The meta-ethics of law: Book One of Aristotle’s Nicomachean Ethics
Upload
khangminh22Category
view
1download
0
Session One
MRCP-PACESETHICS & COMMUNICATION SKILLS
MRCP-PACES/Medical Ethics & Communication Skills/Dr Zein/2013Copyright: KM-426122-613404

1. Ethical issues: Respect for Patient Autonomy Consent Confidentiality/Disclosure/Public interest Justice
2. Public protection:a- Driving;
Epilepsy Diabetes Mellitus and TIA and Heart disease
b- GU infections/Communicable diseases: HIV TB HBV
3. Breaking Bad News
4. Medico legal issues: Resuscitation/DNR Advance directives Brain death & persistent vegetative state Coroner referral Euthanasia Postmortem examination Organs donation Religious bioethics
5. Counseling: Multiple Sclerosis IHD & Cardiac rehabilitation Cystic Fibrosis Huntington’s Disease Rheumatoid Arthritis Uncontrolled DM Bronchial Asthma/COPD
MRCP-PACES/Medical Ethics & Communication Skills/Dr Zein/2013Copyright: KM-426122-613404

6. Procedures:
Heart-Lung Transplant. CABG Pacemakers Bronchoscopy Endoscopy
7. Updated NICE Guidelines:
Beta-Interferon in MS Infliximab (anti-TNF) in RA & CD
MRCP-PACES/Medical Ethics & Communication Skills/Dr Zein/2013Copyright: KM-426122-613404

Layman English:
Feel edgy (an edge): NervousInvalid: Terminally ill Low: DepressedGive way: CollapseHead piece: BrainFainting: Syncope Giddiness: VertigoFits/Shakes: Epilepsy/ConvulsionsRinging in ears: TinnitusBack passage: Anus Bottom: ButtocksPhlegm: SputumTubes: LungsPuffed/Puffy: BreathlessHeart attack: MIThe Welfare: Social servicesGet the sack: Lose jobPuffed up: SwollenTummy/belly: Stomach/bowel Gullet: Oesophagus Feels sick: NauseatedBeen sick: VomitedWind: Flatulence - To belch: Send wind from stomach - To part: ,, ,, anusToilets: Motions/stoolsWater: UrineKeep wanting to go: FrequencyTo get up at night: NocturiaA growth: A mass, cancer (also: the big C)Lose: MensesPictures/Imaging: X-RaysTemperature: FeverGet back/Flare: RelapsesTo be looking/to turn the corner: ImprovesTo be laid up: Confined to bedTo find one’s legs: Start walks after illness To have a bad turn: Becomes suddenly illTo have a bug: To catch a virus/infectionTo lose one’s nature: Becomes impotentTo go steady: To have a regular partner
(Ref: English for Overseas Doctors)
MRCP-PACES/Medical Ethics & Communication Skills/Dr Zein/2013Copyright: KM-426122-613404

The British Health System
Guidelines & Policies: The General Medical Council (GMC) The National Institute of Clinical Excellence (NICE) The Scottish Intercollegiate Guidelines Network (SIGN) The Royal Colleges
Hospitals (NHS): SHO, SpR, Consultants The GPs The Social Services System The Home Health Care Preventive Section, CICD The Legal Advisor, the Coroner system, etc Occupational health services & rehabilitation The Nursing teams:
- Specialist nurses (diabetes, Asthma,)- District nurses- Teams (e.g. McMillan team) - Nursing homes
Voluntary agencies Support groups & Societies (MS)
MRCP-PACES/Medical Ethics & Communication Skills/Dr Zein/2013Copyright: KM-426122-613404

Station 4: ETHICS and COMMUNICATION
Candidate’s Instructions:
o You will be given 5 minutes before entering the examination room to read a scenario & to make your plan of action. On hearing the bell, enter the room & begin the consultation.
o You will have 14 minutes to interview the patient/actor & one minute after he/she leaves the room to organize your thoughts and to prepare yourself forthe discussion with the examiners.
o Don’t re-take history from the patient and don’t examine him/her.
In this section some scenarios will be presented & will be followed by a suggestion on howto approach similar situations when you, hopefully face them in your actual examination.This will be preceded by short talks emphasizing essential ethical & legal issues and some important guidelines e.g. DVLA, INF in MS, End of life decisions etc.A comprehensive knowledge of UK law is not required from overseas candidates; however,they are expected to know in broad terms relevant ethical & legal principles.Many candidates fail this section of the PACES examination not as a result of its difficulty, but because they fail to prepare to it adequately. On the other hand, many of the successful ones feel that with good preparation, success in this section is probably more predictable than in any other section of this exam.
***The key sentence to success is “Practice & practice till mastering”
MRCP-PACES/Medical Ethics & Communication Skills/Dr Zein/2013Copyright: KM-426122-613404

Station 4: ETHICS and COMMUNICATION
USEFUL HINTS
When given the scenario outside the examination rooms STUDY it carefully & decide at first which ethical/communication principle is being tested.Then on the provided paper write down the points that you would like to discuss with the patient/actor & the plan of action needed to manage the given problem.
On entering the exam. room, start by greeting the examiners then sit facing the patient, greet her/him & introduce self and explain role e.g. “ Hello Mrs. X. I’m doctor Y, the medical SHO who is looking after your husband”. Then agree the purpose of the interview “We are here today to discuss the result of his bone imaging. Is that right? Would you like to discuss any other issue?”
Maintain good eye-to-eye contact with the patient & put him/her at ease.
Start the interview with open-ended questions “e.g. what do you know about your husband’s condition?” or “I learned from your GP’s letter that you have had a seizure last weekend, can you tell me more about that?”
Use close-ended questions as the interview progresses.
Provide clear & understandable explanations
Avoid using jargons
At the end of the interview:
- Agrees a clear course of action with the patient - Summarizes
- Check understanding (e.g. “what message you will take home with
you?” or “what are you going to tell the other members of the family?”) - Shake hands & say goodbye.
MRCP-PACES/Medical Ethics & Communication Skills/Dr Zein/2013Copyright: KM-426122-613404

PRINCIPLES OF MEDICAL ETHICS
The 4 Principles of Medical Ethics1. Respect for Patient Autonomy2. Beneficence3. Non-maleficence4. Justice
1. Respecting the patient’s Autonomy: (wishes & self-rule)Autonomy: means self rule i.e.(the capacity to think, decide & act freely and independently). It is the patient’s right to be involved in any decision about his health.This requires that the health professionals help patients in making their own decisions and respect & follow these decisions. Respect of autonomy implies that doctors treat competentpatients in accordance with their informed choices, even if these conflict with the doctor’s beliefs.
2. Beneficence: (doing good to & promoting of what is best for the patient.)This entails doing what is best for the patient.In most situations 1&2 lead to the same conclusions, however, the two principles conflict when a competent pt. chose a course of action that is not in his/her best interests.* If such a conflict arises (Autonomy vs. Beneficence):
1. Make sure that the patient is competent2. Explain the possible consequences of his choice (e.g. refusal of treatment)3. Suggest discussing others (a friend, family member, etc) & a senior colleague4. Respect the patient's autonomy
3. Non-maleficence: (do no harm, need to avoid harm)With regard to treatment & procedures, the potential goods & harms and their possibilities must be weighed up to decide what, overall, is in the patient s best interest. * *These two last principles imply that:
1. Treatment must be thought likely to be successful OR that,2. Potential benefits overweight potential risks.
4. Justice: (fairness in provision of health care)Refers to the duty of the doctor to the whole society.
A. Patients with similar situation should get accessibility to similar health care.B. When determining what level of care should be available to one set of patients, we
should take into account the effect of such use of resources on other patients (i.e. wemust try to distribute limited resources fairly). Using these resources to aggressivelytreat a terminally ill patient is potentially depriving others of the treatment.
MRCP-PACES/Medical Ethics & Communication Skills/Dr Zein/2013Copyright: KM-426122-613404

*Sometimes the patient's autonomy conflicts with the "Public Interest". In such a case the latter must be respected; as your role for the whole society is more superiorto respecting the patient's autonomy.
CONSENTING PATIENTS
Types of Consent:1. Expressed: Written or verbal agreement for the procedure2. Implied: e.g. the patient’s action in response to a request for exam.3. Statuary: When the law requites a particular consent e.g. IVF
Elements of valid consent:VALID CONSENT =
Understanding (Competent patient + Appropriate Information)+ Voluntary decision (i.e. without coercion)
True informed consent requires that the patient does not merely passively assents to the doctor’s decision, but specifically authorizes the doctor to initiate the medical plan.
Information to be provided to the patient: Diagnosis/Prognosis Uncertainty about the diagnosis/need for further investigations Purpose, details & expected outcome of procedures Likely benefits & probability of success Possible side-effects & complications
Techniques:- Use illustrations, written or visual aids for explanation- Allow a relative/a friend to attend if the patient agrees - Involve other staff e.g. a nurse- Give a balanced view- Allow sufficient time for reflection & decision-making
Consent in English law:What is Competence (Capacity)?A competent patient must fulfill the following requirements & demonstrate them repeatedlyand consistently:
Understands a simple explanation of his/her medical condition, treatment and expected outcome.
Is able to reason about specific goals of treatment & choose to act on the best of such reasoning.
Communicates his/her choice & the reason for this choice. Understands the consequences of such choice.
MRCP-PACES/Medical Ethics & Communication Skills/Dr Zein/2013Copyright: KM-426122-613404
N.B. - A patient should not be regarded as incompetent merely because he makes a decision that is against his best interest. - Competence is “function specific”
Consent cont’d…
(1) Competent patient:A. A competent patient may refuse any, even life-saving treatment.
Anything done without the patient’s consent, even touching, is battery (for which damage may be awarded). In contrast to negligence, the patient doesn’t need to prove that he/she has suffered harm as a result of the battery for damages to be awarded.
B. The patient should be given information about the nature of the procedure or other medical interventions (otherwise battery), common & rare side-effects, benefits & reasonable alternatives (otherwise negligence: failure to give appropriate information to the patient before choosing to accept/refuse a treatment or a diagnostic test.
(2) Incompetent patient: Possible approaches:
A. Doctors should act in the best interests of patients.Relatives & friends may be approached as a source of information to judge the patient’s best interests, but can’t give or withhold consent (i.e. there is no proxy consent for an incompetent adult patient).NB: Tutor dative (Partnership giving)
B. Substituted judgment: What treatment option would the patient choose if he become competent?To answer this question, Consider:
- The patient’s previously expressed preference - His general values & backgrounds- The doctor’s experience with other patients
C. Advance Directives: Should be respected after ensuring that the patient was competent & had all the relevant information and that he had considered the clinical situation that has arisen.D. Involve hospital’s legal adviser/apply to the Court if:
There are differences of opinions/controversy in therapy.
Examination/testing & treatment without consent:
1. For life-saving procedures when the patient is unconscious/incompetent to indicate his/her wishes.
2. Where a patient is incapable of giving consent as a result of a mental illness, the treatment should be based on the patient’s “best interest" principle.
MRCP-PACES/Medical Ethics & Communication Skills/Dr Zein/2013Copyright: KM-426122-613404

3. Where a minor (<18 years of age) is a ward of Court & the Court decides that a specific treatment should be given in the child’s “best interest”.
SESSION TWO
MRCP-PACES/Medical Ethics & Communication Skills/Dr Zein/2013Copyright: KM-426122-613404

Useful Skills in Breaking Bad News
BBN Step-by-step: (1)Preparation:
Before talking to the patient / relative:- Have all the facts available; ensure privacy, uninterrupted interview, etc- Make sure that support is available from an experienced nurse, a relative / friend or an appropriate religious support- Find out with whom you are going to speak/Any relatives around?
(2) Check awareness:Establish the patient/relative’s current knowledge e.g. “Have you any thoughts of what might be causing your / her pain or problem? --- What you understand from all the teststhat were carried out? --- Have you any idea of what’s going wrong with you?”This will help to judge the gap between the person’s perception & the reality.Is more information wanted & how much?“Would you like me to explain a bit more? Do you like to know everything? Don’t force information into the patient.
(3) Give a “warning shot”:“I am afraid that it looks rather more serious”Then pause to allow the pt to prepare for the news. The pt will then ask for clarificationor re-maintain an eye contact when ready to listen to more.Then give further details, to narrow the gap step-by-step. Avoid information overload& the use of jargons. Speak out slowly & clearly.
(3)Pausing & acknowledging distress:Don’t be afraid of silence.Allow time for the bad news to be absorbed & the response to occur.Wait for a signal that the pt. is ready to re-engage in the conversation.Actively acknowledge distress “I can see that what you have heard has made you very upset”
(4) Encourage ventilation of feelings:This is the key phase in items of pt satisfaction with the interview. It also gives you the chance to show empathy.
MRCP-PACES/Medical Ethics & Communication Skills/Dr Zein/2013Copyright: KM-426122-613404

(5) Reactions to the bad news:Crying:Avoid looking embarrassed & let the pt know that this is understandable & normal behavior, also avoid speaking whilst the patient is recovering his composure.Have tissues available
Anger: Anger is from the bad news & is not against you. Remain objective, stay calm & don’t get defensive. Denial/disbelief:A useful coping mechanism. e.g. “Are you sure that he is dead? Could there have been some mistake e.g. identification?Are you sure that these reports are mine?"Firmly, but gently, reassure the person.
Quilt: e.g. “I should have made him come to the hospital earlier!”
(6) Discussing prognosis:(Key advice: Be honest & realistic- Avoid giving specific time frames.)
**Commonly asked Q’s about death & dying:
“Am I going to die?”“I am afraid that your cancer is so advanced, that it is likely to shorten your life”
“How long have I got?”A useful framework is “I can not tell exactly. It may be months rather than years, but it is unlikely to be a few weeks”A better approach might be: “Different cancers behave differently in different people & it isn’t possible to predict exactly how they behave in each individual”+ Encourage hope: “Let us look foreword e.g. symptom control, a birthday, X-mas etc”
MRCP-PACES/Medical Ethics & Communication Skills/Dr Zein/2013Copyright: KM-426122-613404

Collusion with relatives:“Don’t tell him doctor, the news will kill him."
When requested by relatives not to tell the patient: 1) Acknowledge their concerns & stress. Explain that you will handle the matter
sensitively.2) Outline the ethical position often helps. e.g. “ Your husband(the pt.) has the right to
know if he wants, but I will not force the information on him.”3) Stress that it is best to be open now about the situation rather than risking the
distrust of the patient if he found out at a later stage.
Then explain that telling him about the bad news is not all bad “He might have things to do, specific people to be around, some wills to tell, planning for the journey, etc”
(6) Identifying other concerns: - Elicit all the pt’s main concerns (e.g. pain relief chemotherapy, surgery etc.)
before giving advice or further information. - Reassurance can be given that every effort will be made to help the patient e.g. giving the best possible care, helping pain relief etc. - Don’t give a false reassurance about the future. - Foster hope but don’t allow misunderstanding treatment for cure.
(7) Summarizes,& Check understanding frequently:
e.g. “What message you are taking home with you?” “What you are going to tell the other members of the family?”
(8) Ensure continuity of care/support:
Support: e.g. “ We will do our best to make you/him as comfortable as possible” Explain the potential treatment available & share with him/her the management
plan e.g. radiotherapy for bone metastasis, feeding etc Offer availability
(Document in the patient’s medical records)
MRCP-PACES/Medical Ethics & Communication Skills/Dr Zein/2013Copyright: KM-426122-613404

Useful Strategies in BBN:
Always respect the patient autonomy. Don’t discuss his condition with relatives without his consent.
Honesty is the best policy. Don’t tell the pt more than he/she wants to know Never give a specific time period Don’t take all the hope away; find some reason to be optimistic e.g. encourages
the pt to look foreword to a particular event such as a birthday, a period of remission or pain-free death. However, you should never give a false hope.
Pitfalls in Breaking Bad News:
BBN without exploring the patient's willingness to know them Being unsure of the information to give to the patient BBN too early without preparing the patient by a reasonable "warning shot" Delaying the bad news in a fear of the patient reactions Getting shaky or hesitant when asked direct Qs by the patient like "Is it cancer?" Or
"Is she going to die?" Remember to break the BN at an appropriate time & to leave adequate amount of
time to deal with the patient's reactions, other concerns, or discussing other relevant issues e.g. DNR, Postmortem, etc
MRCP-PACES/Medical Ethics & Communication Skills/Dr Zein/2013Copyright: KM-426122-613404

Session Three
MRCP-PACES/Medical Ethics & Communication Skills/Dr Zein/2013Copyright: KM-426122-613404

Counseling for an HIV testing
Objectives of Pretest discussion:
1. To clarify why the patient have to be tested & what are his expectations2. To provide information on technical aspects of the test3. To provide information on possible implications of the test 4. To educate about risks of transmission & risk reduction
Consenting for HIV testing:- In most cases informed consent is sought. Written consent is only required from blood donors and for life insurance.- Implied consent can be assumed when an individual is requesting to be tested.- When testing a seriously ill patient in order to make a diagnosis, the doctor should act in “the patient’s best interest”. Informed consent should normally be obtained.
Pretest Counseling:
Technical aspects of the HIV test:A simple, clear & jargon-free explanation of the test should be given to the patient. Written materials should be available as some individuals may like to defer the test.Examples of information that patients need to be told:- It is a simple blood test & its result will be available the same day.- It reflects the HIV status in the previous three months (explain in a simple language
MRCP-PACES/Medical Ethics & Communication Skills/Dr Zein/2013Copyright: KM-426122-613404
Pretest discussion checklist Introduce yourself & clearly identify your role Assess risk factors & explore HIV/AIDS Explain the test procedures Discuss potential advantages/disadvantages Discuss coping with the test results Identify personal, social & medical support systems Discuss how to protect sexual partner(s) in the meantime (safer sex and/or
safer drug use) If a female, discuss pregnancy & fertility Check who the patient like to tell & who has already been told
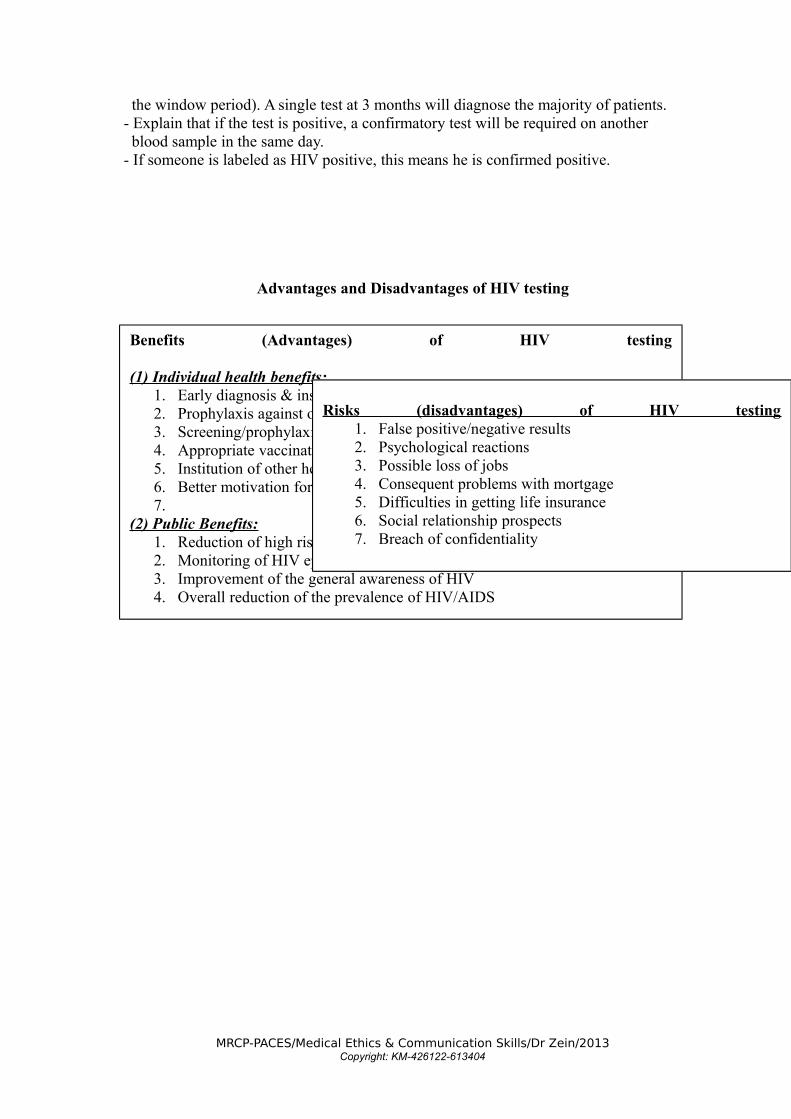
the window period). A single test at 3 months will diagnose the majority of patients. - Explain that if the test is positive, a confirmatory test will be required on another blood sample in the same day. - If someone is labeled as HIV positive, this means he is confirmed positive.
Advantages and Disadvantages of HIV testing
MRCP-PACES/Medical Ethics & Communication Skills/Dr Zein/2013Copyright: KM-426122-613404
Benefits (Advantages) of HIV testing
(1) Individual health benefits:1. Early diagnosis & institution of anti-retroviral therapy2. Prophylaxis against opportunistic infections e.g. PCP3. Screening/prophylaxis against TB, STD, etc4. Appropriate vaccinations5. Institution of other health measures6. Better motivation for safer sex and drugs use7.
(2) Public Benefits:1. Reduction of high risk behaviors & attitudes2. Monitoring of HIV epidemiology3. Improvement of the general awareness of HIV4. Overall reduction of the prevalence of HIV/AIDS
Risks (disadvantages) of HIV testing1. False positive/negative results2. Psychological reactions3. Possible loss of jobs4. Consequent problems with mortgage 5. Difficulties in getting life insurance6. Social relationship prospects7. Breach of confidentiality

HIV: Introduction to discussion
- A discussion of diagnostic possibilities & results of investigations to date may help.- Check awareness of: - Nature of the test - Difference between HIV and AIDS
- Risk factors/risk reduction methods- If there is evidence of HIV, the patient should be told of this.- Ask him/her if there are any thoughts as to what the illness might be? - Enquire about risk factors in an indirect way e.g. marital status, sexual activities, partner(s)/, exposure to high risk behaviors, PH/ STD, travel abroad, drug use, blood transfusion etc- Ask about any previous test or recent blood donation.- Ask if he would like to have an HIV test performed? Educate:- Methods of transmission, risk factors & how to reduce them.- That every day social & domestic activities are safe.- That the patient will have continued medical care regardless of the test result.- Discuss advantages & disadvantages of testing and how he/she will cope with result.- Inform of the availability of social & psychological support.
Confidentiality:- Patients can be reassured that their HIV results will only be seen for “Medical” reasons by doctors& nurses involved in their care.- Samples may be labeled “High Risk” & phrases like “Low T4 Count” or “Retroviral Illness” may be used.- Reassure the patient that the front of the notes will not be changed to identify the infection. (See section 2of NHS Venereal Disease Regulation 1974)- It is important to discuss with patient who they want to made aware of their illness e.g. a partner, family doctor etc- As a general rule, information is best disclosed on “A Need to Know” only.
MRCP-PACES/Medical Ethics & Communication Skills/Dr Zein/2013Copyright: KM-426122-613404

HIV: Giving the result
If the result is POSITIVE:
o BBN: --- Shock, anger denial etc ----- EMPATHYo IS IT HIV OR AIDS?o Plan of action:o – What is the next step? o – Who will be looking after the patient? o – What further tests need to be done? o – Any therapeutic measures/interventions?o – With whom the patient wishes to share the information?o – Educate: safer sex, injecting practices etc o – Be ready to answer the patient’s questions & queries, e.g. “How long have I been infected?” In this case the patient wanted to discuss who else might have been infectedo – Give written informationo – Provide the patient with a list of voluntary agencies, support groups, and social work facilities.
If the result is NEGATIVE:
o Advice to repeat the test after 3 months (The Window Period)o Asserting safer sexual or injecting practices (Risk Reduction)o Clearly emphasizes to the patient that a negative test does not mean that he/she is
immune against HIV infection unless the present practice is modified.
Needle-stick injuries: (See attachment)
MRCP-PACES/Medical Ethics & Communication Skills/Dr Zein/2013Copyright: KM-426122-613404

Session Four
MRCP-PACES/Medical Ethics & Communication Skills/Dr Zein/2013Copyright: KM-426122-613404

End of Life Decisions & Terminal Care
Discussing Resuscitation Status & DNR with patients and relatives
Justifications for making Do- Not- Resuscitate (DNR) decisions:1. When a fully-informed competent patient asks not to be resuscitated2. A poor quality of life following a successful CPR is anticipated3. Futility: the chances of the patient surviving CPR are so low that it can be regarded
futile. This is a clinical decision, which doesn’t need involvement of the patient, & there is no obligation to attempt CPR in such cases. Examples: disseminating malignancies, septicaemia, severe HF etc
A DNR decision isn’t necessary to discuss with patients:1. If the patient is incompetent 2. If the decision was made on grounds of futility3. If a competent patient indicates that he/she doesn’t wish to discuss it4. This may also be justified in competent patients, without obtaining consent, if
decision is based on basis of “poor quality of life”.
Discussing DNR decision with patients & relatives:1. Competent patients:
- The discussion should aim at determining the patient’s views of his/her quality of life.
- Relatives should only be involved in discussion with the patient’s consent. - Relatives may be discussed if the decision is made on “Poor quality of life” Basis & the patient don't like to discuss the issue. 2. Incompetent patients: - The doctor should decide on the “Best interest” of the patient. - Relatives & friends can be discussed for the purpose of getting a better idea of the patient’s wishes and also to determine whether there is an Advance Directive (Living will)
What facts need to be told to the patient? - The patient should be fully informed about the diagnosis & prognosis - That CPR is usually unsuccessful. - About 10 – 20% survive to leave the hospital & for one year afterwards - The possibility of survival with a neurological damage should be pointed out. However, these are relatively uncommon; 1 –2% survives in a Permanent Vegetative State (PVS) - Elderly patients with chronic illnesses have < 5% chance of survival to discharge. - Ascertain that the patient understand that if they have a cardio-respiratory arrest & they don’t have CPR, they will almost certainly die. - That a DNR is a Consultant decision.
MRCP-PACES/Medical Ethics & Communication Skills/Dr Zein/2013Copyright: KM-426122-613404

Session Five
MRCP-PACES/Medical Ethics & Communication Skills/Dr Zein/2013Copyright: KM-426122-613404

Sudden Death of a family member(A special form of breaking bad news that requires great empathy)
(A) The interview with the relative; Breaking the bad news:Preparation: - Check your facts about the deceased per son, his illness, etc.
- Put him at ease. - Make sure that support is available (an experienced nurse/other health professional, a relative/friend, religious support, etc).
(1) Introduce your self, explain role & identify the relative. Also check whether other relatives are around / need to attend the interview.
(2) Establish his current information/ knowledge of the situation:
(3) Give a warning shot :
(4) Wait for his response, then BBN: - Don’t wait too long as this will aggravate the agony. - Be ready to confirm direct questions e.g. “Is he dead?” - If there is no direct question: Use a clear & simple language to give a brief description of the illness and explain that treatment/resuscitation hasn’t been successful & the patient has died.
(5) Give relatives the chance to ventilate . Express empathy & give more details when needed. - Insure & show continued care and support to the family. E.g. – Offer transport to home, give details of contact with the department for more explanation etc. - Allow accessability to the deceased body, it is important for some people to see and hold their dead loves ones & to keep a lock of their hair. - Provide clear explanation of any visible injuries
(9) Always Summarize & check understanding.
MRCP-PACES/Medical Ethics & Communication Skills/Dr Zein/2013Copyright: KM-426122-613404
(B) A Request for Organ Donation:
A. Many relatives ask about organ donation.B. Otherwise you can sensitively & at the suitable time, bring the issue for discussion. This can be addressed in many ways; one approach is to ask whether the deceasedhad expressed any wishes/advanced directive in this regard (check also if he has a donor card). You can also invite the discussion by telling other people’s experiences e.g. “Some people in a situation similar to yours like to make good to their loved ones by donating their organs to some patient who are in desperate need of them.” “His internal organs can be used for other patients who need them to maintain their lives”
Re. Corneal Donation: The eyes must be removed within 6 hours if the corneas are to be donated. Contact the eye hospital. If death has to be reported to Coroner, his/her permission must be obtained
before organs are donated. (C) Requesting permission for a Postmortem Examination:
-Approach in a sensitive & understanding manner that allows relatives to make well- informed decisions. - Explain the specific reason for the PM request & the benefits of PM exam. - The request should be made in a way that doesn’t put pressure on relatives. - Relatives should be given enough time to think about the issue & to discuss
with other members of the family if they wish to do so. - Try to explore relative’s misconceptions regarding PM & to find out the reasons for refusal and then to clarify them(refer to information box ). - Relatives should be informed of the PM results as soon as possible.
- Clinicians should be: - Able to anticipate & cope with the concerns and reactions of relatives at the time of bereavement. - Aware of the possible cultural/religious impacts related to death, funeral arrangements & attitude towards PM. - Aware of the administrative procedures. - Able to explain the difference between medico legal & academic PM. (NB. In non-medico legal PM consent is required from the next of kin). - Able to consider possible alternatives in case of PM refusal E.g. limited PM, laproscopic/endoscopic exam. etc - Be aware of deaths reportable to the Coroner!
MRCP-PACES/Medical Ethics & Communication Skills/Dr Zein/2013Copyright: KM-426122-613404

MRCP-PACES/Medical Ethics & Communication Skills/Dr Zein/2013Copyright: KM-426122-613404
Reasons for consent for a Postmortem examination:1- To establish the precise cause of death2- To confirm the diagnosis3- To help others / medical researches etc4- To respect the wishes of the deceased / family 5- Organ donation
Reasons for refusal of Postmortem:1- Concerns about disfigurement of the deceased2- Interference with funeral arrangements3- Lack of information about the reason for PM4- Religious / Cultural (e.g. Muslims, Jews, Afro-
Caribbean’s, Christian Scientists)5- Respect for the deceased & their wishes 6- Too upset to consider it 7- A desire to finish things as soon as possible8- Objection from other family members
Deaths reportable to the Coroner:1- The deceased wasn’t seen by a doctor within 14 days prior to death2- If the death:
A. Is of suspicious circumstances, there is a history of violence or may be linked with an accident
B. May be linked with an abortionC. Is related to a medical procedure or treatmentD. Had occurred during an operation or before full recovery from anesthesia (or
in any way related to anesthesia)E. Is due to lack of medical careF. Is due to industrial disease or in any way related to the deceased
employment.G. Occurred during or shortly after detention in police or prison custody.
3. The actions of the deceased may have contributed to his death.

COUNSELING RELATIVES FOR A POSTMORTEM EXAMINATION
If a relative is concerned about PM examination: Speak to the relative aiming at: exploring their main concerns about PM, improving their understanding & give justifications and benefits of PM exam. e.g.- The PM may provide useful information that was not available when the deceased was alive.- The PM results may assist relatives overcoming their grieving reaction. It may lead to peace of mind by knowing the cause of death & that the appropriate care was given.- The PM can be beneficial, not only to medical profession, but also to the family & the society in general (give examples)- Medical profession can gain vital feedback about accuracy of diagnosis, effects of treatments, etc.
(1) Reassurance re. disfigurement: The PM exam. is similar to a surgical operation & is carried out by
medically-qualified pathologists. The outward appearance of the deceased would not be altered in ant way
& no external markers would be visible apart from incision scar.
(2) Reassurance re. possible interference with funeral arrangements: PM exam. will only need a short time to perform. In urgent cases, the PM can be expedited.The mortuary staff can liaise with the funeral director to release the bodyin a reasonable time.
MRCP-PACES/Medical Ethics & Communication Skills/Dr Zein/2013Copyright: KM-426122-613404

MRCP-PACES/Medical Ethics & Communication Skills/Dr Zein/2013Copyright: KM-426122-613404
THE BENEFITS OF PM
A. For the relatives: Knowledge of the precise cause of death / Confirmation of the diagnosis. Reassurance & peace of mind. Alleviation of guilt by reassurance that death
was inevitable & that all the needed care was provided. Identification of possible hereditary conditions. Helping others e.g. organ donation. Assistance in advances in medical knowledge. Insurance & compensation claims.
B. For the medical profession: To establish the precise cause of death. Gives a feedback about the accuracy of the clinical diagnosis. Aids in medical audit & risk management. Enables researches & advancement in knowledge. Improves accuracy of epidemiological statistics.
C. For the society: Improvement of accuracy of epidemiological statistics. Organ donation. Identification & prevention of environmental and occupational hazards /
infectious diseases & epidemics. Improvement of medical knowledge.

Session Six
MRCP-PACES/Medical Ethics & Communication Skills/Dr Zein/2013Copyright: KM-426122-613404

COUNSELLING
Guidelines for Giving Information to a Patient (1) Check how much information to give. E.g. test result, diagnosis, management plan, advice on life style, etc “Would you like to know the result of your bone scan? Do you want to discuss any thing else?” Then explain accordingly.
(2) Summarizes the patient’s problems. E.g. “ You have told me that your Asthma isn’t as well controlled as it used to be. Is that’s right?”
(3) Check the patient’s Understanding of his condition. E.g. “Have any thoughts of what might be the cause of this problem?”
(4) Outline the Structure of the interview. E.g. “Now we are going to discuss several things: 1 st: what I think is wrong with you. 2 nd: what further tests we need to do, and lastly: what treatment I’m going to give you. Is that’s ok?”
(5) Use appropriate language: - Describe and explain each piece of information- Give the most important information first. - Use short sentences.- Be specific.- Avoid medical jargons
(6) Use drawings when appropriate.
(7) Explore the patient’s views: E.g. “Perhaps you could tell me what you think about that”
(8) Negotiate management. If necessary, help the patient in making his decision
(9) Check understanding: E.g. “Well, Mr. James, I seem to have given you lots of information. Would you like to just go over what we have said?”
(10) Summarizes.
MULTIPLE SCLEROSIS
MRCP-PACES/Medical Ethics & Communication Skills/Dr Zein/2013Copyright: KM-426122-613404

What should the patient be told?- Ask the patient if he/she have “Any thoughts about what might be wrong with you?” “Any particular condition worries you?”- BBN step-by-step- Educate: what is MS- Check understanding “What are you going to tell your family?”- Consequences:
Difficult to get life insurance or promotion at work Alteration of life style Psychological & emotional burden
- Positive aspects of diagnosis: NOT a brain tumour & NOT a mental disease Benefits of early diagnosis & treatment with Interferon beta & copolymer
- Early follow-up appointment: To give the patient the chance of asking questions in a calmer state of mind.- Provide support & information:
Written information, videos Specialist nurse Social worker Occupational therapist for self-support measures Local MS society- shouldn’t be rushed as an early visit may be depressing for a
newly-diagnosed patient
What information to give? MS is a chronic disease affecting 1:1000 of UK population Cause is NOT known At present NO medical cure, but there are treatments which can help many
symptoms Course: -Variable & is very difficult to predict.
- Different in each individual - Initially may be relapsing & remitting with full recovery between the attacks. Length of relapses (flares) is 24 hrs.-12 months. Rate of relapses is around 1:100/year. Relapses are more common in the first 5 years & particularly the first year. - May become progressive at any time, secondary progression affects 40% patients by 10 years & 60% by 15 years. Progression is not inevitable. - Primary progression from the onset occurs in 10-20% cases. - There is a clear relationship between progression & late age of onset - Foster hope by giving examples of good predictive features applicable to the patient.
MRCP-PACES/Medical Ethics & Communication Skills/Dr Zein/2013Copyright: KM-426122-613404

Employment:
Different studies: - In the first 5 years: up to 50% were in full work & 70% capable of some work - By 15 years: 10-25% were in full work & 40% of long-term survivals are capable of some useful activity. Spastic paraparesis is the major cause of loss of work. More patients could work from home.
Life expectancy:
- Is strongly predicted by the degree of the disability.- Death isn’t directly caused by MS but results from infective complications- Life expectancy was found to be only 6-7 years less than population without MS for the ages 20-50 & this is even less after the age of 50.- Many individuals have normal life expectancy.
Pregnancy:
- Fertility isn’t reduced- No increased risk of abortion or stillbirth- No specific complications of labour- No contra-indications to breast feeding- There is slight risk of relapse during the first 3 months after delivery.
Genetics:MS doesn’t occur more common in relatives than in general population. The risk of a child being affected is 1-4%.
Self-help measures:- No specific diet alters the course of MS.- Symptoms may be aggravated or induced with exertion. Advice to avoid excessive fatigue, but otherwise to continue normal activities.
MRCP-PACES/Medical Ethics & Communication Skills/Dr Zein/2013Copyright: KM-426122-613404

HUNTINGTON’S DISEASE - Progressive chorea & dementia in middle life are the hallmark- Onset: 30-50 years. Prevalence is 1:20000 . AD with full penetrance.- Mutation in the short arm of Ch 4 with variable expression of CAG- repeat in exon1. This results in translation of an extended glutamine sequence in huntingtin; the protein product of the gene.
Pathology:- Cerebral atrophy with marked loss of neurons in the CN&P. - Changes in neurotransmitters
Course:
- Progressive illness & death occurs between 10-20 years of onset.- NOT a cancer & NOT a psychiatric disorder- Initial symptoms: personality or behavioral changes, uncontrolled aggression or sexual behavior. Serious depression is common & suicide is a risk. Later- rigidity & akinesia - bed ridden & emaciated - death- NO cure.- NO treatment to arrest the disease although phenothiazines(e.g. sulpiride) may reduce chorea. Tetrabenzine helps to control movements.- Chronicity & disability - psychological impact on family: Consider residential care- Supporting the family is essential.
Family Screening:
- Children of patients have 1:2 chance of having the disease & their children have 1:4 risk- Using molecular genetics. Blood DNA samples are required from as much family members as possible.- Mutation analysis (accurate &specific) is available for pre-symptomatic testing of family members. Centers performing these tests have a common nationally agreed protocol for counseling.- Pre-natal diagnosis is possible.
MRCP-PACES/Medical Ethics & Communication Skills/Dr Zein/2013Copyright: KM-426122-613404
MRCP-PACES/Medical Ethics & Communication Skills/Dr Zein/2013Copyright: KM-426122-613404

MRCP-PACES
Station 2: HISTORY TAKING
(SHOULD BE PROBLEM-FOCUSED & WELL STRUCTURED WITH SPECIAL CONSIDERATION TO SOCIAL CIRCUMSTANCES)
THE 3 MAIN TASKS:
1. OPENING THE ENCOUNTER:
- Greet by name- Introduce, explain role- Agrees the agenda- Explain note-taking
2. MAIN DISCUSSION
- Gathering information- The main skillful task to promote disclosure- ICE (Ideas, Concerns & Expectations)
3. CLOSURE:
- Encourage the patient to ask questions & express Ideas, Concerns & Expectations (ICE)
- Counsel on health promotion- Agree a mutually satisfactory plan and follow up. - Check understanding & Correct when necessary.- Goodbye & Offer availability.
MRCP-PACES/Medical Ethics & Communication Skills/Dr Zein/2013Copyright: KM-426122-613404

MRCP-PACES
Station 2: HISTORY TAKING
A. Opening the encounter:
Engagement (Starting the interview):
- Great by name- Introduce yourself & Explain your role- Build good rapport- Agrees the agenda- Explain note-taking
B. Gathering the information:
Presenting Complaint (PC):
- Elicit the main presenting problem(s).- Any other problem?
HPC:- Full detailed h/o each complaint from onset to date.- Clarify each problem before moving to the next.- Appropriately use open & close-ended questions.- Nature: e.g." Would you tell me more about the problem/symptom"- Onset: "When it started?"- Duration: "How long it lasted?"- Pattern: - Continuous/Intermittent - Episodic (frequency, severity & duration of each episode)- Course to date:(static, progressive, or improving)- Precipitating/Relieving factors.- Associated symptoms.- Patient's view/perception of his/her problem: "Any thoughts of what
might be causing this problem?"- "Do you want to add anything which I might forget to ask about?"- Effect of symptom/problem on quality of life?- Summarize.
PMH:- Open Q: "What about your health otherwise?"- Similar problem?- Specific: DM, HTN, HD, BA, etc - Hospitalizations & Operations
FH:- Open Q: "What about the health of your family?"- All 1st degree health (parents, siblings, children)- If any death: Age & cause of death.- Specific: DM, HTN, HD, BA, etc
MRCP-PACES/Medical Ethics & Communication Skills/Dr Zein/2013Copyright: KM-426122-613404

DH:- Ask about the drug's list.- Enquire about each drug:- Dose, frequency, duration- Does it help?- Compliance. - SE: "Have you experienced any problem with this drug?"- Any recent change in medications?
ROS (Review of systems):- Always ask about: general wellbeing, fever, appetite, wt
loss/gain, rashes, - Briefly enquire about each body system.- Then ask in more depth about affected system.
SOCIAL Hist. (SH):1. Occupation: Present & previous" What do you do for living?" If unemployed,
ask about pensions.2. Marital status: ?partner(s), sexual life/orientation3. Smoking.4. ALCOHOL: Detailed: quantity, type, and frequency. CAGE5. Finance: income support, invalidity benefits, other allowances & adequacy
of these.6. Availability of Support: Practical & emotional: Home help, district nurse,
social worker, occupational therapy, etc7. Impact of problem: Ability to work, coping with daily activities, mood,
personal relations, etc8. House: flats, steps, modifications9. Activities of daily living: ?Coping, help10. Hobbies? animals, sports11. Travel: 12. Diet.13. Immunization & prophylaxis.
MRCP-PACES/Medical Ethics & Communication Skills/Dr Zein/2013Copyright: KM-426122-613404

Alcohol history:- Drinking habits: What type? How much? How frequent?
For how long?- Quantity:
1 UNIT alcohol = 1/2 Pint of beer = 1 glass of wine = 1 measure of spirit
- CAGE test: C: Have you ever felt the need to C ut down on drinking? A: ,, ,, ,, ,, A nnoyed by criticism on drinking? G: ,, ,, ,, had G uilty feeling about drinking? E: ,, ,, ,, taken alcohol the first thing in the morning? ( E ye opener)
Drugs:- What about recreational drugs?- Have you ever injected drugs? Shared needled?- Marijuana "pot"- Cocaine "coke"- Heroin, others- Are you using them now? How often?
Smoking:- Do you smoke? Have you ever smoked?- Type, amount, for how long?- Did you ever try to quit?
MRCP-PACES/Medical Ethics & Communication Skills/Dr Zein/2013Copyright: KM-426122-613404

3. Closure:
Check Understanding:"It seems we discussed many issues, and I need to make sure that we havethe same understanding, so:
- What message you take home with you?- What you will tell to a family member(s) if they asked?"
Agrees a clear "Plan of action":Investigations, management, hospitalization, etc
Dispose Appropriately:In the closing portion of the interview, you may:
- Inform the patient of your opinion about the illness (diagnosis, management, prognosis)
- Encourage the patient to ask Qs & to express concerns- Negotiate a mutually satisfactory plan- Counsel about health promotion- Offer advice including follow-up- Any Qs?- Offer availability- Thank & say goodbye
MRCP-PACES/Medical Ethics & Communication Skills/Dr Zein/2013Copyright: KM-426122-613404
COMMUNICATION SKILLS
Useful Skills to promote disclosure
Eye contact:Established at the onset of the interview & maintained at reasonable intervals throughout the consultation. Re-establish when the patient mention important piece of information.
Acknowledging & exploring verbal cues:By that you reflect that you are interested in the patient problem.
Non-verbal cues:Pick, address, explore & acknowledge them.e.g. "You looks anxious, can u bear to say why?"
Open-directive Qs:You can gather lot of information by using open-ended Qs.These are the type of Qs their answers are not yes & no.e.g." Can u tell me more about your bowel problem?"
Closed-ended Qs:These are used when a specific piece of information is needed.e.g. "Does the pain go anywhere else?"
Control & Sensitive redirection:Gently control the interview. If the patient raised a relevant issue while you are discussing another important one, you can suggest postponing the issue till u finish with the first one. However, if the issue raised is not important or irrelevant, you can suggest leaving it for another session.
Negotiation:Always negotiate your plans with the patient & try to reach an agreement. However, if you failed to do so, the priority is for the patient's agenda.
Precision:e.g. " You say u have been suffering dizziness. Can u describe exactly what happens when u experience this?"
Empathy:Use I & you.e.g." I could imagine how that experience had affected you""I understand your concerns about your job""I can see that it is hard for you to care for your dad & the 2 kids"
MRCP-PACES/Medical Ethics & Communication Skills/Dr Zein/2013Copyright: KM-426122-613404

Educational guesses:Share them with the patient.e.g. "When we are talking I got the feeling that your diabetes had affected your job & that ulooks rather worried of loosing it"
Facilitation & Silence:Facilitation: by nodding or by saying" yes, I see, go on, uh-huh, or what else" & by looking attentively to the patient.Never get panic because of silence. This important for both of you & the patient to organize thoughts and to think of "what is next?"
Repetition:Used to foster elaboration. You can repeat the patient's last sentence e.g." chest pain?"
Clarification:You have to clarify any information you are not clear about.e.g." I'm not sure I understand. Would u explain it again?""Do u mean…?" "Could you explain to me what you u mean by light-headed?"
Encouragement & Support:- Fine. That's great. You're doing fine, carry on.- You have put great effort to help your sick mum.- I'm happy that you're working hard to control your BP.
MRCP-PACES/Medical Ethics & Communication Skills/Dr Zein/2013Copyright: KM-426122-613404

MRCP-PACESStation 2: HISTORY TAKING
SUGGESTED STRATIGY
In the 5 mins before entering the examination room, make your plan in the provided sheet of paper:
1. OPENING- Introduce yourself, Role- Privacy- Agenda- Any relative to attend- Explain note taking
2. MAIN DISCUSSION- PC- HPC- ROS- PMH- FH- DH- SH
3. CLOSUING- Agreeing a plan of action- Checking understanding- Disposal
PAIN: SOCRATES Site Onset Character Radiation Association Time (duration) Exacerbating/Relieving Severity
MRCP-PACES/Medical Ethics & Communication Skills/Dr Zein/2013Copyright: KM-426122-613404

MRCP-PACES
The Most Common Case Histories
o Abdominal pain o (IBD)o Jaundice/CLD/PBC o Malabsorption/ Diarrohea - Coeliac o Headache o Epilepsy o TIA (funny turns)/CVAo IHD/CAD/CHFo SOB/Palpitations(PAF)o BA/COPDo Pulmonary fibrosiso Bronchiectasis/CFo DMo Goitre/thyroid diseaseo Pyrexia/Diaaohea following foreign travelo Arthritis/RA, SLEo HBV/HIVo Leukemia/Lymphoma
MRCP-PACES/Medical Ethics & Communication Skills/Dr Zein/2013Copyright: KM-426122-613404

MRCP-PACES/Medical Ethics & Communication Skills/Dr Zein/2013Copyright: KM-426122-613404
Copyright © 2022 FDOKUMEN