
Eradicating leprosy in Saudi Arabia: Outcome of a ten-year surveillance (2003-2012)
7
Eradicating leprosy in Saudi Arabia: Outcome of a ten-year surveillance (2003e2012) Abdullah Assiri a , Saber Yezli a , Tamara Tayeb a , Malak Almasri a , Afolabi E. Bamgboye a,b , Ziad A. Memish a, * ,1 a Ministry of Health, Riyadh, Saudi Arabia b Department of Epidemiology and Medical Statistics, University of Ibadan, Ibadan, Nigeria Received 14 June 2014; received in revised form 3 September 2014; accepted 1 October 2014 KEYWORDS Mycobacterium leprae; Eradication; Epidemiology; Public health Summary Background: The Kingdom of Saudi Arabia (KSA) has a sentinel surveillance system on leprosy for effective monitoring of the disease. Methods: A retrospective epidemiological analysis of all cases of leprosy captured by the sur- veillance system between 2003 and 2012 was conducted. Results: Over the 10-year period, there were 242 reported cases of leprosy in KSA, 67% of which were in those aged between 15 and 44 years of age. Males accounted for over 77% of all cases and non-Saudi nationals, dominated by Indians, and represented 57.4% of the total cases. Just over half of the cases were paucibacillary leprosy, and 9% were grade 2 disability. Makkah region accounted for nearly 42% of all cases. Annual trends showed an overall decline in the yearly cases and prevalence of the disease from 41 cases (0.018 per 10,000 population) in 2003 to 15 cases (0.005 per 10,000 population) in 2012. Conclusion: KSA needs to strengthen the leprosy surveillance systems, as well as health care and community education about the disease which will help effective monitoring, early detec- tion and treatment of the disease. Moreover, the role or migrants in the importation of the dis- ease needs to be addressed to achieve and maintain eradication. ª 2014 Elsevier Ltd. All rights reserved. 1. Introduction Leprosy is a public health problem because of its long incubation period, difficulties in its diagnosis, its trans- mission potential and its capacity to cause permanent disabilities with their social consequences of discrimina- tion and stigma [1e3]. Worldwide prevalence of leprosy has fallen substantially in the past 50 years due to * Corresponding author. Ministry of Health, Riyadh 11176, Saudi Arabia. Tel.: þ96 6505483515. E-mail address: [email protected] (Z.A. Memish). 1 College of Medicine, Alfaisal University, Riyadh, Saudi Arabia. + MODEL Please cite this article in press as: Assiri A, et al., Eradicating leprosy in Saudi Arabia: Outcome of a ten-year surveillance (2003e2012), Travel Medicine and Infectious Disease (2014), http://dx.doi.org/10.1016/j.tmaid.2014.10.002 http://dx.doi.org/10.1016/j.tmaid.2014.10.002 1477-8939/ª 2014 Elsevier Ltd. All rights reserved. Available online at www.sciencedirect.com ScienceDirect journal homepage: www.elsevierhealth.com/journals/tmid Travel Medicine and Infectious Disease (2014) xx,1e7
-
Upload
independent -
Category
Documents
-
view
1 -
download
0
Transcript of Eradicating leprosy in Saudi Arabia: Outcome of a ten-year surveillance (2003-2012)

Eradicating leprosy in Saudi Arabia: Outcomeof a ten-year surveillance (2003e2012)
Abdullah Assiri a, Saber Yezli a, Tamara Tayeb a, Malak Almasri a,Afolabi E. Bamgboye a,b, Ziad A. Memish a,*,1
a Ministry of Health, Riyadh, Saudi Arabiab Department of Epidemiology and Medical Statistics, University of Ibadan, Ibadan, Nigeria
Received 14 June 2014; received in revised form 3 September 2014; accepted 1 October 2014
KEYWORDSMycobacteriumleprae;Eradication;Epidemiology;Public health
Summary Background: The Kingdom of Saudi Arabia (KSA) has a sentinel surveillance systemon leprosy for effective monitoring of the disease.Methods: A retrospective epidemiological analysis of all cases of leprosy captured by the sur-veillance system between 2003 and 2012 was conducted.Results: Over the 10-year period, there were 242 reported cases of leprosy in KSA, 67% ofwhich were in those aged between 15 and 44 years of age. Males accounted for over 77% ofall cases and non-Saudi nationals, dominated by Indians, and represented 57.4% of the totalcases. Just over half of the cases were paucibacillary leprosy, and 9% were grade 2 disability.Makkah region accounted for nearly 42% of all cases. Annual trends showed an overall declinein the yearly cases and prevalence of the disease from 41 cases (0.018 per 10,000 population)in 2003 to 15 cases (0.005 per 10,000 population) in 2012.Conclusion: KSA needs to strengthen the leprosy surveillance systems, as well as health careand community education about the disease which will help effective monitoring, early detec-tion and treatment of the disease. Moreover, the role or migrants in the importation of the dis-ease needs to be addressed to achieve and maintain eradication.ª 2014 Elsevier Ltd. All rights reserved.
1. Introduction
Leprosy is a public health problem because of its longincubation period, difficulties in its diagnosis, its trans-mission potential and its capacity to cause permanentdisabilities with their social consequences of discrimina-tion and stigma [1e3]. Worldwide prevalence of leprosyhas fallen substantially in the past 50 years due to
* Corresponding author. Ministry of Health, Riyadh 11176, SaudiArabia. Tel.: þ96 6505483515.
E-mail address: [email protected] (Z.A. Memish).
1 College of Medicine, Alfaisal University, Riyadh, Saudi Arabia.
+ MODEL
Please cite this article in press as: Assiri A, et al., Eradicating leprosy in Saudi Arabia: Outcome of a ten-year surveillance (2003e2012),Travel Medicine and Infectious Disease (2014), http://dx.doi.org/10.1016/j.tmaid.2014.10.002
http://dx.doi.org/10.1016/j.tmaid.2014.10.0021477-8939/ª 2014 Elsevier Ltd. All rights reserved.
Available online at www.sciencedirect.com
ScienceDirect
journal homepage: www.elsevierhealth.com/journals / tmid
Travel Medicine and Infectious Disease (2014) xx, 1e7

international, national and sub national campaigns, andthe disease has been eliminated globally according to theWHO’s definition [4,5]. Introduction of MTD, improvedearly diagnosis and treatment, integration of primaryleprosy services and effective collaborations and part-nerships have led to a considerable reduction in leprosyburden. Nevertheless, new cases continue to occur inalmost all endemic countries and high-burden pockets canexist against a low-burden background. Official figuresfrom 115 countries show the global registered prevalenceof leprosy at 189,018 at the end of 2012 and during thesame year 232,857 new cases were reported. Of these 95%were from 16 countries (mainly in Asia, Africa, and SouthAmerica) [6].Leprosy is a chronic granulomatous infection,principally affecting the skin and peripheral nerves,caused by the obligate intracellular organism Mycobacte-rium leprae [1,2]. The damage to peripheral nerves re-sults in sensory and motor impairment with characteristicdeformities and disability [1]. Most people withleprosy are non-infectious as the mycobacteriumremains intracellular. Patients with lepromatous leprosy,however, excrete M. leprae from their nasal mucosa andskin and are infectious [3]. The mode of transmission isstill not conclusively proven, although person-to-personspread via nasal droplets is believed to be the mainroute [7].
Leprosy is more common among males than females.This is a well reported fact of leprosy epidemiology and isnot thought to be related to under diagnosis in women,although in some countries it is accentuated by delayedpresentation by female patients, which results inhigher rates of deformity [2]. Generally, after the age ofpuberty, the male to female ratio of leprosy range be-tween 1.5 and 2:1 [2]. However the proportion of femalesamong new cases of leprosy can fluctuate by country. Forexample, in 2010, the proportion of females among newcases ranged from 57.5% in Liberia to 20.8% in Madagascar[6].
There are 2 systems used to classify leprosy patients.The Ridley-Jopling system [8] uses clinical and histopath-ological features and the bacteriological index. Thedifferent categories (tuberculoid leprosy, lepromatousleprosy and borderline leprosy) correlate with the activityof the host immune response. The WHO introduced asimplified classification system that uses the number ofskin lesion to classify disease to simplify diagnosis, facili-tate treatment, and decentralize leprosy services to pri-mary health units as much as possible. This system usesthe term paucibacillary (PB) when a person has up tofive lesions, and multibacillary (MB) for more than 5 lesions[1].
Patients with MB leprosy are more infectious than thosewith PB leprosy: the risk of disease in contacts of cases withMB leprosy is twice as high as that in contacts of patientswith PB leprosy [3]. In addition, patients with MB leprosyhave a higher risk of developing reversal reactions andimpairment of nerve function [9]. And if these patientsrelapse, they resume the ability to transmit the organism toothers [3]. This WHO classification is widely used to guidetreatment decisions.
The diagnosis of leprosy remains a clinical one and iscomplicated by the long incubation period and the
unavailability of laboratory investigation methods. It canbe difficult to diagnose leprosy especially in non-endemicregions or where the prevalence is very low. Late diag-nosis leads to continued transmission and to increased riskof disability [10]. Factors associated with late diagnosisinclude delay by patients in presenting especially due tostigma and delay by health services in making a diagnosis[3]. Multidrug therapy (MDT), which is effective in eradi-cating M. leprae in most patients, was introduced inthe early 1980s after the emergence of resistance todapsone-only regimens [11]. In 1995, a resolution waspassed to provide free MDT to all leprosy patients world-wide [3].
Treatment of leprosy in KSA is free for all Saudi patients.However, non-Saudi patients are treated for only onemonth and then deported to their countries of origin inaccordance with the law in the Saudi Arabia. They areadvised to continue treatment in their home countrieswhile Saudi patients continue to receive treatments in theirregions. Complicated cases of leprosy are referred to IbnSina hospital, the only reference hospital in Saudi Arabia forthe treatment of leprosy. This hospital is located in theMakkah region where the country has the largest concen-tration of both legal and illegal immigrants.
The World Health Assembly passed a resolution in 1991to “eliminate leprosy as a public health problem” by 2000;it defined elimination as reducing prevalence to less than 1case per 10,000 population [4]. Elimination of leprosyglobally was achieved in the year 2000 and the disease hasbeen eliminated from 119 countries out of the 122 where itwas considered as a public health problem in 1985 [5,12].However, leprosy was not eliminated from all countries andpockets of high endemicity in some areas of many countriesstill exist and transmission continues. A consensus has beenreached by the WHO that close disease surveillance forleprosy is necessary, and a new target was introduced. Thenew target stressed that the number of new cases withgrade 2 disability in 2015 should be 35% lower than in 2010[13].
Leprosy is known to have existed in Saudi Arabia for avery long time and as part of the worldwide eradicationprogram of the disease, the country has made leprosy oneof the notifiable diseases since 1963 [14].
Previous reports on leprosy in Saudi Arabia showedincidence of the disease to be within the WHO’s definitionof 1 case per 10,000 population for countries classified asbeing in the phase of elimination [13,15]. Nevertheless,new cases of leprosy are registered yearly in the countrysuggesting that Saudis continue to be infected. Thereforean improved epidemiological surveillance system forcapturing all cases of leprosy in the country was establishedin 2003. This surveillance system was designed to alsoinclude zero-cases reporting and active case findings toassure close monitoring of the disease. Also as part of thepublic health interventions, the treatment of leprosy caseswas integrated in the nationwide network of Primary HealthCare Centers.
The objective of this paper is to give an epidemiologicaldescription of all cases of leprosy reported in KSA over aten-year period and to estimate its yearly incidence. Thiswill help identify any challenge to the successful elimina-tion of leprosy in the Kingdom.
2 A. Assiri et al.+ MODEL
Please cite this article in press as: Assiri A, et al., Eradicating leprosy in Saudi Arabia: Outcome of a ten-year surveillance (2003e2012),Travel Medicine and Infectious Disease (2014), http://dx.doi.org/10.1016/j.tmaid.2014.10.002
2. Method
This is a retrospective epidemiological study of all newlyregistered cases of leprosy captured in the country’ssurveillance system over a 10-year period from 2003 to2012.
2.1. The surveillance system
Saudi Arabia is divided into 20 health regions or ‘districts’.The leprosy surveillance system covers all the health fa-cilities in these regions. Submission of monthly reports ofall new cases of leprosy seen in any health clinic in thehealth regions to the central public health office in theMinistry of Health (MoH) in Riyadh is mandatory. Even if nocase of leprosy was detected in any of the regions in agiven month this will still be reported as zero-cases. Thereports include all the demographic characteristics of thepatient as well as any contact screening and epidemio-logical evaluation carried out. Names, age, gender, na-tionality, type of leprosy, treatment status, disability andcontacts are the main items of information in the reportingforms.
2.2. Case definition and disease classification
The diagnosis of leprosy follows the WHO definition of aperson having one or more of ‘hypo pigmented or reddishskin lesion(s) with definite loss of sensation; damage to theperipheral nerves, as demonstrated by loss of sensation andweakness of the muscles of hands, feet or face and positiveskin smears. Also, the WHO clinical classification of thetypes of leprosy based on the number of skin lesions and
thickened nerves are used in all the health facilities inSaudi Arabia. Paucibacillary leprosy (up to five lesions) ormultibacillary leprosy (more than five skin lesions) [1]. TheWHO 0e2 disability grading system was used to classify thedegree of disability of leprosy patients. Those with noanesthesia and visible deformity or damage are grade ‘0’,those with anesthesia but no visible deformity or damage tohand and feet are grade ‘1’ and those with visible deformityor damage to hands and feet or severe visual impairmentare grade ‘2’ [16].
2.3. Data analysis
The data was summarized using simple descriptive statis-tical tools such as proportions, and results presented intables and graphs. The spatial distribution of cases ofleprosy was shown in a regional map of Saudi Arabia. Theincidence rates per 10,000 population were also calculated.
2.4. Ethics statement
The study did not require an ethical approval because itwas a retrospective analysis of data from the leprosy sur-veillance system. The database is hosted at the departmentof Preventive Medicine, Ministry of Health, Riyadh, SaudiArabia, under the authority of the Public Health Direc-torate. All data were de-identified before being madeavailable for analysis.
3. Results
Over the 10-year surveillance period there were 242 casesof leprosy reported to the central public health office in the
Table 1 Characteristics of leprosy cases in Saudi Arabia (2003e2012).
Characteristics All cases Cases per year
N Z 242 (%) 2003 2004 2005 2006 2007 2008 2009 2010 2011 2012
Age<1 0 0.00 0 0 0 0 0 0 0 0 0 01e4 1 0.41 0 1 0 0 0 0 0 0 0 05e14 3 1.24 0 0 0 1 0 2 0 0 0 015e44 162 66.9 32 16 20 12 13 12 13 17 16 11"45 76 31.4 10 14 11 11 7 9 2 5 3 4GenderMale 187 77.2 35 23 21 20 15 15 11 18 16 13Female 55 22.7 7 8 10 4 5 8 4 4 3 2NationalitySaudi 103 42.5 24 12 10 12 9 12 10 5 6 3Non-Saudi 139 57.4 18 19 21 12 11 11 5 17 13 12Type of leprosyPaucibacillary 124 50.8 26 12 14 8 6 14 14 13 7 9Multibacillary 118 48.7 16 19 17 16 14 8 1 9 12 6Degree of DisabilityGrade 0 182 75.2 37 17 15 15 18 22 14 19 16 9Grade 1 38 15.7 3 10 8 8 1 1 1 3 2 1Grade 2 22 9.09 2 4 8 1 1 0 0 0 1 5Total cases 242 100 42 31 31 24 20 23 15 22 19 15
Eradicating leprosy in Saudi Arabia 3+ MODEL
Please cite this article in press as: Assiri A, et al., Eradicating leprosy in Saudi Arabia: Outcome of a ten-year surveillance (2003e2012),Travel Medicine and Infectious Disease (2014), http://dx.doi.org/10.1016/j.tmaid.2014.10.002
Saudi MoH (Table 1). Most cases (98.3%) were in personspost puberty ("15 years old) with 162 cases (67%) in thoseaged between 15 and 44 years of age. No cases wereidentified in children less than 1 year old. Seventy-seven%of cases were in males, and 57% of cases were in non-Saudi nationals. PB leprosy accounted for slightly morecases than MB at 51%. Most cases (75%) were identified asgrade 0 disability, followed by grade 1, then grade 2.
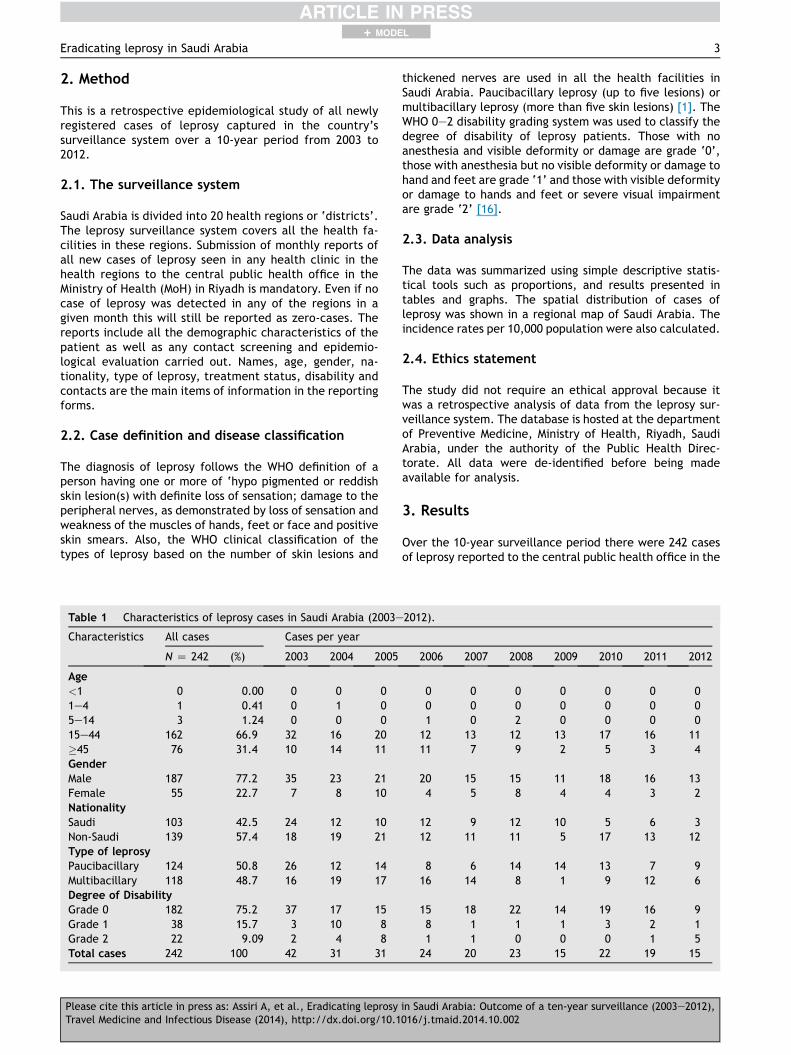
Analysis of the yearly trends of cases showed an overalldecline in the yearly cases between 2003 and 2012, withthe highest number of cases reported between 2003 and2005 (Table 1). Only 15 cases were reported in 2012compared to 41 in 2003. A steady decrease in incidence ofleprosy in Saudi Arabia was seen over the study period(Table 2). Incidence declined from 0.018 per 10,000 popu-lation in 2003 to 0.005 per 10,000 population in 2012.
Cases were dominated by males for all years with anoverall male:female ratio of 3.4:1. However this ratiofluctuated between the years from as low as 1.9:1 in 2008to as high as 6.5:1 in 2012. Similarly, most cases wereamong those aged between 15 and 44 years old, followed bythose aged 45 years or older. The number of cases amongthe latter group have significantly declined in the secondhalf of the surveillance period compared to the first half (23vs 53, p Z 0.016). This is less apparent for the 15e44 yearold group (79 vs 93, p Z 0.3). Less than 2% of all cases werein children younger than 15 years old, and over the 10-yearsurveillance period, only one case of leprosy (reported in2004) was among children less than 5 years old.
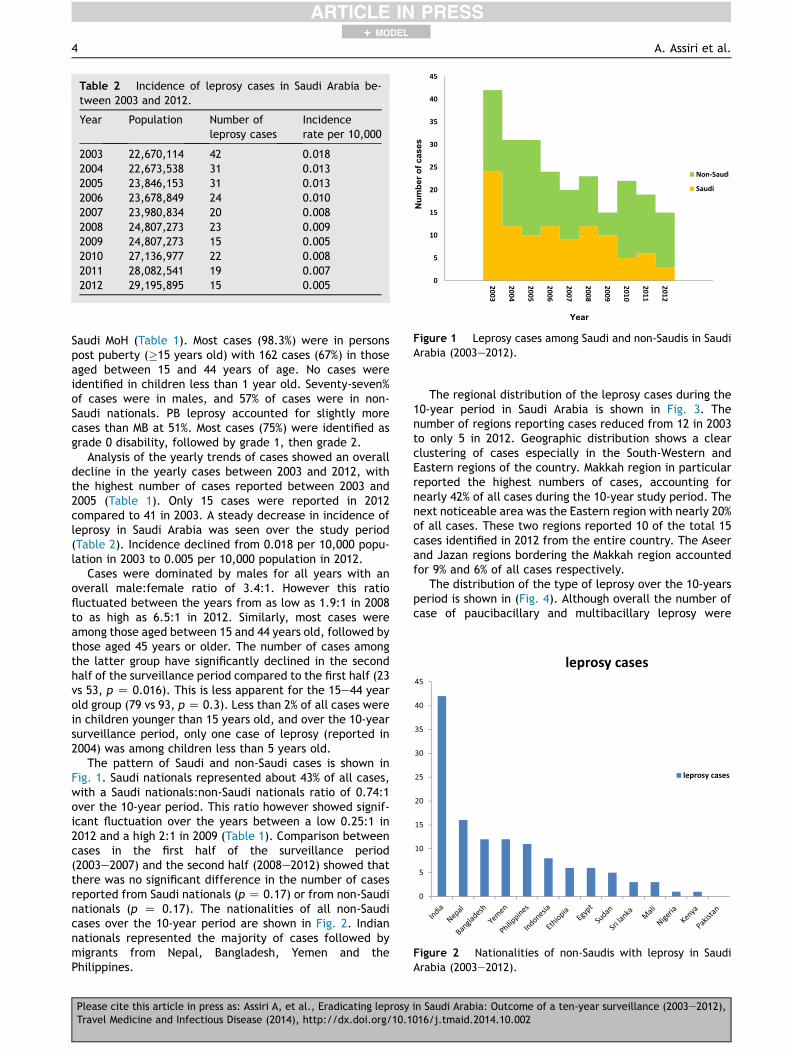
The pattern of Saudi and non-Saudi cases is shown inFig. 1. Saudi nationals represented about 43% of all cases,with a Saudi nationals:non-Saudi nationals ratio of 0.74:1over the 10-year period. This ratio however showed signif-icant fluctuation over the years between a low 0.25:1 in2012 and a high 2:1 in 2009 (Table 1). Comparison betweencases in the first half of the surveillance period(2003e2007) and the second half (2008e2012) showed thatthere was no significant difference in the number of casesreported from Saudi nationals (p Z 0.17) or from non-Saudinationals (p Z 0.17). The nationalities of all non-Saudicases over the 10-year period are shown in Fig. 2. Indiannationals represented the majority of cases followed bymigrants from Nepal, Bangladesh, Yemen and thePhilippines.
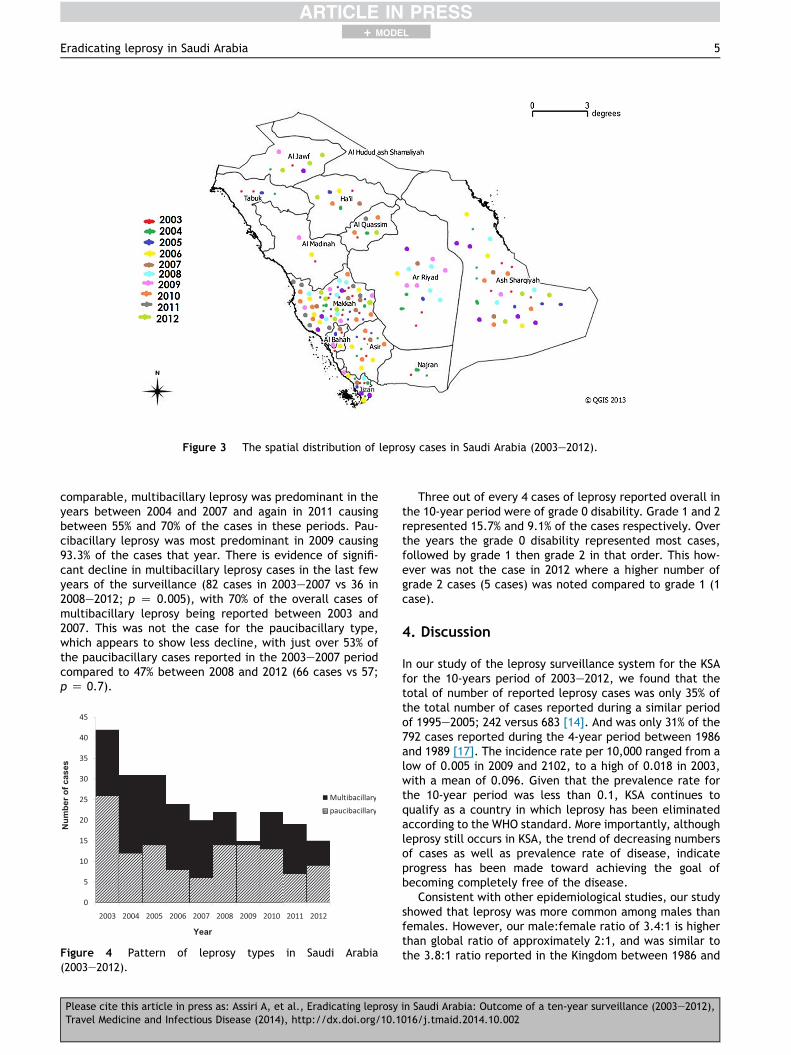
The regional distribution of the leprosy cases during the10-year period in Saudi Arabia is shown in Fig. 3. Thenumber of regions reporting cases reduced from 12 in 2003to only 5 in 2012. Geographic distribution shows a clearclustering of cases especially in the South-Western andEastern regions of the country. Makkah region in particularreported the highest numbers of cases, accounting fornearly 42% of all cases during the 10-year study period. Thenext noticeable area was the Eastern region with nearly 20%of all cases. These two regions reported 10 of the total 15cases identified in 2012 from the entire country. The Aseerand Jazan regions bordering the Makkah region accountedfor 9% and 6% of all cases respectively.
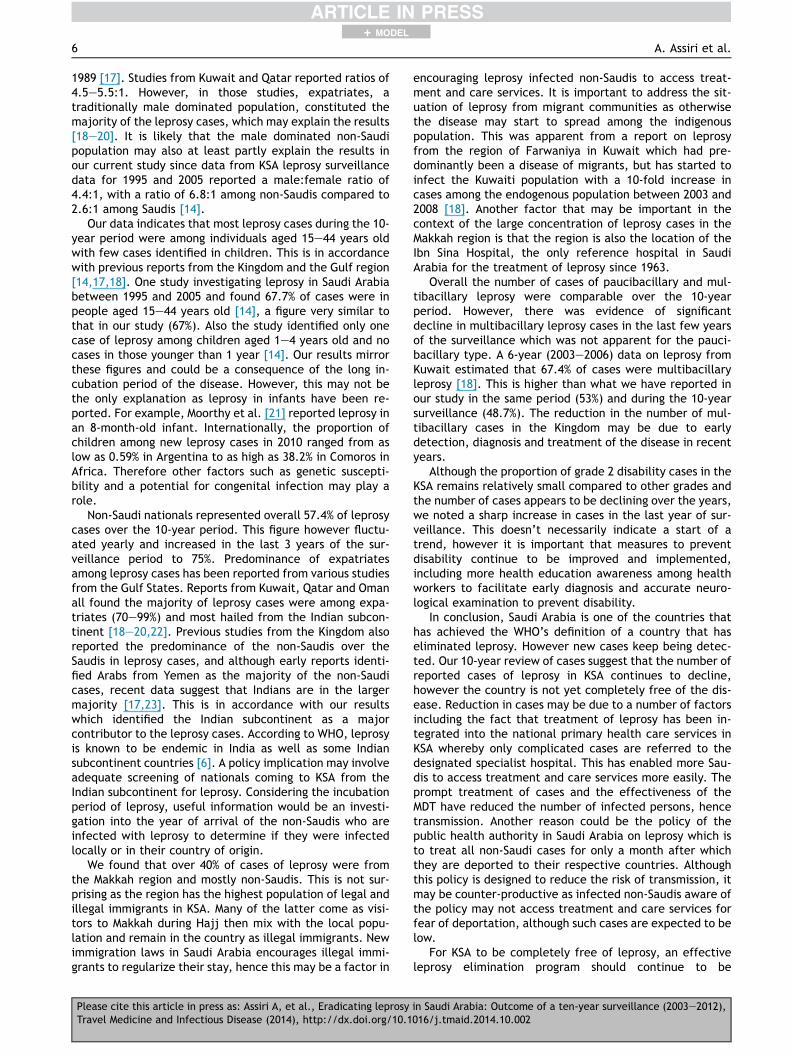
The distribution of the type of leprosy over the 10-yearsperiod is shown in (Fig. 4). Although overall the number ofcase of paucibacillary and multibacillary leprosy were
Table 2 Incidence of leprosy cases in Saudi Arabia be-tween 2003 and 2012.
Year Population Number ofleprosy cases
Incidencerate per 10,000
2003 22,670,114 42 0.0182004 22,673,538 31 0.0132005 23,846,153 31 0.0132006 23,678,849 24 0.0102007 23,980,834 20 0.0082008 24,807,273 23 0.0092009 24,807,273 15 0.0052010 27,136,977 22 0.0082011 28,082,541 19 0.0072012 29,195,895 15 0.005
Figure 1 Leprosy cases among Saudi and non-Saudis in SaudiArabia (2003e2012).
Figure 2 Nationalities of non-Saudis with leprosy in SaudiArabia (2003e2012).
4 A. Assiri et al.+ MODEL
Please cite this article in press as: Assiri A, et al., Eradicating leprosy in Saudi Arabia: Outcome of a ten-year surveillance (2003e2012),Travel Medicine and Infectious Disease (2014), http://dx.doi.org/10.1016/j.tmaid.2014.10.002
comparable, multibacillary leprosy was predominant in theyears between 2004 and 2007 and again in 2011 causingbetween 55% and 70% of the cases in these periods. Pau-cibacillary leprosy was most predominant in 2009 causing93.3% of the cases that year. There is evidence of signifi-cant decline in multibacillary leprosy cases in the last fewyears of the surveillance (82 cases in 2003e2007 vs 36 in2008e2012; p Z 0.005), with 70% of the overall cases ofmultibacillary leprosy being reported between 2003 and2007. This was not the case for the paucibacillary type,which appears to show less decline, with just over 53% ofthe paucibacillary cases reported in the 2003e2007 periodcompared to 47% between 2008 and 2012 (66 cases vs 57;p Z 0.7).
Three out of every 4 cases of leprosy reported overall inthe 10-year period were of grade 0 disability. Grade 1 and 2represented 15.7% and 9.1% of the cases respectively. Overthe years the grade 0 disability represented most cases,followed by grade 1 then grade 2 in that order. This how-ever was not the case in 2012 where a higher number ofgrade 2 cases (5 cases) was noted compared to grade 1 (1case).
4. Discussion
In our study of the leprosy surveillance system for the KSAfor the 10-years period of 2003e2012, we found that thetotal of number of reported leprosy cases was only 35% ofthe total number of cases reported during a similar periodof 1995e2005; 242 versus 683 [14]. And was only 31% of the792 cases reported during the 4-year period between 1986and 1989 [17]. The incidence rate per 10,000 ranged from alow of 0.005 in 2009 and 2102, to a high of 0.018 in 2003,with a mean of 0.096. Given that the prevalence rate forthe 10-year period was less than 0.1, KSA continues toqualify as a country in which leprosy has been eliminatedaccording to the WHO standard. More importantly, althoughleprosy still occurs in KSA, the trend of decreasing numbersof cases as well as prevalence rate of disease, indicateprogress has been made toward achieving the goal ofbecoming completely free of the disease.
Consistent with other epidemiological studies, our studyshowed that leprosy was more common among males thanfemales. However, our male:female ratio of 3.4:1 is higherthan global ratio of approximately 2:1, and was similar tothe 3.8:1 ratio reported in the Kingdom between 1986 and
Figure 3 The spatial distribution of leprosy cases in Saudi Arabia (2003e2012).
Figure 4 Pattern of leprosy types in Saudi Arabia(2003e2012).
Eradicating leprosy in Saudi Arabia 5+ MODEL
Please cite this article in press as: Assiri A, et al., Eradicating leprosy in Saudi Arabia: Outcome of a ten-year surveillance (2003e2012),Travel Medicine and Infectious Disease (2014), http://dx.doi.org/10.1016/j.tmaid.2014.10.002
1989 [17]. Studies from Kuwait and Qatar reported ratios of4.5e5.5:1. However, in those studies, expatriates, atraditionally male dominated population, constituted themajority of the leprosy cases, which may explain the results[18e20]. It is likely that the male dominated non-Saudipopulation may also at least partly explain the results inour current study since data from KSA leprosy surveillancedata for 1995 and 2005 reported a male:female ratio of4.4:1, with a ratio of 6.8:1 among non-Saudis compared to2.6:1 among Saudis [14].
Our data indicates that most leprosy cases during the 10-year period were among individuals aged 15e44 years oldwith few cases identified in children. This is in accordancewith previous reports from the Kingdom and the Gulf region[14,17,18]. One study investigating leprosy in Saudi Arabiabetween 1995 and 2005 and found 67.7% of cases were inpeople aged 15e44 years old [14], a figure very similar tothat in our study (67%). Also the study identified only onecase of leprosy among children aged 1e4 years old and nocases in those younger than 1 year [14]. Our results mirrorthese figures and could be a consequence of the long in-cubation period of the disease. However, this may not bethe only explanation as leprosy in infants have been re-ported. For example, Moorthy et al. [21] reported leprosy inan 8-month-old infant. Internationally, the proportion ofchildren among new leprosy cases in 2010 ranged from aslow as 0.59% in Argentina to as high as 38.2% in Comoros inAfrica. Therefore other factors such as genetic suscepti-bility and a potential for congenital infection may play arole.
Non-Saudi nationals represented overall 57.4% of leprosycases over the 10-year period. This figure however fluctu-ated yearly and increased in the last 3 years of the sur-veillance period to 75%. Predominance of expatriatesamong leprosy cases has been reported from various studiesfrom the Gulf States. Reports from Kuwait, Qatar and Omanall found the majority of leprosy cases were among expa-triates (70e99%) and most hailed from the Indian subcon-tinent [18e20,22]. Previous studies from the Kingdom alsoreported the predominance of the non-Saudis over theSaudis in leprosy cases, and although early reports identi-fied Arabs from Yemen as the majority of the non-Saudicases, recent data suggest that Indians are in the largermajority [17,23]. This is in accordance with our resultswhich identified the Indian subcontinent as a majorcontributor to the leprosy cases. According to WHO, leprosyis known to be endemic in India as well as some Indiansubcontinent countries [6]. A policy implication may involveadequate screening of nationals coming to KSA from theIndian subcontinent for leprosy. Considering the incubationperiod of leprosy, useful information would be an investi-gation into the year of arrival of the non-Saudis who areinfected with leprosy to determine if they were infectedlocally or in their country of origin.
We found that over 40% of cases of leprosy were fromthe Makkah region and mostly non-Saudis. This is not sur-prising as the region has the highest population of legal andillegal immigrants in KSA. Many of the latter come as visi-tors to Makkah during Hajj then mix with the local popu-lation and remain in the country as illegal immigrants. Newimmigration laws in Saudi Arabia encourages illegal immi-grants to regularize their stay, hence this may be a factor in
encouraging leprosy infected non-Saudis to access treat-ment and care services. It is important to address the sit-uation of leprosy from migrant communities as otherwisethe disease may start to spread among the indigenouspopulation. This was apparent from a report on leprosyfrom the region of Farwaniya in Kuwait which had pre-dominantly been a disease of migrants, but has started toinfect the Kuwaiti population with a 10-fold increase incases among the endogenous population between 2003 and2008 [18]. Another factor that may be important in thecontext of the large concentration of leprosy cases in theMakkah region is that the region is also the location of theIbn Sina Hospital, the only reference hospital in SaudiArabia for the treatment of leprosy since 1963.
Overall the number of cases of paucibacillary and mul-tibacillary leprosy were comparable over the 10-yearperiod. However, there was evidence of significantdecline in multibacillary leprosy cases in the last few yearsof the surveillance which was not apparent for the pauci-bacillary type. A 6-year (2003e2006) data on leprosy fromKuwait estimated that 67.4% of cases were multibacillaryleprosy [18]. This is higher than what we have reported inour study in the same period (53%) and during the 10-yearsurveillance (48.7%). The reduction in the number of mul-tibacillary cases in the Kingdom may be due to earlydetection, diagnosis and treatment of the disease in recentyears.
Although the proportion of grade 2 disability cases in theKSA remains relatively small compared to other grades andthe number of cases appears to be declining over the years,we noted a sharp increase in cases in the last year of sur-veillance. This doesn’t necessarily indicate a start of atrend, however it is important that measures to preventdisability continue to be improved and implemented,including more health education awareness among healthworkers to facilitate early diagnosis and accurate neuro-logical examination to prevent disability.
In conclusion, Saudi Arabia is one of the countries thathas achieved the WHO’s definition of a country that haseliminated leprosy. However new cases keep being detec-ted. Our 10-year review of cases suggest that the number ofreported cases of leprosy in KSA continues to decline,however the country is not yet completely free of the dis-ease. Reduction in cases may be due to a number of factorsincluding the fact that treatment of leprosy has been in-tegrated into the national primary health care services inKSA whereby only complicated cases are referred to thedesignated specialist hospital. This has enabled more Sau-dis to access treatment and care services more easily. Theprompt treatment of cases and the effectiveness of theMDT have reduced the number of infected persons, hencetransmission. Another reason could be the policy of thepublic health authority in Saudi Arabia on leprosy which isto treat all non-Saudi cases for only a month after whichthey are deported to their respective countries. Althoughthis policy is designed to reduce the risk of transmission, itmay be counter-productive as infected non-Saudis aware ofthe policy may not access treatment and care services forfear of deportation, although such cases are expected to below.
For KSA to be completely free of leprosy, an effectiveleprosy elimination program should continue to be
6 A. Assiri et al.+ MODEL
Please cite this article in press as: Assiri A, et al., Eradicating leprosy in Saudi Arabia: Outcome of a ten-year surveillance (2003e2012),Travel Medicine and Infectious Disease (2014), http://dx.doi.org/10.1016/j.tmaid.2014.10.002
implemented. Some aspects of this program include thestrengthening of the surveillance system to capture allcases for effective monitoring and control of the disease.The continuing provision of standard MDT through primaryhealth care facilities, training of general health staff inleprosy diagnosis and treatment and the early treatmentand referral of leprosy complications is essential. Appro-priate community health education, that leprosy is treat-able before disability occurs, is an important component ofleprosy control to promote early presentation before theappearance of impairment of nerve function and disability.Moreover, the role or migrants in the importation of thedisease needs to be addressed. Medical examination ofexpatriates, especially those coming from endemic coun-tries, on arrival and periodic check-ups at regular intervalsmay help achieve early diagnosis and treatment of thesepatients and thus prevent the spread of the disease in thecountry.
Funding
None.
Conflict of interest
None to declare.
References
[1] Walker SL, Lockwood DN. Leprosy. Clin Dermatol 2007;25:165e72.
[2] Britton WJ, Lockwood DN. Leprosy. Lancet 2004;363:1209e19.[3] Rodrigues LC, Lockwood DN. Leprosy now: epidemiology,
progress, challenges, and research gaps. Lancet Infect Dis2011;11:464e70.
[4] World Health Assembly. Leprosy resolution WHA 44.9, 44thworld health assembly. 1991.
[5] World Health Organisation (WHO). Weekly epidemiologicalrecord: global leprosy situation, 2000e2001. 2002. ReportNo.: vol. 77 No. 1.
[6] World Health Organisation (WHO). Weekly epidemiologicalrecord: global leprosy situation, 2012. 2012. Report No.: vol.87 No. 34.
[7] Hatta M, van Beers SM, Madjid B, Djumadi A, de Wit MY,Klatser PR. Distribution and persistence of Mycobacteriumleprae nasal carriage among a population in which leprosy isendemic in Indonesia. Trans R Soc Trop Med Hyg 1995;89:381e5.
[8] Ridley DS, Jopling WH. Classification of leprosy according toimmunity. A five-group system. Int J Lepr Other Mycobact Dis1966;34:255e73.
[9] Croft RP, Nicholls PG, Steyerberg EW, Richardus JH, Cairns W,Smith S. A clinical prediction rule for nerve-function impair-ment in leprosy patients. Lancet 2000;355:1603e6.
[10] Burki T. Old problems still mar fight against ancient disease.Lancet 2009;373:287e8.
[11] World Health Organization (WHO). Chemotherapy of leprosyfor control programmes. World Health Organ Tech Rep Ser1982;675:1e33.
[12] World Health Organization (WHO). Leprosy: fact sheet no.101. 2014. Available from: http://www.who.int/mediacentre/factsheets/fs101/en/.
[13] World Health Organisation (WHO). Weekly epidemiologicalrecord: global leprosy situation, 2005. 2005. Report No.: vol.80 No. 34.
[14] Al AF, Al AK. Leprosy in Saudi Arabia. Lepr Rev 2007;78:405e8.[15] Noordeen SK. Elimination of leprosy as a public health prob-
lem: progress and prospects. Bull World Health Organ 1995;73:1e6.
[16] Brandsma JW, Van Brakel WH. WHO disability grading: oper-ational definitions. Lepr Rev 2003;74:366e73.
[17] Ibrahim MA, Kordy MN, Aiderous AH, Bahnassy A. Leprosy inSaudi Arabia, 1986e89. Lepr Rev 1990;61:379e85.
[18] Al-Mutairi N, Al-Doukhi A, Ahmad MS, El-Khelwany M, Al-Haddad A. Changing demography of leprosy: Kuwait needs tobe vigilant. Int J Infect Dis 2010;14:e876e80.
[19] Mahmoud SF, Azadeh B. Leprosy in Qatar. Int J Dermatol 1991;30:125e6.
[20] al-Kandari S, al-Anezi A, Pugh RN, al-Qasaf F, al-Abyad S.Leprosy in Kuwait: an epidemiological study of new cases. AnnTrop Med Parasitol 1990;84:513e22.
[21] Moorthy KV, Desikan KV. Indeterminate leprosy in an infant.Lepr Rev 2006;77:377e80.
[22] Scrimgeour EM, Mehta FR, Suleiman AJ. Infectious and tropicaldiseases in Oman: a review. Am J Trop Med Hyg 1999;61:920e5.
[23] Sebai ZH. An epidemiological study of leprosy and leprosy carein Saudi Arabia. Saudi Med J 1980;1:133e40.
Eradicating leprosy in Saudi Arabia 7+ MODEL
Please cite this article in press as: Assiri A, et al., Eradicating leprosy in Saudi Arabia: Outcome of a ten-year surveillance (2003e2012),Travel Medicine and Infectious Disease (2014), http://dx.doi.org/10.1016/j.tmaid.2014.10.002




















