Empiric use of Linezolid in febrile hematology and hematopoietic stem cell transplantation patients...
6
1 2 Empiric use of linezolid in febrile hematology and hematopoietic stem 3 cell transplantation patients colonized with vancomycin-resistant 4 Enterococcus spp 5 Luiz F. Lisboa Q1 a , Bianca G. Miranda b , Marjorie B. Vieira b , Frederico L. Dulley c , 6 Guilherme G. Fonseca c , Thais Guimara ˜es d , Anna S. Levin b , Maria A. Shikanai-Yasuda b , 7 Silvia F. Costa b, * 8 a Transplant Infectious Diseases, Department of Medicine, University of Alberta, Edmonton, Canada 9 b Department of Infectious Diseases, Faculty of Medicine, University of Sao Paulo, Av. Dr. Eneas de Carvalho Aguiar, 470, Sao Paulo, 054030-000, SP, Brazil 10 c Discipline of Hematology, Faculty of Medicine, University of Sao Paulo, Sao Paulo, Brazil 11 d Infection Control Committee, Hospital das Clı´nicas, University of Sao Paulo, Sao Paulo, Brazil 12 13 14 1. Introduction 15 Q2 Vancomycin-resistant Q3 Enterococcus spp (VRE) infections in 16 hematology and hematopoietic stem cell transplant (HSCT) 17 patients have been gaining attention given the overall increasing International Journal of Infectious Diseases xxx (2015) e1–e6 A R T I C L E I N F O Article history: Received 3 October 2014 Received in revised form 28 January 2015 Accepted 2 February 2015 Keywords: Linezolid VRE Hematology Bone marrow transplant S U M M A R Y Objectives: We conducted a retrospective study on the impact of the empiric use of linezolid on mortality in vancomycin-resistant Enterococcus spp (VRE)-colonized hematology and hematopoietic stem cell transplantation (HSCT) patients. Methods: VRE-colonized inpatients for whom complete data were available (n = 100) were divided into two groups: those who received empiric linezolid in the course of fever refractory to broad-spectrum antibiotics, replacing the glycopeptide utilized for the previous 48 h, and those who did not (control group). All patients were followed until hospital discharge or death. The impact of linezolid and risk factors for all-cause mortality were evaluated; variables with p < 0.10 were analyzed in a multivariate model. A Kaplan–Meier survival analysis was done to compare survival among febrile patients colonized by VRE who received empiric linezolid with patients who did not receive linezolid. Results: Patients empirically prescribed linezolid were generally younger (median age 33 vs. 44 years; p = 0.008) and more likely to be recipients of an allogeneic HSCT (24 (68.6%) vs. 24 (36.9%); p = 0.009) than patients who did not receive the drug. Fourteen (21.5%) VRE bloodstream infections were diagnosed, all in patients who did not receive empiric linezolid (p = 0.002). In-hospital mortality was comparable in empiric linezolid and non-linezolid users (19 (54.3%) vs. 27 (41.5%), respectively; p = 0.293). The Kaplan–Meier survival analysis showed no significant difference in survival comparing the group that received linezolid to the group that did not (p = 0.72). Graft-versus-host disease (GVHD; odds ratio (OR) 5.90, 95% confidence interval (CI) 1.46–23.79; p = 0.012) and persistence of neutropenia (OR 6.93, 95% CI 1.72–27.94; p = 0.0065) were independent predictors of all-cause in-hospital death in HSCT patients, and persistence of neutropenia in non-HSCT patients (OR 8.12, 95% CI 1.22–53.8; p = 0.030). Conclusions: The empiric use of linezolid in VRE-colonized hematology patients had no impact on mortality, which appeared rather to be associated with the persistence of neutropenia in general and GVHD in the HSCT group. ß 2015 The Authors. Published by Elsevier Ltd on behalf of International Society for Infectious Diseases. This is an open access article under the CC BY-NC-SA license (http://creativecommons.org/licenses/by- nc-sa/4.0/). * Corresponding author. Tel.: +55 11 3061 7030. E-mail address: [email protected] (S.F. Costa). G Model IJID 2260 1–6 Please cite this article in press as: Lisboa LF, et al. Empiric use of linezolid in febrile hematology and hematopoietic stem cell transplantation patients colonized with vancomycin-resistant Enterococcus spp. Int J Infect Dis (2015), http://dx.doi.org/10.1016/ j.ijid.2015.02.001 Contents lists available at ScienceDirect International Journal of Infectious Diseases jou r nal h o mep ag e: w ww .elsevier .co m /loc ate/ijid http://dx.doi.org/10.1016/j.ijid.2015.02.001 1201-9712/ß 2015 The Authors. Published by Elsevier Ltd on behalf of International Society for Infectious Diseases. This is an open access article under the CC BY-NC-SA license (http://creativecommons.org/licenses/by-nc-sa/4.0/).
Transcript of Empiric use of Linezolid in febrile hematology and hematopoietic stem cell transplantation patients...

1
2 Empiric use of linezolid in febrile hematology and hematopoietic stem3 cell transplantation patients colonized with vancomycin-resistant4 Enterococcus spp
5 Luiz F. LisboaQ1a, Bianca G. Miranda b, Marjorie B. Vieira b, Frederico L. Dulley c,
6 Guilherme G. Fonseca c, Thais Guimaraes d, Anna S. Levin b, Maria A. Shikanai-Yasuda b,7 Silvia F. Costa b,*
8 a Transplant Infectious Diseases, Department of Medicine, University of Alberta, Edmonton, Canada
9 bDepartment of Infectious Diseases, Faculty of Medicine, University of Sao Paulo, Av. Dr. Eneas de Carvalho Aguiar, 470, Sao Paulo, 054030-000, SP, Brazil
10 cDiscipline of Hematology, Faculty of Medicine, University of Sao Paulo, Sao Paulo, Brazil
11 d Infection Control Committee, Hospital das Clınicas, University of Sao Paulo, Sao Paulo, Brazil
12
13 141. Introduction
15Q2Vancomycin-resistantQ3
Enterococcus spp (VRE) infections in
16hematology and hematopoietic stem cell transplant (HSCT)
17patients have been gaining attention given the overall increasing
International Journal of Infectious Diseases xxx (2015) e1–e6
A R T I C L E I N F O
Article history:
Received 3 October 2014
Received in revised form 28 January 2015
Accepted 2 February 2015
Keywords:
Linezolid
VRE
Hematology
Bone marrow transplant
S U M M A R Y
Objectives: We conducted a retrospective study on the impact of the empiric use of linezolid on mortality
in vancomycin-resistant Enterococcus spp (VRE)-colonized hematology and hematopoietic stem cell
transplantation (HSCT) patients.
Methods: VRE-colonized inpatients for whom complete data were available (n = 100) were divided into
two groups: those who received empiric linezolid in the course of fever refractory to broad-spectrum
antibiotics, replacing the glycopeptide utilized for the previous 48 h, and those who did not (control
group). All patients were followed until hospital discharge or death. The impact of linezolid and risk
factors for all-cause mortality were evaluated; variables with p < 0.10 were analyzed in a multivariate
model. A Kaplan–Meier survival analysis was done to compare survival among febrile patients colonized
by VRE who received empiric linezolid with patients who did not receive linezolid.
Results: Patients empirically prescribed linezolid were generally younger (median age 33 vs. 44 years;
p = 0.008) and more likely to be recipients of an allogeneic HSCT (24 (68.6%) vs. 24 (36.9%); p = 0.009)
than patients who did not receive the drug. Fourteen (21.5%) VRE bloodstream infections were
diagnosed, all in patients who did not receive empiric linezolid (p = 0.002). In-hospital mortality was
comparable in empiric linezolid and non-linezolid users (19 (54.3%) vs. 27 (41.5%), respectively;
p = 0.293). The Kaplan–Meier survival analysis showed no significant difference in survival comparing
the group that received linezolid to the group that did not (p = 0.72). Graft-versus-host disease (GVHD;
odds ratio (OR) 5.90, 95% confidence interval (CI) 1.46–23.79; p = 0.012) and persistence of neutropenia
(OR 6.93, 95% CI 1.72–27.94; p = 0.0065) were independent predictors of all-cause in-hospital death in
HSCT patients, and persistence of neutropenia in non-HSCT patients (OR 8.12, 95% CI 1.22–53.8;
p = 0.030).
Conclusions: The empiric use of linezolid in VRE-colonized hematology patients had no impact on
mortality, which appeared rather to be associated with the persistence of neutropenia in general and
GVHD in the HSCT group.
� 2015 The Authors. Published by Elsevier Ltd on behalf of International Society for Infectious Diseases.
This is an open access article under the CC BY-NC-SA license (http://creativecommons.org/licenses/by-
nc-sa/4.0/).
* Corresponding author. Tel.: +55 11 3061 7030.
E-mail address: [email protected] (S.F. Costa).
G Model
IJID 2260 1–6
Please cite this article in press as: Lisboa LF, et al. Empiric use of linezolid in febrile hematology and hematopoietic stem cell
transplantation patients colonized with vancomycin-resistant Enterococcus spp. Int J Infect Dis (2015), http://dx.doi.org/10.1016/
j.ijid.2015.02.001
Contents lists available at ScienceDirect
International Journal of Infectious Diseases
jou r nal h o mep ag e: w ww .e lsev ier . co m / loc ate / i j id
http://dx.doi.org/10.1016/j.ijid.2015.02.001
1201-9712/� 2015 The Authors. Published by Elsevier Ltd on behalf of International Society for Infectious Diseases. This is an open access article under the CC BY-NC-SA
license (http://creativecommons.org/licenses/by-nc-sa/4.0/).

18 prevalence of VRE colonization and infection in some countries,1–3
19 and the high morbidity and mortality in this patient population.4
20 Colonization of the gastrointestinal tract with VRE is postulated to
21 precede VRE infection.5–9 Bloodstream infection (BSI) due to VRE,
22 in particular, has been linked to increased mortality in this
23 population.10–14 VRE-attributable mortality, however, is difficult
24 to ascertain due to the severity of illness of the underlying disease
25 in these patients.15–17
26 Anti-VRE antibiotic drugs have reportedly been advocated as
27 empirical agents for the treatment of febrile neutropenia among
28 VRE-colonized patients,6,18,19 even though data supporting their
29 empirical use in this setting are largely lacking. Resistance to
30 linezolid among VRE, on the other hand, has been reported,20–22
31 and is directly associated with its consumption,22 thus warranting
32 the investigation of this approach to ensure an adequate rationale
33 for the empiric use of linezolid in VRE-colonized patients.
34 A retrospective study of the impact of empiric use of linezolid
35 and risk factors for all-cause mortality in hematology and HSCT
36 patients colonized by VRE was performed.
37 2. Methods
38 2.1. Design
39 This retrospective study was performed to assess the outcomes
40 of the empiric use of linezolid (Pfizer, NY, USA), prescribed in
41 accordance with the literature recommendations (adult patients,
42 600 mg intravenous (IV) every 12 h; pediatric patients, 10 mg/kg
43 IV every 8 h), in the course of persistent febrile episodes in
44 hematology and HSCT adult and pediatric patients admitted to the
45 Hematology and Bone Marrow Transplant wards of the Hospital
46 das Clınicas da Universidade de Sao Paulo (Sao Paulo, Brazil). VRE-
47 colonized patients admitted between January 2005 and May
48 2007 were considered eligible. Complete paper charts and
49 electronic records holding microbiological data were necessary
50 for inclusion in the study; these were available for 100 patients.
51 A case series describing baseline characteristics and outcomes of
52 VRE-colonized patients receiving linezolid empirically and
53 patients who did not receive this antibiotic (considered the
54 control group) was recorded; risk factors associated with
55 in-hospital mortality were evaluated. The study was approved
56 by the institutional research ethics board (CAPPesq – Ethics
57 Commission for the Analyses of Research Projects, Hospital das
58 Clınicas da Universidade de Sao Paulo).
59 2.2. Setting
60 The study was conducted in a 900-bed tertiary-care teaching
61 hospital in Sao Paulo, Brazil, encompassing a joint unit with eight
62 bone marrow transplant and 15 hematology beds. Local protocols
63 for the treatment of febrile neutropenia in place at the time were
64 largely based on the 1997 guidelines of the Infectious Diseases
65 Society of America (IDSA)23 and did not advocate the routine use of
66 anti-VRE drugs in VRE-colonized patients. Infectious diseases
67 specialists restrict access to linezolid through an individual case
68 assessment as part of the institutional antimicrobial stewardship
69 program. During the study period, the empiric use of linezolid was
70 considered on a case-basis for VRE-colonized patients upon
71 persistence of fever after 48 h of use of broad Gram-negative
72 bacilli antibiotic coverage and a glycopeptide antibiotic. Whenever
73 linezolid was prescribed, glycopeptide antibiotics were immedi-
74 ately discontinued. Antibiotic therapy was de-escalated and
75 optimized according to microbiological data and was continued
76 for the standard recommended duration according to the site of
77 infection, or for that recommended in the absence of confirmed
78 infection. Discontinuation of antimicrobial therapy, in the absence
79of isolation of a causative agent, was contingent on completing a
80minimum of 5 days of treatment and on resolution of fever and
81recovery of neutrophil counts for 72 h (absolute neutrophil counts
82(ANC) >0.5 � 109 cells/l Q4). Specimens for microbiological diagnosis
83were collected routinely prior to administration or upon changes in
84antimicrobial therapy.
852.3. Data collection
86Microbiological data and infection control and medical records
87were reviewed by three investigators (BGM, LFL, SFC). Infections
88were defined according to the Centers for Disease Control and
89Prevention nosocomial infection criteria.24 The following variables
90were compared between the case and control groups: age, length
91of hospital stay, underlying hematological disease, type of HSCT,
92the presence of mucositis or graft-versus-host disease (GVHD) as
93diagnosed by the assisting hematologist and recorded on the
94patient’s chart, Multinational Association of Supportive Care in
95Cancer (MASCC) risk index score,25 use of a central venous catheter
96(CVC), site of infection, laboratory tests including ANC and platelet
97counts, duration and severity of neutropenia, and linezolid
98prescription information. The patients were followed from hospital
99admission until the first of the following events: in-hospital death
100or discharge from the hospital.
1012.4. VRE surveillance
102VRE rectal/peri-anal screening swabs were taken routinely
103upon admission and were repeated weekly, until colonization was
104documented or until hospital discharge. Surveillance cultures were
105seeded directly in VRE-selective medium containing 6 mg/ml of
106vancomycin. Identification and susceptibility testing, including
107ampicillin and linezolid susceptibility testing, were performed for
108all specimens using automated (Vitek; bioMerieux, Hazelwood,
109MO, USA) and/or disk diffusion methods, the latter following the
110methodology established by the Clinical and Laboratory Standards
111Institute (CLSI).
1122.5. Statistical analysis
113Data analyses were performed using PASW Statistics 18 (SPSS
114Inc., Chicago, IL, USA). The two-tailed Fisher’s exact test was used
115for categorical variables and the Mann–Whitney U-test was used
116for continuous variables. Logistic regression models were devel-
117oped to identify factors independently associated with in-hospital
118mortality. All non-overlapping variables with p < 0.1 on univariate
119analysis and that fitted a biological rationale were entered into the
120model in a single step. The logistic regression model obtained was
121also applied for subgroup analysis (non-HSCT vs. HSCT). A p-value
122<0.05 was considered to be statistically significant. A Kaplan–
123Meier survival analysis was done to compare survival among
124febrile hematology and HSCT patients colonized by VRE who
125received empiric linezolid with patients who did not receive
126linezolid.
1273. Results
1283.1. Setting
129A total of 1535 patients were admitted to the hematology
130and bone marrow transplant wards during the study period. VRE
131are endemic to these medical units; the period studied was
132delimited to exclude VRE outbreaks, and no linezolid-resistant
133strains were observed during the study period. The median
134length of hospitalization prior to VRE colonization was 10 days
135(range 0–61 days).
L.F. Lisboa et al. / International Journal of Infectious Diseases xxx (2015) e1–e6e2
G Model
IJID 2260 1–6
Please cite this article in press as: Lisboa LF, et al. Empiric use of linezolid in febrile hematology and hematopoietic stem cell
transplantation patients colonized with vancomycin-resistant Enterococcus spp. Int J Infect Dis (2015), http://dx.doi.org/10.1016/
j.ijid.2015.02.001

136 3.2. Patterns of empiric linezolid usage
137 Demographic and clinical characteristics of the patients are
138 shown in Table 1. Patients empirically prescribed with linezolid
139 (total of 35 patients) were generally younger (median age 33 vs.
140 44 years; p = 0.008) and more likely to be recipients of allogeneic
141 HSCT (24 (68.6%) vs. 24 (36.9%) patients; p = 0.009) than patients
142 who did not receive this drug (total of 65 patients). GVHD was
143 similarly distributed in both groups – nine (25.75%Q5 ) in the linezolid
144 group and nine (13.9%) in the non-linezolid group (p = 0.175) – and
145 affected the following sites: the skin in six patients (33%), the
146 gastrointestinal tract in five (28%), the lungs in two (11%), and the
147 liver in two (11%). No patients receiving linezolid empirically
148 developed VRE infections (all of these patients had cultures
149 collected prior to their first dose which remained negative).
150 Fourteen patients (14%) in the control group developed a first
151 episode of BSI due to VRE, justifying the targeted use of linezolid. Of
152 these, 13 (92.5%) episodes were caused by Enterococcus faecium
153 and one (7.1%) by Enterococcus faecalisQ6 , with all isolates – including
154 E. faecalis – also resistant to ampicillin on disk diffusion testing and
155 microdilution method. An additional five patients in the control
156 group received linezolid for other indications (three urinary and
157 two respiratory tract infections with VRE as the only isolate).
158 Patients receiving linezolid empirically had a lower predicted
159 mortality at hospital admission (median MASCC risk index score
160 21 in cases vs. 16 in controls; p = 0.021). All-cause in-hospital
161 mortality, nonetheless, was statistically similar in the two groups:
162 54.3% (n = 19) in the empiric linezolid group vs. 41.5% (n = 27) in
163 the non-linezolid group (p = 0.293) (Table 1).
164 Neutropenia at admission and persistent neutropenia (ANC
165 <0.5 � 109/l at hospital discharge/death) were seen in similar
166 proportions, whereas severe neutropenia during hospital stay
167(ANC <0.1 � 109/l) was less commonly observed among those in
168the empiric linezolid group (n = 6, 17%) than in the non-linezolid
169group (n = 24, 36.9%) (p = 0.043) (Table 2).
170The empiric use of linezolid had no impact on the overall
171mortality (odds ratio (OR) 1.67, 95% confidence interval (CI) 0.73–
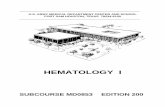
1723.82; p = 0.293) (Table 2). The Kaplan–Meier survival analysis
173showed no significant difference in survival between hematology
174and HSCT febrile patients colonized by VRE who received empiric
175linezolid and those who did not (p = 0.72) (Figure 1 Q7). In a logistic
176regression model, the risk factors independently associated with
177death were the presence of GVHD (OR 3.69, 95% CI 1.13–12.04;
178p = 0.030) and persistent neutropenia (OR 6.46, 95% CI 2.20–19.10;
179p = 0.0007). When mortality was assessed exclusively in recipients
180of allogeneic HSCT using the model that included GVHD, ANC at
181admission, platelets at admission, Hodgkin lymphoma present
182only in patients undergoing HSCT, and persistent neutropenia, the
183following were confirmed as independent predictors of death:
184GVHD (OR 5.90, 95% CI 1.46–23.79; p = 0.012) and persistent
185neutropenia (OR 6.93, 95% CI 1.72–27.94; p = 0.0065). The
186regression model without GVHD and Hodgkin lymphoma applied
187to non-HSCT patients suggested persistent neutropenia as the only
188independent predictor of in-hospital mortality (OR 8.12, 95% CI
1891.22–53.85; p = 0.030).
1904. Discussion
191The importance of VRE colonization to guide the empiric use
192of antibiotics in febrile neutropenia remains a matter of
193debate.7,15–17,24,25 The 2010 IDSA guidelines for the use of
194antimicrobial agents in neutropenic patients with cancer
195recommend considering the initial use of linezolid or daptomycin
196for febrile neutropenic VRE-colonized patients treated in
Table 1
Clinical and demographic characteristics of hematology and HSCT patients colonized with vancomycin-resistant Enterococcus spp (VRE) according to the pattern of linezolid
prescriptiona
Variables Empiric use of linezolid (n = 35) No use of linezolid (n = 65) p-Value
Age, years, median (range) 33 (2–67) 44 (1–77) 0.008
Sex, female, n (%) 18 (51.4) 24 (36.9) 0.204
E. faecium colonization, n (%) 25 (71.4) 51 (78.5) 0.468
Time to VRE colonization, days, median (range) 10 (0–46) 8 (0–61) 0.893
Underlying disease, n (%)
Acute leukemia 17 (48.6) 31 (47.7) 1.000
Chronic leukemia 4 (11.4) 2 (3.1) 0.180
Aplastic anemia 1 (2.9) 4 (6.2) 0.655
Fanconi anemia 2 (5.7) 0 0.120
Non-Hodgkin lymphoma 7 (20.0) 12 (18.5) 1.000
Hodgkin lymphoma 0 5 (7.7) 0.159
Multiple myeloma 2 (5.7) 5 (7.7) 1.000
Myelodysplastic syndrome 0 4 (6.2) 0.295
Other 2 (5.7) 2 (3.1) 0.610
HSCT, n (%) 28 (80.0) 34 (52.3) 0.009
Allogeneic 24 (68.6) 24 (36.9) 0.003
Autologous 4 (11.4) 10 (15.4) 0.765
GVHD, n (%) 9 (25.7) 9 (13.8) 0.175
Mucositis, n (%) 6 (17.1) 17 (26.2) 0.455
Central venous catheter, n (%) 33 (94.3) 61 (93.8) 1.000
ANC at admission, �109/l, median (range) 0.9 (0–21.1) 1.1 (0–19.1) 0.781
ANC at discharge/death, �109/l, median (range) 1.8 (0–34.4) 2.1 (0–127) 0.544
Neutropenia at admission (neutrophils <0.5 �109/l, n (%) 14 (40.0) 29 (44.6) 0.678
Severe neutropenia during hospital stay (neutrophils <0.1 �109/l), n (%) 6 (17.1) 24 (36.9) 0.043
Persistent neutropenia (neutrophils <0.5 � 109/l), n (%) 13 (37.1) 17 (26.2) 0.263
Platelets at admission, �109/l, median (range) 30 (1–144) 28 (1–546) 0.951
Platelets at discharge/death, �109/l, median (range) 32 (3–218) 33 (2–624) 0.624
VRE BSI, n (%) 0 14 (21.5) 0.002
MASCC at admission, median (range) 21 (10–23) 16 (0–23) 0.021
Length of stay, days, median (range) 29 (3–99) 27 (4–134) 0.416
In-hospital mortality, n (%) 19 (54.3) 27 (41.5) 0.293
HSCT, hematopoietic stem cell transplant; GVHD, graft-versus-host disease; ANC, absolute neutrophil count; BSI, bloodstream infection; MASCC, Multinational Association of
Supportive Care in Cancer risk index score.a Fisher’s exact test was used for comparisons of categorical variables and the Mann–Whitney U-test was used for comparisons of continuous variables.
L.F. Lisboa et al. / International Journal of Infectious Diseases xxx (2015) e1–e6 e3
G Model
IJID 2260 1–6
Please cite this article in press as: Lisboa LF, et al. Empiric use of linezolid in febrile hematology and hematopoietic stem cell
transplantation patients colonized with vancomycin-resistant Enterococcus spp. Int J Infect Dis (2015), http://dx.doi.org/10.1016/
j.ijid.2015.02.001

197 hospitals with high rates of VRE endemicity, particularly if the
198 patient’s condition is unstable or if the patient has positive blood
199 culture results suspicious for VRE.26 Our study, however,
200 suggests that the empiric use of linezolid in febrile hematology
201 and HSCT patients colonized by VRE does not have an impact on
202mortality. More importantly, it indicates that persistent neutro-
203penia is a risk factor for mortality for both HSCT and non-HSCT
204patients, and that GVHD is a relevant factor associated with
205mortality in VRE-colonized HSCT patients. Thus, the use of
206empiric linezolid in colonized VRE neutropenic patients should
Table 2
Risk factors associated with mortality among 100 hematology and HSCT patients colonized by vancomycin-resistant Enterococcus spp (VRE)a
Variables Died (n = 46) Survived (n = 54) Univariate analysis Multivariate analysis
OR (95% CI) p-Value OR (95% CI) p-Value
Age, years, median (range) 44 (3–77) 34 (1–66) 0.105
Sex, female, n (%) 23 (50.0) 19 (35.2) 1.84 (0.82–4.11) 0.158
E. faecium colonization, n (%) 33 (71.7) 43 (79.6) 0.65 (0.26–1.63) 0.482
Underlying diseases, n
Acute leukemia 21 27 0.84 (0.38–1.85) 0.692
Chronic leukemia 4 2 2.48 (0.43–14.18) 0.410
Aplastic anemia 3 2 1.81 (0.29–11.36) 0.659
Fanconi anemia 1 1 1.18 (0.07–19.37) 1.000
Non-Hodgkin lymphoma 9 10 1.07 (0.39–2.91) 1.000
Hodgkin lymphoma 0 5 0.060
Multiple myeloma 2 5 0.44 (0.08–2.41) 0.447
Myelodysplastic syndrome 3 1 3.70 (0.37–36.83) 0.331
Other 3 1 3.70 (0.37–36.83) 0.331
HSCT, n (%) 30 (65.2) 32 (59.3) 1.29 (0.57–2.91) 0.680
Allogeneic 26 (56.5) 22 (40.7) 1.89 (0.85–4.19) 0.160
Autologous 4 (8.7) 10 (18.5) 0.42 (0.12–1.44) 0.247
GVHD, n (%) 12 (26.1) 6 (11.1) 2.82 (0.96–8.26) 0.069 3.69 (1.13–12.04) 0.030
Mucositis, n (%) 12 (26.1) 11 (20.4) 1.38 (0.54–3.51) 0.634
Central venous catheter, n (%) 43 (93.5) 51 (94.4) 0.84 (0.16–4.39) 1.000
ANC at admission, �109/l, median (range) 0.535 (0–16) 2.35 (0–21.1) 0.099 0.51
Neutropenia at admission (neutrophils <0.5 � 109/l), n (%) 22 (47.8) 21 (38.9) 1.44 (0.65–3.194) 0.421
Severe neutropenia (neutrophils <0.1 � 109/l), n (%) 16 (34.8) 14 (25.9) 1.52 (0.64–3.60) 0.385
Persistent neutropenia (neutrophils <0.5 � 109/l), n (%) 23 (50) 7 (13.0) 6.71 (2.51–17.93) <0.001 6.46 (2.20–19.10) 0.007
Platelets at admission, �109/l, median (range) 23 (1–546) 31 (1–436) 0.044 0.914
VRE BSI, n (%) 8 (17.4) 6 (11.1) 1.68 (0.53–5.27) 0.400
Empiric use of linezolid, n (%) 19 (41.3) 16 (29.6) 1.67 (0.73–3.82) 0.293
Length of stay, days, median (range) 32 (3–134) 27 (6–110) 0.478
MASCC at admission, median (range) 16.5 (8–23) 21 (0–23) 0.306
HSCT, hematopoietic stem cell transplant; OR, odds ratio; CI, confidence interval; GVHD, graft-versus-host disease; ANC, absolute neutrophil count; BSI, bloodstream
infection; MASCC, Multinational Association of Supportive Care in Cancer risk index score.a Fisher’s exact test was used for comparisons of categorical variables and the Mann–Whitney U-test was used for comparisons of continuous variables. Non-overlapping
variables with p < 0.1 in the univariate analysis fitting a biological rationale were included in the binary logistic regression model.
Figure 1. Kaplan–Meier analysis comparing the survival of 100 febrile hematology and HSCT patients colonized by VRE who received or did not receive empiric linezolid. The
red line represents the patients who did not receive linezolid and the green line patients who received linezolid.
L.F. Lisboa et al. / International Journal of Infectious Diseases xxx (2015) e1–e6e4
G Model
IJID 2260 1–6
Please cite this article in press as: Lisboa LF, et al. Empiric use of linezolid in febrile hematology and hematopoietic stem cell
transplantation patients colonized with vancomycin-resistant Enterococcus spp. Int J Infect Dis (2015), http://dx.doi.org/10.1016/
j.ijid.2015.02.001

207 be rethought and further studies with controlled trials are
208 needed to better understand the role of the use of linezolid in this
209 situation.
210 This study has several limitations. The design was retrospective,
211 it included a small number of patients with a short duration of
212 follow-up, and may express the local data; however, it appears that
213 the use of empiric linezolid in febrile hematology and HSCT patients
214 should be reconsidered and confirmed by controlled studies.
215 Although, the linezolid group did not develop VRE BSI, our data
216 do not support a clear association of VRE BSI with increased
217 mortality. Thus, it seems that VRE infections, which were treated
218 with linezolid, were likely markers of the overall severity of illness
219 in the patients with microbiologically confirmed infections. In this
220 regard, available evidence suggests that short courses of linezolid
221 have an acceptable safety profile regarding myelotoxicity,31–33 and
222 comparable, if not superior survival in VRE BSI when compared to
223 other VRE-active agents.32,33
224 Clinical studies have shown that colonization is an important
225 risk factor for BSI among hematology patients.19,27 The dysregula-
226 tion of innate immune defenses through broad-spectrum antibi-
227 otic use, and the consequent depletion of commensal bacteria,
228 seems to play a key role.28 In an animal model, colonization by VRE
229 was significantly higher after a course of antibiotics; interestingly,
230 this phenomenon was prevented by stimulation of the innate
231 immune receptor, toll-like receptor 5 (TLR5), through systemic
232 administration of flagellin, a structural component of Gram-
233 negative bacteria.29 A shift in the intestinal microflora towards an
234 Enterococcus-predominant microbiota was documented in asso-
235 ciation with antibiotic use and preceded the occurrence of VRE BSI
236 in HSCT recipients.5,8 As transplant patients typically have more
237 intensive antimicrobial exposure, this may account for the high
238 rates of VRE colonization in HSCT patients seen in our study.
239 Previous reports have found an association between VRE BSI
240 and decreased survival,10–13 leading to some advocating empiric
241 VRE therapy during periods of fever and neutropenia in colonized
242 hematology patients.4,6,19 Conflicting data, however, have failed to
243 support this association, suggesting that VRE infection is simply a
244 marker of a poor prognosis.16,17 Although retrospective, our data
245 corroborate the latter, showing that despite the patients who did
246 not receive empiric linezolid therapy having lower MASCC scores,
247 being sicker, and developing VRE BSI, the mortality was similar in
248 the two groups and that the crude mortality was independently
249 associated with GVHD in HSCT patients and with persistent
250 neutropenia in both HSCT and non-HSCT patients. These indepen-
251 dent risk factors are markers of severity of illness in the patients
252 and have previously been associated with bacterial infection and
253 mortality in this type of patient.34,35
254 Although, none of the isolates in the present study was resistant
255 to linezolid, resistance to linezolid among VRE has been
256 reported,20–22 and the spread of resistance is a concern worldwide;
257 this reinforces the importance of the rational use of linezolid in
258 neutropenic patients.
259 In conclusion, the empiric use of linezolid in the course of
260 refractory fever based on the data observed in this study would
261 unlikely modify the in-hospital mortality of VRE-colonized
262 hematology and HSCT patients, which rather seems to be
263 associated with GVHD and the persistence of neutropenia.
264 Uncited referenceQ8
265 30.
266 Acknowledgements
267 We thank Mariuza Basso, RN, for assistance with the VRE
268 surveillance and the collection and compiling of data.
269Funding source: This study was carried out with our own
270background resources.
271Conflict of interest: None of the authors have any conflicts of
272interest to disclose relevant to this work.
273Author contributions: Concept and design (LFL, BGM, SFC), data
274collection (LFL, BGM, MBV, SFC, TG), data analysis and interpreta-
275tion (LFL, MBV, BGM, SFC), drafting of the manuscript (LFL, BGM,
276SFC), critical review of the manuscript (MBV, FLD, GGF, TG, ASSL,
277MASY), final approval of manuscript for publication (LFL, BGM,
278MBV, FLD, GGF, TG, ASSL, MASY, SFC).
279References
2801. Sader HS, Moet GJ, Jones RN. Antimicrobial resistance among Gram-positive281bacteria isolated in Latin American hospitals. J Chemother 2009;21:611–20.2822. Zhao C, Sun H, Wang H, Liu Y, Hu B, Yu Y, et al. Antimicrobial resistance trends283among 5608 clinical Gram-positive isolates in China: results from the Gram-284Positive Cocci Resistance Surveillance program (2005-2010). Diagn Microbiol285Infect Dis 2012;73:174–81.2863. Irfan S, Idrees F, Mehraj V, Habib F, Adil S, Hasan R. Emergence of carbapenem287resistant Gram negative and vancomycin resistant Gram positive organisms in288bacteremic isolates of febrile neutropenic patients: a descriptive study. BMC289Infect Dis 2008;8:80.2904. Vydra J, Shanley RM, George I, Ustun C, Smith AR, Weisdorf DJ, et al. Entero-291coccal bacteremia is associated with increased risk of mortality in recipients of292allogeneic hematopoietic stem cell transplantation. Clin Infect Dis 2012;55:293764–70.2945. Taur Y, Xavier JB, Lipuma L, Ubeda C, Goldberg J, Gobourne A, et al. Intestinal295domination and the risk of bacteremia in patients undergoing allogeneic296hematopoietic stem cell transplantation. Clin Infect Dis 2012;55:905–14.2976. Matar MJ, Tarrand J, Raad I, Rolston KV. Colonization and infection with298vancomycin-resistant Enterococcus among patients with cancer. Am J Infect299Control 2006;34:534–6.3007. Rolston KV, Jiang Y, Matar M. VRE fecal colonization/infection in cancer301patients. Bone Marrow Transplant 2007;39:567–8.3028. Ubeda C, Taur Y, Jenq RR, Equinda MJ, Son T, Samstein M, et al. Vancomycin-303resistant Enterococcus domination of intestinal microbiota is enabled by anti-304biotic treatment in mice and precedes bloodstream invasion in humans. J Clin305Invest 2010;120:4332–41.3069. Miyazaki S, Fujikawa T, Kobayashi I, Matsumoto T, Tateda K, Yamaguchi K.307Development of systemic bacteraemia after oral inoculation of vancomycin-308resistant enterococci in mice. J Med Microbiol 2001;50:695–701.30910. DiazGranados CA, Jernigan JA. Impact of vancomycin resistance on mortality310among patients with neutropenia and enterococcal bloodstream infection.311J Infect Dis 2005;191:588–95.31211. DiazGranados CA, Zimmer SM, Klein M, Jernigan JA. Comparison of313mortality associated with vancomycin-resistant and vancomycin-suscepti-314ble enterococcal bloodstream infections: a meta-analysis. Clin Infect Dis3152005; 41:327–33.31612. Ghanem G, Hachem R, Jiang Y, Chemaly RF, Raad I. Outcomes for and risk factors317associated with vancomycin-resistant Enterococcus faecalis and vancomycin-318resistant Enterococcus faecium bacteremia in cancer patients. Infect Control Hosp319Epidemiol 2007;28:1054–9.32013. Kraft S, Mackler E, Schlickman P, Welch K, Depestel DD. Outcomes of therapy:321vancomycin-resistant enterococcal bacteremia in hematology and bone mar-322row transplant patients. Support Care Cancer 2011;19:1969–74.32314. Suppli M, Aabenhus R, Harboe ZB, Andersen LP, Tvede M, Jensen JU. Mortality in324enterococcal bloodstream infections increases with inappropriate antimicro-325bial therapy. Clin Microbiol Infect 2011;17:1078–83.32615. Avery R, Kalaycio M, Pohlman B, Sobecks R, Kuczkowski E, Andresen S, et al.327Early vancomycin-resistant Enterococcus (VRE) bacteremia after allogeneic328bone marrow transplantation is associated with a rapidly deteriorating clinical329course. Bone Marrow Transplant 2005;35:497–9.33016. Dubberke ER, Hollands JM, Georgantopoulos P, Augustin K, DiPersio JF, Mundy331LM, et al. Vancomycin-resistant enterococcal bloodstream infections on a332hematopoietic stem cell transplant unit: are the sick getting sicker? Bone333Marrow Transplant 2006;38:813–9.33417. Todeschini G, Tecchio C, Borghero C, D’Emilio A, Pegoraro E, de Lalla F, et al.335Association between Enterococcus bacteraemia and death in neutropenic336patients with haematological malignancies. J Infect 2006;53:266–73.33718. Liss BJ, Vehreschild JJ, Cornely OA, Hallek M, Fatkenheuer G, Wisplinghoff H,338et al. Intestinal colonisation and blood stream infections due to vancomycin-339resistant enterococci (VRE) and extended-spectrum beta-lactamase-producing340Enterobacteriaceae (ESBLE) in patients with haematological and oncological341malignancies. Infection 2012;40:613–9.34219. Weinstock DM, Conlon M, Lovino C, Aubrey T, Gudiol C, Riedel E, et al.343Colonization, bloodstream infection, and mortality caused by vancomycin-344resistant Enterococcus early after allogeneic hematopoietic stem cell trans-345plant. Biol Blood Marrow Transplant 2007;13:615–21.34620. Dibo I, Pillai SK, Gold HS, Baer MR, Wetzler M, Slack JL, et al. Linezolid-resistant347Enterococcus faecalis isolated from a cord blood transplant recipient. J Clin348Microbiol 2004;42:1843–5.
L.F. Lisboa et al. / International Journal of Infectious Diseases xxx (2015) e1–e6 e5
G Model
IJID 2260 1–6
Please cite this article in press as: Lisboa LF, et al. Empiric use of linezolid in febrile hematology and hematopoietic stem cell
transplantation patients colonized with vancomycin-resistant Enterococcus spp. Int J Infect Dis (2015), http://dx.doi.org/10.1016/
j.ijid.2015.02.001

349 21. Fossati M, Cappelli B, Biral E, Chiesa R, Biffi A, Ossi C, et al. Fatal vancomycin-350 and linezolid-resistant Enterococcus faecium sepsis in a child undergoing allo-351 geneic haematopoietic stem cell transplantation for beta-thalassaemia major.352 J Med Microbiol 2010;59(Pt 7):839–42.353 22. Scheetz MH, Knechtel SA, Malczynski M, Postelnick MJ, Qi C. Increasing inci-354 dence of linezolid-intermediate or -resistant, vancomycin-resistant Enterococ-355 cus faecium strains parallels increasing linezolid consumption. Antimicrob356 Agents Chemother 2008;52:2256–9.357 23. Hughes WT, Armstrong D, Bodey GP, Brown AE, Edwards JE, Feld R, et al.358 1997 guidelines for the use of antimicrobial agents in neutropenic patients with359 unexplained fever. Infectious Diseases Society of America. Clin Infect Dis360 1997;25:551–73.361 24. Garner JS, Jarvis WR, Emori TG, Horan TC, Hughes JM. CDC definitions for362 nosocomial infections, 1988. Am J Infect Control 1988;16:128–40.363 Bach PB, Malak SF, Jurcic J, Gelfand SE, Eagan J, Little C, Sepkowitz KA. Impact of364 infection by vancomycin-resistant Enterococcus on survival and resource365 utilization for patients with leukemia. Infect Control Hosp Epidemiol 2002;23:366 471–4.367 25. Klastersky J, Paesmans M, Rubenstein EB, Boyer M, Elting L, Feld R, et al. The368 Multinational Association for Supportive Care in Cancer risk index: a multina-369 tional scoring system for identifying low-risk febrile neutropenic cancer370 patients. J Clin Oncol 2000;18:3038–51.371 Kamboj M, Chung D, Seo SK, Pamer EG, Sepkowitz KA, Jakubowski AA, Papa-372 nicolaou G. The changing epidemiology of vancomycin-resistant Enterococcus373 (VRE) bacteremia in allogeneic hematopoietic stem cell transplant (HSCT)374 recipients. Biol Blood Marrow Transplant 2010;16:1576–81.375 26. Freifeld AG, Bow EJ, Sepkowitz KA, Boeckh MJ, Ito JI, Mullen CA, et al. Clinical376 practice guideline for the use of antimicrobial agents in neutropenic patients377 with cancer: 2010 update by the Infectious Diseases Society of America. Clin378 Infect Dis 2011;52:e56–93.
37927. Bossaer JB, Hall PD, Garrett-Mayer E. Incidence of vancomycin-resistant en-380terococci (VRE) infection in high-risk febrile neutropenic patients colonized381with VRE. Support Care Cancer 2010;19:231–7.38228. Brandl K, Plitas G, Mihu CN, Ubeda C, Jia T, Fleisher M, et al. Vancomycin-383resistant enterococci exploit antibiotic-induced innate immune deficits. Nature3842008;455:804–7.38529. Kinnebrew MA, Ubeda C, Zenewicz LA, Smith N, Flavell RA, Pamer EG.386Bacterial flagellin stimulates toll-like receptor 5-dependent defense against387vancomycin-resistant Enterococcus infection. J Infect Dis 2010;201:534–43.38830. Olivier CN, Blake RK, Steed LL, Salgado CD. Risk of vancomycin-resistant389Enterococcus (VRE) bloodstream infection among patients colonized with390VRE. Infect Control Hosp Epidemiol 2008;29:404–9.39131. Hogan HL, Hachem RY, Neuhauser M, Raad II, Coyle E. Clinical experience392of linezolid in bone marrow transplantation patients. J Pharm Pract3932010;23:352–7.39432. Cohen N, Mihu CN, Seo SK, Chung D, Chou J, Heller G, Papanicolaou GA.395Hematologic safety profile of linezolid in the early periengraftment period396after allogeneic stem cell transplantation. Biol Blood Marrow Transplant3972009;15:1337–41.39833. McKinnell JA, Patel M, Shirley RM, Kunz DF, Moser SA, Baddley JW. Observa-399tional study of the epidemiology and outcomes of vancomycin-resistant En-400terococcus bacteraemia treated with newer antimicrobial agents. Epidemiol401Infect 2011;139:1342–50.40234. Richters A, van Vliet M, Peer PG, Verweij PE, Laros-van Gorkom BA, et al.403Incidence of and risk factors for persistent Gram-positive bacteraemia and404catheter-related thrombosis in haematopoietic stem cell transplantation. Bone405Marrow Transplant 2014;49:264–9.40635. Demiraslan H, Sevim M, Pala C, Durmaz S, Berk V, Kaynar L, et al. Risk factors407influencing mortality related to Stenotrophomonas maltophilia infection in408hematology–oncology patients. Int J Hematol 2013;97:414–20.
L.F. Lisboa et al. / International Journal of Infectious Diseases xxx (2015) e1–e6e6
G Model
IJID 2260 1–6
Please cite this article in press as: Lisboa LF, et al. Empiric use of linezolid in febrile hematology and hematopoietic stem cell
transplantation patients colonized with vancomycin-resistant Enterococcus spp. Int J Infect Dis (2015), http://dx.doi.org/10.1016/
j.ijid.2015.02.001