Emergency nurses and disaster response: An exploration of South Australian emergency nurses’...
8
Australasian Emergency Nursing Journal (2011) 14, 87—94 available at www.sciencedirect.com journal homepage: www.elsevier.com/locate/aenj RESEARCH Emergency nurses and disaster response: An exploration of South Australian emergency nurses’ knowledge and perceptions of their roles in disaster response Karen S. Hammad, BN(Hons), GradDipEmergNurs, RN a,∗ , Paul Arbon, PhD, MEd Studies, Grad Dip Health Ed, Dip Ed, BSc RN a , Kristine M. Gebbie, DrPH, RN b a Flinders University, School of Nursing and Midwifery, Flinders Drive, Bedford Park, SA 5042, Australia b CUNY Hunter College, School of Nursing, Park Avenue, NY, USA Received 7 July 2010; received in revised form 1 September 2010; accepted 7 October 2010 KEYWORDS Emergency nurse; Disaster; Disaster education; Disaster training; Emergency department; Previous disaster response; Disaster knowledge nurse Summary The word ‘disaster’ for many people conjures up images of well publicized events such as 9/11 (2001), the London bombings (2005), Hurricane Katrina (2005) and more recently the Haiti earthquake (2010). For Australians, the impact of disasters closer to our shores has been felt through such incidents as the Bali bombings (2002 and 2005) and the Boxing Day Tsunami (2004). Significant events that have occurred on Australian soil include Cyclone Tracey (1974), the Granville Rail disaster (1977) and Ash Wednesday bushfires (1983). Natural disasters such as flooding, cyclones and bushfires continue to impact Australian communities. However, to date Australia has avoided a large scale disaster event that has overwhelmed the health care system. A mixed method approach underpins this study. Both quantitative and qualitative data was collected through a self report questionnaire. Quantitative data has provided statistic evidence to support the findings, while the qualitative data has allowed for a richer understanding of nurses’ perceptions. The population for this study is South Australian emergency nurses working in public hospital emergency departments in metropolitan Adelaide. Three key themes emerged from the data. Firstly, South Australian emergency nurses have had minimal previous disaster experience (either through a real event or simulated exercises). Second, although a large number of nurses have completed what they perceive to be disaster education and training, questions were raised regarding the appropriateness, relevance and ∗ Corresponding author. E-mail address: karen.hammad@flinders.edu.au (K.S. Hammad). 1574-6267/$ — see front matter © 2010 College of Emergency Nursing Australasia Ltd. Published by Elsevier Ltd. All rights reserved. doi:10.1016/j.aenj.2010.10.002
Transcript of Emergency nurses and disaster response: An exploration of South Australian emergency nurses’...
Australasian Emergency Nursing Journal (2011) 14, 87—94
avai lab le at www.sc iencedi rec t .com
journa l homepage: www.e lsev ier .com/ locate /aenj
RESEARCH
Emergency nurses and disaster response: Anexploration of South Australian emergency nurses’knowledge and perceptions of their roles indisaster response
Karen S. Hammad, BN(Hons), GradDipEmergNurs, RNa,∗,Paul Arbon, PhD, MEd Studies, Grad Dip Health Ed, Dip Ed, BSc RNa,Kristine M. Gebbie, DrPH, RNb
a Flinders University, School of Nursing and Midwifery, Flinders Drive, Bedford Park, SA 5042, Australiab CUNY Hunter College, School of Nursing, Park Avenue, NY, USA
Received 7 July 2010; received in revised form 1 September 2010; accepted 7 October 2010
KEYWORDSEmergency nurse;Disaster;Disaster education;Disaster training;Emergencydepartment;Previous disasterresponse;Disaster knowledgenurse
Summary The word ‘disaster’ for many people conjures up images of well publicized eventssuch as 9/11 (2001), the London bombings (2005), Hurricane Katrina (2005) and more recentlythe Haiti earthquake (2010). For Australians, the impact of disasters closer to our shores hasbeen felt through such incidents as the Bali bombings (2002 and 2005) and the Boxing DayTsunami (2004). Significant events that have occurred on Australian soil include Cyclone Tracey(1974), the Granville Rail disaster (1977) and Ash Wednesday bushfires (1983). Natural disasterssuch as flooding, cyclones and bushfires continue to impact Australian communities. However,to date Australia has avoided a large scale disaster event that has overwhelmed the health caresystem.
A mixed method approach underpins this study. Both quantitative and qualitative data wascollected through a self report questionnaire. Quantitative data has provided statistic evidenceto support the findings, while the qualitative data has allowed for a richer understanding of
nurses’ perceptions. The population for this study is South Australian emergency nurses workingin public hospital emergency departments in metropolitan Adelaide.Three key themes emerged from the data. Firstly, South Australian emergency nurses havehad minimal previous disaster experience (either through a real event or simulated exercises).Second, although a large number of nurses have completed what they perceive to be disastereducation and training, questions were raised regarding the appropriateness, relevance and
∗ Corresponding author.E-mail address: [email protected] (K.S. Hammad).
1574-6267/$ — see front matter © 2010 College of Emergency Nursing Australasia Ltd. Published by Elsevier Ltd. All rights reserved.doi:10.1016/j.aenj.2010.10.002

88 K.S. Hammad et al.
availability of such education. Third, South Australian emergency nurses have a low level ofdisaster knowledge. The findings from this study are relevant not only for emergency nurses, butfor all health professionals involved in disaster response. In particular for those who have hadminimal disaster response experience and limited exposure to disaster education and trainingopportunities. This study suggests a disaster training program for South Australian emergencynurses would be beneficial. The need for future research into appropriate disaster education andtraining for health professionals is highlighted by the study.
ncy N
I
B
Thedoitwtsowets
dtbpMarc
tmcro
atseeairp
P
Tcdpweer
M
S
Aqtdtetmq
P
Public hospitals were the focus of this study and the EDof eight public hospitals in metropolitan Adelaide provide
© 2010 College of Emergereserved.
What is known about the topic?
• There is an abundance of disaster related literature,but very little regarding emergency nurses and disas-ter. Particularly with regards to their knowledge andperception their role in disaster response.
What this paper adds or contributes?
• This paper adds to the body of knowledge regardingemergency nurses and disasters. This is particularlyrelevant to disaster education and training, previousdisaster response experience and disaster knowledgeamongst South Australian emergency nurses. It isanticipated that this study will provide a founda-tion into future studies aimed at better preparingemergency nurses for disaster response.
ntroduction
ackground
o date Australia has avoided a catastrophic disaster thatas overwhelmed the health care system.1—3 Such anvent would have a considerable impact on the emergencyepartment (ED) which is considered to be at the front linef the hospital response.4 Emergency nurses play a vital rolen executing the department disaster plan and providingreatment for disaster victims.5—8 It is expected that nursesorking in the ED have the necessary skills and experience
o effectively manage every day emergencies and chaoticituations. However, little is understood about what skillsr experience they need in order to respond effectivelyhen the every day work of the ED is amplified by a disastervent. Such an event could significantly impact a systemhat is already struggling with the daily effects of staffinghortages and overcrowding.
Definitions of the word ‘disaster’ can be found in abun-ance and ‘vary according to who is studying the topic andhe discipline to which the persons conducting the studyelong’.9 Because of the wide range of definitions, for theurposes of this paper, the definition provided by Emergency
anagement Australia (EMA), the Australian governmentgency responsible for coordinating the Commonwealth’sesponse to disaster, was utilised; ‘A serious disruption toommunity life that threatens or causes death or injury intnwi
ursing Australasia Ltd. Published by Elsevier Ltd. All rights
hat community and/or damage to property, the environ-ent and/or economic activity that is beyond the day to day
apacity of the prescribed statutory authorities and whichequires special mobilisation and organisation of resourcesther than those normally available to those authorities’.10
A review of the literature demonstrated that therere only a small amount of studies that directly relateo emergency nurses and disasters. Existing research thatpecifically informs emergency nurses and disasters hasxplored willingness to respond,6 needs and concerns ofmergency nurses,11 emergency department response12,13
nd the experiences of emergency nurses who have beennvolved in disaster response.14—16 There is no currentesearch that explores emergency nurses’ knowledge anderceptions of their roles in disaster response.
urpose of study
his study was conducted with the aim of enhancing theurrent body of knowledge regarding emergency nurses andisaster response. It was anticipated that the study wouldrovide a foundation for further research into determininghat type of disaster education and training would benefitmergency nurses. The study explores South Australian (SA)mergency nurses’ knowledge and preparedness for disasteresponse in the acute setting.
ethod
tudy design
questionnaire was chosen as the data collection tool. Theuestionnaire elicited both qualitative and quantitative datahrough different questioning styles. In an effort to gain aeeper understanding of nurses’ opinions, open ended ques-ions were included in the questionnaire. The use of opennded questions allowed participants to use their own wordshus providing a deeper understanding of the population thatay not have been gained from the use of a quantitativeuestionnaire alone.
articipants and setting
he setting for this research. South Australian emergencyurses were chosen as the population for this study. Thereere 4432 critical care/emergency nurses employed in SA
n 2007.17 At the time the study was conducted there were
R
D
Argntan5fisAinocs
scon(tfesCi(cim
Emergency nurses and disaster response
588 Registered Nurses (RN) employed in public hospital EDin metropolitan Adelaide. This number includes nurses whowere on leave at the time the survey was circulated.
Ethics
Approval to conduct the proposed research was initiallysought from individual department heads, Clinical ServiceCoordinators and Nurse Managers. Ethics approval was thengained from research committees representing each of theeight different sites.
Data collection
A self designed questionnaire was chosen as the data collec-tion tool for this study. A thorough search did not identifyan existing survey tool that would suit the purposes ofthis study. The questionnaire was piloted amongst a group(n = 10) of senior emergency nurses. Following this, minorgrammatical changes were made to the questionnaire. Thequestionnaire was circulated to RN via individual pigeonholes. RN had a period of four weeks to complete the ques-tionnaire and return it to a designated box in the ED.
The questionnaire incorporated five main areas of ques-tioning; demographics, knowledge, awareness, previousdisaster response experience and roles of nurses in disas-ters. As data was collected it was entered verbatim onto aMicrosoft Excel database. Missing responses from the datawere also noted in the database.
Data analysis
Data was analyzed using sum, percentage, frequency distri-butions and measures of central tendency. Thematic analysiswas also used for the analysis of all the open ended and short
answer questions. Individual words, word combinations andthemes were manually extracted from the data and cate-gorized. Both explicit and implicit themes were extractedfrom the data.hbdn
Table 1 Participants responses to knowledge test on disaster mis
Statement Respon
Disasters kill people without respect for social classor economic status in a disaster.
100%, n
Most people behave rationally in a disaster. 100%, nThe poor and marginalized are more at risk of death
than the rich people or the middle classes in adisaster.
99%, n =
Looting is a common problem following disasters. 99% n =All victims of a CBR (chemical biological radiological)
incident will be decontaminated at the scene of anincident prior to their arrival to hospital.
97%, n =
Un-buried dead bodies will create a disease epidemicfollowing a disaster.
97% n =
The majority of casualties from a disaster will arriveto your emergency department via the SAAS (SAAmbulance Service).
99%, n =
89
esults
emographic data
total of 588 questionnaires were circulated, 194 wereeturned resulting in a response rate of 32.9%. The demo-raphic findings paint a profile of emergency nurses that isot dissimilar from the state and national nursing popula-ion. Emergency nurses in this study are aged between 21nd 59 years with an average age of 36 years. 65% (n = 112) ofurses have been working in their current ED between 0 andyears and over half (52%, n = 98) have been employed in theeld of emergency nursing for 0—5 years. Most nurses in thistudy (77%, n = 136) work seven or more shifts a fortnight.lthough females account for the majority of the nurses
n this study, the proportion of males was double that ofational and state averages. Nearly one quarter (23%, n = 39)f the emergency nurse participants in this study are male,ompared with a national average for nurses in all fields andpecialties combined, of 9.6%.17
Level one RN make up the bulk of participants in thistudy (77%, n = 132). In SA there are six RN and Midwifelassifications.18 A level one RN is the lowest classificationn the hierarchy.18 Level one RN include new graduates andurses who do not hold managerial positions. There were 16%n = 27) level two/Clinical Nurses. Nurses in this classifica-ion provide advanced nursing services and are accountableor their own practice standards, activities delegated to oth-rs and the guidance and development of less experiencedtaff.18 There were 6% (n = 10) level three/Clinical Practiceonsultant nurses. In broad terms these nurses provide clin-
cal nursing expertise and leadership.18 There was only 1%n = 1) level four/Advanced nurse in this study. Nurses in thislassification may practice beyond the usual extent of nurs-ng scope of practice and are autonomous clinical decisionakers, working independently and collaboratively in the
ealth care system.18 There were no level five or level sixanded RN in this study. The nurses in this classification areirectors of health units and directors of nursing.18 The largeumber of level one and two RN is an indication that most
conceptions.
se rate Correct answer Agree (%) Disagree (%)
= 194 Disagree 94 6
= 194 Agree 12 88193 Agree 43 57
194 Disagree 92 8191 Disagree 25 75
191 Disagree 86 14
193 Disagree 27 73
90 K.S. Hammad et al.
Who nurses take orders from during a disaster response
0 10 20 30 40 50 60
emergency services (n=2)
hospital executive (n=6)
medical (n=16)
medical/nursing (n=34)
nursing (n=35)
unclear (n=86)
percentage of nurses
Fa
nw
D
Tftttdab(4k
ttrcwwsoo
indatoea
D
HoctM((M
When participants last attended disaster training
05
101520253035
<6 months(n=11)
>6months(n=56)
>12months(n=40)
>2 years(n=43)
none (n=35)
perc
enta
ge o
f par
ticip
ants
F
(et(ep
dana1
P
Tprip(a(intar
tinvolved in a disaster exercise during their current employ-ment. While a further 22% (n = 39) have been involved inonly one disaster exercise at their present employment (seeFig. 3). The majority of these nurses have been working in
Percentage of nurses who have been involved in a disaster exercise in their current employment
no
once22%
twice5%
three +9%
nooncetwice
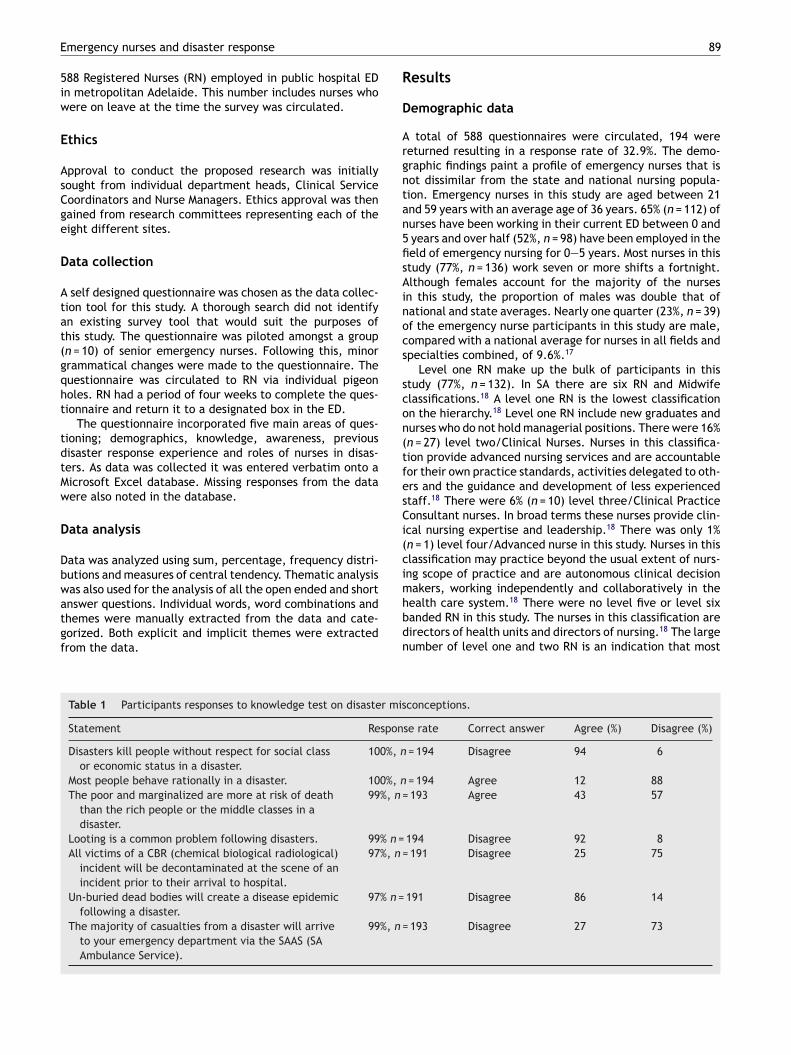
igure 1 Who nurses believe they will take orders from duringdisaster response.
urses in this study are involved in direct patient care andill play a significant role in disaster response.
isaster knowledge and awareness
he questionnaire started with a knowledge ‘test’ adaptedrom a study by Alexander.19 The purpose of this was to cap-ure the participants’ attention and focus them toward theopic at hand — disaster response. Participants were askedo agree or disagree with seven statements which wereesigned to test the participants’ knowledge of common dis-ster misconceptions. A percentage score was establishedy determining how many nurses responded correctly. 15%n = 30) scored above the chosen pass mark of 50%, with only% (n = 8) scoring 100%. Most nurses (85%, n = 164) failed thenowledge test with a score of less than 50% (see Table 1).
Nurses appeared to be unclear regarding command struc-ure (see Fig. 1). Almost half (48%, n = 86) were unclear aso who they would take orders from during a response. Manyesponses to this question were ambiguous regarding thehain of command or the official title of the person theyould take orders from. The suggestion by nurses that theyould take their orders jointly from nursing and medical
taff (19%, n = 34) indicates not only confusion as to whorders would be taken from, but also may lead to confusionn the floor.
Nurses also displayed confusion regarding their likely rolen a disaster. Responses fell into four categories: typicalursing roles or allocations (29%, n = 49), dependant on theisaster and the day (14%, n = 24), general roles (49%, n = 83)nd ‘other’ (8%, n = 4). Again, response were vague referringo general nursing duties such as; ‘treating patients’, ‘caref injured patients’ and ‘clinical care’, or to general allncompassing titles such as: ‘senior nurse’, ‘junior nurse’nd ‘Registered Nurse’.
isaster education and training
ospital education sessions were the most common formf disaster related education/training that nurses hadompleted (69%, n = 134). Other forms of disaster educa-ion/training included; post graduate studies (33%, n = 64);
ajor Incident Medical Management and Support Course13%, n = 25); Emergo Train (10%, n = 20); online education7%, n = 13); military training (5%, n = 9) and Emergencyanagement Australia courses (5%, n = 9). Just under half
Fd
frequency of training
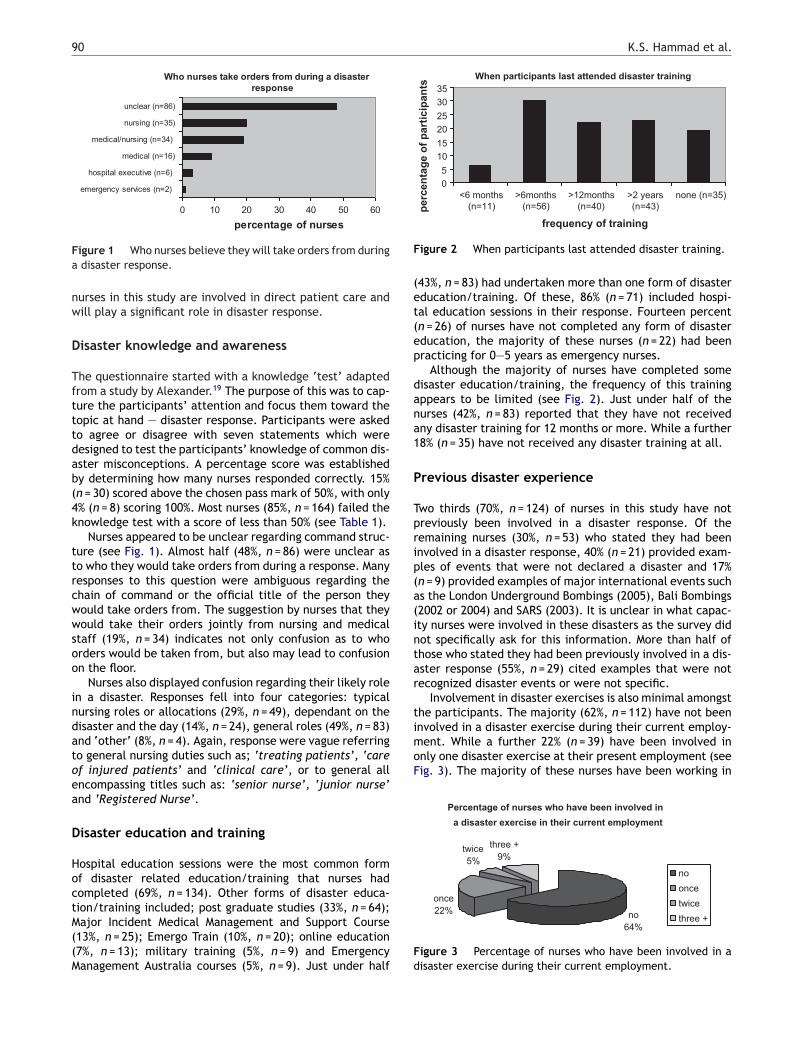
igure 2 When participants last attended disaster training.
43%, n = 83) had undertaken more than one form of disasterducation/training. Of these, 86% (n = 71) included hospi-al education sessions in their response. Fourteen percentn = 26) of nurses have not completed any form of disasterducation, the majority of these nurses (n = 22) had beenracticing for 0—5 years as emergency nurses.
Although the majority of nurses have completed someisaster education/training, the frequency of this trainingppears to be limited (see Fig. 2). Just under half of theurses (42%, n = 83) reported that they have not receivedny disaster training for 12 months or more. While a further8% (n = 35) have not received any disaster training at all.
revious disaster experience
wo thirds (70%, n = 124) of nurses in this study have notreviously been involved in a disaster response. Of theemaining nurses (30%, n = 53) who stated they had beennvolved in a disaster response, 40% (n = 21) provided exam-les of events that were not declared a disaster and 17%n = 9) provided examples of major international events suchs the London Underground Bombings (2005), Bali Bombings2002 or 2004) and SARS (2003). It is unclear in what capac-ty nurses were involved in these disasters as the survey didot specifically ask for this information. More than half ofhose who stated they had been previously involved in a dis-ster response (55%, n = 29) cited examples that were notecognized disaster events or were not specific.
Involvement in disaster exercises is also minimal amongsthe participants. The majority (62%, n = 112) have not been
64%three +
igure 3 Percentage of nurses who have been involved in aisaster exercise during their current employment.

ds
piuimhrikqints
D
TpscfttHaapettw
ssAfutta(atacptpta
ta
Emergency nurses and disaster response
their current ED for between 0 and 5 years. Of those thathave never been involved in a disaster exercise in their cur-rent employment 12% (n = 22) have been working in theircurrent ED for between 6 and 20 years.
Discussion
Three key findings emerged from the data. Firstly South Aus-tralian emergency nurses have had limited previous disasterresponse experience (real event or simulated exercise).Secondly, although the majority of nurses appear to havecompleted disaster education and training, questions havebeen raised regarding the appropriateness and relevanceof this education. The third main finding from the study isthat South Australian emergency nurses have a low level ofdisaster knowledge.
Previous disaster response experience
South Australian emergency nurses have had minimal expo-sure to disaster response. This is demonstrated through thefindings of this study as well as by existing literature.1—3,20—22
Of the nurses in this study who stated they had been involvedin a disaster response, only a small number cited examplesof true disasters all of which had occurred internationally.Although this would provide insight for nurses regardingthe realities of disaster response, expectations will differslightly with regards to policies and procedures of a disasterresponse within the Australian health care system.
Where nurses responded that they had been involved indisaster response and did not indicate a recognized disasterevent, responses were non specific and included examplessuch as; ‘bus crash’, ‘organophosphate exposure’, and ‘EDevacuation’. These responses are comparable with findingspublished by Duong and demonstrate a limited understand-ing by nurses of the true meaning of a disaster.20
With minimal previous disaster response experience theimportance of exercises to provide nurses with insight intothe realities of disaster response is highlighted. Disasterexercises provide nurses with a realistic expectation of howa disaster event would progress which also provides themwith the opportunity to test systems and protocols that willbe relied on in a real life situation. Programs such as EmergoTrain24 provide health professionals with exercises run inreal time that essentially mimic the flow of a real disasterevent. It is important for hospitals to maintain frequency inscheduling their exercises. Regular disaster drills, will keeppatterns ingrained and staff prepared.23
Although the Australian government has not publishedany guidelines regarding the frequency or nature of disastertraining for hospitals, international guidelines do exist.25,26
The Joint Commission on the Accreditation of Health Organi-zations (JCAHO) has set expectations regarding emergencyplanning and minimum numbers of exercises annually. 26 TheAustralian equivalent of JCAHO, the Australian Council onHealth Care Standards (ACHS) also provides an accreditationprogram for health care organizations to ensure safety and
quality improvement. The ACHS has determined that hospi-tals need to maintain safe practice and a safe environmentfor employees, consumers/patients and visitors with regardsto emergency and disaster management.27 However theremstp
91
oes not appear to be any guidelines as to what hospitalshould do to ensure this.
Previous exposure to disaster events creates a betterrepared and more confident workforce.15,28—34 Due to min-mal exposure to disasters South Australian nurses may havenrealistic expectations of disaster response. A more seriousmplication is that involvement in future disaster responseay contribute to a high rate of stress reactions and mental
ealth issues for emergency nurses. Previous studies haveeported that nurses who have been previously involvedn disaster response had the advantage of experience andnowledge, which resulted in diminished feelings of inade-uacy and fear.15 On a background of minimal involvementn disaster response, regular disaster exercises will provideurses with knowledge of what to expect, realistic expecta-ions and a feeling that they are prepared to handle a similarituation in the future.
isaster education and training
he primary source of disaster related education is from hos-ital education sessions (74%, n = 143). Hospital educationessions are site based, providing a low cost option of edu-ation delivery to the workforce. These sessions meet a needor the staff that require education, and almost certainly forhe individual hospitals that need to fulfill certain accredita-ion requirements, by providing low cost, on site education.ospital education sessions are not centrally administerednd therefore vary from hospital to hospital; making dis-ster education inconsistent amongst the emergency nurseopulation. It remains unclear as to what exactly hospitalducation sessions entail, who runs them, what qualifica-ions they have, how frequently the sessions are run, whathe content is or how evidence based it is as this informationas not captured by the questionnaire.
The fact that the majority of nurses have completedome sort of disaster education does paint the provi-ion of disaster education/training for nurses in Southustralia in a positive light. What remains unclear is therequency of disaster training. Disaster plans need to bepdated regularly to allow for system changes and staffurnover. Disaster education and training should reflecthis and be provided regularly so that health profession-ls are kept abreast of latest changes. Despite this, 42%n = 83) of nurses reported that they have not receivedny disaster training for 12 months or more. While a fur-her 18% (n = 35) have not received any disaster trainingt all. This number has decreased somewhat since Duongonducted her study in 2006 where 39% (n = 60) of theopulation had never attended disaster training or educa-ion and therefore suggests either an improvement in therovision of disaster education with time or the percep-ion by nurses that the education they have received isdequate.20
Where nurses were provided with room at the end ofhe questionnaire to comment further on emergency nursingnd disaster more than half of the responses (55%, n = 23)
ade mention of disaster education and training. Thesetatements revolved around limited availability of training,he need for appropriate training, the need for a largerroportion of staff to attend training and a lack of commit-

9
mStri
etsfpcdtsoae
D
Apoceahilkt
osTtpifithtocibi
hCOtktnMvll
trlam
R
R
Tdtnbtlctsesc
R
ItMhostaEdcmaai
L
Tiwmac
C
Te
2
ent from state government and hospital administrators.imilar comments were also scattered throughout the ques-ionnaires. This is an indication that nurses feel they are noteceiving enough disaster education/training, a feeling thats supported by the findings of the study.
On a background of minimal previous disaster responsexperience (real or simulated) health professionals needo be provided with appropriate education and training,o as to better prepare them. This would be informed byuture research aimed at identifying what current trainingrograms provide as well as barriers for nurses seeking edu-ation and training. It appears however, that provision ofisaster education and training is at best haphazard acrosshe board. There is no distinct structure in the provision oftandard education for all nurses. Although a large numberf nurses have completed education, it remains uncertains to the appropriateness, frequency or content of currentducation/training models.
isaster knowledge
low level of global knowledge was demonstrated by theoor performance in the knowledge test at the beginningf the questionnaire. Common belief in disaster miscon-eptions is an effective barrier to the teaching of disasterducation.19 This needs to be considered when determiningppropriate and effective disaster education and training forealth professionals in the future. An overwhelming major-ty of participants failed the knowledge test with a score ofess than 50%. This suggests a low level of general disasternowledge and may act as a potential barrier to effectiveraining.
Perhaps one of the most obvious indicators of the lackf disaster knowledge exhibited by the nurses is the confu-ion that exists surrounding roles and command structure.his demonstrates a lack of understanding around local prac-ices. Widespread confusion regarding local policies andractices during disaster response raises questions regard-ng the content of current education and training. Theailure to educate on local practices could have interest-ng implications on the floor during a disaster response ifhere is not a correctly delineated command structure orealth professionals are unsure of their role. Regular disas-er drills would provide nurses with a clear understandingf the local response, including roles, responsibilities andommand structure. An understanding of the local responses essential to ensuring that nurses are prepared.23 Thisecomes even more vital on the current background of min-mal exposure to disaster response.
Competencies for RN responding to mass casualty eventsave been published internationally.35,36 The Internationalouncil of Nurses (ICN) in association with the World Healthrganisation (WHO) has published Disaster Nursing Compe-encies that provide guidance on the range and level ofnowledge, attitude and skills for nursing in disaster.37 Inhe absence of a set of core competencies for Australianurses responding to disasters.22 The Australian Nursing and
idwifery Council (ANMC) has set guidelines which pro-ide information regarding legal parameters of practice,icensure and competencies.38 According to these guide-ines, nurses should be able to describe or be familiar withaeit
K.S. Hammad et al.
he chain of command in emergency response, emergencyesponse functions and roles and demonstrate them in regu-arly performed drills.38 If the above mentioned findings arenything to go by, South Australian emergency nurses do noteet either the ANMC or the ICN standards.
ecommendations
ecommendations for future research
he paucity of literature regarding emergency nurses andisasters demonstrates a significant gap and need for fur-her research into understanding the role of emergencyurses and disasters. The study demonstrates the associationetween disaster response experience and disaster educa-ion and training and the effect that inconsistencies andimitations in these areas can have on overall knowledge andonfidence. Future research will be informed by examininghe availability, content, cost and process of relinquishingtaff for disaster education and training, as well as furtherxploring the role of emergency nurses in disasters. Doingo may assist in helping to create a better prepared andonfident workforce.
ecommendations for clinical practice
t is time the Australian government gave more commitmento the preparedness of frontline health care professionals.inimum standards for disaster preparedness of Australianospitals need to be determined. This will ensure an amountf standardization in disaster preparedness, not only on atate level but also nation wide. A set of minimum compe-encies for nurses needs to be determined and adhered tolso. In the absence of this it is important that individualD and hospitals ensure that staff are exposed to adequateisaster education and are involved in regular disaster exer-ises. By doing so, hospitals will be ensuring that staff haveore realistic expectations of disaster response as well as
ppropriate knowledge and understanding of local practicesnd policies. More importantly, staff will feel more confidentn their ability to respond effectively.
imitations
he findings discuss the type of disaster education and train-ng that nurses have completed but fail to determine exactlyhat the stated education or training involves. The involve-ent of study participants in previous disaster response was
lso explored, however the study fails to identify in whatontext participants were involved in the response.
onclusion
here is an expectation among the wider community thatmergency nurses will be prepared and will cope with a dis-
ster situation; dealing with emergencies is what they dovery day, it is what they have been trained to do. Whats overlooked however is that a disaster event will amplifyhe everyday work of the ED and nurses will be exposed to
/
Emergency nurses and disaster response
large numbers of patients presenting within shorter periodsof time. Combined with this is the affect of the disasterevent on the community at large as well as the individualnurse and their ability and willingness to respond.
South Australian emergency nurses have had minimalexposure to disasters (through real events or simulatedexercises) to provide them with realistic expectations oftheir role in disaster response. This highlights the need forappropriate and consistent disaster education and train-ing. However, the study demonstrates that South Australianemergency nurses have not received appropriate or consis-tent disaster education and training. These may be factorscontributing to an overall low level of disaster knowledgeand confusion regarding local policies and practice, amongstSouth Australian emergency nurses.
The study demonstrates that South Australian emergencynurses have not been adequately prepared for disasterresponse and highlights not only the importance of futureresearch regarding disaster education and training, but alsothe immediate need for individual hospitals, governmentorganizations and peak health bodies to address disaster andemergency preparedness for frontline health professionals.Australia has so far escaped a large scale disaster eventthat has overwhelmed the health care system. When theinevitable happens, it is essential that front line health pro-fessionals, including emergency nurses feel confident andare prepared to respond.
Provenance and competing interests
No competing interests declared. This paper was not com-missioned.
Funding
No funding was used for this study.
Acknowledgements
Many thanks go to the emergency nurses who took time outof their already busy work days to complete the question-naire.
References
1. Templeman D, Bergin A. Taking a punch: building a moreresilient Australia. Australian Strategic Policy Institute2008:1—22.
2. Bergin A, Khosa R. Are we ready — healthcare preparednessfor catastrophic terrorism. Australian Strategic Policy Institute2007;(4):1—18.
3. Bradt D, Abraham K, Franks R. A strategic plan for disastermedicine in Australia. Emergency Medicine 2003;15:271—82.
4. Schriver J, Talmadge R, Chuong R, Hedges J. Emergency nurs-ing: historical, current and future roles. Journal or EmergencyNursing 2003;29:431—9.
5. Reilly M, Markenson D. Education and training of hospital work-ers: who are essential personnel during a disaster? Prehospitaland Disaster Medicine 2009;24(3):239—45.
6. Considine J, Mitchell B. Chemical, biological and radiological(CBR) incidents: preparedness and perceptions of emergencynurses in disasters. The Journal of Disaster Studies, Policy andManagement 2009:482—97.
93
7. Veneema T. Expanding educational opportunities in disasterresponse and emergency preparedness for nurses. Nursing Edu-cation Perspectives 2006;27(2):93—9.
8. Langan JC, James DC. Preparing nurses for disaster manage-ment. USA: Pearson/Prentice Hall; 2005. p. 3.
9. World Association for Disaster and Emergency Medicine(WADEM). Health disaster management: guidelines for eval-uation and research in the Utstein style. In: Sundnes KO,Birnbaum ML, editors. Chapter 1: Introduction, prehospitaland disaster medicine, vol. 17 (Suppl. 3). 2003. p. 17.
10. Emergency Management Australia (EMA). Australian emer-gency management terms thesaurus; 2009. http://library.ema.gov.au/emathesaurus/tr idx68.htm [accessed 26.08.10].
11. French E, Sole ML, Fowler Byers J. A comparison ofnurses’ needs/concerns and hospital disaster plans follow-ing Florida’s Hurricane Floyd. Journal of Emergency Nursing2002;28:111—7.
12. Behney A, Breit M, Phillips C. Pediatric mass casualty: are youready? Journal of Emergency Nursing 2006;32(3):241—5.
13. Farquharson C, Baguley K. Responding to the Severe AcuteRespiratory Syndrome (SARS) outbreak: lessons learned in aToronto emergency department. Journal of Emergency Nursing2003;29(3):222—8.
14. Taylor RM, O’Connor B, St Leone M, Stoner Halpern J. Thevoice of experience: Australian nurses caring for victims of BaliBombing disaster. Management and Response 2003;1(1):2—7.
15. Riba S, Reches S. When terror is routine: how Israeli nurses copewith multi-casualty terror. Online Journal Issues in Nursing2002;7(3):6. http://www.nursingworld.org/ MainMenuCate-gories/ANAMarketplace/ANAPeriodicals/OJIN/TableofContentsVolume72002/No3Sept2002/IsraeliNursesandTerror.aspx[accessed 26.08.10].
16. Amundson S, Burkle A. Golden minutes: the Oklahoma bomb-ing — two ED nurses stories. Journal of Emergency Nursing1995;21:401—7.
17. Australian Institute of Health and Welfare(AIHW) Nursing and Midwifery Labor Force; 2007.http://www.aihw.gov.au/mediacentre/2009/mr20091016.cfmaccessed on 16/10/2009 [accessed 16.01.10].
18. Nursing and Midwifery SA. Career structure implementation;2010. http://www.nursingsa.com/prof career.php [accessed24.08.10].
19. Alexander D. Misconceptions as a barrier to teaching about dis-asters. Prehospital and Disaster Medicine 2007;22(2):95—103.
20. Duong KS. Disaster education and training of emergency nursesin South Australia. Australasian Emergency Nursing Journal2009;12:86—92.
21. Emergency Management Australia (EMA). EMA disastersdatabase. http://www.ema.gov.au/ema/emaDisasters.nsf[accessed 15.02.10].
22. Arbon P, Bobrowski C, Zeitz K, Hooper C, Williams J, ThitchenerJ. Australian nurses volunteering for the Sumatra—Andamanearthquake and tsunami of 2004: a review of experienceand analysis of data collected by the tsunami volunteerhotline. Australasian Emergency Nursing Journal 2006;9:171—8.
23. Burstein JL. The myths of disaster education. Annals of Emer-gency Medicine 2006;47(1):50—2.
24. Emergo Train System (ETS). http://www.emergotrain.com/Home/tabid/36/Default.aspx [accessed 13.02.10].
25. Caldicott D, Edwards N. Medical preparation for terror-ism in Australia — is luck running out for ‘‘The LuckyCountry’’? Prehospital and Disaster Medicine 2003;18(2):57—65.
26. Powers M. Evaluation of hospital-based disaster education.Journal of Emergency Nursing 2007;33:79—82.
27. Australian Council on Healthcare Standards (ACHS). Nationalreport on health services accreditation performance. ACHS

9
4NSW; 2007—2008. http://www.achs.org.au/NAR [accessed01.11.2010].
28. Suserud BO, Haljamae H. Acting at a disaster site: experiencesexpressed by Swedish nurses. Journal of Advanced Nursing1996;25:155—62.
29. O’Sullivan TL, Dow D, Turner M, Lemyre L, Corneil W,Krewski D, Phillips K, Amaratunga CA. Disaster and emergencymanagement: Canadian nurses’, perceptions of preparednesson hospital front lines. Prehospital and Disaster Medicine2008;23(3):s11—8.
30. Nasrabadi AN, Naji H, Mirzabeigi G, Dadbakhs M. Earthquakerelief: Iranian nurses’ responses in Bam 2003, and lessons.Learned International Nursing Review 2003;54:13—8.
31. Ammartyothin S, Ashkenasi I, Schwartz D, Leiba A, Nakash G,Pelts MA, Goldberg A, Bar-Dayan Y. Medical response of a physi-cian and two nurses to the mass-casualty event resulting in thePhi Phi Islands from the tsunami. Prehospital Disaster Medicine
2006;21(3):212—4.32. Mitani S, Kuboyama K, Shirakawa T. Nursing in sudden onsetdisasters: factors and information that affect participation.Prehospital Disaster Medicine 2003;18(4):359—66.
K.S. Hammad et al.
33. James D, Duarte V. Disaster preparedness of Colorado nurses.Clinical Simulation in Nursing Education 2006;2:e59—64.
34. Lau PF, Lau CC. A disaster drill in Hong Kong. Accident andEmergency Nursing 1996;5:34—8.
35. Nursing Emergency Preparedness Education Coalition (NEPEC).Educational competencies for registered nurses respond-ing to mass casualties incidents; 2003, July. http://www.nursing.vanderbilt.edu/incmce/competencies.html [accessed14.02.10].
36. Gebbie K, Qureshi K. Emergency and disaster preparedness:core competencies for nurses: what every nurse should but maynot know. American Journal of Nursing 2002;102(1):46—51.
37. International Council of Nurses (ICN). Disaster nursingcompetencies; 2009. http://www.icn.ch/publications/free-publications/free-publications.html [accessed 26.08.10].
38. Australian Nursing and Midwifery council (ANMC). The respon-sibilities of nurses and midwives in the event of a declared
national emergency. http://www.anmc.org.au/userfiles/file/guidelines and position statements/The %20Responsibili-ties%20of%20Nurses%20and%20Midwives%20in%20the%20Evenet%20of%20a%20Declared%20National.pdf [accessed 23.06.10].