Elements of renal injury in patients with varicose ulcer. Preliminary study
62
ROMANIAN JOURNAL OF INTERNAL MEDICINE Volume 49 No. 3, 2011 CONTENTS REVIEWS GH. GLUHOVSCHI, CRISTINA GLUHOVSCHI, A. VLAD, R. TIMAR, F. BOB, SILVIA VELCIOV, GH. BOZDOG, LIGIA PETRICA, Diabetic nephropathy and multiorgan protection. Part I...................................................................... 163 ORIGINAL ARTICLES C. MORNOŞ, L. PETRESCU, D. COZMA, S. PESCARIU, ANIKO MORNOŞ, ADINA IONAC, The influence of left bundle branch-block and cardiac dyssynchrony on 2D-strain parameters in patients with heart failure complicating ischemic cardiomyopathy .................................................................................................................................................. 179 C. TOMULEASA, S. ŞUŞMAN, OLGA SORIŢÃU, OFELIA MOŞTEANU, TEODORA POP, B. PETRUSHEV, G. KACSÓ, R. BUIGÃ, M. TANŢĂU, A. IRIMIE, Stem-like cells in colorectal oncology................................................................. 189 VIOLETA ŞAPIRA, INIMIOARA MIHAELA COJOCARU, GABRIELA SOCOLIUC, GABRIELA LILIOS, M. GRIGORIAN, ELVIRA CRAIU, M. COJOCARU, Glutathione reductase levels in patients with unstable angina ................................. 197 SILVIA VELCIOV, GH. GLUHOVSCHI, V. FEIER, VIRGINIA TRANDAFIRESCU, LIGIA PETRICA, CRISTINA GLUHOVSCHI, F. BOB, GH. BOZDOG, FLORICA GADALEAN, CARMEN FLORESCU, MARIA BOBU, ANDREEA CHILIBAN, Elements of renal injury in patients with varicose ulcer. Preliminary study ............................. 202 ALEXANDRINA LIZICA DUMITRESCU, CARMEN TOMA, VIORICA LASCU, Investigating the use of specific cognitive emotion regulation strategies in response to the experience of gingival bleeding ............................................. 207 CASE REPORTS INIMIOARA MIHAELA COJOCARU, GABRIELA SOCOLIUC, VIOLETA ŞAPIRA, ALEXANDRA BASTIAN, MARILENA ALEXIANU, M. MOLDOVAN, Dermatomyositis and polyradiculoneuritis, a rare association ................ 217 ROM. J. INTERN. MED., 2011, 49, 3, 161–222
-
Upload
independent -
Category
Documents
-
view
1 -
download
0
Transcript of Elements of renal injury in patients with varicose ulcer. Preliminary study

ROMANIAN JOURNAL
OF
INTERNAL MEDICINE
Volume 49 No. 3, 2011
CONTENTS
REVIEWS
GH. GLUHOVSCHI, CRISTINA GLUHOVSCHI, A. VLAD, R. TIMAR, F. BOB, SILVIA VELCIOV, GH. BOZDOG,
LIGIA PETRICA, Diabetic nephropathy and multiorgan protection. Part I...................................................................... 163
ORIGINAL ARTICLES
C. MORNOŞ, L. PETRESCU, D. COZMA, S. PESCARIU, ANIKO MORNOŞ, ADINA IONAC, The influence of left
bundle branch-block and cardiac dyssynchrony on 2D-strain parameters in patients with heart failure complicating
ischemic cardiomyopathy.................................................................................................................................................. 179
C. TOMULEASA, S. ŞUŞMAN, OLGA SORIŢÃU, OFELIA MOŞTEANU, TEODORA POP, B. PETRUSHEV, G. KACSÓ,
R. BUIGÃ, M. TANŢĂU, A. IRIMIE, Stem-like cells in colorectal oncology................................................................. 189
VIOLETA ŞAPIRA, INIMIOARA MIHAELA COJOCARU, GABRIELA SOCOLIUC, GABRIELA LILIOS, M. GRIGORIAN,
ELVIRA CRAIU, M. COJOCARU, Glutathione reductase levels in patients with unstable angina................................. 197
SILVIA VELCIOV, GH. GLUHOVSCHI, V. FEIER, VIRGINIA TRANDAFIRESCU, LIGIA PETRICA, CRISTINA
GLUHOVSCHI, F. BOB, GH. BOZDOG, FLORICA GADALEAN, CARMEN FLORESCU, MARIA BOBU,
ANDREEA CHILIBAN, Elements of renal injury in patients with varicose ulcer. Preliminary study ............................. 202
ALEXANDRINA LIZICA DUMITRESCU, CARMEN TOMA, VIORICA LASCU, Investigating the use of specific
cognitive emotion regulation strategies in response to the experience of gingival bleeding ............................................. 207
CASE REPORTS
INIMIOARA MIHAELA COJOCARU, GABRIELA SOCOLIUC, VIOLETA ŞAPIRA, ALEXANDRA BASTIAN,
MARILENA ALEXIANU, M. MOLDOVAN, Dermatomyositis and polyradiculoneuritis, a rare association................ 217
ROM. J. INTERN. MED., 2011, 49, 3, 161–222


REVIEWS
Diabetic Nephropathy and Multiorgan Protection. Part I
GH. GLUHOVSCHI1, CRISTINA GLUHOVSCHI1, A.VLAD2, R. TIMAR2, F. BOB1, SILVIA VELCIOV1, GH. BOZDOG1, LIGIA PETRICA1
1Clinic of Nephrology, 2Diabetes Clinic Emergency Hospital, Timişoara, Romania
Diabetic nephropathy, one of the most important complications of diabetes mellitus, requires during its evolution protective measures defined as renoprotective. Since the complications of diabetes mellitus are not limited to diabetic nephropathy and as this is frequently associated with heart complications that require protective measures defined as cardioprotective, neurologic measures that require neuroprotection of the retina, of the large vessels etc., much more complex protective measures are necessary.
The metabolic complications that are usually at the basis of the other complications at the level of the cell also impose measures of protection.
Such an approach can have important practical consequences. It is a well-known fact that most patients with chronic kidney disease – CKD – do not reach final stages as in the meantime they decease because of cardiovascular diseases.
Consequently, cardioprotective measures have to be associated with renoprotective ones, as well as protective measures that address other organs, in close connection with protective measures at metabolic level.
The protective measures must also address to microcirculation, diabetic nephropathy being a disease that primarily affects microcirculation. Diabetes mellitus also frequently affects the large vessels, the circulatory system being usually affected in its complexity.
The paper represents a synthesis of multiorganprotective measures in diabetic nephropathy, in diabetes mellitus, respectively, the concept of multiorgan protection finding in this disease an ideal domain of expression.
The first part gives the main multiorgan measures: monitoring of blood pressure and, mainly, protection by means of the renine aldosterone (RAAS) system, multiorgan by intensive monitoring of glycaemia and by treatment of proteinuria.
The second part presents the other protective measures used in diabetic nephropathy.
Key words: diabetic nephropathy, renine aldosterone system.
CHRONIC KIDNEY DISEASE IN DIABETES MELLITUS
(DIABETIC NEPHROPATHY) AND MULTIORGAN PROTECTION
Multiorgan protection represents a complex system of protective measures addressed to the organism as a whole and comprises reno-, cardio-, and neuroprotective measures, as well as protective measures concerning other organs. These are addressed to the organism at cellular and biochemical level too (Gluhovschi et al.) [1].
The kidney benefits from protective measures defined as renoprotective measures. Chronic kidney disease (CKD) is not limited to the kidney, but it also associates cardiovascular and cerebral invol-vement. It is well known, however, that the vast majority of the patients with CKD do not reach stage 5 CKD where they might benefit from renal
replacement therapies. These patients die frequently in stages 3-4 CKD through cardiovascular disease. Also, cardiovascular diseases play an important role in the course of CKD.
Cerebrovascular accidents like stroke are observed frequently. Therefore, the renoprotective measures are associated to cardio- and neuro-protective measures.
Inflammatory processes are strongly related to oxidative stress within the frames of CKD. Multiple metabolic processes which occur in CKD are reflected upon the functions of the organism at cellular and biochemical level and thus require adequate protective measures.
The organism possesses a well-developed circulatory system within the brain, the heart, the kidney and other organs, which realises an integrated unit.
ROM. J. INTERN. MED., 2011, 49, 3, 163–177

Gh. Gluhovschi et al. 2
164
Thus, the vascular system risk factors involve its structural components, mainly the endothelium in various organs, especially those with rich vascularization, such as the brain, the heart, and the kidney. One example would be hypertension, in the frames of which target-organ involvement focuses prominently. The lipid metabolism disorders produce lesions in the vessels of these organs, which benefit from a rich circulation governed by an increased perfusion pressure. Therefore, the protective measures have in view not only the vascular system of a single organ, but of all organs with a rich vascular bed. This is the case with the brain, the heart and the kidney which benefit from organ-protective measures such as reno-, cardio-, and neuroprotective measures linked into the concept of multiorgan protection [1].
Moreover, the metabolic disorders in the course of diabetes mellitus (DM) have direct con-sequences on vessels and at the level of various organs.
DM, due to the abnormalities of the carbo-hydrate metabolism, as well as other disorders, such as those of the lipid metabolism, inflame-matory mechanisms, oxidative stress, etc., causes important modifications in the structure and function of organs and tissues. These multiple mechanisms involve the vascular system at the level of the large sized vessels, as well as at the level of micro-circulation. The main lesion in the latter territory involves especially the endothelium.
Other vascular risk factors, such as haemo-dynamic mechanisms, aggravate the lesions in the vascular system.
The carbohydrate metabolism disorders exert a direct consequence at cellular level, which influences the functionality of the organism as a whole. One example would be the action of glucose upon proteins, followed by an important process of protein glycosylation. Haemoglobin glycosylation is a parameter used in the monitoring of the therapy in the course of DM. Excessive glycosylation may represent a stimulating factor for fibrosis. The association of vascular involvement in DM with its deriving metabolic abnormalities at the tissue level contributes to very complex lesions in various organs.
The kidney represents an organ with a very rich vascularization displaying the ability to draw 20% of the cardiac output. DM involves mainly the
microcirculation in the kidney, but also occasionally it may affect large-sized arteries, through a process of atherosclerosis. Concomitantly, renal structures are affected at the cellular level, namely the mesangium. Consequently, lesions of glomerular sclerosis may occur, mainly of diabetic glomerulo-sclerosis, which lead to renal failure and the requirement of renal replacement therapies.
Renal involvement in the course of DM implies the development of chronic kidney disease (CKD) which is defined as diabetic nephropathy (DN). Thus, renoprotective measures become man-datory in order to impede the occurrence of this complication, as well as its evolution.
Due to the fact that DN is associated with other vascular complications within the heart, the brain, retina and the periphery arteries, cardio- and neuroprotective measures are also required. These measures are paralleled by protective measures at cellular and metabolic level.
DN is one of the most severe complications of DM. It is assumed that nearly one third of patients with DM develop nephropathy and DN remains the most common cause of end-stage renal disease (ESRD). Lifetime risk for developing DN with progression to ESRD is roughly equivalent in type 1 and type 2 DM [2]. The necessity for protective measures at cellular and molecular level resides within the fact that hyperglycaemia activates various inflammatory pathways, both directly and via gene transcription. These processes induce oxidative stress, reactive oxygen species, fibrotic factors (such as TGF beta), activation of renin angiotensin system, and advanced glycation end-products, thus leading collectively to podocyte injury, malfunction, apoptosis, and protein deposition in the extracellular matrix of the nephron, with subsequent albumin loss [3].
Also, elevated hyperglycaemia may induce epigenetic complications, as well. In addition, other clinical factors include genetic predisposition, obesity, blood pressure, high lipids and smoking, which add to the role of progression in DN [3].
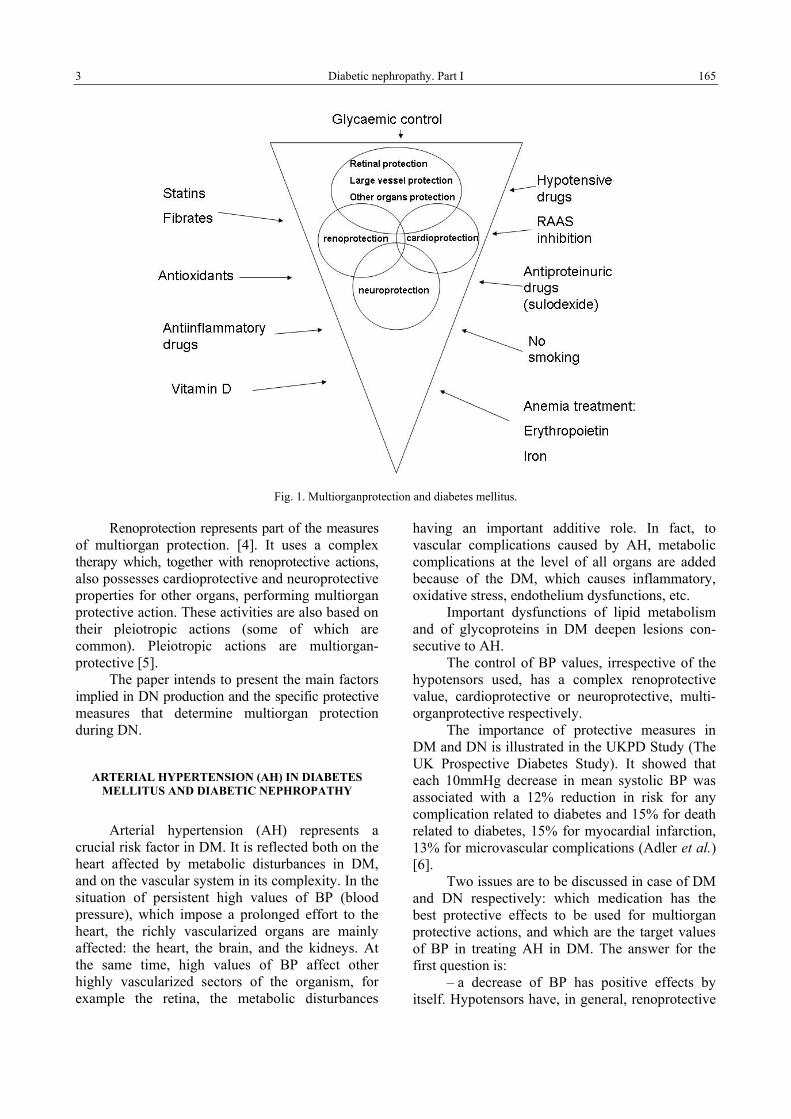
In the course of diabetic CKD complex organ-protective measures are required, such as reno-, cardio-, and neuroprotective measures, to which cellular and molecular protective measures should be added. All these configure the concept of multiorgan protection, DN being a condition which might benefit from these complex measures (Fig. 1).
3 Diabetic nephropathy. Part I
165
Fig. 1. Multiorganprotection and diabetes mellitus.
Renoprotection represents part of the measures of multiorgan protection. [4]. It uses a complex therapy which, together with renoprotective actions, also possesses cardioprotective and neuroprotective properties for other organs, performing multiorgan protective action. These activities are also based on their pleiotropic actions (some of which are common). Pleiotropic actions are multiorgan-protective [5].
The paper intends to present the main factors implied in DN production and the specific protective measures that determine multiorgan protection during DN.
ARTERIAL HYPERTENSION (AH) IN DIABETES MELLITUS AND DIABETIC NEPHROPATHY
Arterial hypertension (AH) represents a crucial risk factor in DM. It is reflected both on the heart affected by metabolic disturbances in DM, and on the vascular system in its complexity. In the situation of persistent high values of BP (blood pressure), which impose a prolonged effort to the heart, the richly vascularized organs are mainly affected: the heart, the brain, and the kidneys. At the same time, high values of BP affect other highly vascularized sectors of the organism, for example the retina, the metabolic disturbances
having an important additive role. In fact, to vascular complications caused by AH, metabolic complications at the level of all organs are added because of the DM, which causes inflammatory, oxidative stress, endothelium dysfunctions, etc.
Important dysfunctions of lipid metabolism and of glycoproteins in DM deepen lesions con-secutive to AH.
The control of BP values, irrespective of the hypotensors used, has a complex renoprotective value, cardioprotective or neuroprotective, multi-organprotective respectively.
The importance of protective measures in DM and DN is illustrated in the UKPD Study (The UK Prospective Diabetes Study). It showed that each 10mmHg decrease in mean systolic BP was associated with a 12% reduction in risk for any complication related to diabetes and 15% for death related to diabetes, 15% for myocardial infarction, 13% for microvascular complications (Adler et al.) [6].
Two issues are to be discussed in case of DM and DN respectively: which medication has the best protective effects to be used for multiorgan protective actions, and which are the target values of BP in treating AH in DM. The answer for the first question is:
– a decrease of BP has positive effects by itself. Hypotensors have, in general, renoprotective

Gh. Gluhovschi et al. 4
166
and multiorgan protective actions by decreasing BP. They differ as far as their protective action is concerned because of the complexity of their actions (for example, the antiproteinuric effect), mainly pleiotropic actions. The most complex action is that of the inhibitors of the renin-angio-tensin-aldosteron system (RAAS), these being considered at present as first line medication in treating AH in DM. Sometimes, the use of several hypotensors is necessary for controlling BP. In these cases, one associates RAAS inhibitors with other drugs with complementary effects, especially pleiotropic ones, of these hypotensors, and secondary effects of these associations are taken into consideration.
The answer to the second question is still in discussion. DN is frequently associated with AH. Having in view their severity and complications, in DM a dominant idea is the fact that its control must bring about lower values of BP, that is the concept of “lower is better”. At present this concept is being reconsidered. The JNC recommendations are similar to the guidelines from American Diabetes Association (ADA), which has also recommended that BP in diabetes be controlled to levels of 130/80 mmHg or lower (although the available data are somehow inconsistent to justify lower target level than 130/80 mmHg). Rigorous control of BP is very important for reducing the progress-sion of DN to ESRD. If proteinuria exceeds 1g/24h and serum creatinine has increased levels, BP levels should reach 125/75 mmHg. These recom-mendations, however, each support evidence from randomized clinical trials.The target BP levels of 130/80mmHg in type 2 DM should be recon-sidered.Thus, three new studies support a level of 110 mmHg for systolic BP.
The main study, ACCORD BP trial, under-lines that intensive, antihypertensive therapy did not significantly reduce primary cardiovascular outcome and the rate of death from any cause [7].
The ACCORD Study group reveals that targeting a systolic BP of less than 120 mmHg as compared with less than 140 mmHg did not reduce the incidence of cardiovascular events in patients with type 2 DM. The benefit was only on stroke reduction.
Systolic BP target below 120 mmHg in patients with type 2 DM is not justified by evidence.
The concept that in hypertension “the lower the better” is under consideration by the INVEST (International Verapamil Trandolapril Study).[8]
and ONTARGET (Ramipril Global Endpoint Trial) studies [9].Other authors maintain these observations:
don’t change the BP limits in diabetes [10].
Outgoing studies, as well as future studies, will decide the utility of changes in the present approach of BP therapy.
Currently, it is considered that ACEIs or ARBs are now standard therapy in patients with DN.
DN is frequently associated with AH. The latter may aggravate the evolution of the disease and contributes to the recurrence of major com-plications, such as cardiac, cerebral and retinal complications, etc. BP control exerts not only reno-protection, but also cardio- and neuroprotection, within multiorgan protection, respectively.
At present a goal systolic blood pressure < 130 mmHg is considered appropriate for most patients with diabetes, which should be treated to diastolic blood pressure < 80 mmHg.
INHIBITORS OF THE RENIN ANGIOTENSIN SYSTEM
ACE-I and ARB
RAAS is involved in regulating BP via both systemic action and renal-level action, by self-regulation of circulation at this level, respectively. There exists also a local renin-angiotensin system, whose role in regulating BP has not been clearly defined yet.
DN is accompanied by high values of BP that can have unfavourable effects at renal, cerebral and cardiovascular circulatory level, as well as at the level of other vascular sectors. Controlling BP will have at this level nephroprotective, cardioprotective and neuroprotective effects, respectively multiorgan protective effects.
The control of BP ensures these effects. Some of the hypotensor drugs have complex protective effects that go beyond the protective background achieved by diminishing BP. Among these are the inhibitors of the RAAS. Some of these inhibitors are the ACE-Is and the ARBs. Lately, one has introduced renin inhibitors in the treatment of AH.
The renin-angiotensin system inhibitors are hypotensors used with predilection in the treatment of DN. ACE-I and BRA, beside hypotensor effects, have also beneficial effects on proteinuria.
Since DN associated HTA with proteinuria, the use of these preparations is recommended both in monotherapy and in association.
The pleiotropic effects of the inhibitors of the RAAS increase responsiveness to insulin and complete both the hypotensor action and the antiproteinuric action. At the same time, these

5 Diabetic nephropathy. Part I
167
pleiotropic actions complete organ protective actions, that is renoprotective, cardioprotective and neuro-protective actions.
For hypotensor antiproteinuric and pleiotropic effects, the inhibitors of the renin-angiotensin system are considered first line drugs in the treatment of DN.
The main renoprotective effect is due to the control of BP.
The objective is reaching values of 130/ 80mmHg.
Renoprotective action
The renoprotective effect reflected in the slowing down of the progression of DN is more evident in patients with a lower value of BP, between 110–119 mmHg, and the urinary excretion higher than 1g/day.
However, a systolic BP under 110 mmHg may be associated with a higher risk for kidney disease progression.
The renin system inhibitors are mainly recom-mended for patients with DM and proteinuria.
Their use is also recommended for normo-tensive patients with DM and without proteinuria. Lisinopril shows a decline in renal function in normotensive diabetic patients with micro or normo-albuminuria (Chaturverdi and EUCLID group) [11].
Secondary effects are minimal. We should mention that these medicines do not interfere with the metabolism of lipids.
Some authors recommend using inhibitors of the renin system for patients with diabetic nephropathy without AH. In normotensive patients with type 1 DM with microalbuminuria, micro-albuminuria diminishes. It was noticed that Captopril reduces the risk of nephropathy in type 1 patients with microalbuminuria, a fact demonstrated by the Microalbuminuria Captopril Study Group [12].
The use of ACE-I is recommended in patients with type 1 DM and microalbuminuria, even if they are normotensive [13].
In patients with type 2 DM the evidence for ACE use in normotensive patients with micro-albuminuria is not as conclusive at this point, but it is accumulating (Ravid et al.) [13]. They are attributed a role in reducing the incidence of new onset type 2 DM.
ACE-I and ARB have a renoprotective effect on the development of progressive diabetic nephro-pathy due to type 1 and type 2 diabetes. The protective effect regards the progression of micro-albuminuria and macroalbuminuria.
The CALM study showed that the decrease of BP in patients with type 2 DM is smaller with individual administration than with their association.
The ONTARGET study does not recommend associated treatment with ACE-I and ARB.
Their secondary effects impose precaution in their use: hyperkalemia, an increase of azotate retention to creatinine values higher than 6 mg%.
In case BP cannot be controlled with ACE-I and ARB, association with other hypotensors is recommended.
The most often recommended association is ACE-I or ARB with a long-acting dihydropiridine preparation (the ACCOMPLISH study)[14]. One can also recommend an association with carvedilol (the GEMINI study) [15].
They are associated with diuretic preparations in cases of kidney damage with cardiac decompen-sation. Association with a loop diuretic (furosemide) is preferable. Chlortalidone indicated by the ALLHAT study has not entered current practice. Other preparations that can be used for association are beta-blockers, for example metoprolol.
There are also studies regarding the association of the ACE-I with the calcium channel blockers (enalopril and nisoldipine in the ABCD trial).[16].
Cardioprotective action
ACE-I have cardioprotective effects highlighted both in type 1 and in type 2 DM patients.
In patients with DN and type 1 DM this effect was found by the Collaborative Study referring to Captopril.
The ABCD study, performed on patients with type 1 DM, has highlighted cardioprotective effects (decrease in left ventricular mass and fatal or non-fatal acute myocardial infarction) of enalapril, more favourable as compared to those produced by nisol-dipine. The HOPE Study (Heart Outcomes Prevention Evaluation study) demonstrated that ramipril produces significant lowering of mortality due to cardiovascular disease and reduction in total mortality in patients with type 2 DM [17].
The renoprotective effects of ARBs have been analyzed in several studies: The RENAAL study did not find statistically significant effects on fatal cardiovascular events as far as Losartan was concerned, as compared to placebo [18]. Nor have Berl and collaborators found cardioprotective effects in type 2 DM and overt nephropathy patients treated with Irbesartan, as compared to those treated with amlodipine or placebo, in addition to conventional therapy (IDNT trial) [19].
Gh. Gluhovschi et al. 6
168
It is considered that ARBs are renoprotective (but not cardioprotective in patients with type 2 DM and overt nephropathy or microalbuminuria)..
However, telmisartan has cardioprotective effects. It protects myocardium from ischemic reperfusion injury in diabetic rats partly because of the activation of PPAR-gamma. ONTARGET study remarks that telmisartan was equivalent to ramipril in patients with vascular disease or high risk of diabetes (ONTARGET investigators). Telmisartan is the only ARB that has been shown to reduce cardiovascular risk in at-risk cardiovascular patients.
No cardiovascular or renal benefits from dual therapy over monotherapy in high vascular risk patients with low glomerular filtration rate or albuminuria was found (A post hoc analysis result from the ONTARGET and TRANSCEND studies).
Analysis of eighty-five trials (MEDLINE, EMBASE and Renal Health Library-21708 patients), performed by Maione, has shown that their effects on mortality and fatal cardiovascular disease are uncertain [20].
Maione appreciates that there is lack of evidence in support of using the combination. But this association has antiproteinuric effects and its combination in people with albuminuria and cardiovascular risk factors is warranted [20].
Neuroprotection
The main lesion of the nervous system in DM is the stroke. RAAS inhibitors act both on systemic circulation and on cerebral circulation. Brain is regulated independently of peripheral RAAS.
The RAAS antagonists have neuroprotective action by means of controlling BP and by their pleiotropic effects.
ACE-I and ARBs may delay the development of atherosclerosis and increase plaque stability.
Experimental studies have shown that tel-misartan prevents ischemic brain damage with PPAR- gamma activation in diabetic mice. Beneficial effects on stroke are partly due to activation of PPAR –gamma, as well as AT1 receptor blockade.
The neuroprotective effects have mainly been highlighted by the studies HOPE (in type 2DM, under treatment with ramipril), ONTARGET (ramipril, telmisartan and combinations of the two). Other trials have also shown neuroprotective effects of inhibitors: the UKPDS trial (captopril or atenolol), the ADVANCE trial (perindopril-indapamid), the ABCD trial (enalapril or nisoldipine).
ARBs, alone or combined with ACE-I, are slightly more effective than treatment based on ACE-I alone.
The use of ACE-I before stroke provides vasoprotective effects resulting in less severe strokes.
Renoprotective effect of ACE-I as compared to ARB
DETAIL STUDY has shown that telmisartan is comparable to enalapril in reducing the decline in glomerular filtration rate and providing reno-protection in patients with type 2 DM and nephropathy.
Dual therapy RAAS- inhibitors
Combined therapy with lisinopril and can-desartan has higher effects on lowering BP in type 2 DM than monotherapy. Similar results are reported about associating valsartan and aliskiren/ captopril.
Antiproteinuric effects in DM are also reported as far as protein excretion of combined ACE-I/ARB is concerned; it lowers proteinuria more than monotherapy with one of these medicines does (The CALM Study).
Associations of aliskiren and losartan have similar effects. They lower proteinuria, the hypo-tensor effect being less important (The AVOID trial).
At present, associations of ACE-ARB are not recommendable in practice. The association of protective effects with Aliskiren has not yet been established, it is still being studied.
Renoprotective effects regarding progression to ESRD are under study. VALID and VA NEPHRON trials are still under study too.
No renoprotective effects are reported in non-proteinuric patients.
The ONTARGET Study found that in most patients without significant proteinuria, having increased cardiovascular events risk, nephroangio-sclerosis and ischemic renal disease, the association does not improve renal and cardiovascular outcomes, and it is associated with increased risk of adverse effects.
The ONTARGET Study has shown that there is no additional advantage (but there is some harm coming from the combination of telmisartan and ramipril used in full doses for this population, as compared with ramipril alone.
It is considered however that patients with refractory hypertension, particularly if coexisting with proteinuria, could benefit from combining ACEi and ARB with good monitoring..
Direct renin inhibitor- Aliskiren
Treatment with inhibitors of the RAAS (ACE-Is and ARBs) is associated with incomplete

7 Diabetic nephropathy. Part I
169
inhibition of the system, a fact which may be responsible for residual organ damage. Moreover, this phenomenon produces an increase of plasma renin activity, which is also observed after diuretics use.
Administered as monotherapy or associated to ARBs, aliskiren reduces the above mentioned effects. Thus, it displays renal and cardioprotective effects, both in animals and in humans.
The AVOID study evaluated the renoprotective effects of the association of aliskiren with losartan in the control of hypertension in patients with DM and DN. It has been concluded that aliskiren may have renoprotective effects that are independent of BP control.
Aliskiren attenuates high-glucose induced extracellular matrix synthesis and prevents apoptosis in cultured mouse podocytes.
Also, aliskiren reduces albuminuria and oxidative stress, and elevates GFR in Japanese patients with advanced DN.
Renoprotective properties leading to a reduction of proteinuria and to a delay of renal failure progression were observed in patients with diabetic and non-diabetic nephropathy. Aliskiren may offer the additional opportunity to inhibit progression of atherosclerosis at tissue level.
Currently, the outgoing study ALTITUDE (Aliskiren Trial in type 2 DM using Cardio-Renal Endpoints) is assessing renal and cardiovascular morbidity, and will further define whether aliskiren provides additional benefits beyond RAAS inhibition and lowering of BP in DM.
Aldosterone antagonists
Aldosterone antagonists represent, together with ACE-I, ARB and renin inhibitors, a category of RAAS inhibitors.
Their use in the treatment of DM or DN, respectively, is reflected in the treatment of AH and especially of proteinuria. Through this, aldo-sterone antagonists have renoprotective effects. Spironolactone and an aldosterone receptor antagonist, eplerenone, are used.
Aldosterone antagonists are usually used associated with other hypotensors, including other RAS inhibitors. One must consider controlling potassium level as an association of aldosterone antagonists with other inhibitors of RAAS increases the risk of hyperkalemia. Beside hypotensive and diuretic effects of aldosterone antagonists, one must pay attention to other effects classified as pleiotropic, as well.
Analysing a group of patients with DN treated with lisinopril, losartan or spironolactone,
Mehdi et al. have found similar degrees of lowering BP in all groups.
They noticed the greatest antiproteinuric effect with spironolactone, as compared to placebo.
Addition of spironolactone to an ACE-I or Ang II blocker is associated with a marked additive effect of aldosterone antagonist. This is present when they are associated in dual or triple therapy. It is to be noted the aldosterone antagonists have cardioprotective effects that are associated to renoprotective effects.
Association of RAAS inhibitors with other hypotensors
In case BP cannot be controlled with ACE-I and ARB, association with other hypotensors is recommended.
The most often recommended association is ACE-I or ARB with long-acting dihydropiridine preparations (The ACCOMPLISH Study), enalapril and nisoldipine (the ABCD trial), benazapril and amlodipine (The SHIELD trial, delapril and mani-dipine (The MORE Trial),verapamil and trandalopril (The BENEDICT Trial), benazepril with either amlodipine or hydrochlorothiozide (The GUARD Study).
One can also recommend an association of ACE-I or ARB with carvedilol or metoprolol (The Gemeni Study), alpha blockers associated with ACE-I, cilazapril associated with doxazosin.
In practice, one frequently uses associations of tiazidic diuretics with SRAA blockers.
Losartan/hydrochlorothiazide was effectively and safely used with Japanese patients, currently not in BP goal with a regimen including ARBs or ACE-I.
Candesartan associated with hydrochloro-thiazide (MEDICA trial) and perindopril with indapamide (ADVANCE –trial).
Multiorgan protective action of associations of RAAS inhibitors with other hypotensors is in study.
Renoprotective, cardioprotective, neuroprotec-tive and other effects, multiorgan protective effects included, are also under study.
THE CONTROL OF GLYCAEMIA AND MULTIORGAN PROTECTION
Correct treatment of glycaemia, that is intensive glycaemic control, represents the corner-stone of DN therapy.
The control of glycaemia has an important multiorgan protective role. It has a renoprotective

Gh. Gluhovschi et al. 8
170
effect expressed either in reduced risks of developing a DN or in reduced risks of progression of an established DN to ESRD.
Hyperglycaemia represents the main element involved in DN. The other factors involved intervene in close relationship with it. Correct control of glycaemia decreases the risk of developing or worsening of an established DN.
The control of glycaemia also has important cardioprotective and neuroprotective effects, protecttive effects against developing diabetic retinopathy and protective effects on other organs. One of the important protective effects is at cellular and molecular level.
At present, intensive treatment in the control of glycaemia in patients with DM is being discussed.
The glycaemic control and type 1 DM Renoprotective effects
The control of glycaemia by intensive treatment and renoprotective effects in DN and type 1 DM has been assessed mainly in the DCCT and EDIC studies.
The prospective study Diabetes Control and Complications Trial (DCCT) assessed the favourable role of intensive therapy with insulin, as compared to conventional treatments. The study pointed out that the new onset microalbuminuria, as well as the new onset macroalbuminuria, were significantly reduced in patients with intensive therapy than in the control group [21]. This argues for a superior renoprotective effect of the control of hyper-glycaemia by means of intensive treatment.
The EDIC study (Epidemiology of Diabetes Interventions and Complications) continued the DCCT study. It pointed out that the new onset microalbuminuria, as well as the new onset macro-albuminuria, were more reduced in patients with intensive therapy than in patients with conventional therapy. This shows that the renoprotective effect over time is superior in the first group [22].
Regarding the progression of the disease from the intensive control group, a smaller number of established microalbuminuria patients, at the moment when the DCCT study started, progressed to macroalbuminuria.
In patients with macroalbuminuria, benefits of aggressive therapy were not present.
Cardioprotection
DCCT did not show a significant reduction in cardiovascular events with intensive control. EDIC trial showed a delayed benefit. After ten years, the
patients in the previous intensive group had significantly fewer cardiovascular events than those in the standard one.
Diabetic retinopathy The DCCT study pointed to a beneficial
effect of intensive therapy with insulin in patients with type 1 DM. The incidence of new retinopathy was 12% as compared to 54% in the control group. This therapy had a favourable effect on its pro-gression, as well.
In case of advanced retinopathy, the protective effect is minimal; in some cases this effect has not been seen at all.
Neuroprotection
The neuroprotective effect of the control of glycaemia was pointed out by the DCCT study. This demonstrated beneficial clinical effects both on nervous conduction and on the autonomous dysfunction.
Intensive therapy delays the onset and slows the progression of diabetic nephropathy.
The benefits of former intensive insulin treatment persisted for 13–14 years after DCCT close-out, fact that pleads for a durable effect of prior intensive treatment on neuropathy (Albers et al.) [23].
Type 2 DM Renoprotection
Intensive treatment has a renoprotective effect. This has been evaluated by several studies.
The UKPDS (United Kingdom Prospective Diabetes Study) highlighted a risk reduction in microvascular disease. UKPDS – post-trial study – has shown that this risk of microvascular disease persisted in intensively treated patients.
The Kumamoto Study highlighted a lower incidence of development or progression of nephro-pathy (Ohkubo et al.) [24]. Intensive glycaemic control can delay the onset and progression of diabetic microvascular complications in Japanese patients with type 2 DM.
ADVANCE trial demonstrated that intensive therapy led to lower the incidence of nephropathy.
Contrary to the above mentioned con-siderations, the VADT study did not show a reduction in the incidence of DN in intensively treated patients. Microvascular complications were minimally effected by intensive glucose control [25].
Glycaemic control also improves hyper-filtration.

9 Diabetic nephropathy. Part I
171
The renoprotective effect of glycaemic control in DN by pancreas or islet cell trans-plantation is highlighted by several studies. Islet cell transplantation is associated with less progress-sion of microvascular complications than intensive medical therapy (DN, retinopathy and neuropathy). Thus, the decline rate in glomerular filtration is slower after islet cell transplantation than after medical therapy. Fioretto et al. found reversal of diabetic nephropathy after pancreas transplantation [26].
Effects on the cardiovascular system
Studies on the effects of intensive glycaemic control on the cardiovascular system have not obtained uniform results. It is considered that whether intensive glucose lowering prevents macrovascular disease and major cardiovascular events remains unclear. The UKPDS post trial study assessed the results of a 10-year follow-up. It was found that tight control of a younger newly diagnosed patient with type 2 DM may have cardiovascular benefits several years later. Primary analysis found a borderline statistically significant reduction between intensive and conventional treatment [27].
The ACCORD, ADVANCE and VADT trials have not demonstrated the existence of a sig-nificant reduction of cardiovascular events by intensive treatment of type 2 DM patients as compared to patients under conventional treatment.
In 2008, the intensive blood sugar lowering arm of ACCORD study was halted due to a higher number of total and cardiovascular deaths.
Pioglitazone has cardiovascular protective effects. This would not be due to better glycaemic control, but to its pleiotropic effects.
In order to analyse whether intensive treatment is beneficial, Ray et al. performed a meta-analysis of live prospective randomized controlled trials of 33,040 participants. They found that intensive therapy compared with standard glycaemic control significantly reduced coronary events without an increased risk of death [28].
Neuroprotection
Meta–analyses of studies evaluating the effect of intensive glucose control on major adverse cardiovascular events in patients with type 2 DM from 1990 to 2009 highlighted that intensive glycaemic control did not affect mortality or non-fatal stroke.
The Kumamoto study highlighted the fact that patients with intensive therapy manifested
significant improvement in the median nerve con-duction velocity. Glycaemic correction after islet cell transplantation associated with intensive medical therapy has shown a non-significant trend for improved nerve conduction velocity.
Diabetic retinopathy
The Kumamoto study highlighted a lower incidence of development of progression of retino-pathy in patients with glycaemic control by inten-sive therapy [24].
Islet transplantation produces a slower progress-sion of retinopathy as compared to intensive medical therapy.
The VADT study found no significant dif-ferences in retinopathy, major nephropathy or neuropathy between patients with intensive glycaemic control and with conventional therapy (Duckworth et al.). The ADVANCE study also found no significant effect on retinopathy.
Analysing microvascular benefits of intensive therapy, Ismail-Beigi et al. consider that these should be weighed against the increase in total and cardiovascular disease mortality, increased weight gain and high risk for severe hypoglycaemia.
Herati considers that maintenance of normal blood glucose remains the cornerstone of treatment of DM and DN.
The multiorgan protective effects of the control of glycaemia are related to:
– A1c levels in patients. The objective considered is obtaining values of A1c lower than or equal to 7.0%
– a sustained period of glycaemic control for a lengthy period of time
– the effect of strict control of glycaemia is reflected in other risk factors as well: obesity, hypertriglyceridaemia, AH.
One should mention that the effect of con-trolling glycaemia can continue after its cessation, a fact that was highlighted by the DCCT trial. It is described as “metabolic memory”.
Control of glycaemia with thiazolidindiones and their multiorgan protective effect
Thiazolidindiones (TZ) act as PPAR agonists (rosiglitazone and pioglitazone) or they are double agonists, alpha and gamma (example, aglitazar). The PPAR receptors are spread at the level of several organs, which could explain their complex action.
TZ act in controlling glycaemia by increasing insulin sensitivity and by preserving beta cell

Gh. Gluhovschi et al. 10
172
function, insulin secretion respectively. They are used as monotherapy or are associated with met-formin, sulphonylurea, or insulin, obtaining thus a more efficient control of glycaemia.
The renoprotective effects have been high-lighted in experimental studies in humans too.
Pre-treatment with rosiglitazone attenuates cisplatin induced renal damage in mice. Rosigli-tazone has a favourable effect on human proximal tube epithelial cells in culture medium.
Pioglitazone ameliorates renal injury through anti inflammatory mechanisms in type 2 diabetic rats.
In humans, activation of the PPAR gamma by TZ is generally considered beneficial for amelio-ration of diabetic complications in type 2 DM and may be effective in delaying and even preventing CKD in patients with type 2 diabetes.
Petrica et al. found that rosiglitazone had nephroprotective effects in normo-albuminuric patients with type 2 DM (Petrica et al.) [29].
Rosiglitazone and pioglitazone reduce urinary albumin excretion in type 2 diabetic patients.
Pioglitazone has been attributed cardio-protective effects.
Experimentally, pioglitazone attenuates left ventricular hypertrophy and fibrosis in rats with salt-sensitive hypertension. The studies of Yasuda et al. pointed out that in rabbits, pioglitazone reduces myocardial infarction size.
One has found beneficial effects of piogli-tazone on the cardiovascular apparatus of humans. PERISCOPE randomized control trial pointed out that patients treated with pioglitazone had a significantly lower rate of progression of coronary atherosclerosis as compared with those treated with glimperide (Mazzone et al.) [30].
A meta-analysis of 19 trials made by Lincoff et al. has shown that pioglitazone is associated with a significantly lower risk of death, myocardial infarction or stroke in patients with type 2 DM. It was found out that the risk of heart failure is increased [31].
Rosiglitazone appears to have no cardio-protective effect; on the contrary, it is incriminated for producing noxious cardiovascular effects. A Meta-analysis of 42 trials appreciates that rosiglita-zone has increased risks of myocardial infarction (MI) and deaths caused by cardiovascular causes [32].
The risk for MI was noticed in patients with DM during the RECORD study [33].
PPAR gamma exerts its renoprotective action by lowering blood pressure. PRAR gamma activators
down regulate angiotensin II type 1 receptors in vascular smooth muscle cells.
However, the action of TZ on the heart has not yet been completely elucidated. Experimen-tally, it has been found that rosiglitazone has beneficial effects on the heart: rosiglitazone attenuates myocardial remodelling in spontaneously hyper-tensive rats. On the other hand, Saraogi et al. find that rosiglitazone and pioglitazone aggravate doxo-rubicin-induced cardiomyopathy in Wistar rats (Saraogi et al.) [34].
Neuroprotective effects
Experimental studies on rats demonstrated neuroprotective effects of rosiglitazone after traumatic brain injury. Favourable neuroprotective results are reported in rats after pioglitazone traumatic brain injury.
According to Friedrich, the effects of rosiglita-zone on cerebrovascular ischemic events suggest benefits, although far from being statistically significant. Pioglitazone reduces the composite of all cause mortality nonfatal myocardial infarction and stroke in patients with type 2 diabetes who have a high risk of macrovascular events. Rosiglita-zone had both renoprotective effects and neuro-protective effects in normo-albuminuric patients with type 2 DM (Petrica et al.) [35,37].
The multiorganprotective action of TZ is based on anti-apoptotic, anti-inflammatory and anti-oxidative effects.
Aleglitazar, a dual PPAR-alfa and PPAR gamma agonist, has potential simultaneous treatment of hyperglycaemia and dislipidaemia in patients with type 2 diabetes mellitus.
The associations metformin-pioglitazone and metformin-rosiglitazone proved safe and effective for patients with type 2 DM and metabolic syn-drome. The association metformin-pioglitazone brings about an additional lowering of plasma lipoproteins, which the rosiglitazone combination does not.
It was demonstrated that, in rats, the association between sirolimus and rosiglitazone has renoprotective effects in DN.
PROTEINURIA – MICROALBUMINURIA IN THE CONTEXT OF MULTIORGAN PROTECTION
Increased urinary protein excretion in DN is an early-set clinical-biologic manifestation of diabetic nephropathy and is manifested in microalbumi-nuria.
11 Diabetic nephropathy. Part I
173
DN passes through several stages: normo-albuminuria, microalbuminuria and macroalbumi-nuria.
Patients with DZ must undergo screening for an early finding of patients with ND, who will be subject to a therapy meant at preventing its evolution.
Several factors are implied in producing proteinuria, or microalbuminuria, respectively:
– Modification of glomerular capillary per-meability, microalbuminuria arising from increased passage of albumin through the glomerular fil-tration barrier.
– Podocytopathy [36] – Tubular lesions [37] – Increase in the number of large pores/
liming size selectivity. – Decrease staining for heparin sulphate, the
major component of the charge barrier. Microalbuminuria would reflect a systemic
endothelial and vascular disorder [36]. Numerous studies in different patient
populations have suggested that, in addition to renal disease, microalbuminuria is an important risk factor for cardiovascular diseases and early cardiovascular mortality in patients with and without diabetes and for hypertension.
Thus HOPE (Heart Outcomes Prevention Evaluation) study finds that the presence of albuminuria was associated with increased risk of myocardial infarction, stroke or cardiovascular death with or without diabetes.Other studies showing the relationship between albuminuria and cardio-vascular risk are LIFE trial and PREVEND [38] [39].
Microalbuminuria is an early marker of diabetic nephropathy and an independent risk factor for cardiovascular disease.
Endothelial dysfunction predicts modification in brain vasculature being related to affecting cerebrovascular reactivity, diabetic cerebral micro-angiopathy and to intima media thickness in the common carotid artery [40]. Microalbuminuria is a major factor for progesssive renal failure in DN. Reduction of albuminuria is a major target for renoprotective therapy in both type 1 and type 2 diabetes.
De Zeeuw et al. consider that the higher the albuminuria is, the higher is the renal risk in patients with type 2 diabetic nephropathy [41].
The treatment of microalbuminuria-proteinuria in ND – a component of multiorgan protection.
The main therapeutical means used are represented by:
– Inhibiting treatment of SRAA, that uses mainly ACE-I, ARB or an association of the two,
and, lately, aliskiren and aldosterone antagonists. This represents the main treatment used for con-trolling both proteinuria-microalbuminuria and HTA.
– Sulodexide – Strict control of glycaemia
Inhibitors of the renine-angiotensine-aldosterone system (RAAS)
A blockade of RAAS is a treatment of choice. According to Karalliedde and Viberti these drugs have successfully halted or delayed progression in nephropathy and have restored elevated rates of albumin excretion to normal values, even when blood pressure decrease was minimal 42].
Renoprotective effects in type 1 DM are shown by:
Microalbuminuria Captopril Study that has highlighted the fact that use of Captopril prevents the occurrence of overt nephropathy in patients with type 1 DM and microalbuminuria. Data on the efficacy of ARB in patients with type 1 diabetes and albuminuria are lacking [13].
In type II DM, the studies HOPE-trial/ ramipril), IDNT (Irbesartan) and RENAAL (LOSARTAN) have shown that ACE-I and ARB may delay progression of microalbuminuria in patients with both microalbuminuria and overt proteinuria [41][43][44].
It also seems reasonable to institute therapy with ACE-I or ARB, if the patient is normotensive, for those patients who have microalbuminuria or overt nephropathy.
Another renoprotective objective is reduction of residual albuminuria to the lowest achievable level.
Dual RAAS blockade (ACE-I and ARB) increases antiproteinuric effects. The favourable effect of dual RAAS blockade on albuminuria proved its efficiency in type 1 DM with ND (ramipril + telmisartan).
Dual therapy is not to be applied routinely to patients with low or moderate risk of progressive kidney disease: normoalbuminuria or micro-albuminuria with preserved glomerular filtration rate. Clinicians should carefully weigh the potential risk and benefits of dual blockade on individual basis.
Cardioprotective effects
Several studies ONTARGET and PREVEND demonstrated cardioprotective effects associated with reduction of microalbuminuria (telmisartan was as effective as ramipril).
Cardiac affection associated with the renal one in DZ is known as cardiorenal disease.

Gh. Gluhovschi et al. 12
174
Karalliedde and Viberti pose the question if pro-teinuria in DM is a bystander or a pathway to cardiorenal for diabetic kidney disease. There is convincing epidemiologic and experimental evidence to assign clinical albuminuria as a surrogate end point, but for lower levels of albuminuria (micro-albuminuria or normoalbuminuria) the evidence is inconclusive or not available. Karalliedde and Viberti consider that albuminuria of any degree is unlikely to be causally related to diabetic cardio-vascular disease [42]. Neuroprotective effects of RAAS inhibition were demonstrated by the HOPE, PROGRESS, ONTARGET trials. These renoprotec-tive effects were parallel with neuroprotective effects, with decrease of microalbuminuria, respectively.
The use of inhibitors of aldosterone and of renine inhibitor Aliskiren are still being assessed. These are associated in the treatment of micro-albuminuria and proteinuria with ACE-I and ARB. Thus, Aliskiren added to losartan reduced al-buminuria and renal dysfunction. AVOID trials are under study (they assess renoprotective effects of dual blockade and RAAS by adding treatment with aliskiren) and ALTITUDE, that assesses the benefits of adding aliskiren to conventional treatment in-cluding either ACE-I or ARB [45][46]).
Addition of aldosterone blockade to RAAS blockade resulted in 30% reduction of mean pro-teinuria together with decreases in systolic and diastolic blood pressure.Similar results have been obtained for the nephritic syndrome [47].
The effect of spironolactone associated with an ACE-I on albuminuria in patients with hyper-tension and diabetic nephropathy was found to be independent of blood pressure reduction.
Adding aldosterone to ACE-I also has protective effects on the heart, thus contributing to cardioprotective measures. The participation of the aldosteron blockade to the RAS blockade maximises multiorgan protective actions.
Sulodexide and diabetic nephropathy
Alterations of glycoproteins that affect the capillaries and the meantime have been noticed in ND. A decrease in the content of heparin-sulphate of GBM has also been noticed.
Specific structure alterations in heparin sulphate are associated with early diabetic nephro-pathy.
Exogenous GAG act to restore glycoprotein present in reduced amounts in the glomerular basement membrane and mesangium of diabetic animal models.
Sulodexide is an antiproteinuric medicine. The treatment with dose-dependent Sulodexide
reduces albuminuria in patients with type 1 and type 2 diabetes, both with microalbuminuria and with macroalbuminuria (Gambaro et al.) [48]. Gluhovschi et al. notice antiproteinuric effects of sulodexide in nephropathies other than ND, like primitive glomerulonephrites. (Gluhovschi et al.) [49].
Sulodexide has effects added to those of ACE-I in patients with ND. It has been noticed that the effect of sulodexide on proteinuria is long-lasting and additive to the ACE inhibitory effect.
GAG therapy apparently intervenes associated with good control of blood pressure values in preventing the progression of DN in NIDM.
The combination of ACE-I and GAGs could synergistically inhibit the TGF-beta axis in the kidney, thus the possibility of preventing glomerulo-sclerosis could increase.
Cardioprotective and neuroprotective, respect-tively multiorganprotective effects, will be discussed in the chapter on endothelial dysfunctions.
Other therapies control
– The value of intensive glycaemia control is unproven in relation to microalbuminuria, and further prospective studies are required.
– Intensive insulin therapy may not slow the rate of progressive renal injury, once macro-albuminuria or overt proteinuria has developed.
– Antiproteinuric effects have also been found in hypolipemiant treatments with fenofibrate.
– Statins administration has not shown clear benefits in reducing microalbuminuria. Some positive results are reported.
Colhoun et al. report that the results of the Collaborative Atorvastatin Diabetes Study (CARDS Trial) failed to show differences in the incidence of albuminuria and regression of albuminuria in diabetic patients (Colhoun et al.) [50].
Administration of pentoxifyline in type 2 DN patients under long treatment with ARB produces a significant additive antiproteinuric effect associated with a reduction of urinary TNF- alfa excretion.
Ruboxistaurin – a selective protein kinase C inhibitor was noted to decrease microalbuminuria. It is being assessed.
It is to be noted that these therapies have a moderate antiproteinuric effect, this antiproteinuric effect completing their multiorganprotective action.
CONCLUSION
The medication used in the treatment of DN, and mainly the RAAS inhibitors, are remarkable

13 Diabetic nephropathy. Part I
175
for their effects on the control of AH, for their multi-organ protective effects, as well as for their antiproteinuric effects.
The studies presented in this paper have demonstrated that the RAAS inhibitors can prevent both the appearance of DN and its development. They have protective effects on the complications of DN, having cardioprotective and neuroprotective effects, and protective effects on other organs as well. These measures are due both to their direct
effects on BP and proteinuria and to their numerous pleiotropic effects, which have an important impact in the general pathogeny of DM and its com-plications.
Correct treatment of glycaemia, that is intensive glycaemic control, represents the corner-stone of DN therapy.
An important renoprotective measure, but with multiorganprotective involvement, is the control of proteinuria.
Nefropatia diabetică, una din complicaţiile cele mai importante ale diabetului
zaharat, necesită în cursul evoluţiei sale măsuri protective definite ca renoprotective. Complicaţiile diabetului zaharat nu se rezumă la nefropatia diabetică, întrucât aceasta se asociază frecvent cu complicaţii cardiace ce necesită măsuri protective definite ca şi cardioprotecţie, neurologice ce necesită neuroprotecţie, retiniene, ale vaselor mari, etc. Se impun măsuri protective mult mai complexe.
Complicaţiile metabolice care stau de obicei la baza celorlalte complicaţii cu implicaţii la nivel celular impun şi ele măsuri de protecţie. Necesitatea de a privi organismul ca un tot unitar a determinat măsuri protective complexe care se încadrează în conceptul de multiorganprotecţie.
O astfel de abordare poate avea consecinţe practice importante. Este un fapt cunoscut că majoritatea bolnavilor cu boală cronică de rinichi (CKD- chronic kidney disease) nu ajung în stadiul final întrucât decedează pe parcurs prin boli cardiovasculare. În consecinţă, măsurile cardioprotective trebuie să se asocieze cu cele renoprotective ca de altfel şi cu măsurile protective care se adresează altor organe în strânsă corelaţie cu măsurile protective la nivel metabolic.
De asemenea, măsurile protective trebuie să se adreseze microcirculaţiei, nefropatia diabetică fiind o boală care afectează în primul rând microcirculaţia. Diabetul zaharat interesează totodată frecvent vasele mari, sistemul circulator fiind afectat de obicei în complexitatea sa.
Lucrarea reprezintă o sinteză a măsurilor multiorganprotective din nefropatia diabetică, respectiv din diabetul zaharat, conceptul de multiorganprotecţie găsind în această boală cadrul ideal de exprimare.
Ea reprezintă în prima parte principalele măsuri multiorganprotective: controlul hipertensiunii arteriale şi în primul rând protecţia prin intermediul sistemului renină angiotensină aldosteron (RAAS), multiorganprotecţia prin controlul intensiv al glicemiei cât şi cea prin tratamentul proteinuriei.
În cea de a 2-a parte se prezintă celelalte măsuri protective utilizate în nefropatia diabetică.
Corresponding author: Prof.Dr.Gh.Gluhovschi Nephrology Department, University of Medicine and Pharmacy, Timişoara E-mail: [email protected]
REFERENCES
1. GLUHOVSCHI G., BOZDOG G., PETRICA L., SCHILLER A., TRANDAFIRESCU V., VELCIOV S., GLUHOVSCHI C., BOB F., Multi-organ protection, From nephroprotection, cadioprotection, neuroprotection to multi-organ protection. Nefrologia (Madrid), 2004, XXIV, 6, 519–534.
2. RITZ E., ORTH S.R., Nephropathy in patients with type 2 diabetes mellitus. N. Engl. J.l999, 341, 1127–1133.

Gh. Gluhovschi et al. 14
176
3. CHOUDHURY D., TUNCEL M., LEVY M., Diabetic nephropathy a multifacet target of new therapies. Discov.Med. 2010, 10, 54, 406–415.
4. GLUHOVSCHI G., BOZDOG G., PETRICA L., SCHILLER A., TRANDAFIRESCU V., VELCIOV S., GLUHOVSCHI C., BOB F., Nephroprotection, part of multi-organ protection. Timişoara Medicală 2006, 56, 23, 190–197.
5. GLUHOVSCHI G., GLUHOVSCHI C., BOB F. VELCIOV S.,TRANDAFIRESCU V., PETRICA L., BOZDOG G., Multiorgan-protective actions of blockers of the renin-angiotensin system, statins and erythropoietin: common pleiotropic effects in reno-, cardio and neuroprotection. Acta Clinica Belgica 2008, 63, 3, 152–169.
6. ADLER A.I., STRATTON I.M., NEIL H.A., YUDKIN I.S., MATTEWS D.R., CULL C.A., WRICHT A.D., TURNER R.C., HOLMAN R.R., Association of systolic blood pressure with macrovascular and microvascular complications of type 2 diabetes (UKPDS 36) prospective observation study. BMJ 2000, 321, 412–419.
7. ACCORD Study Group. Cushman W.C., Evans G.W., Byington R.P., Goff D.C., Grimm R.H. Jr., Cutler J.A., Simons Morton D.G., Basile J.N., Corson M.A., Probstfield J.L., Katz L., Peterson I., Friedewald W.T., Buse J.B., Bigger J.T., Gerstein H.C., Ismail-Beigi F. Collaborators (1238). Effects of intensive blood-pressure control in type 2 diabetes mellitus. N. Engl. J.Med. 2010, 362, 17, 1575–1585.
8. REBOLDI G., GENTILE G., ANGELI F., VERDECHIA P., Optimal therapy in hypertensive subjects with diabetes mellitus. Curr Aheroscler Rep 2011, 13, 2, 176–186.
9. SLEIGHT P. et al., ONTARGET Investigators. Prognostic value of blood pressure in patients with high vascular risk in the Ongoing Telmisartan Alone and in combination with Ramipril Global Endpoint Trial study. J.Hypertens 2009, 27, 1360–1369.
10. BJOREK S., Don’t change the blood pressure limit in diabetes. Lakartidingen 2010, 107, 49, 3146–3147 (Pub.Med.). 11. CHATUVEDI N., The Euclid Study group. Randomised placebo-controlled trial of lisinopril in normotensive patients with
insulin-dependent diabetics and normoalbuminuria or microalbuminuria. Lancet 1999, 349, 9068, 1787–1992. 12. VIBERTI G., MOGENSEN C.E., GROOP L.C., PAULS J.F., Effect of captopril on progression to clinical proteinuria in
patients with insulin-dependent diabetes mellitus and microalbuminuria. European Microalbuminuria Captopril Study Group JAMA 1994, 271, 275–279.
13. RAVID M., BROSH D., LEVI Z., BAR-DAYAN Z., RAVID D., RACHMANI R., Enalapril to attenuate decline in renal function in normotensive, normoalbuminuric patients with type 2 diabetes mellitus. A randomized control trial. Ann Intern Med 1998, 128 (12): 982–988.
14. JAMERSON K., BAKRIS G.L., WUN C.C., DAHLOF B., LEFKOWITZ M., MANFREDA S., PITT B., VELAZQUEZ E.J., WEBER M.A., Rationale and design of the avoiding cardiovascular events through combination therapy in patients living with systolic hypertension (ACCOMPLISH) trial: the first randomized controlled trial to compare the clinical outcome effects of first-line combination therapies in hypertension. Am. J. Hypertens 2004, 17, 9, 793–801.
15. WRIGHT J.T., BAKRIS G.L., BELL D.S., FONSECA V., KATHOLI R.E., MCGILL J.B. et al., Lowering blood pressure with beta-blockers in combination with other renin-angiotensin system blockers in patients with hypertension and type 2 diabetes: result from GEMINI trial. J Clin Hypertens (Greenwich) 2007, 9, 11, 842–849.
16. SCHRIER R.W., ESTACIO R.O., MEHLER P.S., HIATT W.R., Appropriate blood pressure control in hypertensive and normotensive type 2 diabetes mellitus: a summary of the ABCD trial. Nat. Clin Pract. Nephrol 2007, 3, 8, 428–438.
17. Heart Outcomes Prevention Evaluation Study Investigators (2000). Effects of ramipril on cardiovascular and microvascular outcomes in people with diabetes mellitus: results of the HOPE Study and MICRO-HOPE substudy. Lancet 2000, 355, 253–259.
18. BRENNER B.M., COOPER M.E., DEZEEUW D., KEANE W.F., MITCH W.F., PARVING H.H. et al., Study Investigators. Effects of losartan on renal and cardiovascular outcomes in patients with type 2 diabetes and nephropathy. Ann Intern Med 2003, 138, 7, 542–549.
19. BERL T., HUNSICKER L.G., LEWIS J.B., PFEFFER M.B., PORUSH J.G., KOULEAU J.L. et al., Collaborative Study Group. Impact of achieved blood pressure on cardiovascular outcomes in the Irbesartan Diabetic Nephropathy Trial. J Am Soc Nephrol, 2005, 16, 7, 2170–2179.
20. MAIONE A., NAVANEETHAN S.D., GRAZIANO G., MITCHELL R., JOHNSON D., MANN J.F. et al., Angiotensin-converting enzyme inhibitors, angiotensin receptor blockers and combined therapy in patients with micro- and macro-albuminuria and other cardiovascular risk factors: a systematic review of randomised controlled trials. Nephrol Dial Transplant, 2011, 26, 9, 2723–2726.
21. The effect of intensive treatment of diabetes on the development and progression of long-term complications in insulin-dependent diabetes melitus. The Diabetes Control and Complications Trial Research Group. N.Engl. J.Med. 1993, 329, 14, 977–986.
22. Sustained effect of intensive treatment of type 1 diabetes mellitus on development and progression of diabetic nephropathy: the Epidemiology of Diabetes Intervention and Complications (EDIC) Study. JAMA 2003, 290, 2159–2167.
23. The Diabetes Control and Complications Trial research group. The effect of Intensive diabetes therapy on development and progression of neuropathy. Ann Intern Med. 1995, 122, 561–568.
24. OHKUBO Y., KISHIKAWA A., ARAKI E., MIYATA T., ISAMI S., MOTOYOSHI S., Intensive insulin therapy prevents with noninsulin-dependent diabetes mellitus. A randomised prospective 6-year study. Diabetes Res Clin Pract 1995, 28, 103–117.
25. DUCKWORTH W., ABRAIRA C., MORILA T., RECTA D., EMMANUELE N., REAVEN P.D. et al., Glucose control and vascular complications in veteran with type 2 diabetes. N.Engl J.Med. 2009, 360, 2, 129–139.
26. FIORETTO P., SUTHERLAND D.E., NAJALIAN B., MAUER M., Remodeling of renal interstitial and tubular lesions in pancreas transplant recipients. Kidney Int. 2006, 69, 5, 907–912.
27. UK Prospective Diabetes Study (UKPDS), Group Intensive Blood-glucose control with sulphonylureas or insulin compared with conventional treatment and risk of complications in patients with type 2 diabetes (UKPDS 33), Lancet 1998, 352, 837–853.
15 Diabetic nephropathy. Part I
177
28. RAY K.K., SESHASAI S.R., WIJASURIYA S., SIVAKUMARAN R., NETHERCOTT S., PREISS D., ERGON S., SATTAR N., Effect of intensive control of glucose on cardiovascular outcomes and death in patients with diabetes mellitus: a meta-analysis of randomised controlled trials. Lancet 2009, 373, 9677, 1765–1772.
29. PETRICA L., PETRICA M., VLAD A., JIANU D.C., GLUHOVSCHI G., IANCULESCU C. et al., Nephro-and neuroprotective effects of rosiglitazone versus glimepiride in normalbuminuric patients with type 2 diabetes mellitus : a randomized controlled trial. Wien.Klin Wochenschr 2009, 121 (23–24) 765–775.
30. MAZZONE T., MEYER P.M., FEINSTEIN S.B., DAVIDSON M.H., KONDOS G.T., D´AGOSTINO SR.R.P. et al., Effect of pioglitazone compared with glimepiride on carotide-media thickness in type 2 diabetes. A Randomized trial. JAMA 2006, 296, 21, 2572–2581.
31. LINCOFF A.M., WOLSKI K., NICHOLIS S.J., NISSEN S.E., Pioglitazone and risk of cardiovascular events in patients with type 2 diabetes mellitus a meta-analysis of randomized trials. JAMA 2007, 298, 10, 1180–1188.
32. NISSEN S.E., WOLSKI K., Effect of rosiglitazone on the risk of myocardial infarction and death from cardiovascular causes. N.Eng. J.Med. 2007, 356, 2457.
33. PSATY B.M., FURBERG C.D., The record on rosiglitazone and the risk of myocardial infarction. N Engl J Med. 2007, 5, 357(1):67–69.
34. SARAOGI P., PILLAI K.K., SING B.K., DUBEY K., Rosiglitazone and pioglitazone aggravate doxorubicin induced cardiomyopathy in Wistar rats. Biomed Pharmacother 2010, Dec 35.
35. PETRICA L., VLAD A., PETRICA M., JIANU C.D., GLUHOVSCHI G., GADALEAN F. et al., Pioglitazone delays proximal tubule dysfunction and improves cerebral vessels endothelial dysfunction in normoalbuminuric patients with type 2 diabetes mellitus. Diabetes Res Clin Pract 2011 (Epub ahead of print).
36. ZIYADECH F.N., WOLF G., Pathogenesis of podocytopathy and proteinuria in diabetic glomerulopathy. Curr. Diabetes Rev. 2008, 4, 1, 39–45.
37. PETRICA L., PETRICA M., VLAD A., JIANU D.C., GLUHOVSCHI G., IANCULESCU G. et al., Proximal tubule dysfunction is dissociated from endothelial dysfunction in normalbuminuric patients with type 2 diabetes. Nephron Clin Pract 2011, 118, c 155–c 164.
38. WACHTELL K., IBSEN H., OLSEN M.H., BORCH-JOHNSEN K., LINDHOLM L.H., MOGENSEN C.E. et al., Albuminuria and cardiovascular risk in hypertensive patients with left ventricular hypertrophy: the LIFE Study. Ann Intern Med 2003, 139, 11, 901–906.
39. VERHAVE J.C., HILLEGE H.L., BURGERHOL J.G., NAVIS G., DE ZEEUW D., DE JONG P.E., PREVEND Study Group, Cardiovascular risk factors are differently associated with urinary albumin excretion in men and women. J.Am.Soc Nephrol 2003, 15, 5, 1330–1335.
40. PETRICA L., PETRICA M., MUNTEANU M., VLAD A., BOB F., GLUHOVSCHI C. et al., Cerebral microangiopathy in patients with non-insulin-dependent diabetes mellitus. Ann.Acad.med. Singapore 2007, 36, 4, 259–266.
41. DE ZEEUW D., REMUZZI G., PARVING H.H., KEANE W.F., ZHANG Z., SHAHINFAR S. et al., Proteinuria a target for renoprotection in patients with type 2 diabetic nephropathy: lessons from RENAL. Kidney Int 2004, 65, 6, 2309–2320.
42. KARALLIEDDE J., VIBERTI G., Proteinuria in diabetes: bystander or pathway to cardiorenal disease? J.Am.Soc. Nephrol 2010, 21, 12, 2020–2027.
43. Mc QUEEN M.J., LONN E., GERSTEIN H.C., BOSCH J., YUSUF S., The HOPE (Heart Outcomes Prevention Evaluation) Study and its consequences. Scand J. Clin.Lab. Invest Suppl 2005, 240, 143–156.
44. CROOM K.F., CURRAN M.P., GOA K.L., PERR C.M., Irbesartan: a review of its use in hypertension and in the management of diabetic nephropathy. Drugs, 2004, 64, 9, 999–1028.
45. PERSSON F., LEWIS J.B., ROSSING P., HOLLENBERG N.K., PARVING H.H., AVOID Study investigators, Impact of baseline renal function on the efficacy and safety of aliskiren added to losartan in patients with type 2 diabetes and nephropathy. Diabetes Care 2010, 33, 11, 2304–2309.
46. PARVING H.H., BRENNER B.M., MC MURRAY J.J., DE ZEEUW, HAFFNER S.M., SOLOMON S.D. et al., Aliskiren trial in type 2 diabetes using cardio-renal endpoints (ALTITUDE): rationale and study design. Nephrol. Dial.Transplant 2009, 24, 5, 1663–1671.
47. SCHJOEDT K.J., ROSSING K., JUHL T.R., BOOMSMA F., TARNOW L., ROSSING P., PARVING H.H., Beneficial impact of spironolactone on nephrotic stage albuminuria in diabetic nephropathy. Kidney Int 2006, 70, 536–542.
48. GAMBARO G., Van DER WOUDE F.J., Glycosaminoglycans. Use in treatment of diabetic nephropathy. J.Am.Soc. Nephrol.2000, 11, 359–368.
49. GLUHOVSCHI G.H., SCHILLER A.D., RAICA M., PETRICA L., TRANDAFIRESCU V., VELCIOV S. et al., The effects of the therapy with natural glycosaminoglycans (Sulodexide) on proteinuria in different types of glomerulonephrites. Facta Universitatis (Nis) 2001, 8, 1, 26–30.
50. COLHOUN H.M., BETTERIDGE D.J., DURRINGTON P.N., HITMAN G.A., NEIL H.A., LIVINGSTONE S.J. et al., Effects of atorvastatin on kidney outcomes and cardiovascular disease in patients with diabetes: an analysis from the Collaborative Atorvastatin Diabetes Study (CARDS). Am.J.Kidney Dis 2009, 54, 5, 810–819.
Received August 4, 2011


ORIGINAL ARTICLES
The Influence of Left Bundle Branch-Block and Cardiac Dyssynchrony on 2D-strain Parameters in Patients with Heart Failure Complicating Ischemic Cardiomyopathy
C. MORNOŞ1,2, L. PETRESCU1,2, D. COZMA1,2, S. PESCARIU1,2, ANIKO MORNOŞ1, ADINA IONAC1,2
1Institute of Cardiovascular Diseases, Timişoara, Romania 2“Victor Babeş” University of Medicine and Pharmacy, Timişoara, Romania
Coronary artery disease is the underlying cause in approximately two-thirds of patients with heart failure. Torsional and longitudinal deformations are essential components of left ventricular (LV) performance. Electric conduction defects can reduce LV ejection fraction (LVEF) and decrease cardiac output.
Aim. To investigate the influence of left bundle branch-block (LBBB) and cardiac dyssynchrony on 2D-strain parameters in patients with HF complicating ischemic cardiomyopathy.
Methods. We analyzed 106 consecutive patients with HF complicating ischemic cardiomyopathy, in sinusal rhythm. LV strain, LV twist and LV torsion were measured by echocardiographic 2D-strain imaging. LV dyssynchrony was assessed using validated tissue Doppler parameters. Patients were divided into three groups: HF with normal LVEF (group 1), HF with reduced LVEF without LBBB (group 2) and with LBBB (group 3).
Results. LVEF, LV strain, LV torsion and LV twist were significantly better in group 1 (each p < 0.01). In group 3, LV torsion and LV twist were significantly lower compared to group 2 (0.80 ± 0.4 vs. 1.21 ± 0.23°/cm, p = 0.007, and 5.18 ± 2.4 vs. 8.31 ± 1.5°, p = 0.004, respectively), but LV strain and LVEF were not different between group 3 and 2 (–4.91 ± 2.3 vs. –6.28 ± 1.8%, p = 0.056, and 30.6 ± 8.8 vs. 34.4 ± 8.3%, p = 0.11, respectively). Cardiac dyssynchrony induces a reduction of all 2D-strain analyzed parameters (each p < 0.05).
Conclusion. In HF complicating ischemic cardiomyopathy, LBBB and cardiac dyssynchrony induce a reduction of LV strain, torsion and twist. In patients with reduced LVEF, LBBB induces predominantly a significant reduction of LV torsion and LV twist, while LV strain was apparently not influenced.
Key words: Heart failure, left bundle branch-block, global longitudinal strain, Left ventricular twist, left ventricular torsion.
Coronary artery disease (CAD) is believed to be the underlying cause in approximately two-thirds of patients with heart failure (HF) [1]. Left ventricular (LV) function results from the contraction and relaxation of helically oriented myofibres [2][3]. LV torsion and global longitudinal strain (LV strain) are essential components of cardiac performance [2][4–9]. With technical improvements in the temporal and spatial resolutions of two-dimensional (2D) echocardiography, the myocardial deformation and rotation can now be measured using the 2D-strain with the speckle tracking method [4–8][10–13]. This technique might provide a useful means for the detection of subtle changes in LV systolic function which could be caused by myocardial ischemia [14][15]. Several studies have confirmed that ischemia reduces LV longitudinal strain and LV rotation [14–18].
Approximately one third of patients with HF present with conduction disturbances that result in a QRS of greater than 120 ms. Most commonly (in approximately 25% of HF patients) this is exhibited
as a left bundle branch block (LBBB) pattern. This percentage is significantly higher than the estimated 1.5% prevalence of LBBB in the general patient population [19]. Electric conduction defects in HF are associated with a decrease in contractile per-formance [1][9][19][20]. LBBB can reduce global LV ejection fraction (LVEF) and decrease cardiac output, mean arterial pressure, and dP/dt in patients with or without cardiac disease [19]. Epidemiological studies have identified LBBB as an independent risk factor for cardiac mortality [1][9][19–21]. Cardiac asynchrony is highly prevalent for patients with LV dysfunction but there is a very poor agreement among the different methods used to detect it. A variety of echocardiographic parameters has been proposed in LV asynchrony evaluation [5][9] [20–25]. Tissue Doppler imaging is validated and considered the golden standard to determine the LV systolic desynchronization [5][21–25], but Lafitte et al. showed that 49% of HF patients had both positive and negative criteria for LV dyssynchrony during echocardiography [26].
ROM. J. INTERN. MED., 2011, 49, 3, 179–188
C. Mornoş et al. 2 180
The purpose of our study was to evaluate the influence of LBBB and cardiac dyssynchrony on 2D-strain parameters in patients with HF com-plicating ischemic cardiomyopathy.
METHODS
We analyzed 129 consecutive patients in sinus rhythm with a history of symptomatic HF [20] and ischemic cardiomyopathy [27] defined by a history of myocardial infarction (MI) or coronary revascularization, patients with ≥ 75% stenosis of left main or proximal left anterior descending artery, or patients with ≥ 75% stenosis of two or more epicardial vessels.
Twenty three patients were excluded for inadequate echocardiographic images, acute MI within 30 days before the echocardiography, primary valvular heart disease (defined as severe aortic or mitral insufficiency or severe stenosis of any heart valve), valvular prosthesis, congenital heart disease, paced rhythm or right bundle-branch block. The 106 remaining patients were included in the analysis and represented the study population.
All study participants underwent clinical examination, 12-lead electrocardiogram, transthoracic echocardiogram and coronary angiography. The QRS duration was determined by automated computerized measurements and confirmed manually. LBBB was defined according to AHA/ACCF/HRS guidelines: the QRS duration was ≥ 120 ms, with presence of broad monophasic R wave in I, or V5 and V6, absence of Q waves in leads I, V5, and V6, and the displacement of the ST segment and T waves in opposite direction to the major deflection of the QRS complex [28].
Echocardiography Conventional echocardiography was performed
with an ultrasonographic system (Vivid 7 General Electric, Milwaukee, WI) equipped with a multi-frequency transducer (M3S 1.5–4.0 MHz), in accordance to current guidelines [29]. All images were digitally stored and off-line analyzed with EchoPac PC Dimension software (GE Medical). LVEF was calculated from apical two- and four-chamber views, using LV volumes by the modified biplane Simpson rule, in accordance to the guide-lines [29].
Colour Tissue Doppler of the LV was obtained from the apical four chambers, two-chamber, and long-axis views were acquired at high frame rates [5][22–25]. For each plane, at least three consecutive cardiac cycles were acquired during breath hold. Long-axis Tissue Doppler velocities were assessed from six basal and six
mid-segments in the septal, anteroseptal, anterior, lateral, posterior, and inferior walls, for a total of 12 segments. The mean basal myocardial peak systolic (S’) velocities were calculated in six basal segments. Time to peak systolic velocity (Ts) was measured from the beginning of the QRS complex to the peak myocardial systolic velocity within the ejection period, without the impact of isovolumic contraction velocity measurement. The following LV dyssynchrony parameters were derived using cut-off values previously published:
– absolute difference in Ts between any two of the four basal septal, lateral, inferior, and anterior LV segments (∆Ts – 4), with sig-nificant dyssynchrony defined as ≥65 ms [22];
– absolute difference in Ts between any two of the six basal LV segments (∆Ts – 6), with significant dyssynchrony defined as ≥ 110 ms [24];
– absolute difference in Ts between any 2 of the 12 LV (6 basal and 6 mid) segments (∆Ts – 12), with significant dyssynchrony defined as ≥ 100 ms [23];
– standard deviation of Ts of the 12 LV segments (Ts – SD), with significant dys-synchrony defined as ≥ 32.6 ms [23][25].
As studies had previously shown the presence of both positive and negative criteria for LV dys-synchrony within the same individual depending on the type of parameter used [21][26], we derived a composite dyssynchrony score ranging from 0 to 4 to determine the value of combining the above four different dyssynchrony parameters, with a value of 1 or 0 given to each positive or negative parameter. Thus, a dyssynchrony score of 0 means that all four parameters were negative, and a dyssynchrony score of 4 means that all four dyssynchrony para-meters were positive [21].
Cardiac rotation was computed using speckle tracking echocardiography. Grayscale digital cine loops triggered to QRS complexes were acquired from two LV short-axis planes: at LV basal level with the cross-section as circular as possible (identified by the mitral valve) and at apical level (distally to the papillary muscles with an optimized transducer position to ensure a proper, circular short-axis cut with no papillary muscles present) [5][11][12]. In each plane, three cardiac consecutive cycles were recorded during breath-hold at a frame rate of 70–100 frames/s and stored on hard disk for subsequent off-line analysis. The LV twist curve was generated by calculating the difference between apical and basal rotations at each corresponding time point. The peak difference between rotation angles at the apex and base was used in our study. Peak LV torsion was derived from LV twist divided by LV diastolic longitudinal length as

3 Left bundle branch-block in patients with heart failure
181
previously described [10][12]. Speckle tracking echocardiography was also used for myocardial deformation measurements. Longitudinal peak systolic strain was determined from apical planes (four-, three- and two-chamber view) in a 16 LV segments model. Value of LV strain was obtained by averaging all 16 LV segments [6][13]. Off-line analysis was performed by two observers blinded to clinical data.
Patients were divided into three groups: group 1 including 32 patients with HF with normal LVEF (≥ 50%), group 2 including 44 patients with HF with reduced LVEF (< 50%) without LBBB, and group 3 including 30 patients with HF with reduced LVEF and LBBB. The study was approved by local institutional review boards. Informed written consent was obtained from all patients.
Statistical analysis Numeric variables are presented as mean
value ± standard deviation (SD) and compared using Student’s t-tests or analysis of variance, as appropriate. Categorical variables as absolute values and percentages were compared with χ2 tests. Receiver operating characteristic (ROC) curves were constructed to determine optimal sensitivity and specificity. Variability was calculated as the absolute difference between two measurements divided by
the mean of the two measurements. All statistical analyses used the software package SPSS version 11.5 (SPSS Inc, Chicago, IL). A p value of < 0.05 was accepted as statistically significant.
RESULTS
The study included 106 consecutive patients with HF complicating ischemic cardiomyopathy, in sinus rhythm. The mean age of our patients was 58 ± 14 years, 41 were women, 68% presented previous MI, one third with anterior localization, 63% of patients presented more than one vessel CAD, and the mean LV ejection fraction was 37 ± 12%. Characteristics of the study population are presented in Table I. Compared to group 2 and 3, in group 1 the severity of CAD, the LV volume, the QRS duration and the incidence of severe mitral regurgitation were lower. Between group 2 and 3 it was not a significant difference regarding the incidence of previous myocardial infarction (MI), anterior and inferior localization of previous MI, incidence of 2 or 3 vessel CAD, and treatment. In group 3 the LV and QRS complexes were larger and the incidence of severe mitral regurgitation was greater.
Table I Characteristics of the study population
Variables Total n = 106
Group 1 n = 32
Group 2 n = 44
Group 3 n = 30
Age, years 58 ± 14 61 ± 15 57 ± 13 56 ± 14 Hypertension, n (%) 84 (79%) 26 (82%) 35 (80%) 23 (77%) Diabetes, n (%) 46 (43%) 12 (38%)*,** 20 (45%) 14 (47%) Dyslipidemia, n (%) 79 (74%) 23 (72%) 33 (74%) 23 (77%) Smoker, n (%) 54 (51%) 13 (40%)*,** 22 (50%) 19 (63%) Previous MI, n (%) 72% (68%) 19 (59%)*,** 31 (70%) 22 (73%) Anterior MI, n (%) 35 (33%) 6 (19%)*,** 17 (38%) 12 (40%) Inferior MI, n (%) 23 (21%) 9 (28%)*,** 9 (20%) 5 (17%) Lateral MI, n (%) 19 (18%) 4 (12%)*,** 8 (18%)** 7 (23%) 1 vessel CAD, n (%) 43 (40%) 21 (66%)*,** 14 (31%)** 8 (27%) 2 vessels CAD, n (%) 38 (36%) 9 (28%)*,** 17 (39%) 12 (40%) 3 vessels CAD, n (%) 25 (23%) 2 (6%)*,** 13 (29%) 10 (33%) Severe functional MR, n (%) 26 (24%) 3 (9%)*,** 13 (29%)** 11 (37%) LV diastolic volume index, ml/m2 101 ± 32 69 ± 21*,** 104 ± 34** 132 ± 41 LV systolic volume index, ml/m2 63 ± 27 29 ± 9*,** 68 ± 23** 92 ± 29 QRS complex, ms 112 ± 16 91 ± 13*,** 102 ± 11** 152 ± 28 Dyssynchrony score 1.56 ± 1.5 0.41 ± 0.17*,** 1.31 ± 1.07** 3.49 ± 0.47 Medication
Beta-blockers, n (%) 99 (93%) 31 (97%)** 41 (93%) 27 (90%) ACEI/ARB, n (%) 97 (91%) 30 (94%) 40 (91%) 27 (90%) Antiplatelet therapy, n (%) 103 (97%) 32 (100%)* 42 (95%) 29 (97%) Statin, n (%) 104 (98%) 30 (94%)*,** 44 (100%) 30 (100%) Diuretics, n (%) 94 (88%) 24 (75%)*,** 41 (93%) 29 (97%) Digitalis, n (%) 18 (17%) 0 (0%)*,** 10 (23%) 8 (26%)
* p < 0.05 vs. Group 2 ** p < 0.05 vs. Group 3
Legend: ACEI/ARBA = angiotensin-converting enzyme inhibitors/angiotensin receptor blocking agents; CAD = coronary artery disease; MI = myocardial infarction, MR = mitral regurgitation.

C. Mornoş et al. 4 182
In group 1 the LVEF (58 ± 5.9%), LV strain (–14.2 ± 3.5%), LV torsion (1.95 ± 0.66°/cm) and LV twist (13.1 ± 4.1°) were significantly better (each p < 0.001) compared to group 2 and 3 (Fig. 1). In patients with LBBB and reduced LVEF (group 3), LV torsion and LV twist were significantly lower compared to group 2 (0.80 ± 0.4 vs. 1.21 ± 0.23°/cm, p = 0.007, and 5.18 ± 2.4
vs. 8.31 ± 1.5°, p = 0.004, respectively), but LV strain and LVEF were not different between group 3 and 2 (–4.91 ± 2.3 vs. –6.28 ± 1.8%, p = 0.056, and 30.6 ± 8.8 vs. 34.4 ± 8.3%, p = 0.09, respectively) as shown in Fig. 1. Inter-observer variability was 7.9 ± 2.3% for LV strain, 8.49 ± 4.3% for LV twist and 9.63 ± 4.9% for LV torsion, respectively.
Fig. 1. Comparison of mean left ventricular (LV) ejection fraction (a), global LV longitudinal strain (b), LV twist (c) and LV torsion
(d) among groups. See text for a definition of groups. * p < 0.05.
Cardiac asynchrony is highly prevalent for patients with LV dysfunction, but there is a very poor agreement among the different methods used to detect it [26]. The mean dyssynchrony score was maximal in group 3 (3.49 ± 0.47). LV dyssynchrony was considered present by all four proposed criteria in 18 patients (17%), present by any three criteria also in 18 patients (17%), present by any two criteria in 11 patients (10%), and present by only one criterion in 17 patients (16%). Thus, 40% of patients (42 patients) had no evidence of LV asyn-chrony on any criteria. In patients with HF with reduced LVEF, intraventricular dyssynchrony was
present in 16 (36%) to 33 (75%) patients in the group without LBBB and in 29 (87%) to 30 (100%) in the LBBB group, depending on the utilized method.
If we divided our patients according to the numbers of asynchrony criteria, 40% patients presented no dyssynchrony criteria (group A), 26% of patients had 1 or 2 criteria (group B) and 34% presented 3 or 4 dyssynchrony criteria (group C). Comparisons of LVEF, S’ wave, LV global longitudinal strain, LV twist and LV torsion, among dyssynchrony groups are shown in Table II. Patients of group C had the worst 2D-strain parameters at echocardiographic examination.

5 Left bundle branch-block in patients with heart failure
183
Table II Comparisons of left ventricular (LV) ejection fraction, mean basal myocardial peak systolic velocities (S’), LV global longitudinal
strain, LV twist and LV torsion, among dyssynchrony groups. Group A = patients with no dyssynchrony criteria, Group B = patients with one or two dyssynchrony criteria, Group C = patients with three or four dyssynchrony criteria
Variables Group A n = 42
Group B n = 28
Group C n = 36
Dyssynchrony score 0 *,** 1.41 ± 1.07** 3.45 ± 0.51 LV ejection fraction, % 53 ± 12*,** 36 ± 8** 29 ± 8 S’ wave, cm/s 8.2 ± 2.9*,** 6.1 ± 1.4** 4.8 ± 1.2 LV longitudinal strain, % –12.2 ± 4.7*,** –6.4 ± 1.9** –5.1 ± 2.0 LV twist, ° 12.7 ± 3.0*,** 7.7 ± 1.4** 5.4 ± 2.1 LV torsion, °/cm 1.9 ± 0.5*,** 1.1 ± 0.3** 0.8 ± 0.3
* p < 0.01 vs. Group B ** p < 0.01 vs. Group C
Using the ROC analysis to evaluate the accuracy of LV strain, LV torsion, LV twist, LVEF and S’ to identify patients with different dyssyn-crony scores (all four or at least three/two/one criteria of dyssynchrony), the area under ROC-curve (AUC) was every time maximal for LV twist (0.89, 0.90, 0.91 and 0.95 respectively, each p < 0.001) (Figs. 2–5). A statistical comparison of
the ROC curves demonstrates no significant differences between LV twist and LV torsion (each p > 0.05). The optimal cut-off to predict the presence of all four echocardiographic criteria of dyssyncrony was 7.25 for LV twist (sensitivity of 88% and a specificity of 86%) and 0.94°/cm for LV torsion (sensitivity of 84% and a specificity of 85%).
Fig. 2. Receiver operating characteristic (ROC) curves for left ventricular (LV) strain, LV torsion, LV twist, LV ejection fraction (LVEF) and mean basal myocardial peak systolic velocity (S’) to identify patients with all four criteria of dyssynchrony.
Area under the ROC curve (AUC) was 0.89 (95% confidence interval – CI = 0.83–0.95, p < 0.001) for LV twist, AUC = 0.86 (95% CI = 0.77–0.95, p < 0.001) for LV torsion, AUC = 0.78 (95% CI = 0.67–0.89, p < 0.001) for LV strain,
AUC = 0.75 (95% CI = 0.63–0.87, p < 0.001) for S’, AUC = 0.73 (95% CI = 0.63–0.87, p < 0.001) for LVEF.

C. Mornoş et al. 6 184
Fig. 3. Receiver operating characteristic (ROC) curves for left ventricular (LV) strain, LV torsion, LV twist, LV ejection fraction
(LVEF) and mean basal myocardial peak systolic velocity (S’) to identify patients with at least three criteria of dyssynchrony. Area under the ROC curve (AUC) was 0.90 (95% confidence interval – CI = 0.85–0.95, p < 0.001) for LV twist,
AUC = 0.88 (95% CI = 0.82–0.94, p < 0.001) for LV torsion, AUC = 0.81 (95% CI = 0.74–0.88, p < 0.001) for LV strain, AUC = 0.79 (95% CI = 0.71–0.88, p < 0.001) for S’, AUC = 0.79 (95% CI = 0.75–0.89, p < 0.001) for LVEF.
Fig. 4. Receiver operating characteristic (ROC) curves for left ventricular (LV) strain, LV torsion, LV twist, LV ejection
fraction (LVEF) and mean basal myocardial peak systolic velocity (S’) to identify patients with at least two criteria of dyssynchrony. Area under the ROC curve (AUC) was 0.91 (95% confidence interval – CI = 0.85–0.96, 0.001) for LV twist, AUC = 0.87 (95% CI = 0.80–0.94, p < 0.001) for LV torsion, AUC = 0.84 (95% CI = 0.77–0.92, p < 0.001) for LV strain,
AUC = 0.80 (95% CI = 0.72–0.89, p < 0.001) for S’, AUC = 0.85 (95% CI = 0.78–0.93, p < 0.001) for LVEF.

7 Left bundle branch-block in patients with heart failure
185
Fig. 5. Receiver operating characteristic (ROC) curves for left ventricular (LV) strain, LV torsion, LV twist, LV ejection fraction
(LVEF) and mean basal myocardial peak systolic velocity (S’) to identify patients with at least one criterion of dyssynchrony. Area under the ROC curve (AUC) was 0.95 (95% confidence interval – CI = 0.91–0.99, p < 0.001) for LV twist,
AUC = 0.93 (95% CI = 0.88–0.98, p < 0.001) for LV torsion, AUC = 0.87 (95% CI = 0.79–0.95, p < 0.001) for LV strain, AUC = 0.78 (95% CI = 0.68–0.88, p < 0.001) for S’, AUC = 0.90 (95% CI = 0.84–0.96, p < 0.001) for LVEF.
DISCUSSION
An important finding of this study was that LBBB and cardiac dyssynchrony induce a reduction of all 2D-strain analyzed parameters in patients with HF complicating ischemic cardiomyopathy, in sinus rhythm. In the subgroup with reduced LVEF, the presence of LBBB predominantly induces a significant reduction of LV torsion and LV twist, while LV strain was apparently not influenced.
The ventricles consist of a single myofiber band starting to the right ventricle just below the pulmonary valve, forming a double helix extending to the LV, where it attaches to the aorta [3]. In the LV wall, myofiber geometry changes smoothly from a right-handed helix in the subendocardium, to a left-handed helix in the subepicardium and the helix angle varies from positive at the endocardium to negative at the epicardium [2][3]. LV twist is an essential component of systolic function and con-tributes to an efficient ejection, necessary to produce physiological stroke volumes [4][7][8][13]. Speckle tracking imaging allows accurate measurement of the magnitude, timing, and dynamics of LV twist and shows excellent correlation with magnetic resonance imaging data [4]. LV longitudinal strain reflects LV long axis function, controlled pre-
dominantly by subendocardial fibres [2][6]. Altered LV ventricular geometry resulting from cardiac remodeling (fibrosis, dilatation, wall thinning, and reduction in fiber angles) is associated with reduction of the systolic twist and longitudinal strain [8][9][15].
A variety of factors contribute to abnormalities in HF with preserved LVEF, pulmonary congestion could be caused by transient “reversible” episodes of ischemia, which impair LV relaxation and elevate LV filling pressures [1]. The impairment of subendocardial contractile function may be second-dary to subendocardial fibrosis, asymptomatic sub-endocardial infarction, or reduced subendocardial perfusion. The net effect is reduced longitudinal strain, increased LV torsion and the preservation of EF [7][13]. In our study, the global LV longitudinal strain was reduced, but it was lower than previously reported values in patients with HF and normal LVEF [7,13], probably caused by sig-nificant CAD.
The inner myocardium is known to be most susceptible to myocardial ischemia and is the major component responsible for long-axis function. Several studies have confirmed the fact that ischemia reduces both LV longitudinal strain and also the LV rotation [14–18]. All our patients presented a significant CAD; this could explain
C. Mornoş et al. 8 186
why in this study, in patients with reduced LVEF the LV strain was similarly reduced, regardless of LBBB presence. The geometric apical remodeling accompanied by the changes of contractile performance can result in the loss of shearing and less twisting for ejection and suction. Both left anterior descending artery and left circumflex artery ischemia produced similar effects on the dynamics of apex rotation. Some authors propose that although the left circumflex artery does not feed the apex directly, its occlusion affects large areas of muscle fibers, that contribute to the observed changes in apex rotation [30]. Nagle et al. reported a significant reduction in apical rotation in patients with MI [17]. Loss of LV twist is mainly due to a decrease in apical rotation, which represents the dominant contribution to LV twist.
Electric conduction defects in HF are associated with a real decrease in contractile performance, development or prolongation of mitral regurgitation, and wasted cardiac work, as a result of develop-ment in mechanical asynchrony [19]. Some authors showed that asynchronous electrical activation is associated with a redistribution of regional blood flow [19]. These electrical alterations translate into abnormal myocardial metabolism and redirection of regional coronary perfusion, that could be deleterious in patients with underlying CAD [1]. The mechanisms responsible for changes in torsion dynamics for the patients without CAD might be related to LV dilatation, remodeling of cardiac myocytes and connective tissue matrix, and in-creased electrical dyssynchrony. LBBB contributes to a vicious circle of LV wall stress, asymmetric hypertrophy, and dilatation, that progressively deteriorates LV function [19]. Increasing LV diameters might affect torsion; in normal LV volumes although the angles of inclination of the subendocardial and subepicardial fibers are ap-proximately equal (but opposite in sign), physio-logical torsion during systole is dominated by the subepicardial fibers because of their larger radii (and longer lever arms). LV dilatation tends to increase the radii of both the subendocardial and subepicardial layers, thus allowing a relatively greater contribution from the subendocardium to the net torsion moment and decreasing maximal torsion [18]. In our patients with CAD, the presence of LBBB induces a significant reduction of LV torsion and LV twist, while LV strain is apparently not influenced. This supplementary reduction of LV torsion and twist induced by LBBB could be related to the larger volumes of LV and/or to the greater functional mitral regurgitation.
As previously reported, MI associated with ischemic mitral regurgitation resulted in greater perturb-bations in LV torsion and recoil than MI without ischemic mitral regurgitation [18].
LBBB may have a causative role, mediated through the resulting intra-ventricular asynchrony, in the deterioration of cardiac function and the development of cardiac remodeling and HF. Our results showed that 43% of our analyzed patients exhibited combinations of both positive and negative criteria for LV dyssynchrony and only 28% of patients with dyssynchrony (defined by tissue Doppler parameters) had concordance in all four LV dyssynchrony parameters. In this study, LV twist and LV torsion showed a good accuracy to detect patients with all four criteria of LV dys-synchrony. Ng et al. demonstrated in a recent study that after non-ST elevation MI without congestive HF, the presence of impaired LV systolic function (measured as mean S’) independently predicted the severity of early LV dyssynchrony [21]. In our study, the accuracy of S’ and LV strain to predict LV dyssynchrony was lower than the accuracy of LV twist and LV torsion, probably due to the different inclusion criteria. Our observations were consistent with those of Lamia et al who showed that LV torsion is primarily altered by dyssynchrony and cardiac resynchronization therapy that restores LV performance also restores torsion [9].
Our results should be considered in the context of several limitations. The number of patients in this study was relatively small; however, we were able to reach several significant observations. Selection bias is possible since our study was performed in a tertiary centre where evaluations were performed in a referral base. By current echo-cardiographic techniques, this method is challenging, particularly with respect to determining the distance between slices, but also to our approach of detailed strain and rotation mapping. However, given the recent advances in three-dimensional echocardio-graphic imaging, it is likely that simultaneous calculation of global LV strain, twist and torsion will be feasible in the near future. The infarct size was not analyzed, but the global strain methods are recently shown as probably the best available tools for assessment of global infarct size in the clinical setting [15]; in our groups 2 and 3, the global longitudinal strain was comparable. In this study no patient had normal EF and LBBB, and it was often unknown for how long a LBBB has been present. The process of remodeling of the LV may be more distinct in a patient with a long lasting LBBB, than in a patient with a new onset LBBB.

9 Left bundle branch-block in patients with heart failure
187
CONCLUSION
This preliminary study indicates that in patients with HF complicating ischemic cardio-myopathy, the presence of LBBB and/or cardiac dyssynchrony is associated with a significant reduction of longitudinal and rotational LV defor-mation, with probably impact on the intravetricular vortex mechanism. In the subgroup of patients with
reduced LVEF, the presence of LBBB induces predominantly a reduction of LV torsion and LV twist, while LV strain is apparently not influenced. LV twist and LV torsion showed a good accuracy to detect patients with criteria of LV dyssynchrony. However, the widespread clinical applicability of 2D strain-derived parameters has yet to be confirmed in future studies.
___________________________________________________________________ Etiologia pentru aproximativ două treimi dintre pacienţii cu insuficienţă
cardiacă (IC) este reprezentată de către boala coronariană. Torsiunea şi deformarea longitudinală reprezintă componente esenţiale ale performanţei ventriculului stâng (VS). Anomaliile de conducere electrică pot reduce fracţia de ejecţie a VS (FEVS) şi debitul cardiac.
Scop. Analizarea influenţei blocului major de ramură stângă (BRS) şi a asincronismului cardiac asupra parametrilor 2D-strain la pacienţii cu IC de etiologie ischemică.
Material şi metodă. Au fost analizaţi 106 pacienţi consecutivi cu IC de etiologie ischemică, în ritm sinusal. Prin ecocardiografie 2D-strain au fost determinaţi strainul, twistul şi torsiunea VS. Desincronizarea cardiacă a fost apreciată utilizând parametrii Doppler tisular consacraţi. Pacienţii au fost împărţiţi în trei grupuri: IC cu FEVS normală (grup 1), IC cu FEVS scăzută, fără BRS (grup 2) şi respectiv cu BRS (grup 3).
Rezultate. FEVS, strainul, torsiunea şi twistul VS au fost superioare în grupul 1 (fiecare p<0.01). În grupul 3, torsiunea şi twistul VS au fost semnificativ mai reduse comparativ cu grupul 2 (0.80 ± 0.4 versus 1.21 ± 0.23°/cm, p = 0.007, respectiv 5.18 ± 2.4 vs. 8.31 ± 1.5°, p = 0.004), însă strainul VS şi FEVS nu au prezentat diferenţe semnificative între grupurile 3 şi 2 (–4.91 ± 2.3 vs. –6.28 ± 1.8%, p = 0.056, respectiv 30.6 ± 8.8 vs. 34.4 ± 8.3%, p = 0.11). Prezenţa asincro-nismului cardiac induce reducerea tuturor parametrilor 2D-strain analizaţi (fiecare p < 0.05).
Concluzii. În IC de etiologie ischemică, prezenţa BRS şi a desincronizării cardiace induce o reducere a strainului, torsiunii şi twistului VS. La pacienţii cu FEVS scăzută, prezenţa BRS determină predominant o reducere a torsiunii şi twistului VS, în timp ce strainul este aparent mai puţin influenţat. ___________________________________________________________________
Acknowledgement. This work was supported by CNCSIS–UEFISCU, project number PN II/RU code PD 526/2010.
Conflict of interest: none declared.
Corresponding author: C. Mornoş, MD Institute of Cardiovascular Diseases, 13 A, Str G.Adam, Timişoara, Romania E-mail: [email protected] Tel: 004025620735, Fax: 0040256207362
REFERENCES
1. GHEORGHIADE M., SOPKO G., DE LUCA L. et al., Navigating the crossroads of coronary artery disease and heart failure. Circulation 2006; 114 (11): 1202–13.
2. SENGUPTA P.P., TAJIK J.A., CHANDRASEKARAN K., KHANDHERIA B.K., Twist mechanics of the left ventricle: principles and application. J Am Coll Cardiol Img 2008; 1 (3): 366–376.
3. TORRENT-GUASP F., BALLESTER M., BUCKBERG G.D. et al., Spatial orientation of the ventricular muscle band: physiologic contribution and surgical implications. J Thorac Cardiovasc Surg 2001; 122 (2): 389–392.
4. HELLE-VALLE T., CROSBY J., EDVARDSEN T. et al., New noninvasive method for assessment of left ventricular rotation: speckle tracking echocardiography. Circulation 2005; 112 (20): 3149–3156.

C. Mornoş et al. 10 188
5. TESKE A.J., DE BOECK B.W., MELMAN P.G., SIESWERDA G.T., DOEVENDANS P.A., CRAMER M.J., Echocardiographic quantification of myocardial function using tissue deformation imaging, a guide to image acquisition and analysis using tissue Doppler and speckle tracking. Cardiovascular Ultrasound 2007; 5: 27.
6. REISNER S.A., LYSYANSKY P., AGMON Y., MUTLAK D., LESSICK J., FRIEDMAN Z., Global longitudinal strain: a novel index of left ventricular systolic function. J Am Soc Echocardiogr 2004; 17 (6): 630–633.
7. PHAN T.T., SHIVU G.N., ABOZGUIA K., GNANADEVAN M., AHMED I., FRENNEAUX M., Left ventricular torsion and strain patterns in heart failure with normal ejection fraction are similar to age-related changes. Eur J Echocardiogr 2009; 10 (6): 793–800.
8. MELUZIN J., SPINAROVA L., HUDE P. et al., Left ventricular mechanics in idiopathic dilated cardiomyopathy: systolic-diastolic coupling and torsion. J Am Soc Echocardiogr 2009; 22 (5): 486–93.
9. LAMIA B., TANABE M., TANAKA H., KIM H.K., GORCSAN J.R.D., PINSKY M.R., Left ventricular systolic torsion correlates global cardiac performance during dyssynchrony and cardiac resynchronization therapy. Am J Physiol Heart Circ Physiol 2011, 300 (3): 853–8.
10. NOTOMI Y., LYSYANSKY P., SETSER R.M. et al., Measurement of ventricular torsion by two-dimensional ultrasound speckle tracking imaging. J Am Coll Cardiol 2005; 45 (12): 2034–2041.
11. WANG J., KHOURY D.S., YUE Y., TORRE-AMIONE G., NAGUEH S.F., Left ventricular untwisting rate by speckle tracking echocardiography. Circulation 2007; 116 (22): 2580–2586.
12. VAN DALEN B.M., VLETTER W.B., SOLIMAN O.I., TEN CATE F.J., GELEIJNSE M.L., Importance of transducer position in the assessment of apical rotation by speckle tracking echocardiography. J Am Soc Echocardiogr 2008; 21 (8): 895–898.
13. WANG J., KHOURY D.S., YUE Y., TORRE-AMIONE G., NAGUEH S.F., Preserved left ventricular twist and circumferential deformation, but depressed longitudinal and radial deformation in patients with diastolic heart failure. Eur Heart J 2008; 29 (10): 1283–1289.
14. CHOI J.O., CHO S.W., SONG Y.B. et al., Longitudinal 2D strain at rest predicts the presence of left main and three vessel coronary artery disease in patients without regional wall motion abnormality. Eur J Echocardiogr 2009; 10 (5): 695–701.
15. GJESDAL O., HELLE-VALLE T., HOPP E. et al., Noninvasive separation of large, medium, and small myocardial infarcts in survivors of reperfused ST-elevation myocardial infarction: a comprehensive tissue Doppler and speckle-tracking echocardiography study. Circ Cardiovasc Imaging 2008; 1 (3): 189–96.
16. HELLE-VALLE T., REMME E.W., LYSEGGEN E. et al., Clinical assessment of left ventricular rotation and strain: a novel approach for quantification of function in infarcted myocardium and its border zones. Am J Physiol Heart Circ Physiol 2009; 297 (1): H 257–67.
17. NAGEL E., STUBER M., LAKATOS M., SCHEIDEGGER M.B., BOESIGER P., HESS O.M., Cardiac rotation and relaxation after anterolateral myocardial infarction. Coron Artery Dis 2000; 11 (3): 261–7.
18. TIBAYAN F.A., RODRIGUEZ F., LANGER F. et al., Alterations in left ventricular torsion and diastolic recoil after myocardial infarction with and without chronic ischemic mitral regurgitation. Circulation, 2004; 110 (11 Suppl 1): II 109–14.
19. ZANNAD F., HUVELLE E., DICKSTEIN K. et al., Left bundle branch block as a risk factor for progression to heart failure. Eur J Heart Fail 2007; 9 (1): 7–14.
20. DICKSTEIN K., COHEN-SOLAL A., FILIPPATOS G. et al., ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure 2008: the Task Force for the Diagnosis and Treatment of Acute and Chronic Heart Failure 2008 of the European Society of Cardiology. Developed in collaboration with the Heart Failure Association of the ESC (HFA) and endorsed by the European Society of Intensive Care Medicine (ESICM). Eur Heart J 2008; 29 (19): 2388–442.
21. NG A.C., TRAN D.A.T., ALLMAN C., VIDAIC J., LEUNG D.Y., Prognostic implications of left ventricular dyssynchrony early after non-ST elevation myocardial infarction without congestive heart failure. Eur Heart J 2010; 31 (3): 298–308.
22. BAX J.J., BLEEKER G.B., MARWICK T.H. et al., Left ventricular dyssynchrony predicts response and prognosis after cardiac resynchronization therapy. J Am Coll Cardiol 2004; 44: 1834–1840.
23. YU C.M., LIN H., ZHANG Q., SANDERSON J.E., High prevalence of left ventricular systolic and diastolic asynchrony in patients with congestive heart failure and normal QRS duration. Heart 2003; 89: 54–60.
24. NOTABARTOLO D., MERLINO J.D., SMITH A.L. et al., Usefulness of the peak velocity difference by tissue Doppler imaging technique as an effective predictor of response to cardiac resynchronization therapy. Am J Cardiol 2004; 94: 817–820.
25. YU C.M., FUNG J.W.-H., CHAN C.K. et al., Comparison of efficacy of reverse remodeling and clinical improvement for relatively narrow and wide QRS complexes after cardiac resynchronization therapy for heart failure. J Cardiovasc Electrophysiol 2004; 15: 1058–1065.
26. LAFITTE S., BORDACHAR P., LAFITTE M. et al., Dynamic ventricular dyssynchrony: an exercise-echocardiography study. J Am Coll Cardiol 2006; 47: 2253–2259.
27. FELKER G.M., SHAW L.K., O’CONNOR C.M., A standardized definition of ischemic cardiomyopathy for use in clinical research. J Am Coll Cardiol 2002; 39: 210–8.
28. SURAWICZ B., CHILDERS R., DEAL BJ. et al., AHA/ACCF/HRS recommendations for the standardization and interpretation of the electrocardiogram: part III: intraventricular conduction disturbances: a scientific statement from the American Heart Association Electrocardiography and Arrhythmias Committee, Council on Clinical Cardiology; the American College of Cardiology Foundation; and the Heart Rhythm Society: endorsed by the International Society for Computerized Electro-cardiology. Circulation 2009; 119 (10): e 235–40.
29. LANG R.M., BIERIG M., DEVEREUX R.B. et al., Recommendations for chamber quantification. Eur J Echocardiography 2006; 7 (2): 79–108.
30. GIBBONS KROEKER C.A., TYBERG J.V., BEYAR R., Effects of load manipulations, heart rate, and contractility on left ventricular apical rotation. An experimental study in anesthetized dogs. Circulation 1995; 92 (1): 130–41.
Received August 10, 2011

Stem-like Cells in Colorectal Oncology
C. TOMULEASA1,2, S. ŞUŞMAN2,3, OLGA SORIŢĂU1, OFELIA MOŞTEANU2,4, TEODORA POP2,4, B. PETRUSHEV2, G. KACSÓ2,5, R. BUIGÃ3, M. TANŢĂU2,4, A. IRIMIE2,6
Departments of 1Immunology, 3Pathology,5Radiotherapy and 6Surgery, “Ion Chiricuţa” Oncology Institute, Cluj-Napoca
2“Iuliu Haţieganu” University of Medicine and Pharmacy, Cluj-Napoca 4“Octavian Fodor” Regional Institute of Gastroenterology and Hepatology
Although the treatment for colorectal cancer has seen considerable progress during the past few years, the mortality associated with this type of tumor remains high. This article presents the existing methods of treatment, focusing on the new treatments made possible by the advances in the field of normal and tumor stem cells. Starting from the normal architecture of the colon and the properties of the cells identified in it, we sought to present a few notions concerning these cells which have a direct relevance for both pathology and treatment. The manner in which they divide (symmetrically or asymmetrically) as well as the molecules which control their circulation through the body are just a few examples which are likely to influence the treatment of colorectal cancer in the future.
Key words: Cancer stem-like cells, colorectal cancer, resistance to chemotherapy.
COLORECTAL CANCER. EPIDEMIOLOGY AND CURRENT MANAGEMENT
Colorectal cancer is the third most common cancer in both men and women, the available epidemiological data showing that this type of cancer is the second most diagnosed neoplasia as well as the second cause of cancer mortality [1]. In Europe the 5-year survival is far lower at 56.2% than other high-incidence high-mortality cancers such as 79.0% and 77.4% for breast and prostate cancers, while the American data show an average of 65.5% 5-year survival. Even if survival has increased from less than 50% diagnosed in 1990–1994, the incidence has increased in part because of Westernization of the diet [2][3].
The tumor node metastasis (TNM) staging system from the American Joint Committee on Cancer/International Union Against Cancer remains the most reliable prognostic indicator for patients with colorectal cancer [4]. A variety of pathology, molecular and proteic markers have also been shown to be important in prognostics, indepen-dently of TNM stage. These factors include venous and lymphatic invasion, tumor grade, perineural invasion, loss of heterozygosity at 18q or mutations in p53. Also, microsatellite instability status is an attribute categorizing colorectal oncogenesis into the two major pathways: the microsatellite stable and microsatellite instable, the last one including both sporadic and hereditary Lynch syndrome [5].
The combined-modality care of the patient with colon or rectal cancer demands a team approach. While patients with tumors limited to the muscularis propria are cured by surgery in more than 90% of cases, those with cancers penetrating through the bowel wall or involving the regional lymph nodes have a substantial risk of relapse after surgical resection alone. This is the very reason why adjuvant chemotherapy remains the backbone of oncology treatment. For decades, the fluorouracil (5-FU)/leucovorin combination was standard for metastatic cancer of the colon but within the last decade, new agents have led to an improvement in both response rate and median overall survival rate. These regimens include FOLFOX (oxaliplatin, leucovorin and infusional 5-FU) and FOLFIRI (irinotecan, leucovorin and 5-FU) in the first-line setting with protocol-specified crossover to the other regimen as second-line therapy [6]. The addition of a biologic agent to chemotherapy was found to be tolerable and improved the survival curves. Following the US Food and Drug Adminis-tration (FDA) approval of bevacizumab, an anti-vascular endothelial growth factor (VEGF) mono-clonal antibody, for use in combination with first-line intravenous 5-FU chemotherapy, many clinicians combined bevacizumab with FOLFOX or FOLFIRI [7][8]. Another biological agent, cetuximab, an anti-epidermal growth factor receptor (EGFR) monoclonal antibody, was investigated in randomized trials and proven superior regarding progression-free survival
ROM. J. INTERN. MED., 2011, 49, 3, 189–196

C. Tomuleasa et al. 2 190
time by the phase III CRYSTAL study [9]. In a subgroup analysis of the trial, van Cutsem et al. also suggested that the clinical benefit of cetuximab is confined to patients who have KRAS wild-type tumor.
For rectal cancer, radiotherapy plays an im-portant in the multimodal treatment setting, given to the primary tumor and lymph nodes in order to promote R0 resectability, when talking about the neoadjuvant treatment plans. Patients with pT3 and/or N1/2 disease may also benefit from post-operative radiotherapy, with a reported improvement of the survival rate with about 10% [10].
FROM NORMAL HISTOLOGY AND PHYSIOLOGY TO COLORECTAL CANCER
The goal to elucidate cellular mechanisms that link genetic changes to the development of colorectal cancer is a formidable task because it involves a complex process that occurs in crypts (very complex themselves), it develops over a long period of time and involves a multitude of causes, contributory elements and risk factors. Colorectal cancer is initiated by Wnt-pathway-activating mutations in genes such as adenomatous polyposis coli (APC) and, as in many cancers, the cell of origin remains relatively elusive.
The anatomy of the intestinal crypts (Fig. 1) is uniquely suited to study adult stem cells and their niche. Each crypt contains long lived stem cells intermingled with Paneth cells in the small intestine and with goblet cells in the colon. These cells divide every day, being called crypt base columnar cells and their daughter cells constitute the transit-amplifying crypt compartment. Transit amplifying cells divide every 12 to 16 hours, reside within the crypts and undergo several rounds of cell division while migrating upwards. When a transit amplifying cell reaches the crypt-villus junction, it differentiates while continuing its upward migration and initiating mutations in colorectal malignancies target Wnt pathway components, most frequently the negative regulator APC (Fig. 2). This will result in the constitutive activation of a Wnt target gene program that drives the formation of bening adenomas [11–12].
Vogeltein’s theory has been improved by later research (Figs. 3,4), especially by the hypothesis of stem cell overpopulation and adenoma development. Morphologically, adenomatous crypts are wider and longer than normal ones, indicating that the total crypt cell population has expanded. Adeno-matous epithelium has a relatively immature, undifferentiated phenotype that resembles the proliferative epithelium found in the bottom on-
third of normal crypts. This proves that the proli-ferative cell population expands to replace the entire crypt population and that the distribution of S-phase cells is shifted upward to the luminal surface of adenomatous crypts [13][14]. A further displacement of the rapidly proliferating cell population and a further shift in the distribution of S-phase cells toward the crypt top is testable by immunohistochemical staining of colon tissue sections using antibodies against available colonic markers, such as CD133, CD44 or Lgr5, and against rapidly proliferating cells (i.e. Ki67) [15].
While a few tumors develop very rapidly, most do over many years or even decades. A malignant tumor requires mutations that confer a tumor cell the ability to overcome the multiple intrinsic and extrinsic mechanisms that the human body possesses to prevent the breakdown of homeo-stasis. Mutations that cause aberrant cell proliferation are key aspects of oncogenesis and still most DNA damage is quickly repaired. Also, because somatic cells are dependent on homeostatic signals, the mutation that disrupts an epithelial cells’ interaction with the basal lamina can trigger apoptosis or replicative senescence. Considering that the immune system also plays a role in cancer progression, we might say that all the anti-cancer initiation and progression systems act as a selective force that promotes somatic evolution of different clonal sub-species [16].
Cancer can be considered a phenotypic selection of multiple advantageous traits by a specific environment rather than an expansion of individual mutant genotypes. In tumor cell biology, as well as in evolutionary biology, selection is applied at the phenotypic level and cellular pheno-types in tumors are the result of the integration of the genotype with the microenviron-ment. Tumor cells acquire a number of traits as the neoplasm progresses to malignancy. Traits described by Baylin and Pupa et al. [17–18], include self-sufficiency in growth signals, insensitivity to anti-growth signals, evasion of apoptosis, angiogenesis, limitless rep-licative potential and the ability to invade the surrounding tissues.
A rather unconventional but as close to reality as possible way to see cancer is “Game theory”, an ecological mathematical tool used by ecologists to address cancer, evolution of cooperation between the tumor cell and the surrounding environment and the network of metastasis. Game theory, initially introduced by Nash in the 1950s to study human behavior and economy [19], was expanded to study interactions between individuals in the same species to determine the evolutionary dynamics of the population. In the past decade mathematical
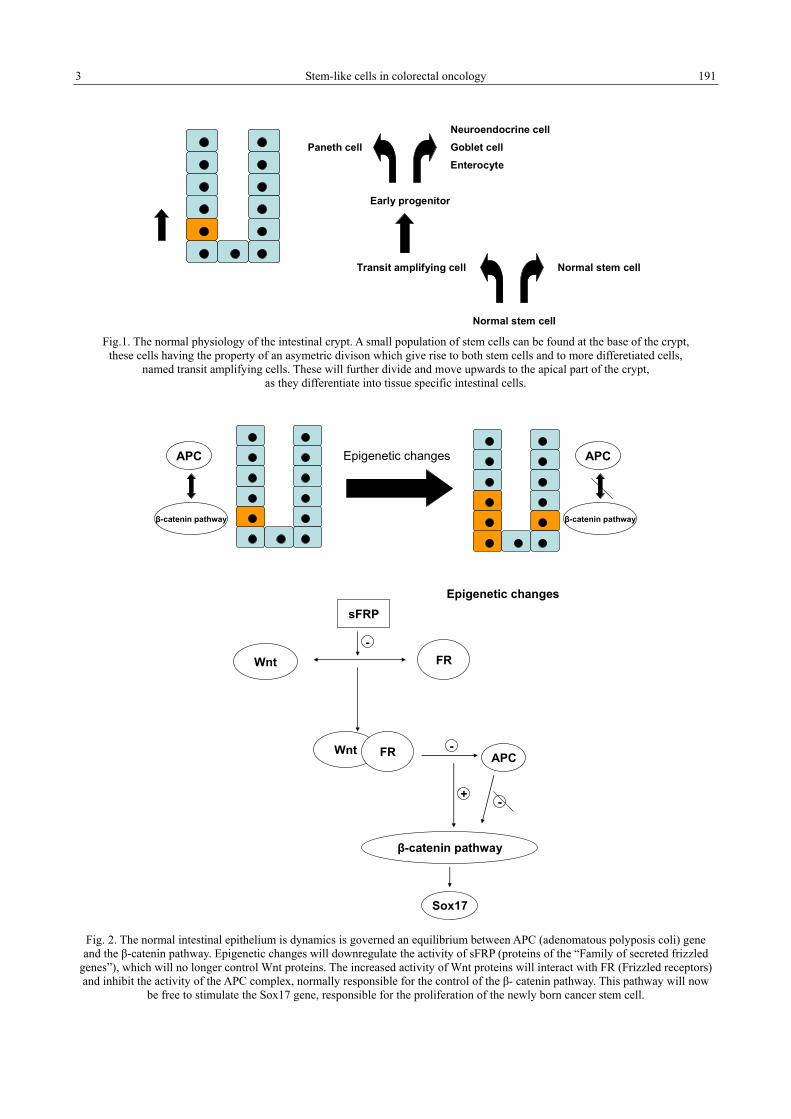
3 Stem-like cells in colorectal oncology
191
Normal stem cellTransit amplifying cell
Early progenitor
Normal stem cell
Paneth cellNeuroendocrine cellGoblet cellEnterocyte
Fig.1. The normal physiology of the intestinal crypt. A small population of stem cells can be found at the base of the crypt,
these cells having the property of an asymetric divison which give rise to both stem cells and to more differetiated cells, named transit amplifying cells. These will further divide and move upwards to the apical part of the crypt,
as they differentiate into tissue specific intestinal cells.
APC
β-catenin pathway
Epigenetic changes APC
β-catenin pathway
Wnt FR
sFRP
-
Wnt FR APC-
+
β-catenin pathway
-
Sox17
Epigenetic changes
Fig. 2. The normal intestinal epithelium is dynamics is governed an equilibrium between APC (adenomatous polyposis coli) gene and the β-catenin pathway. Epigenetic changes will downregulate the activity of sFRP (proteins of the “Family of secreted frizzled
genes”), which will no longer control Wnt proteins. The increased activity of Wnt proteins will interact with FR (Frizzled receptors) and inhibit the activity of the APC complex, normally responsible for the control of the β- catenin pathway. This pathway will now
be free to stimulate the Sox17 gene, responsible for the proliferation of the newly born cancer stem cell.

C. Tomuleasa et al. 4 192
IL-1, IL-6, VEGFIL-2, HGF, IFN-γ
Irritable bowel syndrome
Fig. 3. Correlations between irritable bowel syndrome and the cancer stem cell niche in colorectal tumours.
Normal epithelium
Aberrant cryptfoci
Earlyadenoma
Intermediateadenoma
LateAdenoma
Carcinoma
Distant metastasis
APC downregulation;β - catenin activation
Microstalliteinstability
K-ras mutation
Smad 4
p 53 alteration
CXCR4 activation;Epithelila-mesenchymaltransition
Fig. 4. Slight modification to Vogeltein’s model for colorectal carcinogenesis.
oncologists have started using evolutionary game theory to study somatic evolution in cancer, which requires formally defining the relevant cell pheno-types present during invasion and metastasis and the interplay between these elements in relation to a fitness payoff. The theory has successfully demon-strated the emergence of phenotypes capable of unconstrained growth, avoiding apoptosis, acidifying the microenvironment, promoting angiogenesis and invasion [20–22].
STEM CELL NICHE AND METASTASIS
The epithelial cells in the colon are a cell population undergoing a constant process of re-
generation. In order to strictly regulate this process, there has to be a balance between proliferation, differentiation, senescence and apoptosis, a central role being played by the stem cells located at this level [23].
At the level of the colon, these cells are situated in the basal compartment of the crypts. Just like the other adult stem cells, it is assumed that these cells are surrounded by a niche consisting of mesenchymal structures, which ensure the preservation of their characteristic properties as stem cells [24].
The studies conducted in the attempt to determine the clonal origin of colonic crypts have indicated that although during their embryological development the cells that constitute the crypts are

5 Stem-like cells in colorectal oncology
193
polyclonal, in a later stage they become mono-clonal, possibly through the positive selection of a dominant clone or following the segregation of the cell lines caused by the fission of the crypts, which occurs quite frequently during the development of the colon. This observation has led to the notion of a crypt cycle. Thus, crypts have a limited lifespan which, in the case of mice, has been established at two years [25–26].
Because the fission of the crypts begins at the base, where we also find the colonic stem cells, it is assumed that they play a major role in this process. Thus, customarily, the cell population generated by one stem cell would lead to the formation of an entire colonic crypt. Normally, competition between the cell populations coming from different stem cells is moderate and leads to an increase in the number of crypts. In the case of a malignant trans-formation, the increased proliferation of the cells coming from the tumor stem cell leads to an aggressive, unbalanced competition with the other cells, which come from normal colonic stem cells. This time, the consequence is not the formation of colonic stem cells, but an anarchic proliferation of crypts, leading to an architecture typical of malignant tumors [27–30].
This behavior can explain the architecture of colonic metastases in which crypts were identified, provided that the migrated cell has properties similar to those of the colonic stem cells capable of generating an entire crypt [31]. One of the important characteristics that define a stem cell is asymmetrical division. In this case, the division of a stem cell generates a cell identical to the original one and a cell that would differentiate. Following this division, one of the cells would take the place of the initial cell in the niche, and the other would leave the niche and differentiate [32].
During a malignant transformation, this normal process of asymmetrical division can turn into a process of symmetrical division, with the con-secutive increase in the number of stem cells and without the possibility for the microenvironment to provide a niche for these cells, which would be absolutely necessary for the preservation of their properties [33].
This could lead, in some of these cells, to the activation of certain mechanisms that would allow them to migrate towards other areas in the body, where they could find a suitable microenvironment. The molecular mechanisms involved in this migration process seem to be the same as the ones employed by the normal stem cells, best invest-tigated among them being the CXCL12-CXCR4 axis [34–36].
The activation of this axis determines the cells to move towards areas in the body where previous cellular damage triggered the release of CXCL12, a chemoattractant for normal or tumor stem cells whose surface shows an expression of CXCR4. After reaching this level, displaying increased proliferation properties following the dis-turbance in the cellular cycle, the tumor cells will begin to generate structures with an architecture similar to that of the original tumor from which they migrated [37–40].
TARGETED MOLECULAR THERAPIES
A key focus of cancer research is the under-standing of molecular changes that underly tumor initiation and progression. One of the most promising pathways to targeting CSC is the induction of differentiation with the loss of self-renewal capacity. This is the case of acute promyelocytic leukemia, where retinoic acid has significantly increased the efficacy of chemotherapy. This proof principle is that differentiation agents may be the most promising path to developing effective, nontoxic therapies. Inhibitors of Wnt signaling, such as ICG-001, par-ticularly the CREB-Binding Protein (CBP) pathway, show promising in vivo and in vitro efficacy without toxicity, as well as arsenic trioxide that sensitizes CSC to standard chemotherapy [41][42].
CD44 is a widely expressed protein with an important role in cell-to-cell and cell-to-matrix interactions. Though normally expressed at the base of dividing crypts in the proliferative zone, during inflammation and neoplastic proliferation the distribution of CD44 expression extends to the luminal surface. In a mouse model of acute myeloid leukemia, Jin et al. used a CD44-activating antibody and resulted in reversal of differentiation blockade [43]. Todaro et al. have recently described the autocrine production of IL-4 by CD133 + colon cancer stem-like cells [44]. Even if the cell isolates were resistant to 5-FU or oxaliplatin, the ability to decrease tumorigenic growth was increased when cells were first treated with monoclonal antibodies anti-IL-4. Colon cancer stem cells may also be targeted by natural products, such as curcumin (diferuloylmethane) – the major active ingredient of Curcuma longa. Curcumin inhibits the growth of transformed cells, suppresses initiation, promotion and progression of colon carcinogenesis in com-bination with either 5-FU or FOLFOX [45].
Cancers are extremely heterogeneous in terms of the frequency and types of mutations and the high degree of diversity among human colorectal

C. Tomuleasa et al. 6 194
cancers suggests that individualized treatment strategies hold great promise in future clinical experiments. Radioimmunotherapy is an emerging technology with thus only two FDA-approved protocols, both targeted against non-Hodgkin’s lymphoma. Abraham et al. report a set of nine different decapeptides which when labeled with the β-emitter 32P bound to cell lines derived from a panel of different colorectal adenocarcinomas [46]. The most efficient 32P-labeled decapeptide resulted in permanent incorporation of radioisotope into colon adenocarcinoma cellular proteins at a rate over 100 times greater than in cell lines derived from other cancers.
Telomerase, the research of whom has won Blackburn, Greider and Szostak the 2009 Nobel Prize in Physiology or Medicine, is a ribonucleo-protein considered as a potential target of cancer therapy because of its preferential expression in tumors. Telomerase, whose activity is generally underdetectable in normal somatic cells and ex-pressed in most tumors, has two major components and several associated proteins essential for proper cell function. The first major component is the human telomerase RNA (hTER) to serve as the template on which telomeric repeats are added to the ends of the chromosomes and the second component is the human telomerase reverse trans-criptase (hTERT) catalytic sub-unit. In anticancer therapy, the promoter of the hTERT gene is used to restrict the expression of suicide gene or toxin to telomerase positive tumor cells. Using hTERT-derived peptides or hTERT RNA, cytotoxic T cell responses and tumor immunity are elicited. Due to the fact the normal cells lack telomerase activity they are kept intact and adverse effects are minimal [47][48].
Gene-based therapeutics based on the concept of oncolytic virus therapy also hold considerable promise. Viruses have adapted through a millenium of evolution to effectively invade lysed cells through various mechanisms. The research team led by Galanis at Mayo Clinic in Rochester uses strains of the attenuated measles virus Edmoston (MV-Edm) vaccine lineage that can preferentially infect and destroy cancer cells while sparing the healthy tissue. To facilitate monitoring viral gene expression and replication, the oncolytic strains are engineered to express soluble marker peptides, such as the human carcinoembryonic antigen [49][50].
Another approach that has been introduced recently in the clinic to reduce primary tumor and metastasis load is targeting of the angiogenesis process. As neovascularization depends largely on VEGF signaling, several strategies have been
developed to disrupt this signaling pathway. Small molecule tyrosine kinase inhibitors and antibodies against VEGF receptors can block activation. A phase III clinical trial showed that blocking VEGF with a humanized anti-VEGF antibody in com-bination with standard chemotherapy will increase overall and progression-free survival of patients with metastatic colorectal cancer [51].
Plerixafor, also known as AMD3100, is a bicyclam molecule which binds reversibly to CXCR4. Even though initially developed as a potential therapeutic agent against HIV, preclinical data have shown that AMD3100 blocks CXCL12 binding of CXCR4 and as a result it inhibits SDF-1α-induced calcium flux and chemotaxis. Clinical trials have demonstrated that Plerixafor is effective for the mobilization of peripheral blood stem cells for use in autologous haematopoietic stem cell transplantation, but blocking the same CXCR4-CXCL12 axis can also play an important role in the control of CSC dissemination from the primary prostate lesion and metastasis. New drugs such as CTCE-9908 are currently undergoing preclinical confirmation in this setting [52].
CONCLUSION
Although the treatment of colorectal cancer has seen considerable progress during the past few years, the mortality associated with this type of tumor remains high. The integration of paradigms coming from various fields, such as evolutionary dynamics and mathematical oncology, has increased our understanding of the manner in which tissues are organized and operate. This has opened new perspectives in what concerns the genesis of various pathological processes, especially of malignant tumors. Nowadays we are witnessing a new approach to treatment, and this time the target is a small cell population – tumor stem cells – deemed responsible for the resistance to treatment and for the metas-tasis. That is why current efforts are directed towards the understanding of the biology of this type of cells and of the differences between them and normal stem cells, in an attempt to find more effective treatments that would also have less significant side-effects. Plarixafor, an inhibitor of the CXCR4-CXCL12 axis, is a prime example of a drug that manages to inhibit the metastasis, its use being determined by the discovery of the molecules that control the traffic of normal and tumor stem cells in the body. Alongside the already familiar methods of treatment, it is hoped that in future these molecules, as well as some new ones, would help decrease the mortality in patients suffering from colon cancer.

7 Stem-like cells in colorectal oncology
195
În ciuda progreselor remarcabile obţinute de-a lungul ultimilor ani în terapia cancerului colorectal, mortalitatea şi morbiditatea asociată acestei neoplazii rămân foarte ridicate. În acest articol sunt prezentate în mod succint principalele strategii de tratament, bazate pe cercetarea fundamentală şi în special pe conceptul de celula I tumorală cu proprietăţi stem-like. Bazându-ne pe histologia clasică a colonului şi pe proprietăţile celulelor ce formează ţesuturile acestei componente a tractului digestiv, am dorit să prezentăm câteva noţiuni de bază ale celulei stem, cu implicaţii directe profunde atât pentru morfopatologia locală cât şi pentru tratament. Tipul de diviziune (simetrică ori asimetrică), precum şi moleculele ori citochinele care coordonează mobilitatea celulei în torentul sangvin sunt doar câteva dintre factorii care pot influenţa terapia cancerului colorectal în viitorul apropiat.
Correspondig author: C. TOMULEASA, MD Department of Immunology, “Ion Chiricuţa” Oncology Institute “Iuliu Haţieganu” University of Medicine and Pharmacy 34–35, Republicii Str. 400015, Cluj-Napoca, Romania
REFERENCES
1. FERLAY J., AUTIER P., BONIOL M., HEANUE M., COLOMBET M., BOYLE P., Estimates of the cancer incidence and mortality in Europe in 2006. Ann Oncol.,2007; 18 (3): 581–592.
2. KANAVOS P., SCHURER W., The dynamics of colorectal cancer management in 17 countries. Eur J Health Econ 2010; 10 (Suppl 1):S115–S129.
3. VERDECCHIA A., FRANCISCI S., BRENNER H. et al., Recent cancer survival in Europe: a 2000-02 period analysis of EUROCARE-4 data. Lancet Oncol 2007; 8 (9): 784–796.
4. COMPTON C.C., GREENE F.L., The staging of colorectal cancer: 2004 and beyond. CA Cancer J Clin 2004; 54: 295–308. 5. ZLOBEC I., LUGLI A., Invasive front of colorectal cancer: Dynamic interface of pro-/anti-tumor factors. World J Gastroenterol
2009; 15 (47): 5898–5906. 6. TOURNIGAND C., ANDRÉ T., ACHILLE E. et al., FOLFIRI followed by FOLFOX6 or the reverse sequence in advanced
colorectal cancer: a randomized GERCOR study. J Clin Oncol 2004; 22: 229–237. 7. HURWITZ H., FEHRENBACHER L., NOVOTNY W. et al., Bevacizumab plus irinotecan, fluorouracil and leucovorin for
metastatic colorectal cancer. N Engl J Med 2004; 350: 2335–2342. 8. 8.SALTZ L.B., CLARKE S., DIAZ-RUBIO E. et al., Bevacizumab in combination with oxaliplatin-based chemotherapy as first-
line therapy in metastatic colorectal cancer: a randomized phase III study. J Clin Oncol 2008; 26: 2013–2019. 9. VAN CUTSEM E., KÖHNE C.H., HITRE E. et al., Cetuximab and chemotherapy as initial treatment for metastatic colorectal
cancer. N Engl J Med 2009; 360: 1408–1417. 10. NAGY V.M., Updating the management of rectal cancer. J Gastrointestin Liver Dis 2008; 17 (1): 69–74. 11. BARKER N., VAN DE WETERING M., CLEVERS H., The intestinal stem cell. Genes Dev 2008; 22: 1856–1864. 12. JONES S., CHEN W.D., PARMIGIANI G. et al., Comparative lesion sequencing provides insights into tumor evolution. Proc
Natl Acad Sci USA 2008; 105: 4283–4288. 13. BOMAN B.M., FIELDS J.Z., CAVANAUGH K.L., GUETTER A., RUNQUIST O.A., How dysregulated colonic crypt
dynamics cause stem cell overpopulation and initiate colon cancer. Cancer Res 2008; 68 (9): 3304–3313. 14. FEARON E.R., VOGELSTEIN B., A genetic model for colorectal tumorigenesis. Cell 1990; 61 (5):759–767. 15. CHOI D., LEE H.W., HUR K.Y. et al., Cancer stem cell markers CD133 and CD24 correlate with invasiveness and
differentiation in colorectal adenocarcinoma. World J Gastroenterol 2009; 15 (18): 2258–2264. 16. MORI Y., YIN J., SATO F. et al., Identification of genes uniquely involved in frequent microsatellite instability colon
carcinogenesis by expression profiling combined with epigenetic scanning. Cancer Res 2004; 64: 2434–2438. 17. BAYLIN S.B., Stem cells, cancer and epigenetics (October 31, 2009), StemBook, ed. The Stem Cell Research Community,
StemBook, doi/10.3824/stembook.1.50.1, http://www.stembook.org. 18. PUPA S.M., MÉNARD S., FORTI S., TAGLIABUE E., New insights into the role of extracellular matrix during tumor onset
and progression. J Cell Physiol 2002; 192: 259–267. 19. NASH J.F., Equilibrium Points in N-Person Games. Proc Natl Acad Sci USA 1950; 36 (1): 48–49. 20. VINCENT T.L., GATENBY R.A., An evolutionary model for initiation, promotion, and progression in carcinogenesis. Int
J Oncol 2008; 32 (4): 729–737.

C. Tomuleasa et al. 8 196
21. BASANTA D., SIMON M., HATZIKIROU H., DEUTSCH A., Evolutionary game theory elucidates the role of glycolysis in glioma progression and invasion. Cell Prolif 2008; 41: 980–987.
22. STRAND D.W., FRANCO O.E., BASANTA D., ANDERSON A.R.A., HAYWARD S.W., Perspectives on tissue interactions in development and disease. Curr Mol Med 2010.
23. TSE J.C., KALLURI R., Mechanisms of metastasis: epithelial-to-mesenchymal transition and contribution of tumor microenvironment. J Cell Biochem 2007; 101: 816–829.
24. DALERBA P., DYLLA S.J., PARK I.K. et al., Phenotypic characterization of human colorectal cancer stem cells. Proc Natl Acad Sci U S A 2007;104: 10158–10163.
25. RICCI-VITIANI L., LOMBARDI D.G., PILOZZI E. et al., Identification and expansion of human colon-cancer initiating cells. Nature 2007; 445: 111–115.
26. POLYAK K., HAHN W.C., Roots and stems: stem cells in cancer. Nat Med 2006; 12: 296–300. 27. BALLINGER A.B., ANGGIANSAH C., Colorectal cancer. BMJ 2007; 335: 715–718. 28. MAREEL M., LEROY A., Clinical, cellular, and molecular aspects of cancer invasion. Physiol Rev 2003; 83: 337–376. 29. SUBRAMANIAM V., GARDNER H., JOTHY S., Soluble CD44 secretion contributes to the acquisition of aggressive tumor
phenotype in human colon cancer cells. Exp Mol Pathol 2007; 83: 341–346. 30. MURPHY P.M., Chemokines and the molecular basis of cancer metastasis. N Engl J Med 2001; 345: 833–835. 31. DUFFY M.J., VAN DALEN A., HAGLUND C., HANSSON L., HOLINSKI-FEDER E., KLAPDOR R. et al., Tumour markers
in colorectal cancer: European group on tumour markers (EGTM) guidelines for clinical use. Eur J Cancer 2007, 43: 1348–1360. 32. OGINO S., BRAHMANDAM M., CANTOR M., NAMGYAL C., KAWASAKI T., KIRKNER G. et al., Distinct molecular
features of colorectal carcinoma with signet ring cell component and colorectal carcinoma with mucinous component. Mod Pathol 2006; 19 (1): 59–68.
33. DEBRUYNE P.R., BRUYNEEL E.A., KARAGUNI I.M., LI X., FLATAU G., MÜLLER O. et al., Bile acids stimulate invasion and haptotaxis in human colorectal cancer cells through activation of multiple oncogenic signaling pathways. Oncogene 2002; 21: 6740–6750.
34. ZEELENBERG I.S., RUULS-VAN STALLE L., ROOS E., The chemokine receptor CXCR4 is required for outgrowth of colon carcinoma micrometastases. Cancer Res 2003; 63: 3833–3839.
35. KOSHIBA T., HOSOTANI R., MIYAMOTO Y. et al., Expression of stromal cell-derived factor 1 and CXCR4 ligand receptor system in pancreatic cancer: a possible role for tumor progression. Clin Cancer Res 2000; 6: 3530–3535.
36. TAICHMAN R.S., COOPER C., KELLER E.T. et al., Use of the stromal cell-derived factor-1/CXCR4 pathway in prostate cancer metastasis to bone. Cancer Res 2002; 62: 1832–1837.
37. LIANG Z., YOON Y., VOTAW J. et al., Silencing of CXCR4 blocks breast cancer metastasis. Cancer Res 2005; 65: 967–971. 38. OTTAIANO A., FRANCO R., AIELLO TA. et al., Overexpression of both CXC chemokine receptor 4 and vascular endothelial
growth factor proteins predicts early distant relapse in stage II–III colorectal cancer patients. Clin Cancer Res., 2006, 12: 2795–2803. 39. KIM J., TAKEUCHI H., LAM S.T. et al., Chemokine receptor CXCR4 expression in colorectal cancer patients increases the
risk for recurrence and for poor survival. J Clin Oncol., 2005, 23: 2744–2753. 40. SCHIMANSKI C.C., SCHWALD S., SIMIANTONAKI N. et al., Effect of chemokine receptors CXCR4 and CCR7 on the
metastatic behavior of human colorectal cancer. Clin Cancer Res., 2005, 11: 1743–1750. 41. EMAMI K.H., NGUYEN C., MA H. et al., A small molecule inhibitor of beta-catenin/CREB-binding protein transcription. Proc
Natl Acad Sci USA 2004; 101: 12682–12687. 42. TOMULEASA C., SORITAU O., POP T. et al., Arsenic trioxide plus cisplatin/ interferon α-2b/ doxorubicin/ capecitabine in
vitro combination chemotherapy for hepatocellular carcinoma. J Dig Dis 2010. 43. JIN L., HOPE K.J., ZHAI Q., SMAJDA-JOFFE F., DICK J.E., Targeting of CD44 eradicates human acute myeloid leukemic
cells. Nat Med 2006; 12: 1167–1174. 44. TODARO M., ALEA M.P., DI STEFANO A.B. et al., Colon cancer stem cells dictate tumor growth and resist cell death by
production of interleukin-4. Cell Stem Cell 2007; 1: 389–402. 45. YU Y., KANWAR S.S., PATEL B.B., NAUTIYAL J., SARKAR F.H., MAJUMDAR A.P.N., Elimination of colon cancer stem-
like cells by the combination of curcumin and FOLFOX. Transl Oncol 2009; 2: 321–328. 46. ABRAHAM J.M., CHENG Y., HAMILTON J.P. et al., Generation of small 32P-labeled peptides as a potential approach to
colorectal cancer therapy. PloS One 2008; 3 (6): e2508–e2514. 47. KOGA S., HIROHATA S., KONDO Y. et al., A novel telomerase-specific gene therapy: gene transfer of caspase-8 utilizing the
human telomerase catalytic subunit gene promoter. Hum Gene Ther 2000; 11: 1397–1406. 48. KOMATA T., KANZAWA T., KONDO Y., KONDO S., Telomerase as a therapeutic target for malignant gliomas. Oncogene
2002; 21: 656–663. 49. GALANIS E., HARTMANN L.C., CLIBY W.A. et al., Phase I trial of intraperitoneal administration of an oncolytic measles
virus strain engineered to express carcinoembryonic antigen for recurrent ovarian cancer. Cancer Res 2010; 70 (3): 875–882. 50. MSAOUEL P., DISPENZIERI A., GALANIS E., Clinical testing of engineered oncolytic measles virus strains in the treatment
of cancer: an overview. Curr Opin Mol Ther 2009; 11 (1): 43–53. 51. IVY S.P., WICK J.Y., KAUFMAN B.M., An overview of small-molecule inhibitors of VEGFR signaling. Nat Rev Clin Oncol
2009; 6 (10): 569–579. 52. MATSUSSUE R., KUBO H., HISAMORI S. et al., Hepatic stellate cells promote liver metastasis of colon cancer cell by the
action of SDF-1/CXCR4 axis. Ann Surg Oncol 2009; 16 (9): 2645–2653.
Received August 10, 2011

Glutathione Reductase Levels in Patients with Unstable Angina
VIOLETA ŞAPIRA1,3, INIMIOARA MIHAELA COJOCARU2,3, GABRIELA SOCOLIUC3, GABRIELA LILIOS1, M. GRIGORIAN1, ELVIRA CRAIU1, M. COJOCARU4
1 “Ovidius” University, Faculty of Dental Medicine and Faculty of General Medicine, Constanţa, Romania 2 “Carol Davila” University of Medicine and Pharmacy, Bucharest
3 Department of Neurology, “Colentina” Clinical Hospital, Bucharest 4 “Titu Maiorescu” University, Faculty of Medicine, Bucharest, Romania
Experimental evidence suggests that free-radical damage and antioxidant defense may play an important role in the pathogenesis of coronary heart disease. We have examined the association between plasmatic glutathione reductase (GR) levels and the prognosis of patients with unstable angina. We have evaluated 37 patients, under the age of 75, diagnosed with unstable angina and 19 healthy volunteers. The patients were divided into two groups: the first group – 10 patients with unstable angina with readmission in the following 6 months – and the second group – 27 patients with unstable angina and favourable evolution. GR was measured in dynamics during hospitalization period. After discharge, the patients were monitored and the following data were recorded: months of follow-up, death due to cardiovascular cause and onset of major cardiovascular events. In patients with unstable angina there was a statistically significant higher increase of GR on admission to the values of the control group (p < 0.0001). Subsequently, plasmatic levels begin to decline, so that at discharge, the GR is similar to the control group. Plasmatic levels of GR were statistically significantly lower in patients with unstable angina without cardiovascular event than in patients with readmission in the following months (p < 0.05). In conclusion, patients who experienced unstable angina and without cardiovascular events during follow-up had lower GR plasmatic levels and that GR activity was an independent predictor of cardiovascular events during follow-up.
Key words: unstable angina, oxidative stress, glutathione reductase (GR).
Cardiovascular disease, especially coronary artery disease, is responsible for the highest mortality rate in Romania [1].
Oxidative stress plays a major role in initiation, propagation and rupture of atherosclerotic plaque. The condition of oxidative stress is an im-balance in the rate at which the intracellular content of reactive oxygen species (ROS, free radicals) increases relative to the capacity of the cell to eliminate free radicals [2][3]. Oxidative stress alters normal endothelial function, supporting proinflam-matory, prothrombic, proliferative and vasoconstrictor mechanism that support the atherogenic process.
Thus measuring oxidative stress by various markers can predict the development of various future catastrophic events like myocardial infarction, stroke, etc., since cardiovascular diseases are emerging as the major cause of morbidity and mortality and their relation with the oxidative stress is the near emerging concept. Natural antioxidant
mechanisms of the human body include enzymes like superoxide dismutase (SOD), glutathione peroxidase (GPx), glutathione reductase (GR) which can react with various free radicals and detoxify them [3].
Glutathione-reductase is a major antioxidant factor that plays an important role in the develop-ment of the redox-cycle. Glutathione-reductase is mediating the transformation of oxidified glutathione into reduced glutathione maintaining adequate levels of cellular glutathione, involved in a large number of reactions, resulting in several biochemical com-pounds that are part of essential cellular compounds, or are participants in the development of cellular metabolic processes.
We have examined the association between GR serum levels and the prognosis of patients with unstable angina. GR is responsible for the existence of glutathione (GSH) molecule, a crucial antioxidant against oxidative stress reagents.
ROM. J. INTERN. MED., 2011, 49, 3, 197–201

Violeta Şapira et al. 2 198
MATERIAL AND METHODS
We have evaluated 37 patients, age under 75, consequently hospitalized in the Cardiology Clinic of Emergency Clinic Hospital of Constanta, during May 2008 – May 2009, diagnosed with unstable angina (UA) and 19 healthy volunteers (without cardiovascular disorders, hypercholesterolemia, diabetes and non-smoking), sex- and age-matched – control group.
The patients were informed about the study protocol and a written consent was obtained from each patient. All the patients were diagnosed and evaluated by the same clinical and paraclinical protocol: medical history, physical examination, 12-lead electrocardiography, biochemical analyses.
The patients were divided into two groups: the first group – 10 patients with unstable angina with readmission in the following 6 months and the second group – 27 patients with unstable angina with favourable evolution.
Glutathione reductase activity was measured over a fixed time: T1 – in the first 24 hours after hospital admission, T2 – at 48 hours and T3 – at discharge. After discharge, the patients were monitored by means of a telephone survey, a personal interview, a chart consultation or any other combination of these methods. The following data was recorded: months of follow-up, death due to cardiovascular cause and onset of major cardio-vascular events (MACEs) defined as cardiac death, readmission with acute coronary syndrome or the need for coronary revascularization.
Plasma GR activity was determined using colorimetric method [4], a kit provided by Randox Laboratories Ltd. having the number GR2368 from the notebook. The principle of the method is based on the reaction in which GR catalyses the reduction of glutathione disulfide (GSSG) in the presence of NADPH, which is oxidised to NADP+.
NADPH + H+ + GSSG →GR NADP+ + 2 GSH,
where GSH – reduced glutathione
The decrease of absorbance at 340 nm is measured using Eppendorff ECOM 6122 analyzer.
All data are presented as the mean and standard deviation (SD), continuous data analyzed using Student test for independent samples. The hazard ratio and their 95 percent confidence intervals are reported. The p-value is two-sided; a
p-value of less 0.05 was considered to indicate statistical significance.
RESULTS AND DISCUSSION
The study’s results are presented as tables and graphs.
In patients with unstable angina, it is observed an increase, that is statistically significant, of GR at the moment of admission in hospital (Table I, Fig. 1). Afterwards, the plasmatic level is decreasing, so that at the moment of discharge the level of GR is similar to that of the control group.
Considering patients with unstable angina and unfavourable evolution, the plasmatic level of GR is significantly increased from the moment of admission, and even during hospitalization, the plasmatic levels are starting to decrease, so that at discharge the values remain up-raised significantly compared to that of the control group (Table II, Fig. 2).
On the contrary, in patients with unstable angina and favourable evolution, the increased levels at admission in hospital decrease rapidly during hos-pitalization so that at discharge after hospitalization the level of GR is similar with that of the control group (Table III).
We notice out of Table IV that the plasmatic levels of GR in patients with unstable angina and unfavourable evolution is elevated as compared to the values recorded in patients with favourable evo-lution, at moments T2 and T3 of the admission in hospital.
Glutathione reductase catalyses the reduction of oxidized GSSG to GSH. Cysteinyl residue of GSH offers a nucleophilic thiol, which is important in the detoxification of electrophilic mobilities and meta-bolically produced oxidizing agents and GSH is a substrate for the enzyme GPx and glutathione S-transferase. GSH is converted to GSSG and GSSG is reduced back to GSH by an NADPH dependent enzyme GR [2]. In the present study GR levels were found to be significantly increased in all the groups when compared with group control.
Antioxidant enzyme activity changes rapidly during an acute coronary event, with increased production of reactive oxygen species and depressed antioxidant reserves in the first 6–12 hours [5], up- regulation of enzyme activity 1–2 days after onset
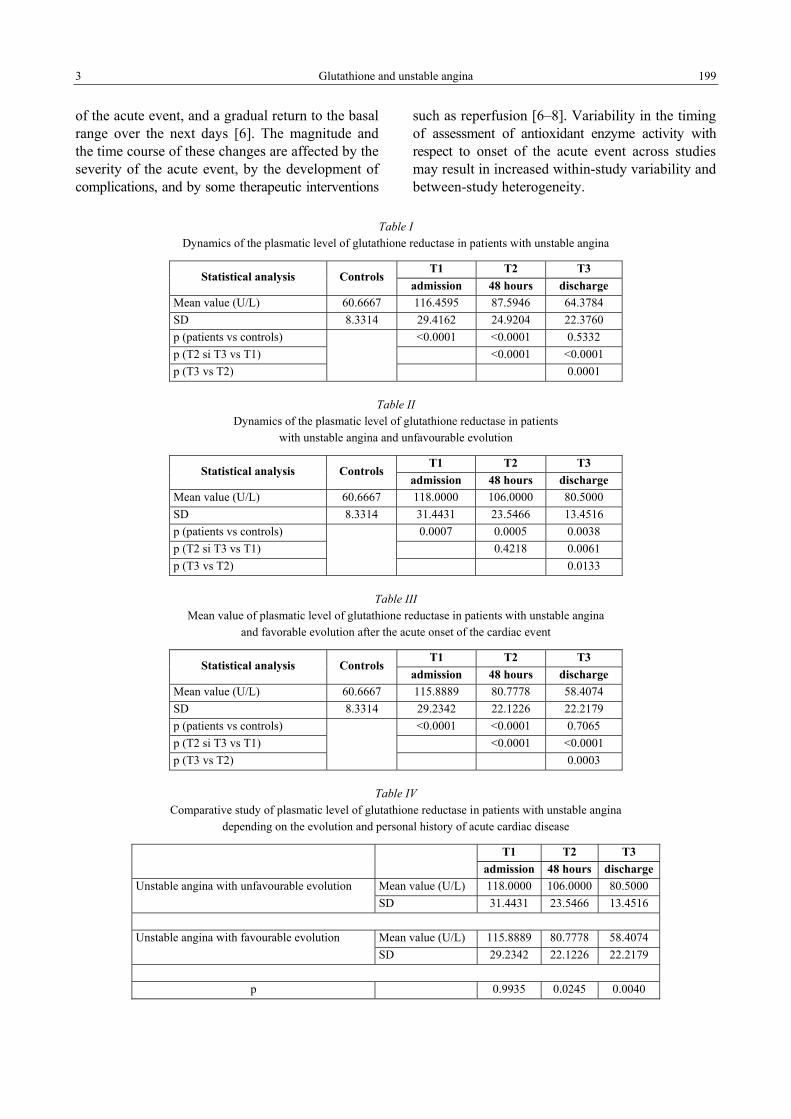
3 Glutathione and unstable angina 199
of the acute event, and a gradual return to the basal range over the next days [6]. The magnitude and the time course of these changes are affected by the severity of the acute event, by the development of complications, and by some therapeutic interventions
such as reperfusion [6–8]. Variability in the timing of assessment of antioxidant enzyme activity with respect to onset of the acute event across studies may result in increased within-study variability and between-study heterogeneity.
Table I Dynamics of the plasmatic level of glutathione reductase in patients with unstable angina
T1 T2 T3 Statistical analysis Controls
admission 48 hours discharge Mean value (U/L) 60.6667 116.4595 87.5946 64.3784 SD 8.3314 29.4162 24.9204 22.3760 p (patients vs controls) <0.0001 <0.0001 0.5332 p (T2 si T3 vs T1) <0.0001 <0.0001 p (T3 vs T2) 0.0001
Table II Dynamics of the plasmatic level of glutathione reductase in patients
with unstable angina and unfavourable evolution
T1 T2 T3 Statistical analysis Controls
admission 48 hours discharge Mean value (U/L) 60.6667 118.0000 106.0000 80.5000 SD 8.3314 31.4431 23.5466 13.4516 p (patients vs controls) 0.0007 0.0005 0.0038 p (T2 si T3 vs T1) 0.4218 0.0061 p (T3 vs T2) 0.0133
Table III Mean value of plasmatic level of glutathione reductase in patients with unstable angina
and favorable evolution after the acute onset of the cardiac event
T1 T2 T3 Statistical analysis Controls
admission 48 hours discharge Mean value (U/L) 60.6667 115.8889 80.7778 58.4074 SD 8.3314 29.2342 22.1226 22.2179 p (patients vs controls) <0.0001 <0.0001 0.7065 p (T2 si T3 vs T1) <0.0001 <0.0001 p (T3 vs T2)
0.0003
Table IV Comparative study of plasmatic level of glutathione reductase in patients with unstable angina
depending on the evolution and personal history of acute cardiac disease
T1 T2 T3 admission 48 hours discharge
Mean value (U/L) 118.0000 106.0000 80.5000 Unstable angina with unfavourable evolution SD 31.4431 23.5466 13.4516
Mean value (U/L) 115.8889 80.7778 58.4074 Unstable angina with favourable evolution SD 29.2342 22.1226 22.2179
p 0.9935 0.0245 0.0040

Violeta Şapira et al. 4 200
0
20
40
60
80
100
120
T1 - admission T2 - 48 hours T3 - discharge
U/L
Controls Patients Fig. 1. Glutathione reductase levels in patients with unstable angina as compared to control group.
0
20
40
60
80
100
120
T1 - admission T2 - 48 hours T3 - discharge
U/L
Controls Patients with readmission Patiens without readmission Fig. 2. Glutathione reductase levels in patients with unstable angina depending on the evolution
and personal history of acute cardiac disease.
CONCLUSION
The reactive oxygen species (ROS), including free radicals, are involved in cardiovascular disease. The ROS are common by-products of many oxidative biochemical and physiological
processes. These results may be related to reflect oxidative injury in patients with unstable angina.
Patients who experienced unstable angina and without cardiovascular events during follow-up had lower GR serum levels and that GR activity was an independent predictor of events during follow-up.

5 Glutathione and unstable angina 201
Dovezile experimentale sugerează că efectul nociv al radicalilor liberi şi mecanismele de apărare antioxidantă pot juca un rol important în patogenia bolilor coronariene. A fost examinată asocierea dintre nivelurile plasmatice ale glutation reductazei (GR) şi prognosticul pacienţilor cu angină instabilă. Au fost evaluaţi 37 pacienţi, cu vârsta sub 75 de ani, diagnosticaţi cu angină instabilă şi 19 subiecţi sănătoşi. Pacienţii au fost împărţiţi în două grupe: primul grup – 10 pacienţi cu angină instabilă, cu reinternare în următoarele 6 luni – şi al doilea grup – 27 de pacienţi cu angină instabilă şi evoluţie favorabilă. GR a fost măsurată în dinamică, pe durata spitalizării. După externare, pacienţii au fost monitorizaţi şi au fost înregistrate următoarele date: perioada de monitorizare, decesul prin cauze cardiovasculare şi noi evenimente majore cardiovasculare. Pacienţii cu angină instabilă au prezentat creşterea înalt semnificativ statistic a GR la internare faţă de valorile determinate la grupul martor (p < 0,0001). Ulterior, nivelul seric începe să scadă, astfel că la externare, nivelul GR este similar cu al grupului martor. Concentraţiile plasmatice ale GR au fost semnificativ statistic mai mici la pacienţii cu angină instabilă fără evenimente cardiovasculare comparativ cu pacienţii cu reinternare (p < 0,05). În concluzie, pacienţii care au prezentat angină instabilă fără evenimente cardiovasculare în perioada de monitorizare au prezentat niveluri serice ale GR mai scăzute, iar activitatea GR a fost un factor de predicţie independent pentru evenimentele cardiovasculare în perioada de monitorizare.
Corresponding author: Senior lecturer Violeta Şapira MD, PhD “Ovidius” University, Faculty of Dental Medicine, Constanţa, Romania
E-mail: [email protected]
REFERENCES
1. TATU-CHIŢOIU G., ARSENESCU-GEORGESCU C., BABEŞ C., CINTEZĂ M., CRAIU E., DATCU D.M. et al., Raportul registrului român pentru infarctul miocardic acut cu supradenivelare de ST (RO-STEMI) (1997–2008). Rev. Română de Cardiologie, 2009, XXIX; 3: 182–206.
2. HARRISON D.G., Cellular and molecular mechanisms of endothelial cells dysfunction. J. Clin. Invest., 1997, 100: 2153–2157. 3. JAWALEKAR S.L., KULKARNI U.J., SURVE V.T., DESHMUKH Y.A., Role of oxidants and anti oxidants in patients with
cardiovascular diseases. Asian J. Med. Sci., 2010, 2 (4): 181–184. 4. GOLDBERG D.M., SPOONER R.J., Glutathione reductase. In: Bergmeyer H.U., ed. Methods in Enzymology, 1983, vol. 3,
Basel: Verlag Chemie: 258–265. 5. GIORDANO F.J., Oxygen, oxidative stress, hypoxia, and heart failure. J Clin Invest. 2005; 115 (3): 500–508. 6. HORIUCHI M., TSUTSUI M., TASAKI H. et al., Upregulation of vascular extracellular superoxide dismutase in patients with
acute coronary syndromes. Arterioscler Thromb Vasc Biol. 2004; 24 (1): 106–111. 7. BÉARD T., CARRIÉ D., BOYER M.J. et al., Production of oxygen free radicals in myocardial infarction treated by
thrombolysis. Analysis of glutathione peroxidase, superoxide dismutase and malondialdehyde [in French]. Arch Mal Coeur Vaiss. 1994; 87 (10): 1289–1296.
8. ZACHARA B.A., UKLEJA-ADAMOWICZ M., NARTOWICZ E. et al., Increased plasma glutathione peroxidase activity in patients with acute myocardial infarction. Med Sci Monit. 2001; 7 (3): 415–420.
Received July 22, 2011

Elements of Renal Injury in Patients with Varicose Ulcer. Preliminary Study
SILVIA VELCIOV 1, GH. GLUHOVSCHI 1, V. FEIER2, VIRGINIA TRANDAFIRESCU1, LIGIA PETRICA1, CRISTINA GLUHOVSCHI1, F. BOB1, GH. BOZDOG1, FLORICA GADALEAN1, CARMEN FLORESCU2,
MARIA BOBU1, ANDREEA CHILIBAN1
1Nephrology Department, 2Dermatology Department, University of Medicine and Pharmacy, Timişoara, Romania
The kidney may be affected in the processes of microbial, viral, parasitic infections. Knowledge of renal disease during chronic infection, with a different location than the throat, is of particular importance for the practicing physician for the detection and prevention of impaired renal function.
Chronic kidney disease recovered in the early stages can prevent the progression of renal function decline.
We studied a total of 85 patients with varicose ulcers with a mean age of 66.78 ± 12.09 years, hospitalized in the Clinic of Dermatology and a control group consisting of 110 apparently healthy individuals.
Urinary abnormalities have been detected in 26 (30%) of patients studied. GFR < 60 ml / min have been detected in 14 (17%) of patients studied. CRF stage II have been detected in 36 (42%) of patients studied. We detected recurrent varicose ulcer in 2 (2%) of patients studied. In two (2%) of patients
during hospitalization we found a decrease in GFR by 15 and 12 ml/min, accompanied by an increase in serum creatinine from 0.7 mg % to 1 mg % in one patient and in another patient from 1.5 mg % to 2 mg %.
Urinary abnormalities detected in patients with both acute and recurrent erysipelas warn about renal impairment and the need for monitoring of the renal patients with varicose ulcers.
Key words: varicose ulcer, proteinuria, hematuria, glomerulonephritis, CRD.
Venous ulcers are chronic inflammations. Chronic ulcers often affect the legs, in 80% of cases in association with chronic venous insufficiency. Venous ulcers affect the lower half of the leg. Although they are sometimes large, venous ulcers are superficial compared with the other types. Stasis ulcers have a wet granular base with irregular edges. Tissues near these cancers show signs of stasis dermatitis. Venous ulcers can sometimes become infected. Gram-positive germs that are more frequently involved: Staphylococcus aureus methicillin-sensitive and methicillin-resistant streptococcus, pneumo-coccus) and gram negative (Enterobacter, Serratia, Citrobacter, Acinetobacter, Providencia, Proteus, Morganella) [1]. Gram-negative germs are more frequently detected in patients with chronic ulcers. In chronic ulcers most commonly involved is Pseudomonas, followed by Staphylococcus aureus resistant to methicillin.
The streptococcal species were isolated from patients with acute ulcers. Streptococcal skin infections have been incriminated in the production
of acute glomerulonephritis. There have been described even acute glomerulonephritis epidemics as a consequence of streptococcal skin infections. In the production of skin infections not only group A streptococci are involved but also other types of streptococci. Even if streptococcus group A β hemolytic (pyogenes) is the usual agent, other agents, such as group B streptococci, C, G, and a variety of other bacteria may be the basis of skin infections. Chronic infections may be associated with glomerular damage.
Glomerulonephritis has been described in association with chronic infection of prosthetic material permanently implanted in the circulatory system [2].
Griffin et al. described proliferative glomerulo-nephritis with acute renal failure secondary to osteomyelitis and staphylococcal infection [3].
There has also been described glomerulo-nephritis associated with staphylococcal infections caused by Staphylococcus aureus methicillin-resistant [4]. Koyama described cases of glomerular nephro-
ROM. J. INTERN. MED., 2011, 49, 3, 202–206
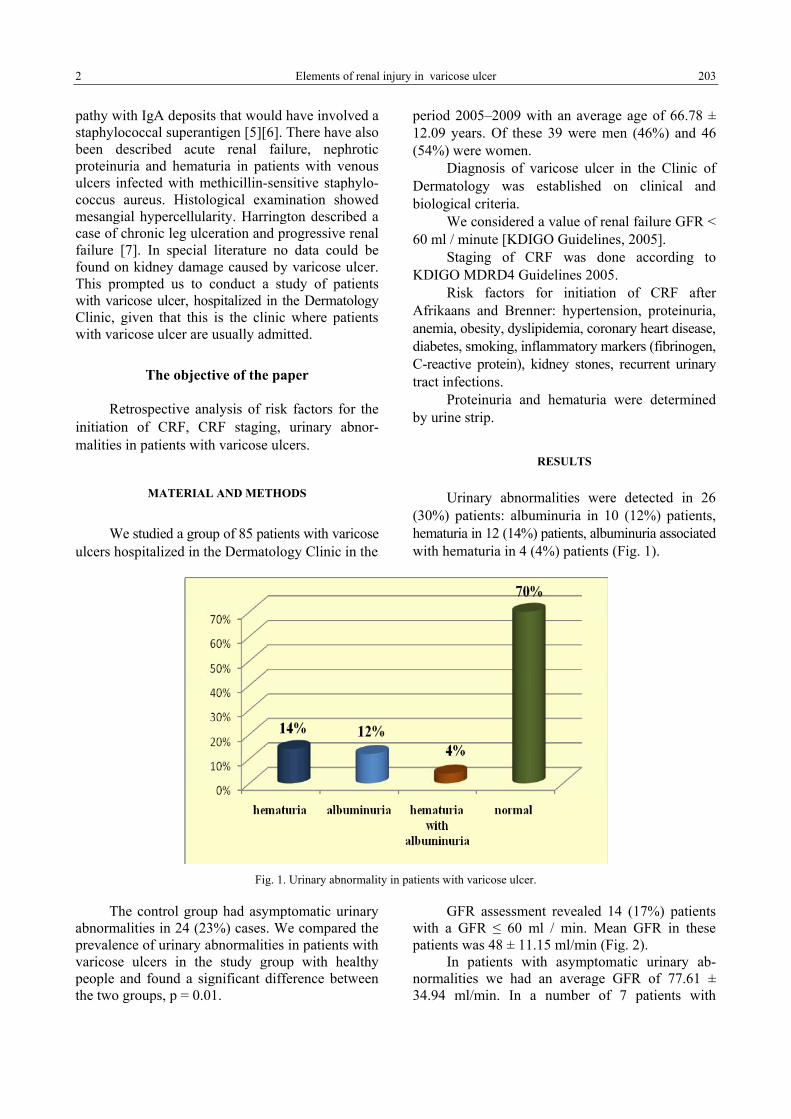
2 Elements of renal injury in varicose ulcer 203
pathy with IgA deposits that would have involved a staphylococcal superantigen [5][6]. There have also been described acute renal failure, nephrotic proteinuria and hematuria in patients with venous ulcers infected with methicillin-sensitive staphylo-coccus aureus. Histological examination showed mesangial hypercellularity. Harrington described a case of chronic leg ulceration and progressive renal failure [7]. In special literature no data could be found on kidney damage caused by varicose ulcer. This prompted us to conduct a study of patients with varicose ulcer, hospitalized in the Dermatology Clinic, given that this is the clinic where patients with varicose ulcer are usually admitted.
The objective of the paper
Retrospective analysis of risk factors for the initiation of CRF, CRF staging, urinary abnor-malities in patients with varicose ulcers.
MATERIAL AND METHODS
We studied a group of 85 patients with varicose ulcers hospitalized in the Dermatology Clinic in the
period 2005–2009 with an average age of 66.78 ± 12.09 years. Of these 39 were men (46%) and 46 (54%) were women.
Diagnosis of varicose ulcer in the Clinic of Dermatology was established on clinical and biological criteria.
We considered a value of renal failure GFR < 60 ml / minute [KDIGO Guidelines, 2005].
Staging of CRF was done according to KDIGO MDRD4 Guidelines 2005.
Risk factors for initiation of CRF after Afrikaans and Brenner: hypertension, proteinuria, anemia, obesity, dyslipidemia, coronary heart disease, diabetes, smoking, inflammatory markers (fibrinogen, C-reactive protein), kidney stones, recurrent urinary tract infections.
Proteinuria and hematuria were determined by urine strip.
RESULTS
Urinary abnormalities were detected in 26 (30%) patients: albuminuria in 10 (12%) patients, hematuria in 12 (14%) patients, albuminuria associated with hematuria in 4 (4%) patients (Fig. 1).
Fig. 1. Urinary abnormality in patients with varicose ulcer.
The control group had asymptomatic urinary abnormalities in 24 (23%) cases. We compared the prevalence of urinary abnormalities in patients with varicose ulcers in the study group with healthy people and found a significant difference between the two groups, p = 0.01.
GFR assessment revealed 14 (17%) patients with a GFR ≤ 60 ml / min. Mean GFR in these patients was 48 ± 11.15 ml/min (Fig. 2).
In patients with asymptomatic urinary ab-normalities we had an average GFR of 77.61 ± 34.94 ml/min. In a number of 7 patients with

Silvia Velciov et al. 3 204
asymptomatic urinary abnormalities we detected a GFR < 60ml/min, respectively 45.58 ± 13.12 ml/min.
Assessment of renal function by calculating MDRD GFR revealed four stages of CRF following distribution: stage 1 CRF 35 patients (41%), CRF 36 stage 2 patients (42%), CRF 13 stage 3 patients (16%), stage 4 CRF 1 patient (1%), and stage 5 patients CRF 0. Evaluation of risk factors for CKD revealed: hypertension in 39 (46%) patients, diabetes in 6 (7%) patients, UTI in 11 (13%) patients, proteinuria in 14 (16%) patients, coronary artery
disease 22 (26%) patients, obesity in two (2%) patients, dyslipidemia in three (3%) patients, anemia 3 (3%) patients, fibrinogen increased to 74 (87%) patients, urolithiasis 3 (3%) patients.
Varicose ulcer site was the following: uni-lateral in 82 (96%) patients, bilateral in three (4%) patients.
Distribution depending on the number of ulcers was: single in 78 (92%) patients and multiple in 7 (8%) patients. In a number of two (2%) patients we found readmission for recurrent varicose ulcer.
Fig. 2. Prevalence of patients with eGFR < 60ml/min.
Distribution of patients after ulcer etiology was as follows: venous ulcer in 81 (95%) patients, arterio-venous ulcers in three (4%) patients, a neuropathic ulcer (1%) patient.
They followed local and systemic antibiotic therapy in a total of 63 (74%) patients and only topical antibiotic antibiotic treatment in a total of 22 (26%) patients. Treatment consisted of systemic antibiotic erythromycin in 18 (29%) patients, gentamicin in 11 (17%) patients, Chloramphenicol in 19 (30%) patients, 9 Ciprofloxacin (14%) patients and 6 Augmentin (10%) patients.
Two (2%) of patients during hospitalization found a decrease in GFR by 15 and 12 ml/min, accompanied by an increase in seric creatinine from 0.7 mg % to 1 mg% in one patient and in another patient from 1.5 mg % to 2 mg %.
DISCUSSION
Our study showed urinary abnormalities in patients with varicose ulcer from the Clinics: Dermatology Clinic over a period of 5 years.
The control group of apparently healthy persons had had asymptomatic urinary abnormalities in 25 (23%).
The prevalence of asymptomatic urinary ab-normalities was higher in patients with varicose ulcer and it was higher in patients with erysipelas compared to healthy persons.
Our study evaluating the group of patients with varicose ulcers, skin diseases from the clinic, showed changes in the relationship with urinary pathology, mainly microhematuria and proteinuria. These urinary changes, hematuria and proteinuria fall under asymptomatic urinary abnormalities, a particular form of glomerular disease manifestation.
They were mostly represented by isolated hematuria in 12 (14%) patients and isolated proteinuria in 10 (12%) patients.
The association of hematuria and proteinuria has been found in 4% patients.
There have been cases of glomerulonephritis in relation to chronic bacterial infections. Thus Probst describes cases of patients with chronic bacterial infections (osteomyelitis, infected vascular

4 Elements of renal injury in varicose ulcer 205
prostheses) without endocarditis who developed renal failure accompanied by glomerulonephritis [8].
Tevlin described a case of IgA nephropathy manifested by microscopic hematuria, proteinuria, acute renal failure in a patient with chronic osteo-myelitis. The patient had normal renal function and urine examination without modifications, before the development of osteomyelitis. Complete era-dication of osteomyelitis by amputation resulted in resolution of urinary changes and restitution of renal failure [9].
In our study two (2%) of patients during hospitalization found a decrease in GFR by 15 and 12 ml/min, accompanied by an increase in seric creatinine from 0.7 mg% to 1 mg % in one patient and in another patient from 1.5 mg % to 2 mg%. Acute renal failure has been shown by Probst et al. in a patient with varicose ulcer [8].
Functional impairment was reported in 14 (16%) of patients studied, GFR < 60mL/min. As a cross-section study we did not have any previous data of impairment of renal function for a period of three months for employment in a stage 1 CRD, according to KDIGO MDRD4 2005 Guidelines for chronic kidney disease staging. We detected CRD stage 2 in 36 (42%) of patients studied. We detected only 13 (15%) patients in stage 3 and a single patient in CRD 4 stage. We detected no patient in stage 5 CRD.
In the special literature there have been cases of varicose ulcers in patients with chronic renal failure. Yates described a case of varicose ulcer in a patient with diabetes and chronic renal failure [1].
Perhaps chronic renal failure may contribute to the persistence of chronic bacterial infections in chronic ulcers and the likes of varicose ulcer. Also in chronic renal failure we can describe a patient's elevated inflammatory status. Data from literature shows that varicose ulcer affects adults, but its prevalence is higher in patients aged 60–80 years. In our study group the average age of patients was 66.78 ± 2.09 a year, consistent with the literature data.
Knowledge of CRD and CRD framing stage is very important for antibiotic treatment of ulcers in patients with impaired renal function. These patients require optimal hydration and avoidance of nephrotoxic antibiotics and dosage adjustment based on the degree of renal function impairment.
Moderate hypertension increases the risk for kidney disease in patients without proteinuria, hematuria, or reduced GFR, the risk is clearly in-creased in patients with severe or malignant hypertension (Hannedouche) [10]. We found a correlation between blood pressure and GFR, r = 0.3818.
In the presence of CRF, hypertension is a major progression. Progression rate is even greater than more severe hypertension. Proteinuria is a major risk factor for progression of renal disease. Proteinuria is an even greater degradation rate of renal function. Persistence of proteinuria promotes progression of renal function deterioration (Keane) [11]. Hematuria was present only in 18% patients. Prevalence of proteinuria and hematuria indicates urinary anomalies that could be represented by a glomerular disease in relation to varicose ulcers.
A cross-section study can detect a glomerular disease, but dynamic studies are needed to assess the dynamics and framing of these cases with respect to the urinary abnormalities. The presence of varicose ulcer relapse could lead to repeated and possibly chronic glomerular disease.
This study reveals that the presence of renal failure in patients with varicose ulcers should require a dynamic analysis of these patients. Bridging the presence of urinary abnormalities and renal failure in patients with varicose ulcer is of great importance for the prognosis of these patients.
Patients require an active admittance and a dynamic evaluation of both GFR and urinary ab-normalities.
CONCLUSIONS
Varicose ulcer can be accompanied by glomerular involvement.
The most frequent biological syndrome is represented by asymptomatic urinary abnormalities, isolated hematuria, isolated proteinuria, or hematuria associated with proteinuria. Recurrent varicose ulcer is associated more frequently with asym-ptomatic urinary abnormalities. GFR is also lower in patients with chronic varicose ulcer. Recurrent varicose ulcer can lead to progression of pre-existing glomerular disease.
Rinichiul poate fi afectat în procesele infecţioase microbiene, virale,
parazitare. Cunoaşterea afectării renale din cursul infecţiilor cronice cu altă localizare decât cea faringiană, are o importanţă deosebită pentru medicul practician pentru decelarea acestora şi prevenirea alterării funcţiei renale.

Silvia Velciov et al. 5 206
Boala cronică de rinichi decelată în stadiile iniţiale poate preveni progresia declinului funcţiei renale.
Am studiat un număr de 85 pacienţi cu ulcer varicos cu vârsta medie 66.78 ± 12.09 ani, internaţi în Clinica de Dermatologie precum şi un lot martor constând din 110 persoane aparent sănătoase.
Anomalii urinare am decelat la 26 (30%) dintre pacienţii studiaţi. RFG < 60 ml/min am decelat la 14 (17%) dintre pacienţii studiaţi. BCR stadiul 2 am decelat la 36 (42%) dintre pacienţii studiaţi. Ulcer varicos recidivant am decelat la 2 (2%) dintre pacienţii studiaţi. La 2 (2%) dintre pacienţi pe parcursul spitalizării am constatat o scădere a
RFG cu 15 şi respectiv 12 ml/min, însoţită şi de o creştere a creatininei serice de la 0.7 mg % la 1 mg % la un pacient, iar la alt pacient de la 1.5 mg % la 2 mg %.
Anomaliile urinare decelate atât la pacienţii cu erizipel acut cât şi recidivat atrag atenţia asupra afectării renale în ulcerul varicos precum şi necesitatea monitorizării din punct de vedere renal a pacienţilor cu ulcer varicos.
Corresponding author: Silvia Velciov Nephrology Dept., Univ. of Medicine and Pharmacy Timişoara, Romania E-mail: [email protected]
REFERENCES
1. YATES C., MAY K., HALE T., ALLARD B., ROWLINGS N., FREEMAN A., HARRISON J., McCANN J., WRAIGHT B.P., Wound Chronicity, Inpatient Care, and Chronic Kidney Disease Predispose to MRSA Infection in Diabetic Foot Ulcers, Diabetes Care , 2009, 32 (10): 1907–1909.
2. COLEMAN M., BURNETT J., BARRATT L.J., DUPONT P., Glomerulonephritis associated with chronic bacterial infection of a dacron arterial prosthesis. Clin Nephrol. 1983; 20 (6): 315–20.
3. GRIFFIN M.D., BJORNSSON J., ERICKSON S.B., Diffuse proliferative glomerulonephritis and acute renal failure associated with acute staphylococcal osteomyelitis. J Am Soc Nephrol, 1997; 8: 1633–1639.
4. SATOSKAR A.A., NADASDY G., PLAZA H.A., SEDMAK D., SHIDHAM G., HEBERT L., NADASDY T., Staphylococcus Infection-Associated Glomerulonephritis Mimicking IgA Nephropathy. Clin J Am Soc Nephrol, 2006; 1: 1179–1186.
5. KOYAMA A., KOBAYASHI M., YAMAGUCHI N., YAMAGATA K., TAKANO K., NAKAJIMA M. et al., Glomerulo-nephritis associated with MRSA infection: A possible role of bacterial superantigen. Kidney Int, 1995; 47: 207–216.
6. KOYAMA A., SHARMIN S., SAKURAI H., SHIMIZU Y., HIRAYAMA K., USUI J. et al., Staphylococcus aureus cell envelope antigen is a new candidate for the induction of IgA nephropathy. Kid Int, 2004; 66: 121–1327.
7. HARRINGTON J.T., COLVIN R.B., Case 12-1994 – A 72-Year-Old Man with Chronic Leg Ulceration and Progressive Renal Failure. NEMJ, 1994; 330: 847–854.
8. PROBST W., BLUMBERG A., Glomerulonephritis in chronic bacterial infections. Schweiz Med Wochenschr. 1987; 21; 117 (8): 265–9.
9. TEVLIN M.T., WALL B.M., COOKE C.R., Reversible renal failure due to IgA nephropathy associated with osteomyelitis. Am J Kidney Dis. 1992; 20 (2): 185–8.
10. HANNEDOUCHE T., CHAUVEAU P., KALOU F., ALBOUZE G., LACOUR B., JUNGERS P., Factors affecting progression in advanced chronic renal failure. Clin Nephrol 1993; 39: 312–320.
11. KEANE W.F., Proteinuria: Its clinical importance and role in progressive renal disease. Am J Kidney Dis, 2000; 35: S97–S105.
Received January 25, 2011

Investigating the Use of Specific Cognitive Emotion Regulation Strategies in Response to the Experience of Gingival Bleeding
ALEXANDRINA LIZICA DUMITRESCU1, CARMEN TOMA2, VIORICA LASCU2
1University of Tromsø, Norway 2“Carol Davila” University of Medicine and Pharmacy, Bucharest, Romania
The present study focuses on the extent to which undergraduates use specific cognitive emotion regulation strategies in response to the experience of the gingival bleeding.
Material and Methods. The present study sample consisted of 190 first year dental students. The questionnaire included information about socio-demographic factors, behavioral variables and self-reported oral health status. To measure the specific emotional cognitive strategies, the Cognitive Emotion Regulation Questionnaire (CERQ) was used.
Results. Self-reported gingival bleeding was associated with statistical significant higher values of self-blame and rumination. Participants who evaluated their self-reported gingival condition as poor/very poor scored higher values on rumination, catastrophising and lower on positive reappraisal, when compared with students with excellent gingival condition. Multiple linear regression analyses revealed that presence of gingival bleeding was an independent determinant of self-blame, rumination and putting into perspective. Among participants with positive self-reported gingival bleeding, reason for dental visits was significantly correlated with positive refocusing, planning, positive reappraisal, putting into perspective and catrastrophizing. Positive reappraisal was found to be a mediating variable in the relationship between gingival status and reason for dental visits. Thus, positive reappraisal helps to explain the association between gingival status and reason for dental visits.
Conclusions. Helping patients to challenge these maladaptive cognitive emotion regulation strategies may therefore play an important role on the focus and content of (preventive) oral health behaviour interventions to be developed for patients with gingival and periodontal disease.
Key words: rumination, emotions, self-blame, gingival bleeding.
Emotions have long been viewed as passions that come and go, more or less of their own accord [1]. Emotion regulation refers to the processes by which we influence which emotions we have, when we have them, and how we experience and express them [2]. Although this definition is inherently broad, there is functional utility in distinguishing emotion from emotion regulation. Specifically, strategies individuals use to alter their emotions affect not only their current emotional experience, but also broader emotional, cognitive, and inter-personal functioning [3].
The concept of cognitive emotion regulation can be understood as the cognitive way of managing the intake of emotionally arousing information and refers to the cognitive part of coping. Although the capacity of cognitive emotion regulation is universal, individual differences exist in the specific thoughts or cognitions by means of which people regulate their emotions in response to life experiences. Cognitive emotion regulation is therefore widely assumed to be an important issue with regard to
mental health [4]. In the literature nine con-ceptually different cognitive emotion regulation strategies were distinguished: Self-blame, referring to thoughts of putting the blame of what you have experienced on yourself [example item: “I feel that I am the one to blame for it”); Other-blame, referring to thoughts of putting the blame of what you have experienced on the environment or another person (example item: “I feel that others are to blame for it”); Rumination or focus on thought, referring to thinking about the feelings and thoughts associated with the negative event (example item: “I often think about how I feel about what I have experienced”); Catastrophizing, referring to thoughts of explicitly emphasizing the terror of what you have experienced (example item: “I often think that what I have experienced is the worst that can happen to a person”); Putting into Perspective, referring to thoughts of brushing aside the seriousness of the event/emphasizing the relativity when comparing it to other events (example item: “I tell myself there are worse things in life”);
ROM. J. INTERN. MED., 2011, 49, 3, 207–215

Alexandrina Lizica Dumitrescu et al. 2 208
Positive Refocusing, referring to thinking about joyful and pleasant issues instead of thinking about the actual event (example item: “I think of some-thing nice instead of what has happened”); Positive Reappraisal, referring to thoughts of creating a positive meaning to the event in terms of personal growth (example item: “I think I can learn something from the situation”); Acceptance, referring to thoughts of accepting what you have experienced and resigning yourself to what has happened (example item: “I think that I have to accept that this has happened”) and Planning, referring to thinking about what steps to take and how to handle the negative event (example item: “I think about a plan of what I can do best”) [5][6].
In general, the results suggest that by using cognitive styles such as Rumination, Catastrophizing and Self-blame people may be more vulnerable to emotional problems than others, while other outcomes suggest that by using other styles, such as Positive Reappraisal people may be less vulnerable. These results indicate that important targets for intervention might be found on the basis of cognitive emotion regulation research [4]. A number of recent studies have confirmed the existence of strong relationships between the use of these strategies and emotional problems, depression, anxiety and psychological distress [5–12].
As a large number of papers have indicated that stress, depression and anxiety appear to affect perio-dontal health, shown by more plaque accumulation and gingival inflammation [13][14], the aim of the present study was to evaluate the interrelationship between gingival status, cognitive emotion regulation and oral health behaviours.
METHODS
Sample The subjects of the study were 190 first year
dental students at the University of Medicine and Pharmacy […] who were invited consecutive to this cross-sectional survey using the two anonymous questionnaires, at the beginning of the 2009/2010 academic year. All students selected for the survey answered the questionnaire. A total score was calculated based on the response on each statement. The subjects gave their informed consent to participate in the study. The mean age (S.D.) of medical students was 19.25 (1.26) years old. The percentage of female students was high in the sample (73.7%).
Instruments and measures Data were collected through a Romanian self-
administered questionnaire and the CERQ scale. A structured, anonymous questionnaire was specifically developed for this study and addressed the following: 1. socio-demographic factors (age, gender); 2. per-ceived oral health status (dental health, non-treated caries, extracted teeth, satisfaction by appearance of own teeth, dental pain, gingival condition, gum bleeding); 3. oral health habits (toothbrushing, flos-sing, mouthrinse frequency, dental visiting) [15–17].
To measure the specific cognitive strategies students used in relation to their oral health status, the Cognitive Emotion Regulation Questionnaire (CERQ) was used [11]. The CERQ is a 36-item questionnaire, consisting of the following nine conceptually distinct subscales, each consisting of four items. Items are measured on a 5-point Likert scale ranging from 1 (almost) never) to 5 (almost) always). Individual subscale scores are obtained by summing up the scores belonging to the particular subscale (ranging from 4 to 20). The higher the subscale score, the more a specific cognitive strategy is used. Earlier studies on the CERQ have provided empirical support to the allocation of items to nine subscales by means of principal com-ponent analyses and have shown that the subscales have good internal consistencies, with alphas ranging from 0.67 to 0.90 [2][5][11]. In the present study, the subscales also appear to have good internal consistencies, with alphas ranging from 0.66 to 0.87 (Table I). As the Acceptance subscale had a Cronbach’s alpha of 0.39 it was removed from further study analysis. Table I also displays the means and standard deviations of the CERQ-sub-scales. It was revealed that the theoretically more adaptive cognitive strategies (such as Positive Refocusing, Positive Reappraisal, Planning and Putting into Perspective) were reported to have been used more often than the less adaptive strategies (such as Catastrophizing, Self-blame and Other-blame). The highest mean scores were found for the reporting of the cognitive strategies of ‘Planning’ and ‘Positive Reappraisal’. ‘Catas-trophizing’ and ‘Other-blame’ were reported to have been used as cognitive strategy less often.
Statistical analysis Descriptive statistics and statistical analyses
were performed with computerized statistical package (SPSS 17.0, Inc., Chicago, USA) software. The internal consistency of the CERQ subscales was examined using Cronbach's α. Descriptive statistics were used on all variables. We assessed
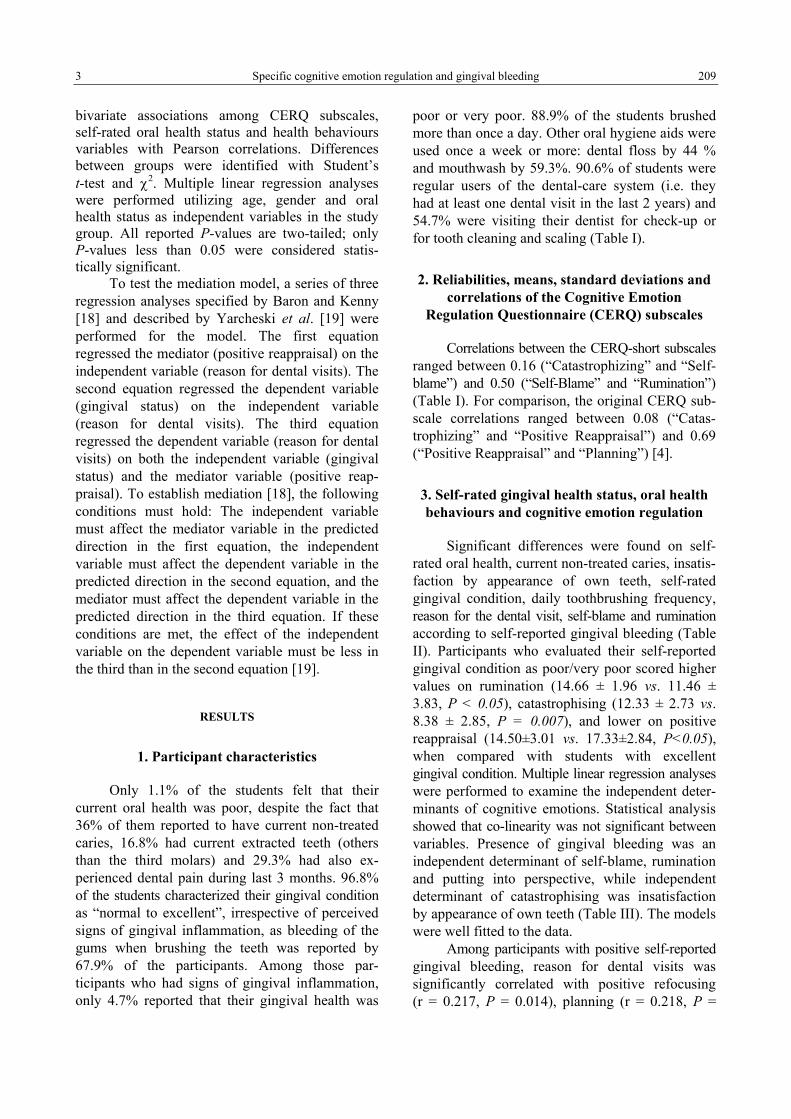
3 Specific cognitive emotion regulation and gingival bleeding 209
bivariate associations among CERQ subscales, self-rated oral health status and health behaviours variables with Pearson correlations. Differences between groups were identified with Student’s t-test and χ2. Multiple linear regression analyses were performed utilizing age, gender and oral health status as independent variables in the study group. All reported P-values are two-tailed; only P-values less than 0.05 were considered statis-tically significant.
To test the mediation model, a series of three regression analyses specified by Baron and Kenny [18] and described by Yarcheski et al. [19] were performed for the model. The first equation regressed the mediator (positive reappraisal) on the independent variable (reason for dental visits). The second equation regressed the dependent variable (gingival status) on the independent variable (reason for dental visits). The third equation regressed the dependent variable (reason for dental visits) on both the independent variable (gingival status) and the mediator variable (positive reap-praisal). To establish mediation [18], the following conditions must hold: The independent variable must affect the mediator variable in the predicted direction in the first equation, the independent variable must affect the dependent variable in the predicted direction in the second equation, and the mediator must affect the dependent variable in the predicted direction in the third equation. If these conditions are met, the effect of the independent variable on the dependent variable must be less in the third than in the second equation [19].
RESULTS
1. Participant characteristics
Only 1.1% of the students felt that their current oral health was poor, despite the fact that 36% of them reported to have current non-treated caries, 16.8% had current extracted teeth (others than the third molars) and 29.3% had also ex-perienced dental pain during last 3 months. 96.8% of the students characterized their gingival condition as “normal to excellent”, irrespective of perceived signs of gingival inflammation, as bleeding of the gums when brushing the teeth was reported by 67.9% of the participants. Among those par-ticipants who had signs of gingival inflammation, only 4.7% reported that their gingival health was
poor or very poor. 88.9% of the students brushed more than once a day. Other oral hygiene aids were used once a week or more: dental floss by 44 % and mouthwash by 59.3%. 90.6% of students were regular users of the dental-care system (i.e. they had at least one dental visit in the last 2 years) and 54.7% were visiting their dentist for check-up or for tooth cleaning and scaling (Table I).
2. Reliabilities, means, standard deviations and correlations of the Cognitive Emotion
Regulation Questionnaire (CERQ) subscales
Correlations between the CERQ-short subscales ranged between 0.16 (“Catastrophizing” and “Self-blame”) and 0.50 (“Self-Blame” and “Rumination”) (Table I). For comparison, the original CERQ sub-scale correlations ranged between 0.08 (“Catas-trophizing” and “Positive Reappraisal”) and 0.69 (“Positive Reappraisal” and “Planning”) [4].
3. Self-rated gingival health status, oral health behaviours and cognitive emotion regulation
Significant differences were found on self-rated oral health, current non-treated caries, insatis-faction by appearance of own teeth, self-rated gingival condition, daily toothbrushing frequency, reason for the dental visit, self-blame and rumination according to self-reported gingival bleeding (Table II). Participants who evaluated their self-reported gingival condition as poor/very poor scored higher values on rumination (14.66 ± 1.96 vs. 11.46 ± 3.83, P < 0.05), catastrophising (12.33 ± 2.73 vs. 8.38 ± 2.85, P = 0.007), and lower on positive reappraisal (14.50±3.01 vs. 17.33±2.84, P<0.05), when compared with students with excellent gingival condition. Multiple linear regression analyses were performed to examine the independent deter-minants of cognitive emotions. Statistical analysis showed that co-linearity was not significant between variables. Presence of gingival bleeding was an independent determinant of self-blame, rumination and putting into perspective, while independent determinant of catastrophising was insatisfaction by appearance of own teeth (Table III). The models were well fitted to the data.
Among participants with positive self-reported gingival bleeding, reason for dental visits was significantly correlated with positive refocusing (r = 0.217, P = 0.014), planning (r = 0.218, P =

Alexandrina Lizica Dumitrescu et al. 4 210
0.013), positive reappraisal (r = 0.314, P < 0.0001), putting into perspective (r = 0.307, P < 0.0001) and catrastrophizing (r = –0.226, P = 0.010).
Pearson correlations were used to examine the relationship between gingival status and reason for dental visits among study participants and to test one cognitive emotion variable, positive reap-
praisal, that theoretically mediate this relationship. Positive correlations were found between gingival status and reason for dental visits (r = 0.18, P < 0.05), between gingival status and positive reap-praisal (r = 0.21, P = 0.003) and between positive reappraisal and reason for dental visits (r = 0.18, P < 0.05).
Table I Means, standard deviations, Cronbach’s Alpha and interscale correlations (N = 213)
Self-blame
Acceptance
Rumination Positive refocusing
Planning Positive reappraisal
Putting into perspective
Catastrophising Blaming others
Self-blame 1 Acceptance 0.126 1 Rumination 0.500** 0.274** 1 Positive refocusing –0.047 0.164* 0.172* 1 Planning 0.164* –0.009 0.231** 0.425** 1 Positive reappraisal –0.004 0.049 0.126 0.501** 0.488** 1 Putting into perspective 0.024 0.202** 0.068 0.294** 0.189** 0.408** 1 Catastrophising 0.160* 0.101 0.238** –0.201** –0.163* –0.306** –0.362** 1 Blaming others –0.112 –0.058 0.009 –0.059 –0.191** –0.126 –0.047 0.414** 1 Mean 13.44 13.03 13.87 14.54 16.74 16.03 14.64 9.67 9.58 Standard deviations 2.68 5.20 3.24 2.93 2.27 3.04 3.74 3.00 3.16 Cronbach’s alpha 0.66 0.39 0.85 0.72 0.74 0.82 0.87 0.62 0.82
*P < 0.05; **P < 0.01
Table II Participants characteristics stratified by presence of gingival bleeding
Total sample
No gingival bleeding group
(n = 61)
Gingival bleeding group
(n = 129)
n (%) n (%) n (%)
P
Self-rated oral health status Very good/Excellent dental health 62 (32.6) 27 (44.3) 36 (27.3) 0.020 Current non-treated caries 68 (36) 15 (24.6) 54 (41.2) 0.025 Current extracted teeth 32 (16.8) 7 (11.5) 25 (18.9) NS Insatisfaction by appearance of own teeth 71 (37.6) 15 (25) 57 (43.2) 0.015 Toothache during last 3 months 55 (29.3) 18 (30.5) 37 (28.4 NS Very good/Excellent gingival condition 92 (48.4) 38 (62.3) 56 (42.4) <0.0001 Oral health-related behaviours Daily toothbrushing frequency: once a day or less 21 (11.1) 3 (5.1) 18 (13.7) 0.055 Flossing frequency: never 95 (50.3) 27 (45) 69 (52.3) NS Mouthrinse frequency: never 60 (31.7) 15 (25) 47 (35.6) NS Last dental visit: more than 2 years ago 18 (9.5) 5 (8.2) 13 (9.80 NS Reason for the dental visit: when treatment is needed or when pain 86 (45.3 22 (36.1) 64 (48.4) 0.017 Cognitive emotion regulation Self-blame 13.42±2.65 12.80±2.82 13.72±2.51 0.039 Rumination 13.86±3.23 12.82±3.36 14.35±3.02 0.002 Positive refocusing 14.49±3.02 14.37±2.99 14.57±3.01 NS Planning 16.72±2.29 17.04±2.03 16.60±2.38 NS Positive reappraisal 16.10±3.05 16.06±3.12 16.11±2.99 NS Putting into perspective 14.62±3.74 14.10±3.82 14.90±3.68 NS Catastrophising 9.60±3.06 9.31±2.93 9.74±3.10 NS Blaming others 9.46±3.07 9.54±3.29 9.51±2.99 NS

5 Specific cognitive emotion regulation and gingival bleeding 211
Table III Summary of the multiple regression analyses predicting cognitive emotion regulation subscales from oral health status
Variable
Predictors B S.E. t P
Age –0.135 0.157 –0.861 0.390 Gender 0.810 0.458 1.768 0.079 Current non-treated caries 0.439 0.439 1.002 0.318 Current extracted teeth –0.022 0.527 –0.042 0.967 Insatisfaction by appearance of own teeth 0.370 0.431 0.859 0.391 Toothache during last 3 months –0.051 0.154 –0.333 0.740
Self-blame
Presence of gingival bleeding 0.126 0.063 2.018 0.045 Age 0.015 0.181 0.082 0.935 Gender 2.153 0.527 40.081 0.000 Current non-treated caries 0.319 0.505 0.631 0.529 Current extracted teeth 0.835 0.607 1.375 0.171 Insatisfaction by appearance of own teeth 0.535 0.496 1.079 0.282 Toothache during last 3 months –0.238 0.178 –1.338 0.183
Rumination
Presence of gingival bleeding 0.210 0.072 2.913 0.004 Age 0.063 0.179 0.352 0.725 Gender 0.592 0.523 1.133 0.259 Current non-treated caries 0.750 0.501 1.497 0.136 Current extracted teeth –0.312 0.602 –0.519 0.604 Insatisfaction by appearance of own teeth 0.074 0.492 0.150 0.881 Toothache during last 3 months 0.084 0.176 0.475 0.636
Positive refocusing
Presence of gingival bleeding 0.038 0.072 0.534 0.594 Age 0.175 0.134 1.307 0.193 Gender 0.292 0.391 0.746 0.456 Current non-treated caries 0.961 0.375 2.562 0.011 Current extracted teeth –0.160 0.450 –0.354 0.723 Insatisfaction by appearance of own teeth –0.165 0.368 –0.448 0.655 Toothache during last 3 months 0.121 0.132 0.918 0.360
Planning
Presence of gingival bleeding –0.036 0.054 –0.672 0.503 Age 0.046 0.180 0.254 0.799 Gender 0.438 0.525 0.834 0.405 Current non-treated caries –0.075 0.503 –0.148 0.883 Current extracted teeth –0.135 0.605 –0.223 0.824 Insatisfaction by appearance of own teeth –0.781 0.494 –1.580 0.116 Toothache during last 3 months –0.054 0.177 –0.307 0.759
Positive reappraisal
Presence of gingival bleeding –0.002 0.072 –0.024 0.981 Age –0.381 0.218 –1.746 0.083 Gender 0.694 0.637 1.089 0.278 Current non-treated caries –0.227 0.610 –0.372 0.711 Current extracted teeth 0.156 0.733 0.212 0.832 Insatisfaction by appearance of own teeth –1.142 0.599 –1.906 0.058 Toothache during last 3 months –0.112 0.215 –0.522 0.602
Putting into perspective
Presence of gingival bleeding 0.176 0.087 2.025 0.044 Age 0.267 0.179 1.490 0.138 Gender 0.037 0.524 0.071 0.943 Current non-treated caries 0.707 0.502 1.407 0.161 Current extracted teeth –0.012 0.603 –0.020 0.984 Insatisfaction by appearance of own teeth 1.218 0.493 2.471 0.014 Toothache during last 3 months –0.007 0.177 –0.041 0.967
Catastrophising
Presence of gingival bleeding 0.045 0.072 0.629 0.530 Age 0.153 0.183 0.839 0.403 Gender –0.808 0.534 –1.514 0.132 Current non-treated caries –0.031 0.512 –0.061 0.952 Current extracted teeth –0.014 0.614 –0.023 0.982 Insatisfaction by appearance of own teeth 0.380 0.502 0.756 0.451 Toothache during last 3 months 0.156 0.180 0.864 0.389
Blaming others
Presence of gingival bleeding –0.026 0.073 –0.352 0.725

Alexandrina Lizica Dumitrescu et al. 6 212
Results for testing the mediational model (see Fig. 1) indicated that in the first regression equation, gingival status influenced positive reappraisal, F (1, 188) = 8.86, P = 0.003, explaining 4.5% of the variance in positive reappraisal. In the second regression equation, gingival status positively influenced reasons for dental visits, F (1, 188) = 6.26, P < 0.05, explaining 3.22% of the variance in reason for dental visits. In the third regression equation, positive reappraisal positively influenced reasons for dental visits (t = 6.59, P = 0.012), explaining 3.32% of the variance in reason for dental visits. In this third equation, which included both gingival status and positive reappraisal, gingival status added 2.08% to the explained variance in reasons for dental visits beyond the
3.32% contributed by positive reappraisal. With positive reappraisal present, the proportion of variance in reasons for dental visits accounted for by gingival status was reduced from 3.22% to 2.08%, and the standardized regression coefficient was decreased from 0.180 to 0.148, as derived from the second to the third equation. Although gingival status still had a statistically significant influence on reasons for dental visits in the third equation (t = 5.264, P = 0.006), the loss of 2.08% of explained variance in reasons for dental visits by gingival status was due to the mediation of positive reappraisal. These results indicate that positive reappraisal is one mediator in the relationship between gingival status and reasons for dental visits.
Fig.1. Results of testing the positive reappraisal mediation model.
DISCUSSION
To our knowledge, this is the first study to examine the interrelationship between gingival status and cognitive emotion regulation. Self-reported gingival bleeding was associated with statistical significant higher values of self-blame and rum-mination. Participants who evaluated their self-reported gingival condition as poor/very poor scored higher values on rumination, catastrophising and lower on positive reappraisal, when compared with students with excellent gingival condition.
The findings suggested that strongly Self-Blame, Ruminating and Catastrophizing in response to having gingival bleeding and poor self-rated gingival health status should be considered as maladaptive cognitive emotion regulation strategies. These findings fit in with findings in general
population samples where the same strategies were related to maladjustment [4][20] .Challenging these maladaptive cognitive emotion regulation strategies may therefore play an important role in inter-vention strategies to be developed for patients with gingivitis and periodontal disease. Rumination is a method of coping with negative mood that involves self-focused attention. According to Response Styles Theory (RST) [21], it is characterized by self-reflection as well as a repetitive and passive focus on one’s negative emotions. Rumination is associated with some physiological measures of elaboration of negative information. Numerous experimental and correlational studies have shown that rumination predicts greater depressive symptoms, predicts the onset, the severity as well as the length of depressive episodes and mediates the gender difference in depressive symptoms [20–24].
Positive reappraisal

7 Specific cognitive emotion regulation and gingival bleeding 213
Relationships between rumination and various kinds of psychopathology, including symptoms of depression, social phobia (post-event processing), trauma symptoms, anxiety, worry, hallucinations and panic disorder have also been reported [25–30]. The present results suggest a strong impact for a cognitive coping style of rumination in young patients with gingivitis, fitting in the previous findings of Dumitrescu & Kawamura [31] who showed that impaired oral health status tended to be associated with higher levels of depression and hopelessness in adults. Further, an important place in the findings is reserved for the cognitive coping strategies: positive refocusing, planning, positive reappraisal and putting into perspective to the oral health behaviours.
Although previous studies have shown that coping strategies, such as problem-focused coping behavior and locus of control, are related to poorer periodontal status, conclusions about various con-structs in general tend to refer to separate research traditions [32–36]. The present study showed that, generally speaking, all cognitive coping strategies were reported to be related to gingival health behavior. The cognitive coping strategies self-blame, rumination and positive reappraisal were shown to play the most important role related to the gingival health status and symptoms of gingival bleeding. Positive reappraisal was found to be a mediating variable in the relationship between gingival status and reason for dental visits. Thus, positive reappraisal helps to explain the association between gingival status and reason for dental visits. As described by Gross [37][38], reappraisal, one commonly used strategies for down-regulating emotion, comes early in the emotion-generative process. It consists of changing the way a situation is construed so as to decrease its emotional impact and behavioral expression [37][38].
A limitation of the design was that the detection of oral health status had to be made on the basis of self-reported evaluations, which may have caused some bias. In addition, the results are based on cross-sectional data. In future, longitudinal design should be performed to study individual developmental changes in time. In future research, it is important to reach other groups, too, because it is reasonable to assume that, for example, in clinical adult samples other patterns of cognitive coping strategies will be used. A strong point in this study has been the use of a large sample of young participants. Another important aspect is that, as far as we know, it is probably one of the first studies to focus on the extent to which the use of certain maladaptive cognitive coping strategies may be related to the severity of self-rated oral health.
Although a clear relationship has been shown between cognitive coping strategies and symptoms of oral health status and behaviour, the present study does not allow to draw conclusions about the directions of influence. Circular causal mechanisms may also be at work, which would make both assumptions true at the same time. Still, whatever the directions of influence may be; on the basis of the present study it might be argued that the use of certain cognitive coping strategies are related to gingival health status and oral health behaviours [11].
Challenging these maladaptive cognitive emotion regulation strategies may therefore play an important role on the focus and content of (pre-ventive) oral health behaviour interventions to be developed for patients with gingivitis and periodontal disease. No previous study has examined the mediator effect of positive reappraisal in the relationship between gingival status and reason for dental visits. Thus, the finding in the present study contributes to the knowledge base regarding the aforementioned association for this age-group.
Scopul studiului. Studiul prezent a fost focalizat pe studierea modului în care studenţii utilizează strategiile emoţionale cognitive ca răspuns la apariţia sângerării gingivale.
Material şi Metoda. Grupul de studiu a fost format din 190 de studenţi din anul întâi care au completat un chestionar ce include informaţii despre factorii socio-demografici, variabilele comportamentale, auto-raportarea stării de sănătate orală şi Chestionarul de reglare cognitivă a emoţiilor (Cognitive Emotion Regulation Questionnaire CERQ).
Rezultate. Auto-raportarea sângerării gingivale a fost în mod semnificativ asociată cu niveluri crescute de auto-învinovăţire şi ruminare. Participanţii care au evaluat condiţia lor gingivală ca fiind proastă/foarte proastă au prezentat

Alexandrina Lizica Dumitrescu et al. 8 214
valori mai ridicate ale ruminării, catastrofării şi mai reduse ale revalorificării pozitive. Analizele de regresie liniara multiplă au relevant faptul că prezenţa sângerării gingivale a fost un factor determinant independent al auto-culpabilizării, ruminării şi punerii în perspectivă. Participanţii ce au raportat sângerare gingivală au evidenţiat corelaţii semnificative între motivul vizitelor la medicul dentist şi reorientarea pozitivă, planificarea, reconsiderarea pozitivă, punerea în perspectivă şi catastrofarea. Reevaluarea pozitivă s-a dovedit a fi un mediator în relaţia dintre starea de sănătate gingivală şi motivul vizitelor la medicul dentist.
Concluzii. Schimbarea strategiilor de reglare emoţională cognitivă maladaptivă joacă un rol important în conţinutul intervenţiilor asupra îmbunătăţirii obi-ceiurilor de igienă orală la pacienţii cu afecţiuni gingivale şi parodontale. __________________________________________________________________
Corresponding author: Alexandrina L. Dumitrescu DDS, PhD, BA Psychology Associate Professor Institute of Clinical Dentistry, Faculty of Medicine, University of Tromsø 9037 Tromsø, Norway Phone: +47 77 64 91 34 Mobile: +47 93 65 11 78 Fax: +47 77 64 91 01 E-mail: [email protected]
REFERENCES
1. GROSS J.J., JOHN O.P., Individual differences in two emotion regulation processes: implications for affect, relationships, and well-being. J Pers Soc Psychol, 2003, 85, 348–62.
2. GROSS J.J., The Emerging Field of Emotion Regulation: An Integrative Review. Rev Gen Psychol, 1998, 2, 271–299. 3. MOORE S.A., ZOELLNER L.A., MOLLENHOLT N., Are expressive suppression and cognitive reappraisal associated with
stress-related symptoms? Behav Res Ther, 2008, 46, 993–1000. 4. GARNEFSKI N., KRAAIJ V., Relationships between cognitive emotion regulation strategies and depressive symptoms: a
comparative study of five specific samples. Pers Individ Dif, 2006, 40, 1659–1669. 5. GARNEFSKI N., KRAAIJ V., SPINHOVEN P., Negative life events, cognitive emotion regulation and depression. Pers Individ
Dif, 2001, 30, 1311–1327. 6. GARNEFSKI N., KOOPMAN H., KRAAIJ V., TEN CATE R., Brief report: Cognitive emotion regulation strategies and
psychological adjustment in adolescents with a chronic disease. J Adolesc, 2009, 32, 449–54. 7. SLEE N., GARNEFSKI N., VAN DER LEEDEN R., ARENSMAN E., SPINHOVEN P., Cognitive-behavioural intervention
for self-harm: randomised controlled trial. Br J Psychiatry, 2008, 192, 202–11. 8. KRAAIJ V., GARNEFSKI N., VLIETSTRA A., Cognitive coping and depressive symptoms in definitive infertility: a
prospective study. J Psychosom Obstet Gynaecol, 2008, 29, 9–16. 9. KRAAIJ V., PRUYMBOOM E., GARNEFSKI N., Cognitive coping and depressive symptoms in the elderly: a longitudinal
study. Aging Ment Health, 2002, 6, 275–81. 10. GARNEFSKI N., BAAN N., KRAAIJ V., Psychological distress and cognitive emotion regulation strategies among farmers
who fell victim to the foot-and-mouth crisis. Pers Individ Dif, 2005, 38, 1317–1327. 11. GARNEFSKI N., LEGERSTEE J., KRAAIJ V.V., VAN DEN KOMMER T., TEERDS J., Cognitive coping strategies and
symptoms of depression and anxiety: a comparison between adolescents and adults. J Adolesc, 2002, 25, 603–11. 12. EFTEKHARI A., ZOELLNER L.A., VIGIL S.A., Patterns of emotion regulation and psychopathology. Anxiety Stress Coping,
2009, 20, 1–15. 13. DUMITRESCU A.L., Psychological perspectives on the pathogenesis of periodontal disease. Rom J Intern Med, 2006, 44, 241–60. 14. DUMITRESCU A.L, WRIGHT C., Psychological pathways in the pathogenesis of periodontal disease. In: Etiology and
Pathogenesis of Periodontal Disease, A.L. Dumitrescu Springer, 1st Edition, 2009, p. 245–265. 15. CHRISTENSEN L.B., JEPPE-JENSEN D., PETERSEN P.E., Self-reported gingival conditions and self-care in the oral health
of Danish women during pregnancy. J Clin Periodontol, 2003, 30, 949–53. 16. HONKALA S., AL-ANSARI J., Self-reported oral health, oral hygiene habits, and dental attendance of pregnant women in
Kuwait. J Clin Periodontol, 2005, 32, 809–14. 17. STÅHLNACKE K., SÖDERFELDT B., UNELL L., HALLING A., AXTELIUS B., Perceived oral health: changes over 5 years in
one Swedish age-cohort. Community Dent Oral Epidemiol, 2003, 31, 292–9. 18. BARON R.M., KENNY D.A., The moderator-mediator variable distinction in social psychological research: conceptual,
strategic, and statistical considerations. J Pers Soc Psychol, 1986, 51, 1173–82. 19. YARCHESKI A., MAHON N.E., YARCHESKI T.J., Social support and well-being in early adolescents: the role of mediating
variables. Clin Nurs Res, 2001, 10, 163–81.

9 Specific cognitive emotion regulation and gingival bleeding 215
20. NOLEN-HOEKSEMA S., PARKER L.E., LARSON J., Ruminative coping with depressed mood following loss. J Pers Soc Psychol, 1994, 67, 92–104.
21. NOLEN-HOEKSEMA S., Sex differences in unipolar depression: Evidence and theory. Psychol Bull, 1987, 101, 259–282. 22. NOLEN-HOEKSEMA S., The role of rumination in depressive disorders and mixed anxiety/depressive symptoms. J Abnorm
Psychol, 2000, 109, 504–511. 23. NOLEN-HOEKSEMA S., MORROW J., A prospective study of depression and posttraumatic stress symptoms after a natural
disaster: the 1989 Loma Prieta earthquake. J Pers Soc Psychol, 1991, 61, 115–121. 24. TREYNOR W., GONZALEZ R., NOLEN-HOEKSEMA S., Rumination Reconsidered: A Psychometric Analysis. Cognit Ther
Res, 2003, 27, 247–259. 25. SMITH J.M., ALLOY L.B., A roadmap to rumination: a review of the definition, assessment, and conceptualization of this
multifaceted construct. Clin Psychol Rev, 2009, 29, 116–28. 26. OTTAVIANI C., SHAPIRO D., DAVYDOV D.M., GOLDSTEIN I.B., MILLS P.J., The autonomic phenotype of rumination.
Int J Psychophysiol, 2009, 72, 267–75. 27. ROELOFS J., ROOD L., MEESTERS C., TE DORSTHORST V., BÖGELS S., ALLOY L.B., NOLEN-HOEKSEMA S., The
influence of rumination and distraction on depressed and anxious mood: a prospective examination of the response styles theory in children and adolescents. Eur Child Adolesc Psychiatry, 2009, 18, 635–42.
28. TAKANO K., TANNO Y., Self-rumination, self-reflection, and depression: self-rumination counteracts the adaptive effect of self-reflection. Behav Res Ther, 2009, 47, 260–4.
29. JONES N.P., PAPADAKIS A.A., HOGAN C.M., STRAUMAN T.J., Over and over again: rumination, reflection, and promotion goal failure and their interactive effects on depressive symptoms. Behav Res Ther, 2009, 47, 254–9.
30. PEARSON M., BREWIN C.R., RHODES J., MCCARRON G., Frequency and nature of rumination in chronic depression: a preliminary study. Cogn Behav Ther, 2008, 37, 160–8.
31. DUMITRESCU A.L., KAWAMURA M., Exploring the relationships between sense of hopelessness, worry, self-rated oral health status, and behavior in a Romanian adult population. J Contemp Dent Pract, 2009, 10, 34–41.
32. GENCO R.J., HO A.W., GROSSI S.G., DUNFORD R.G., TEDESCO L.A. Relationship of stress, distress and inadequate coping behaviors to periodontal disease. J Periodontol, 1999, 70, 711–23.
33. WIMMER G., JANDA M., WIESELMANN-PENKNER K., JAKSE N., POLANSKY R., PERTL C., Coping with stress: its influence on periodontal disease. J Periodontol, 2002, 73, 1343–51.
34. WIMMER G., KÖHLDORFER G., MISCHAK I., LORENZONI M., KALLUS K.W., Coping with stress: its influence on periodontal therapy. J Periodontol, 2005, 76, 90–8.
35. HUGOSON A., LJUNGQUIST B., BREIVIK T., The relationship of some negative events and psychological factors to periodontal disease in an adult Swedish population 50 to 80 years of age. J Clin Periodontol, 2002, 29, 247–53.
36. NEWTON T., Specification and analysis of the effects of coping in research on the relationship between psychosocial stress and periodontal disease. J Clin Periodontol, 2005, 32, 1141–2.
37. GROSS J.J., Antecedent- and response-focused emotion regulation: divergent consequences for experience, expression, and physiology. J Pers Soc Psychol, 1998, 74, 224–37.
38. GROSS J.J., Emotion regulation: affective, cognitive, and social consequences. Psychophysiology, 2002, 39, 281–91.
Received July 7, 2011


CASE REPORT
Dermatomyositis and Polyradiculoneuritis, a Rare Association
INIMIOARA MIHAELA COJOCARU1, GABRIELA SOCOLIUC2, VIOLETA ŞAPIRA2, ALEXANDRA BASTIAN3, MARILENA ALEXIANU3, M. MOLDOVAN4
1“Carol Davila” University of Medicine and Pharmacy, Department of Neurology, Colentina Clinical Hospital, Bucharest, Romania 2Department of Neurology, “Colentina” Clinical Hospital, Bucharest, Romania
3Neuropathology Laboratory, “Colentina” Clinical Hospital, Bucharest, Romania 4“Elias” Emergency University Hospital, Bucharest, Romania
The association between dermatomyositis and polyradiculoneuritis is rarely citated in the speciality literature. Our patient had at first a disorder that looked like dermatomyositis, then she associated polyradiculoneuritis. At the presentation to our hospital the two diseases were combined, being very difficult to differentiate. The discrimination between these two had been made by performing a muscular biopsy and EMG studies. This emphasizes once again their importance in defining the muscular impairment from the neurogenic one.
Keywords: dermatomyositis; polyradiculoneuritis; muscular biopsy; electromyography.
CASE REPORT
P. L., 59 years old, female, a school teacher, with no previous illness history, suffered in December 2010 acute mild myalgias treated initially with nonsteroid antiinflammatory medication. Ap-parently this treatment was not successful, therefore in several weeks the symptoms intensified, restrained her walking and were accompanied by extreme fatigue that forced her to present to the hospital. She was admitted in an Internal Medicine Department in January. At that time one could observe a purplish non itchy rash disposed in plaques on patient’s face, posterior thorax and limbs.
The blood tests found an inflammatory syndrome, hepatocytolysis, high level of anti- HCV antibodies. The treatment administered was anti-allergic (antihistamines) as the skin eruption was considered of allergic origin and she was discharged home.
After 2 weeks our patient had 20 diarrheaic stools in 48 hours and she presented once again for hospitalization. The physical examination undergone found myalgias with functional disability, decrease in strength in the left limbs, livedo reticularis on arms and thorax. The laboratory findings at that time were those of neutrophilic leucocytosis and lymphopenia, and raised values of seric creatinin kinase (CK 20.000 IU/L), lactate dehydrogenase (LDH 1224 IU/L) and aspartate aminotransferase
(AST 415 IU/L). She received pulse therapy with Solu-Medrol 1g daily, but that induced an increase in her glycemic values.
A neurology consultant stated for dermato-myositis and further on, the seric infestations with Trichinella, Chlamydia, Borrelia, Adenovirus, Myco-plasma, Coxsackie had been excluded.
The blood search for various antibodies (anti-smooth muscle, anti-nuclear, anti-mitochondrial, anti-Sm, anti-Jo) was negative; only the anti dsDNA were slightly positive.
During the hospitalization in the Internal Medicine Department disphagia for solids and liquids appeared and the need for a specific neurological care became obvious. The patient was transferred to our clinic where the neurologist noted disphagia for liquids and solids, the impossibility for neck flexion on the pillow, the shoulders were immobile, the motor strength in the superior limbs was 3/5, in both hip flexors 2/5 and in the thigh abductors 2/5, deep-tendon reflexes were absent, Babinski’s sign was absent. The nerve roots irritation tests were positive both on superior and inferior limbs and the sensory examination was normal. A rash was present on the anterior and posterior thorax. At that point acute polyradiculoneuritis and dermatomyositis had to be considered possible diagnostics.
The blood test performed in our clinic revealed an elevation in the CK level (5511 IU/L), in the LDH level (732 IU/L), in AST level (278 IU/L)
ROM. J. INTERN. MED., 2011, 49, 3, 217–221

Inimioara Mihaela Cojocaru et al. 2 218
and the absence of cryoglobulins. The blood count neutrophilic leucocytosis without lymphopenia. As the diarrhea episode was not elucidated and the link between polyradiculoneuritis and Campylobacter sp. was quoted, antibodies against Campylobacter jejuni and Campylobacter fetus were searched for, but they proved to be negative [1] [2]. A lumbar puncture showed a high protein level (1.2 g/L) and albuminocytologic dissociation and an electroneuro-graphic study was carried out [3]. The electroneuro-graphy had a denervation aspect, with decreased nerve conduction studies and was compatible with acute polyradiculoneuritis, the acute motor axonal neuropathy (AMAN) variant.
The diagnostic of dermatomyositis at a 59 years old patient imposed a tumor screening and thorax and abdomen CT scan was performed and tumor markers were searched for [4][5]. They all proved to be negative.
A muscle biopsy from the right quadriceps femoris muscle was sampled and the result was that of muscular lesions of neurogenic origin (Figs. 1–6).
The final diagnostic for this patient was Dermatomyositis and Acute Polyradiculoneuritis (AMAN form). The treatment administered was IG IV, cyclophosphamide pulse-therapy, and gluco-corticoids [6]. The patient’s physical state slowly improved and she walked in canes at her discharge home.
At three, respectively at six months follow-up the EMG performed to our patient showed a predominant proximal myopathic aspect and glucocorticoids were recommended.
DISCUSSION
The association of dermatomyositis with polyradiculoneuritis is rarely seen in human medical literature. The link between polyradiculoneuritis and polymyositis and the infection with Neospora caninum, a protozoan that affects new born puppies neuromuscular system is citated only in two cases [7][8].
Dermatomyositis (polymyositis) is characterized by skin lesions and muscular weakness. The erythema may be difusse or localized, the rash may be slightly elevated and smooth or scaly and localised frequently on the forehead, V of the neck and shoulders, chest and back, forearms and lower legs, elbows and knees, medial malleoli. The skin
changes may precede or may follow the muscular syndrome.
In this case we must consider dermatomyositis as one of the illnesses. The judgement was made on the base of the clinical data, a muscular lysis syndrome, a skin rash and on the negative cancer screening.
In particular to this case, we must point out the association between polymyositis and poly-radiculoneuritis, the last most probably due to a viral infection.
The regular aspect of EMG in polymyositis is that of short-duration, low-amplitude polyphasic units on voluntary activation and increased spon-taneous activity with fibrillations, complex repetitive discharges, and positive sharp waves [9]. It is a test useful to identify the presence of active or chronic myopathy and to exclude neurogenic disorders. EMG also shows evidence of muscle irritability and it is helpful in indicating which muscle groups are the most suitable target for muscle biopsy [10].
In our particular case the electroneurographic aspect was neurogenic, with decreased motor velocity on nerve conduction studies, suggestive for the AMAN form of the disease.
The histopathologic aspect found at this patient was that of denervation, whereas in the classic form of polymyositis the findings are of muscle fibers in varying stages of inflammation, necrosis, and regeneration, focal endomysial infil-tration by mononuclear cells. Inflammatory infiltrates can be diffuse or focal, sometimes confined to the peri- and endomysium, but usually interspersed between the individual muscle fibres as well [10]. The infiltrates consisted largely of small mono-nuclear cells, occasional plasma cells, histiocytes, and polymorphonuclear leucocytes. The inflammatory changes were less marked in longstanding disease.
Later in the course of polymyositis, muscle-cell degeneration, fibrosis, and regeneration may be observed.
Selective type II fibre atrophy and muscular infarcts can be seen. It can also be remarked a high level of muscular degeneration and regeneration; the fibre degeneration or the inflammatory infiltration may prevail in a muscular biopsy.
The particular aspect of the muscular biopsy in our patient can be due to the association of acute polyradiculoneuritis to the glucocorticoid therapy administered before the biopsy to be sampled.

3 Dermatomyositis and polyradiculoneuritis 219
Fig. 1. Size variability of the muscular fibres; elongated and angular fibres. Hematoxylin-eosin (HE), ob. 20.
Fig. 2. Elongated and angular muscular fibres. HE, ob. 40.
Fig. 3. Lack of inflammatory infiltrate, elongated and angular muscular fibres. HE, ob. 40.

Inimioara Mihaela Cojocaru et al. 4 220
Fig. 4. Small groups of atrophic muscular fibres. HE, ob. 20.
Fig. 5. Muscular fibres in necrobiosis. HE, ob. 20.
Fig. 6. Atrophic fibres at the fascicle periphery. HE, ob. 20.

5 Dermatomyositis and polyradiculoneuritis 221
CONCLUSION
One of this case’s particularities is the association between two neuromuscular diseases (dermatomyositis and polyradiculoneuritis), the onset symptoms being those compatible to derma-tomyositis.
The second particularity is that both the neuro-physiological examination and the muscular biopsy were suggestive for peripheric nerves impairment.
In order to obtain an accurate result, the muscular biopsy must be performed close to the disorder onset, before starting the glucocorticoid treatment.
Asocierea dintre dermatomiozita acută şi poliradiculonevrita inflamatorie acută este rară, fiind sporadic citată în literatura de specialitate. Pacienta a prezentat iniţial simptomatologie de tip dermatomiozită, ulterior asociind un tablou de poliradiculonevrită. La internarea în Clinica de Neurologie cele două boli erau intricate, fiind greu de diferenţiat. Deosebirea dintre cele două afecţiuni s-a bazat pe biopsia musculară şi pe examenul EMG. Aceasta subliniază încă o dată importanţa acestor teste în diferenţierea afectării musculare de cea neurogenă.
Corresponding author: Senior lecturer Inimioara Mihaela Cojocaru MD, PhD, Department of Neurology
“Colentina” Clinical Hospital, 19–21, Şos. Ştefan cel Mare 020125, Bucharest, Romania E-mail: [email protected]
REFERENCES
1. JACOBS B.C., ROTHBARTH P.H., VAN DER MECHE F.G. et al., The spectrum of antecedent infections in Guillain-Barre syndrome: a case-control study. Neurology. Oct 1998; 51 (4): 1110–1115.
2. VAN DER MECHE F.G., VISSER LH., JACOBS B.C. et al., Guillain-Barre syndrome: multifactorial mechanisms versus defined subgroups. J Infect Dis. Dec 1997; 176 (Suppl 2): S99–S102.
3. ASBURY A.K., CORNBLATH D.R., Assessment of current diagnostic criteria for Guillain-Barré syndrome.Ann Neurol. 1990; 27 (Suppl): S21–S24.
4. AIRIO A., PUKKALA E., ISOMAKI H., Elevated cancer incidence in patients with dermatomyositis: a population based study. J Rheumatol. 1995; 22 (7): 1300–1303.
5. HILL C.L., ZHANG Y., SIGURGEIRSSON B. et al., Frequency of specific cancer types in dermatomyositis and polymyositis: a population-based study. Lancet. 2001; 357 (9250): 96–100.
6. HENGSTMAN G.J., VAN DEN HOOGEN F.H., VAN ENGELEN B.G., Treatment of the inflammatory myopathies: update and practical recommendations. Expert Opin Pharmacother. 2009; 10 (7): 1183–1190.
7. LIU J.R., ZHANG M., XU B. et al., Polymyositis associated with Guillain-Barre' syndrome: one cases report. Zheijang Da Xue Xue Bao Yi Xue Xue Ban 2004; 33 (2): 184–185.
8. McGLENNON N.J., JEFFERIES A.R., CASAS C., Polyradiculoneuritis and polymyositis due to a toxoplasma-like protozoan: diagnosis and treatment . Journal of Small Animal Practice 1990; 31: 102–104.
9. TROJANORG W., Quantitative electromyography in polymyositis: a reappraisal. Muscle Nerve. 1990; 13 (10): 964–971. 10. KALLIABAKOS D., PAPPAS A., LAGOUDIANAKIS E. et al., A case of polymyositis associated with papillary thyroid
cancer: a case report. Cases Journal. 2008; 1: 289. 11. HANS A. SCHWARZ, SLAVIN G. et al., Muscle biopsy in polymyositis and dermatomyositis: a clinicopathological study.
Annals Rheumatic Diseases, 1980, 39: 500–507.
Received July 22, 2011