
Electrophysiological Indices of Automatic and Controlled Auditory Information Processing in...
11
Electrophysiological Indices of Automatic and Controlled Auditory Information Processing in First-Episode, Recent-Onset and Chronic Schizophrenia Daniel S.G. Umbricht, John A. Bates, Jeffrey A. Lieberman, John M. Kane, and Daniel C. Javitt Background: Deficits in amplitudes of auditory event-related potentials (ERP) indexing preattentive, automatic (mismatch negativity, MMN) and controlled, attention-dependent (N2, P3) auditory information processing have been well described in chronic schizophrenia. Normal MMN, but deficient N2 and P3 have been reported in first-episode patients. No study has investigated these ERPs concurrently in first-episode patients; thus, reported differences in MMN, N2 and P3 generation may reflect differences in patient samples rather than genuine differences in abnormal generation of these ERPs. Methods: We recorded MMN, N2 and P3 in 26 first-episode patients, 25 recent-onset patients within 1.5 to 5 years after first admission, 25 chronic patients and 39 healthy controls. Results: Recent-onset and chronic, but not first-episode patients showed reduced MMN. However, among first-episode patients those with low premorbid educational achievement demonstrated significantly reduced MMN. All patient groups showed pronounced N2 deficits and, to a variable extent, abnormalities in P3 generation. Conclusions: Abnormalities in N2 and P3 generation appear to reflect premorbid neuropathology, whereas MMN deficits may index both ongoing disease processes associated with illness progression as well as premorbid neurocognitive impairment. ERPs may provide tools to assess static and progressive neuropathology in schizophrenia. These findings need confirmation in longitudinal studies. Key Words: Schizophrenia, event-related potentials, mismatch negativity, N2, P3, cognition C ognitive deficits constitute a core feature of schizophrenia that – broadly defined - not only include abnormalities in higher cognitive domains, but also extend to information processing at the sensory and preattentive level (Braff and Geyer 1990; Freedman et al 1983). Thus, in schizophrenia deficits have been demonstrated in the amplitudes of the event-related poten- tials mismatch negativity (MMN), N2 and P3. MMN is a preatten- tive auditory event-related potential (ERP) that is automatically generated when a stimulus is presented that violates invariant characteristics of the recent auditory past (Näätänen 1995) be they simple physical features (e.g frequency, duration, intensity) of the stimuli or more abstract rules of stimulus presentation (Näätänen 1995; Schröger 1997; Ritter et al 1995). Any incoming auditory stimulus is compared against a template, or memory trace, of the regularity or invariance extracted from the recent presentation of standard stimuli. If a violation, i.e. mismatch occurs, MMN is elicited. In the absence of such a memory trace no MMN is generated. Thus, MMN generation indexes auditory sensory memory and reflects context-dependent information processing at the level of the auditory sensory cortex (Näätänen et al 2001). Since the first report of deficient MMN in 1991 by Shelley et al (1991), numerous studies on MMN in chronic schizophrenic patients have replicated these findings (for a review see Um- bricht and Krljes 2005). Indeed, in a recent meta-analysis a mean effect size of .99 was found (Umbricht and Krljes 2005) – a large deficit by common standards. Moreover, MMN deficits are not observed in other major mental illnesses such as bipolar disorder or major depression (Catts et al 1995; Hirsch et al 2002; Umbricht et al 2003) suggesting that they may be fairly specific to schizo- phrenia. There are scant data on the presence of MMN abnormalities close to illness onset. Javitt et al (2000) reported deficient MMN generation in patients who were within 1.5 years of their first episode. In contrast, Salisbury et al (2002) observed normal MMN generation in first-episode patients. Thus, whether MMN deficits are present at illness onset remains controversial. In contrast to MMN, P3 generation is abnormal in first-episode patients (Brown et al 2002; Hirayasu et al 1998; Salisbury et al 1998). P3, unlike MMN whose generation is largely independent of the subject’s attention, is considered an attention-dependent event-related potential that is generated whenever a behaviorally relevant target stimulus embedded in irrelevant standard stimuli is detected. The generation of P3 is preceded by N2 – another ERP that is considered attention-dependent and believed to reflect stimulus categorization (Ritter et al 1979, 1983; Simson et al 1976, 1977a, 1977b). Most studies found N2 deficits to be present both in first– episode and chronic schizophrenia (Brown et al 2002; Salisbury et al 1994) with one study reporting normal N2 in patients tested close to their first-episode (Hirayasu et al 1998). The results in first-episode patients suggest that deficits in MMN, N2 and P3 may manifest different aspects of neuropatho- logical processes in schizophrenia: MMN deficits may only develop with illness progression within the first years of illness and thus manifest illness-related changes of the neural networks involved in its generation, whereas N2 and P3 deficits may point to abnormalities present premorbidly or developing in the very early stages of the illness prior to or around the initial manifes- tation of overt psychotic symptoms. Conversely, MMN deficits may – like N2 and P3 - also relate to premorbid pathology and be static. Thus, abnormal MMN at illness onset may index a more pervasive cortical pathology and only be observed in a subgroup From Exploratory Clinical Development (DSGU), Translational Medicine, No- vartis Pharma AG, Basel, Switzerland; Department of Psychiatry (JAB, JMK), Zucker-Hillside Hospital, Glen Oaks; Department of Psychiatry (JAL), College of Physicians and Surgeons, Columbia University, New York State Psychiatric Institute, New York; Program in Cognitive Neuro- science and Schizophrenia (DCJ), Nathan Kline Institute for Psychiatric Research, Orangeburg, New York. Address reprint requests to Dr. Daniel S.G. Umbricht, Novartis Pharma AG, Translational Medicine, Exploratory Clinical Development, WSJ-27.6.057, 4056 Basel, Switzerland; E-mail: [email protected]. Received April 22, 2005; revised August 10, 2005; accepted August 25, 2005. BIOL PSYCHIATRY 2006;59:762–772 0006-3223/06/$32.00 doi:10.1016/j.biopsych.2005.08.030 © 2006 Society of Biological Psychiatry
-
Upload
independent -
Category
Documents
-
view
5 -
download
0
Transcript of Electrophysiological Indices of Automatic and Controlled Auditory Information Processing in...
ECFD
BMNitM2RwdCbt
Kn
Cp1bttgcto(atponspe
(p
F
A
R
0d
lectrophysiological Indices of Automatic andontrolled Auditory Information Processing inirst-Episode, Recent-Onset and Chronic Schizophrenia
aniel S.G. Umbricht, John A. Bates, Jeffrey A. Lieberman, John M. Kane, and Daniel C. Javitt
ackground: Deficits in amplitudes of auditory event-related potentials (ERP) indexing preattentive, automatic (mismatch negativity,MN) and controlled, attention-dependent (N2, P3) auditory information processing have been well described in chronic schizophrenia.ormal MMN, but deficient N2 and P3 have been reported in first-episode patients. No study has investigated these ERPs concurrently
n first-episode patients; thus, reported differences in MMN, N2 and P3 generation may reflect differences in patient samples ratherhan genuine differences in abnormal generation of these ERPs.
ethods: We recorded MMN, N2 and P3 in 26 first-episode patients, 25 recent-onset patients within 1.5 to 5 years after first admission,5 chronic patients and 39 healthy controls.esults: Recent-onset and chronic, but not first-episode patients showed reduced MMN. However, among first-episode patients thoseith low premorbid educational achievement demonstrated significantly reduced MMN. All patient groups showed pronounced N2eficits and, to a variable extent, abnormalities in P3 generation.onclusions: Abnormalities in N2 and P3 generation appear to reflect premorbid neuropathology, whereas MMN deficits may indexoth ongoing disease processes associated with illness progression as well as premorbid neurocognitive impairment. ERPs may provide
ools to assess static and progressive neuropathology in schizophrenia. These findings need confirmation in longitudinal studies.ey Words: Schizophrenia, event-related potentials, mismatchegativity, N2, P3, cognition
ognitive deficits constitute a core feature of schizophreniathat – broadly defined - not only include abnormalities inhigher cognitive domains, but also extend to information
rocessing at the sensory and preattentive level (Braff and Geyer990; Freedman et al 1983). Thus, in schizophrenia deficits haveeen demonstrated in the amplitudes of the event-related poten-ials mismatch negativity (MMN), N2 and P3. MMN is a preatten-ive auditory event-related potential (ERP) that is automaticallyenerated when a stimulus is presented that violates invariantharacteristics of the recent auditory past (Näätänen 1995) behey simple physical features (e.g frequency, duration, intensity)f the stimuli or more abstract rules of stimulus presentationNäätänen 1995; Schröger 1997; Ritter et al 1995). Any incominguditory stimulus is compared against a template, or memoryrace, of the regularity or invariance extracted from the recentresentation of standard stimuli. If a violation, i.e. mismatchccurs, MMN is elicited. In the absence of such a memory traceo MMN is generated. Thus, MMN generation indexes auditoryensory memory and reflects context-dependent informationrocessing at the level of the auditory sensory cortex (Näätänent al 2001).
Since the first report of deficient MMN in 1991 by Shelley et al1991), numerous studies on MMN in chronic schizophrenicatients have replicated these findings (for a review see Um-
rom Exploratory Clinical Development (DSGU), Translational Medicine, No-vartis Pharma AG, Basel, Switzerland; Department of Psychiatry (JAB,JMK), Zucker-Hillside Hospital, Glen Oaks; Department of Psychiatry(JAL), College of Physicians and Surgeons, Columbia University, NewYork State Psychiatric Institute, New York; Program in Cognitive Neuro-science and Schizophrenia (DCJ), Nathan Kline Institute for PsychiatricResearch, Orangeburg, New York.
ddress reprint requests to Dr. Daniel S.G. Umbricht, Novartis Pharma AG,Translational Medicine, Exploratory Clinical Development, WSJ-27.6.057,4056 Basel, Switzerland; E-mail: [email protected].
eceived April 22, 2005; revised August 10, 2005; accepted August 25, 2005.
006-3223/06/$32.00oi:10.1016/j.biopsych.2005.08.030
bricht and Krljes 2005). Indeed, in a recent meta-analysis a meaneffect size of .99 was found (Umbricht and Krljes 2005) – a largedeficit by common standards. Moreover, MMN deficits are notobserved in other major mental illnesses such as bipolar disorderor major depression (Catts et al 1995; Hirsch et al 2002; Umbrichtet al 2003) suggesting that they may be fairly specific to schizo-phrenia.
There are scant data on the presence of MMN abnormalitiesclose to illness onset. Javitt et al (2000) reported deficient MMNgeneration in patients who were within 1.5 years of their firstepisode. In contrast, Salisbury et al (2002) observed normal MMNgeneration in first-episode patients. Thus, whether MMN deficitsare present at illness onset remains controversial.
In contrast to MMN, P3 generation is abnormal in first-episodepatients (Brown et al 2002; Hirayasu et al 1998; Salisbury et al1998). P3, unlike MMN whose generation is largely independentof the subject’s attention, is considered an attention-dependentevent-related potential that is generated whenever a behaviorallyrelevant target stimulus embedded in irrelevant standard stimuliis detected. The generation of P3 is preceded by N2 – anotherERP that is considered attention-dependent and believed toreflect stimulus categorization (Ritter et al 1979, 1983; Simson etal 1976, 1977a, 1977b). Most studies found N2 deficits to bepresent both in first– episode and chronic schizophrenia (Brownet al 2002; Salisbury et al 1994) with one study reporting normalN2 in patients tested close to their first-episode (Hirayasu et al1998).
The results in first-episode patients suggest that deficits inMMN, N2 and P3 may manifest different aspects of neuropatho-logical processes in schizophrenia: MMN deficits may onlydevelop with illness progression within the first years of illnessand thus manifest illness-related changes of the neural networksinvolved in its generation, whereas N2 and P3 deficits may pointto abnormalities present premorbidly or developing in the veryearly stages of the illness prior to or around the initial manifes-tation of overt psychotic symptoms. Conversely, MMN deficitsmay – like N2 and P3 - also relate to premorbid pathology and bestatic. Thus, abnormal MMN at illness onset may index a more
pervasive cortical pathology and only be observed in a subgroupBIOL PSYCHIATRY 2006;59:762–772© 2006 Society of Biological Psychiatry

opcgr2n
rreg
Mciic
M
S
mags(Oi(fPhwariaetmcdD
irl(db1pD
t
C
fa1
D.S.G. Umbricht et al BIOL PSYCHIATRY 2006;59:762–772 763
f patients – possibly those who demonstrate more premorbidrecursors of schizophrenia or those who are prone to develophronic schizophrenia, both of which may relate to a differentenetic background. Such a view could be explain why MMN inelatives of chronic patients is significantly reduced (Michie et al002; Jessen et al 2001) while first episode patients overall showormal MMN.
However, no study has investigated MMN, N2 and P3 concur-ently in first-episode patients raising the possibility that theeported differences in MMN, N2 and P3 generation in first-pisode patients reflect differences in patient samples rather thanenuine differences in abnormal generation of these ERPs.
This study addressed this issue by concurrently investigatingMN, N2 and P3 in groups of first-episode, recent-onset and
hronic patients. In addition, the questions were explored: i) if MMNn first-episode patients predicted initial treatment response; and ii)f MMN deficits could result from a more symptomatic illnessourse and/or were related to premorbid functioning.
ethods and Materials
ubjectsThis study was conducted in the Psychiatric Research Depart-
ent of the Zucker Hillside Hospital, Glen Oaks, New York, andpproved by the Internal Review Board of this institution. Fourroups were investigated: 1) Subjects participating in the Pro-pective Study of Psychobiology in First-Episode Schizophrenia‘First-episode study’) at the Zucker Hillside Hospital in Glenaks, New York (Bilder et al 2000; Lieberman et al 1992, 1993),
n whom ERPs were acquired within 6 months of first admissionin all but two patients ERPs were recorded within 4 weeks ofirst admission) and referred to as first-episode patients; 2)atients also participating in the same first-episode study whoad been followed for at least 18 months in the study when ERPsere acquired, and termed recent-onset patients; 3) Chronicmbulatory schizophrenic patients who were partially treatmentefractory, recruited for a double-blind treatment study compar-ng clozapine to risperidone (Schooler et al 1999) and referred tos ‘chronic patients’ (ERPs were obtained during the baselinevaluation of these patients); 4) A normal control group recruitedhrough announcements in local newspapers and within theedical center. Control subjects were free of mental disorders,
urrent substance use disorder or a history of substance depen-ence as determined by the Structured Clinical Interview forSM-III-R, nonpatient version.Subjects in the first-episode study were admitted to the hospital
npatient service for a first-episode of psychotic illness havingeceived less than 12 prior weeks of cumulative lifetime neuro-eptic treatment. They satisfied Research Diagnostic CriteriaRDC)(Spitzer et al 1978) for schizophrenia or schizoaffectiveisorder. Further details of ascertainment and treatment haveeen published elsewhere (Bilder et al 2000; Lieberman et al992;1993). In the chronic patient group the diagnosis of schizo-hrenia was established by the Structured Clinical Interview forSM-III-R (SCID) (Spitzer et al 1999).The purpose of the study was explained to all subjects in lay
erms. Written consent was obtained from all subjects.
linical RatingsPatients in the first-episode study were rated on the Schedule
or Affective Disorders and Schizophrenia Change � Psychosisnd Disorganization Scale (SADS-C�PD) (Spitzer and Endicott
978), the Scale for the Assessment of Negative Symptoms(SANS) (Andreasen 1983) and the Clinical Global ImpressionScale (CGI) (Guy 1976). Chronic patients were rated on theanchored version of the Brief Psychiatric Rating Scale (BPRS)(Woerner et al 1988), the SANS and the CGI. The CGI rating, theSANS total score and the sum of the SADS and BPRS items‘severity of hallucinations’/ ‘hallucinations’ and ‘severity of delu-sions’/‘unusual thought content’ (in both scales a scale of 1-7 wasused), respectively, were used to compare the symptom severityof the patient groups. In most cases the clinical rating wasperformed within 7 days of the ERP recording.
Premorbid Educational AchievementAs an overall index of premorbid intellectual level and perfor-
mance, information about the educational level achieved wasobtained in patients and scored as 0 � college or postgraduatetraining, 1 � some college, 2 � high school graduate, 3 � somehigh school, 4 � 8th grade, 5 � 6th – 7th grade, 6 � not beyond5th grade. For the analysis patients were grouped into those withscores 0 and 1 and those scoring higher (this information wasavailable in 21 first-episode, 24 recent-onset and 25 chronicpatients). In addition, in patients participating in the first-episodestudy the Premorbid Adjustment Scale (PAS) (CannonSpoor et al1982) was completed at baseline by using information both frompatients and family members. The PAS has sections coveringchildhood, early adolescence, late adolescence, and adulthood;the scores on items for each section were averaged to provide amean score for each age category.
Treatment ResponseFor patients in the first-episode study, clinical ratings obtained
every two weeks were available. Treatment response was de-fined as a CGI rating of “much” or “very much” improved plus arating of 3 (mild) or less on the following SADS-C� PDI items:severity of delusions, severity of hallucinations, impaired under-standability, derailment, illogical thinking, bizarre behavior. Theseratings had to be sustained for 8 consecutive weeks.
For the first-episode patients the time to initial response ordrop out was calculated. In the recent-onset group the total timein an acute exacerbation since first hospitalization up to the ERPrecording was calculated as the sum of weeks during which thepatient did not meet response criteria.
Auditory Test ParadigmsPassive Auditory Paradigm (MMN). Auditory stimuli con-
sisted of 100 ms, 1000 Hz standard tones intermixed with 100 ms,1500 Hz frequency deviant tones and 250 ms, 1000 Hz durationdeviant tones. All stimuli had rise/fall time of 5 msec. Stimuliwere presented in a fixed order (4 standards, 1 frequencydeviant, 4 standards, 1 duration deviant) with an stimulus onsetasynchrony (SOA) of 300 msec and presented through foaminsert earphones at a nominal intensity of 75 dB sound pressurelevel (SPL). Stimuli were presented in four blocks with 1000stimuli each totaling 4000 stimuli including 3200 standards, 400frequency deviants and 400 duration deviants. During presenta-tion of the auditory test paradigm subjects performed a visual AXcontinuous performance test to distract their attention from theauditory stimuli.
Active Auditory Paradigm (N2, P3). Standard stimuli of 1000Hz, 100 msec duration were presented intermixed with deviantstimuli of 1500 Hz, 100 msec at a SOA of 500 msec. Rise/fall timewas 5 msec. Deviants were pseudorandomly presented with aprobability of .125. However, at least 3 standards preceded
each deviant. A total of 1000 stimuli were presented (875www.sobp.org/journal
siwRod
N2ra
T
A
D
SSPM
BSPSPPPPCSHS8
c
764 BIOL PSYCHIATRY 2006;59:762–772 D.S.G. Umbricht et al
w
tandards, 125 deviants). Stimuli were presented through foamnsert earphones at nominal intensity of 75 dB SPL. Patientsere instructed to press a button after each deviant tone.esponses were coded as correct when the button pressccurred within 200 to 800 msec after the presentation of theeviant stimulus.
EEG Recordings. EEG recordings were acquired with aEUROSCAN SCAN system (El Paso, Texas) and obtained from9 scalp locations, consisting of standard 10/20 placements plusight and left mastoid placement along with an EOG electrodettached to the right outer canthus. An electrode placed on the
Table 1. Demographics
HealthyControls
First EpisPatien
n 39 26M/F 26/13 19/7Age 30.5 � 7.1 23.9 � 5Race 27 W/7 B/5 O 19 W/12 B
M, male; F, female; W, white; B, black; O, other.aSignificantly different from Healthy Controls.
able 2. Clinical Characteristics
First EpisPatien
ge at First Hospitalization (y) 23.9 � 5Min 16.2 M
uration of Illness (y) .05 � .Min 0 MaxWeeks: 2.7 �Min 0 Max
everity of Illness (CGI) 4.0 � 1ANS Total Score 9.7 � 4ositive Symptomsa 6.4 � 3edication StatusTypical Antipsychotic 2Atypical Antipsychotic 20Benzodiazepines 4Anticonvulsants 1Lithium 2Antidepressants 2Antiparkinsonian 9Other 10
aseline Psychopathology and Premorbid Functioningeverity of Illness (CGI) 5.0 � .ositive Symptomsa 12.7 � 4ANS Total Score 11.4 � 4AS Childhood 1.2 � .AS Early Adolescence 1.5 � 1AS Late Adolescence 1.6 � 1AS Adulthood 1.4 � 1ollege/Postgraduate Education 14%ome College 43%igh School Graduation 0%ome High School 29%th Grade 14%
CGI, Clinical Global Impression Scale; SANS, Schedule for the AssessmenaSum of SADS items ‘severity of delusions’ and ‘severity of hallucination
ontent’ and ‘hallucinations’ in chronic patients (scale 1–7 for both rating scbRecent onset sig. different from both first episode and chronic patientscRecent onset patients sig. different from first episode patients.
dFirst episode patients sig. different from recent onset and chronic patients.ww.sobp.org/journal
nose served as reference. Electrode impedance was kept below5 k�. Activity was amplified with a band pass of .1-30 Hz (24 dBdown) and digitized continuously at a sampling rate of 200 Hz.Digital tags were obtained to all auditory stimuli.
For MMN analyses epochs were constructed that consisted of a100 msec prestimulus baseline and a 500 msec poststimulus interval.For the analyses of N2 and P3 epochs consisted of a 250 msecprestimulus baseline and a 750 msec poststimulus interval. Epochswith amplitudes exceeding � 75 �V at any electrode wereexcluded from averaging. Epochs were averaged off-line for eachsubject and stimulus type. For the MMN analyses only standards
Recent OnsetPatients
ChronicPatients
26 2514/12 17/8
30.3 � 6.7 39.0 � 8.6a
9 W/11 B/6 O 12 W/10 B/2 O
Recent OnsetPatients Chronic Patients Sig.
26.9 � 6.6 23.1 � 6.9 p � .9.6 Min 17.8 Max 39.8 Min 13 Max 41
3.4 � 1.5 16 � 6.9 p � .001Min 1.6 Max 7.0 Min 6.1 Max 30.8Months: 41.0 � 17.6Min 19.1 Max 84.2
2.8 � 1.3 4.5 � .9 p � .001b
7.0 � 2.5 8.7 � 2.0 p � .01c
3.1 � 2.0 7.7 � 2.5 p � .001b
10 16 p � .01d
15 137 6
10 5 p � .05c
7 311 9 p � .05c
22 17– 7
5.1 � .914.0 � 4.1
8.6 � 3.3 p � .011.4 � 1.11.6 � .91.9 � .92.0 � .9
8%75%
4%13%
0%
egative Symptoms; PAS, Psychosocial Adjustment Scale.st-episode and recent onset patients; sum of BPRS items ‘unusual thought
.
odets
.5a
/41 O
odets
.5ax 361.56.3
25.4.5.5.0
9.8.2
7.1.1.2
t of N’ in firales).

tawlw
awidlMMwrts
apa
S
ew(c[CgtfRt
R
S
c
D.S.G. Umbricht et al BIOL PSYCHIATRY 2006;59:762–772 765
hat were not preceded by deviants were averaged. For thenalysis of N2 and P3, only epochs to correctly identified targetsere averaged. N2 and P3 averages were filtered with an 8 Hz
ow pass filter to remove any alpha activity. All averages wavesere digitally detrended to remove any linear trend.MMN average waveforms were mathematically referenced to
n average-mastoid reference prior to area measurements. MMNaveforms were then obtained by subtracting waveforms elic-
ted by standards from waveforms elicited by frequency - oruration-deviant stimuli. Mean amplitude was measured within aatency window of 100 to 200 msec poststimulus for frequencyMN and between 200-300 msec poststimulus for durationMN. N2 and P3 mean amplitudes were measured within latencyindows of 150 to 250 msec and 250 to 400 msec poststimulus,
espectively. N2 was measured from the difference wave (ERP toarget stimulus minus ERP to standard stimulus); P3 was mea-ured from the ERP to the target stimulus.
The minimum sweeps that had to be available for averagingnd inclusion in the analysis was set to 70 for the MMN in theassive auditory paradigm and to 15 for N2 and P3 in the activeuditory paradigm.
tatistical AnalysesMean amplitudes of MMN, N2 and P3 were evaluated at
lectrodes F7, F3, Fz, F4, F8, T3, C3, Cz, C4, T4, T5, P3, Pz, P4, T6ith the help of a repeated measure (rm) analysis of variance
ANOVA) with anterior-posterior electrode location (frontal vs.entral vs. parietal chain) and coronal electrode location (far leftF7, T3, T5] vs. left [F3, C3, P3] vs. midline [Fz, Cz, Pz] vs. right [F4,4, T4] vs. far right [F8, T4, T6]) as within-subject factors androup as between factor. In the case of the MMN analysis MMNype (frequency vs. duration) was an additional within-subjectactor. Since age differed significantly between groups (seeesults), age was used as covariate in all analyses. All correla-ions reported are Pearson correlations.
esults
ubjectsTwenty-six first-episode patients, 25 recent-onset patients, 25
Table 3. Correlations of MMN, N2 and P3 with Patient C
Patients in First-Episode Study OnlyPAS ChildhoodPAS Early AdolescencePAS Late AdolescencePAS AdulthoodPAS Item ‘Education’Duration of any Symptom Prior to First AdmissionDuration of Psychotic Symptoms Prior to First AdmissioAge at First HospitalizationDuration of IllnessCGIDelusionsHallucinationsNegative Symptoms (SANS Total Score)
CGI, Clinical Global Impression Scale; SANS, ScheduleAdjustment Scale; MMN, mismatch negativity.
ap � 0.05.bp � 0.01.
hronic patients and 39 healthy controls were recruited for this
study. Sample characteristics are given in Table 1. Age, but notsex or race ratios, differed significantly between groups (seeTable 1).
Clinical characteristics and the medication status of the patientgroups are given in Tables 2 and 3. Recent-onset patients were ratedas significantly less ill and symptomatic than the two other groups.Among patients participating in the first-episode study PsychosocialAdjustment Scale (PAS) childhood, early and late adolescence andadulthood scores did not differ significantly between first-episodeand recent-onset patients (see Table 2). Also, upon first admissionillness severity did not differ between first-episode and recent-onsetpatients, although patients in the first-episode group showed signif-icantly higher negative symptoms. Significantly more patients in therecent-onset group than in the two other groups had attended somecollege prior to illness onset.
Significantly fewer first-episode patients were treated withtypical antipsychotics than either recent-onset or chronic pa-tients. Recent-onset patients received significantly more oftenanticonvulsants and antidepressants than first-episode patients.
Passive Auditory ParadigmMismatch Negativity. For all patients more than 70 sweeps
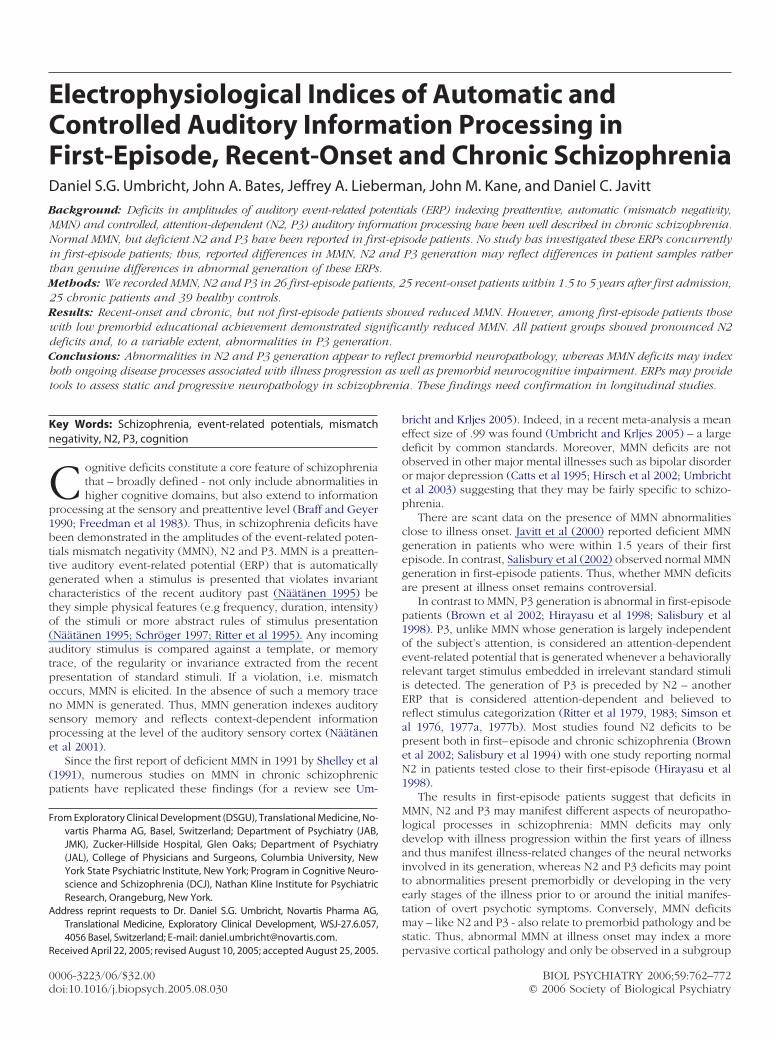
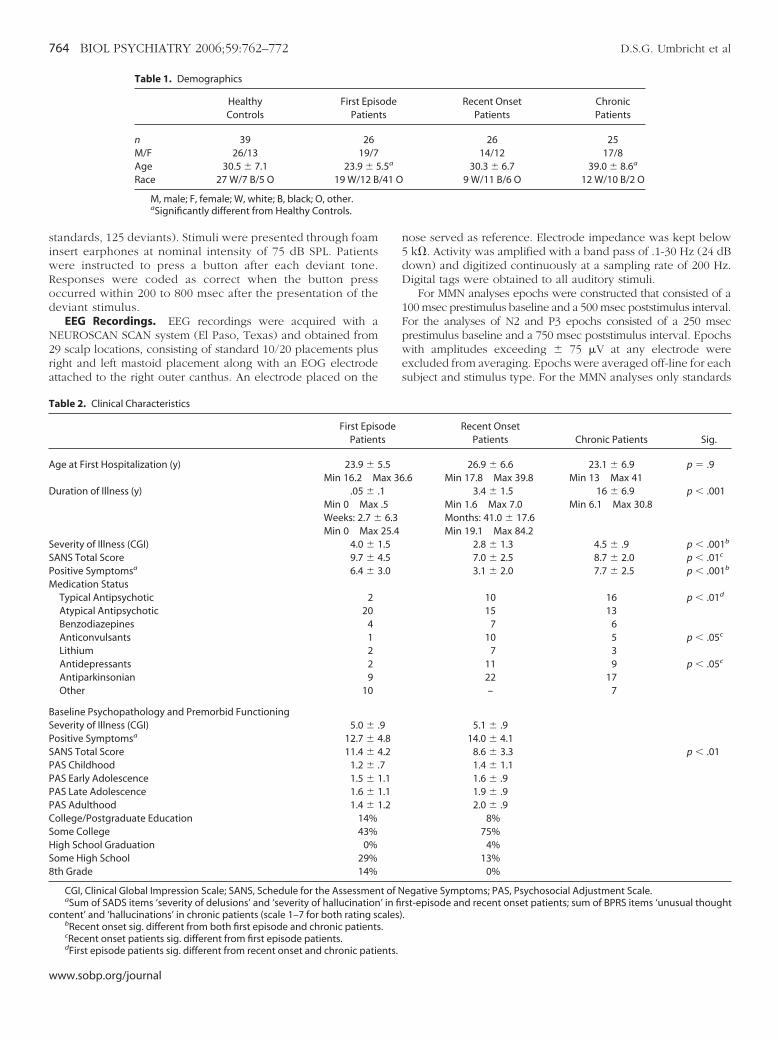
were available for averaging in the MMN paradigm. Mean MMNwas significantly smaller in recent-onset and chronic patientsthan in healthy controls; chronic patients also differed signifi-cantly from first-episode patients (effect of group: F3,111 � 7.08,p � .001; post-hoc LSD p � .05; see Figures 1-3). There was asignificant interaction of group x anterior-posterior electrodelocation (F6,222 � 3.455, p � .005). Post-hoc tests demonstratedsignificant differences at all coronal electrode chains betweenhealthy controls and recent-onset and chronic patients, respec-tively (post-hoc LSD tests of rm ANOVAS for each electrodechain: all p � .05). Separate rm ANOVAs for each MMN typedemonstrated significant group effects for frequency (F3,111 �5.383, p � .005) and duration MMN (F3,111 � 5.340, p � .005).Frequency MMN was significantly larger in healthy controls thanin recent-onset and chronic patients, and in first-episode patientscompared to chronic patients (post-hoc LSD p � .05); post-hoctests showed significantly larger duration MMN in healthy con-
cteristics
FrequencyMMN
DurationMMN N2 P3
�.03 �.20 .50b .03�.15 �.22 .29 .07�.02 �.03 .14 .22�.32 �.13 .13 .12
.31a .40b �.11 �.09
.04 �.17 .46 .2�.01 �.28 .42 .17�.26 �.13 .12 �.05
.19 .19 .08 .05�.05 �.01 .03 �.13�.12 �.12 .02 �.01
.03 �.01 .11 �.18�.35a �.19 .14 .21
e Assessment of Negative Symptoms; PAS, Psychosocial
hara
n
for th
trols than in chronic patients, in first-episode patients than in
www.sobp.org/journal
cM.Meo
ity (M
766 BIOL PSYCHIATRY 2006;59:762–772 D.S.G. Umbricht et al
w
hronic patients and a trend for a significantly larger durationMN in healthy controls than in recent-onset patients (p �
06). Further analyses showed that frequency and durationMN in chronic patients significantly differed at all coronallectrodes chains from healthy controls (see Figure 3). Recent-nset patients showed significantly smaller frequency MMN at
Figure 1. Mismatch negativ
Figure 2. Mismatch negativity (M
ww.sobp.org/journal
all electrode chains and significantly smaller duration MMN atthe central electrode chain compared to healthy controls(Figure 3).
In the recent-onset group MMN amplitudes did not differbetween patients who received atypical antipsychotics (n � 15)and those on typical antipsychotics (n � 9; in the first-episode
MN) to frequency deviants.
MN) to duration deviants.

aot
gsaed
thf
F(C
D.S.G. Umbricht et al BIOL PSYCHIATRY 2006;59:762–772 767
nd chronic group the number of patients who received typicalr atypical antipsychotics, respectively, was too low for a statis-ical comparisons).
We conducted a median split of the first-episode patientroup using both frequency and duration MMN and performed aurvival analysis with time to remission as the dependent vari-ble. None of the survival analyses showed significant differ-nces in time to remission between patients with frequency oruration MMN above or below the median.
In recent-onset patients, the correlation between the totalime each patients had been in an acute exacerbation since firstospitalization prior to the ERP recording was significant for
igure 3. Mean amplitudes of frequency and duration mismatch negativityMMN) across electrodes in the frontal (F7, F3, Fz, F4, F8), central (T3, C3, Cz,4, T4) and parietal (T5, P3, Pz, P4, T6) electrode chains.
requency MMN (r � .4, p � .05), but not duration MMN.
However, after removal of an outlier the correlation was nolonger significant.
Associations and CorrelationsFrequency MMN correlated with negative symptoms across all
patients. However, greater MMN amplitude was associated withhigher negative symptom ratings. Further analyses revealed that thisassociation was only present in first-episode patients. Mean MMNwas significantly associated with educational level achieved acrossall patients (effect of education: F1,64 � 9.426, p � .01, aftercovarying for age at first hospitalization: F1,61 � 5.613, p � .05).Across all patients frequency and duration MMN were signifi-cantly greater in patients who had at least attended some collegecompared to those who had not (frequency MMN: F1,64 � 8.786,p � .01; duration MMN: F1,64 � 5.094, p � .05). Post-hoc analysesdemonstrated that the effect of education for both frequency andduration MMN was only significant in the first-episode, but notthe recent-onset or chronic group (effect of education in first-episode patients: frequency MMN: F1,19 � 6.942, p � .05;duration MMN: F1,19 � 5.959, p � .05). Covarying for age at first
Figure 4. Frequency and duration mismatch negativity (MMN) at electrode
Fz, Cz, and Pz by educational achievement.www.sobp.org/journal
srsbtMs
A
a
Fp
768 BIOL PSYCHIATRY 2006;59:762–772 D.S.G. Umbricht et al
w
ymptom among first episode (FE) patients did not change theseesults. First-episode patients who had not attended collegehowed significantly smaller duration and frequency MMN thanoth normal controls and first-episode patients who had at-ended college (frequency MMN: F2,57 � 3.167, p � .05; durationMN: F2,57 � 3.382, p � .05 (see Figure 4) and did not differ
ignificantly from recent-onset or chronic patients.
ctive Auditory ParadigmFor the N2 and P3 analyses, fewer than 15 sweeps survived
rtifact rejection in 9 patients (1 first-episode, 9 chronic patients)
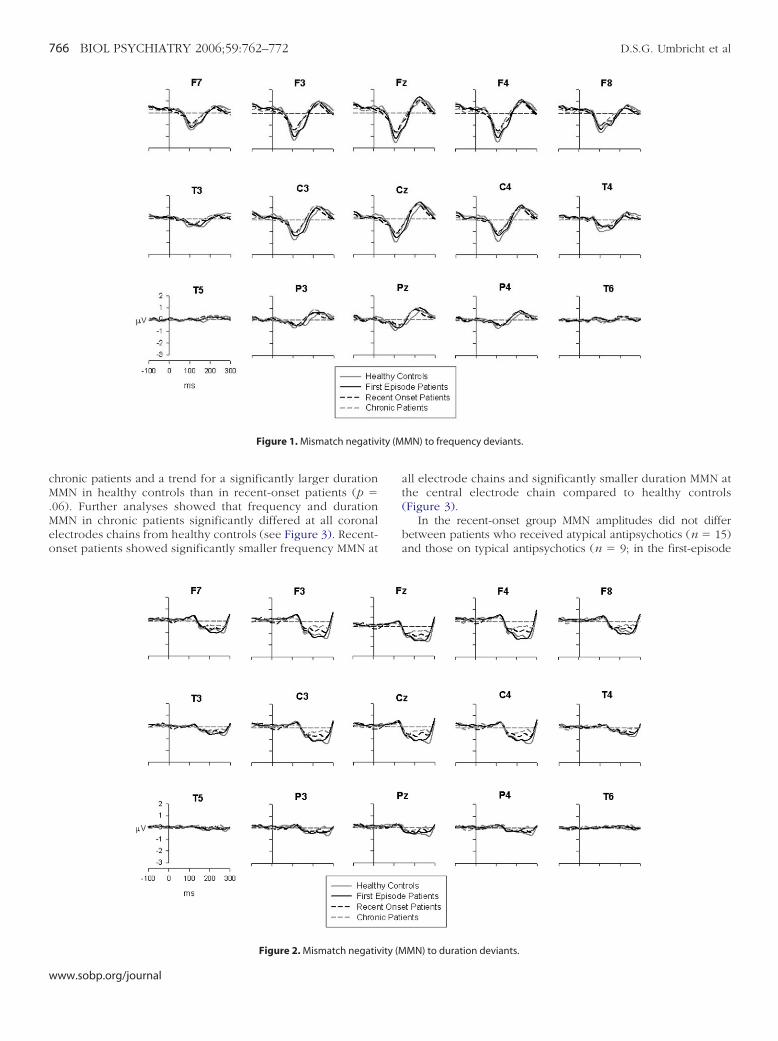
igure 5. N2 at electrode Fz. Note the virtual absence of the N2 wave in allatient groups.
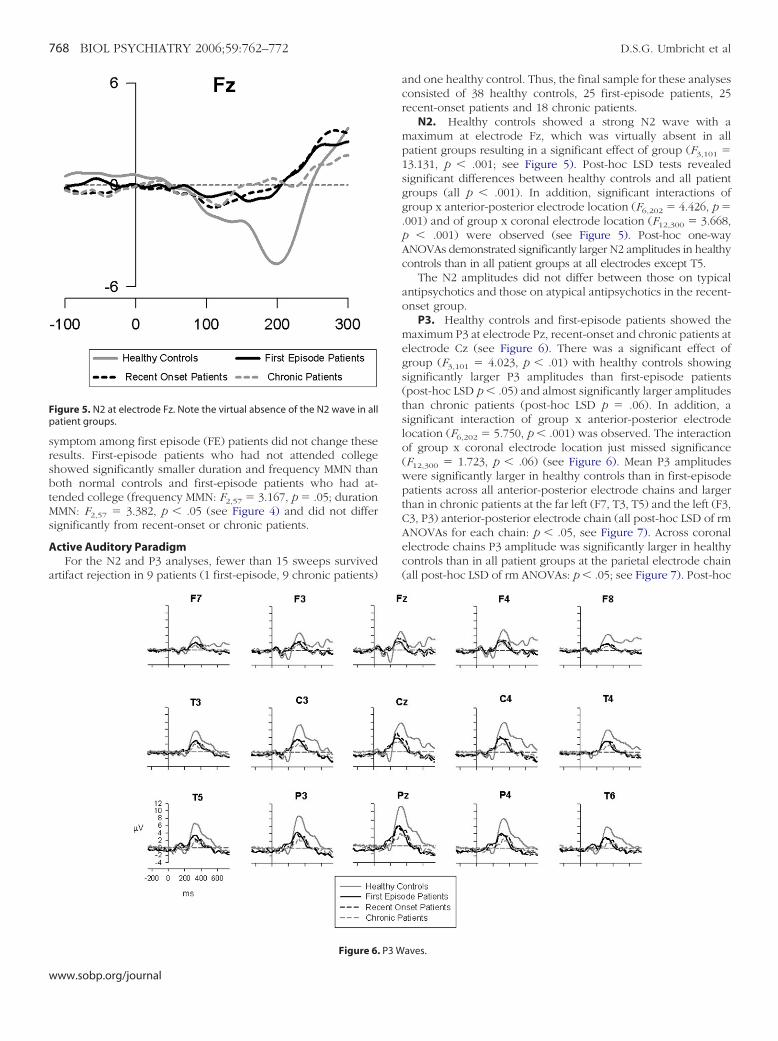
Figure 6. P3 W
ww.sobp.org/journal
and one healthy control. Thus, the final sample for these analysesconsisted of 38 healthy controls, 25 first-episode patients, 25recent-onset patients and 18 chronic patients.
N2. Healthy controls showed a strong N2 wave with amaximum at electrode Fz, which was virtually absent in allpatient groups resulting in a significant effect of group (F3,101 �13.131, p � .001; see Figure 5). Post-hoc LSD tests revealedsignificant differences between healthy controls and all patientgroups (all p � .001). In addition, significant interactions ofgroup x anterior-posterior electrode location (F6,202 � 4.426, p �.001) and of group x coronal electrode location (F12,300 � 3.668,p � .001) were observed (see Figure 5). Post-hoc one-wayANOVAs demonstrated significantly larger N2 amplitudes in healthycontrols than in all patient groups at all electrodes except T5.
The N2 amplitudes did not differ between those on typicalantipsychotics and those on atypical antipsychotics in the recent-onset group.
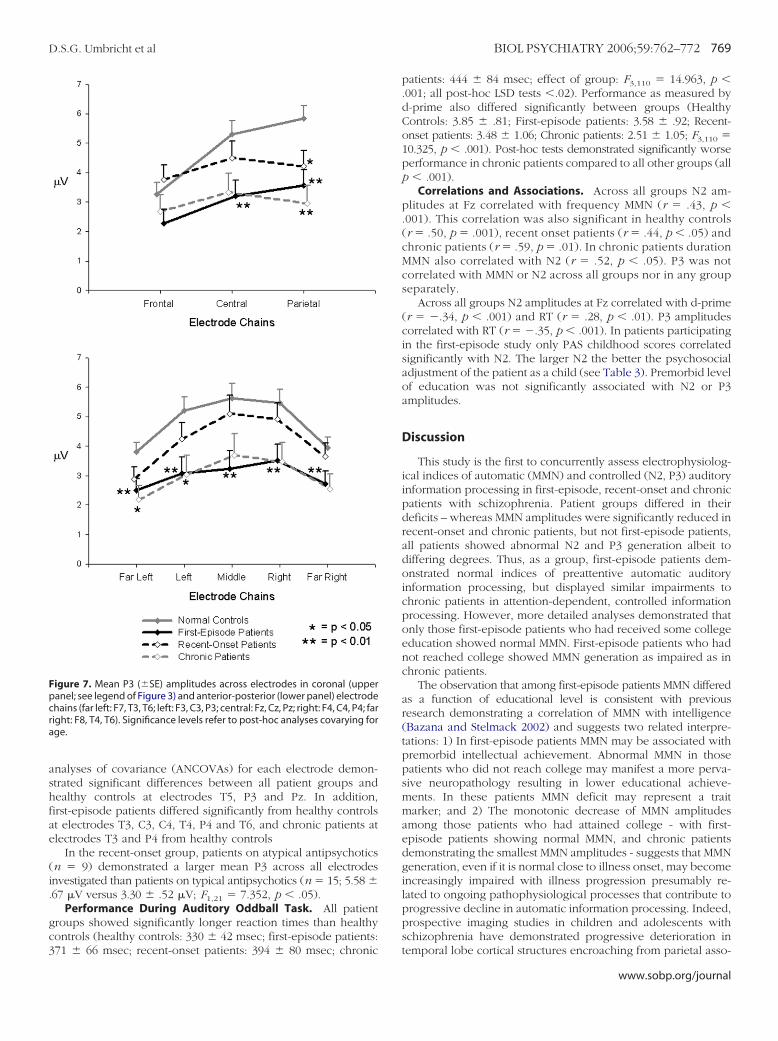
P3. Healthy controls and first-episode patients showed themaximum P3 at electrode Pz, recent-onset and chronic patients atelectrode Cz (see Figure 6). There was a significant effect ofgroup (F3,101 � 4.023, p � .01) with healthy controls showingsignificantly larger P3 amplitudes than first-episode patients(post-hoc LSD p � .05) and almost significantly larger amplitudesthan chronic patients (post-hoc LSD p � .06). In addition, asignificant interaction of group x anterior-posterior electrodelocation (F6,202 � 5.750, p � .001) was observed. The interactionof group x coronal electrode location just missed significance(F12,300 � 1.723, p � .06) (see Figure 6). Mean P3 amplitudeswere significantly larger in healthy controls than in first-episodepatients across all anterior-posterior electrode chains and largerthan in chronic patients at the far left (F7, T3, T5) and the left (F3,C3, P3) anterior-posterior electrode chain (all post-hoc LSD of rmANOVAs for each chain: p � .05, see Figure 7). Across coronalelectrode chains P3 amplitude was significantly larger in healthycontrols than in all patient groups at the parietal electrode chain(all post-hoc LSD of rm ANOVAs: p � .05; see Figure 7). Post-hoc
aves.
ashfae
(i.
gc3
Fpcra
D.S.G. Umbricht et al BIOL PSYCHIATRY 2006;59:762–772 769
nalyses of covariance (ANCOVAs) for each electrode demon-trated significant differences between all patient groups andealthy controls at electrodes T5, P3 and Pz. In addition,irst-episode patients differed significantly from healthy controlst electrodes T3, C3, C4, T4, P4 and T6, and chronic patients atlectrodes T3 and P4 from healthy controls
In the recent-onset group, patients on atypical antipsychoticsn � 9) demonstrated a larger mean P3 across all electrodesnvestigated than patients on typical antipsychotics (n � 15; 5.58 �67 �V versus 3.30 � .52 �V; F1,21 � 7.352, p � .05).
Performance During Auditory Oddball Task. All patientroups showed significantly longer reaction times than healthyontrols (healthy controls: 330 � 42 msec; first-episode patients:
igure 7. Mean P3 (�SE) amplitudes across electrodes in coronal (upperanel; see legend of Figure 3) and anterior-posterior (lower panel) electrodehains (far left: F7, T3, T6; left: F3, C3, P3; central: Fz, Cz, Pz; right: F4, C4, P4; faright: F8, T4, T6). Significance levels refer to post-hoc analyses covarying forge.
71 � 66 msec; recent-onset patients: 394 � 80 msec; chronic
patients: 444 � 84 msec; effect of group: F3,110 � 14.963, p �.001; all post-hoc LSD tests �.02). Performance as measured byd-prime also differed significantly between groups (HealthyControls: 3.85 � .81; First-episode patients: 3.58 � .92; Recent-onset patients: 3.48 � 1.06; Chronic patients: 2.51 � 1.05; F3,110 �10.325, p � .001). Post-hoc tests demonstrated significantly worseperformance in chronic patients compared to all other groups (allp � .001).
Correlations and Associations. Across all groups N2 am-plitudes at Fz correlated with frequency MMN (r � .43, p �.001). This correlation was also significant in healthy controls(r � .50, p � .001), recent onset patients (r � .44, p � .05) andchronic patients (r � .59, p � .01). In chronic patients durationMMN also correlated with N2 (r � .52, p � .05). P3 was notcorrelated with MMN or N2 across all groups nor in any groupseparately.
Across all groups N2 amplitudes at Fz correlated with d-prime(r � �.34, p � .001) and RT (r � .28, p � .01). P3 amplitudescorrelated with RT (r � �.35, p � .001). In patients participatingin the first-episode study only PAS childhood scores correlatedsignificantly with N2. The larger N2 the better the psychosocialadjustment of the patient as a child (see Table 3). Premorbid levelof education was not significantly associated with N2 or P3amplitudes.
Discussion
This study is the first to concurrently assess electrophysiolog-ical indices of automatic (MMN) and controlled (N2, P3) auditoryinformation processing in first-episode, recent-onset and chronicpatients with schizophrenia. Patient groups differed in theirdeficits – whereas MMN amplitudes were significantly reduced inrecent-onset and chronic patients, but not first-episode patients,all patients showed abnormal N2 and P3 generation albeit todiffering degrees. Thus, as a group, first-episode patients dem-onstrated normal indices of preattentive automatic auditoryinformation processing, but displayed similar impairments tochronic patients in attention-dependent, controlled informationprocessing. However, more detailed analyses demonstrated thatonly those first-episode patients who had received some collegeeducation showed normal MMN. First-episode patients who hadnot reached college showed MMN generation as impaired as inchronic patients.
The observation that among first-episode patients MMN differedas a function of educational level is consistent with previousresearch demonstrating a correlation of MMN with intelligence(Bazana and Stelmack 2002) and suggests two related interpre-tations: 1) In first-episode patients MMN may be associated withpremorbid intellectual achievement. Abnormal MMN in thosepatients who did not reach college may manifest a more perva-sive neuropathology resulting in lower educational achieve-ments. In these patients MMN deficit may represent a traitmarker; and 2) The monotonic decrease of MMN amplitudesamong those patients who had attained college - with first-episode patients showing normal MMN, and chronic patientsdemonstrating the smallest MMN amplitudes - suggests that MMNgeneration, even if it is normal close to illness onset, may becomeincreasingly impaired with illness progression presumably re-lated to ongoing pathophysiological processes that contribute toprogressive decline in automatic information processing. Indeed,prospective imaging studies in children and adolescents withschizophrenia have demonstrated progressive deterioration in
temporal lobe cortical structures encroaching from parietal asso-www.sobp.org/journal

cepgsitfofnlutirdwtfipd
gera2Kc1tsittdiB1drpP
bw1rtifctwaHgdpt
770 BIOL PSYCHIATRY 2006;59:762–772 D.S.G. Umbricht et al
w
iation areas into temporal lobe structures over time (Thompsont al 2001; Jacobsen et al 1998). Furthermore, in an ongoingrospective study of MMN in first-episode patients the emer-ence of MMN deficits with illness progression has been ob-erved (Salisbury et al 2004). However, in the recent-onset groupn our study the total time spent in an acute exacerbation prior tohe ERP recording was not correlated with MMN deficits. Thisinding is obviously severely limited by the cross-sectional naturef this study. An alternative view of the overall normal MMN inirst-episode patients holds that this group includes patients withormal MMN who show a favorable illness course and are lessikely represented in samples of chronic patients resulting inndetectable MMN deficits in first-episode groups. Chronic pa-ients may thus represent a more homogenous sample concern-ng the genetics of MMN deficits. This could explain why MMN inelatives of chronic schizophrenic patients is significantly re-uced (Jessen et al 2001; Michie et al 2002). This assumptionould predict that patients with normal MMN show a different
reatment course. However, in our study first-episode patients’requency and duration MMN was not associated with time tonitial remission. To the extent that time to initial remission isredictive of future illness course, these results would favor aeterioration of MMN generation with illness progression.
With regard to N2 all patient groups essentially failed toenerate this potential, consistent with previous studies in first-pisode and chronic schizophrenia that reported significanteduction of N2 wave for the auditory (Alain et al 2001; Brown etl 2002; Bruder et al 2001; Hirayasu et al 1998; O’Donnell et al004; Salisbury et al 1994) and visual modality (Alain et al 1998;ayser et al 1999). Given the evidence that N2 indexes stimuluslassification (Ritter et al 1979, 1983; Simson et al 1976, 1977a,977b) the reduction of N2 in patients and its association withask performance suggest that schizophrenic patients demon-trate abnormalities in this important step of information process-ng which may be related to neuroanatomical abnormalities inhe superior temporal gyrus and in other gray matter structures ofhe temporal lobes (O’Donnell et al 1993). All patient groups alsoemonstrated reduced generation of P3 replicating prior findingsn first-episode and chronic schizophrenia (for reviews seeramon et al 2004; Salisbury et al 1998; Ford 1999; McCarley et al991; Pritchard 1986). While first-episode and chronic patientsiffered significantly from healthy controls at all electrodes,ecent-onset patients demonstrated significantly smaller P3 am-litudes only at left-side and midline parietal electrodes (P3, T5,z) when compared to controls.
P3 deficits in first-episode patients (Brown et al 2002; Salis-ury et al 1998) and relatives of schizophrenic patients (Black-ood 2000; Ebmeier et al 1990; Kimble et al 2000; Weisbrod et al999;Winterer et al 2003a, 2003b) suggest that reduced P3epresents a vulnerability marker for schizophrenia. However, inhe recent-onset patient group the mean P3 across all electrodesnvestigated was not significantly reduced possibly due to theact that those patients who were treated with atypical antipsy-hotics demonstrated significantly larger P3 amplitudes thanhose on typical antipsychotics. This observation is consistentith the enhancement of P3 amplitude after treatment withtypical antipsychotics (Schall et al 1998; Umbricht et al 1998).owever, even this group demonstrated a left-sided deficit in P3eneration consistent with previous reports of pronounced P300eficit on the left side (McCarley et al 1993; Salisbury et al 1998),resumably associated with neuroanatomical abnormalities in
he left superior temporal gyrus (McCarley et al 1993).ww.sobp.org/journal
The significant abnormalities in attention-dependent informa-tion processing in first-episode patients concur with significantimpairments across various cognitive domains in these patients(Bilder et al 2000; Hoff et al 1992). Prospective studies of subjectswho developed schizophrenia indicate that some of these defi-cits are present already in childhood or precede the overt onsetof the illness by years (Cannon et al 1999, 2002; Cornblatt et al1999; Davidson et al 1999; Fuller et al 2002; Rabinowitz et al2000; Reichenberg et al 2002; Weiser et al 2002). Whetherabnormalities in N2 and P3 generation are present premorbidlyhas not been investigated. However, associations of N2 deficitswith poor premorbid adjustment (Levitt et al 1996) and of P3deficits with presumed markers of a neurodevelopmental originof schizophrenia (Hegerl et al 1995) suggest that these ERPdeficits may indeed reflect premorbid neuropathology.
In conclusion, our results suggest that in schizophrenic pa-tients deficits in the generation of MMN, N2 and P3 representboth premorbid pathology, possibly of neurodevelopmentalorigin (MMN in patients with poor educational achievement; N2,P3), as well as progressive neuropathological changes that maydevelop with illness progression (MMN in those with goodeducational achievement).
Our study has several limitations. First-episode patients werenot studied in a medication-free status. Thus, we cannot rule outthe possibility that pharmacologic treatment may have improvedMMN generation accounting for the lack of MMN deficits in thefirst-episode group. However, this is not consistent with thepresence of MMN deficits in the recent-onset and chronic groupswho received pharmacological treatment as well. Moreover,previous studies have failed to demonstrate effects of typical oratypical antipsychotics on MMN (Schall et al 1998; Umbricht et al1998, 1999). Given the evidence that atypical antipsychoticsseem to improve P3 generation (Schall et al 1998; Umbricht et al1998, 1999), and medication withdrawal in chronic patients hasbeen associated with a worsening of P3 (Ford et al 1994), thedeficit in P3 generation in recent-onset patients may have beeneven larger had they been studied in a medication free status. Inaddition, the chronic patients were drawn from a different studythat used different ratings scales for positive symptoms. Thus, afull assessment of potential correlations of ERPs and positivesymptomatology was not possible.
This research was supported by a grant from the NationalAlliance for Research on Schizophrenia and Depression (NARSAD)to DSGU and United States Public Health Service grants MH-41960,MH-00537 and MH-41646 from the National Institute of MentalHealth.
Alain C, Cortese F, Bernstein LJ, He Y, Zipursky RB (2001): Auditory featureconjunction in patients with schizophrenia. Schizophr Res 49:179 –191.
Alain C, Hargrave R, Woods DL (1998): Processing of auditory stimuli during visualattention in patients with schizophrenia. Biol Psychiatry 44:1151–1159.
Andreasen NC (1983): The Scale of the Assessment of Negative Symptoms(SANS). Iowa City: The University of Iowa.
Bazana PG, Stelmack RM (2002): Intelligence and information processing during anauditorydiscriminationtaskwithbackwardmasking:anevent-relatedpotentialanalysis. J Personality Soc Psychology 83:998–1008.
Bilder RM, Goldman RS, Robinson D, Reiter G, Bell L, Bates JA, et al (2000):Neuropsychology of first-episode schizophrenia: initial characterizationand clinical correlates. Am J Psychiatry 157:549 –559.
Blackwood D (2000): P300, a state and a trait marker in schizophrenia. Lancet355:771–772.
Braff DL, Geyer MA (1990): Sensorimotor gating and schizophrenia. Arch Gen
Psychiatry 47:181–188.
B
B
B
C
C
C
C
C
D
E
F
F
F
F
G
H
H
H
H
J
J
J
K
D.S.G. Umbricht et al BIOL PSYCHIATRY 2006;59:762–772 771
ramon E, Rabe-Hesketh S, Sham P, Murray RM, Frangou S (2004): Meta-analysis of the P300 and P50 waveforms in schizophrenia. Schizophr Res70:315–329.
rown KJ, Gonsalvez CJ, Harris AW, Williams LM, Gordon E (2002): Target andnontarget ERP disturbances in first episode vs. chronic schizophrenia.Clin Neurophysiol 113:1754 –1763.
ruder GE, Kayser J, Tenke CE, Friedman M, Malaspina D, Gorman JM (2001):Event-related potentials in schizophrenia during tonal and phoneticoddball tasks: relations to diagnostic subtype, symptom features andverbal memory. Biol Psychiatry 50:447– 452.
annon M, Caspi A, Moffitt TE, Harrington H, Taylor A, Murray RM, et al(2002): Evidence for early-childhood, pan-developmental impairmentspecific to schizophreniform disorder: results from a longitudinal birthcohort. Arch Gen Psychiatry 59:449 – 456.
annon M, Jones P, Huttunen MO, Tanskanen A, Huttunen T, Rabe-HeskethS, et al (1999): School performance in Finnish children and later develop-ment of schizophrenia: a population-based longitudinal study. Arch GenPsychiatry 56:457– 463.
annonSpoor HE, Potkin SG, Wyatt RJ (1982): Measurement of premorbidadjustment in chronic schizophrenia. Schizophr Bull 8:470 – 484.
atts SV, Shelley AM, Ward PB, Liebert B, McConaghy N, Andrews S, et al(1995): Brain potential evidence for an auditory sensory memory deficitin schizophrenia. Am J Psychiatry 152:213–219.
ornblatt B, Obuchowski M, Roberts S, Pollack S, Erlenmeyer-Kimling L(1999): Cognitive and behavioral precursors of schizophrenia. Dev Psy-chopathol 11:487–508.
avidson M, Reichenberg A, Rabinowitz J, Weiser M, Kaplan Z, Mark M(1999): Behavioral and intellectual markers for schizophrenia in appar-ently healthy male adolescents. Am J Psychiatry 156:1328 –1335.
bmeier KP, Potter DD, Cochrane RH, Mackenzie AR, MacAllister H, BessonJA, et al (1990): P300 and smooth eye pursuit: concordance of abnormal-ities and relation to clinical features in DSM-III schizophrenia. Acta Psy-chiatr Scand 82:283–288.
ord JM (1999): Schizophrenia: the broken P300 and beyond. Psychophysi-ology 36:667– 682.
ord JM, White PM, Csernansky JG, Faustman WO, Roth WT, Pfefferbaum A(1994): ERPs in schizophrenia: effects of antipsychotic medication. BiolPsychiatry 36:153–170.
reedman R, Adler LE, Waldo MC, Pachtman E, Franks RD (1983): Neurophys-iological evidence for a defect in inhibitory pathways in schizophrenia:comparison of medicated and drug-free patients. Biol Psychiatry 18:537–551.
uller R, Nopoulos P, Arndt S, O’Leary D, Ho BC, Andreasen NC (2002):Longitudinal assessment of premorbid cognitive functioning in patientswith schizophrenia through examination of standardized scholastic testperformance. Am J Psychiatry 159:1183–1189.
uy W (1976): Clinical Global Impression Scale EDCEU Assessment Manual:United States Department of Health, Education and Welfare, pp 218-222.
egerl U, Juckel G, Muller-Schubert A, Pietzcker A, Gaebel W (1995): Schizo-phrenics with small P300: a subgroup with a neurodevelopmental dis-turbance and a high risk for tardive dyskinesia? Acta Psychiatr Scand91:120 –125.
irayasu Y, Asato N, Ohta H, Hokama H, Arakaki H, Ogura C (1998): Abnor-malities of auditory event-related potentials in schizophrenia prior totreatment. Biol Psychiatry 43:244 –253.
irsch SR, Krljes S, Baldeweg T (2002): Diagnostic ability of mismatch nega-tivity to differentiate between schizophrenia and bipolar disorder.Schizophr Res 53:18.
off AL, Riordan H, O’Donnell DW, Morris L, DeLisi LE (1992): Neuropsycho-logical functioning of first episode schizophreniform patients. Am J Psy-chiatry 149:898 –903.
acobsen LK, Giedd JN, Castellanos FX, Vaituzis AC, Hamburger SD, Kumra S,et al (1998): Progressive reduction of temporal lobe structures in child-hood-onset schizophrenia. Am J Psychiatry 155:678 – 685.
avitt DC, Shelley AM, Silipo G, Lieberman JA (2000): Deficits in auditory andvisual context-dependent processing in schizophrenia: Defining thepattern. Arch Gen Psychiatry 57:1131–1137.
essen F, Fries T, Kucharski C, Nishimura T, Hoenig K, Maier W, et al (2001):Amplitude reduction of the mismatch negativity in first-degree relativesof patients with schizophrenia. Neurosci Lett 309:185–188.
ayser J, Bruder GE, Friedman D, Tenke CE, Amador XF, Clark SC, et al (1999):Brain event-related potentials (ERPs) in schizophrenia during a word
recognition memory task. Int J Psychophysiol 34:249 –265.Kimble M, Lyons M, O’Donnell B, Nestor P, Niznikiewicz M, Toomey R (2000):The effect of family status and schizotypy on electrophysiologic mea-sures of attention and semantic processing. Biol Psychiatry 47:402– 412.
Levitt JJ, O’Donnell BF, McCarley RW, Nestor PG, Shenton ME (1996): Corre-lations of premorbid adjustment in schizophrenia with auditory event-related potential and neuropsychological abnormalities. Am J Psychiatry153:1347–1349.
Lieberman JA, Alvir JM, Woerner MG, Degreef G, Bilder RM, Ashtari M, et al(1992): Prospective study of psychobiology in first-episode schizophre-nia at Hillside Hospital. Schizophr Bulletin 18:351–371.
Lieberman JA, Jody DN, Geisler SH, Alvir JM, Loebel A, Szymanski S, et al(1993): Time course and biologic correlates of treatment response infirst-episode schizophrenia. Arch Gen Psychiatry 50:369 –376.
McCarley RW, Faux SF, Shenton M, Nestor PG, Adams J (1991): Event-relatedpotentials in schizophrenia: their biological and clinical correlates and anew model of schizophrenic pathophysiology. Schizophr Res 4:209 –231.
McCarley RW, Shenton ME, O’Donnell BF, Faux SF, Kikinis R, Nestor PG, et al(1993): Auditory P300 abnormalities and left posterior superior temporalgyrus volume reduction in schizophrenia. Arch Gen Psychiatry 50:190 –197.
Michie PT, Innes-Brown H, Todd J, Jablensky AV (2002): Duration mismatchnegativity in biological relatives of patients with schizophrenia spec-trum disorders. Biol Psychiatry 52:749 –758.
Näätänen R (1995): The mismatch negativity: a powerful tool for cognitiveneuroscience. Ear & Hearing 16:6 –18.
Näätänen R, Tervaniemi M, Sussman E, Paavilainen P, Winkler I (2001): “Prim-itive intelligence” in the auditory cortex. Trends Neurosci 24:283–288.
O’Donnell BF, Shenton ME, McCarley RW, Faux SF, Smith RS, Salisbury DF, etal (1993): The auditory N2 component in schizophrenia: relationship toMRI temporal lobe gray matter and to other ERP abnormalities. BiolPsychiatry 34:26 – 40.
O’Donnell BF, Vohs JL, Hetrick WP, Carroll CA, Shekhar A (2004): Auditoryevent-related potential abnormalities in bipolar disorder and schizo-phrenia. Int J Psychophysiol 53:45–55.
Pritchard WS (1986): Cognitive event-related potential correlates of schizo-phrenia. Psychological Bulletin 100:43– 66.
Rabinowitz J, Reichenberg A, Weiser M, Mark M, Kaplan Z, Davidson M(2000): Cognitive and behavioural functioning in men with schizophre-nia both before and shortly after first admission to hospital. Cross-sec-tional analysis. Br J Psychiatry 177:26 –32.
Reichenberg A, Weiser M, Rabinowitz J, Caspi A, Schmeidler J, Mark M, et al(2002): A population-based cohort study of premorbid intellectual, lan-guage, and behavioral functioning in patients with schizophrenia,schizoaffective disorder, and nonpsychotic bipolar disorder. Am J Psychi-atry 159:2027–2035.
Ritter W, Deacon D, Gomes H, Javitt DC, Vaughan HG, Jr (1995): The mis-match negativity of event-related potentials as a probe of transientauditory memory: a review. Ear & Hearing 16:52– 67.
Ritter W, Simson R, Vaughan HG, Jr (1983): Event-related potential correlatesof two stages of information processing in physical and semantic dis-crimination tasks. Psychophysiology 20:168 –179.
Ritter W, Simson R, Vaughan HG, Jr, Friedman D (1979): A brain event relatedto the making of a sensory discrimination. Science 203:1358 –1361.
Salisbury DF, Kuroki N, Kasai K, Shenton ME, McCarley RW (2004): MismatchNegativity as an index of peri-onset cortical reduction in schizophrenia.Biol Psychiatry 55:Supplement 1, 221S.
Salisbury DF, O’Donnell BF, McCarley RW, Shenton ME, Benavage A (1994):The N2 event-related potential reflects attention deficit in schizophre-nia. Biol Psychol 39:1–13.
Salisbury DF, Shenton ME, Griggs CB, Bonner-Jackson A, McCarley RW(2002): Mismatch negativity in chronic schizophrenia and first-episodeschizophrenia. Arch Gen Psychiatry 59:686 – 694.
Salisbury DF, Shenton ME, Sherwood AR, Fischer IA, Yurgelun-Todd DA,Tohen M, et al (1998): First-episode schizophrenic psychosis differs fromfirst-episode affective psychosis and controls in P300 amplitude over lefttemporal lobe. Arch Gen Psychiatry 55:173–180.
Schall U, Catts SV, Chaturvedi S, Liebert B, Redenbach J, Karayanidis F, et al(1998): The effect of clozapine therapy on frontal lobe dysfunction inschizophrenia: neuropsychology and event-related potential measures.Int J Neuropsychoph 1:19 –29.
Schooler NR, Marder SR, Kane J, Chengappa KN, Wirshing WC, Umbricht D(1999): Clozapine and risperidone: A 29-week randomized clinical trial.
Schizophr Res 36:296.www.sobp.org/journal

S
S
S
S
S
S
S
S
T
772 BIOL PSYCHIATRY 2006;59:762–772 D.S.G. Umbricht et al
w
chröger E (1997): On the detection of auditory deviations: A pre-attentiveactivation model. Psychophysiology 34:245–257.
helley AM, Ward PB, Catts SV, Michie PT, Andrews S, McConaghy N (1991):Mismatch negativity: an index of a preattentive processing deficit inschizophrenia. Biol Psychiatry 30:1059 –1062.
imson R, Vaughan HG, Jr, Ritter W (1977a): The scalp topography of poten-tials in auditory and visual Go/NoGo tasks. Electroencephalogr Clin Neu-rophysiol 43:864 – 875.
imson R, Vaughan HG, Jr, Ritter W (1976): The scalp topography of poten-tials associated with missing visual or auditory stimuli. Electroencepha-logr Clin Neurophysiol 40:33– 42.
imson R, Vaughn HG, Jr, Ritter W (1977b): The scalp topography of poten-tials in auditory and visual discrimination tasks. Electroencephalogr ClinNeurophysiol 42:528 –535.
pitzer RL, Endicott J (1978): Schedule for Affective Disorders and Psychosisand Disorganization, 3rd ed. New York, NY: Biometric Research Division,New York State Psychiatric Institute.
pitzer RL, Endicott J, Robins E (1978): Research Diagnostic Criteria: Ratio-nale and reliability. Arch Gen Psychiatry 35:773–782.
pitzer RL, Williams JBW, Gibbon M, First MB (1999): Structured Clinical Inter-view for DSM-III-R - Patient Version. Washington DC: American PsychiatricPress.
hompson PM, Vidal C, Giedd JN, Gochman P, Blumenthal J, Nicolson R, et al(2001): Mapping adolescent brain change reveals dynamic wave of ac-
celerated gray matter loss in very early-onset schizophrenia. PNAS 98:11650 –11655.ww.sobp.org/journal
Umbricht D, Javitt DC, Novak GP, Bates JA, Pollack S, Lieberman J, et al(1998): Effects of clozapine on auditory event-related potentials inschizophrenia. Biol Psychiatry 44:716 –725.
Umbricht D, Javitt DC, Novak GP, Bates JA, Pollak S, Lieberman J, et al (1999):Effects of risperidone on auditory event-related potentials in schizo-phrenia. Int J Neuropsychoph 2:229 –304.
Umbricht D, Koller R, Schmid L, Skrabo A, Grubel C, Huber T, et al (2003): Howspecific are deficits in mismatch negativity generation to schizophrenia?Biol Psychiatry 53:1120 –1131.
Umbricht D, Krljes S (2005): Mismatch Negativity in Schizophrenia: A meta-analysis. Schizophr Res 76:1–23.
Weisbrod M, Hill H, Niethammer R, Sauer H (1999): Genetic influence onauditory information processing in schizophrenia: P300 in monozygotictwins. Biol Psychiatry 46:721–725.
Weiser M, Knobler HY, Noy S, Kaplan Z (2002): Clinical characteristics ofadolescents later hospitalized for schizophrenia. Am J Med Genet 114:949 –955.
Winterer G, Coppola R, Egan MF, Goldberg TE, Weinberger DR (2003a):Functional and effective frontotemporal connectivity and genetic riskfor schizophrenia. Biol Psychiatry 54:1181–1192.
Winterer G, Egan MF, Raedler T, Sanchez C, Jones DW, Coppola R, et al(2003b): P300 and genetic risk for schizophrenia. Arch Gen Psychiatry60:1158 –1167.
Woerner MG, Manuzza S, Kane JM (1988): Anchoring the Brief Psychiatric
Rating Scale; an aid to improve reliability. Psychopharmacol Bull 24:112–117.



















