Efficacy and safety of the selective 11β-HSD-1 inhibitors MK-0736 and MK-0916 in overweight and...
11
Research Article Efficacy and safety of the selective 11b-HSD-1 inhibitors MK-0736 and MK-0916 in overweight and obese patients with hypertension Sukrut Shah, PhD, RPh * , Anne Hermanowski-Vosatka, MD, PhD, Kendra Gibson, RN, MSN, MBA, Rae Ann Ruck, RN, BSN, Gang Jia, PhD, John Zhang, PhD, Peggy M.T. Hwang, PhD, Nicholas W. Ryan, PharmD, Ronald B. Langdon, PhD, and Peter U. Feig, MD Merck Sharp & Dohme Corp., Rahway, New Jersey, USA Manuscript received November 24, 2010 and accepted January 31, 2011 Abstract 11b-hydroxysteroid dehydrogenase type 1 (11b-HSD1) may be involved in several abnormalities associated with the metabolic syndrome. This study evaluated the antihypertensive efficacy and safety of two 11b-HSD1 inhibitors, MK-0736 and MK-0916, in overweight-to-obese hypertensive patients. Patients aged 18–75 years with sitting diastolic blood pressure (SiDBP) 90–104 mm Hg, systolic BP <160 mm Hg (after washout of prior antihypertensive medications), and BMI 27 to <41 kg/m 2 were randomized to receive 2 or 7 mg/d MK-0736, 6 mg/d MK-0916, or placebo for 12 weeks (n ¼ 51–54/group). Patients with BMI 20 to <27 kg/m 2 received 6 mg/d MK-0916 or placebo for 24 weeks (n ¼ 19/group). The primary endpoint was placebo-adjusted change from baseline in trough SiDBP in patients treated for 12 weeks with 7 mg/d MK-0736. The primary endpoint was not met (placebo-adjusted reduction ¼ 2.2 mm Hg; P ¼ .157). With 7 mg/d MK-0736, placebo-adjusted LDL-C decreased by 12.3%, high-density lipoprotein cholesterol by 6.3%, and body weight by 1.4 kg. Both 11b-HSD1 inhibitors were generally well tolerated. In overweight-to-obese patients with hypertension, reduction in SiDBP with MK-0736 was not statistically significant. Nonetheless, MK-0736 was well tolerated and did appear to modestly improve other BP endpoints, LDL-C, and body weight. J Am Soc Hypertens 2011;5(3):166–176. Ó 2011 American Society of Hypertension. All rights reserved. Keywords: Metabolic syndrome; dyslipidemia; low-density lipoprotein cholesterol; ambulatory blood pressure monitoring. Introduction Although hypertension is well recognized as a major risk factor for development of cardiovascular and renal disease, it is often inadequately treated and new modes of therapy for hypertension are needed. 1–3 There is considerable interest in the possibility that hypertension and/or other components of the metabolic syndrome 4 may be favorably altered through inhibition of the enzyme 11b-hydroxyste- roid dehydrogenase type 1 (11b-HSD1). 5–8 This enzyme is highly active in the liver and is expressed by many other tissues, including the adipocytes in omental fat. In these tissues, it converts the inactive glucocorticoids cortisone and dehydrocorticosterone into the active hormones cortisol and corticosterone. It is thought that, via this action, locally elevated levels of active glucocorticoids may play key roles in the control of blood pressure (BP), blood levels of glucose and lipids, and the growth of adipose tissue. 7,9 MK-0916 and MK-0736 are 2 experimental 11b-HSD1 inhibitors that have been developed as potential treatments for hyperglycemia, hypertension, and other metabolic syndrome components. A Phase I pharmacodynamic study has shown that the dosages of 2 and 7 mg/d MK-0736 inhibit hepatic 11b-HSD1 by about 85% and 95%, S.S. and A.H.-V. are co-first authors. Funding/support: This study was sponsored by Merck Sharp & Dohme Corp., a subsidiary of Merck & Co., Inc., Whitehouse Station, NJ, and registered as NCT00274716 on ClinicalTrials.gov . Conflict of interest: All authors are current or former employees of Merck Sharp & Dohme Corp. *Corresponding author: Sukrut Shah, PhD, RPh, Merck Sharp & Dohme Corp., RY34A-204, 126 E. Lincoln Avenue, P.O. Box 2000, Rahway, NJ 07065–0900, USA. Tel: þ1 (732) 594–1351; fax: þ1 (732) 594–7381. E-mail: [email protected] 1933-1711/$ - see front matter Ó 2011 American Society of Hypertension. All rights reserved. doi:10.1016/j.jash.2011.01.009 Journal of the American Society of Hypertension 5(3) (2011) 166–176
-
Upload
independent -
Category
Documents
-
view
1 -
download
0
Transcript of Efficacy and safety of the selective 11β-HSD-1 inhibitors MK-0736 and MK-0916 in overweight and...
Journal of the American Society of Hypertension 5(3) (2011) 166–176
Research Article
Efficacy and safety of the selective 11b-HSD-1 inhibitors MK-0736and MK-0916 in overweight and obese patients with hypertension
Sukrut Shah, PhD, RPh*, Anne Hermanowski-Vosatka, MD, PhD,Kendra Gibson, RN, MSN, MBA, Rae Ann Ruck, RN, BSN, Gang Jia, PhD, John Zhang, PhD,
Peggy M.T. Hwang, PhD, Nicholas W. Ryan, PharmD, Ronald B. Langdon, PhD,and Peter U. Feig, MD
Merck Sharp & Dohme Corp., Rahway, New Jersey, USA
Manuscript received November 24, 2010 and accepted January 31, 2011
Abstract
11b-hydroxysteroid dehydrogenase type 1 (11b-HSD1) may be involved in several abnormalities associated with the metabolicsyndrome. This study evaluated the antihypertensive efficacy and safety of two 11b-HSD1 inhibitors, MK-0736 and MK-0916,in overweight-to-obese hypertensive patients. Patients aged 18–75 years with sitting diastolic blood pressure (SiDBP) 90–104mm Hg, systolic BP <160 mm Hg (after washout of prior antihypertensive medications), and BMI �27 to <41 kg/m2 wererandomized to receive 2 or 7 mg/d MK-0736, 6 mg/d MK-0916, or placebo for 12 weeks (n ¼ 51–54/group). Patients withBMI �20 to <27 kg/m2 received 6 mg/d MK-0916 or placebo for 24 weeks (n ¼ 19/group). The primary endpoint wasplacebo-adjusted change from baseline in trough SiDBP in patients treated for 12 weeks with 7 mg/d MK-0736. The primaryendpoint was not met (placebo-adjusted reduction ¼ 2.2 mm Hg; P ¼ .157). With 7 mg/d MK-0736, placebo-adjustedLDL-Cdecreased by 12.3%, high-density lipoprotein cholesterol by 6.3%, and bodyweight by 1.4 kg. Both 11b-HSD1 inhibitorswere generally well tolerated. In overweight-to-obese patients with hypertension, reduction in SiDBP with MK-0736 was notstatistically significant. Nonetheless, MK-0736 was well tolerated and did appear to modestly improve other BP endpoints,LDL-C, and body weight. J Am Soc Hypertens 2011;5(3):166–176. � 2011 American Society of Hypertension. All rightsreserved.Keywords: Metabolic syndrome; dyslipidemia; low-density lipoprotein cholesterol; ambulatory blood pressure monitoring.
Introduction
Although hypertension is well recognized as a major riskfactor for development of cardiovascular and renal disease,it is often inadequately treated and new modes of therapyfor hypertension are needed.1–3 There is considerable
S.S. and A.H.-V. are co-first authors.Funding/support: This study was sponsored by Merck Sharp &
Dohme Corp., a subsidiary of Merck & Co., Inc., WhitehouseStation, NJ, and registered as NCT00274716 on ClinicalTrials.gov.
Conflict of interest: All authors are current or formeremployees of Merck Sharp & Dohme Corp.
*Corresponding author: Sukrut Shah, PhD, RPh,Merck Sharp&Dohme Corp., RY34A-204, 126 E. Lincoln Avenue, P.O. Box2000, Rahway, NJ 07065–0900, USA. Tel: þ1 (732) 594–1351;fax: þ1 (732) 594–7381.
E-mail: [email protected]
1933-1711/$ - see front matter � 2011 American Society of Hypertensdoi:10.1016/j.jash.2011.01.009
interest in the possibility that hypertension and/or othercomponents of the metabolic syndrome4 may be favorablyaltered through inhibition of the enzyme 11b-hydroxyste-roid dehydrogenase type 1 (11b-HSD1).5–8 This enzymeis highly active in the liver and is expressed by many othertissues, including the adipocytes in omental fat. In thesetissues, it converts the inactive glucocorticoids cortisoneand dehydrocorticosterone into the active hormones cortisoland corticosterone. It is thought that, via this action, locallyelevated levels of active glucocorticoids may play key rolesin the control of blood pressure (BP), blood levels ofglucose and lipids, and the growth of adipose tissue.7,9
MK-0916 and MK-0736 are 2 experimental 11b-HSD1inhibitors that have been developed as potential treatmentsfor hyperglycemia, hypertension, and other metabolicsyndrome components. A Phase I pharmacodynamic studyhas shown that the dosages of 2 and 7 mg/d MK-0736inhibit hepatic 11b-HSD1 by about 85% and 95%,
ion. All rights reserved.

167S. Shah et al. / Journal of the American Society of Hypertension 5(3) (2011) 166–176
respectively, and that 2mg/dMK-0736 and 6mg/dMK-0916are approximately equipotent with respect to inhibition ofhepatic 11b-HSD1 (H. Wright, E. Lai, J. Stone, andL. Caro, unpublished data, June 2006). Evidence that theseagents may be antihypertensive has come from animalstudies and a previous clinical trial.10 In the spontaneouslyhypertensive rat, it was found that treatment with an11b-HSD1 inhibitor for 14 days lowered mean BP by 12%,compared with treatment by vehicle alone. In an obesity-prone rat model (which tends to be modestly hypertensive),treatment with this same inhibitor for 8 days decreased meanBP from 121 to 113mmHg (D. Shevell and L.-Y. Pai, unpub-lished observation, June 2006).
In a recent clinical trial, treatment with MK-0916 for 12weeks at 6 mg/d (the highest dosage tested) was associatedwith significant reductions in the secondary endpoints ofmean BP and body weight, compared with placebo inpatients with type 2 diabetes and metabolic syndrome,although fasting plasma glucose (the primary endpoint)was not significantly lowered.10 The patients in thisprevious study were only mildly hypertensive, with 55%receiving ongoing antihypertensive therapy, and yet treat-ment with MK-0916 led to reductions from baseline of7.9 and 5.4 mm Hg in systolic and diastolic BP, respec-tively, relative to placebo.
The present study was focused primarily on evaluation ofMK-0736 rather than MK-0916 because the latter is a potentinducer of CYP3A4 at therapeutic doses, and therefore nota preferred drug development candidate. The primary purposeof the present study was to test for BP-lowering efficacy ofMK-0736 in overweight and obese nondiabetic patientswith mild-to-moderate hypertension. Patients randomized toreceive MK-0736 were treated for 12 weeks and patientsrandomized to receive MK-0916 were treated for 24 weeks;the findings throughWeek 12 (primary endpoint) are reportedherein. Study endpoints included trough sitting systolic anddiastolic BP (SiSBP and SiDBP, respectively), 24-hour ambu-latory BP measurements (ABPM), body weight, atherogeniclipid levels, and waist circumference. The primary efficacyhypothesis was that treatment for 12 weeks with 7 mg MK-0736 once daily, compared with placebo, results in signifi-cant, dose-dependent lowering of mean trough SiDBP inoverweight-to-obese nondiabetic patients with mild-to-moderate hypertension.
Methods
Patients
Eligible patients were male or female, 18 to 75 years ofage, with body mass index (BMI) lower than 41 kg/m2 anda history of essential hypertension that was or was notbeing treated at the time of screening. Entry into the studywas contingent upon having, after completing a placeborun-in period with washout of prior antihypertensive
medications (see below), a mean SiSBP lower than 160mm Hg and a mean SiDBP 90 mm Hg or higher and 104mm Hg or lower.
Patients with known or suspected secondary hypertensionwere excluded, as were patients with malignant hyperten-sion, history of stroke, cardiac dysfunction, hyperglycemia,endocrinologic dysfunction (eg, Cushing’s syndrome),abnormal levels of thyroid-stimulating hormone, persistentlyelevated creatine phosphokinase (greater than three-fold theupper limit of normal), alanine aminotransferase (ALT), oraspartate aminotransferase (AST; greater than two-fold theupper limit of normal), low-density lipoprotein cholesterol(LDL-C) higher than 160 mg/dL, triglycerides higher than350 mg/dL, serum creatinine higher than1.8 mg/dL, activeliver disease, history of malabsorption or major surgeryinvolving gastric or intestinal bypass, positive test for humanimmunodeficiency virus, or neoplastic disease. Patients wereexcluded if chronically taking more than 2 antihypertensiveagents or any medication with a narrow therapeutic range(such as digoxin, warfarin, phenytoin, and antiarrhythmicagents). Also excluded were patients who had taken anyglucocorticoid-containing or androgen-containing medica-tion within the prior 4 weeks (except for patients on stabledaily doses of nasally administered steroids for treatmentof allergic rhinitis) and patients on or likely to require treat-ment with medications that inhibit or are metabolized bycytochrome P450 3A4. Patients on stable doses of statins(for at least 6 weeks before randomization), antidepressants(such as fluoxetine and amitriptyline), noncyclical estrogenreplacement therapy, finasteride, dutasteride, weight-lossmedications, or nonsteroidal anti-inflammatory agents (forat least 3 months before randomization) were included.Female patients were required to be either postmenopausalor surgically sterile.
Study Design
This was a multinational, randomized, parallel-treatment,double-blind, placebo-controlled study (registered on www.ClinicalTrials.gov as NCT00274716) in which the primaryassessment of efficacy and safety was made at 12 weeks.Patients were enrolled at 33 sites in 4 countries (UnitedStates, New Zealand, Australia, and South Africa). Theprimary therapy period was December 22, 2005, to January19, 2007. This study was conducted in accordance with prin-ciples of Good Clinical Practice and was approved by theappropriate institutional review boards and regulatoryagencies.
One week after initial screening, eligible patients enteredinto a single-blind placebo run-in period lasting 2 to 6 weeks,depending on whether washout of prior medication wasrequired. Upon completion of this run-in period, patientswere stratified by baseline BMI into a higher-BMI stratum(�27 kg/m2 and <41 kg/m2, the primary study population)and a lower-BMI stratum (�20 and <27 kg/m2). The

168 S. Shah et al. / Journal of the American Society of Hypertension 5(3) (2011) 166–176
higher-BMI patients were then randomized (usinga computer-generated schedule) into treatment groups thatreceived 2 mg of MK-0736, 7 mg of MK-0736, 6 mg ofMK-0916, or image-matched placebo once each morning(1:1:1:1). Lower-BMI patients were randomized to receive6 mg of MK-0916 or placebo once each morning (1:1). Alllower-BMI patients were required to participate in two24-hour intervals of ABPM and some higher-BMI patientswere asked to participate as well, so that BP response inlower-BMI and higher-BMI patients could be compared.
After the first 2 weeks of double-blind treatment, patientswere discontinued if they persistently had any of thefollowing conditions: mean trough SiSBP higher than 170or lower than 100 mm Hg, mean trough SiDBP higherthan 110 or lower than 50 mm Hg, a more than 30 mmHg increase from baseline in mean trough SiSBP or morethan 15 mm Hg increase in mean trough SiDBP, symptomsof hypotension, a difference of more than 20 mm Hgbetween sitting and standing systolic BP or more than 10mm Hg with regard to diastolic BP.
Efficacy Assessments
Trough BP was measured in the clinic during morningvisits (22–26 hours after the previous morning’s dose)that were repeated every 2 weeks during the double-blindtreatment period. The measurements were made using anautomated blood pressure monitor (Lifesource ModelUA-787 AC, A&D Medical, San Jose, CA). Twenty-fourhour ABPM was performed using a SpaceLabs 90207Oscillometric device (Medifacts Ltd. Core LaboratoryResearch Services, Rockville, MD).11,12 This assessmentwas done twice during the study: once at baseline, in the24-hour interval that preceded randomization, and againat Week 12. Ambulatory BP measurements were obtainedeach 20 minutes during daytime (6:00 AM to 10:00 PM),and each 30 minutes during nighttime (10:00 PM to6:00 AM). Accuracy of the ABPM was verified by concur-rent measurements made in the clinic.
The primary efficacy endpoint was change from baselinein trough SiDBP compared with placebo in higher-BMIpatients with hypertension treated for 12 weeks with7 mg/d MK-0736. Additional endpoints included changefrom baseline, compared with placebo, in trough SiSBPin patients treated with 7 mg/d MK-0736; the correspond-ing means in patients treated with 2 mg/d MK-0736 and6 mg/d MK-0916 (in higher-BMI patients alone and inhigher- and lower-BMI patients combined); BP changesobserved in these treatment groups by 24-hour ABPM(including separate averages for daytime and nighttimeABPM); and changes in body weight, waist circumference,plasma levels of low-density lipoprotein cholesterol(LDL-C), high-density lipoprotein cholesterol (HDL-C),and triglycerides. Body weight was measured in duplicateusing a standardized Tanita scale (Model BWB-800-AS;
Tanita Corp., Arlington Heights, IL) at all sites. All labora-tory analyses were performed by PPD Global Central Labo-ratories (Highland Heights, KY, and Zaventem, Belgium).
Safety and tolerability were assessed by review of clin-ical and laboratory adverse experiences, laboratory values,vital signs, and 12-lead electrocardiography. Becausecortisol can act as a negative feedback inhibitor of thehypothalamic-pituitary-adrenal axis (HPA), blood levelsof the adrenal androgens androstenedione, dehydroepian-drosterone (DHEA), and dehydroepiandrosterone sulfate(DHEA-S) were measured in all patients, free testosteronewas measured in women, and the female patients weremonitored for symptoms of virilization (body hair growthand acne). Body hair assessments were done by the inves-tigator at 11 body sites using the Ferriman-Gallweymethod.13 It was predefined that a change from 7 or lessto higher than 7 in the Ferriman-Gallwey total androgen-dependent score would be regarded as meaningful. Globalassessments of acne were performed by the investigatorand by the patient based on visual inspection of the face.14
Statistical Analysis
Efficacy outcomes were analyzed using populationsdefined for each endpoint as the set of all randomized patientswho received at least 1 dose of study medication and forwhom a baseline measurement and at least 1 postrandomiza-tion measurement were available. The primary endpoint,change from baseline in SiDBP at week 12, was evaluatedusing an analysis of covariance (ANCOVA) model thatincluded treatment group (7 mg/d MK-0736, 2 mg/dMK-0736, 6 mg/d MK-0916, or placebo) and participationin ABPM (yes or no) as class variables and baseline meantrough SiDBP as a continuous covariate. This ANCOVAprovided values for least-square mean (LS-mean) differ-ences, adjusted for baseline, between actively treated andplacebo-treated groups, and nominal P values not adjustedfor multiplicity. Secondary endpoints (including bodyweight, blood LDL-C, HDL-C, triglycerides, and waistcircumference) and data from ABPM were analyzed usingANCOVAwith the same class variables and each respectiveendpoint’s baseline values as covariates. A step-downsequence of inference testing was prespecified to preservethe overall Type 1 error rate for the primary hypothesis.The first step in this sequencewas to test for significant effecton SiDBP of treatment for 12 weeks with 7 mg/d MK-0736compared with placebo; subsequent testing was contingenton finding that this primary endpoint was met. Values formissing data were imputed by the method of last observationcarried forward. The analysis of data from the 2 lower-BMIpatient groups was solely descriptive. Mean values forsystolic and diastolic ABPMwere calculated as theweightedmeans of all valid BP readings made during each 24-hourinterval of ABPM and during the daytime and nighttimeportions thereof.
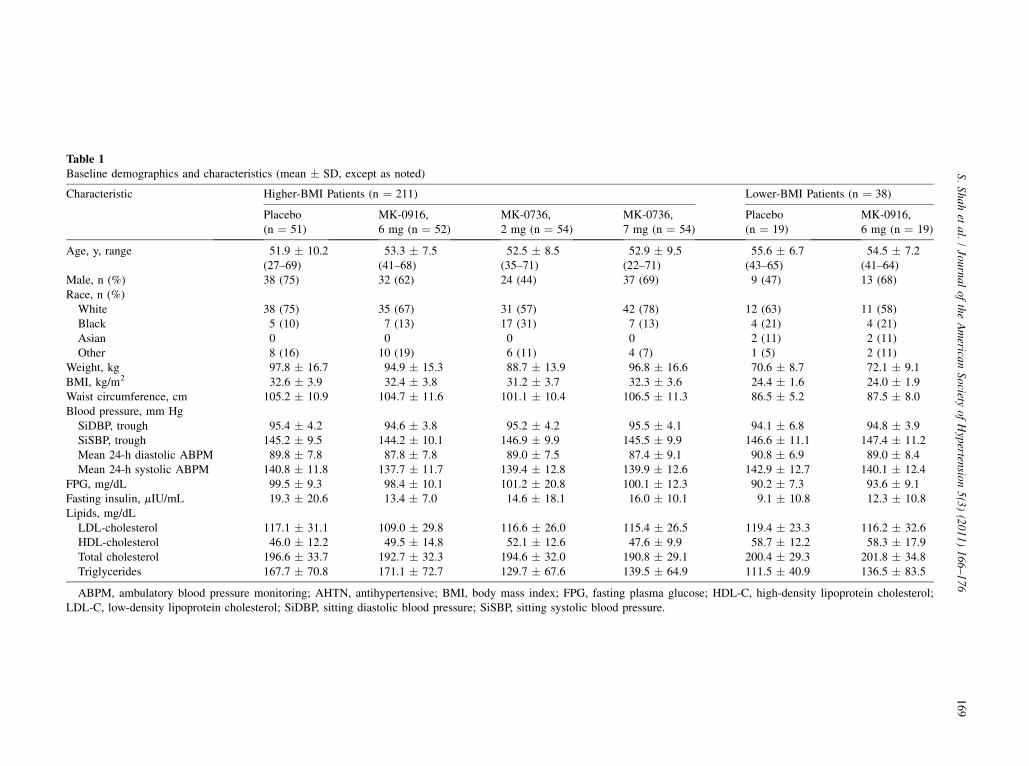
Table 1Baseline demographics and characteristics (mean � SD, except as noted)
Characteristic Higher-BMI Patients (n ¼ 211) Lower-BMI Patients (n ¼ 38)
Placebo(n ¼ 51)
MK-0916,6 mg (n ¼ 52)
MK-0736,2 mg (n ¼ 54)
MK-0736,7 mg (n ¼ 54)
Placebo(n ¼ 19)
MK-0916,6 mg (n ¼ 19)
Age, y, range 51.9 � 10.2(27–69)
53.3 � 7.5(41–68)
52.5 � 8.5(35–71)
52.9 � 9.5(22–71)
55.6 � 6.7(43–65)
54.5 � 7.2(41–64)
Male, n (%) 38 (75) 32 (62) 24 (44) 37 (69) 9 (47) 13 (68)Race, n (%)White 38 (75) 35 (67) 31 (57) 42 (78) 12 (63) 11 (58)Black 5 (10) 7 (13) 17 (31) 7 (13) 4 (21) 4 (21)Asian 0 0 0 0 2 (11) 2 (11)Other 8 (16) 10 (19) 6 (11) 4 (7) 1 (5) 2 (11)
Weight, kg 97.8 � 16.7 94.9 � 15.3 88.7 � 13.9 96.8 � 16.6 70.6 � 8.7 72.1 � 9.1BMI, kg/m2 32.6 � 3.9 32.4 � 3.8 31.2 � 3.7 32.3 � 3.6 24.4 � 1.6 24.0 � 1.9Waist circumference, cm 105.2 � 10.9 104.7 � 11.6 101.1 � 10.4 106.5 � 11.3 86.5 � 5.2 87.5 � 8.0Blood pressure, mm HgSiDBP, trough 95.4 � 4.2 94.6 � 3.8 95.2 � 4.2 95.5 � 4.1 94.1 � 6.8 94.8 � 3.9SiSBP, trough 145.2 � 9.5 144.2 � 10.1 146.9 � 9.9 145.5 � 9.9 146.6 � 11.1 147.4 � 11.2Mean 24-h diastolic ABPM 89.8 � 7.8 87.8 � 7.8 89.0 � 7.5 87.4 � 9.1 90.8 � 6.9 89.0 � 8.4Mean 24-h systolic ABPM 140.8 � 11.8 137.7 � 11.7 139.4 � 12.8 139.9 � 12.6 142.9 � 12.7 140.1 � 12.4
FPG, mg/dL 99.5 � 9.3 98.4 � 10.1 101.2 � 20.8 100.1 � 12.3 90.2 � 7.3 93.6 � 9.1Fasting insulin, mIU/mL 19.3 � 20.6 13.4 � 7.0 14.6 � 18.1 16.0 � 10.1 9.1 � 10.8 12.3 � 10.8Lipids, mg/dLLDL-cholesterol 117.1 � 31.1 109.0 � 29.8 116.6 � 26.0 115.4 � 26.5 119.4 � 23.3 116.2 � 32.6HDL-cholesterol 46.0 � 12.2 49.5 � 14.8 52.1 � 12.6 47.6 � 9.9 58.7 � 12.2 58.3 � 17.9Total cholesterol 196.6 � 33.7 192.7 � 32.3 194.6 � 32.0 190.8 � 29.1 200.4 � 29.3 201.8 � 34.8Triglycerides 167.7 � 70.8 171.1 � 72.7 129.7 � 67.6 139.5 � 64.9 111.5 � 40.9 136.5 � 83.5
ABPM, ambulatory blood pressure monitoring; AHTN, antihypertensive; BMI, body mass index; FPG, fasting plasma glucose; HDL-C, high-density lipoprotein cholesterol;LDL-C, low-density lipoprotein cholesterol; SiDBP, sitting diastolic blood pressure; SiSBP, sitting systolic blood pressure.
169
S.Shah
etal.
/Journal
ofthe
American
Societyof
Hypertension
5(3)(2011)
166–176
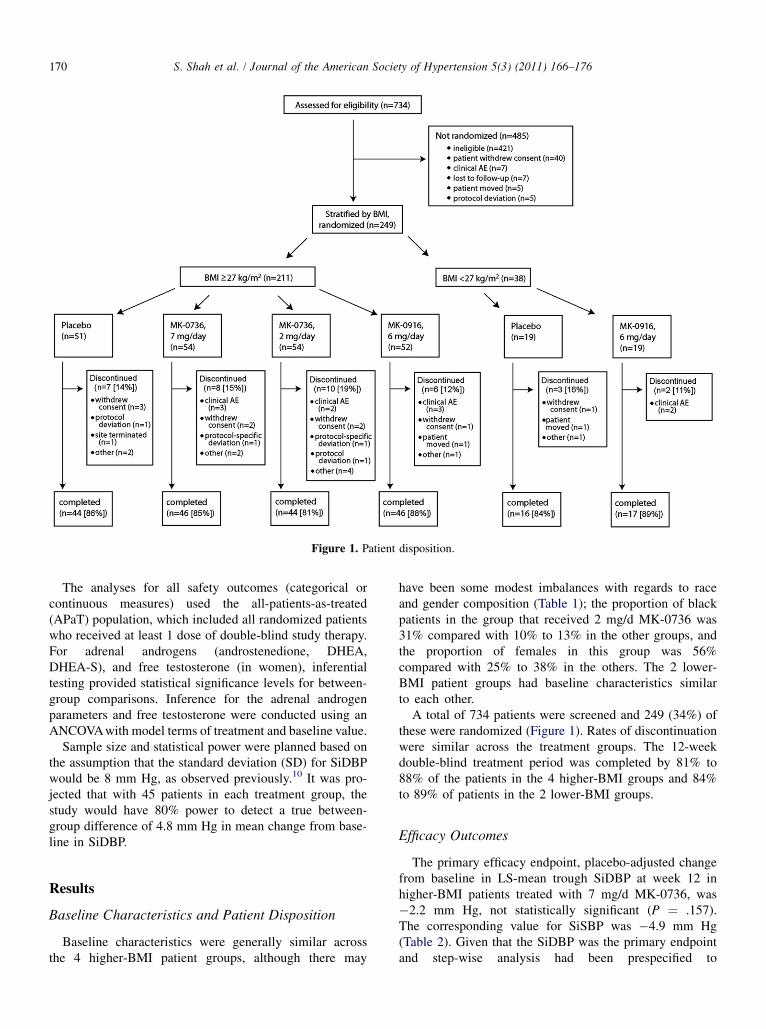
Figure 1. Patient disposition.
170 S. Shah et al. / Journal of the American Society of Hypertension 5(3) (2011) 166–176
The analyses for all safety outcomes (categorical orcontinuous measures) used the all-patients-as-treated(APaT) population, which included all randomized patientswho received at least 1 dose of double-blind study therapy.For adrenal androgens (androstenedione, DHEA,DHEA-S), and free testosterone (in women), inferentialtesting provided statistical significance levels for between-group comparisons. Inference for the adrenal androgenparameters and free testosterone were conducted using anANCOVAwith model terms of treatment and baseline value.
Sample size and statistical power were planned based onthe assumption that the standard deviation (SD) for SiDBPwould be 8 mm Hg, as observed previously.10 It was pro-jected that with 45 patients in each treatment group, thestudy would have 80% power to detect a true between-group difference of 4.8 mm Hg in mean change from base-line in SiDBP.
Results
Baseline Characteristics and Patient Disposition
Baseline characteristics were generally similar acrossthe 4 higher-BMI patient groups, although there may
have been some modest imbalances with regards to raceand gender composition (Table 1); the proportion of blackpatients in the group that received 2 mg/d MK-0736 was31% compared with 10% to 13% in the other groups, andthe proportion of females in this group was 56%compared with 25% to 38% in the others. The 2 lower-BMI patient groups had baseline characteristics similarto each other.
A total of 734 patients were screened and 249 (34%) ofthese were randomized (Figure 1). Rates of discontinuationwere similar across the treatment groups. The 12-weekdouble-blind treatment period was completed by 81% to88% of the patients in the 4 higher-BMI groups and 84%to 89% of patients in the 2 lower-BMI groups.
Efficacy Outcomes
The primary efficacy endpoint, placebo-adjusted changefrom baseline in LS-mean trough SiDBP at week 12 inhigher-BMI patients treated with 7 mg/d MK-0736, was�2.2 mm Hg, not statistically significant (P ¼ .157).The corresponding value for SiSBP was �4.9 mm Hg(Table 2). Given that the SiDBP was the primary endpointand step-wise analysis had been prespecified to
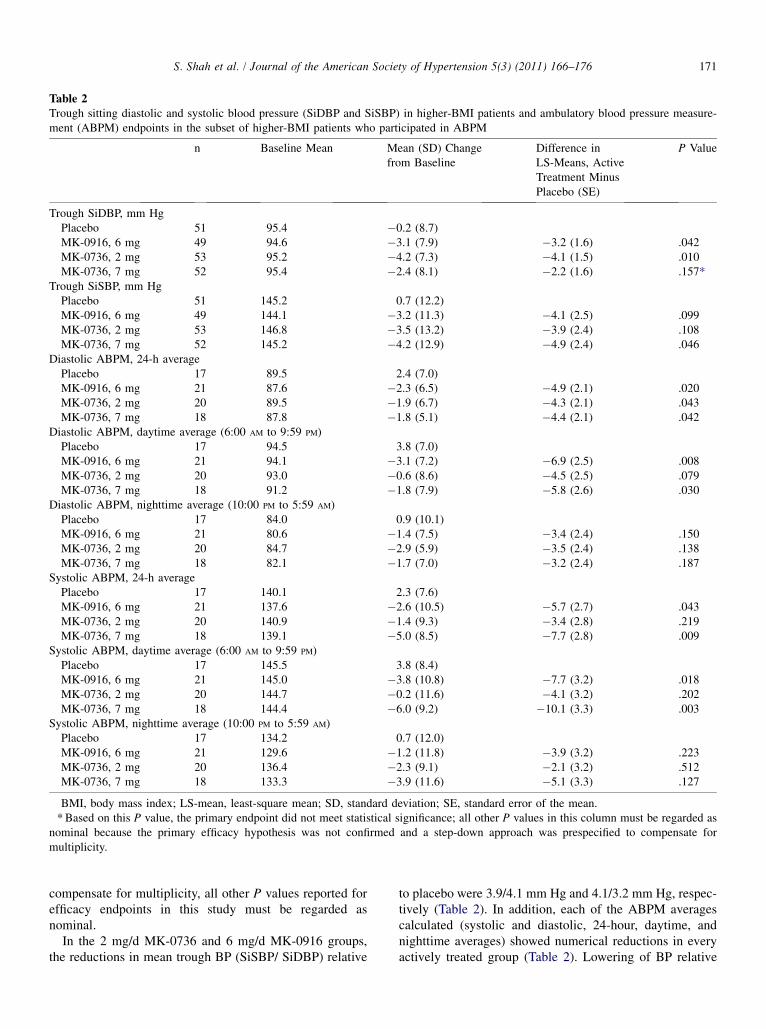
Table 2Trough sitting diastolic and systolic blood pressure (SiDBP and SiSBP) in higher-BMI patients and ambulatory blood pressure measure-ment (ABPM) endpoints in the subset of higher-BMI patients who participated in ABPM
n Baseline Mean Mean (SD) Changefrom Baseline
Difference inLS-Means, ActiveTreatment MinusPlacebo (SE)
P Value
Trough SiDBP, mm HgPlacebo 51 95.4 �0.2 (8.7)MK-0916, 6 mg 49 94.6 �3.1 (7.9) �3.2 (1.6) .042MK-0736, 2 mg 53 95.2 �4.2 (7.3) �4.1 (1.5) .010MK-0736, 7 mg 52 95.4 �2.4 (8.1) �2.2 (1.6) .157*
Trough SiSBP, mm HgPlacebo 51 145.2 0.7 (12.2)MK-0916, 6 mg 49 144.1 �3.2 (11.3) �4.1 (2.5) .099MK-0736, 2 mg 53 146.8 �3.5 (13.2) �3.9 (2.4) .108MK-0736, 7 mg 52 145.2 �4.2 (12.9) �4.9 (2.4) .046
Diastolic ABPM, 24-h averagePlacebo 17 89.5 2.4 (7.0)MK-0916, 6 mg 21 87.6 �2.3 (6.5) �4.9 (2.1) .020MK-0736, 2 mg 20 89.5 �1.9 (6.7) �4.3 (2.1) .043MK-0736, 7 mg 18 87.8 �1.8 (5.1) �4.4 (2.1) .042
Diastolic ABPM, daytime average (6:00 AM to 9:59 PM)Placebo 17 94.5 3.8 (7.0)MK-0916, 6 mg 21 94.1 �3.1 (7.2) �6.9 (2.5) .008MK-0736, 2 mg 20 93.0 �0.6 (8.6) �4.5 (2.5) .079MK-0736, 7 mg 18 91.2 �1.8 (7.9) �5.8 (2.6) .030
Diastolic ABPM, nighttime average (10:00 PM to 5:59 AM)Placebo 17 84.0 0.9 (10.1)MK-0916, 6 mg 21 80.6 �1.4 (7.5) �3.4 (2.4) .150MK-0736, 2 mg 20 84.7 �2.9 (5.9) �3.5 (2.4) .138MK-0736, 7 mg 18 82.1 �1.7 (7.0) �3.2 (2.4) .187
Systolic ABPM, 24-h averagePlacebo 17 140.1 2.3 (7.6)MK-0916, 6 mg 21 137.6 �2.6 (10.5) �5.7 (2.7) .043MK-0736, 2 mg 20 140.9 �1.4 (9.3) �3.4 (2.8) .219MK-0736, 7 mg 18 139.1 �5.0 (8.5) �7.7 (2.8) .009
Systolic ABPM, daytime average (6:00 AM to 9:59 PM)Placebo 17 145.5 3.8 (8.4)MK-0916, 6 mg 21 145.0 �3.8 (10.8) �7.7 (3.2) .018MK-0736, 2 mg 20 144.7 �0.2 (11.6) �4.1 (3.2) .202MK-0736, 7 mg 18 144.4 �6.0 (9.2) �10.1 (3.3) .003
Systolic ABPM, nighttime average (10:00 PM to 5:59 AM)Placebo 17 134.2 0.7 (12.0)MK-0916, 6 mg 21 129.6 �1.2 (11.8) �3.9 (3.2) .223MK-0736, 2 mg 20 136.4 �2.3 (9.1) �2.1 (3.2) .512MK-0736, 7 mg 18 133.3 �3.9 (11.6) �5.1 (3.3) .127
BMI, body mass index; LS-mean, least-square mean; SD, standard deviation; SE, standard error of the mean.* Based on this P value, the primary endpoint did not meet statistical significance; all other P values in this column must be regarded as
nominal because the primary efficacy hypothesis was not confirmed and a step-down approach was prespecified to compensate formultiplicity.
171S. Shah et al. / Journal of the American Society of Hypertension 5(3) (2011) 166–176
compensate for multiplicity, all other P values reported forefficacy endpoints in this study must be regarded asnominal.
In the 2 mg/d MK-0736 and 6 mg/d MK-0916 groups,the reductions in mean trough BP (SiSBP/ SiDBP) relative
to placebo were 3.9/4.1 mm Hg and 4.1/3.2 mm Hg, respec-tively (Table 2). In addition, each of the ABPM averagescalculated (systolic and diastolic, 24-hour, daytime, andnighttime averages) showed numerical reductions in everyactively treated group (Table 2). Lowering of BP relative
172 S. Shah et al. / Journal of the American Society of Hypertension 5(3) (2011) 166–176
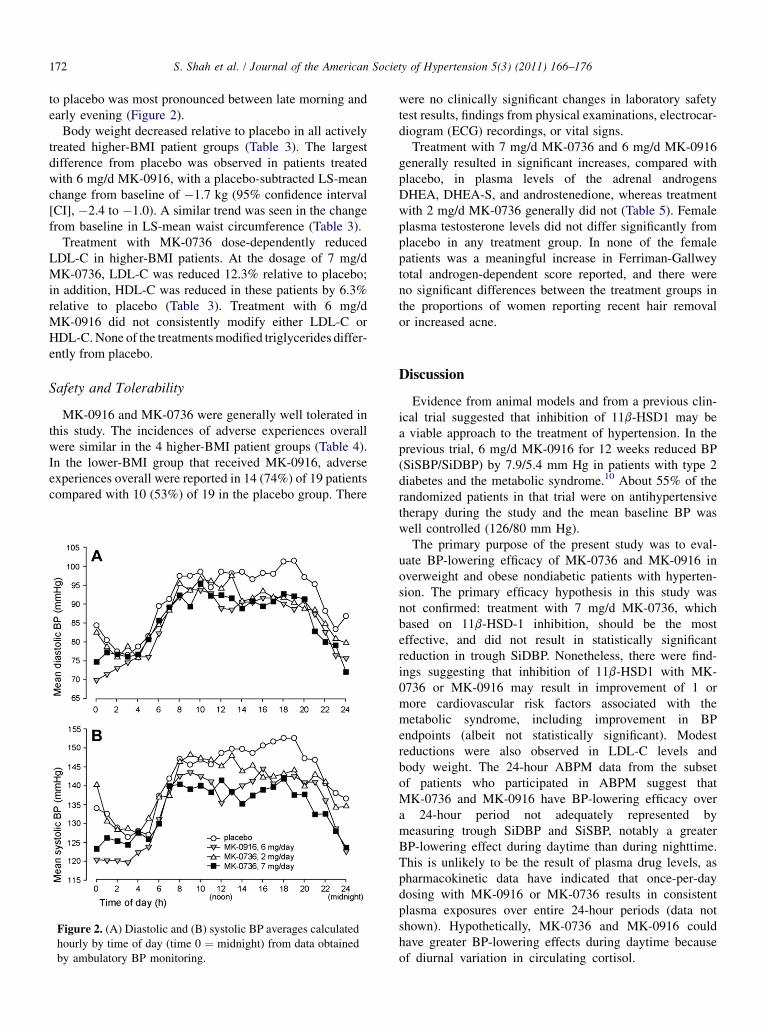
to placebo was most pronounced between late morning andearly evening (Figure 2).
Body weight decreased relative to placebo in all activelytreated higher-BMI patient groups (Table 3). The largestdifference from placebo was observed in patients treatedwith 6 mg/d MK-0916, with a placebo-subtracted LS-meanchange from baseline of �1.7 kg (95% confidence interval[CI], �2.4 to �1.0). A similar trend was seen in the changefrom baseline in LS-mean waist circumference (Table 3).
Treatment with MK-0736 dose-dependently reducedLDL-C in higher-BMI patients. At the dosage of 7 mg/dMK-0736, LDL-C was reduced 12.3% relative to placebo;in addition, HDL-C was reduced in these patients by 6.3%relative to placebo (Table 3). Treatment with 6 mg/dMK-0916 did not consistently modify either LDL-C orHDL-C. None of the treatmentsmodified triglycerides differ-ently from placebo.
Safety and Tolerability
MK-0916 and MK-0736 were generally well tolerated inthis study. The incidences of adverse experiences overallwere similar in the 4 higher-BMI patient groups (Table 4).In the lower-BMI group that received MK-0916, adverseexperiences overall were reported in 14 (74%) of 19 patientscompared with 10 (53%) of 19 in the placebo group. There
Figure 2. (A) Diastolic and (B) systolic BP averages calculatedhourly by time of day (time 0 ¼ midnight) from data obtainedby ambulatory BP monitoring.
were no clinically significant changes in laboratory safetytest results, findings from physical examinations, electrocar-diogram (ECG) recordings, or vital signs.
Treatment with 7 mg/d MK-0736 and 6 mg/d MK-0916generally resulted in significant increases, compared withplacebo, in plasma levels of the adrenal androgensDHEA, DHEA-S, and androstenedione, whereas treatmentwith 2 mg/d MK-0736 generally did not (Table 5). Femaleplasma testosterone levels did not differ significantly fromplacebo in any treatment group. In none of the femalepatients was a meaningful increase in Ferriman-Gallweytotal androgen-dependent score reported, and there wereno significant differences between the treatment groups inthe proportions of women reporting recent hair removalor increased acne.
Discussion
Evidence from animal models and from a previous clin-ical trial suggested that inhibition of 11b-HSD1 may bea viable approach to the treatment of hypertension. In theprevious trial, 6 mg/d MK-0916 for 12 weeks reduced BP(SiSBP/SiDBP) by 7.9/5.4 mm Hg in patients with type 2diabetes and the metabolic syndrome.10 About 55% of therandomized patients in that trial were on antihypertensivetherapy during the study and the mean baseline BP waswell controlled (126/80 mm Hg).
The primary purpose of the present study was to eval-uate BP-lowering efficacy of MK-0736 and MK-0916 inoverweight and obese nondiabetic patients with hyperten-sion. The primary efficacy hypothesis in this study wasnot confirmed: treatment with 7 mg/d MK-0736, whichbased on 11b-HSD-1 inhibition, should be the mosteffective, and did not result in statistically significantreduction in trough SiDBP. Nonetheless, there were find-ings suggesting that inhibition of 11b-HSD1 with MK-0736 or MK-0916 may result in improvement of 1 ormore cardiovascular risk factors associated with themetabolic syndrome, including improvement in BPendpoints (albeit not statistically significant). Modestreductions were also observed in LDL-C levels andbody weight. The 24-hour ABPM data from the subsetof patients who participated in ABPM suggest thatMK-0736 and MK-0916 have BP-lowering efficacy overa 24-hour period not adequately represented bymeasuring trough SiDBP and SiSBP, notably a greaterBP-lowering effect during daytime than during nighttime.This is unlikely to be the result of plasma drug levels, aspharmacokinetic data have indicated that once-per-daydosing with MK-0916 or MK-0736 results in consistentplasma exposures over entire 24-hour periods (data notshown). Hypothetically, MK-0736 and MK-0916 couldhave greater BP-lowering effects during daytime becauseof diurnal variation in circulating cortisol.
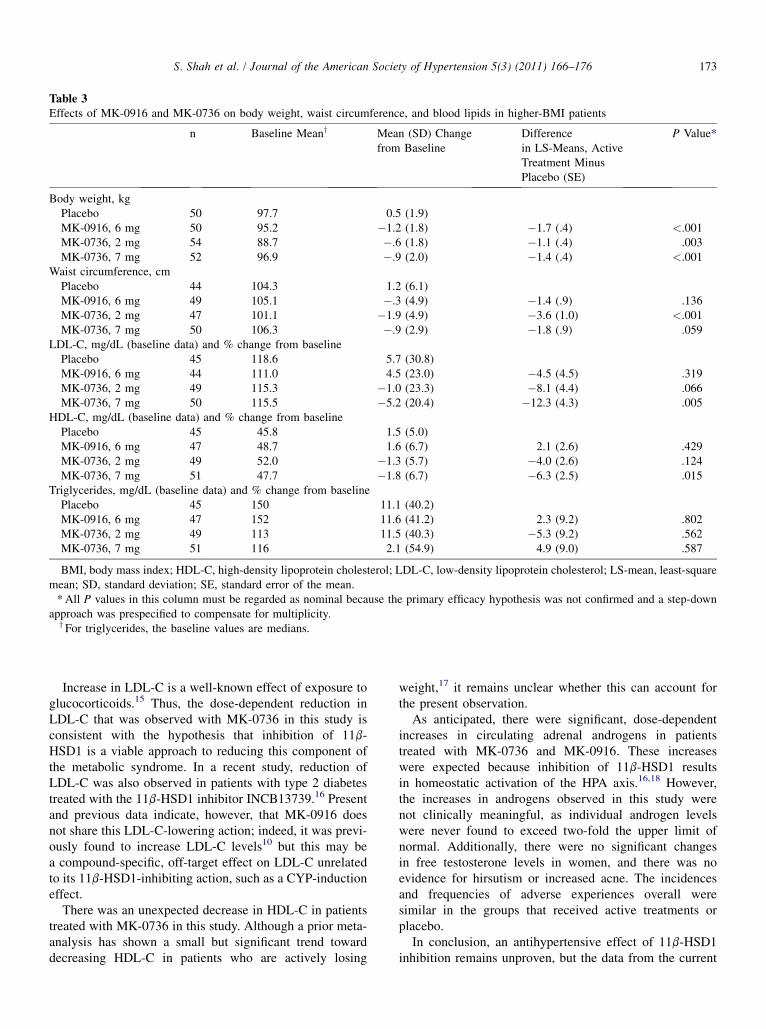
Table 3Effects of MK-0916 and MK-0736 on body weight, waist circumference, and blood lipids in higher-BMI patients
n Baseline Meany Mean (SD) Changefrom Baseline
Differencein LS-Means, ActiveTreatment MinusPlacebo (SE)
P Value*
Body weight, kgPlacebo 50 97.7 0.5 (1.9)MK-0916, 6 mg 50 95.2 �1.2 (1.8) �1.7 (.4) <.001MK-0736, 2 mg 54 88.7 �.6 (1.8) �1.1 (.4) .003MK-0736, 7 mg 52 96.9 �.9 (2.0) �1.4 (.4) <.001
Waist circumference, cmPlacebo 44 104.3 1.2 (6.1)MK-0916, 6 mg 49 105.1 �.3 (4.9) �1.4 (.9) .136MK-0736, 2 mg 47 101.1 �1.9 (4.9) �3.6 (1.0) <.001MK-0736, 7 mg 50 106.3 �.9 (2.9) �1.8 (.9) .059
LDL-C, mg/dL (baseline data) and % change from baselinePlacebo 45 118.6 5.7 (30.8)MK-0916, 6 mg 44 111.0 4.5 (23.0) �4.5 (4.5) .319MK-0736, 2 mg 49 115.3 �1.0 (23.3) �8.1 (4.4) .066MK-0736, 7 mg 50 115.5 �5.2 (20.4) �12.3 (4.3) .005
HDL-C, mg/dL (baseline data) and % change from baselinePlacebo 45 45.8 1.5 (5.0)MK-0916, 6 mg 47 48.7 1.6 (6.7) 2.1 (2.6) .429MK-0736, 2 mg 49 52.0 �1.3 (5.7) �4.0 (2.6) .124MK-0736, 7 mg 51 47.7 �1.8 (6.7) �6.3 (2.5) .015
Triglycerides, mg/dL (baseline data) and % change from baselinePlacebo 45 150 11.1 (40.2)MK-0916, 6 mg 47 152 11.6 (41.2) 2.3 (9.2) .802MK-0736, 2 mg 49 113 11.5 (40.3) �5.3 (9.2) .562MK-0736, 7 mg 51 116 2.1 (54.9) 4.9 (9.0) .587
BMI, body mass index; HDL-C, high-density lipoprotein cholesterol; LDL-C, low-density lipoprotein cholesterol; LS-mean, least-squaremean; SD, standard deviation; SE, standard error of the mean.*All P values in this column must be regarded as nominal because the primary efficacy hypothesis was not confirmed and a step-down
approach was prespecified to compensate for multiplicity.y For triglycerides, the baseline values are medians.
173S. Shah et al. / Journal of the American Society of Hypertension 5(3) (2011) 166–176
Increase in LDL-C is a well-known effect of exposure toglucocorticoids.15 Thus, the dose-dependent reduction inLDL-C that was observed with MK-0736 in this study isconsistent with the hypothesis that inhibition of 11b-HSD1 is a viable approach to reducing this component ofthe metabolic syndrome. In a recent study, reduction ofLDL-C was also observed in patients with type 2 diabetestreated with the 11b-HSD1 inhibitor INCB13739.16 Presentand previous data indicate, however, that MK-0916 doesnot share this LDL-C-lowering action; indeed, it was previ-ously found to increase LDL-C levels10 but this may bea compound-specific, off-target effect on LDL-C unrelatedto its 11b-HSD1-inhibiting action, such as a CYP-inductioneffect.
There was an unexpected decrease in HDL-C in patientstreated with MK-0736 in this study. Although a prior meta-analysis has shown a small but significant trend towarddecreasing HDL-C in patients who are actively losing
weight,17 it remains unclear whether this can account forthe present observation.
As anticipated, there were significant, dose-dependentincreases in circulating adrenal androgens in patientstreated with MK-0736 and MK-0916. These increaseswere expected because inhibition of 11b-HSD1 resultsin homeostatic activation of the HPA axis.16,18 However,the increases in androgens observed in this study werenot clinically meaningful, as individual androgen levelswere never found to exceed two-fold the upper limit ofnormal. Additionally, there were no significant changesin free testosterone levels in women, and there was noevidence for hirsutism or increased acne. The incidencesand frequencies of adverse experiences overall weresimilar in the groups that received active treatments orplacebo.
In conclusion, an antihypertensive effect of 11b-HSD1inhibition remains unproven, but the data from the current
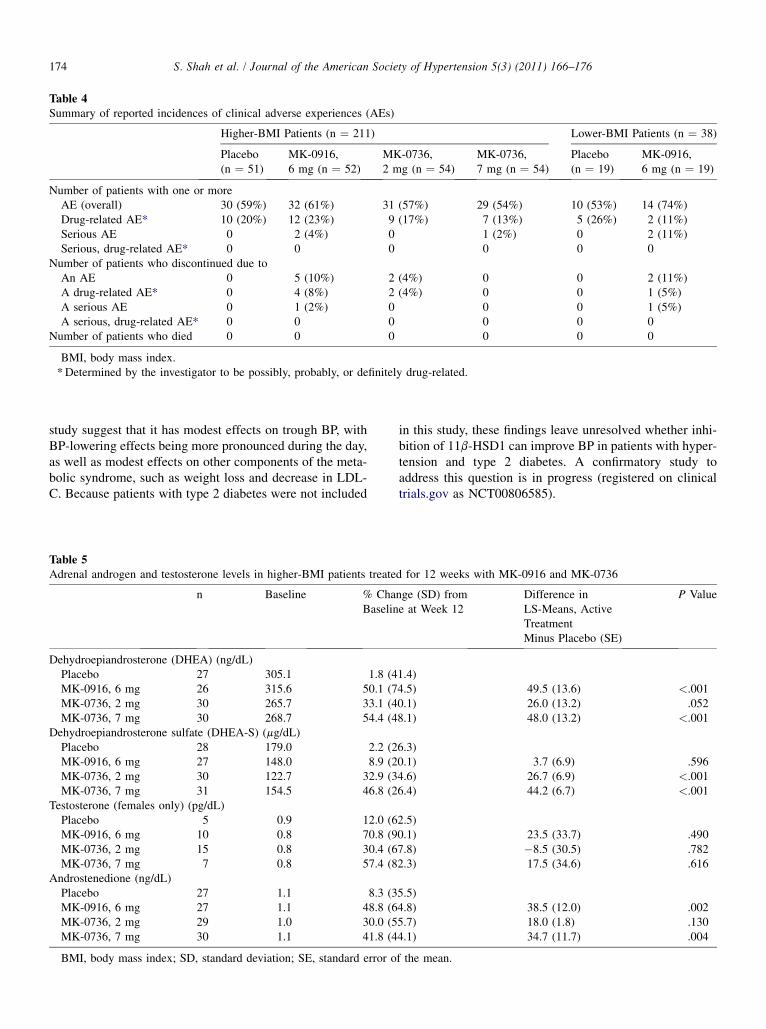
Table 4Summary of reported incidences of clinical adverse experiences (AEs)
Higher-BMI Patients (n ¼ 211) Lower-BMI Patients (n ¼ 38)
Placebo(n ¼ 51)
MK-0916,6 mg (n ¼ 52)
MK-0736,2 mg (n ¼ 54)
MK-0736,7 mg (n ¼ 54)
Placebo(n ¼ 19)
MK-0916,6 mg (n ¼ 19)
Number of patients with one or moreAE (overall) 30 (59%) 32 (61%) 31 (57%) 29 (54%) 10 (53%) 14 (74%)Drug-related AE* 10 (20%) 12 (23%) 9 (17%) 7 (13%) 5 (26%) 2 (11%)Serious AE 0 2 (4%) 0 1 (2%) 0 2 (11%)Serious, drug-related AE* 0 0 0 0 0 0
Number of patients who discontinued due toAn AE 0 5 (10%) 2 (4%) 0 0 2 (11%)A drug-related AE* 0 4 (8%) 2 (4%) 0 0 1 (5%)A serious AE 0 1 (2%) 0 0 0 1 (5%)A serious, drug-related AE* 0 0 0 0 0 0
Number of patients who died 0 0 0 0 0 0
BMI, body mass index.*Determined by the investigator to be possibly, probably, or definitely drug-related.
174 S. Shah et al. / Journal of the American Society of Hypertension 5(3) (2011) 166–176
study suggest that it has modest effects on trough BP, withBP-lowering effects being more pronounced during the day,as well as modest effects on other components of the meta-bolic syndrome, such as weight loss and decrease in LDL-C. Because patients with type 2 diabetes were not included
Table 5Adrenal androgen and testosterone levels in higher-BMI patients treate
n Baseline % ChaBaselin
Dehydroepiandrosterone (DHEA) (ng/dL)Placebo 27 305.1 1.8 (4MK-0916, 6 mg 26 315.6 50.1 (7MK-0736, 2 mg 30 265.7 33.1 (4MK-0736, 7 mg 30 268.7 54.4 (4
Dehydroepiandrosterone sulfate (DHEA-S) (mg/dL)Placebo 28 179.0 2.2 (2MK-0916, 6 mg 27 148.0 8.9 (2MK-0736, 2 mg 30 122.7 32.9 (3MK-0736, 7 mg 31 154.5 46.8 (2
Testosterone (females only) (pg/dL)Placebo 5 0.9 12.0 (6MK-0916, 6 mg 10 0.8 70.8 (9MK-0736, 2 mg 15 0.8 30.4 (6MK-0736, 7 mg 7 0.8 57.4 (8
Androstenedione (ng/dL)Placebo 27 1.1 8.3 (3MK-0916, 6 mg 27 1.1 48.8 (6MK-0736, 2 mg 29 1.0 30.0 (5MK-0736, 7 mg 30 1.1 41.8 (4
BMI, body mass index; SD, standard deviation; SE, standard error o
in this study, these findings leave unresolved whether inhi-bition of 11b-HSD1 can improve BP in patients with hyper-tension and type 2 diabetes. A confirmatory study toaddress this question is in progress (registered on clinicaltrials.gov as NCT00806585).
d for 12 weeks with MK-0916 and MK-0736
nge (SD) frome at Week 12
Difference inLS-Means, ActiveTreatmentMinus Placebo (SE)
P Value
1.4)4.5) 49.5 (13.6) <.0010.1) 26.0 (13.2) .0528.1) 48.0 (13.2) <.001
6.3)0.1) 3.7 (6.9) .5964.6) 26.7 (6.9) <.0016.4) 44.2 (6.7) <.001
2.5)0.1) 23.5 (33.7) .4907.8) �8.5 (30.5) .7822.3) 17.5 (34.6) .616
5.5)4.8) 38.5 (12.0) .0025.7) 18.0 (1.8) .1304.1) 34.7 (11.7) .004
f the mean.
175S. Shah et al. / Journal of the American Society of Hypertension 5(3) (2011) 166–176
Acknowledgments
The authors acknowledge Hamish Wright, LuzelenaCaro, Lee-Yuh Pai and Diane Shevell of Merck. We alsoacknowledge Dr Steven Heymsfield (Pennington Biomed-ical Research Center) and the participating investigatorsand institutions for their valuable contributions: CapitalClinical Research Center, Olympia, WA: Dr Eric J. Klein;Green & Seidner Family Practice: Dr Michael R. Green;Pro Health Physicians Inc.: Dr Anthony M. Roselli; HealthTrends Research, LLC: Dr Boris Kerzner; University ofAlabama at Birmingham, Birmingham, AL (Departmentof Vascular Biology & Hypertension): Dr David A. Cal-houn; Charlotte Clinical Research: Dr Gregory V. Collins;Coastal Carolina Research Center: Dr Cynthia BecherStrout; International Institute of Clinical Research: DrDavid A. Claassen; Covance Clinical Research: Dr FrankH. Farmer, Jr; Abbott Clinical Research: Dr Raul E. Gaona,Sr; University Clinical Research, Inc.: Dr Larry I. Gilder-man; Safe Harbor Clinical Research: Dr Ronald M. Gil-man; Ohio Clinical Research: Dr Terence Isakov; SFBCInternational, Inc.: Dr Kenneth C. Lasseter; PiedmontMedical Research: Dr Thomas Willard Littlejohn III;Family Physicians, PA: Dr Cecilia L. McKeown-Biagas;The Greater Fort Lauderdale Heart Group Research: DrAlan L. Niederman; Warminster Medical Associates:Dr Robert Topkis; Clinical Research Associates, Inc.: DrMichael Miller; Arroyo Seco Research, Inc.: Dr Henry P.Sideropoulos; Valley Medical Center: Dr John L. Stoker;Apex Research Institute: Dr Charles N. Morcos; J. LewisResearch, Inc.: Dr Randall L. Watson; Radiant Research–Tacoma: Dr Wayne E. Larson; Clifton-Wallington MedicalGroup: Dr Piotr Z. Imiolek; Cedar Crosse Research Center:Dr Danny H. Sugimoto; Cardiovascular Research, Auck-land City Hospital: Dr Jocelyne R. Benatar; ChristchurchSchool of Medicine & Health Sciences: Dr Mark Richards;Canterbury Geriatric Medical Research Trust, PrincessMargaret Hospital: Dr Nigel Leslie Gilchrist; TaurangaHospital, Department of Medical Research: Dr AnthonyNeil Graham; Cardiology Clinical Trials, Waikato Hospital:Dr Denis Hugo Friedlander; Dunedin Hospital–CardiologyDepartment: Associate Professor Gerald Wilkins; Austra-lian Clinical Research Centre 3: Dr Andrew Lowy; Mar-oondah Hospital–Eastern Clinical Research: Dr MurrayGerstman; Emeritus Research: Dr James McDonald; Bris-bane South Clinical Research Center: Dr MaureenMcKeirnan; GrooteSchuur Hospital: Professor Brian Ray-ner; Vincent Palotti Hospital: Dr E. Lloyd; Dr Louis vanZyl; TREAD Research, Tygerberg Hospital: Professor Les-ley Jean Burgess; FPA Clinical Research: Dr ChristopherM. Chappel; Diabetes & Glandular Disease Research Asso-ciates: Dr Mark S. Kipnes; Adviso Medical Research: DrDominador L. Dayon, Jr.; Endocrine Research Associates:Dr Raymond F. Grenfell, Jr; National Clinical Research –Richmond, Inc.: Dr John Arthur Hoekstra; Bensalem
Medical Practice: Dr Kenneth Alan Morris; Quick CareMedical: Dr Neeja Misra; Texas Center for Drug Develop-ment, Inc.: Dr Jerry Ray Mitchell; Atta California MedicalGroup, Inc.: Dr Alberto Odio; Community Research, Cin-cinnati, OH: Dr Antoinette A. Pragalos; Riser MedicalAssociates: Dr James Riser; Research & CardiovascularCorp.: Dr Jose B. Vazquez-Tanus.
References
1. Kearney PM, Whelton M, Reynolds K, Muntner P,Whelton PK, He J. Global burden of hypertension:analysis of worldwide data. Lancet 2005;365:217–23.
2. Feig PU, Roy S, Cody RJ. Antihypertensive drug devel-opment: current challenges and future opportunities.J Am Soc Hypertens 2010;4:163–73.
3. Galzerano D, Capogrosso C, Di Michele S, Bobbio E,Paparello P, Gaudio C. Do we need more than justpowerful blood pressure reductions? New paradigmsin end-organ protection. Vasc Health Risk Manag2010;6:479–94.
4. Expert Panel on Detection, Evaluation, and Treatmentof High Blood Cholesterol in Adults. Executivesummary of the third report of the national cholesteroleducation program (NCEP) expert panel on detection,evaluation, and treatment of high blood cholesterol inadults (Adult Treatment Panel III). JAMA 2001;285:2486–97.
5. Thieringer R, Hermanowski-Vosatka A. Inhibition of11b-HSD1 as a novel treatment for the metabolicsyndrome: do glucocorticoids play a role? Expert RevCardiovasc Ther 2005;3:911–24.
6. Wamil M, Seckl JR. Inhibition of 11b-hydroxysteroiddehydrogenase type 1 as a promising therapeutic target.Drug Discov Today 2007;12:504–20.
7. Cooper MS, Stewart PM. 11b-hydroxysteroid dehydro-genase type 1 and its role in the hypothalamus-pituitary-adrenal axis, metabolic syndrome, andinflammation. J Clin Endocrinol Metab 2009;94:4645–54.
8. Morton NM. Obesity and corticosteroids: 11b-hydrox-ysteroid type 1 as a cause and therapeutic target inmetabolic disease. Mol Cell Endocrinol 2010;316:154–64.
9. Tomlinson JW, Walker EA, Bujalska IJ, Draper N,Lavery GG, Cooper MS, et al. 11b-hydroxysteroiddehydrogenase type 1: a tissue-specific regulator ofglucocorticoid response. Endocr Rev 2004;25:831–66.
10. Feig PU, Shah S, Hermanowski-Vosatka A, Plotkin D,Springer M, Donahue S, et al. Effects of an11b-hydroxysteroid dehydrogenase type 1 (HSD1)inhibitor, MK-0916, in patients with type 2 diabetesmellitus and metabolic syndrome. Diabetes ObesMetab 2011 [Epub ahead of print].
176 S. Shah et al. / Journal of the American Society of Hypertension 5(3) (2011) 166–176
11. O’Brien E, Mee F, Atkins N, O’Malley K. Accuracy ofthe SpaceLabs 90207 determined by the British Hyper-tension Society protocol. J Hypertens 1991;9:573–4.
12. O’Brien E, Waeber B, Parati G, Staessen J, Myers MG.Blood pressure measuring devices: recommendationsof the European Society of Hypertension. BMJ 2001;322:531–6.
13. Ferriman D, Gallwey JD. Clinical assessment of bodyhair growth in women. J Clin Endocrinol Metab1961;21:1440–7.
14. Allen BS, Smith JG Jr. Various parameters for gradingacne vulgaris. Arch Dermatol 1982;118:23–5.
15. Sweetman SC. Corticosteroids. In: Sweetman SC,editor. Martindale—The complete drug reference.
34th ed. London: Pharmaceutical Press; 2005.p. 1068–71.
16. Rosenstock J, Banarer S, Fonseca VA, Inzucchi SE,Sun W, Yao W, et al. The 11-b-hydroxysteroid dehy-drogenase type 1 inhibitor INCB13739 improveshyperglycemia in patients with type 2 diabetes inade-quately controlled by metformin monotherapy. Dia-betes Care 2010;33:1516–22.
17. Dattilo AM, Kris-Etherton PM. Effects of weightreduction on blood lipids and lipoproteins: a meta-analysis. Am J Clin Nutr 1992;56:320–8.
18. Harno E, White A. Will treating diabetes with11b-HSD1 inhibitors affect the HPA axis? TrendsEndocrinol Metab 2010;21:619–27.