Efficacy and Safety of Immediate-Release Methylphenidate Treatment for Preschoolers With ADHD
10
Copyright @ 2006 American Academy of Child and Adolescent Psychiatry. Unauthorized reproduction of this article is prohibited. Efficacy and Safety of Immediate-Release Methylphenidate Treatment for Preschoolers With ADHD LAURENCE GREENHILL, M.D., SCOTT KOLLINS, PH.D., HOWARD ABIKOFF, PH.D., JAMES MCCRACKEN, M.D., MARK RIDDLE, M.D., JAMES SWANSON, PH.D., JAMES MCGOUGH, M.D., SHARON WIGAL, PH.D., TIM WIGAL, PH.D., BENEDETTO VITIELLO, M.D., ANNE SKROBALA, M.A., KELLY POSNER, PH.D., JASWINDER GHUMAN, M.D., CHARLES CUNNINGHAM, PH.D., MARK DAVIES, M.P.H., SHIRLEY CHUANG, M.S., AND TOM COOPER, M.A. ABSTRACT Objective: The Preschool ADHD Treatment Study (PATS) was a NIMH-funded, six-center, randomized, controlled trial to determine the efficacy and safety of immediate-release methylphenidate (MPH-IR), given t.i.d. to children ages 3 to 5.5 years with attention-deficit/hyperactivity disorder (ADHD). Method: The 8-phase, 70-week PATS protocol included two double-blind, controlled phases, a crossover-titration trial followed by a placebo-controlled parallel trial. The crossover- titration phase`s primary efficacy measure was a combined score from the Swanson, Kotkin, Atkins, M-Flynn, and Pelham (SKAMP) plus the Conners, Loney, and Milich (CLAM) rating scales; the parallel phase`s primary outcome measure was excellent response, based on composite scores on the Swanson, Nolan, and Pelham (SNAP) rating scale. Results: Of 303 preschoolers enrolled, 165 were randomized into the titration trial. Compared with placebo, significant decreases in ADHD symptoms were found on MPH at 2.5 mg (p G .01), 5 mg (p G .001), and 7.5 mg (p G .001) t.i.d. doses, but not for 1.25 mg (p G .06). The mean optimal MPH total daily dose for the entire group was 14.2 T 8.1 mg/day (0.7 T 0.4 mg/kg/day). For the preschoolers (n = 114) later randomized into the parallel phase, only 21% on best-dose MPH and 13% on placebo achieved MTA-defined categorical criterion for remission set for school-age children with ADHD. Conclusions: MPH-IR, delivered in 2.5-, 5-, and 7.5-mg doses t.i.d., produced significant reductions on ADHD symptom scales in preschoolers compared to placebo, although effect sizes (0.4Y0.8) were smaller than those cited for school-age children on the same medication. J. Am. Acad. Child Adolesc. Psychiatry, 2006;45(11):1284Y1293. Key Words: preschool, attention-deficit/ hyperactivity disorder, psychopharmacology, treatment, adverse events. Accepted October 25, 2005. Dr. Greenhill and Posner, Mr. Davies (retired), Mr. Cooper, Ms. Skrobala, and Ms. Chuang are with the New York State Psychiatric Institute, Columbia University; Dr. Kollins is with Duke University, Durham, NC; Dr. Abikoff is with the New York University Child Study Center, New York; Dr. Riddle is with Johns Hopkins University, Baltimore; Dr. Ghuman is with the University of Arizona, Tucson; Dr. Cunningham is with McMaster University, Hamilton, Ontario, Canada; Drs. McCracken and McGough are with the University of California, Los Angeles; Drs. Swanson, T. Wigal, and S. Wigal are with the University of California, Irvine; and Mr. Cooper is also with the Nathan Kline Institute, Orangeburg, NY; Dr. Vitiello is with the National Institute of Mental Health, Bethesda, MD. This research was supported by a cooperative agreement between the National Institute of Mental Health and the following institutions: University of California, Irvine (U01 MH60833), Duke University Medical Center (U01 MH60848), NYSPI/Columbia University (U01 MH60903), New York University Child Study Center (U01 MH60943), University of California, Los Angeles (U01 MH60900), and Johns Hopkins University (U01 MH60642). The opinions and assertions contained in this report are the private view of the authors and are not to be construed as official or as reflecting the views of the National Institute of Mental Health, the National Institutes of Health, or the Department of Health and Human Services. Correspondence to Dr. Laurence Greenhill, Division of Child and Adolescent Psychiatry, New York State Psychiatric Institute, 1051 Riverside Drive, New York, NY 10032; e-mail: [email protected]. 0890-8567/06/4511-1284Ó2006 by the American Academy of Child and Adolescent Psychiatry. DOI: 10.1097/01.chi.0000235077.32661.61 SPECIAL SECTION 1284 J. AM. ACAD. CHILD ADOLESC. PSYCHIATRY, 45:11, NOVEMBER 2006
-
Upload
independent -
Category
Documents
-
view
5 -
download
0
Transcript of Efficacy and Safety of Immediate-Release Methylphenidate Treatment for Preschoolers With ADHD

Copyright @ 2006 American Academy of Child and Adolescent Psychiatry. Unauthorized reproduction of this article is prohibited.
Efficacy and Safety of Immediate-ReleaseMethylphenidate Treatment for Preschoolers
With ADHD
LAURENCE GREENHILL, M.D., SCOTT KOLLINS, PH.D., HOWARD ABIKOFF, PH.D.,
JAMES MCCRACKEN, M.D., MARK RIDDLE, M.D., JAMES SWANSON, PH.D.,
JAMES MCGOUGH, M.D., SHARON WIGAL, PH.D., TIM WIGAL, PH.D.,
BENEDETTO VITIELLO, M.D., ANNE SKROBALA, M.A., KELLY POSNER, PH.D.,
JASWINDER GHUMAN, M.D., CHARLES CUNNINGHAM, PH.D., MARK DAVIES, M.P.H.,
SHIRLEY CHUANG, M.S., AND TOM COOPER, M.A.
ABSTRACT
Objective: The Preschool ADHD Treatment Study (PATS) was a NIMH-funded, six-center, randomized, controlled trial to
determine the efficacy and safety of immediate-release methylphenidate (MPH-IR), given t.i.d. to children ages 3 to 5.5
years with attention-deficit/hyperactivity disorder (ADHD). Method: The 8-phase, 70-week PATS protocol included two
double-blind, controlled phases, a crossover-titration trial followed by a placebo-controlled parallel trial. The crossover-
titration phase`s primary efficacy measure was a combined score from the Swanson, Kotkin, Atkins, M-Flynn, and Pelham
(SKAMP) plus the Conners, Loney, and Milich (CLAM) rating scales; the parallel phase`s primary outcome measure was
excellent response, based on composite scores on the Swanson, Nolan, and Pelham (SNAP) rating scale. Results: Of
303 preschoolers enrolled, 165 were randomized into the titration trial. Compared with placebo, significant decreases in
ADHD symptoms were found on MPH at 2.5 mg (p G .01), 5 mg (p G .001), and 7.5 mg (p G .001) t.i.d. doses, but not for
1.25mg (p G .06). Themean optimal MPH total daily dose for the entire group was 14.2 T 8.1 mg/day (0.7 T 0.4 mg/kg/day).
For the preschoolers (n = 114) later randomized into the parallel phase, only 21% on best-dose MPH and 13% on placebo
achieved MTA-defined categorical criterion for remission set for school-age children with ADHD. Conclusions: MPH-IR,
delivered in 2.5-, 5-, and 7.5-mg doses t.i.d., produced significant reductions on ADHD symptom scales in preschoolers
compared to placebo, although effect sizes (0.4Y0.8) were smaller than those cited for school-age children on the same
medication. J. Am. Acad. Child Adolesc. Psychiatry, 2006;45(11):1284Y1293. Key Words: preschool, attention-deficit/
hyperactivity disorder, psychopharmacology, treatment, adverse events.
Accepted October 25, 2005.Dr. Greenhill and Posner, Mr. Davies (retired), Mr. Cooper, Ms. Skrobala,
and Ms. Chuang are with the New York State Psychiatric Institute, ColumbiaUniversity; Dr. Kollins is with Duke University, Durham, NC; Dr. Abikoff iswith the New York University Child Study Center, New York; Dr. Riddle iswith Johns Hopkins University, Baltimore; Dr. Ghuman is with the Universityof Arizona, Tucson; Dr. Cunningham is with McMaster University, Hamilton,Ontario, Canada; Drs. McCracken and McGough are with the University ofCalifornia, Los Angeles; Drs. Swanson, T. Wigal, and S. Wigal are with theUniversity of California, Irvine; and Mr. Cooper is also with the Nathan KlineInstitute, Orangeburg, NY; Dr. Vitiello is with the National Institute of MentalHealth, Bethesda, MD.This research was supported by a cooperative agreement between the National
Institute of Mental Health and the following institutions: University of
California, Irvine (U01 MH60833), Duke University Medical Center (U01MH60848), NYSPI/Columbia University (U01 MH60903), New YorkUniversity Child Study Center (U01 MH60943), University of California,Los Angeles (U01MH60900), and JohnsHopkins University (U01MH60642).The opinions and assertions contained in this report are the private view of
the authors and are not to be construed as official or as reflecting the views of theNational Institute of Mental Health, the National Institutes of Health, or theDepartment of Health and Human Services.Correspondence to Dr. Laurence Greenhill, Division of Child and Adolescent
Psychiatry, New York State Psychiatric Institute, 1051 Riverside Drive, NewYork, NY 10032; e-mail: [email protected].
0890-8567/06/4511-1284�2006 by the American Academy of Childand Adolescent Psychiatry.
DOI: 10.1097/01.chi.0000235077.32661.61
S P E C I A L S E C T I O N
1284 J . AM. ACAD. CHILD ADOLESC. PSYCHIATRY, 45:11, NOVEMBER 2006

Copyright @ 2006 American Academy of Child and Adolescent Psychiatry. Unauthorized reproduction of this article is prohibited.
Attention-deficit/hyperactivity disorder (ADHD) inpreschool children has been treated with the samepsychostimulants that have become the first-linetreatment for the disorder in school-age children. Yetthe safety and efficacy of methylphenidate (MPH) inpreschoolers with ADHD is unproven. This is becauseonly 10 single-site, small, randomized studies of MPHinvolving a total of 240 preschoolers with ADHD havebeen conducted (Greenhill, 1998; Kollins et al., 2006).Results from these 10 preschool treatment studies aremixed, with 6 reporting good efficacy and safety withMPH treatment, 2 failing to demonstrate significantdifferences between MPH and placebo (Barkley et al.,1984; Cohen, 1981), and 2 reporting higher rates ofadverse events compared with older children (Firestoneet al., 1998; Handen et al., 1999), especially MPH-associated social withdrawal.
These early preschool MPH trials were single-site,short-duration, small-sample studies that used diversediagnostic methods. Teacher data were not included, andthere was no follow-up. Study doses were not based ondose-ranging trials or pharmacokinetic studies in chil-dren of comparable ages. Such methodological problemspreclude pooling of data for a meta analyses of the safetyand efficacy of MPH in this age range (Greenhill, 1998).Even so, MPH has become the most commonly usedpharmacological agent for ADHD presenting beforeage 6, and its use increased during the 1991Y1995 era(Zito et al., 2000). This trend has occurred in spite ofthe labeling by the U.S. Food and Drug Administrationthat indicates that the medication should not be usedin children younger than 6 years of age.
There are no published pharmacokinetic studies ofMPH in preschool children with ADHD by the date ofthis publication that could help estimate safe andeffective dose ranges for this vulnerable population. Theneed for efficacy, safety, and dose-ranging data led tothe Preschool ADHD Treatment Study (PATS).
The PATS trial was designed as a randomized,multicenter clinical trial that included a double-blind,placebo-controlled titration phase followed by a double-blind, placebo-controlled parallel-design phase. Thesetwo phases were designed to evaluate the efficacy andsafety of MPH for preschoolers with ADHD. Thespecific aims of the study, design, rationale for choicesmade, and research methods are detailed by Kollins et al.(2006). This report focuses on the two efficacy phases ofthe PATS: the 5-week titration phase that determined
the effective dose range of MPH and the double-blind,parallel-group controlled efficacy trial that comparedbest dose MPH to placebo.
METHOD
Subjects
Participants were recruited without regard to sex, race, orethnicity at six academic sites (Columbia University, DukeUniversity, Johns Hopkins University, New York University,University of California, Irvine, and University of California, LosAngeles) from clinics, paid and public service advertisements innewspapers and on the radio, primary care physicians, nurseryschools, day care centers, and kindergartens. Telephone screening of1,915 referrals determined that 1,272 families (66%) were eligible;of those, 553 (43% of eligible) signed consent, and 303 (24% ofeligible) met inclusion criteria during the period between February2001 and April 2003.
Details on inclusion and exclusion criteria are presented byKollins et al. in this issue. Briefly, to be included, the children had tomeet the following criteria: stimulant naBve, children of both sexes,ages 3 to 5.5 years with a DSM-IV consensus diagnosis of ADHD(American Psychiatric Association, 1994) based on the DiagnosticInterview Schedule for Children IV-Parent Version (Schaffer et al.,1996) and semistructured interview; combined or predominantlyhyperactive subtype; an impairment scale score G55 on theChildren`s Global Assessment Scale (Shaffer et al., 1983);hyperactive-impulsive subscale T score of 65 (1.5 SDs above theage- and sex-adjusted means) on both the Revised Conners Parent(Conners et al., 1998a) and Teacher (Conners et al., 1998b) RatingScales; Full Scale IQ equivalent of 970 on the Differential AbilityScales (Elliott, 1990); participation in a preschool, day care groupsetting, or other school program at least 2 half-days per week with atleast eight same-age peers; and the same primary caretaker for atleast 6 months before screening.
Children were excluded if there was current evidence ofadjustment disorder, pervasive developmental disorders, psychosis,significant suicidality, or other psychiatric disorder in addition toADHD that required treatment with additional medication; currentstimulant or cocaine abuse in a relative living in the home; aconfounding medical condition; inability of the parent to under-stand or follow study instructions, or history of bipolar disorder inboth biological parents.
Diagnostic and Assessment Baseline Measures
Baseline diagnoses of ADHD and associated comorbidities wereestablished using the Diagnostic Interview Schedule for ChildrenIV-Parent Version and a semistructured clinical interview con-ducted by a child psychiatrist or psychologist, as described byKollins et al. in this issue. Data from parent and teacher ratingscales, Autism Screener, Differential Ability Scales score, DiagnosticInterview Schedule for Children IV-Parent Version, and clinicalinterview were summarized in an anonymized narrative andsubsequently circulated for review in a weekly consensus diagnosisteleconference involving all of the clinicians from each site.Unanimous agreement was required for diagnosis.
After a preliminary telephone review of inclusion and exclusioncriteria, parents were invited to visit the clinic to obtain consent. Allparents/guardians viewed a slide show presentation of the study and
METHYLPHENIDATE EFFICACY IN PATS
1285J . AM. ACAD. CHILD ADOLESC. PSYCHIATRY, 45:11, NOVEMBER 2006

Copyright @ 2006 American Academy of Child and Adolescent Psychiatry. Unauthorized reproduction of this article is prohibited.
then were asked to read and sign written informed consent forms.They also were reconsented before entering each of the other sevenphases of the 70-week study. The institutional review board at eachof the six sites approved the study protocol and all consentprocedures. Central monitoring was performed by the Data andSafety Monitoring Board of the National Institute of Mental Health.
Once consented, families flowed through study phases assummarized in the CONSORT chart (Fig. 1). Of the 303 familieseligible, 165 were randomized into the crossover-titration trial. Asshown in Table 1, the randomized group met the main study criteriafor preschool age, severe ADHD, had comorbidities, and a normalIQ, with a mean age (SD) of 4.4 (0.68), and a mean (SD)Differential Ability Scales General Ability Score of 97 (16). Theywere predominantly male (73%). Symptom scores were severe, witha mean (SD) parent CPRS ADHD symptom rating of 22.27 (3.5),at a T score of 77, and a Child Global Assessment Scale (Shafferet al., 1983) score of 46.79 (4.3). Oppositional defiant disorder(52%) was the most common comorbidity, followed by commu-nication disorder (22%), anxiety disorder (including specificphobia, 16%), and elimination disorder (8%).
Study Design
Those preschoolers who were eligible to enter the controlledmedication phases were those who continued to meet ADHDseverity criteria after 10 weeks of parent training. They entered asequential, open-label, safety lead-in phase in which the daily intakeof MPH was increased over 1 week through the dose range from1.25 mg b.i.d. to 7.5 mg t.i.d.
Generic MPH was purchased by grant funds for the double-blindphases of the study and was milled by a U.S. Food and DrugAdministration manufacturing pharmacy into similar-appearingcapsules of different dose strengths. Before receiving the study drug,the eligible preschoolers were randomly assigned to one of a series ofdose sequences that included weekly doses of 1.25, 2.5, 5.0, or7.5 mg MPH-IR or placebo on a t.i.d. schedule. Randomization wasdone centrally at the coordinating site using a computerizedstratified randomization, 1:1:1:1 starting dose allocation ratio, usinga randomized, balanced, crossover protocol designed to avoid ordereffects. A second randomization to active MPH or to placebo wasperformed before entering the parallel-design, placebo-controlledphase. Except in emergencies, clinicians remained blind to the dosesequences. Blinding was maintained for the primary dependentmeasures until after the best dose was determined or as needed.
Children who had tolerated all open MPH doses in the lead-inphase then entered the 5-week, double-blind, crossover-titration onalgorithms used to find best dose in the MTA study (Greenhill et al.,1996). Subjects were randomized to one of five sequences of fourdifferent MPH doses (1.25, 2.5, 5, 7.5 mg) and placeboadministered t.i.d. in identical capsules for 1 week each. Parentand teacher dose-response rating scale graphs were prepared andblindly evaluated by two study clinicians who determined thechild`s best dose by identifying the week with the optimallyminimized ADHD symptoms and medication side effects.
The primary outcome measure for the titration phase chosen apriori was a composite formed by standardizing and thencombining parent and teacher Conners, Loney, and Milich(CLAM) and Swanson, Kotkin, Atkins, M-Flynn, and Pelham(SKAMP) rating scales (Swanson et al., 1998) to reflect overallmedication response for each dose across settings. This datareduction approach was used previously to measure effects in theMTA titration trial (Greenhill et al., 2001) and at the end of the 14-
month MTA study (MTA Cooperative Group, 1999). The primaryefficacy measure for the parallel phase was borrowed from theBexcellent responder^ criterion using a combination of parent andteacher Swanson, Nolan, and Pelham (SNAP) ratings scales(Swanson et al., 2001).
Afterward, following a 1-day washout, subjects were randomlyassigned to their best dose or to placebo for a 4 week, double-blind,placebo-controlled, parallel-design efficacy trial. Parent and teacherSNAP questionnaires (Swanson, 1992) were collected to monitorADHD symptoms and determine responder status.
Medication Monitoring
MPH administration followed a manual-based procedure tomaintain fidelity to the protocol across the six performance sites.Families had one pharmacotherapist throughout the study. Inaddition to assessing the preschooler`s clinical status, response tomedication, and adverse events during 20- to 40-minute medicationvisits, pharmacotherapists followed the general guidelines for best-practice parameters for the MPH treatment of ADHD, collectingblood pressures and pulses twice at each visit, collecting spontaneousresponses of parents to a nonsystematic general inquiry about thechild`s health, and a parent-scored drug-specific checklist of adverseevents first developed in the MTA study.
Data Analyses
The Nathan Kline Institute served as the data managementcenter. Data entry and verification, data transfer, confidentiality andsecurity, backup and storage, and initial data analyses wereconducted at this site. All analyses were run using the intent-to-treat principle (i.e., each observation obtained for the child was usedin the analysis including those from children who entered each ofthe two phases under consideration and did not complete thephase). The statistical analytic plan and power analysis wereprepared during the planning phase of the study. Specific scientifichypotheses with the corresponding statistical hypotheses wereincluded in the analytic plan. The null hypothesis tested was thatthere were no significant differences in outcome measures betweenthe randomly assigned treatment groups. The primary outcomemeasure for the crossover phase was the combined parent-teacherscalar report using the CLAM/SKAMP; the primary outcomemeasure for the parallel group phase of the study was excellentresponder status, a binary response variable, defined using theSNAP. A mixed-effects linear random regression model was used toestimate parameters and test hypotheses for the crossover phase.Parameters were estimated and tested using SAS Proc Mixed (SASInstitute, Cary, NC). A fixed effect for site was included; randomeffects were the slope of the regression of the CLAM/SKAMP ondose and child-specific random error. The average slope of theregression of the CLAM/SKAMP on the dose of MPH was testedagainst the value 0 to test the null hypothesis of no relationshipbetween dose and clinical improvement. The difference in the ratesof excellent response between children on placebo or best doseduring the 4-week parallel group phase was tested using a logisticregression model. The model was tested using SAS Proc Logisticwith fixed effects included for site. For hypotheses regarding theprimary outcomes, all power analyses assumed that statisticalsignificance (type I error rate) is set at 5%; all tests are two-tailed; byconvention, adequate power is achieved at 80% or better.Simplifying assumptions were made for the calculation of powerfor analysis of the crossover-titration trial, including the assumption
GREENHILL ET AL.
1286 J . AM. ACAD. CHILD ADOLESC. PSYCHIATRY, 45:11, NOVEMBER 2006

Copyright @ 2006 American Academy of Child and Adolescent Psychiatry. Unauthorized reproduction of this article is prohibited.
Fig. 1 PATS CONSORT chart depicting numbers of patients participating at each phase.
METHYLPHENIDATE EFFICACY IN PATS
1287J . AM. ACAD. CHILD ADOLESC. PSYCHIATRY, 45:11, NOVEMBER 2006

Copyright @ 2006 American Academy of Child and Adolescent Psychiatry. Unauthorized reproduction of this article is prohibited.
TABLE 1Characteristics of the Sample
VariablePassed Caseness
(n = 303)Enrolled in CrossoverTitration (n = 165)
Enrolled in Parallel Trial(n = 114)
Subject VariablesAge,a yr, mean (SD) 4.41 (0.70) 4.74 (0.69) 4.76 (0.70)Male, no. (%) 229 (76) 122 (74) 85 (75)Ethnicity, no. (%)
White 190 (63) 104 (63) 74 (65)Black or African American 58 (19) 29 (18) 19 (17)Hispanic or Latino 47 (16) 29 (18) 19 (17)Asian 6 (2) 2 (1) 1 (0.9)American Indian or Alaskan Native 2 (0.7) 1 (0.6) 1 (0.9)
Group educational activity, no. (%)Public nursery 11 (4) 4 (2) 2 (2)Public kindergarten 34 (11) 19 (12) 15 (13)Private/parochial nursery 67 (22) 35 (21) 29 (25)Private/parochial kindergarten 10 (3) 3 (2) 0 (0)Special school for preschoolers with learning problems 27 (9) 15 (9) 9 (8)Day care 48 (16) 23 (14) 12 (11)Play group 1 (0.3) 0 (0) 0 (0)Prenursery 6 (2) 3 (2) 1 (0.9)Prekindergarten 91 (30) 60 (36) 45 (39)Not in school, play group, or day care 8 (3) 3 (2) 1 (0.9)
Conners Teacher Rating Scale, mean (SD)Inattention 16.78 (5.53) 17.85 (5.40) 17.6 (5.15)Hyperactivity 21.71 (3.65) 22.27 (3.48) 22.29 (3.49)Total 38.52 (8.03) 40.16 (7.67) 39.95 (7.49)
Conners Parent Rating Scale, mean (SD)Inattention 15.20 (5.87) 15.39 (5.84) 14.84 (5.81)Hyperactivity 20.17 (4.63) 20.43 (4.62) 20.55 (4.69)Total 35.43 (9.08) 35.91 (8.92) 35.48 (8.85)
Differential Ability Scales IQ, mean (SD) 99.06 (18.30) 97.93 (17.67) 97.45 (16.11)CGAS Impairment Scale, mean (SD) 47.33 (4.07) 46.79 (4.26) 47.35 (4.20)ADHD subtype, no. (%)
Hyperactive-impulsive 75 (25) 39 (24) 29 (25)Combined 228 (75) 126 (76) 85 (75)
Comorbidity (clinical evaluation), no. (%)Oppositional-defiant disorder 158 (52) 90 (55) 60 (53)Communication disorder 66 (22) 33 (20) 25 (22)Elimination disorder (i.e., encopresis, enuresis) 24 (8) 14 (8) 8 (7)Specific phobia (i.e., animals, needles, social phobia) 23 (8) 11 (7) 8 (7)Anxiety disorder (i.e., separation, generalized,
posttraumatic stress disorder)23 (8) 17 (10) 12 (11)
Developmental coordination disorder 10 (3) 7 (4) 6 (5)Conduct disorder 7 (2) 5 (3) 3 (3)Pica 6 (2) 3 (2) 1 (0.9)Adjustment disorder 4 (1) 1 (0.6) 1 (0.9)Reactive attachment disorder 3 (1) 3 (2) 2 (2)Obsessive-compulsive disorder 2 (0.7) 1 (0.6) 1 (0.9)Sleepwalking disorder 1 (0.3) 1 (0.6) 1 (0.9)
Parent/Family VariablesHigh school graduate, no. (%)
Mother 288/297 (97) 154/161 (96) 107/11 (96)Father 242/250 (97) 130/133 (98) 91/93 (98)
GREENHILL ET AL.
1288 J . AM. ACAD. CHILD ADOLESC. PSYCHIATRY, 45:11, NOVEMBER 2006

Copyright @ 2006 American Academy of Child and Adolescent Psychiatry. Unauthorized reproduction of this article is prohibited.
that the within-individual correlation among the repeated measures,week 1 to week 5, is constant (r = 0.60).
To evaluate the clinical significance of the impact of treatment onoutcome, effect sizes (Cohen`s d, the standardized difference of themeans) are calculated as d = MC/SD pooled, where MC is thedifference between means in the active and placebo conditions, andSD pooled is the pooled SD for the active and placebo conditions(Rosenthal et al., 2000). The sample size was set to detect an effectsize of at least 0.45. We anticipated that the parent`s report ofoutcome would show smaller differences than the teacher`s report.
For the crossover phase, the smallest slope detectable withadequate power is 0.020 standardized units on the CLAM/SKAMPper milligram of MPH. Over a 22.5-mg range from placebo to themaximum dose of 22.5 mg, this slope translates to an effect size of0.45 (0.020 slope * 22.5 mg) for comparison of placebo and thehighest dose. For the double-blind parallel phase, children wererandomized equally to best dose of MPH or placebo. Before thestudy, we planned to recruit 120 children to be randomized, so thatdifferences in response rates in excess of 28% (e.g., 36% response forchildren on placebo and 64% response for children on MPH) couldbe detected with adequate power (83%). We anticipated that thedifference would be substantially larger than 28%.
RESULTS
Primary Outcomes
Crossover Phase. Mean (SD) composite SKAMP/CLAM scores are presented by dose level for both thecrossover-titration and parallel phases in Table 2.
During the crossover-titration, random-coefficientregression analyses of composite SKAMP/CLAM scoresidentified a statistically significant linear trend withdose (F1,156 = 51.45, p G .0001). In addition, the2.5-mg (F1,148 = 4.26, p G .001), 5-mg (F1,150 = 4.96,
p G .001), and 7.5-mg (F1,126 = 6.36, p G .001) dosesgiven t.i.d. also were associated with significantlyreduced ADHD symptom scores compared to placeboon the primary outcome measure. The 1.25-mg t.i.d.dose differed from placebo at the trend level only(F1,146 = 1.8, p G .06).
By the end of titration, blind ratings classified 7 (4%)preschoolers as nonresponders (4%); 14 (8%) as placeboresponders; 24 (15%) as best responding to 1.25 mg t.i.d.(0.2 mg/kg/day); 26 (16%) as best responding to 2.5 mgt.i.d. (0.4 mg/kg/day); 30 (18%) as best responding to5 mg t.i.d. (0.8 mg/kg/day); 36 (22%) as best respondingto 7.5 mg t.i.d. (1.2 mg/kg/day); and 7 (4%) as bestresponding to 10 mg t.i.d. (1.3 mg/kg/day). The mean ofoptimal MPH total daily doses was 14.2 T 8.1 mg (0.7 T0.4 mg/kg/day). There was no significant correlationbetween age and MPH absolute dose or MPH dose byweight.
The clinical significance of MPH treatment onoutcome during the titration trial was evaluated bycalculating effect sizes relative to placebo for the scalarcomposite SKAMP/CLAM ratings. Effect sizes forMPH during titration with doses of 1.25, 2.5, 5, and7.5 mg t.i.d. were 0.16, 0.34, 0.43, and 0.72,respectively. Effect sizes for MPH doses during theparallel phase (1.25, 2.5, 5, and 7.5 mg versus placebo)were 0.22, 0.48, 0.52, and 0.87, respectively.
Separate examination of the composite SKAMP/CLAM ratings by informants indicated that teacher
TABLE 1Continued
VariablePassed Caseness
(n = 303)Enrolled in CrossoverTitration (n = 165)
Enrolled in Parallel Trial(n = 114)
Employed, no. (%)Mother 213/295 (72) 120/160 (75) 80/110 (73)Father 214/287 (75) 112/158 (71) 80/109 (73)
Welfare, no. (%) 22/275 (8) 13/148 (9) 7/98 (7)Married, no. (%) 184/297 (62) 98/163 (60) 68/112 (61)Hollingshead socioeconomic status, mean (SD) 47.20 (9.56) 47.01 (9.58) 47.61 (9.45)Family composition, no. (%)
2 parents 246 (76) 130 (79) 91 (80)1 parent 57 (18) 35 (21) 22 (19)
Note: Employed refers to the proportion of the sample whose parents held full- or part-time jobs, were unemployed and looking for work, orwere full- or part-time students; married refers to those with intact two-parent families (married or common law). CGAS = Clinical GlobalAssessment Scale.
a Age at screening for the passed caseness group and age at baseline at the beginning of the medication trial for the enrolled in crossovertitration and enrolled in parallel trial groups.
METHYLPHENIDATE EFFICACY IN PATS
1289J . AM. ACAD. CHILD ADOLESC. PSYCHIATRY, 45:11, NOVEMBER 2006
Copyright @ 2006 American Academy of Child and Adolescent Psychiatry. Unauthorized reproduction of this article is prohibited.
ratings (F1,139 = 39.64, p G .0001) show a greatersensitivity to the medication effects than parent ratings(F1,156 = 35.83, p G .0001). Teacher ratings also yieldeda significant dose effect when children were taking1.25 mg (F1,104 = 23.38, p G .0192), but parent ratingsdid not, as shown in Figure 2.Parallel Phase. Only 13/61 (22%) of subjects
randomized to best-dose MPH and 7/53 (13%) ofthose randomized to placebo met criteria for excellentresponse on the SNAP composite score, a difference thatdid not reach statistical significance ( p G .3). Thisoutcome may have been related to attrition, with 36(32%) patients leaving the parallel phase before comple-tion (33 had behavioral deterioration, 2 declined study
participation, and 1 had medication-related side effects).This included 24 of 53 (45%) randomized to placebo,and 9 of 61 (15%) randomized to best-dose MPH.
In an additional post hoc, intent-to-treat, lastobservation carried forward analysis, we used theprimary efficacy composite SNAP rating of the parallelphase as a continuous measure to supplement thecategorical approach cited above. This revealed sig-nificantly (p G .02) lower mean symptom scores forthose randomized to MPH (1.49, n = 61) versusplacebo (1.79, n = 52). The significant advantage forbest dose was maintained for completers` compositescores between those assigned to MPH (1.39, n = 51)versus placebo (1.76, n = 26, p G .049). Attrition from
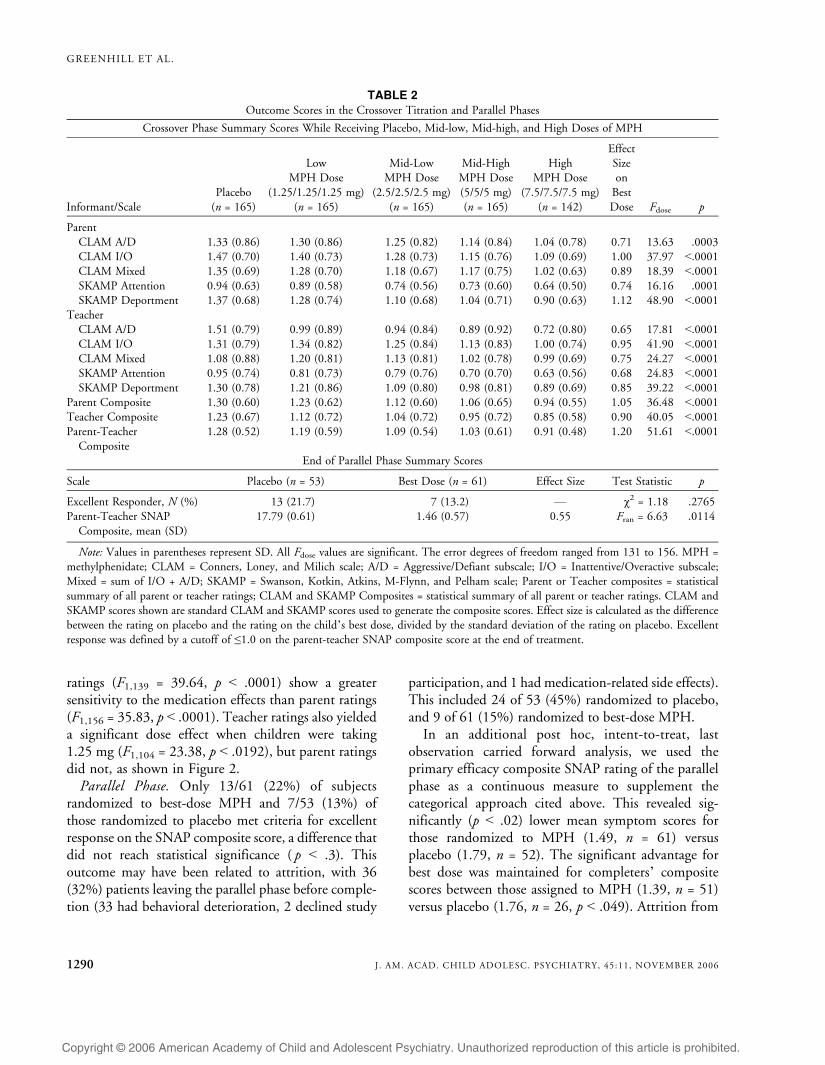
TABLE 2Outcome Scores in the Crossover Titration and Parallel Phases
Crossover Phase Summary Scores While Receiving Placebo, Mid-low, Mid-high, and High Doses of MPH
Informant/ScalePlacebo
(n = 165)
LowMPH Dose
(1.25/1.25/1.25 mg)(n = 165)
Mid-LowMPH Dose
(2.5/2.5/2.5 mg)(n = 165)
Mid-HighMPH Dose(5/5/5 mg)(n = 165)
HighMPH Dose
(7.5/7.5/7.5 mg)(n = 142)
EffectSizeon
BestDose Fdose p
ParentCLAM A/D 1.33 (0.86) 1.30 (0.86) 1.25 (0.82) 1.14 (0.84) 1.04 (0.78) 0.71 13.63 .0003CLAM I/O 1.47 (0.70) 1.40 (0.73) 1.28 (0.73) 1.15 (0.76) 1.09 (0.69) 1.00 37.97 G.0001CLAM Mixed 1.35 (0.69) 1.28 (0.70) 1.18 (0.67) 1.17 (0.75) 1.02 (0.63) 0.89 18.39 G.0001SKAMP Attention 0.94 (0.63) 0.89 (0.58) 0.74 (0.56) 0.73 (0.60) 0.64 (0.50) 0.74 16.16 .0001SKAMP Deportment 1.37 (0.68) 1.28 (0.74) 1.10 (0.68) 1.04 (0.71) 0.90 (0.63) 1.12 48.90 G.0001
TeacherCLAM A/D 1.51 (0.79) 0.99 (0.89) 0.94 (0.84) 0.89 (0.92) 0.72 (0.80) 0.65 17.81 G.0001CLAM I/O 1.31 (0.79) 1.34 (0.82) 1.25 (0.84) 1.13 (0.83) 1.00 (0.74) 0.95 41.90 G.0001CLAM Mixed 1.08 (0.88) 1.20 (0.81) 1.13 (0.81) 1.02 (0.78) 0.99 (0.69) 0.75 24.27 G.0001SKAMP Attention 0.95 (0.74) 0.81 (0.73) 0.79 (0.76) 0.70 (0.70) 0.63 (0.56) 0.68 24.83 G.0001SKAMP Deportment 1.30 (0.78) 1.21 (0.86) 1.09 (0.80) 0.98 (0.81) 0.89 (0.69) 0.85 39.22 G.0001
Parent Composite 1.30 (0.60) 1.23 (0.62) 1.12 (0.60) 1.06 (0.65) 0.94 (0.55) 1.05 36.48 G.0001Teacher Composite 1.23 (0.67) 1.12 (0.72) 1.04 (0.72) 0.95 (0.72) 0.85 (0.58) 0.90 40.05 G.0001Parent-Teacher
Composite1.28 (0.52) 1.19 (0.59) 1.09 (0.54) 1.03 (0.61) 0.91 (0.48) 1.20 51.61 G.0001
End of Parallel Phase Summary Scores
Scale Placebo (n = 53) Best Dose (n = 61) Effect Size Test Statistic p
Excellent Responder, N (%) 13 (21.7) 7 (13.2) V #2 = 1.18 .2765Parent-Teacher SNAP
Composite, mean (SD)17.79 (0.61) 1.46 (0.57) 0.55 Fran = 6.63 .0114
Note: Values in parentheses represent SD. All Fdose values are significant. The error degrees of freedom ranged from 131 to 156. MPH =methylphenidate; CLAM = Conners, Loney, and Milich scale; A/D = Aggressive/Defiant subscale; I/O = Inattentive/Overactive subscale;Mixed = sum of I/O + A/D; SKAMP = Swanson, Kotkin, Atkins, M-Flynn, and Pelham scale; Parent or Teacher composites = statisticalsummary of all parent or teacher ratings; CLAM and SKAMP Composites = statistical summary of all parent or teacher ratings. CLAM andSKAMP scores shown are standard CLAM and SKAMP scores used to generate the composite scores. Effect size is calculated as the differencebetween the rating on placebo and the rating on the child`s best dose, divided by the standard deviation of the rating on placebo. Excellentresponse was defined by a cutoff of e1.0 on the parent-teacher SNAP composite score at the end of treatment.
GREENHILL ET AL.
1290 J . AM. ACAD. CHILD ADOLESC. PSYCHIATRY, 45:11, NOVEMBER 2006

Copyright @ 2006 American Academy of Child and Adolescent Psychiatry. Unauthorized reproduction of this article is prohibited.
the parallel phase was significantly correlated withelevated composite SNAP scores (p G .009), suggestingthat parents withdrew their children from the studybecause of a lack of medication response.
Effect sizes for active MPH doses during the parallelphase were 0.22 for 1.25 mg t.i.d., 0.48 for 2.5 mg t.i.d.,0.52 for 5 mg t.i.d., and 0.87 for 7.5 mg t.i.d..
Safety and Tolerability
Ninety-two percent of preschoolers tolerated MPHdoses in the open safety lead-in phase (see Wigal et al.,2006). Fourteen children left during the lead-in,crossover-titration, and parallel phases because ofadverse events, with 9 of 14 leaving because ofemotionality or irritability. Five side effects occurredmore frequently on the high MPH doses than onplacebo or low MPH doses: appetite loss, troublesleeping, stomachaches, social withdrawal, and lethargy(dull/tired/listless). During the crossover-titrationphase, high blood pressure was reported on eightoccasions and tachycardia was reported on at least onemeasurement.
Although 36 participants dropped out of the parallelphase, only one discontinued because of a drug-relatedadverse event. Weight velocity decreases were evidentafter the preschool children had completed both thetitration and parallel phases and are described in thereport by Swanson et al. (2006).
There were eight serious adverse events in the entirestudy, but only one, a possible seizure, was thought tobe related to medication. There were no episodes ofmania, hypomania, depression, or suicidality.
DISCUSSION
The PATS trial determined the optimal MPH dosesfor 147 children between 3 and 5.5 years withsymptoms of severe ADHD, the efficacy of MPH,as well as their safety profile on MPH. The multisiteteam enrolled 303 preschoolers with severe DSM-IVADHD over 3 years. One hundred sixty-five of thesepreschoolers with ADHD entered the multisite,randomized MPH clinical trial. The behavioral outcomemeasure used in this study shows that preschoolers withADHD do benefit from treatment with MPH.
Preschoolers with severe ADHD responded to 7.5 to30 mg of MPH (total daily dose). Treatment wasinitiated at low doses, although higher doses wererequired for maintenance. The children`s mean optimaldose at the end of titration was 14.22 T 8.1 mg/day(0.7 T 0.4 mg/kg/day). Randomized into a paralleldesign comparing the optimized MPH dose in the formof active drug or placebo, more children taking theactive drug showed a decrease of ADHD symptomsthan did those on placebo.
Despite the statistically significant and clinicallymeaningful improvements in ADHD symptoms withMPH, effect sizes for this medication in PATS aresmaller than those reported in the MTA study ofschool-age children. Factor scores derived from CLAMratings showed an MPH effect size of 0.35 for parentsand 0.43 for teachers. The MTA reported effect sizes of0.52 and 0.75, respectively, on the same measures(Greenhill et al., 2001). For the CLAM attention (IO)subscale, the PATS best-dose effect sizes for parents was0.54 and for teachers was 0.66, whereas in the MTAstudy, they were 0.63 and 1.31, respectively. However,rating attention in preschoolers is more difficult than inschool-age children because the task set in mostpreschool educational settings emphasizes socialization,not attending to cognitive tasks.
Does the lower effect size for MPH treatment inPATS suggest a different response in preschoolers?Matching responses across the age range between thesetwo studies is difficult. The PATS trial was a morecomplex study than the MTA study, with interlocking,interdependent phases (eight versus two), multiplereconsenting during the trial, an option to Bskip out of^double-blind phases and go directly to maintenance,and increased attrition from the controlled phases. Thisattrition may have lowered the estimate of MPH
Fig. 2 Methylphenidate dose-response curve in preschool children withattention-deficit/hyperactivity disorder (N = 165). CLAM = Conners,Loney, and Milich scale; SKAMP = Swanson, Kotkin, Atkins, M-Flynn, andPelham scale.
METHYLPHENIDATE EFFICACY IN PATS
1291J . AM. ACAD. CHILD ADOLESC. PSYCHIATRY, 45:11, NOVEMBER 2006

Copyright @ 2006 American Academy of Child and Adolescent Psychiatry. Unauthorized reproduction of this article is prohibited.
efficacy in PATS. Another interpretation is thatpreschoolers benefit less from MPH than do theirschool-age counterparts. More research will be neces-sary to settle this question.
The MTA study also differed from PATS in theMPH dose range tested. The PATS protocol wasrestricted by the Data and Safety Monitoring Board tototal daily doses of 3.75 to 30 mg, narrower than the15- to 50-mg range used in the MTA study. This couldhave artificially truncated the upper range of optimalMPH treatment daily doses required to optimally treatsome of the preschoolers in our study.
Limitations
PATS had to overcome several limitations. First, thestudy design did not support retention. Negativeexpectancy of deterioration on placebo, repeatedreconsent procedures, and the always available optionto skip directly into open maintenance underminedparental willingness to stick with the research protocol.Parents in this study also may have been more nervousabout medication side effects. They may have beenmore likely to withdraw the child for adverse events thatwould have been tolerated in a school-age child. It isdifficult to determine whether PATS` attrition rate wasthe result of more MPH side effects, more wary parents,or a combination of the two.
Another problem arose in the controlled parallelphase with the choice of an Ball-or-nothing^ categoricaloutcome measure criterion for remission we used todefine our excellent responders. Although more chil-dren on active drug met this strict responder criterionthan did those assigned to placebo, the difference didnot reach significance. Failure to meet this remissioncriterion does not mean that MPH is ineffective inpreschoolers with ADHD. Rather, the failure to remitmay be caused by the severity of the ADHD symptomsin this study. As a group, they were more severelyimpaired than the school-age children recruited for theMTA study. Furthermore, it is not known whetherremission of ADHD symptoms on the SNAP meansthat the preschool children treated have any lessimpairment. This caution is supported by our posthoc analyses of SNAP scores at the end of the parallelphase, which indicated improvement on MPH com-pared with placebo.
Third, the dose-optimizing titration trial used acrossover design could have been confounded by
carryover effects. We sought to reduce this problemby collecting parent and teacher ratings after 7 days oneach treatment condition. This should have reduced theimpact of the any carryover effects from the previousweek`s dose.
Fourth, the PATS dose optimization algorithm wascomplex and thus is not readily transportable intoclinical practice. PATS employed MPH-IR, not theonce-daily, long-duration, controlled-release formula-tions ubiquitous in clinical practice. Long-durationpreparations may be more palatable to preschoolersthan MPH-IR because these new medications can besprinkled on food.
Clinical Implications
PATS data suggest that preschoolers with ADHDneed to start with low MPH doses. Treatment may bestbegin using MPH-IR at 2.5 mg b.i.d. and then beincreased to 7.5 mg t.i.d. during the course of 1 week.The mean optimal total daily MPH dose forpreschoolers was 14.2 T 8.1 mg/day, lower than themean found in school-age children in the MTA study(Greenhill et al., 2001). Replication of this finding witha study design that includes higher MPH doses isneeded because it goes against the commonly heldnotion that smaller children actually require higherdoses than can be predicted by their weight.
PATS is the first controlled multisite trial to addressthe question of the safety and efficacy of MPH inpreschool children with ADHD. Preschoolers withADHD in PATS tolerated MPH, although higher ratesof emotional lability on drug were noted. Treatmenteffect sizes were smaller than those reported in school-age children (Greenhill et al., 2001; MTA StudyCooperative Group, 1999). Nonetheless, this is one ofthe first controlled studies that shows an advantage oflow MPH doses (1.25 mg t.i.d.) over placebo in theclassroom setting. Additional reports from PATS in thisissue address patterns of MPH-related adverse events inpreschoolers (T. Wigal et al.), the long-term impact ofMPH on preschooler`s growth (Swanson et al.), and thepharmacokinetics of MPH in preschool children(McGough et al.).
The authors acknowledge the following members of the PATSGroup: University of California, Irvine: Annamarie Stehli, M.S.,Marc Lerner, M.D., Ken Steinhoff, M.D., Robin Epstein, M.D.,Steve Simpson, M.A., Ron Kotkin, Ed.D., Audrey Kapelinsky,L.C.S.W., Joey Trampush, Ben Thorp; Duke University Medical
GREENHILL ET AL.
1292 J . AM. ACAD. CHILD ADOLESC. PSYCHIATRY, 45:11, NOVEMBER 2006

Copyright @ 2006 American Academy of Child and Adolescent Psychiatry. Unauthorized reproduction of this article is prohibited.
Disclosure: The authors` relationships with for-profit enterprises for theperiod 2000Y2006 are as follows: Dr. Kollins: Cephalon, Pfizer,Psychogenics, Shire, Eli Lilly, New River Pharmaceuticals, McNeil;Dr. Greenhill: Eli Lilly, Shire Pharmaceuticals, Cephalon, McNeil,Celltech, Novartis, Sanofi Aventis, Otsuka, Janssen; Dr. Swanson:Cephalon, Eli Lilly, Janssen, McNeil, Novartis, Shire, UCB; Dr. S.Wigal: McNeil, Cephalon, Shire, Eli Lilly; Dr. Abikoff: McNeil, Shire,Eli Lilly, Pfizer, Celltech, Novartis; Dr. McCracken: Eli Lilly, Wyeth,Shire, Pfizer, McNeil, Novartis, Bristol-Myers Squibb, Janssen;Dr. Riddle: Pfizer; Dr. McGough: Eli Lilly, McNeil, Novartis,Shire, Pfizer, New River Pharmaceuticals; Dr. Posner: GlaxoSmith-Kline, Forest Laboratories, Eisai Inc., AstraZeneca Pharmaceuticals,Johnson & Johnson, Abbott Laboratories, Wyeth Research, OrganonUSA, Bristol-Myers Squibb, Sanofi-Aventis, Cepalon, Novartis, ShirePharmaceuticals, and UCB Pharma; Dr. T. Wigal: Cephalon, EliLilly, McNeil, Shire; Mr. Davies: Pfizer, Amgen, Johnson & Johnson,Wyeth, Merck, GlaxoSmithKline, Bard. Dr. Cunningham receivescompensation for talks and workshops regarding the COPE program.The other authors have no financial relationships to disclose.
REFERENCES
American Psychiatric Association (1994), Diagnostic and Statistical Manualof Mental Disorders, 4th edition (DSM-IV). Washington, DC: AmericanPsychiatric Association
Barkley RA, Karlsson J, Strzelecki E, Murphy JV (1984), Effects of age andRitalin dosage on the mother-child interactions of hyperactive children.52:750Y758
Cohen NJ (1981), Evaluation of the relative effectiveness of methylpheni-date and cognitive behavior modification in the treatment ofkindergarten-aged hyperactive children (1981). J Abnorm Child Psychol9:43Y54
Conners CK, Sitarenios G, Parker J, Epstein J (1998a), The Revised ConnersParent Rating Scale (CPRS-R): factor structure, reliability, and criterionvalidity. J Abnorm Child Psychol 26:257Y268
Conners CK, Sitarenios G, Parker J, Epstein J (1998b), Revision andrestandardization of the Conners Teacher Rating Scale (CTRS-R): factorstructure, reliability and criterion validity. J Abnorm Child Psychol26:279Y293
Elliott CD (1990), Differential Ability Scales, Harcourt Assessment
Corporation, San Antonio, TX; http://harcourtassessment.com/haiweb/Cultures/enUS/Products/Product+Detial.htm?CD_ProductID=015-8067-959 and CS_Category=Adolescents and CS_Catalog=TPC-USCatalog. Accessed November 9, 2005
Firestone P, Musten LM, Pisterman S, Mercer J, Bennett S (1998), Short-term side effects of stimulant medication are increased in preschoolchildren with attention-deficit/hyperactivity disorder: a double-blindplacebo-controlled study. J Child Adolesc Psychopharmacol 8:13Y25
Greenhill LL (1998), The use of psychotropic medication in preschoolers:indications, safety, and efficacy. Can J Psychiatry 43:576Y581
Greenhill LL, Abikoff HB, Arnold LE et al. (1996), Medication treatmentstrategies in the MTA study: relevance to clinicians and researchers. J AmAcad Child Adolesc Psychiatry 35:1304Y1313
Greenhill LL, Swanson JM, Vitiello B et al. (2001), Impairment anddeportment responses to different methylphenidate doses in childrenwith ADHD: the MTA titration trial. J Am Acad Child AdolescPsychiatry 40:180Y187
Handen BL, Feldman HM, Lurier A, Murray PJ (1999), Efficacy ofmethylphenidate among preschool children with developmentaldisabilities and ADHD. J Am Acad Child Adolesc Psychiatry 38:805Y812
Kollins S, Greenhill L, Swanson J, Wigal S, Abikoff H, McCracken J, RiddleM, Swanson J, McGough J, Vitiello B, Wigal T, Skrobala A, Posner K,Ghuman J, Davies M, Cunningham C, Bauzo A (2006), Rationale,design, and methods of the Preschool ADHD Treatment Study (PATS).J Am Acad Child Adolesc Psychiatry 45:1275Y1283
McGough J, McCracken J, Swanson J, Riddle M, Kollins S, Greenhill L,Abikoff H, Davies M, Chuang S, Wigal T, Wigal S, Posner K,Skrobala A, Kastelic E, Ghuman J, Cunningham C, Shigawa S,Moyzis R, Vitiello B (2006), Pharmacogenetics of methylphenidateresponse in preschoolers with ADHD. J Am Acad Child AdolescPsychiatry 45:1314Y1322
MTA Cooperative Group (1999), A 14-month randomized clinical trial oftreatment strategies for attention-deficit/hyperactivity disorder. TheMTA Cooperative Group. Multimodal Treatment Study of Childrenwith ADHD. Arch Gen Psychiatry 56:1073Y1086
Rosenthal R, Rosnow R, Rubin DB (2000), Contrasts and Effect Sizes inBehavioral Research. Cambridge, UK: Cambridge University Press
Schaffer D, Fisher P, Lucas C (1996), The NIMH Diagnostic InterviewSchedule for Children Version 4.0 (DISC-4.0). New York: Ruane Centerfor Early Diagnosis, Division of Child Psychiatry, Columbia University
Shaffer D, Gould MS, Brasic J et al. (1983), A Children`s Global AssessmentScale (CGAS). Arch Gen Psychiatry 40:1228Y1231
Swanson JM (1992), School-Based Assessments and Interventions for ADDstudents. Irvine, CA: K.C. Publications
Swanson J, Greenhill L, Wigal T, Kollins S, Stehli A, Davies M, Chuang S,Vitiello B, Skrobala A, Posner K, Abikoff H, Oatis M, McCracken J,McGough J, Riddle M, Ghuman J, Cunnigham C, Wigal S (2006),Stimulant-related reductions of growth rates in the PATS. J Am AcadChild Adolesc Psychiatry 45:1304Y1313
Swanson J, Wigal S, Greenhill L et al. (1998), Objective and subjectivemeasures of the pharmacodynamic effects of Adderall in the treatment ofchildren with ADHD in a controlled laboratory classroom setting.Psychopharmacol Bull 34:55Y60
Swanson JM, Kraemer HC, Hinshaw SP et al. (2001), Clinical relevance ofthe primary findings of the MTA: success rates based on severity ofADHD and ODD symptoms at the end of treatment. J Am Acad ChildAdolesc Psychiatry 40:168Y179
Wigal T, Greenhill L, Chuang S, McGough J, Vitiello B, Skrobala A,Swanson J, Wigal S, Abikoff H, Kollins S, McCracken J, Riddle M,Posner K, Ghuman J, Davies M, Thorp B, Stehli A (2006), Safety andtolerability of methylphenidate in preschool children with ADHD. J AmAcad Child Adolesc Psychiatry 45:1294Y1303
Zito JM, Safer DJ, dosReis S, Gardner JF, Boles M, Lynch F (2000), Trendsin the prescribing of psychotropic medications to preschoolers. JAMA283:1025Y1030
Center: Allan Chrisman, M.D., Ave Lachiewicz, M.D., PriscillaGrissom, Ph.D., Desiree Murray, Ph.D., Rebecca McIntyre, M.A.;NYSPI/Columbia University: Janet Fairbanks, M.D., Pablo H.Goldberg, M.D., John K. Burton, M.D., Lena S. Kessler, Tova Ferro,Ph.D.; New York University Child Study Center: Tracey Rawls,M.A., Roy Boorady, M.D.; Mark Krushelnycky, M.D.; MelvinOatis, M.D., Daphne Anshel, Ph.D.; Lori Evans, Ph.D.; Universityof California, Los Angeles: Caroly Pataki, M.D.; Robert Suddath,M.D., Melissa Del`Homme, Ph.D., Jennifer Cowen, M.A., KeriVasquez, Cynthia Whitham, M.S.W.; Johns Hopkins University:Golda Ginsburg, Ph.D., Elizabeth Kastelic, M.D., MargaretSchlossberg, Ph.D., Richard D`Alli, M.D., Alexander M. Scharko,M.D., Deidre Everist; NYSPI Statistical Support: Shirley Chuang,M.S; Nathan Kline Institute: Thomas Cooper, M.A., Jim Robinson,M.Ed., Terri DeSouza, R.N., M.P.A., Rita Lindberg, M.S.; NationalInstitute of Mental Health: Joanna Chisar. The authors are gratefulfor the technical support of James Robinson and his staff (NathanKline Institute) for preparing the study interview forms.
METHYLPHENIDATE EFFICACY IN PATS
1293J . AM. ACAD. CHILD ADOLESC. PSYCHIATRY, 45:11, NOVEMBER 2006