
Efficacy and safety of evolocumab (AMG 145), a fully human monoclonal antibody to PCSK9, in...
11
..................................................................................................................................................................................... ..................................................................................................................................................................................... CLINICAL RESEARCH Lipids Efficacy and safety of evolocumab (AMG 145), a fully human monoclonal antibody to PCSK9, in hyperlipidaemic patients on various background lipid therapies: pooled analysis of 1359 patients in four phase 2 trials Evan A. Stein 1 * , Robert P. Giugliano 2 , Michael J. Koren 3 , Frederick J. Raal 4 , Eli M. Roth 5 , Robert Weiss 6 , David Sullivan 7 , Scott M. Wasserman 8 , Ransi Somaratne 8 , Jae B. Kim 8 , Jingyuan Yang 8 , Thomas Liu 8 , Moetaz Albizem 8 , Rob Scott 8 , and Marc S. Sabatine 2 , for the PROFICIO Investigators 1 Metabolic and Atherosclerosis Research Centre, Cincinnati, OH, USA; 2 TIMI Study Group, Brigham and Women’s Hospital, Boston, MA, USA; 3 Jacksonville Centre for Clinical Research, Jacksonville, FL, USA; 4 Carbohydrate & Lipid Metabolism Research Unit, University of Witwatersrand, Johannesburg, South Africa; 5 Sterling Research Group, Cincinnati, OH, USA; 6 Maine Research Associates, Auburn, ME, USA; 7 Department of Clinical Biochemistry, Royal Prince Alfred Hospital, Camperdown, Australia; and 8 Amgen Inc., Thousand Oaks, CA, USA Received 22 November 2013; revised 8 January 2014; accepted 30 January 2014; online publish-ahead-of-print 4 March 2014 Aims Prior trials with monoclonal antibodies to proprotein convertase subtilizin/kexin type 9 (PCSK9) reported robust low density lipoprotein cholesterol (LDL-C) reductions. However, the ability to detect potentially beneficial changes in other lipoproteins such as lipoprotein (a), triglycerides, high-density lipoprotein cholesterol (HDL-C), and apolipopro- tein (Apo) A1, and adverse events (AEs) was limited by sample sizes of individual trials. We report a pooled analysis from four phase 2 studies of evolocumab (AMG 145), a monoclonal antibody to PCSK9. Methods and results The trials randomized 1359 patients to various doses of subcutaneous evolocumab every 2 weeks (Q2W) or 4 weeks (Q4W), placebo, or ezetimibe for 12 weeks; 1252 patients contributed to efficacy and 1314, to safety analyses. Mean per- centage (95% CI) reductions in LDL-C vs. placebo ranged from 40.2% (44.6%, 35.8%) to 59.3% (63.7%, 54.8%) among the evolocumab groups (all P , 0.001). Statistically significant reductions in apolipoprotein B (Apo B), non-high-density lipo- protein cholesterol (non-HDL-C), triglycerides and lipoprotein (a) [Lp(a)], and increases in HDL-C were also observed. Adverse events (AEs) and serious AEs with evolocumab were reported in 56.8 and 2.0% of patients, compared with 49.2% and 1.2% with placebo. Adjudicated cardiac and cerebrovascular events were reported in 0.3 and 0% in the placebo and 0.9 and 0.3% in the evolocumab arms, respectively. Conclusion In addition to LDL-C reduction, evolocumab, dosed either Q2W or Q4W, demonstrated significant and favourable changes in other atherogenic and anti-atherogenic lipoproteins, and was well tolerated over the 12-week treatment period. ----------------------------------------------------------------------------------------------------------------------------------------------------------- Keywords Proprotein convertase subtilizin/kexin type 9 † Low-density lipoprotein cholesterol † Randomized controlled trials Introduction One of the cornerstones for reducing cardiovascular disease (CVD) morbidity and mortality is reduction of low-density lipoprotein cholesterol (LDL-C). 1,2 Although the great majority of the evidence has been obtained from statin-based randomized outcome trials, 3,4 it is also supported by similar reductions in CVD with other agents such as bile acid sequestrants and immediate release nicotinic acid. 5,6 *Corresponding author. Tel: +1 8596533141, Email: [email protected] Published on behalf of the European Society of Cardiology. All rights reserved. & The Author 2014. For permissions please email: [email protected] European Heart Journal (2014) 35, 2249–2259 doi:10.1093/eurheartj/ehu085 by guest on June 12, 2016 http://eurheartj.oxfordjournals.org/ Downloaded from
-
Upload
independent -
Category
Documents
-
view
1 -
download
0
Transcript of Efficacy and safety of evolocumab (AMG 145), a fully human monoclonal antibody to PCSK9, in...
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
CLINICAL RESEARCHLipids
Efficacy and safety of evolocumab (AMG 145),a fully human monoclonal antibody to PCSK9,in hyperlipidaemic patients on various backgroundlipid therapies: pooled analysis of 1359 patientsin four phase 2 trialsEvan A. Stein1*, Robert P. Giugliano2, Michael J. Koren3, Frederick J. Raal4, Eli M. Roth5,Robert Weiss6, David Sullivan7, Scott M. Wasserman8, Ransi Somaratne8, Jae B. Kim8,Jingyuan Yang8, Thomas Liu8, Moetaz Albizem8, Rob Scott8, and Marc S. Sabatine2,for the PROFICIO Investigators1Metabolic and Atherosclerosis ResearchCentre, Cincinnati, OH, USA; 2TIMI Study Group, Brigham and Women’s Hospital, Boston, MA, USA; 3Jacksonville Centre for Clinical Research,Jacksonville, FL, USA; 4Carbohydrate & Lipid Metabolism ResearchUnit, Universityof Witwatersrand, Johannesburg, South Africa; 5Sterling ResearchGroup, Cincinnati, OH, USA; 6MaineResearch Associates, Auburn, ME, USA; 7Department of Clinical Biochemistry, Royal Prince Alfred Hospital, Camperdown, Australia; and 8Amgen Inc., Thousand Oaks, CA, USA
Received 22 November 2013; revised 8 January 2014; accepted 30 January 2014; online publish-ahead-of-print 4 March 2014
Aims Prior trials with monoclonal antibodies to proprotein convertase subtilizin/kexin type 9 (PCSK9) reported robust lowdensity lipoprotein cholesterol (LDL-C) reductions. However, the ability to detect potentially beneficial changes inother lipoproteins such as lipoprotein (a), triglycerides, high-density lipoprotein cholesterol (HDL-C), and apolipopro-tein (Apo) A1, and adverse events (AEs) was limited by sample sizes of individual trials. We report a pooled analysis fromfour phase 2 studies of evolocumab (AMG 145), a monoclonal antibody to PCSK9.
Methodsand results
The trials randomized 1359 patients to various doses of subcutaneous evolocumab every 2 weeks (Q2W) or 4 weeks(Q4W), placebo, or ezetimibe for 12 weeks; 1252 patients contributed to efficacy and 1314, to safety analyses. Mean per-centage (95% CI) reductions in LDL-C vs. placebo ranged from 40.2% (44.6%, 35.8%) to 59.3% (63.7%, 54.8%) among theevolocumab groups (all P , 0.001). Statistically significant reductions in apolipoprotein B (Apo B), non-high-density lipo-protein cholesterol (non-HDL-C), triglycerides and lipoprotein (a) [Lp(a)], and increases in HDL-C were also observed.Adverseevents (AEs) and seriousAEswith evolocumabwere reported in 56.8 and2.0% ofpatients, comparedwith 49.2%and 1.2% with placebo. Adjudicated cardiac and cerebrovascular events were reported in 0.3 and 0% in the placebo and0.9 and 0.3% in the evolocumab arms, respectively.
Conclusion In addition toLDL-Creduction, evolocumab, dosedeither Q2WorQ4W,demonstratedsignificant and favourablechangesin other atherogenic and anti-atherogenic lipoproteins, and was well tolerated over the 12-week treatment period.
- - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - -Keywords Proprotein convertase subtilizin/kexin type 9 † Low-density lipoprotein cholesterol † Randomized controlled trials
IntroductionOne of the cornerstones for reducing cardiovascular disease (CVD)morbidity and mortality is reduction of low-density lipoprotein
cholesterol (LDL-C).1,2 Although the great majority of the evidencehas been obtained from statin-based randomized outcome trials,3,4 itis also supported by similar reductions in CVD with other agents suchas bile acid sequestrants and immediate release nicotinic acid.5,6
*Corresponding author. Tel: +1 8596533141, Email: [email protected]
Published on behalf of the European Society of Cardiology. All rights reserved. & The Author 2014. For permissions please email: [email protected]
European Heart Journal (2014) 35, 2249–2259doi:10.1093/eurheartj/ehu085
by guest on June 12, 2016http://eurheartj.oxfordjournals.org/
Dow
nloaded from
However, there is still a large unmet need for additional LDL-C redu-cing agents because existing therapies may not be well tolerated andnot all treated patients can achieve LDL-C goals.7,8
Based on biology and human genetics, proprotein convertase sub-tilizin/kexin type 9 (PCSK9) provides a new and compelling target forLDL-C lowering therapy.9 Over the last year, early clinical trials withmonoclonal antibodies have confirmed this approach with rapid anddramatic LDL-C reductions.10–17 Potentially beneficial trends inother lipids and lipoproteins, such as triglycerides, lipoprotein (a)[Lp(a)], and high-density lipoprotein cholesterol (HDL-C), wereobserved, but the precision of those estimates and the capacity toexamine for consistency across clinically important subgroups, suchas gender, age, and background lipid therapy, were limited by thesample sizes in each trial.
As part of the Program to Reduce LDL-C and Cardiovascular Out-comes Following Inhibition of PCSK9 in Different Populations (PRO-FICIO), over 1300 patients from 4 randomized, placebo-controlledphase 2 trials11 –14 were pooled into a single data set to betterassess efficacy, safety, and tolerability of evolocumab (AMG 145).
Methods
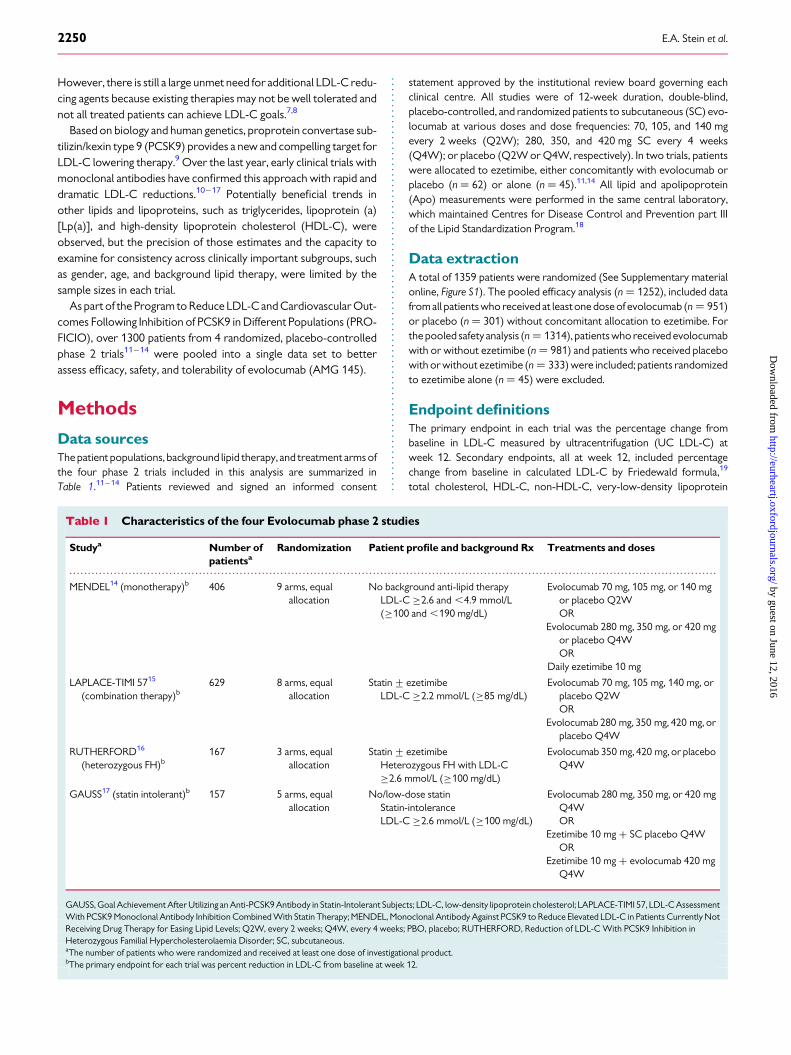
Data sourcesThe patient populations, background lipid therapy, and treatment arms ofthe four phase 2 trials included in this analysis are summarized inTable 1.11 –14 Patients reviewed and signed an informed consent
statement approved by the institutional review board governing eachclinical centre. All studies were of 12-week duration, double-blind,placebo-controlled, and randomized patients to subcutaneous (SC) evo-locumab at various doses and dose frequencies: 70, 105, and 140 mgevery 2 weeks (Q2W); 280, 350, and 420 mg SC every 4 weeks(Q4W); or placebo (Q2W or Q4W, respectively). In two trials, patientswere allocated to ezetimibe, either concomitantly with evolocumab orplacebo (n ¼ 62) or alone (n ¼ 45).11,14 All lipid and apolipoprotein(Apo) measurements were performed in the same central laboratory,which maintained Centres for Disease Control and Prevention part IIIof the Lipid Standardization Program.18
Data extractionA total of 1359 patients were randomized (See Supplementary materialonline, Figure S1). The pooled efficacy analysis (n ¼ 1252), included datafromall patients who received at leastone dose of evolocumab (n ¼ 951)or placebo (n ¼ 301) without concomitant allocation to ezetimibe. Forthe pooled safety analysis (n ¼ 1314), patients who received evolocumabwith or without ezetimibe (n ¼ 981) and patients who received placebowith or without ezetimibe (n ¼ 333) were included; patients randomizedto ezetimibe alone (n ¼ 45) were excluded.
Endpoint definitionsThe primary endpoint in each trial was the percentage change frombaseline in LDL-C measured by ultracentrifugation (UC LDL-C) atweek 12. Secondary endpoints, all at week 12, included percentagechange from baseline in calculated LDL-C by Friedewald formula,19
total cholesterol, HDL-C, non-HDL-C, very-low-density lipoprotein
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Table 1 Characteristics of the four Evolocumab phase 2 studies
Studya Number ofpatientsa
Randomization Patient profile and background Rx Treatments and doses
MENDEL14 (monotherapy)b 406 9 arms, equalallocation
No background anti-lipid therapyLDL-C ≥2.6 and ,4.9 mmol/L(≥100 and ,190 mg/dL)
Evolocumab 70 mg, 105 mg, or 140 mgor placebo Q2WOR
Evolocumab 280 mg, 350 mg, or 420 mgor placebo Q4WOR
Daily ezetimibe 10 mg
LAPLACE-TIMI 5715
(combination therapy)b629 8 arms, equal
allocationStatin+ ezetimibe
LDL-C ≥2.2 mmol/L (≥85 mg/dL)Evolocumab 70 mg, 105 mg, 140 mg, or
placebo Q2WOR
Evolocumab 280 mg, 350 mg, 420 mg, orplacebo Q4W
RUTHERFORD16
(heterozygous FH)b167 3 arms, equal
allocationStatin+ ezetimibe
Heterozygous FH with LDL-C≥2.6 mmol/L (≥100 mg/dL)
Evolocumab 350 mg, 420 mg, or placeboQ4W
GAUSS17 (statin intolerant)b 157 5 arms, equalallocation
No/low-dose statinStatin-intoleranceLDL-C ≥2.6 mmol/L (≥100 mg/dL)
Evolocumab 280 mg, 350 mg, or 420 mgQ4WOR
Ezetimibe 10 mg + SC placebo Q4WOR
Ezetimibe 10 mg + evolocumab 420 mgQ4W
GAUSS, Goal Achievement After Utilizing an Anti-PCSK9 Antibody in Statin-Intolerant Subjects; LDL-C, low-density lipoprotein cholesterol; LAPLACE-TIMI 57, LDL-C AssessmentWith PCSK9 Monoclonal Antibody Inhibition Combined With Statin Therapy; MENDEL, Monoclonal Antibody Against PCSK9 to Reduce Elevated LDL-C in Patients Currently NotReceiving Drug Therapy for Easing Lipid Levels; Q2W, every 2 weeks; Q4W, every 4 weeks; PBO, placebo; RUTHERFORD, Reduction of LDL-C With PCSK9 Inhibition inHeterozygous Familial Hypercholesterolaemia Disorder; SC, subcutaneous.aThe number of patients who were randomized and received at least one dose of investigational product.bThe primary endpoint for each trial was percent reduction in LDL-C from baseline at week 12.
E.A. Stein et al.2250
by guest on June 12, 2016http://eurheartj.oxfordjournals.org/
Dow
nloaded from
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Table 2 Patient demographics and lipid parameters at baseline
Placebo Evolocumab Totala
Q2W(n 5 123)
Q4W(n 5 178)
Q4W 1 EZEQD (n 5 32)
70 mg Q2W(n 5 124)
105 mg Q2W(n 5 125)
140 mg Q2W(n 5 123)
280 mg Q4W(n 5 156)
350 mg Q4W(n 5 210)
420 mg Q4W(n 5 213)
420 mgQ4W 1 EZE QD(n 5 30)
N 5 1359
Age, years, mean (SD) 57.4 (9.9) 54.4 (12.0) 62.4 (6.6) 56.3 (11.8) 54.9 (11.6) 58.9 (11.7) 57.5 (10.7) 55.9 (13.0) 56.1 (12.1) 62.0 (7.2) 56.4 (11.7)
Age ,65 years, n (%) 95 (77.2) 135 (75.8) 18 (56.3) 90 (72.6) 96 (76.8) 81 (65.9) 111 (71.2) 150 (71.4) 151 (70.9) 17 (56.7) 987 (72.6)
Women, n (%) 67 (54.5) 103 (57.9) 18 (56.3) 74 (59.7) 58 (46.4) 81 (65.9) 86 (55.1) 117 (55.7) 111 (52.1) 23 (76.7) 764 (56.2)
Race, n (%)
White 107 (87.0) 158 (88.8) 28 (87.5) 105 (84.7) 104 (83.2) 106 (86.2) 127 (81.4) 185 (88.1) 185 (86.9) 24 (80.0) 1164 (85.7)
Black 14 (11.4) 7 (3.9) 2 (6.3) 13 (10.5) 13 (10.4) 13 (10.6) 18 (11.5) 15 (7.1) 21 (9.9) 1 (3.3) 126 (9.3)
Other 2 (1.6) 13 (7.3) 2 (6.3) 6 (4.8) 6 (4.8) 4 (3.2) 11 (7.1) 10 (4.8) 7 (3.3) 5 (16.7) 63 (4.6)
Statin use, n (%) 78 (63.4) 133 (74.7) 6 (18.8) 78 (62.9) 78 (62.4) 78 (63.4) 84 (53.8) 139 (66.2) 141 (66.2) 4 (13.3) 819 (60.3)
Ezetimibe use, n (%) 5 (4.1) 41 (23.0) 0 (0.0) 6 (4.8) 8 (6.4) 7 (5.7) 7 (4.5) 44 (21.0) 42 (19.7) 0 (0.0) 160 (11.8)
Lipid parameters, mean (SD)
UC LDL-C,b
mmol/L 3.39 (0.72) 3.64 (0.96) 4.73 (0.94) 3.34 (0.66) 3.43 (0.77) 3.31 (0.65) 3.68 (1.10) 3.74 (1.09) 3.74 (1.15) 5.03 (1.55) 3.64 (1.01)
Calc LDL-C,c
mmol/L 3.37 (0.75) 3.60 (0.99) 4.68 (0.92) 3.31 (0.70) 3.37 (0.79) 3.25 (0.66) 3.62 (1.10) 3.69 (1.13) 3.68 (1.17) 5.01 (1.54) 3.59 (1.03)
Total-C, mmol/L 5.48 (0.93) 5.64 (1.10) 7.10 (1.01) 5.39 (0.82) 5.47 (0.91) 5.35 (0.76) 5.77 (1.28) 5.75 (1.23) 5.76 (1.29) 7.23 (1.69) 5.68 (1.16)
HDL-C, mmol/L 1.42 (0.46) 1.36 (0.42) 1.57 (0.49) 1.41 (0.44) 1.39 (0.46) 1.41 (0.39) 1.42 (0.46) 1.34 (0.40) 1.34 (0.43) 1.55 (0.50) 1.39 (0.43)
Non-HDL-C,mmol/L 4.05 (0.85) 4.27 (1.10) 5.53 (1.04) 3.98 (0.78) 4.08 (0.88) 3.93 (0.69) 4.35 (1.23) 4.41 (1.21) 4.42 (1.33) 5.68 (1.57) 4.3 (1.13)
Total-C/HDL-Cratio 4.14 (1.15) 4.51 (1.65) 4.91 (1.55) 4.12 (1.20) 4.29 (1.41) 4.02 (1.07) 4.41 (1.46) 4.62 (1.64) 4.71 (1.91) 5.09 (2.42) 4.44 (1.55)
VLDL-C, mmol/L 0.65 (0.40) 0.64 (0.40) 0.8 (0.37) 0.64 (0.33) 0.65 (0.34) 0.63 (0.27) 0.67 (0.36) 0.67 (0.38) 0.68 (0.40) 0.66 (0.27) 0.66 (0.37)
Apo B, g/L 1.04 (0.18) 1.11 (0.25) 1.38 (0.22) 1.03 (0.17) 1.05 (0.20) 1.02 (0.17) 1.12 (0.27) 1.14 (0.28) 1.15 (0.29) 1.39 (0.33) 1.11 (0.25)
Apo A1, g/L 1.57 (0.30) 1.51 (0.30) 1.71 (0.32) 1.56 (0.29) 1.54 (0.30) 1.57 (0.27) 1.58 (0.31) 1.52 (0.27) 1.51 (0.29) 1.63 (0.29) 1.55 (0.29)
Apo B/Apo A1ratio 0.69 (0.17) 0.77 (0.27) 0.84 (0.23) 0.69 (0.18) 0.71 (0.20) 0.67 (0.16) 0.74 (0.22) 0.78 (0.26) 0.79 (0.28) 0.88 (0.33) 0.75 (0.24)
Triglycerides,mmol/L 1.51 (0.76) 1.50 (0.82) 1.85 (0.74) 1.46 (0.62) 1.55 (0.72) 1.50 (0.64) 1.58 (0.72) 1.60 (0.81) 1.61 (0.82) 1.48 (0.63) 1.55 (0.75)
Lipoprotein(a),median (IQrange), nmol/L
47.0 (16.0,176.0)
42.0 (14.0,132.0) 58.5 (5.5, 140.5) 46.0 (14.0, 136.0) 40.0 (12.0, 151.0) 43.5 (14.0, 141.0) 37.0 (12.0, 130.0) 36.0 (10.0, 127.0) 41.0 (14.5, 152.5) 39.0 (14.0, 187.0) 40.0 (13.0, 144.0)
FreePCSK9, ng/mL 413.7 (125.2) 470.5 (165.6) 389.9 (90.9) 385.6 (113.0) 398 (104.5) 411.7 (117.8) 402.9 (135.0) 459.5 (164.0) 468.3 (158.9) 379.4 (110.9) 427.5 (143.1)
Apo A1, apolipoprotein A1; Apo B, apolipoprotein B; calc, calculated; EZE, ezetimibe; HDL-C, high-density lipoprotein cholesterol; IQ, interquartile; LDL-C, low-density lipoprotein cholesterol; PCSK9, proprotein convertase subtilizin/kexintype 9;IQ, interquartile; Q2W, every 2 weeks; Q4W, every 4 weeks; SC, subcutaneous; Total-C, total cholesterol; UC LDL-C, LDL-C measured by preparative ultracentrifugation; VLDL-C, very low-density lipoprotein cholesterol.aIncludes all randomized and dosed patients from the four clinical trials.bLDL-C measured by preparative ultracentrifugation.cLDL-C calculated by the Friedewald formula.
Efficacyand
safetyofevolocum
ab2251
by guest on June 12, 2016 http://eurheartj.oxfordjournals.org/ Downloaded from
cholesterol (VLDL-C), Apo B, Apo A1, Lp(a), triglycerides, and the ratiosof total cholesterol/HDL-C and Apo B/Apo A1. Exploratory analysisincluded LDL-C, Apo B, HDL-C, and Apo A1 response by gender, age(, and ≥65 years), statin or no-statin background therapy andabove or below the mean baseline LDL-C at entry of 3.64 mmol/L(140.6 mg/dL). The incidence of adjudicated events of death (all-causeand cardiovascular); cardiac ischaemic events (myocardial infarction,hospitalization for unstable angina, and coronary revascularization);hospitalization for heart failure; and cerebrovascular events wereassessed throughout the trials. All cardiovascular-related events werepre-specified for blinded adjudication by an academically based clinicalevents committee. Key safety endpoints included the incidence oftreatment-emergent adverse events (AEs), treatment-related AEs,safety laboratory values, and the incidence of anti-evolocumab antibodies(binding and if positive, neutralizing).
Statistical analysisPatients were analysed in the treatment group to which they were rando-mized. All efficacy endpoints of lipid parameters were analysed using theanalysis of covariance model (ANCOVA) within each dosing regimen(Q2W or Q4W) to assess the efficacy of evolocumab dose groups com-pared with placebo, with last observation carried forward imputation formissing data, a significance level of 0.05, and no adjustment for multiplecomparisons. The ANCOVA model includes treatment group and acommon stratification factor used in each study (screening LDL values,130 mg/dL or not). Safety analyses were conducted using descriptivestatistics. Safety data were reported as observed. All analyses were per-formed with SAS/STATw, version 9.2 (SAS Institute, Cary, NC, USA).
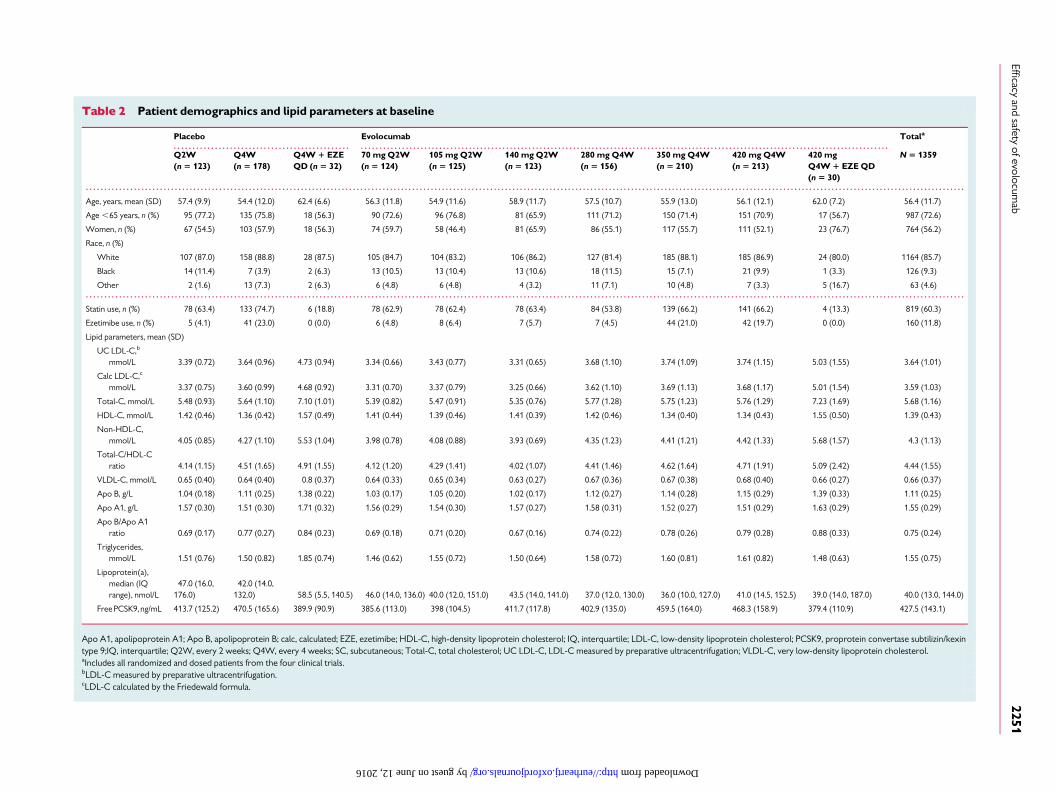
ResultsPatient demographics, baseline statin and ezetimibe therapy, and lipidlevels are shown in Table 2. The mean+ standard deviation (SD) agewas 56.4+ 11.7 years, 56.2% were women, and 85.7% were white.At baseline, a total of 60.3% of patients were taking a statin and11.8% were taking ezetimibe; the baseline mean+ SD baseline UCLDL-C was 3.64+ 1.01 mmol/L (141+39 mg/dL).
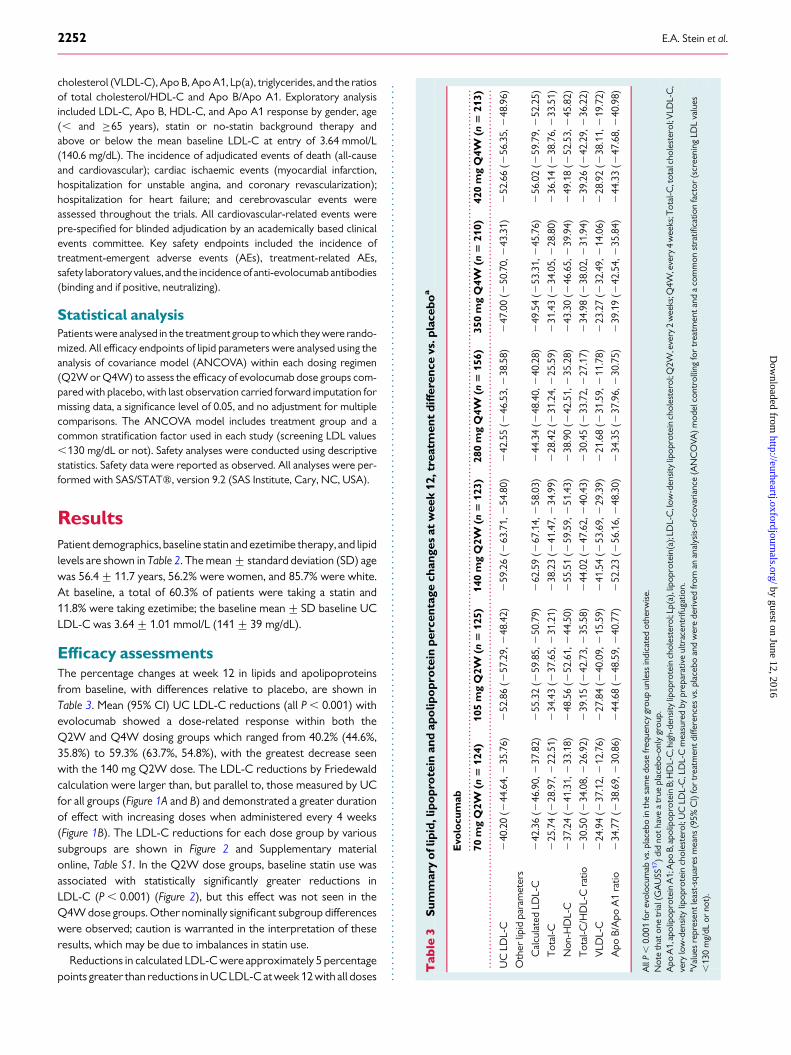
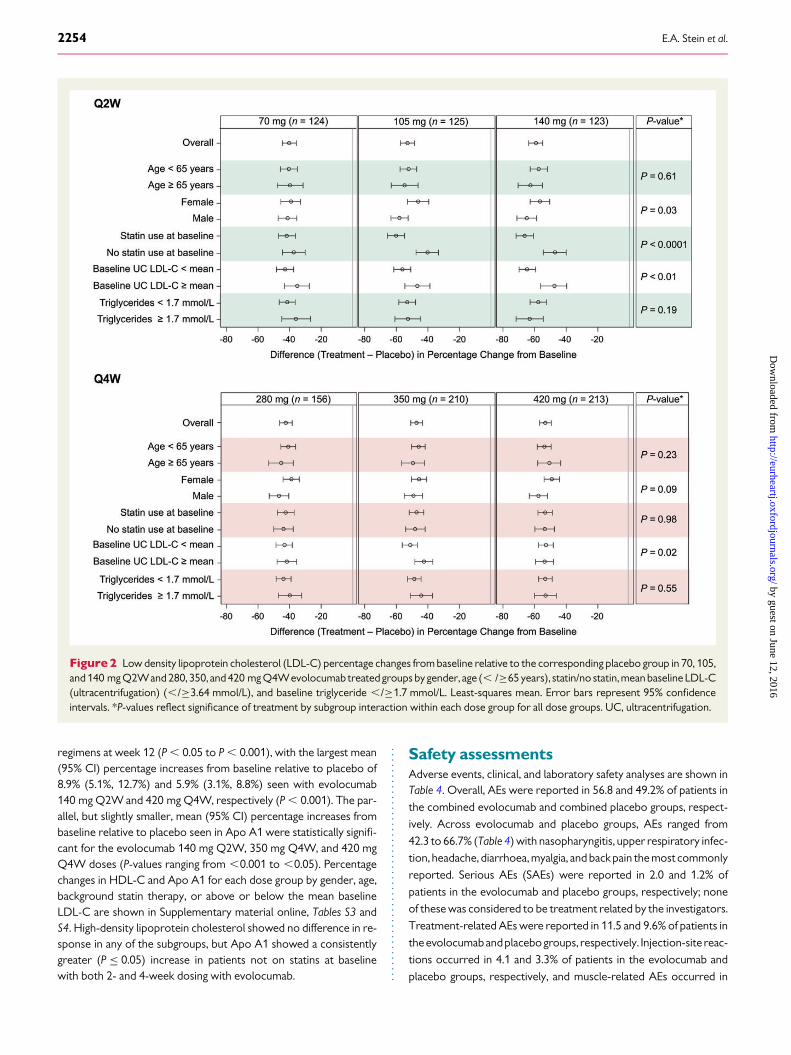
Efficacy assessmentsThe percentage changes at week 12 in lipids and apolipoproteinsfrom baseline, with differences relative to placebo, are shown inTable 3. Mean (95% CI) UC LDL-C reductions (all P , 0.001) withevolocumab showed a dose-related response within both theQ2W and Q4W dosing groups which ranged from 40.2% (44.6%,35.8%) to 59.3% (63.7%, 54.8%), with the greatest decrease seenwith the 140 mg Q2W dose. The LDL-C reductions by Friedewaldcalculation were larger than, but parallel to, those measured by UCfor all groups (Figure 1A and B) and demonstrated a greater durationof effect with increasing doses when administered every 4 weeks(Figure 1B). The LDL-C reductions for each dose group by varioussubgroups are shown in Figure 2 and Supplementary materialonline, Table S1. In the Q2W dose groups, baseline statin use wasassociated with statistically significantly greater reductions inLDL-C (P , 0.001) (Figure 2), but this effect was not seen in theQ4W dose groups. Other nominally significant subgroup differenceswere observed; caution is warranted in the interpretation of theseresults, which may be due to imbalances in statin use.
Reductions in calculated LDL-C were approximately 5 percentagepoints greater than reductions in UC LDL-C atweek 12 with all doses
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
..
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
....
.
Tab
le3
Sum
mar
yo
flip
id,l
ipo
pro
tein
and
apo
lipo
pro
tein
perc
enta
gech
ange
sat
wee
k12
,tre
atm
ent
diff
eren
cevs
.pla
cebo
a
Evo
locu
mab
70m
gQ
2W(n
512
4)10
5m
gQ
2W(n
512
5)14
0m
gQ
2W(n
512
3)28
0m
gQ
4W(n
515
6)35
0m
gQ
4W(n
521
0)42
0m
gQ
4W(n
521
3)
UC
LDL-
C2
40.2
0(2
44.6
4,2
35.7
6)2
52.8
6(2
57.2
9,2
48.4
2)2
59.2
6(2
63.7
1,2
54.8
0)2
42.5
5(2
46.5
3,2
38.5
8)2
47.0
0(2
50.7
0,2
43.3
1)2
52.6
6(2
56.3
5,2
48.9
6)
Oth
erlip
idpa
ram
eter
s
Cal
cula
ted
LDL-
C2
42.3
6(2
46.9
0,2
37.8
2)2
55.3
2(2
59.8
5,2
50.7
9)2
62.5
9(2
67.1
4,2
58.0
3)2
44.3
4(2
48.4
0,2
40.2
8)2
49.5
4(2
53.3
1,2
45.7
6)2
56.0
2(2
59.7
9,2
52.2
5)
Tot
al-C
225
.74
(228
.97,
222
.51)
234
.43
(237
.65,
231
.21)
238
.23
(241
.47,
234
.99)
228
.42
(231
.24,
225
.59)
231
.43
(234
.05,
228
.80)
236
.14
(238
.76,
233
.51)
Non
-HD
L-C
237
.24
(241
.31,
233
.18)
248
.56
(252
.61,
244
.50)
255
.51
(259
.59,
251
.43)
238
.90
(242
.51,
235
.28)
243
.30
(246
.65,
239
.94)
249
.18
(252
.53,
245
.82)
Tot
al-C
/HD
L-C
ratio
230
.50
(234
.08,
226
.92)
239
.15
(242
.73,
235
.58)
244
.02
(247
.62,
240
.43)
230
.45
(233
.72,
227
.17)
234
.98
(238
.02,
231
.94)
239
.26
(242
.29 ,
236
.22)
VLD
L-C
224
.94
(237
.12,
212
.76)
227
.84
(240
.09,
215
.59)
241
.54
(253
.69,
229
.39)
221
.68
(231
.59,
211
.78)
223
.27
(232
.49,
214
.06)
228
.92
(238
.11,
219
.72)
Apo
B/A
poA
1ra
tio2
34.7
7(2
38.6
9,2
30.8
6)2
44.6
8(2
48.5
9,2
40.7
7)2
52.2
3(2
56.1
6,2
48.3
0)2
34.3
5(2
37.9
6,2
30.7
5)2
39.1
9(2
42.5
4,2
35.8
4)2
44.3
3(2
47.6
8,2
40.9
8)
All
P,
0.00
1fo
rev
oloc
umab
vs.p
lace
boin
the
sam
edo
sefr
eque
ncy
grou
pun
less
indi
cate
dot
herw
ise.
Not
eth
aton
etr
ial(
GA
USS
17 )
did
noth
ave
atr
uepl
aceb
o-on
lygr
oup.
Apo
A1,
apol
ipop
rote
inA
1;A
poB,
apol
ipop
rote
inB;
HD
L-C
,hig
h-de
nsity
lipop
rote
inch
oles
tero
l;Lp
(a),
lipop
rote
in(a
);LD
L-C
,low
-den
sity
lipop
rote
inch
oles
tero
l;Q
2W,e
very
2w
eeks
;Q4W
,eve
ry4
wee
ks;T
otal
-C,t
otal
chol
este
rol;
VLD
L-C
,ve
rylo
w-d
ensi
tylip
opro
tein
chol
este
rol;
UC
LDL-
C,L
DL-
Cm
easu
red
bypr
epar
ativ
eul
trac
entr
ifuga
tion.
a Val
ues
repr
esen
tlea
st-s
quar
esm
eans
(95%
CI)
for
trea
tmen
tdiff
eren
ces
vs.p
lace
boan
dw
ere
deri
ved
from
anan
alys
is-o
f-co
vari
ance
(AN
CO
VA)
mod
elco
ntro
lling
for
trea
tmen
tand
aco
mm
onst
ratifi
catio
nfa
ctor
(scr
eeni
ngLD
Lva
lues
,13
0m
g/dL
orno
t).
E.A. Stein et al.2252
by guest on June 12, 2016http://eurheartj.oxfordjournals.org/
Dow
nloaded from
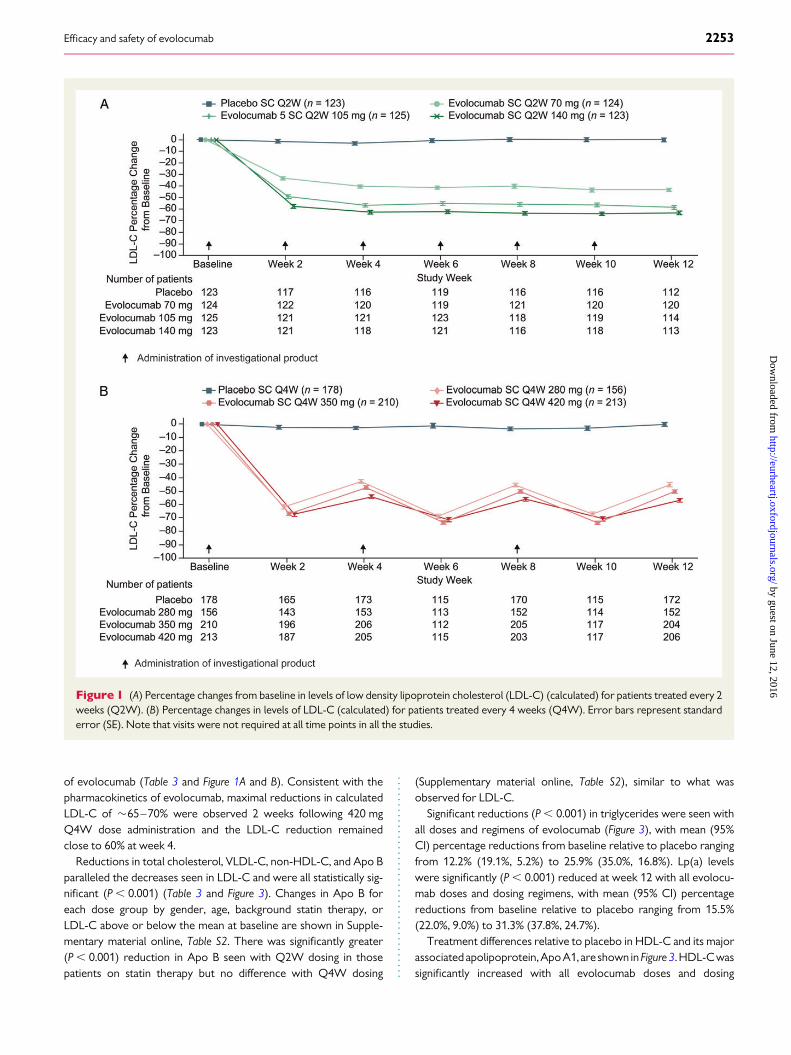
of evolocumab (Table 3 and Figure 1A and B). Consistent with thepharmacokinetics of evolocumab, maximal reductions in calculatedLDL-C of �65–70% were observed 2 weeks following 420 mgQ4W dose administration and the LDL-C reduction remainedclose to 60% at week 4.
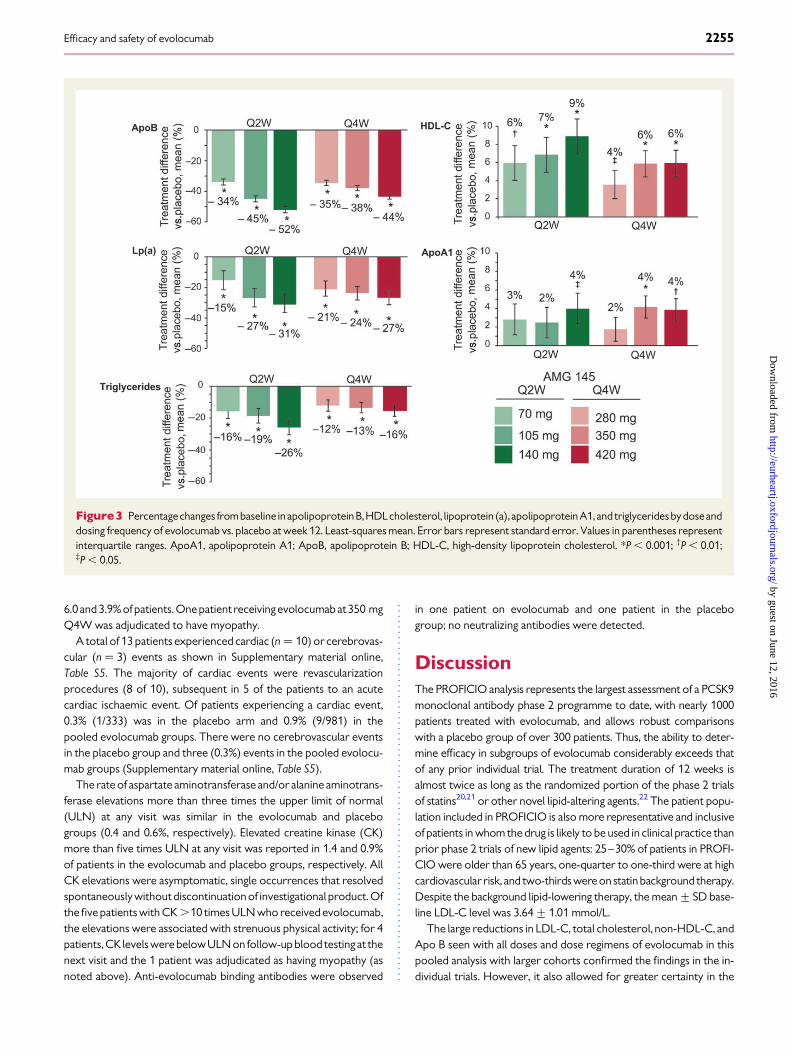
Reductions in total cholesterol, VLDL-C, non-HDL-C, and Apo Bparalleled the decreases seen in LDL-C and were all statistically sig-nificant (P , 0.001) (Table 3 and Figure 3). Changes in Apo B foreach dose group by gender, age, background statin therapy, orLDL-C above or below the mean at baseline are shown in Supple-mentary material online, Table S2. There was significantly greater(P , 0.001) reduction in Apo B seen with Q2W dosing in thosepatients on statin therapy but no difference with Q4W dosing
(Supplementary material online, Table S2), similar to what wasobserved for LDL-C.
Significant reductions (P , 0.001) in triglycerides were seen withall doses and regimens of evolocumab (Figure 3), with mean (95%CI) percentage reductions from baseline relative to placebo rangingfrom 12.2% (19.1%, 5.2%) to 25.9% (35.0%, 16.8%). Lp(a) levelswere significantly (P , 0.001) reduced at week 12 with all evolocu-mab doses and dosing regimens, with mean (95% CI) percentagereductions from baseline relative to placebo ranging from 15.5%(22.0%, 9.0%) to 31.3% (37.8%, 24.7%).
Treatment differences relative to placebo in HDL-C and its majorassociated apolipoprotein, ApoA1, are shown in Figure 3. HDL-Cwassignificantly increased with all evolocumab doses and dosing
Figure 1 (A) Percentage changes from baseline in levels of low density lipoprotein cholesterol (LDL-C) (calculated) for patients treated every 2weeks (Q2W). (B) Percentage changes in levels of LDL-C (calculated) for patients treated every 4 weeks (Q4W). Error bars represent standarderror (SE). Note that visits were not required at all time points in all the studies.
Efficacy and safety of evolocumab 2253
by guest on June 12, 2016http://eurheartj.oxfordjournals.org/
Dow
nloaded from
regimens at week 12 (P , 0.05 to P , 0.001), with the largest mean(95% CI) percentage increases from baseline relative to placebo of8.9% (5.1%, 12.7%) and 5.9% (3.1%, 8.8%) seen with evolocumab140 mg Q2W and 420 mg Q4W, respectively (P , 0.001). The par-allel, but slightly smaller, mean (95% CI) percentage increases frombaseline relative to placebo seen in Apo A1 were statistically signifi-cant for the evolocumab 140 mg Q2W, 350 mg Q4W, and 420 mgQ4W doses (P-values ranging from ,0.001 to ,0.05). Percentagechanges in HDL-C and Apo A1 for each dose group by gender, age,background statin therapy, or above or below the mean baselineLDL-C are shown in Supplementary material online, Tables S3 andS4. High-density lipoprotein cholesterol showed no difference in re-sponse in any of the subgroups, but Apo A1 showed a consistentlygreater (P ≤ 0.05) increase in patients not on statins at baselinewith both 2- and 4-week dosing with evolocumab.
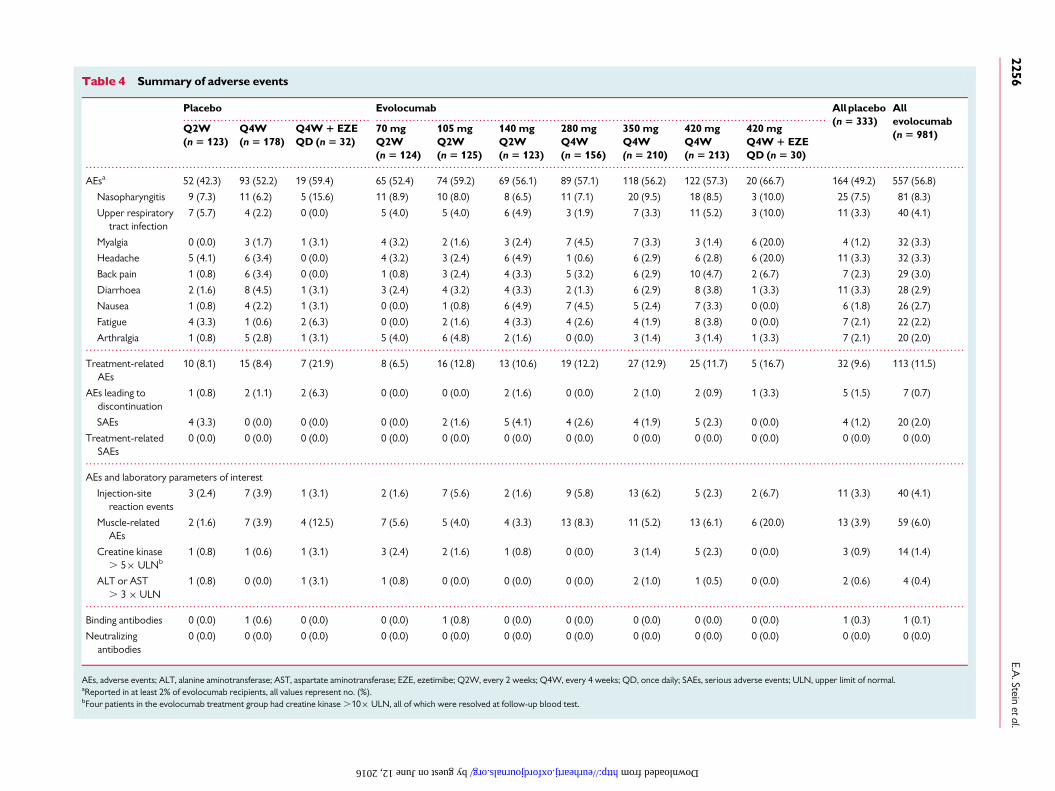
Safety assessmentsAdverse events, clinical, and laboratory safety analyses are shown inTable 4. Overall, AEs were reported in 56.8 and 49.2% of patients in
the combined evolocumab and combined placebo groups, respect-
ively. Across evolocumab and placebo groups, AEs ranged from
42.3 to 66.7% (Table 4) with nasopharyngitis, upper respiratory infec-
tion, headache, diarrhoea, myalgia, and back pain the most commonly
reported. Serious AEs (SAEs) were reported in 2.0 and 1.2% of
patients in the evolocumab and placebo groups, respectively; none
of these was considered to be treatment related by the investigators.
Treatment-related AEs were reported in 11.5 and 9.6% of patients in
the evolocumabandplacebogroups, respectively. Injection-site reac-
tions occurred in 4.1 and 3.3% of patients in the evolocumab and
placebo groups, respectively, and muscle-related AEs occurred in
Figure 2 Low density lipoprotein cholesterol (LDL-C) percentage changes from baseline relative to the corresponding placebo group in 70, 105,and 140 mg Q2Wand 280, 350, and 420 mg Q4Wevolocumab treated groups by gender, age (, /≥65 years), statin/no statin, mean baseline LDL-C(ultracentrifugation) (,/≥3.64 mmol/L), and baseline triglyceride ,/≥1.7 mmol/L. Least-squares mean. Error bars represent 95% confidenceintervals. *P-values reflect significance of treatment by subgroup interaction within each dose group for all dose groups. UC, ultracentrifugation.
E.A. Stein et al.2254
by guest on June 12, 2016http://eurheartj.oxfordjournals.org/
Dow
nloaded from
6.0 and 3.9%of patients. Onepatient receiving evolocumab at350 mgQ4W was adjudicated to have myopathy.
A total of 13 patients experienced cardiac (n ¼ 10) or cerebrovas-cular (n ¼ 3) events as shown in Supplementary material online,Table S5. The majority of cardiac events were revascularizationprocedures (8 of 10), subsequent in 5 of the patients to an acutecardiac ischaemic event. Of patients experiencing a cardiac event,0.3% (1/333) was in the placebo arm and 0.9% (9/981) in thepooled evolocumab groups. There were no cerebrovascular eventsin the placebo group and three (0.3%) events in the pooled evolocu-mab groups (Supplementary material online, Table S5).
The rate of aspartate aminotransferase and/or alanine aminotrans-ferase elevations more than three times the upper limit of normal(ULN) at any visit was similar in the evolocumab and placebogroups (0.4 and 0.6%, respectively). Elevated creatine kinase (CK)more than five times ULN at any visit was reported in 1.4 and 0.9%of patients in the evolocumab and placebo groups, respectively. AllCK elevations were asymptomatic, single occurrences that resolvedspontaneously without discontinuation of investigational product. Ofthe five patients with CK .10 times ULN who received evolocumab,the elevations were associated with strenuous physical activity; for 4patients, CK levels werebelowULN on follow-up blood testing at thenext visit and the 1 patient was adjudicated as having myopathy (asnoted above). Anti-evolocumab binding antibodies were observed
in one patient on evolocumab and one patient in the placebogroup; no neutralizing antibodies were detected.
DiscussionThe PROFICIO analysis represents the largest assessment of a PCSK9monoclonal antibody phase 2 programme to date, with nearly 1000patients treated with evolocumab, and allows robust comparisonswith a placebo group of over 300 patients. Thus, the ability to deter-mine efficacy in subgroups of evolocumab considerably exceeds thatof any prior individual trial. The treatment duration of 12 weeks isalmost twice as long as the randomized portion of the phase 2 trialsof statins20,21 or other novel lipid-altering agents.22 The patient popu-lation included in PROFICIO is also more representative and inclusiveof patients in whom the drug is likely to be used in clinical practice thanprior phase 2 trials of new lipid agents: 25–30% of patients in PROFI-CIO were older than 65 years, one-quarter to one-third were at highcardiovascular risk, and two-thirds were on statinbackground therapy.Despite the background lipid-lowering therapy, the mean+SD base-line LDL-C level was 3.64+1.01 mmol/L.
The large reductions in LDL-C, total cholesterol, non-HDL-C, andApo B seen with all doses and dose regimens of evolocumab in thispooled analysis with larger cohorts confirmed the findings in the in-dividual trials. However, it also allowed for greater certainty in the
Figure3 Percentagechanges from baseline in apolipoproteinB,HDLcholesterol, lipoprotein (a), apolipoproteinA1, and triglyceridesbydoseanddosing frequency of evolocumab vs. placebo at week 12. Least-squares mean. Error bars represent standard error. Values in parentheses representinterquartile ranges. ApoA1, apolipoprotein A1; ApoB, apolipoprotein B; HDL-C, high-density lipoprotein cholesterol. *P , 0.001; †P , 0.01;‡P , 0.05.
Efficacy and safety of evolocumab 2255
by guest on June 12, 2016http://eurheartj.oxfordjournals.org/
Dow
nloaded from
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Table 4 Summary of adverse events
Placebo Evolocumab All placebo(n 5 333)
Allevolocumab(n 5 981)
Q2W(n 5 123)
Q4W(n 5 178)
Q4W 1 EZEQD (n 5 32)
70 mgQ2W(n 5 124)
105 mgQ2W(n 5 125)
140 mgQ2W(n 5 123)
280 mgQ4W(n 5 156)
350 mgQ4W(n 5 210)
420 mgQ4W(n 5 213)
420 mgQ4W 1 EZEQD (n 5 30)
AEsa 52 (42.3) 93 (52.2) 19 (59.4) 65 (52.4) 74 (59.2) 69 (56.1) 89 (57.1) 118 (56.2) 122 (57.3) 20 (66.7) 164 (49.2) 557 (56.8)
Nasopharyngitis 9 (7.3) 11 (6.2) 5 (15.6) 11 (8.9) 10 (8.0) 8 (6.5) 11 (7.1) 20 (9.5) 18 (8.5) 3 (10.0) 25 (7.5) 81 (8.3)
Upper respiratorytract infection
7 (5.7) 4 (2.2) 0 (0.0) 5 (4.0) 5 (4.0) 6 (4.9) 3 (1.9) 7 (3.3) 11 (5.2) 3 (10.0) 11 (3.3) 40 (4.1)
Myalgia 0 (0.0) 3 (1.7) 1 (3.1) 4 (3.2) 2 (1.6) 3 (2.4) 7 (4.5) 7 (3.3) 3 (1.4) 6 (20.0) 4 (1.2) 32 (3.3)
Headache 5 (4.1) 6 (3.4) 0 (0.0) 4 (3.2) 3 (2.4) 6 (4.9) 1 (0.6) 6 (2.9) 6 (2.8) 6 (20.0) 11 (3.3) 32 (3.3)
Back pain 1 (0.8) 6 (3.4) 0 (0.0) 1 (0.8) 3 (2.4) 4 (3.3) 5 (3.2) 6 (2.9) 10 (4.7) 2 (6.7) 7 (2.3) 29 (3.0)
Diarrhoea 2 (1.6) 8 (4.5) 1 (3.1) 3 (2.4) 4 (3.2) 4 (3.3) 2 (1.3) 6 (2.9) 8 (3.8) 1 (3.3) 11 (3.3) 28 (2.9)
Nausea 1 (0.8) 4 (2.2) 1 (3.1) 0 (0.0) 1 (0.8) 6 (4.9) 7 (4.5) 5 (2.4) 7 (3.3) 0 (0.0) 6 (1.8) 26 (2.7)
Fatigue 4 (3.3) 1 (0.6) 2 (6.3) 0 (0.0) 2 (1.6) 4 (3.3) 4 (2.6) 4 (1.9) 8 (3.8) 0 (0.0) 7 (2.1) 22 (2.2)
Arthralgia 1 (0.8) 5 (2.8) 1 (3.1) 5 (4.0) 6 (4.8) 2 (1.6) 0 (0.0) 3 (1.4) 3 (1.4) 1 (3.3) 7 (2.1) 20 (2.0)
Treatment-relatedAEs
10 (8.1) 15 (8.4) 7 (21.9) 8 (6.5) 16 (12.8) 13 (10.6) 19 (12.2) 27 (12.9) 25 (11.7) 5 (16.7) 32 (9.6) 113 (11.5)
AEs leading todiscontinuation
1 (0.8) 2 (1.1) 2 (6.3) 0 (0.0) 0 (0.0) 2 (1.6) 0 (0.0) 2 (1.0) 2 (0.9) 1 (3.3) 5 (1.5) 7 (0.7)
SAEs 4 (3.3) 0 (0.0) 0 (0.0) 0 (0.0) 2 (1.6) 5 (4.1) 4 (2.6) 4 (1.9) 5 (2.3) 0 (0.0) 4 (1.2) 20 (2.0)
Treatment-relatedSAEs
0 (0.0) 0 (0.0) 0 (0.0) 0 (0.0) 0 (0.0) 0 (0.0) 0 (0.0) 0 (0.0) 0 (0.0) 0 (0.0) 0 (0.0) 0 (0.0)
AEs and laboratory parameters of interest
Injection-sitereaction events
3 (2.4) 7 (3.9) 1 (3.1) 2 (1.6) 7 (5.6) 2 (1.6) 9 (5.8) 13 (6.2) 5 (2.3) 2 (6.7) 11 (3.3) 40 (4.1)
Muscle-relatedAEs
2 (1.6) 7 (3.9) 4 (12.5) 7 (5.6) 5 (4.0) 4 (3.3) 13 (8.3) 11 (5.2) 13 (6.1) 6 (20.0) 13 (3.9) 59 (6.0)
Creatine kinase. 5× ULNb
1 (0.8) 1 (0.6) 1 (3.1) 3 (2.4) 2 (1.6) 1 (0.8) 0 (0.0) 3 (1.4) 5 (2.3) 0 (0.0) 3 (0.9) 14 (1.4)
ALT or AST. 3 × ULN
1 (0.8) 0 (0.0) 1 (3.1) 1 (0.8) 0 (0.0) 0 (0.0) 0 (0.0) 2 (1.0) 1 (0.5) 0 (0.0) 2 (0.6) 4 (0.4)
Binding antibodies 0 (0.0) 1 (0.6) 0 (0.0) 0 (0.0) 1 (0.8) 0 (0.0) 0 (0.0) 0 (0.0) 0 (0.0) 0 (0.0) 1 (0.3) 1 (0.1)
Neutralizingantibodies
0 (0.0) 0 (0.0) 0 (0.0) 0 (0.0) 0 (0.0) 0 (0.0) 0 (0.0) 0 (0.0) 0 (0.0) 0 (0.0) 0 (0.0) 0 (0.0)
AEs, adverse events; ALT, alanine aminotransferase; AST, aspartate aminotransferase; EZE, ezetimibe; Q2W, every 2 weeks; Q4W, every 4 weeks; QD, once daily; SAEs, serious adverse events; ULN, upper limit of normal.aReported in at least 2% of evolocumab recipients, all values represent no. (%).bFour patients in the evolocumab treatment group had creatine kinase .10× ULN, all of which were resolved at follow-up blood test.
E.A.Stein
etal.2256
by guest on June 12, 2016 http://eurheartj.oxfordjournals.org/ Downloaded from
assessment of dose-related reductions and confirmed maximalreductions are achieved with the 140 mg Q2W dosing. In addition,while the maximal LDL-C reductions seen after 2 weeks with 350and 420 mg dosing were the same, the 420 mg dose maintained agreater LDL-C reduction for a longer period as measured 4 weekspost-dose. The large number of patients per treatment group alsoallowed for statistically significant changes to be seen in triglycerides,Lp(a), HDL-C, and Apo A1. Despite average baseline triglyceridelevels in PROFICIO of slightly ,1.70 mmol/L (150 mg/dL), statistic-ally significant reductions of 26 and 16% were seen with the highestdoses used in the Q2W and Q4W dosing regimens, respectively.As is well documented with statins, which also upregulate LDL recep-toractivity, triglyceride reductions aredependent toa largeextentonbaseline triglycerides.23 Future trials that include patients with higherbaseline triglycerides may help better determine the therapeutic po-tential for evolocumab in more severely hypertriglyceridaemicpatients and if a dose-related effect exists as for statins. The largecohorts provide solid and robust confirmation of the significant re-duction in Lp(a) with evolocumab (P , 0.001 for each dose vs.placebo) seen in the individual phase 2 trials with evolocumab. In add-ition, these results also confirm trends observed in smaller studieswith another PCSK9 monoclonal antibody, alirocumab.16,17,24
The magnitude of effect of evolocumab on the HDL parameters,HDL-C, and Apo A1 was somewhat unexpected because of thelarge proportion of patients already on statin therapy, which alsoraises HDL-C, and with relatively high baseline HDL-C levels[range, 1.3421.42 mmol/L (51.7–54.7 mg/dL) for the pooled effi-cacy analysis population]. Thus, the further statistically significantHDL-C increase of �9% with 140 mg Q2W and �6% with420 mg Q4W represents an additional potentially favourable effectof therapy. Associated with the HDL-C increases was a uniform in-crease in Apo A1 with all doses of evolocumab, which reached�4% (P , 0.05 to P , 0.001) with the highest doses in each dosingregimen. Thus, in terms of the overall lipid profile, evolocumabappears to provide a superior effect on LDL-C, non-HDL-C, ApoB, Lp(a), and HDL-C than even the highest doses of the most effectivestatins.25 Whether these changes in lipid biomarkers translate intoreductions in CVD events and outcomes will be assessed over thenext few years in the 22 500 patient evolocumab trial, Further Car-diovascular Outcomes Research With PCSK9 Inhibition in SubjectsWith Elevated Risk [FOURIER (NCT01764633)].26
In terms of safety assessment, PROFICIO provides 225 patient-years of exposure to evolocumab and comparison with 70 patient-years of treatment with placebo in these double-blind studies. Theoverall AE rate was slightly higher with evolocumab (56.8%) thanplacebo (49.2%), but when individual AEs were compared, no differ-ences or trends in any organ system were seen. There was also a lowrate of AEs leading to discontinuation (0.7% with evolocumab and1.5% with placebo) and no dose- or dose frequency-related trendsnoted with evolocumab. Although SAEs during the trial were alsoslightly greater in those treated with evolocumab than placebo (2.0vs. 1.2%, respectively), there were no SAEs determined to betreatment-related by investigators in either group. The tolerabilityof SC administration was excellent irrespective of dosing frequency,with injection site reactions reported in 4.1% of evolocumab-treatedpatients and in 3.3% of placebo-treated patients. This tolerabilitycontrasts significantly with the only approved SC-administered
lipid-lowering agent, mipomersen, an Apo B antisense drug givenonce weekly, with which a high rate (92%) of injection-site reactionswas observed.
The hepatic function and muscle-related enzyme measurementsare reassuring as neither showed any signals of toxicity in this large,but short duration, study analysis. The inclusion in PROFICIO of atrial in which the entry criteria required documented evidence ofmuscle-related AEs on prior statin therapy and patients who wererandomized to evolocumab or ezetimibe (i.e. no placebo-only arm)provided a large number of patients ‘sensitized’ to this side effect.Thus, the relatively low reported rate of muscle-related AEs withevolocumab, which was not significantly different from placebo, pro-vides further evidence of the importance of the drug for statin-aversepatients. A total of 0.3% of placebo-treated patients experienced acardiac event compared with 0.9% treated with evolocumab.However, the phase 2 programme was not designed to evaluate car-diovascular outcomes and the aforementioned proportions repre-sent a total of only 13 patients experiencing a cardiac orcerebrovascular event. Nonetheless, the imbalance indicates theneed for continued close, independent monitoring for cardiac andcerebrovascular events during the phase 3 programme. Reassuringly,genetic association studies have demonstrated lower rates of CVDevents in patients carrying loss-of-function PCSK9 variants.27 The de-finitive evaluation of pharmacologic PCSK9 inhibition on cardiovas-cular events will have to wait for the results from the ongoingFOURIER trial.26
LimitationsPROFICIO examined two different patient populations across thefour studies, patients with and without background statin therapy.Despite the large patient population, it has limitations specificallyfor assessing safety. The trials were all of 12 weeks’ duration andthus were unable to determine the safety of a drug that will likelybe administered for life after patients commence therapy; resultsfrom an ongoing open-label extension study will provide additionalsafety data. In addition, short-term trials with highly motivated andmonitored patients in which the drug is administered in a researchclinic may not be an optimal setting to fully evaluate the acceptanceof, and long-term compliance with, a lipid-lowering agent thatrequires SC administration. These issues will be explored further inthe phase 3 programme.
ConclusionsThe PROFICIO analysis confirms the large and rapid reductionsachievable in Apo B and its related lipoproteins, LDL-C, VLDL-C,and non-HDL-C seen in individual trials with evolocumab. Thepooled analysis further provides new and additional data on the pro-longed effect of the 420 mg Q4W dose on LDL-C and the robustdecreases in triglycerides and Lp(a). Our results also substantiatethe statistically significant, if moderate, increases in the anti-atherogenic lipoprotein HDL-C and Apo A1. The large pooledsafety analysis of 981 patients treated with evolocumab, albeit foronly 12 weeks, did not reveal any new or unexpected safety signals.These results support large-scale phase 3 trials of evolocumab, in-cluding a cardiovascular outcomes trial.
Efficacy and safety of evolocumab 2257
by guest on June 12, 2016http://eurheartj.oxfordjournals.org/
Dow
nloaded from
Supplementary materialSupplementary Material is available at European Heart Journal online.
AcknowledgementsWe thank Miranda Tradewell, PhD, of Complete Healthcare Com-munications, Inc. (whose work was funded by Amgen Inc.) andMeera Kodukulla, PhD, of Amgen Inc. for editorial support.
FundingThis work was supported by Amgen, Inc.
Conflict of interest: E.A.S. has received consulting fees from Amgen,BMS/Adnexus Therapeutics, Genentech, Regeneron, and Sanofirelated to PCSK9 inhibitors and his institution has received researchfunding related to PCSK9 clinical trials from Amgen, Alnylam, BMS/Adnexus Therapeutics, Genentech, Sanofi, and Regeneron. M.J.K. is anemployee of Jacksonville Centre for Clinical Research, which hasreceived research grants from Amgen. F.J.R. has received consultingfees from Amgen and Sanofi related to PCSK9 inhibitors, and his institu-tion has received research funding related to PCSK9 inhibitor clinicaltrials from Amgen and Sanofi. E.M.R. has received fees as a speaker forMerck, AstraZeneca, and Amarin, and as a consultant to Regeneronand Sanofi. R.W. has no conflicts of interest to disclose.
D.S. has received research funding from Amgen, Abbott Products,AstraZeneca, Merck, Sharp and Dohme, and Sanofi Aventis; he has alsoreceived funding for educational programs from Abbott Products, Astra-Zeneca, Merck, Sharp, and Dohme, Pfizer Australia, and Roche andtravel support from Merck, Sharp, and Dohme. He served on advisoryboards for Abbott Products, Merck, Sharp, and Dohme, and Pfizer Austra-lia. S.M.W., R.S., J.B.K., J.Y., T.L., M.A., and R.S. are employees of Amgen Inc.and have received Amgen stock/stock options. R.P.G. and M.S.S. havereceived research grant support through Brigham and Women’s Hospitalfor theLAPLACE-TIMI57trial fromAmgen,andhaveservedasconsultantsfor Amgen. R.P.G. has received honoraria for consulting from Regeneronand Sanofi and also received research grant support through Brighamand Women’s Hospital, and honoraria for consulting and CME lecturesfrom Daiichi-Sankyo and Merck. M.S.S. has also received research grantsupport through Brigham and Women’s Hospital from AstraZeneca,AstraZeneca/Bristol-Myers Squibb Alliance, Bristol-Myers Squibb/Sanofi-Aventis Joint Venture, Daiichi-Sankyo, Eisai, Genzyme, GlaxoS-mithKline, Intarcia, Merck, Sanofi-Aventis, and Takeda, and received hon-oraria for consulting from Aegerion, Amgen, AstraZeneca/Bristol-MyersSquibb Alliance, Bristol-Myers Squibb, GlaxoSmithKline, Intarcia, Merck,Pfizer, Sanofi-Aventis, and Vertex.
References1. Third Report of the National Cholesterol Education Program (NCEP) Expert Panel
on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (AdultTreatment Panel III) final report. Circulation 2002;106:3143–3421.
2. Task Force for the Management of Dyslipidaemias of the European Society of Car-diology, The European Atherosclerosis Society, Catapano AL, Reiner Z, DeBacker G, Graham I, Taskinen MR, Wiklund O, Agewall S, Alegria E, Chapman MJ,Durrington P, Erdine S, Halcox J, Hobbs R, Kjekshus J, Perrone Filardi P,Riccardi G, Storey RF, Wood D, E. S. C. Committee for Practice Guidelines, Com-mittees. ESC/EAS Guidelines for the management of dyslipidaemias: the TaskForce for the Management of Dyslipidaemias of the European Society of Cardiology(ESC) and the European Atherosclerosis Society (EAS). Atherosclerosis 2011;217:S1–S44.
3. Cholesterol Treatment Trialists C, Baigent C, Blackwell L, Emberson J, Holland LE,Reith C, Bhala N, Peto R, Barnes EH, Keech A, Simes J, Collins R. Efficacy and safety ofmore intensive lowering of LDL cholesterol: a meta-analysis of data from 170,000participants in 26 randomised trials. Lancet 2010;376:1670–1681.
4. Ridker PM, Danielson E, Fonseca FA, Genest J, Gotto AM Jr, Kastelein JJ, Koenig W,Libby P, Lorenzatti AJ, MacFadyen JG, Nordestgaard BG, Shepherd J, Willerson JT,Glynn RJ, Jupiter Study Group. Rosuvastatin to prevent vascular events in menand women with elevated C-reactive protein. N Engl J Med 2008;359:2195–2207.
5. Canner PL, Berge KG, Wenger NK, Stamler J, Friedman L, Prineas RJ, Friedewald W.Fifteen year mortality in Coronary Drug Project patients: long-term benefit withniacin. J. Am Coll Cardiol 1986;8:1245–1255.
6. The Lipid ResearchClinics CoronaryPrimary PreventionTrial results. I. Reduction inincidence of coronary heart disease. JAMA 1984;251:351–364.
7. Waters DD, Brotons C, Chiang CW, Ferrieres J, Foody J, Jukema JW, Santos RD,Verdejo J, Messig M, McPherson R, Seung KB, Tarasenko L, Lipid Treatment Assess-ment Project I. Lipid treatment assessment project 2: a multinational survey to evalu-ate the proportion of patients achieving low-density lipoprotein cholesterol goals.Circulation 2009;120:28–34.
8. Bruckert E, Hayem G, Dejager S, Yau C, Begaud B. Mild to moderate muscular symp-toms with high-dosage statin therapy in hyperlipidemic patients—the PRIMO study.Cardiovasc Drugs Ther 2005;19:403–414.
9. Stein EA, Swergold GD. Potential of proprotein convertase subtilisin/kexin type 9based therapeutics. Curr Atheroscler Rep 2013;15:310.
10. Dias CS, Shaywitz AJ, Wasserman SM, Smith BP, Gao B, Stolman DS, Crispino CP,Smirnakis KV, Emery MG, Colbert A, Gibbs JP, Retter MW, Cooke BP, Uy ST,Matson M, Stein EA. Effects of AMG 145 on low-density lpoprotein cholesterollevels: Results from 2 randomized, double-blind, placebo-controlled, ascending-dose phase 1 studies in healthy volunteers and hypercholesterolemic subjects onstatins. J Am Coll Cardiol 2012;60:1888–1898.
11. Koren MJ, Scott R, Kim JB, Knusel B, Liu T, Lei L, Bolognese M, Wasserman SM. Effi-cacy, safety, and tolerability of a monoclonal antibody to proprotein convertase sub-tilisin/kexin type 9 as monotherapy in patients with hypercholesterolaemia(MENDEL): a randomised, double-blind, placebo-controlled, phase 2 study. Lancet2012;380:1995–2006.
12. Giugliano RP, Desai NR, Kohli P, Rogers WJ, Somaratne R, Huang F, Liu T,Mohanavelu S, Hoffman EB, McDonald ST, Abrahamsen TE, Wasserman SM,Scott R, Sabatine MS. Efficacy, safety, and tolerability of a monoclonal antibody toproprotein convertase subtilisin/kexin type 9 in combination with a statin in patientswith hypercholesterolaemia (LAPLACE-TIMI 57): a randomised, placebo-controlled, dose-ranging, phase 2 study. Lancet 2012;380:2007–2017.
13. Raal F, Scott R, Somaratne R, Bridges I, Li G, Wasserman SM, Stein EA. Low-densitylipoprotein cholesterol-lowering effects of AMG 145, a monoclonal antibody toproprotein convertase subtilisin/kexin type 9 serine protease in patients withheterozygous familial hypercholesterolemia: The Reduction of LDL-C WithPCSK9 Inhibition inHeterozygous Familial Hypercholesterolemia Disorder (RUTH-ERFORD) Randomized Trial. Circulation 2012;126:2408–2417.
14. Sullivan D, Olsson AG, Scott R, Kim JB, Xue A, Gebski V, Wasserman SM, Stein EA.Effect of a monoclonal antibody to PCSK9 on low-density lipoprotein cholesterollevels in statin-intolerant patients: The GAUSS Randomized Trial. JAMA 2012;308:2497–2506.
15. McKenney JM, Koren MJ, Kereiakes DJ, Hanotin C, Ferrand AC, Stein EA. Safety andefficacy of a monoclonal antibody to proprotein convertase subtilisin/kexin type 9serine protease, SAR236553/REGN727, in patients with primary hypercholesterol-emia receiving ongoing stable atorvastatin therapy. J Am Coll Cardiol 2012;59:2344–2353.
16. Stein EA, Mellis S, Yancopoulos GD, Stahl N, Logan D, Smith WB, Lisbon E,Gutierrez M, Webb C, Wu R, Du Y, Kranz T, Gasparino E, Swergold GD. Effect ofa monoclonal antibody to PCSK9 on LDL cholesterol. N Engl J Med 2012;366:1108–1118.
17. Roth EM, McKenney JM, Hanotin C, Asset G, Stein EA. Atorvastatin with or withoutan antibody to PCSK9 in primary hypercholesterolemia. N Engl J Med 2012;367:1891–1900.
18. Myers GL, Cooper GR, Winn CL, Smith SJ. The Centres for Disease Control-National Heart, Lung and Blood Institute Lipid Standardization Program. An ap-proach to accurate and precise lipid measurements. Clin Lab Med 1989;9:105–135.
19. Friedewald WT, Levy RI, Fredrickson DS. Estimation of the concentration of lowdensity lipoprotein cholesterol in plasma, without use of the preparative ultracentri-fuge. Clin Chem 1972;18:499–502.
20. Hunninghake D, Miller VT, Palmer RH, Schonfeld G, Stein EA et al. (Lovastatin StudyGroup II). Therapeutic response to lovastatin (mevinolin) in nonfammilial hyper-cholesterolemia: a multicenter study. JAMA 1986;256:2829–2834.
21. Nawrocki JW, Weiss SR, Davidson MH, Sprecher DL, Schwartz SL, Lupien PJ,Jones PH, Haber HE, Black DM. Reduction of LDL cholesterol by 25% to 60% inpatients with primary hypercholesterolemia by atorvastatin, a new HMG-CoA re-ductase inhibitor. Arterioscler Thromb Vasc Biol 1995;15:678–682.
22. Stein E. Results of phase I/II clinical trials with ezetimibe, a novel selective cholesterolabsorption inhibitor. Eur Heart J Suppl 2001;3(Suppl E):E11–E16.
23. Stein EA, Lane M,Laskarzewski P. Comparisonof statins inhypertriglyceridemia.Am JCardiol 1998;81:66B–69B.
E.A. Stein et al.2258
by guest on June 12, 2016http://eurheartj.oxfordjournals.org/
Dow
nloaded from

24. Stein EA, Gipe D, Bergeron J, Gaudet D, Weiss R, Dufour R, Wu R, Pordy R. Effect ofa monoclonal antibody to PCSK9, REGN727/SAR236553, to reduce low-densitylipoprotein cholesterol in patients with heterozygous familial hypercholesterol-aemia on stable statin dose with or without ezetimibe therapy: a phase 2 randomisedcontrolled trial. Lancet 2012;380:29–36.
25. Jones PH, Davidson MH, Stein EA, Bays HE, McKenney JM, Miller E, Cain VA,Blasetto JW, Group SS. Comparison of the efficacy and safety of rosuvastatinversus atorvastatin, simvastatin, and pravastatin across doses (STELLAR* Trial).Am J Cardiol 2003;92:152–160.
26. Further Cardiovascular Outcomes Research With PCSK9 Inhibition in SubjectsWith Elevated Risk (FOURIER; NCT01764633). http://www.clinicaltrials.gov/ct2/show/NCT01764633?term=fourier&rank=1 (26 February 2013).
27. Ference BA, Yoo W, Alesh I, Mahajan N, Mirowska KK, Mewada A, Kahn J, Afonso L,Williams KA Sr, Flack JM. Effect of long-term exposure to lower low-densitylipoprotein cholesterol beginning early in life on the risk of coronary heartdisease: a Mendelian randomization analysis. J Am Coll Cardiol 2012;60:2631–2639.
Efficacy and safety of evolocumab 2259
by guest on June 12, 2016http://eurheartj.oxfordjournals.org/
Dow
nloaded from




















