
Effects of rehabilitative training and anti-inflammatory treatment on functional recovery and...
7
Effects of rehabilitative training and anti-inflammatory treatment on functional recovery and cellular reorganization following stroke Susan Liebigt, Nadja Schlegel, Julia Oberland, Otto W. Witte, Christoph Redecker, Silke Keiner ⁎ Hans Berger Department of Neurology, Jena University Hospital, Erlanger Allee 101, D-07747 Jena, Germany abstract article info Article history: Received 15 August 2011 Revised 1 November 2011 Accepted 25 November 2011 Available online 8 December 2011 Keywords: Indometacin Minocycline Skilled reaching training Sensorimotor cortex Post-ischemic inflammation plays a critical role in cellular reorganization and functional recovery after stroke. We therefore address the hypothesis whether anti-inflammatory treatment with either indometacin or minocycline combined with rehabilitative training improve functional recovery and influence perilesional cellular response following focal cortical infarcts. Using the photothrombosis model in adult rats, focal corti- cal infarcts were induced in the fore- and hindlimb sensorimotor cortex. Inflammatory processes were blocked by intraperitoneal application of indometacin or minocycline twice daily during the first 2 weeks of the experiment. Immediately after the infarct, the animals received a daily session of skilled reaching train- ing of the impaired forelimb. In addition, Bromodeoxyuridine (BrdU) was administrated for 5 sequential days post infarct. Proliferation and differentiation of astrocytes, microglia, immature and mature neurons in the perilesional zone were immunocytochemically quantified at days 14 and 42. Functional recovery was assessed in a sensorimotor walking task preoperatively and 4, 14 and 28 days post surgery. Combined reha- bilitative training and indometacin or minocycline strongly improved sensorimotor performance and signif- icantly reduced the number of proliferating microglia compared to reaching training alone. Furthermore, the combination increased the survival of proliferating astrocytes and, moreover, minocycline increased the doublecortin-positive cells in the perilesional zone. Anti-inflammatory drug application combined with reha- bilitative training demonstrates improved functional recovery and significantly modifies proliferation and survival of distinct glial and neuronal subpopulations in the direct vicinity of cortical infarcts compared to reaching training alone. © 2011 Elsevier Inc. All rights reserved. Introduction Sensorimotor impairments are the most common disabilities caused by stroke (Thom et al., 2006). Recent experimental studies in rodents have shown that physical activity, exposure to an enriched environment, and daily reaching training of the impaired forelimb improves functional recovery after focal ischemic infarcts, although, these processes are often insufficient to restore normal levels of func- tion (Dobkin, 2004; Keiner et al., 2008). On the other hand, basic and clinical research provides evidence that inflammatory mechanisms play a central role both in the pathogenesis and during functional re- covery following stroke (Kriz and Lalancette-Hebert, 2009; Liu et al., 2007). We recently demonstrated (Keiner et al., 2008) that rehabilita- tive training of the impaired forelimb alone alters the cellular response in the perilesional zone with a prominent reduction of pro- liferating microglia. These results encouraged us to investigate whether enhanced functional recovery following infarct can be further promoted via a pharmacological reduction of microglia. Hence, we combined skilled reaching training of the impaired fore- limb as described previously (Keiner et al., 2008) with additional treatment using indometacin or minocycline. Previous studies (Chu et al., 2010; Hoehn et al., 2005) have demonstrated that both drugs inhibit microglial activity after stroke. Using this approach, we pro- vide evidence that rehabilitative training in combination with anti- inflammatory treatment enhanced functional recovery and modified the complex postlesional cellular reorganization in the direct vicinity of the infarct. Materials and methods Photothrombotic infarction The study was conducted in accordance with the animal care guidelines issued by the National Institute of Health and by the Insti- tutional Animal Care and Use Committee. Photothrombotic infarcts were induced in a total of 50 male Wistar rats (3 months old, 250– 300 g) in the forelimb and hindlimb sensorimotor cortex. The animals were anesthetized with 2.0–3.5% isofluran in a mixture of oxygen/ nitrous oxide (30%/70%), placed in a stereotactic frame and illuminat- ed with a cold light source (KL 1500, Schott, Jena, Germany) by a Experimental Neurology 233 (2012) 776–782 ⁎ Corresponding author. Fax: + 49 3641 9325902. E-mail address: [email protected] (S. Keiner). 0014-4886/$ – see front matter © 2011 Elsevier Inc. All rights reserved. doi:10.1016/j.expneurol.2011.11.037 Contents lists available at SciVerse ScienceDirect Experimental Neurology journal homepage: www.elsevier.com/locate/yexnr
Transcript of Effects of rehabilitative training and anti-inflammatory treatment on functional recovery and...

Experimental Neurology 233 (2012) 776–782
Contents lists available at SciVerse ScienceDirect
Experimental Neurology
j ourna l homepage: www.e lsev ie r .com/ locate /yexnr
Effects of rehabilitative training and anti-inflammatory treatment on functionalrecovery and cellular reorganization following stroke
Susan Liebigt, Nadja Schlegel, Julia Oberland, Otto W. Witte, Christoph Redecker, Silke Keiner ⁎Hans Berger Department of Neurology, Jena University Hospital, Erlanger Allee 101, D-07747 Jena, Germany
⁎ Corresponding author. Fax: +49 3641 9325902.E-mail address: [email protected] (S. Ke
0014-4886/$ – see front matter © 2011 Elsevier Inc. Alldoi:10.1016/j.expneurol.2011.11.037
a b s t r a c t
a r t i c l e i n f oArticle history:Received 15 August 2011Revised 1 November 2011Accepted 25 November 2011Available online 8 December 2011
Keywords:IndometacinMinocyclineSkilled reaching trainingSensorimotor cortex
Post-ischemic inflammation plays a critical role in cellular reorganization and functional recovery afterstroke. We therefore address the hypothesis whether anti-inflammatory treatment with either indometacinor minocycline combined with rehabilitative training improve functional recovery and influence perilesionalcellular response following focal cortical infarcts. Using the photothrombosis model in adult rats, focal corti-cal infarcts were induced in the fore- and hindlimb sensorimotor cortex. Inflammatory processes wereblocked by intraperitoneal application of indometacin or minocycline twice daily during the first 2 weeksof the experiment. Immediately after the infarct, the animals received a daily session of skilled reaching train-ing of the impaired forelimb. In addition, Bromodeoxyuridine (BrdU) was administrated for 5 sequential dayspost infarct. Proliferation and differentiation of astrocytes, microglia, immature and mature neurons in theperilesional zone were immunocytochemically quantified at days 14 and 42. Functional recovery wasassessed in a sensorimotor walking task preoperatively and 4, 14 and 28 days post surgery. Combined reha-bilitative training and indometacin or minocycline strongly improved sensorimotor performance and signif-icantly reduced the number of proliferating microglia compared to reaching training alone. Furthermore, thecombination increased the survival of proliferating astrocytes and, moreover, minocycline increased thedoublecortin-positive cells in the perilesional zone. Anti-inflammatory drug application combined with reha-bilitative training demonstrates improved functional recovery and significantly modifies proliferation andsurvival of distinct glial and neuronal subpopulations in the direct vicinity of cortical infarcts compared toreaching training alone.
© 2011 Elsevier Inc. All rights reserved.
Introduction
Sensorimotor impairments are the most common disabilitiescaused by stroke (Thom et al., 2006). Recent experimental studiesin rodents have shown that physical activity, exposure to an enrichedenvironment, and daily reaching training of the impaired forelimbimproves functional recovery after focal ischemic infarcts, although,these processes are often insufficient to restore normal levels of func-tion (Dobkin, 2004; Keiner et al., 2008). On the other hand, basic andclinical research provides evidence that inflammatory mechanismsplay a central role both in the pathogenesis and during functional re-covery following stroke (Kriz and Lalancette-Hebert, 2009; Liu et al.,2007). We recently demonstrated (Keiner et al., 2008) that rehabilita-tive training of the impaired forelimb alone alters the cellularresponse in the perilesional zone with a prominent reduction of pro-liferating microglia. These results encouraged us to investigatewhether enhanced functional recovery following infarct can befurther promoted via a pharmacological reduction of microglia.
iner).
rights reserved.
Hence, we combined skilled reaching training of the impaired fore-limb as described previously (Keiner et al., 2008) with additionaltreatment using indometacin or minocycline. Previous studies (Chuet al., 2010; Hoehn et al., 2005) have demonstrated that both drugsinhibit microglial activity after stroke. Using this approach, we pro-vide evidence that rehabilitative training in combination with anti-inflammatory treatment enhanced functional recovery and modifiedthe complex postlesional cellular reorganization in the direct vicinityof the infarct.
Materials and methods
Photothrombotic infarction
The study was conducted in accordance with the animal careguidelines issued by the National Institute of Health and by the Insti-tutional Animal Care and Use Committee. Photothrombotic infarctswere induced in a total of 50 male Wistar rats (3 months old, 250–300 g) in the forelimb and hindlimb sensorimotor cortex. The animalswere anesthetized with 2.0–3.5% isofluran in a mixture of oxygen/nitrous oxide (30%/70%), placed in a stereotactic frame and illuminat-ed with a cold light source (KL 1500, Schott, Jena, Germany) by a
777S. Liebigt et al. / Experimental Neurology 233 (2012) 776–782
fiberoptic bundle (3.0 mm diameter, skull 0.0 mm anterior to bregmaand 1.0 mm lateral to the midline) for 20 min. Before switching onthe light, a photosensitive dye Rose Bengal (1.3 mg/0.1 kg bodyweight at a concentration of 10 mg/ml in 0.9% NaCl; Sigma-Aldrich,Taufkirchen, Germany) was injected through a femoral vein catheter.After surgery the animals were returned to their cage and placedunder 12 h light/12 h dark conditions.
Experimental design
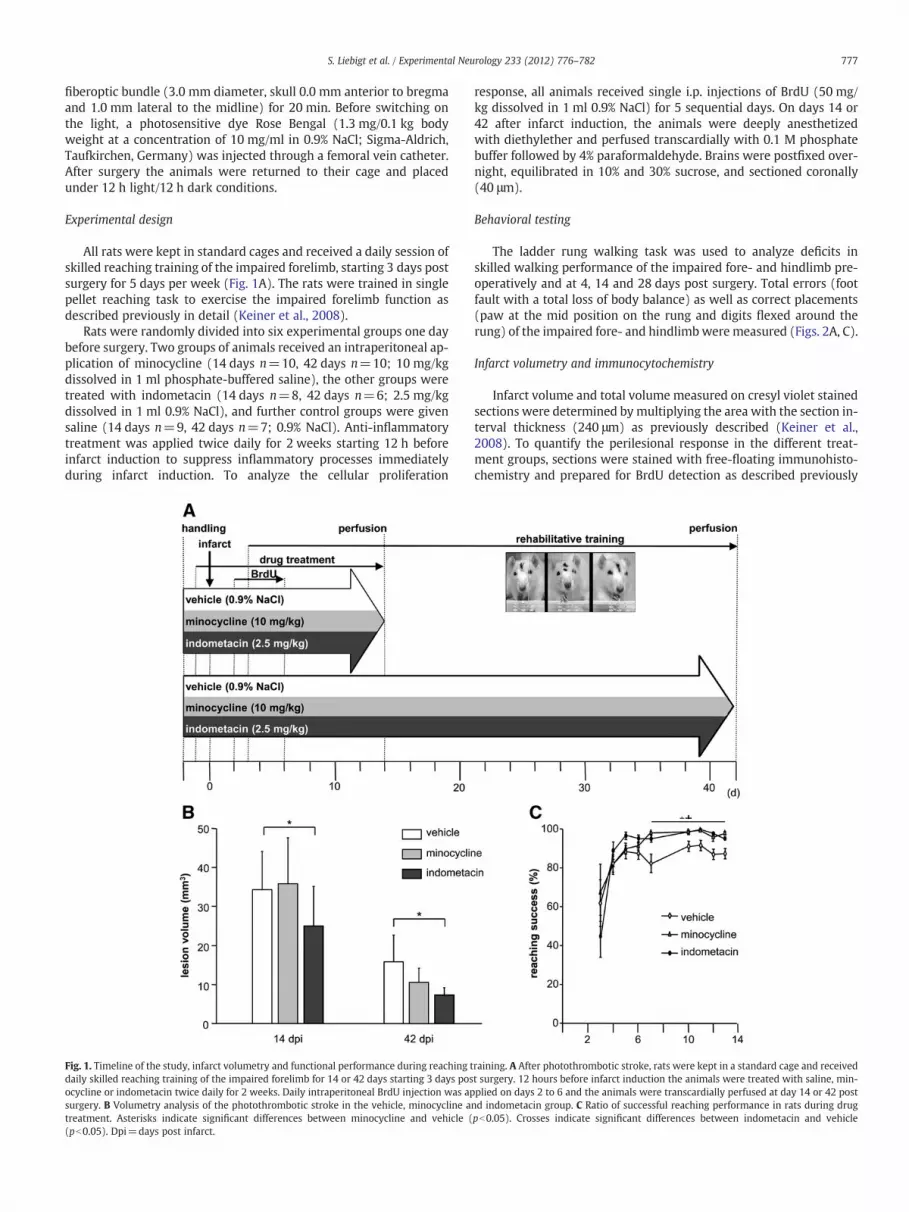
All rats were kept in standard cages and received a daily session ofskilled reaching training of the impaired forelimb, starting 3 days postsurgery for 5 days per week (Fig. 1A). The rats were trained in singlepellet reaching task to exercise the impaired forelimb function asdescribed previously in detail (Keiner et al., 2008).
Rats were randomly divided into six experimental groups one daybefore surgery. Two groups of animals received an intraperitoneal ap-plication of minocycline (14 days n=10, 42 days n=10; 10 mg/kgdissolved in 1 ml phosphate-buffered saline), the other groups weretreated with indometacin (14 days n=8, 42 days n=6; 2.5 mg/kgdissolved in 1 ml 0.9% NaCl), and further control groups were givensaline (14 days n=9, 42 days n=7; 0.9% NaCl). Anti-inflammatorytreatment was applied twice daily for 2 weeks starting 12 h beforeinfarct induction to suppress inflammatory processes immediatelyduring infarct induction. To analyze the cellular proliferation
Fig. 1. Timeline of the study, infarct volumetry and functional performance during reaching tdaily skilled reaching training of the impaired forelimb for 14 or 42 days starting 3 days posocycline or indometacin twice daily for 2 weeks. Daily intraperitoneal BrdU injection was apsurgery. B Volumetry analysis of the photothrombotic stroke in the vehicle, minocycline atreatment. Asterisks indicate significant differences between minocycline and vehicle ((pb0.05). Dpi=days post infarct.
response, all animals received single i.p. injections of BrdU (50 mg/kg dissolved in 1 ml 0.9% NaCl) for 5 sequential days. On days 14 or42 after infarct induction, the animals were deeply anesthetizedwith diethylether and perfused transcardially with 0.1 M phosphatebuffer followed by 4% paraformaldehyde. Brains were postfixed over-night, equilibrated in 10% and 30% sucrose, and sectioned coronally(40 μm).
Behavioral testing
The ladder rung walking task was used to analyze deficits inskilled walking performance of the impaired fore- and hindlimb pre-operatively and at 4, 14 and 28 days post surgery. Total errors (footfault with a total loss of body balance) as well as correct placements(paw at the mid position on the rung and digits flexed around therung) of the impaired fore- and hindlimb were measured (Figs. 2A, C).
Infarct volumetry and immunocytochemistry
Infarct volume and total volume measured on cresyl violet stainedsections were determined by multiplying the area with the section in-terval thickness (240 μm) as previously described (Keiner et al.,2008). To quantify the perilesional response in the different treat-ment groups, sections were stained with free-floating immunohisto-chemistry and prepared for BrdU detection as described previously
raining. A After photothrombotic stroke, rats were kept in a standard cage and receivedt surgery. 12 hours before infarct induction the animals were treated with saline, min-plied on days 2 to 6 and the animals were transcardially perfused at day 14 or 42 postnd indometacin group. C Ratio of successful reaching performance in rats during drugpb0.05). Crosses indicate significant differences between indometacin and vehicle
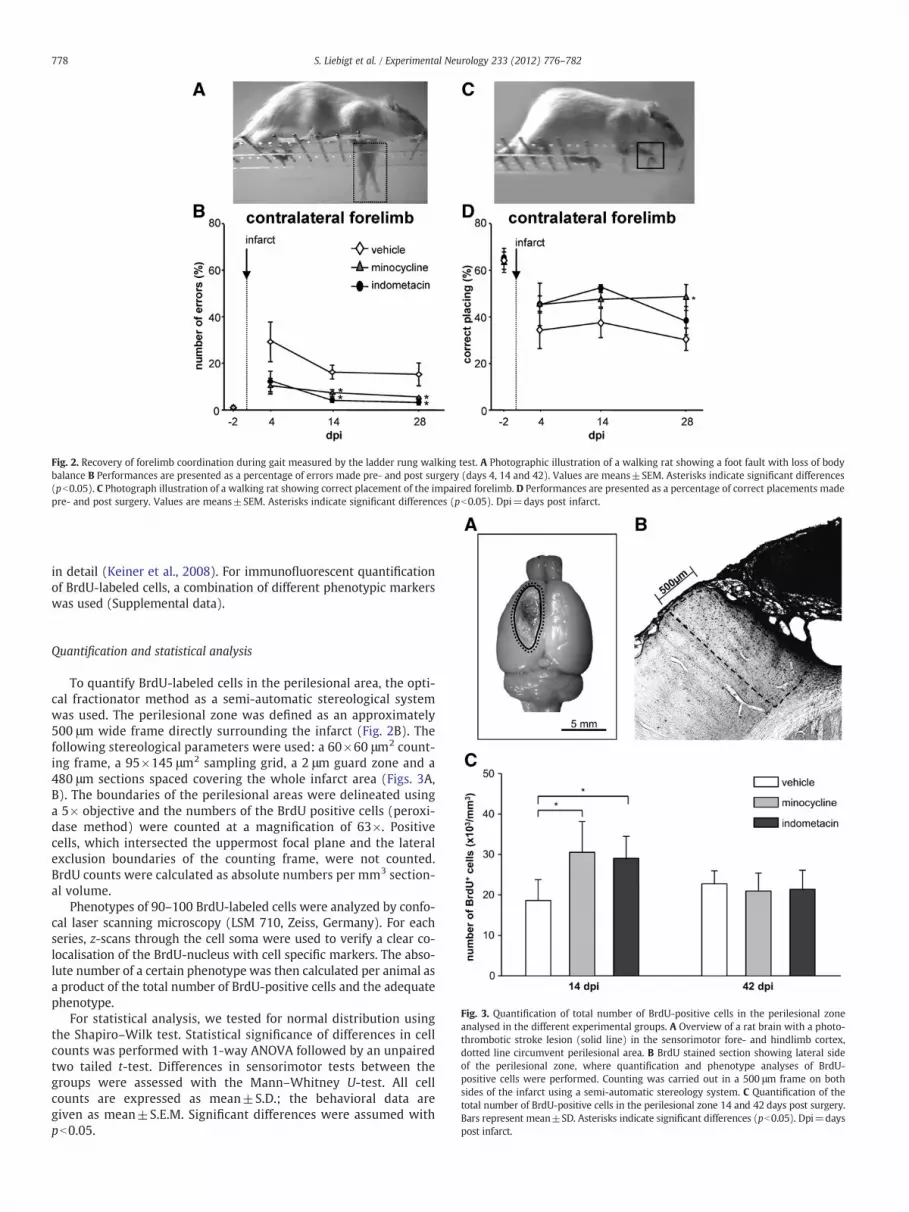
Fig. 2. Recovery of forelimb coordination during gait measured by the ladder rung walking test. A Photographic illustration of a walking rat showing a foot fault with loss of bodybalance B Performances are presented as a percentage of errors made pre- and post surgery (days 4, 14 and 42). Values are means±SEM. Asterisks indicate significant differences(pb0.05). C Photograph illustration of a walking rat showing correct placement of the impaired forelimb. D Performances are presented as a percentage of correct placements madepre- and post surgery. Values are means±SEM. Asterisks indicate significant differences (pb0.05). Dpi=days post infarct.
778 S. Liebigt et al. / Experimental Neurology 233 (2012) 776–782
in detail (Keiner et al., 2008). For immunofluorescent quantificationof BrdU-labeled cells, a combination of different phenotypic markerswas used (Supplemental data).
Fig. 3. Quantification of total number of BrdU-positive cells in the perilesional zoneanalysed in the different experimental groups. A Overview of a rat brain with a photo-thrombotic stroke lesion (solid line) in the sensorimotor fore- and hindlimb cortex,dotted line circumvent perilesional area. B BrdU stained section showing lateral sideof the perilesional zone, where quantification and phenotype analyses of BrdU-positive cells were performed. Counting was carried out in a 500 μm frame on bothsides of the infarct using a semi-automatic stereology system. C Quantification of thetotal number of BrdU-positive cells in the perilesional zone 14 and 42 days post surgery.Bars represent mean±SD. Asterisks indicate significant differences (pb0.05). Dpi=dayspost infarct.
Quantification and statistical analysis
To quantify BrdU-labeled cells in the perilesional area, the opti-cal fractionator method as a semi-automatic stereological systemwas used. The perilesional zone was defined as an approximately500 μm wide frame directly surrounding the infarct (Fig. 2B). Thefollowing stereological parameters were used: a 60×60 μm2 count-ing frame, a 95×145 μm2 sampling grid, a 2 μm guard zone and a480 μm sections spaced covering the whole infarct area (Figs. 3A,B). The boundaries of the perilesional areas were delineated usinga 5× objective and the numbers of the BrdU positive cells (peroxi-dase method) were counted at a magnification of 63×. Positivecells, which intersected the uppermost focal plane and the lateralexclusion boundaries of the counting frame, were not counted.BrdU counts were calculated as absolute numbers per mm3 section-al volume.
Phenotypes of 90–100 BrdU-labeled cells were analyzed by confo-cal laser scanning microscopy (LSM 710, Zeiss, Germany). For eachseries, z-scans through the cell soma were used to verify a clear co-localisation of the BrdU-nucleus with cell specific markers. The abso-lute number of a certain phenotype was then calculated per animal asa product of the total number of BrdU-positive cells and the adequatephenotype.
For statistical analysis, we tested for normal distribution usingthe Shapiro–Wilk test. Statistical significance of differences in cellcounts was performed with 1-way ANOVA followed by an unpairedtwo tailed t-test. Differences in sensorimotor tests between thegroups were assessed with the Mann–Whitney U-test. All cellcounts are expressed as mean±S.D.; the behavioral data aregiven as mean±S.E.M. Significant differences were assumed withpb0.05.

779S. Liebigt et al. / Experimental Neurology 233 (2012) 776–782
Results
Morphology of photothrombotic infarcts
All animals had typical photothrombotic infarcts involving alllayers of the sensorimotor fore- and hindlimb cortex. Only animalsthat had received indometacin showed a significant decline in lesionvolume at days 14 and 42 compared to vehicle (Fig. 1B).
Functional recovery
At the beginning of daily reaching training, all animals demon-strated functional impairments of the contralateral forelimb. Reach-ing success significantly increased between 82% and 98%, 1 weekafter drug application. During the second week, anti-inflammation-treated animals showed significantly better reaching success (99%)compared to standard animals (91%) (Fig. 1C).
After photothrombotic stroke, all animals showed impairment incoordination for the ladder rung walking test compared to baseline.Vehicle-treated animals showed significantly more placing errorscompared to minocycline- and indometacin-treated groups at days14 and 28 post-lesion (Fig. 2B). Minocycline showed a significantlybetter performance of correct placements for impaired forelimb com-pared to vehicle (Fig. 2D), whereas no differences of hindlimb coordi-nation after indometacin- or minocycline-treatment were detected ateach time point.
Proliferation of microglia and astrocytes in the perilesional zone
The intraperitoneal application of indometacin or minocyclinerevealed prominent differences in the stereological quantification ofBrdU-positive cells in the perilesional area 14 days after photothrombotic
Fig. 4. Immunocytochemical quantification of microglia in the perilesional zone in the diffehigh resolution of a z-stack scan, scale bar 10 μm) of double-labeled sections stained withpositive cells in the perilesional zone at days 14 and 42 after the infarct. Bars represent me
infarction (Fig. 3C). Both drugs strongly increased BrdU-labeled cells thatreached significance compared to the vehicle group. Forty-two days postinfarct, the number of BrdU-positive cells showed no differences betweenthe groups.
Intraperitoneal application of minocycline or indometacin differen-tially influenced the phenotypic differentiation of BrdU-positive cellsat days 14 and 42. Bothminocycline and indometacin-treatment signif-icantly reduced proliferating microglia expressing CD68 in the perile-sional zone at the early time point after infarct induction (Fig. 4).No differences were detected between the drug-treated animals. Atday 42, only a few BrdU-CD68-microglia survived and treatment-dependent differences were absent.
Furthermore, BrdU-labeled cells were characterized for coexpres-sion of the astrocytic marker GFAP (Fig. 5). The majority of BrdU-positive cells in the perilesional zone were identified as proliferatingastroglia. The total number of BrdU-GFAP-positive astrocytes signifi-cantly differed between the indometacin-treated animals and vehicleat day 14 post surgery. Finally, a significant increase of proliferatingGFAP-positive astrocytes was detected between the drug-treated an-imals and vehicle group at day 42 post-lesion. Further immunocycto-chemical analysis of BrdU-S100β astrocytes revealed an increase inthe indometacin group but not in the minocycline group comparedto standard controls at day 14 after surgery, whilst the total numberof BrdU-S100β did not significantly differ between the experimentalgroups at day 42 (data not shown).
Proliferation of DCX-positive cells in the perilesional zone
We also observed a significant number of BrdU-positive cellsexpressing the immature neuronal marker doublecortin (DCX) afterminocycline-treatment compared to vehicle at day 14 (Figs. 6A, B).Ablation of DCX-expressing cells in the subventricular zone or
rent experimental groups. A Confocal images (left: overview, scale bar 100 μm; right:antibodies against BrdU (red) and CD68 (green). B Quantification of the BrdU-CD68-an±SD. Asterisks indicate significant differences (pb0.05). Dpi=days post infarct.

Fig. 5. Immunocytochemical quantification of astrocytes in the perilesional zone in the different experimental groups. A Confocal images (left: overview, scale bar 100 μm; right:high resolution of a z-stack scan, scale bar 10 μm) of double-labeled sections stained with antibodies against BrdU (red) and GFAP (green). B Quantification of the BrdU-GFAP-positive cells in the perilesional zone at days 14 and 42 after the infarct. Bars represent mean±SD. Asterisks indicate significant differences (pb0.05). Dpi=days post infarct.
Fig. 6. Immunocytochemical quantification of DCX-positive neuroblasts and BrdU-NeuN positive neurons in the perilesional zone in the different experimental groups. A A highresolution z-stack scan of double-labeled sections stained with antibodies against BrdU (red) and DCX (green), scale bar=10 μm. B Quantification of the BrdU-DCX-positive andBrdU-NeuN-positive cells in the perilesional zone at days 14 and 42 after the infarct. Bars represent mean±SD. Asterisks indicate significant differences (pb0.05). C/D A high res-olution z-stack scan of double-labeled sections stained with antibodies against BrdU (red) and NeuN (blue) and BrdU (red) and HuC/D (green), scale bar=10 μm. Dpi=days postinfarct.
780 S. Liebigt et al. / Experimental Neurology 233 (2012) 776–782

781S. Liebigt et al. / Experimental Neurology 233 (2012) 776–782
dentate gyrus increased infarct size and sensorimotor deficits afterfocal cortical infarcts, indicating that this subpopulation of cells is in-volved in functional recovery (Jin et al., 2010). Furthermore, immu-nocytochemistry against the mature neuronal marker, NeuNrevealed only a small number of BrdU-NeuN-positive cells in the min-ocycline group reaching significance compared to vehicle. Additionalanalysis of the mature neuronal marker HuC/D confirmed this result(Figs. 6B, C, D).
Discussion
Rehabilitative training in combination with anti-inflammatorytreatment following focal cortical infarcts leads to a better functionalrecovery of the impaired forelimb associated with significant changesof cellular response in the perilesional zone. In the acute phase of in-flammation, skilled reaching training and indometacin or minocyclineapplication strongly diminished proliferating microglia, while mino-cycline additionally increased the number of proliferating DCX-positive cells. Furthermore, 6 weeks after infarct, there is enhancedsurvival of new born astrocytes and detection of a small number ofnewly-generated neurons.
Previous studies have shown that rehabilitative training alone im-proved the functional performance after stroke in a similar manner tonon-specific stimulation via exposure to an enriched environment orspecific reaching training of the impaired forelimb (Biernaskie andCorbett, 2001; Keiner et al., 2008; Metz andWhishaw, 2002). Anotherapproach to improve sensorimotor function after stroke is to applyanti-inflammatory drugs like minocycline or indometacin. Chu et al.(2007) treated ischemic animals with minocycline and showedlong-term improvement of sensorimotor deficits in multiple tests,for example, limb placing, foot fault, and the adhesive tape test. In an-other study, chronic treatment with minocycline for a period of1 month additionally reduced the functional impairment followingfocal cortical infarcts in a battery of behavioral tests (Liu et al., 2007).Further, Hewlett and Corbett (2006) reduced long-term functional def-icits after interval application of minocycline detected by means of thestaircase reaching test and cylinder forelimb asymmetry task. More-over, in human acute stroke, minocycline leads to a significantly betterfunctional outcome compared to placebo (Lampl et al., 2007). To ourknowledge, this is the first study combining anti-inflammatory drugtreatment with rehabilitative training of the impaired forelimb follow-ing focal cortical infarcts. Using this combined approach, we detecteda strong improvement of forelimb motor recovery in the ladder rungwalking test compared to skilled reaching training alone.
Furthermore, in the present study rehabilitative training and indo-metacin treatment significantly reduced cortical infarct volume.However, total infarct volume has long been used as a measure of in-jury and predictor of outcome after stroke (Friel and Nudo, 1998;Rogers et al., 1997; Saver et al., 1999). In our study, we detected a de-crease of infarct volume after rehabilitative training combined withindometacin-treatment, which correlates with functional recovery.Compared to these findings, although minocycline did not change in-farct volume, there was improved functional outcome. This observa-tion further underlines that infarct volume is not an ideal outcomepredictor after stroke.
The study was designed to analyze the cellular correlates of anti-inflammatory treatment and rehabilitative training in detail. Inorder to suppress the microglial response effectively, we appliedindometacin and minocycline 12 h prior to the infarct. Our data sug-gest that this approach significantly suppresses microglial prolifera-tion and correlates with improved functional recovery. However, toanswer the question whether this concept also functions in the clini-cal context, additional experiments are required comprising the ap-plication of indometacin and minocycline shortly after stroke.
It iswell known that activatedmicroglia following ischemia functionin a complex manner, which involves tissue repair such as secretion of
neuroprotective molecules, or induction of cytotoxic molecules leadingto tissue damage. In our study, minocycline, a semi-synthetic antibioticwas used due to its neuroprotective properties including the modula-tion of microgliosis by a decline of nitric oxide, cytokine, cyclooxygen-ase production and 5-lipoxygenase (Chu et al., 2007; Dawson et al.,1998; Samdani et al., 1997; Tikka et al., 2001; Yrjanheikki et al., 1999).The non-steroidal indometacin, on the other hand, prevents activationof the cyclooxygenase (COX1 and COX2) enzymes and is agonistic tothe transcription factor, peroxisome proliferator-activated receptor γ,which inhibits the elaboration of proinflammatory cytokine inmicrogliaand shifts the balance from cell death to survival in the inflammatoryenvironment (Mitchell et al., 1993).
In the present study, we detected a highly significant decrease of pro-liferating microglia on combining forelimb training with minocycline orindometacin compared to skilled reaching training alone. In our previousstudy (Keiner et al., 2008), we also detected a significant reduction ofmicroglia, albeit at a lower rate, which were induced alone due to fore-limb training or an enriched environment. Several studies have shownthat suppression or modulation of microglia is correlated with an im-provement of functional recovery after ischemia (Keiner et al., 2008;Stirling et al., 2004), confirming present study results. However, to date,this finding only confirms a correlation and is no proof of causality.
We further detected changes in the survival of proliferating astro-cytes. Combining minocycline or indometacin and rehabilitativetraining increased the survival of GFAP-positive astrocytes to higherlevels compared to skilled reaching training alone. Furthermore indo-metacin increased the proliferation of GFAP- and S100β-astrocytes2 weeks post lesion In accordance to our results, Hoehn et al.(2005) analyzing the effects of indometacin in the striatum and cor-tex after middle cerebral occlusion (MCAO), also showed a significantincrease in the number of proliferating GFAP-positive astrocytes inthe indometacin-treated group compared to controls. It is wellknown, that GFAP contributes to the formation of the glial scar andthat loss of the intermediate filament protein results in infarctgrowth, indicating a stabilizer role for GFAP.
The present study further demonstrates that the number of DCX-positive cells after skilled reaching training in the perilesional areais additionally raised by minocycline treatment and is associatedwith a small number of newly-generated neurons after infarct induc-tion. However, it is not likely that these newborn neurons have afunctional implication or that they are integrated in the existing net-work. Previous studies described an association of DCX with the mi-gration of cerebral cortical neurons, as well as an important role formicrotubulin stabilization in nuclear translocation, growth cone dy-namics, and in the regulation of microtubulin dynamics. However,the role of DCX in the cerebral cortex as a possible neurogenic markeris still unclear. Bloch and colleagues described four different DCX-populations with respect to the morphology and marker-expressionin their analysis of DCX expression in the cerebral cortex of adulthumans and nonhuman primates (Bloch et al., 2011). Indeed, DCX-positive cells in the cortex show neural progenitor properties involv-ing synaptic plasticity and glia-to-neuron signaling. In addition,transgenic-ablation of DCX-expression in the dentate gyrus as wellas the subventricular zone by Jin et al. (2010) was associated withdeficits in functional recovery after stroke.
Minocycline has been reported to be a well tolerated drug with agood safety record and robust neuroprotective effects after ischemicstroke (Yong et al., 2004). However there are some reports associat-ing minocycline with exacerbating properties (Matsukawa et al.,2009). Previous studies (Chiu et al., 1998; Nagarajan and Lam,2000) described an increase of intracranial pressure and tense bulg-ing of the fontanels in young human infants after minocycline treat-ment. Furthermore, Tsuji and colleagues (Tsuji et al., 2004) haveshown a deterioration of hypoxic-ischemic brain injury in neonatalmice, whereas these side effects were absent in rats. The underlyingmechanisms are still unclear but some indications that minocycline

782 S. Liebigt et al. / Experimental Neurology 233 (2012) 776–782
inhibits endothelial proliferation, affects PGE2 and COX-2 in variousways between mice and rats after cerebral infarct, and impairs mito-chondrial functions are apparent (Attur et al., 1999; Guerin et al.,1992; Yrjanheikki et al., 1999). Spells of dizziness and gastrointestinalproblems have been described in stroke patients when levels rise to100 mg. Compared to minocycline, indometacin decreases the cere-bral blood flow after ischemia potentially by vasoconstriction. It isstill controversially discussed whether cerebral hypoperfusion leadsto ischemic damage (Godoy et al., 2005; Rasmussen, 2005).
Conclusions
We demonstrate herein that treatment with indometacin or min-ocycline combined with rehabilitative training of the impaired func-tion substantially modulates perilesional cellular plasticity followingfocal cortical infarcts and contributes to a better functional recovery.Our data suggest that anti-inflammatory co-medication supports theefficacy of rehabilitation following stroke. Hence, it seems worth-while to establish whether this concept also functions in the clinicalcontext using application protocols for indometacin and minocyclineshortly after stroke.
Funding
Scholarship program of the Ernst-Abbe-Foundation Jena (IZKFscholarship program to S.L. and N.S., junior research program J12 toS.K.) and GermanMinistry of Education and Research (BMBF program‘Cell-based, regenerative therapies’, 01GN0977 to C.R.).
Supplementary materials related to this article can be found on-line at doi:10.1016/j.expneurol.2011.11.037.
Acknowledgments
We are grateful to Mrs N. Kroegel for editing the manuscript.
References
Attur, M.G., Patel, R.N., Patel, P.D., Abramson, S.B., Amin, A.R., 1999. Tetracycline up-regulates COX-2 expression and prostaglandin E2 production independent of itseffect on nitric oxide. J. Immunol. 162, 3160–3167.
Biernaskie, J., Corbett, D., 2001. Enriched rehabilitative training promotes improvedforelimb motor function and enhanced dendritic growth after focal ischemic inju-ry. J. Neurosci. 21, 5272–5280.
Bloch, J., Kaeser,M., Sadeghi, Y., Rouiller, E.M., Redmond, D.E., Brunet, J.F., 2011. Doublecortin-positive cells in the adult primate cerebral cortex and possible role in brain plasticity anddevelopment. J. Comp. Neurol. 519, 775–789.
Chiu, A.M., Chuenkongkaew, W.L., Cornblath, W.T., Trobe, J.D., Digre, K.B., Dotan, S.A.,Musson, K.H., Eggenberger, E.R., 1998. Minocycline treatment and pseudotumorcerebri syndrome. Am. J. Ophthalmol. 126, 116–121.
Chu, L.S., Fang, S.H., Zhou, Y., Yu, G.L., Wang, M.L., Zhang, W.P., Wei, E.Q., 2007. Minocy-cline inhibits 5-lipoxygenase activation and brain inflammation after focal cerebralischemia in rats. Acta Pharmacol. Sin. 28, 763–772.
Chu, L.S., Fang, S.H., Zhou, Y., Yin, Y.J., Chen,W.Y., Li, J.H., Sun, J., Wang,M.L., Zhang,W.P.,Wei,E.Q., 2010.Minocycline inhibits 5-lipoxygenase expression and accelerates functional re-covery in chronic phase of focal cerebral ischemia in rats. Life Sci. 86, 170–177.
Dawson, T.M., Sasaki, M., Gonzalez-Zulueta, M., Dawson, V.L., 1998. Regulation of neu-ronal nitric oxide synthase and identification of novel nitric oxide signaling path-ways. Prog. Brain Res. 118, 3–11.
Dobkin, B.H., 2004. Strategies for stroke rehabilitation. Lancet Neurol. 3, 528–536.
Friel, K.M., Nudo, R.J., 1998. Recovery of motor function after focal cortical injury in pri-mates: compensatory movement patterns used during rehabilitative training.Somatosens. Mot. Res. 15, 173–189.
Godoy, D.A., Biestro, A., Puppo, C., 2005. Does indomethacin cause cerebral ischemia?Acta Anaesthesiol. Scand. 49, 1577–1578.
Guerin, C., Laterra, J., Masnyk, T., Golub, L.M., Brem, H., 1992. Selective endothelialgrowth inhibition by tetracyclines that inhibit collagenase. Biochem. Biophys.Res. Commun. 188, 740–745.
Hewlett, K.A., Corbett, D., 2006. Delayed minocycline treatment reduces long-termfunctional deficits and histological injury in a rodent model of focal ischemia. Neu-roscience 141, 27–33.
Hoehn, B.D., Palmer, T.D., Steinberg, G.K., 2005. Neurogenesis in rats after focal cerebralischemia is enhanced by indomethacin. Stroke 36, 2718–2724.
Jin, K., Wang, X., Xie, L., Mao, X.O., Greenberg, D.A., 2010. Transgenic ablation ofdoublecortin-expressing cells suppresses adult neurogenesis and worsens strokeoutcome in mice. Proc. Natl. Acad. Sci. U. S. A. 107, 7993–7998.
Keiner, S., Wurm, F., Kunze, A., Witte, O.W., Redecker, C., 2008. Rehabilitative therapiesdifferentially alter proliferation and survival of glial cell populations in the perile-sional zone of cortical infarcts. Glia 56, 516–527.
Kriz, J., Lalancette-Hebert, M., 2009. Inflammation, plasticity and real-time imagingafter cerebral ischemia. Acta Neuropathol. 117, 497–509.
Lampl, Y., Boaz, M., Gilad, R., Lorberboym, M., Dabby, R., Rapoport, A., Anca-Hershkowitz,M., Sadeh, M., 2007. Minocycline treatment in acute stroke: an open-label,evaluator-blinded study. Neurology 69, 1404–1410.
Liu, Z., Fan, Y., Won, S.J., Neumann, M., Hu, D., Zhou, L., Weinstein, P.R., Liu, J., 2007.Chronic treatment with minocycline preserves adult new neurons and reducesfunctional impairment after focal cerebral ischemia. Stroke 38, 146–152.
Matsukawa, N., Yasuhara, T., Hara, K., Xu, L., Maki, M., Yu, G., Kaneko, Y., Ojika, K., Hess,D.C., Borlongan, C.V., 2009. Therapeutic targets and limits of minocycline neuro-protection in experimental ischemic stroke. BMC Neurosci. 10, 126.
Metz, G.A., Whishaw, I.Q., 2002. Cortical and subcortical lesions impair skilled walkingin the ladder rung walking test: a new task to evaluate fore- and hindlimb step-ping, placing, and co-ordination. J. Neurosci. Methods 115, 169–179.
Mitchell, J.A., Akarasereenont, P., Thiemermann, C., Flower, R.J., Vane, J.R., 1993. Selec-tivity of nonsteroidal antiinflammatory drugs as inhibitors of constitutive and in-ducible cyclooxygenase. Proc. Natl. Acad. Sci. U. S. A. 90, 11693–11697.
Nagarajan, L., Lam, G.C., 2000. Tetracycline-induced benign intracranial hypertension. J.Paediatr. Child Health 36, 82–83.
Rasmussen, M., 2005. Treatment of elevated intracranial pressure with indomethacin:friend or foe? Acta Anaesthesiol. Scand. 49, 341–350.
Rogers, D.C., Campbell, C.A., Stretton, J.L., Mackay, K.B., 1997. Correlation betweenmotor impairment and infarct volume after permanent and transient middle cere-bral artery occlusion in the rat. Stroke 28, 2060–2065.
Samdani, A.F., Dawson, T.M., Dawson, V.L., 1997. Nitric oxide synthase in models offocal ischemia. Stroke 28, 1283–1288.
Saver, J.L., Johnston, K.C., Homer, D., Wityk, R., Koroshetz, W., Truskowski, L.L., Haley,E.C., 1999. Infarct volume as a surrogate or auxiliary outcome measure in ischemicstroke clinical trials. Stroke 30, 293–298.
Stirling, D.P., Khodarahmi, K., Liu, J., McPhail, L.T., McBride, C.B., Steeves, J.D., Ramer,M.S., Tetzlaff, W., 2004. Minocycline treatment reduces delayed oligodendrocytedeath, attenuates axonal dieback, and improves functional outcome after spinalcord injury. J. Neurosci. 24, 2182–2190.
Thom, T., Haase, N., Rosamond, W., Howard, V.J., Rumsfeld, J., Manolio, T., Zheng, Z.J.,Flegal, K., O'Donnell, C., Kittner, S., Lloyd-Jones, D., Goff Jr., D.C., Hong, Y., Adams,R., Friday, G., Furie, K., Gorelick, P., Kissela, B., Marler, J., Meigs, J., Roger, V., Sidney,S., Sorlie, P., Steinberger, J., Wasserthiel-Smoller, S., Wilson, M., Wolf, P., 2006.Heart disease and stroke statistics—2006 update: a report from the AmericanHeart Association Statistics Committee and Stroke Statistics Subcommittee. Circu-lation 113, e85–e151.
Tikka, T., Fiebich, B.L., Goldsteins, G., Keinanen, R., Koistinaho, J., 2001. Minocycline, atetracycline derivative, is neuroprotective against excitotoxicity by inhibiting acti-vation and proliferation of microglia. J. Neurosci. 21, 2580–2588.
Tsuji, M., Wilson, M.A., Lange, M.S., Johnston, M.V., 2004. Minocycline worsenshypoxic-ischemic brain injury in a neonatal mouse model. Exp. Neurol. 189,58–65.
Yong, V.W., Wells, J., Giuliani, F., Casha, S., Power, C., Metz, L.M., 2004. The promise ofminocycline in neurology. Lancet Neurol. 3, 744–751.
Yrjanheikki, J., Tikka, T., Keinanen, R., Goldsteins, G., Chan, P.H., Koistinaho, J., 1999. Atetracycline derivative, minocycline, reduces inflammation and protects againstfocal cerebral ischemia with a wide therapeutic window. Proc. Natl. Acad. Sci.U. S. A. 96, 13496–13500.




















