Effectiveness of a Web-Based Application to Monitor Health-Related Quality of Life
13
Effectiveness of a Web-Based Application to Monitor Health-Related Quality of Life WHAT’S KNOWN ON THIS SUBJECT: Monitoring and discussion of patient-reported outcomes in clinical practice facilitates good communication between the patient and treating physician. However, studies on the use of health-related quality of life patient- reported outcomes in pediatric clinical practice are scarce. WHAT THIS STUDY ADDS: A web-based application to systemically monitor health-related quality of life problems in pediatric rheumatology is effective in increasing awareness of psychosocial topics of the patient and the patient ’ s family, contributing to increased satisfaction of the pediatric rheumatologist with the care provided during consultation. abstract BACKGROUND AND OBJECTIVE: Monitoring health-related quality of life (HRQoL) by using electronic patient-reported outcomes (ePROs) has been only minimally evaluated in pediatrics. Children with juvenile idiopathic arthritis (JIA) are at risk for HRQoL problems. The aim of this study was to investigate the effectiveness of ePROs in clinical pediatric rheumatology care. METHODS: All children (aged 0–18 years) with JIA visiting any of the 4 pediatric rheumatology clinics in Amsterdam between February 2009 and February 2010 were eligible for this sequential cohort intervention study. Before an outpatient consultation, children (aged 8–18 years) or parents (of children aged 0–7 years) completed web-based questionnaires. The resulting ePROfile was provided to the pediatric rheumatologist (PR). The study was divided into a control period in which the ePROfile was not discussed during consultation, and an intervention period in which the ePROfile was provided and discussed during consultation. Effectiveness was evaluated in terms of communication about different HRQoL topics, referral to a psychologist, and satisfaction with the consultations. RESULTS: Out of the eligible JIA patients, 176 (65%) participated in the study. Use of the ePROfile increased discussion of psychosocial topics (P , .01), as well as the PR’ s satisfaction with provided care during consultation (P , .01). The use of ePROfiles did not affect referrals to a psychologist or parental satisfaction. Parents and PRs evaluated the use of the ePROfile as positive in 80% to 100% of the consultations. CONCLUSIONS: Our web-based application to systemically monitor HRQoL problems in pediatric rheumatology contributed significantly to communication about psychosocial issues in a positive way. We recommend implementation of ePROs in pediatric clinical practice. Pediatrics 2013;131:e533–e543 AUTHORS: Lotte Haverman, MSc, a Marion A.J. van Rossum, MD, PhD, b,c Mira van Veenendaal, MD, b J. Merlijn van den Berg, MD, PhD, b,c Koert M. Dolman, MD, PhD, d,e Joost Swart, MD, c,e Taco W. Kuijpers, MD, PhD, b and Martha A. Grootenhuis, PhD a a Psychosocial Department and b Department of Pediatric Hematology Immunology & Infectious Disease, Academic Medical Center, Emma Children’ s Hospital, Amsterdam, Netherlands; c Department of Pediatric Rheumatology, Reade (Jan van Breemen location), Amsterdam, Netherlands; d Department of Pediatrics, Sint Lucas Andreas Hospital, Amsterdam, Netherlands; and e Department of Pediatric Rheumatology, VU University Medical Centre, Amsterdam, Netherlands KEY WORDS health-related quality of life, electronic patient reported outcomes, juvenile idiopathic arthritis, clinical practice ABBREVIATIONS CHAQ—Childhood Health Assessment Questionnaire ePRO—electronic patient-reported outcome HRQoL—health-related quality of life JIA—juvenile idiopathic arthritis PedsQL—Pediatric Quality of Life Inventory PR—pediatric rheumatologist PRO—patient-reported outcome TAPQOL—TNO-AZL Preschool Children’ s Health-Related Quality of Life VAS—visual analog scale All authors made substantial contributions to the conception and design of the study and to the interpretation of data. Ms Haverman collected the data. The analyses were performed by Ms Haverman and Dr Grootenhuis. All authors helped to draft the article or review it critically for important intellectual content. All authors gave final approval of the version to be published. www.pediatrics.org/cgi/doi/10.1542/peds.2012-0958 doi:10.1542/peds.2012-0958 Accepted for publication Sep 25, 2012 Address correspondence to Lotte Haverman, MSc, Emma Children’ s Hospital AMC, Meibergdreef 9, Room A3-241, 1105 AZ Amsterdam, Netherlands. E-mail: [email protected] PEDIATRICS (ISSN Numbers: Print, 0031-4005; Online, 1098-4275). Copyright © 2013 by the American Academy of Pediatrics FINANCIAL DISCLOSURE: The authors have indicated they have no financial relationships relevant to this article to disclose. FUNDING: Supported by Pfizer BV Pharmaceuticals and AGIS Healthcare. PEDIATRICS Volume 131, Number 2, February 2013 e533 ARTICLE by guest on April 6, 2016 Downloaded from
-
Upload
independent -
Category
Documents
-
view
2 -
download
0
Transcript of Effectiveness of a Web-Based Application to Monitor Health-Related Quality of Life

Effectiveness of a Web-Based Application to MonitorHealth-Related Quality of Life
WHAT’S KNOWN ON THIS SUBJECT: Monitoring and discussion ofpatient-reported outcomes in clinical practice facilitates goodcommunication between the patient and treating physician.However, studies on the use of health-related quality of life patient-reported outcomes in pediatric clinical practice are scarce.
WHAT THIS STUDY ADDS: A web-based application to systemicallymonitor health-related quality of life problems in pediatricrheumatology is effective in increasing awareness of psychosocialtopics of the patient and the patient’s family, contributing toincreased satisfaction of the pediatric rheumatologist with thecare provided during consultation.
abstractBACKGROUND AND OBJECTIVE: Monitoring health-related quality oflife (HRQoL) by using electronic patient-reported outcomes (ePROs)has been only minimally evaluated in pediatrics. Children with juvenileidiopathic arthritis (JIA) are at risk for HRQoL problems. The aim of thisstudy was to investigate the effectiveness of ePROs in clinical pediatricrheumatology care.
METHODS: All children (aged 0–18 years) with JIA visiting any of the 4pediatric rheumatology clinics in Amsterdam between February 2009 andFebruary 2010 were eligible for this sequential cohort intervention study.Before an outpatient consultation, children (aged 8–18 years) or parents(of children aged 0–7 years) completed web-based questionnaires. Theresulting ePROfile was provided to the pediatric rheumatologist (PR). Thestudy was divided into a control period in which the ePROfile was notdiscussed during consultation, and an intervention period in which theePROfile was provided and discussed during consultation. Effectivenesswas evaluated in terms of communication about different HRQoL topics,referral to a psychologist, and satisfaction with the consultations.
RESULTS: Out of the eligible JIA patients, 176 (65%) participated in thestudy. Use of the ePROfile increased discussion of psychosocial topics(P , .01), as well as the PR’s satisfaction with provided care duringconsultation (P , .01). The use of ePROfiles did not affect referrals toa psychologist or parental satisfaction. Parents and PRs evaluated theuse of the ePROfile as positive in 80% to 100% of the consultations.
CONCLUSIONS: Our web-based application to systemically monitorHRQoL problems in pediatric rheumatology contributed significantlyto communication about psychosocial issues in a positive way. Werecommend implementation of ePROs in pediatric clinical practice.Pediatrics 2013;131:e533–e543
AUTHORS: Lotte Haverman, MSc,a Marion A.J. van Rossum,MD, PhD,b,c Mira van Veenendaal, MD,b J. Merlijn van denBerg, MD, PhD,b,c Koert M. Dolman, MD, PhD,d,e JoostSwart, MD,c,e Taco W. Kuijpers, MD, PhD,b and Martha A.Grootenhuis, PhDa
aPsychosocial Department and bDepartment of PediatricHematology Immunology & Infectious Disease, Academic MedicalCenter, Emma Children’s Hospital, Amsterdam, Netherlands;cDepartment of Pediatric Rheumatology, Reade (Jan vanBreemen location), Amsterdam, Netherlands; dDepartment ofPediatrics, Sint Lucas Andreas Hospital, Amsterdam, Netherlands;and eDepartment of Pediatric Rheumatology, VU UniversityMedical Centre, Amsterdam, Netherlands
KEY WORDShealth-related quality of life, electronic patient reportedoutcomes, juvenile idiopathic arthritis, clinical practice
ABBREVIATIONSCHAQ—Childhood Health Assessment QuestionnaireePRO—electronic patient-reported outcomeHRQoL—health-related quality of lifeJIA—juvenile idiopathic arthritisPedsQL—Pediatric Quality of Life InventoryPR—pediatric rheumatologistPRO—patient-reported outcomeTAPQOL—TNO-AZL Preschool Children’s Health-Related Quality of LifeVAS—visual analog scale
All authors made substantial contributions to the conceptionand design of the study and to the interpretation of data. MsHaverman collected the data. The analyses were performed byMs Haverman and Dr Grootenhuis. All authors helped to draftthe article or review it critically for important intellectualcontent. All authors gave final approval of the version to bepublished.
www.pediatrics.org/cgi/doi/10.1542/peds.2012-0958
doi:10.1542/peds.2012-0958
Accepted for publication Sep 25, 2012
Address correspondence to Lotte Haverman, MSc, EmmaChildren’s Hospital AMC, Meibergdreef 9, Room A3-241, 1105 AZAmsterdam, Netherlands. E-mail: [email protected]
PEDIATRICS (ISSN Numbers: Print, 0031-4005; Online, 1098-4275).
Copyright © 2013 by the American Academy of Pediatrics
FINANCIAL DISCLOSURE: The authors have indicated they haveno financial relationships relevant to this article to disclose.
FUNDING: Supported by Pfizer BV Pharmaceuticals and AGISHealthcare.
PEDIATRICS Volume 131, Number 2, February 2013 e533
ARTICLE
by guest on April 6, 2016Downloaded from

Juvenile idiopathic arthritis (JIA) isarthritis of unknownetiologywithonsetbefore age 16. It is the most commonrheumatic disease in childhood, af-fecting 0.07 to 4.01 per 1000 childrenworldwide1 and is a major cause ofchildhood disability. These children areat risk for a lower health-related qualityof life (HRQoL) compared with healthypeers.2–7 To obtain comprehensive in-sight into the consequences of theirdisease, the use of physical measuresis not sufficient. To provide effectivetreatment and support, it seems es-sential to evaluate the patient’s HRQoL inclinical practice.5
The use of HRQoL patient-reportedoutcomes (PROs) in daily clinicalpractice has received increased atten-tion. Routine assessment of HRQoL ina clinical setting facilitates early rec-ognition of lowered HRQoL in adultpatients.8–14 Physicians generally regardthe use of PROs as a valuable addition todaily health care.10 Research on the useof PROs to improve patient satisfactionwith the care they receive is still chal-lenging.8,11,13,15
In the context of a chronically ill child’sdevelopment, all domains of HRQoL(physical, social, emotional, and cogni-tive functioning) need to be addressed,and the developmental trajectory needsmonitoring. Using PROs in daily clinicalpractice can be a helpful tool to discussthese issues systematically and providetailored interventions if needed. How-ever, research on the use of PROs inpediatrics is still scarce.16–18 Onestudy showed that the use of PROsimproved care satisfaction in adoles-cents with diabetes.18 Engelen et aldemonstrated that PROs increaseddiscussion of emotional and psycho-social functioning and improved iden-tification of emotional problems inpediatric oncology.17,19,20
The aim of this study was to investi-gate the effectiveness of a web-based intervention that provided an
electronic PRO (ePRO) to the pediatricrheumatologist (PR) during consul-tation. The ePROwhichwas completedat home just before consultationincludes generic HRQoL scores anddisease-specific information on thefunctional ability of the patient withJIA. Outcomes of effectiveness werecommunication about HRQoL, referrals,and satisfaction with the providedcare. In addition, users evaluated theePRO.
METHODS
Participants
All children (aged 0–18 years) with JIAwho visited the following pediatricrheumatology centers in Amsterdamwere approached: Emma Children’sHospital AMC, VUMedical Centre, Reade(Jan van Breemen location), and theSint Lucas Andreas Hospital. All 5 PRsat the 4 centers participated.
Intervention
The intervention consisted of providingHRQoL scores of the patient (ePROfile,Fig 1) and scores on functional ability(ePROfile, Fig 2) to the PR during con-sultation, focusing on identifying, moni-toring, and discussing HRQoL problems.For that purpose, the child or parentcompleted online questionnaires justbefore consultation, at home by usingthe KLIK Web site (www.hetklikt.nu). Theanswers were then automatically con-verted to an ePROfile and keyed to col-ors, with red (“often” and “almostalways”) indicating that a child experi-enced problems with an issue, orange(“sometimes”) representing mild prob-lems, or green (“never” and “almostnever”) indicating no reported prob-lems. The development of the ePROfilehas taken several steps, as described inEngelen et al 201019 and Haverman et al2011.21
The PR retrieved the patient’s ePROfiledirectly from the Web site. The items
and sum scores were shown on thecomputer screen and provided theopportunity to discuss the results di-rectly with the child and parents.
To optimize the effectiveness, all PRswere trained in the use of the PROfile.19,21
Design and Procedure
Asequential cohortdesignwasused.19,21
Patients took part in either the controlor intervention group, depending onthe date of consultation; if a patientparticipated in the control group, thatpatient was no longer eligible for par-ticipation in the intervention group.All PRs first participated in the con-trol group (control period: February2009–April 2009; online questionnairecompleted by the patient, but theePROfile was not provided to the PR)and thereafter in the interventiongroup (intervention period: May 2009–February 2010; online questionnairecompleted by the patient, and theePROfile was provided to the PR). Theintervention period was longer thanthe control period because we had theopportunity to extend the researchproject. As a result, more patients wereincluded in the intervention groupcompared with the control group, andtherefore in the intervention group, theePROfile could be discussed in 2 con-secutive consultations.
Randomization was not desirable, be-cause it could result in the provision ofextra attention to HRQoL issues in thecontrol group (contamination).8,13
Children and parents were invited bymail toparticipate in thestudywhen theconsultation date was planned. Theyreceived a username and password bye-mail to log in on the KLIK Web site.21
Each user of the Web site has a uniquelogin name and is automatically givenaccess to a specific secure section ofthe Web site. The Web site only allowsthe pediatricians to see the results fortheir own patients, and therefore, theprivacy of the patients is guaranteed.
e534 HAVERMAN et alby guest on April 6, 2016Downloaded from

FIGURE 1The ePROfile: generic HRQoL scores.
ARTICLE
PEDIATRICS Volume 131, Number 2, February 2013 e535by guest on April 6, 2016Downloaded from

FIGURE 2The ePROfile: functional ability.
e536 HAVERMAN et alby guest on April 6, 2016Downloaded from

The security and functions of the KLIKWeb site are extensively described inHaverman et al 2011.21
To assess the effectiveness of the in-tervention, shortly after the consulta-tion, the parents and the PR completedan online questionnaire about theHRQoL topics discussed, referrals, andtheir satisfaction with the consultation,again by using the Web site. In addition,parents and PRs evaluated the ePROfilein the intervention period.
All patients and/or parents gave in-formed consent, and themedical ethicscommittees of all participating centersapproved the study.
Measures
HRQoL Questionnaires
The Netherlands Organisation for Ap-plied Scientific Research-AcademischZiekenhuis Leiden (TNO-AZL) PreschoolChildren Quality of Life (TAPQOL)22,23
was used to measure parent-reportedHRQoL in children aged 0 to 5 years. TheTAPQOL is a Dutch proxy report, ge-neric, and multidimensional HRQoL in-strument. The 43 items are clusteredinto 12 multi-item scales, with higherscores indicating better HRQoL. Thecompletion time is ∼5 to 10 minutes,and the psychometric properties aresatisfactory. The Pediatric Quality ofLife Inventory (PedsQL) Generic CoreScale24,25 was used to measure genericHRQoL in older children: PedsQL self-report form (children aged 8–18) andPedsQL parent-report form (childrenaged 6 and 7).
Disease-specific Questionnaires
Disease-specific symptoms were as-sessed with a self-composed ques-tionnaire (Table 1) based on theDISABKIDS arthritis module.26 Theanswers to these items were onlyreported in the ePROfile. The datawere not used for sum scores orgroup comparisons.
The Dutch version of the Childhood He-alth Assessment Questionnaire (CHAQ)27
was used tomeasure functional ability.28
A 100-mm visual analog scale (VAS) wasused for the evaluation of pain andoverall well-being.
Communication About HRQoL
After every consultation, the PRs andthe parents scored whether the fol-lowing 12 HRQoL topics were discussed(yes/no): Condition/Energy, Sports,Autonomy, Pain/Physical Problems, Useof Medicine, Sleep, Eating/Drinking,Emotions, Family, Contact With Peers,School and Cognition, and Attendanceat School. These topics represented the4 HRQoL domains in the ePROfile.
Referrals
PRs reported referral to a psychologistafter each consultation. Scoreswere ona dichotomy scale (0 = no referral, 1 =referral).
Satisfaction
After the consultation, the satisfactionof the PR and the parentswas assessed
with the adapted version of the PatientSatisfaction Questionnaire.19,29,30 Thequestions, answered on a 100-mm VAS(0 = not at all satisfied to 100 = verysatisfied), referred to satisfaction withrespect to (1) meeting needs, (2) activeinvolvement, (3) provided information,(4) (emotional) support, and (5) overallsatisfaction with care provided duringthe consultation. Parents completedthe 5 questions about the functioningof the PR and the overall consultation;PRs completed these questions forboth child (3 items) and parent (3items) and overall satisfaction (1 item).
Evaluation of the ePROfile
After the first and second consultationsin the intervention period, the parents,children, and PRs completed an ad hocdesigned5-point (PRsandparents)or3-point (child) scale questionnaire abouttheir experience with the ePROfile.Parents and PRs were asked if theyregarded the ePROfile as useful, un-necessary, clarifying, practical, emo-tional, or unpleasant (5-point scale;“totally agree” to “disagree”). Children($8 years) were asked if discussingtheir answers with the pediatricianwas nice, unpleasant, normal, tense,stupid, delightful, or sad (3-point scale;“yes,” “a little,” and “no”).
Parents were also asked if the ePROfilehelped them or their child gain insightinto the child’s HRQoL (5-point scale;“totally agree” to “disagree”) and if theePROfile correctly reflected the HRQoLof their child (“yes” or “no”). In addi-tion, we asked them to rate the use ofthe ePROfile during the consultation on10-point scale: 0 = very negative to 10 =very positive.
Sociodemographic and MedicalInformation
Parents completed an online ques-tionnaire about sociodemographics atthe start of the study.Medical datawereassessed by the PR during the
TABLE 1 A Self-Composed Questionnaire toMeasure Disease-SpecificSymptoms of JIA
Disease-specific questionsDo your joints feel stiff in the morning?Do you feel tired more quickly than your peers?Does JIA interfere with you having a good time
when spending time with your friends?How often did you have pain in the last week?Does pain stop you from doing things you enjoy?Are you able to do all sports you would like to do?Are you able to do all hobbies you would like to
do?Does your family take into account that you have
JIA?Do your friends take into account that you have
JIA?Do people at school take into account that you
have JIA?MedicationDo you have to use medication for your JIA?If yes, do you experience side effects from the
medication?Do you dread taking/getting your medication?
SchoolHave you had to stay back a year at school?In the past 3 mo, howmany dayswere you absent
from school?
ARTICLE
PEDIATRICS Volume 131, Number 2, February 2013 e537by guest on April 6, 2016Downloaded from

consultation. Somesociodemographics(child age and gender, parental countryof birth) andmedical informationaboutnonparticipants were retrieved frommedical files.
Statistical Analysis
SPSS version 18.0 (IBM SPSS Statistics,IBM Corporation, Armonk, NY) wasused. First, sociodemographic andmedical differences between partic-ipants and nonparticipantswere testedas well as differences between thecontroland interventiongroup,byusingindependent t tests (age), x2 test (agegroups, gender, parental country ofbirth, JIA subtype, medication, PRs), andMann-Whitney tests (physician diseaseactivity rating: VAS score, disease du-ration). Differences in HRQoL scoresbetween control and interventiongroups were analyzed with independentt tests and the difference in CHAQ scoreswith the Mann-Whitney test.
Second, the effect of the intervention(ePROfile) was examined by testingdifferences between the control andintervention group on the outcomemeasures. x2 tests were used forcommunication (topics discussed) andreferrals; satisfaction was analyzed byusing analysis of variance by groupand age. Descriptive statistics wereused for the evaluation of the ePROfile.To adjust for multiple testing, we useda P value of ,.01.
RESULTS
Participants
Two hundred seventy-three childrenwith JIA and their parents wereapproached to participate in this study.The patients were included if thequestionnaires were completed beforeconsultation and either the parents orthe PR completed the questionnairesafter consultation. Eventually, 176(64.5%) patients completed the onlinequestionnaires; the mean age forpatients was 11.6 (SD 4.5) years and
66.8%were girls. Participating patientswere younger than the nonparticipants(mean 11.6 vs 13.22; P , .01), and, asa result, disease duration (years) in theparticipants was shorter (4.0 vs 4.8;P , .05). The participating parentswere born in the Netherlands moreoften (79.5% vs 66.0%; P , .01) com-pared with the nonparticipants.7
During the control period, 67 patientsparticipated. In the intervention period,109 patients participated; 40 patientshad 1 consultation, and 69 patients had2 consultations.
Despite differences in age, the distribu-tion of the different age categories be-tween thecontrol and interventiongroupdid not differ significantly (Table 2).
Regarding HRQoL in patients aged 0 to 5years, no differences were found be-tween the control and interventiongroups. However, the patients aged 6 to18 years in the intervention group
reported better functioning in schoolcomparedwith the patients aged 6 to 18in the control group (mean 63.9 vs 71.7;P , .05).
Regarding disease specific symptomsofJIA, functionalability (CHAQ),andpainscore (VAS), no differences were foundbetween the control and interventiongroup. However, the control groupreported a worse overall well-beingscore (VAS; mean 27.7 vs 26.6; P, .05).
All PRs participated in the control aswell as the intervention groups. The 5PRs managed, respectively, 9%, 16%,20%, 21%, and 34% of the patients. Nosignificant differences in the distribu-tion of the patients over the PRs werefound between the control and the in-tervention group.
Communication About HRQoL
According to the parents, the topics of“emotions” and “family”were discussed
TABLE 2 Sociodemographics and Disease Characteristics of the Control and Intervention Groups
Control Intervention
N Mean, %, or median (range) N Mean, %, or median (range)
Age, y, mean (SD)a 67 13.0 (4.2) 109 10.8 (4.5)Age group (%), y0–5 y 6 9.0 22 20.26–7 y 3 4.5 10 9.28–12 y 21 33.3 42 38.513–18 ya 37 55.2 35 32.1
Gender (female), % 48 71.6 73 67.0Country of birth parents(Netherlands), %
56 83.6 84 78.5
JIA subtype, %Oligoarticular JIA, persistent 13 19.4 26 23.9Oligoarticular JIA, extended 10 14.9 14 12.8Polyarticular JIA, RF negative 29 43.3 43 39.4Polyarticular JIA, RF positive 3 4.5 4 3.7Systemic JIA 0 0 8 7.3Enthesitis related arthritis 9 13.4 8 7.3Undifferentiated JIA 3 4.5 4 3.7Chronic arthritis with other
autoimmune inflammatorydisease
0 0 2 1.8
Medication use, %DMARDs 59 88.1 81 74.3Biologicals (anti-TNF) with DMARDs 11 16.4 10 9.2No medication 3 4.5 12 11.0
Physician disease activity (VAS scorerange 0–100), median (range)
67 17.0 (0.0–76.0) 109 16.5 (0.0–94.0)
Disease duration (y), median (range) 67 3.6 (0.44–14.12) 108 3.0 (0.28–14.82)
DMARD, disease modifying antirheumatic drug; RF, rheumatoid factor.a P , .01.
e538 HAVERMAN et alby guest on April 6, 2016Downloaded from

more often in the intervention group (i2)than in the control group (Table 3).
In addition, according to the PRs, thetopics “family” and “contact with peers”were more often discussed in the in-tervention group (i1 and i2) than in thecontrol group. “Emotions” were dis-cussed more often in the first consul-tation compared with the control group.
Referrals
The PR referred 3.0% of the controlpatients to a psychologist comparedwith 9.2%of the patients during thefirstintervention consultation (i1) and 4.3%during the second intervention con-sultation (i2).
Satisfaction
Parents’ satisfaction with the careprovided during consultation in theintervention group did not differ fromthat in the control group (Fig 3).
The PRs reported that they were moresatisfied with the provided care duringthe consultations in the domains ofemotional support for parents andchild, meeting the needs of the child,and in overall satisfaction with theprovided care during the consultationin thefirst interventionconsultation (i1)and the second intervention consulta-tion (i2; Fig 4) compared with the con-trol period. The PRs also reported to bemore satisfied about the provided in-formation to the child in the secondintervention consultation (i2) com-pared with the control period.
Evaluation of the ePROfile
Overall, the evaluation of the use of theePROswas positive. In 88% (i1) and 80%(i2) of the consultations, the parentsregarded the ePROfile as useful. In 57%,theyregarded theePROfileashelpful forthemselves and in 60% of the con-sultations as helpful for their child. In94% of the first intervention consulta-tion (i1) and in 91% of the second in-tervention consultation (i2), parents
judged that the PROfile reflected theirchild’s HRQoL adequately. The parents(i1 and i2 combined) evaluated thePROfile with a median of 8 on a 10-pointscale (range 4–10).
The PRs regarded the provided PROfileas useful in 95.1% of intervention con-sultations 1 (i1) and 100% of inter-vention consultations 2 (i2).
The children reported that discussingtheePROfilewith thePRwas “normal” in97.9% of the first intervention con-sultations (i1) and in 82.8% of thesecond intervention consultations (i2)(Table 4).
DISCUSSION
Our study shows that providing in-formation to PRs on patient HRQoL,disease-specific symptoms, and func-tional ability with an ePROfile leads to
significantly more discussion of emo-tional and social functioning duringconsultation and improves the PR’ssatisfaction with the provided care. Theuse of the ePROfile during consultationseems to result in more psychosocialreferrals. Overall parents, children,and PRs evaluate the use of the ePRO-file positively.
Our findings of the use of the ePROfileregarding communication correspondwith the findings in previous PROstudies in adult8,10,31 and pediatric17
medical settings. With the use of anePROfile, emotions, family, and contactwith peers were discussed signifi-cantly more often during consultationsthan without the use of an ePROfile. It isimportant to discuss HRQoL systemat-ically in daily clinical practice to iden-tify problems early. Timely, tailoredinterventions by psychologists or
TABLE 3 Communication Reported by PR and Parents: Percentage of Consultations in Which theHRQoL Topics Are Discussed: Control (C) Versus Intervention Group First Consultation(i1) and Control Versus Intervention Group Second Consultation (i2)
C i1 i2
n % n % n %
ParentsCondition/energy 50 86.2 75 86.2 51 89.5Sports 51 87.9 76 87.4 50 87.7Autonomy 29 50.0 53 60.9 33 57.9Pain/physical problems 57 98.3 87 100.0 56 98.2Use of medicine 57 98.3 86 98.8 56 98.2Sleep 22 37.9 40 46.0 26 45.6Eating/drinking 14 24.1 32 36.8 21 36.8Emotions 22 37.9 46 52.9 40 70.2a
Family 12 20.7 27 31.0 26 45.6b
Contact with peers 20 34.5 37 42.5 33 57.9School and cognition 42 72.4 50 57.5 33 57.9Attendance at school 25 43.1 42 48.3 21 36.8
PRCondition/energy 62 92.5 92 89.3 59 92.2Sports 64 95.5 97 94.2 62 96.9Autonomy 32 47.8 52 50.5 39 60.9Pain/physical problems 64 95.5 102 99.0 64 100.0Use of medicine 63 94.0 96 93.2 61 95.3Sleep 18 26.9 39 37.9 20 31.3Eating/drinking 7 10.4 23 22.3 12 18.8Emotions 33 49.3 71 68.9b 43 67.2Family 10 14.9 36 35.0b 30 46.9a
Contact with peers 25 37.3 62 61.2b 43 67.2a
School and cognition 55 82.1 67 65.0 40 62.5Attendance at school 39 58.2 53 51.5 38 59.4
Parents: C, n = 58; i1, n = 87; i2, n = 57. PR: C, n = 67; i1, n = 103; i2, n = 6.a P = .001.b P # .01.
ARTICLE
PEDIATRICS Volume 131, Number 2, February 2013 e539by guest on April 6, 2016Downloaded from

social workers can then be offeredwhen needed. Although solving prob-lems in social and emotional function-ing is not the main scope of apediatrician, the discussion of HRQoLtopics can itself lead to a decrease innegative feelings or feelings of in-security.32
Despite a trend toward more psycho-social referrals (3% of the control
consultations compared with 9% of theintervention consultations), the use ofthe ePROfile did not result in a signifi-cant increase in the percentage ofreferrals. This corresponds with thefindings in earlier studies.8,10,17 Overall,based on systematic reviews, PROs areseen as most efficient and effective inimproving communication about psy-chosocial issues.33,34
The PRs reported increased satisfac-tion with the provided care duringconsultation if the ePROfile was used.This finding is confirmed by the resultsshowing that PRs regarded the ePROfileas useful in almost all consultations(95%–100%). This positive evaluationof the ePROfile by health care workersis in line with former findings in adulthealth care,8,9,35 but to date, this hasnot been reported in pediatric clinicalcare.
The results regarding parental satis-faction with the provided care duringconsultation were not unequivocal. Al-though the majority of the parentsregarded the ePROfile as useful in theconsultation (80%–88%) and parentsevaluated the ePROfile with a highscore (8 out of 10), the use of theePROfile did not seem to influence pa-rental satisfaction. This may be due toa ceiling effect,10,15 which is indicatedby the high satisfaction score in thecontrol group. This phenomenon wasalso observed in other studies evalu-ating the use of PROs on patient satis-faction,10,17 whereas the study of De Witet al (2008) recorded improved
FIGURE 3Satisfaction with the consultation reported by the parents: control (C) versus intervention group firstconsultation (i1) and control group versus intervention group second consultation (i2). Range 0 to 100.No significant differences to analysis of variance by group and age (control versus intervention group;P, .01) between the control group and the intervention group were found. C (n5 60), i1 (n5 85), i2(n5 57): these numbers are smaller than the number of participating patients because some childrenvisited the PR without their parents.
FIGURE 4Satisfaction with the consultation reported by the PR about the parent, child, and consultation: control (C) versus intervention group first consultation (i1) andcontrol group versus intervention group second consultation (i2). Range 0 to 100. * Difference at P, .01 according to analysis of variance by group and age(control versus intervention group). ** Difference at P#.001 according to analysis of variance by group and age (control versus intervention group). C (n = 66;n = 60), i1 (n = 99; n = 80), i2 (n = 61; n = 50): these numbers are smaller than the number of participating patients because some children visited the PRwithout their parents or the patient was not old enough to participate in the consultation.
e540 HAVERMAN et alby guest on April 6, 2016Downloaded from
satisfaction with care in adolescentswith diabetes by including HRQoLscores in routine clinical practice.18
Taken together, our results show thatusing ePROs for children with JIA wasappreciated by parents and PRs andthat its use has a positive effect oncommunication about psychosocialissues and on PR satisfaction withprovided care. A strength of ourePROfile is that it includes all relevantdomains for the provision of clinicalcare to children with JIA.36,37 It is welldocumented that children with JIA areat risk for a low HRQoL and that pain,physical functioning, school absence,and the subjective burden of medica-tion use are the main predictorsof their HRQoL.7 The ePROfile in-corporated all these aspects as well asinformation on specific symptoms ofJIA and general well-being.
A limitation of our study was the pos-sible confounding influence of theprovision of the questionnaires to thecontrol group. Therefore, our controlgroup can also be considered an at-
tention control group. In future re-search, it would be interesting to add acontrol group under only standard carewithout the use of questionnaires.8,9
Furthermore, it should be consideredthat we did not include HRQoL as anoutcome measure. In our opinion, theduration of our study was too short toestablish any differences in HRQoL. Inaddition, to avoid contamination, wedid not randomize our study partic-ipants. A sequential cohort design wasconsidered most suitable for the KLIKstudy.17 A fourth limitation is that we didnot determine the association betweenHRQoL scores and communication. Infuture research, it would be interestingto investigate the influence of HRQoLscores on the items discussed by, forexample, audiotaping the consultations.
Because all patients with JIA in care inthe district of Amsterdam were invitedto participate in this study and onlysmall differences in characteristicswere found between participants andnonparticipants, we believe that ourfindings can be generalized to all chil-
dren with JIA. Furthermore, our find-ings are in line with previous results inpediatrics17,18 and in adult oncology.8,10,12
We therefore think that the imple-mentation of the ePROfile in pediatricsis justified in daily clinical practice forchildrenwith different types of diseases.
The ePROfile is nowbeing implementedin clinical care in our hospitals. Theimplementation of a web-based e-PROfile in clinical practice creates newchallenges and opportunities for care,as is extensively described in the In-ternational Society for Quality of LifeResearch guidelines and in otherstudies.38 In our study, the use of theePROfile was feasible. In the Nether-lands, which has the highest rate ofInternet access in Europe, the useof the Internet to provide PROs39 isan efficient medium for monitoringHRQoL in daily clinical practice. Thecompletion of the HRQoL question-naire takes only 10 minutes,40 anddiscussing HRQoL issues in clinicalpractice does not seem to increase theduration of the consultation.10,17,31
Depending on a patient’s health careneeds, members of a multidisciplinaryteam can use the ePROfile individuallyor during multidisciplinary team con-sultation. In addition, parent-reportedoutcomes can be useful supplemen-tary components in the care of chroni-cally ill children and their families.41,42
CONCLUSIONS
Our multicenter study is a valuable ad-dition to the few studies on feedbackusing ePROs in pediatric settings. Inconclusion, a web-based application tosystemically monitor HRQoL problems inpediatric rheumatology is effective inincreasing discussion about psychoso-cial topics and satisfaction with theprovided care by the PR. Therefore, werecommend implementation of theePROfile indailyclinicalpractice, todetectHRQoL problems at an early stage and toprovide timely and tailored interventions.
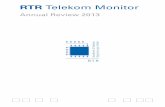
TABLE 4 Evaluation of the Use of the PROfile During the Control Consultation (C), InterventionGroup First Consultation (i1), and Intervention Group Second Consultation (i2)
Parents PRs
i1 (n = 65) i2 (n = 46) i1 (n = 102) i2 (n = 64)
n % n % n % n %
Useful 57 87.7 37 80.4 97 95.1 64 100.0Unnecessary 6 9.2 5 10.8 2 2.0 1 1.6Clarifying 48 73.8 28 60.9 90 88.2 60 93.8Practical 54 83.0 34 73.9 95 93.2 64 100.0Emotional 11 16.9 6 13.0 8 7.8 2 3.2Unpleasant 0 0.0 3 6.5 1 1.0 1 1.6
Children
i1 (n = 48) i2 (n = 35)
n % n %
Nice 41 58.4 30 85.7Unpleasant 1 2.1 2 5.7Normal 47 97.9 29 82.8Tense 10 20.9 4 11.4Stupid 4 8.4 2 5.7Delightful 36 75.1 31 88.6Sad 5 10.4 4 11.5
The percentages in the table represent the answer categories “totally agree” and “partly agree.” i1 (n = 65, n = 102, n = 48), i2(n = 46, n = 64, n = 35): these numbers are smaller than the number of participating patients because some children visitedthe PR without their parents or the patient was not old enough to participate in the consultation.
ARTICLE
PEDIATRICS Volume 131, Number 2, February 2013 e541by guest on April 6, 2016Downloaded from

ACKNOWLEDGMENTSWethankall thechildren,parents,nursesand nurse practitioners, and the othermedical staffwhoparticipated in theKLIK
study. In addition, we thank HeleenMaurice-Stam for her statistical supportand her valuable comments on the man-uscript, BioMedia/Artsen voor Kinderen
for the web design used in this study,and Hedy van Oers and Perrine Limpergfor supporting the implementationof theePROfile in daily clinical practice.
REFERENCES
1. Prince FH, Otten MH, van Suijlekom-Smit LW.Diagnosis and management of juvenile id-iopathic arthritis. BMJ. 2010;341:c6434
2. Grootenhuis MA, Koopman HM, Verrips EG,Vogels AG, Last BF. Health-related quality oflife problems of children aged 8-11 yearswith a chronic disease. Dev Neurorehabil.2007;10(1):27–33
3. Gutiérrez-Suárez R, Pistorio A, CespedesCruz A, et al; Pediatric Rheumatology In-ternational Trials Organisation (PRINTO).Health-related quality of life of patientswith juvenile idiopathic arthritis comingfrom 3 different geographic areas. ThePRINTO multinational quality of life cohortstudy. Rheumatology (Oxford). 2007;46(2):314–320
4. LeBovidge JS, Lavigne JV, Donenberg GR,Miller ML. Psychological adjustment ofchildren and adolescents with chronic ar-thritis: a meta-analytic review. J PediatrPsychol. 2003;28(1):29–39
5. Sawyer MG, Whitham JN, Roberton DM,Taplin JE, Varni JW, Baghurst PA. The re-lationship between health-related quality oflife, pain and coping strategies in juvenileidiopathic arthritis. Rheumatology (Ox-ford). 2004;43(3):325–330
6. Shaw KL, Southwood TR, Duffy CM, McDonaghJE. Health-related quality of life in adoles-cents with juvenile idiopathic arthritis. Ar-thritis Rheum. 2006;55(2):199–207
7. Haverman L, Grootenhuis MA, van den BergJM, et al. Predictors of Health-RelatedQuality of Life in Children and AdolescentsWith Juvenile Idiopathic Arthritis: Resultsfrom a Web-based Survey. Hoboken, NJ: Ar-thritis Care Res; 2012
8. Velikova G, Booth L, Smith AB, et al. Mea-suring quality of life in routine oncologypractice improves communication and pa-tient well-being: a randomized controlledtrial. J Clin Oncol. 2004;22(4):714–724
9. Velikova G, Keding A, Harley C, et al.Patients report improvements in continuityof care when quality of life assessmentsare used routinely in oncology practice:secondary outcomes of a randomisedcontrolled trial. Eur J Cancer. 2010;46(13):2381–2388
10. Detmar SB, Muller MJ, Schornagel JH,Wever LD, Aaronson NK. Health-related
quality-of-life assessments and patient-physician communication: a randomizedcontrolled trial. JAMA. 2002;288(23):3027–3034
11. Taenzer P, Bultz BD, Carlson LE, et al. Impactof computerized quality of life screening onphysician behaviour and patient satisfac-tion in lung cancer outpatients. Psy-chooncology. 2000;9(3):203–213
12. Gutteling JJ, Darlington AS, Janssen HL,Duivenvoorden HJ, Busschbach JJ, de ManRA. Effectiveness of health-related quality-of-life measurement in clinical practice:a prospective, randomized controlled trialin patients with chronic liver disease andtheir physicians. Qual Life Res. 2008;17(2):195–205
13. Snyder CF, Aaronson NK. Use of patient-reported outcomes in clinical practice.Lancet. 2009;374(9687):369–370
14. Rubenstein LV, McCoy JM, Cope DW, et al.Improving patient quality of life with feed-back to physicians about functional status.J Gen Intern Med. 1995;10(11):607–614
15. Darby C. Patient/parent assessment of thequality of care. Ambul Pediatr. 2002;2(suppl4):345–348
16. Varni JW, Burwinkle TM, Lane MM. Health-related quality of life measurement in pe-diatric clinical practice: an appraisal andprecept for future research and applica-tion. Health Qual Life Outcomes. 2005;3:34
17. Engelen V, Detmar S, Koopman H, et al.Reporting health-related quality of lifescores to physicians during routine follow-up visits of pediatric oncology patients: is iteffective? Pediatr Blood Cancer. 2012;58(5):766–774
18. de Wit M, Delemarre-van de Waal HA,Bokma JA, et al. Monitoring and discussinghealth-related quality of life in adolescentswith type 1 diabetes improve psychosocialwell-being: a randomized controlled trial.Diabetes Care. 2008;31(8):1521–1526
19. Engelen V, Haverman L, Koopman H, et al.Development and implementation of a pa-tient reported outcome intervention (QLIC-ON PROfile) in clinical paediatric oncologypractice. Patient Educ Couns. 2010;81(2):235–244
20. Engelen V, van Zwieten M, Koopman H, et al.The influence of patient reported outcomes
on the discussion of psychosocial issues inchildren with cancer. Pediatr Blood Cancer.2012;59(1):161–166
21. Haverman L, Engelen V, van Rossum MA,Heymans HS, Grootenhuis MA. Monitoringhealth-related quality of life in paediatricpractice: development of an innovative web-based application. BMC Pediatr. 2011;11:3
22. Fekkes M, Theunissen NC, Brugman E, et al.Development and psychometric evaluationof the TAPQOL: a health-related quality oflife instrument for 1–5-year-old children.Qual Life Res. 2000;9(8):961–972
23. Fekkes M, Bruil J, Vogels T. TAPQOL Manual.Leiden, Netherlands: TNO Prevention andHealth; 2003
24. Varni JW, Burwinkle TM, Seid M, Skarr D.The PedsQL 4.0 as a pediatric populationhealth measure: feasibility, reliability, andvalidity. Ambul Pediatr. 2003;3(6):329–341
25. Engelen V, Haentjens MM, Detmar SB,Koopman HM, Grootenhuis MA. Health re-lated quality of life of Dutch children: psy-chometric properties of the PedsQL in theNetherlands. BMC Pediatr. 2009;9:68
26. Baars RM, Atherton CI, Koopman HM,Bullinger M, Power M; DISABKIDS group.The European DISABKIDS project: de-velopment of seven condition-specificmodules to measure health related qual-ity of life in children and adolescents.Health Qual Life Outcomes. 2005;3:70
27. Singh G, Athreya BH, Fries JF, Goldsmith DP.Measurement of health status in childrenwith juvenile rheumatoid arthritis. ArthritisRheum. 1994;37(12):1761–1769
28. Wulffraat N, van der Net JJ, Ruperto N, et al;Paediatric Rheumatology International Tri-als Organisation. The Dutch version of theChildhood Health Assessment Question-naire (CHAQ) and the Child Health Ques-tionnaire (CHQ). Clin Exp Rheumatol. 2001;19(4 suppl 23):S111–S115
29. Ong LM, Visser MR, Lammes FB, de Haes JC.Doctor-patient communication and cancerpatients’ quality of life and satisfaction.Patient Educ Couns. 2000;41(2):145–156
30. Zandbelt LC, Smets EM, Oort FJ, Godfried MH,de Haes HC. Satisfaction with the outpatientencounter: a comparison of patients’ andphysicians’ views. J Gen Intern Med. 2004;19(11):1088–1095
e542 HAVERMAN et alby guest on April 6, 2016Downloaded from

31. Santana MJ, Feeny D, Johnson JA, et al.Assessing the use of health-related qualityof life measures in the routine clinical careof lung-transplant patients. Qual Life Res.2010;19(3):371–379
32. de Haes H, Bensing J. Endpoints in medicalcommunication research, proposinga framework of functions and outcomes.Patient Educ Couns. 2009;74(3):287–294
33. Valderas JM, Kotzeva A, Espallargues M,et al. The impact of measuring patient-reported outcomes in clinical practice:a systematic review of the literature. QualLife Res. 2008;17(2):179–193
34. Marshall S, Haywood K, Fitzpatrick R. Im-pact of patient-reported outcome mea-sures on routine practice: a structuredreview. J Eval Clin Pract. 2006;12(5):559–568
35. Detmar SB, Aaronson NK. Quality of lifeassessment in daily clinical oncology
practice: a feasibility study. Eur J Cancer.1998;34(8):1181–1186
36. Filocamo G, Consolaro A, Schiappapietra B,et al. A new approach to clinical care ofjuvenile idiopathic arthritis: the JuvenileArthritis Multidimensional Assessment Re-port. J Rheumatol. 2011;38(5):938–953
37. Feldman BM, Grundland B, McCullough L,Wright V. Distinction of quality of life, healthrelated quality of life, and health status inchildren referred for rheumatologic care. JRheumatol. 2000;27(1):226–233
38. Snyder CF, Aaronson NK, Choucair AK, et al.Implementing patient-reported outcomesassessment in clinical practice: a review ofthe options and considerations. Qual LifeRes. 2012;21(8):1305–1314
39. Guyatt GH, Ferrans CE, Halyard MY, et al;Clinical Significance Consensus MeetingGroup. Exploration of the value of health-related quality-of-life information from
clinical research and into clinical practice[published correction appears in Mayo ClinProc. 2007;82(12)1579]. Mayo Clin Proc.2007;82(10):1229–1239
40. Varni JW, Limbers CA, Burwinkle TM, BryantWP, Wilson DP. The ePedsQL in type 1 andtype 2 diabetes: feasibility, reliability, andvalidity of the Pediatric Quality of Life In-ventory Internet administration. DiabetesCare. 2008;31(4):672–677
41. Hatzmann J, Heymans HS, Ferrer-i-CarbonellA, van Praag BM, Grootenhuis MA. Hiddenconsequences of success in pediatrics: pa-rental health-related quality of life—resultsfrom the Care Project. Pediatrics. 2008;122(5). Available at: www.pediatrics.org/cgi/content/full/122/5/e1030
42. Committee on Hospital Care and Institutefor Patient- and Family-Centered Care. Patient-and family-centered care and the pedia-trician’s role. Pediatrics. 2012;129(2):394–404
ARTICLE
PEDIATRICS Volume 131, Number 2, February 2013 e543by guest on April 6, 2016Downloaded from

DOI: 10.1542/peds.2012-0958; originally published online January 6, 2013; 2013;131;e533Pediatrics
Berg, Koert M. Dolman, Joost Swart, Taco W. Kuijpers and Martha A. GrootenhuisLotte Haverman, Marion A.J. van Rossum, Mira van Veenendaal, J. Merlijn van den
LifeEffectiveness of a Web-Based Application to Monitor Health-Related Quality of
ServicesUpdated Information &
/content/131/2/e533.full.htmlincluding high resolution figures, can be found at:
References
/content/131/2/e533.full.html#ref-list-1at:This article cites 40 articles, 10 of which can be accessed free
Citations /content/131/2/e533.full.html#related-urls
This article has been cited by 7 HighWire-hosted articles:
Subspecialty Collections
/cgi/collection/health_information_technology_subHealth Information Technologythe following collection(s):This article, along with others on similar topics, appears in
Permissions & Licensing
/site/misc/Permissions.xhtmltables) or in its entirety can be found online at: Information about reproducing this article in parts (figures,
Reprints /site/misc/reprints.xhtml
Information about ordering reprints can be found online:
rights reserved. Print ISSN: 0031-4005. Online ISSN: 1098-4275.Grove Village, Illinois, 60007. Copyright © 2013 by the American Academy of Pediatrics. All and trademarked by the American Academy of Pediatrics, 141 Northwest Point Boulevard, Elkpublication, it has been published continuously since 1948. PEDIATRICS is owned, published, PEDIATRICS is the official journal of the American Academy of Pediatrics. A monthly
by guest on April 6, 2016Downloaded from

DOI: 10.1542/peds.2012-0958; originally published online January 6, 2013; 2013;131;e533Pediatrics
Berg, Koert M. Dolman, Joost Swart, Taco W. Kuijpers and Martha A. GrootenhuisLotte Haverman, Marion A.J. van Rossum, Mira van Veenendaal, J. Merlijn van den
LifeEffectiveness of a Web-Based Application to Monitor Health-Related Quality of
/content/131/2/e533.full.html
located on the World Wide Web at: The online version of this article, along with updated information and services, is
of Pediatrics. All rights reserved. Print ISSN: 0031-4005. Online ISSN: 1098-4275.Boulevard, Elk Grove Village, Illinois, 60007. Copyright © 2013 by the American Academy published, and trademarked by the American Academy of Pediatrics, 141 Northwest Pointpublication, it has been published continuously since 1948. PEDIATRICS is owned, PEDIATRICS is the official journal of the American Academy of Pediatrics. A monthly
by guest on April 6, 2016Downloaded from