Effectiveness of a hand hygiene promotion strategy using alcohol-based handrub in 6 intensive care...
7
Effectiveness of a hand hygiene promotion strategy using alcohol-based handrub in 6 intensive care units in Colombia Lena Barrera, MD, MSc, a,b Walter Zingg, MD, c Fabian Mendez, MD, PhD, a and Didier Pittet, MD, MS c,d Cali, Colombia; and Geneva, Switzerland Background: Hand hygiene is an effective strategy for the prevention of health care-associated infection (HAI). We investigated the effect of a hand hygiene promotion strategy introducing alcohol-based handrub (AHBR) on the incidence of HAI in a university hospital in Colombia. Methods: A Prospective cohort study was performed in 6 intensive care units from January 2001 to December 2005. HAI were iden- tified using standard US Centers for Disease Control and Prevention definitions. Alcohol-based handrub dispensers were installed between February and June 2002. Results: Total ABHR consumption was 5,794 L (mean, 28.9 L per 1,000 patient-days) and significantly increased over time (19.2% per year; P , .001). Of 14,516 patients cumulating 166,498 patient-days, 2,398 (16.5%) acquired a total of 3,490 HAI episodes (20.9 per 1,000 patient-days). Incidence densities for central line-associated bloodstream infection (CLABSI), ventilator- associated pneumonia, and urinary tract infections were 7.7, 10.6, and 3.6 episodes per 1,000device-days, respectively. A signif- icant decrease was observed for CLABSI (212.7% per year; P , .001) with low nurse-to-patient ratio independently associated with infection (odds ratio, 1.11; 95% confidence interval: 1.07-1.16; P , .001). Conclusion: Improved hand hygiene measured by increased ABHR consumption resulted in CLABSI reduction. Low nurse- to-patient ratio is independently associated with HAI in an upper-middle income country. Key Words: Hand hygiene; alcohol-based handrub; health care-associated infections; central line-associated bloodstream infec- tions; Acinetobacter baumannii; methicillin-resistant Staphylococcus aureus; MRSA. Copyright ª 2011 by the Association for Professionals in Infection Control and Epidemiology, Inc. Published by Elsevier Inc. All rights reserved. (Am J Infect Control 2011;39:633-9.) Health care workers’ (HCW) hands are the most important source of health care-associated infection (HAI), 1-4 and hand hygiene is a critical strategy for pre- vention. 5,6 However, compliance with hand hygiene is low, especially among physicians. 5,7-10 The introduction of alcohol-based handrub (ABHR) has improved hand hygiene compliance because its use has several advan- tages over handwashing in daily practice. 5,7,11,12 Most reports of the successful introduction of ABHR have been conducted in high-income countries, 5,7,13-16 and data from low- and middle income countries on the efficacy of hand hygiene promotion, including the introduction of ABHR, are sparse. 17-19 In 2001, the directorate of the University Hospital of Valle in Cali, Colombia, decided to introduce ABHR for hand hygiene in an attempt to control an ongoing outbreak due to Acinetobacter baumannii. The objective of this study was to monitor prospectively the effect of a hand hygiene promotion strategy including the intro- duction of ABHR on HAI and more specifically on device-associated HAIs, such as central line-associated bloodstream infections (CLABSI), ventilator-associated pneumonia (VAP), and urinary tract infections (UTI). We also compare our findings with the results of pub- lished studies in high-income countries. METHODS Setting A prospective cohort study was conducted from Jan- uary 2001 to December 2005 in the intensive care units (ICU) of the University Hospital of Valle, Cali, Colombia. From the Department of Internal Medicine and School of Public Health, University of Valle, Cali, Colombia a ; Epidemiology Unit, University Hos- pital of Valle, Cali, Colombia b ; Infection Control Program, University of Geneva Hospitals and Faculty of Medicine, Geneva, Switzerland c ; and World Health Organization Collaborating Center on Patient Safety, d University of Geneva Hospitals and Faculty of Medicine, Geneva, Switzerland. Address correspondence to Didier Pittet, MD, MS, professor, Infection Control Program, University of Geneva Hospitals and Faculty of Medicine, 4 Rue Gabrielle Perret-Gentil, 1211 Geneva 14, Switzerland. E-mail: [email protected]. Conflicts of interest: None to report. 0196-6553/$36.00 Copyright ª 2011 by the Association for Professionals in Infection Control and Epidemiology, Inc. Published by Elsevier Inc. All rights reserved. doi:10.1016/j.ajic.2010.11.004 633
-
Upload
independent -
Category
Documents
-
view
3 -
download
0
Transcript of Effectiveness of a hand hygiene promotion strategy using alcohol-based handrub in 6 intensive care...

FUpGWUS
ACM
E
C
0
CCr
d
Effectiveness of a hand hygienepromotion strategy using alcohol-basedhandrub in 6 intensive care unitsin Colombia
Lena Barrera, MD, MSc,a,b Walter Zingg, MD,c Fabian Mendez, MD, PhD,a and Didier Pittet, MD, MSc,dCali, Colombia; and Geneva, Switzerland
romniveital oeneorlnivewitz
ddrontedi
-mai
onfl
196
opyonteser
oi:1
Background: Hand hygiene is an effective strategy for the prevention of health care-associated infection (HAI). We investigated theeffect of a hand hygiene promotion strategy introducing alcohol-based handrub (AHBR) on the incidence of HAI in a universityhospital in Colombia.Methods: A Prospective cohort study was performed in 6 intensive care units from January 2001 to December 2005. HAI were iden-tified using standard US Centers for Disease Control and Prevention definitions. Alcohol-based handrub dispensers were installedbetween February and June 2002.Results: Total ABHR consumption was 5,794 L (mean, 28.9 L per 1,000 patient-days) and significantly increased over time (19.2%per year; P , .001). Of 14,516 patients cumulating 166,498 patient-days, 2,398 (16.5%) acquired a total of 3,490 HAI episodes(20.9 per 1,000 patient-days). Incidence densities for central line-associated bloodstream infection (CLABSI), ventilator-associated pneumonia, and urinary tract infections were 7.7, 10.6, and 3.6 episodes per 1,000 device-days, respectively. A signif-icant decrease was observed for CLABSI (212.7% per year; P, .001) with low nurse-to-patient ratio independently associated withinfection (odds ratio, 1.11; 95% confidence interval: 1.07-1.16; P , .001).Conclusion: Improved hand hygiene measured by increased ABHR consumption resulted in CLABSI reduction. Low nurse-to-patient ratio is independently associated with HAI in an upper-middle income country.Key Words: Hand hygiene; alcohol-based handrub; health care-associated infections; central line-associated bloodstream infec-tions; Acinetobacter baumannii; methicillin-resistant Staphylococcus aureus; MRSA.
Copyright ª 2011 by the Association for Professionals in Infection Control and Epidemiology, Inc. Published by Elsevier Inc. All rightsreserved. (Am J Infect Control 2011;39:633-9.)
Health care workers’ (HCW) hands are the mostimportant source of health care-associated infection(HAI),1-4 and hand hygiene is a critical strategy for pre-vention.5,6 However, compliance with hand hygiene islow, especially among physicians.5,7-10 The introductionof alcohol-based handrub (ABHR) has improved handhygiene compliance because its use has several advan-tages over handwashing in daily practice.5,7,11,12 Most
the Department of Internal Medicine and School of Public Health,rsity of Valle, Cali, Colombiaa; Epidemiology Unit, University Hos-f Valle, Cali, Colombiab; Infection Control Program, University ofva Hospitals and Faculty of Medicine, Geneva, Switzerlandc; andd Health Organization Collaborating Center on Patient Safety,d
rsity of Geneva Hospitals and Faculty of Medicine, Geneva,erland.
ess correspondence to Didier Pittet, MD, MS, professor, Infectionrol Program, University of Geneva Hospitals and Faculty ofcine, 4 Rue Gabrielle Perret-Gentil, 1211 Geneva 14, Switzerland.
icts of interest: None to report.
-6553/$36.00
right ª 2011 by the Association for Professionals in Infectionrol and Epidemiology, Inc. Published by Elsevier Inc. All rightsved.
0.1016/j.ajic.2010.11.004
reports of the successful introduction of ABHR havebeen conducted in high-income countries,5,7,13-16 anddata from low- and middle income countries on theefficacy of hand hygiene promotion, including theintroduction of ABHR, are sparse.17-19
In 2001, the directorate of the University Hospital ofValle in Cali, Colombia, decided to introduce ABHR forhand hygiene in an attempt to control an ongoingoutbreak due toAcinetobacter baumannii. The objectiveof this studywas tomonitor prospectively the effect of ahand hygiene promotion strategy including the intro-duction of ABHR on HAI and more specifically ondevice-associated HAIs, such as central line-associatedbloodstream infections (CLABSI), ventilator-associatedpneumonia (VAP), and urinary tract infections (UTI).We also compare our findings with the results of pub-lished studies in high-income countries.
METHODS
Setting
A prospective cohort study was conducted from Jan-uary 2001 to December 2005 in the intensive care units(ICU) of the University Hospital of Valle, Cali, Colombia.
633

634 Barrera et al. American Journal of Infection ControlOctober 2011
The institution is a 715-bed teaching hospital serving apopulation of 4.1 million and a referral center withinthe Colombian Health Services System. The followingICUs were included in the study: general (internal med-icine and cardiovascular surgery), 10 beds; trauma,8 beds; neurosurgery, 4 beds; burn, 15 beds; pediatric(PICU), 7 beds; and neonatology (NICU), 40 beds. Base-line data from 2001 were retrieved retrospectively fromexisting surveillance records. The study protocol wasapproved by the Institutional Review Board.
HAI were identified using standard US Centers forDisease Control and Prevention (CDC) definitions.20,21
Incidence rates were reported as incidence densities:events per 1,000 patient-days for all HAI and per1,000 device-days for specific device-associated infec-tions (CLABSI, VAP, and UTI). Central venous catheterand tracheal tube utilization was defined as totaldevice-days per total patient-days. ABHR use was quan-tified in liters per 1,000 patient-days per month. HCW’swork experience was defined as the mean of annualperson-years per unit. The proportion of temporaryworkers was defined as the monthly rate of temporaryworkers per unit. Nurse-to-patient ratio was defined asbeds per nurse per shift. Mortality was defined as crudein-hospital mortality. HAI-associated mortality wasdefined as in-hospital death from HAI.
Intervention
Between February and June 2002, ABHR dispenserswere introduced in the ICUs simultaneous to educa-tional sessions including information on hand hygieneand practical instructions on how to use ABHR. EachICU bed/place was equipped with a dispenser, and bot-tles (500 mL) were replaced twice weekly. The ABHRformulation consisted of 67% ethanol and skin emol-lients and was produced in-house by the hospital phar-macy. ICU teams were also provided with quarterlyfeedback about their HAI rates. There was no specificstrategy for CLABSI prevention, in particular no intra-venous line placement teams, change in line care, orthe use of technologies such as impregnated cathetersor chlorhexidine sponges.
Surveillance activities
Prospective daily surveillance included HAI anddevice use (central lines, tracheal tubes, urinary cathe-ters). Information on ABHR consumption, work experi-ence, temporary workers, and nurse-to-patient ratiowas retrieved from the pharmacy database, human re-sources, and the nursing coordination register, respec-tively. Daily surveillance was conducted by trainedinfection control nurses and an epidemiology team us-ing predefined case report forms.22 The following var-iables were collected: age; sex; length of ICU stay;
device-days; type and date of onset of HAI; anddeath. The primary outcome parameters were HAI andCLABSI, VAP, and UTI. The secondary outcome parame-ter was ABHR consumption.5 Variables such as workexperience and nurse-to-patient ratio were tested forindependent association with HAI.23 Disagreementsbetween infection control nurses and members of theepidemiology team on infection surveillance were dis-cussed at weekly meetings with the study physician.All final case report forms were validated by the studyphysician (L.I.B.) before data entry.
Statistical analysis
Incidence and incidence densities of HAI, CLABSI,VAP, and UTI were computed for the different ICUs.Annual trends and risk for HAI and CLABSI were com-pared using Poisson regression.24,25 Because compli-ance with ABHR use may have varied between theICUs, as did patient populations, we adjusted for intra-group correlation by specifying each unit as a cluster.Two sided P values of .05 were considered statisticallysignificant. Results were reported as correlation coeffi-cients for trends and incidence rate ratios for risk anal-ysis. Data were analyzed using STATA version 10 (StataCorporation, College Station, TX).
RESULTS
Between January 2001 and December 2005, a totalof 14,516 patients cumulating 166,498 patient-dayswere hospitalized in the study ICUs. Main patient andICU characteristics are summarized in Table 1. Lengthof ICU stay averaged 11.5 (64.4) days and varied mark-edly according to the type of ICU (Table 1). Central ve-nous catheter utilization ranged between 10% (burnunit) and 74% (trauma ICU). Endotracheal tube utiliza-tion ranged between 14% (NICU) and 70% (traumaICU). There was no significant trend toward increasedor reduced device utilization over time. Crude mortalitywas 20.5% (2,975/14,516), and HAI-associated mortal-ity was 5.3% (775/14,516) without significant trendover time (P 5 .436).
A total of 5794 L of ABHR was distributed by the hos-pital pharmacy for an average of 43.2 L per 1,000patient-days between 2001 and 2005. Monthly ABHRuse increased linearly from February 2002 (19.2%per year; P , .001) (Fig 1).
Overall, 16.5% (2,398/14,516 patients) developedHAI over the study period, with proportions varyingfrom 9.5% to 21.4% according to the type of ICU(Table 1). A total of 3,490 HAIs was detected among2,398 patients. Among HAI patients, 896 (31.3%)were identified with 2 or more infections. The overallincidence and incidence density were 24 per 100 pa-tients and 20.9 per 1,000 patient-days, respectively.
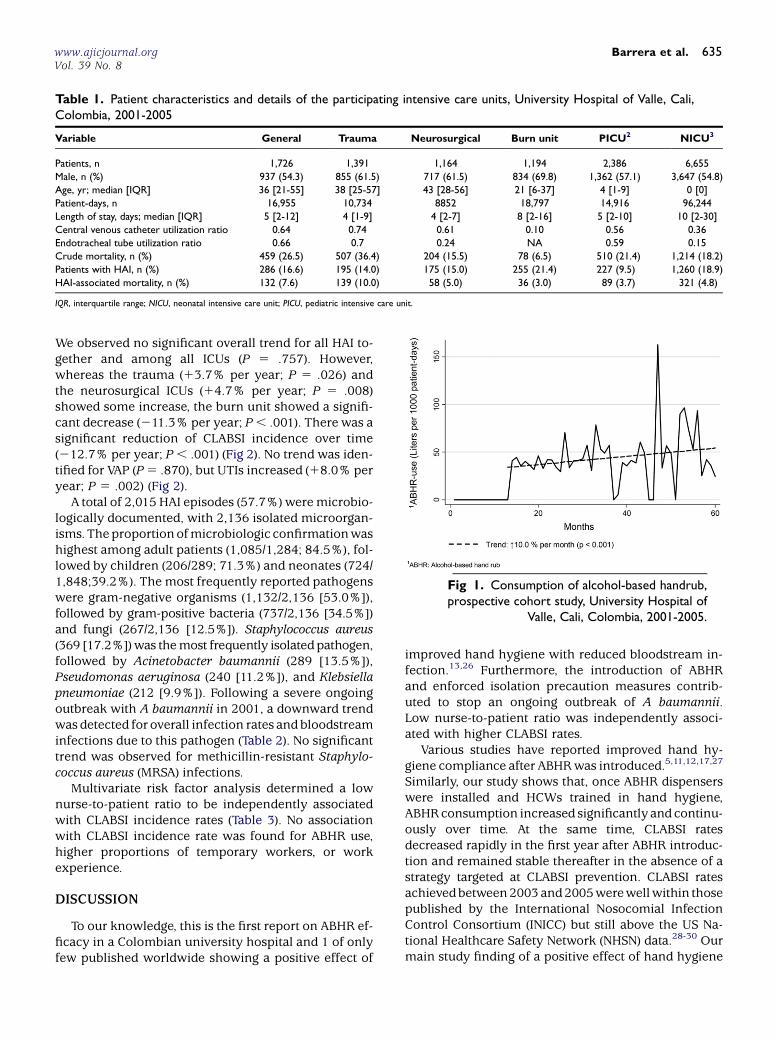
Table 1. Patient characteristics and details of the participating intensive care units, University Hospital of Valle, Cali,Colombia, 2001-2005
Variable General Trauma Neurosurgical Burn unit PICU2 NICU3
Patients, n 1,726 1,391 1,164 1,194 2,386 6,655
Male, n (%) 937 (54.3) 855 (61.5) 717 (61.5) 834 (69.8) 1,362 (57.1) 3,647 (54.8)
Age, yr; median [IQR] 36 [21-55] 38 [25-57] 43 [28-56] 21 [6-37] 4 [1-9] 0 [0]
Patient-days, n 16,955 10,734 8852 18,797 14,916 96,244
Length of stay, days; median [IQR] 5 [2-12] 4 [1-9] 4 [2-7] 8 [2-16] 5 [2-10] 10 [2-30]
Central venous catheter utilization ratio 0.64 0.74 0.61 0.10 0.56 0.36
Endotracheal tube utilization ratio 0.66 0.7 0.24 NA 0.59 0.15
Crude mortality, n (%) 459 (26.5) 507 (36.4) 204 (15.5) 78 (6.5) 510 (21.4) 1,214 (18.2)
Patients with HAI, n (%) 286 (16.6) 195 (14.0) 175 (15.0) 255 (21.4) 227 (9.5) 1,260 (18.9)
HAI-associated mortality, n (%) 132 (7.6) 139 (10.0) 58 (5.0) 36 (3.0) 89 (3.7) 321 (4.8)
IQR, interquartile range; NICU, neonatal intensive care unit; PICU, pediatric intensive care unit.
Fig 1. Consumption of alcohol-based handrub,prospective cohort study, University Hospital of
Valle, Cali, Colombia, 2001-2005.
www.ajicjournal.orgVol. 39 No. 8
Barrera et al. 635
We observed no significant overall trend for all HAI to-gether and among all ICUs (P 5 .757). However,whereas the trauma (13.7% per year; P 5 .026) andthe neurosurgical ICUs (14.7% per year; P 5 .008)showed some increase, the burn unit showed a signifi-cant decrease (211.3% per year; P, .001). There was asignificant reduction of CLABSI incidence over time(212.7% per year; P, .001) (Fig 2). No trend was iden-tified for VAP (P5 .870), but UTIs increased (18.0% peryear; P 5 .002) (Fig 2).
A total of 2,015 HAI episodes (57.7%) weremicrobio-logically documented, with 2,136 isolated microorgan-isms. Theproportionofmicrobiologic confirmationwashighest among adult patients (1,085/1,284; 84.5%), fol-lowed by children (206/289; 71.3%) and neonates (724/1,848;39.2%). The most frequently reported pathogenswere gram-negative organisms (1,132/2,136 [53.0%]),followed by gram-positive bacteria (737/2,136 [34.5%])and fungi (267/2,136 [12.5%]). Staphylococcus aureus(369 [17.2%])was themost frequently isolatedpathogen,followed by Acinetobacter baumannii (289 [13.5%]),Pseudomonas aeruginosa (240 [11.2%]), and Klebsiellapneumoniae (212 [9.9%]). Following a severe ongoingoutbreak with A baumannii in 2001, a downward trendwasdetected foroverall infection rates and bloodstreaminfections due to this pathogen (Table 2). No significanttrend was observed for methicillin-resistant Staphylo-coccus aureus (MRSA) infections.
Multivariate risk factor analysis determined a lownurse-to-patient ratio to be independently associatedwith CLABSI incidence rates (Table 3). No associationwith CLABSI incidence rate was found for ABHR use,higher proportions of temporary workers, or workexperience.
DISCUSSION
To our knowledge, this is the first report on ABHR ef-ficacy in a Colombian university hospital and 1 of onlyfew published worldwide showing a positive effect of
improved hand hygiene with reduced bloodstream in-fection.13,26 Furthermore, the introduction of ABHRand enforced isolation precaution measures contrib-uted to stop an ongoing outbreak of A baumannii.Low nurse-to-patient ratio was independently associ-ated with higher CLABSI rates.
Various studies have reported improved hand hy-giene compliance after ABHRwas introduced.5,11,12,17,27
Similarly, our study shows that, once ABHR dispenserswere installed and HCWs trained in hand hygiene,ABHRconsumption increased significantly and continu-ously over time. At the same time, CLABSI ratesdecreased rapidly in the first year after ABHR introduc-tion and remained stable thereafter in the absence of astrategy targeted at CLABSI prevention. CLABSI ratesachievedbetween2003 and2005werewellwithin thosepublished by the International Nosocomial InfectionControl Consortium (INICC) but still above the US Na-tional Healthcare Safety Network (NHSN) data.28-30 Ourmain study finding of a positive effect of hand hygiene

Fig 2. Trends of health care-associated infections, prospective cohort study, University Hospital of Valle, Cali,Colombia, 2001-2005.
636 Barrera et al. American Journal of Infection ControlOctober 2011
on infection as shown by increased use of ABHR and de-creased CLABSI confirms similar findings, such as thoseby Pessoa-Silva et al.13 Whereas those authors observeda significant reduction among clonally-related patho-gens only, and thus proving the positive effect of handhygiene on pathogen cross transmission, we detectedan overall reduction of all CLABSI episodes.
Although the effect ofABHRonCLABSI reductionwasencouraging, we did not observe a similar effect on VAPor UTI. Our VAP rates, although lower compared to themost recent INICC report, remained stable over timewith no upward or downward trend.28,29 In contrast toCLABSI where hand hygiene ismore likely to play ama-jor role in prevention,13,26,31 variables other than handhygiene are likely to bemore important as part of amul-timodal intervention strategy for VAP prevention.32,33 Incontrast, UTI rates increased, although only in 2005, fol-lowing low rates reported for several years.28,29 Unfor-tunately, we have no explanation for this trend.
Simultaneous to the installation of ABHR dispensers,HCWs were offered education on the efficacy of handhygiene and trained in the use of ABHR in daily prac-tice. Furthermore, units were given regular feedback
about their HAI rates. Education and performance feed-back are widely used in HAI prevention, and their effi-cacy has been well demonstrated.5,7,17,34 Becauseeducation and performance feedback often go togetherwith the introduction of ABHR, it is difficult to distin-guish among their single effect on infection preven-tion.5,13,17 The same is true for our study, and, thus,we cannot further contribute to this study question.
The most important gram-negative pathogen associ-ated with HAI in our study was A baumannii. Prior tothe introduction of ABHR, institutional policy was al-ready set to place patients colonized or infected withA baumannii in contact isolation.35 However, ABHRuse contributed to terminate the outbreak and reduceA baumannii infection rates by almost 50%. AlthoughABHR use concomitant to hand hygiene improvementhas been repeatedly shown to reduce MRSA infec-tions,5,15,36-38 our overall rates did not change withthe sole exception of the NICU where a significantdownward trend was detected.
Our observation of low nurse-to-patient ratio beingindependently associated with CLABSI confirms datafrom Hugonnet et al39 and others40 describing staffing

Table 2. Infection trends for Acinetobacter baumannii and methicillin-resistant Staphylococcus aureus among participatingICUs, prospective cohort study, University Hospital of Valle, Cali, Colombia, 2001-2005
Year General Trauma Neurosurgical Burn unit PICU NICU Total
Acinetobacter baumannii: incidence density (infections per 1,000 patient-days)
2001 6.6 5.3 5.6 5.7 2.6 0.6 2.5
2002 3.8 7.2 1.7 1.6 1.1 0.1 1.3
2003 3.8 4.1 1.2 3.1 1.3 0.1 1.3
2004 3.2 2.8 1.1 3.2 0.9 0.3 1.2
2005 5.3 6.2 1.2 2.8 0.6 0.2 1.5
Trend No trend 29.3% 215.5% 218.4% No trend No trend 28.4%
P value ns .012 .017 ,.001 ns ns .022
MRSA: Incidence density (infections per 1,000 patient-days)
2001 5.4 2.4 3.0 2.2 3.0 2.2 2.7
2002 5.3 4.8 2.3 2.1 1.8 0.6 1.7
2003 5.0 3.6 4.4 1.4 0.3 0.6 1.5
2004 1.4 4.3 2.7 1.7 0.9 1.1 1.5
2005 6.5 6.7 8.9 2.3 1.3 0.6 2.3
Trend 29.0% No trend 112.3% No trend No trend 229.8% No trend
P value .022 ns .004 ns ns .001 ns
MRSA, methicillin-resistant Staphylococcus aureus; NICU, neonatal intensive care unit; PICU, pediatric intensive care unit; Trend, change of incidence density per year.
Table 3. Risk factors for central line-associated bloodstream infection, prospective cohort study, University Hospital ofValle, Cali, Colombia, 2001-2005
Variable
Univariate analysis Multivariate analysis
IRR 95% CI P value IRR 95% CI P value
Year* 0.88 0.80-0.96 .006 0.89 0.80-0.98 .015
Use of ABHR 1.00 0.99-1.00 .241 – – –
Work experience 0.98 0.92-1.00 .552 – – –
Temporary workers* 0.99 0.98-1.00 .143 – – –
Nurse-to-patient ratio* 1.12 1.09-1.15 ,.001 1.11 1.07-1.16 ,.001
ABHR, alcohol-based handrub consumption in liters per 1,000 patient-days; CI, confidence interval; IRR, incidence rate ratio.
*Included in the multivariate analysis.
www.ajicjournal.orgVol. 39 No. 8
Barrera et al. 637
as a key determinant of HAI in critically ill patients.This finding is important because most informationabout staffing in the context of HAI comes from high-income countries39-41; our data strongly suggest thatunderstaffing may be a universal problem in all hospi-tal settings, irrespective of available resources.
The current study has several limitations. We did notperformdirect observationof handhygiene, recommen-ded as the gold standard for compliance monitoring,7
and only monitored ABHR consumption. The latteris considered as a surrogate marker for compliance5
but is recognized to be inferior to direct hand hygieneobservation.7 Only direct hand hygiene observationcan reveal whether ABHR was used at appropriatetimes42 and whether the introduction of ABHR wasequally associatedwith increased or decreased recourseto soap and water handwashing. Furthermore, the
ethanol content of our ABHRproductwas only 67%. An-other product, preferably containing $80% alcohol,7
may have been more effective in HAI reduction.In conclusion, we demonstrate that ABHR use has
the potential to reduce CLABSI rates rapidly and witha sustained effect when accompanied by educationand feedback. Although we could not demonstrate apositive effect against MRSA, we did show that im-proved hand hygiene together with contact precautionmeasures has the potential to stop outbreaks due toA baumannii. The at-risk analysis highlighted alsothat low nurse-to-patient ratio is as an independentrisk factor in upper-middle income countries, similarto high-income countries.
We thank Hilda Mary Gomez, Sandra Ossa, Magnolia Diaz, Alejandro Zu~niga, JulietaJaramillo, Ernesto Martinez, and Luz Marina Cuellar for their support, and RosemarySudan for editorial assistance.

638 Barrera et al. American Journal of Infection ControlOctober 2011
References
1. Pittet D, Allegranzi B, Sax H, Dharan S, Pessoa-Silva CL, Donaldson L,
et al. Evidence-based model for hand transmission during patient
care and the role of improved practices. Lancet Infect Dis 2006;6:
641-52.
2. Ehrenkranz NJ, Alfonso BC. Failure of bland soap handwash to pre-
vent hand transfer of patient bacteria to urethral catheters. Infect
Control Hosp Epidemiol 1991;12:654-62.
3. Marples RR, Towers AG. A laboratory model for the investigation of
contact transfer of micro-organisms. J Hyg (Lond) 1979;82:237-48.
4. Grundmann H, Hori S, Winter B, Tami A, Austin DJ. Risk factors for
the transmission of methicillin-resistant Staphylococcus aureus in an
adult intensive care unit: fitting a model to the data. J Infect Dis
2002;185:481-8.
5. Pittet D, Hugonnet S, Harbarth S, Mourouga P, Sauvan V, Touveneau S,
et al. Effectiveness of a hospital-wide programme to improve compli-
ance with hand hygiene. Infection Control Programme. Lancet 2000;
356:1307-12.
6. Boyce JM, Pittet D. Guideline for hand hygiene in health-care settings.
Recommendations of the Healthcare Infection Control Practices Ad-
visory Committee and the HICPAC/SHEA/APIC/IDSA Hand Hygiene
Task Force. Society for Healthcare Epidemiology of America/Associa-
tion for Professionals in Infection Control/Infectious Diseases Society
of America. MMWR Recomm Rep. 2002;51:1-45, quiz CE1-4.
7. World Health Organization. WHO guidelines for hand hygiene in
health care. Geneva: World Health Organization; 2009.
8. Pittet D, Simon A, Hugonnet S, Pessoa-Silva CL, Sauvan V, Perneger
TV. Hand hygiene among physicians: performance, beliefs, and percep-
tions. Ann Intern Med 2004;141:1-8.
9. Pittet D. Improving compliance with hand hygiene in hospitals. Infect
Control Hosp Epidemiol 2000;21:381-6.
10. O’Boyle CA, Henly SJ, Larson E. Understanding adherence to hand hy-
giene recommendations: the theory of planned behavior. Am J Infect
Control 2001;29:352-60.
11. Bischoff WE, Reynolds TM, Sessler CN, Edmond MB, Wenzel RP.
Handwashing compliance by health care workers: the impact of intro-
ducing an accessible, alcohol-based hand antiseptic. Arch Intern Med
2000;160:1017-21.
12. Girard R, Amazian K, Fabry J. Better compliance and better tolerance
in relation to a well-conducted introduction to rub-in hand disinfec-
tion. J Hosp Infect 2001;47:131-7.
13. Pessoa-Silva CL, Hugonnet S, Pfister R, Touveneau S, Dharan S, Posfay-
Barbe K, et al. Reduction of health care associated infection risk in ne-
onates by successful hand hygiene promotion. Pediatrics 2007;120:
e382-90.
14. Sax H, Uckay I, Richet H, Allegranzi B, Pittet D. Determinants of good
adherence to hand hygiene among healthcare workers who have ex-
tensive exposure to hand hygiene campaigns. Infect Control Hosp Ep-
idemiol 2007;28:1267-74.
15. Grayson ML, Jarvie LJ, Martin R, Johnson PD, Jodoin ME, McMullan C,
et al. Significant reductions in methicillin-resistant Staphylococcus au-
reus bacteraemia and clinical isolates associated with a multisite,
hand hygiene culture-change program and subsequent successful
statewide roll-out. Med J Aust 2008;188:633-40.
16. Johnson PD, Martin R, Burrell LJ, Grabsch EA, Kirsa SW, O’Keeffe J,
et al. Efficacy of an alcohol/chlorhexidine hand hygiene program in a
hospital with high rates of nosocomial methicillin-resistant Staphylococ-
cus aureus (MRSA) infection. Med J Aust 2005;183:509-14.
17. Allegranzi B, Sax H, Bengaly L, Richet H, Minta DK, Chraiti MN, et al.
Successful implementation of the World Health Organization hand hy-
giene improvement strategy in a referral hospital in Mali, Africa. Infect
Control Hosp Epidemiol 2010;31:133-41.
18. Allegranzi B, Pittet D. Healthcare-associated infection in developing
countries: simple solutions to meet complex challenges. Infect Con-
trol Hosp Epidemiol 2007;28:1323-7.
19. Marra AR, D’Arco C, Bravim Bde A, Martino MD, Correa L, Silva CV,
et al. Controlled trial measuring the effect of a feedback intervention
on hand hygiene compliance in a step-down unit. Infect Control Hosp
Epidemiol 2008;29:730-5.
20. Garner JS, Jarvis WR, Emori TG, Horan TC, Hughes JM. CDC defini-
tions for nosocomial infections, 1988. Am J Infect Control 1988;16:
128-40.
21. Horan TC, Emori TG. Definitions of key terms used in the NNIS Sys-
tem. Am J Infect Control 1997;25:112-6.
22. Horan TC, Gaynes RP. Surveillance of noscomial infections. In: Mayhall
CG, editor. Hospital epidemiology and infection control. 3rd ed.
Philadelphia: Lippincott Williams & Wilkins; 2004. p. 1559-702.
23. Hugonnet S, Villaveces A, Pittet D. Nurse staffing level and nosocomial
infections: empirical evaluation of the case-crossover and case-time-
control designs. Am J Epidemiol 2007;165:1321-7.
24. Berry JG, Harrison JE. A guide to statistical methods for injury surveil-
lance. Adelaide: Australian Institute of Health and Welfare; 2005.
25. Lizan-Garcia M, Peyro R, Cortina M, Crespo MD, Tobias A. Nosoco-
mial infection surveillance in a surgical intensive care unit in Spain,
1996-2000: a time-trend analysis. Infect Control Hosp Epidemiol
2006;27:54-9.
26. Zingg W, Imhof A, Maggiorini M, Stocker R, Keller E, Ruef C. Impact of
a prevention strategy targeting hand hygiene and catheter care on the
incidence of catheter-related bloodstream infections. Crit Care Med
2009;37:2167-73 quiz 80.
27. Pittet D. Improving adherence to hand hygiene practice: a multidisci-
plinary approach. Emerg Infect Dis 2001;7:234-40.
28. Edwards JR, PetersonKD,Mu Y, Banerjee S, Allen-Bridson K, Morrell G,
et al. National Healthcare Safety Network (NHSN) report: data sum-
mary for 2006 through 2008, issued December 2009. Am J Infect Con-
trol 2009;37:783-805.
29. Rosenthal VD, Maki DG, Jamulitrat S, Medeiros EA, Todi SK, GomezDY,
et al. International Nosocomial Infection Control Consortium (INICC)
report, data summary for 2003-2008, issued June 2009. Am J Infect
Control. 2010;38:95-104.e2.
30. Moreno CA, Rosenthal VD, Olarte N, Gomez WV, Sussmann O,
Agudelo JG, et al. Device-associated infection rate and mortality in
intensive care units of 9 Colombian hospitals: findings of the Interna-
tional Nosocomial Infection Control Consortium. Infect Control
Hosp Epidemiol 2006;27:349-56.
31. Eggimann P, Harbarth S, Constantin MN, Touveneau S, Chevrolet JC,
Pittet D. Impact of a prevention strategy targeted at vascular-access
care on incidence of infections acquired in intensive care. Lancet
2000;355:1864-8.
32. Bouadma L, Mourvillier B, Deiler V, Le Corre B, Lolom I, R�egnier B,
et al. A multifaceted program to prevent ventilator-associated pneu-
monia: impact on compliance with preventive measures. Crit Care
Med 2010;38:789-96.
33. Pittet D, Zingg W. Reducing ventilator-associated pneumonia: when
process control allows outcome improvement and even benchmark-
ing. Crit Care Med;38:983-4.
34. Rosenthal VD, Guzman S, Pezzotto SM, Crnich CJ. Effect of an in-
fection control program using education and performance feedback
on rates of intravascular device-associated bloodstream infections
in intensive care units in Argentina. Am J Infect Control 2003;31:
405-9.
35. Trick WE, Vernon MO, Welbel SF, Demarais P, Hayden MK, Weinstein
RA. Multicenter intervention program to increase adherence to hand
hygiene recommendations and glove use and to reduce the incidence
of antimicrobial resistance. Infect Control Hosp Epidemiol 2007;28:
42-9.
36. Brown SM, Lubimova AV, Khrustalyeva NM, Shulaeva SV, Tekhova I,
Zueva LP, et al. Use of an alcohol-based hand rub and quality improve-
ment interventions to improve hand hygiene in a Russian neonatal in-
tensive care unit. Infect Control Hosp Epidemiol 2003;24:172-9.

www.ajicjournal.orgVol. 39 No. 8
Barrera et al. 639
37. Gordin FM, Schultz ME, Huber RA, Gill JA. Reduction in nosoco-
mial transmission of drug-resistant bacteria after introduction of
an alcohol-based handrub. Infect Control Hosp Epidemiol 2005;
26:650-3.
38. Ng PC, Wong HL, Lyon DJ, So KW, Liu F, Lam RK, et al. Combined use
of alcohol hand rub and gloves reduces the incidence of late onset in-
fection in very low birthweight infants. Arch Dis Child Fetal Neonatal
Ed 2004;89:F336-40.
39. Hugonnet S, Chevrolet JC, Pittet D. The effect of workload on infec-
tion risk in critically ill patients. Crit Care Med 2007;35:76-81.
40. Fridkin SK, Pear SM, Williamson TH, Galgiani JN, Jarvis WR. The role
of understaffing in central venous catheter-associated bloodstream in-
fections. Infect Control Hosp Epidemiol 1996;17:150-8.
41. Needleman J, Buerhaus P, Mattke S, Stewart M, Zelevinsky K. Nurse-
staffing levels and the quality of care in hospitals. N Engl J Med 2002;
346:1715-22.
42. Sax H, Allegranzi B, Uckay I, Larson E, Boyce J, Pittet D. ‘‘My five mo-
ments for hand hygiene’’: a user-centred design approach to under-
stand, train, monitor and report hand hygiene. J Hosp Infect 2007;
67:9-21.