
Effect of tumor size on the prognosis of carcinoma of the uterine cervix treated with irradiation...
11
2796 Effect of Tumor Size on the Prognosis of Carcinoma of the Uterine Cervix Treated With Irradiation Alone Carlos A. Perez, MD,* Perry W. Grigsby, MD,* Shriram M. Nene, H. Marvin Camel, MD,t Andrew Galakafos, MD,t Ming-Shian Kao, MD,t and Mary Ann Locketf, MBA* The authors conducted a retrospective analysis of 1178 patients with histologically proven invasive carcinoma of the uterine cervix treated with irradiation alone. The minimum follow-up time was 3 years. The 10-year ac- tuarial pelvic failure rate in Stage IB was 6% for tumors less than 3 cm, 15% for tumors 3 to 5 cm, and 30% for tumors more than 5 cm (P = 0.0018). The 10-year actuar- ial pelvic failure rate in Stage IIA was 10% for tumors less than 3 cm, 28% for tumors 3 to 5 cm, and 20% for tumors more than 5 cm (P = 0.09). Stage IIB unilateral nonbulky tumors (less than 5 cm) had a 20% pelvic fail- ure rate compared with 28% for bilateral lesions and 35% for unilateral bulky tumors (more than 5 cm) (P = 0.35). In Stage IIB, pelvic failures were greater when disease extended into the lateral parametrium (30%) compared with medial parametrial involvement only (17%) (P = 0.01). In Stage I11 unilateral nonbulky tumors, the pel- vic failure rate was 28% compared with 45% to 50% for unilateral bulky lesions (P = 0.002). Bilateral parametrial disease in Stage IIB did not increase the pelvic failure rate (21% in both subgroups) (P = 0.83), whereas in Stage 111, bilateral parametrial involvement was associated with a 48% pelvic failure rate versus 28% for unilateral extension (P 5 0.01). Five-year disease-free survival (DFS) rates for IB tumors less than or equal to 3 cm was 90% versus 67% for tumors more than 3 cm (P = 0.01). In Stage IIA tumors less than or equal to 3 cm, 5-year DFS was 70% versus 45% for tumors more than 3 cm. Patients with Stage IIB nonbulky tumors (less than or equal to 5 cm in diameter) had better 10-year DFS (65% to 70%) compared with those with bilateral bulky tumors (45% to Presented at the 75th Annual Meeting of the American Radium Society, Montreal, Canada, May 4-8, 1991. From the *Radiation Oncology Center, Mallinckrodt Institute of Radiology, and the tDivision of Gynecologic Oncology, Department of Obstetrics and Gynecology, Barnes Hospital, Washington Univer- sity School of Medicine, St. Louis, Missouri. Address for reprints: Carlos A. Perez, MD, Radiation Oncology Center, 4511 Forest Park, St. Louis, MO 63108. Accepted for publication January 31, 1992. 55%) (P = 0.10). Stage I11 patients with unilateral non- bulky tumors had a 55% 10-year DFS compared with 35% to 40% for bulky tumors or bilateral parametrial involve- ment (P = 0.002). The authors concluded that clinical stage and size of tumor are critical factors in the progno- sis, therapy selection, and evaluation of results in carci- noma of the uterine cervix. Cancer 1992; 69:2796-2806. Definitive radiation therapy has been shown to be ef- fective in treating patients with carcinoma of the uter- ine cervix.'-3 Tumor control and survival in Stage I and IIA are comparable when patients are adequately treated with either definitive irradiation or radical sur- gery. Several prognostic factors have been identified that have a profound influence on outcome. Some are related to host characteristics (age, Karnofsky perfor- mance status, and hemoglobin level), tumor (stage and volume, histologic type, depth of stromal invasion, and vascular permeation), or therapy factors (technique and dose of irradiati~n).~-~ This report updates previous article^^-^ and ana- lyzes in detail the effect of tumor size on the outcome of definitive irradiation in the treatment of invasive carci- noma of the uterine cervix. Materials and Methods The records of 11 78 patients with histologically proven carcinoma of the uterine cervix (intact uterus) (Stages IB, 11, 111, and IVA) who were treated with definitive irradiation alone at the Mallinckrodt Institute of Radiol- ogy, Barnes Hospital, Washington University School of Medicine, between January 1959 and December 1986 were retrospectively reviewed. The results of 17 addi- tional patients with Stage IIIA disease (56% survived 5 years without tumor) were not included even though the results were similar to those of the Stage IIIB group. Patients with carcinoma of the cervical stump were also
-
Upload
independent -
Category
Documents
-
view
1 -
download
0
Transcript of Effect of tumor size on the prognosis of carcinoma of the uterine cervix treated with irradiation...

2796
Effect of Tumor Size on the Prognosis of Carcinoma of the Uterine Cervix Treated With Irradiation Alone Carlos A. Perez, MD,* Perry W. Grigsby, MD,* Shriram M. Nene, H . Marvin Camel, MD,t Andrew Galakafos, MD,t Ming-Shian Kao, MD,t and Mary Ann Locketf, MBA*
The authors conducted a retrospective analysis of 1178 patients with histologically proven invasive carcinoma of the uterine cervix treated with irradiation alone. The minimum follow-up time was 3 years. The 10-year ac- tuarial pelvic failure rate in Stage IB was 6% for tumors less than 3 cm, 15% for tumors 3 to 5 cm, and 30% for tumors more than 5 cm (P = 0.0018). The 10-year actuar- ial pelvic failure rate in Stage IIA was 10% for tumors less than 3 cm, 28% for tumors 3 to 5 cm, and 20% for tumors more than 5 cm (P = 0.09). Stage IIB unilateral nonbulky tumors (less than 5 cm) had a 20% pelvic fail- ure rate compared with 28% for bilateral lesions and 35% for unilateral bulky tumors (more than 5 cm) ( P = 0.35). In Stage IIB, pelvic failures were greater when disease extended into the lateral parametrium (30%) compared with medial parametrial involvement only (17%) ( P = 0.01). In Stage I11 unilateral nonbulky tumors, the pel- vic failure rate was 28% compared with 45% to 50% for unilateral bulky lesions ( P = 0.002). Bilateral parametrial disease in Stage IIB did not increase the pelvic failure rate (21% in both subgroups) (P = 0.83), whereas in Stage 111, bilateral parametrial involvement was associated with a 48% pelvic failure rate versus 28% for unilateral extension (P 5 0.01). Five-year disease-free survival (DFS) rates for IB tumors less than or equal to 3 cm was 90% versus 67% for tumors more than 3 cm (P = 0.01). In Stage IIA tumors less than or equal to 3 cm, 5-year DFS was 70% versus 45% for tumors more than 3 cm. Patients with Stage IIB nonbulky tumors (less than or equal to 5 cm in diameter) had better 10-year DFS (65% to 70%) compared with those with bilateral bulky tumors (45% to
Presented at the 75th Annual Meeting of the American Radium Society, Montreal, Canada, May 4-8, 1991.
From the *Radiation Oncology Center, Mallinckrodt Institute of Radiology, and the tDivision of Gynecologic Oncology, Department of Obstetrics and Gynecology, Barnes Hospital, Washington Univer- sity School of Medicine, St. Louis, Missouri.
Address for reprints: Carlos A. Perez, MD, Radiation Oncology Center, 4511 Forest Park, St. Louis, MO 63108.
Accepted for publication January 31, 1992.
55%) (P = 0.10). Stage I11 patients with unilateral non- bulky tumors had a 55% 10-year DFS compared with 35% to 40% for bulky tumors or bilateral parametrial involve- ment ( P = 0.002). The authors concluded that clinical stage and size of tumor are critical factors in the progno- sis, therapy selection, and evaluation of results in carci- noma of the uterine cervix. Cancer 1992; 69:2796-2806.
Definitive radiation therapy has been shown to be ef- fective in treating patients with carcinoma of the uter- ine cervix.'-3 Tumor control and survival in Stage I and IIA are comparable when patients are adequately treated with either definitive irradiation or radical sur- gery. Several prognostic factors have been identified that have a profound influence on outcome. Some are related to host characteristics (age, Karnofsky perfor- mance status, and hemoglobin level), tumor (stage and volume, histologic type, depth of stromal invasion, and vascular permeation), or therapy factors (technique and dose of irradiati~n).~-~
This report updates previous article^^-^ and ana- lyzes in detail the effect of tumor size on the outcome of definitive irradiation in the treatment of invasive carci- noma of the uterine cervix.
Materials and Methods
The records of 11 78 patients with histologically proven carcinoma of the uterine cervix (intact uterus) (Stages IB, 11, 111, and IVA) who were treated with definitive irradiation alone at the Mallinckrodt Institute of Radiol- ogy, Barnes Hospital, Washington University School of Medicine, between January 1959 and December 1986 were retrospectively reviewed. The results of 17 addi- tional patients with Stage IIIA disease (56% survived 5 years without tumor) were not included even though the results were similar to those of the Stage IIIB group. Patients with carcinoma of the cervical stump were also

Effect of Tumor Size on Uterine Cervix CAIPerez et al. 2797
excluded. Thirty-six patients with Stage IIB disease and 18 patients with Stage IIIB disease on whom an extra- peritoneal pelvic lymphadenectomy was performed be- fore 1964 in a study assessing the effect of irradiation on the pelvic lymph nodes were included. None of the patients had undergone any other surgical procedure. Patients with periaortic lymph nodes were assigned to the respective clinical stage (IB [7 patients], IIA [l pa- tient], IIB [9 patients], IIIB [13 patients], and IV [l pa- tient]), disregarding periaortic lymph node metastases. These patients were treated in a manner similar to the others, except for irradiation to the periaortic lymph nodes (approximately 5000 cGy tumor dose in 5 weeks). More than 90% of the tumors were epidermoid carcinoma, approximately 6% were adenocarcinoma, 2% were adenosquamous carcinoma, and less than 1 YO were other histologic types.
Patients were initially evaluated with physical and pelvic examinations, routine blood count, chemistry profile, chest radiograph, and intravenous pyelogram. Lymphangiograms were performed on selected Stage IB and IIA patients and in most patients with advanced stages until 1984, when computed tomography was in- creasingly used. Barium enema was routinely per- formed in patients with Stage IIB or higher or in those with lower stages who had lower intestinal symptoms. Multiple-punch biopsies of the cervix were obtained for all patients, and dilatation and curettage was frequently performed at the time of first implant. Patients were jointly staged by the staffs of Radiation Oncology and Gynecological Oncology according to the International Federation of Gynecology and Obstetrics (FIGO) classi- fication with modifications. When there was a disagree- ment, the patient was assigned to the less-advanced stage. lo
Based on information in the radiation oncology re- cords, the size of the tumor (cm) was retrospectively coded in Stage IB and IIA patients. In Stages IIB and 111, the tumors were classified as bulky (more than 5 cm) or not bulky (less than or equal to 5 cm in diameter) and whether parametrial involvement was unilateral or bi- lateral. Stage IIB lesions were additionally categorized according to the involvement of the medial or the lat- eral parametrium. In some patients, particularly those treated before 1970, tumor description in the records was not sufficient to adequately estimate the tumor vol- ume and they are classified as unspecified.
Cases were followed-up periodically by the staffs of both divisions for at least 3 years or until death. Me- dian follow-up time in surviving patients was 11 years (minimum, 3 years; maximum, 23 years). Information was available for 97% of the patients from institutional records, from letter or telephone contact with the refer- ring physician, or occasionally through direct communi-
cation with the patient or relatives. Cases lost to follow- up were withdrawn at that time from the risk groups.
Recurrences were classified as cervical (local), mar- ginal (in the vagina), parametrial (all three included as pelvic failures), or distant metastases (outside the pelvis).
Irradiation Techniques
Although general treatment policies were followed, therapy was individualized depending on the tumor stage and configuration, geometry of the pelvic organs, age of the patient (5% to 10% reduction for those older than 65 years of age), previous history of pelvic inflam- matory disease or surgical procedures (5% to 10% dose reduction), and the judgment of the physician.
As previously de~cribed,~ patients were treated with high-energy photons, initially 22 MV (betatron) and later 18 to 25 MV from linear accelerators (1000 cGy to 2000 cGy to whole pelvis plus 4000 cGy to para- metria with midline step wedge or rectangular block). Irradiation was administered through anteroposterior (AP) and posteroanterior (PA) 15 X 15 cm portals for Stage IB and IIA or through 18 X 15 cm portals in pa- tients with Stages IIB, 111, and IV to include a greater volume of the common iliac lymph nodes. Fraction- ation was 180 cGy to 200 cGy tumor dose daily, five fractions per week.
Brachytherapy
Until 1965, the Ter-Pogossian applicator (Washington University, St. Louis, MO) or original Fletcher applica- tor was used. Since then, Fletcher-Suit afterloading ap- plicators have been routinely used. The standard load- ing has been 20-10-10 mgRaEq sources in the tandem with additional 10 mgRaEq sources for deeper cavities and 20 mgRaEq sources in the 2 cm diameter vaginal colpostats. Radium sources were replaced with 'OCo in 1960 and with 137Cs in 1971. Regardless of the isotope used, all doses were prescribed in RaEqmg-h, and doses to point A and pelvic nodes were calculated. The dose rate at point A was approximately 60 cGy/hour to 70 cGy/hour. Point A was defined as 2 cm above the vagi- nal fornix and 2 cm lateral to the tandem. Dose to pelvic lymph nodes was calculated at 2 cm above the vaginal fornix and 6 cm lateral to the tandem on a tilted coronal plane along the axis of the tandem and midpoint of the long axes of the vaginal ovoids.
Usually two intracavitary insertions were carried out. In most patients, the first intracavitary insertion was done after administration of 1000 cGy to 2000 cGy to the pelvis. A second insertion was performed 2 to 3 weeks later, depending on tumor regression, with the patient continuing external irradiation during this time.

2798 CANCER Iune I , 1992, Volume 69, No. 11
When necessary, a third insertion was carried out at the completion of the external therapy.
The prescription for brachytherapy doses varied from 6500 to 7500 mgRaEq-h for Stage IB to 8000 to 8500 mgRaEq-h for Stages IIB and 111. In the more ad- vanced stages, it was sometimes necessary to adminis- ter 4000 cGy to the whole pelvis, in which case the total intracavitary dose was reduced to 6000 mgRaEq-h. These techniques delivered a total dose to point A of 6000 cGy to 8000 cGy in Stages IB and IIA and 7000 cGy to 9500 cGy in Stages JIB, 111, and IV. The dose to the pelvic lymph nodes ranged from 4500 cGy to 7000 cGy. The policies of treatment by stage have been previ- ously de~cribed.~ The variation in doses was partially due to physician preference, an adjustment in dosime- try factorsg before 1971, and modifications of therapy based on applicator loading, tumor volume, stage, and tumor response to the course of irradiation.
After the records were reviewed, doses in cGy to point A and the lateral pelvic wall were determined from external beam calculations at central axis and iso- dose curves for brachytherapy. From a biologic stand- point, there may have been difference in the lethal ef- fects and repair of sublethal damage between continu- ous low-dose-rate brachytherapy and high-dose-rate fractionated external irradiation. Because all patients were treated with the same techniques, however, physi- cal doses from both modalities were added without ad- ditional corrections.
Data Analysis
Analysis of clinical data was done using a VAX 8600 (Digital Equipment Corp., Maynard, MA) computer and BMDP Statistical Software (University of Califor- nia Press, Los Angeles, CA). All survival curves and survival functions used the actuarial life table as ap- plied by Cutler and Ederer." Survival time was calcu- lated from the date of therapy initiation.
Test statistics were carried out using generalized Wilcoxon (Breslow) log-rank test, generalized Savage (Mantel-Cox) test, and Tarone-Ware Trend
analysis was performed by the Tarone method.14 Sur- vival analysis with covariates was based on the Cox form of the proportional hazards regression m0de1.I~
Results
Survival and Patterns of Failure
The actuarial 5-year disease-free survival (DFS) rates were 85% for Stage 1,70% for Stage IIA, 72% for Stage IIB, and 52% for Stage 111. There were no long-term survivors among the 20 patients with Stage IVA disease (Table 1).
The anatomic location and overall incidence of fail- ures are shown in Table 1. In Stage IB, there was 9.6% incidence of pelvic recurrence and 17.5% incidence of distant metastases. In Stages IIA and IIB, the overall incidence of pelvic recurrences was 20% and the overall incidence of distant metastases was approximately 30%. In Stage 111, the overall pelvic recurrence rate was 41% and the overall distant metastases rate was 42% (75% to 80% for both in Stage IVA). The actuarial 10- year failure rate was 10% in Stage IB, 21% in Stages IIA and IIB, 44% in Stage 111, and 85% in Stage IVA.
Pelvic Failure Rate as Function of Stage and Tumor Sire
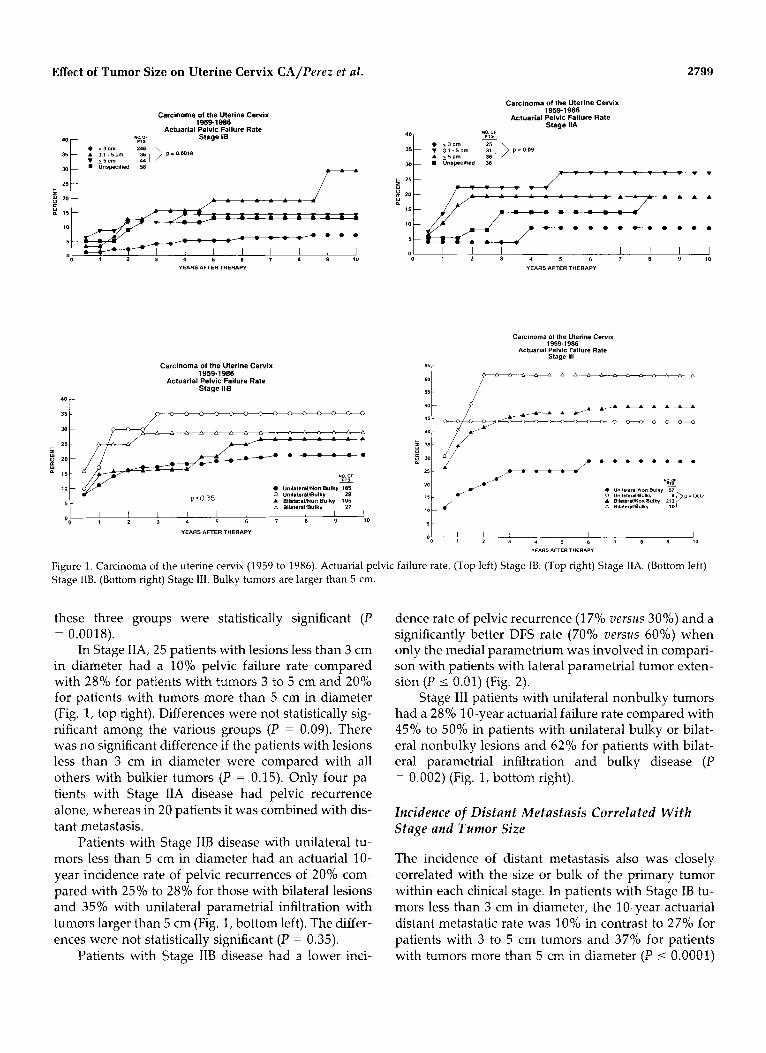
In 116 patients with Stage IB disease with small lesions diagnosed by conization and in whom relatively mini- mal residual tumor was noted after this procedure, 6% had pelvic failures (three alone and four combined with distant metastasis). The incidence was similar to that in 130 patients with tumors less than 3 cm in diameter, and they are shown as one group in Figure 1, top left. In contrast, in 36 patients with tumors 3 to 5 cm in diame- ter, the pelvic failure rate was approximately 15% (one alone and six combined with distant metastasis). In 44 patients with lesions more than 5 cm in diameter, one failed in the pelvis only and five had pelvic failure com- bined with distant metastasis for an actuarial rate of 20% at 5 years and 30% at 10 years. Differences among
Table 1. Carcinoma of the Uterine Cervix: Disease-Free Survival and Incidence of Tumor Recurrence
5-year disease-free Site of recurrence
No. of survival Pelvic oniy Pelvic + distant Total pelvic Distant metastases Stage patients rate (YO) (Yo) metastases (YO) failures (YO) only (YO)
IB 384 85 6 (2) 31 (8) 37 (10) 36 (9) IIA 128 70 4 (3) 20 (16) 24 (19) 24 (19) IIB 353 72 38 (11) 43 (12) 81 (23) 54 (15) I11 293 52 48 (16) 73 (25) 121 (41) 54 (18) IVA 20 0 3 (15) 12 (60) 15 (75) 4 (20)
Effect of Tumor Size on Uterine Cervix CA/Perez et al. 2799
Carcinoma of the Uterine Cervix 19591986
Actuarial Pelvic Failure Rate Stage IIA
Carcinoma of the Uterine Cervix 1959-1986
Actuarial Pelvic Failure Rate NO OF Stage IB
::! 00 1 2 3 4 5 6 7 8 9 10
YEARSAFTERTHERAPV
Carcinoma of the Uterine Cervix 1959-1 986
Actuarial Pelvic Failure Rate Stage llB
0 1 2 3 4 5 6 7 8 9 10 YEARSAFTERTHERAPY
Carcinoma of the Uterine Cervix 1959-1986
Actuarial Pelvic Failure Rate Stage 111
a-
35 - >-'
30-
25 -
YI
. "",ll,lr~l,*O" Bulky 57
&~;~;;~:'& 2,:;)D'ooz 5 - b 8,1.,Lr.lm"ll" 10)
p 20-
15-
10 UnilalerallNon Bulky 185 0 Unil~br~l/Bulky 29
-
' 0 1 2 3 1 5 6 7 8 9 10
YEARS AFTER THERAPY
"EARSAFTERTHERAPY
Figure 1. Carcinoma of the uterine cervix (1959 to 1986). Actuarial pelvic failure rate. (Top left) Stage IB. (Top right) Stage IIA. (Bottom left) Stage IIB. (Bottom right) Stage 111. Bulky tumors are larger than 5 cm
these three groups were statistically significant (P
In Stage IIA, 25 patients with lesions less than 3 cm in diameter had a 10% pelvic failure rate compared with 28% for patients with tumors 3 to 5 cm and 20% for patients with tumors more than 5 cm in diameter (Fig. 1, top right). Differences were not statistically sig- nificant among the various groups (P = 0.09). There was no significant difference if the patients with lesions less than 3 cm in diameter were compared with all others with bulkier tumors (P = 0.15). Only four pa- tients with Stage IIA disease had pelvic recurrence alone, whereas in 20 patients it was combined with dis- tant metastasis.
Patients with Stage IIB disease with unilateral tu- mors less than 5 cm in diameter had an actuarial 10- year incidence rate of pelvic recurrences of 20% com- pared with 25% to 28% for those with bilateral lesions and 35% with unilateral parametrial infiltration with tumors larger than 5 cm (Fig. 1, bottom left). The differ- ences were not statistically significant (P = 0.35).
Patients with Stage IIB disease had a lower inci-
= O.OOl8). dence rate of pelvic recurrence (1 7% versus 30%) and a significantly better DFS rate (70% versus 60%) when only the medial parametrium was involved in compari- son with patients with lateral parametrial tumor exten- sion (P I 0.01) (Fig. 2).
Stage 111 patients with unilateral nonbulky tumors had a 28% 10-year actuarial failure rate compared with 45% to 50% in patients with unilateral bulky or bilat- eral nonbulky lesions and 62% for patients with bilat- eral parametrial infiltration and bulky disease (P = 0.002) (Fig. 1, bottom right).
Incidence of Distant Metastasis Correlated W i t h Stage and Tumor Size
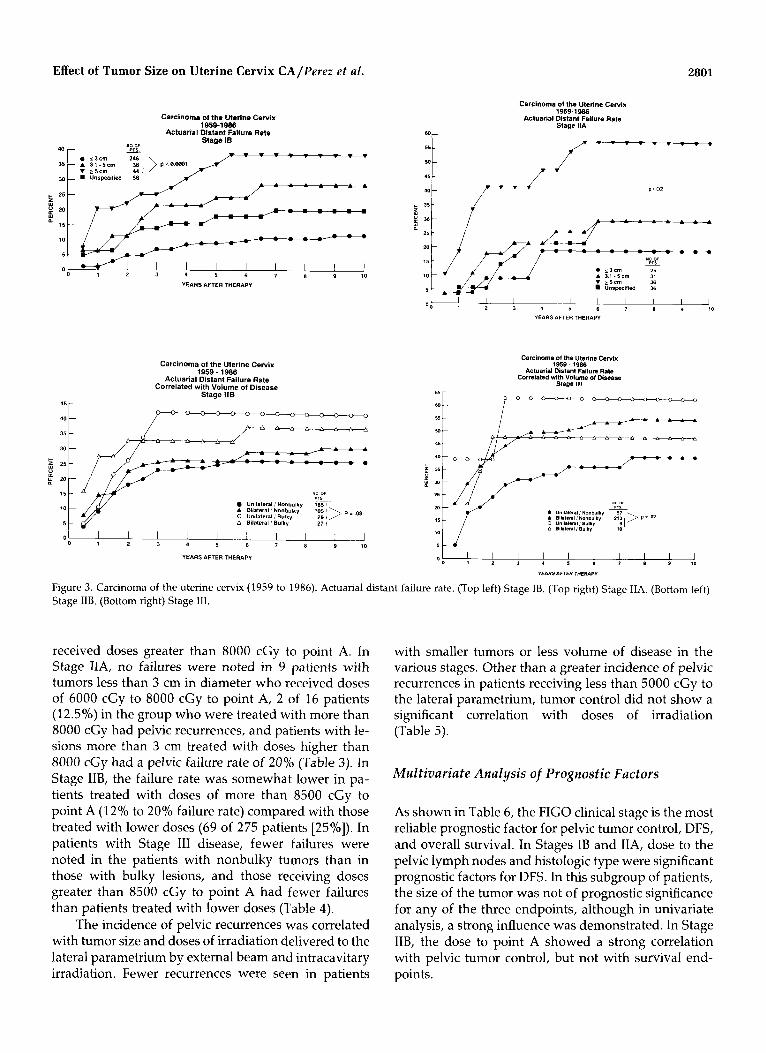
The incidence of distant metastasis also was closely correlated with the size or bulk of the primary tumor within each clinical stage. In patients with Stage IB tu- mors less than 3 cm in diameter, the 10-year actuarial distant metastatic rate was 10% in contrast to 27% for patients with 3 to 5 cm tumors and 37% for patients with tumors more than 5 cm in diameter (P I 0.0001)

2800 CANCER June I , 1992, Volume 69, No. 11
CARCINOMA OF THE UTERINE CERVIX, STAGE I1 MIR (19501SW)
ACTUARIAL PELVIC FAILURE RATE MEDIAL Vs. LATERAL PARAYETRIAL INVOLVEMENT
CARCINOMA OF THE UTERINE CERVIX, STAGE II B YIR 1959-lW)
MEDIAL vs. LATERAL PARAYETRIAL INVOLVEMENT DISEASE L E E SURVIVAL
H Y.dl.1 Rnmelrlum 1&2 H LM.r.1 Fwamnrlum W4 - :,,, p I .01
o 1 a 3 4 5 6 I a 9 %o YEARS AFTER THERAPY
Figure 2. (Top) Actuarial pelvic failure rate and (bottom) disease free survival correlated with medial uersus lateral parametrial involvement.
(Fig. 3, top left). In Stage IIA disease, the 10-year ac- tuarial incidence of distant metastasis was 18% for pa- tients with lesions less than 3 cm in diameter, 30% for patients with 3 to 5 cm tumors, and 57% for patients with tumors more than 5 cm in diameter ( P = 0.02) (Fig. 3, top right).
In Stage IIB, patients with nonbulky tumors showed a 20% to 25% incidence rate of distant metas- tasis in contrast to 40% for bulky lesions, regardless of whether they had unilateral or bilateral parametrial in- volvement (Fig. 3, bottom left). In Stage 111 tumors, the incidence of distant metastasis was 35% for unilateral nonbulky tumors, 45% to 50% for bilateral tumors, and 60% for unilateral bulky tumors (Fig. 3, bottom right).
Disease-Free and Actuarial Survival Correlated W i t h Tumor Size
Patients with Stage IB tumors less than 3 cm in diameter had a 10-year DFS rate of approximately 90% com- pared with 65% to 75% for those with larger lesions. Differences were statistically significant (P < 0.001)
(Fig. 4, top left). In patients with Stage IIA disease, those with tumors less than 5 cm in diameter had a 10-year DFS rate of 70% to 80% compared with 40% for those with lesions more than 5 cm. The differences were statistically significant ( P = 0.028) (Fig. 4, top right). Less effect of tumor size on DFS was seen in patients with Stage IIB and I11 disease (Fig. 4, bottom left and right), although patients with unilateral non- bulky tumors in both stages had a better survival rate (70% and 55%, respectively) than those with larger or bilateral tumors (50% to 60% in Stage IIB and 35% to 40% in Stage 111). These findings are probably related to the higher incidence of distant metastases in all sub- groups.
As reported previ~usly,~, '~ because a large propor- tion of patients with carcinoma of the cervix are older women, many will die of intercurrent disease although they are cured of their tumors. Nevertheless, in Stage IB and IIA disease, overall survival was significantly in- fluenced by the tumor size (Stage IB patients with le- sions less than 3 cm in diameter had a 10-year actuarial survival rate of more than 80% compared with 60% for those with larger lesions [P < 0.00011). In Stage IIA, there was no significant difference in the 10-year sur- vival rate for patients with lesions smaller or larger than 3 to 5 cm (approximately 60% survival); however, in 36 patients with tumors more than 5 cm in diameter, the 10-year survival rate was 38% ( P = 0.02). Whereas in Stage IIB no significant correlation was found between the volume of tumor and survival, in Stage 111 those with unilateral nonbulky lesions had a better 5-year survival rate (55%) compared with patients with more extensive lesions (35%), although at 10 years the differ- ence in survival for both groups disappeared (30%).
Correlation of Doses of Irradiation, Tumor Site, and Pelvic Tumor Control
These data must be interpreted with caution because this is not a dose-seeking Phase I1 randomized study, but a retrospective review in which the doses of irradia- tion were influenced by clinical judgment, philosophy of the treating physician, tumor size, and heterogeneity of the tumor. In lesions less than 3 cm in diameter, the pelvic recurrence rate was 5% to 8.7%, regardless of the doses of irradiation. In tumors more than 3 cm in diame- ter, the failure rate ranged from 7.7% to 9%, with 7000 cGy to 8000 cGy to point A to 31% with more than 8000 cGy (Table 2). These findings most likely are a reflection of the larger doses that were prescribed for larger tumors, the characteristics of which cannot be fully determined from the retrospective review. A higher number of pelvic recurrences were noted in pa- tients with tumors more than 3 cm in diameter who
Effect of Tumor Size on Uterine Cervix CAIPerez e t al .
15
€0-
55
Y)-
45
4.-
5 - 3 -
c = - 25
211
I5
10
5 -
2801
-
-
-
- NO o / - ~ P T I
-
-
40 i_l 35
15
10
5
0
O5 r
Carcinoma of the Uterine Cervix
Actuarial Distant Failure Rate Stage I6
1959-1986
YO or mTI - - - - - - - -
+ - - - - - - A
1 2 3 4 5 6 7 8 9 10
YEARS AFTER THERAPY
Carcinoma of the Uterine Cervix 1959 - t 986
Actuarial Distant Failure Rate Correlated with Volume of Disease
Stage I 1 6
35 401 15
10
5
NO 01
Unllaleral INOnbulky 1 8 5 , A Bilateral I Nonbuiky 105 \ \ 0 Unilateral I Bulky 29 , / A Bilateral I Bulky 27 ,
V r L .
Carcinoma of the Uterine Cervix 1959-1986
Actuarial Distant Fallure Rate Stage IIA
40 r/ P i 0 2
"0 OF
0 1 3 c m A 3 1 - 5 c m 31 . L S C m 36
U"*pc,l,ed 36
YEARSAFTERTHERAPY
I I I I I I I I I l l YEARS AFTER THERAPY O O 1 2 3 . 5 (i 7 8 9 10
YEARSAFTERTHERAPY
Figure 3. Carcinoma of the uterine cervix (1959 to 1986). Actuarial distant failure rate. (Top left) Stage IB. (Top right) Stage IIA. (Bottom left) Stage IIB. (Bottom right) Stage 111.
received doses greater than 8000 cGy to point A. In Stage IIA, no failures were noted in 9 patients with tumors less than 3 cm in diameter who received doses of 6000 cGy to 8000 cGy to point A, 2 of 16 patients (12.5%) in the group who were treated with more than 8000 cGy had pelvic recurrences, and patients with le- sions more than 3 cm treated with doses higher than 8000 cGy had a pelvic failure rate of 20% (Table 3). In Stage IIB, the failure rate was somewhat lower in pa- tients treated with doses of more than 8500 cGy to point A (12% to 20% failure rate) compared with those treated with lower doses (69 of 275 patients [25%]). In patients with Stage 111 disease, fewer failures were noted in the patients with nonbulky tumors than in those with bulky lesions, and those receiving doses greater than 8500 cGy to point A had fewer failures than patients treated with lower doses (Table 4).
The incidence of pelvic recurrences was correlated with tumor size and doses of irradiation delivered to the lateral parametrium by external beam and intracavitary irradiation. Fewer recurrences were seen in patients
with smaller tumors or less volume of disease in the various stages. Other than a greater incidence of pelvic recurrences in patients receiving less than 5000 cGy to the lateral parametrium, tumor control did not show a significant correlation with doses of irradiation (Table 5).
Multiuariate Analysis of Prognostic Factors
As shown in Table 6, the FIG0 clinical stage is the most reliable prognostic factor for pelvic tumor control, DFS, and overall survival. In Stages IB and IIA, dose to the pelvic lymph nodes and histologic type were significant prognostic factors for DFS. In this subgroup of patients, the size of the tumor was not of prognostic significance for any of the three endpoints, although in univariate analysis, a strong influence was demonstrated. In Stage IIB, the dose to point A showed a strong correlation with pelvic tumor control, but not with survival end- points.

2802 CANCER Iune 2,2992, Volume 69, No. 11
I I I I L I I I I I
Carcinoma of the Uterine Cervix 1959-1986
Disease Free Survival by lhmor Size
I I I I I I I I I J
Carcinoma of the Uterine Cervix 19591986
Disease Free Survlval bv Tumor Slze
Carcinoma of the Uterine Cervix 19591986
Disease Free Survival Stase llB
100
m
260
P' 10
Stage IIA .
0 6 3 c m
v 2 5 c m UnWec,llied 56
0 1 2 1 4 5 YEARSIFTERTHERAPY
'OOh 80
Carcinoma of the Uterine Cervix 1959-1986
Disease Free Survival Stage 111
UnilalerrllNon Bulky 57 0 UnilaleraliBvlky
40
$1020 00 VEARSAFTERTHERAPV
Figure 4. Carcinoma of the uterine cervix (1959 to 1986). Disease-free survival correlated with tumor size. (Top left) Stage IB. (Top right) Stage IIA. (Bottom left) Stage IIB. (Bottom right) Stage 111. Bulky tumors are larger than 5 cm.
Discussion
Several prognostic factors, including tumor stage and size, patient age, performance status, and presence of metastatic pelvic/periaortic lymph nodes, affect thera- peutic outcome in patients with carcinoma of the uter- ine ~ e r v i x . ~ , ' ~ The current analysis emphasizes the im- portance of detailed assessment of tumor characteristics within each clinical stage in the selection of therapy and evaluation of the results of irradiation. A better under- standing of these factors will lead to more rational thera-
peutic strategies to optimize doses of irradiation alone or combined with another modality, which will yield the highest pelvic tumor control with acceptable mor- bidity. This approach has been advocated by Fletcher' and other^^,'^,'^ and should involve the definition of appropriate doses of irradiation for a given tumor vol- ume (not clinical stage) in specific patients (according to age and Karnofsky performance status), choice of irra- diation alone or combined with surgery (bulky tumors and endometrial extension), or the potential use of ef- fective cytotoxic agents (when adequately tested in pro- spective clinical trials).20-22
Table 2. Carcinoma of the Uterine Cervix Stage IB: Correlation of Pelvic Recurrences With Dose to Medial Parametrium (Point A) and Size of Primary Tumor
Dose to medial parametrium (cGy) < 3 ( O h ) * 3 to 5 ( O h ) * > 5 (Yo)* Unspecified*
Size of lesion (cm)
5 6000 4/50 (8) 0/5 0/6 1/12 (8.3)
7001-8000 4/75 (5.3) 1/11 (9.1) 1/13 (7.7) 2/17 (11.8) > 8000 6/69 (8.7) 6/19 (31.6) 5/22 (22.7) 3/17 (17.6)
6001-7000 3/50 (6) o/ 1 0/3 0/11
* Number with recurrences/number with that size tumor receiving that dose.

Effect of Tumor Size on Uterine Cervix CA/Perez et al . 2803
Table 3. Carcinoma of the Uterine Cervix Stage IIA: Correlation of Pelvic Recurrences With Dose to Medial Parametrium (Point A) and Size of Primary Tumor
Dose to medial parametrium (cGy) < 3 (Yo))" 3 to 5 (%)* > 5 (Yo)* Unspecified ( O h ) *
Size of lesion (cm)
5 6000 0/1 0/4 1/3 2/7 (28.6)
7001-8000 0/2 3/10 (30) 3/8 (37.5) 1/8 (12.5) 6001-7000 0/6 1/1 1/2 0/8
> 8000 2/16 (12.5) 3/15 (20) 4/22 (18.2) 3/13 (23.1) * Number with recurrences/number with that size tumor receivin2 that dose.
Many reports have shown significant differences in pelvic tumor control, incidence of distant metastasis, DFS, and overall survival in patients with carcinoma of the cervix treated with various modalities. In patients treated with a radical hysterectomy, there has been a significant correlation of the previously mentioned pa- rameters with the size of the primary tumor. For exam- ple, Delgado et reported a DFS rate of 94% for patients with Stage IB occult disease, 85.5% for patients with tumors less than or equal to 3 cm, and 68.4% for patients with tumors greater than 3 cm in diameter. Piver and C h ~ n g ~ ~ noted that 5-year survival rate in Stage IB carcinoma of the cervix treated with radical hysterectomy correlated with size of the lesion (84% for patients with tumors less than 1 cm in diameter, 90% for patients with tumors 2 to 3 cm in diameter, 65.9% for patients with tumors 4 to 5 cm in diameter, and 60% for patients with tumors more than 6 cm in diameter). In Stage IIA, the corresponding values were 8l.8%, 72%, 38%, and 41%, respectively. Chung et de- scribed a 92% 5-year survival rate in 83 patients with Stage IB and IIA disease with tumors less than 4 cm in diameter compared with 47% in 15 patients with tu- mors larger than 4 cm. The corresponding local recur- rence rates were 5% and 40%, and the distant metasta- sis rates were 1% and 40%. Van Nagell et ~ 1 . ~ ~ reported 5 YO tumor recurrence after radical hysterectomy and pelvic lymphadenectomy in lesions less than 2 cm in diameter compared with 24% in tumors 2 to 5 cm in diameter. Underwood et noted 89% corrected 5- year survival rate in 11 patients with tumors less than 6
cm in diameter treated with radical hysterectomy in contrast to 75% in 8 patients with tumors more than 6 cm.
Parametrial extension was found to be a detrimen- tal prognostic factor by Inoue and Okumura28 in 628 cases of carcinoma of the cervix treated with radical hysterectomy and pelvic lymphadenectomy. Similar findings have been reported with irradiation alone by others, as well as in our current analysis, correlating tumor control, distant metastasis, and survival with the size of the cervical carcinoma. Van Nagell et ~ 1 . ~ ~ de- scribed a 6% tumor recurrence rate in lesions less than 2 cm in diameter compared with 11 YO in tumors 2 to 5 cm and 86% in seven patients with tumors more than 5 cm. Homesley et described a 95% 5-year survival rate in patients with Stage I disease less than 4 cm in diame- ter compared with 67% for larger tumors. Kapp et u I . ~ ' reported a 5-year survival rate of 88% in patients with Stage IB tumors less than 3 cm in diameter compared with 75% with larger lesions. In Stage IIA and IIB, the 5-year rates were 80% for the small tumors and 65% for larger lesions. The local recurrence rates were not re- ported by these authors.
Lanciano et ~ l . , ~ in an analysis of 1558 patients with squamous cell carcinoma of the uterine cervix treated in the Patterns of Care Study, reported 4-year survival rates of 81% in Stage I, 67% in Stage IIA, 65% in Stage IIB, and 40% in Stage 111. The infield failure rates were 8% (Stage I), 19% (Stage 11), and 47% (Stage 111). Pa- tients with Stage I nonbulky tumors had a 4-year sur- vival rate of 82% (92 of 535) in contrast to 75% (12 of
Table 4. Carcinoma of the Uterine Cervix: Correlation of Pelvic Failures With Total Dose of Irradiation to Point A and Tumor Size
Stage IIB Stage I11 Total dose to point A (cGy) Nonbulky (%)* Bulky (Yo)* Nonbulky (%)* Bulky (Yo)*
18/25 (72) - I 6000 9/12 (75) 0/2
6001-8500 48/223 (21.5) 12/38 (31.6) 65/170 (38.2) 7/11 (63.6) > 8500 7/59 (11.9) 3/15 (20) 24/70 (34.3) 3/7 (42.9)
* Number with recurrences/number with that size tumor receiving that dose

2804 CANCER June 2, 2992, Volume 69, No. 11
Table 5. Carcinoma of the Uterine Cervix: Correlation of Pelvic Failures With Total Dose of Irradiation to Lateral Parametrium and Tumor Size
Stage IB (cm) Stage IIA (cm) Stage IIB Stage III Dose to lateral parametrium Nonbulky Nonbulky kGy) < 3 (%)* z 3 (%)* < 3 (%)* ;r 3 (%)* (%) * Bulky (%)* (YO) * Bulky (%)*
5 4000 2/27 (7.4) 1/3 (33.3) 1/8 (12.5) 2/3 (66.7) 6/10 (60) - 10/13 (77) - 4001-5000 4/84 (4.8) 2/11 (18.2) 2/23 (8.7) 0/3 7/52 (13.5) 2/10 (20) 22/48 (45.8) 0/1 5001-6500 11/145 (7.6) 4/20 (20) 9/42 (21.4) 3/14 (21.4) 12/89 (13.5) 4/14 (28.6) 28/75 (37.3) 1/3 (33.3)
> 6500 6/74 (8.1) 5/17 (29.4) 5/24 (20.8) 2/8 (25) 39/143 (27.3) 9/31 (29) 47/129 (36.4) 9/14 (64.3) * Number with recurrences/number with that size tumor receiving that dose.
46) for those with bulky lesions (the infield failure rates were 6% and IS%, respectively). In Stage IIB patients with unilateral parametrial disease, the 4-year survival rate was 70% in contrast to 52% in those with bilateral parametrial involvement (the corresponding infield fail- ure rates were 17% and 31%, respectively). Although the numbers are different, the data are in accord with those reported by Coia et aL3' for 565 patients treated in 1978 in the same study. The 4-year actuarial survival rates were 58% for unilateral and 47% for bilateral par- ametrial involvement, and the failure rates were 32% and 45%, respectively.
Flet~her,~' in his M. D. Anderson staging classifica- tion of carcinoma of the cervix, separated those with medial parametrial extension (so-called Stage IIA) from those with lateral parametrial disease (Stage IIB). As in our experience, patients with medial parametrial in- volvement had a lower incidence of pelvic recurrences and higher survival than those with involvement of the lateral parametrium.
Stehman et a1 .6 analyzed 626 patients with carci- noma of the cervix (clinical Stages 11, 111, or IVA) who were treated with irradiation and other modalities in several Gynecologic Oncology Group protocols. Tumor size more than 6 cm in diameter was found to be an important prognostic factor for progression-free sur- vival or overall survival. However, the presence of bilat- eral parametrial involvement was a significant prog- nostic factor for survival but not for progression-free interval. In our analysis and in a previous report by Kovalic et a1.,33 no significant prognostic influence of unilateral or bilateral parametrial disease (64% versus 61% 10-year DFS, P = 0.06) was seen in patients with Stage IIB nonbulky tumors. However, patients with bulky tumors, whether unilateral or bilateral, had a greater incidence of pelvic recurrences and distant me- tastasis and decreased survival compared with patients with nonbulky lesions. In Stage 111, patients with unilat- eral nonbulky tumors exhibited a 25% pelvic failure rate and 57% 10-year DFS rate compared with 45% to
Table 6. Multivariate Analysis of Prognostic Factors
P values of endpoints
Variable Pelvic tumor Disease- f ree Overall control survival survival
Stage IB-IIA FIGO stage (IB-IIA) 0.002% 0.001* 0.002* Dose to lateral pelvic nodes 0.060 0.003' 0.729 Dose to point A 0.486 0.880 0.780 Size of tumor 0.749 0.891 0.787
Age 0.785 0.346 0.001* Histologic type 0.954 0.026* 0.168
Stage IIB-111 FIGO stage (IIB-111) 0.001* 0.001* 0.001* Dose to point A 0.054* 0.292 0.570
Age 0.045* 0.227 0.027* Parametrial disease (unilateral versus bilateral) 0.083 0.080 0.114 Dose to lateral pelvic nodes 0.111 0.350 0.109 No. of intracavitary insertions 0.303 0.202 0.230
FIGO: International Federation of Gynecology and Obstetrics. * Significant.

Effect of Tumor Size on Uterine Cervix CA/Perez et al . 2805
62% recurrence rate and 35% DFS rate for patients with bilateral parametrial or bulky disease. Lanciano et aL5 reported a higher 4-year survival rate in patients with Stage 111 Unilateral parametrial involvement (44% in 182 patients) compared with those with bilateral para- metrial disease (34% in 45 patients) ( P = 0.4), contrary to our experience in which these patients had similar DFS rates (35% to 40%). The infield pelvic failure rates were 43% and 52%, respectively, which were similar to those in our analysis.
A few previously reported studies have attempted to correlate pelvic tumor control with doses of irradia- tion. In our experience and that of Lanciano ef al.,5 in- creasing the doses to the paracervical tissues from 7500 cGy to 8500 cGy or to the lateral pelvic wall from 5000 cGy to 6000 cGy did not significantly affect tumor con- trol probability in Stages I or 11. Lanciano et ~ l . , ~ how- ever, observed a lower pelvic failure rate (36%) in pa- tients with Stage I11 treated with paracentral doses more than 8500 cGy compared with lower doses (46% to 56%) ( P = 0.01).
Some inconsistencies in these correlations are most likely related to the retrospective nature of the studies; doses were prescribed by physicians using clinical judg- ment, with higher doses being given to bulky, more extensive tumors or those that did not show satisfactory tumor regression at the end of the standard prescribed therapy. Heterogeneity of the patients (age, Karnofsky performance status, and hemoglobin levels) and tumor cellular characteristics made it extremely difficult to ac- curately correlate doses of irradiation with tumor con- trol probability. The point calculations used may not necessarily coincide with the anatomic location of the tumor or the entire volume of the pelvic organs at risk, and the volume irradiated to specific dose levels was extremely difficult to quantitate with existing treatment planning systems.
From this analysis, we conclude that clinical stage continues to be the strongest prognostic factor in pa- tients with carcinoma of the uterine cervix. Size/vol- ume of disease is an important prognostic factor within each stage and should be carefully evaluated to select the optimal therapy that will achieve the highest pelvic tumor control with the lowest morbidity and to evalu- ate therapeutic results. To acquire valid correlations of tumor control with irradiation doses, it will be neces- sary to conduct properly stratified prospective Phase I1 dose escalation studies for various tumor stages and volumes. Also, three-dimensional dose distributions and dose volume histograms will be required to en- hance the quality of the data.
References 1. Fletcher GH, ed. Textbook of Radiotherapy, ed. 3. Philadelphia:
Lea & Febiger, 1980.
2.
3.
4.
5.
6.
10.
11.
12.
13.
14.
15.
16.
17.
18.
19.
20.
21.
22.
23.
Hanks GE, Herring DF, Kramer S. Patterns of care outcome stud- ies: Results of the national practice in cancer of the cervix. Cancer 1983; 51:959-967. Perez CA, Camel HM, Kuske RR et a / . Radiation therapy alone in the treatment of carcinoma of the uterine cervix: A 20-year experience. Gynecol Oncol 1986; 23:127-140. Bush RS. The significance of anemia in clinical radiation ther- apy. Int ] Radiat Oncol Biol Phys 1986; 12:2047-2050. Lanciano RM, Won M, Coia LR, Hanks GE. Pretreatment and treatment factors associated with improved outcome in squa- mous cell carcinoma of the uterine cervix: A final report of the 1973 and 1978 Patterns of Care Studies. Int ] Radia t Oncol Biol Phys 1991; 20:667-676. Stehman FB, Bundy BN, DiSaia PJ, Keys HM, Larson JE, Fowler WC. Carcinoma of the cervix treated with radiation therapy: 1. A multivariate analysis of prognostic variables in the Gynecologic Oncology Group. Cancer 1991; 67:2776-2785. Perez CA, Breaux S, Madoc-Jones H et a/. Radiation therapy alone in the treatment of carcinoma of uterine cervix: I. Analysis of tumor recurrence. Cancer 1983; 51:1393-1402. Perez CA, Camel HM, Kuske RR et a / . Radiation therapy alone in the treatment of carcinoma of the uterine cervix: A 20-year experience. Gynecol Oncol 1986; 23:127-140. Perez CA, Fox S, Lockett MA et al . Impact of dose in outcome of irradiation alone in carcinoma of the uterine cervix (intact uterus): Analysis of two different methods. Int ] Radia t Oncol Biol Phys 1991; 21:925-933. Kottmeier HL. Classification and staging of malignant tumors in the female pelvis. ]ourtinl of the Zntertintional Federatioti Gytzaeco- logy atid Obstetrics 1971; 9:172-179. Cutler SJ, Ederer F. Maximum utilization of the life table method in analyzing survival. ] Chron Dis 1958; 8:699-711. Miller RG Jr. Survival Analysis. New York: John Wiley & Sons, 1981. Tarone R, Ware J . On distribution free tests for equality of sur- vival distributions. Biometrika 1977; 64:156-160. Tarone R. Tests for trend in life table analysis. Biometrika 1975;
Cox DR. Regression models and life tables. ] Roy Stat Sac 1972; 34(Series B):187-220. Arneson AN, Williams CF. Long-term follow-up observations in cervical cancer. A m ] Obstet Gynecol 1960; 80:775-790. Perez CA, Kao MS. Radiation therapy alone or combined with surgery in the treatment of barrel-shaped carcinoma of the uter- ine cervix. In t Rad ia t Oncol Biol Phys 1985; 11:1903-1909. Mendenhall WM, McCarty PJ, Morgan LS, Chafe WE. Stage IB-IIA-B carcinoma of the cervix 2 6 cm diameter managed with irradiation: Is adjuvant hysterectomy beneficial? (Abstr). Int ] Radia t Oticol Biol Phys 1990; 19(Suppl 1):127. Thoms WW, Eifel PJ, Delclos L e t al . Bulky endocervical carci- nomas of the uterine cervix: A 23 year experience at the M.D. Anderson Cancer Center (Abstr). Znt ] Radia t Oncol B i d Phys 1990; 19(Suppl 1):127. Perez CA, Kuske RR, Camel HM et al . Analysis of pelvic tumor control and impact on survival in carcinoma of the uterine cervix treated with radiation therapy alone. Znt ] Radia t Oncol Biol Phys
Stehman FR, Bundy RN, Keys H, Currie JL, Mortel R, Creasman WT. A randomized trial of hydroxyurea versus misonidazole adjunct to radiation therapy in carcinoma of the cervix: A prelim- inary report of a Gynecologic Oncology Group study. A m ] Ob- stet Gynecol 1988; 159:87-94. Thomas G, Dembo A, Fyles A et a / . Concurrent chemoradiation in advanced cervical cancer. Gynecol Oncol 1990; 38:446-451. Delgado G, Bundy B, Zaino R, Sevin B-U, Creasman WT, Major
621679-682.
1988; 14:613-621.

2806 CANCER June I , 1992, Volume 69, No. 11
24.
25.
26.
27.
28.
F. Prospective surgical-pathological study of disease-free inter- val in patients with stage IB squamous cell carcinoma of the cervix: A Gynecologic Oncology Group study. Gynecol Oncol
Piver MS, Chung WS. Prognostic significance of cervical lesion size and pelvic node metastases in cervical carcinoma. Obstet Gynecof 1975; 46(5):50?-510. Chung CK, Nahhas WA, Stryker JA, Curry SL, Abt AB, Mortel R. Analysis of factors contributing to treatment failures in stages IB and IIA carcinoma of the cervix. Am I Obstet Gynecol 1980;
van Nagell JR Jr, Rayburn W, Donaldson ES e t al . Therapeutic implications of patterns of recurrence in cancer of the uterine cervix. Cancer 1979; 44:2354-2361. Underwood PB, Wilson WC, Kreutner A, Miller MC 111, Murphy E. Radical hysterectomy: A critical review of twenty-two years’ experience. Am Obstet Gynecol 1979; 134:889-898. Inoue T, Okumura M. Prognostic significance of parametrial ex- tension in patients with cervical carcinoma Stages IB, IIA, and IIB. Cancer 1984; 54:1?14-1719.
1990; 38:352-357.
138~550-556.
29. Homesley HD, Raben M, Blake DD el al . Relationship of lesion size to survival in patients with stage IB squamous cell carci- noma of the cervix uteri treated by radiation therapy. Surg Gyne- col Oncof 1980; 150:529-531.
30. Kapp DS, Fischer D, Guitierrez E, Kohorn El, Schwartz PE. Pre- treatment prognostic factors in carcinoma of the uterine cervix: A multivariable analysis of the effect of age, stage, histology and blood counts on survival. Int Radiat Or~cof B i d Phys 1983; 9:445-455.
31. Coia L, Won M, Lanciano R, Marcia1 VA, Martz K, Hanks G. The patterns of care outcome study for cancer of the uterine cervix: Results of the Second National Practice Survey. Cancer 1990; 66:2451-2456. Fletcher GH. Cancer of the uterine cervix: Janeway Lecture Attiericari lournal oflioentgrriolog!y Radium Therapy Nuclear Medi- cirie 1971; 111:225-242. Kovalic JL, Perez CA, Grigsby PW, Lockett MA. The effect of volume of disease in patients with carcinoma of the uterine cer- vix. In t ] Radiat Oncol Biol Phys 1991; 21:905-910.
32.
33.




















