
Effect of mandibular mobilization on electromyographic signals in muscles of mastication and static...
13
Dear Author, Here are the final proofs of your article. Please check the proofs carefully. All communications with regard to the proof should be sent to bmcproductionteam2@spi- global.com. Please note that at this stage you should only be checking for errors introduced during the production process. Please pay particular attention to the following when checking the proof: - Author names. Check that each author name is spelled correctly, and that names appear in the correct order of first name followed by family name. This will ensure that the names will be indexed correctly (for example if the author’s name is ‘Jane Patel’, she will be cited as ‘Patel, J.’). - Affiliations. Check that all authors are cited with the correct affiliations, that the author who will receive correspondence has been identified with an asterisk (*), and that all equal contributors have been identified with a dagger sign (†). - Ensure that the main text is complete. - Check that figures, tables and their legends are included and in the correct order. - Look to see that queries that were raised during copy-editing or typesetting have been resolved. - Confirm that all web links are correct and working. - Ensure that special characters and equations are displaying correctly. - Check that additional or supplementary files can be opened and are correct. Changes in scientific content cannot be made at this stage unless the request has already been approved. This includes changes to title or authorship, new results, or corrected values. How to return your corrections Returning your corrections via online submission: - Please provide details of your corrections in the online correction form. Always indicate the line number to which the correction refers. Returning your corrections via email: - Annotate the proof PDF with your corrections. - Send it as an email attachment to: [email protected]. - Remember to include the journal title, manuscript number, and your name when sending your response via email. Note: in order to ensure timely publication, if we do not hear from you within 48 hours we may take the decision to sign-off the article on your behalf and proceed to publication. After you have submitted your corrections, you will receive email notification from our production team that your article has been published in the final version. All changes at this stage are final. We will not be able to make any further changes after publication. Kind regards, BioMed Central Production Team 2
-
Upload
independent -
Category
Documents
-
view
2 -
download
0
Transcript of Effect of mandibular mobilization on electromyographic signals in muscles of mastication and static...
Dear Author, Here are the final proofs of your article. Please check the proofs carefully. All communications with regard to the proof should be sent to [email protected]. Please note that at this stage you should only be checking for errors introduced during the production process. Please pay particular attention to the following when checking the proof: - Author names. Check that each author name is spelled correctly, and that names appear in the
correct order of first name followed by family name. This will ensure that the names will be indexed correctly (for example if the author’s name is ‘Jane Patel’, she will be cited as ‘Patel, J.’).
- Affiliations. Check that all authors are cited with the correct affiliations, that the author who will receive correspondence has been identified with an asterisk (*), and that all equal contributors have been identified with a dagger sign (†).
- Ensure that the main text is complete. - Check that figures, tables and their legends are included and in the correct order. - Look to see that queries that were raised during copy-editing or typesetting have been resolved. - Confirm that all web links are correct and working. - Ensure that special characters and equations are displaying correctly. - Check that additional or supplementary files can be opened and are correct. Changes in scientific content cannot be made at this stage unless the request has already been approved. This includes changes to title or authorship, new results, or corrected values. How to return your corrections Returning your corrections via online submission: - Please provide details of your corrections in the online correction form. Always indicate the line
number to which the correction refers. Returning your corrections via email: - Annotate the proof PDF with your corrections. - Send it as an email attachment to: [email protected]. - Remember to include the journal title, manuscript number, and your name when sending your
response via email. Note: in order to ensure timely publication, if we do not hear from you within 48 hours we may take the decision to sign-off the article on your behalf and proceed to publication. After you have submitted your corrections, you will receive email notification from our production team that your article has been published in the final version. All changes at this stage are final. We will not be able to make any further changes after publication. Kind regards, BioMed Central Production Team 2
1 STUDY PROTOCOL Open Access
2 Effect of mandibular mobilization on3 electromyographic signals in muscles of4 mastication and static balance in individuals with5 temporomandibular disorder: study protocol for6 a randomized controlled trial7 Yasmin El-Hage2*†, Fabiano Politti2†, Dowglas F Magalhães de-Sousa1, Carolina Marciela Herpich1,8 Igor Phillip dos-Santos Gloria1, Cid André Fidelis de-Paula Gomes2, Ana Paula Amaral1, Nívea Cristina de-Melo2,9 Thais Correa da-Silva2, Eric Edmur Camargo Arruda1, Cesar Ferreira Amorim3, Inaê Caroline Gadotti4,10 Tabajara Oliveira Gonzalez2, Fausto Berzin5, Sandra Kalil Bussadori1, Marília Barbosa Santos Garcia1,11 Bruno Roberto Borges Barbosa1 and Daniela Aparecida Biasotto-Gonzalez11213141516
17 Abstract
18 Background: The stomatognathic system and dysfunction in this system may be related to postural control.19 The proposal of the present study is to assess the effect of mandibular mobilization in individuals with20 temporomandibular disorder using surface electromyography of the muscles of mastication and21 stabilometric variables.
22 Methods/Design: A randomized, controlled, blind, clinical trial will be carried out, with the participants divided23 into three groups: 1) facial massage therapy (control group), 2) nonspecific mandibular mobilization and 3) specific24 mandibular mobilization. All groups will be assessed before and after treatment using the Research Diagnostic25 Criteria for Temporomandibular Disorders, surface electromyography of the masseter and temporal muscles and26 stabilometry. This study is registered with the Brazilian Registry of Clinical Trials (RBR9x8ssz).
27 Discussion: A large number of studies have employed surface electromyography to investigate the function/28 dysfunction of the muscles of mastication and associations with signs and symptoms of temporomandibular29 disorders. However, it has not yet been determined whether stabilometric variables offer adequate reliability in30 patients with this disorder. The results of the proposed study will help determine whether specific and/or31 nonspecific mandibular mobilization exerts an effect on the muscles of mastication and postural control. Moreover,32 if an effect is detected, the methodology defined in the proposed study will allow identifying whether the effect is33 local (found only in the muscles of mastication), global (found only in postural control) or generalized.
34 Keywords: Temporomandibular joint disorders, Electromyography, Postural balance, Complementary therapy,
35Physical therapy modalities
* Correspondence: [email protected]†Equal contributors2Department of Physical Therapy, Universidade Nove de Julho (UNINOVE),Av. Dr. Adolfo Pinto, 109. Água Branca, São Paulo, SP 05001-100, BrazilFull list of author information is available at the end of the article
TRIALS
© 2013 El-Hage et al.; licensee BioMed Central Ltd. This is an Open Access article distributed under the terms of the CreativeCommons Attribution License (http://creativecommons.org/licenses/by/2.0), which permits unrestricted use, distribution, andreproduction in any medium, provided the original work is properly cited.
El-Hage et al. Trials 2013, 14:316http://www.trialsjournal.com/content/14/1/316
36 Background37 Correlations between dental occlusion and bodily balance38 have recently been analyzed [1-4]. The possibility of an as-39 sociation between conditions affecting the stomatognathic40 system, such as temporomandibular disorder (TMD), and41 postural problems have also been investigated [1,5-8].42 Deviations in global posture lead to bodily adaptations43 and realignments, which can affect the organization44 and function of the temporomandibular joint (TMJ)45 [9]. Moreover, the effect of alterations in the muscles of46 mastication and dentoalveolar ligaments on the stoma-47 tognathic system can lead to a perturbation of visual48 stabilization, generating postural imbalance [2].49 Constant oscillations (body sway) occur to maintain50 balance. Afferent (sensory) signals originate from pro-51 prioceptive, tactile, vestibular and visual receptors. Pro-52 prioception of the mandibular system emerges from the53 muscles of mastication (due to changes in the mandible54 position), receptors of the TMJ (due to rotation and/or55 translation of the condyles) and dentoalveolar ligaments56 (due to changes in occlusal contacts) and is determined57 by the trigeminal nerve [1,2,10-13].58 Contact between the jaws is maintained by ligaments59 and muscles, including the masseter and temporal60 muscles. When these muscles are in tonic equilibrium,61 the mandible is at rest [2,14]. This mandibular resting62 position can be altered by different circumstances, such63 as occlusal interferences, TMD, the position of the head64 and body and emotional tension [14]. Electromyography65 (EMG) has evidenced a relationship between the stomatog-66 nathic system and cervical spine and how head movements67 [15], changes in body posture [14], occlusal contact pattern68 and the vertical dimension of the teeth [15-18] can69 alter EMG activity in the muscles of mastication and70 affect the mandibular resting position. Indeed, EMG71 activity in the muscles of mastication at rest in indi-72 viduals with TMD may be greater than that found in73 individuals without this disorder, indicating muscle74 hyperactivity [19-21].75 Studies have suggested that massaging the muscles76 of mastication, joint mobilization, manual therapy,77 mandibular exercises, biofeedback and the application78 of electrophysical resources may be effective in the79 treatment of TMD [22-26]. Joint mobilization has proven80 effective at reducing pain, disability and local ischemia81 [27], breaking fibrous adhesions, enhancing the extensi-82 bility of non-contractile structures, increasing the range83 of motion, enhancing the transmission of afferent infor-84 mation through the stimulation of mechanoreceptors and85 stimulating proprioception and the production of synovial86 fluid [27,28]. The use of joint mobilization has been tested87 on individuals with TMD, in whom a reduction in pain88 and increased mandibular range of movement (ROM)89 have been reported [29-32].
90Massage has proven effective at diminishing EMG91activity and pain [19,21], preventing the formation of92connective tissue adherences, enhancing the production93and circulation of endogenous opioids [19], increasing94local blood flow, facilitating the elimination of residual95substances and extracellular fluid, improving the nutrition96of myofibrils and promoting relaxation and a sensation of97wellbeing [33,34]. Massaging the muscles of mastication98has been administered to patients with TMD, leading to a99reduction in pain, an increase in mandibular ROM and a100decrease in EMG activity in the muscles [21,35].101Postural control may be related to afferent signals of102the trigeminal nerve, which depend on information from103receptors of the stomatognathic complex (dentoalveolar104ligaments, muscle and joint receptors). Moreover, TMD105may alter muscle activity and the positioning of structures106of the stomatognathic system, interfering in the infor-107mation transmitted for the control of posture. Thus,108relaxation of the muscles of mastication (as assessed109through surface EMG) and the alignment of joint110structures (assessed through a clinical exam) may alter111afference from the receptors of the stomatognathic112system, thereby affecting postural control (assessed113through stabilometry). Based on this hypothesis, the114aim of the proposed study is to determine the effect of115facial massage and mandibular mobilization on EMG116activity of the muscles of mastication and static balance117in individuals with TMD.
118Methods/Design119Overview of research design120A randomized, controlled, blind, clinical trial is proposed121to study the effects of specific and nonspecific man-122dibular mobilization. The participants will be allocated123to three groups through a randomization process using124opaque envelopes. Each group will receive a specific125form of treatment for TMD. The control group (CG)126will receive massage therapy and those submitted to127joint mobilization will be divided into two groups: the128specific mobilization group (SMG) and the nonspecific129mobilization group (NMG). Evaluations will be carried130out before and after treatment using the Research Diag-131nostic Criteria for Temporomandibular Disorders (RDC/132TMD), EMG of the masseter and temporal muscles and133stabilometry.134After screening, individuals with TMD (based on the135RDC/TMD) will be selected. The study will be divided136into three types of treatment, three evaluations and two137phases, to which all individuals will be submitted:
138Evaluation 1: randomization of treatment with139allocation to treatment groups, stabilometric analysis140and EMG analysis, with the administration of the141protocol for the respective treatment.
El-Hage et al. Trials 2013, 14:316 Page 2 of 11http://www.trialsjournal.com/content/14/1/316
142 Evaluation 2: second stabilometric and EMG evaluation143 immediately following respective treatment.144 Treatment phase: treatment following respective protocol.145 Evaluation 3: third stabilometric and EMG evaluation146 and second administration of the RDC/TMD147 questionnaire.
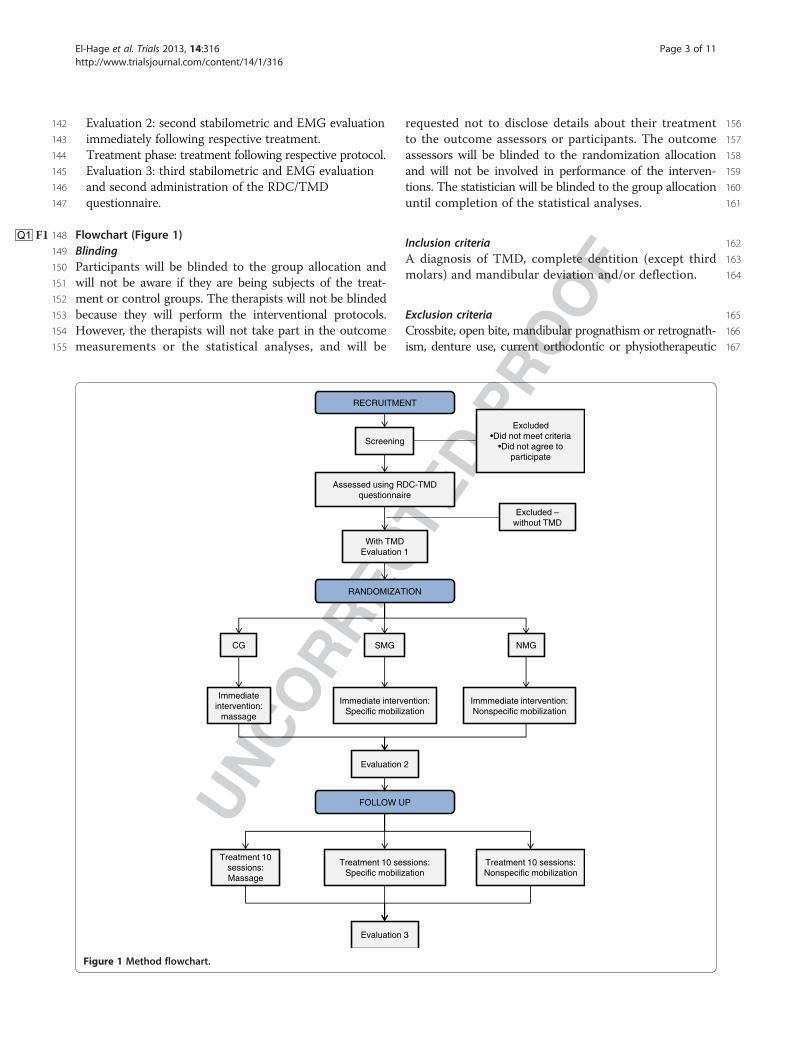
148 FlowchartQ1 (FigureF1 1)149 Blinding150 Participants will be blinded to the group allocation and151 will not be aware if they are being subjects of the treat-152 ment or control groups. The therapists will not be blinded153 because they will perform the interventional protocols.154 However, the therapists will not take part in the outcome155 measurements or the statistical analyses, and will be
156requested not to disclose details about their treatment157to the outcome assessors or participants. The outcome158assessors will be blinded to the randomization allocation159and will not be involved in performance of the interven-160tions. The statistician will be blinded to the group allocation161until completion of the statistical analyses.
162Inclusion criteria163A diagnosis of TMD, complete dentition (except third164molars) and mandibular deviation and/or deflection.
165Exclusion criteria166Crossbite, open bite, mandibular prognathism or retrognath-167ism, denture use, current orthodontic or physiotherapeutic
Screening
Excluded•Did not meet criteria
•Did not agree to participate
Assessed using RDC-TMD questionnaire
Excluded –without TMD
With TMDEvaluation 1
RANDOMIZATION
CG NMG
Immediateintervention:
massage
Evaluation 2
Treatment 10 sessions:Massage
Treatment 10 sessions:Nonspecific mobilization
Evaluation 3
FOLLOW UP
RECRUITMENT
SMG
Immediate intervention:Specific mobilization
Immmediate intervention:Nonspecific mobilization
Treatment 10 sessions:Specific mobilization
Figure 1 Method flowchart.
El-Hage et al. Trials 2013, 14:316 Page 3 of 11http://www.trialsjournal.com/content/14/1/316
168 treatment, neurological disorder that may affect balance,169 use of orthopedic insoles.
170 Ethical considerations171 The proposed study received approval from the local172 Human Research Ethics Committee under process173 number 457625 dated 28 September 2011. The study174 will be conducted in compliance with the norms that175 regulate research involving human subjects contained176 in Resolution number 196/97 of the Brazilian National177 Health Council and is registered with the Brazilian178 Registry of Clinical Trials (RBR9x8ssz). All participants179 will be informed regarding the objectives and procedures180 of the study and will be asked to sign a statement of181 informed consent agreeing to participate.
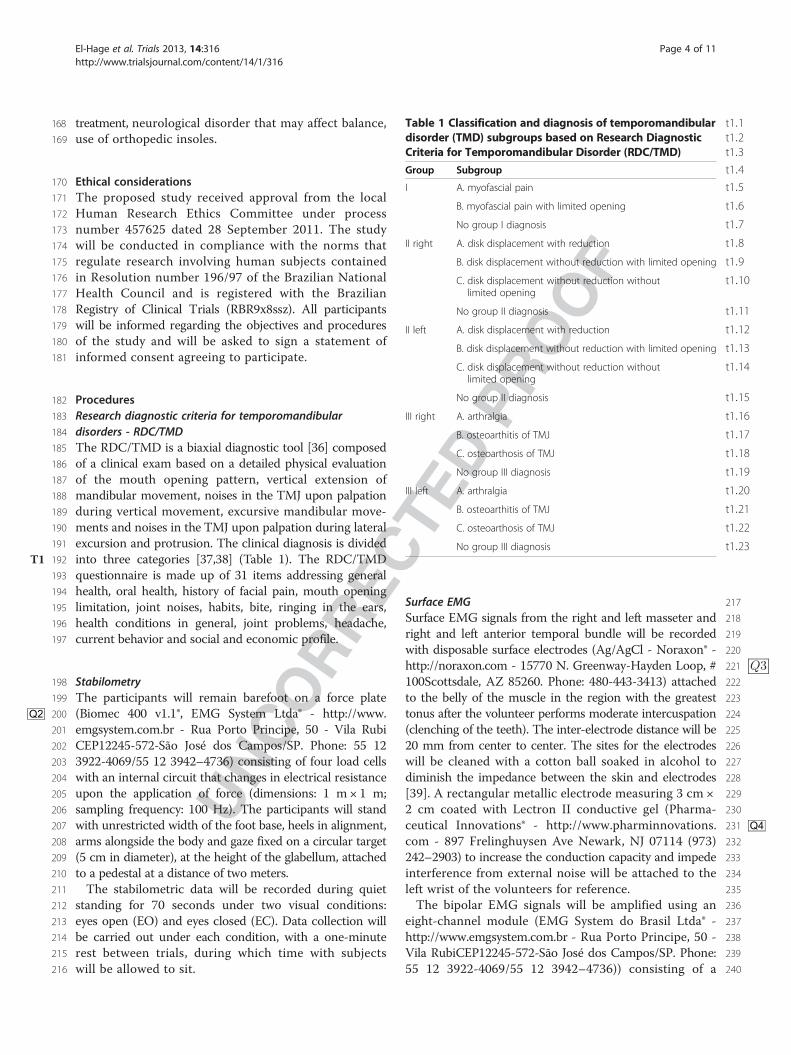
182 Procedures183 Research diagnostic criteria for temporomandibular184 disorders - RDC/TMD185 The RDC/TMD is a biaxial diagnostic tool [36] composed186 of a clinical exam based on a detailed physical evaluation187 of the mouth opening pattern, vertical extension of188 mandibular movement, noises in the TMJ upon palpation189 during vertical movement, excursive mandibular move-190 ments and noises in the TMJ upon palpation during lateral191 excursion and protrusion. The clinical diagnosis is divided192 into three categories [37,38] (TableT1 1). The RDC/TMD193 questionnaire is made up of 31 items addressing general194 health, oral health, history of facial pain, mouth opening195 limitation, joint noises, habits, bite, ringing in the ears,196 health conditions in general, joint problems, headache,197 current behavior and social and economic profile.
198 Stabilometry199 The participants will remain barefoot on a force plate200 (Biomec 400 v1.1®, EMG System Ltda® -Q2 http://www.201 emgsystem.com.br - Rua Porto Principe, 50 - Vila Rubi202 CEP12245-572-São José dos Campos/SP. Phone: 55 12203 3922-4069/55 12 3942–4736) consisting of four load cells204 with an internal circuit that changes in electrical resistance205 upon the application of force (dimensions: 1 m ! 1 m;206 sampling frequency: 100 Hz). The participants will stand207 with unrestricted width of the foot base, heels in alignment,208 arms alongside the body and gaze fixed on a circular target209 (5 cm in diameter), at the height of the glabellum, attached210 to a pedestal at a distance of two meters.211 The stabilometric data will be recorded during quiet212 standing for 70 seconds under two visual conditions:213 eyes open (EO) and eyes closed (EC). Data collection will214 be carried out under each condition, with a one-minute215 rest between trials, during which time with subjects216 will be allowed to sit.
217Surface EMG218Surface EMG signals from the right and left masseter and219right and left anterior temporal bundle will be recorded220with disposable surface electrodes (Ag/AgCl - Noraxon® -
Q3221http://noraxon.com - 15770 N. Greenway-Hayden Loop, #222100Scottsdale, AZ 85260. Phone: 480-443-3413) attached223to the belly of the muscle in the region with the greatest224tonus after the volunteer performs moderate intercuspation225(clenching of the teeth). The inter-electrode distance will be22620 mm from center to center. The sites for the electrodes227will be cleaned with a cotton ball soaked in alcohol to228diminish the impedance between the skin and electrodes229[39]. A rectangular metallic electrode measuring 3 cm !2302 cm coated with Lectron II conductive gel (Pharma-231ceutical Innovations® - Q4http://www.pharminnovations.232com - 897 Frelinghuysen Ave Newark, NJ 07114 (973)233242–2903) to increase the conduction capacity and impede234interference from external noise will be attached to the235left wrist of the volunteers for reference.236The bipolar EMG signals will be amplified using an237eight-channel module (EMG System do Brasil Ltda® -238http://www.emgsystem.com.br - Rua Porto Principe, 50 -239Vila RubiCEP12245-572-São José dos Campos/SP. Phone:24055 12 3922-4069/55 12 3942–4736)) consisting of a
t1:1Table 1 Classification and diagnosis of temporomandibulart1:2disorder (TMD) subgroups based on Research Diagnostict1:3Criteria for Temporomandibular Disorder (RDC/TMD)t1:4Group Subgroup
t1:5I A. myofascial pain
t1:6B. myofascial pain with limited opening
t1:7No group I diagnosis
t1:8II right A. disk displacement with reduction
t1:9B. disk displacement without reduction with limited opening
t1:10C. disk displacement without reduction withoutlimited opening
t1:11No group II diagnosis
t1:12II left A. disk displacement with reduction
t1:13B. disk displacement without reduction with limited opening
t1:14C. disk displacement without reduction withoutlimited opening
t1:15No group II diagnosis
t1:16III right A. arthralgia
t1:17B. osteoarthitis of TMJ
t1:18C. osteoarthosis of TMJ
t1:19No group III diagnosis
t1:20III left A. arthralgia
t1:21B. osteoarthitis of TMJ
t1:22C. osteoarthosis of TMJ
t1:23No group III diagnosis
El-Hage et al. Trials 2013, 14:316 Page 4 of 11http://www.trialsjournal.com/content/14/1/316
241 conditioner with a band pass filter with cut-off frequencies242 of 20 to 1000 Hz, an amplifier gain of 1,000 and a243 common mode rejection ratio > 120 dB. All data will244 be acquired and processed using a 16-bit analog to245 digital converter (EMG System do Brasil Ltda® - http://246 www.emgsystem.com.br - Rua Porto Principe, 50 - Vila247 RubiCEP12245-572-São José dos Campos/SP. Phone: 55248 12 3922-4069/55 12 3942–4736)) at a sampling frequency249 of 2 kHz.250 For the recording of the EMG signals, the participants251 will remain seated in a chair with feet apart and hands252 resting on the lower limbs. To standardize the EMG253 potentials of the four muscles analyzed with tooth contact,254 two strips of Parafilm M® (American National Can TM,255 Chicago, IL, USA) will be folded into five parts (3 mm256 in thickness) and positioned on the first and second257 mandibular molars (bilateral) of each subject [40]. Four258 seconds of maximum voluntary clenching (MVC) will259 be recorded three times, with a three-minute interval260 between readings.261 After five minutes of rest, the recording of EMG activity262 will be performed three times successively under the263 following conditions: i) rest position: the subjects will be264 asked to relax and maintain the maxillary and mandibular265 teeth without contact; ii) maximal intercuspation (iso-266 metric): the subjects will be ask to clench the teeth as hard267 as possible and maintain the same level of contraction268 (tooth contact); and iii) chewing (isotonic): the subjects269 will be instructed to mildly and symmetrically bite270 down (chew) on the two strips of Parafilm M® (positioned271 bilaterally) in time with a metronome adjusted to 60272 beats per minute.273 For the EMG signals recorded in rest position and274 during chewing, a two-minute interval will be allowed275 between readings. For maximal intercuspation, a five-276 minute interval between readings will be used. The data277 collection time will be 15 seconds for the rest position278 and chewing condition and 8 seconds for maximal279 intercuspation.
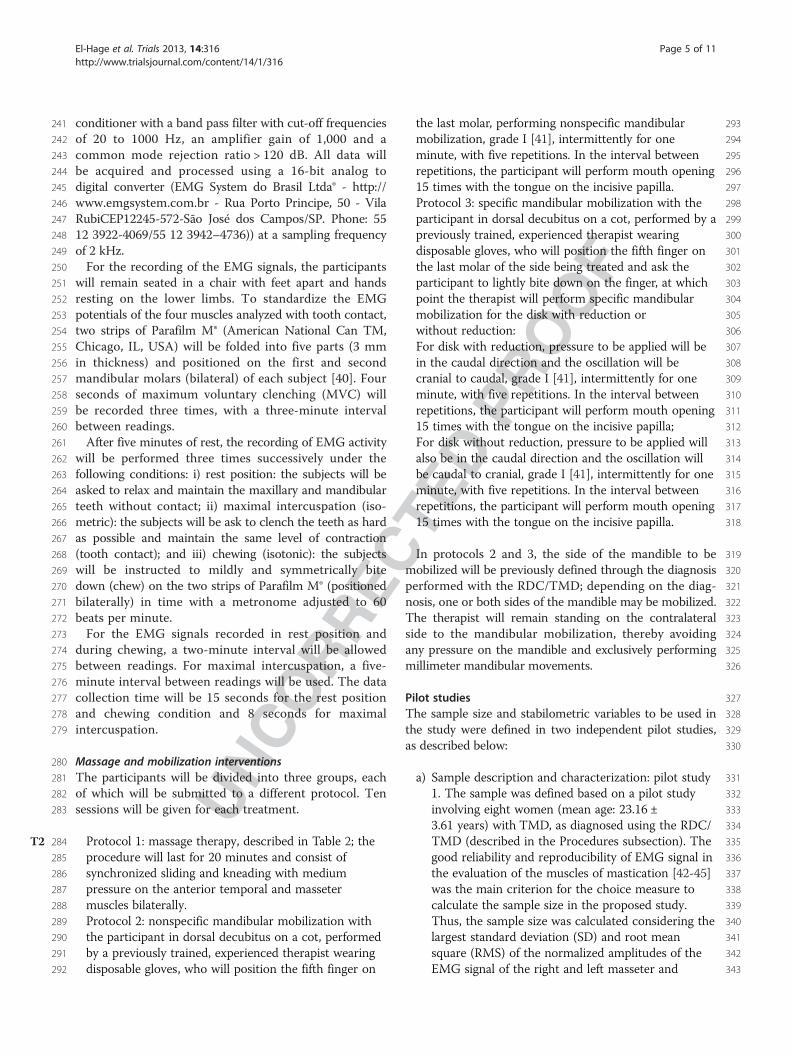
280 Massage and mobilization interventions281 The participants will be divided into three groups, each282 of which will be submitted to a different protocol. Ten283 sessions will be given for each treatment.
284 Protocol 1: massage therapy, described in TableT2 2; the285 procedure will last for 20 minutes and consist of286 synchronized sliding and kneading with medium287 pressure on the anterior temporal and masseter288 muscles bilaterally.289 Protocol 2: nonspecific mandibular mobilization with290 the participant in dorsal decubitus on a cot, performed291 by a previously trained, experienced therapist wearing292 disposable gloves, who will position the fifth finger on
293the last molar, performing nonspecific mandibular294mobilization, grade I [41], intermittently for one295minute, with five repetitions. In the interval between296repetitions, the participant will perform mouth opening29715 times with the tongue on the incisive papilla.298Protocol 3: specific mandibular mobilization with the299participant in dorsal decubitus on a cot, performed by a300previously trained, experienced therapist wearing301disposable gloves, who will position the fifth finger on302the last molar of the side being treated and ask the303participant to lightly bite down on the finger, at which304point the therapist will perform specific mandibular305mobilization for the disk with reduction or306without reduction:307For disk with reduction, pressure to be applied will be308in the caudal direction and the oscillation will be309cranial to caudal, grade I [41], intermittently for one310minute, with five repetitions. In the interval between311repetitions, the participant will perform mouth opening31215 times with the tongue on the incisive papilla;313For disk without reduction, pressure to be applied will314also be in the caudal direction and the oscillation will315be caudal to cranial, grade I [41], intermittently for one316minute, with five repetitions. In the interval between317repetitions, the participant will perform mouth opening31815 times with the tongue on the incisive papilla.
319In protocols 2 and 3, the side of the mandible to be320mobilized will be previously defined through the diagnosis321performed with the RDC/TMD; depending on the diag-322nosis, one or both sides of the mandible may be mobilized.323The therapist will remain standing on the contralateral324side to the mandibular mobilization, thereby avoiding325any pressure on the mandible and exclusively performing326millimeter mandibular movements.
327Pilot studies328The sample size and stabilometric variables to be used in329the study were defined in two independent pilot studies,330as described below:
331a) Sample description and characterization: pilot study3321. The sample was defined based on a pilot study333involving eight women (mean age: 23.16 ±3343.61 years) with TMD, as diagnosed using the RDC/335TMD (described in the Procedures subsection). The336good reliability and reproducibility of EMG signal in337the evaluation of the muscles of mastication [42-45]338was the main criterion for the choice measure to339calculate the sample size in the proposed study.340Thus, the sample size was calculated considering the341largest standard deviation (SD) and root mean342square (RMS) of the normalized amplitudes of the343EMG signal of the right and left masseter and
El-Hage et al. Trials 2013, 14:316 Page 5 of 11http://www.trialsjournal.com/content/14/1/316
344temporal muscles. The data were collected during345maximum intercuspation for eight seconds before346(T0) and after five sessions of nonspecific347mobilization (T1). Considering a statistical power of3480.80, the right temporal muscle determined the349largest sample (13 individuals (T0 = 1.19; T1 = 1.08;350SD = 0.14)). The sample will be made up of male and351female individuals, between 18 and 36 years of age,352selected based on the eligibility criteria and353diagnosed with TMD based on the RDC/TMD.354b) Stabilometric analysis: pilot study 2 after the355definition of the sample size, a second pilot study356was conducted to determine the stabilometric357variables that exhibit the best within-day and358between-day reproducibility. Fifteen female subjects359with TMD, as diagnosed by the RDC/TMD360(described in Procedures subsection), were recruited.361The subjects had a mean age of 20.13 (± 6.19) years,362mean height of 1.64 cm (± 0.06) and mean body363weight of 61.08 Kg (± 9.72). Each participant364completed two test sessions on two different days.365All sessions were performed in the same laboratory366environment by the same examiners, with a seven-367day interval between sessions. Each session consisted368of two successive trials of quiet upright stance, with369a rest period of approximately 60 seconds between370trials. The stabilometric data were recorded for37170 seconds under two visual conditions: eyes open372(EO) and eyes closed (EC). For the analysis of the373stabilometric variables, the initial 10 seconds were374discarded to avoid initial transients and anticipation375effects. Two collections were carried out under each376visual condition, with a one-minute rest between377collections (session 1). The order of the visual378conditions (EO and EC) was randomly determined379to control for the learning effect.380c) The justification for two collections under each381visual condition is based on the fact that three trials382were initially planned for each visual condition, but383the first five individuals selected for this initial study384reported discomfort and fatigue. Thus, new tests385were carried out with the same participants with a386one-day interval and the trials were reduced to two387under each visual condition, with no report of any388discomfort. The possibility of diminishing the time389to less than 60 seconds was not considered due to
t2:1 Table 2 Twenty-minute facial massage protocolt2:2 performed bilaterallyt2:3 Surface sliding 3 minutes
t2:4 Circular movements in counter-clockwise direction
t2:5 Anterior bundle of temporal muscle
t2:6 Kneading 3 minutes
t2:7 Kneading in cranial-caudal direction
t2:8 Upper fibers of masseter muscle
t2:9 Return of hands to initial position with continuoust2:10 caudal-cranial sliding of suprahyoid musculature
t2:11 Surface sliding 1 minute
t2:12 Circular movements in counter-clockwise direction
t2:13 Anterior bundle of temporal muscle
t2:14 Kneading 1 minute
t2:15 Kneading in cranial-caudal direction
t2:16 Upper fibers of masseter muscle
t2:17 Return of hands to initial position with continuoust2:18 caudal-cranial sliding of suprahyoid musculature
t2:19 Surface sliding 1 minute
t2:20 Circular movements in counter-clockwise direction
t2:21 Anterior bundle of temporal muscle
t2:22 Kneading 1 minute
t2:23 Kneading in cranial-caudal direction
t2:24 Upper fibers of masseter muscle
t2:25 Return of hands to initial position with continuoust2:26 caudal-cranial sliding of suprahyoid musculature
t2:27 Deep sliding 3 minutes
t2:28 Circular movements in counter-clockwise direction
t2:29 Anterior bundle of temporal muscle
t2:30 Kneading 3 minutes
t2:31 Kneading in cranial-caudal direction
t2:32 Upper fibers of masseter muscle
t2:33 Return of hands to initial position with continuoust2:34 caudal-cranial sliding of suprahyoid musculature
t2:35 Deep kneading 1 minute
t2:36 Circular movements in counter-clockwise direction
t2:37 Anterior bundle of temporal muscle
t2:38 Kneading 1 minute
t2:39 Kneading in cranial-caudal direction
t2:40 Upper fibers of masseter muscle
t2:41 Return of hands to initial position with continuoust2:42 caudal-cranial sliding of suprahyoid musculature
t2:43 Deep sliding 1 minute
t2:44 Circular movements in counter-clockwise direction
t2:45 Anterior bundle of temporal muscle
t2:46 Kneading 1 minute
t2:47 Kneading in cranial-caudal direction
Table 2 Twenty-minute facial massage protocolperformed bilaterally (Continued)
t2:48Upper fibers of masseter muscle
t2:49Return of hands to initial position with continuoust2:50caudal-cranial sliding of suprahyoid musculature
t2:51Finalization with light touch
El-Hage et al. Trials 2013, 14:316 Page 6 of 11http://www.trialsjournal.com/content/14/1/316

390 the indication of using at least 90 seconds of data391 collection for each trial [46]. Moreover, it has been392 demonstrated that, under the eyes closed condition,393 reliability is lesser for short sampling and rises as the394 individual adapts [47]. Thus, the measurements of395 center of pressure (CoP) of these five individuals396 were not considered and only two trials under each397 visual condition were performed in this pilot study398 to maintain the integrity of the participants in the399 study.The tests were repeated after a one-week400 interval (session 2). All details regarding the401 equipment and analysis of the stabilometric data are402 described in the Procedures and Signal processing403 subsections, respectively.
404 Signal processing405 Stabilometric parameters406 Displacement from the center of pressure (CoP) in the407 anteroposterior (AP) and mediolateral (ML) directions408 will be used to analyze body sway, as in the preliminary409 study (pilot study 2). CoP data will be filtered with a410 Butterworth low-pass filter with a cut-off frequency of411 10 Hz [46]. Postural sway will be quantified by means of412 two common scale-dependent variables: CoP sway area413 as an indicator for magnitude of CoP movements and414 CoP mean velocity and frequency as indicators of the415 efficiency of postural control. As an indicator for the416 regularity of CoP movements, a scale-independent variable417 denominated sample entropy (SaEn) will be used. Each418 parameter is briefly described below:
419 – Sway area (cm2) will be estimated by fitting an420 ellipse to the CoP data (AP versus ML) that421 encompasses 95% of the data; [48]422 – Mean velocity (cm/s) of the CoP in both AP and423 ML directions will be calculated by taking the total424 distance traveled and dividing it by the time of the425 trial; [49]426 – Frequency (Hz) of CoP displacement will be427 determined by the frequency at which 80% of the428 CoP spectral power is below. The 80% value was429 chosen based on the study by Baratto et al. (2002)430 [50], who suggest that this value is a better431 discriminator for CoP data than other spectral432 measurements;433 – SaEn is a method for quantifying the regularity of a434 time series [51,52] and reflects the conditional435 probability that two sequences of ‘m’ consecutive436 data points that are similar to each other will remain437 similar when one more consecutive point is438 included. Being ‘similar’ means that the value of a439 specific measure of distance is less than ‘r’.440 Therefore, SaEn is a function of m and r parameters441 [53]. The embedding dimension, m, and the
442tolerance distance, r, will be set to m = 3 and r = 30%443of standard deviation of the data sequence [54]. To444render an outcome for the scale-independent SaEn,445the CoP data in both AP and ML directions will be446normalized to unit variance by dividing the time-447series in question by their respective standard448deviation [55]. Values close to zero indicate greater449regularity, while values closer to two indicate greater450entropy in the signal being analyzed. In the present451study, a decrease in sample entropy (that is, more452regular sway fluctuations) will be interpreted as a453decrease in the effectiveness of postural control.
454Surface electromyographic data455Five seconds of the signal will be used for the calculation456of the root mean square (RMS) of the amplitude, with457the two initial seconds and final one second of the eight-458second reading discarded. For data recorded in the resting459position and during maximal intercuspation, the RMS460will be calculated using a 200 ms moving window.461The data recorded during chewing will be normalized462by the peak EMG recorded from the same isotonic trial463(dynamic mean method). The amplitude of the signal464obtained in the resting position and during maximal465intercuspation will be expressed as percentage of the466average RMS recorded in the three readings during467maximum voluntary contraction (MVC) (%MVC).468All stabilometric and EMG signals will be processed469performing specific routines carried out in the Matlab470program, version 7.1 (The MathWorks Inc., Natick,471MA, USA).
472Data analysis473The Shapiro-Wilk test will be used to test the data with474regard to Gaussian distribution. Data that demonstrate475parametric distribution will be expressed as mean and476standard deviation (SD) values. Data with nonparametric477distribution will be expressed as median and inter-quartile478interval. Either repeated-measure ANOVA or Friedman’s479test will be used for the intra-group analysis and either480one-way ANOVA or the Kruskal-Wallis test will be used481for the inter-group analysis of data with parametric and482non-parametric distribution, respectively.
483Reliability484Data on the CoP measures obtained in two sessions with-485out any type of intervention (pilot study 2) are expressed486as mean and SD. Some test results revealed non-normal487distribution. Thus all data were log-transformed prior to488analyses to negate the effects of heteroscedasticity [56].489The reliability of each CoP-based measure was quantified490using intraclass correlation coefficients (ICC) [57], 95%491confidence intervals (CI) and the standard error of the492mean (SEM) [58]. For the purposes of this study, the ICC
El-Hage et al. Trials 2013, 14:316 Page 7 of 11http://www.trialsjournal.com/content/14/1/316
493 was interpreted using the following criteria: 0.00 to 0.39494 (poor), 0.40 to 0.59 (fair), 0.60 to 0.74 (good) and 0.75495 to 1.00 (excellent) [59]. The SEM was used to express496 reliability in absolute values, with a lower SEM denoting497 greater reliability of the measurement, whereas a high498 SEM indicates a high level of error and implies the499 non-reproducibility of the tested values.
500All data were analyzed using the Statistical Package for501the Social Sciences (SPSS - Q5http://www-01.ibm.com/soft-502ware/analytics/spss/ - IBM Corporation 1 New Orchard503Road Armonk, New York 10504–1722 United States504914-499-1900 Version 17.
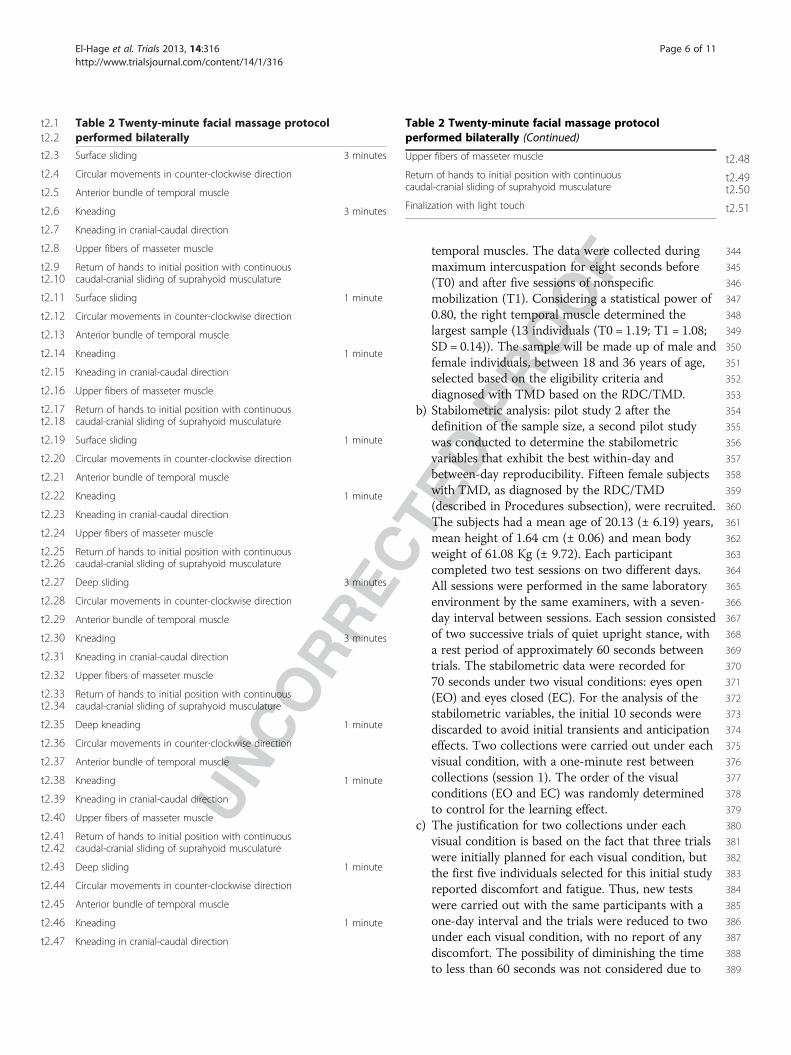
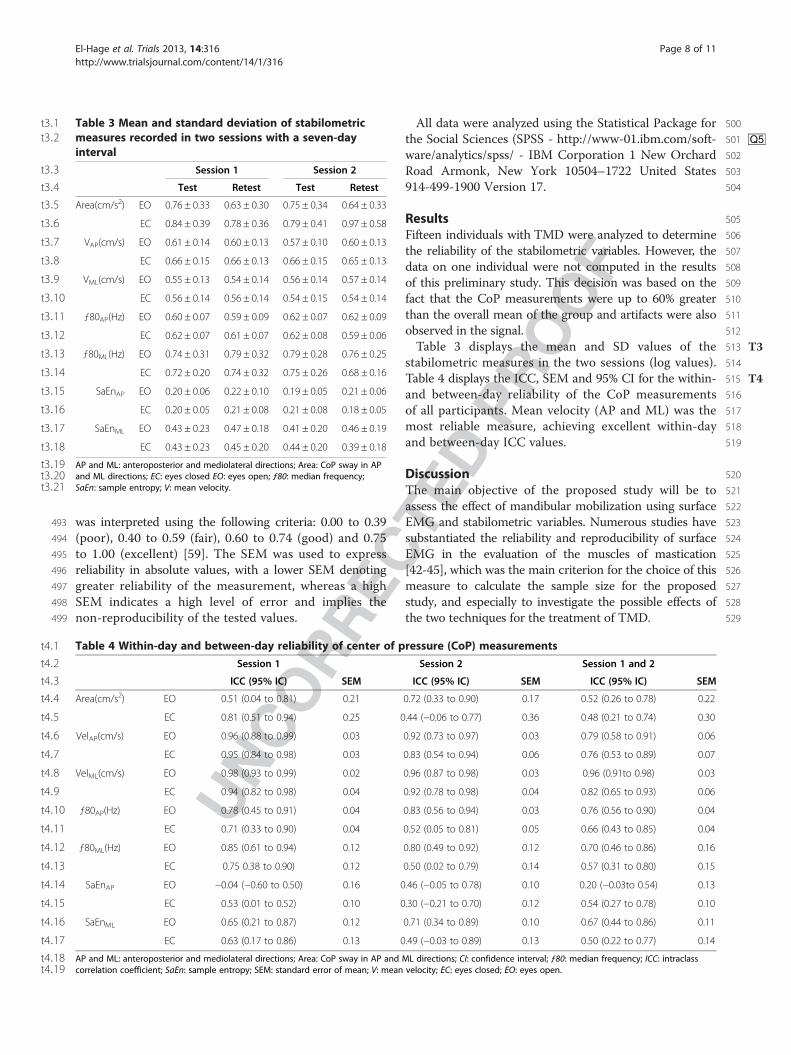
505Results506Fifteen individuals with TMD were analyzed to determine507the reliability of the stabilometric variables. However, the508data on one individual were not computed in the results509of this preliminary study. This decision was based on the510fact that the CoP measurements were up to 60% greater511than the overall mean of the group and artifacts were also512observed in the signal.513Table T33 displays the mean and SD values of the514stabilometric measures in the two sessions (log values).515Table T44 displays the ICC, SEM and 95% CI for the within-516and between-day reliability of the CoP measurements517of all participants. Mean velocity (AP and ML) was the518most reliable measure, achieving excellent within-day519and between-day ICC values.
520Discussion521The main objective of the proposed study will be to522assess the effect of mandibular mobilization using surface523EMG and stabilometric variables. Numerous studies have524substantiated the reliability and reproducibility of surface525EMG in the evaluation of the muscles of mastication526[42-45], which was the main criterion for the choice of this527measure to calculate the sample size for the proposed528study, and especially to investigate the possible effects of529the two techniques for the treatment of TMD.
t3:1 Table 3 Mean and standard deviation of stabilometrict3:2 measures recorded in two sessions with a seven-day
intervalt3:3 Session 1 Session 2
t3:4 Test Retest Test Retest
t3:5 Area(cm/s2) EO 0.76 ± 0.33 0.63 ± 0.30 0.75 ± 0.34 0.64 ± 0.33
t3:6 EC 0.84 ± 0.39 0.78 ± 0.36 0.79 ± 0.41 0.97 ± 0.58
t3:7 VAP(cm/s) EO 0.61 ± 0.14 0.60 ± 0.13 0.57 ± 0.10 0.60 ± 0.13
t3:8 EC 0.66 ± 0.15 0.66 ± 0.13 0.66 ± 0.15 0.65 ± 0.13
t3:9 VML(cm/s) EO 0.55 ± 0.13 0.54 ± 0.14 0.56 ± 0.14 0.57 ± 0.14
t3:10 EC 0.56 ± 0.14 0.56 ± 0.14 0.54 ± 0.15 0.54 ± 0.14
t3:11 ƒ80AP(Hz) EO 0.60 ± 0.07 0.59 ± 0.09 0.62 ± 0.07 0.62 ± 0.09
t3:12 EC 0.62 ± 0.07 0.61 ± 0.07 0.62 ± 0.08 0.59 ± 0.06
t3:13 ƒ80ML(Hz) EO 0.74 ± 0.31 0.79 ± 0.32 0.79 ± 0.28 0.76 ± 0.25
t3:14 EC 0.72 ± 0.20 0.74 ± 0.32 0.75 ± 0.26 0.68 ± 0.16
t3:15 SaEnAP EO 0.20 ± 0.06 0.22 ± 0.10 0.19 ± 0.05 0.21 ± 0.06
t3:16 EC 0.20 ± 0.05 0.21 ± 0.08 0.21 ± 0.08 0.18 ± 0.05
t3:17 SaEnML EO 0.43 ± 0.23 0.47 ± 0.18 0.41 ± 0.20 0.46 ± 0.19
t3:18 EC 0.43 ± 0.23 0.45 ± 0.20 0.44 ± 0.20 0.39 ± 0.18
t3:19 AP and ML: anteroposterior and mediolateral directions; Area: CoP sway in APt3:20 and ML directions; EC: eyes closed EO: eyes open; ƒ80: median frequency;t3:21 SaEn: sample entropy; V: mean velocity.
t4:1 Table 4 Within-day and between-day reliability of center of pressure (CoP) measurementst4:2 Session 1 Session 2 Session 1 and 2
t4:3 ICC (95% IC) SEM ICC (95% IC) SEM ICC (95% IC) SEM
t4:4 Area(cm/s2) EO 0.51 (0.04 to 0.81) 0.21 0.72 (0.33 to 0.90) 0.17 0.52 (0.26 to 0.78) 0.22
t4:5 EC 0.81 (0.51 to 0.94) 0.25 0.44 (!0.06 to 0.77) 0.36 0.48 (0.21 to 0.74) 0.30
t4:6 VelAP(cm/s) EO 0.96 (0.88 to 0.99) 0.03 0.92 (0.73 to 0.97) 0.03 0.79 (0.58 to 0.91) 0.06
t4:7 EC 0.95 (0.84 to 0.98) 0.03 0.83 (0.54 to 0.94) 0.06 0.76 (0.53 to 0.89) 0.07
t4:8 VelML(cm/s) EO 0.98 (0.93 to 0.99) 0.02 0.96 (0.87 to 0.98) 0.03 0.96 (0.91to 0.98) 0.03
t4:9 EC 0.94 (0.82 to 0.98) 0.04 0.92 (0.78 to 0.98) 0.04 0.82 (0.65 to 0.93) 0.06
t4:10 ƒ80AP(Hz) EO 0.78 (0.45 to 0.91) 0.04 0.83 (0.56 to 0.94) 0.03 0.76 (0.56 to 0.90) 0.04
t4:11 EC 0.71 (0.33 to 0.90) 0.04 0.52 (0.05 to 0.81) 0.05 0.66 (0.43 to 0.85) 0.04
t4:12 ƒ80ML(Hz) EO 0.85 (0.61 to 0.94) 0.12 0.80 (0.49 to 0.92) 0.12 0.70 (0.46 to 0.86) 0.16
t4:13 EC 0.75 0.38 to 0.90) 0.12 0.50 (0.02 to 0.79) 0.14 0.57 (0.31 to 0.80) 0.15
t4:14 SaEnAP EO !0.04 (!0.60 to 0.50) 0.16 0.46 (!0.05 to 0.78) 0.10 0.20 (!0.03to 0.54) 0.13
t4:15 EC 0.53 (0.01 to 0.52) 0.10 0.30 (!0.21 to 0.70) 0.12 0.54 (0.27 to 0.78) 0.10
t4:16 SaEnML EO 0.65 (0.21 to 0.87) 0.12 0.71 (0.34 to 0.89) 0.10 0.67 (0.44 to 0.86) 0.11
t4:17 EC 0.63 (0.17 to 0.86) 0.13 0.49 (!0.03 to 0.89) 0.13 0.50 (0.22 to 0.77) 0.14
t4:18 AP and ML: anteroposterior and mediolateral directions; Area: CoP sway in AP and ML directions; CI: confidence interval; ƒ80: median frequency; ICC: intraclasst4:19 correlation coefficient; SaEn: sample entropy; SEM: standard error of mean; V: mean velocity; EC: eyes closed; EO: eyes open.
El-Hage et al. Trials 2013, 14:316 Page 8 of 11http://www.trialsjournal.com/content/14/1/316
530 Regarding CoP measurements, however, it is not yet531 possible to determine whether stabilometric variables offer532 adequate reproducibility in patients with TMD. The533 reliability of CoP variables has generally been analyzed534 in healthy adults and elderly individuals [60] or those535 with associated diseases [61,62], but no such studies are536 found involving patients with TMD. This led to the need537 to conduct the aforementioned pilot study to test the538 reproducibility of the data and determine the collection539 protocol for the stabilometric variables idealized in540 the project. The preliminary execution of this project541 also contributed to an adjustment of the data collection542 protocol regarding the number of trials per session543 based on the participants’ reports of discomfort, as544 described above.545 Studies have demonstrated that the number of recorded546 tests exerts an effect on the reliability of CoP measure-547 ments used to assess postural control during quiet548 standing (static posture) [60-63]. Although the results549 of this study indicate that CoP-based measurements550 have quite diverse levels of reliability, mean velocity was551 the most reliable measure with regard to within-day552 and between-day readings, which is consistent with553 earlier reports [46,60,61,63,64]. Within-day reliability was554 generally better than between-day reliability. Moreover,555 the reliability of CoP measurements was also influenced556 by the visual condition (eyes open and eyes closed). The557 ICC was greater under the eyes open condition for mean558 velocity and median frequency (ƒ80) in the two directions559 (AP and ML). The visual influence on postural control560 demonstrates a specific characteristic among individuals561 with TMD, as higher overall reliability values have previ-562 ously been demonstrated under the eyes closed condition563 compared to eyes open [49,65,66].564 The weakest index regarding reliability was the SaEn,565 followed by sway area. The variation in ICC among poor,566 fair and good and the high SEM demonstrate that these567 variables should not be considered when investigating568 the possible effects of mandibular mobilization for the569 treatment of TMD.570 The results of this pilot studied showed that mean571 velocity was the most reliable measure, which is consistent572 with earlier reports, and can be selected as a reliable573 postural sway measure. Moreover, the results of the574 proposed study will help determine whether specific575 and/or nonspecific mandibular mobilization exerts an576 effect on the muscles of mastication and postural control.577 Moreover, if an effect is detected, the methodology defined578 in the proposed study will allow identifying whether the579 effect is local (found only in the muscles of mastication),580 global (found only in postural control) or generalized.
581 Trial status582 This trial is currently recruiting patients.
583Abbreviations584Ag/AgCl: Silver/silver chloride; ANOVA: Analysis of variance;585AP: Anteroposterior; CG: Control group; CI: Confidence interval; CoP: Center586of pressure; COPAP: Anteroposterior center of pressure; COPML: Mediolateral587center of pressure; EC: Eyes closed; EMG: Electromyography; EO: Eyes open;588f80: Median frequency; ICC: Interclass correlation coefficient; ML: Mediolateral;589MVC: Maximum voluntary contraction; NMG: Nonspecific mobilization group;590RDC/TMD: Research Diagnostic Criteria for Temporomandibular Disorders;591RMS: Root mean square; ROM: Range of movement; SaEn: Sample entropy;592SD: Standard deviation; SEM: Standard error of mean;593EMG: Electromyography; SPSS: Satistical package for social sciences;594TMD: Temporomandibular disorder; TMJ: Temporomandibular joint.
595Competing interests596The authors declared that they have no competing interests.
597Authors’ contributions598YE submitted the manuscript. YE, FP, DABG, TO and CAFPG drafted the599original protocol. TO, FP, ICG and DABG contributed to the study design.600FP, DABG and YE performed the sample size calculation and description601of the data processing. DFMS, SKB, FB - dentists in charge of screening602and application of diagnostic criteria; CAFPG and IPSG - in charge of603stabilometry and electromyography; EECA, CMH, NCM, TCS - responsible for604the execution of the treatments; FP, YE in charge of the data processing605and analysis; CFA - responsible for equipment used in the study; MBSG606and BRBB - in charge of patients recruitment and performed the reviews607of the manuscript; APA - translated the manuscript to English; DABG -s in608charge of the laboratory and coordination of the study. All authors read609and approved the final manuscript.
610Acknowledgments611To all involved in the study, the team, participants, Nove de Julho612University (UNINOVE), and Fundação de Amparo à Pesquisa do Estado613de São Paulo (FAPESP).
614Funding615The study is funded by Fundação de Amparo à Pesquisa do Estado de São616Paulo (FAPESP).
617Author details6181Postgraduate Program in Rehabilitation Sciences, Laboratório de619Biodinâmica do Movimento Humano, Universidade Nove de Julho620(UNINOVE), Av. Dr. Adolfo Pinto, 109 Água Branca, São Paulo, SP 05001-100,621Brazil. 2Department of Physical Therapy, Universidade Nove de Julho622(UNINOVE), Av. Dr. Adolfo Pinto, 109. Água Branca, São Paulo, SP 05001-100,623Brazil. 3Master’s Program in Physical Therapy, Universidade da Cidade de São624Paulo (UNICID), Rua Cesáreo Galeno, 475. Tatuapé, São Paulo, SP 03071-000,625Brazil. 4Department of Physical Therapy, Florida International University (FIU),626AHC3-427, 11200S.W. 8th Street, Miami, FL 33199, USA. 5College of Dentistry,627State University of Campinas, Morphology, Av. Limeira, 901 Caixa Postal 52,628Piracicaba, SP, Brazil.
629Received: 9 January 2013 Accepted: 3 September 2013630Published: 1 October 2013
631References1. 632Bracco P, Deregibus A, Piscetta R: Effects of different jaw relations on
633postural stability in human subjects. Neurosci Lett 2004, 356:228–230.2. 634Dawson PE: New definition for relating occlusion to varying
635conditions of the temporomandibular joint. J Prostetic Dentistry 1995,63674(7):619–627.
3. 637Huggare J, Harkness E: Association between head posture and dental638occlusion. J Dent Res 1993, 72:255.
4. 639Nobili A, Adversi R: Relationship between posture and occlusion: a640clinical experimental investigation. J Craniomandibular Pract 1996,64114:274–285.
5. 642Braun BL: Postural differences between asymptomatic men and643women and craniofacial pain patients. Arch Phys Med Rehabil 1991,64472:653–656.
El-Hage et al. Trials 2013, 14:316 Page 9 of 11http://www.trialsjournal.com/content/14/1/316

6.645 Ferrario VF, Sforza C, Schimitz JH, Taroni A: Occlusion and center of foot646 pressure variation: is there a relationship? J Prosthetic Dentistry 1996,647 76:302–308.
7.648 Palano D, Molinari G, Capeletto M, Guidetti G, Vernole B: The role of649 stabilometry in assessing the correlations between craniomandibular650 disorders and equilibrium disorders. Bulletin du Groupèment International651 pour la Recherché Scientifique en Stomatologie & Odondologie 1994, 37:23–26.
8.652 Palano D, Molinari G, Capeletto M, Guidetti G, Vernole B: The use of the653 computer-assisted stabilometry in the diagnosis of craniomandibular654 disorders. Bulletin du Groupèment International pour la Recherché Scientifique655 en Stomatologie & Odondologie 1994, 37:19–22.
9.656 Saito ET, Akashi PMH, Sacco ICN: Global body posture evaluation in657 patients with temporomandibular joint disorder. Clinics 2009, 64(1):35–39.
10.658 Buisseret-Delmas C, Compoint C, Delfini C, Buisseret P: Organisation of659 reciprocal connections between trigeminal and vestibular nuclei in the660 rat. J Comp Neurol 1999, 401:153–168.
11.661 Gangloff P, Perrin PP: Unilateral trigeminal anesthesia modifies postural662 control in human subjects. Neurosci Lett 2002, 330:179–182.
12.663 Milani RS, De-Pierre DD, Lapeyre L, Pourreyron L: Relationship between664 dental occlusion and posture. J Craniomandibular Pract 2000, 18:127–134.
13.665 Eriksson PO, Zafar H, Nordh E: Concomitant mandibular and head-neck666 movements during jaw opening-closing in man. J Oral Rehabil 1998,667 25:859–870.
14.668 Tingey EM, Buschang MA, Throckmorton GS: Mandibular rest position: a669 reliable position by head support and body posture. Am J Orthod670 Dentofacial Orthop 2001, 120:614–622.
15.671 Ceneviz C, Mehta NR, Forgione A, Sands MJ, Abdallah EF, Lobo SL, Mavroudi672 S: The immediate effect of changing mandibular position on the EMG673 activity of the masseter, temporalis, sternocleidomastoid, and trapezius674 muscles. J Craniomandibular Pract 2006, 24:237–244.
16.675 Landulpho ABE, Silva WAE, Silva FA, Vitti M: Electromyographic evaluation676 of masseter and anterior temporalis muscles in patients with677 temporomandibular disorders following interocclusal appliance678 treTMJent. J Oral Rehabil 2004, 31:95–98.
17.679 Zuñiga C, Miralles R, Mena B, Montt R, Moran D, Santander H, Moya H:680 Influence of variation in jaw posture on sternocleidomastoid and681 trapezius electromyographic activity. Cranio 1995, 13(3):157–162.
18.682 Ferrario VF, Sforza C, Dellavia C, Tartaglia GM: Evidence of an influence of683 asymmetrical occlusal interferences on the activity of the684 sternocleidomastoid muscle. J Oral Rehabil 2003, 30:34–40.
19.685 Capellini VK, Souza GS, Faria CRS: Massage therapy in the management of686 myogenic TMD: a pilot study. J Appl Oral Sci 2006, 14:21–26.
20.687 Pinho JC, Caldas FM, Mora MJ, Santana-Penin U: Electromyographic activity688 in patients with temporomandibular disorders. J Oral Rehabil 2000,689 27(1):985–990.
21.690 Biasotto-Gonzalez DA, Bérzin F: Electromyographic study of patients with691 masticatory muscles disorders, physiotherapeutic treTMJent (massage).692 Braz J Oral Sci 2004, 3(10):516–521.
22.693 Kalamir A, Pollard H, Vitiello AL, Bonello R: Manual therapy for694 temporomandibular disorders: a review of the literature. J Bodyw Mov695 Ther 2007, 11:84–90.
23.696 Crider AB, Glaros AG: A meta-analysis of EMG biofeedback treTMJent of697 temporomandibular disorders. J Orofac Pain 1999, 13(1):29–37.
24.698 Gray RJM, Quayle AA, Hall CA, Schofield MA: Physiotherapy in the699 treTMJent of temporomandibular joint disorders: a comparative study of700 four treTMJent methods. Br Dent J 1994, 176(7):257–261.
25.701 Michelotti A, Parisini F, Farella M, Cimino R, Martina R: Muscular702 physiotherapy in patients with temporomandibular disorders. Controlled703 clinical Trial. Minerva Stomatological 2000, 49(11–12):541–548.
26.704 Van der-Glas HW, Buchner R, Van-Grootel RJ: Comparison of treTMJent705 options for myogenous temporomandibular dysfunction. Nederlands706 Tijdschrft voor Tandheelkunde 2000, 107(12):505–512.
27.707 Simons DG: Clinical and etiological update of myofacial pain from trigger708 points. J Musculoskel Pain 1996, 4:97–125.
28.709 Pertille A, Macedo AB, Dibai AVF, Rêgo EM, Arrais LDF, Negri JR, Teodori710 RM: Immediate effects of bilateral grade III mobilization of the711 talocrural joint on the balance of elderly women. J Manipulative Physiol712 Therapeut. in press.
29.713 Taylor M, Suvinen T, Reade P: The effect of grade IV distraction714 mobilization on patients with temporomandibular pain-dysfunction715 disorder. Physiother Theory Pract 1994, 10(3):129–136.
30. 716Nicolakis P, Erdogmus CB, Kollmitzer J, Kerschan-Schindl K, Sengstbratl M,717Nuhr M, Crevenna R, Fialka-Moser V: Long-term outcome after treTMJent718of temporomandibular joint osteoarthritis with exercise and manual719therapy. Cranio 2002, 20(1):23–27.
31. 720Furto ES, Cleland JA, Whitman JM, Olson KA: Manual physical therapy721interventions and exercise for patients with temporomandibular722disorders. Cranio 2006, 24(4):283–291.
32. 723Cameli E, Sheklow SL, Blommenfeld I: Comparative study of repositioning724splint therapy and passive manual range of motion techniques for725anterior displaced temporomandibular discs with unstable excursive726reduction. Physiotherapy 2001, 87:26–36.
33. 727Ali HM: Diagnostic criteria for temporomandibular joint disorders: a728physiotherapist’s perspective. Physiotherapy 2002, 88:421–426.
34. 729Michelotti A, Steens MH, Farella M, Parisini F: Short-term effects of730physiotherapy versus counseling for the treTMJent of myofascial pain of731the jaw muscles. J Oral Rehabil 2002, 29(9):874.
35. 732Katsoulis J, Richter M: Efficacité de la physiothérapie spécialisée sur les733Sadam musculaires. Revue de stomatologie et de chirurgie maxillo-faciale7342008, 109:9–14.
36. 735Dworkin SF, Leresche L: Research diagnostic criteria for736temporomandibular disorders: review, criteria, examinations and737specifications, critique. J Craniomandibular disorders 1992, 6:301–355.
37. 738Lucena 1BS, Kosminsky M, Costa 1, Góes PSA: Validation of the Portuguese739version of the RDC/TMD axis II questionnaire. Braz Oral Res 2006,74020(4):312–317.
38. 741Schiffman EL, Ohrbach R, Truelove EL, Feng T, Anderson GC, Pan W,742Gonzalez YM, John MT, Sommers E, List T, Velly AM, Kang W, Look JO: The743revised research diagnostic criteria for temporomandibular disorders:744methods used to establish and validate revised axis I diagnostic745algorithms. J orofacial pain 2010, 24(1):63–78.
39. 746De-Luca CJ: The use of surface electromyography in biomechanics.747J Appl Miomech 1997, 13(2):135–163.
40. 748Biasotto-Gonzalez DA, Bérzin F, Costa JM, Gonzalez TO: Electromyographic749study of stomatognathic system muscles during chewing of different750materials. Electromyogr Clin Neurophysiol 2010, 50:121–127.
41. 751Maitland GD: Principle techniques. In Maitlan’s Vertebral Manipulation.7526th edition. London: Publisher:Butterworth-Heineman; 2001:171–182.
42. 753Ferrario V, Sforza C, D’Addona A, Miani A: Reproducibility of EMG754measures: a statistical analysis. J Oral Rehabil 1991, 18:513–521.
43. 755Buxbaum J, Mylinski N, Parente FR: Surface EMG reliability using spectral756analysis. J Oral Rehabil 1996, 23(1l):77I–775I.
44. 757Castroflorio T, Icardi K, Torsello F, Deregibus A, Debernardi C, Bracco P:758Reproducibility of surface EMG in the human masseter and anterior759temporalis muscle areas. J Craniomandibular Pract 2005, 23(2):130–137.
45. 760De-Felício CM, Sidequersky FV, Tartaglia GM, Sforza C: Electromyographic761standardized indices in healthy Brazilian young adults and data762reproducibility. J Oral Rehabil 2009, 36(8):577–583.
46. 763Ruhe A, Fejer R, Walker B: The test-retest reliability of center of pressure764measures in bipedal static task conditions - a systematic review of the765literature. Gait & posture 2010, 32:436–445.
47. 766Le-Cliar K, Riach C: Postural stability measures: what to measure and for767how long. Clinical Biomechanics 1996, 11:176–178.
48. 768Oliveira LF, Simpson DM, Nadal J: Calculation of area of stabili-metric signals769using principal component analysis. Physiol Meas 1996, 17:305–312.
49. 770Doyle TL, Newton RU, Burnett AF: Reliability of traditional and fractal771dimension measures of quiet stance center of pressure in young,772healthy people. Arch Phys Med Rehabil 2005, 86:2034–2040.
50. 773Baratto L, Morasso PG, Re C, Spada G: A new look at posturographic774analysis in the clinical context: sway-density versus other775parameterization techniques. Mot Control 2002, 6:246–270.
51. 776Lake DE, Richman JS, Griffin MP, Moorman JR: Sample entropy analysis of777neonatal heart rate variability. Am J Physiol Regul Integr Comp Physiol 2002,778283:789–797.
52. 779Richman JS, Moorman JR: Physiological time-series analysis using780approximate entropy and sample entropy. Am J Physiol Heart Circ Physiol7812000, 278:H2039–4.
53. 782Costa M, Peng CK, Goldberger AL, Hausdor JM: Multiscale entropy analysis783of human gait dynamics. Physica 2003, 330(A):53–60.
54. 784Ramdani S, Seigle B, Lagarde J, Bouchara F, Bernard PL: On the use of785sample entropy to analyze human postural sway data. Med Eng Phys7862009, 31:1023–1031.
El-Hage et al. Trials 2013, 14:316 Page 10 of 11http://www.trialsjournal.com/content/14/1/316
55.787 Lamoth CJC, Van-Heuvelen MJG: Sports activities are reflected in the local788 stability and regularity of body sway: older ice-skaters have better789 postural control than inactive elderly. Gait Posture 2012, 35:489–493.
56.790 Sturnieks DL, Arnold R, Lord SR: Validity and reliability of the Swaymeter791 device for measuring postural sway. Biomed Central Geriatrics 2011, 11:63.
57.792 Shrout PE, Fleiss JL: Intraclass correlations: uses in assessing rater793 reliability. Psychol Bull 1979, 86:420–428.
58.794 Bruton A, Conway JH, Holgate ST: Reliability: what is it and how is it795 measured? Physiotherapy 2000, 86(2):94–99.
59.796 Cicchetti DV, Sparrow SS: Developing criteria for establishing inter-rater797 reliability of specific items: application to assessment of adaptive798 behavior. Am J Ment Defic 1981, 86:127–137.
60.799 Lin D, Seol H, Nussbaum MA, Madigan ML: Reliability of COP-based postural800 sway measures and age-related differences. Gait Posture 2008, 28:337–342.
61.801 Salavati M, Hadian MR, Mazaheri M, Negahban H, Ebrahimi I, Talebian S,802 Jafari AH, Sanjari MA, Sohani SM, Parnianpour M: Test-retest reliability of803 center of pressure measures of postural stability during quiet standing804 in a group with musculoskeletal disorders consisting of low back pain,805 anterior cruciate ligament injury and functional ankle instability. Gait806 Posture 2009, 29:460–464.
62.807 Maribo T, Stengaard-Pedersen K, Jensen LD, Andersen NT, Schiøttz-Christense808 B: Postural balance in low back pain patients: intra-session reliability of809 center of pressure on a portable force platform and of the one leg stand810 test. Gait Posture 2011, 34:213–217.
63.811 Pinsault N, Vuillerme N: Test-retest reliability of center of foot pressure812 measures to assess postural control during unperturbed stance.813 Med Eng Phys 2009, 31:276–286.
64.814 Raymakers JA, Samson MM, Verhaar HJJ: The assessment of body sway815 and the choice of stability parameter(s). Gait Posture 2005, 21:48–58.
65.816 Bauer C, Groger I, Rupprecht R, Gassmann KG: Intrasession reliability of817 force platform parameters in community-dwelling older adults.818 Arch Phys Med Rehabil 2008, 89:1977–1982.
66.819 Harringe ML, Halvorsen K, Renstrom P, Wermer S: Postural control measured820 as the center of pressure excursion in young female gymnasts with low821 back pain or lower extremity injury. Gait Posture 2008, 28(1):38–45.
822 doi:10.1186/1745-6215-14-316823 Cite this article as: El-Hage et al.: Effect of mandibular mobilization on824 electromyographic signals in muscles of mastication and static825 balance in individuals with temporomandibular disorder: study826 protocol for a randomized controlled trial. Trials 2013 14:316.
Submit your next manuscript to BioMed Centraland take full advantage of:
• Convenient online submission
• Thorough peer review
• No space constraints or color figure charges
• Immediate publication on acceptance
• Inclusion in PubMed, CAS, Scopus and Google Scholar
• Research which is freely available for redistribution
Submit your manuscript at www.biomedcentral.com/submit
El-Hage et al. Trials 2013, 14:316 Page 11 of 11http://www.trialsjournal.com/content/14/1/316
Author Query Form
Journal: Trials
Title: Effect of mandibular mobilization on electromyographic signals in muscles ofmastication and static balance in individuals with temporomandibular disorder: studyprotocol for a randomized controlled trial
Authors: Yasmin El-Hage, Fabiano Politti, Dowglas F Magalhães de-Sousa, Carolina -Marciela Herpich, Igor Phillip dos-Santos Gloria, Cid André Fidelis de-Paula Gomes, Ana -Paula Amaral, Nívea Cristina de-Melo, Thais Correa da-Silva,Eric Edmur Camargo Arruda, Cesar Ferreira Amorim, Inaê Caroline Gadotti, Tabajara -Oliveira Gonzalez, Fausto Berzin, Sandra Kalil Bussadori, Marília Barbosa Santos Garcia,Bruno Roberto Borges Barbosa, Daniela Aparecida Biasotto-Gonzalez
Article: 1745-6215-14-316
Dear Authors,
During production of your paper, the following queries arose. Please respond to these by annotating your proofs withthe necessary changes/additions. If you intend to annotate your proof electronically, please refer to the E-annotationguidelines. We recommend that you provide additional clarification of answers to queries by entering your answers onthe query sheet, in addition to the text mark-up.
Query No. Query Remark
Q1 Figure: Figure 1 is cited in the section header. Although this is not against thejournal standards, we suggest that it should be modified as it is not visuallypleasing. Otherwise, please advise us on how to proceed.
Q2 URL: Please check that the following URLs are working. If not, please providealternatives: http://www.emgsystem.com.br
Q3 URL: Please check that the following URLs are working. If not, please providealternatives: http://noraxon.com
Q4 URL: Please check that the following URLs are working. If not, please providealternatives: http://www.pharminnovations.com
Q5 URL: Please check that the following URLs are working. If not, please providealternatives: http://www-01.ibm.com/software/analytics/spss/




















