
Multicollinearity in genetic effects for weaning weight in a beef cattle composite population
Upload
independentCategory
view
2download
0
Effect of a nursing-implemented sedation protocol onweaning outcome*
Susana Arias-Rivera, RN; Maria del Mar Sanchez-Sanchez, RN; Rosa Santos-Dıaz, RN;Juana Gallardo-Murillo, RN; Raquel Sanchez-Izquierdo, RN; Fernando Frutos-Vivar, MD;Niall D. Ferguson MD, MSc; Andres Esteban, MD, PhD
Sedative and analgesic medica-tions are commonly used incritically ill patients, especiallyin those who are mechanically
ventilated (1). The need for continuousadministration of sedatives has been as-sociated with longer durations of me-chanical ventilation and stay in the in-tensive care unit (ICU) (2). Severalapproaches, such as daily interruptionof sedatives infusions (3), or the imple-mentation of a sedation protocol to ad-just the sedatives to a target sedationlevel (4 –9), have been proposed to
shorten the time to arousal and, as aconsequence, the duration of mechani-cal ventilation.
Several studies have shown significantpositive effects of a sedation protocol onduration of mechanical ventilation (4–8),although these findings are not universal(9). Some of these studies have reporteddifferences in the duration of mechanicalventilation between survivors and non-survivors and between tracheostomizedand nontracheostomized patients; itcould be possible that mismatching ofthese subgroups between interventiongroups influenced the final results. Ourobjective was to determine the effect ofthe implementation of a sedation proto-col, including only mechanically venti-lated patients who were ready to wean.Our hypothesis was that if the nursingstaff could manage the sedation of thesepatients, then they would be more awakewhen they met criteria to perform a spon-taneous breathing trial and, therefore,could be extubated earlier. The primaryoutcome was the duration of intubation.Some of the results of this study havebeen reported previously in the form ofan abstract (10).
MATERIALS AND METHODS
Design and Setting
This before-and-after study was performedin the 18-bed medical-surgical ICU in the Hos-pital Universitario de Getafe (Madrid, Spain)with a patient/nurse ratio of 2:1 or 3:1. Ourunit is a closed unit managed by ten full-timeattending physicians and six residents of crit-ical care medicine; the nurses are full-timeand part-time permanent staff. Patients olderthan age 18 yrs with an expected duration ofmechanical ventilation longer than 48 hrs andwho were intubated were included at admis-sion to the ICU. Patients were excluded fromthe study if, during their course of ventilation,they met one of the following conditions: du-ration of mechanical ventilation less than 48hrs, tracheostomy before extubation, anddeath or transfer to another hospital. Patientswere excluded if they had previously been en-rolled in the study. The Ethics committee ofthe Hospital Universitario de Getafe waivedthe need for informed consent.
Protocol
Consecutive patients were prospectivelyenrolled during two 17-month periods sepa-rated by a 4-month interval during which the
*See also p. 2199.From the Intensive Care Unit & Burn Unit, Hospital
Universitario de Getafe; Madrid, Spain and CIBER En-fermedades Respiratorias (SAR, MSS, RSD, JGM, RSI,FFV, AE); and Interdepartmental Division of CriticalCare Medicine, and Department of Medicine, Divisionof Respirology (NDF), University Health Network, Uni-versity of Toronto, Toronto, Canada.
Supported, in part, by grant 03/1177 of Fondo deInvestigaciones Sanitarias, Red GIRA (G03/063) andRed RESPIRA (C03/11) from Instituto de Salud CarlosIII, Spain.
For information regarding this article, E-mail:[email protected]
Copyright © 2008 by the Society of Critical CareMedicine and Lippincott Williams & Wilkins
DOI: 10.1097/CCM.0b013e31817bfd60
Objective: To evaluate the effect of the implementation of anursing-driven protocol of sedation on duration of intubation.
Design: Before-and-after prospective study.Setting: 18-bed medical-surgical intensive care unit.Patients: Patients receiving mechanical ventilation longer than
48 hrs who were ready to wean.Interventions: During the observational period, sedatives and
analgesics were adjusted according to physicians’ orders. Duringthe intervention period, sedatives and analgesics were adjustedby nurses according to an algorithm-based sedation guideline,including a sedation scale.
Measurements and Main Results: A total of 356 patients wereincluded in the study (176 patients in the observational period and189 patients in the intervention period). There were no significantdifferences in the duration of intubation between the two periods
(median, 7 [interquartile range, 5–13] days vs. 7 [interquartilerange, 5–9] days). In a Kaplan-Meier analysis, the probability ofsuccessful extubation was higher during the intervention periodthan during the observational period (log-rank � 0.02). During theintervention period, patients were more awake without a signif-icant increment in the nurse workload; however, there was nosignificant decrease in the total doses of sedatives and analgesicsadministered.
Conclusions: The implementation of a nursing-driven protocolof sedation may improve the probability of successful extubationin a heterogeneous population of mechanically ventilated pa-tients. (Crit Care Med 2008; 36:2054–2060)
KEY WORDS: nursing process; clinical nursing research; seda-tives; mechanical ventilation; weaning; nursing workload
2054 Crit Care Med 2008 Vol. 36, No. 7

investigative team trained the nursing staff inthe use of the chosen sedation score: GlasgowComa Score modified by Cook and Palma(GCS-CP) (11), also known as the Cook seda-tion scoring system (Appendix). During thefirst period (from June 2001 to November2002), no protocol of sedation was applied(observational period). All aspects of sedationwere ordered by the treating physicians;nurses could not make changes in the seda-tion regimen without a physician’s written orverbal order. During this period, no sedationscore was used to guide the level of sedation.The investigative team prospectively recorded theGCS-CP at 8 a.m. and 3 p.m. To minimize theimpact on existing sedation delivery practices,the bedsides nurses and physicians were un-aware of this assessment. During the secondperiod (April 2003 to August 2004), a sedationprotocol was used (intervention period). Thetypes of sedatives and analgesics were deter-mined by the treating physician. Nurseswere required to change the doses of con-tinuous intravenous infusions to achieve thesedation target: GCS-CP between 8 and 13points. As part of this objective, nurses re-corded the sedation score hourly. Treatingphysicians could deviate from the protocol ifthey believed that it was necessary for the man-agement of the patient; this included the admin-istration of intravenous boluses of sedatives, an-algesics, or neuromuscular blockers.
Patients received midazolam or propofolfor sedation and morphine for analgesia dur-ing both periods of the study. During the in-tervention period, the administration of seda-tion and analgesia was as follows: a)midazolam: sedation with midazolam wasstarted with an intravenous bolus of 5 mgevery 5 mins until target sedation wasachieved. This dose was continued by an in-travenous infusion at a rate of 0.15 mg/kg/hr.In patients with poor tolerance, the infusionrate was increased 2.5 mg every 5 mins untilthe target level of sedation was reached. Inpatients with a GCS-CP lower than target level(8–13 points), nurses decreased the infusion2.5 mg every 5 mins until the target level wasattained; b) propofol: sedation with propofolwas started with an intravenous bolus of 30mg every 5 mins until target sedation wasachieved. Subsequently, an intravenous infu-sion at a rate of 1.5 mg/kg/hr was started. If apatient was uncomfortable the infusion ratewas increased 20 mg every 5 mins until thetarget level of sedation was achieved. In pa-tients with a GCS-CP lower than 8 points,nurses decreased the infusion by 30 mg every5 mins until the target level was achieved; c)morphine: when physicians considered thatthe patients required analgesia, an intrave-nous continuous infusion of morphine at arate of 0.03 mg/kg/hr was started. This infu-
sion was increased at step of 1 mg each 15mins until an optimal level of analgesia wasreached, according to a Visual Analog Scale ofpain. This protocol was not applied while pa-tients were receiving continuous infusions ofneuromuscular blockers.
Mechanical ventilation weaning practicesdid not differ between the two periods. A spon-taneous breathing trial with T-piece, continu-ous positive airway pressure or pressure sup-port of 7 cm H2O (12), was performed when
the attending physician considered that thepatient was in a stable condition and ready tobe weaned from the ventilator. Patients wereextubated within the next 120 mins if theyshowed good clinical tolerance of the sponta-neous breathing trial (13). Successful extuba-tion was defined as removal of the endotra-cheal tube without subsequent reintubationwithin 48 hrs. The criteria used to judgeneed for reintubation were: hypercapnia; re-spiratory acidosis; decrease in the oxygen
Figure 1. Flow chart of the study. MV, mechanical ventilation.
Table 1. Baseline characteristics of patients at inclusion in the study
Observational PeriodN � 176
Intervention PeriodN � 189 p Value
Age, years, mean (SD) 65 (17) 65 (15) .84Female, n (%) 62 (35%) 56 (30%) .25Simplified Acute Physiology Score II,
points, mean (SD)43 (14) 40 (13) .04
Addictions, n (%) .20Tobacco 4 (18%) 8 (25%)Alcohol 16 (2%) 24 (4%)Illegal drugs 2 (1%) —
Reason for mechanical ventilation,n (%)
Exacerbation of chronic pulmonarydisease
29 (16.5) 14 (7%) .007
Coma 15 (8.5%) 19 (10%) .61Acute respiratory failure 132 (75%) 156 (82.5%) .08
Cause of acute respiratory failure,n (%)
Congestive heart failure 38 (22%) 64 (34%) .009Sepsis 28 (16%) 20 (11%) .13Postoperative 16 (9%) 29 (15%) .07Pneumonia 17 (10%) 12 (6%) .24Heart arrest 4 (2%) 4 (2%) 1.00Acute respiratory distress syndrome 3 (2%) — .11Aspiration 1 (1%) — .48Trauma 11 (6%) 10 (5%) .55Other cause 14 (8%) 17 (9%) .72
2055Crit Care Med 2008 Vol. 36, No. 7

saturation to �85 percent, despite the use ofa high fraction of inspired oxygen; signs ofrespiratory-muscle fatigue; changes in men-tal status; hypotension, with a systolic bloodpressure �90 mm Hg for more than 30 minsdespite adequate volume challenge, the use ofvasopressors, or both; or copious secretions thatcould not be adequately cleared or that wereassociated with acidosis, hypoxemia, or changesin mental status. The final decision to reintubatewas made by the treating physician.
Data Collection
The following data were prospectively re-corded during both phases of the study: demo-graphic data (age, sex, weight, height), addic-tions (illegal drugs, alcohol, tobacco), mainreason for admission, Simplified Acute Physi-
ology Score (SAPS II), date of admission, dateof intubation, date of the first spontaneousbreathing trial, date of extubation, reintuba-tion, tracheostomy, ventilator-free days (14),and date and status at discharge from the ICU.Each day throughout the period of mechanicalventilation, we recorded the GCS-CP at 8 a.m.and 3 p.m., nursing workload estimated bythe Nine Equivalents of Nurse Manpowerscore (NEMS) (15), total daily dose of mida-zolam, propofol, and morphine, use of otherintravenous sedatives and neuromuscularblockers, and accidental removal of tubesand catheters.
Statistical Analysis
SPSS version 13 (SPSS Inc., Chicago, IL)was used to perform the statistical analysis. Con-
tinuous variables are expressed as mean (SD) ormedian (interquartile range) as appropriate. Cat-egorical variables are reported as number andproportion. Comparisons between periods wereperformed using Student’s t-test or Mann-Whitney test for quantitative variables and thechi-square test and Fisher’s exact test for cate-gorical variables. The probability of successfulextubation over time in each period was esti-mated according to the Kaplan-Meier methodand compared by the log-rank test.
Using our ICU database, we observed thatthe mean duration of mechanical ventilationof patients ventilated longer than 48 hrs was10 (SD 7) days. Accordingly, we determinedthat the sample size needed to show a reduc-tion of 2 days in intubation duration with analpha error of 0.05 and a power of 80% wouldbe 151 patients in each period.
RESULTS
From 685 potentially eligible pa-tients, 365 patients were included inthe study: 176 patients in the observa-tional period, and 189 patients in theintervention period (Fig. 1). Baselinecharacteristics are shown in Table 1.During the observational period, therewas a higher proportion of patientswith exacerbation of chronic obstruc-tive pulmonary disease and a lower per-centage of patients with acute respira-tory failure caused by congestive heart
Figure 2. Kaplan-Meier plot of the cumulative probability of successful extubation in both groups: interventional group (thin line) and observational group(thick line).
Table 2. Comparison of variables related to primary objective
Observational PeriodN � 176
Intervention PeriodN � 189 p Value
Days of intubationMean (SD) 10 (7) 8 (5) 0.07Median (interquartile range) 7 (5, 13) 7 (5, 9) 0.36
Days of weaningMean (SD) 4 (4) 3 (3) 0.04Median (interquartile range) 1 (2, 5) 1 (2, 4) 0.36
Ventilator-free daysMean (SD) 17 (9) 19 (7) 0.02Median (interquartile range) 22 (13, 24) 22 (19, 24) 0.39
Reintubation, n (%) 32 (18%) 26 (14%) 0.25
2056 Crit Care Med 2008 Vol. 36, No. 7
failure. There were significant differ-ences in illness severity at admission:SAPS II 43 points (SD 14) in the obser-vational period vs. 40 points (SD 13) inthe intervention period.
Main Outcome
Table 2 shows the comparison of theprimary outcome of the study. We ob-served an insignificant trend toward ashorter duration of intubation in the in-tervention period and, as a consequence,more ventilator-free days. There was asignificant (log-rank test � 0.02) in-crease in successful extubation duringthe intervention period (Fig. 2).
Secondary Outcomes
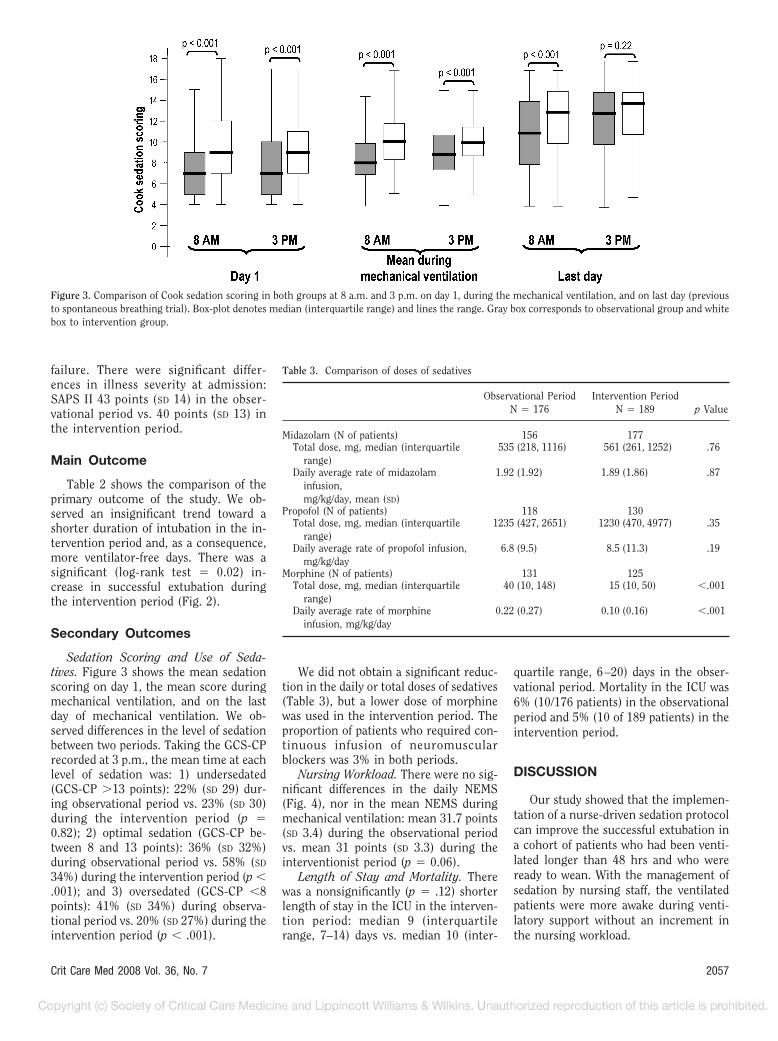
Sedation Scoring and Use of Seda-tives. Figure 3 shows the mean sedationscoring on day 1, the mean score duringmechanical ventilation, and on the lastday of mechanical ventilation. We ob-served differences in the level of sedationbetween two periods. Taking the GCS-CPrecorded at 3 p.m., the mean time at eachlevel of sedation was: 1) undersedated(GCS-CP �13 points): 22% (SD 29) dur-ing observational period vs. 23% (SD 30)during the intervention period (p �0.82); 2) optimal sedation (GCS-CP be-tween 8 and 13 points): 36% (SD 32%)during observational period vs. 58% (SD
34%) during the intervention period (p �.001); and 3) oversedated (GCS-CP �8points): 41% (SD 34%) during observa-tional period vs. 20% (SD 27%) during theintervention period (p � .001).
We did not obtain a significant reduc-tion in the daily or total doses of sedatives(Table 3), but a lower dose of morphinewas used in the intervention period. Theproportion of patients who required con-tinuous infusion of neuromuscularblockers was 3% in both periods.
Nursing Workload. There were no sig-nificant differences in the daily NEMS(Fig. 4), nor in the mean NEMS duringmechanical ventilation: mean 31.7 points(SD 3.4) during the observational periodvs. mean 31 points (SD 3.3) during theinterventionist period (p � 0.06).
Length of Stay and Mortality. Therewas a nonsignificantly (p � .12) shorterlength of stay in the ICU in the interven-tion period: median 9 (interquartilerange, 7–14) days vs. median 10 (inter-
quartile range, 6–20) days in the obser-vational period. Mortality in the ICU was6% (10/176 patients) in the observationalperiod and 5% (10 of 189 patients) in theintervention period.
DISCUSSION
Our study showed that the implemen-tation of a nurse-driven sedation protocolcan improve the successful extubation ina cohort of patients who had been venti-lated longer than 48 hrs and who wereready to wean. With the management ofsedation by nursing staff, the ventilatedpatients were more awake during venti-latory support without an increment inthe nursing workload.
Figure 3. Comparison of Cook sedation scoring in both groups at 8 a.m. and 3 p.m. on day 1, during the mechanical ventilation, and on last day (previousto spontaneous breathing trial). Box-plot denotes median (interquartile range) and lines the range. Gray box corresponds to observational group and whitebox to intervention group.
Table 3. Comparison of doses of sedatives
Observational PeriodN � 176
Intervention PeriodN � 189 p Value
Midazolam (N of patients) 156 177Total dose, mg, median (interquartile
range)535 (218, 1116) 561 (261, 1252) .76
Daily average rate of midazolaminfusion,mg/kg/day, mean (SD)
1.92 (1.92) 1.89 (1.86) .87
Propofol (N of patients) 118 130Total dose, mg, median (interquartile
range)1235 (427, 2651) 1230 (470, 4977) .35
Daily average rate of propofol infusion,mg/kg/day
6.8 (9.5) 8.5 (11.3) .19
Morphine (N of patients) 131 125Total dose, mg, median (interquartile
range)40 (10, 148) 15 (10, 50) �.001
Daily average rate of morphineinfusion, mg/kg/day
0.22 (0.27) 0.10 (0.16) �.001
2057Crit Care Med 2008 Vol. 36, No. 7

Although we did not observe signifi-cant differences between periods in dura-tion of ICU stay, we showed a trend sim-ilar to that reported in previous studies(4–8). Probable reasons explaining theabsence of significant differences couldbe: 1) design of the study: the design of abefore-and-after study and an insufficientsample size, with differences in the pop-ulation included in both periods; 2) asatisfactory baseline practice of sedationdelivery in the observation period beforeimplementation of the protocol; and 3)differences in the sedatives administered.
One possible limitation of the studymight be that there was no randomiza-tion. We chose a before–after design be-cause the patient/nurse ratio is alwaysgreater than the one in our unit, and arandomized, controlled trial would havemeant that one nurse could have been incharge of two or more patients random-ized to different arms. The knowledge ofthe protocol of the intervention groupwould have inadvertently led to contam-ination in the observational group. Addi-tionally, we could have had an insuffi-cient sample size. We calculated thesample size by using the mean durationof intubation in the historical record ofour unit as a reference, and this time wassimilar (10 days) to that observed in theobservational group. In addition, we in-cluded more patients in both periods to
compensate for possible losses. As a con-sequence of the design, we do not have aperfect matching of patients in both pe-riods. During the observational period,we included more patients with an exac-erbation of a chronic obstructive pulmo-nary disease and fewer patients with con-gestive heart failure. It might be arguedthat this could be a reason for the differ-ence in the duration of mechanical ven-tilation between the two periods. How-ever, in a previous study by our group,patients with a chronic obstructive pul-monary disease did not have a longerduration of mechanical ventilation com-pared with other patients without thisdiagnosis (16). Also, there were differ-ences in the severity of illness at admis-sion to the ICU: higher SAPS II in theobservation period. However, to ourknowledge, no study has related the se-verity of illness at admission to weaningoutcome. The patients included in ourstudy were patients who improved from thecondition for which they were ventilated,and we speculate that their illness severityat the moment they started weaning wassimilar in both groups, because they metstandard readiness to wean criteria. Unfor-tunately, we did not calculate the SAPS IIscore at this time point.
Second, it does not seem that thebaseline practice of sedation was ade-quate. In the observational period, we ob-
served that almost half of the patientswere oversedated and only 36% of pa-tients were in the optimal level of seda-tion defined for this study. The imple-mentation of the protocol allowed for themajority of the patients to be in the op-timal range of the sedation score. Finally,we did not find any differences in thetypes of sedative used. In any case, previ-ous studies (4, 6) did not find any differencein the duration of mechanical ventilationbetween patients treated with propofol ver-sus midazolam. Thus, it seems most likelythat the protocol resulted in a better titra-tion of sedation, but that sedative doseswere not lower because of differences inpatient tolerance and drug requirementsbetween the two study periods.
No assessment of delirium was providedin the study because the sedation scaleused, as with all sedation scales, did notaddress this issue. Although delirium hasan elevated incidence in mechanically ven-tilated patients, it has not been directlylinked to weaning outcome (17); however,this area needs further investigation.
In conclusion, in our before–after study,the implementation of a nursing-drivenprotocol of sedation improved the probabil-ity of successful extubation among a heter-ogeneous population of mechanically ven-tilated patients. These results and theeffects of such a protocol on duration of
Figure 4. Daily mean (SEM) of the Nine Equivalents of Nurse Manpower score (NEMS) in both groups: intervention group (white box) and observationalgroup (gray box).
2058 Crit Care Med 2008 Vol. 36, No. 7

ventilation may warrant confirmation ina cluster-randomized, controlled trial.
REFERENCES
1. Arroliga A, Frutos-Vivar F, Hall J, et al: Use ofsedatives and neuromuscular blockers in acohort of patients receiving mechanical ven-tilation. Chest 2005; 128:496–506
2. Kollef MH, Levy NT, Ahrens TS, et al: The useof continuous i.v. sedation is associated withprolongation of mechanical ventilation.Chest 1998; 114:541–548
3. Kress JP, Pohlman AS, O’Connor MF, HallJB. Daily interruption of sedative infusions incritically ill patients undergoing mechanicalventilation. N Engl J Med 2000; 342:1471–1477
4. Brook AD, Ahrens TS, Schaiff R, et al: Effectof a nursing-implemented sedation protocolon the duration of mechanical ventilation.Crit Care Med 1999; 27:2609–2615
5. Brattebø G, Hofoss D, Flaatten H, et al: Effectof a scoring system and protocol for sedationon duration of patients’ need for ventilatorsupport in a surgical intensive care unit. BMJ2002; 324:1386–1389
6. De Jonghe B, Bastuji-Garin S, Fangio P, et al:Sedation algorithm in critically ill patientswithout acute brain injury. Crit Care Med2005; 33:120–127
7. Chanques G, Jaber S, Barbotte E, et al: Im-pact of systematic evaluation of pain andagitation in an intensive care unit. Crit CareMed 2006; 34:1691–1699
8. Quenot JP, Ladoire S, Devoucoux F, et al:Effect of a nurse-implemented sedation pro-tocol on the incidence of ventilator-associ-ated pneumonia. Crit Care Med 2007; 35:2031–2036
9. Elliott R, McKinley S, Aitken LM, et al: Theeffect of an algorithm-based sedationguideline on the duration of mechanicalventilation in an Australian intensive careunit. Intensive Care Med 2006; 32:1506 –1514
10. Arias-Rivera S, Sanchez-Sanchez MM, Santos-Dıaz R, et al: Effect of a nursing-imple-mented sedation protocol based on the Glas-gow Coma Score modified by Cook andPalma. Proc Am Thorac Soc 2006; 3:A301
11. Cook S, Palma O: Propofol as a sole agent forprolonged infusion in intensive care. J DrugDev 1989; 4(Suppl 2):65–67
12. Esteban A, Alia I, Gordo F, et al: Extubation
outcome after spontaneous breathing trialswith T-tube or pressure support ventilation.Am J Respir Crit Care Med 1997; 156(2 Pt1):459–465
13. Esteban A, Alia I, Tobin MJ, et al: Effect ofspontaneous breathing trial duration on out-come of attempts to discontinue mechanicalventilation. Am J Respir Crit Care Med 1999;159:512–518
14. Schoenfeld DA, Bernard GR, ARDS Net-work: Statistical evaluation of ventilator-free days as an efficacy measure in clinicaltrials of treatments for acute respiratorydistress syndrome. Crit Care Med 2002;30:1772–1777
15. Reis Miranda D, Moreno R, Iapichino G: Nineequivalents of nursing manpower use score(NEMS). Intensive Care Med 1997; 23:760–765
16. Esteban A, Anzueto A, Frutos F, et al: Char-acteristics and outcomes in adult patientsreceiving mechanical ventilation: A 28-dayinternational study. JAMA 2002; 287:345–355
17. Boles JM, Bion J, Connors A, et al: Weaningfrom mechanical ventilation. Eur Respir J2007; 29:1033–1056
2059Crit Care Med 2008 Vol. 36, No. 7

APPENDIX
A, Algorithm of administration of midazolam during the intervention period. GCS, Glasgow CookScore. B, Algorithm of administration of propofol during the intervention period.
Glasgow Coma Score modified by Cook andPalma
Points
Eyes openSpontaneously 4In response to speech 3In response to pain 2None 1
Response to nursing proceduresObeys commands 5Purposeful movements 4Non-purposeful flexion 3Non-purposeful extension 2None 1
CoughSpontaneous strong 4Spontaneous weak 3On suction only 2None 1
RespirationObeys commands 5Spontaneous intubated 4Spontaneous intermittent mandatory
ventilator triggering3
Respiration against ventilator 2No respiratory efforts 1
2060 Crit Care Med 2008 Vol. 36, No. 7
Copyright © 2022 FDOKUMEN




















