Ecology and epidemiology of anthrax in cattle and humans in Zambia
10
Instructions for use Title Ecology and epidemiology of anthrax in cattle and humans in Zambia Author(s) Siamudaala, Victor M.; Bwalya, John M.; Munang'andu, Hetron M.; Sinyangwe, Peter G.; Banda, Fred; Mweene, Aaron S.; Takada, Ayato; Kida, Hiroshi Citation Japanese Journal of Veterinary Research, 54(1): 15-23 Issue Date 2006-05-31 Doc URL http://hdl.handle.net/2115/13690 Right Type bulletin Additional Information There are other files related to this item in HUSCAP. Check the above URL. Hokkaido University Collection of Scholarly and Academic Papers : HUSCAP
Transcript of Ecology and epidemiology of anthrax in cattle and humans in Zambia

Instructions for use
Title Ecology and epidemiology of anthrax in cattle and humans inZambia
Author(s)Siamudaala, Victor M.; Bwalya, John M.; Munang'andu,Hetron M.; Sinyangwe, Peter G.; Banda, Fred; Mweene, AaronS.; Takada, Ayato; Kida, Hiroshi
Citation Japanese Journal of Veterinary Research, 54(1): 15-23
Issue Date 2006-05-31
Doc URL http://hdl.handle.net/2115/13690
Right
Type bulletin
AdditionalInformation
There are other files related to this item in HUSCAP. Check theabove URL.
Hokkaido University Collection of Scholarly and Academic Papers : HUSCAP

Ecology and epidemiology of anthrax in cattleand humans in Zambia
Victor M. Siamudaala1),John M. Bwalya2),Hetron M. Munag’andu2),Peter G. Sinyangwe3),Fred Banda4),Aaron S. Mweene2,5)
Ayato Takada6)and Hiroshi Kida5,6)*
(Accepted for publication : May11,2006)
Abstract
Anthrax is endemic in Western and North-western Provinces of Zambia.The disease occurs throughout the year and impacts negatively on the econ-omy of the livestock industry and public health in Zambia. During1989‐1995,there were1,626suspected cases of anthrax in cattle in Western province andof these51were confirmed. There were220cases of human anthrax cases in1990alone and248cases during1991‐1998with19.1% and7.7% case fatalityrates, respectively. Interplay of the ecology of affected areas and anthropo-genic factors seem to trigger anthrax epidemics. Anthrax has drawn consider-able attention in recent years due to its potential use as a biological weapon.In this paper, the history, current status and approaches towards the control ofthe disease in Zambia are discussed. Quarantine measures restrict trade oflivestock and exchange of animals for draught power resulting in poor food se-curity at household levels. Challenges of anthrax control are complex and com-prise of socio-political, economical, environmental and cultural factors. Inade-quate funding, lack of innovative disease control strategies and lack of coop-eration from stakeholders are the major constraints to the control of the dis-
1)Zambia Wildlife Authority, Private Bag1CHILANGA, ZAMBIA2)School of Veterinary Medicine, University of Zambia, P.O BOX32379,LUSAKA, ZAMBIA3)Department of Veterinary and Livestock Development, LUSAKA, ZAMBIA4)Department of Veterinary and Livestock Development, MONGU, ZAMBIA5)Laboratory of Microbiology, Department of Disease Control, Graduate School of Veterinary Medicine, Hok-kaido University, Sapporo060‐0818,Japan6)Research Center for Zoonosis Control, Hokkaido University, Sapporo060‐0818,JapanCorresponding author:H. Kida*
Laboratory of Microbiology, Department of Disease Control, Graduate School of Veterinary Medicine, Hok-kaido University, Sapporo060‐0818,Japan
Tel.:+81‐11‐706‐5207,Fax:+81‐11‐706‐5273E‐mail : [email protected]
Jpn. J. Vet. Res. 54(1):15‐23,2006
REVIEW ARTICLE

Introduction
Infectious diseases in animals confer con-siderable economic losses on the livestock in-dustry in Zambia24,25).Anthrax is endemic inWestern and North-western Provinces ofZambia27,28).Zambia is a landlocked countryin Central Africa with an area of approxi-mately725,600km2.The country is adminis-tratively divided into nine provinces24).Landuse is divided into four general types as fol-lows : i)communal areas with small scale andpeasant agriculture ; ii) commercial farm-land ; iii)urban areas ; and iv)wildlife andforest areas. Zambia has an estimated popula-tion of 10.3 million1) with 1,596,271cattle,24,019sheep,498,173goats,135,045pigs,3,293,730 poultry,2,648 donkeys and27horses6).
Anthrax, an infectious bacterial and usu-ally fatal zoonotic disease11,16,20) is caused by agram-positive endospore-forming bacteriumcalled Bacillus anthracis (B. anthracis) andhas an almost worldwide distribution8,16,22).Anthrax is a re-emerging infection and conse-quently, endemic areas may provide addi-tional sources of alternative strains of B. an-thracis for bioterrorism placing global secu-rity at renewed risk. All mammals appear tobe susceptible to anthrax to some degree, butruminants such as cattle, sheep, and goats arethe most susceptible and commonly affected,followed by horses, and then swine. There arethree forms of anthrax, these being cutaneous,gastrointestinal and inhalational23).Inhala-
tional anthrax resulting from exposure toaerosolized B. anthracis is the most deadlyform of the disease in humans with a mortal-ity rate approaching100%21)even with appro-priate treatment especially if initiated afterclinical symptoms have already progressed. Ithas been used widely in biological warfare in-cluding bioterrorism for decades3,9,19).The re-silience of the B. anthracis endospore com-bined with the potentially lethal nature of thedisease and the efficiency with which it in-fects via an aerosol route make it an ideal bio-logical weapon and consequently issues aboutanthrax have drawn considerable attention inrecent years13,14). The incidences of theanthrax-laced letters that were sent in thewake of the11 September2001 terrorist at-tacks on the World Trade Center and the Pen-tagon that caused5American deaths haveshown renewed potential use of this bacte-rium as a biological weapon15).
Despite its long history in the country,epidemiological and socio-economic data onanthrax is still less valuable in terms of dis-ease emergency preparedness and under-standing the disease in the overall context ofexisting land use practices in endemic areas.The information discussed in this study mayincrease public awareness of the risk factorsand may subsequently help in the formula-tion of disease management options for the ul-timate goal of implementation of regionalrather than local disease control programs.
ease. It is hoped that the information provided here will stimulate continuedawareness for the veterinary and medical authorities to maintain their sur-veillance and capabilities against the disease. This may lead to a culminatingpositive impact on livestock and human health in the southern African region.
Key Words : Anthrax, Disease Control, Livestock, Socio-economic impact, Zam-bia
Epidemiology of anthrax in Zambia16

Materials and Methods
The study involved a review of literatureand reports( including scientific publica-tions)on anthrax in livestock and humans atthe Department of Veterinary and LivestockDevelopment, National Archives and the Cen-tral Veterinary Research Institute in Zambia.The data was also obtained from discussionswith local communities and various veteri-nary professionals in the country.
Anthrax in Livestock
Historical PerspectiveIn Zambia, anthrax was first reported in
1914 in Luambe National Park28).The originof the disease is unknown. During1989‐1995,there were1,626 suspected cases of anthraxin cattle in Western Province and of these51were confirmed. It remains speculative thatmovement of cattle from Southern Africa in-troduced the disease into the country. Live-stock entering the country in early1900 atLivingstone Border were never quarantined.Mandatory quarantine of livestock enteringthe country was only introduced in1931.Dur-
ing the pre-colonial period , anthrax wasbrought under control with epizootic and spo-radic cases limited to Southern and WesternProvinces among the traditional farming sec-tor and was virtually absent in the commer-cial farming community as they vaccinatedtheir animals. The disease was not uncom-mon in Namwala , Mazabuka , Monze andChoma Districts of Southern Province and ,Mongu and Senanga Districts of WesternProvince . The last outbreak of anthrax inSouthern Province was in1987 in MazabukaDistrict. The disease has been rare in Centraland Copperbelt Provinces. Anthrax was re-ported only once in Kafue District of LusakaProvince and Kitwe District of CopperbeltProvince in1928and1971,respectively(Fig-ure1).
Current SituationInitially, confined to Mongu and Senanga
Districts in Western Province , anthrax hasspread to other districts(i.e. Lukulu, Kalabo,Sesheke and Kaoma)in the Province and ad-jacent North-western Province(Kabompo andZambezi Districts).In both provinces the dis-ease is generally confined to the Zambeziplain and is rarely seen in upland areas. An-thrax epidemics are frequent in the dry sea-son and are generally associated with onset ofthe first rains in October/November17,18)whengrazing pasture is limited to the Zambeziplains. The plains are generally low lying andflood during the rain season. The floods usu-ally leave behind deposits of organic materi-als along the riverbanks resulting in the eco-logical conditions described by Van Ness32)
that trigger anthrax epidemics. During thedry season, the grass is short and animals are,thereby, forced to graze very close to theground . This increases chances of animalspicking up anthrax spores in areas whosesoils and pastures are contaminated with the
Figure 1.Map of Zambia showing areas where an-thrax has been reported as well other ma-jor towns.
Victor M. Siamudaala et al. 17

spores.Anthrax epidemics are also common in
areas with inadequate vaccinations . Vacci-nating cattle whilst in the flood plains is diffi-cult as animals scatter over large areas withdifficult terrain . Subsequently, vaccinationcoverage is insufficient resulting in the mush-rooming of cases of anthrax. This phenome-non has led the local communities to believethat the disease is introduced and spreadthrough vaccinations. Consequently, peopleresist vaccination campaigns against anthrax.A large-scale anthrax epidemic ravaged al-most the entire Western Province in 1990.The disease was first reported in November1990 in Lukulu District and quickly spreadfrom these initial foci to other areas along theZambezi Plains reaching Mongu, Kalabo andSenanga Districts and by December of thesame year a total of511cases were recorded.
Disease Diagnosis
All districts in Zambia submit monthlylivestock disease cases to the headquarters ofthe Department of Veterinary and LivestockDevelopment of the Ministry of Agriculture
Food and Fisheries. Field diagnosis of anthraxcases reported in this study was based onclinical signs as described by De Vos7).An-thrax was suspected in all cases of suddendeath with the presence of bloody dischargesfrom all natural orifices of the carcasses. Adefinitive diagnosis was based on laboratoryinvestigation of B. anthracis in stained bloodsmears from infected carcasses and bacterialculture as described by Ebedes10).During theperiod1989‐1995,a total of1,626 suspectedcases of anthrax were reported throughoutWestern Province. The isolation of B. anthra-cis from suspected cases and environmentalsamples are given in Tables1and2,respec-tively.
Anthrax Control
Historically, control measures of anthraxin Zambia comprise annual vaccination of cat-tle and public awareness of the disease. Thevaccine is produced locally by the Central Vet-erinary Laboratory, Department of Veterinaryand Livestock Development, Ministry of Agri-culture, Food and Fisheries. The vaccine hashigh potency and has no side effects. Emer-
Table1.Diagnosis of anthrax in cattle in Western Province of Zambia during1989‐1995
Year
Cases 1989 1990 1991 1992 1993 1994 1995 Total
Suspected 45 747 511 111 208 4 - 1,626
Investigated - - 27 11 44 - 64 146
Confirmed 2 9 7 8 10 - 15 51
% Investigated/Suspected - - 5.3 10.0 21.2 - - 9.0
% Confirmed/Investigated - - 25.9 72.7 22.7 - 23.4 34.9
Table2.Isolation of Bacillus anthracis from environmental samples in Western Province‐1996
Samples
Soil Meat/skin Bone Total
Sample number 1 15 1 17
Positive 1 12 0 13
% Positive 100.0 80.0 0.0 76.5
Epidemiology of anthrax in Zambia18

gency vaccinations of animals at risk are car-ried out during epidemics whilst the generalpublic is advised against salvaging anthraxcarcasses for meat . Inadequate vaccinationcoverage along the Zambezi plains resultingin cases of anthrax has forced local farmers tooppose vaccination campaigns since they be-lieve that the disease is introduced andspread through these vaccinations. Resistanceto anthrax vaccinations was also reportedamong indigenous people , particularly inSouthern Province, during the colonial period.The local people were suspicious of the colo-nial government and considered vaccinationcampaigns as an attempt to kill cattle in orderto create more land for the commercial whitesettlers. Extensive anthrax vaccinations wereonly enforced when the Good Cattle Produc-tion Bounty Scheme came into operation in1949.Even then, the farmers were still reluc-tant to accept the vaccinations until 1960when the increasing incidence of the diseasecompelled them to have their animals vacci-nated.
In other areas, anthrax received little at-tention from farmers compared to other dis-eases such as contagious bovine pleuropneu-monia, rabies, tuberculosis, East Coast feverand trypanosomosis. In1935,Native Authori-ties in Barotseland(now Western Province)did not oppose the free anthrax vaccinationsbut rather requested government to give pri-ority to the control of contagious bovinepleuropneumonia that was difficult to controldue to its sprawling expansion into neigh-bouring Angola.
Quarantine of livestock during anthraxepidemics is difficult to enforce due to the ex-istence of numerous illegal routes. Incinera-tion of carcasses is constrained by inadequatesources of firewood in the flood plains whereanthrax cases frequently occur. Disease epi-demics usually coincide with the farming sea-
son(July-December)and the traditional farm-ers have little or no time to spend on other ac-tivities such as burning of carcasses. Duringthis time the farming community is opposedto vaccination campaigns, as they prefer tocontinue using the animals for ox-draughtpower and milk production than resting theanimals to avoid stress-related immuno-suppression.
Anthrax in Humans
Human cases are a sequel of salvaging ofanthrax carcasses by rural local communitiesto supplement animal protein in their diet .Human cases of anthrax have been reportedin Senanga , Kaoma , Mongu , Kalabo andLukulu Districts in Western Province andZambezi District in North-western Province.
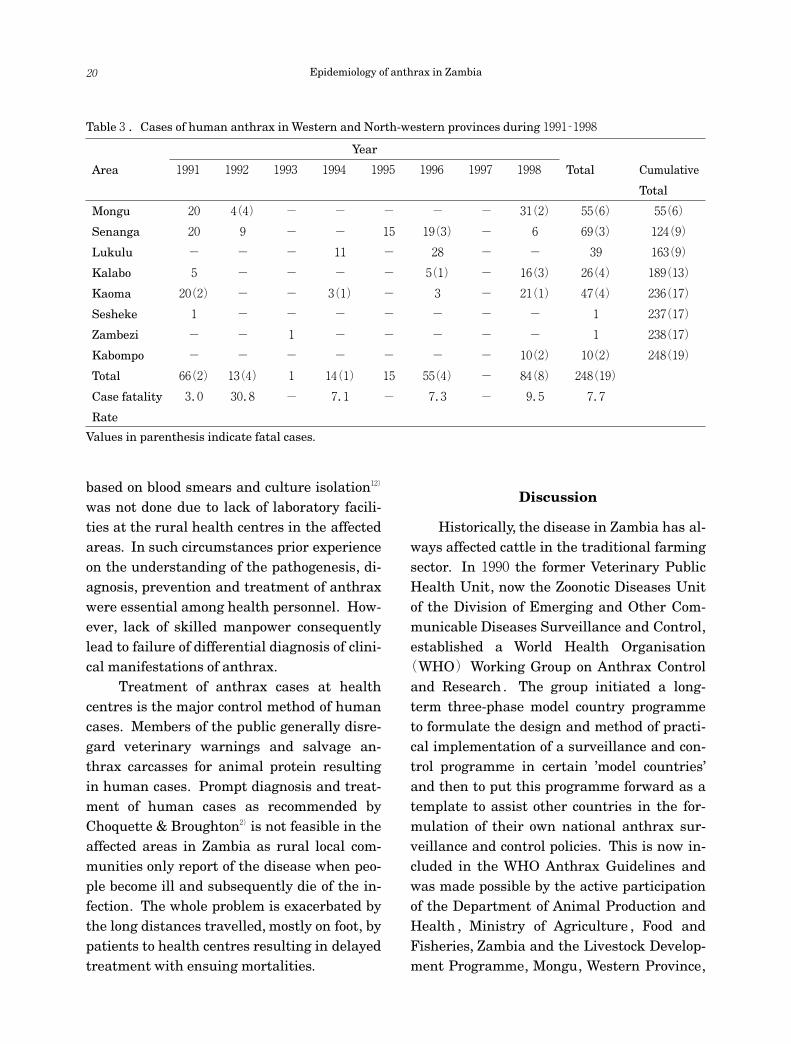
The highest incidence of human caseswas in1990 when about220 cases were re-ported to the veterinary and health officials.The fatality rate among the reported caseswas19.1%.The severely affected Districtswere Mongu, Kalabo, Lukulu and Senanga. Atleast 248 cases were reported in Senanga ,Mongu, Kaoma, Lukulu, Kalabo and SeshekeDistricts in Western Province and Kabompoand Zambezi Districts in North-western Prov-ince between1991and1998.The case fatalityrate among the cases was7.7% while the av-erage annual case fatality rate was7.2%(Ta-ble3).The majority of the reported caseswere intestinal anthrax with only33cases ofcutaneous anthrax. The presenting clinicalsigns in intestinal anthrax were acute gastro-enteritis, diarrhoea, vomiting and abdominalpain while oedema of the face, enlarged pa-rotid lymph nodes and fever were the present-ing clinical signs in cutaneous anthrax.
Diagnosis of the disease in the affectedareas was based on the history and clinicalexamination of the patient. Diagnosis of thedisease using standard laboratory methods
Victor M. Siamudaala et al. 19
based on blood smears and culture isolation12)
was not done due to lack of laboratory facili-ties at the rural health centres in the affectedareas. In such circumstances prior experienceon the understanding of the pathogenesis, di-agnosis, prevention and treatment of anthraxwere essential among health personnel. How-ever, lack of skilled manpower consequentlylead to failure of differential diagnosis of clini-cal manifestations of anthrax.
Treatment of anthrax cases at healthcentres is the major control method of humancases. Members of the public generally disre-gard veterinary warnings and salvage an-thrax carcasses for animal protein resultingin human cases. Prompt diagnosis and treat-ment of human cases as recommended byChoquette & Broughton2)is not feasible in theaffected areas in Zambia as rural local com-munities only report of the disease when peo-ple become ill and subsequently die of the in-fection. The whole problem is exacerbated bythe long distances travelled, mostly on foot, bypatients to health centres resulting in delayedtreatment with ensuing mortalities.
Discussion
Historically, the disease in Zambia has al-ways affected cattle in the traditional farmingsector. In1990 the former Veterinary PublicHealth Unit, now the Zoonotic Diseases Unitof the Division of Emerging and Other Com-municable Diseases Surveillance and Control,established a World Health Organisation(WHO)Working Group on Anthrax Controland Research . The group initiated a long-term three-phase model country programmeto formulate the design and method of practi-cal implementation of a surveillance and con-trol programme in certain ’model countries’and then to put this programme forward as atemplate to assist other countries in the for-mulation of their own national anthrax sur-veillance and control policies. This is now in-cluded in the WHO Anthrax Guidelines andwas made possible by the active participationof the Department of Animal Production andHealth , Ministry of Agriculture , Food andFisheries, Zambia and the Livestock Develop-ment Programme, Mongu, Western Province,
Table3.Cases of human anthrax in Western and North-western provinces during1991‐1998
Year
Area 1991 1992 1993 1994 1995 1996 1997 1998 Total Cumulative
Total
Mongu 20 4(4) - - - - - 31(2) 55(6) 55(6)
Senanga 20 9 - - 15 19(3) - 6 69(3) 124(9)
Lukulu - - - 11 - 28 - - 39 163(9)
Kalabo 5 - - - - 5(1) - 16(3) 26(4) 189(13)
Kaoma 20(2) - - 3(1) - 3 - 21(1) 47(4) 236(17)
Sesheke 1 - - - - - - - 1 237(17)
Zambezi - - 1 - - - - - 1 238(17)
Kabompo - - - - - - - 10(2) 10(2) 248(19)
Total 66(2) 13(4) 1 14(1) 15 55(4) - 84(8) 248(19)
Case fatality 3.0 30.8 - 7.1 - 7.3 - 9.5 7.7
Rate
Values in parenthesis indicate fatal cases.
Epidemiology of anthrax in Zambia20

Zambia, in a model country programme de-signed by the Working Group for the pur-pose29,30,31).
Widely accepted control measures of an-thrax such as vaccinations, public awarenesscampaigns, quarantine and burning or bury-ing of carcasses seem impractical to enforce inthe endemic areas in Zambia. Inadequate co-operation from rural farming communities ex-pressed in form of maximized usage of ani-mals(draught power and milk production),reluctance to bury or burn carcasses and lackof fuel wood to burn carcasses are the majorconstraints to anthrax control . Inadequatetechnical and administrative support is themajor weakness of the government driven an-thrax control programme. Funding and sup-ply of logistics(human resource , transportand cold chain system)are erratic and highlycentralized and based at the National Veteri-nary Office in Lusaka resulting in wastage ofvaluable time completing administrative pro-cedures.
Government has now opted to sub-contract private veterinary practitioners tovaccinate livestock against the disease al-though success from this strategy may beminimal given the lack of systematic qualitycontrol measures to evaluate the performanceof the private sector. Alternative and innova-tive approaches are required to bring anthraxunder control . It is recommended that gov-ernment should adopt a strict and systematicquality control programme of anthrax vacci-nation campaigns, decentralize managementof veterinary resources to operational centerswith timely disbursement of resources thereof,introduce an effective cold-chain system andconduct vaccination campaigns at regular in-tervals when climatic and anthropogenic fac-tors favour their implementation. Work is un-derway to determine the current prevalence ofanthrax in wildlife. Studies on molecular epi-
demiology of the disease should be conductedfor strain identification and differentiationwhich are an essential prerequisite for properepidemiological investigations and under-standing of anthrax. This effort could subse-quently lead to practical implementation ofsurveillance and control programmes not onlyin Zambia but also in the whole of southernAfrica.
References
1)Census estimates.2001.Central Statis-tics Office. Government of the Republic ofZambia.
2)Choquette, L. P. E. and Broughton, E.1981.Anthrax. In : Infectious Diseases ofWild Mammals, 2nd ed . , pp.288‐296,Davis, J. W., Karstad, L. H., and Trainer,D. O. eds., Ames, Iowa, USA. The IowaState University Press.
3)Christopher, G. W., Cieslak, T. J., Palvin, J.A. and Eitzen, E. M.1997.Biological war-fare : a historical perspective. J. Am. Med.Assoc.,278:412‐417
4)Davies, J. C. A.1983.A Major Epidemic ofAnthrax in Zimbabwe, Part II. The Cen-tral African J. Med.,29:8‐12.
5)Davies, J. C. A.1982.A Major Epidemic ofAnthrax in Zimbabwe, Part I. The CentralAfrican J. Med.,28:291‐298.
6)Department of Veterinary and LivestockDevelopment.2001. Annual Reports ,Government Printers, Lusaka, Zambia.
7)De Vos, V.1994.Anthrax. In : InfectiousDiseases of Livestock with Special Refer-ence to Southern Africa, pp.1262‐1289,Coetzer, J. A. W. , Thomson, G. R. andTustin , R. C. eds. , Cape Town , OxfordUniversity Press.
8)Dixon, T., Meselson, M., Guillemin, J. andHanna, P.1999.Medical progress : an-thrax. N. Engl. J. Med.341:815‐826.
9)Dudley, J. P. and Woodford, M. H,2002.
Victor M. Siamudaala et al. 21

Bioweapons , bioterrorism and biodiver-sity : Potential impacts of biologicalweapons attacks on agricultural and bio-logical diversity. Rev. Sci .Tech.Off. Int .Epiz.,21:125‐137.
10)Ebedes, H.1976.Anthrax epizootics inEtosha National Park. Madoqua.,10:99‐118.
11)Hambleton, P., Carman, J. A. and Melling,J.1984.Anthrax : the disease in relationto vaccines. Vaccine., 2:125‐132.
12)Harrison, L. H., Ezzel, J. W., Abshire, T. G.,Kidd , S . and Kaufmann , A . F.1989.Evaluation of ecological tests for diagno-sis of anthrax after an outbreak of cuta-neous anthrax in Paraguay. J. Infect. Dis.,160:706‐710.
13)Ingelsby, T., Henderson, D. A., Bartlett, J.G., Ascher, M. S., Eitzen, E., Friedlander,A. M., Hauer, J., McDade, J., Osterholm M.T., O’Toole, T., Parker, G., Perl T. M., Rus-sell , P. K . , Tonat , K . , for the workinggroup on civilian biodefence.1999.An-thrax as a biological weapon : medicaland public health management. JAMA.,281:1735‐1745.
14)Ingelsby, T. V., O’Toole, T., Henderson, D.A., Bartlett, J. G., Ascher, M. S., Eitzen, E.,Friedlander, A. M., Gerberding, J., Hauer,J., Hughes, J., McDade, J., Osterholm, M.T., Parker, G., Perl, T. M., Russell, P. K.and Tonat, K., for the working group oncivilian biodefense.2002.Anthrax as abiological weapon,2002‐updated recom-mendations for management . JAMA .,287:2236‐2252.
15)Jernigan, D. B., Raghunathan, P. L., Bell,B. P., Brechner, R., Bresnitz, E. A., Butler,J. C., Cetron, M., Cohen, M., Doyle, T.,Fischer, M. , Greene, C. , Grifth , K. S. ,Guarner, J., Hadler, J. L., Hayslett, J. A.,Meyer, R., Petersen, L. R., Phillips, M.,Pinner, R . , Popovic , T. , Quinn , C. P. ,
Reefhuis, J., Reissman, D., Rosenstein, N.,Schuchat , A. , Shieh, W. J. , Siegal , L . ,Swerdlow, D. L., Tenover, F. C., Traeger,M., Ward, J. W., Weisfuse, I., Wiersma, S.,Yeskey, K . , Zaki , S . , Ashford , D . A . ,Perkins, B. A., Ostroff, S. , Hughes, J. ,Fleming, D., Koplan, J. P., Gerberding, J.L . and the National Anthrax Epidemi-ologic Investigation Team.2002.Investi-gation of bioterrorism-related anthrax ,United States,2001:Epidemiologic find-ings. Emerg. Infect. Dis.,8:1019‐1028.
16)Kopcha, M. and Bartlett, P. C.1997.Im-portant zoonoses from direct contact withlivestock. Vet. Med.,92:370‐374.
17)MAFF(Ministry of Agriculture, Food andFisheries).1997.Report on a consul-tancy mission to assess the anthrax situ-ation in Western Province, Zambia.
18)MAFF(Ministry of Agriculture, Food andFisheries).1995.Farmers’ attitudes to-wards the control and prevention of an-thrax in Western Province Zambia. Work-ing paper,95/11.
19)Manchee, R. J., Broster, M. G., Stagg, A. J.,Hibbs, S. E., and Patience, B.1990.Outof the Gruinard Island. Proceedings of theInternational Workshop on Anthrax, Spe-cial supplement., No.68:16‐17.
20)Mbise, A. N., Nsengwa, G. R. M. , andMbasha, E. M. S.1991.Anthrax Epizo-otic in Tarangire National Park Tanza-nia : An Important Disease of Impala ina Period of15Years. Bull. Anim. Hlth .Prod. Africa.,39:45‐50.
21)Meselson, M., Guillemin, J., Hugh-Jones,M. et al.1994.The Sverdlovsk anthraxoutbreak of1979.Science,266:1202‐8.
22)Mitchell, P.1998.Anthrax-The Practitio-ner’s View. State Vet. J.,8:5‐8.
23)Mock, M. and Fouet, A.2001.Anthrax.Ann. Rev. Microbiol.,55:647‐671.
24)Mweene, A. S., Fukushi, H., Pandey, G. S.,
Epidemiology of anthrax in Zambia22

Syakalima, M., Simuunza, M., Malamo,M., Nambota, A., Samui, K. L., Tsubota, T.,Nakazato, Y., Onuma, M. and Yasuda, J.2003.The prevalence of bovineherpesvi-rus‐1 in traditional cattle in southernprovince, Zambia. Rev Sci. Tech. Off. Int.Epiz.,22:873‐877.
25)Mweene, A. S., Pandey, G. S., Sinyangwe,P., Nambota, A., Samui, K. and Kida, H.1996.Viral diseases of livestock in Zam-bia. Jpn. J. Vet. Res.,44:89‐105.
26)Ndyabahinduka, D. G. K., Chu, I. H., Ab-dou, A. H. and Gaifuba, J. K.1984.Anoutbreak of Human Gastrointestinal An-thrax. Ann. Ist. Sanita.,20:205‐208.
27)Tuchili, L. M. and Pandey, G. S.1995.Theimpact of anthrax on wildlife, human andthe environment in Zambia. In : Proceed-ings of the symposium on ‘The effects ofenlargement of domestic animal pastureon the wildlife in Zambia, Suzuki, A. K.,Pandey, G. S. and Nambota, A. Eds,22March1995,Lusaka, Zambia.
28)Tuchili, L. M., Pandey, G. S., Sinyangwe,P. G. and Kaji, T.1993.Anthrax in cattle,wildlife and humans in Zambia. Vet. Rec. ,132:487.
29)Turnbull, P. C. B., Bohm, R., Chizyuka, H.G. B., Fujikura, T., Hugh-Jones, M. E. andMelling, J.1993.Guidelines for the Sur-veillance and Control of Anthrax in Hu-mans and Animals . Geneva : WorldHealth Organisation. WHO/Zoon./93.170.
30)Turnbull, P. C. B., Bohm, R., Doganay, M.,Hugh-Jones, M., Lalitha, M. K. and DeVos, V.1999.Guidelines on Anthrax Sur-veillance and Control . Geneva : WorldHealth Organisation. WHO/EMC/ZDI/98・6.
31)Turnbull, P. C. B., Hugh-Jones, M. E. andCosivi, O.1999.World Health Organiza-tion activities on anthrax surveillanceand control. J. Appl. Microbiol. ,87:318‐320.
32)Van Ness, G. B.1971.Ecology of Anthrax.Science,172:1303‐1307.
Victor M. Siamudaala et al. 23