Relatively optimal control with characteristic polynomial assignment
Upload
independentCategory
view
0download
0
Ebola and Marburg haemorrhagic fever viruses: major scientific
advances, but a relatively minor public health threat for Africa
E. M. Leroy1,2, J-P Gonzalez1 and S. Baize3
1) Centre International de Recherches Medicales de Franceville, Franceville, Gabon, 2) MIVEGEC (IRD 224, CNRS 5290, Universites Montpellier 1), Institut
de Recherche pour le Developpement, Montpellier, France and 3) Unite de Biologie des Infections Virales Emergentes, Institut Pasteur, IFR128-Biosciences
Gerland-Lyon Sud, Lyon, France
Abstract
Ebola and Marburg viruses are the only members of the Filoviridae family (order Mononegavirales), a group of viruses characterized by
a linear, non-segmented, single-strand negative RNA genome. They are among the most virulent pathogens for humans and great
apes, causing acute haemorrhagic fever and death within a matter of days. Since their discovery 50 years ago, filoviruses have caused
only a few outbreaks, with 2317 clinical cases and 1671 confirmed deaths, which is negligible compared with the devastation caused by
malnutrition and other infectious diseases prevalent in Africa (malaria, cholera, AIDS, dengue, tuberculosis …). Yet considerable human
and financial resourses have been devoted to research on these viruses during the past two decades, partly because of their potential
use as bioweapons. As a result, our understanding of the ecology, host interactions, and control of these viruses has improved consid-
erably.
Keywords: Ebola, immunity, Marburg, outbreak, reservoir, vaccine
Clin Microbiol Infect
Corresponding author: E. M. Leroy, Centre International de Re-
cherches Medicales de Franceville, Franceville, Gabon
E-mail: [email protected]
Introduction
Ebola (EBOV) and Marburg (MARV) are the only members
of the Filoviridae family and are among the most virulent
pathogens for humans and great apes. The most virulent spe-
cies of these viruses induce acute haemorrhagic fever and
death within a few days in up to 90% of symptomatic individ-
uals [1,2]. The explosive disease course, high case fatality
rate, and lack of specific treatments or vaccines make EBOV
and MARV a major public health issue for Africa, and a cate-
gory A biothreat [3,4]. In the field, clinical specimens must
be handled according to WHO guidelines on viral haemor-
rhagic fever agents in Africa [5], and analyzed in biosafety
level 4 laboratories.
Research on filoviruses has been closely tied to outbreak
activity. Some advances in the biology and pathogenesis of
MARV and EBOV were made just after the discovery of these
agents, in 1967 and 1976, respectively. The two viruses were
then largely neglected until EBOV re-emerged in 1995 in Kik-
wit, Democratic Republic of Congo (DRC), where it caused a
large outbreak that received considerable media attention
worldwide. The extraordinarily high lethality, multifocal haem-
orrhaging, and specificity to African ecosystems enhanced the
fascination of Ebola for the international community, which
saw this disease as a potential threat in the post-Cold War
context [6]. This partly explains why research on the biology,
epidemiology, ecology and pathophysiology of these viruses
has advanced markedly over the past 15 years, leading
recently to the development of potential antiviral drugs and
candidate vaccines. Yet the overall disease burden of filovirus-
es over the past 45 years is minimal compared with major
infectious diseases such as AIDS, malaria, cholera, dengue and
tuberculosis [7,8]. This paper reviews research advances in
Ebola and Marburg ecology, virus–host interactions and dis-
ease control during the past 15 years.
CL
M3
53
5B
Dispa
tch:
19.4.11
Jour
nal:
CLM
CE:N
athiya
JournalName
ManuscriptNo.
Autho
rRec
eive
d:No.
ofpa
ges:
13PE
:Gay
athr
i
ª2011 The Authors
Clinical Microbiology and Infection ª2011 European Society of Clinical Microbiology and Infectious Diseases
REVIEW 10.1111/j.1469-0691.2011.03535.x
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
32
33
34
35
36
37
38
39
40
41
42
43
44
45
46
47
48
49
50
Filoviruses as Prototypes of EmergingPathogens
An emerging pathogen is defined as either a truly novel or a
hitherto unknown agent, or a pathogen whose incidence has
increased considerably in susceptible populations. EBOV and
MARV fulfil one criterion of this definition, in that they were
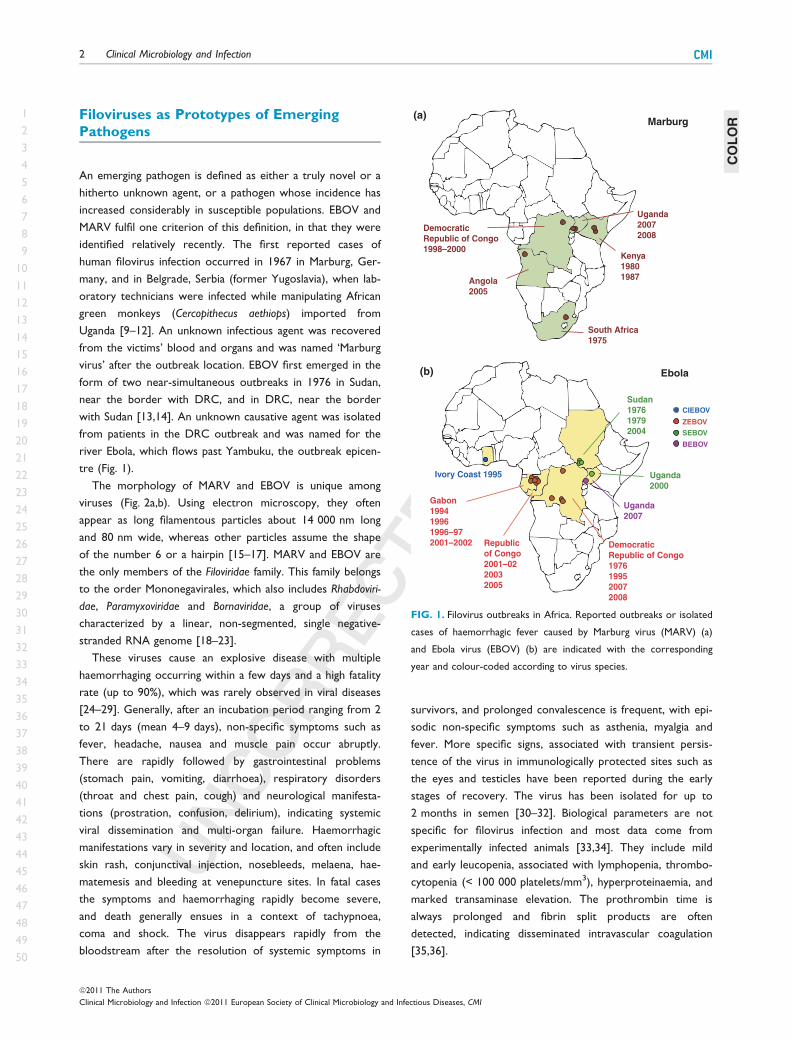
identified relatively recently. The first reported cases of
human filovirus infection occurred in 1967 in Marburg, Ger-
many, and in Belgrade, Serbia (former Yugoslavia), when lab-
oratory technicians were infected while manipulating African
green monkeys (Cercopithecus aethiops) imported from
Uganda [9–12]. An unknown infectious agent was recovered
from the victims’ blood and organs and was named ‘Marburg
virus’ after the outbreak location. EBOV first emerged in the
form of two near-simultaneous outbreaks in 1976 in Sudan,
near the border with DRC, and in DRC, near the border
with Sudan [13,14]. An unknown causative agent was isolated
from patients in the DRC outbreak and was named for the
river Ebola, which flows past Yambuku, the outbreak epicen-
tre (Fig. 1).
The morphology of MARV and EBOV is unique among
viruses (Fig. 2a,b). Using electron microscopy, they often
appear as long filamentous particles about 14 000 nm long
and 80 nm wide, whereas other particles assume the shape
of the number 6 or a hairpin [15–17]. MARV and EBOV are
the only members of the Filoviridae family. This family belongs
to the order Mononegavirales, which also includes Rhabdoviri-
dae, Paramyxoviridae and Bornaviridae, a group of viruses
characterized by a linear, non-segmented, single negative-
stranded RNA genome [18–23].
These viruses cause an explosive disease with multiple
haemorrhaging occurring within a few days and a high fatality
rate (up to 90%), which was rarely observed in viral diseases
[24–29]. Generally, after an incubation period ranging from 2
to 21 days (mean 4–9 days), non-specific symptoms such as
fever, headache, nausea and muscle pain occur abruptly.
There are rapidly followed by gastrointestinal problems
(stomach pain, vomiting, diarrhoea), respiratory disorders
(throat and chest pain, cough) and neurological manifesta-
tions (prostration, confusion, delirium), indicating systemic
viral dissemination and multi-organ failure. Haemorrhagic
manifestations vary in severity and location, and often include
skin rash, conjunctival injection, nosebleeds, melaena, hae-
matemesis and bleeding at venepuncture sites. In fatal cases
the symptoms and haemorrhaging rapidly become severe,
and death generally ensues in a context of tachypnoea,
coma and shock. The virus disappears rapidly from the
bloodstream after the resolution of systemic symptoms in
survivors, and prolonged convalescence is frequent, with epi-
sodic non-specific symptoms such as asthenia, myalgia and
fever. More specific signs, associated with transient persis-
tence of the virus in immunologically protected sites such as
the eyes and testicles have been reported during the early
stages of recovery. The virus has been isolated for up to
2 months in semen [30–32]. Biological parameters are not
specific for filovirus infection and most data come from
experimentally infected animals [33,34]. They include mild
and early leucopenia, associated with lymphopenia, thrombo-
cytopenia (< 100 000 platelets/mm3), hyperproteinaemia, and
marked transaminase elevation. The prothrombin time is
always prolonged and fibrin split products are often
detected, indicating disseminated intravascular coagulation
[35,36].
(a)
(b)
Republic
of Congo
2001–02
2003
2005
Democratic
Republic of Congo
1976
1995
2007
2008
Sudan
1976
1979
2004
Uganda
2000
Ivory Coast 1995
Uganda
2007
Gabon
1994
1996
1996–97
2001–2002
Kenya
1980
1987
South Africa
1975
Democratic
Republic of Congo
1998–2000
Angola
2005
Uganda
2007
2008
CIEBOV
BEBOV
SEBOV
ZEBOV
Marburg
Ebola
FIG. 1. Filovirus outbreaks in Africa. Reported outbreaks or isolated
cases of haemorrhagic fever caused by Marburg virus (MARV) (a)
and Ebola virus (EBOV) (b) are indicated with the corresponding
year and colour-coded according to virus species.
COLOR
2 Clinical Microbiology and Infection CMI
ª2011 The Authors
Clinical Microbiology and Infection ª2011 European Society of Clinical Microbiology and Infectious Diseases, CMI
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
32
33
34
35
36
37
38
39
40
41
42
43
44
45
46
47
48
49
50

Filoviruses: a Questionable Public HealthBurden for Africa
Since their discovery 45 years ago, filoviruses have been
responsible for only a few outbreaks, resulting in 2317 clini-
cal cases and 1671 confirmed deaths (reviewed in Fig. 1 and
Table 1, [37]). Hence, the disease burden of filovirus infec-
tion in Africa is extremely small compared with other infec-
tious diseases and malnutrition.
As said previously, the first MARV outbreak occurred in
Europe and was associated with 31 cases, including 25 pri-
mary cases (i.e. infected directly by animals) with seven
deaths [9–11]. Since then, only sporadic cases have been
reported, in South Africa in 1975 (three cases, one death)
and in Kenya in 1980 (two cases, one death) and 1987 (one
fatal case) [31,38,39]. MARV subsequently caused two large
outbreaks, in 1998–2000 in DRC and in 2004–2005 in
Angola. The longest MARV outbreak hit the Durba area
(eastern DRC) between 1998 and 2000, affecting 154 people
and killing 83% of victims [40]. Most patients worked in
underground gold mines. The Durba outbreak was charac-
terized by the circulation of multiple viral strains, pointing to
multiple independent introductions from the unknown
(a) (b)
(c)
VP40
VP24
NPVP30RNA
VP35LMembrane
GP1,2
trimer
(d)
FIG. 2. 10Ultrastructure and structure of filovirus virons. Particles of various forms are visualized by negative staining by uracyl acetate (a, b). Part
of a rod-shaped particle showing the tubular nucleocapsid and the surface spikes (c). Schematic representation of a filovirion indicating protein
composition, the tubular nucleocapsid and the surface spikes (d). (From Kuhn JH 9. Filoviruses: a compendium of 40 years of epidemiological, clini-
cal, and laboratory studies. In: Calisher CH editor. Springer, Wien, NewYork; 2008).
TABLE 1. List of filovirus outbreaks with the corresponding
location, number of clinical cases and fatality rate
Virus Date Location CasesFatality(%)
Marburg virus 1967 Germany – Yugoslavia 31 231975 South Africa 3 331980 Kenya 2 501987 Kenya 1 100
1998–2000 DRC 154 832005 Angola 252 902007 Uganda 4 252007 Uganda 1 02008 Uganda 1 100
Ebola virusZaire
1976 DRC 318 881977 DRC 1 1001994 Gabon 49 651995 DRC 315 881996 Gabon 37 57
1996–1997 Gabon 60 752001–2002 Gabon and
Republic of Congo123 79
2003 begin Republic of Congo 143 902003 end Republic of Congo 35 83
2005 Republic of Congo 11 752007 DRC 264 712008 DRC 32 47
Ebola virusSudan
1976 Sudan 286 531979 Sudan 34 652000 Uganda 425 532004 Sudan 17 42
Ebola virusCote d’Ivoire
1994 Ivory Coast 1 0
Ebola virusBundibugyo
2007 Uganda 102 42
DRC, Democratic Republic of Congo.
LOW
RESOLUTIO
NCOLOR
FIG
CMI Leroy et al. Ebola and Marburg haemorrhagic fever viruses1
3
ª2011 The Authors
Clinical Microbiology and Infection ª2011 European Society of Clinical Microbiology and Infectious Diseases, CMI
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
32
33
34
35
36
37
38
39
40
41
42
43
44
45
46
47
48
49
50

natural reservoir [29,40,41]. The largest recorded MARV
outbreak occurred in Uige province of northern Angola in
2004–2005 [42]. It was the first recorded outbreak in West
Africa, causing 252 cases and 227 deaths (fatality rate 90%).
Complete genomic characterization showed that the culprit
strain was closely related to previous East African isolates
[42]. Finally, small MARV outbreaks occurred in western
Uganda in 2007 and 2008 among workers in lead and gold
mines of the Kitaka Cave near Ibanda village [43,44]. Two of
the six victims died.
Ebola virus first emerged in the form of two near-simulta-
neous outbreaks in 1976 caused by two different species,
namely Sudan Ebola virus (SEBOV) in Sudan and Zaire Ebola
virus (ZEBOV) in DRC [13,14]. In Sudan, the outbreak was
centred in the Nzara and Maridi and was responsible for 284
cases. The mortality rate was 53%, characteristic of SEBOV
infection. The epicentre of the DRC outbreak was in Yamb-
uku, about 800 km from Maridi. This outbreak resulted in
318 cases with a mortality rate of 89%, characteristic of
ZEBOV infection. Later there was an unconfirmed lethal case
involving a 9-year-old girl living in Tandala, DRC, [45], fol-
lowed by another SEBOV outbreak in 1979, again in Nzara
and Maridi, with 34 cases and 22 deaths [46]. After a 15-year
period in which no further cases were recorded, EBOV
re-emerged in 1994 for a 3-year period. This new phase was
marked by the identification of a new species, Cote d’Ivoire
Ebola virus (CIEBOV), and by four ZEBOV outbreaks. The
only case caused by CIEBOV occurred in 1994, when an eth-
nologist sickened a few days after autopsying a chimpanzee
found dead in the Tai national park in Ivory Coast [47–49].
A large outbreak then occurred in 1995, in and around the
town of Kikwit, south of DRC, with 315 cases and a mortal-
ity rate of 81% [50]. Despite the deployment of more
sophisticated scientific and medical resources than those
available in 1976, this outbreak was as large as the 1976 out-
break, probably because it affected a town with several hun-
dred thousand inhabitants. Three other outbreaks, all as the
result of ZEBOV, struck northeast Gabon between 1994 and
1997 [51–54]. In total, these outbreaks involved 140 cases
and caused 75 deaths. The first occurred in gold-digger
camps located in the heart of the forest. The second out-
break hit the village of Mayibout, located south of Mekouka,
among children who had carried and butchered a chimpan-
zee carcass found in the forest. The third outbreak occurred
in 1996–1997, with 60 cases and 45 deaths over a 6-month
period. Fifteen cases and 11 deaths were recorded in Libre-
ville, the capital of Gabon, and a South African nurse was
infected by a Gabonese physician who had travelled to
Johannesburg. The period 2000–2008 was marked by
repeated ZEBOV outbreaks, SEBOV resurgence, and the dis-
covery of a new species of Ebola virus, Bundibugyo Ebola
virus (BEBOV). Between 2001 and 2005, Gabon and Republic
of Congo (RC) were hit by five ZEBOV outbreaks [55–58].
The first outbreak occurred within the cross-border area
between northeast Gabon and northwest RC, and resulted
in 143 cases and 128 deaths. RC was again affected twice in
2003 (respectively 143 and 35 cases, and 128 and 29 deaths),
and then in 2005 at Etoumbi, where only 11 cases (nine fatal-
ities) were reported. Two outbreaks of Sudan Ebola virus
also occurred during this period. One hit Uganda in 2000,
comprised three foci and was the largest of all recorded
EBOV outbreaks, causing 173 deaths among its 425 victims
[59,60]. A second SEBOV outbreak occurred in Sudan in
2004 in the town of Yambio, located near Nzara and Maridi.
There were 17 cases and seven deaths [61–63]. The latest
species to be discovered, Bundibugyo Ebola virus (BEBOV),
was discovered in 2007 in Uganda, where it was responsible
for a large outbreak [64] with 116 cases and 30 deaths (fatal-
ity rate 26%).
These four EBOV species are all pathogenic for humans
and arose in sub-Saharan Africa. An additional species, Res-
ton Ebola virus (REBOV), was isolated in 1989 from Asian
cynomolgus monkeys (Macaca fascicularis) imported from the
Philippines and housed in a quarantine facility in Reston, Vir-
ginia, USA. The monkeys developed a haemorrhagic disease
associated with high lethality, and subsequent outbreaks
among cynomolgus monkeys were reported in animal facili-
ties in Texas, USA, Italy and the Philippines [39,65–68].
Although no humans fell sick during these episodes, several
monkey handlers in the United States and in the Philippines
were shown to have seroconverted [69,70]. Recently, REB-
OV was also isolated from domestic Philippino swine with a
severe respiratory syndrome and co-infected by porcine
reproductive and respiratory syndrome virus [71].
Filoviral Genes and Proteins
The MARV and EBOV genomes are about 19 000 nucleo-
tides long and are transcribed into eight major subgenomic
mRNAs, which encode seven structural proteins: 3¢ leader,
nucleoprotein (NP), virion protein 35 (VP35), VP40, glyco-
protein (GP), VP30, VP24, and RNA-dependent RNA poly-
merase (L)-5¢ trailer; and one non-structural protein (sGP),
shown in Fig. 2. The central core of the virion is composed
of the ribonucleoprotein complex, which consists of the
genomic RNA molecule encapsulated by NP linked to the
inner matrix proteins VP30 and VP35 and the RNA-depen-
dent RNA polymerase (Fig. 2d). This complex is involved in
transcription and replication [72–74]. The matrix proteins
4 Clinical Microbiology and Infection CMI
ª2011 The Authors
Clinical Microbiology and Infection ª2011 European Society of Clinical Microbiology and Infectious Diseases, CMI
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
32
33
34
35
36
37
38
39
40
41
42
43
44
45
46
47
48
49
50

VP40 and VP24 are linked to the ribonucleoprotein complex
at the inner surface of the lipid bilayer of the viral envelope,
which is derived from the host cell. VP40 and VP24 are
involved in viral nucleocapsid formation, viral budding or
assembly, and host range determination [72,75–82]. The viral
envelope contains only the glycoproteins, organized as tri-
meric spikes (Fig. 2c,d) consisting of two fragments (extracel-
lular protein, GP1, and membrane-anchored protein, GP2)
which result from furin-like enzyme cleavage of precursor
polyproteins and remain linked by a disulphide bond [74,83–
85]. GP binds preferentially to endothelial and monocytic
cells via GP1, mediating target cell entry, inducing endothelial
cell disruption and cytotoxicity in blood vessels in vitro, and
causing immunosuppression in vitro via a retrovirus-like pep-
tide [74,86–94]. EBOV differs from MARV and from other
members of the Mononegavirales in that infected cells
secrete large amounts of a non-structural glycoprotein
(sGP), the primary product of the GP gene, which is
expressed from non-edited mRNA species [93,95,96]. The
role of sGP is poorly understood. Finally, the matrix proteins
VP35 and VP24 seem to play a key role in the pathogenicity
of EBOV and MARV, by inhibiting antiviral responses and
particularly type 1 interferon (IFN) synthesis [97–102].
Filoviruses Genomics
The Filoviridae family comprises two genera, Marburgvirus and
Ebolavirus, and belongs to the order Mononegavirales, a
group of viruses characterized by a genome consisting of a
linear, non-segmented, single negative strand of RNA [18–
23]. Molecular evolutionary analyses of the glycoprotein
genes suggests that EBOV and MARV diverged several thou-
sand years ago [103]. The genus Marburgvirus consists of a
single species, Marburgvirus, comprising five viruses differing
from one another by up to 21% at the nucleotide level, while
there are five known species of Ebolavirus that have different
geographic locations, case fatality rates, and nucleotide
sequence divergences of about 32–41% [16].
Our knowledge of filovirus distribution and diversity may
be limited because EBOV and MARV have only been identi-
fied and characterized in sick or dead humans and animals
[40,42,43,53–56,64,68,71,104–107]. Numerous studies have
attempted to determine the regions of EBOV and MARV cir-
culation. Remotely sensed data and niche ecologic modelling
suggest that filoviruses may circulate within a much wider
region than their outbreak areas [108–111]. Using a sensitive
and specific ELISA method, an overall ZEBOV-specific IgG se-
roprevalence of 15.3% was found in Gabon, the highest ever
reported [112]. The seroprevalence was significantly higher
in forested areas (19.4%) than in grassland (12.4%), savannah
(10.5%) and areas rich in lakes (2.7%). These results are con-
sistent with previous reports of seroprevalence rates ranging
from 1.8% to 21.3% throughout central Africa using poorly
specific immunofluorescence antibody testing 2methods [113–
117]. More convincingly, two recent small serosurveys, based
on the same ELISA as the one we used, have shown high
antibody prevalence in some forested regions of Central
Africa. Indeed, a 9.3% (15/161) prevalence of ZEBOV-specific
IgG was found in unaffected villages surrounding Kikwit a few
weeks after the 1995 outbreak [118], and a 13.2% (25/190)
seroprevalence was found in the Aka Pygmy population in
the Central African Republic, where no ZEBOV outbreaks
have been reported [119]. Such high seroprevalence rates
indicate a high level of ZEBOV circulation in the tropical rain
forest environment and suggest that human rural populations
are highly exposed to the virus, with mild or asymptomatic
infection by outbreak strains [120] or less pathogenic strains,
or simple exposure to inert viral particles.
Filoviruses in Wildlife
Filovirus haemorrhagic fevers are typical zoonotic diseases
transmitted accidentally by direct contact with live or dead
animals. The role of wildlife species in the human epidemiol-
ogy of ZEBOV is only partly understood (Fig. 3). In addition
to its high pathogenicity for humans, ZEBOV has caused
massive outbreaks among gorillas and chimpanzees, killing
thousands of animals during the last decade in parts of Ga-
bon and RC [56,121–125]. Another study conducted in the
Tai forest of Ivory Coast showed that the disappearance of
11 members (26%) of a group of 43 chimpanzees during
November 1994 may have been the result of CIEBOV [126].
Such massive outbreaks in great apes could have major impli-
cations for animal conservation. The identification of multiple
strains during the 2001 Gabon/RC outbreak and the recent
identification of two phylogenetically divergent lineages sug-
gest independent introductions into great ape and human
populations following multiple viral spill-overs from a reser-
voir host [56,107,127]. In this ‘multi-emergence’ hypothesis,
Ebola outbreaks would occur episodically in certain ecologi-
cal conditions caused by habitat disturbances or climatic phe-
nomena [108,109]. Although the idea of multi-emergence
makes no reference to a particular timescale, this theory also
implicitly assumes that ZEBOV was present in Equatorial
Africa long before the first documented outbreak in 1976, as
supported by various serosurveys [128–130].
Although many field and laboratory studies have been
conducted since the first recorded outbreak in an attempt
CMI Leroy et al. Ebola and Marburg haemorrhagic fever viruses1
5
ª2011 The Authors
Clinical Microbiology and Infection ª2011 European Society of Clinical Microbiology and Infectious Diseases, CMI
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
32
33
34
35
36
37
38
39
40
41
42
43
44
45
46
47
48
49
50

to identify the reservoir species of MARV and EBOV, conclu-
sive evidence that bats are natural hosts for filoviruses was
obtained only recently [14,45,131–138]. Antibodies and
nucleotide sequences specific for ZEBOV [127,139] were
detected in the liver and spleen of three fruit bat species in
Gabon and RC (Hypsignathus monstrosus, Epomops franquetti
and Myonycteris torquata), and antibodies and nucleotide
sequences specific for MARV [140,141] were found in a fruit
bat species in Gabon (Rousettus aegyptiacus) and in two insec-
tivorous bat species in DRC (Rhinolophus eloquens and Mini-
opterus inflatus). More recently, MARV was isolated from
cave-dwelling Rousettus aegyptiacus bats in Uganda [43].
Finally, a recent study showed that the 2007 Luebo outbreak
in DRC was linked to massive fruit bat migration, strongly
suggesting that humans could be infected directly by bats
(Fig. 3) [142].
Pathogenesis of Ebola Virus Infection andImmune Responses
Antigen-presenting cells such as dendritic cells and macro-
phages are major EBOV targets [143,144]. Indeed, by their
presence in mucosal tissues and skin, these cells are infected
early and serve as the substrate for the first replicative viral
cycles. Because of their extensive distribution among the dif-
ferent organs and tissues, and their mobility, dendritic cells
and macrophages are probably responsible for viral dissemi-
nation and systemic infection [145]. Intense viral replication
then occurs in secondary lymphoid organs and liver, and the
virus subsequently spreads to hepatocytes, endothelial cells,
fibroblasts and some epithelial cells [146,147]. The pathogen-
esis of filovirus infection is reviewed in Fig. 4.
However, despite widespread viral replication, the
observed damage to endothelia, liver and other organs is not
sufficiently severe to cause terminal shock and death. Endo-
thelial infection is infrequent, occurring in the terminal stages
with no clear evidence of cytopathic effects [36]. Similarly,
although multifocal hepatic necrosis may be linked to viral
replication in liver, the observed hepatocellular lesions can-
not directly lead to death [146,147]. A pathogenic role of
the host response is therefore suspected.
Extensive infection of monocytes and macrophages leads to
aberrant release of inflammatory mediators and chemokines
such as interleukin-1b (IL-1b), tumour necrosis factor-a (TNF-
a), IL-6, IL-15, IL-16, IL-1 receptor antagonist, soluble TNF
receptor, IL-10, NO), IL-8, growth regulated oncogene-a,
CCL3, CCL4, CXCL10, monocyte chemotactic protein-1, and
eotaxin [144,148–151]. This ‘cytokine storm’, particularly
prominent in the terminal stages of the disease in humans and
non-human primates, has dramatic consequences. It is proba-
ble that TNF-a, NO), and other vasoactive compounds play a
crucial role in the associated vascular leakage, by increasing
endothelial permeability, reducing vascular tone, and altering
endothelial cell functions [144,152–154]. In addition, some of
these mediators may induce the expression of adhesion mole-
cules at the surface of endothelial cells, so allowing neutroph-
ils and monocytes to invade sites of infection where they may
cause bystander tissue damage [155]. Infected macrophages
are involved in the coagulopathy and in the induction of dis-
seminated intravascular coagulation by their abundant expres-
sion of tissue factor [35,156,157]. Other consequences of the
massive antigen-presenting cell infection are lymphoid deple-
tion in the spleen, lymph nodes and thymus, and extensive
apoptosis of T lymphocytes and natural killer cells, as
observed in blood and tissues of human and non-human pri-
mate fatalities [145,150,154,158–161]. T-cell death cannot be
the result of a direct viral cytopathic effect, as lymphocytes
are not infected by EBOV, but would rather result from inter-
actions with infected antigen-presenting cells and soluble medi-
Reservoirs of ZEBOV & MARV:
fruit bats species
Intermediary susceptible species:
virus amplification in great apes and duikers
Outbreak
Suspected
Direct
contact
FIG. 3. 11Model of the natural cycle of filovirus. The diagram shows animal-to-human transmissions leading to outbreak appearance. Several Zaire
Ebola virus (ZEBOV) outbreaks appeared when hunters handled the infected carcasses of chimpanzee, gorilla and duiker. Several ZEBOV and
Marburg virus (MARV) outbreaks were suspected to be associated with exposure to fruit bats.
LOW
RESOLUTIO
NCOLOR
FIG
6 Clinical Microbiology and Infection CMI
ª2011 The Authors
Clinical Microbiology and Infection ª2011 European Society of Clinical Microbiology and Infectious Diseases, CMI
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
32
33
34
35
36
37
38
39
40
41
42
43
44
45
46
47
48
49
50

ators [36,150,158]. A viral protein with superantigen activity
might also be involved [162]. Although T-cell depletion proba-
bly induces profound immunosuppression, the consequences
for disease progression are unclear [163,164]. Fatal Ebola
haemorrhagic fever is also associated with defective humoral
responses, with absent specific IgG and barely detectable IgM
[158,165]. This impairment of adaptive immunity may result
from extensive infection of dendritic cells. Indeed, EBOV-
infected dendritic cells produce only a limited panel of cyto-
kines without full activation and maturation, which may impair
their ability to trigger adaptive immunity [143,145,166,167].
Some viral factors are also able to counteract innate
immunity and thereby impede the control of viral replication.
Indeed, VP35 blocks IFN-a/b synthesis by preventing the acti-
vation of interferon regulatory factors 3 and 7
[97,99,101,102,168]. VP35 also interferes with the activation
of dsRNA-dependent protein kinase [169], and, like VP30
and VP40 [170], is a suppressor of RNA silencing [171].
VP24 impairs the nuclear accumulation of tyrosine-phosphor-
ylated signal transducer and activator of transcription 1 and
thereby inhibits IFN-a/b and IFN-c signalling [172,173]. Inhibi-
tion of type I IFN responses seems to be crucial for EBOV
virulence, as viruses that have lost this property by VP35
mutation are attenuated in vitro and in vivo [174,175].
In striking contrast with fatal outcome, effective control of
EBOV infection is associated with balanced immune
responses. A transient and well-regulated inflammatory
response is observed early in the disease not only in patients
that survive, but also in asymptomatic subjects [120,149].
This response may help to control the infection and to
induce specific immunity. An early and robust humoral
response is strongly correlated with survival in symptomatic
patients [158,165]. In asymptomatic EBOV-infected subjects,
antibodies are detected about 3 weeks after infection and in
moderate amounts [120]. In survivors and asymptomatic sub-
jects, high antibody titres persist for years [176]. Although
FIG. 4. A model of pathogenesis of filovirus infection, based on findings with Zaire Ebola virus. Dendritic cells and macrophages are early targets
of filoviruses. The virus spreads from the initial site of infection to secondary lymphoid organs and liver where intense replication takes place.
Then, other cells are infected such as hepatocytes, endothelial cells, fibroblasts and some epithelial cells. The inhibition of type I interferon (IFN)
production by viral proteins leads to relentless viral replication in most organs. The extensive infection of antigen-presenting cells (APC) leads to
altered inflammatory response and uncontrolled release of mediators. This ‘cytokine storm’ contributes to the pathogenesis by attracting inflam-
matory cells towards infected tissues, inducing coagulopathy and increasing endothelial permeability and vascular leakage. In addition, infected
APC and/or soluble factors are responsible for the defective adaptive immunity and the massive apoptosis of T lymphocytes. Multifocal necrosis
of hepatocytes, liver failure, destruction of secondary lymphoid organs and other tissue damage may result from direct cytopathic effects but also
from the host response. Together, these events lead to multi-organ failure, impairment of the vascular system, terminal shock and death.
COLOR
CMI Leroy et al. Ebola and Marburg haemorrhagic fever viruses1
7
ª2011 The Authors
Clinical Microbiology and Infection ª2011 European Society of Clinical Microbiology and Infectious Diseases, CMI
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
32
33
34
35
36
37
38
39
40
41
42
43
44
45
46
47
48
49
50

antibodies probably participate in the control of infection,
their precise role is unclear. Importantly, control of EBOV
infection is also characterized by a lack of T-cell apoptosis
and by the circulation of activated T cells (probably including
cytotoxic T lymphocytes), coinciding with a fall in viraemia
and the disappearance of symptoms [158]. A similar
response also occurs in asymptomatic individuals [177], sug-
gesting that T-cell responses are crucial for controlling the
infection. The factors underlying the radically different out-
comes of EBOV infection are unclear, but may include the
route of infection, the size of the inoculum, the cell types
that are initially infected, previously acquired immunity [112],
heterologous immunity, and MHC status [178]. However, it
is unlikely that outcomes were related to different virus
strains, as no difference was found in the coding sequences
of viruses isolated from survivors and fatalities and different
outcomes can be observed in patients infected with the same
viral source [51,105].
Treatment and Prevention
Although several advances in the treatment and prevention
of EBOV infection have recently been described, there is no
licensed vaccine, and the only way to limit outbreaks is to
isolate patients. The development of therapeutic measures is
hampered not only by the need to manipulate EBOV in bio-
safety level 4 facilities, but also by the limited number of
people affected since the discovery of filoviruses. However,
the increasing frequency of EBOV outbreaks in humans and
great apes [56,122–124] and the recent emergence of new
EBOV species [47,64], give evidence for the intense circula-
tion of EBOV in the endemic area.
The main challenge is to develop a vaccine conferring
cross-protection against heterologous EBOV species, includ-
ing emerging strains, ideally after a single dose. Several vac-
cine candidates have shown good efficacy in non-human
primates over the last 10 years. The use of live viral vectors
or virus-like particles to produce EBOV GP is a promising
approach, providing sterilizing immunity after a single dose
[179–184]. Recent studies have demonstrated the feasibility
of a multivalent vaccine able not only to protect against the
filovirus species used to formulate the candidate
[180,185,186] but also to cross-protect against an emerging
species [187]. However, several concerns must be dealt with
before human use, such as the safety of the viral vector, pos-
sible pre-existing immunity to the vector, and formulation of
a single-dose cross-protective vaccine. Results obtained with
candidate vaccines confirm the major role of T-cell
responses, and of CD8+ T cells in particular, in the control
of filovirus infections, as well as the presence of cross-react-
ing immunogenic epitopes on the viral GP.
A vesicular stomatitis virus-based candidate also has thera-
peutic potential, conferring substantial post-exposure protec-
tion when administered very rapidly to non-human primates
[188,189]. Passive immunization with convalescent plasma or
monoclonal antibodies seems to be ineffective [190–192],
tending to confirm that humoral responses are not primarily
responsible for the control of EBOV infection. Similarly,
recombinant type I IFN administration fails to protect non-
human primates [193]. One promising approach is to manip-
ulate the coagulation system by inhibiting the tissue factor
pathway with a factor VIIa/tissue factor inhibitor [156] or by
activating the natural anticoagulant protein C pathway with
recombinant activated protein C [194]. However, the sur-
vival benefit is limited. Another approach is to target viral
replication with small interfering RNA or antisense oligonu-
cleotides [195–198], although the latter is limited by the
need to use virus species-specific sequences, which are not
known in the early stages of an outbreak.
Conclusions
Substantial advances in our understanding of the ecology of
EBOV and MARV, as well as host–virus interactions and dis-
ease control, have been made during the past two decades.
This period was marked by the first recorded MARV out-
break in West Africa, resurgence of Ebola Sudan in Sudan
and Uganda, the discovery of two new species (Cote d’Ivoire
and Bundibugyo), and escalation of ZEBOV outbreaks in the
border region of Gabon and the Republic of Congo. Bats
have been identified as a major filovirus reservoir, and many
human outbreaks have been shown to have arisen through
the handling of infected chimpanzee and gorilla carcasses.
The 2007 ZEBOV outbreak was linked to fruit bats, although
the precise mechanism of transmission to humans was not
identified. MARV and ZEBOV induce profound suppression
of adaptive immunity, characterized by massive B-lymphocyte
and T-lymphocyte apoptosis largely mediated by the TRAIL
(TNF-related apoptosis-inducing ligand) and Fas pathways. A
recent study suggests that superantigenic activity may be
involved and numerous studies have shown that VP35 and
VP24 play an essential role in ZEBOV suppression of IFN-a/
b production.
Transparency Declaration
Conflicts of interest: nothing to declare.
8 Clinical Microbiology and Infection CMI
ª2011 The Authors
Clinical Microbiology and Infection ª2011 European Society of Clinical Microbiology and Infectious Diseases, CMI
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
32
33
34
35
36
37
38
39
40
41
42
43
44
45
46
47
48
49
50

References
1. Hoenen T, Groseth A, Falzarano D, Feldmann H. Ebola virus: unrav-
elling pathogenesis to combat a deadly disease. Trends Mol Med
2006; 12: 206–215.
2. Sanchez A, Geisbert TW, Feldmann H. Filoviridae: Marburg and Ebo-
la viruses. In: Knipe DM, Howley PM, eds, Fields virology. Philadelphia:
Lippincott Williams and Williams, 2007; 1409–1448.
3. Borio L, Inglesby T, Peters CJ et al. Hemorrhagic fever viruses as
biological weapons: medical and public health management. JAMA
2002; 287: 2391–2405.
4. Centers for Disease Control and Prevention. Bioterrorism agents/
diseases, 2010. Available at: http://wwwbtcdcgov/agent/agentlist-cate-
goryasp#a3 .
5. World Health Organization. Recommendations for management of
viral haemorrhagic fevers in Africa. ?????: World Health Organization,
19854
6. Bray M, Murphy FA. Filovirus research: knowledge expands to meet
a growing threat. J Infect Dis 2007; 196 (suppl. 2): S438–S443.
7. World Health Organization. Ebola haemorrhagic fever – fact sheet
revised in May 2004. Wkly Epidemiol Rec 2004; 79: 435–439.
8. Borchert M, Boelaert M, Sleurs H et al. Viewpoint: filovirus haemor-
rhagic fever outbreaks: much ado about nothing? Trop Med Int Health
2000; 5: 318–324.
9. Smith CEG, Simpson DIH, Bowen ETW. Fatal human disease from
vervet monkeys. Lancet 1967; II: 1119–1121.
10. Martini GA. Marburg agent disease in man. Trans R Soc Trop Med
Hyg 1969; 63: 295–302.
11. Martini GA, Siegert R. Marburg virus disease. New York: Springer,
1971.
12. Slenczka W, Klenk HD. Forty years of Marburg virus. J Infect Dis
2007; 196 (suppl. 2): S131–S135.
13. Smith DIH. Ebola haemorrhagic fever in Sudan, 1976. Bull World
Health Organ 1978; 56: 247–270.
14. Johnson KM. Ebola haemorrhagic fever in Zaire, 1976. Bull World
Health Organ 1978; 56: 271–293.
15. Kiley MP, Regnery RL, Johnson KM. Ebola virus: identification of vir-
ion structural proteins. J Gen Virol 1980; 49: 333–341.
16. Feldmann H, Kiley MP. Classification, structure, and replication of fil-
oviruses. Curr Top Microbiol Immunol 1999; 235: 1–21.
17. Sanchez A, Khan A, Zaki SR, Nabel GJ, Ksiazek TG, Peters CJ. Filo-
viridae: Marburg and Ebola viruses. In: Knipe DM, Howley PM, eds,
Fields virology. Philadelphia: Lippincott Williams & Wilkins, 2001;
1279–1304.
18. Kiley MP, Bowen TW, Eddy GA et al. Filoviridae: taxonomic home
for Marburg and Ebola viruses? Intervirology 1982; 18: 24–32.
19. Regnery RL, Johnson KM, Kiley MP. Virion nucleic acid of Ebola
virus. J Virol 1980; 36: 465–469.
20. Feldmann H, Muhlberger E, Randolf A et al. Marburg virus, a filo-
virus: messenger RNAs, gene order, and regulatory elements of the
replication cycle. Virus Res 1992; 24: 1–19.
21. Muhlberger E, Sanchez A, Randolf A et al. The nucleotide sequence
of the l gene of Marburg virus, a filovirus: homologies with paramyx-
oviruses and rhabdoviruses. Virology 1992; 187: 534–547.
22. Feldmann H, Klenk HD, Sanchez A. Molecular biology and evolution
of filoviruses. Arch Virol 1993; 7: 81–100.5
23. Feldmann H, Nichol ST, Klenk H-D, Peters CJ, Sanchez A. Charac-
terization of filoviruses based on difference in structure and antige-
nicity of the virion glycoprotein. Virology 1994; 199: 469–473.
24. Martini GA. Clinical syndrome. In: MGAaS R, ed. Marburg virus dis-
ease. New York: Springer-Verlag, 1971; 1–9.
25. Smith DH, Francis F, Simpson DIH. African haemorrhagic fever in
southern Sudan, 1976: the clinical manifestations. In: Pattyn SR, ed.
Ebola virus haemorrhagic fever. New York: Elsevier/North-Holland
biomedical press, 1978; 21–26.
26. Peters CJ, Khan AS. Filovirus diseases. In: Klenk HD, ed. Current top-
ics in microbiology and immunology: filovirus disease. Berlin: Springer-
Verlag, 1999; 85–95.
27. Peters CJ, LeDuc JW. An introduction to Ebola: the virus and the
disease. J Infect Dis 1999; 179 (suppl. 1): ix–xvi.
28. Bwaka MA, Bonnet M-J, Calain P et al. Ebola hemorrhagic fever in
Kiwit, Democratic Republic of the Congo: clinical observations in
103 patients. J Infect Dis 1999; 179: S1–S7.
29. Colebunders R, Tshomba A, Van Kerkhove MD et al. Marburg hem-
orrhagic fever in Durba and Watsa, Democratic Republic of the
Congo: clinical documentation, features of illness, and treatment. J
Infect Dis 2007; 196 (suppl. 2): S148–S153.
30. Emond RT, Evans B, Bowen ET, Lloyd G. A case of Ebola virus infec-
tion. Br Med J 1977; 2: 541–544.
31. Smith DH, Isaacson M, Johnson KM et al. Marburg-virus disease in
Kenya. Lancet 1982; I: 816–820.
32. Rowe AK, Bertolli J, Khan AS et al. Clinical, virologic, and immuno-
logic follow-up of convalescent Ebola hemorrhagic fever patients and
their household contacts, Kikwit, Democratic Republic of the
Congo. J Infect Dis 1999; 179: S28–S35.
33. Fisher-Hoch SP, Lloyd G, Platt GS, Simpson DIH. Hematological and
biochemical monitoring of Ebola infection in rhesus monkeys: impli-
cations for patient management. Lancet 1983; 2: 1055–1058.
34. Fisher-Hoch SP, Platt GS, Neild GH et al. Pathophysiology of shock
and hemorrhage in a fulminating viral infection (Ebola). J Infect Dis
1985; 152: 887–894.
35. Geisbert TW, Young HA, Jahrling PB, Davis KJ, Kagan E,
Hensley L. Mechanisms underlying coagulation abnormalities in Ebola
hemorrhagic fever: overexpression of tissue factor in primate
monocytes/macrophages is a key event. J Infect Dis 2003; 188: 1618–
1629.
36. Geisbert TW, Young HA, Jahrling PB et al. Pathogenesis of Ebola
hemorrhagic fever in primate models: evidence that hemorrhage is
not a direct effect of virus-induced cytolysis of endothelial cells. Am
J Pathol 2003; 163: 2371–2382.
37. Kuhn JH. Filoviruses. A compendium of 40 years of epidemiological,
clinical, and laboratory studies. Arch Virol Suppl 2008; 20: 13–360.
38. Gear JS, Cassel GA, Gear AJ et al. Outbreak of Marburg virus dis-
ease in Johannesburg. Br Med J 1975; 4: 489–493.
39. Johnson ED, Johnson BK, Silverstein D et al. Characterization of a
new Marburg virus isolated from a 1987 fatal case in Kenya. Arch
Virol Suppl 1996; 11: 101–114.
40. Bausch DG, Nichol ST, Muyembe-Tamfum JJ et al. Marburg hemor-
rhagic fever associated with multiple genetic lineages of virus. N Engl
J Med 2006; 355: 909–919.
41. Bausch DG, Borchert M, Grein T et al. Risk factors for Marburg
hemorrhagic fever, Democratic Republic of the Congo. Emerg Infect
Dis 2003; 9: 1531–1537.
42. Towner JS, Khristova ML, Sealy TK et al. Marburg virus genomics
and association with a large hemorrhagic fever outbreak in Angola.
J Virol 2006; 80: 6497–6516.
43. Towner JS, Amman BR, Sealy TK et al. Isolation of genetically
diverse Marburg viruses from Egyptian fruit bats. PLoS Pathog 2009;
5: e1000536.
44. Hartman AL, Towner JS, Nichol ST. Ebola and Marburg hemorrhagic
fever. Clin Lab Med 2010; 30: 161–177.
45. Heymann DL, Weisfeld JS, Webb PA, Johnson KM, Cairns T, Ber-
quist H. Ebola hemorrhagic fever: Tandala, 1977–1978. J Infect Dis
1980; 142: 372–376.
46. Baron RC, McCormick JB, Zubeir OA. Ebola virus disease in south-
ern Sudan: hospital dissemination and intrafamilial spread. Bull World
Health Organ 1983; 61: 997–1003.
CMI Leroy et al. Ebola and Marburg haemorrhagic fever viruses1
9
ª2011 The Authors
Clinical Microbiology and Infection ª2011 European Society of Clinical Microbiology and Infectious Diseases, CMI
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
32
33
34
35
36
37
38
39
40
41
42
43
44
45
46
47
48
49
50

47. Le Guenno B, Formenty P, Wyers M, Gounon P, Walker F, Boesch
C. Isolation and partial characterisation of a new strain of Ebola. Lan-
cet 1995; 345: 1271–1274.
48. Le Guenno B, Formenty P, Boesch C. Ebola virus outbreaks in Ivory
Coast and Liberia, 1994–1995. In: Klenk H-D, ed. Current topics in
microbiology and immunology: Marburg and Ebola viruses. Berlin:
Springer-Verlag, 1999; 77–84.
49. Formenty P, Hatz C, Le Guenno B, Stoll A, Rogenmoser P,
Wildmer A. Human infection due to Ebola virus, subtype Cote
d’Ivoire: clinical and biologic presentation. J Infect Dis 1999; 179:
S48–S53.
50. Khan AS, Tshioko FK, Heymann DL et al. The reemergence of Ebola
hemorrhagic fever, Democratic Republic of the Congo, 1995. J Infect
Dis 1999; 179: S76–S86.
51. Georges AJ, Leroy EM, Renaut AA et al. Ebola hemorrhagic fever
outbreaks in Gabon, 1994–1997: epidemiologic and health control
issues. J Infect Dis 1999; 179: S65–S75.
52. Amblard J, Obiang P, Edzang S, Prehaud C, Bouloy M, Le Guenno B.
Identification of the Ebola virus in Gabon in 1994. Lancet 1997; 349:
181–182.
53. Georges-Courbot M-C, Lu C-Y, Lansoud-Soukate J, Leroy E, Baize
S. Isolation and partial molecular characterisation of a strain of Ebola
virus during a recent epidemic of viral haemorrhagic fever in Gabon.
Lancet 1997; 349: 181.
54. Georges-Courbot M-C, Sanchez A, Lu C-Y et al. Isolation and phylo-
genetic characterization of Ebola viruses causing different outbreaks
in Gabon. Emerg Infect Dis 1997; 1: 59–62.
55. Leroy EM, Souquiere S, Rouquet P, Drevet D. Re-emergence of
Ebola haemorrhagic fever in Gabon. Lancet 2002; 359: 712.
56. Leroy EM, Rouquet P, Formenty P et al. Multiple Ebola virus trans-
mission events and rapid decline of central african wildlife. Science
2004; 303: 387–390.
57. Pourrut X, Kumulungui B, Wittmann T et al. The natural history of
Ebola virus in Africa. Microbes Infect 2005; 7: 1005–1014.
58. Formenty P, Leroy EM, Epelboin A et al. Detection of Ebola virus
in oral fluid specimens during outbreaks of Ebola virus hemor-
rhagic fever in the Republic of Congo. Clin Infect Dis 2006; 42: 1521–
1526.
59. Lamunu M, Lutwama JJ, Kamugisha J et al. Containing a haemorrhagic
fever epidemic: the Ebola experience in Uganda (October 2000–Jan-
uary 2001). Int J Infect Dis 2004; 8: 27–37.
60. Okware SI, Omaswa FG, Zaramba S et al. An outbreak of Ebola in
Uganda. Trop Med Int Health 2002; 7: 1068–1075.
61. World Health Organization. Ebola haemorrhagic fever in south
Sudan – update. Wkly Epidemiol Rec 2004; 79: 253.
62. Towner JS, Rollin PE, Bausch DG et al. Rapid diagnosis of Ebola
hemorrhagic fever by reverse transcription-PCR in an outbreak set-
ting and assessment of patient viral load as a predictor of outcome.
J Virol 2004; 78: 4330–4341.
63. Onyango CO, Opoka ML, Ksiazek TG et al. Laboratory diagnosis of
Ebola hemorrhagic fever during an outbreak in Yambio, Sudan, 2004.
J Infect Dis 2007; 196 (suppl. 2): S193–S198.
64. Towner JS, Sealy TK, Khristova ML et al. Newly discovered Ebola
virus associated with hemorrhagic fever outbreak in Uganda. PLoS
Pathog 2008; 4: e1000212.
65. Jahrling PB, Geisbert TW, Dalgard DW et al. Preliminary report: iso-
lation of Ebola virus from monkeys imported to USA. Lancet 1990;
335: 502–505.
66. Dalgard DW, Hardy RJ, Pearson SL et al. Combined simian hemor-
rhagic fever and Ebola virus infection in cynomolgus monkeys. Lab
Anim Sci 1992; 42: 152–157.
67. Hayes CG, Burans JP, Ksiazek TG et al. Outbreak of fatal illness
among captive macaques in the Philippines caused by an Ebola-
related filovirus. Am J Trop Med Hyg 1992; 46: 664–671.
68. Rollin PE, Williams RJ, Bressler DS et al. Ebola (subtype reston)
virus among quarantined nonhuman primates recently imported
from the Philippines to the United States. J Infect Dis 1999; 179:
S108–S114.
69. Miranda MEG, White ME, Dayrit MM, Hayes CG, Ksiazek TG, Bu-
rans JP. Seroepidemiological study of filovirus related to Ebola in the
Philippines. Lancet 1991; 337: 425–426.
70. Miranda ME, Ksiazek TG, Retuya TJ et al. Epidemiology of Ebola
(subtype reston) virus in the Philippines, 1996. J Infect Dis 1999; 179:
S115–S119.
71. Barrette RW, Metwally SA, Rowland JM et al. Discovery of swine as
a host for the reston Ebola virus. Science 2009; 325: 204–206.
72. Huang Y, Xu L, Sun Y, Nabel GJ. The assembly of Ebola virus
nucleocapsid requires virion-associated proteins 35 and 24 and post-
translational modification of nucleoprotein. Mol Cell 2002; 10: 307–
316.
73. Muhlberger E, Weik M, Volchkov VE, Klenk H-D, Becker S. Compari-
son of the transcription and replication strategies of Marburg and
Ebola virus by using artificial replication systems. J Virol 1999; 73: ???–
???. 6
74. Volchkov VE, Volchkova VA, Muhlberger E et al. Recovery of infec-
tious Ebola virus from complementary DNA: RNA editing of the gp
gene and viral cytotoxicity. Science 2001; 291: 1965–1969.
75. Volchkov VE, Chepurnov AA, Volchkova VA, Ternovoj VA, Klenk
HD. Molecular characterization of guinea pig-adapted variants of
Ebola virus. Virology 2000; 277: 147–155.
76. Noda T, Sagara H, Suzuki E, Takada A, Kida H, Kawaoka Y. Ebola
virus vp40 drives the formation of virus-like filamentous particles
along with gp. J Virol 2002; 76: 4855–4865.
77. Han Z, Boshra H, Sunyer JO, Zwiers SH, Paragas J, Harty RN. Bio-
chemical and functional characterization of the Ebola virus vp24 pro-
tein: implications for a role in virus assembly and budding. J Virol
2003; 77: 1793–1800.
78. Watanabe S, Watanabe T, Noda T et al. Production of novel Ebola
virus-like particles from cDNAs: an alternative to Ebola virus gener-
ation by reverse genetics. J Virol 2004; 78: 999–1005.
79. Bamberg S, Kolesnikova L, Moller P, Klenk HD, Becker S. Vp24 of
Marburg virus influences formation of infectious particles. J Virol
2005; 79: 13421–13433.
80. Noda T, Watanabe S, Sagara H, Kawaoka Y. Mapping of the vp40-
binding regions of the nucleoprotein of Ebola virus. J Virol 2007; 81:
3554–3562.
81. Johnson RF, McCarthy SE, Godlewski PJ, Harty RN. Ebola virus
vp35-vp40 interaction is sufficient for packaging 3e-5e minigenome
RNA into virus-like particles. J Virol 2006; 80: 5135–5144.
82. Ruigrok RW, Schoehn G, Dessen A et al. Structural characterization
and membrane binding properties of the matrix protein vp40 of
Ebola virus. J Mol Biol 2000; 300: 103–112.
83. Sanchez A, Trappier SG, Mahy BWJ, Peters CJ, Nichol ST. The vir-
ion glycoproteins of Ebola viruses are encoded in two reading
frames and are expressed through transcriptional editing. Proc Natl
Acad Sci USA 1996; 93: 3602–3607.
84. Volchkov VE, Feldmann H, Volchkova VA, Klenk H-D. Processing of
the Ebola virus glycoprotein by the proprotein convertase furin. Proc
Natl Acad Sci USA 1998; 95: 5762–5767.
85. Volchkov VE, Volchkova VA, Slenczka W, Klenk H-D, Feldmann H.
Release of viral glycoproteins during Ebola virus infection. Virology
1998; 245: 110–119.
86. Volchkov VE, Blinov VM, Netesov SV. The envelope glycoprotein of
Ebola virus contains an immunosuppressive-like domain similar to
oncogenic retroviruses. FEBS Lett 1992; 305: 181–184.
87. Wool-Lewis RJ, Bates P. Characterization of Ebola virus entry by
using pseudotyped viruses: identification of receptor-deficient cell
lines. J Virol 1998; 72: 3155–3160.
10 Clinical Microbiology and Infection CMI
ª2011 The Authors
Clinical Microbiology and Infection ª2011 European Society of Clinical Microbiology and Infectious Diseases, CMI
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
32
33
34
35
36
37
38
39
40
41
42
43
44
45
46
47
48
49
50
88. Yang Z-Y, Delgado R, Xu L et al. Distinct cellular interactions of
secreted and transmenbrane Ebola virus glycoproteins. Science 1998;
279: 1034–1037.
89. Chepurnov AA, Tuzova MN, Ternovoy VA, Chernukhin IV.
Suppressive effect of Ebola virus on T cell proliferation in vitro is
provided by a 125-kDa gp viral protein. Immunol Lett 1999; 68: 257–
261.
90. Yang ZY, Duckers HJ, Sullivan NJ, Sanchez A, Nabel EG, Nabel GJ.
Identification of the Ebola virus glycoprotein as the main viral deter-
minant of vascular cell cytotoxicity and injury. Nat Med 2000; 6:
886–889.
91. Chan SY, Speck RF, Ma MC, Goldsmith MA. Distinct mechanisms of
entry by envelope glycoproteins of Marburg and Ebola (Zaire)
viruses. J Virol 2000; 74: 4933–4937.
92. Chan SY, Empig CJ, Welte FJ et al. Folate receptor-alpha is a cofac-
tor for cellular entry by Marburg and Ebola viruses. Cell 2001; 106:
117–126.
93. Feldmann H, Volchkov VE, Volchkova VA, Stroher U, Klenk HD.
Biosynthesis and role of filoviral glycoproteins. J Gen Virol 2001; 82:
2839–2848.
94. Yaddanapudi K, Palacios G, Towner JS et al. Implication of a retrovi-
rus-like glycoprotein peptide in the immunopathogenesis of Ebola
and Marburg viruses. FASEB J 2006; 20: 2519–2530.
95. Volchkova VA, Feldmann H, Klenk H-D, Volchkov VE. The non-
structural small glycoprotein sgp of Ebola virus is secreted as an
antiparallel-orientated homodimer. Virology 1998; 250: 408–414.
96. Dolnik O, Volchkova V, Garten W et al. Ectodomain shedding of the
glycoprotein gp of Ebola virus. EMBO J 2004; 23: 2175–2184.
97. Basler CF, Mikulasova A, Martinez-Sobrido L et al. The Ebola virus
vp35 protein inhibits activation of interferon regulatory factor 3. J
Virol 2003; 77: 7945–7956.
98. Hartman AL, Towner JS, Nichol ST. A C-terminal basic amino acid
motif of Zaire Ebola virus vp35 is essential for type I interferon
antagonism and displays high identity with the RNA-binding domain
of another interferon antagonist, the ns1 protein of influenza A
virus. Virology 2004; 328: 177–184.
99. Cardenas WB, Loo YM, Gale M Jr et al. Ebola virus vp35 protein
binds double-stranded RNA and inhibits alpha/beta interferon pro-
duction induced by RIG-I signaling. J Virol 2006; 80: 5168–5178.
100. Hartman AL, Bird BH, Towner JS, Antoniadou ZA, Zaki SR, Nichol
ST. Inhibition of IRF-3 activation by vp35 is critical for the high level
of virulence of Ebola virus. J Virol 2008; 82: 2699–2704.
101. Prins KC, Cardenas WB, Basler CF. Ebola virus protein vp35 impairs
the function of interferon regulatory factor-activating kinases IKKep-
silon and TBK-1. J Virol 2009; 83: 3069–3077.
102. Chang TH, Kubota T, Matsuoka M et al. Ebola Zaire virus blocks
type I interferon production by exploiting the host Sumo modifica-
tion machinery. PLoS Pathog 2009; 5: e1000493.
103. Suzuki Y, Gojobori T. The origin and evolution of Ebola and Mar-
burg viruses. Mol Biol Evol 1997; 14: 800–806.
104. Rodriguez LL, De Roo A, Guimard Y et al. Persistence and genetic
stability of Ebola virus during the outbreak in Kikwit, Democratic
Republic of the Congo, 1995. J Infect Dis 1999; 179: S170–S176.
105. Leroy EM, Baize S, Lansoud-Soukate J, Mavoungou E, Apetrei C.
Sequence analysis of gp, np, vp40 and vp24 genes of Ebola virus from
deceased, survival and asymptomatic infected individuals during 1996
outbreak in Gabon. Comparative studies and phylogenetic character-
ization. J Gen Virol 2002; 83: 67–73.
106. Sanchez A, Rollin PE. Complete genome sequence of an Ebola virus
(Sudan species) responsible for a 2000 outbreak of human disease in
Uganda. Virus Res 2005; 113: 16–25.
107. Wittmann TJ, Biek R, Hassanin A et al. Isolates of Zaire Ebola virus
from wild apes reveal genetic lineage and recombinants. Proc Natl
Acad Sci U S A 2007; 104: 17123–17127.
108. Pinzon JE, Wilson JM, Tucker CJ, Arthur R, Jahrling PB, Formenty P.
Trigger events: enviroclimatic coupling of Ebola hemorrhagic fever
outbreaks. Am J Trop Med Hyg 2004; 71: 664–674.
109. Peterson AT, Bauer JT, Mills JN. Ecologic and geographic distribution
of filovirus disease. Emerg Infect Dis 2004; 10: 40–47.
110. Peterson AT, Carroll DS, Mills JN, Johnson AM. Potential mamma-
lian filovirus reservoirs. Emerg Infect Dis 2004; 10: 2073–2081.
111. Peterson AT, Lash RR, Carroll DS, Johnson KM. Geographic poten-
tial for outbreaks of Marburg hemorrhagic fever. Am J Trop Med Hyg
2006; 75: 9–15.
112. Becquart P, Wauquier N, Mahlakoiv T et al. High prevalence of both
humoral and cellular immunity to Zaire Ebola virus among rural pop-
ulations in Gabon. PLoS ONE 2010; 5: e9126.
113. Ivanoff B, Duquesnoy P, Languillat G et al. Haemorrhagic fever in
Gabon. I. Incidence of Lassa, Ebola and Marburg viruses in Haut-Og-
ooue. Trans R Soc Trop Med Hyg 1982; 76: 719–720.
114. Bouree P, Bergmann JF. Ebola virus infection in man: a serological
and epidemiological survey in the Cameroons. Am J Trop Med Hyg
1983; 32: 1465–1466.
115. Gonzalez JP, Josse R, Johnson ED et al. Antibody prevalence against
haemorrhagic fever viruses in randomized representative Central
African populations. Res Virol 1989; 140: 319–331.
116. Johnson BK, Wambui C, Ocheng D et al. Seasonal variation in anti-
bodies against Ebola virus in Kenyan fever patients. Lancet 1986; 1:
1160.
117. Johnson ED, Gonzalez JP, Georges AJ. Filovirus activity among
selected ethnic groups inhabiting the tropical forest of Equatorial
Africa. Trans R Soc Trop Med Hyg 1993; 87: 536–538.
118. Busico KM, Marshall KL, Ksiazek TG et al. Prevalence of IgG antibod-
ies to Ebola virus in individuals during an Ebola outbreak, Democratic
Republic of the Congo, 1995. J Infect Dis 1999; 179: S102–S107.
119. Gonzalez JP, Nakoune E, Slenczka W, Vidal P, Morvan JM. Ebola and
Marburg virus antibody prevalence in selected populations of the
Central African Republic. Microbes Infect 2000; 2: 39–44.
120. Leroy EM, Baize S, Volchkov VE et al. Human asymptomatic Ebola
infection and strong inflammatory response. Lancet 2000; 355: 2210–
2215.
121. Huijbregts B, De Wachter P, Ndong Obiang S, Akou Ella M. Ebola
and the decline of gorilla Gorilla gorilla and chimpanzee Pan troglodytes
populations in Minkebe forest, northeastern Gabon. Oryx 2003; 37:
437–443.
122. Walsh PD, Abernethy KA, Bermejo M et al. Catastrophic ape
decline in western Equatorial Africa. Nature 2003; 422: 611–614.
123. Rouquet P, Froment J-M, Bermejo M et al. Wild animal mortality
monitoring and human Ebola outbreaks, Gabon and Republic of
Congo, 2001–2003. Emerg Infect Dis 2005; 11: 283–290.
124. Bermejo M, Rodriguez-Teijeiro JD, Illera G, Barroso A, Vila C,
Walsh PD. Ebola outbreak killed 5000 gorillas. Science 2006; 314:
1564.
125. Caillaud D, Levrero F, Cristescu R et al. Gorilla susceptibility to
Ebola virus: the cost of sociality. Curr Biol 2006; 16: R489–R491.
126. Formenty P, Boesch C, Wyers M et al. Ebola virus outbreak among
wild chimpanzees living in a rain forest of Cote d’Ivoire. J Infect Dis
1999; 179 (suppl. 1): S120–S126.
127. Leroy EM, Kumulungui B, Pourrut X et al. Fruit bats as reservoirs of
Ebola virus. Nature 2005; 438: 575–576.
128. Monath TP. Ecology of Marburg and Ebola viruses: speculations
and directions for the future research. J Infect Dis 1999; 179: S127–
S138.
129. Leroy EM, Telfer P, Kumulungui B et al. A serological survey of Ebo-
la virus infection in Central African nonhuman primates. J Infect Dis
2004; 190: 1895–1899.
130. Feldmann H, Wahl-Jensen V, Jones SM, Stroher U. Ebola virus ecol-
ogy: a continuing mystery. Trends Microbiol 2004; 12: 433–437.
CMI Leroy et al. Ebola and Marburg haemorrhagic fever viruses1
11
ª2011 The Authors
Clinical Microbiology and Infection ª2011 European Society of Clinical Microbiology and Infectious Diseases, CMI
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
32
33
34
35
36
37
38
39
40
41
42
43
44
45
46
47
48
49
50

131. Arata AA, Johnson B. Approaches towards studies on potential res-
ervoirs of viral haemorrhagic fever in southern Sudan (1977). In: Pat-
tyn SR, ed. Ebola virus haemorrhagic fever. Amsterdam: Elsevier/
Netherland biomedical, 1978; 191–202.
132. Turell MJ, Bressler DS, Rossi CA. Lack of virus replication in arthro-
pods after intrathoracic inoculation of Ebola reston virus. Am J Trop
Med Hyg 1996; 55: 89–90.
133. Swanepoel R, Leman PA, Burt FJ. Experimental inoculation of plants
and animals with Ebola virus. Emerg Infect Dis 1996; 2: 321–325.
134. Breman JG, Johnson KM, van der Groen G et al. A search for Ebola
virus in animals in the Democratic Republic of the Congo and Cam-
eroon: ecologic, virologic, and serologic surveys, 1979–1980. J Infect
Dis 1999; 179: S139–S147.
135. Reiter P, Turell M, Coleman R et al. Field investigations of an out-
break of Ebola hemorrhagic fever, Kikwit, Democratic Republic of the
Congo, 1995: arthropod studies. J Infect Dis 1999; 179: S148–S154.
136. Leirs H, Mills JN, Krebs JW et al. Search for the Ebola virus reser-
voir in Kikwit, Democratic Republic of the Congo: reflections on a
vertebrate collection. J Infect Dis 1999; 179: S155–S163.
137. Formenty P, Jahrling P, Rossi C et al. Search for the Ebola virus res-
ervoir in Taı forest, Cote d’Ivoire: 1996–1997, preliminary results.
XIth International Congress of Virology. Sydney, Australia, 1999.
138. Morvan JM, Deubel V, Gounon P et al. Identification of Ebola virus
sequences present as RNA or DNA in organs of terrestrial small
mammals of the Central African Republic. Microbes Infect 1999; 1:
1193–1201.
139. Pourrut X, Delicat A, Rollin PE, Ksiazek TG, Gonzalez JP, Leroy EM.
Spatial and temporal patterns of Zaire Ebola virus antibody preva-
lence in the possible reservoir bat species. J Infect Dis 2007; 196
(suppl. 2): S176–S183.
140. Towner JS, Pourrut X, Albarino CG et al. Marburg virus infection
detected in a common African bat. PLoS ONE 2007; 2: e764.
141. Swanepoel R, Smit SB, Rollin PE et al. Studies of reservoir hosts for
Marburg virus. Emerg Infect Dis 2007; 13: 1847–1851.
142. Leroy EM, Epelboin A, Mondonge V et al. Human Ebola outbreak
resulting from direct exposure to fruit bats in Luebo, Democratic
Republic of Congo, 2007. Vector Borne Zoonotic Dis 2009; 6: 723–
728.
143. Mahanty S, Hutchinson K, Agarwal S, McRae M, Rollin PE, Pulendran
B. Cutting edge: impairment of dendritic cells and adaptive immunity
by Ebola and Lassa viruses. J Immunol 2003; 170: 2797–2801.
144. Stroher U, West E, Bugany H, Klenk H-D, Schnittler H-J, Feldmann
H. Infection and activation of monocytes by Marburg and Ebola
viruses. J Virol 2001; 75: 11025–11033.
145. Geisbert TW, Hensley L, Larsen T et al. Pathogenesis of Ebola hem-
orrhagic fever in cynomolgus macaques: evidence that dendritic cells
are early and sustained targets of infection. Am J Pathol 2003; 163:
2347–2370.
146. Ryabchikova EI, Kolesnikova LV, Luchko SV. An analysis of features
of pathogenesis in two animal models of Ebola virus infection. J Infect
Dis 1999; 179: S199–S202.
147. Baskerville A, Fisher-Hoch SP, Neild GH, Dowsett AB. Ultrastruc-
ture pathology of experimental Ebola haemorrhagic fever virus infec-
tion. J Pathol 1985; 147: 199–209.
148. Gupta M, Mahanty S, Ahmed R, Rollin PE. Monocyte-derived human
macrophage and peripheral blood mononuclear cells infected with
Ebola virus secrete MIP-1a and TNF-a and inhibit poly-IC-induced
IFN-a in vitro. Virology 2001; 284: 20–25.
149. Baize S, Leroy EM, Georges AJ et al. Inflammatory responses in Ebo-
la virus-infected patients. Clin Exp Immunol 2001; 128: 163–168.
150. Wauquier N, Becquart P, Padilla C, Baize S, Leroy EM. Human fatal
Zaire Ebola virus infection is associated with an aberrant innate
immunity and massive lymphocyte apoptosis. PLoS Negl Trop Dis
2010; 4: e837.
151. Villinger F, Rollin PE, Brar SS et al. Markedly elevated levels of inter-
feron (IFN)-gamma, IFN-alpha, interleukin (IL)-2, IL-10, and tumor
necrosis factor-a associated with fatal Ebola virus infection. J Infect
Dis 1999; 179: S188–S191.
152. Feldmann H, Bugany H, Mahner F, Klenk HD, Drenckhahn D,
Schnittler HJ. Filovirus-induced endothelial leakage triggered by
infected monocytes/macrophages. J Clin Invest 1996; 70: 2208–
2214.
153. Schnittler HJ, Feldmann H. Molecular pathogenesis of filovirus infec-
tions: role of macrophages and endothelial cells. Curr Top Microbiol
Immunol 1999; 235: 175–204.
154. Hensley L, Young HA, Jahrling PB, Geisbert TW. Proinflammatory
response during Ebola virus infection of primate models: possible
involvement of the tumor necrosis factor receptor superfamily.
Immunol Lett 2002; 80: 169–179.
155. Gerszten RE, Garcia-Zepeda EA, Lim Y-C et al. MCP-1 and IL-8 trig-
ger firm adhesion of monocytes to vascular endothelium under flow
conditions. Nature 1999; 398: 718–723.
156. Geisbert TW, Hensley L, Jahrling PB et al. Treatment of Ebola virus
infection with a recombinant inhibitor of factor VII/tissue factor: a
study in rhesus monkeys. Lancet 2003; 362: 1953–1958.
157. Ruf W. Emerging roles of tissue factor in viral hemorrhagic fever.
Trends Immunol 2004; 25: 461–464.
158. Baize S, Leroy EM, Georges-Courbot M-C et al. Defective humoral
responses and extensive intravascular apoptosis are associated with
fatal outcome in Ebola virus-infected patients. Nat Med 1999; 5:
423–426.
159. Baize S, Leroy EM, Mavoungou E, Fisher-Hoch SP. Apoptosis in fatal
Ebola infection. Does the virus toll the bell for the immune system?
Apoptosis 2000; 5: 5–7.
160. Geisbert TW, Hensley LE, Gibb TR, Steele KE, Jaax NK, Jahrling PB.
Apoptosis induced in vitro and in vivo during infection by Ebola and
Marburg viruses. Lab Invest 2000; 80: 171–186.
161. Reed DS, Hensley LE, Geisbert JB, Jahrling PB, Geisbert TW. Deple-
tion of peripheral blood T lymphocytes and NK cells during the
course of Ebola hemorrhagic fever in cynomolgus macaques. Viral
Immunol 2004; 17: 390–400.
162. Leroy EM, Becquart P, Wauquier N, Baize S. Evidence for Ebola
virus superantigen activity. J Virol 2011; ???: ???–???. 7
163. Bradfute SB, Swanson PE, Smith MA et al. Mechanisms and conse-
quences of ebolavirus-induced lymphocyte apoptosis. J Immunol
2010; 184: 327–335.
164. Parrino J, Hotchkiss RS, Bray M. Prevention of immune cell apopto-
sis as potential therapeutic strategy for severe infections. Emerg
Infect Dis 2007; 13: 191–198.
165. Ksiazek TG, Rollin PE, Williams AJ et al. Clinical virology of Ebola
hemorrhagic fever (EHF): virus, virus antigen, and IgG and IgM anti-
body findings among EHF patients in Kikwit, Democratic Republic of
the Congo, 1995. J Infect Dis 1999; 179: S177–S187. 8
166. Bosio CM, Aman MJ, Grogan C et al. Ebola and Marburg viruses rep-
licate in monocyte-derived dendritic cells without inducing the pro-
duction of cytokines and full maturation. J Infect Dis 2003; 188:
1630–1638.
167. Jin H, Yan Z, Prabhakar BS et al. The vp35 protein of Ebola virus
impairs dendritic cell maturation induced by virus and lipopolysac-
charide. J Gen Virol 2010; 91: 352–361.
168. Basler CF, Wang X, Muhlberger E et al. The Ebola virus vp35 pro-
tein functions as a type I IFN antagonist. Proc Natl Acad Sci U S A
2000; 97: 12289–12294.
169. Feng Z, Cerveny M, Yan Z, He B. The vp35 protein of Ebola virus
inhibits the antiviral effect mediated by double-stranded RNA-depen-
dent protein kinase PKR. J Virol 2007; 81: 182–192.
170. Fabozzi G, Nabel CS, Dolan MA, Sullivan NJ. Ebolavirus proteins
suppress the effects of small interfering RNA by direct interaction
12 Clinical Microbiology and Infection CMI
ª2011 The Authors
Clinical Microbiology and Infection ª2011 European Society of Clinical Microbiology and Infectious Diseases, CMI
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
32
33
34
35
36
37
38
39
40
41
42
43
44
45
46
47
48
49
50

with the mammalian RNA interference pathway. J Virol 2011; 85:
2512–2523.
171. Haasnoot J, de Vries W, Geutjes EJ, Prins M, de Haan P, Berkhout
B. The Ebola virus vp35 protein is a suppressor of RNA silencing.
PLoS Pathog 2007; 3: e86.
172. Reid SP, Leung LW, Hartman AL et al. Ebola virus vp24 binds kary-
opherin alpha1 and blocks STAT1 nuclear accumulation. J Virol 2006;
80: 5156–5167.
173. Reid SP, Valmas C, Martinez O, Sanchez A, Basler CF. Ebola virus
vp24 proteins inhibit the interaction of np1-1 subfamily karyopherin
alpha proteins with activated STAT1. J Virol 2007; 81: 13469–13477.
174. Hartman AL, Ling L, Nichol ST, Hibberd ML. Whole-genome
expression profiling reveals that inhibition of host innate immune
response pathways by Ebola virus can be reversed by a single amino
acid change in the vp35 protein. J Virol 2008; 82: 5348–5358.
175. Prins KC, Delpeut S, Leung DW et al. Mutations abrogating vp35
interaction with double-stranded RNA render Ebola virus avirulent
in guinea pigs. J Virol 2010; 84: 3004–3015.
176. Wauquier N, Becquart P, Gasquet C, Leroy EM. Immunoglobulin G
in Ebola outbreak survivors, Gabon. Emerg Infect Dis 2009; 15:
1136–1137.
177. Leroy EM, Baize S, Debre P, Lansoud-Soukate J, Mavoungou E. Early
immune responses accompanying human asymptomatic Ebola infec-
tions. Clin Exp Immunol 2001; 124: 453–460.
178. Wauquier N, Padilla C, Becquart P, Leroy E, Vieillard V. Association
of kir2ds1 and kir2ds3 with fatal outcome in Ebola virus infection.
Immunogenetics 2010; 62: 767–771.
179. Bukreyev A, Rollin PE, Tate MK et al. Successful topical respiratory
tract immunization of primates against Ebola virus. J Virol 2007; 81:
6379–6388.
180. Geisbert TW, Geisbert JB, Leung A et al. Single-injection vaccine
protects nonhuman primates against infection with Marburg virus
and three species of Ebola virus. J Virol 2009; 83: 7296–7304.
181. Jones SM, Feldmann H, Stroher U et al. Live attenuated recombinant
vaccine protects nonhuman primates against Ebola and Marburg
viruses. Nat Med 2005; 11: 786–790.
182. Sullivan NJ, Geisbert TW, Geisbert JB et al. Accelerated vaccination
for Ebola virus haemorrhagic fever in non-human primates. Nature
2003; 424: 681–684.
183. Sullivan NJ, Geisbert TW, Geisbert JB et al. Immune protection of
nonhuman primates against Ebola virus with single low-dose adenovi-
rus vectors encoding modified gps. PLoS Med 2006; 3: e177.
184. Warfield KL, Swenson DL, Olinger GG, Kalina WV, Aman MJ, Bavari
S. Ebola virus-like particle-based vaccine protects nonhuman pri-
mates against lethal Ebola virus challenge. J Infect Dis 2007; 196 (sup-
pl. 2): S430–S437.
185. Pratt WD, Wang D, Nichols DK et al. Protection of nonhuman pri-
mates against two species of Ebola virus infection with a single com-
plex adenovirus vector. Clin Vaccine Immunol 2010; 17: 572–581.
186. Swenson DL, Wang D, Luo M et al. Vaccine to confer to nonhuman
primates complete protection against multistrain Ebola and Marburg
virus infections. Clin Vaccine Immunol 2008; 15: 460–467.
187. Hensley LE, Mulangu S, Asiedu C et al. Demonstration of cross-pro-
tective vaccine immunity against an emerging pathogenic Ebolavirus
species. PLoS Pathog 2010; 6: e1000904.
188. Geisbert TW, Daddario-DiCaprio KM, Williams KJ et al. Recombi-
nant vesicular stomatitis virus vector mediates postexposure protec-
tion against Sudan Ebola hemorrhagic fever in nonhuman primates. J
Virol 2008; 82: 5664–5668.
189. Feldmann H, Jones SM, Daddario-DiCaprio KM et al. Effective post-
exposure treatment of Ebola infection. PLoS Pathog 2007; 3: e2.
190. Geisbert TW, Hensley L, Geisbert JB, Jahrling PB. Evidence against
an important role for infectivity-enhancing antibodies in Ebola virus
infections. Virology 2002; 293: 15–19.
191. Jahrling PB, Geisbert JB, Swearengen JR, Larsen T, Geisbert TW.
Ebola hemorrhagic fever: evaluation of passive immunotherapy in
nonhuman primates. J Infect Dis 2007; 196 (suppl. 2): S400–S403.
192. Mupapa K, Massamba M, Kibadi K et al. Treatment of Ebola hemor-
rhagic fever with blood transfusions from convalescent patients. J
Infect Dis 1999; 179: S18–S23.
193. Jahrling PB, Geisbert TW, Geisbert JB et al. Evaluation of immune
globulin and recombinant interferon-a2b for treatment of experi-
mental Ebola virus infections. J Infect Dis 1999; 179: S224–S234.
194. Hensley LE, Stevens EL, Yan SB et al. Recombinant human activated
protein c for the postexposure treatment of Ebola hemorrhagic
fever. J Infect Dis 2007; 196 (suppl. 2): S390–S399.
195. Geisbert TW, Lee AC, Robbins M et al. Postexposure protection of
non-human primates against a lethal Ebola virus challenge with RNA
interference: a proof-of-concept study. Lancet 2010; 375: 1896–1905.
196. Warfield KL, Swenson DL, Olinger GG et al. Gene-specific counter-
measures against Ebola virus based on antisense phosphorodiamidate
morpholino oligomers. PLoS Pathog 2006; 2: e1.
197. Warren TK, Warfield KL, Wells J et al. Antiviral activity of a small-
molecule inhibitor of filovirus infection. Antimicrob Agents Chemother
2010; 54: 2152–2159.
198. Warren TK, Warfield KL, Wells J et al. Advanced antisense thera-
pies for postexposure protection against lethal filovirus infections.
Nat Med 2010; 16: 991–994.
CMI Leroy et al. Ebola and Marburg haemorrhagic fever viruses1
13
ª2011 The Authors
Clinical Microbiology and Infection ª2011 European Society of Clinical Microbiology and Infectious Diseases, CMI
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
32
33
34
35
36
37
38
39
40
41
42
43
44
45
46
47
48
49
50

Author Query Form
Journal: CLM
Article: 3535
Dear Author,
During the copy-editing of your paper, the following queries arose. Please respond to these by marking up your
proofs with the necessary changes/additions. Please write your answers on the query sheet if there is insufficient
space on the page proofs. Please write clearly and follow the conventions shown on the attached corrections
sheet. If returning the proof by fax do not write too close to the paper’s edge. Please remember that illegible
mark-ups may delay publication.
Many thanks for your assistance.
Query
reference
Query Remarks
Q1 AUTHOR: A running head short title was not supplied; please
check if this one is suitable and, if not, please supply a short title
of up to 40 characters that can be used instead.
Q2 AUTHOR: Please confirm that this is the correct expansion of
IFAT
Q3 AUTHOR: Please check this website address and confirm that it
is correct. (Please note that it is the responsibility of the
author(s) to ensure that all URLs given in this article are correct
and useable.)
Q4 AUTHOR: Please provide the address for reference [5].
Q5 AUTHOR: Please check the issue for reference [22].
Q6 AUTHOR: Please provide the page range for reference [73].
Q7 AUTHOR: Please provide the volume number, page range for ref-
erence [162].
Q8 AUTHOR: Please check authors name for reference [165].
Q9 AUTHOR: Please confirm that permission has been granted to
reproduce this figure
Q10 AUTHOR: Figure 2 has been saved at a low resolution of 244 dpi.
Please resupply at 300 dpi. Check required artwork specifications
at http://authorservices.wiley.com/submit_illust.asp?site=1
Q11 AUTHOR: Figure 3 has been saved at a low resolution of 214 dpi.
Please resupply at 300 dpi. Check required artwork specifications
at http://authorservices.wiley.com/submit_illust.asp?site=1
MARKED PROOF
Please correct and return this set
Instruction to printer
Leave unchanged under matter to remain
through single character, rule or underline
New matter followed by
or
or
or
or
or
or
or
or
or
and/or
and/or
e.g.
e.g.
under character
over character
new character
new characters
through all characters to be deleted
through letter or
through characters
under matter to be changed
under matter to be changed
under matter to be changed
under matter to be changed
under matter to be changed
Encircle matter to be changed
(As above)
(As above)
(As above)
(As above)
(As above)
(As above)
(As above)
(As above)
linking characters
through character or
where required
between characters or
words affected
through character or
where required
or
indicated in the margin
Delete
Substitute character or
substitute part of one or
more word(s)Change to italics
Change to capitals
Change to small capitals
Change to bold type
Change to bold italic
Change to lower case
Change italic to upright type
Change bold to non-bold type
Insert ‘superior’ character
Insert ‘inferior’ character
Insert full stop
Insert comma
Insert single quotation marks
Insert double quotation marks
Insert hyphen
Start new paragraph
No new paragraph
Transpose
Close up
Insert or substitute space
between characters or words
Reduce space betweencharacters or words
Insert in text the matter
Textual mark Marginal mark
Please use the proof correction marks shown below for all alterations and corrections. If you
in dark ink and are made well within the page margins.
wish to return your proof by fax you should ensure that all amendments are written clearly
Copyright © 2022 FDOKUMEN