
EatSafe Cohort Methodology and Protocol - PDF Server
28
EatSafe: Evidence and Action Towards Safe, Nutritious Food EatSafe Cohort Methodology and Protocol July 2021
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of EatSafe Cohort Methodology and Protocol - PDF Server
EatSafe: Evidence and Action Towards Safe, Nutritious Food
EatSafe Cohort Methodology and Protocol
July 2021
2
This EatSafe report presents evidence that will help engage and empower consumers and market actors to better obtain safe nutritious food. It will be used to design and test consumer-centered food safety interventions in informal markets through the EatSafe program. Recommended Citation: Global Alliance for Improved Nutrition. 2021. EatSafe Cohort Methodology Report. A USAID EatSafe Project Document. Acknowledgements: This protocol was written by Elisabetta Lambertini and Stella Nordhagen, with contributions from Eric Djimeu Wouabe, with useful feedback on prior drafts provided by Eva Monterrosa, Caroline Smith DeWaal, Bonnie McClafferty, and Nwando Onuigbo-Chatta. Agreement Number: 7200AA19CA00010/ Project Year 1 output Project Start Date and End Date: July 31, 2019 to July 30, 2024 USAID Technical Office: Bureau for Food Security (BFS)/Office of Market and Partnership Innovations (MPI) Agreement Officer Representative (AOR): Lourdes Martinez Romero Submission Date: MAY 2021. Revised: JULY 2021.
For additional information, please contact:
Bonnie McClafferty, EatSafe Project Director Global Alliance for Improved Nutrition (GAIN) 1701 Rhode Island Ave NW Washington, D.C. 20026 Email: [email protected] Caroline Smith DeWaal, EatSafe Deputy Director Global Alliance for Improved Nutrition (GAIN) 1701 Rhode Island Ave NW Washington, D.C. 20026 Email: [email protected] This document is produced by the Global Alliance for Improved Nutrition (GAIN) and made possible by the generous support of the American people through the support of the U.S. Agency for International Development (USAID). Its contents are the sole responsibility of the Global Alliance for Improved Nutrition (GAIN) and do not necessarily reflect the views of USAID or the U.S. Government.
3
TABLE OF CONTENTS
ACRONYMS 4 1. 5 2. 5 3. 7
3.1. Study objectives 7
3.2. Research Questions 7
3.2.1. Consumers 8
3.2.2. Vendors 9
3.3 Study location 10
3.4 Market selection 10
3.5. Key Food Commodities 11
3.6. Food Safety Intervention 12
3.7. Data collection overview 12
3.8. Study participants 13
3.9. Sample Size 15
3.10. Tool development, interviewer training, and field operations 16
3.11. Study participant recruitment 19
3.12. Assignment into intervention arms 20
4. 21 5. 22 6. ETHICAL CONCERNS: CONSENT, RISKS, AND ADVERSE EVENTS 22 REFERENCES 24
LIST OF TABLES Table 1. Market Selection Criteria 11 Table 2. Sample Size Calculations for the Cohort Study 16
4
ACRONYMS
Below is a list of all acronyms and abbreviations used in this document.
ANCOVA
ANOVA
DALY
FBD
FES
FTF
GAIN
ILRI
IRB
KAP
LMIC
PIP
USAID
USD
Analysis of Covariance
Analysis of Variance
Disability-Adjusted Life Years
Foodborne Disease
Focused Ethnographic Study
Feed the Future
Global Alliance for Improved Nutrition
International Livestock Research Institute
Institutional Review Board
Knowledge, Attitudes, and Practices
Low- and Middle-income country
Program Impact Pathway
United States Agency for International Development
U.S. Dollars
5
1. GOALS OF THE STUDY
The overarching goal of this study is to gather evidence on food safety1 knowledge, attitudes, and practices (KAPs) in traditional markets in low- and middle-income countries (LMICs), and specifically in Nigeria. It will do so by assessing knowledge, attitudes or feelings, and actions or behaviors related to food-related choices and food safety among both consumers and vendors in traditional markets in the city of Birnin-Kebbi, Kebbi state, Nigeria. The study will take a broad dietary and market hygiene approach, including the seven commodity categories that are addressed by the EatSafe risk assessment and focused ethnographic study for Nigeria: maize, cowpeas, soy, rice, aquaculture fish, fresh vegetables, and beef (termed “Key Commodities” in the remainder of this document).
The main data collection tools will be semi-structured surveys, complemented by direct observations. Data will be collected before and after the implementation of a behavior change intervention, and if appropriate during the implementation of the intervention. The intervention (or set of interventions) will aim to improve consumer and vendor awareness of food safety, increase its salience as an issue for them, increase motivation to demand or provide safer food, and influence attitudes and practices related to food safety, with focus on behaviors related to purchasing and selling nutritious food in traditional food markets. The difference between baseline and end line levels, across a treatment group (receiving the interventions) and a control group (not receiving the interventions) for individual-level interventions, will be used to evaluate the potential impact of the intervention. This protocol focuses on the methods of data collection at baseline and end line.
The intervention is currently under design and will be refined based on evidence developed by EatSafe during the formative research phase, which includes findings of the baseline cohort data (this protocol) and a focused ethnographic study (FES). The overall results of the cohort study will be used to inform the design of future food safety interventions and improve future food safety policy and programming in traditional markets, in Nigeria and elsewhere.
2. BACKGROUND AND RATIONALE
For a food to be safe, it must be free of disease-causing pathogens, parasites, chemical contaminants, or adulterants. Unfortunately, many foods (globally and in Nigeria) are not safe. Foodborne disease is responsible for an estimated 600 million illnesses and 420,000 premature deaths annually, worldwide (2). About one third of diarrheal disease cases can be attributed to food (3), and diarrheal disease is not only a major determinant of undernutrition (4–9) but also of mortality (10,11). The majority of the foodborne burden falls on those living in low- and middle-income countries (LMICs) (3,10), who make up about 75% of deaths from
1 Food safety is defined as the assurance that food will not cause harm to the consumer when it is prepared or eaten according to its intended use (1).
6
foodborne illness (despite comprising only 41% of the global population). This is particularly true for Africa, where the per-capita burden of foodborne disease is about 27 times that of Europe or North America (2). Young children are particularly susceptible, shouldering about 40% of the burden (2). This is particularly troubling in settings with high burdens of malnutrition, as diarrheal disease can exacerbate childhood malnutrition (4–9). Such is the case in Nigeria, which suffers from persistent malnutrition, with 36.8% of children under 5 stunted and 18% wasted (12).
Foodborne hazards2 can both cause acute illness and raise the risk of sequelae or long-term and chronic disease. For example, both aflatoxins and arsenic have been associated with cancer (13,14). Foodborne illnesses also entail economic costs, due to sickness and loss of life, treatment costs, and impacts on trade. The World Bank estimates these at about $20 billion USD per year (15). Several past studies have shown high levels (contamination in up to 100% of samples) of risk and hazard for numerous foods sold in informal markets in Nigeria, with contamination in up to 100% of samples (16). The region containing Nigeria (AFR-D) has the highest per capita burden of foodborne illness, in disability-adjusted life years (DALYs), with most of this being due to diarrheal disease agents, followed by helminths (2).3 Nigeria, as a transitioning lower-middle-income country with considerable urbanisation, falls into the category of country for which food safety concerns are generally at their most critical due to rapid economic, demographic, and dietary change but limited food safety management capacities (15).
Informal markets, where a large share of consumers in LMICs purchase their foods (17), can be especially risky for foodborne hazards. This is due to poor market infrastructure, including limited access to potable water (18), poor hygienic conditions (19,20), and poor storage practices (21), among others (22). Several studies in Nigeria have concluded that vendors have poor food hygiene knowledge and/or practices (e.g., (23–25)). For example, a 2010 study found that 23.8% of street food vendors in Owerri prepared food in unhygienic conditions, 42.86% did not use aprons, 47.62% handled food with bare hands and 61.9% handled money while serving food (26). Others, however, have found that vendors have moderate to good knowledge and/or practices (27–29). Some have found high levels of knowledge but poor practices (30,31). Studies of Nigerian consumers have generally found poor knowledge regarding food safety practices, and awareness of foodborne illnesses (32,33).
Improving food safety in informal markets in Nigeria will require understanding (and potentially shaping) the motivations, attitudes, beliefs, and practices that shape the decisions of both consumers and food vendors, in order to enable consumers to demand safer food and vendors to deliver it (34,35). While there have been several prior studies of consumer and
2 These include viruses, bacteria, protozoa, helminths (worms), hazardous chemicals, and hazardous radionuclides, in forms or amounts that may cause adverse health impacts upon ingestion. 3 AFR-D countries: Algeria, Angola, Benin, Burkina Faso, Cameroon, Cape Verde, Chad, Comoros Equatorial Guinea, Gabon, Gambia, Ghana, Guinea, Guinea-Bissau, Liberia, Madagascar, Mali, Mauritania, Mauritius, Niger, Nigeria, Sao Tome and Principe, Senegal, Seychelles, Sierra Leone, Togo. Nigeria is the most populous among AFR-D countries.
7
especially vendors’ knowledge and practice related to food safety in Nigeria (36), a recent review (37) noted that these tended to focus on only consumers or vendors (not both) and on street foods and similar prepared foods. They also did not generally assess the salience of food safety as a concern, relative to other concerns, or the cultural and socioeconomic issues that might influence food safety-related behaviors such as intra-household gender norms. In addition, the main documented interventions for food safety in Nigeria focused on training vendors or food handlers (e.g., (38–40)). There have been few or no studies aiming to leverage the power of consumer demand as a force to improve food safety in Nigeria. This is despite the fact that consumer demand has been a major driver of safer food in middle- and high-income countries (41–43).
Improving food safety also requires testing new interventions and verifying how well they work, which the EatSafe program will do in its second phase (hypothesis testing), based on the outcomes of the first formative research phase (hypothesis generating). The cohort study outlined here supports both phases. Specifically, this cohort study seeks to: (1) assess knowledge, attitudes or beliefs, and actions or practices relevant to food safety among both food consumers and vendors in three informal markets in Kebbi, Nigeria; and (2) assess how these change after an intervention to impact consumers’ and vendors’ awareness and behaviors related to food safety.
3. STUDY DESIGN & METHODS
3.1. Study objectives
The cohort study will play three overarching roles:
1. The baseline will serve as a self-standing cross-sectional survey with the objective of providing a description of food safety in the markets with respect to purchasing habits, attitudes, and choice drivers, which will help inform the detailed design of a food safety intervention;
2. The combined baseline and end line will be used to assess progress along the impact pathway of the intervention;
3. If possible, the baseline and end line (and any other data collection in between) will also serve to track any changes in opinions, experiences, and behaviors over time.
Role 1 will be fulfilled using only the baseline data. To achieve objectives 2 and 3, data from the cohort study baseline and end line will be compared.
3.2. Research Questions
The overarching research questions as well as associated sub-questions that the cohort study wishes to address are presented below, for consumers and vendors, respectively. This
8
protocol and the survey tools used for data collection were developed based on these overarching research questions.
3.2.1. Consumers
What are general attitudes and habits regarding food purchasing decisions?
Domains that will be explored include:
● Characteristics of the food that consumers look for ● Characteristics of the market that consumers see as positive or negative ● Characteristics of shops and vendors that consumer prefer ● Interactions between consumers and vendors.
What are dominant beliefs and attitudes about food safety?
Domains that will be explored include:
● What food or food characteristics are perceived as ‘safe’ or ‘unsafe’ ● What foods, hazards, or illnesses are top concerns for consumers ● Perceptions of vendor behaviors related to food safety ● Beliefs around self-efficacy in avoiding unsafe food.
What factors affect consumers’ decisions about food safety in traditional markets?
Domains that will be explored include:
● What food characteristics are important for consumers when deciding if food is safe or not
● Relative importance of food safety vs. other food attributes as criteria for food choice (e.g. price, nutritional properties, taste)
● Relative importance of cleanliness and other vendor characteristics as criteria for selecting a vendor to buy food from
● Market characteristics that affect consumer preferences on where to shop.
Do gender and family dynamics influence food safety and ability to manage risks? Domains that will be explored include:
● Whether gender roles are associated with food purchase and preparation ● Who in the family decides what food to purchase ● Gender as a factor in consumer preferences related to food characteristics ● Gender as a factor in consumer preferences related to vendors and shops ● Whether consumers are more likely to discuss food quality and safety with vendors,
based on their and the vendor’s gender.
9
What information sources are used to obtain information relevant to food safety?
Domains that will be explored include:
● Who consumers trust when seeking information about food and health ● What media channels are most frequently used to access information ● Which organizations consumers trust to take action to improve food safety ● Consumers’ exposure to information on food safety or food and health via different
media channels.
3.2.2. Vendors
What are general attitudes and habits regarding food vending decisions?
Domains that will be explored include:
● What foods vendors regularly sell at the market ● What market characteristics motivate vendors to sell at that market ● What are the relationships between consumers and vendors, as perceived by
vendors? Do vendors talk to consumers about characteristics of the food that are important to the consumers?
● What features of their shop or their behavior towards customers vendors strive to maintain
● What desired food characteristics vendors look for when they buy from suppliers
What are dominant beliefs and attitudes about food safety?
Domains that will be explored include:
● What food or food characteristics are perceived as ‘safe’ or ‘unsafe’ ● What foods, hazards, or illnesses are top concerns for vendors ● Perceptions of consumer needs and demands related to food quality and safety ● Beliefs and preferences around selecting safe food, keeping food safe at the market,
and maintaining shop hygiene. What factors affect vendors’ decisions about food safety in traditional markets?
Domains that will be explored include:
● What food characteristics are important for vendors when deciding if food is safe or not
● Importance of cleanliness and other supplier characteristics as criteria for selecting a supplier to buy food from
● What interactions with consumers or consumer demand are important in affecting vendor behaviors relevant to food safety
● What aspects of the interaction between vendors and market management affects vendor behaviors relevant to food safety
10
How does gender influence food safety behaviors for vendors?
Domains that will be explored include:
● Whether gender is associated with selling specific foods ● Whether gender affects how the shop is managed, for example in regard to hygiene
practices or ability to select food from suppliers ● Whether vendor gender impacts consumers’ perception of the vendor and the food
they sell ● Whether vendors are more likely to discuss food quality and safety with consumers,
based on their and the consumer’s gender.
What information sources are used to obtain information about food safety?
Domains that will be explored include:
● Who vendors trust when seeking information about food quality or other information needed for their business
● What media channels are most frequently used to access information ● Which organizations vendors interact with and trust to provide services or
information related to food quality and safety ● Vendors’ exposure to information on food quality and safety via different media
channels.
3.3 Study location
The study will be conducted in Kebbi state, Nigeria. Within Kebbi state, the study will focus on traditional markets within the Birnin Kebbi urban area, the largest urban area in the state. The geographic focus was determined in consultation with key local stakeholders, based on local priorities and alignment with existing policies and programs.
The following criteria were used to select the chosen geographic area: city being within a Feed the Future Zone of Influence; undernutrition being prevalent in the state; the Key Commodities being widely consumed in the city; the city being of sufficient size to have multiple markets, the city and state having sufficient security to allow for the work to take place safely. Within Kebbi state, the urban area of Birnin Kebbi was prioritized based on size (with the preference for a city, large enough to have multiple markets but small enough to facilitate research), security, and other relevant factors.
3.4 Market selection
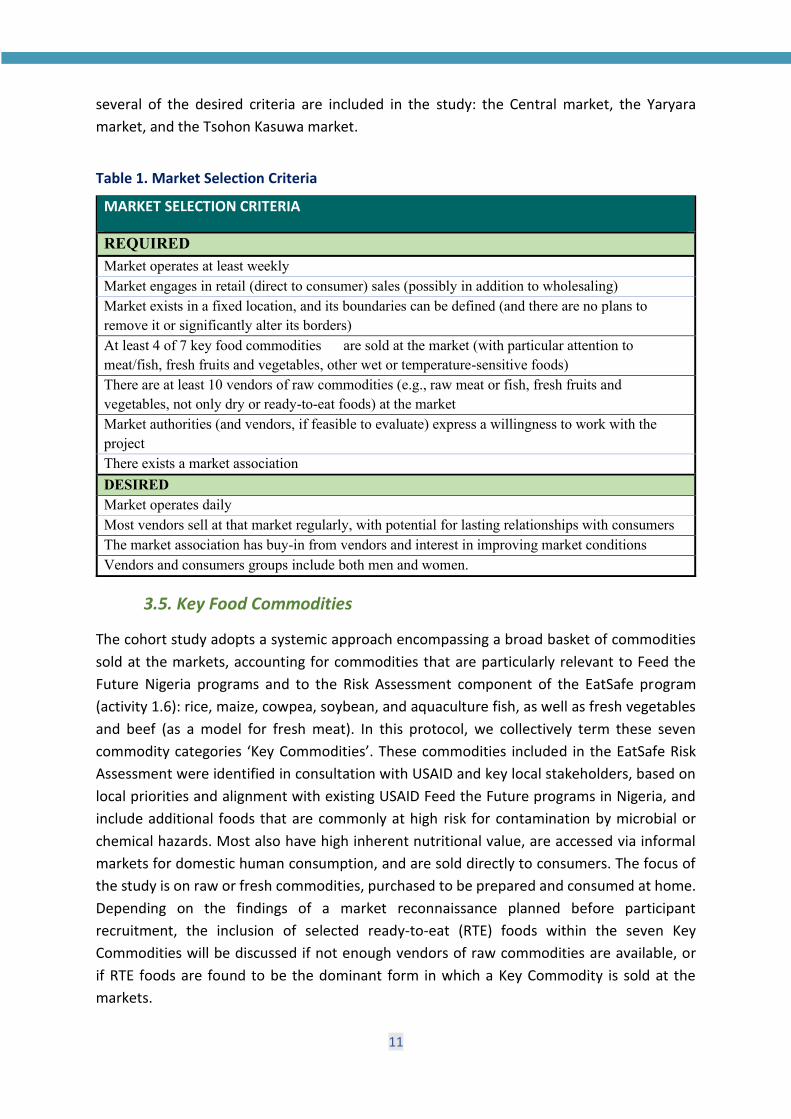
Within the urban area of Birnin Kebbi, open air fresh food markets included in the study have been identified based on a set of criteria related to the goals of the research and the nature of the intervention (see Table 1 below). Three markets meeting all required criteria and
11
several of the desired criteria are included in the study: the Central market, the Yaryara market, and the Tsohon Kasuwa market.
Table 1. Market Selection Criteria
MARKET SELECTION CRITERIA
REQUIRED Market operates at least weekly Market engages in retail (direct to consumer) sales (possibly in addition to wholesaling) Market exists in a fixed location, and its boundaries can be defined (and there are no plans to remove it or significantly alter its borders) At least 4 of 7 key food commodities are sold at the market (with particular attention to meat/fish, fresh fruits and vegetables, other wet or temperature-sensitive foods) There are at least 10 vendors of raw commodities (e.g., raw meat or fish, fresh fruits and vegetables, not only dry or ready-to-eat foods) at the market Market authorities (and vendors, if feasible to evaluate) express a willingness to work with the project There exists a market association DESIRED Market operates daily Most vendors sell at that market regularly, with potential for lasting relationships with consumers The market association has buy-in from vendors and interest in improving market conditions Vendors and consumers groups include both men and women.
3.5. Key Food Commodities
The cohort study adopts a systemic approach encompassing a broad basket of commodities sold at the markets, accounting for commodities that are particularly relevant to Feed the Future Nigeria programs and to the Risk Assessment component of the EatSafe program (activity 1.6): rice, maize, cowpea, soybean, and aquaculture fish, as well as fresh vegetables and beef (as a model for fresh meat). In this protocol, we collectively term these seven commodity categories ‘Key Commodities’. These commodities included in the EatSafe Risk Assessment were identified in consultation with USAID and key local stakeholders, based on local priorities and alignment with existing USAID Feed the Future programs in Nigeria, and include additional foods that are commonly at high risk for contamination by microbial or chemical hazards. Most also have high inherent nutritional value, are accessed via informal markets for domestic human consumption, and are sold directly to consumers. The focus of the study is on raw or fresh commodities, purchased to be prepared and consumed at home. Depending on the findings of a market reconnaissance planned before participant recruitment, the inclusion of selected ready-to-eat (RTE) foods within the seven Key Commodities will be discussed if not enough vendors of raw commodities are available, or if RTE foods are found to be the dominant form in which a Key Commodity is sold at the markets.
12
3.6. Food Safety Intervention
A set of behavior change interventions (here: “intervention”) to improve demand, attitudes, and practices related to food safety will be implemented in the markets included in the study and/or the associated market basins (i.e., urban areas where market customers live). The i ntervention is likely to involve both market vendors and consumers, as the dynamic between the two groups – as well as within each group – may be key to how consumer demand is expressed and how it affects practices. Intervention activities will be defined in full detail after the results of the baseline survey have been analyzed. The findings from the baseline of this cohort study, along with information from the literature and results of the EatSafe Focused Ethnographic Study (FES), stakeholder consultations, risk assessment, story sourcing, and reviews of existing literature and prior interventions will be used to inform the detailed design of the intervention. The intervention is expected to be designed in the months following the completion of the cohort study baseline.
A general program impact pathway (PIP) outlining hypothesized outcomes of an intervention is also under development in support of intervention design and has informed the development of this protocol. To assess the progress of the intervention and its likelihood of achieving an impact, the cohort study will aim to track key indicators related to attitudes and behaviors for both consumers and vendors. These indicators are included in the survey tool or can be calculated from survey answers.
3.7. Data collection overview
The study will assess consumer and vendor knowledge, attitudes, and behaviors related to food safety and how these change over time, through an overall pre-post cohort study structure. The cohort will be followed over the course of the study, from before (baseline) to shortly after the end of the intervention period (endline). Structured surveys, administered to market vendors and consumers, will be the primary data collection approach. Surveys will be complemented by direct behavior observations of vendors at the market (as well as features of the shop and appearance of the vendor), performed before the survey for a subset of vendors. Full data collection will be repeated at least twice: before intervention (baseline), and after intervention (end line). Data collection will consist of a multi-module questionnaire (available as a separate document, see summary in Section 3.11), complemented by direct observations using a checklist (see Section 3.11 and Appendix 1). Data collection at midline (to be discussed, contingent upon resource availability and congruency with the chosen intervention), will be administered to all or a sub-sample of cohort participants after several months of intervention implementation to track progress and coverage of the intervention. The midline survey will involve a much shorter subset of the survey, with additional focused questions to assess intervention coverage and perception. Midline data will be used to course-correct the intervention, if needed.
13
For interventions targeting individuals or small groups (e.g., trainings), differences from baseline to end line will be compared between a treatment group (targeted by one or a set of interventions outlined in Section 3.7) and a comparison control group. For larger-scale interventions such as any mass media messaging or engagement, if used, it is recognized that there will be no true ‘comparison group,’ as all individuals in the study area could be reached by such interventions. As such, data analysis will examine the difference between baseline and end line only.
The data collection is structured as a cohort design, with the same group of individuals being surveyed at baseline and end line. Attrition up to 15% is anticipated and accounted for in sample size determinations (Section 3.10). If attrition is significantly higher, or follow-up becomes logistically unfeasible, the study will revert to a pre-post structure based on a repeated cross-sectional survey, i.e., groups of different individuals will be surveyed at baseline and end line. The intervention is expected to begin approximately six months after completion of the baseline survey. Thus, participants will be exposed to the intervention for at least 18 months before the end line assessment. Before the endline data collection, the contact information of respondents (phone numbers) will be checked to ensure it is still current. In case a phone number is not valid anymore, reasonable effort will be applied to find the respondent using their market location (for vendors) or address (for vendors and consumers). In case attrition is above 15% for any reason, a new power analysis will be conducted, and a new round of enrollment may be carried out to complement the cohort.
3.8. Study participants There will be two main groups of participants: consumers that purchase food at the study markets, and vendors that sell food at the study markets. The two cohorts will be distinct groups from those that participated in the FES.
Consumers eligible for enrolment in the study are defined as those who shop in at least one target market, at least once a month on average, and have primary or shared responsibility for purchasing food for their household. Within each household, one respondent (the ‘primary shopper’) will be interviewed. In the case that one member of the household is the ‘primary shopper’ and another is the ‘primary food preparer’, only the ‘primary shopper’ will be enrolled. The consumer cohort will be stratified by market and by gender, with care that consumers purchasing all Key Commodity categories are included.
Inclusion criteria for consumers are:
● Be 18 years of age or above (completed years) ● Have primary or shared responsibility for purchasing food for their household ● Shop at a target market at least once in the average month ● Purchase at least one Key Commodity at a target market, and preferably three or more ● Be able and willing to give informed consent
14
Exclusion criteria for consumers are:
● Be a food vendor at the target market ● Reselling part or all of the food purchased at the target market (not including buying
some food for a neighbour or a relative) ● Planning to move far from the market or stop shopping at the market in the next two
years ● Be a participant in the EatSafe Focused Ethnographic Study (FES) ● Another member of the household that shares primary food shopping responsibilities
is already enrolled in the cohort study (the person with primary responsibilities should be preferentially enrolled)
● Not being able to communicate verbally in English or Hausa ● Not being willing to share contact information for follow-up ● Being a vendor or hawker of street or ready to eat foods ● Being a vendor or hawker selling outside the boundaries of the market
Vendors eligible for enrolment in the study are defined as key staff of a market shop or stall, that regularly perform key vending operations which may include those relevant for food safety (such as restocking and arranging food for display, temporary storage for the day or shift, preparing food if relevant, conducting transactions with customers, upkeeping the stall, cleaning the stall and any tools through the day, storing the food at closing time). Only vendors interfacing directly with consumers will be included. Only one vendor per shop/stall/business will be enrolled (note: in this document the term “vendor” is used to indicate a person, but it should map 1-1 to a shop or vending business). Ownership of the business per se is not a discriminant for eligibility, i.e., owners, managers, and employees in a food vending business can be eligible. However, to be eligible vendors need to both be “hands on” in performing day-to-day vending actions, and have decision power on how the shop operates, such as which suppliers to buy from, how food is arranged, when and how the shop is cleaned, how customers are treated, and how to handle any consumer complaints. In practice, shop managers or owner-managers are most likely to fulfil these roles. The vendor cohort will be stratified by commodity categories, market, and by gender.
Inclusion criteria for vendors are:
● Be 18 years of age or above (completed years) ● Selling food within the boundaries of the study market ● The vendor or the business where the vendor works sells food at the market at least
one day per week ● Selling at least one Key Commodity4 regularly (at least once per average week) in a
target market
4 The Key Commodity(-ies) should be a main product and a sizeable portion of what the shop sells, not only a niche product. It is acceptable if the grains and legumes in the seven Key Commodities are sold among several other products.
15
● Be a primary vendor in the shop or food vending business, i.e. (a) being physically present in the shop/business for at least half of average business hours in a week, (b) interact directly with consumers during transactions, and (c) be a primary decider of how the shop/stall operates (e.g. which suppliers to buy from, which tools or equipment is used, how the food is arranged in the shop).
● Having sold food at the study market for at least 3 months ● Be able and willing to give informed consent
Exclusion criteria for vendors are:
● Planning to move far from the market or stop selling food at the market in the next two years
● Be a participant in the EatSafe Focused Ethnographic Study (FES) ● Another vendor in the same food vending business is already enrolled in the cohort
study (the person with primary responsibilities in the operation of the business should be preferentially enrolled)
● The business sells only snacks or food that is not bought home and consumed at home ● Not being able to communicate verbally in English or Hausa ● Not being willing to share contact information for follow-up.
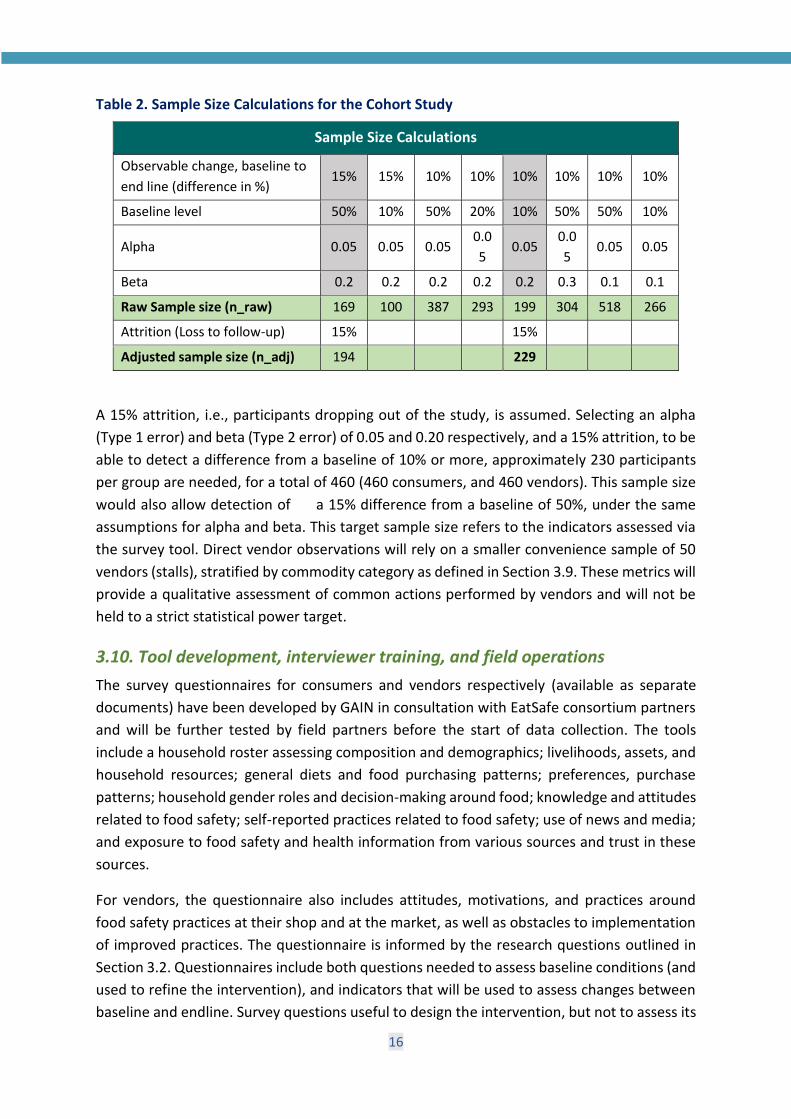
3.9. Sample Size We base our sample size calculations on the ability to detect an absolute difference of at least 15% in the intervention group compared to the control group, e.g., in the percentage of respondents that report practicing key behaviors around food choices. In the absence of data for this area and population, we can make assumptions on the baseline prevalence: 50% is a conservative baseline prevalence, while a 10% baseline is less stringent (because it would lead to a lower sample size needed to meet the same alpha and beta constraints). Based on a two-sided test, the table below indicates the different sample sizes that would be required to obtain predetermined levels of alpha (probability of false positives) and power (1- probability of false negatives), based on different assumptions. Calculations were carried out using the power.prop.test function in the R software. The calculated sample size (n_raw) refers to the number of participants per arm, i.e., for each of the intervention and control groups. Hence, this value needs to be doubled to yield the total number of participants to enroll in the baseline survey.
16
Table 2. Sample Size Calculations for the Cohort Study
Sample Size Calculations
Observable change, baseline to end line (difference in %)
15% 15% 10% 10% 10% 10% 10% 10%
Baseline level 50% 10% 50% 20% 10% 50% 50% 10%
Alpha 0.05 0.05 0.05 0.05
0.05 0.05
0.05 0.05
Beta 0.2 0.2 0.2 0.2 0.2 0.3 0.1 0.1
Raw Sample size (n_raw) 169 100 387 293 199 304 518 266
Attrition (Loss to follow-up) 15% 15%
Adjusted sample size (n_adj) 194 229
A 15% attrition, i.e., participants dropping out of the study, is assumed. Selecting an alpha (Type 1 error) and beta (Type 2 error) of 0.05 and 0.20 respectively, and a 15% attrition, to be able to detect a difference from a baseline of 10% or more, approximately 230 participants per group are needed, for a total of 460 (460 consumers, and 460 vendors). This sample size would also allow detection of a 15% difference from a baseline of 50%, under the same assumptions for alpha and beta. This target sample size refers to the indicators assessed via the survey tool. Direct vendor observations will rely on a smaller convenience sample of 50 vendors (stalls), stratified by commodity category as defined in Section 3.9. These metrics will provide a qualitative assessment of common actions performed by vendors and will not be held to a strict statistical power target.
3.10. Tool development, interviewer training, and field operations The survey questionnaires for consumers and vendors respectively (available as separate documents) have been developed by GAIN in consultation with EatSafe consortium partners and will be further tested by field partners before the start of data collection. The tools include a household roster assessing composition and demographics; livelihoods, assets, and household resources; general diets and food purchasing patterns; preferences, purchase patterns; household gender roles and decision-making around food; knowledge and attitudes related to food safety; self-reported practices related to food safety; use of news and media; and exposure to food safety and health information from various sources and trust in these sources.
For vendors, the questionnaire also includes attitudes, motivations, and practices around food safety practices at their shop and at the market, as well as obstacles to implementation of improved practices. The questionnaire is informed by the research questions outlined in Section 3.2. Questionnaires include both questions needed to assess baseline conditions (and used to refine the intervention), and indicators that will be used to assess changes between baseline and endline. Survey questions useful to design the intervention, but not to assess its
17
impact may be removed from the endline survey tool. To determine approximate household wealth, a series of questions needed to construct the Poverty Probability Index (44) are included. A dietary consumption survey, customized to focus on the Key Commodities due to the need to limit the survey to below an hour in length, will provide information to assess potential foodborne exposure and to track which food forms and combinations are preferred by consumers.
The tool for recording vendor observations (also available as a separate document) has been developed by GAIN, with feedback from consortium partners. The checklist includes characteristics of the shop or stall that are directly related to hygiene and food safety, as well as vendor appearance and vendor behaviors related to shop management and interaction with customers. The checklist is informed by existing Codex Alimentarius guidelines for food safety and hygiene in markets or street-vended foods (46–52). General market and environmental conditions, such as waste management, presence of toilet facilities, or availability of clean water for washing hands and food have been recorded as part of market reconnaissance visits and are not included in this tool.
A data collection partner (Ipsos Nigeria Limited) will implement all aspects of data collection. The survey will be translated into Hausa, so that interviewees could select their language of preference. The answers will be translated back into English before data analysis. The survey will be administered using an in-field computer-assisted personal interviewing (CAPI) data entry program. Before deployment, the questionnaire will be field tested to obtain feedback on question clarity and cultural appropriateness, as well as to define most common answers to be pre-coded. Each interviewer will conduct at least one, and ideally two pilot interviews with representatives of the target groups (consumers and vendors), at markets other than the study markets, that they will interview. Each survey module should be tested at least once by survey managers, and at least twice with real-world participants. The pilot tests will provide feedback on how questions are interpreted, allow correction of any unclear phrasing, and allow further customization of the survey to the local settings. A detailed pilot report will be produced and used to revise and finalize the survey tools. Both the pre-pilot and post-pilot version of the survey tool will be translated in Hausa. The CAPI interface will also be tested for functionality and congruence with the “paper” tool.
Locally recruited and experienced data collectors, fluent in Hausa and English, will be rigorously trained to ensure standardized data collection. This will follow standard training approaches and instructions for all standard survey questions/modules (i.e., WHO/UNICEF/USAID FANTA for dietary assessments). Performance criteria will be established that all data collectors must pass before being permitted to collect data for the study. A GAIN research team member will be present during part of the training and tool testing, in order to provide an introduction to EatSafe and the cohort study goal, as well as to oversee the activities.
18
All data will be collected in the field using Ipsos’ iField Applications for data collection, an integrated case management and data collection application with capabilities for fieldwork management and quality control. The data collection application will be loaded on tablets or mobile phones. Data will be uploaded to a secure web-based platform using mobile phone or Wi-Fi networks, which will help avoid data entry errors and allow for instant aggregation and real-time quality control. Data collectors will also be supervised closely in the field by an experienced data collection supervisor. Supervisors and a research manager will review data in real time (via the online platform) and debrief with data collectors to identify and correct any errors. To aid with follow-up and supervision, GPS coordinates will be logged for each house or shop surveyed, and phone numbers will be collected for all participants.
Survey data collection will preferentially occur at the respondent’s home, or in a convenient public location that offers privacy. For vendor, based on reconnaissance information it is unlikely that they will allow for the interview to occur at their domicile. We will allow for data collection at the market, albeit less than ideal in terms of distractions and possible spill-over to other vendors. As much as possible, enumerator will invite the vendor to step away from their shop and be interviewed in a quiet area of the market, or near the market. The specific location and conditions of the interview will be noted.
For the direct observation of vendor activities one observer, upon receiving consent from the food vendor, will position themselves close to the stall, so as to be able to clearly witness vendors’ actions including interactions with consumers, without disturbing vendor’s activities or being noted by customers in a way that changes the interaction with vendors (e.g. they should be sitting on the side or back of the stall, as if texting on their phone). Shop characteristics and vendor appearance will be noted at the beginning of the observation. Vendor actions will be observed and noted for one full hour. During this time, the observer will not talk to the vendor, except to reposition themselves if needed. Shop features can be noted before or after the observation time. Observers will record both the occurrence of a specific behavior at any time during the observation period, and the number of occurrences. If multiple vendors at a stall interact with customers, the observer will follow one vendor only, making sure the selected vendor is active and performing food handling or preparation activities. The observed vendor should be at the stall and actively working for the entirety of the 1-hour observation (with the exception of taking a bathroom break or a short phone call). In case the observation is interrupted before 45 uninterrupted minutes have passed, a second 1-hr observation period will be conducted. As an exception, observations that lasted between 45 and 60 minutes before a major interruption will be considered complete, but less than 5% of observations should fall in this category.

19
3.11. Study participant recruitment 3.11.1. Consumers
For consumers, a market reconnaissance will provide an overall estimate of the number of consumers visiting the market each day, what days and times are busy or not, and which sectors of the market are most popular, as well as other characteristics that support recruitment activities. Recruitment of consumers purchasing Key Commodities at each target market will be carried out by positioning recruiters at strategic points where consumer purchase Key Commodities (e.g., near vendors of Key Commodities), as informed by the market reconnaissance, and by approaching consumers after their purchase or as they leave the market. All consumers seen to be purchasing at least one Key Commodity will be eligible for potential participation in the study. If needed, consumers not seen to purchase any Key Commodities at the time of the enrolment screening will be asked whether they ever purchase those foods at that market; if responding affirmatively, they will be considered eligible. Depending on market size, at least two recruitment rounds will be carried out for each market, or as many times as is needed to obtain the required sample size. Market recruitment visits will be at different times and on different days, including on a main market day, to limit bias in recruitment. During recruitment, a member of the study team will explain to eligible consumers what participation would entail. For those who agree to participate, contact information will be collected and enumerators will arrange to interview them in person at home at a mutually agreed day and time. Interviewers will note the number and basic characteristics (gender, age category) of consumers who do not agree to participate, to understand potential biases in participant self-selection. Once a sampling frame of eligible participants is created, participants will be selected randomly, in alignment with overall sample size and stratification by gender and market, with consideration to giving adequate representation to key commodity categories. Target stratification by gender is 50-50%, slightly oversampling women, based on approximate observations that women make 40-45% of the consumer population across the three markets. Given the importance of gender as a variable, ability to compare the answers of men vs. women was given priority over (approximate) representativeness of the consumer population (which, if needed, could be reconstructed by weighing results). Stratification by market will be based on relative market size, estimated in terms of number of vendors.
3.11.2. Vendors
Before participant recruitment, the study will include a thorough market reconnaissance to assess the number of vendors per commodity, their distribution throughout the market, and other relevant characteristics in support of recruitment activities. Only vendors selling food within the perimeter of the market will be considered for recruitment, i.e., excluding street food vendors outside the perimeter of the market. At a first level of screening, all vendors seen to be selling at least one Key Commodity will be considered eligible for potential participation in the study. If needed to meet sample size targets, food vendors not selling any

20
Key Commodities at the time of the census will be asked whether they regularly sell any of them at that market; if responding affirmatively, they will be considered eligible for potential participation. This enumeration will allow estimation of the relative proportion of vendors that sell different Key Commodities. This information will be used so that the enrolled vendors are distributed across categories encompassing all Key Commodities (grains and legumes; fresh vegetables; fresh beef; and aquaculture fish), in numbers approximately representative of the proportion of different Key Commodity vendors in the larger market population. Vendors that do not have fixed structures (e.g., a stall, table, or other fixed structure) and may move around the market during a vending day (e.g., using a movable cart, or carrying baskets) will be considered eligible, if they meet inclusion criteria. At a second level of screening, all other inclusion criteria will be assessed. The screening will allow to establish a comprehensive sampling frame to draw from, within the limitations of the overall number of vendors operating in the three study markets. The vendor cohort of participants will be stratified at three levels: (1) at market level (three study markets, based on the relative size of the market, estimated as number of vendors), (2) by gender, and (3) by food categories (either the Key Commodities or three broader categories including the seven Key Commodities). Quotas for stratification will be defined based on a vendor count carried out before enrollment. During recruitment, a member of the study team will explain to eligible vendors what participation would entail. For those who agree to participate, contact information will be collected, and enumerators will arrange to interview them in person, either at their home or other location affording sufficient privacy, excluding the market, at a mutually agreed day and time. Interviewers will also note the number and basic characteristics (gender, age category) of vendors who do not agree to participate, to understand potential biases in participant self-selection.
3.12. Assignment into intervention arms For interventions that involve individuals as the unit of intervention (e.g., trainings), individual participants will be randomly assigned to either the intervention or the control group. The populations of vendors across the three study markets will be considered as one study population, and similarly consumers enrolled from the three markets will be considered as one study population. As such, the study will not be clustered. It is recognized that there is a chance of “intervention spill over” across vendors, in particular if their stalls are located next to each other. Based on preliminary market mapping, it appears that in all three study markets, vendors of a commodity category are clustered together. As such, it may not be possible to mitigate the confounding impact of intervention spill over by selecting vendors whose stalls are far from each other. GPS coordinates of each enrolled vendor will be collected, and the relative position of vendors mapped and accounted for in the analysis and interpretation of results. The same will be done for consumers, although it is expected that consumers’ dwellings will be spread throughout a broader area.
21
For an intervention involving the entire market or the entire participant group (e.g., media campaigns), no assignment will occur as the entire group will receive the intervention. All three study markets will receive such intervention; hence the analysis will be based on pre/post comparisons, without clusters.
4. DATA PROCESSING AND ANALYSIS
Upon completion of data collection for the baseline survey and back-translation of answers into English, the data will be cleaned, labelled, and analyzed using simple descriptive statistics. Characteristics of the study population will be examined using descriptive statistics both as a whole and by sub-groups, according to various variables potentially including market, gender, and socioeconomic status. Outcome (dependent) variables will be the survey answers and will take various forms, depending on the survey question, including percent of respondents answering “yes” or selecting an item in a multiple-choice question; categorical variables representing selection within multiple choice options; ranked categorical variables, e.g., from likert scales; and continuous or discrete numerical variables, e.g., amount of a specific food consumed. Established statistical tests (e.g., t tests, Chi-squared tests, or ANOVA) will be used to compare between groups. Generalized linear mixed models will be developed for selected outcomes (KAPs measures) to assess the significance of factors and potential confounders, including those listed above. Analyses will be performed using widespread statistical software, such as R (45) or STATA v.15 (StataCorp, College Station, TX, USA).
For interventions with individual participants as the unit of intervention, Intent-to-treat analyses will assess whether the intervention improved changes in all outcomes using fixed-effects, difference-in-differences models with individuals as a fixed effect. We will use generalized linear mixed models (e.g., logistical regression) to compare the magnitude of pre/post change in KAPs between the intervention vs. control group. Data from the baseline and endline surveys will be used. Intervention impact will be assessed based on the sign and significance of a dummy variable representing the interaction between the data collected at the end line and being in the intervention group. We will examine models both including different independent variables and without, to test for potential confounding. Independent variables to be considered will include sociodemographic characteristics, in particular those found to impact KAP output variables in the baseline data.
For larger-scale interventions involving an entire market, or an entire market basin (for consumers), a pre/post analytical framework for prospective cohort studies will be applied to baseline and end line data. Comparison between outcomes variables means for a group (where groups refer to the entire vendor study group across the three markets, and the entire consumer study group recruited in the three markets) will be assessed using a simple difference in the same outcomes collected at the baseline and the end line. Various approaches, including Analysis of Variance (ANOVA), Analysis of Covariance (ANCOVA), t-test, and chi square test comparing the group pre-post difference in outcomes.
22
5. DATA MANAGEMENT AND SUBJECT CONFIDENTIALITY
A Data Management SOP document will be developed to document procedures from data collection to analysis and archival, and to outline best practices to be followed in managing the data pipeline. All data collected in the study will be linked by identifiers and will be treated with strict confidentiality throughout and beyond the duration of the trial, with identifier-linked data available only to selected study investigators. Individual identifiers will not be accessible to the data analysts and will be accessed by a data manager only in case respondent identity disambiguation is necessary (e.g., to make sure a respondent is not counted twice). Data will be anonymized before being formatted for archival in a database. The database will be archived in multiple formats, including .csv, on secure GAIN servers. The final datasets will also be archived on a physical support. All analyses and papers will report results in aggregate format to prevent any possible identification of individual identity; names will be collected in the survey only to ensure accountability of the survey team and non-duplication in the data/interviewing, as well as follow-up in the end line survey; they will be disposed of for analysis and replaced with anonymous ID numbers.
All source data is expected to be in electronic form. Written data will be collected via a secure online platform. As soon as they are received, data will be backed up to a secure server at the GAIN country or headquarters offices. Access will be granted only to members of the research team, or selected individuals with the permission and under the supervision of the GAIN research team. Any paper forms will be preserved for 3 years after the end of the research and then destroyed by shredding. After the end of the study, de-identified data will be made available publicly (open access) in line with the requirements of the donor and the Nigerian government.
6. ETHICAL CONCERNS: CONSENT, RISKS, AND ADVERSE EVENTS
The survey protocol will ensure complete adherence to research ethics. The principles of voluntary participation, confidentiality, do no harm, and respect will always be upheld. A process of verbal informed consent (translated into local languages, as needed) will be used. Vendors and consumers eligible to be enrolled in the study will be explained the study objectives, procedures, and all associated potential risks and benefits, as well as how data will be protected. They will have the opportunity to have their questions answered and to refuse to take part in all or any part of the study. This study will not be collecting highly sensitive data or biochemical specimens.
The research should not involve any situation that might result in physical or emotional harm to the respondents as a result of their participation in the survey. Subjects participating in the study will be exposed to no greater than minimal risks, not exceeding those associated with a normal interview. An interview visit is likely to take 60 to 90 minutes in total for the survey,
23
during which participants will not be able to carry out other activities. During direct vendor observations, which will last approximately 75 minutes in total, vendors will be able to perform regular vending operations. It is possible that the presence of an observer may cause the vendor to modify their behavior, but no increase in risk is anticipated. In terms of benefits, participants will receive a thank-you token for their time, in the form of a small amount of phone credit. All those in the intervention arms will benefit from the subsequent interventions, which are expected to benefit consumers and vendors alike. In the medium-long term, those in non-intervention arms should also benefit from an improved enabling environment for food safety, due to greater consumer and vendor awareness within the same markets.
Ethical clearance for the research will be sought from the National Health Ethics Research Committee of Nigeria, Federal Ministry of Health, Nigeria. The application for ethical clearance will be submitted by Ipsos Nigeria Limited, contracted for this study. It is very unlikely that problems or adverse events will occur in connection with this study. Ipsos Nigeria Limited will seek at all times to minimize any risk arising from working in the field and will take on the responsibility for the security and Duty of Care to ensure the safety and wellbeing of all field personnel, including making appropriate security arrangements. If any problems do occur in the study sites, they will be addressed by the supervising consultant with the assistance and support of GAIN personnel, who will record the incident and response. Any such issues will be brought to the Project Director’s notice within a week; if needed, the investigators will then file a report with the IRB. The research will take place in the context of the COVID-19 pandemic. As such, we will adjust methods to protect the safety of the research staff and participants. This will be done in full compliance with the requirements of the local IRB and informed by best practices emerging from studies elsewhere. This is likely to include: both interviewer and interviewee using hand sanitizer before the interview, both wearing masks throughout the interview, holding interviews in the open air where possible, and ensuring social distancing between interviewer and interviewee. All research travel and training activities will also be carried out in line with local COVID-19-related restrictions.
24
REFERENCES
1. FAO, WHO. Risk Management and Food Safety: Report of a Joint FAO/WHO Consultation [Internet]. Rome: Food and Agriculture Organization of the United Nations; 1997. Available from: http://www.fao.org/3/W4982E/W4982E00.htm
2. Havelaar AH, Kirk MD, Torgerson PR, Gibb HJ, Hald T, Lake RJ, et al. World Health Organization Global Estimates and Regional Comparisons of the Burden of Foodborne Disease in 2010. PLOS Medicine. 2015 Dec 3;12(12):e1001923.
3. Grace D. Food Safety in Low- and Middle-Income Countries. IJERPH. 2015 Aug 27;12(9):10490–507.
4. Guerrant RL, Schorling JB, McAuliffe JF, de Souza MA. Diarrhea as a cause and an effect of malnutrition: diarrhea prevents catch-up growth and malnutrition increases diarrhea frequency and duration. Am J Trop Med Hyg. 1992 Jul;47(1 Pt 2):28–35.
5. Schaible UE, Kaufmann SHE. Malnutrition and Infection: Complex Mechanisms and Global Impacts. PLOS Medicine. 2007 May 1;4(5):e115.
6. Newell DG, Koopmans M, Verhoef L, Duizer E, Aidara-Kane A, Sprong H, et al. Food-borne diseases — The challenges of 20years ago still persist while new ones continue to emerge. International Journal of Food Microbiology. 2010 May 30;139:S3–15.
7. Tauxe RV. Emerging foodborne diseases: an evolving public health challenge. Emerg Infect Dis. 1997;3(4):425–34.
8. Mead PS, Slutsker L, Dietz V, McCaig LF, Bresee JS, Shapiro C, et al. Food-related illness and death in the United States. Emerg Infect Dis. 1999;5(5):607–25.
9. Checkley W, Buckley G, Gilman RH, Assis AM, Guerrant RL, Morris SS, et al. Multi-country analysis of the effects of diarrhoea on childhood stunting. Int J Epidemiol. 2008 Aug;37(4):816–30.
10. Kirk MD, Pires SM, Black RE, Caipo M, Crump JA, Devleesschauwer B, et al. World Health Organization Estimates of the Global and Regional Disease Burden of 22 Foodborne Bacterial, Protozoal, and Viral Diseases, 2010: A Data Synthesis. PLOS Medicine. 2015 Dec 3;12(12):e1001921.
11. Fischer Walker CL, Aryee MJ, Boschi-Pinto C, Black RE. Estimating Diarrhea Mortality among Young Children in Low- and Middle-Income Countries. PLOS ONE. 2012 Jan 3;7(1):e29151.
12. National Population Commission (NPC), ICF. Nigeria Demographic and Health Survey 2018. Abuja, Nigeria, and Rockville, Maryland, USA: NPC and ICF; 2019.
13. Liu Y, Chang C-CH, Marsh GM, Wu F. Population attributable risk of aflatoxin-related liver cancer: systematic review and meta-analysis. Eur J Cancer. 2012 Sep;48(14):2125–36.
14. Oberoi S, Barchowsky A, Wu F. The global burden of disease for skin, lung, and bladder cancer caused by arsenic in food. Cancer Epidemiol Biomarkers Prev. 2014 Jul;23(7):1187–94.
15. Jaffee S, Henson S, Unnevehr L, Grace D, Cassou E. The Safe Food Imperative: Accelerating Progress in Low- and Middle-Income Countries [Internet]. The World Bank; 2018 [cited 2020
25
Mar 27]. 208 p. (Agriculture and Rural Development). Available from: https://doi.org/10.1596/978-1-4648-1345-0
16. Grace D, Alonso S, Mutua F, Roesel K, Lindahl J, Amenu K. Food safety investment expert advice: Burkina Faso, Ethiopia, Nigeria. Nairobi: International Livestock Research Institute; 2018.
17. Tschirley D, Reardon T, Dolislager M, Snyder J. The Rise of a Middle Class in East and Southern Africa: Implications for Food System Transformation: The Middle Class and Food System Transformation in ESA. J Int Dev. 2015 Jul;27(5):628–46.
18. Cortese RDM, Veiros MB, Feldman C, Cavalli SB. Food safety and hygiene practices of vendors during the chain of street food production in Florianopolis, Brazil: A cross-sectional study. Food Control. 2016 Apr;62:178–86.
19. Gadaga TH, Samende BK, Musuna C, Chibanda D. The microbiological quality of informally vended foods in Harare, Zimbabwe. Food Control. 2008 Aug;19(8):829–32.
20. Muyanja C, Nayiga L, Brenda N, Nasinyama G. Practices, knowledge and risk factors of street food vendors in Uganda. Food Control. 2011 Oct;22(10):1551–8.
21. Alves da Silva S, Cardoso R de CV, Góes JÂW, Santos JN, Ramos FP, Bispo de Jesus R, et al. Street food on the coast of Salvador, Bahia, Brazil: A study from the socioeconomic and food safety perspectives. Food Control. 2014 Jun;40:78–84.
22. Macheka L, Manditsera FA, Ngadze RT, Mubaiwa J, Nyanga LK. Barriers, benefits and motivation factors for the implementation of food safety management system in the food sector in Harare Province, Zimbabwe. Food Control. 2013 Nov;34(1):126–31.
23. Aluko OO, Ojeremi TT, Olaleke DA, Ajidagba EB. Evaluation of food safety and sanitary practices among food vendors at car parks in Ile Ife, southwestern Nigeria. Food Control. 2014 Jun;40:165–71.
24. Andy E, Mangai, Kayong E, Afoi B, Goshit J, Kasang N, et al. Assessment of Practice of Food Safety and Hygiene among Food Vendors within Jos North Local Government Area of Plateau State, Nigeria. International Journal of Medical and Health Research. 2015;1(2).
25. Okojie PW, Isah EC. Food hygiene knowledge and practices of street food vendors in Benin City, Nigeria. Int J Consum Stud. 2019 Nov;43(6):528–35.
26. Chukuezi C. Food Safety and Hyienic Practices of Street Food Vendors in Owerri, Nigeria. Studies in Sociology of Science. 2010;1(1).
27. Agwu ACO, Akpan UE, Obiageli U-IF, Kalu IO, Nkwa AA, Okorie EA, et al. Assessment of Food Hygiene Practices in Abia State, South East Nigeria. American Journal of Food, Nutrition and Health. 2018;8(3).
28. Ezenwoko AZ, Awosan KJ, Oche MO, Makusidi MA, Abubakar BG, Raji IA. Knowledge and Practices Related to Food Hygiene among Food Handlers in Sokoto, Nigeria. International Journal of Tropical Disease & Health. 2017;26(1).
29. Odipe OE, Olalekan RM, Sanchez ND, Funmilayo AA, Edewor O-P, Lateefat HM, et al. Assessment of Environmental Sanitation, Food Safety Knowledge, Handling Practice among
26
Food Handlers of Bukateria Complexes in Iju Town, Akure North of Ondo-State, Nigeria. ACTA Sciientific Nutritional Health. 2019;3(6).
30. Iwu AC, Uwakwe KA, Duru CB, Diwe KC, Chineke HN, Merenu IA, et al. Knowledge, Attitude and Practices of Food Hygiene among Food Vendors in Owerri, Imo State, Nigeria. 2017;5.
31. Lawan UM, Iliyasu Z, Abubakar S, Gajida AU, Abdussalam A. Personal and food hygiene practices of subsistence food vendors operating in Kano metropolis, northwestern Nigeria. International Journal of Medical Science and Public Health. 2015;4(2).
32. Adebowale OO, Kassim IO. Food safety and health: a survey of rural and urban household consumer practices, knowledge to food safety and food related illnesses in ogun state. Epidemiology Biostatistics and Public Health. 2017;14(3).
33. Awoyemi AO, Ajiboy MN, Adesiji GB, Kayode AO. Food safety knowledge among farming households in Irepodun local government area, Kwara State, Nigeria. Agricultural Science and Technology. 2019;11(2).
34. Ortega DL, Tschirley DL. Demand for food safety in emerging and developing countries: A research agenda for Asia and Sub-Saharan Africa. Journal of Agribusiness in Developing and Emerging Economies. 2017 Jan 1;7(1):21–34.
35. Chamhuri N, Batt PJ. Exploring the Factors Influencing Consumers’ Choice of Retail Store When Purchasing Fresh Meat in Malaysia. International Food and Agribusiness Management Review. 2013;16.
36. GAIN. Global Alliance for Improved Nutrition. EatSafe - Evidence and Action Towards Safe, Nutritious Food; Consumer and Vendor Perspectives and Practices Related to Food Safety in Nigeria: A Review. 2020.
37. Nordhagen S. Consumers’ and Vendors Perspectives on Food Safety in Nigeria: A Review. Geneva; 2020.
38. Grace D, Dipeolu M, Olawoye J, Ojo E, Odebode S, Agbaje M, et al. Evaluating a group-based intervention to improve the safety of meat in Bodija Market, Ibadan, Nigeria. Trop Anim Health Prod. 2012 Sep;44(S1):61–6.
39. Ituma B, Akpa C, Iyare O. Food Hygiene Knowledge, Practice and Safety Training Intervention among Food Handlers in Abakaliki, Nigeria. AJMAH. 2017 Jan 10;7(3):1–7.
40. Umar A, Mande A, Umar J. The Effect of food hygiene training among street food vendors in Sabon Gari Local Government Area of Kaduna State, Nigeria. Sub-Saharan Afr J Med. 2018;5(1):20.
41. Arnade C, Calvin L, Kuchler F. Consumer Response to a Food Safety Shock: The 2006 Food-Borne Illness Outbreak of E. coli O157: H7 Linked to Spinach. Review of Agricultural Economics. 2009 Dec;31(4):734–50.
42. Guh S, Xingbao C, Poulos C, Qi Z, Jianwen C, von Seidlein L, et al. Comparison of cost-of-illness with willingness-to-pay estimates to avoid shigellosis: evidence from China. Health Policy and Planning. 2007 Nov 12;23(2):125–36.
27
43. Ortega DL, Wang HH, Olynk NJ, Wu L, Bai J. Chinese Consumers’ Demand for Food Safety Attributes: A Push for Government and Industry Regulations. American Journal of Agricultural Economics. 2012 Jan;94(2):489–95.
44. IPA. Poverty Probability Index (PPI) [Internet]. 2020 [cited 2020 Apr 6]. Available from: https://www.povertyindex.org/about-ppi
45. R Core Team. R: A language and environment for statistical computing. R Foundation for Statistical Computing, Vienna, Austria. https://www.R-project.org/ [Internet]. 2020. Available from: https://www.R-project.org/
46. Codex Alimentarius Commission. Guidelines for the design of control measures for street-vended foods in Africa [Internet]. 1997 [cited 2020 Sep 2]. Available from: http://www.fao.org/3/w6419e/w6419e05.htm
47. WHO. World Health Organization. A guide to healthy food markets [Internet]. 2006. Available from: www.who.int/foodsafety/publications/capacity/healthymarket_guide.pdf
48. Codex Alimentarius Commission. CODEX Revised Regional Code of Hygienic Practice for the Preparation and Sale of Street Foods (Latin America and the Caribbean) CAC/RCP 43R-1995/Revised in 2001 [Internet]. 2001. Available from: http://www.fao.org/fao-who-codexalimentarius/sh-proxy/en/?lnk=1&url=https%253A%252F%252Fworkspace.fao.org%252Fsites%252Fcodex%252FStandards%252FCXC%2B43R-1995%252FCXP_043Re.pdf
49. Codex Alimentarius Commission. CODEX Regional Code of Hygienic Practice for Street-Vended Foods in Asia, CXC 76R-2017 [Internet]. 2017. Available from: http://www.fao.org/fao-who-codexalimentarius/sh-proxy/en/?lnk=1&url=https%253A%252F%252Fworkspace.fao.org%252Fsites%252Fcodex%252FStandards%252FCXC%2B76R-2017%252FCXP_076Re.pdf
50. WHO. World Health Organization, Food Safety Unit, Division of Food and Nutrition. Essential Safety Requirements for Street-Vended Foods [Internet]. 1996. Available from: https://www.who.int/foodsafety/publications/street-vended-food/en/
51. FAO, Food and Agriculture Organization of the United Nations. The Informal Food Sector: Municipal support policies for operators. [Internet]. 2003. Available from: http://www.fao.org/3/y4312e/y4312e.pdf
52. WHO. World Health Organization. Basic Steps to Improve the Safety of Street-Vended Food; INFOSAN Information Note no. 3/2010; WHO, 30 June 2010. [Internet]. 2010. Available from: https://www.who.int/foodsafety/fs_management/No_03_StreetFood_Jun10_en.pdf

28




















