Early, single chlorhexidine application reduces ventilator-associated pneumonia in trauma patients
8
Care of the Critically Ill Early, single chlorhexidine application reduces ventilator-associated pneumonia in trauma patients Mary Jo Grap, PhD, RN, ACNP, FAAN a, *, Cindy L. Munro, PhD, RN, ANP, FAAN a , V. Anne Hamilton, RN, MS a , R. K. Elswick Jr, PhD b , Curtis N. Sessler, MD, FCCM, FCCP c , Kevin R. Ward, MD d a Adult Health and Nursing Systems Department of the School of Nursing, Virginia Commonwealth University, Richmond, Virginia b Department of Biostatistics of the School of Medicine, Virginia Commonwealth University, Richmond, Virginia c Division of Pulmonary and Critical Care Medicine of the Department of Internal Medicine of the School of Medicine, Virginia Commonwealth University, Richmond, Virginia d Department of Emergency Medicine of the School of Medicine, Virginia Commonwealth University, Richmond, Virginia article info Article history: Received 27 July 2010 Revised 7 January 2011 Accepted 11 January 2011 Online 16 March 2011 Keywords: Chlorhexidine Oral care Ventilator-associated pneumonia abstract Background: Ventilator-associated pneumonia (VAP) is an important complication of mechanical ventilation and is particularly common in trauma, burn, and surgical patients. Interventions that kill bacteria in the oropharynx reduce the pool of viable organisms available for translocation to the lung and thereby lessen the likelihood of developing VAP. Repeated administration of chlorhexidine (CHX) to the mouth and oropharynx has been shown to reduce the incidence of VAP, but use of a single dose has not been studied. This randomized, controlled clinical trial tested an early (within 12 hours of intubation) application of CHX by swab versus control (no swab) on oral microbial flora and VAP. Methods: A total of 145 trauma patients requiring endotracheal intubation were randomly assigned to the intervention (5 mL CHX) or control group. VAP (Clinical Pulmonary Infection Score [CPIS] 6) was evaluated on study admission and at 48 and 72 hours after intubation. Results: A total of 145 patients were enrolled; 71 and 74 patients were randomized to intervention and control groups, respectively. Seventy percent of the patients were male, and 60% were white; their mean age was 42.4 years (18.2). A significant treatment effect was found on CPIS both from admission to 48 hours (P ¼ .020) and to 72 hours (P ¼ .027). In those subjects without pneumonia at baseline (CPIS < 6), 55.6% of the control patients (10/18) had developed VAP by 48 or 72 hours versus only 33.3% of the intervention patients (7/21). Funding: TriService Nursing Research Program, TSNRP MDA-905-03-1-TS02, M.J.G., Principal Investigator. * Corresponding author: Mary Jo Grap, PhD, RN, ACNP, FAAN, Professor, School of Nursing, Virginia Commonwealth University, Box 980567, Richmond, VA 23298-0567. E-mail address: [email protected] (M. J. Grap). 0147-9563/$ - see front matter Ó 2011 Elsevier Inc. All rights reserved. doi:10.1016/j.hrtlng.2011.01.006
Transcript of Early, single chlorhexidine application reduces ventilator-associated pneumonia in trauma patients

Care of the Critically Ill
Early, single chlorhexidine application reducesventilator-associated pneumonia in trauma patients
Mary Jo Grap, PhD, RN, ACNP, FAANa,*, Cindy L. Munro, PhD, RN, ANP, FAANa,V. Anne Hamilton, RN, MSa, R. K. Elswick Jr, PhDb,
Curtis N. Sessler, MD, FCCM, FCCPc, Kevin R. Ward, MDd
aAdult Health and Nursing Systems Department of the School of Nursing, Virginia Commonwealth University, Richmond, VirginiabDepartment of Biostatistics of the School of Medicine, Virginia Commonwealth University, Richmond, Virginia
cDivision of Pulmonary and Critical Care Medicine of the Department of Internal Medicine of the School of Medicine, Virginia Commonwealth
University, Richmond, VirginiadDepartment of Emergency Medicine of the School of Medicine, Virginia Commonwealth University, Richmond, Virginia
a r t i c l e i n f o
Article history:Received 27 July 2010Revised 7 January 2011Accepted 11 January 2011Online 16 March 2011
Keywords:ChlorhexidineOral careVentilator-associatedpneumonia
Funding: TriService Nursing Research Progr* Corresponding author: Mary Jo Grap, PhD,
980567, Richmond, VA 23298-0567.E-mail address: [email protected] (M. J. Gr
0147-9563/$ - see front matter � 2011 Elsevidoi:10.1016/j.hrtlng.2011.01.006
a b s t r a c t
Background: Ventilator-associated pneumonia (VAP) is an importantcomplication of mechanical ventilation and is particularly common intrauma, burn, and surgical patients. Interventions that kill bacteria in theoropharynx reduce the pool of viable organisms available for translocationto the lung and thereby lessen the likelihood of developing VAP. Repeatedadministration of chlorhexidine (CHX) to the mouth and oropharynx hasbeen shown to reduce the incidence of VAP, but use of a single dose has notbeen studied. This randomized, controlled clinical trial tested an early(within 12 hours of intubation) application of CHX by swab versus control(no swab) on oral microbial flora and VAP.
Methods: A total of 145 trauma patients requiring endotracheal intubation wererandomly assigned to the intervention (5 mL CHX) or control group. VAP (ClinicalPulmonary Infection Score [CPIS] � 6) was evaluated on study admission and at48 and 72 hours after intubation.
Results: A total of 145 patients were enrolled; 71 and 74 patients wererandomized to intervention and control groups, respectively. Seventypercent of the patients were male, and 60% were white; their mean age was42.4 years (�18.2). A significant treatment effect was found on CPIS bothfrom admission to 48 hours (P ¼ .020) and to 72 hours (P ¼ .027). In thosesubjects without pneumonia at baseline (CPIS < 6), 55.6% of the controlpatients (10/18) had developed VAP by 48 or 72 hours versus only 33.3% ofthe intervention patients (7/21).
am, TSNRP MDA-905-03-1-TS02, M.J.G., Principal Investigator.RN, ACNP, FAAN, Professor, School of Nursing, Virginia Commonwealth University, Box
ap).
er Inc. All rights reserved.

h e a r t & l ung 4 0 ( 2 0 1 1 ) e 1 1 5ee 1 2 2e116
Conclusion: an early, single application of CHX to the oral cavity significantlyreduces CPIS and thus VAP in trauma patients.
Cite this article: Grap, M. J., Munro, C. L., Hamilton, V. A., Elswick, R. K., Sessler, C. N., & Ward, K. R. (2011,
SEPTEMBER/OCTOBER). Early, single chlorhexidine application reduces ventilator-associated pneumonia
in trauma patients. Heart & Lung, 40(5), e115-e122. doi:10.1016/j.hrtlng.2011.01.006.
Pneumonia is a common complication of mechanicalventilation (ventilator-associated pneumonia [VAP]),occurring in up to 25% of ventilated patients.1 VAP isresponsible for 90% of nosocomial infections in thispatient population,2 greatly adding to cost,3,4 durationof mechanical ventilation,5 intensive unit care (ICU)length of stay,6 hospital length of stay,7 and mortality.3
One of the most critical risk factors for the devel-opment of nosocomial pneumonia in patients whoare endotracheally intubated is colonization ofthe oropharynx.8 Growth of potentially pathogenicbacteria in dental plaque provides a nidus of infectionfor microorganisms that have been shown to beresponsible for the development of VAP.9 Bacterialcolonization of the oropharynx in the mechanicallyventilated critically ill patient increases after intuba-tion, with a predominance of gram-negative organ-isms. Early reduction of the number of viableorganisms in the oral cavity after intubation with anoral care intervention is an attractivemethod to reducethe risk of development of VAP.
Chlorhexidine (CHX), an oral antiseptic agent, hasbeen evaluated for its effect on the incidence of noso-comial pneumonia, including 2 recent meta-anal-yses.10,11 In an analysis of 7 trials (2144 patients) on theeffect of oral application of antiseptics (CHX or povi-done iodine) on VAP rates, Chan et al10 found that theincidence of VAP was significantly reduced with eitherantiseptic. Chlebicki and Safdar11 specifically evalu-ated the efficacy of topical CHX applied to theoropharynx versus placebo or standard care for VAPand found that in 7 randomized controlled trials (RCTs)CHX significantly reduced VAP (P ¼ .02), with thegreatest benefit in cardiac surgery patients. Five of theseven trials in these two analyses were the same. Ina recent RCT that evaluated both mechanical (tooth-brushing) and pharmacologic (CHX) oral interventionsto reduced VAP, Munro et al12 found that CHX alonereduced the incidence of VAP among subjects whowere without pneumonia at baseline (P ¼ .0065),whereas toothbrushing had no effect on VAP. Whensubjects with and without pneumonia at baseline wereanalyzed together, no effect of either CHX (P ¼ .69) ortoothbrushing (P ¼ .95) on VAP was found. Wehypothesized that the use of an early, single applica-tion of CHX, an economic and easy to administerintervention, also may be effective in reducing VAP.
Patients who are at especially high risk for thedevelopment of VAP include trauma, burn, neurosur-gical, and surgical patients.13 Therefore, the primaryaim of this study was to test the effect of an early,
single application of CHX on the development of VAPafter traumatic injury.
Methods and Materials
Design and Sample
This randomized, 2-group (intervention and control)clinical trial evaluated the use of an early (within 12hours of intubation), single application of CHX (.12%solution) by swab to the oral cavity in trauma patients,on the development of VAP. The study was conductedat Virginia Commonwealth University Health System,in Richmond, Virginia, in its 983-bed medical centerhousing a level 1 trauma center. The subjects wererandomized to a treatment group or control group(usual care) using a block randomization scheme.Patients who were intubated in the emergencydepartment, in the field, or in route to the emergencydepartment or in the prehospital setting were eligiblefor enrollment if enrolled within 12 hours of intuba-tion. The 12-hour time period was chosen as a reason-able amount of time to obtain consent from the traumapatient’s legally authorized representative becausemost patients were sedated and unable to give consent.In addition, the first 12 hours of intubation is a clini-cally feasible time period for application of CHX, ratherthan closer to intubation time, when lifesaving inter-ventions are the priority. Patients were excluded if theyhad previous endotracheal tube placement in the last48 hours (because reintubation has been shown to bea significant risk factor for the development of VAP),14
a clinical diagnosis of pneumonia at the time of intu-bation, or burn injuries (because it is difficult todiscriminate inhalation injury from VAP). Patients whowere edentulous were also excluded because dentalplaque is a major target for the intervention.
CHX Intervention and Usual CareOne 5 mL dose of CHX solution (.12%) was applied tothe oral cavity by swab. Although 15 mL is the CHXrecommended dose for an oral rinse in alert patients,our pilot data15 and others16 show that as little as 2 mLis adequate to cover the oral cavity using a researcher-applied swabbing technique. In addition, aspiration ofthe solution in this obtunded population is a risk.Therefore, to ensure complete coverage while usinga minimum amount of solution, we chose a 5 mL dosein this protocol. By using a standardized protocol that

h e a r t & l ung 4 0 ( 2 0 1 1 ) e 1 1 5ee 1 2 2 e117
had been tested in our pilot study,15 all areas of the oralcavity were covered, including the anterior and poste-rior pharynx, gums, teeth, tongue, and buccal mucosa.In the pilot study,15 we tested the effect of in vitro CHXon VAP pathogens, Staphylococcus aureus, Streptococcuspneumoniae, and Pseudomonas Aeruginosa, and foundluxuriant growth of S. aureus and S. pneumoniae at 107
cfu/mL in the absence of CHX and complete inhibi-tion of growth of these organisms on plates treatedwith CHX. However, a single application of CHX did noteliminate growth of P. aeruginosa on blood agar plates;the extremely high initial titer of organisms (undilutedculture > 1010 cfu/mL) may have reduced the effec-tiveness of the drug in this experiment.
The control group received standard endotrachealintubation and oral care that did not include CHX. Afterintubation, ICU staff nurses provided oral comfort carefor all subjects (control and intervention groups) as pertheir usual practice. Data related to frequency and typeof oral comfort measures provided by ICU nursing staffwere documented from nurses’ entries on the ICU flowsheet. In a previous study of oral care practices,17 wefound that oral care practices were not differentbetween the 2 units where trauma patients werelocated (surgical trauma ICU and neuroscience ICU).Respiratory therapy equipment and care are alsostandardized across these 2 units.
Measurement of Key Variables
Development of VAPVAP is defined as pneumonia occurring in a mechan-ically ventilated patient that was neither present nordeveloping at the time of intubation; thus, clinicalevidence of VAP occurs 48 hours or more after intu-bation.18,19 A graded clinical tool was used in this studyto measure the development of VAP. The ClinicalPulmonary Infection Score (CPIS)20 consists of 6parameters: temperature, white blood cell count,tracheal secretions, oxygenation (calculated by PAO2/FIO2), chest radiograph (radiologist’s report), andtracheal aspirate culture. The tracheal secretions scoreis an estimation of the total secretions per day and iscalculated on the basis of the nurse’s estimate of thequantity of secretions from 0 to 4 (none, scant, small,moderate, large [as routinely documented on the ICUflowsheet]) for each aspiration and then totaled fora 24-hour period. The tracheal aspirate culture wasevaluated using a microscopic examination (Gramstain) and semiquantitative culture of endotrachealsecretions. Each parameter is assigned points (0-2), andthe final score ranges from 0 to 12 (VAP � 6). The CPISallows a description of the development of VAP overtime, enhancing the ability to describe the effect ofa single, early application of CHX.20-24
Additional Data CollectionData were also collected on additional VAP risk factorsto provide a comprehensive description of the studysample and equivalence of groups. On study
enrollment, subject demographics, Acute Physiology,Age, and Chronic Health Evaluation25 (APACHE III),Trauma‑Injury Severity Score (TRISS),26 and oral healthstatus (number of teeth decayed,missing, filled [DMF])27
were collected. The TRISS method26 is a standardapproach for evaluating the probability of traumasurvival and includes the Trauma Score, the InjurySeverity Score, and the patient’s age. Daily data up to 72hours after intubation included ventilatory support data(ventilator mode, rate, type of support, positive end-expiratory pressure, pressure support ventilation, FIO2,PAO2, and SAO2), enteral nutrition data (presence, route,rate, type of enteral nutrition, and highest daily gastricpH), time and number of mouth care interventions,presence of antibiotic, histamine blocker, proton-pumpinhibitors, antacid, and vasopressor therapy during thestudy period.
Procedures
Consent for study participation was obtained from thesubject’s legally authorized representative. All baselineclinical data were collected at the time of studyenrollment, including components for the CPIS. Endo-tracheal aspiration of sputum for culture and gramstain (for the CPIS) was obtained using a single-use,sterile catheter based on hospital procedure (nosaline was used) and when the patient required endo-tracheal tube suctioning as close to the required timeframe as possible. Subjects remained in the study for72 hours after intubation or until extubation if extu-bated before 72 hours. This time period was chosen onthe basis of the length of time of increased risk ofdevelopment of early VAP after intubation28 and dataconcerning the length of efficacy of a single CHXintervention indicating that an early, single dose ofCHX will likely have its greatest effect on the incidenceof early colonization and early VAP.28-31 Componentsfor the CPIS were collected at admission to the studyand at 48 and 72 hours after study enrollment.
Data Analysis
Comparison of baseline variables in the study groupswas done to assess group equivalence. The CPIS wasused for comparison of VAP in the 2 study groups. Anypatient with a CPIS score at 48 or 72 hours was includedin the analysis. The CPIS data were compared usinga random effects, repeated-measures analysis ofcovariance model. The model included effects forintervention group, time, group by time interaction,covariates of severity score (TRISS) and illness severity(APACHE III), and a random effect for patient. All modelassumptions, including normality of the residuals,equal variance of the residuals, and homogeneity ofthe covariate slopes, were tested.

Screenedn= 2369
h e a r t & l ung 4 0 ( 2 0 1 1 ) e 1 1 5ee 1 2 2e118
Results
Met inclusion criteria Did not meet inclusion criterian= 477 n=1892
1363 Not intubated/trach 253 Intubated > 24 hours 85 Less than 18 yrs old60 Reintubated in last 48 hrs76 Other/Prisoners29 Pneumonia on admission26 Facial trauma
Unable to obtain consent Consent obtainedn= 325 n=152
197 family not available76 other reasons 52 refused
Patients enrolled (n=152)Randomized to group assignment
n=7 lost to follow up or ineligible after enrollment 1 family withdrew subject2 had significant oral trauma; unable to evaluate1 transferred to another institution1 off the unit for extended time period1 intubated > 12 hours1 reintubated within last 48 hours
Subjects used in initial analysis (n=145)n=85 not included in final analysis
70 extubated prior to 48 hrs of intubation15 with incomplete data for CPIS (VAP)
Subjects used in final analysis (n=60)
Figure 1 e Study flow. CPIS, Clinical PulmonaryInfection Score; VAP, ventilator-associatedpneumonia.
Subjects
A total of 152 subjects were enrolled in the study, but 7were lost to follow-up (Figure 1). Of the remaining 145randomized patients, 71 and 74 were randomized tointervention and control groups, respectively. Seventypercent of the patients were male, and 60% were white.The mean age was 42.4 years (�18.2), mean APACHE IIIscorewas66.6 (�29.8),andaverageprobabilityofsurvival(TRISS) for the enrolled sample was 62%. Characteristicsof thesampleare shown inTable 1.Of these145 subjects,75 were still endotracheally intubated at 48 hours, with63 subjects having data at 72 hours. Reasons for attritionincluded extubation, missing CPIS values, and subjectdeath (Figure 1). As a result, there were 60 subjects whohad CPIS scores either at 48 (n¼ 56) or 72 hours (n¼ 48),and were thus part of the final analysis. Comparison ofthe 60 patients in this analysis sample with thoseenrolled but not included in the analysis (n ¼ 85) foundno significant differences in baseline variables (race, ICUtype, intubation process, intubation location, age, DMF,APACHE III, and TRISS) (Table 2). In addition, no differ-ence was found between the groups in the AbbreviatedInjuryScore, a subscaleof theTRISS that identifies injurylocation, for any injury site including chest and headinjuries.
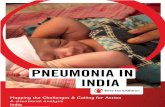
CHX Effect on VAPThere were no significant differences between groupsat study admission for any clinical characteristicexcept for a greater number of male patients in theintervention group (Table 2) and higher CPIS scores(5.36 (�2.53) for intervention versus 3.95 (�1.83) forcontrol, P ¼ .023). By controlling for the difference inCPIS on admission to the study, a significant treatmenteffect on CPIS both from admission to 48 hours (P ¼.020) and to 72 hours (P ¼ .027) was found. The least-square CPIS means and standard errors from therandom effect repeated-measures analysis are pre-sented in Table 2 and Figure 2. Figure 2 shows that theCPIS from the control group increased over time incontrast with CPIS from the intervention group, whichstayed steady over time. Although the CPIS differedbetween groups on study admission, this differencewas controlled for in the analysis by comparing thechange from admission to 48 and 72 hours. In thosesubjects without pneumonia (CPIS < 6) at baseline (n ¼39), 55.6% of the control patients (10/18) had developedVAP by 48 or 72 hours versus only 33.3% of the inter-vention patients (7/21).
Discussion
This randomized, clinical trial evaluated the use of anearly, single dose of CHX in reducing VAP in trauma
patients. The study subjects were representative of thetrauma population, being primarily male with a meanage of 43 years and a mean probability of traumasurvival of 62%.
A single, early application of CHX was found toreduce VAP in this sample of trauma patients whoremained intubated at 48 to 72 hours. The greatest VAPincidence occurs in trauma, burn, neurosurgical,2 andsurgical patients compared with other patient pop-ulations.32 In addition, patients who undergo traumaor surgery of the head, neck, thorax, or abdomen havebeen shown to be at increased risk.2,33,34 Therefore,reducing VAP in this high-risk population may signifi-cantly improve patient outcomes.
The pathogenesis of VAP is thought to resultprimarily from the leakage of contaminated oropha-ryngeal secretions around the endotracheal tube cuffand into the lung. Thus, reducing contamination oforal secretions is a reasonable prevention strategy. Inaddition, oral flora changes within the first 48 hours ofcritical illness from the usual predominance of strep-tococci to more potentially pathogenic microbes,which have been shown to contribute to VAP.31,35-37
Therefore, it is not surprising that an early interven-tion (within 24 hours) to reduce oral pathogenicbacteria as described reduces the incidence of VAP.However, this is the first evaluation of a single dose ofCHX in reducing VAP.

Table 1 e Characteristics of enrolled sample and patients with 48- or 72-hour data
Enrolled sample n ¼ 145 Patients with 48- or 72-hour data n ¼ 60
Gender, No. (%)Female 44 (30.34) 22 (36.67)Male 101 (69.66) 38 (63.33)
Race, No. (%)Asian 1 (.69) 1 (1.67)Black/African American 55 (37.93) 25 (41.67)Other 2 (1.38) 2 (3.33)White 87 (60.0) 32 (53.33)
ICU, No. (%)NSICU 54 (37.24) 23 (38.33)STICU 91 (62.76) 37 (61.67)
Intubation process, No. (%)Elective: no patient distress 21 (14.58) 7 (11.67)Emergent: immediate 81 (56.25) 33 (55.00)Urgent: non-elective 42 (29.17) 20 (33.33)
Age, mean � SD 42.36 � 18.22 43.27 � 17.90DMF, mean � SD 7.43 � 9.74 7.83 � 9.54Apache III, mean � SD 65.64 � 29.84 66.53 � 27.86TRISS, mean � SD .62 � .38 .61 � .38Length of intubation (d), mean � SD 5.05 � 5.82 9.71 � 6.27ICU LOS (d), mean � SD 12.53 � 14.56 19.97 � 17.58
NSICU, Neuroscience intensive care unit; STICU, surgical trauma intensive care unit; DMF, number of decayed missing filledteeth; TRISS, Trauma Injury Severity Score; ICU, intensive care unit; LOS, length of stay; SD, standard deviation.
h e a r t & l ung 4 0 ( 2 0 1 1 ) e 1 1 5ee 1 2 2 e119
Others have examined the effectiveness of repeatedoral care interventions in preventing VAP providedover time, either before or after endotracheal tubeintubation, both mechanical (toothbrushing) andpharmacologic (CHX, povidone-iodine). Two recentmeta-analyses have evaluated the effect of oraldecontamination on the incidence of VAP. Chan et al10
reviewed 11 trials with 3242 patients. Seven trialsdemonstrated significantly reduced VAP with oralapplication of antiseptics (CHX or povidone iodine),whereas 4 trials did not. When the results of the 11trials were pooled, VAP rates were lower in thosereceiving either method of oral decontamination,although duration of mechanical ventilation, ICUlength of stay, and mortality were not reduced byeither method.10 A meta-analysis by Chlebicki andSafdar11 to evaluate the efficacy of CHX in VAPprevention found that in 7 RCTs CHX significantlyreduced VAP (P ¼.02); the greatest benefit was found incardiac surgery patients.
In the only RCT to date that evaluated bothmechanical (toothbrushing) and pharmacologic (CHX)oral interventions implemented up to 7 days afterintubation, Munro et al12 found that in 249 subjects,CHX alone reduced VAP among subjects who werewithout pneumonia at baseline (P ¼ .0065), whereastoothbrushing had no effect on VAP. When subjectswith and without pneumonia at baseline wereanalyzed together, no effect of either CHX (P ¼ .6903) ortoothbrushing (P ¼ .95) was found. However, in thosewithout pneumonia at baseline, the CPIS increasedfrom day 1 to 3 in both the control and the CHX groups,but the amount of CPIS increase was greater in thecontrol group (2.0 increase) than in the CHX group
(.8 increase), showing a difference between groups ofCPIS increase of 10% (12-point CPIS scale), a potentiallyclinically significant difference.12 We found similardifferences between the groups in CPIS from baselineto 48 or 72 hours that also represent clinically mean-ingful differences in the CPIS. At 48 hours, the controlgroup’s CPIS increased from admission by .97, whereasthe CHX group’s CPIS decreased by .38 (>11% differencein CPIS). Similarly, at 72 hours the control group CPISincreased from admission to by 1.49, whereas the CHXgroup CPIS increase was only .11 (also >11% differencein CPIS).
Other procedures in which a tube is passed througha contaminated area into a sterile area (eg, insertion ofvascular lines, urinary tract catheters, chest tubes)include cleaning the area before tube insertion toreduce procedure-associated contamination. Duringthe endotracheal intubation procedure, organismsmay be dragged by the tube from the contaminatedoropharynx to the lung. Therefore, reducing thenumber of microorganisms in the mouth pre-intubation by application of CHX may also provideprotection against VAP. To date, however, evaluationof CHX use immediately before intubation has notbeen reported, although an RCT (clinicaltrials.govNCT00893763) is presently in process.
Although 152 patients were enrolled in this study,the number available for analysis was smaller. Becausewe did not focus our enrollment on patients who werelikely to be intubated for longer periods of time, butenrolled all patients who met the study criteria, themajority of subjects not included were extubatedbefore the first CPIS measurement at 48 hours. Inter-ventions to reduce the duration of mechanical

Table 2 e Characteristics of patients with 48- or 72-hour data by group
Control n ¼ 24 CHX n ¼ 36 P value
Gender, No. (%) .02Female 13 (54.17) 9 (25.0)Male 11 (45.83) 27 (75.0)
Race, No. (%) .92White 13 (54.17) 19 (52.78)Non-white 11 (45.83) 17 (47.22)
ICU, No. (%) .67NSICU 10 (41.67) 13 (36.11)STICU 14 (58.33) 23 (63.89)
Intubation process, No. (%) .81Elective: no patient distress 3 (12.5) 4 (11.11)Emergent: immediate 12 (50.0) 21 (58.33)Urgent: non-elective 9 (37.5) 11 (30.56)
Intubation location, No. (%) .84ED 8 (33.3) 15 (41.7)OR 5 (20.8) 5 (13.9)ICU 7 (29.2) 9 (25.0)In the field or in transport 4 (16.7) 7 (19.4)
Age, mean � SD 41.92 � 19.77 44.17 � 16.77 .65DMF, mean � SD 7.00 � 9.54 8.39 � 9.64 .58Apache III, mean � SD 60.46 � 23.45 70.69 � 30.14 .15TRISS, mean � SD .66 � .37 .58 � .39 .46Abbreviated Injury ScoreChest, mean � SD 2.17 � 1.74 2.59 � 1.65 .35Head/face, mean � SD 2.25 � 1.80 2.35 � 1.72 .83
CPIS at admission* 3.99 � .47 5.30 � .39 .020CPIS at 48 h* 4.96 � .48 4.92 � .39 .020y
CPIS at 72 h* 5.48 � .51 5.41 � .41 .027y
Length of intubation (d), mean � SD 9.79 � 6.62 9.66 � 6.14 .94ICU LOS (d), mean � SD 21.38 � 22.18 19.08 � 14.23 .66
CHX, Chlorhexidine; NSICU, neuroscience intensive care unit; STICU, surgical trauma intensive care unit; DMF, number ofdecayedmissing filled teeth; TRISS, Trauma Injury Severity Score; CPIS, Clinical Pulmonary Infection Score; LOS, length of stay;ED, emergency department; ICU, intensive care unit; OR, operating room; SD, standard deviation.*Adjusted means and standard errors from random effects, repeated-measures analysis of covariance model.yP value from comparing the group means from admission to 48 and 72 hours.
h e a r t & l ung 4 0 ( 2 0 1 1 ) e 1 1 5ee 1 2 2e120
ventilation have been a recent focus in critical care,and our medical center, similar to others, has seena reduction in days of intubation overall. Even thoughthe number analyzed was small, differences betweenthe intervention and control groups were still found.Although we did find a difference in the likelihood ofdeveloping VAP, we did not find any difference induration of mechanical ventilator or ICU days betweenthe groups.
At the time this 3-year study began, the CPIS was anacceptedmethod of evaluating VAP, but since that time2 authors have reported conflicting findings in thecritically ill. Because the pulmonary inflammationassociated with thoracic injury or sepsis may not beable to be differentiated from pneumonia, Croce et al38
compared the CPIS in 158 trauma patients who hada CPIS calculated at the time of bronchoscopy withbronchial alveolar lavage. VAP required> 105 colonies/mLon quantitative bronchial alveolar lavage for diagnosis.Patients with < 105 colonies/mL were diagnosed withsystemic inflammatory response syndrome. Theyfound, using a CPIS > 6 as the threshold for VAP,a sensitivity of 61% and a specificity of 43%. However,
most recently, Pelosi et al39 investigated the role of theCPIS in the detection VAP in 58 patients with severebrain injury. They found that the CPIS increased at theday of VAP diagnosis, compared with study entry(median, 6.6 vs 1.5, P< .001; sensitivity, 97%; specificity,100%), whereas other serum inflammatory markers(C-reactive protein and serum amyloid A) did notchange. They also reported that deterioration inoxygenation and changes in tracheal secretions werethe main determinants of CPIS changes and suggestedthat CPIS may help detect the patients with early VAP.
A more recent systematic review of VAP diagnosis40
described major limitations of the literature validatingCPIS for diagnosing VAP, that is, bronchial alveolarlavage culture is not a true gold standard, the CPIScalculation has been modified by some authors,different cutoff points were used to diagnose VAP, andsome interobserver variation exists.40 Tomanage theseissues in our study, we used the CPIS as originallydescribed by Pugin et al,20 and 1 observer (pulmonolo-gist), who was blinded to the subject’s group assign-ment, evaluated all chest radiographs. Because of theconcern about the use of the CPIS in trauma patients,

Admission 24 hours 48 hours 72 hours
SIPC
3.0
3.5
4.0
4.5
5.0
5.5
6.0
6.5
ControlCHX
Adjusted or Least Square Means and standard error bars*
*From the Figure, it can be seen that the CPIS from the control group rose over time in contrast to CPIS from the intervention group which stayed steady over time. Although the CPIS differed between groups on study admission, this difference was controlled for in the analysis by comparing the change from Admission to 48 and 72 hours. A significant treatment effect on CPIS both from admission to 48 hrs (p=0.020) and to 72 hrs (p=0.027) was found.
Figure 2 e CPIS means from repeated-measuresanalysis. CHX, Chlorhexidine; CPIS, ClinicalPulmonary Infection Score.
h e a r t & l ung 4 0 ( 2 0 1 1 ) e 1 1 5ee 1 2 2 e121
we also compared the type of injury between the 2groups and found no difference in the incidence ofchest or head injury (Abbreviated Injury Score).
However, because it is difficult to distinguish thepulmonary inflammation of sepsis from VAP, it mayalso be difficult to attribute all the differences in CPIS tothe development of VAP alone. Therefore, replicationof this RCT of an early application of CHX may bewarranted.
Conclusions
The use of an early, single application of CHX to theoral cavity may significantly reduce VAP in traumapatients. Because compliance with repeated daily oralcare interventions may be difficult, especially in thefirst 24 to 48 hours of critical illness when other life-threatening priorities may take preference, the use ofan easily administered, single oral swab applicationmay be a useful alternative to reduce VAP in themechanically ventilated population. This interventionis particularly attractive because it is technicallysimple to perform, low cost, and rapidly administered.However, the results of this single study should bereplicated in a large, multicenter RCT.
References
1. Tablan OC, Anderson LJ, Arden NH, Breiman RF,Butler JC, McNeil MM. Guideline for prevention ofnosocomial pneumonia. The Hospital InfectionControl Practices Advisory Committee. Am J InfectControl 1994;22:247-92.
2. Chevret S, Hemmer M, Carlet J, Langer M. Incidenceand risk factors of pneumonia acquired in intensivecare units. Results from amulticenter prospectivestudy on 996 patients. European Cooperative Groupon Nosocomial Pneumonia. Intensive Care Med 1993;19:256-64.
3. Kappstein I, Schulgen G, Beyer U, Geiger K,Schumacher M, Daschner FD. Prolongation of hospitalstay and extra costs due to ventilator- associatedpneumonia in an intensive care unit. Eur J ClinMicrobiol Infect Dis 1992;11:504-8.
4. Haley RW, Schaberg DR, Crossley K, Von Allmen SD,McGowan JE Jr. Extra charges and prolongation ofstay attributable to nosocomial infections:a prospective interhospital comparison. Am J Med1981;70:51-8.
5. Kollef MH, Wragge T, Pasque C. Determinants ofmortality and multiorgan dysfunction in cardiacsurgery patients requiring prolonged mechanicalventilation. J Hosp Infect 1995;107:1395-401.
6. Rodriguez JL, Gibbons KJ, Bitzer LG, Dechert RE,Steinberg SM, Flint LM. Pneumonia: incidence, riskfactors, and outcome in injured patients. J Trauma1991;31:907-12.
7. Craven DE, Steger KA. Nosocomial pneumonia inmechanically ventilated adult patients: epidemiologyand prevention in 1996. Semin Respir Infect 1996;11:32-53.
8. Fourrier F, Duvivier B, Boutigny H, Rourrel-Delvallez M, Chopin C. Colonization of dental plaque:a source of nosocomial infections in intensive careunit patients. Crit Care Med 1998;26:301-8.
9. Scannapieco FA, Stewart EM, Mylotte JM.Colonization of dental plaque by respiratorypathogens in medical intensive care patients. CritCare Med 1992;20:740-5.
10. Chan EY, Ruest A, Meade MO, Cook DJ. Oraldecontamination for prevention of pneumonia inmechanically ventilated adults: systematic reviewand meta-analysis. BMJ 2007;334:889.
11. Chlebicki MP, Safdar N. Topical chlorhexidinefor prevention of ventilator-associated pneumonia:a meta-analysis. Crit Care Med 2007;35:595-602.
12. Munro CL, Grap MJ, Jones DJ, McClish DK, Sessler CN.Chlorhexidine, toothbrushing, and preventingventilator-associated pneumonia in critically illadults. Am J Crit Care 2009;18:428-37.
13. Edwards JR, Peterson KD, Mu Y, Banerjee S, Allen-Bridson K, Morrell G, et al. National Healthcare SafetyNetwork (NHSN) report: data summary for 2006through 2008, issued December 2009. Am J InfectControl 2009;37:783-805.
14. Cook DJ, Walter SD, Cook RJ, Griffith LE, Guyatt GH,Leasa D, et al. Incidence of and risk factors forventilator-associated pneumonia in critically illpatients. Ann Intern Med 1998;129:433-40.
15. Grap MJ, Munro CL, Elswick RK Jr, Sessler CN,Ward KR. Duration of action of a single, early oralapplication of chlorhexidine on oral microbial flora inmechanically ventilated patients: a pilot study. HeartLung 2004;33:83-91.
16. Francis JR, Hunter B, Addy M. A comparison of threedelivery methods of in handicapped children. I.Effects on plaque, gingivitis, and toothstaining.J Periodontol 1987;58:451-5.
17. Grap MJ, Munro CL, Ashtiani B, Bryant S. Oral careinterventions in critical care: frequency anddocumentation. Am J Crit Care 2003;12:113-8.

h e a r t & l ung 4 0 ( 2 0 1 1 ) e 1 1 5ee 1 2 2e122
18. Kollef MH. The prevention of ventilator associatedpneumonia. N Engl J Med 1999;340:627-34.
19. Meduri GU. Diagnosis of ventilator-associatedpneumonia. Infect Dis Clin North Am 1993;7:295-329.
20. Pugin J, Auckenthaler R, Mili N, Janssens JP, Lew PD,Suter PM. Diagnosis of ventilator-associatedpneumonia by bacteriologic analysis ofbronchoscopic and nonbronchoscopic “blind”bronchoalveolar lavage fluid. Am Rev Respir Dis 1991;143:1121-9.
21. Papazian L, Thomas P, Garbe L, Guignon I, Thirion X,Charrel J, et al. Bronchoscopic or blind samplingtechniques for the diagnosis of ventilator-associatedpneumonia. Am J Res Crit Care Med 1995;152:1982-91.
22. Abele HM, Dauber A, Bauernfeind A, Russwurm W,Seyfarth MI, Gleich P, et al. Decrease in nosocomialpneumonia in ventilated patients by selectiveoropharyngeal decontamination (SOD). IntensiveCare Med 1997;23:187-95.
23. Cook D, Guyatt G, Marshall J, Leasa D, Fuller H, Hall R,et al. A comparison of sucralfate and ranitidine forthe prevention of upper gastrointestinal bleedingin patients requiring mechanical ventilation.Canadian Critical Care Trials Group. N Engl J Med1998;338:791-7.
24. Singh N, Gayowski T, Wagener MM, Marino IR.Pulmonary infiltrates in liver transplant recipientsin the intensive care unit. Transplantation 1999;67:1138-44.
25. Knaus WA, Wagner DP, Draper EA, Zimmerman JE,Bergner M, Bastos PG, et al. The APACHE III prognosticsystem. Risk prediction of hospital mortality forcritically ill hospitalized adults. Am J Respir Crit CareMed 1991;100:1619-36.
26. Boyd CR, Tolson MA, Copes WS. Evaluating traumacare: the TRISS method. Trauma Score and the InjurySeverity Score. J Trauma 1987;27:370-8.
27. Munro CL, Grap MJ, Jablonski R, Boyle A. Oral healthmeasurement in nursing research: state of thescience. Biol Res Nurs 2006;8:35-42.
28. Schwartz SN, Dowling JN, Benkovic C, DeQuittner-Buchanan M, Prostko T, Yee RB. Sources of gram-negative bacilli colonizing the tracheae of intubatedpatients. J Infect Dis 1978;138:227-31.
29. van Lunsen DM, de Soet JJ, Weerheijm KL, Groen HJ,Veerkamp JS. Effects of dental treatment and singleapplication of a 40% varnish on mutans Streptococciin young children under intravenous anaesthesia.Caries Res 2000;34:268-74.
30. Carret L, Reverdy ME, Lafforgue C, Falson F,Fleurette J, Freney J. Kinetics of chlorhexidine on
intact skin following a single application. Pathol Biol1997;45:737-40.
31. Cardenosa Cendrero JA, Sole-Violan J, Bordes BA,Noguera CJ, Arroyo FJ, Saavedra SP, et al. Role ofdifferent routes of tracheal colonization in thedevelopment of pneumonia in patients receivingmechanical ventilation. Am.J.Respir.Crit. Care Med1999;116:462-70.
32. NNIS. National Nosocomial Infections Surveillance(NNIS) System Report, Data Summary from October1986-April 1998. Washington, DC: U.S. Department ofHealth and Human Services; 1998. 1-25.
33. Celis R, Torres A, Gatell JM, Almela M, Rodriguez-Roisin R, Agusti-Vidal A. Nosocomial pneumonia.A multivariate analysis of risk and prognosis. J HospInfect 1988;93:318-24.
34. George DL. Epidemiology of nosocomial pneumoniain intensive care unit patients. Clin Chest Med 1995;16:29-44.
35. Garrouste OM, Chevret S, Arlet G, Marie O,Rouveau M, Popoff N, et al. Oropharyngeal or gastriccolonization and nosocomial pneumonia in adultintensive care unit patients. A prospective studybased on genomic DNA analysis. Am J Respir Crit CareMed 1997;156:1647-55.
36. Bonten MJ, Bergmans DC, Ambergen AW, deLeeuw PW, van der Geest S, Stobberingh EE, et al. Riskfactors for pneumonia, and colonization ofrespiratory tract and stomach in mechanicallyventilated ICU patients. Am J Res Crit Care Med 1996;154:1339-46.
37. Ewig S, Torres A, el-Ebiary M, Fabregas N,Hernandez C, Gonzalez J, et al. Bacterial colonizationpatterns in mechanically ventilated patients withtraumatic and medical head injury. Incidence, riskfactors, and association with ventilator-associatedpneumonia. Am J Respir Crit Care Med 1999;159:188-98.
38. Croce MA, Swanson JM, Magnotti LJ, Claridge JA,Weinberg JA, Wood GC, et al. The futility of theclinical pulmonary infection score in trauma patients.J Trauma 2006;60:523-7.
39. Pelosi P, Barassi A, Severgnini P, Gomiero B, Finazzi S,Merlini G, et al. Prognostic role of clinical andlaboratory criteria to identify early ventilator-associated pneumonia in brain injury. Am J RespirCrit Care Med 2008;134:101-8.
40. Rea-Neto A, Youssef NC, Tuche F, Brunkhorst F,Ranieri VM, Reinhart K, et al. Diagnosis of ventilator-associated pneumonia: a systematic review of theliterature. Crit Care 2008;12:R56.