Early Intervention to Preempt Major Depression Among Older Black and White Adults
9
Early Intervention to Preempt Major Depression Among Older Black and White Adults Charles F. Reynolds, III, M.D. Stephen B. Thomas, Ph.D. Jennifer Q. Morse, Ph.D. Stewart J. Anderson, Ph.D. Steven Albert, Ph.D. Mary Amanda Dew, Ph.D. Amy Begley, M.A. Jordan F. Karp, M.D. Ariel Gildengers, M.D. Meryl A. Butters, Ph.D. Jacqueline A. Stack, M.S.N. John Kasckow, M.D., Ph.D. Mark D. Miller, M.D. Sandra C. Quinn, Ph.D. Objective: The study objective was to assess the efficacy of problem- solving therapy for primary care (PST-PC) for preventing episodes of major depression and mitigating depressive symptoms of older black and white adults. The comparison group received dietary coaching. Methods: A total of 247 participants (90 blacks, 154 whites, and three Asians) with subsyndromal depressive symptoms were recruited into a randomized depression prevention trial that compared effects of individually delivered PST-PC and dietary coaching on time to major depressive episode and level of depressive symptoms (Beck Depression Inventory) over two years. Cumulative intervention time averaged 5.526.0 hours in each study arm. Results: The two groups did not differ significantly in time to major de- pressive episodes, and incidence of such episodes was low (blacks, N=8, 9%; whites, N=13, 8%), compared with published rates of 20%–25% over one year among persons with subsyndromal symptoms and receiving care as usual. Participants also showed a mean decrease of 4 points in de- pressive symptoms, sustained over two years. Despite greater burden of depression risk factors among blacks, no significant differences from whites were found in the primary outcome. Conclusions: Both PST-PC and dietary coaching are potentially effective in protecting older black and white adults with subsyndromal depressive symptoms from developing episodes of major depression over two years. Absent a control for con- current usual care, this conclusion is preliminary. If confirmed, both interventions hold promise as scalable, safe, nonstigmatizing interventions for delaying or preventing episodes of major depression in the nation’s increasingly diverse older population. (Psychiatric Services in Advance, March 17, 2014; doi: 10.1176/appi.ps.201300216) M ajor depressive disorder is prevalent, with adequate treatment difficult to ac- cess and only partially successful in averting years lived with disability (1). In later life, particularly, major de- pressive disorder has public health im- portance because of its prevalence and associated disability, morbidity, health care costs, and mortality, especially among primary care outpatients and people from racial-ethnic minority groups (2). Major depressive disorder is also a risk factor for dementia (3). The limitations of treatment underscore the need to develop public health– relevant approaches to prevent depres- sion and its downstream consequences for high-risk older adults. Elderly adults who are from racial- ethnic minority groups show partic- ular vulnerability to common mental illnesses. Older blacks, for example, endorse significantly greater depressive symptoms than whites (4) and bear a higher burden of risk of depression rooted in social and medical disadvan- tages (5): more disability, greater health risks (including obesity, smoking, and substance use disorders), lower edu- cation attainment, and lower likeli- hood of marriage (6). Blacks also have a higher incidence of dementia (7), and preventing depression may delay or prevent dementia (8). In addition, inequalities in the utilization of mental health services and the treatment rate Dr. Reynolds, Dr. Morse, Dr. Dew, and Ms. Begley through Dr. Miller are with the Department of Psychiatry, University of Pittsburgh School of Medicine (Western Psychiatric Institute and Clinic), Pittsburgh, Pennsylvania (e-mail: [email protected]). Dr. Kasckow is also with the Department of Behavioral Health, Veterans Affairs Pittsburgh Health Care System. Dr. Thomas and Dr. Quinn are with the Center for Health Equity, University of Maryland, College Park. Dr. Anderson is with the Department of Biostatistics, University of Pittsburgh Graduate School of Public Health. Dr. Albert is with the Depart- ment of Behavioral and Community Health Science, University of Pittsburgh. PSYCHIATRIC SERVICES IN ADVANCE 1
Transcript of Early Intervention to Preempt Major Depression Among Older Black and White Adults

Early Intervention to PreemptMajor Depression AmongOlder Black andWhite AdultsCharles F. Reynolds, III, M.D.Stephen B. Thomas, Ph.D.Jennifer Q. Morse, Ph.D.Stewart J. Anderson, Ph.D.Steven Albert, Ph.D.Mary Amanda Dew, Ph.D.Amy Begley, M.A.
Jordan F. Karp, M.D.Ariel Gildengers, M.D.Meryl A. Butters, Ph.D.Jacqueline A. Stack, M.S.N.John Kasckow, M.D., Ph.D.Mark D. Miller, M.D.Sandra C. Quinn, Ph.D.
Objective: The study objective was to assess the efficacy of problem-solving therapy for primary care (PST-PC) for preventing episodes ofmajor depression and mitigating depressive symptoms of older black andwhite adults. The comparison group received dietary coaching.Methods:Atotal of 247 participants (90 blacks, 154 whites, and three Asians) withsubsyndromal depressive symptoms were recruited into a randomizeddepression prevention trial that compared effects of individually deliveredPST-PC and dietary coaching on time to major depressive episode andlevel of depressive symptoms (BeckDepression Inventory) over two years.Cumulative intervention time averaged 5.526.0 hours in each study arm.Results: The two groups did not differ significantly in time to major de-pressive episodes, and incidence of such episodes was low (blacks, N=8,9%; whites, N=13, 8%), compared with published rates of 20%–25% overone year among persons with subsyndromal symptoms and receiving careas usual. Participants also showed a mean decrease of 4 points in de-pressive symptoms, sustained over two years. Despite greater burden ofdepression risk factors among blacks, no significant differences fromwhites were found in the primary outcome.Conclusions:Both PST-PC anddietary coaching are potentially effective in protecting older black andwhite adults with subsyndromal depressive symptoms from developingepisodes of major depression over two years. Absent a control for con-current usual care, this conclusion is preliminary. If confirmed, bothinterventions hold promise as scalable, safe, nonstigmatizing interventionsfor delaying or preventing episodes of major depression in the nation’sincreasingly diverse older population. (Psychiatric Services in Advance,March 17, 2014; doi: 10.1176/appi.ps.201300216)
Major depressive disorder isprevalent, with adequatetreatment difficult to ac-
cess and only partially successful inaverting years lived with disability (1).In later life, particularly, major de-pressive disorder has public health im-portance because of its prevalence andassociated disability, morbidity, healthcare costs, and mortality, especiallyamong primary care outpatients andpeople from racial-ethnic minoritygroups (2). Major depressive disorderis also a risk factor for dementia (3).The limitations of treatment underscorethe need to develop public health–relevant approaches to prevent depres-sion and its downstream consequencesfor high-risk older adults.
Elderly adults who are from racial-ethnic minority groups show partic-ular vulnerability to common mentalillnesses. Older blacks, for example,endorse significantly greater depressivesymptoms than whites (4) and bear ahigher burden of risk of depressionrooted in social and medical disadvan-tages (5): more disability, greater healthrisks (including obesity, smoking, andsubstance use disorders), lower edu-cation attainment, and lower likeli-hood of marriage (6). Blacks also havea higher incidence of dementia (7),and preventing depression may delayor prevent dementia (8). In addition,inequalities in the utilization of mentalhealth services and the treatment rate
Dr. Reynolds, Dr. Morse, Dr. Dew, and Ms. Begley through Dr. Miller are with theDepartment of Psychiatry, University of Pittsburgh School of Medicine (WesternPsychiatric Institute and Clinic), Pittsburgh, Pennsylvania (e-mail: [email protected]).Dr. Kasckow is also with the Department of Behavioral Health, Veterans Affairs PittsburghHealth Care System. Dr. Thomas and Dr. Quinn are with the Center for Health Equity,University of Maryland, College Park. Dr. Anderson is with the Department of Biostatistics,University of Pittsburgh Graduate School of Public Health. Dr. Albert is with the Depart-ment of Behavioral and Community Health Science, University of Pittsburgh.
PSYCHIATRIC SERVICES IN ADVANCE 1

for depression continue to grow (9) andare compounded by barriers of trust,stigma, and shortages of providers whohave the same race-ethnicity as theirpatients (10).Mildly symptomatic individuals are
at highest risk of developing episodesof major depression (11–13). Bereave-ment, social isolation, sleep distur-bance, disability, previous depression,and female gender are important riskfactors for depression among oldercommunity residents (14). Per the In-stitute of Medicine, focusing depres-sion prevention for mildly symptomaticpersons (“indicated” prevention) mayhave the greatest efficiency from a pub-lichealthperspective,witha lowernum-ber needed to treat to prevent oneincident case (14,15).The dearth of randomized controlled
prevention trials with older adults,however, raises the question of whichinterventions to use. Older patients,especially blacks, prefer psychosocialinterventions to antidepressant medi-cation for treatment of depression (16).Moreover, antidepressant medications,while effective in severe depression,appear to show minimal benefit rela-tive to placebo in mild depression (17),although the notion that mild depres-sion does not respond to antidepres-sant medication is not settled (18).Problem-solving therapy for primary
care (PST-PC) is a brief interventionwith antidepressant treatment efficacythat is deliverable by non–mental healthclinicians in primary care (19,20). Itdelays or prevents depression of olderadults with macular degeneration (21)and after stroke (22). The antidepres-sant and depression-preventing effectsof PST-PCmay bemediated by a seven-step approach to better problem solv-ing (including behavioral activation),leading to improved self-efficacy andresilience, together with reductionin learned helplessness (23).In designing this trial, we sought
a culturally acceptable, active com-parison intervention to control fornonspecific effects of time and atten-tion inherent in PST-PC. The choice ofcoaching in healthy dietary practicesgrew out of field data collected from1,244 black participants in the HealthyBlack Family Project at the Universityof Pittsburgh’s Graduate School ofPublic Health, in which many of the
respondents with high levels of stresswere either overweight (45%) or obese(50%). Our Community ResearchAdvisory Board endorsed the choiceof dietary coaching as an active controlarm and as a culturally acceptablestrategy consistent with clinical equi-poise and one that would facilitaterecruitment of black participants(many of whom were not receivingprimary care services) more easily thantreatment as usual or a no-interventioncontrol.
Our primary study hypothesis wasthat PST-PC would reduce incidentepisodes of major depression by 50%over two years compared with dietarycoaching. Our second hypothesis wasthat participants in PST-PC wouldreport more and better sustained de-cline in depressive symptoms com-pared with dietary coaching.
MethodsInformed consent, screening,assessment, and enrollmentThe protocol was overseen by a datasafety monitoring board and reviewedand approved annually by the Univer-sity of Pittsburgh’s Institutional Re-view Board.
Beginning in September 2006, andextending over a period of 42 months,we enrolled a sample of 247 partic-ipants: 154 (62%) whites, 90 (36%)blacks, and three (1%) Asians. To re-cruit participants with subsyndromaldepressive symptoms, we screenedindividuals who were 50 or older,using the Center for Epidemiolog-ical Studies Depression Scale (CES-D) (24) and requiring a score of 11or greater and an absence of a majordepressive episode during the pre-vious year. We administered theStructured Clinical Interview forDSM-IV Disorders (SCID) (25) torule out current major depressivedisorder. Participants were also re-quired to have a Mini-Mental Statescore of 24 or higher, to excludeprobable dementia (26). An episodeof alcohol or other substance usedisorder within the past 12 monthsand a history of bipolar disorder, otherpsychotic disorder, or neurodegenera-tive disorder also were conditions forstudy exclusion. Recruitment pathwaysto study participation differed forblacks and whites, largely reflecting
the different settings in which help-seeking takes place. For example, themajor source for recruiting white par-ticipants was referrals from primarycare practices, whereas for blackparticipants the major source wascommunity-based agencies, includ-ing black churches.
RandomizationA project statistician randomly assignedparticipants to either the PST-PC ordietary coaching condition, usingpermuted-block randomization stratifiedby the presence or absence of a historyof major depression (because a pasthistory is a strong risk factor for futureepisodes) and by site of recruitment—primary care, community agencies, orspecialty mental health care. Random-ization accounted for the differentsociodemographic characteristics ofparticipants (including race), recruit-ment site, and the possibility that re-cruitment site could influence rates ofoccurrence of major depressive epi-sodes. Random assignment was com-municated by the statistician to theproject co-coordinator but concealedfrom independent evaluators. Therewere no instances of breaking the blind.
InterventionsBoth interventions—PST-PC and di-etary coaching—had similar numbersof sessions (six to eight sessions) andsemiannual boosters (lasting 30–45minutes at three, nine, and 15months).Both interventions were provided byinterventionists in individual sessions.Interventionists were trained in ourNational Institute of Mental Health–sponsored center for depression pre-vention and treatment of older adults.Both interventions included homeworkassignments and monitoring of adher-ence, and they focused on concernsidentified by each participant.
The experimental group receivedmanualized PST-PC. To teach themodel to participants, the first sessionlasted an hour, and the subsequentsessions lasted 30 minutes each (totaltime 4.5561.46 hours of PST-PC and3.9262.19 hours of dietary coaching).
Participants in the control condi-tion received coaching in healthyeating practices. Using a manualizededucational intervention, interven-tionists reviewed general nutrition
2 PSYCHIATRIC SERVICES IN ADVANCE

guidelines, including the U.S. De-partment of Agriculture food pyra-mid; helped with preparing weeklymenus and grocery lists; saved cou-pons for food items; and reviewedfood intake since last visit. Topicsdiscussed included access to healthyfood, cost of food, meal preparation,culturally specific and acceptablefoods, and specific topics raised byparticipants.Interventionists were six white social
workers and mental health nurses. Thesame interventionists delivered bothPST-PC and dietary coaching, to avoidconfounding intervention with clini-cian effects. To ensure fidelity of in-tervention delivery, we randomlyselected 20% of audiotapes of inter-vention sessions for evaluation, and wesupervised groups and gave one-on-one feedback to the interventionists.PST-PC adherence ratings assessingquality were completed by the in-tervention supervisor, who used twosessions for each case, an early session(sessions 1–3) and a later session(sessions 4–8). Once ratings werecompleted, corrective feedback wasprovided. Most sessions (N=41 of 56,73%) of both study conditions wererated as adherent. A treatment fidelityscale was also developed to documentthe absence of intervention contami-nation effects. With this scale, ratingswere completed on seven consecutiveminutes of the session, starting fiveminutes into the session. Two ratersindependently rated the sessions forthe presence of PST-PC and dietarycoaching elements. Using blind rat-ings, we found the two interventions tobe highly discriminable (k=.91), eventhough they were delivered by thesame interventionists. Interventionswere delivered primarily face to facein settings the participants chose: pri-mary care offices, community agen-cies, and participants’ homes. About9% (N=173 of 1,884) of sessions weredelivered over the telephone.
OutcomesThe primary outcome was incidentepisodes of major depression, per theSCID section for mood disorders(25), administered by independentevaluators blind to randomized in-tervention assignment at baseline(time 1), at the end of intervention,
and every three months subsequentlyuntil 24 months, for a total of ninetime points. Also assessed at the sametime points were levels of depressivesymptoms (Beck Depression Inven-tory [BDI]) (27) and health-relatedquality of life (Medical OutcomesStudy 12-Item Short Form) (28).Other domains of assessment encom-passed coexisting general medicalillness per total score on the Cumu-lative Illness Rating Scale for Geri-atrics (CIRS-G) (29), problem-solvingskills (Social Problem Solving Inven-tory [SPSI], a self-report measure ofproblem-solving style) (30), and anx-iety (Brief Symptom Inventory [BSI])(31). (Outcomes other than depres-sion will be reported elsewhere.)
Data analysisOutcomes analyses were conductedby study statisticians operating in-dependently of the investigators andblind to study arm. All analyses wereperformed on the basis of the intent-to-treat principle so that comparisonswere made according to the assignedintervention groups. All data wereexamined for normality before theanalyses; transformations were usedwhere necessary. Baseline demo-graphic and clinical differencesbetween participants by randomassignment and by race were testedwith t tests for continuous variablesand chi square tests with continuitycorrection for categorical variables.Kaplan-Meier curves were used toillustrate the effects of PST-PC anddietary coaching on incidence ofmajor depressive episodes. Formalinferences between groups weremade with log-rank tests if five ormore events were expected in botharms or with Fisher’s exact testsotherwise. Multivariate Cox propor-tional hazard models were used toexplore the strongest predictors ofmajor depressive disorder.
To compare depression levels (BDI),we first tested whether baseline dif-ferences were present between in-tervention groups. In cases where nodifferences were apparent, we thenused a mixed-models approach tocompare the trajectories of the vari-ables over time between the groups. Ifthere was a significant baseline differ-ence between groups, we used the
baseline value as a covariate in thefitted models. To characterize andcompare the trajectories betweenPST-PC and dietary coaching, weused mixed models examining inter-vention, time, time squared, and thepotential interactions among inter-vention and the time variables. Inanalyses involving race, we includedrace and the interactions among raceand other variables. We documentedreasons for missing data and handledmissing data using mixed-model anal-yses. Formal tests were conducted todetermine whether the missingness ofdata was random.
To examine effects of problemsolving on depressive symptoms, weconducted exploratory analyses andincluded SPSI score as a time-varyingcovariate in the whole-group longitu-dinal model. To examine the possibil-ity of bidirectional relationship of SPSIscore and depressive symptoms, wealso examined SPSI scores as outcome,using the same model of treatment,time, and treatment3 time effects butincluding BDI scores as a time-varyingcovariate.
ResultsThe groups did not differ in socio-demographic, general health, cogni-tive, mental health, and recruitmentpathways (Table 1). Primary care re-ferrals provided the main source ofenrollment, followed by recruitmentin community-based agencies and byself-referral in response to print andon-air advertisements.
Participant descriptive dataBlack participants differed signifi-cantly from whites in having feweryears of formal education, greaterlikelihood of not living with a spouseor partner, less likelihood of beingemployed, lower household income,greater rate of obesity, lower generalhealth–related quality of life, lowerscores on cognitive screening mea-sures, and lower rate of current anxietydisorder (Table 2). Despite the greaterburden of social and medical disadvan-tages, black participants did not differfrom whites on preintervention mea-sures of emotional distress (CES-D),depression (BDI), or anxiety (BSI) andproportion with a history of majordepressive disorder. Participants were
PSYCHIATRIC SERVICES IN ADVANCE 3

Table 1
Characteristics of older adults receiving problem-solving therapy for primary care (PST-PC) or dietary coaching
PST-PC(N=125)
Dietary coaching(N=122)
Characteristic Total N N % N % Test statistic df p
SociodemographicAge (M6SD years) 247 65.8610.9 65.4611.0 t=.28 245 ..778Female 247 86 69 90 74 x2=.52 1 ..470Race 247Asian/Pacific Islander 2 2 1 1 ..541a
Black 42 34 48 39White 81 65 73 60
Education (M6SD years) 247 14.462.8 14.762.7 t=–.78 245 ..436Marital statusCohabiting or married 247 58 46 56 46 x2=1.68 3 ..640Divorced or separated 21 17 27 22Never married 17 14 12 10Widowed 29 23 27 22
Employed 247 52 42 47 39 x2=.13 1 ..716Median household income (M6SD $) 243 50,511625,787 45,545621,599 t=1.62 241 ..105
General healthCumulative Illness RatingScale (M6SD score)Totalb 245 7.763.6 8.064.2 t=–.60 243 ..550Countc 246 4.962.1 5.062.4 t=–.48 244 ..628Heart and vasculard 246 2.061.5 1.961.5 t=.60 244 ..549
Body mass indexTotal (M6SD) 245 30.566.6 30.667.3 t=–.07 243 ..942$30 points (obesity indicator) 245 57 46 62 52 x2=.68 1 ..411
Rand Health Status Inventory (M6SD)e
Physical health component 207 41.3611.8 42.9611.8 t=–.95 205 ..342Mental health component 207 42.469.8 43.769.0 t=–1.04 205 ..297
Cognition: Mini-Mental Status Examination(M6SD)f 246 28.161.7 28.461.5 t=–1.38 244 ..170
Mental healthHamilton Rating Scale for Depression (M6SD)g 246 11.664.0 10.863.5 t=1.68 244 ..094Center for Epidemiologic Studies DepressionScale (M6SD)h 246 21.968.3 20.467.5 t=1.48 244 ..141
Beck Depression Inventory (M6SD)i 233 11.165.9 9.965.5 t=1.60 231 ..110Brief Symptom Inventory anxiety (M6SD)j 235 .56.5 .56.5 t=–.16 233 ..875History of major depressive disorder 41 33 42 34 x2=.02 1 ..892History of anxiety disorder 27 22 25 20 x2=.00 1 ..954Current anxiety disorder 27 22 33 27 x2=.72 1 ..395Social Problem Solving Inventory (M6SD)k
Total 214 99.8613.7 103.1613.0 t=–1.82 212 ..070Positive problem orientation 229 95.8616.4 99.8614.7 t=–1.92 227 ..056
Referral sourceCommunity outreachl 22 18 24 20 x2=3.54 5 ..618Mental health specialist 5 4 5 4Primary care 53 43 57 47Research (research program or registry) 13 11 12 10Self-referred (media, brochure, presentation,peer educator) 23 19 13 11
Word of mouth 7 6 10 8
a Fisher exact p value reportedb Possible scores range from 0 to 52, with higher scores indicating more medical burden.c Possible scores range from 0 to 13, with higher scores indicating more medical burden.d Possible scores range from 0 to 8, with higher scores indicating more medical burden.e Possible scores range from 0 to 100, with higher scores indicating better health.f Possible scores range from 0 to 30, with higher scores indicating more cognitive impairment.g Possible scores range from 0 to 52, with higher scores indicating more depressive symptoms.h Possible scores range from 0 to 60, with higher scores indicating more depressive symptoms.i Possible scores range from 0 to 63, with higher scores indicating more depressive symptoms.j Possible scores range from 0 to 4, with higher scores indicating more anxiety symptoms.k Possible scores for Total range from 29 to 139 and those for positive problem orientation range from 52 to 135, with higher scores on each scaleindicating better problem solving.
l Referrals came from the Kingsley Center, Healthy Black Family Project, Healthy Hearts and Souls, grocery store screening, or a barbershop.
4 PSYCHIATRIC SERVICES IN ADVANCE

Table 2
Characteristics of older adults receiving problem-solving therapy for primary care (PST-PC) or dietary coaching, byrace
Whites(N=154)
Blacks(N=90)
Characteristic Total N N % N % Test statistic df pa
SociodemographicAge (M6SD years) 244 65.5611.7 65.869.7 t=.24 242 ..813Female 244 104 68 70 78 x2=2.44 1 ..118Education (M6SD years) 244 15.262.8 13.362.2 t=–5.56 242 ,.001Marital status 244 x2=21.74 3 ,.001Cohabiting or married 88 57 25 28Divorced or separated 22 14 25 28Never married 12 8 16 18Widowed 32 21 24 27
Employed 244 71 46 27 30 x2=5.48 4 ,.019Median household income (M6SD $) 240 58,273623,210 31,003613,137 t=–10.16 238 ,.001
General healthCumulative Illness RatingScale (M6SD score)Totalb 242 7.463.8 8.464.0 t=1.89 240 ..059Countc 243 4.862.2 5.262.2 t=1.60 241 ..109Heart and vasculard 243 1.861.5 2.161.5 t=1.34 241 ..181
Body mass indexTotal (M6SD) 242 29.166.4 33.067.0 t=4.34 240 ,.001$30 points (obesity indicator) 242 60 39 57 63 x2=11.95 1 ,.001
Rand Health Status Inventory (M6SD)e
Physical health component 204 43.9611.3 38.8612.0 t=–3.00 202 ,.004Mental health component 204 42.969.2 43.369.9 t=.27 202 ..788
Cognition: Mini-Mental Status Examination(M6SD)f 243 28.761.3 27.461.8 t=–6.61 241 ,.001
Mental healthHamilton Rating Scale for Depression(M6SD)g 243 10.963.7 11.763.8 t=1.64 241 ..101
Center for Epidemiologic StudiesDepression Scale (M6SD)h 243 21.168.0 21.367.9 t=.19 241 ..851
Beck Depression Inventory (M6SD)i 230 10.665.3 10.466.4 t=–.22 228 ..829Brief Symptom Inventory anxiety(M6SD)j 232 .56.5 .56.5 t=–.41 230 ..684
History of major depressive disorder 244 54 35 28 31 x2=.24 1 ..623History of anxiety disorder 244 30 19 22 24 x2=.56 1 ..452Current anxiety disorder 244 45 29 14 16 x2=5.06 1 ,.025Social Problem Solving Inventory (M6SD)k
Total 212 100.3613.4 103.7613.4 t=1.80 210 ..073Positive problem orientation 227 95.9615.2 100.9616.1 t=2.38 225 ,.018
Referral source 244 x2=89.62 5 ,.001Community outreachl 4 3 42 47Mental health specialist 7 5 3 3Primary care 95 62 15 17Research (research program or registry) 19 12 6 7Self-referred (media, brochure,presentation, or peer educator) 22 14 14 16
Word of mouth 7 5 10 11
a Fisher exact p value reportedb Possible scores range from 0 to 52, with higher scores indicating more medical burden.c Possible scores range from 0 to 13, with higher scores indicating more medical burden.d Possible scores range from 0 to 8, with higher scores indicating more medical burden.e Possible scores range from 0 to 100, with higher scores indicating better health.f Possible scores range from 0 to 30, with higher scores indicating more cognitive impairment.g Possible scores range from 0 to 52, with higher scores indicating more depressive symptoms.h Possible scores range from 0 to 60, with higher scores indicating more depressive symptoms.i Possible scores range from 0 to 63, with higher scores indicating more depressive symptoms.j Possible scores range from 0 to 4, with higher scores indicating more anxiety symptoms.k Possible scores for Total range from 29 to 139 and those for positive problem orientation range from 52 to 135, with higher scores on each scaleindicating better problem solving.
l Referrals came from the Kingsley Center, Healthy Black Family Project, Healthy Hearts and Souls, grocery store screening, or a barbershop.
PSYCHIATRIC SERVICES IN ADVANCE 5

similar on SPSI scores (30) regardlessof race, with the exception thathigher positive problem orientation(a measure of active coping andresilience) was evident among blackparticipants. More whites than blackshad a current anxiety disorder, de-spite lower social and medical burdenamong whites.
Survival analysis of time tomajor depressive episodeParticipants in PST-PC and dietarycoaching did not differ significantly intime to major depressive episodes.Moreover, we observed similar in-cidence between black participants(N=8 of 90, 9%; 95% confidenceinterval [CI]=4%–17%) and whiteparticipants (N=13 of 154, 8%;CI=5%214%) and similar incidenceas well by recruitment site (mentalhealth specialty, N=7 of 67, 10%;CI=4%219%; community agencies,N=5 of 62, 8%; CI=3%218%; andprimary care practices, N=9 of 111,8%; CI=4%215%). Multivariate Coxproportional hazard models identi-fied the two strongest predictors ofincident episodes: greater cumulativemedical comorbidity (total CIRS-Gscore, hazard ratio [HR]=1.18, CI=1.07–1.31) and greater severity of depressivesymptoms (BDI score, HR=1.17,CI=1.09–1.25). Every 1-unit increasein total CIRS-G score increasedhazard of an event by 18%, and a 1-unit increase on the BDI increasedhazard by 17%.The overall dropout rate was 24%
(N=59 of 247) and did not differby study arm or race. Thus similarpercentages of blacks (N=62, 69%)and whites (N=102, 66%) completedthe study, experienced the onset ofmajor depressive episodes (blacks,N=8, 9%; whites, N=13, 8%), diedduring the trial (blacks, N=2, 2%;whites, N=3, 2%; no suicides), ordropped out because of loss of interestor respondent burden, participant re-location, or additional diagnosis(blacks, N=18, 20%; whites, N=36,23%). We observed no differences inage, race, or baseline severity of de-pressive symptoms between partic-ipants who completed the trial andthose who did not. However, a higherpercentage of women compared withmen completed the trial (women,
N=144 of 176, 82%; men, N=44 of71, 62%; x2=9.90, df=1, p,.001).Comparable percentages of male andfemale participants were randomlyassigned to each study arm.
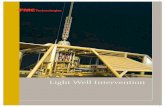
Symptom burdenParticipants in both arms experiencedon average a 4-point drop in depressivesymptoms (BDI), with improvementssustained over two years of follow-up.Black and white participants demon-strated similar patterns of responses toPST-PC and dietary coaching onmeasures of depressive symptoms(Figure 1).
Both interventions were associatedwith similar and sustained improve-ments on total scores of the SPSI,a composite measure of active copingand negative problem orientation(avoidant coping, impulsivity, andrational problem solving) (30,32) be-fore and after treatment. SPSI scorewas a significant covariate in ourlongitudinal model of BDI scores.An increase (improvement) in SPSIscore was associated with a decreasein depressive symptoms (b=–.0306.003, t=–9.80, df=799, p,.001). Con-versely, when examining SPSI scoresas outcome using the same model oftreatment, time, and treatment 3time effects, and including BDI asa covariate, we found a bidirectionalrelationship such that depressivesymptom scores were also a significanttime-varying covariate of SPSI. A de-crease in depression symptoms wasassociated with an increase (improve-ment) in SPSI score (b=–.6546.062,t=–10.56, df=799, p,.001).
DiscussionBoth PST-PC and dietary coachingare potentially effective in protectingolder black and white adults overa two-year period from the persis-tence of depressive symptoms (aver-age of 4-point drop in BDI scores)and from the concomitant risk posedby persistent subsyndromal depres-sive symptoms for incident episodesof major depression. However, in theabsence of a concurrent, usual-carecontrol, this conclusion should beregarded as preliminary.
Compared with previously pub-lished rates of incident major depres-sion among persons with subsyndromal
symptoms receiving usual care (20%–
25% over one year) (24–27), the ap-parent protective effect against majordepression is noteworthy. We madea pragmatic decision not to control forcare as usual (in effect a control fortime’s passage, because treatment asusual is often no treatment at all) forseveral reasons, namely that manyblack participants lacked primary careservices, our community advisory boardwarned that it could be a barrierto participation, and other studiesof treatment as usual, includingour own (33), have observed thatsubsyndromal depressive symptomstend to persist under conditions ofusual care—not improving and put-ting individuals at risk of majordepressive disorder and deterioratingquality of life (33–37).
For example, in our study of suicideprevention for the primary care el-derly population (34), older adultswith subsyndromal symptoms underconditions of usual care had greaterthan a fivefold increased risk of con-version to major depressive disorderwithin one year, compared with thosewithout such symptoms (33,35). Sim-ilarly, in a Dutch study of 170 olderprimary care patients aged 75 andolder with subthreshold symptoms ofdepression and anxiety, a stepped-careintervention (which included problem-solving therapy) reduced the incidenceof depressive and anxiety disorders by50% over one year relative to care asusual (24% versus 12%) (36). A similarresult was reported in the MANAStrial (25% versus 12.3%) in a mixed-aged sample of primary care patients inGoa, India (37). Our data showed anincidence of major depression among21 of 247 persons (9%) over two yearsand among 13 of 247 persons (5%)over one year, similar to the Dutch andIndian observations. This observationcontrasts with a published rate of20%225% having major depressiveepisodes over two years, based on thestudies cited above, in which partic-ipants were recruited mainly in pri-mary care settings.
A separate but related observationis that our sample was recruited fromboth primary care clinic and commu-nity sites (in order to oversampleblack participants). Because incidencemay differ according to locus of
6 PSYCHIATRIC SERVICES IN ADVANCE

recruitment, we stratified the ran-domization to intervention group bylocus of recruitment. We did not,however, detect different incidenceas a function of primary care,community-based, or mental healthspecialty recruitment. Moreover, ourcommunity-referred participants weremostly black, and black participantscarried a higher burden of risk ofmajor depression than white partic-ipants did (Table 2).Contrary to our study hypothesis,
we observed in both PST-PC anddietary coaching comparable and sus-tained reductions in depressive symp-toms over time. Dietary coachingprovided more than a control forface-to-face contact. It was by design
an active control intervention in itsown right, coaching participants toaddress the challenges of implement-ing healthy dietary practices, withhomework assignments. Participants inthis group reported both improvementsin depressive symptoms and inproblem-solving skills. Dietary coach-ing’s active-coping component, as wellas social contact, may have protectedagainst depression. Participants re-ceived assistance in tackling a problemassociated with managing health issues.With the higher positive problem-solving orientation of black participants,dietary coaching fit culturally with lifeexperience of having to problemsolve and cope even in the absenceof many resources. Dietary coaching
also did not pose the issues of safety,stigma, and financial burden associ-ated with long-term antidepressantpharmacotherapy.
In our longitudinal modeling ofcovariation between BDI scores andSPSI scores, we observed that in-creasing (improving) scores on theSPSI predicted lower depressionscores and vice versa—that fallingdepression scores predicted increas-ing (improving) scores on the SPSI.This finding suggests the possibility ofa bidirectional effect (that is, betterproblem solving leads to improve-ment in depression, and improvementin depression leads to better problemsolving). However, this inference shouldbe seen as preliminary, because SPSI
Figure 1
Two-year BDI scores of older adults receiving problem-solving therapy for primary care (PST-PC) or dietary coachinga
PST-PCDiet
PST-PCDiet
PST-PCDiet
14
12
10
8
6
4
2
0
BDI s
core
14
12
10
8
6
4
2
0
BDI s
core
14
12
10
8
6
4
2
0
BDI s
core
Pre 6*Post 9 12*
Months Months
Months15 18* 21 24
Pre 6*Post 9 12* 15 18* 21 24
69 5746 47 51 50 51 4072
6061 5951 50 55 49 52 53
Pre 6*Post 9 12* 15 18* 21 24
PST-PC N=Diet N= 45 3837 34 38 33 34 36
404031 2625 22 25 26 27 27PST-PC N=
Diet N=
115 9684 82 90 84 86 86114
10194 8778 73 82 77 81 82PST-PC N=
Diet N=
Whites Blacks
a Participants in both conditions demonstrated similar improvement in depressive symptoms, as measured with the Beck Depression Inventory (BDI).Asterisks indicate when a booster session was given. The top panel is for the overall group of 247, which included three Asian participants. There wasa significant quadratic effect and linear time effects (F=75.91, dfs=1 and 1,356, p,.001, and F=159.57, dfs=1 and 1,356, p,.001, respectively) but nosignificant intervention or intervention 3 time effects. Examination of race as a moderator (bottom panels) showed baseline racial differences betweeninterventions, and covarying the model for baseline score (Pre) resulted in a significant time effect (F=26.78, dfs=1 and 1,115, p,.001) forpostintervention (Post) through two years, but no other significant effects. BDI scores can range from 0 to 63, with higher scores indicating moredepressive symptoms. Vertical lines represent standard errors.
PSYCHIATRIC SERVICES IN ADVANCE 7

scores and BDI scores are very likely tohave shared variance based on theirintrinsic definitions and constructs.This study breaks new ground
in indicated depression preventionresearch with an active control condi-tion for the effects of attention, face-to-face time, and support, two years offollow-up, and an adequate number ofblack participants to explore effectsof race on patterns of incident de-pression, trajectory of symptoms, andchanges in health-related quality oflife over two years. Most studies ofdepression prevention have not usedan active comparator, have followedpatients for shorter periods (generallyone year), and have not had sufficientracial or ethnic diversity in their studygroups to examine variability relatedto sociocultural characteristics. Bothinterventions in this trial were foundto be acceptable to blacks and whites,with comparably low rates of non-adherence and dropout over twoyears.
ConclusionsRecruitment and retention of blackparticipants were facilitated by part-nerships with community championsfor the study, the nonuse of antide-pressant medication, low respondentburden, and conduct of the study incommunity settings (including partic-ipants’ homes), rather than in a med-ical setting. Lifestyle interventionssuch as dietary coaching may be moreculturally appropriate and acceptablein racial-ethnic minority communi-ties, regardless of income. These areimportant strategic considerations forreaching underserved individuals atrisk of major depression, given thatcultural beliefs and stigma contributeto low utilization of mental health careamong older individuals from racial-ethnic minority groups. At a time ofincreasing shortages of mental healthprofessionals dedicated to workingwith older adults (36), it is plausiblethat PST-PC and dietary coachingmay be amenable to delivery by layhealth counselors (peer supporters)with the same racial-ethnic back-ground as the community they serve,increasing the scalability of theseinterventions in impoverished areasand utility to federally qualified com-munity health centers or other pri-
mary care settings where nurses orhealth educators could fill this role.Thus the results of this study may beparticularly pertinent to the integra-tion of primary care and behavioralhealth services, especially for olderpatients whose increasing generalmedical comorbidity places them athigh risk of developing major de-pressive disorders.
Acknowledgments and disclosures
This work was supported by grants P60MD000207, P30 MH090333, UL1RR024153,and UL1TR000005 from the National Instituteof Mental Health and National Institutes ofHealth, by the University of Pittsburgh MedicalCenter Endowment in Geriatric Psychiatry, andby the Commonwealth of Pennsylvania. Thiswork is registered on ClinicalTrials.gov asNCT00326677.
Dr. Reynolds reports receiving pharmaceuticalsupport for National Institutes of Health–sponsored research studies from Bristol-MyersSquibb, Forest, Pfizer, and Lilly. He is the co-inventor of Psychometric Analysis of thePittsburgh Sleep Quality Index (licensed in-tellectual property PRO10050447). Dr. Karpreports receipt of medication supplies fromPfizer and Reckitt Benckiser for investigator-initiated studies. Dr. Butters has receivedremuneration fromGlaxoSmithKline for perform-ing neuropsychological services. Dr. Kasckowhas received assistance from Robert BoschHealth Care, Inc., for software-related costsfor a research project. The other authors reportno competing interests.
References
1. Cuijpers P, Beekman ATF, Reynolds CF,III: Preventing depression: a global prior-ity. JAMA 307:1033–1034, 2012
2. Reynolds CF, III, Cuijpers P, Patel V, et al:Early intervention to reduce the globalhealth and economic burden of major de-pression in older adults; in Annual Reviewof Public Health. Edited by Fielding JE,Brownson RC, Green LW. Palo Alto, Calif,Annual Reviews, 2012
3. Diniz BS, Butters MA, Albert SM, et al:Late-life depression and risk of vasculardementia and Alzheimer’s disease: sys-tematic review and meta-analysis ofcommunity-based cohort studies. BritishJournal of Psychiatry 202:329–335, 2013
4. Jang Y, Borenstein AR, Chiriboga DA,et al: Depressive symptoms among AfricanAmerican and white older adults. Journals ofGerontology: Series B, Psychological Sciencesand Social Sciences 60:P313–P319, 2005
5. Sriwattanakomen R, McPherron J, ChatmanJ, et al: A comparison of the frequencies ofrisk factors for depression in older black andwhite participants in a study of indicatedprevention. International Psychogeriatrics22:1240–1247, 2010
6. Mental Health: Culture, Race and Eth-nicity: A Supplement to Mental Health: A
Report of the Surgeon General. Rockville,Md, Department of Health and HumanServices, 2001
7. Shadlen MF, Siscovick DS, Fitzpatrick AL,et al: Education, cognitive test scores, andblack-white differences in dementia risk.Journal of the American Geriatrics Society54:898–905, 2006
8. Barnes DE, Yaffe K: The projected effectof risk factor reduction on Alzheimer’sdisease prevalence. Lancet Neurology 10:819–828, 2011
9. Williams DR: Race, stress, and mentalhealth; in Minority Health in America:Findings and Policy Implications FromCommonwealth Fund Minority HealthSurvey. Edited by Hogue CJR, HargravesMA, Collis KS. Baltimore, Johns HopkinsUniversity Press, 2000
10. Steffens DC, Artigues DL, Ornstein KA,et al: A review of racial differences in ge-riatric depression: implications for care andclinical research. Journal of the NationalMedical Association 89:731–736, 1997
11. Cuijpers P, de Graaf R, van Dorsselaer S:Minor depression: risk profiles, functionaldisability, health care use and risk of de-veloping major depression. Journal of Af-fective Disorders 79:71–79, 2004
12. Muñoz RF, Ying YW, Bernal G, et al:Prevention of depression with primary carepatients: a randomized controlled trial.American Journal of Community Psychol-ogy 23:199–222, 1995
13. Smit F, Ederveen A, Cuijpers P, et al:Opportunities for cost-effective preventionof late-life depression: an epidemiologicalapproach. Archives of General Psychiatry63:290–296, 2006
14. Cole MG: Evidence-based review of riskfactors for geriatric depression and briefpreventive interventions. Psychiatric Clin-ics of North America 28:785–803, 2005
15. Schoevers RA, Smit F, Deeg DJH, et al:Prevention of late-life depression in primarycare: do we know where to begin? AmericanJournal of Psychiatry 163:1611–1621, 2006
16. Cooper-Patrick L, Gallo JJ, Gonzales JJ,et al: Race, gender, and partnership in thepatient-physician relationship. JAMA 282:583–589, 1999
17. Fournier JC, DeRubeis RJ, Hollon SD,et al: Antidepressant drug effects and de-pression severity: a patient-level meta-analysis.JAMA 303:47–53, 2010
18. Stewart JA, Deliyannides DA, HellersteinDJ, et al: Can people with nonsevere majordepression benefit from antidepressantmedication? Journal of Clinical Psychiatry73:518–525, 2012
19. Unützer J, Katon W, Callahan CM, et al:Collaborative care management of late-lifedepression in the primary care setting:a randomized controlled trial. JAMA 288:2836–2845, 2002
20. Nezu AM, Nezu CM: Problem solving ther-apy. Journal of Psychotherapy Integration 11:187–205, 2001
21. Rovner BW, Casten RJ, Hegel MT, et al:Preventing depression in age-related macular
8 PSYCHIATRIC SERVICES IN ADVANCE

degeneration. Archives of General Psychiatry64:886–892, 2007
22. Robinson RG, Jorge RE, Moser DJ, et al:Escitalopram and problem-solving therapyfor prevention of poststroke depression:a randomized controlled trial. JAMA 299:2391–2400, 2008
23. Alexopoulos GS, Raue P, Areán PA:Problem-solving therapy versus supportivetherapy in geriatric major depression withexecutive dysfunction. American Journal ofGeriatric Psychiatry 11:46–52, 2003
24. Radloff LS: The CES-D Scale: a self-report depression scale for research in thegeneral population. Applied PsychologicalMeasurement 1:385–401, 1977
25. First M, Spitzer RL, Gibbon M, et al:Structured Clinical Interview for DSM-IVAxis II Personality Disorders (SCID-II),Version 2.0. New York, New York StatePsychiatric Institute, 1994
26. Folstein MF, Folstein SE, McHugh PR:“Mini-Mental State”: a practical method forgrading the cognitive state of patients for theclinician. Journal of Psychiatric Research 12:189–198, 1975
27. Beck AT, Ward CH, Mendelson M, et al:An inventory for measuring depression.Archives of General Psychiatry 4:561–571,1961
28. Ware J: SF-36 Health Survey. Manual andInterpretation Guide 2. Boston, HealthInstitute, New England Medical Center,Nimrod Press, 1997
29. Miller MD, Paradis CF, Houck PR, et al:Rating chronic medical illness burden ingeropsychiatric practice and research: ap-plication of the Cumulative Illness RatingScale. Psychiatry Research 41:237–248, 1992
30. D’Zurilla TJ, Nezu AM: Development andpreliminary evaluation of the SocialProblem-Solving Inventory. PsychologicalAssessment 2:156–163, 1990
31. Derogatis LR, Melisaratos N: The BriefSymptom Inventory: an introductory report.Psychological Medicine 13:595–605, 1983
32. D’Zurilla TJ, Nezu AM: Problem-SolvingTherapy: A Positive Approach to ClinicalIntervention. New York, Springer, 2007
33. Lyness JM, Heo M, Datto CJ, et al: Out-comes of minor and subsyndromal de-
pression among elderly patients in primarycare settings. Annals of Internal Medicine144:496–504, 2006
34. Bruce ML, Ten Have TR, Reynolds CF,III, et al: Reducing suicidal ideation anddepressive symptoms in depressed olderprimary care patients: a randomizedcontrolled trial. JAMA 291:1081–1091,2004
35. Lyness JM, Yu Q, Tang W, et al: Risks fordepression onset in primary care elderlypatients: potential targets for preventiveinterventions. American Journal of Psychi-atry 166:1375–1383, 2009
36. van’t Veer-Tazelaar PJ, van Marwijk HW,van Oppen P, et al: Stepped-care pre-vention of anxiety and depression in latelife: a randomized controlled trial. Ar-chives of General Psychiatry 66:297–304,2009
37. Patel V, Weiss HA, Chowdhary N, et al:Effectiveness of an intervention led bylay health counsellors for depressive andanxiety disorders in primary care in Goa,India (MANAS): a cluster randomisedcontrolled trial. Lancet 376:2086–2095,2010
PSYCHIATRIC SERVICES IN ADVANCE 9