
Randomised controlled trial of group cognitive behavioural therapy for comorbid anxiety and...
8
Randomised controlled trial of group cognitive behavioural therapy for comorbid anxiety and depression in older adults q Viviana M. Wuthrich * , Ronald M. Rapee Centre for Emotional Health, Department of Psychology, Macquarie University, Sydney 2109, Australia article info Article history: Received 5 June 2013 Received in revised form 2 September 2013 Accepted 4 September 2013 Keywords: Anxiety Depression Transdiagnostic Cognitive behavioural therapy Older age abstract Anxiety and depression are commonly comorbid in older adults and are associated with worse physical and mental health outcomes and poorer response to psychological and pharmacological treatments. However, little research has examined the effectiveness of psychological programs to treat comorbid anxiety and depression in older adults. Sixty-two community dwelling adults aged over 60 years with comorbid anxiety and depression were randomly allocated to group cognitive behavioural therapy or a waitlist condition and were assessed immediately following and three months after treatment. After controlling for cognitive ability at pre-treatment, cognitive behaviour therapy resulted in significantly greater reductions, than waitlist, on symptoms of anxiety and depression based on a semi-structured diagnostic interview rated by clinicians unaware of treatment condition. Significant time by treatment interactions were also found for self-report measures of anxiety and depression and these gains were maintained at the three month follow up period. In contrast no significant differences were found be- tween groups on measures of worry and well-being. In conclusion, group cognitive behavioural therapy is efficacious in reducing comorbid anxiety and depression in geriatric populations and gains maintain for at least three months. Ó 2013 The Authors. Published by Elsevier Ltd. All rights reserved. Objective Epidemiological studies show that depression and anxiety are common disorders throughout the lifespan and that they are typically comorbid (Beekman et al., 1998; Kessler et al., 1996). Research indicates considerable overlap of these disorders in terms of risk factors (Vink, Aartsen, & Schoevers, 2008), phenomenology (Watson et al., 1995), and genetic factors, particularly for General- ized Anxiety Disorder (GAD) and Major Depressive Disorder (MDD) (Kendler, Gardner, Gatz, & Pedersen, 2007). Rates of comorbid anxiety and depression in older adults are similar to those in younger populations, with as many as 35% of primary care patients with major depression also reporting a life time history of an anxiety disorder and 23% reporting a current comorbid anxiety disorder (Lenze et al., 2000). In a community sample, 47% of older adults who met criteria for major depression also met criteria for an anxiety disorder and 23% with an anxiety disorder also met criteria for a comorbid major depressive disorder (Beekman et al., 2000). In older adults, the presence of both anxiety and depression is associated with worse outcomes than either disorder alone including increased risk of cognitive decline and dementia (DeLuca et al., 2005), more severe depression and increased suicide rates (Cohen, Gilman, Houck, Szanto, & Reynolds, 2009; Lenze et al., 2000) and a chronic course (Almeida et al., 2012). Given the high prevalence of comorbid anxiety and depression, research indicating that comorbidity is associated with worse outcomes, and the large overlap in symptom profiles and risk factors, it is important to pay more attention to the comorbid presentation and treatment of these disorders in older adults. Recent reviews of psychological treatments for depression in older adults indicate that cognitive behavioural therapy (CBT) is as effective as in younger adults and is superior to waitlist, care-as- usual, placebo and other control groups, with moderate to large effect sizes (mean d ¼ 0.72) (Cuijpers, van Straten, & Smit, 2006; Mackin & Arean, 2005; Serfaty, Haworth, Blanchard, Buszewicz, & King, 2009). Reviews for psychological treatment of primary anxi- ety demonstrate the effectiveness of relaxation, supportive therapy, and CBT in older adults (Ayers, Sorrell, Thorp, & Wetherell, 2007; Nordhus & Pallesen, 2003). Hendriks et al. conducted a system- atic review and meta-analysis of CBT for anxiety disorders in older adults and concluded that CBT was superior to waitlist and active q This is an open-access article distributed under the terms of the Creative Commons Attribution-NonCommercial-No Derivative Works License, which per- mits non-commercial use, distribution, and reproduction in any medium, provided the original author and source are credited. * Corresponding author. Tel.: þ61 2 9850 4866; fax: þ61 2 9850 8062. E-mail addresses: [email protected] (V.M. Wuthrich), Ron.Rapee@ mq.edu.au (R.M. Rapee). Contents lists available at ScienceDirect Behaviour Research and Therapy journal homepage: www.elsevier.com/locate/brat 0005-7967/$ e see front matter Ó 2013 The Authors. Published by Elsevier Ltd. All rights reserved. http://dx.doi.org/10.1016/j.brat.2013.09.002 Behaviour Research and Therapy 51 (2013) 779e786
Transcript of Randomised controlled trial of group cognitive behavioural therapy for comorbid anxiety and...

lable at ScienceDirect
Behaviour Research and Therapy 51 (2013) 779e786
Contents lists avai
Behaviour Research and Therapy
journal homepage: www.elsevier .com/locate/brat
Randomised controlled trial of group cognitive behavioural therapyfor comorbid anxiety and depression in older adultsq
Viviana M. Wuthrich*, Ronald M. RapeeCentre for Emotional Health, Department of Psychology, Macquarie University, Sydney 2109, Australia
a r t i c l e i n f o
Article history:Received 5 June 2013Received in revised form2 September 2013Accepted 4 September 2013
Keywords:AnxietyDepressionTransdiagnosticCognitive behavioural therapyOlder age
q This is an open-access article distributed undeCommons Attribution-NonCommercial-No Derivativemits non-commercial use, distribution, and reproductthe original author and source are credited.* Corresponding author. Tel.: þ61 2 9850 4866; fax
E-mail addresses: [email protected] (mq.edu.au (R.M. Rapee).
0005-7967/$ e see front matter � 2013 The Authorshttp://dx.doi.org/10.1016/j.brat.2013.09.002
a b s t r a c t
Anxiety and depression are commonly comorbid in older adults and are associated with worse physicaland mental health outcomes and poorer response to psychological and pharmacological treatments.However, little research has examined the effectiveness of psychological programs to treat comorbidanxiety and depression in older adults. Sixty-two community dwelling adults aged over 60 years withcomorbid anxiety and depression were randomly allocated to group cognitive behavioural therapy or awaitlist condition and were assessed immediately following and three months after treatment. Aftercontrolling for cognitive ability at pre-treatment, cognitive behaviour therapy resulted in significantlygreater reductions, than waitlist, on symptoms of anxiety and depression based on a semi-structureddiagnostic interview rated by clinicians unaware of treatment condition. Significant time by treatmentinteractions were also found for self-report measures of anxiety and depression and these gains weremaintained at the three month follow up period. In contrast no significant differences were found be-tween groups on measures of worry and well-being. In conclusion, group cognitive behavioural therapyis efficacious in reducing comorbid anxiety and depression in geriatric populations and gains maintainfor at least three months.
� 2013 The Authors. Published by Elsevier Ltd. All rights reserved.
Objective anxiety disorder and 23% with an anxiety disorder also met criteria
Epidemiological studies show that depression and anxiety arecommon disorders throughout the lifespan and that they aretypically comorbid (Beekman et al., 1998; Kessler et al., 1996).Research indicates considerable overlap of these disorders in termsof risk factors (Vink, Aartsen, & Schoevers, 2008), phenomenology(Watson et al., 1995), and genetic factors, particularly for General-ized Anxiety Disorder (GAD) and Major Depressive Disorder (MDD)(Kendler, Gardner, Gatz, & Pedersen, 2007). Rates of comorbidanxiety and depression in older adults are similar to those inyounger populations, with as many as 35% of primary care patientswith major depression also reporting a life time history of ananxiety disorder and 23% reporting a current comorbid anxietydisorder (Lenze et al., 2000). In a community sample, 47% of olderadults whomet criteria for major depression alsomet criteria for an
r the terms of the CreativeWorks License, which per-
ion in any medium, provided
: þ61 2 9850 8062.V.M. Wuthrich), Ron.Rapee@
. Published by Elsevier Ltd. All righ
for a comorbid major depressive disorder (Beekman et al., 2000).In older adults, the presence of both anxiety and depression is
associated with worse outcomes than either disorder aloneincluding increased risk of cognitive decline and dementia (DeLucaet al., 2005), more severe depression and increased suicide rates(Cohen, Gilman, Houck, Szanto, & Reynolds, 2009; Lenze et al.,2000) and a chronic course (Almeida et al., 2012). Given the highprevalence of comorbid anxiety and depression, research indicatingthat comorbidity is associated with worse outcomes, and the largeoverlap in symptom profiles and risk factors, it is important to paymore attention to the comorbid presentation and treatment ofthese disorders in older adults.
Recent reviews of psychological treatments for depression inolder adults indicate that cognitive behavioural therapy (CBT) is aseffective as in younger adults and is superior to waitlist, care-as-usual, placebo and other control groups, with moderate to largeeffect sizes (mean d ¼ 0.72) (Cuijpers, van Straten, & Smit, 2006;Mackin & Arean, 2005; Serfaty, Haworth, Blanchard, Buszewicz, &King, 2009). Reviews for psychological treatment of primary anxi-ety demonstrate the effectiveness of relaxation, supportive therapy,and CBT in older adults (Ayers, Sorrell, Thorp, & Wetherell, 2007;Nordhus & Pallesen, 2003). Hendriks et al. conducted a system-atic review and meta-analysis of CBT for anxiety disorders in olderadults and concluded that CBT was superior to waitlist and active
ts reserved.

V.M. Wuthrich, R.M. Rapee / Behaviour Research and Therapy 51 (2013) 779e786780
control conditions for anxiety and comorbid depression symptoms,but only superior to waitlist conditions for worry severity(Hendriks, Oude Voshaar, Keijsers, Hoogduin, & Van Balkom, 2008).A recent meta-analysis of CBT for anxiety disorders in older adultsfound that CBT was only marginally more effective than activecontrol conditions and called for approaches to increase the effec-tiveness of CBT for anxiety in older adults (Gould, Coulson, &Howard, 2012). They suggested that targeting comorbidity mightincrease therapeutic outcomes.
Despite the high prevalence of comorbid anxiety and depres-sion, and the particularly negative outcomes associated with thiscomorbidity, there is a striking absence of studies that have focusedon the psychosocial treatment of comorbid anxiety and depressionin older adults. Sallis et al. (1983) compared the effectiveness ofthree treatment conditions: relaxation training, pleasant eventscheduling and rational disputing, and a self-disclosure discussiongroup on comorbid anxiety and depression in older adults. Theyfound that depression reduced from pre to post in all conditionsequally, while improvements in anxiety symptoms only occurred inthe placebo condition. A major limitation of this study is that thesample size was small (n ¼ 24) and lacked the statistical power todetect anything less than a very large difference between activetreatments. To our knowledge, no other published trial has spe-cifically investigated the efficacy of group CBT for comorbid anxietyand depression in older adults.
The majority of studies have focused on the treatment of pri-mary depression or anxiety and not their comorbidity, and reportthat the presence of a comorbid disorder reduces the effectivenessof treatment for the primary disorder. For example, comorbidanxiety has been shown to delay and reduce treatment responseto both pharmacological and psychological treatments fordepression (Andreescu et al., 2007; Andreescu et al., 2009; Arnowet al., 2007; Cohen et al., 2009; Gum, Arean, & Bostrom, 2007;Hegel et al., 2005), and comorbid depression has been demon-strated to reduce the effectiveness of psychological treatment forprimary anxiety in some studies (Schuurmans et al., 2009), buthas not been found to impact on effectiveness in others (Wetherellet al., 2005).
Further, psychological treatments for primary depression havetypically failed to produce significant reductions in comorbidanxiety symptomatology (Dombrovski et al., 2006; Gum et al.,2007; Serfaty et al., 2009). In contrast, psychological therapy tar-geting geriatric anxiety typically results in simultaneous reductionsin post-treatment depression (Barrowclough et al., 2001;Gorenstein et al., 2005; Mohlman et al., 2003; Mohlman &Gorman, 2005; Stanley et al., 2003; Wetherell, Gatz, & Craske,2003). However, limitations of these studies include that somestudies have excluded individuals with clinically severe depression(Gorenstein et al., 2005; Mohlman et al., 2003; Mohlman &Gorman, 2005), many studies have only included a small numberwith comorbid depression, and none have reported post-treatmentchanges in mood disorder diagnostic severity using a clinicalinterview, so it is unclear whether these anxiety treatments pro-duce diagnostically significant change in both anxiety anddepressive disorders. Given that comorbidity reduces the effec-tiveness of treatments targeting one disorder only (the primarydisorder) and is associated with worse long term outcomes, aprogram that addresses the core features of both disorders mightbe more efficacious.
The aim of the current study was to conduct a randomisedcontrolled trial to evaluate the efficacy of group CBT program tar-geting comorbid anxiety and depression in older adults. The pri-mary aim was to establish the program’s basic efficacy bycomparing it to a comparable waitlist condition. The primaryoutcome was changes in diagnostic severity for both the anxiety
and depressive disorders. Secondary outcomes included changeson self-reported anxiety, depression and life interference. Weincluded individuals whomet criteria or subclinical criteria for botha mood and an anxiety disorder. We hypothesized that the CBTconditionwould result in significant improvements on all symptommeasures from pre to post treatment and that these gains would bemaintained at the 3 month follow up.
Methods
Participants
Sixty-two community dwelling participants aged 60e84 (meanage ¼ 67.44, SD ¼ 6.19, 22 ¼ male, 40 ¼ female) were recruited viaadvertisements in local newspapers. Participants attended theCentre for Emotional Health, Macquarie University, Sydney,Australia for assessment and treatment. All participants met DSM-IV criteria or subclinical criteria (see below for definition) for bothan anxiety and a mood disorder, with either anxiety or mood beingthe primary (most interfering) problem. In fact, the vast majority ofthe sample met full DSM-IV criteria for both an anxiety disorderand a mood disorder with either problem being primary (N ¼ 55),with the remaining 7 participants having at least subclinical levelsof anxiety, depression or both. Exclusion criteria were: aged under60 years, unable to read a newspaper, current self-harm, activesuicidal intent, psychosis, or bipolar disorder. All participants wereasked to refrain from engaging in additional treatment from atherapist or making changes to their medication status during thecourse of the trial.
Measures
Diagnostic clinical interviewParticipants completed the Anxiety Disorders Interview
Schedule for DSM-IV (ADIS: Di Nardo, Brown, & Barlow, 1994), asemi-structured interview for diagnosing anxiety and relateddisorders including mood disorders according to DSM-IV criteriaon a 0e8 severity rating scale where ratings of 4 and above areconsidered of clinical severity and meet diagnostic status. Thisinterview was administered by five different graduate students inclinical psychology formally trained on the ADIS and given regularsupervision to discuss diagnostic decisions. The primary disorderwas defined as the one that most interfered with the person’s life.In this study, participants with clinical severity ratings of 3 orabove for their main anxiety disorder and main mood disorderwere included in the study, as we were interested in also treatingsubclinical anxiety and depression; however, 89% of the samplemet full diagnostic criteria for both an anxiety and mood disorder.The interviews were videotaped for reliability purposes and 25%were recoded after the study’s completion for the purpose ofreliability coding. Inter-rater reliability (k) for agreement on thepresence of a disorder in the diagnostic profile was k ¼ 1.0 (100%agreement) for mood disorder, k ¼ 1.0 (100% agreement) forgeneralized anxiety disorder and k ¼ 0.81 (92% agreement) forsocial phobia.
Cognitive assessmentAddenbrooke Cognitive Examination-Revised (ACE-R: Mioshi,
Dawson, Mitchell, Arnold, & Hodges, 2006), is a brief rating scalefor dementia that assesses five cognitive domains, namely atten-tion/orientation, memory, verbal fluency, language and visuospa-tial abilities. Research indicates good sensitivity and specificity forcut off scores of 88 (sensitivity ¼ 0.94, specificity ¼ 0.89) and 82(sensitivity ¼ 0.84, specificity ¼ 1.0) (Mioshi et al., 2006).

Table 1Outline of session content of Ageing Wisely program.
Session Session content Homework content
1 Introduction, psychoeducation,myths about ageing
Read over session notes
2 Motivation to change & goalsetting, mood monitoring,identifying presence of thoughtsin situations
Mood monitoring
3 Activity scheduling, linkingthoughts and feelings
Activity scheduling, pluspreviously presented skill
4 Identifying unhelpfulthoughts, problem solving
Identifying thoughts, problemsolving, plus previouslypresented skills
5 Cognitive restructuring Cognitive restructuring, pluspreviously presented skills
6 Common barriers to cognitiverestructuring, using cognitiverestructuring to deal withloneliness and low motivation
Previously presented skills
7 Review of goals, reviewof skills taught so far
Previously presented skills
8 Graded exposure andreducing avoidance
Graded exposure, pluspreviously presented skills
9 Graded exposure,assertiveness andcommunication
Assertiveness practice, pluspreviously presented skills
10 Sleep strategies Sleep strategies, plus previouslypresented skills
11 Dealing with lossand bereavement
Previously presented skills
12 Review goals and skills,relapse prevention
Previously presented skills
V.M. Wuthrich, R.M. Rapee / Behaviour Research and Therapy 51 (2013) 779e786 781
Self-report measuresThe following questionnaires were administered at pre-
treatment, post-treatment and 3 month follow up.Geriatric Depression Scale (GDS: Yesavage et al., 1983), a 30 item
self-report measure of depression symptoms developed for olderadults. It has high internal consistency, reliability, sensitivity andspecificity in inpatient, outpatient and nursing home residents withzero to moderate cognitive impairment (Jongenelis et al., 2005;Yesavage et al., 1983). Internal consistency in this sample wasalpha ¼ .86.
The Centre for Epidemiological Studies e Depression Scale (CES-D:Radloff, 1977), a 20 item questionnaire that assesses depressionsymptoms over the past week. This questionnaire has been shownto be reliable and valid in elders (Beekman et al., 1997; Haringsma,Engels, Beekman, & Spinhoven, 2004). Internal consistency in thissample was alpha ¼ .90.
The Geriatric Anxiety Inventory (GAI: Pachana et al., 2007), a 20item measure of anxiety symptoms developed for older adults. Ithas been shown to have adequate internal consistency, test-retestreliability and concurrent validity (Pachana et al., 2007). Internalconsistency in this sample was alpha ¼ .89.
The Penn State Worry Questionnaire (PSWQ: Meyer, Miller,Metzger, & Borkovec, 1990) is a measure of worry that has shownadequate internal consistency and convergent validity in elderlypatients with GAD and controls (Stanley, Novy, Bourland, Beck, &Averill, 2001). Internal consistency in this sample was alpha ¼ .84.
The Short Form e 12 version 1 Mental Health Subscale (SF12:Ware, Kosinski, & Keller, 1996), is a general measure of mentalhealth status. The SF12 has been demonstrated to be reliable andvalid in older populations (Jakobsson, 2007). The internal consis-tency in this sample was alpha ¼ .83.
Group CBT programThe Ageing Wisely group program consisted of 12 � 2 h sessions
conducted by the lead author and two graduate students in clinical
psychology receiving regular supervision, with 6e8 group mem-bers. Groups had one or two therapists with the second therapistbeing largely an observer. The program included generic CBT skillssuch as psycho-education, problem-solving, cognitive restructur-ing, sleep hygiene, assertiveness training, and graded exposurewhich is a core skill for treatment of anxiety, and activity sched-uling which is a core skill for the treatment of depression. Theprogram was designed for older adults with skills were presentedover several sessions, including significant repetition, large font,and case examples of older adults focused on problems relevant tothis life stage such as worry about dementia, physical disability,bereavement and loneliness. Due to the transdiagnostic aim of thisprogram, all skills were presented with examples for a depressivetype of problem and an anxious problem (mainly worry or socialevaluation concern). Similarly, graded exposure was presentedwith examples for a range of anxiety problems including worry,social anxiety and specific phobia. Cognitive restructuring was acore component of the program and was introduced over thecourse of 4 weeks, and then practiced as homework each week,with considerable attention paid to establishing links betweenthoughts and feelings. A highly structured cognitive restructuringform was used that included the following sections: Situation,Thoughts, Evidence Collecting and Helpful Replacement Thought.The Evidence Collecting section included seven questions to helpidentify relevant evidence including: “What would a friend say?”,“What can my past tell me about my ability to cope here?”, “Howlikely is it that it will really happen?”, and “What alternatives arethere to this situation?” See Table 1 for an outline of the sessioncontent. The program included a detailed structured participantand therapist workbook that included all material presented duringthe sessions, and all homework exercises. Skills were taught with amixture of didactic teaching, group discussions and role play. Therewas a large emphasis on home practice with a weekly review ofhomework and homework forms for each new and previouslypresented skill included in their manual each week.
Procedure
Ethical approval was obtained through theMacquarie UniversityHuman Research Ethics Committee. After participants completedconsent forms, they completed the pre-assessment questionnairesand provided demographic and medical information. Then theycompleted the ACE-R cognitive examination and ADIS diagnosticinterview. Participants were randomly assigned, following simplerandomization procedures (computerized random numbers), to 1of 2 treatment groups of 12 weeks duration (CBT or waitlist) inblocks of 8 participants. At the end of the 12 weeks, participantsagain completed post-treatment assessments including diagnosticinterviews (rated by clinicians unaware of condition allocation),cognitive assessments and questionnaires. Those in the waitlistcondition were then offered group treatment and those whocompleted the group program completed the assessments againthree months after the treatment ended.
Data analysis
Data analysis was conducted using SPSS (version 19, SPSS Inc.,USA). All analyses were conducted as intent-to-treat and as such allparticipants were analysed in the group to which they were rand-omised. For partially completed self-report questionnaires, data forthe missing items were generated using the Expectation-Maximization algorithm. This algorithm computes probabilities foreach possible completion of the missing data using the current pa-rameters to form aweighted set that is then used to provide the newparameter estimates (Do & Batzoglou, 2008). For participants who

V.M. Wuthrich, R.M. Rapee / Behaviour Research and Therapy 51 (2013) 779e786782
did not start or complete treatment, missing values were imputedusing the Multiple Imputation procedure (Schafer & Graham, 2002;Sinharay, Stern, & Russell, 2001). Using this procedure, pre-treatment group allocation, ADIS severity scores and questionnaireitems were used to generate 20 sets of imputed data and the pooleddata were used to predict missing scores.
Differences between groups on continuous measures (pre,post, follow up) were examined using hierarchical mixed modelscontaining random intercept and random slope terms as well asfixed effects for treatment received. In order to run mixed modelanalyses in SPSS for the multiple imputation pooled dataset, thevan Ginkel macro (van Ginkel, 2010) was used to calculate the Fvalues, standard errors, p-values, and degrees of freedom for thegroup (CBT, waitlist) by time (pre, post, follow-up) interactions.Differences between groups on diagnostic status were examinedusing the chi-squared statistic to report recovery rates from pre topost assessment. The flow of participants through the study ispresented in Fig. 1.
Fig. 1. Consort diagram of parti
Results
The mean number of sessions attended of the twelve weekprogramwas 9.31 (SD ¼ 3.11). Our sample size allowed us to detecta medium effect size (Cohen’s d > 0.4) with adequate power (90%).
Baseline measures
The groups did not differ significantly in terms of any de-mographic features (e.g. age, income, education), pre-assessmentACE-R or pre-assessment questionnaires, except that the severityof the primary problem was significantly higher for the CBT con-dition than the waitlist condition at pre-assessment. See Table 2 formore details. Means on self-report questionnaires fell over (GAI,GDS, CES-D) or close to (PSWQ) cut-offs recommended for clinicalseverity, corroborating the ADIS severity ratings that the sampleswere clinically impaired but not extreme. Although there was nostatistical difference between the means of the total ACE-R scores
cipants through the study.

Table 2Demographic data across conditions intent-to-treat (SD in parenthesis).
Demographic CBT (N ¼ 27) Waitlist (N ¼ 35)
Sex, % female 66.66 62.86Age M ¼ 66.92
(SD ¼ 5.93)M ¼ 67.80(SD ¼ 6.53)
Highest educationlevel, %
Primary school 7.4 0High school 22.22 29.41TAFE/trade 33.33 38.24University degree 37.04 32.35Family income, %>$80,000 4.00 6.25$40,000e80,000 33.00 25$15, 000e40,000 36.00 37.5$0e15,000 28.00 31.25Country of birth, %Australia/New Zealand 59.26 62.86Asian 7.40 5.71Europe 25.92 20.00Africa/Middle East 11.11 5.71South America 0 5.70Marital Status, %Married/partnered 55.55 42.86Widowed 3.70 20.00Separated/divorced 37.04 28.57Single, never married 3.70 8.57Employment status, %Full time employed 14.81 0Part-time employed/
semi-retired18.52 20.00
Retired 55.55 62.86Unemployed/
unable to work7.40 8.57
Home duties 3.70 8.57Taking psychotropic
medication, %22.2 20.0
ACE-R Total Score M ¼ 90.33 (SD ¼ 5.37) M ¼ 91.38 (SD ¼ 5.18)GDS M ¼ 17.98 (SD ¼ 6.18) M ¼ 16.50 (SD ¼ 5.99)CES-D M ¼ 26.21 (SD ¼ 8.07) M ¼ 22.66 (SD ¼ 10.96)GAI M ¼ 11.62 (SD ¼ 4.72) M ¼ 9.49 (SD ¼ 5.43)PSWQ M ¼ 53.75 (SD ¼ 12.39) M ¼ 49.33 (SD ¼ 13.06)SF12 (Mental) M ¼ 43.69 (SD ¼ 9.22) M ¼ 42.15 (SD ¼ 6.69)ADIS primary
disorder severityM ¼ 6.37 (SD ¼ 0.653) M ¼ 5.80 (SD ¼ 1.16)*
Principal diagnoses, %GAD 40.74 28.57SOC 14.81 5.71SPEC 3.70 0PTSD 3.70 5.71MDD 18.52 22.86DYS 11.11 17.14ADNOS 3.70 2.86MDNOS 3.70 17.14Secondary diagnoses, %GAD 25.93 34.29SOC 14.81 14.29SPEC 3.70 5.71PTSD 0 2.86OCD 0 2.86MDD 33.33 14.29DYS 14.81 8.57ADNOS 7.40 2.86MDNOS 0 5.71
Note: Based on original dataset, M ¼ Mean, SD ¼ Standard Deviation, ACE-R ¼ Addenbrooke Cognitive Examination Revised, ADIS ¼ Anxiety Disorder Inter-view Schedule, GDS ¼ Geriatric Depression Scale, CES-D ¼ Centre for Epidemio-logical Studies Depression Scale, GAI ¼ Geriatric Anxiety Inventory, PSWQ ¼ PennState Worry Questionnaire, SF12 ¼ Short Form 12, GAD ¼ Generalized anxietydisorder; SOC ¼ Social Phobia; SPEC ¼ Specific phobia; PTSD ¼ Post traumatic stressdisorder; OCD ¼ Obsessive Compulsive Disorder, MDD ¼ Major Depressive Disor-der; DYS ¼ Dysthymia; ADNOS ¼ Anxiety Disorder Not Otherwise Specified;MDNOS ¼ Mood Disorder Not Otherwise Specified, *F (1,61) ¼ 5.32, p ¼ 0.03 (allother differences between groups were non-significant, ANOVAs p > .05).
V.M. Wuthrich, R.M. Rapee / Behaviour Research and Therapy 51 (2013) 779e786 783
for the two treatment groups, F(1,60) ¼ 0.32, p ¼ .574, becausecognitive ability varied (range 73e98) and pre-treatment cognitionmay be important for the ability to learn and implement CBT(Johnco, Wuthrich, & Rapee, 2013), pre-assessment cognition wasstatistically controlled in all further analyses. Three participantshad ACE-R scores <82 and therefore had likely dementia.
Diagnostic severity across time and condition
Using mixed model analyses on the pooled data, the interactionbetween time (pre, post) and group (CBT, waitlist) for the clinicianrated severity of the primary problem was significant,F(1,47.95) ¼ 17.36, p < .001, demonstrating a significant improve-ment with treatment compared to waitlist. Estimated marginalmeans, standard errors and within group effect sizes for all mixedmodel analyses are presented in Table 3.
To compare the efficacy of the CBT program in reducing anxietyand depression separately, we coded the primary problem as eitheranxiety or mood. Mixed model analysis failed to demonstrate asignificant interaction between time (pre, post), group(CBT, waitlist), and primary problem type (anxiety, mood), F(1,45.38) ¼ .632, p ¼ .431. This indicated that the CBT group programdid not statistically differ in its efficacy in reducing primary anxietyand primary mood problems.
Questionnaire measures across time and condition
Mixed model analyses indicated significant time by group in-teractions on the GDS, F(1, 50.88) ¼ 8.86, p ¼ .004, CES-D, F(1,53.23)¼ 7.90, p¼ .007, and the GAI, F(1, 55.65)¼ 7.40, p¼ .009.1 In allcases self-reported anxiety and depression symptoms reduced signif-icantlymore in theCBTcondition thanwaitlist. Incontrast, thegroupbytime interaction was not significant for the PSWQ, F(1, 54.95) ¼ 0.57,p¼ .452, or the SF12 Mental scale, F(1,51.39)¼ .000, p ¼ .988.
Evaluation of treatment maintenance
Mixed model analyses were used to determine whether thebenefits from treatment were retained at the follow up period forthe CBT condition controlling for ACER scores at pre-assessment(there was no follow up data for the waitlist condition as partici-pants received CBT immediately after the post assessment). For theclinician-rated severity of the primary problem there was a sig-nificant main effect of time, F(2, 49.53) ¼ 35.23, p < .001, whereseverity of the primary problemwas significantly reduced from preto post treatment, t(42.12) ¼ 8.00, p < .001, but not from post tofollow-up, t(33.60) ¼ 1.23, p ¼ .22. See Table 4. To check whetherthe efficacy of the CBT program differed for anxiety symptomscompared to depressive symptoms over time, we examined theinteraction between time (pre, post, follow up) and primaryproblem type (anxiety, mood) and found a non-significant inter-action, F(2, 48.12) ¼ .293, p ¼ .75, indicating that reductions insymptoms over time were not statistically different for symptomsof depression or anxiety.
For the majority of self-report measures, the mixed modelanalysis indicated a significant change over time that was main-tained at follow-up: GDS, F(2, 49.31) ¼ 21.04, p < .001, pre to posttreatment reduction, t(46.39) ¼ 5.49, p < .001, post to follow up,t(44.71) ¼ �.29, p ¼ .77, CES-D, F(2, 49.48) ¼ 34.52, p < .001, pre topost treatment reduction, t(47.38) ¼ 7.29, p < .001, post to followup, t(45.96) ¼ .10, p ¼ .93, GAI, F(2, 49.79) ¼ 9.46, p < .001, pre to
1 A Bonferroni adjustment was made to account for multiple comparisons,alpha ¼ .01 (.05/5).
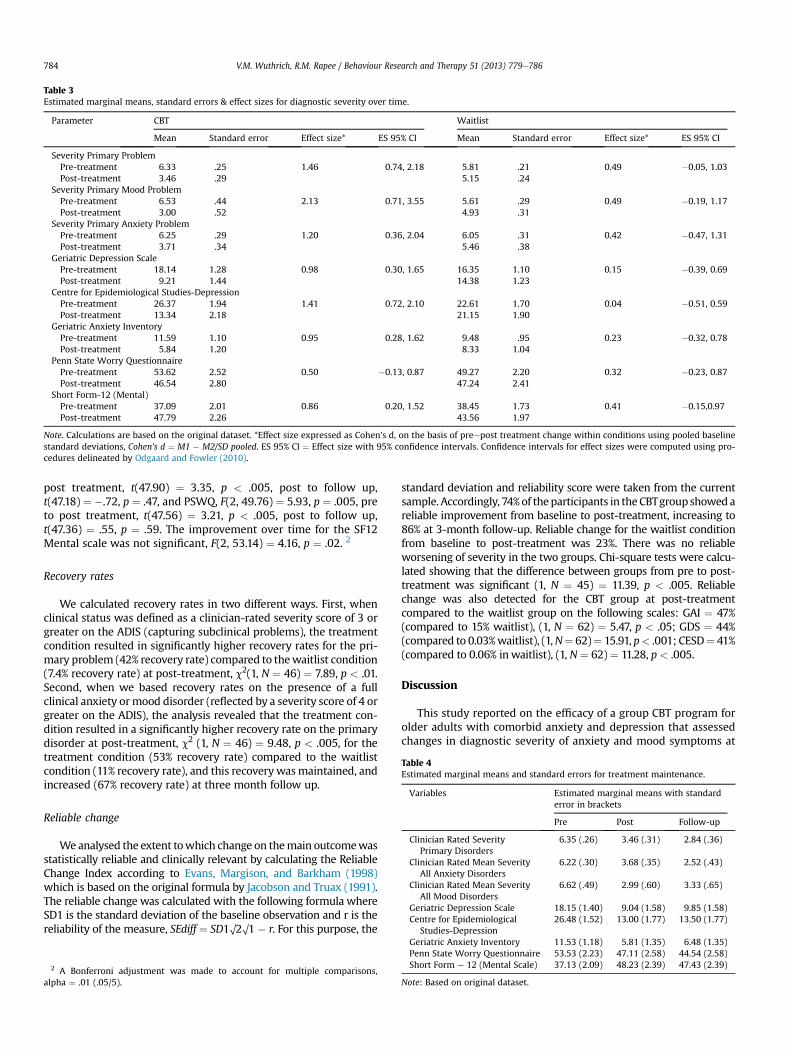
Table 3Estimated marginal means, standard errors & effect sizes for diagnostic severity over time.
Parameter CBT Waitlist
Mean Standard error Effect size* ES 95% CI Mean Standard error Effect size* ES 95% CI
Severity Primary ProblemPre-treatment 6.33 .25 1.46 0.74, 2.18 5.81 .21 0.49 �0.05, 1.03Post-treatment 3.46 .29 5.15 .24
Severity Primary Mood ProblemPre-treatment 6.53 .44 2.13 0.71, 3.55 5.61 .29 0.49 �0.19, 1.17Post-treatment 3.00 .52 4.93 .31
Severity Primary Anxiety ProblemPre-treatment 6.25 .29 1.20 0.36, 2.04 6.05 .31 0.42 �0.47, 1.31Post-treatment 3.71 .34 5.46 .38
Geriatric Depression ScalePre-treatment 18.14 1.28 0.98 0.30, 1.65 16.35 1.10 0.15 �0.39, 0.69Post-treatment 9.21 1.44 14.38 1.23
Centre for Epidemiological Studies-DepressionPre-treatment 26.37 1.94 1.41 0.72, 2.10 22.61 1.70 0.04 �0.51, 0.59Post-treatment 13.34 2.18 21.15 1.90
Geriatric Anxiety InventoryPre-treatment 11.59 1.10 0.95 0.28, 1.62 9.48 .95 0.23 �0.32, 0.78Post-treatment 5.84 1.20 8.33 1.04
Penn State Worry QuestionnairePre-treatment 53.62 2.52 0.50 �0.13, 0.87 49.27 2.20 0.32 �0.23, 0.87Post-treatment 46.54 2.80 47.24 2.41
Short Form-12 (Mental)Pre-treatment 37.09 2.01 0.86 0.20, 1.52 38.45 1.73 0.41 �0.15,0.97Post-treatment 47.79 2.26 43.56 1.97
Note. Calculations are based on the original dataset. *Effect size expressed as Cohen’s d, on the basis of preepost treatment change within conditions using pooled baselinestandard deviations, Cohen’s d ¼ M1 � M2/SD pooled. ES 95% CI ¼ Effect size with 95% confidence intervals. Confidence intervals for effect sizes were computed using pro-cedures delineated by Odgaard and Fowler (2010).
V.M. Wuthrich, R.M. Rapee / Behaviour Research and Therapy 51 (2013) 779e786784
post treatment, t(47.90) ¼ 3.35, p < .005, post to follow up,t(47.18) ¼ �.72, p ¼ .47, and PSWQ, F(2, 49.76) ¼ 5.93, p ¼ .005, preto post treatment, t(47.56) ¼ 3.21, p < .005, post to follow up,t(47.36) ¼ .55, p ¼ .59. The improvement over time for the SF12Mental scale was not significant, F(2, 53.14) ¼ 4.16, p ¼ .02. 2
Table 4Estimated marginal means and standard errors for treatment maintenance.
Recovery rates
We calculated recovery rates in two different ways. First, whenclinical status was defined as a clinician-rated severity score of 3 orgreater on the ADIS (capturing subclinical problems), the treatmentcondition resulted in significantly higher recovery rates for the pri-mary problem (42% recovery rate) compared to thewaitlist condition(7.4% recovery rate) at post-treatment, c2(1, N ¼ 46) ¼ 7.89, p < .01.Second, when we based recovery rates on the presence of a fullclinical anxiety ormood disorder (reflected by a severity score of 4 orgreater on the ADIS), the analysis revealed that the treatment con-dition resulted in a significantly higher recovery rate on the primarydisorder at post-treatment, c2 (1, N ¼ 46) ¼ 9.48, p < .005, for thetreatment condition (53% recovery rate) compared to the waitlistcondition (11% recovery rate), and this recoverywasmaintained, andincreased (67% recovery rate) at three month follow up.
Variables Estimated marginal means with standarderror in brackets
Pre Post Follow-up
Clinician Rated SeverityPrimary Disorders
6.35 (.26) 3.46 (.31) 2.84 (.36)
Clinician Rated Mean SeverityAll Anxiety Disorders
6.22 (.30) 3.68 (.35) 2.52 (.43)
Clinician Rated Mean SeverityAll Mood Disorders
6.62 (.49) 2.99 (.60) 3.33 (.65)
Geriatric Depression Scale 18.15 (1.40) 9.04 (1.58) 9.85 (1.58)Centre for Epidemiological
Studies-Depression26.48 (1.52) 13.00 (1.77) 13.50 (1.77)
Reliable change
Weanalysed the extent towhich change on themain outcomewasstatistically reliable and clinically relevant by calculating the ReliableChange Index according to Evans, Margison, and Barkham (1998)which is based on the original formula by Jacobson and Truax (1991).The reliable change was calculated with the following formula whereSD1 is the standard deviation of the baseline observation and r is thereliability of the measure, SEdiff ¼ SD1O2O1 � r. For this purpose, the
2 A Bonferroni adjustment was made to account for multiple comparisons,alpha ¼ .01 (.05/5).
standard deviation and reliability score were taken from the currentsample. Accordingly, 74%of theparticipants in theCBTgroupshowedareliable improvement from baseline to post-treatment, increasing to86% at 3-month follow-up. Reliable change for the waitlist conditionfrom baseline to post-treatment was 23%. There was no reliableworsening of severity in the two groups. Chi-square tests were calcu-lated showing that the difference between groups from pre to post-treatment was significant (1, N ¼ 45) ¼ 11.39, p < .005. Reliablechange was also detected for the CBT group at post-treatmentcompared to the waitlist group on the following scales: GAI ¼ 47%(compared to 15% waitlist), (1, N ¼ 62) ¼ 5.47, p < .05; GDS ¼ 44%(compared to 0.03%waitlist), (1,N¼ 62)¼ 15.91, p< .001; CESD¼ 41%(compared to 0.06% inwaitlist), (1, N ¼ 62) ¼ 11.28, p < .005.
Discussion
This study reported on the efficacy of a group CBT program forolder adults with comorbid anxiety and depression that assessedchanges in diagnostic severity of anxiety and mood symptoms at
Geriatric Anxiety Inventory 11.53 (1.18) 5.81 (1.35) 6.48 (1.35)Penn State Worry Questionnaire 53.53 (2.23) 47.11 (2.58) 44.54 (2.58)Short Form e 12 (Mental Scale) 37.13 (2.09) 48.23 (2.39) 47.43 (2.39)
Note: Based on original dataset.

V.M. Wuthrich, R.M. Rapee / Behaviour Research and Therapy 51 (2013) 779e786 785
pre-treatment, post-treatment, and follow up periods. Compared towaitlist, older adults receiving treatment demonstrated significantimprovements according to clinician reported severity of primaryanxiety and mood problems. Importantly, the degree of improve-ment in primary anxiety and primary mood problems was similarindicating that the program successfully targeted both disorders. Inaddition, we found significant improvements in self-reported rat-ings of anxiety and depression following CBT but not waitlist. All ofthese changes were maintained three months following the end oftreatment. These improvements resulted in recovery rates of theprimary clinical problem of 52% in the treatment group comparedto 11% of the waitlist group that were maintained three monthslater. Further, significant reliable change was shown by 74% of CBTparticipants compared to 23% of waitlist participants on clinicianrated severity of their main problem and by 40e50% of CBT par-ticipants compared with <1%e15% of participants on waitlist onself report measures.
Despite these improvements, we failed to find a significantgroup by time interaction on the PSWQ and the SF12 Mental scale.The relatively minimal change on the PSWQ relative to strongchanges seen on other measures is interesting and in contrast tomost other studies on GAD in older adults. One possible conclusionis that although the treatment package focused heavily on cognitiverestructuring skills it did not satisfactorily target symptoms ofworry. Given that a large portion of our sample were diagnosedwith GAD, post-hoc analyses were conducted to compare changesin clinician-rated severity between those with primary GAD andthose with other primary anxiety or mood disorders. The resultsshowed a non-significant group by time interaction, F(2,47.09) ¼ 0.10, p ¼ .908, and a non-significant time effect,F(2,26.32) ¼ 0.65, p ¼ 0.53. Because these non-significant com-parisons may be affected by a lack of power, we also examinedwhether there was a significant main effect of time on GAD severityfor those treated with CBT, and found a significant effectF(2,13.81) ¼ 9.14, p < .005. These results suggest that this programwas effective for individuals with GAD, but for some reason thePSWQ did not detect these improvements when examined for allindividuals in the trial. The fact that the PSWQ has been shown tohave only moderate test-retest reliability (Hopko et al., 2003;Stanley et al., 2001) and a different factor structure in older sam-ples compared to younger samples (Knight, McMahon, Skeaff, &Green, 2008) might also contribute to these findings.
The failure to find significant change on the SF12 Mental scalewith treatmentmight reflect the broad nature of this scale and a lifeinterference measure more targeted at impairment associated withanxiety and depression in older adults might have identifiedstronger differences. Although there was sufficient power in thisstudy to detect medium effects, changes on the PSWQ and SF12may reflect smaller effects that weren’t detected in this sample.Further research is needed with larger sample sizes.
It is important to note that the CBT program showed similareffects in reducing symptoms of both anxiety and depression. Thus,in line with our aims, it appears that the program was able toadequately target both disorders in this population. Given highrates of comorbidity, the vast overlap in symptoms, and previousfindings that comorbidity is generally associated with worsetreatment outcomes in single disorder treatment studies, researchshould continue to focus on treating these disorders together. Thisresult is in line with recent work that has demonstrated that CBTcan be used in older adults with subclinical levels of anxiety anddepression in a preventative role, with results lasting at least twoyears (van’t Veer-Tazelaar et al., 2011; van’t Veer-Tazelaar et al.,2009). The direction is also consistent with recent moves amongprograms for younger adults that aim to target broader emotionaldistress rather than individual disorders (Farchione et al., 2012).
Limitations of the study include that treatmentwas compared toa waitlist control and not an active intervention that controlled forother nonspecific therapy factors. Socializing with others and beingheard by an empathetic therapist are important nonspecific ther-apeutic factors that are present in a group therapy format and mayhave accounted for some of the treatment effects. Therefore futureresearch needs to compare group CBT with a placebo group con-dition that specifically controls for potential nonspecific therapyfactors or with other group based psychological treatments in orderto determine whether the specific components associated with theCBT program are specifically responsible for the efficacy of theintervention. Further, the power achieved in this study was prob-ably too low to detect small differences in treatment efficacy forworry severity and life interference, or to detect differences in theeffectiveness of the program for anxiety versus mood symptoms.The study also had a relatively short follow up period of 3 months.Previous research has shown maintenance of treatment gains forspecific disorders among older adults up to 12 months (Stanleyet al., 2003) so it is unlikely that the effects reported here woulddissipate with time, but demonstration of this maintenance withina comorbid populationwould be valuable. Finally, this study lackedformal treatment adherence and therapist competence measures.Instead these issues were monitored by weekly supervision ses-sions with study authors, but should be included in future studies.
Overall this study meets a need to develop an efficacioustransdiagnostic psychological treatment program to tackle theproblem of comorbid anxiety and depression in older adults.Tackling both disorders at once is likely to be cost-effective andproduce superior outcomes to treatments that focus on the primarydisorder only. Given the negative consequences of anxiety anddepression in older adults, interventions such as this may help toreduce the risk of these negative outcomes and produce lastingbenefits for older individuals.
Acknowledgements
This project was funded by a Macquarie University ResearchDevelopment Grant and was registered with the Australian NewZealand Clinical Trials Registry and allocated the ACTRN number:ACTRN12611000528954. Thank you to Dr. Alan Taylor for statisticaladvice.
References
Almeida, O. P., Draper, B., Pirkis, J., Snowdon, J., Lautenschlager, N. T., Byrne, G., et al.(2012). Anxiety, depression, and comorbid anxiety and depression: risk factorsand outcome over two years. International Psychogeriatrics, 24, 1622e1632.
Andreescu, C., Lenze, E. J., Dew, M. A., Begley, A. E., Mulsant, B. H.,Dombrovski, A. Y., et al. (2007). Effect of comorbid anxiety on treatmentresponse and relapse risk in late-life depression: controlled study. BritishJournal of Psychiatry, 190, 344e349.
Andreescu, C., Lenze, E. J., Mulsant, B. H., Wetherall, J. L., Begley, A. E., Mazumdar, S.,et al. (2009). High worry severity is associated with poorer acute and mainte-nance efficacy of antidepressants in late-life depression. Depression and Anxiety,26, 266e272.
Arnow, B. A., Blasey, C., Manber, R., Constantino, M. J., Markowitz, J. C., Klein, D. N.,et al. (2007). Dropouts versus completers among chronically depressed out-patients. Journal of Affective Disorders, 97, 197e202.
Ayers, C. R., Sorrell, J. T., Thorp, S. R., & Wetherell, J. L. (2007). Evidence-basedpsychological treatments for late-life anxiety. Psychology and Aging, 22, 8e17.
Barrowclough, C., King, P., Colville, J., Russell, E., Burns, A., & Tarrier, N. (2001).A randomized trial of the effectiveness of cognitive-behavioral therapy andsupportive counseling for anxiety symptoms in older adults. Journal ofConsulting and Clinical Psychology, 69, 756e762.
Beekman, A. T. F., Bremmer, M. A., Deeg, D. J. H., Van Balkom, A. J. L. M., Smit, J. H., DeBeurs, E., et al. (1998). Anxiety disorders in later life: a report form the LongitudinalAging Study Amsterdam. International Journal of Geriatric Psychiatry, 13, 717e726.
Beekman, A. T. F., de Beurs, E., van Balkom, A., Deeg, D. J. H., van Dyck, R., & vanTilburg, W. (2000). Anxiety and depression in later life: co-occurrence andcommunality of risk factors. American Journal of Psychiatry, 157, 89e95.
V.M. Wuthrich, R.M. Rapee / Behaviour Research and Therapy 51 (2013) 779e786786
Beekman, A. T. F., Deeg, D. J. H., Braam, A., Van Limbeek, J., Braam, A. W., Vries, De,et al. (1997). Criterion validity of the centre for epidemiological studiesdepression scale (CES-D): results from a community-based sample of oldersubjects in the Netherlands. Psychological Medicine, 27, 231e235.
Cohen, A., Gilman, S. E., Houck, P. R., Szanto, K., & Reynolds, C. F. (2009). Socio-economic status and anxiety as predictors of antidepressant treatmentresponse and suicidal ideation in older adults. Social Psychiatry and PsychiatricEpidemiology, 44, 272e277.
Cuijpers, P., van Straten, A., & Smit, F. (2006). Psychological treatment of late-lifedepression: a meta-analysis of randomised controlled trials. InternationalJournal of Geriatric Psychiatry, 21, 1139e1149.
DeLuca, A. K., Lenze, E. J.,Mulsant, B.H., Butters,M.A., Karp, J. F., Dew,M.A., et al. (2005).Comorbid anxietydisorder in late lifedepression: associationwithmemorydeclineover four years. International Journal of Geriatric Psychiatry, 20, 848e854.
Di Nardo, P. A., Brown, T. A., & Barlow, D. H. (1994). Anxiety disorders interviewschedule for DSM-IV. Boston: Center for Stress and Anxiety Related Disorders,Boston University.
Do, C. B., & Batzoglou, S. (2008). What is the expectation maximization algorithm?Nature Biotechnology, 26, 897e899.
Dombrovski, A. Y., Blakesley-Ball, R. E., Mulsant, B. H., Mazumdar, S., Houck, P. R.,Szanto, K., et al. (2006). Speed of improvement in sleep disturbance and anxietycompared with core mood symptoms during acute treatment of depression inold age. American Journal of Geriatric Psychiatry, 14, 550e554.
Evans, C., Margison, F., & Barkham, M. (1998). The contribution of reliable andclinically significant change methods to evidence-based mental health. EvidenceBased Mental Health, 1, 70e72.
Farchione, T. J., Fairholme, C. P., Ellard, K. K., Boisseau, C. L., Thompson-Hollands, J.,Carl, J. R., et al. (2012). Unified protocol for transdiagnostic treatment of emotionaldisorders: a randomized controlled trial. Behavior Therapy, 43, 666e678.
van Ginkel, J. R. (2010). SPSS syntax for applying rules for combining multivariateestimates in multiple imputation. MI-MUL2.sps [computer software]. Retrieved:05.02.13 http://www.socialsciences.leiden.edu/educationandchildstudies/childandfamilystudies/organisation/staffcfs/van-ginkel.html.
Gorenstein, E. E., Kleber, M. S., Mohlmann, J., DeJesus, M., Gorman, J. M., & Papp, L. A.(2005). Cognitive-behavioural therapy for management of anxiety andmedicationtaper in older adults. American Journal of Geriatric Psychiatry, 13, 901e909.
Gould, R. L., Coulson, M. C., & Howard, R. J. (2012). Efficacy of cognitive behavioraltherapy for anxiety disorders in older people: a meta-analysis and meta-regression of randomized controlled trials. Journal of the American GeriatricsSociety, 60, 218e229.
Gum, A. M., Arean, P. A., & Bostrom, A. (2007). Low-income depressed older adultswith psychiatric comorbidity: secondary analyses of response to psychotherapyand case management. International Journal of Geriatric Psychiatry, 22, 124e130.
Haringsma, R., Engels, G. I., Beekman, A. T. F., & Spinhoven, P. H. (2004). The cri-terion validity of the center for epidemiological studies depression scale (CES-D) in a sample of self-referred elders with depressive symptomatology. Inter-national Journal of Geriatric Psychiatry, 19, 558e563.
Hegel, M. T., Unutzer, J., Tang, L., Arean, P. A., Katon, W., Noel, P. H., et al. (2005).Impact of comorbid panic and posttraumatic stress disorder on outcomes ofcollaborative care for late-life depression in primary care. American Journal ofGeriatric Psychiatry, 13, 48e58.
Hendriks, G. J., Oude Voshaar, R. C., Keijsers, G. P. J., Hoogduin, C. A. L., & VanBalkom, A. J. L. M. (2008). Cognitive-behavioural therapy for late-life anxietydisorders: a systematic review and meta-analysis. Acta Psychiatrica Scandinav-ica, 117, 403e411.
Hopko, D. R., Stanley, M. A., Reas, D. L., Wetherall, J. L., Beck, J. G., Novy, D. M., et al.(2003). Assessing worry in older adults: confirmatory factor analysis of thePenn State Worry Questionnaire and psychometric properties of an abbreviatedmodel. Psychological Assessment, 15, 173e183.
Jacobson, N. S., & Truax, P. (1991). Clinical significance: a statistical approach todefining meaningful change in psychotherapy research. Journal of Consultingand Clinical Psychology, 59, 9e12.
Jakobsson, U. (2007). Using the 12-item short form health survey (SF-12) to mea-sure quality of life among older people. Aging Clinical and Experimental Research,19, 457e464.
Johnco, C., Wuthrich, V. M., & Rapee, R. M. (2013). The role of cognitive flexibility incognitive restructuring skill acquisition among older adults. Journal of AnxietyDisorders, 27, 576e584.
Jongenelis, K., Pot, A. M., Eisses, A. M. H., Gerritsen, D. L., Derksen, M.,Beekman, A. T. F., et al. (2005). Diagnostic accuracy of the original 30-item andshortened versions of the Geriatric Depression Scale in nursing home patients.International Journal of Geriatric Psychiatry, 20, 1067e1074.
Kendler, K. S., Gardner, C. O., Gatz, M., & Pedersen, N. L. (2007). The sources of co-morbidity between major depression and generalised anxiety disorder in aSwedish national twin sample. Psychological Medicine, 37, 453e462.
Kessler, R. C., Nelson, C. B., McGonagle, K. A., Liu, J., Swartz, M., & Blazer, D. G. (1996).Comorbidity of DSM-III-R major depressive disorder in the general population: re-sults from theUSNational Comorbidity Survey.British Journal of Psychiatry, 30, 8e21.
Knight, R. G., McMahon, J., Skeaff, C., & Green, T. J. (2008). Normative data forpersons over 65 on the Penn State Worry Questionnaire. New Zealand Journal ofPsychology, 37, 4e9.
Lenze, E. J., Mulsant, B. H., Shear, M. K., Schulberg, H. C., Dew, M. A., Begley, A. E.,et al. (2000). Comorbid anxiety disorders in depressed elderly patients. Amer-ican Journal of Psychiatry, 157, 722e728.
Mackin, R. S., & Arean, P. A. (2005). Evidence-based psychotherapeutic interventionsfor geriatric depression. Psychiatric Clinics of North America, 28, 805e820.
Meyer, T. J., Miller, M. L., Metzger, R. L., & Borkovec, T. D. (1990). Development andvalidation of the Penn State Worry Questionnaire. Behaviour Research andTherapy, 28, 487e495.
Mioshi, E., Dawson, K., Mitchell, J., Arnold, R., & Hodges, J. R. (2006). The Adden-brooke’s Cognitive Examination Revised (ACE-R): a brief cognitive test battery fordementia screening. International Journal of Geriatric Psychiatry, 21, 1078e1085.
Mohlman, J., Gorenstein, E. E., Kleber, M., deJesus, M., Gorman, J. M., & Papp, L. A.(2003). Standard and enhanced cognitive behavior therapy for late life gener-alized anxiety disorder: two pilot investigations. American Journal of GeriatricPsychiatry, 11, 24e32.
Mohlman, J., & Gorman, J. M. (2005). The role of executive functioning in CBT: apilot study with anxious older adults. Behaviour Research and Therapy, 43,447e465.
Nordhus, I. H., & Pallesen, S. (2003). Psychological treatment of late-life anxiety: anempirical review. Journal of Consulting and Clinical Psychology, 71, 643e651.
Odgaard, E. C., & Fowler, R. L. (2010). Confidence intervals for effect sizes: compli-ance and clinical significance in the Journal of Consulting and Clinical Psy-chology. Journal of Consulting and Clinical Psychology, 78, 287e297.
Pachana, N. A., Byrne, G. J., Siddle, H., Koloski, N., Harley, E., & Arnold, E. (2007).Development and validation of the geriatric anxiety inventory. InternationalPsychogeriatrics, 19, 103e114.
Radloff, L. S. (1977). The CES-D scale: a self-report depression scale for research inthe general population. Applied Psychological Measurement, 1, 385e401.
Sallis, J. F., Lichenstein, K. L., Clarkson, A. D., Stalgaitis, S., & Campbell, M. (1983).Anxiety and depression management for the elderly. International Journal ofBehavioral Geriatrics, 1, 3e12.
Schafer, J. L., & Graham, J. W. (2002). Missing data: our view of the state of the art.Psychological Methods, 7, 147e177.
Schuurmans, J., Comijs, H., Emmelkamp, P. M. G., Weijnen, I. J. C., van den Hout, M.,& van Dyck, R. (2009). Long-term effectiveness and prediction of treatmentoutcome in cognitive behavioral therapy and sertraline for late-life anxietydisorders. International Psychogeriatrics, 21, 1148e1159.
Serfaty, M. A., Haworth, D., Blanchard, M., Buszewicz, M., & King, M. (2009). Clinicaleffectiveness of individual cognitive behavioral therapy for depressed olderpeople in primary care: a randomized control trial. Archives of General Psychi-atry, 66, 1332e1340.
Sinharay, S., Stern, H. S., & Russell, D. (2001). The use of multiple imputation for theanalysis of missing data. Psychological Methods, 6, 317e329.
Stanley, M. A., Beck, J. G., Novy, D. M., Averill, P. M., Swann, A. C., Diefenbach, G. J.,et al. (2003). Cognitive-behavioral treatment of late-life generalized anxietydisorder. Journal of Consulting and Clinical Psychology, 71, 309e319.
Stanley, M. A., Novy, D. M., Bourland, S. L., Beck, J. G., & Averill, P. M. (2001).Assessing older adults with generalised anxiety: a replication and extension.Behaviour Research and Therapy, 39, 221e235.
van’t Veer-Tazelaar, P. J., van Maruiijk, H. W., Van Oppen, P., Van der Horst, H. E.,Smit, F., Cuijpers, P., et al. (2011). Prevention of late-life anxiety and depressionhas sustained effects over 24 months: a pragmatic randomized trial. AmericanJournal of Geriatric Psychiatry, 19, 230e239.
van’t Veer-Tazelaar, P. J., van Maruiijk, H. W., van Oppen, P., van Hout, H. P., van derHorst, H. E., Cuijpers, P., et al. (2009). Stepped-care prevention of anxiety anddepression in late life. Archives of General Psychiatry, 66, 297e304.
Vink, D., Aartsen, M. J., & Schoevers, R. A. (2008). Risk factors for anxiety anddepression in the elderly: a review. Journal of Affective Disorders, 106, 29e44.
Ware, J. E., Kosinski, M., & Keller, S. D. (1996). A 12-item short-form health survey:construction of scales and preliminary tests for reliability and validity. MedicalCare, 34, 220e233.
Watson, D., CLark, L. A., Weber, K., Assenheimer, J. S., Strauss, M. E., &McCormick, R. A. (1995). Testing a tripartite model, II: exploring the symptomstructure of anxiety and depression in student, adult, and patient samples.Journal of Abnormal Psychology, 104, 15e25.
Wetherell, J. L., Gatz, M., & Craske, M. G. (2003). Treatment of generalisedanxiety disorder in older adults. Journal of Consulting and Clinical Psychol-ogy, 71, 340e341.
Wetherell, J. L., Hopko, D. R., Diefenbach, G. J., Averill, P. M., Beck, J. G., Craske, M. G.,et al. (2005). Cognitive-behavioral therapy for late-life generalized anxietydisorder: who gets better? Behavior Therapy, 36, 147e156.
Yesavage, J. A., Brink, T. L., Rose, T. L., Lum, O., Huang, V., Adley, M., et al. (1983).Development and validation of a geriatric depression screening scale: a pre-liminary report. Journal of Psychiatric Research, 1, 37e49.




















