
Durable remissions with autologous stem cell transplantation for high-risk HIV-associated lymphomas
20
doi:10.1182/blood-2004-04-1532 Prepublished online September 23, 2004; Joseph Rosenthal, Joseph Alvarnas and Stephen J Forman Amrita Krishnan, Arturo Molina, John Zaia, David Smith, Debbie Vasquez, Neil Kogut, Peter M Falk, HIV-associated lymphomas Durable remissions with autologous stem cell transplantation for high risk (1881 articles) Transplantation (4217 articles) Neoplasia (1734 articles) Free Research Articles (3716 articles) Clinical Trials and Observations Articles on similar topics can be found in the following Blood collections http://bloodjournal.hematologylibrary.org/site/misc/rights.xhtml#repub_requests Information about reproducing this article in parts or in its entirety may be found online at: http://bloodjournal.hematologylibrary.org/site/misc/rights.xhtml#reprints Information about ordering reprints may be found online at: http://bloodjournal.hematologylibrary.org/site/subscriptions/index.xhtml Information about subscriptions and ASH membership may be found online at: digital object identifier (DOIs) and date of initial publication. the indexed by PubMed from initial publication. Citations to Advance online articles must include final publication). Advance online articles are citable and establish publication priority; they are appeared in the paper journal (edited, typeset versions may be posted when available prior to Advance online articles have been peer reviewed and accepted for publication but have not yet Copyright 2011 by The American Society of Hematology; all rights reserved. 20036. the American Society of Hematology, 2021 L St, NW, Suite 900, Washington DC Blood (print ISSN 0006-4971, online ISSN 1528-0020), is published weekly by For personal use only. by guest on June 6, 2013. bloodjournal.hematologylibrary.org From
-
Upload
independent -
Category
Documents
-
view
1 -
download
0
Transcript of Durable remissions with autologous stem cell transplantation for high-risk HIV-associated lymphomas
doi:10.1182/blood-2004-04-1532Prepublished online September 23, 2004;
Joseph Rosenthal, Joseph Alvarnas and Stephen J FormanAmrita Krishnan, Arturo Molina, John Zaia, David Smith, Debbie Vasquez, Neil Kogut, Peter M Falk, HIV-associated lymphomasDurable remissions with autologous stem cell transplantation for high risk
(1881 articles)Transplantation � (4217 articles)Neoplasia �
(1734 articles)Free Research Articles � (3716 articles)Clinical Trials and Observations �
Articles on similar topics can be found in the following Blood collections
http://bloodjournal.hematologylibrary.org/site/misc/rights.xhtml#repub_requestsInformation about reproducing this article in parts or in its entirety may be found online at:
http://bloodjournal.hematologylibrary.org/site/misc/rights.xhtml#reprintsInformation about ordering reprints may be found online at:
http://bloodjournal.hematologylibrary.org/site/subscriptions/index.xhtmlInformation about subscriptions and ASH membership may be found online at:
digital object identifier (DOIs) and date of initial publication. theindexed by PubMed from initial publication. Citations to Advance online articles must include
final publication). Advance online articles are citable and establish publication priority; they areappeared in the paper journal (edited, typeset versions may be posted when available prior to Advance online articles have been peer reviewed and accepted for publication but have not yet
Copyright 2011 by The American Society of Hematology; all rights reserved.20036.the American Society of Hematology, 2021 L St, NW, Suite 900, Washington DC Blood (print ISSN 0006-4971, online ISSN 1528-0020), is published weekly by
For personal use only. by guest on June 6, 2013. bloodjournal.hematologylibrary.orgFrom
Durable Remissions with Autologous Stem Cell Transplantation for high-risk HIV-associated Lymphomas
Amrita Krishnan, M.D., Arturo Molina, M.D., M.S., John Zaia, M.D., David Smith, Ph.D., Debbie Vasquez, R.N., Neil Kogut, M.D., Peter M. Falk, M.D., Joseph Rosenthal, M.D., Joseph Alvarnas, M.D., Stephen J. Forman, M.D.
City of Hope Hematologic Neoplasia Program
City of Hope Cancer CenterDivision of Hematology and Hematopoietic Stem Cell Transplantation1500 East Duarte RoadDuarte CA 91010
Short Title: Long Term Remission in High-risk HIV-Associated LymphomaScientific Heading: TransplantationCorresponding Author: Amrita Krishnan MD City of Hope Cancer Center
1500 East Duarte Road Duarte CA 90101
Fax 626 301 8973 tel 626 359 8111 ext62645 Email [email protected]
Research Support: The work was supported in part by United States Public Health Service Grants CA30206, CA33572, AI38592, MO1 RR-43 from the General Clinical Research Center branch of the National Center for Research Resources, National Institutes of Health. AK was the recipient of a Lymphoma Research Foundation of America Fellowship Award. AM was the recipient of an American Cancer Society Clinical Oncology Career Development Award.
Abstract word Count: 192Word Count: 3017
Blood First Edition Paper, prepublished online September 23, 2004; DOI 10.1182/blood-2004-04-1532
Copyright © 2004 American Society of Hematology
For personal use only. by guest on June 6, 2013. bloodjournal.hematologylibrary.orgFrom

Abstract
The treatment of HIV-associated lymphoma has changed since the widespread use of highly
active antiretroviral therapy. HIV infected individuals can tolerate more intensive chemotherapy
as they have better hematologic reserves and fewer infections. This has led to higher response
rates in patients with HIV-associated Hodgkin’s (HD) or non-Hodgkin’s lymphoma (NHL)
treated with chemotherapy in conjunction with antiretroviral therapy. However, for patients with
refractory or relapsed disease, salvage chemotherapy still offers little chance of long-term
survival.
In the non-HIV setting, patients with relapsed HD or NHL have a better chance of long term
remission with high dose chemotherapy with autologous stem cell rescue (ASCT) compared with
conventional salvage chemotherapy. In a prior report we demonstrated that this approach is well
tolerated in patients with underlying immunodeficiency from HIV infection. Furthermore,
similar engraftment to the non-HIV setting and low infectious risks have been observed. Herein,
we expand upon this early experience with the largest single institution series of twenty patients.
With long-term followup we demonstrate that ASCT can lead to an 85% progression free
survival which suggests that this approach may be potentially curative in select patients with
relapsed HIV associated HD or NHL.
For personal use only. by guest on June 6, 2013. bloodjournal.hematologylibrary.orgFrom
The incidence of Hodgkin’s (HD) and non-Hodgkin’s lymphoma (NHL) in HIV infected
individuals is much greater than in the HIV negative population.1,2 In earlier decades the
treatment of lymphoma in the setting of immune deficiency was far less successful than in the
HIV negative patient.3 This was in part due to the poor hematologic reserves of HIV infected
patients but also due to higher rates of infection and higher rates of relapse of the lymphoma.
The advent of highly active antiretroviral therapy (HAART) altered the natural history of HIV
infection by reducing the incidence of opportunistic infections and improving the underlying
immune deficiency.4In addition, combining HAART with chemotherapy or consolidating
chemotherapy with HAART has increased remission rates in both HIV-associated Hodgkin’s and
non-Hodgkin’s lymphoma.5,6Recent studies have also confirmed that the International Prognostic
Index (IPI) is applicable to patients treated with HAART and chemotherapy.7For HIV infected
lymphoma patients with high-risk features as defined by the IPI, relapse rates are still high after
conventional chemotherapy. Furthermore, for HIV infected patients with either relapsed HD or
NHL the current salvage chemotherapy regimens offer little chance of long term survival.
In the HIV negative setting, studies have shown that high dose therapy with autologous stem cell
transplant (ASCT) is the optimal therapy for relapsed HD and NHL.8,9,10 As the procedure related
mortality of ASCT has decreased, ongoing studies are exploring its use in high-risk first
remission patients.10Now that HIV infected individuals have markedly improved immune and
hematologic function, the use of both solid organ and ASCT is being explored in patients with
underlying immunodeficiency and concomitant malignancy or organ dysfunction.11-15Herein we
report the City of Hope Comprehensive Cancer Center experience on the largest single
institution series of patients with HIV-associated lymphomas undergoing ASCT. Our initial
For personal use only. by guest on June 6, 2013. bloodjournal.hematologylibrary.orgFrom
experience demonstrated the feasibility of this approach in terms of stem cell mobilization,
engraftment and low regimen related toxicity.16 Now with long term follow up in a larger series
of patients we demonstrate that ASCT can provide durable remissions in a subset of these high-
risk patients.
Patients, Materials, and Methods
Patients
HIV positive patients with NHL who failed to achieve complete remission (CR) after standard
dose front line chemotherapy or had a chemosensitive relapse (PR or CR) after an initial CR
were eligible. HIV NHL patients with high-risk disease in first CR as defined by the IPI were
also eligible. Patients with HD with a chemotherapy sensitive relapse were eligible. All
pathology was reviewed at the City of Hope by a hematopathologist. Inclusion criteria were the
institutional standard criteria for ASCT- cardiac ejection fraction >50% by either MUGA scan or
echocardiogram, 24hour urine creatinine clearance >60cc/minute, diffusion capacity>50%
predicted, liver function tests <2X normal, <10% bone marrow involvement with lymphoma and
no CNS involvement with lymphoma. Patients with prior positive CSF cytology were eligible if
the CSF cleared with intrathecal therapy. Positive hepatitis serology was not an exclusion criteria
but required further evaluation including a liver biopsy. Initially, the first five patients were
required to have an absolute CD4 count of >100/mcl at the time of lymphoma diagnosis or
recurrence. However, this requirement was deleted for subsequent patients. All patients had to
have an HIV viral load of <10,000cp/ml by RT-PCR at enrollment. Patients had to be free of
opportunistic infections for one year prior to enrollment except for treatment responsive thrush,
For personal use only. by guest on June 6, 2013. bloodjournal.hematologylibrary.orgFrom
mycobacterium and herpes infections. All patients had to be receiving highly active antiretroviral
therapy (HAART). The City of Hope’s institutional review board approved the protocol and
informed consent was obtained from each patient in accordance with institutional guidelines.
Treatment
Patients in first remission had peripheral blood stem cells (PBSC) collected upon recovery from
standard front line chemotherapy or after cyclophosphamide (2g/m2) plus G-CSF(10µg/kg) for
stem cell priming. Patients in partial remission (PR) or with relapsed disease received a variety
of salvage chemotherapy regimens. Those who demonstrated chemotherapy response had PBSC
collected upon recovery from another cycle of the same chemotherapy. Details of stem cell
collection have been previously outlined.16 In order to avoid myelosuppression, patients on
trimethoprim sulfamethoxazole were changed to inhaled pentamidine for pneumocystis
prophylaxis prior to stem cell collection. A minimum of 5x106 CD 34+ cells/kg was collected.
The first five patients had additional stem cells collected for use in gene therapy trials.
Two high dose therapy regimens were utilized. A chemotherapy based regimen of carmustine
150mg/m2/daily (day –5 to –7), etoposide 60mg/kg adjusted body weight (day-4)
cyclophosphamide 100mg/kg ideal body weight (day-2), or a radiation based regimen of
fractionated total body irradiation (FTBI)to a total dose of 1200cGy, etoposide 60mg/kg (day-4),
cyclophosphamide 100mg/kg ideal body weight (day-2). Patients less than 55 years of age with
bulky disease or extranodal disease who had not received prior radiation were offered the FTBI
based regimen. Two patients who received the chemotherapy based regimen received involved
For personal use only. by guest on June 6, 2013. bloodjournal.hematologylibrary.orgFrom
field radiation post ASCT. PBSC were thawed and reinfused on day 0. Only one patient did not
receive the entire collection as he had extremely high cell doses. A back up product of 12X10 6
CD34+cells/kg was reserved. G-CSF 5ug/kg was started on day+1. Antibacterial prophylaxis
was with levofloxacin 500mg daily, antifungal prophylaxis consisted of either fluconazole
400mg/day or amphotericin. 0.1-0.15mg/kg/day, and antiviral prophylaxis was with acyclovir
5mg/kg twice daily until day+25. All patients were maintained on their HAART regimen.
RESULTS
Between March 1998 and August 2003, twenty patients with HIV-associated lymphomas were
enrolled. Median age at ASCT was 44 years (range 11-68). The majority had relapsed disease
or failed to achieve a CR with front line therapy, 7 in 1st relapse, 2 in 2nd relapse, 5 in 1st PR.
Four patients with a high-risk IPI score were in first CR and one in 2nd and 3rd CR respectively.
The histologic subtypes, and chemotherapy regimens are listed in table 1. Patients received a
median of 2 chemotherapy regimens prior to ASCT (range 1-4).
The median CD4 count at lymphoma diagnosis was 174cells/mcl (range 30-500) and median
viral load at lymphoma diagnosis was 26,120 cp/ml (range 500-1,300,000). At study entry
seventeen patients had undetectable viral loads, and the remaining three had a viral load ranging
between 700-6500 cp/ml. The median CD4 count at study entry was 175 cells/mcl (range 25-
1064). Fifteen patients were on a protease inhibitor based regimen and the remainder on a non-
nucleoside reverse transcriptase inhibitor based regimen. One patient had concomitant hepatitis
B infection. His liver biopsy prior to ASCT showed no evidence of cirrhosis.
For personal use only. by guest on June 6, 2013. bloodjournal.hematologylibrary.orgFrom
A median of 10.6X106 CD34+ cells/kg were collected after a median of 4 days of apheresis.
One patient required prolonged apheresis (10days). No significant toxicity in terms of rise in
HIV viral load or opportunistic infections were seen during apheresis.
Seventeen patients received the chemotherapy based conditioning regimen and three received the
radiation based regimen. Antiretroviral therapy was given to all patients from the start of
conditioning onwards, but only nine were able to tolerate it throughout. The remainder were
intolerant due to gastrointestinal toxicity such as nausea in the majority, or mucositis in the FTBI
patients. The same HAART regimen was restarted in all but two patients after a median of 21
days. One patient did not resume his antiretroviral therapy as he developed multiorgan failure.
Another patient was changed from the two nucleoside reverse transcriptase inhibitors (NRTI)
Zidovudine and Lamivudine and one nonnucleoside reverse transcriptase inhibitor (NNRTI)
Nevirapine to Abacavir, Lamivudine and Efavirenz. The majority of patients were able to
resume HAART by two months post ASCT with the exception of one who had persistent nausea
and noncompliance that was in part ascribed to depression. Genotyping was not performed prior
to the resumption of HAART. All patients engrafted at a median of eleven days for neutrophil
engraftment (range 9-23). The markedly delayed engraftment of twenty three days was in the one
patient who was on Zidovudine as part of his HAART regimen.
Other treatment related toxicities included liver function abnormalities in the majority of
patients, grade 1-2 in 16, and grade 3-4 in three. One of these patients, the oldest in the series,
age 68, ultimately developed cardiomyopathy and renal failure and died at day+22 post ASCT.
For personal use only. by guest on June 6, 2013. bloodjournal.hematologylibrary.orgFrom
The other recovered uneventfully and the third had late hepatoxicity over ten months post ASCT
that responded to a change in his antiretroviral regimen, Two patients developed an engraftment
syndrome manifest as high temperatures, hypotension, skin rash and fluid retention. Both
responded to corticosteroids. Interstitial pneumonitis that was ascribed to the carmustine
developed in one patient and was successfully treated with corticosteroids. Pericarditis
presumed to be secondary to cyclophosphamide was seen in one patient and was treated with
nonsteroidals and a five day course of low dose prednisone. This same patient also developed
transient atrial fibrillation that was treated with medical therapy. Another patient with a history
of supraventricular (SVT) arrhythmias prior to the transplant developed recurrent SVT and had
to be cardioverted. The patient who had delayed engraftment post ASCT developed subdural
hematomas during a period of thrombocytopenia after a lumbar puncture. They ultimately
required surgical drainage. He also developed hemorrhagic cystitis that responded to bladder
irrigation.
Early infectious complications prior to engraftment included gram positive bacteremias in four
patients and fever and neutropenia in eight patients. One patient had vancomycin resistant
enterococcus isolated from a bronchoalveolar lavage. Post engraftment, opportunistic infections
were more common. Two patients who were not compliant with prophylaxis developed
pneumocystis pneumonia. One of these patients also developed pulmonary aspergillus after
steroid treatment for his pneumocystis. One patient never had documented pneumocystis but
was treated empirically for this after a chest xray demonstrated interstitial infiltrates. Two
patients developed disseminated herpes zoster. Cytomegalovirus retinitis developed in one
patient and two had asymptomatic viremia All patients responded to therapy. At a year post
For personal use only. by guest on June 6, 2013. bloodjournal.hematologylibrary.orgFrom

ASCT one patient acquired hepatitis C which was found upon evaluation of liver function
abnormalities.
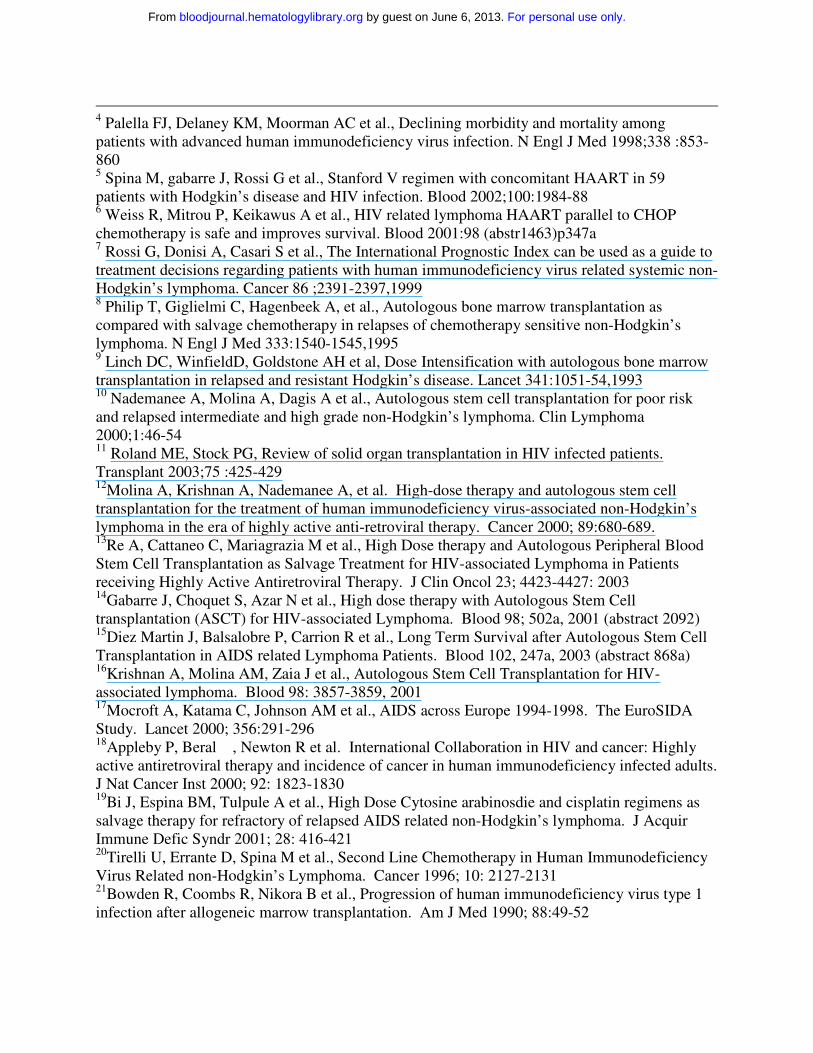
The underlying HIV infection did not worsen as a result of the transplant. While CD4 counts
nadired at approximately 6 months post transplant, they recovered to pretransplant levels by one
year in all patients (figure 1). The median CD4 count at one year was 187 cells/mcl and 472
cells/mcl at two years. The HIV viral load tended to fluctuate, in part due to prolonged
noncompliance with HAART in one patient. The majority (76%) had undetectable viral loads at
one year (range 0-500,000 cp/mL). Two of the four with detectable viral loads at one year were
undetectable at study enrollment. However, one of these patients did not resume HAART until
one year post ASCT. Ten of the seventeen long term survivors required changes in their
antiretroviral regimen during the observation period due to viral failure.
Median length of follow up is 31.8 months (range 5.5-70). Seventeen of the twenty patients are
alive and in remission. One patient with a follow up of 5.5 months had a positive PET scan at his
100 day restaging but no CAT scan correlation. Two patients died of relapsed lymphoma early
post transplant (2months, 4months). One patient died of regimen related toxicity at day+22. The
progression free survival (PFS) is 85%(95% CI 69-100) and overall survival 85% for the entire
group. (figure 2) For the patients transplanted beyond 1st CR the OS is 81%(95% CI 62-100)
(figure 3) and PFS is 81% (69-100).
Discussion
For personal use only. by guest on June 6, 2013. bloodjournal.hematologylibrary.orgFrom
ASCT has become an accepted standard of care for patients with relapsed aggressive NHL and
certain patients with relapsed HD. The mortality of this procedure has declined to the point that
we are now performing transplants in older patients as well as those with other co-morbid
illnesses. However, this has not become a standard of care with HIV lymphoma despite
significant advances in the treatment of HIV infection. Patients are living longer and suffering
from fewer opportunistic infections.
Notably, in the current era, despite the use of HAART, lymphoma remains a major cause of
morbidity and mortality in HIV infected individuals. 17,18 While the use of concomitant
chemotherapy and HAART has increased remission rates and improved survival, options for
patients with refractory or relapsed lymphoma are limited.19,20 Results even in the HAART era
with salvage therapy have been poor. For example, in a group of thirteen patients with refractory
or relapsed HIV-NHL, seven of whom were on protease inhibitor based therapy, all treated with
ESHAP (etoposide, cisplatinum, cytarabine, solumedrol), median survival was only 7.1
months.19An even shorter median survival in the pre-HAART era was reported from an Italian
group who treated 21 patients with HIV-NHL either refractory to primary chemotherapy or in
first relapse. Five of the nineteen evaluable patients achieved a CR (26%), median survival in the
CR patients was 13months but for the entire cohort median survival was only 2.1 months.20
Thus, for these high-risk patients, better treatment options are clearly needed.
Prior to the advent of HAART, HIV infection was considered a contraindication to both solid
organ and stem cell transplantation. Certainly this was borne out by the early allogeneic
transplant experience in HIV infected patients, which was characterized by high rates of
For personal use only. by guest on June 6, 2013. bloodjournal.hematologylibrary.orgFrom
opportunistic infections.21,22 However, as our understanding of how to administer antimicrobial
prophylaxis in conjunction with antiretroviral therapy has improved, centers have revisited the
issues of transplantation in patients with HIV lymphoma.
One of the early series of ASCT was from France. Gabarrre et al., used both radiation and
chemotherapy based conditioning regimens for a group of patients with HIV HD and NHL14
They included multiply relapsed patients as well as primary refractory patients. Infectious
complications were similar to our series, with opportunistic infections induding CMV viremia
noted. Six of the fourteen were (43%) alive at the time of reporting with the longest follow up
being 31 months. Another series, a multi institutional trial from Italy was performed using a
standard chemotherapy based conditioning regimen of BEAM (carmustine,cytarabine,
etoposide,melphalan).13 They too included refractory as well as relapsed patients. The patients
received debulking chemotherapy prior to ASCT, though details of disease status at the time of
ASCT were not provided. Sixteen patients were enrolled on the trial and analyzed on an intent to
treat basis. Fifteen patients underwent stem cell collection. Three patients failed to mobilize
adequate stem cells for ASCT. Of the remaining twelve, two had disease progression before
ASCT, one did not proceed to ASCT and one did and subsequently died of progressive disease
4months post ASCT. Ten other patients went on to ASCT of which nine were evaluable at the
time of reporting. Median follow up is short (8 months) but eight patients achieved a CR or PR
post ASCT. Median disease free survival and overall survival of the cohort undergoing ASCT
was 11 months and eighteen months respectively. Projected two year overall survival for the
entire group is 39%.
For personal use only. by guest on June 6, 2013. bloodjournal.hematologylibrary.orgFrom
The most recent series reported from Spain included many 1st CR patients.15 However, their
definition of 1st CR also included patients who required more than one line of chemotherapy to
achieve a CR as well as Burkitt’s type lymphoma who were initially undertreated and then
achieved CR with other therapy. All patients but one were in CR at the time of ASCT. The
majority received BEAM as the conditioning regimen, Median followup is 21 months (range 1-
28). Disease free survival was 73%. Infectious complications were similar to all other series and
included one case of herpes zoster and once case of pulmonary aspergillus.
The reported experiences mirror some of the challenges in treating these patients. For example,
difficulty in stem cell mobilization. Based on the same experience in two patients, our
antiretroviral regimens were modified. Specifically patients cannot be on an antiretroviral
regimen containing zidovudine pre or post ASCT and not on trimethroprim sulfamethoxazole for
pneumocystis prophylaxis pre stem cell collection. Post transplant, all groups report similar
infectious complications, such as herpes zoster. This too has led to a modification in our post
ASCT care in that all patients after discharge are now maintained on oral acyclovir for at least
one year.
The varied results reported in these series may in part reflect patient selection. For example the
inclusion of chemotherapy refractory patients in the French series, as well as patients with
multiple relapses may have played a factor in the lower disease free survival in this study.
Similarly, the Italian series analyzed all patients with HIV lymphoma who were considered for
transplant. Not surprisingly they demonstrated a markedly better survival in the patients who
went onto to ASCT, moreover, the median survival of this subgroup is similar to the other series.
For personal use only. by guest on June 6, 2013. bloodjournal.hematologylibrary.orgFrom
Our experience is unique in that it is a single institution experience and provides the longest
follow up. Patient selection may have played a bias in our good results in that most patients had
to demonstrate chemotherapy sensitive disease, but we too included multiply relapsed patients as
well as those patients not in CR after first line chemotherapy. Moreover, our transplant selection
criteria in regards to the underlying lymphoma are no different than in our HIV negative
lymphoma patients. In fact we consider the HIV infection to be akin to a chronic illness that can
be managed with appropriate prophylaxis and surveillance. However, we do require that eligible
patients must have well controlled HIV infection as manifest by low HIV viral loads to optimize
the chance of stem cell mobilization and minimize infectious risks. The other series do not
include this criteria though the Italian series did require a CD4 count of greater than 100/mcl and
an effective HAART regimen. Hence one can postulate that in part, the superior disease free
survival in our series is mediated by well controlled HIV infection. Certainly in the nontransplant
setting, studies have demonstrated that the use of HAART is an independent prognostic factor
for event free survival in HIV NHL.23,24 The experience of all the centers suggests that ASCT
should be considered earlier after demonstration of chemotherapy sensitivity for those in first
relapse or with primary refractory disease, as the procedure can be performed with low
procedural related mortality. Further research is needed for those with high-risk first CR. Our
long term follow up confirms that ASCT can provide durable remissions and can be a potentially
curative option for those with otherwise dismal prognosis with conventional therapy.
1 Levine AM Hodgkin’s Disease in the setting of human immunodeficiency virus infection. J Natl Cancer Inst Monogr 1998;23:37-422 Levine AM Acquired Immune deficiency syndrome related lymphoma;clinical aspects.Semin Oncol 2000;27:442-4533 Kaplan LD, Straus DJ, Testa MA et al., Low dose compared with standard dose m-BACOD chemotherapy for non-Hodgkin’s lymphoma associated with human immunodeficiency virus infection. N Engl J Med 1997;336:1641-48
For personal use only. by guest on June 6, 2013. bloodjournal.hematologylibrary.orgFrom
4 Palella FJ, Delaney KM, Moorman AC et al., Declining morbidity and mortality among patients with advanced human immunodeficiency virus infection. N Engl J Med 1998;338 :853-8605 Spina M, gabarre J, Rossi G et al., Stanford V regimen with concomitant HAART in 59 patients with Hodgkin’s disease and HIV infection. Blood 2002;100:1984-886 Weiss R, Mitrou P, Keikawus A et al., HIV related lymphoma HAART parallel to CHOP chemotherapy is safe and improves survival. Blood 2001:98 (abstr1463)p347a7 Rossi G, Donisi A, Casari S et al., The International Prognostic Index can be used as a guide to treatment decisions regarding patients with human immunodeficiency virus related systemic non-Hodgkin’s lymphoma. Cancer 86 ;2391-2397,19998 Philip T, Giglielmi C, Hagenbeek A, et al., Autologous bone marrow transplantation as compared with salvage chemotherapy in relapses of chemotherapy sensitive non-Hodgkin’s lymphoma. N Engl J Med 333:1540-1545,19959 Linch DC, WinfieldD, Goldstone AH et al, Dose Intensification with autologous bone marrow transplantation in relapsed and resistant Hodgkin’s disease. Lancet 341:1051-54,199310 Nademanee A, Molina A, Dagis A et al., Autologous stem cell transplantation for poor risk and relapsed intermediate and high grade non-Hodgkin’s lymphoma. Clin Lymphoma 2000;1:46-5411 Roland ME, Stock PG, Review of solid organ transplantation in HIV infected patients. Transplant 2003;75 :425-42912Molina A, Krishnan A, Nademanee A, et al. High-dose therapy and autologous stem cell transplantation for the treatment of human immunodeficiency virus-associated non-Hodgkin’s lymphoma in the era of highly active anti-retroviral therapy. Cancer 2000; 89:680-689.13Re A, Cattaneo C, Mariagrazia M et al., High Dose therapy and Autologous Peripheral Blood Stem Cell Transplantation as Salvage Treatment for HIV-associated Lymphoma in Patients receiving Highly Active Antiretroviral Therapy. J Clin Oncol 23; 4423-4427: 200314Gabarre J, Choquet S, Azar N et al., High dose therapy with Autologous Stem Cell transplantation (ASCT) for HIV-associated Lymphoma. Blood 98; 502a, 2001 (abstract 2092)15Diez Martin J, Balsalobre P, Carrion R et al., Long Term Survival after Autologous Stem Cell Transplantation in AIDS related Lymphoma Patients. Blood 102, 247a, 2003 (abstract 868a)16Krishnan A, Molina AM, Zaia J et al., Autologous Stem Cell Transplantation for HIV-associated lymphoma. Blood 98: 3857-3859, 200117Mocroft A, Katama C, Johnson AM et al., AIDS across Europe 1994-1998. The EuroSIDA Study. Lancet 2000; 356:291-29618Appleby P, Beral , Newton R et al. International Collaboration in HIV and cancer: Highly active antiretroviral therapy and incidence of cancer in human immunodeficiency infected adults. J Nat Cancer Inst 2000; 92: 1823-183019Bi J, Espina BM, Tulpule A et al., High Dose Cytosine arabinosdie and cisplatin regimens as salvage therapy for refractory of relapsed AIDS related non-Hodgkin’s lymphoma. J Acquir Immune Defic Syndr 2001; 28: 416-42120Tirelli U, Errante D, Spina M et al., Second Line Chemotherapy in Human Immunodeficiency Virus Related non-Hodgkin’s Lymphoma. Cancer 1996; 10: 2127-2131 21Bowden R, Coombs R, Nikora B et al., Progression of human immunodeficiency virus type 1 infection after allogeneic marrow transplantation. Am J Med 1990; 88:49-52
For personal use only. by guest on June 6, 2013. bloodjournal.hematologylibrary.orgFrom

22Contu L, La Nasa G, Arras M et al., Allogeneic bone marrow transplantation combined with multiple anti-HIV 1 treatment in a case of AIDS. Bone Marrow Transplantation 1993; 12: 669-67123Navarro J, Ribera J, Oriol A et al., Influence of highly active anti-retroviral therapy on response to treatment and survival in patients with acquired immunodeficiency syndrome related non-Hodgkin’s lymphoma treated with cyclophosphamide, hydroxydoxorubicin, vincristine and prednisone. Br J Hem 2001; 112: 909-91524Hoffman C, Wolf E, Fatkenheuer G et al., Response to highly active antiretroviral therapy strongly predicts outcome in patients with AIDS related lymphoma. AIDS 2003; 17: 1521-1529.
For personal use only. by guest on June 6, 2013. bloodjournal.hematologylibrary.orgFrom
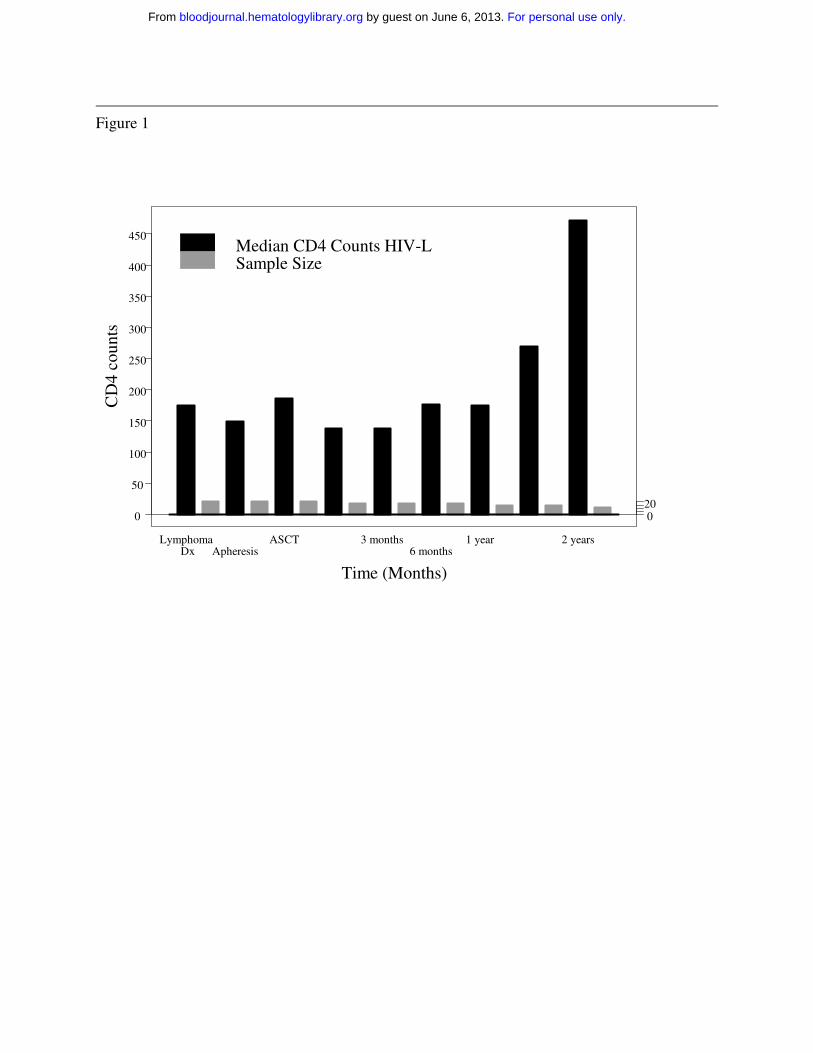
Figure 1
Lymphoma Dx Apheresis
ASCT 3 months6 months
1 year 2 years
Time (Months)
0
50
100
150
200
250
300
350
400
450
0 20
CD
4 co
unts
Median CD4 Counts HIV-LSample Size
For personal use only. by guest on June 6, 2013. bloodjournal.hematologylibrary.orgFrom
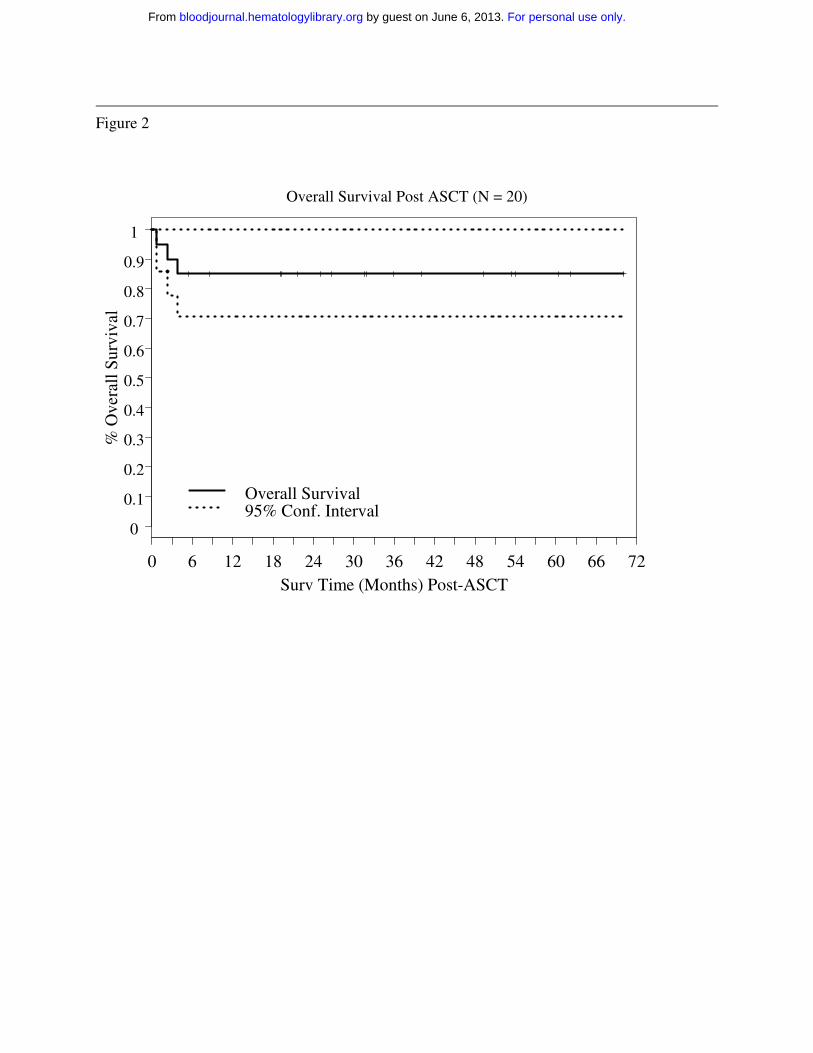
Figure 2
Overall Survival Post ASCT (N = 20)
Surv Time (Months) Post-ASCT0 6 12 18 24 30 36 42 48 54 60 66 72
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1
% O
vera
ll Su
rviv
al
Overall Survival95% Conf. Interval
For personal use only. by guest on June 6, 2013. bloodjournal.hematologylibrary.orgFrom
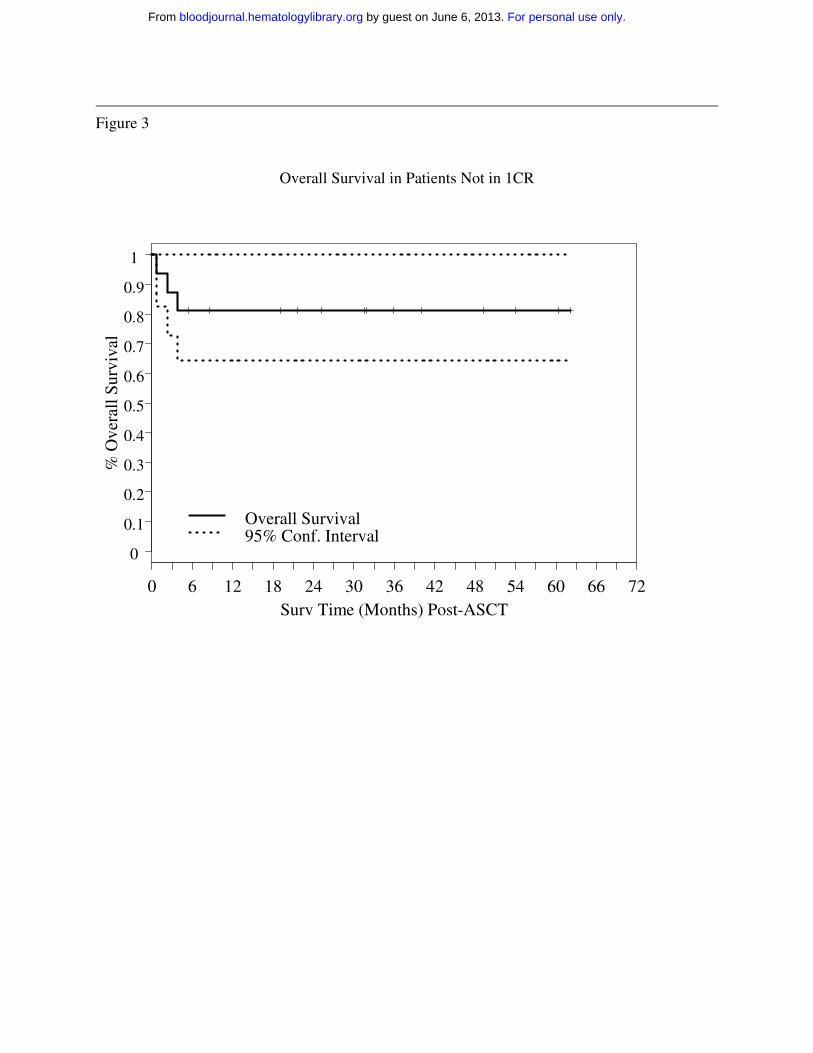
Figure 3
Overall Survival in Patients Not in 1CR
Surv Time (Months) Post-ASCT0 6 12 18 24 30 36 42 48 54 60 66 72
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1
% O
vera
ll Su
rviv
al
Overall Survival95% Conf. Interval
For personal use only. by guest on June 6, 2013. bloodjournal.hematologylibrary.orgFrom
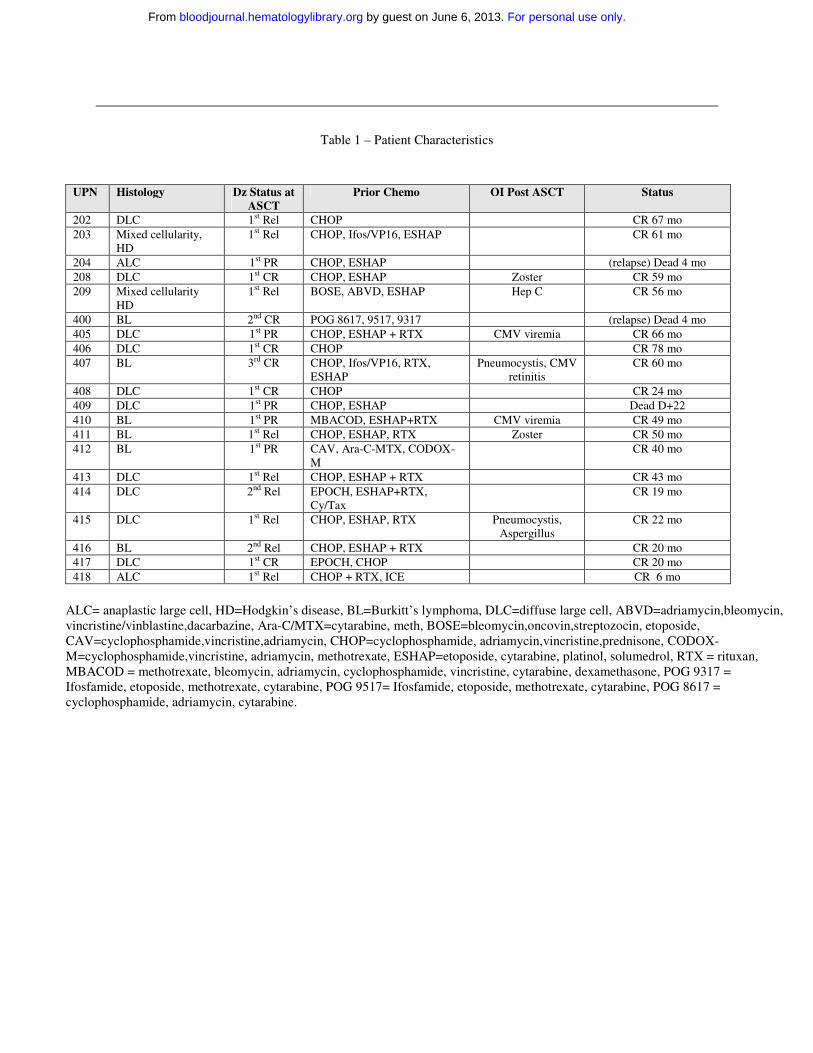
Table 1 – Patient Characteristics
UPN Histology Dz Status at ASCT
Prior Chemo OI Post ASCT Status
202 DLC 1st Rel CHOP CR 67 mo203 Mixed cellularity,
HD1st Rel CHOP, Ifos/VP16, ESHAP CR 61 mo
204 ALC 1st PR CHOP, ESHAP (relapse) Dead 4 mo208 DLC 1st CR CHOP, ESHAP Zoster CR 59 mo209 Mixed cellularity
HD1st Rel BOSE, ABVD, ESHAP Hep C CR 56 mo
400 BL 2nd CR POG 8617, 9517, 9317 (relapse) Dead 4 mo405 DLC 1st PR CHOP, ESHAP + RTX CMV viremia CR 66 mo406 DLC 1st CR CHOP CR 78 mo407 BL 3rd CR CHOP, Ifos/VP16, RTX,
ESHAPPneumocystis, CMV
retinitisCR 60 mo
408 DLC 1st CR CHOP CR 24 mo409 DLC 1st PR CHOP, ESHAP Dead D+22410 BL 1st PR MBACOD, ESHAP+RTX CMV viremia CR 49 mo411 BL 1st Rel CHOP, ESHAP, RTX Zoster CR 50 mo412 BL 1st PR CAV, Ara-C-MTX, CODOX-
MCR 40 mo
413 DLC 1st Rel CHOP, ESHAP + RTX CR 43 mo414 DLC 2nd Rel EPOCH, ESHAP+RTX,
Cy/TaxCR 19 mo
415 DLC 1st Rel CHOP, ESHAP, RTX Pneumocystis, Aspergillus
CR 22 mo
416 BL 2nd Rel CHOP, ESHAP + RTX CR 20 mo417 DLC 1st CR EPOCH, CHOP CR 20 mo418 ALC 1st Rel CHOP + RTX, ICE CR 6 mo
ALC= anaplastic large cell, HD=Hodgkin’s disease, BL=Burkitt’s lymphoma, DLC=diffuse large cell, ABVD=adriamycin,bleomycin, vincristine/vinblastine,dacarbazine, Ara-C/MTX=cytarabine, meth, BOSE=bleomycin,oncovin,streptozocin, etoposide, CAV=cyclophosphamide,vincristine,adriamycin, CHOP=cyclophosphamide, adriamycin,vincristine,prednisone, CODOX-M=cyclophosphamide,vincristine, adriamycin, methotrexate, ESHAP=etoposide, cytarabine, platinol, solumedrol, RTX = rituxan, MBACOD = methotrexate, bleomycin, adriamycin, cyclophosphamide, vincristine, cytarabine, dexamethasone, POG 9317 = Ifosfamide, etoposide, methotrexate, cytarabine, POG 9517= Ifosfamide, etoposide, methotrexate, cytarabine, POG 8617 = cyclophosphamide, adriamycin, cytarabine.
For personal use only. by guest on June 6, 2013. bloodjournal.hematologylibrary.orgFrom




















