
Drug attitude in adolescents: A key factor for a comprehensive assessment
10
Drug Attitude in Adolescents A Key Factor for a Comprehensive Assessment Silvia Molteni, MD,* Giovanni Giaroli, MD,Þþ Giorgio Rossi, MD,§ Mario Comelli, MSc,|| Maneesh Rajendraprasad, MD,Þ and Umberto Balottin, MD*§ Abstract: Objective: Very few studies have evaluated the subjective experience (SE) in children and adolescents treated with antipsychotics. The present study aimed to evaluate the SE of antipsychotics in ado- lescents diagnosed with different psychiatric conditions and to identify explanatory variables of adolescents’ SE and compliance with treatment. Methods: The Drug Attitude Inventory (DAI) was used to evaluate SE in 67 adolescents in 2 different countries (Italy and United Kingdom). Compliance was measured using a Likert scale completed by both patients and parents. To evaluate other parameters correlated to the SE, the following scales were administered: Clinical Global Impression Scale, Children’s Global Assessment Scale, Extrapyramidal Symptoms Rating Scale, Barnes Akathisia Rating Scale, and EuroQoL (for quality of life). Multiple and logistic regression analyses were applied. Results: No significant difference in drug attitude was found between psychotic and nonpsychotic patients. Our results showed a highly sig- nificant association between DAI and compliance (Spearman index, 0.33; P = 0.005); for all other variables, DAI associated significantly only with quality of life (r = 0.25; P = 0.03). The multivariable analysis confirmed the presence of a strong association between compliance and DAI (P = G0.001). In our sample, drug attitude was the only variable found to be correlated with the compliance, whereas extrapyramidal adverse effects showed an only marginally significant association. Conclusions: Our observations provide confirmation, also in adoles- cents, that drug attitude is strongly correlated with treatment compliance and underline the need in clinical assessments to always consider the patient’s viewpoint. Key Words: Drug Attitude Inventory (DAI), subjective experience, compliance, adolescence, antipsychotic drugs, psychosis (J Clin Psychopharmacol 2014;34: 99Y108) T he use of antipsychotic (AP) drugs is a cornerstone of the treatment of adolescents with severe mental disorders. 1Y3 Unfortunately, the compliance to psychotropic medications in this group of patients is often far from optimal. 4 In 1963, Sarwer-Foner, 5 exploring the psychodynamic mechanisms of neuroleptic drugs, stated that ‘‘The therapeutic effect as compared to the pharmacological effect on the patient is due not to the pharmacological action alone, but the way this physiological action psychologically influences the patient’s defences in terms of the patient’s total situation.’’ Although increasing knowledge in the field of psychophar- macology has resulted in more effective treatments and reduced relapse rates, 6 the percentage of nonadherence to treatment is still high. 7,8 The issue of subjective experience (SE) of treatment with APs and its relevance to therapeutic outcome came to prominence in the early 1990s. 9,10 In 1989, Awad 11 suggested that various factors contribute to the response to APs. According to his conceptual framework, subjective interpretation of the physiological changes accompa- nying medication can alter the clinical outcome of the treatment, as well as the severity of the adverse effects and the patient’s be- havioral response. With the studies of Jaspers, 12 SE became, and has since remained, a key focus of psychopathology, due to the need to give priority to the subjective point of view, particularly in adolescents. Subjective experience is defined as the patient’s perception or ‘‘inner sense’’ of his own body, mind, relations with others, disease, and treatment. 10 Although the importance of SE in adults treated with APs is amply demonstrated, 13Y16 to date, very few studies have evaluated this aspect in children/adolescents. In 2005, Schimmelmann et al 17 used the Subjective Well- Being under Neuroleptic Treatment scale 18 to study 20 adoles- cents affected by early-onset psychosis under treatment with second-generation APs. In this sample, SE was found to be negatively associated with adverse effects, in particular neuro- logical adverse effects and sedation. In a study by Fraguas et al, 19 drug attitude evaluated at baseline with the 10-item version of Drug Attitude Inventory 20 (DAI-10) was significantly related to all-cause AP treatment discontinuation in a sample of adolescents with a first episode of psychosis. Nevertheless, the specific association between drug attitude and treatment discontinuation was not significant. Townsend et al 21 found a low but significant correlation between the DAI and compliance in a sample of 122 adolescents with Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition, Text Revised (DSM-IV-TR) Axis I disorders treated with different psychotropic drugs. The early identification of a negative attitude to medication would, in fact, make it easier to identify factors favoring noncompliance and therefore con- tributing to the development of acute psychosis, suicidal idea- tion and, ultimately, a negative outcome. Finally, Floersch et al 22 used the Teen Subjective Experience of Medication Interview to collect qualitative data on SE in 20 adolescents treated with different psychiatric medications. The patients’ experiences were found to be mediated by the following complex social dynamics: family, cultural and personal influences and opinions, their own attitude to the diagnosis, and aspects of the physician-patient relationship. Our hypothesis is that SE is a key element to be taken into account for a comprehensive assessment of adolescent patients being treated with AP medications. This could also play a funda- mental role in understanding patients’ adherence to AP treatment. ORIGINAL CONTRIBUTION Journal of Clinical Psychopharmacology & Volume 34, Number 1, February 2014 www.psychopharmacology.com 99 From the *Child Neuropsychiatry Unit, Department of Brain and Behavioral Sciences, University of Pavia, Pavia, Italy; †North East London NHS Founda- tion Trust, Ilford; ‡Department of Psychosis Studies, Institute of Psychiatry, King’s College London, London, UK; §Child Neuropsychiatry Unit, IRCCS C. Mondino National Institute of Neurology Foundation; and ||Biostatistics Unit, Department of Brain and Behavioral Sciences, University of Pavia, Pavia, Italy. Received November 12, 2012; accepted after revision May 1, 2013. Reprints: Umberto Balottin, MD, Child Neurology and Psychiatry Unit, IRCCS C. Mondino National Institute of Neurology Foundation, Via Mondino 2, 27100 Pavia, Italy (e<mail: [email protected]). Copyright * 2014 by Lippincott Williams & Wilkins ISSN: 0271-0749 DOI: 10.1097/JCP.0000000000000035 Copyright © 2013 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
Transcript of Drug attitude in adolescents: A key factor for a comprehensive assessment

Drug Attitude in AdolescentsA Key Factor for a Comprehensive Assessment
Silvia Molteni, MD,* Giovanni Giaroli, MD,Þþ Giorgio Rossi, MD,§Mario Comelli, MSc,|| Maneesh Rajendraprasad, MD,Þ and Umberto Balottin, MD*§
Abstract: Objective: Very few studies have evaluated the subjectiveexperience (SE) in children and adolescents treated with antipsychotics.The present study aimed to evaluate the SE of antipsychotics in ado-lescents diagnosed with different psychiatric conditions and to identifyexplanatory variables of adolescents’ SE and compliance with treatment.Methods: The Drug Attitude Inventory (DAI) was used to evaluate SEin 67 adolescents in 2 different countries (Italy and United Kingdom).Compliance was measured using a Likert scale completed by bothpatients and parents. To evaluate other parameters correlated to the SE,the following scales were administered: Clinical Global ImpressionScale, Children’s Global Assessment Scale, Extrapyramidal SymptomsRating Scale, Barnes Akathisia Rating Scale, and EuroQoL (for qualityof life). Multiple and logistic regression analyses were applied.Results: No significant difference in drug attitude was found betweenpsychotic and nonpsychotic patients. Our results showed a highly sig-nificant association between DAI and compliance (Spearman index,0.33; P = 0.005); for all other variables, DAI associated significantlyonly with quality of life (r = 0.25; P = 0.03). The multivariable analysisconfirmed the presence of a strong association between compliance andDAI (P = G0.001). In our sample, drug attitude was the only variablefound to be correlated with the compliance, whereas extrapyramidaladverse effects showed an only marginally significant association.Conclusions: Our observations provide confirmation, also in adoles-cents, that drug attitude is strongly correlated with treatment complianceand underline the need in clinical assessments to always consider thepatient’s viewpoint.
Key Words: Drug Attitude Inventory (DAI), subjective experience,compliance, adolescence, antipsychotic drugs, psychosis
(J Clin Psychopharmacol 2014;34: 99Y108)
The use of antipsychotic (AP) drugs is a cornerstone of thetreatment of adolescents with severe mental disorders.1Y3
Unfortunately, the compliance to psychotropic medications inthis group of patients is often far from optimal.4
In 1963, Sarwer-Foner,5 exploring the psychodynamicmechanisms of neuroleptic drugs, stated that ‘‘The therapeuticeffect as compared to the pharmacological effect on the patientis due not to the pharmacological action alone, but the way thisphysiological action psychologically influences the patient’sdefences in terms of the patient’s total situation.’’
Although increasing knowledge in the field of psychophar-macology has resulted in more effective treatments and reducedrelapse rates,6 the percentage of nonadherence to treatment is stillhigh.7,8
The issue of subjective experience (SE) of treatment withAPs and its relevance to therapeutic outcome came to prominencein the early 1990s.9,10
In 1989, Awad11 suggested that various factors contribute tothe response to APs. According to his conceptual framework,subjective interpretation of the physiological changes accompa-nying medication can alter the clinical outcome of the treatment,as well as the severity of the adverse effects and the patient’s be-havioral response.
With the studies of Jaspers,12 SE became, and has sinceremained, a key focus of psychopathology, due to the need to givepriority to the subjective point of view, particularly in adolescents.Subjective experience is defined as the patient’s perceptionor ‘‘inner sense’’ of his own body, mind, relations with others,disease, and treatment.10
Although the importance of SE in adults treated with APsis amply demonstrated,13Y16 to date, very few studies haveevaluated this aspect in children/adolescents.
In 2005, Schimmelmann et al17 used the Subjective Well-Being under Neuroleptic Treatment scale18 to study 20 adoles-cents affected by early-onset psychosis under treatment withsecond-generation APs. In this sample, SE was found to benegatively associated with adverse effects, in particular neuro-logical adverse effects and sedation.
In a study by Fraguas et al,19 drug attitude evaluated atbaseline with the 10-item version of Drug Attitude Inventory20
(DAI-10) was significantly related to all-cause AP treatmentdiscontinuation in a sample of adolescents with a first episodeof psychosis. Nevertheless, the specific association betweendrug attitude and treatment discontinuation was not significant.Townsend et al21 found a low but significant correlation betweenthe DAI and compliance in a sample of 122 adolescents withDiagnostic and Statistical Manual of Mental Disorders, FourthEdition, Text Revised (DSM-IV-TR) Axis I disorders treated withdifferent psychotropic drugs. The early identification of anegative attitude to medication would, in fact, make it easierto identify factors favoring noncompliance and therefore con-tributing to the development of acute psychosis, suicidal idea-tion and, ultimately, a negative outcome.
Finally, Floersch et al22 used the Teen Subjective Experienceof Medication Interview to collect qualitative data on SE in 20adolescents treated with different psychiatric medications. Thepatients’ experiences were found to be mediated by the followingcomplex social dynamics: family, cultural and personal influencesand opinions, their own attitude to the diagnosis, and aspects ofthe physician-patient relationship.
Our hypothesis is that SE is a key element to be taken intoaccount for a comprehensive assessment of adolescent patientsbeing treated with AP medications. This could also play a funda-mental role in understanding patients’ adherence to AP treatment.
ORIGINAL CONTRIBUTION
Journal of Clinical Psychopharmacology & Volume 34, Number 1, February 2014 www.psychopharmacology.com 99
From the *Child Neuropsychiatry Unit, Department of Brain and BehavioralSciences, University of Pavia, Pavia, Italy; †North East London NHS Founda-tion Trust, Ilford; ‡Department of Psychosis Studies, Institute of Psychiatry,King’s College London, London, UK; §Child Neuropsychiatry Unit, IRCCS C.Mondino National Institute of Neurology Foundation; and ||Biostatistics Unit,Department of Brain and Behavioral Sciences, University of Pavia, Pavia, Italy.Received November 12, 2012; accepted after revision May 1, 2013.Reprints: Umberto Balottin, MD, Child Neurology and Psychiatry Unit,
IRCCS C. Mondino National Institute of Neurology Foundation, ViaMondino 2, 27100 Pavia, Italy (e<mail: [email protected]).
Copyright * 2014 by Lippincott Williams & WilkinsISSN: 0271-0749DOI: 10.1097/JCP.0000000000000035
Copyright © 2013 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.

Therefore, we conducted a naturalistic and observational studyaiming to (a) identify explanatory variables of SE among a seriesof selected clinical variables, (b) test for a statistically significantcorrelation between SE of APs and compliance with treatment,and (c) evaluate which variables most influenced compliance.
Because of the failure of previous studies to evaluate SE inpatients with different psychiatric conditions, another objectiveof our study was to compare the SE in patients diagnosed withschizophrenia and other psychotic disorders and in patients withother psychiatric diagnoses.
METHODSThe sample for this naturalistic and observational cross-
sectional study, designed to evaluate SE of APs in adolescents,was recruited from 3 different Child and Adolescent MentalHealth Services (CAMHSs): South Essex Partnership UniversityNHS Foundation Trust (SEPT) UK; CAMHS, North East LondonFoundation Trust, UK; and Unit of Child Neurology and Neuro-psychiatry, C. Mondino National Institute of Neurology Founda-tion, IRCCS, Pavia Italy.
The study was approved by the relevant local ethics com-mittees and has been carried out in accordance with the Dec-laration of Helsinki.
We aimed to recruit all patients referred to these CAMHSsand prescribed an AP.
All patients and their families were given written infor-mation (age appropriate) about the study and were required toprovide their written consent to participate.
Of a total of 80 patients contacted between February 2010and July 2011, 67 agreed to participate in the study.
Patients included were aged between 14 and 19 years, hada DSM IV-TR Axis I or Axis II disorder, and had been undertreatment with the same AP for at least the previous month at astable dose; we excluded patients with acute psychosis (posi-tive and negative syndrome scale23 [PANSS], 970), learningdisability, substance abuse, or organic psychosis. Conversely,psychiatric comorbidity and concurrent use of other psycho-tropic medications was accepted and recorded.
Principal Variables
Subjective ExperienceThe longer version of DAI (DAI-3020) was used to evalu-
ate the adolescents’ attitude to APs. This scale has a total of 30dichotomous items (requiring a true/false response). The in-strument has a total score range of j30 to +30. A positive ornegative total score indicates, respectively, a positive or negativesubjective attitude.
According to the study of Hogan et al,20 DAI is a mixtureof patient’s subjective response and experience of medication(DAI-SR) and attitudes to medication (AM). Therefore, DAIcan be also divided into these 2 subscores.
ComplianceA simple 4-point questionnaire (Likert-type), with separate
versions for administration to patients and caregivers, was de-veloped to investigate patient compliance with the prescribedtreatment: 1, I never take my medication (absence of compli-ance); 2, I forget to take my medication more than once a week(poor compliance); 3, I sometimes forget, but less than once aweek (moderate compliance); and 4, I always take my medication(excellent compliance). This approach, also used by Townsendet al,21 was preferred to proxy measures, which are not necessarilymore reliable. The caregivers and patients completed the measuresseparately.
Secondary Variables
Demographic and Clinical VariablesData on patients’ primary and comorbid diagnoses were
collected from parents and clinical notes; we also noted pa-tients’ age and sex, parents and patients’ years of education,pharmacological therapy (APs) and any concurrent psychotro-pic medication, duration of illness, date of starting current APtreatment and current AP dosage, and weight changes.
The diagnoses were confirmed using the Mini Interna-tional Neuropsychiatric Interview24 and the Structured ClinicalInterview for DSM Axis II Personality Disorders (SCID-II).25
Positive and negative syndrome scale was used to evaluate theseverity of psychopathology in patients with psychosis.
Adverse EffectsAll patients underwent a complete neurological examina-
tion. The Extrapyramidal Symptoms Rating Scale (ESRS)26
was used to assess the presence of extrapyramidal symptoms(EPSs) due to AP therapy; this scale is designed to detect arange of EPSs that can be associated with treatment with APs.Of these, akathisia is a highly distressing symptom in adoles-cents which can impact greatly on SE of therapy. In view of this,we analyzed it separately using a semistructured interview, theBarnes Akathisia Rating Scale (BARS).27 This instrument givesratings for both the clinician’s and the patient’s impressions(BARS1 and BARS2).
Global Functioning and Disease SeverityDisease severity was evaluated using the Clinical Global
Impression (CGI) Scale28 and the Children’s Global AssessmentScale (CGAS).29
Quality of LifeAs an indicator of quality of life, current well-being was
measured using EuroQoL, a 0 to 100 visual analog scale.30
Sample SizeTo detect correlations of at least 0.4 between quantitative
variables, with > = 0.05 and sample size equal to 67, the powerof the study is 0.9.
Statistical AnalysisBetween-groups comparisons of quantitative variables
were performed using the t test. Correlations were computed bythe Pearson or Spearman correlation coefficient as appropriate.
To evaluate the effect of all the factors that may influenceDAI-30 scores, we estimated a multiple regression model, usingthe penalized least squares technique. All the explanatoryvariables were kept in the model whatever their P values are.To calculate the fraction of estimated variance due to eachexplanatory variable, the corresponding multiple R2 increasewas used.
To evaluate the factor influencing the compliance, a pro-portional odds logistic model was estimated using the penalizedmaximum likelihood method.31,32
BARS2 scores were categorized as ‘‘mild’’ and ‘‘moderate-severe’’ (we pooled the scale’s second and third categories, toavoid excessively small subgroups). For the same reason,BARS1 was dichotomized as absent/present. Equivalent dosewas classified into 3 categories to give account the nonlinearityof its effect.
The data were analyzed by means of R.33
Molteni et al Journal of Clinical Psychopharmacology & Volume 34, Number 1, February 2014
100 www.psychopharmacology.com * 2014 Lippincott Williams & Wilkins
Copyright © 2013 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.

RESULTS
Characteristics of the SampleA total of 67 adolescents (mean age, 16.6 [1.4] years),
referred as outpatients or inpatients to the 3 participating centersbetween February 2010 and July 2011, met the inclusion criteriaand were included in the study.
The DAI was filled out during the treatment (all patientshad been under treatment with APs from at least 1 month at astable dose). The psychopathological assessment (CGAS, CGI,and PANSS) was carried out at least 1 month after the beginningof the treatment (on average 9.02 months [SD, 10 months]). Allthe scales, questionnaires, and evaluations (DAI, Likert scale forcompliance, PANSS, CGAS, CGI, ESRS, BARS, and EuroQol)were filled out at this time in 1 single assessment during ascheduled follow-up visit.
The sample was made up of 33 (49.25%) men and 34(50.75%) women; 30 (44.78%) of whom were Italian and 37(55.22%) British.
The patients’ diagnoses were based on the DSM IV-TRcriteria and confirmed through administration of the Mini In-ternational Neuropsychiatric Interview and the SCID-II.
Thirty-six (53.73%) adolescents were diagnosed withpsychotic disorders (cases) (schizophrenia in 12, brief psychoticdisorder in 6, schizoaffective disorder in 8, and psychosis NOSin 10), and 31 (46.27%) with nonpsychotic psychiatric disorders(controls).
Psychiatric comorbidity was present in 35.8% of the sample(10 cases and 14 controls).
Sixty-four patients were receiving second-generation APs:31 risperidone (mean dosage, 4.40 [3.87] mg), 15 aripiprazole(11.03 [6.21] mg), 9 quetiapine (455.56 [187.82] mg), 7olanzapine (11.6 [7.67] mg), 1 clozapine (350 mg), and 1amisulpiride (500). The other 3 patients were taking the first-generation AP, haloperidol (2.13 [1.03] mg). Nearly half ofthe patients (49.25%) were concomitantly receiving drugs otherthan APs, mainly antidepressants.
Antipsychotics’ equivalent dose was comparable in cases andcontrols (high dosage, 69% vs 58%;moderate dosage, 25% vs 26%).
Other demographic and clinical characteristics of the sampleare presented in Table 1.
Adverse Effects of TreatmentsSixty (89.6%) patients recorded a weight gain ranging from
1 to 20 kg (mean, 5.18 [4.8] kg). Of the remaining 7 patients, allof whom lost weight, 6 were being treated with aripiprazole and1 with quetiapine.
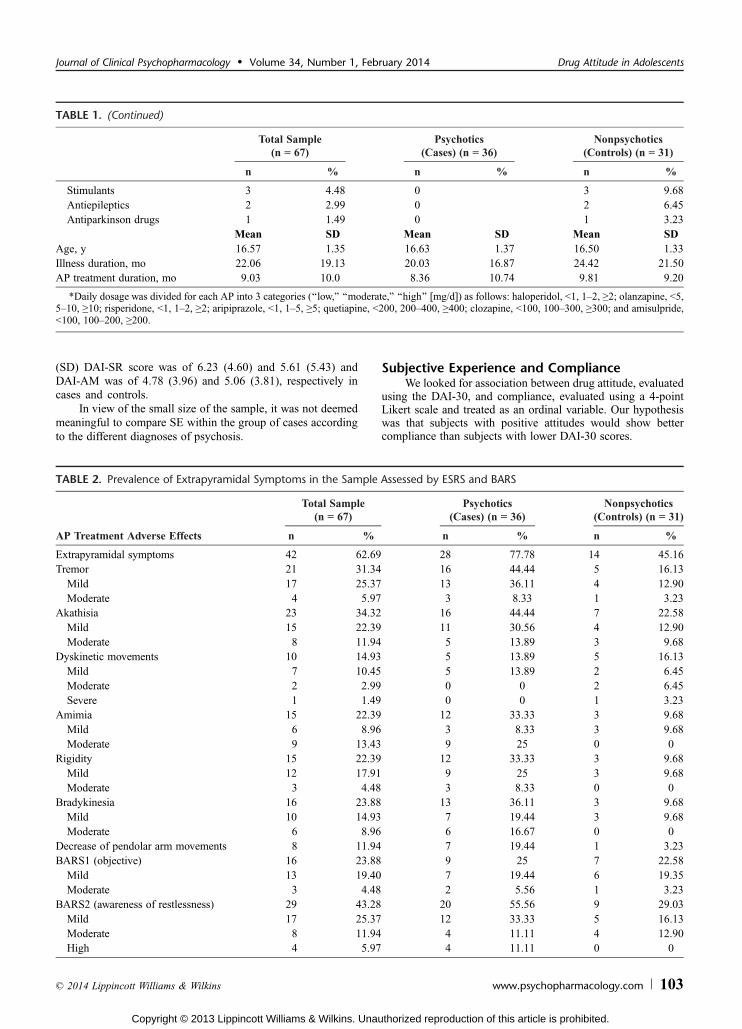
Forty-two (62.7%) patients presented EPSs; of these,28 were affected by psychosis and 14 by other disorders. Themain EPSs, each present in more than a quarter of the sample,were akathisia (34.3%) and tremor (31.3%). In addition, morethan 20% of the patients presented bradykinesia and amimia.With the sole exception of a patient receiving haloperidol whodeveloped severe dyskinesias (high frequency and amplitude),all adverse effects were mild or moderate in severity. Table 2provides more details of the therapeutic adverse effectsobserved.
Disease SeverityAdministration of the CGAS resulted in a mean global
functioning score, in the whole sample, of 54.7 (15.6); the valuewas slightly lower in the cases (51.5 [15]) than in the controls(58.5 [15.6]).
Disease severity, evaluated using the clinician-rated CGI,was found to be mild or moderate (34.3% and 32.8%, respec-tively) in most of the patients, whereas smaller proportions werealmost normal, borderline, markedly, or severely mentally ill(4.5%, 14.9%, 11.9%, and 1.5%, respectively).
The patients with psychosis had a mean total PANSS scoreof 59.47 (9.56) (range, 40Y70). Analysis of the 3 PANSS sub-scales revealed the following mean scores: 14.14 (4.9) on thepositive scale, 16.08 (6.08) on the negative scale, and 29.25(4.96) on the general psychopathology scale.
Quality of LifeThe mean EuroQoL score calculated in the whole sample
was 64.03 (19.31). Patient-reported quality of life was found tobe slightly lower in the cases than in the controls, respectively,62.08 (19.43) versus 66.29 (19.24).
ComplianceIn 62 (93%) patients, there was agreement between the
patient-reported degree of compliance and the level reported byparents/caregivers. In the other 5 subjects (3 cases and 2 con-trols), the patients reported lower levels of adherence comparedwith what was reported by their parent/caregiver. Given thatexploration of the patient’s viewpoint is the primary objective ofthis study, we decided, despite this discrepancy, to include theresponses of these 5 patients in the subsequent analyses.
Of the 67 patients taking part in this study, 44 (65.67%)gave a score of 4 (excellent compliance), 17 (25.37%) a score of3 (moderate compliance), and 6 (8.96%) a score of 2 (poorcompliance). The mean compliance score was 3.57 (0.66).
In the cases, compliance was found to be excellent in 24,moderate in 10, and poor in 2 patients; mean compliance in thisgroup was 3.61 (0.60).
In the control group, compliance was excellent in 20 pa-tients, moderate in 7, and poor in 4; the controls recorded amean (SD) compliance score of 3.52 (0.72).
DAI-30The mean DAI-30 score in the whole sample was 13.06
(8.67), ranging from j12, recorded in 1 control, to +28,recorded in 2 subjects with psychosis.
Five (7.46%) of the 67 participants gave a negative score (j2,j2,j4,j8, andj12) and the other 62 (92.6%) a positive score.
Of the subjects recording a positive SE of treatment withAPs (DAI-30 score, 90), 18 had scores of 1 to 10, 26 recordedscores of 11 to 20, and 18 had scores in the 21 to 30 range.
Subjective Experience: Comparison of Casesand Controls
With the exception of 1 patient (DAI-30 score of j2), allthe cases showed a positive drug attitude: 13 (36.1) recordedscores of 1 to 10, 13 (36.1%) scores of 11 to 20, and 9 (25%)scores in the 21 to 30 range.
Negative attitudeswere recorded by 4members of the controlgroup (DAI-30 scores ofj12,j8,j4, andj2, respectively); ofthe other controls, 5 (16.1%) recorded scores of 1 to 10, 13(41.9%) scores of 11 to 20, and 9 (29%) scores of 21 to 30.
Overall, the cases and controls recorded mean (SD) DAI-30 scores of 13.28 (8.13) and 12.80 (9.4), respectively.
No significant difference in SE, evaluated using DAI-30,was found between the psychotic and nonpsychotic patients(P = 0.8).
Also, DAI subscores did not prove to be statistically dif-ferent in cases and controls (both P = 0.7): in particular, mean
Journal of Clinical Psychopharmacology & Volume 34, Number 1, February 2014 Drug Attitude in Adolescents
* 2014 Lippincott Williams & Wilkins www.psychopharmacology.com 101
Copyright © 2013 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
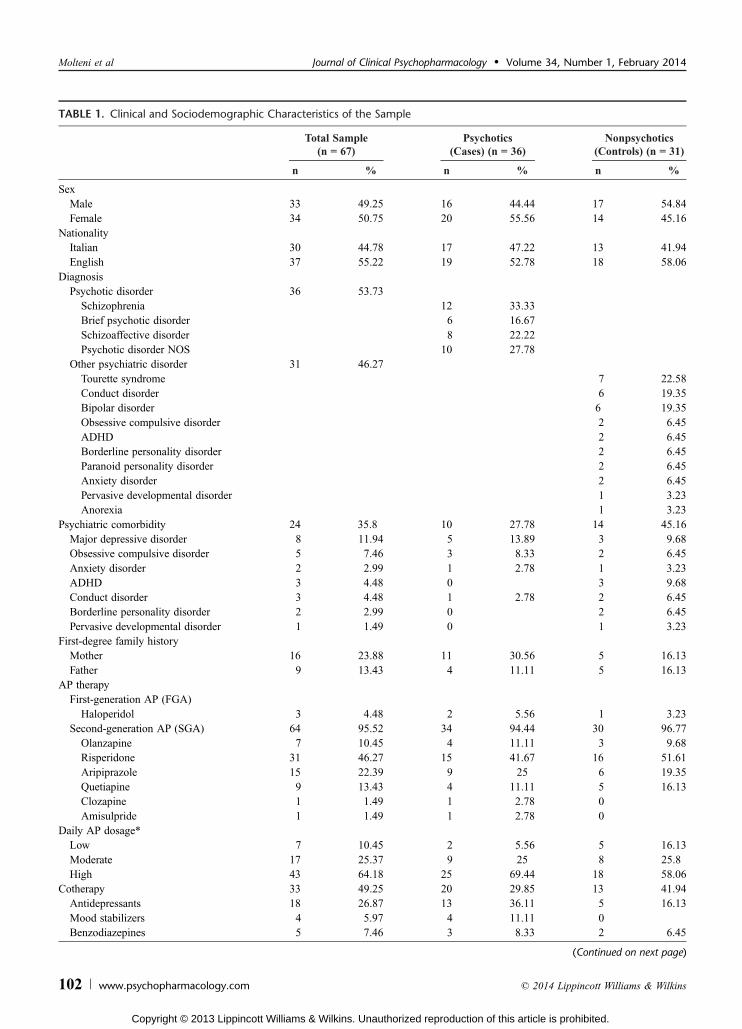
TABLE 1. Clinical and Sociodemographic Characteristics of the Sample
Total Sample(n = 67)
Psychotics(Cases) (n = 36)
Nonpsychotics(Controls) (n = 31)
n % n % n %
SexMale 33 49.25 16 44.44 17 54.84Female 34 50.75 20 55.56 14 45.16
NationalityItalian 30 44.78 17 47.22 13 41.94English 37 55.22 19 52.78 18 58.06
DiagnosisPsychotic disorder 36 53.73
Schizophrenia 12 33.33Brief psychotic disorder 6 16.67Schizoaffective disorder 8 22.22Psychotic disorder NOS 10 27.78
Other psychiatric disorder 31 46.27Tourette syndrome 7 22.58Conduct disorder 6 19.35Bipolar disorder 6 19.35Obsessive compulsive disorder 2 6.45ADHD 2 6.45Borderline personality disorder 2 6.45Paranoid personality disorder 2 6.45Anxiety disorder 2 6.45Pervasive developmental disorder 1 3.23Anorexia 1 3.23
Psychiatric comorbidity 24 35.8 10 27.78 14 45.16Major depressive disorder 8 11.94 5 13.89 3 9.68Obsessive compulsive disorder 5 7.46 3 8.33 2 6.45Anxiety disorder 2 2.99 1 2.78 1 3.23ADHD 3 4.48 0 3 9.68Conduct disorder 3 4.48 1 2.78 2 6.45Borderline personality disorder 2 2.99 0 2 6.45Pervasive developmental disorder 1 1.49 0 1 3.23
First-degree family historyMother 16 23.88 11 30.56 5 16.13Father 9 13.43 4 11.11 5 16.13
AP therapyFirst-generation AP (FGA)
Haloperidol 3 4.48 2 5.56 1 3.23Second-generation AP (SGA) 64 95.52 34 94.44 30 96.77
Olanzapine 7 10.45 4 11.11 3 9.68Risperidone 31 46.27 15 41.67 16 51.61Aripiprazole 15 22.39 9 25 6 19.35Quetiapine 9 13.43 4 11.11 5 16.13Clozapine 1 1.49 1 2.78 0Amisulpride 1 1.49 1 2.78 0
Daily AP dosage*Low 7 10.45 2 5.56 5 16.13Moderate 17 25.37 9 25 8 25.8High 43 64.18 25 69.44 18 58.06
Cotherapy 33 49.25 20 29.85 13 41.94Antidepressants 18 26.87 13 36.11 5 16.13Mood stabilizers 4 5.97 4 11.11 0Benzodiazepines 5 7.46 3 8.33 2 6.45
(Continued on next page)
Molteni et al Journal of Clinical Psychopharmacology & Volume 34, Number 1, February 2014
102 www.psychopharmacology.com * 2014 Lippincott Williams & Wilkins
Copyright © 2013 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
(SD) DAI-SR score was of 6.23 (4.60) and 5.61 (5.43) andDAI-AM was of 4.78 (3.96) and 5.06 (3.81), respectively incases and controls.
In view of the small size of the sample, it was not deemedmeaningful to compare SE within the group of cases accordingto the different diagnoses of psychosis.
Subjective Experience and ComplianceWe looked for association between drug attitude, evaluated
using the DAI-30, and compliance, evaluated using a 4-pointLikert scale and treated as an ordinal variable. Our hypothesiswas that subjects with positive attitudes would show bettercompliance than subjects with lower DAI-30 scores.
TABLE 1. (Continued)
Total Sample(n = 67)
Psychotics(Cases) (n = 36)
Nonpsychotics(Controls) (n = 31)
n % n % n %
Stimulants 3 4.48 0 3 9.68Antiepileptics 2 2.99 0 2 6.45Antiparkinson drugs 1 1.49 0 1 3.23
Mean SD Mean SD Mean SDAge, y 16.57 1.35 16.63 1.37 16.50 1.33Illness duration, mo 22.06 19.13 20.03 16.87 24.42 21.50AP treatment duration, mo 9.03 10.0 8.36 10.74 9.81 9.20
*Daily dosage was divided for each AP into 3 categories (‘‘low,’’ ‘‘moderate,’’ ‘‘high’’ [mg/d]) as follows: haloperidol, G1, 1Y2, Q2; olanzapine, G5,5Y10, Q10; risperidone, G1, 1Y2, Q2; aripiprazole, G1, 1Y5, Q5; quetiapine, G200, 200Y400, Q400; clozapine, G100, 100Y300, Q300; and amisulpride,G100, 100Y200, Q200.
TABLE 2. Prevalence of Extrapyramidal Symptoms in the Sample Assessed by ESRS and BARS
Total Sample(n = 67)
Psychotics(Cases) (n = 36)
Nonpsychotics(Controls) (n = 31)
AP Treatment Adverse Effects n % n % n %
Extrapyramidal symptoms 42 62.69 28 77.78 14 45.16Tremor 21 31.34 16 44.44 5 16.13Mild 17 25.37 13 36.11 4 12.90Moderate 4 5.97 3 8.33 1 3.23
Akathisia 23 34.32 16 44.44 7 22.58Mild 15 22.39 11 30.56 4 12.90Moderate 8 11.94 5 13.89 3 9.68
Dyskinetic movements 10 14.93 5 13.89 5 16.13Mild 7 10.45 5 13.89 2 6.45Moderate 2 2.99 0 0 2 6.45Severe 1 1.49 0 0 1 3.23
Amimia 15 22.39 12 33.33 3 9.68Mild 6 8.96 3 8.33 3 9.68Moderate 9 13.43 9 25 0 0
Rigidity 15 22.39 12 33.33 3 9.68Mild 12 17.91 9 25 3 9.68Moderate 3 4.48 3 8.33 0 0
Bradykinesia 16 23.88 13 36.11 3 9.68Mild 10 14.93 7 19.44 3 9.68Moderate 6 8.96 6 16.67 0 0
Decrease of pendolar arm movements 8 11.94 7 19.44 1 3.23BARS1 (objective) 16 23.88 9 25 7 22.58Mild 13 19.40 7 19.44 6 19.35Moderate 3 4.48 2 5.56 1 3.23
BARS2 (awareness of restlessness) 29 43.28 20 55.56 9 29.03Mild 17 25.37 12 33.33 5 16.13Moderate 8 11.94 4 11.11 4 12.90High 4 5.97 4 11.11 0 0
Journal of Clinical Psychopharmacology & Volume 34, Number 1, February 2014 Drug Attitude in Adolescents
* 2014 Lippincott Williams & Wilkins www.psychopharmacology.com 103
Copyright © 2013 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.

The results revealed a highly significant association of SEwith compliance (Spearman index, 0.33, P = 0.005).
Other CorrelationsTesting for correlations between each ESRS-identified
EPS and SE evaluated using the DAI-30 failed to reveal statis-tically significant associations (P 9 0.05).
Analysis of akathisia using the BARS confirmed the ab-sence of associations between this symptom and drug attitude inall the subscales.
Quality of life, evaluated using EuroQoL, was significantlycorrelated with SE (r = 0.25; P = 0.03). Instead, no correlationemerged with the other variables considered (disease severity,global functioning and positive/negative psychotic symptomsand general psychopathology in subjects with psychosis).
Multivariable Analysis
Subjective ExperienceBecause of the small sample size, we restricted the analysis
to the most important clinical variables (sex, diagnosis, weightchange, compliance with treatment, CGAS, CGI, EuroQol,EPS, BARS1, and BARS2).
Table 3 shows the results of the analysis.The following variables had statistically significant effects
on DAI-30: compliance (the subjects with better complianceshowed a better drug attitude) and weight change (the subjectswith higher weight gains had lower DAI-30 scores). The effectsof all the other variables, after elimination of confounding, werenot significant.
To understand the model, it is important to note the DAI-30score changes due to unitary variations of the single explanatoryvariables.
The multivariable analysis confirmed the presence of astrong association between compliance and SE: compared withsubjects showing poor compliance, those with moderate or ex-cellent compliance recorded 10-point and 14-point increases inthe DAI-30 score, respectively. Moreover, in our model, the
variable compliance explained 25% of the variation of drugattitude.
Having EPSs was not found to significantly influence SE(the presence of these symptoms causing an only minimalchange in the DAI-30 score). Analysis of the BARS scores re-vealed that subjects recording moderate clinician-rated akathisiashowed a 5-point DAI-30 score reduction compared with thosewithout akathisia. Instead, DAI-30 scores were not influencedby patient-rated akathisia.
Patients’ drug attitudes were found to be influenced bytheir quality of life: subjects with 50-point differences in theirEuroQol scores (eg, 30 vs 80) showed an approximately 4-pointdifference in their DAI-30 scores.
Note that each kilogram gained corresponded to a 0.3-point DAI-30 score decrease. In other words, patients under-going a rather common weight gain (eg, 10 kg) are predicted toshow a substantial change in their DAI-30 score (eg, 3 points).
Leaving aside small variations probably due to residualoverfitting, the influence of disease severity (CGI score) ondrug attitude can be resumed as follows: it is satisfactory inpatients in remission from acute illness (those with the lowestCGI scores) and in the severely or extremely ill patients (highestCGI scores). It is disappointing in those falling between these 2clinical extremes.
There emerged no clinically significant effect of diagnosisor sex on drug attitude, evaluated both with the univariate andthe multivariable approach.
The association between the variables that were found to bestatistically associated in the model with the whole DAI-30 andthe 2 DAI subscores was also tested.
DAI-SR and DAI-AM by themselves have shown astatistically significant association with compliance to treatment(P = 0.005 and P = 0.0001, respectively) in the same way asthe whole DAI-30. No association has been found with weightchange.
ComplianceGiven the strong association between SE and compliance
emerging from the multivariable analysis, we used a multivari-able approach to analyze how compliance changed in oursample.
The model included the following explanatory variables:diagnosis, equivalent dose, weight change, presence of EPSs,CGAS, CGI, DAI-30, EuroQol, BARS1, and BARS2 scores(Table 4).
The model had a predictive capacity, calculated as the areaunder the generalized receiver operating characteristic curve31
of 0.82.The DAI-30 score was the only variable found to be cor-
related with and capable of significantly influencing compli-ance, whereas EPSs showed an only marginally significantassociation. In our model, drug attitude, evaluated with DAI-30,explained almost 20% of the variation of compliance.
To better illustrate the model used in this study, we list aseries of typical patients and their probability to fall into thedifferent compliance categories.
For this purpose, several variables were kept constant:weight change, 4, equivalent dose, ‘‘high’’; BARS1 and BARS2,absent in all patients. We distinguished between the following:
- patients with reasonable health (CGAS, 65; EuroQol, 77; CGI,borderline)
- patients with poor health (CGAS, 44; EuroQol, 5; CGI, marked)
TABLE 3. Model for Explaining SE Evaluated Using the DAI-30
Effect P
Sex, female vs male j1.53 0.40Diagnosis, other vs psychosis j1.23 0.48Weight change* j0.32 0.05CGAS 0.09 0.21CGI, borderline vs normal 0.28 0.94CGI, mild vs normal j4.63 0.20CGI, moderate vs normal j0.63 0.87CGI, marked vs normal j4.68 0.29CGI, severely vs normal 2.38 0.66Compliance, 3 vs 2* 9.77 0.001Compliance, 4 vs 2* 13.58 G0.0001EuroQol 0.08 0.08EPSs 0.99 0.64BARS1 j2.56 0.12BARS2 j0.08 0.95
Variation of DAI-30 determined by unitary variation of each ex-planatory variable.
*Variables with statistical significant effects.
Molteni et al Journal of Clinical Psychopharmacology & Volume 34, Number 1, February 2014
104 www.psychopharmacology.com * 2014 Lippincott Williams & Wilkins
Copyright © 2013 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
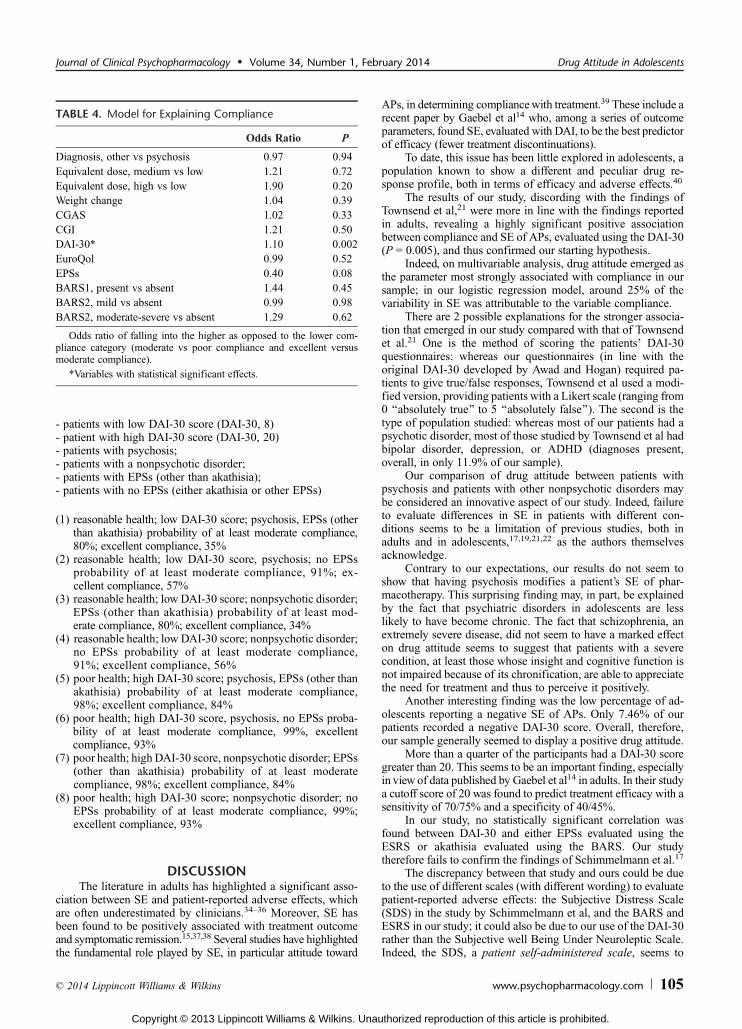
- patients with low DAI-30 score (DAI-30, 8)- patient with high DAI-30 score (DAI-30, 20)- patients with psychosis;- patients with a nonpsychotic disorder;- patients with EPSs (other than akathisia);- patients with no EPSs (either akathisia or other EPSs)
(1) reasonable health; low DAI-30 score; psychosis, EPSs (otherthan akathisia) probability of at least moderate compliance,80%; excellent compliance, 35%
(2) reasonable health; low DAI-30 score, psychosis; no EPSsprobability of at least moderate compliance, 91%; ex-cellent compliance, 57%
(3) reasonable health; low DAI-30 score; nonpsychotic disorder;EPSs (other than akathisia) probability of at least mod-erate compliance, 80%; excellent compliance, 34%
(4) reasonable health; low DAI-30 score; nonpsychotic disorder;no EPSs probability of at least moderate compliance,91%; excellent compliance, 56%
(5) poor health; high DAI-30 score; psychosis, EPSs (other thanakathisia) probability of at least moderate compliance,98%; excellent compliance, 84%
(6) poor health; high DAI-30 score, psychosis, no EPSs proba-bility of at least moderate compliance, 99%, excellentcompliance, 93%
(7) poor health; high DAI-30 score, nonpsychotic disorder; EPSs(other than akathisia) probability of at least moderatecompliance, 98%; excellent compliance, 84%
(8) poor health; high DAI-30 score; nonpsychotic disorder; noEPSs probability of at least moderate compliance, 99%;excellent compliance, 93%
DISCUSSIONThe literature in adults has highlighted a significant asso-
ciation between SE and patient-reported adverse effects, whichare often underestimated by clinicians.34Y36 Moreover, SE hasbeen found to be positively associated with treatment outcomeand symptomatic remission.15,37,38 Several studies have highlightedthe fundamental role played by SE, in particular attitude toward
APs, in determining compliancewith treatment.39 These include arecent paper by Gaebel et al14 who, among a series of outcomeparameters, found SE, evaluated with DAI, to be the best predictorof efficacy (fewer treatment discontinuations).
To date, this issue has been little explored in adolescents, apopulation known to show a different and peculiar drug re-sponse profile, both in terms of efficacy and adverse effects.40
The results of our study, discording with the findings ofTownsend et al,21 were more in line with the findings reportedin adults, revealing a highly significant positive associationbetween compliance and SE of APs, evaluated using the DAI-30(P = 0.005), and thus confirmed our starting hypothesis.
Indeed, on multivariable analysis, drug attitude emerged asthe parameter most strongly associated with compliance in oursample; in our logistic regression model, around 25% of thevariability in SE was attributable to the variable compliance.
There are 2 possible explanations for the stronger associa-tion that emerged in our study compared with that of Townsendet al.21 One is the method of scoring the patients’ DAI-30questionnaires: whereas our questionnaires (in line with theoriginal DAI-30 developed by Awad and Hogan) required pa-tients to give true/false responses, Townsend et al used a modi-fied version, providing patients with a Likert scale (ranging from0 ‘‘absolutely true’’ to 5 ‘‘absolutely false’’). The second is thetype of population studied: whereas most of our patients had apsychotic disorder, most of those studied by Townsend et al hadbipolar disorder, depression, or ADHD (diagnoses present,overall, in only 11.9% of our sample).
Our comparison of drug attitude between patients withpsychosis and patients with other nonpsychotic disorders maybe considered an innovative aspect of our study. Indeed, failureto evaluate differences in SE in patients with different con-ditions seems to be a limitation of previous studies, both inadults and in adolescents,17,19,21,22 as the authors themselvesacknowledge.
Contrary to our expectations, our results do not seem toshow that having psychosis modifies a patient’s SE of phar-macotherapy. This surprising finding may, in part, be explainedby the fact that psychiatric disorders in adolescents are lesslikely to have become chronic. The fact that schizophrenia, anextremely severe disease, did not seem to have a marked effecton drug attitude seems to suggest that patients with a severecondition, at least those whose insight and cognitive function isnot impaired because of its chronification, are able to appreciatethe need for treatment and thus to perceive it positively.
Another interesting finding was the low percentage of ad-olescents reporting a negative SE of APs. Only 7.46% of ourpatients recorded a negative DAI-30 score. Overall, therefore,our sample generally seemed to display a positive drug attitude.
More than a quarter of the participants had a DAI-30 scoregreater than 20. This seems to be an important finding, especiallyin view of data published by Gaebel et al14 in adults. In their studya cutoff score of 20 was found to predict treatment efficacy with asensitivity of 70/75% and a specificity of 40/45%.
In our study, no statistically significant correlation wasfound between DAI-30 and either EPSs evaluated using theESRS or akathisia evaluated using the BARS. Our studytherefore fails to confirm the findings of Schimmelmann et al.17
The discrepancy between that study and ours could be dueto the use of different scales (with different wording) to evaluatepatient-reported adverse effects: the Subjective Distress Scale(SDS) in the study by Schimmelmann et al, and the BARS andESRS in our study; it could also be due to our use of the DAI-30rather than the Subjective well Being Under Neuroleptic Scale.Indeed, the SDS, a patient self-administered scale, seems to
TABLE 4. Model for Explaining Compliance
Odds Ratio P
Diagnosis, other vs psychosis 0.97 0.94Equivalent dose, medium vs low 1.21 0.72Equivalent dose, high vs low 1.90 0.20Weight change 1.04 0.39CGAS 1.02 0.33CGI 1.21 0.50DAI-30* 1.10 0.002EuroQol 0.99 0.52EPSs 0.40 0.08BARS1, present vs absent 1.44 0.45BARS2, mild vs absent 0.99 0.98BARS2, moderate-severe vs absent 1.29 0.62
Odds ratio of falling into the higher as opposed to the lower com-pliance category (moderate vs poor compliance and excellent versusmoderate compliance).
*Variables with statistical significant effects.
Journal of Clinical Psychopharmacology & Volume 34, Number 1, February 2014 Drug Attitude in Adolescents
* 2014 Lippincott Williams & Wilkins www.psychopharmacology.com 105
Copyright © 2013 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.

focus more on evaluating the subjective distress linked to EPSs.Therefore, the use of the SDS and SWN by Schimmelmann et alcould explain why they found a stronger association betweensubjective distress and drug attitude.
The finding, on univariate analysis, of a positive associa-tion between SE and quality of life (P = 0.03) was another in-teresting finding of our study that confirmed, in adolescents,what has already been observed in adults.41 It has to be pointedout, however, that this association was much weaker thanexpected and was not confirmed on multivariable analysis (P =0.08), this fact is possibly suggesting that variables influencingthe quality of life, such as disease severity, are actually deter-mining the effect of SE on quality of life. Moreover, althoughEuroQol is a standardized instrument frequently used to evaluatequality of life, it is not specific for schizophrenia and might notbe very sensitive to detect relevant relationship in schizophrenia.
Contrary to the findings of previous studies in adults, wefound no positive correlation between drug attitude and patientglobal functioning.
In our patients, weight change seemed to influence SE toAPs far more negatively than the more classically studied adverseeffects of APs treatment (in particular, EPSs and akathisia). It islikely that, as often observed in clinical practice, weight change isassociated with a greater level of subjective distress in adoles-cents, who are going through a period in which their body imageis changing drastically. It thus seems fundamental, throughouttreatment, to monitor patients closely for weight changes and re-lated metabolic complications and for possible associated sub-jective distress.
An interesting, although nonsignificant, disease severity-related pattern of SE emerged in our study. Drug attitude wasfound to correlate positively with disease severity in the patientswho were in remission from acute illness (those with the lowestCGI scores) and in the severely or extremely ill ones (highestCGI scores), but negatively in those falling between these 2extremes. Our data therefore indicate a need for closer moni-toring of SE of drug treatments in this latter group.
Given the strong association between SE and complianceemerging from the multivariable analysis, we used a multivari-able approach to establish how the single variables affect com-pliance. The results of this analysis confirmed our initialhypothesis: of the variables analyzed, the DAI-30 score wasfound to be the only one significantly associated with compli-ance. Our data show that SE is a key variable correlated withpatient compliance with treatment, more important than othervariables classically considered fundamental, such as adverseeffects of APs (EPS and weight gain).
To illustrate our model for explaining treatment compli-ance, we calculated the probabilities, for a series of hypotheticalpatients, of presenting at least moderate compliance or excellentcompliance and found SE, as assessed using the DAI-30, to bethe variable with the greatest influence on treatment compli-ance. Indeed, in our model, drug attitude explained almost 20%of the variation in compliance.
Although EPSs tended to reduce compliance, particularlyin patients with a negative drug attitude; conversely in patientswith a positive SE, the negative effect of EPSs was far lessmarked. It thus seems that changes in compliance are due not somuch to the objective presence of EPS, as to the worse SE thatmay result from them.
Thus, the influence of the patient’s diagnosis on compli-ance (as on SE) seemed to be negligible.
Akathisia, both clinician-rated akathisia and moderate orsevere patient-rated akathisia, had a positive effect on compliance,showing a trend similar to that of disease severity (the greater the
severity of the akathisia, the greater the patient’s level of compli-ance). Adolescents possibly consider this symptom a componentof their disease rather than a treatment adverse effect.
LIMITATIONS OF THE STUDYA main limitation of this study was the small sample
size, which is due to the inclusion and exclusion criteriaused. Many subjects were excluded because they had mentalretardation or a history of learning disabilities. Because thisstudy used self-administered scales that had to be completedindependently by the participants, the inclusion of indi-viduals with an IQ less than or equal to 70 might have madeit difficult to establish whether inability to understand theitems influenced the responses. However, the exclusion ofpatients with mental retardation strengthens the validity ofour results.
The inclusion of patient with concurrent use of other psy-chotropic medications may also be considered a limitation. Aspecific statistical analysis was conducted: when the presence ofa concurrent medication was included among the explanatoryvariables, both the model for explaining SE and the one forcompliance were not substantially influenced.
The use of a self-administered scale to evaluate com-pliance is another limitation of this study. Furthermore, wedid not use objective methods for evaluating compliance (countingtablets, recording drug prescriptions, measuring plasma concen-trations of drugs); the patients were merely required to indicatetheir level of adherence to their treatment regimen.
In addition, because this was a naturalistic, observationalcross-sectional study, we were not able to assess the stability,over time, of drug attitude and treatment compliance.
On the other hand, studies, like this one, that analyze in-dividuals referred to mental health services are important asthey provide a realistic picture of patients needing treatment.Furthermore, the previously mentioned limitations, which inour view do not affect the clinical validity of the study, arejustified by the lack of previous studies in this field and by theexploratory nature of this work.
CONCLUSIONSOur observations provide confirmation that drug attitude is
a key element to understand treatment compliance in adoles-cents. Our data underline the need, when making clinical as-sessments and proposing and monitoring drug treatments, toalways consider the patient’s viewpoint.
A simple instrument, like the DAI-30, capable of measur-ing patient’s drug attitude could constitute an additional re-source enabling clinicians to make a more comprehensiveassessment and to improve their care of psychiatric patients,allowing the latter to become more involved and to take anactive part in treatment decisions. As shown in the literature,patient perception of the treatment is a crucial factor in deter-mining outcome.
We believe that clinical improvements can be achievedonly through strong physician-patient alliances in which thephysician is open to exploring, and also willing to understand,the patient’s attitude to treatment and the healing process. Thisis the perspective from which we conducted this study.
AUTHOR DISCLOSURE INFORMATIONDr Giaroli has served as consultant to Shire and received
honoraria as a speaker and received financial support to attend
Molteni et al Journal of Clinical Psychopharmacology & Volume 34, Number 1, February 2014
106 www.psychopharmacology.com * 2014 Lippincott Williams & Wilkins
Copyright © 2013 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
medical meetings from Eli Lilly, Janssen, and Phlynn Pharma.Dr Rossi served as a principal investigator in Shire studySPD503-316 in 2011 and as an investigator in Eli Lilly studyB4Z-IT- LICY in 2006. The other authors declare no funding orconflicts of interest.
REFERENCES
1. Findling RL, Steiner H, Weller EB. Use of antipsychotics in childrenand adolescents. J Clin Psychiatry. 2005;66(suppl 7):29Y40.
2. Correll CU. Antipsychotic use in children and adolescents:minimizing adverse effects to maximize outcomes.J Am Acad Child Adolesc Psychiatry. 2008;47(1):9Y20.
3. Vitiello B, Correll C, van Zwieten-Boot B, et al. Antipsychoticsin children and adolescents: increasing use, evidence for efficacyand safety concerns. Eur Neuropsychopharmacol.2009;19(9):629Y635.
4. Swanson J. Compliance with stimulants for attention-deficit/hyperactivitydisorder: issues and approaches for improvement. CNS Drugs.2003;17(2):117Y131.
5. Sarwer-Foner GJ. On the mechanisms of the action of neurolepticdrugs: a theoretical psychodynamic explanation.Recent Adv Biol Psychiatry. 1963;6:217Y232.
6. Leucht S, Tardy M, Komossa K, et al. Antipsychotic drugs versusplacebo for relapse prevention in schizophrenia: a systematic reviewand meta-analysis. Lancet. 2012;379(9831):2063Y2071.
7. Lambert M, Conus P, Cotton S, et al. Prevalence, predictors,and consequences of long-term refusal of antipsychotictreatment in first-episode psychosis. J Clin Psychopharmacol.2010;30(5):565Y572.
8. Velligan DI, Weiden PJ, Sajatovic M, et al. The expert consensusguideline series: adherence problems in patients with seriousand persistent mental illness. J Clin Psychiatry.2009;70(suppl 4):1Y46.
9. Awad AG, Hogan TP. Subjective response to neuroleptics and thequality of life: implications for treatment outcome. Acta Psychiatr
Scand Suppl. 1994;380:27Y32.
10. Balestrieri M, Giaroli G, Mazzi M, et al. Performance of theItalian version of the subjective well-being under neuroleptic(SWN) scale in schizophrenic outpatients. Pharmacopsychiatry.2006;39(3):81Y84.
11. Awad AG. Drug therapy in schizophreniaVvariability ofoutcome and prediction of response. Can J Psychiatry.1989;34(7):711Y720.
12. Jaspers K. Allgemeine Psychopathologie. Berlin: Springer Verlag;1959. Berlin. Italian edition: Roma: Il Pensiero Scientificoeditore; 1964.
13. Karow A, Naber D. Subjective well-being and quality of life underatypical antipsychotic treatment. Psychopharmacology (Berl).2002;162(1):3Y10.
14. Gaebel W, Riesbeck M, von Wilmsdorff M, et al. Drug attitudeas predictor for effectiveness in first-episode schizophrenia: resultsof an open randomized trial (EUFEST). Eur Neuropsychopharmacol.2010;20(5):310Y316.
15. Ritsner M, Gibel A, Perelroyzen G, et al. Quality of life outcomesof risperidone, olanzapine, and typical antipsychotics amongschizophrenia patients treated in routine clinical practice: anaturalistic comparative study. J Clin Psychopharmacol. 2004;24(6):582Y591.
16. Lambert M, Schimmelmann BG, Schacht A, et al. Differential3-year effects of first- versus second-generation antipsychotics
on subjective well-being in schizophrenia using marginal structuralmodels. J Clin Psychopharmacol. 2011;31(2):226Y230.
17. Schimmelmann BG, Paulus S, Schacht M, et al. Subjective distressrelated to side effects and subjective well-being in first admittedadolescents with early-onset psychosis treated with atypicalantipsychotics. J Child Adolesc Psychopharmacol. 2005;15(2):249Y258.
18. Naber D. A self-rating to measure subjective effects of neurolepticdrugs, relationships to objective psychopathology, quality of life,compliance and other clinical variables. Int Clin Psychopharmacol.1995;10(suppl 3):133Y138.
19. Fraguas D, Llorente C, Rapado-Castro M, et al. Attitude towardantipsychotic medication as a predictor of antipsychotic treatmentdiscontinuation in first-episode early-onset psychosis. Rev PsiquiatrSalud Ment. 2008;1(1):10Y17.
20. Hogan TP, Awad AG, Eastwood R. A self-report scale predictive of drugcompliance in schizophrenics: reliability and discriminative validity.Psychol Med. 1983;13(1):177Y183.
21. Townsend L, Floersch J, Findling RL. Adolescent attitudes towardpsychiatric medication: the utility of the Drug Attitude Inventory.J Child Psychol Psychiatry. 2009;50(12):1523Y1531.
22. Floersch J, Townsend L, Longhofer J, et al. Adolescent experienceof psychotropic treatment. Transcult Psychiatry. 2009;46(1):157Y179.
23. Kay SR, Fiszbein A, Opler LA. The positive and negativesyndrome scale (PANSS) for schizophrenia. Schizophr Bull.1987;13(2):261Y276.
24. Sheehan DV, Lecrubier Y, Sheehan KH, et al. The Mini-InternationalNeuropsychiatric Interview (M.I.N.I.): the development and validationof a structured diagnostic psychiatric interview for DSM-IV andICD-10. J Clin Psychiatry. 1998;59(suppl 20):22Y33.
25. First MB, Gibbon M, Spitzer RL, et al. Structured Clinical Interview for
DSM-IV Axis II Personality Disorders, (SCID-II). Washington, DC:American Psychiatric Press, Inc; 1997.
26. Chouinard G, Margolese HC. Manual for the Extrapyramidal SymptomRating Scale (ESRS). Schizophr Res. 2005;76(2Y3):247Y265.
27. Barnes TR. A rating scale for drug-induced akathisia. Br J Psychiatry.1989;154:672Y676.
28. GuyW. ECDEU. Assessment Manual for Psychopharmacology, revised.
U.S. Department of Health, Education, and Welfare publication
(ADM), 76-338. Rockville, MD: National Institute of Mental Health;1976:218Y222.
29. Shaffer D, Gould MS, Brasic J, et al. A children’s global assessmentscale (CGAS). Arch Gen Psychiatry. 1983;40(11):1228Y1231.
30. EuroQol Group. EuroQolVa new facility for the measurement ofhealth-related quality of life. Health Policy. 1990;16:199Y208.
31. Harrell FE. Regression Modeling Strategies. New York, NY: SpringerVerlag Inc; 2001.
32. Babyak MA. What you see may not be what you get: a brief,nontechnical introduction to overfitting in regression-type models.Psychosom Med. 2004;66:(3): 411Y421.
33. R: A language and environment for statistical computing [computer
program]. Version 2.13.1. Vienna, Austria: R Foundation for StatisticalComputing, R Core Team; 2011.
34. Mizrahi R, Bagby RM, Zipursky RB, et al. How antipsychotics work:the patients’ perspective. Prog Neuropsychopharmacol Biol Psychiatry.2005;29(5):859Y864.
35. Gervin M, Browne S, Garavan J, et al. Dysphoric subjective responseto neuroleptics in schizophrenia: relationship to extrapyramidalside effects and symptomatology. Eur Psychiatry.1999;14(7):405Y409.
Journal of Clinical Psychopharmacology & Volume 34, Number 1, February 2014 Drug Attitude in Adolescents
* 2014 Lippincott Williams & Wilkins www.psychopharmacology.com 107
Copyright © 2013 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.

36. Seale C, Chaplin R, Lelliott P, et al. Antipsychotic medication, sedationand mental clouding: an observational study of psychiatricconsultations. Soc Sci Med. 2007;65(4):698Y711.
37. de Haan L, Nimwegen L, Amelsvoort T, et al. Improvement ofsubjective well-being and enduring symptomatic remission,a 5-year follow-up of first episode schizophrenia.Pharmacopsychiatry. 2008;41(4):125Y128.
38. Murawiec S, Boutros NN. Correlation between early subjectiveresponse to antipsychotics and the number of hospitalizations andhospitalization days in a period of 10Y11 years in schizophreniapatients. Neuropsychobiology. 2012;66(2):120Y125.
39. Yang J, Ko YH, Paik JW, et al. Symptom severity and attitudestoward medication: impacts on adherence in outpatients withschizophrenia. Schizophr Res. 2012;134(2Y3):226Y231.
40. Correll CU, Penzner JB, Parikh UH, et al. Recognizing andmonitoring adverse events of second-generation antipsychoticsin children and adolescents. Child Adolesc Psychiatr Clin N Am.2006;15:177Y206.
41. Hofer A, Kemmler G, Eder U, et al. Quality of life inschizophrenia: the impact of psychopathology, attitude towardmedication, and side effects. J Clin Psychiatry.2004;65(7):932Y939.
Molteni et al Journal of Clinical Psychopharmacology & Volume 34, Number 1, February 2014
108 www.psychopharmacology.com * 2014 Lippincott Williams & Wilkins
Copyright © 2013 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.




















