Download - eSocialSciences
278
-
Upload
khangminh22 -
Category
Documents
-
view
1 -
download
0
Transcript of Download - eSocialSciences


Database for Disease Burden EstimationMalaria, Filaria, Dengue & Diarrhoeal Diseases
Indian Council of Medical Research inCollaboration with WHO India Country Offiece
2006

Participating Centres
Malaria Research Centre Dr.Ashwini KumarNew Delhi Dr.A.P. Dash
Vector Control Research Centre Dr.K.KrishnamoorthyPondicehrry Dr.L.K.Das
Mr.K.T.HarichandrakumarDr.Krishna KumariDr.P.K.Das
Centre for Research in Medical Dr.Lalitha KabilanEntomology, Madurai Dr. S.C.Tewari
Dr.RajendranDr.A.P.Dash
National Institute of Cholera and Dr. B.MannaEnteric Diseases, Kolkata Dr.Alok Deb
Dr.S.K.Bhattacharya
Co-ordinating Unit Dr. Lalit KantICMR, New Delhi Dr. Ambujam Nair Kapoor
Professional Guidance
Dr. V.I. Mathan, Chair-in-Epidemiology, National Institute of Epidemiology,Indian Council of Medical Research
Ms. Sujatha Rao, National Commission on Macroeconomics & Health, India,Ministry of Health & F.W.
Dr. Arvind Pandey, Director, National Institute of Medical Statistics , DelhiProf. K.Ramachandran, ChennaiDr. PSS Sunder Rao, Consultant, Leprosy Mission Trust India, New DelhiMr.Sunil Nandraj, NPO, WHO
The study was carried out with support from World Health Organization, India Country Office.
(iii)

Contents
1. Summary --------------------------------------------------------------------------1
Part-A : Literature Survey
2. Malaria -------------------------------------------------------------------------- 11
3. Filaria ---------------------------------------------------------------------------- 31
4. Dengue -------------------------------------------------------------------------- 61
5. Diarhoeal Diseases ------------------------------------------------------------ 71
Part-B: Annotated Bibliography
6. Malaria -------------------------------------------------------------------------- 95
7. Filaria ---------------------------------------------------------------------------149
8. Dengue -------------------------------------------------------------------------197
9. Diarhoeal Diseases -----------------------------------------------------------215
(v)

(vi)
GLOSSARY
ADL - AdenolymphangitisAPHS - Andhra Pradesh Health SurveyCFR - Case Fatality RateDALY - Disability Adjusted Life Years.NVBDCP - National Vector Borne Disease Control ProgrammeDEC - Diehyl CarbamazineDF - Dengue FeverDHF - Dengue Hemorrhagic FeverDSS - Dengue Shock SyndromeDWs - Disability WeightsGBD - Global Burden of DiseaseLF - Lymphatic FilariasisMCCD - Medically Certified Cause of DeathNFCP - National Filaria Control ProgrammePHC - Primary Health CentreSCD - Survey of Cause of DeathSFR - Slide Falciparum RateSMMR - Specific Malaria Mortality RatioSPR - Slide Positivity RateYLD - Years lived with disabilityYLL - Years of Life Lost
In 1993, the World Development Report presented Disability Adjusted Life-years(DALYs) as a measure of global burden of disease. It summarized conditions of illhealth due to various diseases of varying severity and disability and different durationsinto one composite index for quantifying disease. The methodology used wasdeveloped by Murray and Lopez.Years of life lost from premature death and yearsof life lived with disabilities were combined to derive DALY as a single indicator.Publication of the original GBD Study in 1993-1996, prompted countries to applythe methods to estimate disease burden. Majority have followed the essentialprinciples and methodology initially proposed by Murray and Lopez and theseestimates have been used as a method of health prioritization at national level.
Communicable diseases continue to remain as a major public health concern, inIndia. There is no comprehensive data on the burden of disease due to communicablediseases in the country. Estimation of disease burden requires information aboutdiseases, their incidences, consequence, causation and trends. This informationfor communicable diseases is limited in India. The only estimates of burden ofdisease in terms of DALY as an indicator for the country as a whole are thoseavailable from the GBD which was first estimated for the year 1990; the data wasre-analyzed in 2000.
In order to make more realistic estimates of disease burden, it is essential that Indiagenerate its own data. To begin with the Indian Council of Medical Research decidedto create a database on available literature on morbidity and mortality in India forcommunicable diseases. Since data requirements for calculation of DALYs areextensive, it was decided to undertake this exercise for four infections namely malaria,filarial, dengue and diarrhoeal diseases.
The following ICMR centres participated in the study:1. Malaria : Malaria Research Centre, Delhi2. Filaria : Vector Control Research Centre, Pondicherry3. Dengue : Centre for Research in Medical Entomology,
Madurai4. Diarrhoeal Diseases : National Institute of Cholera and Enteric
Diseases, Kolkatta
Summary
1

2
Summary
There are many issues in the estimation of DALY. These include availability ofepidemiological data in terms of space, time and quality, data satisfyingmethodological standards, disability weights and their validity and information onthe disease dynamics. It is therefore essential to examine these issues. This reportdeals with the data base compiled from the literature and other sources on incidenceor prevalence of diseases, inferences on disease dynamics, demographic data and allrelevant information that are useful to carry out estimation of DALY for the selectedfour diseases.
For each infection studied, the data available from published and unpublishedsources were collected for each component of the data requirement for calculationof DALYs viz.:1. Life expectancy;2. Years of Life Lost (cause specific mortality pattern, age weighting and discounting;3. Years Lived in Disability (age at onset of disease, duration of disease, disease
sequelae); and4. Disability weight.
The Report of the study is in two parts – Part A gives the findings of the literaturesurvey, the limitations of the database and the data gaps for each infection; Part B isthe annotated bibliography for each of the four infections.
The centres reviewed the published and unpublished information on the four identifiedinfections. The review showed several limitations of the available data. Valid andreliable cause of death is an essential input for estimation of disease burden. InIndia, cause of death statistics is incomplete. Some information on cause of deathfor rural areas used to be collected for rural areas through the Survey of Cause ofDeath –rural scheme which operated till 1998. Thereafter cause of death was to beincorporated as a component of Sample Registration scheme. This is yet to beoperationalized. There is gross under reporting of data from the routine reporting forthese infections under the national programmes. Incidence data on diseases are notreadily available. The limitations in the available data for each of the four infectionswere identified and is summarized below.
Limitations of the Studies for Estimation of DALY and Data GapsThe limitations of available information for estimation of DALYs and the data gapsfor each infection are as follows:

3
Summary
MALARIA1. Demographic Data
! Full Census Report of 2001 needed.! Life Expectancy Tables India
2. Morbidity dataIncidence Studies! Gap in malaria incidence reported by NVBDCP and WHO.! Many longitudinal studies suggest poor surveillance and discrepancy in
incidence to the extent of 68-98%.! Lack of information on clinically treated malaria.! Non-notification of clinically treated cases hence not included in the incidence
statistics.! Lack of malaria incidence by Age–sex at national, sub national, districts and
PHC level according to GBD age classes.Prevalence Studies! Malaria cases according to uniform age classes used for DALYs estimation
not available.! Information lacking on the extent of asymptomatic malaria in stable malaria
zones of the country.! Lack of information on prevalence of malaria in the town through independent
studies.3. Mortality Data
! Deaths are grossly under reported.! Non reporting of registered and medically certified cause of death by some
states as a result incomplete information is available in Medical Certificationof Cause of Death (MCCD) report.
! Data on cause of death generated through Sample Registration Survey-ruralon the basis of verbal autopsy not yet available.
! Lack of information on Deaths at exact ages in both sexes in most of theresearch studies.
4. Sequelae! Lack of information on duration of disease sequelae such as anaemia and for
neurological disorders due to complicated malaria.5. Disability Weights
! Lack of Disability Weights for different sequelae in different paradigms ofmalaria in India except for the State of Andhra Pradesh.
! Lack of information as to how asymptomatic malaria and drug resistant P.falciparum impacts duration of disability.

4
Summary
FILARIA! Epidemiologial data on age and genderwise incidence of disease, Age and
gender wise prevalence of disease are not available! Information on remission rates of disease sequelae and transition rates of
disease sequelae are not available! No literature is available to suggest that mortality could be attributable to
LF. In recent years, however, there are indications that patients with LFsuccumb to sudden overwhelming septicemia due to acute ADL attackstherefore cause of death studies LF are urgently required.
! Disability for all sequelae age and gender wise is not available. This is beingcurrently undertaken
DENGUE! In most of the published / unpublished reports either one or many parameters
(case incidence with age & sex specific, and duration of onset of disease)required for BoD estimation are lacking. True incidence could not be obtainedsince proper diagnostic facilities are lacking in most of hospitals at districtlevel (urban and rural setup).
! To record causes of death (COD) in the case of dengue is difficult due tounavailability of proper diagnostic tools.
! Hospitalized DHF cases and deaths have been reported annually. In recentyears, progressively more outpatient and inpatient care has been provided bythe private sector. Case reporting from the private sector is incomplete.
! DHF cannot be diagnosed using clinical judgment alone. Laboratory testsare needed to correctly identify a case of DHF and, ideally, virologic orserologic tests to confirm it. Laboratory equipment to perform a completearray of diagnostic tests is often not available
! The case definitions differ among health officials, with some reporting onlylaboratory-confirmed cases whereas others reporting clinically diagnosedcases as well. Some report cases and deaths from DF & DHF separately,other report DHF combined. Problems of over and under diagnosis,incomplete reporting and delays also weaken surveillance for dengue.
! Proper surveillance of dengue should also include the monitoring of serotypescirculating in the population. The introduction of a new serotype may be animportant indicator of future epidemics of DHF. In many places, laboratoriesneed considerable strengthening to monitor circulating serotypes.

5
Summary
DIARRHOEAL DISEASESProblems with morbidity data
Definition of diarrhoea! Many publications did not mention how they defined an episode of diarrhoea.Recall period! Different studies used different recall periods to obtain information on
diarrhoea. Influence of using different recall periods to get such data hasbeen studied in rural Tamil Nadu, South India. It was found that there couldbe considerable under-reporting of diarrhoeal morbidity when the recall periodexceeded 3 days.
Non-availability of age-/sex-stratified data! Most of the data are available for the child population; few studies have
reported data for all ages or for !5 years population (without any further agegrouping). Even fewer studies reported data according to the gender.
Outbreak data! Data from outbreak investigations are not suitable for estimating disease
burden at the community level, as these data tend to give higher estimatesfor obvious reasons.
Problems with mortality data! Under-reporting of deaths! Problems in ascertainment of cause of death
It was not clear how deaths due to diarrhoea were defined in different studiesthat reported data on diarrhoeal mortality. Only one study used a cleardefinition - “ A death was considered diarrhoea-related if the child haddiarrhoea in the week before death, and there was no obvious cause of deathunrelated to diarrhoea”, provided by the WHO (WHO/CDD/SER/86.2).
! Non-availability of death certificates! Questionable reliability and validity of verbal autopsy! Mortality data for hospitalized cases! Usually, the more severe and complicated cases are admitted to the hospital
– thus, mortality is expected to be higher among hospitalized cases; on theother hand, due to the care that those patients receive in the hospital, themortality could be lower than that would be expected among similar patientsin the community who are not hospitalized
! Mortality data from outbreaksWhile mortality from diarrhoea tends to be higher during the outbreaks thanthe usual situations, for mortality among hospitalized cases, the issue is alittle complex.

6
Summary
Problems with disability data" Compared to morbidity and mortality, fewer studies reported diarrhoea
duration. Most data on duration was obtained from hospital-based clinicaltrials, which were conducted under stringent experimental conditions, andthus, the duration was likely to be less than that might occur under usualfield conditions.
" There were almost no data from community or hospital-based studies ondisability weights for diarrhoea, which is likely to be different across theplaces, depending on social, cultural, economic, and many such characteristicsof the populations.
Estimation of DALY for setting priorities has been criticized on account of issuesconcerning quality of data used as well as issues such as disability weights anddiscounting. As has been indicated above, the published data of scientific reports donot have a standard definition of specific infectious diseases, case definition andseverity, seasonality varies across studies or studies relate to outbreak investigations.
There are variations in providing incidence, prevalence and mortality rates by ageand sex and samples studied are not representative samples. Also, data from routinereporting under disease control programme are usually under reported.
The draft report of the literature survey was discussed in an expert group meetingand the following recommendation were made:(i) The information on morbidity/mortality from existing health care system is
not sufficient to be used for a State level/national diseases burden estimation.There is no exact information on corrective factor for incidence/prevalence,age, duration that can be applied to existing data. Therefore, review of existingdata from published/unpublished studies is inadequate to make a meaningfulconclusion.
(ii) Alternative systems need to be established to get enough information. Thefollowing suggestions were made for consideration :a. The Ministry needs to develop one integrated data collection system usingmodern information technology. Assistance from Infosys/Wipro/Tata etc.could be sought. ICMR should be used for technical assistance.b. Develop a mechanism for involvement of medical colleges to improvequality. ICMR can provide technical inputs for quality.c. The Integrated Disease Surveillance project (IDSP) will be implemented.Additional inputs that can be provided into IDSP need be looked at liketraining and information technology.

7
Summary
d. ICMR could form an expert committee and develop a common protocolfor disease burden estimation. WHO SEARO, USAID and other internationalorganizations could be involved so that the protocol is internationallyaccepted. Institutes to be involved and budget may then be worked out.ICMR could come in as a technical organization. The mechanism should bea part of the health system.
(iii) A small group could be formed by Ministry of Health and ICMR to look intothe above suggestions, identify what needs to be done so that in 2-3 yearsthe data for disease burden estimation can be obtained on a regular basis.

Part-A
Literature Survey

IntroductionMalaria disease is of great socio-economic significance and is considered as one ofthe three major public health challenges to mankind in addition to tuberculosis andHIV. Seven diseases viz., pneumonia, diarrhoea, HIV, tuberculosis, measles, hepatitisB and malaria account for 85% of Global infectious disease burden [1,2]. Malariaafflicts some 90 countries and territories and almost half of them are in Africa Southof Sahara. While there are 300-500 million malaria cases per year as per the WHO,36% of the total population of the world i.e. 2020 million is exposed to the risk ofcontracting malaria. In South Eastern Asian Region of WHO, out of the 1.4 billionpeople living in 11 countries (land area 8,466,600 sq. km i.e. 6% of global area), 1.2billion people are exposed to the risk of malaria and most of them are in India [3]. In1990 it was estimated that out of population of 843.7 million, 75, 240 and 500million people were at high, moderate and low risk of contracting malaria in thecountry respectively. Situation has not changed much since then. The reported malariaincidence in India is around 2 million cases and 1000 deaths/annum whereas estimatedincidence is 20 million with 19500 to 20000 deaths (WHO).
In the World Development Report of 1993 on investing in health for estimation ofglobal burden of disease for the 1990, a summary measure ‘Disability Adjusted LifeYear Lost’ (DALY) for expressing state of health was introduced. Ever since thenthe interest in computation of DALYs has gradually increased. Estimation of diseaseburden in terms of DALY has been viewed more appropriate, as it takes into accountboth years of life lost due to pre-mature deaths on account of disease as well as yearslived with disability due to morbidity in the population. As an end point, estimationof burden of malaria would be of great significance from the perspective of a healthPlanner/Administrator as it would become a parameter for problem based stratificationand prioritizing resource allocation for disease control at National and sub-nationallevel. It has been estimated by the WHO that India lost 577,000 DALYs in 1998 outof total loss of 1.6 million DALYs in the SEAR of WHO and of 39.267 million inthe world [4]. As expected African continent suffered the most with 34.506 millionDALYs lost on account of malaria with staggering 961,000 deaths in 1998.
Disease Burden studies have been completed in some countries and many othershave taken initiative to take up such studies at both national and subnational level.The World Health Organization has been promoting such efforts through technical
Malaria
11

12
Malaria
and monetory support. In India, ICMR has taken initiative and scientists were trainedon disease burden estimation in Institute of Health Systems at Hyderabad in 2001.The present inquiry was funded by the WHO from its biennium budget as a part of aproject entitled ‘Studies on estimation of disease burden of identified infectiousdiseases’. One of the four diseases selected was malaria. As a first step efforts weredirected to collect and review literature from as many sources as possible to assessthe availability of data from published epidemiological studies carried out in thecountry that are crucial for disease burden estimation and to identify data gaps thatneed generation through specific studies. The results of this study have been presentedin this report.
MethodologyOnline Search: Different websites were accessed and useful information related tostudy was downloaded. The words used for online search were DALY/DALYs,malaria, incidence, malaria morbidity, mortality, sequelae, P. falciparum incidence,malaria in India, malaria DALYs, etc.
Published and Unpublished Reports: A search for literature on incidence andprevalence of malaria, different sequelae, in different parts of India was carried out.Relevant publications in national and International journals were searched. 108published articles were collected and about 80 publications relevant to Malaria diseaseestimation study have been reviewed in the report. Besides some unpublished articlesand project reports were also obtained. In addition, information on epidemiology ofmalaria was collected from books and compilations on malaria both at national andInternational level. Three documents published by WHO and one by National VectorBorne Diseases Control Programme were also acquired. For population estimates,reports on Census of India 1991 and 2001 were obtained in the form of publisheddocuments and CDs from the Office of Registrar General and Census Commissioner,Govt. of India. Website http://www.censusindia.net was also searched for informationon population in India, Indian states and districts. Detailed report on Medicalcertification of cause of death 1997 was obtained from the Office of the RegistrarGeneral of India, Ministry of Home affairs. A report on state of health in Indiapublished by an NGO was collected. Malaria data generated during NFHS-II wasalso obtained.
Literature ReviewDemographic Data: One of the most important pre-requisite for disease burdenestimation is population data of a given country, states, districts, cities and villageswhere such study has been planned. In India the population census is conducted

13
Malaria
every decennial and the last census was conducted in 2001. In the census report,population distributed by age-sex and also in convenient age classes is available,which can be readily used for disease burden studies. Population data of decennialcensuses of 1991 and 2001 for the entire country, state and districts have beencompiled by the Directorate General of Census Operations, Govt. of India and itssubordinate offices located in all the states. This complete set of data has beencollected for 1991 census. Age and sex wise distribution of population in differentstates and Union territories of India is available in 1991 Census report, provisionalpopulation report on 2001 census is available.
Following documents can be obtained from the Office of Registrar General & CensusCommissioner, India.
a. Census of India 1991 (series I: Part IV A): Socio-cultural tables Volume Ib. Census of India 1991 (series I: Part IV A): Socio-cultural tables Volume IIc. Census of India 2001(series 31:Goa):Provisional population totals: paper-1
of 2001.d. Census of India 2001(series 31:Goa):Provisional population totals: paper-2
of 2001.e. Census of India 1991 (series 6: Part IV-B ii - Goa): Religion: Table C-9.f. Census of India 1991 (series 6: Paper –1-Goa): Provisional population totals.g. Census of India 1991 (Series 6: Part IV A-C Series): Socio-cultural tables.
1. Census of India 2001 (Paper 1 of 2001 supplement) Provisional populationtotals: Series I: India.
2. Census of India 2001:Primary Census Abstracts
Malaria Incidence in IndiaThe incidence data of malaria for different states of India is available with the NationalVector Borne Diseases Control Programme (earlier NAMP). District wiseepidemiological data from 1985-1995, and similar data for states and India from1961 to 1995 is available in the document entitled “Epidemiology and control ofmalaria in India in 1996” by Sharma et al., [5]. The data includes population, bloodsmear examined, positive cases, P. falciparum and P. vivax cases, Pf%, Annual bloodexamination rate (ABER), Annual Parasite Index (API), SPR, SfR and deaths due tomalaria. However malaria incidence by age and sex has not been documented.
It is noteworthy that malaria incidence data presented in the above document is asreported by different states to NVBDCP on the basis of active and passive surveillanceand there is no indication whether it also includes clinically treated cases. Such apossibility appears remote as according to the definition of malaria followed by

14
Malaria
NVBDCP, only slide confirmed cases are being included in malaria statistics. Thereis no separate information available on slide confirmed and clinically treated casesin the private sector as they are rarely, if at all, notified to the health authorities sothat they became part of the incidence statistics. Further, it has been pointed out onthe basis of number of research studies that all the blood smears collected may notbe examined and a backlog usually existed. Hence based on reported SPR and backlogof unexamined slides alone, it was estimated that 11,70,664 cases were missed in 10years from 1971 to 80 and therefore on an average 97,555 cases were missed annuallyand not reported in the annual incidence [6].
A hospital based study showed how reliable was the clinical diagnosis alone for thetreatment of malaria as it was found that with clinical judgment alone the SPR was24% as compared to 52% when microscopic diagnosis was done showing a gap of28% [7]. On the basis of parallel longitudinal research studies carried out in somestates, doubts have also been expressed in several publications on the reliability ofmalaria data generated on the basis of routine surveillance, which shows a huge gap of68 to 98% between the reported and actual incidence of malaria. Following studiesbear evidence about gaps in the malaria incidence. Choudhury et al., [8] had studiedmalaria problem in 10 districts of U.P. and found that as against 725 cases (SPR : 5.47%)detected by their team, the state machinery had reported only 194 cases (SPR : 1.46%)showing high discrepancy in reported and the real incidence of malaria.
Reports have also been published on misdiagnosis of malaria in India e.g. in a studyin Gujarat, 6.7% slides were found misdiagnosed as a result 1262 malaria caseswere missed in 9 PHCs which would mean that instead of reported API of 5.9, itshould have been 9.0 [9]. In an earlier study conducted in Kharhkoda PHC in districtSonepat in Haryana and Kichha PHC in district Nainital of U.P., a huge gap wasfound between the incidence of malaria (63 cases) reported by the Kichha PHC andthat detected (1784 cases) in a longitudinal research study. Interestingly no case ofPf was detected by the PHC although 23 (including 3 mix infections) were detectedin the parallel surveys. Similarly in Kharkhoda PHC, a total of 7117 cases (SPR43.2%; SFR 30.46%) were detected during research study as against 183 (SPR 12.6%;SFR 5.5%) detected in PHC conducted surveys. This once again showed glaring gapbetween the reported and real incidence of malaria. Besides in mass blood surveys,additional 438 cases in Kichha PHC and 2375 cases were detected in KharkhodaPHC [10]. In yet another study, Malhotra et al., [11] showed that there were 2623cases (SPR:58.66% and SFR:34.58%) as compared to 49 cases (SPR:5.27% andSFR:1.61%) reported by PHC indicating gross under reporting of malaria. In 1988,a survey in Bisra PHC near Rourkela revealed that SPR for malaria was 26.3% and

15
Malaria
SFR 15.8% as compared to 7.6% and 3.8% reported by the PHC indicating therebythat large proportion of malaria cases were being missed by the PHC and malariacases were much more than being reported [12]. In a recent study conducted inAhmedabad, it has been found that in the hospital admitted patients, there were37,431 cases against 4119 cases reported [13].
The WHO has estimated 15 million cases of malaria with 19500 to 20000 deaths inIndia annually as against 1.6-3 million cases and around 1000 deaths reported byNVBDCP [14]. Hence the official estimates on morbidity and mortality cannot berelied upon for DALY estimation but on the basis of well-planned pilot studies, theincidence reported by NVBDCP could be used after applying necessary correction.Another problem is that incidence data is not readily available according to age andsex-wise distribution that would match GBD template for the estimation of YLD.When available, it is not according to the smaller age groups recommended in GlobalBurden of Diseases studies. On the other hand, hardly any published studies showdistribution of malaria according to the age classes prescribed in GBD study, hence theavailable secondary data is also of limited use. The distribution of malaria amongstdifferent ages and sexes in different eco-epidemiological zones is likely to differ. Henceproperly planned seasonal point prevalence studies would be necessary to fill the existinggap.
Prevalence studiesAvailable literature reveals that most of the point prevalence studies carried out inthe country were for the purpose of outbreak/epidemic investigations. Only a fewpoint prevalence studies have been carried out during normal malaria transmissionseason in different parts of the country. The age classification has also been usedarbitrarily by different workers. For example Srivastava et al., [15] in their report onmalaria in Buhari PHC of Surat have distributed malaria according to <1, 1-4, 5-9,10-14, 15-29 and >30 years age groups in both sexes. They showed that while inmale children of 1-4 year age, SPR was 80%, it was 21.92 % in >30 years adults.Almost similar trend was noticed in females in different age classes. On the otherhand Shukla et al. [16] investigated outbreak of malaria in Moradabad, U.P. anddistributed malaria cases age-wise together for both sexes. The age groups were <1,1-5, 5-15, 15-25, 25-50 and 51 & above and found SPR of 80% in infants whichdeclined gradually over other age classes to 57.1% in the age group of > 51 years.Dhiman et al., [17] chose yet another classification of age groups to group malariacases in Bahraich district of Uttar Pradesh and their age classes were <5 years (SPR19.2%), 6-14 (28.84%), 15-25 years (12.5%) and > 25years (39.4%) which meansmalaria showed increasing trend with age which was contrary to the earlier studies
16
Malaria
referred above. In a study in Shankargarh in Allahabad district, it was found thatmalaria was high in all the age groups of both sexes e.g. 47% amongst infants and50% in children of 1-4 year age followed by 57% in 4-8 years, 57% in 8-14 yearsand 52% above 14 years [18]. They also found that Pf gametocytaemia ranged from15.7 to 24.8% amongst these patients and only 56% were symptomatic cases.
Prakash et al., [19], in a village based study in Sonitpur in Assam, have reported highprevalence of malaria with SPR ranging from 39.7 to 50% and spleen rate in children<10 years 51.3%. The P. falciparum proportion varied from 95 to 100%. In Kamrupdistrict of Assam, Dev and Sharma [20] reported perennial transmission of malariawith SPR ranging from 22.9% to 36.5% with proportion of Pf 74%. High incidence ofmalaria was reported in all the months amongst all age groups including infants.
Singh and Khare [21] have analyzed epidemiological situation of malaria in MadhyaPradesh from 1976 to 1996 and reported that annual parasite incidence ranged from1.94 to 19.4 and the problem was severe in densely forested tribal areas (API range:10.99 to 18.71; SPR range 8.10 to 11.74%) followed by forested areas (API range:3.74 to 6.95; SPR range 3.69 to 5.80%), forest fringe area (API range: 2.24 to 4.07;SPR range 2.15 to 3.34%) and Deforested area (API range: 1.78 to 2.51; SPR range1.74 – 2.14%).
A malaria outbreak was investigated by Prakash et al, [22] in Titabor PHC in Jorhatdistrict of Assam, which revealed that SPR and SFR during mass survey were 16.1and 14.5% respectively with P. falciparum contributing to 90% cases. Individuals>15 years of age suffered less (SPR 11.0%) as compared to younger age groups(SPR 22.9%). Males suffered relatively more (SPR=14.7%) than females(SPR=7.5%). In Boko area of Assam, Nandi et al., [23] found that 30.5% tribals hadmalaria and Pf% was 94.4%. The SPR was highest in May at 43.8%. The glandpositivity for sporozoite in An. minimus was observed throughout the year indicatingperennial transmission. Another study carried out in Boko area by Dutta et al., [24]showed that out of 120 blood slides collected 61 were positive (SPR = 50.83% andSFR= 42.5%). It was also found that 17 asymptomatic cases were detected fromamongst 59 healthy looking children with SPR and SFR of 28.8% and 25.4%respectively. Infant parasite rate was 75% in this area although only 4 blood smearsamongst infants could be taken of which 3 were positive. Similar to the above study,Prakash et al., [25] found that sporozoite rate of An. minimus was as high as 6.5%. InSonitpur, Assam, Prakash et al., [26] investigated outbreak of malaria and foundsituation alarming (SPR:42.9%, SFR: 42.5%, Pf% : 99.1% and spleen rate 50.6%).

17
Malaria
In Morigaon district of Assam, malaria outbreak was investigated by Dev et. al.,[27]. They found that 68% of the blood smears were positive for malaria (Pf:87%).Age and sex wise distribution of malaria cases detected in mass survey revealed that44% children below 4 years age had malaria while 45% in the age group 5-14 and38% from 15 and above age group suffered from malaria.
In a study carried out in ethnic communities in Assam and Arunachal Pradesh, Duttaet al., [28] found that incidence was quite high amongst tribals with proportion of P.falciparum 80%. The slide positivity for malaria in apparently healthy school goingchildren was 7.25 to 17.46%. Problem of malaria was high in infants and children(44.11%) in Rabha, Bodokachari area and decreased with the age (14.7%). Whereas,it was high in children <10 years of age (21.09%) and then reduced in 10-20 yearsage group (11.4%) followed by another rise in >20 years adults (24.4%) in Karbiethnic communities. In Arunachalis, on the other hand, it was 25.27% in children<10 years (25.3%) followed by 42.62% in 10-20 year of age and then declined onceagain to 20.3% in > 20 years of age. Dutta et al., [29] conducted a study onepidemiological situation of malaria in Tengakhat PHC in Dibrugarh district in Assam.In this area they found that malaria was seasonal (1987-89: SPR ranged from 12.9 to28.5% and SFR from 10.78 to 25.01%) and all age groups suffered from malaria.The attack rate (Cases per 1000 pop.) was the least (9.07) in infants but highest inchildren (53.98%) and in the higher age groups it ranged from 11.97 to 35.19%.They found that An. dirus was the principal vector of malaria in this area.
Dev and Phukan [30] have studied problem of malaria in the tea estates ofBrahmaputra Valley of Assam and found high prevalence rate of falciparum malaria(66%). The SPR ranged from 0-61% in different circles and Pf% ranged from 0-100% and it was concluded that the tea estates in the North block had more malariaand predominance of P. falciparum than the southern block which had greaterproportion of P. vivax. In another study Dev [31] found that malaria incidence washigh in hamlets close to Tarajulie Tea Estate in Sonitpur district of Assam. The An.minimus sporozoite positivity was 4.23% in the human dwellings in these hamlets.Infant parasite rate and infant falciparum rates were 22.2% and 18.2% respectively.In the other age groups SPR and SFR were 24.5% and 21.9% for 1-5 years children,39.8 and 32.6% in 5-15 years, 42.6 and 31.5% in >15 years. Overall SPR and SFRamongst these tribals inhabiting hamlets were 34.9 and 27.7% respectively. Das etal., [32] investigated malaria outbreak in Tamulpur PHC, Assam and found that outof 250 people screened in 4 villages, 158 were positive (63.2%) and Pf incidencewas very high i.e. 93.7% and SFR was also high 59.2%.
18
Malaria
Dutta and Bhattacharya [33] conducted a malaria survey in some parts of Namsangcircle of Tirap district, Arunachal Pradesh and found that SPR was 26.84% in a sampleof 190 blood smears examined and SFR was 21.05%. They analyzed malaria accordingto age groups below 1, 1-10, 11-20, 21-30, 31-50 and >51 years in both sexes andfound that while SPR was nil in infants and low in persons >50 years age, it graduallyincreased up to 30 years of age.
A study conducted on epidemiology of malaria in tribal Rajmahal Range, Biharshowed that the slide positivity rate was 25.1% and Pf% was 64.2. Age wisedistribution showed that SPR in children was 25% and it increased to 34.4% in 6-10years age group and 37.7% in 11-15 years age group [34]. In Lakhimpur district,Assam, Das et al., [35] found that in forest fringed villages the SPR was 46.5%, SFR28.1% while Pf% was 60.4%. Malaria greatly affected children below 5 years(SPR:47.6%), and in the higher age groups SPR ranged from 30.9% to 64.3% showingthereby alarming situation created by the outbreak of malaria. Prakash et al., [26]studied malaria problem in forest fringed areas in Dibrugarh district Assam andfound that SPR% was 47, SFR was 39.0% while Pf% was 83.1. Age and sex wisedistribution showed that infants suffered the maximum in this area (SPR:69.2%)while malaria problem was also acute in other age groups (SPR range 36.1 to 60.7%).
Mohapatra et. al. [36] have highlighted the importance of younger age groups duringepidemic in Tamalpur, Assam and found out that children between 3 and 12 years ofage who were treated and recovered continued to harbour gametocytes and transmitmalaria as gametocyte reservoirs. Kamal and Das [37] found in Darang district ofAssam that peak transmission of malaria was between May and October and SPRranged from 2.3-45.67% in different months with predominance of P. falciparum(91.7%) as found in other studies. The worst affected age groups were 0-1 and 21-30years although all age groups suffered from malaria (SPR 11.65% to 19.09%).
P. malariae has always been under-reported although this species can cause chronicinfection spanning many decades and could impair renal function. In a study, Pandaet al., [38] reported that P. malariae proportion was 2% in tribal Bastar district andmore than 60% had gametocytes indicating that these were old infections. In a detailedstudy, Yadav et al., [39] found 82 cases (1.1%) of P. malariae in Bisra PHC out oftotal 7363 malaria cases detected in Sundergarh district of Orissa. In 13 cases P.malariae co-existed with P. falciparum and/or P. vivax species.
There is scanty information on malaria in urban areas of the country although townscontribute about 15% of total malaria in India [40]. In 1982, malaria problem in

19
Malaria
labour hutment in Delhi was investigated and it was found that 39.6% fever caseshad malaria of which 16.3% had P. falciparum infections. Age and sex wisedistribution showed that malaria was prevalent in all age classes of both sexes [41].While overall infant parasite rate was 7.83%, it was as high as 94.1% in age group of15-24 years. However, a study conducted in Faridabad showed, [42] that Faridabadtown contributed 38.7% of total malaria and 38.2% Pf malaria in the entire Faridabaddistrict. Malaria could also be an occupational hazard for the construction workerswho live close to the construction complex in the hutment and are exposed to thevector bites that may be breeding in the stagnant water in these complexes. Thework force itself serves as reservoir of infection. For example, in Delhi Adak et al.,[43] studied outbreak of malaria in a hotel construction site and found SPR of 60.1%SFR of 44.1% and Pf% of 73.5.
Considering the enormity of the malaria problem in different ecotypes and paradigmsin India, specially designed cross sectional point prevalence studies according toage classes covering both sexes specified in GBD study would be necessary to estimatemalaria incidence at local (Village), PHC, district, sub-national (state) and nationallevel.
Mortality dataMalaria has all along been known as one of the most important factors responsibledirectly or indirectly for infant and child mortality in areas where the disease ishighly prevalent. In pre-independent India the toll was one million during normalyears and two million during epidemic years. Christopher in 1924[44] had said inthe fifth Indian Science Congress “All men must die, but it is to be hoped that eachwill have a run for his money, so to speak, and live to a reasonable age, say 50years”. Its interpretation meant that an average man must live a fruitful life of atleast fifty years so as to contribute substantially towards economic well being of thecommunity. Thus if mortality at an early age is of sufficient magnitude, expectationsof life in the community is shortened and the work force is relatively small.
Malaria mortality steeply declined in India from 1 million cases/annum up to 1940safter eradication programme was launched in 1958. The National Vector BorneDisease Control Programme reported 879, 666, 1057, 946 and 938 deaths due tomalaria from 1997 to 2001 showing a Specific Malaria Mortality Ratio (SMMR)of 0.30 to 0.48 in these years which is one of the lowest in the world (WHOwebsite). In the recent years deaths are however being regularly reported duringout breaks and epidemics of malaria. The cause of some of the outbreaks/epidemicshas been investigated in detail and studies published. For example, in Negoyi and

20
Malaria
Tilhar PHCs of Shahjahanpur district, there were 249 and 96 deaths respectivelydue to malaria in just three months. Fever surveys revealed that SPR was 75.3%,SFR was 72.4% and Pf% was 96%. Following this epidemic, intensive malariacontrol measures were initiated in 1984 and 1985. The follow up study revealedthat incidence of malaria continued to be cause of concern in spite of four roundsof HCH spraying in 1984 and 1985 [45].
In 1983, sudden deaths were reported in an epidemic that hit Meerut district villagesin U.P. where incidence of malaria was determined and 32 deaths were investigated[46]. It was found that SPR (76.2%) and Pf% (95.3) were alarming. Falciparummalaria was 100% in Jangethi village and 93%, 92.1%, and 94.5% in Dayampur,Dobka and Zakhera villages respectively. Contrary to these findings, the PHC recordsshowed very poor surveillance and confirmed malaria cases. Even mass contactslides of 113 villagers whose relatives had died in the epidemic also showed SFR of45.1%.
In 1990s malaria epidemics have brought in their wake sudden wave of mortality inIndia. For example, in Rajasthan state alone 447 deaths were reported in Barmer,Bikaner, Jodhpur and Jaisalmer where 108, 94, 69 and 56 deaths were reported by theofficial machinery [47].
Mathur et al., [48] reported 47 deaths in Barmer district of Rajasthan in 1990 and theyalso found out high infectivity among infants and paediatric groups and there waspossibility of deaths amongst these age groups, which could not be verified. Infantparasite rate was found to be 40%, child parasite rate (60%) and adult parasite rate of58%. Mukhopadhyay et al., [49] have reported 79 deaths due to malaria from 1990 to1996 in Calcutta. The SPR in fever cases was 47.94% while Pf% varied from 0.5% inJune 1996 to 82.3% in Dec. 1996.
In Goa accelerated construction activities led to active transmission and outbreaksduring which deaths were constantly reported from 1990 to 2003 (Goa State NAMP:personal communication).
Following 139 fever related deaths in Bahraich district of Uttar Pardesh, it was foundduring investigation that 33.8 % fever cases had malaria and P. falciparum was88.4% of the total cases. Malaria affected all the age groups [17].
Mohapatra et al., [50] have reported high incidence of malaria in an investigation inTamulpur PHC in district Nalbari, Assam following 30 deaths. The asymptomatic

21
Malaria
malaria was high 19.5% while the SPR and SFR was 26.1 and 19.2% respectively.The deaths were maximum (73.2%) in children below 10 years.
It is well known that pregnant women constitute an important risk group for malariainfection, which may cause abortion, still-births, intra-uterine growth retardation(IUGR) and pre-mature labour. Besides it may be the cause of cerebral malaria,severe anaemia and maternal mortality. In a hospital based study in Bikaner, Kocharet al., [51] found that mortality rate in P. falciparum cases was highly significant inpregnant women (37.8%) in comparison to non-pregnant women (14.81%) atp<0.001. Similarly, cerebral malaria (75.55%), severe anaemia (< 5g%) 20%, hepatic(13.3%) and renal failure (20%) were more in pregnant women than non-pregnantfemales at 32.92%, 4.11%, 9.05% and 6.17% respectively.
In Vellore, a 10% mortality was observed in 98 P. falciparum cases admitted intertiary care hospital )[52]. In a malaria outbreak investigation in Bahraich districtof Uttar Pradesh with predominant P. falciparum (88.4%), Dhiman et al., [17] foundthat fever related deaths were 57.5% out of 139 in >25 year age group and in othergroups i.e. <5, 6-14 and 15–25 years were 17.9%, 20.8% and 3.6% respectively.
In another study in Madhya Pradesh, Shukla et al., [53] studied complicated Pfmalaria in the Govt. Medical College Jabalpur and found that out of 1783 patientsadmitted with fever 152 (8.5%) had cerebral malaria. Of these 39 (25.6%) diedand majority of them were in 16-40 years age group. Mortality was significantlyhigher in patients with hyper-parasitaemia, hypoglycemia, and delayed diagnosisand comatose condition was the main determinant of death.
Talking about the current status of mortality on account of malaria reported in India,the National Vector Borne Disease Control Programme (earlier NMEP/NAMP)reports around 1000 deaths per annum against 19500 to 20000 estimated by WHO.Other than these sources, there are scanty reports on deaths due to malaria. Theavailable information is from Hospital based studies and case fatality rate of 8 to30% has been reported in admitted cases in different phases of complications. Hencethis data if used for extrapolation for case fatality estimation would lead tooverestimation of death and thus erroneous for calculation of YLL component onwhich DALY estimates depend much greater than YLD component. Personalcommunication with experts has revealed that Case fatality rate of malaria in Indiais much lesser than that in Africa as revealed by SMMR of 0.3 to 0.48, which theyattribute to the better health facilities and better clinical management in India. But acritical assessment of medically certified cause of deaths report published by Ministry

22
Malaria
of Home affairs suggests that there were 3572 deaths reported in various categoriesof hospitals due to malaria when only 15% of the total registered deaths weremedically certified [54]. A simple conversion to 100% certification would mean thatthere would be 23813 deaths. Further, if state wise correction was applied based onmalarial deaths and proportion of deaths medically certified out of total registereddeaths, the malaria deaths in India would at least be 71396 in the year 1997 asagainst 879 reported by national programme in 1997. It may be noted that MCCD-1997 report did not include deaths statistics of Bihar, Assam, Gujarat, West Bengaland J &K due to unavailability. It is noteworthy that all these states except J & K areendemic to malaria. Had there been reporting of deaths from these states the malarialdeaths would have been higher than 71396. Hence available data on deaths isincomplete. This shows a huge gap between reported and actual deaths due to malaria.
The latest information on deaths available with Registrar General of Births and Deathsis of 1997, hence data for the subsequent years is not available. Moreover, the firstSample Registration Survey (rural) on the basis of verbal autopsy is in progress andits report will be available after mid 2004. It is therefore necessary to generate reliableinformation on deaths in carefully planned studies that would bring out reliableestimates of deaths at exact ages in both sexes, which are necessary for YLL (yearsof life lost due to malaria) computation in disease burden studies.
SequalaeThere are two recognized sequalae of malaria i.e. anaemia and neurological sequelae.It may be mentioned that according to GBD, there is 50% anaemia in < 5 years agechildren and 25% between age 5-14 due to malaria. In Vellore, a study has shownthat anaemia (haemoglobin of <8g %) was 33% i.e. in 17 out of 51 complicated Pfcases admitted in the hospital. In Jabalpur, 12.38% complicated pf patients, whoimproved after admission, were anaemic as against 82% who died. In case of pregnantVs non pregnant malaria patients, severe anaemia (<5g%) was reported in 20% asagainst 4.1% in non pregnant malaria patients [51]. In another hospital based studyin Vellore, anaemia (<8g%) was observed in 30% of 284 cases (including 33% of 98P. falciparum cases, 19% of 28 mixed infections and none in the 158 P. vivax cases).
In Jabalpur, Madhya Pradesh, Shukla et al., [53] found that 14 out of 113 cerebralmalaria patients who improved had severe anaemia while amongst 32 of 39 whodied had severe anaemia indicating thereby high association with mortality incomplicated Pf cases. In a study conducted on malaria in pregnancy and its effectson foetus in a tribal area of Koraput district, Orissa by Das [55], it was found that Hbconcentration declined to 8.4g/dl (range 7.2-10.2 g/dl) at full term and parturition

23
Malaria
from its initial level of 9.6 g/dl (range 7.2-12.8 g/dl). There was significant difference(p<0.05) in Hb concentration among the trimesters of pregnancy. In a similar studyconducted in Nigeria, a significantly high anaemia was observed in pregnant womenthan in the non pregnant women suffering from malaria [56].
There is further need to search for literature on anaemia in both uncomplicated andcomplicated Pf cases. Random, sample based, cross sectional surveys are necessaryto find out extent and duration of anaemia. As far as neurological deficiency isconcerned, none of the published studies contained information about neurologicalsequelae except the GBD study. Neurological sequelae were reported in 1.3 per1000 episodes of malaria. These have to be determined under Indian conditions insome sentinel sites. Neurologists who routinely handle malaria cases could also beconsulted about their opinion.
Disability studiesDisability weights decide what duration of life lived in good health should beconsidered lost as equivalent to one year spent in disability of particular severity.The weights are on a scale of 0-1 with 1 for state equivalent to death and 0 for stateof optimal health. Disability weights are best assigned by community e.g. in case ofmalaria to classical episodes, anaemia and neurological sequalae on the basis ofsubjective valuation/societal preferences for different health states. None of the studiesin literature reviewed provided this information corresponding to these diseaseconditions except the Global Burden of Disease (GBD) studies and Andhra PradeshHealth Survey (APHS) [57]. The DWs in GBD studies for malarial episodes (0.172-0.211), anaemia (0.012-0.013) and neurological sequela (0.581) were quite differentthan APHS being 0.47-0.503 for malaria episodes, 0.435-0.436 for anaemia and0.579 for neurological sequela. This suggests that community perception is likely tobe different in different malaria endemic zones and epidemiological situation.
Data GapsDemographic data! Full census report of census of India 2001 needed.! Life Expectancy Tables: India.Incidence data! Gap in malaria incidence reported by NVBDCP and WHO.! Many longitudinal studies suggest poor surveillance and discrepancy in incidence
to the extent of 68-98%.! Lack of information on clinically treated malaria.

24
Malaria
! Non-notification of clinically treated cases hence not included in the incidencestatistics.
! Lack of Age–sex distribution of malaria cases at national, sub national, districtsand PHC level according to GBD age classes.
Prevalence data! Malaria cases according to uniform age classes used for DALYs estimation
not available.! Information lacking on the extent of asymptomatic malaria in stable malaria
zones of the country.! Lack of information on prevalence of malaria in the town through independent
studies.Death Statistics! Deaths are grossly under reported.! Non reporting of registered and medically certified cause of death by some states
as a result incomplete information is available in MCCD report.! Data on cause of death generated through Sample Registration Survey-rural on
the basis of verbal autopsy not yet available.! Lack of information on Deaths at exact ages in both sexes in most of the studies.Sequelae! Lack of information on duration of disease sequalae such as anaemia and for
neurological disorders due to complicated malaria.Disability weights! Lack of Disability Weights for different sequalae in different paradigms of malaria
in India except for Andhra Pradesh.! Lack of information as to how Chloroquine resistant P. falciparum malaria impacts
duration of disability.
The review of literature, shows that :Data from systematically planned on longitudinal studies where an effort has beenmade to compare the incidence/prevalence data collected during the study with thatcollected during routine surveillance activity. These studies suggest that there is hugegap between the data generated during routine surveillance and the estimated incidence.
Several studies, were conducted following outbreaks or epidemics for investigationpurpose and results published. These involved point prevalence, fever surveys orMass surveys but deaths wherever occurred were not thoroughly investigated.
There are some hospital based studies wherein extent of complicated malaria, clinicalsigns and symptoms as well as case fatality rate due to malaria have been documented.

25
Malaria
In none of the studies reviewed, effort has been made to collect information on malariadiagnosis and treatment in private sector covering pathological labs and private medicalpractitioners treating cases purely on clinical signs and symptoms. In many studies,age and sex distribution of cases have been mentioned wherein age groups have beenselected arbitrarily and therefore comparison between them is difficult. In many studiesreviewed, malaria incidence is not divided according to sexes.
Studies to be used for estimation of malaria disease burdenIn the first instance WHO estimates of incidence and deaths due to malaria in Indiacan be used for projecting DALYs estimation in India. Disability weights and averageduration of cases can be as per GBD study for international comparison althoughweights can also be used measured during Andhra Pradesh Health Survey.
Alternatively DALYs lost due to malaria in India can be estimated using WHO dataon incidence and estimation of deaths from MCCD and SRS-rural records.
Study conducted by Yadav et al (2003)[13] in Ahmedabad wherein true incidence ofmalaria cases and deaths have been estimated can be used for DALYs estimation inthat city having population of 3 million. The age and sex distribution of incidenceand deaths is needed to generate DALYs. DWs as proposed in GBD/APHS can beused for the purpose as they are not locally generated as yet.
There are many studies conducted in Assam following outbreaks wherein authorshave estimated incidence through special point prevalence surveys and the age-sexdistribution of the cases has been shown for that particular population. These studieswould be useful for DALYs estimation if detailed data on deaths attributable tomalaria is made available by the programme on request.
General recommendations! Access to local, state and national data (networking with NVBDCP and ICMR
institutes)! Epidemiological surveillance for incidence/prevalence estimation.! Completeness of Cause of death statistics: accessing data from various sources.! Disease specific recommendations.! Networking and functional relationship with National Programme for data sharing
and DALYs estimation.! Pilot scale project on estimation of malaria DALYs in low, moderate and high
transmission zones preceded by prevalence studies on age-gender distributionof malaria.

26
Malaria
! Completeness of Cause of Death statistics and creation of database on malariamortality at district, state and National level.
! Disability weights estimation through Health valuation surveys.! Questionnaire based study on duration of sequelae taking expert opinion.! Estimation of extent of clinically treated malaria in private and govt. sector.! Studies on the extent of asymptomatic malaria in stable malaria zones and its
effect on duration of disability.! Studies on true incidence of malaria.! Limitations of the studies for DALY estimation
Source of data and method of collectionIn most of the publications reviewed during the present study, point prevalence surveysboth fever and mass surveys and longitudinal studies have been carried out. Somepublications clearly show wide gap between the reported and true incidence of malaria.In some studies attempt has been made to estimate true incidence of malaria bygathering information from different sources such as routine surveillance, hospitalrecords from both private and Govt. hospitals. Most of the studies which were carriedout to investigate outbreaks/epidemics following deaths, carried out fever and masssurveys but did not collect and analyse information on deaths attributable to malariabut mention merely numbers of dead. This is the major limitation of the studiescarried out.
Limitation of data base for DALY calculationThe limitations observed on the basis of Review of literature are on all frontsstarting from true incidence to death attributable to malaria as these are thebackbones for eastimation of DALYs lost. The incidence data of the nationalprogramme has serious limitations as pin pointed by various studies reviewed.Since Years lost due to malaria is a major component of DALYs estimation, deathsdue to malaria and their proper estimation is of paramount importance. Duringthis study, MCCD records were analysed wherein deaths due to malaria in differentstates of India as well as according to age and sex have been given. From thissingle source one can clearly see that there is huge gap between the reported deathsand medically certified deaths attributable to malaria. It has been estimated that at100% certification of all deaths, the malarial deaths may have been over 71000 in1997. The SRS Report (rural) on verbal autopsy could further add to the cases. Inthis regard it is pertinent to mention that the figures of National Programme cannot be relied upon for the estimation of DALYs unless a correction factor is appliedto arrive at convincing death figure and checking the incidence and mortality datafor internal consistency using DISMOD. For disability weights either fresh health

27
Malaria
valuation need to be conducted or GBD values could be used till such time localweights become available for disease seqaelae.
Publications reviewed1. Murray CJL and Lopez AD (1996). Evidence-based health policy—Lessons from the Global Burden of
Disease Study. Science 274:740-743.2. Murray CJL, Lopez AD (1997). The Global Burden of Disease 1990-2020: Alternative projections of
mortality and disability by cause for eight regions. Lancet, 349: 1498-1504.3. Kondrashin, A. V. (1992). Malaria in WHO Southeast Asia Region. Indian J. Malariol. 29: 129-160.4. Park, K. (2000). Preventive and Social Medicine. Publ. Banarsidas Bhanot Publishers, Jabalpur, India PP.
189-199.5. Sharma, R. S., G. K. Sharma and G. P. S. Dhillon (1996). Epidemiology and Control of malaria in India-
1996.National malaria Eradication Programme, New Delhi. pp: 752.6. Sharma, V. P. (1982). Observations on the incidence of malaria in India. Indian J. Malariol. 19: 57-58.7. Gautam, A. S., R. C. Sharma, V. P. Sharma and G. K. Sharma (1991). Importance of Clinical Diagnosis of
malaria in National Malaria Control Programme. Indian J. Malariol. 28: 183-187.8. Choudhury, D. S., V. P. Sharma, S. C. Bhalla, S. S. Agarwal and S. K. Das (1987). Malaria prevalence in
patients attending primary health centres in ten districts of Uttar Pradesh. Indian J. Malariol. 24:79-83.9. Gautam, A. S., R. C. Sharma, R. M. Bhat and D. K. Gupta (1992). Microscopic Diagnosis of malaria in
Kheda District of Gujarat. Indian J. Malariol. 29:83-87.10. Sharma, V. P., D. S. Choudhury, M. A. Ansari, M. S. Malhotra, P.K.B. Menon, R. K. Razdan and C. P.
Batra (1983). Studies on the true incidence of malaria in Kharkhoda (district Sonepat, Haryana) and Kichha(district Nainital, U.P.) Primary Health Centres. Indian J. Malariol. 20:21-34.
11. Malhotra, M. S., R. P. Shukla and V. P. Sharma (1985). Studies on the incidence of malaria in Gadarpurtown of terrain, Distt. Nainital, U.P. Indian J. Malariol. 22: 57-60.
12. Ghosh, S. K., A. Kumar, S. K. Chand and D. S. Choudhury (1989). A prelimnary malaria survey in BisraPHC, district Sundergarh, Orissa. Indian J. Malariol. 26:167-170.
13. Yadav, R. S., R. M. Bhat, V. K. Kohli and V. P. Sharma (2003). The burden of malaria in Ahmedabad city,India: a retrospective analysis of reported cases and deaths. Ann. Trop. Med. Parasitol. 97 (8): 793-802.
14. Sharma, V. P. (1999). Current scenario of malaria in India. Parasitologia 41: 349-353.15. Srivastava, H. C., Rajni Kant, R. M. Bhat, S. K. Sharma and V. P. Sharma (1995). Epidemiological
observations on malaria in villages of Buhari PHC, Surat, Gujarat. Indian J. Malariol. 32: 140-152.16. Shukla, R. P., S. N. Sharma and S. K. Bhat (2002). Malaria outbreak in Bhojpur PHC of District Moradabad,
Uttar Pardesh, India. J. Com. Dis., 34(2):118-123.17. Dhiman, R. C., C. R. Pillai and S. K. Subbarao (2001). Investigation of malaria outbreak in Bahraich
district. Indian J. Med. Res., 113:186-191.18. Yadav, R. N., S. N. Tewari, P. K. Tayagi, A. K. Kulsreshtha and Anil Prakash (1993). Malaria in Shankargarh
PHC, Allahabad district (U.P.): A clinical report. Indian J. Malariol. 30: 9-16.19. Prakash, A., P. K. Mohapatra, D. R. Bhattacharyya, P. Doloi and J. Mahanta (1997a). Changing malaria
endemicity – a village based study in Sonitpur, Assam. J. Commun. Dis. 29(2):175-178.20. Dev, V. and Sharma, V. P. (1995). Persistent transmission of malaria in Sonapur PHC, Kamrup district,
Assam. J. Parasitic Dis. 19:65-68.21. Singh, N. and K. K. Khare (1999). Forest malaria in Madhya Pradesh: Changing Scenario of disease and
its vectors. J. Parasitic Dis. 23: 105-112.22. Prakash Anil, P. K. Mohapatra, D. R. Bhattacharyya, C. K. Sharma, B. K. Goswami, N. C. Hazarika and J.
Mahanta (2000a). Epidemiology of malaria outbreak (April/May, 1999) in Titabor Primary Health Centre,district Jorhat (Assam). Indian J. Med. Res. 111:121-126.

28
Malaria23. Nandi, J., S. P. Mishra., R. Rajagopal, and M. V. V. L. Narasimham (1993). Present perspectives of
malaria transmission in Boko area of Assam. J. Com. Dis., 25(1): 18-2624. Dutta, P. D. R. Bhattacharyya, S. A. Khan, C. K. Sharma and B. K. Goswami (1994). Some observations
on malaria in Boko PHC of Kamrup District. Assam. J. Com. Dis., 26(1): 52-55.25. Prakash Anil, P. K. Mohapatra, and V. K. Srivastava (2000b). Vector incrimination in Tamalpur primary
health centre, district Nalbari, Lower Assam during malaria outbreak 1995. Indian J. Med. Res. 103:146-149.26. Prakash A., D. R. Bhattacharyya, P. K. Mohapatra and J. mahanta (1997b). Seasonal prevalence and malaria
transmission in a forest fringed village of Assam, India. Indian J. Malariol. 34: 117-125.27. Dev, V., M. A. Ansari, C. R. Hira and K. Barman (2001). An outbreak of Plasmodium falciparum malaria
due to Anopheles minimus in Central Assam, India. Indian J. Malariol. 38:32-38.28. Dutta, P., A. M. Khan and J. Mahanta (1999). Problem of malaria in relation to Socio-cultural diversity in
some ethnic communities of Assam and Arunachal Pradesh. J. Parasitic Dis. 23: 101-104.29. Dutta, P., D. R. Bhattacharyya and L. P. Dutta (1991). Epidemiological observations on malaria in some
parts of Tengakhat PHC, Dibrugargh district, Assam. J. Com. Dis., 28: 121-128.30. Dev, V. and Phookan, S. (1996). Malaria prevalence in tea estates of Brahmaputra Valley of Assam, India.
J. Parasitic. Dis. 20:189-192.31. Dev, V. (1996). Malaria survey in Tarajulie tea estate and adjoining hamlets in Sonitpur district, Assam.
Indian J. Malariol. 33: 21-29.32. Das, N. G., I. Baruah, S. Kamal, P. K. Sarkar, S. C. Das and K. Santhanam (1997). An epidemiological and
Entomological investigation on malaria outbreak at Tamalpur PHC, Assam. Indian J. malariol. 34: 164-170.33. Dutta, P. and Bhattacharyya D. R. (1990). Malaria survey in some parts of Namsang circle of Tirap district,
Arunachal Pradesh. J. Com. Dis., 22(2): 92-97.34. Das, N. G., M. Bhuyan and S. C. Das (2000). Entomological and epidemiological studies on malaria in
Rajmahal range, Bihar. Indian J. Malariol. 37:88-96.35. Das, N. G., I. Baruah and S. C. Das (2002). Situation of malaria in forest fringed villages of North lakhimpur
district, Assam. Indian J. Malariol. 39:43-47.36. Mohapatra, P. K., A. Prakash, D. R. Bhattacharyya and J. Mahanta (1998). Epidemiological importance of
younger age group during malaria epidemic in PHC Tamalpur, Assam. J. Commun. Dis. 30(4): 229-232.37. Kamal, S. and S. C. Das (2001). Epidemiological observations on malaria in some parts of Darang district,
Assam. Indian J. Malariol. 38: 25-31.38. Panda, R., K. V. S. Verma and S. J. Rehman (1990). Present status of Plasmodium malariae infection in
Bastar District (M. P.). J. Com. Dis., 22 (3): 185-190.39. Yadav, R.S., V. P. Sharma, S. K. Ghosh and A. Kumar (1990). Quartan malaria-An investigation on the
incidence of Plasmodium malariae in Bisra PHC, District Sundergarh, Orissa. Indian J. Malariol. 27:85-94.40. Kumar, A. (1997). Urban Malaria and its control in India. J. Parasitic Dis. 21: 83-88 (Review Article).41. Sharma, V. P., H. C. Uprety, P. K. Srivastava and R. K. Chandrahas (1985a). Studies on malaria transmission
in hutments of Delhi. Indian J. Malariol. 22: 77-84.42. Sharma, S. N. (1993). Malaria in stone quarry area in Faridabad Complex (Haryana). Indian J. Malariol.
30:113-117.43. Adak, T., C. P. Batra, P. K. Mittal and V. P. Sharma (1994). Epidemiological study of malaria outbreak in
a hotel construction site in Delhi. Indian J. Malariol. 31: 126-131.44. Christopher, S. R. (1924). What disease costs India: Statement of the problem before medical research in
India. Indian Med. Gaz., 59: 196-200.45. Sharma, V. P., R. K. Chandrahas, B. N. Nagpal and P. K. Srivastava (1985b). Follow up studies of Malaria
epidemic in villages of Shahjahanpur district, U.P. Indian J. Malariol. 22:119-121.45a.Bryant, J. (1969). Health in Developing World. (Cornell University Press, London).46. Ansari, M. A., V. P. Sharma, R. K. Razdan and C. P. Batra (1986). Malaria situation in Meerut district
villages (U. P.). Indian J. Malariol. 23:147-150.

29
Malaria47. Sharma, V. P. (1996). Re-emergence of malaria in India. Indian J. Med. Res. 103:26-45.48. Mathur, K. K., G. Harpalani, N. L. Kalra, G. G. K. Murthy and M. V. V. L. Narasimham (1992). Epidemic
of malaria in Barmer District (Thar Desert) of Rajasthan during 1990. Indian J. Malariol. 29:1-10.49. Mukhopadhyay, A. K., P. Karmakar, A. K. Hati and P. Dey (1997). Recent epidemiological status of malaria
in Calcutta Municipal Corporation area, West Bengal. Indian J. Malariol. 34: 188-196.50. Mohapatra, P. K., A. Prakash, H. K. Das, J. Mahanta and V. K. Srivastava (1995). Malaria outbreak in
Lower Assam: An epidemiological appraisal. J. Parasitic Dis. 19: 175-178.51. Kochar, D. K., I. Thanvi, A. Joshi, Subhakaran, S. Aseri and B. I. Kumawat (1998). Falciparum malaria
and Pregnancy. Indian J. Malariol. 35: 123-130.52. Herris V. K., V. S. Richard, E. Mathai, U. Sitaram, K. V. Kumar, A. M. Cherian, S. M. Amelia and G. Anand
(2001). A study on clinical profile of Falciparum malaria in a tertiary care hospital in south India. Indian J.Malariol. 38: 19-24.
53. Shukla, M. M., Neeru Singh, M. P. Singh, B. M. Tejwani, D. K. Srivastava and V. P. Sharma (1995).Cerabral malaria in Jabalpur, India. Indian J. Malariol. 32: 70-75.
54. Anonymous (2001). Medical Certification of cause of death-1997. Publ. Office of the Registrar General,India, Ministry of Home Affairs, New Delhi. pp. 143.
55. Das, L. K. (2000). Malaria during pregnancy and its effects on Foetus in a Tribal Area of Koraput district,Orissa. Indian J. Malariol. 37: 11-17.
55a. Das, D. B., R. N. Satpathy, P. C. Satpathy, J. K. Patnaik and B. S. Das (1992). Incidence of hypoglycaemiain children with severe Plasmodium falciparum malaria around Rourkela, Orissa state. Indan J. Med. Res.[A]95: 79-83.
56. Egwunyenga, O. A., J. A. Ajayi and D. D. Duhlinska-Popova (1997). Malaria in pregnancy in Nigerians:seasonality and relationship to splenomegaly and anaemia. Indian J. Malariol. 34: 17-24.
57. Mahapatra, P. (2001). Estimating National Burden of Disease: The burden of disease in Andhra Pradesh1990s. Publ. Institute of Health Systems, Hyderabad.pp 259.
58. Ray, A. P. (1981). Some aspects of the socio-economic impact of malaria and its control. Indian J. Malariol.18: 12-20.
59. Sinton, J. A. What malaria costs India (1935). Hlth. Bull. No. 26, Malaria Bureau No. 13 (Govt. of IndiaPress)
60. Rao, G. R. (1928). Economic significance of malaria to an industrial concern: A Railway. Indian Med.Gaz., 63: 568-573.
61. Winslow, C.E.A. (1951). The cost of sickness and the price of Health. WHO Monograph Series No. 7, Geneva.62. Newman, P. (1965). Malaria Eradication and Population growth (School of public health, University of
Michigan, USA)63. Barlow, R. (1968). The economic effects of malaria eradication, Ceylone (University of Michigan press,
Ann Arbor Michigan, USA).64. Pattanayak, S., V. P. Sharma, N. L. Kalra, V. S. Orlov and R. S. Sharma (1994). Malaria paradigms in India
and control strategies. Indian J. Malariol. 31: 141-199.65. Sharma, G. K. (1996). Malaria and its control in India. VIII. Rajasthan-year wise and epidemiological data
and parameters (1975 and 1976) (Directorate of National Malaria Eradication Programme. Ministry ofHealth and Family Welfare, New Delhi): 165-166.
66. Shukla, R. P., A. C. Pandey and A. Mathur (1995). Investigations of malaria outbreak in Rajasthan. IndianJ. Malariol. 32: 119-128.
67. Tayagi, B. K., S. P. Yadav, R. Sachdev and P. K. Dam (2000). Malaria outbreak in the Indira Gandhi NaharPariyojana Command area in Jaisalmer District, Thar Desert, India. J. Commun. Dis. 33 (2): 88-95.
68. Chandrahas, R. K. and V. P. Sharma (1983). Malaria Epidemic in Shahjahanpur (U.P.). Indian J. Malariol.20: 163-166.
69. Prasad, R. N., K. J. Virk., T. Sharma and G.D.P. Dutta (1992). Malaria Epidemic in Baniyani village,district Farrukhabad (U.P.). Indian J. Malariol. 29: 219-234.
30
Malaria70. Singh, N. and V. P. Sharma (1989). Persistent malaria transmission in Kundaim block, district Jabalpur
(M.P.). Indian J. Malariol. 26: 1-7.71. Chopra, R. N. (1933). Indigenous drugs of India (The Art Press, 20 British India Street, Calcutta).72. Shiv Lal, G. P. S. Dhillon and R. S. Sharma (Unpublished report). Impact of malaria control on our
national economy. National Malaria Eradication Programme, 22 Sham Nath Marg, Delhi-110 054.73. Yadav, R.S., S. K. Ghosh, S. K. Chand and A. Kumar (1991). Prevalence of malaria and economic loss in
two major iron ore mines in Sundergarh district, Orissa. Indian J. Malariol. 28:105-113.74. Bhati, P. G., V. S. Malviya, Rajni Kant, H. C. Srivastava, S. K. Sharma and V. P. Sharma (1996). Socio-
economic aspects of malaria in Kheda District, Gujarat. Indian J. Malariol. 33:200-208.75. Kondrachine and Trigg (1997). Importance of Clinical Diagnosis of malaria in National Malaria Control
Programme. Indian J. Malariol. 28: 183-187.
Books/documents Referreds1. Anonymous (1991). Census of India 1991: Series I-India-Socio-cultural tables. Vol. 2, Part IV A-C Series.
Pub. Registrar General and Census Commissioner, India. pp:395.2. Anonymous (1991). Census of India 1991: Series 6: Part IV A-C Series-Goa-Socio-cultural Tables). Publ.
Directorate of Census Operations, Goa -pp:953. Anonymous (1991). Census of India 1991: Series 6: Part IV –B (ii): Religion- Tables C-9). Publ. Directorate
of Census Operations, Goa -pp:384. Anonymous (2001). Census of India 2001: Series 31-Goa-Provisional Populationa Totals. Paper 1 of 2001.
Publ. Director of Census Operations, Goa -pp:43.5. Anonymous (2001). Census of India 2001: Series 31-Goa-Provisional Populationa Totals. Paper 2 of 2001.
Publ. Director of Census Operations, Goa -pp:676. Bruce Chwatt, L. J. (1985). Essential Malariology.II Edition.Publ. William Heinemann Medical Books
Ltd. London. pp. 452.7. Mahapatra, P. (2001). Estimating National Burden of Disease: The burden of disease in Andhra Pradesh
1990s. Publ. Institute of Health Systems, Hyderabad. pp 259.8. Malaria: Prinicples and practice of Malariology (1988). Eds. Wernsdorfer W. H. and McGregor, I. Churchill
Livingstone Publ. Edinburgh, London, Melbourne and New York. Vol 1:pp 1-912.9. Malaria: Prinicples and practice of Malariology (1988). Eds. Wernsdorfer W. H. and McGregor, I. Churchill
Livingstone Publ. Edinburgh, London, Melbourne and New York. Vol 2:pp 913-1818.10. Park, K. (2000). Preventive and Social Medicine. Publ. Banarsidas Bhanot Publishers, Jabalpur, India PP.
189-199.11. Sharma, R. S., G. K. Sharma and G. P. S. Dhillon (1996). Epidemiology and Control of malaria in India-
1996.National malaria Eradication Programme, New Delhi. pp:752.12. WHO (2001) National Burden of Disease Studies: A Practical Guide-Global Program on Evidence for
Health Policy, WHO, Geneva.
Important Website Accessedhttp://www.censusindia.nethttp://www.namp.gov.inhttp://www.nicd.orghttp://www.who.india.orghttp://www.whosea.orghttp://www.ncbi.nim.nih.govhttp://www.who.int/health_topics/malaria.

Information about the distribution and prevalence of a disease is essential for ameaningful discussion of its public health importance1. For a country like India,resource constraints for health sector (5.2% of GDP of which, government allocationof only 17%, while the rest by public) (NHP, GOI, 2002) is a major problem. Inorder to reallocate this meagre resources, it necessiates prioritisation of diseases ofpublic health importance for their control. Studies and estimates on Global Burdenof Disease (GBD) using a common scale such as disability adjusted life years lost(DALY) are being carried out2. To facilitate evidence-based decision making, globalburden due to Lymphatic Filariasis (LF) was estimated using DALY by the GBDstudy group for the year1992 with figures for India out3. As India being the secondlargest country contributing about 45% of the global burden4, DALY estimates wereupdated untill 1998. Then onwards, no separate estimate was available for India,but included under SEAR countries. The data available with the Indian Nationalcontrol programmes against LF was used by the GBD study group.
Although WHO estimates provide an indication of the numerical scale of the problemglobally, information on the finer details is scarce like information on age and gender
Filaria
DALY input Data component
Life Table (a) 5 year age interval & sex wise population(b) 5 year age interval & sex wise death rate (ASDR).
Years of Life Lost (YLL) (a) Cause Specific Mortality Pattern (CSMP) (5 year age inter-val & sex wise).
(b) Age weighting and discounting; if required.
Years Lived in Disability (a) Age at onset of disease ( disease sequelae).(YLD)* (b) Duration of disease (disease sequelae).Incidence Based YLD (IYLD) (5 year age interval & sex wise).Prevalence Based YLD (PYLD) 5 year age interval & sex wise prevalence of disease (dis-
ease sequelae)
Disability weight GBD disability weights by disease sequelae, age(5 year age interval) and gender class.
Applying DISMOD to check the 5 year age interval populationinternal consistency of prevalence ASDR Incidence or prevalence of disease sequelaedata. Remission rate of disease sequelae
Relative RiskCase Fatality Rate
* Incidence based data is ideal for for calculation of YLD. However, in its absence, prevalence data can be usedby incidence*duration per year.
31

32
Filaria
differences in infection and disease pattern5, on prevalence of different disease signs(sequalae), assessment of morbidity management and severity levels etc.
As the realistic estimates of DALY largely depend on the availability and qualityof demographic, descriptive epidemiological data and disease mortality data, thisstudy aims at reviewing the literature addressing (1) availability of data on LFdisease prevalence (overall and sequale wise), age and gender distribution ofdisease, data on mortality and relative risk on life expectancy morbiditymanagement and natural history (remission pattern, conversion from infection todisease, duration of irreversible sequale) and severity of the disease sequale, (2)identification of data gaps and (3) recommedations, if any, on data to be generated.
Data Components required to estimate the disease Burden using DALY asa Summary Measure :The data required to calculate different compoents if DALY is given in the table.Demographical data relating to age and gender wise population, age specific deathrate and cause specific mortality rate and epidemiological data relating to age andgender specific incidence or prevalence along with the duration of health state ofa given disease are required for the estimation of DALY. Disability weight fordifferent health state is another important data required. In addition, data is requiredon remission, transition, case fatality and relative risk to check the internalconsistency of data using DISMOD software.
Methodology of literature surveyEpidemiological data on lymphatic filariasis due to W.bancrofti in India wereextracted from publications and reports through computer literature searches andscrutiny of published and unpublished reports compiled at VCRC. In all cases, themost recent publications were given priority. However, some crucial publicationsnecessary for the earlier estimation of NBD for LF were also considered.
Sources of literature survey:1. Pubmed: online search2. Pubmed: Pubmed central (NLM)3. VCRC : Library4. VCRC:Filaria web site5. Manuals and reports: published and unpublished6. Data available with state units of National Programme (NFCP)7. Personal discussions with the experts.

33
Filaria
FINDINGS OF LITERATURE SURVEY
Epidemiological data
DISEASE PREVALENCE
Table 1. Number of research publications fromdifferent states and UTs of India on LymphaticFilariasis
States State/ No.UT References
Andhra Pradesh State 11Arunachal Pradesh State 0Assam State 3Bihar State 14Jharkhand StateGoa State 0Gujarat State 3Haryana State 1Himachal Pradesh State 0Jammu & Kashmir State 2Karnataka State 4Kerala State 19Madhya Pradesh State 8Chhatisgarh StateMaharashtra State 7Manipur State 1Meghalaya State 1Mizoram State 1Nagaland State 1Orissa State 24Punjab State 2Rajasthan State 3Sikkim State 0Tamil Nadu State 24Tripura State 0Uttar Pradesh State 11Uttaranchal StateWest Bengal State 8Andaman & Nicobar Islands UT 8Chandigarh UT 1Dadra & Nagar Haveli UT 2Daman & Diu UT 0Delhi UT 2Lakshadweep UT 2Pondicherry UT 4National 7Total 174
India
Reports on the prevalence of filarialdisease are available for different statesdepending on the completion of thedelimitations surveys carried out by theNational Filaria Control Programme(NFCP) launched in 1955. Out of a totalof 593 districts (as per 2001 census), 466districts have been covered under thesurvey till date. Apart from the annualreport of NFCP6, publications are availableon the filarisis situation in India and arebeing updated from time to time7-11.Filariasis caused by Wuchereria bancroftiand Brugia malayi have been reportedfrom 261 districts from 23 States andUnion Terriorities and the population atrisk of infection is reported to 454million12. Details of the survey results andpopulation at risk including estimatedcases of filarial disease is given in Table 2.
Filaria surveys were also carried out in 9states (Hariyana, Himachal Pradesh, Jammu& Kashmir, Manipur, Meghalaya,Nagaland, Punjab, Rajasthan and Tirupura)and one Union Territory (Chandigarh)hitherto believed to be non-endemic showedpresence of mf carriers but were importedexcept in Nagaland where indigenous caseswere recorded 13.
This based on the available data collectedover a period of several decades andextrapolating the results to the whole
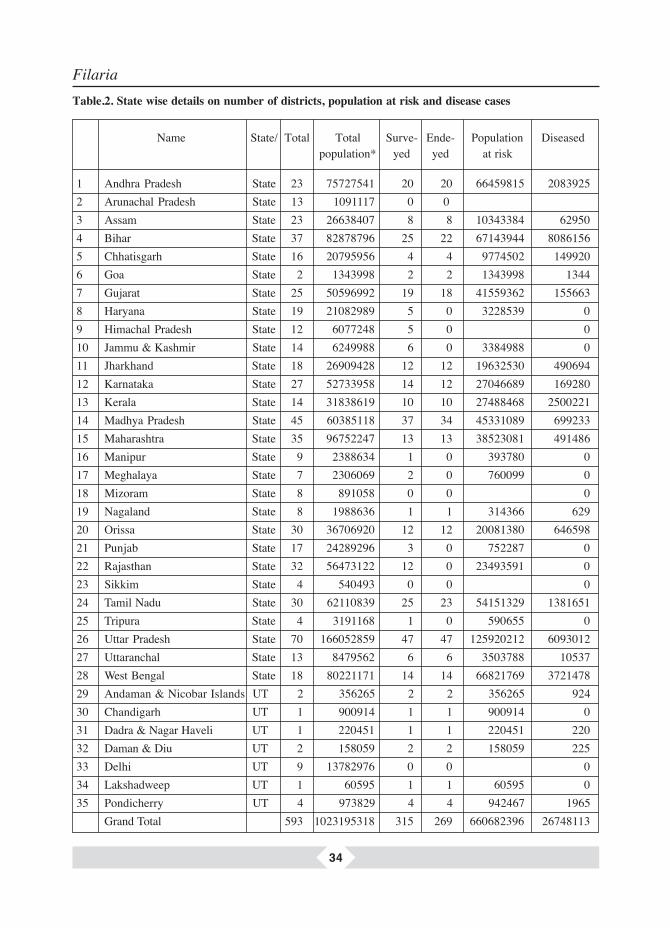
34
Filaria
1 Andhra Pradesh State 23 75727541 20 20 66459815 20839252 Arunachal Pradesh State 13 1091117 0 0 3 Assam State 23 26638407 8 8 10343384 629504 Bihar State 37 82878796 25 22 67143944 80861565 Chhatisgarh State 16 20795956 4 4 9774502 1499206 Goa State 2 1343998 2 2 1343998 13447 Gujarat State 25 50596992 19 18 41559362 1556638 Haryana State 19 21082989 5 0 3228539 09 Himachal Pradesh State 12 6077248 5 0 010 Jammu & Kashmir State 14 6249988 6 0 3384988 011 Jharkhand State 18 26909428 12 12 19632530 49069412 Karnataka State 27 52733958 14 12 27046689 16928013 Kerala State 14 31838619 10 10 27488468 250022114 Madhya Pradesh State 45 60385118 37 34 45331089 69923315 Maharashtra State 35 96752247 13 13 38523081 49148616 Manipur State 9 2388634 1 0 393780 017 Meghalaya State 7 2306069 2 0 760099 018 Mizoram State 8 891058 0 0 019 Nagaland State 8 1988636 1 1 314366 62920 Orissa State 30 36706920 12 12 20081380 64659821 Punjab State 17 24289296 3 0 752287 022 Rajasthan State 32 56473122 12 0 23493591 023 Sikkim State 4 540493 0 0 024 Tamil Nadu State 30 62110839 25 23 54151329 138165125 Tripura State 4 3191168 1 0 590655 026 Uttar Pradesh State 70 166052859 47 47 125920212 609301227 Uttaranchal State 13 8479562 6 6 3503788 1053728 West Bengal State 18 80221171 14 14 66821769 372147829 Andaman & Nicobar Islands UT 2 356265 2 2 356265 92430 Chandigarh UT 1 900914 1 1 900914 031 Dadra & Nagar Haveli UT 1 220451 1 1 220451 22032 Daman & Diu UT 2 158059 2 2 158059 22533 Delhi UT 9 13782976 0 0 034 Lakshadweep UT 1 60595 1 1 60595 035 Pondicherry UT 4 973829 4 4 942467 1965 Grand Total 593 1023195318 315 269 660682396 26748113
Name State/ Total Total Surve- Ende- Population Diseasedpopulation* yed yed at risk
Table.2. State wise details on number of districts, population at risk and disease cases

35
Filaria
population of a district could lead to vastly exagerated number of patients. The needfor exploring the ways and means of obtaining more accurae and recent estimates.Data on the prevalence of cases is also availabe for atleast 31 districts where massdrug administration is being implemented. Research studies are yet another sourceof data on disease prevalence. Literature on the prevalence of LF disease in differentstates is given in the following section.
Another source of data is from the Control units (206) and night clinics (198) of theNational Filaria Control Programme. These units are established to control LF through
Andhra Pradesh State 66459815 525000 2 29 4 4.57Arunachal Pradesh StateAssam State 10343384 27000 1 1 0 0Bihar State 67143944 731000 2 35 38 1.79Chhatisgarh State 9774502Goa State 1343998 31000 0 4 6 0Gujarat State 41559362 340000 0 9 7 0.02Haryana State 3228539 Himachal Pradesh State Jammu & Kashmir State 3384988 Jharkhand State 19632530 Karnataka State 27046689 63000 1 6 19 7.37Kerala State 27488468 389000 2 16 9 1.07Madhya Pradesh State 45331089 64000 3 9 8 1.26Maharashtra State 38523081 568000 6 16 10 0.97Manipur State 393780 Meghalaya State 760099 Mizoram State Nagaland State 314366 Orissa State 20081380 210000 2 15 15 16.68Punjab State 752287 Rajasthan State 23493591 Sikkim State Tamil Nadu State 54151329 822000 1 21 42 0.05Tripura State 590655 Uttar Pradesh State 125920212 637000 2 29 34 6.26Uttaranchal State 3503788 West Bengal State 66821769 133000 4 10 3 11.81Andaman & Nicobar Islands UT 356265 5000 1 1 1 0.04Chandigarh UT 900914 Dadra & Nagar Haveli UT 220451 Daman & Diu UT 158059 3000 2 2 0.21Delhi UT Lakshadweep UT 60595 1000 1 0 0Pondicherry UT 942467 47000 0 2 0 0.45Grand Total 660682396 4596000 27 206 198 1.5
Table 3. Statewise population protected by the NFCP10
Name State/ Population Population Survey Control Clin DiseaseUT at risk Protected Units Units ics prevalence

36
Filaria
vector control and case detection and treatment. Each unit covers about 50,000population and the entire population is being covered to screen for infection anddisease in a target period of 2 and half years. The data on prevalence indicate theimpact of the intervention and the limitation of this data is that it pertains to onlyareas under interventions (Table 3).
PondicherryThe earliest published study available on the LF disease in Pondicherry is by Dattain a Girls Mission School14. However, a detailed scientific study of NFCP was fromfilaria survey in Pondicherry settlements in 1957, published in 196015. This studyincluded only 4 disease sequale: acute attack (adenolymphangitis, ADL) (1%),hydrocele (2.7%), lymphoedema (1.7%) and chyluria (0.2%). In an integrated Vectorconrtrol demonstration project in Pondicherry the LF disease survey indicated thatthe prevalence of hydrocele was very high (86.9%) ADL, Lymphoedema(Lymphoedema and elephantiasis) and chyluria prevalence were 6.1, 7 and 18.5%16&17. Prevalence of these sequale were assessed in selected localities in which itwas observed that ADL, hydrocele, lymphoedema and chyluria was 0.2, 11.9, 1.9and 1.2% respectively 18&19. The latest research study conducted on the prevalenceon LF disease in Pondicherry was in the year 1992 again in selected localities20 inwhich it was shown that the ADL (0.4%), hydrocele (17.3%), lymphoedema (1.8%)and chyluria (0.2%). The overall prevalence of LF disease in these studies variedbetween 4.7% and 9.7%.
It is observed from the available studies that the overall disease prevalence hasincreased over the years. Prevalence of hydrocele has increased over the years whereasthat of lymphoedema remained stable and a decline was observed in chyluria.Hydrocele, the major manifestations in males was confirmed due to LF (13)21. Therewas no record of other clinical manifestations of LF like tropical pulmonaryeosinophilia (TPE), microscopic haematuria and mono-articular arthritis inPondicherry as observed in other parts of India.The major limitation of these studieswere 5 decade old data and restricted study area. NFCP survey in all the four districtsduing the year 1988 showed that disease was prevalent only in two districts rangingfrom 0.09 to 3.03.
KeralaBrugia malayi : In the hill tribes of Kerala, endemic for Brugia malayi infection,the microfilaria and disease rates have undergone a remarkable reduction. The mfrate has declined from 25.9% in 1957 to 6% in 1979 whereas the disease rate hasdeclined from 28.9% to 6.7% sduring the same period22. However,the mf (23.8-44.8%) and disease rates (28.6-96.6%) were very high in the same populationduring 1930s23. In one article, the results of earlier studies (1937, 1955, 1976,

37
Filaria
1986) on infection and disease in this area was compared and it was observed thatthe infection rate has reduced from 21 to 2% and disease rate from 24 to 10% overa period of 50 years24. In another study in semi urban community in the state, itwas observed that the mf rate was 5.55 and disease rate 3.6%25. In a recent study,it was observed that the disease rate 9.5 in Shertallai region of the state26. Trend ofmalayan filariasis in selected areas of Kerala27 and its epidemiology were alsoreported28&29.
W. bancrofti : In areas with W.bancrofti infection, the mf rate was 14.4, diseaserate 15% (with hydrocele 3.7%) and endemity 28%30. In another survey carriedout in urban areas, it was observed that mf rate was 0.48 and disease rate 0.25%21.In a recent survey, the mf rate was found to be 1.51%32. Disease prevalence basedon sample surveys carried out in different localities in the state was reported atdifferent time points33-45. Occurrence of adenolymphangitis, an acure episodic attackdue to filarial infection has also been reported inlcuding its managementtechniques46-50.
Uttar Pradesh (UP) and UttranchalStudies are available from 1950s in Uttar Pradesh. A survey carried out betweenMay-August, 1956 in Ballia district of UP showed that the disease rate ranged between19.87 (rural) and 34.5% (urban) area51. Another study showed an overall diseaserate of 34.47%, the majority of the patients were presented with hydrocele (58.8%)followed by lymphoedema (33.56%)52.
In a study carried out in 18 villages in 5 PHC areas has shown that the W.bancroftimf rate, filarial disease rate and endemicity rates were were 10.1, 11.4% and 18.8%respectively53. Studies carried out in 1960s, both in rural and urban areas, it wasobserved that in rural areas of Sitapur district, mf rate and disease rate were 3.96 and1.66% rspectively whereas in urban areas of Sitapur town mf rate and disease ratewere 5.09 and 2.75 respectively54&55. In the urba area, it was observed that 91 (of116) had hydrocele, 27 lymphoedema and 5 had chyluria. In the rural area, 77 (of109) had hydrocele, 19 lymphoedema and 15 had chyluria. Chand et.al., had carriedout a number of studies in 1960s in different districts of Utta Pradesh56-60. It wasobserved in Gorakhpur district that the mf rate was 13.15, and disease rate 11.9%. Atotal of 71.5% had hydrocele, others had lymphoedema with 22.2% lower limbinvolvement. There was no case of chyluria. In a recent study carried out in Varanasiregion of UP has revealed that the mf rate is between 9-14% and prevalence ofelephantiasis of leg between 3.1 to 7.3%61. Investigations were also carried out onthe filariasis problem in Balia district62.

38
Filaria
OrissaIn a very recent epidemiological study, carried out in Satyabadi PHC (Puri district)of Orissa, it was observed that the mf rate was 14.8 for ( 13.3 for W.bancrofti, 1.4for B.malayi and 0.09 for mixed infections). and disease rate 19.8% (12.85% acuteand 6.97% chronic manifestations). Filaria tropical pulmonary eosiniphilia (0.47%),microscopic haematuria (0.5%) and monoarticular arthritis(0.24%) are also observedin this are63.
In a survey in Chudamani area of Balasore district in 1989, 6.8 per cent were casesfound to harbour mf; 19 cases (of 36) had Brugia malayi, 4 Wuchereria bancroftiand 5 cases had mixed infection. In 8 cases, species could not be ascertained. For thefirst time after 1955, a focus of B. malayi has been detected in Orissa64. Kar andothers65-68 found that the overall prevalences of clinical disease and infection in bothmainlanders (34.18 and 14.4%) and tribals (25.47 and 17.9%) were comparable.However, both annual average adenolymphangitic attack rate (1.77 year-1) and theprevalence of chronic filarial disease (22.6%) amongst tribals were significantlylower.
In another study carried out in Puri district, the prevalence of microfilaria was found tobe 7.3 per cent and the disease rate 9.5 per cent69. Data collected from 60 villages inOrissa, areas are classified into low, high, hyper and holo endemic levels. The meanmf rates were found to be 2.7, 6.8, 12.0, and 16.0, and disease rates 4.9, 10.2, 18.9 and35.1 respectively at four endemicity levels70. In a study, 15.6% were found to haveasymptomatic haematuria (Grade I haematuria-14.7%, Grade II-0.6%, Grade-III 0.3%)71.Babu and others72 reported the prevalence of disease due to lymphatic filariasis inKhurda district of Orissa was significantly higher in males (14.79%) than females(10.04%). However, elephantiasis is more prevalent in females, and adenolymphangitisis more prevalent in males than females. Results on the prevalence of disease infectionin different parts of the state were also available at different time points73-80.
West BengalA survey carried out in 1996 in Nemari village in Burdwan district of West Bengalshowed that mf and disease rates were 0.8 (36/4512) and 1.41% (64/4512). Out of64 cases, elephantiasis in 8, lymphangitis in 14, lymphoedema in 8, lymphvarix in 9and hydrocele alongwith epididymoorchitis in 25 cases were observed81. The mfand disease rates percent worked out to be 0.914 and 1.87 respectively. The earliestages showing mf and disease manifestations were 3 and 11 respectively. The maleand female ratio in terms of mf carriers and chronic cases worked out to be 1.4:1 and1:282. There have been few studies on the disease among the tribal populations of the

39
Filaria
state. In a study in tribal and non-tribal populations living in Bankura district revealedthat the tribal subjects had lower prevalence of microfilaraemia (3.17% v. 8.86%)and of symptomatic filariasis (5.92% v. 13.74%) than the non-tribal, filariasisendemicity (8.95% v 22.12%)83.In Bagdogra town, district Darjeeling (West Bengal),Wuchereria bancrofti,mf rate was 2.32% (males and females were 2.84% and 1.79% respectively). The age of these positives ranged from 5-45 years. The mf rate washighest (4.46%) in the age group of 20-29 years. Disease and filarial endemicityrates were 0.33% and 2.65% respectively. During 1976 survey in the same town, mfrate was 1.6% and disease rate was nil84. As a part of the on-going National FilariaControl Programme, National Filaria Day was observed in Purulia district of WestBengal on 26th Nov 2000 with an extensively organized mass DEC consumptioncampaign preceded by IEC activities and followed by mopping up operations. Diseaseprevalence among population covered showed 0.1% hand swelling, 0.6 to 0.8% legswelling, while 1.1% of males had hydrocele83. The clinical spectrum of bancroftianfilariasis86 and occurrence of malayan filariasis in coastal areas of West Bengal87
have also been reported.
Andaman Nicobar islandsA filariasis survey, carried out in 1993 in Nicobar islands showed the mean diseaseprevalence of 1.9%88. Subsequent surevy showed very low prevalence of filarialdisease (83). Another study in the Little Andaman island, covering a population of12,247 in 12 of the 13 villages showed that infection due to Wuchereria bancroftiwas found only in 3 villages with microfilaria (mf) rate ranging from 1.02 to 6.45per cent89. Only one of 2788 individuals examined was found to have clinicalmanifestation. (0.24%). Other studies on filariasis reported only the prevalence ofinfection90-9390-93. Sub periodic bancroftian filariasis occurs only in this group ofislands in India.
PunjabA filariasis survey was conducted in 1998 in Pathankot town of Punjab covering apopulation of 28, 041. A total of 2136 blood smears were collected from migratoryand local inhabitants. Microfilaria (Mf) rate and mean Mf density was 1.19 and15.05 respectively. Disease rate was nil. All the 20 microfilaria carriers detectedwere from other filaria endemic states. Wuchereria bancrofti was the only infectionencountered. These findings were compared to earlier surveys in the same area andother non-endemic areas. Non-endemic areas continue to be non-endemic for filariasisdespite considerable increase in mf rate among migratory population and vectordensity94. Incidence of filariasis among industrial population was reported fromAmritsar95.

40
Filaria
Andhra PradeshThe earliest report from Andra Pradesh was from Nellore district which showed adisease prevalence of 1.16%96. Subsequently the results of delimitation surveys ofNFCP were available for 20 districts out of total 23 districts97-106. A review on thesurvey conducted between 1955 and 59 by the NFCP6 has summarized the prevalenceof infection and disease in 20 districts in AP7. A study on Filariasis control in ruralareas through detection and treatment with diethylcarbamazine107, undertaken in therural areas of Srikakulam (1.8 Million) and Vizianagaram (0.89 Million) of AndhraPradesh showed that this chemotherapeutic method of control of filaria in rural areasis feasible and acceptable to society. During first round of detection and treatment20,300 mf carriers (90.6 per cent of detected) and 6,588 disease persons (86 per centof detected) in Srikakulam and 7,097 mf carriers (94.8 per cent of detected) and1,436 disease persons (93.4 per cent of detected) in Vizian. The mf rate and diseaserates were 2.1 and 0.57 in Srikakulam and 1.35 and 0.2 in Vizianagaram respectively.This based on mass screening of individuals and not on sample surveys as beingdone under delimitation surveys of NFCP.
The impact of different control measures viz.antilarval measures, antilarval measuresalong with selective treatment of microfilaria (mf ) carriers with diethylcarbamazine(DEC), selective treatment of mf carriers with DEC only, and total populationtreatment with DEC, on the incidence and prevalence of filariasis in villages wasmeasured. In Penikeru, the mf prevalence rate before treatment was 10.8 per cent,and afterwards 7.2 percent; ( P>0.05), In Alameru , the mf prevalence rate beforetreatment was 14.0 percent, and after wards 8.5 percent (P< 0.01), ; in Angara , itdeclined from 16.0 to 7.2 percent ( P< 0.01); and in West Kandrika , the mf prevalencerate declined from 15.5 to 13.8 percent ( P>0.05) 104.
Tamil NaduThere are 30 districts in Tamil Nadu and data on the prevalence of filarial disease isavailable from the annual report of NFCP (1989). Filaria surveys were carried out inMadras108 and some rural areas109&110. Filariasis is prevalent in 13 districts. Data onfilarial disease prevalence are availale from NFCP delimitation survey (annual report1989), NFCP control units and MDA programme111. Data from the delimitation surveyshowed that disease was recorded from 15 districts, ranging from 0.06 to 8.01 percent.Data from the MDA programme showed that the disease prevalence ranged from0.02 to 0.35 in different districts based on line listing of cases (Department of PublicHealth, personnal communication). Data is also available from the NFCP controlunits on the prevalence of disease from 21 control units and 42 night clinics111.

41
Filaria
KarnatakaResults of NFCP survey6 in 19 districts showed the prevalence in 17 distircts rangingfrom 0.01 to 2.71 percent. Filariasis prevalence is very low in Karnataka. Surveycarried out in Bangalore slum areas showed very low (0.03%) disease prevalence112.Risk of filariasis transmission in Bangalore city has also been reported113&114.
LakshadweepDisease prevalence was found to range between 0.08 and 27.7 with an average of15.5% among the population of 11846 covered under the survey115&116.
AssamInfection in Upper Assam was reported to be 10.3%117. Other studies report onlyprevalence of microfilaraemia118&119. NFCP6 report showed that five of the six districtssurveyed were endemic with disease prevalence ranging from 0.15 to 1.60 %.
Bihar and JharkhandDelimitation survey of the NFCP6 showed the prevalence of disease in 35 districtswith the disease rate ranging from 0.9 to 30.14%. Survey carried out in Patna120 showedthe prevalence of disease among 30.1%. Another survey conducted in Bhagalpur townshowed that the disease prevalent among 17.11% of the urban population and 7.9 % ofthe rural population121&122. Results were also available for three more districts123-129.
MaharastraResults of the survey6 carried out in urban areas of 15 districts showed that diseaseprevalence ranged from 0.09 to 7.6% while in the rural areas disease was reportedfrom 11 districts with the disease rate ranging from 0.04 to 5.65%. The disease ratewas found to be 3.6% in Bombay city130. Data are also available for some localitiesin Bombay urban area131-133.
GujaratAs per the survey carried out in 20 districts in Gujarat by the NFCP6 duing 1958-1987, disease was reported from 16 districts with disease rate raning from 0.01 to8.8%134. Another survey carrie out in 1984 in Valsad district showed that the diseaseprevalence was between 0.2 and 0.4%135&136.
Madhya PradeshData on the prevalence of disease is available based on the delimitation survey ofNFCP for 39 districts and in most of the districts it is below 1%. In the districts

42
Filaria
where filarial disease prevalence is above 1%, it ranged between 2.1 and 9.7%.Chand and others carried out a survey in 1996 in the tribals of Panna showed verylow mf prevalence137. Reports were also available on disease prevalece for otherdistricts138-142.
Prevalence of filarial disease has been reported from Goa (0.1%), Daman (0.12) andDiu (0.2%) from the delimitation survey carried out in 1988 by the NFCP6. Data ondisease prevalence from Dadar & Nager Havali143&144 are also available, but verylow prevalence (0.1 to 0.3%).
Non endemic States/Union TerritoriesFilarial disease has not yet been reported from 2 (Delhi and Chandigarh) of the sevenUnion Territorines and 11 states (Tripura, Mizoram, Sikkim, Rajasthan, Punjab,Manipur, Maharastra, 1India6. However special surveys in the army camps and slumsin Delhi showed prevalence of diseased cases145,146. In Jamu and Kashmir, survey wascarried out in Srinagar and Baramulla town showing the prevalence of infection amongarmy personnels147. The indigenous population of Rajasthan do not have filarial infectionor disease13. In a study, it was observed that the migratory labour population (mostlyfrom U.P, Bihar and Orissa) had a microfilaria rate of 4% with mean density of 16.5and disease rate of 2%148. Prevalence of vector species has also been reported149.
Natural history and disease dynamics
Disease sequalaeStudies available in India from 1955 onwards have reported 3 main chronicmanifestations of lymphatic filariasis, hydrocele, lymphoedema and chyluria andone acute manifestation, acute adenolymphangits (ADL). However, othermanifestaions also have been reported in Orissa showed the following63, 150, 151:
1. Hydrocele 59.0%2. Lymphoedema of limbs 38.6%3. Chyluria 1.2%4. Microscopic haematuria/proteinuria 0.5%5. Tropical Pulmonary Eosiniphilia 0.47%6. Mono-articular arthritis 0.24%
The asymptomatic microfilaraemics harbouring a very large number of parasites(even 20,000 or more per microlitre of blood) commonly have microscopic

43
Filaria
haematuria or proteinuria152. In a study conducted on 363 suspected filarialpatients attending the surgery out patient division of the MGIMS, Sevegram,the disease was significantly higher in males (86%) than in females (14%).Majority (52.9%) of the cases were in the age group of 11-30 years. Thedistribution of cases into three different grades of infection showed, 52.6%,33.3% and 14.1% of the cases having acute (grade I), sub-acute (grade II) andchronic (grade III) stages of infection respectively. While 73% of the caseshad genital manifestations, 23% were with lymphatic obstruction in limbs andthe rest of the 4% suffered from manifestations like cellulitis, abscesses,haematuria and chyluria153.
Prevalence of disease according to age and genderThe disease rates were higher in all age classes in 1992 and monotonicallyincrease in disease prevalence with age was observed in both the surveys of1987 and 1992 whereas in was less rapid upto the age of 31-40 years in 1957study. It was observed in all these studies that hydrocele is the major clinicalmanifestation of LF. Gender specific analysis showed that the disease rate issignificantly higher in males than females and hydrocele is the major clinicalmanifestation of LF in males and lymphoedema in females in Pondicherry.Prevalence of chronic manifestations are age dependent in both genders whereasacute attacks were age-independent154. Though some studies are available onmicrofilaria distribution in children155&156 the disease pattern in them is notavailable.
Estimation of loss and gain rates of infectionTransition from infection to disease is crucial in forecasting disease recruitmentover a period of time and estimating disease prevalence. In two studies carriedout in VCRC, it was observed that the rate of loss of infection is statisticallyhigher than that of the gain rate. In one study the rate of loss of infection wasestimated to be 0.4822 per 1000 and gain rate of 0.019 whereas in anotherstudy these figures were 0.67 and 0.062 respectively (VCRC Annual report,1999). In a study using a reversible catalytic model to estmate the rate of lossand gain of infection, it was observed that the instantaneous rate of loss ofinfection is independent of age while the rate of gain of infection exhibits aconvex age profile (peak at 16-20 years) and the mean expected life span ofadult Wuchereria bancrofti to be 5.4 years157. In a subsequent estimate, it wasshown that the mean expected life span of adult Wuchereria bancrofti variesbetween 2.1-5.0 years158.

44
Filaria
Infection to diseaseRecent studies in India on Wuchereria bancrofti and Brugia malayi have shown thatmicrofilaria carriers who subsequently become amicrofilaraemic are at higer risk ofdeveloping chronic disease159,163. The cumulative exposure and its relationship havebeen carried out164,165. In a study carried out in Pondicherry, it was observed thatabout 11% of the population at risk develop lymphoedema and age prevalence of thepopulation at risk correspond to the age prevalence of lymphoedema in males butnot in females159. In another study, 23% of amicrofilaremic males were reported tobe at risk to develop hydrocele. These findings of Pondicherry studies are similarwith that carried out elsewhere, 17.24%150 of a microfilaremics and 23%151 developedhydrocele. It was observed that only 5.7% of microfilariae carriers develophydrocele151.
In Pondicherry it was observed that the prevalence of disease and hydrocele inmicrofilaraemic individuals (9.4% and 20.0% respectively) was higher comparedto that observed in amicrofilaraemic persons (6.4% and 11.2% respectively). TheRelative Risk (RR) of parasite carriers developing disease (any manifestations)was marginally higher compared to amicrofilaraemic persons (1.18). However,the RR of developing hydrocele manifestation due to microfilaraemia was muchgreater (1.5 times) compared to amicrofilaraemic persons. The Attributable Risk(AR) due to microfilaraemia for developing hydrocele was 0.05. This suggeststhat although the risk is high in mf carriers, there might be alternate route of infectedpersons developing disease without becoming microfilaraemic166. All these studieswere based on long term community based observeations and follow-up of
Age Infection Disease Among Hydrocele Among
mf + ves mf - ves mf + ves mf - ves
Among Loss/Gain Gain Loss Gain Loss Gain Loss Gain Loss
0-14 0.00 0.06 - 0.00 0.00 0.00 - - -
0.00
15-39 0.00 0.12 1.00 0.25 1.00 0.15 - 0.33 -
0.32
>=40 0.25 0.13 0.00 0.00 0.67 0.10 - 0.00 0.50
0.26
Total 0.10 0.12 0.50 0.13 0.69 0.11 - 0.25 0.50
0.24
45
Filaria
microfilaria carriers rendered negative after treatment with a standard course ofdiethylcarbamazine (DEC).
In an unpublished study at VCRC, the rate of loss and gain of infection and disease fromamong microfilaria positives and negatives is given as follows (VCRC unpublished data).
Age at onset of diseaseThe earliest ages showing mf and disease manifestations were 3 and 11 respectively.The male and female ratio in terms of mf carriers and chronic cases worked out to be1.4:1 and 1:2167. In a study carried out in Shertallai in Brugian filariasis, it wasobserved that the mean age at onset of Grade I (recent oedema), was 29 years whereasGrade II (persistent oedema without skin change) was 34 years and Grade III & IV(persistent oedema with skin change) oedema was 44 years168.
Duration of disease sequaleIn W. bancrofti infection the mean number of adenolymphangitis (ADL) attacks asco-morbidity in one year was 4.9, 5.5 and 10.4 in patients with grade I, grade II andgrade III lymphoedema respectively. The mean duration of oedema was 47.4 ± 5.9days, 6.2 ± 0.5 and 8.6 ± 0.9 year in patients with grade I, grade II and grade IIIlymphoedema respectively169-171. These figures for B.malayi infection were 0.9, 2.5and 5.1 (ADL attacks) and 0.1, 13.6 and 28.7 (mean duration of lymphoedema)172.The gap in the mean age between grades roughly indicates the duration of eachsequalae which was found to be 0.3 years, 6.1 years & 3.5 years for grade I, II and IIIrespectively for W.Bancrofti170,173.
Disability weightDisability Weights (DW) of different disease sequale of LF are crucial for estimatingprevalencec based “Years Lived with Disabilty”(PYLD) component of DALY. Thespectrum of clinical manifestation of this disease varies from acute manifestation of fewdays’ duration to chronic irreversible life-long disabling sequale of lymphoedema andelephantiasis174. Disability weights provided by Global Burden of Disease (GBD) studygroup is available3 for only two disease sequelae viz., lymphoedema and hydrocelethrough expert rating. Epidemiologically, progression of LF disease shows clear stagesof acute and chronic manifestations with different sequelae and the pattern of morbidityvaries with the type of manifestation. Therefore it is logical to consider these categoriesof disease manifestations seperately for determining the disability weight for a morerealistic estimate of DALY. No literature is available on the disability weights for anyother sequale except lymphoedema and hydrocele (>15 cm).

46
Filaria
Though a few qualitative studies are available on the estimated costs of treatment toLF patients175-177, the impact of functional impairement LF in a labour population178
and the economic burden of LF in India179, studies on quantification of disabilitydue to different sequelae of LF in terms of disability weight is not currentlyavailable.The disability weights used by global burden of disease (GBD) are basedon experts’ rating2 (Murray et.al., 1994). In the changed international scenario, ithas been recommended to have community ratings. The GBD DW for differentsequale available are as follows:
Disease sequale Disability weight by age group (years)
0-4 5-14 15-44 45-59 60+
Hydrocele >15cm 0.066 0.070 0.075 0.075 0.075
Lymphoedema 0.067 0.080 0.113 0.128 0.119
Data have to be generated for DW for acute attacks, different grades of lymphoedema,hydrocele less than 15 cm diameter, chyluria, microscopic haematuria, tropicalpulmonary eosiniplilia and mono-articular arthritis. Secondly, community ratedvalues will be preferred in welfare states instead of experts values. Nationallyagrreable values of DW should be used for comaprison across the diseases.
Mortality due to LF: Cause of death (CoD)Clinical presentations and natural history of LF indicate that either case fatality ormortality attributable to the disease is a matter of debate. Age specific death rate (ASDR)is a crucial parameter for estimation of Years of Life Lost (YLL) component of DALY.LF is classifed under 74.0 of international classification of disease-10th version (ICD-10) and the clinical presentation and natural history of LF suggests that no mortalitycan be attributable to this disease and therefore, GBD estimates put YLL to be zero.No literature is available to suggest that mortality could be attributable to this disease.However, in recent years there have been indications that patients with LF succumb tosudden overwhelming septicaemia due to acute attacks ADL (personal communications,Dr. Manokaran, Apollo hospital, Chennai, Dr. Ambika Arasu, Vijaya hospital ,Chennaiand Dr. R.K.Shenoy, Allepey medical college hospital). Therefore, CoD studies areurgently required in LF disease. However, considering the duration of the irreversibledisabled conditions arising out of accumulation of lymph in the extremities andsuperimposed with repeated dermal bacterial/ fungal infections, the risk of loweredage at death if any in comparison to people without the disease need to be studied.

47
Filaria
Table 4. Progress of Surveys on Disease Prevalence in India.
Year Total District Endemic Population Mf Disease SourceDistricts surveyed District at risk. rate rate
1960 60 58 64 24 4.4 Ramakrishnan, et al,19601970 290 152 ? 131 11.3 8 Rao et al, 19761976 290 162 ? 236 18 14 Sharma et al,19771981 296 218 157 304 21.7 15.84 Sharma et al,19831989 301 243 174 367 25 19 NFCP Annual report2001 466 289 257 472 30.9 23.4 WHO, 2001
In a study carried out in VCRC suggests that the mean age (68 years) at death of patientswith LF is significantly lower than that without (74 years) LF (VCRC unpublished data).Relative Risk (RR) of earlier age at death due to LF should be looked into.
Limitations of data base for DALY calculationData from NFCPThe major limitation is that there is no data available on morbidity in terms of diseaseincidence due to lymphatic filariasis as the chronic cases are irreversible and are notregistered under conventional case detection methods. However data on diseaseprevalence is available for different communities/districts. This is based on samplesurveys conducted by NFCP under delimination survey. The survey design followedin this survey is to get an estimate representing a given state. But the limitations inthis data bases include a) survey is conducted at different time periods (Table 4) andhence current situation is not available, b) still more than 100 “endemic” districtsare to be surveyed c) no age, gender and manifestation (grade) wise breakups are notavailable and d) current figures are extrapolated estimates. The other source ofprevalence data is from the control units (Table 3).
Data from operational programme of MDAMass drug (DEC) administration (MDA) programme has been launched in India ona pilot scale to assess the operational feasibility and impact of MDA in controllinglymphatic filariasis. It was started in 13 districts in 7 states and subsequently expandedto 31 districts. One of the activities is to enumerate the population and enlist thecases with disease manifestation. This can be considered as recent data on LF diseaseprevalence. Unpublished report obtained from the Govt. of Tamil Nadu was used toestimate the disease burden. Unlike prevalence survey results, this data base givesabsolute number of cases suffereing from LF. The limitation of this data is that datais not available for all the endemic states and age, gender and manifestation wisebreakups are not available in the summary report. Further, enlisting of LF cases is

48
Filaria
done by posing querries and not by physical examination and therefore there isevery chance for underestimation of cases, particulary hydrocele cases.
Data from research studiesData on LF disease prevalence is also availble from research studies. Research studiesare being conducted for specific objectives and therefore the results do not reflectthe actual prevalence of LF in the study area. Also, survey methodology is not uniformas it is generally designed to address the research question.
Analysis of dataDisease burden due to LF was estimated in terms of DALY using data from differentsources. Two disease sequale viz, hydrocele and lymphoedema were used and thedisability weight for these two manifestations derived by the Global Disease Burdenstudy group was used. Using descriptive epidemiological analysis, age and genderspecific prevalence was calcualted for different data sets. Acute manifestation(adenolymphangitis) has been included for the estimation. The number of diseasecases was estimated from the prevalence data assuming that there was no change inthe prevalence and the cases are in proportion to population growth. The prevalencefor the new districts (bifurcation) was assumed to be that of parent district. Usingthe prevalence data from the delimitation survey units, DALY was calculated foreach state and for the Nation (Table 5 and Fig. 1).
Data qualityData quality was assessed using DISMOD soft ware. The assumptions made in thismodel are remission rate as 0 and transition rate as 1 (Odema mostly remainirreversible) and all the infected become diseased. But comparision of age specificprevalence with estimated incidence did not show any trend (Fig. 2 & 3). Use ofDISMOD to assess the internal consistency of the data needs to be explored further.
Comparison of dataData obtained from different sources are compared and the results are shown intable 6 and 7. The results suggest that NFCP data showed a higher prevalence whichwas assessed during 1950s, while the current situation was much lower. Comparisonof prevalence assessed by NFCP in 1957 was lower than that reported in a researchstudy in Pondicherry. While the prevalence of lymphoedema remains unchanged,there has be four to five fold increase in the prevalence of hydrocele. This could bedue to improvement in screening procedure and acceptability of the community forphysical examination. These analyses suggest that source of data on LF prevalenceis important to be considered while making disease burden estimates.

49
FilariaTable 5. State wise disease burden due to LF
Name Total Population Diseased DALY1 Andhra Pradesh 75727541 2083925 1733072 Arunachal Pradesh 10911173 Assam 26638407 62950 52354 Bihar 82878796 8086156 6724755 Chhatisgarh 20795956 149920 124686 Goa 1343998 1344 1127 Gujarat 50596992 155663 129468 Haryana 21082989 0 09 Himachal Pradesh 6077248 0 010 Jammu & Kashmir 6249988 0 011 Jharkhand 26909428 490694 4080812 Karnataka 52733958 169280 1407813 Kerala 31838619 2500221 20792814 Madhya Pradesh 60385118 699233 5815115 Maharashtra 96752247 491486 4087416 Manipur 2388634 0 017 Meghalaya 2306069 0 018 Mizoram 891058 0 019 Nagaland 1988636 629 5220 Orissa 36706920 646598 5377321 Punjab 24289296 0 022 Rajasthan 56473122 0 023 Sikkim 540493 0 024 Tamil Nadu 62110839 1381651 11490325 Tripura 3191168 0 026 Uttar Pradesh 166052859 6093012 50671727 Uttaranchal 8479562 10537 87628 West Bengal 80221171 3721478 30949229 Andaman & Nicobar Islands 356265 924 7730 Chandigarh 900914 0 031 Dadra & Nagar Haveli 220451 220 1832 Daman & Diu 158059 225 1933 Delhi 13782976 0 034 Lakshadweep 60595 0 035 Pondicherry 973829 1965 163 Grand Total 1023195318 26748113 2224472
**Descriptive epidemiology from Pondicherry studyLymphoedema - 20.1 %Hydrocele – 79.1 %

50
Filaria

51
Filaria
NFCP Data MDA (operational)Hydrocele Lymph Total Hydrocele Lymph Total
Oedema OedemaMale 1103939 68317 1172256 21720 5181 26901Female 209395 209395 9360 4236Total 1103939 277712 1381651 8728 14541 36261
Table 6. Number of case obtained from different data sources in Tamil Nadu
Difference 38 times lower
Data gaps
Type of data Required Available (A)/Not available(NA)
Demography Age and gender wise census population AAge specific death rate (ASDR) A
Epidemio- Age and gender wise incidence of disease NA (to be initiatedlogical data using DISMOD)
Age and gender wise prevalence of disease AInc./Prev. of all disease sequale NARemission Rates of disease sequale. Transition NARates of disease sequale NA
Data on mortality ASDR: male and female NA (to be initiated )due to LFDisability weight DW for all sequale: age and gender wise NA (under study)
Table 7. Data from different source
Parameters NFCP (1957) VCRC (1986) VCRC (1992)Disease rate 4.7 6.7 9.9ADL 1.0 0.2 0.04Lymphoedema 1.9 1.9 1.8Hydrocele 2.7 11.9 17.3

52
Filaria
RecommendationsEpidemiological" Disease prevalence data of NFCP can be used provided as method of data
collection was uniformly used in the Nation wide survey. However, details onage classes and gender were not available. This can be obtained from the rawdata through colloborative approach with NFCP. Therefore, it is recommendedto include NFCP as one of the partners in networking. It is recommended that ifthe data is made available, analysis can be carried out by the VCRC to identifyendemic states by mapping already known endemic districts. Data on currentprevalence of LF need to be generated. As this is a pre-requisite to implementthe proposed MDA programme by the NVBDC, this task can be planned jointlyby evolving appropriate method.
" Extrapolation of epidemiological data to whole population to get the actual numberof cases is erroneous. Therefore, a delimitation survey could be undertaken toknow the endemic districts before extrapolation of data at district level.
" Data on disease remission and mortality are not available. Studies have beenproposed to generate these informations.
" As there are some difficulties encountered in the application of DISMOD, forlymphatic filariasis, it could be refined by incorporating data from the above studies.
Disability weight" Only expert rated Disability Weights are available and the issue needs to be
assesed as to whose perspective should be used" Need for a nationally agreeable disability weight" Both expert as well as community rated DW need to be derived and compared. A
multicentric study using a common protocol by the particpating institutes maybe useful to avoid duplication and to derive more realistic values on disabilityweight.
" All disease sequale of LF need to be considered for deriving disability.
Publications reviewed1. Anonymous (1993). Investing Heath: World Development Indicators in World Health Development Report,
Oxford University Press, Oxford.2. Murray CJL (1994). Quantifying the burden of disease: the technical basis for disability adjusted life years.
Bulletin of the WHO, 72(3): 429-445.3. Murray C.J.L:and Lopez A.D 1996. The global burden of disease.A comprehensive assessment of mortality
and disability from diseases, injuries and risk factors in 1990 and projected to 2020. Boston:HarvardSchool of Public Health

53
Filaria4. Das, P. K., Ramaiah, K. D., Augustin, D. J., Kumar, A. (2001). Towards elimination of lymphatic filariasis
in India. Trends in Parasitology, 17(10):457-605. Brabin, B.J., Ginny, M., Alpers, M., Brabin, T., Eggelte and Kaay, V.D. 1990. Failure of chloroquine
prophylaxis for falciparum malaria in pregnant women in Medange, Papua New Guinea. Ann. Trop. Med.Parasitol., 84:1-9
6. National Filaria Control Programme, India, Annual Report 1989.7. Ramakrishnan, S. P., Raghavan, N. G. S., Krishnaswami, A. K., Nair, C. P., Basu P, C. and Dalip, Singh.
National filaria control programme in India: a review (1955-59). Ind J Malar 14: 457-94.8. Sharma, M. I. D. (1976). Problem of filariasis in India. J Commu Dis 8: 95-100.9. Sharma, S. P., M. Das, et al. (1977). “Current estimates of filariasis problem in India.” J Comm Dis
9:111-6.10. Sharma, S.P., Biswas, H. and Sexana, N.B.L. (editors) (1995). National Filaria control programme – India.
Operational manual, Delhi, National Malaria Eradication Programme11. Sharma, S.P., Biswas, H., Das, M., Dwivedi, S.R. (1983). Present status of filariasis problem in India. J
Commu Dis, 15:53-6012. World Health Organization. (2002). Lymphatic filariasis. Weekly epidemiological record, 77(16):125-13213. Rao, C.K., Russel, S. and Das, M. (1976). Filariasis problem in non-endemic states – India. J Commu Dis,
8:221-2914. Datta, S.P., 1960. Filarial survey in mission girls hostels in Pondicherry Town. Bull Natn Soc India Malar
8:131-36.15. Nair, P. 1960. Filariasis in centrally administrated areas. PartI. Filaria surveys of Pondicherry settlement.
Ind J Malariol 14:233-52.16. Rajagopalan, P. K., P. K. Das, et al. (1988). Evaluation of integrated vector control measures on filariasis
transmission in Pondicherry. Indian J Med Res 87: 434-9.17. Rajagopalan, P. K., P. K. Das, et al. (1989). Bancroftian filariasis in Pondicherry, south India: 1. Pre-
control epidemiological observations. Epidemiol Infect 103: 685-92.18. Pani, S.P, L.K Das, N Balakrishnan, C Sadanandane, A.R Rajavel, S Subramanian, and P Vanamail. 1989.
A study on the clinical manifestations of Bancroftian filariasis in Pondicherry. Indian Medical GazetteCXXII (4):111-115.
19. Pani, S.P, J Yuvaraj, P Vanamail, V Dhanda, E Michael, B.T Grenfell, and D.A.P Bundy. 1995. Episodicadenolymphangitis and lymphoedema in patients with bancroftian filariasis. Transactions of the RoyalSociety of Tropical Medicine and Hygiene 89 (1):72-74.
20. Surendran, K, S.P Pani, M.B Soudarssanane, D.K Srinivasa, P.C Bordolai, and S Subramanian. 1996.Natural history, trend of prevalence and spectrum of manifestations of bancroftian filarial disease inPondicherry (South India). Acta Tropica 61 (1):9-18.
21. Sivam, S., Jayanthi, S, Anannthakrishnan, N., Elango, E., Yuvaraj, J., Hoti, S.L. and Pani, S.P. (1995). Tropicalvaginal hydoroceles; are they all filarial in origin. Southeast Asian J Trop Med Pub Hlth, 26(4):739-742
22. Chandrasekharan A, Balaraman K, Rao CK. 1981.Decline in brugian filariasis in hill tribe settlements ofKerala. Indian J Med Res.73 Suppl: 82-6
23. Iyenger MOT, 1938. Studies on the epidemiology of filariasis. Indian Med Res Memoir: 30.24. Rajagopalan PK,Panicker KN, Pani SP.1989. Impact of 50 years of vector control on the prevalence of
Brugia malayi in Shertallai area of Kerala state.Indian J Med Res.89: 418-2525. Jain, D. C.; Chandrasekharan, A.; Sethumadhavan, K. V.; Johny, V. M.; Cherian, C.; Ghosh, T. K.: 1989.
Epidemiology of brugian filariasis in a rural community of Kerala State. J Commun Dis 21(1): 27-3326. Pani, S. P.; Krishnamoorthy, K.; Rao, A. S.; Prathiba, J. 1990. Clinical manifestations in malayan filariasis
infection with special reference to lymphoedema grading. Indian J Med Res. 91: 200-7

54
Filaria27. Russel, S., M. Das, et al. (1976). Trend of malayan filariasis in selected areas of Kerala State. J Commun
Dis., 8: 203-209.28. Jain DC,Chandrasekharan A, Sethumadhavan KV,Johny VM,Cherian C,Ghosh TK.1989a. Epidemiology
of brugian filariasis in a rural community of Kerala State.J Commun Dis. 21(1): 27-33.29. Raghavan, N. G.; Pattanayak, S.1963. Studies on the Epidemiology of B. Malayi Filariasis in Kerala State.
Periodicity of the Microfilariae. Indian J Malariol., 17:285-291.30. Nair, C. P. 1962. Filariasis in Kerala State. VII. Survey of Ponani (Palghat District).Indian J Malariol., 16: 47-6231. Pattanayak, S.; Chandrasekhar, A.1963. Filariasis in Kerala State: Filaria Survey of Kottayam Municipality.
Indian J Malariol., 17: 273-732. Rajendran G, Panicker KN, Krishnamoorthy K, Sabesan S, Snehlatha, Radhakrishnan R.1997.Current
status of filariasis in Chavakad taluk, Trichur district, Kerala. J Commun Dis., 29(4): 333-43.33. Nair, C. P. 1969. Filariasis survey on Vaikom municipality in Kerala state. J Commun Dis 1: 59-70.34. Joseph, C. and Peethambaran, P.1963. A Filariasis Survey of Trichur (Kerala State). Indian J Malariol.,
17:33-3635. Joseph, G.; Prasad, B. G.1967. An epidemiological study of filariasis in the coastal belt of Kerala State.
Indian J Med Res. 55(11): 1259-7236. Pillay, M. K. and M. A. V. Menon (1957). Filariasis in the State of Kerala. Bull Nat Soc Ind Mal Mosq
Borne Dis 5: 191-5.37. Jain DC, Menon PK, Sethumadhavan KV,Johny VM,Ghosh TK.1989b. Epidemiology of bancroftian
filariasis in a semi-urban community of Kerala State. J Commun Dis.21(4): 265-7138. Arunachalam N, Mariappan T, Vijayakumar KN, Sabesan S, Panicker K N.1996. Mattancherry urban
agglomeration, a diminishing focus of lymphatic filariasis in Kerala. J Commun Dis.28(3): 168-70.39. Singh, J., N. G. S. Raghavan, et al. (1956). Filariasis in Travancore-Cochin State. 1 Ennakulam and
Mattancherri. Ind J Malar 10: 219-38.40. Cruickshank, J. A. and R. E. Wright (1914). Filariasis in Cochin. Indian J Med Res 1: 741-85.41. Day, F. (1860). Elephantiasis arabum or ‘Cochin leg’. Madras Q J Med Sci 1: 37-53.Bibliography of
Filariasis and Elephantiasis, South Pacific Commission III42. Galliard, H. (1958). The filarial aetiology of elephantiasis ‘Cochin leg’ in Travancore (India). Presse Med
66: 755-57.43. Nair, C. P., R. Roy, et al. (1960). Filariasis in Kerala State. VI. Filaria survey of Fort Cochin Municipality.
Ind J Malariol 14: 223-31.44. Ragharan, N. G. S., C. P. Nair, et al. (1958). Filariasis in Travancore-Cochin (Kerala State). III. Hilltribe
settlements in Quilon and Trivandrum districts. IV. Filarial survey of Eriyad Panchayat, Craganore Taluk.Ind J Malariol 12: 183-93.
45. Singh, J., A. K. Krishnaswami, et al. (1956). Filariasis in Travancore-Cochin State. II Shertallai Taluk. BullNat Soc Ind Mal Mosq Dis Ind J Malariol 10: 317-25.
46. Shenoy, R. K., V. Kumaraswami, et al. (1992). Ivermectin for the treatment of periodic malayan filariasis:a study of efficacy and side effects following a single oral dose and retreatment at six months. Ann TropMed Parasitol 86: 271-8.
47. Shenoy, R. K., V. Kumaraswami, et al. (1993). A comparative study of the efficacy and tolerability of singleand split doses of ivermectin and diethylcarbamazine in periodic brugian filariasis. Ann Trop Med Parasitol87: 459-67.
48. Shenoy, R. K. (2002). Management of disability in lymphatic filariasis—an update. J Commun Dis34(1): 1-14.

55
Filaria49. Suma, T. K., R. K. Shenoy, et al. (2002). Efficacy and sustainability of a footcare programme
in preventing acute attacks of adenolymphangitis in Brugian filariasis. Trop Med Int Health7(9): 763-6.
50. Suma, T. K., R. K. Shenoy, et al. (2003). A qualitative study of the perceptions, practices and socio-psychological suffering related to chronic brugian filariasis in Kerala, southern India. Ann Trop MedParasitol 97(8): 839-45.
51. Gujral JS 1958. Urban, semi-urban and rural filariasis in Ballia district, Uttara Pradesh. Ind J Malariol 12(2), June: 101-8.
52. Singh, M. V. (1960). Geographical distribution of filariasis in Uttar Pradesh. Ind J Malariol 14: 379-86.53. Prasad RN, Das MK et.al., 1993. Prevalence of filariasis in rural areas of Shahjahanpur district (UP).
Indian J Med Res 97: 112-4.54. Singh MV, Rastigi KC, Singh RP and Srivastava VK. 1963a. Observations on the urban filariasis in
Sitapur town (Uttara Pradesh). Ind J Malariol 17(4) December: 357-363.55. Singh MV, Rastigi KC, Singh RP and Srivastava VK. 1963b. Observations on the rural filariasis in
Sitapur town (Uttara Pradesh). Ind J Malariol 17(4) December :303-310.56. Chand Diwan, Singh MV, Vyas LC 1961a. Filariasis in Ghazipur district, Uttara Pradesh. Ind J Malariol
15: 21-9.57. Chand Diwan, Singh MV, Vyas LC 1961b. Filariasis in Deoria district, Uttara Pradesh. Ind J Malariol
15: 31-8.58. Chand Diwan, Singh MV, Vyas LC 1961c. Filariasis in Ghazipur district, Uttara Pradesh. Ind J Malariol
15: 21-9.59. 53 Chand Diwan, Singh MV, Vyas LC 1961d. Filariasis in Bahraich district, Uttara Pradesh. Ind J Malariol
15: 175-84.60. Chand Diwan, Singh MV, Vyas LC 1962. Filariasis in Gorakhput district, Uttara Pradesh. Ind J Malariol
16(3) September: 269-76.61. Sharma S, Sharma M and Rathaur S. 1999. Bancroftian filariasis in the Varanasi region of north India: an
epidemioloical study. Annals of Tropical Medicine & Parasitology 93 (4): 379-387.62. Rahman J, Singh MV, Gujral JS 1957. Investigation of filariasis problem in Ballia district, Uttara Pradesh.
Ind J Malariol 11 (2), June: 163-67.63. Chhotray, G. P., M. Mohapatra, et al. (2001). A clinico-epidemiological perspective of lymphatic filariasis
in Satyabadi block of Puri district, Orissa. Indian J Med Res 114: 65-71.64. Rath, R. N., R. K. Das, et al. (1984). Bancroftian filariasis in two selected rural communities in Puri
district: Orissa—a comparative study of filariometric data. J Commun Dis 16: 104-12.65. Kar S K, Mania J, Kar PK. 1993. Clinical filarial disease in two ethnic endemic communities of Orissa,
India. J Trop Med Hyg 96 (5): 311-666. Kar, S. K. (1986). Epidemiological study on lymphatic filariasis in an endemic zone of Orissa. J Commun
Dis 18: 312.67. Kar, S. K. and J. Mania (1993). Tropical pulmonary eosinophilia in an Orissa village. Natl Med J
India 6: 64-7.68. Kar, S. K., J. Mania, et al. (1993). Prevalence of lymphatic nodule in a bancroftian endemic population.
Acta Trop 55: 53-60.69. Kumar A, Dash AP,Mansing GD.1994. Prevalence of filariasis in rural Puri, Orissa. J Commun Dis 26(4):
215-20.70. Kumar A. 1996. Human filariasis: infection rate as the uniform measurable criterion for filarial endemicity.
J Commun Dis.28(3):163-771. ChhotrayGP, Ranjit MR, Mohapatra M.2000. Occurrence of asymptomatic microscopic haematuria in a
filarial endemic area of Orissa, India. J Commun Dis 32(2): 85-93.

56
Filaria72. Babu BV, Acharya AS, Mallick G, Jangid PK, Nayak AN, Satyanarayana K. 2001. Lymphatic filariasis in
Khurda district of Orissa, India: an epidemiological study. Southeast Asian J Trop Med Public Health.32(2): 240-3
73. Kumar, A. and S. K. Chand (1990). Prevalence of Wuchereria bancrofti infection in some coastal villagesof Ganjam, Orissa. J Commun Dis 22: 209-12.
74. Mahapatra, G. S. (1961). Filariasis in Orissa. J Assoc Physics India 9: 677-684.75. Rao, S. S. (1936). Filariasis in Patnagarh (Orissa Feudatory State). Ind J Med Resch 23: 871-879.76. Rath, R. N., B. N. Mohapatra, et al. (1989). Detection of a new focus of Brugia malayi infection in Orissa.
J Commun Dis 21: 39-40.77. Richards, V. (1873). Elephantiasis arabum; being a sketch of the disease as it exists in Northern Orissa; its
treatment and influence on opium eating. Indian Ann Med Sci 15: 342-75.78. Russel, S., A. R. Rao, et al. (1980). Disappearance of some Brugia malayi foci from Madhya Pradesh,
Orissa and Tamil Nadu and co-existence of Malayan and Bancroftian filariasis in some pockets. J CommunDis 12: 183-7.
79. Sabharwal, K. K., B. B. Purohit, et al. (1975). Filariasis in India-facts and figures. Part ix-Orissa. J CommunDis 7: 364-368.
80. Sahu, K. C. (1963). Clinical observations on some dermal manifestation of filariasis in Orissa and theirresponse to Uni-carbazan Forte (tablet). Indian J Derm 8: 119-21.
81. Chandra G, Hati AK.1996. Filariasis survey in a rural area of West Bengal. J Commun Dis. 28(3): 206-8.82. Raina VK, Joshi MC, Singh S, Joshi RD, Bhattacharjee KK, Kumar A, Verghese T. 1990. Epidemiology of
Brugia malayi infection and its co-existence with Wuchereria bancrofti in and around Sillaberia PHC,District Midnapur, West Bengal. J Commun Dis.22(3): 205-8.
83. Rudra SK, Chandra G. 2000. Comparative epidemiological studies on lymphatic filariasis, between tribal andnon-tribal populations of Bankura district, West Bengal, India. Ann Trop Med Parasitol. 94(4): 365-72.
84. Singh S, Bora D, Sharma RC, Datta KK. 2002. Bancroftian filariasis in Bagdogra town, district Darjeeling(West Bengal). J Commun Dis.34(2): 110-7.
85. Haldar A, Mundle M, Haldar S, Biswas AK, Mitra SP, Mahapatra BS.2001. Mass DEC campaign forfilariasis in a hyper endemic district of West Bengal. J Commun Dis. 33 (3): 192-7.
86. Dondero TJ Jr., Bhattacharya NC, Black HR, Chowdhury AB, Gubler DJ, Inui TS, Mukerjee M.1976.Clinical manifestations of Bancroftian filariasis in a suburb of Calcutta, India. Am J Trop Med Hyg.25(1): 64-73.
87. Bera DK, Banerjee P.1996. A lymphatic filarial survey revealing a focus of Brugia malayi in the coastalregion of west Bengal. J Indian Med Assoc. 94(8): 296-7, 310.
88. Tewari, S. C., J. Hiriyan, et al. (1995). Epidemiology of subperiodic Wuchereria bancrofti infection in theNicobar Islands, India. Trans R Soc Trop Med Hyg 89: 163-6.
89. Shriram, A. N., M. V. Murhekar, et al. (2002). Prevalence of diurnally subperiodic bancroftian filariasisamong the Nicobarese in Andaman and Nicobar Islands, India: effect of age and gender. Trop Med IntHealth 7(11): 949-54.
90. Shriram, A. N., A. P. Sugunan, et al. (1996). Little Andaman Island, a new focus of infection with nocturnallyperiodic Wuchereria bancrofti. Indian J Med Res 104: 166-70.
91. Das, M., S. Russel, et al. (1975). Filariasis in Andaman and Nicobar Islands. Part II. Periodicity of microfilariaof Wuchereria bancrofti. J Comm Dis 7: 251-256.Helminthological Abstracts (Series A) 1976
92. Kalra, N. L. (1974). Filariasis among aborigines of Andaman and Nicobar Islands. 1. Detection ofnon-periodic bancroftian filariasis among Nicabarese of Nancowry group of Nicobar Islands. J CommunDis 6: 40-56.

57
Filaria93. Kalra, N. L. (1976). Filariasis among aborigines of Andaman and Nicobar Islands. II Filaria survey of
Shompens of Greater Nicobars and Onges of Little Andamans. J Commun Dis Delhi 8: 51-9.94. Singh, S., D. Bora, et al. (2000). A study of filarial transmission in a non-endemic area of Pathankot
(Punjab). J Commun Dis 32(1): 61-4.95. Sangha, H.K. and Chitkara, N.L. (1974). Incidence of filarisis in the industrial population of Amritsar.
Indian J Path & Bact, 18:41-4596. Farooq, M. and M. Qutubuddin (1946). Epidemiology of filariasis in certain parts of H.E.H. the Nizam’s
State. Ind Med Gaz 81: 470-4.97. Naidu, C. R. (1962). Filariasis control in Andhra Pradesh. Bull Nat Soc Ind Malar Mosquit Dis 10: 69-90.98. Briender, S., P. C. Basu, et al. (1967). Filariasis in India-Facts and Figures Part I-Andhra Pradesh. Bull Ind
Soc Mal Com Dis 4: 65.99. Rao, C. K., K. K. Datta, et al. (1980). Epidemiological studies on bancroftian filariasis in East Godavari
district (Andhra Pradesh): baseline filariometric indices. Indian J Med Res 71: 712-20.100. Narasimham, M. V., C. Krishna Rao, et al. (1983). Some clinical aspects of bancroftian filariasis in East
Godavari district, Andhra Pradesh. Indian J Med Res 78: 631-5.101. Biswas, H., S. P. Sharma, et al. (1989). Filariasis control in rural areas through detection and treatment
with diethylcarbamazine. J Commun Dis 21: 272-81.102. Patnaik, S. K., P. K. Rao, et al. (1991). Some epidemiological and clinical aspects of bancroftian filariasis
in coastal Andhra Pradesh. Indian J Public Health 35: 123-5.103. Rao, C. K., K. Ramaprasad, et al. (1981). Epidemiology of bancroftian filariasis in East Godavari district
(Andhra Pradesh)—incidence of tropical pulmonary eosinophilia. Indian J Med Res 74: 517-23.104. Rao, C. K., K. R. Prasad, et al. (1982b). Impact of control measures on prevalence and incidence of
bancroftian filariasis in East Godavari district (Andhra Pradesh). Indian J Med Res 75: 515-20.105. Rao, C. K., K. R. Prasad, et al. (1982a). Prevalence and incidence rates of microfilaraemia and filaria
disease in the East Godavari district of Andhra Pradesh. Indian J Med Res 75: 23-7.106. Singh, B., P. C. Basu, et al. (1967). Filariasis in India-facts and figures. I Andhra Pradesh. (B.A.). Bull
Indian Soc Mal Com Dis 4: 65-8.107. Biswas, H., S. P. Sharma, et al. (1989). “Filariasis control in rural areas through detection and treatment
with diethylcarbamazine.” J Commun Dis 21: 272-81.108. Hyma, B., A. Ramesh, et al. (1989). Lymphatic filariasis in Madras, India. Soc Sci Med 29: 983-90.109. Ramaiah KD, Pani SP, Balakrishnan N, Sadanandane C, Das L K, Mariappan T, Rajavel AR, Vanamail P,
Subramanian S. 1989. Prevalence of bancroftian filariasis & its control by single course of diethylcarbamazine in a rural area in Tamil Nadu. Indian J Med Res. 89: 184-91.
110. Sarma, R. V., R. S. Vallishayee, et al. (1987). Prevalence survey of filariasis in two villages in Chingleputdistrict of Tamil Nadu. Indian J Med Res 85: 522-30.
111. Government of Tamil Nadu, Unpublished report on the prevalence of chronic cases during the enumerationof households for MDA (2003)
112. Ann. (1973). Filaria survey in the slums of Bangalore City Corporation. J Commun Dis 5: 1-7.113. Raghuvir Rao, L. (1961). A note on the natural transmission of Wuchereria bancrofti in Bangalore (Mysore
State). Bull Nat Soc India Malaria Other Mosquito Borne Dis 9: 209-11.114. Vadhera, K. K. (1970). A filariasis survey among recruits in Bangalore. Armed Forces Med J India 26:
158-61.115. Rao, C. K., P. P. Rao, et al. (1981). Control of bancroftian filariasis with common salt medicated with
diethylcarbamazine in Lakshadweep. Indian Journal of Medical Research 73: 865-873.116. Subramaniam, H., H. Ramoo, et al. (1958). Filariasis survey in the Laccadive Minicoy and Amindiri Islands,
Madras state. Ind J Malar 12: 115-27.

58
Filaria117. Khan, A. M., P. Dutta, et al. (1999). Lymphatic filariasis in two distinct communities of upper Assam. J
Commun Dis 31(2): 101-6.118. Dutta, P., B. K. Gogoi, et al. (1995). Filariasis in the labour population of a tea estate in Upper Assam.
Indian J Med Res 101: 245-6.119. Prakash, A., P. K. Mohapatra, et al. (1998). Bancroftian filariasis in Namrup tea estate, district Dibrugarh,
Assam. Indian J Public Health 42(4): 103-7, 112.120. Kant, L., S. K. Sen, et al. (1956). Filariasis in Patna (Bihar) Part I. Ind J Malariology
10: 199-217.121. Varma, B. K., V. P. Sinha, et al. (1960). Filariasis in Sultanganj and its suburbs (Bihar). Bull Nat Soc India
Malar 8: 149-52.122. Varma, B. K., N. L. Dass, et al. (1961a). Filariasis in the rural population around Bhagalpur Town. Part II.
Ind J Malar 15: 293-99.123. Varma, B. K., N. L. Dass, et al. (1961b). Studies on the incidence and transmission of filariasis in Bhagalpur
Town (Bihar). Ind J Malar 15: 185-94.124. Varma, B. K., R. M. Prasad, et al. (1962). Studies on the incidence and transmission of filariasis in Monghyr
(Bihar). Indian J Malariol 16: 17-26.125. Varma, B. K., V. P. Sinha, et al. (1964a). Observation on mass therapy with diethylcarbamazine for filaria
control in Bhagalpur District, Bihar. Patna J Med 38: 76-80.126. Varma, B. K. and V. P. Sinha (1964b). Studies on mass therapy with diethylcarbamazine for filaria control
in Monghyr, Bihar. Patna J Med 38: 329-336.127. Verma, B. K., V. P. Sinha, et al. (1960). Filariasis in Sultan Ganj and its suburbs (Bihar). Bull Nat Soc Ind
Mal Mosq Dis 8: 149-52.128. Raghavan, N. G. S., S. Birendar, et al. (1967). “Filariasis in India-Facts and Figures. Part III-Bihar.” Bull
Ind Soc Mal Com Dis 4: 155-6.129. Korke, V. T. (1930). Observations on the characters of filarial endemic areas in Bihar and Orissa. Part VI.
Ind J Med Res 18: 333-6.130. Patel (1986). Filariasis. Proceedings of a seminar. Bombay, 12 May 1986. J Commun Dis 18: 223-319.131. Gupta, K. K. (1988). Prevalence of filariasis among naval community residing in Navy Nagar, Bombay.
Indian J Public Health 32: 160-1.132. Sant, M. V., W. N. Gatlewar, et al. (1974). Epidemiological and biochemical studies in filariasis in four
villages near Bombay. Prog Drug Res 18: 269-75.133. Patel, T. B. and P. B. Paranjpey (1958). Observations on mass therapy with diethylcarbamazine (hetrazan)
for filaria control in Bombay State. Ind J Malar 12: 171-82.134. Singh, B., P. C. Basu, et al. (1967). Filariasis in India. Facts and figures: IV Gujarat. Bull Indian Soc
Malaria Commun Dis 4: 260-3.Biological Abstracts 1969135. Raina, V. K., G. J. Kosare, et al. (1984). Impact of diethylcarbamazine treatment of selective microfilaria
carriers and filarial cases under rural filaria control project in Valsad district, Gujarat. J Commun Dis 16:247-9.
136. Sharma, S. P., H. Biswas, et al. (1984). Control of Bancroftian filariasis with diethylcarbamazine in ruralareas of Valsad district, Gujarat State. J Commun Dis 16:282-6.
137. Chand G, Pandey GD,Tiwary RS.1996.Prevalence of Wuchereria bancrofti infection among the tribals ofPanna district of Madhya Pradesh.J Commun Dis., 28(4): 304-7
138. Park, J. E. (1961). Filariasis in Rewa Division, Madhya Pradesh. Ind J Pub Health 5:114-21.139. Park, J. E. (1962a). Filariasis in Chhatarpur district Madhya Pradesh. Ind J Med Sci 16: 604-612.140. Park, J. E. (1962b). Filariasis in Datia district, Madhya Pradesh. J Assoc Physns India 10: 25-29.Tropical
Diseases Bulletin 1963

59
Filaria141. Park, J. E. (1962c). Filariasis in Satna district, Madhya Pradesh. Bull Nat Soc Ind Matar Mosqu Dis 10: 3-10.142. Raghavan, N. G. S., B. Singh, et al. (1967). Filariasis in India-Facts and figures. Part VI Madhya Pradesh.
Bull Indian Soc Mal Com Dis 4: 385-90.143. Raina VK, Joshi MC, Joshi RD, Singh Sukhvir, Yadava RL, Ashok Kumar. Filaria Situation in the Union
Territory of Dadra & Nagar Haveli. 1991. J Commmu Dis 23: 182-184.144. Russel, S., C. K. Rao, et al. (1982). Filariasis in Dadra and Nagar Haveli. J Commun Dis
14: 157-60.145. Verma, R. N. and M. S. Bhoparai (1969). Transmission of filariasis amongst the army personnel in Delhi.
J Comm Dis Delhi 1: 270-3.146. Raina, V. K., V. C. Tripathi, et al. (1992). Status of lymphatic filariasis in some select slum clusters of
Delhi. J Commun Dis 24: 92-6.147. Raina, V. K., C. K. Rao, et al. (1985). Status of lymphatic filariasis transmission in Srinagar and Baramulla
towns—Jammu and Kashmir state. J Commun Dis 17: 92-3.148. Sharma, R. S., V. K. Raina, et al. (1986). A filariasis survey among the migratory labourers at Alwar,
Rajasthan. J Commun Dis 18: 287-90.149. Verma, K. V., V. Joshi, et al. (1991). Studies on mosquito vector species in indoor habitats of desert and
non-desert regions of Rajasthan. J Commun Dis 23: 263-9.150. Beuria, M.K., Bal, M.S., Mandal, N.N. and Das, M.K. 2002. Antigneamia at 10 years after
diethylcarbamazine treatment of a symptomatic micorfilaraemic individual: marginal conversion to infection-free state. Parasitol Immunology, 24:109-111.
151. Sahoo, P.K., Baboo, J.J.G., Satapathy, A.K., Mohanthy, M.C., Das, B.K., Acharya, A.S., Misra,N. andRavindran,B. 2002. Bancroftian filariasis:a 13-year followup study of asymptomatic microfilaria carriersand endemic normals in Orissa, India. Parasitology, 124:191-201.
152. Dreyer, G., E. A. Ottesen, et al. (1992). “Renal abnormalities in microfilaremic patients with Bancroftianfilariasis.” Am J Trop Med Hyg 46: 745-51.
153. Mehta, V. K., H. Lohar, et al. (1999). «Surgical filariasis: immunoscreening for filarial IgG antibodiesusing Wuchereria bancrofti microfilarial excretory-secretory antigen.» J Commun Dis 31(1): 35-40.
154. Pani, S. P., N. Balakrishnan, et al. (1991). “Clinical epidemiology of bancroftian filariasis: effect of ageand gender.” Trans R Soc Trop Med Hyg 85: 260-4.
155. Das, P. K., A. Sirvidya, et al. 1997. “Wuchereria bancrofti microfilaraemia in children in relation to parentalinfection status.” Transactions of the Royal Society of Tropical Medicine and Hygiene 91(6): 677-679.
156. Ramaiah, K. D. and K. N. Vijay Kumar (2000). “Effect of lymphatic filariasis on school children.” ActaTrop 76(2): 197-9.
157. Vanamail P, Subramanian S, Das PK, Pani SP, Rajagopalan PK, Bundy DA, Grenfell BT. 1989. Estimationof age-specific rates of acquisition and loss of Wuchereria bancrofti infection.Trans R Soc Trop MedHyg.83(5): 689-93
158. Vanamail P, Subramanian S, Das PK, Pani SP, Rajagopalan PK.1990. Estimation of fecundic life span ofWuchereria bancrofti from longitudinal study of human infection in an endemic area of Pondicherry (southIndia).Indian J Med Res.91: 293-7.
159. Srividya, A., S. P. Pani, et al. (1991). “The dynamics of infection and disease in bancroftian filariasis.”Trans R Soc Trop Med Hyg 85: 255-9.
160. Sabesan, S., K. Krishnamoorthy, et al. (1991). “The dynamics of microfilaraemia and its relation withdevelopment of disease in periodic Brugia malayi infection in south India.” Epidemiol Infect 107: 453-63.
161. Chan, M.S, A Srividya, R.A Norman, S.P Pani, K.D Ramaiah, P Vanamail, E Michael, P.K Das, and D.A.PBundy. 1998. EPIFIL: a dynamic model of infection and disease in lymphatic filariasis. The AmericanJournal of Tropical Medicine and Hygiene 59 (4):606-614.

60
Filaria162. Vanamail P, Ramaiah K D, Pani SP, Das P K, Grenfell BT, Bundy DA.1996. Estimation of the fecund life
span of Wuchereria bancrofti in an endemic area. Trans R Soc Trop Med Hyg.90(2): 119-21.163. Subramanian, S., P. Vanamail, et al. (1989). “A simple deterministic model for host-parasite relationship
in Wuchereria bancrofti infection & its relevance to parasite regulation in human host.” Indian J MedRes 89: 411-7.
164. Das PK, Srividya A, Pani SP, Ramaiah KD, Vanamail P, Dhanda V.1994. Cumulative exposure and itsrelationship with chronic filarial disease in bancroftian filariasis. Southeast Asian J Trop Med PublicHealth.25(3):516-21
165. Grenfell, B. T., P. K. Das, et al. (1990). “Frequency distribution of lymphatic filariasis microfilariae inhuman populations: population processes and statistical estimation.” Parasitology 3: 417-27.
166. Pani, S. P., P. Vanamail, et al. (1994). “Micro-spatial variation in filarial disease and risk of developingdisease associated with microfilaremia in urban situation.” Southeast Asian J Trop Med Public Health25: 719-23.
167. Raina, V. K., M. C. Joshi, et al. (1990). “Epidemiology of Brugia malayi infection and its co-existencewith Wuchereria bancrofti in and around Sillaberia PHC, District Midnapur, West Bengal.” J CommunDis 22: 205-8.
168. Pani, S.P, K Krishnamoorthy, J Prathiba, and A.S Rao. 1989. Diethylcarbamazine and supportive measuresfor the treatment of brugian filariasis. National Medical Journal of India 2 (6):260-263.
169. Pani, S.P, and A Srividya. 1995. Clinical manifestations of bancroftian filariasis with special reference tolymphoedema grading. Indian Journal of Medical Research 102 (9):114-118.
170. Pani, S.P, J Yuvaraj, P Vanamail, V Dhanda, E Michael, B.T Grenfell, and D.A.P Bundy. 1995. Episodicadenolymphangitis and lymphoedema in patients with bancroftian filariasis. Transactions of the RoyalSociety of Tropical Medicine and Hygiene 89 (1):72-74.
171. Ramaiah, K. D., K. Ramu, et al. (1996). “Epidemiology of acute filarial episodes caused by Wuchereriabancrofti infection in two rural villages in Tamil, Nadu, south India.” Trans-R-Soc-Trop-Med-Hyg 90(6):639-43
172. Pani, S.P, K Krishnamoorthy, A.S Rao, and J Prathiba. 1990. Clinical manifestations in malayanfilariasis infection with special reference to lymphoedema grading. Indian Journal of Medical Research91 (5):200-207.
173. Pani, S.P, and R Lall. 1998. Clinical Features, Pathogenesis and Management of Lymphatic Filariasis.ICMR Bulletin 28 (5):41-51.
174. Pani, S.P, and V Dhanda. 1994. Natural-history and dynamics of progression of clinical manifestation offilariasis. Tropical Diseases:Molecular Biology and Control Strategies:1-8.
175. Krishnamoorthy, K. (1999). “Estimated costs of acute adenolymphangitis to patients with chronicmanifestations of bancroftian filariasis in India.” Indian J Public Health 43(2): 58-63
176. Nanda, B. and K. Krishnamoorthy (2003). “Treatment seeking behaviour and costs due to acute and chronicforms of lymphatic filariasis in urban areas in south India.” Trop Med Int Health 8(1): 56-9.
177. Ramaiah, K. D., K. Ramu, et al. (1998). “Direct and indirect costs of the acute form of lymphatic filariasisto households in rural areas of Tamil Nadu, south India.” Trop Med Int Health 3(2): 108-15.
178. Ramaiah, K. D., M. P. Radhamani, et al. (2000a). “The impact of lymphatic filariasis on labour inputs insouthern India: results of a multi-site study.” Ann Trop Med Parasitol 94(4): 353-64.
179. Ramaiah, K. D., P. K. Das, et al. (2000b). “The economic burden of lymphatic filariasis in India.” ParasitolToday 16(6): 251-3.
IntroductionDengue is presently the most important human viral disease transmitted by arthropods.An estimated 50 to 100 million cases of dengue fever (DF), and 250 – 500 thousandcases of dengue haemorrhagic fever (DHF) and dengue shock syndrome (DSS)occur globally each year1. Dengue has been endemic in south and southeast Asia forat least 200 years2 . As per the WHO report in Asia great majority of reported casesare hospitalized cases of dengue haemorrhagic fever. The burden of severe diseaseremains proportionately much greater in the affected countries. There is a need tocompile all the available data from different sources to understand the true magnitudeof BoD due to dengue. A review of literature was made for the past 10-15 years tocreate a data base from the available sources which will be helpful to estimate theBoD due to dengue in India.
MethodologyA. Descriptive epidemiologyTo understand the descriptive epidemiology of dengue related to estimation of BoDof dengue following online and off line important reports / documents were referred:
i). Online searchB. Data required to estimate disability adjusted life year (DALY)
Dengue
1 www.medlineplus.gov Bibliography on Dengue2 www.ncbi.nlm.nih.gov Bibliography on Dengue3 www.indmed.nic.in Bibliography on Dengue4 www.who.int/health_topics Dengue diseases5 www.medwebplus.com/search ? Diseases incl. Dengue6 www.virology.net Viral diseases and dengue7 www.whoindia.org Indian Dengue outbreak8 www.who.int/ctd/dengue/burdens.html Dengue disease burden9 www.who.int/ctd/dengue/whodocs.htm Dengue references10 www.who.int/emc/diseases/ebola/denguepublications/ Dengue Publications
index.html11 www3.who.int/whosis/menu.cfm?path=whosis.burden WHO NBD: A practical
&language=English guide
61

62
Dengue
a) Primary1. Disability incidence, disability duration, age of onset and distribution of
severity class.2. Mortality, age & sex at onset of disease, cause of death.
b) Secondary1. Age specific incidence of dengue fever (DF), dengue hemorrhagic fever
(DHF) and dengue shock syndrome (DSS).2. Age specific dengue mortality.3. Duration of hospitalization for DF, DHF and DSS.4. Total number of cases requiring admission versus number of cases treated as
outpatients.5. Total domiciliary episodes versus episodes requiring care of health centers.6. Total episodes in rural settings versus urban settings.
C. Case definitionThe case definition of dengue is very essential as disease symptoms match withseveral other viral diseases and unless the diagnosis is not correct, it is very difficultto determine the disability estimate as well as true incidence of dengue. Thereforecase definition is important and this should be uniformly followed by the private aswell as public health sectors.
Dengue fever (DF)As per the WHO criteria3 classical dengue fever is a disease of older children andadults. It is characterized by the sudden onset of fever and specific signs andsymptoms including retro-orbital pains, muscle pain (myalgia) and joint pain(arthralgia) and rash. Temperature may rise to 102 to 105º F and may last for 2 to7 days. In some cases the fever may drop and then return in 12 to 24 hours (saddle-back fever).
Dengue hemorrhagic fever (DHF)The following must be present in DHF: Fever lasting 2-7 days occasionally biphasic,haemorrhagic tendencies, evidence of plasma leakage, thrombocytopenia (< 100000/cmm) and hepatomagaly.
Dengue Shock Syndrome (DSS)With above mentioned symptoms (DHF) plus rapid and weak pulse, narrow pulsepressure (<20mm mercury), Hypotension for age, cold clammy skin and restlessness.

63
Dengue
Detection of Dengue casesDengue cases could be detected and confirmed only by serological tests on the supportof the above mentioned case definitions of DF, DHF and DSS. Many infections,especially in young children, are asymptomatic, or minimally symptomatic. Thesemay be detectable only by the demonstration of dengue antibodies in sera of persons4,5.Confirmation made by isolation of dengue virus, by tissue culture or RT-PCRbioassay.
Literature reviewIn order to create a data base on dengue disease burden, we reviewed 25 publishedarticles related to BoD. All these articles were critically reviewed and abstracts ofeach is provided with comments on availability of data related to BoD. Most ofthese articles addresses dengue epidemics/ outbreaks or some follow up work onhospital based studies. Mahapatra (2001) made maiden attempt in India to estimateDALY for several diseases taking one of the Indian states, Andhra Pradesh (AP) asa study area. But during his study period no death due to dengue was recordedeither in urban or rural areas of AP. Hence DALY value remained very low (221DALY) taking only YLD values (no YLL). Indrayan6 attempted to overcome thedifficulties for incomplete data for BoD but he also emphasized basic data eg., agespecific incidence and onset of disease is highly essential. An authentic source ofmorbidity and mortality data on dengue is available (state wise) with National VectorBorne Disease Control Programme (NVBDCP), New Delhi. Data during the periodof 1996 to 2003 has been illustrated in Table 1. However, the incidences/deathsrecorded were without onset of disease, age and sex specific details. This data wascompiled from the information received from health department of individual stateswhere data was only computed on hospital based incidences with age and sex details.However, some of the states viz., Kerala have recently started recording all theparameters which may be helpful in future to estimate BoD.
Data on incidence / morbidityDF is a complex viral disease with high rate of morbidity (>90%) which is difficultto distinguish from other febrile illness. The descriptive epidemiology of DF matcheswith hepatitis, malaria, leptospirosis, typhoid and other viral fever3,5. Common urbanpopulation were prone to be infected by dengue virus and causing DF may not reportedto the referral hospital where facility are available for the diagnosis of DF. Denguefever can be diagnosed only by serological investigation for which facilities areavailable only in large tertiary care facilities. This emphasizes that true incidenceand prevalence of dengue cases are not available in India. The duration and age of

64
Dengue
onset of disease is one of the important parameters for the estimation of YLD6.Hence, estimating the true morbidity rate is extremely difficult from currentlyavailable data.
For instance, in Madhya Pradesh, out of 312 febrile cases admitted to the hospital,202 (65%) of them had dengue infection and all the age groups were affected5.Thisinformation was not included in the NVBDCP report resulting in incompleteness ofthe case details. Similarly 1998, Tamil Nadu reported cases of dengue from Chennai,Erode and Coimbatore districts. In Chennai city alone there were 94 cases (CRMEAnnual report – 2002-03). In Coimbatore area, 20 hospitalized cases were testedand all were positive for dengue7. This area was silent for dengue in the past. Butaccording to NVBDCP reports, only 35 cases and 5 deaths were there in TamilNadu for the year 1998. which shows the under reporting of cases from the state.The estimation of dengue burden utilizing this information may not be realistic. Toestimate actual burden of disease true incidence are very essential. In hospital basedstudies duration of illness which is one of the parameter essential for calculating theDALY was missing.
C- Cases ; D- Deaths
Table 1. Dengue cases in India : 1996- 2003 (source NVBDCP, Delhi)
States 1996 1997 1998 1999 2000 2001 2002 2003C D C D C D C D C D C D C D C D
Andra Pradesh 0 0 0 0 0 0 0 0 5 0 1 0 61 3 95 5Bihar 0 0 0 0 0 0 0 0 0 0 0 0 1 0 0 0Chandigarh 0 0 0 0 0 0 0 0 0 0 0 0 15 0 0 0Delhi 10252 423 273 1 333 5 168 2 180 2 322 3 42 0 2882 35Goa 0 0 0 0 0 0 0 0 0 0 1 0 0 0 14 2Gujarat 0 0 5 0 0 0 92 0 29 0 69 0 40 0 249 9Haryana 1631 54 54 0 14 0 3 0 2 0 260 5 3 0 83 6Karnataka 123 5 262 4 115 3 39 0 196 0 220 0 428 1 1226 7Kerala 0 0 0 0 6 0 0 0 0 0 41 0 219 2 3546 68Maharastra 3068 5 249 5 193 5 59 12 66 3 54 2 370 18 481 39Orissa 0 0 0 0 11 0 0 0 0 0 0 0 0 0 0Punjab 806 32 23 3 0 0 419 1 91 1 49 0 27 2 848 13Rajasthan 0 0 18 1 2 0 1 0 0 0 1452 35 163 5 292 3Tamil Nadu 491 16 264 21 33 5 135 2 81 1 729 8 392 0 1274 8Uttar Pradesh 146 10 29 1 0 0 28 0 0 0 21 0 0 0 730 8Total 16517 545 1177 36 707 18 944 17 650 7 3219 53 1761 31 11720 203

65
Dengue
Mortality dataThere are several reports of epidemics in India since 1960s but no mortalitywas recorded, as most of the epidemics were not due to DHF and DSS. Mostof the states in India have reported dengue fever outbreaks right from north,Jammu & Kashmir to the south of Kerala, from eastern state, West-Bengal towest Rajasthan 8-17. In the year 1970, in Kanpur18 dengue like illness wasreported but no DHF cases were reported. Similarly in 1967 during the outbreakof dengue in Delhi9, only classical DF cases were reported. It is to be notedthat all these epidemics were reported mainly from urban areas and dengueinfection was confirmed only by serological investigations. Usually oneserotype (very rarely two) was reported to be involved in these epidemics. In196315 an explosive epidemic with haemorrhagic symptoms occurred in Kolkatawith significant number of deaths due to circulatory collapse, which was mainlydue to Chikungunya .
After 1980, outbreaks of DHF/DSS occurred in many places19-24. Delhi sufferedanother major dengue outbreak of DHF/DSS in 1996 during which 10252 cases and423 deaths were recorded. The average CFR was 7.525-27, and in the same year inthe capital of UP, Lucknow the CFR was 3.8 (highest was 47%)28. Recently, in theyear 2003 several urban localities of Delhi, Gujarat, Karnataka, Kerala, Maharastra,Punjab, Tamil Nadu, UP, Delhi (source by National Vector-Borne Disease ControlProgramme [NVBDCP], Delhi) recorded high incidence with low mortality rate. Inlast two decades, the occurrence of DHF/DSS have increased in India29, withinvolvement of the multi-serotypes. Dengue is not limited to the urban areas, but ithas been spreading to rural areas of India since 199030-36. Silent dengue transmissionof all four dengue serotypes have been demonstrated in a rural area during an inter-epidemic period37. Hence these information are not useful in estimating the diseaseburden. Therefore it suggested that emphasis should be made to incorporate genderwise and age wise mortality and morbidity data and to record the duration of illnessin all the outbreak investigations.
Age & sex specific dataIn all the above mentioned studies, age, sex-specific case incidence and mortalitydata were not available. However, in only one of the studies carried out in Delhiduring 199838 where morbidity data was recorded with age and sex but duration ofonset illness was found missing which is essential for the estimation of BoD. Mostof these studies are outbreak investigation and information need for BoD are notfocused.

66
Dengue
Underestimation
Dengue Infected CasesThe mortality and morbidity mainly depends upon the reported cases in the stateand national health systems. Table 1 showed the details of the cases and deathsrecorded in India from 1996 to 2003 (source NVBDCP, Delhi). Out of total 35states in India, only 15 states are reporting dengue cases. Of these, 6 states are highlyendemic. Dengue continues to emerge in areas previously untouched and diseasecontinues to spread to newly urbanized areas infested with mosquito vectors. Thereis sudden increase in incidence in 2003 when 11,720 cases with 203 deaths werereported, but the number of states reporting cases remain same.
Cause of deathDHF and DSS are the virulent form of dengue virus infection which are the maincause of mortality in dengue disease. The overall mortality in DHF and DSS casesranges from 3.8% to 7.5%. In hospital admitted cases it rises to 47%. However, asper the national record on mortality by NVBDCP the average CFR ranges between1.1 (year 2000) and 3.3 (year 1996). As the diagnostic facility are lacking, the truerecord of cause of death are not available. The cause of death is also mislead andthe sources of MCCD, SCD-rural are not sufficient to give the information aboutmortality. In view of the above, it is extremely difficult to estimate the true diseaseburden due to lack of information on mortality in the case of Dengue disease.
In Tamil Nadu State during a period of 5 years from 1998 to 2002, the total numberof dengue cases were 1370 with 16 deaths having average CFR value of 1.17 (Tables2 & 3). However, the records of only one of the referral hospitals in Chennai viz.,Institute of Child Health, Egmore (which would be covering population of about 6million in and around Chennai city when compared to Tamil Nadu population of 60million) showed during the same period (1998-2002) a total of 389 cases and 29 deathswith an average CFR of 7.46. This is about seven times higher when compared therate (1.17) recorded for Tamil Nadu by national programme NVBDCP, Delhi (Table3). This indicates that indepth investigations of the DF cases to be made to get thetrue incidence of dengue in different states of the country. It is clearly evident thatmost of the published / unpublished reports are mostly hospital based studies whichmainly focuses on the confirmation of dengue or on clinical investigation. Studieson descriptive epidemiology will be more appropriate and useful for the estimationof disease burden. Recently, in Kerala epidemic, date of onset of fever and detailslike age, sex, duration etc., are being included in the case sheet summary.

67
Dengue
Data gaps
a. Major lacunae for the estimation of morbidity and mortality (to estimate the BoD)1. In most of the published / unpublished reports either one or many parameters
(case incidence with age & sex specific, and duration of onset of disease)required for BoD estimation are lacking. True incidence could not be obtainedsince proper diagnostic facilities are lacking in most of hospitals at districtlevel (urban and rural setup).
2. To record causes of death (COD) in the case of dengue is difficult due tounavailability of proper diagnostic tools.
b. Surveillance systems and Problems in IndiaHospitalized DHF cases and deaths have been reported annually. In recent years,progressively more outpatient and inpatient care has been provided by the privatesector. Case reporting from the private sector is incomplete. A system should bedeveloped so that all the practitioners from the private sector also shouldcommunicate the reports periodically.
As a result of above factors, a number of problems confound an accurate assessmentof the illness burden imposed by dengue :
Source Age groups Number of Number of Case Fatality(years) Cases Deaths Rate (CFR)
<1 99 14 14.14
1-5 153 14 9.15
ICH, 6-10 115 0 0
Chennai 11-15 21 1 4.76
16-20 0 0 0
Total 389 29 7.45
Table 2. Hospital based study: Age wise CFR of dengue recorded during 1998-2002 (5years) in ICH,Chennai
Table 3: Comparison of CFR recorded in Tamil Nadu by two different sources (ICH, Chennai andNVBCD, Delhi) during 1998- 2002 (5 years)
Source Number of Cases Number of Deaths Case Fatality Rate (CFR)ICH, Chennai 389 29 7.45NVBDC, New Delhi 1370 16 1.17
68
Dengue
" The symptoms of dengue fever (DF) are difficult to distinguish from othercommon febrile illnesses. DF and DHF may not be suspected or recognized.
" DHF cannot be diagnosed using clinical judgment alone. Laboratory tests areneeded to correctly identify a case of DHF and, ideally, virologic or serologictests to confirm it. Laboratory equipment to perform a complete array of diagnostictests is often not available.
" The case definitions differ among health officials, with some reporting onlylaboratory-confirmed cases whereas others reporting clinically diagnosed casesas well. Some report cases and deaths from DF & DHF separately, other reportDHF combined. Problems of over and under diagnosis, incomplete reportingand delays also weaken surveillance for dengue.
" Proper surveillance of dengue should also include the monitoring of serotypescirculating in the population. The introduction of a new serotype may be animportant indicator of future epidemics of DHF. In many places, laboratoriesneed considerable strengthening to monitor circulating serotypes.
Recommendations" National / State level networking facilities to be made to record the dengue cases
with age and sex specific details on morbidity and mortality." It is suggested a sample of fever cases in all the district headquarter hospital may
be screened / diagnosed for dengue virus infection and the result could beextrapolated to determine the true case incidence.
" Special emphasise should be made to record for age, sex and onset of disease neededfor the calculation of YLD. Disability weight of GBD is to be taken into consideration,as calculation of disability weight of each area is very cumbersome exercise.
" All district and referral hospitals should follow uniformly the case definition asper the WHO criteria.
" Dengue disease should be included under “Notifiable Diseases” on national level,so that all the mortality and morbidity due to dengue could be recorded by allmedical practitioners.
" Most of the asymptomatic cases are not recorded hence to determine truedisability, a module needed to estimate the transition probability.
References cited1. WHO 1997. Dengue haemorrhagic fever: diagnosis, treatment, prevention and control-2nd ed. World Health
Organization, Geneva, 1-84.2. Vijayarani H, Gajanana A. 2000. Low rate of Japanese encephalitis infection in rural children in Thanjavur
district (Tamil Nadu), an area with extensive paddy cultivation. Indian Journal of Medical Research 111,212-214.
69
Dengue3. Rigau-Perez, J G , Clarke, G C , Gubler, D J, Reiter, P, Sanders, E J, and Vomdam, A V 1998 Dengue and
dengue haemorrhagic fever. Lancet 325 : 971- 977.4. Gubler, D J 1998. The global pandemic of dengue /dengue haemorrhagic fever: Current status and
prospects for the future. Ann. Acad. Medicine: 27 227- 234.5. Parida MM, Dash PK, Upadhyay C, Saxena P & Jana AM. 2002. Serological and virological investigation
of an outbreak of dengue fever in Gwalior, India. Indian Journal of Medical Research 116, 248-254.6. Indrayan A. (Provisional Draft). A simple explanation of the Burden of Disease Methodology: Procedure
to estimate DALYs from incomplete data. Division of Biostatistics and Medical Informatics, Delhi UniversityCollege of Medical Sciences, Delhi.
7. Singh J, Balakrishnan N, Bhardwaj M, Amuthadevi P, George EG, Subramani K, Soundararajan K, AppavooNC, Jain DC, Ichhpujani RL, Bhatia R, Sokhey J. 2000. Silent spread of dengue and dengue haemorrhagicfever to Coimbatore and Erode districts in Tamil Nadu, India, 1998: need for effective surveillance tomonitor and control the disease. Epidemiol Infect. 125(1): 195-200.
8. Mathew T, Suri JC, Suri NK, Bhola SR, Arora RR, Lal P, Raichaudhari AN, Mathur KK, Gupta JP. 1977.Investigation on an epidemic of dengue in Jammu, 1974. Indian J Med Res. 65(5): 613-22.
9. Balaya S, Paul SD, Lima LVD and Pavri KV.1969. Investigation of an outbreak of dengue in Delhi. IndianJ Med Res. 57: 767-74.
10. Chadurvedi UC, Mathur AK, Chandra D, Khan AM, Mehrotra RML. 1970. Dengue haemorrhagic illnessat Hardoi, UP. Bull. WHO. 43: 289-293.
11. Padbidri VS, Dandawate CN, Goverdhan MK, Bhat UK, Rodrigues FM, D’Lima LV, Kaul HN, Guru PY,Sharma R, Gupta NP. 1973. An investigation of the aetiology of the 1971 outbreak of febrile illness inJaipur City, India. Indian J Med Res. 61(12): 1737-43.
12. Ghosh SN, Sheikh BH. Investigations on the outbreak of dengue fever in Ajmer City, Rajasthan in 1969.PartII: Result of serological tests. 1974. Indian J Med Res. 62(4): 523-33.
13. Rao GL, Khasnis CG, Rodrigues FM, Gupta NP, Shah CB, Guru PY, Pinto BD. 1981. Investigation of the1975 dengue epidemic in Amalner town of Maharashtra. Indian J Med Res. 74:156-63.
14. Rodrigues FM, Patankar MR, Banerjee K, Bhatt PN, Goverdhan MK, Pavri KM, Vittal M. 1972. Etiologyof the 1965 epidemic of febrile illness in Nagpur city, Maharashtra State, India. Bull World Health Organ.46(2): 173-9.
15. Ramachandra Rao T and Anderson CR 1964. Concluding review on the papers on the outbreak of febrileillness with haemorrhagic manifestations in Calcutta. Indian J Med Res: 52 727-734
16. Shanmugam J & Raveendranath M. 1980. Serological evidence of arboviral infection (flavivirus) inKerala. Indian Journal of Medical Research, 72:779-784.
17. Carey DE, Myers RM, Reuben R, Rodrigues FM. 1966. Studies on dengue in Vellore, South India. Am JTrop Med Hyg. 15(4): 580-7.
18. Chadurvedi UC, Mathur AK, Chandra D, Khan AM, Mehrotra RML. 1970. Dengue haemorrhagic illnessat Hardoi, UP. Bull. WHO. 43: 281-287.
19. Acharya SK, Buch P, Irshad M, Gandhi BM, Joshi YK, Tandon BN.1988. Outbreak of Dengue fever inDelhi. Lancet. Dec 24-31;2(8626-8627):1485-6.
20. Srivastava VK, Suri S, Bhasin A, Srivastava L, Bharadwaj M. 1990. An epidemic of dengue haemorrhagicfever and dengue shock syndrome in Delhi: a clinical study. Ann Trop Paediatr. 10(4): 329-34.
21. Mahadev PV, Kollali VV, Rawal ML, Pujara PK, Shaikh BH, Ilkal MA, Pathak V Dhanda V, RodriguesFM, Banerjee K. 1993. Dengue in Gujarat state, India during 1988 & 1989. Indian J Med Res. 97:135-44.
22. Bhattacharjee N, Mukherjee KK, Chakravarti SK, Mukherjee MK, De PN, Sengupta M, Banik GB,Bhowmick P, Sinha SK, Chakraborty MS. 1993. Dengue haemorrhagic fever (DHF) outbreak in Calcutta—1990. J Commun Dis.25(1):10-4.

70
Dengue23. Cherian T, Ponnuraj E, Kuruvilla T, Kirubakaran C, John TJ, Raghupathy P. 1994. An epidemic of dengue
haemorrhagic fever & dengue shock syndrome in & around Vellore. Indian J Med Res. 100:51-6.24. Kabilan L, Balasubramanian S, Keshava SM, Thenmozhi V, Sekar G, Tewari SC, Arunachalam N, Rajendran
R, Satyanarayana K. 2003. Dengue disease spectrum among infants in the 2001 dengue epidemic in Chennai,Tamil Nadu, India. J Clin Microbiol. 41(8): 3919-21.
25. Dar L, Broor S, Sengupta S, Xess I, Seth P. 1999. The first major outbreak of dengue hemorrhagic fever inDelhi, India. Emerg Infect Dis. 5(4): 589-90.
26. Anuradha S, Singh NP, Rizvi SN, Agarwal SK, Gur R, Mathur MD. 1998. The 1996 outbreak of denguehemorrhagic fever in Delhi, India. Southeast Asian J Trop Med Public Health. 29(3): 503-6.
27. Aggarwal A, Chandra J, Aneja S, Patwari AK, Dutta AK. 1998. An epidemic of dengue hemorrhagic feverand dengue shock syndrome in children in Delhi. Indian Pediatr. 35(8): 727-32.
28. Agarwal R, Kapoor S, Nagar R, Misra A, Tandon R, Mathur A, Misra AK, Srivastava KL, Chaturvedi UC.1999. A clinical study of the patients with dengue hemorrhagic fever during the epidemic of 1996 atLucknow, India. Southeast Asian J Trop Med Public Health. 30(4): 735-40
29. Panda MM, Dash PK, Upadhyay C, Saxena P, Jana AM. 2002. Serological & virological investigation ofan outbreak of dengue fever in Gwalior, India. Indian Journal of Medical Research. 116, 248-252.
30. Jamaluddain M, Saxena VK. 1997. First outbreak of Dengue fever in a typical rural area of Haryana statein northern India. J Commun Dis. 29(2): 169-70.
31. Kumar A, Sharma SK, Padbidri VS, Thakare JP, Jain DC, Datta KK. An outbreak of dengue fever in ruralareas of northern India. 2001. J Commun Dis. 33(4): 274-81.
32. Mehendale SM, Risbud AR, Rao JA, Banerjee K. 1991.Outbreak of dengue fever in rural areas of Parbhanidistrict of Maharashtra (India). Indian J Med Res. 93:6-11.
33. Mahadev PV, Kollali VV, Rawal ML, Pujara PK, Shaikh BH, Ilkal MA, Pathak V Dhanda V, RodriguesFM, Banerjee K. 1993. Dengue in Gujarat state, India during 1988 & 1989. Indian J Med Res. 97:135-44.
34. Norman G, Theodre A, Joseph A. 1991. An insular outbreak of dengue fever in a rural south Indian village.J Commun Dis. 23(3):185-90.
35. Abdul Kader MS, Kandaswamy P, Appavoo NC, Anuradha. 1997. Outbreak and control of dengue in avillage in Dharmapuri, Tamil Nadu. J Commun Dis. 29(1): 69-71.
36. Victor TJ, Malathi M, Gurusamy D, Desai A, Ravi V, Narayanasamy G, Anuradha L, Rani C, KrishnamurthyP. 2003. Dengue fever outbreaks in two villages of Dharmapuri district in Tamil Nadu. Indian J Med Res.116:133-9.
37. Tewari SC, Thenmozhi V, Katholi CR, Manavalan R, Munirathinam A & Gajanana A 2004. Denguevector prevalence and virus infection in a rural area in south India. Tropical Medicine and InternationalHealth: in press.
38. Sharma RS, Panigrahi N, Kaul SM, Shivlal, Barua K & Bhardwaj M. 1999. Status report on DF/DHFduring 1998 in the national capital territory of Delhi, India. Dengue Bulletin 23:109-112.

Demographic DataWest Bengal
Relevant data from Census of India, 2001The data from 2001 census of India show that West Bengal has a total population of802,21,171 of which 577,34,690 (71.97%) live in the rural areas and 224,86,481(28.03%) live in the urban areas [3]. As of now, since no data are available on theage- and sex-distribution of these populations, we may rely on such data from the1991 census, assuming similar age- and sex distributions for the 2001 population.These data should be updated as 2001 distributions are made available.
Relevant data from Census of India, 1991 :During the 1991 census, the rural-urban distribution (72.52% and 27.48%,respectively) of total population in West Bengal was similar to that found in 2001census. In the rural areas, under-5 and 5+ years population consisted of 12.76% and87.24%, whereas in the urban areas, these figures were 8.15% and 91.85%,respectively [4]. The age distribution of the population in the country in 1991 was asfollows -
Applying the age distribution of Census 1991 data to Census 2001 data, the followingresults would be obtained - in the rural areas, 7366946 (12.76%) are below 5 years
Diarrhoeal Diseases
age Total Rural Urban
Groups Male Female Both Male Female Both Male Female Both(yrs)0-4 12.0 12.4 12.2 12.6 12.9 12.7 10.4 11.0 10.75-9 13.2 13.4 13.3 13.7 13.7 13.7 11.7 12.2 11.910-14 11.9 11.6 11.8 12.1 11.6 11.9 11.4 11.7 11.515-19 9.7 9.1 9.4 9.5 8.8 9.2 10.3 10.1 10.220-24 8.6 9.2 8.9 8.2 8.9 8.5 9.9 10.0 9.925.29 7.9 8.6 8.3 7.7 8.3 8.0 8.7 9.5 9.130-44 18.4 18.2 18.3 17.7 17.8 17.7 20.6 19.2 19.945-59 10.8 10.4 10.6 10.7 10.6 10.7 10.7 9.7 10.360+ 6.8 6.8 6.8 7.2 7.0 7.1 5.5 6.0 5.6
Age distribution (%) of total and rural / urban population: Census of India, 1991
71

72
Diarrhoeal Diseases
and 50367744 (87.24%) are 5 years or older. The corresponding figures in the urbanareas are 1832648 (8.15%) and 20653833 (91.85%). However, as noted earlier, theseshould be updated once 2001 census data are available.
Data on morbidity from diarrhoeal diseasesFor estimation of disease burden, incidence rather than prevalence data are useful.However, incidence data are not easy to obtain, and thus, sometimes we may have todepend on prevalence data. Of course, there had been a number of community-basedlongitudinal studies in different parts of West Bengal and other states in India, whichshowed varied incidence data depending on situations in which the estimates were made.These wide arrays of data obtained through different data sources are presented below:
Incidence Data
West BengalThe findings from several studies have indicated a declining trend in diarrhoealmorbidity and mortality among under-5 children over the last two decades in WestBengal as well as in other parts of India, which has also been noted in a recentreview on diarrhoeal diseases in India [7]. The study results, in ascending order ofstudy period, are below:
During 1985, a study among under-5 children in two rural ICDS blocks of WestBengal showed a high incidence of diarrhoea – 4.7 episodes/child/year in one blockand 4.1 episodes/child/year in another [6]. However, this higher incidence might bea reflection of the post-epidemic period of shigellosis in West Bengal in 1984, whenespecially the young children were affected and the shigella strains were resistant tothe commonly available drugs and antibiotics [61,33].
A cohort of rural children below 4 years was prospectively observed in three villagesnear Kolkata in West Bengal during August 1992 - December 1994. In this study, theoverall incidence of diarrhoea among these children was 1.7 episodes/child/year;the incidences of mucoid diarrhoea and dysentery in this cohort were 0.8 and 0.2episodes/child/year, respectively. Children aged 6-11 months had a higher incidenceof mucoid diarrhoea (1.3 episodes/child/year) [77].
During 1997-98, in a study in rural West Bengal, the incidence of diarrhoea amongchildren aged 6-47 months was 1.15 episodes/child/year, which was reduced to 0.56episodes/child/year after vitamin A supplementation [5]. Incidences in specific age

73
Diarrhoeal Diseases
groups among these children have been provided under the reference section, butthese estimates were obtained after the vitamin A intervention.
During 1998-99, while studying gender differences in health care seeking behaviourin a rural community of West Bengal, the overall incidence of diarrhoea (detectedthrough weekly surveillance for one year) among children less than 5 years were1.49 episodes/child/year; among boys and girls the figures were 1.44 and 1.54respectively [70].
During the same period (1998-99), a community-based observational study wasconducted in an urban slum area of Kolkata where diarrhoeal episodes among low-and normal-birth weight babies were detected through weekly surveillance. Amongthe low-birth weight babies, the incidence of diarrhoea was 0.5 episodes/child/yearamong the exclusively breast-fed babies and 4.1 episodes/child/year among the early-weaned babies. For the normal birth weight babies, the incidence was 0.5 episodes/child/year among the exclusively breast-fed babies and 1.3 episodes/child/year amongearly-weaned babies [67].
In 1999, during a study to observe the impact of zinc supplementation on diarrhoealmorbidity among rural children (6-41 months) in West Bengal, the incidence ofdiarrhoea in placebo group was 1.67 episodes/child/year. The episodes were detectedthrough weekly surveillance [65].
A similar intervention study in an urban slum area of Kolkata (during 1999-2001)showed the incidence among the placebo group to be 1.93 episodes/child/year; thisstudy followed a birth cohort of 100 low birth weight children until 1 year of age anddata were collected through active weekly surveillance [68]. Although this studyshowed a slightly higher incidence (compared to the previous studies conductedduring the similar period mentioned above), it included only low birth weight infantsin whom the incidence is expected to be higher [58,67].
To determine the effect of a single megadose of vitamin A supplementation to Indianmothers on morbidity of breast-fed young infants delivered in the hospital, a studywas undertaken in a tertiary care hospital in Kolkata during early 2000. The infantsof these mothers were followed up from birth until 6 months of age. Among thebreast-fed infants up to 6 months of age, the incidence of diarrhoea in the placebogroup (babies of mothers that did not receive vitamin A supplementation) was 1.61episodes/child/year [69].

74
Diarrhoeal Diseases
During 2003, three community-based studies were conducted to estimate theincidence of diarrhoea – two studies in the urban slum areas of Kolkata, while anotherstudy in a rural population of West Bengal. Unpublished data from these three studiesare as follows :a. In two urban slum areas of Kolkata, covering more than 57,000 population of all
ages, incidence of diarrhoea was estimated by weekly follow up. The overallincidence was 0.4 episodes/child/year, while the incidences among <5 and 5+years age groups were 1.2 and 0.33 episodes/person/year, respectively [62]. Thissurvey was conducted during the low season for occurrence of diarrhoea, andthus, the incidence was probably underestimated.
b. A similar study was conducted in another urban slum, using 2-week recall foroccurrences of diarrhoea in a population of about 30,000 (all ages). Here also, thesurvey was conducted during the low season, and the incidences (episodes/child/year) were – overall: 0.3, among <5 years: 1.1 and among 5+ years: 0.2 [63].
c. In the rural West Bengal, another study was conducted, covering more than 26,000population of all ages, and using 1-week recall to obtain data on diarrhoealepisodes. This survey covered both low and high seasons for diarrhoea, and theincidences (episodes/child/year) among this rural population were – overall: 0.72,among <5 years: 1.71 and among 5+ years: 0.63 [64].
Other statesData from other parts of India was collected mainly to get an idea about the situationat the national level. We also wanted to compare such data with the observations inWest Bengal, having admitted that direct comparison of such data across differentstates may not be very useful. These data are presented below –
As in West Bengal, during the earlier period (1984-’85), a study in rural Haryanaalso showed a higher incidence among 0-3 yrs children (5.48 episodes/child/year,range: 4.19 to 5.98) [8], and the incidence was also higher in a later study in urbanslums in New Delhi (8.6 episodes/child/year in placebo group) among 6-30 monthold children [9].
In 1988, children aged 6-47 months were followed up for one year in villages of Faridabad,Haryana where the sanitary condition was very poor. Mean diarrhoeal incidence amongthese children, as detected through 2-week recall, was 2.88 episodes/child/year [79].
In 1990s, one study in rural Alwar district demonstrated an incidence of 2.27 episodes/child/year among under-5 children [10].

75
Diarrhoeal Diseases
During the same period, another survey in three slum areas in Delhi revealed anoverall incidence of diarrhoea in the 2 weeks period preceding the survey to be 29.1episodes per 1000 people (0.76 episodes/person/year); among under-5 children, theincidence was 60.2 episodes per 1000 children (1.56 episodes/child/year), whereasamong the adults the incidence was lower - 13.8 episodes per 1000 people (0.39episodes/person/year) [78].
Prevalence DataUsefulness and Limitations of Prevalence DataUsually, prevalence data may not be useful directly in estimating the burden of thedisease. However, in absence of reliable incidence data, or to supplement availableincidence data, we can make use of the prevalence data for indirectly estimating theincidence, provided we also have data on duration of the disease. Of course, wehave to make certain, sometimes doubtful, assumptions (e.g. a steady-state population)to do this; nevertheless, we can at least get some measurement on incidence.
Prevalence of Diarrhoea
West BengalThere were a number of studies in West Bengal that revealed prevalence data inseveral districts.
In 1986, a study was conducted in an urban Muslim slum community in West Bengal tostudy nutritional status and prevalence of common infections among children up to 5years of age. It was revealed that the prevalence of diarrhoea among the under-nourishedchildren was 52.8%, whereas it was 40.5% among the normally nourished children [72].
During the similar period (April 1985 – January 1987), a study conducted amongunder-5 children in two rural ICDS blocks in West Bengal showed a higher prevalence(18.1% and 15.7%) [6]. The differences in these two studies could be due to thefollowing factors – in the Muslim urban slum communities, the prevalence ofdiarrhoea (and also other communicable diseases) is expected to be higher due toovercrowding, poor sanitary and hygienic conditions, often contaminated food andwater etc. [76,78], whereas in the ICDS blocks prevalence of such diseases is expectedto be lower than the average, because of maternal and child health services providedthrough the ICDS program [48,54,84].
The prevalence of diarrhoea among under-5 children in three districts of West Bengalduring early 1990s was 14.2% in Howrah, 5.9% in Hooghly (data collected in non-monsoon season) and 14.5% in south 24-Parganas [11].

76
Diarrhoeal Diseases
In a flood-prone area in rural West Bengal, the prevalence of diarrhoea amongpopulation of all ages during the pre-flood season in 1998 was 11.9%; the prevalencewas 8.6% in non-flood prone area in the same study [12].
In 1999, in a study to observe the impact of zinc supplementation on diarrhoealmorbidity among rural children (6-41 months) in West Bengal, the percentage ofchildren suffering from diarrhoea in the placebo group was 30.8% [65].
Other statesIn 1986, a hospital survey in the pediatrics ward of Command Hospital in Pune,Maharashtra, revealed that 26.2% of all admissions in the ward was due to diarrhoea[74]. However, this might not reflect the community situation of occurrence ofdiseases in children, because only a single hospital was studied and due to differentialrates of presentation and admission to the hospital.One study in Mumbai slum areas during 1980s showed a prevalence of diarrhoea ofapproximately 50% among under-5 children [73].
Another study among the slum and pavement dwellers of all ages in Mumbai during2000, showed that the prevalence of diarrhoea was 61.4% [71].
Slightly higher prevalence was noted in rural Chandigarh – during monsoons in1996, the prevalence among <5 years children was 23.2% [41].
During 1998-2002, a cluster-randomized trial was conducted in Haryana to determinethe effect of community interventions (promotion of exclusive breastfeeding) ondiarrheal illness and growth among a birth cohort of infants born during the study.The prevalence of diarrhoea was assessed among those infants at 3 months and 6months of age. Summary of the results were as follows [42]:
Intervention ControlCommunities Communities
At age 3 months -Children with diarrhoea in previous24 hours 17% 21%7 days 22% 30%
At age 6 months -Children with diarrhoea in previous24 hours 21% 19%7 days 25% 28%
Effect of intervention on diarrhoea morbidity during the first 6 months of life

77
Diarrhoeal Diseases
Data from Outbreak InvestigationsBesides the community- and hospital-based studies, there are other data availablefrom investigations of outbreaks of diarrhoeal diseases in West Bengal and otherIndian states. Morbidity and mortality estimates from these outbreak investigationswill obviously be higher than the usual non-outbreak situations. Nonetheless, thesedata will also be important to consider since outbreaks of diarrhoea still continue tooccur from time to time and add to the overall burden of diarrhoeal diseases in thecommunities.
Outbreak of Diarrhoeal Diseases in West BengalIn March 1984, an outbreak of acute bacillary dysentery was investigated in onevillage in Hooghly district in West Bengal, where 47% of all families had at leastone member affected. The overall attack rate was 97 per 1000 and it was higher (227per 1000) among the infants [33].
Since late 1992 till early 1993, Kolkata and its neighboring areas experienced alarge outbreak of acute watery diarrhoea caused by Vibrio cholerae O139 [30,32].The epidemic predominantly affected the adult population, but attack rate could notbe estimated since the base population was not known [15].
During September-October 2000, an outbreak of acute watery diarrhoea caused byVibrio cholerae O139 occurred in one Kolkata Municipal Corporation area. It wasthe first outbreak of Vibrio cholerae O139 in Kolkata since the widespread epidemicin 1992. It affected mostly the adult population and the attack rate (all ages) was7.1% [66].
Outbreak of Diarrhoeal Diseases in Other StatesDuring July-September 1978, an outbreak of acute gastroenteritis occurred inManipur, involving all age groups. The outbreak was caused by Vibrio choleraebiotype ElTor. Initially, the case-fatality among patients aged <5 years and ³5 yearswere 20 per 1000 and 19 per 1000 respectively. With promotion and distribution ofORS in the affected areas, the case-fatality came down after 3 months – 7 per 1000and 6 per 1000, respectively, in the two age groups [31].
In rural South India, two outbreaks of acute watery diarrhoea occurred during 2000.The attack rates in these two outbreaks were 10.03% and 15.53% [27].
Morbidity data that may be used for estimating diarrhoeal disease burden inWest Bengal :

78
Diarrhoeal Diseases
From the data presented above, it appears that an acceptable range for incidence ofdiarrhoea among under-5 children might be 1.15 – 1.71 episodes/child/year; dataare very scarce for incidence among ³5 years population – especially, age group-wise data, though it is well known that incidence of diarrhoea varies widely acrossage groups and gender. From the available sources, it may be assumed that theincidence among ³5 years population would be around 0.6 episodes/person/year.
MortalityMortality data are required to calculate YLL part of the DALYs. Similar to themorbidity data, literature search also revealed wide variations in mortality estimatesin different studies and a declining trend over the years.
West BengalAmong the community-based studies, a study among the under-5 children in tworural ICDS blocks in West Bengal in 1985 showed a cause-specific death due todiarrhoea of 2.8 per 1000 in both the blocks; the overall under-5 mortality was 11.5per 1000 in one block and 9.0 per 1000 in another [6].
Among children under 5 years admitted to the DTTU of a tertiary care hospital inKolkata, the case-fatality from diarrhoea was reported to be 18/1000 in 1991 and17/1000 in 1992 [16].
In the DTTU of the Infectious Diseases Hospital, Kolkata, a retrospective analysisof hospital records were carried out for 1989-1993. The case-fatality of diarrhoeaamong all age groups were 45 per 1000 in 1989 and 25 per 1000 in 1993. Among theunder-5 children, the case-fatality was 127 per 1000 in 1989, which came down to21 per 1000 in 1992 [83].
As reported to the Department of Health, Government of West Bengal, the case-fatalityfrom diarrhoea came down from 5.88 per 1000 in 1995 to 0.73 per 1000 in 2001 [13].
On the other hand, data for hospitalized cases at Infectious Diseases Hospital, Kolkatashowed a case-fatality of 30.99 per 1000 in 1992, which came down to 8.98 per1000 in 2002 [14].
Other StatesIn a cohort of North Indian children, the case-fatality was found to vary with durationof diarrhoeal episodes – for durations of <7 days, 7-13 days, and ³14 days, the case-fatality was 6/1000, 8/1000, and 119.4/1000, respectively [17].

79
Diarrhoeal Diseases
In urban slums of Patna, Bihar, diarrhoea was responsible for 8.82% of infant mortalityand 37.5% of 1-6 years mortality; here, the IMR was 64.6 per 1000 live births, and1-3 years and 3-6 years mortality were 11.3/1000 and 9.1/1000, respectively [18].
Higher figures were reported from rural Aligarh – diarrhoea caused 21.2% of infantmortality and 32.2% of 1-5 years mortality, and IMR in that area was 79.3 per 1000live births and mortality in 1-<2 years and 2-<5 years were 29.6/1000 and 16.2/1000, respectively [19,80].
Diarrhoeal mortality during OutbreaksAn outbreak of acute bacillary dysentery occurred in 1984 in West Bengal. In onevillage in Hooghly district, 47% of all families had at least one case. The outbreakwas caused by Shigella dysenteriae Type 1, which was found to be resistant to mostcommonly used drugs. The case-fatality among the patients (all ages) in that villagewas 22 per 1000 [33].
During the 1993 outbreak of Vibrio cholerae O139 in Kolkata, data from the patientsadmitted to the Infectious Diseases Hospital, Kolkata showed a higher case-fatality(around 25 per 1000), which was similar in patients aged £10 years or >10 years,although slightly higher case-fatality was noted among the female patients in bothage groups [15]. Such higher case-fatality was not unexpected since this was a newstrain introduced in the community at that time.
In September 1997, an outbreak of acute watery diarrhoea occurred in the Maldadistrict of West Bengal, involving about 30,000 population. Among the hospitalizedcases, the case-fatality was 10.55 per 1000 [28].
In July 1998, an explosive outbreak of cholera (caused by Vibrio cholerae O1)occurred in Malda district in West Bengal, affecting 15 blocks and 2 municipal areas.During investigation, case-fatality among the affected population (all ages) was foundto be 17 per 1000 [29].
Mortality data that may be used for estimating diarrhoeal disease burden inWest BengalMost of the data on mortality due to diarrhoea in West Bengal were available either forhospitalized cases only or from outbreaks of diarrhoea in different parts of the state.One community-based study reported an overall cause-specific death due to diarrhoeaof 2.8 per 1000 population. Since this study was conducted about two decades ago (in

80
Diarrhoeal Diseases
1985), we may have to rely on case-fatality data (0.73 per 1000 population of all ages)reported in 2001 by the Department of Health, Govt. of West Bengal.
Data on Life Expectancy at Different Ages
West BengalRegarding life expectancy, data from Sample Registration System determines a lifeexpectancy of 61.4 years at birth, 62.9 years at age 5, 40.4 years at age 30 etc. [20].These could be applied during calculation of YLL due to diarrhoea, especially whenage-stratified morbidity and mortality data are not available for all age groups. Thefollowing table shows life expectancy at different ages in West Bengal: [20]
Age (years) Life Expectancy (years)
0 (at birth) 61.41 64.95 62.910 58.620 49.430 40.440 31.550 23.060 15.870 10.3
West Bengal: Life expectancy
Data on disability from diarrhoeal diseasesTo assess disability due to diarrhoea, two kinds of information are required - data onduration of diarrhoea and data on disability weights for diarrhoea. For disabilityweight, we relied on data used in the estimation of global burden of diseases. Dataavailable from various sources on duration of diarrhoeal episodes are presented below:
Data on Duration of Diarrhoea
West BengalA hospital-based case-control study was conducted with 243 cases and 136 controls(total 279 children) to determine the risk factors for development of dehydrationamong children with diarrhoea. Children up to 2 years with diarrhoea were recruitedat the Infectious Diseases Hospital, Kolkata during October 1991 to June 1993. Pre-admission duration of diarrhoea was 26.0±19.4 hours among cases and 27.4±20.7among controls. Duration of diarrhoea after hospitalization was not available [35].

81
Diarrhoeal Diseases
Adult (18-55 years) male hospitalized patients with acute watery diarrhoea and severedehydration were included in a randomized controlled trial at the Infectious DiseasesHospital, Kolkata during March 1993 to September 1994. Findings in the control(no antibiotic) group (n=29) were as follows: pre-admission duration of diarrhoea =10±4 hours, and post-admission duration of diarrhoea = 55±24 hours [24], givingthe mean total duration of diarrhoea of 65 hours or 2.75 days.
Children (aged 1-10 years) admitted to the Infectious Diseases Hospital, Kolkatawith history suggestive of acute bacillary dysentery were included in a clinical trialbetween April 1993 and October 1994. In Nalidixic acid group (n=27), duration ofdysentery was 1.8±1.1 days before admission and 3.7±0.8 days after treatment. InNorfloxacin group (n=32), the duration was 2.0±0.9 days before admission and2.7±0.9 days after treatment [26].
A randomized controlled clinical trial was conducted at the same hospital betweenAugust 1993 and March 1996 to compare the effects of different ORS formulations onclinical course of diarrhoea. Adult (18-55 years) hospitalized males with waterydiarrhoea and severe dehydration were included. In the control (WHO-ORS) group(n=30), the duration of diarrhoea was 10.9±5.9 hours before admission and 46.9±11.9hours after admission [23] - thus, the total mean duration was 57.8 hours (2.41 days).
Another similar randomized controlled clinical trial of ORS was conducted at theInfectious Diseases Hospital, Kolkata during May 1995 to June 1996. The treatmentgroup received rice-based ORS while the control group received standard WHO-ORS. The results in the control group were as follows [22]:
Among adult males (18-55 years) with diarrhoea of <24 hours duration and severedehydration, the pre-admission duration of diarrhoea was 8.42±2.21 hours and post-admission duration of diarrhoea was 45.68±6.91 hours (total mean duration amongadults = 54.10 hours or 2.25 days).
Among children aged 3 to 12 years with acute watery diarrhoea and severedehydration, the pre-admission duration of diarrhoea was 9.2±6.6 hours and post-admission duration of diarrhoea was 35.95 ±7.37 hours (total mean duration amongchildren = 45.15 hours or 1.88 days).
Adult (18-55 years) male patients hospitalized at the I.D. Hospital, Kolkata withacute watery diarrhoea of <24 hours duration and severe dehydration were included

82
Diarrhoeal Diseases
between September 1995 and March 1996 to observe the effects of different serotypesof V. cholerae on diarrhoeal illness.
The results were as follows [25]:
Characteristics O139 (n = 10) O1(n = 15) Non-O1 Non-O139(n = 11)
Age(years) 32.5"11.5 30.3"8.3 28.6"9.1Diarr. duration 11.8"5.4 11.7"6.2 8.4"4.8(pre-adm, hrs)Diarr. duration 50.9"9.5 29.0"10.9 35.9"10.1(post-adm, hrs)
Vibrio cholera
The total mean durations in the three groups were - 62.7 hours (2.61 days), 40.7hours (1.69 days) and 44.3 hours (1.85 days), respectively.
Another randomized controlled clinical trial conducted at the Infectious DiseasesHospital, Kolkata during August 1995 to May 1998. The trial compared three ORSformulations: WHO-ORS (as control group) and Glucose-based hypo-osmolar ORSand Rice-based hypo-osmolar ORS. Male children aged 2 to 10 years with acutewatery diarrhoea of <24 hours duration and severe dehydration were included. Inthe control (WHO-ORS) group, the pre-admission duration of diarrhoea was8.92±3.29 hours and post-admission duration of diarrhoea was 38.47 ±3.89 hours(total mean duration was 47.39 hours or 1.97 days) [21].
Duration of Diarrhoea
Other StatesIn the villages of Haryana, one study reported an average duration of diarrhoealepisodes ranging from 3.87 to 4.16 days among children 0-3 years of age [8].
Another study was conducted among children aged 1-5 years in an urban slum areaof New Delhi to see the effects of vitamin a supplementation. At baseline (beforesupplementation), the mean duration of diarrhoea in the vitamin A group (n-451)was 3.1 days, while in the placebo group the mean duration was 3.2 days [86].However, only children with diarrhoea of less than 7 days duration were included inthe study. Duration of diarrhoea after treatment was not available.

83
Diarrhoeal Diseases
In 2003, one study was conducted in the Govt. Medical College in Nagpur todetermine the effects of zinc and copper supplementation among children aged 6 to59 months. Here also, children with duration of diarrhoea of less than 7 days wereincluded in the study. The total (pre-+ post-admission) mean duration of diarrhoeawas 4.48 days in the control group that did not receive the supplementation [87].
Data on Duration of Diarrhoea During OutbreaksIn rural south India, the median duration was 5 days during two outbreaks of acutewatery diarrhoea [27],
Data on Disability Weights due to DiarrhoeaAs mentioned earlier, disability weights for diarrhoea could be adopted from theGlobal Burden of Disease (GBD) study, which are as follows [92]:
Severity weights Indicator conditions
0.00 – 0.02 Vitiligo on face; Weight-for height <2 SD
0.02 – 0.12 Watery Diarrhoea; Severe anaemia
0.12 – 0.24 Infertility; Rheumatoid arthritis
0.24 – 0.36 Below-knee amputation; Deafness
0.36 – 0.50 Rectovaginal fistula; Down’s syndrome
0.50 – 0.70 Major depression; Blindness; Paraplegia
0.70 – 1.00 Active psychosis; Dementia; Quadriplegia
In one study on cost-effectiveness of zinc and copper supplementation to reducediarrhoeal morbidity among young (6-59 months) children in Nagpur, disabilityweights between 0.4 and 0.6 were used (based on clinical severity) to estimate DALYsfor diarrhoeal diseases [87]. This study did not consider parameters like perceiveddisability to perform daily work and other activities.
Data on duration of diarrhoea that may be used for estimating diarrhoeal diseaseburden in West Bengal:
In West Bengal, all data came from hospital-based clinical trials, where the reportedmean duration of diarrhoea in different studies ranged from 1.69 to 2.75 days. Insuch strictly supervised setting, the duration is likely to be less than that is expectedin the usual community settings. Including the data obtained from other states, itappears that the mean duration of diarrhoea among children would be between 3 and4.5 days for acute watery diarrhoea and 4.7 to 5.5 days for acute dysentery.

84
Diarrhoeal Diseases
Gaps in information on diarrhoeal diseasesValid and reliable information must be generated at the primary level of health caresystem and they should be analyzed by a comprehensive systems approach [50]. Inmost studies, apart from questions about reliability of the data – e.g., reliability ofverbal autopsy method to ascertain causes of death – age and sex stratified data arenot available. There will also be inadequate registration of deaths as well as influenceof different recall periods used in different studies in measuring the morbidity andmortality estimates, as shown in one study from rural Tamil Nadu [41]. Additionally,impact of past interventions on diarrhoeal morbidity and mortality is often not knownquantitatively, and peoples’ perception about severity of the disease and disabilityalso remains unclear.
Data Gaps
Problems with morbidity data :a) Definition of diarrhoea
Many publications did not mention how they defined an episode of diarrhoea. Itis likely that the definitions used in various publications were not consistent,and thus, data across different publications might not be directly comparable.In many times, mothers or some other family members are asked about theoccurrence of an episode of diarrhoea in the children. Without probing andproviding a clear definition for diarrhoea, mothers’ judgment about a diarrhoealepisode is prone to give erroneous information, as detected by a study conductedin Punjab in 1991 [49]. While measuring the occurrence of diarrhoea, this maylead to misclassification in an unpredictable way.
b) Recall periodDifferent studies used different recall periods to obtain information on diarrhoea.Influence of using different recall periods to get such data has been studied inrural Tamilnadu, South India. It was found that there could be considerable under-reporting of diarrhoeal morbidity when the recall period exceeded 3 days. Theestimated extent of under-reporting for various recall periods were – 15%, 26%and 45% with 3-, 6- and 7-13 days of recall period, respectively [75]. If this istrue, then probably most studies underestimated the morbidity and mortality fromdiarrhoea to the extent mentioned above.
c) Non-availability of age-/sex-stratified dataAs noted above, most of the data are available for the child population; fewstudies have reported data for all ages or for ³5 years population (without anyfurther age grouping). Even fewer studies reported data according to the gender.

85
Diarrhoeal Diseases
d) Outbreak dataAs mentioned earlier, data from outbreak investigations are not suitable forestimating disease burden at the community level, as these data tend to givehigher estimates for obvious reasons.
Problems with mortality data1. Under-reporting of deaths
Under-reporting is a problem in most of the parts in the country. From theavailable data the extent of under-reporting of deaths ranged from 13% [84] tomore than 30% [56].
2. Problems in ascertainment of cause of deathIt was not clear how deaths due to diarrhoea were defined in different studiesthat reported data on diarrhoeal mortality. Only one study [6] used a cleardefinition - “ A death was considered diarrhoea-related if the child had diarrhoeain the week before death, and there was no obvious cause of death unrelated todiarrhoea”, provided by the WHO (WHO/CDD/SER / 86.2). Other factors relatedto this problem are as follows -- Non-availability of death certificates:
Very often death certificates are not available, even when deaths occur in thehospital. In a study to ascertain cause of death, it was noted that for almost95% of the hospital deaths, no death certificate was available [56].
- Reliability of verbal autopsy:Many studies reported cause of death based on verbal autopsies, the reliabilityand validity of which are quite debatable [59,88-91].
3. Mortality data for hospitalized cases4. Mortality data from outbreaks
While mortality from diarrhoea tends to be higher during the outbreaks than theusual situations, for mortality among hospitalized cases, the issue is a littlecomplex. Usually, the more severe and complicated cases are admitted to thehospital – thus, mortality is expected to be higher among hospitalized cases; onthe other hand, due to the care that those patients receive in the hospital, themortality could be lower than that would be expected among similar patients inthe community who are not hospitalized.
Problems with disability dataCompared to morbidity and mortality, fewer studies reported diarrhoea duration.Most data on duration was obtained from hospital-based clinical trials, which were

86
Diarrhoeal Diseases
conducted under stringent experimental conditions, and thus, the duration was likelyto be less than that might occur under usual field conditions.
There were almost no data from community or hospital-based studies on disabilityweights for diarrhoea, which is likely to be different across the places, depending onsocial, cultural, economic, and many such characteristics of the populations.
The wide variability in estimates of morbidity, mortality, or disability due to diarrhoeadiscussed so far could be explained by differential distribution of various determinants thatput the people at different risks for suffering or dying from diarrhoea. Some of the importantdeterminants as identified through several studies include prevalence of malnutrition, poorwater supply and sanitation system, poor personal hygiene, inadequate breast feeding andearly weaning, inadequate knowledge about ORT and feeding during diarrhoea etc.[7,11,16,35-44,51,52,57]. The organism responsible for causing diarrhoea is also animportant factor that can determine morbidity and mortality from diarrhoea [31,45,46].Regarding mortality, it is well established that apart from many other factors, type of diarrhoeais an important determinant. In 1996, a review of data on diarrhoeal deaths in the developingcountries revealed that acute diarrhoea, dysentery, and non-dysenteric persistent diarrhoeawere responsible for 35%, 20%, and 45% of the total diarrhoeal deaths, respectively [81].Another review of 1990 hospital records from one of the referral pediatric hospital inKolkata revealed that annual hospital death rates of children suffering from acute waterydiarrhoea, dysentery, and persistent diarrhoea were 13.6%, 18.2%, and 25.9%, respectively[82], while data from another review showed that 47% of the infant diarrhoeal deaths inIndia were due to persistent diarrhoea [85]. These information may be useful while calculatingthe overall number of diarrhoeal deaths.
RecommendationsOn the basis of the literature review as described above, we propose the followingmeasures that could facilitate availability of data as relevant to estimation of diseaseburden due to diarrhea are proposeda. Regular collection, compilation and reporting of data on diarrhoeal morbidity,
mortality, and disability at the government level.b. Analyzing and reporting of such data by age, gender, rural/urban areas for
government data as well data from different studies.c. Use of uniform age grouping system to facilitate comparison across studies.d. Provide clear definitions for “diarrhoea”, “deaths due to diarrhoea” and such
other relevant terms.

87
Diarrhoeal Diseases
e. Conduct more community-based studies using sound methodologies that canprovide results that are more generalizable.
While conducting studies, try to assess extent of reporting errors or misclassification,especially when diarrhoeal episodes are recorded through recall or causes of deathare assessed through verbal autopsies.
References1. Census of India, 2001. www.censusindia.net2. Census of India, 1991. www.censusindia.net3. Bhattacharya SK. Progress in the prevention and control of diarrhoeal diseases since Independence. Natl
Med J India 2003; 16 Suppl 2: 15-9.4. Sircar BK, Deb BC, Sengupta PG, Mondal S, Gupta DN, Sarkar S, Sikder SN, Ghosh S, Saha NC, Pal SC.
An operational study on implementation of oral rehydration therapy in a rural community of West Bengal,India. Indian J Med Res 1991; 93: 297-302.
5. Pal SC. Dysentery: an overview. Still problems to resolve. Dialogue Diarrhoea. 1986 Jun;(25):4.6. Sengupta PG, Mandal S, Sen D, Das P, Deb BC, Pal SC. Multidrug resistant epidemic shigellosis in a
village in west Bengal, 1984. Indian J Public Health. 1990 Jan-Mar;34(1):15-9.7. Gupta DN, Sircar BK, Sengupta PG, Ghosh S, Banu MK, Mondal SK, Saha DR, De SP, Sikdar SN,
Manna B, Dutta S, Saha NC. Epidemiological and clinical profiles of acute invasive diarrhoea with specialreference to mucoid episodes: a rural community-based longitudinal study. Trans R Soc Trop Med Hyg.1996 Sep-Oct;90(5):544-7.
8. Sircar BK, Ghosh S, Sengupta PG, Gupta DN, Mondal SK, Sur D, Deb M, Manna B, Bhattacharya SK.Impact of vitamin A supplementation to rural children on morbidity due to diarrhoea. Indian J Med Res2001; 113: 53-9.
9. Pandey A, Sengupta PG, Mondal SK, Gupta DN, Manna B, Ghosh S, Sur D, Bhattacharya SK. Genderdifferences in healthcare-seeking during common illnesses in a rural community of West Bengal, India. JHealth Popul Nutr. 2002 Dec;20(4):306-11.
10. Sur D, Mondal SK, Gupta DN, Ghosh S, Manna B, Sengupta PG. Impact of Breastfeeding on WeightGain and Incidence of Diarrhea. Among Low Birth Weight Infants of an Urban Slum of Calcutta. IndianPediatrics 2001; 38: 381-384.
11. Gupta DN, Mondal SK, Ghosh S, Rajendran K, Sur D, Manna B. Impact of zinc supplementation ondiarrhoeal morbidity in rural children of West Bengal, India.Acta Paediatr. 2003 May;92(5):531-6.
12. Sur D, Gupta DN, Mondal SK, Ghosh S, Manna B, Rajendran K, Bhattacharya SK. Impact of zincsupplementation on diarrheal morbidity and growth pattern of low birth weight infants in kolkata, India: arandomized, double-blind, placebo-controlled, community-based study. Pediatrics. 2003 Dec;112(6 Pt1):1327-32.
13. Hirve S, Ganatra B. A prospective cohort study on the survival experience of under five children in ruralwestern India. Indian Pediatr. 1997 Nov;34(11):995-1001.
14. Basu S, Sengupta B, Paladhi PK. Single megadose vitamin A supplementation of Indian mothers andmorbidity in breastfed young infants. Postgrad Med J. 2003 Jul;79(933):397-402.
15. Unpublished data. “Surveillance for Cholera and Typhoid Fever in eastern Kolkata, India”. ICMR-IVICollaborative Project, Kolkata, West Bengal. 2003.
16. Unpublished data. Surveillance under DBT-project at NICED, Kolkata. 2003.

88
Diarrhoeal Diseases17. Unpublished data. NICED project entitled “An operational study on effect of zinc supplementation on
reduction of diarrhoeal morbidity among rural children”. 200318. Lal S. Surveillance of acute diarrhoeal diseases at village level for effective home management of diarrhoea.
Indian J Public Health. 1994 Apr-Jun;38(2):65-8.19. Bhandari N, Bahl R, Taneja S, Strand T, Molbak K, Ulvik RJ, Sommerfelt H, Bhan MK. Substantial
reduction in severe diarrheal morbidity by daily zinc supplementation in young north Indian children.Pediatrics 2002; 109(6): e86.
20. Anand K, Sundaram KR, Lobo J, Kapoor SK. Are diarrheal incidence and malnutrition related in underfive children? A longitudinal study in an area of poor sanitary conditions. Indian Pediatr. 1994Aug;31(8):943-8.
21. Singh J, Gowriswari D, Chavan BR, Patiat RA, Debnath AC, Jain DC, Sharma RS, Sharma RC, DattaKK. Diarrhoeal diseases amongst children under five. A study in rural Alwar. J Commun Dis. 1992Sep;24(3):150-5.
22. Lal P, Bansal AK, Aggarwal CS, Taneja DK, Gogia V. Incidence of diarrhoea and some related environmentaland behavioural factors in Jhuggis of Delhi. Indian J Public Health. 1996 Apr-Jun;40(2):35-7.
23. Ray SK, Roy P, Deysarkari S, Lahiri A, Mukhopadhaya BB. A cross sectional study ofundernutrition in 0-5 yrs. age group in an urban community. Indian J Matern Child Health. 1990Apr-Jun;1(2):61-2.
24. Gupta P, Murali MV, Seth A. Epidemiology of diarrhea in urban slums.Indian Pediatr. 1998Feb;35(2):147-51.
25. Sharma A, Gupta S. Impact of ICDS on health and nutritional status of children. Indian J Matern ChildHealth 1993; 4(1): 27-30.
26. Biswas AB, Basu M, Das KK, Biswas R. (Dr. P. C. Sen Award on rural health practice). Infant and earlychildhood mortality in some rural ICDS blocks of west Bengal. Indian J Public Health. 1993 Jul-Sep;37(3):81-6
27. Singh SP, Reddy DC, Mohapatra SC, Gaur SD. Study of infant and childhood mortality in an ICDS blockof eastern U.P. Indian J Public Health. 1993 Apr-Jun;37(2):61-5.
28. Ray SK, Kumar S, Saha I, Dasgupta S. Utilisation of ORT during diarrhoea in three districts of WestBengal. Indian J Public Health. 1994 Apr-Jun;38(2):73-6.
29. Mondal NC, Biswas R, Manna A. Risk factors of diarrhoea among flood victims: a controlled epidemiologicalstudy. Indian J Public Health 2001; 45(4): 122-7.
30. Mahendraker AG, Dutta PK, Urmil AC, Moorthy TS. A study of medico social profile of under five childrensuffering from diarrhoeal diseases. Indian J Matern Child Health. 1991;2(4):127-30.
31. Kothari G. Diarrhoea in urban slums: Bombay. Dialogue Diarrhoea. 1987 Dec;(31):4-5.32. Kumar Karn S, Harada H. Field survey on water supply, sanitation and associated health impacts in urban
poor communities—a case from Mumbai City, India. Water Sci Technol. 2002;46(11-12):269-75.33. Bhatia V, Swami HM, Bhatia M, Bhatia SP. Attitude and practices regarding diarrhoea in rural community
in Chandigarh. Indian J Pediatr 1999; 66(4): 499-503.34. Bhandari N, Bahl R, Mazumdar S, Martines J, Black RE, Bhan MK; Infant Feeding Study Group. Effect of
community-based promotion of exclusive breastfeeding on diarrhoeal illness and growth: a clusterrandomised controlled trial. Lancet 2003; 361(9367): 1418-23.
35. Bhattacharya SK, Bhattacharya MK, Nair GB, Dutta D, Deb A, Ramamurthy T, Garg S, Saha PK, Dutta P,Moitra A, Mandal BK, Shimada T, Takeda Y, Deb BC. Clinical profile of acute diarrhoea cases infectedwith the new epidemic strain of Vibrio cholerae O139: designation of the disease as cholera. J Infect 1993;27(1): 11-5.
36. Bhattacharya SK, Goswami AG, Bhattacharya MK, Dutta D, Deb A, Deb M, Sircar BK, Chowdhury AS,Das KP, Nair GB. Epidemic of Vibrio cholerae 0139 in Calcutta. Indian J Med Res. 1994 Nov;100:213-6.

89
Diarrhoeal Diseases37. Bhattacharya SK, Goswami AG, Bhattacharya MK, Dutta D, Deb A, Deb M, Sircar BK, Chowdhury AS,
Das KP, Nair GB. Epidemic of Vibrio cholerae 0139 in Calcutta. Indian J Med Res 1994; 100: 213-6.38. Sur D, Sengupta PG, Mondal SK, Dutta P, Gupta DN, Ghosh S, Pandey A, Ramamurthy T, Bhattacharya
SK. A localised outbreak of Vibrio cholerae O139 in Kolkata, West Bengal. Indian J Med Res. 2002Apr;115:149-52.
39. Sircar BK, Saha MR, Deb BC, Singh PK, Pal SC. Effectiveness of oral rehydration salt solution (ORS)in reduction of death during cholera epidemic. Indian J Public Health. 1990 Jan-Mar;34(1):68-70.
40. Kang G, Ramakrishna BS, Daniel J, Mathan M, Mathan VI. Epidemiological and laboratory investigationsof outbreaks of diarrhoea in rural South India: implications for control of disease. Epidemiol Infect 2001;127(1): 107-12.
41. Singh K, Kumar K. Mothers’ concept of the ideal number, colour and consistency of stools of their infants.Indian J Matern Child Health 1993; 4(2): 62-3.
42. Ramakrishnan R, Venkatarao T, Koya PK, Kamaraj P. Influence of recall period on estimates ofdiarrhoea morbidity in infants in rural Tamilnadu. Indian J Public Health. 1999 Oct-Dec;43(4):136-9.
43. Sengupta B, Dasgupta S, Saha I, Mandal AK, Palodhi PK. Experience in running a DiarrhoealTraining cum Treatment Unit (DTTU) in a state teaching hospital in Calcutta. J Indian Med Assoc1998; 96(4): 104-5, 108.
44. Kumar S, Debnath A, Goswami A. Some aspects of Diarrhoea Training and Treatment Unit in InfectiousDiseases Hospital, Calcutta. Indian J Public Health. 1994 Apr-Jun;38(2):81-6.
45. State Bureau of Health Intelligence, 2002. Govt. of West Bengal.46. Bhandari N, Bhan MK, Sazawal S. Mortality associated with acute watery diarrhea, dysentery and persistent
diarrhea in rural north India. Acta Paediatr.1992; 381 :111 –11647. Choudhary SR, Jayaswal ON. Infant and early childhood mortality in urban slums under ICDS scheme—
a prospective study. Indian Pediatr. 1989 Jun;26(6):544-9.48. Khalique N, Sinha SN, Yunus M, Malik A. Early childhood mortality—a rural study. J R Soc Health. 1993
Oct;113(5):247-9.49. Khalique N, Sinha SN, Yunus M, Malik A. Certain aspects of infant mortality - a prospective study in a
rural community. Indian J Matern Child Health. 1992 Jul-Sep;3(3):85-8.50. Bhattacharya MK, Ghosh S, Mukhopadhyay AK, Deb A, Bhattacharya SK. Outbreak of cholera caused by
Vibrio cholerae 01 intermediately resistant to norfloxacin at Malda, West Bengal. J Indian Med Assoc2000; 98(7): 389-90.
51. Sur D, Dutta P, Nair GB, Bhattacharya SK. Severe cholera outbreak following floods in a northern districtof West Bengal. Indian J Med Res. 2000 Nov;112:178-82.
52. Awasthi S, Pande VK. Cause-specific mortality in under fives in the urban slums of Lucknow, north India.J Trop Pediatr. 1998 Dec;44(6):358-61.
53. Indrayan A, Wysocki MJ, Kumar R, Chawla A, Singh N. Estimates of the years-of-life-lost due to the top ninecauses of death in rural areas of major states in India in 1995. Natl Med J India. 2002 Jan-Feb;15(1):7-13.
54. Mirza NM, Macharia WM, Wafula EM, Agwanda RO, Onyango FE. Verbal autopsy: a tool for determiningcause of death in a community. East Afr Med J 1990; 67(10): 693-8.
56. Gajalakshmi V, Peto R, Kanaka S, Balasubramanian S.Verbal autopsy of 48 000 adult deaths attributableto medical causes in Chennai (formerly Madras), India. BMC Public Health 2002; 2(1): 7.
55. Bang AT, Bang RA. Diagnosis of causes of childhood deaths in developing countries by verbal autopsy:suggested criteria. The SEARCH Team. Bull World Health Organ 1992; 70(4): 499-507.
56. Maude GH, Ross DA.The effect of different sensitivity, specificity and cause-specific mortality fractionson the estimation of differences in cause-specific mortality rates in children from studies using verbalautopsies. Int J Epidemiol 1997; 26(5): 1097-106.

90
Diarrhoeal Diseases57. SRS based abridged life tables, 1988-’92. Govt. of West Bengal.58. Bhattacharya SK, Bhattacharya MK, Manna B, Dutta D, Deb A, Dutta P, Goswami AG, Dutta A, Sarkar S,
Mukhopadhaya A, Krishnan T, Naik TN, Nair GB. Risk factors for development of dehydration in youngchildren with acute watery diarrhoea: a case-control study. Acta Paediatr 1995; 84(2): 160-4.
59. Dutta D, Bhattacharya SK , Bhattacharya MK, Deb A, Deb M, Manna B, Moitra A, Mukhopadhyay AK,Nair GB. Efficacy of norfloxacin and doxycycline for treatment of Vibrio cholerae O139 infection. JAntimicrob Chemother 1996; 37: 575-81.
60. Bhattacharya SK, Bhattacharya MK, Dutta D, Dutta S, Deb M, Deb A, Das KP, Koley H, Nair GB. Double-blind, randomized clinical trial for safety and efficacy of norfloxacin for shigellosis in children. Acta Paediatr1997; 86(3): 319-20.
61. Bhattacharya MK, Bhattacharya SK, Dutta D, Deb AK, Deb M, Dutta A, Saha Choudhury A, Nair GB,Mahalanabis D. Efficacy of oral hyposmolar glucose-based and rice-based oral rehydration salt solutionsin the treatment of cholera in adults. Scand J Gastroenterol 1998; 33(2): 159-63.
62. Dutta D, Bhattacharya MK, Deb A, Chowdhury AS, Nair GB, Ramakrishna BS, Bhattacharya SK. Uncookedrice powder in oral rehydration solution: an alternative to glucose or cooked rice powder. Indian J Med Res1998; 107: 257-62.
63. Bhattacharya MK, Dutta D, Bhattacharya SK, Deb A, Mukhopadhyay AK, Nair GB, Shimada T, Takeda Y,Chowdhury A, Mahalanabis D. Association of a disease approximating cholera caused by Vibrio choleraeof serogroups other than O1 and O139. Epidemiol Infect 1998; 120(1): 1-5.
64. Dutta D, Bhattacharya MK, Deb AK, Sarkar D, Chatterjee A, Biswas AB, Chatterjee K, Nair GB,Bhattacharya SK. Evaluation of oral hypo-osmolar glucose-based and rice-based oral rehydration solutionsin the treatment of cholera in children. Acta Paediatr 2000; 89(7): 787-90.
65. Bhandari N, Bhan MK, Sazawal S. Impact of massive dose of vitamin A given to preschool children withacute diarrhoea on subsequent respiratory and diarrhoeal morbidity. BMJ 1994; 309: 1404-7.
66. Patel AB, Dhande LA, Rawat MS. Economic evaluation of zinc and copper use in treating acute diarrhoeain children: a randomized controlled trial. Cost Eff Resour Alloc 2003; 1(1): 7-16.
67. Murray CJ, Lopez AD. Global mortality, disability, and the contribution of risk factors: Global Burden ofDisease Study. Lancet 1997; 349(9063): 1436-42.
68. World Health Organization WHO. Office of Information. Cholera: ancient scourge on the rise. WHOannounces global plan for cholera control. (25 April 1991). WHO Feature 1991; (154): 1-3.
69. Diarrhoeal diseases control programme. Diarrhoea Dialogue 1980; 1(1): 6.70. World Health Organization WHO. Division of Diarrhoeal and Acute Respiratory Disease Control. Rational
management of diarrhoea in children. Essent Drugs Monit 1991; (11):10-1.71. Srivastava RN. Editorial-programme for control of diarrhoeal diseases. J Indian Assoc Commun Dis 1982;
5(3-4): 48-9.72. Mondal SK, Gupta PG, Gupta DN, Ghosh S, Sikder SN, Rajendran K, Saha MR, Sircar BK, Bhattacharya
SK. Occurrence of diarrhoeal diseases in relation to infant feeding practices in a rural community in WestBengal, India. Acta Paediatr 1996; 85(10): 1159-62.
73. Crook N, Malaker CR. Child mortality in new industrial localities and opportunities for change: a survey inan Indian steel town. Health Transit Rev. 1992 Oct;2(2):165-76.
74. Sarkar K. Role of oral rehydration therapy in controlling epidemic of cholera and watery diarrhoea. JIndian Med Assoc. 2003 Jun;101(6):379-80, 386.
75. Zodpey SP, Deshpande SG, Ughade SN, Kulkarni SW, Shrikhande SN, Hinge AV. A prediction model formoderate or severe dehydration in children with diarrhoea. J Diarrhoeal Dis Res 1999; 17(1): 10-6.
76. Ghosh S, Sengupta PG, Gupta DN, Mondal SK, Goswami M, Bhattacharya SK, Sircar BK. Maternalknowledge on risk behavioural practices and it’s association with diarrhoea in a rural community of WestBengal, India. J Commun Dis 1998; 30(4): 251-5.

91
Diarrhoeal Diseases77. Badari S, Gopal YS, Devaramani SC. Infant mortality, its components and correlates: findings from a
longitudinal study in rural Karnataka, India. Genus. 1991 Jan-Jun;47(1-2):89-108.78. Niyogi SK, Saha MR, De SP. Enteropathogens associated with acute diarrhoeal diseases.Indian Public
Health. 1994 Apr-Jun;38(2):29-32.79. Saha DR, Gupta DN, Sengupta PG, Mondal SK, Ghosh S, Saha NC, Sikder SN, Sircar BK. Intestinal
parasitism: a childhood problem in rural Bengal. J Commun Dis. 1995 Sep;27(3):170-4.80. Bhan MK, Bhandari N, Bhatnagar S, Bahl R. Epidemiology & management of persistent diarrhoea in
children of developing countries. Indian J Med Res. 1996 Jul;104:103-14.81. Dutta P, Mitra U, Rasaily R, Bhattacharya SK, Bhattacharya MK, Manna B, Gupta A, Kundu B. Assessing
the cause of in-patients pediatric diarrheal deaths: an analysis of hospital records. Indian Pediatr. 1995Mar;32(3):313-21.
82. Victora CG, Huttly SR, Fuchs SC, Barros FC, Garenne M, Leroy O, Fontaine O, Beau JP, Fauveau V,Chowdhury HR, et al. International differences in clinical patterns of diarrhoeal deaths: a comparison ofchildren from Brazil, Senegal, Bangladesh, and India. J Diarrhoeal Dis Res. 1993 Mar;11(1):25-9.
83. Bhargava I. Review of mother and child health programmes and targets in light of the national healthpolicy. ICCW News Bull 1987; 35(4-5): 2-6.

Part-B
Annotated Bibliography

1. Microscopic Diagnosis of Malaria in Kheda District of Gujarat
A.S. GAUTAM, R.C. SHARMA, R.M. BHATT and D.K. GUPTA.
Indian Journal of MalariologyVol. 29, June 1992, pp. 83-87.
A study conducted in 1990 revealed that 2% (range 0.6-4.8) of negative bloodsmears were mislabeled as positive, and 6.7% of positive blood smears weremislabeled as negative. A result of such mislabeling would lead to inadequatetreatment of a large number of patients. Hence there is need to look into thetraining aspect and system of supervision of laboratory technicians. The presentsystem of cross-checking of blood smears at different levels also needs to bereviewed. A study which could address itself to these needs is indicated.
Salient Findings: The study has highlighted the discrepancies in examination ofblood smears by detecting both false negative and positive smears in appreciablenumbers and suggests the corrected figure of API based on discrepancy rates.The study also finds out the reasons for the discrepancy.
Comments: This study assumes importance in finding out gap between thereported and true incidence of malaria and suggests the importance of crosschecking of slides on regular basis.
2. Studies on the True Incidence of Malaria in Kharkhoda (District Sonepat,Haryana) and Kichha (District Nainital, U.P.) Primary Health Centres
V.P. SHARMA, D.S. CHOUDHURY, M.A. ANSARI. M.S. MALHOTRA.P.K.B. MENON, R.K. RAZDAN and C.P. BATRA
Indian Journal of MalariologyVol. 20, June 1983, 21-34
Malaria
95

96
Malaria
Intensive surveillance revealed that malaria incidence was extremely high inKichha and Kharkhoda PHCs. The study also revealed that NMEP’s surveillancewas recording a small number of malaria cases, and that the ongoing surveillancewas missing the vivax and falciparum malaria peaks and was not sensitive enoughto reveal the real effect of spraying. The study was useful in organizing malariacontrol operations in Kharkhoda PHC and pointed out that small focus offalciparum malaria should be stamped out from Kichha PHC. The importance ofbetter surveillance is emphasized in the present day context of malaria control.
Salient Findings: This study highlights glaring gap between the reported andtrue incidence of malaria in two PHCs, one situated in Haryana and another inUttar Pradesh. The parallel malaria surveys suggested that routine surveillancewas missing >95% cases which was alarming. Seasonal distribution of malariahas been presented in both the PHCs studied.
Comments: The study is comprehensive in bringing to light the gap between reportedand true incidence of malaria, which is its greatest strength. It suggests that there isserious limitation of official figures of malaria and should not be relied upon for theestimation of disease burden. From disease burden estimation point of view, howeverage and sex wise distribution of incidence data has not been provided in the study.Deaths if any due to malaria have also not been mentioned.
3. Studies on the Incidence of Malaria in Gadarpur town of Terai, Distt.Nainital, U.P .
M.S. MALHOTRA, R.P. SHUKLA and V.P. SHARMA
Indian Journal of MalariologyVol. 22, June 1985, pp. 57-60.
Terai region of district Nainital (U.P.) is well known for green revolution. Earlyattempts to colonize Terai were unsuccessful mainly because of high morbidityand mortality due to malaria. The situation took a dramatic turn with theavailability of DDT in malaria control. Initially between 1947 to 1949 threecolonization units were opened in Terai. These units inter alia made important

97
Malaria
contributions in determining the dosage of DDT and the frequency of itsapplication. Subsequently, these units were merged and made NMEP unit. As aresult of spraying under NMEP malaria was eradicated from Terai by the mid1960’s. Control of malaria resulted in the conversion of vast jungles intoagricultural farms and simultaneous growth of agro-industries. To increaseagricultural production, Govind Ballabh Pant University of Agriculture andTechnology was established in 1960 and several dams were constructed forirrigation. Today the area is well irrigated by a network of canals and theirtributaries and artesian wells. In late 1960s malaria resurgence started throughoutTerai, as it did in other parts of the country. To tackle this situation, the Governmentof India in 1977 implemented the Modified Plan of Operations (MPO). Oneobjective of the MPO was to provide protection to the green revolution. In orderto study the impact of the MPO in Terai region, a field station of the MalariaResearch Centre was opened in 1979.
Early studies revealed the occurrence of 29 mosquito species belonging to 8genera, and that A. minimus was absent and A. stephensi was represented by afew specimens (Nagpal el al. 1983). A. culicifacies was found throughout Teraiin good densities. It is resistant to DDT and BHC and breeds in innumerablesites mostly associated with irrigation systems (Sharma el al. 1983a). Studies in1981-82 revealed that malaria in Terai was mainly due to P. vivax and there wasa small focus of P. falciparum (Sharma el al. 1983b). A. culicifacies and A.f1uviatilis were incriminated as vectors of malaria (Choudhury, 1984).
Gadarpur town is situated in Terai. It has a population of about 6500. The townis an important centre of commerce and people from surrounding villages visitGadarpur for shopping and medical help. It has a primary health centre (PHC)and several private practitioners. A one year sampling study (1982-83) revealedthat Gadarpur PHC villages were endemic for malaria and that the incidence offalciparum malaria was extremely high (Choudhury el al. 1983a). In vivo testsshowed decreased sensitivity of P. falciparum to chloroquine (Choudhury et al.1983b). During the same period, a study on the incidence of malaria in Gadarpurtown was undertaken by continuously monitoring the same population for a oneyear period. Results of the study are reported in this paper. Before the start ofstudy, a census was made and all houses were numbered. Active surveillancewas started in April, 1982 and continued till March, 1983. During a one yearperiod, surveillance was intensified by deploying additional staff so as not to

98
Malaria
miss any fever case. Mass blood surveys were also done during April-August.All fever cases were given presumptive treatment (600 mg chloroquine or 4tablets adult dose) followed by radical treatment as per the drug policy of theNMEP (Sharma, 1984). Blood smears were stained with JSB stain and at least100 fields of thick film were examined before declaring the slide as negative.Parasite identification was confirmed by thin film examination.
Active surveillance revealed extremely high incidence of malaria throughoutthe year, except for 2 months during the extreme winters. In April almost allinfections were due to P. vivax followed by a drop to low numbers in October-March. There was a sudden increase in falciparum cases in August peaking inSeptember followed by decline to low numbers during the winter months. Anotable feature was the complete absence of P. malariae, which used to occur ingood proportions (about 17%) before the colonization of Terai. There were only8 mixed (Pv+Pf) infections in one year. Slide positivity rate remained highthroughout the study period and averaged 58.66% (range 32.43-90.43) and SFRaveraged 34.58% reaching as high as 88.04% in November. During mass bloodsurveys, a total of 1798 blood smears were collected from April to August. 1982.Of these 299 were P. vivax, 12 P. falciparum and 2 mixed infections. The SPRwas 17.38%. There was therefore a high proportion of atypical malaria cases inthe community. During the same period NMEP recorded a total of 49 malariacases (34 Pv + 14 Pf and I mixed). The SPR and SFR was 5.27 and 1.61respectively. It was therefore obvious that NMEP’s surveillance was not adequateand a large number of parasite positive cases were being missed. Improvedsurveillance and good spraying, targeted to achieve about 80% coverage, isrecommended to contain malaria in Terai.
Salient Findings: This is one year study, which shows huge gap between thereported incidence and the one longitudinally estimated during parallel activesurveillance.
Comments: This study indicates that data compiled through routine surveillancecan not be relied upon for the estimation of disease burden. In this study incidencedata has not been analysed age and sex wise and there is no mention of deathsdue to malaria if any in this region during the period of study.

99
Malaria
4. A Preliminary Malaria Survey in Bisra PHC, District Sundergarh, Orissa
S.K. GHOSH, A. KUMAR , S.K. CHAND and D.S. CHOUDHURY
Indian Journal of MalariologyVol. 26, September 1989, pp. 167-170.
Bisra PHC is located in Sundergarh district of Orissa between 22°10' and 22020’North latitude and 84°50' and 8505' East longitude. It is surrounded by Singhbhumhill range in the North and in the East, Rourkela town in the West and villagesunder Birkera PHC in the South. Villages in Singhbhum hill range were highlyendemic for malaria (Watts, 1924; Christophers, 1925; Senior White and Das,1938). Malaria has returned with vengeance in this area. The spraying is poorand surveillance is inadequate. During 1986 and 1987 the SPR and SfR of BisraPHC varied from 9 to 12 and 8 to 12 (Source: DMO). Health Department; OrissaGovt. suggested that Malaria Research Centre should open its field station tostudy the feasibility of the bioenvironmental control of malaria in Bisra PHC,because of persistent malaria transmission and the fact that spraying was notacceptable to the community. At the time of opening of field station a preliminarysurvey of malaria situation was carried out in Bisra PHC. Results of this studyare reported in this paper.
Bisra PHC HQs is located 15 kms from Rourkela town. The PHC (rural) has atotal area of 147 sq kms with 71 villages having a population of 46,072 (1981census). Each village is further split into small hamlets locally known as ‘tolas’which are often far from each other.
The land is mostly undulating interspersed with low hillocks having sparse forests.River “Koel’ runs along the northern limits of the PHC and four streams runningthrough the PHC area feed the river. The area receives an annual normal rainfallof 165 cms, mostly during the monsoon months. During the non-monsoon monthsthe land, however, remains dry and thus a large number of bed pools are formedin the streams and river, which support heavy Anopheles culicifacies breeding.Most of the inhabitants are aboriginals belonging to Gram, Munda, Kharia, Kisan,Bhuyia, Binjhia, Gonds, Khonds, Santhal, Lohar and Baraik tribes in order ofprevalence. Some migrants particularly from Bihar, Rajasthan and Uttar Pradeshhave settled in and around Bisra town. The main occupation is agriculture, which

100
Malaria
largely depends on monsoons and during the rest of the year the people areengaged in labour work in industries or railways. Thus there is a daily flux ofpopulation between Bisra PHC villages and Rourkela town.
Although the establishment of Rourkela Steel Plant has transformed this areaboth economically and ecologically, malaria continues to persist as a major healthproblem.
A preliminary survey was conducted in the first fortnight of April 1988 in orderto determine the present status of malaria in Bisra PHC. Active fever survey wascarried out in nine villages within a radius of 15 kms from the PHC HQs. Thesevillages were Dareikela, Kapranda, Tulsikani, Barsuan, Bhangurkela, Bijadihi,Jabaghat, Sarubahal and Dhadari.
Blood smears were collected, stained with JSB stain and examined for thepresence of malaria parasites. Adult patients with malaria were treated withchloroquine (900 mg for P. vivax and P. malariae and 1500 mg for P. falciparum).The children received proportionately low dosages. Spleens of primary schoolchildren (age below 9 yrs) were also examined for enlargement. Adult anophelinemosquitoes were collected in eight riverine and four non-riverine villages withthe help of suction tubes both in the morning (0600 hrs to 0800 hrs) and in theevening (1800 hrs to 2000 hrs). The mosquitoes were identified and dissectedfor the presence of sporozoites.
Fever surveys were carried out in nine villages and a total of 95 blood smears werecollected. Of these, 26 (SPR 26.3%) were positive for malaria showing a ParasiteIndex (PI) of 3.61. Among the positives, 9 were P. vivax, 15 P. falciparum and 1P. malariae. This is the first report of P. malariae from this area. Table 1 showsthat SPR, SfR and PI recorded in this survey were much higher than that of theNMEP surveillance conducted from March to May in the corresponding andprevious years. This may be the result of better case detection during the survey.Out of 42 school children examined only 3 (7.1%) showed enlarged spleens.
A case of cerebral malaria was also detected in a boy of 5 years. At the time ofblood smear collection, the patient had high fever associated with rigor andconvulsions. The boy was under antibiotic therapy (ampicillin) by a localpractitioner. On examination, the blood smear showed P. falciparum rings. The

101
Malaria
boy was treated with chloroquine and recovered. It may be noted that there wasthe death of a 22 year old woman in the neighbourhood, apparently due tomalignant tertian malaria, a week before the detection of this case.
A total of 2210 mosquitoes belonging to five species viz., An. culicifacies, An.annularis, An. subpictus, An. vagus and An. splendidus were collected duringthe survey. Of all the anophelines, An. culicifacies was the most abundant species(89.2%). It was observed that villages adjacent to the river Koel had an average63.1 man hour density (MHD) of An. culicifacies as compared to 6.9 in the non-riverine villages, and the same was also true in the case of other anophelinespecies. A single specimen of An. splendidus was also collected from a riverinevillage. None of the 1973 An. culicifacies dissected showed gut or gland infection.This might be due to very low humidity (RH 30%) in April in this area resultingin reduced longevity.
Senior White and Das (1938) incriminated An. fluviatilis, An. minimus, An. varunaand An. culicifacies from Singhbhum hills and concluded that the first threespecies were mostly responsible for malaria transmission in this area and therole of An. culicifacies was of very little significance. During the present study,however, An. fluviatilis, An. minimus and An. varuna were not encountered. Theabsence of these erstwhile vectors and the prevailing malaria endemicity suggeststhat studies are required on the role of An. culicifacies in the malaria transmissionin this region. It may be mentioned that recently Nagpal and Sharma (1986) haveincriminated An. culicifacies in the transmission of malaria in six districts ofOrissa. Studies on the susceptibility status of P. falciparum to chloroquine shouldalso be taken up.
Salient findings: The point prevalence survey shows huge gap between reportedincidence and the estimated incidence through fever surveys. The SPR was 26.3%in surveys as compared to 7.6% recorded by PHC. Similarly SfR was 15.8 versus3.8%. For the first time P. malariae was also reported from this area.
Comments: The study suggests that malaria incidence was much higher thanbeing reported. This study once again suggests that for DALYs estimation, theincidence data of routine surveillance can not be relied upon to work out DALYs.Age and sex wise distribution of cases was not presented. Although a case ofcerebral malaria was reported during this limited duration survey, no informationon deaths was available from this area.

102
Malaria
5. The burden of malaria in Ahmedabad city, India: a retrospective analysisof reported cases and deaths
R. S. YADAV, R. M. BHATT, V. K. KOHLI and V. P. SHARMA
Annals of Tropical Medicine & Parasitology,Vol. 97, No.8, 793-802 (2003)
Owing to the paucity of accurate information on the burden of malaria in urbanIndia, a retrospective, epidemiological study was carried out in Ahmedabad city,which has a population of about 3 million. Surveillance data for the years 1965-1998 showed a gradual resurgence of malaria between 1967 to 1976, followed bywaves of low and high incidences. Plasmodium vivax always predominated butthe proportion of cases attributed to P. falciparum increased markedly from 1983.When the surveillance data and health records of the major public and privatehealth facilities in the city were analysed, for the period between 1991 and 1998,P. vivax was found to account for 69% of all malaria cases and P. falciparum forthe other 31 %. The incidence of infection with each Plasmodium species showedseasonal variation, with that of P. vivax increasing from January to September butthen declining as the incidence of P. falciparum increased. The age-specificdifferences seen in incidence were not statistically significant (P= 0.7). The annualnumbers of malaria-attributable deaths were strongly correlated with the incidenceof P. falciparum (r = 0.88). The malaria incidence detected (37,431 cases,representing a mean annual incidence of 12.2 cases/1000) was nine times greaterthan that officially reported (4119 cases, or 1.3 cases/1000 each year). Similarly,the annual malaria-attributable mortality detected (22 deaths/million) was far higherthan that officially notified (0.3death/million). The results of the retrospectiveanalysis not only provide a more accurate, baseline estimate of the burden of malariain an urban area of India but also clearly indicate the need for a much more efficienthealth-information system, for recording and managing malaria in such a setting.
Salient Features: This is a comprehensive study in which malaria data spanning8 years (1991-98) has been collected from Municipal corporation clinics, privateand govt. hospitals in Ahmedabad town in Gujarat having 3 million population.True incidence of malaria has been estimated on the basis of malaria cases reportedby UMS (Urban Malaria Scheme) and data retrieved from hospital recordscovering 14 hospitals and 85 clinics including both parasitologically confirmed

103
Malaria
and clinically treated malaria cases. The seasonal trends of cases and age andsex wise distribution of malaria has been studied. Deaths due to malaria for thestudy period have been compiled from the records.
Comments: The data is useful in estimation of DALYs lost in Ahmedabad citybased on estimated cases and age and sex wise distribution of malaria. However,age and sex specific distribution of malarial deaths has not been presented whichis crucial for YLL estimation. Contacts have been established with the seniorauthor of the paper Dr. Yadav to compile the data in necessary format forestimation of DALYs lost due to malaria in Ahmedabad city.
6. Epidemiological Observations on Malaria in Villages of Buhari PHC, Surat,Gujarat
H.C. SRIVASTAVA, RAJNI KANT, R.M. BHATT, S.K. SHARMA and V.P.SHARMA
Indian Journal of Malar1ologyVol. 32, December 1995. pp. 140-152
Investigations were carried out in the villages of Buhari PHC, Surat district,Gujarat to determine factors responsible for high prevalence of P. falciparum.The area is well-known for sugarcane cultivation, industrialization and frequentmovement of labourers. The slide positivity rate (44.24%) and P. fa1ciparuminfections (95.37%) were significantly high. The children of 5-9 yrs of age groupsuffered maximum from malaria. The infection in children was found associatedwith splenomegaly also. High falciparum infection (82.35%) was found inlabourers camping near villages out of which 90% afebrile cases were reportedwhich were silent carriers and source of transmission. Chloroquine was effectivein 75% cases despite of existence of resistant falciparum strain. Among sevenanopheline species encountered, An. culicifacies was predominant and foundbreeding in most of the breeding sites. The status of the insecticide spray and itsreceptivity among the community were poor. The investigation led to theconclusion that adequate measures are required to deal with migratory labourers,improper insecticide coverage, poor surveillance and a mass ignorance.
Salient Findings: This is a detailed epidemiological study carried out at PHClevel covering 6 villages. Point prevalence parasitological data has been presented

104
Malaria
village wise. Age and sex wise distribution of malaria has been presented in 6age classes. The study shows high incidence of malaria in children and malariadeclines >30 years age group.
Comments: The study is useful in studying case distribution according to ageand sex in Surat district and for comparison with other studies carried out inGujarat and rest of India through meta-analysis.
7. Malaria Outbreak in Bhojpur PHC of District Moradabad, Uttar Pradesh,India.
R.P. SHUKLA, S.N. SHARMA AND S.K. BHAT
J. Commun. Dis. 34 (2) 2002: 118
Based on the reports of 18 fever related deaths in Bhojpur Primary Health Centre(PHC) of Moradabad. District (UP), a study was undertaken during Septemberand October, 2000 to explore the possibility of outbreak of malaria in the areaand the reasons of the outbreak. The slide positivity rate (SPR) and slidefalciparum rate (SFR) in active fever surveys were found to be 84.7% and 82.2%respectively. Among children the average enlarged spleen and spleen rate were1.9 and 27.4 per cent respectively. The mortality rate of Anopheles culicifaciesin DDT, Malathion and Deltamethrin was 42.5, 86.7 and cent per cent respectively.The results of the study revealed that the outbreak was of malaria withpredominance of Plasmodium falciparum causing several deaths in the affectedvillages. The investigation revealed that there was disruption of surveillance andsupervision of malaria activities.
Salient Findings: In this study high incidence of malaria and Pf was found inthree villages where deaths had been reported. The spleen rate in children washigh. Age wise distribution of malaria was presented in 6 classes and maximumincidence was found in infants and children and it gradually declined in adults>15 years of age.
Comments: Although in this study age wise distribution of malaria gives anindication that severe transmission was going on but sex wise distribution was

105
Malaria
not given. This data however can be made use of in meta-analysis of agedistribution of cases in Uttar Pradesh particularly in Moradabad area.
8. Investigation of malaria outbreak in Bahraich district, Uttar Pradesh
DHIMAN, C.R. PILLAI & S.K. SUBBARAO
Indian J Med Res 113, May 2001, pp 186-191
Background & objectives: Based on the reports of 139 fever related deaths inJarwal primary health centre (PHC) of Bahraich district, Uttar Pradesh (UP)during April to September 1999, a study wasundertaken to explore the possibilityof outbreak of Plasmodium falciparum malaria in the area and reasons of outbreak.
Methods: The study was undertaken during September-October 1999 in Bahraichdistrict, UP. The study included a parasitological and an entomological survey.Blood slides from fever cases were collected and examined following standardprocedures for detection of species and stage of parasite. The resting adultmosquitoes were collected from human dwellings and cattle sheds from selectedvillages. Susceptibility status of Anopheles culicifacies to 4 per cent DDT and0.05 per cent deltamethrin was determined under laboratory conditions followingthe WHO procedure. In vitro drug sensitivity of P. falciparum to chloroquinewas also estimated.
Results: Overall slide positivity rate (SPR) was found to be 33.8 with apreponderance of P. falciparum (88.4%). There was an outbreak of Pf malaria inJarwal and surrounding areas as well. Foci of P. falciparum malaria were foundin Jarwal, Fakharpur and Hazoorpur PHCs around Kaisarganj PHC. In addition,P. falciparum cases, were also reported from Motipur and Tejwapur.
Interpretation & conclusion: Poor surveillance of affected areas resulting in lowannual parasite incidence (API), lack of insecticidal spray in the currently affectedPHCs as the API was less than 2 and development of resistance in P. falciparumto chloroquine were found as the possible reasons for the outbreak. It isrecommended that surveillance be strengthened in all PHCs of Bahraich districtto contain further extension of malaria in northeastern UP.

106
Malaria
Salient Findings: In this study, the villages where fever related deaths occurredhad high proportion of P. falciparum. Age wise break up of 139 deaths havebeen analysed and most (57%) were found in > 25 years age group followed by20.8% in children 6-14 years. These deaths were reported from a population of2570. The age distribution of cases shows malaria to be high in children <14yearsrange 19.23 to 28.84% while > 25 years it was still higher at 39.4% and in thisage group maximum deaths also occurred. Malaria affected equally both thesexes with ratio of 1.08:1.0 between males and females.
Comments: The study is important in highlighting that in the Eastern part ofUttar Pradesh state during an out break/epidemic, people > 25years of age wereaffected more by malaria as indicated by the incidence and death data. This is incontrast with other studies, such as the one conducted by Shukla et al., 2002,where malaria affected children more than higher age groups. Thus suggestingthat meta analysis of age-sex distribution of malaria would be necessary orregional approach may have to be followed to work out DALYs within a state ora geaographical region.
9. Malaria in Shankargarh PHC, Allahabad District (U.P.): A Clinical Report
R. N. YADAV, S. N. TIWARI, P. K. TYAGI, A. K. KULSHRESTHA and ANILPRAKASH
Indian Journal of MalariologyVol. 30, March 1993, pp. 9-16.
A longitudinal study of malaria incidence recorded at malaria clinic of MRC,Shankargarh, during 1988-1991 showed the immense popularity of the clinic inquarry area. In clinical cases, SPR and SfR gradually increased from 45.6 and18.2 in 1988 to 52.5 and 34.5 respectively in 1991. Increase in malaria casesduring the reporting period was mainly contributed by P. falciparum cases. Peaksof vivax and falciparum malaria were recorded in September and Octoberrespectively. Extended transmission in Shankargarh region might be attributedto the influx of quarry labourers after post-monsoon season. SfR for 0 to 1-yearage group malaria cases was found to be relatively low as compared to the higherage groups. Only 56 per cent of malarial-positive patients reported in the clinichad fever.

107
Malaria
Salient Findings: Clinic data of 4 years has been analysed age and sex wise inage groups of 0-1, 1-4, 4-8, 8-14 and >14 years. It reveals high incidence in allage groups including infants (SPR 44.6 in males and 49.8 I females). Symptomspresented by the P. vivax and P. falciparum have also been analysed. P. falciparumincidence was high and Pf gametocyte carriers (gametocyte rate : 24.8%) werefound in all age groups from Jan. to March and Aug. to Dec.
Comments: Although age and sex wise distribution of malaria cases has beenshown, a broad category of age class > has been created. The incidence data is ofuse to work out YLD in different age classes and both sexes.
10. Changing malaria endemicity -a village based study in Sonitpur, Assam
ANIL PRAKASH, P.K. MOHAPATRA, D.R. BHATTACHARYYA, P. DOLOIAND J. MAHANTA
J. Commun. Dis. 29 (2) :175-178 (1997)
Sporadic outbreaks of malaria have occurred in several districts of Assam in the1980’s. A widespread malaria epidemic, in 1995 however swept many parts ofthe state causing high mortality. Following reports of unusual rise in malariacases and deaths during April, May 1996 from several Primary Health Centres .-.UHCs) of district Sonitpur, Assam, we undertook a study of the epidemiologicaland entomological factors responsible for them in one of the worst affected PHCsviz. PHC North Jamuguri and the findings are presented here.
PHC North Jamuguri is situated near Tezpur town separated from ArunachalPradesh by a forest belt measuring about 980 hectares and its southern boundarylimited by Brahamaputra river. The study was conducted in Vijaypur-Najraparvillage. The village with a population of 608 is situated in the foothill adjoiningthe forest belt and is surrounded by tea gardens, is canal irrigated and has severalperennial streams flowing through it. The village recorded the highest increase(863%) of API in last five years.
The study methods included: (1) retrospective analysis of the spray andepidemiological data in regard to the PHC and the study village. (2) Mass blood

108
Malaria
survey, of about 40.6% of the village population. (3) Spleen survey (4) Anophelinecollection and dissection. During 5 years the least number of malaria cases wererecorded in 1991 SPR, 5.05). Thereafter, rise in malaria incidence was phenomenalas the API increased by 585% i.e. from 5.4 in 1991 to 37.0 in 1995. Proportionof P. falciparum cases varied between 22 and 47% during this period. Malariacases were recorded throughout the year with a distinct peak in May-June.Amongst the 14 NMEP sections of this PHC four northernmost sections borderingthe forest belt were the most malarious. Between 1991 and 1993 no malariapositive case was reported from study village. However, 130 malaria positives(Pf 17.7%) in 1994 and 58 malaria positives (Pf 24.1%) in 1995 were recordedin the village. In 1996, till May, a total of 57 malaria cases had been reportedwhich included 11 Pf and 46 Pv cases.
The spray coverage when calculated on the basis of total population variedbetween 4.2% (1994-II round) to 37.3%. In the blood survey 247 persons out of608 population of the study village were screened. Malaria parasite was detectedin 106 smears (SPR 42.9) of which 105 had P. falciparum infection (pf 99.1 %)including two cases of mixed infection. Of the 106 positives 64 (60.4%) werebelow 20 years of age and not much difference was observed in age or sex specificSPR (Table). Of 247 persons covered in the survey 138 had fever or recent feverhistory (fever attack rate 55.9%). In this category 71 persons were found positive(SPR 51.4). Amongst the remaining 109 healthy afebrile persons without anyother symptoms 35 were found malaria positives (SPR 32.1). Palpable spleenwas found in 125 persons (Spleen Rate 50.6%). Spleen Rate did not vary muchwith the age. Of the 106 malaria positives 78 were also found spleen positives(73.6%) while amongst 141 microscopically negative cases palpable spleen wasfound in 47 (33.3%) persons.
In entomological studies, 5 anopheline species were collected from the studyvillage. An. vagus was the predominant species (> 70% in the indoor collections).Density of indoor resting An. minimus was extremely low. Suitable adultspecimens of An. minimus (n = 2), An. culicifacies (n = 10), An. annularis (n = 7)and An. Vagus (n = 24) were dissected but none was found sporozoite positive.Poorly maintained irrigation canal, perennial streams with grassy margins,periodomestic ditches, wells, paddy fields and freshly dug roadside pits werepotential breeding habitats of anophelines in and around the study village.Breeding of An. minimus and An. culicifacies was detected in irrigation canal aswell as in streams.

109
Malaria
The time lag between blood slide collection from the field and administration ofradical treatment was found to be high, varying between 3 and 4 weeks. Theprojection of malaria parasite species distribution in the study area by the PHCwas at variance with our findings. While in 1996 till May only 11 out of 57positives were declared as P. falciparum in the study village by the PHC oursurvey revealed Pf percentage to be 99.1.
PHC North Jamuguri, hypo to moderately endemic PHC for malaria with highreceptivity until early 1990s, has been maintaining high endemicity of malariaparticularly in its northern foothill sections adjoining the forest belt since 1993.The increased endemicity was traced to large scale immigration of people fromhigh malarious areas of Assam into the adjoining forest belt in the north of PHCsince late 1992. These immigrants have now settled in this forest after its clearanceand started mixing up with local population. In these forest settlements organisedmalaria control activities are lacking. This population movement fromhyperendemic areas into a receptive but low endemic area might have increasedthe parasitic reservoir and perhaps also introduced newer strains of malaria insurrounding villages thus, making PHC N. Jamuguri vulnerable, ultimatelyresulting in enhanced transmission and creating a permanent epidemic type ofsituation in local residents from 1993 onwards as described by Verdrager. Severalmalaria epidemics in the past have been traced to migration in Orissa, MadhyaPradesh, South Bihar and Rajasthan. The epidemiological data of the PHC clearlypoint towards the unstable malaria situation, due to the prevailing persistenttransmission, which seems to be in the process of stabilization. This observationis supported by, more or less, similar SPR & spleen rates in children and adultsas obtained in the present study.
Salient findings: In this paper the authors have highlighted that following anoutbreak in Assam and reports of deaths due to malaria, the village of Sonitpurin Assam had accelerated incidence of malaria as cases per 1000 populationincreased by 585% in 1995 as compared to 1991. Age distribution of malariashowed that all ages were affected as SPR ranged from 38.0 to 50% and spleenrate was also high and large number of asymptomatic cases were detected.Whereas, the PHC data showed only about 19% Pf cases, the authors found thePf% to be 99.1.
Comments: The study points to the fact that proper diagnosis of malaria was notbeing done by the PHC, there was significant rise in malaria. The spleen rate and

110
Malaria
asymptomatic carriers revealed long history of transmission in the area due towhich deaths might have occurred. Unfortunately number of reported deathshave not been mentioned.
11. Persistent Transmission of Malaria in Sonapur PHC, Kamrup District,Assam
V. DEV AND V.P. SHARMA
Journal of Parasitic DiseasesVol. 19, June 1995, pp. 65 -68
Data on morbidity due to malaria were collected in villages of Sonapur PHCfor the period from January 1988 till December, 1992 through active casedetection. Slide positivity rate in fever cases ranged from 22.93% to 36.46%,and majority (over 74%) were Plasmodium falciparum infections. Malariacases were recorded during all months including those in (0-1) Yr age group,however, there was a consistent high rise in number of cases beginning Maytill September corresponding to monsoon season. The transmission of malariawas perennial and persistent supported by Anopheles minimus and An.fluviatilis. An. minimus was prevalent and sporozoite infections were recordedfor most part of the year, thus this species was re-established as the majorvector. An. fluviatilis occurred in low density and sporozoite infections wereonly seasonal (winter months). High morbidity was attributed due to difficultterrain, low socio-economic conditions, and inadequate interventionmeasures.
Salient findings: In this epidemiological study it has been shown that malaria isperennial in Sonapur PHC of Kamrup district, Assam and it was being transmittedby two vectors Anopheles minimus and An. fluviatilis. The API (85 to 160) andPf% (>74%) were very high.
Comments: Monthly trend of cases has been presented. Age and sex wisedistribution of cases were not separated in the PHC.

111
Malaria
12. Forest Malaria in Madhya Pradesh: Changing Scenario of Disease and itsVectors
N. SINGH* AND K.K. KHARE**
Journal of Parasitic DiseasesVol. 23, December 1999, pp. 105-112
Madhya Pradesh lies in the geographical heart of India. With an area of4,42,841 square kilometers it is the largest state in the country having highesttribal population. It is rural, agricultural state where irrigation facilities arenil. Forests occupy 35% of the total land area of the state and about 22% ofthe total forest area of the country. Large areas have undulating terrain whichremain inaccessible during the rainy season, which is the main transmissionseason of malaria. Persistent malaria is the characteristic feature in mostforested areas and both Plasmodium vivax and P. falciparum are prevalent.However, the proportion of P. falciparum is on increase regularly and theemergence of drug resistance in P. falciparum has further compounded theproblem. Sociological and ecological factors, movement within the forestsand migration are other important features in the dynamics of forest malariatransmission.
Salient Findings: Malaria Incidence data of Madhya Pradesh has been presentedfrom 1976 to 1996. Epidemiological situation of malaria has been analysed infour ecological settings viz., Dense Forests, Forests, Forest fringe and Deforestedarea; highest in the dense forests and lowest in the deforested areas. Deaths dueto malaria ranging from 8-48 per annum have been provided from 1986-1996for the whole state.
Comments: This paper gives details of incidence data of 20 years of MadhyaPradesh, which can be used for disease burden estimation retrospectively providedage-sex distribution of malaria is determined in four different epidemiologicalsettings identified by the authors. Another limitation id that age and sex wisedistribution of deaths has not been provided which is necessary for DALYsestimation.

112
Malaria
13. Epidemiology of malaria outbreak (April/May, 1999) in Titabor PrimaryHealth Centre, district Jorhat (Assam).
ANIL PRAKASH, P.K. MOHAPATRA, D.R. BHATTACHARYYA, C.K.SHANNA, B.K. GOSWAMI, N.C. HAZARIKA & J. MAHANTA
Indian J Med Res 111, Apri12000, pp 121-126
An investigation was undertaken of a malaria outbreak in the Primary HealthCentre Titabor, district Jorhat, Assam during May / June 1999. The fever rate inthe community since March 1999, was 44.4 per cent with an average case loadof 2.5 per family. The fever cases peaked in the third week of May. Slide positiveand slide falciparum rates in mass blood survey, in the study village were 16.1and 14.5 per cent respectively with 90 per cent infection of Plasmodiumfalciparum. Males (SPR 17.5%) suffered relatively more than females (SPR14.7%). Malaria prevalence was significantly less in individuals above 15 yr ofage (SPR 11.0% ) as compared to those below 15 yr (SPR 22.9%). Prevalence ofmalaria as well as mosquito densities in different clusters of the village wereinversely related to the distance from the forested Naga hills. Anopheles minimusand A. dirus were collected in good numbers with comparatively higher densitiesof the former. Several factors like unusual climatic conditions, inadequatesurveillance, unsatisfactory laboratory services and inadequate indoor residualinsecticide spray were instrumental for the outbreak.
Salient Features: In this paper results of a malaria survey following an outbreakin Assam have been presented. There was predominance of P. falciparum. Ageand sex wise distribution of malaria suggested greater incidence in children < 15years of age as compared to > 15 years.
Comments: Malaria cases were distributed according to 4 age groups viz., <5,6-10, 11-15 and >15. Sex wise cases were separated which as in many otherstudies suggested more males than females suffered from malaria.
14. Present Perspectives of Malaria Transmission in Boko Area of Assam
J. NANDI, S.P. MISRA, R. RAJAGOPAL, M.V.V.L. NARASIMHAM
J. Com. Dis., 25(1) : 18-26, 1993

113
Malaria
A longitudinal study on malaria transmission was conducted from January 1984to December 1988 in three villages in Boko PHC of Assam, where indoor residualDDT spray was withdrawn during the period of study. Anopheline faunacomprising of 19 species was identified and their seasonal density estimated.Anopheles philippinensis was the predominant species followed by An. minimus.The principal role of An. minimus in the transmission of malaria and predilectionfor indoor resting in this area was clearly evident. Though An. dirus and An.fluviatilis were found in low density, sporozoite infection was detected in themalong with An. minimus. The high malaria incidence predominantly withPlasmodium falciparum was closely related to sporozoite infection in the vectorsand their densities. The biting cycle of An. minimus was maximum in the firsthalf of the night.
Salient Findings: The work correlates anopheline infection with malariaincidence in different months in Boko area of Assam. In this 5 yearsepidemiological study, it was shown that malaria is perennial problem in thisarea although peak occurs in May to July and SPR continues to remain above20% in the rest of the months.
Comments: This is a detailed study in which 3 vectors have been incriminatedfor their role in malaria transmission in Boko area of Assam. The data on malariaincidence has not been presented in detail and age and sex wise distribution ofcases is not shown.
15. Vector incrimination in Tamulpur primary health centre, district Nalbari,lower Assam during malaria outbreak 1995
A. PRAKASH, P.K. MOHAPATRA & V.K. SRIVASTAVA
Indian J Med Res 103, March 1996, pp 146-149
A widespread outbreak of malaria occurred in different districts of lower Assamin April, 1995. Entomological investigations were carried out in Primary HealthCentre Tamulpur. The worst hit area of Nalbari district. Of thc nine anophelinespecies collected, Anopheles minimus was incriminated as the malaria vector,with sporozoite rate of 6.5 per cent. The slow moving streamlets were identifiedas thc sole breeding places of An. minimus.

114
Malaria
Salient findings: Anopheles minimus was incriminated as vector.
Comments: No epidemiological data is provided except comments that thisstudy was carried out after an out break occurred in Lower Assam.
16. Seasonal Prevalence of Anopheles dirus and Malaria Transmission in aForest Fringed Village of Assam, India
ANIL PRAKASH, D.R. BHATTACHARYYA, P.K. MOHAPATRA and J.MAHANTA
Indian Journal of MalariologyVol. 34. September 1997. pp. 117-125.
Seasonal abundance of Anopheles dirus (s.l.) and malaria prevalence in anisolated forest fringed village was monitored at monthly intervals duringAugust 1995 to July 1996. An. dirus was the only vector species detectedduring the study period. Its density pattern showed distinct seasonality withthe peak occurring in the month of July and very low number during cool drymonths. Positive correlation (r=0.721) was found between the density of An.dirus and the amount of rainfall occurring two weeks prior to the collections.Overall sporozoite rate of 1.6% and parous rate of 64.7% were found in thestudy. Malaria transmission closely followed the density pattern of An. dirusand was seasonal with slide positivity rate and P. falciparum percentage of47 and 83% respectively. Mean malaria prevalence was higher (p < 0.05) infemales.
Salient findings: Incidence of malaria in villages of Dibrugarh district inAssam, age and sex wise distribution of cases, seasonal prevalence havebeen presented. Vector An. dirus was incriminated in different months in1995 and 1996.
Comments: The study is useful in the estimation of DALYs lost due to malariain Assam as meta-analysis of malaria cases distributed in different age groups inboth the sexes could help in comparison of trends in other studies.

115
Malaria
17. An Outbreak of Plasmodium falciparum Malaria due to Anopheles minimusin Central Assam, India.
V. DEV, M.A. ANSARI, C.R. HIRA and K. BARMAN
Indian Journal of MalariologyVol. 38, March-June 2001, pp. 32-38.
Epidemiological investigations were conducted in Nellie subcentre, PHC Jhargaon,under Morigaon district (Assam). The results of fever cases revealed 68 per centslide positivity rate (SPR) and 40 per cent slide falciparum rate (SfR). The Pfproportion was >87 per cent and remaining cases were P. vivax infections. An.minimus was incriminated as a malaria vector during the study period. Thesporozoite rate was 3.08 per cent. The indoor man mosquito contact was 35 perbait/night as against 23 in outdoors. Results of susceptibility test revealed that thevector was still susceptible to both DDT and malathion at discriminating dosages.The study revealed that inadequate surveillance and vector control measures werecontributing factors for malaria outbreak. In view of this, insecticide treated netsmay be introduced to provide cost-effective control of malaria.
Salient Findings: During this outbreak investigation, high proportion of malariacases amongst fever cases (68%) and 40% amongst mass blood surveys. Malariacases have been presented for three age groups viz., 0-4, 5-14 and >15.
Comments: sex wise cases not presented, pf was the predominant species.
18. Problem of Malaria in Relation to Socio-Cultural Diversity in Some EthnicCommunities of Assam and Arunachal Pradesh
P. DUTTA, A.M. KHAN AND J. MAHANTA
Journal of Parasitic DiseasesVol. 23, December 1999,pp. 101-104
Epidemiological studies conducted in some of the tribal inhabited areas of Assamand Arunachal Pradesh reveal that malaria is comparatively high among tribalpopulation. Plasmodium falciparum malaria is predominant over P. vivax

116
Malaria
constituting more than 80% of the total positive cases. All the age groups andboth sexes are affected by malaria. Slide positivity rate among apparently healthyschool children of different ethnic groups ranged from 7.25 to 17.46%. Factorsaffecting high attack rate in different ethnic communities were found to bedifferent. Human ecology, socioeconomic status and housing pattern facilitateman-mosquito contact in some and in others socio-cultural habits, poor healthfacilities and non acceptability of mosquito control measures are responsible forhigh transmission of malaria in these communities.
Salient findings: The study which is conducted in three PHCs in Assam borderingthree districts of Arunachal Pradesh, Nagaland and Meghalya inhabited bydifferent ethnic tribes shows high incidence amongst children and declining withthe increasing ages. The study high lights the presence of afebrile school childrenharbouring malaria in all the three PHCs ranging from 7.5 to 17.5% more beingin males than female children. The age and sex wise break up has been given for<10, 10-20 and > 20 age groups.
Comments: The study is useful in Disease burden estimation particularly YLDpart and if age and sex specific deaths were given it would have been possible tocompute YLL component as well.
19. Epidemiological Observations on Malaria in some parts of Tengakhat PHC,Dibrugarh District, Assam
P. DUTTA, D. R. BHATTACHARYYA and L. P. DUTTA
Indian Journal of MalariologyVol. 28, June 1991, pp. 121-128.
A three-year study carried out in 44 villages (pop. 17,938) reveals seasonaltransmission of malaria i.e., from June to November. The incidence of malariawas high in the year 1988 in comparison to that of 1987 and 1989. P. falciparumwas the predominant species. The population, living in forest fringe areas weremore prone to malaria than the rest. Anopheles nigerrimus, An. kochi, An. karwariand An. philippinensis were most abundant among the 16 anopheline speciescollected. Known vectors of malaria such as An. minimus, An. philippinensis,An. annularis and An. dirus were detected. An. dirus was incriminated as vectorduring this study.

117
Malaria
Salient Findings: Three year epidemiological data was compared, age distributionof malaria has been presented in six age groups for both sexes, An. dirus wasincriminated as vector. Seasonal build up of vector in relation to malaria caseshas been presented.
Comments: The study presents epidemiological data of Dibrugarh district andis useful in working out DALYs based on incidence data presented and age andsex wise distribution of cases presented.
20. Malaria Prevalence in Tea Estates of Brahmaputra Valley of Assam, India
V. DEV AND S. PHOOKAN
Journal of Parasitic DiseasesVol. 20, December 1996, pp. 189-192
Malaria prevalence in tea estates under various circles .of Assam BranchIndian Tea Association has been reported. P. falciparum (PC) was thepredominant parasite species (>66% ) in most tea estates located on theNorth bank of Brahmaputra river whereas on the South bank, in Nagaonand Jorhat Circles, P. vivax outnumbered Pf cases. Outbreak of malariawas attributed due to migration of labourers between gardens and itsadjoining villages. For effective malaria/Pf containment, insecticideimpregnated bed nets were advocated along with early case detection andprompt treatment.
Salient Findings: This study which was carried out in 10 circles and 30 tea estateshighlighted the presence of malaria with SPR ranging from (0-61%) and Pf%up to 100% which indicated malaria was a significant problem in most of the teastates in Assam.
Comments: In this study although 16302 smears were examined for malariaand 6672 were positive (40.92%), unfortunately age sex distribution of caseswas not presented which would have been useful in estimating YLD in tea estatesof Assam. Moreover no data on deaths, if there were any, has been made availablein the paper.
118
Malaria
21. Malaria Survey in Tarajulie Tea Estate and Adjoining Hamlets in SonitpurDistrict, Assam
V. DEV
Indian Journal of MalariologyVol. 33. March 1996. pp. 21-29.
Malaria survey in Tarajulie tea estate (TE) and its adjoining hamlets revealedthat Pf was the predominant parasite species (79%) and morbidity was alarming.Malaria positive cases were recorded in all age groups including infants. However,morbidity was much pronounced in the hamlets than among garden dwellers.Mostly Anopheles minimus were recorded in the day resting collections fromhuman dwellings (indoor) and in overnight man biting catches in the hamlets.From these collections. An. minimus was incriminated and the sporozoite infectionrate was found to be 4.23 per cent. An. minimus were not recorded in the gardenpremises. Thus morbidity in the garden population was attributed to the movementof labourers to and fro between hamlets and the garden premises. The hamletsserved as reservoirs for malaria infection.
Salient findings: In this study the author has compared age wise distribution ofmalaria in the passive collection with age and sex wise distribution of cases onthe basis of mass blood surveys. Malaria has been divided in four age categoriesi..e. <1, 1-5, 5-15 and > 15 years. Migration pattern has been studied and An.minimus was incriminated as vector. Malaria cases was found to be much morein the Tarajulie tea estate than in the adjoining hamlets.
Comments: The study is restricted to a Tea Estate in Assam and its adjoininghamlet and incidence of malaria presented in 5 age groups can be used to studyage distribution of malaria in Sonitpur district of Assam and to workout DALYs.
22. An Epidemiological and Entomological Investigation on malaria Outbreakat Tamulpur PHC, Assam
N.G. DAS. I. BARUAH. S. KAMAL. P.K. SARKAR. S.C. DAS and K.SANTHANAM
Indian Journal of MalariologyVol. 34, September 1997. pp. 164-170.

119
Malaria
Northeast India is well-known for endemicity of malaria. In spite of controlmeasures adopted by National Malaria Eradication Programme (NMEP), theincidence of malaria is increasing day-by-day. This may be due to chloroquineresistant strains of Plasmodium falciparum, difficult terrains, favourable climaticconditions for mosquito breeding, high man-vector contact and low socio-economic status. Chloroquine resistance of P. falciparum have been reportedearlier from Assam, Arunachal Pradesh. Meghalaya and Nagaland by severalworkers. Moreover, recent studies carried out by Jana-Kara et al. and Prakash etal. found P. falciparum the most dominant species of malarial parasites in Assam.In India, about two million cases of malaria are being reported every year by theNMEP. P. falciparum contributes about 35 per cent of total malaria in the country.It is worth mentioning that northeastern region contributes about one-eighth ofthe entire Plasmodium falciparum load of the country.Anopheles dirus and An. minimus are the efficient malaria vectors of northeasternregion. An. minimus, which seems to have either disappeared or scarce in thisregion due to constant insecticidal spray, rapid urbanization, from several statesof northeastern region and re-established its role in malaria transmission.
During April-June, 1995 there was a malaria outbreak in Goalpara. Nalbari andSonitpur districts of Assam, which resulted in heavy casualities. This laboratoryundertook an investigation covering epidemiological and entomological aspectsof malaria in four worst affected villages under Tamulpur PHC in Nalbari districtof Assam.
Tamulpur PHC under Nalbari district lies on northwest part of Assam, sharingan international border with Bhutan. Tamulpur PHC comprises many villagesdominated by local Bodos. Assamese and some migrated population from Nepal.It is a low-lying area and the paddy cultivation is the main occupation of thevillagers. Houses are made up of thatched roofs and walls of split bamboos withmud-plaster. The area is intersected with katcha nallahs, streams with aquaticvegetations, ditches, ponds and paddy fields which provide ideal breeding habitatsfor mosquitoes. The worst malaria affected villages namely, Baitamari, Sontola,Sorubelbari, and Kalabari under Tamulpur PHC were selected for the presentstudy.
Blood slides were collected from the fever cases of all the four villages. Theywere stained and examined under microscope in the field laboratory for rapid

120
Malaria
detection of malarial parasites and early treatment. Epidemiological parameters,such as SPR, SfR, Pf%. age and sex-wise distribution of malaria infection werecalculated and analysed.
Adult mosquitoes were collected from the human dwellings and cattle shedsfrom 1800 to 0600 hrs with the help of 6 volt battery operated CDC miniaturelight traps (Communicable Disease Centre, USA). Simultaneously, two hourlycollection of mosquitoes were done from dusk-to-dawn to determine the peakbiting hour of the vector species. Resting collection of mosquitoes was alsomade in human huts from 0500 to 0700 hrs with the help of aspirator tubes. Thecollected mosquitoes were identified in the field camp using standard keys. Man-hour and per trap night (PTN) density were calculated for important malariavectors. Alive female Anopheles species were dissected to determine their paritystatus by counting the number of dilatations in the overioles and to detectsporozoite infection in the salivary glands.
In epidemiological study, a total of 250 blood slides were collected from thefever cases out of the total study population of about 2834. Of these, 158 bloodslides were found positive for malaria indicating 63.2 per cent positivity rate.Plasmodium falciparum was the most dominant species which formed 93.7 percent and P. vivax contributed 6.3 per cent of the total cases. Similarly, highincidence of P. falciparum was reported earlier from different geographical areasof Assam by several investigators. Analysis of data revealed a little difference inthe incidence of malaria among male and female population indicating slidepositivity rate of 59.8 and 66.4% respectively which is in conformity with theearlier findings of Dutta and Bhattacharyya. Among the four villages, the highestslide positivity rate (SPR) was recorded in Sorubelbari (77.3) followed by Sontola(66.7), Baitamari (59.0) and Kalbari (48.4). Cent per cent P. falciparum caseswere recorded in Sontola, while 93.2, 88.2 and 86.7% in Baitamari, Sorubelbariand Kalbari respectively. .
Maximum number of positive cases of malaria was recorded in the age group of1-10 yrs and minimum in the age group of 51 yrs and above (Table 1). Dutta andRajvir13 also reported high incidence of malaria among children up to the age of14 yrs in north Indian districts. Altogether 6,208 mosquitoes belonging to 19species under 5 genera namely, Anopheles (9), Aedes (2), Armigeres (I), Culex(5) and Mansonia (2) were collected from human dwellings and cattle sheds in19 trap nights (Table 2). The major species encountered were Culex vishnui

121
Malaria
group (3891), Cx. malayi (935), Anopheles vagus (341), An. annularis (195),Cx. bitaeniorhynchus (107) and An. minimus (105). Anophelines formed 16.45per cent of the total collections. Per trap night density of anophelines in humandwelling and cattle shed were 42.33 and 55.88 respectively. Among anophelines,An. vagus was the dominant species (33.4%) followed by An. annularis (19.10%).An.culicifacies (10.68%) and An. minimus (10.28%) (Table 3). Per trap nightcollection of known malaria vectors namely An. annularis, An. culicifacies andAn. minimus were relatively high in cattlesheds than in human dwellings. Similarobservations were made from the other parts of northeastern region. These specieswere found to rest indoor with a man hour density of 1.53. 0.83 and 0.57respectively. The study on the biting activity of malaria vectors revealed that An.minimus starts biting from 2200 hrs and continued up to 0400 hrs with a peakbetween midnight and 0200 hrs. In contrast. Bhatnagar et al. found peak bitingof An. minimus in the first part of night during dry season and late part of night inthe wet season in foothills of Nagaland. Similarly. High density of An. minimuswas observed from 2000 to 0400 hrs with a peak between midnight and 0200 hrsin Tuichang9 and between 2200 and 2400 hrs in Tlabongl6 in south Mizoramduring wet season. In confirmation of earlier observations of Bhatt et al.l,7 thepresent study also revealed that An. annularis and An. culicifacies bites throughoutthe night With a peak biting activity between 2200 and 0200 hrs. A total of 98An. culicifacies, 91 An. minimus and 41 An. annularis were dissected but nonewas found positive for sporozoites in the salivary glands. High parity rate of An.minimus (73%), An. culicifacies (70%) and An. annularis (65%) indicate theirpotentiality as vector(s) in the present epidemic. Prakash et al. confirmed therole of An. minimus as a vector during the same epidemic at Tamulpur. Profusebreeding of An. culicifacies and An. minimus was found in the grassy margins ofslow flowing katcha nallahs, streams and paddy fields. Das et al. reported thebreeding of An. minimus from streams/rivers in Mizoram. Vas Dev has observedthe breeding of An. minimus in the streams/streamlets in the grassy margins andpaddy fields, while An. culicifacies only in paddy fields in Sonapur, Assam.
An. minimus and An. culicifacies were found susceptible to 4% DDT as cent percent mortality was observed within two hours of holding (recovery) period. Incase of An. annularis, 82% mortality was recorded after 24 h of recovery periodwhich required further verification for its resistant status. However, resistanceof this species to 4% DDT had been already reported from Tezpur.
High parasitic load in the community, high density and long survival of vector(s}may be responsible for the present outbreak of malaria at Tamalpur. Unlike other

122
Malaria
parts of the country, the major malaria vectors are still susceptible to 4% DDT inAssam. Thus, reasonable coverage and methodical spray of insecticides coupledwith the reduction of parasitic load in the community may be effective oncontrolling malaria in the region present outbreak of malaria at Tamulpur.
Salient Findings: Very high incidence (SPR 63%) of malaria was found duringinvestigation of malaria outbreak in Tumulpur PHC in Nalbari district of Assam.Age wise distribution of cases has been given for 6 age groups. Sex wisedistribution of cases is not given.
Comments: If the sex wise distribution were known, the study would have beenmore useful. Nevertheless it can be used for case distribution.
23. Malaria Survey in Some Parts of Namsang Circle of Tirap District,Arunachal Pradesh
P. DUTTA AND D. R. BHATTACHARYYA
J. Com. Dis., 22 (2): 92-97, 1990
A study on malaria conducted in Namsang Circle of Tirap District (ArunachalPradesh) during April-October 1986 revealed that the malaria incidence due toPlasmodium falciparum was considerably high. RII level of chloroquine resistancewas also found among the P. falciparum cases studied by WHO In-vivo test. Inentomological survey, Anopheles maculates was collected more than other 10anopheline species were encountered. A. minimus was detected and incriminatedas a vector species.
Salient findings: In this study age and sex wise distribution of malaria in Tiraphas been given and SPR and SfR have been calculated for both sexes in 6 agegroups including <1, 1-10, 11-20, 21-30, 31-50 and 51 and above.
Comments: The sample size of blood examined in this point prevalence studywas although small, yet the study indicates that malaria was maximum in 11-20age group followed by 21-30 years age.

123
Malaria
24. Entomological and Epidemiological Studies on Malaria in Rajmahal Range,Bihar
N.G. DAS, M. BHUYAN and S.C. DAS
Indian Journal of MalariologyVol. 37, September-December 2000, pp. 88-96.
The epidemiological investigations carried out in six tribal villages in Rajmahalrange hill in south Bihar revealed average slide positivity rate (SPR) 25.1ranging between 9.8 and 37.8 per cent. Plasmodium falciparum was thedominant parasite, which accounted 64.2 per cent of the total infections. Resultsof mass blood survey indicated the presence of high percentage of asymptomaticcarriers of malaria parasites in the local populace. In an entomological survey,25 species of mosquitoes under five genera were collected in 20 trap nights.The average density of mosquitoes recorded was 230.6 per trap night. Anophelesmosquitoes alone accounted 72.8 per cent of the total collection whereas malariavectors Anopheles maculatus, An. minimus, An. philippinensis, An. varuna andAn. annularis accounted 32.8 per cent of the total anophelines collected. Bothanopheline and culicine mosquitoes were found susceptible to DDT (4 percent) and malathion (5per cent) in 30 min exposure. Dissection of malariavectors An. minimus, An. maculates and An. philippinensis revealed very highpercentage of parity rate (77.8 per cent), which gives a strong indication abouttheir vectorial status in the transmission of malaria. Poor socio-economiccondition, lack of sense of hygiene worsen the situation in the presence ofasymptomatic carriers.
Salient findings: In this study malaria incidence has been reported in tribal villagesand entomological investigations have been done.
Comments: The authors have segregated cases in 5 age classes <5, 6-10, 11-15, 16-20 and >21 years of age groups but not for each sex within theseclasses. The total cases have been divided amongst male and females. Thestudy is useful in making age wise assessment of malaria incidence in thisregion.

124
Malaria
25. Epidemiological importance of younger age group during malaria epidemicin PHC Tamulpur, Assam
P.K. MOHAPATRA, ANIL PRAKASH, D.R BHATTACHARYYA ANDJ. MAHANTA*
J. Commun. Dis. 30(4) 229-232
An investigation of a malaria epidemic was carried out in Tamulpur PrimaryHealth Centre, district Nalbari, Assam during April 1995. The analysis revealedthat children between 3 and 12 years of age, who were treated and who recoveredclinically from fever during the epidemic were instrumental in the progressionof the epidemic by acting as Plasmodium falciparum gametocyte reservoirs.Special efforts are required for treatment of children below 12 years during anepidemic.
Salient findings: This study shows how following an epidemic, malaria parasitereservoir is created and asymptomatic carriers silently promote transmission.
Comments: Age and sex wise distribution of malaria cases with and withouthistory of fever are segregated to show gametocyte carriers amongst asymptomaticcases and their possible role in enhancing transmission. The study suggests thatasymptomatic malaria which may exist in significant proportions could causeextended disability and subnormal performance in the patients.
26. Epidemiological Observations on Malaria in Some Parts of Darrang District,Assam
S. KAMAL and S.C. DAS
Indian Journal of MalariologyVol. 38, March-June 2001, pp. 25-31
A study on malaria conducted in tribal villages of Darrang district, Assam duringApril 1994 to March 1995 revealed that the malaria incidence due to Plasmodiumfalciparum was considerably high. Slide positivity rate (SPR) ranged between

125
Malaria
2.3 to 45.67 per cent with transmission from May to October. P. falciparum wasthe dominant species (91.7 per cent ) followed by P. vivax (7.25 per cent) andmixed infection (Pv +Pf = 1.05 per cent). Malaria cases were recorded throughoutthe year in all the age groups including infants, however, age groups between 0-1 and 21-30 years were more affected. Among 17 anophelines collected,Anopheles vagus, An. jamesii, An. crawfordi and An. minimus were the mostabundant species. Known vectors of malaria like An. annularis, An. culicifacies,An. minimus, An. philippinensis and An. varuna were detected. Perennialtransmission of malaria was attributed to low socio-economic conditions, poorsurveillance and inadequate intervention measures.
Salient Findings: On the basis of surveys conducted in 4 villages of Darangdistrict, age distribution of malaria has been presented for 7 age groups viz., <1,1-10, 11-20, 21-30, 31-40, 41-50 and >51.
Comments: The data presented gives indication of age distribution of malaria,although gender wise distribution is not presented. The study along with other studiesconducted can be of help in meta-analysis of age distribution of malaria in Assam.
27. Present Status of Plasmodium malariae Infection in Bastar District (M.P.)
R. PANDA, K. V. S. VERMA.. AND S. J. RAHMAN.
J. Com. Dis., 22 (3): 185-190. 1990
Plasmodium malariae infection was detected in Bastar district (M.P.) duringmalaria survey in 1981-83. The data collected during the survey was comparedwith the earlier records of P. malariae infection in the area. From the data it canbe seen that the infection in this area has declined due to the ecological/developmental activities undertaken by Government. All the cases were foundto be indigenous and approximately 62 per cent infection was found in age groupof 10-14 years irrespective of sex. More than 60 per cent of P. malariae infectionswere positive for gametocytes. Three day regimen of 4-amino-quinolines for thetreatment was found quite effective.
Salient Findings: The paper highlights the presence of indigenously transmittedP. malariae which was 2% of the total cases although Pf proportion was 74%and Pv 24%. The authors have also analysed 13 cases according to age and sexes

126
Malaria
and found that 61.5% cases of Pm were detected below 14 years of age. Therewas no difference between the sexes.
Comments: The paper presents incidence of P. malariae, which is distributedin pockets in India and perhaps underestimated. The species can cause chronicinfection with the involvement of kidneys and may cause long disability as adisease sequela. Age and sex wise distribution of the cases is useful althoughsample size is small.
28. Quartan Malaria-An Investigation on the Incidence of Plasmodium malariaein Bisra PHC, District Sundargarh, Orissa
R.S. YADAV. V .P .SHARMA .S.K. GHOSH and A. KUMAR
Indian Journal of MalariologyVol. 27, June 1990, pp. 85-94.
A longitudinal study on the incidence of P. malariae was taken up from September1988 to December 1989 in Bisra block, District Sundargarh, Orissa covering38,615 population, which is mainly tribal. The area is a known hard-coremalarious region in the Garhjat hill range in eastern India. In this study, out of22,217 blood smears examined through weekly active surveillance, 7362 (33.1%)were found malaria parasite positive. Out of the total positive cases, 82 (1.1%)were P. malariae. These occurred mostly (91.4%) in persons below 40 years ofage and children below 9 years accounted for 36.6% of total quartan malariacases. In this age group the disease was found to be associated with splenomegaly(average enlarged spleen 2.07; spleen rate 45.9%) and 9 out of 13 mixed infectionsof P. malariae with P. falciparum and/or P. vivax were detected from this agegroup. This is the first report of quartan malaria from this area.
Salient findings: This study highlights the quantum of P. malariae in atribal pocket in Bisra, District Sundergarh. Although it constituted 1.1%(82 cases) either alone or in combination with other two prevalent species,P. malariae was in good proportion (36.6%) in chronic form in children <9 years having high rate of splenomegaly. The young age of many patientswith P. malariae and mixed infection with other species was suggestive ofrecent indigenous transmission.

127
Malaria
The incidence was 2.12 per 1000 population which is appreciably high.
Comments: The study suggests that disability due to P. malariae may be formuch longer duration when it causes chronic infection than other two species Pvand Pf especially when they cause acute infections and there are greater chancesof detection and treatment. In DALYs estimation therefore this factor should begiven due consideration. Age distribution of cases and its relation withparasiaemia has been shown.
29. Studies on Malaria Transmission in Hutments of Delhi
V.P. SHARMA, H. C. UPRETY, P.K. SRIVASTAVA and R.K. CHANDRAHAS
Indian Journal of MalariologyVol. 22, December 1985, pp. 77-84.
Parasitological surveys in the itinerant labour camps of Delhi revealed that malariawas one of the most common causes of morbidity. P. vivax cases start early inspring and reach high numbers in August-September. During the same period, asudden spurt in falciparum malaria results in high morbidity due to falciparumand vivax malaria. In later months, the incidence of P. vivax goes down butfalciparum malaria remains at that level till the onset of extreme winter. A.stephensi was incriminated as the vector in September 1983. Studies broughtout the importance of hutments in the epidemiology of malaria in Delhi.
Salient findings: This is one year longitudinal study during which 7191 smearswere collected and 2851 (39%) were positive for malaria with Pf% of 16.31.Age and sex wise distribution of malaria revealed males of 15-24 years sufferedthe most whereas females of 9-14 years suffered the most. Overall male sufferedmore than females.
Comments: Malaria was high in the hutment in 1982-83. Age and sex wiseincidnce has been presented. P. vivax was predominant. Study is useful inretrospective estimation of DALYs during outbreak as population data accordingto different ages and sexes has been provided in this comprehensive study.

128
Malaria
30. Malaria in Stone Quarry Area of Faridabad Complex (Haryana)
S.N. SHARMA
Indian Journal of MalariologyVol. 30, September 1993, pp. 113-117.
An analysis of five-year (1987-91) epidemiological data showed that the stonequarries contributed, on an average, 38.7% of malaria cases to the total ofFaridabad Town and 11.6% total of Faridabad district. Various malariometricindices like Annual Parasite Incidence (API), Anua1 Blood Examination Rate(ABER), Slide Positivity Rate (SPR) and Slide falciparum Rate (SfR) wereanalysed to assess the endemicity of disease, and attempts were made to comparethem with the malaria parameters of the town and then of the district. Migrantpopulation working as labour in stone quarries resides in areas conducive tomalaria and hence the need for intensive control measures.
Salient Findings: The paper highlights the incidence of malaria in stone quarriesworkers who were migrants from neighbouring states and their contribution tothe Faridabad district of Haryana. Annual incidence of Faridabad district,Faridabad complex and stone quarry area has been presented from 1987 to 1991.
Comments: The data is of limited use for estimation of DALYs as there is nomention of age and sex wise distribution of incidence cases. Deaths due to malariaif any have not been mentioned.
31. Epidemiological Study of Malaria Outbreak in a Hotel Construction Site ofDelhi
T. ADAK. C.P. BATRA. P.K. MITTAL and V.P. SHARMA
Indian Journal of MalariologyVol.31. September 1994, pp. 126-131.
Delhi is situated in the malaria epidemic zone of Indian subcontinent. Focaloutbreaks of malaria have been reported in different parts of Delhi as a result

129
Malaria
of unplanned urbanization and industrialization with aggregation of largemigratory labour. An in-depth account of prevailing mosquitogenic potentialin Delhi and urgent remedial measures for malaria control programme forthe capital city have been recommended by Kalra and Sharma in 1987.However, the incidence of malaria is increasing progressively and the othermost disturbing feature is the appearance of chloroquine resistant P.falciparum and reported resistance to long acting sulphonamide/pyrimethamine combination.
An outbreak of febrile illness was detected during October 1992 in a five starhotel construction site in South Delhi. Owing to this an epidemiologicalinvestigation was initiated for precise determination of the causative agent ofthe fever epidemic, estimation of its magnitude, to determine the mechanism ofits transmission and consequences. The first report of the fever was recorded on22 October 1992 at Malaria Research Centre Clinic. Subsequently,epidemiological investigations were carried out approximately for one monthduring October-November 1992 in the hutments located within and around thehotel construction site. Information was collected during the epidemiologicalstudy pertaining to demography and source of labour immigration, fevermorbidity, diagnosis and treatment, mosquito species prevalence and vectorincrimination. The fever morbidity of labour population were recorded by door-to-door surveillance of hutments in and around the construction site and thediagnosis of malaria was made by microscopic examination of blood smearswith standard JSB staining. All P. vivax positive cases were treated with 900 mgof chloroquine in divided doses, whereas P. falciparum positive cases were treatedwith 1500 mg chloroquine and doses for infants and children were adjustedaccordingly.
Adult mosquito collections were carried out both at early morning (0600-0900hrs) and at night (2100-0100 hrs) by hand collection technique. All watercollections in and around the study area were searched for larval breeding. Larvaewere collected using laddIes and pippets and reared in the laboratory forsubsequent species identification. Adult vectors collected from the study sitewere dissected for detection of oocysts and sporozoites. Eggs from individualprogeny of An. stephensi were checked for number of ridges in the egg float toidentify mysorensis/type form14.15.

130
Malaria
A total of 462 migrant labourer population involved in construction activitieshailing from 51 districts belonging to eight states of India and neighbouringcountry Nepal were screened. They were living with extremely poor communityfacilities in the basement and sub-basement of the hotel. Out of 462 peoplesurveyed 52% migrants were from Uttar Pradesh, 21% from Bihar, 15% fromOrissa, 5% from Rajasthan and rest 7% were from other states of the country.Some of these labourers had paid frequent visits to their native places in thepreceding two years. On an average the migrants had stayed at their native placesfor 8 to 10 weeks.
Results of blood smear examination of fever cases among these labourers andthose living in the hutments around the hotel revealed high incidence of malaria.Blood smears from a total of 188 fever cases were examined for the presence ofparasitaemia. Out of which 113 cases were found positive. Of these 83 werepositive for P. falciparum, 27 for P. vivax and 3 had mixed infection.
Larval surveys revealed the presence of Culex spp. Aedes aegypti and An.subpictus breeding besides An. stephensi, in three types of water collections i.e.curing tanks, stagnant water used for curing of roof and borrow- pits createdwithin the project. Adult mosquito collection included Culex quinquefasciatus,Aedes aegypti, An. subpictus and An. stephensL Of these, two An. stephensiwere incriminated for gland and for gut infection. Among the two common vectorspecies, An. culicifacies and An. stephensi prevalent in Delhi, the lalter has beenfound to be associated with focal outbreaks particularly in construction sites,due to its high breeding potential . Similarly, in the present epidemic, An. stephensiwas found to be involved in active transmission even at very low density. It maybe mentioned that egg ridge revealed the presence of An. stephensi type form(ridge number > 16).
Magnitude of malaria morbidity did not show any correlation with the state ofimmigration in the present epidemic, suggesting that different levels of malariaimmunity in the one labour population, if existed was not of any protectivesignificance. In the present investigation 13.76% of the total labour populationwere from 4 hardcore districts of Orissa namely Dhenkanal, Sambalpur, Kalahandiand Sundergarh from where Pf resistant cases have been reported. In our studytwo Pf resistant cases were suspected suggesting malaria infection being importedto Delhi through these labourers leading to focal outbreak.

131
Malaria
Salient findings: The study suggests high incidence of malaria in a constructioncomplex in migrant labour with the evidence of chloroquine resistance.Themoxomg of labour from many states with different endemicities to malariaresulted in epidemic with SPR > 60%.
Comments: The paper shows the accelerated transmission of malaria in aconstruction complex. Data has been presented for hotel construction site,settlement colony and labour colony but age sex wise distribution of cases hasnot been given. The study suggests that malaria in urban areas could be asignificant problem particularly development zones in construction complexes.
32. Follow up Studies of Malaria Epidemic in Villages of Shahjahanpur District,U.P.
V.P. SHARMA, R.K. CHANDRAHAS, B.N. NAG PAL and P.K. SRIVASTAVA
Indian Journal of MalariologyVol. 22, December 1985, pp. 119-121
During 1983 deaths occurred due to malaria in 38 villages of Shahjahanpur district(Negoyi and Tilhar PHCs). Within three months (August to October) there were249 deaths in Negoyi PHC and 96 deaths in Tilhar PHC from all causes. Soonafter the report of deaths, Malaria Research Centre (MRC) undertookepidemiological studies in eight affected villages of Negoyi PHC. Studies revealedthat despite intensive antimalaria measures undertaken by the NMEP, the slidepositivity rate (SPR) in the fever survey was 75.3% and Pf% was 96.1. Resultsof blood smear examination of the family members of the deceased in 5 villagesshowed that out of 396 blood smears collected, 214 were positive for P. falciparumand 9 for P. vivax. Therefore, the likely cause of most of the deaths was falciparummalaria (Chandrahas and Sharma, 1983). This was the situation of malaria whenthe villages were sprayed with 3 rounds of BHC at 200 mg/m2 in 1983. To preventfurther deaths, the National Malaria Eradication Programme (NMEP) undertookadditional malaria control measures in the affected villages by giving fever radicaltreatment (FRT) and mass radical treatment (MRT) in the affected villages during1983 and 1984.

132
Malaria
During 1984, NMEP further intensified anti-malaria work in the affected villages.This was done by improving the spraying, surveillance arid drug distributionsystem. During 1984 a special round of BHC was sprayed in March followed bythree other rounds of BHC. A similar spraying schedule is being followed in1985. Antimalarial drugs were easily available in villages through the drugdistribution centres and the fever treatment depots. Radical treatment of theparasite positive cases was administered more effectively. The impact of thesemeasures was checked by the MRC during 1984 and 1985. Results of this studyare briefly summarized below.
Parasitological surveys were carried out in six villages in September-October 1984 and in eight villages in May 1985. During 1984, 247 bloodsmears were collected from the fever cases. Of these, 114 slides werepositive for the malaria parasite viz., 27 P. vivax and 87 P. falciparum. Theslide positivity rate (SPR) averaged 46.2 (range 31.5-65.4%). Mass bloodsurvey was carried out in 3590 population during the same period. A totalof 1317 blood smears were collected. Of these, 88 blood smears werepositive for P. vivax and 179 for P. falciparum. The SPR was 20.3 and Pf%was 67.0. During May 1985 before the commencement of the transmissionseason, 145 blood smears were collected from fever cases. Of these 57were positive for malaria parasites i.e. 54 for P. vivax and 3 for P. falciparumand the SPR was 39.3%. Following the 1983 epidemic, observation in 1984revealed that intensive antimalaria measures were not effective ininterrupting transmission and observation during May 1985 confirmed thatthe parasite load in the community was high with moderate to high vectordensities and that any significant change in the disease incidence or itspattern is unlikely to occur. Under the circumstances a change in the malariacontrol strategy is warranted.
Salient Findings: The study reveals that there was high incidence of malaria inthe 38 villages of Shahjahanpur in Uttar Pradesh state in 1985 despite antimalarialmeasures undertaken in 1983 and 1984.
Comments: No age and sex wise distribution of incidence cases and deathshave been provided. The study as such would be of limited values in the estimationof DALYs estimation.

133
Malaria
33. Malaria Situation in Meerut district Villages, U. P.
M.A. ANSARI, V.P. SHARMA, R.K. RAZDAN and C.P. BATRA
Indian Journal of MalariologyVol. 23, December 1986, pp. 147-150.
Following news of deaths due to malaria, an investigation into the causes wascarried out in Rohta and Jani PHCs. Results of the study are reported below.
Blood smears from fever cases and contacts of deceased patients were collected.Children between 2-12 years were examined for spleen enlargement. Anophelinemosquitoes were dissected for gut or gland infection. Susceptibility of A.culicifacies adults to insecticides was tested following the WHO procedure.
Parasitological surveys were carried out for a few days in each village andprevalence of malaria was compared with the data collected by the DMO forthat month (Table I). The incidence of falciparum malaria was extremely high inall the affected villages. In November 1983, of the 311 blood smears collectedfrom fever cases, 237 were positive for malaria parasite. The slide positivity ratewas 76.2% and parasite formula was 4.21% P. vivax, 95.3% P. falciparum and0.4% mixed infection. During the next transmission season in July and August1984, 687 slides were collected from fever cases and 335 were positive formalaria. The slide positivity rate was 48.7% and parasite formula was 38.5% P.vivax, 60.2% P. falciparum and 1.19% mixed infection. Falciparum malaria was100 per cent in Jangethi village and 93.02%. 92.1% and 94.5% in Dayampur.Dobka and Zakhera villages respectively. Malaria cases recorded by the DistrictMalaria Officer based on active case detection (ACD) at an interval of 15 dayswere negligible because of poor surveillance and/or laboratory services. It mayalso be noted that ACD would miss afebrile cases and half of the cases detectedwere afebrile and asymptomatic.
Further proof of high endemicity to malaria was obtained by examination ofenlarged spleen and blood tests of children between 2-12 years. Of the 305 childrenexamined from Jangethi. Dayampur and Zakhera villages. 56 had enlarged spleen.The average spleen (AS) was 0.26, 1.15 and 0.84 in Jangethi. Dayampur andZakhera villages respectively. Similarly the proportion of afebrile cases found

134
Malaria
positive for malaria parasite was 22.2. 53.8 and 55.0 per cent in Jangethi,Dayampur and Zakhera villages respectively.
During investigations 32 deaths were investigated from Jangethi, Dayampur andZakhera villages. Results of blood smears collected from the houses of thedeceased revealed that out of 113 slides collected. 51 were positive for P.falciparum. The most likely cause of these deaths was probably malaria, a situationsimilar to Shahjahanpur (Chandrahas and Sharma. 1983; Sharma et al., 1985)and Bareilly (Ansari et al.1984).
Entomological observations revealed that among the anopheline mosquitoes A.culicifacies, A. stephensi, A. annularis, A. pallidus and A. subpictus were thecommonly encountered species. During November 1983, A. culicifacies was thedominant species and the per man hour (PMH) densities ranged between 8.8 to24.6, whereas A. stephensi populations were negligible.During July-August 1984very high A. culicifacies densities ranging between 18.0 to 113.0 wereencountered. Dissection of A. culicifacies revealed four positive mosquitoes outof 816 dissected from Jangethi village. A. culicifacies was therefore responsiblefor maintaining high malaria trans-mission.
Salient findings: This investigative study suggests that there was high incidenceof malaria as against very less according to the records of Jani and Rohta PHCsin Meerut District. The incidence was high and spleen was enlarged in goodproportion of children.
Comments: The study is yet another example of under reporting of malariacases. The age and sex wise distribution of malaria cases has not been presented.Although study mentions investigation of 32 deaths, no information on age andsex wise deaths was presented.
34. Epidemic of Malaria in Barmer District (Thar Desert) of Rajasthan during1990
K.K. MATHUR, G. HARPALANI, N.L. KALRA, G.G.K. MURTHY andM. V. V. L. NARASIMHAM
Indian Journal of MalariologyVol. 29, March 1992, pp. 1-10.

135
Malaria
Barmer district of Rajasthan in Thar desert and hitherto a hypoendemic area formalaria came in the grip of a severe malaria epidemic during 1990. The epidemicoccurred as an aftermath of floods, preceded by normal rains during 1988 and1989 after a prolonged drought phase. The epidemic was spread over the wholedistrict including Barmer town. Annual Parasite Incidence (API) and AnnualFalciparum Incidence (AFI) for the district touched record figures of 17.20 and5.83 respectively while for the Barmer town they were 36.5 and 14.0 respectively.Out of the eight PHCs, Baitu PHC was the Worst affected where the two indicestouched all-time high figures of 55.3 and 19.6 per cent respectively. A total of122 infants were reported Positive for malaria, of which 103 were contributedby Baitu PHC alone. Eighty per cent infant positivity was spread over Septemberand November, indicating a high rate of transmission. A total of 47 deaths due tocerebral malaria were reported. However, in view of the high infectivity amonginfants and paediatric groups there was a strong possibility of deaths amongthese groups, which could not be verified.
Entomological findings revealed that a sudden increase in An. culicifaciesdensities due to extensive breeding potential, as a sequel to floods, activated thetransmission, which was maintained at a low level by An. stephensi, predominantin this desert region. Other factors which contributed to the intensity and extentof epidemic were the return of drought-migrated population from malarious areas,low cattle density, malaria non-immune population, inadequate and poor spraycoverage and delayed radical treatment. Insecticide adult susceptibility testsrevealed a high degree of resistance in An. stephensi against DDT and dieldrin.
Salient Findings: The study highlights the build up of epidemic in BarmerRajasthan due to flooding. Malaria incidence of Barmer district from 1977 to1990 has been provided and presented in relation to rainfall. Factors responsiblefor epidemic have been elucidated. Incidence data of 12 PHCs has been mentionedfrom years 1984 to 1990. Age and sex wise malaria cases have been presentedfor Baitu PHC.
Comments: The study provides incidence data of Barmer district for 14 years. Ageand sex wise distribution has been provided. Study reports 47 deaths due to malariabesides which there were unconfirmed deaths in infants. 87% of deaths were foundto be above 16 years of age. Convulsions, neck rigidity and anaemia were common.Although details of age and sex wise distribution of deaths is not provided yet thedata is of value in estimation of malaria burden in Barmer district of Rajasthan.

136
Malaria
35. Recent Epidemiological status of malaria in Calcutta Municipal CorporationArea, West Bengal
A.K. MUKHOPADHYAY, P. KARMAKAR. A.K. HATI and P. DEY
Indian Journal of MalariologyVol. 34, December 1997, pp. 188-196.
In Calcutta, Plasmodium falciparum cases and death due to malaria showremarkably increasing trend since 1990. The incidence of P. falciparum malariahas increased more than eleven folds in 1996 in comparison to 1990, with 0, 0,0, 3, 7, 52 and 17 deaths in 1990, 1991, 1992, 1993, 1994, 1995 and 1996respectively. Situation is more serious than what it is projected in official recordsas annual blood examination rate (ABER) in Calcutta Municipal area is poor,varying from 1.5 to 3.9 in 1993 and 1996 respectively. This is further evidentfrom the fact that in a study area in 19 months (January 1995 to July 1996) theslide positivity rate (SPR) was 47.94% on an average 28.72% suffer from P.falciparum infection (as low as 0.5% in June 1996 and as high as 71.5% inNovember 1996). For the first time resistance of P. falciparum to chloroquinehas been noted at RII and RIII level. The response of the same parasite strain tosulfa-pyrimetharnine combination drug is very much promising. Fresh infectionis occurring in all the months of the year and the favourable period is from Julyto November 1995 that is corroborating with Container index and Breteau indexrelated to the vector mosquito Anopheles. Susceptibility status of An. stephensiindicates that the mosquito species has acquired resistance to DDT, BHC,propoxure and malathion but is still susceptible to fenthion and deltamethrin.
Salient Findings: This paper highlights epidemic of malaria in Calcutta citywherein deaths were reported from 1993 to 1996. The data of annual incidencecases and deaths in West Bengal and Calcutta city has been given from 1990 to1997. The monthly data of 1995 an 1996 has been presented which indicatesperennial transmission and high SPR (27.6 to 69.4%) in different months. The P.falciparum strain showed resistance to chloroquine up to RIII level.
Comments: The incidence and death data will be helpful but it would have beenof more value from Disease burden estimation point of view had there been ageand sex wise distribution of malaria cases and deaths.
137
Malaria
36. Malaria outbreak in lower Assam: An Epidemiological Appraisal
P. K. MOHAPATRA, A. PRAKASH, H.K. DAS, J. MAHANTA AND V.K.SRIVASTAVA
Journal of Parasitic DiseasesVol. 19, December 1995, pp. 175-178
A widespread outbreak of malaria in lower Assam during 1995 was investigatedin a worst hit Primary Health Centre (PHC) Tamulpur of district Nalbari. ThisPHC reported 30 deaths mostly in children under 10 years of age. The incidenceof fever in the study population since the onset of epidemic was 41.2% with anaverage case load of 2.6 per family. The outbreak started from last week of Marchand reached its peak in the third week of April. The majority of cases (56%)were below 20 years of age. The commonest symptom complex (fever, chill andrigor with headache) was presented by 61.2% cases. The blood slide examinationof the study population irrespective of fever status showed SPR and SfR of 26.1and 19.2 respectively. The asymptomatic malaria was as high as 19.5%. A highmosquitogenic potential coupled with surveillance failure, poor laboratory serviceand high refusal for DDT spray by the community were identified as the factorsresponsible for the outbreak.
Salient findings: The paper highlights steep rise in the incidence in TamalpurPHC in 1995. The 30 reported deaths have been presented age group wise andmaximum deaths were reported from children below 10 years of age.
Comments: Malaria incidence of 5 years (1991-94) has been presented prior tosevere epidemic in 1995. Age wise distribution of deaths has been given but sexwise not mentioned with in thse gae categories.
37. A Study on Clinical Profile of Falciparum Malaria in a Tertiary Care Hospitalin South India
V.K. HARRIS, VIJAY S. RlCHARD, ELIZABETH MATHAI, USHA SITARAM,K. VIJAYA KUMAR, A.M. CHERIAN, S.M. AMELIA and G. ANAND
Indian Journal of MalariologyVol. 38, March-June 2001, pp. 19-24.

138
Malaria
Malaria continues to be a major problem in tropical countries. To study theclinical features and complications of malaria in a tertiary care hospital in southIndia, records of 183 patients were analysed. Among 86 patients with P.falciparum and mixed infection, 24 (28 per cent) had cerebral malaria and 32(37 per cent) had hyperbilirubinemia. Twenty-three out of 32 (72 per cent) patientswith jaundice had direct hyperbilirubinemia and elevated liver enzymessuggesting hepatocellular damage. Mortality of the order of 10 per cent wasseen only in P. falciparum malaria. High incidence of hepatic involvement andhepatorenal failure were the unusual features observed in the study.
Salient Findings: In this hospital based study the case fatality rate of 10% wasobserved. 28% of Pf cases had cerebral malaria. The most notable feature is that32 (18%) of the total cases (29 i.e 41% all Pf and 3 i.e. 19% mix) had Jaundiceand 30% had anaemia (<8 g%). The cases were from Tamil Nadu, Andhra Pradesh,Karnataka, Kerala, West Bengal, Orissa, Assam and Tripura.
Comments: The study is useful in estimating case fatality rate and causes ofmalaria mortality. It brings to light high proportion of Jaundice and anaemiacases thus useful in knowing sequelae due to malaria. The limitation of the studyis that age and sex distribution of malaria cases both with and withoutcomplications, and deaths have not been presented.
38. Cerebral malaria in Jabalpur, India.
M.M. SHUKLA. NEERU SINGH. M.P. SINGH. B.M. TE.JWANI, D.K.SRIVASTAVA and V.P. SHARMA
Indian Journal of MalariologyVol. 32. June 1995, pp. 70- 75.
A total of 1783 patients were admitted in Govt. Medical College Hospital Jabalpurwith fever in 1993. Out of these 152 (8.5%) patients had cerebral malaria ofwhich 39 (25.6%) patients died. Age and sex-wise break-up indicated that malessuffered more (p<0.01) from malaria and majority of patients belonged to 16-40yrs age-group. Mortality was significantly higher in patients with hyper-parasitaemia, hypoglycaemia and delayed diagnosis and treatment. Comatosecondition was the main determinant of death.

139
Malaria
Salient findings: This hospital based study highlights the age and sex wisedistribution of malaria cases admitted with different complications of P.falicparum. It also gives account and numbers of patients showing varioussymptoms and other clinical findings such as bleeding, severe anaemia, renalfailure, jaundice, hypoglycaemia, hyper-parasitaemia and unconsciousness/comaand those who died due to various complications.
Comments: This is very useful study in that it gives case fatality rate amongstcomplicated malaria cases and various disease manifestations. It also mentionsproportion of patients suffering from anaemia which is an important sequelae.However there is no mention of neurological disorder amongst acomatose patientswho might have been followed up after treatment.
39. Malaria during Pregnancy and its Effects on Foetus in a Tribal Area ofKoraput District,Orissa
L.K. DAS
Indian Journal of MalariologyVol .37,March-June2000,pp.II-I7.
Malaria during pregnancy and its maternal and foetal complications was studiedin Koraput district of Orissa-a tribal area, endemic for malaria. A total of 209pregnant women with 738 pregnancy months were studied. The parasitic indexamong the pregnant women ranged between 10.8 and 25.6 per cent with peakincidence during post-monsoon months. There was a significant difference inparasite incidence between the primi- and multigravidae (p<0.05) but differencewas not observed between the trimesters. The mean haemoglobin (Hb)concentration declined to 8.4 g/dl (range 7.2-10.2 g/dl) at full-term and parturitionfrom its initial level of 9.6 g/dl (range 7.2-12.8 g/dl). There was a significantdifference (p<0.05) in Hb concentration among the trimesters of pregnancy. Therewas no significant difference in the outcome of pregnancies in women with orwithout malaria prarasites in their peripheral blood. There was no significantdifference in Hb concentrations between malaria parasite positive and negativepregnant women (p>0.05). Significant difference was observed in the proportionof new born positives from mothers with or without malaria parasites indicatinga high degree of transplacental transmission. The overall foetal mortality rate

140
Malaria
was 21.5 per cent. The miscarriage, stillbirth, premature delivery leading to foetaland neonatal along with perinatal mortality constituted for 24.4, 13.3, 20 and 17.7 per cent of all mortalities respectively.
Salient Findings: This is a comprehensive study carried out in 32 villages inKoraput wherein 209 pregnant women were enrolled. In the study a significantdifference of malaria was found between primigravidae and multiparae. Theproportion of Pf species varied from 66.7 to 90.9% and the rest were P. vivax.Interestingly there was no significant difference found between parasite positiveand negative women. In this study malaria did not influence the outcome ofpregnancy as and malaria infection in the newborns.
Comments: Malaria is considered as an important factor for stillbirths, low birthweights and maternal mortality in Africa as many studies suggest. In the presentstudy however, the author has not found any association between malaria(predominantly Pf) and the outcome of pregnancy. The study highlights thatmalaria is a significant problem in pregnant women and new born in tribal areaswhich are generally hyper to holoendemic with predominance of P. falciparum.
40. Incidence of hypoglycaemia in children with falciparum malaria aroundRourkela, Orissa state.
D.B. DAS, R.N. SATPATHY, P.C.SATPATHY, J.K. PATNAIK & B.S. DAS
Indian J Med Res [A] 95, March 1992, pp 79-83
To determine the incidence of hypoglycaemia in children suffering from severefalciparum malaria, 23 patients from Rourkela (Orissa), were investigated. Plasmaglucose and immunoreactive insulin were estimated before and at hourly intervalsduring quinine infusion. No child had hypoglycaemia at the time of admission.Correlation between parasite count and prequinine plasma glucose was notsignificant. In the period of quinine infusion, 20 patients showed fall in plasmaglucose during all the three hours (p<0.05. p<0.01, p<0.01 at the end of 1st, 2nd,and 3rd h respectively) but the decrease to hypoglycaemic level (plasma glucose< 40 mg/dl) was observed in only one child. Concomitant increase in plasmainsulin was noticed in 18 of these patients. Decrease in plasma glucose andincrease in plasma insulin was found to correlate well (rTM-0.78, p<0.001).

141
Malaria
Hypoglycaemia was found to be an infrequent complication of severe falciparummalaria in children from the area studied. Though decrease in plasma glucosewas observed after quinine infusion, it was less severe and did not reach thehypoglycaemic level.
Salient Findings: This is a hospital based study where in hypoglycaemia wasmonitored in complicated P. falciparum cases. The authors have found thathypoglycaemia is not encountered in complicated cases and only post quinineinfusion there is drop in glucose levels that too not to hypoglycaemic levels.
Comments: This study is although of limited value in disease burden estimation,yet suggests that hypoglycaemia is not a severe complication in complicatedcases and unlike anaemia and neurological sequelae, do not cause disability.
41. Investigation of Malaria Outbreak in Rajasthan
R.P. SHUKLA, A.C. PANDEYA and A. MATHUR
Indian Joumal of MalariologyVol. 32, September 1995. pp. 119-12E
Jaisalmer and Barmer districts in the Thar Desert of Rajasthan experienced anunprecedented rains during 1994 leading to an outbreak of malaria. Investigationswere carried out at three sites in two districts (i) Pokaran PHC and (ii) NachanaPHC in Jaisalmer district and Dhorimana in Barmer district during November1994. Epidemiological and entomological studies in Pokaran PHC revealed thepresence of small foci of stable malaria. These foci were maintained by largebodies of water (ponds/lakes) drained from surrounding areas and spread over 1to 5 sq km. slide positivity rate (SPR), slide falciparum rate (SfR) and childspleen rate (SR) were 60.1, 56.9 and 86.9%, respectively with 3, deaths reported.Adjoining villages experienced epidemic reporting deaths fed by the reservoirfrom these stable foci. An. culicifacies and An. stephensi were the major malariavectors.
Nachana PHC recorded stable malaria foci of irrigation malaria due to introductionof Indira Gandhi Canal (IGC). SPR, SFR and SR recorded were 52.35, 50.58

142
Malaria
and 80.8%, respectively. Transmission appeared to be maintained by An.stephensi. An. culicifacies and An. fluviatilis in relays. An. fluviatilis seem tohave established breeding in silted grassy margins of IGC. Dhorimana PHC inborder district was also found to be a stable malaria focus although with lowmalaria indices. However, An. culicifacies and expanded breeding potential ofAn. stephensi were the main factors in maintaining malaria endemicity in theregion.
Salient Findings: The study was carried out post epidemic in Jaisalmer and Barmer.Mass surveys and spleen surveys were carried out in three villages. The studyshowed higher SPR and SfR than reported from the area. Also the spleen rate washigh. 3 deaths were reported from the earlier recoeds from Pokaran villages.
Comments: Although some 600 cases were detected during the mass surveys,age and sex wise distribution has not been mentioned. The prevalence datasimilarly from three study villages has also not been analysed age and sex wise.There is no detail of 3 cases of deaths. Hence the study will be of limited use forestimation of disease burden.
42. Malaria Outbreak in the lndira Gandhi Nahar Pariyojna Command areain Jaisalmer District, Thar Desert, India.
B.K. TYAGI, S.P. YADAV, R. SACHDEV AND P.K. DAM
J. Commun. Dis. 33(2):88
A focal outbreak of malaria occurred in the villages situated close to the mainIndira Gandhi canal near Ramgarh in Jaisalmer district, western Rajasthan.Stagnation of water over a month’s period in the main canal as well as longstanding rain water in the form of expansive lakes near these villages formedvast breeding grounds for the vectors like Anopheles culicifacies, along with A.stephensi already breeding in the ‘tanka’ and ‘beri’ in the epidemic-hit villages.Rapid mass blood surveys along with other entomological and parasitologicalinvestigations were conducted in four of the ten affected villages, viz., Seuva,Raghwa, Raimala and Sadhna. A total of 992 specimens belonging to four vectorspecies were sampled, namely, A. stephensi (47.4%), A. culicifacies (41.0%), A.subpictus (11.2%) and A. annularis (0.4%). Epidemiologically, about one-fourth

143
Malaria
of the examined persons were positive (SPR 25.5%), although Plasmodiumfalciparum dominated the parasitaemia (49.5%). Available data are indicativeof changed malariological scenario in the lndira Gandhi Nahar Pariyojnacommand area, where epidemics are regular features every year.
Salient Findings: This publication is based on epidemic investigation in Rajasthanin 4 villages. This epidemiological study tries to pinpoint causes of malariaepidemic in Jaisalmer district. The malaria data of mass survey has been presentedvillage wise and age and sex distribution of cases with splenomegaly have beenpresented. Symptoms presented by patients have been analysed.
Comments: The study is of limited value for the estimation of DALYs . Age andsex distribution of incidence cases is lacking as also information on deaths thatmight have accompanied the epidemic.
43. Malaria Epjdemic in Shahjahanpur (U.P.)
R.K. CHANDRAHAS and V. P. SHARMA,
Indian Journal of MalariologyVol. 20, Dec. 1983, pp. 163-166.
Following 253 deaths in 28 villages of Negoyi PHC and 96 deaths from 10villages of Tilar PHC of Shahjahanpur district of Ut tar Pradesh during Augustto October 1983, an investigation was carried out by the Malaria Research Centreduring 3rd week of October to determine the cause of these unusual deaths.These PHCs are located at about 25 Km North of Shahjahanpur town. The datacollected from the state health authorities revealed that these unusual deathsstarted occurring from first week of August and continued till the third week ofOctober 1983 with maximum number of deaths during mid September. Theaffected villages were situated in canal irrigated zone and had innumerableseepages and rain water collection sites. The team carried out survey of fevercases in 8 out of the 28 affected villages in Negoyi PHC. Two villages locatedoutside the affected area were also surveyed. Of a total of 377 blood smearscollected and examined, 284 were found positive for malaria parasites givingthe slide positivity rate of 75.33. Of the total positives, 273 (96.1 %) were due toP. falciparum. Blood smears were also collected from the family members of

144
Malaria
the deceased in 5 villages. Out of 396 blood smears collected, 214 were positivefor malaria, the SPR being 54.04. P. falciparum was found in 204 out of 214positives (95.32%).
It may be noted that a few days before this investigation was undertaken, theU.P. Health Department had completed administration of Mass Radical Treatment(MRT) in all the affected villages by the end of September 1983. Theadministration of Fever Radical Treatment (FRT) was in progress at the time ofinvestigations during the third week of October 1983. Therefore, it was surprisingto find such a high rate of falciparum malaria even after these treatments: Therewere 38 deaths among infants out of a total of 349 deaths (10.8%) in 11 out of 38affected villages in both the Primary Health Centres. Only two infant blood smearswere collected during the fever survey of which the one collected from Parsonavillage was positive for P. falciparum.
The investigations revealed an epidemic outbreak of falciparum malaria in thesevillages. It is quite reasonable to surmise that some of the unusual deaths recordedearlier were due to falciparum infection. The investigations also revealed thatthere was a complete breakdrown of surveillance in these areas and acute shortageof anti-malarials and microslides with the Multipurpose Workers (MPW) andother supervisory staff. The Shahjahanpur episode is of great public healthimportance. It highlighted the value of good surveillance, insecticidal sprayingtargeted to achieve at least 75 to 80% coverage and improved laboratory servicesin fulfilling the objectives of the Modified Plan of Operations (MPO) of theNational Malaria Eradication Programme (NMEP).
Salient findings: The study shows that in a post epidemic phase malariaincidence particularly P. falciparum was very high in all the age groups andboth sexes in two PHCs where investigation was done. Contact slides takenfrom the relatives of the diseased also showed high incidence of falciparummalaria. The analysis of deaths due to malaria revealed that 38 deaths out of349 were in infants.
Comments: Age and sex wise incidence has been given which is useful inestimation of disease burden. The age and sex wise distribution of malariadeaths has not been given although it has been shown that deaths in infantswere 10.8%.

145
Malaria
44. Malaria Epidemic in Baniyani Village, District Farrukhabad (U.P.)
R.N. PRASAD, K.J. VIRK, T. SHARMA AND G.D.P. DUTTA
Indian Journal of MalariologyVol. 29, December 1992, pp. 219-224
Many deaths recorded in village Baniyani of Talgram PHC of District Farukhabad,U.P. during August to November 1991, which is the malaria transmission seasonin this area. Integrated measures like one-round spraying of DDT and HCH, sixround fogging of malathion and six time application of Baytex in mosquito breedingsites, were adopted by the Health Department of the U.P. Govt. to avert an epidemic.Investigations carried out by Malaria Research Centre during November andDecember 1991 showed low mosquito densities and larval positivity but very highincidence of malaria in the village. No case of malaria was recorded by surveillanceworker of the Health Department of the state Govt. before the outbreak of thedisease. However, high slide falciparum rate (51.57%), child parasite rate (40.0%),infant parasite rate (66.66%) and spleen rate (82.9%) in the village clearly indicatedhyperendemic conditions in the area and hence deaths recorded in the village duringthe malaria transmission period could be due to malaria only. Major factorsresponsible for the deaths due to malaria in the village were poor surveillance,faulty diagnosis, and low literacy and socio-economic status of the villagers.
Salient findings: This is yet another study pointing to poor surveillance and highincidence of malaria especially the Pf in an outbreak/epidemic situation. It alsopoints to the fact that 32 deaths were reported from the study village by the PHCattributed to Hyperthermia and other causes. But local physicians reported 45deaths due to malaria.
Comments: The current investigative study is not of much significance in malariadisease burden estimation in rural UP as it is restricted to a village where suddendeaths were reported. Age and sex wise cases of malaria incidence and deathshave not been mentioned.
45. Persistent Malaria Transmission in Kundam Block, District Jabalpur (M.P.)
NEERU SINGH and V.P.SHARMA
Indian Journal of MalariologyVol. 26, March 1989, pp. 1-7.

146
Malaria
Malaria survey was undertaken in 7 villages of Kundam PHC from August 1987to July 1988. Epidemiological findings revealed high spleen (20-70), child parasite(40-85) and infant parasite rates (20-75) in the area. P. falciparum was thepredominant species and unchecked malaria transmission continued almostthroughout the year. The study of month wise distribution of positive cases andthe period during which intensive intervention measures were undertaken revealedthat despite an extra round of HCH and intensive chemotherapeutic measures,there was no marked decrease in the prevalence of malaria.
Salient findings: This study shows glaring gap between the reported and estimatedincidence of malaria detected through point prevalence surveys and comparedwith routine surveillance undertaken by the control programme. The month wisedata in infants and children suggest perennial transmission due to consistentlyhigh incidence. The spleen rates in children were also high 47.5 to 49.8% indifferent seasons which also suggest long duration of transmission.
Comments: This study focuses on persistent transmission of malaria in an ethnictribe inhabited area in Jabalpur district of Madhya Pradesh. The gap betweenreported and estimated incidence can help in determining correction factor.Although data has been segregated in infants (SPR 20-70%) and children from1-10 years (SPR 44 to 85%), in the higher age groups incidence is not shown.No information on deaths has been provided which normally accompanyepidemics such as this.
46. Prevalence of Malaria and Economic Loss in two Major Iron Ore Mines inSundargarh District, Orissa.
R.S. YADAV, S.K. GHOSH, S.K. CHAND and A. KUMAR
Indian Journal of MalariologyVol. 28, June 1991, pp. 105-113.
A cross-sectional study on malaria was undertaken in May 1989 in the settlementsof Kalta and Barsuan iron ore mines situated in a hilly area of Sundargarh district.Fever surveys revealed slide positivity rates of 33.9% and 34.8% in Kalta andBarsuan, respectively. Malaria infection rates as recorded through mass bloodsurveys in the resident population were 23.5 and 13.8%, respectively. Children

147
Malaria
up to 9 years age suffered most from malaria and in the age group of 2-9 years37.3%, children had enlarged spleens with an average enlarged spleen (AES)index of 1.7. P. falciparum was the most prevalent species followed by P. vivaxand P. malariae. Malaria vectors viz., An. fluviatilis and An. culicifacies werepresent in high densities. The present paper also brings out the economic lossdue to malaria to the mining industry.
Salient findings: The study highlights prevalence of malaria and economic lossdue to disease to the iron ore mining industry in Orissa. On the basis of pointprevalence surveys, mass blood surveys and hospital admissions, it was foundthat malaria was much higher in children than the other gae groups.
Comments: This study is quite comprehensive as it not only analyses the hospitaldata but also finds prevalence of malaria in mine workers and their families. Theage distribution of malaria has been presented although incidence according togender has not been presented. This study could be of use in assessing reliabilityof state malaria data from forested areas of Orissa especially similar to this areainhabited by tribals, where the study was conducted.
47. Socio-economic Aspects of Malaria in Kheda District, Gujarat
P.G. BHATI. V.S. MALAVIYA. RAJNI KANT. H.C. SRNASTAVA, S.K.SHARMA and V.P, SHARMA
Indian Journal of MalariologyVol. 33. December 1996. pp. 200-208
Study on the socio-cultural factors and economic loss due to malaria in rural andurban areas of Kheda district, Gujarat revealed that factors such as education,profession, income, housing pattern, social groups, water storage and treatmentseeking behaviour play an important role in malaria transmission. However, thedifference of these components in respect to malaria cases between rural andurban areas were statistically insignificant. Mean monetary loss per malariaepisode was found to be more in urban area (Rs. 393.59) as compared to rural(Rs. 157.59). The study also suggests the importance of socio-cultural factors inimplementing any community health programme. Health education is needed tomake the people aware and health conscious for prevention of disease at theirown level.

148
Malaria
Salient Findings: This is a proforma based study carried out to estimate economicloss due to malaria in a rural and an urban pocket in Kheda district of Gujarat. Ithas been suggested that economic loss due to in urban area is more than doubleas compared to urban area which was attributed to more wage loss, treatmentcost, special diet and mean man days lost than in rural area.
Comments: The study is not of much direct help in estimation of DALYs butwill be of good value if economic loss is to be worked out due to malaria basedon DALYs lost estimated for Gujarat state.

Filaria
1. Mattancherry urban agglomeration, a diminishing focus of lymphaticfilariasis in Kerala.
ARUNACHALAM N, MARIAPPAN T, VIJAYAKUMAR KN, SABESAN S,PANICKER K N.
J Commun Dis.28(3): 1996168-70.
Parasitological survey conducted recently in Mattancherry, Kerala showed alow prevalence of microfilariae (mf), with a mf rate of 1.81%, compared tothat of 1956 when the mf rate was 14.7%. No brugian infection was encounteredin the present investigation, though both bancroftian and brugian infectionswere reported earlier. Culex quinquefasciatus, the vector of bancroftian filariasiswas the most predominant (93.3%) mosquito species, and its infection andinfectivity rates were 0.76% and 0.54% respectively. Mansonioides spp., thevectors of brugian filariasis constituted only 0.2% of the total mosquitoes andwith no infection. The overall reduction in the prevalence of mf cases andvector infection rates over the years is attributed to the continued activities ofthe National Filaria Control Programme. The disappearance of brugian filariasiscould mainly be due to the drastic reduction in the Mansonioides breedinghabitats, as a result of rapid urbanization coupled with improved socio economicconditions.
2. Treatment costs and work time loss due to episodic adenolymphangitis inlymphatic filariasis patients in rural communities of Orissa, India.
BABU, B. V. AND A. N. NAYAK
Trop Med Int Health 8(12): (2003). 1102-9.
Data on expenditure on treatment and loss of work along with otherepidemiological information were collected through a 1-year surveillance of113 acute episodes of ADL from 72 individuals of the study population(5.42%).
149

150
Filaria
3. The economic loss due to treatment costs and work loss to individuals withchronic lymphatic filariasis in rural communities of Orissa, India.
BABU, B. V., A. N. NAYAK, ET AL.
Acta Trop 82(1): (2002).31-8.
This paper is based on 1 year round case control study to investigate the economicburden, in terms of treatment costs and loss of work to people affected withchronic lymphatic filariasis in rural communities of Orissa, Eastern India. Aroundthree-fourths of the chronic patients have sought treatment for their conditionand spent, on average an amount of INR 396 (approximately US$ 8.7) per year.The major component of the expenditure is the cost of medicines. The data onloss of work time due to chronic condition reveal that the total absenteeism tothe work is significantly higher among chronic filariasis patients than controls.The total number of working hours spent per day by patients and controls are4.94 and 6.06, respectively with a significant difference. The total absenteeismand the total number of working hours per day are influenced significantly bydisease condition and other personal characteristics, namely age, sex and familytype. The chronic patients lose a total of 68 days of work per year, which isequivalent to 19% of the total working time of the year. The present results showthat the chronic conditions of lymphatic filariasis pose considerable burden onthe patient, family and community.
4. Lymphatic filariasis in Khurda district of Orissa, India: an epidemiologicalstudy. Southeast
BABU, B. V., A. S. ACHARYA, ET AL.
Asian J Trop Med Public Health (2001). 32(2): 240-3.
A cross-sectional survey was undertaken to determine the prevalence of diseasedue to lymphatic filariasis in Khurda district of Orissa, India. The total diseaseattributable to filariasis was significantly higher in males (14.79%) than females(10.04%). However, elephantiasis is more prevalent in females, andadenolymphangitis is more prevalent in males than their counterparts. Theprevalences of various forms of the disease are age dependent in both sexes.About one-seventh of men and women of higher age groups suffered from chronic

151
Filaria
debilitation forms of the disease. The study suggests that overt clinical forms oflymphatic filariasis constitute a major public health problem in the study area.
5. A lymphatic filarial survey revealing a focus of Brugia malayi in the coastalregion of west Bengal.
BERA DK, BANERJEE P..
J Indian Med Assoc. 94(8): 1996, 296-7, 310.
Random night blood samples were examined from 528 subjects in an endemiczone of lymphatic filariasis, in the coastal region of West Bengal. There were136 cases out of 528 who were symptomatic, with or without recurrent episodesof fever, lymphangitis and lymphadenitis and with various degrees oflymphoedema. Examination of blood samples revealed microfilaria in 43 casesof which 42 were asymptomatic and only one was symptomatic withlymphoedema. All the microfilariae were of the species Brugia malayi.
6. A lymphatic filarial survey revealing a focus of Brugia malayi in the coastalregion of west Bengal.
BERA DK, BANERJEE P.
J Indian Med Assoc. 94(8): 1996.296-7, 310.
Random night blood samples were examined from 528 subjects in an endemiczone of lymphatic filariasis, in the coastal region of West Bengal. There were136 cases out of 528 who were symptomatic, with or without recurrent episodesof fever, lymphangitis and lymphadenitis and with various degrees oflymphoedema. Examination of blood samples revealed microfilaria in 43 casesof which 42 were asymptomatic and only one was symptomatic withlymphoedema. All the microfilariae were of the species Brugia malayi.
7. Filariasis control in rural areas through detection and treatment withdiethylcarbamazine.
BISWAS, H., S. P. SHARMA, ET AL.
J Commun Dis 21(4): (1989).272-81.

152
Filaria
During first round of detection and treatment 20,300 mf carriers (90.6 per centof detected) and 6,588 disease persons (86 per cent of detected) in Srikakulamand 7,097 mf carriers (94.8 per cent of detected) and 1,436 disease persons (93.4per cent of detected) in Vizianagaram were treated with DEC tablets. These areaswere again surveyed after five years and detected cases were treated with DECwith coverage of treatment ranging from 82.3 per cent to 95 per cent for both mf& disease cases and decline in mf and disease rate was noted to be 52.4 per centand 50.9 per cent respectively in Srikakulam and 42.2 per cent for mf rate inVizianagaram. The mf reduction was appreciably high (50 per cent or more) in11 PHCs of Srikakulam and 4 PHCs of Vizianagaram. The mf rate reductionwas the highest in the age group of 1 to 4 year indicating that the transmissionhas been cut down significantly. The vector infection rate showed reduction by50 per cent during second round of detection and treatment as compared to firstround, indicating significant reduction in transmission potential.
8. Epifil: a dynamic model of infection and disease in lymphatic filariasis.
CHAN MS, SRIVIDYA A, NORMAN RA, PANI SP, RAMAIAH KD,VANAMAIL P, MICHAEL E,,DAS PK, BUNDY DA.
Am J Trop Med Hyg.59(4): 1998, 606-14.
The lack of a quantitative framework that describes the dynamic relationshipsbetween infection and morbidity has constrained efforts aimed at the community-level control of lymphatic filariasis. In this paper, we describe the developmentand validation of EPIFIL, a dynamic model of filariasis infection intensity andchronic disease. Infection dynamics are modeled using the well establishedimmigration-death formulation, incorporating the acquisition of immunity toinfective larvae over time. The dynamics of disease (lymphodema and hydrocele)are modeled as a catalytic function of a variety of factors, including worm loadand the impact of immunopathological responses. The model was parameterizedusing age-stratified data collected from a Bancroftian filariasis endemic area inPondicherry in southern India. The fitted parameters suggest that a relativelysimple model including only acquired immunity to infection and irreversibleprogression to disease can satisfactorily explain the observed infection and diseasepatterns. Disease progression is assumed to be a consequence of worm induceddamage and to occur at a high rate for hydrocele and a low rate for lymphodema.This suggests that immunopathology involvement may not be a necessarycomponent of observed age-disease profiles. These findings support a centralrole for worm burden in the initiation and progression of chronic filarial disease.

153
Filaria
9. Filariasis survey in a rural area of West Bengal.
CHANDRA G, HATI AK.
J Commun Dis. 1996, 28(3): 206-8.
Survey carried out in Nemari village in Burdwan district of WestBengal showedthat mf and disease rates were 0.8 (36/4512) and 1.41%(64/4512). Out of 64cases, elephantiasis in 8, lymphangitis in 14, lymphoedema in 8, lymphvarix in9 and hydrocele alongwith epididymoorchitis in 25 cases were observed.
10. A clinico-epidemiological perspective of lymphatic filariasis in Satyabadiblock of Puri district, Orissa.
CHHOTRAY, G. P., M. MOHAPATRA, ET AL.
Indian J Med Res (2001).114: 65-71.
The prevalence of microfilaraemia was observed to be 14.8 per cent; 13.3 percent Wuchereria bancrofti, 1.4 per cent Brugia malayi and 0.09 per cent hadmixed infections. Geometric mean microfilaraemia density (infected personsonly) was found to be 1288 per ml in case of W. bancrofti and 204 per ml in caseof B. malayi. The disease rate was observed to be 19.8 per cent; 12.85 per centhad acute manifestations and 6.97 per cent had chronic manifestations.INTERPRETATION & CONCLUSION: The rate of acute disease manifestationswas observed to be significantly higher (P < 0.001) than chronic manifestations.There was a male preponderence among the affected individuals (P < 0.001).The interesting observations of the study were the occurrence of occult filarialmanifestations viz., tropical pulmonary eosinophilia (TPE) in 0.47 per cent casesand other associated manifestations like asymptomatic microscopic haematuria,monoarticular arthritis and filarial associated respiratory diseases in 0.50, 0.24and 0.19 per cent of cases respectively. The present study indicates that the areais highly endemic for lymphatic filariasis with active transmission.
11. A clinico-epidemiological perspective of lymphatic filariasis in Satyabadiblock of Puri district, Orissa.
CHHOTRAYGP, MOHAPATRA M, ACHARYA AS, RANJIT MR.
Indian J Med Res. 2001.114: 65-71.

154
Filaria
The prevalence of microfilaraemia was observed to be 14.8 per cent; 13.3 percent Wuchereria bancrofti, 1.4 per cent Brugia malayi and 0.09 per cent hadmixed infections. The disease rate was observed to be 19.8 per cent; 12.85 percent had acute manifestations and 6.97 per cent had chronic manifestations. Theinteresting observations of the study were the occurrence of occult filarialmanifestations viz., tropical pulmonary eosinophilia (TPE) in 0.47 per cent casesand other associated manifestations like asymptomatic microscopic haematuria,monoarticular arthritis and filarial associated respiratory diseases in 0.50, 0.24and 0.19 per cent of cases respectively.
12. Occurrence of asymptomatic microscopic haematuria in a filarial endemicarea of Orissa
CHHOTRAYGP, RANJIT MR, MOHAPATRA M
India. J Commun Dis 32(2): 2000.85-93.
15.6% were found to have asymptomatic haematuria (Grade I-14.7%, Grade II-0.6%, Grade-III 0.3%). The prevalence of asymptomatic microscopic haematuriawas observed to have positive statistical correlation with mf status (P < 0.001),filarial antigenaemia (Ag) (P < 0.001), antibody (Ab) (P < 0.001) and circulatingimmunocomplex antigen (CIC-Ag) (P < 0.001). The prevalence was also foundto be increased with the progression of the disease process i.e. from endemicnormal to chronic manifestations. None of the cases having Grade-II and IIIhaematuria cases revealed any gross renal pathological lesions, when subjectedto special investigations like X-ray, IVP, cystoscopy and urethroscopy.
13. Towards elimination of lymphatic filariasis in India.
DAS PK, RAMAIAH KD, AUGUSTIN DJ, KUMAR A.
Trends Parasitol.17(10). 2001, 457-60.
The global initiatives to eliminate lymphatic filariasis as a public health problemby the year 2020 have generated a great deal of debate in India, the largest endemiccountry. This has led to a shift in the focus from control to elimination of thedisease. Although the campaign to eliminate filariasis has begun, much moreneeds to be done. Several recent research studies have provided an insight into

155
Filaria
various operational issues and prospects of elimination of lymphatic filariasis.In this article, the current scenario, recent research results, logistics and theprospects of eliminating lymphatic filariasis in India will be discussed.
14. Wuchereria bancrofti microfilaraemia in children in relation to parentalinfection status.
Das PK, Sirvidya A,Vanamail P, Ramaiah K D, Pani SP,Michael E, Bundy DA.
Trans R Soc Trop Med Hyg. 1997, 91(6): 677-9.
A total of 946 families with 2302 children was surveyed for microfilaraemia dueto Wuchereria bancrofti. The prevalence of microfilaraemia among offspringborn to microfilaraemic parents was significantly higher than in those born toamicrofilaraemic parents (P = 0.0049; relative risk = 3.40). However, there wasno statistically significant difference between the prevalence of microfilaraemiain children born to microfilaraemic mothers or microfilaraemic fathers, suggestingthat parental (not only maternal) infection is the important risk factor, and it maybe exposure within the household which is important. Logistic regression analysesalso confirmed that the risk of infection for offspring born to eithermicrofilaraemic mothers or microfilaraemic fathers was higher than that foroffspring born to amicrofilaraemic parents and indicated that infection in children< or = 20 years old was primarily dependent on parental infection status andminimally influenced by factors other than household exposure.
15. Cumulative exposure and its relationship with chronic filarial disease inbancroftian filariasis.
DAS PK, SRIVIDYA A, PANI SP, RAMAIAH KD, VANAMAIL P, DHANDA V.
Southeast Asian J Trop Med Public Health. 1994, 25(3):516-21.
Several hypotheses have been put forth about the factors influencing the dynamicsof infection and disease in lymphatic filariasis. However, appropriate validationof these hypotheses by real situation analyses of epidemiological data is lacking.The present analyses examine the relationship between cumulative exposure toinfection and prevalence of disease by utilizing the existing entomological andclinical data collected between 1981 and 1986 in Pondicherry, South India,

156
Filaria
endemic for bancroftian filariasis. While there was a significant negativeassociation when the cumulative exposure was correlated with total prevalenceof disease (r = 0.70, p = 0.024) as well as hydrocele alone (r = 0.74, p = 0.014),a significant positive association was found with prevalence of lymphedema (r =0.72, p = 0.018). These results suggest that hydrocele development follows earlyafter exposure, but prolonged exposure could result either in development oflymphedema or immune tolerance resulting in microfilaremia. These could alsosuggest that the pathomechanisms in development of hydrocele and lymphedemacould follow different pathways. Implications of the present findings are discussedin light of the various hypotheses put forward by earlier studies.
16. Clinical manifestations of Bancroftian filariasis in a suburb of Calcutta
DONDERO TJ JR., BHATTACHARYA NC, BLACK HR, CHOWDHURY AB,GUBLER DJ, INUI TS, MUKERJEE M.
India. Am J Trop Med Hyg. 1976, 25(1): 64-73.
Interviews and physical examinations for filarial disease were conducted inHowrah near Calcutta, West Bengal, India, in a study area where long termquantitative entomological studies have disclosed high intensity, year roundexposure to Wuchereria bancrofti. Little elephantiasis or other serious filariasis-related disease was noted, but half the males over 20 years of age had genitallesions of various types. Ninety-two percent of households had at least one residentwith microfilaremia or presumptive clinical evidence of filarial disease.
17. Filariasis in the labour population of a tea estate in Upper Assam.
DUTTA, P., B. K. GOGOI, ET AL
Indian J Med Res (1995) 101: 245-6.
Preliminary random and mass blood surveys undertaken between 2000-0100 hin a tea garden of Upper Assam revealed more than 8 per cent positivity formicrofilaria (mf) of Wuchereria bancrofti. The mf carriers were considerablyhigh among males (73) as compared to females (48). Culex quinquefasciatuswas incriminated as a vector with man hour density of 68.5 in human dwellings(indoors). The detection of mf in children who had never moved from the area

157
Filaria
and filaria larvae in vector mosquitoes collected from human dwellings indicatethat indigenous transmission is going on in the garden and that filariasis hasbecome a local health problem.
18. Evidence of sex variations in microfilaraemia and fluorescent antibody titrelevel at puberty in a bancroftian filariasis endemic area.
DUTTA, S. N. AND H. J. DIESFELD
J Commun Dis (1994), 26(1): 43-51.
1101 children and young adults between 2 and 17 years age, residing inBancroftian filariasis endemic area of the Jharia Coalfields in Bihar, wereexamined by Indirect Immunofluorescent Test (IIFT) against Dipetalonema Vitae.The results, along with those of two night blood surveys conducted in the samearea, covering 2148 and 2246 persons respectively, are reported. In the prepubertalage groups there was no statistically significant variation in the percentage ofchildren showing positive antibody titre in either sex, but a sudden fall of morethan 50 per cent in the antibody level was observed in females at the onset ofpuberty. This did not occur in males. Analysis of the night blood results alsoindicated a remarkable fall in microfilaria rate and density in females at theonset of puberty and a low level was then maintained over the whole of the childbearing age. No such change was observable in males. Sex differences in thesusceptibility of the host to helminthic infections is well-known and in animalexperiments the effect of sex hormones in modifying such susceptibility hasbeen established. In human filariasis the probable part played by the male andfemale sex hormones in bringing about abrupt changes in immunoresponse andinfection rate at the onset of puberty is discussed.
19. Evidence of sex variations in microfilaraemia and fluorescent antibody titrelevel at puberty in a bancroftian filariasis endemic area.
DUTTA, S. N. AND H. J. DIESFELD
J Commun Dis (1994), 26: 43-51.
1101 children and young adults between 2 and 17 years age, residing inBancroftian filariasis endemic area of the Jharia Coalfields in Bihar, were

158
Filaria
examined by Indirect Immunofluorescent Test (IIFT) against Dipetalonema Vitae.The results, along with those of two night blood surveys conducted in the samearea, covering 2148 and 2246 persons respectively, are reported. In the prepubertalage groups there was no statistically significant variation in the percentage ofchildren showing positive antibody titre in either sex, but a sudden fall of morethan 50 per cent in the antibody level was observed in females at the onset ofpuberty. This did not occur in males. Analysis of the night blood results alsoindicated a remarkable fall in microfilaria rate and density in females at theonset of puberty and a low level was then maintained over the whole of the childbearing age. No such change was observable in males. Sex differences in thesusceptibility of the host to helminthic infections is well-known and in animalexperiments the effect of sex hormones in modifying such susceptibility hasbeen established. In human filariasis the probable part played by the male andfemale sex hormones in bringing about abrupt changes in immunoresponse andinfection rate at the onset of puberty is discussed.
20. Naturally acquired concomitant infections of bancroftian filariasis andhuman plasmodia in Orissa.
GHOSH, S. K. AND R. S. YADAV
Indian J Malariol (1995). 32: 32-6.
Blood smears collected from fever cases for detection of malaria parasites duringdaytime showed concomitant infections of Wuchereria bancrofti from 1989 to1991 in Bisra PHC of district Sundargarh, Orissa. Of the total 51,448 bloodsmears examined, 18,444 (35.84%) were positive for malaria parasites whichcomprised 3401 (18.44%) Plasmodium vivax, 14,524 (78.75%) P. falciparum,156 (0.84%) P. malariae and 363 (1.97%) mixed plasmodial infections. Only240 (0.46%) cases were positive for W. bancrofti, of which 160 (66.67%) werefrank microfilariae (mf) cases, while 80 (33.33%) showed concomitant infectionswith malaria parasites. Filariasis was less prevalent in lower age-groups. Malariaincidence in people below thirty years was higher compared to older people, onthe contrary, mf incidence was more in people above 15 yrs or more age.Microfilariae density was within 1-7 parasites per 10 microliters blood. About90% mf cases were within the range of 1-4 per 10 microliters blood. Mean malariaparasitaemia in concomitant infection cases was 9574 per microliters blood(median 5955; range 35 to 49,500). Presence of diurnal microfilaraemia needsfurther investigation.

159
Filaria
21. Naturally acquired concomitant infections of bancroftian filariasis andhuman plasmodia in Orissa
GHOSH, S. K. AND R. S. YADAV
Indian J Malariol 1995, 32: 32-6.
Blood smears collected from fever cases for detection of malaria parasites duringdaytime showed concomitant infections of Wuchereria bancrofti from 1989 to1991 in Bisra PHC of district Sundargarh, Orissa. Of the total 51,448 bloodsmears examined, 18,444 (35.84%) were positive for malaria parasites whichcomprised 3401 (18.44%) Plasmodium vivax, 14,524 (78.75%) P. falciparum,156 (0.84%) P. malariae and 363 (1.97%) mixed plasmodial infections. Only240 (0.46%) cases were positive for W. bancrofti, of which 160 (66.67%) werefrank microfilariae (mf) cases, while 80 (33.33%) showed concomitant infectionswith malaria parasites. Filariasis was less prevalent in lower age-groups. Malariaincidence in people below thirty years was higher compared to older people, onthe contrary, mf incidence was more in people above 15 yrs or more age.Microfilariae density was within 1-7 parasites per 10 microliters blood. About90% mf cases were within the range of 1-4 per 10 microliters blood. Mean malariaparasitaemia in concomitant infection cases was 9574 per microliters blood(median 5955; range 35 to 49,500). Presence of diurnal microfilaraemia needsfurther investigation.
22. Frequency distribution of lymphatic filariasis microfilariae in humanpopulations: population processes and statistical estimation.
GRENFELL BT, DAS PK, RAJAGOPALAN PK, BUNDY DA.
Parasitology. 1990.101 Pt 3: 417-27.
This paper uses simple mathematical models and statistical estimation techniquesto analyse the frequency distribution of microfilariae (mf) in blood samples fromhuman populations which are endemic for lymphatic filariasis. The theoreticalanalysis examines the relationship between microfilarial burdens and theprevalence of adult (macrofilarial) worms in the human host population. Themain finding is that a large proportion of observed mf-negatives may be ‘true’zeros, arising from the absence of macrofilarial infections or unmated adult

160
Filaria
worms, rather than being attributable to the blood sampling process. Thecorresponding mf distribution should then follow a Poisson mixture, arising fromthe sampling of mf positives, with an additional proportion of ‘true’ mf-zeros.This hypothesis is supported by analysis of observed Wuchereria bancrofti mfdistributions from Southern India, Japan and Fiji, in which zero-truncated Poissonmixtures fit mf-positive counts more effectively than distributions including theobserved zeros. The fits of two Poisson mixtures, the negative binomial and theSichel distribution, are compared. The Sichel provides a slightly better empiricaldescription of the mf density distribution; reasons for this improvement, and adiscussion of the relative merits of the two distributions, are presented. The impacton observed mf distributions of increasing blood sampling volume and extractionefficiency are illustrated via a simple model, and directions for future work areidentified.
23. Haldar A, Mundle M, Haldar S, Biswas AK, Mitra SP, Mahapatra BS.
MASS DEC CAMPAIGN FOR FILARIASIS IN A HYPER ENDEMICDISTRICT OF WEST BENGAL.
J Commun Dis. 2001, 33 (3): 192-7.
As a part of the on-going National Filaria Control Programme, National FilariaDay was observed in Purulia district of West Bengal on 26th Nov 2000 with anextensively organized mass DEC consumption campaign preceded by IECactivities and followed by mopping up operations. Disease prevalence amongpopulation covered showed 0.1% hand swelling, 0.6 to 0.8% leg swelling, while1.1% of males had hydrocele.
Hyma, B., A. Ramesh, et al. (1989). “Lymphatic filariasis in Madras, India.” SocSci Med 29: 983-90.This study examines the state of mosquito-borne lymphaticfilariasis in Madras, Tamil Nadu, in southern India during the 1970s and into the1980s. In its various forms it remains a public health problem of considerablemagnitude in many tropical countries and affects both rural and urban populations[1. World Health Organization (Third Report). Expert Committee on Filariasis.Tech. Rep. Ser. No. 542, p. 7, 1974]. Here problems of delimiting the spatialextent of morbidity in Madras are discussed and sample survey data are examinedwhich suggest that the disease is prevalent throughout the city to varying extentsand that community health education is still inadequate.

161
Filaria
24. Epidemiology of bancroftian filariasis in a semi-urban community of KeralaState.
JAIN DC, MENON PK, SETHUMADHAVAN KV,JOHNY VM,GHOSH TK.
J Commun Dis.21(4): 1989, 265-71
A community-based longitudinal study was initiated in 1983 in a semi-urbanarea, endemic for bancroftian filariasis to determine the incidence and prevalence,natural history and clinical pattern of filarial infection and also to study the impactof control measures on it. The base-line filariometric indices observed duringthe initial clinico-parasitological survey and entomological observations madeduring the first 12 months of this study are highlighted in this paper. 5.5 per centof the examined population had microfilaraemia with average infestation of 8.1per 20 cmm. The microfilaraemia found to have significant (P less than 0.001)relationship with age, but not with sex (P greater than 0.05). The filarial diseasewhich had the prevalence of 3.6 per cent showed a significant (P less than 0.001)relationship to both age and sex. The youngest microfilaria (mf) carrier was of 2years and with filarial swelling was of 6 years age. A significant (P less than0.001) relationship of educational status and family size was observed with diseasewhile it was non-significant (P greater than 0.05) with microfilaraemia. With theincrease in per capita income of the individuals, a significant decrease in numberof persons with microfilaraemia (P less than 0.01) as well as with disease (P lessthan 0.05) was noted. Culex quinquifasciatus, the vector for this infection wasprevalent throughout the period of observation with highest density in September.Vector infection and infectivity rates ranged from 0 to 4.4 per cent and 0 to 2.2per cent respectively.
25. Epidemiology of brugian filariasis in a rural community of Kerala State.
JAIN DC,CHANDRASEKHARAN A, SETHUMADHAVAN KV,JOHNYVM,CHERIAN C,GHOSH TK.
J Commun Dis, 1989., 21(1): 27-33.
The baseline clinico-parasitological parameters collected during the initial surveyand the entomological observations made during the first year as a part of alongitudinal study undertaken in a brugian endemic rural community are presented

162
Filaria
in this paper. Out of the total (11.604) examined population, 8.1 per cent hadmicrofilaraemia and 7.6 per cent had filarial disease. A highly significant (P lessthan 0.001) relationship of age was observed with microfilaraemia and the disease.The filarial disease rate showed no significant difference between two sexeswhile the microfilaria (Mf) rate was significantly (P less than 0.001) higher inmales than females. A significant (P less than 0.001) relationship ofmicrofilaraemia as well as of filarial disease was found with the income and theeducational status of the individual. The mf and the disease rates did not differby the family size except those families with 1-3 members. However, therelationship of family size was found to be significant (P less than 0.001) withdisease and non-significant (P greater than 0.05) with microfilaraemia. The vectorswere prevalent throughout the year but the infection was mostly confined toMansonia annulifera.
26. Clinical filarial disease in two ethnic endemic communities of Orissa,
KAR S K, MANIA J, KAR PK.
India. J Trop Med Hyg 1993. 96 (5): 311-6.
The overall prevalences of clinical disease and infection in both mainlanders(34.18 and 14.4%) and tribals (25.47 and 17.9%) were comparable. However,both annual average adenolymphangitic attack rate (1.77 year-1) and theprevalence of chronic filarial disease (22.6%) amongst tribals were significantlylower. No true elephantiasis was observed in tribals.
27. Clinical filarial disease in two ethnic endemic communities of Orissa,
KAR S K, MANIA J, KAR PK.
India. J Trop Med Hyg ,1993.96 (5): 311-6
The overall prevalences of clinical disease and infection in both mainlanders(34.18 and 14.4%) and tribals (25.47 and 17.9%) were comparable. However,both annual average adenolymphangitic attack rate (1.77 year-1) and theprevalence of chronic filarial disease (22.6%) amongst tribals were significantlylower. No true elephantiasis was observed in tribals.

163
Filaria
28. Tropical pulmonary eosinophilia in an Orissa village.
KAR SK, MANIA J.
Natl Med J India 1993.6(2): 64-7.
We were able to screen 1754 (91%) out of 1918 villagers who were more than 5years old and found 69 cases who had typical clinical features of tropicalpulmonary eosinophilia. Only 6 (0.34%) of these had eosinophil counts above3000 per cmm and were considered to have the disease. Only 2 of the 6 hadassociated filarial lesions, one had microfilaraemia and 3 had typical chest X-ray changes. The mean (+/- SD) titres for filaria specific IgG (0.355 +/- 0.315 v.0.120 +/- 0.092) and total IgE (0.455 +/- 0.316 v. 0.114 +/- 0.075) weresignificantly higher in cases with tropical pulmonary eosinophilia than in controlsubjects. The level of eosinophilia was related neither to the patients’ immunestatus nor to the severity of the radiological lesions. All cases recovered aftertherapy with diethylcarbamazine. CONCLUSION. Tropical pulmonaryeosinophilia is not uncommon in this community in Orissa where filariasis isendemic. However, the syndrome is rarely associated with clinical filarial lesions.
29. Tropical pulmonary eosinophilia in an Orissa village
KAR, S. K. AND J. MANIA
Natl Med J India(1993). 6: 64-7.
We were able to screen 1754 (91%) out of 1918 villagers who were more than 5years old and found 69 cases who had typical clinical features of tropicalpulmonary eosinophilia. Only 6 (0.34%) of these had eosinophil counts above3000 per cmm and were considered to have the disease. Only 2 of the 6 hadassociated filarial lesions, one had microfilaraemia and 3 had typical chest X-ray changes. The mean (+/- SD) titres for filaria specific IgG (0.355 +/- 0.315 v.0.120 +/- 0.092) and total IgE (0.455 +/- 0.316 v. 0.114 +/- 0.075) weresignificantly higher in cases with tropical pulmonary eosinophilia than in controlsubjects. The level of eosinophilia was related neither to the patients’ immunestatus nor to the severity of the radiological lesions. All cases recovered aftertherapy with diethylcarbamazine. CONCLUSION. Tropical pulmonaryeosinophilia is not uncommon in this community in Orissa where filariasis isendemic. However, the syndrome is rarely associated with clinical filarial lesions.

164
Filaria
30. Clinical filarial disease in two ethnic endemic communities of Orissa, India.
KAR, S. K., J. MANIA, ET AL.
J Trop Med Hyg (1993).96: 311-6.
To evaluate the possible role of ethnicity in susceptibility to filarial infection, acomparative study of the prevalence of filarial infection was initiated in anendemic village inhabited by two ethnic populations of mainlanders and tribals.An age and sex matched sampled population of 591 mainlanders and 106 tribalswas studied by detailed clinical and parasitological (60 mm3 blood) examinations.Sera collected from both population groups (26 each) matched for clinical stageof infection were analysed for humoral immune responses such as antifilarialIgG, circulating filarial antigen and immune complex level. The overallprevalences of clinical disease and infection in both mainlanders (34.18 and14.4%) and tribals (25.47 and 17.9%) were comparable. However, both annualaverage adenolymphangitic attack rate (1.77 year-1) and the prevalence of chronicfilarial disease (22.6%) amongst tribals were significantly lower. No trueelephantiasis was observed in tribals. No significant difference was observed intheir humoral immune response, although the antifilarial antibody of IgG classin all stages of filarial infection was lower in tribals than in mainlanders. Theresults did not reveal any difference in susceptibility to filarial infection in theethnic groups. The paucity of progressive lesions observed in tribals possiblyreflects a difference in the anatomy of lymphatics or genetic or immunoregulatorymechanisms, that needs further study.
31. Prevalence of lymphatic nodule in a bancroftian endemic population
KAR, S. K., J. MANIA, ET AL.
Acta Trop (1993).55: 53-60.
Prevalence and clinical manifestation of lymphatic nodule in natural course ofbancroftian filariasis was evaluated in a representative population of 2837 of adefined endemic community of Orissa. Detailed clinical and parasitologicalexamination of study subjects revealed high disease (35.6%) and mf rate (15.8%)and mean microfilariae density (GM: 15.3 +/- 5.1 per 60 mm3 of blood) in thecommunity. Lymphatic filarial nodule was manifested in 216 (7.6%) subjects in
165
Filaria
different spectrum of filarial infection including endemic normals andasymptomatic mf carriers. Significant proportion of cases with acute filarialdisease in the community manifested nodule. Significant proportion of caseswith nodule had microfilaraemia (33.3%) as compared to that of community.However highest frequency of nodule was observed amongst microfilaraemicswith lowest density of microfilaraemia in the community (P < 0.05.). This possiblyindicates microfilariae clearance from circulation as a consequence of death ofadult parasite. The above observations suggest that lymphatic nodules maymanifest as an early and/or the only clinical sign of bancroftian filariasis. Thismight have been mediated through either the attempt of the immuno-competenthost to kill the adult parasite in a similar fashion that is effected through DEC orby death of the mature parasite in its natural process of attrition.
32. Lymphatic filariasis in two distinct communities of upper Assam
KHAN, A. M., P. DUTTA, ET AL.
J Commun Dis (1999).31(2): 101-6.
Current status of bancroftian filariasis among two distinct communities of UpperAssam was evaluated. High prevalence (10.3% mf rate) in tea workersdescendents of tribals migrated from endemic states such as Orissa, Bengal,Uttar Pradesh and southern states of India, were recorded. Among non tea workers(indigenous population) significantly low mf rate was found in spite of the factthat both the communities are living in close vicinity and in similar ecologicaland mosquitogenic conditions. Culex quinquefasciatus was incriminated as vectorin the areas of both the communities. A group of recent migrants of Bihar andBengal living in the locality of non tea worker population were also foundmicrofilaraemic. Significantly lower infection rate in non tea worker populationappears to be associated with host susceptibility to the infection. Familialclustering in microfilaraemic subjects noticed in tea workers group also suggestsinvolvement of racial susceptibility to infection.
33. Prevalence of filariasis in rural Puri, Orissa.
KUMAR A, DASH AP,MANSING GD.
J Commun Dis,1994, 26(4): 215-20.

166
Filaria
Prevalence of filariasis in 8 randomly selected villages of Puri district was studied.782 persons were examined. The prevalence of microfilaria was found to be 7.3per cent and the disease rate 9.5 per cent. The mf rate was higher in males (8.8per cent) than the females (5.7 per cent) and similarly the disease rate were 10.6per cent and 8.3 per cent respectively in the two sexes.
34. Human filariasis: infection rate as the uniform measurable criterion forfilarial endemicity.
KUMAR, A.
JCommunDis (1996).28(3): 163-7 Iissn: 0019-5138.
The endemicity classification based on filariasis infection rate is suggested. Basedon the filariometric data collected from 60 villages in Orissa, areas are classifiedinto low, high, hyper and holo endemic levels. Suggested endemicity levels arefound to correlate very well with the filariometric indices. The mean mf rateswere found to be 2.7, 6.8, 12.0, and 16.0, and disease rates 4.9, 10.2, 18.9 and35.1 respectively at four endemicity levels. It is suggested that the proposedclassification may uniformly be used in mapping areas for endemicity so as tohelp direct public health control interventions in a judicious manner.
35. Prevalence of Wuchereria bancrofti infection in some coastal villages ofGanjam, Orissa.
KUMAR, A. AND S. K. CHAND
J Commun Dis (1990).22: 209-12.
The endemicity of filariasis was assessed in 42 villages of coastal KeluapalliPHC in Ganjam District of Orissa. Prevalence was found to vary greatly betweenextreme coastal and subcoastal villages. The infection was non existent in 12coastal villages. Age and sexwise distribution of filariasis cases have beenanalysed and presented.
36. Prevalence of filariasis in rural Puri, Orissa.
Kumar, A., A. P. Dash, et al.
J Commun Dis(1994). 26: 215-20.

167
Filaria
Prevalence of filariasis in 8 randomly selected villages of Puri district was studied.782 persons were examined. The prevalence of microfilaria was found to be 7.3per cent and the disease rate 9.5 per cent. The mf rate was higher in males (8.8per cent) than the females (5.7 per cent) and similarly the disease rate were 10.6per cent and 8.3 per cent respectively in the two sexes. The mf rate wasconsiderably lower (4.6 per cent) in the population using mosquito nets regularlyas compared to irregular users (8.2 per cent) and never users (9.0 per cent).Similarly persons with ‘normal’ clothing had lower mf rate (5.0 per cent) thanthose using ‘medium’ clothing (7.6 per cent) and “minimum” clothing (8.9 percent). The mf rate and disease rate correlate well (r = .65). The Culexquinquefasciatus Say constituted the main bulk (65 per cent) of mosquitocollection in this area with a density of 17 per man hour.
Lymphatic filariasis in Khurda district of Orissa, India: an epidemiological study.Southeast Asian J Trop Med Public Health. 32(2): 240-3. A cross-sectional surveywas undertaken to determine the prevalence of disease due to lymphatic filariasisin Khurda district of Orissa, India. The total disease attributable to filariasis wassignificantly higher in males (14.79%) than females (10.04%). However,elephantiasis is more prevalent in females, and adenolymphangitis is moreprevalent in males than their counterparts
37. Re-assessing the global prevalence and distribution of lymphatic filariasis.
MICHAEL, E., D. A. BUNDY, ET AL.
Parasitology (1996)112 ( Pt 4): 409-28.
This paper estimates the global burden of lymphatic filariasis based on a reviewof the published literature on infection and disease surveys. A method foraggregating and projecting prevalence data from individual studies to national,regional and global levels, which also facilitates the estimation of gender andage-specific burdens, is presented. The method weights in favour of the larger,and hence presumbably more reliable, studies and relies on estimated empiricalrelationships between gender, age, infection and disease in order to correct studieswith incomplete data. The results presented here suggest that although the overallprevalence of filariasis cases is 2.0% globally (approximately totalling 119 millioncases), the disease continues to be of considerable local importance, particularlyin India and Sub-Saharan Africa. Estimates by age and gender clearly show that,

168
Filaria
unlike other helminth infections, filariasis is mainly a disease of the adult andolder age-classes and appears to be more prevalent in males. This work suggeststhat the derivation of more accurate estimates of the burden of filariasis willrequire a better understanding of both the epidemiology and the spatial aspectsof infection and disease. It also suggests that filariasis is preventable based on ageographically targeted strategy for control.
38. Relative abundance of Culex quinquefasciatus (Diptera: Culicidae) withreference to infection and infectivity rate from the rural and urban areas ofEast and West Godavari districts of Andhra Pradesh, India.
MURTY, U. S., K. S. SAI, ET AL.
Southeast Asian J Trop Med Public Health (2002) 33(4): 702-10.
This paper describes the seasonal abundance of Culex quinquefasciatus in therural and urban areas of the East and West Godavari districts (EGDT and WGDT)of Andhra Pradesh, India. The per man-hour density (PMHD) was collected fromseven units in EGDT and two units in WGDT, which comprised rural and urbanareas. The highest infection and infectivity rates were found in the rural areas ofRajahmundry (43.6%) and Amalapuram (13.2%) respectively. In urban areas,the highest infection and infectivity rates were found in Rajahmundry: 7.5% and3.6% respectively. There was considerable difference in the infection rate andinfectivity rates between the rural areas and urban areas in each unit.
39. Treatment seeking behaviour and costs due to acute and chronic forms oflymphatic filariasis in urban areas in south India.
NANDA B, KRISHNAMOORTHY K.
Trop Med Int Health., 2003, 8(1): 56-9.
Previous estimates on the economic burden of lymphatic filariasis (LF) in Indiaand elsewhere were primarily based on studies in rural areas. We investigatedthe treatment costs due to acute and chronic forms of LF in urban areas, wherenearly one-third of the affected people live. Almost 98% of the patients withacute episodes of adenolymphangitis (ADL) underwent treatment and 49% ofchronic patients also received treatment. The average treatment cost per ADL

169
Filaria
episode (n = 108) was Rs 22.21 +/- 53.84 (US dollars 0.46 +/- 1.12). The overall(n = 200) treatment costs incurred by a chronic patient per visit were Rs 16.71 +/- 62.36 (US dollars 0.35 +/- 1.30); for those who paid (n = 98) they were Rs34.10 +/- 85.90 (US dollars$ 0.71 +/- 1.79). These costs are considerably higherthan in rural areas. Government health centres and private practitioners wereimportant considerably more expensive than those from government healthfacilities. sources of treatment. Treatments received from private practitionerswere The cost of medicine accounted for 44% and 50% of the total expenditureon treatment for acute and chronic disease patients, respectively. The medicalpersonnel from these treatment sources need to be trained on the new morbiditymanagement methods, which are likely to be more effective than the currentmethods of treatment.
40. EPIFIL: the development of an age-structured model for describing thetransmission dynamics and control of lymphatic filariasis.
NORMAN RA, CHAN MS, SRIVIDYA A, PANI SP, RAMAIAH KD,VANAMAIL P, MICHAEL E, DAS PK, BUNDY DA.
Epidemiol Infect., 2000, 124(3): 529-41.
Mathematical models of transmission dynamics of infectious diseases provide auseful tool for investigating the impact of community based control measures.Previously, we used a dynamic (constant force-of-infection) model for lymphaticfilariasis to describe observed patterns of infection and disease in endemiccommunities. In this paper, we expand the model to examine the effects of controloptions against filariasis by incorporating the impact of age structure of the humancommunity and by addressing explicitly the dynamics of parasite transmissionfrom and to the vector population. This model is tested using data for Wuchereriabancrofti transmitted by Culex quinquefasciatus in Pondicherry, South India.The results show that chemotherapy has a larger short-term impact than vectorcontrol but that the effects of vector control can last beyond the treatment period.In addition we compare rates of recrudescence for drugs with differentmacrofilaricidal effects.
41. Rapid assessment procedures (RAP) for lymphatic filariasis.
PANI S P, SRIVIDYA A, KRISHNAMOORTHY K, DAS PK, DHANDA V.
Natl Med J India., 1997, 10(1): 19-22

170
Filaria
New strategies are emerging for control of filariasis in terms of chemotherapyand vector control. Field application of these tools requires mapping andprioritization of filaria-endemic areas and quantification of the infection/ diseaseburden. Available procedures are time-consuming, costly and have poorsensitivity. Therefore, rapid assessment procedures need to be developed to assessthe disease burden as well as monitor and evaluate control programmes.METHODS: Data collected on different variables from 25 areas in India andelsewhere were used. The relationship between prevalence of human infectionand vector infection rate was analysed quantitatively. Due to lack of independentsamples, only qualitative analysis was carried out between other epidemiologicalvariables such as infection and disease prevalence in relation to age, gender andmanifestation. RESULTS: There was a significant positive correlation betweenvector infection rate and infection prevalence in humans, suggesting that vectorinfection can be used as an indicator in the rapid assessment of infectionprevalence. Scatter plots showed that community screening may be limited tothe age group of 11-30 years for infection prevalence and 20-50 years for diseaseprevalence. Further, clinical surveys may be limited to only hydrocele prevalencewhich may be sufficient to predict the total disease. This can also be used as analternative method by the community itself for delimiting endemic areas. Vectorinfection rate may be used as an indicator for rapid assessment of human infection.Alternatively, blood smear examination could be limited to the age group of 11-30 years. For a rapid survey of the diseases, males in the age group of 20-50years could be examined only for hydrocele.
42. Clinical epidemiology of bancroftian filariasis: effect of age and gender.
PANI SP, BALAKRISHNAN N, SRIVIDYA A, BUNDY DA, GRENFELL BT.
Trans R Soc Trop Med Hyg, 1991.85(2): 260-4.
A cross-sectional survey was used to determine the prevalence of disease (n =6493) and microfilaraemia (n = 24,946) due to Wuchereria bancrofti inPondicherry, south India. The total disease attributable to filariasis wassignificantly higher in males (13.67%) than females (2.26%), due to theoccurrence of hydrocele in males. While the prevalence of chronic signs wasclearly age-dependent in both sexes, that of acute signs was independent of age.Thus the age and gender structure of the survey sample will crucially influenceapparent prevalence. Examination of the gender differences in the point

171
Filaria
prevalence of disease in 12 areas of India showed a significant relationshipbetween occurrence of disease and gender, but this relationship did notsignificantly differ between northern and southern Indian populations. The studysuggested that the failure to appreciate the importance of age and gender in diseaseprevalence has led to misconception about disease patterns in India.
43. Clinical manifestations of bancroftian filariasis with special reference tolymphoedema grading.
PANI SP, SRIVIDYA A.
Indian J Med Res. , 1995, 102: 114-8.
We report on some aspects of progression of chronic disease and its associationwith acute manifestations with special reference to grades of lymphoedema inbancroftian filariasis. These analyses were based on the clinical history and clinicalfindings of 1300 individuals at the time of their first visit to the filariasis clinic ata centre in south India. The mean number of adenolymphangitis (ADL) attacksin one year was 4.9 +/- 1.7, 5.5 +/- 0.9 and 10.4 +/- 3.2 in patients with grade I,grade II and grade III lymphoedema respectively. The mean duration of oedemawas 47.4 +/- 5.9 days, 6.2 +/- 0.5 and 8.6 +/- 0.9 yr in patients with grade I, gradeII and grade III lymphoedema respectively. These findings suggest that theprogression of lymphoedema from one grade to the next in bancroftian filariasisis associated with increased frequency of ADL attacks.
44. Micro-spatial variation in filarial disease and risk of developing diseaseassociated with microfilaremia in urban situation.Southeast Asian
PANI SP, VANAMAIL P, SRIVIDYA A, DAS PK, DHANDA V.
J Trop Med Public Health, 25(4): 1994.719-23.
Clinical and parasitological surveys were carried out concurrently during 1986in Pondicherry. The analyses showed that there was no significant micro-spatialvariation in prevalence of total diseases (acute and chronic) and the manifestationssuch as hydrocele and lymphedema in the different zones and stations ofPondicherry urban area, a stable endemic area. Analyses on different filariometricindices in different stations showed a significant correlation between disease

172
Filaria
and mf prevalence (r = 0.4106; p = 0.037). The prevalence of disease andhydrocele in microfilaremic individuals (9.4% and 20.0% respectively) was highercompared to that observed in amicrofilaremic persons (6.4% and 11.2%respectively). The relative risk (RR) of parasite carriers developing disease (anymanifestations) was marginally higher compared to amicrofilaremic persons(1.18). However, the RR of developing hydrocele manifestation due tomicrofilaremia was much greater (1.5) compared to amicrofilaremic persons.The attributable risk (AR) due to microfilaremia for developing hydrocele was0.05. This suggests that although the risk is high in mf carriers, there might bealternate ways of developing disease without the infected person becomingmicrofilaremic. The limitations of point prevalence data on understandingcomplex dynamics of infection and disease are discussed.
45. Episodic adenolymphangitis and lymphoedema in patients with bancroftianfilariasis.Trans R
PANI SP, YUVARAJ J, VANAMAIL P, DHANDA V, MICHAEL E, GRENFELLBT, BUNDY DA.
Soc Trop Med Hyg. 1995.89(1). 72-4.
In order to explore the relationship between acute and chronic disease, age-specificdata on the frequency and duration of episodic adenolymphangitis (ADL) inpatients with 3 defined grades of lymphoedema in bancroftian filariasis wereexamined. The age distribution of grades I and II exhibited a convex age profile,but that of grade III showed a monotonic increase. The mean duration of oedemaincreased with its grade (grade I, 0.3 years; grade III, 9.9 years). The mean numberof ADL episodes in the previous year for all cases was 4.2 and it increased withgrade (grade I, 2.4 and grade III, 6.2). The mean duration of each ADL episodefor all cases was 4.1 d and it was independent of grade and age. The mean periodlost to ADL episodes in the previous year was 17.5 d; it increased from 9.4 dwith grade I to 28.5 d with grade III. The results imply that there is a dynamicprogression through the grades of lymphoedema and that the frequency of ADLepisodes is positively associated with this progression. However, the study designcould not separate cause from effect.
173
Filaria
46. Clinical manifestations in malayan filariasis infection with special referenceto lymphoedema grading.
PANI SP,KRISHNAMOORTHY K, RAO AS, PRATHIBA J.
Indian J Med Res, 1990. 91: 200-7.
In a door-to-door survey in Shertallai area of Kerala state in southern India,7,766 persons were examined for clinical manifestations of filariasis. Theprevalence of disease was 9.85 per cent and chronic persistent oedema (grade-II) was the predominant clinical presentation in both sexes. There was nosignificant difference in the age prevalence of disease between the sexes. Incidenceof episodic filarial fever was higher (4.73/1000) compared to other manifestations(2.49/1000) in children aged 5-15 yr and hence this may be an useful indicator ofthe degree of occurrence of fresh cases of clinical filariasis. Classification ofpatients with lymphoedema into three grades showed that 1.65 per cent of thoseexamined had developed lymphoedema within 6 months. Persistence of oedema(grade II) for prolonged period (13.64 +/- 1.17 yr) without skin changes indicatedthat the development of elephantiasis is a slow process. The clinical picture ofmalayan filariasis is similar to that reported elsewhere in the world except forthe rarity of abscess formation is inguinal area.
47. Clinical manifestations in malayan filariasis infection with special referenceto lymphoedema grading.
PANI, S. P.; KRISHNAMOORTHY, K.; RAO, A. S.; PRATHIBA, J.
Indian J Med Res. 1990.91: 200-7
In a door-to-door survey in Shertallai area of Kerala state in southern India,7,766 persons were examined for clinical manifestations of filariasis. Theprevalence of disease was 9.85 per cent and chronic persistent oedema (grade-II) was the predominant clinical presentation in both sexes. There was nosignificant difference in the age prevalence of disease between the sexes. Incidenceof episodic filarial fever was higher (4.73/1000) compared to other manifestations(2.49/1000) in children aged 5-15 yr and hence this may be an useful indicator ofthe degree of occurrence of fresh cases of clinical filariasis. Classification ofpatients with lymphoedema into three grades showed that 1.65 per cent of those

174
Filaria
examined had developed lymphoedema within 6 months. Persistence of oedema(grade II) for prolonged period (13.64 +/- 1.17 yr) without skin changes indicatedthat the development of elephantiasis is a slow process. The clinical picture ofmalayan filariasis is similar to that reported elsewhere in the world except forthe rarity of abscess formation is inguinal area.
48. Bancroftian filariasis in Namrup tea estate, district Dibrugarh, Assam
PRAKASH, A., P. K. MOHAPATRA, ET AL.
Indian J Public Health (1998).42(4): 103-7, 112.
Filariasis survey in a randomly selected tea estate of district Dibrugrah revealed6.7% infection of Wuchereria bancrofti in labour population with microfilaria(mf) rate of 7.6% in males and 5.9% in females. The mf rate increasedprogressively with the age which however, dropped in 31-40 age group of malesand in 41-50 age group of females. Chronic filariasis diseases rate was 2.7%.The involvement of genitals in manifesting chronic filariasis was significantlyhigher than of the lower extremities. Infection and infectivity rates in the vectormosquito, Culex quinquefasciatus were 6.1% and 4.6% respectively with meanL3 load per infective mosquito of 8.5. Drains, land, peridomestic ditches werechief breeding habitats of Cules quinquefasciatus in the tea estate.
49. Epidemiology of Brugia malayi infection and its co-existence withWuchereria bancrofti in and around Sillaberia PHC, District Midnapur,West Bengal.
RAINA VK, JOSHI MC, SINGH S, JOSHI RD, BHATTACHARJEE KK,KUMAR A, VERGHESE T.
J Commun Dis. 1990, 22(3): 205-8.
Of 2186 persons investigated in thirteen villages of Sillaberia PHC, 19 werefound to be infected with Brugia malayi and only one person harbouredmicrofilaria (mf) of Wuchereria bancrofti. Similarly 41 persons exhibited signsand symptoms of chronic filariasis. The mf and disease rates percent worked outto be 0.914 and 1.87 respectively. The earliest ages showing mf and diseasemanifestations were 3 and 11 respectively. The male and female ratio in terms ofmf carriers and chronic cases worked out to be 1.4:1 and 1:2 respectively.

175
Filaria
50. Status of lymphatic filariasis in some select slum clusters of Delhi
RAINA, V. K., V. C. TRIPATHI, ET AL.
J Commun Dis (1992).24: 92-6.
Filaria surveys conducted in some select slum clusters namely Hari Nagar,Yamuna pusht near Vijaya Ghat along the Ring Road and Timarpur in Delhiduring 1989, 1991 and 1992 respectively, covering a population of approximately5000 slum dwellers revealed the presence of bancroftian microfilaria (mf) carriersand disease cases. The mf and disease rates (per cent) in these three slum areaswere in the order of 6.3, 2.2, 3.7 and 1.4, 0.5 and 0.1 respectively. The mf densityvaried from 3.1 to 12.3 per 20 cumm. blood. High ten man hour densities ofCulex quinquefasciatus (581) in Yamuna pusht followed by (355) in Timarpurwere recorded during entomological investigations. Hari Nagar accounted forleast ten man hour density of Cx. quinquefasciatus (160), because collectionwas made during winter months (November-December). The dissection of Cx.quinquefasciatus did not reveal any human filarial infection except in Yamunapusht where out of 139 only one Cx. quinquefasciatus was found infective.
51. Bancroftian filariasis in Pondicherry, south India: 1. Pre-controlepidemiological observations.
RAJAGOPALAN PK, DAS PK, SUBRAMANIAN S, VANAMAIL P,RAMAIAH KD.
Epidemiol Infect. 1989.103(3): 685-92.
A 5-year Integrated Vector Management (IVM) project was implemented inPondicherry, South India, for the control of Bancroftian filariasis. The efficacyof the IVM strategy was compared with routine control strategy under the nationalprogramme. The present paper describes the pre-control epidemiological featuresof filariasis as determined by a mass blood survey in 1981. Of 24946 personsexamined 8.41% were microfilaraemic. Microfilaraemia prevalence washomogeneous throughout the study area. The prevalence and intensity ofmicrofilaraemia were age dependent, and increased monotonically until about20 years, following which there was a decline until about 40 years to becomerelatively stable in older age classes. The gender profiles of both prevalence and

176
Filaria
intensity of microfilaraemia showed no difference between the sexes until about15 years of age, following which both were higher in males compared to females.The distribution of microfilarial counts was overdispersed, indicating aggregationof adult worms.
52. Impact of 50 years of vector control on the prevalence of Brugia malayi inShertallai area of Kerala state.
RAJAGOPALAN PK,PANICKER KN, PANI SP.
Indian J Med Res., 1989,89: 418-25
This article examines the long term effects of vector control on the prevalence ofB. malayi infection and disease, by comparing the results of 3 earlier studies(1934, 1955, 1976) in one area of south India with a recent (1986) survey. Thedata indicate that disease and infection prevalence have declined continuouslyover the last 50 years. Infection has declined (from 21 to 2%) more markedlythan disease (from 24 to 10%). Age-specific data indicate that this difference isdue to the irreversibility of the clinical signs and the long term survival of diseasedcohorts. The results indicate that the prevalence of clinical brugian filariasis canbe reduced using vector control and that such control programmes cannot beevaluated in short term or by using crude morbidity statistics.
53. Current status of filariasis in Chavakad taluk, Trichur district, Kerala.
RAJENDRAN G, PANICKER KN, KRISHNAMOORTHY K, SABESAN S,SNEHLATHA,RADHAKRISHNAN R.
J Commun Dis. 1997.29(4): 333-43.
A sample survey using parasitological, clinical and entomological indicators wascarried out in all the 18 administrative units of Chavakad taluk, Trichur district,Kerala, India to assess the current filariasis situation. Cluster sampling procedurewas followed to screen individuals. Both Wuchereria bancrofti and Brugia malayispecies were found to be prevalent in this taluk. Microfilaria (mf) carriers withW. bancrofti were detected in eight areas while B. malayi was recorded onlyfrom one area. The two species were found to co-exist in another area. Thehighest infection rate registered for W. bancrofti was 1.51 while it was 0.3 for B.

177
Filaria
malayi. Infection due to W. bancrofti constituted 87.88% of the total 33microfilaria cases. Prevalence of B. malayi was very low. Cases with clinicalmanifestation of filariasis were recorded in all the four areas surveyed. The presenttrend in the prevalence of infection (mf) and disease showed a decline in boththe species when compared to earlier surveys of 1960s. At least 11 areas are stillendemic for filariasis in this taluk. Although prevalence of mf was recorded forthe first time in one of the areas viz., Elavalli, the rate was only 0.16%.Entomological surveys revealed the presence of 14 mosquito species, of whichCulex quinquefasciatus contributed 84.85% and Mansonia 0.77%. While C.quinquefasciatus was recorded in all the 18 areas, Mansonia spp were foundonly in 8 areas. Only C. quinquefasciatus was found to harbour differentdevelopmental stages of W. bancrofti, with overall infection and infectivity ratesof 1.94 and 0.97 respectively. The possible reason for the decline in vector densityand infection in man are postulated.
54. Prevalence of bancroftian filariasis & its control by single course of diethylcarbamazine in a rural area in Tamil Nadu.
RAMAIAH KD, PANI SP, BALAKRISHNAN N, SADANANDANE C, DASL K, MARIAPPAN T, RAJAVEL AR, VANAMAIL P, SUBRAMANIAN S.
Indian J Med Res. 1989.89: 184-91.
The prevalence of microfilaraemia, clinical spectrum of bancroftian filariasisand vector potential were studied in Vettavalam village in North Arcot district ofTamil Nadu. The prevalence of microfilaraemia (mf rate) and disease (diseaserate) was found to be 11.7 and 11.09 per cent respectively. Hydrocele was thedominant clinical sign in males and lymphoedema in females.
55. The impact of lymphatic filariasis on labour inputs in southern India: resultsof a multi-site study.
RAMAIAH KD, RADHAMANI MP,JOHN KR, EVANS DB,GUYATT H,JOSEPH A,DATTA M, VANAMAIL P.
Ann Trop Med Parasitol. 2000.94(4): 353-64
A multi-site study was undertaken, in the rural areas of three districts in TamilNadu state, in southern India, to examine the impact of acute and chronic forms

178
Filaria
of lymphatic filariasis, caused by infection with Wuchereria bancrofti, on labourinputs. More than half of the acute episodes of adenolymphangitis (ADL) observedin the study communities caused total disability. The mean (S.D.) time that eachADL case was able to allocate to economic activity each day during these acuteepisodes was much less than seen in the controls matched for sex, age andoccupation [0.97 (2.36) v. 4.48 (3.82) h; P < 0.01]. The acute disease also severelyaffected domestic activities, with female ADL cases spending only 1.54 (2.12)h/day on domestic activity, compared with 4.18 (2.61) h by controls. The subjectswith chronic filariasis also spent significantly less time in economic activitythan their matched controls [4.40 (3.79) v. 5.13 (3.83) h/day; P < 0.01). Althoughthe acute episodes have a dramatic effect on the productivity of the affectedindividual, the labour loss caused by chronic disease is more serious, as themanifestations of chronic disease mostly affect the most productive age-groups,persist for life and are mostly irreversible. The adverse impact of acute and chronicfilariasis was observed in males and females, farmers and non-farmers and duringthe rainy, winter and summer seasons. It is estimated that about 3.8% of thepotential labour inputs of the men and 0.77% of those of the women were lostbecause of lymphatic filariasis. In addition to this loss, the total economic burdenof the disease must include the costs of treatment and other health care and ofthe resources spent on control programmes. Estimates of the disease burden arelikely to be useful in determining the costs and benefits of the recently launchedcampaign to eliminate lymphatic filariasis.
56. Prevalence of bancroftian filariasis & its control by single course of diethylcarbamazine in a rural area in Tamil Nadu.
RAMAIAH, K. D., S. P. PANI, ET AL.
Indian J Med Res (1989).89: 184-91.
The prevalence of microfilaraemia, clinical spectrum of bancroftian filariasisand vector potential were studied in Vettavalam village in North Arcot district ofTamil Nadu. The effectiveness of selective therapy with diethyl carbamazine(DEC) in controlling filariasis in rural areas was also evaluated. The prevalenceof microfilaraemia (mf rate) and disease (disease rate) was found to be 11.7 and11.09 per cent respectively. Hydrocele was the dominant clinical sign in malesand lymphoedema in females. The density of the vector Culex quinquefasciatuswas 25.44 females/man-hour, and the infection and infectivity rates were 18.16

179
Filaria
and 1.09 per cent respectively. All mf carriers detected after the mass bloodsurvey were given a single course of DEC at the dosage of 6 mg/kg of body wt/day for 12 days. Only 61.6 per cent of them took the full course of DEC treatment.DEC therapy brought down the mf rate from 11.7 to 5.84 per cent after onemonth. In the absence of further treatment, there was no significant change in mfprevalence after one year.
57. Impact of control measures on prevalence and incidence of bancroftianfilariasis in East Godavari district (Andhra Pradesh).
RAO, C. K., K. R. PRASAD, ET AL.
Indian J Med Res (1982). 75: 515-20.
The impact of different control measures viz.antilarval measures, antilarvalmeasures along with selective treatment of microfilaria (mf ) carriers withdiethylcarbamazine (DEC), selective treatment of mf carriers with DEC only,and total population treatment with DEC, on the incidence and prevalence offilariasis in villages was measured. In Penikeru, the mf prevalence rate beforetreatment was 10.8 per cent, and afterwards 7.2 percent; ( P>0.05), In Alameru ,the mf prevalence rate before treatment was 14.0 percent, and after wards 8.5percent (P< 0.01), ; in Angara , it declined from 16.0 to 7.2 percent ( P< 0.01);and in West Kandrika , the mf prevalence rate declined from 15.5 to 13.8 percent( P>0.05).
58. Detection of a new focus of Brugia malayi infection in Orissa.
RATH RN, MOHAPATRA BN, DAS B.
J Commun Dis(1989) 21(1): 39-40.
526 people were surveyed in a village called Chudamani, in Balasore district ofOrissa, for detection of asymptomatic microfilaria (mf) carriers. Of these 36 (6.8per cent) were cases found to harbour mf; 19 cases had Brugia malayi, 4Wuchereria bancrofti and 5 cases had mixed infection. In 8 cases, species couldnot be ascertained. For the first time after 1955, a focus of B. malayi has beendetected in Orissa.
180
Filaria
59. Pulmonary eosinophilia in children: report of a school survey in rural TamilNadu in India.
RAY, D. AND R. ABEL
J Trop Pediatr (1994).40: 49-51.
During the period of 1981-82 in a survey of 21 schools in four villages of NorthArcot Ambedkar District of Tamil Nadu, amongst a population of 4282 childrenwe detected 92 with respiratory symptoms and blood eosinophilia greater than1000 per cumm. Sixty-eight students had associated worn infestation, majoritywith hookworm followed by giardia. Altogether 37 children had blood eosinophiliaabove 2000 per cumm and had symptoms of cough, dyspnoea, and wheezeconsistent with pulmonary eosinophilia. Fourteen of the children with pulmonaryeosinophilia had eosinopenic remission with deworming alone. Six of them, onthe other hand, responded to diethyl carbamazine (DEC) alone and 17 others,following deworming, required further DEC therapy for successful eosinopenicremission, thus warranting a diagnosis of Tropical Pulmonary Eosinophilia (TPE).
60. Epidemiology of pulmonary eosinophilia in rural south India—a prospectivestudy, 1981-86
RAY, D., R. ABEL, ET AL.
J Epidemiol Community Health (1993). 47: 469-74
Eosinopenic remission was documented in 135 of 182 cooperative patients whowere considered to have tropical pulmonary eosinophilia and agreed to be treatedwith diethylcarbamazine. CONCLUSIONS—This study found that tropicalpulmonary eosinophilia, either alone or with worm infestation, was a major causeor morbidity in this rural population.
61. Comparative epidemiological studies on lymphatic filariasis, between tribaland non-tribal populations of Bankura district, West Bengal,
RUDRA SK, CHANDRA G.
India. Ann Trop Med Parasitol, 2000, 94(4): 365-72.

181
Filaria
That which is known mostly relates to Calcutta and its suburbs, and there havebeen few studies on the disease among the tribal populations of the state. Thepresent study was designed to compare the epidemiology of filariasis in tribaland non-tribal populations living in Bankura district. The results revealed thatthe tribal subjects had not only lower prevalence of microfilaraemia (3.17% v.8.86%) and of symptomatic filariasis (5.92% v. 13.74%) than the non-tribal,Filariasis endemicity, measured as the percentage of subjects with microfilaraemiaand/or disease, was therefore much lower among the tribal subjects (8.95%)than the non-tribal (22.12%).
62. The dynamics of microfilaraemia and its relation with development of diseasein periodic Brugia malayi infection in south India.
SABESAN S, KRISHNAMOORTHY K, PANICKER KN,VANAMAIL P.
Epidemiol Infect 1991, .107(2): 453-63.
Rates of acquisition and loss of Brugia malayi microfilaraemia were estimatedusing the parasitological data of a cohort of population in Shertallai, South India.The rate of acquisition of microfilaraemia was found to be dependent on age butnot gender. The decline in the rate of acquisition of microfilaraemia in adultsabove 35 years could be due to the development of acquired immunity. Themean reproductive lifespan for the periodic Brugia malayi adult female wormwas estimated to be 3.4 years and it was independent of host age and gender. Theage-specific estimated proportion of population at risk (microfilaria carriers wholost their microfilaria in course of time) of developing lymphoedemaapproximately mirrored the observed age specific prevalence of lymphoedemain the study population. On an average, 99% of population at risk developeddisease in different endemic areas is compared and its epidemiologicalsignificance is discussed.
63. Mapping of lymphatic filariasis in India.
SABESAN S, PALANIYANDI M, DAS PK, MICHAEL E..
Ann Trop Med Parasitol,. 2000,94(6): 591-606.
The derivation of detailed epidemiological maps, at the relevant spatial resolution,is being increasingly recognized as vital to the effective design and

182
Filaria
implementation of successful programmes for the control of parasites and theirvectors. Geographical information systems (GIS) and a recently complieddatabase on the distribution of lymphatic filariasis in India have now been usedto develop the first maps at district-level (i.e. the level at which control againstthis parasite will be enacted in India) of filariasis endemicity in this country. Thederived maps indicate both the substantial extent as well as the marked variabilityin the geographical distribution of this disease in India. The causative infectionand/or the symptomatic disease were detected in most (257) of the 289 districtssurveyed up to 1995. Currently there may be up to 27.09 million microfilaraemics,20.83 million cases of symptomatic filariasis, and about 429.32 millionindividuals potentially at risk of infection in the country. Probability mapping,based on data quantiles, clearly indicates that the risk of filarial infection inIndia is not constant throughout the country but exhibits strong regional trends.Filariasis in general may be a particular problem of the eastern half of the country.The results indicate the potentially vital role that GIS-based mapping approachescan play in the development of filariasis-control campaigns in India and elsewhere.
64. Present status of filariasis problem in India.
SHARMA, S.P., BISWAS, H., DAS, M., DWIVEDI, S.R.
Journal of communicable diseases, (1983).15:53-60.
From results of earlier surveys ( of which the exact survey design and samplesizes are not available) it is estimated that on 1 March 1981 about 304 millionpeople in India lived in areas known to be endemic for bancroftian or malayanfilariasis.About 222 million lived in rural areas and 82 million in urban areas;about 22 million had microfilaraemia and about 16 million showed signs offilariasis.
65. A preliminary study of filariasis related acute adenolymphangitis with specialreference to precipitating factors and treatment modalities.Southeast Asian
SHENOY RK,SANDHYA K, SUMA TK, KUMARASWAMI V.
J Trop Med Public Health. ,1995,26(2):301-5.
Episodic adenolymphangitis (ADL) is one of the important clinical manifestationsof lymphatic filariasis. Recurrent ADLs contribute to the progress of the disease

183
Filaria
and also have important socioeconomic implications since they cause significantloss of man days. The present study was conducted in order to identify theprecipitating factors responsible for ADL attacks and also to examine the differentmodalities of treatment. Sixty-five individuals with filariasis related ADL attacks,who are residents of Alleppey district (endemic for Brugia malayi) were studied.All efforts were taken to identify the precipitating factors for ADLs in theseindividuals. They were hospitalized for a period of five days or more. All ofthem received symptomatic antipyretic/antiinflammatory therapy and topicalantibiotic/antifungal treatment of the affected limbs. They were then randomlyallocated to one of the following four regimens: group I - symptomatic alone;group II - symptomatic plus antibiotics; group III - symptomatic followed bydiethylcarbamazine citrate (DEC) and group IV - symptomatic plus antibioticfollowed by DEC. Patients in groups III and IV received DEC every three monthsup to one year. There was a significant relationship between the number of ADLattacks and the grade of edema. Presence of focus of infection in the affectedlimb could be identified in 28 of the 65 patients. In the majority of patients (48)response to treatment was rapid (resolution in less than five days). Neitherantibiotics nor DEC (given at intervals of three months) appeared to alter thefrequency of ADL attacks. On the otherhand simple hygienic measures combinedwith good foot care and local antibiotic/antifungal cream application (whererequired), were effective in reducing the number of ADL attacks.
66. Little Andaman Island, a new focus of infection with nocturnally periodicWuchereria bancrofti
SHRIRAM, A. N., A. P. SUGUNAN, ET AL.
Indian J Med Res (1996).104: 166-70.
A filariasis survey was carried out for the first time in the Little Andaman island,covering a population of 12,247 in 12 of the 13 villages. Infection due toWuchereria bancrofti was found only in 3 villages with microfilaria (mf) rateranging from 1.02 to 6.45 per cent. Observations on the appearance of mf inperipheral blood showed that the parasite is nocturnally periodic form with apeak at 2000 h. The infection was prevalent only among the settlers from Biharand Bangladesh and none of the local tribal population was affected. Carriersincluded 18 males and 4 females. Their age ranged from 6 to 50 yr. Only one of2788 individuals examined was found to have clinical manifestation. (0.24%).

184
Filaria
Epidemiological investigations and vector studies indicates local transmission.Thus, this island appears as a new focus of infection.
67. Prevalence of diurnally subperiodic bancroftian filariasis among theNicobarese in Andaman and Nicobar Islands, India: effect of age andgender.
SHRIRAM, A. N., M. V. MURHEKAR, ET AL.
Trop Med Int Health(2002). 7(11): 949-54.
We conducted a cross-sectional survey to assess the prevalence of disease andmicrofilaraemia caused by diurnally subperiodic strain of Wuchereria bancroftitransmitted by day biting Aedes niveus in Teressa Island, remotely located in theNicobar district of Andaman and Nicobar Islands. Lymphatic filariasis is aconsiderable public health problem on this island with an overall endemicityrate of 16.2%. There was a gradual increase in microfilaraemia prevalence withage, reaching a plateau above 30 years. Both the microfilaraemia and diseaserates were significantly higher in males (14.7% and 5.2%) than females (8.6%and 1.5%, P < 0.001). The age and gender specific distribution of chronicmanifestations show a gradual increase with age, whereas acute disease startedto occur from age 40 in males. Hydrocele (84.6%) was the commonest diseasemanifestation among males, whereas lymphoedema was the only manifestationencountered among females. As vector control measures are not practicable inthis setting, chemotherapy using diethylcarbamazine (DEC) is the only potentialoption to control this disease.
68. Bancroftian filariasis in Bagdogra town, district Darjeeling (West Bengal).
SINGH S, BORA D, SHARMA RC, DATTA KK.
J Commun Dis. , 2002. 34(2): 110-7.
Filaria endemicity is probably gradually increasing over the years in Bagdogratown, district Darjeeling (West Bengal). Of 1511 night blood smears examined,35 were found positive for Wuchereria bancrofti (mf rate 2.32%). The microfilaria(mf) rates for males and females were 2.84% and 1.79 % respectively. The ageof these positives ranged from 5-45 years. The mf rate was highest (4.46%) in

185
Filaria
the age group of 20-29 years. All mf carriers were local residents of Bagdograand Wuchereria bancrofti was only the infection encountered. Mean microfilariadensity was 7.71 per 20 cmm. of blood, whereas Median microfilaria density(MFD50) was 21 per 20 cmm. of blood. Disease and filarial endemicity rateswere 0.33% and 2.65% respectively. During 1976 survey in the same town, mfrate was 1.6% and disease rate was nil.
69. Tropical vaginal hydroceles: are they all filarial in origin? Southeast Asian
SIVAM N S, JAYANTHI S, ANANTHAKRISHNAN N, ELANGOA,YUVARAJ J, HOTI SL, PANI S P.
J Trop Med Public Health. ,1995,26(4): 739-42.
Hydrocele of the tunica vaginalis testis has been conventionally used as anabsolute indicator of filarial disease in most clinical surveys. The prevalence offilarial etiology in 100 consecutive hydroceles was studied using clinical,parasitological, histopathological and immunological parameters. Filarial etiologycould be proved in 57% of hydrocele cases using major criteria: presence ofmicrofilaria in hydrocele fluid, presence of chyle in hydrocele fluid, demonstrationof adult worm in tunica, ratio of fluid antibody titer to serum antibody titer morethan 2 and presence of filarial antigen in hydrocele fluid. The results of othertests in these 57 cases were used to define the minor criteria. In the other 43cases, based on the minor criteria, 12 hydroceles could be classified as likely tobe due to filariasis and the rest were probably non-filarial. Thus only 69% ofhydroceles were definitely or probably filarial.
70. Utility of the force of infection model for assessing changes in the dynamicsof bancroftian filarial infections.Southeast Asian
SRIVIDYA A, DAS PK.
J Trop Med Public Health. ,1994,.25(1): 201-7
Force of infection is measured in terms of the number of effective contacts thathave been introduced into the population by infective vectors. The utility ofsuch a measure in describing the dynamics of bancroftian filarial infection wastested. Force of infection (beta) incorporating the durations of patent period and

186
Filaria
pre-patent period was estimated for different age classes (assuming that it isconstant in that particular age class) and it was found that the predicted post-control prevalences were close to the observed figures. Utility of Remme’s modelin areas with different transmission levels is discussed. It was examined whetherthe empirical function generally used in helminth infections to describe thefunctional relationship between beta and age could be used for lymphatic filariasis.The relationship between the two was not adequately described by the function.Force of infection, when compared with rate of acquisition calculated usinglongitudinal data, showed that this measure could be used as a crude estimate ofrate of acquisition in places which do not have longitudinal data sets.
71. Frequency distribution of Brugia malayi microfilariae in human populations.
SRIVIDYA A, KRISHNAMOORTHY K, SABESAN S, PANICKER K N,GRENFELL BT, BUNDY D A..
Parasitology. 1991, 102 Pt 2: 207-12
This study examines the effects of host age and sex on the frequency distributionof Brugia malayi infections in the human host. Microfilarial (mf) counts for a largedata base on the epidemiology of brugian filariasis in Shertallai, Kerala, SouthIndia are analysed. Frequency distributions of microfilarial counts partitioned byage are successfully described by zero-truncated negative binomial distributions,fitted by maximum likelihood. This analysis provides estimates of the proportionof mf-positive individuals who are identified as negative due to sampling errors,allowing the construction of corrected mf age-prevalence curves, which indicatethat the observed prevalence may under-estimate the true figures by between 18and 47%. There is no evidence from these results for a decrease in the degree ofover-dispersion of parasite frequency distributions with host age, such as might beproduced by the acquired immunity to infection. This departure from the pattern inbancroftian filariasis (where there is evidence of such decreases in over-dispersion;Das et al. 1990) is discussed in terms of the long history of filariasis control (andconsequently low infection prevalence) in Shertallai.
72. Development of rapid assessment procedures for the delimitation oflymphatic filariasis-endemic areas.
SRIVIDYA A, LALL R, RAMAIAH KD, RAMU K, HOTI SL, PANI SP, DAS PK..
Trop Med Int Health. 2000, 5(1): 64-71.

187
Filaria
Lymphatic filariasis caused by Wuchereria bancrofti is a major public healthproblem in 73 tropical and subtropical countries including India. Delimitationof endemic areas is essential to plan control operations. The current method ofnight blood survey (NBS) for delimitation is cumbersome, time-consuming andexpensive. Therefore, there is a need to develop assessment procedures whichcan rapidly delimit endemic areas. For this purpose we evaluated three procedures:direct interviewing of key informants using structured questionnaires, an indirectmethod of a self-administered questionnaires to key informants and physicalexamination by health workers for the presence of chronic filarial disease. Thirtyrural communities in a filariasis-endemic region in Cuddalore district in TamilNadu State in southern India constituted the study population. The determinationof filariasis endemicity in the village communities assessed by the aboveprocedures was compared in terms of rapidity, specificity, sensitivity and costwith the microfilaria rate and disease rate obtained by night blood sample surveyand clinical examination by physicians. Prevalence score, control preferencescore and weighted mean number of cases with filarial disease per village werecalculated using the key informant questionnaire techniques. While the prevalenceand control preference score showed low sensitivity and moderate specificity,weighted mean number of cases showed high sensitivity and moderate specificityin identifying endemic villages. The prevalence of disease as determined by thephysical examination of a sample population by health workers was highlysensitive in identifying communities endemic for filariasis. The degree ofassociation between the disease rates estimated by physician and trained healthworkers was significant (r = 0.56; P < 0.05). These observations suggest that theweighted mean number of cases per village obtained through key informanttechniques may be considered at a primary level to crudely identify endemicareas, followed by physical examination by health workers for filariasis, since itis relatively cheap and rapid.
73. A geostatistical analysis of the geographic distribution of lymphatic filariasisprevalence in southern
SRIVIDYA A,MICHAEL E, PALANIYANDI M, PANI SP, DAS PK.
India. Am J Trop Med Hyg. 2002, 67(5): 480-9.
Gaining a better understanding of the spatial population structure of infectiousagents is increasingly recognized as being key to their more effective mappingand to improving knowledge of their overall population dynamics and control.

188
Filaria
Here, we investigate the spatial structure of bancroftian filariasis distributionusing geostatistical methods in an endemic region in Southern India. Analysis ofa parasite antigenemia prevalence dataset assembled by sampling 79 villagesselected using a World Health Organization (WHO) proposed 25 x 25 km gridsampling procedure in a 225 x 225 km area within this region was comparedwith that of a corresponding microfilaraemia prevalence dataset assembled bysampling 119 randomly selected villages from a smaller subregion located withinthe main study area. A major finding from the analysis was that once large-scalespatial trends were removed, the antigenemia data did not show evidence for theexistence of any small-scale dependency at the study sampling interval of 25km. By contrast, analysis of the randomly sampled microfilaraemia data indicatedstrong spatial contagion in prevalence up to a distance of approximately 6.6kms, suggesting the likely existence of small spatial patches or foci of transmissionin the study area occurring below the sampling scale used for sampling theantigenemia data. While this could indicate differences in parasite spatialpopulation dynamics based on antigenemia versus microfilaraemia data, the resultmay also suggest that the WHO recommended 25 x 25 km sampling grid forrapid filariasis mapping could have been too coarse a scale to capture and describethe likely local variation in filariasis infection in this endemic location andhighlights the need for caution when applying uniform sampling schemes indiverse endemic regions for investigating the spatial pattern of this parasiticinfection. The present results, on the other hand, imply that both small-scalespatial processes and large-scale factors may characterize the observed distributionof filariasis in the study region. Our preliminary analysis of a mountain rangeassociated large-scale trend in the antigenemia data suggested that a nonlinearrelationship of infection prevalence with elevation might be a factor behind suchobserved global spatial patterns. We conclude that geostatistic methods canprovide a powerful framework for carrying out the empirical investigation andanalysis of parasite spatial population structure. This study shows that theirsuccessful application, however, will crucially depend on our gaining a morethorough understanding of the appropriate geographic scales at which spatialstudies should be carried out.
74. The dynamics of infection and disease in bancroftian filariasis.
SRIVIDYA A,PANI SP, RAJAGOPALAN PK, BUNDY DA, GRENFELL BT..
Trans R Soc Trop Med Hyg. 1991,85(2): 255-9

189
Filaria
This study examines the relationship between the dynamic of Wuchereriabancrofti infection and the development of chronic lymphatic disease. Datasets from Pondicherry, south India, and Calcutta are used to estimate the age-specific proportion of the endemic population which has converted frommicrofilaria positive to amicrofilaraemia, and is assumed to be at risk of disease.For men, but not women, the age-prevalence profile of the estimated population‘at risk’ is shown to correspond closely to the observed age-prevalence ofchronic lymphatic disease in the same community. For both sexes, andindependent of age, approximately 11% of the population at risk eventuallydevelop lymphoedema. These observations suggest that filariasis endemicpopulations consist of those individuals who remain amicrofilaraemic andasymptomatic, and those who progress through the sequence: uninfected,microfilaraemic, amicrofilaraemic, to develop irreversible obstructive lymphaticpathology.
75. Past exposure and the dynamics of lymphatic filariasis infection in youngchildren.
SRIVIDYA A, DAS PK, SUBRAMANIAN S, RAMAIAH KD,GRENFELL BT,MICHAEL E,BUNDY DA.
Epidemiol Infect. 1996. 117(1): 195-201.
This study utilizes parallel, longitudinal entomological and parasitological datacollected during a 5-year vector control programme in Pondicherry, South India,to quantify Wuchereria bancrofti transmission from the vector to the humanpopulation. A simple mathematical model, derived from the standard catalyticmodel, is used to examine the hypothesis that current infection prevalence inyoung children is a dynamical function of their cumulative past exposure toinfective bites. Maximum likelihood fits of the model to the observed data indicatea constant child infection rate with age, above a threshold representing the pre-patent period, or equivalently, the cumulative biting intensity required to producepatent infections. Extrapolation of the model allows the crude estimation of theequilibrium microfilaria age-prevalence curve due to control. The results suggestthat vector control alone may have little impact on the overall age-prevalence ofinfection even when sustained for long periods. These observations are discussedin terms of the likely impact of density dependent mechanisms, such as acquiredimmunity, on model predictions.

190
Filaria
76. Bancroftian filariasis in Pondicherry, south India: 2. Epidemiologicalevaluation of the effect of vector control.
SUBRAMANIAN S, PANI SP, DAS PK, RAJAGOPALAN PK.
Epidemiol Infect. 1989. 103(3): 693-702.
This article examines the evaluation of a bancroftian filariasis control programmeundertaken in Pondicherry from 1981-5. Integrated vector management wasapplied in one half of the town, and routine operations under the nationalprogramme (larviciding and chemotherapy) continued in the comparison area.The programme was evaluated by monitoring relative change in theepidemiological statistics of both populations. The results indicate that therewas significant reduction in prevalence of microfilaraemia in juveniles in thecontrolled area. An apparent reduction in intensity of microfilaraemia was alsoobserved but this was a consequence of the reduction in prevalence, since thedensity of microfilariae remained unchanged. The results suggest that primaryconstraints on the epidemiological evaluation of the vector control of filarasisare the longevity and the population characteristics of the parasite.
77. Natural history, trend of prevalence and spectrum of manifestations ofBancroftian filarial disease in Pondicherry (South India).
SURENDRAN K, PANI SP, SOUDARSSANANE MB,SRINIVASA DK,BORDOLAI PC, SUBRAMANIAN S
Acta Trop. 1996. 61(1): 9-18.
The study examines the changes in the disease parameters of lymphatic filariasisover a period of time based on three surveys during 1957, 1986 and 1992 inPondicherry, South India. The overall prevalence of filarial disease in the threesurveys was 4.7, 6.7 and 9.9% respectively. It was significantly higher in males(1957:5.3%; 1986:13.7%; 1992:18.8%) when compared to females (1957:3.8%;1986:2.3%; 1992:2.7%) in all the three surveys (P <0.05). The overall prevalenceof acute adenolymphangitis declined from 1.0 in 1957 to 0.2 in 1986 and 0.04%in 1992. While the prevalence of hydrocele showed an increasing trend from 2.7in 1957 to 11.9 in 1986 and 17.3% in 1992, the prevalence of lymphoedema (1.9in 1957; 1.9 in 1986 and 1.8% in 1992) was stable over the same period. The

191
Filaria
prevalence of disease was relatively higher in all age groups of both male andfemale population in 1992 when compared either to 1957 or 1986. Similarly amonotonic increase in the prevalence of hydrocele was observed in all age groupsin 1992 when compared to previous surveys. The implications of the changes inprevalence of the chronic manifestations when compared to the changes in theacute manifestations over a period of 35 years are discussed.
78. Epidemiology of subperiodic Wuchereria bancrofti infection in the NicobarIslands, India
TEWARI, S. C., J. HIRIYAN, ET AL.
Trans R Soc Trop Med Hyg (1995). 89: 163-6.
Diurnally subperiodic filariasis due to Wuchereria bancrofti has been reportedfrom tribal populations in the Nancowry group of islands in the Andaman andNicobar Islands, India. This was confirmed in a survey carried out during themonsoon season in 1993. Microfilariae were detected in the peripheral bloodthroughout a 24 h period with a peak at 18:00. The microfilaria (mf) rate rangedfrom 1.2% to 18.7%, with a low disease rate (mean = 1.9%). Incidence of mfwas low in children less than 10 years old (3.5%), but increased with increasingage. Culex (Culex) quinquefasciatus was present at a very low density. Aedes(Finlaya) niveus and Aedes (Stegomyia) malayensis were the only speciescommonly biting man. The former was incriminated as a vector, and foundnaturally infected with W. bancrofti (infection and infectivity rates 1.1% and0.9% respectively). After experimental feeding on donors, W. bancrofti developedto L3 stage larvae in A. niveus but failed to develop in A. malayensis and A.aegypti.
79. Estimation of the fecund life span of Wuchereria bancrofti in an endemicarea.
VANAMAIL P, RAMAIAHK D, PANI SP, DAS P K, GRENFELL BT,BUNDY DA.
Trans R Soc Trop Med Hyg. 1996. 90(2): 119-21.
A stochastic approach appropriate for general use in endemic communities wasapplied to estimate the average yearly instantaneous rate of loss of Wuchereria

192
Filaria
bancrofti microfilaraemia from infected individuals, and gain by uninfectedindividuals, from longitudinal data. This method was shown to give similar results(i.e., the rate of loss was independent of age, while the rate of gain differedsignificantly between age classes) to a previously used method based ontransmision interruption, provided that the intersurvey interval was > 5 years.The method was used to estimate the fecund life span of W. bancrofti in anendemic area at 5 years. The results suggest that the life span is at the lower endof previous estimates.
80. Estimation of age-specific rates of acquisition and loss of Wuchereriabancrofti infection.
VANAMAIL P, SUBRAMANIAN S, DAS PK, PANI SP, RAJAGOPALANPK, BUNDY DA, GRENFELL BT.
Trans R Soc Trop Med Hyg. 1989. 83(5): 689-93.
This study uses a reversible catalytic model to estimate the age-specific rates of gainand loss of Wuchereria bancrofti infection from data collected during a controlprogramme in Pondicherry, South India. The data describe the infection status in1981 and 1986 of two cohorts of individuals, one living in an area where vectorreduction had been achieved, and the other in a comparable endemic area. The rateof loss of infection in the absence of reinfection is estimated for the cohort in thecontrol area, and the rate of gain of infection by the cohort in the endemic areaestimated by substitution in the model. The mean expected life span of patent infectionis estimated to be 5.4 years. The instantaneous rate of loss of infection is independentof age, while the rate of gain of infection exhibits a convex age-profile, peaking inthe 16-20 year age-class. The reduced rate of gain in adults is largely attributable tothe increasing proportion of potentially resistant individuals with clinical disease.The results suggest that the age-distribution of bancroftian filariasis is primarilydetermined by age-dependency in the rate of acquisition of infection.
81. Estimation of age-specific rates of acquisition and loss of Wuchereriabancrofti infection.
VANAMAIL P, SUBRAMANIAN S, DAS PK, PANI SP, RAJAGOPALANPK, BUNDY DA, GRENFELL BT.
Trans R Soc Trop Med Hyg. 1989, 83(5): 689-93.

193
Filaria
This study uses a reversible catalytic model to estimate the age-specific rates ofgain and loss of Wuchereria bancrofti infection from data collected during acontrol programme in Pondicherry, South India. The data describe the infectionstatus in 1981 and 1986 of two cohorts of individuals, one living in an areawhere vector reduction had been achieved, and the other in a comparable endemicarea. The rate of loss of infection in the absence of reinfection is estimated forthe cohort in the control area, and the rate of gain of infection by the cohort inthe endemic area estimated by substitution in the model. The mean expected lifespan of patent infection is estimated to be 5.4 years. The instantaneous rate ofloss of infection is independent of age, while the rate of gain of infection exhibitsa convex age-profile, peaking in the 16-20 year age-class. The reduced rate ofgain in adults is largely attributable to the increasing proportion of potentiallyresistant individuals with clinical disease. The results suggest that the age-distribution of bancroftian filariasis is primarily determined by age-dependencyin the rate of acquisition of infection.
82. Estimation of fecundic life span of Wuchereria bancrofti from longitudinalstudy of human infection in an endemic area of Pondicherry (south India).
VANAMAIL P, SUBRAMANIAN S, DAS PK, PANI SP, RAJAGOPALAN PK.
Indian J Med Res. 1990.91: 293-7.
The fecundic life span of adult female W. bancrofti was estimated by longitudinalstudy of microfilaraemia in a cohort of population (7,525) in Pondicherry. Theestimation was based on a deterministic model, using the rate of loss in infection.The life span of the parasite was 10.2 yr without chemotherapy, while it wasreduced to 5.3 yr following diethyl-carbamazine therapy. The analysis of meanmicrofilarial counts in microfilaraemic persons without chemotherapy indicatesthat the rate of production of microfilaria by the adult female is stable at least fora period of five years.
83. A mathematical analysis of various factors involved in transmission ofbancroftian filariasis in Pondicherry.
VANAMAIL P, SUBRAMANIAN S,RAJAGOPALAN PK.
Indian J Med Res 1990. 91:289-92.

194
Filaria
The variation of clumping factor in microfilaraemia among different age groupswas observed in Pondicherry for 1981 and 1986. The clumping factor wasminimum in the age group 0-5 yr and it was maximum in 16-20 yr group in 1981and 21-25 yr in 1986. The variation in clumping factor resembled the changes inmicrofilaria (mf) rate. Multiple linear regression analysis showed that the multiplecorrelation between mf rate and the other parameters i.e., median microfilarialdensity (MFD50), clumping factor in human population, and, infection rate andinfectivity rate in vector population was highly significant. The relationshipbetween filariometric indices in human host and vector population may providethe basis on which a mathematical model on transmission of filariasis could bedeveloped.
84. Estimation of the fecund life span of Wuchereria bancrofti in an endemic area.
VANAMAIL P,RAMAIAH KD, PANI SP, DAS PK, GRENFELL BT,BUNDY DA.
Trans R Soc Trop Med Hyg, 1996..90(2): 119-21.
A stochastic approach appropriate for general use in endemic communities wasapplied to estimate the average yearly instantaneous rate of loss of Wuchereriabancrofti microfilaraemia from infected individuals, and gain by uninfectedindividuals, from longitudinal data. This method was shown to give similar results(i.e., the rate of loss was independent of age, while the rate of gain differedsignificantly between age classes) to a previously used method based ontransmision interruption, provided that the intersurvey interval was > 5 years.The method was used to estimate the fecund life span of W. bancrofti in anendemic area at 5 years. The results suggest that the life span is at the lower endof previous estimates.
85. Microfilariae in cytologic smears: a report of six cases
VARGHESE, R., C. V. RAGHUVEER, ET AL.
Acta Cytol (1996). 40(2): 299-301.
Filariasis is a major public health problem in tropical countries, including India.Despite this high incidence, it is unusual to find microfilariae in fine needleaspiration cytology. (FNAC) smears and body fluids. Six cases of filariasis

195
Filaria
diagnosed by FNAC are reported. cases. In case 1, a thyroid aspirate from a 23-year-old female showed a microfilaria with colloid and thyroid follicular cells.In case 2, pericardial fluid from a 50-year-old male with breathlessness and chestpain showed clusters of malignant cells and many microfilariae. In case 3, abronchial aspirate from a 55-year-old male with fever and chest pain showedaggregates of acute inflammatory cells and a microfilaria. Cases 4 and 5 werelymph node aspirates from a 29-year-old male and 3-year-old female. Both smearsshowed microfilariae in a background of reactive lymphoid cells. In case 6, FNACfrom a 21-year-old female with a cystic swelling in the breast showed clusters ofmicrofilariae, lymphocytes and granular debris. conclusion: In three of the sixcases microfilariae were the cause of symptoms, whereas in the other three cases,microfilariae were associated with other diseases, including malignancy. Thus,careful screening of FNAC smears might be helpful in detecting microfilariae,even in asymptomatic patients.

1. Dengue disease spectrum among infants in the 2001 dengue epidemic inChennai, Tamil Nadu, India.
KABILAN L, BALASUBRAMANIAN S, KESHAVA SM, THENMOZHI V,SEKAR G, TEWARI SC, ARUNACHALAM N, RAJENDRAN R,SATYANARAYANA K.
J Clin Microbiol. 2003 Aug;41(8):3919-21.
An investigation in a referral pediatric hospital has indicated that during a recentdengue outbreak in Chennai, Tamil Nadu, India, dengue in infancy constituted20% of total dengue virus infections with low mortality rates in this hospital. Indeveloping countries, strengthening of dengue management capabilities athospitals can prevent dengue-related deaths in infants.
Comments: BoD related information like morbidity data, sex details are lacking.
2. Serological and virological investigation of an outbreak of dengue fever inGwalior, India.
PARIDA MM, DASH PK, UPADHYAY C, SAXENA P & JANA AM. PARIDAMM, DASH PK, UPADHYAY C, SAXENA P, JANA AM
Indian Journal of Medical Research 2002. 116, 248-254
Background & Objectives: An outbreak of febrile illness occurred betweenSeptember to November 2001 in Gwalior, Madhya Pradesh affecting individualsmostly in the age group < 30 yr. A total of 312 febrile indoor patients suspectedto have dengue infection were investigated.
Methods: The investigation included examination of blood samples from patientsfor dengue specific IgM and IgG antibodies, isolation of virus in suckling mousepups and in C(6/36) cell line followed by confirmation and typing through reversetranscriptase-PCR and nested PCR.
Dengue
197

198
Summary
Results: The serological analysis of the 312 samples indicated 65 per centpositivity of which 21 per cent are of recent infection as indicated by the presenceof IgM antibody and 78 per cent are found to be secondary in nature by showingthe presence of IgG and/or IgM antibodies. The RT-PCR analysis of patients’sera employing dengue virus group specific conserved amplimer confirmed theetiological agent as dengue complex by showing the characteristic 511 bpamplicons. None of the antibody positive samples were found to be positive byRT-PCR. A total of 13 (6%) samples positive by RT-PCR, were processed forvirus isolation in mouse pups and in C(6/36) cells. Of these 9 samples (80%)were confirmed positive for virus isolation as identified by RT-PCR.
Interpretation & Conclusion: The typing of isolates by nested PCR employingserotype specific amplimer revealed 119 bp amplicon characteristic of denguevirus type-2 and thus confirming the outbreak attributed to dengue virus type-2.
Comments: Dengue outbreak had taken place in Madya Pradesh during the year2001. But this information was not listed in the NVBDCP, Delhi report. OtherBoD related informations are missing in this paper.
3. Dengue fever outbreaks in two villages of Dharmapuri district in TamilNadu.
VICTOR TJ, MALATHI M, GURUSAMY D, DESAI A, RAVI V,NARAYANASAMY G, ANURADHA L, RANI C, KRISHNAMURTHY PINSTITUTE OF VECTOR CONTROL & ZOONOSES, HOSUR, INDIA.
Indian J Med Res. 2002 Oct;116: 133-9.
Background & Objectives: Dengue fever is an important public health problemin India. In recent years this disease has extended to rural areas also due to rapidurbanization. In Tamil Nadu, fever outbreaks were reported in two villages ofDharmapuri district during May and September 2001 with clinical symptomssuggestive of dengue fever. Epidemiological, virological and entomologicalinvestigations were carried out in these two villages to ascertain the etiology ofthe outbreaks. METHODS: Paired serum samples were collected from febrilepatients clinically suspected to have dengue and were tested for the presence ofIgM antibodies to dengue virus by MAC ELISA. Samples were also tested byDengue Duo IgM/IgG rapid strip. Surveys of larval and adult Aedes mosquitoes

199
Dengue
were carried out before and after anti-larval and anti-adult measures wereimplemented. Female Ae. aegypti mosquitoes collected in Mampatti village weretested individually for the presence of dengue-2 viral antigen by indirectimmunofluorescence assay (IIFA). In addition, two pools of female Ae. aegyptimosquitoes were tested for the presence of dengue viral antigen by ELISA andthen subjected to Toxo-IFA system for demonstration of dengue virus. RESULTS:A total of 124 and 267 fever cases with clinical symptoms and signs suggestiveof dengue were reported in Kadumuchandiram and Mampatti villages ofDharmapuri district, respectively. Serodiagnosis revealed that 13 of 31 and 14 of52 patients tested were positive for dengue-2 virus by MAC ELISA inKadumuchandiram and Mampatti villages respectively. Dengue Duo rapid striptest also detected 14 (of 31 tested) patients positive for dengue virus specificIgM antibodies in Kadumuchandiram village and 8 (of 12 tested) in Mampattivillage. Application of temephos and fogging with pyrethrum 2 per cent extractwere found to be effective against immatures and adults respectively. Both thepools of Ae. aegypti tested for the presence of dengue viral antigen were positiveby ELISA and one mosquito (tested individually) was positive by IIFA.Supernatants of two pools were found to be positive for dengue-2 virus by Toxo-IFA. INTERPRETATION & CONCLUSION: Virological and serologicalinvestigations confirmed that the outbreaks of fever were due to dengue virusinfection. High breeding of Ae. aegypti in the study villages, detection of dengue-2 viral antigen and isolation of dengue-2 virus in Ae. aegypti mosquitoesconfirmed the etiology.
Comments: During the 2001, 391 febrile cases from Dharmapuri district referredto the hospital, Of 83 patients tested, 32.5% were found with dengue infection.Age specific case details and disability duration is missing.
4. An outbreak of dengue fever in rural areas of northern India.
KUMAR A, SHARMA SK, PADBIDRI VS, THAKARE JP, JAIN DC,DATTA KK.
J Commun Dis. 2001 Dec;33(4):274-81.
During the past few decades, epidemics of dengue fever are causing concern inseveral South-East Asian countries including India. The rural areas of Hissardistrict of Haryana state, situated about 170 km North-West of Delhi, experienced

200
Dengue
an outbreak of febrile illness during July-August 1996. A total of 13 villages ineight affected primary health centres reported fever cases. The clinical,epidemiological and entomological findings indicated that the present episodewas due to dengue fever. The aetiological agent of the current outbreak, theDEN-2 virus, was isolated from 12 acute-phase sera specimens. Though, in therecent past outbreaks have been reported from the rural areas of southern andwestern India, the present episode is the first outbreak being reported from therural areas of northern India. The increasing frequency of dengue fever outbreaksin rural areas of various Indian states reflects the changing life style of the ruralpopulation as a result of urbanization process and calls for a suitable preventionand control policy based on strengthened surveillance, appropriate healtheducation to the community coupled with proper training of health personnel.
Comments: Incomplete information. First outbreak report from rural areas ofnorthern India in 1996. Case incidence, mortality & morbidity and disabilityduration etc., data are lacking.
5. Dengue fever epidemic in Chennai—a study of clinical profile and outcome.
NARAYANAN M, ARAVIND MA, THILOTHAMMAL N, PREMA R,SARGUNAM CS, RAMAMURTY N.
Indian Pediatr. 2002 Nov;39(11):1027-33.
Children with dengue fever presenting to the Institute of Social Pediatrics,Government Stanley Hospital, during the months of October to December 2001,were prospectively followed up for clinical profile and outcome. Commonestclinical features were fever, vomiting, bleeding, body pain and hepatomegaly.Elevated liver enzymes and low platelet counts were common laboratory findingsin dengue. Hepatomegaly, positive tourniquet test, elevated haematocrit andthrombocytopenia were more common in DHF and DSS group. Retro-orbitalpain was slightly more in DHF and DSS groups and there was a tendency forDSS to present at an earlier age. There was no correlation between platelet countsand bleeding in classical dengue cases.
Comments: DHF/DSS case incidence (morbidity) among hospitalized childrenin Chennai during 2001 was reported. Mostly clinical information. Disabilityduration is missing which is essential for DALY estimation.

201
Dengue
6. Experience in adult population in dengue outbreak in Delhi.
TRIPATHI BK, GUPTA B, SINHA RS, PRASAD S, SHARMA DK.
J Assoc Physicians India. 1998 Mar;46(3):273-6.
Comment in: J Assoc Physicians India. 1999 Jun;47(6):653-4.
A dengue outbreak has recently hit the Indian capital. We studied the clinicalprofile of adult patients. Five hundred and sixty patients of dengue infectionwere admitted in a specially created ward according to the criteria laid down byWHO. Haematemesis (28.28%), epistaxis (26.78%) and malena (14.28%) weresome of the common presentations. Similarly lymphadenopathy, especiallycervical (30.89%), palatal rashes (26.96%) and hepatomegaly (23.75%) werethe most commonly encountered findings on physical examination. Most of thecases were of dengue fever with haemorrhage and only 2.5% cases were classifiedunder dengue haemorrhagic fever or dengue shock syndrome. The averagehospital stay was 3.4 days but only 9.8 hours in the eleven patients who died,suggesting their late arrival in preterminal situation giving little time forresuscitation. Thrombocytopenia was not a feature and only 12.85% patientshad platelet count less than 70,000/cmm. Most of the patients who were admittedwith thrombocytopenia, showed normalization in their platelet counts in nextfew days. Serological examination demonstrated evidence of recent dengueinfection in 41.17% patients. Few patients required blood or platelet concentratetransfusion. Eleven patients died, three due to DIC, one of intracranialhaemorrhage and seven due to massive gastric haemorrhage. Rest of the patientsrecovered completely. Thus we can conclude that recent outbreak in Delhi wasof dengue fever with haemorrhage and mortality was very low in patients whocame early to the hospital.
Comments: Of the 560 adult patients admitted to the hospital at Delhi, duringthe 2001, 47.2% of had dengue infection. 2.5 % had DHF and Three-fourth ofthe DHF patients died. AGE / Sex specific cases incidence due to DF/DHF/DSSare not mentioned.

202
Dengue
7. Epidemiological and entomological investigation in dengue outbreak areaof Ahmedabad district.
JOSHI PT, PANDYA AP, ANJAN JK.
J Commun Dis. 2000 Mar;32(1):22-7.
Epidemiological and Entomological investigations conducted in seven affectedvillages of Sanand and Viramgam Talukas of Ahmedabad district revealed thatall age groups and both the genders were affected. 33.33% blood samples ofpatients showed seropositivity suggesting dengue infection Similarly, Denguevirus antigen was detected in 7 Females Ae. aegypti out of 2 Males and 26 Femalestested by indirect immunofluroscent technique. Aedes aegypti populationmeasured by various parameters i.e. Premise index (32.16%), Receptacle index(26.15%) and infested receptacle index (0.36%) were above the critical limit.Aedes aegypti population is susceptible to 5% Malathion. The findings suggestthe fever outbreak was of dengue. Co-related evidences indicated the possiblerole of dengue 2 virus in the outbreak.
Comments: AGE/Sex specific cases incidence due to DF/DHF/DSS & disabilityduration is missing.
8. Silent spread of dengue and dengue haemorrhagic fever to Coimbatore andErode districts in Tamil Nadu, India, 1998: need for effective surveillanceto monitor and control the disease.
SINGH J, BALAKRISHNAN N, BHARDWAJ M, AMUTHADEVI P, GEORGEEG, SUBRAMANI K, SOUNDARARAJAN K, APPAVOO NC, JAIN DC,ICHHPUJANI RL, BHATIA R, SOKHEY J.
Epidemiol Infect. 2000 Aug;125(1):195-200
Dengue fever (DF) or dengue haemorrhagic fever (DHF) has not previously beenreported in Coimbatore and Erode districts in Tamil Nadu in India. In 1998, 20hospitalized cases of fever tested positive for dengue virus IgM and/or IgGantibodies. All of them had dengue-compatible illness, and at least four hadDHF. Two of them died. Sixteen cases were below 10 years of age. The caseswere scattered in 15 distantly located villages and 5 urban localities that had a

203
Dengue
high Aedes aegypti population. Although the incidence of dengue-like illnesshas not increased recently, almost 89% (95/107) of samples from healthy personsin the community tested positive for dengue IgG antibodies. The study showedthat dengue has been endemic in the area, but was not suspected earlier. Astrong laboratory-based surveillance system is essential to monitor and controlDF/DHF.
Comments: AGE/Sex specific cases incidence due to DF/DHF/DSS & disabilityduration is missing.
9. A clinical study of the patients with dengue hemorrhagic fever during theepidemic of 1996 at Lucknow, India.
AGARWAL R, KAPOOR S, NAGAR R, MISRA A, TANDON R, MATHURA, MISRA AK, SRIVASTAVA KL, CHATURVEDI UC.
Southeast Asian J Trop Med Public Health. 1999 Dec;30(4):735-40
This paper describes the clinical findings in 206 patients with dengue fever (DF)or with dengue hemorrhagic fever (DHF) during the epidemic of 1996 at Lucknow.The age group affected most was 11 to 30 years and 21% of the patients wereless than 10 years old. The male:female ratio was 1.9:1. The onset was abrupt inall the patients, severe frontal headache was observed in 97%, myalgia in 90%,skin rash in 40%, vomiting in 29% and arthralgia in knee and hip joints in 9%.Anuria was seen in two patients. Lymphadenopathy was noted in 14%,hepatomegaly in 4%, being associated with mild jaundice in one patient, andsplenomegaly in 2% of the patients. Involvement of the heart and lungs was seenin one patient each and no case with encephalitis was recorded. Hemorrhagesfrom various sites were observed in 54% patients and 17 patients had profoundshock. The commonest bleeding site was gums. Profound shock was precededby various warning signs, the commonest being sudden hypotension. Amongthe patients with profound shock the mortality was 47% while the overall fatalityrate was 3.8%. A number of the risk factors existed for a long time in this part ofthe world, but what precipitated the present epidemic at this time, is not known.
Comments: This is a hospital-based investigation. True case incidence is notknown. Age wise morbidity details are not mentioned. Demographic detailsare missing.

204
Dengue
10. Dengue virus infection during post-epidemic period in Delhi, India.
VAJPAYEE M, MOHANKUMAR K, WALI JP, DAR L, SETH P, BROOR S.
Southeast Asian J Trop Med Public Health. 1999 Sep;30(3):507-10.
Dengue fever (DF) and dengue hemorrhagic fever (DHF) are major public healthproblems in India. During the period following an epidemic, a study was carriedout using virological and serological tests for confirmation of suspected cases ofdengue virus infection in fever cases presenting to the All India Institute of MedicalSciences. Serum samples of suspected DF/DHF cases were processed fromJanuary to December 1997. In 37 samples from patients with fever of less thann5-day duration, received on ice, virus isolation was attempted in C6/36 clone ofAedes albopictus cell line, followed by indirect fluorescent antibody stainingwith monoclonal antibodies to dengue viruses 1 to 4. One hundred and forty-three serum samples from patients with more than 5 days fever were tested fordengue specific IgM antibody by either MAC-ELISA or a rapidImmunochromatographic assay. Dengue virus type 1 was demonstrated by culturein 8 (21.6%) of 37 serum samples and IgM antibody could be detected in 42(29.4%) of the 143 serum samples by the serological methods. The peak of denguevirus infection was seen from September to November 1997.
Comments: Hospital base study. Description of duration of onset of denguefever attempted.
11. Dengue haemorrhagic fever in children in the 1996 Delhi epidemic
KABRA SK, JAIN Y, PANDEY RM, MADHULIKA, SINGHAL T, TRIPATHIP, BROOR S, SETH P, SETH V. DEPARTMENT OF PEDIATRICS
Trans R Soc Trop Med Hyg. 1999 May-Jun;93(3):294-8.
An epidemic of dengue haemorrhagic fever (DHF) occurred in Delhi in 1996.A total of 240 children between the age of 4 months to 13 years of either sex,admitted in one hospital, were evaluated. Two hundred and sixteen (90%)children were from Delhi. A clinical diagnosis of dengue fever (DF) was madein 25 (10%), dengue fever with unusual bleeding (DFB) in 22 (9%), DHF in80 (33%) and dengue shock syndrome (DSS) in 113 (47%) of the children

205
Dengue
strictly according to the WHO classification. The age peaked at 8 years. Therewas no association between various grades of severity of illness and age-groupsthough girls suffered from more severe illness. No association between severityof malnutrition and severity of illness was observed. Tourniquet test waspositive in 40% with DF, 18% with DFB, 62% with DHF and 64% with DSS.In DSS haematemesis was present in 55 (49%), epistaxis in 39 (35%), melaenain 27 (24%) and ecchymosis in 34 (30%) patients. Children diagnosed as DFBhad haematemesis and epistaxis in 12 (55%) and 10 (45%) respectively.Intravenous fluid requirement was clearly less in DFB patients than in DHF/DSS patients. Unusual clinical features in the form of jaundice were presentin 7 (6%), hepatic encephalopathy in 6 (5%) and dengue encephalopathy in 6(5%) patients. Dengue 2 virus was isolated from 10 of the 50 patients forwhom viral culture was done on C6/36 clone of Aedes albopictus cell line.Eighteen patients suffering from DSS died giving an overall case fatality of7.5%. The mortality rate in DHF/DSS was 9.3%. It is further suggested thatDFB is a distinct entity. Most patients could be classified by the WHOclassification if a retrospective packed cell volume was used to assesshaemoconcentration. We suggest that development of area-specific criteriafor diagnosis and management is desirable.
Comments: This is a hospital-based investigation. True case incidence is notknown. Age wise morbidity details are not mentioned. Demographic details aremissing.
12. The first major outbreak of dengue hemorrhagic fever in Delhi, India.
DAR L, BROOR S, SENGUPTA S, XESS I, SETH P.
Emerg Infect Dis. 1999 Jul-Aug;5(4):589-90.
India An outbreak of dengue hemorrhagic fever/dengue shock syndrome (DHS/DSS) occurred in 1996 in India in and near Delhi. The cause was confirmed asdengue virus type 2, by virus cultivation and indirect immunofluorescence withtype-specific monoclonal antibodies. This is the largest such outbreak reportedfrom India, indicating a serious resurgence of dengue virus infection
Comments: Outbreak investigation of DHF &DSS cases. No other BoDinformation are available.

206
Dengue
13. The 1996 outbreak of dengue hemorrhagic fever in Delhi, India.
Anuradha S, Singh NP, Rizvi SN, Agarwal SK, Gur R, Mathur MD..
Southeast Asian J Trop Med Public Health. 1998 Sep;29(3):503-6.
A major outbreak of dengue hemorrhagic fever (DHF) affected more than 10,000people in Delhi and neighboring areas in 1996. The outbreak started in September,peaked in October to November and lasted till early December. The clinical andlaboratory data of 515 adult patients admitted to Lok Nayak Hospital, New Delhiwere reviewed. Fever (100%), myalgias and malaise (96%), abdominal pain(10.2%) and vomiting (8.7%) were the prominent presenting features.Hemorrhagic manifestations were seen in all patients- a positive tourniquet test(21.2%), scattered petechial rash (23.07%), confluent rash (2.7%), epistaxis(38.4%), gum bleeds (28.06%) and hematemesis (22.86%) being the majorbleeding manifestations. Hepatomegaly was observed in 96% of the patients.Laboratory investigations revealed thrombocytopenia, hemoconcentration andleukopenia. Serological confirmation with a microcapture ELISA technic wasdone in 143/515 patients. The mortality rate was 6.6% and, multiple bleedingmanifestations, severe thrombocytopenia, hypoproteinemia and dengue shocksyndrome (DSS) were associated with a higher mortality.
Comments: More than 10,000 cases were reported. This is only hospital-basedstudy consisting of only 515 patients. Age and sex wise morbidity data are notmentioned.
14. Dengue haemorrhagic fever in adults: a prospective study of 110 cases.
WALI JP, BISWAS A, HANDA R, AGGARWAL P, WIG N, DWIVEDI SN.
Trop Doct. 1999 Jan;29(1):27-30.
One hundred and ten adult patients hospitalized with dengue haemorrhagic fever(DHF) during the recent outbreak in North India were prospectively studied. Ofthese, 48 (43.6%) were grade I, 40 (36.4%) grade II, 10 (9.1%) grade III and 12(10.9%) grade IV DHF. Dengue shock syndrome (DSS) was seen in 22 (20%)patients. Fever, headache, myalgias and arthralgias were the common symptomsseen in 100%,80.9%, 76.2% and 52.3% patients, respectively. Spontaneous

207
Dengue
bleeding was seen in62 patients (56.4%) with muco cutaneous bleeding beingthe most common (46patients). Gastrointestinal bleeding was seen in 38 (34.5%)patients. In as many as 40 patients, the haemorrhagic manifestations occurredafter the fever had come down. Fifty-five patients (50%) required platelettransfusions. Twelve patients died, giving a mortality rate of 10.9% in the presentstudy. Prompt recognition and supportive treatment can be lifesaving.
Comments: This is also a hospital-based study consisting of only 110 adultpatients. Age and sex wise information not available.
15. An epidemic of dengue hemorrhagic fever and dengue shock syndrome inchildren in Delhi.
AGGARWAL A, CHANDRA J, ANEJA S, PATWARI AK, DUTTA AK.
Indian Pediatr. 1998 Aug;35(8):727-32.
Objective: To study clinical profiles and outcome of children of dengue hemorrhagicfever (DHF) and dengue shock syndrome (DSS) during 1996 Delhi epidemic.DESIGN: Retrospective study. SETTING: Hospital based study. METHODS:Children hospitalized from September to November 1996 were studied. All patientswere diagnosed, managed and monitored according to a standard protocol.RESULTS: One hundred and thirty four children (80 (60%) males and 54 (40%)females) were studied. Sixty (45%) children were less than 6 years of age of which12 presented during infancy. There were 92 (67%) cases of DHF and 42 (33%)cases of DSS. Common symptoms were fever (93%), abdominal pain (49%) andvomiting (68%). The commonest hemorrhagic manifestation was hematemesis(39%) followed by epistaxis (36%) and skin bleeds (33%). Hepatomegaly wasobserved in 97 (72%) cases and splenomegaly in 25 (19%). Serology was positive(IgM hemaglutination antibody titres > 1: 160) for dengue type 2 in 31 (80%) of 39patients in whom sera was tested during the acute phase of illness. Mortality was6%. Hematocrit 40% was observed in only 25 (18%) patients and hence themanagement protocol was based on clinical signs and symptoms and not onhematocrit. CONCLUSIONS: A management protocol of DHF/DSS in which fluidtherapy is not based on haematocrit values needs to be formulated.
Comments: This is also a hospital-based study consisting of only 134 childrenaffected due to during the epidemic in 1996. BoD related informations are notreported.

208
Dengue
16. Incidence of dengue fever in relation to climatic factors in Ludhiana, Punjab
RAM S, KHURANA S, KAUSHAL V, GUPTA R, KHURANA SB.
Indian J Med Res. 1998 Oct;108:128-33.
An outbreak of dengue fever occurred in Ludhiana in 1996 and 1997. A total of505 patients who attended the hospital attached to Dayanand MedicalCollege,Ludhiana were clinically diagnosed to have dengue fever. Of these, 460cases were noticed between October and December 1996 while during 1997only 45 dengue fever cases were observed. Serological examination using dengueIgG and IgM blot was performed with single serum samples of 189 patients. Ofthese, 129 serum samples were detected positive for anti dengue antibodies.Twenty eight patients died in the dengue epidemic, 12 of whom suffered fromdengue haemorrhagic fever (DHF) and six with dengue shock syndrome (DSS).Male patients outnumbered the female patients. Seasonal and cyclic pattern ofthe disease incidence was observed.
Comments: Hospital based study. Disability duration is missing.
17. Dengue haemorrhagic fever outbreak in October-November 1996 inLudhiana, Punjab, India
KAUR H, PRABHAKAR H, MATHEW P, MARSHALLA R, ARYA M.
Indian J Med Res. 1997 Jul;106:1-3.
An epidemic of haemorrhagic fever broke out in Ludhiana in October andNovember 1996. Persons of all age groups were affected with preponderance ofyoung adults. Haemorrhagic manifestations like rashes, epistaxis, bleeding fromthe gums and haematemesis were observed. The cause of fever was investigated.Serum samples collected at random from 71 patients were tested by ELISA fordengue types 1-4 IgM antibodies. These were positive in 96.7 per cent of cases.Immunoblot testing for IgM and IgG for all serotypes of dengue virus werepositive in 90.2 and 73.2 per cent of the serum samples respectively. Thehaemorrhagic fever was serologically proven to be due to dengue virus.
Comments: An epidemic investigation; all age groups were affected withpreponderance of young adults. No other BoD details reported.

209
Dengue
18. The 1993 epidemic of dengue fever in Mangalore, Karnataka state, India.
PADBIDRI VS, ADHIKARI P, THAKARE JP, ILKAL MA, JOSHI GD,PEREIRA P, GUTTIKAR SN, WALHEKAR BD, CHOWTA N, HEGDE BM.
Southeast Asian J Trop Med Public Health. 1995 Dec;26(4):699-704.
An epidemic of febrile illness with hemorrhagic manifestations occurred in certainparts of Mangalore city, Karnataka state, India, from the last week of July 1993.The epidemic reached its peak by mid-August and then started declining. Sporadiccases, however, continued to occur till early December. About 200 cases werereported covering all age groups and both sexes. The cases presented with pyrexia,myalgia, arthralgia and headache. Palatal petechiae, magenta colored tongue withcentral coating, maculopapular rash and facial flush were observed as classicalsigns. The tourniquet test was positive in 12% of the cases. Hemorrhage wasobserved in the form of epistaxis (2 cases), subconjunctival hemorrhage (2 cases)or purpura (3 cases). There were no deaths which were attributable to the epidemic.Five strains of dengue (DEN-2) virus were recovered from the acute-phase sera.Dengue virus-specific IgM type of antibodies were detected in 29/116 (25%) sera.Breeding of Aedes aegypti was observed in some of the areas where cases hadoccurred. No virus was isolated from any of the field-caught Ae. aegypti mosquitoes.
Comments: This is an epidemic investigation study. BoD information like agespecific mortality is missing.
19. An epidemic of dengue haemorrhagic fever & dengue shock syndrome in &around Vellore. Cherian
T, PONNURAJ E, KURUVILLA T, KIRUBAKARAN C, JOHN TJ,RAGHUPATHY P.
Indian J Med Res. 1994 Aug;100:51-6.
This report describes an epidemic of dengue haemorrhagic fever/dengue shocksyndrome (DHF/DSS) in the North Arcot Ambedkar district and the adjoiningdistricts in Tamil Nadu and Andhra Pradesh. Nineteen children who fulfilled theclinical criteria for the diagnosis of DHF/DSS were admitted to the ChristianMedical College Hospital, Vellore, during June through November, 1990. Theclinical presentation was similar to that described in South-east Asian children

210
Dengue
and the case fatality rate was 26.3 per cent. Serology was confirmatory or suggestiveof recent dengue virus infection in 16 children, uninterpretable in 2 and notconsistent with recent dengue virus infection in 1 child. All children over 1 yr ofage had very high antibody titres suggesting a secondary response whereas infantshad lower titres consistent with primary response. The occurrence of recurrentepidemics in this region in the last few years with associated high case fatalityemphasizes the urgent need for public health measures to curtail further epidemics.
Comments: This report describes an epidemic of dengue haemorrhagic fever/dengue shock syndrome (DHF/DSS) in the North Arcot Tamil Nadu and AndhraPradesh. Clinical study.
20. Dengue haemorrhagic fever (DHF) outbreak in Calcutta-1990.
BHATTACHARJEE N, MUKHERJEE KK, CHAKRAVARTI SK,MUKHERJEE MK, DE PN, SENGUPTA M, BANIK GB, BHOWMICK P,SINHA SK, CHAKRABORTY MS.
J Commun Dis. 1993 Mar;25(1):10-4.
An outbreak of Dengue Haemorrhagic Fever (DHF) occurred in Calcutta betweenSeptember and December, 1990. Children and young adults were the majorvictims. Haemorrhagic manifestations and shocks were the main features in mostof the hospitalised cases. Five mouse pathogenic agents were isolated from 105acute cases and all were identified as DEN-3. HI and CF test with 55 paired serarevealed evidence of dengue infection in 33 (60 per cent) and flavivirus groupreaction including dengue in 17 (30.9 per cent). It was for the first time, thatDEN-3 was considered to be the etiologic agent for DHF in Calcutta.
Comments: No details regarding mortality and duration of disability. Childrenand young adults are affected.
21. Dengue haemorrhagic fever in children in Delhi.
KABRA SK, VERMA IC, ARORA NK, JAIN Y, KALRA V
Bull World Health Organ. 1992;70(1):105-8.
An epidemic of dengue haemorrhagic fever occurred in Delhi during 1988. Atotal of 21 paediatric patients with dengue haemorrhagic fever/dengue shock

211
Dengue
syndrome were evaluated from September to November 1988. All the patientshad fever, restlessness, ecchymotic spots and ascites. Pleural effusion occurredin 19 patients (90%), and 18 (86%) exhibited each of the following: vomiting,thrombocytopenia, and haemoconcentration. Hepatomegaly was observed in 15patients (71%) and splenomegaly in three (14%). Titres of haemagglutinationinhibition (HI) antibodies against dengue virus type 2 were raised in all the 15cases from whom sera were collected during the acute stage. Convalescent serafrom five patients had increased titres of HI antibodies to dengue virus type 2.The remaining 10 cases exhibited raised IgM antibody levels against denguevirus type 2. The fatality rate for serologically proven cases was 13% (2 of 15patients), while for all patients (including those diagnosed clinically (6) andserologically (15)) it was 33.3% (7 of 21). Patients who survived had no sequelae,except one who had transient hypertension that lasted for two weeks.
PIP: An epidemic of dengue hemorrhagic fever occurred in Delhi during 1988.A total of 21 pediatric patients with that illness or dengue shock syndrome wereevaluated from September-November 1988. All patients had fever, restlessness,ecchymotic spots, and ascites. Pleural effusion occurred in 19 patients (90%)and 18 (86%) exhibited each of the following: vomiting, thrombocytopenia,and hemoconcentration. Hepatomegaly was observed in 15 patients (71%) andsplenomegaly in 3 (14%). Titers of hemagglutination inhibition (HI)antibodiesagainst dengue virus type 2 were raised in all 15 cases from whomsera were collected during the acute stage. Convalescent sera from 5 patientshad increased titers of HI antibodies to dengue virus type 2. The remaining 10cases exhibited raised IgM antibody levels against dengue virus type 2. Thefatality rate for serologically proven cases was 13% (2 of 15 patients) while forall patients (including those diagnosed clinically [n=6] and serologically [n=15]),it was 33.3% (7 of 21). Patients who survived had no sequelae, except 1 whohad transient hypertension which continued for 2 weeks. author’s modified.
Comments: Hospital based study. Serological investigation. BoD related detailsnot reported.
22. An insular outbreak of dengue fever in a rural south Indian village.
NORMAN G, THEODRE A, JOSEPH A.
J Commun Dis. 1991 Sep;23(3):185-90.
In mid 1990, an epidemic of fever affected a single village in Kaniyambadi Block,South India. The illness was characterized by a fever of approximately five days

212
Dengue
duration, accompanied by headache, chills, sweating and muscle pain. The overallattack rate was 22.5 per cent. The attack rate was uniform across the various agegroups and between the sexes. Testing of the acute and convalescent serumsamples obtained from cases showed a serological response to dengue virus.The Aedes house index in the village was found to be 36 per cent with toiletsserving as active breeding sites. Adjacent villages studied showed similarly highrates of Aedes prevalence, although no cases of the same fever were seen. Sinceprevious exposure to dengue increases the risk for epidemics of denguehemorrhagic fever and dengue shock syndrome, health education on methods ofAedes control is continuing.
Comments: All age group was affected; average duration of fever (disability)was 5 days, other BoD information is lacking.
23. Outbreak of dengue fever in rural areas of Parbhani district of Maharashtra(India).
MEHENDALE SM, RISBUD AR, RAO JA, BANERJEE K.
Indian J Med Res. 1991 Jan;93:6-11.
Outbreak of dengue fever in Chikalthana, Pimpalgaon and Waloor villages inParbhani district of Maharashtra (India) were investigated. Clinically, the illnesswas typical of dengue fever except for the absence of maculopapular rash. Atotal of 42 acute, 14 late acute, 73 convalescent and 19 sera from contacts werecollected. Of the 15 virus isolates, 12 were identified as dengue virus type 2 and1 as dengue virus type 1. Serological tests confirmed the etiological role of denguevirus in the outbreak. House-to-house survey was carried out in Chikalthana andPimpalgaon villages. Overall, 15.09 per cent of the surveyed population wasaffected during the outbreak and attack rate was higher at Pimpalgaon. A tendencyof water storage was observed in the households and concomitant entomologicalstudies proved Aedes aegypti breeding. Higher prevalence of dengue fever wasnoted among larger families and in families that had two or more patients, thecommonest duration between the first and the last patient was often less than 5days.
Comments: Outbreak investigation. Higher prevalence of dengue fever was notedamong larger families and in families that had two or more patients, the

213
Dengue
commonest duration between the first and the last patient was often less than 5days. BoD information is incomplete.
24. Clinical & virological study of dengue fever outbreak in Jalore city,Rajasthan 1985
CHOUHAN GS, RODRIGUES FM, SHAIKH BH, ILKAL MA, KHANGAROSS, MATHUR KN, JOSHI KR, VAIDHYE NK.
Indian J Med Res. 1990 Nov;91:414-8.
An epidemic of acute febrile illness caused by dengue virus occurred in Jaloretown, in south-west Rajasthan, in April and May, 1985. Most patients had classicalsigns and symptoms of dengue fever or had only a mild atypical febrile illness. Afew patients had in addition haemorrhagic manifestations/shock or encephalitis.Virological studies (carried out by the National Institute of Virology, Pune) showedthat dengue type 3 virus was the main etiological agent. This is the first reportedoutbreak of dengue in the arid zone in western Rajasthan, that occurred in summer(April-May) in contrast to other parts of India, where such outbreaks arecommonly reported after the rains (between August and November).
Comments: Report on epidemic investigation. Incidence & disability durationdetails are missing.
25. An epidemic of dengue haemorrhagic fever and dengue shock syndrome inDelhi: a clinical study.
SRIVASTAVA VK, SURI S, BHASIN A, SRIVASTAVA L, BHARADWAJ M.
Ann Trop Paediatr. 1990;10(4):329-34
Twenty-four cases of dengue haemorrhagic fever/dengue shock syndromewere studied in Delhi in the months of September and October, 1988. Themajority of these cases were boys aged 6-10 years. Classical symptoms ofdengue (fever, headache, aesthesia, myalgia) occurred in all the patients.Digestive symptoms (nausea, vomiting, anorexia, abdominal pain andhepatomegaly) were also common. Haemorrhagic manifestations were presentin 41.7% of the cases. Of these, 90% had gastrointestinal haemorrhages. Shock

214
Dengue
occurred in 17 cases (70.8%). Thrombocytopenia and prolongation ofcoagulation profile were found in 62.5% of cases. Three patients (12.5%)who presented with encephalopathy died. The other 21 patients recoveredafter an average period of 2-8 days.
Comments: Disability duration is given. Clinical study limited to pediatricpopulation.

1. Census of India, 2001. www.censusindia.net
2. Census of India, 1991. www.censusindia.net
3. Progress in the prevention and control of diarrhoeal diseases sinceIndependence.
BHATTACHARYA SK.
Natl Med J India 2003; 16 Suppl 2: 15-9.
Acute diarrhoeal diseases constitute one of the major health problems amongyoung children in India. It was estimated in 1978 that 1.5 million children underthe age of 5 years die due to diarrhoea every year, which declined to 0.6-0.7million in the estimate revised in 1992. A similar declining trend has also beennoted in hospitalized cases in Calcutta (present Kolkata) during 1980-95 as wellas from other parts of India. Even today, cholera epidemics occur regularly inIndia. The cholera epidemic caused by a novel strain of Vibrio cholerae, designatedas V. cholerae 0139 Bengal in 1992 and multidrug-resistant shigellosis in easternIndia in 1984 are matters of grave concern. The launching of the NationalDiarrhoeal Diseases Control Programme (CDD) in 1978, based on a three-tierapproach, is of great importance. The rate of use of oral rehydration salt (ORS)solution and oral rehydration therapy (ORT) remain suboptimal in India. In spiteof the launching of the ‘Ganga Action Plan’ and the ‘National River Action Plan’,India faces a major problem of diarrhoeal diseases. Lack of safe water supply,poor environmental sanitation, improper disposal of human excreta and poorpersonal hygiene help to perpetuate and spread diarrhoeal diseases in India. Sincediarrhoeal diseases are caused by 20-25 pathogens, vaccination, though anattractive disease prevention strategy, is not feasible. However, as the majorityof childhood diarrhoeas are caused by V. cholerae, Shigellae dysenteriae type 1,rotavirus and enterotoxigenic Escherichia coli (E. coli) which have a highmorbidity and mortality, vaccines against these organisms are essential for thecontrol of epidemics. A strong political will with appropriate budgetary allocationis essential for the control of childhood diarrhoeal diseases in India, a formidabletask in a country with a population of over 1 billion.
Diarrhoeal Diseases
215

216
Diarrhoeal Diseases
4. An operational study on implementation of oral rehydration therapy in arural community of West Bengal, India
SIRCAR BK, DEB BC, SENGUPTA PG, MONDAL S, GUPTA DN, SARKARS, SIKDER SN, GHOSH S, SAHA NC, PAL SC.
Indian J Med Res 1991; 93: 297-302.
Study period: 22 months (April 1985 – January 1987)Study area: Two ICDS Blocks (rural) in Hooghly district, West Bengal –Study block : Polba; Pop=216 825 (<5yrs=30000; 13.8%)Control block: Pandua; Pop=200 553 (<5yrs=28000; 14.0%)
Baseline data (among <5 years):POLBA PANDUA
Prevalence of diarrhoea (2-wk recall): 18.1 15.7Incidence* among <5yrs (ep/child/yr): 4.7 4.1Diarrhoea-related mortality** (per 1000): 2.8 2.8Overall under-5 mortality (per 1000): 11.5 9.0
*The high incidence recorded during the initial survey might be a reflection ofthe post-epidemic period of shigellosis in West Bengal.**A death was considered diarrhoea-related if the child had diarrhoea in theweek before death, and there was no obvious cause of death unrelated to diarrhoea.[WHO/CDD/SER/86.2]
5. Dysentery: an overview. Still problems to resolve.
PAL SC.
Dialogue Diarrhoea. 1986 Jun;(25):4.
This article reviews the global situation with regard to bacillary dysentery, withparticular emphasis on findings from the recent epidemic in West Bengal. Infectionis by the fecal-oral route and generally spread by person-to-person transmission.Serious epidemics caused by the multiple-drug-resistant Shigella shigae haveoccurred recently in Bangladesh, Somalia, South India, Burma, Sri Lanka, Nepal,Bhutan, Rwanda, and Zaire. In each situation, dysentery attacked over 10% of

217
Diarrhoeal Diseases
the population and killed 2-10% of hospitalized cases. In 1984, a dysenteryepidemic spread rapidly throughout West Bengal, especially among youngchildren, and was resistant to most commonly available drugs and antibiotics. Amass media campaign was initiated which emphasized boiling or chlorinationof drinking water, covering feces with soil, protecting food from flies, avoidingexposed raw vegetables and cut fruits, and hand washing. However, thesemeasures were difficult to implement and the epidemic subsided only gradually.Scientific knowledge about the exact mode of transmission of the pathogen, themechanisms of pathogenicity, and the actual cause of death in dysentery casescould contribute to the development of practical public health interventions andan effective vaccine.
6. Multidrug resistant epidemic shigellosis in a village in West Bengal, 1984.
SENGUPTA PG, MANDAL S, SEN D, DAS P, DEB BC, PAL SC.
Indian J Public Health. 1990 Jan-Mar;34(1):15-9.
In March 1984, epidemiologists investigated an outbreak of acute bacillarydynsentery (February 17-March 29) in Dhamasin village in Hooghly district inWest Bengal, India. 47% of all families had at least 1 case. Secondary casesoccurred in 14 families. Further a family of 10 family had 7 members fall ill. 91of 937 people in Dhamasin acquired dysentery (attack rate=9.7%). Children 12months old suffered more than other age groups (attack rate=22.7%) and incidencefell with age. The overall case fatality rate was 2.2%. Number of stools rangedfrom 10-70/day. Unqualified local allopathic doctors or private practitionerstreated most cases with at least 1 antibiotic. Local health authorities did notbegin control measures until March 20. They treated all cases with oral rehydrationsolution and enteroquinol and thalazol. Laboratory personnel isolated Shigelladysenteriae, especially type 1, in 31.8% of the 22 stool samples. The next highestisolation rate (27.3%) was for S. shigae. All S. dysenteriae type 1 isolatesdemonstrated resistance to ampicillin, tetracycline, streptomycin,chloramphenicol, and co-trimoxazole. They were sensitive to nalidixic acid,gentamicin, and kanamycin, however. The investigators concluded that S.dynsenteriae was responsible for the epidemic. The index case brought it intothe village and it spread due to poor sanitation facilities, improper disposal offeces, and indiscriminate defecation. In addition, village was experiencing ascarcity of drinking and domestic water. Moreover flies which transmit Shigella

218
Diarrhoeal Diseases
were abundant. The low infective dose required to induce illness furtherexacerbated the situation since event the best precautions could not preventtransmission.
Relevant findings:An outbreak of dysentery was investigated in a rural area of West Bengal in1984. Among 937 subjects of all ages, the overall attack rate was 97 per 1000population, whereas among infants the attack rate was 227 per 1000 infants. Theoverall case-fatality was 2.2%.
Comments: Outbreak situation in a rural area.
7. Epidemiological and clinical profiles of acute invasive diarrhoea withspecial reference to mucoid episodes: a rural community-basedlongitudinal study.
GUPTA DN, SIRCAR BK, SENGUPTA PG, GHOSH S, BANU MK,MONDAL SK, SAHA DR, DE SP, SIKDAR SN, MANNA B, DUTTAS, SAHA NC
Trans R Soc Trop Med Hyg. 1996 Sep-Oct;90(5):544-7.
A study was carried out in 3 villages near Calcutta, India, having a populationof 5464, between August 1992 and December 1994. A cohort of rural childrenbelow 4 years of age was prospectively observed to determine the clinico-epidemiological aspects of mucoid diarrhoea and examine propensity toinvasiveness. Overall, the incidence of diarrhoea was 1.7 episodes/child/year,and that of mucoid and bloody dysentery was 0.8 and 0.2 episodes/child/year, respectively. Children aged 6-11 months had a higher incidence ofmucoid diarrhoea (1.3 episodes/child/year) and the peak season occurred inJune and July. Multivariate analysis using logistic regression showed thatmucoid diarrhoea and bloody dysentery were closely similar in both clinicaland laboratory findings, including raised faecal leucocyte count (> 10/highpower microscope field [hpf]). However, abdominal pain occurred morefrequently in bloody dysentery than in mucoid diarrhoea. Faecal leucocytecount (> 10/hpf) can therefore be used as an indicator for invasiveness ofmucoid diarrhoea at the community level.

219
Diarrhoeal Diseases
8. Impact of vitamin A supplementation to rural children on morbidity due todiarrhoea.
SIRCAR BK, GHOSH S, SENGUPTA PG, GUPTA DN, MONDAL SK, SURD, DEB M, MANNA B, BHATTACHARYA SK.
Indian J Med Res 2001; 113: 53-9.
Randomized double-blind community-based intervention trial.Interventions: High vit. A – 200 000 IU (n=212), Low vit. A – 50 000 IU(n=192)Outcome: Incidence of diarrhoea in children groups (Diarr: >=3 loose/waterystools in 24 hrs)Study area: Four villages, about 10 km from KolkataAge: All children <4 years , with H/O full-term normal delivery
Table: Incidence of diarrhoea (among 6-47 m) during one year period beforeand after intervention:Before supplementation: 1.15 ep/ch/yrAfter supplementation: 0.56 ep/ch/yr [IRR (95% CI): 0.49 (0.40 – 0.59)] [8]
Age Group Incidence in Vit. A Suppl. Group IRR 95% CI of IRR
(Months) 200 000 IU (n=212) 50 000 IU (n=192)
6-11 0.49 1.16 0.42 0.10-1.6712-23 0.74 0.65 1.14 0.72-1.8124-35 0.59 0.63 0.94 0.57-1.5536-47 0.26 0.30 0.87 0.38-1.9548-59 0.35 0.22 1.59 0.61-4.0760-71 0.14 0.10 1.40 0.23-8.41
Overall (6-71) 0.48 0.46 1.05 0.79-1.40
Table: Age-specific incidence (ep/child/yr) of diarhoea (during one year follow-up after intervention):
9. Gender differences in healthcare-seeking during common illnesses in a ruralcommunity of West Bengal, India.
PANDEY A, SENGUPTA PG, MONDAL SK, GUPTA DN, MANNA B, GHOSHS, SUR D, BHATTACHARYA SK.
J Health Popul Nutr. 2002 Dec;20(4):306-11.

220
Diarrhoeal Diseases
This follow-up observational study examined gender disparities in seekinghealthcare and in home management of diarrhoea, acute respiratory infections,and fever among 530 children (263 boys and 267 girls) aged less than five yearsin a rural community of West Bengal, India, from June 1998 to May 1999. Of790 episodes detected by a weekly surveillance, 380 occurred among boys and410 among girls. At the household level, girls were less likely to get home fluidsand oral rehydration solutions (ORS) during diarrhoea. Qualified healthprofessionals were consulted more often (p = 0.0094) and sooner for boys thanfor girls (8.3 +/- 4.5 hours vs 21.2 +/- 9.5 hours), for which parents also travelledlonger distances (3.3 km for boys vs 1.6 km for girls). Expenditure per treatedepisode (Rs 76.76 +/- 69.23 in boys and Rs 44.73 +/- 67.60 in girls) differedsignificantly (p = 0.023). Results of logistic regression analysis showed thatchance of spending more money was 4.2 [confidence interval (CI) 1.6-10.9]times higher for boys. The boys were 4.9 (CI 1.8-11.9) times more likely to betaken early for medical care and 2.6 (CI 1.2-6.5) times more likely to be seen byqualified allopathic doctors compared to girls. Persistence of gender disparitiescalls for effective interventions for correction.
Relevant findings:Among under-5 children in rural West Bengal, the incidence of diarrhoea was1.49 episodes/ child/year overall-it was 1.44 episodes/child/year among boysand 1.54 episodes/child/year among girls.
10. Impact of Breastfeeding on Weight Gain and Incidence of Diarrhea. AmongLow Birth Weight Infants of an Urban Slum of Calcutta.
SUR D, MONDAL SK, GUPTA DN, GHOSH S, MANNA B, SENGUPTA PG.
Indian Pediatrics 2001; 38: 381-384.
A community based observational study was conducted between April ’98 andMarch ’99, on a birth cohort of fifty LBW (<2500 g) babies, identified from theslum area situated in east Calcutta with a population of about 10,000. Fifty NBWnewborn babies selected from the same area and matched for age and sex servedas controls. A standardized pre-designed questionnaire was used to obtain familydetails including basic demographic and socio-epidemiological data. Weeklysurveillance was carried out for detection of diarrhea.
Relevant findings:Incidence of diarrhoea in the two groups (LBW and NBW):Among the low-birth weight babies, the incidence of diarrhoea was 0.5 episodes/

221
Diarrhoeal Diseases
child/year among the exclusively breast-fed babies and 4.1 episodes/child/yearamong the early-weaned babies. Among the normal birth weight babies, theincidence was 0.5 episodes/child/year among the exclusively breast-fed babiesand 1.3 episodes/child/year among early-weaned babies.
11. Impact of zinc supplementation on diarrhoeal morbidity in rural childrenof West Bengal, India.
GUPTA DN, MONDAL SK, GHOSH S, RAJENDRAN K, SUR D, MANNA B.
Acta Paediatr. 2003 May;92(5):531-6.
Aim: To determine the role of zinc supplementation in reducing diarrhoealmorbidity in children. METHODS: A randomized, double-blind, community-based intervention study was conducted in 280 rural children aged between 6and 41 mo. Children were randomly allocated into three groups. One groupreceived a daily dose of 10 mg zinc for 5 d wk(-1), another group received 50 mgzinc once weekly and the remaining group received placebo. Zinc wassupplemented for 16 wk from November 1999. Diarrhoeal episodes were detectedby weekly surveillance during the supplementation period. RESULTS: Eightydiarrhoeal episodes were detected among 59 children in all 3 groups. The groupswere compared with each other at baseline and as regard to the outcome variable(incidence of diarrhoea). The proportion of children suffering from diarrhoeaduring the period was significantly lower in the zinc-supplemented groups (15.8%in daily and 16.5% in weekly group) than in the placebo group (30.8%). Theincidence of diarrhoea in the daily and weekly zinc-supplemented groups was0.68 and 0.69 episodes child(-1) y(-1), and that in the placebo group was 1.67episodes child(-1) y(-1) (relative risk 0.41, 95% confidence interval 0.24-0.71).Diarrhoeal incidence of < 4 d duration was found to occur significantly lessoften in the supplemented groups. There was no difference in diarrhoeal incidencebetween the daily and weekly zinc-supplemented children. There were no detectedadverse reactions in any of the supplemented groups.
CONCLUSION: The study indicates that zinc supplementation is effective inreducing diarrhoeal morbidity when administered either daily or in a weeklyschedule.
Relevant findings:Among children aged 6-41 months in rural areas of West

222
Diarrhoeal Diseases
Bengal, the incidence of diarrhoea (in the placebo group) was 1.67 episodes/child/year and the prevalence was 30.8%.
12. Impact of zinc supplementation on diarrheal morbidity and growth patternof low birth weight infants in kolkata, India: a randomized, double-blind,placebo-controlled, community-based study.
SUR D, GUPTA DN, MONDAL SK, GHOSH S, MANNA B, RAJENDRANK, BHATTACHARYA SK.
Pediatrics. 2003 Dec;112(6 Pt 1):1327-32.
OBJECTIVE: To assess the impact of zinc supplementation on diarrheal morbidityand growth pattern of low birth weight (LBW) infants. METHODOLOGY: In arandomized, double-blind, placebo-controlled, community-based study conductedin the Tiljala slum of eastern Kolkata, India, between 1999 and 2001, a birthcohort of 100 LBW infants was randomly allocated into either an interventiongroup receiving 1 mL daily dose of 5 mg of elemental zinc as zinc sulfate invitamin B complex-based syrup or a placebo group receiving an identical placeboof 1 mL of vitamin-based syrup from birth up to 1 completed year of age. Activeweekly surveillance was conducted for detection of diarrhea. Anthropometricmeasurements of each child were recorded once every month as close to thechild’s birth date as possible. Data were analyzed by using statistical softwarepackages SPSSPC+ 4.0 (SPSS, Inc, Chicago, IL) and Epi Info 6.0 (Centers forDisease Control and Prevention, Atlanta, GA). RESULTS: Among the zinc-supplemented group, diarrheal incidence of 1.36 episodes per child per year wereobserved, whereas it was 1.93 episodes per child per year among the placebogroup, giving a relative risk of 1.4 (95% confidence interval: 1.02-2.00). Lineargrowth and weight for age showed significant differences between thesupplemented and placebo groups only at the end of 1 year. Interestingly, theimpact of zinc supplementation was masked to a large extent by the protectiveaction of breastfeeding. CONCLUSIONS: The study showed that zincsupplementation had a beneficial impact on the incidence of diarrhea and alsoweight gain among LBW infants.
Relevant findings:Incidence of diarrhoea among low-birth weight babies in an urban slum area ofKolkata, as assessed by active weekly surveillance, was 1.93 episodes per childper year (among the placebo group).
Comments: Study conducted among low birth weight babies.

223
Diarrhoeal Diseases
13. A prospective cohort study on the survival experience of under five childrenin rural western India.
HIRVE S, GANATRA B.
Indian Pediatr. 1997 Nov;34(11):995-1001.
OBJECTIVE: To study the role of birth weight, nutrition, immunization andother medical as well as social factors in determining child survival. DESIGN: Aprospective cohort study. SETTING: 45 villages in Shirur Development Blockin Pune District in Maharashtra. METHODS: A cohort of 4129 children werefollowed from birth till 5 years of age. Weight and length/height of the child wasmeasured at birth and at 3 monthly home visits. Information was also obtainedon common childhood morbidities, immunization status and other bio-medicalfactors. Cause of death was ascertained by verbal autopsy. RESULTS: Theneonatal, infant and underfive mortality was rates were estimated to be 37, 60and 79 per 1000 live births, respectively. Diarrhea and ARI contributed to themajor mortality burden. The Kaplan Meier Survival curve showed a sharp fall inthe neonatal period, a less rapid decline in the post-neonatal period followed bya marginal fall in the post-infancy period till 5 years age. Girls had a bettersurvival in the early neonatal period but the trend reversed in the late neonatalperiod. Normal birth weight children had better survival curves compared tolow birth weight children. Survival improved with increasing birth order.Multivariate analysis revealed that birth weight, immunization status, andmother’s and child’s nutritional status influenced infant and under five mortality.CONCLUSION: Birth weight continues to exert its influence not only on survival/mortality in early life but even as late as 5 years of age. Strategies to improvechild survival should include immunization and breastfeeding.
14. Single megadose vitamin A supplementation of Indian mothers andmorbidity in breastfed young infants.
BASU S, SENGUPTA B, PALADHI PK.
Postgrad Med J. 2003 Jul;79(933):397-402.
BACKGROUND AND OBJECTIVE: In developing countries low maternalvitamin A stores combined with increased demands of pregnancy and lactation

224
Diarrhoeal Diseases
may lead to its deficiency in breastfed infants. This study evaluates the effects ofmaternal supplementation with a high dose of vitamin A on the serum retinollevels of exclusively breastfed infants, and their morbidity in the first six monthsof life. SETTING: Hospital based. STUDY DESIGN: Randomised controlledtrial. SUBJECTS AND METHODS: Mothers of the test group (n=150) wereorally supplemented with a single dose of retinol (209 micro mol) soon afterdelivery and were advised exclusive breastfeeding for six months. Beforesupplementation retinol levels were estimated in the mothers’ and newborns’blood, and in colostrum. On follow up, breastmilk and infants’ serum retinolcontents were assessed monthly for six months. Retinol level <0.7 micro mol/lindicated vitamin A deficiency. Morbidity patterns like vitamin A deficiency,diarrhoea, febrile illnesses, acute respiratory infection, measles, and ear infectionwere also studied and compared between the two groups. RESULTS:Presupplement mean maternal serum retinol levels were 0.98 and 0.92 micromol/l and mean breastmilk levels were 3.85 and 3.92 micro mol/l in the test andcontrol groups respectively (p>0.05). Mean cord blood retinol levels were alsocomparable (0.68 v 0.64 micro mol/l). After supplementation, the test groupshowed a rise in mean breastmilk retinol content (12.08 v 2.96 micro mol/l)which remained significantly higher for four months. The infants’ mean serumretinol level, initially 322.06% of the baseline value, was significantly higher forfive months. In the control group, significant numbers of mothers and infantsshowed deficient breastmilk and serum retinol throughout the follow up (p<0.01).Decreased incidence and duration of various diseases were also found in the testgroup suggesting lesser morbidity. CONCLUSION: Maternal supplementationwith single megadose vitamin A is an effective strategy for vitamin A prophylaxisof exclusively breastfed infants of 0-6 months.
Relevant findings:Among infants up to 6 months of age, the incidence of diarrhoea (in the placebogroup) was 1.61 episodes/child/year.
Comment: Hospital-based study. Base population not known.
15. Unpublished data. “Surveillance for Cholera and Typhoid Fever in easternKolkata, India”. ICMR-IVI Collaborative Project, Kolkata, West Bengal. 2003.
Household survey in two urban slums of Kolkata during 2003, covering 57099population of all ages. Information about diarrhoeal morbidity and mortality
225
Diarrhoeal Diseases
were obtained through 1-week recall during the survey and verbal autopsy,respectively.
Relevant findings:Incidence of diarrhoea (as episodes/person/year) - Overall:0.4, among <5 yrs: 1.2, among ³5 yrs: 0.33. Proportionate mortality due todiarrhoea (all ages): 8.0%
Comments:Survey was conducted during off-season for diarrhoea - thus, the morbiditymeasure is probably under-estimated. Reliability of verbal autopsy not assessed.
16. Unpublished data. Surveillance under DBT-project at NICED, Kolkata. 2003.
Household survey in one urban slum of Kolkata was conducted during 2003,covering about 30000 populations of all ages. Information about diarrhoealmorbidity were obtained through 2-week recall during the survey.
Relevant findings:Incidence of diarrhoea (as episodes/person/year) -Overall : 0.3, among <5 years: 1.1, among ³5 years: 0.2
Comments:Survey was conducted during off-season for diarrhoea - thus, themorbidity measure is probably under-estimated. Some errors due to recall biasmay not be ruled out.
17. Unpublished data. NICED project entitled “An operational study on effectof zinc supplementation on reduction of diarrhoeal morbidity among ruralchildren”. 2003
Household survey in rural areas of West Bengal was conducted during 2003,covering 26395 populations of all ages. Information about diarrhoeal morbiditywere obtained through 1-week recall during the survey.
Relevant findings: Incidence of diarrhoea (as episodes/person/year) -Overall : 0.72, among <5 years: 1.71, among ³5 years: 0.63
Comments: Survey was conducted both during season and off-season fordiarrhoea.

226
Diarrhoeal Diseases
18. Surveillance of acute diarrhoeal diseases at village level for effective homemanagement of diarrhoea.
LAL S.
Indian J Public Health. 1994 Apr-Jun;38(2):65-8.
In Kathura community development block in Haryana state, India, village levelvolunteers (Anganwadis) and health teams promoted oral rehydration andcontinued feeding during diarrheal episodes. Between April 1984 and March1985, 37 anganwadis followed 2278 children aged 0-3 years and recordeddiarrheal episodes and weight to measure the incidence of acute diarrhea amongthese rural children and to gather baseline information with which they candetermine interventions and perform an area specific evaluation. The incidenceof diarrhea was greatest among the infants (75.46%), followed by the 1-2 yearolds (67.25%) and 2-3 year olds (51%). The average number of diarrheal episodesper child was 2.56 (2.33-2.63). The number of episodes per year was 5.48 (4.19-5.98). The average duration of diarrheal episodes ranged from 3.87 to 4.16. Thus,the number of days lost due to diarrhea ranged from 16.2 to 23. Infants (0-12months) were most likely to lose at least 300 g during diarrhea (20% vs. 6.43%for 1-2 years and 7.26% for 2-3 years). They were also less likely to either maintainor gain weight during a diarrheal episode (80% vs. 93.57% and 93.74%,respectively). The overall case fatality rate was 1.27%. It was higher amonginfants than among 1-3 year olds (1.8% vs. 0.75%). These results suggest that,even though there are still frequent diarrheal episodes during infancy and earlychildhood, the anganwadis and health teams were rather successful at trainingmost mothers how to manage diarrhea in homes since weight loss and the casefatality rate were minimal. They also indicate that diarrhea surveillance is beingintegrated into child development services at the village level.
19. Substantial reduction in severe diarrheal morbidity by daily zincsupplementation in young north Indian children.
BHANDARI N, BAHL R, TANEJA S, STRAND T, MOLBAK K, ULVIK RJ,SOMMERFELT H, BHAN MK.
Pediatrics 2002; 109(6): e86.
OBJECTIVE: To evaluate the impact of 4 months of daily zinc supplementationon the incidence of severe and recurrent diarrhea in children 6 to 30 months of

227
Diarrhoeal Diseases
age. METHODS: A double-blind, randomized, placebo-controlled trial wasconducted on children who were identified by a door-to-door survey to be aged6 to 30 months and residing in the urban slum of Dakshinpuri, New Delhi. Theywere randomized to receive daily zinc gluconate (elemental zinc 10 mg to infantsand 20 mg to older children) or placebo. A field attendant administered the syrupdaily at home for 4 months except on Sundays, when the mother did so. Onebottle that contained 250 mL was kept in the child’s home and replaced monthly.Field workers visited households every seventh day during the 4-month follow-up period. At each visit, information was obtained for the previous 7 days onhistory of fever, number and consistency of stools, and presence of cough. Whenthe child was ill, illness characteristics and treatment seeking outside the homewere determined. If the child had diarrhea or vomiting, then dehydration wasassessed. At household visits, 2 packets of oral rehydration salts were givenwhen a child had diarrhea. Children who visited the study clinic spontaneouslyfor illness or were referred by the field workers were treated according to thestandard national program guidelines. Antibiotics were advised only for diarrheawith bloody stools or for associated illnesses. For using generalized estimatingequations for longitudinal analysis of a recurring event such as diarrhea, thefollow-up data for each child was divided into 17 child-periods of 7 days eachand presence or absence of an incident episode of diarrhea or severe diarrheawithin each 7-day period was coded. This method of analysis does not assumeindependence of events and therefore prevents underestimation of variance thatresults because of correlation of morbidity within the same child. A logisticgeneralized estimating equations model with exchangeable correlationcovariance-variance matrix was then used to estimate the effect size. RESULTS:Zinc or placebo doses were administered on 88.8% and 91.2%, respectively, ofstudy days during the 4 months of follow-up. There was a small but significantincrease in the average number of days with vomiting in the zinc group (4.3[standard deviation (SD): 5.8] vs 2.6 [SD 3.9] days; difference in means: 1.7[95% confidence interval (CI): 1.3-2.1] days). At the baseline, mean plasma zincwas 62.0 microg/dL (SD: 14.3 microg/dL) in the zinc and 62.0 microg/dL (SD:11.2 microg/dL) in the placebo group; 45.8% and 42%, respectively, had lowplasma zinc levels below 60 microg/dL. At the end of the study, plasma zinclevels were substantially higher in the zinc group (ratio of geometric means:1.94 [95% CI: 1.86-2.03]) and the proportion with low plasma zinc was lower(difference in proportions: -46.7% [95% CI: -41.8% to -51.4%]). The incidenceof diarrhea during follow-up was lower in the zinc-supplemented as comparedwith the placebo group (odds ratio [OR]: 0.88; 95% CI: 0.82-0.95). The beneficialimpact of zinc was greater on the incidence of diarrhea with progressively

228
Diarrhoeal Diseases
increasing duration: episodes of diarrhea that lasted 1 to 6 days (OR: 0.92; 95%CI: 0.85-1.00), 7 to 13 days (OR: 0.79; 95% CI: 0.65-0.95), and > or =14 days(OR: 0.69; 95% CI: 0.48-0.98). The impact was also greater on the incidence ofepisodes with progressively higher stool frequency: 3 to 5 stools per day (OR:0.90; 95% CI: 0.83-0.98), 6 to 9 stools per day (OR: 0.87; 95% CI: 0.77-0.98),and > or =10 per day (OR: 0.77; 95% CI: 0.63-0.94). In the zinc group,significantly more children experienced no diarrheal episode during the studyperiod (risk ratio [RR]: 1.22; 95% CI: 1.02-1.44). Furthermore, substantiallyfewer children (RR: 0.51; 95% CI: 0.36-0.73) experienced recurrent diarrhea,defined as >6 diarrheal episodes in the follow-up period as compared with childrenin the placebo group. The number of children who were hospitalized for anycause tended to be lower in the zinc group, but the difference was not statisticallysignificant (1.79% vs 2.43%; RR: 0.74; 95% CI: 0.43-1.27). The baseline meanplasma copper (microg/dL) was similar in the 2 groups (difference in means:1.6; 95% CI: -2.9 to 6.1). The end study plasma copper levels were significantlylower in the zinc group (difference in means: -15.5; 95% CI: -19.9 to - 11.1).CONCLUSIONS: Zinc supplementation substantially reduced the incidence ofsevere and prolonged diarrhea, the 2 important determinants of diarrhea-relatedmortality and malnutrition. This intervention also substantially reduced theproportion of children who experienced recurrent diarrhea. Prompt measures toimprove zinc status of deficient populations are warranted. The potentialapproaches to achieve this goal include food fortification, dietary diversification,cultivation of plants that are zinc dense or have a decreased concentration ofzinc absorption inhibitors, and supplementation of selected groups of children.Future studies should assess the impact of increased zinc intakes on childhoodmortality in developing countries. For facilitating intervention, there is a need toobtain reliable estimates of zinc deficiency, particularly in developing countries.The functional consequences of the effect of various doses of zinc on plasmacopper levels merits additional study.
20. Are diarrheal incidence and malnutrition related in under five children? Alongitudinal study in an area of poor sanitary conditions.
ANAND K, SUNDARAM KR, LOBO J, KAPOOR SK.
Indian Pediatr. 1994 Aug;31(8):943-8.
This study was conducted in Atali and Garkhera villages of Faridabad district ofHaryana to assess the relationship between diarrheal incidence and malnutrition.

229
Diarrhoeal Diseases
Two hundred and fifty children in the age group of 6-47 months were followed upfor one year from June 1988. History of diarrheal episodes was ascertained byfortnightly home visits. Nutritional status (weight for age) of the children wasassessed at the beginning of the study and at every four monthly interval. Themean diarrheal incidence was 2.88 +/- 1.28 episodes per child year. The pre-valenceof moderate to severe malnutrition in the children was 35% out of which 8.8%were severely malnourished. Although severely malnourished children had 0.56more episodes of diarrhea in a year compared to normally nourished, the differencewas not statistically significant. Similarly, number of episodes of diarrhea also didnot affect the subsequent nutritional status of the children. The possible reason forthis could be that in areas of poor sanitary conditions, nutritional status may notplay an important role in increasing the susceptibility of children to diarrhea.
21. Diarrhoeal diseases amongst children under five. A study in rural Alwar.
SINGH J, GOWRISWARI D, CHAVAN BR, PATIAT RA, DEBNATH AC, JAINDC, SHARMA RS, SHARMA RC, DATTA KK.
J Commun Dis. 1992 Sep;24(3):150-5.
A house to house survey was done in three villages of district Alwar covering 875children under five years age. Two week incidence of diarrhoea morbidity was2.27 episodes/child/year taking into consideration the seasonal correction factor.The incidence decreased with increase of age. Incidence was found significantlymore in children of illiterate mother (p < 0.05). Children of poor socio-economicconditions as determined by occupational status (labourers) suffered significantlymore often from diarrhoea as compared to children of higher socio-economic status(agriculturist and others). Fifty per cent episodes of diarrhoea were treated withantibiotics, and only one child was given ORS. It is a matter of concern. About 3.7per cent mothers washed their hands before preparing meals while, 1.6 per centwashed their hands after toilet. Only 2 per cent mothers had the knowledge ofpreparing the home made salt sugar solution. An intensive health educationcampaign is therefore, necessary for health professionals as well as mothers.
Relevant findings: Among children <5 years in a rural area, the incidence ofdiarrhoea was 2.27 episodes/child/year.
Comment: Survey conducted in Alwar district.

230
Diarrhoeal Diseases
22. Incidence of diarrhoea and some related environmental and behaviouralfactors in Jhuggis of Delhi.
LAL P, BANSAL AK, AGGARWAL CS, TANEJA DK, GOGIA V.
Indian J Public Health. 1996 Apr-Jun;40(2):35-7.
The incidence of diarrhea was assessed in a survey conducted among 6285 personsliving in 1090 households in 3 Jhuggi clusters in Delhi, India. The survey revealedan overall incidence of diarrhea in the 2 weeks preceding the interview of 29.1/1000. This rate was higher among children under 5 years of age (60.2/1000) thanamong adults (13.8/1000). Dysentery was present in 13.1% of cases. Drinkingwater sources identified by respondents were community tap (53.0%), municipalwater tankers (34.4%), and hand pumps (12.6%). Water was stored in openbuckets kept on the floor without a ladle to draw it in 70.5% of households.68.9% of adults were using public latrines and 22.9% defecated in open fields.Only 20.8% of children used latrines, however. Hand washing after defecationwas practiced by 96.2%, while 76.5% washed their hands before meals. Althoughthis survey documented substantial improvements in sources of water supplyand hand-washing practices, the unsafe household storage of water and defecationby children in fields and drains remain problematic.
23. A cross sectional study of undernutrition in 0-5 yrs. age group in an urbancommunity.
RAY SK, ROY P, DEYSARKARI S, LAHIRI A, MUKHOPADHAYA BB.
Indian J Matern Child Health. 1990 Apr-Jun;1(2):61-2.
The study aim was to determine the extent of malnutrition among young childrenin an urban Muslim slum community in India in 1986. The sample included 103families and 88 children 0-5 years old. 57.95% of the children wereundernourished: 40.91% at Grade I, 14.77% at Grade II, and 2.27% at Grade III.75% of infants were undernourished. The relationship between age and nutritionalstatus was not statistically significant, but the association between sex andnutritional status was significant. 68.88% of females and 46.53% of males wereundernourished. 64.71% of the undernourished and 51.35% of the nourishedhad illiterate parents. 70% of children with 3 or more siblings and 58.85% of

231
Diarrhoeal Diseases
children with less than 3 siblings were undernourished. 41.18% of theundernourished had upper respiratory tract infections, 52.82% had diarrhea, and97.37% had parasitic infections. The respective proportions for nourished childrenwere 59.46%, 40.54%, and 78.57%. Statistically significant differences occurredonly for parasitic infections.
Relevant findings:Among the under-5 children of urban Muslim families in WestBengal in 1986, the prevalence of diarrhoea was 40.5% among well-nourishedchildren and 52.8% among malnourished children.
Comments: Community survey done in 1986 and within selected community.
24. Epidemiology of diarrhea in urban slums.
GUPTA P, MURALI MV, SETH A.
Indian Pediatr. 1998 Feb;35(2):147-51.
Findings are presented from an assessment of the impact of potable water supply,mother’s literacy, toilet type, socioeconomic status, family size, housing, hygienicpractices, and malnutrition upon the frequency of diarrheal episodes amongchildren of low socioeconomic status living in the urban slums of East Delhi,India. The mothers of 450 consecutive children with acute diarrhea attending theUCMS and GTB Hospital’s Diarrhea Treatment-cum-Training Unit (DTTU)clinic were included in the study. The mothers were 17-40 years old, of meanage 25.8 years, while their children were 1-98 months old, of mean age 18 months.The 450 children in the study experienced 726 episodes of diarrhea during thepreceding month, with 205 of the children having more than 1 episode.Multivariate logistics analysis determined that malnutrition and poor hygienicpractices were important, significant factors increasing children’s risk of multiplebouts of diarrhea.
25. Impact of ICDS on health and nutritional status of children
SHARMA A, GUPTA S.
Indian J Matern Child Health 1993; 4(1): 27-30.
The Integrated Child Development Services (ICDS) in India comprises health,nutrition, and education human resource development in 1745 rural, 716 tribal,

232
Diarrhoeal Diseases
and 235 urban projects in about 45% of community development blocks of thecountry. Research studies have found that in ICDS areas there were fewer childrensuffering from Grades S II and IV malnutrition compared with non ICDS areasand the percentage of normal children has increased. 6.8% of children aged 0-3years and 4.0% of children aged 3-6 years in ICDS areas were in Grades III and IVof malnutrition. The ICDS treatment for malnutrition is administration of 16-20gm of protein and about 600 calories and monitoring monthly; there are 13.9 millionchildren presently receiving supplementary nutrition in the ICDS program. Thenutrition program in general aims to provide health and nutrition inputs to expectantmothers throughout the gestation period in order to prevent low birth weight babies;the nutrition supplement distribution has improved, but chronic malnutrition amongpregnant mothers persists. The ICDS program provides regular health checkups,immunization, detection of malnutrition, treatment of diarrhea, and deworming ofand for children. These services have contributed to improved health among childrenin ICDS areas. The infant mortality rate (IMR) of 71.3/1000 live births in 1992 inICDS areas was found to be lower than national estimates in 1989. In ICDS projectsmore than 3 years old, IMR was found to be 84.5; further decline in IMR in 1990were found in projects older than 5 years. Morbidity and mortality have been fundto be higher in non-ICDS areas, and declines have been observed in ICDS areas.The incidence of vaccine preventable diseases was not found to have declined inICDS areas, in spite of increased immunization. ICDS provides anganwadicommunity workers (AWWs) and services through a network of Primary HealthCenters and subcenters, which are not optimally used. However, when comparedwith non-ICDS areas, prenatal services are used by 71.9% of the pregnantpopulation compared with 40% in a non-ICDS control group. In 1992, there was90% coverage of children aged 0-6 years with health check ups; this level of usagemay be due to the availability of medicine kits through AWWs. ICDS providespotential for enhancing the survival of children.
26. Infant and early childhood mortality in some rural ICDS blocks of west Bengal.
BISWAS AB, BASU M, DAS KK, BISWAS R. (DR. P. C. SEN AWARD ONRURAL HEALTH PRACTICE).
Indian J Public Health. 1993 Jul-Sep;37(3):81-6.
This one year prospective study was carried out to determine the CBR, CDR anddifferent underfive mortality rates in some selected rural ICDS blocks of West

233
Diarrhoeal Diseases
Bengal and also to find out the common causes of infant and childhood mortalityin these areas. It was revealed that most of the above mentioned indicators inICDS blocks were considerably lower than that of National figures, but more orless similar to those of rural Bengal as recorded in routine Govt. reports. Comparedto the picture of rural West Bengal, both still birth & perinatal mortality rateswere found higher in all ICDS blocks. The causes of mortality trends amongunder fives’ were found similar to that of rural India pattern i.e. prematurity,acute respiratory infections and diarrhoea being the leaders. Neonates, whocontributed the largest share of infant mortality died mainly due to prematurity.So, observations like high perinatal mortality & still birth rates, huge proportionof neonatal death during infancy, same IMR but low 5MR, and death of neonatesdue to prematurity etc. claim the necessity of improving maternal component ofICDS services, their nutritional care in particular.
27. Study of infant and childhood mortality in an ICDS block of eastern U.P.
SINGH SP, REDDY DC, MOHAPATRA SC, GAUR SD
Indian J Public Health. 1993 Apr-Jun;37(2):61-5.
This analysis aims to determine the extent of underreporting of births and deaths byanganwadi workers (AWW) in Barhaj Mahen project area in Eastern Uttar Pradeshstate, India, in 1988, and to identify the birth rate and childhood mortality rate. Causesof mortality are identified. The project area is known to have a high infant mortalityrate. Data were obtained from 11 AWW areas serving a population of 10,206. Samplingfollowed the random cluster technique. Initial household data collection missed 309births (36.6%) but only 10/72 deaths (13.9%). 35.5% of male and 37.8% of femalebirths were unreported. 14.6% of male and 12.9% of female deaths were unreported.18 neonatal and 5 postneonatal infants died. Early neonatal mortality was 45.3/1000live births, and neonatal mortality was 58.3. Infant mortality was 74.7, and maternalmortality was 6.5/1000 live births. Respiratory infections accounted for the highestmortality (25.9%). Other cause of death were diarrhea (22.3%), fever (14.8%),prematurity (8.1%), tetanus (7.4%), and accident (3.7%). The total death rate (7.2/1000) was lower than the national average. The birth rate in project areas of UttarPradesh was almost the same as the national average. Postneonatal mortality showedthe lowest rates compared to Uttar Pradesh and the nation. Since this study area hadbeen included in the Integrated Child Development Services (ICDS) since 1981, it islikely that the lower child mortality reflects the emphasis on ICDS services.Underreporting of deaths is considered to be marginal.

234
Diarrhoeal Diseases
Relevant findings:Household survey involving 10206 subjects of all ages in anICDS project area in U.P., India was conducted during 1988-’89. In the 0-6 yearage group, overall mortality was 16.3 per 1000, of which 22.3% were duediarrhoea. The extent of under-reporting of deaths was assessed to be 13.9%.
28. Utilisation of ORT during diarrhoea in three districts of West Bengal.
RAY SK, KUMAR S, SAHA I, DASGUPTA S.
Indian J Public Health. 1994 Apr-Jun;38(2):73-6.
In the early 1990s, a baseline survey was conducted in 3 districts of West Bengal,India, to determine the magnitude of diarrhea among children less than 5 years oldand the rates of oral rehydration therapy (ORT) use and continuing feeding rate.The districts included Howrah, Hooghly, and 24-Parganas (South). Diarrheaprevalence was much lower in Hooghly than in Howrah and 24-Parganas (S) (5.9%vs. 14.2% and 14.5%, respectively; p 0.05). Since the survey was conducted duringthe non-monsoon season in Hooghly when diarrhea incidence tends to be low, thedifference was likely due to seasonal variation. ORT use rates were 80.8% inHowrah, 70.7% in Hooghly, and 65% in 24-Parganas (S) which were much higherthan those in Hibar (13%), Orissa (27%), and Assam (10%) in 1987 (p 0.05).Children in Howrah were much more likely to receive WHO recommended ORSthan those in Hooghly and 24-Parganas(S) (40.9% vs. 28% and 29.6%, respectively;p 0.05). ORS access rates ranged from 24.9% in 24-Parganas(S) to 36.3% inHowrah, which are lower than the WHO targeted access rate of oral rehydrationsalts (ORS) (80%). The continuing feeding rates were 60.1% in Howrah, 62.7% inHooghly, and 55.5% in 24-Parganas (S). The proportion of children who receivedeither less food or no food during a diarrheal episode were still rather high (38.9%in Howrah, 37.3% in Hooghly, and 42.4% in 24-Parganas(S) but lower than thosein other Indian districts (57-66%) in 1987. These findings show that India’s ChildSurvival and Safe Mother Programme has much to accomplish to reach the goal of70% reduction of deaths and 25% reduction of cases by the year 2000.
29. Risk factors of diarrhoea among flood victims: a controlled epidemiological study.
MONDAL NC, BISWAS R, MANNA A.
Indian J Public Health 2001; 45(4): 122-7.
The concept and practice of ‘disaster preparedness and response’, instead oftraditional casualty relief, is relatively new. Vulnerability analysis and health

235
Diarrhoeal Diseases
risks assessment of disaster prone communities are important prerequisites ofmeaningful preparedness and effective response against any calamity. In thiscommunity based study, the risk of diarrhoeal disease and its relatedepidemiological factors were analysed by collecting data from two selected floodprone block of Midnapur district of West Bengal. The information was comparedwith that of another population living in two non-flood prone blocks of the samedistrict. The study showed that diarrhoeal disease was the commonest morbidityin flood prone population. Some behaviours, like use of pond water for utensilwash and kitchen purpose, hand washing after defecation without soap, improperhand washing before eating, open field defecation, storage of drinking water inwide mouth vessels etc. were found to be associated with high attack rate ofdiarrhoea, in both study and control population during flood season compared topre-flood season. Attack rates were also significantly higher in flood pronepopulation than that of population in non-flood prone area during the same season.Necessity of both community education for proper water use behaviour andpersonal hygiene along with ensuring safe water and sanitation facilities of floodaffected communities were emphasized.
Relevant findings:Household survey of 899 subjects of all ages in a rural area,with 2-week recall period to assess morbidity from diarrhoea was conducted in1998. Prevalence of diarrhoea was 11.9% in flood-prone areas and 8.6% in non-flood prone areas (during “pre-flood” season).
Comments: Survey conducted in flood-prone area.
30. A study of medico social profile of under five children suffering fromdiarrhoeal diseases.
MAHENDRAKER AG, DUTTA PK, URMIL AC, MOORTHY TS.
Indian J Matern Child Health. 1991;2(4):127-30.
In India, 76 of 290 children (26.2%) under five admitted to the pediatric wardsof Command Hospital Pune during April-October 1986 suffered from variousdiarrheal diseases. Boys were more likely to be afflicted with a diarrheal diseasethan girls (63.16% vs. 36.84%). Health workers made home visits after hospitaldischarge. Diarrheal illness was more frequent among the lower socioeconomicclasses than the upper classes (65.81% for social class III and 22.37% for social

236
Diarrhoeal Diseases
class IV vs. 3.94-7.88 for social classes I-II; p 0.001). The incidence of diarrheawas inversely proportional to maternal literacy status (42.1% for illiteracy, 32.89%for primary school, 10.53% for middle school, 9.21% for secondary school, and5.27% for higher education). A family size of no more than 4 was associatedwith a higher incidence of diarrhea than larger family sizes (72.36% vs. 25% for5-6; 2.64% for 6; p 0.05). Yet, diarrhea was more common in overcrowdedhouseholds than in non-crowded households (73.68% vs. 26.32%; p 0.05). Themost common signs and symptoms in children with diarrheal diseases weredehydration (78.95%), fever (75%), and vomiting (73.68%). Children youngerthan 24 months who were exclusively breast fed made up a smaller proportionof diarrhea cases than their counterparts who were not exclusively breast fed(20.75% vs. 79.25%). Most diarrheal disease cases (67-92%) suffered fromvarious grades of malnutrition. Laboratory personnel isolated pathogenicorganisms from only 36.84% of cases. The most common pathogens were Ascarislumbricoides (10.54% of all cases), Giardia lamblia (7.89%), and Campylobacterjejuni (5.26%). 50% of mothers did not know anything about oral rehydrationtherapy (ORT). Of the mothers who did know about it, only 26.32% were usingORT. These findings highlight the great need for health education on ORT formothers.
Relevant findings:Among all under-5 children admitted in a hospital pediatricward, the prevalence of diarrhoea was 26.2%.
Comment: Hospital survey done in 1986; may not reflect community situationdue to differential rates of presentation and admission to the hospital. One singlehospital was surveyed.
31. Diarrhoea in urban slums: Bombay
KOTHARI G.
Dialogue Diarrhoea. 1987 Dec;(31):4-5.
Bombay is one of the most developed, cosmopolitan cities in India. Yet nearly 1/2 of the population live in slums characterized by unhygienic living conditions,overcrowding, poor housing, and lack of basic amenities. People living in theslums are more vulnerable to communicable diseases and malnutrition. Childrenunder age 3 suffer form diarrhea and dysentery. It is common practice to withholdbreast milk and food during diarrhea to give unsuitable home remedies. The

237
Diarrhoeal Diseases
incidence of infectious diarrhea is greatest at the time of weaning. A surveycarried out in the slums of Bombay found that 35-40% of mothers start workingagain soon after giving birth. The infant is bottle-fed with formula milk dilutedwith contaminated water by older sisters or brothers. Many families do not useoral rehydration therapy (ORT) for diarrhea. Educated mothers are more receptiveto health education messages on the importance of breast feeding, immunization,and simple hygienic measures. In a study of families visiting Lyari GeneralHospital in Karachi situated in an urban slum they were asked about diarrheaand ORT. Most of the children attending were 5 years old with some malnutrition,almost 1/2 of them with diarrhea. Nearly 50% of the parents believed it was dueto ignorance about hygiene, 18% gave other reasons such as artificial milk orteething, and 34% had no idea about its etiology. For correct diarrhea treatmentdrugs and ORT were favored by 63; drugs alone by 29; and ORT alone by 5.When asked specifically about ORT, 55 said that they would use oral rehydrationsalts, (ORS), and 13 states they would use salt sugar solution. Over 40 of thefamilies had access to radio or TV as a source of knowledge about ORS. ORTeach year saves millions of young children.
Relevant findings: In children <5 years in an urban slum in Mumbai, theprevalence of diarrhoea was approximately 50%.
Comments: Field survey done in Mumbai about two decades ago.
32. Field survey on water supply, sanitation and associated health impacts inurban poor communities—a case from Mumbai City, India
KUMAR KARN S, HARADA H.
Water Sci Technol. 2002;46(11-12):269-75.
A field survey was conducted on four slum, squatter and pavement dwellercommunities of Mumbai City, India with a total sample size of 1,070 households.Study revealed extremely low water consumption pattern averaging merely 30 l/c x d, no sewerage and safe excreta disposal facilities manifested by highoccurrence of water-borne diseases. The annual diarrhoeal, typhoid and malariacases were estimated to 614, 68 and 126 per thousand populations respectively.At point prevalence scale, at least 30% of all morbidity can be accounted for bywater-related infections. In addition to the impacts of neighborhood water

238
Diarrhoeal Diseases
pollution and sanitation, such diseases were also found positively correlated withlow water consumption and poverty related factors as, poor housing and familyincome. Analysis of variance also revealed intra-poor gradient both in livingstandards and health conditions on which the pavement dwellers were observedto be the greatest sufferers of all.
Relevant findings:Among the slum and pavement dwellers of all ages in Mumbai,India, the prevalence of diarrhoea was 61.4%.
33. Attitude and practices regarding diarrhoea in rural community inChandigarh.
Bhatia V, Swami HM, Bhatia M, Bhatia SP.
Indian J Pediatr 1999; 66(4): 499-503.
The present study on diarrhoea, its prevalence, practices and awareness of motherswas conducted in 120 randomly selected households in the rural area ofChandigarh during monsoons in 1996. Inspite of access to safe drinking waterand latrines in 83% and 74% of the households in the village respectively, theprevalence rate of diarrhoea in 181 under five children was observed to be 23.2%.Majority (88.1%) of children had treatment for diarrhoea whereas only half(54.8%) of children were given oral rehydration solution. 86.7% of the motherswere aware of ORS but only 18.7% could tell the correct method of its preparation.A large number of respondents implicated a variety of food items responsible fordiarrhoea and restricted them during the episodes.
34. Effect of community-based promotion of exclusive breastfeeding ondiarrhoeal illness and growth: a cluster randomised controlled trial.
BHANDARI N, BAHL R, MAZUMDAR S, MARTINES J, BLACK RE, BHAN MK;
Lancet 2003; 361(9367): 1418-23.
BACKGROUND: Exclusive breastfeeding is recommended until age 6 months.We assessed the feasibility, effectiveness, and safety of an educational interventionto promote exclusive breastfeeding for this length of time in India. METHODS:

239
Diarrhoeal Diseases
We developed the intervention through formative research, pair-matched eightcommunities on their baseline characteristics, and randomised one of each pairto receive the intervention and the other to no specific intervention. We trainedhealth and nutrition workers in the intervention communities to counsel mothersfor exclusive breastfeeding at multiple opportunities. We enrolled 1115 infantsborn in the 9 months after training-552 in the intervention and 473 in the controlcommunities. Feeding at age 3 months, and anthropometry and of diarrhoeaprevalence at age 3 months and 6 months were assessed. All analyses were byintention to treat. FINDINGS: We assessed 483 and 412 individuals at 3 monthsin the intervention and control groups, respectively, and 468 and 412 at 6 months.At 3 months, exclusive breastfeeding rates were 79% (381) in the interventionand 48% (197) in the control communities (odds ratio 4.02, 95% CI 3.01-5.38,p<0.0001). The 7-day diarrhoea prevalence was lower in the intervention than inthe control communities at 3 months (0.64, 0.44-0.95, p=0.028) and 6 months(0.85, 0.72-0.99, p=0.04). The mean weights and lengths, and the proportionwith weight-for-height or height-for-age Z scores of 2 or less, at age 3 monthsand 6 months did not differ much between groups. Intervention effect on exclusivebreastfeeding, diarrhoeal morbidity, and anthropometry at age 6 months in thelow-birthweight subgroup was similar to that for all births. INTERPRETATION:Promotion of exclusive breastfeeding until age 6 months in a developing countrythrough existing primary health-care services is feasible, reduces the risk ofdiarrhoea, and does not lead to growth faltering.
35. Clinical profile of acute diarrhoea cases infected with the new epidemicstrain of Vibrio cholerae O139: designation of the disease as cholera.
BHATTACHARYA SK, BHATTACHARYA MK, NAIR GB, DUTTA D, DEBA, RAMAMURTHY T, GARG S, SAHA PK, DUTTA P, MOITRA A, MANDALBK, SHIMADA T, TAKEDA Y, DEB BC.
J Infect 1993; 27(1): 11-5.
A total of 113 patients suffering from acute watery diarrhoea caused by the novelepidemic strain of Vibrio cholerae non-O1, currently assigned to a new serogroupO139, were investigated in order to determine the clinical presentation of thenew epidemic strain causing outbreaks of cholera-like infection in the Indiansubcontinent. Estimations of electrolyte concentration in serum and stool were

240
Diarrhoeal Diseases
also performed in a representative number of the above cases. The clinical featuresand blood and stool biochemical parameters of V. cholerae serogroup O139diarrhoeal patients were indistinguishable from those in typical cholera, exceptfor 44.3% cases infected by O139 had abdominal cramps. In view of the above,we propose to designate the disease caused by V. cholerae O139 as cholera.
36. Epidemic of Vibrio cholerae 0139 in Calcutta.
BHATTACHARYA SK, GOSWAMI AG, BHATTACHARYA MK, DUTTA D,DEB A, DEB M, SIRCAR BK, CHOWDHURY AS, DAS KP, NAIR GB.
Indian J Med Res. 1994 Nov;100:213-6.
As one of large outbreaks of cholera-like illness in the Indian subcontinent,Calcutta and its neighbouring areas experienced an unprecedented epidemic dueto a new strain of V. cholerae non-01, designated as V. cholerae 0139 Bengal,since January 1993. This epidemic predominantly affected the adult populationof Calcutta as evidenced by the hospitalization of more adults at the InfectiousDisease Hospital, Calcutta (IDH), which bore the main brunt of the epidemic inand around Calcutta. During the peak of the epidemic about 180 to 300 diarrhoeapatients were admitted daily at the IDH. Of the 807 patients screened, 407 werepositive for V. cholerae 0139 and majority (82.8%) of the cases were > 10 yr ofage. Severe dehydration was recorded in 85.5 per cent of the cases.
37. Epidemic of Vibrio cholerae 0139 in Calcutta.
BHATTACHARYA SK, GOSWAMI AG, BHATTACHARYA MK, DUTTA D,DEB A, DEB M, SIRCAR BK, CHOWDHURY AS, DAS KP, NAIR GB.
Indian J Med Res 1994; 100: 213-6.
As one of large outbreaks of cholera-like illness in the Indian subcontinent,Calcutta and its neighbouring areas experienced an unprecedented epidemic dueto a new strain of V. cholerae non-01, designated as V. cholerae 0139 Bengal,since January 1993. This epidemic predominantly affected the adult populationof Calcutta as evidenced by the hospitalization of more adults at the InfectiousDisease Hospital, Calcutta (IDH), which bore the main brunt of the epidemic inand around Calcutta. During the peak of the epidemic about 180 to 300 diarrhoea

241
Diarrhoeal Diseases
patients were admitted daily at the IDH. Of the 807 patients screened, 407 werepositive for V. cholerae 0139 and majority (82.8%) of the cases were > 10 yr ofage. Severe dehydration was recorded in 85.5 per cent of the cases.
Relevant findings:Hospital-based surveillance among all age group patientsadmitted with diarrhoea at the Infectious Diseases Hospital, Kolkata, during 1993.
Age group Gender # Admission # Death Case-fatality (per 1000)<=10 years Male 5123 119 23.23
Female 3699 94 25.41Total 8822 213 24.14
>10 years Male 20583 508 24.68Female 15117 404 26.72Total 35700 912 25.55
All ages Male 25706 627 24.39Female 18816 498 26.47TOTAL 44522 1125 25.27
Comments:The study was conducted during the Vibrio cholerae O139 epidemicin Kolkata when 50.43% of the faecal samples examined were positive for V.cholerae O139, which produced more severe disease and high fatality becausethe organism was newly introduced into the communities.
38. A localised outbreak of Vibrio cholerae O139 in Kolkata, West Bengal.
SUR D, SENGUPTA PG, MONDAL SK, DUTTA P, GUPTA DN, GHOSH S,PANDEY A, RAMAMURTHY T, BHATTACHARYA SK.
Indian J Med Res. 2002 Apr;115:149-52.
BACKGROUND & OBJECTIVES: An explosive outbreak of diarrhoeal diseasewhich occurred in the Baishnabghata, Patuli area of Kolkata MunicipalCorporation during September 28 to October 12, 2000, was investigated by ateam from the National Institute of Cholera and Enteric Diseases, Kolkata, toidentify the causative agent and determine the antimicrobial susceptibility pattern.METHODS: Clinical and epidemiological data were collected from domiciliarycases and also from patients attending two medical camps that had been set up

242
Diarrhoeal Diseases
for the purpose. Stool and water samples were collected for isolation ofdiarrhoeagenic pathogens. RESULTS: A total of 710 cases of diarrhoea occurredwith an attack rate of 7.1 per cent; majority were adults. All 6 faecal samples and2 water samples collected, were positive for Vibrio cholerae O139. The strainswere uniformly (100%) susceptible to the commonly used drugs for cholera suchas tetracycline, norfloxacin, ciprofloxacin, co-trimoxazole and nalidixic acid butresistant (100%) to furazolidone and ampicillin. INTERPRETATION &CONCLUSION: This is the first localised outbreak of V. cholerae O139 in Kolkatasince the devastating epidemic in 1992. Extensive chlorination of all water sourcesresulted in a dramatic decline of the outbreak. The appearance of resistance in V.cholerae O139 to furazolidone is a matter of great concern since this drug isused for the treatment of cholera in children and pregnant women.
Relevant findings:During investigation of a diarrhoeal outbreak in one KolkataMunicipal Corporation area with about 10000 population, the attack rate ofdiarrhoea was 71 per 1000 population.
Comment: Findings refer to outbreak situation (outbreak of V. cholerae O139).
39. Effectiveness of oral rehydration salt solution (ORS) in reduction of deathduring cholera epidemic.
SIRCAR BK, SAHA MR, DEB BC, SINGH PK, PAL SC.
Indian J Public Health. 1990 Jan-Mar;34(1):68-70.
Between July-September 1978, an outbreak of gastroenteritis among all agegroups (total of 4469 reported cases) occurred in various villages in the CentralDistrict of Manipur State, India including Imphal. Upon notification of theepidemic, health workers distributed oral rehydration salt solution (ORS)generously so people could begin taking ORS as soon as any diarrhea appeared.Researchers from the National Institute of Cholera and Enteric Diseasesinvestigated 92 active cases who were either in the hospital or the community.They collected the data from records of the Regional Medical College, theDirectorate of Public Health in Imphal, Primary Health Centers in Thoubal andKakching, and by visiting active cases at home. 45.7% of fecal samples and47.6% of river water samples tested positive for Vibrio cholerae biotype ElTor.The case fatality rates fell significantly during the 3 months from 2% for 5 year

243
Diarrhoeal Diseases
old children to 0.7% to no deaths at all and 1.9% for 5 year old people to 0.6% tono deaths (p.05). The overall case fatality rate was just 0.8% (36 deaths), it washigher for 5 year old children than it was for 5 year old people (1% vs. 0.7%).Data on earlier cholera epidemics in Manipur were not available, but theresearchers found the case fatality rates in cholera epidemics (ElTor) before ORSvaried from 22-24%. In fact, they believed this cholera epidemic to be the 1stuse of ORS under field conditions which happened to result in a case fatalityrate of 1%.
40. Epidemiological and laboratory investigations of outbreaks of diarrhoea inrural South India: implications for control of disease.
KANG G, RAMAKRISHNA BS, DANIEL J, MATHAN M, MATHAN VI.
Epidemiol Infect 2001; 127(1): 107-12.
Two epidemics of acute, watery diarrhoea in villages in North Arcot district,India, were investigated. The attack rates were 10.03 and 15.53 per 100population, the median duration was 5 days and enteric pathogens werepresent in 56.8% and 60.3% of specimens from the two villages, but nopredominant pathogen was identified. Examination of stools from a 20%age-stratified random sample of the population of one of the villages afterthe epidemic found 22.9% of asymptomatic subjects excreted bacterialenteric pathogens. Despite the high background of enteric pathogen carriage,the isolation rates for shigellae, enteropathogenic Escherichia coli andShiga-toxin producing E. coli were significantly higher (P < 0.001, P <0.02, P < 0.05) during the epidemic. The epidemics may have been causedby faecal contamination of well water following rain. Point-of-usetechniques for water disinfection may be most effective for preventing suchoutbreaks, but further research into the development of appropriatetechnology is required.
Relevant findings: Attack rates during the two epidemics were 10.03 and15.33 per 100 population; the median duration of each episode was 5days.
Comments: Survey conducted during outbreak situation in South India.

244
Diarrhoeal Diseases
41. Mothers’ concept of the ideal number, colour and consistency of stools oftheir infants.
SINGH K, KUMAR K.
Indian J Matern Child Health 1993; 4(2): 62-3.
PIP: In August-December 1991, the same investigator interviewed the mothersof 20 infants under 6 months old presenting at the outpatient department ofS.G.T.B. Hospital in Amritsar in the Punjab, India, to study their extent of wrongbeliefs about their infants bowel movements. 95% of infants were under 4 monthsold. 85% of the babies were males, reflecting the Indian bias of seeking medicalcare for males but not for females. Mothers fully breast fed 65% of the infants.Daily stool frequency ranged from 2 to more than 15. 35% and 40% of mothersbelieved the ideal number of daily stools should be 1-2 and 2-4, respectively.90% of the mothers thought the stools were too loose or watery. 35% of motherswere concerned because the stools were yellow-green or green. Yet, the stool ofbreast fed infants is often yellow-green or green. All mothers thought stoolsshould be formed and yellow. 8 mothers used various medications to controlwhat they thought to be diarrhea. These medications included Pectokab,Janamghutti, Streptomagma, Piptal drops, and enterovioform tablets. 2 mothersreceived advice to stop breast feeding and to give cows milk or infant formula.These findings showed the need to counsel mothers about infant stools, includingtheir frequency, color and consistency, during prenatal and immunization visits.All health care workers should know about normal bowel movement patterns ininfants.
42. Influence of recall period on estimates of diarrhoea morbidity in infants inrural Tamilnadu.
RAMAKRISHNAN R, VENKATARAO T, KOYA PK, KAMARAJ P.
Indian J Public Health. 1999 Oct-Dec;43(4):136-9.
Data collected on 689 infants, in a study to assess the incidence of diarrhoea andacute respiratory infections during infancy, is used here to quantify the extent ofunder-reporting in diarrhoea morbidity surveys. The study area consisted of twocontiguous primary health centres in Villupuram health unit district in Tamil

245
Diarrhoeal Diseases
Nadu, South India. Each day of infancy was assigned a recal period and proportionof diarrhoeal days for various recall period computed. The proportion of diarrhoeawas 11.3%, 12.0% and 11.2% for zero, one and two days of recall period,respectively, after which the proportion decreased. The under-reporting ofdiarrhoea was approximately 15%, 26% and 45% with three, six and 7-13 daysof recall period, respectively. As there is considerable under-reporting of diarrhoeamorbidity when recall period exceeds three days, it would be best to collectinformation on diarrhoea at least twice a week in diarrhoeal morbidity surveys.
43. Experience in running a Diarrhoeal Training cum Treatment Unit (DTTU)in a state teaching hospital in Calcutta.
SENGUPTA B, DASGUPTA S, SAHA I, MANDAL AK, PALODHI PK.
J Indian Med Assoc 1998; 96(4): 104-5, 108.
The Diarrheal Training with Treatment Unit (DTTU) was established in theDepartment of Pediatrics, NRS Medical College and Hospital, in Calcutta, India,in 1990, to promote use of oral rehydration therapy (ORT) in diarrhea in children0-5 years of age. To evaluate the success of this effort, a retrospective reviewwas conducted of the 4349 child diarrhea cases presenting to DTTU in 1991-92.3919 children (90.1%) were dehydrated at admission; the nondehydrated casesreceived counseling only and were discharged. 3202 children (73.6%) withdiarrhea-related dehydration were successfully treated with ORT; intravenousfluids were administered in 598 (15.3%) of these cases. 717 children (16.5%)required hospital admission; 83.4% of these children received intravenous fluids.The proportion of diarrhea cases requiring antibiotics decreased from 13.5% in1991 to 6.8% in 1992. Case fatality was 1.8% in 1991 and 1.7% in 1992. Theactual cost of treatment was Rs. 1,50,048 in 1991 and Rs. 91,178 in 1992. Theseamounts represent savings of Rs. 6,00,912 and 5,77,867, respectively, over whatwould have been the costs if all cases had been treated on an inpatient basis withintravenous fluids and antibiotics. These findings confirm the effectiveness ofDTTU’s strategy of ORT management of children with diarrheal dehydrationcombined with proper training and motivation of both mothers and health workers.
Relevant findings: Among under-5 children, case-fatality was 1.8% in 1991 and1.7% in 1992.
Comments: Expected to be low in a DTTU setting.

246
Diarrhoeal Diseases
44. Some aspects of Diarrhoea Training and Treatment Unit in InfectiousDiseases Hospital, Calcutta.
KUMAR S, DEBNATH A, GOSWAMI A.
Indian J Public Health. 1994 Apr-Jun;38(2):81-6.
An analys is of hospital admission records and case histories from 1989 to 1993and interviews with hospital administrators, physicians, and mothers ofhospitalized patients were conducted to examine the benefits of establishing theDiarrhoea Treatment and Training Unit (DTU) in June 1991 at the InfectiousDiseases Hospital in Calcutta, India. The case fatality rate of all diarrhea patientsfell between 1989 and 1993 from 4.5% to 2.5%. Among patients less than 5years old, it ranged from 12.7% in 1989 to 2.1% in 1992. The proportion of totalcases successfully managed by using oral rehydration therapy (ORT) increasedfrom 37% to 78.9% between 1991 and 1993. In 1989-1990, the hospital used12,740 and 14,640 units of intravenous (IV) fluids. By 1993, it used only 7200units of IV fluids. The use of packets of oral rehydration salts increased from6000 in 1989 to 24,000 in 1993 (23,000 in 1993). Antibiotic use fell considerably(1989-1993, 100-31.5% of cases). The cost of treating each diarrhea patientdecreased from Rs.84.50 to Rs.19.10. Before the DTU, the hospital did not allowmothers and other family members to stay with children who had diarrhea. Thus,young children could not be breast fed. Now, mothers stay with the children toadminister ORT and to continue breast feeding. DTU staff train mothers in howto administer ORT and to continue it at home, to feed during and after diarrhea,and to recognize danger signs. These findings show that setting up the DTUreduced the case fatality rate of diarrhea patients and the cost of diarrhea treatment.They indicate the need to establish DTUs in major hospitals and ORT corners inall block primary health centers in the state.
Relevant findings:A retrospective analysis of hospital records of InfectiousDiseases Hopital, Kolkata during 1989-1993 revealed that overall case-fatalitydue to diarrhoea was 45 per 1000 in 1989 and 25 per 1000 in 1993. Amongunder-5 children with diarrhoea, the case-fatality was 127 per 1000 in 1989,which came down to 21 per 1000 in 1992.
Comments: Hospital-based data.

247
Diarrhoeal Diseases
45. State Bureau of Health Intelligence, 2002. Govt. of West Bengal.
(a) Urban Registration System. Government of West Bengal. 2000
Records analysis of vital records from selected urban areas West Bengal wasperformed in 2000. Population of all ages were included in the analysis.
Relevant findings:Proportionate mortality due to diarrhoea among under-5children: 9.1%
Comments:Areas covered may not be representative of all urban areas in WestBengal. Magnitude of under-reporting of deaths and errors in causeascertainment are not known.
(b) Records analysis of selected Government District Hospital Records in WestBengal in 2001 was done for all age groups.
Relevant findings:Proportionate mortality due to diarrhoea (all ages): 5.23%
Comments: Data from 11 out of 18 districts were included. Hospitalized casesin government hospitals may not represent all such cases in the districts.
(c) Table: Case-fatality from diarrhoeal diseases as reported to Dept. of Health, Govt.of West Bengal.
Year Case-fatality (per 1000)
1995 5.881996 3.561997 2.621998 5.051999 2.442000 1.082001 0.73
46. Unpublished data. Infectious Diseases Hospital, Kolkata. 2003
Table: Case-fatality from diarrhoeal diseases at the Infectious Diseases Hospital,Kolkata, West Bengal.

248
Diarrhoeal Diseases
47. Mortality associated with acute watery diarrhea, dysentery and persistentdiarrhea in rural north India.
BHANDARI N, BHAN MK, SAZAWAL S.
Acta Paediatr.1992; 381 :111 –116
Mortality associated with diarrhea was investigated in a longitudinallyfollowed cohort of children under 6 years of age in rural North India. Duringthe followup, 1663 episodes of diarrhea and 23 diarrhea-related deaths wererecorded in 1467 children followed up for 20 months. The case fatality ratewas 0.56% for acute watery diarrhea, 4.27% for dysentery, and 11.94% fornon-dysenteric persistent diarrhea. Most of the episodes lasted less than aweek; 5.2% became persistent (duration 14 days). The case fatality rate wassimilar in episodes of 1 and 2 weeks duration (0.64% and 0.8%) and increasedto 13.95% for persistent episodes. Of the total 86 persistent episodes, 22.1%were dysenteric; the case fatality rate for such dysenteric persistent episodeswas 21.1% and for watery persistent diarrhea 11.4%. Diarrheal attack rateswere similar among different nutritional groups, but diarrheal case fatalityrates progressively increased with increasing severity of malnutrition; thesewere 24 times higher in children with severe malnutrition (7.48%) comparedto those normally nourished (0.31%). With availability and use of oralrehydration therapy, dysentery and persistent diarrhea emerge as major causesof diarrhea-related mortality, with underlying malnutrition as a key associatedfactor.
Year Case-fatality (per 1000)1992 30.991993 25.321994 21.871995 24.341996 15.591997 10.371998 11.811999 10.012000 7.542001 8.382002 8.98

249
Diarrhoeal Diseases
48. Infant and early childhood mortality in urban slums under ICDS scheme—a prospective study.
CHOUDHARY SR, JAYASWAL ON.
Indian Pediatr. 1989 Jun;26(6):544-9.
The infant and early childhood mortality, its causes and associated factors werestudied prospectively, in twelve Anganwadi centres, situated in urban slums ofPatna from 1st January, 1987 to 31st December, 1987. A strict recording of birthsand deaths was done by Anganwadi workers, with monthly verifications byauthors. The causes of death were established on the basis of clinical andcorroborative enquiry from the parents. The birth rate was found to be 29.25,death rate 13.1, infant mortality rate 64.65/1000. Neonatal and post neonatalmortality rates were 49.42/1000 and 15.21/1000, respectively. Mortality inchildren between 1-3 years (11.3/1000) was higher in comparison to that of 3-6years (9.1/1000). Low birth weight (25.52%) and perinatal infection (23.52%)were the major causes of infant mortality followed by respiratory infection (11.76)and diarrhea (8.82%). Diarrhea (37.5%), respiratory infection (15.62%) andaccidents and burns (12.5%) were major killers in children between 1-6 years.Mortality in males was higher than females in infancy. Risk factors associatedwith infant mortality included extremes of maternal age (less than 20 and greaterthan 30 years), multiparity and illiterate mothers.
49. Early childhood mortality—a rural study.
KHALIQUE N, SINHA SN, YUNUS M, MALIK A. J
R Soc Health. 1993 Oct;113(5):247-9.
The present study was conducted in 9 villages of Rural Health Training Centre,Jawan, Aligarh, India, having 1792 registered families. The infant mortality ratewas 79.3 per 1000 live births. Higher mortality in children between 1-2 years(29.6/1000) in comparison to 2-5 years (16.2/1000) reflected the highervulnerability of children below 2 years. Diarrhoea (21.2%) and neonatal factors(21.2%) were the major cause of infant mortality followed by pneumonia (18.2%)and tetanus (15.1%). Diarrhoea (32.2%), pneumonia (22.6%) and malnutrition(12.9%) were the major killers in children between 1-5 years. Mortality in females

250
Diarrhoeal Diseases
was higher than males in infancy. Risk factors associated with infant mortalityincluded extremes of maternal age (< 20+ > 35 years) primipara or multiparaand illiterate mothers.
50. Certain aspects of infant mortality — a prospective study in a ruralcommunity.
KHALIQUE N, SINHA SN, YUNUS M, MALIK A.
Indian J Matern Child Health. 1992 Jul-Sep;3(3):85-8.
A prospective study on infant mortality was conducted in the field practice area ofRural Health Training Center (RHTC), Jawan, Aligarh. A sample of 1792 registeredfamilies in 9 villages under RHTC with a population of 12,118 were selected. Thehousehold survey was done in March 1989 by a questionnaire on type and compositionof family, socioeconomic status, family environment, age, parity, and interval betweenthe births. All live births and infant deaths in these villages during the period of April1989 to March 1990 were considered. There were 416 births in the study year, givinga birth rate of 34.02/1000 mid-year population. Male and female births were 52.8%and 47.12%, respectively. 33 infants died during the period, giving an infant mortalityrate of 79.32/1000 live births. Infant deaths equalled 39.4% for males and 60.6% forfemales. Neonatal and postneonatal deaths made up 63.6% and 36.4%, respectively.33.3% of the neonatal deaths occurred in the first 24 hours, 23.8% in the next 6 days,and 42.9% beyond this period. The mortality risk was high in 5th and higher paritybirths and lowest in 2nd to 4th parity births. Diarrhea (21.2%), pneumonia (18.18%),tetanus (15.15%), prematurity (9.1%), and unqualified fever (9.1%) constituted maincauses of infant death. Pneumonia and prematurity were responsible for more than70% of infant deaths. In the 2nd to 4th parity groups, diarrhea and tetanus were themain causes. Deaths during the first 24 hours were mainly caused by birth injury,while, during the next 6 days, pneumonia and tetanus were the leading causes. Beyondthis period, in addition to the above causes, diarrhea played a major role. In thepostnatal period, diarrhea, pneumonia, and malnutrition were the main causes. Toreduce infant mortality further, training of health workers, strengthening of deliverysystems, maximum utilization of existing health infrastructure, environmental hygieneand health education regarding oral rehydration, and control of respiratory infectionare needed.
Relevant findings:Household survey in rural Aligarh (U.P.) was conducted among12118 subjects of all ages in 1989. The IMR in this population was 79.32 per

251
Diarrhoeal Diseases
1000 live births, of which 21.2% were due to diarrhoea. Diarrhoeal deaths amonginfants were 16.8 per 1000.
Comments: Household survey conducted in Aligarh, U.P.
51. Outbreak of cholera caused by Vibrio cholerae 01 intermediately resistantto norfloxacin at Malda, West Bengal.
BHATTACHARYA MK, GHOSH S, MUKHOPADHYAY AK, DEB A,BHATTACHARYA SK.
J Indian Med Assoc 2000; 98(7): 389-90
During the end of September 1997, an unusual outbreak of severe dehydratingwatery diarrhoea cases and deaths were reported from Malda town. Vibriocholerae 01 El tor, the causative agent responsible for this episode was isolatedfrom 56.5% of cases sampled. Three of the five drinking water samples werealso positive for V cholerae 01. Majority of cases were adults. Isolated strainswere uniformly resistant to furazolidone and intermediately to norfloxacin.Indiscriminate use of antibiotic should be discouraged for development ofmultidrug resistant strains.
52. Severe cholera outbreak following floods in a northern district of WestBengal.
SUR D, DUTTA P, NAIR GB, BHATTACHARYA SK.
Indian J Med Res. 2000 Nov;112:178-82.
BACKGROUND & OBJECTIVES: An explosive epidemic of cholera in thedistrict of Malda in the state of West Bengal, was induced by devastating floodsresulting from overflowing of the two main rivers of the district, at the end ofJuly 1998, affecting 15 blocks and 2 municipalities. Diarrhoeal outbreak occurredaround the middle of August after receding of the flood waters. Within two weeksof its onset, the outbreak spread throughout the district. An investigation wasconducted to understand the epidemiological characteristics, identify theetiological agent, rationalise clinical management and suggest control measures.METHODS: The team visited the Block Primary Health Centres, surrounding

252
Diarrhoeal Diseases
the affected villages and also the district hospital. Morbidity and mortality datawere collected and 88 patients were interviewed and examined clinically.Epidemiological and clinical observations were recorded. Rectal swabs werecollected from both hospitalised and domiciliary cases. RESULTS: During theperiod between August and October 1998, 16,590 cases were reported with 276deaths (case fatality rate of 1.7%). Twenty one of 29 (72%) rectal swabs werepositive for Vibrio cholerae O1, biotype ElTor, serotype Ogawa. All the strainswere sensitive to tetracycline, norfloxacilin, ciprofloxacilin, gentamycin,chloramphenicol but resistant to furazolidine, co-trimoxazole, nalidixic acid,streptomycin and ampicilin. INTERPRETATION & CONCLUSIONS:Observations of the present study identified the epidemiological and clinicaldeficiencies in the management of the outbreak and recommendations wereelaborated for its effective control.
Relevant findings: Case-fatality: 1.% (all ages)
Comment:Data from outbreak of cholera in one district.
53. Cause-specific mortality in under fives in the urban slums of Lucknow, northIndia.
AWASTHI S, PANDE VK.
J Trop Pediatr. 1998 Dec;44(6):358-61.
We recorded the causes of death in the preceding 3 years in a slum population of24,196 children less than 5 years of age in Lucknow, North India. Of 1469 deathsrecorded, 298 were stillbirths. For each death, a ‘verbal autopsy’ was conductedby interviewing the parents to ascertain the cause of death. 71.8 per cent ofdeaths were at home; 94.5 per cent of hospital deaths had no death certificate.Excluding stillbirths, 69.9 per cent of deaths were in the first year of life. Leadingcauses of death in the neonatal period were prematurity (38.5 per cent) and tetanus(36.4 per cent). Beyond the neonatal period, the leading causes of death werepneumonia (23.4 per cent), diarrhoeal disease (20.9 per cent), and malnutritionand/or anaemia (11.4 per cent). The existent mortality-recording system wasunder-reporting at least one third of the deaths. We conclude that stillbirths andneonatal mortality can be reduced by improved antenatal and natal care. In thepostnatal period, since most of the mortality is due either to infective diseases or

253
Diarrhoeal Diseases
malnutrition, interventions to improve the nutritional status of preschool childrencan reduce this.
54. Estimates of the years-of-life-lost due to the top nine causes of death inrural areas of major states in India in 1995.
INDRAYAN A, WYSOCKI MJ, KUMAR R, CHAWLA A, SINGH N.
Natl Med J India. 2002 Jan-Feb;15(1):7-13.
BACKGROUND: Years-of-life-lost (YLL) contribute nearly two-thirds of thedisability-adjusted life-years (DALYs) worldwide and are especially Importantfor India where infant and child mortality is still high. These were estimated forIndia under the Global Burden of Disease study for the year 1990. No estimatesare available for the different states of India. We aimed to prepare state-wiseestimates of YLL for different causes of death in rural areas and to determine thecauses responsible for a higher burden in different states. METHOD: Percentagedeaths of the top 9 causes reported in the Registrar-General’s Survey of Causesof Deaths (Rural)—1995 in 13 major states of India and different age groupswas applied to the expected number of total deaths. The life lost according to thestandard life-table was age-weighted and discounted using the methodology ofthe Global Burden of Disease 1990 study. The causes of death were based on layreporting which otherwise seem reliable. RESULTS: The all-cause YLL in ruralIndia in 1995 were 207 per 1,000 population. The minimum was 74 in Keralaand maximum 276 in Madhya Pradesh. Pneumonia was the top cause responsiblefor 15 YLL. The inter-state variation was high as Tamil Nadu had only 1.6 andUttar Pradesh 30.5 YLL from this cause. Cancers were a uniform burden acrossthe states. Heart attack, and bronchitis and asthma cut across the more and lessdeveloped states. Suicides were a heavy burden in Andhra Pradesh and vehicularaccidents in Haryana and Rajasthan. Bihar, Gujarat, Madhya Pradesh, Orissa,Rajasthan and Uttar Pradesh had communicable and nutritional conditions aspredominant causes while Kerala and Punjab had non-communicable diseasesas the predominant cause of YLL due to premature mortality. CONCLUSION:These results provide a new perspective about the causes of death that needmore attention in rural areas of different states of India. These will also helpprioritize areas which require more inputs at the state-level and hence will beuseful for health policymakers.

254
Diarrhoeal Diseases
55. Verbal autopsy: a tool for determining cause of death in a community.
MIRZA NM, MACHARIA WM, WAFULA EM, AGWANDA RO, ONYANGO FE.
East Afr Med J 1990; 67(10): 693-8.
Verbal autopsy was used to determine causes of death in 239 children under theage of 5 years. The diagnosis derived from verbal autopsy was corroboratedwith hospital diagnosis in 39 cases. There was concurrence of diagnosis in 72%of the cases. Using the diagnosis of bronchopneumonia to validate the method,verbal autopsy was found to have a sensitivity of 71%, specificity of 92%, apositive predictive value of 85%. Reliability index of agreement was 0.654. Recallperiod up to 29 months after death was found to be reliable.
56. Verbal autopsy of 48 000 adult deaths attributable to medical causes inChennai (formerly Madras), India.
GAJALAKSHMI V, PETO R, KANAKA S, BALASUBRAMANIAN S.
BMC Public Health 2002; 2(1): 7.
BACKGROUND: In the city of Chennai, India, registration of the fact of deathis almost complete but the cause of death is often inadequately recorded on thedeath certificate. A special verbal autopsy (VA) study of 48 000 adult deaths inChennai during 1995-97 was conducted to arrive at the probable underlying causeof death and to measure cause specific mortality rates for Chennai. METHODS:Trained non-medical graduates with at least 15 years of formal educationinterviewed the surviving family members or an associate of the deceased towrite a report on the complaints, symptoms, signs, duration and treatment detailsof illness prior to death. Each report was reviewed centrally by two physiciansindependently. The reliability was assessed by comparing deaths attributed tocancer by VA with records in Vital Statistics Department and Chennai CancerRegistry. RESULTS: The VA reduced the proportion of deaths attributed tounspecified medical causes and unknown causes from 37% to 7% in early adultlife and middle age (25-69 yrs) and has yielded fewer unspecified causes (only10%) than the death certificate. The sensitivity of VA to identify cancer was 94%in the age group 25-69. CONCLUSION: VA is practicable for deaths in earlyadult life or middle age and is of more limited value in old age. A systematic

255
Diarrhoeal Diseases
program of VA of a representative sample of deaths could assign broad causesnot only to deaths in childhood (as has previously been established) but also todeaths in early adult life and middle age.
57. Diagnosis of causes of childhood deaths in developing countries by verbalautopsy: suggested criteria.
BANG AT, BANG RA. THE SEARCH TEAM.
Bull World Health Organ 1992; 70(4): 499-507.
In the absence of medical certification of deaths in developing countries, layreporting and verbal autopsy have emerged as useful alternative methods forcollecting data on causes of death. Of these, verbal autopsy offers advantagesand is widely used in field studies and child survival programmes. However,because uniform and valid criteria for the diagnosis of common causes of deathare lacking, comparison of the results of different studies becomes meaningless.This article proposes such a set of criteria for the cause of death among neonatesand for those aged 1-59 months. The criteria are based on the findings of earliervalidation studies, a Delphi survey and the experience gained from performing1000 verbal autopsies in Gadchiroli, India. The emergence of such standardizedcriteria of causes of death should be of immense value for health planning,monitoring and evaluation purposes and for interregional comparisons.
58. The effect of different sensitivity, specificity and cause-specific mortalityfractions on the estimation of differences in cause-specific mortality ratesin children from studies using verbal autopsies
MAUDE GH, ROSS DA..
Int J Epidemiol 1997; 26(5): 1097-106.
BACKGROUND: Verbal autopsies (VA) are increasingly being used indeveloping countries to determine causes of death, but little attention is generallygiven to the misclassification effects of the VA. This paper considers the effectof misclassification on the estimation of differences in cause-specific mortalityrates between two populations. METHODS: The bias in the percentage differencein cause-specific mortality between two populations has been explored under

256
Diarrhoeal Diseases
two different models: i) assuming that mortality from all other causes does notdiffer between the two populations; ii) allowing for a difference in mortalityfrom all other causes. The bias is described in terms of the sensitivity andspecificity of the VA diagnosis and the proportion of mortality due to the causeof interest. Methods for adjustment of sample size and adjusting the estimate ofeffect are also explored. RESULTS: The results are illustrated for a range ofplausible values for these parameters. The bias is more extreme as both sensitivityand specificity fall, and is particularly affected even by a small loss of specificity.The bias also increases as the proportion of all deaths due to the cause of interestdecreases, and is affected by the size of the true change in mortality due to thecause of interest relative to the change in mortality from other causes. Calculationsfrom existing data suggest prohibitively large sample sizes may often be requiredto detect important differences in cause-specific mortality rates in studies usingexisting VA. CONCLUSIONS: Highly specific VA tools are needed beforeobserved differences in cause-specific mortality can be interpreted. Loss of powerdue to misclassification may obscure real differences in cause-specific mortality.
59. SRS based abridged life tables, 1988-’92. Govt. of West Bengal.
60. Risk factors for development of dehydration in young children with acutewatery diarrhoea: a case-control study.
BHATTACHARYA SK, BHATTACHARYA MK, MANNA B, DUTTA D, DEBA, DUTTA P, GOSWAMI AG, DUTTA A, SARKAR S, MUKHOPADHAYA A,KRISHNAN T, NAIK TN, NAIR GB.
Acta Paediatr 1995; 84(2): 160-4.
In a case-control study to understand the risk factors for development of life-threatening dehydration, a total of 379 children comprising 243 cases (moderateor severe dehydration) and 136 controls (non or mild dehydration) up to 2 yearsof age suffering from acute watery diarrhoea were studied. By univariate analysis,the presence of vibrios in stool, withdrawal of breast feeding during diarrhoea,not giving fluids, including oral rehydration solution (ORS), during diarrhoea,frequent purging ( > 8/day), vomiting ( > 2/day) and undernutrition were identifiedas risk factors. However, by multivariate analysis after controlling forconfounders, withdrawal of breast feeding during diarrhoea (odds ratio (OR) =

257
Diarrhoeal Diseases
6.8, p < 0.00001) and not giving ORS during diarrhoea (OR = 2.1, p < 0.006)were identified as significant risk factors. The confounding variables which alsocontributed significantly to increasing the risk were age ( < or = 12 months; OR= 2.7, p = 0.001), frequent purging ( > 8/day; OR = 4.1, p < 0.00001), vomiting( > 2/day; OR = 2.4, p = 0.001) and severe undernutrition (%median < or = 60weight-for-age of Indian Academy of Paediatrics classification; OR = 3.1, p =0.001). We feel that these findings will be useful for Global and NationalDiarrhoeal Diseases Control Programmes for formulating intervention strategiesfor preventing death due to diarrhoeal dehydration.
Relevant findings: Hospital-based case-control study with 243 cases and 136controls (total 279 children).Children up to 2 years with diarrhoea were included during October 1991 toJune 1993.Pre-admission duration of diarrhoea among was 26.0±19.4 hours among casesand 27.4±20.7 among controls.
61. Efficacy of norfloxacin and doxycycline for treatment of Vibrio choleraeO139 infection.
DUTTA D, BHATTACHARYA SK , BHATTACHARYA MK, DEB A, DEB M,MANNA B, MOITRA A, MUKHOPADHYAY AK, NAIR GB.
J Antimicrob Chemother 1996; 37: 575-81.
An open randomised controlled clinical trial with 160 adults with acute waterydiarrhoea and severe dehydration compared the efficacy of varying regimens ofnorfloxacin and doxycycline for the treatment of cholera caused by Vibrio cholerae0139 Bengal. Data were analysed for the 111 patients who were faeces culturepositive for V. cholerae 0139. In addition to rehydration therapy, 28 patientsreceived 300 mg of doxycycline as a single dose on admission, 26 patientsreceived norfloxacin 400 mg bd for three days, 28 patients received a singledose of 800 mg of norfloxacin and 29 patients received no antibiotic (controlgroup). Patients in the three treatment groups and control group had comparablecharacteristics on admission. All three treatment groups had reduced stool output,duration of diarrhoea and fluid intake compared with the control group. Multidosenorfloxacin treatment significantly reduced stool output, duration of diarrhoeaand fluid requirement compared with the other regimens.

258
Diarrhoeal Diseases
Relevant findings:Adult (18-55 years) male hospitalized patients with acutewatery diarrhoea and severe dehydration were included during March 1993 toSeptember 1994.
Findings in control (no antibiotic) group (n=29):Age (years): 33±11Pre-admission duration of diarrhoea: 10±4 hoursPost-admission duration of diarrhoea: 55±24 hous
Comments: Hospital-based clinical trial
62. Double-blind, randomized clinical trial for safety and efficacy of norfloxacinfor shigellosis in children.
BHATTACHARYA SK, BHATTACHARYA MK, DUTTA D, DUTTA S, DEBM, DEB A, DAS KP, KOLEY H, NAIR GB.
Acta Paediatr 1997; 86(3): 319-20.
In a randomized, double-blind clinical trial, the efficacy and safety of norfloxacinwere compared with nalidixic acid in the treatment of shigellosis in children.Out of 59 cases, Shigella spp. were isolated from 8 cases in the nalidixic acidgroup and 14 cases in the norfloxacin group. The norfloxacin group hadsignificantly less duration of diarrhoea and presence of blood in stool as comparedto the nalidixic acid group. No joint problem was encountered in this study at upto 4 months follow-up. Norfloxacin is safe and effective and showed no cartilagetoxicity on short-term follow-up.
Relevant findings:Hospitalized children aged 1-10 years with history suggestive of acute bacillarydysentery were included between April 1993 and October 1994.In Nalidixic acid group (n=27):Mean age = 2.6±1.9 years, duration of dysentery was 1.8±1.1 days beforeadmission and 3.7±0.8 days after treatment.In Norfloxacin group (n=32):Mean age = 4.0±3.0 years, duration of dysentery was 2.0±0.9 days beforeadmission and 2.7±0.9 days after treatment.
Comments:Hospital-based clinical study, done under supervision.
259
Diarrhoeal Diseases
63. Efficacy of oral hyposmolar glucose-based and rice-based oral rehydrationsalt solutions in the treatment of cholera in adults.
BHATTACHARYA MK, BHATTACHARYA SK, DUTTA D, DEB AK, DEBM, DUTTA A, SAHA CHOUDHURY A, NAIR GB, MAHALANABIS D.
Scand J Gastroenterol 1998; 33(2): 159-63.
BACKGROUND: Recent animal experiments and clinical trials have shownthat both osmolarity and rice as the organic components are important factorsfor net intestinal absorption of an oral rehydration salt solution. METHODS: Ina controlled clinical trial 123 male adult patients with severe cholera, after initialrehydration with intravenous Ringer’s lactate solution, were randomly assignedto receive one of the four oral rehydration salt solutions: WHO ORS, ORScontaining 70 mmol/l Na+ and 16.2 g/l glucose, rice ORS containing 50 g/l riceand 90 mmol/l Na+, and rice ORS containing 50 g/l rice and 70 mmol/l Na+. Allpatients received 300 mg of doxycycline as a single dose. RESULTS: Patientswho received rice-low-sodium ORS subsequently had lower (P < 0.05) stooloutput, ORS consumption, and diarrhoea duration than the other three ORSgroups. CONCLUSIONS: We conclude that rice-based low-sodium ORS issuperior for treating adult cholera.
Relevant findings:Randomized controlled clinical trial, conducted betweenAugust 1993 and March 1996.Adult (18-55 years) hospitalized males with watery diarrhoea and severedehydration were included.Findings in WHO-ORS group (n=30):Mean age = 34.0±9.3 years; Duration of diarrhoea was 10.9±5.9 before admissionand 46.9±11.9 after admission.
Comments: Hospital-based clinical trial
64. Uncooked rice powder in oral rehydration solution: an alternative to glucoseor cooked rice powder.
DUTTA D, BHATTACHARYA MK, DEB A, CHOWDHURY AS, NAIR GB,RAMAKRISHNA BS, BHATTACHARYA SK.
Indian J Med Res 1998; 107: 257-62.

260
Diarrhoeal Diseases
Glucose-based or rice-based ORS is the standard treatment in acute dehydratingdiarrhoea. However, glucose may not be easily available in remote villages andthe rice needs to be cooked for rice-based ORS. We embarked on a study toexamine whether uncooked rice powder could be used as an alternative to glucoseor cooked rice powder in ORS. Initially, 50 adult male patients (aged 18 to 55 yr)were randomized to receive glucose-ORS or uncooked rice ORS, in two equalgroups. Subsequently, 20 male children (aged 3 to 12 yr) were also enrolled inthe study and received either WHO-ORS or study ORS. All the adult patientsand the children could be successfully rehydrated with ORS containing uncookedrice powder. As compared to WHO-ORS, the study ORS significantly reducedstool output (6.60 +/- 1.24 vs. 5.88 +/- 1.34 l), ORS intake (9.17 +/- 1.54 vs 8.24+/- 1.69 l) and duration of diarrhoea (45.68 +/- 6.91 vs 41.32 +/- 6.03 h). Inchildren also similar results were obtained. No clinical complication (e.g.,vomiting, abdominal pain etc.) or abnormality in serum electrolyte concentrationswas encountered either in the adults or in the children. Uncooked rice powdercontaining ORS can be considered as an alternative to glucose-based ORS orrice-based ORS.
Relevant findings:Randomized controlled clinical trial conducted at the InfectiousDiseases Hospital, Kolkata during May 1995 to June 1996.Two treatment groups: WHO-ORS and Rice-ORSStudy-I: Adult males (18-55 years) with diarrhoea of <24 hours duration andsevere dehydration were included.In WHO-ORS group (n=25): Mean age = 29.24±7.11 years; Pre-admissionduration of diarrhoea = 8.42±2.21 hours and post-admission duration of diarrhoea= 45.68±6.91 hours.Study-II: Children aged 3 to 12 years with acute watery diarrhoea and severedehydration were included.Similar two treatment groups.In WHO-ORS group (n=10): Mean age = 5.8±1.6 years; Pre-admission durationof diarrhoea = 9.2±6.6 hours and post-admission duration of diarrhoea = 35.95±7.37 hours.
Comments: Hospital-based clinical trial

261
Diarrhoeal Diseases
65. Association of a disease approximating cholera caused by Vibrio choleraeof serogroups other than O1 and O139.
BHATTACHARYA MK, DUTTA D, BHATTACHARYA SK, DEB A,MUKHOPADHYAY AK, NAIR GB, SHIMADA T, TAKEDA Y,CHOWDHURY A, MAHALANABIS D.
Epidemiol Infect 1998; 120(1): 1-5.
One hundred and six patients suffering from severe dehydrating diarrhoea werestudied of whom 36 patients were positive for Vibrio cholerae. Out of 36, 15 werepositive for V. cholerae O1, 10 for V. cholerae O139 and 11 for V. cholerae non-O1 non-O139. O1 and O139 were positive for the 301-bp ctxA amplicon and 471-bp tcpA amplicon indicating that the strains possessed toxigenic capability whereasno non-O1 non-O139 strain possessed ctxA or tcpA genes. Post-admission severityof purging and amount of ORS required were less in the V. cholerae non-O1 non-O139 group (P < 0.05) compared to the V. cholerae O1 and O139 groups. It appearsfrom this study that a cholera-like clinical condition can be caused in the absenceof CT as exemplified by strains of non-O1 non-O139.
Relevant findings:Adult (18-55 years) male hospitalized patients with acutewatery diarrhoea of <24 hours duration and severe dehydration were includedbetween September 1995 and March 1996.
Characteristics O139 (n = 10) O1(n = 15) Non-O1 Non-O139(n = 11)
Age(years) 32.5"11.5 30.3"8.3 28.6"9.1Diarr. duration 11.8"5.4 11.7"6.2 8.4"4.8(pre-adm, hrs)Diarr. duration 50.9"9.5 29.0"10.9 35.9"10.1(post-adm, hrs)
Vibrio cholera
66. Evaluation of oral hypo-osmolar glucose-based and rice-based oralrehydration solutions in the treatment of cholera in children.
DUTTA D, BHATTACHARYA MK, DEB AK, SARKAR D, CHATTERJEEA, BISWAS AB, CHATTERJEE K, NAIR GB, BHATTACHARYA SK.
Acta Paediatr 2000; 89(7): 787-90.

262
Diarrhoeal Diseases
In a randomized controlled clinical trial, the efficacy of a low-sodium low-glucose oral rehydration solution (ORS) and a low-sodium rice-based ORS wascompared with standard WHO glucose ORS in the treatment of severe cholerain children aged 2-10y. In total, 120 children were evaluated for the study, ofwhom 58 patients were positive for Vibrio cholerae and were included in thestudy. Of these 58 cases, 19 received rice-based hypo-osmolar ORS, 20 receivedWHO-ORS and 19 received glucose-based hypo-osmolar ORS. The clinicalcharacteristics (age, preadmission duration of diarrhoea, frequency of stool beforeadmission, incidence of vomiting, body weight and volume of initial fluidrequirement) were comparable in the three treatment groups. All patients receivedtetracycline in a dose of 50 mg/kg/d of body weight in 4 divided doses for 3 d.Conclusions: Patients who received rice-based hypo-osmolar ORS hadsubsequently reduced (p < 0.05) stool output, ORS consumption and diarrhoeaduration than the patients who received either WHO-ORS or glucose-based hypo-osmolar ORS.
Relevant findings:Randomized controlled clinical trial conducted at the InfectiousDiseases Hospital, Kolkata during August 1995 to May 1998.Three treatment groups: WHO-ORS and Glucose-based hypoosmolar ORS andRice-based hypoosmolar ORS.Male children aged 2 to 10 years with acute watery diarrhoea of <24 hours durationand severe dehydration were included.Similar two treatment groups.In WHO-ORS group (n=20): Mean age = 4.37±1.87 years; Pre-admission durationof diarrhoea = 8.92±3.29 hours and post-admission duration of diarrhoea = 38.47±3.89 hours.
Comments: Hospital-based clinical trial
67. Impact of massive dose of vitamin A given to preschool children with acutediarrhoea on subsequent respiratory and diarrhoeal morbidity.
BHANDARI N, BHAN MK, SAZAWAL S.
BMJ 1994; 309: 1404-7.
Objective—To assess the impact of vitamin A supplementation on morbidity
263
Diarrhoeal Diseases
from acute respiratory tract infections and diarrhoea. DESIGN—Double blindrandomised placebo controlled field trial.Setting—An urban slum area in New Delhi, India. SUBJECTS—900 childrenaged 12-60 months attending a local health facility for acute diarrhoea of lessthan seven days’ duration randomly allocated to receive vitamin A 200,000 IU orplacebo.Main Outcome Measures—Incidence and prevalence of acute lower respiratorytract infections and diarrhoea during the 90 days after termination of the enrolmentdiarrhoeal episode measured by twice weekly household surveillance.
Results—The incidence (relative risk 1.07; 95% confidence interval 0.92 to 1.26)and average number of days spent with acute lower respiratory tract infectionswere similar in the vitamin A supplementation and placebo groups. Amongchildren aged 23 months or less there was a significant reduction in the incidenceof measles (relative risk 0.06; 95% confidence interval 0.01 to 0.48). Theincidence of diarrhoea was also similar (relative risk 0.95; 0.86 to 1.05) in thetwo groups. There was a 36% reduction in the mean daily prevalence of diarrhoeaassociated with fever in the vitamin A supplemented children older than 23months.Conclusions—Results were consistent with a lack of impact on acute lowerrespiratory tract related mortality after vitamin A supplementation noted in othertrials and a possible reduction in the severity of diarrhoea.
68. Economic evaluation of zinc and copper use in treating acute diarrhoea inchildren: a randomized controlled trial.
PATEL AB, DHANDE LA, RAWAT MS.
Cost Eff Resour Alloc 2003; 1(1): 7-16.
Background: The therapeutic effects of zinc and copper in reducing diarrhealmorbidity have important cost implications. This health services research studyevaluated the cost of treating a child with acute diarrhea in the hospital, theimpact of micronutrient supplementation on the mean predicted costs and itscost-effectiveness as compared to using only standard oral rehydration solution(ORS), from the patient’s and government’s (providers) perspective.Methods: Children aged 6 months to 59 months with acute diarrhea were randomlyassigned to receive either the intervention or control. The intervention was a

264
Diarrhoeal Diseases
daily dose of 40 mg of zinc sulfate and 5 mg of copper sulfate powder dissolvedin a liter of standard ORS (n = 102). The control was 50 mg of standard ORSpowder dissolved in a liter of standard ORS (n = 98). The cost measures werethe total mean cost of treating acute diarrhea, which included the direct medical,the direct non-medical and the indirect costs. The effectiveness measures werethe probability of diarrhea lasting leq; 4 days, the disability adjusted life years(DALYs) and mortality.
Results: The mean total cost of treating a child with acute diarrhea was US $14 ofwhich the government incurred an expenditure of 66%. The factors that increasedthe total were the number of stools before admission (p = 0.01), fever (p = 0.01),increasing grade of dehydration (p = 0.00), use of antibiotics (p = 0.00), use ofintra-venous fluids (p = 0.00), hours taken to rehydrate a child (p = 0.00), theamount of oral rehydration fluid used (p = 0.00), presence of any complications (p= 0.00) and the hospital stay (p = 0.00). The supplemented group had a 8% lowercost of treating acute diarrhea, their cost per unit health (diarrhea lasting leq; 4days) was 24% less and the incremental cost-effectiveness ratio indicated costsavings (in Rupees) with the intervention [-452; 95%CI (-11306, 3410)]. Howeverthese differences failed to reach conventional levels of significance.Conclusions: An emphasis on the costs and economic benefits of an alternativetherapy is an important aspect of health services research. The cost savings andthe attractive cost-effectiveness indicates the need to further assess the role ofmicronutrients such as zinc and copper in the treatment of acute diarrhea in alarger and more varied population.
69. Global mortality, disability, and the contribution of risk factors: GlobalBurden of Disease Study.
MURRAY CJ, LOPEZ AD.
Lancet 1997; 349(9063): 1436-42.
Background: Prevention and control of disease and injury require informationabout the leading medical causes of illness and exposures or risk factors. Theassessment of the public-health importance of these has been hampered by thelack of common methods to investigate the overall, worldwide burden. The GlobalBurden of Disease Study (GBD) provides a standardised approach toepidemiological assessment and uses a standard unit, the disability-adjusted lifeyear (DALY), to aid comparisons.Methods: DALYs for each age-sex group in each GBD region for 107 disorderswere calculated, based on the estimates of mortality by cause, incidence, averageage of onset, duration, and disability severity. Estimates of the burden andprevalence of exposure in different regions of disorders attributable tomalnutrition, poor water supply, sanitation and personal and domestic hygiene,

265
Diarrhoeal Diseases
unsafe sex, tobacco use, alcohol, occupation, hypertension, physical inactivity,use of illicit drugs, and air pollution were developed. FINDINGS: Developedregions account for 11.6% of the worldwide burden from all causes of death anddisability, and account for 90.2% of health expenditure worldwide.Communicable, maternal, perinatal, and nutritional disorders explain 43.9%;non-communicable causes 40.9%; injuries 15.1%; malignant neoplasms 5.1%;neuropsychiatric conditions 10.5%; and cardiovascular conditions 9.7% ofDALYs worldwide. The ten leading specific causes of global DALYs are, indescending order, lower respiratory infections, diarrhoeal diseases, perinataldisorders, unipolar major depression, ischaemic heart disease, cerebrovasculardisease, tuberculosis, measles, road-traffic accidents, and congenital anomalies.15.9% of DALYs worldwide are attributable to childhood malnutrition and 6.8%to poor water, and sanitation and personal and domestic hygiene.Interpretation: The three leading contributors to the burden of disease arecommunicable and perinatal disorders affecting children. The substantial burdensof neuropsychiatric disorders and injuries are under-recognised. Theepidemiological transition in terms of DALYs has progressed substantially inChina, Latin America and the Caribbean, other Asia and islands, and the middleeastern crescent. If the burdens of disability and death are taken into account,our list differs substantially from other lists of the leading causes of death. DALYsprovide a common metric to aid meaningful comparison of the burden of riskfactors, diseases, and injuries.
PIP: The Global Burden of Disease Study used the disability-adjusted life-year(DALY) to compare death and disability from various disorders in developingand developed countries. In 1990, developing countries carried almost 90% ofthe global disease burden yet were recipients of only 10% of global health carefunding. The highest disease burdens were in sub-Saharan Africa (21.4% of globaltotal) and India (20.9%). Communicable, maternal, perinatal, and nutritionaldisorders (group 1 causes) predominated in sub-Saharan Africa (65.9% of burden),while noncommunicable diseases (group 2 causes) accounted for 80% of theburden in established market economies; injuries (group 3) did not differsubstantially across regions. The ratio of group 2 to group 1 disorders can beused as a measure of the epidemiologic transition. Group 2 disorders alreadysurpass group 1 disorders in China, Latin America, and the Caribbean. On aglobal level, group 1, 2, and 3 causes accounted for 43.9%, 40.9%, and 15.1%,respectively, of DALYs. Overall, the top 3 causes of DALYs in 1990 were lowerrespiratory infections, diarrheal diseases, and perinatal disorders (low birth weightand birth asphyxia or birth trauma). In developed countries, these causes were

266
Diarrhoeal Diseases
ischemic heart disease, unipolar major depression, and cerebrovascular diseases.Malnutrition was the risk factor responsible for the greatest loss of DALYs(15.9%), followed by poor water supply, sanitation, and personal hygiene (6.8%).
70. Cholera: ancient scourge on the rise. WHO announces global plan for choleracontrol.
WORLD HEALTH ORGANIZATION WHO. OFFICE OF INFORMATION.(25 APRIL 1991).
WHO Feature 1991; (154): 1-3.
Vibrio cholerae spreads quickly via contaminated water and food, especially inareas with a poor health and sanitation infrastructure. Its enterotoxin inducesvomiting and huge amounts of watery diarrhea leading to severe dehydration. 80-90% of cholera victims during an epidemic can use oral rehydration salts. A choleraepidemic is now spreading through Latin America threatening 90-120 million people(started in January 1991), particularly those in urban slums and rural/mountainousareas. As of mid April 1991, there were more than 177,000 new reported cases in12 countries and 78% of these cases and more than 1200 deaths were limited to 5countries: Brazil, Chile, Colombia, Ecuador, and Peru, WHO’s Global CholeraControl Task Force coordinates global cholera control efforts to prevent deaths inthe short term and to support infrastructure development in the long term. Itsmembers are specialists in disease surveillance, case management, water andsanitation, food safety, emergency intervention, and information and education.WHO’s Director General is asking for the support of the international communityin cholera control activities. These activities’ costs are considerable. For example,Peru needs about US$ 60 million in 1992 to fulfill only the most immediate demandsof rehabilitation and reconstruction of the infrastructure. Costs of infrastructurecapital throughout Latin America is almost US$ 5 thousand million/year over thenext 10 years. It is indeed an effective infrastructure which ultimately preventscholera. Cholera is evidence of inadequate development, so to fight it, we mustalso fight underdevelopment and poverty.
71. Diarrhoeal diseases control programme.
Diarrhoea Dialogue 1980; 1(1): 6.
Objectives and activities of the Diarrhoeal Disease Control Programme launchedby WHO in 1978 are described. The programme aims to reduce mortality and

267
Diarrhoeal Diseases
malnutrition due to diarrhoea by making available oral rehydration salts andtraining in the treatment and prevention of diarrhoeal diaseses. Research on thecauses, prevention and treatment of diarrhoeal diseases is also being organizedwith the collaboration of national and international agencies.
72. World Health Organization WHO. Division of Diarrhoeal and AcuteRespiratory Disease Control. Rational management of diarrhoea in children.
Essent Drugs Monit 1991; (11): 10-1.
Most health professionals in developing and developed countries consider oralrehydration therapy (ORT) to be the most effective treatment for diarrhea. Anestimated 1,500 million episodes of diarrhea occur annually and 3 million of theseresults in death of children 5 years old. Caretakers must give increased amounts offluids (rice water, tea, and gruel) to children with diarrhea to prevent dehydration.If they become dehydrated, caretakers must take them to a health workers so he/she can assess and treat them with oral rehydration solution (ORS) or, in the caseof severe dehydration, rehydrate them intravenously. Drugs should not be used totreat diarrhea cases. Nevertheless, surveys in 4 Asian nations indicated that druguse ranged from 22-68% of diarrhea episodes and ORS use ranged only from 9-21%. Drug use is very expensive. In fact, Peru spent US$2 million on antidiarrhealsin 1988- 1989. Further, drugs often make up 40% of health care costs in developingcountries, so ORS use reduces these costs. Indeed drug us deflects from correctcase management of diarrhea. In addition, drugs have no proven value for acutediarrhea. They do not decrease the fluid loss responsible for death and may evenhave serious side effects, such as central nerve depression and gastrointestinaltoxicity. If health workers suspect cholera or dysentery, however, they can administereffective and relatively inexpensive antibiotics. Since the early 1980s, almost alldeveloping countries had a national control of diarrheal disease program. In severalcountries, hospital admission rates for diarrhea fell 61% and the case fatality ratefell 71% after ORT introduction. Some hospitals have even saved as much as 60%in costs due to these declines. WHO has a book available which covers rationaluse of drugs in managing acute diarrhea in children.
73. Editorial-programme for control of diarrhoeal diseases.
SRIVASTAVA RN.
J Indian Assoc Commun Dis 1982; 5(3-4): 48-9.
Outlines the Program for Control of Diarrheal Diseases (CDD) funded by the

268
Diarrhoeal Diseases
World Health Organization (WHO) and active in 70 developing countries.Components include the use of oral rehydration therapy (a solution of glucoseand salts in water), administered both in hospital and at home; expandingepidemiological surveillance and epidemic control; encouraging preventivematernal and child care practices such as continued breast feeding andnutritious foods; improving water supplies and sanitation; and stressing healtheducation for the mother or attendant, especially during a diarrheal episode.CDD was initiated after research on the etiology and epidemiology of acutediarrhea found that dehydration was the only cause of death in almost allfatal cases, and that the role of antibiotics and antidiarrheal drugs in controland treatment is limited.
74. Occurrence of diarrhoeal diseases in relation to infant feeding practices ina rural community in West Bengal, India.
MONDAL SK, GUPTA PG, GUPTA DN, GHOSH S, SIKDER SN,RAJENDRAN K, SAHA MR, SIRCAR BK, BHATTACHARYA SK.
Acta Paediatr 1996; 85(10): 1159-62.
In a rural community-based prospective study, diarrhoea in relation to the feedingpatterns of a cohort of infants was studied. A total of 148 infants between theages of 0 and 2 months were enrolled and followed until the completion of 1year of age. Survival analysis showed that by the fourth month of age exclusivebreastfeeding dropped by 75%. The proportion of complementary breastfeedingincreased from 18.6 to 52.9% during the same period and to 83.7% by the eighthmonth. This study clearly highlights the tendency for early switch over fromexclusive breastfeeding to complementary breastfeeding. Early weaning wasassociated with an incidence rate ratio (IRR) of 3.02 (95% CI 1.043-8.802). TheIRR of 3.02 and its confidence limits (1.043-8.02) suggest a significant protectiveeffect of exclusive breastfeeding against diarrhoea in infants. The results of thisstudy indicate that promotion of exclusive breastfeeding has a potential role toreduce the incidence of diarrhoea amongst infants. The findings of this studywill be useful for Diarrhoeal Disease Control Programme in reducing diarrhoealmorbidity.
Relevant findings: IRR for diarrhoea among infants: 3.02 (Early weaning vs.Exclusive breast feeding)

269
Diarrhoeal Diseases
75. Child mortality in new industrial localities and opportunities for change: asurvey in an Indian steel town.
CROOK N, MALAKER CR.
Health Transit Rev. 1992 Oct;2(2):165-76.
The hypothesis of this study of infant mortality in an Indian steel town is thatthe government can intervene, by providing clean water and sanitation, cleanair, and decent housing, and reduce mortality. The objectives were to estimatemortality for a nonmetropolitan city with a heavy industrial base and toidentify mortality differentials and their social or environmental influences.1500 households were sampled in Durgapur, which is reported to have lowerthan the national average mortality (6.7/1000 in 1980-82 for the crude urbandeath rate and 48/1000 live births for infant mortality in 1983). Householdswere stratified into official low grade housing in the steel township and intobustees, or huts, in spontaneous housing. A detailed description of the sampleand the housing types is provided. The Brass method was used to estimateinfant mortality rate (IMR) and child mortality. Life table measures weregenerated using the West model of the Coale-Demeny life tables. IMR wasestimated at 46/1000 for townships and 70/1000 for bustee areas. Theweighted sample of IMR for the working class population within the citywas estimated at 54/1000, which is similar to IMR in Calcutta. This infantmortality was the lowest among Durgapur’s urban population. Occupation-differentiated IMR was the greatest; i.e., 30.4/1000 for skilled workers and83/1000 for lower occupations. Literacy differences were also apparent, withliterate mothers showing an IMR of 83/1000, and with the completion ofprimary school, showing an IMR of 43.1/1000. Those with an inside toilethad an IMR of 67.5/1000 and those with an outside toilet an IMR of 96.5/1000. Access to drinking water showed a similar pattern. Construction featuresof housing also showed slight differences; floor construction was consideredimportant as an indicator of dampness, but was not measured. Occupation,access to safe drinking water, and maternal education were the most important,statistically independent variables in the child survival model in the busteeor township areas. The policy should thus be directed to providing safedrinking water and sanitation in unplanned areas as a cost-effective strategyhaving a substantial impact on child survival. Other interventions are desirableif funding is available.

270
Diarrhoeal Diseases
76. Role of oral rehydration therapy in controlling epidemic of cholera andwatery diarrhoea.
SARKAR K. J
Indian Med Assoc. 2003 Jun;101(6):379-80, 386.
Oral rehydration therapy (ORT) is basically oral administration of liquidcontaining various electrolytes in specific proportions to prevent and treatdehydration. This treatment facilitates safe and optimal absorption of water andessential electrolytes such as sodium chloride, sodium bicarbonate and potassiumchloride in dehydrated patients. Successful ORT was experienced in cholerapatients in Kolkata and Dhaka which was followed by the development of oralrehydration salt (ORS). This procedure can be safely implemented at home. ORTreduced mortality rate both in cholera and non-cholera watery diarrhoea. Thevarious health authorities must support preparedness before pre-positioning ofadequate stocks of ORS packets for emergency situations. Health workers shouldhave been the knowledge to prepare ORS solutions.
77. A prediction model for moderate or severe dehydration in children withdiarrhoea.
ZODPEY SP, DESHPANDE SG, UGHADE SN, KULKARNI SW,SHRIKHANDE SN, HINGE AV. J
Diarrhoeal Dis Res 1999; 17(1): 10-6.
A hospital-based unmatched case-control study (387 cases and 387 controls)was carried out at the Government Medical College Hospital, Nagpur, India, todevise and validate a risk-scoring system for predicting the development ofmoderate or severe dehydration in children, aged less than five years, with acutewatery diarrhoea. On unconditional multiple logistic regression, 12 risk factors—infancy, minority religion, undernutrition, not washing hands by mother beforepreparation of food, frequency of stools > 8/day, frequency of vomiting > 2/day,measles in previous 6 months, withdrawal of breast-feeding/other feedings,withdrawal of fluids during diarrhoea, not giving oral rehydration solutions (ORS),home available fluids and both during diarrhoea—were significant. Based onregression coefficients, these factors were ascribed statistical weights of 5, 5, 4,

271
Diarrhoeal Diseases
4, 22, 9, 11, 13, 5, 5, 5, and 7 respectively. The receiver-operating characteristiccurve suggested a total score of 48 to be the best cut-off for predicting thedevelopment of moderate or severe dehydration. At this cut-off, the sensitivity,specificity, positive predictive value, Cohen’s kappa, and overall predictiveaccuracy were 0.81, 0.81, 0.81, 0.61, and 0.86 respectively. If substantiated byfurther validation, this system can be used for predicting the development ofdehydration at the earlier stage, thereby reducing the mortality associated withlife-threatening dehydration.
78. Maternal knowledge on risk behavioural practices and it’s association withdiarrhoea in a rural community of West Bengal, India.
GHOSH S, SENGUPTA PG, GUPTA DN, MONDAL SK, GOSWAMI M,BHATTACHARYA SK, SIRCAR BK.
J Commun Dis 1998; 30(4): 251-5.
Knowledge of rural mothers related to five diarrhoeagenic risk behaviours,identified in an earlier study, was ascertained. A high proportion of mothers (67%-79%) had knowledge about risk of bottle feeding, non-use of soap for cleaningfeeding containers, storage of drinking water in wide-mouthed vessels andindiscriminate disposal of children’s faeces. However, only around 31% ofmothers were aware about danger of using pond water for cleaning feedingcontainers. Risk behavioural practices were less amongst mothers who hadknowledge about them. Risk of diarrhoea amongst children of mothers havingrisk practice without knowledge as compared to those who utilised theirknowledge to avoid risk practice was found significantly higher (p < or = 0.005)except for bottle feeding (p = 0.330). The results of this study indicate that childrencan be protected significantly from diarrhoea if mothers’ diarrhoeagenicbehaviours can be altered through educational intervention.
79. Infant mortality, its components and correlates: findings from a longitudinalstudy in rural Karnataka, India.
BADARI S, GOPAL YS, DEVARAMANI SC.
Genus. 1991 Jan-Jun;47(1-2):89-108.
Researchers began following 1920 pregnant women (3rd trimester) from 5primary health centers (PHCs) in Bangalore Division of Karnataka State in India

272
Diarrhoeal Diseases
between August 1977-November 1977 to determine the infant mortality rate(IMR), its components, and correlates. Auxiliary nurse midwives followed themonce a week during the 1st month after delivery and then once a month until theindex child either died or reached 1 year. Male infants were more likely to diethan female infants (113 vs. 90; p.05), especially in the neonatal period (76 vs.48; p.01). Further IMR was highest among 15-19 year old mothers and 35-44year old mothers (115 and 128 respectively compared to 87-101 for all othermothers). Infants of birth order 2 had the lowest IMR (85 vs. 102-109 for otherorders). Parental education was inversely correlated with IMR, especially mother’seducation. For example, the IMR for mothers with no education was 115compared to 60 for those with at least 5 years of education (p.01). Father’seducation was significant at .05. Mothers who lived on at least 20 acres ofcultivable land owned by the family (determinant of economic status) exhibitedan IMR of 23 while the IMR for those whose family owned no land was 111(p.1). Mothers who had experienced a previous stillbirth were more apt toexperience infant death than those who had not had a previous stillbirth (150 vs.90; p.05). Untrained traditional birth attendants delivered 69% of all live births.IMR for these infants was considerably higher than that for trained attendants(108 vs. 87; p.1). Most women delivered at home and IMR was much higher forhome births than institution births (103 vs. 89), especially after the 1st 28 days(43 vs. 11; p.1). The IMR was highest at Pavagada PHC (130) and lowest atDoddaballapur PHC (83). Policy makers should consider these findings provewhen formulating suitable policies to reduce infant mortality.
80. Enteropathogens associated with acute diarrhoeal diseases.
NIYOGI SK, SAHA MR, DE SP.
Indian Public Health. 1994 Apr-Jun;38(2):29-32.
Five types of Escherichia coli are responsible for as much as 25% of all diarrhealdiseases in developing countries. They tend to be transmitted via contaminatedfoods, particularly weaning foods, and water. They include enterotoxigenic,enteropathogenic, enteroadherent, enteroinvasive, and enterohemorrhagic E.coli. Shigella species are responsible for 10-15% of acute diarrheas in childrenless than 5 years old and the most common etiologic agents of childhooddysentery. Shigellosis is common in the warm season. An outbreak of shigelladysentery in West Bengal, India, had a high attack rate in children less than 5

273
Diarrhoeal Diseases
years old and was resistant to many drugs. Nontyphoid Salmonella speciescause watery diarrhea with nausea, cramps, and fever. Worldwide, variousSalmonella strains exhibit resistance to ampicillin, chloramphenicol, and co-trimoxazole. Campylobacter jejuni produces watery diarrhea which, in 33% ofcases and 1-2 days after onset, contains blood and mucus. Many normal healthychildren in developing countries are carriers of C. jejuni. Vibrio cholerae O1 isendemic in parts of Africa and Asia (e.g., 5-10% of hospitalized diarrheapatients). The ElTor cholera biotype is responsible for the 7th pandemic. Otherbacterial enteropathogens are Aeromonas species, Bacteroides fragilis, andProvidencia alcalifaciens. Rotavirus is a major cause of sporadic and epidemicdiarrhea among 6-23 month olds. Its incidence peaks in cold or dry seasons.Other viral enteropathogens are Norwalk virus, adenoviruses, astroviruses, andcoronaviruses. In India, the prevalence of Entamoeba histolytica varies from3.6% to 47.4%. It occurs equally in high and low socioeconomic classes. Giardialamblia usually infects 1-5 year old children. Its transmission routes are food,water, and the fecal-oral route. Cryptosporidia produce acute watery diarrhea,especially in children less than 2 years old. Cryptosporidia diarrhea is commonamong AIDS patients. Oral rehydration therapy and proper feeding during andafter diarrhea reduces deaths from diarrhea.
81. Intestinal parasitism: a childhood problem in rural Bengal.
SAHA DR, GUPTA DN, SENGUPTA PG, MONDAL SK, GHOSH S, SAHANC, SIKDER SN, SIRCAR BK. J
Commun Dis. 1995 Sep;27(3):170-4.
A study was undertaken to assess the parasitic infection rate in a ruralcommunity of West Bengal amongst children below four years of agesuffering from gastrointestinal complaints. A total of 221 faecal sampleswere examined during November 1992 to April 1994. G. lamblia (17.2%)and E. histolytica (8.1%) were the predominant protozoas, whereas E.vermicularis (12.2%) and A. lumbricoides (8.1%) were found to be commonamongst helminthic infection. A significantly lower infection rate wasobserved in children below one year (24.4 per cent) as compared to olderage groups (66.4 per cent).

274
Diarrhoeal Diseases
82. Epidemiology & management of persistent diarrhoea in children ofdeveloping countries.
BHAN MK, BHANDARI N, BHATNAGAR S, BAHL R.
Indian J Med Res. 1996 Jul;104:103-14.
Diarrhoea that begins acutely but lasts longer than two weeks is defined to be persistent.Revised estimates in developing countries including India showed that acute diarrhoeaaccounts for 35 per cent, dysentery 20 per cent and non-dysenteric persistent diarrhoea(PD) for 45 per cent of total diarrhoeal deaths. PD also often changes marginalmalnutrition to more severe forms. Factors that increase the risk of acute diarrhoeabecoming persistent have been identified in India and other developing countries.These include antecedent malnutrition, micronutrient deficiency particularly for zincand vitamin A, transient impairment in cell mediated immunity, infection with enteroaggregative Escherichia coli and cryptosporidium, sequential infection with differentpathogens and lack of exclusive breast feeding during the initial four months of lifeparticularly use of bovine milk. Several issues regarding the management of persistentdiarrhoea in hospitalized children in India have been resolved. Diets providing modestamounts of milk mixed with cereals are well tolerated. In those who fail on suchdiets providing carbohydrate as a mixture of cereals and glucose or sucrose hastenrecovery. The role of antimicrobial agents and individual micronutrients in PD iscurrently being investigated. A management algorithm appropriate for India andother developing countries has been developed and found to substantially reducecase fatality in hospital settings to about 2-3 per cent. Recent epidemiological andclinical research related to persistent diarrhoea is also reviewed.
Relevant findings:A review of data about diarrhoeal deaths in the developingcountries (including India) was done. It revealed that acute diarrhoea, dysentery,and non-dysenteric persistent diarrhoea were responsible for 35%, 20%, and45% of total diarrhoeal deaths, respectively.
83. Assessing the cause of in-patients pediatric diarrheal deaths: an analysis ofhospital records.
DUTTA P, MITRA U, RASAILY R, BHATTACHARYA SK,BHATTACHARYA MK, MANNA B, GUPTA A, KUNDU B.
Indian Pediatr. 1995 Mar;32(3):313-21.

275
Diarrhoeal Diseases
Records of all the diarrheal patients up to the age of 5 years who were admittedto and died in Dr. B.C. Roy Memorial Hospital for Children, Calcutta, betweenJanuary and December 1990 were analyzed. The records were reviewed toassess the relative importance of three clinical types of diarrhea (acute waterydiarrhea, acute dysentery and persistent diarrhea) as the causes of mortality.Annual hospital death rates of children suffering from acute watery diarrhea,dysentery and persistent diarrhea were 13.6%, 18.2% and 25.9%, respectively.Overall death rates in dysentery (p = 0.03) and persistent diarrhea groups (p <.00001) were significantly higher than watery diarrhea group. Maximum deathsoccurred among children aged between 7 and 36 months in all categories ofdiarrhea. Shigella infected children had higher case fatality rate. In acute waterydiarrhea, 30.9% cases were assigned to associated causes of death whereas thesame could be assigned to 92.6% and 93.2% cases in dysentery and persistentdiarrhea group, respectively. Deaths occurred in most of the cases who hadbronchopneumonia as underlying cause, septicemia as immediate cause andprotein calorie malnutrition as associated cause and these were most frequentlyassociated in patients suffering from dysentery and persistent diarrhea. Only2.0% children suffering from acute watery diarrhea had dehydration at thetime of death. Significantly, a high percentage of deaths occurred amongmalnourished children who suffered from dysentery (54.4%) and persistentdiarrhea. These data suggest that Diarrheal Disease Control Programme shouldalso give emphasis on management of non watery, non-dehydrating type ofdiarrhea with complications.
Relevant findings:Analysis of 1990 in-patients records of one pediatric referralhospital in Kolkata showed that annual hospital death rates were 13.6% for acutewatery diarrhoea cases,18.2% for dysentery cases, and 25.9% for cases with persistent diarrhoea.
Comments: Data pertain to admitted cases in a pediatric referral hospital.
84. International differences in clinical patterns of diarrhoeal deaths: acomparison of children from Brazil, Senegal, Bangladesh, and India.
VICTORA CG, HUTTLY SR, FUCHS SC, BARROS FC, GARENNE M,LEROY O, FONTAINE O, BEAU JP, FAUVEAU V, CHOWDHURY HR, ETAL. J DIARRHOEAL DIS RES. 1993 MAR;11(1):25-9.

276
Diarrhoeal Diseases
Population-based data on deaths due to diarrhoea among children less than 5years of age were obtained from areas of Brazil (227 deaths), Senegal (531),Bangladesh (236) and India (146). Fatal episodes of diarrhoea were classified aseither acute diarrhoea, dysentery, or persistent diarrhoea based on their durationand on the presence or absence of blood in the stools. Persistent diarrhoeaaccounted for over 60% of infant diarrhoeal deaths in Brazil, 47% in India, 36%in Senegal, and 26% in Bangladesh. In the latter two studies, over one-half ofinfant diarrhoeal deaths were due to acute watery episodes. Among children 1-4years old dying from diarrhoea, persistent episodes were the most common inSenegal and India, whereas dysentery was the leading pattern in Bangladesh.These differences may be related to the use of oral rehydration therapy and theutilisation of health care, as well as to environmental characteristics, and arerelevant for planning control strategies. Further data are required from otherparts of the less developed world.
Relevant findings: Data about diarrhoeal morbidity and mortality among under-5 children in four countries (India, Brazil, Senegal, and Bangladesh) werereviewed. In India, 47% of infant diarrhoeal deaths were found to be due topersistent diarrhoea.
85. Review of mother and child health programmes and targets in light of thenational health policy.
BHARGAVA I.
ICCW News Bull 1987; 35(4-5): 2-6.
India has awarded a high priority to increasing the availability and acceptabilityof maternal-child health services such as immunization, family planning, infantnutrition, and control of diarrhea. To achieve the desired impact, these activitiesshould be targeted at areas of greatest priority—e.g., minimum perinatal care,low birth weight infants, maternal undernutrition, growth of children in the 1st 2years of life, and acute respiratory infections. Careful attention should be givento identifying those at highest risk, whether for biomedical, social, or economicreasons. Also important are nonprogrammatic activities such as group education,in-service training, curriculum development, and management courses for healthworkers. Although India has performed quantitative assessments of its maternal-child health program, a qualitative analysis has yet to be performed. This should

277
Diarrhoeal Diseases
consist of a critical appraisal of whether quantified objectives have been met.The evaluation process should ensure the desired information is available, verifyits relevance, assess its adequacy, and evaluate effectiveness. For such a systemto work, valid and reliable information must be generated at the primary level ofthe health care system and analyzed by a comprehensive systems approach.