
Skin diseases associated with Malassezia yeasts: Facts and controversies
Upload
independentCategory
view
5download
0
+ Models
MYCMED-447; No. of Pages 6
ORIGINAL ARTICLE/ARTICLE ORIGINAL
Do Malassezia species play a role inexacerbation of scalp psoriasis?Les levures Malassezia jouent-elles un role dans les poussees dupsoriasis du cuir chevelu ?
E. Gomez-Moyano *, V. Crespo-Erchiga, L. Martínez-Pilar,D. Godoy Diaz, S. Martínez-García, M. Lova Navarro,A. Vera Casaño
Dermatology, Carlos Haya Hospital, Plaza Hospital Civil, s/n 29009 Malaga, Spain
Received 28 April 2013; received in revised form 7 October 2013; accepted 7 October 2013
KEYWORDSPsoriasis;Malassezia;Skin disease;Exacerbations
SummaryIntroduction. — Clinical expression of psoriasis is in part dependent on external factors, such asdrugs, microorganisms or stress. However convincing evidence of the role of Malassezia speciesin the pathogenesis of the psoriasis is still lacking.Patients and methods. — Samples taken from scalp skin of 40 psoriatic patients and the samenumber of healthy individuals were observed under direct microsocopic examination andcultured on modified Dixon agar.Results. — Direct microscopy examination of psoriatic scalp scales was positive in 30 (75%)patients; while it was positive in only 12 (30%) healthy subjects (P = 0.003). Half of the culturesfrom healthy subjects showed no growth of colonies, but only 8 (15%) of psoriatic patients werenegative. When an exacerbation has occurred in the previous weeks, pseudohyphaes wereobserved in 12 (40%) patients, Malassezia globosa was isolated in 18 (45%) patients andMalassezia restricta was isolated in 12 (30%) patients. In the group of patients having stablelesion, without any exacerbation in the previous weeks, no pseudohypahes were observed,M. globosa was not isolated, M. restricta was isolated in 4 (10%), and cultures were negative in 6of them (15%).Conclusions. — Malassezia species form an integral part of normal cutaneous microflora inhumans, however we found that during the episodes of exacerbation of the disease the presenceof these yeasts, and particularly M. globosa, was increased.# 2013 Elsevier Masson SAS. All rights reserved.
Journal de Mycologie Médicale (2014) xxx, xxx—xxx
* Corresponding author.E-mail address: [email protected] (E. Gomez-Moyano).
Available online at
ScienceDirectwww.sciencedirect.com
1156-5233/$ — see front matter # 2013 Elsevier Masson SAS. All rights reserved.
Please cite this article in press as: Gomez-Moyano E, et al. Do Malassezia species play a role in exacerbation of scalp psoriasis?. Journal DeMycologie Médicale (2014), http://dx.doi.org/10.1016/j.mycmed.2013.10.007
http://dx.doi.org/10.1016/j.mycmed.2013.10.007

+ Models
MYCMED-447; No. of Pages 6
MOTS CLÉSPsoriasis ;Malassezia ;Les maladies de la peau ;Détérioration
Resume
Introduction. — L’expression clinique du psoriasis dépend partiellement de facteurs externes,comme les médicaments, certains microorganismes ou même le stress. Jusqu’à présent, le rôledes levures Malassezia dans la pathogenèse du psoriasis n’était pas bien établi.Patients et methodes. — Des échantillons ont été obtenus par grattage de la peau du cuirchevelu chez 40 malades de psoriasis, ainsi que de 40 sujets témoins sains. Dans tous les cas, on apratiqué un examen direct avec du KOH et des cultures sur milieu de Dixon modifié.Resultats. — L’examen direct des lésions de psoriasis a été positif chez 30 (75 %) des malades,n’étant positif que chez 12 (30 %) des sujets témoins ( p = 0,003). Jusqu’à la moitié des culturesdes échantillons de sujets témoins restèrent négatives, n’étant négatives par contre que pour 8(15 %) de celles des malades de psoriasis. Chez les malades ayant eu une poussée dans lessemaines précédentes, on observait du pseudomycélium dans 12 (40 %) des cas, et on a isoléMalassezia globosa dans 18 (45 %) et Malassezia restricta dans 12 cas (30 %). Par contre, chez lesmalades ayant des lésions stables, n’ayant subi aucune poussée, on n’a pas observé depseudomycélium à l’examen, et on n’a pas isolé M. globosa, et seulement restricta dans 4(10 %). Les cultures restèrent négatives dans 6 (15 %) de ces malades.Conclusions. — Les levures Malassezia font partie de la microflore cutanée normale chez leshumains. Dans certaines maladies cutanées elles peuvent jouer un rôle plus ou moins établi. Dansle psoriasis du cuir chevelu, nous avons remarqué une augmentation de la présence de ceslevures, et en particulier de M. globosa, en relation avec les poussées de la maladie.# 2013 Elsevier Masson SAS. Tous droits réservés.
2 E. Gomez-Moyano et al.
Introduction
The psoriasis is considered as a genetic controlled disease,and its expression is in part dependent on external factors,such as drugs, microorganisms or stress. Microorganisms suchas Malassezia, B—haemolytic streptococci, Staphylococcusaureus and Candida albicans have been suggested as externaltriggers releasing factors which serve as superantigens, andstimulate T cells to initiate the pathogenic events of psoriasis[21,31].
Lipophilic yeast of the genus Malassezia are commensalsof the microbiota found on normal skin of many warmblooded vertebrates, although they are also associated withseveral skin diseases and even systemic infections [8]. Theetiological role of Malassezia yeast in pytiriasis versicolor isunquestioned; the organism found in the lesions is predomi-nantly in its mycelial phase [11,12]. Different studies indi-cate that Malassezia may also be involved in thepathogenesis of psoriasis [3,25]. Cell fragments of Malasse-zia topically applied to the skin of psoriatic patients inducednew psoriatic plaques [22]. Furthermore, it has been obser-ved that Malassezia folliculitis can evolve into guttata pso-riatic lesions [6], and cases of psoriasis exacerbation maycoincide with pityriasis versicolor [23]. Besides the involve-ment of this genus in psoriasis is supported by the beneficialeffect of both oral and topical ketoconazole, followed byreduction of yeasts [15,28]. Morever, the reduction in thenumber of Malassezia on the skin during treatment corre-lates with clinical improvement of scalp psoriasis. Althoughthe antimycotic drugs may act against Malassezia yeast in adirect way [15], these drugs can suppress Malassezia inducedproliferation of lymphocytes in psoriatic patients and alsoreduce the response to the antigenic stimulation in skinlesions [1,29]. This effect is also achieved with other immu-nosuppressive drugs or modern biological therapies in pso-riasis [32].
More recent studies have indicated that Malassezia yeastscause exacerbation of psoriasis by triggering the release of
Please cite this article in press as: Gomez-Moyano E, et al. Do MalassezMycologie Médicale (2014), http://dx.doi.org/10.1016/j.mycmed.201
cytokines, in particular interleukin 8, through a Toll-likereceptor 2 mediated pathway [7], upregulating transforminggrowth factor beta 1 and heat shock protein 70 expression inkeratinocytes [8] and activating complement and recruitingneutrophils as well as inducing immune cell migration to thedermis [9].
These findings suggest that there are several mechanismsby which Malassezia yeasts may contribute to exacerbatepsoriasis, but still remains unclear whether these microor-ganisms are able to initiate the development of psoriasislesions. In contrast, the aetiological role of these yeasts inother superficial dermatoses such as pytiriasis versicolor,seborrheic dermatitis and Malassezia folliculitis is unques-tionable and has been widely documented [3,10,19].
The isolation and identification of Malassezia species onthe scalp in patients with psoriasis may help to designtreatment strategies in these patients, and optimize resour-ces in such chronic disease. On the other hand it could help toknow more about the pathogenesis of psoriasis.
Patients and methods
Patients
This prospective study was carried out at the Department ofDermatology of Carlos Haya Hospital in Malaga (Spain),between January and December 2011. Forty patients withpsoriasis (22 women and 18 men; age range: 15—70 years)and the same number of healthy individuals (22 women and18 men; age range: 15—71 years) were included in the study.We included only those individuals who had not used anytopical and oral treatment in the previous two months, andthe patients having used shampoo with selenium, zinc pyri-thione, lithium succinate, azoles or ciclopirox.
All the subjects gave their written informed consent, andthe study was approved by the ethics committee of CarlosHaya Hospital. A questionnaire was used to obtain informa-tion about the medical history of each individual.
ia species play a role in exacerbation of scalp psoriasis?. Journal De3.10.007
+ Models
MYCMED-447; No. of Pages 6
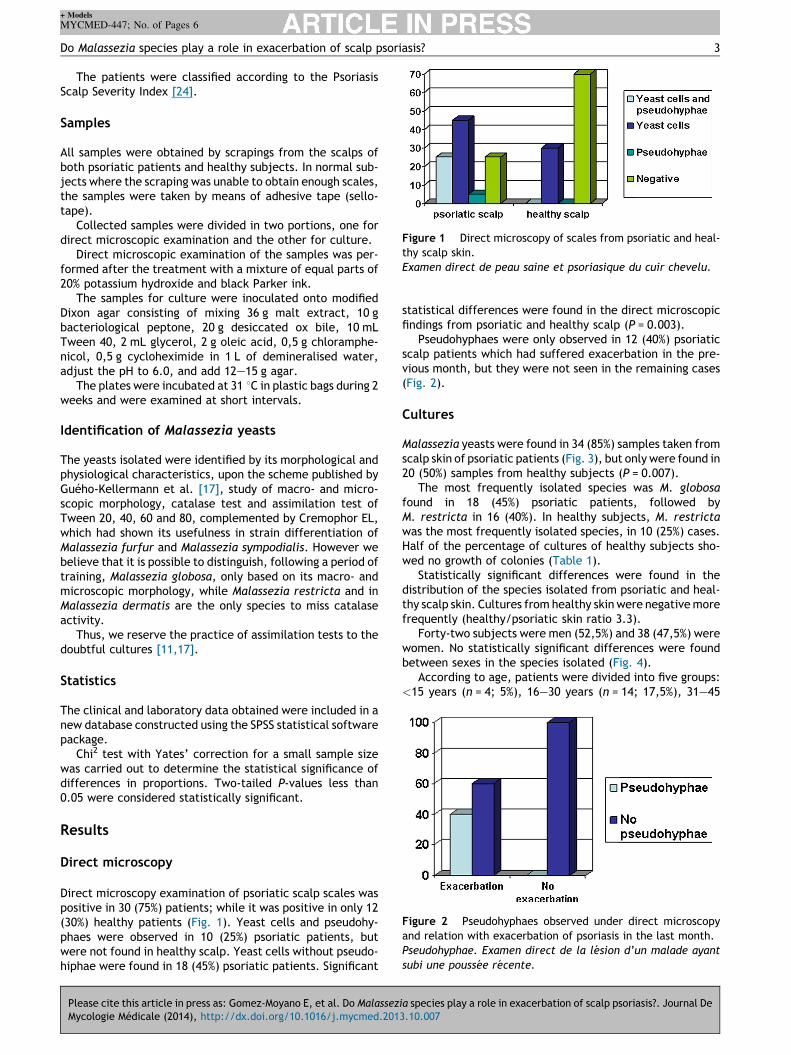
Figure 1 Direct microscopy of scales from psoriatic and heal-thy scalp skin.Examen direct de peau saine et psoriasique du cuir chevelu.
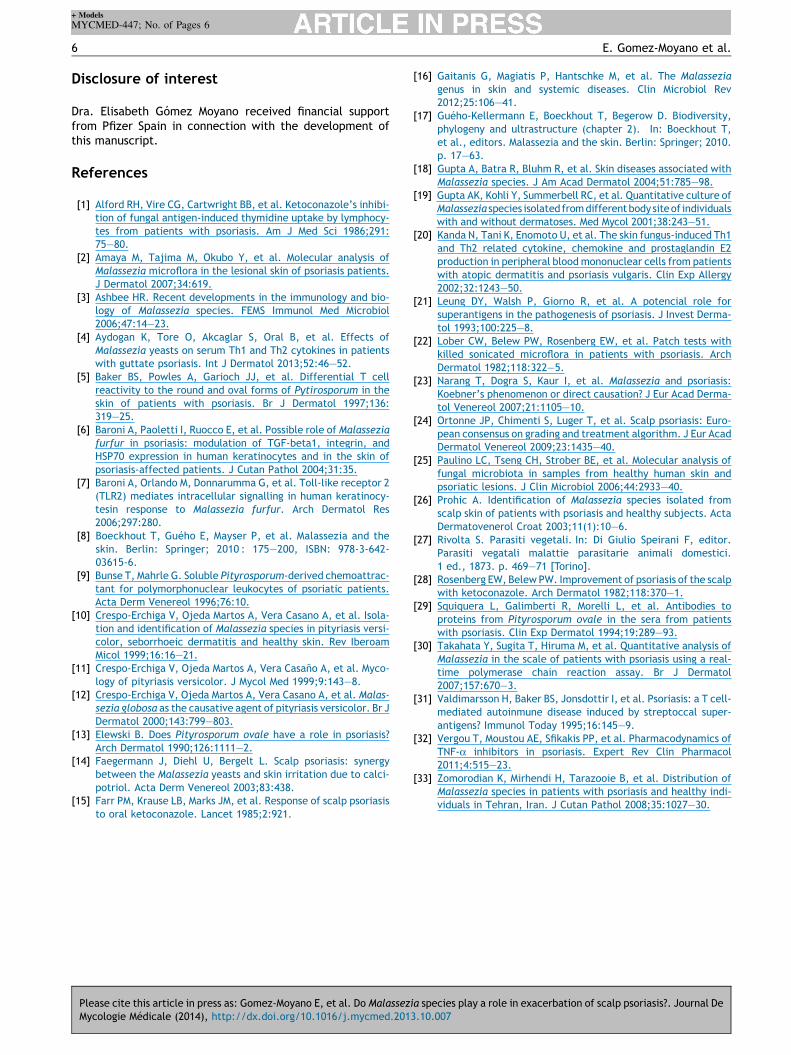
Figure 2 Pseudohyphaes observed under direct microscopyand relation with exacerbation of psoriasis in the last month.Pseudohyphae. Examen direct de la lesion d’un malade ayantsubi une poussee recente.
Do Malassezia species play a role in exacerbation of scalp psoriasis? 3
The patients were classified according to the PsoriasisScalp Severity Index [24].
Samples
All samples were obtained by scrapings from the scalps ofboth psoriatic patients and healthy subjects. In normal sub-jects where the scraping was unable to obtain enough scales,the samples were taken by means of adhesive tape (sello-tape).
Collected samples were divided in two portions, one fordirect microscopic examination and the other for culture.
Direct microscopic examination of the samples was per-formed after the treatment with a mixture of equal parts of20% potassium hydroxide and black Parker ink.
The samples for culture were inoculated onto modifiedDixon agar consisting of mixing 36 g malt extract, 10 gbacteriological peptone, 20 g desiccated ox bile, 10 mLTween 40, 2 mL glycerol, 2 g oleic acid, 0,5 g chloramphe-nicol, 0,5 g cycloheximide in 1 L of demineralised water,adjust the pH to 6.0, and add 12—15 g agar.
The plates were incubated at 31 8C in plastic bags during 2weeks and were examined at short intervals.
Identification of Malassezia yeasts
The yeasts isolated were identified by its morphological andphysiological characteristics, upon the scheme published byGuého-Kellermann et al. [17], study of macro- and micro-scopic morphology, catalase test and assimilation test ofTween 20, 40, 60 and 80, complemented by Cremophor EL,which had shown its usefulness in strain differentiation ofMalassezia furfur and Malassezia sympodialis. However webelieve that it is possible to distinguish, following a period oftraining, Malassezia globosa, only based on its macro- andmicroscopic morphology, while Malassezia restricta and inMalassezia dermatis are the only species to miss catalaseactivity.
Thus, we reserve the practice of assimilation tests to thedoubtful cultures [11,17].
Statistics
The clinical and laboratory data obtained were included in anew database constructed using the SPSS statistical softwarepackage.
Chi2 test with Yates’ correction for a small sample sizewas carried out to determine the statistical significance ofdifferences in proportions. Two-tailed P-values less than0.05 were considered statistically significant.
Results
Direct microscopy
Direct microscopy examination of psoriatic scalp scales waspositive in 30 (75%) patients; while it was positive in only 12(30%) healthy patients (Fig. 1). Yeast cells and pseudohy-phaes were observed in 10 (25%) psoriatic patients, butwere not found in healthy scalp. Yeast cells without pseudo-hiphae were found in 18 (45%) psoriatic patients. Significant
Please cite this article in press as: Gomez-Moyano E, et al. Do MalassezMycologie Médicale (2014), http://dx.doi.org/10.1016/j.mycmed.201
statistical differences were found in the direct microscopicfindings from psoriatic and healthy scalp (P = 0.003).
Pseudohyphaes were only observed in 12 (40%) psoriaticscalp patients which had suffered exacerbation in the pre-vious month, but they were not seen in the remaining cases(Fig. 2).
Cultures
Malassezia yeasts were found in 34 (85%) samples taken fromscalp skin of psoriatic patients (Fig. 3), but only were found in20 (50%) samples from healthy subjects (P = 0.007).
The most frequently isolated species was M. globosafound in 18 (45%) psoriatic patients, followed byM. restricta in 16 (40%). In healthy subjects, M. restrictawas the most frequently isolated species, in 10 (25%) cases.Half of the percentage of cultures of healthy subjects sho-wed no growth of colonies (Table 1).
Statistically significant differences were found in thedistribution of the species isolated from psoriatic and heal-thy scalp skin. Cultures from healthy skin were negative morefrequently (healthy/psoriatic skin ratio 3.3).
Forty-two subjects were men (52,5%) and 38 (47,5%) werewomen. No statistically significant differences were foundbetween sexes in the species isolated (Fig. 4).
According to age, patients were divided into five groups:<15 years (n = 4; 5%), 16—30 years (n = 14; 17,5%), 31—45
ia species play a role in exacerbation of scalp psoriasis?. Journal De3.10.007

+ Models
MYCMED-447; No. of Pages 6
Figure 3 Cultures in modified Dixon medium of scales inhealthy and psoriatic patients.Cultures dans du milieu de Dixon modifie de squames de sujetstemoins et psoriasiques.
Figure 4 Malassezia species distribution from psoriatic andnon-psoriatic scalp according to patient sex.Distribution des especes de Malassezia dans le cuir chevelu desmalades et des sujets temoins par rapport a leur sexe.
Figure 5 Malassezia species distribution from psoriatic andnon-psoriatic scalp skin according to patient age.Distribution des especes de Malassezia dans le cuir chevelu desmalades et des sujets temoins par rapport a leur age.
4 E. Gomez-Moyano et al.
years (n = 32,40%), 46—60 years (n = 10; 12,5%) and >61years (n = 20; 25%). No statistically significant differenceswere found between groups of age in the species isolated(Fig. 5).
Four groups were formed according the duration of thedisease: psoriasis developed since less than one year (n = 6;15%), between 1 and 5 years (n = 18; 45%), between 5 and 10years (n = 4; 10%) and more than 10 years (n = 12; 30%). Nostatistically significant differences were found between fourgroups of duration of the psoriasis and the species isolated.
Two groups were formed according PASI: less than 10(n = 26; 65%) and more than 10 (n = 14; 35%). No statisticallysignificant differences were found.
Patients were divided into three severity groups accordingto the Psoriasis Scalp Severity Index (Fig. 6), as follows [23]:
� mild scalp psoriasis. Affects <50% of the scalp. Milderythema, mild scaling, mild pruritus and minimal thick-ness (n = 10; 25%);� moderate scalp psoriasis. Affects <50% of the scalp.
Moderate erythema, moderate scaling, mild to moderatepruritus and moderate thickness (n = 24; 60%);
Please cite this article in press as: Gomez-Moyano E, et al. Do MalassezMycologie Médicale (2014), http://dx.doi.org/10.1016/j.mycmed.201
Table 1 Malassezia species obtained from scalp skin ofpatients with psoriasis and normal subjects.Especes de Malassezia isolees du cuir chevelu de sujetstemoins et psoriasiques.
Malassezia species Psoriaticscalp skin
Healthyscalp skin
M. globosa 18 6M. restricta 16 10M. sympodialis 0 4M. furfur 0 0M. sloofiae 0 0M. obtusa 0 0M. pachydermatis 0 0Negative 6 20
Total 40 40
� severe scalp psoriasis. Affects >50% of the scalp. Severeerythema, severe scaling, moderate to severe pruritus,evidence of hair loss with scarring, very thick, and hairlineon forehead involvement (n = 6; 15%).
We found statistically significant difference in the dis-tribution of Malassezia species isolated in three severitygroups (P = 0.009). M. restricta and negative cultures werefound in patients with mild and moderate psoriasis, whereasM. globosa was found more frequently in patients withmoderate and severe scalp psoriasis. Negative cultures werenot found in severe scalp psoriasis.
ia species play a role in exacerbation of scalp psoriasis?. Journal De3.10.007
Figure 6 Malassezia species distribution from psoriatic scalpskin according to the severity scalp involvement.Distribution des especes de Malassezia dans le cuir chevelu desmalades par rapport a la severite de l’affection.

+ Models
MYCMED-447; No. of Pages 6
Figure 7 Malassezia species distribution from psoriatic scalpskin according to the presence of exacerbation psoriasis in thelast month.Distribution des especes de Malassezia dans le cuir chevelu desmalades par rapport a les poussees de psoriasis dans le moisprecedente.
Do Malassezia species play a role in exacerbation of scalp psoriasis? 5
Two groups were formed according to the presence ofscalp psoriasis exacerbation in the last month. Whenexacerbation had happened (n = 30; 75%), M. globosa wereisolated in 18 (45%) patients and M. restricta were isolatedin 12 (30%) patients. When it was not present (n = 10; 25%),M. globosa was not isolated, M. restricta was isolated in 4(10%) patients, and cultures were negative in 6 patients(15%). We found statistically significant difference inthe distribution of Malassezia species isolated accordingthe exacerbation (P = 0.000). M. restricta and negativecultures were found in patients without exacerbationscalp psoriasis, whereas M. globosa were found morefrequently in patients with exacerbation scalp psoriasis(Fig. 7).
Discussion
There is evidence that psoriasis is principally a T cell media-ted skin disease. However little is known about the initialstimulus that leads to the abnormal T cell activation.Although psoriasis is a non-contagious disorder, the role ofMalassezia species in this pathogenesis is still not fullyunderstood, but different studies suggest that these lipophi-lic yeasts might be a trigger factor in the exacerbation ofpsoriatic lesions [6,7,30,33].
Rivolta made the first association of the lipophilic yeastsand psoriasis in 1873, and he named them Cryptococcuspsoriasis [27]. Although later several reports indicated thatMalassezia yeast are able to elicit psoriatic lesions in bothhuman and animals [9,13,22,26], the role of these micro-organisms in psoriasis is still undetermined.
The identification of Malassezia yeasts to a species level isof a doubtful value in the diagnosis of skin diseases becausethe same species can be a part of normal cutaneous microfl-ora in humans. However, it is of great importance to deter-mine which species are associated with certain skin diseasesand whether the spectrum varies with clinical data, bodysite, origin of the population, severity and extent of thelesions. . . [26].
Different studies showed that the pathologic response isspecies-specific [18]. It has also been shown that the anti-fungal agent ketoconazole can potentially affect psoriasis
Please cite this article in press as: Gomez-Moyano E, et al. Do MalassezMycologie Médicale (2014), http://dx.doi.org/10.1016/j.mycmed.201
directly by its antifungal action against Malassezia yeast orindirectly by suppressing Malassezia induced lymphocytic-mediated immune responses [15,22,28].
In normal skin Malassezia may downregulate the inflam-matory response, allowing them to live as commensals. Incontrast, in atopic dermatitis and psoriasis, Malassezia yeastmay elicit an inflammatory response that contributes to themaintenance of lesions [16]. A key area for future research isto determine ways in which the inflammatory cycle can bebroken and how the exacerbation of these diseases can becontrolled or prevented. However, the initial encouragingresults for the treatment of scalp psoriasis with antifungaldrugs have not been established in subsequent studies[15,28].
In the present study, the rate of positive cultures waslower in the controls than in patients, and similar resultswere found by Prohic [26]. In another recent studies usingmolecular analysis [2,33], the average number of Malasseziaspecies detected in the scalp was lower in the controls thanin patients. These observations also support the previouslyreported recommendation of using antifungal therapy forscalp psoriasis [14,15,26,28].
We found that the predominant species in psoriasis scalpof our patients was M. globosa, isolated in 45% of cases. Ourresults are in agreement with report by Rosenberg and Belew[28], Farr et al. [15], Gupta et al. [19] and Prohic [26].M. globosa was found more frequently in patients withmoderate and severe scalp psoriasis, whereas M. restrictawas found in mild psoriasis and healthy skin. When exacerba-tion of psoriasis was present in the last month, M. globosawas the most frequently isolated species. M. restricta andnegative cultures were found in patients without exacerba-tion scalp psoriasis. M. globosa in its mycelial phase has beenconfirmed to be the causative agent of pytiriasis versicolor[11,12]. Our study suggests that M. globosa in its yeast phaseis the commonest species in scalp psoriasis, and similarresults were found in Bosnia [26]. When a recent exacerba-tion had happened we observed yeasts and pseudohyphaes oronly pesudohyphae under direct microscopy examination.Pseudohyphaes were not observed in the remaining patientswith stable lesions.
Psoriasis is also known to have a strong genetic compo-nent. Therefore, research has investigated immune reac-tions in patients with psoriasis. It has been shown that theseindividuals have immunological responses to both Malasseziayeasts and to proteins derived from them. T cells reactive tothe yeasts have been isolated from lesional skin [5] and it hasbeen demonstrated that antibodies to the yeasts are presentin serum taken from patients with psoriasis, but not fromcontrol subjects [20,28].
Although Malassezia is part of normal cutaneous microfl-ora in humans, in our study and other studies [26] the rate ofpositive cultures is higher in patients with psoriasis comparedwith the healthy subjects. However the complex pathoge-nesis of psoriasis and the ambiguous therapeutic potential ofantimycotic drugs support only a secondary role, possiblythat of an exacerbating factor, for Malassezia yeast inpsoriasis [4,16]. Ours results suggest that M. globosa mayexacerbate the inflammatory and hyperproliferative changesobserved in scalp psoriasis. Further studies are needed toclarify the relationship between psoriasis and Malasseziayeasts.
ia species play a role in exacerbation of scalp psoriasis?. Journal De3.10.007
+ Models
MYCMED-447; No. of Pages 6
6 E. Gomez-Moyano et al.
Disclosure of interest
Dra. Elisabeth Gómez Moyano received financial supportfrom Pfizer Spain in connection with the development ofthis manuscript.
References
[1] Alford RH, Vire CG, Cartwright BB, et al. Ketoconazole’s inhibi-tion of fungal antigen-induced thymidine uptake by lymphocy-tes from patients with psoriasis. Am J Med Sci 1986;291:75—80.
[2] Amaya M, Tajima M, Okubo Y, et al. Molecular analysis ofMalassezia microflora in the lesional skin of psoriasis patients.J Dermatol 2007;34:619.
[3] Ashbee HR. Recent developments in the immunology and bio-logy of Malassezia species. FEMS Immunol Med Microbiol2006;47:14—23.
[4] Aydogan K, Tore O, Akcaglar S, Oral B, et al. Effects ofMalassezia yeasts on serum Th1 and Th2 cytokines in patientswith guttate psoriasis. Int J Dermatol 2013;52:46—52.
[5] Baker BS, Powles A, Garioch JJ, et al. Differential T cellreactivity to the round and oval forms of Pytirosporum in theskin of patients with psoriasis. Br J Dermatol 1997;136:319—25.
[6] Baroni A, Paoletti I, Ruocco E, et al. Possible role of Malasseziafurfur in psoriasis: modulation of TGF-beta1, integrin, andHSP70 expression in human keratinocytes and in the skin ofpsoriasis-affected patients. J Cutan Pathol 2004;31:35.
[7] Baroni A, Orlando M, Donnarumma G, et al. Toll-like receptor 2(TLR2) mediates intracellular signalling in human keratinocy-tesin response to Malassezia furfur. Arch Dermatol Res2006;297:280.
[8] Boeckhout T, Guého E, Mayser P, et al. Malassezia and theskin. Berlin: Springer; 2010 : 175—200, ISBN: 978-3-642-03615-6.
[9] Bunse T, Mahrle G. Soluble Pityrosporum-derived chemoattrac-tant for polymorphonuclear leukocytes of psoriatic patients.Acta Derm Venereol 1996;76:10.
[10] Crespo-Erchiga V, Ojeda Martos A, Vera Casano A, et al. Isola-tion and identification of Malassezia species in pityriasis versi-color, seborrhoeic dermatitis and healthy skin. Rev IberoamMicol 1999;16:16—21.
[11] Crespo-Erchiga V, Ojeda Martos A, Vera Casaño A, et al. Myco-logy of pityriasis versicolor. J Mycol Med 1999;9:143—8.
[12] Crespo-Erchiga V, Ojeda Martos A, Vera Casano A, et al. Malas-sezia globosa as the causative agent of pityriasis versicolor. Br JDermatol 2000;143:799—803.
[13] Elewski B. Does Pityrosporum ovale have a role in psoriasis?Arch Dermatol 1990;126:1111—2.
[14] Faegermann J, Diehl U, Bergelt L. Scalp psoriasis: synergybetween the Malassezia yeasts and skin irritation due to calci-potriol. Acta Derm Venereol 2003;83:438.
[15] Farr PM, Krause LB, Marks JM, et al. Response of scalp psoriasisto oral ketoconazole. Lancet 1985;2:921.
Please cite this article in press as: Gomez-Moyano E, et al. Do MalassezMycologie Médicale (2014), http://dx.doi.org/10.1016/j.mycmed.201
[16] Gaitanis G, Magiatis P, Hantschke M, et al. The Malasseziagenus in skin and systemic diseases. Clin Microbiol Rev2012;25:106—41.
[17] Guého-Kellermann E, Boeckhout T, Begerow D. Biodiversity,phylogeny and ultrastructure (chapter 2). In: Boeckhout T,et al., editors. Malassezia and the skin. Berlin: Springer; 2010.p. 17—63.
[18] Gupta A, Batra R, Bluhm R, et al. Skin diseases associated withMalassezia species. J Am Acad Dermatol 2004;51:785—98.
[19] Gupta AK, Kohli Y, Summerbell RC, et al. Quantitative culture ofMalassezia species isolated from different body site of individualswith and without dermatoses. Med Mycol 2001;38:243—51.
[20] Kanda N, Tani K, Enomoto U, et al. The skin fungus-induced Th1and Th2 related cytokine, chemokine and prostaglandin E2production in peripheral blood mononuclear cells from patientswith atopic dermatitis and psoriasis vulgaris. Clin Exp Allergy2002;32:1243—50.
[21] Leung DY, Walsh P, Giorno R, et al. A potencial role forsuperantigens in the pathogenesis of psoriasis. J Invest Derma-tol 1993;100:225—8.
[22] Lober CW, Belew PW, Rosenberg EW, et al. Patch tests withkilled sonicated microflora in patients with psoriasis. ArchDermatol 1982;118:322—5.
[23] Narang T, Dogra S, Kaur I, et al. Malassezia and psoriasis:Koebner’s phenomenon or direct causation? J Eur Acad Derma-tol Venereol 2007;21:1105—10.
[24] Ortonne JP, Chimenti S, Luger T, et al. Scalp psoriasis: Euro-pean consensus on grading and treatment algorithm. J Eur AcadDermatol Venereol 2009;23:1435—40.
[25] Paulino LC, Tseng CH, Strober BE, et al. Molecular analysis offungal microbiota in samples from healthy human skin andpsoriatic lesions. J Clin Microbiol 2006;44:2933—40.
[26] Prohic A. Identification of Malassezia species isolated fromscalp skin of patients with psoriasis and healthy subjects. ActaDermatovenerol Croat 2003;11(1):10—6.
[27] Rivolta S. Parasiti vegetali. In: Di Giulio Speirani F, editor.Parasiti vegatali malattie parasitarie animali domestici.1 ed., 1873. p. 469—71 [Torino].
[28] Rosenberg EW, Belew PW. Improvement of psoriasis of the scalpwith ketoconazole. Arch Dermatol 1982;118:370—1.
[29] Squiquera L, Galimberti R, Morelli L, et al. Antibodies toproteins from Pityrosporum ovale in the sera from patientswith psoriasis. Clin Exp Dermatol 1994;19:289—93.
[30] Takahata Y, Sugita T, Hiruma M, et al. Quantitative analysis ofMalassezia in the scale of patients with psoriasis using a real-time polymerase chain reaction assay. Br J Dermatol2007;157:670—3.
[31] Valdimarsson H, Baker BS, Jonsdottir I, et al. Psoriasis: a T cell-mediated autoinmune disease induced by streptoccal super-antigens? Immunol Today 1995;16:145—9.
[32] Vergou T, Moustou AE, Sfikakis PP, et al. Pharmacodynamics ofTNF-a inhibitors in psoriasis. Expert Rev Clin Pharmacol2011;4:515—23.
[33] Zomorodian K, Mirhendi H, Tarazooie B, et al. Distribution ofMalassezia species in patients with psoriasis and healthy indi-viduals in Tehran, Iran. J Cutan Pathol 2008;35:1027—30.
ia species play a role in exacerbation of scalp psoriasis?. Journal De3.10.007
Copyright © 2022 FDOKUMEN














