Dietary Habits and Supplement Use in Relation to National Pregnancy Recommendations: Data from the...
18
Dietary Habits and Supplement Use in Relation to National Pregnancy Recommendations: Data from the EuroPrevall Birth Cohort E. M. Oliver • K. E. C. Grimshaw • A. A. Schoemaker • T. Keil • D. McBride • A. B. Sprikkelman • H. S. Ragnarsdottir • V. Trendelenburg • E. Emmanouil • M. Reche • A. Fiocchi • A. Fiandor • A. Stanczyk-Przyluska • J. Wilczynski • M. Busacca • S. T. Sigurdardottir • R. Dubakiene • O. Rudzeviciene • G. D. Vlaxos • K. Beyer • G. Roberts Ó Springer Science+Business Media New York 2014 Abstract Assessing maternal dietary habits across Eur- ope during pregnancy in relation to their national preg- nancy recommendations. A collaborative, multi-centre, birth cohort study in nine European countries was con- ducted as part of European Union funded EuroPrevall project. Standardised baseline questionnaire data included details of food intake, nutritional supplement use, exposure to cigarette smoke during pregnancy and socio-demo- graphic data. Pregnancy recommendations were collected from all nine countries from the appropriate national or- ganisations. The most commonly taken supplement in pregnancy was folic acid (55.6 % Lithuania–97.8 % Spain) and was favoured by older, well-educated mothers. Vita- min D supplementation across the cohort was very poor (0.3 % Spain–5.1 % Lithuania). There were significant differences in foods consumed in different countries during pregnancy e.g. only 2.7 % Dutch mothers avoided eating peanut, while 44.4 % of British mothers avoided it. Some countries have minimal pregnancy recommendations i.e. Lithuania, Poland and Spain while others have similar, very specific recommendations i.e. UK, the Netherlands, Iceland, Greece. Allergy specific recommendations were associated with food avoidance during pregnancy [relative rate (RR) 1.18 95 % CI 0.02–1.37]. Nutritional supplement recommendations were also associated with avoidance (RR 1.08, 1.00–1.16). Maternal dietary habits and the use of dietary supplements during pregnancy vary significantly E. M. Oliver and K. E. C. Grimshaw have contributed equally to this work. E. M. Oliver (&) Á K. E. C. Grimshaw Á G. Roberts Clinical and Experimental Sciences Academic Unit, Level F, South Academic Block, Faculty of Medicine, Southampton General Hospital, University of Southampton, Tremona Road, Southampton, SO16 6YD, UK e-mail: [email protected] A. A. Schoemaker Á A. B. Sprikkelman Department of Paediatric Respiratory Medicine and Allergy, Emma Children’s Hospital Academic Medical Center, Amsterdam, The Netherlands T. Keil Á D. McBride Institute of Social Medicine, Epidemiology and Health Economics, Charite ´ - Universita ¨tsmedizin Berlin, Berlin, Germany T. Keil Institute of Clinical Epidemiology and Biometry, University of Wu ¨rzburg, Wu ¨rzburg, Germany H. S. Ragnarsdottir Faculty of Nursing, University of Iceland, Reykjavı ´k, Iceland H. S. Ragnarsdottir Department of Immunology, Landspitali - National University Hospital, Reykjavı ´k, Iceland V. Trendelenburg Á K. Beyer Department of Paediatric Pneumology and Immunology, Charite ´ - Universita ¨tsmedizin Berlin, Berlin, Germany E. Emmanouil Allergy Department, 2nd Pediatric Clinic, University of Athens, Athens, Greece M. Reche Á A. Fiandor Department of Allergy, Hospital la Paz, Madrid, Spain A. Fiocchi Á M. Busacca Division of Allergy, Pediatric Department, Bambino Gesu ` Pediatric Hospitaln, Piazza S. Onofrio 4, Rome, Holy See, Vatican City, Italy 123 Matern Child Health J DOI 10.1007/s10995-014-1480-5
-
Upload
independent -
Category
Documents
-
view
2 -
download
0
Transcript of Dietary Habits and Supplement Use in Relation to National Pregnancy Recommendations: Data from the...

Dietary Habits and Supplement Use in Relation to NationalPregnancy Recommendations: Data from the EuroPrevall BirthCohort
E. M. Oliver • K. E. C. Grimshaw • A. A. Schoemaker • T. Keil •
D. McBride • A. B. Sprikkelman • H. S. Ragnarsdottir • V. Trendelenburg •
E. Emmanouil • M. Reche • A. Fiocchi • A. Fiandor • A. Stanczyk-Przyluska •
J. Wilczynski • M. Busacca • S. T. Sigurdardottir • R. Dubakiene •
O. Rudzeviciene • G. D. Vlaxos • K. Beyer • G. Roberts
� Springer Science+Business Media New York 2014
Abstract Assessing maternal dietary habits across Eur-
ope during pregnancy in relation to their national preg-
nancy recommendations. A collaborative, multi-centre,
birth cohort study in nine European countries was con-
ducted as part of European Union funded EuroPrevall
project. Standardised baseline questionnaire data included
details of food intake, nutritional supplement use, exposure
to cigarette smoke during pregnancy and socio-demo-
graphic data. Pregnancy recommendations were collected
from all nine countries from the appropriate national or-
ganisations. The most commonly taken supplement in
pregnancy was folic acid (55.6 % Lithuania–97.8 % Spain)
and was favoured by older, well-educated mothers. Vita-
min D supplementation across the cohort was very poor
(0.3 % Spain–5.1 % Lithuania). There were significant
differences in foods consumed in different countries during
pregnancy e.g. only 2.7 % Dutch mothers avoided eating
peanut, while 44.4 % of British mothers avoided it. Some
countries have minimal pregnancy recommendations i.e.
Lithuania, Poland and Spain while others have similar,
very specific recommendations i.e. UK, the Netherlands,
Iceland, Greece. Allergy specific recommendations were
associated with food avoidance during pregnancy [relative
rate (RR) 1.18 95 % CI 0.02–1.37]. Nutritional supplement
recommendations were also associated with avoidance (RR
1.08, 1.00–1.16). Maternal dietary habits and the use of
dietary supplements during pregnancy vary significantlyE. M. Oliver and K. E. C. Grimshaw have contributed equally to this
work.
E. M. Oliver (&) � K. E. C. Grimshaw � G. Roberts
Clinical and Experimental Sciences Academic Unit, Level F,
South Academic Block, Faculty of Medicine, Southampton
General Hospital, University of Southampton, Tremona Road,
Southampton, SO16 6YD, UK
e-mail: [email protected]
A. A. Schoemaker � A. B. Sprikkelman
Department of Paediatric Respiratory Medicine and Allergy,
Emma Children’s Hospital Academic Medical Center,
Amsterdam, The Netherlands
T. Keil � D. McBride
Institute of Social Medicine, Epidemiology and Health
Economics, Charite - Universitatsmedizin Berlin, Berlin,
Germany
T. Keil
Institute of Clinical Epidemiology and Biometry, University of
Wurzburg, Wurzburg, Germany
H. S. Ragnarsdottir
Faculty of Nursing, University of Iceland, Reykjavık, Iceland
H. S. Ragnarsdottir
Department of Immunology, Landspitali - National University
Hospital, Reykjavık, Iceland
V. Trendelenburg � K. Beyer
Department of Paediatric Pneumology and Immunology,
Charite - Universitatsmedizin Berlin, Berlin, Germany
E. Emmanouil
Allergy Department, 2nd Pediatric Clinic, University of Athens,
Athens, Greece
M. Reche � A. Fiandor
Department of Allergy, Hospital la Paz, Madrid, Spain
A. Fiocchi � M. Busacca
Division of Allergy, Pediatric Department, Bambino Gesu
Pediatric Hospitaln, Piazza S. Onofrio 4, Rome, Holy See,
Vatican City, Italy
123
Matern Child Health J
DOI 10.1007/s10995-014-1480-5

across Europe and in some instances may be influenced by
national recommendations.
Keywords Pregnancy recommendations � Folic acid �Vitamin D � Iron
Introduction
The lifestyle choices a woman makes during pregnancy and
pre-pregnancy have important implications for her unborn
child. There is evidence that inappropriate nutrition and poor
perinatal growth are associated with increased risk of respi-
ratory disease, atopy, coronary heart disease, stroke, type 2
diabetes, adiposity, the metabolic syndrome and osteoporosis
in later life [1–5]. Promoting good health and nutrition during
pregnancy has beneficial effects for both mother and child and
is reflected by the World Health Organisations guidance on
improving pregnancy health outcomes [6–10]. This guidance
is in place to help countries make informed decisions on
appropriate nutrition actions. European countries have spe-
cific national recommendations which may or may not
incorporate this guidance and range from simply recom-
mending daily calorie requirements in pregnancy (e.g. in
Poland and Lithuania [11, 12]) to much more detailed rec-
ommendations concerning both general health and food safety
(e.g. in the UK and the Netherlands [13–15]). To date, a
comparison of recommendations across Europe and how
maternal habits may be influenced by them has not been made.
Such data would help assess the effectiveness of existing
pregnancy health policies and may help inform decisions
regarding the implementation of new recommendations or
how best to amend existing recommendations.
The aim of this paper is to describe maternal dietary
habits during pregnancy of women participating in the
EuroPrevall birth cohort [a multicentre research project
funded by the European Union (EU) investigating food
allergy] [16] and relate this to their national pregnancy
recommendations.
Methods
The methodology of the EuroPrevall birth cohort study has
been described in detail previously [16]. Only the aspects
relevant for this paper will be reiterated here. In summary,
the study was a collaborative multi-centre study of research
institutions from nine countries in Europe. They were
chosen to give a geographic spread across the European
continent. The regions were Nordic (Reykjavik, Iceland),
Maritime (Amsterdam, Netherlands and Southampton,
United Kingdom), Central European (Berlin, Germany;
Lodz, Poland and Vilnius, Lithuania) and the Mediterra-
nean region (Madrid, Spain; Milan, Italy and Athens,
Greece). Each centre obtained approval from their own
governing ethics committee or review board before com-
mencing recruitment. Infants were recruited from October
2005 to February 2010. Written informed consent was
obtained from all mothers (and fathers where required) at
time of recruitment after which a standardised baseline
questionnaire was administered by a trained interviewer.
All questionnaires were translated into the language of
each centre and validated by back translation.
The comprehensive baseline questionnaire included ques-
tions on socio-demographic characteristics and maternal diet
during pregnancy. Full details and a first comparison of data at
recruitment/birth are published elsewhere [16, 17]. Gesta-
tional age when the questionnaire was completed was not
collected, but according to the study protocol it had to be
completed after 28 weeks gestation, or if after delivery, to
limit recall bias the infant was to be younger than 4 weeks of
age. The maternal diet questions only asked the mother
whether they ate a particular food/food group rather than detail
of specific foods or food group eaten. They were then asked
the additional question as to whether they had eaten more, less,
or the same amount of that food during pregnancy compared to
when they were not pregnant. If the mothers reported that they
did not eat the food, they were asked whether they had ever
eaten it or whether they were just avoiding it during preg-
nancy. Mothers were coded as ‘stopped eating’ if she avoided
eating the food for the whole duration of her pregnancy. If she
only avoided for a limited period i.e. first trimester when
possibly feeling nauseous she would have been coded as
‘limiting intake’. If a mother avoided at least three or more
food/groups throughout the whole of pregnancy rather than a
limited period is suggests that factors other than taste prefer-
ence may be influencing behaviour. The foods/food groups
detailed in the questionnaire were: milk and other dairy pro-
ducts; soy and soy products; eggs and foods containing eggs;
peanuts and foods containing peanuts; tree nuts and food
A. Stanczyk-Przyluska
Department of Pediatrics, Clinical Immunology and Cardiology,
Medical University of Lodz, Lodz, Poland
J. Wilczynski
Department of Fetal-Maternal Medicine and Gynecology, Polish
Mothers Memorial Hospital Research Institute, Lodz, Poland
S. T. Sigurdardottir
Department of Immunology, Faculty of Medicine, Landspitali-
National University of Iceland, Reykjavık, Iceland
R. Dubakiene � O. Rudzeviciene
Faculty of Medicine, Vilnius University, Vilnius, Lithuania
G. D. Vlaxos
Department of Obstetrics and Gynecology, Alexandra Hospital,
University of Athens, Athens, Greece
Matern Child Health J
123
containing tree-nuts; fish and fish products; shellfish and foods
containing shellfish; cereals and cereal products; vegetables;
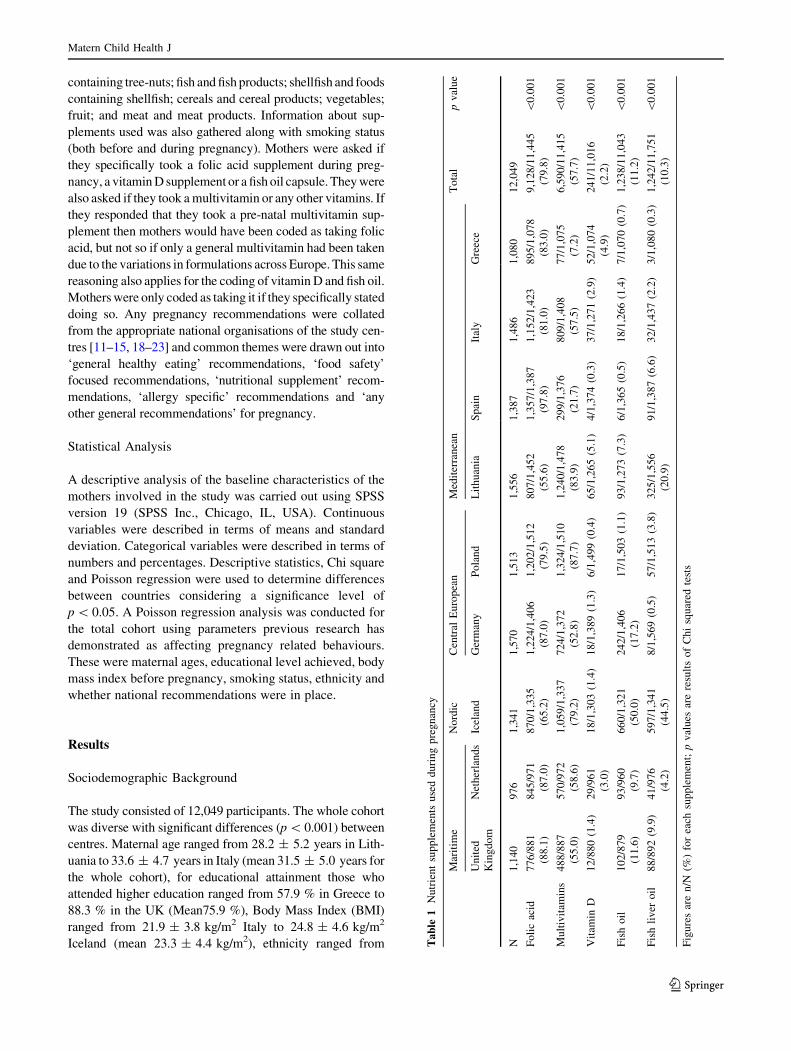
fruit; and meat and meat products. Information about sup-
plements used was also gathered along with smoking status
(both before and during pregnancy). Mothers were asked if
they specifically took a folic acid supplement during preg-
nancy, a vitamin D supplement or a fish oil capsule. They were
also asked if they took a multivitamin or any other vitamins. If
they responded that they took a pre-natal multivitamin sup-
plement then mothers would have been coded as taking folic
acid, but not so if only a general multivitamin had been taken
due to the variations in formulations across Europe. This same
reasoning also applies for the coding of vitamin D and fish oil.
Mothers were only coded as taking it if they specifically stated
doing so. Any pregnancy recommendations were collated
from the appropriate national organisations of the study cen-
tres [11–15, 18–23] and common themes were drawn out into
‘general healthy eating’ recommendations, ‘food safety’
focused recommendations, ‘nutritional supplement’ recom-
mendations, ‘allergy specific’ recommendations and ‘any
other general recommendations’ for pregnancy.
Statistical Analysis
A descriptive analysis of the baseline characteristics of the
mothers involved in the study was carried out using SPSS
version 19 (SPSS Inc., Chicago, IL, USA). Continuous
variables were described in terms of means and standard
deviation. Categorical variables were described in terms of
numbers and percentages. Descriptive statistics, Chi square
and Poisson regression were used to determine differences
between countries considering a significance level of
p \ 0.05. A Poisson regression analysis was conducted for
the total cohort using parameters previous research has
demonstrated as affecting pregnancy related behaviours.
These were maternal ages, educational level achieved, body
mass index before pregnancy, smoking status, ethnicity and
whether national recommendations were in place.
Results
Sociodemographic Background
The study consisted of 12,049 participants. The whole cohort
was diverse with significant differences (p \ 0.001) between
centres. Maternal age ranged from 28.2 ± 5.2 years in Lith-
uania to 33.6 ± 4.7 years in Italy (mean 31.5 ± 5.0 years for
the whole cohort), for educational attainment those who
attended higher education ranged from 57.9 % in Greece to
88.3 % in the UK (Mean75.9 %), Body Mass Index (BMI)
ranged from 21.9 ± 3.8 kg/m2 Italy to 24.8 ± 4.6 kg/m2
Iceland (mean 23.3 ± 4.4 kg/m2), ethnicity ranged from Ta
ble
1N
utr
ien
tsu
pp
lem
ents
use
dd
uri
ng
pre
gn
ancy
Mar
itim
eN
ord
icC
entr
alE
uro
pea
nM
edit
erra
nea
nT
ota
lp
val
ue
Un
ited
Kin
gd
om
Net
her
lan
ds
Icel
and
Ger
man
yP
ola
nd
Lit
hu
ania
Sp
ain
Ital
yG
reec
e
N1
,14
09
76
1,3
41
1,5
70
1,5
13
1,5
56
1,3
87
1,4
86
1,0
80
12
,04
9
Fo
lic
acid
77
6/8
81
(88
.1)
84
5/9
71
(87
.0)
87
0/1
,33
5
(65
.2)
1,2
24
/1,4
06
(87
.0)
1,2
02
/1,5
12
(79
.5)
80
7/1
,45
2
(55
.6)
1,3
57
/1,3
87
(97
.8)
1,1
52
/1,4
23
(81
.0)
89
5/1
,07
8
(83
.0)
9,1
28
/11
,44
5
(79
.8)
\0
.00
1
Mu
ltiv
itam
ins
48
8/8
87
(55
.0)
57
0/9
72
(58
.6)
1,0
59
/1,3
37
(79
.2)
72
4/1
,37
2
(52
.8)
1,3
24
/1,5
10
(87
.7)
1,2
40
/1,4
78
(83
.9)
29
9/1
,37
6
(21
.7)
80
9/1
,40
8
(57
.5)
77
/1,0
75
(7.2
)
6,5
90
/11
,41
5
(57
.7)
\0
.00
1
Vit
amin
D1
2/8
80
(1.4
)2
9/9
61
(3.0
)
18
/1,3
03
(1.4
)1
8/1
,38
9(1
.3)
6/1
,49
9(0
.4)
65
/1,2
65
(5.1
)4
/1,3
74
(0.3
)3
7/1
,27
1(2
.9)
52
/1,0
74
(4.9
)
24
1/1
1,0
16
(2.2
)
\0
.00
1
Fis
ho
il1
02
/87
9
(11
.6)
93
/96
0
(9.7
)
66
0/1
,32
1
(50
.0)
24
2/1
,40
6
(17
.2)
17
/1,5
03
(1.1
)9
3/1
,27
3(7
.3)
6/1
,36
5(0
.5)
18
/1,2
66
(1.4
)7
/1,0
70
(0.7
)1
,23
8/1
1,0
43
(11
.2)
\0
.00
1
Fis
hli
ver
oil
88
/89
2(9
.9)
41
/97
6
(4.2
)
59
7/1
,34
1
(44
.5)
8/1
,56
9(0
.5)
57
/1,5
13
(3.8
)3
25
/1,5
56
(20
.9)
91
/1,3
87
(6.6
)3
2/1
,43
7(2
.2)
3/1
,08
0(0
.3)
1,2
42
/11
,75
1
(10
.3)
\0
.00
1
Fig
ure
sar
en
/N(%
)fo
rea
chsu
pp
lem
ent;
pv
alu
esar
ere
sult
so
fC
hi
squ
ared
test
s
Matern Child Health J
123
72.2 % Caucasian in the Netherlands to 99.9 % in Poland and
Lithuania (mean 93.3 %) and smoking during pregnancy
ranged from 16.3 % in UK to 34.7 % in Greece (mean
24.4 %)). A fuller description of the cohort has previously
been published [17].
Intake Differences Across Europe
There was significant variation in both the nature and fre-
quency of nutrient supplements taken in different countries
(p \ 0.001) (Table 1). The most commonly taken supple-
ment was folic acid with 79.8 % of all mothers reporting
taking it at some point during their pregnancy. The highest
uptake was in Spain and the UK (97.8, 88.1 % respec-
tively) and lowest in Lithuania (55.6 %). 57.7 % of
mothers supplemented their diet with a multivitamin [range
7.2 % (Greece)–87.7 % (Poland)]. Reported vitamin D
supplementation was low for the whole cohort at 2.2 %
[range 0.3 % (Spain)–5.1 % (Lithuania)]. Fish oil and fish
liver oil supplementation was below 21 % for all countries
except Iceland where 94.5 % of mothers took one of these
supplements.
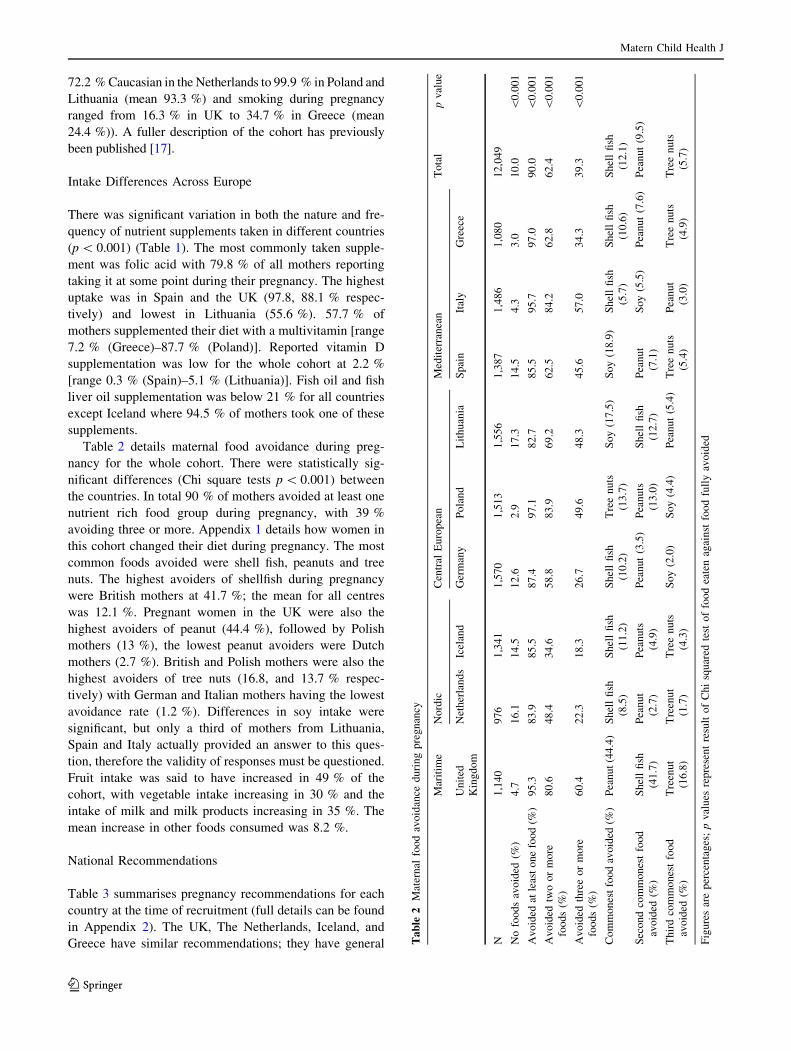
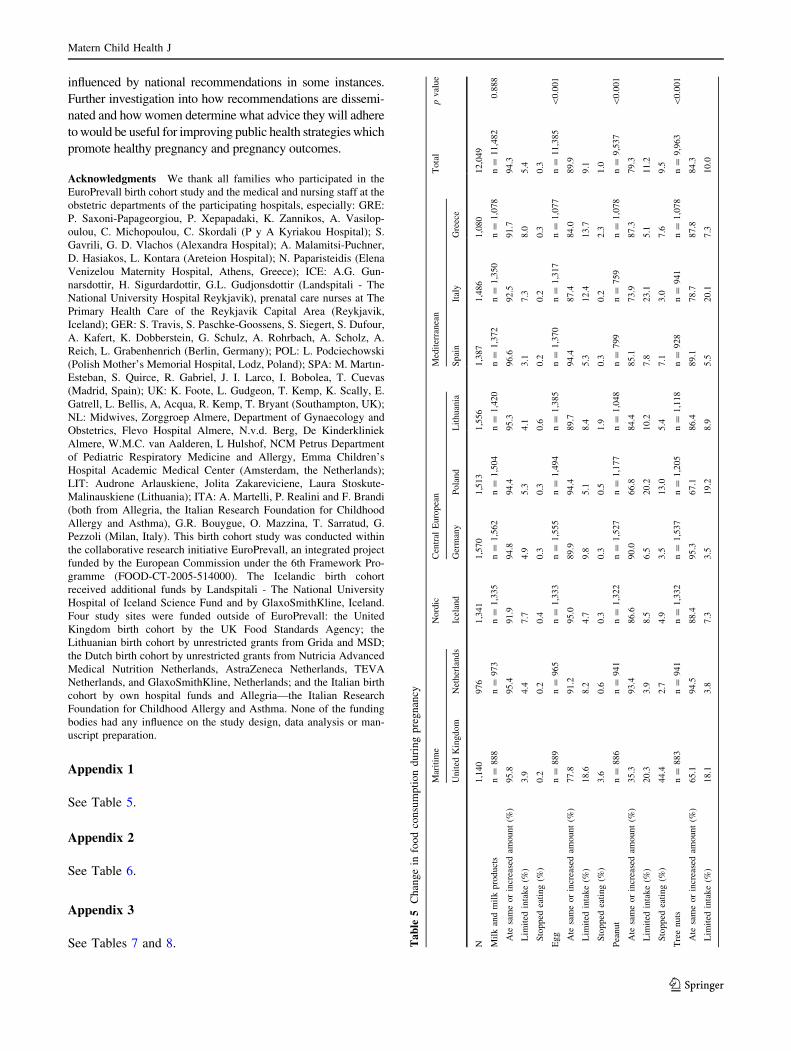
Table 2 details maternal food avoidance during preg-
nancy for the whole cohort. There were statistically sig-
nificant differences (Chi square tests p \ 0.001) between
the countries. In total 90 % of mothers avoided at least one
nutrient rich food group during pregnancy, with 39 %
avoiding three or more. Appendix 1 details how women in
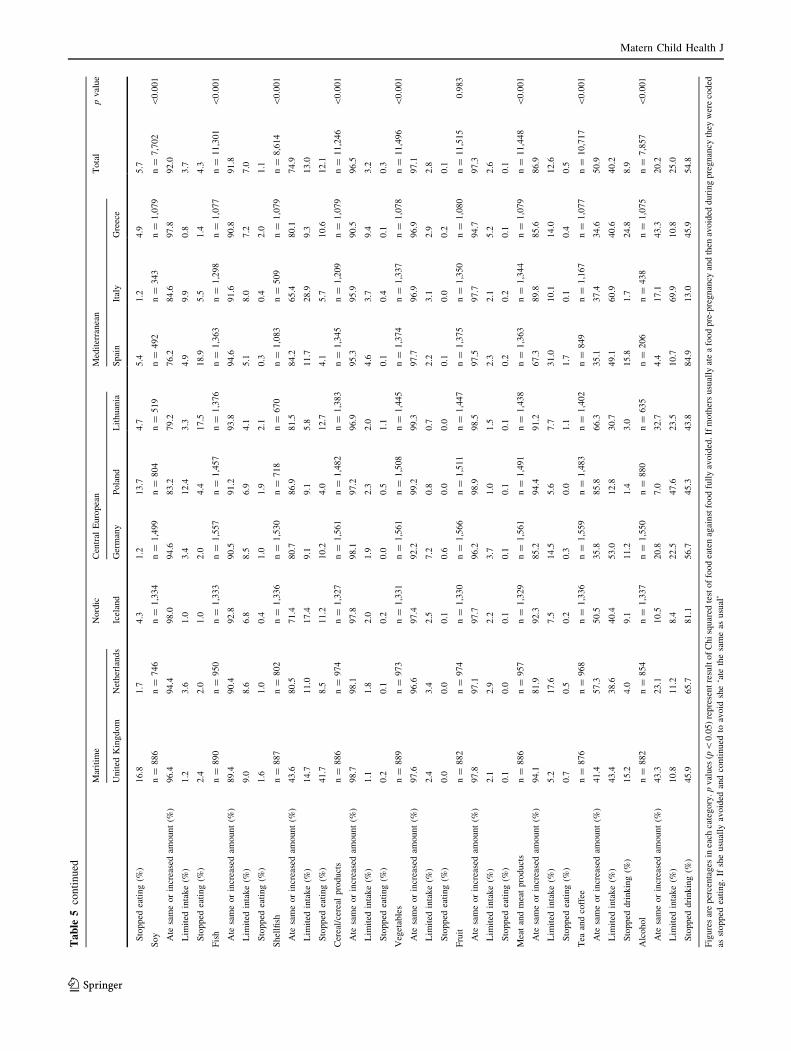
this cohort changed their diet during pregnancy. The most
common foods avoided were shell fish, peanuts and tree
nuts. The highest avoiders of shellfish during pregnancy
were British mothers at 41.7 %; the mean for all centres
was 12.1 %. Pregnant women in the UK were also the
highest avoiders of peanut (44.4 %), followed by Polish
mothers (13 %), the lowest peanut avoiders were Dutch
mothers (2.7 %). British and Polish mothers were also the
highest avoiders of tree nuts (16.8, and 13.7 % respec-
tively) with German and Italian mothers having the lowest
avoidance rate (1.2 %). Differences in soy intake were
significant, but only a third of mothers from Lithuania,
Spain and Italy actually provided an answer to this ques-
tion, therefore the validity of responses must be questioned.
Fruit intake was said to have increased in 49 % of the
cohort, with vegetable intake increasing in 30 % and the
intake of milk and milk products increasing in 35 %. The
mean increase in other foods consumed was 8.2 %.
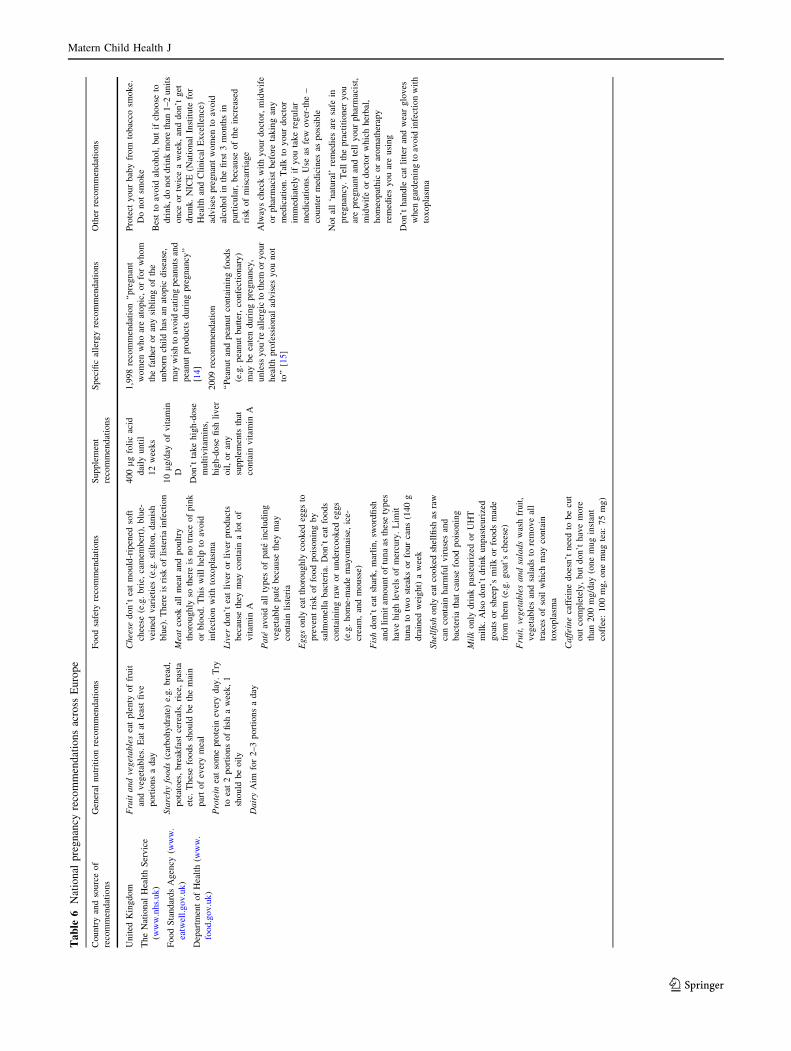
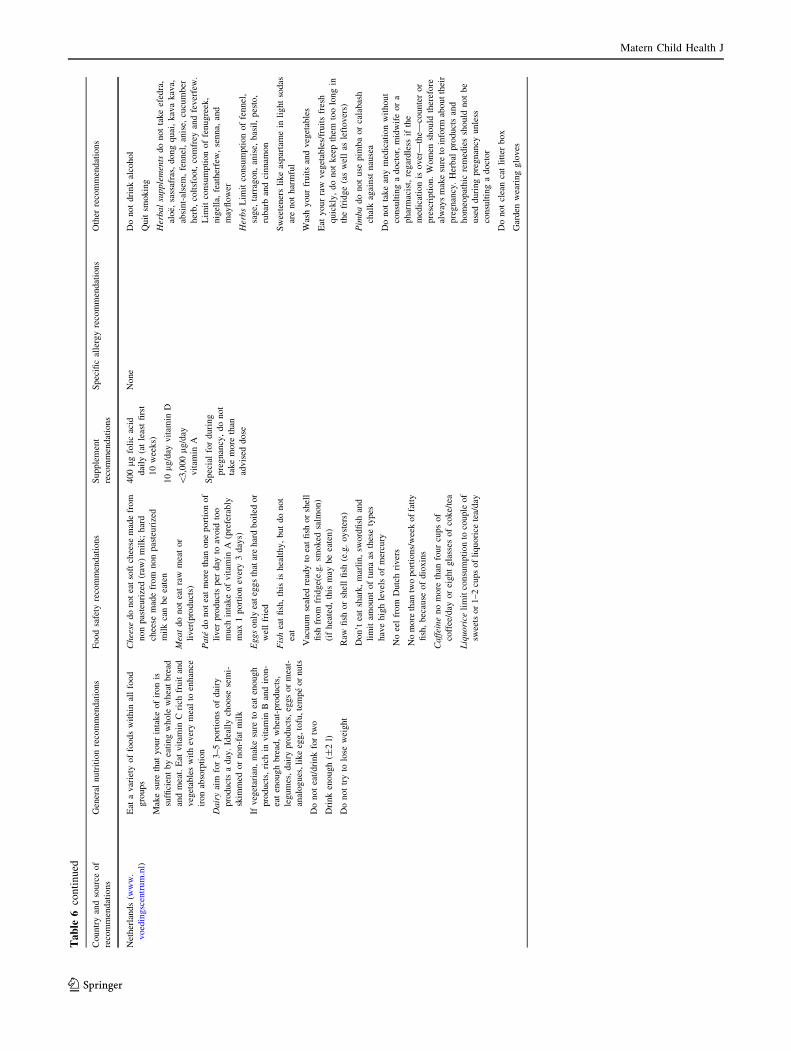
National Recommendations
Table 3 summarises pregnancy recommendations for each
country at the time of recruitment (full details can be found
in Appendix 2). The UK, The Netherlands, Iceland, and
Greece have similar recommendations; they have general Ta
ble
2M
ater
nal
foo
dav
oid
ance
du
rin
gp
reg
nan
cy
Mar
itim
eN
ord
icC
entr
alE
uro
pea
nM
edit
erra
nea
nT
ota
lp
val
ue
Un
ited
Kin
gd
om
Net
her
lan
ds
Icel
and
Ger
man
yP
ola
nd
Lit
hu
ania
Sp
ain
Ital
yG
reec
e
N1
,14
09
76
1,3
41
1,5
70
1,5
13
1,5
56
1,3
87
1,4
86
1,0
80
12
,04
9
No
foo
ds
avo
ided
(%)
4.7
16
.11
4.5
12
.62
.91
7.3
14
.54
.33
.01
0.0
\0
.00
1
Av
oid
edat
leas
to
ne
foo
d(%
)9
5.3
83
.98
5.5
87
.49
7.1
82
.78
5.5
95
.79
7.0
90
.0\
0.0
01
Av
oid
edtw
oo
rm
ore
foo
ds
(%)
80
.64
8.4
34
.65
8.8
83
.96
9.2
62
.58
4.2
62
.86
2.4
\0
.00
1
Av
oid
edth
ree
or
mo
re
foo
ds
(%)
60
.42
2.3
18
.32
6.7
49
.64
8.3
45
.65
7.0
34
.33
9.3
\0
.00
1
Co
mm
on
est
foo
dav
oid
ed(%
)P
ean
ut
(44
.4)
Sh
ell
fish
(8.5
)
Sh
ell
fish
(11
.2)
Sh
ell
fish
(10
.2)
Tre
en
uts
(13
.7)
So
y(1
7.5
)S
oy
(18
.9)
Sh
ell
fish
(5.7
)
Sh
ell
fish
(10
.6)
Sh
ell
fish
(12
.1)
Sec
on
dco
mm
on
est
foo
d
avo
ided
(%)
Sh
ell
fish
(41
.7)
Pea
nu
t
(2.7
)
Pea
nu
ts
(4.9
)
Pea
nu
t(3
.5)
Pea
nu
ts
(13
.0)
Sh
ell
fish
(12
.7)
Pea
nu
t
(7.1
)
So
y(5
.5)
Pea
nu
t(7
.6)
Pea
nu
t(9
.5)
Th
ird
com
mo
nes
tfo
od
avo
ided
(%)
Tre
enu
t
(16
.8)
Tre
enu
t
(1.7
)
Tre
en
uts
(4.3
)
So
y(2
.0)
So
y(4
.4)
Pea
nu
t(5
.4)
Tre
en
uts
(5.4
)
Pea
nu
t
(3.0
)
Tre
en
uts
(4.9
)
Tre
en
uts
(5.7
)
Fig
ure
sar
ep
erce
nta
ges
;p
val
ues
rep
rese
nt
resu
lto
fC
hi
squ
ared
test
of
foo
dea
ten
agai
nst
foo
dfu
lly
avo
ided
Matern Child Health J
123

nutrition recommendations about a healthy diet, with
guidelines on the intake of fruit, vegetable, dairy and car-
bohydrate plus very specific recommendations with a par-
ticular focus on food safety. Although Germany has similar
recommendations concerning food safety and supplemen-
tation there are no specific general nutrition guidelines. The
most common supplement recommendation across all
countries was to take 400 lg folic acid/day to prevent
neural tube defects (NTDs) [15, 18, 21–26], followed by
the recommendation to supplement dietary intake with
10 lg/day of vitamin D [13, 15, 21, 23]. Across the
countries, only the UK had a specific recommendation
regarding allergy and peanut intake at the time of data
collection [27, 28]. Germany recommended no restrictions
of allergenic foods during pregnancy [19]. Lithuania had
no recommendations specific to pregnant women and rec-
ommendations in Poland, Spain and Italy were sparse.
Spain suggested eating a varied, balanced diet and rec-
ommended a few nutrient supplements (but no dosage is
provided). Italy only recommended an increased calorie
intake with a few suggested nutrient supplements and
Poland had no specific dietary recommendations other
than calorie intake and a few nutrient supplement
recommendations.
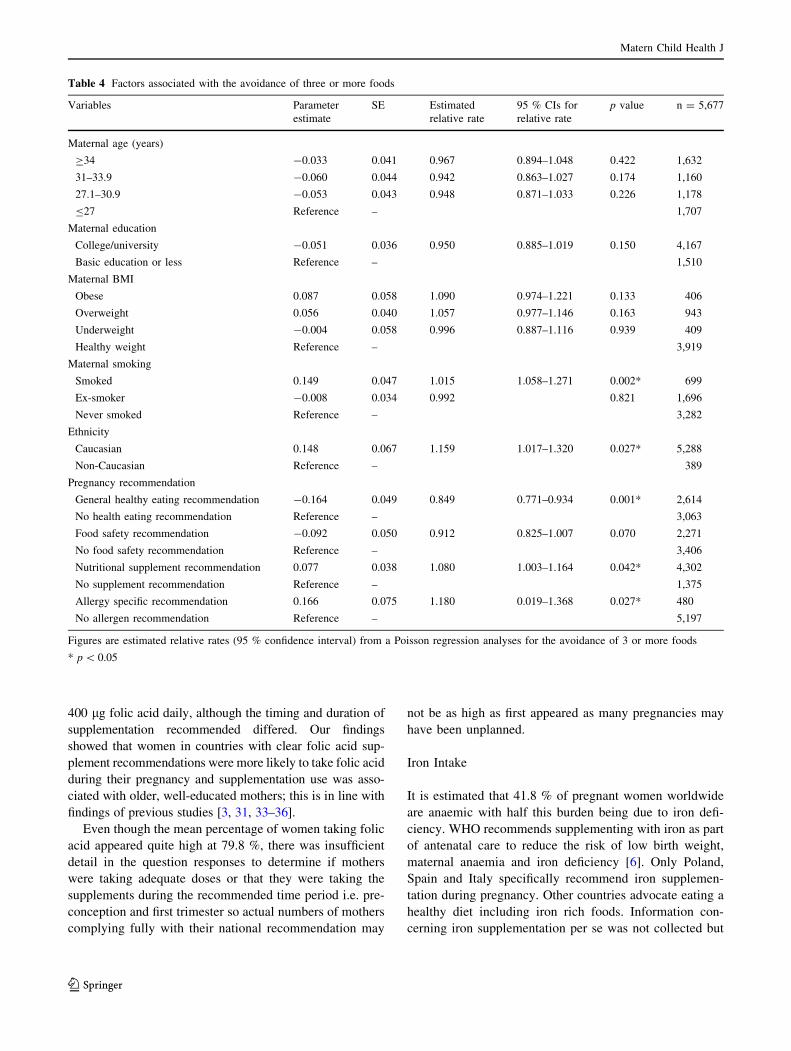
Influence of National Recommendations
Poisson regression analysis showed that having an allergy
specific pregnancy recommendation was associated with a
much higher estimated relative rate (RR) of avoidance of
three or more foods (RR 1.18 95 % CI 0.02–1.37), so too
was having nutritional supplement recommendations (RR
1.08, 1.00–1.16) (Table 4). Having general healthy eating
recommendations was associated with a lower rate of
avoiding three or more foods (0.85, 0.77–0.93). Smoking
and Caucasian mothers were more likely to avoid 3 foods
or more also. Analyses showed that mothers were more
likely to take folic acid when recommendations to do so
were in place (RR 1.22 95 % CI 1.15–1.29). Folic acid was
more likely to be taken by older (RR 1.12, 1.05–1.18),
well-educated mothers (RR 1.09, 1.03–1.15); no factors
were associated with vitamin D recommendation compli-
ance (Appendix 3).
Discussion
This study has shown that intakes of various food groups
and dietary supplements during pregnancy vary signifi-
cantly across Europe. In some countries pregnancy rec-
ommendations are minimal and are no different to general
nutrition guidelines aimed at their whole population. Other
countries have specific recommendations for pregnancy
which appear to be associated with certain eating behav-
iours/supplement use. The WHO guidance for nutrition in
pregnancy covers iron, iodine, folate, vitamin D, vitamin A
and calcium [6–10] and has been applied in some coun-
tries, particularly for folate, vitamin D and iron. In some
parts of Europe iodine deficiency is a major public health
problem [7, 29] but only Germany and Poland recom-
mended women to supplement with iodine during preg-
nancy. However, specific detail of iodine supplementation
was not collected as part of this study so will not be con-
sidered further in this manuscript.
Folic Acid Intake
Folic acid is a vital nutrient throughout life but is particularly
important during periods of growth, especially pregnancy. It
is well documented that peri-conceptual folic acid intake
reduces the risk of pregnancies being affected by NTDs [30,
31]. The prevalence of NTDs varies across EU and is cur-
rently reported from 0.4 to 2.0/1,000 births, unfortunately
national representative data on prevalence is not available for
all countries [32]. All countries in the cohort apart from
Lithuania and Greece advised women of childbearing age
who might become pregnant to supplement their diet with
Table 3 Summary of national pregnancy recommendations
General recommendations
How to eat a healthy diet UK, Netherlands, Iceland, Greece,
Germanya, Spain
An increased calorie intake Italy
Safety recommendations
Shellfish, egg, cheeses and
meat
UK, Netherlands, Greece, Germanyb,
Iceland
Liver UK, Netherlands, Iceland,
Caffeine UK, Netherlands, Iceland, Greece,
Germany
Alcohol consumption UK, Netherlands, Iceland, Greece,
Germany, Spain
Micronutrient recommendations
Take 400 lg folic acid/day UK, Netherlands, Iceland, Italy,
Germany, Spainc, Poland
Take 10 lg vitamin D/day UK, Netherlands, Iceland, Italyd
Take iron Poland, Spainc, Italy
Allergy specific
recommendation about
peanut
UK
a No specific guidelines (implemented new specific guidelines in
2011)b No recommendations for egg and shellfishc This country does not specify dosaged Only for those not exposed to sunlight or not consuming dairy
Matern Child Health J
123
400 lg folic acid daily, although the timing and duration of
supplementation recommended differed. Our findings
showed that women in countries with clear folic acid sup-
plement recommendations were more likely to take folic acid
during their pregnancy and supplementation use was asso-
ciated with older, well-educated mothers; this is in line with
findings of previous studies [3, 31, 33–36].
Even though the mean percentage of women taking folic
acid appeared quite high at 79.8 %, there was insufficient
detail in the question responses to determine if mothers
were taking adequate doses or that they were taking the
supplements during the recommended time period i.e. pre-
conception and first trimester so actual numbers of mothers
complying fully with their national recommendation may
not be as high as first appeared as many pregnancies may
have been unplanned.
Iron Intake
It is estimated that 41.8 % of pregnant women worldwide
are anaemic with half this burden being due to iron defi-
ciency. WHO recommends supplementing with iron as part
of antenatal care to reduce the risk of low birth weight,
maternal anaemia and iron deficiency [6]. Only Poland,
Spain and Italy specifically recommend iron supplemen-
tation during pregnancy. Other countries advocate eating a
healthy diet including iron rich foods. Information con-
cerning iron supplementation per se was not collected but
Table 4 Factors associated with the avoidance of three or more foods
Variables Parameter
estimate
SE Estimated
relative rate
95 % CIs for
relative rate
p value n = 5,677
Maternal age (years)
C34 -0.033 0.041 0.967 0.894–1.048 0.422 1,632
31–33.9 -0.060 0.044 0.942 0.863–1.027 0.174 1,160
27.1–30.9 -0.053 0.043 0.948 0.871–1.033 0.226 1,178
B27 Reference – 1,707
Maternal education
College/university -0.051 0.036 0.950 0.885–1.019 0.150 4,167
Basic education or less Reference – 1,510
Maternal BMI
Obese 0.087 0.058 1.090 0.974–1.221 0.133 406
Overweight 0.056 0.040 1.057 0.977–1.146 0.163 943
Underweight -0.004 0.058 0.996 0.887–1.116 0.939 409
Healthy weight Reference – 3,919
Maternal smoking
Smoked 0.149 0.047 1.015 1.058–1.271 0.002* 699
Ex-smoker -0.008 0.034 0.992 0.821 1,696
Never smoked Reference – 3,282
Ethnicity
Caucasian 0.148 0.067 1.159 1.017–1.320 0.027* 5,288
Non-Caucasian Reference – 389
Pregnancy recommendation
General healthy eating recommendation -0.164 0.049 0.849 0.771–0.934 0.001* 2,614
No health eating recommendation Reference – 3,063
Food safety recommendation -0.092 0.050 0.912 0.825–1.007 0.070 2,271
No food safety recommendation Reference – 3,406
Nutritional supplement recommendation 0.077 0.038 1.080 1.003–1.164 0.042* 4,302
No supplement recommendation Reference – 1,375
Allergy specific recommendation 0.166 0.075 1.180 0.019–1.368 0.027* 480
No allergen recommendation Reference – 5,197
Figures are estimated relative rates (95 % confidence interval) from a Poisson regression analyses for the avoidance of 3 or more foods
* p \ 0.05
Matern Child Health J
123

there was a huge range in the use of multivitamins across
the cohort from 7.2 % in Greece to 87.7 % in Poland and it
is uncertain to what extent their use contributes to mini-
mising iron deficiency risk.
Vitamin D Intake
In recent years prevalence estimates of rickets and other
features of vitamin D deficiency have been increasing. It
has been estimated that upwards of 50 % of both children
and adults in Europe, United States, Canada, Mexico, Asia,
Australia and New Zealand have vitamin D deficiency [37,
38]. The main risk factors for deficiency are those that
inhibit the body’s production of vitamin D in the skin,
which includes dark-pigmentation, too little exposure to
sunlight, clothes that limit exposure of skin, living in lati-
tudes above 40�, season of the year, use of sunscreen,
environmental pollution, ageing and dietary consumption
[9]. Pregnant women are identified as being a particularly
high-risk group. Even in Mediterranean countries where
there is abundant sunshine, studies have shown vitamin D
deficiency in pregnant women and their infants to be a
problem, particularly in winter months [39–43]. Despite
this, only four of the nine countries in the cohort specifi-
cally recommended pregnant women to take vitamin D,
possibly on the assumption that sunshine exposure is ade-
quate. Some countries such the USA and Canada have
mandatory fortification of milk and margarine since vita-
min D is only found in a few foods (e.g. oily fish and egg
yolk). In Europe the UK allows optional fortification of a
number of foods such as margarine and breakfast cereals
with other countries having limited or restricted use of
fortification [44] and therefore dietary sources may not be
sufficient [45, 46]. In the UK, the Scientific Advisory
Committee on Nutrition (SACN) state they are concerned
that vitamin D ‘recommendations are overlooked by health
professionals, as well as the general public’ [47, 48]. This
study provides data to support this concern for the UK, The
Netherlands, Iceland and Italy where a recommendation is
in place as mean supplementation was only 2.2 %. In these
countries the message is clearly not getting through to the
majority of women. There is currently much debate con-
cerning maternal vitamin D and its associations with var-
ious health outcomes [9, 50]. This contradictory evidence
may be why some countries don’t have a specific recom-
mendation. However for those that do, the recommendation
is clearly not being disseminated effectively.
Foods Consumed and Avoided
We have found that variation of food intake between coun-
tries in the EuroPrevall birth cohort does seem to be asso-
ciated with national recommendations. For example, the UK
and Greece recommend to ‘only eat thoroughly cooked egg’
and they had the highest proportion of mothers who limited
egg intake, which may be due to people’s preference for a
runny yolk or may be indicative of women receiving the
message that eggs are not safe and thinking that it is best to
avoid them altogether. The UK also recommends the
avoidance of raw shell fish and they have the highest num-
bers of avoiders of shell fish. The same recommendation is in
place in the Netherlands and Greece and even though
avoidance is lower compared to the UK, it is their most
commonly avoided food. Although no fish oil recommen-
dations are in place, perhaps due to insufficient evidence,
there were big differences in intake across Europe with
intake being particularly high in Iceland (94.5 %) compared
to the cohort mean (21.5 %). This study was unable to
determine whether mothers who did not consume fish oils
were achieving the recommended PUFA intakes during
pregnancy [49–51] but it is known that the Mediterranean
diet recommends moderate to high intake of fish [52].
The UK was the only country to have a specific allergy
recommendation about peanut. At the time of data collec-
tion, the Department of Health advice of 1998 was still in
place. This advice stated ‘‘pregnant women who are atopic,
or for whom the father or any sibling of the unborn child has
an atopic disease, may wish to avoid eating peanuts and
peanut products during pregnancy’’ [27]. This recommen-
dation seemed to influence behaviour as peanut was avoided
by 44 % of respondents. Analyses showed that having this
specific recommendation increased the likelihood of
mothers to avoid three or more foods. It is often perceived
that ‘good’ mothers should manage and avoid all risks to
protect their baby [53]. This particularly appears true in the
UK, where many mothers avoid certain foods such as shell
fish, peanuts and eggs. Many mothers may have avoided
three or more foods to try and avoid ‘risk’ to their baby even
if they had no need to (they or family were not atopic). This
allergy specific advice was amended in 2009 after the evi-
dence base was considered not strong enough to continue
recommending avoidance [28]. It would be interesting to
see if the UK avoidance rate is now more in line with
countries such as Germany which did not recommend any
avoidance of allergenic foods during pregnancy and have
avoidance rates of 3 foods or more of 26.7 %.
If a nation had nutritional supplement recommendations,
mothers were more likely to avoid foods perceived as
‘risky’ which supports the hypothesis that mothers are
trying to do the best for their baby and avoid risk whether
that involved food avoidance or food supplementation
which fits within the protection motivation theory [54].
This is also backed up by the fact that having general
healthy eating recommendations in place for pregnancy
reduced the risk of food avoidance as it encouraged women
to have a broad, balanced diet.
Matern Child Health J
123

Even though some countries had very similar recom-
mendations, differences in food avoidance were consider-
able. In all countries women received some verbal and
written information on diet and dietary supplements at their
first pre-natal appointment. The UK, Germany, Spain, the
Netherlands and Iceland also had government websites
where women could access information. Some had periodic
nationwide health campaigns. The observed differences
seen in adherence to recommendations may have been due
to cultural differences in how health messages were per-
ceived or it may be that the method of delivery of the
national recommendations was more effective in some
countries than others, or it could be that certain recom-
mendations are being overlooked by health professionals.
Strengths and Weaknesses
Strengths of the EuroPrevall birth cohort project are its
provision of unique data, its large sample size and the
standardised data collection throughout the entire cohort
which covers all the climatic regions of Europe. The
questionnaire had been translated and back translated to
ensure uniformity so data between countries was compa-
rable. Potential limitations of this work were with ques-
tionnaire design. The questionnaire did not record amounts
of supplements taken per day, additionally they also did not
record the week and month supplements were used as has
been done in other studies or levels of consumption, so it
could not be determined if consumption was appropriate for
requirements during pregnancy. Additionally, reporting
bias may have occurred if women didn’t know what their
multivitamin contained. However, the mean percentage
taking a multivitamin was still only 58 %. Our findings may
have also been affected by social desirability bias when
reporting folic acid or prenatal multivitamin use. Another
limitation was that we did not know how national and local
health authorities, health professionals and media imple-
mented or emphasised national recommendations nor did
we ask if mothers were aware of any pregnancy recom-
mendations and why they took nutritional supplements or
avoided certain foods. Therefore we were not able to look at
any effect there may have been on how recommendations
were disseminated within a population. Consequently any
observed associations need to be interpreted with caution.
Finally some limitations regarding the representativeness of
the cohort could exist as study centres were mostly located
in large cities and therefore may not represent the general
population of these countries as a whole [18].
Public Health Implications
Findings of this study are useful for advising countries how
mothers are behaving during pregnancy in relation to
pregnancy recommendations that may or may not be in
place. It has highlighted differences between countries and
indicated where more detailed studies which look at con-
sumption of specific food groups or supplements during
pregnancy and their impact on the health and development
of their children need to be undertaken.
As already highlighted, a large number of women across
Europe are not supplementing their diet with folic acid. It may
be that some nations have diets that are traditionally high in
foods which are a good source of folate and so supplementation
is deemed unnecessary but this may not be the case. For those
countries who do not currently recommend folic acid supple-
mentation it may be prudent to assess routine folate intake
within the population and if this is found to be sub-optimal then
to advise folate-rich foods and/or supplementation for women
of child-bearing age and during early pregnancy. For those
countries who already recommend supplementation there is
variability in compliance. Further investigation into how
information is disseminated and perceived would be helpful to
inform public health strategies. However, it would be prudent
to not only target vulnerable groups such as the less educated
and young, but perhaps all women of child bearing age to
ensure adequate levels at conception. Many countries have had
campaigns to increase knowledge and the use of folic acid
supplements, but results are varied [31, 55–59]. Voluntary
fortification of foods with folic acid is common in Europe but
there is wide variation in levels added to foodstuffs and man-
datory fortification has not been implemented in any EU
country [32]. However, to improve women’s pre-conception
folate status the strategy of a legislative approach and man-
datory fortification of foods with folic acid may be something
these countries may wish to consider.
The level of vitamin D supplementation, particularly
where there is a recommendation to do so is of concern.
Clearly this recommendation is not being disseminated
efficiently and further investigation into how women access
information and how they determine which recommenda-
tions they will and will not adhere to needs to be conducted.
For countries where a recommendation is currently not in
place it may be prudent to investigate whether promoting
supplementation is a worthwhile public health strategy.
This study shows that having any advice that suggests the
avoidance of a food or food group for any reason increases the
risk of food avoidance. Consequently, to avoid unnecessary
food avoidance it is important that such advice is introduced
only after strong evidence of a population health value.
Conclusions
This study has demonstrated that maternal dietary habits i.e.
food avoidance and the use of dietary supplements during
pregnancy varies significantly across Europe and may be
Matern Child Health J
123
influenced by national recommendations in some instances.
Further investigation into how recommendations are dissemi-
nated and how women determine what advice they will adhere
to would be useful for improving public health strategies which
promote healthy pregnancy and pregnancy outcomes.
Acknowledgments We thank all families who participated in the
EuroPrevall birth cohort study and the medical and nursing staff at the
obstetric departments of the participating hospitals, especially: GRE:
P. Saxoni-Papageorgiou, P. Xepapadaki, K. Zannikos, A. Vasilop-
oulou, C. Michopoulou, C. Skordali (P y A Kyriakou Hospital); S.
Gavrili, G. D. Vlachos (Alexandra Hospital); A. Malamitsi-Puchner,
D. Hasiakos, L. Kontara (Areteion Hospital); N. Paparisteidis (Elena
Venizelou Maternity Hospital, Athens, Greece); ICE: A.G. Gun-
narsdottir, H. Sigurdardottir, G.L. Gudjonsdottir (Landspitali - The
National University Hospital Reykjavik), prenatal care nurses at The
Primary Health Care of the Reykjavik Capital Area (Reykjavik,
Iceland); GER: S. Travis, S. Paschke-Goossens, S. Siegert, S. Dufour,
A. Kafert, K. Dobberstein, G. Schulz, A. Rohrbach, A. Scholz, A.
Reich, L. Grabenhenrich (Berlin, Germany); POL: L. Podciechowski
(Polish Mother’s Memorial Hospital, Lodz, Poland); SPA: M. Martın-
Esteban, S. Quirce, R. Gabriel, J. I. Larco, I. Bobolea, T. Cuevas
(Madrid, Spain); UK: K. Foote, L. Gudgeon, T. Kemp, K. Scally, E.
Gatrell, L. Bellis, A, Acqua, R. Kemp, T. Bryant (Southampton, UK);
NL: Midwives, Zorggroep Almere, Department of Gynaecology and
Obstetrics, Flevo Hospital Almere, N.v.d. Berg, De Kinderkliniek
Almere, W.M.C. van Aalderen, L Hulshof, NCM Petrus Department
of Pediatric Respiratory Medicine and Allergy, Emma Children’s
Hospital Academic Medical Center (Amsterdam, the Netherlands);
LIT: Audrone Arlauskiene, Jolita Zakareviciene, Laura Stoskute-
Malinauskiene (Lithuania); ITA: A. Martelli, P. Realini and F. Brandi
(both from Allegria, the Italian Research Foundation for Childhood
Allergy and Asthma), G.R. Bouygue, O. Mazzina, T. Sarratud, G.
Pezzoli (Milan, Italy). This birth cohort study was conducted within
the collaborative research initiative EuroPrevall, an integrated project
funded by the European Commission under the 6th Framework Pro-
gramme (FOOD-CT-2005-514000). The Icelandic birth cohort
received additional funds by Landspitali - The National University
Hospital of Iceland Science Fund and by GlaxoSmithKline, Iceland.
Four study sites were funded outside of EuroPrevall: the United
Kingdom birth cohort by the UK Food Standards Agency; the
Lithuanian birth cohort by unrestricted grants from Grida and MSD;
the Dutch birth cohort by unrestricted grants from Nutricia Advanced
Medical Nutrition Netherlands, AstraZeneca Netherlands, TEVA
Netherlands, and GlaxoSmithKline, Netherlands; and the Italian birth
cohort by own hospital funds and Allegria—the Italian Research
Foundation for Childhood Allergy and Asthma. None of the funding
bodies had any influence on the study design, data analysis or man-
uscript preparation.
Appendix 1
See Table 5.
Appendix 2
See Table 6.
Appendix 3
See Tables 7 and 8. Ta
ble
5C
han
ge
info
od
con
sum
pti
on
du
rin
gp
reg
nan
cy
Mar
itim
eN
ord
icC
entr
alE
uro
pea
nM
edit
erra
nea
nT
ota
lp
val
ue
Unit
edK
ingdom
Net
her
lands
Icel
and
Ger
man
yP
ola
nd
Lit
huan
iaS
pai
nIt
aly
Gre
ece
N1,1
40
976
1,3
41
1,5
70
1,5
13
1,5
56
1,3
87
1,4
86
1,0
80
12,0
49
Mil
kan
dm
ilk
pro
duct
sn
=888
n=
973
n=
1,3
35
n=
1,5
62
n=
1,5
04
n=
1,4
20
n=
1,3
72
n=
1,3
50
n=
1,0
78
n=
11,4
82
0.8
88
Ate
sam
eor
incr
ease
dam
ount
(%)
95.8
95.4
91.9
94.8
94.4
95.3
96.6
92.5
91.7
94.3
Lim
ited
inta
ke
(%)
3.9
4.4
7.7
4.9
5.3
4.1
3.1
7.3
8.0
5.4
Sto
pped
eati
ng
(%)
0.2
0.2
0.4
0.3
0.3
0.6
0.2
0.2
0.3
0.3
Egg
n=
889
n=
965
n=
1,3
33
n=
1,5
55
n=
1,4
94
n=
1,3
85
n=
1,3
70
n=
1,3
17
n=
1,0
77
n=
11,3
85
\0.0
01
Ate
sam
eor
incr
ease
dam
ount
(%)
77.8
91.2
95.0
89.9
94.4
89.7
94.4
87.4
84.0
89.9
Lim
ited
inta
ke
(%)
18.6
8.2
4.7
9.8
5.1
8.4
5.3
12.4
13.7
9.1
Sto
pped
eati
ng
(%)
3.6
0.6
0.3
0.3
0.5
1.9
0.3
0.2
2.3
1.0
Pea
nut
n=
886
n=
941
n=
1,3
22
n=
1,5
27
n=
1,1
77
n=
1,0
48
n=
799
n=
759
n=
1,0
78
n=
9,5
37
\0.0
01
Ate
sam
eor
incr
ease
dam
ount
(%)
35.3
93.4
86.6
90.0
66.8
84.4
85.1
73.9
87.3
79.3
Lim
ited
inta
ke
(%)
20.3
3.9
8.5
6.5
20.2
10.2
7.8
23.1
5.1
11.2
Sto
pped
eati
ng
(%)
44.4
2.7
4.9
3.5
13.0
5.4
7.1
3.0
7.6
9.5
Tre
enuts
n=
883
n=
941
n=
1,3
32
n=
1,5
37
n=
1,2
05
n=
1,1
18
n=
928
n=
941
n=
1,0
78
n=
9,9
63
\0.0
01
Ate
sam
eor
incr
ease
dam
ount
(%)
65.1
94.5
88.4
95.3
67.1
86.4
89.1
78.7
87.8
84.3
Lim
ited
inta
ke
(%)
18.1
3.8
7.3
3.5
19.2
8.9
5.5
20.1
7.3
10.0
Matern Child Health J
123
Ta
ble
5co
nti
nu
ed
Mar
itim
eN
ord
icC
entr
alE
uro
pea
nM
edit
erra
nea
nT
ota
lp
val
ue
Unit
edK
ingdom
Net
her
lands
Icel
and
Ger
man
yP
ola
nd
Lit
huan
iaS
pai
nIt
aly
Gre
ece
Sto
pped
eati
ng
(%)
16.8
1.7
4.3
1.2
13.7
4.7
5.4
1.2
4.9
5.7
Soy
n=
886
n=
746
n=
1,3
34
n=
1,4
99
n=
804
n=
519
n=
492
n=
343
n=
1,0
79
n=
7,7
02
\0.0
01
Ate
sam
eor
incr
ease
dam
ount
(%)
96.4
94.4
98.0
94.6
83.2
79.2
76.2
84.6
97.8
92.0
Lim
ited
inta
ke
(%)
1.2
3.6
1.0
3.4
12.4
3.3
4.9
9.9
0.8
3.7
Sto
pped
eati
ng
(%)
2.4
2.0
1.0
2.0
4.4
17.5
18.9
5.5
1.4
4.3
Fis
hn
=890
n=
950
n=
1,3
33
n=
1,5
57
n=
1,4
57
n=
1,3
76
n=
1,3
63
n=
1,2
98
n=
1,0
77
n=
11,3
01
\0.0
01
Ate
sam
eor
incr
ease
dam
ount
(%)
89.4
90.4
92.8
90.5
91.2
93.8
94.6
91.6
90.8
91.8
Lim
ited
inta
ke
(%)
9.0
8.6
6.8
8.5
6.9
4.1
5.1
8.0
7.2
7.0
Sto
pped
eati
ng
(%)
1.6
1.0
0.4
1.0
1.9
2.1
0.3
0.4
2.0
1.1
Shel
lfish
n=
887
n=
802
n=
1,3
36
n=
1,5
30
n=
718
n=
670
n=
1,0
83
n=
509
n=
1,0
79
n=
8,6
14
\0.0
01
Ate
sam
eor
incr
ease
dam
ount
(%)
43.6
80.5
71.4
80.7
86.9
81.5
84.2
65.4
80.1
74.9
Lim
ited
inta
ke
(%)
14.7
11.0
17.4
9.1
9.1
5.8
11.7
28.9
9.3
13.0
Sto
pped
eati
ng
(%)
41.7
8.5
11.2
10.2
4.0
12.7
4.1
5.7
10.6
12.1
Cer
eal/
cere
alpro
duct
sn
=886
n=
974
n=
1,3
27
n=
1,5
61
n=
1,4
82
n=
1,3
83
n=
1,3
45
n=
1,2
09
n=
1,0
79
n=
11,2
46
\0.0
01
Ate
sam
eor
incr
ease
dam
ount
(%)
98.7
98.1
97.8
98.1
97.2
96.9
95.3
95.9
90.5
96.5
Lim
ited
inta
ke
(%)
1.1
1.8
2.0
1.9
2.3
2.0
4.6
3.7
9.4
3.2
Sto
pped
eati
ng
(%)
0.2
0.1
0.2
0.0
0.5
1.1
0.1
0.4
0.1
0.3
Veg
etab
les
n=
889
n=
973
n=
1,3
31
n=
1,5
61
n=
1,5
08
n=
1,4
45
n=
1,3
74
n=
1,3
37
n=
1,0
78
n=
11,4
96
\0.0
01
Ate
sam
eor
incr
ease
dam
ount
(%)
97.6
96.6
97.4
92.2
99.2
99.3
97.7
96.9
96.9
97.1
Lim
ited
inta
ke
(%)
2.4
3.4
2.5
7.2
0.8
0.7
2.2
3.1
2.9
2.8
Sto
pped
eati
ng
(%)
0.0
0.0
0.1
0.6
0.0
0.0
0.1
0.0
0.2
0.1
Fru
itn
=882
n=
974
n=
1,3
30
n=
1,5
66
n=
1,5
11
n=
1,4
47
n=
1,3
75
n=
1,3
50
n=
1,0
80
n=
11,5
15
0.9
83
Ate
sam
eor
incr
ease
dam
ount
(%)
97.8
97.1
97.7
96.2
98.9
98.5
97.5
97.7
94.7
97.3
Lim
ited
inta
ke
(%)
2.1
2.9
2.2
3.7
1.0
1.5
2.3
2.1
5.2
2.6
Sto
pped
eati
ng
(%)
0.1
0.0
0.1
0.1
0.1
0.1
0.2
0.2
0.1
0.1
Mea
tan
dm
eat
pro
duct
sn
=886
n=
957
n=
1,3
29
n=
1,5
61
n=
1,4
91
n=
1,4
38
n=
1,3
63
n=
1,3
44
n=
1,0
79
n=
11,4
48
\0.0
01
Ate
sam
eor
incr
ease
dam
ount
(%)
94.1
81.9
92.3
85.2
94.4
91.2
67.3
89.8
85.6
86.9
Lim
ited
inta
ke
(%)
5.2
17.6
7.5
14.5
5.6
7.7
31.0
10.1
14.0
12.6
Sto
pped
eati
ng
(%)
0.7
0.5
0.2
0.3
0.0
1.1
1.7
0.1
0.4
0.5
Tea
and
coff
een
=876
n=
968
n=
1,3
36
n=
1,5
59
n=
1,4
83
n=
1,4
02
n=
849
n=
1,1
67
n=
1,0
77
n=
10,7
17
\0.0
01
Ate
sam
eor
incr
ease
dam
ount
(%)
41.4
57.3
50.5
35.8
85.8
66.3
35.1
37.4
34.6
50.9
Lim
ited
inta
ke
(%)
43.4
38.6
40.4
53.0
12.8
30.7
49.1
60.9
40.6
40.2
Sto
pped
dri
nkin
g(%
)15.2
4.0
9.1
11.2
1.4
3.0
15.8
1.7
24.8
8.9
Alc
ohol
n=
882
n=
854
n=
1,3
37
n=
1,5
50
n=
880
n=
635
n=
206
n=
438
n=
1,0
75
n=
7,8
57
\0.0
01
Ate
sam
eor
incr
ease
dam
ount
(%)
43.3
23.1
10.5
20.8
7.0
32.7
4.4
17.1
43.3
20.2
Lim
ited
inta
ke
(%)
10.8
11.2
8.4
22.5
47.6
23.5
10.7
69.9
10.8
25.0
Sto
pped
dri
nkin
g(%
)45.9
65.7
81.1
56.7
45.3
43.8
84.9
13.0
45.9
54.8
Fig
ure
sar
eper
centa
ges
inea
chca
tegory
.p
val
ues
(p\
0.0
5)
repre
sent
resu
ltof
Chi
squar
edte
stof
food
eate
nag
ainst
food
full
yav
oid
ed.If
moth
ers
usu
ally
ate
afo
od
pre
-pre
gnan
cyan
dth
enav
oid
edduri
ng
pre
gnan
cyth
eyw
ere
coded
asst
opped
eati
ng.
Ifsh
eusu
ally
avoid
edan
dco
nti
nued
toav
oid
she
‘ate
the
sam
eas
usu
al’
Matern Child Health J
123
Ta
ble
6N
atio
nal
pre
gn
ancy
reco
mm
end
atio
ns
acro
ssE
uro
pe
Countr
yan
dso
urc
eof
reco
mm
endat
ions
Gen
eral
nutr
itio
nre
com
men
dat
ions
Food
safe
tyre
com
men
dat
ions
Supple
men
t
reco
mm
endat
ions
Spec
ific
alle
rgy
reco
mm
endat
ions
Oth
erre
com
men
dat
ions
Unit
edK
ingdom
The
Nat
ional
Hea
lth
Ser
vic
e
(ww
w.n
hs.
uk
)
Food
Sta
ndar
ds
Agen
cy(w
ww
.
eatw
ell.
gov.u
k)
Dep
artm
ent
of
Hea
lth
(ww
w.
food.g
ov.u
k)
Fru
itand
veget
able
sea
tple
nty
of
fruit
and
veg
etab
les.
Eat
atle
ast
five
port
ions
aday
Sta
rchy
foods
(car
bohydra
te)
e.g.
bre
ad,
pota
toes
,bre
akfa
stce
real
s,ri
ce,
pas
ta
etc.
Thes
efo
ods
should
be
the
mai
n
par
tof
ever
ym
eal
Pro
tein
eat
som
epro
tein
ever
yday
.T
ry
toea
t2
port
ions
of
fish
aw
eek,
1
should
be
oil
y
Dair
yA
imfo
r2–3
port
ions
aday
Chee
sedon’t
eat
mould
-rip
ened
soft
chee
se(e
.g.
bri
e,ca
mem
ber
t),
blu
e-
vei
ned
var
ieti
es(e
.g.
stil
ton,
dan
ish
blu
e).
Ther
eis
risk
of
list
eria
infe
ctio
n
Mea
tco
ok
all
mea
tan
dpoult
ry
thoro
ughly
soth
ere
isno
trac
eof
pin
k
or
blo
od.
This
wil
lhel
pto
avoid
infe
ctio
nw
ith
toxopla
sma
Liv
erdon’t
eat
liver
or
liver
pro
duct
s
bec
ause
they
may
conta
ina
lot
of
vit
amin
A
Pate
avoid
all
types
of
pat
ein
cludin
g
veg
etab
lepat
ebec
ause
they
may
conta
inli
ster
ia
Eggs
only
eat
thoro
ughly
cooked
eggs
to
pre
ven
tri
skof
food
pois
onin
gby
salm
onel
labac
teri
a.D
on’t
eat
foods
conta
inin
gra
wor
under
cooked
eggs
(e.g
.hom
e-m
ade
may
onnai
se,
ice-
crea
m,
and
mouss
e)
Fis
hdon’t
eat
shar
k,
mar
lin,
sword
fish
and
lim
itam
ount
of
tuna
asth
ese
types
hav
ehig
hle
vel
sof
mer
cury
.L
imit
tuna
totw
ost
eaks
or
four
cans
(140
g
dra
ined
wei
ght)
aw
eek
Shel
lfish
only
eat
cooked
shel
lfish
asra
w
can
conta
inhar
mfu
lvir
use
san
d
bac
teri
ath
atca
use
food
pois
onin
g
Mil
konly
dri
nk
pas
teuri
zed
or
UH
T
mil
k.
Als
odon’t
dri
nk
unpas
teuri
zed
goat
sor
shee
p’s
mil
kor
foods
mad
e
from
them
(e.g
.goat
’sch
eese
)
Fru
it,
veget
able
sand
sala
ds
was
hfr
uit
,
veg
etab
les
and
sala
ds
tore
move
all
trac
esof
soil
whic
hm
ayco
nta
in
toxopla
sma
Caff
eine
caff
eine
does
n’t
nee
dto
be
cut
out
com
ple
tely
,but
don’t
hav
em
ore
than
200
mg/d
ay(o
ne
mug
inst
ant
coff
ee:
100
mg,
one
mug
tea:
75
mg)
400
lg
foli
cac
id
dai
lyunti
l
12
wee
ks
10
lg/d
ayof
vit
amin
D
Don’t
take
hig
h-d
ose
mult
ivit
amin
s,
hig
h-d
ose
fish
liver
oil
,or
any
supple
men
tsth
at
conta
invit
amin
A
1,9
98
reco
mm
endat
ion
‘‘pre
gnan
t
wom
enw
ho
are
atopic
,or
for
whom
the
fath
eror
any
sibli
ng
of
the
unborn
chil
dhas
anat
opic
dis
ease
,
may
wis
hto
avoid
eati
ng
pea
nuts
and
pea
nut
pro
duct
sduri
ng
pre
gnan
cy’’
[14]
2009
reco
mm
endat
ion
‘‘P
eanut
and
pea
nut
conta
inin
gfo
ods
(e.g
.pea
nut
butt
er,
confe
ctio
nar
y)
may
be
eate
nduri
ng
pre
gnan
cy,
unle
ssyou’r
eal
lerg
icto
them
or
your
hea
lth
pro
fess
ional
advis
esyou
not
to’’
[15]
Pro
tect
your
bab
yfr
om
tobac
cosm
oke.
Do
not
smoke
Bes
tto
avoid
alco
hol,
but
ifch
oose
to
dri
nk,
do
not
dri
nk
more
than
1–2
unit
s
once
or
twic
ea
wee
k,
and
don’t
get
dru
nk.
NIC
E(N
atio
nal
Inst
itute
for
Hea
lth
and
Cli
nic
alE
xce
llen
ce)
advis
espre
gnan
tw
om
ento
avoid
alco
hol
inth
efi
rst
3m
onth
sin
par
ticu
lar,
bec
ause
of
the
incr
ease
d
risk
of
mis
carr
iage
Alw
ays
chec
kw
ith
your
doct
or,
mid
wif
e
or
phar
mac
ist
bef
ore
takin
gan
y
med
icat
ion.
Tal
kto
your
doct
or
imm
edia
tely
ifyou
take
regula
r
med
icat
ions.
Use
asfe
wover
-the
–
counte
rm
edic
ines
asposs
ible
Not
all
‘nat
ura
l’re
med
ies
are
safe
in
pre
gnan
cy.
Tel
lth
epra
ctit
ioner
you
are
pre
gnan
tan
dte
llyour
phar
mac
ist,
mid
wif
eor
doct
or
whic
hher
bal
,
hom
eopat
hic
or
arom
ather
apy
rem
edie
syou
are
usi
ng
Don’t
han
dle
cat
litt
eran
dw
ear
glo
ves
when
gar
den
ing
toav
oid
infe
ctio
nw
ith
toxopla
sma
Matern Child Health J
123
Ta
ble
6co
nti
nu
ed
Countr
yan
dso
urc
eof
reco
mm
endat
ions
Gen
eral
nutr
itio
nre
com
men
dat
ions
Food
safe
tyre
com
men
dat
ions
Supple
men
t
reco
mm
endat
ions
Spec
ific
alle
rgy
reco
mm
endat
ions
Oth
erre
com
men
dat
ions
Net
her
lands
(ww
w.
voed
ingsc
entr
um
.nl)
Eat
avar
iety
of
foods
wit
hin
all
food
gro
ups
Mak
esu
reth
atyour
inta
ke
of
iron
is
suffi
cien
tby
eati
ng
whole
whea
tbre
ad
and
mea
t.E
atvit
amin
Cri
chfr
uit
and
veg
etab
les
wit
hev
ery
mea
lto
enhan
ce
iron
abso
rpti
on
Dair
yai
mfo
r3–5
port
ions
of
dai
ry
pro
duct
sa
day
.Id
eall
ych
oose
sem
i-
skim
med
or
non-f
atm
ilk
Ifveg
etar
ian,
mak
esu
reto
eat
enough
pro
duct
s,ri
chin
vit
amin
Ban
dir
on-
eat
enough
bre
ad,
whea
t-pro
duct
s,
legum
es,
dai
rypro
duct
s,eg
gs
or
mea
t-
anal
ogues
,li
ke
egg,to
fu,te
mpe
or
nuts
Do
not
eat/
dri
nk
for
two
Dri
nk
enough
(±2
l)
Do
not
try
tolo
sew
eight
Chee
sedo
not
eat
soft
chee
sem
ade
from
non
pas
teuri
zed
(raw
)m
ilk;
har
d
chee
sem
ade
from
non
pas
teuri
zed
mil
kca
nbe
eate
n
Mea
tdo
not
eat
raw
mea
tor
liver
(pro
duct
s)
Pate
do
not
eat
more
than
one
port
ion
of
liver
pro
duct
sper
day
toav
oid
too
much
inta
ke
of
vit
amin
A(p
refe
rably
max
1port
ion
ever
y3
day
s)
Eggs
only
eat
eggs
that
are
har
dboil
edor
wel
lfr
ied
Fis
hea
tfi
sh,
this
ishea
lthy,
but
do
not
eat
Vac
uum
seal
edre
ady
toea
tfi
shor
shel
l
fish
from
frid
ge(
e.g.
smoked
salm
on)
(if
hea
ted,
this
may
be
eate
n)
Raw
fish
or
shel
lfi
sh(e
.g.
oyst
ers)
Don’t
eat
shar
k,
mar
lin,
sword
fish
and
lim
itam
ount
of
tuna
asth
ese
types
hav
ehig
hle
vel
sof
mer
cury
No
eel
from
Dutc
hri
ver
s
No
more
than
two
port
ions/
wee
kof
fatt
y
fish
,bec
ause
of
dio
xin
s
Caff
eine
no
more
than
four
cups
of
coff
ee/d
ayor
eight
gla
sses
of
coke/
tea
Liq
uori
celi
mit
consu
mpti
on
toco
uple
of
swee
tsor
1–2
cups
of
liquori
cete
a/day
400
lg
foli
cac
id
dai
ly(a
tle
ast
firs
t
10
wee
ks)
10
lg/d
ayvit
amin
D
\3,0
00
lg/d
ay
vit
amin
A
Spec
ial
for
duri
ng
pre
gnan
cy,
do
not
take
more
than
advis
eddose
None
Do
not
dri
nk
alco
hol
Quit
smokin
g
Her
bal
supple
men
tsdo
not
take
efed
ra,
aloe,
sass
afra
s,dong
quai
,kav
akav
a,
absi
nt-
alse
m,
fennel
,an
ise,
cucu
mber
her
b,
colt
sfoot,
com
frey
and
fever
few
.
Lim
itco
nsu
mpti
on
of
fenugre
ek,
nig
ella
,fe
ather
few
,se
nna,
and
may
flow
er
Her
bs
Lim
itco
nsu
mpti
on
of
fennel
,
sage,
tarr
agon,
anis
e,bas
il,
pes
to,
rubar
ban
dci
nnam
on
Sw
eete
ner
sli
ke
aspar
tam
ein
light
sodas
are
not
har
mfu
l
Was
hyour
fruit
san
dveg
etab
les
Eat
your
raw
veg
etab
les/
fruit
sfr
esh
quic
kly
,do
not
kee
pth
emto
olo
ng
in
the
frid
ge
(as
wel
las
left
over
s)
Pim
ba
do
not
use
pim
ba
or
cala
bas
h
chal
kag
ainst
nau
sea
Do
not
take
any
med
icat
ion
wit
hout
consu
ltin
ga
doct
or,
mid
wif
eor
a
phar
mac
ist,
regar
dle
ssif
the
med
icat
ion
isover
—th
e—co
unte
ror
pre
scri
pti
on.
Wom
ensh
ould
ther
efore
alw
ays
mak
esu
reto
info
rmab
out
thei
r
pre
gnan
cy.
Her
bal
pro
duct
san
d
hom
eopat
hic
rem
edie
ssh
ould
not
be
use
dduri
ng
pre
gnan
cyunle
ss
consu
ltin
ga
doct
or
Do
not
clea
nca
tli
tter
box
Gar
den
wea
ring
glo
ves
Matern Child Health J
123

Ta
ble
6co
nti
nu
ed
Countr
yan
dso
urc
eof
reco
mm
endat
ions
Gen
eral
nutr
itio
nre
com
men
dat
ions
Food
safe
tyre
com
men
dat
ions
Supple
men
t
reco
mm
endat
ions
Spec
ific
alle
rgy
reco
mm
endat
ions
Oth
erre
com
men
dat
ions
Icel
and
Dir
ecto
rate
of
Hea
lth,
Rey
kja
vik
,Ic
elan
d.
htt
p:/
/
ww
w.l
andla
eknir
.is/
utg
efid-
efni/
skja
l/it
em11446/
Dep
artm
ent
of
Ante
nat
alC
are,
Dir
ecto
rate
of
Hea
lth
and
The
Icel
andic
food
and
vet
erin
ary
Auth
ori
tyhtt
p:/
/ww
w.
landla
eknir
.is/
utg
efid-e
fni/
skja
l/it
em18504/
Eat
avar
iety
of
foods
wit
hin
all
food
gro
ups
Aim
atfi
ve
port
ions
of
fruit
san
d/o
r
veg
etab
les/
day
Eat
ing
food
rich
inir
on
on
adai
lybas
is
should
be
enough
tom
eet
the
incr
ease
d
nee
d
Low
fat
dai
rypro
duct
sar
ere
com
men
ded
Dri
nk
2–3
gla
sses
of
pas
teuri
zed
mil
k/
day
(or
equiv
alen
tam
ount
of
oth
er
dai
rypro
duct
s).
Idea
lly
choose
sem
i-
skim
med
or
non-f
atm
ilk.
For
those
wom
enw
ho
don’t
eat
dai
rypro
duct
s
they
are
reco
mm
ended
toco
nsu
me
pro
duct
sen
rich
edw
ith
calc
ium
.
1,0
00
mg
calc
ium
isth
ere
com
men
ded
dai
lyin
take
for
pre
gnan
tw
om
en
Mea
tdo
not
eat
raw
mea
t
Eggs
avoid
raw
eggs.
Fulm
aran
dfu
lmar
eggs
are
tobe
avoid
edbec
ause
of
conta
min
ants
.G
uil
lem
ot
eggs
should
not
be
eate
nm
ore
than
once
aw
eek
Liv
erav
oid
liver
,pat
ean
dsh
eep
liver
sausa
ge
due
tohig
hle
vel
sof
vit
amin
A
Fis
his
reco
mm
ended
atle
ast
2ti
mes
a
wee
kbut
avoid
:R
awfi
sh,
cod
liver
,
shar
k,
sword
fish
and
larg
ehal
ibut
([1.8
mor
60
kg).
Tuna
fish
stea
kan
d
ora
nge
roughy
should
not
be
eate
n
more
than
once
aw
eek
bec
ause
of
conta
min
ants
Fis
hoil
avoid
poll
ock
fish
oil
due
tohig
h
level
sof
vit
amin
A
Caff
eine
dri
nk
no
more
than
1–2
cups
of
coff
eea
day
or
3–4
cups
of
tea.
Itis
pre
fera
ble
toco
nsu
me
cola
san
d
ener
gy
dri
nks
inm
oder
atio
n
Foli
caci
d400
lg
dai
ly,
4w
eeks
bef
ore
pre
gnan
cy
and
unti
lth
e12th
wee
k.
Itis
also
advis
edto
eat
foods
rich
info
late
s
10
lg/d
ayvit
amin
D
800
lg
dai
ly
reco
mm
ended
inta
ke
of
vit
amin
A
Cod
liver
oil
is
reco
mm
ended
asa
good
sourc
efo
rA
and
Dvit
amin
,
5m
l/day
Ifw
om
enar
eta
kin
g
cod
liver
oil
and
takin
gm
ult
ivit
amin
choose
mult
ivit
amin
that
do
not
conta
in
vit
amin
A
Iron
supple
men
tsar
e
not
reco
mm
ended
unle
ssit
’snee
ded
None
Itis
reco
mm
ended
toav
oid
alco
hol
alto
get
her
duri
ng
pre
gnan
cy
Wom
enar
ead
vis
edto
stop
smokin
gan
d
are
info
rmed
about
the
ben
efits
of
non-
smokin
gpre
gnan
cy
Wom
enar
ere
com
men
ded
not
tota
ke
any
med
icat
ion
wit
hout
consu
ltin
ga
doct
or,
mid
wif
eor
aphar
mac
ist,
regar
dle
ssif
the
med
icat
ion
is‘o
ver
the
counte
r’or
pre
scri
pti
on.
Wom
en
should
ther
efore
alw
ays
mak
esu
reto
info
rmab
out
thei
rpre
gnan
cy
Her
bal
pro
duct
san
dhom
eopat
hic
rem
edie
ssh
ould
not
be
use
dduri
ng
pre
gnan
cyunle
ssco
nsu
ltin
ga
doct
or
Expec
ting
moth
ers
are
reco
mm
ended
at
leas
t30
min
of
physi
cal
acti
vit
y/d
ay
Good
den
tal
hygie
ne
isem
pth
asis
ed
duri
ng
pre
gnan
cy
Incr
ease
dhygie
ne
around
food
is
reco
mm
ended
duri
ng
pre
gnan
cyas
har
mfu
lbac
teri
aan
dpar
asit
esca
n
affe
ctth
ehea
lth
of
both
moth
eran
d
chil
d
Matern Child Health J
123
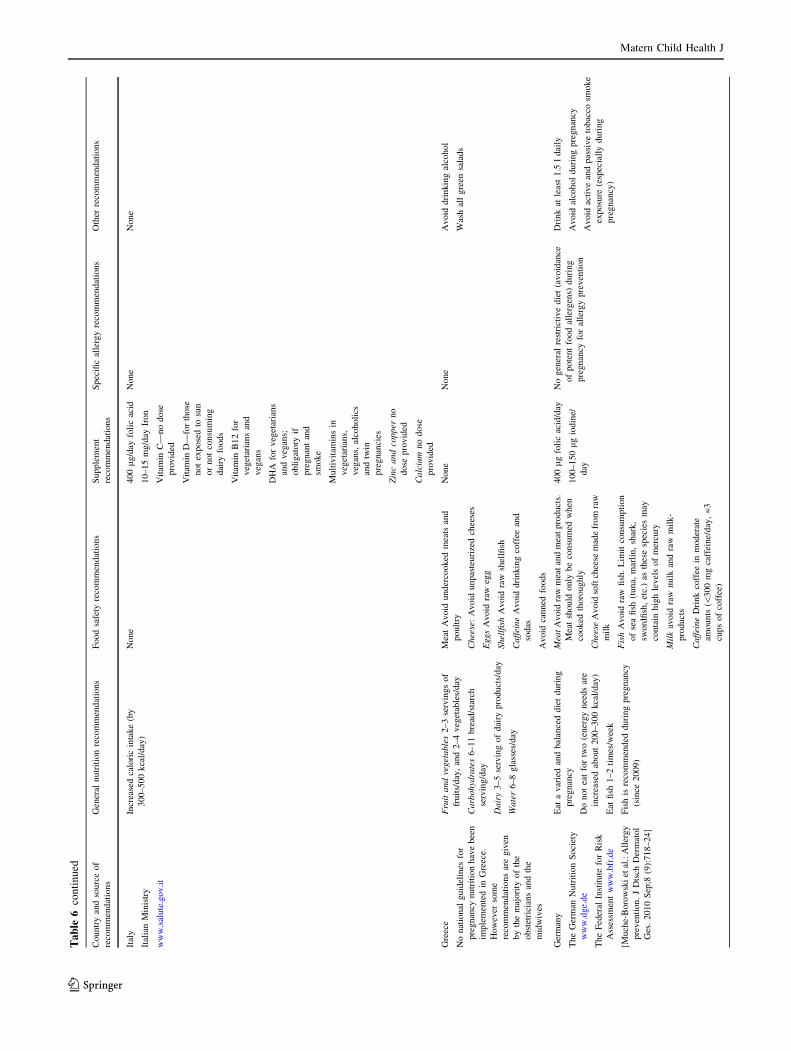
Ta
ble
6co
nti
nu
ed
Countr
yan
dso
urc
eof
reco
mm
endat
ions
Gen
eral
nutr
itio
nre
com
men
dat
ions
Food
safe
tyre
com
men
dat
ions
Supple
men
t
reco
mm
endat
ions
Spec
ific
alle
rgy
reco
mm
endat
ions
Oth
erre
com
men
dat
ions
Ital
y
Ital
ian
Min
istr
y
ww
w.s
alute
.gov.i
t
Incr
ease
dca
lori
cin
take
(by
300–500
kca
l/day
)
None
400
lg/d
ayfo
lic
acid
10–15
mg/d
ayIr
on
Vit
amin
C—
no
dose
pro
vid
ed
Vit
amin
D—
for
those
not
expose
dto
sun
or
not
consu
min
g
dai
ryfo
ods
Vit
amin
B12
for
veg
etar
ians
and
veg
ans
DH
Afo
rveg
etar
ians
and
veg
ans;
obli
gat
ory
if
pre
gnan
tan
d
smoke
Mult
ivit
amin
sin
veg
etar
ians,
veg
ans,
alco
holi
cs
and
twin
pre
gnan
cies
Zin
cand
copper
no
dose
pro
vid
ed
Calc
ium
no
dose
pro
vid
ed
None
None
Gre
ece
No
nat
ional
guid
elin
esfo
r
pre
gnan
cynutr
itio
nhav
ebee
n
imple
men
ted
inG
reec
e.
How
ever
som
e
reco
mm
endat
ions
are
giv
en
by
the
maj
ori
tyof
the
obst
etri
cian
san
dth
e
mid
wiv
es
Fru
itand
veget
able
s2–3
serv
ings
of
fruit
s/day
,an
d2–4
veg
etab
les/
day
Carb
ohyd
rate
s6–11
bre
ad/s
tarc
h
serv
ing/d
ay
Dair
y3–5
serv
ing
of
dai
rypro
duct
s/day
Wate
r6–8
gla
sses
/day
Mea
tA
void
under
cooked
mea
tsan
d
poult
ry
Chee
se:
Avoid
unpas
teuri
zed
chee
ses
Eggs
Avoid
raw
egg
Shel
lfish
Avoid
raw
shel
lfish
Caff
eine
Avoid
dri
nkin
gco
ffee
and
sodas
Avoid
canned
foods
None
None
Avoid
dri
nkin
gal
cohol
Was
hal
lgre
ensa
lads
Ger
man
y
The
Ger
man
Nutr
itio
nS
oci
ety
ww
w.d
ge.
de
The
Fed
eral
Inst
itute
for
Ris
k
Ass
essm
ent
ww
w.b
fr.d
e
[Much
e-B
oro
wsk
iet
al.:
All
ergy
pre
ven
tion.
JD
tsch
Der
mat
ol
Ges
.2010
Sep
;8(9
):718–24]
Eat
avar
ied
and
bal
ance
ddie
tduri
ng
pre
gnan
cy
Do
not
eat
for
two
(ener
gy
nee
ds
are
incr
ease
dab
out
200–300
kca
l/day
)
Eat
fish
1–2
tim
es/w
eek
Fis
his
reco
mm
ended
duri
ng
pre
gnan
cy
(sin
ce2009)
Mea
tA
void
raw
mea
tan
dm
eat
pro
duct
s.
Mea
tsh
ould
only
be
consu
med
when
cooked
thoro
ughly
Chee
seA
void
soft
chee
sem
ade
from
raw
mil
k
Fis
hA
void
raw
fish
.L
imit
consu
mpti
on
of
sea
fish
(tuna,
mar
lin,
shar
k,
sword
fish
,et
c.)
asth
ese
spec
ies
may
conta
inhig
hle
vel
sof
mer
cury
Mil
kav
oid
raw
mil
kan
dra
wm
ilk-
pro
duct
s
Caff
eine
Dri
nk
coff
eein
moder
ate
amounts
(\300
mg
caff
eine/
day
,=
3
cups
of
coff
ee)
400
lg
foli
cac
id/d
ay
100–150
lg
iodin
e/
day
No
gen
eral
rest
rict
ive
die
t(a
void
ance
of
pote
nt
food
alle
rgen
s)duri
ng
pre
gnan
cyfo
ral
lerg
ypre
ven
tion
Dri
nk
atle
ast
1.5
ldai
ly
Avoid
alco
hol
duri
ng
pre
gnan
cy
Avoid
acti
ve
and
pas
sive
tobac
cosm
oke
exposu
re(e
spec
iall
yduri
ng
pre
gnan
cy)
Matern Child Health J
123
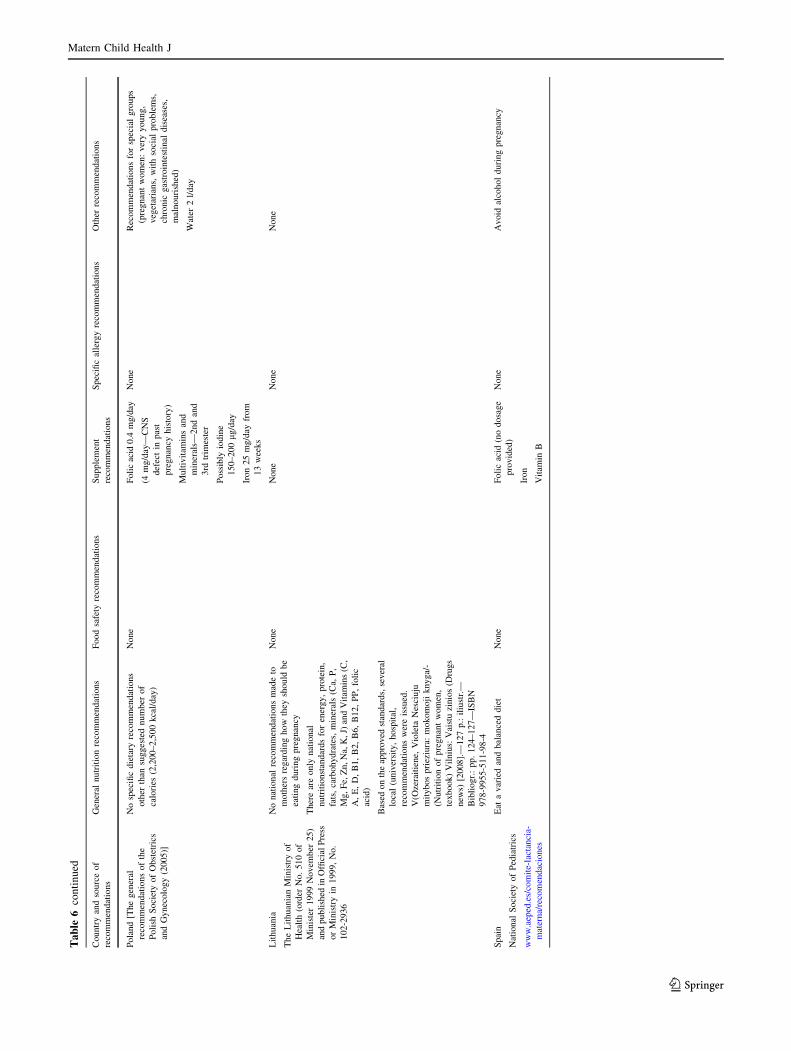
Ta
ble
6co
nti
nu
ed
Countr
yan
dso
urc
eof
reco
mm
endat
ions
Gen
eral
nutr
itio
nre
com
men
dat
ions
Food
safe
tyre
com
men
dat
ions
Supple
men
t
reco
mm
endat
ions
Spec
ific
alle
rgy
reco
mm
endat
ions
Oth
erre
com
men
dat
ions
Pola
nd
[The
gen
eral
reco
mm
endat
ions
of
the
Poli
shS
oci
ety
of
Obst
etri
cs
and
Gynec
olo
gy
(2005)]
No
spec
ific
die
tary
reco
mm
endat
ions
oth
erth
ansu
gges
ted
num
ber
of
calo
ries
(2,2
00–2,5
00
kca
l/day
)
None
Foli
cac
id0.4
mg/d
ay
(4m
g/d
ay—
CN
S
def
ect
inpas
t
pre
gnan
cyhis
tory
)
Mult
ivit
amin
san
d
min
eral
s—2nd
and
3rd
trim
este
r
Poss
ibly
iodin
e
150–200
lg/d
ay
Iron
25
mg/d
ayfr
om
13
wee
ks
None
Rec
om
men
dat
ions
for
spec
ial
gro
ups
(pre
gnan
tw
om
en:
ver
yyoung,
veg
etar
ians,
wit
hso
cial
pro
ble
ms,
chro
nic
gas
troin
test
inal
dis
ease
s,
mal
nouri
shed
)
Wat
er2
l/day
Lit
huan
ia
The
Lit
huan
ian
Min
istr
yof
Hea
lth
(ord
erN
o.
510
of
Min
iste
r1999
Novem
ber
25)
and
publi
shed
inO
ffici
alP
ress
or
Min
istr
yin
1999,
No.
102-2
936
No
nat
ional
reco
mm
endat
ions
mad
eto
moth
ers
regar
din
ghow
they
should
be
eati
ng
duri
ng
pre
gnan
cy
Ther
ear
eonly
nat
ional
nutr
itio
nst
andar
ds
for
ener
gy,
pro
tein
,
fats
,ca
rbohydra
tes,
min
eral
s(C
a,P
,
Mg,
Fe,
Zn,
Na,
K,
J)an
dV
itam
ins
(C,
A,
E,
D,
B1,
B2,
B6,
B12,
PP
,fo
lic
acid
)
Bas
edon
the
appro
ved
stan
dar
ds,
sever
al
loca
l(u
niv
ersi
ty,
hosp
ital
,
reco
mm
endat
ions
wer
eis
sued
.
V(O
zera
itie
ne,
Vio
leta
Nes
ciuju
mit
ybos
pri
eziu
ra:
mokom
oji
knyga/
-
(Nutr
itio
nof
pre
gnan
tw
om
en,
texbook)
Vil
niu
s:V
aist
uzi
nio
s(D
rugs
new
s)[2
008].
—127
p.:
iliu
str.
—
Bib
liogr.
:pp.
124–127—
ISB
N
978-9
955-5
11-9
8-4
None
None
None
None
Spai
n
Nat
ional
Soci
ety
of
Ped
iatr
ics
ww
w.a
eped
.es/
com
ite-
lact
anci
a-
mat
erna/
reco
men
dac
iones
Eat
avar
ied
and
bal
ance
ddie
tN
one
Foli
cac
id(n
odosa
ge
pro
vid
ed)
Iron
Vit
amin
B
None
Avoid
alco
hol
duri
ng
pre
gnan
cy
Matern Child Health J
123
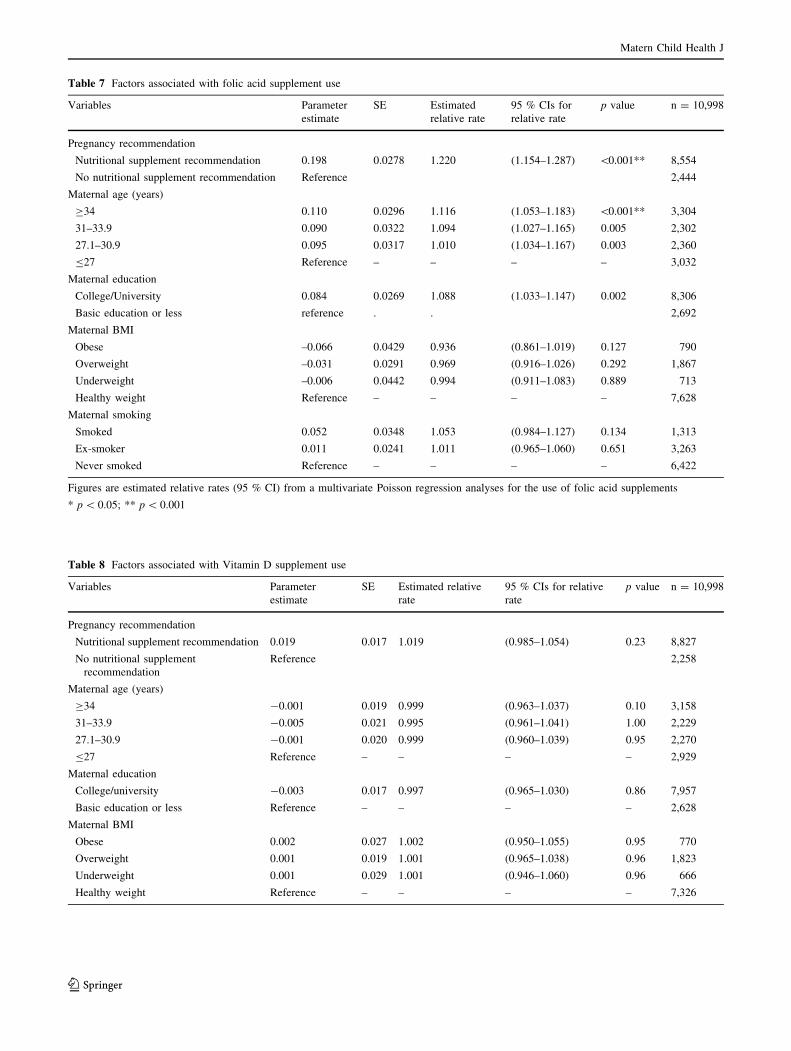
Table 7 Factors associated with folic acid supplement use
Variables Parameter
estimate
SE Estimated
relative rate
95 % CIs for
relative rate
p value n = 10,998
Pregnancy recommendation
Nutritional supplement recommendation 0.198 0.0278 1.220 (1.154–1.287) \0.001** 8,554
No nutritional supplement recommendation Reference 2,444
Maternal age (years)
C34 0.110 0.0296 1.116 (1.053–1.183) \0.001** 3,304
31–33.9 0.090 0.0322 1.094 (1.027–1.165) 0.005 2,302
27.1–30.9 0.095 0.0317 1.010 (1.034–1.167) 0.003 2,360
B27 Reference – – – – 3,032
Maternal education
College/University 0.084 0.0269 1.088 (1.033–1.147) 0.002 8,306
Basic education or less reference . . 2,692
Maternal BMI
Obese –0.066 0.0429 0.936 (0.861–1.019) 0.127 790
Overweight –0.031 0.0291 0.969 (0.916–1.026) 0.292 1,867
Underweight –0.006 0.0442 0.994 (0.911–1.083) 0.889 713
Healthy weight Reference – – – – 7,628
Maternal smoking
Smoked 0.052 0.0348 1.053 (0.984–1.127) 0.134 1,313
Ex-smoker 0.011 0.0241 1.011 (0.965–1.060) 0.651 3,263
Never smoked Reference – – – – 6,422
Figures are estimated relative rates (95 % CI) from a multivariate Poisson regression analyses for the use of folic acid supplements
* p \ 0.05; ** p \ 0.001
Table 8 Factors associated with Vitamin D supplement use
Variables Parameter
estimate
SE Estimated relative
rate
95 % CIs for relative
rate
p value n = 10,998
Pregnancy recommendation
Nutritional supplement recommendation 0.019 0.017 1.019 (0.985–1.054) 0.23 8,827
No nutritional supplement
recommendation
Reference 2,258
Maternal age (years)
C34 -0.001 0.019 0.999 (0.963–1.037) 0.10 3,158
31–33.9 -0.005 0.021 0.995 (0.961–1.041) 1.00 2,229
27.1–30.9 -0.001 0.020 0.999 (0.960–1.039) 0.95 2,270
B27 Reference – – – – 2,929
Maternal education
College/university -0.003 0.017 0.997 (0.965–1.030) 0.86 7,957
Basic education or less Reference – – – – 2,628
Maternal BMI
Obese 0.002 0.027 1.002 (0.950–1.055) 0.95 770
Overweight 0.001 0.019 1.001 (0.965–1.038) 0.96 1,823
Underweight 0.001 0.029 1.001 (0.946–1.060) 0.96 666
Healthy weight Reference – – – – 7,326
Matern Child Health J
123

References
1. Pike, K., Rose-Zerilli, M., Osvald, E., Inskip, H., Godfrey, K.,
Crozier, S., et al. (2011). The relationship between infant lung
function and the risk of wheeze in the pre-school years. Pediatric
Pulmonology, 46, 75–82.
2. Pike, K., Crozier, S., Lucas, J., Inskip, H., Roberts, G., & God-
frey, K. (2010). Patterns of and infant growth are related to atopy
and wheezing disorders at age 3 years. Thorax, 65, 1099–1106.
3. Inskip, H., Crozier, S., Godfrey, K., Borland, S., Cooper, C., &
Robinson, S. (2009). Women’s compliance with nutrition and
lifestyle recommendations before pregnancy: General population
cohort study. British Medical Journal, 338, b481.
4. Gluckman, P., Hanson, M., Cooper, C., & Thornburg, K. (2008).
Effect of in utero and early-life conditions on adult health and
disease. New England Journal of Medicine, 35(1), 61–73.
5. Godfrey, K., & Barker, D. (1995). Maternal nutrition in relation
to fetal and placental growth. European Journal of Obstetrics,
Gynecology, and Reproductive Biology, 61, 15–22.
6. WHO. (2012). Guideline. Daily iron and folic acid supplemen-
tation in pregnant women. Geneva: World Health Organization
(cited February 12, 2014). http://www.who.int/elena/titles/daily_
iron_pregnancy/en/index.html.
7. WHO. (2007). Iodine deficiency in Europe: A continuing public
health problem. WHO and UNICEF (cited February 12, 2014).
http://www.who.int/nutrition/publications/micronutrients/iodine_
deficiency/en/.
8. WHO. (2011). Guideline: Vitamin A supplementation in pregnant
women. Geneva: World Health Organization (cited February 12,
2014). http://www.who.int/nutrition/publications/micronutrients/
guidelines/vas_pregnant/en/.
9. WHO. (2012). Guideline: Vitamin D supplementation in preg-
nant women. Geneva: World Health Organization (cited February
12, 2014). http://www.who.int/elena/titles/vitamind_supp_preg
nancy/en/.
10. WHO. (2013). Guideline: Calcium supplementation in pregnant
women. Geneva: World Health Organization (cited February 12,
2014). http://www.who.int/elena/titles/calcium_pregnancy/en/.
11. The Lithuanian Ministry of Health Order No. 510. (1999). http://
www.sam.lt.
12. Spaczynski, M. (2005). Recommendations of the Polish Society
of Obstetrics and Gynaecology for prenatal care in normal
pregnancy. Ginekologia Polska, 76(7), 517–527.
13. The Food Standards Agency. (2012). Eat well, be well (cited
February 12, 2014). http://www.eatwell.gov.uk/ageandstages/
pregnancy/.
14. The National Health Service. (2012) (cited February 12, 2014).
http://www.nhs.uk/conditions/pregnancy-and-baby/.
15. The Netherlands Pregnancy Recommendations. (2012) (cited
February 12, 2014). http://www.voedingscentrum.nl.
16. Keil, T., McBride, D., Grimshaw, K., Niggemann, B., Xepapa-
daki, P., & Zannikos, K. (2010). The multinational birth cohort of
Europrevall: Background, aims and methods. Allergy, 20(65),
482–490.
17. McBride, D., Keil, T., Grabenhenrich, L., Dubakiene, R., Dras-
utiene, G., & Fiocchi, A. (2012). The Europrevall birth cohort
study on food allergy: Baseline characteristics of 12,000 new-
borns and their families from nine European countries. Pediatric
Allergy and Immunology, 23(3), 230–239.
18. SpanishNationalSocietyofPediatrics. (2012) (citedFebruary12,2014).
http://www.aeped.es/comite-lactancia-materna/recomendaciones.
19. The German Nutrition Society. 2012 (cited February 12, 2014).
http://www.dge.de.
20. Italian Ministry Pregnancy Guidelines. (2010). http://www.
archeo.salute.gov.it/indexEnglish.jsp.
21. Italian Ministry Pregnancy Guidelines. (2007). http://www.salute.
gov.it.
22. Department of Antenatal Care, Directorate of Health and The Ice-
landic food and veterinary Authority. (2012) (cited February 12,
2014). http://www.landlaeknir.is/utgefid-efni/skjal/item18504/.
23. Directorate of Health, Reykjavik, Iceland. (2012) (cited February
12, 2014). http://www.landlaeknir.is/utgefid-efni/skjal/item11446.
24. Scientific Advisory Committee on Nutrition. (2006). Folate and
disease prevention. London: Stationery Office. (cited February
12, 2014). http://www.sacn.gov.uk/pdfs/folate_and_disease_pre
vention_report.pdf.
25. Bundesinstitut fur Risikobewertung (BfR) und Arbeitskreis Jo-
dmangel (AKJ): Jod, Folsaure und Schwangerschaft - Ratschlage
fur Arzte. (2006).
26. Drews, K., Spaczynski, M., Br1zert, J., Breborowicz, G., Cele-
wicz, Z., Czajkowski, K., et al. (2006). Rekomendacje Zarz1du
G3ownego PTG w zakresie opieki przedporodowej w ci1>y o
prawid3owym przebiegu. Ginekol Dypl; T.8 Wyd. Specjalne,
59–66.
27. COT report on Peanut Allergy. Department of Health. (1998)
(cited February 12, 2014). http://www.food.gov.uk.
28. Department of Health. (2009). UK Government advice on peanut
consumption during early life and allergy risk (cited February 12,
2014). http://www.food.gov.uk/safereating/allergyintol/
peanutspregnancy.
29. Bath, S., Walter, A., Taylor, A., Wright, J., & Rayman, M.
(2014). Iodine deficiency in pregnant women living in the South
East of the UK: The influence of diet and nutritional supplements
on iodine status. British Journal of Nutrition, 111(9), 1622–1631.
30. MRC Vitamin Study Research Group. (1991). Prevention of
neural tube defects: Results of the MRC vitamin study. Lancet,
338(131), 137.
31. Knudsen, V., Orozova-Bekkevold, I., Rasmussen, L., Mikkelsen,
T., Michaelsen, K., & Olsen, S. (2004). Low compliance with
recommendations on folic acid use in relation to pregnancy: Is
Table 8 continued
Variables Parameter
estimate
SE Estimated relative
rate
95 % CIs for relative
rate
p value n = 10,998
Maternal smoking
Smoked -0.001 0.022 0.999 (0.956–1.044) 0.98 1,273
Ex-smoker -0.001 0.016 0.999 (0.967–1.027) 0.83 3,095
Never smoked Reference – – – – 6,217
Figures are estimated relative rates (95 % CI) from a multivariate Poisson regression analyses for the use of vitamin D supplements
* p \ 0.05
Matern Child Health J
123

there a need for fortification? Public Health Nutrition, 7(7),
843–850.
32. EFSA. (2009). ESCO report prepared by the EFSA Scientific
Cooperation Working Group on Analysis of risks and benefits of
fortification of food with folic acid. EFSA (European Food Safety
Authority). http://www.efsa.europa.eu/en/supporting/pub/3e.htm.
33. Crozier, S., Robinson, S., Borland, S., Godfrey, K., Cooper, C., &
Inskip, H. (2009). Do women change their health behaviours in
pregnancy? Findings from the Southampton Women’s survey.
Paediatric and Perinatal Epidemiology, 23(5), 446–453.
34. Matthews, F., Yudkin, P., Smith, R., & Neil, A. (2000). Nutrient
intake during pregnancy: The influence of smoking and age.
Journal of Epidemiology and Community Health, 54, 17–23.
35. Erkkola, M. (1998). Folate, vitamin D and iron intakes are low
among pregnant Finnish women. European Journal of Clinical
Nutrition, 52, 742–748.
36. Arkkola, T., Uusitalo, U., Pietikainen, M., Metsala, J., Kronberg-
Kippila, C., Erkkola, M., et al. (2006). Dietary intake and use of
dietary supplements in relation to demographic variables among
pregnant Finnish women. British Journal of Nutrition, 96(5),
913–920.
37. Holick, M. (2007). Vitamin D deficiency. New England Journal
of Medicine, 357, 266–281.
38. Dini, C., & Bianchi, A. (2012). The potential role of vitamin D
for prevention and treatment of tuberculosis and infectious dis-
eases. Annali dell Istituto Superiore di Sanita, 48(3), 319–327.
39. Adami, S., Romagnoli, E., Carnevale, V., Scillitani, A., Giusti,
A., Rossini, M., et al. (2011). Guidelines on prevention and
treatment of vitamin D deficiency. Reumatismo, 63(3), 129–147.
40. Nicolaidou, P., Hatzistamatiou, Z., Papadopoulou, A., Kaleyias,
J., Floropoulou, E., Lagona, E., et al. (2006). Low vitamin D
status in mother–newborn pairs in Greece. Calcified Tissue
International, 78, 337–342.
41. Challa, A., Ntourntoufi, A., Cholevas, V., Bitsori, M., Galanakis,
E., & Andronikou, S. (2005). Breastfeeding and vitamin D status
in Greece during the first 6 months of life. European Journal of
Pediatrics, 164, 724–729.
42. Carnevale, V., Modoni, S., Pileri, M., Di Giorgio, A., Chiodini, I.,
Minisola, S., et al. (2001). Longitudinal evaluation of vitamin D
status in healthy subjects from southern Italy: Seasonal and gender
differences. Osteoporosis International, 12(12), 1026–1030.
43. Yeste, D., & Carrascosa, A. (2003). Nutritional rickets in child-
hood: Analysis of 62 cases. Medical Clinica (Barcelona), 121(1),
23–27.
44. Calvo, M., Whiting, S., & Barton, C. (2005). Symposium: Vita-
min D insufficiency: A significant risk factor in chronic diseases
and potential disease-specific biomarkers of vitamin D suffi-
ciency. The Journal of Nutrition, 135, 310–316.
45. de Lourdes Samaniego-Vasesken, M., Alonso-Aperte, E., &
Varela-Moreiras, G. (2012). Vitamin food fortification today.
Food & Nutrition Research, 56, 5459–5468.
46. Czech-Kowalska, J., Dobrzanska, A., Gruszfeld, D., Zochowska,
A., Malinowska, E., Golkowska, M., et al. (2008). High
prevalence of neonatal vitamin D deficiency—Rationale for
reevaluation of vitamin D supplementation during pregnancy.
Archives of Perinatal Medicine, 14(4), 18–22.
47. Scientific Advisory Committee on Nutrition, Update on Vitamin
D. (2007). Norwich: The Stationery Office (cited February 12,
2014). http://www.sacn.gov.uk/reports_postion_statements/.
48. Hypponen, E., & Boucher, B. (2010). Avoidance of vitamin D
deficiency in pregnancy in United Kingdom: The case for a
unified approach in National policy. British Journal of Nutrition,
104, 309–314.
49. Scientific Advisory Committee on Nutrition & Committee on
Toxicity. (2004). Advice on fish consumption: Benefits and risks.
London, UK: The Stationary Office.
50. EFSA Panel on Dietetic Products, Nutrition and Allergies.
(2010). Scientific opinion on dietary reference values for fats,
including saturated fatty acids, polyunsaturated fatty acids and
cholesterol. EFSA Journal, 8, 1461.
51. Joint FAO/WHO Expert consultation on fats and fatty acids in
human nutrition. (2010). Fats and fatty acids in human nutrition:
Report on expert consultation. Rome, Italy: Food and Agriculture
Organization.
52. Arvaniti, F., Priftis, K., Papadimitriou, A., Papadopoulos, M.,
Roma, E., Kapsokefalou, M., et al. (2011). Adherence to the
Mediterranean type of diet is associated with lower prevalence of
asthma symptoms, among 10–12 years old children: The PAN-
ACEA study. Pediatric Allergy and Immunology, 22, 283–289.
53. McDonald, K., Amir, L., & Davey, M. (2011). Maternal bodies
and medicines: A commentary on risk and decision-making of
pregnant and breastfeeding women and health professionals.
BMC Public Health, 25(11 Suppl 5), 1–8.
54. McMath, B. F., & Prentice-Dunn, S. (2005). Protection motiva-
tion theory and skin cancer risk. The role of individual differ-
ences in responses to persuasive appeals. Journal of Applied
Social Psychology, 35, 621–635.
55. Department of Health. (2000). Folic acid and the prevention of
disease. Report on health and social subjects no. 50. London: The
Stationary Office.
56. McDonald, R., Johnson, Z., Doyle, A., & Sayers, G. (1999).
Determinants of folic acid knowledge and use amongst antenatal
women. Journal of Public Health Medicine, 21, 145–149.
57. McGovern, E., Moss, H., Grewal, G., Taylor, A., Bjornsson, S., &
Pell, J. (1997). Factors affecting the use of folic acid supplements
in pregnant women in Glasgow. British Journal of General
Practice, 47, 635–637.
58. Van der Pal-de Bruin, K., de Walle, H., Jeeninga, W., de Rover,
C., Cornel, M., & de Jong-van den Berg, L. (2000). The Dutch
‘Folic acid campaign’—Have the goals been achieved? Paedi-
atric and Perinatal Epidemiology, 14, 111–117.
59. Chan, A., Pickering, J., Haan, E., Netting, M., Burford, A., &
Johnson, A. (2001). ‘Folate before pregnancy’: The impact on
women and earth professionals of a population-based health
promotion campaign in South Australia. Medical Journal of
Australia, 174, 631–636.
Matern Child Health J
123