Diarrhoeal Disease and its Control* - WHO | World Health ...
29
Bull. Org. mond. Sante 1960 Bull. Wld Hlth Org. 23, 73-101 Diarrhoeal Disease and its Control* NELSON K. ORDWAY, M.D. 1 The diarrhoeal diseases are an important cause of illness throughout the world and a leading cause of death among infants and young children. Unfortunately, the greatest wealth of clinical material is found where the facilities for its study are least available. This article deals with a number of the many problems which therefore arise. The etiology is multiple, and often obscure. The relationship between the diarrh9eal diseases and malnu- trition is as yet.far from being elucidated. Many epidemiological questions require an answer. There is no standard treatment. Prevention, it is universally agreed, depends largely upon improvement in environmental sanitation, especially upon the provision of a safe and adequate supply of piped water, but this apparently simple measure is.fraught with difficulties. Much remains to be done before anything like satisfactory control of this group of diseases can be achieved. " Diarrhoeal disease" is a conglomerate term which covers the disease states in which diarrhoea is a major sign. High prevalence of diarrhoeal disease is associated with inadequacy of personal and public hygienic facilities, and with crowding, poverty, and malnutrition. As a public health problem, concern is chiefly with infants and young children because of the high morbidity and mortality in this age-group. Programmes for the control of diarrhoeal disease must be designed to promote (a) improvement of personal and public hygiene, so as to lower morbidity, and (b) early and effective treatment of affected individuals, so as to lower mortality. CLINICAL CONSIDERATIONS Pathological physiology of diarrhoeal disease Diarrhoea is conceived of as a disturbance of intestinal motility and absorption which, once and by whatever means initiated, may become self- perpetuating as a disease through the production of dehydration and profound cellular disturbances, * Revised version of a paper submitted to the WHO Expert Committee on Diarrhoeal Diseases, November 1958; also to be published, in Spanish, in the Boletin de la Oficina Sanitaria Panamericana. 1 Professor of Pediatrics, Yale University School of Medicine; Pediatrician-in-Chief, University Division, Grace- New Haven Community Hospital, New Haven, Conn., USA. which in turn favour the continuing passage of liquid stools. This state of disturbed intestinal physiology is seen with greatest frequency and in greatest severity in infants and young children, particularly in association with malnutrition. The initiating factor may be considered in the vast majority of instances to be a primary infection of the intestinal tract. Expressed in simple terms, dehydration is a state of depletion of body water and electrolytes, chiefly sodium and chloride. In severe diarrhoeal disease, fever and vomiting are frequent, and these in turn accentuate the loss of body fluids. Since diarrhoea occurs chiefly in hot weather, the losses may be still further aggravated by sweating. The almost inevitable accompanying acidosis is countered by over-breathing, which further contributes to the loss of water. The function of the kidneys, which normally maintain homeostasis of the internal environment through selective excretion of water and electrolytes, soon becomes compromised because of reduction of renal blood flow. As dehydration becomes more severe, consciousness becomes clouded and the patient appears " toxic ". Clinical types of diarrhoeal disease The sign " diarrhoea " varies from the passage of a slightly increased number of stools of greater than normal water content to the almost continuous passage of large quantities of liquid material. The 903 -73
-
Upload
khangminh22 -
Category
Documents
-
view
4 -
download
0
Transcript of Diarrhoeal Disease and its Control* - WHO | World Health ...

Bull. Org. mond. Sante 1960Bull. Wld Hlth Org. 23, 73-101
Diarrhoeal Disease and its Control*NELSON K. ORDWAY, M.D. 1
The diarrhoeal diseases are an important cause of illness throughout the world and aleading cause of death among infants and young children. Unfortunately, the greatestwealth of clinical material is found where the facilities for its study are least available.This article deals with a number ofthe many problems which therefore arise. The etiology ismultiple, and often obscure. The relationship between the diarrh9eal diseases and malnu-trition is as yet.far from being elucidated. Many epidemiological questions require ananswer. There is no standard treatment. Prevention, it is universally agreed, dependslargely upon improvement in environmental sanitation, especially upon the provision of asafe and adequate supply of piped water, but this apparently simple measure is.fraughtwith difficulties. Much remains to be done before anything like satisfactory control of thisgroup of diseases can be achieved.
" Diarrhoeal disease" is a conglomerate termwhich covers the disease states in which diarrhoeais a major sign. High prevalence of diarrhoealdisease is associated with inadequacy of personaland public hygienic facilities, and with crowding,poverty, and malnutrition. As a public healthproblem, concern is chiefly with infants and youngchildren because of the high morbidity and mortalityin this age-group. Programmes for the control ofdiarrhoeal disease must be designed to promote(a) improvement of personal and public hygiene, soas to lower morbidity, and (b) early and effectivetreatment of affected individuals, so as to lowermortality.
CLINICAL CONSIDERATIONS
Pathological physiology of diarrhoeal disease
Diarrhoea is conceived of as a disturbance ofintestinal motility and absorption which, once andby whatever means initiated, may become self-perpetuating as a disease through the productionof dehydration and profound cellular disturbances,
* Revised version of a paper submitted to the WHOExpert Committee on Diarrhoeal Diseases, November 1958;also to be published, in Spanish, in the Boletin de la OficinaSanitaria Panamericana.
1 Professor of Pediatrics, Yale University School ofMedicine; Pediatrician-in-Chief, University Division, Grace-New Haven Community Hospital, New Haven, Conn.,USA.
which in turn favour the continuing passage ofliquid stools. This state of disturbed intestinalphysiology is seen with greatest frequency and ingreatest severity in infants and young children,particularly in association with malnutrition. Theinitiating factor may be considered in the vastmajority of instances to be a primary infection of theintestinal tract.
Expressed in simple terms, dehydration is a stateof depletion of body water and electrolytes, chieflysodium and chloride. In severe diarrhoeal disease,fever and vomiting are frequent, and these in turnaccentuate the loss of body fluids. Since diarrhoeaoccurs chiefly in hot weather, the losses may bestill further aggravated by sweating. The almostinevitable accompanying acidosis is countered byover-breathing, which further contributes to theloss of water. The function of the kidneys, whichnormally maintain homeostasis of the internalenvironment through selective excretion of waterand electrolytes, soon becomes compromised becauseof reduction of renal blood flow. As dehydrationbecomes more severe, consciousness becomes cloudedand the patient appears " toxic ".
Clinical types of diarrhoeal disease
The sign " diarrhoea " varies from the passageof a slightly increased number of stools of greaterthan normal water content to the almost continuouspassage of large quantities of liquid material. The
903 -73
N. K. ORDWAY
associated clinical disease is to a considerable extentconditioned by the associated factors briefly out-lined above, and is further affected by the quantityand composition of the fluids offered to the patient.The clinical picture may thus vary from that of aninfant who is passing a few liquid stools but isotherwise not apparently ill to the child who isseverely dehydrated and even comatose. Thevariety of terms that have been applied to differentclinical forms of diarrhoea has given rise to a nomen-clature based on largely unjustified etiological andpathological preconceptions, confusing enoughwithin any one language but exasperatingly complexwhen similar words in related languages are usedwith divergent meanings. In English the word" dysentery " is used as a descriptive term for severediarrhoea, but implies as well diarrhoeal diseasedue to Shigella. In Latin America, " enterocolitis "commonly refers to the passage of stools containingblood, pus, and mucus; " dispepsia" to diarrhoeawithout inflammatory elements but associated withvomiting and at times with dehydration; and" toxicosis " to a severe clinical condition character-ized by clouding or loss of consciousness and cardio-vascular collapse.The clinical picture may be at best only roughly
related to the type of inciting agent and there arefrequent exceptions. The presence of blood and pusin the stools is classically associated with Shigellainfection but occurs also with acute, severe Sal-monella infection. On the other hand, diarrhoeaassociated with Shigella may be characterized byonly a few watery stools. In a recently reportedstudy of cases of diarrhoea attributed to viruses,Ramos-Alvarez & Sabin (1958) noted the presenceof blood in the stools of seven of 34 patients withalleged virus diarrhoea as well as in those of oneof six patients with Shigella or Salmonella infections.Enteropathogenic Escherichia coli infections, by wayof contrast, are almost uniformly stated not to beassociated with the presence of blood in the stools.An exception is a contradictory report from Chile(Rodriguez et al., 1956) attributing two-thirds of54 cases of " enterocolitis " to infection with E. coli.
CLASSIFICATION OF DIARRHOEAL DISEASE
An international classification of causes of death,necessarily dependent on diagnostic terms used overthe world, is at once beset by difficulties because ofthe variety of these terms. This is particularly truein the case of a disease complex as variable as
diarrhoea, as illustrated in the foregoing section.Difficulties in classification also derive from thefact that the International Classification of Diseasesoffers at the same time etiological, topographical,symptomatic, and age-specific categories. Thus,diarrhoea may appear as a disease due to a specificmicro-organism, a morbid condition of the gastro-intestinal tract, a symptomatic gastro-intestinaldisturbance, or a disorder of early infancy.The confusion in the classification of diarrhoeal
diseases resulting from the multiple diagnosticterms used in Latin American countries has beenpointed out by Verhoestraete & Puffer (1958). Theynote that " toxicosis " is used frequently to signifya specific clinical entity, essentially the result ofsevere and rapid dehydration from diarrhoealdisease. When toxicosis is stated as the cause ofdeath for children under one year, the cause hasbeen assigned in the International Classification ofDiseases (sixth revision) to the group, " ill-defineddiseases peculiar to early infancy "; and for thoseone year and over it has been coded to " ill-definedand unknown causes ". Thus, reported death-rates from diarrhoeal disease have been greatlyinfluenced by the use of the term toxicosis. Whento this confusion are added the facts that diarrhoeahas been extensively attributed to the presence ofintestinal parasites, and that in most parts of theworld it is associated with severe malnutrition,it is clear that deaths due to or significantly asso-ciated with diarrhoeal disease may appear in manycategories in the International Classification.
It must be appreciated that although, as hasbeen pointed out, certain difficulties are encountered,a standard framework like the International Listis necessary for world-wide study. The list issubject to continuous study, and regular revisionsat 10-year intervals permit changes in accordancewith medical progress.The national mortality statistics to be cited
consist of the categories designated gastritis, duo-denitis, enteritis, and colitis (code numbers 543,571 and 572 of the 1948 revision), since these con-stitute the great bulk of cases, are most frequentlyused throughout the world, and are most nearlycomparable to categories 119 and 120, diarrhoeaand enteritis, in the 1938 revision of the InternationalList. While this group does not include diarrhoeaof the newborn (764), diarrhoea of children twoyears of age and over (785.6), or deaths due toSalmonella (042) or Shigella (045), the omissionsdo not seriously affect the conclusions.
74
DIARRHOEAL DISEASE AND ITS CONTROL 75
MAGNITUDE OF THE PROBLEM OF
DIARRHOEAL DISEASE
Incompleteness and inaccuracy of statisticsNational statistics, while showing that the problem
of diarrhoeal disease is world-wide, none the lessprobably minimize the true magnitude of mortalityfrom diarrhoeal disease, for there is gross under-reporting.
Under-reporting of births and deaths is commonin most of the world. As an example, but 60 000births of an estimated 308 000 were registered inMorocco in 1955.1 Reporting of births and deathswas found to be grossly inaccurate by Weir et al.(1952) in Egyptian villages in 194849: " In the firstyear at Sindbis an infant mortality rate of 325.8deaths under 1 year of age per 1000 Jive births anda crude death rate of 32 per 1000 population werereported. This contrasted sharply with infant deathrates ranging from 80 to 161 and crude death ratesfrom 12 to 23 in the other four villages... whichwere remote from the health center." While thereported birth-rate ranged from 44 to 50 births per1000 population, the true birth-rate ranged from56 to 61 per 1000.A more recent detailed study of Egyptian com-
munities in which registration is required by lawrevealed failure to register up to 71 % of births, 77%of deaths, and 91% of infant deaths.2 The degree ofunder-registration increased with the distance fromthe local health centre, at the most but a little overthree kilometres. These Egyptian data, compiled inareas of high diarrhoea morbidity and mortality,show the inevitable concomitants: high birth-rate,high over-all mortality, and high infant mortality.Duly reported deaths may be incorrectly certified
as to cause. A major potential source of inaccuracyis the certification of deaths in many countries ofthe world by non-medical registrars. Of 25 countriesin the Americas supplying statistical information forthe XV Pan American Sanitary Conference (PanAmerican Sanitary Bureau, 1958), 13 reportedmedical certification of fewer than 60% of deathsin 1955 or 1956; the percentages of medical certifica-tion ranged as low as 12.1 % in El Salvador and13.0% in Guatemala.Some of the possible errors in non-medical
certification are illustrated by data from the Institute
Youssef ben Abbes-unpublished information.2 Poulton, E. M. (1957) The status of maternal and child
health in the Eastern Mediterranean and adjacent areas(unpublished working document of the WHO RegionalOffice for the Eastern Mediterranean).
of Nutrition of Central America and Panama(INCAP) showing the discrepancies in a series of222 deaths between causes of death reported by layregistrars and by a trained visitor who interviewedthe dead child's family within two days of demise(Behar et al., 1958). The official statistics showed21 deaths due to disease of the digestive system,58 to intestinal parasites, none to kwashiorkor, and41 to ill-defined and unknown causes. After in-vestigation, 37 deaths were considered due todiseases of the digestive system, none to intestinalparasites, 40 to kwashiorkor, and 17 to ill-definedcauses. Thus, the diarrhoeal diseases and deficiencystates would appear to be much more importantcauses of mortality than is apparent from officialstatistics, with intestinal parasites grossly overstated.Even death certification by physicians does not
ensure accuracy. The reported percentage of infantdeaths in Warsaw attributed to diarrhoea roseabruptly from 19 %Y in 1949 and 1950 to 39%in 1951, following a review by W. Winnicka 3 of therecords of all infant deaths in 1951 (Bielicka et al.,1956).
Mortality
Notwithstanding difficulties in classification, under-reporting, and inaccuracies in certification of causeof death, statistics from all over the world documentthe pre-eminent position of diarrhoea as a killer ofinfants and young children. Indeed, in the light ofthe foregoing discussions, the reported statistics areall the more impressive. Representative data follow.
Latin America. The magnitude of the problem inthe western hemisphere has been clearly presentedby Verhoestraete & Puffer (1958). Diarrhoealdisease was found to be the leading cause of deathin eight of the 17 countries forwarding data for theXIV Pan American Sanitary Conference in 1954, andamong the five principal causes in four other coun-tries of the Americas. Additional evidence regardingthe importance of diarrhoeal disease was presentedin an analysis of the principal causes of death ininfancy (under one year) and in early childhood(one to four years) in ten selected countries. Dia-rrhoea was noted to be the principal or a majorcause of death in most, with rates as high as 150times the comparable rates in the USA.The staggering toll of lives claimed by diarrhoea
in Latin America is vividly illustrated by reportsfrom small communities. In the " house-to-house"
' Personal communication, 1958.
N. K. ORDWAY
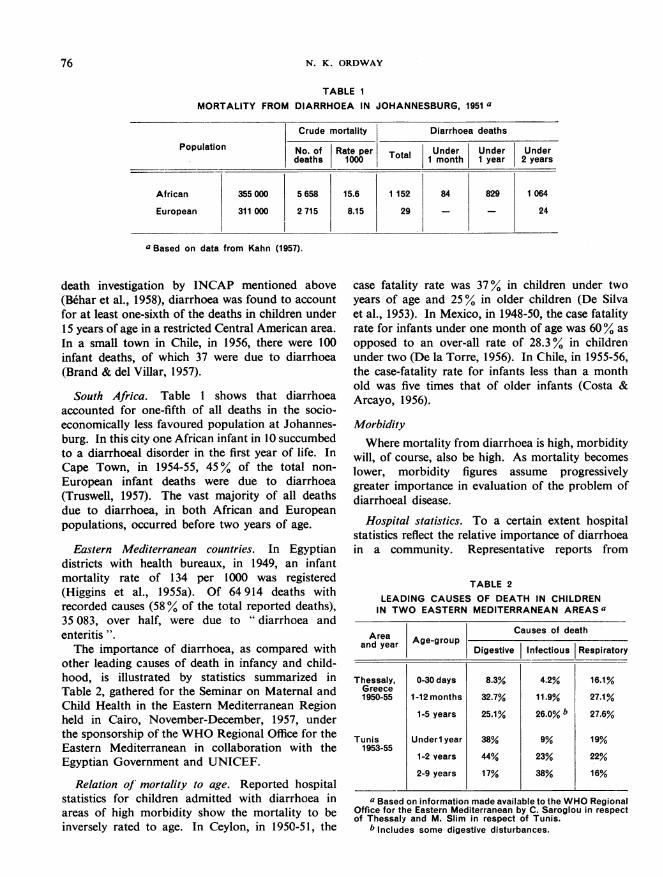
MORTALITY FROMTABLE I
DIARRHOEA IN JOHANNESBURG, 1951 a
Crude mortality Diarrhoea deaths
Population No. of Rate per Total Under Under Underdeaths 1000 1 month 1 year 2 years
African 355 000 5 658 15.6 1 152 84 829 1 064
European 311 000 2 715 8.15 29 - - 24
a Based on data from Kahn(1957).a Based on data from Kahn (1957).
death investigation by INCAP mentioned above(Behar et al., 1958), diarrhoea was found to accountfor at least one-sixth of the deaths in children under15 years of age in a restricted Central American area.
In a small town in Chile, in 1956, there were 100infant deaths, of which 37 were due to diarrhoea(Brand & del Villar, 1957).
South Africa. Table 1 shows that diarrhoeaaccounted for one-fifth of all deaths in the socio-economically less favoured population at Johannes-burg. In this city one African infant in 10 succumbedto a diarrhoeal disorder in the first year of life. InCape Town, in 1954-55, 45% of the total non-
European infant deaths were due to diarrhoea(Truswell, 1957). The vast majority of all deathsdue to diarrhoea, in both African and Europeanpopulations, occurred before two years of age.
Eastern Mediterranean countries. In Egyptiandistricts with health bureaux, in 1949, an infantmortality rate of 134 per 1000 was registered(Higgins et al., 1955a). Of 64 914 deaths withrecorded causes (58 % of the total reported deaths),35 083, over half, were due to "diarrhoea andenteritis ".The importance of diarrhoea, as compared with
other leading causes of death in infancy and child-hood, is illustrated by statistics summarized inTable 2, gathered for the Seminar on Maternal andChild Health in the Eastern Mediterranean Regionheld in Cairo, November-December, 1957, underthe sponsorship of the WHO Regional Office for theEastern Mediterranean in collaboration with theEgyptian Government and UNICEF.
Relation of mortality to age. Reported hospitalstatistics for children admitted with diarrhoea inareas of high morbidity show the mortality to beinversely rated to age. In Ceylon, in 1950-51, the
case fatality rate was 37% in children under twoyears of age and 25% in older children (De Silvaet al., 1953). In Mexico, in 1948-50, the case fatalityrate for infants under one month of age was 60% asopposed to an over-all rate of 28.3% in childrenunder two (De la Torre, 1956). In Chile, in 1955-56,the case-fatality rate for infants less than a monthold was five times that of older infants (Costa &Arcayo, 1956).
MorbidityWhere mortality from diarrhoea is high, morbidity
will, of course, also be high. As mortality becomeslower, morbidity figures assume progressivelygreater importance in evaluation of the problem ofdiarrhoeal disease.
Hospital statistics. To a certain extent hospitalstatistics reflect the relative importance of diarrhoeain a community. Representative reports from
TABLE 2LEADING CAUSES OF DEATH IN CHILDREN
IN TWO EASTERN MEDITERRANEAN AREAS a
Causes of deathard ear Age-group -__________
and year Age-group Digestive Infectious Respiratory
Thessaly, 0-30 days 8.3% 4.2% 16.1%Greece1950-55 1-12 months 32.7% 11.9% 27.1%
1-5 years 25.1% 26.0% b 27.6%
Tunis Underl year 38% 9% 19%1953-55
1-2 vears 44% 23% 22%
2-9 years 17% 38% 16%
a Based on information made available to the WHO RegionalOffice for the Eastern Mediterranean by C. Saroglou in respectof Thessaly and M. Slim in respect of Tunis.
b Includes some digestive disturbances.
76
DIARRHOEAL DISEASE AND ITS CONTROL 77
individual hospitals show almost half the admissionsof children in Colombo, Ceylon, in 1950-51 to havebeen for intestinal parasitism or diarrhoea (De Silvaet al., 1953); in Beirut, in 1954-55, one-third werefor diarrhoea.1 Also in Beirut, of over 60 000 sickchildren seen at polyclinics, 18 %-35% complainedof diarrhoea, the higher percentages during thesummer months. In the municipal hospitals of NewYork City, in 1952, by way of contrast, fewer than2% of children's admissions were for diarrhoea(Fraenkel & Erhardt, 1955).
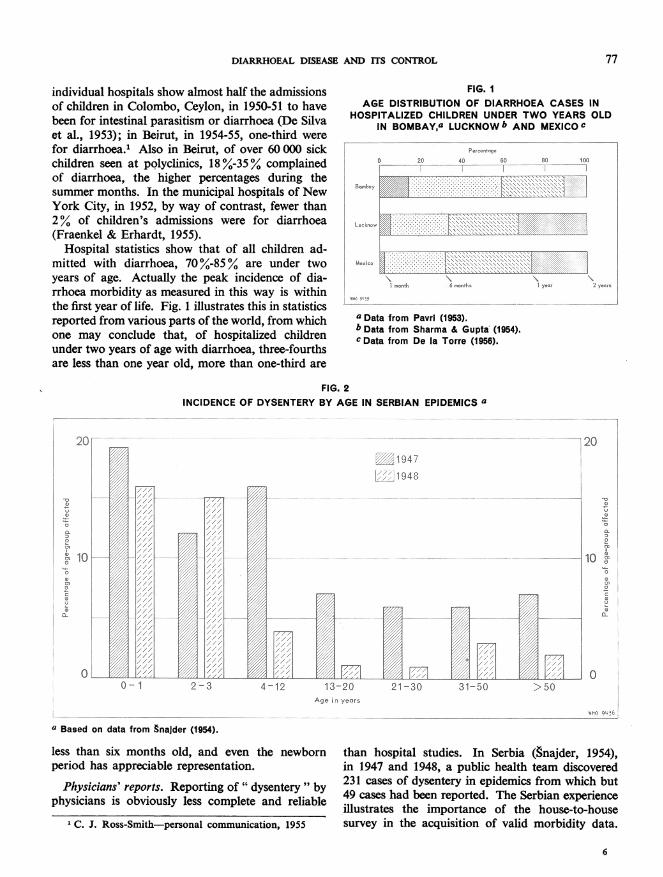
Hospital statistics show that of all children ad-mitted with diarrhoea, 70 %-85% are under twoyears of age. Actually the peak incidence of dia-rrhoea morbidity as measured in this way is withinthe first year of life. Fig. 1 illustrates this in statisticsreported from various parts of the world, from whichone may conclude that, of hospitalized childrenunder two years of age with diarrhoea, three-fourthsare less than one year old, more than one-third are
FIG. IAGE DISTRIBUTION OF DIARRHOEA CASES IN
HOSPITALIZED CHILDREN UNDER TWO YEARS OLDIN BOMBAY,a LUCKNOW b AND MEXICO c
o 3 40so as 100~ ----'- - ,
----------
1 . .) y..
_ .3
UeAq. ...~~~~~~~~~~~~~~~V.:...'.01.%.....
a Data from Pavri (1953).b Data from Sharma & Gupta'(1954).c Data from De la Torre (1956).
FIG. 2INCIDENCE OF DYSENTERY BY AGE IN SERBIAN EPIDEMICS a
0-1 2-0-2. 1-0 13 15 5
a Basd on ata fom Snlder 1954)
*0
10 1
U
/L ~~~~~~~~~0
0-1 2-3 4-12 '13-20 21-30 31-50 >50oAge in years
WHO ,'#,6
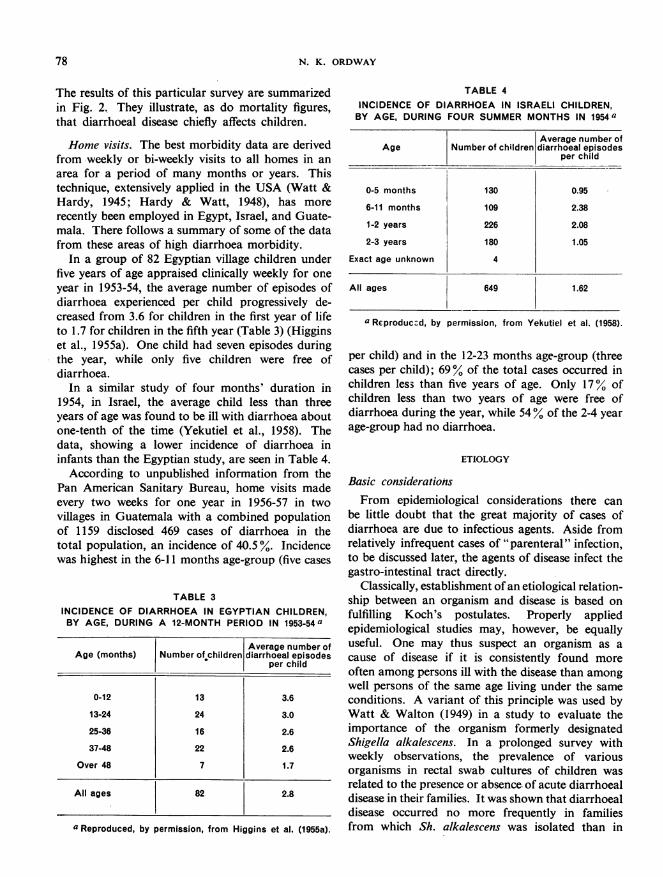
a Based on data from Snajder (1954).
less than six months old, and even the newbornperiod has appreciable representation.
Physicians' reports. Reporting of " dysentery " byphysicians is obviously less complete and reliable
1 C. J. Ross-Smith-personal communication, 1955
than hospital studies. In Serbia (gnajder, 1954),in 1947 and 1948, a public health team discovered231 cases of dysentery in epidemics from which but49 cases had been reported. The Serbian experienceillustrates the importance of the house-to-housesurvey in the acquisition of valid morbidity data.
6
N. K. ORDWAY
The results of this particular survey are summarizedin Fig. 2. They illustrate, as do mortality figures,that diarrhoeal disease chiefly affects children.
Home visits. The best morbidity data are derivedfrom weekly or bi-weekly visits to all homes in anarea for a period of many months or years. Thistechnique, extensively applied in the USA (Watt &Hardy, 1945; Hardy & Watt, 1948), has morerecently been employed in Egypt, Israel, and Guate-mala. There follows a summary of some of the datafrom these areas of high diarrhoea morbidity.
In a group of 82 Egyptian village children underfive years of age appraised clinically weekly for oneyear in 1953-54, the average number of episodes ofdiarrhoea experienced per child progressively de-creased from 3.6 for children in the first year of lifeto 1.7 for children in the fifth year (Table 3) (Higginset al., 1955a). One child had seven episodes duringthe year, while only five children were free ofdiarrhoea.
In a similar study of four months' duration in1954, in Israel, the average child less than threeyears of age was found to be ill with diarrhoea aboutone-tenth of the time (Yekutiel et al., 1958). Thedata, showing a lower incidence of diarrhoea ininfants than the Egyptian study, are seen in Table 4.According to unpublished information from the
Pan American Sanitary Bureau, home visits madeevery two weeks for one year in 1956-57 in twovillages in Guatemala with a combined populationof 1159 disclosed 469 cases of diarrhoea in thetotal population, an incidence of 40.5%. Incidencewas highest in the 6-11 months age-group (five cases
TABLE 3INCIDENCE OF DIARRHOEA IN EGYPTIAN CHILDREN,BY AGE, DURING A 12-MONTH PERIOD IN 1953-54 a
Average number ofAge (months) Number of.children diarrhoeal episodes
per child
0-12 13 3.6
13-24 24 3.0
25-36 16 2.6
37-48 22 2.6
Over 48 7 1.7
All ages 82 2.8
a Reproduced, by permission, from Higgins et al. (1955a).
TABLE 4INCIDENCE OF DIARRHOEA IN ISRAELI CHILDREN,BY AGE, DURING FOUR SUMMER MONTHS IN 1954a
Average number ofAge Number of children diarrhoeal episodes
per child
0-5 months 130 0.95
6-11 months 109 2.38
1-2 years 226 2.08
2-3 years 180 1.05
Exact age unknown 4
All ages 649 1.62
a Reproduc:d, by permission, from Yekutiel et al. (1958).
per child) and in the 12-23 months age-group (threecases per child); 69% of the total cases occurred inchildren less than five years of age. Only 17% ofchildren less than two years of age were free ofdiarrhoea during the year, while 54% of the 2-4 yearage-group had no diarrhoea.
ETIOLOGY
Basic considerationsFrom epidemiological considerations there can
be little doubt that the great majority of cases ofdiarrhoea are due to infectious agents. Aside fromrelatively infrequent cases of "parenteral" infection,to be discussed later, the agents of disease infect thegastro-intestinal tract directly.
Classically, establishment of an etiological relation-ship between an organism and disease is based onfulfilling Koch's postulates. Properly appliedepidemiological studies may, however, be equallyuseful. One may thus suspect an organism as acause of disease if it is consistently found moreoften among persons ill with the disease than amongwell persons of the same age living under the sameconditions. A variant of this principle was used byWatt & Walton (1949) in a study to evaluate theimportance of the organism formerly designatedShigella alkalescens. In a prolonged survey withweekly observations, the prevalence of variousorganisms in rectal swab cultures of children wasrelated to the presence or absence of acute diarrhoealdisease in their families. It was shown that diarrhoealdisease occurred no more frequently in familiesfrom which Sh. alkalescens was isolated than in
78
DIARRHOEAL DISEASE AND ITS CONTROL
families with intestinal flora containing no knownpathogens. By contrast, the attack rates weretwice as great or more in families from whichSh. paradysenteriae Flexner sp., Sh. sonnei, or Sal-monella species were cultured. It was concludedthat Sh. alkalescens could not be incriminated as acause of diarrhoea any more than organismsnormally considered saprophytic.
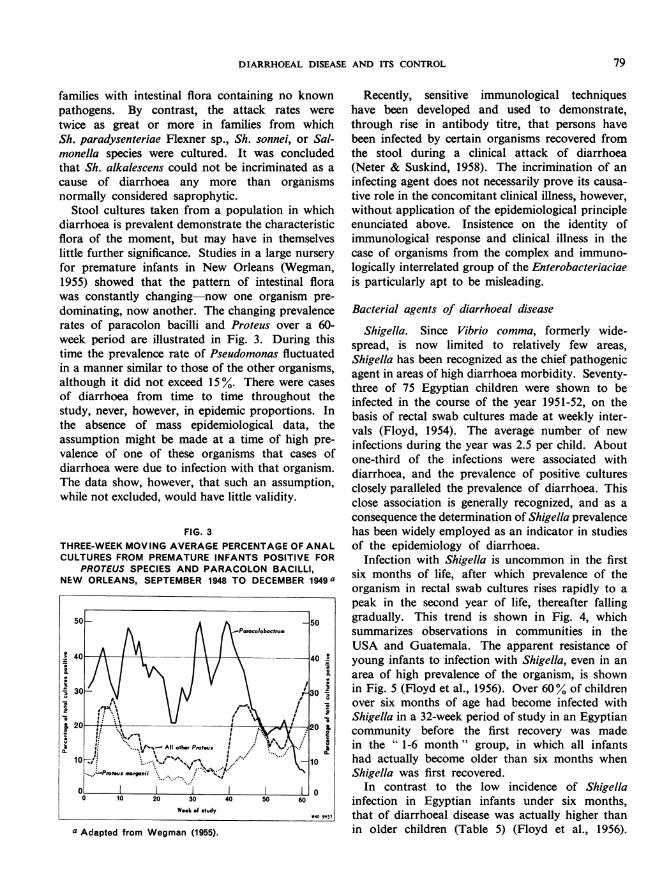
Stool cultures taken from a population in whichdiarrhoea is prevalent demonstrate the characteristicflora of the moment, but may have in themselveslittle further significance. Studies in a large nurseryfor premature infants in New Orleans (Wegman,1955) showed that the pattern of intestinal florawas constantly changing now one organism pre-dominating, now another. The changing prevalencerates of paracolon bacilli and Proteus over a 60-week period are illustrated in Fig. 3. During thistime the prevalence rate of Pseudomonas fluctuatedin a manner similar to those of the other organisms,although it did not exceed 15%. There were casesof diarrhoea from time to time throughout thestudy, never, however, in epidemic proportions. Inthe absence of mass epidemiological data, theassumption might be made at a time of high pre-valence of one of these organisms that cases ofdiarrhoea were due to infection with that organism.The data show, however, that such an assumption,while not excluded, would have little validity.
FIG. 3THREE-WEEK MOVING AVERAGE PERCENTAGE OF ANALCULTURES FROM PREMATURE INFANTS POSITIVE FOR
PROTEUS SPECIES AND PARACOLON BACILLI,NEW ORLEANS, SEPTEMBER 1948 TO DECEMBER 1949 a
40A VI40
1 O
0 10 20 30 40 s 60
Week of study
-o 9*3
a Adapted from Wegman (1955).
Recently, sensitive immunological techniqueshave been developed and used to demonstrate,through rise in antibody titre, that persons havebeen infected by certain organisms recovered fromthe stool during a clinical attack of diarrhoea(Neter & Suskind, 1958). The incrimination of aninfecting agent does not necessarily prove its causa-tive role in the concomitant clinical illness, however,without application of the epidemiological principleenunciated above. Insistence on the identity ofimmunological response and clinical illness in thecase of organisms from the complex and immuno-logically interrelated group of the Enterobacteriaciaeis particularly apt to be misleading.
Bacterial agents of diarrhoeal disease
Shigella. Since Vibrio comma, formerly wide-spread, is now limited to relatively few areas,Shigella has been recognized as the chief pathogenicagent in areas of high diarrhoea morbidity. Seventy-three of 75 Egyptian children were shown to beinfected in the course of the year 1951-52, on thebasis of rectal swab cultures made at weekly inter-vals (Floyd, 1954). The average number of newinfections during the year was 2.5 per child. Aboutone-third of the infections were associated withdiarrhoea, and the prevalence of positive culturesclosely paralleled the prevalence of diarrhoea. Thisclose association is generally recognized, and as aconsequence the determination of Shigella prevalencehas been widely employed as an indicator in studiesof the epidemiology of diarrhoea.
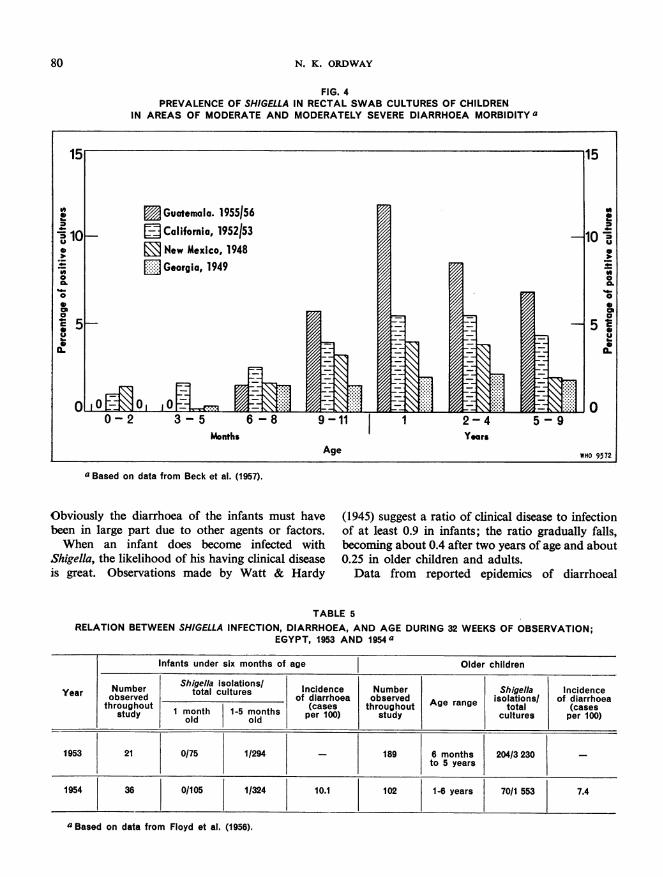
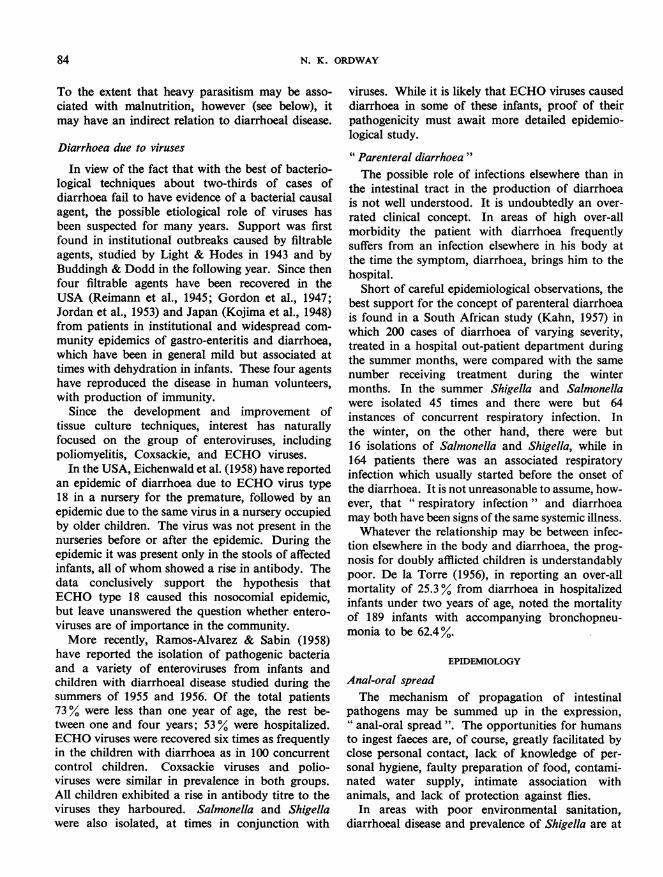
Infection with Shigella is uncommon in the firstsix months of life, after which prevalence of theorganism in rectal swab cultures rises rapidly to apeak in the second year of life, thereafter fallinggradually. This trend is shown in Fig. 4, whichsummarizes observations in communities in theUSA and Guatemala. The apparent resistance ofyoung infants to infection with Shigella, even in anarea of high prevalence of the organism, is shownin Fig. 5 (Floyd et al., 1956). Over 60% of childrenover six months of age had become infected withShigella in a 32-week period of study in an Egyptiancommunity before the first recovery was madein the " 1-6 month " group, in which all infantshad actually become older than six months whenShigella was first recovered.
In contrast to the low incidence of Shigellainfection in Egyptian infants under six months,that of diarrhoeal disease was actually higher thanin older children (Table 5) (Floyd et al., 1956).
79
N. K. ORDWAY
FIG. 4PREVALENCE OF SHIGELLA IN RECTAL SWAB CULTURES OF CHILDREN
IN AREAS OF MODERATE AND MODERATELY SEVERE DIARRHOEA MORBIDITY a
a Based on data from Beck et al. (1957).
Obviously the diarrhoea of the infants must havebeen in large part due to other agents or factors.When an infant does become infected with
Shigella, the likelihood of his having clinical diseaseis great. Observations made by Watt & Hardy
(1945) suggest a ratio of clinical disease to infectionof at least 0.9 in infants; the ratio gradually falls,becoming about 0.4 after two years of age and about0.25 in older children and adults.Data from reported epidemics of diarrhoeal
TABLE 5RELATION BETWEEN SHIGELLA INFECTION, DIARRHOEA, AND AGE DURING 32 WEEKS OF OBSERVATION;
EGYPT, 1953 AND 1954a
Infants under six months of age Older children
Year | Number Shigella soulations/ Incidence Number Shigella Incidenceobserved total_cultures _of diarrhoea observed Age an isolations/ of diarrhoeathroughout (cases throughout A rage total (cases|study
I monthldonth per 100) study cultures per 100)
1953 21 0/75 1/294 _ 189 6 months 204/3 230 -
to 5 years
1954 36 0/105 1/324 10.1 102 1-6 years 70/1 553 7.4
a Based on data from Floyd et al. (1956).
80
DIARRHOEAL DISEASE AND ITS CONTROL
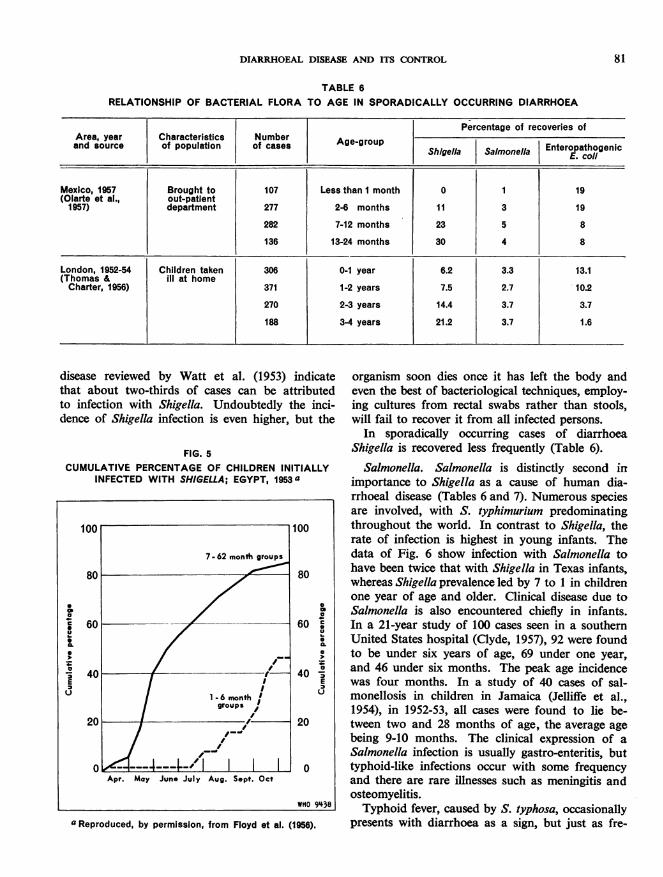
TABLE 6RELATIONSHIP OF BACTERIAL FLORA TO AGE IN SPORADICALLY OCCURRING DIARRHOEA
Percentage of recoveries ofArea, year Characteristics Number Age-roand source | of population | of cases g g -g up | Shigella Salmonella Enteropathogenic
E. coill
Mexico, 1957 Brought to 107 Less than I month 0 1 19(Olarte et al., out-patient1957) department 277 2-6 months 11 3 19
282 7-12 months 23 5 8
136 13-24 months 30 4 8
London, 1952-54 Children taken 306 0-1 year 6.2 3.3 13.1(Thomas & ill at homeCharter, 1956) 371 1-2 years 7.5 2.7 10.2
270 2-3 years 14.4 3.7 3.7
188 3-4 years 21.2 3.7 1.6
disease reviewed by Watt et al. (1953) indicatethat about two-thirds of cases can be attributedto infection with Shigella. Undoubtedly the inci-dence of Shigella infection is even higher, but the
FIG. 5CUMULATIVE PERCENTAGE OF CHILDREN INITIALLY
INFECTED WITH SHIGELLA; EGYPT, 1953a
a
a.
S.
a
60 @0
-fa
40 ,E
20
0
WHO 9438
a Reproduced, by permission, from Floyd et al. (1956).
organism soon dies once it has left the body andeven the best of bacteriological techniques, employ-ing cultures from rectal swabs rather than stools,will fail to recover it from all infected persons.
In sporadically occurring cases of diarrhoeaShigella is recovered less frequently (Table 6).
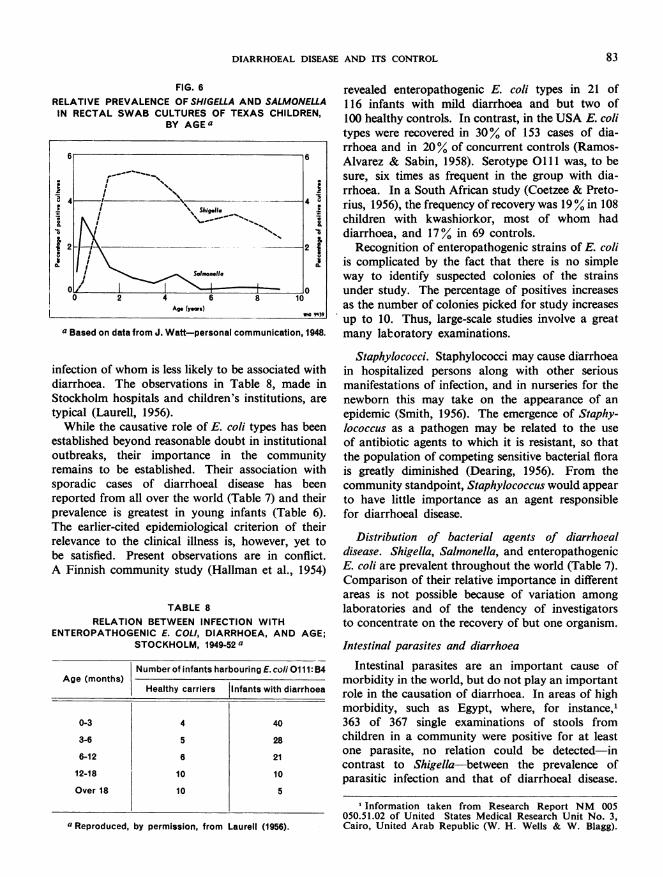
Salmonella. Salmonella is distinctly second inimportance to Shigella as a cause of human dia-rrhoeal disease (Tables 6 and 7). Numerous speciesare involved, with S. typhimurium predominatingthroughout the world. In contrast to Shigella, therate of infection is highest in young infants. Thedata of Fig. 6 show infection with Salmonella tohave been twice that with Shigella in Texas infants,whereas Shigella prevalence led by 7 to 1 in childrenone year of age and older. Clinical disease due toSalmonella is also encountered chiefly in infants.In a 21-year study of 100 cases seen in a southernUnited States hospital (Clyde, 1957), 92 were foundto be under six years of age, 69 under one year,and 46 under six months. The peak age incidencewas four months. In a study of 40 cases of sal-monellosis in children in Jamaica (Jelliffe et al.,1954), in 1952-53, all cases were found to lie be-tween two and 28 months of age, the average agebeing 9-10 months. The clinical expression of aSalmonella infection is usually gastro-enteritis, buttyphoid-like infections occur with some frequencyand there are rare illnesses such as meningitis andosteomyelitis.Typhoid fever, caused by S. typhosa, occasionally
presents with diarrhoea as a sign, but just as fre-
81
N. K. ORDWAY
quently with constipation. It is a disease of lowermortality than diarrhoeal disease and affects chieflyolder children. Of 205 cases of typhoid fever inchildren up to 12 years of age (Taneja & Ghai,1957), there were but 18 under three years of age,the youngest of whom was nine months old; abouttwo-thirds of the children were over six years ofage.
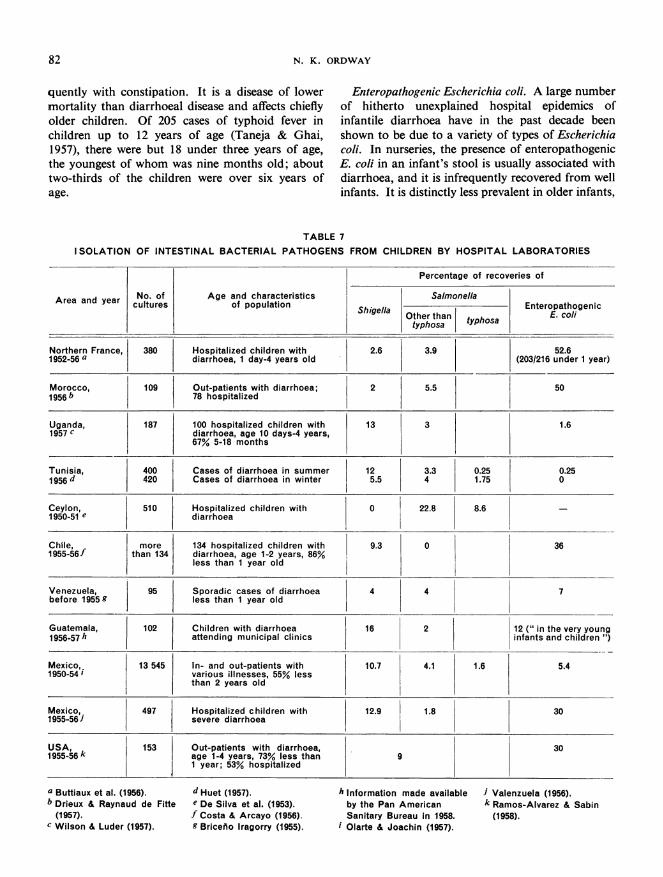
Enteropathogenic Escherichia coli. A large numberof hitherto unexplained hospital epidemics ofinfantile diarrhoea have in the past decade beenshown to be due to a variety of types of Escherichiacoli. In nurseries, the presence of enteropathogenicE. coli in an infant's stool is usually associated withdiarrhoea, and it is infrequently recovered from wellinfants. It is distinctly less prevalent in older infants,
TABLE 7I SOLATION OF INTESTINAL BACTERIAL PATHOGENS FROM CHILDREN BY HOSPITAL LABORATORIES
Percentage of recoveries of
Area and year No. of Age and characteristics Salmonellayearcultures | _ Shigel osaEnteropathogenicArea andcultures of population Shigella ~~~Other than typhosa E. co/i
typhosa
Northern France, 380 Hospitalized children with 2.6 3.9 52.61952-56 a diarrhoea, 1 day-4 years old (203/216 under 1 year)
Morocco, 109 Out-patients with diarrhoea; 2 5.5 501956b 78 hospitalized
Uganda, 187 100 hospitalized children with 13 3 1.61957 c diarrhoea, age 10 days-4 years,
67% 5-18 months
Tunisia, 400 Cases of diarrhoea in summer 12 3.3 0.25 0.251956 d 420 Cases of diarrhoea in winter 5.5 4 1.75 0
Ceylon, 510 Hospitalized children with 0 22.8 8.6 -
1950-51 e diarrhoea
Chile, more 134 hospitalized children with 9.3 0 361955-56f than 134 diarrhoea, age 1-2 years, 86%
less than 1 year old
Venezuela, 95 Sporadic cases of diarrhoea 4 4 7before 1955k less than 1 year old
Guatemala, 102 Children with diarrhoea 16 2 12 (" in the very young1956-57*h 1 attending municipal clinics infants and children )
Mexico, 13 545 In- and out-patients with 10.7 4.1 1.6 5.41950-54 i various illnesses, 55% less
than 2 years old
Mexico,. 497 Hospitalized children with 12.9 1.8 301955-56J severe diarrhoea
USA, 153 Out-patients with diarrhoea, 301955-56k age 1-4 years, 73% less than 9
1 year; 53% hospitalized
a Buttiaux et al. (1956).b Drieux & Raynaud de Fifte
(1957).c Wilson & Luder (1957).
d Huet (1957).e De Silva et al. (1953).f Costa & Arcayo (1956).g Briceno Iragorry (1955).
h Information made availableby the Pan AmericanSanitary Bureau in 1958.
i Olarte & Joachin (1957).
i Valenzuela (1956).k Ramos-Alvarez & Sabin
(1958).
82
DIARRHOEAL DISEASE AND ITS CONTROL 83
FIG. 6RELATIVE PREVALENCE OF SHIGELLA AND SALMONELLAIN RECTAL SWAB CULTURES OF TEXAS CHILDREN,
BY AGE a
6 6
4 4
2 2
ifcinowhmileslkltobasoiate wth
typical(Laurell, 1956). onell
o I
WhilethecausatierolewsWHOE.clitpe9asbe
astablshedonbeyfomnd resoaft-eroaommun icaittion,al48
inections tof who istabsslishelyTohei association withdiarrhoea.asee observationsliniTable hasmadein
prevalenc h.italsan young infants areTypicalearlier-citelld epidemi al crti ote
Whlevne tohecausaicalrolnessE cois typeesr,a beentbestablisfied. Preyond raonbledoubtare institutioct.
outbreaks,Finnisheircommprtaesnthetcomm ya 19
inections tof who istalesshielyTohei associatedn withsoaicaeofdiarrhoea.lTedoservtosiable 8,hadeein
Stockholme hospiretalstand chidrn'sinfnstitTions, are
TABLE 8RELATION BETWEEN INFECTION WITH
ENTEROPATHOGENIC E. COLI, DIARRHOEA, AND AGE;STOCKHOLM, 1949-52 a
Number of infants harbouring E. coli 0111: B4Age (months)
Healthy carriers Infants with diarrhoea
0-3 4 40
3-6 5 28
6-12 6 21
12-18 10 10
Over 18 10 5
a Reproduced, by permission, from Laurell (1956).
revealed enteropathogenic E. coli types in 21 of116 infants with mild diarrhoea and but two of100 healthy controls. In contrast, in the USA E. colitypes were recovered in 30% of 153 cases of dia-rrhoea and in 20% of concurrent controls (Ramos-Alvarez & Sabin, 1958). Serotype 0111 was, to besure, six times as frequent in the group with dia-rrhoea. In a South African study (Coetzee & Preto-rius, 1956), the frequency of recovery was 19% in 108children with kwashiorkor, most of whom haddiarrhoea, and 17% in 69 controls.
Recognition of enteropathogenic strains of E. coliis complicated by the fact that there is no simpleway to identify suspected colonies of the strainsunder study. The percentage of positives increasesas the number of colonies picked for study increasesup to 10. Thus, large-scale studies involve a greatmany laboratory examinations.
Staphylococci. Staphylococci may cause diarrhoeain hospitalized persons along with other seriousmanifestations of infection, and in nurseries for thenewborn this may take on the appearance of anepidemic (Smith, 1956). The emergence of Staphy-lococcus as a pathogen may be related to the useof antibiotic agents to which it is resistant, so thatthe population of competing sensitive bacterial florais greatly diminished (Dearing, 1956). From thecommunity standpoint, Staphylococcus would appearto have little importance as an agent responsiblefor diarrhoeal disease.
Distribution of bacterial agents of diarrhoealdisease. Shigella, Salmonella, and enteropathogenicE. coli are prevalent throughout the world (Table 7).Comparison of their relative importance in differentareas is not possible because of variation amonglaboratories and of the tendency of investigatorsto concentrate on the recovery of but one organism.
Intestinal parasites and diarrhoea
Intestinal parasites are an important cause ofmorbidity in the world, but do not play an importantrole in the causation of diarrhoea. In areas of highmorbidity, such as Egypt, where, for instance,l'363 of 367 single examinations of stools fromchildren in a community were positive for at leastone parasite, no relation could be detected-incontrast to Shigella-between the prevalence ofparasitic infection and that of diarrhoeal disease.
1 Information taken from Research Report NM 005050.51.02 of United States Medical Research Unit No. 3,Cairo, United Arab Republic (W. H. Wells & W. Blagg).
N. K. ORDWAY
To the extent that heavy parasitism may be asso-ciated with malnutrition, however (see below), itmay have an indirect relation to diarrhoeal disease.
Diarrhoea due to viruses
In view of the fact that with the best of bacterio-logical techniques about two-thirds of cases ofdiarrhoea fail to have evidence of a bacterial causalagent, the possible etiological role of viruses hasbeen suspected for many years. Support was firstfound in institutional outbreaks caused by filtrableagents, studied by Light & Hodes in 1943 and byBuddingh & Dodd in the following year. Since thenfour filtrable agents have been recovered in theUSA (Reimann et al., 1945; Gordon et al., 1947;Jordan et al., 1953) and Japan (Kojima et al., 1948)from patients in institutional and widespread com-munity epidemics of gastro-enteritis and diarrhoea,which have been in general mild but associated attimes with dehydration in infants. These four agentshave reproduced the disease in human volunteers,with production of immunity.
Since the development and improvement oftissue culture techniques, interest has naturallyfocused on the group of enteroviruses, includingpoliomyelitis, Coxsackie, and ECHO viruses.
In the USA, Eichenwald et al. (1958) have reportedan epidemic of diarrhoea due to ECHO virus type18 in a nursery for the premature, followed by anepidemic due to the same virus in a nursery occupiedby older children. The virus was not present in thenurseries before or after the epidemic. During theepidemic it was present only in the stools of affectedinfants, all of whom showed a rise in antibody. Thedata conclusively support the hypothesis thatECHO type 18 caused this nosocomial epidemic,but leave unanswered the question whether entero-viruses are of importance in the community.More recently, Ramos-Alvarez & Sabin (1958)
have reported the isolation of pathogenic bacteriaand a variety of enteroviruses from infants andchildren with diarrhoeal disease studied during thesummers of 1955 and 1956. Of the total patients73% were less than one year of age, the rest be-tween one and four years; 53% were hospitalized.ECHO viruses were recovered six times as frequentlyin the children with diarrhoea as in 100 concurrentcontrol children. Coxsackie viruses and polio-viruses were similar in prevalence in both groups.All children exhibited a rise in antibody titre to theviruses they harboured. Salmonella and Shigellawere also isolated, at times in conjunction with
viruses. While it is likely that ECHO viruses causeddiarrhoea in some of these infants, proof of theirpathogenicity must await more detailed epidemio-logical study.
"Parenteral diarrhoea"The possible role of infections elsewhere than in
the intestinal tract in the production of diarrhoeais not well understood. It is undoubtedly an over-rated clinical concept. In areas of high over-allmorbidity the patient with diarrhoea frequentlysuffers from an infection elsewhere in his body atthe time the symptom, diarrhoea, brings him to thehospital.
Short of careful epidemiological observations, thebest support for the concept of parenteral diarrhoeais found in a South African study (Kahn, 1957) inwhich 200 cases of diarrhoea of varying severity,treated in a hospital out-patient department duringthe summer months, were compared with the samenumber receiving treatment during the wintermonths. In the summer Shigella and Salmonellawere isolated 45 times and there were but 64instances of concurrent respiratory infection. Inthe winter, on the other hand, there were but16 isolations of Salmonella and Shigella, while in164 patients there was an associated respiratoryinfection which usually started before the onset ofthe diarrhoea. It is not unreasonable to assume, how-ever, that "respiratory infection" and diarrhoeamay both have been signs of the same systemic illness.Whatever the relationship may be between infec-
tion elsewhere in the body and diarrhoea, the prog-nosis for doubly afflicted children is understandablypoor. De la Torre (1956), in reporting an over-allmortality of 25.3% from diarrhoea in hospitalizedinfants under two years of age, noted the mortalityof 189 infants with accompanying bronchopneu-monia to be 62.4%.
EPIDEMIOLOGY
Anal-oral spreadThe mechanism of propagation of intestinal
pathogens may be summed up in the expression," anal-oral spread ". The opportunities for humansto ingest faeces are, of course, greatly facilitated byclose personal contact, lack of knowledge of per-sonal hygiene, faulty preparation of food, contami-nated water supply, intimate association withanimals, and lack of protection against flies.
In areas with poor environmental sanitation,diarrhoeal disease and prevalence of Shigella are at
84
DIARRHOEAL DISEASE AND ITS CONTROL
a peak during the summer months. Under goodenvironmental sanitary conditions, the summer-time increase in prevalence of diarrhoeal diseasedisappears. Indeed, in a long-term United Statesfamily epidemiological study the peak incidence ofgastro-intestinal upsets has been observed to be inNovember (Dingle et al., 1953). In England a
slight winter-time increase in the frequency ofshigellosis has been attributed in part to the longersurvival of Shigella in public places during coldweather, for instance, on toilet seats (Hutchinson,1956).The role of hand-to-mouth contact becomes
relatively more crucial as community sanitarymeasures improve. In Southampton, England,Shigella was cultured from toilet seats and pupils'hands in school epidemics (Hutchinson, 1956).Studies indicated the probable mechanisms of con-tamination of toilet seats, demonstrated the lackof protection to the hands afforded by toilet tissue,and called attention to the frequency with whichchildren would suck their fingers, even before theirdutiful hand-washing following use of the toilet.A Scottish report of an institutional epidemic dueto drug-susceptible Shigella notes that failure wasmost common in infants under one year of age." Frequent reinfection from faeces, contaminatedhands or linen, is considered to have been an impor-tant factor in failure of cure in this age group"(Johnson & Landsman, 1957).
Intimate personal contact enhances the spread ofenteric infection despite adequate community healthprotection. Watt et al. (1953) noticed in theirCalifornia study a distinctly higher incidence ofShigella infections in infants with infected siblingsthan in only children. In a United States familyepidemiological study (Hodges et al., 1956), gastro-intestinal symptoms were more than twice as
frequent in the late pre-school and early school years
as in infancy and adulthood, presumably reflectingthe effects of closer and more frequent exposure toother children.
Size of infecting dose
In addition to qualitative environmental factors,the importance of quantity of the infecting dose oforganisms deserves particular emphasis. The appli-cation of this concept is well illustrated in the con-trast between the violent reaction of adults, arelatively insusceptible population, to large doses ofSalmonella in episodes of poisoning by contaminatedfoods, and the lack of diarrhoeal disease observed
in a highly susceptible population, prematureinfants in a nursery in New Orleans into whichSalmonella tennessee was introduced by six pre-mature infants transferred from another hospital(Watt et al., 1958). In the ensuing many weeks morethan 30 subsequent isolations were made from otherinfants, nursery personnel, and facilities, such asweighing scales and even a freshly prepared bassinet.During this entire period no infected infant haddiarrhoea. The numbers of organisms were neverlarge and most of the recoveries would not havebeen made unless special cultural techniques hadbeen used. Presumably, thanks to constant pre-cautions on the part of nursing personnel-notablyscrupulous attention to careful hand-washing-theinfants were infected with numbers of organisms sosmall that clinical disease did not appear.
Animal reservoirs of enteric pathogensA word is in order about the special epidemiolo-
gical characteristics of Salmonella. In contrast toShigella, this is basically an animal pathogen and,with the exception of S. typhosa, infection of thehuman organism may be considered accidentallyrelated to our association with animals and animalfood products. It thus tends to be prevalent in foodhandlers and in persons living in association withdomestic animals. It has been recovered from allanimal species cultured, including a pet armadillo(Watt & DeCapito, 1950) and a pet tortoise (Thomas1957); the last is known to have initiated outbreaksof diarrhoeal disease in human contacts.Once introduced into the human population,
Salmonella is spread by the same mechanisms asShigella, as illustrated by numerous reportedhospital nursery outbreaks of diarrhoea due toSalmonella.Though enteropathogenic E. coli types are widely
prevalent in cattle, an animal reservoir appears notto be of epidemiological importance for thispathogen.
Comment on relation between pathogenic agents anddiarrhoeal diseaseShigella is presumably the agent chiefly responsible
for diarrhoeal disease in children and adults in areasof moderate to severe diarrhoea morbidity, and is,under these conditions, a sensitive indicator both ofpersonal and community sanitation and of the pre-valence of diarrhoeal disease. Information con-cerning the agents responsible for diarrhoea ininfants, particularly in the first six months of life, isincomplete. Presumably diarrhoeal episodes in this
85
86 N. K. ORDWAY
age-group are of infectious origin and come aboutthrough the same epidemiological means as Shigellainfections, since the frequency of diarrhoea in younginfants parallels the incidence of diarrhoea in thecommunity. The infecting agents most likely to becausative, on the basis of present information, areE. coli types and viruses.
RELATION OF MALNUTRITION TO
DIARRHOEAL DISEASE
The world's literature emphasizes the almostuniversal association of malnutrition, frequentlysevere, with diarrhoeal disease. Typical is a SouthAfrican analysis of 100 consecutive cases of diarr-hoea: 12 of 17 undernourished children over fivemonths of age had had previous attacks of diarrhoea,as opposed to but nine of 47 adequately nourishedpatients in the same age-group (Truswell, 1957). Thereported experience in communities in Egypt(Higgins et al., 1955a), however, where diarrhoea isrampant and malnutrition is not common, shows thatmalnutrition is not an obligatory concomitant ofdiarrhoea and suggests the desirability of attemptingto define their interrelationships in an effort to viewthem as separate problems. Answers may be soughtto the following questions: 1. Does malnutritionpredispose to gastro-intestinal infection? 2. Isdiarrhoea a sign of severe malnutrition? 3. Doesdiarrhoea lead to malnutrition?Does mnalnutrition predispose to gastro-intestinal
infection ?On theoretical grounds, malnutrition should
indeed greatly lower the resistance of the host toinfection (Chandler, 1957). This is most easilyillustrated in consideration of deficiency of protein,which is necessary for tissue repair, antibodyproduction, and leucocyte production. Since theparasite is in competition with the host for food, lackof protein may react adversely on the parasite aswell. While the parasite may suffer more than thehost when a specific dietary essential, such as avitamin, is lacking, the net balance in malnutritionis usually distinctly to the disadvantage of the host.Well nourished animals tend to have relatively fewectoparasites. Malnourished dogs have been ob-served to deliver hookworms promptly on beinggiven an adequate diet. Chandler (1953b) comments:" One may go so far as to say that severe chronicintestinal nematode infections are unusual, if notimpossible, in an otherwise normal host on anadequate diet."
Despite plausible theoretical preconceptions, how-ever, there is as yet no evidence to support the thesisthat enteric infection occurs with increased frequencyin malnourished persons in areas in which both mal-nutrition and diarrhoeal disease are prevalent. Onthe contrary, in patients with the most extreme formof protein malnutrition-kwashiorkor-enteric in-fection with bacteria and parasites has been en-countered no more frequently than in better nourishedsubjects (Scrimshaw et al., 1956). Observations byCoetzee & Pretorius (1956) in a South Africanhospital are typical: a search was made for entericbacterial pathogens in 108 out-patients withkwashiorkor aged six months to four years, most ofwhom had diarrhoea of short duration, and 69 con-current controls, without gastro-intestinal com-plaints, in the same age-group. The percentage ofpathogens isolated was 28 in the kwashiorkorgroup and 21 in the controls.A sociologist's observation 1 of the common
ingestion of dirt from the household floor by childrenin Guatemala leads one to wonder what the relativefrequency ofpica, a potential mode of infection, maybe in malnourished, as compared with well nourished,children.
Is diarrhoea a sign of severe malnutrition ?
The data reported by Coetzee & Pretorius, citedabove, can logically lead one to conclude, with theauthors, that bacterial pathogens did not play animportant causative role in the diarrhoea of theirpatients with kwashiorkor. Indeed, it is generallyaccepted-without adequate epidemiological evi-dence, however-that recurrent and chronic dia-rrhoea is a sign of this syndrome. Diarrhoea hasbeen observed by Jelliffe, Bras & Stuart (1954) tooccur with comparable frequency in kwashiorkor(protein malnutrition) and marasmus (generalcaloric under-nutrition).
Since morbidity and mortality from diarrhoeaare at their peak at an earlier age than that atwhich kwashiorkor occurs with greatest frequency,conclusions based on observations of the older groupdo not necessarily apply to younger subjects, mostof whom present less striking evidences of mal-nutrition. Interesting light has been shed on thisand other problems by the recently published reportof a 15-months' clinical, bacteriological, and
1 Unpublished report (1957) by J. D. Freedman on socialfactors in the etiology of infantile pluricarencial syndrome(kwashiorkor) in Guatemala.
DIARRHOEAL DISEASE AND ITS CONTROL 87
epidemiological study of children in immigrants'camps in Israel (Yekutiel, 1959).
If, indeed, the gastro-intestinal tract of younginfants is vulnerable to a variety of adverse influenceselsewhere in the body, it is not unreasonable toassume that diarrhoea might be a sign of malnutri-tion at this age. Malnutrition might at least aggra-vate the severity of diarrhoea due to a variety ofprimary etiologies, whether or not it produces itdirectly.
Diarrhoea as a sign of severe vitamin A deficiencyin children 2 1/2 to 9 years of age has been observedby Ramalingaswami (1948). The diarrhoea prompt-ly ceased on administration of vitamin A withoutother therapy.
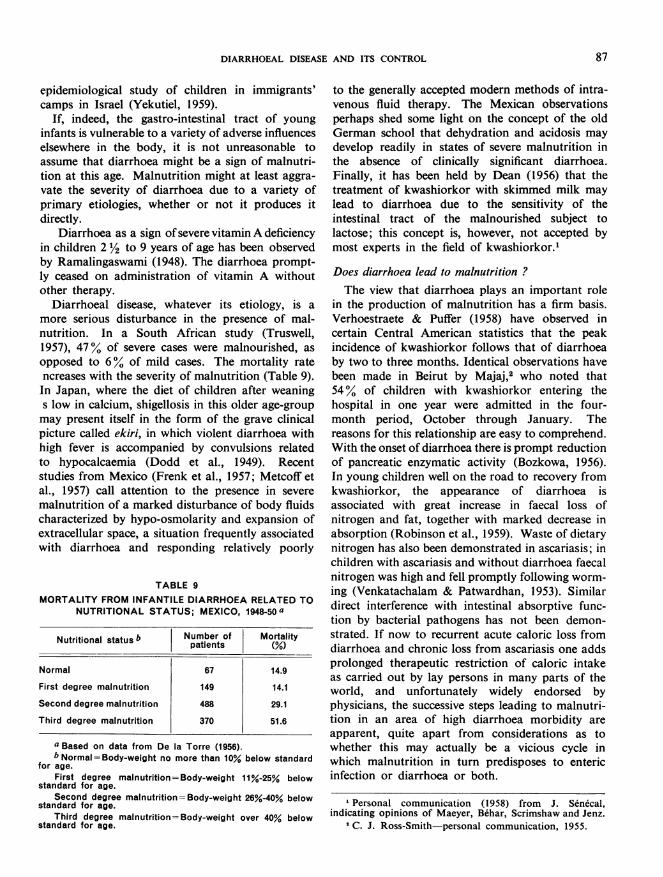
Diarrhoeal disease, whatever its etiology, is amore serious disturbance in the presence of mal-nutrition. In a South African study (Truswell,1957), 47% of severe cases were malnourished, asopposed to 6% of mild cases. The mortality ratencreases with the severity of malnutrition (Table 9).In Japan, where the diet of children after weanings low in calcium, shigellosis in this older age-groupmay present itself in the form of the grave clinicalpicture called ekiri, in which violent diarrhoea withhigh fever is accompanied by convulsions relatedto hypocalcaemia (Dodd et al., 1949). Recentstudies from Mexico (Frenk et al., 1957; Metcoff etal., 1957) call attention to the presence in severemalnutrition of a marked disturbance of body fluidscharacterized by hypo-osmolarity and expansion ofextracellular space, a situation frequently associatedwith diarrhoea and responding relatively poorly
TABLE 9MORTALITY FROM INFANTILE DIARRHOEA RELATED TO
NUTRITIONAL STATUS; MEXICO, 1948-50 a
Nutritional status b Number of Mortalitypatients (%
Normal 67 14.9
First degree malnutrition 149 14.1
Second degree malnutrition 488 29.1
Third degree malnutrition 370 51.6
a Based on data from De la Torre (1956).b Normal=Body-weight no more than 10% below standard
for age.First degree malnutrition=Body-weight 11%-25% below
standard for age.Second degree malnutrition=Body-weight 26%-40% below
standard for age.Third degree malnutrition=Body-weight over 40% below
standard for age.
to the generally accepted modern methods of intra-venous fluid therapy. The Mexican observationsperhaps shed some light on the concept of the oldGerman school that dehydration and acidosis maydevelop readily in states of severe malnutrition inthe absence of clinically significant diarrhoea.Finally, it has been held by Dean (1956) that thetreatment of kwashiorkor with skimmed milk maylead to diarrhoea due to the sensitivity of theintestinal tract of the malnourished subject tolactose; this concept is, however, not accepted bymost experts in the field of kwashiorkor.
Does diarrhoea lead to malnutrition ?The view that diarrhoea plays an important role
in the production of malnutrition has a firm basis.Verhoestraete & Puffer (1958) have observed incertain Central American statistics that the peakincidence of kwashiorkor follows that of diarrhoeaby two to three months. Identical observations havebeen made in Beirut by Majaj,2 who noted that54% of children with kwashiorkor entering thehospital in one year were admitted in the four-month period, October through January. Thereasons for this relationship are easy to comprehend.With the onset of diarrhoea there is prompt reductionof pancreatic enzymatic activity (Bozkowa, 1956).In young children well on the road to recovery fromkwashiorkor, the appearance of diarrhoea isassociated with great increase in faecal loss ofnitrogen and fat, together with marked decrease inabsorption (Robinson et al., 1959). Waste of dietarynitrogen has also been demonstrated in ascariasis; inchildren with ascariasis and without diarrhoea faecalnitrogen was high and fell promptly following worm-ing (Venkatachalam & Patwardhan, 1953). Similardirect interference with intestinal absorptive func-tion by bacterial pathogens has not been demon-strated. If now to recurrent acute caloric loss fromdiarrhoea and chronic loss from ascariasis one addsprolonged therapeutic restriction of caloric intakeas carried out by lay persons in many parts of theworld, and unfortunately widely endorsed byphysicians, the successive steps leading to malnutri-tion in an area of high diarrhoea morbidity areapparent, quite apart from considerations as towhether this may actually be a vicious cycle inwhich malnutrition in turn predisposes to entericinfection or diarrhoea or both.
1 Personal communication (1958) from J. Sen6cal,indicating opinions of Maeyer, Behar, Scrimshaw and Jenz.
2 C. J. Ross-Smith-personal communication, 1955.
N. K. ORDWAY
RELATION OF DIARRHOEAL DISEASE TOSOCIO-ECONOMIC STATUS
Three basic factors are emphasized in virtuallyall discussions of diarrhoeal disease: age (infantsand young children), malnutrition, and low socio-economic status. The last two are obviously inextri-cably interrelated. The last, already implicated inthe discussion of epidemiology, will now be brieflyconsidered with emphasis on sociological factors.
Mortality and morbidity statisticsNowhere is the influence of local contrasts in
socio-economic status more strikingly illustratedthan in South Africa. In Johannesburg, in 1951, theinfant mortality rate from diarrhoea was 35 timeshigher in the African than in the European popula-tion (Table 1) (Kahn, 1957). In 1954-55, diarrhoeacaused 45% of 1069 non-European infant deaths inCape Town as opposed to but 8% of 72 deaths inEuropean infants (Truswell, 1957).
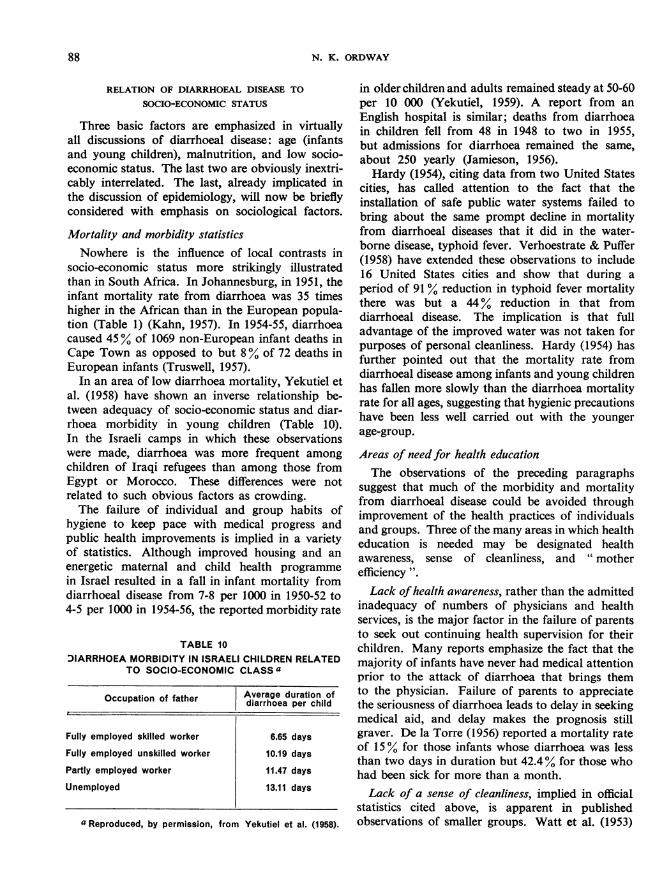
In an area of low diarrhoea mortality, Yekutiel etal. (1958) have shown an inverse relationship be-tween adequacy of socio-economic status and diar-rhoea morbidity in young children (Table 10).In the Israeli camps in which these observationswere made, diarrhoea was more frequent amongchildren of Iraqi refugees than among those fromEgypt or Morocco. These differences were notrelated to such obvious factors as crowding.The failure of individual and group habits of
hygiene to keep pace with medical progress andpublic health improvements is implied in a varietyof statistics. Although improved housing and anenergetic maternal and child health programmein Israel resulted in a fall in infant mortality fromdiarrhoeal disease from 7-8 per 1000 in 1950-52 to4-5 per 1000 in 1954-56, the reported morbidity rate
TABLE 10DIARRHOEA MORBIDITY IN ISRAELI CHILDREN RELATED
TO SOCIO-ECONOMIC CLASS a
Occupation of father Average duration ofOccupationof father diarrhoea per child
Fully employed skilled worker 6.65 days
Fully employed unskilled worker 10.19 days
Partly employed worker 11.47 days
Unemployed 13.11 days
a Reproduced, by permission, from Yekutiel et al. (1958).
in older children and adults remained steady at 50-60per 10 000 (Yekutiel, 1959). A report from anEnglish hospital is similar; deaths from diarrhoeain children fell from 48 in 1948 to two in 1955,but admissions for diarrhoea remained the same,about 250 yearly (Jamieson, 1956).Hardy (1954), citing data from two United States
cities, has called attention to the fact that theinstallation of safe public water systems failed tobring about the same prompt decline in mortalityfrom diarrhoeal diseases that it did in the water-borne disease, typhoid fever. Verhoestrate & Puffer(1958) have extended these observations to include16 United States cities and show that during aperiod of 91 % reduction in typhoid fever mortalitythere was but a 44% reduction in that fromdiarrhoeal disease. The implication is that fulladvantage of the improved water was not taken forpurposes of personal cleanliness. Hardy (1954) hasfurther pointed out that the mortality rate fromdiarrhoeal disease among infants and young childrenhas fallen more slowly than the diarrhoea mortalityrate for all ages, suggesting that hygienic precautionshave been less well carried out with the youngerage-group.
Areas of need for health educationThe observations of the preceding paragraphs
suggest that much of the morbidity and mortalityfrom diarrhoeal disease could be avoided throughimprovement of the health practices of individualsand groups. Three of the many areas in which healtheducation is needed may be designated healthawareness, sense of cleanliness, and " motherefficiency ".Lack ofhealth awareness, rather than the admitted
inadequacy of numbers of physicians and healthservices, is the major factor in the failure of parentsto seek out continuing health supervision for theirchildren. Many reports emphasize the fact that themajority of infants have never had medical attentionprior to the attack of diarrhoea that brings themto the physician. Failure of parents to appreciatethe seriousness of diarrhoea leads to delay in seekingmedical aid, and delay makes the prognosis stillgraver. De la Torre (1956) reported a mortality rateof 15% for those infants whose diarrhoea was lessthan two days in duration but 42.4% for those whohad been sick for more than a month.Lack of a sense of cleanliness, implied in official
statistics cited above, is apparent in publishedobservations of smaller groups. Watt et al. (1953)
88
DIARRHOEAL DISEASE AND ITS CONTROL 89
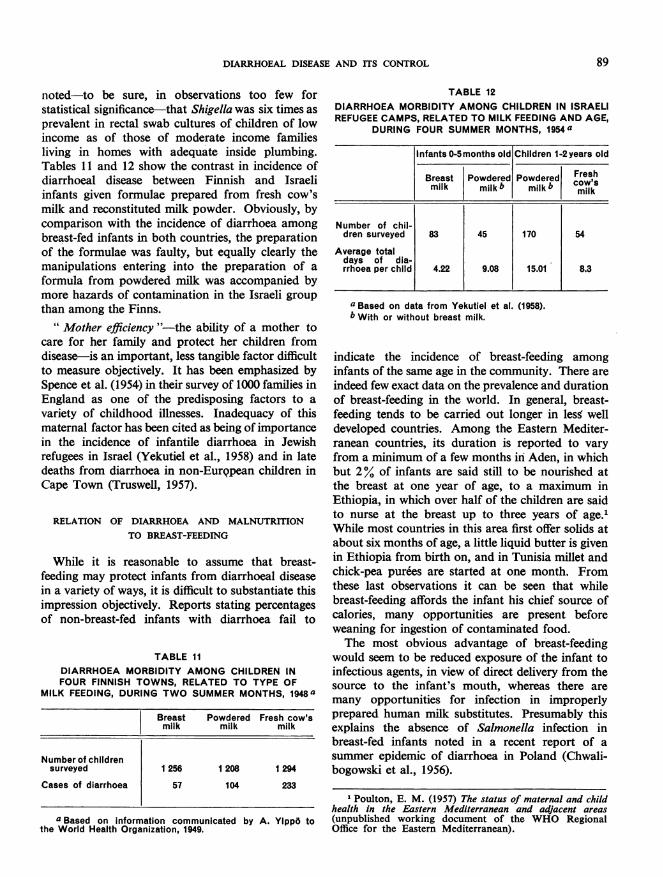
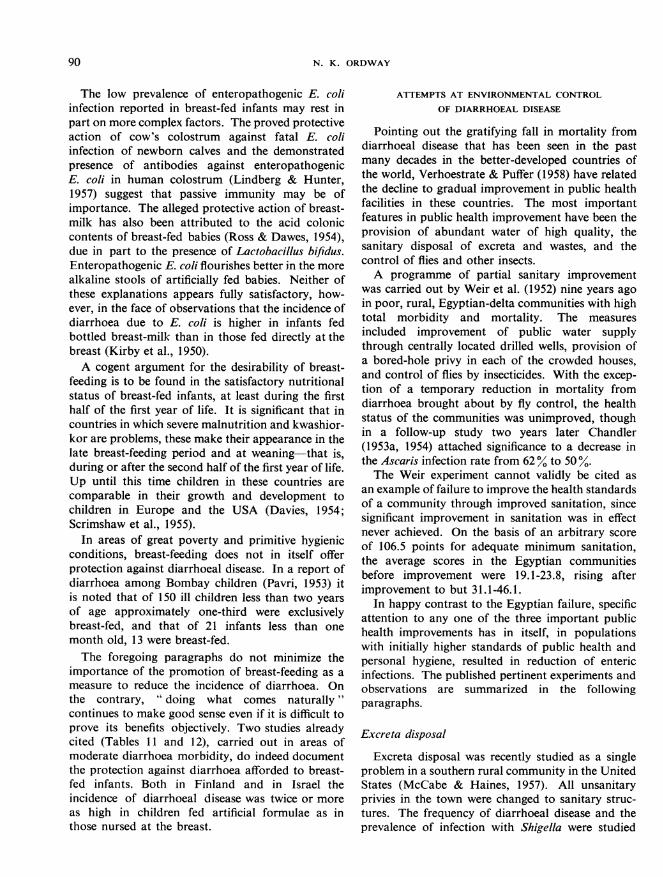
noted-to be sure, in observations too few forstatistical significance-that Shigella was six times asprevalent in rectal swab cultures of children of lowincome as of those of moderate income familiesliving in homes with adequate inside plumbing.Tables 11 and 12 show the contrast in incidence ofdiarrhoeal disease between Finnish and Israeliinfants given formulae prepared from fresh cow'smilk and reconstituted milk powder. Obviously, bycomparison with the incidence of diarrhoea amongbreast-fed infants in both countries, the preparationof the formulae was faulty, but equally clearly themanipulations entering into the preparation of aformula from powdered milk was accompanied bymore hazards of contamination in the Israeli groupthan among the Finns.
" Mother efficiency "-the ability of a mother tocare for her family and protect her children fromdisease-is an important, less tangible factor difficultto measure objectively. It has been emphasized bySpence et al. (1954) in their survey of 1000 families inEngland as one of the predisposing factors to avariety of childhood illnesses. Inadequacy of thismaternal factor has been cited as being of importancein the incidence of infantile diarrhoea in Jewishrefugees in Israel (Yekutiel et al., 1958) and in latedeaths from diarrhoea in non-Eur9pean children inCape Town (Truswell, 1957).
RELATION OF DIARRHOEA AND MALNUTRITIONTO BREAST-FEEDING
While it is reasonable to assume that breast-feeding may protect infants from diarrhoeal diseasein a variety of ways, it is difficult to substantiate thisimpression objectively. Reports stating percentagesof non-breast-fed infants with diarrhoea fail to
TABLE 11DIARRHOEA MORBIDITY AMONG CHILDREN INFOUR FINNISH TOWNS, RELATED TO TYPE OF
MILK FEEDING, DURING TWO SUMMER MONTHS, 1948a
Breast Powdered Fresh cow'smilk milk milk
Number of childrensurveyed 1 256 1208 1 294
Cases of diarrhoea 57 104 233
aBased on information communicated by A. YIppo tothe World Health Organization, 1949.
TABLE 12DIARRHOEA MORBIDITY AMONG CHILDREN IN ISRAELIREFUGEE CAMPS, RELATED TO MILK FEEDING AND AGE,
DURING FOUR SUMMER MONTHS, 1954a
Infants 0-5 months old Children 1-2 years old
Breast Powdered Powdered Freshmilk milk b milk b COW'smilk
Number of chil-dren surveyed 83 45 170 54
Average totaldays of dia-rrhoea per child 4.22 9.08 15.01 8.3
a Based on data from Yekutiel et al. (1958).b With or without breast milk.
indicate the incidence of breast-feeding amonginfants of the same age in the community. There areindeed few exact data on the prevalence and durationof breast-feeding in the world. In general, breast-feeding tends to be carried out longer in less welldeveloped countries. Among the Eastern Mediter-ranean countries, its duration is reported to varyfrom a minimum of a few months in Aden, in whichbut 2% of infants are said still to be nourished atthe breast at one year of age, to a maximum inEthiopia, in which over half of the children are saidto nurse at the breast up to three years of age.'While most countries in this area first offer solids atabout six months of age, a little liquid butter is givenin Ethiopia from birth on, and in Tunisia millet andchick-pea purees are started at one month. Fromthese last observations it can be seen that whilebreast-feeding affords the infant his chief source ofcalories, many opportunities are present beforeweaning for ingestion of contaminated food.The most obvious advantage of breast-feeding
would seem to be reduced exposure of the infant toinfectious agents, in view of direct delivery from thesource to the infant's mouth, whereas there aremany opportunities for infection in improperlyprepared human milk substitutes. Presumably thisexplains the absence of Salmonella infection inbreast-fed infants noted in a recent report of asummer epidemic of diarrhoea in Poland (Chwali-bogowski et al., 1956).
1 Poulton, E. M. (1957) The status of maternal and childhealth in the Eastern Mediterranean and adjacent areas(unpublished working document of the WHO RegionalOffice for the Eastern Mediterranean).
N. K. ORDWAY
The low prevalence of enteropathogenic E. coliinfection reported in breast-fed infants may rest inpart on more complex factors. The proved protectiveaction of cow's colostrum against fatal E. coliinfection of newborn calves and the demonstratedpresence of antibodies against enteropathogenicE. coli in human colostrum (Lindberg & Hunter,1957) suggest that passive immunity may be ofimportance. The alleged protective action of breast-milk has also been attributed to the acid coloniccontents of breast-fed babies (Ross & Dawes, 1954),due in part to the presence of Lactobacillus bifidus.Enteropathogenic E. coli flourishes better in the morealkaline stools of artificially fed babies. Neither ofthese explanations appears fully satisfactory, how-ever, in the face of observations that the incidence ofdiarrhoea due to E. coli is higher in infants fedbottled breast-milk than in those fed directly at thebreast (Kirby et al., 1950).A cogent argument for the desirability of breast-
feeding is to be found in the satisfactory nutritionalstatus of breast-fed infants, at least during the firsthalf of the first year of life. It is significant that incountries in which severe malnutrition and kwashior-kor are problems, these make their appearance in thelate breast-feeding period and at weaning-that is,during or after the second half of the first year of life.Up until this time children in these countries arecomparable in their growth and development tochildren in Europe and the USA (Davies, 1954;Scrimshaw et al., 1955).
In areas of great poverty and primitive hygienicconditions, breast-feeding does not in itself offerprotection against diarrhoeal disease. In a report ofdiarrhoea among Bombay children (Pavri, 1953) itis noted that of 150 ill children less than two yearsof age approximately one-third were exclusivelybreast-fed, and that of 21 infants less than onemonth old, 13 were breast-fed.The foregoing paragraphs do not minimize the
importance of the promotion of breast-feeding as ameasure to reduce the incidence of diarrhoea. Onthe contrary, " doing what comes naturally "continues to make good sense even if it is difficult toprove its benefits objectively. Two studies alreadycited (Tables 11 and 12), carried out in areas ofmoderate diarrhoea morbidity, do indeed documentthe protection against diarrhoea afforded to breast-fed infants. Both in Finland and in Israel theincidence of diarrhoeal disease was twice or moreas high in children fed artificial formulae as inthose nursed at the breast.
ATTEMPTS AT ENVIRONMENTAL CONTROL
OF DIARRHOEAL DISEASE
Pointing out the gratifying fall in mortality fromdiarrhoeal disease that has been seen in the pastmany decades in the better-developed countries ofthe world, Verhoestrate & Puffer (1958) have relatedthe decline to gradual improvement in public healthfacilities in these countries. The most importantfeatures in public health improvement have been theprovision of abundant water of high quality, thesanitary disposal of excreta and wastes, and thecontrol of flies and other insects.A programme of partial sanitary improvement
was carried out by Weir et al. (1952) nine years agoin poor, rural, Egyptian-delta communities with hightotal morbidity and mortality. The measuresincluded improvement of public water supplythrough centrally located drilled wells, provision ofa bored-hole privy in each of the crowded houses,and control of flies by insecticides. With the excep-tion of a temporary reduction in mortality fromdiarrhoea brought about by fly control, the healthstatus of the communities was unimproved, thoughin a follow-up study two years later Chandler(1953a, 1954) attached significance to a decrease inthe Ascaris infection rate from 62% to 50 %.The Weir experiment cannot validly be cited as
an example of failure to improve the health standardsof a community through improved sanitation, sincesignificant improvement in sanitation was in effectnever achieved. On the basis of an arbitrary scoreof 106.5 points for adequate minimum sanitation,the average scores in the Egyptian communitiesbefore improvement were 19.1-23.8, rising afterimprovement to but 31.1-46.1.
In happy contrast to the Egyptian failure, specificattention to any one of the three important publichealth improvements has in itself, in populationswith initially higher standards of public health andpersonal hygiene, resulted in reduction of entericinfections. The published pertinent experiments andobservations are summarized in the followingparagraphs.
Excreta disposal
Excreta disposal was recently studied as a singleproblem in a southern rural community in the UnitedStates (McCabe & Haines, 1957). All unsanitaryprivies in the town were changed to sanitary struc-tures. The frequency of diarrhoeal disease and theprevalence of infection with Shigella were studied
90

DIARRHOEAL DISEASE AND ITS CONTROL
by monthly clinical historical appraisal and rectalswab cultures from over 300 children under tenyears of age, in this community and in neighbouringcontrol communities, before and for eighteen monthsafter the installation of the sanitary privies. Follow-ing the installations, the Shigella infection rate fellfrom 4.7% to 2.8%, while in the same period therate rose from 3.3% to 5.7% in the unimprovedtowns. The improved town also experienced a50% reduction in morbidity from diarrhoea. Thereduction in infection is believed to have beenbrought about through the removal of faeces fromcontact with flies. Although the total fly populationof the village was unchanged, the number of fliesbreeding in privies or visiting privies was greatlyreduced.
Fly control
The importance of flies as carriers of entericorganisms was demonstrated by Floyd & Cook(1953) in Egypt. These workers trapped flies invarious areas and cultured 156 " pools " of 25 flieseach. All but one pool were positive for Escherichiacoli species. Eighteen pools were positive forShigella or Salmonella in a ratio of two to one, whileS. typhosa was found four times. Further studyshowed that a fly may carry Shigella up to 12 daysand Salmonella up to 28 days. The organisms weredemonstrated to multiply while in the fly's intestinaltract. Eggs deposited in infected faeces producedinfected adult flies.
Fly control by insecticides has been significantlybut only temporarily effective in reducing the incid-ence of diarrhoeal disease. In carefully controlledstudies in southern United States communities withmoderate (Lindsay et al., 1953) and moderatelyhigh (Watt & Lindsay, 1948) diarrhoea morbidityand high fly populations, the incidence of bothShigella infection and diarrhoea fell during flycontrol; Salmonella infections were found not to besignificantly affected. Fly control was noted aboveto have been the only one of several partial sanitaryimprovements in Egyptian-delta communities thatresulted in lowered mortality from diarrhoealdisease (Weir et al., 1952).
Fly control by larvicides and insecticides is at bestbut a temporary measure, however, since resistancedevelops within a few months (Weir et al., 1952;Lindsay et al., 1953). The only permanently effectivefly control is sanitary control of breeding-places.Screening is, of course, of local benefit.
Abundance and availability of water
In recognizing the value of water of high qualityfor internal consumption one must emphasize aswell the importance of adequate quantity for externalpurposes: for instance, loosening of infected materialfrom hands, bodies, clothing, utensils, and, theenvironment with the aid of soap and removal ofmost of it through copious rinsing, coupled withsanitary removal of excreta and wastes throughwater-borne sewage disposal systems. Pathogenicorganisms can be so reduced in number throughhand-washing as not to produce infection when theyare carried, directly or indirectly, to the mouth; or,if infection does result, it may be so mild as not tobe expressed as clinical disease.
Frequent, thorough hand-washing, which, asseveral cited observations have implied, is a healthhabit carried out more or less effectively dependingon the individual's training and experience in thefamily or cultural group, requires water which is notonly in adequate supply but readily available. Theimportance of this was demonstrated in two separatestudies carried out by Watt and collaborators inmigrant workers' camps in California (Watt et al.,1953; Hollister et al., 1955). Prevalence of Shigellainfection and frequency of diarrhoeal disease weredirectly related to the distance of the source of waterfrom the house. A similar study by Stewart et al.(1955) carried out later in a southern United Statescommunity in homes without inside plumbingshowed that the prevalence of Shigella in rectal swabcultures of families was 42% higher when thesource of water was relatively far from the housethan when it was close by. Of particular interest isthe observation that proximity of the water was ofgreater importance than its quality. Prevalence ofinfection was approximately the same whethermunicipal water was piped to the area or whetherthe source was an open dug well subject to pollution.
MEDICAL PROPHYLAXIS OF DIARRHOEAL DISEASE
There is no safe or effective immunological orchemoprophylactic method of protecting the indi-vidual exposed to enteric pathogens. A controlledexperiment among Egyptian children in an area ofhigh diarrhoea morbidity showed that Shigellaflexneri 3 vaccine was ineffective in preventinginfection due to this or any other Shigella species(Higgins et al., 1955b). As part of the same ex-periment prophylaxis of shigellosis with sulfadiazine,
91
92N. K. ORDWAY
streptomycin, and oxytetracycline was attempted andfound to be neither practical nor effective in thedosages used (Higgins et al., 1955c). Attempts toprevent diarrhoea and other infections in nurseriesfor premature and full-term newborn infants haveproved uniformly unsatisfactory and complicatedby the appearance of a variety of clinical infections,including diarrhoea, due to the emergence ofresistant organisms such as fungi or Staphylococci,or the appearance of diarrhoea as a sign of intoler-ance of the antibiotic agent used.
TREATMENT OF DIARRHOEAL DISEASE
Treatment of the patient with diarrhoeal diseasefalls into three categories, listed in order of im-portance:
1. Fluid therapy:(a) restoration of deficits of body water andelectrolytes;(b) provision of fluids to offset normal and ab-normal fluid losses, together with provision ofat least minimal caloric requirements.
2. In so far as practical and practicable. pre-
vention or reduction of further abnormal losses offluid from the body (symptomatic treatment).
3. Destruction of the infecting agent.
Fluid therapy
Proper management with water and electrolytes isby all odds the most important feature in the treat-ment of the patient with diarrhoea. The markedreduction of mortality from diarrhoeal diseaseuniversally achieved in hospital practice during thepast twenty years has been almost entirely due tothe application of principles derived from betterunderstanding of the disturbed physiology ofdehydration. In short, modem therapy amounts tothe rapid restoration of most of the child's deficit ofwater and sodium chloride, followed by furtherprovision of more modest amounts of water and salt,together with the addition of potassium and at leastsufficient carbohydrate to minimize the breakdownof body protein during the necessary period ofdiminished caloric intake. While the principles are
simple enough, their practical application may beunsatisfactory owing to failure to recognize the sever-
ity of dehydration in small infants, failure to carry outtherapy with requisite vigour initially, technicaldifficulties in the parenteral administration of fluids
to small infants, and perhaps above all the over-whelming clinical pressures imposed on inadequatenumbers of inadequately equipped professionalpersonnel in areas of high diarrhoea morbidity.While it is generally accepted that rapid intra-
venous administration of fluids is the most effectivetherapy for severely dehydrated infants, for reasonscited above resort has been successfully made inmany rehydration centres to either of two simplertechniques: hypodermoclysis and slow intragastricdrip through a nasogastric tube. The success ofthese forms of therapy is intimately related to theeffectiveness of patient follow-up and will be dis-cussed below in a section devoted to rehydrationcentres.
Quite obviously the simplest means of admi-nistering fluids is by mouth. Repair of dehydrationby the oral route is ordinarily not practicable in theseverely dehydrated baby, because of vomiting,anorexia, fatigue, or drowsiness on the part of theinfant, or fear on the part of the physician ofaggravating the severity of the diarrhoea. Preventionof dehydration, on the other hand-that is, main-tenance of hydration-by adequate administrationof fluids by mouth, is accepted by all physicians asbeing of great value. In practice the baby's milkfeedings are temporarily suspended and electrolytesolutions are given by mouth in their place. Whilethis sort of treatment seems eminently sensible, nocritical objective data are available to indicate thatdehydration appears in a significantly lower per-centage of these infants than in babies not somanaged. An ever-present danger lies in the factthat fluids useful and desirable for successful oralhydration are inadequate nutritionally. When useof these fluids is unnecessarily prolonged, mal-nutrition may be produced or aggravated, as notedin an earlier section. A further danger is that ofimproper dilution of powders or liquid concentrates,resulting in administration to the patient of asolution too high in electrolyte content. Thewidespread promotion of oral hydration as a publichealth measure would require greatly expandedmaternal and child health activities, including largenumbers of trained home visitors.A cogent medical criticism of almost all re-
commended regimens for rehydration-parenteraland oral alike-is that the electrolyte content of thespecial fluids prescribed is excessively high. This isprobably due to two factors: (a) adherence torecommendations of a few years ago, which in thelight of recent knowledge are not satisfactory; and
92
DIARRHOEAL DISEASE AND ITS CONTROL
(b), probably more importantly, widespread con-fusion based on failure of physicians to distinguishbetween requirements for repair of dehydration andfor maintenance of the patient during the phase ofrecovery, whether or not accompanied by thepassage of liquid stools. The electrolyte content offluids for the latter purpose should be considerablylower than for the initial repair.A satisfactory maintenance solution will contain
approximately equivalent amounts of sodium andpotassium, will have an over-all electrolyte con-centration of about 100 milliosmoles per litre, thatis, about one-third the osmotic pressure of normalbody fluids, and will contain carbohydrate inapproximately 5% concentration. The simplestpossible solution, prepared from the chloride saltsof sodium and potassium, is the following, to whichattention was called some years ago (Hardy, 1954):
Sodium chloride .......Potassium chloride ......Syrup of raspberry .....
Water to make .......
1.5 g
2.0 g60 ml
1000 ml
This solution may be offered to infants ad libitumin place of milk mixtures. Dextrose may be sub-stituted for the syrup in amounts of 35 (isotonic) to100 g, in order to make a preparation suitable forparenteral use (Ordway, 1956). Some authoritiesprefer to replace up to half the chloride with phos-phate and bicarbonate; the bicarbonate commonlytakes the form of lactate.
Prevention offurther fluid loss
The first energetic intravenous efforts to combatdehydration are usually attended by rapid reductionin the number and volume of stools. From thispoint on the continued suppression of diarrhoea asa sign is best effected by the further provision offluids to the body by some parenteral route. Con-tinued interdiction of oral feeding, however, notonly imposes the technical difficulties already citedbut is inevitably accompanied by the provision ofinadequate calories. For a short period this is of nogreat import to the patient but one hesitates tocontinue to starve the malnourished subject for morethan a day or two. While some authorities are quiteapprehensive over the dangers from temporaryunder-provision of adequate nutritional needs andare overly zealous for early re-establishment of fulloral feeding, others are so concerned over thecharacter of the stools that they are willing toneglect the infant's nutritional needs until watery
stools have completely disappeared. Each point ofview is logical, and fortunately in the vast majorityof instances treatment can be so designed as partiallyto satisfy both.
Aside from suppression of oral intake no treat-ment has been shown to be effective in reducing lossof water and electrolytes from the body. Variouspharmaceutical agents, such as opium derivatives,are notably ineffectual. Great interest has attachedto a variety of preparations and special formulaecontaining pectin, hemicellulose, and other hygro-scopic agents. Essentially these absorb the waterand electrolytes excreted into the bowel, where toall intents and purposes they are already outside thebody. It remains to be shown that these agents arein any way effective in reducing loss of water fromthe body, even though they may alter the appearanceof the stool and perhaps result in retention of stoolsin the colon for more prolonged periods so that theycannot be seen. The most generally used prepara-tion of this sort in Europe is carrot puree, whichappears to be well tolerated, provides neededcalories and electrolytes, and leaves physician andmother alike with the feeling that something bene-ficial is being done for the baby. Certain proprietaryinfant feeding preparations appear to be equallysatisfactory.The use of acid milks such as yoghourt, lactic
acid milk, vinegar milk, and " acidophilus " milk hasbeen recommended in the belief that throughalteration of bacterial flora in the intestinal tractthey will favourably alter the clinical course ofdiarrhoea. It is likely that the greater virtue of thesepreparations lies in their resistance to bacterial con-tamination in situations of inadequate refrigeration.
Antimicrobial therapy
Shigella. While Shigella may be eliminated fromthe gastro-intestinal tract by a variety of drugs, thepatient's clinical illness is not likely to be greatlyaltered, although its duration may be a day or twoless than in the untreated subject. In view of themagnitude of the disturbance of gastro-entericphysiology and metabolic balance in diarrhoealdisease, the lack of striking clinical response tochemotherapy is not surprising. Since the chiefeffectiveness of antibacterial drugs thus lies intermination of the infection rather than of thediarrhoea, their use is, in a sense, more importantfor the person in the next bed than for the patienthimself.
93
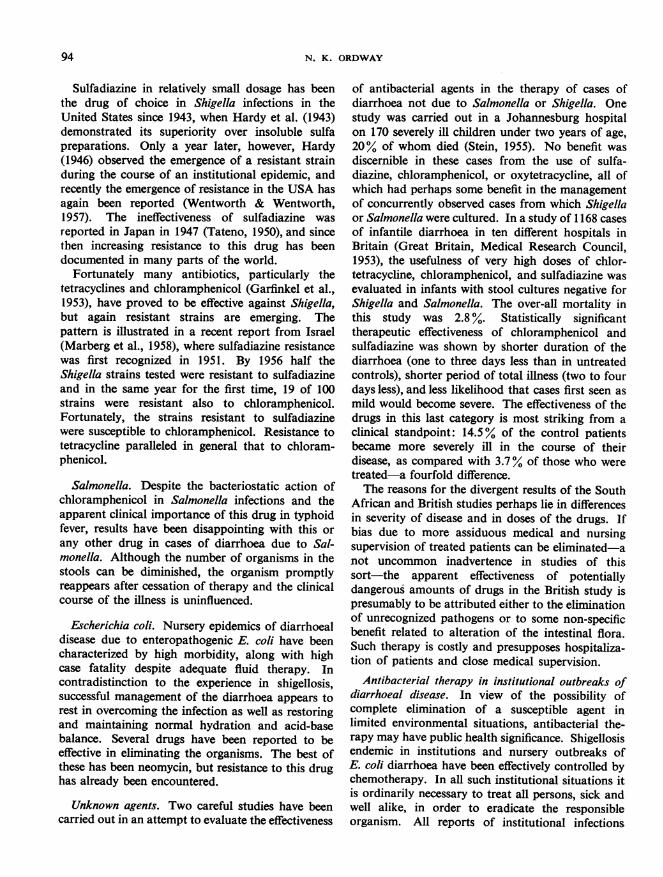
N. K. ORDWAY
Sulfadiazine in relatively small dosage has beenthe drug of choice in Shigella infections in theUnited States since 1943, when Hardy et al. (1943)demonstrated its superiority over insoluble sulfapreparations. Only a year later, however, Hardy(1946) observed the emergence of a resistant strainduring the course of an institutional epidemic, andrecently the emergence of resistance in the USA hasagain been reported (Wentworth & Wentworth,1957). The ineffectiveness of sulfadiazine wasreported in Japan in 1947 (Tateno, 1950), and sincethen increasing resistance to this drug has beendocumented in many parts of the world.
Fortunately many antibiotics, particularly thetetracyclines and chloramphenicol (Garfinkel et al.,1953), have proved to be effective against Shigella,but again resistant strains are emerging. Thepattern is illustrated in a recent report from Israel(Marberg et al., 1958), where sulfadiazine resistancewas first recognized in 1951. By 1956 half theShigella strains tested were resistant to sulfadiazineand in the same year for the first time, 19 of 100strains were resistant also to chloramphenicol.Fortunately, the strains resistant to sulfadiazinewere susceptible to chloramphenicol. Resistance totetracycline paralleled in general that to chloram-phenicol.
Salmonella. Despite the bacteriostatic action ofchloramphenicol in Salmonella infections and theapparent clinical importance of this drug in typhoidfever, results have been disappointing with this orany other drug in cases of diarrhoea due to Sal-monella. Although the number of organisms in thestools can be diminished, the organism promptlyreappears after cessation of therapy and the clinicalcourse of the illness is uninfluenced.
Escherichia coli. Nursery epidemics of diarrhoealdisease due to enteropathogenic E. coli have beencharacterized by high morbidity, along with highcase fatality despite adequate fluid therapy. Incontradistinction to the experience in shigellosis,successful management of the diarrhoea appears torest in overcoming the infection as well as restoringand maintaining normal hydration and acid-basebalance. Several drugs have been reported to beeffective in eliminating the organisms. The best ofthese has been neomycin, but resistance to this drughas already been encountered.
Unknown agents. Two careful studies have beencarried out in an attempt to evaluate the effectiveness
of antibacterial agents in the therapy of cases ofdiarrhoea not due to Salmonella or Shigella. Onestudy was carried out in a Johannesburg hospitalon 170 severely ill children under two years of age,20% of whom died (Stein, 1955). No benefit wasdiscernible in these cases from the use of sulfa-diazine, chloramphenicol, or oxytetracycline, all ofwhich had perhaps some benefit in the managementof concurrently observed cases from which Shigellaor Salmonella were cultured. In a study of 168 casesof infantile diarrhoea in ten different hospitals inBritain (Great Britain, Medical Research Council,1953), the usefulness of very high doses of chlor-tetracycline, chloramphenicol, and sulfadiazine wasevaluated in infants with stool cultures negative forShigella and Salmonella. The over-all mortality inthis study was 2.8%. Statistically significanttherapeutic effectiveness of chloramphenicol andsulfadiazine was shown by shorter duration of thediarrhoea (one to three days less than in untreatedcontrols), shorter period of total illness (two to fourdays less), and less likelihood that cases first seen asmild would become severe. The effectiveness of thedrugs in this last category is most striking from aclinical standpoint: 14.5% of the control patientsbecame more severely ill in the course of theirdisease, as compared with 3.7% of those who weretreated-a fourfold difference.The reasons for the divergent results of the South
African and British studies perhaps lie in differencesin severity of disease and in doses of the drugs. Ifbias due to more assiduous medical and nursingsupervision of treated patients can be eliminated-anot uncommon inadvertence in studies of thissort-the apparent effectiveness of potentiallydangerous amounts of drugs in the British study ispresumably to be attributed either to the eliminationof unrecognized pathogens or to some non-specificbenefit related to alteration of the intestinal flora.Such therapy is costly and presupposes hospitaliza-tion of patients and close medical supervision.
Antibacterial therapy in institutional outbreaks ofdiarrhoeal disease. In view of the possibility ofcomplete elimination of a susceptible agent inlimited environmental situations, antibacterial the-rapy may have public health significance. Shigellosisendemic in institutions and nursery outbreaks ofE. coli diarrhoea have been effectively controlled bychemotherapy. In all such institutional situations itis ordinarily necessary to treat all persons, sick andwell alike, in order to eradicate the responsibleorganism. All reports of institutional infections
94
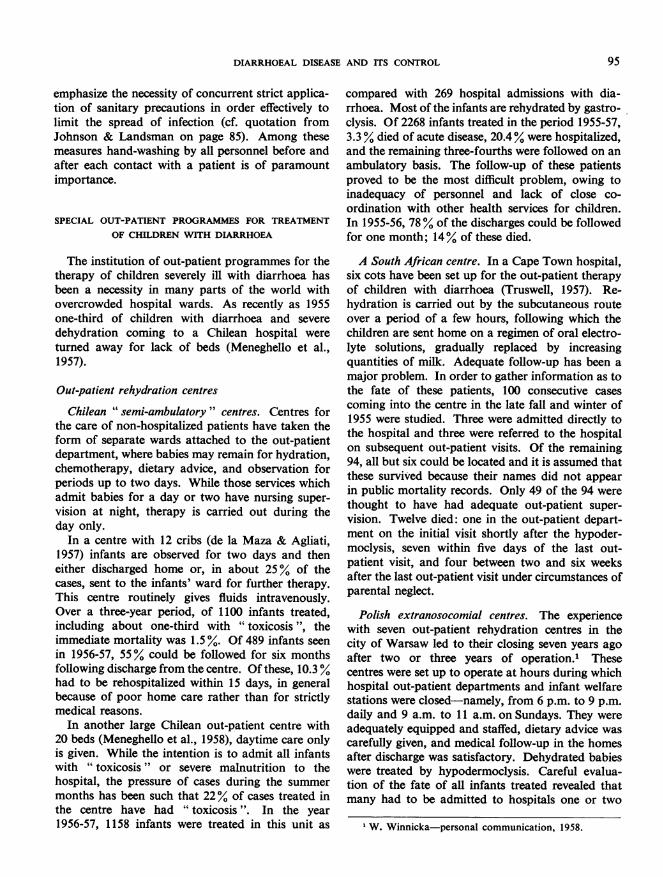
DIARRHOEAL DISEASE AND ITS CONTROL 95
emphasize the necessity of concurrent strict applica-tion of sanitary precautions in order effectively tolimit the spread of infection (cf. quotation fromJohnson & Landsman on page 85). Among thesemeasures hand-washing by all personnel before andafter each contact with a patient is of paramountimportance.
SPECIAL OUT-PATIENT PROGRAMMES FOR TREATMENTOF CHILDREN WITH DIARRHOEA
The institution of out-patient programmes for thetherapy of children severely ill with diarrhoea hasbeen a necessity in many parts of the world withovercrowded hospital wards. As recently as 1955one-third of children with diarrhoea and severedehydration coming to a Chilean hospital wereturned away for lack of beds (Meneghello et al.,1957).
Out-patient rehydration centres
Chilean " semi-ambulatory " centres. Centres forthe care of non-hospitalized patients have taken theform of separate wards attached to the out-patientdepartment, where babies may remain for hydration,chemotherapy, dietary advice, and observation forperiods up to two days. While those services whichadmit babies for a day or two have nursing super-vision at night, therapy is carried out during theday only.
In a centre with 12 cribs (de la Maza & Agliati,1957) infants are observed for two days and theneither discharged home or, in about 25% of thecases, sent to the infants' ward for further therapy.This centre routinely gives fluids intravenously.Over a three-year period, of 1100 infants treated,including about one-third with "toxicosis ", theimmediate mortality was 1.5 %. Of 489 infants seenin 1956-57, 55% could be followed for six monthsfollowing discharge from the centre. Of these, 10.3 %had to be rehospitalized within 15 days, in generalbecause of poor home care rather than for strictlymedical reasons.
In another large Chilean out-patient centre with20 beds (Meneghello et al., 1958), daytime care onlyis given. While the intention is to admit all infantswith " toxicosis " or severe malnutrition to thehospital, the pressure of cases during the summermonths has been such that 22% of cases treated inthe centre have had " toxicosis". In the year1956-57, 1158 infants were treated in this unit as
compared with 269 hospital admissions with dia-rrhoea. Most of the infants are rehydrated by gastro-clysis. Of 2268 infants treated in the period 1955-57,3.3% died of acute disease, 20.4% were hospitalized,and the remaining three-fourths were followed on anambulatory basis. The follow-up of these patientsproved to be the most difficult problem, owing toinadequacy of personnel and lack of close co-ordination with other health services for children.In 1955-56, 78% of the discharges could be followedfor one month; 14% of these died.
A South African centre. In a Cape Town hospital,six cots have been set up for the out-patient therapyof children with diarrhoea (Truswell, 1957). Re-hydration is carried out by the subcutaneous routeover a period of a few hours, following which thechildren are sent home on a regimen of oral electro-lyte solutions, gradually replaced by increasingquantities of milk. Adequate follow-up has been amajor problem. In order to gather information as tothe fate of these patients, 100 consecutive casescoming into the centre in the late fall and winter of1955 were studied. Three were admitted directly tothe hospital and three were referred to the hospitalon subsequent out-patient visits. Of the remaining94, all but six could be located and it is assumed thatthese survived because their names did not appearin public mortality records. Only 49 of the 94 werethought to have had adequate out-patient super-vision. Twelve died: one in the out-patient depart-ment on the initial visit shortly after the hypoder-moclysis, seven within five days of the last out-patient visit, and four between two and six weeksafter the last out-patient visit under circumstances ofparental neglect.
Polish extranosocomial centres. The experiencewith seven out-patient rehydration centres in thecity of Warsaw led to their closing seven years agoafter two or three years of operation.' Thesecentres were set up to operate at hours during whichhospital out-patient departments and infant welfarestations were closed-namely, from 6 p.m. to 9 p.m.daily and 9 a.m. to 11 a.m. on Sundays. They wereadequately equipped and staffed, dietary advice wascarefully given, and medical follow-up in the homesafter discharge was satisfactory. Dehydrated babieswere treated by hypodermoclysis. Careful evalua-tion of the fate of all infants treated revealed thatmany had to be admitted to hospitals one or two
I W. Winnicka-personal communication, 1958.
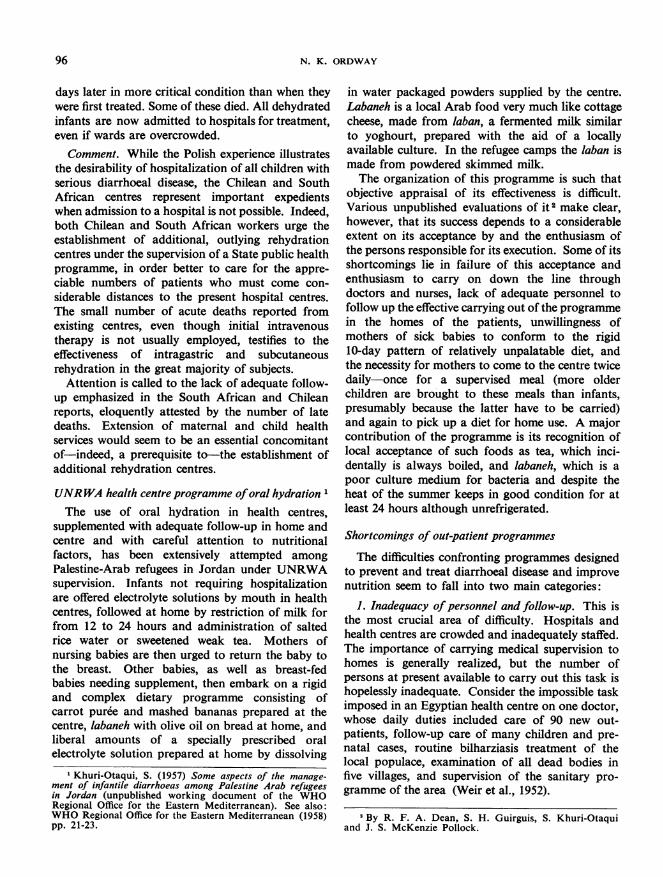
96 N. K. ORDWAY
days later in more critical condition than when theywere first treated. Some of these died. All dehydratedinfants are now admitted to hospitals for treatment,even if wards are overcrowded.
Comment. While the Polish experience illustratesthe desirability of hospitalization of all children withserious diarrhoeal disease, the Chilean and SouthAfrican centres represent important expedientswhen admission to a hospital is not possible. Indeed,both Chilean and South African workers urge theestablishment of additional, outlying rehydrationcentres under the supervision of a State public healthprogramme, in order better to care for the appre-ciable numbers of patients who must come con-siderable distances to the present hospital centres.The small number of acute deaths reported fromexisting centres, even though initial intravenoustherapy is not usually employed, testifies to theeffectiveness of intragastric and subcutaneousrehydration in the great majority of subjects.
Attention is called to the lack of adequate follow-up emphasized in the South African and Chileanreports, eloquently attested by the number of latedeaths. Extension of maternal and child healthservices would seem to be an essential concomitantof-indeed, a prerequisite to-the establishment ofadditional rehydration centres.
UNRWA health centre programme oforal hydrationThe use of oral hydration in health centres,
supplemented with adequate follow-up in home andcentre and with careful attention to nutritionalfactors, has been extensively attempted amongPalestine-Arab refugees in Jordan under UNRWAsupervision. Infants not requiring hospitalizationare offered electrolyte solutions by mouth in healthcentres, followed at home by restriction of milk forfrom 12 to 24 hours and administration of saltedrice water or sweetened weak tea. Mothers ofnursing babies are then urged to return the baby tothe breast. Other babies, as well as breast-fedbabies needing supplement, then embark on a rigidand complex dietary programme consisting ofcarrot puree and mashed bananas prepared at thecentre, labaneh with olive oil on bread at home, andliberal amounts of a specially prescribed oralelectrolyte solution prepared at home by dissolving
1 Khuri-Otaqui, S. (1957) Some aspects of the manage-ment of infantile diarrhoeas among Palestine Arab refugeesin Jordan (unpublished working document of the WHORegional Office for the Eastern Mediterranean). See also:WHO Regional Office for the Eastern Mediterranean (1958)pp. 21-23.
in water packaged powders supplied by the centre.Labaneh is a local Arab food very much like cottagecheese, made from laban, a fermented milk similarto yoghourt, prepared with the aid of a locallyavailable culture. In the refugee camps the laban ismade from powdered skimmed milk.The organization of this programme is such that
objective appraisal of its effectiveness is difficult.Various unpublished evaluations of it 2 make clear,however, that its success depends to a considerableextent on its acceptance by and the enthusiasm ofthe persons responsible for its execution. Some of itsshortcomings lie in failure of this acceptance andenthusiasm to carry on down the line throughdoctors and nurses, lack of adequate personnel tofollow up the effective carrying out of the programmein the homes of the patients, unwillingness ofmothers of sick babies to conform to the rigid10-day pattern of relatively unpalatable diet, andthe necessity for mothers to come to the centre twicedaily-once for a supervised meal (more olderchildren are brought to these meals than infants,presumably because the latter have to be carried)and again to pick up a diet for home use. A majorcontribution of the programme is its recognition oflocal acceptance of such foods as tea, which inci-dentally is always boiled, and labaneh, which is apoor culture medium for bacteria and despite theheat of the summer keeps in good condition for atleast 24 hours although unrefrigerated.
Shortcomings of out-patient programmes
The difficulties confronting programmes designedto prevent and treat diarrhoeal disease and improvenutrition seem to fall into two main categories:
1. Inadequacy ofpersonnel and follow-up. This isthe most crucial area of difficulty. Hospitals andhealth centres are crowded and inadequately staffed.The importance of carrying medical supervision tohomes is generally realized, but the number ofpersons at present available to carry out this task ishopelessly inadequate. Consider the impossible taskimposed in an Egyptian health centre on one doctor,whose daily duties included care of 90 new out-patients, follow-up care of many children and pre-natal cases, routine bilharziasis treatment of thelocal populace, examination of all dead bodies infive villages, and supervision of the sanitary pro-gramme of the area (Weir et al., 1952).
2 By R. F. A. Dean, S. H. Guirguis, S. Khuri-Otaquiand J. S. McKenzie Pollock.
DIARRHOEAL DISEASE AND ITS CONTROL 97
2. Lack of acceptance of hygienic methods. This isusually the result of cultural blocks and inadequatehealth education. It is clear, for instance, that notall the dietary inadequacies of the world are due topoverty alone. The resistance to health progressimposed by ingrained cultural habits has beenemphasized by many observers (Jelliffe, 1957;Solien & Scrimshaw, 1957; Freedman 1) but appearsnot to be generally appreciated. Resistance toalteration of established dietary habits is illustratedby the widespread lack of acceptance of powderedmilk in the area to which it is supplied by UNRWA.Only about 40% of the mothers in this area take theskimmed milk ration to which they are entitled.2 Asociologist (Freedman 1), reporting on the impactof the programme of study and prevention of mal-nutrition in Guatemala, points out that the collectionof blood samples has caused such misunderstandingand resentment that it threatens to compromiseeffective relationship between populace and healthpersonnel. In the treatment of kwashiorkor, inwhich it is important that local dietary customs beradically changed, some Guatemalan hospitals havenot provided parents with the opportunity to visitat meal-times so that they may see their child imp-rove on a diet interdicted at home, or at a time whenthey may talk with the physician in charge of thechild's treatment.
FUTURE ACTION
General objectives and suggested specific measuresEnough is known from what has already been done
to make it possible for future programmes to beeffective in the prevention of diarrhoea morbidityand mortality. Acquisition of further importantepidemiological and etiological data is secondary tothis primary objective.
Obviously programmes of public health improve-ment, particularly in environmental sanitation, mustbe carried forward vigorously. Physicians in allcountries must be educated to the desirability ofemploying more precise nomenclature in the descrip-tion of diarrhoeal disease. Nations must increasinglyrecognize the importance of complete and accurateclassification of causes of disease and death.
Short of these general and long-term objectives,the foregoing review has pointed up several more
Op. cit. (see p. 86).'R. C. Burgess-personal communication, 1956.
limited measures that hold considerable promise ofreducing morbidity and mortality from diarrhoealdisease within present frameworks of socio-economicunder-development. These measures are:
1. Limited sanitary improvements in selectedenvironments:
(a) provision of abundant water in or imme-diately adjacent to homes;
(b) installation of facilities for the sanitarydisposal of human excreta.
2. Attempted prevention of dehydration by earlyoral administration of sugar-electrolyte solutions toinfants and children with diarrhoea.
3. Treatment of dehydration in " semi-ambula-tory " rehydration centres in areas of high diarrhoeamorbidity and inadequate hospital services.
Provision of water
The first of the above measures, representing apreventive rather than a therapeutic approach,merits further discussion.There is urgent need to demonstrate whether the
United States experience of reduced incidence ofdiarrhoea and Shigella infection in environmentswith readily available water can be duplicated in lesswell developed areas of the world, among peoplesunfamiliar with running water and with little or noconception of the rudimentary principles of personalhygiene. Such a study is at present under way inBrazil (Penido, 1959).The importance of developing municipal water
systems was stressed by the Advisory Committee onEnvironmental Sanitation of the Pan AmericanSanitary Bureau at its first meeting in April 1958.The following paragraphs appear in the summaryand recommendations of the committee's report(unpublished):
" Sanitary control of the environment is one of theprincipal means for the prevention of [diarrhoeal andother communicable] diseases, involving chiefly provisionof safe and abundant water, sanitary waste disposal,clean milk and other foods, and adequate housing."A program to carry out large-scale improvement
in all of these phases, simultaneously, does not appearpracticable now or in the immediate future. The Com-mittee believes therefore that a concerted effort should beinitiated as soon as possible on one function which ismost certain to give positive results within a minimumtime at a relatively low per capita cost. Installation of

N. K. ORDWAY
piper water systems throughout populated communities,whether urban or scattered, meets best these criteria.
" Besides direct benefit to health, a water program willalso result in improved and more rapid development ofcommunity housing, industrial and commercial growthand tourist trade-all of which are of great economicimportance to [the Latin American] countries...
" The Committee unanimously recommends that thePan American Sanitary Bureau look to the early initiationof a program for the full-scale, concerted promotion ofpublic water supply systems in the Americas. Such aprogram should envisage:
" 1. Provision of safe and ample water directly intothe homes in concentrated populated areas, by construc-tion of new systems or by the extension and improvementof existing ones...
" 8. Accomplishment of a substantial part of theprogram within a 10-year period with an overall expendi-ture of about $50 per capita. Based on serving anestimated population of 80 million persons, the totalcapital investment is estimated at $4 000 000 000. Thisamount may seem startling at first sight, but it is reason-able considering the area involved, the time for fulldevelopment, the size of the immediate and futurebenefits and the dormant resources in many of thecountries."
Need for further epidemiological knowledgeProgrammes can be designed to yield information,
in addition to the effectiveness of the controlmeasures being tested, on the following unsolvedproblems:
1. The importance of E. coli types as entero-pathogenic agents in the community at large;
2. The etiological significance of viruses;3. The relation in the first year of life between
RtS
Malgre la confusion de la nomenclature, la complexitede la classification et l'insuffisance notoire du nombre desdeclarations, il est incontestable que les maladies diarrh&-iques a etiologie infectieuse sont une cause majeure demorbidite dans le monde entier et la cause principale desdeces chez les nourrissons et les jeunes enfants.
L'infection A Shigella sevit parmi les nourrissons dudeuxieme age, les enfants et les adultes, dans les zones amorbidite diarrheiques moyenne et elevee. Les Salmo-nellae presentent une importance tout A fait secondaire,bien qu'elles soient plus repandues que les Shigellaeparmi les nourrissons. On sait qu'il faut imputer a desEscherichia coli et A certains virus encore insuffisammentetudies les flambees de diarrh6e survenues dans des eta-
diarrhoea and E. coli, viruses, and other micro-biological agents;
4. The relation of malnutrition to diarrhoea;5. The relation of breast-feeding to diarrhoea and
malnutrition;6. More precise definition of sociological factors
such as " mother efficiency ".
Need for trained personnelThe great need for additional personnel, including
physicians, nurses, and engineers, has been re-peatedly pointed out in this review. Of basicimportance are the strengthening of existing maternaland child health organizations and the developmentof new ones. The shortage of trained public healthnurses can be met in part by " nursing auxiliaries ",of whom considerable and growing use is beingmade in Latin America (Ripley & Verhoestraete,1958). These are persons of limited general educa-tional background who can be well trained toassume limited, clearly defined responsibilities in thefield of maternal and child health. It is not unlikelythat such persons, under the guidance of healtheducators as well as nurses and doctors, may beparticularly effective in promoting acceptance ofhealth programmes by lay persons and communities.The counsel of sociologists might be sought with
profit in adapting programmes to communities andin evaluating their effectiveness as experiments inhealth education. In other words, it is suggested thatthe value of epidemiological observations will beenhanced by sociological appraisal, and that theeffectiveness of programmes themselves will beabetted by such review.
UMI_
blissements collectifs. I1 n'est guere probable que les para-sites intestinaux soient par eux-memes une cause frequentede maladie diarrheique.
Les agents pathogenes sont propages par la contami-nation fecale des aliments. On a demontre le r6le jouepar les mains dans la dissemination du materiel conta-mine au cours des epidemies qui eclatent dans les h6pi-taux, les creches et les etablissements scolaires. Le tableauclinique de l'infection est directement en rapport avec laquantite de germes infectants.Dans les zones a forte morbidite diarrheique, la maladie
est presque toujours associee a la malnutrition. S'il estevident que la diarrhee et le parasitisme intestinal quiI'accompagne le plus souvent peuvent aboutir a la mal-
98
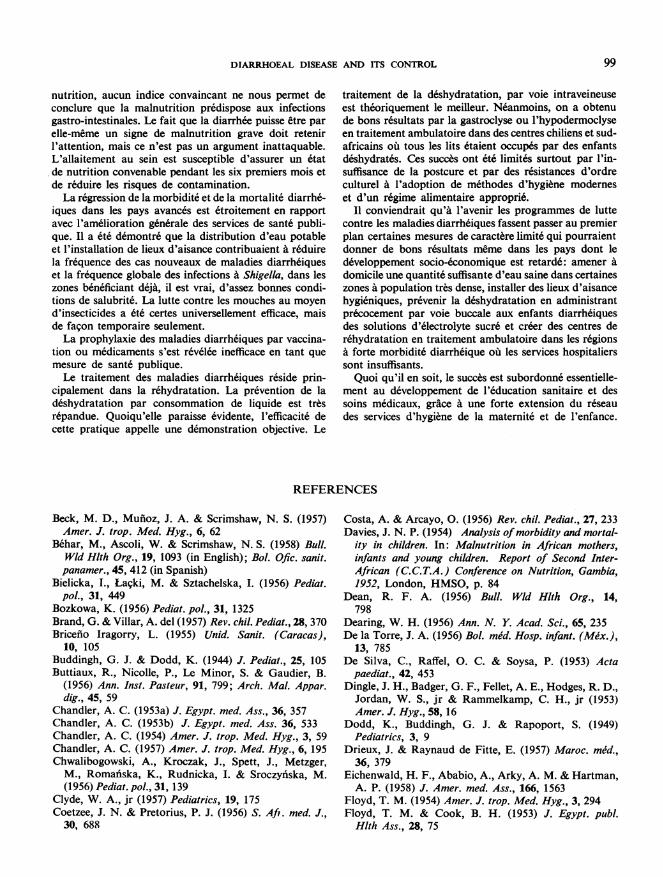
DIARRHOEAL DISEASE AND ITS CONTROL 99
nutrition, aucun indice convaincant ne nous permet deconclure que la malnutrition predispose aux infectionsgastro-intestinales. Le fait que la diarrhee puisse etre parelle-meme un signe de malnutrition grave doit retenirl'attention, mais ce n'est pas un argument inattaquable.L'allaitement au sein est susceptible d'assurer un etatde nutrition convenable pendant les six premiers mois etde reduire les risques de contamination.La regression de la morbidite et de la mortafite diarrhe-
iques dans les pays avances est etroitement en rapportavec I'amelioration generale des services de sante publi-que. I1 a ete demontre que la distribution d'eau potableet l'installation de lieux d'aisance contribuaient a reduirela frequence des cas nouveaux de maladies diarrheiqueset la fr6quence globale des infections a Shigella, dans leszones beneficiant deja, il est vrai, d'assez bonnes condi-tions de salubrite. La lutte contre les mouches au moyend'insecticides a ete certes universellement efficace, maisde facon temporaire seulement.La prophylaxie des maladies diarrheiques par vaccina-
tion ou medicaments s'est revelee inefficace en tant quemesure de sante publique.Le traitement des maladies diarrheiques reside prin-
cipalement dans la r6hydratation. La prevention de ladeshydratation par consommation de liquide est tresrepandue. Quoiqu'elle paraisse evidente, l'efficacite decette pratique appelle une demonstration objective. Le
traitement de la d6shydratation, par voie intraveineuseest theoriquement le meilleur. Neanmoins, on a obtenude bons resultats par la gastroclyse ou l'hypodermoclyseen traitement ambulatoire dans des centres chiliens et sud-africains o'u tous les lits etaient occupes par des enfantsd6shydrates. Ces succes ont et6 limit6s surtout par l'in-suffisance de la postcure et par des resistances d'ordreculturel 'a 'adoption de methodes d'hygiene moderneset d'un regime alimentaire approprie.
I1 conviendrait qu'a l'avenir les programmes de luttecontre les maladies diarrheiques fassent passer au premierplan certaines mesures de caractere limite qui pourraientdonner de bons resultats meme dans les pays dont ledeveloppement socio-economique est retarde: amener adomicile une quantite suffisante d'eau saine dans certaineszones a population tres dense, installer des lieux d'aisancehygieniques, prevenir la deshydratation en administrantprecocement par voie buccale aux enfants diarrh6iquesdes solutions d'electrolyte sucr6 et creer des centres der6hydratation en traitement ambulatoire dans les regionsa forte morbidite diarrheique ou les services hospitalierssont insuffisants.Quoi qu'il en soit, le succts est subordonn6 essentielle-
ment au developpement de l'6ducation sanitaire et dessoins medicaux, grace a une forte extension du reseaudes services d'hygiene de la maternite et de l'enfance.
REFERENCES
Beck, M. D., Munioz, J. A. & Scrimshaw, N. S. (1957)Amer. J. trop. Med. Hyg., 6, 62
Behar, M., Ascoli, W. & Scrimshaw, N. S. (1958) Bull.Wld Hlth Org., 19, 1093 (in English); Bol. Ofic. sanit.panamer., 45, 412 (in Spanish)
Bielicka, I., Lacki, M. & Sztachelska, I. (1956) Pediat.pol., 31, 449
Bozkowa, K. (1956) Pediat. pol., 31, 1325Brand, G. & Villar, A. del (1957) Rev. chil. Pediat., 28, 370Bricefio Iragorry, L. (1955) Unid. Sanit. (Caracas),
10, 105Buddingh, G. J. & Dodd, K. (1944) J. Pediat., 25, 105Buttiaux, R., Nicolle, P., Le Minor, S. & Gaudier, B.
(1956) Ann. Inst. Pasteur, 91, 799; Arch. Mal. Appar.dig., 45, 59
Chandler, A. C. (1953a) J. Egypt. med. Ass., 36, 357Chandler, A. C. (1953b) J. Egypt. med. Ass. 36, 533Chandler, A. C. (1954) Amer. J. trop. Med. Hyg., 3, 59Chandler, A. C. (1957) Amer. J. trop. Med. Hyg., 6, 195Chwalibogowski, A., Kroczak, J., Spett, J., Metzger,
M., Romaiiska, K., Rudnicka, I. & Sroczyniska, M.(1956) Pediat. pol., 31, 139
Clyde, W. A., jr (1957) Pediatrics, 19, 175Coetzee, J. N. & Pretorius, P. J. (1956) S. Aft. med. J.,
30, 688
Costa, A. & Arcayo, 0. (1956) Rev. chil. Pediat., 27, 233Davies, J. N. P. (1954) Analysis ofmorbidity and mortal-
ity in children. In: Malnutrition in African mothers,infants and young children. Report of Second Inter-African (C.C.T.A.) Conference on Nutrition, Gambia,1952, London, HMSO, p. 84
Dean, R. F. A. (1956) Bull. Wld Hlth Org., 14,798
Dearing, W. H. (1956) Ann. N. Y. Acad. Sci., 65, 235De la Torre, J. A. (1956) Bol. mid. Hosp. infant. (Mix.),
13, 785De Silva, C., Raffel, 0. C. & Soysa, P. (1953) Acta
paediat., 42, 453Dingle, J. H., Badger, G. F., Fellet, A. E., Hodges, R. D.,
Jordan, W. S., jr & Rammelkamp, C. H., jr (1953)Amer. J. Hyg., 58,16
Dodd, K., Buddingh, G. J. & Rapoport, S. (1949)Pediatrics, 3, 9
Drieux, J. & Raynaud de Fitte, E. (1957) Maroc. med.,36, 379
Eichenwald, H. F., Ababio, A., Arky, A. M. & Hartman,A. P. (1958) J. Amer. med. Ass., 166, 1563
Floyd, T. M. (1954) Amer. J. trop. Med. Hyg., 3, 294Floyd, T. M. & Cook, B. H. (1953) J. Egypt. publ.
Hlth Ass., 28, 75
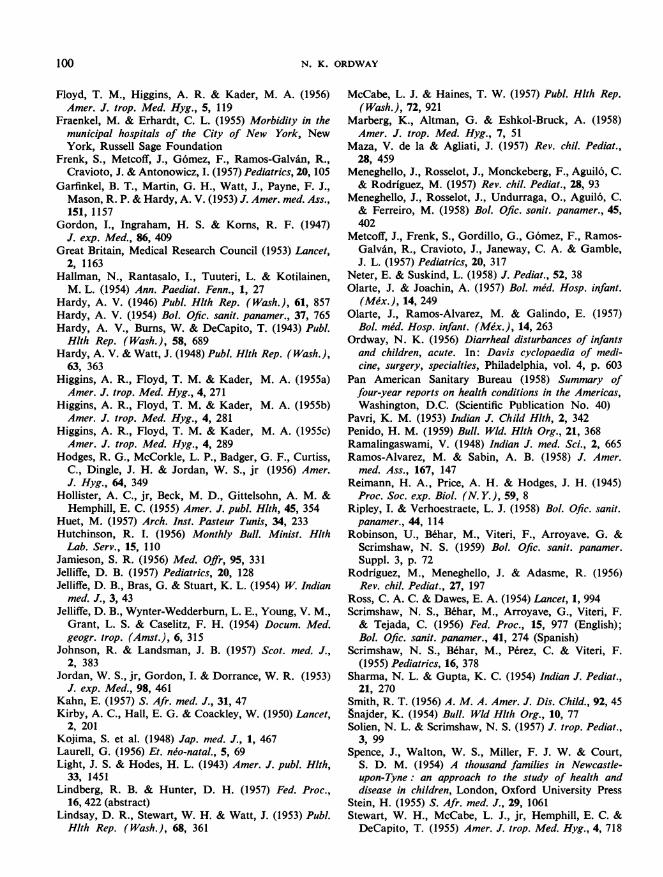
100 N. K. ORDWAY
Floyd, T. M., Higgins, A. R. & Kader, M. A. (1956)Amer. J. trop. Med. Hyg., 5, 119
Fraenkel, M. & Erhardt, C. L. (1955) Morbidity in themunicipal hospitals of the City of New York, NewYork, Russell Sage Foundation
Frenk, S., Metcoff, J., G6mez, F., Ramos-Galvin, R.,Cravioto, J. & Antonowicz, I. (1957) Pediatrics, 20, 105
Garfinkel, B. T., Martin, G. H., Watt, J., Payne, F. J.,Mason, R. P. & Hardy, A. V. (1953) J. Amer. med. Ass.,151, 1157
Gordon, I., Ingraham, H. S. & Korns, R. F. (1947)J. exp. Med., 86, 409
Great Britain, Medical Research Council (1953) Lancet,2, 1163
Hallman, N., Rantasalo, I., Tuuteri, L. & Kotilainen,M. L. (1954) Ann. Paediat. Fenn., 1, 27
Hardy, A. V. (1946) Publ. Hlth Rep. (Wash.), 61, 857Hardy, A. V. (1954) Bol. Ofic. sanit. panamer., 37, 765Hardy, A. V., Burns, W. & DeCapito, T. (1943) Publ.
Hlth Rep. (Wash.), 58, 689Hardy, A. V. & Watt, J. (1948) Publ. Hlth Rep. (Wash.),
63, 363Higgins, A. R., Floyd, T. M. & Kader, M. A. (1955a)Amer. J. trop. Med. Hyg., 4, 271
Higgins, A. R., Floyd, T. M. & Kader, M. A. (1955b)Amer. J. trop. Med. Hyg., 4, 281
Higgins, A. R., Floyd, T. M. & Kader, M. A. (1955c)Amer. J. trop. Med. Hyg., 4, 289
Hodges, R. G., McCorkle, L. P., Badger, G. F., Curtiss,C., Dingle, J. H. & Jordan, W. S., jr (1956) Amer.J. Hyg., 64, 349
Hollister, A. C., jr, Beck, M. D., Gittelsohn, A. M. &Hemphill, E. C. (1955) Amer. J. publ. Hlth, 45, 354
Huet, M. (1957) Arch. Inst. Pasteur Tunis, 34, 233Hutchinson, R. I. (1956) Monthly Bull. Minist. HlthLab. Serv., 15, 110
Jamieson, S. R. (1956) Med. Offr, 95, 331Jelliffe, D. B. (1957) Pediatrics, 20, 128Jelliffe, D. B., Bras, G. & Stuart, K. L. (1954) W. Indian
med. J., 3, 43Jelliffe, D. B., Wynter-Wedderburn, L. E., Young, V. M.,
Grant, L. S. & Caselitz, F. H. (1954) Docum. Med.geogr. trop. (Amst.), 6, 315
Johnson, R. & Landsman, J. B. (1957) Scot. med. J.,2, 383
Jordan, W. S., jr, Gordon, I. & Dorrance, W. R. (1953)J. exp. Med., 98, 461
Kahn, E. (1957) S. Afr. med. J., 31, 47Kirby, A. C., Hall, E. G. & Coackley, W. (1950) Lancet,
2, 201Kojima, S. et al. (1948) Jap. med. J., 1, 467Laurell, G. (1956) Et. nJo-natal., 5, 69Light, J. S. & Hodes, H. L. (1943) Amer. J. publ. Hlth,
33, 1451Lindberg, R. B. & Hunter, D. H. (1957) Fed. Proc.,
16, 422 (abstract)Lindsay, D. R., Stewart, W. H. & Watt, J. (1953) Publ.
Hlth Rep. (Wash.), 68, 361
McCabe, L. J. & Haines, T. W. (1957) Publ. Hlth Rep.(Wash.), 72, 921
Marberg, K., Altman, G. & Eshkol-Bruck, A. (1958)Amer. J. trop. Med. Hyg., 7, 51
Maza, V. de la & Agliati, J. (1957) Rev. chil. Pediat.,28, 459
Meneghello, J., Rosselot, J., Monckeberg, F., Aguil6, C.& Rodriguez, M. (1957) Rev. chil. Pediat., 28, 93
Meneghello, J., Rosselot, J., Undurraga, O., Aguil6, C.& Ferreiro, M. (1958) Bol. Ofic. sonit. panamer., 45,402
Metcoff, J., Frenk, S., Gordillo, G., Gomez, F., Ramos-Galvan, R., Cravioto, J., Janeway, C. A. & Gamble,J. L. (1957) Pediatrics, 20, 317
Neter, E. & Suskind, L. (1958) J. Pediat., 52, 38Olarte, J. & Joachin, A. (1957) Bol. mid. Hosp. infant.
(Mix.), 14, 249Olarte, J., Ramos-Alvarez, M. & Galindo, E. (1957)
Bol. mid. Hosp. infant. (Meix.), 14, 263Ordway, N. K. (1956) Diarrheal disturbances of infantsand children, acute. In: Davis cyclopaedia of medi-cine, surgery, specialties, Philadelphia, vol. 4, p. 603
Pan American Sanitary Bureau (1958) Summary offour-year reports on health conditions in the Americas,Washington, D.C. (Scientific Publication No. 40)
Pavri, K. M. (1953) Indian J. Child Hlth, 2, 342Penido, H. M. (1959) Bull. Wld. Hlth Org., 21, 368Ramalingaswami, V. (1948) Indian J. med. Sci., 2, 665Ramos-Alvarez, M. & Sabin, A. B. (1958) J. Amer.
med. Ass., 167, 147Reimann, H. A., Price, A. H. & Hodges, J. H. (1945)
Proc. Soc. exp. Biol. (N. Y.), 59, 8Ripley, I. & Verhoestraete, L. J. (1958) Bol. Ofic. sanit.panamer., 44, 114
Robinson, U., Behar, M., Viteri, F., Arroyave. G. &Scrimshaw, N. S. (1959) Bol. Ofic. sanit. panamer.Suppl. 3, p. 72
Rodriguez, M., Meneghello, J. & Adasme, R. (1956)Rev. chil. Pediat., 27, 197
Ross, C. A. C. & Dawes, E. A. (1954) Lancet, 1, 994Scrimshaw, N. S., Behar, M., Arroyave, G., Viteri, F.& Tejada, C. (1956) Fed. Proc., 15, 977 (English);Bol. Ofic. sanit. panamer., 41, 274 (Spanish)
Scrimshaw, N. S., Behar, M., Perez, C. & Viteri, F.(1955) Pediatrics, 16, 378
Sharma, N. L. & Gupta, K. C. (1954) Indian J. Pediat.,21, 270
Smith, R. T. (1956) A. M. A. Amer. J. Dis. Child., 92, 45gnajder, K. (1954) Bull. Wld Hlth Org., 10, 77Solien, N. L. & Scrimshaw, N. S. (1957) J. trop. Pediat.,
3, 99Spence, J., Walton, W. S., Miller, F. J. W. & Court,
S. D. M. (1954) A thousand families in Newcastle-upon-Tyne: an approach to the study of health anddisease in children, London, Oxford University Press
Stein, H. (1955) S. Afr. med. J., 29, 1061Stewart, W. H., McCabe, L. J., jr, Hemphill, E. C. &
DeCapito, T. (1955) Amer. J. trop. Med. Hyg., 4, 718
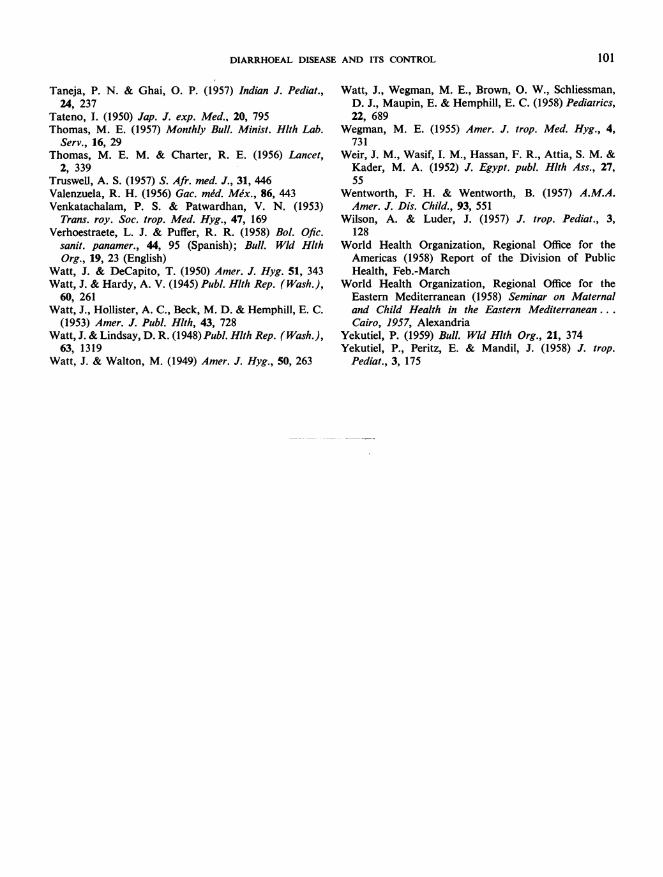
DIARRHOEAL DISEASE AND ITS CONTROL 101
Taneja, P. N. & Ghai, 0. P. (1957) Indian J. Pediat.,24, 237
Tateno, I. (1950) Jap. J. exp. Med., 20, 795Thomas, M. E. (1957) Monthly Bull. Minist. Hlth Lab.
Serv., 16, 29Thomas, M. E. M. & Charter, R. E. (1956) Lancet,
2, 339Truswell, A. S. (1957) S. Afr. med. J., 31, 446Valenzuela, R. H. (1956) Gac. med. Mex., 86, 443Venkatachalam, P. S. & Patwardhan, V. N. (1953)
Trans. roy. Soc. trop. Med. Hyg., 47, 169Verhoestraete, L. J. & Puffer, R. R. (1958) Bol. Ofic.
sanit. panamer., 44, 95 (Spanish); Bull. Wld HlthOrg., 19, 23 (English)
Watt, J. & DeCapito, T. (1950) Amer. J. Hyg. 51, 343Watt, J. & Hardy, A. V. (1945) Publ. Hlth Rep. (Wash.),
60, 261Watt, J., Hollister, A. C., Beck, M. D. & Hemphill, E. C.
(1953) Amer. J. Publ. Hlth, 43, 728Watt, J. & Lindsay, D. R. (1948) Publ. Hlth Rep. (Wash.),
63, 1319Watt, J. & Walton, M. (1949) Amer. J. Hyg., 50, 263
Watt, J., Wegman, M. E., Brown, 0. W., Schliessman,D. J., Maupin, E. & Hemphill, E. C. (1958) Pediatrics,22, 689
Wegman, M. E. (1955) Amer. J. trop. Med. Hyg., 4,731
Weir, J. M., Wasif, I. M., Hassan, F. R., Attia, S. M. &Kader, M. A. (1952) J. Egypt. publ. Hlth Ass., 27,55
Wentworth, F. H. & Wentworth, B. (1957) A.M.A.Amer. J. Dis. Child., 93, 551
Wilson, A. & Luder, J. (1957) J. trop. Pediat., 3,128
World Health Organization, Regional Office for theAmericas (1958) Report of the Division of PublicHealth, Feb.-March
World Health Organization, Regional Office for theEastern Mediterranean (1958) Seminar on Maternaland Child Health in the Eastern Mediterranean...Cairo, 1957, Alexandria
Yekutiel, P. (1959) Bull. Wld Hlth Org., 21, 374Yekutiel, P., Peritz, E. & Mandil, J. (1958) J. trop.
Pediat., 3, 175