
Ex-situ and in-situ selenization of copper-indium and copper-boron thin films

Diagnosis and Management of Ductal Carcinoma In SituAmina Khan, MDLisa A. Newman, MD, MPH*
Address*Breast Care Center, University of Michigan, 1500 East Medical Center Drive, Ann Arbor, MI 48109, USA.E-mail: [email protected]
Current Treatment Options in Oncology 2004, 5:131–144Current Science Inc. ISSN 1527-2729Copyright © 2004 by Current Science Inc.
IntroductionBefore the era of screening mammography, ductalcarcinoma in situ (DCIS) was a rare occurrence, primarilypresented as a palpable mass in the breast. The high ratesof coexisting microinvasive disease within these lesionsresulted in the outdated notion that distinctions betweenDCIS and invasive carcinoma were not clinically relevant.Public health efforts during the 1970s and 1980spromoted early detection of nonpalpable breast cancer
through surveillance mammography. Rapid increases inpopulation-based detection of DCIS were documentedby Ernster et al. [1] in a review of incidence data fromthe Surveillance, Epidemiology, and End Results (SEER)program. Between 1973 and 1983, a 3.9% increase wasseen in the age-adjusted incidence of DCIS annually. From1983 to 1993, these annual increases rose to 17.5%, result-ing in an overall increase in DCIS incidence by 557%.
Opinion statementDuctal carcinoma in situ (DCIS) is a preinvasive form of breast cancer that has increased in incidence over the past 25 years, primarily as a result of mammographically detected microcalcifications. Inadequately treated DCIS carries a risk for evolving into the malig-nant phenotype; however, the magnitude and timeline for this risk are poorly defined. Treatment options include lumpectomy with or without breast irradiation and mast-ectomy. The overall survival rate is 96% to 98% with any of these strategies, but the risk of local recurrence (LR) is highest after lumpectomy alone. Breast irradiation can reduce this risk from levels in excess of 40% to 10% over a 10-year follow-up period. Approximately 50% of all LR from DCIS are invasive lesions. Therefore, the occurrence of a LR after breast-conserving therapy is a potentially greater threat to the patient with DCIS compared to the patient diagnosed with invasive cancer. In patients diag-nosed with invasive cancer, the risk of micrometastatic disease is present from the time of initial diagnosis. In patients with DCIS, the expectation is that a potentially 100% cure rate should be achieved with local therapy alone. Although most DCIS cases compli-cated by LR will be successfully salvaged with prolonged overall survival, it is critically important to take every precaution that will minimize the risk of locally recurrent disease. Therefore, radiation therapy as an adjunct to lumpectomy is essential. A subset of patients with DCIS with low-volume low-grade disease who can be safely treated by lumpectomy alone has not yet been clearly defined. Prospective studies designed to identify this category are ongoing. Inadequate margin control is the most consistent risk factor for LR that has been reported thus far, but there is no universally accepted definition for what constitutes an optimal negative margin distance. Young age at diagnosis, high nuclear grade, and comedonecrosis are other factors that have been implicated as increasing the risk for LR. Tamoxifen can further decrease the rate of new in-breast events on the affected side and in the contralateral breast. Ongoing trials will also define the role of aromatase inhibitors as a risk-reducing strategy.

132 Breast Carcinoma
Data from SEER reveal that DCIS accounts for approx-imately 20% of all breast cancers diagnosed in the UnitedStates, with age-adjusted incidence rates of 30 cases per100,000 women and approximately 47,000 cases detectedeach year [2]. The premalignant nature of DCIS issupported by the median age at diagnosis, which isapproximately 5 to 10 years younger compared to the
average age of an American woman with invasive breastcancer, and by SEER data consistently demonstratingexcellent 5-year survival rates approaching 100%. Further-more, it is likely that recent declines in breast cancermortality rates in the United States, despite a continuedrise in incidence, are largely attributable to successfultreatment of mammographically detected DCIS.
Treatment
• The expansion of preinvasive pathology datasets that accompanied imple-mentation of mammography screening programs led to the contemporary concept of DCIS as a broad array of microscopic patterns. Studies of molec-ular markers reveal that approximately 75% to 80% of DCIS lesions will be positive for expression of the estrogen receptor (ER). High-grade lesions are frequently positive for HER2/neu overexpression, p53, and various indices of proliferation.
• Ductal carcinoma in situ is a function of the continued proliferation of individual cancer cells within discrete ductal units. As long as the cancerous cells are confined within the basement boundary of the ductal structure, they do not have access to the intramammary lymphatics and vascular system, thus they do not have the capacity to metastasize to nodal basins or distant organs. However, persistent accumulation of these cancer cells throughout the ductal tree can result in an extensive volume of involved breast tissue. Within the cross-sectional ductal unit, an early DCIS lesion may appear as papillary projections into the ductal lumen (papillary pattern). Progression of this process can lead to interconnections between these papillary growths within the lumen, giving rise to a lacy cribriform pattern. Once the ductal lumen is completely obliterated by these packed-in cells, the microscopic appearance is described as solid. When the cellular growth outstrips the blood supply, the process of comedonecrosis with calcification deposition ensues. However, the process retains the premalig-nant designation until cancer cells are identified that infiltrate beyond the basement membrane.
• Data from autopsy studies suggest that some DCIS lesions may be latent clinically occult conditions. These series have revealed DCIS present in the breasts of 6% to 18% of women dying from unrelated diseases [3–6]. Four studies provide long-term follow-up information on breast cancer incidence among women with untreated DCIS (Table 1) [7–10]. These datasets were compiled by retrospective reviews of breast biopsies that were initially interpreted as being benign, but they were found to contain foci of DCIS on subsequent re-evaluation. These studies demonstrate that with up to 30 years of follow-up, invasive cancer is detected in approxi-mately 66% of cases, which indicates that a substantial fraction of untreat-ed DCIS lesions progress to infiltrating disease (not necessarily all). These findings are probably only relevant for low-grade DCIS pathology that is easily overlooked and misinterpreted as representing completely benign fibrocystic changes. Some of the DCIS in these biopsies may have been resected in their entirety, thus cured surgically. These data suggest that some DCIS lesions can be managed conservatively with a prolonged control of locoregional and distant disease.
Histopathology
Natural history of ductal carcinoma in situ

Diagnosis and Management of Ductal Carcinoma In Situ Khan and Newman 133
• Holland et al. [11] conducted a detailed study of the mastectomy specimens from 82 DCIS cases by serial sectioning, section mammography, and correla-tive histopathologic evaluations to determine growth patterns and likelihood of multicentric origin. Most of the lesions were confined to one quadrant, and contiguous growth throughout the ductal tree was identified in 26 of 28 comedo cases. The investigators also found frequent discrepancies in the final extent of DCIS measured by histopathology compared to the mammo-graphic measurements. Mammography was especially prone to underesti-mate the extent of disease for micropapillary/cribriform patterns of DCIS compared to the pure comedo pattern. Discrepancies of at least 2 cm were found in eight cases (44%) of the micropapillary/cribriform patterns compared to five cases (12%) of the pure comedo pattern.
• Valuable information regarding growth patterns of DCIS was also contrib-uted by Lagios et al. [12] in studies correlating volume of DCIS-involved breast parenchyma with the likelihood of detecting a focus of invasive cancer. For lesions measuring less than 2.5 cm, the risk of coexisting invasive cancer was very low compared to a 50% risk for DCIS involving more than 2.5 cm of breast tissue.
• Collectively, the studies by Holland et al. [11] and Lagios et al. [12] suggest that DCIS more commonly develops from a single site and extends longitu-dinally throughout the ductal tree. Cross-sectional proliferation and pro-gression to invasive disease occurs concurrently, accounting for the greater prevalence of invasive disease in cases of diffuse DCIS. However, these two growth patterns do not necessarily occur at the same rate, accounting for the occasional detection of pure micropapillary patterns as diffuse low-grade disease throughout the breast compared to comedo patterns as more local-ized lesions. Furthermore, there are likely to be some cases of DCIS that do evolve from separate multifocal/multicentric sites within the breast.
• The heterogeneity of DCIS is also evidenced by the incidence of associated axillary metastases and occasional reports of disease recurrence in the form of distant organ metastases without any site of invasive disease ever being detected. Before the 1980s, management of DCIS was identical to the approach used for invasive cancer and most patients underwent modified radical mastectomy [13]. Axillary metastases are identified in approxi-mately 2% of these cases, even when only pure DCIS was found in the mas-tectomy specimen. A similar proportion of patients with pure DCIS develop distant organ metastases, despite receiving appropriate surgical care [14•]. Although the assumption is that a focus of microinvasive disease must have been missed in the breast tissue sampling, another possi-ble explanation is that rare cases of DCIS may be associated with genetic changes permitting distant dissemination in the absence of microscopic evidence of invasion within the primary affected breast tissue.
Table 1. Studies of long-term outcome after biopsy alone for ductal carcinoma in situ
Study Initial biopsy period Patients, n Follow-up, ySubsequent invasive
cancers, n
Betsill et al. [8] 1940–1950 10 21.6 6 (60%)Rosen et al. [7]
(expansion of Betsill et al. [8] study)1940–1950 15 18 10 (66%)
Page et al. [9] 1950–1968 25 15 7 (28%)Page et al. [10]
(expansion of Page et al. [9] study)1950–1968 28 30 9 (32%)

134 Breast Carcinoma
• More than 90% of DCIS lesions diagnosed today are clinically occult, detected on routine mammographic screening, and microcalcifications are the most common image-detected characteristic. Clinically evident DCIS may present in a myriad of ways: a palpable mass, bloody nipple discharge, and Paget’s disease of the nipple. This report does not include a discussion of management issues specific to Paget’s disease.
• There is a limited correlation between the histopathologic subtype of DCIS and the pattern of associated mammographic calcifications. Comedo-type DCIS is frequently diagnosed as casting calcifications (a linear branching pattern aligned in a ductal distribution). In contrast, noncomedo DCIS is more often associated with a cluster of fine punctate calcifications or a noncalcified mass/asymmetric density. Up to 94% of comedo-type DCIS lesions have mammographic calcifications compared to only 53% of non-comedo lesions [11,15]. The mammographic abnormality (microcalcifica-tions and architectural distortion) should be worked up by diagnostic imaging, such as magnification views, spot compressions, or an ultrasound evaluation. Holland et al. [11] have shown that the mammographic size estimates are more accurate for comedo-type DCIS compared to non-comedo patterns.
• Because most cases of DCIS are nonpalpable, diagnostic biopsies often require some form of image guidance. Available options include fine needle aspiration, core needle biopsy with mammographic and stereotactic or ultrasound guidance, and open surgical biopsy with image-guided wire localization. The same options, with tactile guidance, can be attempted in cases of palpable DCIS. The sensitivity of fine needle aspiration and cytologic diagnosis of DCIS is only 51% to 55% [15]. Stereotactically guided core biopsy with specimen imaging to confirm retrieval of micro-calcifications has sensitivity up to 91% to 94% [15]. Diagnostic yield is optimized by use of larger caliber core needles and vacuum-assisted biopsy devices. Metallic clips should be inserted percutaneously if there is a risk that the entire lesion will be extracted by the cores. These clips would become the target for subsequent wire localization and biopsy. Wire localization to assist surgical excision is also a second-choice diagnostic maneuver if the lesion is not amenable to percutaneous biopsy.
• Because DCIS is largely a disease in which manifestations are confined to in-breast pathology, management strategies focus on various combinations of local therapy: mastectomy, lumpectomy, and breast irradiation. Axillary metastases are sufficiently rare with DCIS that nodal staging with the conventional level I/II lymph node dissection and its associated risk of lymphedema is generally considered unnecessary. However, in cases of extensive DCIS, in which the risk of coexisting invasive disease is signifi-cant, information regarding the axillary nodal status becomes more rele-vant. The advent of lymphatic mapping and sentinel lymph node biopsy has greatly facilitated the handling of this dilemma. Adjuvant systemic therapy provides no survival benefit for pure DCIS because of the exceed-ingly low risk of micrometastases. However, hormonally active medical therapies, such as selective ER modulators and aromatase inhibitors, exert a suppressive effect on abnormal proliferative activity in the breast, thus these agents can be useful in contributing to local control of disease and prevention of new breast primary cancerous events. Table 2 summarizes
Detection and diagnosis
Management

Diagnosis and Management of Ductal Carcinoma In Situ Khan and Newman 135
Tabl
e 2.
Res
ults
of
pros
pect
ive
rand
omiz
ed c
linic
al t
rial
s ev
alua
ting
tre
atm
ent
for
duct
al c
arci
nom
a in
sit
u
NSA
BP B
-06*
Fish
er e
t al
. [16
]EO
RTC
Julie
n et
al.
[17•
•]
and
Bijk
er e
t al
. [21
]N
SABP
B-1
7 Fi
sher
et
al. [
18]
and
Fish
er e
t al
. [20
]
NSA
BP B
-24
Fish
er e
t al
. [19
]
Elig
ibili
ty r
equi
rem
ents
Desi
gned
to
eval
uate
the
saf
ety
ofbr
east
con
serv
atio
n fo
r st
age
I/II
br
east
can
cer
and
inke
d m
argi
n tu
mor
free
Desi
gned
to e
valu
ate
lum
pect
omy
wit
h ve
rsus
wit
hout
bre
ast
XRT;
m
amm
ogra
phic
ally
det
ecte
d DC
IS≤
5 cm
; an
d no
m
argi
nsp
ecif
icat
ion
Desi
gned
to
eval
uate
lum
pect
omy
wit
h ve
rsus
wit
hout
bre
ast
XRT;
DC
IS d
etec
ted
by m
amm
ogra
m
orph
ysic
al e
xam
; an
d in
ked
mar
gin
tum
or f
ree
Desi
gned
to
eval
uate
the
add
ed
bene
fit
of t
amox
ifen
as
adju
vant
th
erap
y fo
r pa
tien
ts w
ith
DCIS
tr
eate
d w
ith
lum
pect
omy
and
brea
st X
RT;
DCIS
det
ecte
d by
m
amm
ogra
m o
r ph
ysic
al e
xam
; an
d in
ked
mar
gin
tum
or f
ree
Aver
age
follo
w-u
p, m
o83
6590
74Ra
ndom
izat
ion
arm
sLu
mp
Lum
p +
XRT
Mas
tect
omy
Lum
pLu
mp
+ XR
TLu
mp
Lum
p +
XRT
Lum
p +
XRT
Lum
p +
XRT
+ta
mox
ifen
Pati
ents
, n
2127
2842
643
740
341
190
290
2Lo
cal r
ecur
renc
es,
n9
(42.
8%)
2 (7
.4%
)0
(0%
)83
(1
9.5%
)54
(1
2.4%
)10
4 (2
5.8%
)47
(1
1.4%
)87
(9
.6%
)63
(7
%)
Inva
sive
loca
l re
curr
ence
s,n
5 of
9
(45%
)1
of 2
(5
0%)
NA37
of
83
(44%
)23
of
54
(45%
)53
of
104
(51%
)17
of
47
(36%
)40
of
87
(46%
)23
of
63
(37%
)Ov
eral
l sur
viva
ll (a
llca
uses
), %
9696
9697
9797
9697
97
Risk
fac
tors
for
lo
calr
ecur
renc
eLa
ck o
f XR
T af
ter
lum
pect
omy
and
com
edon
ecro
sis
Lack
of
XRT;
age
≤ 4
0 ye
ars;
sy
mpt
omat
icDC
IS;
invo
lved
m
argi
ns;
and
solid
/cri
brifo
rm/
com
edo
patt
erns
Lack
of
XRT
and
calc
ific
atio
ns
onm
amm
ogra
mLa
ck o
f ta
mox
ifen
; ag
e <
50ye
ars;
invo
lved
mar
gins
; co
med
onec
rosi
s;an
d sy
mpt
omat
icDC
IS
* Sev
enty
-six
cas
es r
ando
miz
ed in
NSA
BP B
-06
wer
e fo
und
to b
e pu
re D
CIS
on r
etro
spec
tive
pat
holo
gy r
evie
w.DC
IS—
duct
al c
arci
nom
a in
sit
u; E
ORTC
—Eu
rope
an O
rgan
izat
ion
for
Rese
arch
and
Tre
atm
ent
of C
ance
r; L
ump—
lum
pect
omy;
NSA
BP—
Nati
onal
Sur
gica
l Adj
uvan
t Br
east
Pro
ject
; XR
T—br
east
irra
diat
ion.

136 Breast Carcinoma
the results reported by phase III studies designed to compare and contrast DCIS treatment options [16,17••,18–21]. Decisions regarding the optimal choice of therapy for minimal toxicity, morbidity, and disfigurement, whereas durable control of disease is maximized, can be challenging.
Local therapy• Mastectomy was the standard management approach for DCIS until
approximately 25 years ago. During the 1980s, two developments pro-vided the impetus for expanded surgical options in the treatment of this condition: publication of prospective randomized clinical trials from the United States and Europe confirming the safety of breast-conservation therapy as management for early-stage invasive breast cancer and imple-mentation of widespread screening mammography programs and the resulting increased rates of detection for localized foci of DCIS. Despite concerns that DCIS represented a diffuse pattern of disease in the breast, it became increasingly difficult for clinicians to support the paradox of offering breast-sparing treatment to women with invasive palpable breast cancer while women with mammographically detected DCIS were penal-ized with a routine recommendation for mastectomy. Therefore, breast-conservation strategies were explored and have been proven to be onco-logically safe for appropriately selected DCIS cases.
• Mastectomy remains a reasonable treatment option for DCIS, resulting in prolonged disease-free survival. Advances in plastic surgery techniques for immediate or delayed breast reconstruction have further improved the results achieved by mastectomy for DCIS. In certain clinical scenarios, mastectomy remains the preferred approach: diffuse suspicious-appearing microcalcifications; inability to obtain margin control by lumpectomy and re-excision(s); patient contraindication to chest wall irradiation or lack of access to an irradiation facility; patient’s personal preference for mas-tectomy; multiple clinically apparent foci of DCIS that are not amenable to resection within a single margin-negative lumpectomy; and suboptimal tumor-to-breast size ration in which a margin-negative lumpectomy will yield an unacceptable cosmetic result (as defined by the patient).
• Mastectomy and lumpectomy have never been directly compared in a pro-spective randomized trial designed for patients with DCIS. However, compa-rable survival has been confirmed by indirect comparisons from retrospective studies and patients with DCIS that were incidentally included in the National Surgical Adjuvant Breast Project (NSABP) B-06 trial [16]. The B-06 trial was designed to evaluate the outcome of approximately 1800 patients with stage I and II breast cancer randomized to treatment by breast-conservation therapy (with vs without breast irradiation) or mastectomy. The centralized pathology review subsequently identified 78 cases of DCIS that were also randomized and equally divided between the three study arms [16]. The overall survival for all three arms was similar (approximately 96% at 6 years), but the addition of breast irradiation to lumpectomy decreased local recurrence (LR) from 43% to 7% (Table 2).
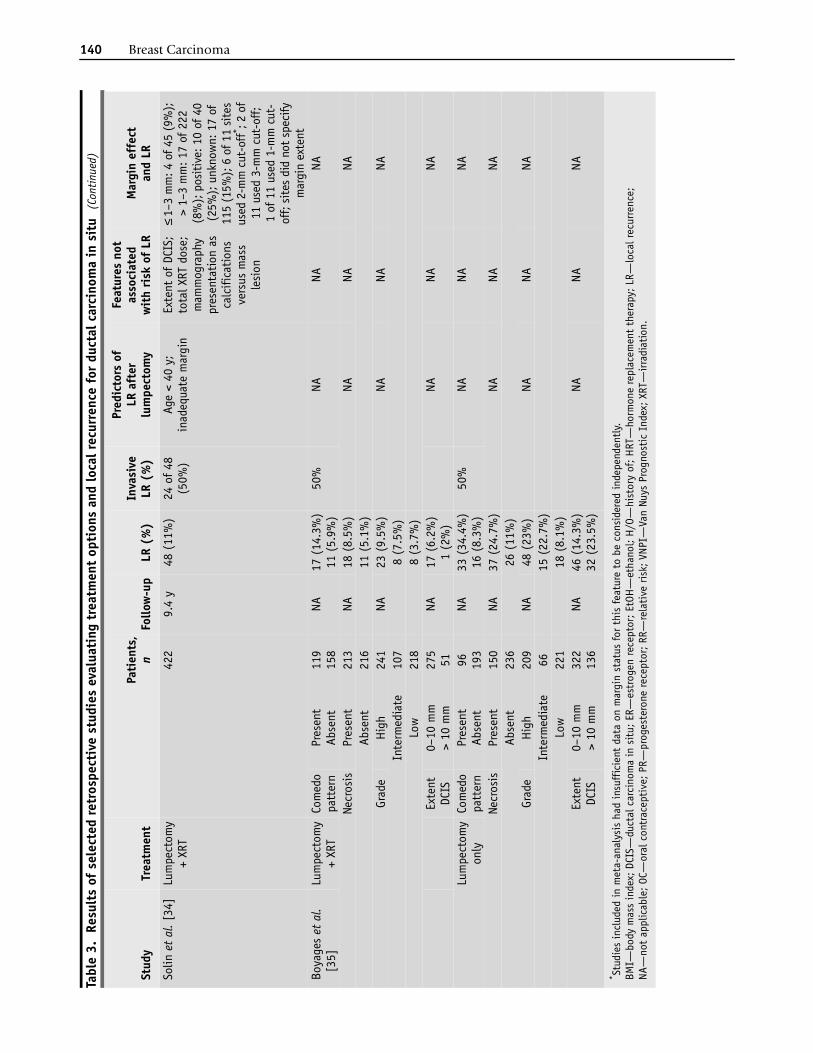
• Table 3 summarizes results of several retrospective studies regarding outcome from DCIS managed by lumpectomy, with or without breast irradiation, and mastectomy [22–28,29••,30–35]. Lumpectomy alone resulted in consistently higher rates of LR (range 8%–34%) compared to patients treated by lumpectomy and breast radiation (range 0%–17%). Risk factors for LR varied between studies, with involved margin status, young age at diagnosis, and high-grade tumors with comedonecrosis being the most commonly cited predictors. Although inadequate margin control

Diagnosis and Management of Ductal Carcinoma In Situ Khan and Newman 137
was frequently implicated in risk for developing LR, there was notable vari-ation between studies regarding the optimal extent of a negative margin. Furthermore, as shown in a meta-analysis of breast-conservation studies for DCIS by Boyages et al. [35], studies published before 1998 often neglected to include margin status in their analyses. In the more recent studies, a negative margin was variously defined as a minimum of 1 mm, 2 mm, or 3 mm of microscopically normal tissue at the inked lumpectomy borders. Regardless of the definition, within studies, the risk of LR was often lower for subsets in which margin control was achieved.
• Another consistent finding between studies was that approximately 50% of all locally recurrent lesions were in the form of invasive disease. This find-ing suggests that the decision to be treated by breast preservation involves a different category of risk that is assumed by the patient with DCIS compared to the patient undergoing lumpectomy for invasive cancer. In patients with invasive cancer undergoing lumpectomy, the risk for distant micrometastases is present from the time of diagnosis and decisions regarding the need for adjuvant systemic therapy are addressed at that time. However, in patients with DCIS treated by breast preservation, there would be no need to consider treatment of micrometastases because DCIS biologically would not be expected to have the ability to extend beyond the local tissue environment of the breast. The development of a LR alters this prognostically favorable situa-tion and affected patients face the risk of breast cancer mortality from distant spread. The proportion of invasive LR was similar for the patients treated by lumpectomy alone versus lumpectomy and irradiation. However, because the risk of LR is lower for the radiated patients, the assumption would be that radiation reduces the incidence of a potentially life-threatening pattern of disease progression. It could be further postulated that mastectomy is the safest treatment for patients with DCIS because of the exceptionally low rate of LR. Although low, this risk is existent, indicating that rare forms of DCIS possess a biologically more aggressive nature [36,37]. At least two retrospective series have confirmed the progressively decreasing risk of LR associated with lumpectomy alone versus lumpectomy and breast irradiation versus mastectomy as treatment for DCIS [22,23].
• In response to concerns regarding the increased risk of converting DCIS into invasive disease through the opportunity of LR after breast-conserving therapy, two prospective randomized trials have been conducted that confirm the safety of lumpectomy (with or without radiation) in terms of prolonged overall survival. The European Organization for Research and Treatment of Cancer (EORTC) trial 10853 and the NSABP B-17 study each randomized nearly 900 patients with DCIS to treatment by lumpectomy or lumpectomy followed by breast irradiation (Table 2) [17••,18,20,21]. The EORTC trial did not specify the extent of margin negativity, and the NSABP study man-dated that there be no cancer cells at the inked surface microscopically. At 65 and 90 months median follow-up time, the EORTC and NSABP studies reported LR rates of 19.5% and 25.8%, respectively, for the lumpectomy arms. In contrast, LR rates for the lumpectomy/irradiation arms were 12.4% and 11.4%, respectively. However, long-term overall survival was similar for the two treatment strategies in both studies at approximately 97%. Cause-specific breast cancer survival is likely even higher for these studies because some participant deaths were related to noncancerous events.
• Because of the expense, inconvenience, and potential adverse effects of irradi-ation, several investigators have attempted to identify subsets of patients with DCIS with sufficiently low-risk lesions that could routinely be treated by lumpectomy alone. The obvious candidates would be small-volume low-grade DCIS with widely negative margins on lumpectomy. Some groups have developed grading systems that stratify patients with DCIS based on

138 Breast Carcinoma
Tabl
e 3.
Res
ults
of
sele
cted
ret
rosp
ecti
ve s
tudi
es e
valu
atin
g tr
eatm
ent
opti
ons
and
loca
l rec
urre
nce
for
duct
al c
arci
nom
a in
sit
u
Stud
yTr
eatm
ent
Pati
ents
, n
Follo
w-u
pLR
(%
)In
vasi
ve
LR (
%)
Pred
icto
rs o
f LR
aft
er
lum
pect
omy
Feat
ures
not
as
soci
ated
w
ith
risk
of
LRM
argi
n ef
fect
an
d LR
Wen
g et
al.
[22]
Lum
pect
omy
+ XR
T38
8.3
y5
(13.
1%)
1 of
5
(20%
)In
adeq
uate
mar
gin;
no
tre
ceiv
ing
XRT
Fam
ily h
isto
ry;
path
olog
ic
subt
ype
≤ 2
mm
: LR
5 o
f 18
(2
8%);
> 2
mm
: LR
6 o
f 44
(14
%)
Lum
pect
omy
only
246
(25%
)2
of 6
(3
3%)
Mas
tect
omy
261
of 2
6 (3
.8%
)1
of 1
(1
00%
)Jh
a et
al.
[23]
Lum
pect
omy
+ XR
T97
88 m
o1
of 9
7
(1%
)3
of 6
(5
0%)
Not
rece
ivin
g XR
TNo
t re
port
edAl
l lum
pect
omie
s pe
rfor
med
wit
h m
argi
ns ≥
5 m
mLu
mpe
ctom
y on
ly31
5 of
31
(16%
)M
aste
ctom
y17
60
(0%
)0
(0%
)H
abel
et
al.
[24]
Lum
pect
omy
+ XR
T29
362
mo
40 (
13.6
%)
18 o
f 40
(4
5%)
Not
rece
ivin
g XR
T;
com
edon
ecro
sis;
BM
I>
31
Age;
par
ity;
H/O
H
RT u
se;
H/O
OC
use;
men
opau
sal
stat
us;
EtOH
Not
repo
rted
Lum
pect
omy
only
248
63 (
25.4
%)
37 o
f 63
(5
9%)
Kest
in e
t al
. [25
]Lu
mpe
ctom
y +
XRT
146
7.2
y13
(9%
)10
of
13
(77%
)Ag
e <
45 y
; tr
ends
(n
otsi
gnif
ican
t)
for
mar
gin
stat
us
and
lack
of
XRT
VNPI
≤ 2
mm
/unk
now
n:
5-y
actu
aria
l rat
e 15
%;
> 2
mm
: 5-
y ac
tuar
ial
rate
6%
Lum
pect
omy
only
315.
9 y
2 (6
%)
1 of
2
(50%
)≤
2 m
m/u
nkno
wn:
5-
y ac
tuar
ial r
ate
17%
; >
2 m
m:
5-y
actu
aria
l ra
te 5
%de
Mas
care
l et
al.
[26]
Lum
pect
omy
+ XR
T15
571
mo
14 (
9%)
24 o
f 46
(5
2%)
Exte
nt o
f DC
ISVN
PINo
t re
port
ed
Lum
pect
omy
only
212
32 (
15.1
%)
* Stu
dies
incl
uded
in m
eta-
anal
ysis
had
insu
ffic
ient
dat
a on
mar
gin
stat
us f
or t
his
feat
ure
to b
e co
nsid
ered
inde
pend
entl
y.BM
I—bo
dy m
ass
inde
x; D
CIS—
duct
al c
arci
nom
a in
sit
u; E
R—es
trog
en r
ecep
tor;
EtO
H—
etha
nol;
H/O
—hi
stor
y of
; H
RT—
horm
one
repl
acem
ent
ther
apy;
LR—
loca
l rec
urre
nce;
NA
—no
t ap
plic
able
; OC
—or
al c
ontr
acep
tive
; PR
—pr
oges
tero
ne r
ecep
tor;
RR—
rela
tive
ris
k; V
NPI—
Van
Nuys
Pro
gnos
tic
Inde
x; X
RT—
irra
diat
ion.

Diagnosis and Management of Ductal Carcinoma In Situ Khan and Newman 139
Chan
et
al.
[27]
Lum
pect
omy
+ XR
T27
47 m
o3
(11%
)0
Inad
equa
te m
argi
n;
nucl
ear
grad
e 3
Adju
vant
the
rapy
≤ 1
mm
: 25
of 6
6 (3
8%);
1.
1–5
mm
: 4 o
f 89
(4%
);
5.1–
10 m
m:
2 of
28
(7%
); 1
0.1–
40 m
m:
1 of
22
(5%
)Lu
mpe
ctom
y on
ly17
829
(16
%)
6 of
29
(21%
)Ne
usch
atz
et a
l. [2
8]Lu
mpe
ctom
y +
XRT
5454
mo
5 (9
%)
Not
repo
rted
Inad
equa
te m
argi
n;
exte
nt o
f DC
IS >
15
mm
Age;
gra
de; V
NPI;
ne
cros
is≤
1 m
m: 7
of 2
8 (2
5%);
>
1 m
m: 4
of 6
8 (6
%);
>
1–10
mm
: 1 o
f 27
(4%
);
> 10
mm
: 3 o
f 41
(7%
)Lu
mpe
ctom
y on
ly55
49 m
o8
(15%
)
Silv
erst
ein
et a
l. [4
6]Lu
mpe
ctom
y +
XRT
280
81 m
o49
(17
.5%
)24
of
49
(49%
)VN
PI;
age
< 40
yNo
t re
port
ed<
1 m
m:
RR 1
2.1;
1–
9 m
m:
RR 6
.4;
≥ 10
mm
: RR
1.0
Lu
mpe
ctom
y on
ly42
670
(16
.4%
)25
of
70
(36%
)Ri
ngbe
rg
et a
l. [3
0]Lu
mpe
ctom
y on
ly12
162
mo
31 (
26%
)13
of
31
(42%
)H
igh-
grad
e hi
stol
ogy;
hi
gh K
i67;
no
ndip
loid
DNA
ER;
PR;
HER
2/ne
u;
Bcl-
2; p
53
Not
repo
rted
Doug
las-
Jone
s et
al.
[31]
Lum
pect
omy
only
115
15 (
13%
)9
of 1
5 (6
0%)
Inad
equa
te m
argi
nVN
PI;
cyto
nucl
ear
grad
eJh
ingr
an
et a
l. [3
2]Lu
mpe
ctom
y +
XRT
150
63 m
o12
(8%
)7
of 1
2 (5
8%)
Hig
h nu
clea
r gr
ade
Age;
mar
gin
stat
us; ex
tent
of
DCI
S;
fam
ily h
isto
ry
Not
repo
rted
Fow
ble
et a
l. [3
3]Lu
mpe
ctom
y +
XRT
110
5.3
y3
(3%
)3
of 3
(1
00%
)Yo
ung
age* ;
in
adeq
uate
mar
gin
tren
ds* ;
too
few
LR
for
stat
isti
cal s
igni
fican
ce
Fam
ily h
isto
ry;
hist
olog
ic
subt
ype
≤ 2
mm
: 1 o
f 20
(5%
);
> 2
mm
: 1
of 6
8 (1
%);
un
know
n: 1
of
22 (
5%)
Tabl
e 3.
Res
ults
of
sele
cted
ret
rosp
ecti
ve s
tudi
es e
valu
atin
g tr
eatm
ent
opti
ons
and
loca
l rec
urre
nce
for
duct
al c
arci
nom
a in
sit
u (
Cont
inue
d)
Stud
yTr
eatm
ent
Pati
ents
, n
Follo
w-u
pLR
(%
)In
vasi
ve
LR (
%)
Pred
icto
rs o
f LR
aft
er
lum
pect
omy
Feat
ures
not
as
soci
ated
w
ith
risk
of
LRM
argi
n ef
fect
an
d LR
* Stu
dies
incl
uded
in m
eta-
anal
ysis
had
insu
ffic
ient
dat
a on
mar
gin
stat
us f
or t
his
feat
ure
to b
e co
nsid
ered
inde
pend
entl
y.BM
I—bo
dy m
ass
inde
x; D
CIS—
duct
al c
arci
nom
a in
sit
u; E
R—es
trog
en r
ecep
tor;
EtO
H—
etha
nol;
H/O
—hi
stor
y of
; H
RT—
horm
one
repl
acem
ent
ther
apy;
LR—
loca
l rec
urre
nce;
NA
—no
t ap
plic
able
; OC
—or
al c
ontr
acep
tive
; PR
—pr
oges
tero
ne r
ecep
tor;
RR—
rela
tive
ris
k; V
NPI—
Van
Nuys
Pro
gnos
tic
Inde
x; X
RT—
irra
diat
ion.
140 Breast Carcinoma
Solin
et
al.
[34]
Lum
pect
omy
+ XR
T42
29.
4 y
48 (
11%
)24
of
48
(50%
)Ag
e <
40 y
; in
adeq
uate
mar
gin
Exte
nt o
f DC
IS;
tota
l XRT
dos
e;
mam
mog
raph
y pr
esen
tati
on a
s ca
lcif
icat
ions
ve
rsus
mas
s le
sion
≤ 1–
3 m
m: 4
of 4
5 (9
%);
>
1–3
mm
: 17
of 2
22
(8%
); p
osit
ive:
10
of 4
0 (2
5%);
unk
now
n: 1
7 of
11
5 (1
5%);
6 o
f 11
site
s us
ed 2
-mm
cut
-off
* ; 2
of
11 u
sed
3-m
m c
ut-o
ff;
1 of
11
used
1-m
m c
ut-
off;
site
s di
d no
t sp
ecify
m
argi
n ex
tent
Boya
ges
et a
l. [3
5]Lu
mpe
ctom
y +
XRT
Com
edo
patt
ern
Pres
ent
Abse
nt11
915
8NA
17 (
14.3
%)
11 (
5.9%
)50
%NA
NANA
Necr
osis
Pres
ent
213
NA18
(8.
5%)
NANA
NAAb
sent
216
11 (
5.1%
)Gr
ade
Hig
h24
1NA
23 (
9.5%
)NA
NANA
Inte
rmed
iate
107
8 (7
.5%
)Lo
w21
88
(3.7
%)
Exte
nt
DCIS
0–10
mm
> 10
mm
275
51NA
17 (
6.2%
)1
(2%
)NA
NANA
Lum
pect
omy
only
Com
edo
patt
ern
Pres
ent
Abse
nt96 19
3NA
33 (
34.4
%)
16 (
8.3%
)50
%NA
NANA
Necr
osis
Pres
ent
150
NA37
(24
.7%
)NA
NANA
Abse
nt23
626
(11
%)
Grad
eH
igh
209
NA48
(23
%)
NANA
NAIn
term
edia
te66
15 (
22.7
%)
Low
221
18 (
8.1%
)Ex
tent
DC
IS0–
10 m
m>
10 m
m32
213
6NA
46 (
14.3
%)
32 (
23.5
%)
NANA
NA
Tabl
e 3.
Res
ults
of
sele
cted
ret
rosp
ecti
ve s
tudi
es e
valu
atin
g tr
eatm
ent
opti
ons
and
loca
l rec
urre
nce
for
duct
al c
arci
nom
a in
sit
u (
Cont
inue
d)
Stud
yTr
eatm
ent
Pati
ents
, n
Follo
w-u
pLR
(%
)In
vasi
ve
LR (
%)
Pred
icto
rs o
f LR
aft
er
lum
pect
omy
Feat
ures
not
as
soci
ated
w
ith
risk
of
LRM
argi
n ef
fect
an
d LR
* Stu
dies
incl
uded
in m
eta-
anal
ysis
had
insu
ffic
ient
dat
a on
mar
gin
stat
us f
or t
his
feat
ure
to b
e co
nsid
ered
inde
pend
entl
y.BM
I—bo
dy m
ass
inde
x; D
CIS—
duct
al c
arci
nom
a in
sit
u; E
R—es
trog
en r
ecep
tor;
EtO
H—
etha
nol;
H/O
—hi
stor
y of
; H
RT—
horm
one
repl
acem
ent
ther
apy;
LR—
loca
l rec
urre
nce;
NA
—no
t ap
plic
able
; OC
—or
al c
ontr
acep
tive
; PR
—pr
oges
tero
ne r
ecep
tor;
RR—
rela
tive
ris
k; V
NPI—
Van
Nuys
Pro
gnos
tic
Inde
x; X
RT—
irra
diat
ion.

Diagnosis and Management of Ductal Carcinoma In Situ Khan and Newman 141
the risk of developing LR. The most popular of these systems is the Van Nuys Prognostic Index (VNPI) developed by Silverstein et al. [38] and based on the detailed pathology analyses and follow-up of several hundred patients with DCIS. This index uses a point system to categorize patients on the basis of nuclear grade (with vs without necrosis), extent of DCIS (≤ 15 mm vs 16–40 mm vs > 40 mm), and margin width (≥ 10 mm vs 1–9 mm vs < 1 mm). Cumulative points resulting in scores of 3 or 4 identify patients that should be safely managed by lumpectomy only, whereas scores of 8 or 9 would be indications for mastectomy. Intermediate scores would be consistent with safe treatment by lumpectomy and irradiation. This index was recently modified to include age (< 40 vs 40–60 vs > 60 years) [29••]. However, several studies have been unable to validate the accuracy of the VNPI as predictive of LR (Table 3). A major disadvantage to the VNPI is that it was developed by retrospective review of treated patients, thus it has some inherent biases. Despite the difficulties in developing a reproducible and accurate scoring system for DCIS, an international and multidisciplinary panel of DCIS experts convened a consensus panel several years ago and collectively decreed that all pathology reports on DCIS should include a description of morphology, nuclear grade, and necrosis [39].
• Several investigative groups have implemented prospective clinical trials designed to evaluate the long-term results of treating highly selected subsets of patients with DCIS by lumpectomy alone. One study conducted by the Dana-Farber/Harvard Cancer Center (Boston, MA) used DCIS grade 1 or 2, size up to 2.5 cm, and final margins of at least 1 cm as eligibility criteria. After an accrual of 157 patients (out of an accrual goal of 200), the early closure of this study was recently reported because of an excessive LR rate [40]. At a median follow-up time of 40 months, 13 patients experienced a LR (nine were invasive recurrences), corresponding to a 5-year rate of 12.5% and a per annum rate of 2.5% per patient-year. A phase III clinical trial imple-mented by the Radiation Therapy Oncology Group, which randomizes small low-grade DCIS to lumpectomy with versus without irradiation and with versus without tamoxifen, is under way.
Regional treatment and management of the axilla• Past studies of mastectomy performed for DCIS revealed axillary metastases
in approximately 2% of DCIS cases. It is commonly assumed that these are related to a focus of invasive disease in the breast that was overlooked on pathologic tissue sampling. This low risk of detecting nodal disease and the wish to minimize risk of lymphedema prompted most surgeons to abandon the routine practice of performing a conventional level I/II axillary lymph node dissection (ALND) in patients with DCIS. For those patients requiring a mastectomy because of diffuse DCIS, the need for axillary staging becomes more relevant because of the associated increased risk of coexisting micro-invasion. In these cases, the standard approach was to include a level I ALND with the mastectomy.
• Integration of the lymphatic mapping technology into breast cancer surgery during the past decade presented a novel and minimally invasive method for detecting axillary metastases. Several investigators have reported their findings from series of patients with DCIS undergoing sentinel lymph node biopsy with interesting results. Intra et al. [41] found axillary metastases in seven of 223 (3.1%) patients with DCIS and Pendas et al. [42] reported a 6% rate of sentinel lymph node positivity in 87 DCIS cases. These increased rates of upstaging patients previously thought to have preinvasive DCIS are inconsistent with established overall long-term survival rates of 98% for

142 Breast Carcinoma
patients with DCIS. However, in both of these series, most sentinel node disease was micrometastatic, detected by immunohistochemistry, and completion ALNDs rarely demonstrated additional metastases in non-sentinel lymph nodes. Therefore, the biologic significance of axillary metastases in this setting is questionable. Because of this uncertainty, the standard of care is to defer axillary staging by lymphatic mapping in DCIS cases managed with breast preservation unless invasion is detected in the lumpectomy specimen, in which case the patient can be returned to the operating room for a subsequent sentinel lymph node biopsy. In contrast, it is not technically feasible to perform a lymphatic mapping procedure after the breast has been removed and a different approach must be used for patients with DCIS undergoing mastectomy. If there is a significant likelihood of a coexisting invasive focus based on prior biopsy findings or based on the extent of DCIS, it is reasonable to perform the lymphatic mapping procedure concomitantly with the mastectomy. Immunohisto-chemistry should not be routinely performed for these cases outside of a clinical trial.
Medical therapy• Because of the high prevalence of ER expression in DCIS lesions and because
the known ability of tamoxifen is to suppress breast ductal proliferative activ-ity, it has been reasonable to explore the use of this selective ER modulator as adjuvant therapy for DCIS. The B-24 study by the NSABP randomized 1800 patients with DCIS to treatment by lumpectomy and irradiation, followed by 5 years of tamoxifen versus placebo (Table 2) [19]. At a median follow-up time of 74 months, tamoxifen was found to result in a significantly lower risk of ipsilateral and contralateral breast cancer events. There were 130 breast cancer events in the placebo arm versus 84 in the arm receiving tamox-ifen, consistent with a 37% reduction for the patients receiving tamoxifen (P = 0.0009). There was no requirement for margin control in this trial and there were fewer ipsilateral breast cancer events in the tamoxifen-treated arm, even among those patients with involved margins.
• The pattern of benefit conferred by tamoxifen in the NSABP B-24 study was notable, with most of the risk reduction occurring in contralateral breast events. Tamoxifen reduced the risk of contralateral invasive and noninvasive disease by 52% (P = 0.01). For ipsilateral breast cancer events, there was a 44% reduction in invasive recurrences (P = 0.03), but the reduction in recurrent DCIS was only 18% (P = 0.43).
• Allred [43] conducted a meticulous study of the ER expression in DCIS lesions from the NSABP arm treated with tamoxifen and reported a close association between the pattern of hormone receptor positivity and the like-lihood of benefit from tamoxifen. With a median follow-up time of 104 months, the rate of LR for ER-positive DCIS was 10% compared to 23% for the ER-negative lesions. However, Allred [43] used a specific grading and interpretation of ER staining by immunohistochemistry. Their findings with regard to DCIS and tamoxifen are biologically plausible and worthy of merit. However, whether their methods can be widely replicated for standardized clinical practice warrants further study.
• The ATAC (anastrozole, tamoxifen, alone or in combination) trial yielded provocative results regarding the activity of the aromatase inhibitor anastro-zole for adjuvant management ER-positive postmenopausal breast cancer. This trial randomized more than 9000 patients with early-stage breast cancer to receive anastrozole, tamoxifen, or the combination of anastrozole with tamoxifen as systemic adjuvant therapy. The risk of contralateral new breast

Diagnosis and Management of Ductal Carcinoma In Situ Khan and Newman 143
cancers was reduced to a significantly greater degree in the anastrozole arm compared to the tamoxifen arm (odds ratio 0.42; P = 0.007) [44••]. These findings prompted the NSABP B-35 study, a phase III trial that randomized postmenopausal patients with DCIS treated by breast-conservation therapy to receive adjuvant tamoxifen versus anastrozole for the prevention of additional breast cancer events [45].
• Ductal carcinoma in situ is a common form of breast cancer and screening mammography has resulted in the realization that this preinvasive disease is quite heterogeneous in presentation, histopathology, and clinical behavior. However, it is a lesion associated with an excellent prognosis and manage-ment is primarily focused on local therapy.
References and Recommended ReadingPapers of particular interest, published recently, have been highlighted as:• Of importance•• Of major importance
1. Ernster VL, Barclay J, Kerlikowske K, et al.: Incidence of and treatment for ductal carcinoma in situ of the breast. JAMA 1996, 275:913–938.
2. Ries L, Eisner M, Kosary CL, et al.: SEER Cancer Statistics Review, 1973-1999. Bethesda: National Cancer Institute; 2002.
3. Nielsen M, Jensen J, Andersen J: Precancerous and cancerous breast lesions during lifetime and at autopsy: a study of 83 women. Cancer 1984, 54:612–615.
4. Nielsen M, Thomsen JL, Primdahl S, et al.: Breast cancer and atypia among young and middle-aged women: a study of 110 medicolegal autopsies. Br J Cancer 1987, 56:814–819.
5. Alpers CE, Wellings SR: The prevalence of carcinoma in situ in normal and cancer-associated breasts. Hum Pathol 1985, 16:796–807.
6. Bhathal PS, Brown RW, Lesueur GC, et al.: Frequency of benign and malignant breast lesions in 207 con-secutive autopsies in Australian women. Br J Cancer 1985, 51:271–278.
7. Rosen PP, Braun DW Jr, Kinne DE: The clinical signifi-cance of pre-invasive breast carcinoma. Cancer 1980, 46:919–925.
8. Betsill WL Jr, Rosen PP, Lieberman PH, et al.: Intraductal carcinoma: long-term follow-up after treatment by biopsy alone. JAMA 1978, 239:1863–1867.
9. Page DL, Dupont WD, Rogers LW, et al.: Intraductal carcinoma of the breast: follow-up after biopsy only. Cancer 1982, 49:751–758.
10. Page DL, Dupont WD, Rogers LW, et al.: Continued local recurrence of carcinoma 15-25 years after a diagnosis of low grade ductal carcinoma in situ of the breast treated only by biopsy. Cancer 1995, 76:1197–1200.
11. Holland R, Hendriks JH, Vebeek AL, et al.: Extent, distri-bution, and mammographic/histological correlations of breast ductal carcinoma in situ. Lancet 1990, 335:519–522.
12. Lagios MD, Westdahl PR, Margolin FR, et al.: Duct carci-noma in situ: relationship of extent of noninvasive disease to the frequency of occult invasion, multi-centricity, lymph node metastases, and short-term treatment failures. Cancer 1982, 50:1309–1314.
13. Albert S, Belle S, Eckert D, et al.: Current surgical management of in situ cancer of the female breast. J Surg Oncol 1982, 20:99–104.
14.• Ernster VL, Barclay J, Kerlikowske K: Mortality among women with ductal carcinoma in situ of the breast in the population-based Surveillance, Epidemiology, and End Results program. Arch Intern Med 2000, 160:953–958.
This study, in conjunction with Ernster et al. [1], provides useful data on the magnitude of DCIS in the United States, in correla-tion with expansion of mammographic screening programs.15. Evans A: The diagnosis and management of pre-invasive
breast disease: radiological diagnosis. Breast Cancer Res 2003, 5:250–253.
16. Fisher ER, Leeming R, Anderson S, et al.: Conservative management of intraductal carcinoma (DCIS) of the breast: collaborating NSABP investigators. J Surg Oncol 1991, 47:139–147.
17.••Julien JP, Bijker N, Fentiman IS, et al.: Radiotherapy in breast-conserving treatment for ductal carcinoma in situ: first results of the EORTC randomised phase III trial 10853. EORTC Breast Cancer Cooperative Group and EORTC Radiotherapy Group. Lancet 2000, 355:528–533.
This phase III clinical trial, similar to the NSABP B-17 proto-col, confirms the safety of breast-conserving therapy for DCIS, but with higher local recurrence rates when lumpectomy is performed alone.18. Fisher ER, Dignam J, Tan-Chiu E, et al.: Pathologic
findings from the National Surgical Adjuvant Breast Project (NSABP) eight-year update of Protocol B-17: intraductal carcinoma. Cancer 1999, 86:429–438.
Conclusions

144 Breast Carcinoma
19. Fisher B, Dignam J, Wolmark N, et al.: Tamoxifen in treatment of intraductal breast cancer: National Surgical Adjuvant Breast and Bowel Project B-24 randomised controlled trial. Lancet 1999, 353:1993–2000.
20. Fisher B, Dignam J, Wolmark N, et al.: Lumpectomy and radiation therapy for the treatment of intraductal breast cancer: findings from National Surgical Adjuvant Breast and Bowel Project B-17. J Clin Oncol 1998, 16:441–452.
21. Bijker N, Peterse JL, Duchateau L, et al.: Risk factors for recurrence and metastasis after breast-conserving therapy for ductal carcinoma in situ: analysis of Euro-pean Organization for Research and Treatment of Cancer Trial 10853. J Clin Oncol 2001, 19:2263–2271.
22. Weng EY, Juillard GJ, Parker RG, et al.: Outcomes and factors impacting local recurrence of ductal carcinoma in situ. Cancer 2000, 88:1643–1649.
23. Jha MK, Avlonitis VS, Griffith CD, et al.: Aggressive local treatment for screen-detected DCIS results in very low rates of recurrence. Eur J Surg Oncol 2001, 27:454–458.
24. Habel LA, Daling JR, Newcomb PA, et al.: Risk of recurrence after ductal carcinoma in situ of the breast. Cancer Epidemiol Biomarkers Prev 1998, 7:689–696.
25. Kestin LL, Goldstein NS, Martinez AA, et al.: Mammo-graphically detected ductal carcinoma in situ treated with conservative surgery with or without radiation therapy: patterns of failure and 10-year results. Ann Surg 2000, 231:235–245.
26. de Mascarel I, Bonichon F, MacGrogan G, et al.: Application of the van nuys prognostic index in a retrospective series of 367 ductal carcinomas in situ of the breast examined by serial macroscopic sectioning: practical considerations. Breast Cancer Res Treat 2000, 61:151–159.
27. Chan KC, Knox WF, Sinha G, et al.: Extent of excision margin width required in breast conserving surgery for ductal carcinoma in situ. Cancer 2001, 91:9–16.
28. Neuschatz AC, DiPetrillo T, Safaii H, et al.: Margin width as a determinant of local control with and without radiation therapy for ductal carcinoma in situ (DCIS) of the breast. Int J Cancer 2001, 96:97–104.
29.••Silverstein MJ: The University of Southern California/Van Nuys prognostic index for ductal carcinoma in situ of the breast. Am J Surg 2003, 186:337–343.
The VNPI is a landmark endeavor to stratify DCIS risk and eligibility for breast-conserving treatment based on discrete clinical and pathologic features.30. Ringberg A, Anagnostaki L, Anderson H, et al.: Cell
biological factors in ductal carcinoma in situ (DCIS) of the breast relationship to ipsilateral local recur-rence and histopathological characteristics. Eur J Cancer 2001, 37:1514–1522.
31. Douglas-Jones AG, Logan J, Morgan JM, et al.: Effect of margins of excision on recurrence after local excision of ductal carcinoma in situ of the breast. J Clin Pathol 2002, 55:581–586.
32. Jhingran A, Kim JS, Buchholz TA, et al.: Age as a predictor of outcome for women with DCIS treated with breast-conserving surgery and radiation: the University of Texas MD Anderson Cancer Center experience. Int J Radiat Oncol Biol Phys 2002, 54:804–809.
33. Fowble B, Hanlon AL, Fein DA, et al.: Results of conser-vative surgery and radiation for mammographically detected ductal carcinoma in situ (DCIS). Int J Radiat Oncol Biol Phys 1997, 38:949–957.
34. Solin LJ, Fourquet A, Vicini FA, et al.: Mammographic-ally detected ductal carcinoma in situ of the breast treated with breast-conserving surgery and definitive breast irradiation: long-term outcome and prognostic significance of patient age and margin status. Int J Radiat Oncol Biol Phys 2001, 50:991–1002.
35. Boyages J, Delaney G, Taylor R: Predictors of local recurrence after treatment of ductal carcinoma in situ: a meta-analysis. Cancer 1999, 85:616–628.
36. Clark L, Ritter E, Glazebrook K, et al.: Recurrent ductal carcinoma in situ after total mastectomy. J Surg Oncol 1999, 71:182–185.
37. Montgomery RC, Fowble BL, Goldstein LJ, et al.: Local recurrence after mastectomy for ductal carcinoma in situ. Breast J 1998, 4:430–436.
38. Silverstein MJ, Lagios MD, Craig PH, et al.: A prognostic index for ductal carcinoma in situ of the breast. Cancer 1996, 77:2267–2274.
39. Consensus conference of the classification of ductal carcinoma in situ. The Consensus Conference Committee. Cancer 1997, 80:1798–1802.
40. Wong J, Gadd M, Gelman R, et al.: Wide excision alone for ductal carcinoma in situ of the breast. Proceedings of the 26th Annual San Antonio Breast Cancer Symposium, Breast Cancer Research and Treatment. San Antonio: San Antonio Breast Cancer Symposium; 2003:15.
41. Intra M, Veronesi P, Mazzarol G, et al.: Axillary sentinel lymph node biopsy in patients with pure ductal carcinoma in situ of the breast. Arch Surg 2003, 138:309–313.
42. Pendas S, Dauway E, Giuliano R, et al.: Sentinel node biopsy in ductal carcinoma in situ patients. Ann Surg Oncol 2000, 7:15–20.
43. Allred DC, Bryant J, Lard S, et al.: Estrogen receptor expression as a predictive marker of the effectiveness of tamoxifen in the treatment of DCIS: findings from NSABP Protocol B-24. Proceedings of the 25th Annual San Antonio Breast Cancer Symposium. San Antonio: San Antonio Breast Cancer Symposium; 2002:30.
44.••Baum M, Budzar AU, Cuzick J, et al.: Anastrozole alone or in combination with tamoxifen versus tamoxifen alone for adjuvant treatment of postmenopausal women with early breast cancer: first results of the ATAC randomised trial. Lancet 2002, 359:2131–2139.
This landmark study demonstrating the benefits of anastro-zole in the adjuvant setting for invasive breast cancer pro-vides the basis for the NSABP B-35 study, which randomizes postmenopausal patients with DCIS to receive anastrozole versus tamoxifen.45. Julian T, Land S, Wolmark N: NSABP B-35: a clinical
trial to compare anastrozole and tamoxifen for post-menopausal patients with ductal carcinoma in situ undergoing lumpectomy with radiation therapy. Breast Dis Yearbook Q 2003, 14:121–122.
46. Silverstein MJ, Lagios MD, Groshen S, et al.: The influence of margin width on local control of ductal carcinoma in situ of the breast. N Engl J Med 1999, 340:1455–1461.
Copyright © 2022 FDOKUMEN




















