Developmental Issues in the Study of Coping
27
INTERNATIONAL JOURNAL OF BEHAVIORAL DEVELOPMENT, 1998, 22 (2), 287–313 Requests for reprints should be sent to Dr Sandra Losoya, Psychology, Arizona State University, Tempe, AZ 85287–1104, USA. This research was supported by grants from the National Science Foundation (DBS–9208375) and the National Institutes of Mental Health (1 R01 HH55052) to the second and third authors and by Research Scientist Development and Research Scientist Awards from the National Institute of Mental Health (K02 MH00903 and K05 M801321) to Nancy Eisenberg. The authors wish to thank the many students who assisted in this study, the parents and children involved, and the principals and teachers in the Child Study and Child Development Laboratories, and in the Tempe, Kyrene, Mesa, and Scottsdale School Districts. q 1998 The International Society for the Study of Behavioural Development Developmental Issues in the Study of Coping Sandra Losoya, Nancy Eisenberg, and Richard A. Fabes Arizona State University, USA Developmental issues generally have been ignored in the study of coping. Thus, the goals of this paper were threefold: (1) to summarise theory in which coping is placed in the larger context of emotion regulation; (2) to review brie y existing literature related to consistency and change in coping, interrelations among coping strategies at different ages, and the relation of coping to the quality of social functioning at different ages; and (3) to summarise data from a longitudinal study pertaining to the aforementioned issues. Coping was relatively consistent across time (over a six-year period); there were some age-related changes in mean levels of children’s adult- reported coping; and there was considerable consistency in interrelations of coping strategies at different ages. In general, relations of coping to social functioning were similar across age, although some age-related changes in patterns were noted. Children’s abilities to cope with stress have been a topic of considerable interest among psychologists in the last decade (Sandler, Wolchik, MacKinnon, Ayers, & Roosa, 1997). Although evidence of the relation of coping to children’s mental health outcomes and adjustment has been accumulating, there are still relatively few data concerning continuity and discontinuity in children’s coping, the interrelations among various types of coping at various ages, or how relations of coping with child outcomes (e.g. adjustment, social competence) change with age. Without developmental data, efforts to improve and increase children’s adaptive coping with stressors are likely to miss the mark. Thus, the purpose of this paper is by guest on December 2, 2015 jbd.sagepub.com Downloaded from
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of Developmental Issues in the Study of Coping
INTERNATIONAL JOURNAL OF BEHAVIORAL DEVELOPMENT, 1998, 22 (2), 287–313
Requests for reprints should be sent to Dr Sandra Losoya, Psychology, Arizona StateUniversity, Tempe, AZ 85287–1104, USA.
This research was supported by grants from the National Science Foundation(DBS–9208375) and the National Institutes of Mental Health (1 R01 HH55052) to the secondand third authors and by Research Scientist Development and Research Scientist Awards fromthe National Institute of Mental Health (K02 MH00903 and K05 M801321) to Nancy Eisenberg.The authors wish to thank the many students who assisted in this study, the parents and childreninvolved, and the principals and teachers in the Child Study and Child DevelopmentLaboratories, and in the Tempe, Kyrene, Mesa, and Scottsdale School Districts.
q 1998 The International Society for the Study of Behavioural Development
Developmental Issues in the Study of Coping
Sandra Losoya, Nancy Eisenberg, and Richard A. FabesArizona State University, USA
Developmental issues generally have been ignored in the study of coping.Thus, the goals of this paper were threefold: (1) to summarise theory in whichcoping is placed in the larger context of emotion regulation; (2) to reviewbrie�y existing literature related to consistency and change in coping,interrelations among coping strategies at different ages, and the relation ofcoping to the quality of social functioning at different ages; and (3) tosummarise data from a longitudinal study pertaining to the aforementionedissues. Coping was relatively consistent across time (over a six-year period);there were some age-related changes in mean levels of children’s adult-reported coping; and there was considerable consistency in interrelations ofcoping strategies at different ages. In general, relations of coping to socialfunctioning were similar across age, although some age-related changes inpatterns were noted.
Children’s abilities to cope with stress have been a topic of considerableinterest among psychologists in the last decade (Sandler, Wolchik,MacKinnon, Ayers, & Roosa, 1997). Although evidence of the relation ofcoping to children’s mental health outcomes and adjustment has beenaccumulating, there are still relatively few data concerning continuity anddiscontinuity in children’s coping, the interrelations among various types ofcoping at various ages, or how relations of coping with child outcomes (e.g.adjustment, social competence) change with age. Without developmentaldata, efforts to improve and increase children’s adaptive coping withstressors are likely to miss the mark. Thus, the purpose of this paper is
by guest on December 2, 2015jbd.sagepub.comDownloaded from

288 LOSOYA, EISENBERG, FABES
threefold. First, we brie�y summarise recent thinking on coping andemotion-related regulation. Second, the literature on the relations ofchildren’s coping to adjustment and social competence is reviewed, as aredata pertaining to developmental consistencies and age-related changes incoping. Third, we brie�y describe a longitudinal study including data oncoping. Speci�cally, we summarise data on inter-individual consistencyacross time and changes in mean levels of children’s coping as reported byteachers over a six-year period, and then present in more detail two types ofdata: (1) interrelations among various types of coping at four ages; and (2)relations of mode of coping to quality of social functioning at four ages.
OVERVIEW
One of the most frequently cited models of coping emerges from the adultliterature wherein coping is de�ned as “constantly changing cognitive andbehavioral efforts to manage speci�c external and/or internal demands thatare appraised as taxing or exceeding the resources of the person” (Lazarus &Folkman, 1984, p. 141). The focus of this model is on strategies used formanaging stressors (e.g. problem-focused coping), as well as those used inthe management of emotional arousal associated with the stressor (e.g.emotion-focused coping). Although there are other important models ofcoping (e.g. primary vs. secondary; Rothbaum, Weisz, & Snyder, 1982;approach vs. avoidance; Roth & Cohen, 1986; monitoring and blunting;Miller, 1987), most theorists acknowledge that the process of coping mayinvolve procedures that are directed at managing the stressor, and/or the selfin relation to the stressor.
Regardless of the differences among coping theorists, it is likely that mostwould agree that coping is motivated by the presence or expectation ofemotion arousal (generally resulting from stress or danger). Indeed, the veryact of coping usually is aimed at regulating the experience of emotion, theemotion-eliciting stressor, and one’s own emotion-related behaviour inresponse to the stressor. Moreover, speci�c emotions tend to have functionalmeanings for individuals and evoke emotion-speci�c coping tendencies(Barrett & Campos, 1987). Although coping behaviours usually are con�nedto behaviours that are effortful and consciously executed (a point whichcould be debated), subtler forms of emotion regulation are involved indealing with everyday events and stress. In any case, many forms of copingare very similar to types of regulation discussed in the emotion-regulationliterature. Thus, a consideration of the literature on emotion regulation perse is germane to a discussion of coping.
Emotion-related regulation pertains to more than merely suppressing orexpressing emotion. As suggested by Campos and his colleagues (Campos,Mumme, Kermoian, & Campos, 1994), emotion-relevant regulation
by guest on December 2, 2015jbd.sagepub.comDownloaded from

DEVELOPMENT OF COPING 289
involves input regulation (involving sensory receptors), central regulation(information or cognitive processing), and output regulation (at theresponse selection or behavioural level). Some form of managementon all levels often may be required when an individual is exposed to astressor.
Eisenberg and Fabes (Eisenberg et al., 1995) recently proposed that thereare at least three interrelated types of emotion regulation relevant to thediscussion of coping and the development of quality of socially competentbehaviour. The �rst is the regulation of internal (experienced) emotion—theprocess of initiating, maintaining, or modulating the occurrence, intensity, orduration of internal feeling states and emotion-related physiologicalprocesses. This kind of regulation is similar to emotion-focused copingdiscussed by Lazarus and Folkman (1984). Many of the strategies used toregulate the experience of emotion are cognitive in nature; for example,individuals may cognitively restructure events in their minds so as to altertheir emotion (e.g. think about a bad experience in a more positive light).Other modes of emotion regulation involve attentional skills discussed bytemperament theorists such as attentional shifting and focusing. Shiftingattention from a negatively evocative stimulus has been shown to reducenegative arousal in a variety of studies (Fabes, Eisenberg, Eisenbud, 1993;Miller & Green, 1985; Rothbart, Ziaie, & O’Boyle, 1992). In addition,individuals can refocus their attention to issues or things that elicit positiveemotion or suppress negative emotion. Finally, regulating experiencedemotion also may include strategies that involve approach or withdrawalfrom a stressor or seeking comfort from others to reduce an aversive internalstate.
The second type of regulation proposed by Eisenberg and Fabes is theregulation of behaviour associated with the experience of emotion,including overt actions toward others as well as facial expressions.Constructs such as behavioural inhibition, impulsivity, and activationalcontrol, which are discussed by temperament and personality theorists (e.g.Derryberry & Rothbart, 1988; Rothbart, Ahadi, & Hershey, 1994), tapindividual differences in the ability to regulate behaviour and also mayindicate tendencies to cope in particular ways. For instance, individuals whoare low in behavioural regulation are likely to enact nonconstructivebehaviour when stressed (e.g. aggression or venting of hostile emotion),whereas those who are well regulated generally react with more constructivemodes of behavioural regulation (e.g. Eisenberg et al., 1994).
The third type of regulation pertinent to the discussion of coping is theregulation of the emotion-eliciting context. This kind of regulation involvesefforts to modify the source of emotional arousal and maps closely on to thekind of problem-focused coping discussed by Lazarus and other copingtheorists. It requires active, approach type behaviour by the individual to
by guest on December 2, 2015jbd.sagepub.comDownloaded from
290 LOSOYA, EISENBERG, FABES
change the source of the problem, although regulation of a stressormay be achieved by seeking instrumental guidance and support fromothers.
In summary, it has become increasingly clear that emotion-related typesof regulation include coping and that coping is an effort at emotionregulation, de�ned broadly. Thus, �ndings from the work on emotionregulation (much in the form of research on temperament and earlysocioemotional functioning) are relevant to an understanding of thedevelopment of coping and its in�uence on later adjustment and socialcompetence.
THE RELATION OF COPING TO SOCIALFUNCTIONING
There is increasing evidence that individual differences in emotionregulation in infancy and toddlerhood are related to later social functioningand adjustment. Temperament theorists have argued that dimensions oftemperament such as early behavioural inhibition relates speci�cally tointernalising problems, whereas temperamental undercontrol relates toexternalising behaviours (Rothbart & Bates, 1997; Biederman et al., 1990;Caspi, Henry, McGee, Mof�tt, & Silva, 1995; Sanson, Oberklaid, Pedlow, &Prior, 1991). Findings on the link between early emotion-relevant regulationand social functioning or adjustment are accumulating, although thepathways and processes involved have yet to be well articulated.
With regard to the literature on coping in later childhood, studies havebegun to demonstrate linkages between particular coping strategies andlater adjustment. For instance, there is evidence that problem-focusedcoping strategies are related to positive developmental outcomes in many(but not all) circumstances. In general, children’s use of problem-focusedcoping strategies has been found to be negatively related to emotional andbehavioural problems (Ayers, Sandler, West, & Roosa, 1996; Dubow, Tisak,Causey, Hryshko, & Reid, 1991; Ebata & Moos, 1991; Glyshaw, Cohen, &Towbes, 1989; Herman-Stahl, Stemmler, & Petersen, 1995; Sandler, Tein, &West, 1994), social problems (Compas, Malcarne, & Fondacoro, 1988), andadolescent health-risk behaviours (McCubbin, Needle, & Wilson, 1985)although not always (see Weisenberg, Schwarzwald, Waysman, Solomon, &Klingman, 1993). Moreover, there is evidence that children who are lessadept at generating problem-focused coping strategies experience moreadjustment problems (Compas et al., 1988; Dubow, et al., 1991). In contrast,frequent use of emotion-focused coping has been related to higher levels ofbehavioural problems and symptoms of anxiety and depression (Compas,Ey, Worsham, & Howell, 1996; Compas et al., 1988; Hoffman, Levy-Shiff,Sohlberg, & Zarizki, 1992), although not in some situations where the
by guest on December 2, 2015jbd.sagepub.comDownloaded from

DEVELOPMENT OF COPING 291
stressor is uncontrollable (Miller & Green, 1985; also see Rudolph, Dennig,& Weisz, 1995).
The �ndings on avoidant coping strategies (which often includebehavioural and cognitive avoidance of stressful thoughts or situations) andtheir relations to social functioning and adjustment are not consistent.Avoidant coping has been linked to higher psychological symptoms for postdivorce children (Sandler et al., 1994), depression (Ebeta & Moos, 1991;Herman-Stahl et al., 1995), anxiety (Lewis & Kliewer, 1996), internalisingproblems (Finnegan, Hodges, & Perry, 1996; Kotchick, Forehand,Armistead, Klein, & Wierson, 1996), conduct disordered behaviour andexternalising problem behaviours (Kotchick et al., 1996; Ebeta & Moos,1991), dif�culty adapting to school (Causey & Dubow, 1993), and substanceuse (Patterson & McCubbin, 1987). In contrast, other researchers �nd thatchildren high in avoidant coping are low in problem behaviours at school(Kliewer, 1991; Eisenberg et al., 1993) and higher in teacher-reported socialcompetence (Kliewer & Sandler, 1993). Moreover, some initial worksuggests that avoidant coping may be linked to social competence more forchildren (particularly girls) high in depressive symptoms (Kliewer &Sandler, 1993). It is possible that avoidant coping is positively related tosocial functioning when the stressful situation is uncontrollable and whenavoidance prevents a negative situation from escalating.
However, as for the broader domain of emotion-focused coping, avoidant/distraction coping strategies may be appropriate in stressful situations thatare uncontrollable (Miller & Green, 1985). For instance, in a study ofpost-Persian Gulf War Israeli children, avoidant coping in response tomissile threat was not related to symptoms. However, in another study,children who had no understanding of who or what was in control of astressor were more likely to use avoidance in response to a painful procedureand were rated as more anxious by parents and clinical observers(Carpenter, 1992). Thus, �ndings on the relations of use of avoidant copingto social and psychological functioning are somewhat mixed. Generally,avoidant coping is related to poorer functioning; however, in some situationsdeemed uncontrollable, the reverse may be true. Moreover, it is possiblethat behavioural avoidance, which often has been part of avoidancemeasures for younger children, is constructive (or at least viewed asconstructive by adults) in situations involving potential con�ict amongchildren.
Other coping strategies such as support-seeking, aggressive coping (e.g.verbal/physical aggression to solve problems or to release feelings), denial,and venting (e.g. yelling, crying, blaming, etc.) also have been found to beassociated with children’s competencies and adjustment. Children’s reportsof having support from signi�cant others has been related to teacher-ratedcompetence among children in the third through �fth grades (Dubow &
by guest on December 2, 2015jbd.sagepub.comDownloaded from
292 LOSOYA, EISENBERG, FABES
Tisak, 1989; Dubow et al., 1991), although it is not clear in work of this type ifchildren actively coped by seeking support. In another study, Garber,Braa�adt, and Weiss (1995) found that children with lower scores on adepression inventory reported using more support-seeking coping inresponse to stressors that involved achievement than those with childrenwith higher depression scores. Eisenberg and her colleagues (1993, 1994)found that, for 4- to 6-year-olds, constructive coping, a composite thatincluded support coping (and instrumental coping) was positively related toteachers’ reports of social competence, but only for boys (support-seekingwas not examined separately). In contrast, nonconstructive coping, acomposite that included aggressive coping and venting (as well as lowavoidance/distraction and cognitive restructuring) was related to low socialcompetence. Similarly, teacher-reported support-seeking was related toteachers’ reports of children’s social competence (Kliewer & Sandler, 1993);however, the relation was not signi�cant when children were the reporters oftheir own coping behaviour. In summary, there is limited work on therelations of children’s coping to social functioning and adjustment.Moreover, the studies that are available differ in methodology and in theoperationalisation of coping, thus making them dif�cult to integrate into acoherent picture.
CONSISTENCY OF COPING IN CHILDHOOD ANDADOLESCENCE
Few researchers have examined inter-individual consistency in children’scoping (i.e. the magnitude of correlations of coping across time in a givensample). However, there are relevant �ndings in the literature on infanttemperament and early socioemotional functioning. For instance,attentional capacities (relevant to cognitive kinds of emotion-focusedcoping) such as attention span, attentional control, or distractibility aremoderately stable in infancy (McDevitt & Carey, 1981). Moreover, aspectsof emotion-relevant regulation such as adaptability and persistence/distractibility evidence moderate consistency from 2 to 12 years and from 3to 13 years (Caspi et al, 1995; Guerin & Gottfried, 1994).
There are few data pertaining to consistency in coping across time orstressors and when consistency has been examined, researchers frequentlyhave assessed reactions to different types of stressors at different times.Thus, it is dif�cult to discern whether coping behaviours are really unstableor change due to differences in measurement. Approach and problem-focused strategies (e.g. information seeking, problem solving) have shownconsistency over 3 months (Causey & Dubow, 1993), 5 months (Glyshaw etal, 1989), 9 months (Compas et al, 1988), and 1 and 2 years (Ebeta & Moos,1994; Dubow et al., 1991). In addition, there is some evidence of inter-
by guest on December 2, 2015jbd.sagepub.comDownloaded from

DEVELOPMENT OF COPING 293
individual consistency across time for cognitive avoidance and emotion-focused coping over comparable time periods (Causey & Dubow, 1993;Compas et al., 1988; Ebeta & Moos, 1994; Glyshaw et al., 1989). Thus, thereis limited evidence of consistency in children’s use of coping, although moststudies involve relatively short time periods.
Age-related Changes in Mean Levels of Children’sCoping
Previous work on emotion regulation in infancy has suggested that there arepredictable developmental changes in the coping strategies used to regulateemotional arousal (Kopp, 1982, 1989). Early infant behaviours such asthumb-sucking, looking at hands, and head turning, as well as reliance oncaregivers serve as primary coping strategies for infants dealing withstressors. By 9–18 months, infants are much better at attentional control andtheir use of coping strategies becomes much more differentiated. Forinstance, older toddlers appear to engage in more self-comfortingbehaviours and problem-focused coping than 12-month-olds (Parritz, 1996)and 12- or 18-month-olds use more self-soothing and self-distraction, andless fussing and gaze aversion, than 6-month-olds for coping with stress(Mangelsdorf, Shapiro, & Marzolf, 1995). Moreover, communicativebehaviours such as pointing and gesturing (which are thought to enhance theregulation of emotion) as well as language, are increasingly employed tocope with stressful situations early in life (Bates, O’Connell, & Shore, 1987;Braungart-Rieker & Stifter, 1996; Kopp, 1989).
At the same time as children’s coping skills become more complex, so dothe stressful situations that they encounter. As children mature, stressorsrange from issues related to separation from caregivers to parental control(Kopp, 1982), entrance into school (Rutter, 1983), peer relations (Fabes &Eisenberg, 1992), and adolescent development. Thus, by preschool and oninto adolescence, the types of coping assessed in research change somewhat.Relevant data pertaining to age-related mean changes in coping areembedded in the few extant longitudinal studies of coping, as well as incross-sectional studies in which coping at different ages is compared. Ingeneral, the �ndings are mixed, although a few patterns have emerged. Forinstance, age-related increases in the use of cognitive types of coping,including emotion-focused coping, avoidant/distraction strategies, cognitivereappraisals, positive self-talk, intrapsychic coping, and attention diversionhave been found (Altshuler & Ruble, 1989; Band & Weisz, 1988; Brown,O’Keefe, Sanders, & Baker, 1986; Bull & Drotar, 1991; Compas, et al., 1988,1996; Ebeta & Moos, 1994; Hoffman et al., 1992; Hoffner, 1993; Kurdek,1987; Weisenberg et al., 1933; Wertlieb, Weigel, & Feldstein, 1987).
by guest on December 2, 2015jbd.sagepub.comDownloaded from
294 LOSOYA, EISENBERG, FABES
Although coping that requires cognitive maturity appears to increase withage, the �ndings for avoidant coping have not been as consistent. Forinstance, in some studies, avoidant coping that is behavioural in nature (e.g.“I left the situation”), as opposed to cognitive avoidance (e.g. “I won’t letmyself think about it”) has been found to be higher among younger thanolder children (Altshuler & Ruble, 1989; Garber et al., 1995). Yet olderchildren report more frequent use of cognitive kinds of avoidant strategies,particularly in situations that they perceive as uncontrollable (Altshuler &Ruble, 1989). Other investigators have found decreases in avoidantstrategies, be they cognitive or behavioural (Sandler et al., 1994), or show noage-related changes at all (Altshuler, Genevro, Ruble, & Bornstein, 1995;Ebeta & Moos, 1994; Stark, Spirito, Williams, & Gueverment, 1989). It maybe that different operationalisations of avoidant coping and variation in theperceived controllability of coping contexts underlie some of theinconsistency in the �ndings (Altshuler & Ruble, 1989; Wertlieb et al., 1987).
Age-related changes in problem-focused types of coping are unclear. Forinstance, Ebeta and Moos (1994) examined approach and avoidance copingin response to stressors experienced in the previous year. At wave 1 andwave 2, older adolescents reported using somewhat more of all approachcoping dimensions (and one avoidance dimension). Others have reportedsimilar age increases in problem-focused types of coping (Bernzweig,Eisenberg, & Fabes, 1993; Brown et al., 1986; Herman-Stahl et al., 1995). Incontrast, other investigators have reported that younger children were morelikely to use more problem-focused coping (Band & Weisz, 1988; Bull &Drotar, 1991; Kliewer, 1991; Roecker, Dubow, & Donaldson, 1996;Weisenberg et al., 1993). Finally, some researchers have found no clearage-related patterns in the use of active approach (including seekinginformation) or problem-focused coping (Altshuler et al., 1995; Altshuler &Ruble, 1989; Compass et al., 1988; Hoffner, 1993; Spirito, Overholser, &Stark, 1989). Additional research, especially using longitudinal samples, isnecessary to delineate age changes in problem-focused coping and todetermine factors (e.g. type of stressor situation) associated with variation inthe �ndings. Moreover, researchers need to address whether the quality (e.g.sophistication, ef�cacy) of problem-focused coping efforts change with age.
Age changes in support-seeking coping also have been found. Someresearchers have reported that kindergarteners engaged in more supportstrategies than did third graders (Bernzweig et al., 1993). Similar resultswere found for 7-year-olds as opposed to 10-year-olds (Kliewer, 1991), for8-year-olds as opposed to 10-year-olds (Ryan, 1989), and for �fth graders asopposed to seventh or tenth graders (Weisenberg et al., 1993). Thus, itappears that in general, reliance on external support decreases with age,although some investigators have noted no age changes (Hoffner, 1993;Spirito et al., 1989).
by guest on December 2, 2015jbd.sagepub.comDownloaded from
DEVELOPMENT OF COPING 295
In summary, some trends emerge from the literature on age changes inchildren’s coping. First, with age, children use more strategies that are moreinner-focused and mentalistic, such as emotion-focused coping. Strategiesthat require more sophisticated cognitive processing are not evident inyoung children’s coping repertoire but emerge with age in childhood.Moreover, with age, children seem to become more independent and beginto move away from relying on others for support.
INTERRELATIONS AMONG COPING STRATEGIESAT DIFFERENT AGES
Only a few researchers have discussed age-related differences in the patternsof inter-correlations among various coping strategies. Kliewer (1991) foundthat coping strategies generally were unrelated to one another, except thatavoidant actions and use of distracting actions were positively related for�fth graders, but not for second graders. This �nding may suggest that olderchildren are more likely than younger children to understand similaritiesamong coping strategies in their functions. Kliewer (1991) also reported thatfor both second and �fth graders, expressing feelings was negatively relatedto cognitive avoidance, and, for second graders, cognitive decision making.
Thus, as children get older, it appears that they may become morediscriminating with regard to their use and understanding of copingstrategies. For instance, in a longitudinal study, Ebeta and Moos (1994)reported that all of the interrelations among coping strategies at Time 1 werepositive and signi�cant. Although most of these relations held one year later,some were no longer signi�cant, for example, the relations of seekingguidance/support with both resigned acceptance and cognitive avoidance(or resigned acceptance coping with problem solving). Nevertheless, the sizeof the correlations generally did not differ greatly across age, perhaps in partbecause the age range of the children was between 12 and 18 years andmeasurements occurred only one year apart.
With a slightly younger and age-restricted sample, Hoffman et al. (1992)reported what appear to be striking differences in the pattern of correlationsamong coping strategies for boys aged 10–11 and 12–13 years. For instance,emotional coping (i.e. “blamed self for what happened”, “got angry withpeople/things that caused the problems”, “told yourself things to makeyourself feel better”) and cognitive coping (i.e. “concentrated on the goodthings”, “tried not to think about it”) were positively related forpreadolescents but were negatively related for adolescents. Similarly,practical coping (instrumental support seeking) was positively related toemotional coping for the younger boys but was negatively related for theolder boys. For both groups, practical coping was positively related tocognitive coping, but the strength of the relation was greater for younger
by guest on December 2, 2015jbd.sagepub.comDownloaded from
296 LOSOYA, EISENBERG, FABES
boys. Unfortunately, emotional coping was a mix of turning emotion inwardand outwardly (e.g. blaming the self, getting angry with others) and cognitivereframing. Thus, it is dif�cult to interpret the �ndings or integrate them withother studies. Clearly, research in which relatively homogeneous measuresof coping are inter-correlated at different ages is needed to examine whetherthere are developmental changes in the interrelations of coping strategies. Arecent study is a good example of the type of research that is needed. Ayerset al. (1996) examined the factor structure for various coping strategies thatwere de�ned in normative ways from interviews with post-divorce childrenaged 9–10 and 11–13 years. The underlying factor structure remained thesame across two age groups. Thus, there was no evidence of change in theinterrelations of coping strategies across this age span. Of course, change inthe structure of coping may be found with samples of children varying morein age.
A LONGITUDINAL STUDY OF COPING
We have conducted a longitudinal study of children’s regulation andemotionality that contained teachers’ reports of coping behaviour inpotential peer con�ict situations over a six-year period. These data providesome interesting descriptive information on coping behaviour from age 4–6to age 10–12 years, at least as perceived by teachers. In addition to examiningchanges in mean groups levels of various kinds of coping at different ages,three kinds of correlational relations were computed: (1) inter-individualstability over time (correlations on a given kind of coping over time); (2)structural consistency (relations of a given kind of coping with other types ofcoping at different ages, which provide insights as to the meaning of a giventype of coping); and (3) correlations with measures of quality of socialfunctioning at different ages, which tap the centrality of a given kind ofcoping for social outcomes at each age.
Participants were part of a six-year longitudinal study with fourassessments, each two years apart (see Eisenberg et al., 1994, 1995, 1997).The children were aged 4–6 years (in preschool or in a kindergartenassociated with a preschool) when the study began and were 10–12 years (infourth, �fth, or sixth grade) at the end of the study. The sample wasapproximately 90% Caucasian and middle class and upper-middle class.Detailed information on the sample is provided in the foregoing references.
The �rst wave of data was collected during two consecutive semesterswhen the children were in preschool or kindergarten classes (thekindergarten was at a preschool). Ninety-three children were involved onesemester or another. The children also were studied two, four, and six yearslater. Only children with data for coping from all time periods were used inthe analyses that are reported in this paper (i.e. 54 children had teacher
by guest on December 2, 2015jbd.sagepub.comDownloaded from

DEVELOPMENT OF COPING 297
coping data at all assessments). The mean ages in months were 65(range 5 54–79), 88 (77–102 range), 108 (97–122), and 132 (121–146) at thefour assessments.
Children’s coping styles were rated by teachers using the same proceduresat all times. Three scenarios about everyday con�icts were presented and theteachers rated the likelihood (1 5 not at all likely; 7 5 extremely likely) thatthe child would engage in each of 9 types of coping as well as “doing nothing”(similar to Kliewer, 1991 and Sandler et al., 1994): (1) instrumental coping(takes some constructive action to improve a problem situation); (2)emotional intervention (cries to elicit assistance from others to help solvethe problem); (3) instrumental aggression (resolves problems throughphysical or verbal aggression); (4) behavioural avoidance (leaves or avoids aproblem situation); (5) behavioural distraction (keeps him/herself busy so asnot to think about the problem); (6) venting emotion (cries to releasepent-up feelings or elicit comfort from others); (7) emotional aggression(uses physical or verbal aggression to release pent-up feelings); (8) cognitiverestructuring (tries to think about the situation in a positive way); and (9)emotional support (talks about his/her problems with friends or a teacher inhope of getting support). The scenarios concerned when the child becamehurt or angry because he/she was made fun of or excluded from play, orbecause a peer purposely destroyed something of the child’s or disrupted thechild’s activities. Concrete examples of each coping behaviour wereprovided (e.g. “Ask the other children why they won’t let him play”).Teachers completed the measure at each of the four time periods; ages 4–6,6–8, 8–10, and 10–12 (see Eisenberg et al., 1993, 1995, 1997).
Using the total sample at each time period, analogous items wereaveraged across the three vignettes. Next, based on conceptualconsideration and correlations, the coping styles were reduced to thefollowing seven coping measures at each of the time periods: (1) aggressivecoping composite—emotional and instrumental aggression; (2) avoidance/distraction coping composite (including behavioural avoidance anddistraction); (3) venting coping composite—venting emotion and emotionalintervention; (4) cognitive restructuring coping; (5) emotional supportcoping; (6) instrumental coping; and (7) doing nothing (see Eisenberg et al.,1993, 1995, 1997; Murphy et al., 1997, for alphas and more details).
Consistency, Change, and Inter-correlations
As reported by Murphy et al. (1997), there was considerable consistency inteachers’ reports of individual differences in some forms of children’scoping, even over several years’ time. For example, reports of instrumentalcoping were signi�cantly related over two, four, and six years, withcorrelations ranging from .26 to .38. Similar consistency was found for
by guest on December 2, 2015jbd.sagepub.comDownloaded from
298 LOSOYA, EISENBERG, FABES
aggressive coping, with correlations ranging from .34 to .43, including acorrelation of .57 over six years. Reports of doing nothing were consistentafter age 4–6 (i.e. from age 6–8 and older), whereas reports of venting ofemotion were signi�cantly correlated over two years’ time, but not longer.Teachers’ reports of positive cognitive restructuring and support seekinggenerally were not consistent over time, whereas avoidant coping wasconsistent over some two- or four-year periods.
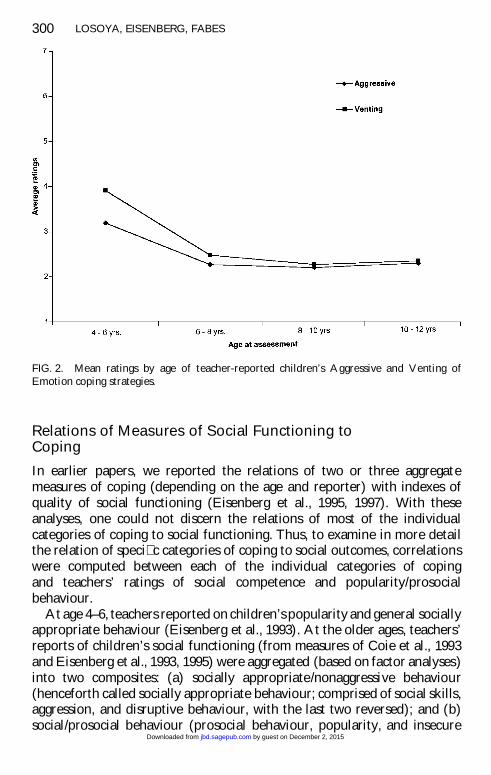
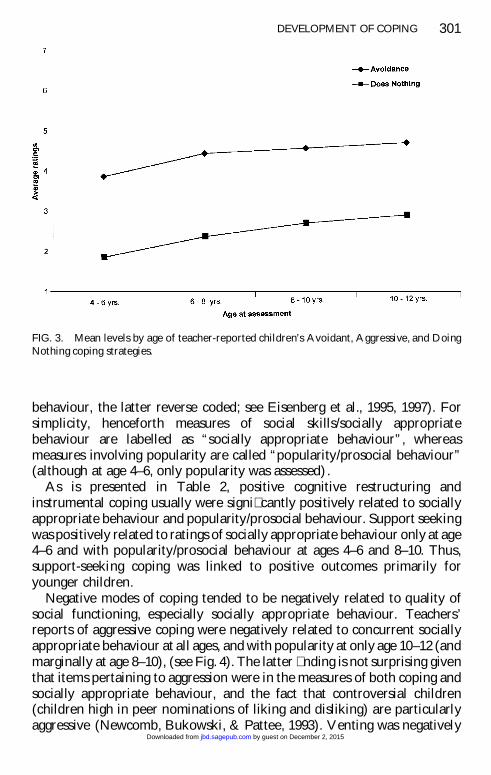
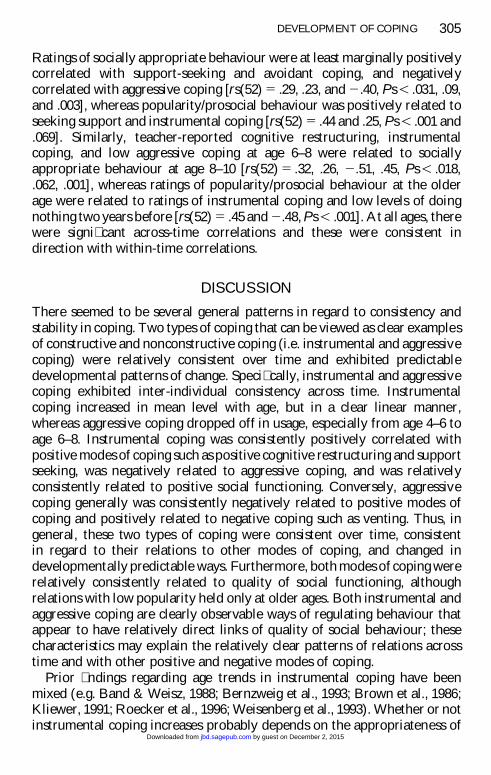
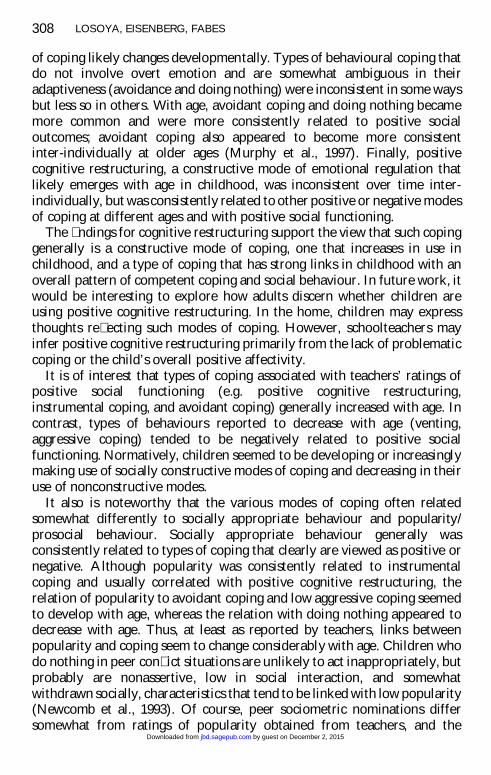
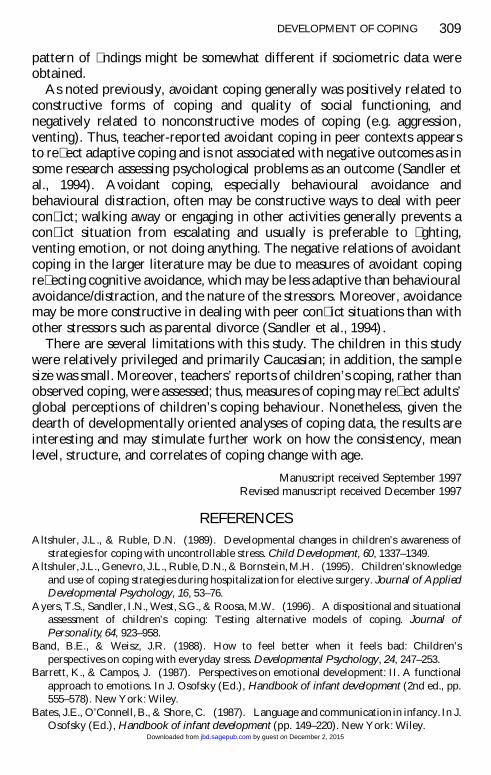
In terms of mean levels of coping, trend analyses indicated teachers’reports of positive cognitive restructuring and instrumental coping increasedover time whereas reports of coping by seeking support �uctuated such thatit dropped off early in elementary school, then increased, and thendecreased again (i.e. there was a cubic trend; see Murphy et al., 1997), (seeFig. 1). Aggressive coping and venting of emotion showed a decrease overtime, particularly from age 4–6 to age 6–8 (see Fig. 2). There also werequadratic trends for aggressive and venting coping. The quadratic trend forventing was slightly stronger than the linear trend and re�ected a sharp dropin venting from age 4–6 to 8–10, followed by very little change from T4 to T5.Finally, reports of doing nothing and avoidant coping increased over time(see Fig. 3), particularly from age 4–6 to 6–8.
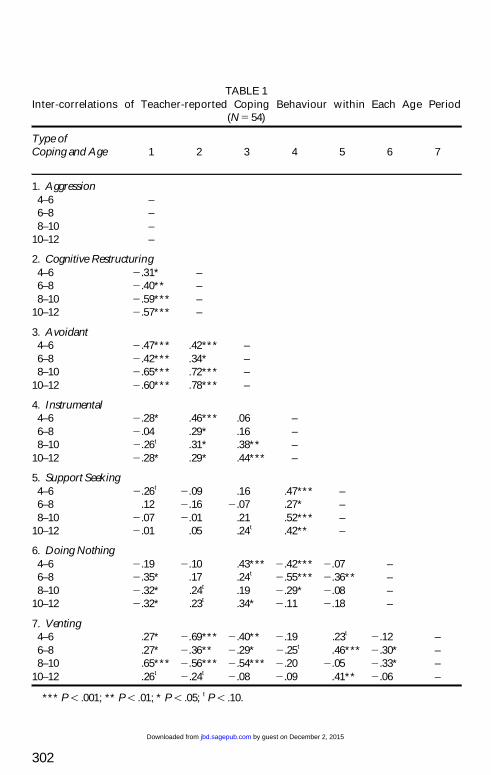
It also was of interest to examine the interrelations of the variouscategories of coping at each time period. When all categories werefactor-analysed, the results varied somewhat with age so it was impossible toconstruct similar composites based on the same factors at each age. Thisproblem apparently occurred because many of the categories of coping weresigni�cantly interrelated, and small changes in the degree of associationcould affect the factor loadings. Indeed, the patterns of correlations weresimilar across the various ages. For example, aggression was positivelyrelated to venting at all four time periods (P , .10 at age 10–12) andnegatively related to avoidant coping and positive cognitive restructuring atall time periods (see Table 1). Aggressive coping also was signi�cantlynegatively related to doing nothing at age 6–8, 8–10, and 10–12, and toinstrumental coping at age 4–6 and 10–12 (and marginally at age 8–10).Furthermore, instrumental coping was positively related to both supportseeking and positive cognitive restructuring at all four time periods, andnegatively related to avoidant coping at the two older ages and doingnothing at ages 4–6 and 10–12. In addition to the aforementionedcorrelations involving avoidant coping, avoidant coping was negativelyrelated to venting at the three younger ages, and positively related topositive cognitive restructuring at all time periods and doing nothing at ages4–6 and 10–12 (and marginally at 6–8). Besides the relations alreadymentioned for venting, venting was at least marginally, negatively correlated
by guest on December 2, 2015jbd.sagepub.comDownloaded from

DEVELOPMENT OF COPING 299
FIG. 1. Mean levels by age of teacher-reported children’s positive coping strategies.
with positive cognitive restructuring at all time periods and positively relatedto doing nothing at three ages.
It is of interest that venting was related only to support seeking at T4,although correlations with venting often were substantial at younger ages.Thus, venting coping seemed to be somewhat less related to other forms ofcoping with age. Moreover, instrumental coping seemed to be somewhatmore consistently positively associated with avoidant coping with age, andless correlated with doing nothing. Thus, with age, instrumental coping wasassociated with avoidant behaviours and cognitions that minimised con�ictbut was negatively related to a passive stance.
In summary, although the pattern of interrelations was fairly consistentover time, there were a few intriguing signs of changes in patterning.Age-related changes in patterning were most evident for venting, a copingbehaviour that probably is deemed by most as more appropriate for youngerthan older children. Moreover, the correlations for emotional supportseeking were not highly consistent in patterning, perhaps because seekingadult emotional support varies in its appropriateness and meaning with theage of the child (as suggested by the cubic trend for mean levels of supportseeking).
by guest on December 2, 2015jbd.sagepub.comDownloaded from
300 LOSOYA, EISENBERG, FABES
FIG. 2. Mean ratings by age of teacher-reported children’s Aggressive and Venting ofEmotion coping strategies.
Relations of Measures of Social Functioning toCoping
In earlier papers, we reported the relations of two or three aggregatemeasures of coping (depending on the age and reporter) with indexes ofquality of social functioning (Eisenberg et al., 1995, 1997). With theseanalyses, one could not discern the relations of most of the individualcategories of coping to social functioning. Thus, to examine in more detailthe relation of speci�c categories of coping to social outcomes, correlationswere computed between each of the individual categories of copingand teachers’ ratings of social competence and popularity/prosocialbehaviour.
At age 4–6, teachers reported on children’s popularity and general sociallyappropriate behaviour (Eisenberg et al., 1993). At the older ages, teachers’reports of children’s social functioning (from measures of Coie et al., 1993and Eisenberg et al., 1993, 1995) were aggregated (based on factor analyses)into two composites: (a) socially appropriate/nonaggressive behaviour(henceforth called socially appropriate behaviour; comprised of social skills,aggression, and disruptive behaviour, with the last two reversed); and (b)social/prosocial behaviour (prosocial behaviour, popularity, and insecure
by guest on December 2, 2015jbd.sagepub.comDownloaded from
DEVELOPMENT OF COPING 301
FIG. 3. Mean levels by age of teacher-reported children’s Avoidant, Aggressive, and DoingNothing coping strategies.
behaviour, the latter reverse coded; see Eisenberg et al., 1995, 1997). Forsimplicity, henceforth measures of social skills/socially appropriatebehaviour are labelled as “socially appropriate behaviour”, whereasmeasures involving popularity are called “popularity/prosocial behaviour”(although at age 4–6, only popularity was assessed).
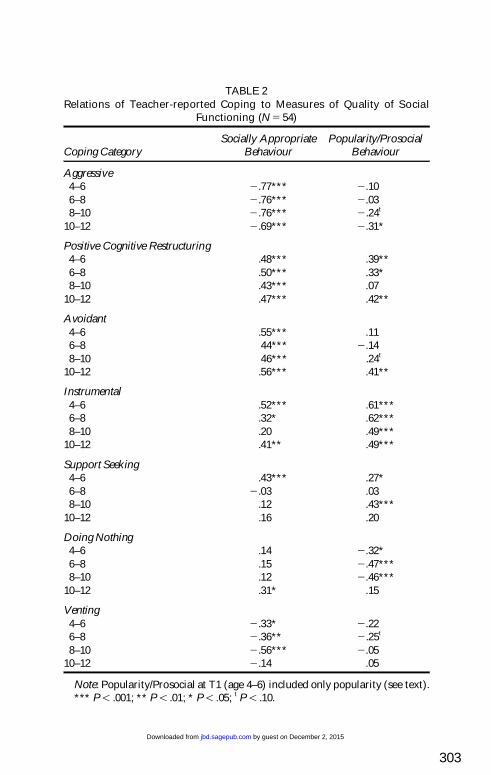
As is presented in Table 2, positive cognitive restructuring andinstrumental coping usually were signi�cantly positively related to sociallyappropriate behaviour and popularity/prosocial behaviour. Support seekingwas positively related to ratings of socially appropriate behaviour only at age4–6 and with popularity/prosocial behaviour at ages 4–6 and 8–10. Thus,support-seeking coping was linked to positive outcomes primarily foryounger children.
Negative modes of coping tended to be negatively related to quality ofsocial functioning, especially socially appropriate behaviour. Teachers’reports of aggressive coping were negatively related to concurrent sociallyappropriate behaviour at all ages, and with popularity at only age 10–12 (andmarginally at age 8–10), (see Fig. 4). The latter �nding is not surprising giventhat items pertaining to aggression were in the measures of both coping andsocially appropriate behaviour, and the fact that controversial children(children high in peer nominations of liking and disliking) are particularlyaggressive (Newcomb, Bukowski, & Pattee, 1993). Venting was negatively
by guest on December 2, 2015jbd.sagepub.comDownloaded from
302
TABLE 1Inter-correlations of Teacher-reported Coping Behaviour within Each Age Period
(N 5 54)
Type of Coping and Age 1 2 3 4 5 6 7
1. Aggression4–6 –6–8 –8–10 –
10–12 –
2. Cognitive Restructuring4–6 2 .31* –6–8 2 .40** –8–10 2 .59*** –
10–12 2 .57*** –
3. Avoidant4–6 2 .47*** .42*** –6–8 2 .42*** .34* –8–10 2 .65*** .72*** –
10–12 2 .60*** .78*** –
4. Instrumental4–6 2 .28* .46*** .06 –6–8 2 .04 .29* .16 –8–10 2 .26t .31* .38** –
10–12 2 .28* .29* .44*** –
5. Support Seeking4–6 2 .26t 2 .09 .16 .47*** –6–8 .12 2 .16 2 .07 .27* –8–10 2 .07 2 .01 .21 .52*** –
10–12 2 .01 .05 .24t .42** –
6. Doing Nothing4–6 2 .19 2 .10 .43*** 2 .42*** 2 .07 –6–8 2 .35* .17 .24t 2 .55*** 2 .36** –8–10 2 .32* .24t .19 2 .29* 2 .08 –
10–12 2 .32* .23t .34* 2 .11 2 .18 –
7. Venting4–6 .27* 2 .69*** 2 .40** 2 .19 .23t 2 .12 –6–8 .27* 2 .36** 2 .29* 2 .25t .46*** 2 .30* –8–10 .65*** 2 .56*** 2 .54*** 2 .20 2 .05 2 .33* –
10–12 .26t 2 .24t 2 .08 2 .09 .41** 2 .06 –
*** P , .001; ** P , .01; * P , .05; t P , .10.
by guest on December 2, 2015jbd.sagepub.comDownloaded from
303
TABLE 2Relations of Teacher-reported Coping to Measures of Quality of Social
Functioning (N 5 54)
Socially Appropriate Popularity/ProsocialCoping Category Behaviour Behaviour
Aggressive4–6 2 .77*** 2 .106–8 2 .76*** 2 .038–10 2 .76*** 2 .24t
10–12 2 .69*** 2 .31*
Positive Cognitive Restructuring4–6 .48*** .39**6–8 .50*** .33*8–10 .43*** .07
10–12 .47*** .42**
Avoidant4–6 .55*** .116–8 44*** 2 .148–10 46*** .24t
10–12 .56*** .41**
Instrumental4–6 .52*** .61***6–8 .32* .62***8–10 .20 .49***
10–12 .41** .49***
Support Seeking4–6 .43*** .27*6–8 2 .03 .038–10 .12 .43***
10–12 .16 .20
Doing Nothing4–6 .14 2 .32*6–8 .15 2 .47***8–10 .12 2 .46***
10–12 .31* .15
Venting4–6 2 .33* 2 .226–8 2 .36** 2 .25t
8–10 2 .56*** 2 .0510–12 2 .14 .05
Note: Popularity/Prosocial at T1 (age 4–6) included only popularity (see text).*** P , .001; ** P , .01; * P , .05; t P , .10.
by guest on December 2, 2015jbd.sagepub.comDownloaded from
304 LOSOYA, EISENBERG, FABES
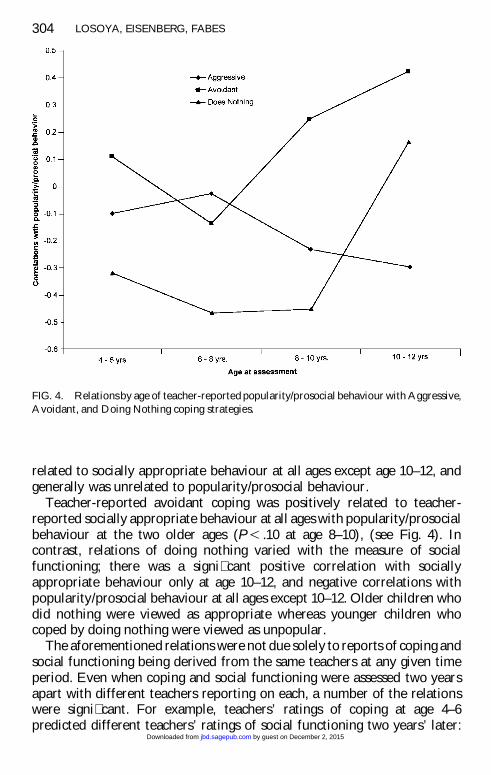
FIG. 4. Relations by age of teacher-reported popularity/prosocial behaviour with Aggressive,Avoidant, and Doing Nothing coping strategies.
related to socially appropriate behaviour at all ages except age 10–12, andgenerally was unrelated to popularity/prosocial behaviour.
Teacher-reported avoidant coping was positively related to teacher-reported socially appropriate behaviour at all ages with popularity/prosocialbehaviour at the two older ages (P , .10 at age 8–10), (see Fig. 4). Incontrast, relations of doing nothing varied with the measure of socialfunctioning; there was a signi�cant positive correlation with sociallyappropriate behaviour only at age 10–12, and negative correlations withpopularity/prosocial behaviour at all ages except 10–12. Older children whodid nothing were viewed as appropriate whereas younger children whocoped by doing nothing were viewed as unpopular.
The aforementioned relations were not due solely to reports of coping andsocial functioning being derived from the same teachers at any given timeperiod. Even when coping and social functioning were assessed two yearsapart with different teachers reporting on each, a number of the relationswere signi�cant. For example, teachers’ ratings of coping at age 4–6predicted different teachers’ ratings of social functioning two years’ later:
by guest on December 2, 2015jbd.sagepub.comDownloaded from
DEVELOPMENT OF COPING 305
Ratings of socially appropriate behaviour were at least marginally positivelycorrelated with support-seeking and avoidant coping, and negativelycorrelated with aggressive coping [rs(52) 5 .29, .23, and 2 .40, Ps , .031, .09,and .003], whereas popularity/prosocial behaviour was positively related toseeking support and instrumental coping [rs(52) 5 .44 and .25, Ps , .001 and.069]. Similarly, teacher-reported cognitive restructuring, instrumentalcoping, and low aggressive coping at age 6–8 were related to sociallyappropriate behaviour at age 8–10 [rs(52) 5 .32, .26, 2 .51, .45, Ps , .018,.062, .001], whereas ratings of popularity/prosocial behaviour at the olderage were related to ratings of instrumental coping and low levels of doingnothing two years before [rs(52) 5 .45 and 2 .48, Ps , .001]. At all ages, therewere signi�cant across-time correlations and these were consistent indirection with within-time correlations.
DISCUSSION
There seemed to be several general patterns in regard to consistency andstability in coping. Two types of coping that can be viewed as clear examplesof constructive and nonconstructive coping (i.e. instrumental and aggressivecoping) were relatively consistent over time and exhibited predictabledevelopmental patterns of change. Speci�cally, instrumental and aggressivecoping exhibited inter-individual consistency across time. Instrumentalcoping increased in mean level with age, but in a clear linear manner,whereas aggressive coping dropped off in usage, especially from age 4–6 toage 6–8. Instrumental coping was consistently positively correlated withpositive modes of coping such as positive cognitive restructuring and supportseeking, was negatively related to aggressive coping, and was relativelyconsistently related to positive social functioning. Conversely, aggressivecoping generally was consistently negatively related to positive modes ofcoping and positively related to negative coping such as venting. Thus, ingeneral, these two types of coping were consistent over time, consistentin regard to their relations to other modes of coping, and changed indevelopmentally predictable ways. Furthermore, both modes of coping wererelatively consistently related to quality of social functioning, althoughrelations with low popularity held only at older ages. Both instrumental andaggressive coping are clearly observable ways of regulating behaviour thatappear to have relatively direct links of quality of social behaviour; thesecharacteristics may explain the relatively clear patterns of relations acrosstime and with other positive and negative modes of coping.
Prior �ndings regarding age trends in instrumental coping have beenmixed (e.g. Band & Weisz, 1988; Bernzweig et al., 1993; Brown et al., 1986;Kliewer, 1991; Roecker et al., 1996; Weisenberg et al., 1993). Whether or notinstrumental coping increases probably depends on the appropriateness of
by guest on December 2, 2015jbd.sagepub.comDownloaded from

306 LOSOYA, EISENBERG, FABES
instrumental and problem-focused approaches in a given situation. Insituations involving potential peer con�ict, problem-focused approachesfrequently may be effective and, consequently, may increase in frequency inchildhood. In instances in which problem-focused coping is not likely toresult in desired outcomes, it may not increase in frequency with age.
Contrast the pattern of �ndings for emotional support seeking and ventingwith aggressive and instrumental coping. Both support seeking and ventingcoping involve emotion, be it overtly expressed or the reason for seekingsupport. Seeking emotional support generally is viewed as positive, at leastat younger ages, whereas venting likely is viewed as negative (see Eisenberget al., 1994). Both types of coping are unstable in various ways. Neither ofthese modes of coping was very consistent inter-individually over time.Moreover, both exhibited strong nonlinear changes in mean levels (althoughthere also was linear trend for venting). Speci�cally, although ventingdecreased with age, most of the decrease occurred over a two-year period, asre�ected in the strong quadratic trend. Support-seeking coping exhibited adistinctly nonlinear (cubic) trend. In addition, relations with other modes ofcoping were not as consistent as for instrumental and aggressive coping.Support-seeking coping was positively related to one of the most positivetypes of coping (instrumental) but was inconsistently correlated or unrelatedto other types of coping. Venting tended to be positively related to negativemodes of coping and negatively related to some positive modes of coping,but relations with other modes of coping were not consistent across age (i.e.there were few signi�cant correlations at age 10–12 years). Finally, bothtypes of coping were more consistently related to quality of socialfunctioning at younger than older ages. The lack of consistency in these twomodes of coping is not surprising because their signi�cance andappropriateness likely change substantially with age. Both were mostcommon in 4- to 6-year-olds and likely are viewed as most appropriate foryounger children. Because of children’s growing coping capacities andincreased peer pressure on children not to cry at school, coping by ventingsimply may be uncommon in the school context by age 10–12. It also isprobable that venting is less noticeable to teachers with age because it is lessfrequently displayed in the elementary than preschool classroom.
Positive cognitive restructuring, avoidant coping, and coping by doingnothing all were a mix of consistency and inconsistency. Positive cognitiverestructuring, viewed as a positive type of coping in many situations, was notvery consistent inter-individually over time, although it did increase in aclear linear fashion with age, was fairly consistently related to various modesof coping at all ages, and was consistently related to positive socialfunctioning. Perhaps the inconsistency across time was due to the factthat positive cognitive restructuring likely develops relatively latedevelopmentally and is emerging for some children in the early school years.
by guest on December 2, 2015jbd.sagepub.comDownloaded from

DEVELOPMENT OF COPING 307
Moreover, cognitive restructuring is a type of emotion regulation that isdif�cult to observe directly, a factor that could also contribute to lowinter-individual consistency across time.
Avoidant coping and doing nothing also were a mix of consistency andinconsistency, but a different mix than for cognitive restructuring. Inter-individual consistencies for both avoidant coping and doing nothing wereobtained over two or four years but not six years. Both increased linearlywith age, although the increase for avoidance was primarily from age 4–6 to6–8 (as re�ected in a quadratic trend). Although relations of avoidant copingwith low aggressive coping and high positive cognitive restructuring wereconsistent at all ages, correlations with other modes of coping variedconsiderably with age. Avoidant coping appeared to change from analternative to venting at a young age to a correlate of active instrumentalcoping at older ages. Inconsistency in relations with other modes of copingwas even more evident for coping by doing nothing than for avoidant coping.Doing nothing appeared to be an alternative to instrumental coping in thepreschool and early school years and an alternative to aggression in the earlyto later school years. Avoidant coping was consistently related to sociallyappropriate behaviour across age; however, correlations with popularitywere evident only at older ages. Doing nothing was positively related tosocially appropriate behaviour only at the oldest age (age 10–12), and wasnegatively related to popularity/prosocial behaviour only at earlier threeages.
Because avoidance and doing nothing likely vary in the degree to whichthey are considered constructive coping by teachers across contexts andperhaps age, perhaps it is not surprising that they show some instabilities intheir inter-individual consistency and relations with other modes of coping.Both avoidant coping and doing nothing seemed to be a component of arelatively constructive pattern of coping at older ages and were associatedwith more positive outcomes at older than younger ages. Avoidant copingand passive coping may be relatively controlled ways of dealing with peercon�ict at older ages, whereas doing nothing may re�ect a lack of alternativecoping strategies among younger children.
In brief, types of coping that involved clearly constructive ornonconstructive behavioural regulation (instrumental and aggressivecoping) seemed to exhibit the most consistency (inter-individually,structurally, and in regard to indexes of social competence), as well asnormative developmental change in the direction of enhanced copingcompetence. Types of emotion-related regulation that involved the directexpression of emotion or attempts to get direct external assistance inregulating emotion (support seeking) were relatively inconsistent at morethan one level and did not exhibit predominantly linear changes in meanlevel with age. As discussed previously, the appropriateness of these modes
by guest on December 2, 2015jbd.sagepub.comDownloaded from
308 LOSOYA, EISENBERG, FABES
of coping likely changes developmentally. Types of behavioural coping thatdo not involve overt emotion and are somewhat ambiguous in theiradaptiveness (avoidance and doing nothing) were inconsistent in some waysbut less so in others. With age, avoidant coping and doing nothing becamemore common and were more consistently related to positive socialoutcomes; avoidant coping also appeared to become more consistentinter-individually at older ages (Murphy et al., 1997). Finally, positivecognitive restructuring, a constructive mode of emotional regulation thatlikely emerges with age in childhood, was inconsistent over time inter-individually, but was consistently related to other positive or negative modesof coping at different ages and with positive social functioning.
The �ndings for cognitive restructuring support the view that such copinggenerally is a constructive mode of coping, one that increases in use inchildhood, and a type of coping that has strong links in childhood with anoverall pattern of competent coping and social behaviour. In future work, itwould be interesting to explore how adults discern whether children areusing positive cognitive restructuring. In the home, children may expressthoughts re�ecting such modes of coping. However, schoolteachers mayinfer positive cognitive restructuring primarily from the lack of problematiccoping or the child’s overall positive affectivity.
It is of interest that types of coping associated with teachers’ ratings ofpositive social functioning (e.g. positive cognitive restructuring,instrumental coping, and avoidant coping) generally increased with age. Incontrast, types of behaviours reported to decrease with age (venting,aggressive coping) tended to be negatively related to positive socialfunctioning. Normatively, children seemed to be developing or increasinglymaking use of socially constructive modes of coping and decreasing in theiruse of nonconstructive modes.
It also is noteworthy that the various modes of coping often relatedsomewhat differently to socially appropriate behaviour and popularity/prosocial behaviour. Socially appropriate behaviour generally wasconsistently related to types of coping that clearly are viewed as positive ornegative. Although popularity was consistently related to instrumentalcoping and usually correlated with positive cognitive restructuring, therelation of popularity to avoidant coping and low aggressive coping seemedto develop with age, whereas the relation with doing nothing appeared todecrease with age. Thus, at least as reported by teachers, links betweenpopularity and coping seem to change considerably with age. Children whodo nothing in peer con�ict situations are unlikely to act inappropriately, butprobably are nonassertive, low in social interaction, and somewhatwithdrawn socially, characteristics that tend to be linked with low popularity(Newcomb et al., 1993). Of course, peer sociometric nominations differsomewhat from ratings of popularity obtained from teachers, and the
by guest on December 2, 2015jbd.sagepub.comDownloaded from
DEVELOPMENT OF COPING 309
pattern of �ndings might be somewhat different if sociometric data wereobtained.
As noted previously, avoidant coping generally was positively related toconstructive forms of coping and quality of social functioning, andnegatively related to nonconstructive modes of coping (e.g. aggression,venting). Thus, teacher-reported avoidant coping in peer contexts appearsto re�ect adaptive coping and is not associated with negative outcomes as insome research assessing psychological problems as an outcome (Sandler etal., 1994). Avoidant coping, especially behavioural avoidance andbehavioural distraction, often may be constructive ways to deal with peercon�ict; walking away or engaging in other activities generally prevents acon�ict situation from escalating and usually is preferable to �ghting,venting emotion, or not doing anything. The negative relations of avoidantcoping in the larger literature may be due to measures of avoidant copingre�ecting cognitive avoidance, which may be less adaptive than behaviouralavoidance/distraction, and the nature of the stressors. Moreover, avoidancemay be more constructive in dealing with peer con�ict situations than withother stressors such as parental divorce (Sandler et al., 1994).
There are several limitations with this study. The children in this studywere relatively privileged and primarily Caucasian; in addition, the samplesize was small. Moreover, teachers’ reports of children’s coping, rather thanobserved coping, were assessed; thus, measures of coping may re�ect adults’global perceptions of children’s coping behaviour. Nonetheless, given thedearth of developmentally oriented analyses of coping data, the results areinteresting and may stimulate further work on how the consistency, meanlevel, structure, and correlates of coping change with age.
Manuscript received September 1997Revised manuscript received December 1997
REFERENCESAltshuler, J.L., & Ruble, D.N. (1989). Developmental changes in children’s awareness of
strategies for coping with uncontrollable stress. Child Development, 60, 1337–1349.Altshuler, J.L., Genevro, J.L., Ruble, D.N., & Bornstein, M.H. (1995). Children’s knowledge
and use of coping strategies during hospitalization for elective surgery. Journal of AppliedDevelopmental Psychology, 16, 53–76.
Ayers, T.S., Sandler, I.N., West, S.G., & Roosa, M.W. (1996). A dispositional and situationalassessment of children’s coping: Testing alternative models of coping. Journal ofPersonality, 64, 923–958.
Band, B.E., & Weisz, J.R. (1988). How to feel better when it feels bad: Children’sperspectives on coping with everyday stress. Developmental Psychology, 24, 247–253.
Barrett, K., & Campos, J. (1987). Perspectives on emotional development: II. A functionalapproach to emotions. In J. Osofsky (Ed.), Handbook of infant development (2nd ed., pp.555–578). New York: Wiley.
Bates, J.E., O’Connell, B., & Shore, C. (1987). Language and communication in infancy. In J.Osofsky (Ed.), Handbook of infant development (pp. 149–220). New York: Wiley.
by guest on December 2, 2015jbd.sagepub.comDownloaded from
310 LOSOYA, EISENBERG, FABES
Bernzweig, J., Eisenberg, N., & Fabes, R.A. (1993). Children’s coping in self- and other-relevant contexts. Journal of Experimental Child Psychology, 55, 208–226.
Biederman, J., Rosanbaum, J.F., Hirshfeld, D.R., Faraone, S.V., Bolduc, E.A., Gersten, M.,Meminger, S.R., Kagan, J., Snidman, N., & Reznick, S. (1990). Psychiatric correlates ofbehavioural inhibition in young children of parents with and without psychiatric disorders.Archives of General Psychiatry, 47, 21–26.
Braungart-Riecker, J.M., & Stifter, C.A., (1996). Infants’ responses to frustrating situations:Continuity and change in reactivity and regulation. Child Development, 67, 1767–1779.
Brown, J.M., O’Keeffe, J., Sanders, S.H., & Baker, B. (1986). Developmental changes inchildren’s cognition to stressful and painful situations. Journal of Pediatric Psychology, 11,343–357.
Bull, B.A., & Drotar, D. (1991). Coping with cancer in remission: Stressors and strategiesreported by children and adolescents. Journal of Pediatric Psychology, 16, 767–782.
Campos, J.J., Mumme, D.L., Kermoian, R., & Campos, R.G. (1994). A functionalistperspective on the nature of emotion. In N.A. Fox (Ed.), The development of emotionregulation: Biological and behavioral considerations. Monographs of the Society forResearch in Child Development, 59, (Serial No. 240, 284–303).
Carpenter, P.J. (1992). Perceived control as a predictor of distress in children undergoinginvasive medical procedures. Journal of Pediatric Psychology, 17, 757–773.
Caspi, A., Henry, B., McGee, R.O., Mof�tt, T.E., & Silva, P.A. (1995). Temperamentalorigins of child and adolescent behaviour problems: From age three to age �fteen. ChildDevelopment, 66, 55–68.
Causey, D.L., & Dubow, E.F. (1993). Negotiating the transition to junior high school: Thecontributions of coping strategies and perceptions of the school environment. Prevention inHuman Services, 10, 59–81.
Coie, J.D., Terry, R., Dodge, K.A., & Underwood, M.K. (1993). A teacher checklist ofchildren’s social behavior. Unpublished manuscript, Duke University.
Compas, B.E., Malcarne, V.L., & Fondacaro, K.M. (1988). Coping with stressful events inolder children and young adolescents. Journal of Consulting and Clinical Psychology, 563,405–411.
Compas, B.E., Ey, S., Worsham, N.L., Howell, D.C. (1996). When mom or dad has cancer: II.Coping, cognitive appraisals, and psychological distress in children of cancer patients. ChildDevelopment, 15, 167–175.
Derryberry, D., & Rothbart, M.K. (1988). Arousal, affect, and attention as components oftemperament. Journal of Personality and Social Psychology, 55, 958–966.
Dubow, E.F., & Tisak, J.T. (1989). The relations between stressful life events and adjustmentin elementary school children: The role of social support and social problem-solving skills.Child Development, 60, 1412–1423.
Dubow, E.F., Tisak, J., Causey, D., Hryshko, A., Reid, G. (1991). A two-year longitudinalstudy of stressful life events, social support, and social problem-solving skills: Contributionsto children’s behavioral and academic adjustment. Child Development, 62, 583–599.
Ebeta, A.T., & Moos, R.H. (1991). Coping and adjustment in distressed and healthyadolescents. Journal of Applied Developmental Psychology, 17, 33–54.
Ebeta, A.T., & Moos, R.H. (1994). Personal, situational, and contextual correlates of copingin adolescence. Journal of Research on Adolescence, 4, 99–125.
Eisenberg, N., Fabes, R.A., Bernzweig, J., Karbon, M., Poulin, R., & Hanish, L. (1993). Therelations of emotionality and regulation to preschoolers’ social skills and sociometric status.Child Development, 64, 1418–1438.
Eisenberg, N., Fabes, R.A., Murphy, B., Maszk, P., Smith, M., & Karbon, M. (1995). The roleof emotionality and regulation in children’s social functioning: A longitudinal study. ChildDevelopment, 66, 1239–1261.
by guest on December 2, 2015jbd.sagepub.comDownloaded from
DEVELOPMENT OF COPING 311
Eisenberg, N., Fabes, R.A., Nyman, M., Bernzweig, J., & Pinuelas, A. (1994). The relationsof emotionality and regulation to children’s anger-related reactions. Child Development, 65,109–128.
Eisenberg, N., Fabes, R.A., Shepard, S.A., Murphy, B.C., Guthrie, I.K., Jones, S., Friedman, J.,Poulin, R., & Maszk, P. (1997). Contemporaneous and longitudinal prediction ofchildren’s social functioning from regulation and emotionality. Child Development, 68,642–664.
Fabes, R.A., & Eisenberg, N. (1992). Young children’s coping with interpersonal anger.Child Development, 63, 116–128.
Fabes, R.A., Eisenberg, N., & Eisenbud, L. (1993). Behavioral and physiological correlatesof children’s reactions to others’ distress. Developmental Psychology, 29, 655–663.
Finnegan, R.A., Hodges, E.V.A., & Perry, D.G. (1996). Preoccupied and avoidant copingduring middle childhood. Child Development, 67, 1318–1328.
Garber, J., Braa�adt, N., & Weiss, B. (1995). Affect regulation in depressed andnondepressed children and young adolescents. Development and Psychopathology, 7,93–115.
Glyshaw, K., Cohen, L.H., & Towbes, L.C. (1989). Coping strategies and psychologicaldistress: Prospective analyses of early and middle adolescents. American Journal ofCommunity Psychology, 17, 607–623.
Guerin, D.W., & Gottfried, A.W. (1994). Developmental stability and change in parentreports of temperament: A ten-year longitudinal investigation from infancy throughadolescence. Merrill-Palmer Quarterly, 40, 334–355.
Guerin, D.W., & Gottfried, A.W. (1994). Temperamental consequences of infantdif�cultness. Infant Behavior and Development, 17, 413–421.
Herman-Stahl, M.A., Stemmler, M., & Petersen, A.C. (1995). Approach and avoidantcoping: Implications for adolescent mental health. Journal of Youth and Adolescence, 24,649–665.
Hoffman, M.A., Levy-Shiff, R., Sohlberg, S.C., & Zarizki, J. (1992). The impact of stress andcoping: Developmental changes in the transition to adolescence. Journal of Youth andAdolescence, 21, 451–469.
Hoffner, C. (1993). Children’s strategies for coping with stress: Blunting and monitoring.Motivation and Emotion, 17, 91–106.
Kliewer, W. (1991). Coping in middle childhood: Relations to competence, type Abehavior, monitoring, blunting, and locus of control. Developmental Psychology, 27,689–697.
Kliewer, W., & Sandler, I.N. (1993). Social competence and coping among children ofdivorce. American Journal of Orthopsychiatry, 63, 432–440.
Kopp, C.B. (1982). Antecedents of self-regulation: A developmental perspective.Development Psychology, 18, 199–214.
Kopp, C.B. (1989). Regulation of distress and negative emotions: A developmental view.Developmental Psychology, 25, 343–354.
Kotchick, B.A., Forehand, R., Armistead, L., Klein, K., & Wierson, M. (1996). Coping withillness: Interrelationships across family members and predictors of psychologicaladjustment. Journal of Family Psychology, 10, 358–370.
Kurdek, L.A. (1987). Gender differences in the psychological symptomatology and copingstrategies of young adolescents. Journal of Early Adolescence, 7, 395–410.
Lazarus, R.S., & Folkman, S. (1984). Stress, appraisal, and coping. New York: Springer.Lewis, H.A., & Kliewer, W. (1996). Hope, coping, and adjustment among children with
Sickle Cell Disease: Tests of mediator and moderator models. Journal of PediatricPsychology, 21, 25–41.
Mangelsdorf, S.C., Shapiro, J.R., & Marzolf, D. (1995). Developmental and temperamentaldifferences in emotion regulation in infancy. Child Development, 66, 1817–1828.
by guest on December 2, 2015jbd.sagepub.comDownloaded from

312 LOSOYA, EISENBERG, FABES
McCubbin, H.I., Needle, R.H., & Wilson, M. (1985). Adolescent health risk behaviors:Family stress and adolescent coping as critical factors. Family Relations, 34, 51–62.
McDevitt, S.C., & Carey, W.B. (1981). Stability of ratings vs. perceptions of temperamentfrom early infancy to 1–3 years. American Journal of Orthopsychiatry, 51, 342–345.
Miller, S.M. (1987). Monitoring and blunting: Validation of a questionnaire to assess styles ofinformation seeking under threat. Journal of Personality and Social Psychology, 52, 345–353.
Miller, S.M., & Green, M.L. (1985). Coping with stress and frustration: Origins, nature, anddevelopment. In M. Lewis & C. Saarni (Eds.), The socialization of emotions (pp. 263–314).New York: Plenum.
Murphy, B.C., Eisenberg, N., Fabes, R.A., Shepard, S., & Guthrie, I. (1997). Consistency andchange in children’s emotionality, regulation, and coping: A longitudinal study. (Manuscriptsubmitted for publication.)
Newcomb, A.F., Bukowski, W.M., & Pattee, L., (1993). Children’s peer relations: Ameta-analytic review of popular, rejected, neglected, controversial, and average sociometricstatus. Psychological Bulletin, 113, 99–128.
Parritz, R. H. (1996). A descriptive analysis of toddler coping in challenging circumstances.Infant Behavior and Development, 19, 171–180.
Patterson, J.M., & McCubbin, H.I. (1987). Adolescent coping style and behaviors:Conceptualization and measurement. Journal of Adolescence, 10, 163–186.
Roecker, C.E., Dubow, E.F., & Donaldson, D. (1996). Cross-situational patterns inchildren’s coping with observed interpersonal con�ict. Journal of Clinical Child Psychology,25, 288–299.
Roth, S., & Cohen, L.J. (1986). Approach, avoidance, and coping with stress. AmericanPsychologist, 41, 813–819.
Rothbaum, F., Weisz, J.R., & Snyder, S.S. (1982). Changing the world and changing the self:A two-process model of perceived control. Journal of Personality and Social Psychology, 42,5–37.
Rothbart, M.K., & Bates, J.E. (1997). Temperament. In W. Damon (Series Ed.) and N.Eisenberg (Volume Ed.), Social, emotional and personality development: Vol. 3. Handbookof child psychology (pp. 105–106). New York: Wiley.
Rothbart, M.K., Ahadi, S.A., & Hershey, K.L. (1994). Temperament and social behavior inchildhood. Merrill-Palmer Quarterly, 40, 21–39.
Rothbart, M.K., Ziaie, H., & O’Boyle, C.G. (1992). Self-regulation and emotion in infancy.New Directions in Child Development, 55, 7–23.
Rudolph, K. D., Dennig, M.D., & Weisz, J.R. (1995). Determinants and consequences ofchildren’s coping in the medical setting: Conceptualization, review, and critique.Psychological Bulletin, 118, 328–357.
Rutter, M. (1983). Stress, coping, and development: Some issues and some questions. In N.Garmezy and M. Rutter (Eds.), Stress, coping, and development in children (pp. 1–42). NewYork: McGraw-Hill.
Ryan, N.M. (1989). Stress-coping strategies identi�ed from school-age children’sperspective. Research in Nursing and Health, 12, 111–122.
Sandler, I.N., Tein, J., & West, S.G. (1994). Coping, stress and the psychological symptoms ofchildren of divorce: A cross-sectional and longitudinal study. Child Development, 65,1744–1763.
Sandler, I.N., Wolchik, S.A., MacKinnon, D., Ayers, T.S., & Roosa, M.W. (1997).Developing linkages between theory and intervention in stress and coping processes. In S.A.Wolchik & I.N. Sandler (Eds.), Handbook of children’s coping: linking theory andintervention(pp. 3–40). New York: Plenum.
Sanson, A., Oberklaid, F., Pedlow, R., & Prior, M. (1991). Risk indicators: Assessment ofinfancy predictors of pre-school behavioral maladjustment. Journal of Child Psychologyand Psychiatry, 37, 185–195.
by guest on December 2, 2015jbd.sagepub.comDownloaded from

DEVELOPMENT OF COPING 313
Spirito, A., Overholser, J., & Stark, L.J. (1989). Common problems and coping strategies II:Findings with adolescent suicide attempters. Journal of Abnormal Psychology, 17, 213–221.
Stark, L.J. Spirito, A., Williams, C.A., & Guevremont, D.C. (1989). Common problems andcoping strategies: I. Findings with normal adolescents. Journal of Abnormal ChildPsychology, 17, 203–212.
Weisenberg, M., Schwarzwald, J., Waysman, M., Solomon, Z., & Klingman, A. (1993).Coping of school-age children in the sealed room during scud missile bombardment andpostwar stress reactions. Journal of Consulting and Clinical Psychology, 61, 462–467.
Wertlieb, D., Weigel, M.A., & Feldstein, M. (1987). Measuring children’s coping. AmericanJournal of Orthopsychiatry, 57, 548–560.
by guest on December 2, 2015jbd.sagepub.comDownloaded from