




Developmental Disabilities: - Continuing Education
355
This activity is developed by a community planning and advisory committee made up of self-advocates and representatives from the following agencies: UCSF, Stanford University, The Arc San Francisco, Golden Gate Regional Center, East Bay Regional Center, State Council on Developmental Disabilities, Support for Families, WITH Foundation, and the California Department of Developmental Services. Photos courtesy of Support for Families, The Arc San Francisco, and Down Syndrome Connection of the Bay Area 19th Annual Developmental Disabilities: Update for Health Professionals Presented by the UCSF SCHOOL OF MEDICINE and the UCSF SCHOOL OF NURSING COURSE CO-CHAIRS Lucy S. Crain, MD, MPH, FAAP Geraldine Collins-Bride, MS, ANP, FAAN March 5-6, 2020 Holiday Inn Golden Gateway San Francisco, California
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of Developmental Disabilities: - Continuing Education

This activity is developed by a community planning and advisory committee made up of self-advocates and representatives from the following agencies: UCSF, Stanford University, The Arc San Francisco, Golden Gate Regional Center, East Bay Regional Center, State Council on Developmental Disabilities, Support for Families, WITH Foundation, and the California Department of Developmental Services. Photos courtesy of Support for Families, The Arc San Francisco, and Down Syndrome Connection of the Bay Area
19th Annual
Developmental Disabilities: Update for Health Professionals
Presented by the
UCSF SCHOOL OF MEDICINE and the UCSF SCHOOL OF NURSING
COURSE CO-CHAIRS Lucy S. Crain, MD, MPH, FAAP Geraldine Collins-Bride, MS, ANP, FAAN
March 5-6, 2020 Holiday Inn Golden Gateway
San Francisco, California

19th Annual Developmental Disabilities: An Update for Health Professionals The 19th annual interdisciplinary conference offers a unique update for primary care and subspecialty health care professionals and others who care for children, youth, and adults with developmental disabilities and complex health care needs. Most medical and health professional education programs inadequately address care for people with developmental and intellectual developmental disabilities, although they represent a growing (and aging) population in the US. The pace of new information and research provides us with exciting opportunities to transform and improve the quality of care provided to these individuals. The conference covers a broad spectrum of developmental disabilities, with special focus on autism spectrum disorders and cerebral palsy in 2020. Our emphasis this year is on communication, self-determination and supported decision-making, transitions from childhood to adulthood, and access to healthcare systems and services from a variety of specialists. We are pleased to also present talks on maximizing potential, mental health, dental care, and advocacy. Presentations by our expert faculty should be of interest to pediatricians, family physicians, nurse clinicians, psychologists, and internists who are involved in the health care of individuals with developmental disabilities, as well as to those in other health-related disciplines including health policy, epidemiology, psychiatry, school health, social work, and case management services. While the conference is designed for health care professionals, we welcome families and individuals with developmental disabilities who wish to learn from the various represented disciplines. Non-profit conference exhibitors feature resources to help our audience better provide care for children, youth, and adults with developmental disabilities. We welcome you to the 19th annual Developmental Disabilities Update Conference and hope that your patients and clients with special health care needs will benefit from your participation. Lucy S. Crain, MD, MPH, FAAP Gerri Collins-Bride, RN, MS, ANP, FAAN Course Co-Chair Course Co-Chair

EDUCATIONAL OBJECTIVES
Upon completion of this program, attendees should be able to:
Discuss state and national advocacy, and policy issues surrounding insurance for those with special needs and creating access to healthcare for children and adults with developmental disabilities in the 21st century;
Discuss current social and cultural disparities, and implications for healthcare access and quality of care for individuals with developmental disabilities;
Counsel individuals and families regarding special needs trusts, self-determination and supported decision-making;
Identify and implement new communication strategies for individuals with developmental and intellectual disabilities;
Provide informed healthcare for people with autism spectrum disorders and other behavioral disorders and develop strategies for appropriate referral;
Describe innovations in dental care for people with DD/ID and make patient recommendations accordingly;
Apply state of the art healthcare for patients with movement disorders to improve quality of life;
Identify the signs of sexual abuse or trafficking, and have strategies to seek intervention;
Counsel patients and families on potentially dangerous new “cures” for developmental disabilities;
Discuss mental health care and be aware of psychopharmacological considerations for people with intellectual and developmental disabilities.
ACCREDITATION
The University of California, San Francisco School of Medicine (UCSF) is accredited by the Accreditation Council for Continuing Medical Education to provide continuing medical education for physicians.
Physicians UCSF designates this live activity for a maximum of 14.50 AMA PRA Category 1 Credits™. Physicians should claim only the credit commensurate with the extent of their participation in the activity.
This CME activity meets the requirements under California Assembly Bill 1195, Continuing Education and Cultural and Linguistic Competency. Family Physicians This Live activity, 19th Annual Developmental Disabilities: Update for Health Professionals, with a beginning date of 03/05/2020, has been reviewed and is acceptable for up to 13.75 Prescribed credit(s) by the American Academy of Family Physicians. Physicians should claim only the credit commensurate with the extent of their participation in the activity. Nurses For the purpose of recertification, the American Nurses Credentialing Center accepts AMA PRA Category 1 Credit™ issued by organizations accredited by the ACCME.

ACCREDITATION, CONT. Physician Assistants AAPA accepts category 1 credit from AOACCME, Prescribed credit from AAFP, and AMA PRA Category 1 Credit™ from organizations accredited by the ACCME. Pharmacists The California Board of Pharmacy accepts as continuing professional education those courses that meet the standard of relevance to pharmacy practice and have been approved for AMA PRA Category 1 Credit™. Psychologists The California Board of Psychology accepts as continuing education those courses that meet the standard of relevance to psychology practice and have been approved for AMA PRA Category 1 Credit™. Psychologists are responsible for reporting their own attendance to the California Board of Psychology. Psychologists from other states should check with their respective licensing boards. Licensed Clinical Social Workers and Marriage & Family Therapists University of California, San Francisco School of Medicine (UCSF) is approved by the California Association of Marriage and Family Therapists to sponsor continuing education for LCSWs, LMFTs, LPCCs, and/or LEPs. UCSF maintains responsibility for this program/course and its content. Course meets the qualifications for 14.50 hours of continuing education credit for LMFTs, LCSWs, LPCCs, and/or LEPs as required by the California Board of Behavioral Sciences. Provider Name: UCSF Approval Number: 64239 No instructor or facilitator is permitted to promote or advocate for a single modality of treatment that is discriminatory or likely to harm clients, based upon current accepted standards of practice. All CAMFT- certified education must provide training on how to treat all clients in an ethically and clinically sound manner.

General Information Attendance Verification/Sign-In Sheet/CME Certificates Please remember to sign-in on the sign-in sheet when you check in at the UCSF Registration Desk on your first day. You only need to sign-in once for the course, when you first check in. After the meeting, you will receive an email from [email protected] with a link to complete your online Course Evaluation / Electronic CME Certificate. The Qualtrics system will send you reminders to complete your CME Certificate Claiming until you complete it. Upon completing the online course evaluation, your CME certificate will be automatically generated on the screen for you to print or save as a PDF. The link will be available for 30 days after the last day of the course. However, after that date the link will expire and you will no longer be able to claim your credits online. You must then contact the Office of CME at [email protected] to receive your certificate. Speaker Survey Your opinion is important to us – we do listen! On Wednesday, March 4th, you should receive an email from [email protected] with a link to access the Speaker Survey. The survey can be completed online in real time during the course and is separate from the Evaluation/CME Certificate. If you did not receive the link, please see the UCSF Registration Desk. Wine and Cheese Reception A networking wine and cheese reception will be held in the lobby restaurant immediately following the conclusion of the lectures from 5:15-6:15pm on Thursday March 5th. Lunches Lunch is provided on Thursday. A list of nearby restaurants is included at the end of the syllabus for Friday. The hotel’s lobby restaurant will offer attendees a special rate if you wish to dine in-house. Security We urge caution with regard to your personal belongings and syllabus books. We are unable to replace these in the event of loss. Please do not leave any personal belongings unattended in the meeting room during lunch or breaks or overnight. Exhibits Exhibits will be available outside the meetingroom during breakfasts, breaks, and the lunch on Thursday March 5th. Final Presentations Final presentations will be available on our course website approximately 1-2 weeks post event. We will contact you when presentations are posted. https://www.ucsfcme.com/2020/MOC20001/slides.html

ACKNOWLEDGEMENTS This educational activity has been supported in part by a grant from Ability Central Philanthropy, a non profit 501(c)3 organization, and support from the California Department of Developmental Services and the UCSF Office of Diversity and Outreach. Ability Central’s Mission To serve as an educator, convener and resource that works collaboratively to ensure communications and information access in service of individuals who are Deaf or disabled.
Program Exhibitors/Resource Center
Alameda County Developmental Disabilities Planning Advisory Council
CBEM
Dance and Fitness Concepts
Disability Rights California
Down Syndrome Connection of the Bay Area
East Bay Regional Center
Golden Gate Regional Center
LEAP Family Home Agency
Pomeroy Recreation & Rehabilitation Center
State Council on Developmental Disabilities
Support for Families
TACT/Redwood Coast Regional Center
The Arc San Francisco
UCSF Office of Developmental Primary Care

Healthy People 2020: Disability and Health
Objective #1: Include in the core of Healthy People 2020 population data systems a standardized set of questions that identify “people with disabilities.” Objective #2: Increase the number of Tribes, States, and the District of Columbia that have public health surveillance and health promotion programs for people with disabilities and caregivers. Objective #3: Increase the proportion of U.S. master of public health (M.P.H.) programs that offer graduate-level courses in disability and health. Objective #4: Reduce the proportion of people with disabilities who report delays in receiving primary and periodic preventive care due to specific barriers. Objective #5: Increase the proportion of youth with special health care needs whose health care provider has discussed transition planning from pediatric to adult health care. Objective #6: Increase the proportion of people with epilepsy and uncontrolled seizures who receive appropriate medical care. Objective #7: Reduce the proportion of older adults with disabilities who use inappropriate medications. Objective #8: Reduce the proportion of people with disabilities who report physical or program barriers to local health and wellness programs. Objective #9: Reduce the proportion of people with disabilities who encounter barriers to participating in home, school, work, or community activities. Objective #10: Reduce the proportion of people with disabilities who report barriers to obtaining the assistive devices, service animals, technology services, and accessible technologies that they need. Objective #11: Increase the proportion of newly constructed and retrofitted U.S. homes and residential buildings that have visitable features. Objective #12: Reduce the number of people with disabilities living in congregate care residences. Objective #13: Increase the proportion of people with disabilities who participate in social, spiritual, recreational, community, and civic activities to the degree that they wish. Objective #14: Increase the proportion of children and youth with disabilities who spend at least 80 percent of their time in regular education programs. Objective #15: Reduce unemployment among people with disabilities. Objective #16: Increase employment among people with disabilities. Objective #17: Increase the proportion of adults with disabilities who report sufficient social and emotional support. Objective #18: Reduce the proportion of people with disabilities who report serious psychological distress. Objective #19: Reduce the proportion of people with disabilities who experience nonfatal unintentional injuries that require medical care. Objective #20: Increase the proportion of children with disabilities, birth through age 2 years, who receive early intervention services in home or community-based settings.
For more information, please visit:
https://www.healthypeople.gov/2020/topics-objectives/topic/disability-and-health

Federal and State Law Regarding Linguistic Access and Services for Limited English Proficient Persons
I. Purpose.
This document is intended to satisfy the requirements set forth in California Business and Professions code 2190.1. California law requires physicians to obtain training in cultural and linguistic competency as part of their continuing medical education programs. This document and the attachments are intended to provide physicians with an overview of federal and state laws regarding linguistic access and services for limited English proficient (“LEP”) persons. Other federal and state laws not reviewed below also may govern the manner in which physicians and healthcare providers render services for disabled, hearing impaired or other protected categories
II. Federal Law – Federal Civil Rights Act of 1964, Executive Order 13166, August 11,
2000, and Department of Health and Human Services (“HHS”) Regulations and LEP Guidance.
The Federal Civil Rights Act of 1964, as amended, and HHS regulations require recipients of federal financial assistance (“Recipients”) to take reasonable steps to ensure that LEP persons have meaningful access to federally funded programs and services. Failure to provide LEP individuals with access to federally funded programs and services may constitute national origin discrimination, which may be remedied by federal agency enforcement action. Recipients may include physicians, hospitals, universities and academic medical centers who receive grants, training, equipment, surplus property and other assistance from the federal government. HHS recently issued revised guidance documents for Recipients to ensure that they understand their obligations to provide language assistance services to LEP persons. A copy of HHS’s summary document entitled “Guidance for Federal Financial Assistance Recipients Regarding Title VI and the Prohibition Against National Origin Discrimination Affecting Limited English Proficient Persons – Summary” is available at HHS’s website at: http://www.hhs.gov/ocr/lep/ . As noted above, Recipients generally must provide meaningful access to their programs and services for LEP persons. The rule, however, is a flexible one and HHS recognizes that “reasonable steps” may differ depending on the Recipient’s size and scope of services. HHS advised that Recipients, in designing an LEP program, should conduct an individualized assessment balancing four factors, including: (i) the number or proportion of LEP persons eligible to be served or likely to be encountered by the Recipient; (ii) the frequency with which LEP individuals come into contact with the Recipient’s program; (iii) the nature and importance of the program, activity or service provided by the Recipient to its beneficiaries; and (iv) the resources available to the Recipient and the costs of interpreting and translation services. Based on the Recipient’s analysis, the Recipient should then design an LEP plan based on five recommended steps, including: (i) identifying LEP individuals who may need assistance; (ii) identifying language assistance measures; (iii) training staff; (iv) providing notice to LEP persons; and (v) monitoring and updating the LEP plan. A Recipient’s LEP plan likely will include translating vital documents and providing either on-site interpreters or telephone interpreter services, or using shared interpreting services with other Recipients. Recipients may take other reasonable steps depending on the emergent or non-emergent needs of the LEP individual, such as hiring bilingual staff who are competent in the skills required for medical translation, hiring staff interpreters, or contracting with outside public or private agencies that provide interpreter services. HHS’s guidance provides detailed examples of the mix of services that a Recipient should consider and implement. HHS’s guidance also establishes a “safe harbor” that Recipients may elect to follow when determining whether vital documents must be translated into other languages. Compliance with the safe harbor will be strong evidence that the Recipient has satisfied its written translation obligations.
In addition to reviewing HHS guidance documents, Recipients may contact HHS’s Office for Civil Rights for technical assistance in establishing a reasonable LEP plan.
III. California Law – Dymally-Alatorre Bilingual Services Act. The California legislature enacted the California’s Dymally-Alatorre Bilingual Services Act (Govt. Code 7290 et seq.) in order to ensure that California residents would appropriately receive services from public agencies regardless of the person’s English language skills. California Government Code section 7291 recites this legislative intent as follows:
“The Legislature hereby finds and declares that the effective maintenance and development of a free and democratic society depends on the right and ability of its citizens and residents to communicate with their government and the right and ability of the government to communicate with them. The Legislature further finds and declares that substantial numbers of persons who live, work and pay taxes in this state are unable, either because they do not speak or write English at all, or because their primary language is other than English, effectively to communicate with their government. The Legislature further finds and declares that state and local agency employees frequently are unable to communicate with persons requiring their services because of this language barrier. As a consequence, substantial numbers of persons presently are being denied rights and benefits to which they would otherwise be entitled. It is the intention of the Legislature in enacting this chapter to provide for effective communication between all levels of government in this state and the people of this state who are precluded from utilizing public services because of language barriers.”
The Act generally requires state and local public agencies to provide interpreter and written document translation services in a manner that will ensure that LEP individuals have access to important government services. Agencies may employ bilingual staff, and translate documents into additional languages representing the clientele served by the agency. Public agencies also must conduct a needs assessment survey every two years documenting the items listed in Government Code section 7299.4, and develop an implementation plan every year that documents compliance with the Act. You may access a copy of this law at the following url: http://www.spb.ca.gov/bilingual/dymallyact.htm

Faculty List
Course Chairs
Lucy S. Crain, MD, MPH, FAAP Professor of Pediatrics (Emerita), UCSF School of Medicine Adjunct Professor of Pediatrics, Stanford University Geraldine Collins Bride, RN, MS, ANP, FAAN Professor and Vice-Chair, Department of Community Health Systems UCSF School of Nursing
Guest Faculty
Tiffani Andrade, MA Assistant Deputy Director, CA Department of Developmental Services, Sacramento, CA
Aaron Carruthers Executive Director, State Council on Developmental Disabilities
Henry Chambers, MD Pediatric Orthopedic Surgeon Professor of Clinical Orthopedic Surgery, University of California, San Diego Program Director, Pediatric Orthopedic Education Southern Family Chair of Cerebral Palsy Program Medical Director, David Sutherland Motion Analysis Laboratory Rady Children’s Hospital San Diego
Melissa Crisp-Cooper Health Advocate, UCSF Office of Developmental Primary Care
Stephen W. Dale, Esq LLM Attorney and Disability Rights Advocate, The Dale Law Firm, PC
Mark Del Monte, JD CEO/Executive Vice President American Academy of Pediatrics (AAP)
Ryan Easterly Executive Director, WITH Foundation
Heidi M. Feldman, MD, PhD Ballinger-Swindells Professor of Developmental and Behavioral Pediatrics, Stanford University School of Medicine
Tyler Fihe Autism Consultant, California
Richard Goldwasser, MD Psychiatric Consultant to Redwood Coast Regional Center and North Bay Regional Center
Susan Goldwasser, MD Psychiatric Consultant to Redwood Coast Regional Center and North Bay Regional Center

Guest Faculty, Cont.
Elizabeth Grigsby Consumer Rights Advocate Golden Gate Regional Center San Francisco, CA
Lauren Libero, PhD Autism Program Specialist, CA Department of Developmental Services, Sacramento, CA
Ben Meisel, MD Medical Director – California Children’s Services, San Francisco Department of Public Health
Catherine Nichols Senior Director of Accessibility Programs, Salesforce
Kristen Pedersen Senior Director, Business Development and Workforce Inclusion, The Arc-San Francisco
Kelly Rinehart, MA, CCC-SLP AAC Specialist Speech/Language Pathologist Augmentative Communication & Technology Services
Katie Savin, MSW, ASW PhD Student, School of Social Welfare, University of California, Berkeley
Hari Srinivasan Undergraduate in Psychology University of California, Berkeley
Mark Starford Director, Board Resource Center
David Teplitz Undergraduate in Political Science University of California, Berkeley
Kecia Weller Disability Rights Advocate; Board Resource Center Abuse Prevention Advisory Team Lead
Allen Wong, DDS, EdD, DABSCD Pacific Dugoni School of Dentistry Professor and Director AEGD Program; Director Hospital Dentistry Program; Global Clinical Advisor, Special Olympics Special Smiles Program
UCSF Faculty (University of California, San Francisco)
Clarissa C. Kripke, MD, FAAFP Professor of Family and Community Medicine; Director, Office of Developmental Primary Care, Department of Family and Community Medicine
Neal Rojas, MD Associate Clinical Professor of Pediatrics; Developmental Behavioral Pediatrician, Division of Developmental Medicine

Disclosures
The following individuals have disclosed they have no financial interest/arrangement or affiliation with any commercial interests who provide products or services relating to their presentation(s) in this continuing medical education activity: Tiffani Andrade, MA Aaron Carruthers Geraldine Collins-Bride, RN, MS, ANP Lucy S. Crain, MD, MPH, FAAP Melissa Crisp-Cooper Stephen W. Dale, Esq., LL.M Mark Del Monte, JD Ryan Easterly Heidi M. Feldman, MD, PhD Tyler Fihe Richard Goldwasser, MD Susan Goldwasser, MD Elizabeth Grigsby
Clarissa C. Kripke, MD, FAAFP Lauren Libero, PhD Ben Meisel, MD Catherine Nichols Kristen Pedersen Kelly Rinehart, MA, CCC-SLP Neal Rojas, MD, MPH Katie Savin, MSW, ASW Hari Srinivasan Mark Starford David Teplitz Kecia Weller Allen Wong, DDS, EdD
The following individuals have disclosed having a financial interest/arrangement or affiliation during the past twelve months with a commercial interest who provides products or services relating to their presentation(s) in this continuing medical education activity. All conflicts of interest have been resolved in accordance with the ACCME Standards for Commercial Support: Hank Chambers, MD Consultant Allergan Consultant Orthopaedics Corp This UCSF CME educational activity was planned and developed to: uphold academic standards to ensure balance, independence, objectivity, and scientific rigor; adhere to requirements to protect health information under the Health Insurance Portability and Accountability Act of 1996 (HIPAA); and, include a mechanism to inform learners when unapproved or unlabeled uses of therapeutic products or agents are discussed or referenced. This activity has been reviewed and approved by members of the UCSF CME Governing Board in accordance with UCSF CME accreditation policies. Office of CME staff, planners, reviewers, and all others in control of content have disclosed they have no relevant financial relationships.

Presented by the UCSF SCHOOL OF MEDICINE and the UCSF SCHOOL OF NURSING
UPCOMING CME COURSES Primary Care Medicine: Update 2020 April 5 – 10, 2020 Wailea Beach Marriott and Spa – Maui, Hawaii 48th Annual Advances in Internal Medicine May 18 – 21, 2020 Holiday Inn Golden Gateway – San Francisco, California 53rd Annual Advances and Controversies in Clinical Pediatrics May 28 – 30, 2020 Parc Central Hotel – San Francisco, California 48th Annual Advances in Internal Medicine June 15 – 18, 2020 UCSF Parnassus Campus – San Francisco, California Essentials of Women's Health: An Integrated Approach to Primary Care and Office Gynecology July 5 – 10, 2020 Westin Hapuna Beach Resort – Big Island, Hawaii Essentials of Primary Care: A Core Curriculum for Ambulatory Practice August 2 – 7, 2020 Resort at Squaw Creek – Lake Tahoe, California Primary Care Medicine: Principles and Practice October 15 – 17, 2020 Hotel Nikko – San Francisco, California Controversies in Women’s Health December 10 – 11, 2020 Hotel Nikko – San Francisco, California ALL COURSES MANAGED BY UCSF Office of Continuing Medical Education 3333 California Street, Room 450, San Francisco, CA 94118 For attendee information call: 415-476-4251 Visit the web site at cme.ucsf.edu

PROGRAM THURSDAY MARCH 5, 2020 7:15‐7:50am Registration and Continental Breakfast 7:50‐8:00 Welcome and Course Overview Lucy S. Crain, MD, MPH, FAAP Geraldine Collins‐Bride, MS, ANP, FAAN
8:00‐8:30 New DDS Programs for People with Developmental Disabilities Tiffani Andrade, MA and Lauren Libero, PhD
8:30‐9:15 The Role of Advocacy to Improve Systems of Care Mark Del Monte, JD
9:15‐9:30 Q & A 9:30‐9:45 Break, Exhibits
9:45‐10:30 Special Needs Trusts, Self Determination and Supported Decision‐Making Stephen Dale, JD 10:30‐11:15 Language Nutrition for Language Health: How to talk to children with autism and
developmental disabilities Heidi M. Feldman, MD, PhD 11:15‐12:05 Who Defines My Quality of Life?
Melissa Crisp‐Cooper and Katie Savin 12:05‐12:15 Q & A
12:15‐1:15pm Lunch (Provided) & Exhibits
1:15‐2:00 The Role of the California State Council On Developmental Disabilities: Advocacy & Systems
Change Aaron Carruthers
2:00‐2:45 What's New with Augmentative Communication and Assistive Technologies Kelly Rinehart, MA, CCC‐SLP
2:45‐3:00 Break, Exhibits
3:00‐4:00 Reimagining the Possible for Non‐Speaking, Autistic People Clarissa Kripke, MD, Hari Srinivasan, David Teplitz, Tyler Fihe
4:00‐4:10 Q & A
4:10‐4:40 Maximizing Potential‐ Understanding the Dimension of Neurodiversity Kristen Pedersen 4:40‐4:45 Q & A
ANNUAL SHRIVER LECTURE & AWARD
4:45‐5:15 Jobs for People with Developmental Disabilities: Making It Happen! Catherine Nichols
5:15‐6:15pm Networking Reception

FRIDAY MARCH 6, 2020
7:15‐7:50am Registration and Continental Breakfast 7:50‐8:00 Welcome and Daily Overview Lucy S. Crain, MD, MPH, FAAP Geraldine Collins‐Bride, MS, ANP, FAAN
8:00‐8:45 California Children’s Services: Nuts and Bolts Ben Meisel, MD 8:45‐9:15 Private Lives, Private Dollars: How Philanthropy Can Address and Enhance Healthcare for
Adults with Developmental Disabilities Ryan Easterly 9:15‐9:30 Q & A
9:30‐9:45 Break, Exhibits 9:45‐10:30 Cerebral Palsy: Personal & Professionals Perspectives Henry Chambers, MD
10:30‐11:15 A Conversation on Cerebral Palsy from Consumers and Professionals Elizabeth Grigsby, Henry Chambers, Ryan Easterly, Ben Meisel 11:15‐11:30 Q & A 11:30‐1:00pm Lunch (On Your Own)
1:00‐1:30 Dangerous or Deadly “Cures” for Autism and Other DD
Neal Rojas, MD, MPH
1:30‐2:00 Dental Care for Children & Adults with DD: Special Considerations Allen Wong, DDS, EdD
2:00‐2:45 Silence is Violence
Mark Starford and Kecia Weller 2:45‐3:00 Q & A 3:00-3:15 Coffee Break
3:15‐4:00 Mental Health Challenges/Psychopharmacology for Individuals with DD Richard Goldwasser, MD and Susan Goldwasser, MD
4:00‐4:15 Q & A
4:15pm Course Adjourns

New DDS Programs for People with Developmental
Disabilities
Tiffani Andrade, Assistant Deputy DirectorDr. Lauren Libero, Autism Specialist
Department of Developmental Services
19th Annual Developmental Disabilities: An Update for Health ProfessionalsMarch 5‐6, 2020
Disclosure
No relevant financial conflicts of interest
Overview
1. Department of Developmental Services
2. Community Development
3. Safety Net
4. AB 2083
5. Self‐Determination Program
6. Promoting Best Practices
Learning Objectives
•Identify major trends in the demographics of individuals served through the developmental services system
•Identify priorities and initiatives for the developmental services system
•Consider future directions for ensuring the use and development of best practices for serving individuals with developmental disabilities in the community
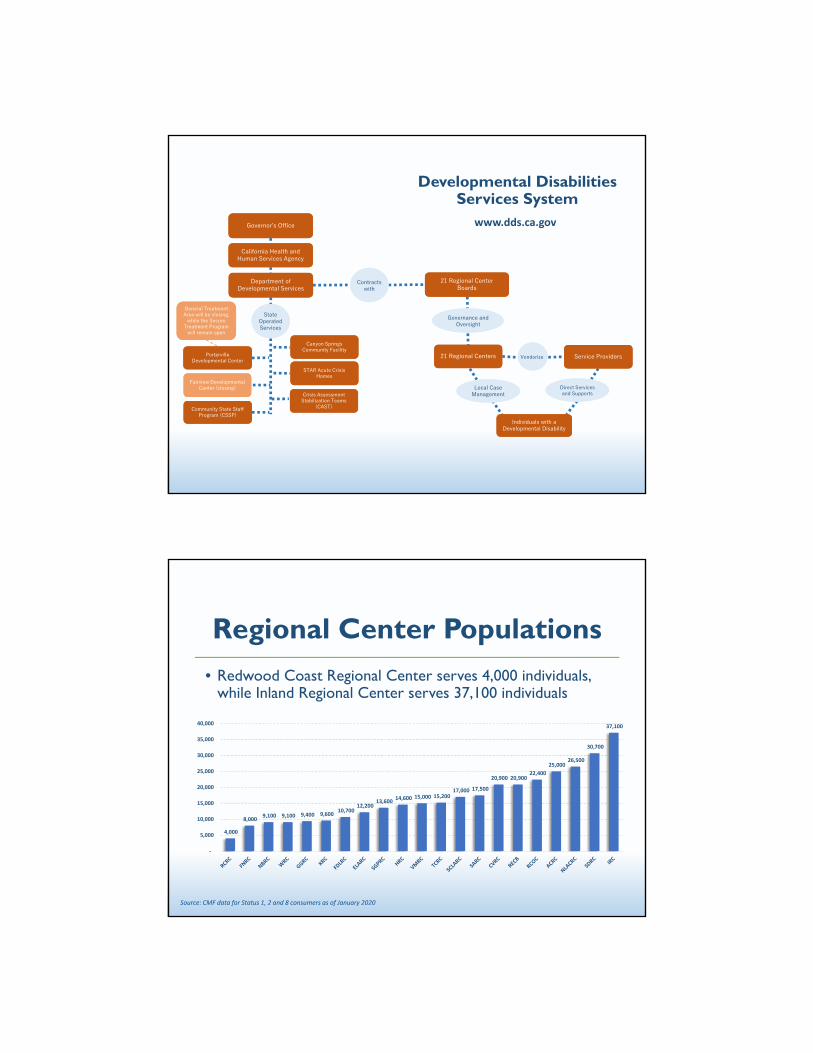
Developmental Disabilities Services System
Governorʼs OfficeGovernorʼs Office
California Health and Human Services Agency
California Health and Human Services Agency
Department of Developmental Services
Department of Developmental Services
Governance and Oversight
Vendorize
Individuals with a Developmental Disability
Individuals with a Developmental Disability
Porterville Developmental Center
Porterville Developmental Center
Canyon Springs Community Facility
Canyon Springs Community Facility
State Operated Services
Crisis Assessment Stabilization Teams
(CAST)
Crisis Assessment Stabilization Teams
(CAST)Community State Staff Program (CSSP)
Community State Staff Program (CSSP)
Contracts with
21 Regional Center Boards
21 Regional Center Boards
STAR Acute Crisis Homes
STAR Acute Crisis Homes
Fairview Developmental Center (closing)
Fairview Developmental Center (closing)
21 Regional Centers21 Regional Centers
Local Case Management
Direct Services and Supports
Service ProvidersService Providers
General Treatment Area will be closing,
while the Secure Treatment Program
will remain open
General Treatment Area will be closing,
while the Secure Treatment Program
will remain open
www.dds.ca.gov
Regional Center Populations• Redwood Coast Regional Center serves 4,000 individuals,
while Inland Regional Center serves 37,100 individuals
4,000
8,000 9,100 9,100 9,400 9,600
10,700 12,200
13,600 14,600 15,000 15,200
17,000 17,500
20,900 20,900 22,400
25,000 26,500
30,700
37,100
‐
5,000
10,000
15,000
20,000
25,000
30,000
35,000
40,000
Source: CMF data for Status 1, 2 and 8 consumers as of January 2020

Who We ServeTotal Population
Source: CMF data for Status 1, 2 and 8 consumers as of December of each year
26,000 33,000 49,000
210,000246,000
302,000
0
50,000
100,000
150,000
200,000
250,000
300,000
350,000
400,000
2009 2014 2019
Early Start (Ages 0 to 2) Lanterman (Ages 3+)
236,000
279,000
351,000
Who We ServePopulation by Age Group
Source: CMF data for Status 1, 2 and 8 consumers as of December of each year
2014 20192009
14%
36%
9%
33%
9%12%
36%
9%
34%
10%14%
37%
8%
32%
9%
Ages 0 to 2 Ages 3 to 17 Ages 18 to 21 Ages 22 to 51 Ages 52 or Older

Who We ServePopulation by Diagnosis
2014 20192009
Source: CDER data for Status 1, 2 and 8 consumers as of December of each yearNote: An individual may have more than one diagnosis and may be counted under multiple diagnoses, i.e., duplicated counts
23%17% 18%
71%
12%
30%
15% 16%
66%
10%
42%
12% 13%
59%
11%
Autism Cerebral Palsy Epilepsy IntellectualDisability
Other
Who We ServePopulation by Ethnicity
2014 20192009
40%
30%
15%
9%
7%
37%
34%
11%
9%
6%
34%
38%
12%
9%
6%
Hispanic
White
Other
Black/AfricanAmerican
Asian
Source: CMF data for Status 1, 2 and 8 consumers as of December of each year

Community Development
• History of Community
Placement Plan (CPP) &
Community Resource
Development Fund (CRDP)
“Bedroom Community” by Christian Jackson
https://www.dds.ca.gov/services/cpp/
Community Development
• New home models:
• Enhanced Behavioral Supports
Home (EBSH)
• Community Crisis Home (CCH)

Safety Net
• Specialized Step-Down homes
• Individualized Intensive Transition services
• STAR and CAST
• START Services
“Cars” by David Tveritenov
AB 2083
• Developing coordinated, timely, and trauma-informed system of care for foster children who have experienced severe trauma
• Development of EBSHs and CCHs for dually-served youth “Ice Cream Cone” by Lisa Chun

Self-Determination Program
• Allows participants the opportunity to have more control in developing their service plans and selecting service providers to better meet their needs
• Starting June 7, 2021 the program will be available to all eligible individuals
https://www.dds.ca.gov/initiatives/sdp/
Promoting Best Practices
• Building expertise of the community
• Ensuring new development is:
• Person-centered
• Trauma-informed
• Culturally and linguistically competent

Promoting Best Practices
• Best practices for specialty care
• Developing services for a changing population
• Developmental Services Task Force
“Horses” by Alex Hannah
TThe Role of Advocacc tto Improve Systems of Care
Mark Del Monte, JDCEO, Executive Vice President
Mark Del Monte, JD has documented he has no financial conflicts to disclose.
Disclosure

"The American Academy of Pediatrics recommends that pediatricians take the steps they would for any potential infectious disease outbreak, including preparing their offices or clinics to adopt standard infection-control practices, collaborating with their local hospital and health systems, and advising families in their practice to stay home from work, school and child care if they are sick. The AAP will continue to advise and update members as the situation evolves," said Dr. Sally Goza.
MissionThe mission of the AAP is to attain optimal physical, mental, and social health and well-being for all infants, children, adolescents, and young adults. To accomplish this mission, the AAP shall support the professional needs of its members.
VisionChildren have optimal health and well-being and are valued by society. Academy members practice the highest quality health care and experience professional satisfaction and personal well-being.
Core ValuesWe believe:
In the inherent worth of all children, they are our most enduring and vulnerable legacy.
Children deserve optimal health and the highest quality health care.
Pediatricians and subspecialists are the best qualified to provide child health care.
Multidisciplinary teams including patients and families are integral to delivering the highest quality health care.
The AAP is the organization to advance child health and well-being and the profession of
AAAP Mission, Vision, Values

children under the age of 18 have special health care needs (19.8%)
hildren (birth to 5 years): 11.4%
d 6-11: 22.7%
d 12-17: 25.1%
s have special health care needs, compared to 17.0 % of girls
children with special health care needs varies among income groups
es below 100 percent of the FPL 16%
hhot: Children with Special Health Care Needs

cians and Health Care Systems Are (or WW For Patients with Developmental Disabi
1 in 5 children has a special health care need
1 in 6 children has a developmental disability
1 in 4 adults has a disability
Systems of care that meet the needs of individuals with disabilities will also
AAhher’seew
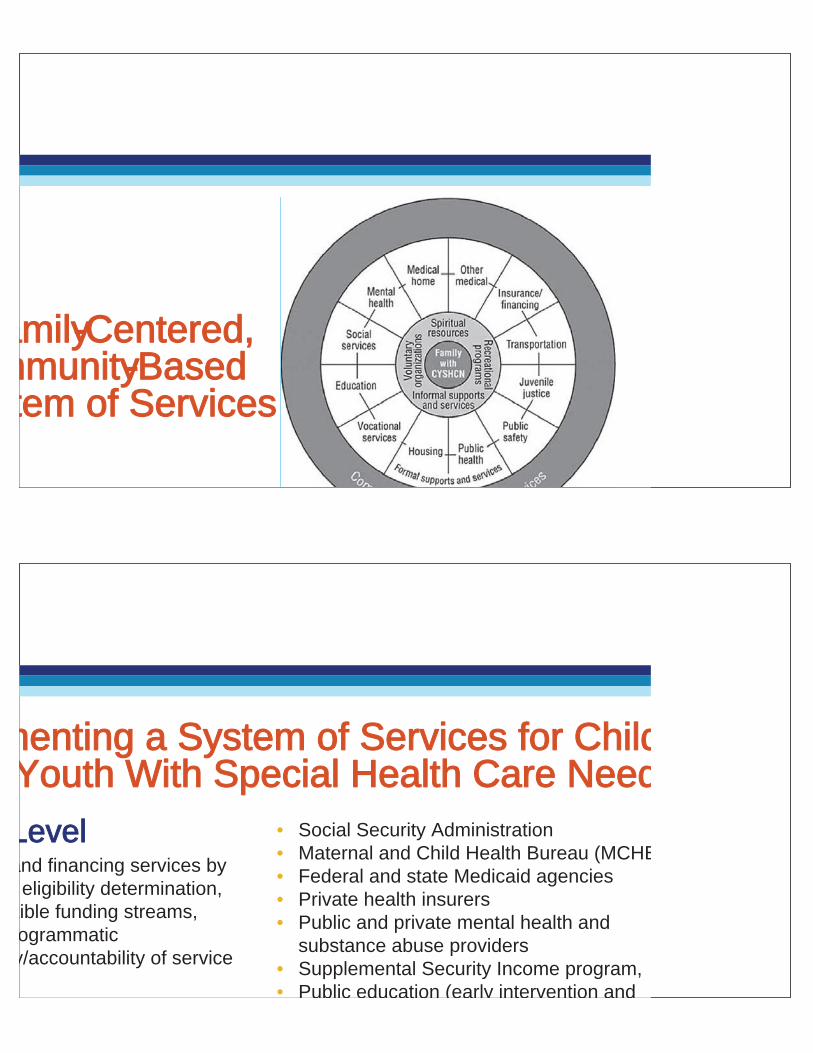
amily-Centered,mmunity-Basedtem of Services
menting a System of Services for Childd Youth With Special Health Care Need
• Social Security Administration• Maternal and Child Health Bureau (MCHB• Federal and state Medicaid agencies• Private health insurers• Public and private mental health and
substance abuse providers• Supplemental Security Income program, • Public education (early intervention and
Leveland financing services by
eligibility determination, xible funding streams, ogrammatic y/accountability of service
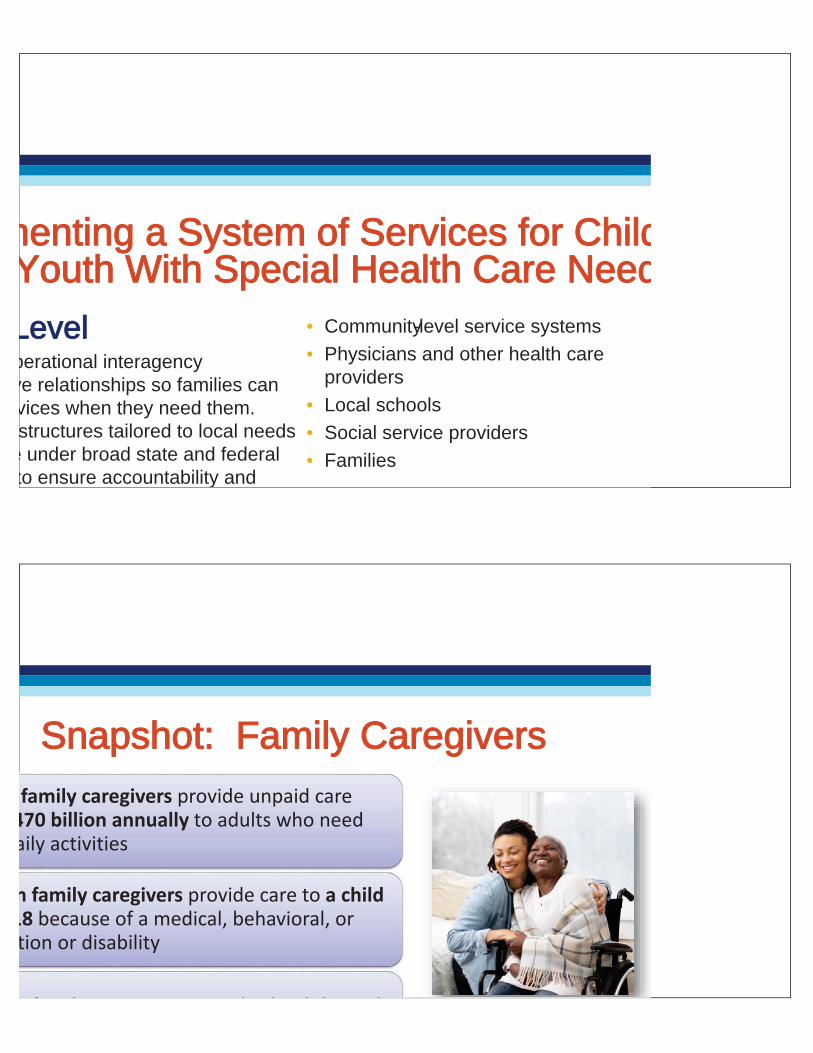
menting a System of Services for Childd Youth With Special Health Care Needd
Levelperational interagency ve relationships so families can vices when they need them. structures tailored to local needs
e under broad state and federal to ensure accountability and
• Community-level service systems
• Physicians and other health care providers
• Local schools
• Social service providers
• Families
family caregivers provide unpaid care 470 billion annually to adults who need aily activities
n family caregivers provide care to a child 18 because of a medical, behavioral, or tion or disability
f l b h d l d
SSnapshot: Family Caregivers

ootional, and ffinancialchallenges
experience emotional strain andmmental health pecially depression
physical health than non-caregivers
propriately recognized, iincluded, and
Snapshot: Family Caregivers
re pprincipal caregivers and center of strength/support
milies are iintegral partners of the health care team
ize and value diversity among patients, families, ns
n the strengths of children and familieswer them to communicate their strengths
families,
s
lies Must Not Only Take Part in Systeeedesign Efforts But Help Guide Them
les for Family Engagement

tt and inform pediatricians and the AAP
AAP think “outside the box” and pprovide missing ctives
he AAP standardize family engagement
siinput from families and youth on strategic areas
s and pprovides family/youth perspective to AAP
missing
ent
egic
tito AAP vvtoeeo
AP FamilY Partnerships Network
UUsing Advocacy to ““Move the Dial”
iivemoting positive legislation:
merican’s With Disabilities Act
ental Health Parity Act
e ABLE Act
e Affordable Care Act
lizing to stop harmful legislation
orts to repeal protections from the
RRegulatory• Replying to proposed rules from the
Social Security Administration, Department of Education, Department of Health and Human Services, etc.
Advocacy Takes Many Forms
ChangingPublicPolicy
Politicalal
ScientificKnowledge
Julius B. Richmond Model: CChanging Public Policy

1) Identify decision makers –Who’s in charge?
2) Build coalitions and set a goal –Find partners and agree
3) Mobilize–Have an action plan
4) CCraft a message and speak out D id t
HHope is Not a Strategy
You work with those with special health caa needs every day…
• You are the expert!
• You know the needs of your patients and thfamilies
• You live with the rules of practice and paym—you know what works and what does not
SSnapshot: Physicians, Nurses and Allied Health Professionals
• Patients and self-advocates
• Family members/caregivers
• Physicians, nurses, allied health professio
• Medical societies and advocacy organiza– We’re stronger together
– People who are affected by a decision or change need to be at the table
AAdvocacy is a Team Sport
anize:Put a face to an issue
rate: Paint a picture of how an issue impacts real ren and families
ttable:Put audiencein the shoes of that person
morable:More than just a number or statistic
yy Are Stories Important to Advocacy?
as 5 minutes:
patient story to frame ocacy
e news, listen to the radio, e paper. Ask yourself, s this affect patients with ental disabilities?”
aacy Opportunities
o,,,,,
h
IIn less than 30 minutes:• Set up google news alerts with ke
words about developmental and intellectual disabilities for your hometown paper
• Set up a social media account andhelp contribute to conversations about caring for those with
AAdvocacy Opportunities

n hour: tter to the editor or op-edcal paperofessional rounds or noon ce presentation on
advocacy article for your
aacy Opportunities
onnnnnnnnnnnnnnnnnnnnnnnnnnnnnn
ral Legislation in the 115th & 116th CongressReauthorizations• Autism CARES Reauthorization Act (P.L. 116-60)• Early Hearing Detection and Intervention Act (P.L. 115-71)• PREEMIE Act (P.L. 115-328)• Congenital Heart Futures Act (P.L. 115-342)
New Legislation• Kevin and Avonte’s Law (added as amendment to the FY18
omnibus appropriations bill -P.L. 115-141)
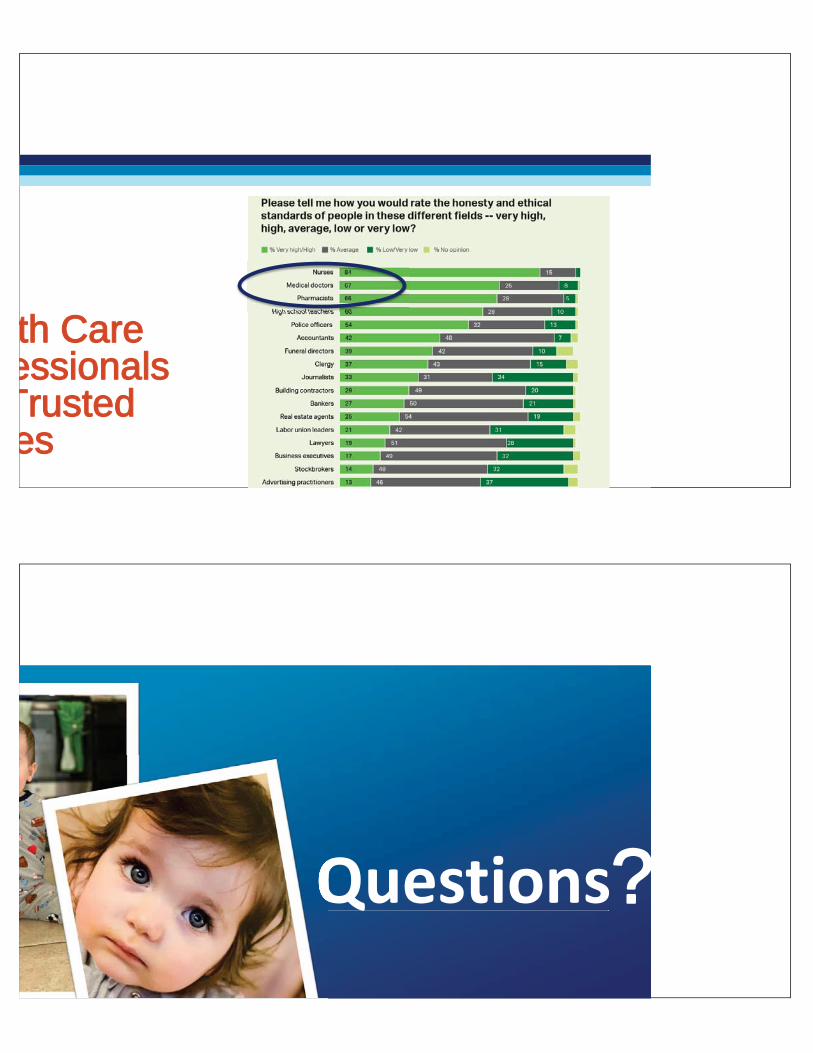
th Care eessionals
Trusted ees
Questions?
Language Nutrition for Language Health How to talk to children with autism and developmental
disabilities
Heidi M Feldman MD PhD
Stanford University
19th Annual Developmental Disabilities: An Update for Health Professionals
March 5, 2020
iversity
Disclosure
• I have no financial disclosures and no conflicts of interest

Inspiration
Classroom observations Clinical visits with families
Learning Objectives: By the conclusion of this talk, participants will be able to
• Define the components of Language Nutrition
• Discuss methods for assessing the language environment of children
• Contrast language nutrition for children who are typically developing and children with autism
• Evaluate the impact of language nutrition on language development in autism
• Advise parents of children with autism about how to talk to their children
Take home messages
1. Nutrition is important for physical development
2. Language nutrition is important for language development
3. Language nutrition is important for language development in children with autism
Language Health in the Information Age

Language in the first 5 years
Adapted from the Asmussen et al., 2019
1 year 2 years 3 years 4 years
Recognizes name
First gestures
~50 words in their
productive vocabularies Word combinations, increasing
grammar complexity, questions and negations
~500 words in their
productive vocabularies Narrative skills
Preliteracy skills
Birth
First words
Variable rates of development: Cross‐sectional data
Size of Productive Vocabulary
n = 4867, English‐speakingFrank, Braginsky, Yurovsky, & Marchman, 2016
Child age in months
600
400
200
0
16 18 20 22 24 26 28 30

Child age in months
Number of
different words
n = 108, English‐speakingPan, Rowe, Singer, Snow, 2005
Variable rates: Longitudinal data
Variability in language development
Maternal depression
Activities in the home
environment
Family income
School district
Caregiver occupation
Caregiver education

Maternal depression
Caregiver occupation
Activities in the home
environment
Family income
School district
Caregiver education
Variability in language development
Language nutrition
1313
Terminology
Child‐directed speech
Infant‐directed speech
Baby talk
Language Nutrition
Input
Hart and Risley (1995) Meaningful Differences• Longitudinal study
• 42 carefully selected US families
• Children 7‐9 months to 3 years
• SES based on parental occupation (upper, middle, lower, welfare)
• Methods: Obtained about 1 hours/day of input; transcribed 1300 samples
• Findings• 86‐98% child words in parent vocabulary
• Dramatic differences in child vocabulary
• Dramatic differences in parent input
• Extrapolations to 30 million word gap
?
What comprises a nutritious language environment?15
1616
Language nutrition
Quantity
• Total words• Total gestures
Quality
• Number of different words• Sentence complexity• Wh‐questions• Talking about past and future
Interaction
• Responsiveness• Expansions• Joint engagement• Intrusiveness• Directiveness

18
Language learning opportunities vary

Old school
19
Advances in assessing language environments
New school
Diurnal variation – Adult Word Counts
8am 12pm 3pm 8pm
1200
800
400
0
Adult Word
Countsin 10 min
(AWC)
20

Diurnal variation – Conversational Turns21
Time8am 12pm 3pm 8pm
30
20
10
0
Conversational Turns
in 10 min(CTC)
2222Language nutrition: key predictor of language outcomes
Child language
Language Nutrition
● English
● French
● Spanish
● Yucatan Maya
● Pre‐term
● Hard of hearing
● Down Syndrome
● Specific Language Impairment

Autism
Variability in trajectories in ASD
n = 106Pickles et al,. 2017
TypicalTypical/Mild delay
Marked delay
Scoping review
Language nutrition as prevention
Type Prevention Define Example
Primary Prevention
Asymptomatic individual gets treatment and never gets the condition
Vaccination
Secondary prevention
Individual at early stage gets treatment and develops mild form of condition
Mammography
Tertiary prevention
Individual with condition gets treatment and has a better functional outcome
Early intervention

Child‐directed speech in ASD
• https://drive.google.com/drive/u/1/my‐drive
Critical questions about language nutrition
Question 1: Compared to language nutrition of healthy and typically developing children, what is the language nutrition to children with autism (and intellectual disability/global developmental delay)?
Question 2: What is the strength of the association between features of the language input and child language outcomes in children with autism?
Question 3: To what extent can intervention change/improve language nutrition and thereby improve child language outcomes?
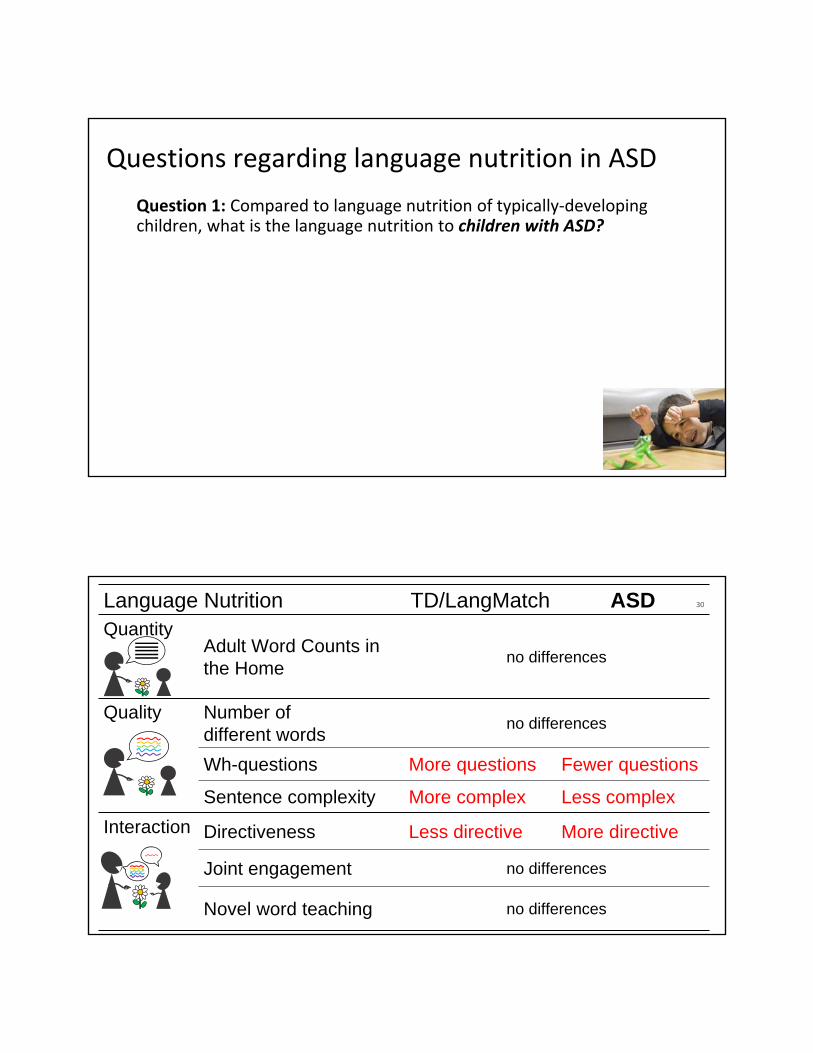
Questions regarding language nutrition in ASD
Question 1: Compared to language nutrition of typically‐developing children, what is the language nutrition to children with ASD?
3030Language Nutrition TD/LangMatch ASDQuantity
Adult Word Counts in the Home
no differences
Quality Number of different words
no differences
Wh-questions More questions Fewer questions
Sentence complexity More complex Less complex
Interaction Directiveness Less directive More directive
Joint engagement no differences
Novel word teaching no differences

3131Language Nutrition TD/LangMatch GDD/IDQuantity
Adult Word Counts at Home
no differences
QualityDescriptions no differences
Encouragement Less encouraging More encouraging
InteractionDirectiveness Less directive More directive
Joint engagement no differences
Tertiary Prevention: ID and ASD
Question 1: Compared to language nutrition of typically‐developing children, what is the language nutrition to children with ID and children with ASD?
Question 2: What is the strength of the association between features of the language nutrition and child language outcomes?
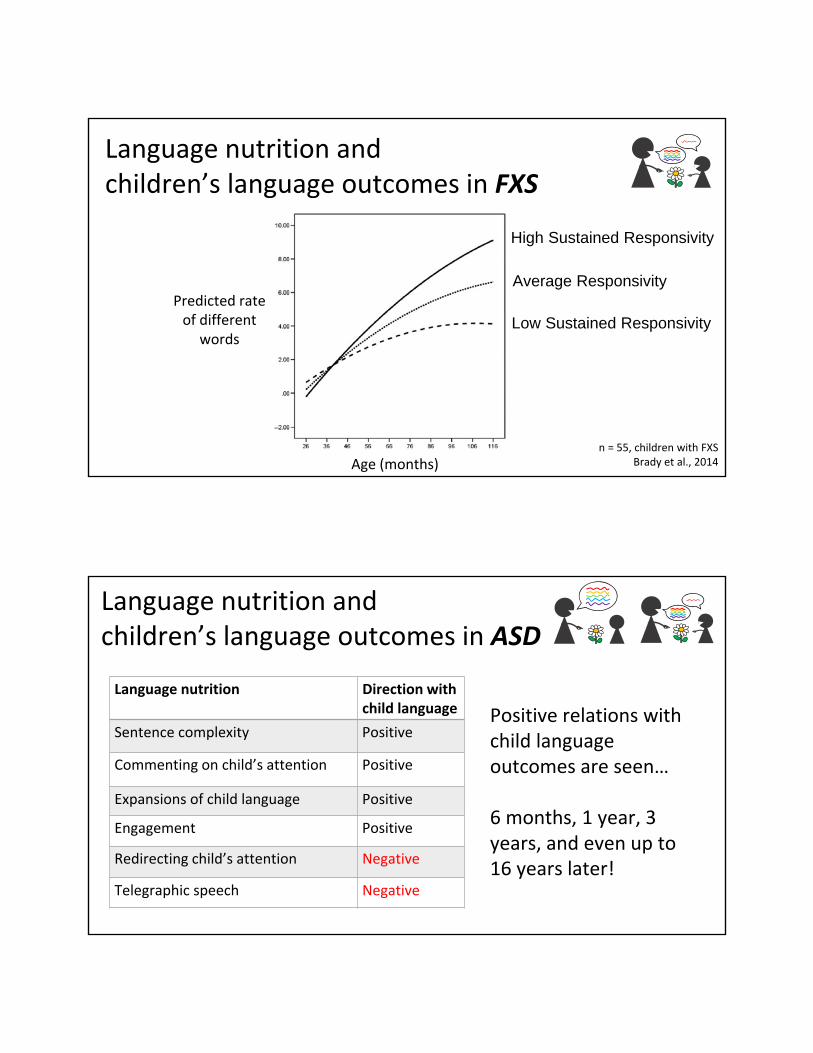
Language nutrition and children’s language outcomes in FXS
n = 55, children with FXSBrady et al., 2014Age (months)
Predicted rate of different
words
High Sustained Responsivity
Average Responsivity
Low Sustained Responsivity
Language nutrition Direction with child language
Sentence complexity Positive
Commenting on child’s attention Positive
Expansions of child language Positive
Engagement Positive
Redirecting child’s attention Negative
Telegraphic speech Negative
Positive relations with child language outcomes are seen…
6 months, 1 year, 3 years, and even up to 16 years later!
Language nutrition and children’s language outcomes in ASD

Tertiary Prevention: ID and ASD
Question 1: Compared to language nutrition of typically‐developing children, what is the language nutrition to children with ID and children with ASD?
Question 2: What is the strength of the association between features of the language nutrition and child language outcomes?
Question 3: To what extent can intervention change/improve language nutrition and thereby improve child language outcomes?
Language nutrition RCTs – Child OutcomesID and ASD: Roberts & Kaiser, 2011
Vocabulary raw mean difference, 95% CI
0
Hedge’s g mean difference, 95% CI
ASD: Nevill et al., 2018
0-1 1
225112.5-225 -112.5

Why modest effect size?
• Children are enrolled in other services. Language nutrition must make a contribution over the other interventions.
• In many studies, the intervention is minimal• Few sessions
• Parent education without child present
• Limited modelling and feedback
• Interventions target one component of language nutrition rather than all 3 components
• Choice of outcome measures: autism symptoms versus language features, structured language rather than communication, lack of functional outcomes
Future Directions for Research
• Conduct RCTs to establish that intervention can change language nutrition and that those changes cause improve outcomes
• Create interventions of language nutrition that include improvements in quantity and quality of language input and quality of verbal interactions
• Evaluate appropriate outcome measures in speech, language, and communication; goal of secondary/tertiary prevention
• Employ interventions that follow recommended practices for language nutrition

Ingredients for successful interventions
Sustained over time
Model language nutrition
Explicit Personal Training
Caregivers and Children Together
Alternative approach to improving nutrition
ReassessmentCustomized FeedbackIndividualized Assessment

Clinical recommendations for families• Be warm and responsive, have fun
• Provide the child with many words and gestures. Repeat those words frequently.
• Follow into the child’s focus of attention.
• Use full sentences, appropriate grammar
• Avoid simplified speech
• Avoid directing and prompting
• Model, using many words in grammatical sentences
• Encourage child’s comprehension
4242
1 2 30 4 5
e.g,. Rowe, 2012; Rowe & Goldin‐Meadow, 2008
Child Age in Years
Use lots of words
Add gestures
Present with warmth and responsiveness
Clinical recommendations for families over time

4343
1 2 30 4 5
e.g,. Rowe, 2012; Rowe & Goldin‐Meadow, 2008
Use a wide variety of different words
Use grammatical sentences
Ask questions
Talk about the past and future
Child Age in Years
Use lots of words
Add gestures
Present with warmth and responsiveness
Clinical recommendations for families over time
Questions? Comments?
Thanks!

Office of Developmental Primary Care
Who Defines MY Quality of Life?:
Perspectives from disability advocatesand their supporters
Melissa Crisp-Cooper Katie Savin, MSWMarch 5-6th, 2020
Office of Developmental Primary Care
Improving health outcomes for people with developmental disabilities.

Disclosures
Thank you to our funders:
Stupski Foundation, WITH Foundation, and Far Northern, Golden Gate, and Redwood Coast Regional Centers.
Thank you to our project partners:
Clarissa Kripke, MD, FAAFP; Jo Cummins; and Patricia Mejia
Office of Developmental Primary Care
Overview
Discussion group organization
Themes- Communication- Assumptions- Changes in or loss of function- Medical decision-making / Advanced Care
Planning- End of life care conversations
Healthcare for people with disabilities - video
Office of Developmental Primary Care

Learning Objectives
Learn from the lived experience of disabled people and their families in health care settings
Identify concerns of these people and families
Understand the variety in definitions of quality of life
Identify the best practices needed to engage in effective health care discussions with disabled people throughout their lifespan
Recognize disability as one feature of an intersectional identity
Office of Developmental Primary Care
14 Participants
7 parents / supporters
5 participants in-person
discussion group
2 phone interviews
7 disabled adult “self advocates”
7 participants in-person discussion
group
Quality Improvement Project Design
Aim: Learn more about the experiences of people with disabilities and their families in accessing the health care system.

Communication
“When I have brought others, especially my parents, the providers tend to direct their questions to them and not me. They take them more seriously. It’s frustrating.”
Office of Developmental Primary Care
Communication
Recommendations:
• Presume competence
• Always address the disabled person
• Explore different communication options, such as visual aids, slowing down the conversation, and using plain language
Office of Developmental Primary Care

Disabled and Beyond: Intersecting Identities
“My primary nurse practitioner sees me as a whole person, including my disability, sexuality, social life, and other medical needs unrelated to my disability.”
Office of Developmental Primary Care
Disabled and Beyond: Intersecting Identities
Recommendations:
• Both advocates and supporters asked that clinicians acknowledge and respect them as whole people when considering the impact of potential treatment.
• Disability as a cultural identity
Office of Developmental Primary Care
Avoiding Assumptions - 1
“I wish medical students had to work in the community so they could see for
themselves what our lives can be. I would like them to see ‘life’.
That it’s not all medical – we have
fun!”
Avoiding Assumptions - 2
Participant Experiences
Negative messages regarding disability can be found everywhere, including medical literature and popular culture
Suggestions for Clinicians
Refer patients to peer‐led groups and/or websites that promote positive disability identity

Avoiding Assumptions - 2
Participant Experiences
Negative messages regarding disability can be found everywhere, including medical literature and popular culture
Suggestions for Clinicians
Refer patients to peer‐led groups and/or websites that promote positive disability identity
Avoiding Assumptions - 3
Suggestions for Clinicians
Ask patients to describe their baseline
Participant Experiences
Members of both groups cautioned clinicians not to confuse a patient’s health status in a hospital setting with their typical baseline
Office of Developmental Primary Care

Avoiding Assumptions - 4
Participant Experiences
Participants expressed the need to respect privacy and personal boundaries
Suggestions for Clinicians
Tell patients what they can expect to happen before starting an exam
Avoiding Assumptions - 5
Participant Experiences
People with disabilities want clinicians to avoid basing treatment options on assumptions about their quality of life
Suggestions for Clinicians
Ask patients what brings value to their lives

Decision-Making
“I brought in her communication device and they were shocked that she could do anything like that.
They had assumed that she was a little lump.”
Office of Developmental Primary Care
Decision Making
Recommendations:
• Increase opportunities for disabled patients’ autonomy as much as possible.
• Disabled patients should be able to choose trusted supporters to help them make medical decisions.
• Decision-making as spectrum vs binary; consider what supports or accommodations can optimize a patient’s capacity to participate in decision-making
Office of Developmental Primary Care

Cultural Humility & Respecting PatientExperiences
“Believe me. I may not have medical training, but I know a lot about my disability. Don’t give up on
me.”
Office of Developmental Primary Care
Cultural Humility & Respecting PatientExperiences
Recommendations:
- Recognize disabled people and their supporters as experts in their care and abilities
- Group members requested that clinicians trust the information and history they provide and correct errors that may exist in the medical chart
- Everyone has unconscious bias – be willing to revise your ideas of what it means to be disabled
Office of Developmental Primary Care
Adapting to Change in Function
“About 10 years ago, I became spinal cord injured. It’s common with CP (cerebral palsy), but
no one spoke to me about it. I had to relearn things. It was heavy.”
Office of Developmental Primary Care
Adapting to Change in Function
Recommendations:
- All people have the capacity to adapt to change and evolving circumstances
- Many members of the advocate group spoke of how aging with a significant developmental disability can be full of unknowns
- Clinicians can help patients by educating them on any disability-specific progressions based on literature and clinical experience
Office of Developmental Primary Care

Visits to the Emergency Department - 1
“People I see more than once are almost always okay. The problem is the ED or people who work
in the hospital. They don’t know who we are. They only see us for our problems and that’s a real
problem.”
Office of Developmental Primary Care
Visits to the Emergency Department - 2
Emergency visits pose unique challenges to disabled patients
- Physicians and medical personnel may be unfamiliar with a patient’s disability, medical history, baseline, or communication style
- Sensory overload due to bright lights and loud noises can impair a disabled person’s capacity to communicate
- Some disabled people are survivors of medical trauma
Office of Developmental Primary Care

Visits to the Emergency Department - 3
Accommodations to consider:
- Reduced wait time
- Better coordination between departments
- Streamlining discharge
Office of Developmental Primary Care
Advanced Care Planning
“Afterward, they kept talking about it, when I was doing well. A social worker came to my house and
her first question was, “Do you want a DNR?” This is when I was doing fine. All I wanted to do
was move away from that conversation.”
Office of Developmental Primary Care

Advanced Care Planning
Recommendations:
- Parents and supporters reported that they want to know that their options are based on neutral medical advice
- Patients want to know that their lives are valued
- Promote opportunities for disabled people to make decisions about what happens to them during a medical emergency and at the end of their lives
Office of Developmental Primary Care
End of Life
“I really appreciated how hard they tried to save her. They gave value to her life.”
Office of Developmental Primary Care

End of Life
Recommendations:
• All lives have value and all deaths will be grieved, regardless of one’s level of functioning at the time of death.
• Disabled people reported concerns that their wishes would not be followed at the end of their lives.
• Along with disability status, many factors impact patients’ relationship to the death and dying process, e.g. religion, family structure and legacy of access to medical care.
Office of Developmental Primary Care
Bridging the Gap Improving Healthcare Access for People with Disabilities
Office of Developmental Primary Care
Resources
White paper available from the ODPC information table, and on the website: https://odpc.ucsf.edu/clinical/patient-centered-care/who-defines-my-quality-of-life-perspectives-from-disability-advocates
Office of Developmental Primary Care
Resources
Office of Developmental Primary Care
Office of Developmental Primary Care: http://odpc.ucsf.edu
My Health Passport:https://odpc.ucsf.edu/clinical/tips-for-organizing-visits/health-passport
Supported Decision-Making: https://odpc.ucsf.edu/advocacy/supported-health-care-decision-making
What I Wish My Doctor Knew About Non-Traditional Communicators:https://odpc.ucsf.edu/advocacy/advice-from-self-advocates/non-traditional-communicators#pdf
What I Wish My Doctor Knew About People Who Accompany us to our Medical Appointments:https://odpc.ucsf.edu/advocacy/advice-from-self-advocates/the-people-who-accompany-us-to-our-medical-appointments#pdf

Office of Developmental Primary Care
Contact us:
Melissa Crisp-Cooper: [email protected] Savin: [email protected]

Special Needs Trusts, Conservatorships and Alternatives including Self Determination and
Supported Decision‐Making
Stephen W. Dale Esq. LL.M
Attorney ‐ Dale Law Firm
Trustee ‐ Golden State Pooled Trust
19th Annual Developmental Disabilities: An Update for Health ProfessionalsMarch 5‐6, 2020
Disclosures
• Nothing to disclose

The Olive‐Green Logbook
In the 1950’s when I was a boy, my father and grandfather worked at Agnews State Hospital, a state
institution dedicated to caring for persons with psychiatric disabilities. My father worked on the wards –
the more clinical side of the institution. My grandfather worked the farm and in those days the farms
were the foundation of State Hospitals. Only later did the State Hospitals transform themselves totally
into clinical warehouses as the medical model replaced the mission of California’s State Hospitals that
for many decades had provided a place of true asylum and community.
In those days, the farms run by California State Hospitals for persons with mental illness operated more
like small communities. This is not to say that barriers did not exist – for many they certainly did – but
for many the farms at the institutions were a true asylum allowing persons with mental illness a place to
find refuge and more importantly community. Many were free to come go as they pleased. It was not
unusual that they would go away for months at a time, and not unusual that they would return. For
those living in the cottages there were no fences and there were no restraints.
The people with mental illnesses lived in cottages on the farm. They cooked, played games, worked and
went to church together. There were no walls or fences, and most were free to come and go as they
pleased. Never did I dream that things would ever be any different – but in fact I was witnessing the end
of an era.
During my boyhood – it was not uncommon that staff would bring their children to work from time to
time. It wasn’t for any other reason than to show their children what they did. It was very common that
staff had picnics – usually as part of the California State Employees Association (CSEA). We would hear
the almost endless speeches from CSEA’s leadership of how the area of mental health care needs more
attention and the quest for licensing the Psychiatric Technician.
Each cottage housed between 12‐18 men. The cottages had no staff assigned to them other than to
perform the tasks that were necessary to meet their needs. First my grandfather and I would go to the
parts of the farms that he was responsible for to make sure all was in order. He would talk to each of the
men as well as staff and ask them how they are doing. He would listen to their stories and share stories
with them. On occasion the men would act strangely, talking to people that were not present, and
twitching methodically. I would ask my grandfather why, and he would usually answer that it was just
their way, and that I should not be afraid. He would tell me that they were just people not much
different from anyone else. As I got older both my father and my grandfather often told me that serving
the people at Agnews was of great importance – and something that was very honorable. This is a lesson
I never forgot.
My grandfather’s last duty of each day was to check the logbooks of each of the cottages and I
remember him going from cottage to cottage looking for an olive‐green bound logbook left with pages
carefully lined by hand, each log carefully placed neatly on a desk. I don’t remember the first time I
accompanied him but I certainly do remember a routine.
My grandfather would look at each logbook and transfer numbers to a clipboard he carried with him and
record how many gallons of milk the cottage needed, how many eggs, how many loaves of bread, how
many lunches for the men working in the fields, how many bags of laundry need to be picked up, and all
the things these men needed for their daily needs. After he recorded all these numbers he would go to

the main hospital and drop off the log to warehouse so the orders would be delivered to each cottage
the next morning.
One day we went to a cottage and the ritual of the log had not been followed. This cottage had a new
resident named Foxy who had some problem that day that had kept him from completing the logbook.
Foxy was distressed and kept repeating a series of words over and over. My grandfather was the most
patient man I have ever met and he reassured Foxy that everything was ok – and beckoned him to
watch my grandfather set up the log. Foxy sat and watched my grandfather as he told Foxy and me and
that the other men are depending on him. He instructed Foxy to follow his instructions exactly. He
emphasized that the wellbeing of each of the men are depending on him and this was a great
responsibility. He asked Foxy if he was up for the challenge. Yes, Foxy replied – and he quickly focused
on fulfilling his duties. Obviously, what I was about to observe was of great importance. So, my
grandfather took out a ruler and pen and instructed Foxy on how to line the book. In the upper right
corner, we need a box large enough to have a line for each man. We need a block for any men going to
clinic the next day and for how many are going off the grounds. Are there any visitors expected?
On the opposite page he lined the page methodically to have a place for what would be needed for the
next day, how many gallons of milk the cottage needed., how many eggs, how many loaves of bread,
how many lunches for the men working in the field, how many bags of laundry need to be picked up
along with any other things these men needed for their daily needs. I followed my grandfather for many
years, I watched him direct his men on how to tend to the animals, how to prune the orchards, and how
to harvest the crops. But at the end of every day, he would go to each cottage and transfer the
information from each olive‐green logbook to his clipboard to drop off at the supply depot.
Fast‐forward to 1973. After I got my psychiatric technician license – I transferred to Napa State Hospital
to a PM shift position on a unit called T11. My charge nurse told me that one of my jobs would be to set
up tomorrow’s log and she could teach me how to do it. I was instructed to finish my charting early so
my education would begin.
I finished my charting at 9 pm leaving me plenty of time to learn this new skill. She pulled out an olive‐
green bound book, with pages all lined in methodically. I was mesmerized by this book – exactly what I
had seen almost 2 decades earlier. She told me that the following instructions must be followed exactly.
First you create a box just big enough for all the staff scheduled. Then you create a series of boxes
where we put the number of gallons of milk we need, how many eggs, how many lunches and how
many dinners. In a very strange way – I felt that there was a direct connection between my grandfather,
my father, to Foxy, and to the many men that depended on each man fulfilling their duty.
Fast forward once again. Today – I am an attorney and trustee that focuses on getting people with
disabilities the things they need. We have no olive‐green logs, but in many ways nothing has changed.
Our challenge today is how to provide the men and women we serve in the community with what they
need. How do they get their milk and bread? How do they get to where they need to be? How do we
ensure that they are free from abuse and neglect, and lead the best quality of life possible? While the
hospitals are long gone as they should be, for me, the job has not changed.
Stephen W. Dale

Learning Objectives
• Explore what a special needs trusts function is, how it works, and ways to minimize loss of control by the beneficiary
• Understand that the trustee of a special needs trust is a fiduciary, and in most cases has no authority to make personal decisions.
• Review the basics of limited conservatorships
• Explore alternatives to a limited conservatorship including• Supported Decision Making
• Powers of Attorney
• Relying on the regional center to make medical decisions
• Health Directives
• Self Determination
• ABLE Accounts
PT2
Special Needs Trusts
A primer
A Primer on Public Benefits
Benefits Based on Entitlements
• Social Security Disability Insurance (SSDI)
• Childhood Disability Benefits (CDB)• Medicare• Special Education
Needs Based Benefits
• Supplemental Security Income (SSI)
• Medi‐Cal• Food stamps, legal aid, and
utility payment assistance• Housing subsidies (H.U.D.
or Section 8)
Supplemental Security Income
SSI is intended to pay for the beneficiary's food, and shelter and nothing more.

The SSI rate as of January 2020 in California is $943.72 a month
Supplemental Security Income
Meet Definition of Disability
Income test determines how much is received.
Resource test determines eligibility
3 Part SSI Test
Special Needs Trust Basics
• The Social Security Administration defines resources for SSI eligibility as cash and any other personal property that an individual owns or has the power to convert to cash, or not legally restricted from using for his or her support and maintenance.
• If an SSI recipient does not own an asset outright and is legally restricted from direct access to the funds, those assets are not considered a resource for benefits eligibility.
Special Needs Trust Basics
• A special needs trust is a contract where the trustee has sole and absolute discretion over the assets in the trust and the beneficiary has none.
• In essence, a special needs trust is a form of a spendthrift trust
• By directing assets otherwise intended for the individual to a special needs trust, you are preventing those assets from counted as an available resource thus preserving his or her eligibility for benefits.

The Ideal Trustee
Will use discretion in the best interest of the disabled beneficiary
Must understand public benefits and keep up with changes in the law
Can wisely invest and conform to all statutory fiduciary requirements
Understands taxes Keeps perfect books Provides advocacy and prevents
abuse Is immortal
12
Financial• Can wisely invest and
conform to all statutory fiduciary requirements
• Understands taxes
Advocacy• Will use discretion in the best
interest of the disabled beneficiary
• Must understand public benefits • Provides advocacy and prevents
abuse
Accountability• Keeps perfect book• Carries insurance, is
bondable or has deep pockets
• Is immortal
Divide These Duties Into Three Categories
13
Model 1The Trustee Directed by a Trust Advisory Committee
• The Trustee manages funds, makes distributions, does taxes, keeps records
• The Trustee is directed by a Trust Advisory Committee which gives guidance on distributions, can amend the trust or replace the Trustee
• Can include a care manager to access the needs of the beneficiary to guide the management team.
14
Trustee
Advisory Committee
Care Manager
Limitations of a Special Needs Trust
• A Trustee of a Special Needs Trust is a fiduciary and not the beneficiaries' guardian of conservator
• Can authorize payment for a beneficiary BUT has no authority to authorize the treatment itself.

Establishing Incapacity
Establishing Actual Incapacity
• All persons over 18 are presumed to have the capacity to make decisions about their personal, financial and medical matters. Prob. Code § 810(a).
• The “mere diagnosis of a mental or physical disorder” is not enough to establish “unsound mind” or lack of capacity to do a certain act. Prob. Code § 811(d).
• To establish incapacity, it must be shown through clear and convincing evidence that the person cannot provide for his/her own personal needs. Prob. Code § 1801(a).

Establishing Actual Incapacity
• A Petitioner must show that a deficit in atleast one of four mental functions rendersthe person unable to make andcommunicate decisions or to understandand appreciate the consequences of thosedecisions. Prob. Code §§ 811‐812, 1801.
• Four mental functions:• Alertness and attention;• Information processing;• Thought processes; and• Ability to modulate mood and affect.
Limited Conservatorships

History of Limited Conservatorships
• Prior law allowed a person with a developmental disability to be conserved with very little due process
• Decisions were made by professionals and not family
• Reform was initiated in part because of the practice of sterilizing persons with developmental disabilities in State Hospitals
Things to Think About
• One of the many difficult decisions that a parent of a developmentally disabled child must make is whether or not to conserve their child when the child turns 18.
• Must balance between allowing your child to make choices for themselves, and authorizing someone to make decisions for them.
• Conserving a person is limiting their civil rights.

Age 18
• Legal decision making authority of the parents ends regardless of the circumstances
• A person is not presumed incompetent merely because of a diagnosis of a developmental disability
Does Every Developmentally Disabled Person Need A Limited Conservatorship?• NO!
• Depends upon the individuals• functional abilities and needs• capacity to care for himself or herself as a
“reasonably prudent” person.
• Consider whether an alternative to conservatorship is appropriate
• A limited Conservatorship is a protective judicial proceeding for persons whose developmental disability substantially impairs their ability to care for themselves or their property.
What is a Limited Conservatorship?
How Is A Conservatorship Established?
• Requires a Petition to the Court, anda hearing, usually 60‐90 days later
• Conservatee must attend unless adoctor certifies he or she cannotattend for medical reasons
• Can be filed shortly before the 18th
birthday, or any time afterwards

How Is A Conservatorship Established?
• Court investigator is appointed and will interview proposed conservatee
• Attorney is appointed for the proposed limited conservatee
• Regional Center report is required
• Proposed conservatee’s opinion is sought
The Role of the Regional Center
• Within 30 days after the filing of a petition, a proposed limited conservatee shall be assessed at a regional center
• The regional center submits a written report of its findings and recommendations
• Provides the court with guidance about the appropriateness of the conservatorship and the suitability of the proposed conservator, if not a natural parent of the proposed conservatee
• Regional Center recommendations are not binding on the court

Powers a Limited Conservator of the Person can Petition for?
• Select the residence of the limited conservatee
• Have access to confidential records and papers
• To consent or withhold consent for marriage
• The right of the limited conservatee to contract
• To give or withhold medical consent
• To control social and sexual contacts
• Decisions concerning the education of the limited conservatee
The Health Insurance Portability and Accountability Act (HIPAA)

What is HIPAA Authorization?
• The HIPAA Privacy Rule (effective since April 14, 2003) introduced standards covering allowable uses and disclosures of health information, including to whom information can be disclosed and under what circumstances protected health information can be shared.
• The HIPAA Privacy Rule permits the sharing of health information by healthcare providers, health plans, healthcare clearinghouses, business associates of HIPAA‐covered entities, and other entities covered by HIPAA Rules under certain circumstances.
• In general terms, permitted uses and disclosures are for treatment, payment, or health care operations.
Alternatives to a Conservatorship

Meet Erica
• Meet Erica
• Receives SSI and Medicaid
• Has no experiencing making actual purchases during her entire life.
• Has significant challenges, but wit the right assistance fully capable of making her own decisions.
Supported Decision Making (SDM)• When a young person with disabilities approaches the age of 18, the family is
often mistakenly told that they must seek conservatorship (guardianship) or they will no longer be able to obtain information or provide guidance and support in the areas of healthcare, education and other services.
• There are a variety of tools commonly used that allow families to continue to provide support to their loved ones.
• While some people with disabilities may need assistance with understanding information, researching and weighing options and making decisions, conservatorship is the most restrictive option available to support these issues. .
• Families are often unaware of potential complications of conservatorship or the alternatives available to support their loved ones.
https://health.ucdavis.edu/mindinstitute/centers/cedd/sdm.html

Supported Decision Making (SDM)
• Supported decision making (SDM) allows people to obtain guidance and support without relinquishing their legal right to make decisions about their lives.
• Using supported decision‐making, a person with a disability chooses a person or a team of trusted people to help understand, make, and communicate their decisions.
• The person may rely heavily on their supporters when making decisions, but the decisions ultimately remain within their control.
• Supported decision‐making is a very flexible process; as the person gains experience, the areas in which they seek support and the people who they choose to support them may change.
https://health.ucdavis.edu/mindinstitute/centers/cedd/sdm.html
Supported Decision Making (SDM)
• Supported decision‐making may include the development of a written statement or formal contract that is written in plain language and is explained using the method the person receiving support understands most clearly.
• The agreement specifies the people who have been chosen as supporters, describes the role of the supporters and the areas that they have been asked to support with.
• Having a contract can be useful to clarify the roles of the supporters and is helpful if the role of the supporter(s) is ever challenged by school staff, medical provider or other professionals.
• There are a range of established tools, ranging from HIPAA releases, power of attorneys, IPPs, and many others, that are frequently used within the supported decision‐ making model.
https://health.ucdavis.edu/mindinstitute/centers/cedd/sdm.html

Powers of Attorney
• A Power of Attorney, in California, is a written instrument where a person designates to someone else to act on the principal's behalf.
• The powers granted to an agent may be extremely broad or for a specific transaction.
Durable Power of Attorney
• A DPA is a relatively easy, inexpensive way to give someone the ability to manage your financial affairs.
• DPA does not give the agent legal access to the principal’s assets for the agent’s own use, and DPAs terminate upon the principal’s death.
• The main disadvantage of the DPA is that it can be subject to abuse because the court does not actively supervise the agent. This is why it is extremely important to choose an agent you trust to capably handle your affairs.

Advance Health Care Directives
• The Advance Health Care Directive, appoints an agent to make health care decisions for the individual who can no longer do so.
• Enables the principal to express his or her wishes about life‐sustaining treatment, anatomical gifts, and other health care issues.
• It is quick and inexpensive.
• It can be undone as quickly if the individual objects
Limitations
• California law does not allow an agent to authorize • Commitment to or placement in a mental health
treatment facility. • Convulsive treatment• Psychosurgery• Sterilization. • Abortion. • Mercy killing, assisted suicide, or euthanasia.

IPP Participation
• On occasion, a parent will initiate a conservatorship of the person because they are being excluded from the regional center process.
• This in most cases is just plain wrong and violates the Lanterman Act
• Family generally have a right to attend so long as it is appropriate
• For instance, if a child expresses they do not want their parent to attend – it is not appropriate
Authorized Representative Assigned by Area Board (Now the State Council)• If the rights or interests of a consumer is not properly protected or
advocated, the local area board may appoint a person or agency as the Authorized Representative.
• The Authorized Representative may participate in IPPs and Fair Hearings

• The director of a regional center or the director’s designee may give consent to medical, dental, and surgical treatment of a regional center client and provide for such treatment if the developmentally disabled person has no parent, guardian, or conservator legally authorized to consent .
Regional Center Director’s Authority to Authorize Medical Treatment under the Lanterman Act
• Although the Lanterman Act does not specify or limit who might be qualified to be designated to make medical decisions, the designee is almost always a regional center staff member.
Regional Center Director’s Authority to Authorize Medical Treatment under the Lanterman Act
ABLE Accounts
• Can be a tool to teach financial literacy
• Allows a SSI or Medi‐Cal recipient ability to purchase items without interfering with benefit eligibility
• Presumes the person with a disability has control, otherwise can be controlled by parent, agent under valid power of attorney or conservatorship.
Self‐Determination• As authorized in Welfare and Institutions Code, Section 4685.8
• The Self‐Determination Program is a delivery system. • It consists of services and supports which are totally selected and directed
voluntary by consumers/families through person‐centered planning, so that the goals of his or her Individual Program Plan (IPP) can be met.
• Participants will be provided with a budget based on the previous year’s history of funding for services. The budget allows participants to purchase the services and supports they want.
• For the first three years, 2,500 people will be selected to participate statewide. This is called the pilot phase.
• After the 3 years, the Self‐Determination Program will be open to everyone who receives regional center services.
Last Thoughts
• Approach should focus on the individual
• Decision‐making rights should never be restricted without considering less least restrictive alternatives.
• In many cases you can mix tools• Example – even with a conservatorship – supported decision making can still
be implemented
• This is an area of development – and we can expect changes in the near future.
Special Needs Trusts, Conservatorships and Alternatives including Self Determination and
Supported Decision‐Making
Stephen W. Dale Esq. LL.M
Attorney ‐ Dale Law Firm
Trustee ‐ Golden State Pooled Trust
19th Annual Developmental Disabilities: An Update for Health ProfessionalsMarch 5‐6, 2020

WELFARE AND INSTITUTIONS CODE - WIC DIVISION 4.5. SERVICES FOR THE DEVELOPMENTALLY DISABLED [4500 - 4885] (Division4.5addedbyStats.1977,Ch.1252.)
CHAPTER 5. Regional Centers for Persons With Developmental Disabilities [4620 -
4669.75] (Chapter5addedbyStats.1977,Ch.1252.)
ARTICLE 2. Regional Center Responsibilities [4640 - 4659.2] (Article2addedbyStats.1977,Ch.1252.)4655. The director of a regional center or his designee may give consent to medical, dental, and surgical treatment of a regional center client and provide for such treatment to be given to the person under the following conditions:
(a) If the developmentally disabled person’s parent, guardian, or conservator legally authorized to consent to such treatment does not respond within a reasonable time to the request of the director or his designee for the granting or denying of consent for such treatment, the director of a regional center or his designee may consent on behalf of the developmentally disabled person to such treatment and provide for such treatment to be given to such person.
(b) If the developmentally disabled person has no parent, guardian, or conservator legally authorized to consent to medical, dental, or surgical treatment on behalf of the person, the director of the regional center or his designee may consent to such treatment on behalf of the person and provide for such treatment to be given to the person. The director of a regional center or his designee may thereupon also initiate, or cause to be initiated, proceedings for the appointment of a guardian or conservator legally authorized to consent to medical, dental, or surgical services.
(c) If the developmentally disabled person is an adult and has no conservator, consent to treatment may be given by someone other than the person on the person’s behalf only if the developmentally disabled person is mentally incapable of giving his own consent.
(AmendedbyStats.1979,Ch.730.)
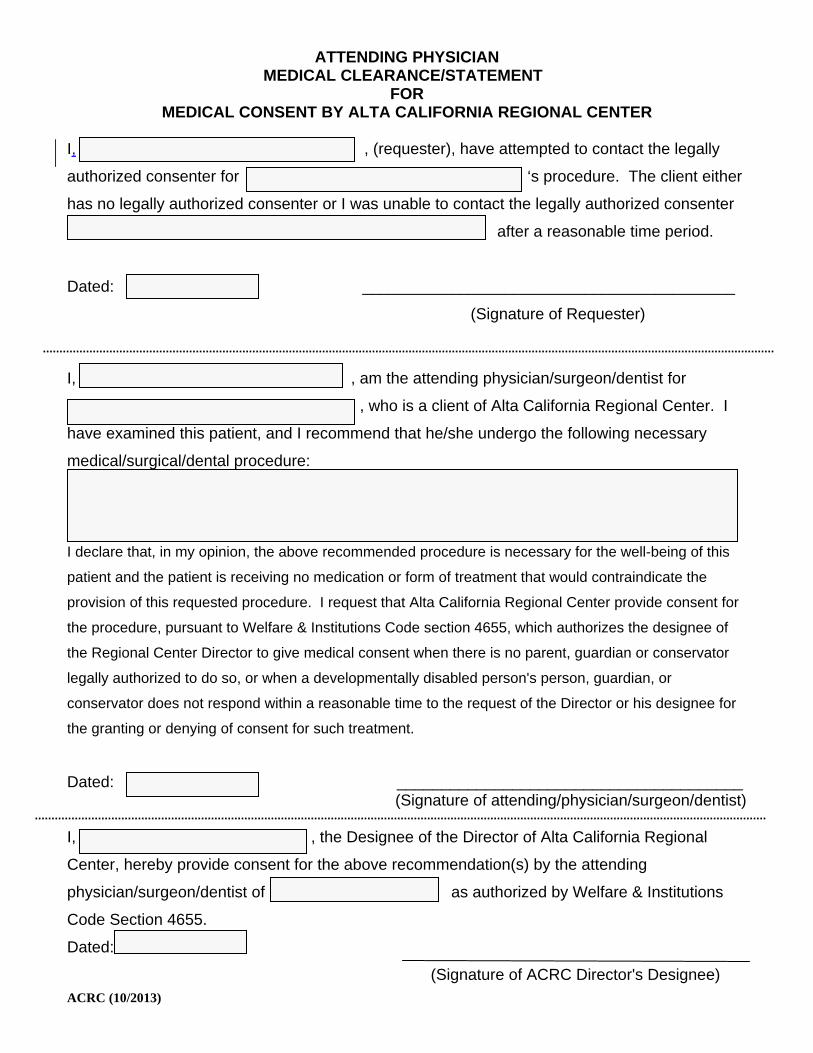
ATTENDING PHYSICIAN MEDICAL CLEARANCE/STATEMENT
FOR MEDICAL CONSENT BY ALTA CALIFORNIA REGIONAL CENTER
ACRC (10/2013)
I, , (requester), have attempted to contact the legally
authorized consenter for ‘s procedure. The client either
has no legally authorized consenter or I was unable to contact the legally authorized consenter
. after a reasonable time period.
Dated: __________________________________________
(Signature of Requester)
I, , am the attending physician/surgeon/dentist for
, who is a client of Alta California Regional Center. I
have examined this patient, and I recommend that he/she undergo the following necessary
medical/surgical/dental procedure:
I declare that, in my opinion, the above recommended procedure is necessary for the well-being of this
patient and the patient is receiving no medication or form of treatment that would contraindicate the
provision of this requested procedure. I request that Alta California Regional Center provide consent for
the procedure, pursuant to Welfare & Institutions Code section 4655, which authorizes the designee of
the Regional Center Director to give medical consent when there is no parent, guardian or conservator
legally authorized to do so, or when a developmentally disabled person's person, guardian, or
conservator does not respond within a reasonable time to the request of the Director or his designee for
the granting or denying of consent for such treatment.
Dated: _______________________________________ (Signature of attending/physician/surgeon/dentist)
I, , the Designee of the Director of Alta California Regional
Center, hereby provide consent for the above recommendation(s) by the attending
physician/surgeon/dentist of as authorized by Welfare & Institutions
Code Section 4655.
Dated:
(Signature of ACRC Director's Designee)
19th Annual Developmental Disabilities: An Update for Health Professionals
Aaron Carruthers, Executive Director
I don’t have anything to disclose

The purpose of this presentation is to describe major changes in motion inside and outside the developmental disabilities service system
Objective 1: SCDDKnow the Role of the State Council on Developmental Disabilities
Objective 2: System Changes ◦ Identify at least 3 Changes Currently Reshaping the
Developmental Disabilities Service Delivery System
Objective 3: Living a Full Life ◦ Identify at least 3 Needs People with IDD Have
Outside the Service Delivery System

State Council on Developmental Disabilities◦ In federal and state◦ Independent state department, funded by Congress ◦ Authority to advocate, build capacity, and change
systems◦ Do this by training people with IDD, their families, and
other advocates, advocating directly ◦ Last year: trained 20,000 people, technical assistance
for 10,000 people ◦ Last year: work impacted 1.9 million Californians
System Growing 5x faster than the state◦ CA grows less than 1% per year◦ IDD service system growing by 5% per year
Governor proposes $9.2 billion for the Department of Developmental Services (DDS)◦ Increase of $1 billion from prior year
368,000 individuals with IDD served through 21 independent regional centers◦ 50 new people enter the system every day

Home and Community Based Settings Final Rule ◦ Issued by the federal Centers for Medicare and
Medicaid Services (CMS) in 2014, implemented by 2022
To get federal funding recipients must be in most integrated setting appropriate◦ Setting is selected by the individual from setting options
including non-disability specific settings ◦ Is integrated and supports access to the greater
community
$2.8 billion at risk to not meet Final Rule
Regional Center Provider Rates ◦ Administration commissioned a study to create
transparency, sustainability, quality◦ Wide variety of services and supports, +150 codes Residential services Day programs Employment programs Independent and supported living
◦ System underfunded by $1.8 billion

Self Determination Program ◦ A different way of receiving services through the
regional center ◦ Provides regional center clients and their families more
flexibility and control in the services ◦ Does not have to be regional center vendored provider ◦ Approved by CMS in June 2018◦ Initial 2,5000 participants◦ Eligible to all 368,000 regional center clients June
2021◦ Currently 150 out of 2,500 in the new program
System growing 5x faster than State Home and Community Based Settings Final
Rule Regional Center Provider Rates Self Determination Program

Housing A crisis within a crisis 100,000 regional center adult clients living with
families 11% of people with disabilities living
independently Need 20,000 housing units
Employment Employment rate of regional center clients
13.6%◦ 4,500 competitive integrated employment◦ 5,400 in group employment ◦ 67,000 in day programs or subminimum wage

Safety Public Safety Power Shutoffs Interactions with law enforcement 3% of sexual assaults against people with IDD
are reported Abuse, neglect, crime◦ 4x – 10x more likely to be victims
Dental care
Housing Employment Safety◦ PSPS ◦ Law enforcement ◦ Sexual assaults, abuse, neglect, crime◦ Dental care

Objective 1: SCDDKnow the Role of the State Council on Developmental Disabilities
Objective 2: System Changes ◦ Identify at least 3 Changes Currently Reshaping the
Developmental Disabilities Service Delivery System
Objective 3: Living a Full Life ◦ Identify at least 3 Needs People with IDD Have
Outside the Service Delivery System
Aaron Carruthers Executive Director State Council on Developmental Disabilities [email protected]

What’s New in AAC & AT?
19th Annual Developmental Disabilities: Update for Health ProfessionalsFriday, March 6, 2020
Kelly Rinehart, M.A., CCC-SLP
disclosures• I am an associate with Augmentative Communication & Technology Services
(ACTS). We provide AAC & AT clinical services and evaluations for infants, toddlers, and school aged children as well adults with congenital and developmental disabilities, as well as mentorship, consultation, and program development.
• ACTS associates, not including myself, developed the CSA tool; I have no financial gain from it.
• I am a lecturer and clinical supervisor at SFSU.
• I worked at the Bridge School, but did not develop the Framing a Future tool and have no financial gain from it.
• I have no relevant financial and no relevant non-financial relationships with UCSF. 2
learning objectives
• Participants will be able to list 1-3 assessments to aid goal setting for individuals with complex communication needs.
• Participants will be able to list at least 3 current technologies in AAC/AT.
• Participants will be able to identify a new iDevice accessibility option.
• Participants will be able to identify 3 funding sources for SGDs.
3
• there are no prerequisites for AAC
• it’s never too early to start
• bilingual individuals do not need to pick a language
• AAC does not interfere with speech development
• get beyond requesting
4

It’s the Goal! Not the Tool!
Multimodal Communication
Access
5
It’s the Goal! Not the Tool!
Multimodal Communication
Access
6
7
It’s the GOAL! Not the tool!

9
www.praacticalaac.org

• http://csa.acts-at.com/
• observations recorded on sampling form
• online tool:
• manual & tips
• sample
• data summary report
• report template 11
12
• means
• functions
• language sample

• https://communicationmatrix.org/
• outlines communication status and progress of early communicators with CCN
• addresses pre-intentional behavior through language use
• looks at a variety of functions: refuse, obtain, social, information
• Spanish version
13
Framing a Future• http://selfdetermined.bridgeschool.org/framing-a-future/
• 65 items in 7 major life areas
• what is important?
• how satisfied are they?
• establish priorities
• steps to address priorities
• examples of modifications on website
• Spanish version 14

adult services
15
It’s the Goal! Not the Tool!
Multimodal Communication
Access
18
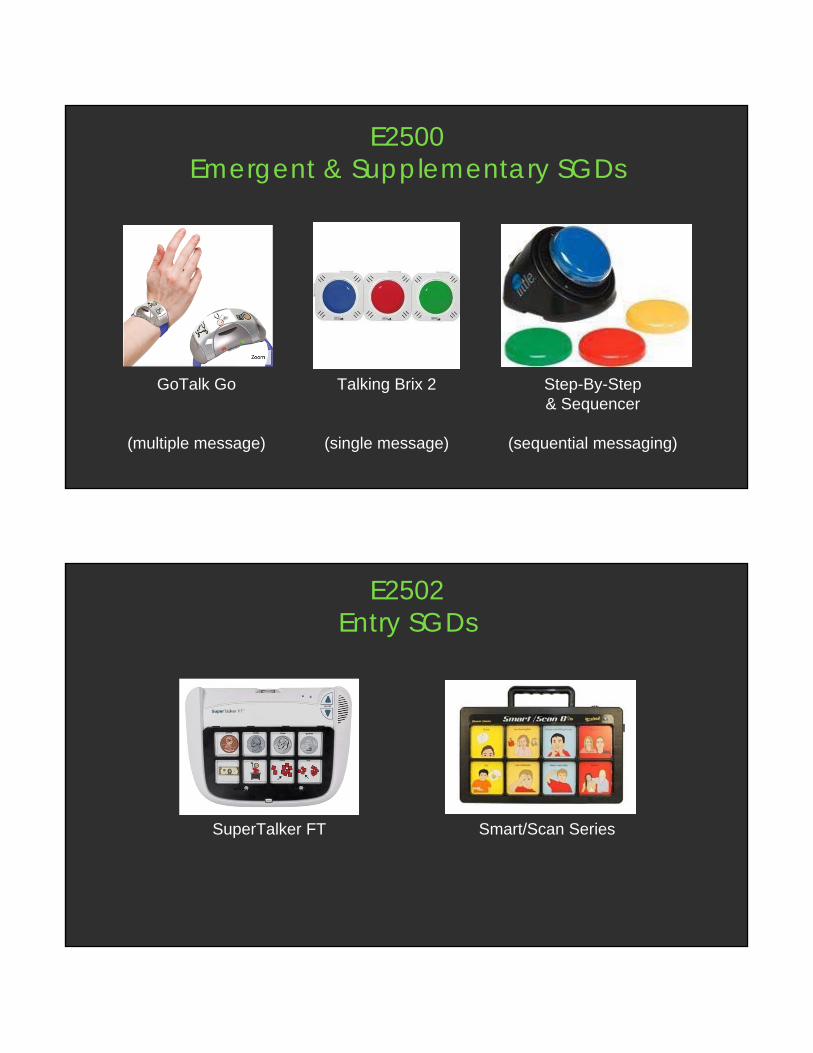
E2500Emergent & Supplementary SGDs
Talking Brix 2
(single message)
Step-By-Step& Sequencer
(sequential messaging)
GoTalk Go
(multiple message)
E2502Entry SGDs
Smart/Scan SeriesSuperTalker FT

E2508/2510Intermediate SGDs
Quicktalker Freestyle(not MediCal) PRC Prio/Mini
(not MediCal)
TouchChat Express
E2510Advanced SGDs
NOVA Chat / Chat Fusion** headpointing
Forbes WinSlate(not MediCal)
Accent(new: Empower software)

E2599Advanced SGDs with eye tracking
Tobii Dynavox i13 & i16 PRC’s Look eye tracking module
Forbes WinSlatew/ Enable Eyes(not MediCal)
medically-based SGD evaluations
25
SGD funding sources•Private Insurance
•California Children’s Services (CCS)
•Medi-Cal
•CPUC Deaf and Disabled Telecommunications Program (DDTP)
•School District
•Low Incidence Funds
•General Education Funds
•Regional Center: funding for SGD evals & replacement evals
26children AND adults http://www.cpuc.ca.gov/sgd/

dedicated/locked devices
unlock codes
27
It’s the Goal! Not the Tool!
Multimodal Communication
Access
32

seating and positioning
• ensure comfort
• ensure safety and stability
• promote & enable functional skills
33
Scanning:selection control
techniques
Blue2 Candycorn
Tapio

sip n puff
SCATIR
string switchmembrane switch
NeuroNodeby Control Bionics
• eye gaze
• EMG
• touch & motion sensors40
• EMG activated switch
brain computer interface (BCI)
42
44

iDevice Scanning
• Switches: External; Screen; Camera (iPad Pro: head tracking, facial movements)
• Recipes (handout)
• Triple click to exit scanning mode
iPad Pro head tracking / facial movements
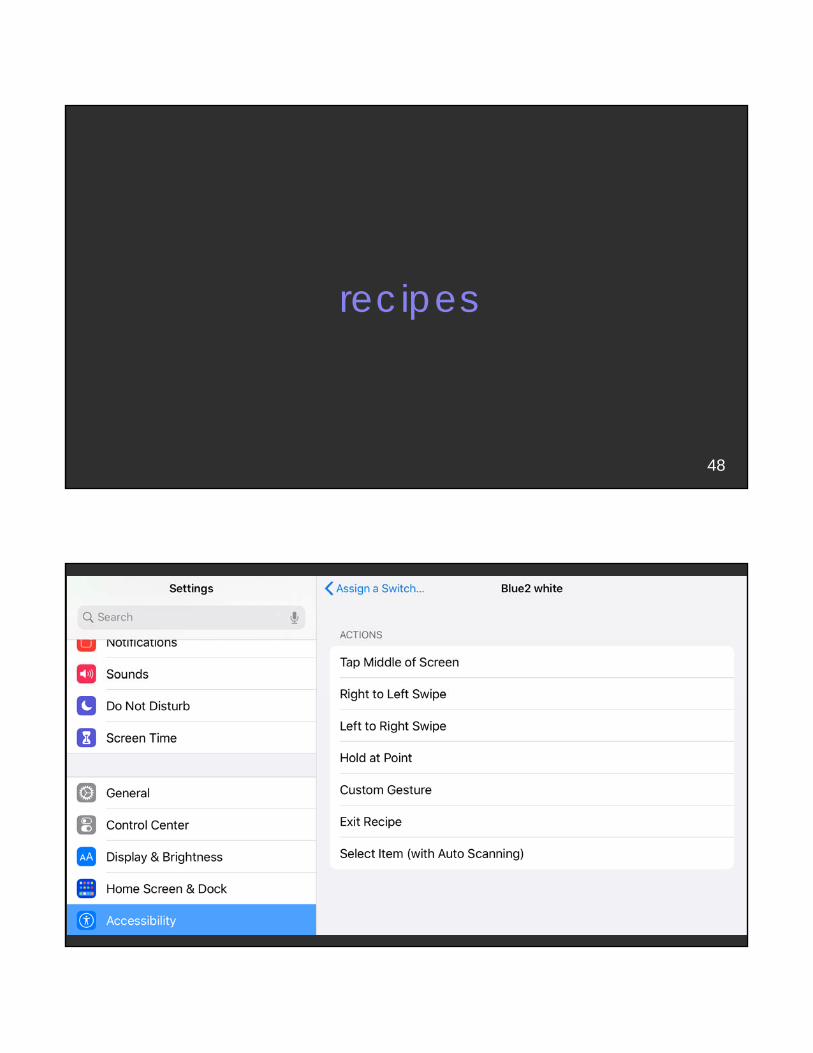
recipes
48
49

50
51

52
Integration with other devices & applications
54

55

National Joint Committee for the Communication Needs of Persons with Severe Disabilities (NJC)
National Joint Committee for the Communication Needs of Persons With Severe Disabilities (NJC)
COMMUNICATION BILL OF RIGHTSAll people with a disability of any extent or severity have a basic right to affect, through communication, the conditions of their existence. Beyond this general right, a number of specific communication rights should be ensured in all daily interactions and interventions involving persons who have severe disabilities. To participate fully in communication interactions, each person has these fundamental communication rights:
1. The right to interact socially, maintain social closeness, and build relationships
2. The right to request desired objects, actions, events, and people
3. The right to refuse or reject undesired objects, actions, events, or choices
4. The right to express personal preferences and feelings
5. The right to make choices from meaningful alternatives
6. The right to make comments and share opinions
7. The right to ask for and give information, including information about changes in routine and environment
8. The right to be informed about people and events in one’s life
9. The right to access interventions and supports that improve communication
10. The right to have communication acts acknowledged and responded to even when the desired outcome cannot be realized
11. The right to have access to functioning AAC (augmentative and alternative communication) and other AT (assistive technology) services and devices at all times
12. The right to access environmental contexts, interactions, and opportunities that promote participation as full communication partners with other people, including peers
13. The right to be treated with dignity and addressed with respect and courtesy
14. The right to be addressed directly and not be spoken for or talked about in the third person while present
15. The right to have clear, meaningful, and culturally and linguistically appropriate communications
For more information, go to the NJC website at: www.asha.org/njc
11220
Brady, N. C., Bruce, S., Goldman, A., Erickson, K., Mineo, B., Ogletree, B. T., Paul, D., Romski, M., Sevcik, R., Siegel, E., Schoonover, J., Snell, M., Sylvester, L., & Wilkinson, K. (2016). Communication services and supports for individuals with severe disabilities: Guidance for assessment and intervention. American Journal on Intellectual and Developmental Disabilities, 121(2), 121-138.

Simplifying Switch Access withSwitch Control Recipes
Apple, iPad, iPhone, and iPod touch are trademarks of Apple Inc., registered in the U.S. and other countries. iOS is a trademark or registered trademark of Cisco in the U.S. and other countries and is used under license.
Updated September 9, 2019 7:05 PM

2
Table of ContentsIntroduction ......................................................................................................................................................................2
What You Need .................................................................................................................................................................2
Getting Started ................................................................................................................................................................3-5
Turn Pages On An eBook................................................................................................................................................6-8
Control Music ...................................................................................................................................................................8-11
Cause and Effect with Garage Band ........................................................................................................................... 12-15
IntroductionWith Switch Control for iOS 13 and iPadOS 13 you can do almost anything with a switch. With this power comes some complexity for the user. The recipes feature found within Switch Control for iOS 13 can greatly simplify switch use on the iPad, iPhone, or iPad touch. To help introduce you to recipes and simplified switch access for the user, we’ve put together a few tutorials.
What You NeedFor all Switch Control Recipe tutorials you will need the following:
• An iPhone or iPod touch with iOS 13 or iPad with iPadOS 13
• A switch interface for your device
- Hook+ iOS Switch Interface: Hook+ is an Apple MFi approved switch interface that provides a reliable wired connection to the iPad, iPhone, or iPod touch via the Lightning connector. Connect one to four wired switches to Hook+ for use with Switch Control. More information at www.ablenetinc.com.
- Blue2 Bluetooth Switch: The Blue2 Bluetooth switch provides single or dual switch access when used with Switch Control. Users can activate the orange and white switch tops, or they can plug in two external switches for activation. More information at More information at www.ablenetinc.com
Hook+ iOS Switch Interface Blue2 Bluetooth Switch

3
Getting StartedBefore you can begin any of the Switch Control Recipe tutorials, you need to make sure that your switch interface is connected to your device and two switches are configured.
SET UP HOOK+ iOS SWITCH INTERFACE
1. Plug switches into Switch Jack 1 and Switch Jack 2 on Hook+
2. On the device go to Settings App > Accessibility > Switch Control
3. Turn Switch Control On
4. Plug Hook+ into the Lightning Connector on your device. Two switches will automatically configure.
5. You are now ready to proceed with the Switch Control Recipe tutorials
After Step 4, you will see these two switches
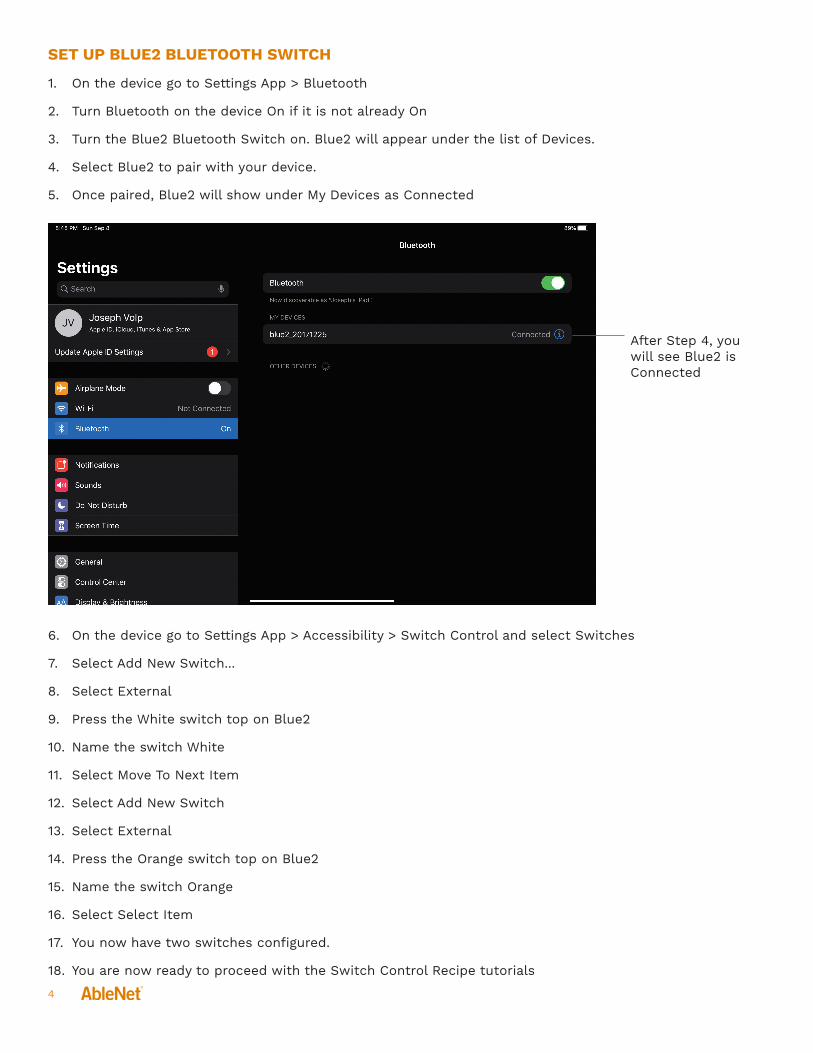
4
SET UP BLUE2 BLUETOOTH SWITCH
1. On the device go to Settings App > Bluetooth
2. Turn Bluetooth on the device On if it is not already On
3. Turn the Blue2 Bluetooth Switch on. Blue2 will appear under the list of Devices.
4. Select Blue2 to pair with your device.
5. Once paired, Blue2 will show under My Devices as Connected
6. On the device go to Settings App > Accessibility > Switch Control and select Switches
7. Select Add New Switch...
8. Select External
9. Press the White switch top on Blue2
10. Name the switch White
11. Select Move To Next Item
12. Select Add New Switch
13. Select External
14. Press the Orange switch top on Blue2
15. Name the switch Orange
16. Select Select Item
17. You now have two switches configured.
18. You are now ready to proceed with the Switch Control Recipe tutorials
After Step 4, you will see Blue2 is Connected

5
For additional details on using the Hook+ iOS Switch Interface or Blue2 Bluetooth Switch with iOS Switch Control, download iOS Accessibility - Switch Control - The Missing User Guide at www.ablenetinc.com.
After Step 16, you will see these two switches

6
Tutorial 1: Turn Pages In An eBookIn this tutorial you will create a Switch Control Recipe that enables the user to turn pages in an eBook forward and backwards with two switches. Before starting, make sure you have completed setting up your Hook+ iOS Switch Interface with two switches or your Blue2 Bluetooth Switch.
1. On the device go to Settings App > Accessibility > Switch Control
2. Turn Switch Control Off. If Switch Control is On, the Recipe will not work correctly.
3. Select Recipes
4. Under Recipes select Turn Pages
5. You will notice that both of your switches were automatically assigned to Right to Left Swipe and Left to Right Swipe
6. Make sure Timeout is turned Off
7. At the top of the screen select Recipes to go back to the main Recipes menu
8. Select Launch Recipe
9. Select Turn Pages
Step 5, if you are using Hook+, in-stead of Orange it will say Next and instead of White it will say Select.
Step 6, make sure Timeout is turned off

7
10. At the top of the screen select Recipes to go back to the main Recipes menu
11. At the top of the screen select Switch Control to go back to the man Switch Control menu
12. Turn Switch Control On
13. When Switch Control turns On, you will see a message appear in the middle of your device screen that says Your switches are configured to use the “Turn Pages” recipe.
After Step 9, you will see this
Step 13, you will see this warning message

8
14. On the device, open the iBooks App
15. Select a book the user would like to read
16. When the user activates the Orange Switch on Blue2 (or if using Hook+, Switch 2 / Next) the page will turn forward. When the user activates the White Switch on Blue2 (or if using Hook+, Switch 1 / Select) the page will turn backwards.
17. Once finished with the eBook, you can turn the Recipe Off, by going to Settings App > Accessibility > Switch Control and turning Switch Control Off. You must ALSO go to Recipes > Launch Recipe and change this back to None.
Tutorial 2: Control MusicIn this tutorial you will learn how to create a custom Switch Control Recipe that can be used to control music. We will be using a paper marker on the device screen to mark where the Skip Track Forward button is located and you will need a small piece of a Post-It-Note to do this. Before starting, make sure you have completed setting up your Hook+ iOS Switch Interface with two switches or your Blue2 Bluetooth Switch.
1. Orient the device in the direction the user will be using it. This is important because we will be marking a specific location on the screen of the device for the Switch Control Recipe.
2. On the device open the Music App
3. Select a song so that the music player controls appear on the screen
4. Using a small piece of the Post-It-Note, mark on the screen where the Skip Track Forward button is located. If you wanted to use the Play/Pause or Skp Track Backwards buttons, you could mark those instead.
Step 4, Post-It-Note marker over Skip Track Forward button

9
5. Exit out of the Music App. Make sure you leave your Post-It-Note marker on the screen of your device.
6. On the device go to Settings App > Accessibility > Switch Control
7. Turn Switch Control Off. If Switch Control is On, the Recipe will not work correctly.
8. Select Recipes
9. Under Recipes select Create New Recipe...
10. Name your recipe Skip Track Forward (if using Blue2, you will need to activate the keyboard button on the side of Blue2 to get the on-screen keyboard to appear)
11. Select Assign a Switch
12. If using Blue2, choose White (or if using Hook+, choose Select)
13. Select Custom Gesture
14. You will be brought to a screen with instructions. Tap on your Post-It-Note marker and then select Save in the upper right corner of the screen.
15. You will now see under Switches that White (or if using Hook+, Select) has been assigned Custom Gesture
16. Make sure Timeout is turned Off
Step 14, Post-It-Note marker showing where the Skip Track Forward button is located

10
17. At the top of the screen select Recipes to go back to the main Recipes menu
18. Select Launch Recipe
19. Select Skip Track Forward
Step 15, the White switch has been assigned a custom gesture (if using Hook+ instead of White you will see Select)
Step 16, make sure Timeout is turned off
After Step 19, you will see this

11
20. At the top of the screen select Recipes to go back to the main Recipes menu
21. At the top of the screen select Switch Control to go back to the man Switch Control menu
22. Turn Switch Control On
23. When Switch Control turns On, you will see a message appear in the middle of your device screen that says Your switches are configured to use the “Skip Track Forward” recipe.
24. On the device, open the Music App. Make sure the device is in the same orientation as it was when you placed your Post-It-Note marker on the screen.
25. Select a song to bring up the music player controls. Make sure the music is playing before giving the device to the user. They will only be able to change the song playing.
26. When the user activates the White switch top on Blue2 (or if using Hook+, Switch 1 / Select) and the song will skip to the next song
27. Once finished with the Music App, you can turn the Recipe Off, by going to Settings App > Accessibility > Switch Control and turning Switch Control Off. You must ALSO go to Recipes > Launch Recipe and change this back to None.
Step 23, you will see this warning message

12
Tutorial 3: Cause and Effect with Garage BandIn this tutorial you will learn how to create a Switch Control Recipe for a simple cause and effect activity using Garage Band. We will be using a paper markers on the device screen to mark where the drums are located and you will need small pieces of a Post-It-Note to do this. Before starting, make sure you have completed setting up your Hook+ iOS Switch Interface with two switches or your Blue2 Bluetooth Switch.
1. Orient the device in the direction the user will be using it. This is important because we will be marking a specific location on the screen of the device for the Switch Control Recipe.
2. On the device open the Garage Band App
3. Under Tracks select Drums
4. Once you select the Drums you will be presented with a full drum set. Place small pieces of the Post-It-Note on three different drums (you can select less or more than three drums to mark).
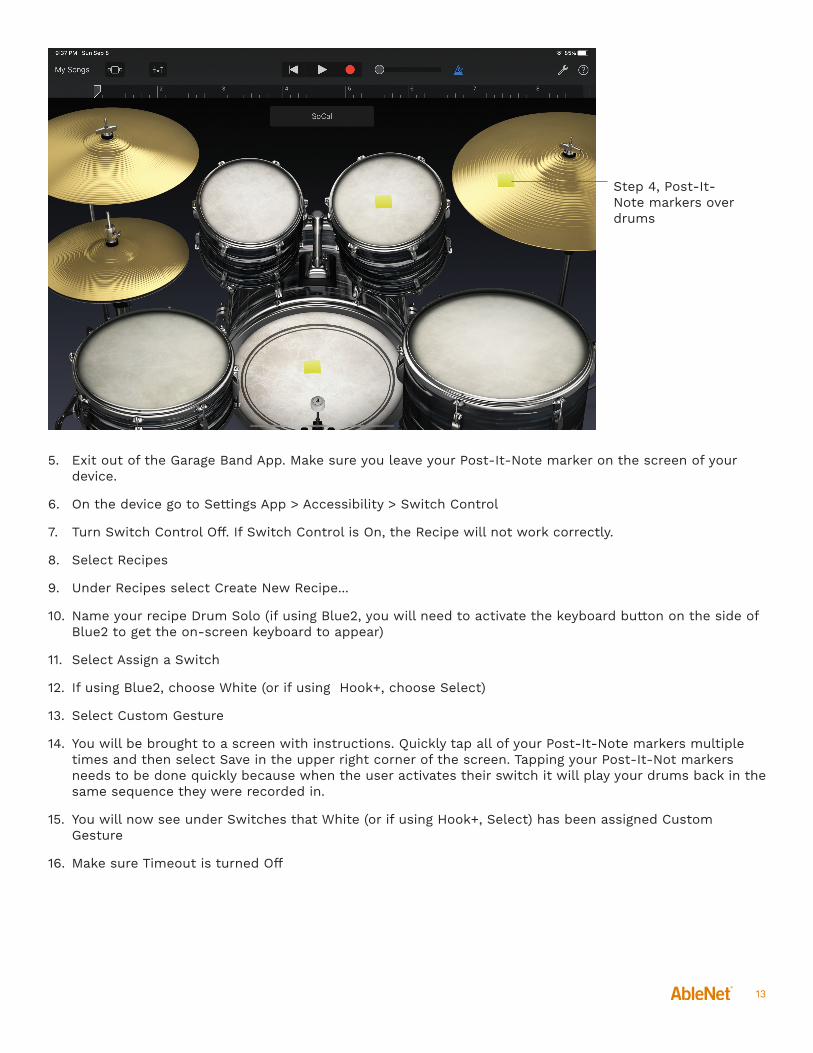
13
5. Exit out of the Garage Band App. Make sure you leave your Post-It-Note marker on the screen of your device.
6. On the device go to Settings App > Accessibility > Switch Control
7. Turn Switch Control Off. If Switch Control is On, the Recipe will not work correctly.
8. Select Recipes
9. Under Recipes select Create New Recipe...
10. Name your recipe Drum Solo (if using Blue2, you will need to activate the keyboard button on the side of Blue2 to get the on-screen keyboard to appear)
11. Select Assign a Switch
12. If using Blue2, choose White (or if using Hook+, choose Select)
13. Select Custom Gesture
14. You will be brought to a screen with instructions. Quickly tap all of your Post-It-Note markers multiple times and then select Save in the upper right corner of the screen. Tapping your Post-It-Not markers needs to be done quickly because when the user activates their switch it will play your drums back in the same sequence they were recorded in.
15. You will now see under Switches that White (or if using Hook+, Select) has been assigned Custom Gesture
16. Make sure Timeout is turned Off
Step 4, Post-It-Note markers over drums
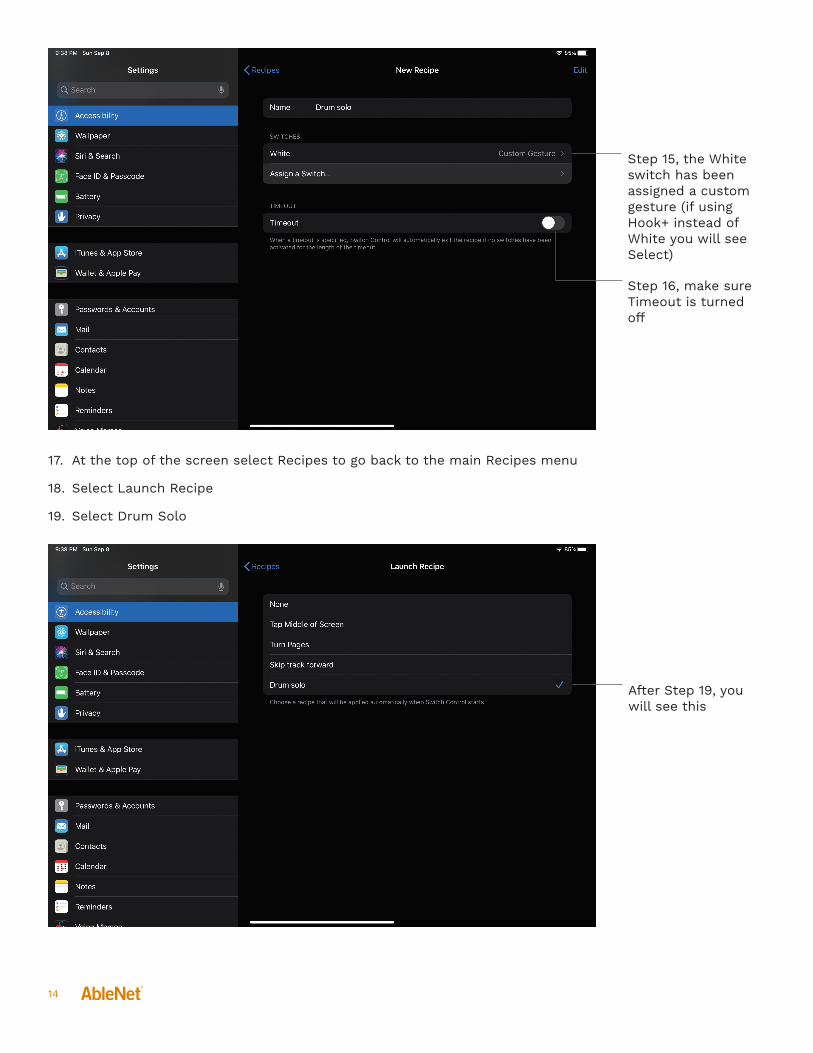
14
17. At the top of the screen select Recipes to go back to the main Recipes menu
18. Select Launch Recipe
19. Select Drum Solo
Step 15, the White switch has been assigned a custom gesture (if using Hook+ instead of White you will see Select)
Step 16, make sure Timeout is turned off
After Step 19, you will see this
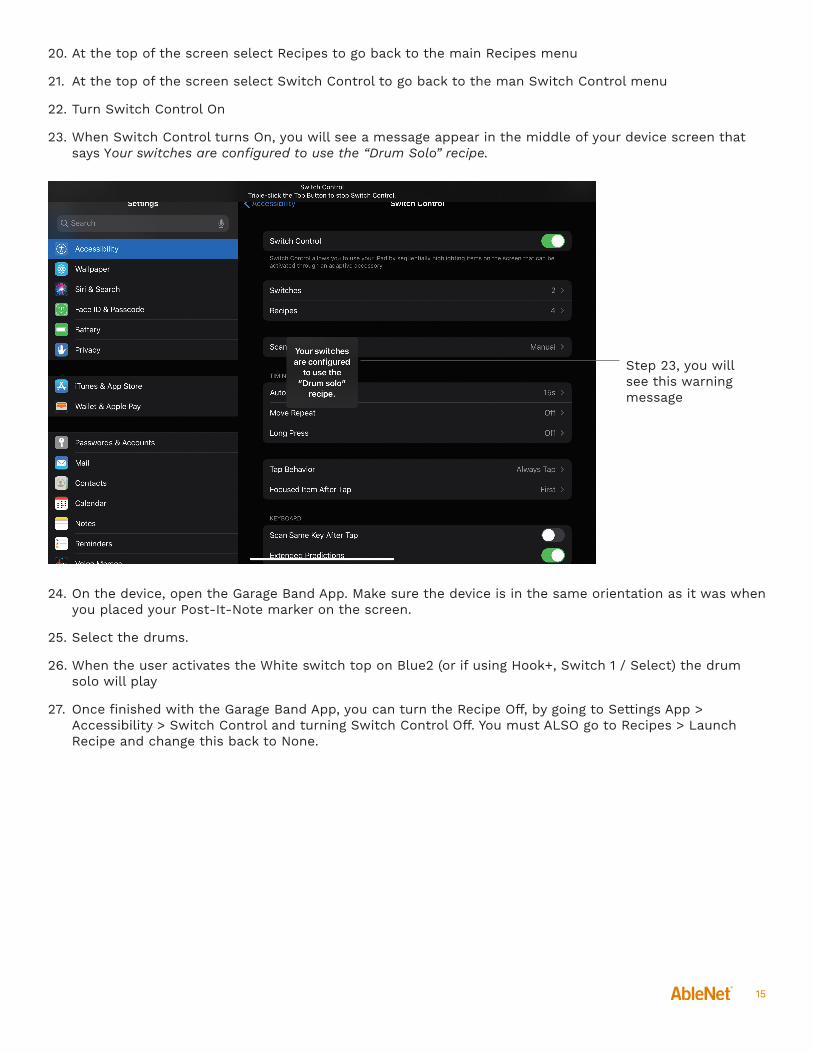
15
20. At the top of the screen select Recipes to go back to the main Recipes menu
21. At the top of the screen select Switch Control to go back to the man Switch Control menu
22. Turn Switch Control On
23. When Switch Control turns On, you will see a message appear in the middle of your device screen that says Your switches are configured to use the “Drum Solo” recipe.
24. On the device, open the Garage Band App. Make sure the device is in the same orientation as it was when you placed your Post-It-Note marker on the screen.
25. Select the drums.
26. When the user activates the White switch top on Blue2 (or if using Hook+, Switch 1 / Select) the drum solo will play
27. Once finished with the Garage Band App, you can turn the Recipe Off, by going to Settings App > Accessibility > Switch Control and turning Switch Control Off. You must ALSO go to Recipes > Launch Recipe and change this back to None.
Step 23, you will see this warning message

UCSF Schoolof Medicine
Department of Familyand Community Medicine
Office of Developmental Primary Care
Reimagining the Possible for Non-Speaking, Autistic People19th Annual Developmental Disabilities: An Update for Health Professionals, March 5-6, 2020
Clarissa Kripke, MD, FAAFPDavid TeplitzHari SrinivasanTyler Fihe
Office of Developmental Primary Care: https://odpc.ucsf.edu/2
Disclosure
We have nothing to disclose.
Office of Developmental Primary Care: https://odpc.ucsf.edu/3
Overview
--Review what we are learning about autism and why it is better accommodated when understood as a neurological issue than a psychological or cognitive one.
--Hear directly from three, nonspeaking, autistic leaders about their experiences and recommendations.
--Discuss what we can do to raise our expectations and reimagine what is possible for nonspeaking or minimally or unreliably speaking autistic people.
Office of Developmental Primary Care: https://odpc.ucsf.edu/4
Sensory-Movement Differences
Self-advocates are telling us we have our paradigm wrong:
Autism, especially for nonspeaking people with dyspraxia, is a neurological issue, not a problem with restricted interests, intellectual disability, or social understanding.
Recap of last year’s talk Autism: Working with Sensory-Movement Differences:
https://www.uctv.tv/shows/Autism-Working-with-Sensory-Movement-Differences-34672
Office of Developmental Primary Care: https://odpc.ucsf.edu/5
Key points about sensory and movement issues in autism?
- Performance does not equal intelligence.
- Not all behavior is communication.
- Intelligence isn’t a fixed trait or capacity.
- Working with sensory and movement differences is more effective than working against them.
- Everybody needs a fluent form of expressive communication.
- Autistic people are routinely underestimated.
Office of Developmental Primary Care: https://odpc.ucsf.edu/6
Resources
- https://unitedforcommunicationchoice.org/
- https://odpc.ucsf.edu/communications-paper
- https://www.callutheran.edu/centers/autism/
- https://communicationfirst.org/

Office of Developmental Primary Care: https://odpc.ucsf.edu/7
Office of Developmental Primary Care500 Parnassus Avenue, Box 0900Tel: 415-476-4641 | Fax: 415-476-6051email: [email protected]: http://odpc.ucsf.edu

2/23/2020
1
REIMAGINING THE
POSSIBLEFOR NON-SPEAKING,
AUTISTIC PEOPLE
DAVID TEPLITZ
ORIENTATION WEEK at U.C. BERKELEY

2/23/2020
2
SABRINA & ME ON HALLOWEEN
A REUNION WITH A FEW OF MY AIDES FROM OVER THE YEARS

2/23/2020
3
A REUNION WITH A FEW OF MY AIDES FROM OVER THE YEARS8TH GRADE GRADUATION ‘09

2/23/2020
4
SKYLINE H.S. GRADUATION ’13

2/23/2020
5

2/23/2020
6
2/23/2020
7
2/23/2020
8
THANKYOU!
DAVID TEPLITZ
2/17/20
1
Reimagining Possibilitiesfor minimally/non-speaking autistics
Hari Srinivasan, Student, UC Berkeley
Disclosure
I have nothing to disclose -Hari Srinivasan
UCSF Office of Continuing Medical Education
19th Annual Developmental Disabilities.
Update for Health Professionals March 5, 2020
• Everyone deserves to wake up to a productive and meaningful life.
• The experiences of a non-speaking autistic used to demonstrate the potential of this marginalized population (~30% of ASD population)
• Some takeaways for professionals towards reimagining the possibilities for this population from the viewpoint of a growth mindset
Overview

2/17/20
2
1. Communication is a mandatory skill2. Developmentally “All-Over-The-Place”3. The Right to Dignity and Inclusion in
Human Society4. Professionals as Game Changerso Educators/Service Providers/ Support
Staffo Health Care Professionalso Case Managers/ Regional Center /
Overseeing Agencies
Learning ObjectivesA Growth Mindset
Reimagining Possibilities
• Student UC Berkeley• Major Psychology, Minor Disability Studies• Minimally-Speaking Autistic who types to communicate
Copyright © 2018 Hari Srinivasan
Introducing Hari
Autism Challenges • Non-speaking, Type to Communicate
• Oral Motor Apraxia• Poor Body Schema• Poor Body Coordination• Sensory Dysregulation
(stims)• Poor Fine Motor (affects
handwriting and self help skills)
• OCD• ADHD• Anxiety and Mood
Regulation

2/17/20
3
• First two non-speaking autistics at UC Berkeley.• Should be the norm and not the exception.
The Experience of College
Where else are you gonna do stuff like this?
Result of Reimagining
2. Communication Breakthrough
1. The Futile Years
3. Reimagining Possibility
4. Road to University
My Journey
My Wasted Years
• Dismal elementary years• No communication ability• Bored, frustrated, depressed à more behaviors

2/17/20
4
Communication Breakthrough
Typing to Communicate
I need more…
Time to Reimagine
Charter High School ValedictorianNational Gold Medal, PublicationInternships
Mainstream Education & more
DSP Accommodations that Enable Education
Examples• Extra Time for Tests• Alternative Media• Reduced Course Load• Laptop/ iPad• Specialized Software• Managing Sensory Environment• Support Aide (Regulation/
Communication/Behavior)• Priority Registration• Distraction Free Setting
2/17/20
5
My Berkeley Experience• Intellectually stimulating classes with amazing Profs• Social Opportunities - group projects, student events,
student parties, Cal Athletics and events• Third semester as Student Instructor for a faculty-
sponsored, semester-long 1-unit course on autism.• Senior Staff Reporter for the Daily Cal• Research Assistant at various Labs • Psi-Chi Honor Society. Golden Key Honor Society
• more …..
Loving learning neuroscience with 800 Students
3rd Semester as Student Teacher for a semester-long class on Autism (w/ 30 students)

2/17/20
6
Daily Californian• 34 Articles• 25 Interviews• Weekly Opinion Column on Autism
‘Typer-Communicators’ on relatable pathsat UC Berkeley
With fellow bear David
• Day Programs after Post Secondary Programs.
• Some ”seem” to manage, others struggle• Day Programs not equipped to handle
challenges of autism• Placeholders à Out of Sight, Out of mind• Where is the chance at a meaningful life.• Worrying scenario
Adult Trajectory(My observations)
2/17/20
7
Manifestations of Depression (Devt. Psychopathology Class, UC Berkeley)
• Acting Out (Behaviors due to frustration)• Apathy (mistaken for
compliant/manageable adults)• Suicide Ideation (Yale Study, Jan 2018)
Prof Steve Hinshaw, “There is a lot at stake”
Observed Result à Depression
Reimagining the PossibleA Growth Mindset
1. Communication is a mandatory skill2. Developmentally “All-Over-The-Place”3. Never TOO Old4. (Reminder): The Right to Dignity and Inclusion in
Human Society5. Professionals as Game Changers• Educators/Service Providers/ Support Staff• Health Care Professionals• Case Managers/ Regional Center / Overseeing
Agencies

2/17/20
8
1. Communication
•Critical Survival Skill•No communication = maladaptive behaviors.•Communication = Coping skills. Access to help•Communication = Resolution of Frustrations.•Communication aids self-determination, seat at table in decision making.•Communication includes thoughts and feelings, goes beyond 100 basic wants
Its about Quality of Life
Movement Perspective + Oral Motor Apraxia
→ Trying to function in a body we can’t quite control.à Presumption of Competence
Medium/Long Term hope → Research/Technology that will make getting out what’s inside our heads easier. AI? Neural Link? Wearable caps?
In the meantime à Communication via AAC Prompt fading is already part of all kinds of therapy. Severe oral-motor apraxia issues and movement disorder may mean significantly longer to prompt fade
2. Developmentally “All-Over-the-Place”
•Brains wired differently. All may not fit neatly into existing Evidence-Based solutions•Open to trying different approaches. Like Edison, if one method does not work, try another.
Einstein- Not everything that counts can be counted and not everything
that’s counted truly counts
Developmentally “All-Over-the-Place”NOT
Developmentally “Delayed”
2/17/20
9
3. Never TOO OLD
•Neuroplasticity of the human brain continues to adulthood.•Learning does not end at the early intervention window•We are never too old to learn and progress.
4. Right to Dignity & Inclusion In Human Society
•We already live with a disability that is overwhelming for us.•Not an unfeeling block of wood
Belonging-ness
Two Viewpoints:•Neurotypicals need exposure to us from early age→ tolerance of us as adults→ future allies to open opportunities for us•If we are kept away, they learn to stigmatize us further.
•ASD individuals need the exposureà to learn to survive in society.à Develop a sense of belonging to the community• Especially need active interaction and small group interaction
2/17/20
10
5. Professionals as Game ChangersEducators / Service Providers/ Support Staff
• Push for AAC Communication that goes beyond “wants”
• Communication helps in long-term self-determination
• Age appropriate materials and activities.• Assume Competence.• Accommodations to enable education and
inclusion
5. Professionals as Game ChangersHealthcare Professionals
• Not everything is “due to Autism” - run other tests and checks. We have comorbidities and healthcare needs too.
• Currently many autistics end up at ER in crisis state.• Standard of HealthCare needed, starting with Nutrition,
Lifestyle, Physical Health Needs, Mental Health Needs, Aging needs. → Long term Quality of Life.
• Accommodations and modifications to environment/procedures to make healthcare accessible.
• Encourage and respect communication by the individual.• Not every maladaptive behavior can be attributed to
communication or compliance.
5. Professionals as Game ChangersCase Managers/ Regional Centers/Agencies….
• Care Burnout: Individuals and Families going from crisis to crisis trying to manage EVERYTHING on own. • Guidance with coordinated planning/support for the individual over MANY aspects of life . • Include a longer term view. • What will life be like at age 50 / 80? • What does person get to wake up to each day?
2/17/20
11
Professionals,YOU ARE GAME CHANGERS!!
•You have enormous training, expertise, and knowledge•This is a population with significant support needs. Only a few have access to a “voice” for self-determination.•Your effort, your passion, and your attitude can make a HUGE difference in our future path.•From our point of view, we need you to HELP US and GUIDE US through this journey.•We DEPEND on you to view us with a growth mindset.
• Far from clear for me.• But my present is better than my past and I can only
hope the same for my future• I dare dream that I can make the path that much
easier for those who follow behind me.•
The Road Ahead
Can the quest for knowledge ever end?Never, answers the mind.Reimagine the possible.
Emotions and the sensory body are sinkholes enroute.Mind urges…
take detours, challenge the sinkholes, we must persevere.have to travel possibilities, open opportunities, and pave new roads
The quest for meaningful life can never end,
Neurotransmitters Flow in this Autism Mind

2/17/20
12
Thank You

1
My name is Tyler. I am 34 years old. I am happy to be here with you today. The topic at hand is vitally important to me and anyone who has a communication impairment. I have autism and with rare exceptions I have never been able to produce functional speech, even as a child. I think one of the most important things teachers, doctors and other professionals, people can do when confronted by someone with a communication impairment is to assume competence. When one has limited output that does not mean there is limited understanding. I was lucky enough at the young age of six to be introduced to facilitated communication, also called supported typing. Therefore, I got a regular education, with accommodations, and completed high school. With a lot of practice I learned to read aloud what I type. Whether you realize it or not producing speech is actually a rather complicated combination of motor movements including breath control. I am not able to automatically get my lips, tongue and mouth in the correct positions and at the same time, organize my thoughts and formulate my message. Typing to communicate has some other real disadvantages. It’s not just what you say, it’s how you say it. When one speaks, other people interpret the voice, in addition to listening to the words. Others pay attention to the timing and pace, how loud you speak, your tone, your inflection and the words you emphasize. This adds meaning to your message. Think about how someone's tone of voice, for example, can indicate sarcasm, anger, affection, or confidence. Most people have experienced a breakdown or misunderstanding when only text is used to communicate. I love being able to speak my own words but you can see that my voice does not help me get my message across. Since high school I have taken a number of college classes and ultimately I plan to earn a bachelors degree and get a job related to social justice. I am not able to manage a full load as my typing is slow but so far I have a 3.8 grade point average for my coursework. Slow and steady can win the race. Typing is ridiculously slow with one finger but motoricaly easier than speech. I always have a lot to say but it can be very challenging to get people to slow down and include me. You speaking people rattle off words at a speed I cannot even begin to match. That is one of the many reasons I formed the support group called Loud Talking Fingers over a decade ago. A group of us typers meet once a month to share our experiences and support each other at our own pace.
2
I now live in my own apartment with 24-hour support staff provided by a supporting living agency. You might think that I have the perfect set up to take control of my life but you would be wrong because I need to be able to communicate to do that. Serving as my communication partner takes time and practice. While individuals on the autism spectrum have areas of common concern and distress, autism expresses itself very differently in every individual on the spectrum .One thing that people on the autism spectrum share is that they experience sensory input very differently than “neurotypical” people do. People on the autism spectrum notice things you normally would not and can’t ignore things you normally can. This means I am often bombarded with sensory information, which you either don’t register or you filter out without thinking. These sensory irregularities can result in people, places and events “innocently” assaulting a person, like me who have such sensitive systems and processing irregularities. That can produces stress in that moment as well as anxiety about where and when the next assault may come. I have a low level of anxiety almost all the time. Sometimes I lose the sensation of the relationship or position of my body parts to each other. To imagine what that might be like, think of trying to walk when your foot has fallen asleep, before the pins and needles and that body part is just numb. That happens to me a lot. In the worst cases I not only lose the sensation of my own body but I also lose my sense of where I am in space. I feel like an astronaut floating in outer space and lost in time. As I type (or point) my partner pulls back on my arm as I move towards my target. This resistance helps me feel my arm and know where I am in space. Usually without this external feedback I cannot hit my intended target, although more and more often I am now typing or pointing reliably with increased independence. I can type on any kind of device or even simply point to letters written on a sheet of paper. Typing means I can choose the exact words I need to express my thoughts. My communication partner needs more skill to support my typing so I also use an app called Touch Chat. My home page looks like this. I have programmed the buttons with commonly needed words and phrases. It is easier for me and easier for my staff to support me as I touch one button rather than typing a whole sentence.
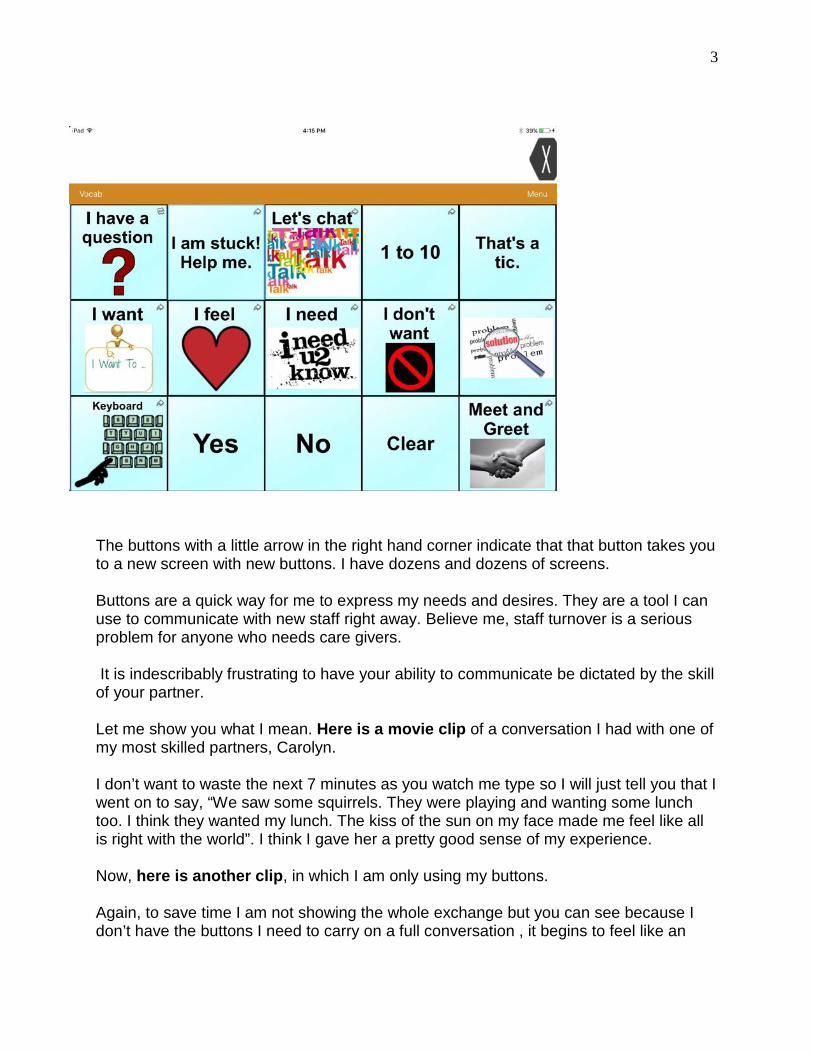
3
The buttons with a little arrow in the right hand corner indicate that that button takes you to a new screen with new buttons. I have dozens and dozens of screens. Buttons are a quick way for me to express my needs and desires. They are a tool I can use to communicate with new staff right away. Believe me, staff turnover is a serious problem for anyone who needs care givers. It is indescribably frustrating to have your ability to communicate be dictated by the skill of your partner. Let me show you what I mean. Here is a movie clip of a conversation I had with one of my most skilled partners, Carolyn. I don’t want to waste the next 7 minutes as you watch me type so I will just tell you that I went on to say, “We saw some squirrels. They were playing and wanting some lunch too. I think they wanted my lunch. The kiss of the sun on my face made me feel like all is right with the world”. I think I gave her a pretty good sense of my experience. Now, here is another clip, in which I am only using my buttons. Again, to save time I am not showing the whole exchange but you can see because I don’t have the buttons I need to carry on a full conversation , it begins to feel like an
4
interrogation rather than a conversation, and I was not really able to share my experience. Sadly this happens with new partners even when I am able to type. Take a look. Not only is communication is a fundamental human right, it is the vehicle by which all other rights are exercised. Communication is at the heart of who we are as human beings. Without communication I am at the mercy of the often misguided benevolence of others. With communication, the possibilities are endless and the world is my oyster.

Maximizing Potential:Neurodiversity at Work
19th Annual Developmental Disabilities: An Update for Health Professionals
March 5‐6, 2020
Kristen PedersenSenior Director, Business Development & Workforce InclusionThe Arc San Francisco
I have no disclosures
Disclosures

We will explore how The Arc San Francisco through partnerships and network building is creating career development for people with intellectual and developmental disabilities throughout the Bay Area and beyond.
Overview
Learning Objectives
• Leveraging resilience training as a tool for success• Models for success to increase inclusion at work• Keys to partnership building in the private sector
Years of disability workforce development
30The Arc San Francisco
85%Corporate and workforce partners
150 Internship placement rate
Maximizing Potential:Neurodiversity at Work
19th Annual Developmental Disabilities: An Update for Health Professionals
March 5‐6, 2020
Kristen PedersenSenior Director, Business Development & Workforce InclusionThe Arc San Francisco

Q & A
19th Annual Developmental Disabilities: An Update for Health Professionals
March 5‐6, 2020
Kristen PedersenSenior Director, Business Development & Workforce InclusionThe Arc San Francisco

Jobs for People with Developmental Disabilities: Making It Happen!
Catherine Nichols, Senior Director Accessibility Programslinkedin.com/in/catherinecnichols
19th Annual Developmental Disabilities: An Update for Health ProfessionalsMarch 5-6, 2020
DisclosureI have nothing to disclose

Program OverviewWorkforce Development for People with Disabilities
At Salesforce, we believe that business can be powerful platforms for social change and that our higher purpose is to drive Equality for all. Disability Inclusion is fundamental to this belief. We have an ambition to become the number one employer for people with disabilities, for the products we sell to be accessible by people with disabilities, and for all persons to have full and equitable access to our offices, our meetings and our events.
+ + +
Learning Objectives
What Salesforce is doing to create Disabilities@Work Programs
Salesforce’s Partnership with The ARC San FranciscoSalesforce’s Autism@Work Programs

Driving Workforce Development: A Long Standing Partnership Between Salesforce and the ARC
Employees from The ARC work in a variety of roles at Salesforce within office services. 50+ ARC / affiliates across SF, NY, Indy, Bellevue, London, Dublin Planned expansions both domestically and globally over the next yearSalesforce employees have sat on The ARC’s board and the organization is a customer
Salesforce Sustainability FY19 Stakeholder Impact Report
The Autism Advantage
Autism @ Work Playbook: Annabi, H., Crooks, E.W., Barnett, N., Guadagno, J., Mahoney, J.R., Michelle, J., Pacilio, A., Shukla, H. and Velasco, J. Autism @ Work Playbook: Finding talent and creating meaningful employment opportunities for people with autism. Seattle, WA: ACCESS-IT, The Information School, University of Washington, 2019. Autism and Health: A Special Report by Autism Speaks 2017
500kAdditional
adults with ASD by 2028
50kHigh School
graduates with ASD per year
17%Complete a 4-year college
degree
85%Unemployment
rate among college grads

Autism@Work Launch
Internal Partners
ExternalPartners
CommittedStaff
BusinessCase
ExecutiveSponsor(s)
Planning
Onboard
Workshop
Neurodiversity Training for Managers
Non-Traditional Interviews
Training and Documentation
Mentoring and Career
Development
Retention
Autism@Work Journey
Recruit
Recruit Candidates
Assess
1-Month Internship

Focus on Agile project management methodologies and teaming in a professional
setting
Autism@Work Journey: One Month Internship
Getting comfortable with the Salesforce office
environment and a daily routine.
Assessing attention to details, including
maintaining documentation and
quality control
Completing a project related to Salesforce
product development in partnership with hiring
teams
College Link Program (CLP)Mission Statement: to help students who have been diagnosed with Autism Spectrum Disorder to transition and succeed in the higher education environment
Preparation
• Complete the Salesforce Career Exploration trail
• Search job descriptions they are interested in
• Update resume to tailor to the job description
Day of the Visit
• Introduction to Salesforce and Salesforce Culture
• Demo of Salesforce
• Mock interviews with Salesforce employees
• Tour of Salesforce
https://www.csueastbay.edu/clp/

California Children’s Services: Nuts & Bolts
Ben Meisel, MD – Medical Director
CCS San Francisco
19th Annual Developmental Disabilities: An Update for Health ProfessionalsMarch 5‐6, 2020
Disclosures
I have nothing to disclose.

Overview & Learning Objectives◦History and Basics – What is California Children’s Services◦ Eligibility
◦ Services
◦ What CCS is NOT!
◦ The Medical Therapy Program
◦Whole Child Model vs Independent Counties vs Dependent Counties
◦Who Can Refer to CCS and HOW?
◦ Life After 21 years old?
CCS – THE BASICSThe History
◦1927 California Crippled Children’s Program◦ Care for children affected by Polio
◦Dept of Health Care Services (DHCS) funding to improve medical care of children and mothers
◦NOT the Department of Developmental Services◦ Separately created in 1979 – Lanterman Act
◦Regional Center Funding

CCS – THE BASICSThe Mission
◦ Making Pediatric Subspecialty Medical Care available to children with eligible medical conditions.
◦ Providing expert Physical Therapy and Occupational Therapy to children with qualifying neuromuscular & musculoskeletal conditions.
◦ To arrange, direct, and pay for specialized medical care, equipment, and rehabilitation for children who qualify.
◦ Improving care and decreasing costs in the long run.
CCS – THE BASICSEligibility
Under 21 years of age.
Permanent resident of the California County where you apply.
Medi‐Cal eligible or Family income < $40,000/yr or Cost >20% AGI
Medically eligible condition “Think Chronic, Lifelong Conditions”◦ Some examples:
◦ Cancers
◦ Sickle cell, Hemophilia, Thalassemia
◦ Intractable seizure disorder
◦ Transplants
◦ Congenital Heart disease

CCS – THE BASICSServices Provided
◦ Specialized Treatment*: ◦ Board Certified Physician Services
◦ Hospital & Surgical Care
◦ Rehabilitation OT/PT
◦ Skilled Nursing
◦ Lab Tests, Radiology
◦ Medical Equipment, Supplies, & Medicines
◦Medical Case Management
◦Medical Therapy Program (MTP) PT & OT separate from public school PT/OT program
◦High Risk Infant Follow‐up (HRIF)
*All medical services must be done by CCS approved providers and at CCS approved institutions, including Special Care Centers.
CCS – THE BASICSWhat CCS is NOT!
NOT Developmental, Behavioral, or Hypotonic conditions
NOT Primary Care Services
NOT Short term hospitalizations or transient health challenges

Medical Therapy Program (MTP)
Medically Necessary PT & OT servicesSpecific musculoskeletal or neuromuscular conditions
Not hypotonic CP
Medical Therapy Units (MTU’S) at public school sites
NO COST to the family
Eligibility for ServicesCCS
Reside in San Francisco
Eligible medical condition
Under 21 yo
Financial
MTP
Reside in San Francisco
Eligible medical condition
Under 21 yo
Based on Physical Exam by Specialist MD (Ortho/Neuro/Rehab)
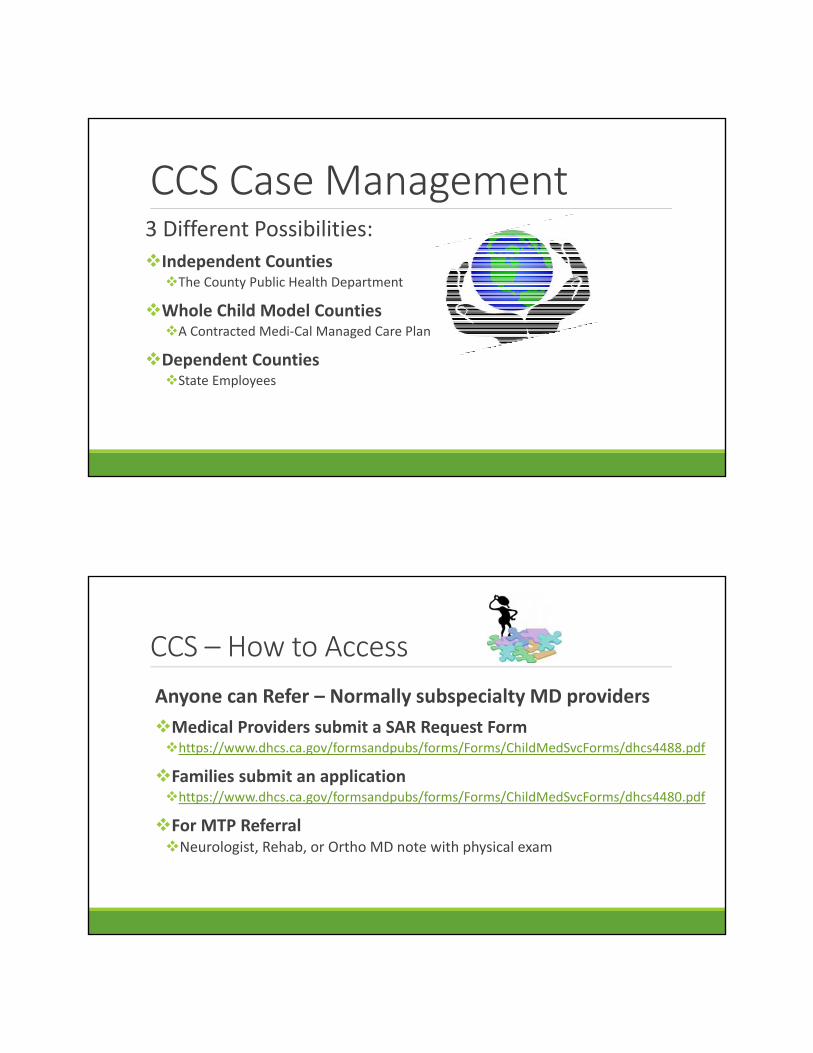
CCS Case Management3 Different Possibilities:
Independent CountiesThe County Public Health Department
Whole Child Model CountiesA Contracted Medi‐Cal Managed Care Plan
Dependent CountiesState Employees
CCS – How to Access
Anyone can Refer – Normally subspecialty MD providers
Medical Providers submit a SAR Request Formhttps://www.dhcs.ca.gov/formsandpubs/forms/Forms/ChildMedSvcForms/dhcs4488.pdf
Families submit an applicationhttps://www.dhcs.ca.gov/formsandpubs/forms/Forms/ChildMedSvcForms/dhcs4480.pdf
For MTP ReferralNeurologist, Rehab, or Ortho MD note with physical exam

Life After 21yoWhen CCS Stops?
There is nothing for adults that replaces CCS
Few Adult Medicine offices have Case Management
Medi‐Cal is supposed to continue care for eligible clients
Regional Center clients get some case management support
Questions
CONTACT US
@30 Van Ness Ave, Suite 210
San Francisco, CA 94102
(415)575‐5700
Ben “Dr. Ben” Meisel – Medical Director◦(415)575‐5738◦[email protected]
Katie Kim – NURSE MANAGER◦(415)575‐5674◦[email protected]

Private Lives, Private Dollars: How Philanthropy Can Address and Enhance Healthcare forAdults with Developmental Disabilities
Ryan Easterly, WITH Foundation
19th Annual Developmental Disabilities: An Update for Health ProfessionalsMarch 5‐6, 2020
Disclosure
• I have no financial conflicts of interest to disclose
1

Overview
• Summary of Philanthropy and Healthcare‐focused giving
• WITH’s Mission, History, & Funding Priorities
• Key Components of Service Delivery / Program Design
• Why THIS matters
Learning Objectives
• Have an understanding of the size and scope of philanthropy and healthcare‐focused giving
• Identify some of the key components of healthcare service delivery that enhance the experience of adults with developmental disabilities

(Image Description: Image of movie character, Jerry Maguire with text at bottom of image that reads: Show me the money!)
2
Established in 2002, the mission of WITH Foundation is to promote the establishment of comprehensive healthcare for adults with developmental disabilities that is designed to address their unique and fundamental needs.
withfoundation.org

KEY COMPONENTS
(Image Description: Graphic of a pile of red question marks)

Cerebral Palsy: A View from Both Sides
Hank Chambers, MDDavid H Sutherland Chair of Cerebral Palsy ProgramRady Children s Hospital San DiegoProfessor of Clinical Orthopedic SurgeryUniversity of California at San Diego
DisclosuresPersonal Disclosures:
Consultant: Allergan Corporation, Orthopediatrics, 3D4Medical Corp.
Institutional Research Support:NIH, Orthopedic Research and Education Foundation, Major League Baseball, Rady Children s Hospital, DePuy Spine, Allergan, Axial Biotech, Ellipse, Alphatec Spine, KFx, Magellan Spine, Zimmer, KCI, Synthes, Syntaxin, K2M,
Institutional Education Support:Rady Children s Hospital, DePuy Spine
Southern Family Cerebral Palsy Center
at Rady Children’s Hospital
Off-Label Use
Botulinum Toxin (Botox, Myobloc, Xeomin, etc) are not approved for use in children for spasticity by the FDA. Dysport has recently received approval for lower extremity spasticity in children
Intrathecal Baclofen is not approved for use in dystonia
However, 50% of all drugs that are used in children are not specifically indicated

Creativity is the ability to hide your sources
Hank Chambers
Creativity is the ability to hide your sources
Albert Einstein

What Is Cerebral Palsy?Is it brain damage due to obstetrical trauma?
Was the baby too big or too small?
Occurs before the age of 3
Cerebral palsy (CP) describes a group of permanent disorders of the development of movement and posture, causing activity limitation, that are attributed to non-progressive disturbances that occurred in the developing fetal or infant brain. The motor disorders of cerebral palsy are often accompanied by disturbances of sensation, perception, cognition, communication, behavior, by epilepsy and by secondary musculoskeletal problems
Epidemiology: The Cerebral PalsiesRisk is 25-30 times in neonates < 1500g
1 in 3 children with VLBW will have CPMost children with CP were not premature10% of <28 week premature patients will have CP
Prevalence in 8 year olds: 3-4 patients/1000 (1 in 278)10,000 new diagnoses each year
Prevalence: ~950,000 Americans with CP
87% 30-year survival rate
Much higher prevalence in black population
There are now more adults with CP than children
Some Statistics
54 million Americans have a disability
72 percent of unemployed adults with disabilities would like to work
Lifetime cost of child born today with CP:
$1 million
Etiology of Cerebral PalsiesPrematurity
Multiple Births: Assistive Reproduction, older mothers, teen pregnancy
Chromosomal and Brain AbnormalitiesGenetic InfluencesMetabolic Influences
HormonalHeatInflammation
Hemostatic DisordersInfection: bacterial, viralTraumaEpigenetic factors such as maternal depressionRemember: Correlation does not imply causation


Tractography
Preventive StrategiesMagnesium Sulfate
Caffeine
Infant and brain cooling
Antiinflammatories
Thyroid Hormone
Erythropoiesis Stimulating Agents
Xenon
Avoidance of toxic substances: nicotine, drugs, alcohol
Question Assistive Reproduction Technology
Prevention of Non accidental Trauma, automobile accidents, near drowning

Career ChoicesUnited Cerebral Palsy Telethon
Pediatric Rotation
Birth of my son, Sean in 1982 while I was an intern
Orthopedic Education
Residency taught me the fundamentals of cerebral palsy care, which essentially was heel cord lengthening, percutaneous adductor and hamstring lengthening and prolonged casting
Therefore these were the procedures that I learned and these were the procedures that my son had.

Fellowship in San DiegoIntroduction to Gait Analysis by Dr. David Sutherland
Other teachers included forward thinkers such as Scott Mubarak and Dennis Wenger who encouraged me to work in the field
Meeting other great thinkers like Freeman Miller, Mike Sussman, Mike Aiona, Jim Gage, Kerr Graham, etc
Gait Analysis
What is gait analysis?
Why is it important for the individual patient and the overall care of children with cerebral palsy?
Why is there a controversy?
Classification SystemsThe diplegia (38%), quadriplegia (23%), hemiplegia(39%) system has poor intra and interobserver reliability
Unilateral vs Bilateral (Surveillance of Cerebral Palsy in Europe)
Levels of ambulation: household, therapy, community also has limitations
Gross Motor Functional Classification System (GMFCS)
Gross Motor Function Measure (GMFM)
Series of tests given to ascertain the level of gross motor involvement in children with cerebral palsy.

GMFCS
GMFCS and Musculoskeletal Problems

Functional Mobility Scale
Function at 5, 50 and 500 meters
Other ClassificationsManual Ability Classification System
For Upper Extremity Problems
Communication Functional Classification SystemI Effective Sender and Receiver with unfamiliar and familiar partnersII Effective but slower paced Sender and/or Receiver with unfamiliar partnersIII Effective Sender and Receiver with familiar partnersIV Inconsistent Sender or Receiver with familiar partnersV Seldom Effective Sender and Receiver even with familiar partners

Dimensions of DisabilityInternational Classification of Functioning, Disability and Health (ICF) WHO
Body FunctionsBody StructuresActivities and ParticipationEnvironmental Factors
Participation

The NCMRR Model of Disablement
Treatment Paradigms
Goal Setting: Realistic and ConcensusTeam ApproachManagement of Movement DisordersTherapies: Physical, Occupational, SpeechRole of TechnologyTiming of Orthopedic SurgeryBony and Soft Tissue Surgery
First We Must Set GoalsIndependenceWorking CommunicationActivities of Daily LivingMobilityWalking
Integrated Treatment Approach in the Child with Cerebral Palsy

TherapiesOccupational
Speech and Language
Management of Drooling
Visual Impairment
Physical Therapy
Neurodevelopmental Therapy
Hippotherapy
Equipment

TechnologyPromise and Challenges
ChallengesCost
Training
Upkeep
Specificity for each child
Robotics
Speech TherapyCommunication Devices
SimpleComputer

MobilityGetting from Point A-Point B
May mean walking, using assistive devices, wheelchairs or the means of accessing private or public transportation
ivate or
Walkers
Rear Entry WalkersReverse WalkersGait Trainers

Rear Entry Walkers
Reverse Walkers

Gait Trainers
Role of Standing

Standers
Wheelchairs
Simple sling chairs
Custom Manual Chairs
Custom Powered Chairs

Mobility: Wheelchairs and Seating Systems
Lifts
Transportation
Other Technologies
Feeding Equipment
Respiratory/Ventilator Equipment
Sporting Equipment (skiing, bicycling, etc)
Many, many others
Medical Management of Cerebral Palsy
Growth Retardation
Seizure Disorders
Management of Reflux
Management of other GI issues such as Gall stones, constipation, dumping after bowel surgery
Kidney Stones
Skin ulceration
Oral Health
Intellectual Disability
Etc. Etc, Etc
Spasticity
Choreo-Athetosis
Ataxia
Dystonia
Movement Disorders

Ataxia

Choreoathetosis
Dystonia and Choreoathetosis

Spasticity vs Dystonia
New understandings of the definitions and therefore the natural history of children with cerebral palsy.cerebral palsy.

Other Important Problems
Loss of Selective Motor Control
Sensory Deficits
WeaknessDelayed Growth and Development
Epilepsy

Current Spasticity Treatment Options: General
Exercise and physical modalities
Systemic drugsDiazepam (Valium)Baclofen (Lioresal)Trihexyphenidyl (Artane)Etc.
Anesthetic and neurolytic injections
PhenolAlcohol
Chemodenervation injections
Botulinum Toxin A, BCannibis CBD Oil

Orthopedic and Neurosurgical Methods
Tendon lengthenings altering the muscle receptors
OsteotomiesLever Arm Syndrome
Neurotomies
Fusion especially spinal fusion stabilizes the trunk
Intrathecal drugs
Intrathecal Baclofen
Selective DorsalRhizotomy
lllllll

Deep Brain Stimulation

Principles of Orthopedic SurgerySingle event, multilevel surgery
Delay surgery as long as possible (> 6 years)
Use spasticity management as adjunct to surgery
Timing of Orthopedic Surgical Interventions
GMFCS Level 1
GMFCS Level 1
• High level physical functioning: spastic hemiplegia, mild spastic diplegia
• Seizures, occasionally
• Learning difficulties
• Behavioral problems
• Autistic spectrum disorders
igh level emiplegia
spastic a

GMFCS Level I
• Mild gait dysfunction
• Many benefit from botulinum toxin
• Few need any orthopaedic surgery
• Too mild for SDR or ITB
• No hip displacement, no scoliosis
• UL Surgery in Hemiplegia
Mild gai
M b toxin
GMFCS Level II
GMFCS Level II
• Mostly spastic diplegia of prematurity
• Some have severe hemiplegia
• Wide range of gait dysfunction
• Significant spasticity
• Significant deformities
• Mild hip disease, no scoliosis
Mostly urity
GMFCS Level II
• Botulinum Toxin very useful
• SDR: a very few , highly selected cases
• No ITB
• Single level orthopaedic surgery: UL & LL
• Hip screening and preventative surgery
• SEMLS: Multilevel surgery
otulinu

GMFCS Level III

GMFCS Level III
• Severe diplegia, mild quadriplegia
• Spastic-dystonia
• Botulinum toxin + Phenol are useful, some ITB
• Hip displacement common & important
• Screen and prevent hip displacement
• Gait correction surgery: hips and feet
legia
Treatment of Lever Arm Syndrome
Femoral OsteotomiesProximalDistal
Tibial rotational osteotomies
Correction of foot valgus

GMFCS Level IV
GMFCS Level IV
• Spastic quadriplegia: mild-moderate
• Spastic-dystonia
• Botox and ITB
• Hip displacement and scoliosis
• Screen and prevent hip displacement
• Orthopaedic surgery for standing, sitting
• May need hip and knee surgery
• Spast
• Spast
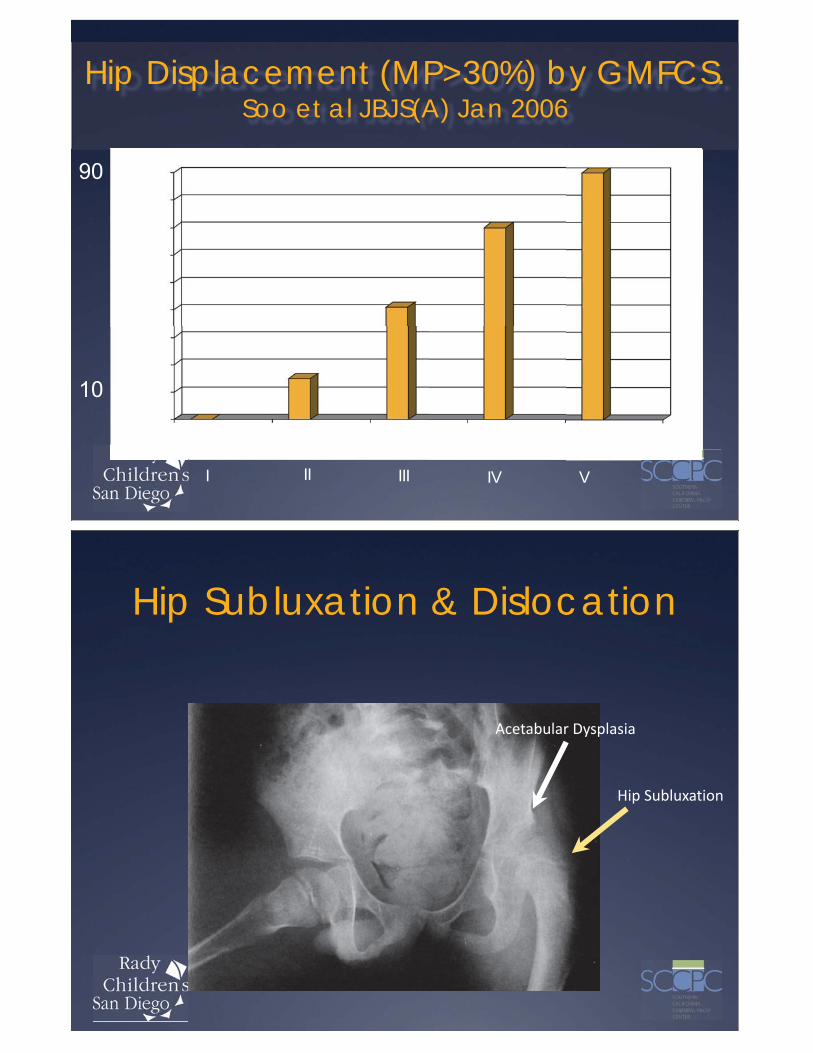
Hip Displacement (MP>30%) by GMFCS. Soo et al JBJS(A) Jan 2006
I II III IV V
Hip Subluxation & Dislocation
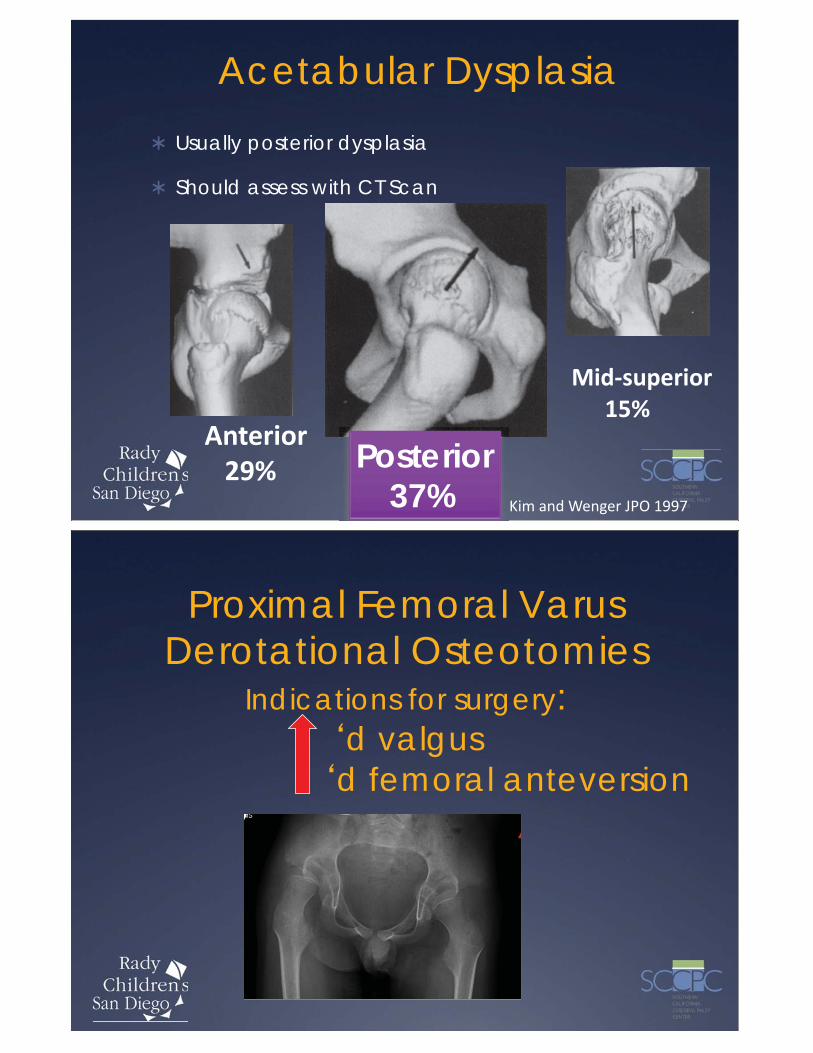
Acetabular DysplasiaUsually posterior dysplasia
Should assess with CT Scan
Posterior37%
Proximal Femoral Varus Derotational Osteotomies
Indications for surgery: d valgus
d femoral anteversion


GMFCS Level V
GMFCS Level V
• Spastic quadriplegia
• Multiple medical co-morbidities
• Significant excess mortality in each decade
• Dystonia, spasticity: Botox, phenol, ITB
• 90% will develop hip disease and scoliosis
• Comfortable sitting
paaaaastttttic qu
Multiple m
GMFCS Level V
• Optimizing health
• Minimizing co-morbidities
• Goal setting
• Hip and spine surveillance
• Preventative, reconstructive surgery
• Child and care giver quality of life
Optimizing
Minimizing
VALGUS OSTEOTOMY
AdvantagesIncreased motionPain relief
DisadvantagesMay be painful

PROXIMAL FEMORAL RESECTION
TOTAL HIP REPLACEMENT
AdvantagesPain reliefMotion
DisadvantagesRe-dislocationDifficultInfection

Shoulder Arthroplasty
Botulinum Toxin for Pain in Dislocated Hips
Current study at Rady Children s Hospital
32 patients with painful dislocated hips or previously surgically treated hips
400 Units of Botox in muscles about the hip (16 separate sites)
Marked improvement in pain in 90%
Must be repeated every 4-5 months.

Fuse Joints for Stability
Orthopedic Surgical Interventions: Spine
Intervention to correct
ScoliosisSpondylolisthesisHyperkyphosisHyperlordosis

Unconventional or Alternative Treatments
Hyperbaric Oxygen
Adeli Suit
Postural Suits
Acupuncture
Biofeedback
Conductive Education
Facilitated Communication
Doman-Delicato
Many, many more
Caregiver StressIncreased physical strain
Higher incidence of back pain
Increased mental strain
More time to care for child, including feeding
Increased marital stress85% divorce rate (in articles, but not true)
Mothers (usually) giving up job/career
Sleep Disorder
Sibling stress

Other Stressors:New Interventions with little or
no evidenceHyperbaric Oxygen
Different therapiesDoman DelicatoConductive TherapyEtc
Stem Cell treatment
Adult Clinic5100 Patients treated in last 25 years.
Multitude of new problems including:Increased painArthritisDifficulty sittingProgression of movement disorderBipolar disease (45% of all my adult patients are on antidepressants)Loss of ambulationCervical Spine ProblemsProgressive Hydrocephalus

Stages of Grief
So, What have I learned in 35 years
Parents are always seeking a cure for their childHyperbaric OxygenStem Cells?????? And $$$$$$
Simple insights lead to great changes in careDefinition of dystoniaGMFCS
Little money available for research
There is a huge disparity between health care for children and adults with disabilities
Treatment is important, but prevention is the real hope
There are true heroes who have no vested interest other than the care of children who have dedicated their careers to the understanding and treatment of this disorder



Thank you

A Conversation on Cerebral Palsy from Consumers and Professionals Elizabeth Grigsby, Henry Chambers, Ryan Easterly, Ben Meisel
_____________________________________________________________________________________
Notes:

Dangerous or Deadly
“Cures” for Autism and
Other Developmental
Disabilities
• Neal Rojas, MD MPH
• Associated Clinical Professor of Pediatrics
• UCSF Department of Pediatrics
• Division of Developmental Medicine
• 19th Annual Developmental Disabilities: An Update for Health Professionals
• March 5‐6, 2020
Disclosures • I have nothing to disclose

Overview
• There are several reports of injuries and deaths related to treatments of children with neurodevelopmental disabilities
• We will review which types of therapies have been associated with this morbidity as well as how patients can be educated to make the safest choices while pursuing treatment for neurodevelopmental disabilities
Learning Objectives
• We will take a health education approach to describing risks and understanding what is prevalent in the treatment world today
• We will then review specific treatments which can cause harm
• We will then discuss a clinical approach which will allow for communication and collaboration in maximizing safety while pursuing efficacy in treating neurodevelopmental disabilities (NDD)
• We will attempt to be humble in also remembering what is considered standard therapy is not always as safe as we’d like to think

Why Parents Chose Dangerous ”Cures”
• Autism is perceived as a severe, life‐long condition, resulting in a poor prognosis.
• Parents, new to the diagnosis, lack knowledge about the disorder, and maybe minimally trained in scientific inquiry.
• Parents must deal with conflicting information and competing perspectives from professionals.
Why Parents Chose ”Cures”
THE FADS ARE OFTEN PRESENTED AS QUICK
FIXES OR CURES.
THERE IS INADEQUATE INFORMATION ABOUT
THE CAUSE OF AUTISM.
MEDS CAN ONLY ALLEVIATE CERTAIN
SYMPTOMS. NO CURE. (METZ ET. AL.)
Role of Media
Often shows preferential coverage of “breakthoughs” or ”miracles”
Rarely able to go into full scientific breakdowns and methods of studies
Often uses strident denunciation of all previous treatments rather than building upon evidence incrementally
Celebrities can hijack attention over science using a very powerful anecdotal ‘human face’ approach to convince patients
Pseudoscience
• ”a collection of beliefs or practices mistakenly regarded as being based on scientific method” (Websters Dictionary)
“a system of theories and methods that has some resemblance to a genuine science but that cannot be considered such. Examples include astrology, numerology, and esoteric magic. ”(APA dictionary)

How Pseudoscience Works
Uses some scientific jargon and concepts as well as research‐based evidence but does not fulfill burden of proof with controlled trials or repeatability
Often relies on very small studies with leaps of faith in logic that they generalize across real clinical applications (APA)
Pseudoscience can move towards Science with increased rigorous study or towards‐>
• Snake Oil‐ Little to no scientific basis but popular due to cultural or persuasive testimonials (Websters)

ASD “Abnormal Physiology” Theories
• Several theories of what may cause ASD are avenues for current therapies:
• These include: Oxidative stress; Inflammation/immune dysfunction; environmental toxins
• These are real lines of scientific inquiry across the globe of ASD researchers
Evidence vs. Theories
• While promising evidence for some treatments exists such as NAC *and Vitamin B12
• Other therapy modalities which ride on these theories such as chelation or hyperbaric oxygen ARE NOT SAFE! (Bent and Hendrin)
Top 5 Most Dangerous Treatments for ASD/NDD
• MMS
• Chelation
• HBOT
• Lupron Therapy aka Chemical Castration
• Stem Cell Therapy
MMS
• “Miracle Mineral Solution” or MMS aka Chlorine Dioxine CD or AKEA• May cause immediate symptoms of esophageal burning
• Long term GI issues because it’s BLEACH! (see poison center reference**)
• Autism Research Institute (ARI) “We advise against using Miracle Mineral Solution. We hope parents will remain critical of unsubstantiated claims that children have recovered or greatly improved in the absence of objective proof. We also strongly encourage any parents who choose to administer MMS to their children to report it to their physician so that side effects can be monitored.”

Dangerous Treatments: Chelation Therapy
• Based on theory that heavy metal toxicity causes autism and other NDD
• Given risks of renal/kidney damage and hypocalcemia/low Calcium (at least one documented death of 5 year old with ASD)
• No evidence of efficacy from Cochran analysis in 2015
• FDA stated that chelators that are sold over the counter as treatments for autism, are dangerous and illegal. They stated that they are potent drugs that carry serious risks—including kidney damage, dehydration, and even death (Tsouderos, 2010).
Dangerous Treatments: Hyperbaric Oxygen
• Hyperbaric Oxygen Therapy (HBOT) used for several other conditions unfortunately lending credibility to it’s use for NDD
• Some studies by HBOT advocates show mixed evidence of efficacy and some behavioral benefits.
• More Common Risks include ear pain, tinnitus, exacerbation of anxiety. Some reports of more severe reactions including hyponatremia/low Sodium and seizures
• Association for Science in Autism Treatment “In conclusion, at this time, there is no quality empirical research, meeting standards of good science, that support the claim that HBOT is effective as a treatment for ASD. Equally important, the logic and fundamental assumption of using HBOT with individuals with ASD (i.e., to treat inflammation of the brain) is not substantiated and deserves skepticism.”

Lupron Therapy/Chemical castration
• Chemical castration.
• Introduced to the world of autism treatment by the now notorious father‐son team of the Geiers. These two, in a 20‐year‐long run of damage, might now be reaching the end of their particular race. The father has had his medical license stripped in several states. That didn't stop the Geiers from filing a patent for their chemical castration protocol.
Stem Cell Therapy
• Also has some coattail credibility due to it’s use in leukemia and recent breakthroughs in blood disorders
• “Stem cell therapy for autism is illegal in the United States, but that hasn’t stopped some from offering this as a treatment for autism in Costa Rica, China, and other countries. There is no evidence that the treatment is safe or effective for autism, and no guarantee that the stem cells used in these countries are even human.” (Autism Science Foundation)
• Self placenta cell therapy protocals exist in U.S. at a prominent research university (these may be safer but do not currently offer a clear path to cure )

Standard Therapy (aka Allopathy)
• Traditional Western Medicine with Biological/Scientific basis requiring proof of efficacy and safety (FDA)
• Unfortunately, this has resulted in mostly just medications for symptoms rather than etiology management (“The Cure”)
• Atypical Antipsychotic medications and neuroleptic medications such as risperidone, aripiprazole, and others are well associated with causing metabolic abnormalities such as insulin resistance and high cholesterol
Standard Interdisciplinary Therapy or Multimodal Treatment• Interdisciplinary work with other types of therapy supporting children
with NDD such as
• Speech Therapy
• Occupational Therapy
• Physical Therapy
• Cognitive Behavioral Therapy
• Other Behavioral Therapies

Integrative Medicine‐CAM Again?
• Given that Allopathy has not offered very much for NDD and ASD especially, the vast majority of families with ASD surveyed tried one or more CAM modalities.
• These are often directed at the common co‐morbid challenges associated with NDD/ASD such as irritability, hyperactivity, sleep problems or GI symptoms.
Integrative Medicine Approach to NDD
• Growing amount of research looking at areas involving
• nutrition,
• supplements,
• mind‐body therapies

References
• Stephen James, Shawn W Stevenson, Natalie Silove, and Katrina Williams, “Chelation for autism spectrum disorder (ASD) Cochrane Database; Cochrane Database Syst Rev. 2015 May; 2015(5): CD010766.
• Mary E. McDonald PhD , Darra Pace EdD , Elfreda Blue PhD & Diane Schwartz EdD ”Critical Issues in Causation and Treatment of Autism: Why Fads Continue to Flourish” 290‐304 | Received 01 Oct 2010, Accepted 07 Mar 2011, Published online: 06 Nov 2012
References
• Plafki C, Peters P, Almeling M, Welslau W, Busch R. Aviat Space Environ Med. Complications and side effects of hyperbaric oxygen therapy.
• 2000 Feb;71(2):119‐24.
• Ghanizadeh A. Hyperbaric oxygen therapy for treatment of children with autism, a systematic review of randomized trials. Med Gas Res. 2012;2(1):13. doi: 10.1186/2045‐9912‐2‐13.[PMC free article] [PubMed] [CrossRef] [Google Scholar]
• Rossignal DA et al. Hyperbaric oxygen treatment in autism spectrum disorders. Medical Gas Research. Published online 2012 Jun 15. doi: 10.1186/2045‐9912‐2‐16

References (continued)
• “Complementary and Alternative Treatments for Autism Part 1: Evidence‐Supported Treatments” Stephen Bent, MD, and Robert L. Hendren, DO AMA Journal of Ethics, April 2015, Volume 17, Number 4: 369‐374
• Complementary and Alternative Treatments for Autism Part 2: Identifying and Avoiding Non‐Evidence‐Based Treatments;Alison Singer, MBA and Ramita Ravi.
• Metz , B. , Mulick , J. A. , & Butler , E. M. ( 2005 ). Autism: A late 20th century fad magnet . In J.Jacobson , R. Foxx , & J. Mulick (Eds.), Controversial therapies for developmental disabilities: Fad, fashion, and science in professional practice (pp. 237 –264 ). Mahwah , NJ : Lawrence Erlbaum .
References
• “The fake cures for autism that can prove deadly” by Frances Ryan, July 13, 2016 The Guardian (US Edition)

Dr. Allen Wong ([email protected])
Dental Care for Children and Adults With DD: Special Considerations
19th Annual Developmental Disabilities: An Update for Health Professionals March 5-6, 2020
Nothing to Disclose
2015 Dr. Allen Wong ([email protected])

Dr. Allen Wong ([email protected])
- ID/DD populations, children and adults - Disparity of care overview - Changes in Dental education - Barriers of care - New sciences in dentistry - New strategies for prevention - New materials for dentistry - Prevention and advocacy
2020 Dr. Allen Wong ([email protected])

2020 Dr. Allen Wong ([email protected])
Patients with special needs: Those patients whose medical, physical, Psychological, cognitive or social situations make it necessary to consider a wide range of assessment and care options in order to provide dental treatment. These individuals include, but are not limited to, people with developmental disabilities, cognitive impairment, complex medical problems, significant physical limitations, and the vulnerable elderly. CODA 2020
Generally, an IQ test score of around 70 or as high as 75 indicates a limitation in intellectual functioning.
• Conceptual skills—language and literacy; money, time, and number concepts; and self-direction.
• Social skills—interpersonal skills, social responsibility, self-esteem, gullibility, naïveté (i.e., wariness), social problem solving, and the ability to follow rules/obey laws and to avoid being victimized.
• Practical skills—activities of daily living (personal care), occupational skills, healthcare, travel/transportation, schedules/routines, safety, use of money, use of the telephone.
Standardized tests can also determine limitations in adaptive behavior, which comprises three skill types:

2015 Dr. Allen Wong ([email protected])

Neurodevelopmental Disorder
Fragile X Syndrome
Down Syndrome
Cerebral Palsy
Autism
Fetal Stroke
ID
2015 Dr. Allen Wong ([email protected])
#1 unmet healthcare need for those with special needs -
Dr. Allen Wong ([email protected])
* Dr Rick Rader study 5y ago
General public ◦ Believes people with ID receive better health care than the general population.
Training of Health Care Professionals ◦ 52% of medical school deans, 53% of dental school deans, 56% of students and 32% of medical residency program directors responded that graduates were “not competent” in treating people with ID.

2-23 Graduates must be competent in providing oral health care within the scope of general dentistry to patients in all stages of life. 2-25 Graduates must be competent in assessing ( and managing ) the treatment needs of patients with special needs.
Dr. Allen Wong ([email protected])
PREDOCTORAL
Intent: An appropriate patient pool should be available to provide experiences that may include patients whose medical, physical, psychological, or social situations make it necessary to consider a wide range of assessment and care options.
Dr. Allen Wong ([email protected])
PREDOCTORAL

The assessment should emphasize the importance of non-dental considerations. These individuals include, but are not limited to, people with developmental disabilities, cognitive impairment, complex medical problems, significant physical limitations, and the vulnerable elderly.
Dr. Allen Wong ([email protected])
Clinical instruction and experience with the patients with special needs should include instruction in proper communication techniques and assessing the treatment needs compatible with the special need.
Dr. Allen Wong ([email protected])

Standard 2-1 Curriculum Content
b) Assess, diagnose and plan for the Provision of multidisciplinary oral health care for a wide variety of patients including Patients with special needs
Dr. Allen Wong ([email protected])
Biases Diagnostic Overshadowing Medication changes ◦ - B12 levels ◦ - Calcium ◦ - Magnesium ◦ + Constipation ◦ + Osteoporosis ◦ + Pneumonia
Dr. Allen Wong ([email protected])
Behavior Complaint Behavior
Complaint
Diagnostic Overshadowing - Blaming a new medical or behavioral problem entirely on an existing disability, for example:
• New behaviors are just due to autism
• Decline in mental function is just due to Down syndrome
• Decline in physical function is just due to Cerebral Palsy
1.5% Profound 3.5% Severe 10% Moderate 85% Mild
Dr. Allen Wong ([email protected])

Pandemic disease Preventable disease Infectious like disease Multifactorial disease
Dr. Allen Wong ([email protected])
CAries Management By Risk Assessment
2015 Dr. Allen Wong ([email protected])

It’s for Everyone…who has teeth
Dr. Allen Wong ([email protected])
New Concept… why now? Old Dental philosophy Consistency… in material taught.. Some common questions Why didn’t my other dentist mention? I can’t afford that kind of care My insurance doesn’t pay for it, I don’t want it I never had problems before with caries
Dr. Allen Wong ([email protected])
Dr. Allen Wong ([email protected])
Blood Pressure Blood Test Insulin test C-reactive protein Urinalysis Temperature
Dr. Allen Wong ([email protected])

Or an idea of Prognosis?
Dr. Allen Wong ([email protected])
Which is NOT a Pattern Recognition of Dental Caries Risk?
2015 Dr. Allen Wong ([email protected])
25% more likely to get a prescription
300% more likely to continue a prescription
46% of psychotropic drugs don’t have a corresponding psychiatric diagnosis
13% of anti-seizure drugs don’t have a corresponding seizure diagnosis
Major Health Risk Categories ◦ Long QT Syndrome (cardiac arrhythmia) ◦ Weight Gain ◦ Osteoporosis (low bone density) ◦ Constipation ◦ Sun Sensitivity ◦ Reflux ◦ Caries (dental cavities) ◦ Dehydration

Dr. Kim Kutsch
Dr. Kim Kutsch
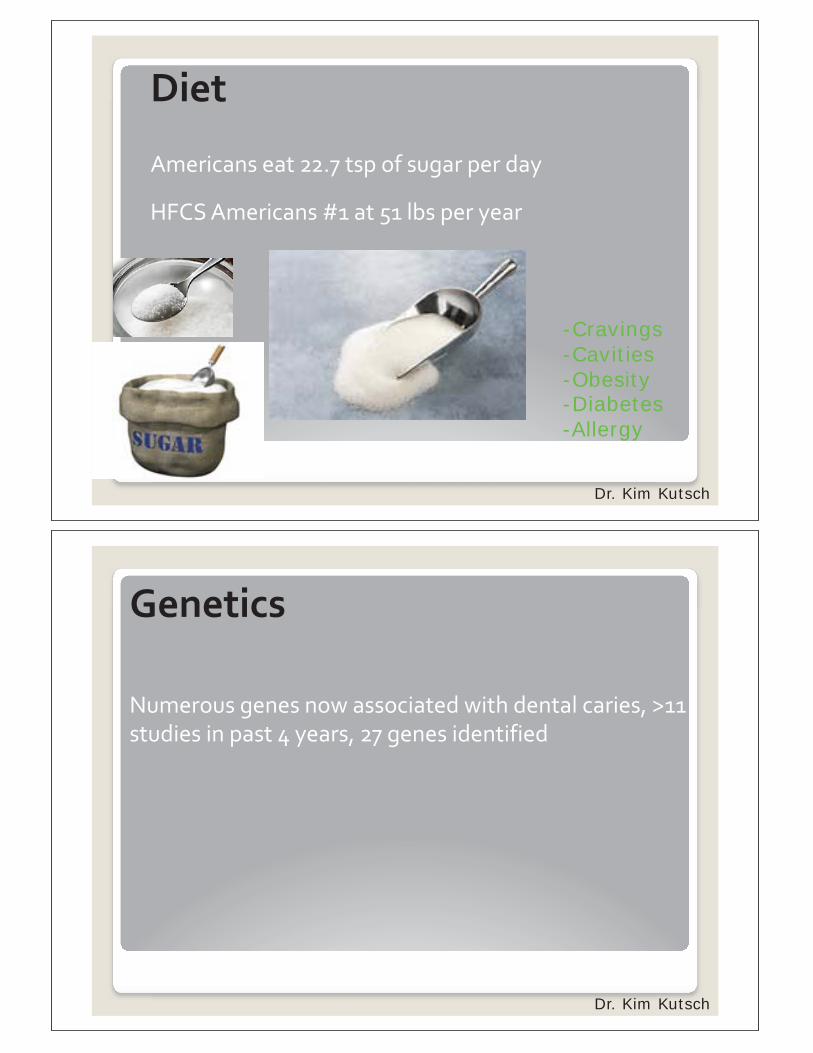
-Cravings -Cavities -Obesity -Diabetes -Allergy
Dr. Kim Kutsch
Dr. Kim Kutsch

Cardiovascular Disease (CAD and Stroke) Poor Pregnancy Outcomes (Fetal Development, low birth wt, pre-term births) Diabetes Bacterial pneumonia (VAP) Orthopedic Implant Failure Kidney Disease
Dr. Allen Wong ([email protected])
The most significant areas identified to date to have a suspected oral systemic
connection are:
Young et al., 2011

Picture
Which is NOT a Factor for Caries Risk Assessment Diagnosis?
A) Disease Indicators B) Socioeconomics Factors C) Biologic Factors D) Protective Factors E) Salivary pH
2015 Dr. Allen Wong ([email protected])

62 J CA Dent Assn. Oct 2007, p 704
A Statistically Validated Caries Risk Assessment Form (13,000 patients)
62
Young DA, Novy BB, Zeller GG, et al. The American Dental Association Caries Classification System for Clinical Practice: A report of the American Dental Association Council on Scientific Affairs. J Am Dent Assoc 2015;146(2):79-86.
9% 50% 77% 88% 100% 100%

Prevention, prevention, prevention Evaluate hard tissue (teeth) , soft tissue (gums) and saliva @ baseline Monitor hard tissue, soft tissue and saliva for changes Follow prescriptions to counteract effects of disease and medications Even MD’s can Fluoride Varnish? (USPSTF)
Dr. Allen Wong ([email protected])
Introduction & Science What is Dental Caries: The New Paradigm Environment is Everything y g
Dr. Allen Wong ([email protected])
Caries Treatment Strategies
Dr. Allen Wong ([email protected])
Restorative plan Antimicrobial Strategies: CHX, PI, Fluoride, Sodium Hypochlorite Remineralization Strategies: Fluoride, ACP-CCP or nano HA Bacteriostatic/Probiotic Strategies: Xylitol pH Strategies: Neutralizing and buffering rinses, sprays, gels, toothpastes, baking soda rinses Behavior Modification: Counsel specific risk factors
Think A, B, C’s
Dr. Allen Wong ([email protected])
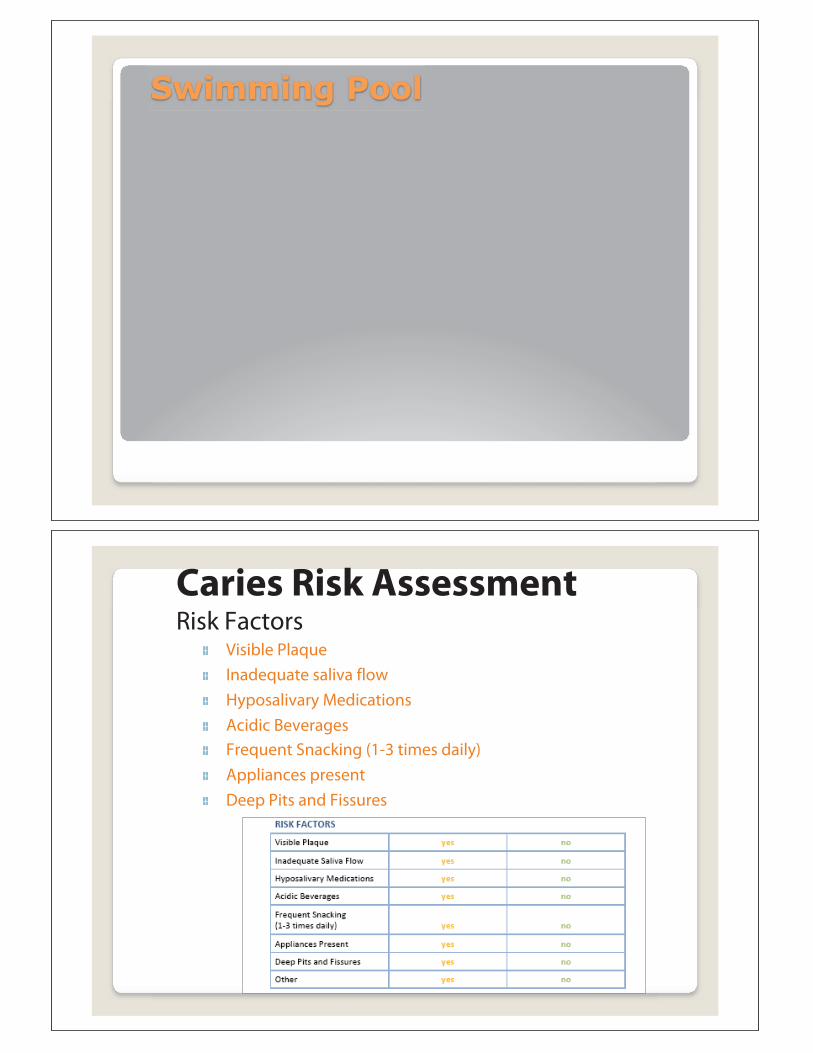
Caries Risk Assessment Risk Factors
Visible Plaque Inadequate saliva flow Hyposalivary Medications Acidic Beverages Frequent Snacking (1-3 times daily) Appliances present Deep Pits and Fissures

Dr. Allen Wong ([email protected])
Grow Teeth? Remineralization 5 factors
1 2 3 4 5
Dr. Allen Wong ([email protected])
SAMPLE CASES

Young et al., 2011

Caries Risk Assessment Form Guide for patient assessment for caries risk Covers all Disease Indicator and Risk
Factors
Caries Risk Assessment
Cavitations Radiographs
Bacterial Test Risk Factors
2012 Dr. Allen Wong ([email protected])
2015 Dr. Allen Wong ([email protected])
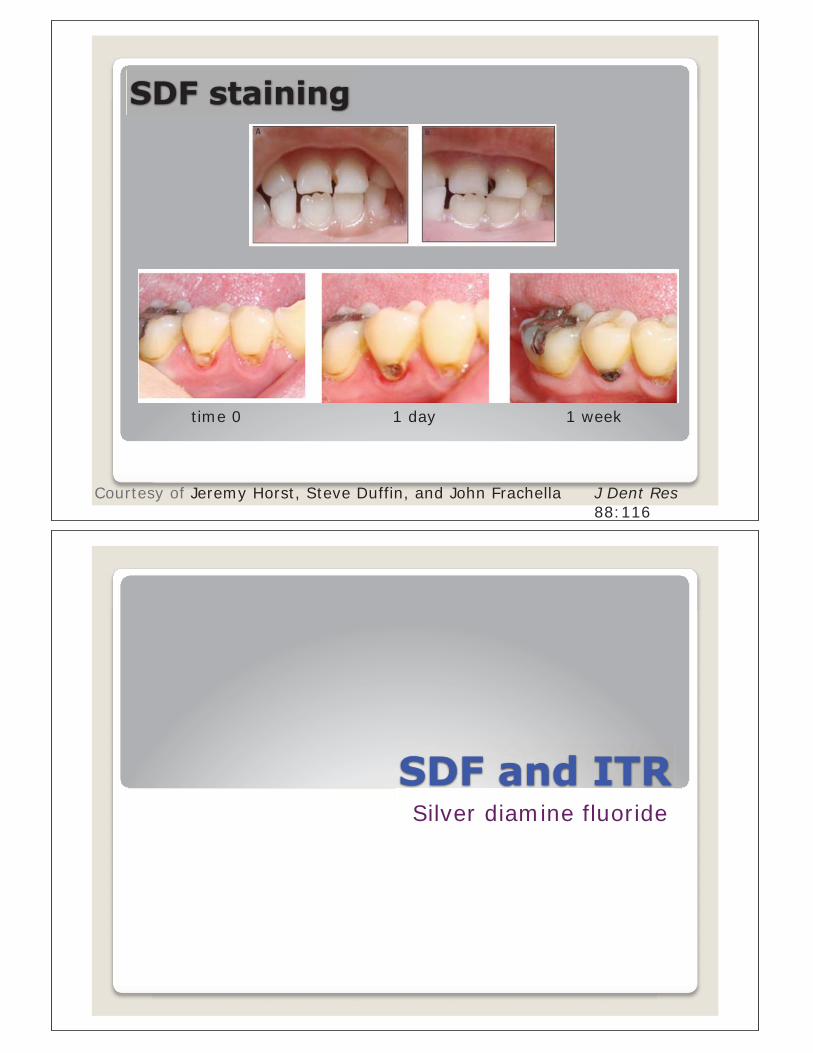
time 0 1 day 1 week
J Dent Res 88:116
Courtesy of Jeremy Horst, Steve Duffin, and John Frachella
Silver diamine fluoride

Courtesy of Steve Duffin
Courtesy of John Frachella

Seton J Scocca 49yom DD
3/29/16
UCSF
Con
sent
Courtesy of Jeremy Horst, Steve Duffin, and John Frachella
Allen’s Thoughts….. New paradigm?
Discuss with office the disparity of care and your willingness to help with the access to issue Schedule an introductory Tour of the Office ( usually early morning-short ) ( desensitize tools, materials, sensory) Send medical forms and have returned a couple days before to review Review the Diagnosis and discuss the goals with the Team At the tour, spend some time with caregiver in reviewing strategies

Set goals for the next meeting based on patients tolerance … desensitize If patient cannot tolerate, don’t force….relationships takes time Talk TO the patient, when possible, SMILE Give homework to caregiver ( such as counting teeth using a cotton swab ) Truly inform..wait…then perform Keep instructions simple Don’t use analogies, many are literal
Think about giving reasonable time markers for the patient ( counting to 10 ) Use picture books or mirrors
Walk in their shoes and understand their journey
Final Cautions
MI Paste (Amorphous Calcium Phosphate)
Xylitol
Chlorhexidine
Special Olympics Oath:
“Let me Win but if I cannot Win; Let me be brave in the attempt”

Kecia Weller & Mark Starford Board Resource Center
19th Annual Developmental Disabilities: An Update for Health Professionals March 5-6, 2020
Kecia Weller & Mark Starford
Disclosure
We have nothing to discloseWe have no financial conflicts of interest

Overview Efforts to address sexual violence - even movements like #MeToo have not focused on people with disabilities.
However, people with disabilities experience sexual violence at a very high rate and have comparatively few resources to support them.
Being silent creates more violence
Overview
This session focuses on sexual assault and violence against persons with intellectual/developmental disabilities.
We will share information about the “epidemic of violence” and provide recommendations about how all of us can decrease victimization

Learning Objectives
1. Identify reasons why people with disabilities face greater risk of sexual violence.
2. Hear recommendations from survivors about what agencies , organizations and providers can do to reduce sexual violence.
3. Learn about new tools that self-advocate leaders developed to help healthcare professionals, and social workers communicate with victims.
Before We Get Started
• This topic can be difficult for many people. Some may have reactions. This is ok
• Some of us have experienced sexual violence. If you are having strong emotions, feel free to leave the room
• Self-care is needed to be an effective advocate
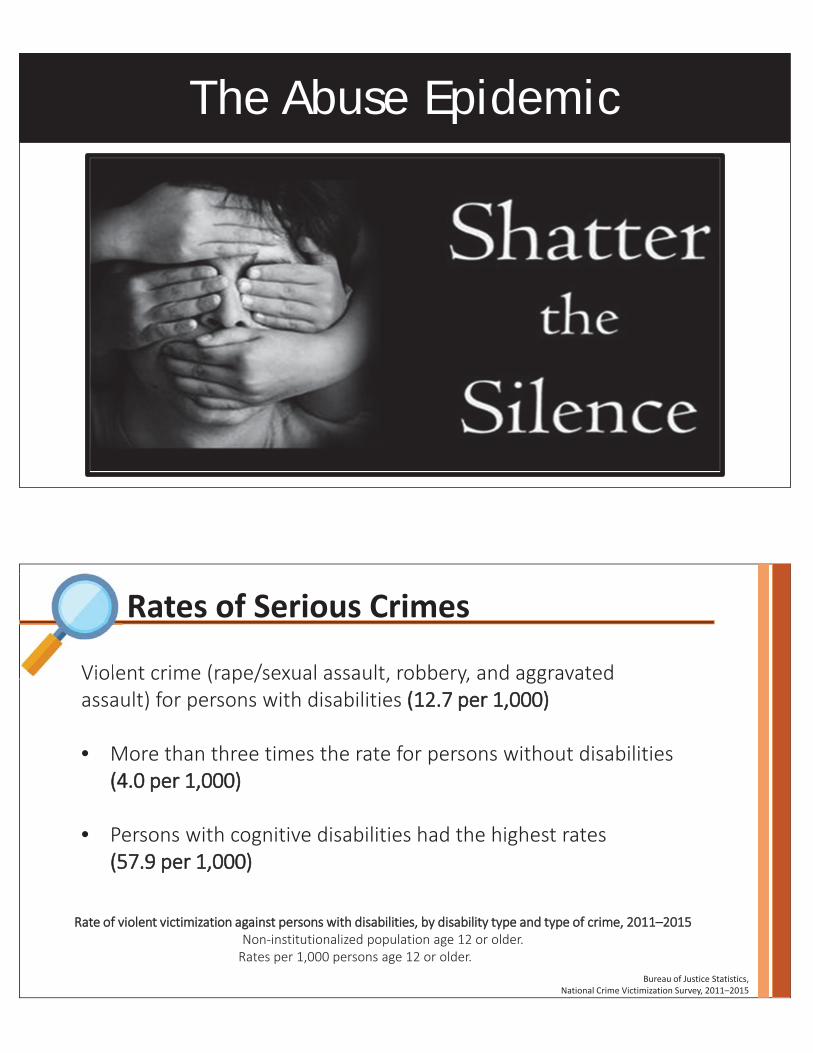
The Abuse Epidemic
Rates of Serious Crimes
Violent crime (rape/sexual assault, robbery, and aggravated assault) for persons with disabilities (12.7 per 1,000)
• More than three times the rate for persons without disabilities (4.0 per 1,000)
• Persons with cognitive disabilities had the highest rates (57.9 per 1,000)
Bureau of Justice Statistics, National Crime Victimization Survey, 2011–2015
Rate of violent victimization against persons with disabilities, by disability type and type of crime, 2011–2015Non-institutionalized population age 12 or older.
Rates per 1,000 persons age 12 or older.
Viole

NPR’s Abused and Betrayed Series
The rate of rape and sexual assault against people with an intellectual disability is mmore than seven times the rate for people without disabilities.
2.18
Abused and Betrayed Series:The Sexual Assault Epidemic No One Talks About
https://www.npr.org/series/575502633/abused-and-betrayed
https://www.npr.org/2018/01/08/570224090/the-sexual-assault-epidemic-no-one-talks-about
Sexual Assault Rates Among People With Developmental Disabilities 2011-2015
Abuse Epidemic

Acquaintance666%
34%
Intimate partnerOther relative
StrangerUnknown
Offender Relationship
70%
Reporting Facts
Domestic Violence & Disability http://www.bflnyc.org/about-us/domestic-violence-disability/
Abuse cases against adults with disabilitiesthat go unreported

• Not seen as credible due to disability
• Many people are told and believe there will be more abuse
• Fear of losing homes, jobs and relationships
• Lack having someone they trust to share with
• Communicate in non-traditional ways
• Taught to be compliant
… as reported by self-advocate survivors
“Without reporting, the cycle of abuse continues” James Meadours
Reporting Dilemma
Ongoing Barriers to Support
Leigh Ann Davis, National Center on Criminal Justice and Disability – The Arc, 2019

• Not taught how to identify abuse
• Sexual violence is a taboo subject that people avoid
• People with I/DD typically live an overprotected life and sheltered from the community
• Abuse that happens in programs is often treated as an employment issue, and not reported
Additional Barriers… as reported by self-advocate leaders
1. Lack of agency focus on the issue
2. Minimal interagency collaboration, data collection and sharing3. Minimal training for healthcare professionals, social workers, and
self-advocates
4. Inadequate follow-up care for victims
5. Materials typically not accessible or in “Plain Language”
6. Lack of communication to victims about what reporting means
SummaryThe abuse epidemic has grown despite
media attention, and alarming statistics

The system failed me!
“I should be able to get the support I need from the system that is set up for people with intellectual/developmental disabilities”
Lack of accommodations and follow-up care make reporting very difficult. As a result, many cases, including mine – are dismissed.
Kecia Weller
Let’s Take a Deeper Look - Survivor ReflectionHealthcare and law enforcement are not receptive
Let’s Talk
…
Topics included:
• Barriers to reducing sexual abuse against persons with disabilities
• Ways to move trauma-informed care forward
• Organizing a “National Peer Support Network”
• Starting a national campaign to increase awareness of sexual assault, identify promising practices and reduce barriers to reporting
1st Annual Convening – NAPSA Conference 2019
• Include survivors in all trainings
• Provide prevention, recognition, and reporting education
• Increase inclusive social connections, communication, and education
• Trust and believe survivors
• Educate health care professionals
• Provide trauma informed services
What Can We Do?
•
•
•
•

Recommendations
1. Increase reporting by healthcare professionals
Provide Training:
Better recognize signs of sexual assault and violence
Mandated Reporter responsibilities
Role of Adult Protective Services
Understand needs of gender non-conforming patients
Use everyday language when speaking with a patient
2. Increase victim understanding of sexual violence
Use short videos in facilitated group discussions
Provide case workers with tools and training to facilitate ACCESSIBLE conversations
Create handouts about sexual violence and victim resources
Assist persons at risk to develop safety plans
Recommendations

3. ProvidersKnow your legal responsibilities
Require reporting training for all employees
Do deeper background checks
When a person reports, provide them privacy
Ensure accommodations are available
Recommendations
Coalition BuildingIdentify and collaborate with organizations that are making a difference
Silence = Violence Network was established by self-advocates, disability organizations and their allies to address abuse against people with disabilities and older persons
Partners work collaboratively to reduce abuse and neglect against older persons and people with disabilities
Leadership is Required….Collaborative leadership & coalition-building to bring innovation and action across a decentralized network

Example: Easy-to-use training tools for Healthcare Providers
Purpose:• Increase patient-centered conversations• Increase community referrals and reporting• Decrease discomfort talking about sexual violence
Talk About Sexual Violence
www.talkaboutsexualviolence.org
Talk About Sexual Violence Video Training
“James Meets with his Doctor”“How to Have the Conversation”James MeadoursKecia Weller Dr. Howard
Phase One Phase Two

• Educate HCPs about accessible communication with patients
• Ensure all HCPs have community resource information available
• Initiate MOUs between APS and regional centers
• Educate community support providers, rape crisis centers
• Conduct ongoing peer led safety training at peer advocacy groups
• Provide resources for self-advocates
Recommendations From Project Advisors
Together We Can
Train
Advocate
Educate
Make a change!

Join the conversation, talk about sexual violence, take action and together we can end the silent epidemic!
Kecia Weller
Contact Information
Kecia Weller [email protected]
Mark Starford [email protected]
NCCJD® www.thearc.org/NCCJD
Talk About Sexual Violence www.talkaboutsexualviolence.org

• Talk About Sexual Violencewww.talkaboutsexualviolence.org
• NCCJD Pathways to Justice®www.nccjdpathwaystojustice.org
• Papers/webinars https://www.thearc.org/NCCJD/publications
• Self-Advocates Leadershiphttps://www.endabusepwd.org/projects/promoting-self-advocates-as-leaders/
• Other Projectshttps://www.endabusepwd.org/projects/
Learn More
Supporting the Adult Protective Services Workforce, UCSFhttps://healthworkforce.ucsf.edu/sites/healthworkforce.ucsf.edu/files/hwrc_aps_report_2.12.2020_FINAL.pdf
The Arc’s Violence, Abuse and Bullying white paperhttps://www.thearc.org/NCCJD/publications
Vera Reporthttps://www.vera.org/publications/sexual-abuse-of-children-with-disabilities-a-national-snapshot
Child Welfare Information Gatewayhttps://www.childwelfare.gov/topics/systemwide/statistics/can/stat-disabilities/
Learn More

Learn More – Human TraffickingCDC resources on sexual violence and trafficking https://www.cdc.gov/violenceprevention/sexualviolence/resources.html
Human Trafficking Report in San Francisco, 2015, City and County of San Francisco, Dept. on the Status of Women https://sfgov.org/dosw/sites/default/files/HT%20Report_FINAL.pdf
Human Trafficking Task Force e-Guide. Office for Victims of Crimehttps://www.ovcttac.gov/taskforceguide/eguide/4-supporting-victims/45-victim-populationsSex
Trafficking of Girls with ID Reid, J.A. Sex Trafficking of Girls with ID. 2018. 30(2 /victims-with-physical-cognitive-or-emotional-disabilities/
Trafficking in Persons Report. US Dept. of State. June 2018. https://www.state.gov/j/tip/rls/tiprpt/
SSilence is ViolenceResources Kecia Weller & Mark Starford
[email protected] Resource Center

As I see it:One of the primary problems with both regional centers and health care providers is the failure to makean APS report when a victim of abuse reports abuse to them. The personnel who work at regionalcenters and health care providers are mandated reporters. Another problem that regional centers andhealth care providers face are inconsistent training or lack of training regarding their mandatory reportingrequirements. A third problem I see with both regional centers and health care providers is that they donot provide enough support to abuse victims.
Like in my own sexual assault case, I was let down because a report was not filed with APS after I sharedmy story. I was not provided with resources to start the recovery process. Regional centers and healthcare providers must provide resources to individuals who have been victimized by a perpetrator.
What I would like regional centers and healthcare providers to do differently• Always report an abuse victimization to APS
• Have mandatory reporting requirement trainings at least every 6 to 12 months for all mandatory reporters
• Provide accessible resources to abuse victims and their trusted allies
• Work with local rape crisis centers to ensure they are trained on how to work with people with intellectual/developmental disabilities
• Make sure SANE Nurses are trained on accessible accommodations
• Refer victims for psychological support services that utilize “Trauma Informed Care”
• Work closely with APS, victim provider agencies and law enforcement agencies
• Provide a “warm handoff” to support agencies
Kecia Weller
Kecia’s Message:
August, 2019NAPSA Conference, Denver, CO.
My Personal Impact Report from the National Convening to Prevent Sexual Violence against People with Intellectual/DevelopmentalDisabilities.
Abuse prevention is so important for all Self Advocates to understand because abuse happens to us 7 times more often than ithappens to people who do not have disabilities.
7 times more – that’s a lot. Here’s something else to think about – once a person with disabilities is abused they are oftenabused many times afterward. That happened to me and to many people I know.
IntroductionI am at the Convening today to help create systematic change in terms of abuse prevention and interagency collaboration for helpingthe survivors of sexual abuse and other kinds of abuse nationally. The Convening is very important because NAPSA, MassachusettsDPPC and the Board Resource Center are collaborating to create a learning environment for survivors of abuse, APS personnel, andother abuse prevention personnel to learn from each other about how to support survivors of abuse with Trauma Informed Care.
Personal outcomesI have made the decision to use my experience as an opportunity to engage in advocacy work and educate others about sexual violenceagainst people with intellectual and developmental disabilities and older persons. I use my leadership role to bring together differentagencies to develop solutions to this problem.

Kecia’s Recommendations:
Increase conversations at advocacy meetingsIncreasing conversations regarding abuse at Self Advocacy Meeting is important. Meeting Self Advocates at their most comfortable meeting isimportant and bring necessary supports to make sure Self Advocates are not traumatized by having an open discussion on abuse prevention.
Topics to Consider:1. Why Abuse Awareness important for Self Advocates to know2. Learn about the different types of abuse and the red flags to each abuse type3. Abuse statistics – know the abuse statistics helps to prevent abuse4. Why it’s important to create a support system to help prevent abuse
How can Self Advocates, case management agencies and DDS benefit frommore open conversations?When Self Advocates, case management agencies and DDS talk openly about abuse prevention, they all come out of their individual silos tocollaborate with each other to create a community against abuse. When all the stakeholders come together for an open discussion on abuseprevention, they will not be duplicating services and will be able to find solutions together.
I believe we can “together” improve the lives of many people. In the end, these are the words I live by:• I DO NOT need to suffer in silence.• I have hope.• I reach out – there are good people who will help.• I advocate for myself, and for others.
All of us deserve to have a safe life, listened to and respected, not bullied.
Resource Links – Vera Institute of Justice, Center on Victimization and Safetyhttps://www.vera.org/centers/victimization and safety
Measuring Capacity to Serve Survivors with Disabilities Two publications developed to measure the capacity of organizations to serve survivors of sexualassault with disabilities. Each presents the performance indicators developed for the specific type of organization—one for rape crisis centers (90 pp) andone for disability organizations (86).
How Safe Are Americans with Disabilities?https://storage.googleapis.com/vera web assets/downloads/Publications/how safe are americans with disabilities/legacy_downloads/How safe areamericans with disabilities fact sheet web.pdf
Full report (39 pp):https://storage.googleapis.com/vera web assets/downloads/Publications/how safe are americans with disabilities/legacy_downloads/How safe areamericans with disabilities web.pdf
https://storage.googleapis.com/vera web assets/downloads/Publications/measuring capacity to serve survivors withdisabilities/legacy_downloads/Rape Crisis Center Implementation Guide.pdf
https://storage.googleapis.com/vera web assets/downloads/Publications/measuring capacity to serve survivors withdisabilities/legacy_downloads/Disability Organization Implementation Guide.pdf

Resource Links –The 1st Annual Convening to Develop a National Vision to Address Sexual Abuses AgainstPersons with Intellectual and Developmental Disabilities Resources List (August 19, 2019)
End Abuse of Persons with Disabilities https://www.endabusepwd.org/community/center on victimization and safety/
Disability and Abuse Project: https://www.endabusepwd.org/community/disability and abuse project/
Sexual Assault
National Sexual Violence Resource Center: https://www.nsvrc.org/
SART Toolkit on Working with Survivors with Disabilities: https://www.nsvrc.org/sarts/toolkit/6 6 Find Help https://www.nsvrc.org/find helpStatistics https://www.nsvrc.org/node/4737 Find Experts https://www.nsvrc.org/experts
RAINN https://www.rainn.org/About Sexual Assault https://www.rainn.org/about sexual assault Safety and Prevention https://www.rainn.org/safety prevention Consulting and Traininghttps://www.rainn.org/consulting services
Illinois Imagines Illinois Imagines was a statewide project to improve services to women with disabilities who have been victims of sexual violence from 20062018. http://icasa.org/resources/illinois imaginesMaterials http://icasa.org/resources/illinois imagines/materials toolkit and other material Resources http://icasa.org/resources/illinois imagines/imaginesresourcesCollaborative Teams http://icasa.org/resources/illinois imagines/collaborative teams
Talk About Sexual ViolenceTalk About Sexual Violence gives healthcare professionals the tools they need for simple, direct, and honest conversations with their patients about the all toocommon experience faced by individuals with intellectual and developmental disabilities (I/DD).https://thearc.org/our initiatives/criminal justice/talk about sexual violence/
Resource Links –The 1st Annual Convening to Develop a National Vision to Address Sexual Abuses AgainstPersons with Intellectual and Developmental Disabilities Resources List (August 19, 2019)
Kecia Weller Blog PostTalk About Sexual Violence: https://thearc.org/talk about sexual violence kecia/
Kecia Weller: “Kecia Weller Demands Justice for Survivors with Disabilities,” Ms. Magazine (March 8, 2019) https://msmagazine.com/2019/03/08/seekingjustice for survivors with disabilities/
James Meadours, Chris Miller, and Kecia Weller Blog PostOn the Front Lines: https://thearc.org/category/from the frontlines/
Mark Starford, Kecia Weller, and Molly KennedyAbuse of People with Disabilities: A Silent Epidemic (YouTube Video – Public Service Announcement) https://www.youtube.com/watch?v=yhLsATwO0o4
James Meadours: States Aim to Halt Sexual Abuse of People with Intellectual Disabilities https://www.npr.org/2018/06/25/623189167/states aim to haltsexual abuse of people with intellectual disabilities
Raising the Voices of Individuals with IDD Podcast(Hogg Foundation for Mental Health, University of Texas) Into the Fold, Episode 54: Abuse, Recovery and Self Advocacy http://hogg.utexas.edu/podcast selfadvocacy idd
Joseph Shapiro, National Public Radio: Abused and Betrayed Serieshttps://www.npr.org/series/575502633/abused and betrayed
Connecting the Dots and Building Collaboration to Support People with Disabilities Who Experience Sexual Violence, Bev Frantz, PhD, Institute on Disabilities,Temple University (The Arc Webinar, 2019) Transcripts, Session Slides, and YouTube link:https://thearc.org/resource/connecting the dots and building collaboration to support people with disabilities who experience sexual violence/
Resource Links –The 1st Annual Convening to Develop a National Vision to Address Sexual Abuses AgainstPersons with Intellectual and Developmental Disabilities Resources List (August 19, 2019)
Using Model Protocols to Guide Criminal Justice Responses to Domestic Violence and Sexual Assault Victims with Disabilities (The Arc’s National Center onCriminal Justice and Disability Webinar)Transcripts, Session Slides, and YouTube link:https://thearc.org/resource/using model protocols to guide criminal justice responses to domestic violence and sexual assault victims with disabilities/
Nevada Coalition to End Domestic and Sexual Violence – Join Advisory Committee: Preventing Sexual Abuse of People with Developmental Disabilitieshttps://www.ncedsv.org/advisory committee individuals with developmental disabilities 2/
Sexual Abuse of Arizonans with Developmental and Other Disabilitieshttps://addpc.az.gov/sites/default/files/media/2019%20ADDPC%20recomendations%20on%20preventing%20abu se_2.pdf
SAFE (Stop Abuse for Everyone) Place, Austin, TXAccessible DV/SA Services for persons with disabilitieshttps://www.safeaustin.org/our services/prevention and education/disability services/
Barrier Free Living:Services and Support for Survivors of Domestic Violence with Disabilities: https://www.bflnyc.org/ Shelter https://www.bflnyc.org/programsservices/#freedom house Counseling/Advocacy https://www.bflnyc.org/programs services/#secret garden
OtherBuilding Partnerships Initiative: Working Together to Protect Persons with Disabilities https://np ma bpi.johnguilfoil.com/building partnerships initiative/
The Board Resource Center: https://www.brcenter.org/index.html
Administration on Intellectual and Developmental Disabilities, Administration on Disabilities, Administration for Community Living, U.S. Department of Healthand Human Services https://acl.gov/about acl/administration disabilities
Resource Links –The 1st Annual Convening to Develop a National Vision to Address Sexual Abuses AgainstPersons with Intellectual and Developmental Disabilities Resources List (August 19, 2019)
Trauma Informed
A Practical Guide for Creating Trauma Informed Disability, Domestic Violence and Sexual Assault OrganizationsWisconsin’s Violence Against Women withDisabilities and Deaf Women Project: Disability Rights Wisconsin, Wisconsin Coalition Against Sexual Assault, Wisconsin Coalition Against Domestic Violence(December 2011) https://www.nsvrc.org/publications/guides/practical guide creating trauma informed disability domestic violence and sexual
Trauma Informed Care and Intellectual and Developmental Disabilities (by Ike Evans | Feb 9, 2017 | Blog, Hogg) Blog, Podcast: http://hogg.utexas.edu/traumaand idd
How Trauma Affects People with Intellectual Disabilities, The Arc (2011) https://thearc.org/wp content/uploads/forchapters/Trauma.pdf
Improving Recovery From Sexual Assault with Trauma Informed Care (June 27, 2019, in From Our Chapters, by The Arc)https://thearc.org/improving recovery from sexual assault the arc nm/
Office for Victims of Crime, Office of Justice Programs, U.S. Department of Justice https://www.ovc.gov
Promising Practices in Serving Crime Victims with Disabilities Toolkit (2008)https://www.ovc.gov/publications/infores/ServingVictimsWithDisabilities_toolkit/collaboration.htmlhttps://www.ovc.gov/publications/infores/ServingVictimsWithDisabilities_bulletin/crime.html
Multidisciplinary Response to Crime Victims with Disabilities: Community Level Replication Guide (2012)https://www.ovc.gov/pubs/victimswithdisabilities/communityguide/index.html
Victims with Disabilities: The Forensic Interview – Techniques for Interviewing Victims with Communication and/or Cognitive Disabilities (Revised 2011)https://www.ovc.gov/publications/infores/pdftxt/VictimsGuideBook.pdf

Mental Health Challenges, Assessment and Psychopharmacology in Individuals with
Developmental Disabilities
Susan Goldwasser M.D.Richard Goldwasser M.D.
Mill Valley, CAChild, Adolescent and Adult Psychiatrists
Consultants to Redwood Coast Regional Center and North Bay Regional Center
We have nothing to disclose

Learning Objectives
• To understand the components of a psychiatric assessment
• Common reasons for psychiatric referral
• To familiarize with psychopharmacology
Learning Objectives
• Identify five reasons for psychiatric referral
• Recognize signs and symptoms of psychosis, cognitive decline and mood disorders in the developmentally disabled populations
• Understand an indication for prescribing SSRI antidepressants, stimulants, and antipsychotics

Part I: Assessments
Susan Goldwasser, M.D.
Why is an individual referred to a psychiatrist?
Some common concerns include:• Aggression• Self injury• Explosive outbursts• Property destruction• Resisting attending school, Adult Day
Programs, previously enjoyable activities• Withdrawal, crying• Change in sleep patterns
Many referrals are because the local mental health provider or clinic refused to do an assessment because the person is non-verbal.
Many physicians assess non-verbal patients
(A) Pediatricians see infants
(B) Neurologists see non-verbal stroke patients
As mental health workers we can and should assess all people who may benefit from our services. Even if they are non-verbal.

Here are some examples of individuals, verbal and nonverbal, I have recently seen for mental health assessments.
(1)AC is a 16 year old non-verbal teen with ASD, ID, ADHD with a long history of aggression, impulsivity and hyperactivity with a recent dramatic escalation in violence and self injury at home and school requiring 2:1 staffing at all times.
(2) HC is a 36 year old man with very limited verbal skills, Down syndrome, ID previously nonviolent, active participant in his Adult Day Program who now has attacked his mother, eloped from his Adult Day Program into traffic and is suspended from the program. He moves furniture blocking doors so his large extended family is prevented from entering or exiting.
(3) SD is a 42 year old woman with very limited verbal skills, Down syndrome, ID previously non violent who has started picking up forks and threatening to stab one housemate during meals when their long term careprovider of 13 years turns her back. She is no longer able to follow directions, she repeats the same question continuously and is no longer able to sort laundry by colors.
(4) AE is a 14 year old verbal boy with ASD, ADHD who has become agitated and more aggressive on stimulants and SSRIs who is increasingly violent toward himself and others at school and home. On 3 occasions he has picked up knives, held them to his throat, and threatened to kill himself and others.

(5) ZJ is a nonverbal 7 year old boy with ASD, ID, PICA who constantly attempts to elope. He is seen with both parents and wears a safety harness (looks like a leash). He is not making cognitive gains at school, has not learned any language/communication skills despite intensive speech therapy or benefitted from applied behavioral analysis therapy. He is increasingly agitated, aggressive and not sleeping.
(6) MRF is a 15 year old boy with ASD who was previously verbal but over the past year has become nonverbal, will type into his iPad, he has become increasingly violent choking his mother and sisters, unable to fall asleep, withdrawn, crying, angry and for the first time has punched a classmate and has been sent home.
Straightforward, right?
Welcome to the Regional Center.
And all these individuals can be scheduled for ONE clinic.
So where to begin?
First of all:
An assessment of a verbal or nonverbal person is essentially the same. The difference is perhaps relying more heavily on collateral information from family members, care providers, therapists, behaviorists, teachers etc. but we need that information for all of our patients.

Reminder:
Just because a person is nonverbal, doesn’t mean they cannot communicate or understand.
Augmentative and Alternative Communication Devices; PEC’s; writing/typing; whispering to trusted person, etc.
We have to be open to the various ways people can communicate.
Prior to doing an assessment, we gather information and review it before the appointment.
1. Our comprehensive questionnaire2. School Information: IEP, psychoeducational
testing, a Connor’s behavior rating scale to have a better idea of teacher concerns about current classroom behavior
3. ABA therapists reports4. Any relevant medical information, labs5. Copies of neuropsych testing if available6. Past assessments

At the appointment, meet with individual and family members, care provider, sometimes service coordinator, respite worker, ABA therapist, teacher.

• Goal: Establish a rapport so patient, family, care providers feel safe, comfortable, confident you will try your best to help them.
• Clarify reason for coming to see us. Establish TARGET symptoms.
• When asking about aggression, self injury, property destruction, tantrums, determine:– Triggers– Frequency– Duration– Location: home, school, community
• Changes in mood as evidenced by crying, withdrawal, loss of interest in previous activities, decline in self care, skills, not making expected gains in school
Team Approach
Past Psychiatric History
• Review psychoeducational testing, reports, etc. • Ask in-depth about past treatments, what has
been helpful. • Explore if there has been physical, emotional,
sexual abuse, witnessed domestic violence• Trauma: accidents, homelessness, etc.• Past:
– major depressive, manic symptoms, suicidal behaviors/attempts, psychiactric hospitalizations
Medical History
Special emphasis on:
• Neuro: – Seizures
– Staring episodes
– Head injury
– Headaches
– Tics
Medical History
• GI– Constipation/diarrhea – Appetite/diet– PICA – eating/mouthing nonfood items– GERD– Encopresis
• GU– Enuresis– menses

Medical History con’t• Sleep
– Initiation (falling asleep)– Snoring/gasping– Frequent awakenings– Sweating/restlessness– Nightmares
• Dental– Last seen?– Sedated dentistry? Able to cooperate with non-sedated
dentistry?• Substances
– ETOH– Drugs– Cigarettes/vaping
• Current Medications:– Compliance
– How they are dispensed
– Side effects: i.e. weight gain, tics, sedation
• Past Medications– Tried/failed
– Side effects?

• Pregnancy/Developmental History– Exposures in utero to drugs and alcohol
• Self Care Skills: hygiene, dressing, toileting, tooth brushing
• Family History: always notable when there is NOTHING reported.– Asking about medical history, emotional issues,
susbtance/alcohol abuse
Social History
• Weapons/guns at home– Locked? Ammunition separate? – 80% school shooters get guns at home
• Food Insecurity• Living Circumstances• SSI/IHSS/Respite/Conserved• Legal issues• Interests• Typical Day

Educational History
• Is the student getting adequate support? ST/OT/Counseling.
• Many families resist special education and child struggles academically and socially because there is not enough expertise and support.
• ADP– So many benefits: cognitive stimulation, vocational
training, socialization, autistic/creative outlet• Many adults are not in programs. Family
fearful, resistant community, does not have appropriate/staffing program, etc.
Mental Status Exam
• Ask the person directly. Even if they are non-verbal and you think they do not understand you.
• Observe facial expression: does the person look sad, happy, fearful, angry, bored?
• Are they wandering around the room, head banging, aggressive towards others?
• To evaluate for psychosis determine if the person is talking to themselves, having an angry conversation when no one is present. Talking and conversation can be vocal utterances rather than words.
• Paranoid ideation may present as no longer wanting to be around family or co-workers, isolating, withdrawl, resisting attending school or Adult Day Program or family social gatherings.

• We try to determine mood, suicidal ideation, homicidal ideation, auditory or visual hallucinations, paranoid ideation ,judgment, insight.
• Observe affect, appearance, eye contact, tics, tremors, gait.
• Listen to speech, vocal tics
Based on all the above, we make our diagnoses, impressions and treatment
recommendations.

Part II: Psychopharmacology
Richard Goldwasser, M.D.
DSM-5: Selected Diagnostic Categories
• Neurodevelopmental Disorders– Intellectual Disabilities– Communication Disorders – Autism Spectrum Disorder– Attention-Deficit/Hyperactivity Disorder– Specific Learning Disorder– Motor Disorders
• Stereotypic Movement Disorders• Tic Disorders
– Other Developmental Disorders

DSM-5
• Schizophrenia Spectrum and Other Psychotic Disorders
• Bipolar and Related Disorders
• Depressive Disorders– Disruptive Mood Dysregulation Disorder
– Major Depressive Disorders
– Persistent Depressive Disorder (Dysthymia)
– Premenstrual Dysphoric Disorder
DSM-5
• Anxiety Disorders– Separation Anxiety Disorder– Social Anxiety Disorder (Social Phobia)– Generalized Anxiety Disorder– Panic Disorder and Specific Phobias
• Obsessive-Compulsive and Related Disorders– Trichotillomania (Hair-Pulling Disorder)– Excoriation (Skin-Picking) Disorder

DSM-5
• Trauma- and Stressor-Related Disorders– Reactive Attachment Disorder– Posttraumatic Stress Disorder
• Dissociative Disorders• Somatic Symptom and Related Disorders
– Conversion Disorder (Functional Neurogological Symptom Disorder)
• Feeding and Eating Disorders – Pica
DSM-5
• Elimination Disorders– Enuresis – Encopresis
• Sleep-Wake Disorders– Insomnia– Sleep Apnea– Restless Leg Syndrome– Parasomnias
• Sexual Dysfunctions• Gender Dysphoria

DSM-5
• Disruptive, Impulse-Control, and Conduct Disorders– Oppositional Defiant Disorder– Intermittent Explosive Disorder– Conduct Disorder
• Substance-Related and Addictive Disorders• Neurocognitive Disorders
– Delirium– Major and Mild Neurocognitive Disorder (e.g. due
to Alzheimer’s Disease)
DSM-5
• Personality Disorders
• Paraphilic Disorders
• Other Mental Disorders
• Medical-Induced Movement Disorders and Other Adverse Effects of Medicaiton
Treatment
• Referrals– Medical (e.g. neurology, GI, ENT, sleep)– Dental– Behavioral Therapy (e.g. ABA)– Psychology (e.g. therapy, testing)– Speech and Language Therapy– Occupational Therapy (e.g. Sensory processing
dysfunction, motor skills)– Physical Therapy– Special Education (Individual Education Plan) – Day Program
Treatment• FDA Approved Medications
– Autism Spectrum Disorder• risperidone (Risperdal)• aripiprazole (Abilify)
– Attention-Deficity Hyperactivity Disorder• Stimulants
– methylphenidate (Ritalin, Concerta, Metadate, QuillichewER, Quillivant ER, Jornay, etc.)
– dextroamphetamine (Dexedrine, Adderall, Adderall XR, Vyvanse, Dyanavel XR)
– atomoxetine (Strattera)– alpha-2-agonists
» clonidine (Catapres, Kapvay)» guanfacine (Tenex, Intuniv)

Treatment• FDA Approved Medications (con’t)
– Depression• SSRI
– fluoxetine (Prozac)– sertraline (Zoloft)– peroxatine (Paxil)– citalopram (Celexa)– escitalopram (Lexapro)– fluoxamine (Luvox)
• SNRI – venlafaxine (Effexor XR)– duloxetine (Cymbalta)– mirtazepine (Remeron)
• Others– trazodone (Desyrel)– bupropion (Wellbutrin)
Treatment
• FDA Approved Medications (con’t)– Anxiety
• SSRIs
• SNRIs
• quetiapine (Seroquel)
• buspirone (Buspar)
• benzodiazepines (lorazepam, clonazepam, diazepam, etc.)

Treatment• FDA Approved Medications (con’t)
– Mood Stabilizers• Lithium• Anti-epileptics
– valproate (Depakote)– carbamazepine (Tegretol)– lamotrigine (Lamictal)
• Anti-psychotics– aripiprazole (Abilitfy)– asenapine (Saphris)– cariprazine (Vraylar)– clozapine (Clozaril)– lurasidone (Latuda)– olanzapine (Zypreza)– quetiapine (Seroquel)– risperidone (Risperdal)– ziprasidone (Geodon)
Treatment
• FDA Approved Medications (con’t)– Tics/Tourette Syndrome
• pimozide (Orap)• haloperidol (Haldol)• risperidone (Risperdal)• aripiprazale (Abilify)• clonidine (Catapres, Kapvay)• guanfacine (Tenex, Intuniv)
– Enuresis• imipramine• desmopressin (DDAVP)

Treatment
• Off-Label Use of Medications– Aggression/Irritability/Impulsivity
• ADHD Rx
• Antipsychotics
• Anti-epileptics (including VPA, CBZ, TPX)
• Lithium
• Beta-blockers
• prazosin (Minipres)
• Amantadine
Treatment
• Off-Label Use of Medications– Self-injurious behavior
• Antipsychotics
• Anti-epileptics
• Anti-hypertensives (alpha-2-agonists, beta blockers)
• Naltrexone

Treatment
• Off-Label Use of Medications– Sleep
• Clonidine
• Trazodone, mirtazepine
• Gabapentin
• Antipsychotics
• Non-prescription– Melatonin, valerian, GABA, diphenhydramine, CBD
Treatment• Medication Side Effects
– Common • Sedation
• insomnia
• increased appetite/weight gain
• decreased appetite/weight loss
• GI (e.g. nausea, constipation, diarrhea)
• dry mouth (xerostomia)
• emotional flattening
Treatment
• Medication side effects– Rare but serious
• Worse mood or behavior – e.g. akathisia/agitation/activation (ADHD, antidepressants,
antipsychotics, anti-epileptics)
– Suicidal ideation (antidepressants, anti-epileptics, atomoxetine)
• Cardiovascular (e.g. change of blood pressure, heart rate, or rhythm)
• Tardive Dyskinesia
Discussing Medications• Including Patient, family, caregivers• Context
– Rx in addition to non-pharmacologic interventions (e.g. behavioral services, therapy, school, day program, medical/dental, etc.)
• Realistic expectations• Conservative vs. aggressive treatment (i.e.
crisis? placement or safety at risk?)– Risks of treatment/non-treatment– Risk of dosing too fast/too slow

Discussing Medications
• Who dispenses/has access? (e.g. concern about diversion of stimulants)
• Monitoring response and side effects (reports from patient, parents, teachers, staff)
• Who decides to adjust dose? (parameters)
Discussing Medications
• Generic vs. brand
• Non-compliance– May indicate side effects
• Follow-up and labs

Polypharmacy
• Avoid if possible
• Common
• Interactions especially with anti-epileptics
• Consult pharmacist, epocrates
Pharmacogenomic testing
• e.g. Genesight, Genomind
• May be helpful, especially if multiple failed medication trials
• Medicaid/MediCal and Medicare will pay

Conclusion
• Psychiatric conditions are common
• Treatment involves a team, whole person approach
• Medications can be a safe and effective part of a comprehensive treatment plan
Resources
• Our emails– [email protected]
• DSM-5: Diagnostic and Statistical Manual of Mental Disorders 2015
• American Academy of Child and Adolescent Psychiatry – www.aacap.org




















