
Antepartum & Intrapartum Management - Continuing Education
374
The Department of Obstetrics, Gynecology and Reproductive Sciences of the University of California, San Francisco School of Medicine presents Antepartum & Intrapartum Management June 5 - 7, 2014 Hotel Nikko San Francisco, CA Course Chairs Julian T. Parer, MD, PhD Professor of Obstetrics, Gynecology and Reproductive Sciences Tekoa L. King, CNM, MPH Associate Clinical Professor, University of California, San Francisco School of Nursing; Deputy Editor, Journal of Midwifery & Women’s Health Judith T. Bishop, CNM, MSN, MPH Professor of Obstetrics, Gynecology and Reproductive Sciences Mary E. Norton, MD Professor of Obstetrics, Gynecology and Reproductive Sciences Aaron B. Caughey, MD, MPP, MPH, PhD Professor and Chair, Department of Obstetrics & Gynecology, Julie Neupert Stott Director, Center for Women’s Health, Oregon Health & Science University, Portland, Oregon University of California, San Francisco School of Medicine
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of Antepartum & Intrapartum Management - Continuing Education

The Department of Obstetrics, Gynecology and Reproductive Sciences of the University of California, San Francisco School of Medicine presents
Antepartum & Intrapartum
Management
June 5 - 7, 2014
Hotel Nikko San Francisco, CA
Course Chairs
Julian T. Parer, MD, PhD Professor of Obstetrics, Gynecology and Reproductive Sciences
Tekoa L. King, CNM, MPH
Associate Clinical Professor, University of California, San Francisco School of Nursing; Deputy Editor, Journal of Midwifery & Women’s Health
Judith T. Bishop, CNM, MSN, MPH
Professor of Obstetrics, Gynecology and Reproductive Sciences
Mary E. Norton, MD Professor of Obstetrics, Gynecology and Reproductive Sciences
Aaron B. Caughey, MD, MPP, MPH, PhD
Professor and Chair, Department of Obstetrics & Gynecology, Julie Neupert Stott Director, Center for Women’s Health, Oregon Health & Science University, Portland, Oregon
University of California, San Francisco School of Medicine
Exhibitors
Hologic
Ob Hospitalist Group
Southwest Medical Books
Wolters Kluwer

University of California, San Francisco School of Medicine Presents
Antrepartum and Intrapartum Management
Course Description Presented by the University of California, San Francisco School of Medicine, this course stresses antepartum and intrapartum assessment and clinical management in obstetrics. On the first day, various aspects of prenatal diagnosis, ultrasound, antepartum conditions, and maternal complications of pregnancy are covered. The second day is largely devoted to fetal heart rate interpretation and management of fetal heart rate patterns. The third day continues with discussions of potential complications of pregnancy and their management. The course is appropriate for physicians, midwives, obstetric nurses, and trainees. The faculty instructors are internationally known through their clinical and basic research, scholarly articles, and texts. The faculty are highly qualified, certified by their respective specialties, and the majority are qualified or eligible for the subspecialty division of Maternal Fetal Medicine of the American Board of Obstetrics and Gynecology. Educational Objectives Upon completion of this course, participants should be able to:
Apply best practices in managing women with obesity during labor; Manage and treat selected maternal medical complications of pregnancy; Implement current assessment and management strategies for Rh sensitization; Describe the clinical implications of fetal heart rate categories; Analyze labor management practices that may lower the primary cesarean section rate; Identify good candidates for a trial of labor after cesarean section.
Accreditation
Physician Credit The University of California, San Francisco School of Medicine (UCSF) is accredited by the Accreditation Council for Continuing Medical Education to provide continuing medical education for physicians. UCSF designates this live activity for a maximum of 18.25 AMA PRA Category 1 Credits™. Physicians should only claim credit commensurate with the extent of their participation in the activity. Nursing Credit For the purpose of recertification the American Nurses Credentialing Center accepts AMA PRA Category 1 Credit™ issued by organizations accredited by ACCME. AMCB Credit ACCME Credit hours in Category 1 are accepted by the Certificate Maintenance Program (CMP) of the American Midwifery Certification Board (AMCB) for programs relevant to midwifery. Certified nurse-midwives and certified midwives attending this program may report 18.00 credit hours.

Accreditation, Continued ACOG Credit The American College of Obstetricians and Gynecologists has assigned 18 cognate credits to this program. Fetal Heart Rate Monitoring The approved credits include 3.75 AMA PRA Category 1 Credits™ towards Fetal Heart Rate Monitoring and Assessment Education. Nursing Pharmacology Continuing Education For the purposes of recertification the American Credentialing Center accepts AMA PRA Category 1 Credits™ issued by organizations accredited by the ACCME. This activity is designated for 2.50 pharmacology credits towards meeting the requirement for nursing pharmacology continuing medical education.

General Information Attendance Verification / CME Certificates Please remember to sign-in on the sign-in sheet when you check in at the UCSF Registration Desk on your first day. You only need to sign-in once for the course, when you first check in. After the meeting, please visit this website to complete the online course evaluation: http://www.ucsfcme.com/evaluation Upon completing the online evaluation, your CME certificate will be automatically generated and emailed to you.
Evaluation Your opinion is important to us – we do listen! We have two evaluations for this meeting. The speaker evaluation is the light yellow hand-out you received in your syllabus when you checked in. Please complete this during the meeting and turn it in to the registration staff at the end of the conference. The overall conference evaluation is online at: http://www.ucsfcme.com/evaluation We request you complete this evaluation within 30 days of the conference in order to receive your CME certificate through this format. Security We urge caution with regard to your personal belongings and syllabus books. Please put your name on the cover of your syllabus. We are unable to replace these in the event of loss. Please do not leave any personal belongings unattended in the meeting room during lunch or breaks or overnight. Lunch Lunch is on your own each day. A list of nearby restaurants is printed in the back of your syllabus. Wine and Cheese Reception You are cordially invited to join us for a Wine and Cheese reception in the Ballroom Foyer on Thursday June 5, 5:30-6:45pm. Going Green We are pleased to announce our efforts to ‘go green’. Currently all marketing materials such as brochures and syllabi are printed only on recycled paper. We need your help – if you would like to see this course provide only an electronic syllabus or make other changes please let us know via your evaluation. Audience Response System Keypads Audience Response System keypads have been provided for your use during the course. Please be sure that you turn your keypad in at the end of each day and pick up a new one each morning. Your assistance is greatly appreciated. Presentations Color PDFs of presentations will be available on our website, www.cme.ucsf.edu, approximately 2-4 weeks post event. We will only post presentations for those authorized by the presenters.

Federal and State Law Regarding Linguistic Access and Services for Limited English Proficient Persons
I. Purpose.
This document is intended to satisfy the requirements set forth in California Business and Professions code 2190.1. California law requires physicians to obtain training in cultural and linguistic competency as part of their continuing medical education programs. This document and the attachments are intended to provide physicians with an overview of federal and state laws regarding linguistic access and services for limited English proficient (“LEP”) persons. Other federal and state laws not reviewed below also may govern the manner in which physicians and healthcare providers render services for disabled, hearing impaired or other protected categories
II. Federal Law – Federal Civil Rights Act of 1964, Executive Order 13166, August 11, 2000, and
Department of Health and Human Services (“HHS”) Regulations and LEP Guidance. The Federal Civil Rights Act of 1964, as amended, and HHS regulations require recipients of federal financial assistance (“Recipients”) to take reasonable steps to ensure that LEP persons have meaningful access to federally funded programs and services. Failure to provide LEP individuals with access to federally funded programs and services may constitute national origin discrimination, which may be remedied by federal agency enforcement action. Recipients may include physicians, hospitals, universities and academic medical centers who receive grants, training, equipment, surplus property and other assistance from the federal government. HHS recently issued revised guidance documents for Recipients to ensure that they understand their obligations to provide language assistance services to LEP persons. A copy of HHS’s summary document entitled “Guidance for Federal Financial Assistance Recipients Regarding Title VI and the Prohibition Against National Origin Discrimination Affecting Limited English Proficient Persons – Summary” is available at HHS’s website at: http://www.hhs.gov/ocr/lep/ . As noted above, Recipients generally must provide meaningful access to their programs and services for LEP persons. The rule, however, is a flexible one and HHS recognizes that “reasonable steps” may differ depending on the Recipient’s size and scope of services. HHS advised that Recipients, in designing an LEP program, should conduct an individualized assessment balancing four factors, including: (i) the number or proportion of LEP persons eligible to be served or likely to be encountered by the Recipient; (ii) the frequency with which LEP individuals come into contact with the Recipient’s program; (iii) the nature and importance of the program, activity or service provided by the Recipient to its beneficiaries; and (iv) the resources available to the Recipient and the costs of interpreting and translation services. Based on the Recipient’s analysis, the Recipient should then design an LEP plan based on five recommended steps, including: (i) identifying LEP individuals who may need assistance; (ii) identifying language assistance measures; (iii) training staff; (iv) providing notice to LEP persons; and (v) monitoring and updating the LEP plan. A Recipient’s LEP plan likely will include translating vital documents and providing either on-site interpreters or telephone interpreter services, or using shared interpreting services with other Recipients. Recipients may take other reasonable steps depending on the emergent or non-emergent needs of the LEP individual, such as hiring bilingual staff who are competent in the skills required for medical translation, hiring staff interpreters, or contracting with outside public or private agencies that provide interpreter services. HHS’s guidance provides detailed examples of the mix of services that a Recipient should consider and implement. HHS’s guidance also establishes a “safe harbor” that Recipients may elect to follow when determining whether vital documents must be translated into other languages. Compliance with the safe harbor will be strong evidence that the Recipient has satisfied its written translation obligations.

In addition to reviewing HHS guidance documents, Recipients may contact HHS’s Office for Civil Rights for technical assistance in establishing a reasonable LEP plan.
III. California Law – Dymally-Alatorre Bilingual Services Act. The California legislature enacted the California’s Dymally-Alatorre Bilingual Services Act (Govt. Code 7290 et seq.) in order to ensure that California residents would appropriately receive services from public agencies regardless of the person’s English language skills. California Government Code section 7291 recites this legislative intent as follows:
“The Legislature hereby finds and declares that the effective maintenance and development of a free and democratic society depends on the right and ability of its citizens and residents to communicate with their government and the right and ability of the government to communicate with them. The Legislature further finds and declares that substantial numbers of persons who live, work and pay taxes in this state are unable, either because they do not speak or write English at all, or because their primary language is other than English, effectively to communicate with their government. The Legislature further finds and declares that state and local agency employees frequently are unable to communicate with persons requiring their services because of this language barrier. As a consequence, substantial numbers of persons presently are being denied rights and benefits to which they would otherwise be entitled. It is the intention of the Legislature in enacting this chapter to provide for effective communication between all levels of government in this state and the people of this state who are precluded from utilizing public services because of language barriers.”
The Act generally requires state and local public agencies to provide interpreter and written document translation services in a manner that will ensure that LEP individuals have access to important government services. Agencies may employ bilingual staff, and translate documents into additional languages representing the clientele served by the agency. Public agencies also must conduct a needs assessment survey every two years documenting the items listed in Government Code section 7299.4, and develop an implementation plan every year that documents compliance with the Act. You may access a copy of this law at the following url: http://www.spb.ca.gov/bilingual/dymallyact.htm

COURSE DIRECTORS
Julian T. Parer, MD, PhD Professor of Obstetrics, Gynecology and Reproductive Sciences Tekoa L King, CNM, MPH Associate Clinical Professor, University of California, San Francisco School of Nursing; Deputy Editor, Journal of Midwifery & Women’s Health Judith T. Bishop, CNM, MSN, MPH Professor of Obstetrics, Gynecology and Reproductive Sciences Mary E. Norton, MD Professor, Department of Obstetrics, Gynecology and Reproductive Sciences Aaron B. Caughey, MD, MPP, MPH, PhD Professor and Chair, Department of Obstetrics & Gynecology, Julie Neupert Stott Director, Center for Women’s Health, Oregon Health & Science University, Portland, Oregon GUEST FACULTY
Natali Aziz, MD, MS Clinical Assistant Professor, Stanford University School of Medicine, Stanford, California Jamie Dolkas, JD Associate Director of Women's Leadership, University of California, Hastings College of the Law Center for Worklife Law Maurice L. Druzin, MD Professor and Vice-Chair; Program Director, Obstetrics and Gynecology Residency Program, Division of Maternal Fetal Medicine, Department of Obstetrics and Gynecology, Stanford University Medical Center; Associate Dean for Academic Affairs, Stanford University School of Medicine, Stanford, California Yasser Y. El-Sayed, MD Professor and Director, Division of Maternal-Fetal Medicine and Obstetrics, Stanford University Medical Center; Obstetrician-in-Chief, Lucile Packard Children’s Hospital, Stanford, California Jeffrey L. Ecker, MD Professor, Obstetrics, Gynecology and Reproductive Biology, Harvard Medical School, Boston, Massachusetts Kimberly D. Gregory, MD, MPH Vice Chair, Women’s Healthcare Quality & Performance Improvement, Department of Obstetrics & Gynecology, Cedars Sinai Medical Center; Professor, David Geffen School of Medicine & UCLA Fielding School of Public Health, Los Angeles, California Deidre J. Lyell, MD Associate Professor, Department of Obstetrics and Gynecology, Stanford University Medical Center, Stanford, California Leonardo M. Pereira, MD, MCR Associate Professor, Division Director of Maternal-Fetal Medicine, Oregon Health & Science University, Portland, Oregon

GUEST FACULTY, CONT. Brian L. Shaffer, MD Assistant Professor, Department of Obstetrics & Gynecology, Division of Maternal-Fetal Medicine, Oregon Health & Science University, Portland, Oregon UCSF FACULTY Michael D. Fox, RN, BSN Clinical Program Director, Change Agent Program Center for the Health Professions Anna Glezer, MD, PhD Assistant Professor, Department of Psychiatry Juan M. Gonzalez, MD, MS Assistant Professor, Department of Obstetrics, Gynecology and Reproductive Sciences Kathryn A. Houston, MD Assistant Professor, Department of Obstetrics, Gynecology and Reproductive Sciences Lena H. Kim, MD Assistant Professor, Department of Obstetrics, Gynecology and Reproductive Sciences Michael S. Policar, MD, MPH Professor, Department of Obstetrics, Gynecology and Reproductive Sciences Patricia A. Robertson, MD Professor and Director of Medical Student Education, Department of Obstetrics, Gynecology and Reproductive Sciences Kirsten E. Salmeen, MD Assistant Professor, Department of Obstetrics, Gynecology and Reproductive Sciences Suzanne M. Seger, CNM, MSN, MTS Associate Professor, Department of Obstetrics, Gynecology and Reproductive Sciences Naomi E. Stotland, MD Associate Professor, Department of Obstetrics, Gynecology and Reproductive Sciences Loretta M. Strachowski, MD Professor, Department of Radiology and Biomedical Imaging; Adjunct Professor, Department of Obstetrics, Gynecology and Reproductive Sciences Mari-Paule Thiet, MD Professor, Department of Obstetrics, Gynecology and Reproductive Sciences Marya G. Zlatnik, MD, MMS Professor, Department of Obstetrics, Gynecology and Reproductive Sciences

Disclosures The following faculty speakers, moderators, and planning committee members have disclosed no financial interest/arrangement or affiliation with any commercial companies who have provided products or services relating to their presentation(s) or commercial support for this continuing medical education activity: Natali Aziz, MD, MS Judith T. Bishop, CNM, MSN, MPH Aaron B. Caughey, MD, MPH, MPP, PhD Jamie Dolkas, JD Maurice L. Druzin, MD Yasser Y. El-Sayed, MD Jeffrey L. Ecker, MD Michael D. Fox, RN, BSN Anna Glezer, MD, PhD Juan M. Gonzalez, MD, MS Kimberly D. Gregory, MD, MPH Kathryn A. Houston, MD Lena H. Kim, MD
Tekoa L. King CNM, MPH Deidre J. Lyell, MD Julian T. Parer, MD, PhD Leonardo M. Pereira, MD Michael S. Policar, MD, MPH Patricia A. Robertson, MD Kirsten E. Salmeen, MD Brian L. Shaffer, MD Suzanne M. Seger, CNM Naomi E. Stotland, MD Lori M. Strachowski, MD Mari-Paule Thiet, MD Marya G. Zlatnik, MD
The following faculty speakers have disclosed a financial interest/arrangement or affiliation with a commercial company who has provided products or services relating to their presentation(s) or commercial support for this continuing medical education activity. All conflicts of interest have been resolved in accordance with the ACCME Standards for Commercial Support: Aaron B. Caughey, MD, MPP, PhD Medical Advisor Ariosa, Cellscape, Mindchild Mary E. Norton, MD Research Support Ariosa, Natera This UCSF CME educational activity was planned and developed to: uphold academic standards to ensure balance, independence, objectivity, and scientific rigor; adhere to requirements to protect health information under the Health Insurance Portability and Accountability Act of 1996 (HIPAA); and, include a mechanism to inform learners when unapproved or unlabeled uses of therapeutic products or agents are discussed or referenced. This activity has been reviewed and approved by members of the UCSF CME Governing Board in accordance with UCSF CME accreditation policies. Office of CME staff, planners, reviewers, and all others in control of content have disclosed no relevant financial relationships.

UCSF Antepartum and Intrapartum Management – Lecture Agenda
F = FHR Credit P = Pharmacology Credit
THURSDAY, JUNE 5, 2014 7:00 - 8:00 am Continental Breakfast 7:30 - 8:10 Registration
8:10 - 8:15 Introduction
Moderator: Julian T. Parer, MD, PhD
8:15 - 8:45 Cell Free Fetal DNA: The Popular Press versus the Mary E. Norton, MD Evidence
8:45 - 9:15 P Rh Disease and Other Alloimmune Hemolytic Lena H. Kim, MD Disorders in Pregnancy: A Fresh Look at an Old Problem
9:15 - 9:45 The Obese Patient During Pregnancy and Labor Naomi E. Stotland, MD
9:45 - 10:05 Questions and Answers
10:05 - 10:25 Break
10:25 - 10:55 The Continuing Controversy Over Screening for Kirsten E. Salmeen, MD Gestational Diabetes
10:55 - 11:25 P Mental Health Disorders in Pregnancy: Anna Glezer, MD, PhD What is Your Responsibility?
11:25 - 11:55 Evidence-Based Techniques for Cesarean Section Marya G. Zlatnik, MD, MMS
11:55 - 12:15 Questions and Answers
12:15 - 1:30 Lunch (individually arranged)
Moderator: Tekoa L. King, CNM, MPH
1:30 - 2:00 Perinatal Care for LGBT Patients: Patricia A. Robertson, MD Is Your Practice Ready?
2:00 - 2:30 P Update on Antibiotics in Intrapartum Obstetrics Natali Aziz, MD, MS
2:30 - 3:00 P Chorioamnionitis: What is the Evidence for Clinical Juan M. Gonzalez, MD Management?
3:00 - 3:20 Questions and Answers
3:20 - 3:40 Break
3:40 - 4:10 Sonographic Criteria for Nonviable Pregnancy in Loretta M. Strachowski, MD the 1st Trimester
4:10 - 4:40 Diagnosis and Management of Arrest Yasser Y. El Sayed, MD Disorders: How Long to Wait? 4:40 - 5:10 TOLAC 2014: Which Patients and Which Centers? Jeffrey L. Ecker, MD
5:10 - 5:30 Questions and Answers
5:30 - 6:45 pm Wine and Cheese Reception
FRIDAY, JUNE 6, 2014 7:00 - 8:00 am Continental Breakfast
Moderator: Mary E. Norton MD
8:00 - 8:30 The Hazards of Placenta Accreta Deirdre J. Lyell, MD
8:30 - 9:00 Twins: Timing and Management of Delivery Mari-Paule Thiet, MD

UCSF Antepartum and Intrapartum Management – Lecture Agenda
F = FHR Credit P = Pharmacology Credit
FRIDAY, JUNE 6, 2014 Cont.
9:00 - 9:30 am Genetic Carrier Screening: Review of the Brian L. Shaffer, MD Old, the New, and the Controversial
9:30 - 9:50 Questions and Answers
9:50 - 10:10 Break
10:10 - 10:40 Are you HIP? Update on ACOG Hypertension in Maurice L. Druzin, MD Pregnancy Task Force
10:40 - 11:10 F Applying the NICHD Categories: Michael D. Fox, RN Case Studies in FHR Monitoring
11:10 - 11:40 Delayed Cord Clamping: What’s it All About? Judith T. Bishop CNM, MSN, MPH
11:40 - 12:00 pm Questions and Answers
12:00 - 1:30 Lunch (individually arranged)
Moderator: Aaron B. Caughey, MD, PhD
1:30 - 2:00 FP Safe and Appropriate Use of Magnesium Sulfate Jeffrey L. Ecker, MD in Obstetrics
2:00 - 2:30 F The Category II Conundrum Tekoa L. King, CNM, MPH
2:30 - 3:00 F Tachysystole: Much Ado about Nothing? Kimberly D. Gregory, MD, MPH
3:00 - 3:20 Questions and Answers
3:20 - 3:40 Break
3:40 - 5:10 F Fetal Heart Rate Monitoring Aaron B. Caughey, MD, PhD Interactive Session with Faculty Panel Jeffrey L. Ecker, MD Kimberly D. Gregory, MD, MPH Julian T. Parer, MD, PhD
5:10 - 5:30 pm Questions and Answers
SATURDAY, JUNE 7, 2014 7:00 - 8:00 am Continental Breakfast
Moderator: Judith T. Bishop, CNM, MSN, MPH
8:00 - 8:30 The Persistent Dilemma of Preterm Delivery Leonardo M. Pereira, MD, MCR
8:30 - 9:00 Nulliparous Term Singleton Vertex Cesareans: Kimberly D. Gregory, MD, MPH Is the Healthy People 2020 Goal Possible?
9:00 - 9:30 Patient Expectations and Preferences: Where Do Kathryn A. Houston, MD They Come From?
9:30 - 9:50 Questions and Answers
9:50 - 10:10 Break
10:10 - 10:40 The Affordable Care Act is Here: Now What? Michael S. Policar, MD, MPH
10:40 - 11:10 Discriminatory Practices in Your Setting Suzanne M. Seger, CNM, MSN, MTS & Jamie Dolkas, JD
11:10 -11:40 Decision-to-Delivery Time in Obstetric Emergencies Aaron B. Caughey, MD, PhD
11:40 - 12:00 pm Questions and Answers
12:00 pm Adjourn

6/5/2014
1
Cell free DNA: The Popular Press vs The EvidenceMary E Norton, MDProfessor of Obstetrics, Gynecology & Reproductive Sciences; UCSFAntepartum and Intrapartum Management
Disclosures
• Principal Investigator of ongoing clinical trial on cfDNA supported by Ariosa Diagnostics
• Unpaid clinical consultant for CellScapeand Natera
• Research support from Natera• No personal financial involvement in any of the cfDNA companies
6/5/2014
2
020406080
100120
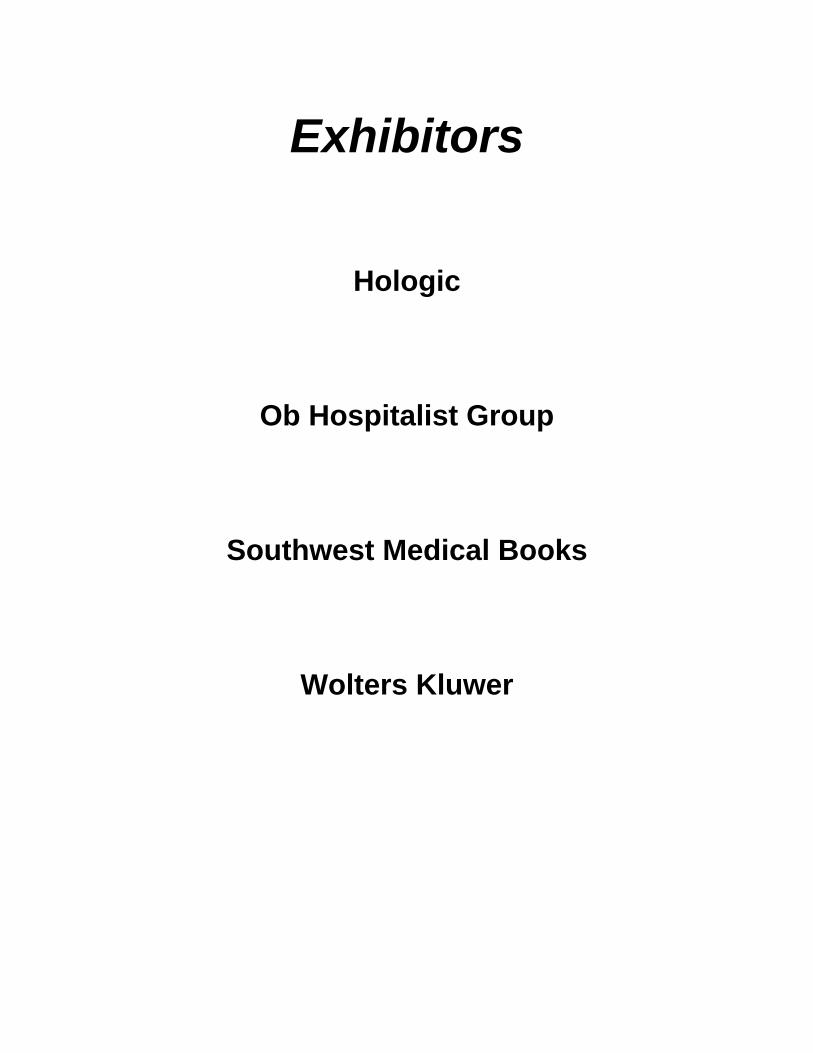
Detection rate of prenatal screening for Down syndrome has
improved over time
Det
ectio
n R
ate
(%)
Cell free fetal DNA• Cell free fetal DNA (cffDNA) is made up of short
segments of fetal DNA (<200 base pairs) that circulate in maternal plasma
• Origin of these fragments is thought to be primarily placenta
Maternal DNA
Fetal DNA
Cell free DNA results from apoptosis

6/5/2014
3
Companies currently offering cfDNAscreening (in order of appearance):
Noninvasive Prenatal Testing (NIPT)
• Detection requires accurate quantification of DNA from a specific chromosome
• Somewhat different methods are utilized by different laboratories
Analysis of fetal DNA
Zhong, X, Holzgreve, W, Glob. libr. women's med 2009
Wts (%)
10099.1 (98.3 - 99.6)2.594.4 (72.7 - 100)1.2100 (63.1 - 100)3.5100 (86.3 - 100)4.1100 (88.4 - 100)1.6100 (71.5 - 100)4.9100 (90.3 - 100)11.0100 (95.6 - 100)1.2100 (63.1 - 100) 1.6100 (71.5 - 100)2.3100 (79.4 - 100)12.0100 (95.9 - 100)6.8100 (92.9 - 100)1.9100 (75.3 - 100)28.498.6 (95.9 - 99.7)5.3100 (91.0 - 100)
50 60 70 80 90100 DR % (95% CI) (%)
11.6100 (95.8 - 100)
Pooled analysis
Verweij et al., 2013 [18]Song et al., 2013 [8]
Nicolaides et al., 2013 [25]Guex et al., 2013 [30]
Zimmerman et al., 2012 [11]Sparks et al., 2012 [36]Norton et al., 2012 [81]
Nicolaides et al., 2012 [8]Lau et al., 2012 [11]
Jiang et al., 2012 [16]Bianchi et al., 2012 [89]Ashoor et al., 2012 [50]Sehnert et al., 2011 [13]
Palomaki et al., 2011 [212]Ehrich et al., 2011 [39]
Chiu et al., 2011 [86]Author DR (95% CI)
0 3 6 9 12 FPR % (95% CI) (%)
0.08 (0.03 - 0.17)
FPR (95% CI) Wts (%)
100
0.00 (0.0 - 0.7) 5.80.00 (0.0 - 0.2) 13.9
0.00 (0.0 - 1.8) 2.70.00 (0.0 - 2.5) 2.00.00 (0.0 - 2.7) 1.80.00 (0.0 - 2.8) 1.80.04 (0 - 0.2) 18.00.00 (0.0 - 0.2) 14.80.00 (0.0 - 3.7) 1.30.00 (0.0 - 0.4) 9.00.00 (0.0 - 0.9) 4.90.00 (0.0 - 1.1) 4.30.00 (0.0 - 10.3) 0.5
0.20 (0.0 - 0.6) 12.60.24 (0.0 - 1.4) 4.92.06 (0.4 - 5.9) 2.0
T21: n=733 11,475 non-T21
Trisomy 21 performance cfDNA testing: meta-analysis (Gil et al, Fetal Diagn Ther, 2014)

6/5/2014
4
Wts (%)
10099.1 (98.3 - 99.6)
2.594.4 (72.7 - 100)1.2100 (63.1 - 100)3.5100 (86.3 - 100)4.1100 (88.4 - 100)1.6100 (71.5 - 100)4.9100 (90.3 - 100)11.0100 (95.6 - 100)1.2100 (63.1 - 100) 1.6100 (71.5 - 100)2.3100 (79.4 - 100)12.0100 (95.9 - 100)6.8100 (92.9 - 100)1.9100 (75.3 - 100)28.498.6 (95.9 - 99.7)5.3100 (91.0 - 100)
50 60 70 80 90100 DR % (95% CI) (%)
11.6100 (95.8 - 100)
Pooled analysis
Verweij et al., 2013 [18]Song et al., 2013 [8]
Nicolaides et al., 2013 [25]Guex et al., 2013 [30]
Zimmerman et al., 2012 [11]Sparks et al., 2012 [36]Norton et al., 2012 [81]
Nicolaides et al., 2012 [8]Lau et al., 2012 [11]
Jiang et al., 2012 [16]Bianchi et al., 2012 [89]Ashoor et al., 2012 [50]Sehnert et al., 2011 [13]
Palomaki et al., 2011 [212]Ehrich et al., 2011 [39]
Chiu et al., 2011 [86]Author DR (95% CI)
0 3 6 9 12 FPR % (95% CI) (%)
0.08 (0.03 - 0.17)
FPR (95% CI) Wts (%)
100
0.00 (0.0 - 0.7) 5.80.00 (0.0 - 0.2) 13.9
0.00 (0.0 - 1.8) 2.70.00 (0.0 - 2.5) 2.00.00 (0.0 - 2.7) 1.80.00 (0.0 - 2.8) 1.80.04 (0 - 0.2) 18.00.00 (0.0 - 0.2) 14.80.00 (0.0 - 3.7) 1.30.00 (0.0 - 0.4) 9.00.00 (0.0 - 0.9) 4.90.00 (0.0 - 1.1) 4.30.00 (0.0 - 10.3) 0.5
0.20 (0.0 - 0.6) 12.60.24 (0.0 - 1.4) 4.92.06 (0.4 - 5.9) 2.0
T21: n=733 11,475 non-T21
Trisomy 21 performance cfDNA testing: meta-analysis (Gil et al, Fetal Diagn Ther, 2014)
DR: 99.1% (98.3 - 99.6)
Wts (%)
10099.1 (98.3 - 99.6)
2.594.4 (72.7 - 100)1.2100 (63.1 - 100)3.5100 (86.3 - 100)4.1100 (88.4 - 100)1.6100 (71.5 - 100)4.9100 (90.3 - 100)11.0100 (95.6 - 100)1.2100 (63.1 - 100) 1.6100 (71.5 - 100)2.3100 (79.4 - 100)12.0100 (95.9 - 100)6.8100 (92.9 - 100)1.9100 (75.3 - 100)28.498.6 (95.9 - 99.7)5.3100 (91.0 - 100)
50 60 70 80 90100 DR % (95% CI) (%)
11.6100 (95.8 - 100)
Pooled analysis
Verweij et al., 2013 [18]Song et al., 2013 [8]
Nicolaides et al., 2013 [25]Guex et al., 2013 [30]
Zimmerman et al., 2012 [11]Sparks et al., 2012 [36]Norton et al., 2012 [81]
Nicolaides et al., 2012 [8]Lau et al., 2012 [11]
Jiang et al., 2012 [16]Bianchi et al., 2012 [89]Ashoor et al., 2012 [50]Sehnert et al., 2011 [13]
Palomaki et al., 2011 [212]Ehrich et al., 2011 [39]
Chiu et al., 2011 [86]Author DR (95% CI)
0 3 6 9 12 FPR % (95% CI) (%)
0.08 (0.03 - 0.17)
FPR (95% CI) Wts (%)
100
0.00 (0.0 - 0.7) 5.80.00 (0.0 - 0.2) 13.9
0.00 (0.0 - 1.8) 2.70.00 (0.0 - 2.5) 2.00.00 (0.0 - 2.7) 1.80.00 (0.0 - 2.8) 1.80.04 (0 - 0.2) 18.00.00 (0.0 - 0.2) 14.80.00 (0.0 - 3.7) 1.30.00 (0.0 - 0.4) 9.00.00 (0.0 - 0.9) 4.90.00 (0.0 - 1.1) 4.30.00 (0.0 - 10.3) 0.5
0.20 (0.0 - 0.6) 12.60.24 (0.0 - 1.4) 4.92.06 (0.4 - 5.9) 2.0
T21: n=733 11,475 non-T21
Trisomy 21 performance cfDNA testing: meta-analysis (Gil et al, Fetal Diagn Ther, 2014)
DR: 99.1% (98.3 - 99.6)FPR: 0.08% (0.03 - 0.17)

6/5/2014
5
NIPT: Clinical ChallengesFalse positives:• Unrecognized or vanishing twin• Placental mosaicism• Low level maternal mosaicism, esp sex chromosomal• Maternal malignancyFalse negatives:• Genetic variants• Placental mosaicismFailed results: • Increased BMI• Failure to extract adequate material• Individual variation in amount of cell free fetal DNA• Fetal aneuploidy
Published Trials of NIPT: failure rates
Trial Failure rate Detection False positive rate
Chiu et al (2011) 11/764 (1.4%) 86/86 3/146 Ehrich et al. (2011) 18/467 (3.8%) 39/39 1/410 Palomaki et al. (2011) 13/1696 (0.8%) 209/212 3/1471Bianchi et al. (2012) 30/532 (3.0%) 89/89 0/404Norton et al (2012) 148/3228 (4.6%) 81/81 1/2888Zimmermann et al (2012) 21/166 (12.6%) 11/11 0/145
All 241/6853 (3.5%) 424/427 (99.3%) 8/5319 (0.15%)
Fetal fraction of DNA and test failure
Up to 5% of samples do not provide a result
o Low fraction fetal DNA, failed sequencing, high variability in counts
o Some association with gestational age (<10 wks) o Low fetal fraction associated with maternal BMI
• 20% at >250 lbs• 50% at >350 lbs
� Low fetal fraction appears to be associated with aneuploidy� Repeating test will provide a result in some cases

6/5/2014
6
Why is NIPT not diagnostic? • Confined Placental Mosaicism• THIS IS A PLACENTAL, AND NOT A FETAL TEST
False positive False negative
NIPT: Trisomy 13 and Trisomy 18Author T13 T18
DR FPR DR FPR
Palomaki ’11 11/12 (92%) 16/1688 (0.97%) 59/59 (100%) 5/1688 (0.28%)
Bianchi ’12 11/14 (79%) 0/488 35/36 (99%) 0/460 (0%)
Norton ’12 --- --- 37/38 (97.4%) 2/2888(0.07%)Zimmermann 2/2 (100%) 0/145 3/3 (100%) 0/145
‘12Porreco ’14 14/16 (92%) 0/3322 36/39 (92%) 0/3322
Bianchi ’14 1/1 (100%) 1/899 (0.1%) 2/2 (100%) 3/1905 (0.2%)
TOTAL 39/45 (87%) 17/6542 (.03%) 172/177 (97%) 10/10,408 (0.1%)
Sex Chromosomal AneuploidyAuthor Cases:
ControlsDR FPR No result
Samango-Sprouse
16:185 92% 0 7%
Bianchi 20:532 75% 0.2% 20%Nicolaides 59:118 88% 0.8% 2.7%Total 95:835 86% 0.6% 10%

6/5/2014
7
Professional Society Opinions: ACOG; ACMG; International Society of Prenatal Diagnosis; National Society of Genetic Counselors
Common themes:
There are recognized benefits, but…• Not diagnostic
o Needs confirmationo “Advanced screening test”
• Only detects common trisomies (vs invasive testing)• Requires comprehensive genetic counseling• Should only be used in validated groups (eg high risk)• Need a low risk study before introducing into general
population screening
6/5/2014
8
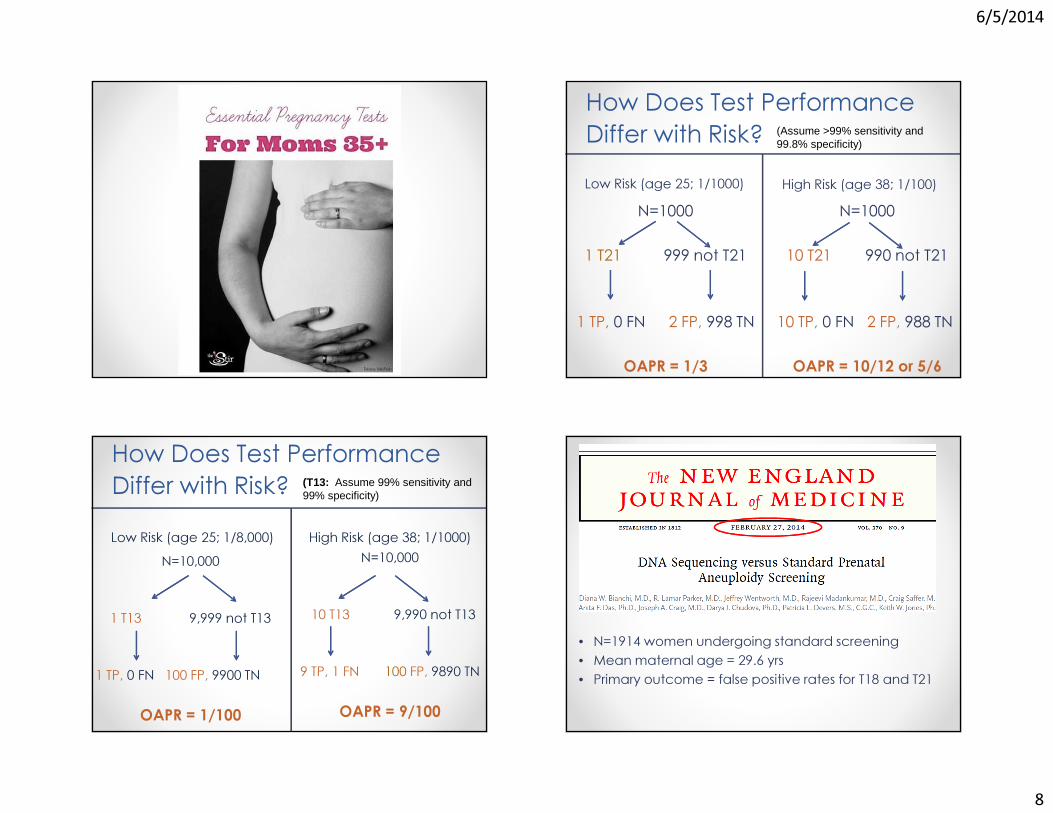
How Does Test Performance Differ with Risk? Low Risk (age 25; 1/1000) High Risk (age 38; 1/100)
N=1000
1 T21 999 not T21
1 TP, 0 FN 2 FP, 998 TN
OAPR = 1/3
N=1000
10 T21 990 not T21
10 TP, 0 FN 2 FP, 988 TN
OAPR = 10/12 or 5/6
(Assume >99% sensitivity and 99.8% specificity)
How Does Test Performance Differ with Risk? Low Risk (age 25; 1/8,000) High Risk (age 38; 1/1000)
N=10,000
1 T13 9,999 not T13
1 TP, 0 FN 100 FP, 9900 TN
OAPR = 1/100
N=10,000
10 T13 9,990 not T13
9 TP, 1 FN 100 FP, 9890 TN
OAPR = 9/100
(T13: Assume 99% sensitivity and 99% specificity)
• N=1914 women undergoing standard screening• Mean maternal age = 29.6 yrs• Primary outcome = false positive rates for T18 and T21

6/5/2014
9
cfDNA vs Standard Screening
Bianchi et al, NEJM, 2014
FPR PPVcfDNA 0.3% 45.5% p<.001Standard 3.6% 4.2%
• Only 8 aneuploidy cases in the cohort (5: T21, 2: T18, and 1: T13)
• All were detected
Where does cfDNA fit?
� Is this an outstanding screening test or an imperfect diagnostic test?� Is this best used as a secondary screening test, or as a first tier screening test?� Are we ready to abandon current screening in favor of cfDNA?
Secretary’s Advisory Committee on Genetics, Health and Society• Analytic validity: ability of test to measure particular genetic characteristics (eg DNA sequence) accurately and reliably in a given specimen
• Clinical validity: test’s accuracy in detecting the presence of, or predicting risk for, a health condition or phenotype
� Clinical utility: balance between health related benefits and harms that can ensue from a genetic test Personalized Medicine 2008

6/5/2014
10
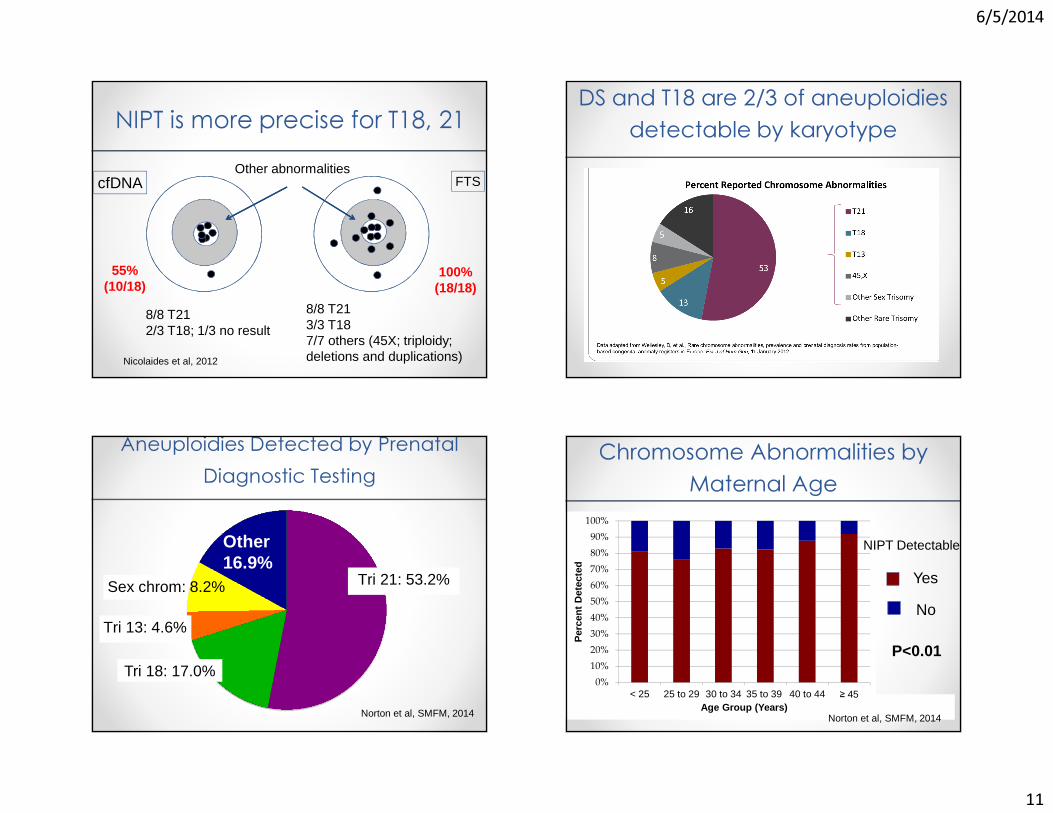
NIPT is more precise for T18, 21
cfDNA Current NT + serum screen
cfDNA Current NT + serum screen
Other abnormalities
NIPT is more precise for T18, 21 NIPT is more precise for T18, 21
cfDNA FTSOther abnormalities
8/8 T212/3 T18; 1/3 no result
8/8 T213/3 T187/7 others (45X; triploidy; deletions and duplications)Nicolaides et al, 2012
6/5/2014
11
NIPT is more precise for T18, 21
cfDNA FTSOther abnormalities
8/8 T212/3 T18; 1/3 no result
8/8 T213/3 T187/7 others (45X; triploidy; deletions and duplications)
55%(10/18)
100%(18/18)
Nicolaides et al, 2012
DS and T18 are 2/3 of aneuploidies detectable by karyotype
Aneuploidies Detected by Prenatal Diagnostic Testing
Tri 21: 53.2%Sex chrom: 8.2%
Tri 13: 4.6%
Tri 18: 17.0%
Other16.9%
Norton et al, SMFM, 2014
Chromosome Abnormalities by Maternal Age
0%10%20%30%40%50%60%70%80%90%
100%
< 25 25 to 29 30 to 34 35 to 39 40 to 44 ≥ 45
Per
cen
t D
etec
ted
Age Group (Years)
NIPT Detectable
Yes
No
P<0.01
Norton et al, SMFM, 2014

6/5/2014
12
NIPT Detection Rate
• ~83% of chromosomal abnormalities detected by current screening can potentially be identified by NIPT
• This varies by maternal ageo Lower detection in younger women (75-80%)o Greater detection in older women, but still only 90%
Disorders potentially detectable by serum screening and NIPTNIPT Current Screening
• Trisomy 21• Trisomy 18• Trisomy 13• Some sex chromosomes
• Trisomy 21• Trisomy 18• Trisomy 13• Some sex chromosomes• Triploidy• Other rare aneuploidies• Congenital heart defects• Noonan syndrome• Neural tube defects• Ventral wall defects• Congenital adrenal hypoplasia• Smith Lemli Opitz syndrome• Steroid sulfatase deficiency• Adverse OB outcomes (IUGR, PreE, PTB)
Disorder Prevalence
Common trisomies(13,18,21)
0.2%
Other chromosomeabnormalities
0.4%
Microdeletions and duplications
1.5%
Mendelian GeneticDisorders
0.4%
Congenital heart defects
0.3%
Other structural defects
3%
Adverse OB outcomes 15-20%Total ~25%
Causes of Birth Defects and Other Adverse Perinatal Outcomes:
It’s Not All Down Syndrome

6/5/2014
13
NIPT: Expanded panelsLaboratories have added other trisomies and microdeletions
• Trisomies 16 and 22• Microdeletion syndromes
o 22q (diGeorge)o 5p (cri-du-chat)o 1p36o 15q (Prader Willi)o 4p (Wolf-Hirshhorn)
What is a microdeletion?• 1MB (megabase) = 1 million base pairs• Microdeletions are 100kb to several MB• Karyotype can usually only visually detect >7-10 MB
Outcome will depend on the size & the genes involved
Microdeletion syndromesSyndrome Frequency Features22q11.2 (DiGeorge)
1/4K Varies: cardiac, palatal, immune, intellectual disability
1q36 1/5-10K Severe intellectual disability (ID), +/- obvious structural
anomaliesAngelman 1/12-20K Severe ID, seizures, speech
delayPrader-Willi 1/10-30K Obesity, ID, behavioral
problemsCri-du-chat 1/20-50K Microcephaly, ID, +/- CHDWolf-Hirshhorn
1/50K ID, seizures, +/- CL/CP

6/5/2014
14
Prevalence in 100,000 Live Births
0
20
40
60
80
100
120
140
53
NIPT for Rare Disorders
N=100,000
2 Wolf-Hirschhorn 99,998 not WHS
2 TP; 0 FN 800 FP; 99,198 TN
OAPR = 1/400
Population Risk = 1/50,000
(Wolf-Hirschhorn, 4p-: Assume 99% sensitivity and 99.2% specificity)
Chromosomal Microarray (CMA) for Prenatal Diagnosis
6/5/2014
15
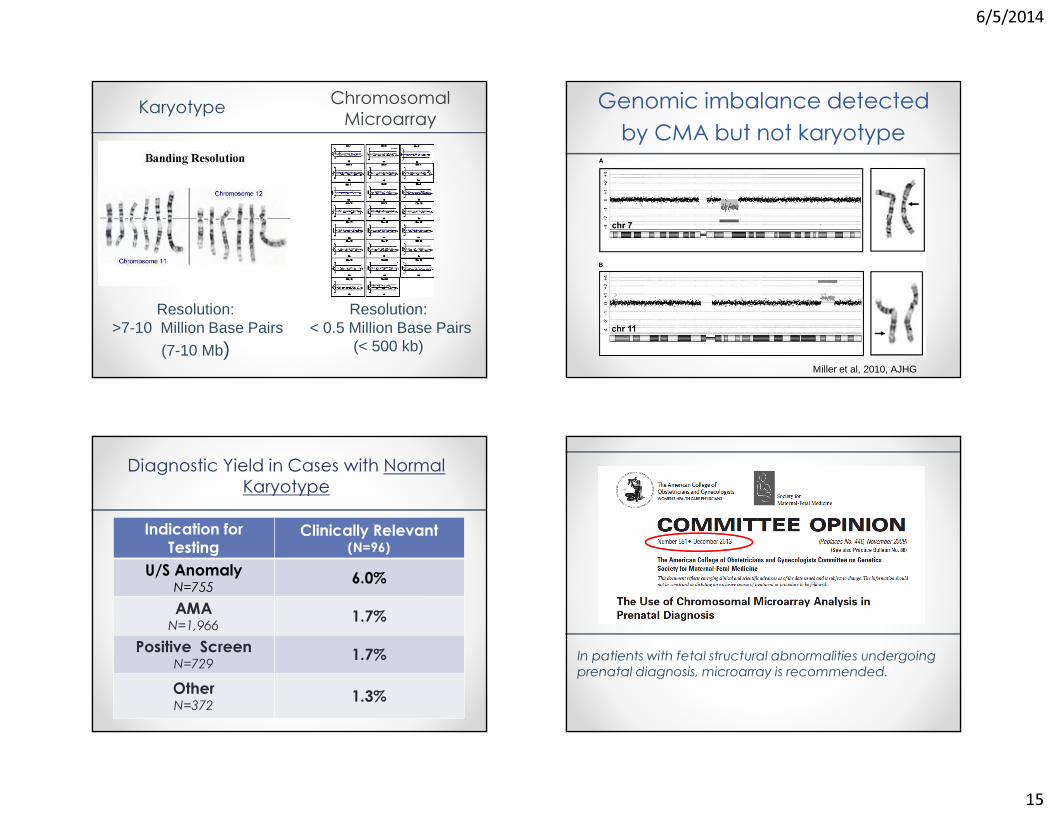
Karyotype
Resolution:>7-10 Million Base Pairs
(7-10 Mb)
Resolution:< 0.5 Million Base Pairs
(< 500 kb)
Chromosomal Microarray Genomic imbalance detected
by CMA but not karyotype
Miller et al, 2010, AJHG
Diagnostic Yield in Cases with Normal Karyotype
Indication for Testing
Clinically Relevant (N=96)
U/S AnomalyN=755 6.0%AMAN=1,966 1.7%
Positive ScreenN=729 1.7%OtherN=372 1.3%
In patients with fetal structural abnormalities undergoing prenatal diagnosis, microarray is recommended.
6/5/2014
16
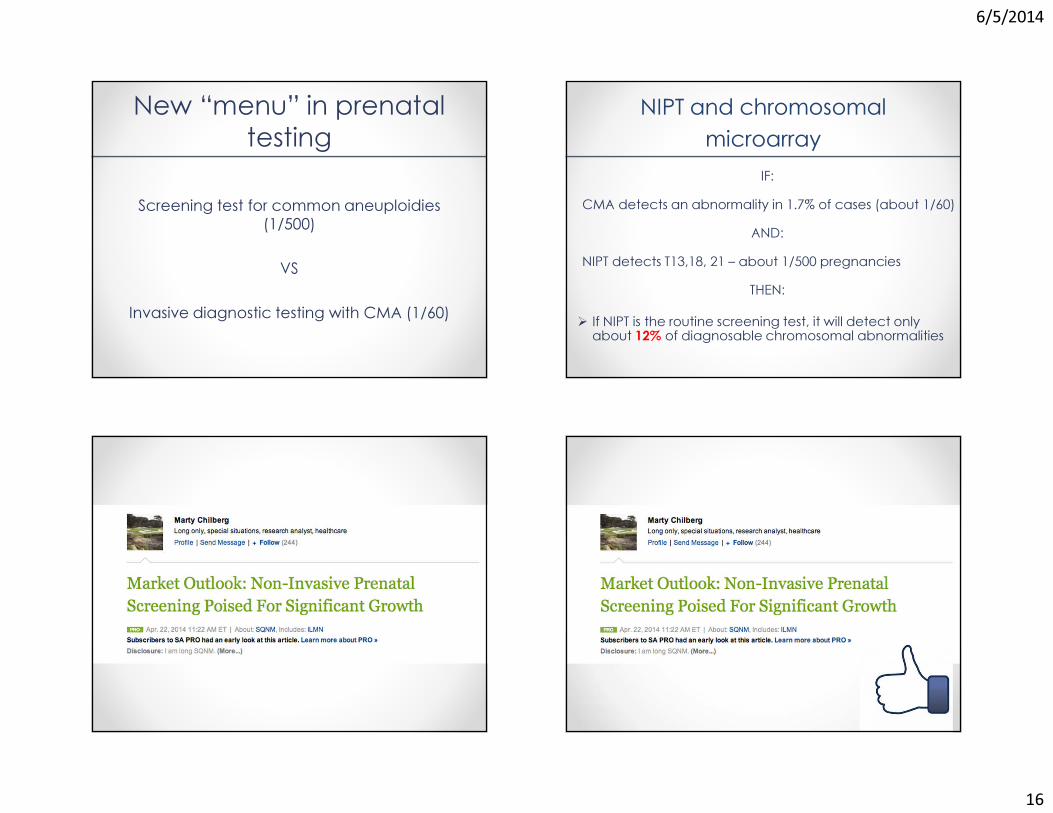
New “menu” in prenatal testing
Screening test for common aneuploidies (1/500)
VS
Invasive diagnostic testing with CMA (1/60)
NIPT and chromosomal microarray
IF:CMA detects an abnormality in 1.7% of cases (about 1/60)
AND:NIPT detects T13,18, 21 – about 1/500 pregnancies
THEN:� If NIPT is the routine screening test, it will detect only about 12% of diagnosable chromosomal abnormalities
6/5/2014
17
Cost sensitivity analysis of NIPT• Calculated marginal costs of Down syndrome detection
compared to current screening
• If NIPT costs $1000, increased cost per case detected is $3.6 million more than first trimester combined screening
� Universal NIPT screening will only become cost effective if costs drop substantially
� Contingent screening of highest risk 10-20% is recommended
Cuckle et al, Prenat Diag 2013
6/5/2014
18
Summary• cfDNA is a better test for Down syndrome than current screeningo For patients that obtain a result, a positive or negative test is near diagnostic
o Test failure indicates an increased risk for aneuploidy• These patients require counseling and follow up
• The detected disorders are fewer than with traditional screening or diagnostic testing
• Patients need to be carefully counseled about the trade-offs of lower false positives but fewer disorders tested
If only it were this simple…
Thank You!

6/5/2014
1
Rh Disease & Other Alloimmune Hemolytic Disorders in Pregnancy: A Fresh Look at an Old
ProblemLena H. Kim, MD
Assistant ProfessorMaternal-Fetal Medicine, UCSF
AIM CONFERENCE: Thursday June 5, 2014
Rh Disease: (& Other Alloimmune Hemolytic Disorders in Pregnancy)
A Fresh Look at an Old Problem
Lena H. Kim, MDAssistant Professor
Maternal-Fetal Medicine, UCSF
AIM CONFERENCE: Thursday June 5, 2014
DISCLOSURES
• I have nothing to disclose.
UCSF
OBJECTIVES
• Rh alloimmunization– Background
– Pathophysiology
– Management
– Treatment
• Other common RBC antibodies

6/5/2014
2
BACKGROUND
• Red blood cells (RBC) have hundreds of antigens
• D antigen is part of the Rhesus blood group– Rh system: D, C, c, E, e, G
• “Rh(-)” is a misnomer– Rh(-) = D(-)
BACKGROUND
• Prevalence of Rh(-)– Basques 30-35%
– Caucasians 15%
– African 4-6%
– Asian <1%
• Prevalence of Rh alloimmunization– 6.8/1000 live births in the U.S. 2003
Moise KJ. Obstet Gynecol 2008;112:164
PATHOPHYSIOLOGY
• Rh(-) mother pregnant with Rh(+) fetus
• Maternal exposure to fetal RBCs
• Maternal B-cells recognize D antigen
• Short-lived IgM response
• Next pregnancy memory B-cells– Rapid development of anti-D IgG antibodies
– IgG antibodies cross the placenta
– Fetal hemolytic anemia
PATHOPHYSIOLOGY
• Possible etiologies of alloimmunization– Fetomaternal hemorrhage
– Blood transfusion error: D antigen variants • T&S Rh(-) but may weakly express D
• Weak D also called Du antigen
• Can cause anti-D antibody production in Rh(-) recipient

6/5/2014
3
PATHOPHYSIOLOGY
• Etiology of unexplained alloimmunization – Unrecognized early miscarriages
• Fetal RBCs express D antigen by day 38 (7w3d)
– Grandmother theory• Rh(+) mother pregnant with female Rh(-) fetus• Mother’s RBCs enter daughter’s circulation at birth• Rh(-) baby develops anti-D antibodies • Anti-D antibodies at 1st T&S in her 1st pregnancy
PATHOPHYSIOLOGY
• Variable amounts of exposure � antibodies
• 1960s study of exposed Rh(-) male prisoners– As little as 0.1 mL � antibodies
– 2 exposures 10 mL + 5 mL � 70% antibodies
– As much a 450 mL � only 80% antibodies
• Slow antibody response 5-15 weeks– 1st pregnancy usually not at risk of fetal anemia
Zipursky & Israels. Can Med Assoc J. 1967;97(21):1245Pollack et al. Transfusion. 1971;11(6):333
PATHOPHYSIOLOGY
• Fetomaternal hemorrhage common
• Maternal presence of 0.01 mL fetal RBCs– 1st trimester 3%
– 2nd trimester 12%
– 3rd trimester 46%
Bowman et al. Fetomaternal transplacental hemorrhage during pregnancy and after delivery. Vox Sang 1986;51:117-21.
PATHOPHYSIOLOGY
• Transplacental passage of maternal antibodies– Anti-D IgG antibodies
• Antibodies opsonize fetal RBCs– Fetal RBC phagocytosis by splenic macrophages
• Hemolytic disease of the fetus or newborn– HDN or HDFN
• Fetal immune hydrops– Erythroblastosis fetalis
• IUFD or neonatal morbidity & mortality
6/5/2014
4
MANAGEMENT
• Prevention– Identify Rh(-) women
• T&S at 1st prenatal visit
• Earlier T&S if bleeding and pregnant
• Consider T&S at preconception counseling visits
– Educate Rh(-) women about Rhogam
– Father of the baby Rh testing• Rh positive � 60% heterozygous
MANAGEMENT
• Rhogam (anti-D immune globulin)– Pooled plasma with high anti-D antibody titer
• Male volunteers purposely sensitized
– 300mcg standard dose• Enough for 15mL fetal RBCs = 30mL whole blood• Covers 10% of average term newborn’s total blood volume
– “Mini-rhogam” 50mcg• 2.5mL fetal RBCs
– Lasts ~12 weeks• 15-20% still have low titer <1:4 at term• Anti-D antibody detection as long as ~26 weeks later
MANAGEMENT
• Rhogam routine dosing in the United States– 300mcg
• 50mcg up through 12 weeks GA
– Recheck antibody screen prior to administration– 28 weeks GA– Postpartum within 72hr of delivery
• Up to 28 days later might still efficacious
• United Kingdom & Canada routine dosing– 100mcg– 28 + 34 weeks GA
Fung et al. J Obstet Gynaecol Can 2003;25(9):765
MANAGEMENT• Rhogam indicated if risk of fetomaternal hemorrhage
– Pregnancy loss: SAB, TAB, ectopic pregnancy
– Threatened abortion: vaginal bleeding
– Invasive procedures• CVS, amniocentesis, MFPR, fetal surgery
– Placental abruption
– Bleeding previa
– Trauma• MVA, ECV
– IUFD

6/5/2014
5
MANAGEMENT
• Rhogam mechanism of action– Anti-D prophylaxis: passive anti-D IgG
– Epitope masking• Fetal RBC D antigens covered by passive anti-D IgG
• Fetal RBCs cleared/destroyed without alloimmunization
• INCOMPLETE epitope masking
– Down-regulation of antigen-specific B cells
MANAGEMENT
• Four rhesus immune globulin brands– RhoGAM® (Ortho-Clinical Diagnostics, NY)
• IM due to IgA contaminants
– HyperRHO® (Talecris, NC)• IM due to IgA contaminants
– Rhophlac® (ABO Pharmaceuticals, CA)• IV or IM (IgG only)
– Win-Rho-SDF® (Cangene Corporation, Canada)• IV or IM (IgG only)
– Thimerosal free
MANAGEMENT
• Before the standard use of rhogam:– High alloimmunization rates
• 2 non-compatible pregnancies � 16%
• After standard use of postpartum rhogam:– Lowered alloimmunization rate � 2%
• And 3rd trimester + Postpartum rhogam:– Even lower alloimmunization rate � 0.1%
MANAGEMENT
• Testing for fetomaternal hemorrhage– Rosette test
• Qualitative � +/- result
– Kleihauer-Betke • Quantitative
• Volume of hemorrhage
• % fetal blood cells x 50

6/5/2014
6
MANAGEMENT - OLD
• Maternal anti-D antibodies � Fetal Rh status– Father of the baby (FOB) Rh status
• Genotype if Rh(+)
• 60% chance heterozygote
• If heterozygote, 50% chance fetus will be Rh(-)
– Amniocentesis if FOB heterozygous or unknown
– Serial anti-D titers q4 wks if fetus Rh(+) or ?• Increase titers to q2 weeks after 24 wks GA
– Laboratory critical titer >1:8 – 1:32
AUDIENCE RESPONSE QUESTION
Maternal serum cell free fetal DNA (NIPT) is useful in the management of Rh alloimmunizationbecause:
Y ou s h
o u ld r u
l . . .
F e ta l g
e n de r a
. . .
N I PT c a
n de t e
c . . .
42%52%
6%
A. You should rule out aneuploidy before considering treatment of fetal anemia
B. Fetal gender affects prognosis
C. NIPT can detect fetal Rh status
MANAGEMENT - NEW
• Maternal anti-D antibodies � Fetal Rh status– Father of the baby (FOB) Rh status
• Genotype if Rh(+)• 60% chance heterozygote• If heterozygote, 50% chance fetus will be Rh(-)
– Amniocentesis if FOB heterozygous or unknown
–Maternal serum cell free fetal DNA– Serial anti-D titers q4 weeks if fetus Rh(+)
• Increase titers to q2 weeks after 24 wks GA
– Laboratory critical titer >1:8 – 1:32
MANAGEMENT - NEW
• Maternal serum cell free fetal DNA– Rh D gene on short arm chromosome 1
– Apoptosis of placental trophoblasts� fetal DNA in maternal system
– Europe using cffDNA routinely for fetal Rh
– Avoid unnecessary rhogam in ~40% of Rh(-)♀– 99.3 – 100% sensitivity
Clausen et al. Transfusion 2012;52(4):752Wikman et al. Obstet Gynecol 2012;120(2Pt1):227

6/5/2014
7
MANAGEMENT - OLD
• Rise in titers or previously affected pregnancy– Referral to MFM for co-management
• Antenatal testing starting at 32 weeks GA
• Amniocentesis for ∆OD450– Bilirubin levels in the amniotic fluid
– Liley curve � Queenan curve
– Predict severity of fetal anemia
Queenan et al. Am J Obstet Gynecol 1993;168:1370
AUDIENCE RESPONSE QUESTION
Moderate to severe fetal anemia can be detected using ultrasound doppler of the:
U mb i l
i c al a r
t e .. .
U mb i l
i c al v e
i n D u
c t us v
e n os u s
Mi d d
l e ce r e
b r a. . .
21%
67%
1%11%
A. Umbilical artery
B. Umbilical vein
C. Ductus venosus
D. Middle cerebral artery
MANAGEMENT - NEW
• Rise in titers or previously affected pregnancy– Referral to MFM for co-management
• Antenatal testing if viable gestational age
• Amniocentesis for ∆OD450– Liley curves to predict severity of fetal anemia
• Middle cerebral artery peak systolic velocity (MCA PSV)
MANAGEMENT - NEW
• MCA PSV– Non-invasive screening for severe fetal anemia
– Weekly ultrasound with doppler > 18 wks GA
– Avoids ~50% of unnecessary PUBS
– Detection of moderate - severe fetal anemia• MCA PSV ≥ 1.5 MoM
• Sensitivity 100%
• False positive rate 12%
• Not validated for >35 weeks gestation
Mari et al. NEJM 2000;342:9-14
6/5/2014
8
TREATMENT
• Percutaneous umbilical blood sampling (PUBS)– Cordocentesis or funipuncture
– Confirm severe anemia
– Calculate ideal transfusion amount
– 1-2% procedure-related rate of fetal death
• Intrauterine transfusion (IUT)
TREATMENT
• Intraperitoneal transfusion – Sir William Liley 1963
• IUT possible with improved ultrasound – Perinatal survival rates ~90%
• Lower if hydrops, ~78%
– Long-term normal neurologic outcomes >90%
– High-risk for needing serial transfusions until 3 months of life due to persistent maternal antibodies
vanKamp et al. Am J Obstet Gynecol 2005;192:171
TREATMENT
• Late preterm/early term delivery– MCA PSV stays <1.5 MoM � 38 week delivery
– Fetal anemia + >35 wks GA � delivery
• Antepartum phenobarbital in certain cases– Maturation of the fetal liver for bilirubin clearance
TREATMENT
• Investigational therapy for women with RH disease & prior severe early fetal anemia– Maternal plasmapheresis
• Single volume plasmapheresis QOD x 3 at 12wks GA
– IVIG following final plasmapheresis• 1g/kg slow infusions 2 days in a row• 1g/kg slow infusion every week until 20wks GA
Ruma et al. Am J Obstet Gynecol 2007;196:138.e1

6/5/2014
9
TREATMENT
• Preconception counseling
• Prevent subsequent pregnancy with HDFN– Future conception with Rh(-) donor sperm – IVF with preimplantation genetic diagnosis
• Father of the baby Rh D heterozygote
– Gestational surrogate
TREATMENT
• Future prevention of severe fetal anemia– Immunization to paternal leukocytes
• Rabbit model
– Ameliorate anti-D response in subsequent pregnancy• Intranasal spray RhD peptides
• Transgenic mouse model
Whitecar et al. Am J Obstet Gynecol 2002;187:977Hall et al. Blood 2005;105:2175
AUDIENCE RESPONSE QUESTION
The number of other non-D RBC antigens that can cause HDFN is:
1
2 -5
6 -1 0 > 10
5%
28%31%
36%A. 1
B. 2-5
C. 6-10
D. >10
OTHER BLOOD GROUP SYSTEMS
• Non-D Rh– E, C, c Mild to severe HDFN
• Lewis & I – Lea and Leb No risk (IgM), routine care– I No risk (IgM), routine care
• Kell– K Mild to severe HDFN– k, Ko, Kpa+b, Jsa+b Low risk, routine care– Transfused blood not cross-matched for Kell
Weinstein L. Clin Obstet Gynecol 1982;25:321

6/5/2014
10
OTHER BLOOD GROUP SYSTEMS
• Duffy– Fya Mild to severe– Fyb, By3 Low risk
• Kidd– Jka Mild to severe– Jkb, Jk3 Low risk
• MNSs– M, S, s, U, Mia Mild to severe– N Low risk
Weinstein L. Clin Obstet Gynecol 1982;25:321
OTHER BLOOD GROUP SYSTEMS
• Due to Rhogam, HDFN due to non-D antibodies↑• ~2% of obstetric patients have non-D antibodies
• Management of women with non-D antibodies– Determine if the antibodies can cause HDFN
– If yes, same as Rh alloimmunization
– Exception is anti-K• Maternal titers do not correlate with risk of HDFN
• If non-D antibodies detected & Rh(-)– Still a Rhogam candidate
THANK YOU
• UCSF MFM Division Director– Dr. Mari-Paule Thiet
• UCSF PUBS/IUT mentors– Dr. Julian T. Parer
– Dr. Larry Rand
• Alloimmunization expert– Dr. Kenneth J. Moise
REFERENCES• ACOG Practice Bulletin 75, August 2006• Bowman et al. Fetomaternal transplacental hemorrhage during pregnancy and after
delivery. Vox Sang 1986;51:117-21. • Clausen et al. Transfusion 2012;52(4):752• Fung et al. J Obstet Gynaecol Can 2003;25(9):765• Hall et al. Blood 2005;105:2175• Mari et al. NEJM 2000;342:9-14• Moise KJ. Obstet Gynecol 2008;112:164• Pollack et al. Transfusion 1971;11(6):333• Queenan et al. Am J Obstet Gynecol 1993;168:1370• Ruma et al. Am J Obstet Gynecol 2007;196:138.e1• vanKamp et al. Am J Obstet Gynecol 2005;192:171• Weinstein L. Clin Obstet Gynecol 1982;25:321• Whitecar et al. Am J Obstet Gynecol 2002;187:977• Wikman et al. Obstet Gynecol 2012;120(2Pt1):227• Zipursky & Israels. Can Med Assoc J 1967;97(21):1245

6/5/2014
1
The Obese Patient During Pregnancy & Labor
Naomi E. Stotland, MDAssociate Professor
Dept. of Obstetrics, Gynecology, and Reproductive Sciences
University of California, San FranciscoSan Francisco General Hospital
No disclosures
Obesity Classification• Class I Obesity – BMI 30 – 34.9
5’4’’ woman who weighs 175 lbs has BMI = 30• Class II Obesity – BMI 35 – 39.9
5’4’’ woman who weighs 205 lbs has BMI = 35• Class III Obesity – BMI ≥ 40
5’4’’ woman who weighs 235 lbs has BMI = 40Don’t “eyeball it” – calculate BMI and write it on the chart
Limitations of BMI• Does not account for body
composition• Muscle weighs more than fat• Isn’t a great proxy for
metabolic health
6/5/2014
2
Etiology of Obesity
Environment
Genetics & Fetal Programming
Behavior/
Psychology
Animal studies have shown similarities in the way the brain responds to classic drugs of abuse (e.g., morphine, alcohol, nicotine) and to sugar (Avena, Rada, and Hoebel 2008).
Obesity is associated with metabolic dysfunction
Obesity
Chronic inflammation
HTN, DM, liver disease
-Some obese have little to no metabolic dysfunction-Many normal weight people have metabolic dysfunction
Early Pregnancy Concerns• Spontaneous abortion• Fetal anomalies, esp neural tube
defects• Difficult U/S

6/5/2014
3
Antepartum Complications• GDM and DM2• Chronic hypertension• Postterm pregnancy• Failed ECV
Intrapartum Complications• Prolonged labor• Lower likelihood of VBAC success• Preeclampsia• Higher rates of cesarean delivery• Anesthetic complications• Macrosomia and shoulder dystocia• Stillbirth
Postpartum Complications• Longer hospital stays
• Infections–Wound infection and endometritis
• Lower rates of breastfeeding
Long-term Risks to Offspring• Obesity• Cardiometabolic diseases • Autism/developmental delay

6/5/2014
4
Fetal Programming• Animal studies support the role of diet during
pregnancy on body composition and metabolism after birth
• Improving diet during pregnancy may have long-term benefits for offspring
Prenatal Care for Obese Women
At first prenatal visit• Screen for DM2 (repeat at 24 wks if neg)• Measure and record BMI in chart• Review weight gain goals and strategies with
patient• Discuss risks especially re: weight gain• If concern for CHTN: baseline Cr, 24hour urine,
LFTs
Fetal growth• Obese women at increased risk for both SGA
and LGA• If fundus easily palpated, can follow fundal
height• If fundus not easily palpated, consider serial
ultrasound for fetal growth

6/5/2014
5
Antenatal Testing• Increased stillbirth risk in obese women• No RCT to support or refute benefit of
antenatal testing, but many recommend it• At SFGH we start weekly NST/AFI at 32 weeks
for women with BMI of 40 or greater
Intrapartum Managment
When to deliver?• No evidence to support nor refute, but we
consider induction of labor at 39-40 weeks in women with BMI ≥ 40, especially if cervix is favorable
• Elevated risk of IUFDIf induction is not progressing after 24+ hours and maternal/fetal status reassuring (and intact membranes), will stop induction and either try again in a few days or wait for spontaneous labor
On admission to L&D• Consult anesthesia on admission• Place internal monitors if needed• Assess IV access• Prepare for shoulder dystocia, especially if
GDM/DM2 or suspected macrosomia• Staffing considerations

6/5/2014
6
Cesarean in the morbidly obese patient
6 weeks post–opTransverse skin incision under the panniculus
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3289484/?report=reader#!po=19.2308
Preparing for cesarean• 20-degree Left lateral tilt is even more important
because of the added weight of the abdominal pannus, but,
• The tilt puts the midline far from the operating surgeon and is ergonomically challenging
• Retraction of the pannus with Montgomery straps and/or extra surgical assistants
• Retraction of the extremely large pannus can cause hypotension, difficult ventilation, and fetal compromise
Cesarean – type of incision and closure?
• No randomized trial of incision type; no evidence that vertical skin is preferable – choose based on surgeon’s preference
• When pannus is massive, a supra-umbilical incision may be considered – transverse or vertical
• Some evidence that vertical incisions are associated with more pain and poorer healing, but study results are mixed
• Vertical incisions may increase the risk of classical uterine incision if access to LUS is limited
6/5/2014
7
Cesarean – type of incision and closure?
• Pre-op antibiotics – at least 2g cefazolin IV• Subcutaneous sutures decrease risk of seroma, but
not good evidence in BMI ≥ 50• Drains not shown to provide benefit and may
increase infection• Staple vs. suture – ongoing clinical trial in obese
women, but current evidence suggests some benefit of suture over staples
• If staples uses, delayed removal may improve outcomes
Prevent difficult extraction of infant• Make all incisions larger than usual – skin,
fascia, and uterus• Have vacuum available since fundal pressure
may be difficult to apply
DVT Prophylaxis?• Mechanical thromboprophylaxis (pneumatic
compression) SCDs pre and post-operatively• Early ambulation
• If BMI>40 consider unfractionated heparin 5000-10000 u q 8-12 hrs
No well designed RTCs to assess risk reduction therefore recommendations is expert opinion
Emergency Cesarean BMI ≥ 40Need to plan for extra time to • move patient to OR table• induce anesthesia, and • do the surgeryAll will take longer, so have to move earlier to C/S especially for fetal indications

6/5/2014
8
Length of labor• First stage of labor takes longer among obese
women• As long as maternal and fetal status
reassuring, may tolerate a slower labor curve in obese patient
• Second stage length NOT associated with BMI (nullips)
Why are cesarean rates so high among obese women?
• Much of this may be iatrogenic • Obese women should be given a chance for a
safe vaginal birth• Allow labor to take longer• Provide continuous labor support (doulas)• Obesity alone (BMI of 30-39/Classes 1-2) may
not “risk a woman out” for midwifery or birth center delivery
Previous C-section:Balancing Risks
Consider patient preferences and values
Advantages of vaginal birthVS.
Risks of unplanned c-sectionROCK
HARD PLACE
Weight Gain During Pregnancy for Obese Women

6/5/2014
9
The IOM Report and GuidelinesIOM Recommendations for Weight Gain in Pregnancy 20 09
Pre-pregnancy BMI (kg/m2)
IOM Recommended Gestational Weight Gain
(kg / lbs)
<18.5 (Underweight) 12.5-18 / 28-40
18.5 – 24.9 (Normal) 11.5-16 / 25-35
25.0 - 29.9 (Overweight) 7-11.5 / 15-25
≥30.0 (Obese) 5-9 / 11-20
Combined effects of obesity & excessive weight gain
• Preeclampsia, macrosomia, and cesarean birth increase with increasing weight gain among obese women
• Some evidence that weight gain <11 lbs decreases these risks, but may also increase risk of SGA
Comparison of weight gain by BMI category between PRAMS 2002-2003, and new IOM guidelines
Does Prenatal Advice on Weight Gain Matter?
• Receiving correct advice about weight gain was associated with actual weight gain within guidelines;
• Receiving no advice about weight gain was associated with gain outside guidelines;
• About a third of women report receiving no advice about how much weight to gain.
Cogswell et al. Obstet Gynecol 1999.Stotland et al. Obstet Gynecol 2005.

6/5/2014
10
Barriers to weight gain counseling
Insufficient nutrition training
Belief that counseling is ineffective
Concern about sensitivity of topic
normalize
CME, dieticians
Literature
What do patients want?
What do patients want?• Women were advised to gain too much weight
or given no advice;
• Providers perceived as being unconcerned about excessive gain;
• Women desire and value weight gain advice from providers
Preliminary Outcome Data (n=93)The Healthy Moms Trial
Vesco et al, Kaiser Portland Presented at The Obesity Society 2012
� DASH diet, caloric restriction, weekly meetings
� Goal: maintain weight within 3%
� Mean pre-pregnancy BMI (36.2 kg/m2)

6/5/2014
11
Preliminary Outcome Data (n=93)The Healthy Moms Trial
Vesco et al, Kaiser Portland Presented at The Obesity Society 2012
� Gain of ≤3% in 28% vs. 10%(OR=3.7, 95% CI [1.1,12.6], p=.04).
� Average gain 4.5 kg vs 8.3 difference=3.7 kg , 95% CI [2.0, 12.2], p<.001.
Summary - Weight Gain Intervention Studies
• Small sample sizes – unknown if impact on outcomes other than weight (GDM, c-section, macrosomia)
• Not powered to exclude possibility of harm from weight restriction
• Diet and exercise can reduce weight gain among obese women
• More intensive (and expensive) interventions may be necessary to see an impact
MANY studies ongoing… Bariatric Surgery & Pregnancy• 220,000 procedures in 2008, ½ in
reproductive-age women• Fewer obesity-related pregnancy
complications post-surgery• Risks of vitamin deficiencies: iron, vitamin
B12, calcium, folic acid, vitamin D

6/5/2014
12
Healthy Diet for Pregnancy: EnhanceComplex Carbohydrates
LegumesSteel cut OatsWhole Grains
FruitsVegetables, especially dark green
Increase fruits and vegetablesIncrease whole grains/fiber
Dietary Advice• Whole-foods diet, high in fiber and nutrients• Reduce or cut out high-calorie, highly-processed, nutrient-
poor foods• Cut out high-calorie beverages including juice• Replace refined grains with whole grains• Replace saturated fat/trans fat with plant-based and fish-
based fats (nuts, avocados, olive oil, salmon)• Legumes – beans, lentils• Supplements: Folic acid, Vitamin D – obese women are
especially deficient in these• Allow patient to choose goal, make a plan, write it down
Exercise/physical activity• At least 30 min/day 5 days a week• Base it on prior level of activity• Walking• Group activities
Summary• Most obese women are gaining too much weight• More research needed to establish safety of minimal
weight gain / weight loss during pregnancy • Excessive weight gain compounds risks of obesity• On L&D, be patient but be prepared!• We can improve outcomes among obese pregnant
women w/ lifestyle interventions (counseling, diet, exercise)

6/5/2014
1
The Continuing Controversy Over Screening for Gestational Diabetes
Kirsten E. Salmeen, MDAssistant Professor
Obstetrics, Gynecology & Reproductive SciencesMaternal-Fetal Medicine
I have nothing to disclose.
GDM & ControversyThe Continuing Controversy Over
Screening for Gestational Diabetes
• The nature of screening tests• Why screening for GDM matters• The major controversies• Possible sources of those controversies• What I think you should do

6/5/2014
2
The Nature of Screening Tests
• Screening is the identification of an asymptomatic disease, harmful condition or risk factor.
• When deciding how to screen, the following must be considered:- Burden of suffering caused by the condition- Therapeutic interventions available - Performance of available screening tests
Fletcher et al. Clinical Epidemiology: The Essentials, 5th Ed, Lippincott Williams & Wilkins 2013
How great is the burden of suffering caused by GDM?
Why should we be concerned with GDM at all?
Overall % RR/ORMacrosomia 20 RR ~1.4
Pre-Eclampsia 15 RR ~1.7Cesarean Section Varies RR ~ 1.2Shoulder Dystocia 3-5 OR ~ 1.2
IUFD ~ 0.05 RR ~ 2
HAPO Study Cooperative Research Group. N Engl J Med. 2008;358(19):1991-2002.Schmidt M et al. Diabetes Care. 2001;24(7):1151-5.Wendland E et al. BMC Pregnancy Childbirth. 2012;31(12):23-36.
Blinded study of ~25,000 women at 15 centers, 9 countriesPrimary predictor: Levels of hyperglycemiaPrimary outcomes: Birth weight > 90%ile, primary CD,
neonatal hypoglycemia, cord-blood C-peptide level
HAPO Study Cooperative Research Group. N Engl J Med. 2008;358(19):1991-2002.

6/5/2014
3
HAPO ResultsIncreasing maternal glycemia is associated with increased risk
of maternal and fetal complications.
HAPO Study Cooperative Research Group. N Engl J Med. 2008;358(19):1991-2002.
How good is the therapeutic intervention for GDM?
Intervention Group N = 485
(%)
Control Group N = 473
(%)Relative Risk p-value
NICU Admission 9 11.6 0.77 (0.51 – 1.18) 0.19
Macrosomia 5.9 14.3 0.41 (0.26 – 0.66) < 0.001Neonatal
Hypoglycemia 5.3 6.8 0.77 (0.44 – 1.36) 0.32
Shoulder Dystocia 1.5 4.0 0.37 (0.14 – 0.97) 0.02
Cesarean Delivery 26.9 33.8 0.79 (0.64 – 0.99) 0.02Preeclampsia or
GHTN 8.6 13.6 0.63 (0.42 – 0.96) 0.01
Landon – Trial of Treatment for GDM
Landon et al. N Eng J Med. 2009;361:1339-48.
Crowther – Trial of Treatment for GDM
Crowther et al. N Engl J Med. 2005;352:2477-86.
Intervention Group N= 490
(%)
Routine Care N= 510
(%)
Adjusted RR or Treatment Effect
Adjusted p-value
*Any serious perinatalcomplication 1 4 0.33 (0.14 – 0.75) 0.01
Admission to NICU 71 61 1.13 (1.03 – 1.23) 0.04
Macrosomia 10 21 0.47 (0.34 – 0.64) < 0.001
Neonatal hypoglycemia 7 5 1.42 (0.87 – 2.32) 0.16
Preeclampsia 12 18 0.7 (0.51 – 0.95) 0.02
Cesarean Delivery 31 32 0.97 (0.81 – 1.16) 0.73* One or more of: death, shoulder dystocia, bone fracture, nerve palsy

6/5/2014
4
Increasing maternal glycemia is associated with worse perinatal outcomes.
Treatment improves outcomes.
What’s the controversy?!
How good are the screening tests for GDM?
(How good is too good?)
GDM Controversies
One-Step Testing v. Two-Step TestingCarpenter Coustan v. National Diabetes Data Group
Universal Screening v. Risk-Based ScreeningEarly Screening v. 24-28 Week ScreeningHemoglobin A1c v. No Hemoglobin A1c
Blood sugar testing for 1 abnormal value v. No testing
GDM Controversies
One-Step Testing v. Two-Step TestingCarpenter Coustan v. National Diabetes Data Group
Universal Screening v. Risk-Based ScreeningEarly Screening v. 24-28 Week ScreeningHemoglobin A1c v. No Hemoglobin A1c
Blood sugar testing for 1 abnormal value v. No testing

6/5/2014
5
One-Step vs. Two-Step Testing
Two-StepStep 1: Non-Fasting, 50 g, 1 hr serum glucose measurement
≥ 130/140 mg/dL� Step 2Step 2: Fasting, 100 g, 3 hr glucose test
2+ abnormal values � GDM
GDM prevalence ~ 5-10%
One-StepFasting, 75 g, 1 & 2 hr serum glucose measurement
1+ abnormal value � GDM
GDM prevalence ~ 20%
GDM Controversies
One-Step Testing v. Two-Step TestingCarpenter Coustan v. National Diabetes Data Group
Universal Screening v. Risk-Based ScreeningEarly Screening v. 24-28 Week ScreeningHemoglobin A1c v. No Hemoglobin A1c
Blood sugar testing for 1 abnormal value v. No testing
Carpenter-Coustan v. NDDGFasting (mg/dL)
1 hr(mg/dL)
2 hr(mg/dL)
3 hr(mg/dL)
GDM Prevalence
National Diabetes Data
Group105 190 165 145 3-4%
Carpenter-CoustanCriteria
95 180 155 140 5-7%
GDM Controversies
One-Step Testing v. Two-Step TestingCarpenter Coustan v. National Diabetes Data Group
Universal Screening v. Risk-Based ScreeningEarly Screening v. 24-28 Week ScreeningHemoglobin A1c v. No Hemoglobin A1c
Blood sugar testing for 1 abnormal value v. No testing
6/5/2014
6
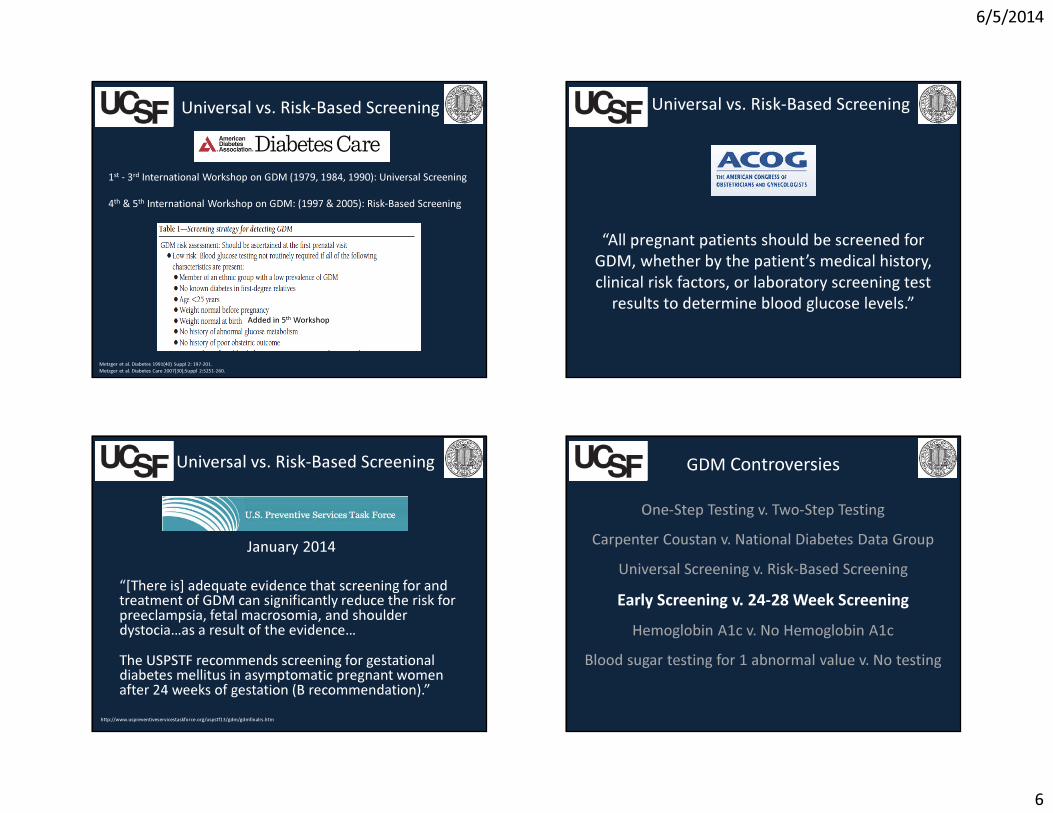
Universal vs. Risk-Based Screening
1st - 3rd International Workshop on GDM (1979, 1984, 1990): Universal Screening
4th & 5th International Workshop on GDM: (1997 & 2005): Risk-Based Screening
Metzger et al. Diabetes 1991(40) Suppl 2: 197-201.Metzger et al. Diabetes Care 2007(30);Suppl 2:S251-260.
Added in 5th Workshop
“All pregnant patients should be screened for GDM, whether by the patient’s medical history, clinical risk factors, or laboratory screening test
results to determine blood glucose levels.”
Universal vs. Risk-Based Screening
Universal vs. Risk-Based Screening
January 2014
“[There is] adequate evidence that screening for and treatment of GDM can significantly reduce the risk for preeclampsia, fetal macrosomia, and shoulder dystocia…as a result of the evidence…The USPSTF recommends screening for gestational diabetes mellitus in asymptomatic pregnant women after 24 weeks of gestation (B recommendation).”
http://www.uspreventiveservicestaskforce.org/uspstf13/gdm/gdmfinalrs.htm
GDM Controversies
One-Step Testing v. Two-Step TestingCarpenter Coustan v. National Diabetes Data Group
Universal Screening v. Risk-Based ScreeningEarly Screening v. 24-28 Week Screening
Hemoglobin A1c v. No Hemoglobin A1cBlood sugar testing for 1 abnormal value v. No testing

6/5/2014
7
Early Screening• Detecting women with pre-existing diabetes
or glucose intolerance (pre-diabetes)
• ACOG: History of GDM, known impaired glucose metabolism, obesity
• ADA: Severe obesity, strong family history, personal history of GDM, impaired glucose metabolism, glucosuria
January 2014
“The USPSTF concludes that the current evidence is insufficient to assess the balance of
benefits and harms of screening for GDM in asymptomatic pregnant women before 24
weeks of gestation.”
http://www.uspreventiveservicestaskforce.org/uspstf13/gdm/gdmfinalrs.htm
GDM Controversies
One-Step Testing v. Two-Step TestingCarpenter Coustan v. National Diabetes Data Group
Universal Screening v. Risk-Based ScreeningEarly Screening v. 24-28 Week Screening
Hemoglobin A1c v. No Hemoglobin A1cBlood sugar testing for 1 abnormal value v. No testing
Diagnosing Type 2 DM:
http://www.diabetes.org/diabetes-basics/diagnosis/?loc=DropDownDB-diagnosisO’Connor et al. Clin Chem Lab Med 2012;50(5):905-9.
A1c ≥ 6.5 � DM2A1c 5.7 – 6.5 � Glucose IntoleranceA1c < 5.7 � Normal
Non-Pregnant 1st Trimester 2nd
Trimester3rd
Trimester
HbA1c % 4.8 – 5.5 (5.2)
4.3 – 5.4 (5.0)
4.4 – 5.4 (4.9)
4.7 – 5.7 (5.1)
Average HbA1c Values Non-Diabetic Women
Hemoglobin A1c

6/5/2014
8
GDM Controversies
One-Step Testing v. Two-Step TestingCarpenter Coustan v. National Diabetes Data Group
Universal Screening v. Risk-Based ScreeningEarly Screening v. 24-28 Week ScreeningHemoglobin A1c v. No Hemoglobin A1c
Blood sugar testing for 1 abnormal value v. No testing
Pregnancy Outcomes for Women with 1 Abnormal Value on 3 hour
McLaughlin et al AJOG 2006;194:e16-19.
Treatment for Patients With 1 Abnormal Value
Fassett et al. AJOG 2007;196:597.e1-597.e4
Sources of Controversy

6/5/2014
9
More Sensitive, Less SpecificFewer women with disease test positive
Fewer women WITHOUT disease test positive
Missing a clinically important diagnosis
More women with disease test positiveMore women WITHOUT disease test positive
Diagnosing women who might not actually have clinically important disease
Sensitivity v Specificity
Less Sensitive, More Specific
One-Step Two-StepCarpenter Coustan National Diabetes Data GroupUniversal Screening Risk-Based Screening
Early Screening 24-28 Week ScreeningHemoglobin A1c No Hemoglobin A1c
Testing for 1 abnormal value No f/u for 1 abnormal valueDichotomization of a continuous process is
bound to result in disagreement
What constitutes disease?
What primary cesarean section rate defines a bad outcome from disease?
HAPO Study Cooperative Research Group. N Engl J Med. 2008;358(19):1991-2002.
Who Decides?

6/5/2014
10
Lack of unambiguous evidence that aggressive diagnosis improves clinically important pregnancy outcomes
• The Landon study included women with 2 abnormal values on a 3-hour
• Studies of treatment are within the confines of strict clinical trials
• No study has compared outcomes between women who rule-in by 1-step approach but rule out by 2-step approach
“Parachutes reduce the risk of injury after
gravitational challenge, but their effectiveness has not
been proved with randomised controlled
trials.”
Worry about the over-medicalization of pregnancy and increased anxiety about diagnosis
Differences in Perceived Goals of Testing
6/5/2014
11
(Probably) the Ultimate Source of Controversy
COSTS BENEFITS
Costs v Benefits1-step screening strategy would:• Increase frequency of GDM 2-3 fold� 15-20%• Annually Add:
– 450,000 patient education visits–1 million prenatal testing appointments–1 million clinic visits
• Increase cost of care for GDM by > $1 billion
What I Think You Should Do

6/5/2014
12
What I Think You Should Do
• Pre-conception planning• Easy access to laboratory services• Universal access to nutritional counseling• Ample time and access to exercise facilities • Appropriate emotional support • Long-term follow up
What I Think You Should Do
CUT THE CONTROVERSY!
One-Step Testing v. Two-Step TestingCarpenter Coustan v. National Diabetes Data Group
Universal Screening v. Risk-Based ScreeningEarly Screening v. 24-28 Week ScreeningHemoglobin A1c v. No Hemoglobin A1c
Blood sugar testing for 1 abnormal value v. No testing
What Is NOT Controversial
Health risks go up with increasing blood sugar. There is no risk of harm from encouraging women to follow a healthy diet and get regular physical activity.SOME portion of women will change their behavior after being made aware of an increased risk of disease.
Determine what testing strategy generally fits your circumstances best
Be flexible!
What I Think You Should Do
6/5/2014
13
Thank You

6/5/2014
1
Mental Health Disorders in Pregnancy:
What is Your Responsibility?Anna Glezer, MD
Assistant Clinical Professor of PsychiatryConsultation-Liaison Service
University of California, San FranciscoJune 5, 2014
Disclosures:None
• Prevalence of MI in Pregnancy• Screening for MI in Pregnancy• Treatment of MI in Pregnancy
Outline• The reproductive years are the most common for
onset of mood disorders• Prevalence rates for depression range from 7-13%• Frequently under-diagnosed
– Similar symptoms to those of normal pregnancy experience
Depression in Pregnancy
6/5/2014
2
• Previous episodes of depression– Risk of recurrence high off of medication
• Limited social support• Marital conflict• Multiple other children• Ambivalence about pregnancy
Risk Factors of Depression in Pregnancy
Poor perinatal outcome- Lower APGAR scores- Higher rates of preterm labor and
delivery complications
Increased rates of substance usePoor nutritionLess follow through with prenatal visitsImpaired sleep
Increase risk of PP Depression
Untreated Depression in Pregnancy
• Prevalence: 9.5% at some point in the pregnancy.– Highest rates in the first trimester (7%)– 2nd Trimester: 2% and 3% in the third trimester.
• Risk Factors: – Previous history of GAD was the strongest predictor– Decreased levels of social support– Less education– History of child abuse
Previous patient questionnaire studies demonstrate higher rates
Generalized Anxiety in Pregnancy
J Affect Disord. 2011 Jun;131(1-3):277-83. Generalized anxiety disorder: course and risk factors in pregnancy.Buist A, Gotman N, Yonkers KA.
• Mixed results during pregnancy– Subgroup with improved symptoms
• Possible anxiolytic effects of progesterone– Subgroup with worsened symptoms
• Requiring higher doses• Increased risk postpartum
Panic Disorder and OCD in Pregnancy

6/5/2014
3
• Extremely rare• Most commonly due to an affective disorder
(depression with psychotic features or bipolar disorder), rarely schizophrenia
Psychosis in Pregnancy• Disordered eating behaviors often improve in
pregnancy, except binging• Prevalence in large recent study:
– Anorexia Nervosa 2.1% (0.3% in last year)– Bulimia Nervosa 3.0% (0.9% in the last year)– Both 1.8% (0.1%) – No differences were found in mean birth weight,
prevalence of a small-for-gestational-age, or premature birth.
• Active Symptoms may be different
Eating Disorders in Pregnancy
BJOG. 2012 Nov;119(12):1493-502. Perinatal outcomes and gestational weight gain in women with eating disorders: a population-based cohort study.Micali N, De Stavola B, dos-Santos-Silva I, Steenweg-de Graaff J, Jansen PW, JaddoeVW, Hofman A, Verhulst FC, Steegers EA, Tiemeier H.
• 2003 National Household Survey on Drug Use and Health indicated that 9.3% of pregnant women used alcohol and 4.3% percent of pregnant women used illicit drugs.
• Pregnancy Risk Assessment Monitoring System (PRAMS) found about 13% (as high as 28% in certain states) of women smoked during the last 3 months of pregnancy.
• Risks associated with the substance and risks associated with the addiction behaviors
Substance Use Disorders in Pregnancy• Who to screen?• When to screen?• How to screen? Which tools?
->Screening for medical conditions (such as thyroid dysfunction)
Screening

6/5/2014
4
• Postpartum screening for depression is now recommended universally
• Awareness of risk factors– Prior mental illness– Psychosocial stressors: un/underemployment,
financial problems, housing issues, lower education
– Family history– Complicated pregnancy or delivery
Who to Screen
• First prenatal visit• First postpartum visit• 4-8 weeks postpartum
When to Screen
• Insufficient data to suggest the use of any one particular scale universally
• Commonly used tools include:– MDQ (Mood Disorders Questionnaire)– PHQ 2 or PHQ 9– Edinburgh Postnatal Depression Scale
How to ScreenEdinburgh Postnatal
Depression Scale

6/5/2014
5
• Thorough medical evaluation for organic cause of symptoms
• In-home supportive services• Treatment
– Therapy -> supportive, cognitive-behavioral, group, family
– Medication
When There Is a Positive Screen• Pharmacotherapy• Psychotherapy
– Individual supportive therapy– CBT/DBT– Group psychotherapy
• Support groups/Mothers’ groups• Psychoeducation
Treatment
• SSRI/SNRI• Wellbutrin• Benzodiazepines• Buspar• Antipsychotic medications• Mood stabilizers
Psychopharmacology• Perinatal Psychiatry (examples include UCSF OB/Psych
Clinic or Mood Assessment Clinic, SFGH High Risk OB Clinic
• General outpatient psychiatry and psychotherapy – Community mental health clinics– Private psychotherapy and psychiatric practices– Psychology Today website– University affiliated clinics (such as UCSF’s Langley Porter)
Resources for Referral
Resource for Education:Womensmentalhealth.org

6/5/2014
6
• Mental illness is common during pregnancy, with depression and anxiety the most prevalent disorders.
• Mental illness during pregnancy is associated with a variety of risks and complications.
• All patients should be screened for mental illness during pregnancy.
• Treatment is available. Pharmacotherapy requires a risk/benefit analysis on effects of untreated/undertreated mental illness versus effects of medication.
Take-Home Points

1
Cesarean Section: Surgical Techniques that Work
Marya G. Zlatnik, MD, MMSMaternal Fetal MedicineUCSF
Hamano, Teisuke. 1880. Kainin no kokoroe (Information on pregnancy). Japanese Woodblock Print Collection, Archives & Special Collections, UCSF Library & Centerfor Knowledge Management.
ZMG1
No Disclosures
Learning Objectives� Review different aspects of C/S technique� Current basis in literature� Evidence-based steps (according to me)
– Berghella, Am J ObGyn 2005, updated 2013 (Dahlke)
– Cochrane, various years– Given time constraints, some data in syllabus
onlyThe way Mother Nature intended….

Slide 1
ZMG1 30 minutes, hides more slides@@@@@@@@@@@@@@@@@@@@@@@@@@@@@@@@@@@@@@@@@@@@@@@@@@@@@@@@@@@@@@@@@@@@@@@@@@@@@@Zlatnik, Marya G., 5/13/2014

2
Cesarean Rates Continue to Rise Cesarean Section Technique� Prophylactic Atbx� Prep� Remove FSE� Abdominal Incision� Bladder flap� Uterine incision� Placental delivery
� Exteriorization of uterus� Uterine incision closure � Peritoneal closure� Irrigation� Fascial closure� Subcutaneous closure� Staples/skin
Prophylactic Antibiotics� Cochrane Review
– 4700 pts– RR 0.42 (95%CI 0.28-
0.65) morbidity/death– Effect bigger if labor
� Decreased fever, SSI, endometritis, UTI, LOS (RR ~0.4)
� No benefit to multi-dosesSmaill Cochrane 2010
Prophylactic Atbx—Fever 1st Generation vs. 2nd or 3rd
Alfirevic Cochrnae 2010Hopkins Cochrane 1999
Same result with Ampicillin vs. Ceph

3
13
Timing of cefazolin: Decreased SSI w/ Preop atbx vs After cord clamp
p= 0.002
p= 0.014
p= 0.020
Kaimal SMFM 2008
0
2
4
6
8
Overall Endometritis Cellulitis
SS
I (%
)2005-2006n= 800
After 2006n= 516
2013 Clinical Practice Guidelines: Antimicrobial Prophylaxis in Surgery
� American Society Health-System Pharmacists, Infectious Diseases Society of America, Surgical Infection Society, Society for Healthcare Epidemiology of America
� Based on pharmacokinetic dosing studies, 1g cefazolin is often not enough
� At UCSF we have transitioned from cefazolin 1g (2g if obese) to cefazolin 2g (3g if BMI >120kg)
� Re-dose if 4> hrs from 1st dose or EBL >1500 cc
Bratzler 2013
Prophylactic Atbx—Extended Spectrum Regimens � RCT adding metronidazole vag gel
– 224 pts; vaginal gel vs placebo gel– Less endometritis (7 vs 17%), trend towards less fever;
no difference in wound infxn, LOS
� Ureasplasma increases risk for C/S SSI– Cephalosporin doesn’t cover– Post-cord-clamp cefotetan plus placebo or
doxy+azithro Andrews 2003
Pitt 2001
16
Extended spectrum Prophylaxis
� UAB study over 14 years– In 2000, IV cefotetan or cefazolin & IV azithro at cord clamp– Decreased endometritis– Decreased wound infections
Tita ObGyn 2009Tita AJOG 2008

4
17
Extended spectrum Prophylaxis?� UCSF rate much lower� Hesitant to extend atbx spectrum for all C/S pts
– Concerns re atbx resistance� Selectively extend atbx spectrum
– eg, pt w/ DM/obesity– Cefazolin 2-3g IV preop + azithro 500mg IV
after cord clamp (mix in 250mL/give over 1 hr )
Abdominal Prep� Several small RCTs: different solutions
– No clear winner– Magann 1993, Brown 1984, Weed 2011
� CHG better than povidone-iodine in G. Surg– Darioche 2010
� Bundled CHG cleanse + OR prep + other interventions � decreased SSI rate– Rauk 2010
Vaginal Prep prior to C/S� Povidone-iodine prep -> decreased endometritis,
esp w/ ROM� No difference in fever or wound complications� ? benefit if already chorio� Possible effect on neonatal thyroid studies� Risk of vaginal lac� Dahlke gives a “B”
– Cochrane 2010, Reid 2001, Rouse 1997, Starr 2005
Remove scalp electrode?� What to do if FSE in place prior to C/S?� Removal if FHR reassuring
– Sensible but little data� If NRFHR? Case reports:
– Mine (unpublished)– Retained for 23 years– Migrated into jejunum– In baby’s scalp(cases all have emergent delivery in common)
Valenzuela 2006Kimm 1992Frederikson-Moller 2011
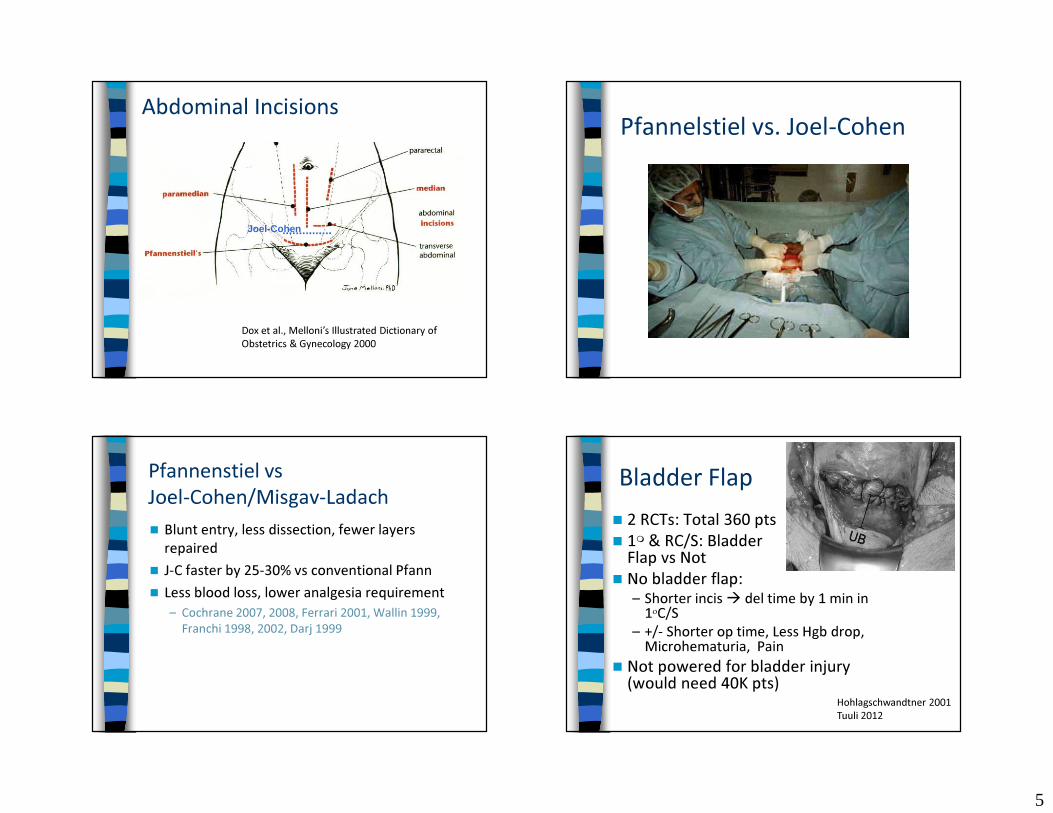
5
Dox et al., Melloni’s Illustrated Dictionary of Obstetrics & Gynecology 2000
Abdominal Incisions
Joel-Cohen
Pfannelstiel vs. Joel-Cohen
Pfannenstiel vs Joel-Cohen/Misgav-Ladach� Blunt entry, less dissection, fewer layers
repaired� J-C faster by 25-30% vs conventional Pfann� Less blood loss, lower analgesia requirement
– Cochrane 2007, 2008, Ferrari 2001, Wallin 1999, Franchi 1998, 2002, Darj 1999
Bladder Flap� 2 RCTs: Total 360 pts� 1� & RC/S: Bladder Blad
Flap vs Not� No bladder flap:
– Shorter incis� del time by 1 min in 1οC/S
– +/- Shorter op time, Less Hgb drop, Microhematuria, Pain
� Not powered for bladder injury (would need 40K pts)
Hohlagschwandtner 2001Tuuli 2012

6
Uterine Incision—Blunt vs. Sharp Extension� RCTs: Blood loss greater with sharp
– More transfusions – Rodriguez 1994, Magann 2002,
Cochrane 2008� Cephalad to caudad
extension– Less blood loss, fewer
extensions– Cromi 2008,
Sekhavat 2010
Uterine Incision: BABE� B: Breathe. Pause before making the
hysterotomy� A: Allis clamps. Use Allis clamps, if needed, to
help elevate the hysterotomy� B: Blunt. Use a single digit to sweep over
hysterotomy bluntly between each scalpel pass
� E: Extend. Extend hysterotomy bluntly (stretch laterally or vertically)
Encarnacion 2012
Placental Delivery

7
Placenta: Manual Removal
� Manual extraction: bigger Hct drop, more endometritis (vs spontaneous)
Cochrane 1995
Anorlu Cochrane 2008
Uterine Exteriorization
Exteriorization of Uterus � Easier repair? (easier to teach) � ? Infection, bleeding risk� Anesthesiologist blames you for emesis� No real differences in complications,
including emesis
Cochrane 2006, 2009
Opening the cervix� To let out evil humours in unlabored C/S� Cochrane review—> no decrease in
febrile morbidity
Cochrane 2011

8
Closure of Uterine Incision: 1 vs. 2 Layers� Short term:
– OR time– Hemostasis/
Blood loss– Endometritis
� Long term:– Scar strength/VBAC risk
Short Term Outcomes: 1 vs. 2 Layer Closure
� Hauth’s RCT, UAB + 9 other studies� No difference in use of extra hemostatic
stitches� Less blood loss� Less post-op pain� 5-7 min shorter OR time
Hauth 1992, Cochrane 2008
1 vs. 2 Layer Closure:Scar Strength� Follow-up from Hauth’s RCT� 906 pts in RCT�164 preg again� 83 previous 1-layer, 81 previous 2-layer� 56/70 vs 64/75 successful VBACs� No difference in PPH, infxn, LOS� One dehiscence in 1-layer group, no
ruptures (power only .07)
Chapman 1997
1 vs. 2 Layer ClosureScar Strength for TOLAC� Retrospective data conflicting whether
rupture risk increased or not� Risk of uterine rupture after 1-layer closure
not significantly different from 2-layer closure overall (OR 1.71; 95% CI 0.66-4.44) – risk increased after locked 1-layer closure (OR 4.96)
but not after unlocked 1-layer closure (OR 0.49) compared w/ 2-layer closure
� Need RCT!Bujold 2002, Dumwald 2003, Roberge 2011

9
Uterine Replacement After Exteriorization Irrigation of Incision
Wound Irrigation� RCT in cattle
– C/S for macrosomia– Wounds irrigated with betadine vs nothing– No difference in wound infections
� Only a few RCTs in humans– Study design flaws– Saline vs nothing– No difference in wound complications, more
nausea with irrigation
de Kruif 1987
Bamigboye, Harrigill 2003Cochrane 2006, Viney 2010
Peritoneal Closure vs. Not� Short term outcomes vs. long term
outcomes� Short-term: Non-closure better
– Shorter OR time– Less fever– Shorter LOS– Trend less analgesia need & wound infection
Bamigboye, Cochrane 2010

10
Long Term Outcomes: Non-Closure of Peritoneum� Cohort & retrospective studies mixed on what
causes fewer adhesions
� 2 pseudo RCT suggest nonclosure better
� 1 RCT non-closure � fewer adhesions
Lyell 2005, Stark 1995, Lyell 2012
Weerawetwat 2004, Komoto 2006
Kapustian 2012
Failure of Wound� Suture breaks� Knot slips (unties)� Viscera protrudes between stitches� Suture tears through fascia (most common)
Knot Slips/Types of Knots� Square� Surgeon’s square (least likely to
slide undone, but can’t tighten after 2nd throw)
� Square slip (can slip, even after 5 throws; inadvertently tied by one-handed technique)
� Granny (not a bad knot, but easy to accidentally make granny slip knot)
� Granny slip (not secure)
Loop-to-Strand Knots (e.g.when tying fascia suture in midline)� 0 & 2-0 Monocryl, 6 throws , stretched until
failure (breakage or slippage)� Loop-to-single strand, sliding knot
– 55-85% untied– 112 newtons to break knot
� Loop-to-single strand, flat square knot– 5-15% untied– 117 newtons to break knot
� Strand-to-single strand, flat square knot– NONE untied– 132 newtons to break knotHurt 2004

11
Failure of WoundType of Suture Material� Metaanalysis from General Surgery lit.� Nonabsorbable vs. absorbable
– NNT = 50 for incisional hernia� Risk of hernia not increased with PDS, is
increased with VicrylHodgson 2000
� Monocryl & Chromic no good for sheep C/SGreenberg 2011
Skin Closure
Skin Closure� Re-approximation of subQ tissue � A few meta-analyses
– Most included > 2cm subQ fat– 3-0 plain gut, mostly running stitch– Decreased wound complications (fewer
hematomas & seromas), NNT = 16� SubQ Drains: a few RCTs
– Probably no benefit to routine useChelmow 2004, Cochrane 2006Ramsey 2005, Al-Inany 2002
Skin Staples or Suture
12
Staples vs. SubQ Suture� A few RCTs, 2 meta-analyses � Staples quicker (by ~5-9 min)� Pts often prefer suture� Sutures fewer wound infections/
breakdowns – NNT 16
� Sew if there is timeFrishman 1997, Tuuli 2011, Clay 2011Mackeen 2014
Conclusions� Yes:
– Prophylactic Atbx (pre-op)– Joel-Cohen or Pfannenstiel– Spontaneous placental
delivery– SubQ closure—yes if > 2cm
fat– Sew skin if you have time
� Surgeon’s choice:– Bladder flap—may skip on
low risk cases – Exteriorization of uterus
for repair
� Awaiting data:– Skin prep – Uterine incision closure—
Jury’s still out – Peritoneal closure—Jury’s
still out– Irrigation subQ
� No: – Uterine incision—sharp
extension – Multi-dose or high-
powered atbx prophylaxis– Granny , slip square, loop-
to–strand knots on fascia
Thank You!

1
Perinatal Care for LGBTQ Patients – Is Your Practice
Ready?
Patricia A. Robertson, MDProfessor
Division of Perinatal Medicine and BiologyDept. of Obstetrics, Gynecology and Reproductive Sciences. UCSF
AIM, 2014
Disclosures
• I have no financial disclosures
Objectives
• Understand unique obstetrical issues for the LGBTQ community
• Assess whether your obstetric practice is welcoming/inclusive to LGBTQ patients and their partners
• Be aware of strategies to be more welcoming/inclusive for LGBTQ parents
Questions
1. What options for reproduction do LGBTQ people have and when is the best time?
2. What medical and social preparation is necessary for the best neonatal outcomes?
3. What are the strategies to preservefertility prior to transitioning F to M or M to F?
4. What are the challenges as LGBTQ parents?
2
Gaybe Boom
• Two to six million children in the United States are being raised by LGBT parents
• Which state has the highest percentage of LGBT couples raising children?
Williams Institute, UCLA
Metro Areas with Highest % of SS Couples Raising Children
• Salt Lake City
• Virginia Beach• San Antonio
• Memphis
• Detroit
Williams Institute, UCLA
Lesbians and Birth
• About 16% of lesbians have given birth(Cochran, 2001)
When Is the Best Time to Have a Baby?
• Support from family and friends
• At your healthiest
• If in a couple, assess if relationship stable and if you both want children
• When you have figured out how to handle the increased responsibility (finances, childcare, insurance)
• When you have the energy
3
The Biologic Clock
• For women
• -once 30 years old, more challenges for
fertility, increased rate of miscarriages• - once 34, birth defect rate increases
significantly
• For men• - increase rate of birth defects once 40
Reproductive Options for Lesbians
• Insemination by known or unknown donor
(donor ID release option at age 18 of child)• Intercourse
• Co-maternity in which one partner donates an egg by IVF, egg is fertilized in the lab and the embryo is placed in the uterus of her partner
Decision re: Known vs. Unknown Donor
• No difference in outcome behaviors of children (Gartrell)
• Children are currently satisfied with the level of contribution of their male donors and do not think of their donors as dads (survey ages 19 – 29; N=11)(Goldberg A and Allen K, 2013)
Breastfeeding in Lesbians
• Goal: exclusive breastfeeding for the first 6 months
• Gartrell’s results
• Option: if in a couple, lactataion induction in the non-bio Mom

4
Children of Lesbian Couples
• No difference in sexual orientation, self-esteem or emotional health compared to heterosexual parented children
• Children of lesbian couples appeared to be less aggressive, more nurturing, more tolerant of diversity, more adrogynous, less behavior issues as teens
Reproductive Options for Gay Men
Intercourse with female gestational carrier or intended female parent
Insemination with female gestational carrier or intended female parent
Surrogacy by IVF via egg donor and gestationalcarrier
If partnered, mixing of sperm prior to IVF or insemination
Reproductive Options for Bisexual People
• Conception within heterosexual relationship
• Options described under lesbian for women
• Options described under gay men for men
MTF Reproductive Potential
• If a transwoman is not taking hormones, she can use her sperm to conceive.
• If she’s been taking hormones longer than 6 months, she might resume sperm production if she pauses for at least 4 months, but there are no guarantees.
• She can give her partner live sperm, or go through a sperm bank.
• Hormones used for transition have not been shown to cause any chromosomal damage.
• Consider the emotional implications for your patient of creating life through the use of her sperm, and be open to discussing them.

5
Practice cultural humility• Admit when you don’t know something
• Commit to an ongoing formal and informal learning process
• Learn about yourself, your biases, your discomforts, your assumptions, and your fears
• Have a sense
of humor
Trans-friendly images
Patrick, Blake, and Matt (2000)
Thomas Beatie (2008)
FTM Reproductive Potential
• If a transman is not taking hormones, he can use his ovaries and/or uterus to conceive.
• If he’s been taking hormones long enough to stop menstruating, he might resume gamete production if he pauses, but there are no guarantees.
• He can use his partner’s sperm, or go through a sperm bank, or his partner can carry his ovum.
• Hormones used for transition have not been shown to cause any chromosomal damage.
• Consider the emotional implications for your patient of being unable to reproduce in a traditionally male way, and be open to discussing them.
In case of emergency
• Encourage your pregnant male patient to prepare for emergencies:– Have a durable power of attorney for health care
form filled out and with him at all times.– Have a brief introductory cheat sheet for new care
providers with him at all times.
I am a manI was born a womanI am a manI am pregnantI have a uterus and will be giving birthPlease call me he
6
Pregnancy Planning for Lesbians,Bisexual Women and Trans Men
• Mammogram if female and 40 yo or older
• Multi-vitamins or prenatal vitamins three months prior to conception
• Consideration of known vs. unknown donor
• Blood work at annual exam to include
rubella antibodies, HIV screen, CF testing, etc.
Assisted Reproductive Technology
• Insemination
- Frozen Sperm- Fresh Sperm
• IUI vs Insemination
In Vitro Fertilization
• Take-home baby rate per cycle (30%)
• Take-home egg donor baby rate (60%)• Cost per cycle: $10,000 to $15,000
• Issues
- Multi-fetal gestation- Increase risk of birth defects
- Increase preterm birth rates
Birthplace
• Home Birth
• Free-standing Birth Center
• Hospital Birth- L and D nurses
- Inclusive for family of choice
- Lactation support/choices

7
Legal Aspects
• Packet available at the National Center for Lesbian Rights
• Issues: if in a couple - parenting rights for each member of the couple, guardian in case of parental death or severe disability, effect of individual state laws on these issues
• Obtain legal counsel prior to conception
Family Constellations
Many and Varied

8
Enhancing Perinatal Care for LGBT Patients
• Quality Improvement Project by Elizabeth Losada MD at Kaiser Oakland
• Create access to centralized source of information about LGBT PG, adoption, foster parenting, support groups
• Write booklet for LGBT enrollees about Kaiser policies about insemination especially re: fresh, frozen sperm and known and unknown donor
Enhancing Care for LGBT Families (cont)
• Create a perception that Kaiser cares for a constellation of families: children’s books and magazines in waiting rooms
• Be sure that prenatal class language is inclusive and not heterosexist re: couples and single Moms; use “support person”
• Have LGBT-friendly forms, with parent #1, parent #2
Enhancing Prenatal Care for LGBT Families
• Offer longitudinal care so do not have to “come out” at each visit
• Prepare LGBT families re: variability in birth certificate forms by county and be clear about the timeline
• Do not marginalize the non-bio mom
• Indicate preferred pronoun on EHR for
trans patients

9
Postpartum Depression
• Up to the first year postpartum
• Diagnosis• Treatment
• Impact on infant
• Partner postpartum depression
LGBT Parenting Issues
• Supportive prenatal and birth environment
• Postpartum Depression
• Family-of-origin, Family-of-choice• Religion
• Schools
• Blended Families• If in a couple, how to share responsibilities
• Parenting Styles
Same-Sex Marriage
• 17 states in the USA
• 60% of the population in states that still deny same-sex marriage
• In MA and CA, same-sex marriage has led to fewer mental health care visits and expenditures for gay men and has reduced psychological distress among LGB adults in legally recognized same-sex relationships
Same Sex Marriage
• Improves access to health insurance for LGBT people (42% of companies extend benefits to LGBT partners) therefore improves disparities slightly
• Strengthens access to health insurance for the 220,000 children being raised by same-sex parents in the United States
N Engl J Med 2014:370:1373-1376

10
Family Constellation
• Family-of-Choice
- partnered or single- co-parent/s
- godparent roles
- grandparent roles• Family-of-Origin
• Friends
Religion
• Discuss ahead of the birth
• If desired, find inclusive communityand one welcoming of children
• Rituals
Schools
• Play Groups
• Preschools
• Elementary Schools- Private vs. Public (Charter v. Traditional)
• Middle Schools
• High Schools • College
Blended Families
• Co-parenting with an ex
• Co-parenting with a new partner without children
• Co-parenting with a new partner with children
• Step-parenting

11
Teens/Young Adults
• Research from Nanette Gartrell
• COLAGE
• Parenting an LGBT teen: research from Caitlin Ryan on accepting vs. rejecting
parent behaviors
• Parenting a straight teen
Remember
You can make a tremendous difference to your LGBTQ patients by having a welcoming/inclusive practice during this vulnerable and joyous time of their starting their families!

1
Updates on Intrapartum Antibiotic Management
Natali Aziz, MD, MSDepartment of Obstetrics and Gynecology
Stanford University School of Medicine
Antepartum and Intrapartum ManagementJune 5, 2014
Disclosures
I have no industry affiliations.
Overview
Group B Streptococcus prophylaxis
Infective endocarditis prophylaxis
PPROM and PTL prophylaxisChorioamnionitis and endometritis
Preoperative prophylaxis– Cesarean delivery – Cerclage, PPTL
Procedural prophylaxis – 3rd/4th degree repair – Manual removal of placenta
GBS Prophylaxis
No GBS resistance to penicillin or ampicillin
GBS susceptibility – Penicillin G, ampicillin, extended-spectrum
penicillins, cephalosporins, vancomycin
Penicillin G is most active agent in vitro
Penicillin preferred – Narrower spectrum of activity– Theoretic reduction of ampicillin-resistant
organism development
Oral treatment NOT recommended CDC/MMWR 2010, Andrews 200

2
GBS Prophylaxis
GBS resistance – Clindamycin: 13-20% – Erythromycin: 25-32%– Trimethoprim-sulfamethoxazole: most isolates
Erythromycin resistance– Erythromycin NO LONGER recommended!
Do not reach fetal tissues reliably
– Often associated with clindamycin resistance– GBS may have inducible resistance to clindamycin – D-zone testing for inducible resistance performed
CDC/MMWR 2010
GBS Prophylaxis
Appropriate maternal vancomycin dosing? – Dosing regimens
Phase 1: 1 g Q 12 hours (CDC 2010 Guidelines)Phase 2: 15 mg/kg Q 12 hours Phase 3: 20 mg/kg Q 8 hours (max individual dose=2 g)
– 55 women: 31 phase 1, 12 phase 2, 12 phase 3
Maternal and neonatal therapeutic levelsPhase 1: 32% and 9%Phase 2: 50% and 33% Phase 3: 83% and 83%
CDC/MMWR 2010, Onwuchuruba 2014
GBS Prophylaxis
GBS intrapartum antibiotic prophylaxis– Penicillin G 5 M, then 2.5-3 M units IV Q 4 hours
PREFERRED over ampicillin
– Ampicillin 2 g IV, then 1 g IV Q 4 hours – Low risk penicillin allergy
Cefazolin 2 g IV, then 1 g IV Q 8 hours
– High risk penicillin allergyAnaphylaxis, angioedema, respiratory distress, urticariaClindamycin 900 mg IV Q 8 hours
– High risk penicillin allergy and clindamycin resistantVancomycin 1 g Q12 hours or 20 mg/kg IV Q8 hours
CDC/MMWR 2010, Onwuchuruba 2014
Infective Endocarditis Prophylaxis
Highest risk of adverse endocarditis outcomes– Prosthetic valve or valve repair material– Previous history of infective endocarditis – Congenital heart disease
Cyanotic CHD (unrepaired), prosthetic material or devise < 6 months, residual defect at or near repair site with prosthetic material or device
– Cardiac transplant patients with regurgitation Due to abnormal valve
American Heart Association 2008, American College of Cardiology 2008, ACOG 2011
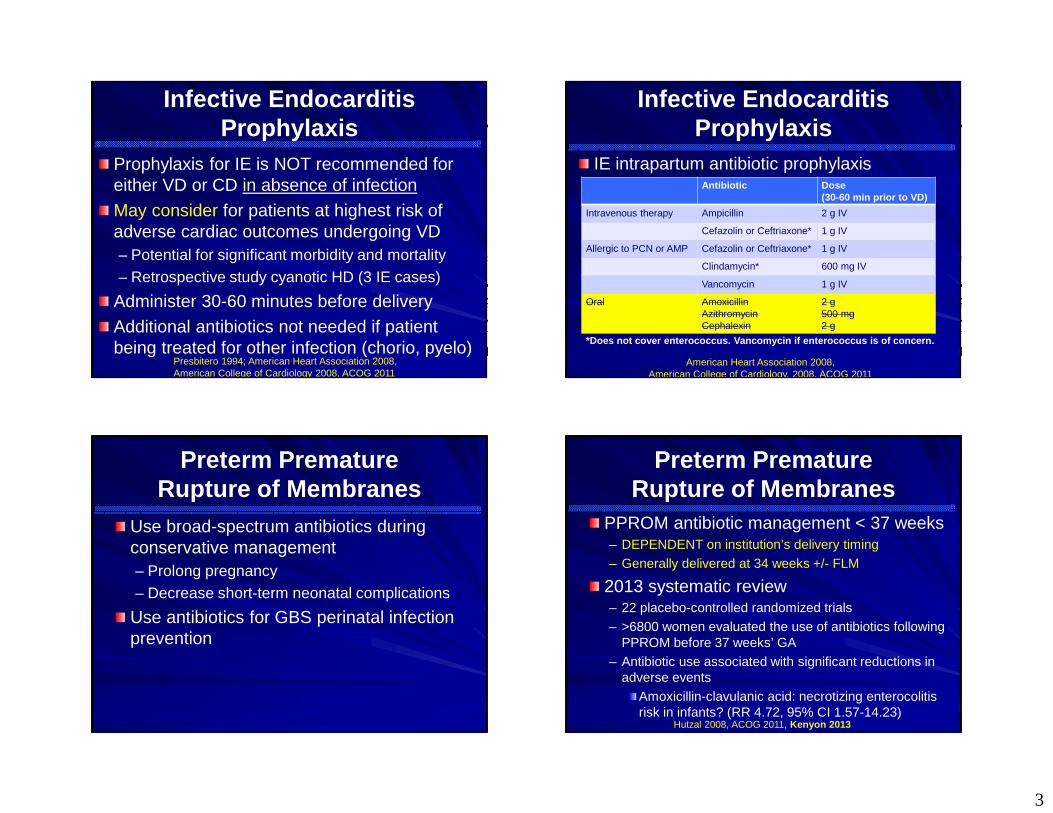
3
Infective Endocarditis Prophylaxis
Prophylaxis for IE is NOT recommended for either VD or CD in absence of infection
May consider for patients at highest risk of adverse cardiac outcomes undergoing VD– Potential for significant morbidity and mortality– Retrospective study cyanotic HD (3 IE cases)
Administer 30-60 minutes before delivery
Additional antibiotics not needed if patient being treated for other infection (chorio, pyelo)
Presbitero 1994; American Heart Association 2008, American College of Cardiology 2008, ACOG 2011
Infective Endocarditis Prophylaxis
IE intrapartum antibiotic prophylaxis
American Heart Association 2008, American College of Cardiology, 2008, ACOG 2011
Antibiotic Dose (30-60 min prior to VD)
Intravenous therapy Ampicillin 2 g IV
Cefazolin or Ceftriaxone* 1 g IV
Allergic to PCN or AMP Cefazolin or Ceftriaxone* 1 g IV
Clindamycin* 600 mg IV
Vancomycin 1 g IV
Oral AmoxicillinAzithromycinCephalexin
2 g500 mg2 g
*Does not cover enterococcus. Vancomycin if enterococcus is of concern.
Preterm Premature Rupture of Membranes
Use broad-spectrum antibiotics during conservative management – Prolong pregnancy– Decrease short-term neonatal complications
Use antibiotics for GBS perinatal infection prevention
Preterm Premature Rupture of Membranes
PPROM antibiotic management < 37 weeks– DEPENDENT on institution’s delivery timing– Generally delivered at 34 weeks +/- FLM
2013 systematic review – 22 placebo-controlled randomized trials – >6800 women evaluated the use of antibiotics following
PPROM before 37 weeks’ GA– Antibiotic use associated with significant reductions in
adverse eventsAmoxicillin-clavulanic acid: necrotizing enterocolitis risk in infants? (RR 4.72, 95% CI 1.57-14.23)
Hutzal 2008, ACOG 2011, Kenyon 2013

4
Preterm Premature Rupture of Membranes
Reduction of perinatal adverse events – Chorioamnionitis (RR 0.66, 95% CI 0.46-0.96) – Infants born in relation to randomization
Within 48 hours (RR 0.71, 95% CI 0.58-0.87) Within 7 days (RR 0.79, 95% CI 0.71-0.89)
– Neonatal infxn (RR 0.67, 95% CI 0.52-0.85)– Surfactant use (RR 0.83, 95% CI 0.72-0.96) – Neonatal oxygen tx (RR 0.88, 95% CI 0.81-0.96)– Abnormal cerebral US prior to hospital discharge
(RR 0.81, 95% CI 0.68-0.98) Hutzal 2008, ACOG 2011, Kenyon 2013
Preterm Premature Rupture of Membranes
PPROM prophylactic antibiotic management when FLM not documented and delivery not imminent <34-37 weeks’ GA – Amp/Amox and erythromycin regimen x 7 days
Amp 2 g IV Q 6 hours and erythromycin 250 mg IV Q 6 hours x 48 hoursThen, amoxicillin 250 mg PO Q 8 hours and erythromycin 333 mg Q 8 hours x 5 days Alternative (no trial)
– Amp 2 g IV Q 6 hours, Azithromycin 1 g PO x 1– Then amoxicillin 500 mg PO Q 8 hours x 5 days
ACOG 2011, Mercer 1997
Preterm Premature Rupture of Membranes
PCN allergic patients (not anaphylaxis) – Replace PCN agent with cefazolin 1 g IV Q8 hrs x 48 hrs– Then cephalexin 500 mg PO QID x 5 days for h/o non-
severe reactions
PCN allergic patients- high risk for anaphylaxis– Anaphylaxis, angioedema, respiratory distress, urticaria– Replace PCN agent with Clindamycin 900 mg IV Q 8 hours
PLUS gentamicin 5 mg/kg daily x 48 hours – Then clindamycin 300 mg PO Q 8 hours x 5 days– USE vancomycin 1 g Q 12 hours or 20 mg/kg Q 8 hours for
GBS +, clindamycin resistance or if GBS unknown status!!! ACOG 2011, Mercer 1997
Preterm Premature Rupture of Membranes
GBS perinatal infection prevention– Regimen with adequate IV GBS coverage for at
least first 48 hours of preterm PROM latency prophylaxis, pending GBS test results obtained on admission
– GBS test results should not affect antibiotic therapy duration for PPROM management
– Intrapartum GBS prophylaxis should then be managed by the results of baseline GBS test at the time of preterm PROM for up to 5 weeks
CDC/MMWR 2010, ACOG 2011
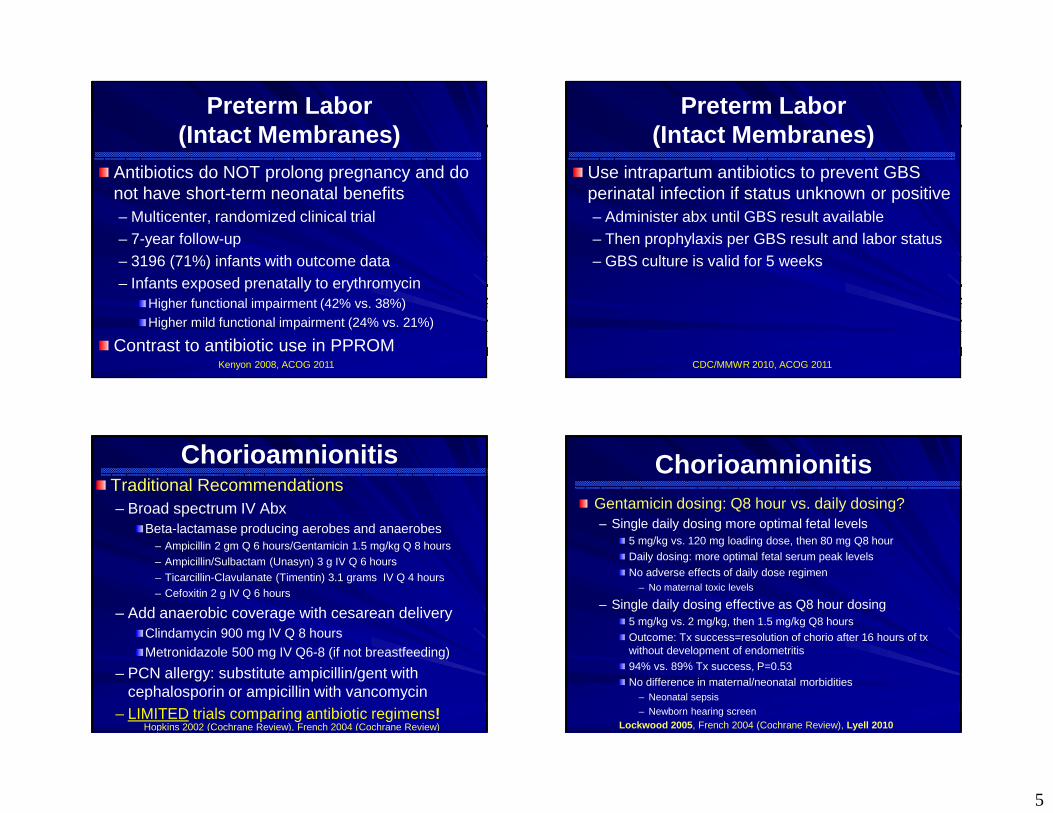
5
Preterm Labor (Intact Membranes)
Antibiotics do NOT prolong pregnancy and do not have short-term neonatal benefits– Multicenter, randomized clinical trial– 7-year follow-up – 3196 (71%) infants with outcome data – Infants exposed prenatally to erythromycin
Higher functional impairment (42% vs. 38%)Higher mild functional impairment (24% vs. 21%)
Contrast to antibiotic use in PPROM Kenyon 2008, ACOG 2011
Preterm Labor (Intact Membranes)
Use intrapartum antibiotics to prevent GBS perinatal infection if status unknown or positive– Administer abx until GBS result available– Then prophylaxis per GBS result and labor status– GBS culture is valid for 5 weeks
CDC/MMWR 2010, ACOG 2011
ChorioamnionitisTraditional Recommendations– Broad spectrum IV Abx
Beta-lactamase producing aerobes and anaerobes– Ampicillin 2 gm Q 6 hours/Gentamicin 1.5 mg/kg Q 8 hours– Ampicillin/Sulbactam (Unasyn) 3 g IV Q 6 hours – Ticarcillin-Clavulanate (Timentin) 3.1 grams IV Q 4 hours– Cefoxitin 2 g IV Q 6 hours
– Add anaerobic coverage with cesarean deliveryClindamycin 900 mg IV Q 8 hours Metronidazole 500 mg IV Q6-8 (if not breastfeeding)
– PCN allergy: substitute ampicillin/gent with cephalosporin or ampicillin with vancomycin
– LIMITED trials comparing antibiotic regimens!Hopkins 2002 (Cochrane Review), French 2004 (Cochrane Review)
ChorioamnionitisGentamicin dosing: Q8 hour vs. daily dosing?– Single daily dosing more optimal fetal levels
5 mg/kg vs. 120 mg loading dose, then 80 mg Q8 hourDaily dosing: more optimal fetal serum peak levels
No adverse effects of daily dose regimen – No maternal toxic levels
– Single daily dosing effective as Q8 hour dosing 5 mg/kg vs. 2 mg/kg, then 1.5 mg/kg Q8 hours Outcome: Tx success=resolution of chorio after 16 hours of tx without development of endometritis94% vs. 89% Tx success, P=0.53No difference in maternal/neonatal morbidities
– Neonatal sepsis
– Newborn hearing screenLockwood 2005, French 2004 (Cochrane Review), Lyell 2010
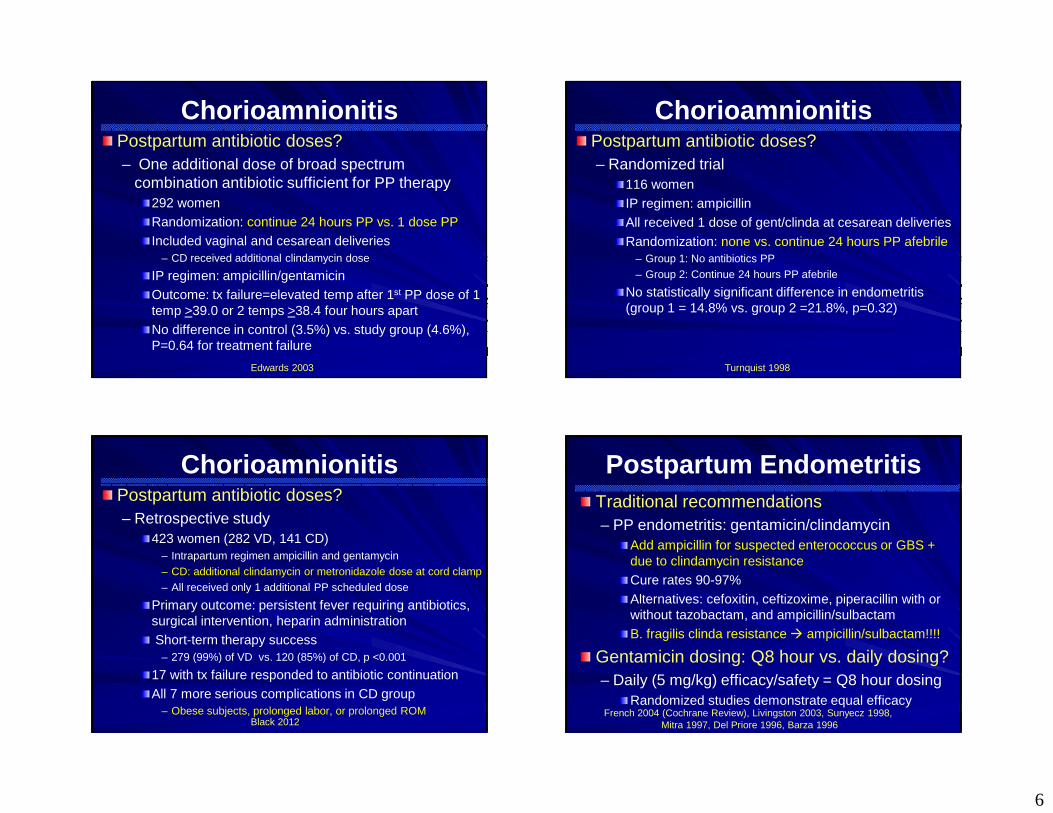
6
ChorioamnionitisPostpartum antibiotic doses?– One additional dose of broad spectrum
combination antibiotic sufficient for PP therapy292 women Randomization: continue 24 hours PP vs. 1 dose PP Included vaginal and cesarean deliveries
– CD received additional clindamycin dose
IP regimen: ampicillin/gentamicinOutcome: tx failure=elevated temp after 1st PP dose of 1 temp >39.0 or 2 temps >38.4 four hours apart No difference in control (3.5%) vs. study group (4.6%), P=0.64 for treatment failure
Edwards 2003
ChorioamnionitisPostpartum antibiotic doses?– Randomized trial
116 women IP regimen: ampicillinAll received 1 dose of gent/clinda at cesarean deliveries
Randomization: none vs. continue 24 hours PP afebrile – Group 1: No antibiotics PP– Group 2: Continue 24 hours PP afebrile
No statistically significant difference in endometritis (group 1 = 14.8% vs. group 2 =21.8%, p=0.32)
Turnquist 1998
ChorioamnionitisPostpartum antibiotic doses?– Retrospective study
423 women (282 VD, 141 CD)– Intrapartum regimen ampicillin and gentamycin– CD: additional clindamycin or metronidazole dose at cord clamp– All received only 1 additional PP scheduled dose
Primary outcome: persistent fever requiring antibiotics, surgical intervention, heparin administration Short-term therapy success
– 279 (99%) of VD vs. 120 (85%) of CD, p <0.001
17 with tx failure responded to antibiotic continuation All 7 more serious complications in CD group
– Obese subjects, prolonged labor, or prolonged ROM Black 2012
Postpartum EndometritisTraditional recommendations– PP endometritis: gentamicin/clindamycin
Add ampicillin for suspected enterococcus or GBS + due to clindamycin resistance Cure rates 90-97% Alternatives: cefoxitin, ceftizoxime, piperacillin with or without tazobactam, and ampicillin/sulbactamB. fragilis clinda resistance � ampicillin/sulbactam!!!!
Gentamicin dosing: Q8 hour vs. daily dosing?– Daily (5 mg/kg) efficacy/safety = Q8 hour dosing
Randomized studies demonstrate equal efficacyFrench 2004 (Cochrane Review), Livingston 2003, Sunyecz 1998,
Mitra 1997, Del Priore 1996, Barza 1996
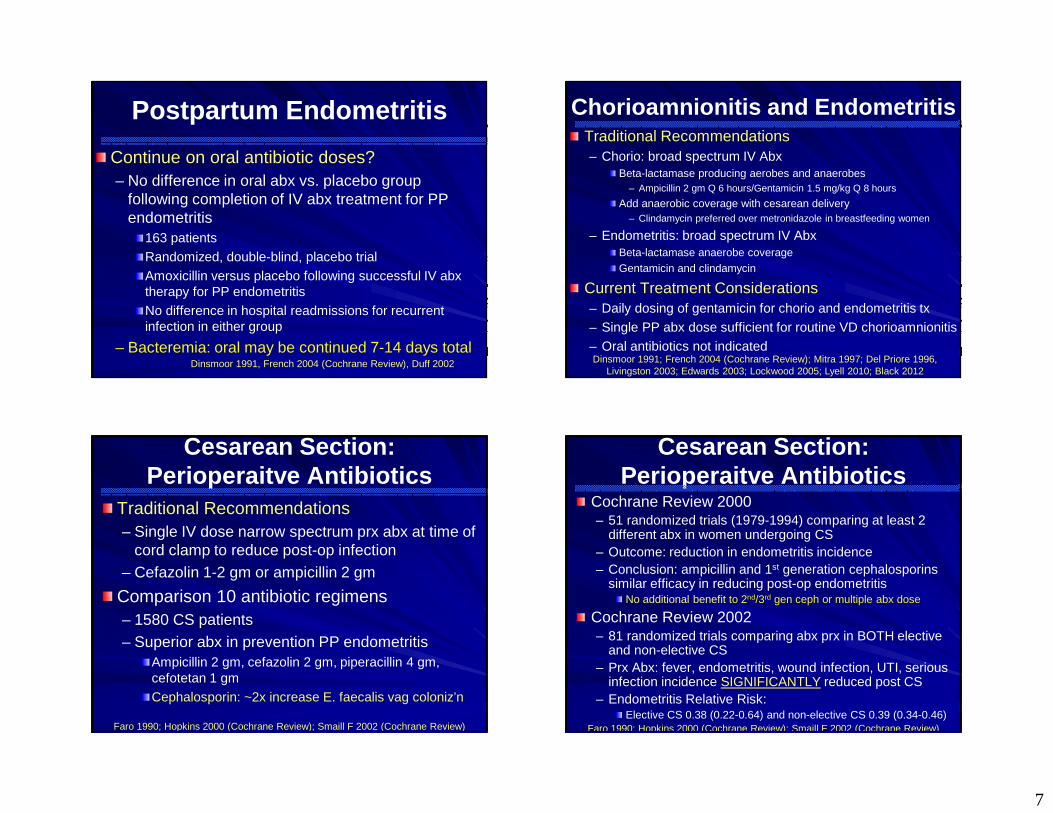
7
Postpartum Endometritis
Continue on oral antibiotic doses?– No difference in oral abx vs. placebo group
following completion of IV abx treatment for PP endometritis
163 patients Randomized, double-blind, placebo trialAmoxicillin versus placebo following successful IV abx therapy for PP endometritisNo difference in hospital readmissions for recurrent infection in either group
– Bacteremia: oral may be continued 7-14 days totalDinsmoor 1991, French 2004 (Cochrane Review), Duff 2002
Chorioamnionitis and EndometritisTraditional Recommendations– Chorio: broad spectrum IV Abx
Beta-lactamase producing aerobes and anaerobes– Ampicillin 2 gm Q 6 hours/Gentamicin 1.5 mg/kg Q 8 hours
Add anaerobic coverage with cesarean delivery– Clindamycin preferred over metronidazole in breastfeeding women
– Endometritis: broad spectrum IV AbxBeta-lactamase anaerobe coverage Gentamicin and clindamycin
Current Treatment Considerations – Daily dosing of gentamicin for chorio and endometritis tx – Single PP abx dose sufficient for routine VD chorioamnionitis – Oral antibiotics not indicatedDinsmoor 1991; French 2004 (Cochrane Review); Mitra 1997; Del Priore 1996,
Livingston 2003; Edwards 2003; Lockwood 2005; Lyell 2010; Black 2012
Cesarean Section: Perioperaitve Antibiotics
Traditional Recommendations– Single IV dose narrow spectrum prx abx at time of
cord clamp to reduce post-op infection – Cefazolin 1-2 gm or ampicillin 2 gm
Comparison 10 antibiotic regimens – 1580 CS patients– Superior abx in prevention PP endometritis
Ampicillin 2 gm, cefazolin 2 gm, piperacillin 4 gm, cefotetan 1 gmCephalosporin: ~2x increase E. faecalis vag coloniz’n
Faro 1990; Hopkins 2000 (Cochrane Review); Smaill F 2002 (Cochrane Review)
Cesarean Section: Perioperaitve Antibiotics
Cochrane Review 2000– 51 randomized trials (1979-1994) comparing at least 2
different abx in women undergoing CS – Outcome: reduction in endometritis incidence – Conclusion: ampicillin and 1st generation cephalosporins
similar efficacy in reducing post-op endometritis No additional benefit to 2nd/3rd gen ceph or multiple abx dose
Cochrane Review 2002 – 81 randomized trials comparing abx prx in BOTH elective
and non-elective CS– Prx Abx: fever, endometritis, wound infection, UTI, serious
infection incidence SIGNIFICANTLY reduced post CS– Endometritis Relative Risk:
Elective CS 0.38 (0.22-0.64) and non-elective CS 0.39 (0.34-0.46)Faro 1990; Hopkins 2000 (Cochrane Review); Smaill F 2002 (Cochrane Review)

8
Cesarean Section: Perioperaitve Antibiotics
Cochrane Review 2010– 86 studies: 13000 women – Non-emergent and emergent CD – Prophylactic antibiotics
Febrile morbidity, wound complications, endometritis reduced Reduction regardless of type of CD (elective vs. emergent) Endometritis reduced by ~60% for all CD and ~75% for elective CDCefazolin and ampicillin similar efficacy
MFMU Network – 9000 women – Term pre-labor CD – Prophylactic antibiotics
Reduction in both endometritis and wound complications
Dinsmoor 2009, Smaill F 2010 (Cochrane Review), ACOG 2011
Cesarean Section: Perioperaitve Antibiotics
Optimal drug timing?– Meta-analysis 6 randomized controlled trials before
procedure vs. intraoperativeN=2313 women and 2345 newbornsResults
– PP endometritis reduced by 41% (RR 0.59, 95% CI 0.37-0.94)
– Non-significant reductions in wound infection, maternal febrile morbidity, neonatal sepsis, neonatal septic work-up, and neonatal intensive care unite admission
Abx prx for CD before skin incision decreased PP endometritis and possibly other infectious morbidities
– Neonatal outcomes not affected adversely!Baaqeel 2013
Cesarean Section: Perioperaitve Antibiotics
Optimal drug choices and timing?– Systematic review 15 studies assessing timing or
use extended-spectrum antibioticsAbx admin before incision OR use of extended-spectrum regimens (azithromycin or metronidazole) after cord clamp reduced post-CS maternal infection by up to 50%
– Two strategies NOT compared with each other!– Effect on neonatal infection or infection with resistant organisms
needs further study
Conclusion: cefazolin alone before incision or addition of extended-spectrum regimen (azithromycin/metronidazole) after cord clamp reduced post-CS maternal infection
– Further studies needed for post-incisional abx addition strategy Andrews 2003; Tita 2008; Tita 2008; Constantine 2008; Tita 2009
Cesarean Section: Perioperaitve Antibiotics
Optimal drug choices?– Women with history of significant PCN or
cephalosporin allergy Anaphylaxis, angioedema, respiratory distress, urticariaClindamycin with aminoglycoside
– Clindamycin 900 mg IV and gentamicin 5 mg/kg IV
– Women already on antibiotics GBS prophylaxis (PCN or ampicillin)
– Consider addition of single dose broad spectrum abx
Chorioamnionitis (ampicillin and gentamicin)– Add clindamycin or change to ampicillin-sulbactam– If B. fragilis resistance to clindamycin� ampicillin-sulbactam!
ACOG 2011; Kenyon 2013 (Cochrane Review)
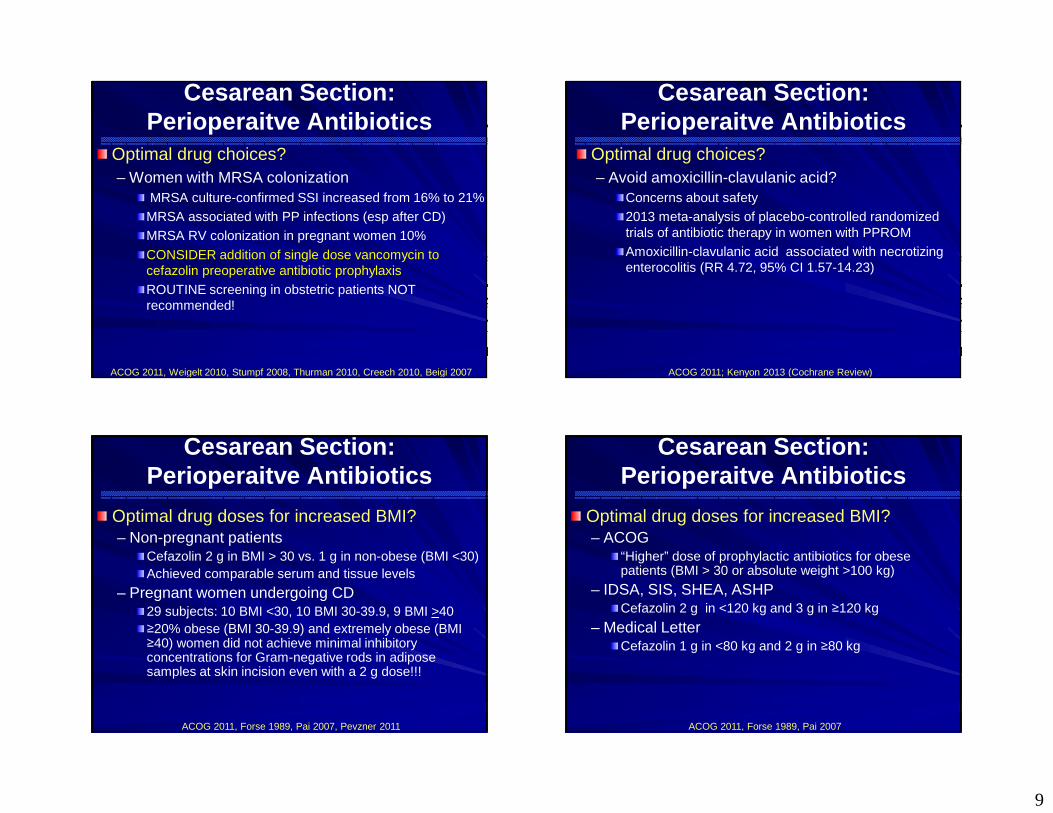
9
Cesarean Section: Perioperaitve Antibiotics
Optimal drug choices?– Women with MRSA colonization
MRSA culture-confirmed SSI increased from 16% to 21%MRSA associated with PP infections (esp after CD)MRSA RV colonization in pregnant women 10%
CONSIDER addition of single dose vancomycin to cefazolin preoperative antibiotic prophylaxis ROUTINE screening in obstetric patients NOT recommended!
ACOG 2011, Weigelt 2010, Stumpf 2008, Thurman 2010, Creech 2010, Beigi 2007
Cesarean Section: Perioperaitve Antibiotics
Optimal drug choices?– Avoid amoxicillin-clavulanic acid?
Concerns about safety 2013 meta-analysis of placebo-controlled randomized trials of antibiotic therapy in women with PPROM Amoxicillin-clavulanic acid associated with necrotizing enterocolitis (RR 4.72, 95% CI 1.57-14.23)
ACOG 2011; Kenyon 2013 (Cochrane Review)
Cesarean Section: Perioperaitve Antibiotics
Optimal drug doses for increased BMI?– Non-pregnant patients
Cefazolin 2 g in BMI > 30 vs. 1 g in non-obese (BMI <30) Achieved comparable serum and tissue levels
– Pregnant women undergoing CD 29 subjects: 10 BMI <30, 10 BMI 30-39.9, 9 BMI >40≥20% obese (BMI 30-39.9) and extremely obese (BMI ≥40) women did not achieve minimal inhibitory concentrations for Gram-negative rods in adipose samples at skin incision even with a 2 g dose!!!
ACOG 2011, Forse 1989, Pai 2007, Pevzner 2011
Cesarean Section: Perioperaitve Antibiotics
Optimal drug doses for increased BMI?– ACOG
“Higher” dose of prophylactic antibiotics for obese patients (BMI > 30 or absolute weight >100 kg)
– IDSA, SIS, SHEA, ASHP Cefazolin 2 g in <120 kg and 3 g in ≥120 kg
– Medical Letter Cefazolin 1 g in <80 kg and 2 g in ≥80 kg
ACOG 2011, Forse 1989, Pai 2007

10
Cesarean Section: Perioperaitve Antibiotics
Optimal drug doses?– Cochrane Review
No additional benefit from multiple prophylaxis dose (OR 0.92, 0.79-1.23) for narrow spectrum regimens randomized trials
– Continuation of broad spectrum regimen for 6-12 hours postoperatively may decrease infection???
Institution-specific patient characteristics?
– Repeat dose recommended if significant blood loss (>1500 cc) or operative time >4 hours
Repeat dosing: Q 1-2 half-lives of the drug in patients with normal renal function Cefazolin therapeutic level: maintained ~3-4 hours
Hopkins 2002 (Cochrane Review); Andrews 2003; Tita 2008; Tita 2008; Tita 2009
Cesarean Section: Perioperaitve Antibiotics
Optimal pre-incision drug administration time?– Varies in OBSTETRIC data
No consistent time window amongst studies
– Extrapolate from general surgical literature 2nd generation cephalosporin (cefuroxime)30-60 minutes most effective in reduction SSI Superior to <30 minutes (aOR 1.95, 1.4-2.8, P<0.001) and 60-120 minutes (aOR 1.74, 1.0-2.9, P=0.035)
Constantine 2008; Tita 2009; Weber 2008; Garey 2006
Cesarean Section: Perioperaitve Antibiotics
Traditional Recommendations– Single IV dose narrow spectrum prx abx at time of
cord clamp to reduce post-op infection – Cefazolin 1-2 gm or ampicillin 2 gm
Summary– Narrow spectrum, longer half-life abx (cefazolin
preferred over ampicillin) before incision associated with reduction post-CS maternal infection
Hopkins 2002; Andrews 2003; Tita 2008; Tita 2008; Constantine 2008; Tita 2009
Cesarean Section: Perioperaitve Antibiotics
Current Treatment Considerations – Cefazolin 1-2 g IV prior to skin incision
Ideally 30-60 minutes prior to procedure
– Single dose sufficient for routine cases– Additional dose for excessive blood loss or
prolonged procedure – Extended spectrum- data still limited
More costly NOT proven to be superior to Cefazolin prior to incision regimen in comparison trials
Hopkins 2002; Andrews 2003; Tita 2008; Tita 2008; Constantine 2008; Tita 2009

11
Cerclage
Insufficient data for perioperative antibiotic administration
ACOG 2011
Postpartum Tubal Ligation
Insufficient data for perioperative antibiotic administration – Exception: vaginal/colpotomy technique
Single dose of prophylactic antibiotic should be administered ~ 30 minutes before procedure
ACOG 2009, Smith 1991
3rd/4th Degree Lacerations
Prophylactic antibiotics at time of 3rd and 4th degree perineal laceration repairs– 147 patients – Randomized to single IV dose of cefotetan or cefoxitin– 27% loss at 2-week follow-up – 8% of Abx group vs. 24% of placebo developed perineal
wound complications by 2 weeks PP (P=0.037)Gross disruption or purulent discharge
– Findings not replicated in meta analysis
Treatment consideration– Administer single dose IV 2nd generation cephalosporin
at time of 3rd or 4th degree perineal laceration repairDuggal 2008, Buppasiri 2010 (Cochrane Review)
Placental Extraction
Insufficient data for antibiotic administration– Antibiotic prophylaxis for reduction of PP
infection prevention in placental extraction and/or curettage for retained placenta???
– Several studies report for CD increased PP endometritis with manual removal of placenta
– No studies assessing antibiotic prophylaxis!!! – ?Extrapolated from gynecology literature and
perinatal HIV literature

12
SummaryGBS
– Consider higher vancomycin dosing, especially in obese patients: 20 mg/kg Q 8 hours (maximum of 2 g each dose)
Infective endocarditis – Antibiotic prx only in highest risk patients without infection PPROM
– Ampicillin/amoxicillin and erythromycin regimen x 7 days – Coverage for GBS! PTL with intact membranes
– Antibiotics NOT recommended for pregnancy prolongation– Erythromycin may be associated with adverse events– Coverage for GBS!
SummaryChorioamnionitis
– Limited comparison abx trials– Daily dosing of gentamicin– Single dose PP sufficient for routine VD chorioamnionitis– CD with prolonged labor course/ROM or obese patients
likely require more than single PP course PP endometritis
– Daily (5 mg/kg) as efficacious/safe as Q8 hour dosing – Oral antibiotics not indicated following successful IV
treatment
SummaryCD preoperative
– Cefazolin 1-2 g IV, 30-60 min prior to skin incision– Higher dose for obese patients!!! – Single dose sufficient for routine cases– Add vancomycin to cefazolin in MRSA-colonized
patient – Re-dose in complicated (large EBL or long OR time)
procedures– PCN severe allergy: clindamycin and gentamicinLimited/insufficient data for cerclage, PPTL, placental manual extraction abx prophylaxis
– Antibiotics generally not recommended
3rd or 4th degree perineal laceration– Consider single dose IV 2nd generation cephalosporin
Acknowledgements
Judith Bishop, CNM, MSN, MPHAaron Caughey, MD, PhDTekoa King, CNM, MPH
Mary Norton, MDJulian Parer, MD, PhD
Gaelen Lombard and UCSF CME office
13
Thank You!Pager: 650-723-8222
Pager ID 23344
Other Antimicrobial Intrapartum Management
Considerations
Genital HSV Suppression
Traditional Recommendations– Acyclovir 400 mg TID for HSV suppression in pregnancy
after 36 weeks until delivery
Valacyclovir prophylaxis– 338 women with history of HSV– Randomized valacyclovir 500mg BID vs. placebo – 36 weeks until delivery – Valacyclovir significantly reduced at delivery
HSV shedding (2% vs. 9%, p=0.02) Recurrent genital HSV (4% vs. 13%, P=0.009) Less CD in treatment group
ACOG 2007; Sheffield 2006; Sheffield 2004; Watts 2003; Scott 2002; Scott 2001;
Genital HSV Suppression
Current Treatment Recommendations– Acyclovir 400 mg TID or Valacyclovir 500 mg
BID HSV suppression in pregnancy after 36 weeks until delivery
Acyclovir less expensive, covered by more insurances Valacyclovir easier compliance dosing
ACOG 2007; Sheffield 2006; Sheffield 2004; Watts 2003; Scott 2002; Scott 2001;

14
Skin/Soft Tissue InfectionsCA-MRSA in Pregnancy
Retrospective chart review – 57 pregnant women with MRSA infections between 2000-2004
Increasing MRSA infection incidenceRF for MRSA infection: multiparity, CD, repeat CDGestational age diagnosed– 2nd trim (46%) > 1st trim > Postpartum > 3rd trim
Lesion sites– Extremities (44%) > buttocks > breast/mastitis > vulva/groin > abdomen
Postpartum lesions – Breast (40%) > incision (30%) > other soft tissue (30%)
96% skin or soft tissue infections 58% recurrent episodes63% required in-patient treatment
Laibl 2005
Vulvar Abscess
www.visualdxhealth.com
Vulvar Abscess162 women with vulvar abscesses16% (26) patients pregnant 64% of cultured abscesses were MRSA40% required inpatient management In-patient treatment more common with comorbidities, larger abscess, systemic illness No difference in inpatient admission or treatment complications in MRSA group Treatment – I&D plus TMP/SMX, vancomycin, or clindamycin
Thurman 2008
Vulvar and Soft Tissue Infections Abscess
Traditional Recommendations: – Gram positive coverage for skin/soft tissue infxn in pregnancy– Cephalexin 500 mg QID x 10 days
Summary– CA-MRSA emergence in obstetric infections– Consider MRSA Coverage – MRSA abscess I&D alone highly effective (90% cure rate)
Post procedure antibiotics may not substantially improve outcome
Current Treatment Considerations– Be aware of local community infectious characteristics– Consider I&D plus TMP/SMX, vancomycin, or clindamycin
Especially if not responsive to routine staph aureas coverage If I&D not effective within 7 days, antibiotics initiation important

15
Mastitis/Breast Abscess
Journal of Midwifery & Womens Health 2007
Mastitis/Breast AbscessRise CA-MRSA mastitis/breast abscessesCA-MRSA >10% of community isolatesRetrospective case series nonpuerperal breast abscess – 44 women – 19% MRSA > Coag neg Staph 16% > MSSA 14%
Case control postpartum mastitis – 27 MSSA and 21 MRSA– Increasing incidence of MRSA mastitis infections – 95% CA-MRSA of 21 MRSA cases– MRSA cases more often multiparous (57%) vs. MSSA (33%)– MRSA less likely to receive appropriate/timely antibiotic tx– Higher temperature with MRSA vs. MSSA (p=0.05)– No significant difference in clinical outcome
Moazzez 2007, Reddy 2007
Mastitis/Breast Abscess
Reddy 2007
Mastitis/Breast Abscess127 women hospitalized with puerperal mastitisMastitis only cultures (n=54)– MSSA (44%) > S. epi (35%) > MRSA (2%)
Mastitis + breast abscess cultures (n=35)– CA-MRSA most common breast abscess organism– MRSA (67%) vs. MSSA (19%)
Women with CA-MRSA inappropriately treated– 56% did NOT receive appropriate antibiotic
Empiric use of ineffective antibiotic DID NOTadversely affect outcomes
Stafford 2008

16
Mastitis/Breast AbscessManagement
CA-MRSA increasingly more common in puerperal mastitis and especially abscesses Continue first line mastitis treatment in routine casesConsider cultures if tx failure, recurrence, high prevalence, RF’sConsider CA-MRSA therapy– Recurrence, tx (beta lactam) failure, abscess, severe infection until
cultures obtained– Local epidemiology – Adjunct drainage or aspiration may be warranted
Treatment/Management for MRSA mastitis– Continue breastfeeding/pumping– TMP/SMX = first line (efficacy, cost, compliance)– Clindamycin and Linezolid 2nd line alternatives– I&D or aspiration/catheter drainage for abscess
Stafford 2008, Reddy 2007, Moazzez 2009
Influenza Testing and Treatment
Antiviral treatment recommended for pregnant women with suspected or confirmed influenza– Regardless of trimester of pregnancy!!!– Women up to 2 weeks PP (including pregnancy loss)!
Do not delay treatment – Negative rapid influenza diagnostic test– Inability to test – While awaiting test results
CDC September 2009; CDC April 2010
Antiviral Summary
Agent Treatment Chemoprophylaxis
Oseltamivir 75 mg PO BID x 5 days
75 mg PO QD x 10 days
Oseltamivir(Acutely ill)
150 mg PO BID x 10 days
Zanamivir Two 5-mg inhalations (10 mg total) BID x 5 days
Two 5-mg inhalations (10 mg total) QD x 10 days
Peramivir(Specific Criteria)
600 mg IV Daily x 5-10 days
CDC 2009, Saleeby 2009

6/5/2014
1
CHORIOAMNIONITIS: WHAT IS THE EVIDENCE FOR CLINICAL MANAGEMENT?Juan M. Gonzalez, MD Assistant Professor Maternal-Fetal Medicine
Department of Ob/Gyn & RSUniversity of California, San Francisco
Disclosures
• No Financial Disclosures
Definition
• Chorioamnionitis
• Amnionitis• Intramamniotic infection
Pathogenesis
• Ascending of cervicovaginal flora• Facilitated by ROM
• Tranplacental• Listeria moncytogenes
• Iatrogenic • Amnio, CVS, fetal surgery

6/5/2014
2
Clin Perinatol. 2010 Jun;37(2):339-54.
EPIDEMIOLOGY
Preterm
• Intramamniotic infection with pPROM• Less than 27 weeks � 41 %• 28 to 36 weeks � 15 %
• Intraamniotic infection 1/3 of spontaneous preterm labor with intact membranes
Clin Obstet Gynecol. 1993 Dec;36(4):795-808.
Am J Obstet Gynecol. 2001 Nov;185(5):1130-6.
Term
• 2 to 4 % term deliveries
• 12 % in labor who undergo a cesarean delivery

6/5/2014
3
Risk Factors
• Low parity • Prolonged labor • Prolonged rupture of membranes • Multiple vaginal examinations in labor (consequence of longer labors)
• Internal fetal monitoring • Genital tract pathogens (STI, GBS, BV)
Microbiology
• Clinical intraamniotic infection • Bacteroides species (25 %)• G. vaginalis (24 %) • GBS (12 %)• Aerobic streptococci (13 %)• E. coli (10%)• Aerobic gram-negative rods (10 %)
J Infect Dis. 1982 Jan;145(1):1-8.
Microbiology
• 35 % of patients with clinical chorioamnionitisyield Mycoplasm hominis
J Infect Dis. 1983 Apr;147(4):650-3.

6/5/2014
4
Clinical Presentation
• Clinical chorioamnionitis
• Subclinical absence of clinical findings:• Most commonly presents as spontaneous preterm labor or pPROM
Clinical Chorioamnionitis
• Maternal fever (oral temp ≥ 38.0C or 100.4F) (all cases)
• At least two of the following: • wbc > 15k (70-90% of cases)• maternal tachycardia (> 100 bpm) (50-80% of cases)• fetal tachycardia (> 160 bpm) (50-80% of cases)• uterine tenderness or foul odor of the amniotic fluid (4-
25% of cases)
Clin Perinatol. 2010 Jun;37(2):339-54.
Test
Clinical parameters
Fever Temperature >100.4 F 95 – 100 sensitiveNewton ER. Clin Obstet Gynecol 1993;36:795
Maternal tachycardia > 100/min 50 – 80% sensitive
Fetal tachycardia >160/min 40 – 70% sensitive
Fundal tenderness Tenderness on palpation 4 – 25% sensitive
Vaginal discharge Foul-smelling discharge 5 – 22% sensitive
Amniocentesis
• Refractory to tocolytics
• pPROM to determine whether induction is indicated
• Discriminate between chorioamnionitis and other causes of fever and abdominal pain
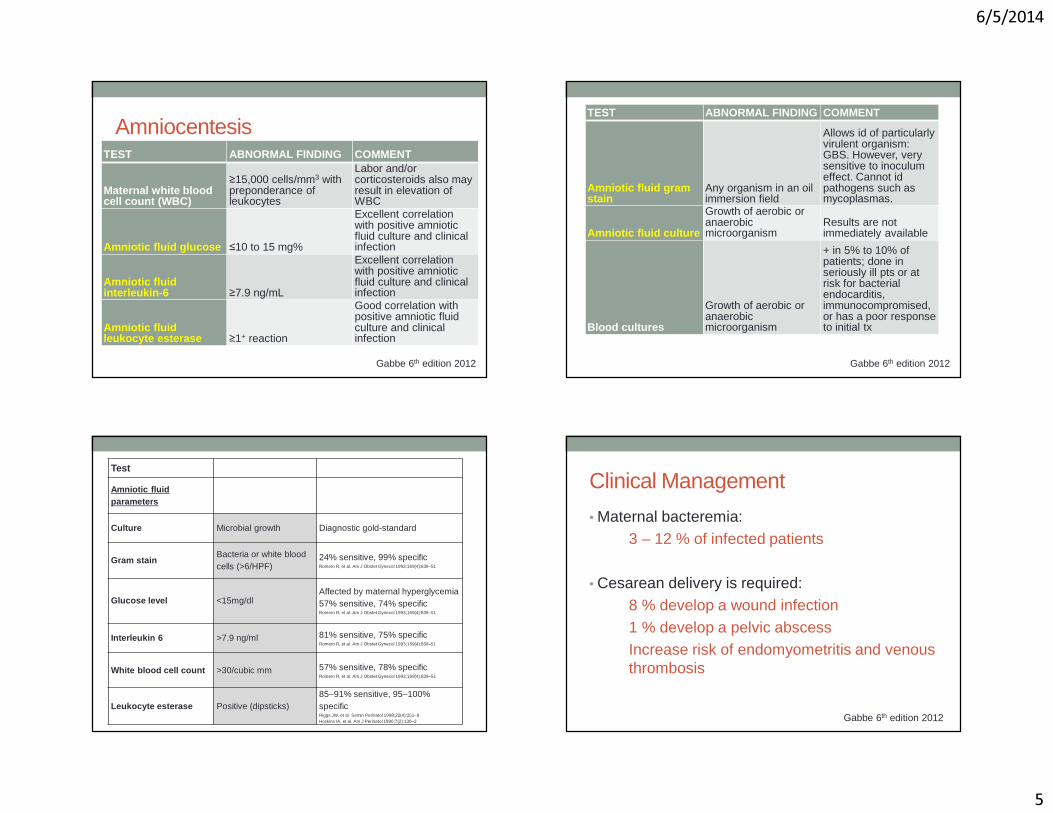
6/5/2014
5
Amniocentesis TEST ABNORMAL FINDING COMMENT
Maternal white blood cell count (WBC)
≥15,000 cells/mm3 with preponderance of leukocytes
Labor and/or corticosteroids also may result in elevation of WBC
Amniotic fluid glucose ≤10 to 15 mg%
Excellent correlation with positive amniotic fluid culture and clinical infection
Amniotic fluid interleukin-6 ≥7.9 ng/mL
Excellent correlation with positive amniotic fluid culture and clinical infection
Amniotic fluid leukocyte esterase ≥1+ reaction
Good correlation with positive amniotic fluid culture and clinical infection
Gabbe 6th edition 2012
TEST ABNORMAL FINDING COMMENT
Amniotic fluid gram stain
Any organism in an oil immersion field
Allows id of particularly virulent organism: GBS. However, very sensitive to inoculum effect. Cannot id pathogens such as mycoplasmas.
Amniotic fluid culture
Growth of aerobic or anaerobic microorganism
Results are not immediately available
Blood cultures
Growth of aerobic or anaerobic microorganism
+ in 5% to 10% of patients; done in seriously ill pts or at risk for bacterial endocarditis, immunocompromised, or has a poor response to initial tx
Gabbe 6th edition 2012
Test
Amniotic fluid parameters
Culture Microbial growth Diagnostic gold-standard
Gram stainBacteria or white blood cells (>6/HPF)
24% sensitive, 99% specificRomero R, et al. Am J Obstet Gynecol 1993;169(4):839–51
Glucose level <15mg/dlAffected by maternal hyperglycemia 57% sensitive, 74% specificRomero R, et al. Am J Obstet Gynecol 1993;169(4):839–51
Interleukin 6 >7.9 ng/ml 81% sensitive, 75% specificRomero R, et al. Am J Obstet Gynecol 1993;169(4):839–51
White blood cell count >30/cubic mm 57% sensitive, 78% specificRomero R, et al. Am J Obstet Gynecol 1993;169(4):839–51
Leukocyte esterase Positive (dipsticks)85–91% sensitive, 95–100% specificRiggs JW, et al. Semin Perinatol 1998;22(4):251–9Hoskins IA, et al. Am J Perinatol 1990;7(2):130–2
Clinical Management
• Maternal bacteremia:3 – 12 % of infected patients
• Cesarean delivery is required: 8 % develop a wound infection 1 % develop a pelvic abscessIncrease risk of endomyometritis and venous thrombosis
Gabbe 6th edition 2012
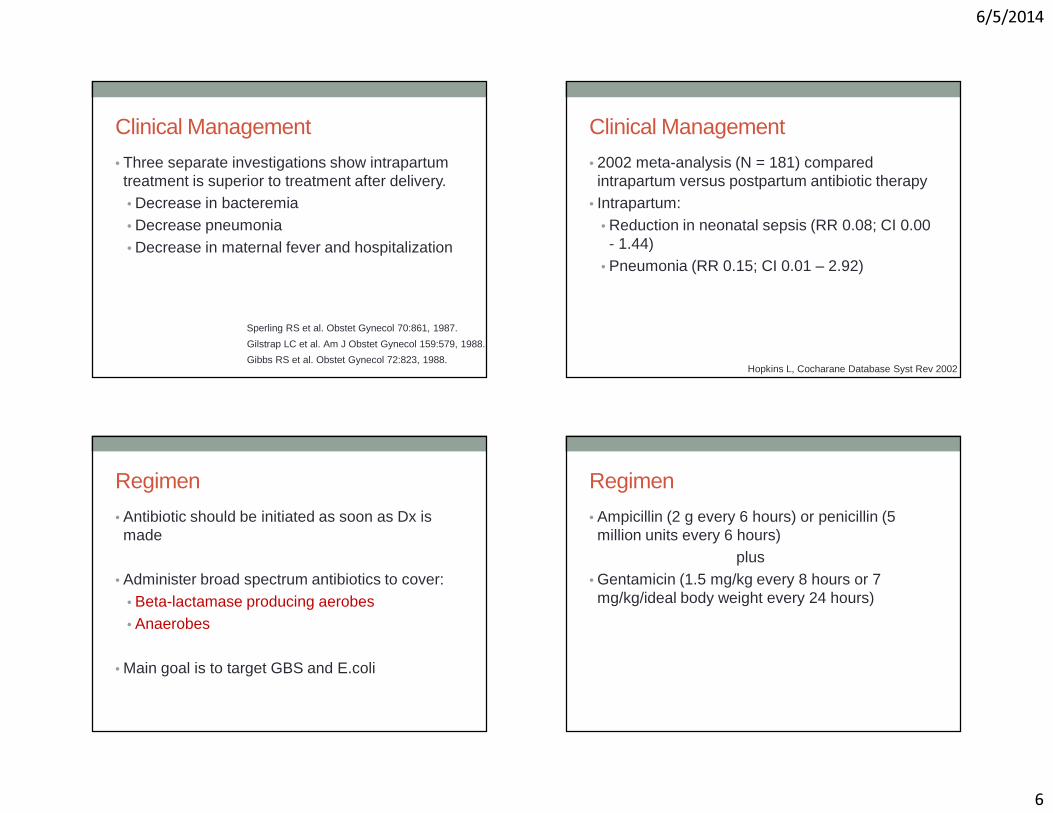
6/5/2014
6
Clinical Management
• Three separate investigations show intrapartumtreatment is superior to treatment after delivery. • Decrease in bacteremia • Decrease pneumonia • Decrease in maternal fever and hospitalization
Sperling RS et al. Obstet Gynecol 70:861, 1987.
Gilstrap LC et al. Am J Obstet Gynecol 159:579, 1988.
Gibbs RS et al. Obstet Gynecol 72:823, 1988.
Clinical Management
• 2002 meta-analysis (N = 181) compared intrapartum versus postpartum antibiotic therapy
• Intrapartum: • Reduction in neonatal sepsis (RR 0.08; CI 0.00 - 1.44)
• Pneumonia (RR 0.15; CI 0.01 – 2.92)
Hopkins L, Cocharane Database Syst Rev 2002
Regimen
• Antibiotic should be initiated as soon as Dx is made
• Administer broad spectrum antibiotics to cover: • Beta-lactamase producing aerobes • Anaerobes
• Main goal is to target GBS and E.coli
Regimen
• Ampicillin (2 g every 6 hours) or penicillin (5 million units every 6 hours)
plus • Gentamicin (1.5 mg/kg every 8 hours or 7 mg/kg/ideal body weight every 24 hours)

6/5/2014
7
Other Regimens
• Ampicillin-sulbactam• 3 grams intravenously every six hours
• Ticarcillin-clavulanate• 3.1 grams intravenously every four hours
• Cefoxitin• 2 grams intravenously every six hours
Regimen • Penicillin-allergic patients
• Substitute ampicillin for:
• Vancomycin 1 gram every 12 hours • If GBS+ and Clinda resistant/resistance unknown: Vancomycin /Gentamicin
OR
• Clindamycin 900 mg every 8 hours • If GBS-negative or Clinda-sensitive GBS: Clindamycin /Gentamicin
Regimen
Chorioamnionitis and Cesarean delivery:
• If Amp/Gent or Vanco/Gent used • add Clindamycin
or • Metronidazole
(ideally prior to skin incision) for anaerobic coverage
Duration Postpartum
• Post-partum management if vaginal delivery: • antibiotics are continued for one dose after delivery unless the
woman is diagnosed with endometritis
No difference in treatment failure or infection-related complications in RCT evaluating:
• single postpartum dose of antibiotics (Amp/Gent in study)
versus
• continuing until 24 hours afebrile postpartum
Edwards et al. Obstet Gynecol 102:957, 2003.

6/5/2014
8
Duration Postpartum • Post-partum management of chorioamnionitis if Cesarean
delivery: • If Amp/Gent or Vanco/Gent used
• add Clindamycin or
• Metronidazole
Edwards’ study included vaginal delivery and cesarean.
Underpowered to compare single-dose vs. continued dose just including Cesarean.
Given the high risk of endometritis in the setting of chorioamnionitis and Cesarean, continue antibiotics until 24 hours afebrile postpartum
Edwards et al. Obstet Gynecol 102:957, 2003.
Regimen
• There is NO evidence for oral antibiotics after discontinuation of parental therapy.
Dinsmoor MJ et al. Obstet Gynecol 1991; 77:60.
Antipyretics
• Maternal fever + fetal acidosis confers a 12.5% risk of neonatal encephalopathy (OR 94, 95 % CI 29 - 307)
• Independent effect:• Fever OR 8.1, 95 % CI 3.5 - 18.6• Neonatal acidosis OR 11.5, 95 % CI 5.0 – 26.5
Impey LW et al Am J Obstet Gynecol 2008; 198:49.
Route of Delivery
• Bactericidal concentrations in fetus one-half to one hour after infusion
• Average time between diagnosis and delivery is 3 to 5 hours
• No evidence that duration of infection correlates with outcomes
Gibbs RS et al Am J Obstet Gynecol 1991; 164:1317
Gilstrap LC 3rd et al Obstet Gynecol Clin North Am 1989; 16:373

6/5/2014
9
Rouse DJ et al Am J Obstet Gynecol 2004; 191:211
Rouse DJ et al Am J Obstet Gynecol 2004; 191:211
• Prolonged first or second stage of labor has been associated with an increased risk of chorioamnionitis
• Whether this relationship is causal is unclear �evolving chorioamnionitis may predispose to longer labor
• Neither chorioamnionitis nor its duration should be an indication for cesarean delivery
ACOG Number 1, March 2014
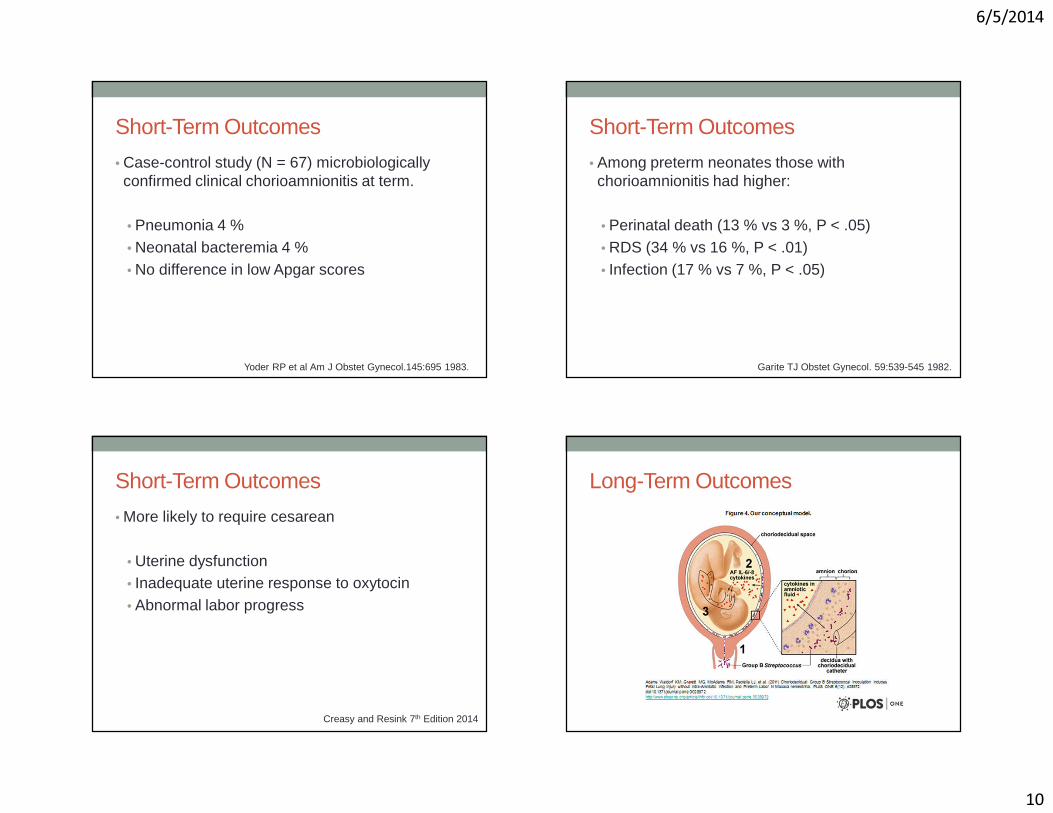
6/5/2014
10
Short-Term Outcomes
• Case-control study (N = 67) microbiologically confirmed clinical chorioamnionitis at term.
• Pneumonia 4 %• Neonatal bacteremia 4 %• No difference in low Apgar scores
Yoder RP et al Am J Obstet Gynecol.145:695 1983.
Short-Term Outcomes
• Among preterm neonates those with chorioamnionitis had higher:
• Perinatal death (13 % vs 3 %, P < .05)• RDS (34 % vs 16 %, P < .01)• Infection (17 % vs 7 %, P < .05)
Garite TJ Obstet Gynecol. 59:539-545 1982.
Short-Term Outcomes
• More likely to require cesarean
• Uterine dysfunction • Inadequate uterine response to oxytocin• Abnormal labor progress
Creasy and Resink 7th Edition 2014
Long-Term Outcomes

6/5/2014
11
Long-Term Outcomes Diagnosis N RR (95% CI)
PRETERM INFANTS
Cerebral Palsy
Clinical chorioamnionitis 11 1.9 (1.4-2.5)
Histologic chorioamnionitis 5 1.6 (0.9-2.7)
Cystic Periventricular Leukomalacia
Clinical chorioamnionitis 6 3.0 (2.2-4.0)
Histologic chorioamnionitis 7 2.1 (1.5-2.9)
CI, confidence interval; RR, relative risk.
Grether JK, Nelson KB JAMA278:207, 1997; Wu YW, Colford JM Jr JAMA284:1417, 2000.
Creasy and Resink 7th edition 2014.
Long-Term Outcomes
Diagnosis N RR (95% CI)
TERM INFANTS
Cerebral Palsy
Clinical chorioamnionitis 2 4.7 (1.3-16.2)
Histologic chorioamnionitis 1 8.9 (1.9-40)
CI, confidence interval; RR, relative risk.
Grether JK, Nelson KB JAMA278:207, 1997; Wu YW, Colford JM Jr JAMA284:1417, 2000.
Creasy and Resink 7th edition 2014.
Prevention
• Ineffective:• Chlorhexidine vaginal washes during labor1
• Antepartum treatment of bacterial vaginosis 2
• Broad-spectrum antibiotics in patients with preterm labor but intact membranes3
Rouse DJ et al Am J Obstet Gynecol. 176:617 1997. 1
Carey JC et al N Engl J Med. 342:534 2000. 2
Egarter C et al Obstet Gynecol. 88:303 1996. 3
Prevention
• Intrapartum prophylaxis to prevent neonatal GBS sepsis decrease chorioamnionitis
• Screening based strategy versus risk-based
Locksmith GJ et al Am J Obstet Gynecol. 180:416 1999.

6/5/2014
12
Prevention
• Active management of laborLopez-Zeno JA et al N Engl J Med. 326:450 1992.
• Induction of labor after PROM at term Mozurkewich EL et al Am J Obstet Gynecol. 89:1035 1997.
• Prophylactic antibiotics in selected patients with pPROM
Mercer BM Lancet. 346:1271 1995.
Prevention
• Largest randomized study found induction with oxytocin induction in PROM • Reduced:
• the time interval between premature rupture of membranes and delivery
• chorioamnionitis• postpartum febrile morbidity• neonatal antibiotic treatments
• Without increasing cesarean deliveries or neonatal infections
ACOG PB Number 107, August 2009.Hannah ME et al N Engl J Med 1996; 334:1005–10.
Prevention • Intravaginal PGE2 for IOL with PROM appears to be safe
and effective
• Randomized study IOL with PROM at term, only 1 dose of intravaginal misoprostol was necessary for successful labor induction in 86%
• No evidence that use of either prostaglandin increases the risk of infection in women with ROM
• Insufficient evidence to guide on use of mechanical dilators in ruptured membranes.
ACOG PB Number 107, August 2009.
Ray DA, Garite TJ. Am J Obstet Gynecol 1992;166:836–43.Sanchez-Ramos L et al Obstet Gynecol 1997;89:909–12.
Prevention • Meta-analysis (N = 6,814) PROM at term compared:
• IOL with prostaglandins or oxytocin • expectant management
• In patients which underwent IOL significant reduction in the risk of:• chorioamnionitis• endometritis• number of neonates requiring admission to NICU
Dare MR et al Cochrane Database of Systematic Reviews 2006, Issue 1. Art. No.: CD005302.

6/5/2014
13
Summary • Chorioamnionitis is polymicrobial
• results from migration of cervicovaginal flora through the cervical canal
• Other causes include transplacental infection • bacteremia • invasive procedures
• Maternal fever ≥100.4 F. • Clinical diagnosis is strengthened by risk factors for the disease
and excluding sources of fever • Nonspecific clinical signs: leukocytosis, maternal and fetal
tachycardia, uterine tenderness, malodorous amniotic fluid
Tita, A et al Clin Perinatol. 2010;37(2):339-354.
Summary
• Amniocentesis may be helpful in cases of diagnostic uncertainty
• Chorioamnionitis may impair myometrialcontractility �can result:• labor abnormalities• need for cesarean delivery (with higher rate of complications)
• postpartum hemorrhage
Tita, A et al Clin Perinatol. 2010;37(2):339-354.
Summary
• Broad spectrum antibiotics should be started at diagnosis to minimize maternal and fetal morbidity.• Vaginal delivery: a single dose of antibiotics after delivery
• Cesarean section: afebrile for at least 24 hours
Tita, A et al Clin Perinatol. 2010;37(2):339-354.
Summary
• In the setting of chorioamnionitis, prompt induction or augmentation of labor• cesarean delivery reserved for standard obstetrical indications
• Immediate cesarean in the setting reassuring intrapartum fetal testing, adequate progress of labor, and administration of antibiotics does not improve neonatal or maternal outcome.
• Adverse neonatal outcomes associated with chorioamnionitis
Tita, A et al Clin Perinatol. 2010;37(2):339-354.

6/6/2014
1
Sonographic Criteria for Nonviable Pregnancy in the 1st Trimester
Lori Strachowski, MDClinical Professor of Radiology, UCSF
Chief of Ultrasound, SFGH
I have no disclosures.
The Article
N Engl J Med October 2013;369:1443-51
Lecture Goals• Detailed overview of update on diagnostic criteria for
nonviable pregnancy early in the first trimester– Panelists– Issue – Objective– Plan– Recommended criteria– Reasoning

6/6/2014
2
The Panelists• Society of Radiologists in Ultrasound (SRU) Multispecialty
Panel on Early First Trimester Miscarriage and Exclusion of a Viable Intrauterine Pregnancy
• 3 Specialties:– Radiologists (7)– Obstetrician-Gynecologists (5)– Emergency Medicine (3)
The Rads
• Peter M. Doubilet, M.D., Ph.D., Brigham and Women’s and Harvard Medical School*
• Carol B. Benson, M.D., Brigham and Women’s/Harvard* • Beryl R. Benacerraf, M.D., Brigham and Women’s/Harvard• Douglas L. Brown, M.D., Mayo Clinic, Rochester• Roy A. Filly, M.D., UCSF• Edward A. Lyons, M.D., Univ of Manitoba, Winnipeg, MB• Dolores H. Pretorius, M.D., UCSD
* primary authors
The OB/Gyn’s
• Tom Bourne, M.B., B.S., Ph.D., Imperial College, London*• Steven R. Goldstein, M.D., NYU School of Medicine• Ilan E. Timor-Tritsch, M.D., NYU School of Medicine• Kurt T. Barnhart, M.D., M.S.C.E., University of Pennsylvania• Misty Blanchette Porter, M.D., Dartmouth
* primary authors
The ER Docs
• Michael Blaivas, M.D., University of South Carolina*• J. Christian Fox, M.D., University of California, Irvine• John L. Kendall, M.D., Denver Health Medical Center
* primary authors
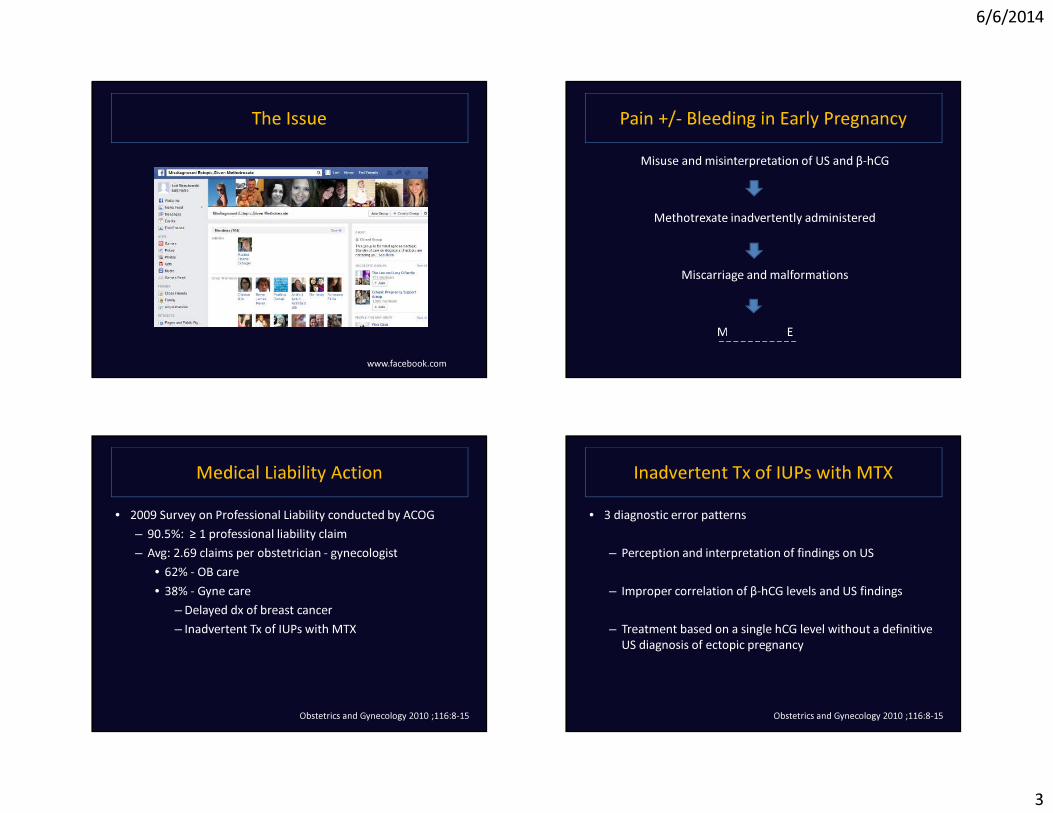
6/6/2014
3
The Issue
www.facebook.com
Pain +/- Bleeding in Early PregnancyMisuse and misinterpretation of US and β-hCG
Methotrexate inadvertently administered
Miscarriage and malformations
MALPRACTICE_ _ _ _ _ _ _ _ _ _ _
Medical Liability Action• 2009 Survey on Professional Liability conducted by ACOG
– 90.5%: ≥ 1 professional liability claim– Avg: 2.69 claims per obstetrician - gynecologist
• 62% - OB care• 38% - Gyne care
– Delayed dx of breast cancer– Inadvertent Tx of IUPs with MTX
Obstetrics and Gynecology 2010 ;116:8-15
Inadvertent Tx of IUPs with MTX• 3 diagnostic error patterns
– Perception and interpretation of findings on US
– Improper correlation of β-hCG levels and US findings
– Treatment based on a single hCG level without a definitive US diagnosis of ectopic pregnancy
Obstetrics and Gynecology 2010 ;116:8-15

6/6/2014
4
US Error Types• Perception:
– Finding seen in retrospect but initially missed• i.e. an early intrauterine gestational sac or yolk sac
• Interpretation:– Findings perceived but incorrectly diagnosed
• i.e. CL of pregnancy interpreted as an EP or an early GS as a pseudo-sac
• Confounding factors for both:– Poor quality images, noncritical image evaluation,
incomplete clinical info
Obstetrics and Gynecology 2010 ;116:8-15
The Objective
First, DO NO HARM
or the least possible
The Plan• Set quality standards for diagnostic tests
• Standardize terminology
• Establish diagnostic criteria – Widely applicable and reproducible– Minimize risk
• Based (in part) on downstream consequences of false positive and false negative results
The Diagnostic Tests: hCG• Human chorionic gonadotropin
– Serum measured with use of WHO 3rd or 4th International Standard
– Positive serum pregnancy test is defined by > 5 mIU/ml
NOTE: low levels of hCG can occur in health non-pregnant patients.

6/6/2014
5
The Diagnostic Tests: US • Minimum quality criteria:
– TVS of uterus and adnexa– TAS for FF and mass high in the pelvis– Oversight by an appropriately trained physician– Performed by providers and interpreted by physicians, all
of whom meet at least minimum training or certification standards
– Scanning equipment permitting adequate visualization of structures early in the first trimester
The Terminology • Viable
• Nonviable
Definition: Viable (vī-ə-bəl)1: capable of living; especially: having attained such form and development as to be normally capable of surviving outside the mother's womb <a viable fetus>
www.Merriam-Webster.com
Definition: Viable (vī-ə-bəl)1: capable of living; especially: having attained such form and development as to be normally capable of surviving outside the mother's womb <a viable fetus>
www.Merriam-Webster.com

6/6/2014
6
Definition: Viable (vī-ə-bəl)1: capable of living; especially: having attained such form and development as to be normally capable of surviving outside the mother's womb <a viable fetus>
2: capable of growing or developing <viable seeds> <viable eggs>
3 a : capable of working, functioning, or developing adequately <viable alternatives> b : capable of existence and development as an independent unit <the colony is now a viable state> c (1) : having a reasonable chance of succeeding <a viablecandidate> (2) : financially sustainable <a viable enterprise>
www.Merriam-Webster.com
Definition: Viable (vī-ə-bəl)1: capable of living; especially: having attained such form and development as to be normally capable of surviving outside the mother's womb <a viable fetus>
2: capable of growing or developing <viable seeds> <viable eggs>
3 a : capable of working, functioning, or developing adequately <viable alternatives> b : capable of existence and development as an independent unit <the colony is now a viable state> c (1) : having a reasonable chance of succeeding <a viablecandidate> (2) : financially sustainable <a viable enterprise>
www.Merriam-Webster.com
The Terminology• Viable:
– A pregnancy is viable if it can potentially result in a liveborn baby.
• Nonviable: – A pregnancy is nonviable if it cannot possibly result in a
liveborn baby. • Ectopic pregnancies and failed intrauterine pregnancies
are nonviable.
The Differential
CurrentlyViable
IUPFailed/Failing
IUP
Ectopic pregnancy
Expectant management MUA, MTX,
+/- surgeryMUA

6/6/2014
7
Currently Viable IUP The Differential
CurrentlyViable
IUPFailed/Failing
IUP
Ectopic pregnancy
Expectant management MUA, MTX,
surgeryMUA
Ectopic Pregnancy
Ov
The Differential
CurrentlyViable
IUPFailed/Failing
IUP
Ectopic pregnancy
Expectant management MUA, MTX,
surgeryMUA
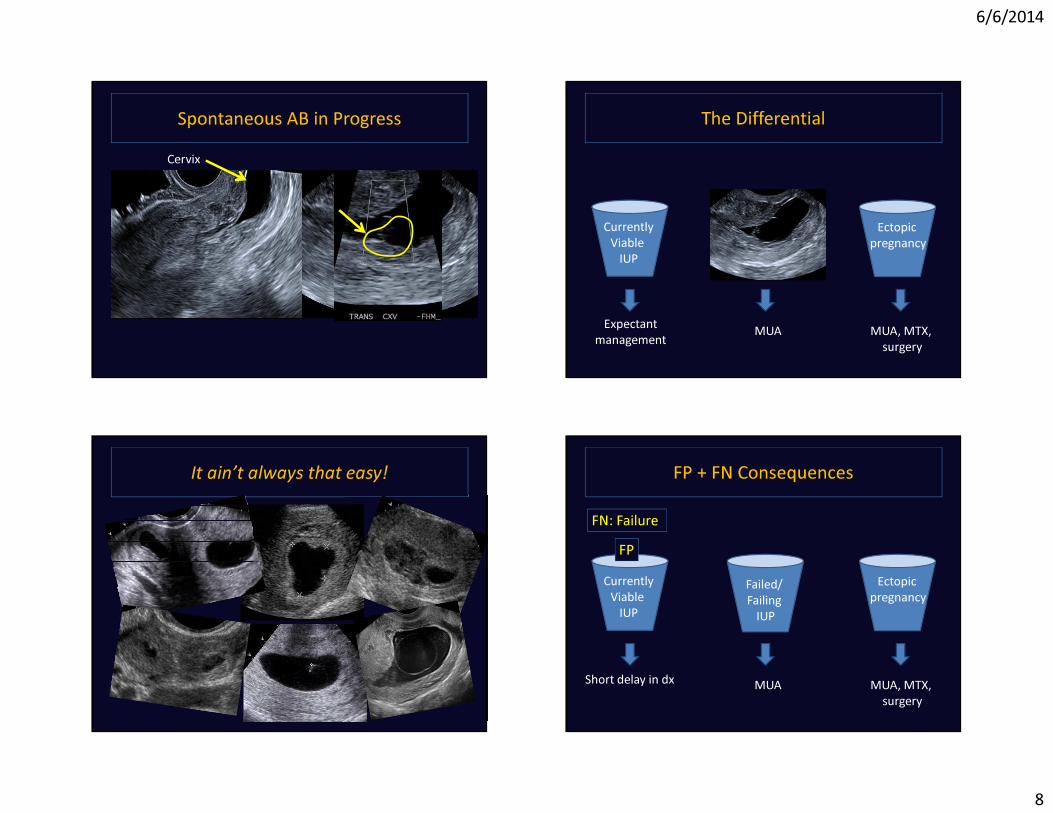
6/6/2014
8
Spontaneous AB in ProgressCervix
The Differential
CurrentlyViable
IUPFailed/Failing
IUP
Ectopic pregnancy
Expectant management MUA, MTX,
surgeryMUA
It ain’t always that easy! FP + FN Consequences
CurrentlyViable
IUPFailed/Failing
IUP
Ectopic pregnancy
Expectant management MUA, MTX,
surgeryMUA
FP
Short delay in dx
FN: Failure

6/6/2014
9
FP + FN Consequences
CurrentlyViable
IUPFailed/Failing
IUP
Ectopic pregnancy
Expectant management MUA, MTX,
surgeryMUAShort delay in dx
Likely non-life-threatening!
FN: EP
FP + FN Consequences
CurrentlyViable
IUPFailed/Failing
IUP
Ectopic pregnancy
Expectant management MUA, MTX,
surgeryMUAShort delay in dx
Likely non-life-threatening!
FN: EP FN: Failure
FP + FN Consequences
CurrentlyViable
IUPFailed/Failing
IUP
Ectopic pregnancy
Expectant management MUA, MTX,
surgeryMUA
FP FP
Short delay in dxLikely non-life-
threatening!
FN: Viable IUP FN: Viable IUP
To “DO NO HARM”1. Criteria for non-viability require
– 100% Specificity– 100% PPV
2. Need more buckets!
or as close as possible

6/6/2014
10
The Expanded Differential
CurrentlyViable
IUPFailed/Failing
IUP
Ectopic pregnancy
Expectant management
MUA, MTX, +/- surgery
MUA
IUP of Uncertain Viability
Pregnancyof
UnknownLocation
The Terminology• Intrauterine pregnancy of uncertain viability:
– If transvaginal ultrasonography shows an intrauterine gestational sac with no embryonic heartbeat and no findings of definite pregnancy failure.
• Pregnancy of unknown location:– Positive pregnancy test and no intrauterine or ectopic
pregnancy is seen on transvaginal US.
Is there a chance of a viable pregnancy?
The Expanded Differential
CurrentlyViable
IUPFailed/Failing
IUP
Ectopic pregnancy
Expectant management
MUA, MTX, +/- surgery
MUA
IUP of Uncertain Viability
Pregnancyof
UnknownLocation
Expectant management
Expectant management
The Expanded Differential
CurrentlyViable
IUPFailed/Failing
IUP
Ectopic pregnancy
Expectant management
MUA, MTX, +/- surgery
MUA
IUP of Uncertain Viability
Pregnancyof
UnknownLocation
Expectant management
Expectant management
Viable IUP
Failure
Short delay in dx
EPIUP
Short delay in dxLikely non-life-
threatening

6/6/2014
11
The Expanded Differential
Failed/Failing
IUPIUP of Uncertain Viability
Pregnancyof
UnknownLocation
Specific criteria and management algorithms
Literature on Nonviable IUP Criteria• Serum beta level
– Largely unreliable given range of normal
• US findings– Size-based criteria
• Embryo without heart motion• GS without an embryo
– Time-based criteria• Appearance of interval findings
Let’s review normal.
vv
US of Early Pregnancy• In order of appearance:
– Intradecidual sign– Double decidual sac sign– Yolk sac– Embryo– Amnion
Gestational sac
(+ heart motion)
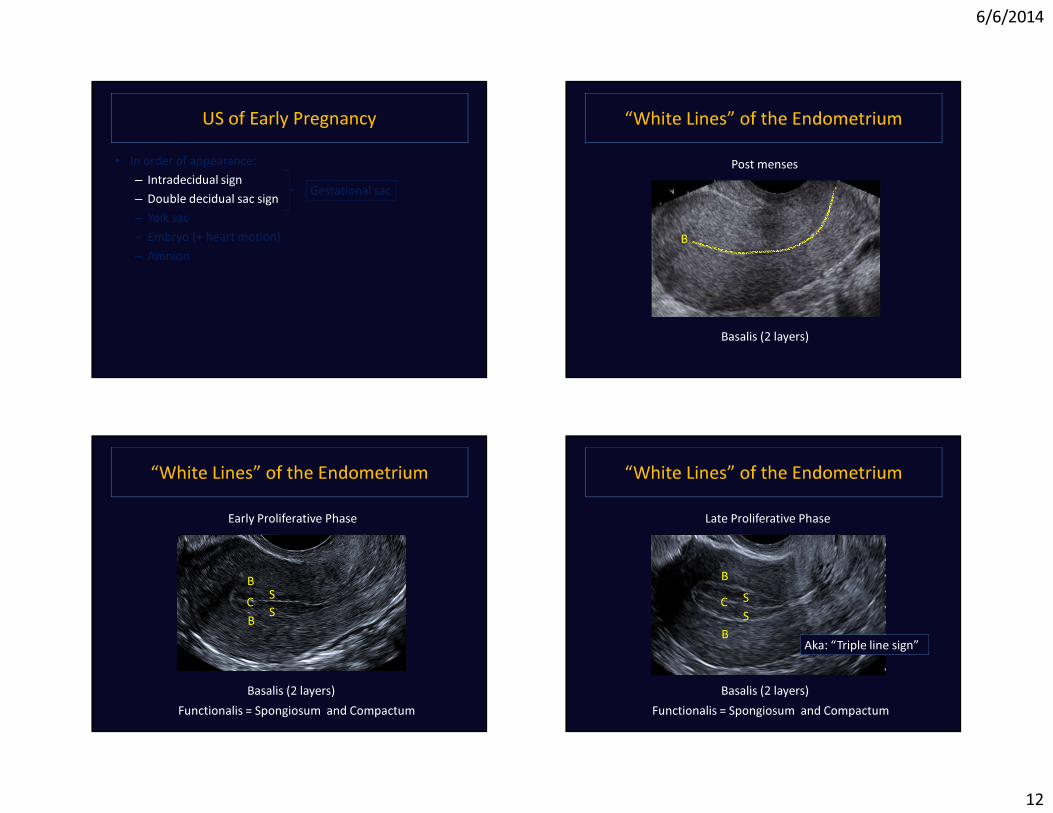
6/6/2014
12
US of Early Pregnancy• In order of appearance:
– Intradecidual sign– Double decidual sac sign– Yolk sac– Embryo– Amnion
Gestational sac
(+ heart motion)
“White Lines” of the EndometriumPost menses
B
Basalis (2 layers)
“White Lines” of the EndometriumEarly Proliferative Phase
Basalis (2 layers) Functionalis = Spongiosum and Compactum
B
BC S
S
“White Lines” of the Endometrium
B
B
C SS
Basalis (2 layers) Functionalis = Spongiosum and Compactum
Late Proliferative Phase
Aka: “Triple line sign”
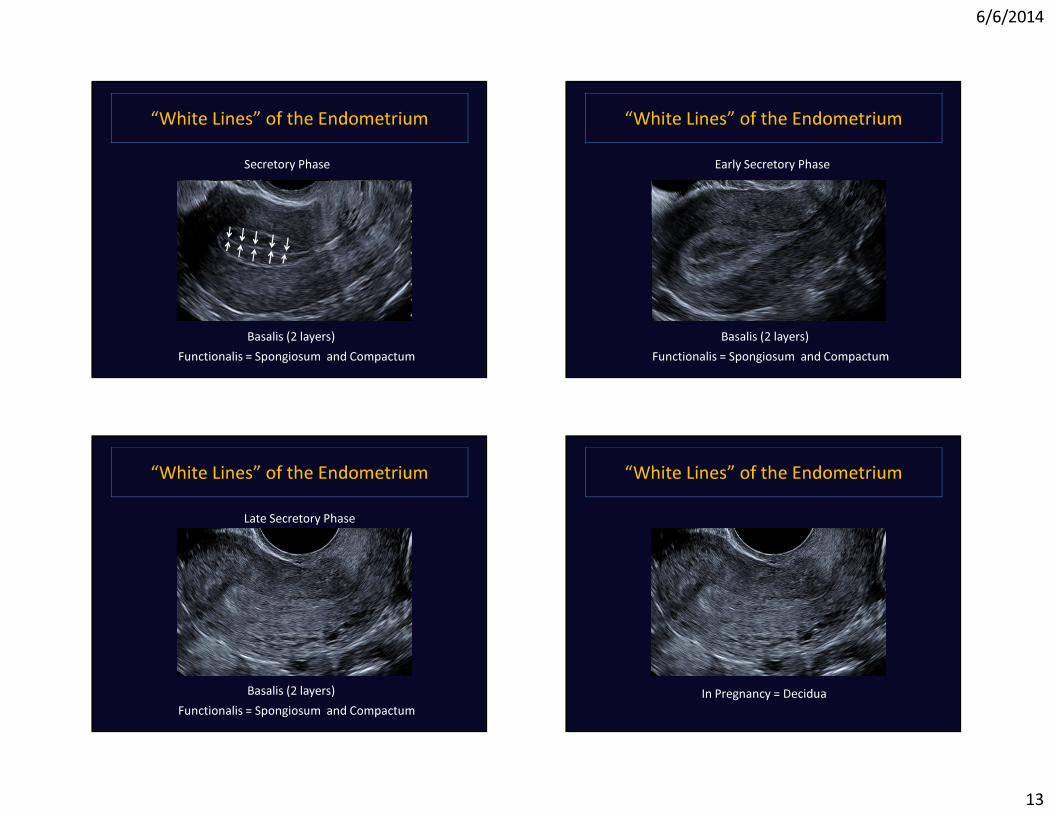
6/6/2014
13
“White Lines” of the EndometriumSecretory Phase
Basalis (2 layers) Functionalis = Spongiosum and Compactum
“White Lines” of the EndometriumEarly Secretory Phase
Basalis (2 layers) Functionalis = Spongiosum and Compactum
“White Lines” of the Endometrium
Basalis (2 layers) Functionalis = Spongiosum and Compactum
Late Secretory Phase
“White Lines” of the Endometrium
Basalis (2 layers) Functionalis = Spongiosum and Compactum
In Pregnancy = Decidua

6/6/2014
14
“White Lines” of the Endometrium
Basalis (2 layers) Functionalis = Spongiosum and Compactum
Blastocyst
In Pregnancy = Decidua
“White Lines” of the Endometrium
Basalis (2 layers) Functionalis = Spongiosum and Compactum
In Pregnancy = Decidua
Intradecidual Sign
Basalis (2 layers) Functionalis = Spongiosum and Compactum
In Pregnancy = Decidua
Intradecidual Sign• ~ 3-4 weeks• US:
– ≥ 2 mm cyst– Thin echogenic rim– Eccentric to central
echogenic line of endometrium
– Occasional “color flash”
Yeh, et.al., Radiology. 1986 Nov;161(2)

6/6/2014
15
Intradecidual Sign: Mimics• Intracavitary fluid• Decidual cysts
– IUP– EP
• Endometrial pathology– Polyps– Cystic hyperplasia– Cancer
Intradecidual Sign
Grows ~ 1mm/day and becomes….
Double Decidual Sac Sign Double Decidual Sac Sign• ~ 5 weeks• US:
– Round/oval fluid collection with 2 echogenic rims• Inner: chorion• Outer: decidua
Bradley, Filly, et.al., Radiology.1982 Apr;143(1)

6/6/2014
16
Double Decidual Sac Sign: Mimic• Pseudogestational sac
– Fluid/blood in endometrial cavity
• US:– Round/oval fluid
collection with 1 echogenic rim = decidua
– Acute angle margins• Associations:
– Implantation bleed– EP (10-20%)
How reliable are these signs?• Intradecidual sac sign
– Sensitivity: 48 - 92 %– Specificity: 66 - 97%
• Double decidual sac sign– Sensitivity: 64 - 95%– Specificity: 85 - 98%
Absent in at least 35% of
gestational sacs
If you see an oval/round intrauterine fluid collection……
It’s a GS until proven otherwise!
“ Therefore, any round or oval fluid collection in a woman with a positive pregnancy test most likely represents an intrauterine
gestational sac and should be reported as such.”
N Engl J Med October 2013;369:1445
Mean Sac Diameter• Diameter of anechoic sac
(excluding echogenic rim)• Measure:
– Greatest length– Perpendicular– Orthogonal greatest
length• Divide by 3
LONG
TRANS
“If this represents a GS, the MSD measures # mm”

6/6/2014
17
Yolk Sac • ~ 5 ½ weeks• US:
– 3-5 mm round, thin echogenic ring
NOTE: Never > 6mm OR thick/solid appearing at this gestational age
IUP MSD
Never to early to date!
IUP MSD
MSD (mm) + 30 = GA (days)i.e. 10 + 30 = 40 days (5 wks, 5 days)
Embryo • ~ 6 weeks• US:
– Adjacent to yolk sac– Present as flickering
heart motion– Grows ~ 1mm/day– Reniform, tadpole
appearance
Crown-rump length (CRL) avgof 2-4 measurements

6/6/2014
18
Amnion• ~ 8 weeks• US:
– Very thin echogenic ring surrounding embryo between yolk sac and chorion of GS
– Fuses with chorion: 12-16 weeks
“2nd skin”
YS
US of Early Pregnancy• In order of appearance:
– Intradecidual sign– Double decidual sac sign– Yolk sac– Embryo– Amnion
Gestational sac
(+ heart motion)
4 criteria definitive for failure
Size-based Criteria for Failure: CRL• Discriminatory CRL = size above which, the absence of cardiac
motion is unequivocal for failure• Historically: 5 mm
– Sensitivity: 50%– Specificity: 100% (95% CI: 90-100%)
• More recent data reports CRL 5-6 mm without heart motion and subsequent viable pregnancy
• Interobserver variability (measurement technique): + 15%• Worst case scenario:
Upper nl CRL (6) + 15% (0.9) = 6.9 mm7.0 mm
#1 Criteria Definitive for Failure• CRL ≥ 7 mm without cardiac
activity – PPV for failure: 100%
“Embryonic demise”
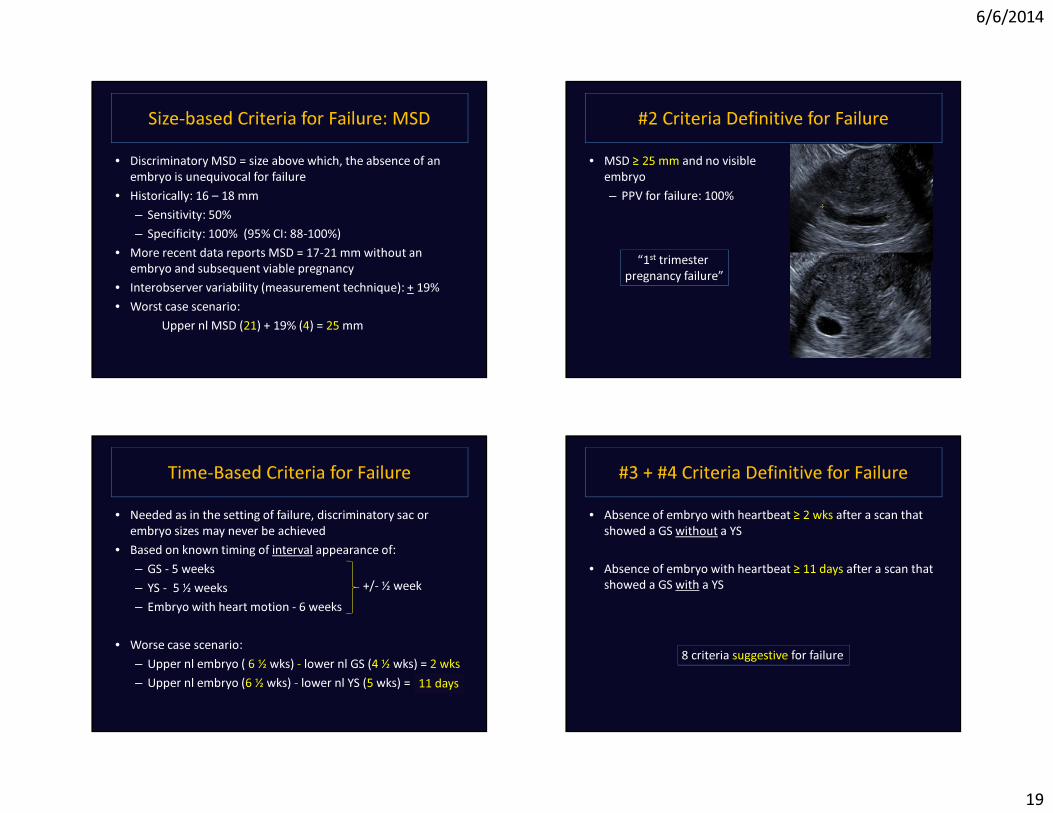
6/6/2014
19
Size-based Criteria for Failure: MSD• Discriminatory MSD = size above which, the absence of an
embryo is unequivocal for failure• Historically: 16 – 18 mm
– Sensitivity: 50%– Specificity: 100% (95% CI: 88-100%)
• More recent data reports MSD = 17-21 mm without an embryo and subsequent viable pregnancy
• Interobserver variability (measurement technique): + 19%• Worst case scenario:
Upper nl MSD (21) + 19% (4) = 25 mm
#2 Criteria Definitive for Failure• MSD ≥ 25 mm and no visible
embryo– PPV for failure: 100%
“1st trimester pregnancy failure”
Time-Based Criteria for Failure• Needed as in the setting of failure, discriminatory sac or
embryo sizes may never be achieved• Based on known timing of interval appearance of:
– GS - 5 weeks – YS - 5 ½ weeks– Embryo with heart motion - 6 weeks
• Worse case scenario:– Upper nl embryo ( 6 ½ wks) - lower nl GS (4 ½ wks) = 2 wks– Upper nl embryo (6 ½ wks) - lower nl YS (5 wks) = 1 ½ wks
+/- ½ week
11 days
#3 + #4 Criteria Definitive for Failure• Absence of embryo with heartbeat ≥ 2 wks after a scan that
showed a GS without a YS
• Absence of embryo with heartbeat ≥ 11 days after a scan that showed a GS with a YS
8 criteria suggestive for failure

6/6/2014
20
Criteria Suggestive of Failure• CRL <7 mm and no heartbeat
• MSD of 16 - 24 mm and no embryo
• Absence of embryo with heartbeat 7–13 days after a GS (-YS)
• Absence of embryo with heartbeat 7–10 days after a GS (+YS)
“When there are findings suspicious for pregnancy failure, follow-up US at 7 to 10 days is generally appropriate.”
Do we really need to wait to call this?
Normal GS and embryo grow ~1 mm/day
Criteria Suggestive of Failure• Empty amnion (amnion seen
adjacent to yolk sac, with no visible embryo)
Criteria Suggestive of Failure• Empty amnion (amnion seen
adjacent to yolk sac, with no visible embryo)
• Enlarged yolk sac (>7 mm)
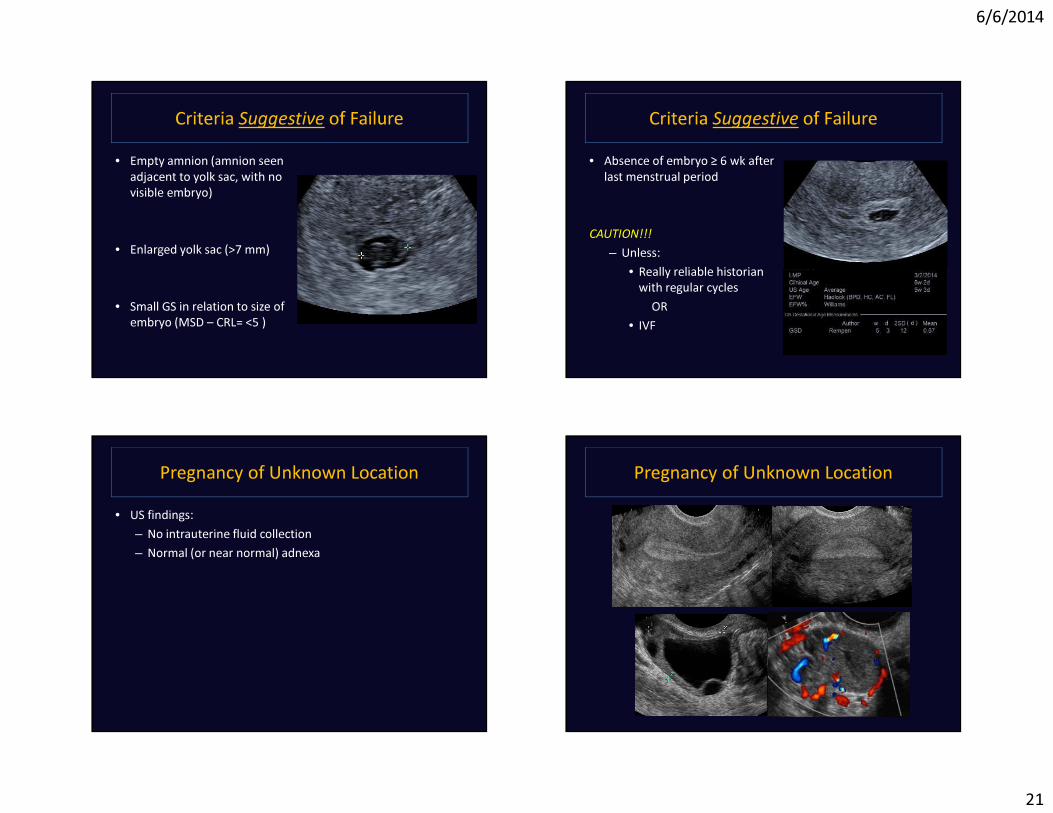
6/6/2014
21
Criteria Suggestive of Failure• Empty amnion (amnion seen
adjacent to yolk sac, with no visible embryo)
• Enlarged yolk sac (>7 mm)
• Small GS in relation to size of embryo (MSD – CRL= <5 )
Criteria Suggestive of Failure• Absence of embryo ≥ 6 wk after
last menstrual period
CAUTION!!!– Unless:
• Really reliable historian with regular cycles
OR• IVF
Pregnancy of Unknown Location• US findings:
– No intrauterine fluid collection– Normal (or near normal) adnexa
Pregnancy of Unknown Location
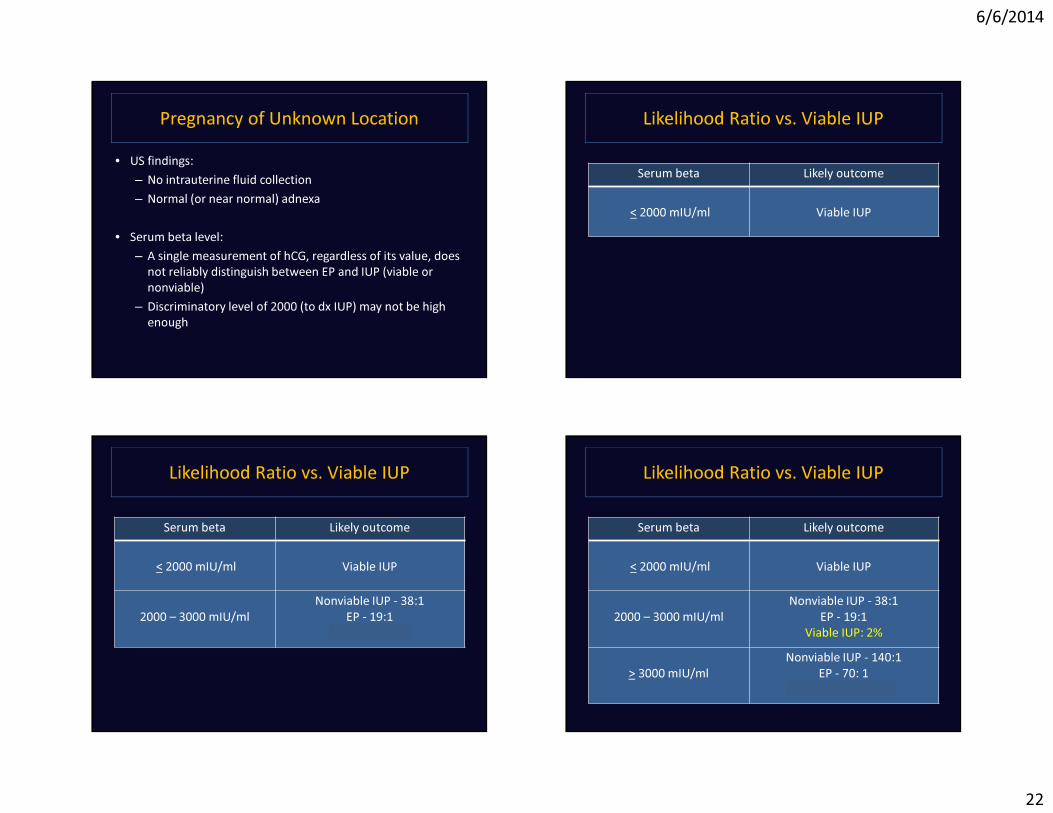
6/6/2014
22
Pregnancy of Unknown Location• US findings:
– No intrauterine fluid collection– Normal (or near normal) adnexa
• Serum beta level:– A single measurement of hCG, regardless of its value, does
not reliably distinguish between EP and IUP (viable or nonviable)
– Discriminatory level of 2000 (to dx IUP) may not be high enough
Likelihood Ratio vs. Viable IUP
Serum beta Likely outcome
< 2000 mIU/ml Viable IUP
Likelihood Ratio vs. Viable IUP
Serum beta Likely outcome
< 2000 mIU/ml Viable IUP
2000 – 3000 mIU/mlNonviable IUP - 38:1
EP - 19:1 Viable IUP: 2%
Likelihood Ratio vs. Viable IUP
Serum beta Likely outcome
< 2000 mIU/ml Viable IUP
2000 – 3000 mIU/mlNonviable IUP - 38:1
EP - 19:1 Viable IUP: 2%
> 3000 mIU/mlNonviable IUP - 140:1
EP - 70: 1Viable IUP: 0.5%
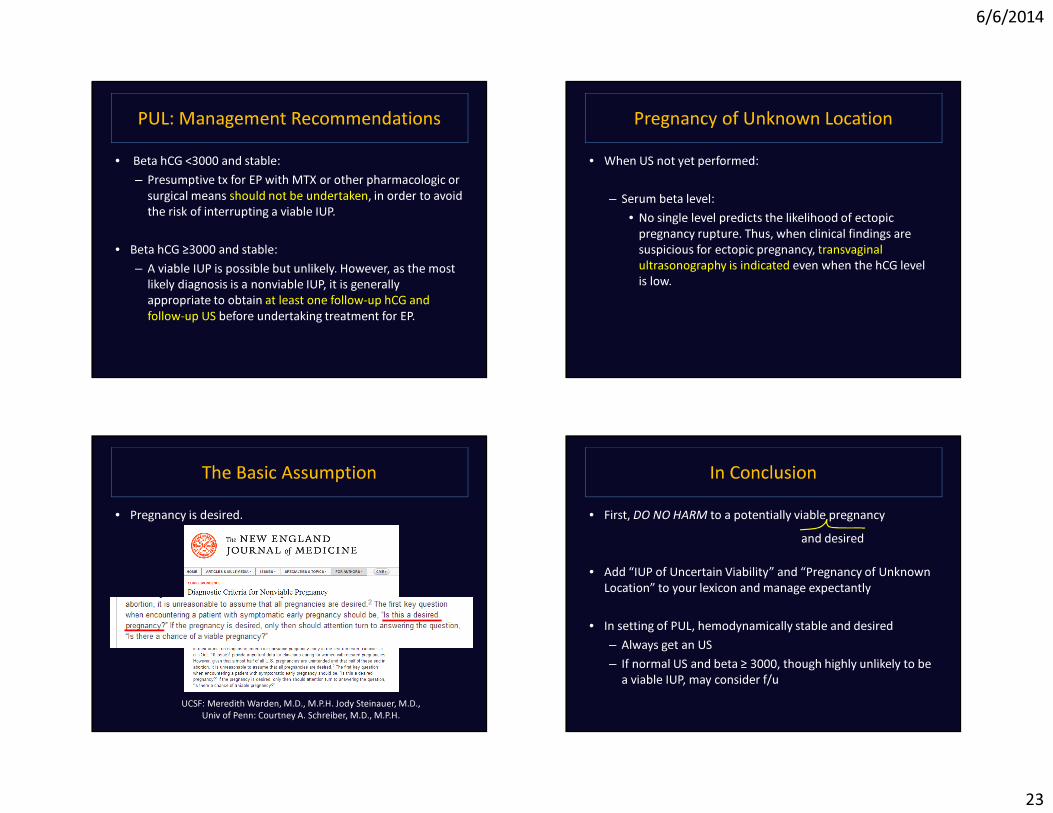
6/6/2014
23
PUL: Management Recommendations• Beta hCG <3000 and stable:
– Presumptive tx for EP with MTX or other pharmacologic or surgical means should not be undertaken, in order to avoid the risk of interrupting a viable IUP.
• Beta hCG ≥3000 and stable:– A viable IUP is possible but unlikely. However, as the most
likely diagnosis is a nonviable IUP, it is generally appropriate to obtain at least one follow-up hCG and follow-up US before undertaking treatment for EP.
Pregnancy of Unknown Location• When US not yet performed:
– Serum beta level:• No single level predicts the likelihood of ectopic
pregnancy rupture. Thus, when clinical findings are suspicious for ectopic pregnancy, transvaginalultrasonography is indicated even when the hCG level is low.
The Basic Assumption• Pregnancy is desired.
UCSF: Meredith Warden, M.D., M.P.H. Jody Steinauer, M.D., Univ of Penn: Courtney A. Schreiber, M.D., M.P.H.
In Conclusion• First, DO NO HARM to a potentially viable pregnancy
• Add “IUP of Uncertain Viability” and “Pregnancy of Unknown Location” to your lexicon and manage expectantly
• In setting of PUL, hemodynamically stable and desired– Always get an US – If normal US and beta ≥ 3000, though highly unlikely to be
a viable IUP, may consider f/u
and desired
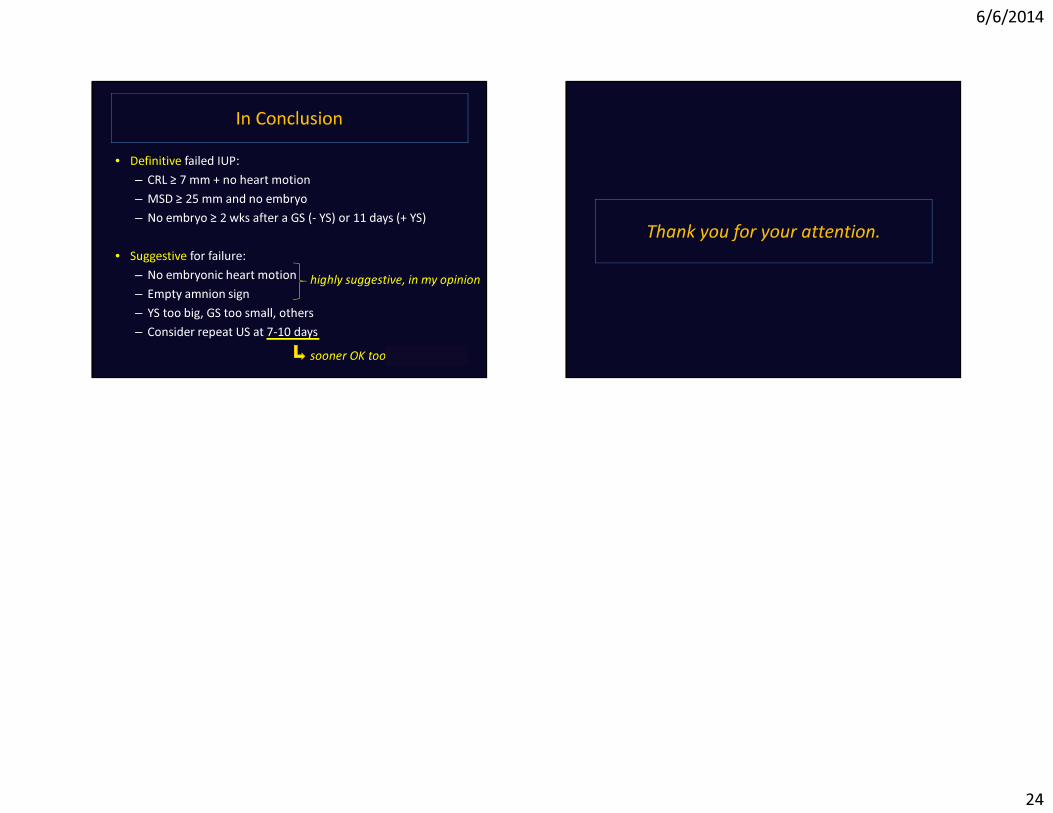
6/6/2014
24
In Conclusion• Definitive failed IUP:
– CRL ≥ 7 mm + no heart motion– MSD ≥ 25 mm and no embryo– No embryo ≥ 2 wks after a GS (- YS) or 11 days (+ YS)
• Suggestive for failure:– No embryonic heart motion– Empty amnion sign– YS too big, GS too small, others– Consider repeat US at 7-10 days
highly suggestive, in my opinion
sooner OK too , in my opinion
Thank you for your attention.

6/6/2014
1
Diagnosis and Management of Arrest Disorders: Duration to Wait
Antepartum and Intrapartum Management ConferenceSan Francisco, California, June 2014
Yasser Y. El-Sayed, M.D.
Professor and DirectorMaternal-Fetal Medicine and Obstetrics
Stanford UniversityObstetrician-in-Chief
Lucile Packard Children’s Hospital
Disclosure
I have nothing to disclose
Stages of Labor
• Seminal work of Emmanuel Friedman– First to depict a labor curve divided into
several stages and phases
– Relationship between duration of labor and cervical dilation as a sigmoid curve
– 622 consecutive primigravid women at term• 500 selected for analysis for sufficient detail

6/6/2014
2
Friedman’s CurveFriedman EA. Obstet Gynecol 1955 Friedman’s Curve
• Nulliparas Limits of Normal: total population (n=500)
• Latent phase: maximum: 20.6 hrs• Transition to active phase: by 4cm• Maximum slope: minimum 1.2 cm/hr
• First stage duration: maximum 28.5 hrs
Friedman’s Curve
• Limits of Normal: Multiparas (n=500)
• Latent phase: maximum: 13.6 hrs
• Transition to active phase: by 4 cm• Maximum slope: minimum 1.5 cm/hr
Friedman EA. Labor in multiparas. A graphicostatistical analysis.1956;8:691-703
First Stage Labor• Latent Phase Duration
– Transition to active phase may occur later than described by Friedman
– 1060 nulliparous and 639 primi- or multi-parous in spontaneous labor, intact membranes at admission
• <50% labors active by 4cm
• 74% active by 5 cm
• “a patient who is not progressing in labor at 4 cm cervical dilation is not necessarily abnormal.”
Peisner and Rosen – Obstet Gynecol 1986

6/6/2014
3
First Stage Labor• 1,329 nulliparous parturients - term, singleton, vertex,
normal birthweight, spontaneous onset of labor, vaginal delivery
– No perceivable change in cervical dilation for 2 hours before 7 cm not uncommon
– No deceleration phase was detected
– 5th percentiles rate of cervical dilation all below 1 c m/hour
Zhang et al. Reassessing the labor curve in nulliparous women. AJOG 2002;187:824-8
First Stage Labor• Retrospective Study from EMR in 19 hospitals across U.S.
• 62,415 parturients
– Singleton, term, spontaneous onset of labor, vertex, vaginal delivery, normal perinatal outcome
– Repeated measures analysis used to construct average labor curves by parity
– Interval-censored regression used to estimate duration of labor• Stratified by cervical dilation at admission and centimeter by centimeter.
– Median and 95th percentiles calculated
Zhang et al. for the Consortium on Safe Labor. Contemporary Patterns of Spontaneous Labor With Normal Neonatal Outcomes.Obstet Gynecol 2010
© 2010 The American College of Obstetricians and Gynecologists. Published by Lippincott Williams & Wilkins, Inc. 2
Contemporary Patterns of Spontaneous Labor With Normal Neonatal Outcomes.Zhang, Jun; PhD, MD et al.Obstetrics & Gynecology. 116(6):1281-1287, December 2010.
Fig. 2. Average labor curves by parity in singleton term pregnancies with spontaneous onset of labor, vaginal delivery, and normal neonatal outcomes. P0, nulliparous women; P1, women of parity 1; P2+, women of parity 2 or higher.Zhang. Contemporary Labor Patterns. Obstet Gynecol 2010.
© 2010 The American College of Obstetricians and Gynecologists. Published by Lippincott Williams & Wilkins, Inc. 2
Contemporary Patterns of Spontaneous Labor With Normal Neonatal Outcomes.Zhang, Jun; PhD, MD et al. Obstetrics & Gynecology. 116(6):1281-1287, December 2010.
Table 2. Duration of Labor in Hours by Parity in Spontaneous Onset of Labor
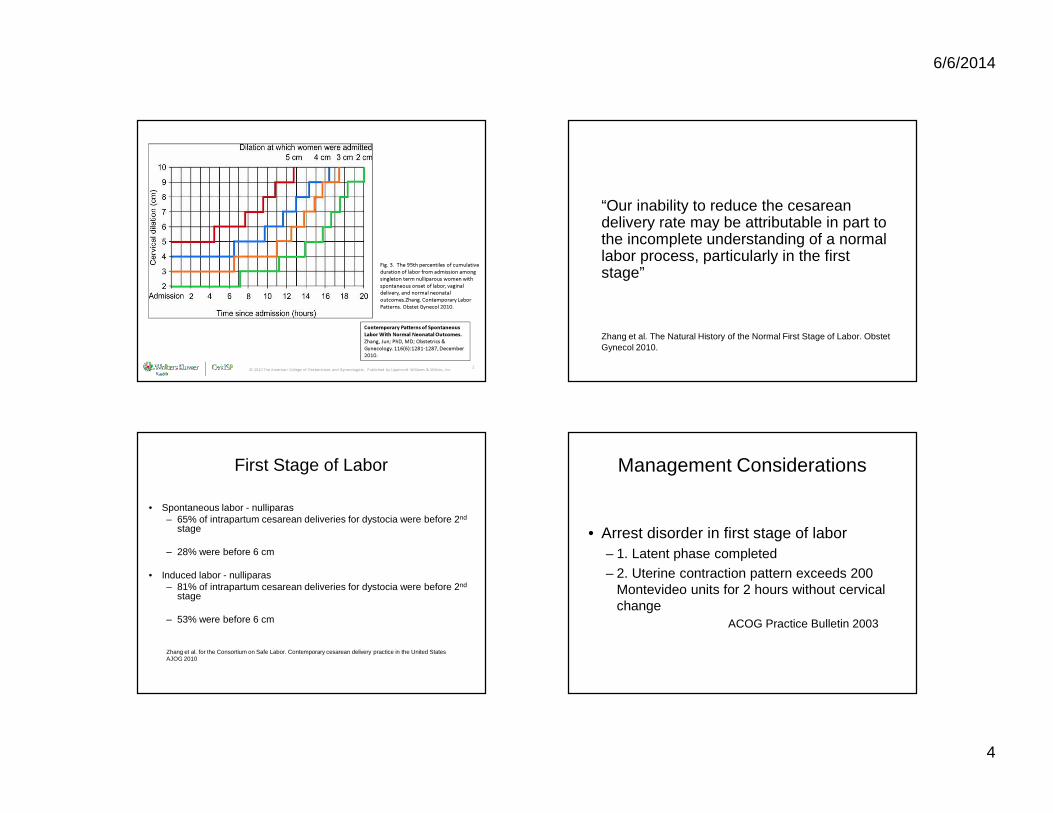
6/6/2014
4
© 2010 The American College of Obstetricians and Gynecologists. Published by Lippincott Williams & Wilkins, Inc. 2
Contemporary Patterns of Spontaneous Labor With Normal Neonatal Outcomes.Zhang, Jun; PhD, MD; Obstetrics & Gynecology. 116(6):1281-1287, December 2010.
Fig. 3. The 95th percentiles of cumulative duration of labor from admission among singleton term nulliparous women with spontaneous onset of labor, vaginal delivery, and normal neonatal outcomes.Zhang. Contemporary Labor Patterns. Obstet Gynecol 2010.
“Our inability to reduce the cesarean delivery rate may be attributable in part to the incomplete understanding of a normal labor process, particularly in the first stage”
Zhang et al. The Natural History of the Normal First Stage of Labor. Obstet Gynecol 2010.
First Stage of Labor
• Spontaneous labor - nulliparas– 65% of intrapartum cesarean deliveries for dystocia were before 2nd
stage
– 28% were before 6 cm
• Induced labor - nulliparas– 81% of intrapartum cesarean deliveries for dystocia were before 2nd
stage
– 53% were before 6 cm
Zhang et al. for the Consortium on Safe Labor. Contemporary cesarean delivery practice in the United States AJOG 2010
Management Considerations
• Arrest disorder in first stage of labor– 1. Latent phase completed
– 2. Uterine contraction pattern exceeds 200 Montevideo units for 2 hours without cervical change
ACOG Practice Bulletin 2003

6/6/2014
5
• Arrest disorder
– At least 4 hours of >200 Montevideo units or
– Minimum of 6 hours of oxytocin if pattern unattainable
– Eventual vaginal delivery rate in group with no progress after 4 hours oxytocin• 56% for nulliparas• 88% for multiparas
– Maternal: chorioamnionitisRouse et al. Obstet Gynecol 1999,
• Extending the minimum period of oxytocin augmentation for active phase arrest from 2 hours to 4 hours appears effective
ACOG Practice Bulletin 2003
First Stage - Duration to Wait
Conclusions• Labor appears to progress more slowly now than before
• More measured, nuanced approach to diagnosis of first stage arrest:
– Adjust management to account for gradual active phase curve in nulliparas
– Adjust management to account for later inflection point in multiparas
– 6 cm is a better landmark for start of active phase
– One size does not fit all - The Connected Staircase• Labor curve based on both parity and admission dilation
• Merriman – 1820 – “The forceps shall never be applied until the ear of the child has
been within the reach of the operator’s fingers for at least six hours.”
• Hamilton – 1861 – “Whenever the os become fully dilated, so that an ear can be
felt, I hold that the danger to the child becomes imminent if allowed to remain undelivered much more than 2 hours.”
Merriman S. A synopsis of of various kinds of difficult parturition, ed.s 3, London 1820.Hamilton G. Classical observations and suggestions in obstetrics. Edinburgh Med J.1861
The Second Stage of Labor

6/6/2014
6
How Long Is Too Long?
• Increase in infant mortality when second stage exceeded 150 minutes
Hellman and Prystowsky AJOG 1952
The Second Stage of LaborFriedman’s Curve
• Limits of Normal: total population* (n=500)– Mean: 0.95 hr.– Median 0.8 hr.
– Statistical maximum: 2.5 hours 2.0 hours (ideal population)
*55% incidence of low or mid-forceps
Friedman EA. Primigravid Labor: a graphicostatistical analyis. Obstet Gynecol 1955
The Second Stage of Labor
• Duration of the second stage of labor– Nulliparas:
• Mean – 54 minutes• 95th %ile -132 minutes• 95th %ile with conduction anesthesia –185 minutes
– Multiparas: • Mean - 19 minutes• 95th%ile- 61 minutes• 95th %ile with conduction anesthesia –131 minutes
Kilpatrick et al. Characteristics of normal labor. Obstet Gynecol 1989
The Second Stage of Labor
• ACOG: Prolonged second stage of labor
– Nulliparas: 2 hours without regional anesthesia3 hours with regional anesthesia
– Multiparas: 1 hour without regional anesthesia
2 hours with regional anesthesia
• ACOG Practice bulletin. Dystocia and augmentation of labor. No 49; Obstet Gynecol 2003
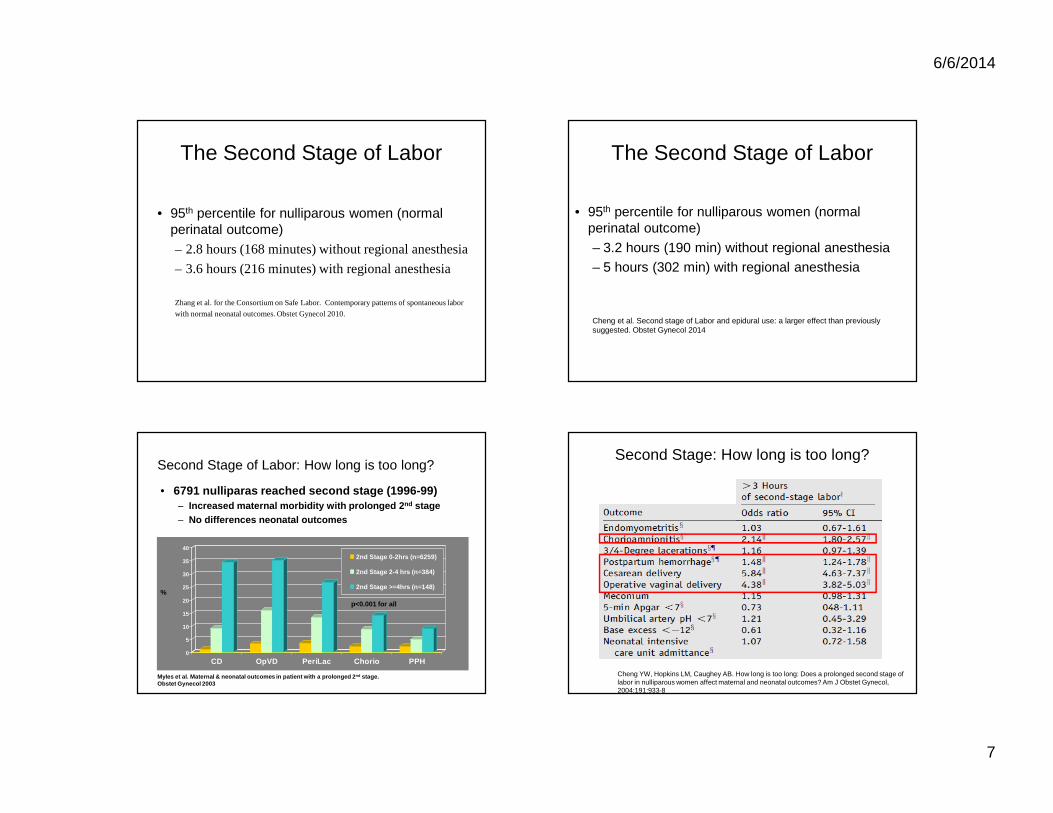
6/6/2014
7
The Second Stage of Labor
• 95th percentile for nulliparous women (normal perinatal outcome)– 2.8 hours (168 minutes) without regional anesthesia
– 3.6 hours (216 minutes) with regional anesthesia
Zhang et al. for the Consortium on Safe Labor. Contemporary patterns of spontaneous labor
with normal neonatal outcomes. Obstet Gynecol 2010.
The Second Stage of Labor
• 95th percentile for nulliparous women (normal perinatal outcome)
– 3.2 hours (190 min) without regional anesthesia– 5 hours (302 min) with regional anesthesia
Cheng et al. Second stage of Labor and epidural use: a larger effect than previously suggested. Obstet Gynecol 2014
Second Stage of Labor: How long is too long?
• 6791 nulliparas reached second stage (1996-99)– Increased maternal morbidity with prolonged 2 nd stage– No differences neonatal outcomes
0
5
10
15
20
25
30
35
40
CD OpVD PeriLac Chorio PPH
2nd Stage 0-2hrs (n=6259)
2nd Stage 2-4 hrs (n=384)
2nd Stage >=4hrs (n=148)%
p<0.001 for all
Myles et al. Maternal & neonatal outcomes in patien t with a prolonged 2 nd stage. Obstet Gynecol 2003
Second Stage: How long is too long?
Cheng YW, Hopkins LM, Caughey AB. How long is too long: Does a prolonged second stage of labor in nulliparous women affect maternal and neonatal outcomes? Am J Obstet Gynecol, 2004;191:933-8
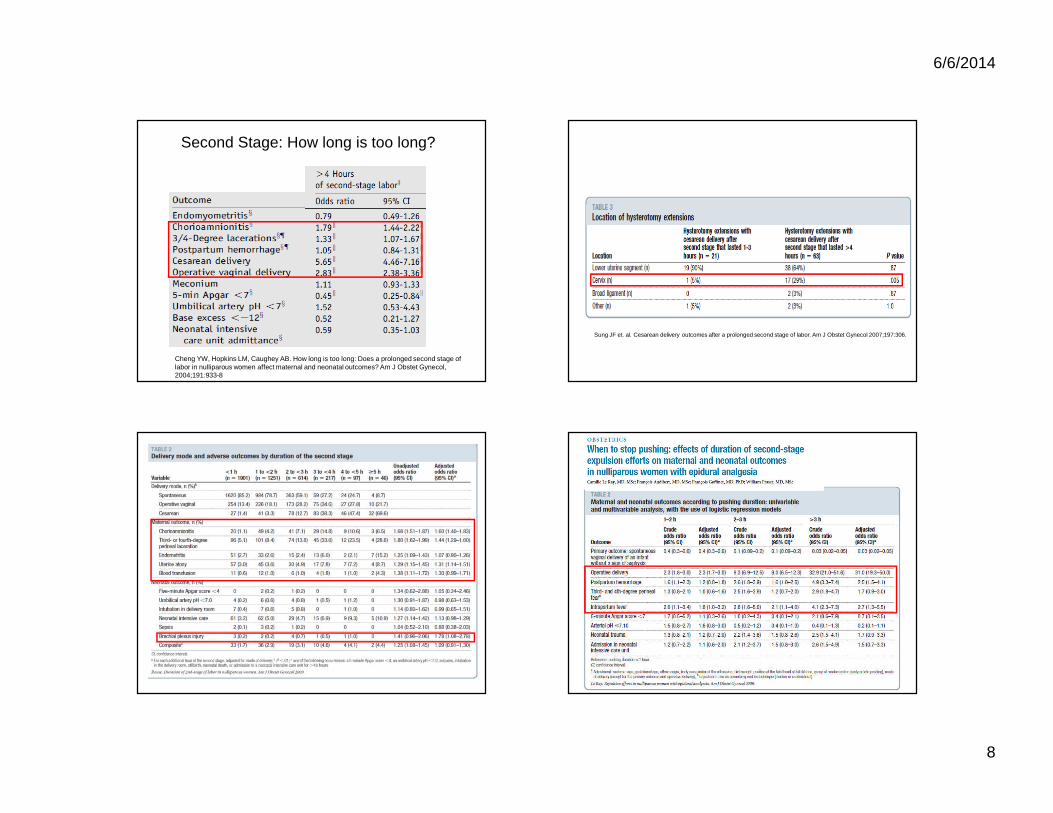
6/6/2014
8
Second Stage: How long is too long?
Cheng YW, Hopkins LM, Caughey AB. How long is too long: Does a prolonged second stage of labor in nulliparous women affect maternal and neonatal outcomes? Am J Obstet Gynecol, 2004;191:933-8
Sung JF et. al. Cesarean delivery outcomes after a prolonged second stage of labor. Am J Obstet Gynecol 2007;197:306.

6/6/2014
9
Second Stage - How long is too long?
If progress is being made, duration of the second stage alone does not mandate intervention by operative delivery
• ACOG Practice bulletin. Dystocia and augmentation of labor. No 49; Obstet Gynecol 2003
© 2009 The American College of Obstetricians and Gynecologists. Published by Lippincott Williams & Wilkins, Inc. 2
Maternal and Perinatal Outcomes With Increasing Duration of the Second Stage of Labor.Allen, Victoria; MD, MSc et al. Obstetrics & Gynecology. 113(6):1248-1258, June 2009.
Cheng et al. Second stage of labor and epidural use. Obstet Gynecol 2014
Second Stage - How long is too long?
• Evidence Mixed– Maternal outcomes worse
• Would earlier cesarean improve?• Association versus causation
– Neonatal outcomes – more clarity?

6/6/2014
10
Second Stage - How long is too long?
• Chorioamnionitis
• Is it that simply longer labor leads to more infections?
OR
• Women with pre-chorio / chorio have longer labors?
Second Stage - How long is too long?
• PPH / Perineal lacerations
• Is it that simply longer labor leads to more bleeding / injury?
OR
• Women with longer second stages eventually are delivered via cesarean / op vag delivery leading to complications?
Second Stage: How long is too long?
• Systematic review:
• Recurrent limitations included:– oversimplified categorization of second stage– inconsistency in study population characteristics, and lack of
control of confounding factors.
• Conclusions: “The primary findings of our review indicated that most of the studies are flawed and do not answer the important questions for maternity caregivers to safely manage prolonged second stage.”
Altman M, Lydon-Rochelle M. Prolonged Second Stage of Labor and Risk of Adverse Maternal and Perinatal Outcomes: A Systematic Review. Birth: Issues In Perinatal Care. December
2006;33(4):315-322.
Second Stage - How long is too long?
• >4 hours second stage– Cesarean delivery rate – 32.8%– Operative vaginal delivery rate – 48.4%– Spontaneous vaginal delivery rate – 18.8%
• > 6 hour second stage– Cesarean delivery rate - 48.4%– Operative vaginal delivery rate - 35.2%– Spontaneous vaginal delivery rate - 16.4 %
Cheng YW, Hopkins LM, Caughey AB. How long is too long: Does a prolonged second stage of labor in nulliparous women affect maternal and neonatal outcomes? Am J Obstet Gynecol, 2004;191:933-8

6/6/2014
11
Second Stage – Duration to WaitConclusions
• Executive Summary SMFM, NICHD, ACOG Workshop. Obstet Gynecol 2012. • 4 hours in a nulliparous woman with epidural• 3 hours in a nulliparous woman without an epidural• 3 hours in a multiparous woman with epidural• 2 hours in a multiparous women without epidural
• Cheng et al. Second stage of Labor and epidural use. Obstet Gynecol 2014• 5 hours in a nulliparous woman with regional anesth esia• 3 hours in a nulliparous woman without regional anesthesia• 3.6 hours in a multiparous woman with epidural• 1.3 hours in a multiparous women without epidural
Second Stage – Duration to WaitConclusions
• Need prospective studies and long term outcomes to address second stage management– 3 hours versus 4 or 5 or 6 hours
• >4 hours in nulliparous woman• Precise determination of actual descent and fetal status• Balanced consideration of maternal and neonatal
complications• Diminished likelihood of spontaneous vaginal delivery• Patient informed preference
THANK YOU

6/6/2014
12
Delayed Pushing - PEOPLE
• Maternal Outcomes
Fraser et al. Multicentered, RTC of delayed pushin g for nulliparas in the second stage with continuous epidural analgesia. Am J Obstet Gynecol 2000
Delayed Push (n=926)
Early Push(n=936)
RR (95% CI)P value
3rd/4th degree lac 9.3 % 9.5 % NS
Fever (38’ C) 8.5% 4.5% 1.88 (1.31-2.71)
EBL>500ml 17.6 % 16.8 % NS
Delayed Pushing - PEOPLE
• Neonatal Outcomes
• No difference – Respiratory, blood cultures, fractures, Apgars
Fraser et al. Multicentered, RTC of delayed pushin g for nulliparas in the second stage with continuous epidural analgesia. Am J Obstet Gynecol 2000
Delayed Push (n=926)
Early Push(n=936)
RR (95% CI)P value
Abnormal uapH (<7.10) 4.5% 1.8% 2.45 (1.35-4.43)
Ventilation 6.9% 6.3% NS
uapH (<7.0) 1.98 (0.36–10.80)
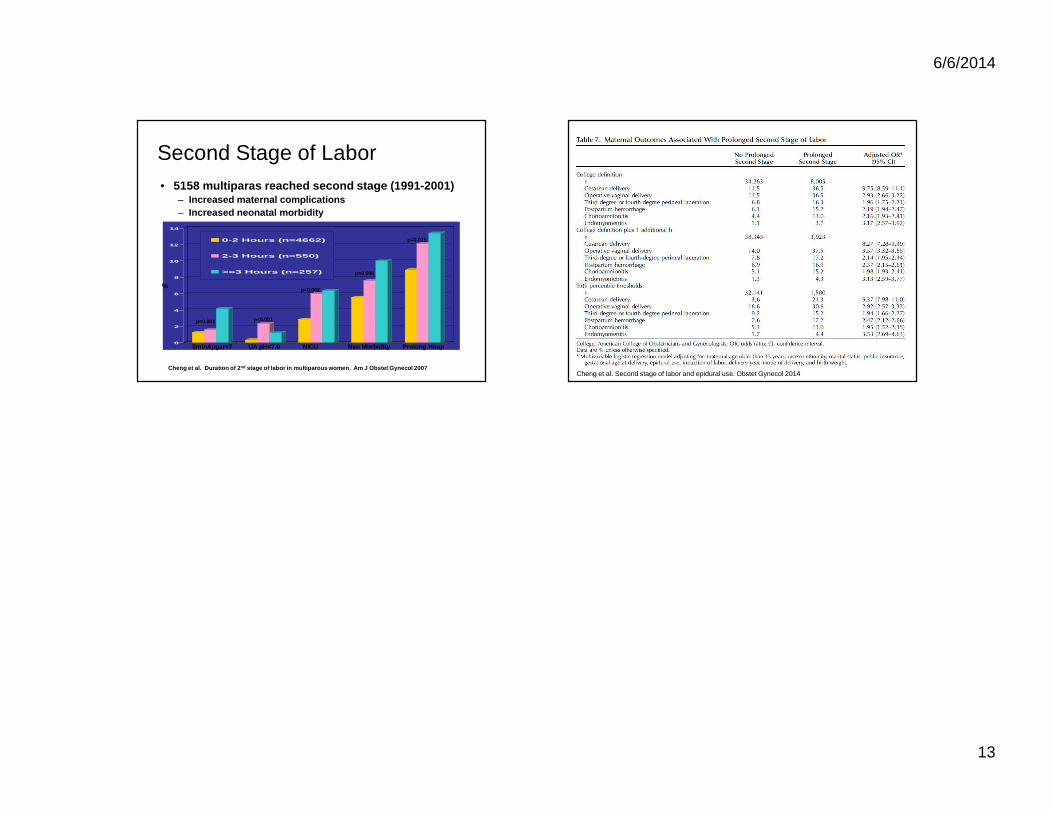
6/6/2014
13
0
2
4
6
8
10
12
14
0-2 Hours (n=4662)
2-3 Hours (n=550)
>=3 Hours (n=257)
Second Stage of Labor• 5158 multiparas reached second stage (1991-2001)
– Increased maternal complications– Increased neonatal morbidity
%
5minApgar<7 UA pH<7.0 NICU Neo M orbidity Prolong Hosp
Cheng et al. Duration of 2 nd stage of labor in multiparous women. Am J Obstet Gynecol 2007
p<0.001 p<0.001
p=0.002
p=0.006
p=0.015
Cheng et al. Second stage of labor and epidural use. Obstet Gynecol 2014
6/6/2014
1
Trial of Labor after Cesarean Delivery: Which Patients? Which
Hospitals?Jeffrey L Ecker, MD
Vincent Memorial Obstetric ServiceMassachusetts General Hospital
Harvard Medical School
Disclosures
• I have not had a cesarean delivery
• I do not get paid more money for doing cesarean deliveries
• I did help write ACOG PB #115
…and have nothing else todisclose
TOLAC: What’s New and What’s Not
• Context and Definitions
• Which Patients?---What’s New in PB 115
• Which Hospitals?: Ethics, Risks and “Immediately Available”
• What’s the Problem?: A Pragmatic Look at the TOLAC map
Context: Trends

6/6/2014
2
Local Data:
• VBAC Rate 2002 = 37%
• VBAC Rate 2012 = 24%
• VBAC Rate 2013 = 20.2%*
* Different Denominator
Context: NIH
Context: NIH
• Conclusions
– Many critical gaps in definitions, outcomes, available data
– “Trial of labor is a reasonable option for many women with one prior cesarean…”
– TOLAC and ERCD have different and important risks for a mother and her fetus
– “This poses a profound ethical dilemma…”

6/6/2014
3
Context:NIH
• Conclusions
– “ We are concerned about the barriers women face in gaining access to clinicians and facilities that are able and willing to offer a trial of labor”
– “We are concerned that medico-legal considerations add to, and in many cases exacerbate, these barriers”
– Recommend that ACOG and SOAP re-examine requirements for resources needed to conduct TOLAC/VBAC
Which Patients?
• Depends on the numbers
– Chances of VBAC if TOLAC
– Chance of morbidity and mortality if TOLAC
– How many planned future pregnancies
Numbers That Patients and Providers Need
• Chance of VBAC if TOLAC: 60-80%
– 74% in summary meta-analysis from AHRQ
60% 74% 80%
Numbers That Patients and Providers Need
• Chance of VBAC modified by several factors
• There are available prediction models
– Will push PPV/NPV 10-20% from average

6/6/2014
4
Numbers That Patients and Providers Need
• Chance of VBAC modified by several factors
• There are available prediction models
– Knowing that chance of VBAC are 95% v 75% v 65% may be important to some decisions
Numbers That Patients and Providers Need
• Risks of TOLAC
– For the mother include risk of hemorrhage, infection, injury to pelvic organs, hysterectomy, death
• Most maternal risks with TOLAC occur when cesarean delivery becomes necessary :risk therefore tied to chances of VBAC
– For the neonate include respiratory complications, infection, HIE, death
Maternal Morbidity and Mortality

6/6/2014
5
Neonatal Morbidity and Mortality TOLAC Outcomes: Not ALL VBACs
Numbers That Patients and Providers Need
• Risk of uterine dehiscence
– 0.3-0.9% for single prior low transverse hysterotomy
– Higher for classical cesarean (data limited, ? 6-10%)
– Reported data limited in some series by including symptomatic rupture and asymptomatic separations and by failure to stratify by type of prior hysterotomy
Immediately Available

6/6/2014
6
“Immediately Available”: Not a Crowd Pleaser
Which Patients?: Most Patients!
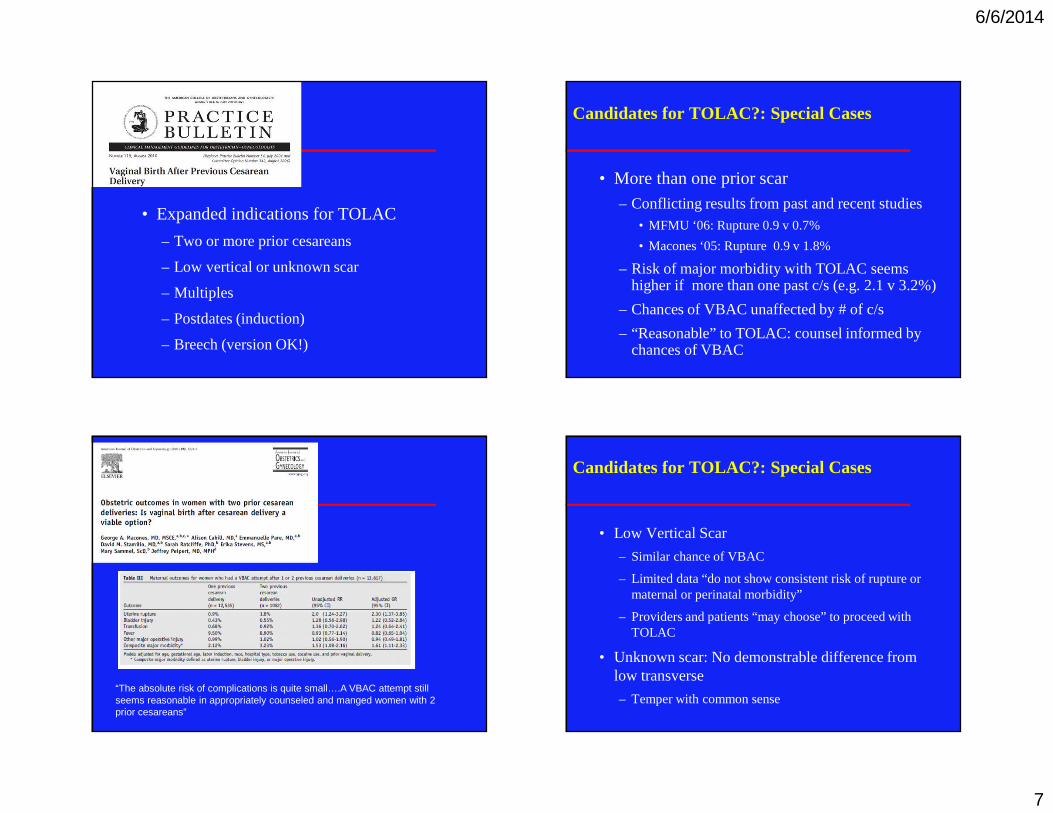
6/6/2014
7
• Expanded indications for TOLAC
– Two or more prior cesareans
– Low vertical or unknown scar
– Multiples
– Postdates (induction)
– Breech (version OK!)
Candidates for TOLAC?: Special Cases
• More than one prior scar
– Conflicting results from past and recent studies• MFMU ‘06: Rupture 0.9 v 0.7%
• Macones ‘05: Rupture 0.9 v 1.8%
– Risk of major morbidity with TOLAC seems higher if more than one past c/s (e.g. 2.1 v 3.2%)
– Chances of VBAC unaffected by # of c/s
– “Reasonable” to TOLAC: counsel informed by chances of VBAC
“The absolute risk of complications is quite small….A VBAC attempt still seems reasonable in appropriately counseled and manged women with 2 prior cesareans”
Candidates for TOLAC?: Special Cases
• Low Vertical Scar
– Similar chance of VBAC
– Limited data “do not show consistent risk of rupture or maternal or perinatal morbidity”
– Providers and patients “may choose” to proceed with TOLAC
• Unknown scar: No demonstrable difference from low transverse
– Temper with common sense

6/6/2014
8
Candidates for TOLAC?: Special Cases
• Twins: Less Likely to choose TOLAC but similar outcomes to singletons
Can We?: Management of TOLAC
• Induction
– Appears to be a gradient of risk of rupture: spontaneous < oxytocin augmentation < oxytocin induction < oxytocin + prostaglandin induction
– Small case series suggest PGE1 should be avoided
– Risk of rupture may increase with increasing doses of oxytocin but indentifying a threshold dose is challenging
Risk of Uterine Rupture: MFMU Study
Landon NEJM, 2005
Drilling Down
Grobman Ob/Gyn, 2007

6/6/2014
9
Drilling Down
Grobman Ob/Gyn, 2007
Can We?: Management of TOLAC
• Induction
– Incremental risk is not large
– “Induction of labor for maternal or fetal indications remains an option for women undergoing TOLAC”
– Prostaglandins
• PGE1 should not be used in the third trimester with past uterine scar
• PGE2 to minimize the risk of rupture, select those with the greatest chance of VBAC and avoid sequential use with oxytocin
Can We?: Management of TOLAC
• Epidural
– Yes: the Geneva convention applies in labor
– Does not appear to reduce VBAC
– Most common sign of rupture is FHR abnormalities
• Version– Limited data suggest it is not contraindicated
– Similar success rates reported

6/6/2014
10
“Immediately Available”: Limits and Arguments
• Available data largely from centers with immediately available
• Comparative data of immediately available to other standards is not available
• Limits access to/availability of TOLAC
Managing TOLAC: Needed Resources
• Emergencies can happen and be unexpected
• Sometimes minutes may make a difference
– With occlusion, cord pH may drop as rapidly as .01/minute
Managing TOLAC: Evidence for Needed Resources

6/6/2014
11
But…Risk, TOLAC and the Ethics of Patient Choice
• Incremental risk likely to be small
• Given likely small absolute risk, respect for autonomyargues that appropriately patients and providers may choose TOLAC in settings with more limited resources
– Counseling/informed consent is key
– Respect for autonomy should not be an excuse to avoid providing resources
Immediately Available?
• “Recommends” that TOLAC be undertaken at facilities where staff are immediately available for emergency care (Level C---expert opinion)
• When “immediate” is not available
– Discuss available resources
– Decision to proceed with TOLAC in such circumstances should be “carefully considered”
– Transfer/referral may be best
Immediately Available?
• Respect for autonomy supports the concept that patients should be allowed to accept increased levels of risk
• No patient should be/can be forced to have a cesarean regardless of facility’s TOLAC resources
• Change in policy is not meant to limit facilities’ appropriate efforts to provide recommended resources or respond to unexpected emergencies
Reactions to PB 115
6/6/2014
12
Reactions to PB 115
“It is unclear how women will be at liberty to choose TOLAC when facilities continue to refuse them this option citing compliance with 2010 guidelines”
• Described a recommendation for “immediately available”
– Hospitals wishing to do VBAC must be prepared for emergency surgery
• Many hospitals still won’t offer VBAC and women won’t have this choice
– Is repeat cesarean under such circumstances, voluntary?
• This is a situation that should be of great concern to obstetricians and the bioethics community
Does Immediately Available Limit TOLAC?
• For some women: Yes– Particularly in rural areas only covered by smaller volume
facilities
• But, as a matter of public health, the issue is not just the number of sites that offer TOLAC but the number of women covered by those sites– Many women deliver at or have ready access to centers
that support TOLAC
• The issue is clearly not all access: at sites that support/encourage TOLAC many chose ERCD
The Conundrum of Access to TOLAC
• Let’s Not Conflate Numbers of TOLAC Centers with Access– One center with 3000 deliveries/year and supporting
TOLAC will provider greater access than 5 centers doing 500 deliveries/year who do not
• I am unaware of a map describing TOLAC centers in relation to U.S. population
• Referral and referral networks are an important, potential solution
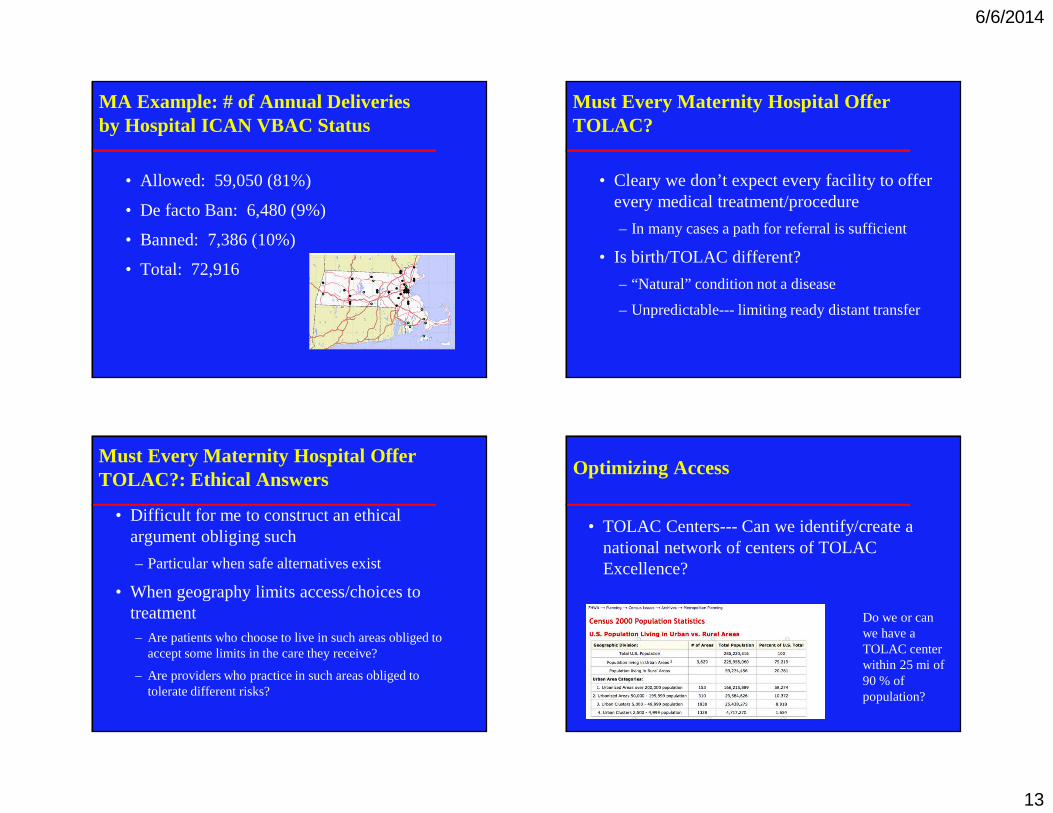
6/6/2014
13
MA Example: # of Annual Deliveries by Hospital ICAN VBAC Status
• Allowed: 59,050 (81%)
• De facto Ban: 6,480 (9%)
• Banned: 7,386 (10%)
• Total: 72,916
Must Every Maternity Hospital Offer TOLAC?
• Cleary we don’t expect every facility to offer every medical treatment/procedure
– In many cases a path for referral is sufficient
• Is birth/TOLAC different?
– “Natural” condition not a disease
– Unpredictable--- limiting ready distant transfer
Must Every Maternity Hospital Offer TOLAC?: Ethical Answers
• Difficult for me to construct an ethical argument obliging such
– Particular when safe alternatives exist
• When geography limits access/choices to treatment– Are patients who choose to live in such areas obliged to
accept some limits in the care they receive?
– Are providers who practice in such areas obliged to tolerate different risks?
Optimizing Access
• TOLAC Centers--- Can we identify/create a national network of centers of TOLAC Excellence?
Do we or can we have a TOLAC center within 25 mi of 90 % of population?

6/6/2014
14
What Are Facilities to Do?
• Make a genuine effort to marshal needed resources to make TOLAC as safe as possible in their setting– In many cases this will mean having resources
immediately available
– This may include antenatal referral of appropriate patient
• Consider plans/protocols for accessing resources whether readily or immediately available– Emergency drills
– Anticipate problems and access resources before emergencies arise
Can We Increase VBAC Rates
• One way to increase national rates of TOLAC/VBAC is to increase uptake/interest among women who are delivering at centers that already support and encourage this option
• Patient Education
– Understand first why don’t patients elect TOLAC
– Then consider how to promote acceptance among appropriate candidates
Conclusion: Nothing New

6/6/2014
15
Definitions
• Trial of Labor (TOLAC):Trial of labor in women who have had a previous cesarean delivery regardless of outcome
• Vaginal Birth After Cesarean (VBAC):Vaginal birth after a prior cesarean delivery
– Not “successful VBAC”
Definitions
• Trial of Labor (TOLAC):Trial of labor in women who have had a previous cesarean delivery regardless of outcome
• Vaginal Birth After Cesarean (VBAC):Vaginal birth after a prior cesarean delivery
– Not “successful VBAC”
Patients choose this
Not this
A Gradient of Risk
Lowest
HighestTOLAC ERCD
VBACVBAC
CS after TOLAC
CS without TOLAC
A Gradient of Risk
Lowest
HighestTOLAC ERCD
VBACVBAC
CS after TOLAC
CS without TOLACPopulation Risk Depends onChances of VBAC

6/6/2014
16
Numbers That Patients and Providers Need
• Chance of VBAC if TOLAC: 60-80%– 74% in summary meta-
analysis from AHRQ
74%
Neonatal Morbidity and Mortality
Moderate Risk ofRespiratory
Complications
Neonatal Morbidity and Mortality
Rare, rare risk ofDeath or HIE
Moderate Risk ofRespiratoryMorbidity
And What About Them Lawyers?
• Shared decision making over time---informedconsent
• Careful documentation
• Willingness to continually re-evaluate plans
The Hazards of Placenta Accreta
Deirdre J. Lyell, MDAssociate Professor, Maternal-Fetal MedicineLucile Packard Children’s Hospital at Stanford
UCSF Antepartum & Intrapartum Management CourseJune 6, 2014
Disclosures
� I have nothing to disclose
Placenta increta is
P l ac e n
t a a t t
a c .. .
P l ac e n
t a i n t
o .. .
P l ac e n
t a t h r
o u. . .
4%
26%
71%A. Placenta attached to the
myometrium
B. Placenta into the myometrium
C. Placenta through the myometrium and serosa
The recommended time to deliver women with accreta is
3 3- 3 4
w ee k s
3 4- 3 5
w ee k s
3 5- 3 6
w ee k s
3 6- 3 7
w ee k s
0%
51%
29%
20%
A. 33-34 weeks
B. 34-35 weeks
C. 35-36 weeksD. 36-37 weeks

Objectives
� Definitions, causes and demographics� Maternal and neonatal hazards� Antenatal diagnosis� Best management practices
Placenta percreta with bladder invasion at cesarean delivery
Belfort et al, Am J Obstet Gynecol, Nov. 2010
www.searchsuccess.net
Definitions, causes and demographics of accreta

http://embryology.med.unsw.edu.au/notes/placenta2.htm
Cause?
� Insufficiently protective/deficient decidua� Lower uterine
segment� Scarring
� Overly invasive trophoblast� Accreta reported in
setting of no known prior scarring
OR
Risk factors
� Myometrial damage/scarring� Prior uterine surgery: cesarean, myomectomy,
dilation and curretage, thermal ablation� Uterine artery embolization, radiation � Asherman Syndrome
� Placenta previa� Submucous fibroids� Multiparity� Advanced maternal age
Risk factors
� Prior uterine surgery (cesarean) and previa:
� After one cesarean, 0.3% (11%-25% if previa)� After two cesareans, 0.6% (40% if previa)� After three cesareans, 2.4% (61% if previa)

Accreta: increasing with cesarean delivery
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%19
60
197
0
197
5
197
8
198
0
198
5
198
6
198
7
198
8
198
9
199
0
199
1
199
2
199
3
199
4
199
5
199
6
199
7
199
8
199
9
200
0
200
1
200
2
200
3
200
4
200
5
200
6
200
7
200
9
201
0
201
1
Cesarean
VaginalbirthAccreta
1/2,510
Accreta1/333
Accreta1/30,000
Accreta: increasing with previa
Risk Factor Increased Risk
Prior placenta previa 8x
Prior cesarean delivery 1.5-15x
Prior suction curretage 1.3x
Age > 35 years 4.7x
Age > 40 years 9x
Multiparity 1.1-1.7x
Non-white (all) 0.3x
Asian 1.9x
Cigarette smoking 1.4-3x
Maternal and neonatal hazards of accreta
Maternal Morbidity: bleeding
� Acute, life threatening bleeding� during pregnancy: 90% previa bleed by 37 weeks� during attempted placental removal� after surgery � renal, cardiac damage, TRALE, death
� 66 cases of cesarean with accreta+� 95% received rbc transfusion� 39% >10 units rbcs 0 to 46 units (mean 10±9)� 11% >20 units rbcs� No differences found among accreta subtypes
� Stottler B. et al, Transfusion, 2011

Maternal Morbidity
� Surgical damage to surrounding organs� Hysterectomy� DVT/PE� Infectious morbidity� Amniotic fluid embolism� Death: 6-7%
� Washecka et al, Hawaii Med J 2002,
� O’Brien et al, Am J Obstet Gynecol 1996
Fetal and Neonatal Morbidity
Fetal Outcomes
� No reported increases in fetal anomalies or IUGR
� Perinatal mortality from maternal hemorrhage in placenta previa:� 25% (1960)� 8-13% (1980s)� 1% (2010 estimate)
Neonatal Outcomes
� Late preterm birth� 34-35 weeks, recommended delivery timing
� NIH: Timing of Indicated Late-Preterm and Early-Term Birth, Spong et al. Obstet Gynecol 2011 August
� National SMFM survey, 2009� 50% deliver at 36 weeks� Northwest: greatest percent of providers who
deliver at 35 weeks� Esakoff et al. JMFNM 2012
� Utah average GA at delivery: 35.4 weeks � Eller at al., BJOG 2009

March 2011, Stanford
� Three prior cesareans� Prior classical
hysterotomy� Prior uterine rupture� Previa, ultrasound
suggestive of accreta� 29 week delivery due
to persistent contractions
Antenatal diagnosis
Ultrasound diagnosis of accreta
� Relatively small studies� Differences in techniques, definitions� Important to consider:� High PPV to justify aggressive management� High NPV to justify less aggressive
management� Cali et al., Ultrasound Obstet Gynecol 2013;41:406-12
Ultrasound diagnosis
� Ultrasound diagnosis, UCSF� PPV 68%� NPV 98%
� Esakoff et al, Ultrasound Obstet Gynecol Mar. 2011
� Placental lakes + <1 mm myometrial thickness� PPV 72%
� Twickler, JMFM 2000
� Numerous coherent vessels in 3D� 97% sensitivity, 92% specificity, PPV 76%
� Shih Ultrasound Obstet Gynecol, 2009
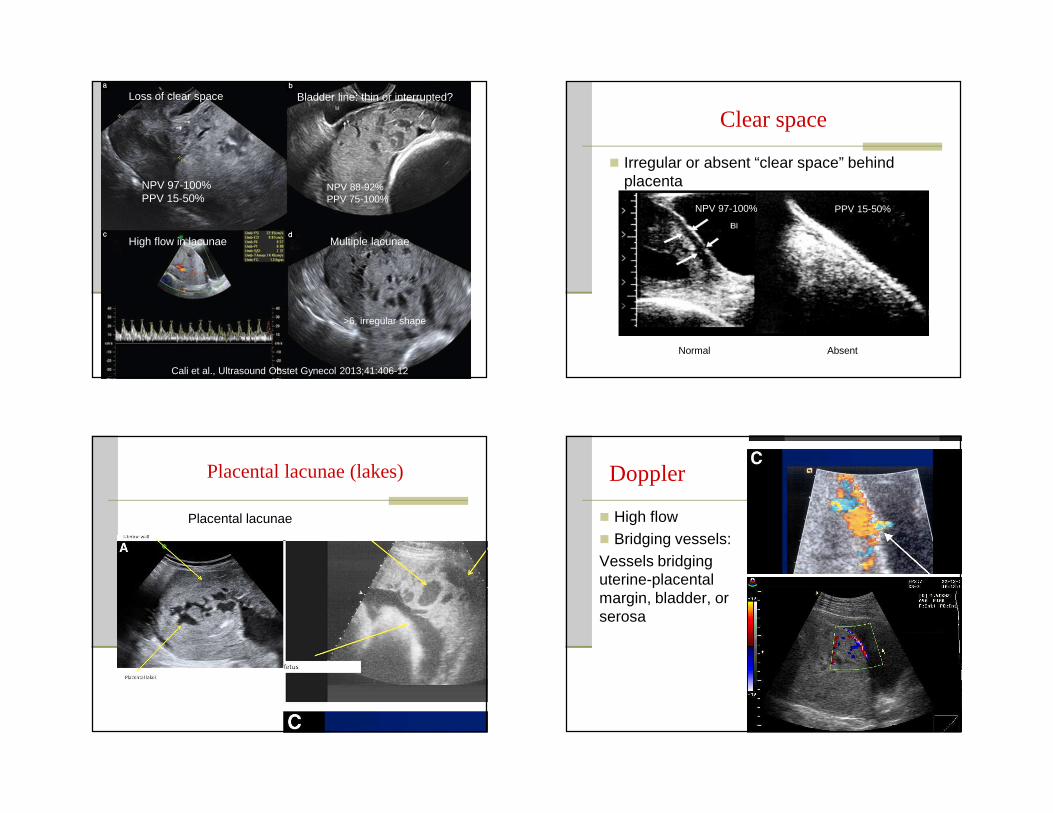
Loss of clear space Bladder line: thin or interrupted?
High flow in lacunae Multiple lacunae
NPV 97-100%PPV 15-50%
NPV 88-92%PPV 75-100%
>6, irregular shape
Cali et al., Ultrasound Obstet Gynecol 2013;41:406-12
Clear space
� Irregular or absent “clear space” behind placenta
Normal Absent
NPV 97-100% PPV 15-50%
Placental lacunae (lakes)
Placental lacunae
Doppler
� High flow� Bridging vessels:Vessels bridging uterine-placental margin, bladder, or serosa
Placental lakes Thin myometrium

Cali et al., Ultrasound Obstet Gynecol 2013
� Using 5 criteria:� Clear space, bladder line, lacunae/flow,
irregular intraplacental vascularization, hypervascular uterine serosa/bladder wall� At least 2 criteria were present in all
accreta/percreta cases� All women without accreta/percreta had 0 or 1
criteria
Antenatal detection of accreta: US
� Ultrasound meta-analysis:� sensitivity 90.72% (95% CI, 87.2-93.6)� specificity 96.94% (95% CI, 96.3-97.5)� LR+ 11.01 (95% CI, 6.1-20.0)� LR-, 0.16 (95% CI, 0.11-0.23)
� Color doppler had the best predictive accuracy
� D’Antonio et al. Ultrasound Obstet Gynecol. 2013 Nov;42(5):509-17
Antenatal detection of accreta: MRI
� MRI: meta-analysis:� sensitivity 94.4% (95% CI 86.0-97.9)� specificity: 84.0% (95% CI 76.0-89.8)� +LR: 5.91 (95% CI 3.73-9.39)� -LR: 0.07 (95% CI 0.02-0.18)
� MRI may be useful for depth and location of invasion
D'Antonio et al. Ultrasound Obstet Gynecol. 2014 Feb 10
� Helpful if ultrasound is inconclusive
Stanford accreta evaluation protocol: US
� Lacunae? Presence and number?� Turbulent flow?� Peak systolic velocity
� Retroplacental clear space� Uterine-serosa bladder wall interface:
hypervascular?� Irregular placental vessels crossing tissue
planes?� Placental location: previa: lateral, posterior?

Serum analytes?
� MS-AFP: associated with increased accreta� Kupferminc MJ et al Obstet Gynecol 1993� Zelop C et al. Obstet Gynecol 1992;80(4):693-4� Dreux S et al. Prenat Diagn 2012;32(10):1010-2
� >2.5 MoM, OR 8.3 (95% CI 1.8-39.3)� free beta hCG >2.5 MoM OR 3.9 (95% CI 1.9-9.9)� Hung et al, Obstet Gynecol, 1999
First trimester: PAPP-A?
� Cleaves IGF from IGF-BP4� Low PAPP-A implicated in poorly invasive
placentation� Elevated PAPP-A seen with overly invasive
placentation?
PAPP-A and accreta
� Retrospective study of 16 accretas, 82 previa controls� Median PAPP-A 1.68 MoM accreta vs. 0.98
previa� Desai N. et al., Prenat Diagn Feb 2014
� CA GDSP and OSHPD linked databases� 37 accretas, 699 previa controls� PAPP-A ≥ 95th%ile (2.63 MoM)� aOR 8.71, 95% CI 2.77 – 27.42 � Lyell et al., SMFM February 2014
Best management practices
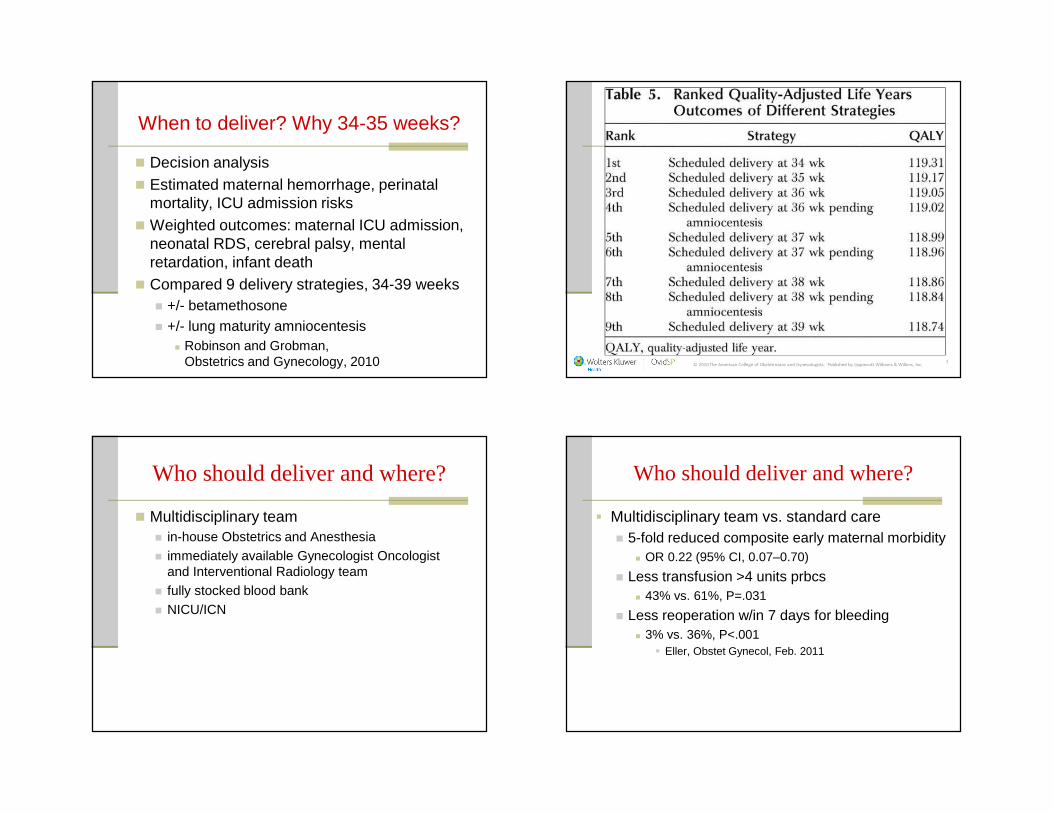
When to deliver? Why 34-35 weeks?
� Decision analysis� Estimated maternal hemorrhage, perinatal
mortality, ICU admission risks� Weighted outcomes: maternal ICU admission,
neonatal RDS, cerebral palsy, mental retardation, infant death
� Compared 9 delivery strategies, 34-39 weeks� +/- betamethosone� +/- lung maturity amniocentesis� Robinson and Grobman,
Obstetrics and Gynecology, 2010 © 2010 The American College of Obstetricians and Gynecologists. Published by Lippincott Williams & Wilkins, Inc. 2
Who should deliver and where?
� Multidisciplinary team� in-house Obstetrics and Anesthesia� immediately available Gynecologist Oncologist
and Interventional Radiology team� fully stocked blood bank � NICU/ICN
Who should deliver and where?
� Multidisciplinary team vs. standard care� 5-fold reduced composite early maternal morbidity� OR 0.22 (95% CI, 0.07–0.70)
� Less transfusion >4 units prbcs � 43% vs. 61%, P=.031
� Less reoperation w/in 7 days for bleeding � 3% vs. 36%, P<.001 � Eller, Obstet Gynecol, Feb. 2011
Delivery: it takes a villageManagement: pre-op
� Large bore I.V. access, availability of high-flow infusion device
� 1-2 MTG equivalents in the room� DVT prophylaxis� Avoidance of hypothermia� Antibiotics one hour prior to delivery� Repeat >1500cc EBL or >3 hours surgery
� I.R.?
Elective hysterectomy?
� Create fundal hysterotomy, deliver � If future childbearing is planned and feasible:� Can await spontaneous placental separation
(do NOT attempt manual separation)
� If proceeding with hysterectomy:� Do not attempt placental removal� Close hysterotomy
Persistent bleeding: temporizing measures
� Diffuse, nonarterial bleeding� Pelvic pressure packing with laparotomy
sponges
� Infrarenal aortic compression� Balloon occlusion or clamping of aorta
reported in extreme cases� Risks: distal thrombosis and ischemia
� “Know when to walk away”

Interval staged surgery
August, 2012, Stanford
Postoperative care
� ICU admission, observation� Correction of coagulopathy, anemia, ongoing
evaluation for bleeding, renal tract injury� Low threshold for re-exploration
Postoperative risks
� Prolonged surgery, massive transfusion, hypotension� Renal, cardiac and other organ dysfunction� Sheehan syndrome � Hyponatremia is an early sign
� Pulmonary edema, TRALE� PE� Infection
Program in Placental Disorders, Stanford
Streamlining Complex Maternal Care for a Safe Delivery for Mothers and
Newborns
Program Goals
� Minimize morbidity and mortality for mother and newborn
� Maximize coordination of care� Research the problem of abnormal
placentation� Data and tissue banks
Coordination for a Safe Delivery
� Maternal-Fetal Medicine� Obstetric Anesthesia� Gynecologic Oncology
� Trauma Surgery� Vascular Surgery� Pediatric Radiology� Interventional Radiology� Adult Critical Care� Neonatal Intensive Care� Transfusion Services� Perinatal Nursing� Pathology
Placenta increta is
A. Placenta attached to the myometrium
B. Placenta into the myometrium
C. Placenta through the myometrium and serosa
The recommended time to deliver women with accreta isA. 33-34 weeks
B. 34-35 weeks
C. 35-36 weeksD. 36-37 weeks

Referrals
� Center for Maternal and Fetal Health� Diagnosis� Consultation� Management
650-724-2221
Prevention
� Avoid first cesarean when possible
The Hazards of Placenta Accreta
Deirdre J. Lyell, MDAssociate Professor, Maternal-Fetal MedicineLucile Packard Children’s Hospital at Stanford
UCSF Antepartum & Intrapartum Management CourseJune 6, 2014

1
+
Twins: Timing and Management of DeliveryMari-Paule Thiet, MD
Director, Division of Maternal-Fetal MedicineVice-Chair of Patient Safety and Quality Assurance
Department of Obstetrics, Gynecology and Reproductive SciencesUniversity of California, San Francisco
+
� I have nothing to disclose
Disclosures
At what gestational age should uncomplicated well grown monochorionic diamniotic twins be delivered?
3 2 w e
e k s
3 4 w e
e k s
3 6 w e
e k s
0%
90%
10%
1. 32 weeks2. 34 weeks3. 36 weeks
Would you allow this patient a trial of labor?35 year old IVF dichorionic diamniotic twin gestation with v/br twin gestation at 36 weeks gestation who presents in preterm labor at 4 cm with intact membranes?
Y es
N o
5%
95%
1. Yes2. No

2
Would you allow her to labor if her first twin has an estimated fetal weight of 5 lbs and the 2nd one has an EFW of 6# and is a footling breech?
Y es
N o
46%
54%
1. Yes2. No
What if the previous patient had a hx of a previous low transverse c/s?
Y es , l a
b o r
N o, c /
s
26%
74%1. Yes, labor2. No, c/s
+
�Define Incidence/scope of problem�Determine optimal gestational age for delivery�Monochorionic vs dichorionic� Plan optimal route of delivery�Delivery considerations�Management of 2nd twin
Objectives + Incidence/Scope of the problem
� Incidence of multiples increasing�ART vs spontaneous�Older gravidas� Risks� Fetal/neonatal complications�Maternal complications
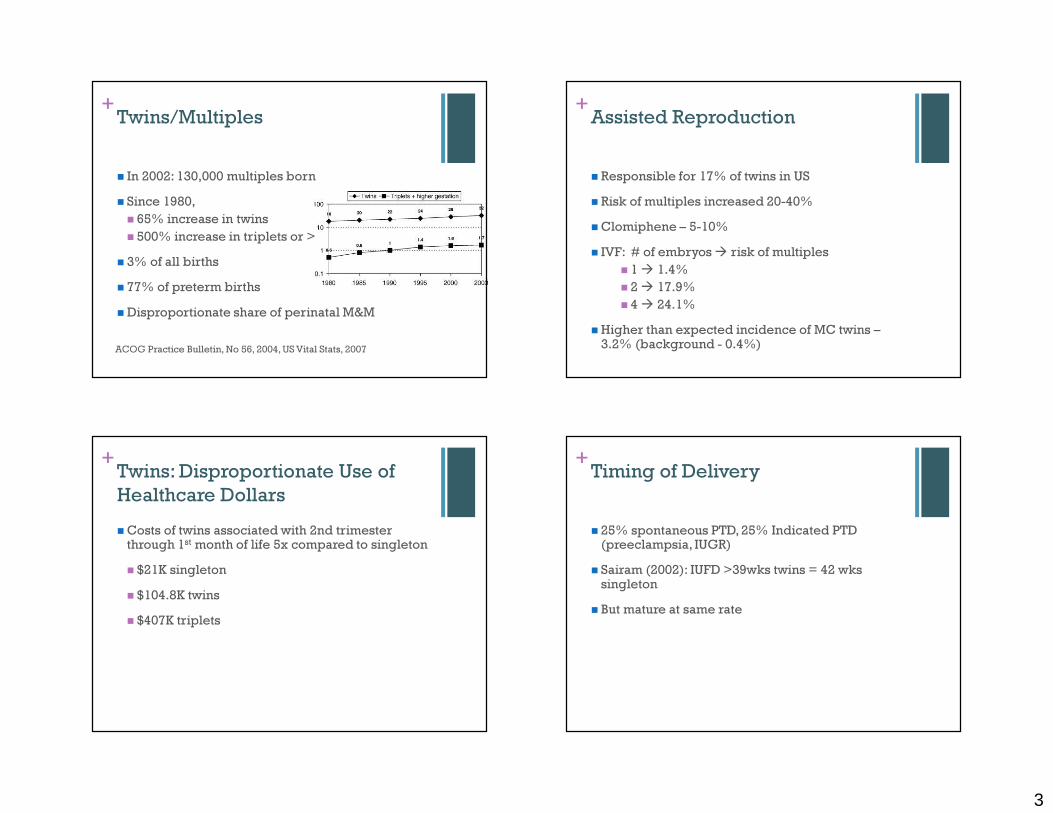
3
+Twins/Multiples
� In 2002: 130,000 multiples born � Since 1980, � 65% increase in twins� 500% increase in triplets or > � 3% of all births� 77% of preterm births�Disproportionate share of perinatal M&M
ACOG Practice Bulletin, No 56, 2004, US Vital Stats, 2007
+Assisted Reproduction
� Responsible for 17% of twins in US� Risk of multiples increased 20-40%�Clomiphene – 5-10%� IVF: # of embryos � risk of multiples� 1 � 1.4%� 2 � 17.9%� 4 � 24.1%
�Higher than expected incidence of MC twins –3.2% (background - 0.4%)
+Twins: Disproportionate Use of Healthcare Dollars�Costs of twins associated with 2nd trimester through 1stmonth of life 5x compared to singleton� $21K singleton� $104.8K twins� $407K triplets
+Timing of Delivery
� 25% spontaneous PTD, 25% Indicated PTD (preeclampsia, IUGR)� Sairam (2002): IUFD >39wks twins = 42 wkssingleton� But mature at same rate

4
+Recommended timing of delivery: Near-term twins(≥34 weeks)� Twin Clinic at Med. Univ. S. Carolina�MFM, U/S, NST, del 37-38 wks� 1987-2010: 1779 twin gestations� 1011 excluded: PTD <34 wks, unsure chorionicity, monoamniotic, anomalies� 768 twin gestations analyzed� 601 di/di: 1 IUFD after 34 wks� 167 mo/di: no IUFDs after 34 wks (only 94 went past 36 wks)
Burgess, American Journal of Obstetrics and Gynecology, 2014
+Neonatal Mortality
Burgess, American Journal of Obstetrics and Gynecology, 2014
+Recommended timing of delivery: Complicated near-term twins(≥34 weeks)
Burgess, American Journal of Obstetrics and Gynecology, 2014
+Recommended timing of delivery: Uncomplicated near-term twins (≥34 weeks)
Burgess, American Journal of Obstetrics and Gynecology, 2014Spong, NICHD consensus, 2011
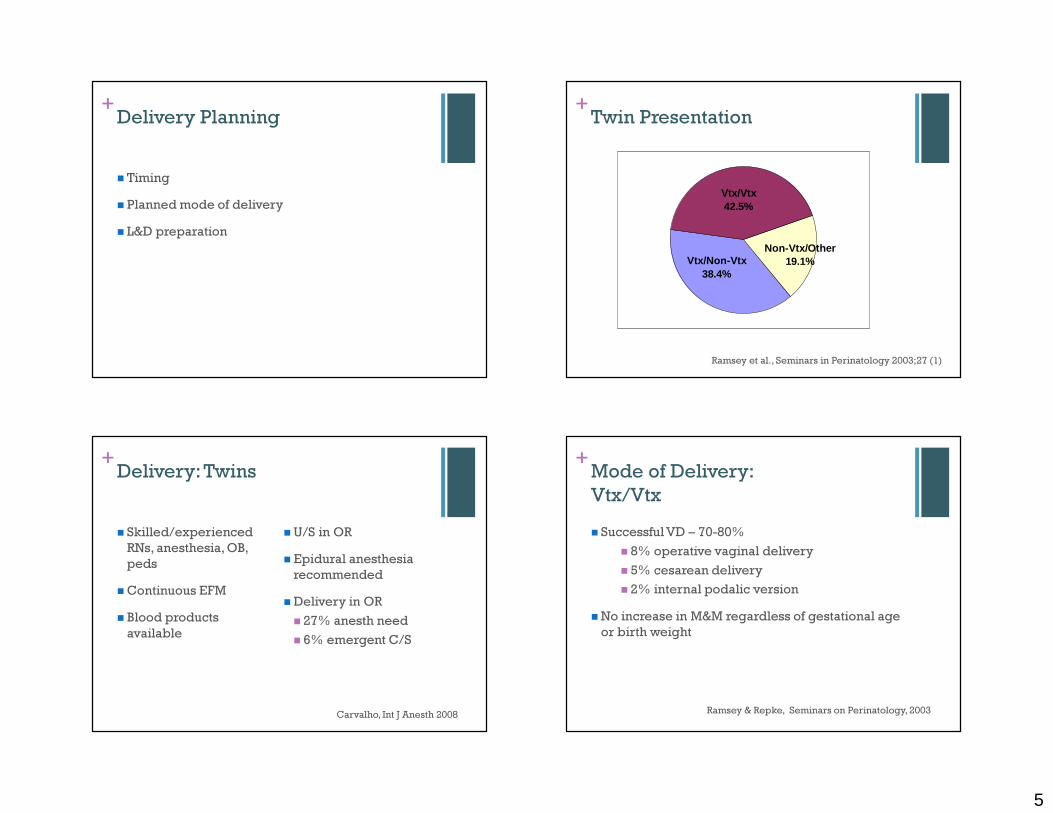
5
+
� Timing� Planned mode of delivery� L&D preparation
Delivery Planning +Twin Presentation
Vtx/Vtx42.5%
Vtx/Non-Vtx38.4%
Non-Vtx/Other19.1%
Ramsey et al., Seminars in Perinatology 2003;27 (1)
+Delivery: Twins
� Skilled/experienced RNs, anesthesia, OB, peds�Continuous EFM� Blood products available
�U/S in OR � Epidural anesthesia recommended�Delivery in OR� 27% anesth need� 6% emergent C/S
Carvalho, Int J Anesth 2008
+Mode of Delivery: Vtx/Vtx� Successful VD – 70-80%� 8% operative vaginal delivery� 5% cesarean delivery� 2% internal podalic version
�No increase in M&M regardless of gestational age or birth weight
Ramsey & Repke, Seminars on Perinatology, 2003

6
+
�Cesarean Delivery generally recommended� Level II-C evidence
Mode of Delivery:Non-Vertex Twin A
+Mode of Delivery:Non-Vertex Second Twin� Retrospective cohort, 1542 twin pairs in Nova Scotia, 1988-2002� 2nd twin greater risk adverse outcome independent of presentation, chorionicity, sex
Armson, B et al. Obstet Gynecol 2006
+
� Retrospective cohort, 858 twin pairs in France, >35 wks, 1st twin cephalic, VD if B <125% A� “Active management of 2nd twin”�Mean intertwin interval (VD) 4.9 minutes� 657 planned VD: 78% V/V, 21% C/C, 0.5% V/C�Neonatal composite morbidity unchanged � (5 vs 4.7%) � Level II evidence
Mode of Delivery:Non-Vertex Second Twin
Schmitz. Obstet Gynecol 2008
+RCT: Mode of DeliveryFirst Twin Cephalic� RCT: planned C/S vs planned VD� Toronto/multi-center� Twins 32+0-38+6 wks� Twin A cephalic� Both alive, with EFWs 1500-4000g� Excluded MA twins, lethal anomalies, previous classical or >1 LTCS �OBs “qualified” per their dept head
Barrett, Twin Birth Study Collab. GroupNEJM 2013
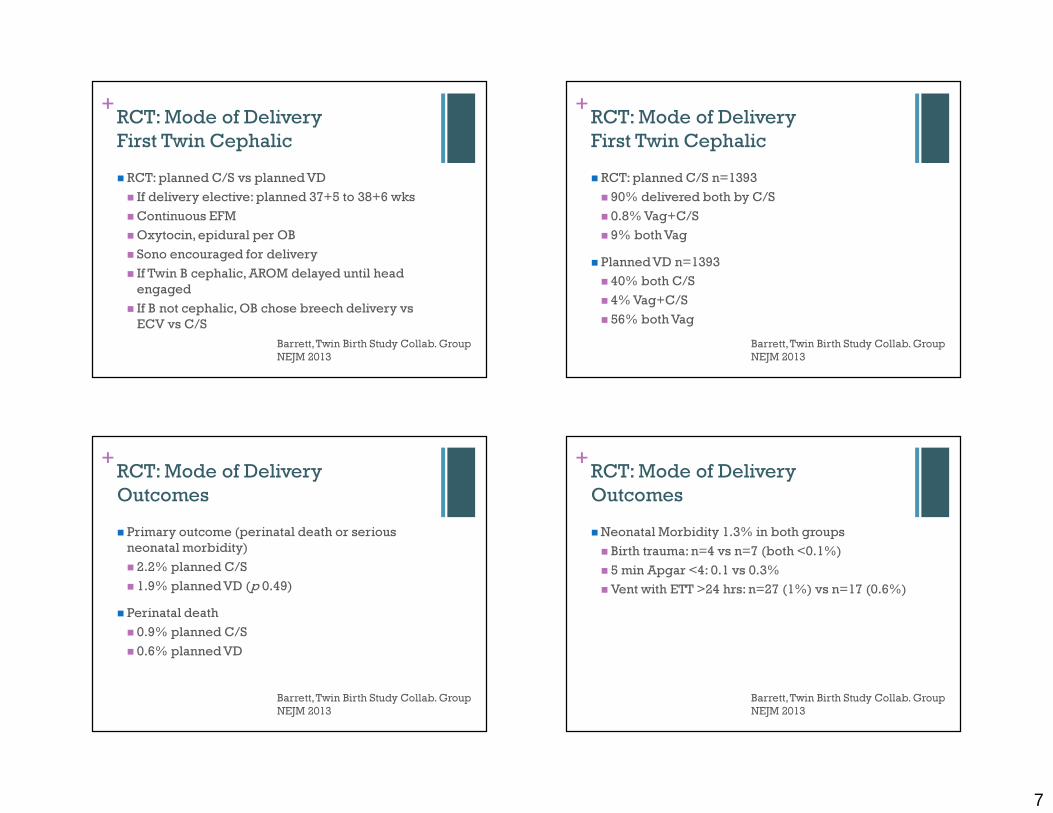
7
+RCT: Mode of DeliveryFirst Twin Cephalic� RCT: planned C/S vs planned VD� If delivery elective: planned 37+5 to 38+6 wks�Continuous EFM�Oxytocin, epidural per OB� Sono encouraged for delivery� If Twin B cephalic, AROM delayed until head engaged� If B not cephalic, OB chose breech delivery vs ECV vs C/S
Barrett, Twin Birth Study Collab. GroupNEJM 2013
+RCT: Mode of Delivery First Twin Cephalic� RCT: planned C/S n=1393� 90% delivered both by C/S� 0.8% Vag+C/S� 9% both Vag� Planned VD n=1393� 40% both C/S� 4% Vag+C/S� 56% both Vag
Barrett, Twin Birth Study Collab. GroupNEJM 2013
+RCT: Mode of Delivery Outcomes� Primary outcome (perinatal death or serious neonatal morbidity)� 2.2% planned C/S� 1.9% planned VD (p 0.49)� Perinatal death� 0.9% planned C/S� 0.6% planned VD
Barrett, Twin Birth Study Collab. GroupNEJM 2013
+RCT: Mode of Delivery Outcomes�Neonatal Morbidity 1.3% in both groups� Birth trauma: n=4 vs n=7 (both <0.1%)� 5 min Apgar <4: 0.1 vs 0.3%�Vent with ETT >24 hrs: n=27 (1%) vs n=17 (0.6%)
Barrett, Twin Birth Study Collab. GroupNEJM 2013

8
+RCT: Mode of Delivery Outcomes�Maternal M&M: 7% vs 8.5% p 0.29�Maternal Mortality: n=1 in each group �Maternal Morbidity:�Hemorrhage: 6% C/S vs 7.8% VD� 3rd or 4th degree: 0% C/S vs 0.3% VD� Infection (wound + non-wound): 3.7% C/S vs 2.6% VD
+RCT: Mode of Delivery
�Conclusion:No benefits of planned cesarean section over planned vaginal delivery for twins between 32-38 weeks if first twin is cephalic
Barrett, Twin Birth Study Collab. GroupNEJM 2013
+Trial of Labor in Twins:Previous Cesarean � Small studies�No increased risk uterine rupture, maternal morbidity� Perinatal mortality not increased after adjusting for confounders
Aaronson, JMFNM 2009 Delaney, JOG Can 2003Sansregret, JOG Can 2003Ford, AJOG 2006Barrett, 2013
+Trial of Labor in Twins: A few studies� 38 TOL� 28 VD� no ruptures; 2 C/S for 2nd twin� repeat C/S had higher SSI morbidity
� 26 TOL� 85% del A vag, 73% del both vag; 71 elective RC/S� No difference in outcomes except LOS
�NIS data: 4705 elective repeat, 1805 TOL� 45% both twins vag� 0.9% uterine rupture rate (= singleton rate)
Delaney, JOG Can 2003Sansregret, JOG Can 2003Ford, AJOG 2006

9
+Twins: A Reasonable Approach
�Deliver at 36-37 wks mo/di, 38 wks di/di� Route of delivery based on presentation & OB experience (no benefit to C/S if you are trained to deliver twins)� Epidural anesthesia, OR delivery w/ U/S, peds, anesthesia, & extra MD/RN help
+
Thank you for your attention.
Questions?
6/6/2014
1
Genetic Carrier Screening: Review of theOld, the New, and the Controversial
Brian L Shaffer, MD6/6/14
Assistant ProfessorDivision of Maternal Fetal Medicine
Oregon Health and Sciences University
Disclosures• I have no relevant financial relationships
Objectives• Carrier Screening: Review tenets• ACOG recommendations – Ethnicity based screening
• Cystic Fibrosis, Hemoglobinopathies, Ashkenazi Jewish Disorders, Fragile X, Spinal Muscular Atrophy
• Expanded carrier screening: “Universal”• Pros and Cons• What to expect
Carrier Screening - Foundation
Independent of family history: Asymptomatic Single gene: autosomal recessive; X-linkedInformed consent: Non-directive
• Natural history of disorder - Severity• Access to quality genetic counseling - Residual risk• Acceptance by screened population - Voluntary
High frequency of carriers in screened population• Geographic ancestry – 1 in 30

6/6/2014
2
Carrier Screening - FoundationQuality test:
• Timely and dependable• Inexpensive/cost efficient • High detection rate – 90%
Availability of intervention: Preconception/Prenatal• Donor sperm/egg; PGD; adoption; forgo pregnancy • Prenatal diagnosis – To carry (and prepare) or not?
Goal: Risk assessment, informed decision makingPublic health implications: Prevention
Case 119 year old G1 8 wks, presents for new OB visit• Ethnicity?• Geographic ancestry?• Her partner is from Mexico • No family history of any genetic disease• In either she or FOB
• Carrier Screening
Case 119 year old G1 8 wks, presents for new OB visit• Ethnicity? • Geographic ancestry?• Her partner is from Mexico • No family history of any genetic disease• In either she or FOB
• Carrier Screening
Case 119 year old G1 8 wks, presents for new OB visit• Ethnicity? • Geographic ancestry?• Her partner is from Mexico • No family history of any genetic disease• In either she or FOB
• Carrier Screening• “ACOG says” ACOG SAYS ?

6/6/2014
3
Case 119 year old G1 8 wks, presents for new OB visit• Ethnicity? • Geographic ancestry?• Her partner is from Mexico • No family history of any genetic disease• In either she or FOB
• Carrier Screening• “ACOG says”
• Cystic FibrosisACOG SAYS ?
Cystic Fibrosis - CFTR• Most common AR disorder among whites (1/2500-3300)• 1/25-29 with no family history is a carrier of a CF gene change
(mutation) or variant � alters function• Pulmonary disease, pancreatic insufficiency, gastrointestinal,
infertility; normal intelligence• Life limiting – ~40 years• ~80% of children with CF are born to parents with no prior
family history of the disease• ACOG: “it is difficult to assign a single ethnicity to affected
individuals… offer to all patients”ACOG Committee Opinion #486, 2011
Case 1 (cont.)19 year old G1 8 wks, presents for new OB visit
• Carrier Screening – negative for 32 mutations• Carrier screening for a gene is needed only once
• “So my baby won’t have cystic fibrosis”• What is a residual risk?• What is the risk of having an affected child?
Group Incidence Carrier risk Detection Residual risk
after negative
Ashkenazi 1/2270 1/24 94% 1/384
Caucasian 1/2500 1/25 88% 1/206
Hispanic 1/13,500 1/58 72% 1/203
African American 1/15,100 1/61 64% 1/171
Asian American 1/35,100 1/94 49% 1/183
Cystic Fibrosis: Incidence, Carrier risks and Detection rates*
* Detection rates derived from using ACMG 23 mutation panel
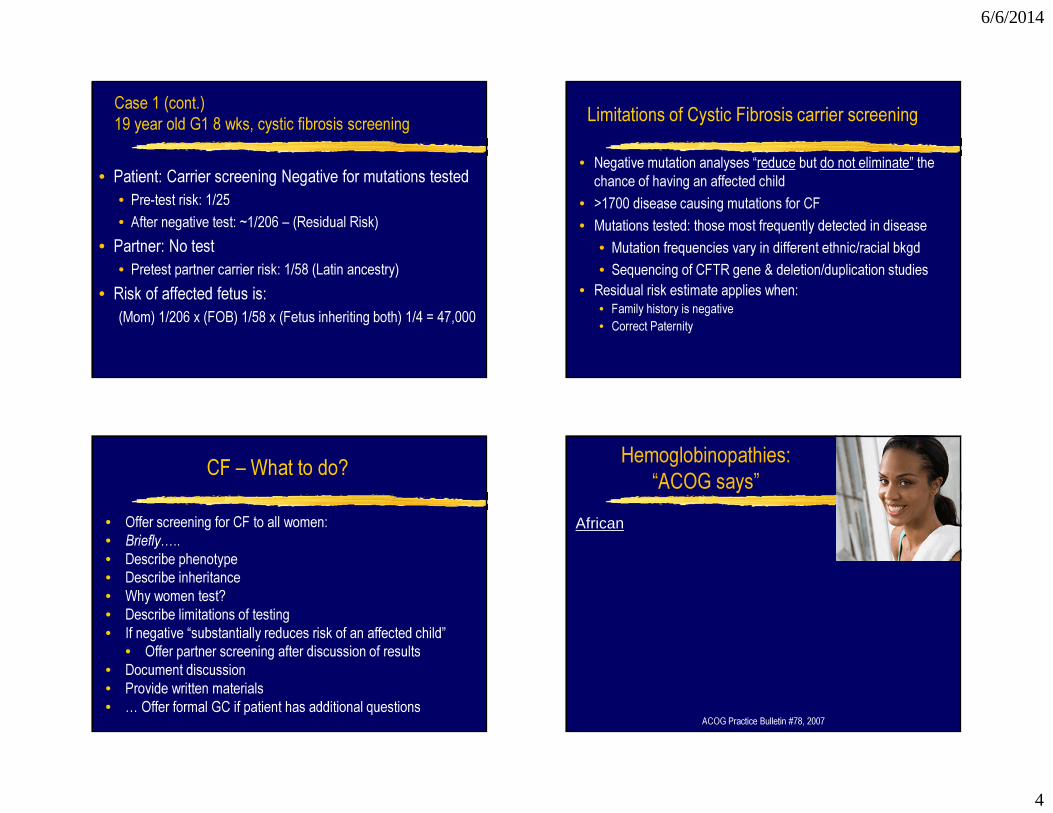
6/6/2014
4
Case 1 (cont.)19 year old G1 8 wks, cystic fibrosis screening
• Patient: Carrier screening Negative for mutations tested• Pre-test risk: 1/25• After negative test: ~1/206 – (Residual Risk)
• Partner: No test• Pretest partner carrier risk: 1/58 (Latin ancestry)
• Risk of affected fetus is:(Mom) 1/206 x (FOB) 1/58 x (Fetus inheriting both) 1/4 = 47,000
Limitations of Cystic Fibrosis carrier screening• Negative mutation analyses “reduce but do not eliminate” the
chance of having an affected child• >1700 disease causing mutations for CF• Mutations tested: those most frequently detected in disease
• Mutation frequencies vary in different ethnic/racial bkgd• Sequencing of CFTR gene & deletion/duplication studies
• Residual risk estimate applies when:• Family history is negative• Correct Paternity
CF – What to do?• Offer screening for CF to all women:• Briefly…..• Describe phenotype• Describe inheritance• Why women test?• Describe limitations of testing• If negative “substantially reduces risk of an affected child”
• Offer partner screening after discussion of results• Document discussion• Provide written materials• … Offer formal GC if patient has additional questions
Hemoglobinopathies:“ACOG says”
African
ACOG Practice Bulletin #78, 2007

6/6/2014
5
Structure of hemoglobin
b1b2
a1a2
a3a4
Beta globin genes Alpha globin genes
Chromosome 11 Chromosome 16
Hemoglobinprotein
Hemoglobinopathies:“ACOG says”
African• Hemoglobin electrophoresis• CBC
ACOG Practice Bulletin #78, 2007ACOG SAYS ?
Hemoglobinopathies:“ACOG says”
African• Hemoglobin electrophoresis• CBC
ACOG Practice Bulletin #78, 2007
Hemoglobinopathies:“ACOG says”
African• Hemoglobin electrophoresis• CBC
Mediterranean• CBC• If Anemia, MCV <80 (microcytic)• Normal iron studies (ferritin)
• Hemoglobin Electrophoresis• Assess for Beta Thalassemia
ACOG Practice Bulletin #78, 2007
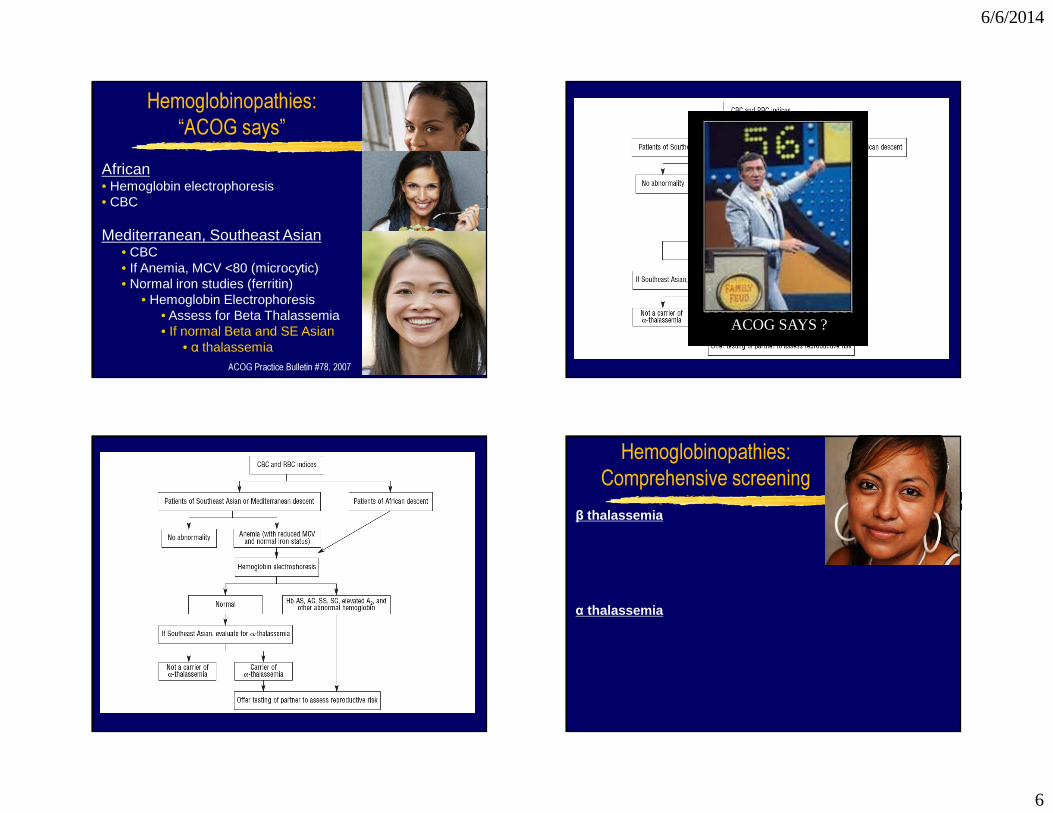
6/6/2014
6
Hemoglobinopathies:“ACOG says”
African• Hemoglobin electrophoresis• CBC
Mediterranean, Southeast Asian• CBC• If Anemia, MCV <80 (microcytic)• Normal iron studies (ferritin)
• Hemoglobin Electrophoresis• Assess for Beta Thalassemia• If normal Beta and SE Asian
• α thalassemiaACOG Practice Bulletin #78, 2007
ACOG SAYS ?
Hemoglobinopathies:Comprehensive screening
β thalassemia
α thalassemia

6/6/2014
7
Hemoglobinopathies:Comprehensive screening
β thalassemia
α thalassemia
Hemoglobinopathies:Comprehensive screening
β thalassemia
α thalassemia
Hemoglobinopathies:Comprehensive screening
β thalassemiaLatin, Middle Eastern, Indian, Pacific Islander, Chinese
• If Anemia, MCV <80, normal iron• Hemoglobin Electrophoresis
α thalassemiaMediterranean (Italy, Greece), East Asia (China), Mid Eastern (Turkey, Pakistan), Central Asia (West India), African
• If Anemia, MCV <80, normal iron• Hemoglobin Electrophoresis nl
• Molecular studies for alpha thal
Case 2 • 26 yo G1P0 at 10 weeks with a younger brother with autism and cognitive disability who “looks different” than other family members. On further questioning her mother had early menopause.
• What is her fetus at risk for?• Why the primary ovarian deficiency in her mother?• What carrier screening should be offered?
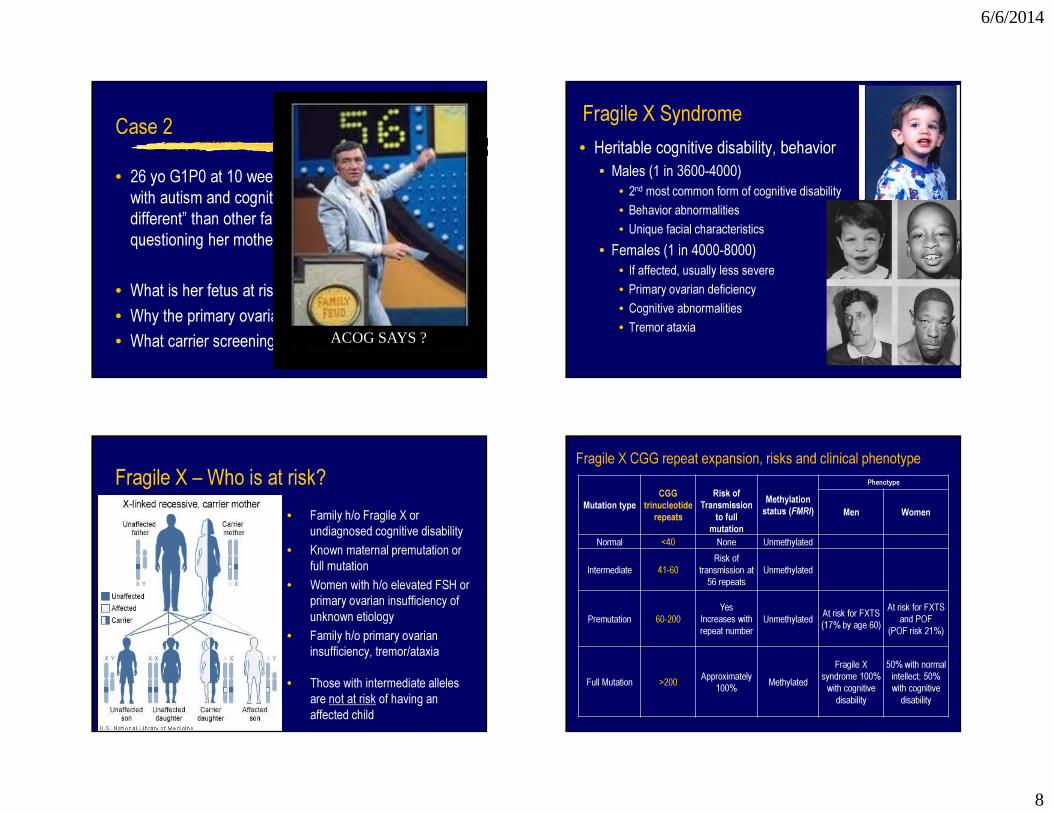
6/6/2014
8
Case 2 • 26 yo G1P0 at 10 weeks with a younger brother with autism and cognitive disability who “looks different” than other family members. On further questioning her mother had early menopause.
• What is her fetus at risk for?• Why the primary ovarian deficiency in her mother?• What carrier screening should be offered?ACOG SAYS ?
Fragile X Syndrome• Heritable cognitive disability, behavior
• Males (1 in 3600-4000)• 2nd most common form of cognitive disability• Behavior abnormalities• Unique facial characteristics
• Females (1 in 4000-8000)• If affected, usually less severe• Primary ovarian deficiency• Cognitive abnormalities• Tremor ataxia
Fragile X – Who is at risk?• Family h/o Fragile X or
undiagnosed cognitive disability• Known maternal premutation or
full mutation• Women with h/o elevated FSH or
primary ovarian insufficiency of unknown etiology
• Family h/o primary ovarian insufficiency, tremor/ataxia
• Those with intermediate alleles are not at risk of having an affected child
Mutation typeCGG
trinucleotide repeats
Risk of Transmission
to full mutation
Methylation status (FMRI)
Phenotype
Men Women
Normal <40 None Unmethylated
Intermediate 41-60Risk of
transmission at 56 repeats
Unmethylated
Premutation 60-200Yes
Increases with repeat number
Unmethylated At risk for FXTS(17% by age 60)
At risk for FXTS and POF
(POF risk 21%)
Full Mutation >200 Approximately 100% Methylated
Fragile X syndrome 100% with cognitive disability
50% with normal intellect; 50% with cognitive disability
Fragile X CGG repeat expansion, risks and clinical phenotype

6/6/2014
9
Mutation typeCGG
trinucleotide repeats
Risk of Transmission
to full mutation
Methylation status (FMRI)
Phenotype
Men Women
Normal <40 None Unmethylated
Intermediate 41-60Risk of
transmission at 56 repeats
Unmethylated
Premutation 60-200Yes
Increases with repeat number
Unmethylated At risk for FXTS(17% by age 60)
At risk for FXTS and POF
(POF risk 21%)
Full Mutation >200 Approximately 100% Methylated
Fragile X syndrome 100% with cognitive disability
50% with normal intellect; 50% with cognitive disability
Fragile X CGG repeat expansion, risks and clinical phenotype
ACOG SAYS ?
Fragile X – Carrier Rate – “ACOG says”• Low risk women (neg family history)
• 1 in 113-300 • Family history of Fragile X
• 1 in 4 (28.8%)• Suspicious family history
• 1 in 83• 1º ovarian insufficiency, ↑ FSH
• As high as 1 in 10
ACOG: No, but if requests, Yes, +GCACOG: Yes, +GC
ACOG: Yes, +GC
ACOG: Yes, +GC
ACOG Committee Opinion #469, 2010
Case 325 year old G1, new OB
• Ashkenazi descent
Case 325 year old G1, new OB
• Ashkenazi descent
ACOG SAYS ?

6/6/2014
10
Case 325 year old G1, new OB
• Ashkenazi descent – “ACOG says”• CF, Tay Sachs, Fam Dysautonomia, Canavan• Others: “made available”
Case 325 year old G1, new OB
• Ashkenazi descent – “ACOG says”• CF, Tay Sachs, Fam Dysautonomia, Canavan• Others: “made available”
Case 325 year old G1, new OB
• Ashkenazi descent – “ACOG says”• CF, Tay Sachs, Fam Dysautonomia, Canavan• Others: “made available”
• Tay Sachs – “ACOG says”• AJ, Fr Canadian (Quebec), Cajun• Leukocyte testing in pregnancy –
• Biochemical• Carrier screening • Refer
ACOG Committee Opinion #442, 2009 ACOG Committee Opinion #318, 2005
Disorder Disease incidence
Carrier frequency
DetectionRate
Tay-Sachs†Canavan†Familial dysautonomia†Cystic fibrosis†Fanconi anemia- group CNiemann-Pick- type AMucolipidosis- type IVBloomGaucher
1/3,0001/6,400-9,1001/3,6001/2,500-3,0001/32,0001/32,0001/62,5001/40,0001/900
1/30-311/40-481/31-321/24-291/891/901/1271/1071/15-18
98% by HEX A enzyme92-99% by DNA98%99%94-97%98-99%94-97%90-95%99%89-95%
French Canadian/Cajun†Tay-Sachs 1/675-360,000 1/13-300 Varies
Table 1-1. Ashkenazi Jewish/East European –Geographic Ancestry-based Carrier Screening
† - ACOG recommends

6/6/2014
11
Case 435 year old G1, IVF
Case 435 year old G1, IVF, requests SMA screening
Case 435 year old G1, IVF, requests SMA screening
ACOG SAYS ?
Case 435 year old G1, IVF, requests SMA screeningSpinal Muscular atrophy (SMA), SMN1• 2nd most common fatal recessive disease• All ethnicities, 1 in 40-60• Motor weakness, paralysis, death - weakness – variable• Education, counseling – logistics, phenotype & genetics• Patient preferences, cost effectiveness“ACOG says” – No, unless request and have formal GCExpanded carrier screening?
ACOG Committee Opinion #432, 2009

6/6/2014
12
Expanded Carrier screening: Why?• All are carriers of recessive conditions – up to 7 diseases• Ethnicity based screening has limitations:
• Difficult to appropriately assign ethnicity (e.g., CF)• Does not identify all who may want prenatal diagnosis
• Technology -- Next generation sequencing• Quick, inexpensive, high fidelity identification of mutations
• Screen many genes for disease causing mutations• Test ~100 genes for known mutations (~400)
• No longer, what can we screen for?• but what should we screen for?
Expanded carrier screen: ControversyIssue Potential Solution
Which diseases?- Severity- Organ affected- Milder phenotype- Adult in onset
ACMG Policy Statement, Genet Med 2013
Expanded carrier screen: Controversy
Most patients at risk: Consider PNDxMild phenotypeVariable expressivityIncomplete penetrance
-- OptionalAdult onset Could impact his/her offspring
-- Must provide consent
Issue Potential Solution
Which diseases?- Severity- Organ affected- Milder phenotype- Adult in onset
ACMG Policy Statement, Genet Med 2013
Expanded carrier screen: ControversyIssue Potential Solution
For a given disorder:- Causative gene- Mutation- Frequencies
Residual risk calculationCarrier frequencyAllele frequency
Risk is less? By how much Doctor?
ACMG Policy Statement, Genet Med 2013

6/6/2014
13
Expanded carrier screen: Controversy
LaboratoriesReport residual riskHow risk was calculatedHigh detection rate
Issue Potential Solution
For a given disorder:- Causative gene- Mutation- Frequencies
Residual risk calculationCarrier frequencyallele frequency
Risk is less? By how much Doctor?
ACMG Policy Statement, Genet Med 2013
Expanded carrier screen: ControversyIssue Potential Solution
Quality testGenotype-PhenotypeFor a mutation
- Mild-severe?- Variant?
ACMG Policy Statement, Genet Med 2013
Expanded carrier screen: Controversy
Laboratories should provide citation regarding the typical clinical course
Issue Potential Solution
Quality testGenotype-PhenotypeFor a mutation
- Mild-severe?- Variant?
ACMG Policy Statement, Genet Med 2013
Expanded carrier screen: ControversyIssue Potential Solution
Informed consentcan’t be obtained
ACMG Policy Statement, Genet Med 2013
6/6/2014
14
Expanded carrier screen: Controversy
Alter processUndergo general pre-test counselingfor both partners
Detailed post test counselingRisk 1 in 4Residual risk
Issue Potential Solution
Informed consentcan’t be obtained
ACMG Policy Statement, Genet Med 2013
Expanded carrier screen: What to expect
• ~25% – carrier one or more conditions• ~0.7% of couples have changes in the same gene
• CF, SMA, Smith-Lemli-Opitz syndrome, Connexin 26• Option of invasive testing
• May find that your patient or father of the baby has “disease”• Incorrect classification of a “mutation”• Reduced penetrance or variable expressivity
Expanded carrier screen: What to do
• Prepare patients for potential results• Preconception period, if possible
• Well woman Gyn visit• Preconception visit
• Perform only once• Formal genetic counseling
• In person, phone, telemedicine
Summary
ACOG: Ethnicity based carrier screenAll women: CFAfrican: Hgb Elec, CBCSE Asian, Mediterranean – CBC, <80; Hgb Elec – β thalassemia
SE Asian – α thalassemiaFamily/Personal history for FraX – carrier screen +GCAshkenazi – CF, TSD, Canavan, Fam dysautonomiaFrench Canadian, Cajun – TSD“I want SMA testing” GC and SMABe prepared for expanded carrier screening

6/6/2014
15
Thank you
ACOG SAYS ?
References1) Carrier Screening Based on Ashkenazi Jewish Ancestry: ACOG committee opinion no. 442: preconception and prenatal carrier screening for genetic diseases in individuals of Eastern European Jewish descent, 2009 .2) Carrier Screening for Hemoglobinopathies American College of Obstetricians and Gynecologists Committee on Obstetrics : ACOG practice bulletin no. 78 Hemoglobinopathies in pregnancy , 2007.3) Carrier Screening for Cystic Fibrosis Committee on Genetics: ACOG committee opinion no. 486: Update on carrier screening for cystic fibrosis, 2011.4) ACOG committee opinion no. 469: carrier screening for fragile X syndrome, 2010. 5) ACOG committee opinion no. 432: Spinal muscular atrophy, 2009 .6) ACOG committee opinion no. 318: Screening for Tay-Sachs disease, 2005 .7) Grody WW, et al; ACMG Policy Statement: ACMG position statement on prenatal/preconception expanded carrier screening; Genet Med 2013.
Heterozygote (Carrier) screening and “ethnicity” or geographic ancestry
All women Cystic fibrosis
Ashkenazi Jewish Tay-Sachs, Canavan disease, familial dysautonomia, make “other” available
African American, African, Mediterranean
Sickle cell anemia
Ethnic group Disease
Heterozygote (Carrier) screening and “ethnicity” or geographic ancestry
Southeast Asian, Mediterranean, African (not African American), Middle Eastern, Indian, Chinese
Alpha thalassemia
Mediterranean, East Asian, Middle Eastern, Central Asia, Far Eastern
Beta thalassemia
All ethnicities? Spinal muscular atrophyExpanded carrier screening
Ethnic groups Disease

6/6/2014
16
DNA REPORT Cystic FibrosisEthnicity: White: Non-HispanicSupplemental indications: Supervision of Other Normal PregnancyPatient Results:Negative for mutations analyzedInterpretation:It is our understanding that this individual has a negative personal and family history of cystic fibrosis (CF). Using the methodology described, this individual is negative for the 23 CF mutation screening test recommended by the American College of Medical Genetics. These results do not rule out the possibility that this individual could be a carrier of a mutation not detected by this test. The following table provides data to be used in the genetic counseling for this individual. Limited information is available for individuals from other ethnic groups. These risks would differ for individuals who have a family history of CF; if this is the case for this patient, please contact the laboratory.Estimated Carrier RiskETHNIC GROUP DETECTION RATE BEFORE TEST AFTER NEG TESTAshkenazi Jewish 94% 1/24 ~1 in 384European Caucasian 88% 1/25 ~1 in 206African American 64% 1/61 ~1 in 171Hispanic American 72% 1/58 ~1 in 203Asian American 49% ~1/94 ~1 in 183Methods: The CFTR gene was tested for the presence of these specific 32 mutations (and benign variants as indicated) by polymerase chain reaction (PCR) and oligoligation assay. The ACMG panel of 23 recommended mutations is shown as the standard mutation panel.

6/6/2014
1
Are you HIP?
Update on ACOG Hypertension inPregnancy Task Force
Maurice L. Druzin, MDProfessor and Vice-Chair
Department of Obstetrics and GynecologyDivision of Maternal Fetal MedicineStanford University Medical Center
Associate Dean for Academic AffairsStanford University School of Medicine
I have no financial disclosures to report
Learning Objectives
� To review the most current recommendations for the diagnosis andmanagement of hypertensive disorders of pregnancy from ACOG and the California Preeclampsia Task Force (PTF) of CMQCC.
� To review the impact of hypertensive disorders of pregnancy on maternal and perinatal morbidity and mortality.
� To delineate the most common causes of maternal morbidity and mortality secondary to hypertensive disorders of pregnancy.
� To outline a management algorithm to optimize care for patients with hypertensive disorders of pregnancy.
Rocket science? Only 4 things Brain surgery?
� Classification: 1)PE
� 2)CHT
� 3)CHT+PE
� 4)GHTN
� Management: 1)BP control
� 2)Seizure prevention
� 3)Delivery- 34 wks,37wks.
� 4)Post partum surveillance
Only 4 things
6/6/2014
2
Executive Summary : Hypertension in Pregnancy
American College of Obstetricians and Gynecologists
James Martin, Jr, MD
Obstet Gynecol 2013;122:1122-31
Improving Health Care Response to Preeclampsia:
A California Quality Improvement Toolkit
Funding for the development of this toolkit was provided by: Federal Title V block grant funding from the California Department of Public Health; Maternal, Child and Adolescent Health Division and Stanford University.
6
Development of the California Toolkit ‘Improving Health Care Response to Preeclampsia’ was funded by the California Department of Public Health (CDPH), Center for Family Health, Maternal Child and Adolescent
Health (MCAH) Division, using federal Title V MCH funds.
Preeclampsia Task Force MembersMaurice Druzin, MD – StanfordElliott Main, MD – CMQCCBarbara Murphy, RN – CMQCCTom Archer, MD – UCSDOcean Berg, RN, CNS – SF General HospitalBrenda Chagolla, RNC, CNS – UC DavisHolly Champagne, RNC, CNS – Kaiser Meredith Drews – Preeclampsia FoundationRacine Edwards-Silva, MD – UCLA Olive ViewKristi Gabel, RNC CNS – RPPC SacramentoThomas Kelly, MD – UCSD
Larry Shields, MD – Dignity HealthNancy Peterson, RNC, PNNP – CMQCCChristine Morton, PhD – CMQCCSarah Kilpatrick, MD – Cedars SinaiRichard Lee, MD – Univ. of Southern CaliforniaAudrey Lyndon PhD, RNC – UC San FranciscoMark Meyer, MD – Kaiser SDValerie Cape – CMQCCEleni Tsigas – Preeclampsia FoundationLinda Walsh, PhD, CNM – UC San FranciscoMark Zakowski, MD – Cedars SinaiConnie Mitchell, MD, MPH – CDPH - MCAH
7
� The incidence of preeclampsia has increased by 25% in the United States during the past two decades.
� Preeclampsia is a leading cause of maternal and perinatal morbidity and mortality , with an estimated 50,000-60,000 preeclampsia-related deaths per year worldwide .
Ref: ACOG – HIP, 2013
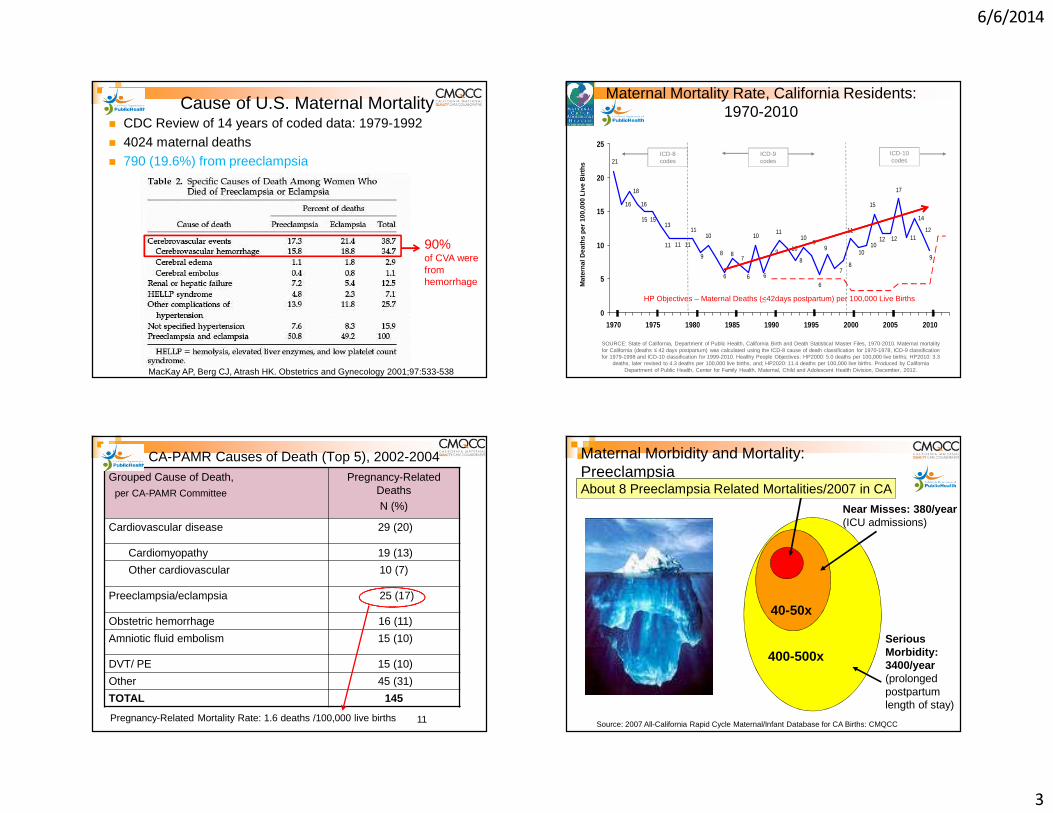
6/6/2014
3
Cause of U.S. Maternal Mortality� CDC Review of 14 years of coded data: 1979-1992� 4024 maternal deaths� 790 (19.6%) from preeclampsia
MacKay AP, Berg CJ, Atrash HK. Obstetrics and Gynecology 2001;97:533-538
90% of CVA were from hemorrhage
16
18
16
13
9 10
8
1011
14
9
12
78 8
1515
99
1011
10
6
666
10
9
11
111111
87
10
11
15
12
17
12
21
0
5
10
15
20
25
1970 1975 1980 1985 1990 1995 2000 2005 2010
HP Objectives – Maternal Deaths (<42days postpartum) per 100,000 Live Births
Mat
erna
l Dea
ths
per
100,
000
Live
Birt
hs
ICD-10 codes
ICD-8 codes
ICD-9 codes
Maternal Mortality Rate, California Residents: 1970-2010
SOURCE: State of California, Department of Public Health, California Birth and Death Statistical Master Files, 1970-2010. Maternal mortality for California (deaths ≤ 42 days postpartum) was calculated using the ICD-8 cause of death classification for 1970-1978, ICD-9 classification for 1979-1998 and ICD-10 classification for 1999-2010. Healthy People Objectives: HP2000: 5.0 deaths per 100,000 live births; HP2010: 3.3
deaths, later revised to 4.3 deaths per 100,000 live births, and; HP2020: 11.4 deaths per 100,000 live births. Produced by California Department of Public Health, Center for Family Health, Maternal, Child and Adolescent Health Division, December, 2012.
CA-PAMR Causes of Death (Top 5), 2002-2004Grouped Cause of Death,
per CA-PAMR Committee
Pregnancy-Related Deaths N (%)
Cardiovascular disease 29 (20)
Cardiomyopathy 19 (13)
Other cardiovascular 10 (7)
Preeclampsia/eclampsia 25 (17)
Obstetric hemorrhage 16 (11)
Amniotic fluid embolism 15 (10)
DVT/ PE 15 (10)
Other 45 (31)
TOTAL 145
Pregnancy-Related Mortality Rate: 1.6 deaths /100,000 live births 11
400-500xSerious Morbidity: 3400/year (prolonged postpartum length of stay)
Maternal Morbidity and Mortality: Preeclampsia
40-50x
Near Misses: 380/year (ICU admissions)
About 8 Preeclampsia Related Mortalities/2007 in CA
Source: 2007 All-California Rapid Cycle Maternal/Infant Database for CA Births: CMQCC
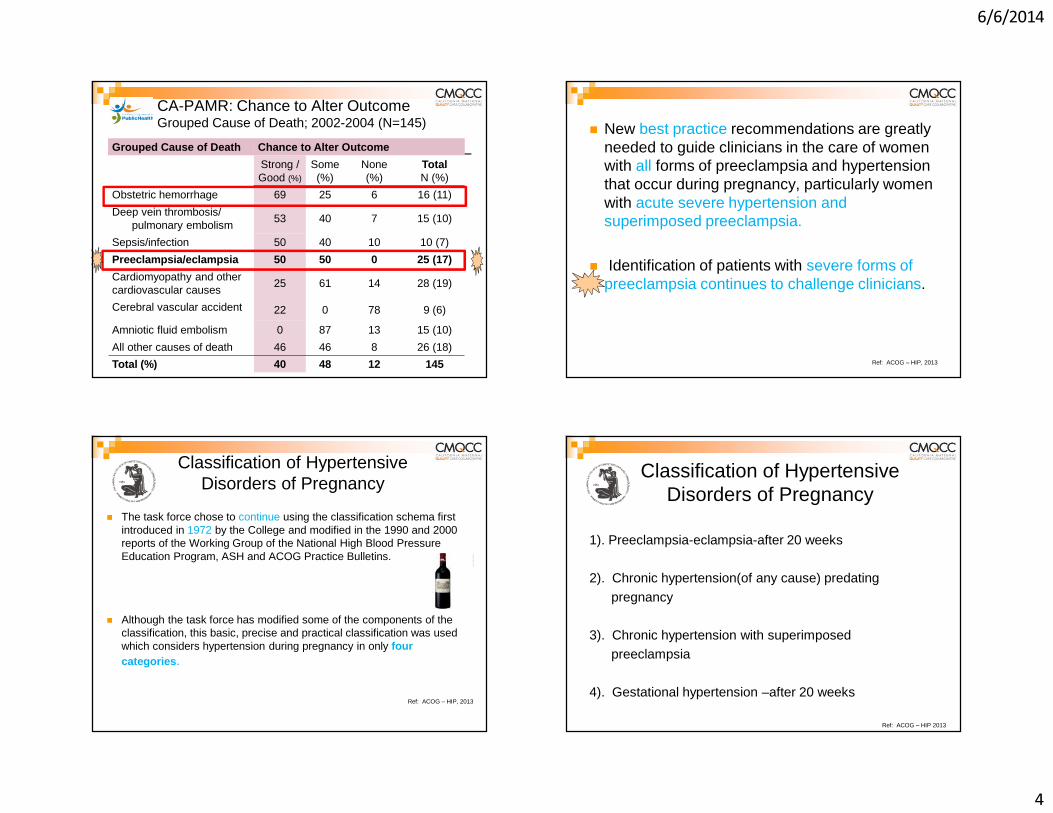
6/6/2014
4
CA-PAMR: Chance to Alter Outcome Grouped Cause of Death; 2002-2004 (N=145)
Grouped Cause of Death Chance to Alter Outcome
Strong /Good (%)
Some(%)
None(%)
Total N (%)
Obstetric hemorrhage 69 25 6 16 (11)
Deep vein thrombosis/pulmonary embolism
53 40 7 15 (10)
Sepsis/infection 50 40 10 10 (7)
Preeclampsia/eclampsia 50 50 0 25 (17)
Cardiomyopathy and other cardiovascular causes
25 61 14 28 (19)
Cerebral vascular accident 22 0 78 9 (6)
Amniotic fluid embolism 0 87 13 15 (10)
All other causes of death 46 46 8 26 (18)
Total (%) 40 48 12 145
� New best practice recommendations are greatly needed to guide clinicians in the care of women with all forms of preeclampsia and hypertension that occur during pregnancy, particularly women with acute severe hypertension and superimposed preeclampsia.
� Identification of patients with severe forms of preeclampsia continues to challenge clinicians.
Ref: ACOG – HIP, 2013
Classification of HypertensiveDisorders of Pregnancy
� The task force chose to continue using the classification schema first introduced in 1972 by the College and modified in the 1990 and 2000 reports of the Working Group of the National High Blood Pressure Education Program, ASH and ACOG Practice Bulletins.
� Although the task force has modified some of the components of the classification, this basic, precise and practical classification was used which considers hypertension during pregnancy in only four categories .
Ref: ACOG – HIP, 2013
Classification of HypertensiveDisorders of Pregnancy
1). Preeclampsia-eclampsia-after 20 weeks
2). Chronic hypertension(of any cause) predating
pregnancy
3). Chronic hypertension with superimposedpreeclampsia
4). Gestational hypertension –after 20 weeks
Ref: ACOG – HIP 2013

6/6/2014
5
Executive Summary: Hypertension in Pregnancy, American College of Obstetricians and Gynecologist, Obstet Gynecol 2013;122:1122-31. Copyright permission received.
Diagnostic Criteria for Preeclampsia
Key Clinical Pearl
Forty percent of patients with new onset hypertension or
new onset proteinuria will develop classic preeclampsia.
Barton JR, Sibai BM. Prediction and prevention of recurrent preeclampsia. Obstet Gynecol. 2008;112(2 PART 1): 359-372.
Key Clinical Pearl
Patients presenting with vague symptoms of:
� headache� abdominal pain� shortness of breath� generalized swelling� complaints of “I just don’t feel right”
should be evaluated for atypical presentations of preeclampsia or “severe features”
Sibai BM, Stella CL. Diagnosis and management of atypical preeclampsia-eclampsia. Am J ObstetGynecol. May 2009;200(5):481 e481-487.
Laboratory Evaluation of Preeclampsia
� Initial lab studies should include:�CBC with platelet count�AST, ALT, LDH (hemolysis)�Creatinine, Bilirubin, Uric acid, Glucose
� For women with acute abdominal pain, add:�Serum amylase, lipase and ammonia

6/6/2014
6
Diagnosis of Severe Preeclampsia
Executive Summary: Hypertension in Pregnancy, American College of Obstetricians and Gynecologist, ObstetGynecol 2013;122:1122-31. Copyright permission received.
*5 grams proteinuria eliminated as a criterion
• Acute onset, persistent (lasting 15 min or more), severe systolic (≥160 mm Hg) or severe diastolic hypertension (≥ 110 mm Hg) or both in pregnant or postpartum women with preeclampsia/eclampsia constitutes a hypertensive emergency* and it is inadvisable to wait 4 hours for treatment.
• If BP is still elevated above threshold after 15 min, treat with antihypertensive medication within 30-60 min.
However…
*Emergent Therapy for Acute-Onset, Severe Hypertension With Preeclampsia or Eclampsia, ACOG Committee Opinion, # 514, December 2011
The Deadly Triad
Severe Preeclampsia -HELLP Syndrome(20%) - Eclampsia (seizures)
Associated with an increased risk of adverse outcomes
such as:� Placental Abruption
� Renal Failure
� Sub-capsular Hepatic Hematoma
� Preterm Delivery
� Fetal or Maternal Death
� Recurrent PreeclampsiaACOG Practice Bulletin #33, Reaffirmed 2012; ACOG Committee Opinion #514, 2012; Tuffnell D, Jankowitcz D, Lindow S, et al. BJOG 2005;112:875-880.
ACOG Executive Summary onHypertension In Pregnancy, Nov 2013
1. The term “mild” preeclampsia is discouraged forclinical classification. The recommended terminology is: a. “preeclampsia without severe features ” (mild)b. “preeclampsia with severe features ” (severe)
2. Proteinuria is not a requirement to diagnose preeclampsia with new onset hypertension.
3. The total amount of proteinuria > 5g in 24 hours has been eliminated from the diagnosis of severe preeclampsia.
4. Early treatment of severe hypertension is mandatory at the threshold levels of 160 mm Hg systolic or 110 mm Hg diastolic.

6/6/2014
7
Cause of U.S. Maternal Mortality� CDC Review of 14 years of coded data: 1979-1992� 4024 maternal deaths� 790 (19.6%) from preeclampsia
MacKay AP, Berg CJ, Atrash HK. Obstetrics and Gynecology 2001;97:533-538
90% of CVA were from hemorrhage
CA-PAMR Final Cause of Death Among Preeclampsia Cases, 2002-2004 (n=25)
Final Cause of Death Number % Rate/100,000
StrokeHemorrhagicThrombotic
16142 12.5%
1.0
Hepatic (liver) Failure 4 16.0% .25Cardiac Failure 2 8.0%Hemorrhage/DIC 1 4.0%Multi-organ failure 1 4.0%ARDS 1 4.0%
How Do Women Die Of Preeclampsia in CA?
26
64%
87.5%
Preeclampsia Mortality Rates in California and UK
Cause of Death among PreeclampsiaCases
CA-PAMR (2002-04)Rate/100,000
Live Births
UK CMACE (2003-05)Rate/100,000
Live Births
Stroke 1.0 .47
Pulmonary/Respiratory .06 .00
Hepatic .25 .19
OVERALL 1.6 .66
The overall mortality rate for preeclampsia in California
is greater than 2 times that of the UK, largely due to differences in deaths
caused by stroke.27
Controlling blood pressure is the optimal intervention
to prevent deaths due to stroke in women with preeclampsia.
Key Clinical Pearl
Over the last decade, the UK has focused QI efforts on aggressive treatment of both systolic and diastolic blood pressure and has demonstrated a reduction in deaths.

6/6/2014
8
� Hypertensive disorders of pregnancy are major contributors to prematurity.
� Despite considerable research, the etiology of preeclampsia remains unclear.
Ref: ACOG – HIP, 2013
Gestational Age Groups of CA-PAMR Deaths, 2002 to 2004
Early Preterm Birth Preeclampsia Deaths: 36% (n=9) were <34 weeks gestation
GESTATIONAL AGE GROUPS
2002-2004 CA-CA CA-PAMR PREECLAMPSIA DEATHS (N=25)
CA-PAMR NON-PREECLAMPSIA DEATHS
N (%) N (%)
<24 weeks 0 (0) 2 (2%)
24-31w6d 2 (8%) 13 (11%)
32-36w6d 12 (48%) -- 56%29 (24%) -- 37%
>37 weeks 11 (44%)76 (63%)
TOTAL 25 120
In patients with severe preterm preeclampsia,
the disease can rapidly progress to significant maternal morbidity and/or
mortality.
Key Clinical Pearl
All patients with severepreeclampsia, irrespective of
gestational age, should have an evaluation by an obstetrician as
soon possible.
Key Clinical Pearl

6/6/2014
9
Expectant Management in Pregnancies with Severe Preeclampsia >24- < 34 Weeks Gestation
With stable maternal/fetal conditions, continued pregnancy should be undertaken only at facilities with adequate maternal and neonatal intensive care resources
Administer corticosteroids for fetal lung maturity benefit
Expectant management recommendations :
ACOG Executive Summary: Hypertension in Pregnancy. Obstet Gynecol 2013;122:1122-31
Maternal Stabilization refers to:� Seizure prophylaxis� BP control� Adequate maternal cardio-pulmonary function
� AND� Consultation with:
� NICU� MFM� Anesthesia and/or � Critical care services
Expectant Management of Pregnancies with Preeclampsia < 34 Weeks Gestation
Management of Suspected Severe Preeclampsia < 34 Weeks Gestation
Proceed to delivery for:• Recurrent severe hypertension despite therapy• Other contraindications to expectant
management
Initial 24-48 hours observation• Initiate antenatal corticosteroids if not previously administered• Initiate 24 hour urine monitoring as appropriate• Ongoing assessment of maternal symptoms, BP, urine output• Daily lab evaluation (minimum) for HELLP and renal function• May observe on an antepartum ward after initial evaluation
Antenatal corticosteroid treatment completed:• Expectant management not contraindicated• Consider ongoing in-patient expectant
management
Adapted from Sibai BM. Evaluation and management of severe preeclampsia before 34 weeks’ gestation. American Journal of Obstetrics & Gynecology, September 2011, pg. 191-198.
No contraindications to expectant management – Short Term
Expectant Management of Pregnancies < 34 Weeks Gestation(From CMQCC Preeclampsia Toolkit, 2013)

6/6/2014
10
ACOG Task Force Recommendations
� For women with mild gestational hypertension, (less than 160/110).
OR
� Preeclampsia without severe features at or beyond 37 0/7 weeks of gestation, delivery rather than continued observation is suggested.
Ref: Koopmans CM, et al. Induction of labour versus expectant monitoring for gestational hypertension or mild preeclampsia after 36 weeks gestation. (HYPITAT). Lancet 2009;374:979-88
Contributing Factor(at least one factor probably or definitely contributed)
PreeclampsiaN (%)
TOTALN (%)
OVERALL 25 (100%) 129 (89%)
PATIENT FACTORS 16 (64%) 104 (72%) Underlying significant medical conditions 8 (50%) 40 (39%)
Delay or failure to seek care 10 (63%) 27 (26%)
Lack of understanding the importance of a health event
9 (56%) 16 (15%)
HEALTHCARE PROFESSIONALS 24 (96%) 115 (79%)
Delay in diagnosis 22 (92%) 62 (54%)
Use of ineffective treatment 19 (79%) 48 (42%)
Misdiagnosis 13 (54%) 36 (31%)
Failure to refer or seek consultation 6 (25%) 26 (23%)
HEALTHCARE FACILITY 12 (48%) 72 (50%)
Factors Contributing to Pregnancy-Related Deaths, CA-PAMR 2002-2004
Key Clinical Pearl
An organized tool to identify “clinical signs ,” of high concern or
triggers can aid clinicians to recognize and respond in a more timely manner to avoid delays in
diagnosis and treatment.
Preeclampsia Early Recognition Tool

6/6/2014
11
Clinical Signs to Watch for:
10.30.13v1
Hamlet, Act III, Scene I
Oh, woe is me, T' have seen what I have seen, see what I see!
ACOG / CMQCC PTFOh, woe is me, T’ have seen what I have
seen, what can I do? 1). BP control2). Seizure prevention3). Delivery 34wks, 37wks4). Post partum surveillance
Yogi Berra
“It ain’t over till it’s over.”
CMQCC/ACOG“It ain’t over till its over, 6 weeks postpartum”
Timing of Pregnancy-Related Deaths, CA-PAMR, 2002 to 2004
68%
8% 12%4% 4% 0% 4%
01020304050607080
0 1 2 3 4 5 6+Number of weeks between baby's birth and maternal death
Perce
nt Pr
eecla
mpsia
Dea
ths
88%
87%
Non-PreeclampsiaDeaths(n=129)
Preeclampsia Deaths(n=25)
96%
89% 63%
17
7
1 1 1
10
0
10
20
30
40
50
60
70
0 1 2 3 4 5 6+P
erce
nt P
regn
ancy
-Rel
ated
Dea
th
Number of weeks between baby’s birth and maternal d eath
6/6/2014
12
Eclampsia: Maternal-Perinatal Outcome In 254 Consecutive Cases over 12 years
� 83,720 deliveries, for an incidence of one in 330
� 49 patients (19%) did not have proteinuria
� 58 patients (23%) did not have hypertension
Sibai BM. Eclampsia VI. Maternal-perinatal outcome in 254 consecutive cases. Am J Obstet Gynecol Sep 163(3):1049-1054; discussion 1054-1065 1990.
Eclampsia: Maternal-Perinatal Outcome In 254 Consecutive Cases over 12 years
� 73(29%) occurred postpartum.
� Over half of postpartum cases, (40 cases/16%) occurred in the late postpartum period(>48 hrs)
� 18 of these 40 cases were normotensive; all 18 had symptoms of headache or visual disturbance
Sibai BM. Eclampsia VI. Maternal-perinatal outcome in 254 consecutive cases. Am J Obstet Gynecol Sep 163(3):1049-1054; discussion 1054-1065 1990.
ACOG Task Force RecommendationsPost Partum Hypertension and Preeclampsia
� For women in whom GHN,PE , or superimposed PE is diagnosed, it is suggested that BP be monitored in the hospital or equivalent outpatient surveillance be performed for at least 72 hours postpartum and again 7-10 days after delivery or earlier in women with symptoms.
PREECLAMPSIA TOOLKIT TREATMENT
RECOMMENDATIONS
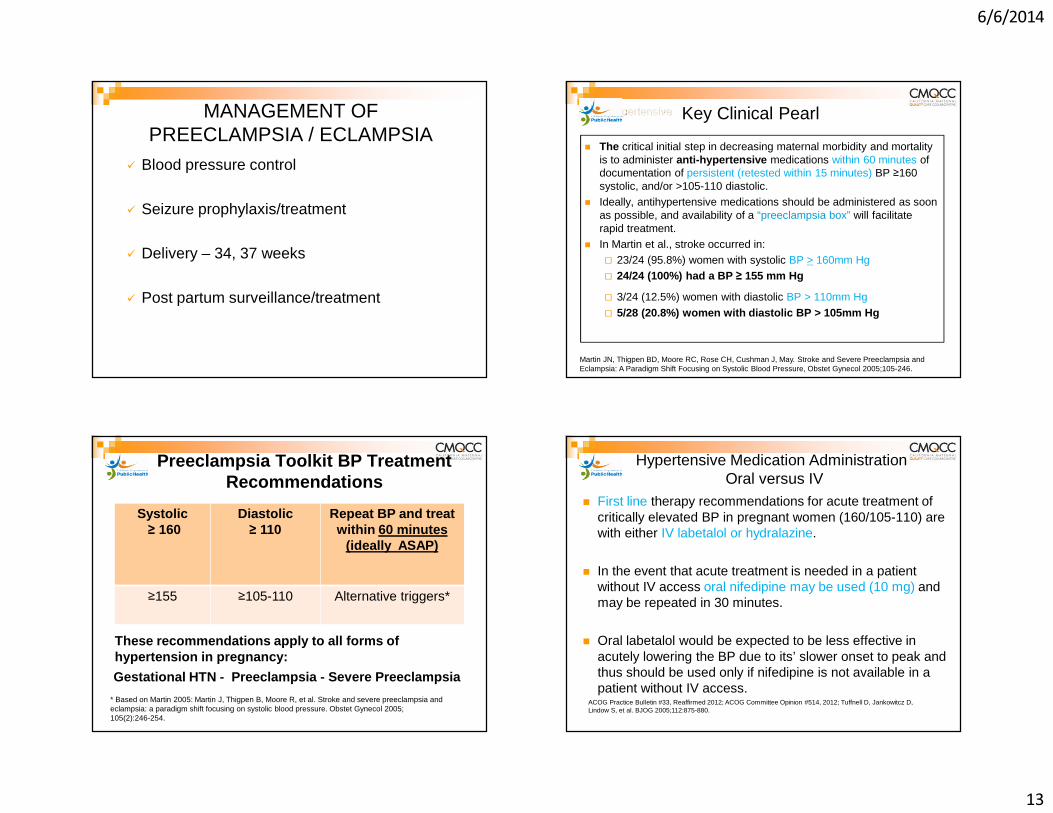
6/6/2014
13
MANAGEMENT OF PREECLAMPSIA / ECLAMPSIA
� Blood pressure control
� Seizure prophylaxis/treatment
� Delivery – 34, 37 weeks
� Post partum surveillance/treatment
Key Clinical Pearl
� The critical initial step in decreasing maternal morbidity and mortality is to administer anti-hypertensive medications within 60 minutes of documentation of persistent (retested within 15 minutes) BP ≥160 systolic, and/or >105-110 diastolic.
� Ideally, antihypertensive medications should be administered as soon as possible, and availability of a “preeclampsia box” will facilitate rapid treatment.
� In Martin et al., stroke occurred in: � 23/24 (95.8%) women with systolic BP > 160mm Hg� 24/24 (100%) had a BP ≥ 155 mm Hg
� 3/24 (12.5%) women with diastolic BP > 110mm Hg
� 5/28 (20.8%) women with diastolic BP > 105mm Hg
Martin JN, Thigpen BD, Moore RC, Rose CH, Cushman J, May. Stroke and Severe Preeclampsia and Eclampsia: A Paradigm Shift Focusing on Systolic Blood Pressure, Obstet Gynecol 2005;105-246.
Preeclampsia Toolkit BP Treatment Recommendations
Systolic≥ 160
Diastolic ≥ 110
Repeat BP and treat within 60 minutes
(ideally ASAP)
≥155 ≥105-110 Alternative triggers*
Gestational HTN - Preeclampsia - Severe Preeclampsia
These recommendations apply to all forms of hypertension in pregnancy:
* Based on Martin 2005: Martin J, Thigpen B, Moore R, et al. Stroke and severe preeclampsia and eclampsia: a paradigm shift focusing on systolic blood pressure. Obstet Gynecol 2005; 105(2):246-254.
Hypertensive Medication AdministrationOral versus IV
� First line therapy recommendations for acute treatment of critically elevated BP in pregnant women (160/105-110) are with either IV labetalol or hydralazine.
� In the event that acute treatment is needed in a patient without IV access oral nifedipine may be used (10 mg) and may be repeated in 30 minutes.
� Oral labetalol would be expected to be less effective in acutely lowering the BP due to its’ slower onset to peak and thus should be used only if nifedipine is not available in a patient without IV access.
ACOG Practice Bulletin #33, Reaffirmed 2012; ACOG Committee Opinion #514, 2012; Tuffnell D, Jankowitcz D, Lindow S, et al. BJOG 2005;112:875-880.

6/6/2014
14
Magnesium Sulfate� Primary effect is via CNS depression� Improves blood flow to CNS via small vessel
vasodilation� Blood pressure after magnesium infusion:
� 6 gm loading then 2 gm/hr.
sBPmm Hg
sBP30 min
sBP120 min
dBPmm Hg
dBP30 min
dBP120 min
Mild Group
145±10
143±13
141±14
87±10
79±9
82±9
Belfort M, Allred J, Dildy G. Magnesium sulfate decreases cerebral perfusion pressure in preeclampsia.Hypertens Pregnancy. 2008;27(4):315-27.
� Magnesium sulfate should not be considered a antihypertensive medication
Magnesium Sulfate in the Management of Preeclampsia
Magpie Trial Collaboration Group . Do women with pre-eclampsia, and their babies, benefit from magnesium sulfate?
� 58% reduction in seizures� 45% reduction in maternal death*� 33% reduction in placental abruption
Altman D, Carroli G, Duley L, et al. The Magpie Trial: a randomized placebo-controlled trial; Lancet 2002;359:1877–90.
*The 45% reduction in maternal death is not statistically significant but clinically important.
Recommendations for Women Who Should Be Treated With Magnesium
Preeclampsia without severe
features
SeverePreeclampsia
Eclampsia
ACOG ** X X
NICE X X
SOGC X* X X
CMQCC X* X X
WHO X X X**ACOG Executive Summary, 2013: for preeclampsia wi thout severe features, it is suggested that magnesium sulfate no t be administered universally for the prevention of eclampsia.
* Should be considered: Numbers needed to treat (NNT) = 109 for “mild” , 63 for “severe”
Key Clinical Pearl
Algorithms for acute treatment of severe hypertension and eclampsia should be readily available or preferably posted in all clinical areas that may encounter pregnant women.

6/6/2014
15
Policy and Procedure: Perinatal Inpatient: IV
Labetalol/Hydralazine for Acute Hypertension
LPCH Approval: March 2014
Labor and Delivery Medication Box and Dose Guidelines for Severe Preeclampsia and Eclampsia
Yogi Berra
“It ain’t over till it’s over.”
CMQCC/ACOG“It ain’t over till its over, 6 weeks postpartum”
� Early post-discharge follow-up recommended for all patients diagnosed with preeclampsia/eclampsia
� Preeclampsia Toolkit recommends post-discharge follow-up:� within 3-7 days if medication was used during labor and
delivery OR postpartum� within 7-14 days if no medication was used
� Postpartum patients presenting to the ED with hypertension, preeclampsia or eclampsia should either be assessed by or admitted to an obstetrical service
Key Clinical Pearls
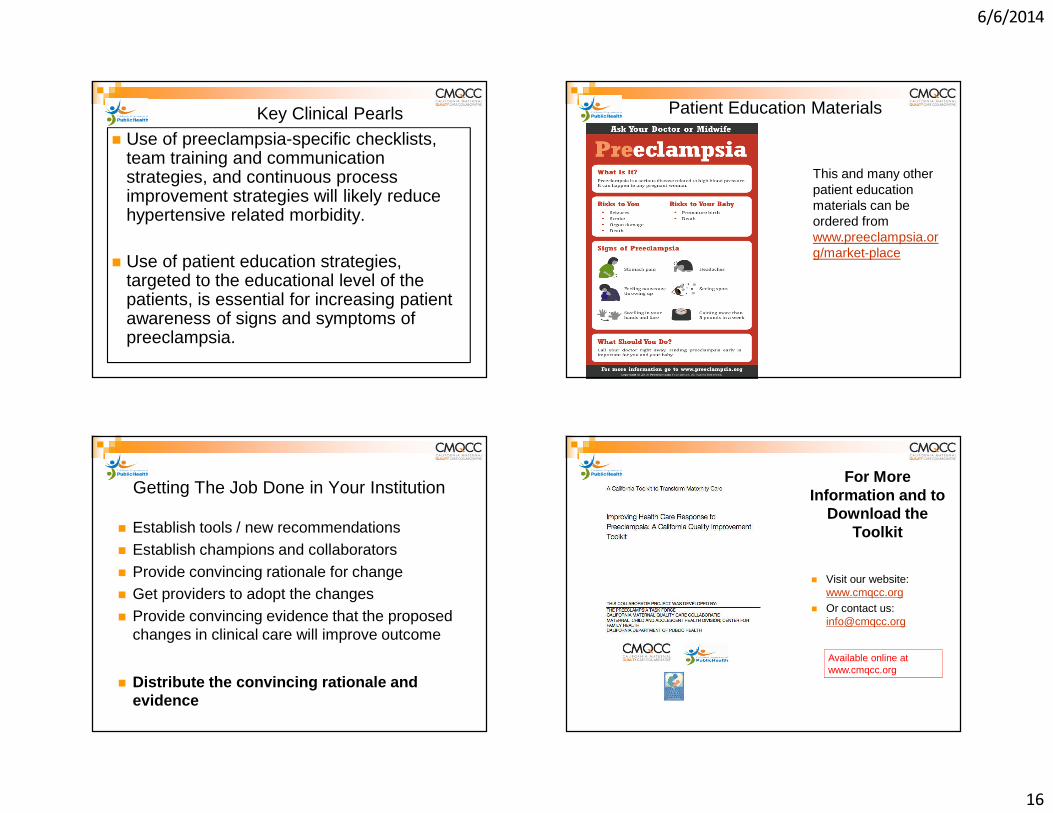
6/6/2014
16
Key Clinical Pearls
� Use of preeclampsia-specific checklists, team training and communication strategies, and continuous process improvement strategies will likely reduce hypertensive related morbidity.
� Use of patient education strategies, targeted to the educational level of the patients, is essential for increasing patient awareness of signs and symptoms of preeclampsia.
Patient Education Materials
This and many other patient education materials can be ordered from www.preeclampsia.org/market-place
Getting The Job Done in Your Institution
� Establish tools / new recommendations� Establish champions and collaborators� Provide convincing rationale for change� Get providers to adopt the changes� Provide convincing evidence that the proposed
changes in clinical care will improve outcome
� Distribute the convincing rationale and evidence
For More Information and to
Download the Toolkit
� Visit our website: www.cmqcc.org
� Or contact us:[email protected]
Available online at www.cmqcc.org
6/6/2014
17
Hot and Sizzling off the press!!
OBGYN News Digital Networkwww.obgynnews.com
Draft recommendations back aspirin for preeclampsia prevention
www.obgynnews.com
By: Elizabeth MechcatieOBGYN News Digital Network
April 10, 2014
Prophylactic low-dose aspirin – 81 mg per day – should be started after 12 weeks’ gestation in women at high risk for developing preeclampsia, according to a draft recommendation issued by the U.S. Preventive Services Task Force in April.
The recommendation applies to asymptomatic pregnant women at increased risk for preeclampsia who have no contraindications to using low-dose aspirin and have not experienced adverse effects associated with aspirin previously.
"The USPSTF found adequate evidence of a reduction in preeclampsia, preterm birth, and IUGR [intrauterine growth restriction] in women at increased risk for preeclampsia who received low-dose aspirin, thus demonstrating substantial benefit," the recommendations state.
In a review of clinical trials, low-dose aspirin (at doses of 50-160 mg per day) reduced the risk of preeclampsia by 24%, the risk of preterm birth by 14%, and the risk of IUGR by 20%. There also was "adequate evidence" that the risks of placental abruption, postpartum hemorrhage, and fetal intracranial bleeding were not increased with low-dose aspirin, the USPSTF statement said.
6/6/2014
18
� The draft recommendations were based on a review of data on low-dose aspirin and preeclampsia in 23 studies of women at high or average risk of preeclampsia, which was published online April 8 in Annals of Internal Medicine (doi: 10.7326/M13-2844).
Dr. E. Albert Reece and Dr. John T. Repke discuss a new paradigm for preeclampsia, a growing problem that requires prompt diagnosis and management to reduce the maternal-fetal morbidity and mortality that it causes.
OBGYN.News – Vol. 49, No. 5 May 2014
My Take
� Contrary to former recommendations, the task force’s new recommendations suggest that use of magnesium sulfate for preeclampsia without severe features (formerly called "mild preeclampsia") may not be needed.
� Although magnesium sulfate may not be warranted in every case, patients can progress so rapidly from having no severe symptoms to developing severe symptoms that it is difficult if not impossible to parse out who would or would not benefit from treatment. Ref: OBGYN News, Vol. 49, No 5.
Repke, JT – A new paradigm for preeclampsia
My Take
� If we try to do so, we run the great risk of not providing the necessary medication to our patients, thereby increasing the chances of maternal morbidity and mortality.
Ref: OBGYN News, Vol. 49, No 5. Repke, JT – A new paradigm for preeclampsia

1
Michael D. Fox RN, BSN
Applying the NICHD Categories Case Studies In Fetal Monitoring II
III
INormal
Abnormal
Indeterminate
NICHD 2008Three - Tier Fetal Heart Rate Interpretation
System
NICHD 2008Three - Tier Fetal Heart Rate Interpretation
System
I
NICHD 2008NICHD 2008
““““Normal””””
Category I• Moderate Variability• FHR 110-160 bpm• No late or variable decelerations •±±±± early decelerations•±±±± accelerations
Category I• Moderate Variability• FHR 110-160 bpm• No late or variable decelerations •±±±± early decelerations•±±±± accelerations
NICHD 2008NICHD 2008Category III• Absent variability with recurrent:
• Late decelerations• Variable decelerations• Bradycardia OR• Sinusoidal pattern
Category III• Absent variability with recurrent:
• Late decelerations• Variable decelerations• Bradycardia OR• Sinusoidal pattern ““““Abnormal”III

2
NICHD 2008NICHD 2008
II““““Indeterminate””””
Category II Tracings
Everything else
Category II Tracings
Everything else
““““The Mess In the Middle””””““““The Mess In the Middle””””
II
III
I
““““Abnormal””””
Indeterminate
““““Normal””””
2008 NICHD 3 Tier System Fails To:
2008 NICHD 3 Tier System Fails To:
• Clearly identify the relationship between FHR patterns and significant acidemia.
• Clearly identify the relationship between FHR patterns and significant acidemia.
• Simplify and make clear the framework for determining the choice and timing of our interventions
• Simplify and make clear the framework for determining the choice and timing of our interventions
2008 NICHD 3 Tier System Fails To:
2008 NICHD 3 Tier System Fails To:
• Clearly identify the relationship between FHR patterns and significant acidemia.
• Clearly identify the relationship between FHR patterns and significant acidemia.
• Simplify and make clear the framework for determining the choice and timing of our interventions
• Simplify and make clear the framework for determining the choice and timing of our interventions
? Minimal FHR variability (with decelerations) should be considered as potentially indicative of fetal acidemia and should be managed accordingly.
Minimal FHR variability (with decelerations) should be considered as potentially indicative of fetal acidemia and should be managed accordingly.
Moderate FHR variability reliably predicts the absence of fetal metabolic acidemia at the time it is observed.Moderate FHR variability reliably predicts the absence of fetal metabolic acidemia at the time it is observed.
Absent FHR variability with decelerations… is abnormal and conveys an increased risk of fetal acidemia at the time it is observed.
Absent FHR variability with decelerations… is abnormal and conveys an increased risk of fetal acidemia at the time it is observed.
NONO
MaybeMaybe
PresumedPresumed
FHR Patterns and AcidemiaFHR Patterns and Acidemia
2008 NICHD Report EFM JOGNN, 37, 1-6; 2008. 2008 NICHD Report EFM JOGNN, 37, 1-6; 2008.
NICHD - ACOG Practice Bulletin #116 November 2010
NICHD - ACOG Practice Bulletin #116 November 2010NICHD - ACOG Practice Bulletin #116 November 2010
Simplify the Framework3 Clinical Categories
Simplify the Framework3 Clinical Categories
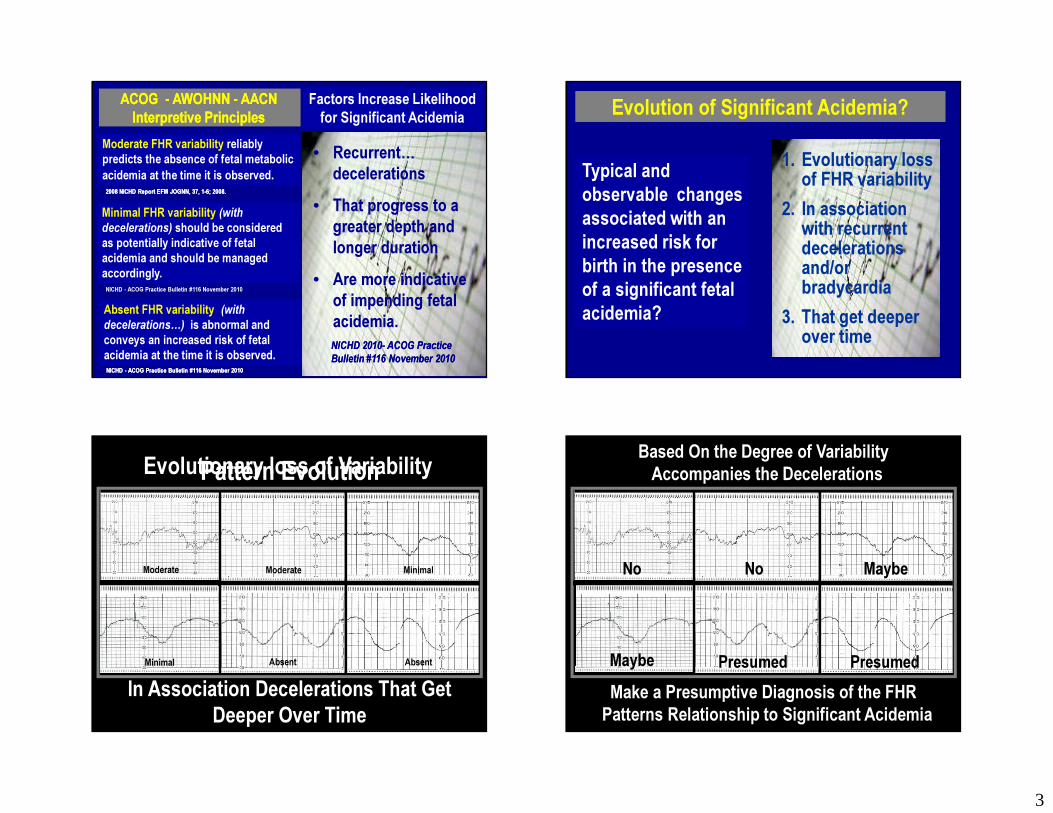
3
Minimal FHR variability (with decelerations) should be considered as potentially indicative of fetal acidemia and should be managed accordingly.
Minimal FHR variability (with decelerations) should be considered as potentially indicative of fetal acidemia and should be managed accordingly.
Moderate FHR variability reliably predicts the absence of fetal metabolic acidemia at the time it is observed.Moderate FHR variability reliably predicts the absence of fetal metabolic acidemia at the time it is observed.
Absent FHR variability ((with decelerations…) is abnormal and conveys an increased risk of fetal acidemia at the time it is observed.
Absent FHR variability ((with decelerations…) is abnormal and conveys an increased risk of fetal acidemia at the time it is observed.
ACOG - AWOHNN - AACN Interpretive Principles
ACOG - AWOHNN - AACN Interpretive Principles
Factors Increase Likelihood for Significant Acidemia
Factors Increase Likelihood for Significant Acidemia
2008 NICHD Report EFM JOGNN, 37, 1-6; 2008. 2008 NICHD Report EFM JOGNN, 37, 1-6; 2008.
NICHD - ACOG Practice Bulletin #116 November 2010
NICHD - ACOG Practice Bulletin #116 November 2010NICHD - ACOG Practice Bulletin #116 November 2010
• Recurrent… decelerations
• That progress to a greater depth and longer duration
• Are more indicative of impending fetal acidemia.NICHD 2010- ACOG Practice Bulletin #116 November 2010NICHD 2010- ACOG Practice Bulletin #116 November 2010
Evolution of Significant Acidemia? Evolution of Significant Acidemia?
Typical and observable changes associated with an increased risk for birth in the presence of a significant fetal acidemia?
Typical and observable changes associated with an increased risk for birth in the presence of a significant fetal acidemia?
1. Evolutionary loss of FHR variability
2. In association with recurrent decelerations and/or bradycardia
3. That get deeper over time
In Association Decelerations That Get Deeper Over Time
Moderate
Absent
Minimal
Pattern EvolutionEvolutionary loss of Variability
Moderate
AbsentMinimal
No No Maybe
Presumed PresumedMake a Presumptive Diagnosis of the FHR Patterns Relationship to Significant Acidemia
Based On the Degree of Variability Accompanies the Decelerations
Maybe
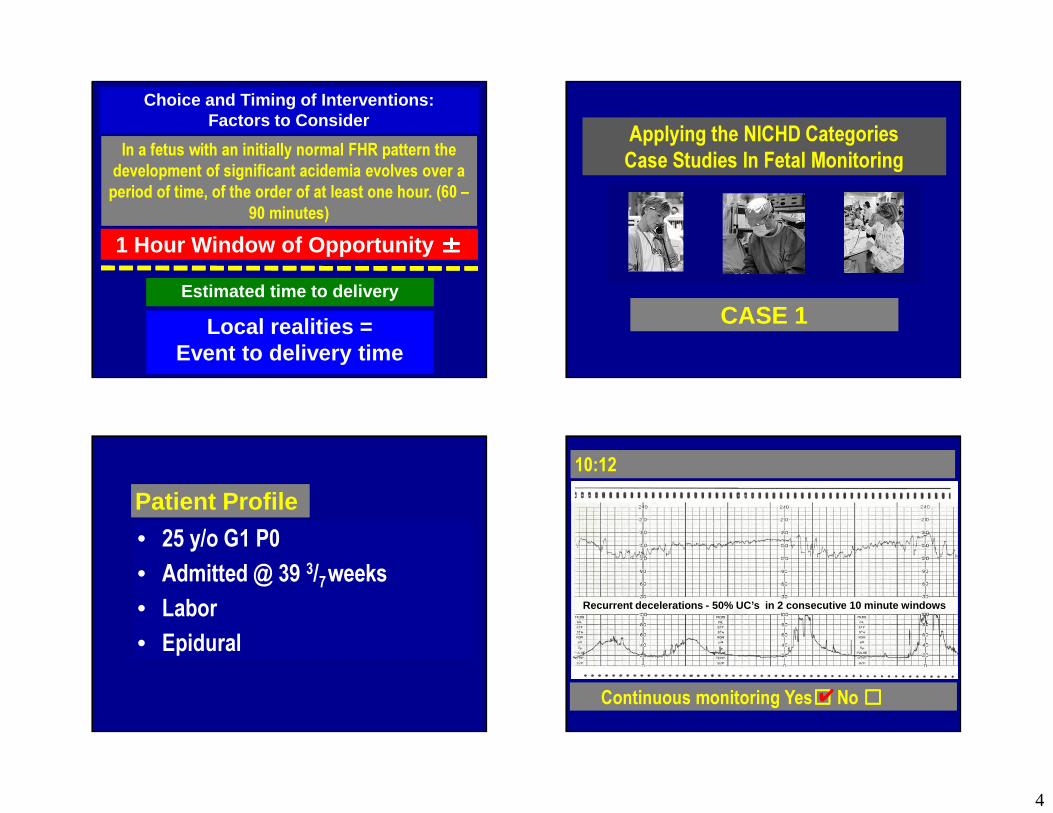
4
In a fetus with an initially normal FHR pattern the development of significant acidemia evolves over a period of time, of the order of at least one hour. (60 –
90 minutes)
In a fetus with an initially normal FHR pattern the development of significant acidemia evolves over a period of time, of the order of at least one hour. (60 –
90 minutes)
Estimated time to deliveryEstimated time to delivery
Local realities = Event to delivery time
Local realities = Event to delivery time
Choice and Timing of Interventions: Factors to Consider
Choice and Timing of Interventions: Factors to Consider
1 Hour Window of Opportunity ±±±±1 Hour Window of Opportunity ±±±±
Applying the NICHD Categories Case Studies In Fetal MonitoringApplying the NICHD Categories Case Studies In Fetal Monitoring
CASE 1CASE 1
Patient ProfilePatient Profile
• 25 y/o G1 P0 • Admitted @ 39 3/7weeks • Labor• Epidural
• 25 y/o G1 P0 • Admitted @ 39 3/7weeks • Labor• Epidural
10:1210:12
Continuous monitoring Yes☐☐☐☐ No ☐☐☐☐Continuous monitoring Yes☐☐☐☐ No ☐☐☐☐✔✔
Recurrent decelerations - 50% UC’s in 2 consecutive 10 minute windows

5
MD/CNM notification Yes☐☐☐☐ No ☐☐☐☐MD/CNM notification Yes☐☐☐☐ No ☐☐☐☐✔✔
10:1210:12
Bedside evaluation Yes☐☐☐☐ No ☐☐☐☐Bedside evaluation Yes☐☐☐☐ No ☐☐☐☐✔✔
10:1210:12
Preparation for Delivery Yes☐☐☐☐ No ☐☐☐☐Preparation for Delivery Yes☐☐☐☐ No ☐☐☐☐✔✔
10:1210:12
Delivery Yes☐☐☐☐ No ☐☐☐☐Delivery Yes☐☐☐☐ No ☐☐☐☐✔✔ MD SVE - Leaves room
10:12 10:12
Complete. Feels urge to push
10:17

6
10:30 13 minutes later10:30 13 minutes later 10:30 18 minutes later10:30 18 minutes later
Ensure ability to rescue fetus Yes☐☐☐☐ No ☐☐☐☐Ensure ability to rescue fetus Yes☐☐☐☐ No ☐☐☐☐✔✔
11:10 40 minutes later11:10 40 minutes later 12:00 50 minutes later12:00 50 minutes later
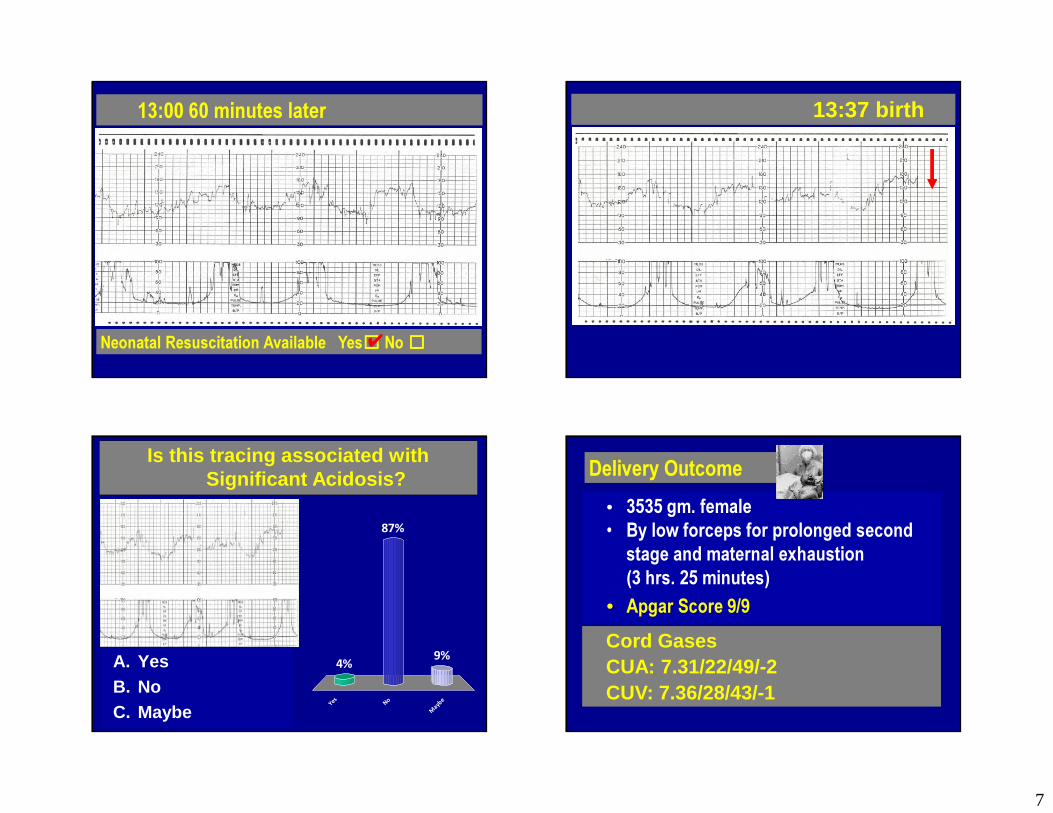
7
13:00 60 minutes later13:00 60 minutes later
Neonatal Resuscitation Available Yes☐☐☐☐ No ☐☐☐☐Neonatal Resuscitation Available Yes☐☐☐☐ No ☐☐☐☐✔✔
13:37 birth13:37 birth
Is this tracing associated with Significant Acidosis?
Y e s N o
M ay b e
4% 9%
87%
A. YesB. NoC. Maybe
A. YesB. NoC. Maybe
Delivery OutcomeDelivery Outcome• 3535 gm. female• By low forceps for prolonged second
stage and maternal exhaustion (3 hrs. 25 minutes)
• Apgar Score 9/9
• 3535 gm. female• By low forceps for prolonged second
stage and maternal exhaustion (3 hrs. 25 minutes)
• Apgar Score 9/9Cord GasesCUA: 7.31/22/49/-2CUV: 7.36/28/43/-1
Cord GasesCUA: 7.31/22/49/-2CUV: 7.36/28/43/-1

8
2006 - Fetal acidemia and electronic fetal heart rate patterns: Is there evidence of an association? J. T. Parer a;T. King a; S. Flanders a; M. Fox a; S. J. Kilpatrick b The Journal of Maternal-Fetal Medicine, Volume 19, Issue 5 May 2006
2006 - Fetal acidemia and electronic fetal heart rate patterns: Is there evidence of an association? J. T. Parer a;T. King a; S. Flanders a; M. Fox a; S. J. Kilpatrick b The Journal of Maternal-Fetal Medicine, Volume 19, Issue 5 May 2006
Moderate FHR variability reliably predicts the absence of fetal metabolic acidemia at the time it is observed.Moderate FHR variability reliably predicts the absence of fetal metabolic acidemia at the time it is observed.2008 NICHD Report EFM JOGNN, 37, 1-6; 2008. 2008 NICHD Report EFM JOGNN, 37, 1-6; 2008.
• 98% of the fetuses with moderate FHR variability, with or without decelerations or second stage bradycardia will be born in the absence of a significant metabolic acidemia, and/or in the presence of neonatal vigor.
•When moderate FHR variability is present at the time of birth < 1% of neonates will be born with an Apgar score <7 at 5 minutes.
• 98% of the fetuses with moderate FHR variability, with or without decelerations or second stage bradycardia will be born in the absence of a significant metabolic acidemia, and/or in the presence of neonatal vigor.
•When moderate FHR variability is present at the time of birth < 1% of neonates will be born with an Apgar score <7 at 5 minutes.
CASE 2CASE 2
Applying the NICHD Categories Case Studies In Fetal MonitoringApplying the NICHD Categories Case Studies In Fetal Monitoring
Patient ProfilePatient Profile
• 16 y/o G1 P0 @ 40 6/7 weeks arrives in triage contracting strongly
• SVE in triage 5/100/-2
• AROM – thick mec
• FSE/IUPC are placed - amnioinfusionbegun
• Complete within 3 hours admission
• 16 y/o G1 P0 @ 40 6/7 weeks arrives in triage contracting strongly
• SVE in triage 5/100/-2
• AROM – thick mec
• FSE/IUPC are placed - amnioinfusionbegun
• Complete within 3 hours admission
Time: 23:50 – complete and pushingTime: 23:50 – complete and pushing

9
00:20: 30 minutes later…00:20: 30 minutes later… 00:40: 20 minutes later…00:40: 20 minutes later…
01:20: 40 minutes later01:20: 40 minutes later 01:30: 10 minutes later01:30: 10 minutes later
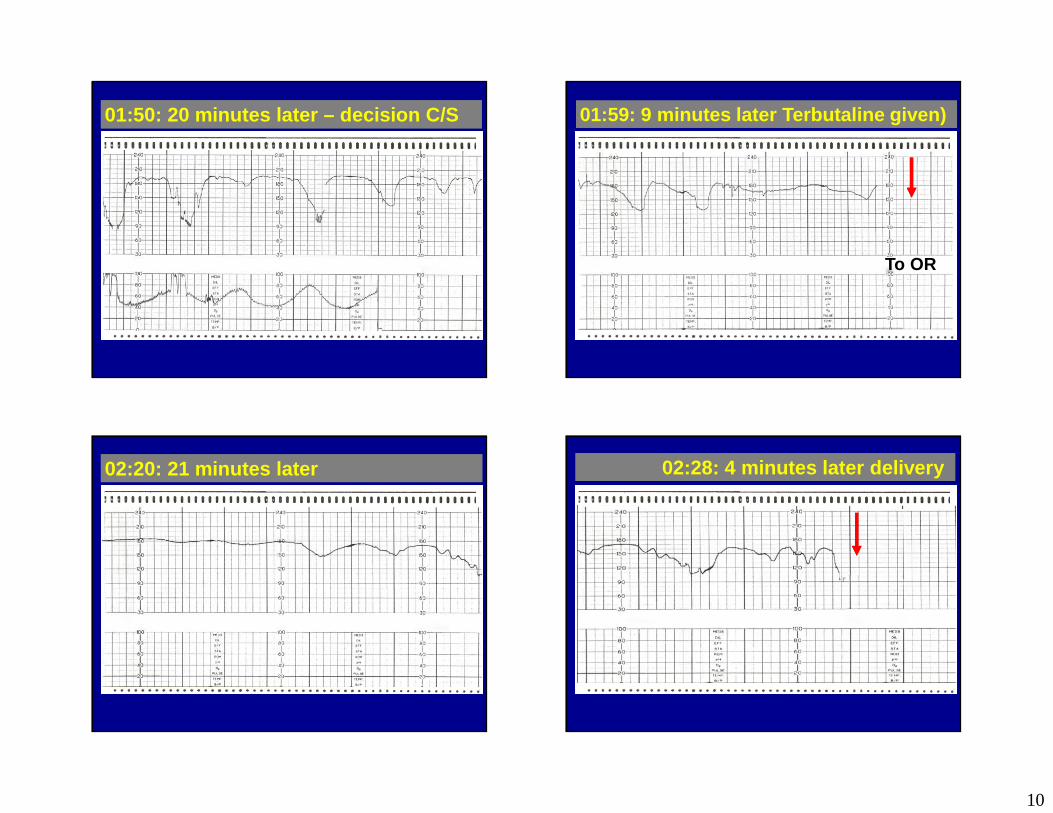
10
01:50: 20 minutes later – decision C/S01:50: 20 minutes later – decision C/S 01:59: 9 minutes later Terbutaline given) 01:59: 9 minutes later Terbutaline given)
To OR
02:20: 21 minutes later 02:20: 21 minutes later 02:28: 4 minutes later delivery 02:28: 4 minutes later delivery
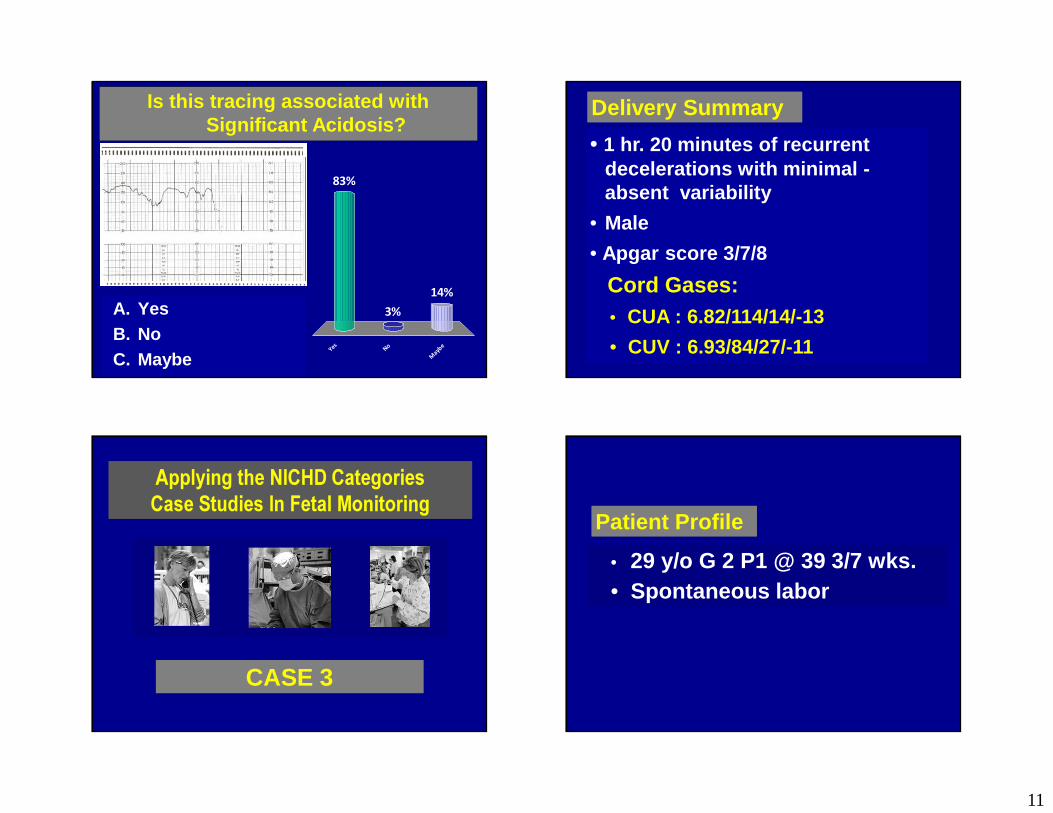
11
Is this tracing associated with Significant Acidosis?
Y e s N o
M ay b e
83%
14%3%A. Yes
B. NoC. Maybe
A. YesB. NoC. Maybe
Delivery SummaryDelivery Summary
• 1 hr. 20 minutes of recurrent decelerations with minimal -absent variability
• Male
• Apgar score 3/7/8
Cord Gases: • CUA : 6.82/114/14/-13
• CUV : 6.93/84/27/-11
• 1 hr. 20 minutes of recurrent decelerations with minimal -absent variability
• Male
• Apgar score 3/7/8
Cord Gases: • CUA : 6.82/114/14/-13
• CUV : 6.93/84/27/-11
Applying the NICHD Categories Case Studies In Fetal MonitoringApplying the NICHD Categories Case Studies In Fetal Monitoring
CASE 3CASE 3
• 29 y/o G 2 P1 @ 39 3/7 wks.• Spontaneous labor• 29 y/o G 2 P1 @ 39 3/7 wks.• Spontaneous labor
Patient ProfilePatient Profile
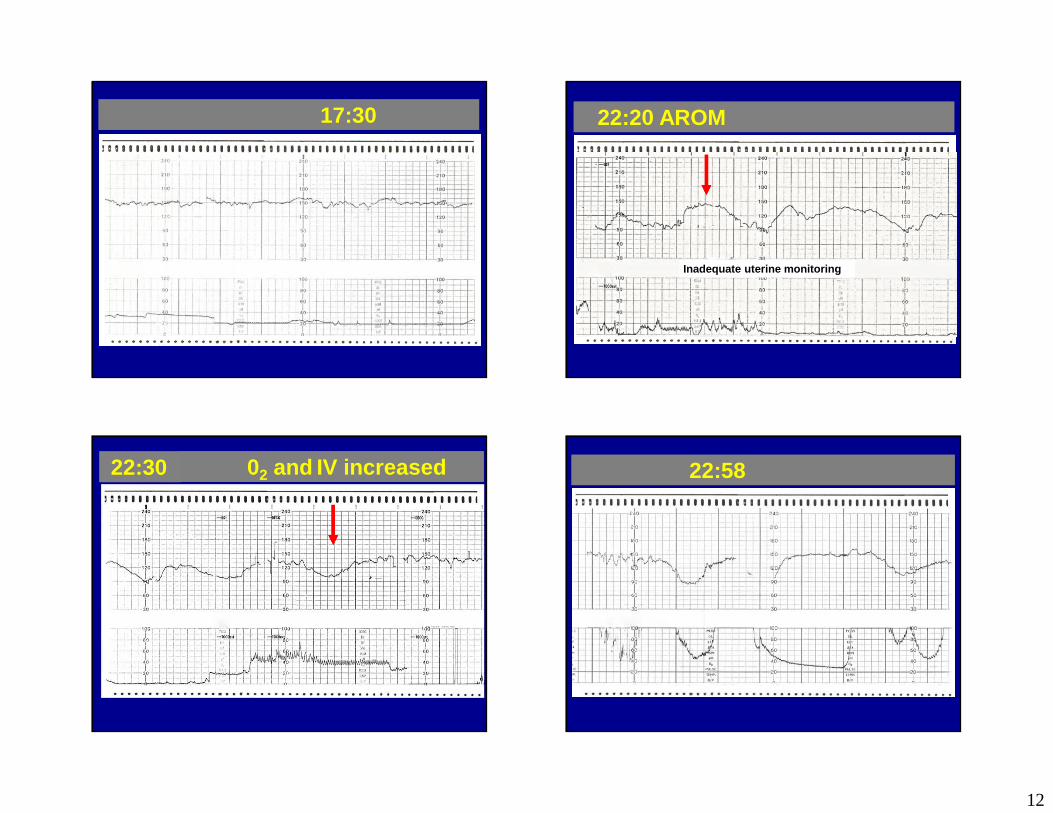
12
17:3017:30 22:20 AROM 22:20 AROM
Inadequate uterine monitoring
22:3022:30 02 and IV increased 02 and IV increased 22:5822:58
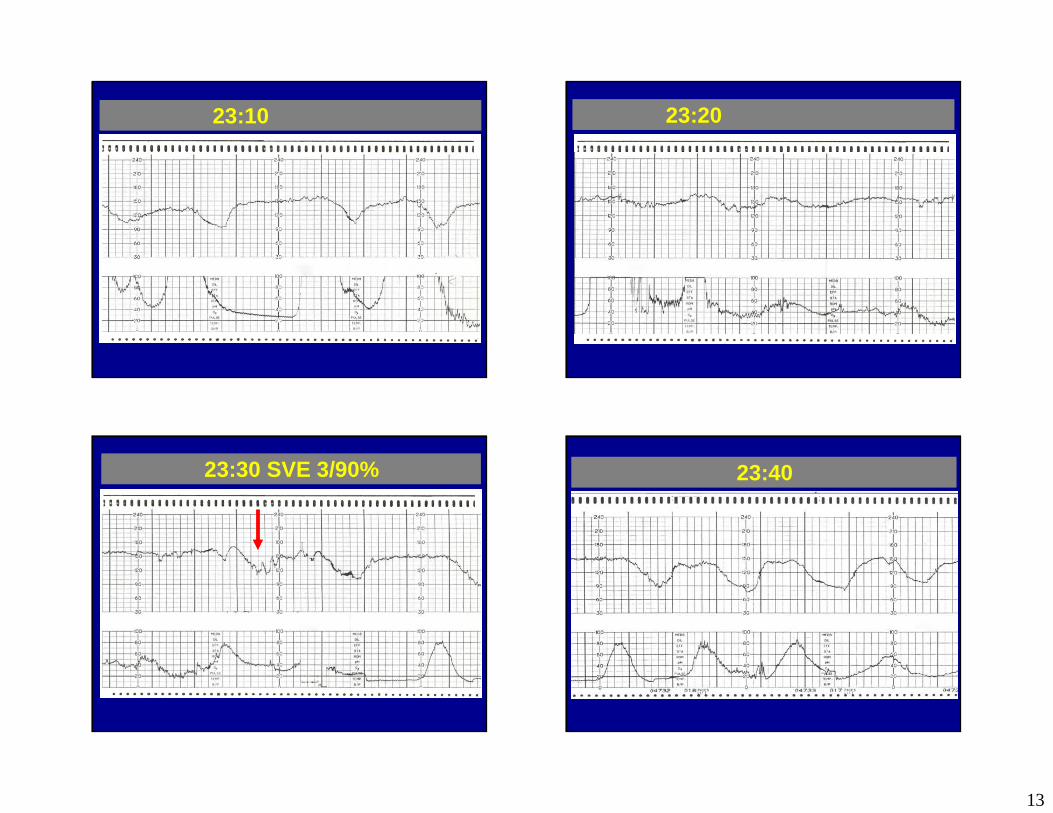
13
23:1023:10 23:2023:20
23:30 SVE 3/90%23:30 SVE 3/90% 23:4023:40
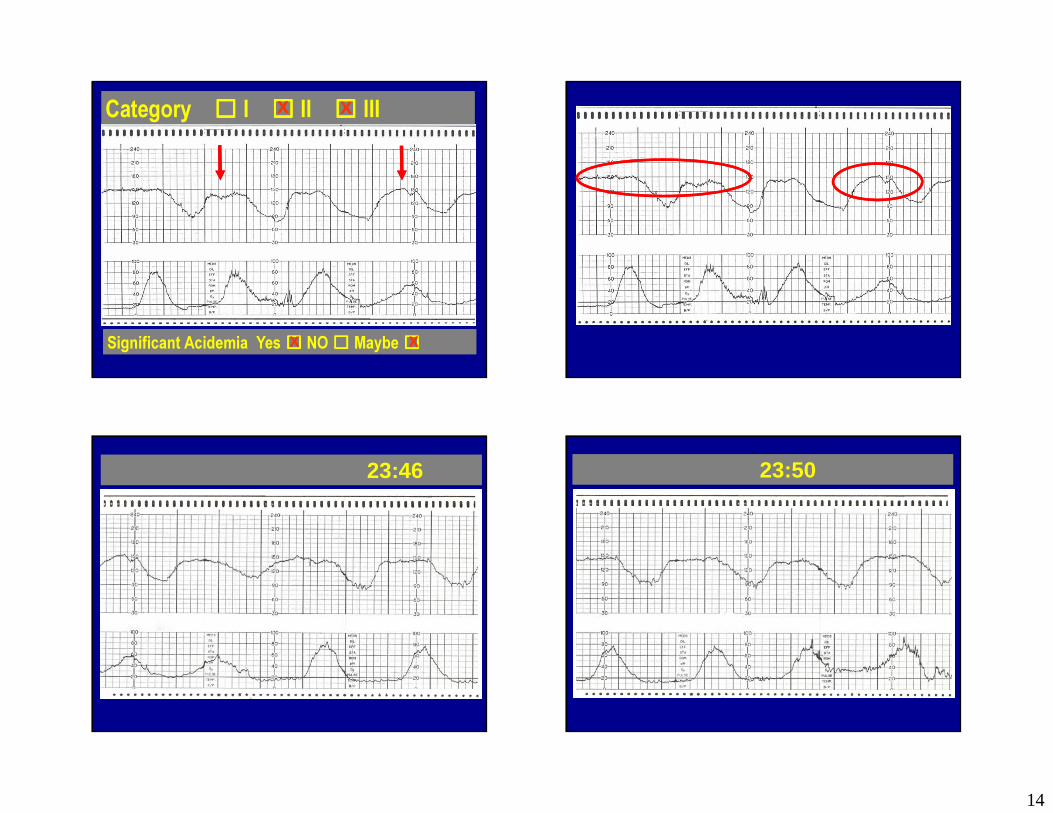
14
Category ☐☐☐☐ I ☐☐☐☐ II ☐☐☐☐ IIICategory ☐☐☐☐ I ☐☐☐☐ II ☐☐☐☐ III
Significant Acidemia Yes ☐☐☐☐ NO ☐☐☐☐ Maybe ☐☐☐☐Significant Acidemia Yes ☐☐☐☐ NO ☐☐☐☐ Maybe ☐☐☐☐
XX XX
XX XX
23:4623:46 23:5023:50

15
24:00 SVE 4 cm – plan C/S24:00 SVE 4 cm – plan C/S 00:03 SQ Terbutaline00:03 SQ Terbutaline To ORTo OR
00:09 Positioned for spinal 00:2000:20 00:28 delivery00:28 delivery
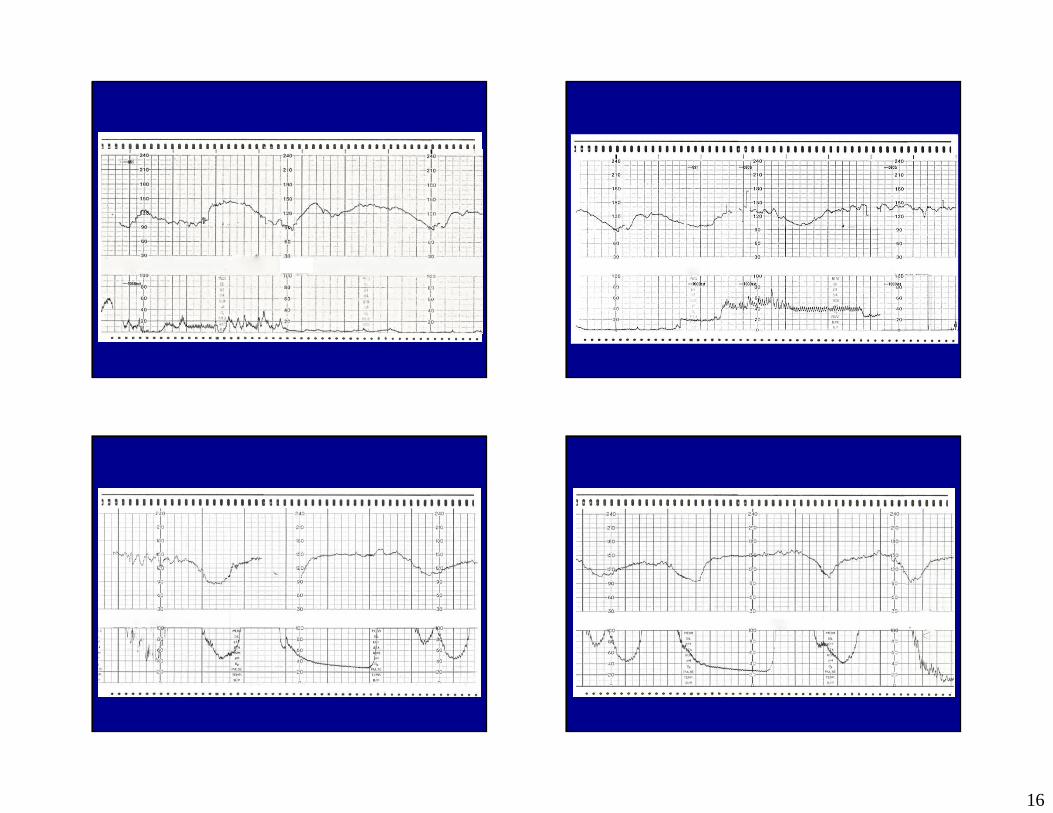
16
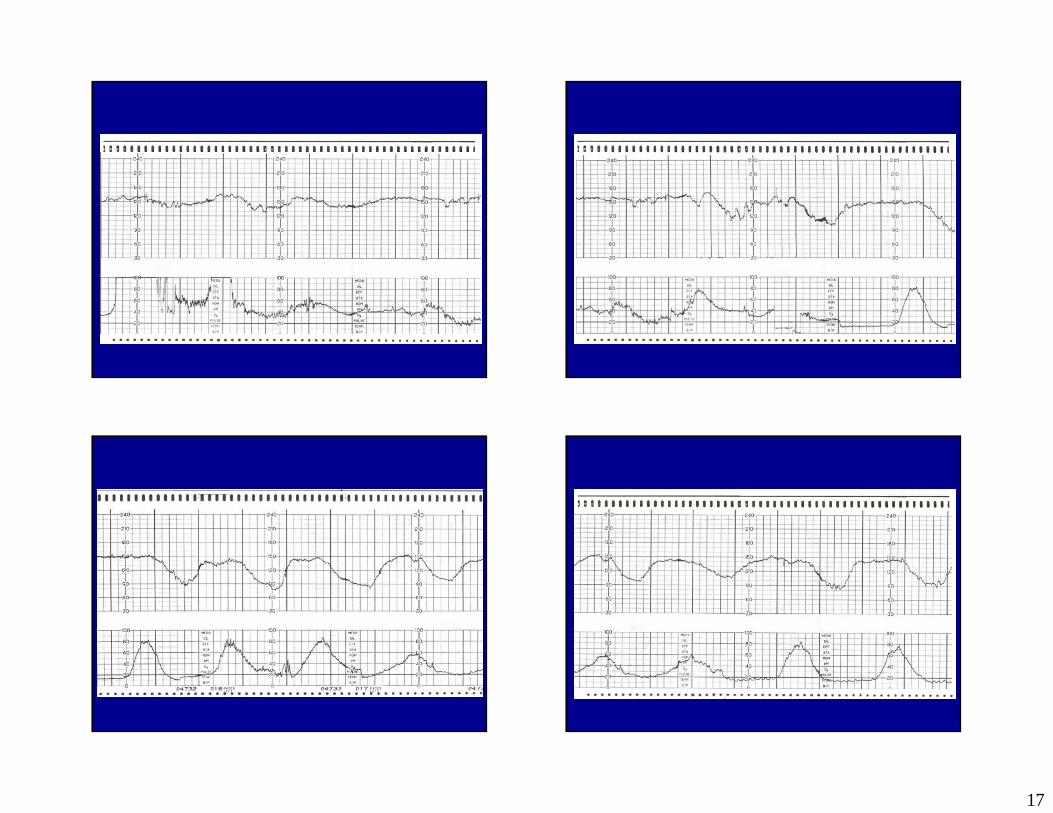
17

18

19
Is this tracing associated with Significant Acidosis?
Y e s N o
M ay b e
12%
41%47%
A. YesB. NoC. Maybe
A. YesB. NoC. Maybe
• C/S for ““““fetal distress. ””””
• 1900 gm. Female • APGARS 5/8.
• C/S for ““““fetal distress. ””””
• 1900 gm. Female • APGARS 5/8.
Birth OutcomeBirth Outcome
Cord GasesCUA:7.17/62/9/-8CUV:7.22/52/16/-7
Cord GasesCUA:7.17/62/9/-8CUV:7.22/52/16/-7

20
(23:40 – 00:03) - 23 minutes minimal variability + recurrent late decelerations(some deep – 60
beats below baseline)
(23:40 – 00:03) - 23 minutes minimal variability + recurrent late decelerations(some deep – 60
beats below baseline)
Local realities = in house surgical team immediate C/S capabilities
Local realities = in house surgical team immediate C/S capabilities
Timing of Interventions: Factors to Consider Timing of Interventions: Factors to Consider
1 Hour Window of Opportunity ±±±±1 Hour Window of Opportunity ±±±±
Estimated time to delivery – presumption remote delivery- 4 cm
Estimated time to delivery – presumption remote delivery- 4 cm
00:03 Restoration of moderate FHR variability immediately before delivery
00:03 Restoration of moderate FHR variability immediately before delivery
SummationSummation
1. FHR decelerations as an independent finding are poorly predictive of complicated outcomes.
1. FHR decelerations as an independent finding are poorly predictive of complicated outcomes.
2. The degree of variability is the most sensitive indicator of the adequacy of oxygen delivery to the fetus at any given moment in time.
2. The degree of variability is the most sensitive indicator of the adequacy of oxygen delivery to the fetus at any given moment in time.
4. A metabolic acidemia typically develops slowly in association with recurrent decelerations and an evolutionary reduction of FHR variability over time.
4. A metabolic acidemia typically develops slowly in association with recurrent decelerations and an evolutionary reduction of FHR variability over time.
3. The deeper the decelerations the > likelihood for developing a significant acidemia.
3. The deeper the decelerations the > likelihood for developing a significant acidemia.
4 Simple Guidelines FHR Monitoring4 Simple Guidelines FHR Monitoring
Fetal acidemia and electronic fetal heart rate patt erns: Is there evidence of an association? J. T.
PARER1, T. KING1, S. FLANDERS1, M. FOX1, & S. J. KI LPATRICK2
Evidence Based Indications For ActionBased on the degree of variability that accompanies the decelerations
MAYBE?
Make a presumptive Diagnosis
YES?NO?
Significant acidemia?

21
� Continuous Observation� Notification� Bedside Evaluation� Prepare for birth� Expedite Birth� Prepare For Neonatal Resuscitation� Prepare to Transfer/Transport
� Continuous Observation� Notification� Bedside Evaluation� Prepare for birth� Expedite Birth� Prepare For Neonatal Resuscitation� Prepare to Transfer/Transport
IntrauterineResuscitation In a fetus with an initially normal FHR pattern
the development of significant acidemia evolves over a period of time, of the order of at
least one hour. (60 – 90 minutes)
In a fetus with an initially normal FHR pattern the development of significant acidemia
evolves over a period of time, of the order of at least one hour. (60 – 90 minutes)
Estimated time to deliveryEstimated time to delivery
Local realities = Event to delivery time
Local realities = Event to delivery time
Timing of Interventions: Factors to Consider Timing of Interventions: Factors to Consider
1 Hour Window of Opportunity ±±±±1 Hour Window of Opportunity ±±±±
Minimal FHR variability (with decelerations) should be considered as potentially indicative of fetal acidemia and should be managed accordingly.
Minimal FHR variability (with decelerations) should be considered as potentially indicative of fetal acidemia and should be managed accordingly.
Moderate FHR variability reliably predicts the absence of fetal metabolic acidemia at the time it is observed.
Moderate FHR variability reliably predicts the absence of fetal metabolic acidemia at the time it is observed.
Absent FHR variability with decelerations… is abnormal and conveys an increased risk of fetal acidemia at the time it is observed.
Absent FHR variability with decelerations… is abnormal and conveys an increased risk of fetal acidemia at the time it is observed.
NONO
MaybeMaybe
PresumedPresumed
Interpretive PrinciplesInterpretive Principles
I
II
III
Relationship AcidemiaRelationship AcidemiaExample: 3 – Tiered System that Integrated Patterns Presumed Relationship Acidemia with the CategoriesExample: 3 – Tiered System that Integrated Patterns Presumed Relationship Acidemia with the Categories
II
III
I
““““Abnormal””””
Indeterminate
““““Normal””””
Integrated 3 Tier SystemIntegrated 3 Tier System• More clearly identify the relationship between FHR patterns and significant acidemia.
• More clearly identify the relationship between FHR patterns and significant acidemia.
•Better clarify how our presumptive diagnosis informs the choice and timing of our interventions.
•Better clarify how our presumptive diagnosis informs the choice and timing of our interventions.
6/6/2014
1
Judith T. Bishop CNM MPHAIM Course
June 6, 2014
�Nothing to disclose
� Aristotle and Hippocrates apparently approved of waiting before tying
� Subject of immediate tying seen in writings of 1600’s (blamed on introduction of male midwives, forceps use )
� First commercial cord clamp “Magennis (1899)” came with strict instructions not to use until cord stopped pulsating
� 1942 Midwifery text: “…the importance of waiting a few miuntes before tying the cord is evident.”
� Delaying cord clamping is a pretty standard Birth Plan request…
� Obstetrics and Gynecology Beckman et al, 2002:“Once the newborn has been delivered it is transported to the warming unit”

6/6/2014
2
� Has for decades been common practice in hospital settings around the world
� This turns the “doing nothing” act of delayed cord clamping (DCC) into the “intervention”
� But this decade has found us cycling around for another look at a more physiologic approach to transition from intrauterine to extra uterine life and benefits that may come with that
� Yao, 1969
� 30% more blood volume
� 50-60% more red blood cells
� (millions of stem cells)
(Yao, 1969 )
� Higher circulating blood volume
� Better systemic blood pressure
� Increased blood flow in superior vena cava
� Increased left ventricular output
� Higher cerebral oxygenation index

6/6/2014
3
� Reduced need for transfusion� Decreased incidence of IVH (up to 50% lower)� Reduced respiratory distress
� Decreased late onset sepsis
In context of no harms (no long term studies)(Hofmeyer,Ibrahim,Kinmon, Mercer, Nelle, Rabe)
Ob’s and Peds coming together to make changes in management based on this data
� UCSF (2012)� WHO (2006,2012)� ACOG (2012)
Have developed recommendations/protocols in support of a 30-120 sec delay for preterm
Primary measurable benefit , well documented by RCT’s and meta-analyses� Newborn: ◦ increased hct/hgb◦ decreased anemia
� 3-6 Months◦ Increased ferritin and total body iron stores◦ Decreased anemia/iron deficiency (Andersson 2011, Hutton 2007, McDonald 2008)
� Iron essential to aspects of brain development
� Lasting cognitive delays, impaired motor development, behavioral effects from iron deficiency with or without anemia
� Although anemia less common in developed world (3-10%), iron deficiency is high (26%)
(Lozoff 1987 2006, Gunnarsson 2007, Thomas 2009)
6/6/2014
4
� Potential that increased iron stores can improve neurodevelopmental outcomes for term infants
� 2012 NIH & Bill&Melinda Gates funded The Infant Brain Study
� 5 year study following effects of placental transfusion on structure and functioning of brain in term infants
� PI is Judith S. Mercer, CNM PhD
� Potential value of increased stem cell transfusion from DCC to have long and short term effects on immunity, host defense, and repair
(Raju 2012)
� Increased birth weight (McDonald, 2013)
� Reduction of weight loss in first days after birth (Indraccolo, 2013)
� Increased duration of breastfeeding(Mercer 2001,2006)
� Term have less risk of transfusion, IVH, late onset sepsis – …
� Still potential for improvement in/support of smoother, more physiologic transition
� (And what’s the harm?...)

6/6/2014
5
Concerns about: � Maternal hemorrhage
� Hypothermia
� Polycythemia & jaundice
� ICC no longer a formal part of Active Management of Third Stage Protocol
� Administering uterotonics =only component w/ evidence (Cotter 2001)
� No evidence that ICC contributes to reduced maternal blood loss
� No studies reporting on blood loss find increase in maternal hemorrhage with DCC
� Now generally accepted that babies don’t automatically need radiant warmers but in fact do better skin to skin with their mothers
� No evidence in any studies reporting on temperature implicating DCC as cause for hypothermia – not even with premies
� Most cited by obs, nurses, and peds alike as reason to avoid DCC
� None of the RCTs since 1980 show a significant association between DCC , clinical jaundice or symptomatic polycythemia
� Hutton and Hassan’s 2007 Meta-analysis of controlled trials (1972-2006) no significant difference in mean bili at 24 or 72 hours
6/6/2014
6
2008, 2013Cochrane review findings ◦ Polycythemia: No difference between groups◦ Clinical jaundice: No difference between groups◦ Jaundice requiring phototherapy: sig more in DCC� 3% of ICC group, 5% of DCC� Risk difference of 2% (2008)
Lower risk (<2%) but still significant in 2013 update
Mercer vs. McDonald!� Mercer argues significance only appears when weight of an unpublished 1996 dissertation of McDonald’s is included� (McDonald is first author of this Cochrane review)� With that study removed, no significant difference in need for treatment appears� Dissertation was included again in 2013 review
� No studies showing significant difference between ICC and DCC in risk for clinically significant polycythemia
� No studies showing significant difference in clinical jaundice
� Increased risk for phototherapy due to DCC is a strongly held belief, not well supported and by inconsistent data
� Worst case scenario appears to be a <2% additional risk for phototherapy without difference in outcome
� Cochrane Conclusion: “A more liberal approach to [DCC]in healthy term infants appears to be warranted..”

6/6/2014
7
“Other” issues/concerns interfering with DCC◦ Nuchal cord◦ Collecting cord blood -� for gases, � for storage, for studies
◦ Getting infants to the warmer / pediatric team if resuscitation seems indicated
� Changed view of “automatic” cutting of nuchal cord
� Danger if cut and delivery does not then proceed � Danger of hypovolemia from tight cord – exactly situation where returning volume (by not cutting) would be an important resuscitative measure
� “Somersault maneuver” leaves cord intact for resuscitation/restoration of blood volume (Schornand Blanco, 1991 Mercer 2005)
� Gases, if required, can be obtained from cord while still attached (Andersson,2012)

6/6/2014
8
� ACOG has stated in Committee Opinion #399, 2008 that:
“collection should not alter routine practice for the timing of umbilical cord clamping”� “A child is not allowed to be a blood donor in this country” (Mercer 2012)
� No studies looking at long term consequences infant “donation” of large amounts of placental blood
� Stem cell banks could be motivated to find other methods to collect the large volume of stem cells left in the placenta (Hutchon 2012)
� Maintaining placental circulation viewed as a part of resuscitation (Dunn 984,Hutchon&Thakur 2008, Mercer&Bewley 2009,Van Rheenen 2011)
� Changing workflow to accommodate assessment and initial resuscitative measures at bedside◦ NRP changes – eg with mec◦ “BASICS” trolley(Bedside Stabilization and Initial Cardiores-piratory Support)
� 20-30 cm length of cord� milking 10 cm/sec, x3-4 times� 30 sec delay = milking in terms of volume of blood transfused in preterm infants (Rabe2011)
� (Rabe 2011, Hosono 2008,9,Erikson-Owens 2012, Upadhyay2013)

6/6/2014
9
� Gravity has an effect
� Raising or lowering by >15-20 cm has effect(Raising or lowering by 10 cm does not)
(Gunther1957, Yao 1969)
� Complete placental transfusion can occur in 30 sec at 40 cm below introitus (Linderkamp1982, Yao1969)
� Evidence that skin to skin◦ Improves physiologic stability of mother & baby◦ Promotes normal brain development◦ Improves successful breastfeeding◦ Facilitates mother infant bonding
(MooreER 2012)
� Blood left in placenta, infant skin to skin� 2012 Cochrane review on this subject found no studies that met inclusion criteria
� Recommend supporting women’s choices in position and time of clamping (but keeping baby below 20 cm above introitus until cord is cut)

6/6/2014
10
� Multicenter, RCT� 190+ in each group, DCC for 2 min� Randomised to held at introitus vs. on mother’s abdomen/chest
� No sig difference between groups using weights as proxy for placental transfusion volume
� WHO 2012–(approx 3 min)
� Vanderbilt 2011-(minimum of 2 min)
� International Consensus on Cardiopulmonary Resuscitation &Resuscitation Council (UK) 2010– (at least 1 min)
� ICC is an intervention without rationale or evidence of benefit� DCC appears to have benefits for Preterm and Term infants with evidence of safety� Concerns for harms, including increased treatment for jaundice and symptomatic polycythemia are unsupported
� Delaying cord clamping for preterm infants ◦ Significant positive short term outcomes◦ increasing institutional and organizational support
Delaying clamping for term newborns� Provides opportunity to affect much larger number with evidence of safety� Supports smooth physiological transition� Substantially increases iron stores in infancy� Keeps baby with the mother� Many other benefits may flow from these?
6/6/2014
11
� Circumstantial barriers can be worked around
� Collaboration between all providers required to make a change in routine practice*Seeing ICC as the intervention in need of defense*

6/6/2014
1
Safe and Appropriate Use of Magnesium in Obstetrics
Jeffrey L Ecker, MD
Massachusetts General Hospital
Harvard Medical School
Disclosures
• I left San Francisco for Boston
• I use magnesium (less and less)
• I have no financial or other disclosures
Epsom Salts: Take a Soak?
• Can soothe the body, mind and soul
– Relax the nervous system
– Cure skin problems
– Draw toxins from the body
• Not actually a salt but a compound
– Magnesium sulfate

6/6/2014
2
Could Lady Sybil have been saved? I honestly do not know, as I am not a doctor, or medical historian, but I am very much fascinated by the subject. Based on my readings, a C-section done early enough could have possibly saved her, so long as the hospital conditions and surgical instruments didn’t give her a terrible illness. As said before, this was a risky procedure back then. Another possibility is intravenous magnesium sulfate, which had just been recently introduced as a treatment for pre-eclampsia.
Magnesium In Obstetrics
• 1906: Horn in Germany suggests treatment of eclamptic seizures with magnesium
• 1926: Lazard uses and publishes series of IV magnesium to treat eclamptic seizures
– 12% v 36% Mortality
• 1974: Pritchard reports 154 consecutive cases of IV+IM magnesium treatment of eclampsia without a death
JAMA, 1926
Safe and Appropriate Use of Magnesium in Obstetrics
• Uses
– Prevention of eclamptic seizures
– Tocolysis
– Neuroprotection
• FDA and other warnings
– ACOG response
• Safety measures

6/6/2014
3
Prevention of Eclampsia: Does It Work?
• Cochrane Review 2011:
– Prevents Maternal Death (2 studies , 10K women)
• RR : 0.54 (.26-1.1)
– Prevents Eclampsia (6 studies, 11 K women)
• RR: 0.41 (.29-.58)
• Risk Difference: -.01
Prevention of Eclampsia
Magnesium for Seizure Prophylaxis: What Dose?
• No one dosing regimen demonstrably better than another
– Loading 4-6 mg/hr IVB
– Continuous: 1-3 mg/hr
• Be mindful of urine output
Magnesium for Seizure Prophylaxis: Which Patients?
• It’s all about NNT
– MAGPIE/Cochrane
• Mild PE: NNT=100
• Severe PE: NNT=60
• “Active” labor has nothing to do with it
• Evaluate /weigh (in your facility) the downside of a seizure

6/6/2014
4
Magnesium for Seizure Prophylaxis: Which Patients?
• Some experts recommend treating all with PE
• ACOG 2013:
“for women with preeclampsia with systolic blood pressure of less than 160 mmHg and a diastolic blood pressure less than 110 mmHg and no maternal symptoms, it is suggested that magnesium sulfate not be administered universally for the prevention of eclampsia” Quality of Evidence—Low, Strength of Recommendation---qualified
What is ACOG’s Favorite Plant?
Magnesium for Tocolysis
• Smooth muscle relaxant
• Observational series suggest a benefit
– “Magnesium sulfate was found to be a successful, inexpensive and relatively non-toxic tocolytic agent that had few side effects.”
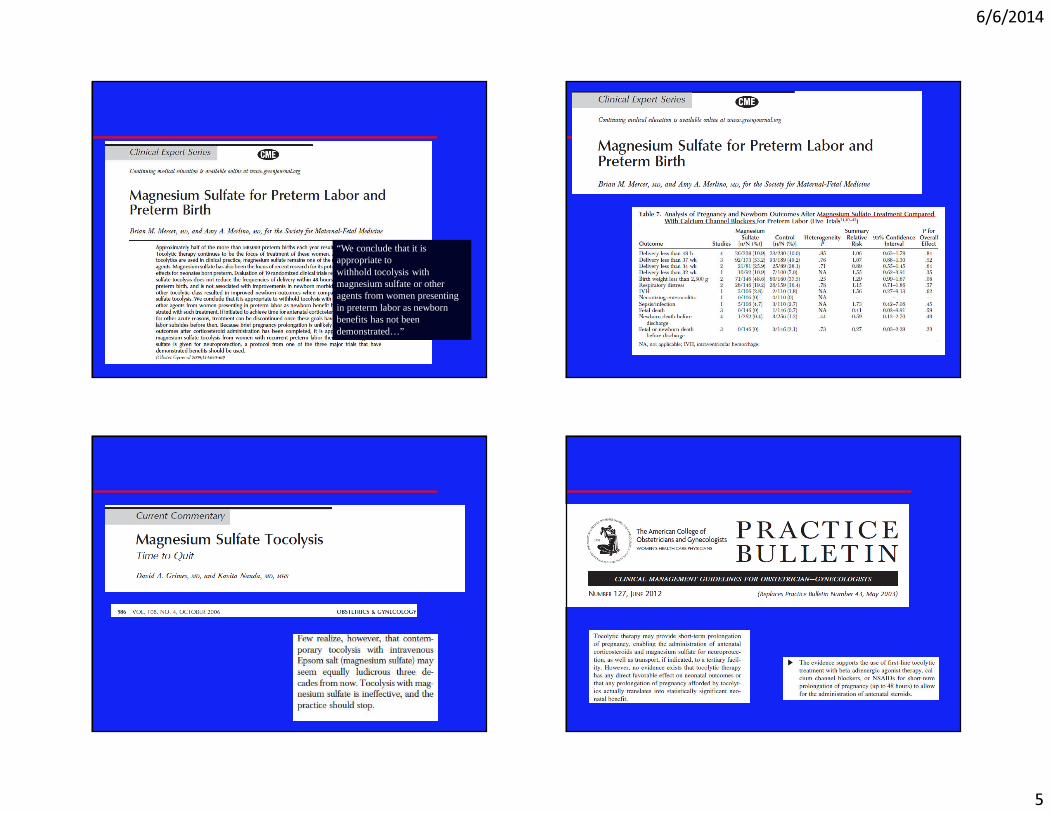
6/6/2014
5
“We conclude that it is appropriate towithhold tocolysis with magnesium sulfate or other agents from women presenting in preterm labor as newborn benefits has not been demonstrated…”
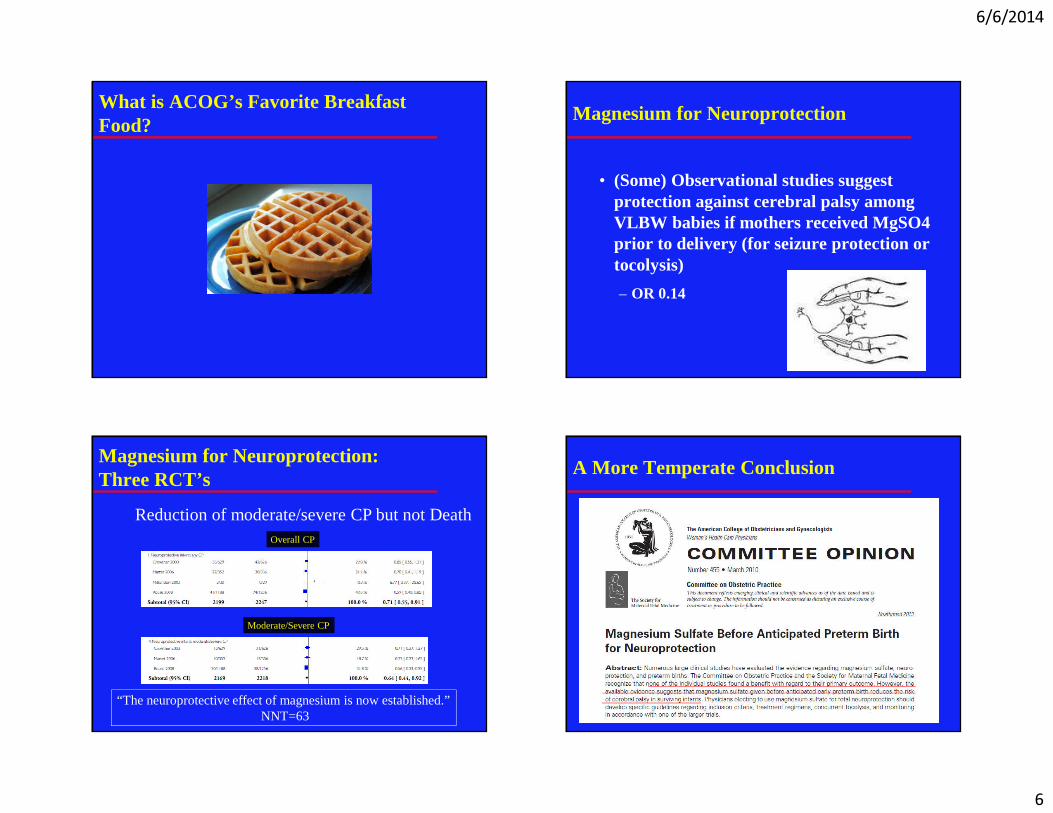
6/6/2014
6
What is ACOG’s Favorite Breakfast Food?
Magnesium for Neuroprotection
• (Some) Observational studies suggest protection against cerebral palsy among VLBW babies if mothers received MgSO4 prior to delivery (for seizure protection or tocolysis)
– OR 0.14
Magnesium for Neuroprotection: Three RCT’s
Reduction of moderate/severe CP but not DeathOverall CP
Moderate/Severe CP
“The neuroprotective effect of magnesium is now established.”NNT=63
A More Temperate Conclusion
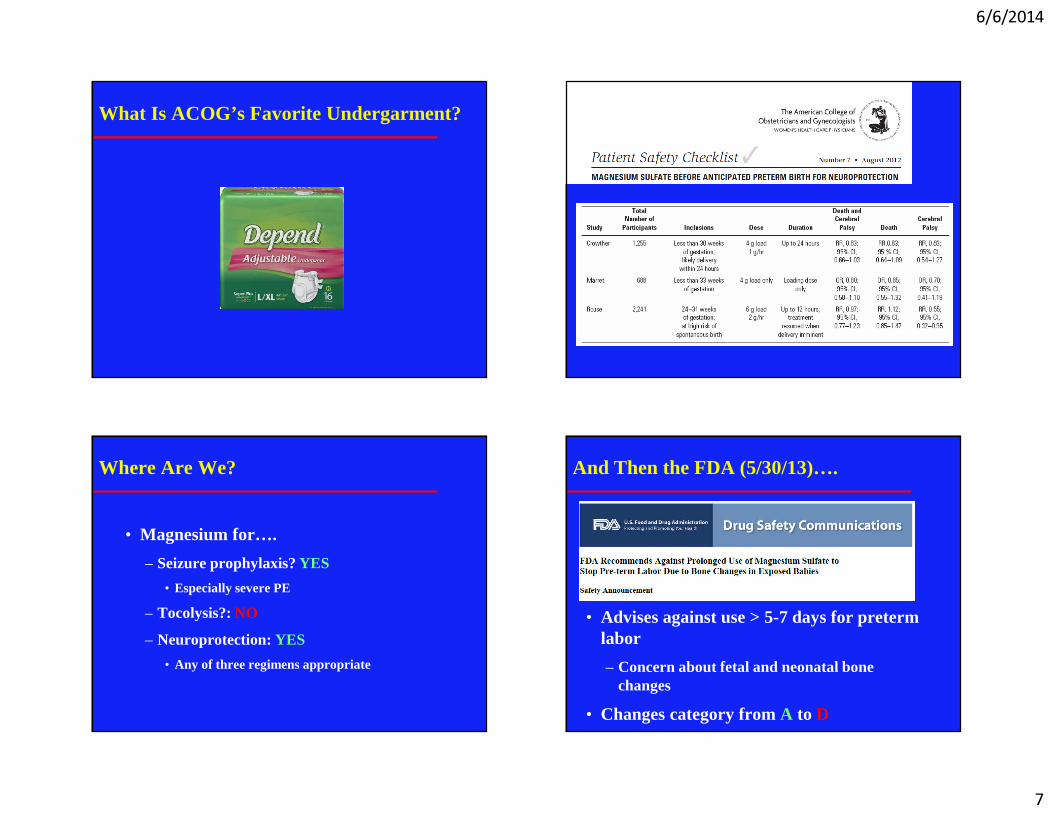
6/6/2014
7
What Is ACOG’s Favorite Undergarment?
• 4 gm IVB over 20 minutes then 1 gm/hr up to 24 hours (Crowther)
• 6 gm IVB over 20-30 minutes then 2 gm/hr (Rouse)
• 4 gm IVB over 30 minutes
Where Are We?
• Magnesium for….
– Seizure prophylaxis? YES
• Especially severe PE
– Tocolysis?: NO
– Neuroprotection: YES
• Any of three regimens appropriate
And Then the FDA (5/30/13)….
• Advises against use > 5-7 days for preterm labor
– Concern about fetal and neonatal bone changes
• Changes category from A to D

6/6/2014
8
But, but……
• No one uses it that long
• Few absolute number of cases of adverse outcome
• Lots of people just look at the letter
• Some benefits
D
In all of these conditions, prolonged use of magnesium sulfate is never indicated. Therefore, the FDA’s change in the pregnancy classification of magnesium sulfate addresses an unindicatedand non-standard use of this medication
Using Magnesium Safely
• Avoid inadvertent toxicity
– Pump not free flowing drip
– Bolus but not continuous infusion if oliguria or decreased renal function
• Know signs and levels of toxicity
• Know the antidote
– Calcium gluconate 1 gm IVP
Magnesium Toxicity
Perinatology.com

6/6/2014
9
Safe Us of Magnesium in Obstetrics
• For seizure prophylaxis
• For neuroprotections
• For less than 48-72 hours
Questions? Objections? Toxic Reactions?
6/6/2014
1
The Category II Conundrum
Tekoa L. King CNM, MPH
June 6, 2014
Disclosure
• I have no financial disclosures related to this talk
What Most of us Think of as a Category 2 Conundrum
3
But what I hope to do today..
Category II Controversy
Category II is a Continuum
Category II Complications
Category II Collaboration
Category II Common sense
4
6/6/2014
2
Objectives
• NICHD Category II– What is the problem?
• Relationship between FHR characteristics and newborn acidemia
• Proposed algorithms for managing category II
• Where do you go from here?
What’’’’s the Problem?
1. There are more than 40 different FHR patterns in Category II
2. Category II is a heterogeneous group of FHR patterns that reflect varying risks for fetal acidemia
Jackson M 2011
What’’’’s the Problem?
1. These are also the FHR patterns seen most frequently in clinical practice
– 22% of time in first stage
– 40% of time in second stage
2. Any clinical setting that wants to use the NICHD 3-tier system has to grapple with how to manage category II tracings
Jackson M 2011
4 Facts Summarize the Relationship Between FHR Patterns and Newborn Acidemia1. Moderate variability is strongly
predictive of neonatal vigor independent of the presence of variant patterns. This pattern has a negative predictive value of 98%-99% for a term fetus
2. Pattern evolution: newborn acidemia with decreasing FHR variability in combination with decelerations develops over a period of time approximating one hour
Parer JT et al 2006
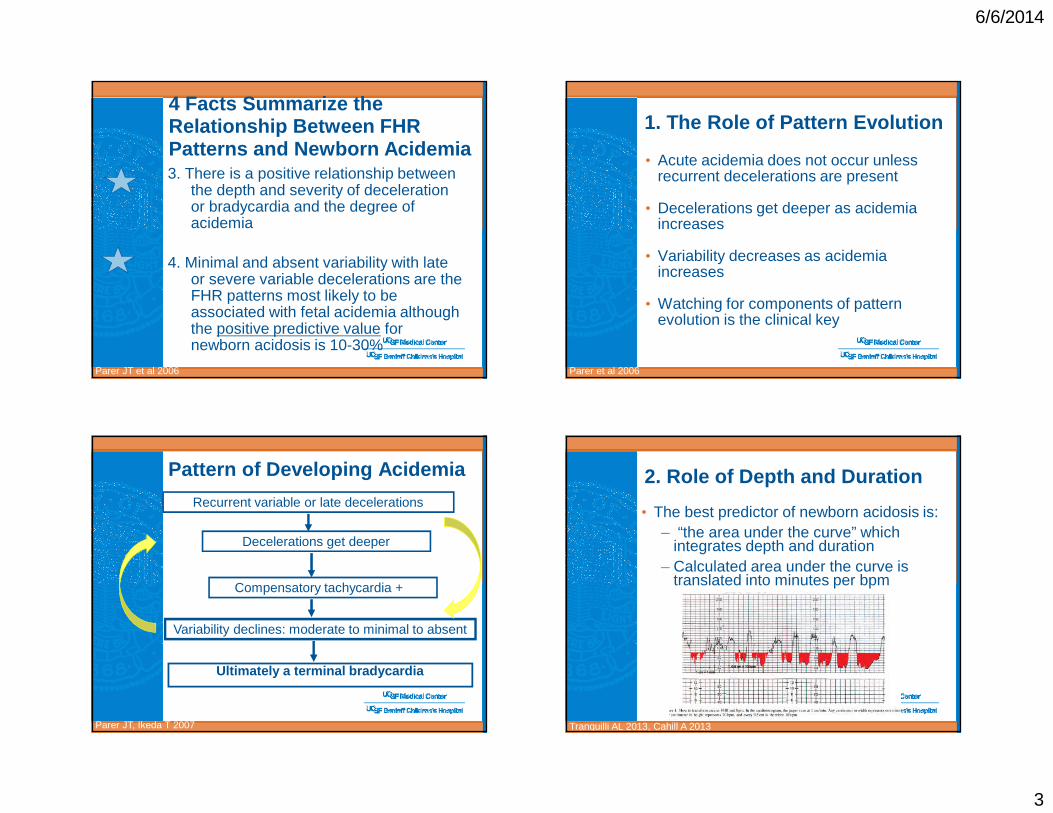
6/6/2014
3
3. There is a positive relationship between the depth and severity of deceleration or bradycardia and the degree of acidemia
4. Minimal and absent variability with late or severe variable decelerations are the FHR patterns most likely to be associated with fetal acidemia although the positive predictive value for newborn acidosis is 10-30%
Parer JT et al 2006
4 Facts Summarize the Relationship Between FHR Patterns and Newborn Acidemia
1. The Role of Pattern Evolution
• Acute acidemia does not occur unless recurrent decelerations are present
• Decelerations get deeper as acidemia increases
• Variability decreases as acidemia increases
• Watching for components of pattern evolution is the clinical key
Parer et al 2006
Pattern of Developing Acidemia
Parer JT, Ikeda T 2007
Ultimately a terminal bradycardia
Recurrent variable or late decelerations
Variability declines: moderate to minimal to absent
Decelerations get deeper
Compensatory tachycardia +/-
2. Role of Depth and Duration
• The best predictor of newborn acidosis is:– “the area under the curve” which
integrates depth and duration– Calculated area under the curve is
translated into minutes per bpm
Tranquilli AL 2013, Cahill A 2013
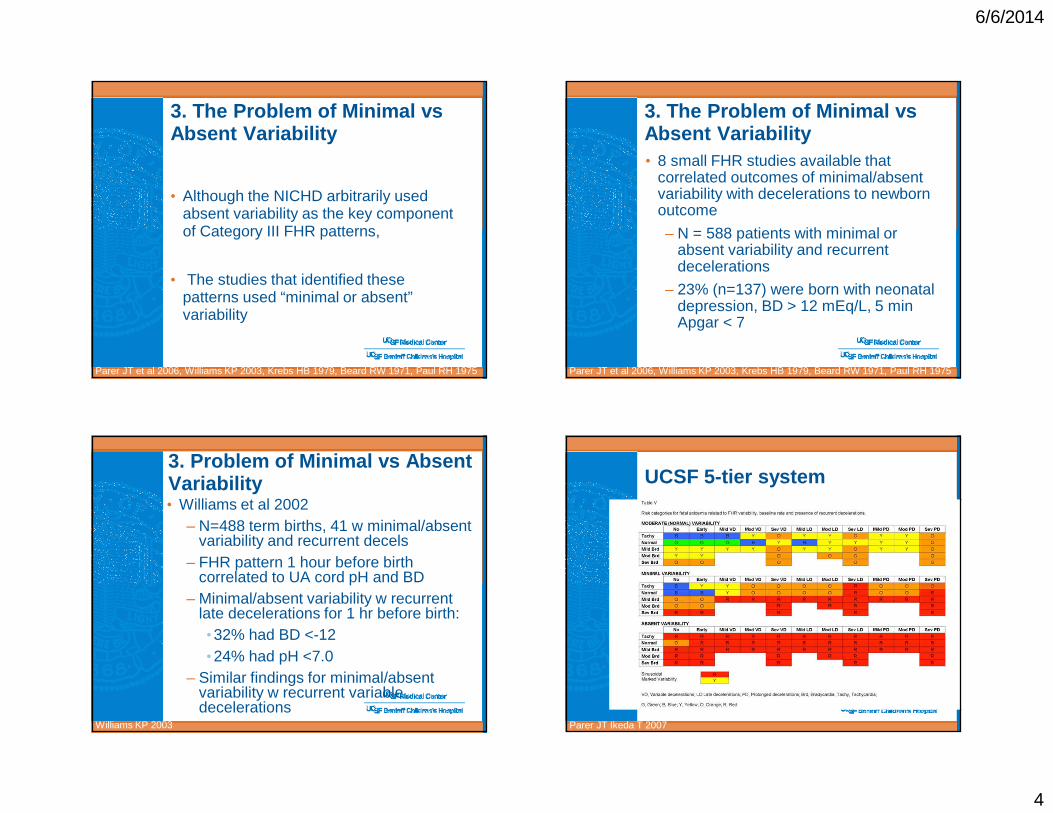
6/6/2014
4
3. The Problem of Minimal vs Absent Variability
• Although the NICHD arbitrarily used absent variability as the key component of Category III FHR patterns,
• The studies that identified these patterns used “minimal or absent” variability
Parer JT et al 2006, Williams KP 2003, Krebs HB 1979, Beard RW 1971, Paul RH 1975
3. The Problem of Minimal vs Absent Variability• 8 small FHR studies available that
correlated outcomes of minimal/absent variability with decelerations to newborn outcome
– N = 588 patients with minimal or absent variability and recurrent decelerations
– 23% (n=137) were born with neonatal depression, BD > 12 mEq/L, 5 min Apgar < 7
Parer JT et al 2006, Williams KP 2003, Krebs HB 1979, Beard RW 1971, Paul RH 1975
3. Problem of Minimal vs Absent Variability• Williams et al 2002
– N=488 term births, 41 w minimal/absent variability and recurrent decels
– FHR pattern 1 hour before birth correlated to UA cord pH and BD
– Minimal/absent variability w recurrent late decelerations for 1 hr before birth:•32% had BD <-12•24% had pH <7.0
– Similar findings for minimal/absent variability w recurrent variable decelerations
Williams KP 2003
UCSF 5-tier system
• Very complicated! • But it does give us the background PhD
thesis version of the relationship between every FHR pattern possible and the corresponding risk of acidemia
• Good for background source material
Parer JT Ikeda T 2007

6/6/2014
5
*Macones et al AJOG 2008:112:661**Position change, increasing IV fluid, reducing uterine activity, modified pushing, etc.
Parer JT Ikeda T 2007
FHR 5-tier app 2012www.obapps.org
Linda Troutfetter RN Petaluma Valley Hospital
How Did The NICHD Guidelines Start Being Used in Practice?
2010: ACOG Practice Bulletin: Now we Have 4 Categories• This algorithm addresses FHR
monitoring from the perspective of the physician BUT…the physician is not usually the first person on the scene….and therefore, this algorithm does not start at the beginning with recommendations for the first responder….the bedside provider

6/6/2014
6
Miller and Miller 2011
• This algorithm incorporates thinking about FHR patterns physiologically but it is a complex version of standard practice and as such, it layers a complex set of mental steps over what we already do.
• May be a good teaching tool for clinicians new to obstetrics
Clark et al 2013
Clark et al 2013 Summary of Category II Algorithms Proposed or In Use• Split Category II into 2 or 3 subcategories
• They base this split on the degree of variability and presence or absence of accelerations
Each of them take into account some of the 3 FHR characteristics that reflect the
development of fetal acidemia that were not addressed by the NICHD 3-tier system
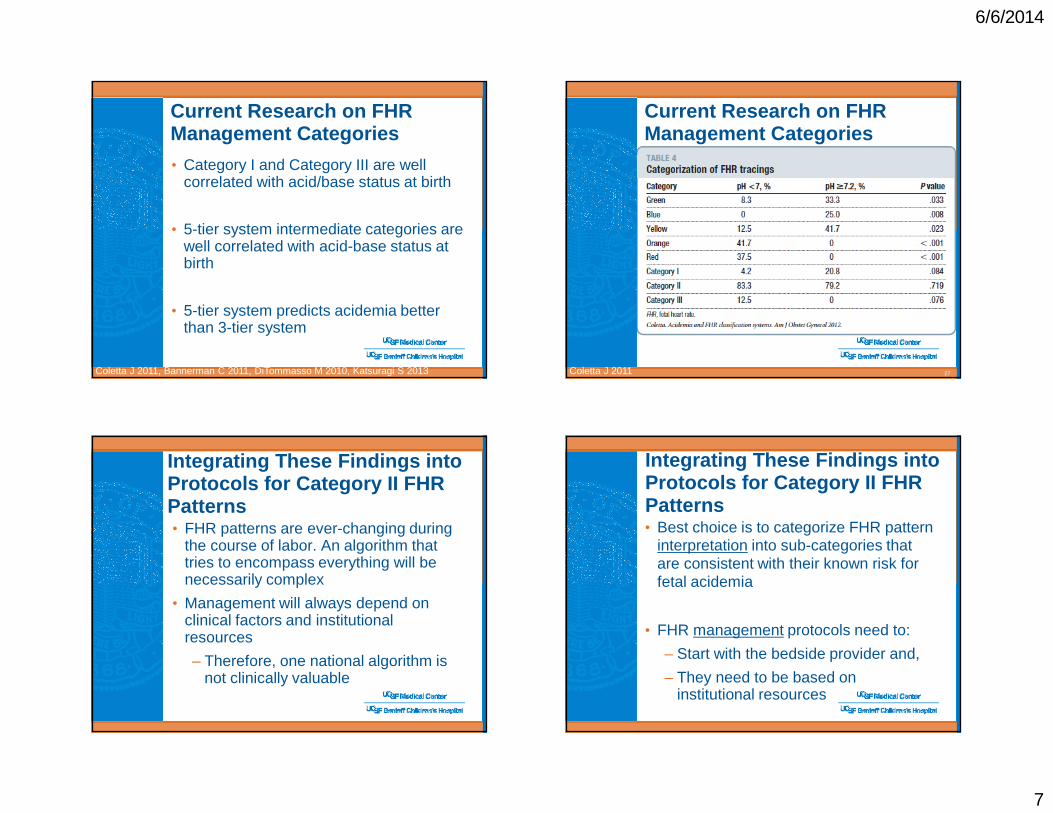
6/6/2014
7
Current Research on FHR Management Categories
Coletta J 2011, Bannerman C 2011, DiTommasso M 2010, Katsuragi S 2013
• Category I and Category III are well correlated with acid/base status at birth
• 5-tier system intermediate categories are well correlated with acid-base status at birth
• 5-tier system predicts acidemia better than 3-tier system
Current Research on FHR Management Categories
27Coletta J 2011
Integrating These Findings into Protocols for Category II FHR Patterns• FHR patterns are ever-changing during
the course of labor. An algorithm that tries to encompass everything will be necessarily complex
• Management will always depend on clinical factors and institutional resources
– Therefore, one national algorithm is not clinically valuable
Integrating These Findings into Protocols for Category II FHR Patterns• Best choice is to categorize FHR pattern
interpretation into sub-categories that are consistent with their known risk for fetal acidemia
• FHR management protocols need to:
– Start with the bedside provider and,
– They need to be based on institutional resources

6/6/2014
8
How do Skilled Clinicians Think?
• Observe
• Evaluate and Get More Information
• Emergent Delivery
Interpretation of Risk Management
5 Categories Based On Clinical Interpretation and Management• 1: No acidemia (Category I)
• 2A: No central fetal acidemia (adequate oxygen) (Category I and II)
• 2B: No central fetal acidemia, but FHR pattern suggests intermittent reductions in O2 which may result in fetal O2 debt (Category II)
• 2C: Fetus potentially on verge of decompensation (Category II)
• III: Evidence of actual or impending damaging fetal asphyxia (Category III)
Parer JT et al 2007, Parer JT & King Tl 2010
Tools for Creating Category II Guidelines
Fox M et al 2000
Tools for Creating Category II Guidelines
MODERATE VARIABILITY
INTERPRETATION MANAGEMENT
• Moderate variability • Normal baseline• Recurrent
decelerations
• Moderate variability
• Tachycardia • No decelerations
• Moderate variability • Tachycardia • Recurrent
decelerations
• Centrally oxygenated• At risk for Pattern
Evolution
• Conservative measures
• Notify clinician in X minutes if unresolved
• Centrally oxygenated• At risk for Pattern
Evolution
• Pattern of developing acidemia
• Conservative measures
• Bedside evaluation by clinician in X minutes
• Conservative measures
• Notify clinician to create plan

6/6/2014
9
Category II Management Based on Pattern Evolution
34
Recurrent decelerations
Variability diminishing
Decelerations getting deeper and/or tachycardia
Conservative measures
Conservative measuresConsult and make a plan for reevaluation in short period of time
Consider delivery in short period of time
Summary
• Current NICHD Category II is not clinically useful
• Algorithms promoted to solve this problem all split Category II into 2 or 3 subcategories for interpretation/management
– Interpretation can be based on the known relationships between FHR patterns and newborn acidemia
– Management has to be based on institutional resources
35
Summary
• Proposed solutions to Category II:
– Consistent in the FHR patterns placed in each subcategories
– Consistent with research on the relationship between FHR patterns and newborn acidemia
– 2 or 3 subcategories
•Acknowledge pattern evolution
• Integrates depth and duration of decelerations
36
Thank YouTekoa L. King CNM, MPH
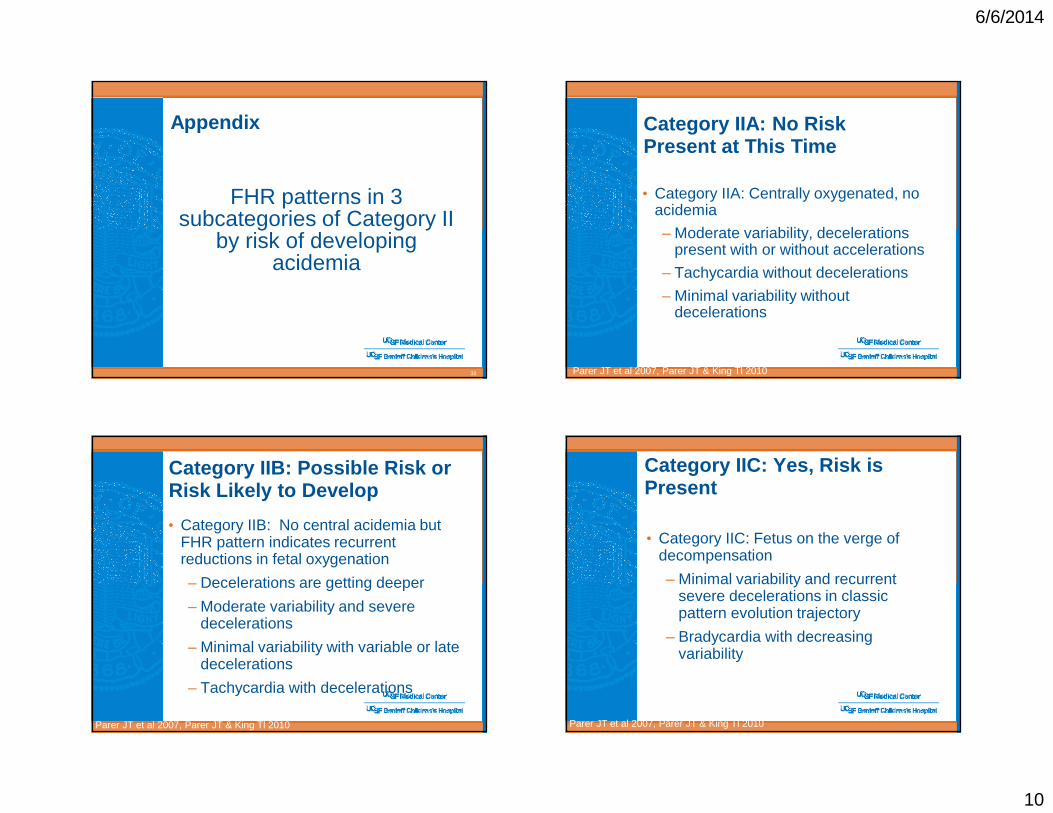
6/6/2014
10
Appendix
FHR patterns in 3 subcategories of Category II
by risk of developing acidemia
38
Category IIA: No Risk Present at This Time
• Category IIA: Centrally oxygenated, no acidemia
– Moderate variability, decelerations present with or without accelerations
– Tachycardia without decelerations
– Minimal variability without decelerations
Parer JT et al 2007, Parer JT & King Tl 2010
Category IIB: Possible Risk or Risk Likely to Develop
• Category IIB: No central acidemia but FHR pattern indicates recurrent reductions in fetal oxygenation
– Decelerations are getting deeper
– Moderate variability and severe decelerations
– Minimal variability with variable or late decelerations
– Tachycardia with decelerations
Parer JT et al 2007, Parer JT & King Tl 2010
Category IIC: Yes, Risk is Present
• Category IIC: Fetus on the verge of decompensation
– Minimal variability and recurrent severe decelerations in classic pattern evolution trajectory
– Bradycardia with decreasing variability
Parer JT et al 2007, Parer JT & King Tl 2010

6/6/2014
11
References
Studies that have evaluated suggested algorithms for
Category IIand
Publications of collaborative FHR protocol development
42
References
• American College of Obstetricians and Gynecologists. Management of Intrapartum Fetal Heart Rate Tracings Practice Bulletin Number 116 November 2010. Obstet Gynecol 2010;116:1232–40
• Bannerman CG, et al. Assessment of the concordance among 2-tier, 3-tier, and 5-tier fetal heart rate classification systems. Am J Obstet Gynecol. 2011 Sep;205(3):288.e1-4. Epub 2011
43
References• Cahill AG, et al. Terminal fetal heart
decelerations and neonatal outcomes. ObstetGynecol. 2013 Nov;122(5):1070-6.
• Coletta J, et al. The 5-tier system of assessing fetal heart rate tracings is superior to the 3-tier system in identifying fetal acidemia. Am J Obstet Gynecol. 2011;206: Dec 22.
• Di Tommaso M,et al. Comparison of five classification systems for interpreting electronic fetal monitoring in predicting neonatal status at birth. J Matern Fetal Neonatal Med. 2013 Mar;26(5):487-90.
44
References
• Elliott C, et al. Graded classification of fetal heart rate tracings: association with neonatal metabolic acidosis and neurologic morbidity. Am J ObstetGynecol. 2010 Mar;202(3):258.e1-8. • Fox M, et al. Fetal Heart Rate Monitoring: Interpretation and collaborative management. J Midwifery Womens Health 2000;45:498-507.• Jackson M, et al. Frequency of fetal heart rate categories and short-term neonatal outcome. Obstet Gynecol 2011;118:803-8
45

6/6/2014
12
References
• Katsuragi S, et al. Immediate newborn outcome and mode of delivery: use of standardized fetal heart rate pattern management. J Matern Fetal Neonatal Med. 2013 Jan;26(1):71-4• MacEachin SR, et al. The fetal heart rate collaborative practice project. Situational awareness in electronic fetal heart rate monitoring; A Kaiser Permanente perinatal patient safety program initiative. J Perinat Neonat Nurs 2009;23:314-23
46
References• Macones GA, et al. National Institute of Child Health and Human Development Research Workshop Report on Electronic fetal heart rate monitoring. Obsetet Gyneocl2008;112:661-6, JOGNN 2008;37:510-15• Miller DA, Miller LA. Electronic fetal heart rate monitoring: applying principles of patient safety. Am J Obstet Gynecol. 2012 Apr;206(4):278-83.• Okai T,et al; Perinatology Committee of the Japan Society of Obstetrics and Gynecology. Intrapartum management guidelines based on fetal heart rate pattern classification. J ObstetGynaecol Res. 2010 Oct;36(5):925-8
47
References• Parer JT, King TL. Fetal heart rate monitoring: the next step. Am J ObstetGynecol 2010;203:520-1• Parer JT, Ikeda T. A framework for standardized management of intrapartum fetal heart rate patterns. Am J ObstetGynecol 2007;197:26e.1-26.e6.• Schnettler WT, et al. A modified fetal heart rate tracing interpretation system for prediction of cesarean section. J MaternFetal Neonatal Med. 2012 Jul;25(7):1055-8
48
References• Soncini E, et al. Intrapartum fetal heart rate monitoring: evaluation of a standardized system of interpretation for prediction of metabolic acidosis at delivery and neonatal neurological morbidity. J Matern Fetal Neonatal Med. 2013 Dec 9• Tranquilli AL, et al. The correlation between fetal bradycardia area in the second stage of labor and acidemia at birth. J Matern Fetal Neonatal Med. 2013 Sep;26(14):1425-9
49

6/6/2014
13
References
• Williams KP, Galerneau F. Intrapartum fetal heart rate patterns in the prediction of neonatal acidemia. Am J Obstet Gynecol2003;188:820-3.
50

1
LEADING THE QUEST FOR HEALTH
Kimberly D. Gregory MD, MPHVice Chair Women’s Healthcare Quality & Performance Improvement
Cedars Sinai Medical Center, Dept Ob/GynProfessor, David Geffen School of Medicine & UCLA School of Public Health
TACHYSYSTOLE…
UCSF June 2014 Disclosures
� I have no financial disclosures
�No off label use of drugs
KD Gregory 5/2014
Objectives
� At the completion of this lecture, participants will be able to …— Describe (and be able to recognize) the different types of
tachysystole— Describe the maternal and neonatal clinical implications of
tachysystole— Describe various treatment options for tachysystole— Describe components of QI program to “cease and desist”
� No more “pitting through it”� No more “pit to distress”
KD Gregory 5/2014
What is tachysystole?
� 2008 NICHD Workshop Report on Electronic Fetal Monitoring— Macones et al; Obstet Gynecol 2008; 112:661-6
� A full description of EFM tracing requires a qualitative and quantitative description of 1. Uterine Contractions2. Baseline fetal heart rate (FHR)3. Baseline FHR variability4. Presence of accelerations5. Periodic or episodic decelerations6. Changes or trends of FHR patterns over time
KD Gregory 5/2014

2
What is Tachysystole?
� 2008 NICHD Workshop Report on Electronic Fetal Monitoring— Macones et al; Obstet Gynecol 2008; 112:661-6
� Uterine Contractions— Number of contractions present in 10 minute window,
averaged over 30 minutes— NORMAL: <5 contractions in 10 min window— TACHYSYSTOLE:>5 contractions in 10 minutes
� TS can be spontaneous or associated with stimulated labor� TS no decelerations vs TS + decelerations
KD Gregory 5/2014
What is tachysystole?
� 2008 NICHD Workshop Report on Electronic Fetal Monitoring— Macones et al; Obstet Gynecol 2008; 112:661-6; — ACOG Practice Bulletin, Obstet Gynecol 2009; 114:192-202
� Uterine Contractions— “the terms hyperstimulation and hypercontractility are not
defined and should be abandoned”
— “other factors such as duration, intensity, and relaxation time between contractions are equally important in clinical practice”
KD Gregory 5/2014
What is Tachysystole?� Kunz et al JOGNN, 2013;42:12-18
— NICHD, ACOG, SMFM, AWHONN� Tachysystole is identified when one or more criteria are present
(30 min increments)1. More than 5 contractions in a 10 min window, averaged over 30 min2. A series of single contractions lasting 2 min or more3. Contractions of normal duration occurring within one minute of each
other (ACOG 2003, Simpson & Creehan 2008)4. Insufficient return of uterine resting tone between contractions via
palpation or intrauterine amniotic pressure above 25 mmHg between contractions via IUPC (Simpson & Creehan)
� Gregory take home point: TS is… TOO MANY CONTRACTIONS!!!
KD Gregory 5/2014
What does Tachysystole look like?
KD Gregory 5/2014
TS, no FHR changes TS + FHR changes
Google images, uterine hyperstimulation
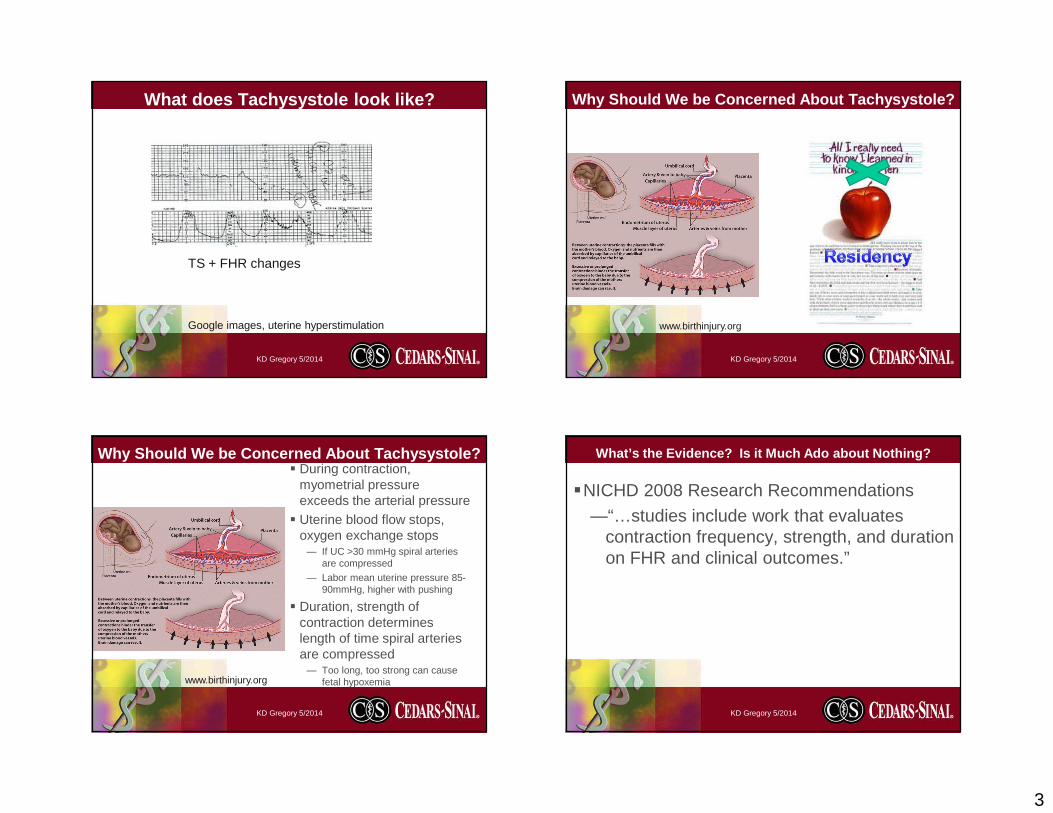
3
What does Tachysystole look like?
KD Gregory 5/2014
TS + FHR changes
Google images, uterine hyperstimulation
Why Should We be Concerned About Tachysystole?
KD Gregory 5/2014
www.birthinjury.org
Why Should We be Concerned About Tachysystole?� During contraction,
myometrial pressure exceeds the arterial pressure
� Uterine blood flow stops, oxygen exchange stops
— If UC >30 mmHg spiral arteries are compressed
— Labor mean uterine pressure 85-90mmHg, higher with pushing
� Duration, strength of contraction determines length of time spiral arteries are compressed
— Too long, too strong can cause fetal hypoxemia
KD Gregory 5/2014
www.birthinjury.org
What’s the Evidence? Is it Much Ado about Nothing?
�NICHD 2008 Research Recommendations
—“…studies include work that evaluates contraction frequency, strength, and duration on FHR and clinical outcomes.”
KD Gregory 5/2014

4
What’s the Evidence? Is it Much Ado about Nothing?
� Bakker et al, AJOG 2007; 196:313.e1-313.e6� Elevated uterine activity increases the risk of fet al acidosis
at birth� Amsterdam, June 1993-July 2004� N=2886 (all cases with IUPC); tracings analyzed via computer
and 2 independent reviewers for each 10 min window for last hour of first stage and all second stage
� Evaluated: relaxation time, duration, amplitude, surface, Mvunits, active planimeter units, and contraction frequency
� Routinely collected blood gases; acidosis defined as pH< 7.11
KD Gregory 5/2014
What’s the Evidence? Is it Much Ado about Nothing?
� Bakker et al, AJOG 2007; 196:313.e1-313.e6
KD Gregory 5/2014
Characteristic First stage(<7.11 vs >7.12)
Second stage(<7.11 vs >7.12)
Shorter avg relax time (sec) 51 vs 63 36 vs 47
Longer contraction duration (sec) 2216 vs 2053 1465 vs 1268
Contraction amplitude (mmHg) 1383 vs 1178 1477 vs 1219
Contraction surface (mmHg x sec) 479 vs 418 442 vs 370
Montevideo units 261 vs 236 442 vs 402
Contraction frequency/10 min 5.0 vs 4.8 5.5 vs 5.2
Conclude: increased uterine activity is significantly associated with higher incidence of umbilical artery pH <7.11
What’s the Evidence? Is it Much Ado about Nothing?
� Simpson & James AJOG 2008; 199:34.e1-34.e5� Effects of oxytocin-induced uterine hyperstimulatio n
during labor on fetal oxygen status and fetal heart rate patterns
� Retrospective study, 56 women with hyperstimulation >30 min defined as <6 or >=6 UC in 10 min
� Evaluated fetal oxygen saturation and FHR patterns
KD Gregory 5/2014
What’s the Evidence? Is it Much Ado about Nothing?
0
10
20
30
40
50
60
Prior 5 min 10 min 15 min 20 min 25 min 30 min
UC <5/10 min
UC=5/10 minUC>=6/10 min
KD Gregory 5/2014
FS
pO2
20% decrease
29% decrease
As contraction frequency increased, effect of fetal oxygen saturation is more pronounced
Simpson & James AJOG 2008; 199:34.e1-34.e5

5
What’s the Evidence? Is it Much Ado about Nothing?
� Simpson & James AJOG 2008; 199:34.e1-34.e5
KD Gregory 5/2014
FSpO2 &FHR
Normal UC<5/10 minN=158
=5 UC/10 minN=102
>= 6 UC/10 minN=56
p
FSpO2 No change 20% dec 29% dec <0.001
Oxytocin mean mU 6.08 9.64 12.03 <0.001
Absent variability (%) 0 1.9 3.6 0.011
Minimal variability (%) 7.6 10.8 16.1 0.011
Accelerations (%) 86.0 77.5 62.5 <0.001
Variables (%) 17.7 29.4 25.0 0.451
Late decelerations (%) 8.9 15.7 26.8 0.032
Prolonged decels (%) 0 3.9 3.6 0.085
Recurrent decels (%) 9.5 21.6 37.5 0.002
What’s the Evidence? Is it Much Ado about Nothing?
� Stewart et al, AJOG 2012; 207:290.e1-6. � Defining uterine tachysystole: how much is too much ?� Prospective cohort study, 584 women undergoing induction of
labor with oral misoprostol (100ug) � Tachysystole >=6 UC in 10 min during first four hours of
induction� Uterine hypertonus—contraction > 120 sec� Evaluated infant condition at birth
— Composite measure: 5 min Apgar<3, pH<7.1, intubation in DR, neonatal seizures, NICU admission or death
KD Gregory 5/2014
What’s the Evidence? Is it Much Ado about Nothing?
� Stewart et al, AJOG 2012; 207:290.e1-6. � Tachysystole during first four hours of misoprostol induction
� 253 (43%) women had at least one 10 min window with >6 UC first 4 hours
� 129 (22%) met criteria averaged over 30 min� 89 (15%) uterine hypertonus
— Stratified into <4, 5, 6, >7 UC or hypertonus—no difference in fetal composite measure
— FHR decelerations were associated with increased number of contractions and hypertonus
� Limitation—elapsed time; conclude self-limited episodes remote from delivery are not harmful
KD Gregory 5/2014
What’s the Evidence? Is it Much Ado about Nothing?
� Kunz et al JOGNN 2013;42:12-18 � Incidence of Uterine Tachysystole in Women Induced w ith
Oxytocin� Retrospective study, 55 women undergoing induction of labor
with oxytocin � Tachysystole >5 UC in 10 min averaged over 30 min � Series of single contractions 2 min or more� UC’s within one min of each other� Insufficient return to baseline (palpation or IUPC >25 mmHg
between contractions
KD Gregory 5/2014

6
What’s the Evidence? Is it Much Ado about Nothing?
� Kunz et al JOGNN 2013;42:12-18 � Mean oxytocin infusion was 9.2 mU/min; median 8 mU/min� Range (0.5-30)
� Duration 4-33.5 hours; mean 13.7 hours� 798.5 hours of strip evaluated/1,597 30-min segments� 661 TS events (41%)
— Most common was fewer than 60 sec between contractions (98%)
— Second most common was >5 in 10 min/30 min (33%)— Series of contractions >120 sec (11%)— Insufficient return to baseline tone (1%)
KD Gregory 5/2014
What’s the Evidence? Is it Much Ado about Nothing?
� Kunz et al JOGNN 2013;42:12-18 � Higher incidence because they used four criteria� Suggest tachysystole is under recognized if limited to single
definition; FHR changes associated with all four definitions � Rates using >5 in 10 min/30 min comparable to prior studies
KD Gregory 5/2014
What’s the Evidence? Is it Much Ado about Nothing?
� Heuser et , AJOG 2013; 209:32e.e1-6. � Tachysystole in term labor: Incidence, risk factors,
outcomes and effect on fetal heart rate tracings� Retrospective cohort study, 10 hospitals March 2007-June
2009; 50,335 term singleton deliveries (spontaneous/induced)� Tachysystole:
— TS in nursing note; UC <=2 min apart; >5 UC in 10 min/30— 100 charts randomly reviewed by authors to validate
� Cesarean delivery� Neonatal complications
KD Gregory 5/2014
What’s the Evidence? Is it Much Ado about Nothing?
� Heuser et , AJOG 2013; 209:32e.e1-6. � 50,335 deliveries; 5363 (10.7%) had at least one TS event� Average duration was approximately 60 min
� 3.7% had TS-FHR changes� 4.3% had TS-Interventions� 1.5% had TS-Delivery expedited (CS or OVD)� Not mutually exclusive
— 8% had 1 event; 2% had 2 events; 1% had 3 or more
KD Gregory 5/2014

7
What’s the Evidence? Is it Much Ado about Nothing?
� Heuser et , AJOG 2013; 209:32e.e1-6. � Oxytocin for induction/augmentation in 37,020 labors (75%);
4591 (12.4%) had at least one TS event� 4.0% had TS-FHR changes� 4.9% had TS-Interventions� 1.5% had TS-Delivery expedited (CS or OVD)� Comparable to entire population� For every 5 mU/min increase in dose, increase RR
— TS 1.12 (1.06-1.13)— TS-F 1.12 (1.09-1.14)
— TS-I 1.16 (1.14-1.18)— TS-D 1.06 (1.02-1.10)
KD Gregory 5/2014
What’s the Evidence? Is it Much Ado about Nothing?
� Heuser et , AJOG 2013; 209:32e.e1-6. � Summary of findings1. 11% of term laboring patients have TS events;
2/3 no change in FHR or interventions2. 25% of patients with TS had unfavorable change in FHR
— FHR improved half the time without intervention— TS increased risk of OVD, NICU admission, composite adverse
neonatal morbidity by 30%
3. 2-3x TS events with any oxytocin; dose response correlation
KD Gregory 5/2014
What’s the Evidence? Is it Much Ado about Nothing?
� Gregory op ed…� There is evidence to suggest…it is much ado about something!� TS is associated with decrease in fetal oxygen saturation
� TS is associated with changes in FHR � TS occurs 10-40% of deliveries
— Oxytocin associated with TS, pervasive use
KD Gregory 5/2014
So what can we do about it?� At the bedside � Hydration� Position change
� Decrease oxytocin/turn oxytocin off� Tocolytic agent
KD Gregory 5/2014

8
So what can we do about it?� Simpson & Dotti AJOG 2008� TS-I: Interventions identified in 148/158 events� 6 decreased oxytocin by ½
— Mean time to resolution = 23 min� 35 stopped oxytocin (d/c oxy)
— Mean time to resolution = 14.2 min� 69 d/c oxy +IVF bolus
— Mean time to resolution = 9.8 min� 38 d/c oxy +IVF bolus+ lateral position
— Mean time to resolution = 6.1 min
KD Gregory 5/2014
So what can we do about it?� At the bedside / hospital / health system� Kunz et al
— “The objective is to integrate an increased awarene ss of uterine tachysystole with evidence-based practice in the titration of oxytocin”
� Gregory op ed…invite you to consider a QI project around dosing oxytocin to prevent tachysystole— 100% hand washing, perioperative ABx— 0 retained objects, surgical site infections— 0 tachysystole events… why not?
KD Gregory 5/2014
QI Program to Eradicate Tachysystole
�Acknowledgements� IHI�Summa Health System�Premier Inc�Ascension Health�Hospital Corporation of
America�Centura Health
KD Gregory 5/2014
Components of TS QI Program1. Rationale2. Multidisciplinary team3. Baseline data: Is TS a problem at your institution?
4. Develop consensus on protocol for oxytocin administration— Standardize (order sets/guidelines) so everyone doing the same thing— Borrow “physiologic dosing” protocol or “low dose” version— Safety checklist (aka “hard stop”)
5. Address team communication
6. Develop audit tool to tract TS events, and define accountability— MD; RN
7. Distribute results8. Refine processes, educate, repeat
KD Gregory 5/2014
9
Components of TS QI Program� Rationale
— Clinical evidence previously discussed— Liability concerns (Simpson & Knox MCN 2009;34:8-14)
� Inappropriate oxytocin use is one of the top 5 areas of preventable perinatal harm
� Oxytocin associated with 22% of claims involving neurologically impaired babies and 15% of claims involving stillbirth or neonatal death
� 50% of paid claims involve allegations of oxytocin misuse—Usually TS—fetal hypoxemia, acidemia, asphyxia
and subsequent brain damage
KD Gregory 5/2014
Components of TS QI Program� Rationale
— Clinical evidence previously discussed— Liability concerns
� FDA black box warning, 1998—Restrict to medically indicated inductions and
augmentations of labor and not used for elective inductions
� Institute for Safe Medication Practices—Oxytocin is a high alert medication, 2007—“heightened risk of causing significant harm if used
in error”
KD Gregory 5/2014
Components of TS QI Program� Rationale� Liability concerns
— “injudicious use of oxytocin” (increased rate despite nonreassuring FHR, or uterine TS) occurred in 68% of cases
— Most cases involving neonatal death or neurologically impaired infant, use of oxytocin decreased chance of successful defense� Hayes & Weinstein AJOG 2008,198:622.e1-622.e7.
KD Gregory 5/2014
Components of TS QI Program� Rationale (Simpson & Knox MCN 2009;34:8-14)� Complications from oxytocin use are commonly dose related� Often involve lack of timely recognition and appropriate
treatment of TS� IVF bolus administration of oxytocin (instead of LR) for FHR
changes or maternal hypotension� Inappropriate elective delivery <39 weeks� Goals of IV oxytocin “affect labor progress by stimulating
contractions of normal intensity, duration, and frequency, and to avoid tachysystole and its potential harmful sequelae. As with other high alert medications, the lowest dose possible to achieve the desired clinical effect should be used ”.
KD Gregory 5/2014

10
Components of TS QI Program� Rationale (Simpson & Knox MCN 2009;34:8-14)� Complications from oxytocin use are not limited to the fetus� Maternal risks include
— Pain— Abruption— Uterine rupture— Unnecessary CS for FHR patterns— Postpartum hemorrhage— Infection— hyponatremia
KD Gregory 5/2014
Components of TS QI Program2. Multidisciplinary team� Include senior management (administration, QI, nursing and
physician leadership)� Include key physician opinion leaders
— Plus recruit MD’s and nurses most likely to be antagonists or known to “push the pit”
— Include early in process—educate and see the evidence as it unfolds� Cooperative management instead of top down or
punitive
KD Gregory 5/2014
Components of TS QI Program3. Baseline data : Is TS a problem at your institution?� Sample a day or a week� Collect data on TS in 30 min increments (whole labor or some
specified time to include both active labor and pushing)� Collect data on FHR tracing, interventions (especially use of
tocolytic)� Collect data on maternal and neonatal outcomes� Collect data by provider (MD and RN)� Compare with normative data sited in literature or…set zero as
goal
KD Gregory 5/2014
Components of TS QI Program4. Develop consensus on protocol for oxytocin administration
— Standard concentration of oxytocin prepared by the pharmacy
— Standardize (order sets/guidelines) so everyone doing the same thing
— Borrow “physiologic dosing” protocol or “low dose” version� Start 1-2 mU/min and increase 1-2 mU/min every 30-60
min based on maternal fetal response
KD Gregory 5/2014

11
Components of TS QI Program4. Develop consensus on protocol for oxytocin administ ration
� Recall oxytocin physiology— Secreted in pulsatile fashion— ½ life of oxytocin 3-12 min; 3-5 ½ lives needed to get to
steady state; should see uterine response within 30-60 min after reaching steady state
— Infusion rate 4-6 mU/min=natural serum levels, spontaneous 1st stage� Hayes & Weinstein, AJOG 2008
KD Gregory 5/2014
Components of TS QI Program4. Develop consensus on protocol for oxytocin administ ration
� Recall oxytocin physiology— At steady state, oxytocin receptors are saturated and
unable to absorb any more; with increasing levels of exogenous oxytocin, the receptor sites become desensitized and are unable to initiate a contraction
—Phaneuf et al J Reprod Fertil 2000;120:91-97— Suggests high dose protocols saturate too quickly
without allowing steady state, and increased risk f or TS
KD Gregory 5/2014
Components of TS QI Program4. Develop consensus on protocol for oxytocin administ ration
� Hayes & Weinstein AJOG 2008 summarize various protocols for induction/augmentation
� Most studies found no difference or slightly longer labor times (1-2 hours) in low dose arm
� Lower cesarean rates in low dose arm (hmm…)� Less TS
KD Gregory 5/2014
Components of TS QI Program4. Develop consensus on protocol for oxytocin administ ration
— Safety checklist (aka “hard stop”)� Specify maximum dose (hard stop)
� Specify contraction frequency goal — (eg. goal of 3-4 contractions in 10 min window that is strong per
palpation or 60 mmHg with IUPC)
� Specify: do not increase oxytocin if adequate labor pattern with adequate cervical change (or stop oxytocin if active phase)
— If no cervical change, continue to increase if category 1 and noTS
� Specify treatment for TS as protocol/nursing practice
— Don’t need to call MD to do interventions— Intervene for TS, don’t wait for FHR changes
KD Gregory 5/2014
Clark et al AJOG 2008;Krening et al JPNN, 2011; Doyle et al JOGNN 2011

12
Components of TS QI Program� Example items for check list (to be reviewed every 15 or 30 min [specify])
KD Gregory 5/2014
Criteria Confirmed Time 1
ConfirmedTime 2…
FHR category 1 or or II with moderate variability 10 of previous 30 min
No more than one late decel in last 30 min
No more than 2 variable decels >60 sec or >60 bpm from baseline in previous 30 min
No more than 5 UC’s in 10 min/30 min
No 2 UC’s greater than 120 sec in 30 min
If IUPC: Mv units <300 mmHg and resting tone <25 mmHg
Clark et al AJOG 2007;197:480.e1-480.e5
Components of TS QI Program5. Address team communication� Team collaboration around goal of “zero TS”� Nurse at the bedside primarily responsible for oxytocin
administration; MD frequently offsite or multitasking� Clinical disagreements about how to manage oxytocin is
frustrating…Algorithm should defer to bedside clinician!
KD Gregory 5/2014
Components of TS QI Program6. Develop audit tool to tract TS events, and define a ccountability� Representative Examples� Was tachysystole present
� How long before intervention� Was protocol followed prior to oxytocin dosage change� Was appropriate interventions implemented within 30 min� If oxytocin stopped, was it restarted per protocol
— (less than 20 min by ½; >20 min, start over)
� RN ID� MD ID� Evidence of appropriate communication between care team� Was chain of command used
KD Gregory 5/2014
Components of TS QI Program7. Distribute results�Acknowledge success of RN/MD’s with zero TS
events�Develop threshold for peer review letter/nursing
performance review monitoring—Look for patterns, recurrent offenders
�Publish (visibly display) unit statistics
KD Gregory 5/2014

13
Components of TS QI Program8. Refine processes, educate, repeat� Re-educate outliers�Unit stats
—De-identify outliers
KD Gregory 5/2014
Can TS QI Program Work?
KD Gregory 5/2014
https://www.google.com/search?q=hamlet+original+book+cover
““one doth
protests too
much”
Successfully implementedMultiple hospitals & health systems
Can TS QI Program Work?
� Clark et al AJOG 2008; 199:105.e1-105.e7� Improved outcomes, fewer cesarean deliveries, and
reduced litigation: results of a new paradigm in pa tient safety
� Total quality improvement program� Team collaboration, communication, standardized protocols,
checklists, peer review� 220,000 deliveries, 120 hospitals, 21 states� Claims/10,000 births decreased from 10 to 6 from 1996-2006� CS rate decreased 24% to 21% 2005 to 2006
KD Gregory 5/2014
Can TS QI Program Work?
� Krening et al JPNN 2012;26:15-24� Oxytocin Administration: The transition to safer m odel of
care� Centura Health, Colorado, 9 hospitals� Initiated Perinatal Services Quality Review Team x system ‘07� Adapted HCA protocols for their institution which included
components of IHI induction/augmentation bundles— Checklist incorporated into EMR; completed q 30 min
� 2009, timeline for rollout x all hospitals
KD Gregory 5/2014
Krening et al JPNN 2012;26:15-24

14
0
2
4
6
8
10
12
Primip
Multip
0%
10%
20%
30%
40%
50%
60%
Hun
dred
s
Incidence of TS
Incidence ofTS
KD Gregory 5/2014
Duration of labor (hrs)
Objectives Met
� At the completion of this lecture, participants will be able to …� Describe (and be able to recognize) the different types of
tachysystole� Describe the maternal and neonatal clinical implications of
tachysystole� Describe various treatment options for tachysystole� Describe components of QI program to “cease and desist”
� No more “pitting through it”� No more “pit to distress”
KD Gregory 5/2014
Take Home Points…LESS IS MORE� Standardized protocol for dose adjustment (“low dose regimen”)� Check lists q ½ hr to confirm FHR ok, no evidence TS� Hold if FHR changes, TS, cervical change
� Bedside clinician (RN) rules� LESS IS MORE
� Labor may be longer…but� Less cesareans
� Less PPH� Less overall neonatal morbidity� Less Liability� LESS IS MORE!
KD Gregory 5/2014
Tachysystole…What’s next?
KD Gregory 5/2014
The horse is already out of the barn…
I predict…

15
Less is more OR enough is enough!
KD Gregory 5/2014
https://www.google.com/search?q=enough+is+enough
http://tutormentorconnection.ning.com/profiles/blog/list?user=2771il57rtuo5
KD Gregory 5/2014

6/7/2014
1
The Persistent Dilemma of Preterm Delivery
Leonardo Pereira MD, MCRAssociate Professor
Division of Maternal Fetal MedicineOregon Health & Science University
Overview
Preterm Birth
Prevalence
Etiology
Current Management ParadigmsPrevention
Therapeutics
Future strategiesPlacental targets
Treatment of IAI
Early vs. late PTB
Preterm BirthPrevalence: 11.5% 2012, reduction last 6 years450,000 births annually
Preterm Birth
Reductions across all ethnic categories

6/7/2014
2
Preterm Birth Preterm Birth
Prevalence: Globally 15 million infants per year
Preterm BirthEtiology
Births
(th
ousa
nds)
Group A - Normal DistributionGroup B – IAI/Pathology
Removed IAI from the OB distribution
Analyzed distribution of remaining births
Remaining births showed normal distribution
Preterm Birth

6/7/2014
3
Births
(th
ousa
nds)
Late Preterm Postterm
Preterm Birth
Late PTB and Posttermpregnancy are opposite ends of normal parturition spectrum
Preterm Birth
Etiology
Early PTB – always pathologic
Late PTB – normal distribution of labor onset, non-pathologic
Preterm Birth
Late PTB
35-37 weeks gestation
~8% of pregnancies; ¾ of all PTB
Growing population
Impact is increasing
Neonatal risks
Healthcare costs
Maternal risks
ALPS trial
Preterm Birth
Current Management Paradigms: Prevention
IM 17-OHP: prior PTB 20-34 weeks
Vaginal Progesterone: CL < 25 mm
Cerclage: prior mid trimester losses, dilated cervix
Pessary: multifetal gestations
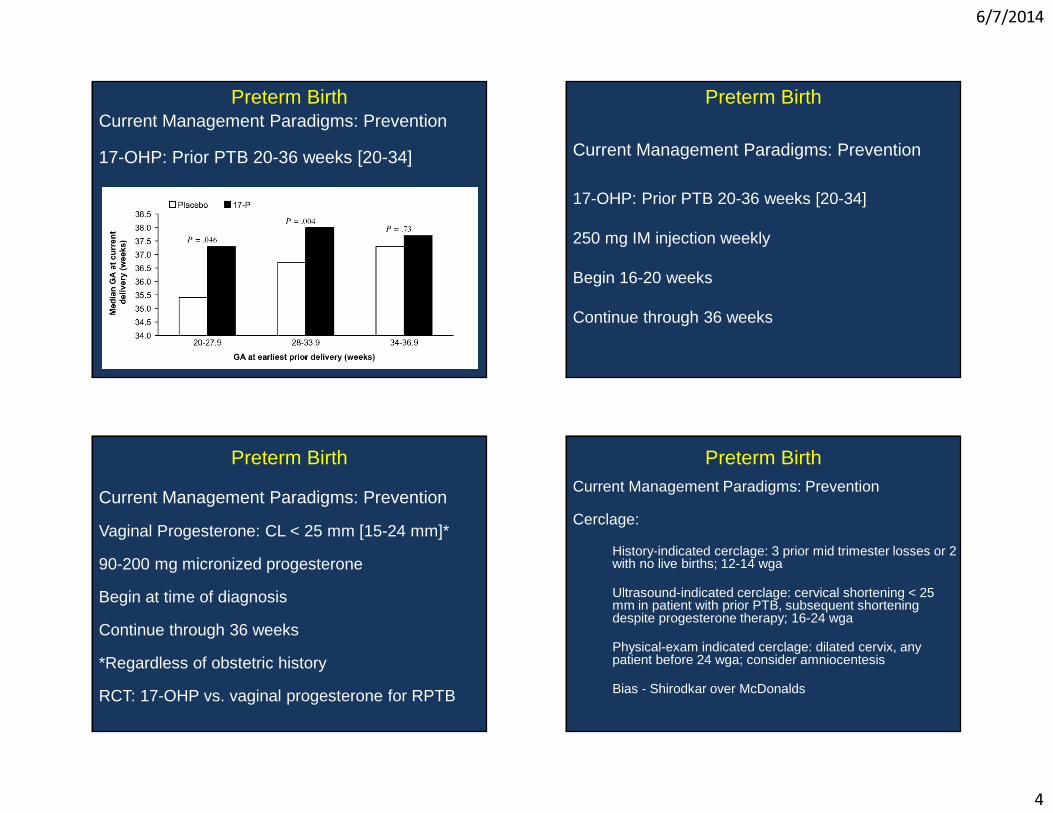
6/7/2014
4
Preterm BirthCurrent Management Paradigms: Prevention
17-OHP: Prior PTB 20-36 weeks [20-34]
Preterm Birth
Current Management Paradigms: Prevention
17-OHP: Prior PTB 20-36 weeks [20-34]
250 mg IM injection weekly
Begin 16-20 weeks
Continue through 36 weeks
Preterm Birth
Current Management Paradigms: Prevention
Vaginal Progesterone: CL < 25 mm [15-24 mm]*
90-200 mg micronized progesterone
Begin at time of diagnosis
Continue through 36 weeks
*Regardless of obstetric history
RCT: 17-OHP vs. vaginal progesterone for RPTB
Preterm BirthCurrent Management Paradigms: Prevention
Cerclage:
History-indicated cerclage: 3 prior mid trimester losses or 2 with no live births; 12-14 wga
Ultrasound-indicated cerclage: cervical shortening < 25 mm in patient with prior PTB, subsequent shortening despite progesterone therapy; 16-24 wga
Physical-exam indicated cerclage: dilated cervix, any patient before 24 wga; consider amniocentesis
Bias - Shirodkar over McDonalds

6/7/2014
5
Preterm Birth
Current Management Paradigms: Prevention
Pessary: multifetal gestations with premature cervical shortening
Not advocating for screening TVUS CL in multifetal gestations but if identified recommend pessary
Preterm BirthPrevention of
Ascending infection - ? role for probiotics
Modulation of inflammatory pathway signaling
Premature cervical changes
Modulation of actin cytoskeletal signaling
Preterm Birth Preterm Birth

6/7/2014
6
Preterm BirthCurrent Management Paradigms: Therapeutics
Tocolysis:
Indomethacin 24-28 weeks
MgSO4: 24-32 weeksCalcium channel blockers: 24-34 weeks
Oxytocin receptor antagonistsIndomethacin 24-28
Indomethacin 24-28
MgSO4 24-32
Ca Channel Blockers 24-34
Ca 32-34MgSO4 28-32
50-100 mg load, then 25 mg q 4-6 hrs PO/PR
6 gm load, then 2 gm/hr
10-20 mg PO q4-6 hrs
Preterm Birth
Current Management Paradigms: Therapeutics
Neuroprotection MgSO4: 24-32 weeksReduction in cerebral palsy
Protocol from NICHD trial recommended in the U.S.
Load 6 gm then 2 gm/hr continuous
If delivery not imminent in 12 hours the D/C
Restart when PTL restarts at 2 gm/hr
Repeat loading dose if > 6 hours from D/C
Preterm Birth
Future strategies
Placental targets
Treatment of IAI
Early/Late PTB
Preterm Birth
Placental targets
Functional MRI – placental modeling, flow, adaptation
Microbubble infusion – measure flow, delivery of therapeutic targets
Modulation of -
innate immune response
apoptosis
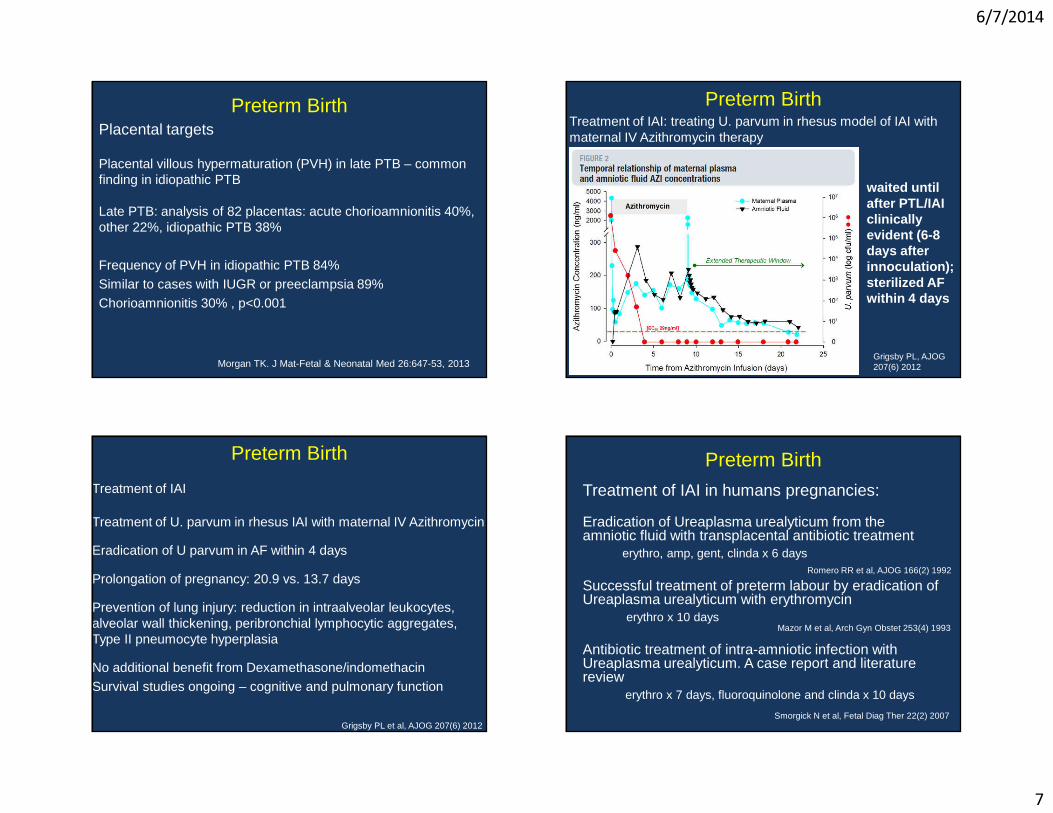
6/7/2014
7
Preterm BirthPlacental targets
Placental villous hypermaturation (PVH) in late PTB – common finding in idiopathic PTB
Late PTB: analysis of 82 placentas: acute chorioamnionitis 40%, other 22%, idiopathic PTB 38%
Frequency of PVH in idiopathic PTB 84%Similar to cases with IUGR or preeclampsia 89%Chorioamnionitis 30% , p<0.001
Morgan TK. J Mat-Fetal & Neonatal Med 26:647-53, 2013
Preterm BirthTreatment of IAI: treating U. parvum in rhesus model of IAI with maternal IV Azithromycin therapy
Grigsby PL, AJOG 207(6) 2012
waited until after PTL/IAI clinically evident (6-8 days after innoculation); sterilized AF within 4 days
Treatment of IAI
Treatment of U. parvum in rhesus IAI with maternal IV Azithromycin
Eradication of U parvum in AF within 4 days
Prolongation of pregnancy: 20.9 vs. 13.7 days
Prevention of lung injury: reduction in intraalveolar leukocytes, alveolar wall thickening, peribronchial lymphocytic aggregates, Type II pneumocyte hyperplasia
No additional benefit from Dexamethasone/indomethacinSurvival studies ongoing – cognitive and pulmonary function
Grigsby PL et al, AJOG 207(6) 2012
Preterm Birth Preterm Birth
Treatment of IAI in humans pregnancies:
Eradication of Ureaplasma urealyticum from the amniotic fluid with transplacental antibiotic treatment
erythro, amp, gent, clinda x 6 days
Successful treatment of preterm labour by eradication of Ureaplasma urealyticum with erythromycin
erythro x 10 days
Antibiotic treatment of intra-amniotic infection with Ureaplasma urealyticum. A case report and literature review
erythro x 7 days, fluoroquinolone and clinda x 10 days
Romero RR et al, AJOG 166(2) 1992
Smorgick N et al, Fetal Diag Ther 22(2) 2007
Mazor M et al, Arch Gyn Obstet 253(4) 1993

6/7/2014
8
Clinical treatment of IAI/PTL limited by
Lack of large well designed trials
Necessity to perform amniocentesis
Inability to determine chronicity of IAI
Preterm Birth
*Need for noninvasive markers or subclinical infection
Births
(th
ousa
nds)
Late Preterm Postterm
Late PTB and Posttermpregnancy are opposite ends of normal parturition spectrum
Preterm Birth
Proteins related to premature or failed initiation of labor
The concept is not novel in medicine:
Endocrinology Hematology (thyroid, diabetes) (platelets, clotting factors)
TSH Factor VIII
Hypothyroidism Graves Disease(hyperthyroidism)
Hemophilia Thrombophilia(stroke)
Preterm Birth Preterm Birth
Challenges of proteomics in late PTB
Findings on pooled samples may not apply to individual cases
Misidentification of proteins is possible
Cost and time of analysis
Need to reproduce findings/validate on separate, large cohorts

6/7/2014
9
Limitation – always get results
You may get the right answer, but are you asking the right question?
Need to ask the right question, in the right way
Importance of validation studies
Clouseau’s postulate
Preterm Birth
1
LEADING THE QUEST FOR HEALTH
Kimberly D. Gregory MD, MPHVice Chair Women’s Healthcare Quality & Performance improvement
Department Obstetrics & GynecologyCedars Sinai Medical CenterProfessor, David Geffen School of Medicine & UCLA School of Public Health
Nulliparous Term Singleton Vertex (NTSV): Is Healthy People 2020 Goal Possible?
KD Gregory 5/2014
Disclosures
�No financial disclosures
�No off-label use of medications
KD Gregory 5/2014
Objectives
�Participants will be able to —Discuss the different strategies for defining normal
and abnormal labor—Describe the risks associated with cesarean
delivery with an emphasis on nulliparous patients—Discuss potential interventions which may help
reduce the risk of having the ‘first’ cesarean delivery and impact the NTSV rate
KD Gregory 5/2014
Why is this important?�Cesarean delivery is the most commonly performed
surgical procedure in the United States�Approximately 1/3 of pregnancies are delivered via
cesarean� In 2010, 26.4% of low risk women underwent a
cesarean—Low risk = nulliparous, term, singleton, vertex
(NTSV)�Over 90% of women undergoing a primary cesarean
in the US will have a repeat cesarean
KD Gregory 5/2014

2
After the first cesarean…
�Maternal risk for complications increase� Intraoperative risks
—Hemorrhage—Injury to viscera
� Bowel� Bladder
—Adhesions
KD Gregory 5/2014
After the first cesarean…� Risks for abnormal placentation increase
— Previa— Accreta
— Increta— Percreta
� Risk of uterine rupture increases— Fetal/Maternal jeopardy
� With all of these, there is an increased risk for:
— Hysterectomy— Blood transfusion— Wound infection/breakdown— DVT
KD Gregory 5/2014
Summary
�The decision to undertake the first cesarean has profound implications on a woman’s future reproductive health
�Much of labor management in the US relies on information based on Friedman’s curves (1955)
�Some of these concepts have been challenged—Review of key concepts introduced throughout the
years regarding labor management
KD Gregory 5/2014
Let’s start with the 1950’s
KD Gregory 5/2014

3
Historical Background�Friedman curve 1955�500 patients
—Ages 13-42 (mostly 20-30)—SVD in 202 (40.4%)—Low forceps in 256 (51.2%)—Mid forceps in 19 (3.8%)—Cesarean delivery 9 (1.8%)
�Augmentation / induction—69 patients (13.8%) received pitocin
� 22 for ‘induction’� 47 for ‘stimulation’
KD Gregory 5/2014
Friedman Curve
� Focused on looking at rate of cervical dilation� Recorded all ‘rectal’ and ‘vaginal’ exams� Dilation plotted over time
� Noted features such as age, pelvis type, fetal presentation, fetal station
Individually plotted by hand!
KD Gregory 5/2014
Characteristic Mean Range StatMaximum
Latent phase (hr) 8.6 1.0-44 20.6
Active phase (hr) 4.9 0.8-34 11.7
Deceleration (hr) 0.9 0.0-14 3.3
Max slope (cm/hr) 3.0 0.4-12 6.8
First stage (hr) 13.3 2.0-58 28.5
Second stage (hr) 0.95 0.0-5.5 2.5
Friedman 1955
Friedman EA. Primagravid Labor: A graphostatistical Analysis. Obstet Gynecol 1955 (6): 567-89.
31 hrs14.3 hrs
95%tile
KD Gregory 5/2014
Friedman Curve – ‘Ideal Labor’
‘Primagravidas whose laborsprogressednormallywithoutIatrogenic tampering.’
Friedman EA. Primagravid Labor: A graphostatistical Analysis. Obstet Gynecol 1955 (6): 567-89.
KD Gregory 5/2014

4
Friedman Curve
� ‘Clinical Inertia’— 46 patients
� Average of 13 hours in latent phase� Average of 12.2 hours in active phase� Second stage was 1.6 hours� Maximum slope was 1.4 cm / hr
— Primary inertia � 21 patients (46%)
— Secondary inertia � 20 patients (43%)
— Reasons:� Excessive medication (46%)� CPD (28%)� Occiput posterior (28%)� Caudal Anesthesia (22%)� Unknown
These people didn’t fit his curves!
KD Gregory 5/2014
On to the 1970’s…
KD Gregory 5/2014
Alternate Ways to Monitor Labor Progress
�Philpott and Castle (1972)
—Cervicograph
� Composed of alert and action lines plotted against time (hours)
—Partograph
KD Gregory 5/2014
Cervicograph
�Founded on Friedman’s work— Low resource conditions— Starts at 3 cm— Alert: close observation— Action: augment/transfer
Philpott & Castle, J Ob Gyn Brit Comm 1972
KD Gregory 5/2014

5
On to the 1990s….
KD Gregory 5/2014
WHO Partograph
�Definition of “active phase”— Shift from “rate of
change” (slope) to specific cm
— 3 cm
KD Gregory 5/2014
Active Phase Labor Arrest
�Rouse et al (1999)
—Prospectively studied a labor-management protocol which mandated at least 4 hours of oxytocin prior to cesarean delivery for active phase arrest
KD Gregory 5/2014
Active Phase Arrest�Term, gravid patients�Spontaneous labor�Active phase arrest
—4 cm dilated —< 1 cm in 2 hours of cervical change
�Excluded:—Malpresentation, prior cesarean deliveries, multiple
gestation, and nonreassuring fetal heart tracings (NRFHT)
KD Gregory 5/2014

6
Active Phase Arrest
�After the diagnosis of active phase arrest, oxytocin was initiated to achieve >200 Mv Units (IUPC)
�Cesarean delivery not performed until 4 hours with adequate MVU—Or a minimum of 6 hours
(if adequacy not achieved)
KD Gregory 5/2014
Active Phase Arrest
Rouse DJ et al. Failed Labor Induction. Obstet Gynecol2011 (117): 267-72. (modified)
Vaginal delivery and infection rate based on laborprogress and time after active phase arrest
KD Gregory 5/2014
Rouse’s Take Home Point: A little more time…
� 2 hours may not be enough time for some women to progress in labor
� A minimum of 4 hours of oxytocin-augmented labor (adequate Mv units) should be allowed
� For women who do not achieve adequate mvu, a minimum of 6 hours of augmentation should be allowed for these patients
KD Gregory 5/2014
Into the 21 st century…
KD Gregory 5/2014

7
REASSESSMENT OF THE FRIEDMAN CURVE (2002)
Zhang J, Troendle JF, Yancey MK. Reassessing the labor curve in nulliparous women. Am J Obstet Gynecol 2002 (187): 824-8.
KD Gregory 5/2014
Reassessing Friedman in the 21 st century
Zhang J, Troendle JF, Yancey MK. Reassessing the labor curve in nulliparous women. Am J Obstet Gynecol 2002 (187): 824-8. (modified)
Comparison of Friedman and Zhang Labor Curves
Study populations
KD Gregory 5/2014
Zhang J, Troendle JF, Yancey MK. Reassessing the labor curve in nulliparous women. Am J Obstet Gynecol 2002 (187): 824-8. (modified
5 cm
Labor Duration (hrs)
Cer
vix
(cm
)
Rate of change based on cervix exam
KD Gregory 5/2014
Zhang Conclusions
�Labor progress may be more gradual than originally thought (especially for nulliparous patients)
�Women may enter active labor between 3-5 cm dilation
�Even the course of the active phase of labor will vary from person to person—May result in a flatter curve
�Friedman’s curve likely represents an individual patient with an ‘ideal’ curve
KD Gregory 5/2014

8
Recap
�Friedman focused on individual progress, defined active labor based on maximum slope rate of change
� Latent phase could be a long time�Philpott & Castle, WHO started curves at 3 cm;
ignored latent phase and/or early labor�Zhang nulliparous slower, mimics Friedman after
active phase; rate of change occurs around 5 cm—Similar population as Friedman; more
contemporaneous cohort—Data started at 3 cm
KD Gregory 5/2014
Safe Labor
�Consortium for Safe Labor*� Large multicenter study�Contemporary women in spontaneous labor undergoing
the ‘usual’ care may:— Take 6 hours to change from 4-5 cm— Take more than 3 hours to change from 5-6 cm— After that point, labor curve is steeper
�Redefine the starting point of active labor from 4 cm to 6 cm
�Does this mean that Friedman’s results are wrong?
*includes patients from CSMC (2002-2008)
KD Gregory 5/2014
Demographics
Safe Labor Consortium 2002-2008
Diverse pop
KD Gregory 5/2014
Zhang et al. Contemp Labor Patterns Obstet Gynecol 2010
Cervical Exam on Admission
95%tile of cumulative duration of spontaneous labor from admission to vaginal delivery
KD Gregory 5/2014

9
Zhang et al. Contemp Labor Patterns. Obstet Gynecol 2010 (modified)
Duration of Labor Based on Exam on Admission
Median (95%tile)
KD Gregory 5/2014
Duration of Labor by Method of Onset
After “active phase” (6 cm) doesn’t matter, all “clinically” the same
“ 6 is the new 4”
KD Gregory 5/2014
Duration of Labor by Method of Onset, Parity
InductionMultipsNullips
SpontaneousMultipsNullips
KD Gregory 5/2014
Implications
� If the definition of active labor is shifted to 6 cm
—many cesarean deliveries performed prior to that point would be considered “latent phase cesareans”
�Arrest of labor diagnosis prior to 6 cm of cervical dilation needs to be considered carefully—Zhang et al
KD Gregory 5/2014

10
58 years later…the discussion about labor continues…Why is this so important?
KD Gregory 5/2014
US Cesarean Rate On the Rise
� US cesarean delivery rate has risen from 6% to approximately 33% between the mid 1950s until now— Based on 2007 data, nearly 27% of low-risk women had a
primary cesarean� Some hospitals have cesarean delivery rates in excess of 50%� Hospitals with lower cesarean delivery rates of 15-20% have
similar outcomes — (high rate has no demonstrated benefit to mother or baby)
KD Gregory 5/2014
NSTV�Cesarean delivery rate for low-risk, nulliparous
women�NSTV = nulliparous, term, singleton, vertex�Portion of cesarean births which has the most
variation — Practitioners— Hospitals— Geographic region
�QI mantra: where there is variation, there is opportunity for improvement
KD Gregory 5/2014
Why are we interested?�Cesarean delivery has profound effects on a
patient’s reproductive life
�Nulliparous women have 4-10 fold increase risk of cesarean deliveries compared to multiparous women
�At least two obstetric practices have been identified which have significant impact on the labor of nulliparous patients:—Induction of labor —Early labor admission
KD Gregory 5/2014

11
What changed between then (50 years ago) and now?
Then Now
KD Gregory 5/2014
Maternal Characteristics
Laughon SK et al. Changes in labor patterns over 50 years. Am J Obstet Gynecol 2012 (206): 419.e1-9. (modified)
Then Now
KD Gregory 5/2014
Labor Characteristics
Laughon SK et al. Changes in labor patterns over 50 years. Am J Obstet Gynecol 2012 (206): 419.e1-9. (modified)
Then Now Difference P value
KD Gregory 5/2014
All things considered, What now?
KD Gregory 5/2014
12
Hmmm…
�OMG…after all this time, is Friedman wrong?
�Given how long “normal” labor can be, are there guidelines to help us correct or reverse the rising cesarean trend—specifically as it relates to NTSV rate?
KD Gregory 5/2014
Characteristics of Labor in NTSV Women Using Different Clinical Models
� SMFM Abstract: Lau G, Gornbein J, El Ibrahim S, Kilpatrick S, Gregory KD.� Characteristics of labor in NTSV women using different clinical models
� The objectives of the study— Null Hypothesis: For NTSV patients, spontaneous labor,
there is no difference between Friedman’s curve and Zhang’s curve� Friedman focused on maximum slope as onset of
active labor� Zhang implied longer time latent phase (6 cm active
labor)
KD Gregory 5/2014
Methods
�Retrospective chart review, CSMC �September 1, 2011- August 30, 2012�Cohort of women; NTSV�Demographics/ Clinical variables
KD Gregory 5/2014
Methods
�Primary Outcome: —Labor curve for NTSV women, spontaneous labor,
vaginal deliveries� Friedman� Zhang et al (CSL)� Lau et al (best fit model derived by statistician
described as “% change”)
KD Gregory 5/2014

13
Demographics of the Spontaneous Labor Group
N=551 Mean
Age(years) 32.1 + 5.2
BMI (admission) 27.8 + 8.6
Bishop 9.9 + 2.3
Gestational Age (weeks) 39.6 + 1.0
Cervical Dilation on admission (cm)
4.5 + 2.5
Cervical Effacement onadmission (%)
85.9 + 5.1
Birthweight (grams) 3306.7 + 6.2
6,500 deliveries at CSMC 2561 NTSV; 551 women in spontaneous labor
KD Gregory 5/2014
Comparison of the three models
Zhang
0.0
2.0
4.0
6.0
8.0
10.0
12.0
8 9 10 11 12 13 14 15 16 17 18 19 20
cervi
cal d
ilatio
n (cm
)
hours from average start of labor
cervical dilation vs average hours from labor start90th, median & 10th dilation percentiles
FriedmanPct chg
ZhangFriedman% change
KD Gregory 5/2014
Comparison of the three models
KD Gregory 5/2014
Model Fit Statistics
Friedman Zhang Percent Chg
R2 59.6 59.1 59.6
Root mean square
2.05 2.07 2.03
Essentially, the models are not all that different
KD Gregory 5/2014

14
Conclusions
�Findings support the null hypothesis�No difference between Friedman or Zhang or our %
change model�Agree with Zhang
—need to re-conceptualize how “long” is “normal labor ”
—how “long” it can take to change 1 cm� depending on exam on admission
KD Gregory 5/2014
�Statistical curves designed to “fit” the data�Very similar, lots of overlap�Make some management suggestions
—Wait longer—Admit later
KD Gregory 5/2014
Examining indications for Primary Cesarean Delivery
Zhang J, et al Contemporary cesarean delivery practice in the United States. Am J Obstet Gynecol 2010 (203):326.e1-10.
KD Gregory 5/2014
How low can we go?
�Spong et al. Obstet Gynecol 2012 (120): 1181-93.� “Preventing the first cesarean delivery”
—Workshop held jointly by NICHD and ACOG in 2012
KD Gregory 5/2014

15
How low can we go?
�Dramatic rise in cesarean deliveries since 1995—Attributable mostly to an increase in primary cesarean
deliveries
�Prompted a review of the available information regarding factors leading to the first cesarean delivery
KD Gregory 5/2014
Labor Management
�Antepartum and intrapartum management decisions have a profound effect on the patient’s likelihood of cesarean delivery
�Diagnosis of failed induction and arrest disorders
KD Gregory 5/2014
Labor Management
�Definition of Failed Induction of Labor�Failure to generate regular contractions (every 3 min)
AND cervical change after at least 24 hours of oxytocin WITH artificial rupture of membranes (if feasible)
Spong et al Obstet Gynecol 2012
KD Gregory 5/2014
Labor Management
�Definition of First Stage Arrest� 6 cm or greater WITH membrane rupture and no
cervical change fora) 4 hr or more with adequate contractions (>200
Mv units)b) 6 hr or more if inadequate contractions
Spong et al Obstet Gynecol 2012
KD Gregory 5/2014

16
Labor Management
�Definition of Second Stage Arrest�No progress (descent OR rotation ) for
a) Nullips: � 4 hrs or more with epidural� 3 hrs or more without epidural
b) Multips:� 3 hrs or more with epidural� 2 hrs or more without epidural
Spong et al Obstet Gynecol 2012
KD Gregory 5/2014
Other Factors
�Patient and physician attitudes and perceptions—Cesarean delivery is relatively safe—Committee recommended discussion of the short-
term and long-term risks as well as benefits of cesarean vs vaginal delivery
KD Gregory 5/2014
Risk of Adverse Maternal and Neonatal Outcomes by Mode of Delivery
Outcome Risk
Maternal Vaginal Delivery Cesarean Delivery
Overall severe morbidity and mortality
0.9% 2.7%
Maternal mortality 3.6:100,000 13.3:100,00
Placental abnormalities Increased with prior cesarean delivery versus vaginal delivery, and risk continues to increasewith each subsequent cesarean delivery
Neonatal
Laceration NA 1.0-2.0%
Respiratory morbidity <1.0% 1.0-4.0% (without labor)
Gregory et al, 2011
KD Gregory 5/2014
Other Factors
�Committee recommended monitoring and providing physician level feedback regarding non-indicated primary cesarean deliveries
KD Gregory 5/2014
17
Labor Management Styles
� Wide variation in cesarean rates among providers likely due to diverse management styles
� EX: Admission in latent labor (cervix < 3 cm dilated)— Early admission itself increases the risk for cesarean — Women requiring earlier admission have an increased risk
of abnormal labor— Early admission may give the impression of a long,
protracted course, and need to “do something”� Recall: Normal labor can be 31 hours
KD Gregory 5/2014
Induction of Labor
� Likelihood of a vaginal delivery is lower after labor induction compared to spontaneous labor—Nulliparous patients—Unfavorable cervix
�Committee recommended to avoid labor induction with an unfavorable cervix unless there is a clear maternal or fetal indication for delivery
KD Gregory 5/2014
Induction of Labor
�Committee recommended allow adequate time to enter into or progress in labor
�Prudent use of labor induction�Use of well-defined criteria should be met prior to
cesarean delivery—Failure of induction—Failure to progress
KD Gregory 5/2014
Primary Cesarean Rates—How Low Can We Go?
�Objective:—Describe the potential reduction in the NTSV
cesarean rate in our own population if we applied the principles outlined in Spong et al.
Lau GW, El Ibrahim S, Li G, Kilpatrick S, Gregory KDUnpublished data
KD Gregory 5/2014
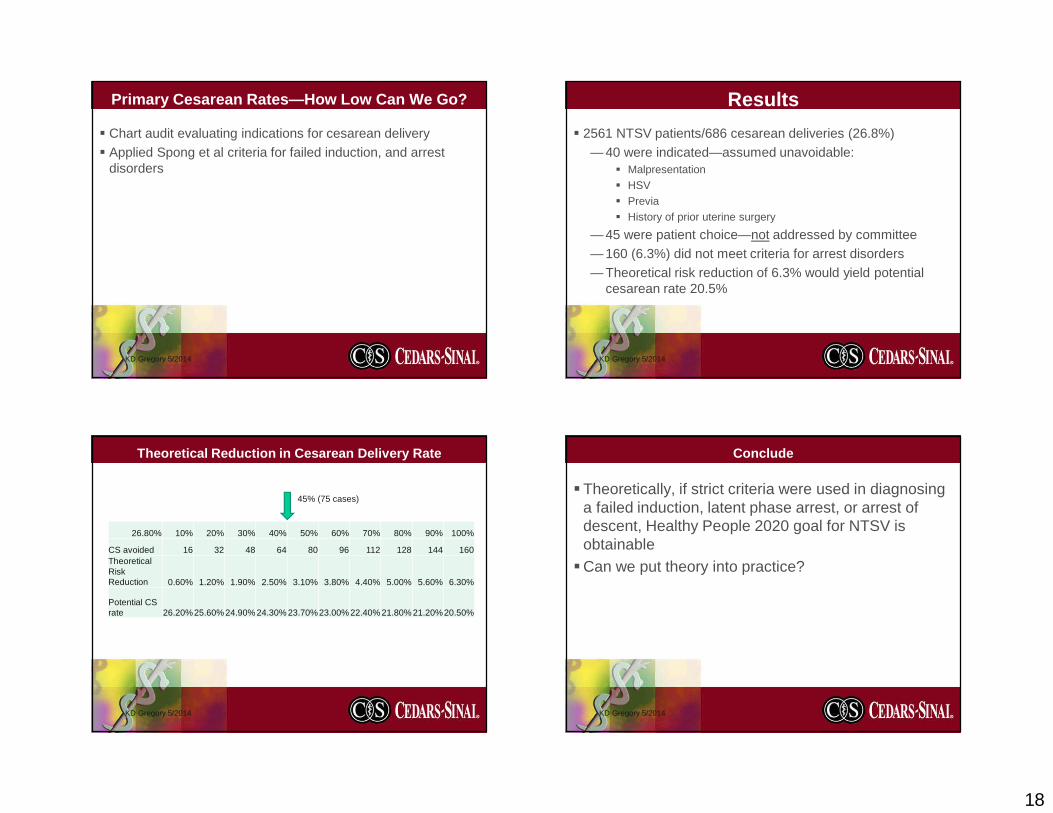
18
Primary Cesarean Rates—How Low Can We Go?
� Chart audit evaluating indications for cesarean delivery� Applied Spong et al criteria for failed induction, and arrest
disorders
KD Gregory 5/2014
Results
� 2561 NTSV patients/686 cesarean deliveries (26.8%)— 40 were indicated—assumed unavoidable:
� Malpresentation� HSV� Previa� History of prior uterine surgery
— 45 were patient choice—not addressed by committee— 160 (6.3%) did not meet criteria for arrest disorders— Theoretical risk reduction of 6.3% would yield potential
cesarean rate 20.5%
KD Gregory 5/2014
Theoretical Reduction in Cesarean Delivery Rate
26.80% 10% 20% 30% 40% 50% 60% 70% 80% 90% 100%
CS avoided 16 32 48 64 80 96 112 128 144 160Theoretical Risk Reduction 0.60% 1.20% 1.90% 2.50% 3.10% 3.80% 4.40% 5.00% 5.60% 6.30%
Potential CS rate 26.20%25.60% 24.90% 24.30% 23.70%23.00% 22.40% 21.80% 21.20%20.50%
45% (75 cases)
KD Gregory 5/2014
Conclude
�Theoretically, if strict criteria were used in diagnosing a failed induction, latent phase arrest, or arrest of descent, Healthy People 2020 goal for NTSV is obtainable
�Can we put theory into practice?
KD Gregory 5/2014

19
Healthy People Goal 2020:� 2000
— Healthy people work group NTSV goal 12 percent� 2010
— When it was clear these goals would not be met, ACOG task force adopted the 25th percentile for primary cesarean section rate as its goal: 15.5 %
� Healthy people goal 2020: MICH-7.1— Reduce cesarean births among low-risk women with no prior
cesarean births— Goal to reduce the rate by 10%— Goal NTSV rate of 23.9%
KD Gregory 5/2014
CMQCC: Median Cesarean Rate by Region 2011
KD Gregory 5/2014
Nulliparous Term Singleton Vertex CesareanGoal: Reduce NTSV rate to 30%
Nulliparous Term Singleton Vertex Cesarean Rate
MetricFY1
4Goal
Jul Aug Sept Oct Nov Dec Jan Feb Mar Apr
% of NTSV women having cesarean
sections30.6 32.5 26.9 27.2 27.0 28.5 26.8 26.7 22.1 23.4 27.2
FY14 Avg. Jul 2013 – . Apr. 2014 rate is 26.8%
36.0% 36.0%
32.3% 33.6%
30.0%
26.7%
22.1% 23.4%
27.2%
0.0%
5.0%
10.0%
15.0%
20.0%
25.0%
30.0%
35.0%
40.0%
2009 2010 2011 2012 2013* Jan-14 Feb-14 Mar-14 Apr-14
CSMC FY14 Goal (30.6%) HP 2020 Goal (23.8%)

20
Progress to-date: PDSA Cycles
Cycle SummaryCycle 1) - Macrosomia Birth weight used to confirm macrosomia as an indication. We found an
acceptable range of error (10-15%) between estimate and actual birth weight.
Cycle 2) - Failed induction Audit of 40 charts revealed 50% of patients being induced underwent a cesarean before meeting criteria for active labor (>4cm dilated).
Cycle 3) - Required Bishop score for induction
18 months of data revealed patients met criteria (physician reported exam consistent with exam on admission)
Cycle 4) - Fetal distress 76/160 charts identified as Category II or III. Reviewers agreed a cesarean was indicated 36/76 cases (47.4%); 14/36 (38.9%) there was an opportunity to alter the outcome.
Cycle 5) - Arrest of dilatation
chart audit revealed an opportunity for improvement in 70% of cases (33/47) where cesarean occurred < 6 cm
Cycle 6) - Spontaneous vs. induced labor
patients who present in spontaneous labor have a shorter labor curve. Physicians should perform fewer inductions and better patient education about what to expect in labor.
Cycle 7) - Patient education
The taskforce identified a gap in patient education information and developed tailored brochures encouraging patients to await spontaneous labor.
Cycle 8) - MD Specific cesarean rates
reports developed and distributed comparing institutional rate with individual physician rates.
Lessons Learned
� Importance of multidisciplinary team, senior management leadership; key physician opinion leaders
� Multifactorial, multi-prong approach
� Maintaining team interest and enthusiasm easier when actively engaged in a “cycle”� Harder to maintain re: sustainability
� Clinical judgment will always play an important role
� Must account for patient specific situations
� Need to improve physician and nursing documentation
� EMR is not a database
Next Steps:
� Continue MD reports biannually� Get educational materials approved
� Labor & Childbirth (aka When to come to the hospital)� Risks and Benefits of Cesarean Delivery
� Data analysis on “6 is the new 4”� Repeat cycle (how well are we doing?)
� Focus: Induction of labor on women with low bishop scores� Look at opportunities for outpatient cervical ripening
� Look at increasing the CSMC VBAC rate� Standardize oxytocin and reduce tachysystole
Closing remarks
� Trend of increasing cesarean deliveries in low risk NTSV patients is concerning
� Concerted active effort, reversible� Big Brother is watching…Consumer Reports (May 2014)� “C-section rates among the hospitals we looked at ranged from a low of 4
percent to a high of 57 percent. ..Read our article on unnecessary C-sections (go to www.consumerreports.org/ cro/csections0514.htm) and our technical report on how we rate hospitals (go to www.consumerreports.org/howweratehospitals)”
KD Gregory 5/2014

21
Closing remarks� Significant decreases in the NTSV cesarean rates may be
possible with critical evaluation of the management of labor— Re-evaluating our assessment of the progression of labor:
� Friedman Curve (1950s)� The partographs (Philpot and Castle, WHO) (1970s-
1990s)� Zhang (2000s)� Regardless of the curve, normal labor can take a long
time!� Readjust patient and provider expectations
— One size does not fit all; Individualized labor curves
KD Gregory 5/2014
Closing Remarks� Re-evaluation of the management of labor in NTSV patients:
— Reducing elective inductions with an unfavorable cervix— Reducing admissions in early/latent labor
— Applying strict criteria in the diagnosis of the following:� Failed induction� Latent phase arrest disorders� Active phase arrest disorders� Arrest of descent
� Patient and provider attitudes and expectations— about the length of labor— And avoid primary elective cesarean deliveries
KD Gregory 5/2014
Ultimate weapon to reduce cesarean delivery…
Motherhood madea man out of me …
KD Gregory 5/2014
Thank You!
Questions?
KD Gregory 5/2014

22
References
� Friedman EA. Primagravid Labor. Obstet Gynecol 1955 (6): 567-89.� Bailit J, Garrett J. Comparison of risk-adjustment methodologies for cesarean delivery rates. Obstet Gynecol 2003; 102:45-51.� Vrouenraets FP, Roumen FJ, Dehing CJ, van den Akker ES, Aarts MJ, Scheve EJ. Bishop score and risk of cesarean delivery after induction of labor in
nulliparous women. Obstet Gynecol 2005; 105: 690-7.� Vahratian A, Zhang J, Troendle JF, Sciscione AC, Hoffman MK. Labor progression and risk of cesarean delivery in electively induced nulliparas. Obstet
Gynecol 2005; 105: 698-704.� Lee L, Hitti J. Is there and association between early labor admission and the risk of cesarean section for dystocia in low risk, nulliparous women? Am J
Obstet Gynecol 2002; 187: S134.� Bailit JL, Dierker L, Blanchard MH, Mercer BM. Outcomes of women presenting in active versus latent phase of spontaneous labor. Obstet Gynecol
2005; 105: 77-9.� Harper LM, Caughey AB, Odibo AO, Roehl KA, Zhao Q, Cahill AG. Normal Progress of Induced Labor. Obstet Gynecol 2012 (119): 1113-8.� Rouse DJ, Weiner SJ, Bloom SL, Varner MW, Spong CY, Ramin SM, Casitis SN, Grobman WA, Sorokin Y, Sciscione A, Carpenter MW, Mercer BM, et
al. Failed Labor Induction. Obstet Gynecol 2011 (117): 267-72.� Gould J, Danielson B, Korst L, Phibbs R, Chance K, Main EK, Wirtschafter D, Stevenson D. Cesarean Delivery Rate and Neonatal Morbidity in a Low-
Risk Population. Obstet Gynecol 2004 (104): 11-19.� Lange AP, Secher NJ, Westergaard JG, Skovgard IB. Prelabor Evaluation of Inducibility. Obstet Gynecol 1982 (60):137-47.� Laughon SK, Zhang J, Grewal J, Sundaram R, Beaver J, Reddy U. Induction of labor in a contemporary obstetric cohort. Am J Obstet Gynecol 2012
(206): 486.31-9� Laughon SK, Branch DW, Beaver J, Zhang J. Changes in labor patterns over 50 years. Am J Obstet Gynecol 2012 (206): 419.e1-9.� Zhang J, Troendle JF, Yancey MK. Reassessing the labor curve in nulliparous women. Am J Obstet Gynecol 2002 (187): 824-8. � Spong CY, Berghella V, Wenstrom KD, Mercer BM, Saade GR. Preventing the First Cesarean Delivery. Obstet Gynecol 2012 (120): 1181-1193. � Neal JL, Lowe NK, Patrick TE, Cabbage LA, Corwin EJ. What is the Slowest-Yet-Normal Cervical Dilation Rate Among Nulliparous Women with
Spontaneous Labor Onset? JOGNN 2010 (39): 361-9.� World Health Organization. World Health Organization partograph in management of labour. Lancet 1994 (343): 1399-404.� Philpott RH and Castle WM. Cervicographs in the management of labour in Primigravidae: I. The Alert Line for Detecting Abnormal Labour. . J Obstet
Gynaecol Br Cwlth. 1972 (79): 592-598.� Philpott RH and Castle WM. Cervicographs in the management of labour in Primigravidae: II. The Action Line and Treatment of Abnormal Labour. . J
Obstet Gynaecol Br Cwlth. 1972 (79): 599-602.� Zhang J, Troendle J, Mikolajczyk R, Sundaram R, Beaver J, and Fraser W. The Natural History of the Normal First of Labor. Obstet Gynecol 2010
(115)): 705-10.
KD Gregory 5/2014

6/7/2014
1
Patient Expectations and Preferences
aka “The Birth Plan”
Kathryn Houston MDAssistant Professor
Department Obstetrics, Gynecology and Reproductive Science
UCSF
Patient Expectations and Preferencesaka “The Birth Plan”
No conflicts of interest to report
Objectives�History of birth plans�Common preferences� Effect on outcomes� Birth plan management
Patient Expectations and Preferencesaka “The Birth Plan”
Birth Plan� Google - 314 million hits� Pubmed – 29 citations
Birth Preferences� Google - 423 million hits� Pubmed- 7 citations
Patient Expectations and Preferencesaka “The Birth Plan”
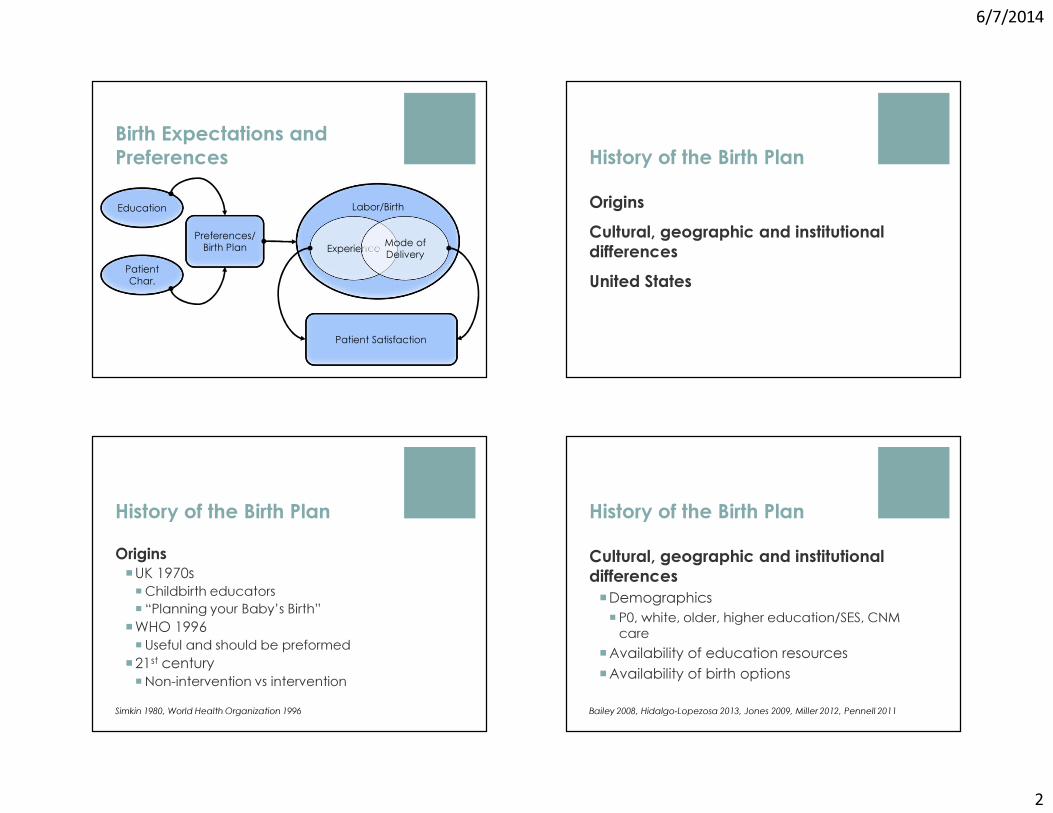
6/7/2014
2
Birth Expectations and PreferencesEducation
Patient Char.
Patient Satisfaction
Preferences/Birth Plan
Labor/Birth
Experience Mode of Delivery
History of the Birth PlanOriginsCultural, geographic and institutional differencesUnited States
History of the Birth PlanOrigins�UK 1970s �Childbirth educators� “Planning your Baby’s Birth”
�WHO 1996�Useful and should be preformed
�21st century�Non-intervention vs intervention
Simkin 1980, World Health Organization 1996
History of the Birth PlanCultural, geographic and institutional differences�Demographics� P0, white, older, higher education/SES, CNM care
�Availability of education resources�Availability of birth options
Bailey 2008, Hidalgo-Lopezosa 2013, Jones 2009, Miller 2012, Pennell 2011

6/7/2014
3
History of the Birth PlanUnited States�Childbirth education�ACOG & AA pediatrics �Cochrane Review
�Healthy People 2010 goal� Increase participation in childbirth classes
� Practice models�More physician/hospital based
American Academy of Pediatrics-The American College of Obstetricians and Gynecologists 2007, Gagnon 2007, Healthy People 2010
What is a Birth Plan?
“A birth plan is an approach to labor, rather than a term for a specific kind of outcome”
� Written or philosophical� Evolves from patients values, desires and concerns of the
birth process� Facilitates communication between patient and provider
� Discussion Birth Plan vs. Hospital Birth Plan
Wagner & Gunning 2006, Kaufman 2007
Common Birth Plan ThemesLogistics
�Venue�Provider�Interventions
�Pain control�Mode of delivery�Infant care
Common Birth Plan ThemesDomains
�CONTROL�Autonomy� Safety� Shared decision making
� Respect� Knowledge

6/7/2014
4
Do preferences affect outcomes?
Provider and patient perceptionsPreferences vs. written birth plan
Do preferences affect outcomes?
Provider and patient perceptions�Wide variation�Worse outcomes - 65% vs 2.4%� Increased CS rates – 66% vs 9%
Expectations�False sense of control�Professional pressure
Grant 2010, Lundgren 2003, Welsh 2013
Do preferences affect outcomes?
Preferences vs. written birth plan�Mixed results�No RCTs�Useful vs no difference� Intapartum care, control
�More critical of provider
Brown 1998, Kuo 2010 Lundgren 2003, Sato 2011, Whitford 1998
Do preferences affect outcomes?
Maternal� Labor interventions� Pain control�Mode of delivery
Neonatal� APGARS� Cord gases
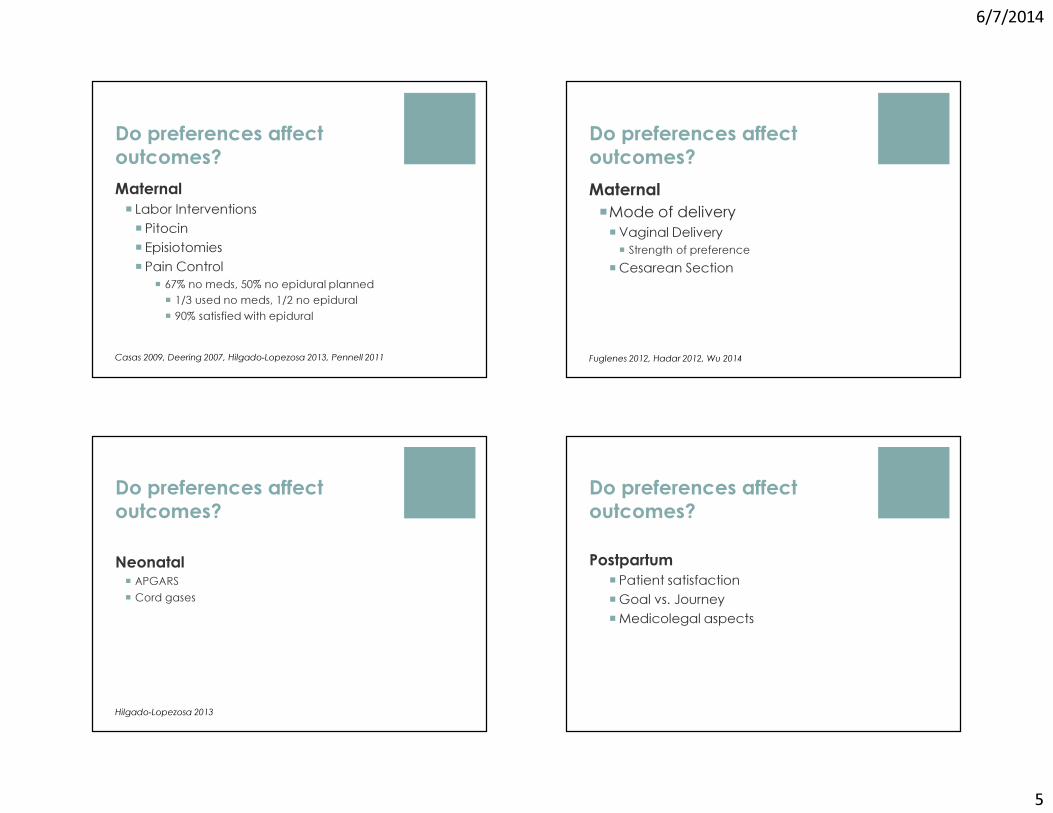
6/7/2014
5
Do preferences affect outcomes?Maternal� Labor Interventions� Pitocin� Episiotomies� Pain Control
� 67% no meds, 50% no epidural planned� 1/3 used no meds, 1/2 no epidural� 90% satisfied with epidural
Casas 2009, Deering 2007, Hilgado-Lopezosa 2013, Pennell 2011
Do preferences affect outcomes?Maternal �Mode of delivery�Vaginal Delivery� Strength of preference
�Cesarean Section
Fuglenes 2012, Hadar 2012, Wu 2014
Do preferences affect outcomes?
Neonatal� APGARS� Cord gases
Hilgado-Lopezosa 2013
Do preferences affect outcomes?Postpartum
� Patient satisfaction�Goal vs. Journey�Medicolegal aspects

6/7/2014
6
Do preferences affect outcomes?Postpartum
�Patient satisfaction� Personal Expectations� Provider support� Provider-patient relationship� Involvement in decision making
Hodnett 2002
Do preferences affect outcomes?Postpartum�Goal vs. Journey�Healthy Mom & Baby�“The perfect birth”�Long term effects�Depression & mode of delivery
Rauh 2012, Sword 2011, Uplong 2006
Do preferences affect outcomes?Postpartum
�Medicolegal aspects�Living will for obstetrics� Provides structured discussion� Reduce conflict/misunderstandings� Address risk� Documentation
�May reduce litigation
Philepsen 2005, Richards 1999
Managing the birth planAdvantages/disadvantages� Patient care/satisfaction� Lots of TIME
Provider vs. patient perspective�Distrust vs. collaboration� Evidenced based practice
Institutional constraints�Hospital policy vs. hospital routine
Epstein 2004
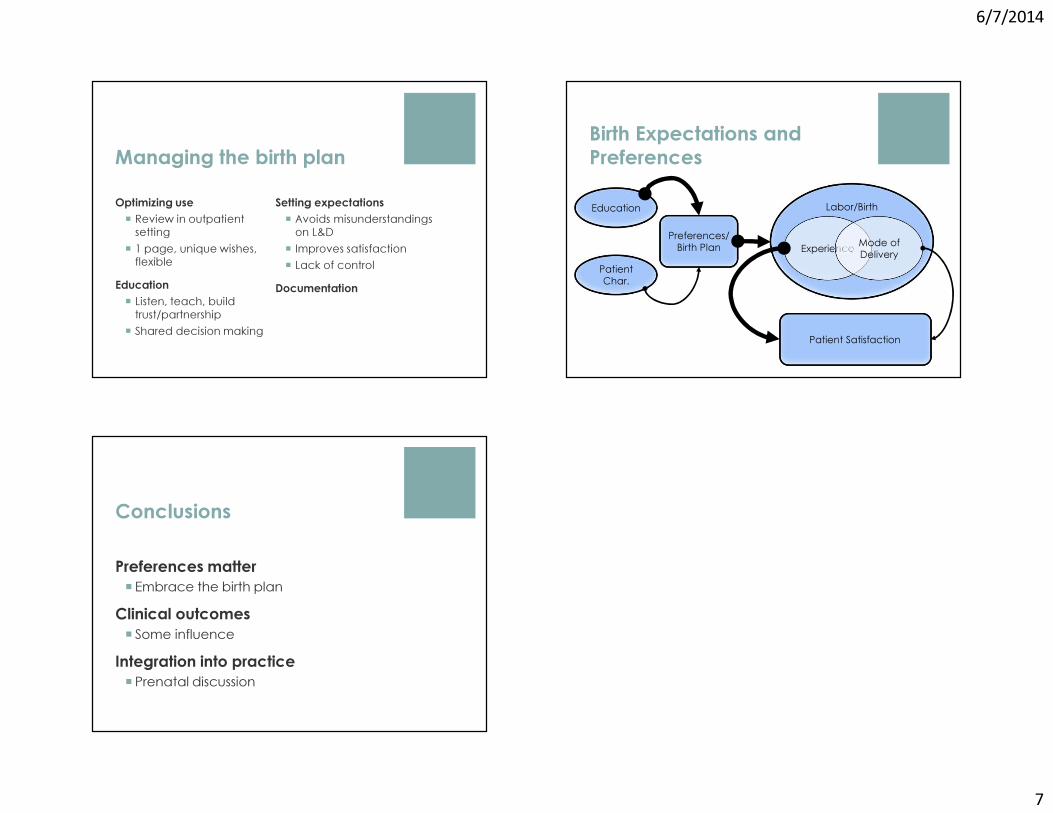
6/7/2014
7
Managing the birth planOptimizing use� Review in outpatient
setting� 1 page, unique wishes,
flexibleEducation� Listen, teach, build
trust/partnership� Shared decision making
Setting expectations� Avoids misunderstandings
on L&D� Improves satisfaction � Lack of control
Documentation
Birth Expectations and PreferencesEducation
Patient Char.
Patient Satisfaction
Preferences/Birth Plan
Labor/Birth
Experience Mode of Delivery
Conclusions
Preferences matter� Embrace the birth plan
Clinical outcomes� Some influence
Integration into practice� Prenatal discussion
6/7/2014
1
UCSF Antepartum and Intrapartum ManagementJune 7, 2014
Michael S. Policar, MD, MPHClinical Professor of Ob,Gyn, & RSUCSF School of [email protected]
No commercial disclosures for this lecture
The Affordable Care Act is Here: Now What?
ACA: What’s Been Done So Far?2010-2013
� Young adults covered on parents plan until 26 years old� No restrictions on pre-existing conditions for children <19� Medicare: rebates and discounts on brand-name
prescription drugs in Part D “doughnut hole”� Ban on lifetime benefit caps and rescissions� Phased-in ban on annual policy limits� Insurance rate increase restrictions
– Plans must spend > 80% of premiums on health care� First dollar coverage of many preventive services (no-cost
sharing…i.e., no deductible or co-payments)

6/7/2014
2
ACA: What Started on 1/1/2014?� Individual requirement to have insurance� State Medicaid expansion� Go-live for health insurance benefits through state health
insurance exchanges (enrollment started 10/1/13)� Essential health benefit (EHB) standards � Insurance market reforms; no rating on health, gender
– No restrictions for adults with pre-existing conditions� Employer shared responsibility penalties
‒ Delayed until 2015
The Individual Mandate� All citizens, legal immigrants 18 and older must have coverage� Tax penalty if no coverage (by 2016)…higher of
– $695/person; up to 3 times for a family, or – 2.5% of household income
� Exemptions granted for– Undocumented persons– No coverage for less than 3 months– Lowest cost plan > 8% personal income (net of subsidies)– Religious objection– Individuals who are incarcerated– Members of Native American tribes– People who have incomes below the tax-filing threshold
($9,750 for single and $27,100 for a family of four)
Women and the Health Care Law in CANational Women’s Law Center and State Partners - April 2013
• In CA, 2.8 million women (24%) women are uninsured – 25% of black women – 35.3% of Hispanic women– Compared to 14% of white women
• Up to 856,000 women in CA will be newly insured once this coverage is fully implemented
• This coverage expansion will reduce uninsurance in California by 39%
Insured through employer
MilitaryVeterans Admin
Undocumentedindividuals
Little or no change
Medicare MedicaidMinor changes
Uninsured Self employedMajor changes
Small business

6/7/2014
3
•Uninsured •Self employed•SB <50 workers
•Small business(50-99 workers)
50%
100%
State Health Insurance Exchanges
Medi-Cal
50%
CA Health Benefit Exchange“Covered California”
Small Business Health Options Program (SHOP)
? ?
Employerbased HI
<50: businesscan purchase<25: businesstax credits
finepay
October 1, 2014 October 2015
Major Changes 2 yr. extension (2016) (19-49)
Insurance Status of Non‐elderly Women in CA
AIM
Household Size If income is less than…
If income between
1 $ 15,867 $ 15, 857-45,9602 $ 21,404 $ 21,404-62,0403 $ 26,952 $ 26,952-78,1204 $ 32,500 $ 32,500-94,2005 $ 38,407 $ 38,047-110,280
You may qualify for
Medi-Cal Premium assistance through Covered CA
Modified Adjusted Gross Income (MAGI) Determines Program Eligibility
6/7/2014
4
Medicaid and Women’s Health Services• Payer for 40-50% of U.S. births• Expansion in Medicaid eligibility to cover adults with
incomes below 138% of the federal poverty level– Previously: “Broke plus something else”– With expansion: men and women with incomes below
$15,867 individual; $32,500 for a family of 4• Federal government will cover 100% of expansion costs
until 2017, then drops to 90% by 2020– Reason for rejection of expansion by many states…
• Creates a “coverage gap” for the poor in 25 states
Medi-Cal Expansion• To be eligible for Medi-Cal Expansion you must be ALL of…
– A U.S. citizen, U.S. national or lawfully present in the U.S.– A resident of California– Less than 65 years old– Have a family income at, or below, 138% of the Federal
Poverty Level– Children of families whose income is at, or below, 250%
of the Federal Poverty Level• All “new” Medi-Cal enrollments via M’cal managed care
Health Insurance Exchanges
� Subsidies for families 138-400% federal poverty level− Premium tax credit (toward purchase of insurance), and− Cost-sharing tax credit (rebate on OOP costs)− 399% FPL: $44,680 individual; $92,200 family of four
� Tax credit applied at enrollment; no wait till taxes filed

6/7/2014
5
Health Insurance Exchanges
Level Plan coversPlatinum 90%Gold 80%Silver 70%Bronze 60%Catastrophic < 30 years old
• Premiums are higher at each level
• Subsidy based on average Silver plan cost
• Out of pocket max= Health Savings Account limit• $5,950 individual• $11,900 family
• Lower out-of-pocket limits if subsidized
Coveredca.com
Alameda Alliance for HealthAnthem Blue Cross of CaliforniaBlue Shield of CaliforniaChinese Community HPContra Costa Health PlanHealth NetKaiser Permanente
L.A. Care Health PlanMolina HealthcareSharp Health PlanValley Health PlanVentura County Health Care PlanWestern Health Advantage
Which Plans Were Selected for Covered CA?

6/7/2014
6
Features of Covered California
• Rates vary by region, by metal level, and age• The following are not factored into rates
– Preexisting conditions– Gender– Smoker vs. non-smoker
• Compared to the small employer market, rates range from 2 percent above the 2013 average premium to 29 percent below the rates in California’s most populous markets
Features of Covered California
� Open enrollment is October 1, 2013 thru March 31, 2014– Next open enrollment is in Oct 2014 for 2015– Earlier if “life-changing event”: loss of job, death of
spouse, birth of child� On-line premium calculator available� Available in 10 languages
http://www.aim.ca.gov
Access For Infants And Mothers Program• Low cost affordable health coverage for middle-income
pregnant women• Cost is 1.5% of net annual income; billed over 12 months• Coverage for pregnant women who…
– Do not have health insurance OR have private insurance with a maternity-only deductible > $500; and,
– Are not eligible for no-cost Medi-Cal or Medicare and,– Have family income above no-cost Medi-Cal; and,– Are less than 30 weeks pregnant

6/7/2014
7
Access For Infants And Mothers Program• Available plans
– SF county: Anthem Blue Cross HMO– Alameda: Anthem Blue Cross HMO– Contra Costa: CC Health Plan; Kaiser Permanente– San Mateo: Kaiser Permanente
• What are the benefits of having AIM as opposed to pregnancy-related restrictive Medi-Cal only?– AIM offers comprehensive benefits, including pregnancy
and non-pregnancy related service
Cost of the AIM ProgramAdjusted Annual Household Income $39,840.00Multiply the Adjusted Annual Household Income by 1.5% to calculate the cost to participate in the AIM program
x 1.5%
Total Annual AIM Contribution $597.60
• No deductibles or copayments
� Specified preventive services must be covered with no cost-sharing (no out-of-pocket costs)
� Applies to private and public programs– (New) Private insurance policies 2010– Medicare, Medicaid 2011– State insurance exchanges 2014
� Improves coverage for preventive services in many individual and small group plans
Reproductive Health
Cancer Healthy Behaviors
Pregnancyrelated
Immunizations Chronicconditions
STI and HIV counseling ; all sexually active F)
Breast Cancer•Mammography
Alcohol S&C •Alcohol S&C
•TdaP, Td booster, •MMR, varicella
CV: HTN,lipids
Ct, GC, Syphilis screening
•Genetic S&C Tobacco C&I •Tobacco C&I
Influenza T2DMscreen
HIV screening (adults at HR; all sexually active F)
•Preventive medicationcounseling
Diet counseling if CVD risk
•Folic acid supplement
•Hepatitis A, B•Meningococcal
Depressionscreen
Contraception(women w/reprocapacity
Cervix:• Cytology• HPV + cytology
Interpersonal and DV S&C
•GDM screen•Rh screen•Anemia screen
•HPV(women 19‐26)
Osteo-porosisscreen
Colorectal: • FOBT, • Colonoscopy,• Sigmoid
Well‐woman visits
•STI screen•Bacteruriascreen
•Pneumococcal•Zoster
Obesity screen; C&I if obese
•Lactation Supports
S&C: screening and counseling C&I: counseling and interventions

6/7/2014
8
Women's Preventive Services
HHS Guideline for Insurance Coverage Frequency
Well-woman visits annually including preconception and prenatal care
• Several visits may be needed to obtain all recommended services, depending on health status, health needs, and other risks
Women's Preventive Services
HHS Guideline for Insurance Coverage FrequencyAll FDA approved contraceptive methods, sterilization procedures, and patient education & counseling for women with reproductive capacity
As prescribed
• All methods must be covered, but not all products• Limited exclusion for religious institutions (e.g., churches)
from providing contraceptive coverage for insured employees
Can Plans Limit Coverage Without Cost-Sharing?
• Plans must cover all of the FDA-approved methods• “Reasonable medical management techniques” are allowed
– Cost-sharing for brand-name drugs– Cost-sharing for out-of-network services– Prescription for over-the-counter methods
• The “Waiver Process”– Allows women to access medically appropriate method
without cost-sharing if plan typically imposes cost-sharing– Usually done through pharmacy pre-authorization
Many Questions…Not Many Answers� If I can’t collect a co-payment, will the Plan pay it?
– In the short term…yes– Over time, most contracting will be with ACOs
� Is there cost-sharing for global OB care?– No cost-sharing for routine prenatal, post-partum visits– Cost-sharing applies to the delivery itself
� If I manage other conditions at a well woman visit, should a co-pay be collected?– Yes, if separate office visit is billed with -25 modifier
6/7/2014
9
When Does the “Contraception As Prevention” Benefit Start?
Definition Cost-sharing?
When is cost-sharing prohibited?
New Plan Created after 8/1/2012
None Now
Non-grandfathered
Created 3/23/10-8/1/12
Yes* Next “new plan year”;mostly by 1/1/2013
Grandfatheredplan
Created before 3/23/2012
Yes* Once plan changes; mostly in 2014
* Unless plan agrees to remove cost sharing earlier than deadline
How Do You Know If You Have First Dollar Coverage for Contraceptives?
• Call “Member Services” at you health plan…the number is on your insurance card
• If you feel you are not receiving benefits to which you are entitled, contact the National Women’s Law Center– 1-866-PILL4US – [email protected]
What’s on The Horizon for Ob-Gyn?• More activity around value-based payments (P4P)• Currently, some health plans and Medicaid programs
incentivize reductions in inductions and C/S rates• Other “hot topics”
– Updated HEDIS criteria for cervical cancer screening intervals
– Hysterectomy indications and rates– Development of post-partum contraceptive metric
Take it Home….• Most individuals and families are now required to have
health insurance or will pay a tax penalty• Women’s heath services will become much more accessible
and clinicians will be paid more reliably going forward• There is “no wrong door” to enter in order to enroll in most
new ACA-related programs • As providers, we owe it to each patient that has no
insurance, or who receives care thru categorical programs, to offer advice regarding health insurance enrollment

6/7/2014
10
Additional Resources• National CMS site for consumer education regarding ACA
– Healthcare.gov• California health insurance marketplace
– Coveredca.com• National Women’s Law Center
– Excellent advice re: accessing preventive services, especially contraception with no cost-sharing benefit
– nwlc.org• Kaiser Family Foundation
– Analysis of the effect of ACA on consumers, providers– kff.org

6/7/2014
1
I Just Need a Note:
Pregnancy Discrimination, Workplace Accommodation, & the
Obstetric Provider’s Role
UCSF/UC Hastings
• Suzanne Seger, MTS, CNM, Associate Clinical Professor UCSF School of MedicineNo disclosures
• Jamie Dolkas, Esq.Director of Women’s Leadership at Center for WorkLifeLaw, UC Hastings College of the LawNo disclosures
Question 1Karen is 32 wks pregnant and works as a baker. She mentions at her prenatal visit that it is becoming more difficult to lift the 50 lb sacks of flour she must use to make products. She is considering stopping work. You should:
T el l h
e r t h e
s . ..
A sk i f
s he h
a s .. .
C ha r t
t he f
u nc . . .
Wr i t e
a n o
t e r . . .
0% 4%
39%
58%A. Tell her the safest plan is to stop workB. Ask if she has spoken to her employer
about the planC. Chart the functions which are becoming
difficult for her and whyD. Write a note reflecting your medical
opinion that it is time to stop work
Question 2The percentage of women who work while on their maternity leave is:
5 % 1 6%
3 4%
4 6%
5%
28%
45%
22%
A. 5%B. 16%C. 34%D. 46%

6/7/2014
2
Question 3Judith is a 31 yo nullipara at 26 weeks of pregnancy. She reports that she is upset about a recent email noting that she would not be promoted due to her pregnancy. She believes her supervisor sent it to her in error.You should:
T el l h
e r t h a
t . ..
D oc u m
e n t t h
e c. . .
A sk h
e r w h
a t s . . .
A ll o f
t he a
b o. . .
0%
19%
48%
33%
A. Tell her that she should sue her employerB. Document the conversation in her chart to
be helpful for later in case she needs itC. Ask her what she wants to do with this
informationD. All of the above
Objectives
• Scope of the problem & significance
• History of pregnancy discrimination laws & protections
• Pregnancy disability leave & eligibility limits
• Effective and clear documentation in the medical record for pregnancy accommodations
Pregnant Women & Work
• 70% of women who are pregnant and/or parenting are in the workplace (EEOC)
40% of mothers are the primary breadwinners for families in the United States today(Glynn, S.J. Center for American Progress 2012)

6/7/2014
3
Pregnancy & Discrimination
• Is not a thing of the past
• Continues to pervade private and public work environments.
Pregnancy Discrimination Cases
• Are on the rise
0
1000
2000
3000
4000
5000
6000
7000
19972010
EEOC Pregnancy Discrimination Charges 2011
Pregnancy & Work
• Very few studies in obstetrics and midwifery on the topic
• Early studies addressed concerns around workplace exposures and teratogens for the fetus

6/7/2014
4
Prevalence?
• In a structured interview study of 165 working women, 69% reported at least one form of workplace adversity during pregnancy
• Higher prevalence in public vs. privately insured women (Cooklin, Rowe & Fisher, 2007)
Low Wage Workers
• Are disproportionately affected.
• Disparities in employment discrimination with the poorest bearing the largest burden.(Terman, 2012, Farrell, Dolkas & Munro, ERA)
Hiring Practices Study
• In a study of interview and hiring practices of candidates with identical resumes, 79% of employers were less likely to hire a mother.
*SOURCE: Shelley J. Correll, Stephen Benard & In Paik, Getting a Job: Is There a Motherhood Penalty?, 112 AM. J. SOC. 1297, 1316 (2007).
Pregnancy & Disability Leave Pearls
• Leave legislation varies state to state
• Leave is FINITE no matter the worker’s circumstance
• Partial wage replacement is usual
• Documentation in the medical record is essential

6/7/2014
5
Pregnancy Leave
• Many workers will not qualify due to the nature of their workplaces
• Not all employers are held to federal and state standards
• California:Supplemental Disability Insurance (SDI)
four weeks before due date & six weeks after for healthy vaginal birth
California Paid Family Leave Act six weeks at 55% pay to care for someone
Family Medical Leave Act 12 weeks unpaid leave with job protection
Three Categories of Pregnancy-Related Legal
Protections At Work
1) Discrimination protections
2) Leave entitlements
3) Pregnancy accommodations
Pregnancy Accommodation Defined
The right of pregnant workers to receive reasonable workplace accommodations for pregnancy-related impairments/disabilities.

6/7/2014
6
Typical Accommodation Requests
• Periodic rest breaks• No standing more than 8 hours• Temporary schedule change – includes fewer
hours or modified hours• Restructuring of job duties• Temporary light duty or transfer to another
position• Leave time to address pregnancy-related
illness
Why Pregnancy Accommodations Are Important
1) Enable pregnant workers to continue working safely and supporting themselves/families
2) Continued employment and associated benefits (health insurance, etc.)
3) Termination and forced unpaid leave causes stress and other problems
4) Big impact on low wage workers who tend to have less flexibility, benefits, and protections
Business Case for Accommodations
Providing an accommodation allows an employee to stay on the job which saves the employer on turnover costs.
Accommodation also promotes worker morale, maintains consistency, and cultivates worker loyalty.
Legal Framework (Federal)1) Title VII of the Civil Rights Act of 1964
(“Title VII”)
2) Family and Medical Leave Act (FMLA) –1993
3) Pregnancy Discrimination Act (PDA) –1978
4) Americans with Disabilities Act (ADA) –1990, amended in 2008
6/7/2014
7
Family and Medical Leave Act12 weeks unpaid, job-protected leave, for employee’s own or immediate family member’s serious illness, or baby-bonding.
To qualify, workers must meet the following requirements:− Covered employer: Must work for employer with 50 or more employees in a 75-mile radius;
− Eligible worker: Must have worked for employer at least 12 months and 1,250 hours in year prior to taking leave. AND
− Taking leave for a qualified reason:� To care for a spouse, child, or parent with a serious health condition;
� For their own serious health condition, or � To bond with a newborn child, newly adopted child, or recently placed foster child.
Protections:− Job protection: Employees who take FMLA leave must be restored to same or equivalent job.
− Benefits: Entitled to continuation of group health benefits (up to 12 weeks); plus retention of accrued benefits and seniority.
− Retaliation: Protection from discrimination and/or retaliation.
FMLA Limitations
1) FMLA has strict coverage requirements –– In order to qualify, a worker must:
• Be taking leave for a qualifying reason (for employee’s own or immediate family member’s serious illness, or baby-bonding),
• Have worked for employer at least 12 months and 1,250 hours in year prior to taking leave;
• Work for an employer with at least 50 employees within a 75-mile radius
– These requirements automatically exclude about half of all workers.
2) Leave under FMLA is unpaid ; federal law does not require paid leave of any kind.– Even when workers are eligible for unpaid leave under the Family
and Medical Leave Act, they often cannot afford to take it.
Accommodations Under the
Pregnancy Discrimination Act
An employer must treat pregnant women with impairments the same as it treats non-pregnant workers with similar impairments.
Thus, an employer must make an accommodation for pregnant employees if the employer has or would have done so for any of its non-pregnant employees.
Americans with Disabilities Act
�Under the ADA, an otherwise qualified employee with a disability is entitled to reasonable accommodations in the workplace
�Although ordinary pregnancy is not an impairment, an impairment that arises due to pregnancy may constitute a disability
6/7/2014
8
Americans with Disabilities Act
As a result of recent 2008 amendments to the ADA, many pregnancy-related impairments are considered disabilities under the ADA:
• Women impaired by pregnancy-related conditions are protected from discriminationon the basis of those impairments; and
• Employers have a duty to make reasonable accommodations to enable pregnant workers to continue working during pregnancy.
ADA Interactive Process
Employer and employee have a duty to participate in “good faith” interactive process to determine appropriate reasonable accommodation.
*Tip: Pregnancy accommodation needs are often met when employer and employee have a conversation about what the employee actually does (as opposed to her job description, which is likely different on paper than in practice) and brainstorm together about how to address her temporary limitations.
Interactive Process Considerations1) What accommodation is requested?
2) What duties can the employee still perform within those restrictions?
3) What are the employee’s job duties/tasks that require an accommodation, and how often are these tasks usually performed?
4) What changes would enable employee to per-form task or accommodate restrictions, such as help from coworkers, or shifting certain duties?
Notes for Work-Related Duty
Can do more harm than good if not written with attention to key components

6/7/2014
9
Clinician Assumptions
• Patients understand their workplace requirements for taking disability leave
• Doctors’ notes carry the same authority in the patient’s workplace as they might in the health care environment
Clinician Challenges
• Time limitations
• Common discomforts or issues not mentioned until patient wants to go on disability
• Patient hope that a note will solve work difficulties
Elements of a Note
• Date, Time, Patient’s condition and its effects on the work duties
• Modifications requested
• That the patient can still perform the essential functions of her job
• Discussion of patient’s knowledge of what she is eligible for
• Discussion of the need to have an interactive process with employer
Common Pregnancy Conditions
Underlying Conditions
Description Othermedical conditions that can producesimilar symptoms
Bodily function affected
Reasonable accommodations
Lumbar lordosis
Pregnant women experience back pain through a variety of mechanisms, including the sway-backed posture (lumbar lordosis) caused by a growing belly and the hormones of pregnancy loosening up the joints, muscle spasms and “Braxton-Hicks” contractions. Pregnancy may also exacerbate pre-existing back problems. Back pain, if severe, can interfere with major life activities (standing, reaching, lifting, or bending).
Back injury; degenerative joint disease; scoliosis; arthritis muscular dystrophy and kidney infection or stones
Musculoskeletal
Use of a heating pad; sitting instead of standing; lifting assistance or limitations; using assistive equipment to lift; modification of the duties of the job, such as temporary light duty
Carpal Tunnel Syndrome
Tingling, pain, numbness and joint stiffness in hands and wrists is common in late pregnancy due to changes in fluid composition and increased amount of pressure on median nerve in wrist. Carpal tunnel syndrome is an impairment that is much more prevalent in pregnant women than the population generally.
Also common in nonpregnant people who do repetitive small motions with hands/ wrists (i.e. typing) or after forearm/ wrist injury
Musculoskeletal; neurological
Occasional breaks from manual tasks or typing; specialized programs that allow for dictation instead of typing
Hyperemesis gravidarum
Pregnant women can have nausea and/ or vomiting that limits their ability to work in certain settings/ certain times of day. Severe nausea and vomiting in pregnancy can result in weight loss, dehydration, and/ or electrolyte imbalance. It occurs most commonly in the first trimester but can extend throughout the entire pregnancy and all day long.
Chemotherapy for cancer; hepatitis; vestibulitis; a variety of GI disorders (gastroparesis, dyspepsia, inflammatory bowel disease)
Digestive
Permission to take more frequent bathroom breaks; permission to eat small snacks during work hours; a cot for lying down; modified schedules
Reprinted by permission of the Yale Law & Policy Re view, Inc., from 32 YALE L. & POL’Y REV. 97 (2013).

6/7/2014
10
“Essential Functions of Her Job”
With Certain Accommodations patient can continue to work!
Case Study
• A pregnant airport security work comes to prenatal clinic & states she needs a note not to wear her bowtie as part of her uniform. She feels as if she cannot breathe. Her supervisor has had her obtain notes for all workplace accommodations from bathroom breaks to water bottles noting he did not want to be perceived as giving her special treatment
A Bad Note Would Say
• Date
• Dear:
• Ms. Blank is our patient and she is pregnant and can’t wear her bowtie as part of her uniform
• Signed name, license number
A Better Note Would Say
• DateDear:
• Ms. Blank is our patient who is pregnant and able to perform the essential functions of her job. She needs an accommodation to not wear her bowtie due to increasing neck girth until {due date}
• Signed, name, license number
6/7/2014
11
Case Study
• A woman is seen for her post partum visit after a preterm birth at 36 weeks. She is six weeks out and her son is struggling with weight gain & breastfeeding. She is stressed as return to work will mean travel that will disrupt breastfeeding and pumping.
A Bad Note Would Say
• Date
• Dear:
• Ms. Blank gave birth and is struggling with breastfeeding. She needs two more additional weeks to be at home with her infant.
• Signed name, license number
A Better Note Would Say
DateDear:Ms. Blank was seen and evaluated in our office today after giving birth to a late preterm infant. This pregnancy complication has affected her infant’s ability to gain weight and breastfeeding. For her sons development, she is requiring an additional two weeks for monitoring for weight gain and will have additional doctors appointments. She is not able to return to work or travel at this time. She will be reevaluated on [date] to assess her readiness to return to work.Signed license number
Pregnancy Accommodation Working Group
• Joint venture UCSF/UC Hastings
• Standardized letters for obstetric providers
• Ongoing work to address pregnancy discrimination and education around work needs for pregnant women

6/7/2014
1
Decision to Incision Timing: Is the 30-minute rule valid?
Aaron B. Caughey, MD, PhD
Professor and ChairDepartment of Obstetrics and Gynecology
Oregon Health & Science [email protected]
Disclosures
� No financial disclosures related to this talk� Medical Advisor to Ariosa, Cellscape, Mindchild� Bob’s Red Mill
Overview
� 30 minute rule?� History
� Biology / pathophysiology� Epidemiology
� Quality Improvement
� Management
Bradycardia

6/7/2014
2
How long would it take to achieve delivery?
1 0 m i
n u te s o
r . . . 1 5
m in u t
e s 2 0
m in u t
e s 3 0
m in u t
e s
L o ng e r
28%
43%
5%7%
17%
A. 10 minutes or less
B. 15 minutes
C. 20 minutesD. 30 minutes
E. Longer
Minimum time until injury?
1 0 m i
n u te s o
r . . . 1 5
m in u t
e s 2 0
m in u t
e s 3 0
m in u t
e s
L o ng e r
46%
22%
7%5%
20%
A. 10 minutes or less
B. 15 minutes
C. 20 minutesD. 30 minutes
E. Longer
Disconnect?
� If injury occurs faster than we can intervene, then why a 30-minute rule?
� Should it be shorter?
The 30 minute rule
� Established as a time threshold for cesarean delivery to occur – 1980s
� ACOG, RCOG, etc
� Became a more prominent rule of the land in the late 1990s
ACOG Committee on Professional Standards for Obstetric-Gynecologic Services. 7th ed.; 1989.Tuffnell et al. BMJ 2001;322:1330–3

6/7/2014
3
VBAC – 1990sWhy 30 minutes?
� Improving outcomes?
� Feasibility?
� Whim?
Prolonged decelerations
J Healthc Risk Manag. 1999 Winter;19(1):11-20.Is the obstetric guideline of 30 minutes from decision to incision for Cesarean delivery clinically significant?Lavery JP1, Janssen J, Hutchinson L.
The time required to extract an infant from a hostile in utero environment is a frequent issue in medical negligence cases. The American College of Obstetricians and Gynecologists and the American Academy of Pediatrics suggest a time guideline of 30 minutes from decision for Cesarean delivery to the beginning (incision) of the procedure. This time frame is based on survey data from hospitals throughout the United States and is not based on clinical outcomes or the pathophysiology of obstetric events .
What time threshold?
� What outcomes are we interested in?
� Mortality� Short-term (neonatal)� Long-term (infant and beyond)
� Morbidity� HIE / CP� Seizures?� Apgars?� Cord gases

6/7/2014
4
Prolonged decelerations
Obstet Gynecol. 2002 Sep;100(3):557-60.The correlation of seizures in newborn infants with significant acidosis at birth with umbilical artery cord gas values.Williams KP1, Singh A.
� 238 neonates w/ UA pH <7.1
� Primary outcome – seizures from HIE
� Examined all gas features� pO2; pCO2; base excess, pH
� pH < 7.0 only was associated in MV model
How long?US, 1995-2005
Cahill AG, et al. Terminal decelerations and outcomes.Obstet Gynecol. 2013 Nov;122(5):1070-6
How long? How long?
Time ≥10 minn=31 (%)
Time <10 minn=920 (%)
P value
Acidemia ≤ 7.10 (n=12) 4 (12.9) 8 (0.9) <0.01Acidemia ≤ 7.05 (n=4) 2 (6.5) 2 (0.2) <0.01APGAR 5min < 7 (n=4) 2 (6.5) 2 (0.2) <0.01Special Care* or NICU Admission (n=38)
5 (16.7) 33 (3.6) <0.01
NICU Admission(n=11) 3 (10.0) 8 (0.9) <0.01
Cahill AG, et al. Terminal decelerations and outcomes.Obstet Gynecol. 2013 Nov;122(5):1070-6

6/7/2014
5
Only Time?
� Are there other features that matter?
� Leung et al – decelerations
� Variability?� Etiology – uterine rupture, abruption, etc.
� Heart rate?
How long?US, 1995-2005
Cahill AG, et al. Terminal decelerations and outcomes.Obstet Gynecol. 2013 Nov;122(5):1070-6
Variability
Decreased variability before bradycardia
Combined with no recovery of the bradycardia mean pH 6.83 +/- 0.16 78% incidence of significant acidosis
Williams K, et al. Obstet Gynecol. 2002 Nov;100(5 Pt 1):951-4.Fetal heart rate parameters predictive of neonatal outcome in the presence of a prolonged deceleration.
Heart Rate
Tranquilli A, et al. J Matern Fetal Neonatal Med. 2013 Sep;26(14):1425-9. The correlation between fetal bradycardia area in the second stage of labor and acidemia at birth.
Time until acidemia
P value
FHR 80s 25 mins <0.01FHR 70s 13 mins <0.01FHR 60s 8 mins <0.01FHR 50s 6 mins <0.01FHR 40s 5 mins <0.01
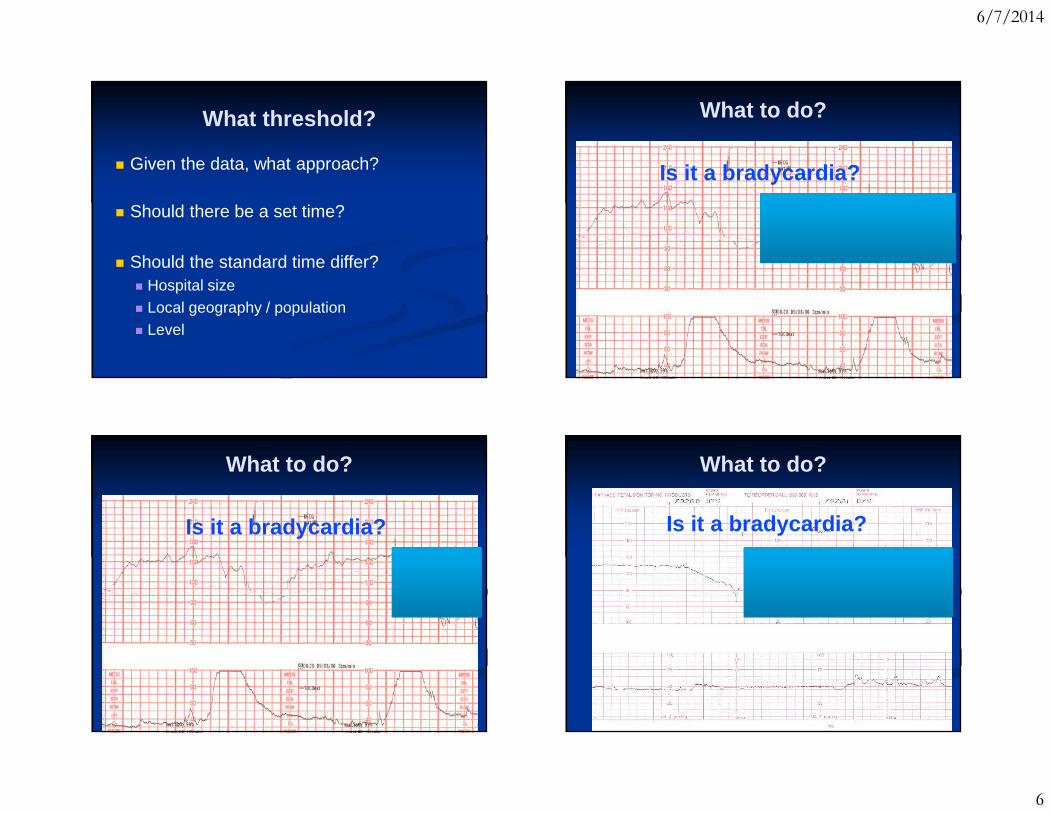
6/7/2014
6
What threshold?
� Given the data, what approach?
� Should there be a set time?
� Should the standard time differ?� Hospital size� Local geography / population� Level
What to do?
Is it a bradycardia?
What to do?
Is it a bradycardia?
What to do?
Is it a bradycardia?Is it a bradycardia?

6/7/2014
7
What to do?
Is it a bradycardia?Is it a bradycardia?
What to do?
Is it a bradycardia?Is it a bradycardia?
What to do?
Is it a bradycardia?Is it a bradycardia?
What to do?
� What is the Baseline status?
� What is the Etiology?
� What needs to be done to achieve Delivery?
� BED

6/7/2014
8
What to do?
� What is the Baseline status?� Decels� Variability� Meconium� Chorioamnionitis� Compromised mother or fetus?� Htn disorder; fetal anomaly; preterm
What to do?
� What is the Etiology?� Abruption� Tachysystole/Tetany� Cord prolapse� Uterine rupture� Maternal� Hypotension (AFE); hypoxic (PE)
� Fetal�Oligo; arrhythmia; rapid descent
What to do?
� What needs to be done to achieve Delivery?�What is the exam? Include position� Parity and prior OB Hx� Patient BMI� EFW� Anesthesia?� OR / staff?
What to do?
� Individual level – BED
� Hospital level� Establish benchmarks� Environment (Geography; Populations)� Engineering (Internal and External)
� Societal level� Encourage collaboration� Public Health

6/7/2014
9
Can we reduce the length of time?
Tuffnell et al. BMJ 2001;322:1330–3
Can we reduce the length of time?
Can we reduce the length of time? Can we reduce the length of time?

6/7/2014
10
What should be done?
� Gather together leadership to discuss
� OB providers (MFM, OB, CNM, FM)
� Measure the outcomes – report the data
� Potentially use QI methods
� Institutionally based (e.g. Lean)
� Establish standards / standard behaviors
What time goal?
As fast as possible!!!
3 0 m i
n u te s ?
2 0
m in u t
e s ?
1 5 m i
n u te s ?
1 0 m i
n u te s ?
11%
27%
40%
22%
A. 30 minutes?
B. 20 minutes?
C. 15 minutes?D. 10 minutes?
Thank You

Upcoming CME Courses
42nd Annual Advances in Internal Medicine June 23 - 27, 2014
San Francisco, California
Essentials of Women's Health: An Integrated Approach to Primary Care and Office Gynecology
Sunday, July 6 – Friday, July 11, 2014 Kohala Coast, Hawaii
Essentials of Primary Care: A Core Curriculum for Ambulatory Practice
August 3 - 8, 2014 North Lake Tahoe, California
Obstetrics and Gynecology Update: What Does the Evidence Tell Us?
October 22 - 24, 2014 San Francisco, California
Primary Care Medicine: Principles and Practice
October 22 - 24, 2014 San Francisco, California
Controversies in Women’s Health
December 11 - 12, 2014 San Francisco, California
Antepartum and Intrapartum Management
June 4 - 6, 2015 San Francisco, California
All Courses Managed by: UCSF Office of Continuing Medical Education
3333 California Street, Room 450, San Francisco, CA 94118 For attendee information call: 415-476-4251
For exhibitor information: 415-476-4253 Visit the web site at www.cme.ucsf.edu