ESSENTIALS OF WOMEN'S HEALTH: - Continuing Education
382
The Division of General Internal Medicine, The Department of Medicine, and The Department of Obstetrics, Gynecology & Reproductive Sciences presents ESSENTIALS OF WOMEN’S HEALTH: AN INTEGRATED APPROACH TO PRIMARY CARE AND OFFICE GYNECOLOGY June 30 – July 5, 2013 Hapuna Beach Prince Hotel Big Island, Hawaii Course Chairs Robert B. Baron, MD, MS Alison F. Jacoby, MD University of California, San Francisco School of Medicine
-
Upload
khangminh22 -
Category
Documents
-
view
1 -
download
0
Transcript of ESSENTIALS OF WOMEN'S HEALTH: - Continuing Education
The Division of General Internal Medicine, The Department of Medicine, and
The Department of Obstetrics, Gynecology & Reproductive Sciences presents
ESSENTIALS OF WOMEN’S HEALTH:
AN INTEGRATED APPROACH TO PRIMARY CARE AND OFFICE GYNECOLOGY
June 30 – July 5, 2013 Hapuna Beach Prince Hotel
Big Island, Hawaii
Course Chairs
Robert B. Baron, MD, MS Alison F. Jacoby, MD
University of California, San Francisco School of Medicine
Acknowledgement of Commercial Support
Exhibitor
Bayer
ESSENTIALS OF WOMEN’S HEALTH: An Integrated Approach to Primary Care and Office Gynecology
June 30 – July 5, 2013 Big Island, Hawaii
SUNDAY, JUNE 30, 2013 4:00 pm Course Registration 5:00 Welcome
Robert B. Baron, MD, MS Alison F. Jacoby, MD
5:10 G Current Controversies in Breast and Cervical Cancer Screening Rebecca Jackson, MD
6:00 G Ovarian Cancer Screening and Principles of Adnexal Mass Evaluation Alison F. Jacoby, MD
7:10 Adjourn
MONDAY, JULY 1, 2013 Moderator: Robert B. Baron, MD, MS 6:30 am Continental Breakfast 7:00 G Current Controversies in Lung, Colon,
and Skin Cancer Screening Jeffrey Tice, MD
7:50 G Prevention of Cardiovascular Disease in Women Robert B. Baron, MD, MS
8:40 Break 9:00 G Management of Hypertension in Women
Eliseo J. Perez‐Stable, MD
9:50 Preventing the Unintended: Update in Contraception Jody Steinauer, MD, MAS
10:40 Adjourn

TUESDAY, JULY 2, 2013 Moderator: Alison F. Jacoby, MD 6:30 am Continental Breakfast 7:00 G What Every Clinician Needs to Know
About Abortion Jody Steinauer, MD, MAS
7:50 Lumps, Bumps, and Pain: Management of Common Breast Disorders Rebecca Jackson, MD
8:40 Common Issues in Pediatric and Adolescent Gynecology Alison F. Jacoby, MD
9:30 Break 9:50 Concurrent Workshops (select one):
A: You Make the Call: Recognizing Common Gynecologic Lesions Alison F. Jacoby, MD LOCATION: Mauka Ballroom
B: Management of Obesity: A Systematic Approach Robert B. Baron, MD, MS LOCATION: Main Ballroom
11:20 Adjourn
WEDNESDAY, JULY 3, 2013 Moderator: Eliseo Perez‐Stable, MD 6:30 am Continental Breakfast 7:00 G Vaccinations for Adult and
Adolescent Women Eliseo J. Perez‐Stable, MD
7:50 G Current Issues in Diabetes Management Robert B. Baron, MD, MS
8:40 G Breast Cancer Evaluation and Treatment Jeffrey Tice, MD
9:30 Break

9:50 Concurrent Workshops (select one):
C: Contraception Challenges: Case Studies and IUD Insertion Practicum Jody Steinauer, MD, MAS LOCATION: Mauka Ballroom
G D: Common Problems in Older Women: Using Geriatric Principles in Everyday Practice Eliseo J. Perez‐Stable, MD LOCATION: Main Ballroom
11:20 Adjourn
THURSDAY, JULY 4, 2013 Moderator: Jeffrey Tice, MD 6:30 am Continental Breakfast 7:00 G Vitamins and Supplements in Women’s Health:
An Evidence‐based Approach Jeffrey Tice, MD
7:50 G New Developments in Osteoporosis Eliseo J. Perez‐Stable, MD
8:40 Abnormal Uterine Bleeding: From Menarche to Menopause Vanessa Jacoby, MD, MAS
9:30 Break 9:50 Concurrent Workshops (select one):
E: Case Studies in Cervical Dysplasia: How Would You Manage These Patients? Rebecca Jackson, MD LOCATION: Mauka Ballroom
F: Clinical Dilemmas in Genetic Testing: A Case‐based Approach Jeffrey Tice, MD LOCATION: Main Ballroom
11:20 am Adjourn
FRIDAY, JULY 5, 2013 Moderator: Rebecca Jackson, MD 6:30 am Continental Breakfast 7:00 Chronic Pelvic Pain:
Current Strategies for Evaluation and Management Rebecca Jackson, MD
7:50 Why Am I Bleeding?
Management of First Trimester Bleeding Alison F. Jacoby, MD
CLOSING ADDRESS:
8:40 G Caring for Challenging Patients in Women’s Health: Insights into Empathy and Professionalism Jody Steinauer, MD, MAS
9:30 Adjourn
G = Geriatric Credit
University of California, San Francisco School of Medicine Presents
Essentials of Women’s Health: An Integrated Approach to Primary Care and Office Gynecology
Increasing appreciation of the unique needs of women patients and women's health care providers has created a need for innovative educational programs on women’s health. This program, designed for family physicians, internists, gynecologists, nurses, nurse practitioners, physician assistants, pharmacists, and all others involved in providing quality health care for women, will provide a practical update on a full range of common but controversial issues in women’s health. The course will serve to enhance the skills of those already working in women’s health as well as help develop new skills for those expanding their work to include more primary care and office gynecology. Developed and taught by UCSF faculty in both primary care internal medicine and obstetrics and gynecology, the course will present an integrated approach to women’s health. Emphasis will be placed on new developments in preventive care and cardiovascular risk factors in women, issues in reproductive health, and clinical strategies in the diagnosis and treatment of common gynecologic complaints and common medical problems of women. Special emphasis will be placed on office skills needed for modern day practice including: enhanced skills in physical examination, common office procedures, clinical nutrition, assessment of new medical technologies, and how to better read the medical literature. The course will use interactive lectures, clinical vignettes, hands‐on workshops, small group discussions, an audience response system and questions and answers. A detailed syllabus will be provided. This course is presented by the Division of General Internal Medicine, Department of Medicine, and the Department of Obstetrics, Gynecology, and Reproductive Sciences and is sponsored by the Office of Continuing Medical Education, University of California, San Francisco.
Educational Objectives
The purpose of this course is to increase competence and improve clinician practice in women’s health. We specifically anticipate improvements in skills and strategies to:
Implement new guidelines in office‐based preventive medicine for prevention and early detection of cancer with clinical exam, pap tests, genetic testing and diagnostic imaging;
Implement new guidelines for prevention and treatment of cardiovascular risk factors in women;
Provide vaccinations to adults and adolescents;
Diagnose and treat common problems in women's health including cervical dysplasia, hypertension, high blood cholesterol, obesity, diabetes, osteoporosis, abnormal uterine bleeding, fibroids, incontinence, ectopic pregnancy, chronic pelvic pain, benign breast disorders, breast cancer, and dementia;
Facilitate counseling and informed decision‐making in contraception and abortion;
Examine patients and perform common office procedures in gynecology;
Diagnose and treat pediatric and adolescent patients with gynecologic concerns;
Provide empathic and professional communication with all patients.
Accreditation
The University of California, San Francisco School of Medicine (UCSF) is accredited by the Accreditation Council for Continuing Medical Education to provide continuing medical education for physicians.
UCSF designates this live activity for a maximum of 20.25 AMA PRA Category 1 CreditsTM.
This CME activity meets the requirements under California Assembly Bill 1195, continuing education and cultural and linguistic competency.
Family Physicians: This Live activity, Essentials of Women's Health: An Integrated Approach to Primary Care and Office Gynecology, with a beginning date of 06/30/2013, has been reviewed and is acceptable for up to 19.75 Prescribed credit(s) by the American Academy of Family Physicians. Physicians should claim only the credit commensurate with the extent of their participation in the activity.
Geriatric Medicine: The approved credits shown above include 11.75 geriatric credits toward meeting the requirement under California Assembly Bill 1820, Geriatric Medicine
ACOG: The American College of Obstetricians and Gynecologists has assigned 21 cognate credits to this program.
General Information
CME Certificates Please complete the sign‐in registration form located at the front desk area of the meeting. Make certain to indicate your total number of credits collected. Visit the below URL to complete the overall course evaluation and receive an electronic certificate immediately. EVALUATION – CME CERTIFICATE ACCESS: www.ucsfcme.com/evaluation Evaluation Your cooperation in completing and returning the course evaluation is an important part of future course planning. The evaluation is the blue packet you received at registration. Please return your evaluation at course completion to the UCSF Registration Desk. Phone Messages Any messages during the conference can be left by calling (808) 880‐1111 and asking for the UCSF “Women’s Health” course. Messages will be posted on the board near the registration desk.

Security We urge caution with regard to your personal belongings and syllabus books. We are unable to replace these in the event of loss. Please do not leave any personal belongings unattended in the meeting room during lunch or breaks.
Federal and State Law Regarding Linguistic Access and Services for Limited English Proficient Persons
I. Purpose. This document is intended to satisfy the requirements set forth in California Business and Professions code 2190.1. California law requires physicians to obtain training in cultural and linguistic competency as part of their continuing medical education programs. This document and the attachments are intended to provide physicians with an overview of federal and state laws regarding linguistic access and services for limited English proficient (“LEP”) persons. Other federal and state laws not reviewed below also may govern the manner in which physicians and healthcare providers render services for disabled, hearing impaired or other protected categories
II. Federal Law – Federal Civil Rights Act of 1964, Executive Order 13166, August 11, 2000,
and Department of Health and Human Services (“HHS”) Regulations and LEP Guidance. The Federal Civil Rights Act of 1964, as amended, and HHS regulations require recipients of federal financial assistance (“Recipients”) to take reasonable steps to ensure that LEP persons have meaningful access to federally funded programs and services. Failure to provide LEP individuals with access to federally funded programs and services may constitute national origin discrimination, which may be remedied by federal agency enforcement action. Recipients may include physicians, hospitals, universities and academic medical centers who receive grants, training, equipment, surplus property and other assistance from the federal government. HHS recently issued revised guidance documents for Recipients to ensure that they understand their obligations to provide language assistance services to LEP persons. A copy of HHS’s summary document entitled “Guidance for Federal Financial Assistance Recipients Regarding Title VI and the Prohibition Against National Origin Discrimination Affecting Limited English Proficient Persons – Summary” is available at HHS’s website at: http://www.hhs.gov/ocr/lep/ . As noted above, Recipients generally must provide meaningful access to their programs and services for LEP persons. The rule, however, is a flexible one and HHS recognizes that “reasonable steps” may differ depending on the Recipient’s size and scope of services. HHS advised that Recipients, in designing an LEP program, should conduct an individualized assessment balancing four factors, including: (i) the number or proportion of LEP persons eligible to be served or likely to be encountered by the Recipient; (ii) the frequency with which LEP individuals come into contact with the Recipient’s program; (iii) the nature and importance of the program, activity or service provided by the Recipient to its beneficiaries; and (iv) the resources available to the Recipient and the costs of interpreting and translation services. Based on the Recipient’s analysis, the Recipient should then design an LEP plan based on five recommended steps, including: (i) identifying LEP individuals who may need assistance; (ii) identifying language assistance measures; (iii) training staff; (iv) providing notice to LEP persons; and (v) monitoring and updating the LEP plan. A Recipient’s LEP plan likely will include translating vital documents and providing either on‐site interpreters or telephone interpreter services, or using shared interpreting services with other Recipients. Recipients may take other reasonable steps depending on the emergent or non‐emergent needs of the LEP individual, such as hiring bilingual
staff who are competent in the skills required for medical translation, hiring staff interpreters, or contracting with outside public or private agencies that provide interpreter services. HHS’s guidance provides detailed examples of the mix of services that a Recipient should consider and implement. HHS’s guidance also establishes a “safe harbor” that Recipients may elect to follow when determining whether vital documents must be translated into other languages. Compliance with the safe harbor will be strong evidence that the Recipient has satisfied its written translation obligations. In addition to reviewing HHS guidance documents, Recipients may contact HHS’s Office for Civil Rights for technical assistance in establishing a reasonable LEP plan.
III. California Law – Dymally‐Alatorre Bilingual Services Act. The California legislature enacted the California’s Dymally‐Alatorre Bilingual Services Act (Govt. Code 7290 et seq.) in order to ensure that California residents would appropriately receive services from public agencies regardless of the person’s English language skills. California Government Code section 7291 recites this legislative intent as follows:
“The Legislature hereby finds and declares that the effective maintenance and development of a free and democratic society depends on the right and ability of its citizens and residents to communicate with their government and the right and ability of the government to communicate with them. The Legislature further finds and declares that substantial numbers of persons who live, work and pay taxes in this state are unable, either because they do not speak or write English at all, or because their primary language is other than English, effectively to communicate with their government. The Legislature further finds and declares that state and local agency employees frequently are unable to communicate with persons requiring their services because of this language barrier. As a consequence, substantial numbers of persons presently are being denied rights and benefits to which they would otherwise be entitled. It is the intention of the Legislature in enacting this chapter to provide for effective communication between all levels of government in this state and the people of this state who are precluded from utilizing public services because of language barriers.”
The Act generally requires state and local public agencies to provide interpreter and written document translation services in a manner that will ensure that LEP individuals have access to important government services. Agencies may employ bilingual staff, and translate documents into additional languages representing the clientele served by the agency. Public agencies also must conduct a needs assessment survey every two years documenting the items listed in Government Code section 7299.4, and develop an implementation plan every year that documents compliance with the Act. You may access a copy of this law at the following url: http://www.spb.ca.gov/bilingual/dymallyact.htm
Faculty List
Program Chairs:
Robert B. Baron, MD, MS Professor of Medicine; Associate Dean for Graduate and Continuing Medical Education; Vice Chief, Division of General Internal Medicine Alison Jacoby, MD Professor of Obstetrics, Gynecology and Reproductive Sciences; Director, UCSF Comprehensive Fibroid Center
Faculty: (University of California, San Francisco)
Rebecca Jackson, MD Chief, SFGH Division Associate Professor, Department of Obstetrics, Gynecology & Reproductive Sciences, and of Epidemiology & Biostatistics Vanessa Jacoby, MD, MAS Assistant Professor of Obstetrics, Gynecology and Reproductive Sciences Eliseo J. Perez‐Stable, MD Professor of Medicine; Chief, Division of General Internal Medicine; Director, Medical Effectiveness Research Center for Diverse Populations Jody Steinauer, MD, MAS Associate Professor, Department of Obstetrics, Gynecology and Reproductive Sciences; Assistant Director, Family Planning Fellowship Jeffrey Tice, MD Associate Professor of Medicine

Disclosure
The following faculty speakers, moderators and planning committee members have disclosed NO financial interest/arrangement or affiliation with any commercial companies who have provided products or services relating to their presentation(s) or commercial support for this continuing medical education activity:
Robert B. Baron, MD, MS none
Alison F. Jacoby, MD none
Rebecca Jackson, MD none
Vanessa Jacoby, MD, MAS none
Eliseo Perez‐Stable, MD none
Jody Steinauer, MD, MAS none
Jeffrey Tice, MD none
The following faculty speakers have disclosed a financial interest/arrangement or affiliation with a commercial company who has provided products or services relating to their presentation(s) or commercial support for this continuing medical education activity. All conflicts of interest have been resolved in accordance with the ACCME Standards for Commercial Support:
N/A This UCSF CME educational activity was planned and developed to: uphold academic standards to ensure balance, independence, objectivity, and scientific rigor; adhere to requirements to protect health information under the Health Insurance Portability and Accountability Act of 1996 (HIPAA); and, include a mechanism to inform learners when unapproved or unlabeled uses of therapeutic products or agents are discussed or referenced. This activity has been reviewed and approved by members of the UCSF CME Governing Board in accordance with UCSF CME accreditation policies. Office of CME staff, planners, reviewers, and all others in control of content have disclosed no relevant financial relationships.
Registrant List
Abela Philip Pollock Pines CA
Ambrose Christa Longmont CO
Banka Raj Fresno CA
Baqai Fauzia Fayetteville NC
Batra Romilla Irvine CA
Beacom Rosalind Drayton Valley AB
Belissary Nicole Modesto CA
Berg Cecelia Herald CA
Berkeley Marsha Los Angeles CA
Brown Tamy El Cerrito CA
Burke Charlotte San Ramon CA
Chan Adrienne Melbourne
Chang Alice Rochester MN
Christman Claudia Kailua Kona HI
Cohen Janet Victoria BC
Collette Ron Burnaby BC
Cooper Michele Huntington Beach CA
Cotulbea Elena Sammamish WA
Daghestani Anas Austin TX
De Castro Jacqueline Hanford CA
Dizon Amy Aiea HI
Dobrotwir Andrew Melbourne VIC
Doney Jessica Chandler AZ
Dureg Karen Aiea HI
Elder Brenda Fort Gibson OK
Feakins Cynthia Redwood City CA
Fitz Emily Monmouth OR
Fored Leigh Stockton CA
Forman Rachel Toronto ON
Francis Rodney Lancaster CA
George Michael Napa CA
Gettel Nadine Puyallup WA
Glick John Longmont CO
Glodowski Jodi Amherst WI
Gravelle Lisa Murray UT
Greer Seldon Roseville CA
Guerra Juan Oakland CA
Harvey Kathryn Corralitos CA
Hasenauer Kevin Scotts Valley CA
Hill Laurie Gaffney SC
Hindia Keya O'Fallon MO
Hobbs June Tigard OR
Humphrey Stinson Kamuela HI
Ienna Larissa Portland OR
Jacklin Sadona Las Vegas NV
Johnson Lisa Anchorage AK
Johnson Susan Martin TN
Jones David Honolulu HI

Kassis Adrienne San Francisco CA
Khalili Tabrizi
Hessam San Diego CA
Klassen Cathlyn Redmond WA
La Saulle Brooke San Francisco CA
Lasher Lisa Paducah KY
Leifer Timothy Pasadena CA
Leung Jennifer San Diego CA
Lewis Leigh Portland OR
Liu Sai‐Ling Nome AK
Lusk James Seattle WA
Mason Danielle Mentone CA
McMillen Douglas Seattle WA
Meals Sam Fairmont MN
Mehta Sonia Northbrook IL
Messner Eric Sunnyvale CA
Miller Terina Oakland CA
Moga Christopher New Prague MN
Mohling Shanti Taos NM
Myles Angela Crossett AR
Nahar Pravin Warners Bay NSW
Nelson Yvonne Kaukauna WI
Pan Jo Costa Mesa CA
Payne Susan Lake Oswego OR
Pearson Lawrence Fallbrook CA
Pena‐Pridmore
M. Rosalie Browns Valley CA
Peyton Michael Drayton Valley AB
Ppowlen Angela Berkeley CA
Purvis Janey Bend OR
Pyant‐DanPullo
Courtney Freeport IL
Raman Srilata Fremont CA
Raymundo Michele Encinitas CA
Reddy Ravi Kaneohe HI
Rojas Joseph Las Vegas NV
Rojas Kirsten Las Vegas NV
Roybal G. Michael Pasadena CA
Saj Marta Naperville IL
San Tun Sabine Kailua Kona HI
Sheets Patrick Rensselaer IN
Shi Michael Livermore CA
Sirotin Nicole Woodside NY
Smith Dana Edmonton AB
Spangler Sherard Charlotte NC
Spencer Paula Happy Valley OR
Stone Barry Provo UT
Sturgeon Treena St. Louis MO
Swift Jean Kamuela HI
Tabas Jeffrey San Francisco CA
Taniguchi Paula Folsom CA
Tannous Rawah Austin TX
Tate Jennifer Longview WA
Tatini Usha Scottsdale AZ
Thiim Christian Irvine CA
Thompson Sharon Phoenix AZ
Ton Kiti Phoenix AZ
Van Dyke Michael Geyserville CA
Walterfang Mark Melbourne
Williams Michael Santa Rosa CA
Wong Juliana Danville CA
Yeturu Sumana Irvine CA
NOTES
Presentation slides will not be used for this session.

6/21/2013
1
Breast & Cervical Cancer Screening:
Updates and Controversies
Rebecca Jackson, MD
Professor, Ob/Gyn & Reproductive Sciences
Epidemiology & Biostatistics
University of California, San Francisco
I have no financial interests to disclose
Part I
Cervical Cancer Screening
1.Why USPSTF and other organizations changed guidelines (interval, start and stop ages)
2.HPV co-testing
3.What to do with HPV +, pap –
4.Which is better: pap or liquid-based cytology
Part II
Breast Cancer Screening
1. Why USPSTF changed guidelines for 40-49 yo women from B to C
2. Risk estimation for 40-49yo
3.Evidence on newer screening techniques: U/S, MRI, digital mammography

6/21/2013
2
Cervical Cancer in US
Pap smears are the most effective screening test ever invented….
Q1: 19 yo brought in by mom for pap. Sexually active since age 15. 4 male sexual partners. In addition to STI screening & counseling on safe sex and birth control, what else would you do?
A. Traditional Pap smear
B. Liquid-based cytology (eg thin prep)
C. HR-HPV only (without cytology)
D. HR-HPV with cytology (ie co-test)
E. Nothing more
Why does pap screening work?
• Sensitivity and specificity of pap/cytology not great
BUT
• The organ is easily accessible for screening
• Natural history is favorable : – precursor exists that is detectable and treatable;
– time course before cancer develops is long
– many opportunities to detect . Even if one test is false negative, get another chance.
• It is cost-effective because many years of life are saved because cancer is actually prevented.

6/21/2013
3
Can we do better?
• Half of cervical cancers occur in women who are not screened or inadequately screened. These women tend to be poor, uninsured, with lack of access to care– A more sensitive test (like many marketed directly
to the public eg Thin Prep), will not fix this problem!
• In poor countries, cervical cancer remains a huge problem.
Can we do better? YES!• False +: Although colposcopy is not that
morbid, false +’s still cause anxiety, labeling, and are costly. – Spacing the screening interval, starting screening
later and HPV typing used correctly in conjunction with cytology, will reduce false +’s and colposcopies
• Over-treatment: Only 30% of untreated CIN3 becomes invasive cancer (over 30 yrs). Destroying all CIN3 =over-treatment. Main harm is preterm delivery. • Smart screening, biomarkers, risk-based
approaches and less aggressive (but still evidence-based) treatment guidelines can help.
Potential adverse effects of LEEPPreterm delivery 70% Low birth weight 82% PPROM 169%
Lancet 2006 367:489-98
Caution: No randomized trials.
Potential adverse effects of cold knife cone
Perinatal mortality 187% Severe preterm delivery 178% Extreme low birthweight 186%
BMJ 2008 Sep 18;337
2012 USPSTF Cx Ca
• STRONGLY RECOMMENDS (“A”)
• Who? Women with cervix, regardless of sexual history
• Begin: Start age 21
• Interval:. 21-29: cytology q 3yr; after 30: can do q 5yr with cyto+HPV or cont’d q 3 yr cyto alone
• End: Age 65 if adequate prior screening (as per
ACS/ASCCP) and not at high risk for cx cancer (HIV, DES, immunocompromised)
• Other: Recommends against any HPV testing in <30yo (“D” grade)

6/21/2013
4
Other US Guidelines very similar
ACS/ASCCP/ASCP (2012)
• Begin: age 21
• Interval: Age 21-29: Q 3yr, HPV as a reflex test not as primary screen. After 30: preferred= cyto + HPV q 5 yrs; cyto alone q 3yrs also ok.
• End: age 65 if 3 nl paps or 2 nl HPV within 10 yrs, most recent within 5yrs. Continue to screen for 20yr after CIN 2/3. Do not resume even if new sex partner
ACOG (2009):
• Same
• 21-29: Q 2yr . After 30, Q 3 yrs if 3 consecutive, satisf normals & not immunocompromised. Co-screen with HPV q 3yr approp if >30yo.
• End: 65-70yo if 3 conseqnls and no abnormals in last 10 yrs
What’s similar• All strongly recommend against starting
before age 21
• None recommends annual screening
• All recommend against HPV alone or as a co-test in women <30 (ok as a reflex test after abnormal pap per ACS/ASCCP)
• All recommend no screening after hyst as long as no history of CIN2+
• All recommend stop at age 65
• None recommend changes in screening for those who’ve had HPV vaccine
What’s new/different?
• Co-test with HPV: – 1st time USPSTF has recommended co-
testing with HPV (ok for women who want to extend interval to 5 yrs)
– ACS/ASCCP: prefers co-test with 5 yr interval; acceptable to do cyto alone q3yr
• F/U after CIN2+: ACS/ASCCP: 20 yrs ACOG: 10 yrs, USPSTF vague
• Criteria to end at age 65: ACS/ASCCP—clearer guidance than others
Why is it ok to delay screening until age 21?
• Cervical cancer extremely rare in younger women
• HPV infection very common immediately after onset of intercourse and 90% is cleared by host within 2 yrs
• When dysplasia does occur in adolescents, it tends to be low grade and transient (90% regression at 3 yr).
– If persists, plenty of time to detect and treat because long progression time of pre-invasive lesions to invasive cancer
• Excision of dysplasia associated with preterm birth
• Labels adolescent with a sexually transmitted infection
• Bottom Line: HPV infection typically cleared without help from us. Screening in adolescents therefore leads to treatment that is largely over-treatment . Harms>>>Benefits

6/21/2013
5
Why is it ok to lengthen the screening interval?
• After several normal tests, very small likelihood of missed disease
• If newly acquired infection, high likelihood of regression and long time to invasion
• The more tests you do, the more false +’s. Mathematical reality: prevalence is low, tests not extremely specific.
21-29yo: The evidence for q 3 yr interval
• ACS/ACSSP: “Annual screening leads to a very small increment in cancers prevented at cost of large excess of unnecessary procedures and treatments.”
• 3 vs 1 yr screening (21-29 yo)– Lifetime risk of cancer death: 0.03/1000 vs
0.05/1000 (decrease of 2 per 100,000)– Lifetime colposcopy rates 2000/1000 vs
760/1000 women (increase of 1240 per 1000)
Why the difference between <30 and >30 yo?
• HR-HPV co-testing becomes clinically useful after age 30
• In <30yo: HPV often positive, often transiently. Therefore, HPV testing not clinically useful.
• > Age 30: HPV positivity more likely to represent persistent HPV which is a significant risk factor for dysplasia/cancer. Conversely, HPV negativity is a strong negative predictor.
Role of HR-HPV testing
• Greater sensitivity, lower specificity, better reproducibility than pap/cytology
• HPV tests may better forecast which women will develop CIN3+
• More sensitive for adeno-ca
• Has potential for increased detection (more sensitive) and increased interval of screening (more predictive of CIN3 risk)
• Harm=increased colpo/treatment. This can be mitigated by increasing interval to 5 yr

6/21/2013
6
ModelingFalse + Colposcopies CIN 2-3 Cancers Cancer
deaths
Cytology q3 years, ages 21-65
350 758 80 8.5 1.55
Cytology q3 years until age 30 then co-testing q5 years
281 625 85 7.1 1.29
Per 1000 women screened over a lifetime.
Modeling studies support similar benefits of co-testing every 5 years and cytology every 3 years, demonstrating small differences in expected cancer cases and cancer deaths.
Co-testing caveats
• HPV has decreased specificity so if we co-screen more often than q5 years, patients will incur greater harm without benefit – Before doing co-test, ensure patient is willing to be
screened every 5 years
• HPV-based strategies also lead to more positives – Some women will need prolonged surveillance
– Some women who would otherwise be able to stop at age 65 will require continued screening beyond age 65
• What to do with HPV+, cytology negative?
Cotesting: what to do with HPV positive/Pap normal women?
About 8-11% of women ages 30-55 in the US will have a positive HPV test (HC2) and a normal Pap test (Ann Int Med April, 2008)
At Kaiser Northern CA, about 3-7% of women ages 30-55 have a positive HPV test (HC2) and a normal Pap test (Obstet Gynecol March 2009)
HPV positive/Pap normal women
Recommendations by ASCCP and ACOG: • Repeat co-test at 12 months.
– If negative q 5yr screening– If still HPV+ or if >= LSIL AS-CUScolposcopy.
2012 ASCCP Guidelines; ObstetGynecol, Apr 2013
Alternate recommendation by ASCCP:• Perform HPV genotype-specific typing for 16 or
16/18. – if positive, perform colposcopy. – If negative, repeat co-test at 12 months.

6/21/2013
7
What’s Better: Pap or LBC?
• N=89,784, cluster RCT– No difference in detection rate (sensitivity) or
PPV, fewer unsatisfactory tests with LBC Conclusion: no difference
• 2nd RCT, different design, similar findings• Evidence based practice center & 2
reviews conclude: no difference in relative or absolute sensitivity or specificity
Siebers, 2009
Conclusions: Cervical Cancer
• Cervical cancer screening in the US is already very successful at decreasing cervical cancer incidence and morbidity
• Now the goal is to decrease harm by decreasing false + and over-treatment:– Start screening later (age 21)
– Screen less often (q 3yr)
– Use HPV co-test to extend interval to 5yr
– Return to traditional pap smear?
Part II
Breast Cancer Screening
1. Why USPSTF changed guidelines for 40-49 yo women from B to C
2. Risk estimation for 40-49yo
3.Evidence on newer screening techniques: U/S, MRI, digital mammography
Q2: 43 yo woman with normal mammo 2 yrs ago but with “extremely dense” breasts. No other breast cancer risk factors. She would like your recommendation re: screening.
A. Wait until age 50 and then get mammo
B. Regular (film) mammo
C. Digital mammo
D. Mammo plus ultrasound
E. Mammo plus MRI

6/21/2013
8
2009 USPSTF recommendations
• 50-74 yo: RECOMMENDS (“B”)• 40-49 yo: Individual decision (ie don’t
offer routinely) (“C”) (was“B” in 2003)
• What? Mammography with or without clinical breast exam
• How often? Every 2 years (was every 1-2 years in 2003)
• When stop? After age 75, evidence is insufficient to make recommendation (“I”)
USPSTF Rec’s: A=strongly recommends; B=recommends; C=no recommendation; D=Recommends against; I=insufficient evidence
2009 Meta-analysis by USPSTF
• 1 new trial specifically in women 40-49
• 1 trial with updated data
Nelson, Annals Int Med, 2009
40-49 yo womenNelson H D et al. Ann Intern Med 2009;151:727-737
2 trials designed to look at women in 40’s
Criticism: Most of these trials include benefits that may have accrued to women due to screening that occurred after the age of 50. On other side: Most were done long ago and mammo technology improved today so benefits may be underestimated. However, modeling studies using updated sensitivity/specificity show same magnitude of benefit
Ratio of Benefits vs Harms• Benefits= decreased mortality, increase in
# life years gained
• Harms (USPSTF doesn’t include financial costs in their analysis)
– screening (radiation risk, pain, inconvenience)
– diagnostic work-up for false positive (49% over 10 mammos, anxiety, 1/3 of total screening cost)
– over-diagnosis (harms assoc with overtreatment, 10-25% of invasive, 34% of DCIS)
• Benefit/Harm ratio varies significantly by patient age

6/21/2013
9
Why the change? Conceptually…
In women 40-49 c/w older women…
• Smaller number of deaths are prevented because: – Lower incidence of breast cancer
– Lower sensitivity of mammography
– Cancers often more aggressive, less treatable
• More false positives– Lower specificity and prevalence lower
positive predictive value & more false positives
Why the change? Numerically….
Tice, Prim Care Clin Office Pract 2009
Why the change from B to C for 40-49 yo’s from 2003 to 2009?
Bottom Line: USPSTF uses absolute benefit, not relative benefit and strongly considers risk of harm to healthy women (which is subjective and debatable).
The USPSTF notes that a "C" grade is a recommendation against routine screening of women aged 40 to 49 years. The Task Force encourages individualized, informed decision making about when to start...
Screening frequency 1 vs 2 yrs
• Similar reduction in mortality with screening every one or two years
• Every two years (compared to annually) maximizes benefits of screening & minimizes harms
Mandelblatt, Annals IM, 2009
6/21/2013
10
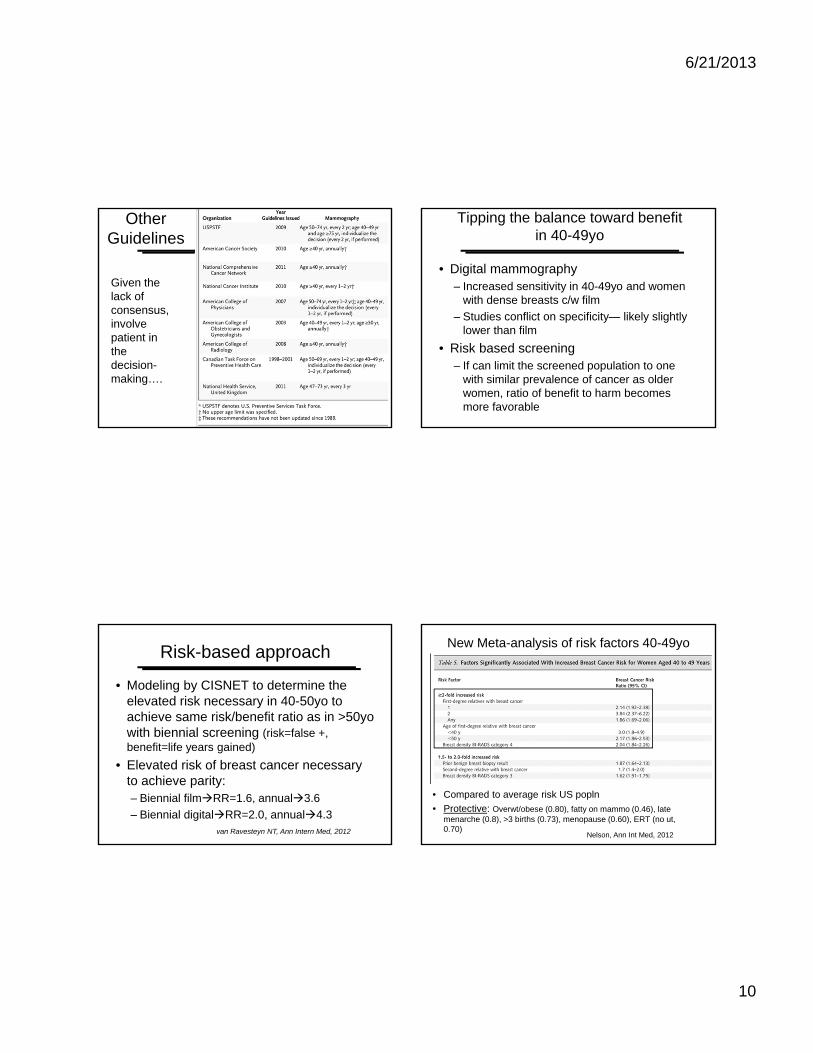
Other Guidelines
Given the lack of consensus, involve patient in the decision-making….
Tipping the balance toward benefit in 40-49yo
• Digital mammography– Increased sensitivity in 40-49yo and women
with dense breasts c/w film
– Studies conflict on specificity— likely slightly lower than film
• Risk based screening– If can limit the screened population to one
with similar prevalence of cancer as older women, ratio of benefit to harm becomes more favorable
Risk-based approach
• Modeling by CISNET to determine the elevated risk necessary in 40-50yo to achieve same risk/benefit ratio as in >50yo with biennial screening (risk=false +, benefit=life years gained)
• Elevated risk of breast cancer necessary to achieve parity:– Biennial filmRR=1.6, annual3.6
– Biennial digitalRR=2.0, annual4.3van Ravesteyn NT, Ann Intern Med, 2012
New Meta-analysis of risk factors 40-49yo
• Compared to average risk US popln
• Protective: Overwt/obese (0.80), fatty on mammo (0.46), late menarche (0.8), >3 births (0.73), menopause (0.60), ERT (no ut, 0.70)
Nelson, Ann Int Med, 2012

6/21/2013
11
New Technologies
• Digital Mammography
• Breast MRI
• Ultrasound plus Mammography
• Thermography?
Digital mammography
• Sensitivity:– Most studies show higher sensitivity in 40-49.
– One large study (DMIST) showed lower sensitivity in women >65yo
• Specificity:– Very mixed: some show no difference, most
show decreased specificity
2 largest US studies: <50yo
DMIST (research study)
• N=42,760 women, 14,335 <50yo
• All women got both digital and film mammo
• One year f/u• Sensitivity: 51% (F) vs
78% (D)• Specificity: both 90%
• Calculated PPV based on 2.8/1000 prevalence: 1.4 vs 2.1%,
BCSC (community based)
• N= 329 260 women, in <50yo: 77,392 digital, 221,696 film
• Women got either digital or film depending on site
• One year f/u• Sensitivity: 76(F) vs 82%(D)
• Specificity: 89.7 vs 88%
• Calc PPV: 2.1 vs 1.9%,
Pisano, NEJM, 2005 Kerlikowske, Ann Int Med, 2011
Bottom Line: Digital
• More sensitive for women<50, extremely dense breasts, ER negative breast cancer
• Easier access, transmission and storage of images, lower average dose of radiation
• Trade-off of slightly lower specificity
• From BCSC: in 10,000, 2 additional breast cancers for 170 additional false positive results

6/21/2013
12
Q2: 43 yo woman with normal mammo 2 yrs ago but with “extremely dense” breasts. No other breast cancer risk factors. She would like your recommendation re: screening.
A. Wait until age 50 and then get mammo
B. Regular (film) mammo
C. Digital mammo
D. Mammo plus ultrasound
E. Mammo plus MRI
Caution: comparing detection rates….
• Studies of new techniques typically compare detection rates
• Key q is : does improved detection lead to overall benefit (decreased mortality/morbidity)
• Observational studies prone to lead-time and length bias
• Earlier treatment may not be better than later– Ex: 10,000 50 yo’s followed for 20 yrs. Without
mammo, 260 will die of breast cancer. With biennial mammo: 223 will die. Screening averted 37 deaths per 10,000 over 20 years = 1 death saved/270 women for 20 years
Ultrasound + Mammo• Potentially useful in dense breasts
• No RCT’s of normal risk women or women with only risk being dense breasts
• Meta-analysis in women with dense breasts: – 6 cohort studies, only 2 included adeq f/u (nec to know
false + and -)– Studies small; few cancers detected (results unstable)– CONCLUSION—more study necessary
• In very high risk women (dense + 1 RF), U/S detected additional 3.7-5/1000, 7-10% biopsy rate
Nothacker BMC Cancer 2009
Berg, JAMA, 2012
MRI + Mammo• For high risk women (BRCA, personal h/o brst ca,
lifetime risk >20%)
• Systematic review– No RCT’s, no studies with long term f/u or mortality,
MRI more sensitive (80-100%) vs 25-59%, less specific 73-93% (3-5 fold higher recall rate)
– Mammo more sensitive for DCIS therefore need both
– Concl: more study needed, unknown if lead time/ length bias or real benefit, screening doesn’t detect nor cure 100% therefore consider risk reducing strategies
• ACS: Annual MRI + mammo for women with lifetime risk >20%
Warner, Ann Int Med, 2008
6/21/2013
13
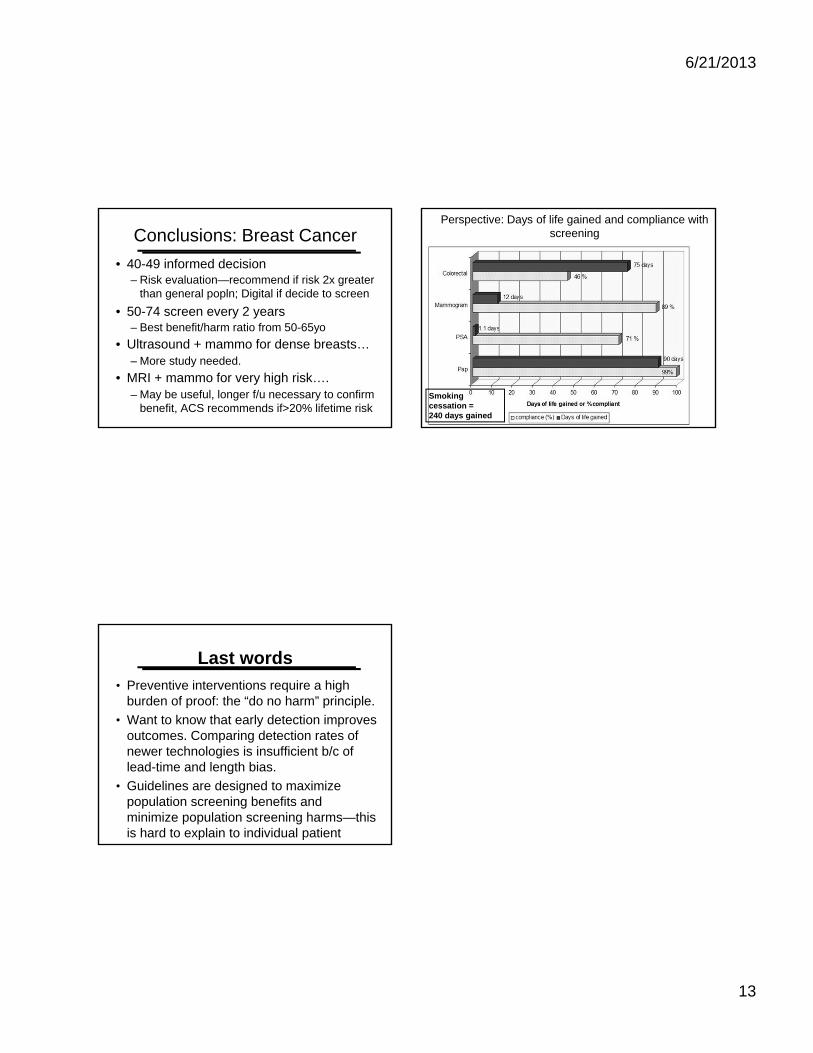
Conclusions: Breast Cancer
• 40-49 informed decision– Risk evaluation—recommend if risk 2x greater
than general popln; Digital if decide to screen
• 50-74 screen every 2 years – Best benefit/harm ratio from 50-65yo
• Ultrasound + mammo for dense breasts… – More study needed.
• MRI + mammo for very high risk…. – May be useful, longer f/u necessary to confirm
benefit, ACS recommends if>20% lifetime risk
Perspective: Days of life gained and compliance with screening
Smoking cessation = 240 days gained
Last words
• Preventive interventions require a high burden of proof: the “do no harm” principle.
• Want to know that early detection improves outcomes. Comparing detection rates of newer technologies is insufficient b/c of lead-time and length bias.
• Guidelines are designed to maximize population screening benefits and minimize population screening harms—this is hard to explain to individual patient

6/21/2013
1
OVARIAN CANCER SCREENINGAND
MANAGEMENT OF ADNEXAL MASSES
Alison Jacoby, MD
UCSF
Learning Objectives
• Review ovarian cancer risk factors
• Discuss ovarian cancer screening alternatives
• Analyze management strategies for premenopausasl and postmenopausal adnexal masses
• Review ACOG guidelines for referring a patient with an adnexal mass to a gyn oncologist
• Compare CA 125 and OVA1 tests
Ovarian Cancer ScreeningCase One
WL is a 54 yr old P0 who presents for an annual exam. She mentions seeing a segment on the evening news last week about improvements in ovarian cancer screening and she would like to be tested.
She is without abdominal complaints and has no family history of gynecologic or gastrointestinal cancers but she would feel better knowing the test was negative.
How would you counsel her?
6/21/2013
2
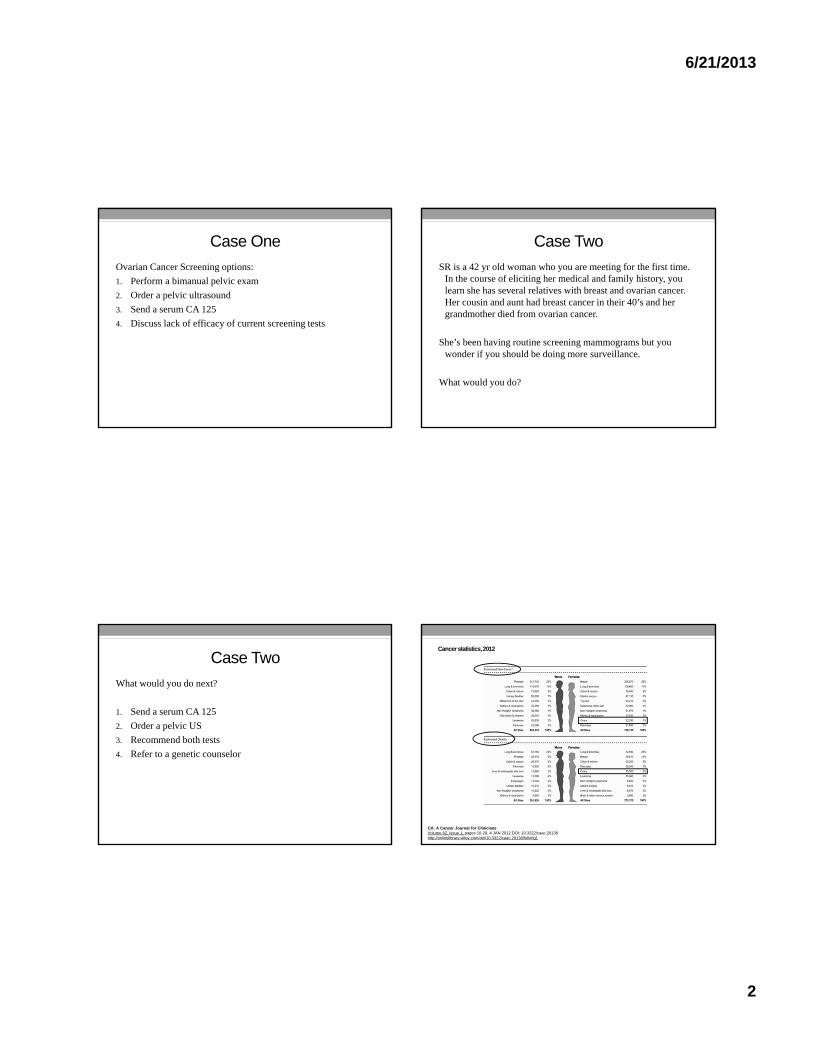
Case One
Ovarian Cancer Screening options:
1. Perform a bimanual pelvic exam
2. Order a pelvic ultrasound
3. Send a serum CA 125
4. Discuss lack of efficacy of current screening tests
Case Two
SR is a 42 yr old woman who you are meeting for the first time. In the course of eliciting her medical and family history, you learn she has several relatives with breast and ovarian cancer. Her cousin and aunt had breast cancer in their 40’s and her grandmother died from ovarian cancer.
She’s been having routine screening mammograms but you wonder if you should be doing more surveillance.
What would you do?
Case Two
What would you do next?
1. Send a serum CA 125
2. Order a pelvic US
3. Recommend both tests
4. Refer to a genetic counselor
Cancer statistics, 2012
CA: A Cancer Journal for CliniciansVolume 62, Issue 1, pages 10-29, 4 JAN 2012 DOI: 10.3322/caac.20138http://onlinelibrary.wiley.com/doi/10.3322/caac.20138/full#fig1

6/21/2013
3
Ovarian Cancer Risk FactorsRR Lifetime Probability (%)*
Familial Ovarian Ca Synd Unknown 30-50
2-3 Relatives w/ Ovarian Ca 4.6 5.5
1 Relative w/ Ovarian Ca 3.1 3.7
No RF’s 1.0 1.8
Past OC use 0.65 0.8
Past Pregnancy 0.5 0.6
Infertility 2.8
Past Breastfeeding 0.8
Tubal Ligation 0.6
* Indicates probability of Ov Ca in a 50 yr old woman
Ovarian Cancer Risk FactorsHormonal and Reproductive Factors
• Nulligravity
• Early menarche (age < 12)
• Late menopause (age >50)
• Endometriosis
• PCOS
Genetic factors- 10-15% of cases
• BRCA mutations
• Lynch II Syndrome
Environmental
• Talc
• Smoking
• Diet ?
• Exercise ?
• Obesity (BMI >30)
Ovarian Cancer Protective Factors
Combined E/P OC’s• 45 studies from 21 countries
• Any use lowers risk compared to non-users
• Longer duration of use assoc’d w/ lower risk reduction
• Protective effect lasts 30 yrs
• No data for non-oral E/P contraceptives (patch, ring)
Hysterectomy and Tubal Ligation• Both reduce RR by 34%
Multiparity
6/21/2013
4
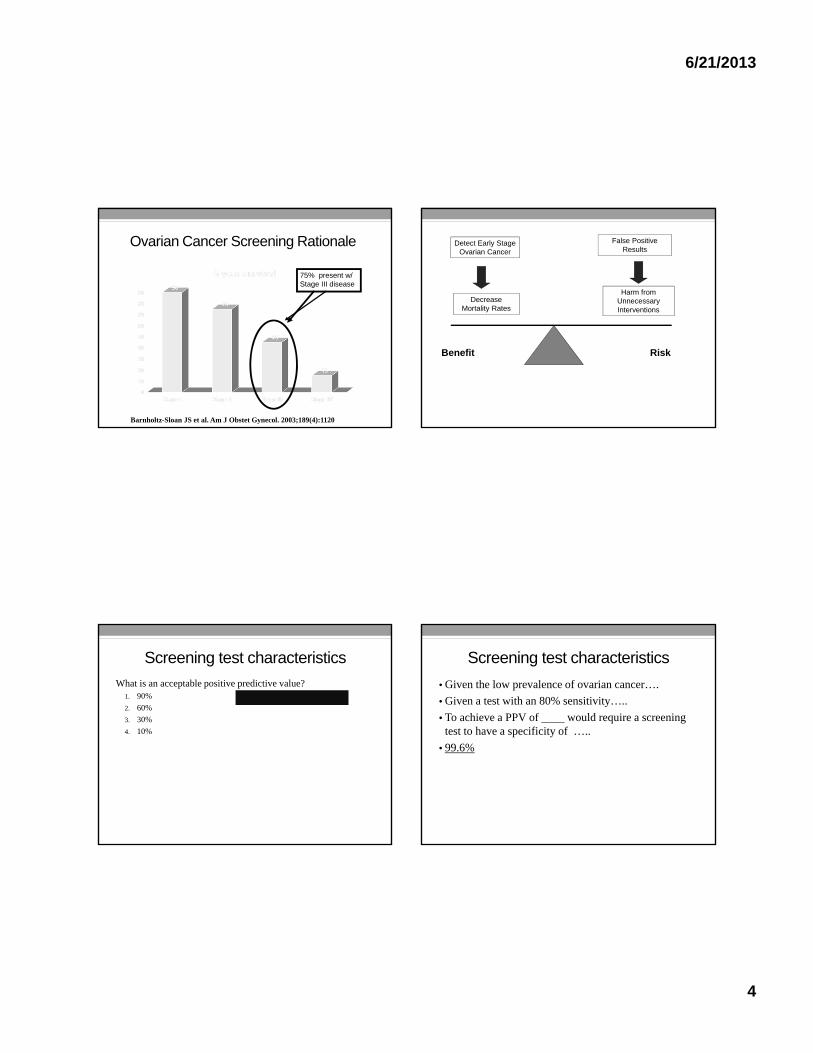
Ovarian Cancer Screening Rationale
75% present w/ Stage III disease
Barnholtz-Sloan JS et al. Am J Obstet Gynecol. 2003;189(4):1120
Benefit Risk
Detect Early Stage Ovarian Cancer
Decrease Mortality Rates
False Positive Results
Harm from Unnecessary Interventions
Screening test characteristics
What is an acceptable positive predictive value?1. 90%
2. 60%
3. 30%
4. 10%
Screening test characteristics
• Given the low prevalence of ovarian cancer….
• Given a test with an 80% sensitivity…..
• To achieve a PPV of ____ would require a screening test to have a specificity of …..
• 99.6%

6/21/2013
5
Potential Screening Tests
• Pelvic examination
• Pap smears
• Tumor markers- CA 125, HE4
• Imaging tests- US, CT
• Combination of modalities
CA 125
• Glycoprotein antigen on tumor cells
• FDA approved for monitoring treatment response and recurrence in women w/ Ov Ca
• Sensitivity
• Early stage disease: 50%
• Advanced stage disease: > 80%
• Specificity: ~68%
• Increased in a variety of benign and malignant conditions
• Endometriosis, fibroids, PID, other cancers, etc.
CA 125
Prostate, Lung, Colorectal, Ovarian Cancer Screening (PLCO) Trial
• >78,000 healthy women, age 55-74
• Randomly assigned to screening or control groups
• Ov Ca Screening: annual serum CA 125, TVUS or both for 5 yrs
• Follow-up for 13 yrs
• At baseline, 436 women had elevated CA 125
• PPV 3.7%
Buys SS, Partridge E, Greene MH, et al. Ovarian cancer screening in the Prostate, Lung, Colorectal and Ovarian (PLCO) Cancer Screening Trial: findings from the initial screen of a randomized trial. Am J Obstet Gynecol. 2005;193(5):1630-9.
Pelvic Ultrasonography
• 4526 women at high risk for Ov Ca screened annually
• After ~13,000 scans, all of the ovarian, fallopian tube and peritoneal cancers identified were Stage III
• NO cases of early disease detected
Fishman DA, et al. Am J Obstet Gynecol. 2005;192(4):1214.

6/21/2013
6
Pelvic Ultrasonography
• 37,293 Asx, low risk women age >50
• Study began in 1987, average f/u 5.8 yrs
• Specificity: 98.5%
• PPV: 8.9%
• NNT: 11 operations performed per case of Ov Ca
• Early detection: 70% of 47 screen-detected Ov Ca cases Stage I or II
• Lower mortality: 5 yr survival for screen-detected vs. unscreened Ov Ca cases: 84.6% vs. 53.7%
van Nagell JR Jr et al. Obstet Gynecol. 2011;118(6):1212.
CT Colonography
• 2869 women screened
• 70 women incidental finding of adnexal abnormality
• Number found to have Ovarian Ca?
• 4 women with normal adnexae dx’d with Ov Ca within 4 yrs
NONE
Pickhardt PJ, Hanson ME Radiology. 2010;257(1):144.
CA 125 and TVUS
Prostate, Lung, Colorectal, Ovarian Cancer Screening (PLCO) Trial
• >78,000 healthy women, age 55-74
• Ov Ca Screening: annual serum CA 125, TVUS or both for 5 yrs
• Follow-up for 13 yrs
• Early detection: NO
• Lower mortality: NO
• High false positive rate: 541 women underwent surgery without a cancer diagnosis
• Harm: 15% had at least 1 serious surgical complication
Case One
WL is a 54 yr old P0 who presents for an annual exam. She mentions seeing a segment on the evening news last week about improvements in ovarian cancer screening and she would like to be tested.
She is without abdominal complaints and has no family history of gynecologic or gastrointestinal cancers but she would feel better knowing the test was negative.
How would you counsel her?
6/21/2013
7
Case One
Ovarian Cancer Screening options:
1. Perform a bimanual pelvic exam
2. Order a pelvic ultrasound
3. Send a serum CA 125
4. Discuss lack of efficacy of current screening tests
Case Two
SR is a 42 yr old woman who you are meeting for the first time. In the course of eliciting her medical and family history, you learn she has several relatives with breast and ovarian cancer. Her cousin and aunt had breast cancer in their 40’s and her grandmother died from ovarian cancer.
She’s been having routine screening mammograms but you wonder if you should be doing more surveillance.
What would you do?
Case Two
What would you do next?
1. Send a serum CA 125
2. Order a pelvic US
3. Recommend both tests
4. Refer to a genetic counselor
Management of Adnexal Masses
6/21/2013
8
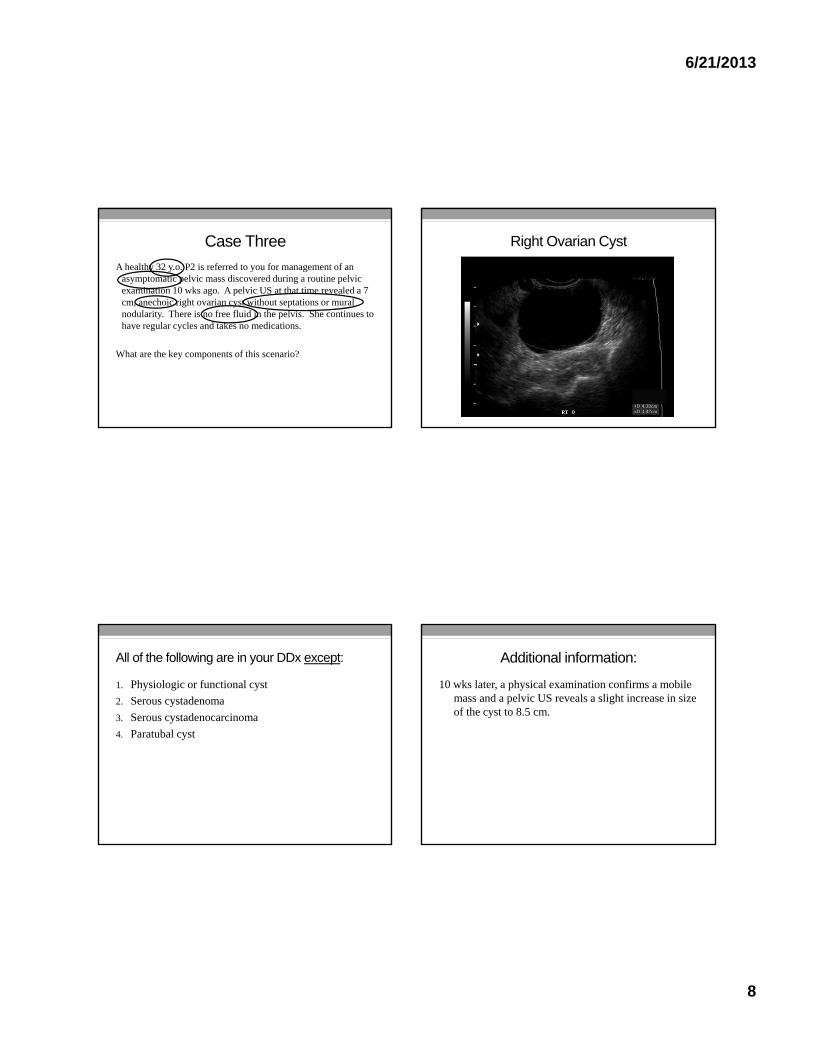
Case Three
A healthy 32 y.o. P2 is referred to you for management of an asymptomatic pelvic mass discovered during a routine pelvic examination 10 wks ago. A pelvic US at that time revealed a 7 cm, anechoic right ovarian cyst without septations or mural nodularity. There is no free fluid in the pelvis. She continues to have regular cycles and takes no medications.
What are the key components of this scenario?
Right Ovarian Cyst
All of the following are in your DDx except:
1. Physiologic or functional cyst
2. Serous cystadenoma
3. Serous cystadenocarcinoma
4. Paratubal cyst
Additional information:
10 wks later, a physical examination confirms a mobile mass and a pelvic US reveals a slight increase in size of the cyst to 8.5 cm.

6/21/2013
9
What is the most likely diagnosis now?
1. Physiologic or functional cyst
2. Serous cystadenoma
3. Serous cystadenocarcinoma
4. Paratubal cyst
What are her options?
• Observation
• Cyst content aspiration
• Laparoscopic ovarian cystectomy
• Laparoscopic oophorectomy
• Check tumor markers and refer to a gyn oncologist
Observation vs. Intervention
• Asymptomatic
• Low likelihood of malignancy
• Risks of surgery
• Natural history suggests growth will continue
• Tissue sample to confirm benign
• Risk for ovarian torsion necessitating urgent surgery
Cyst content aspiration
Easy to accomplish but…..

6/21/2013
10
Cyst content aspiration
Easy to accomplish but…..
• Potential spillage of malignant cells
• Low diagnostic yield
• Reaccumulation of fluid/cyst
Laparoscopic cystectomy
What is the most likely diagnosis now?
1. Physiologic or functional cyst
2. Serous cystadenoma
3. Serous cystadenocarcinoma
4. Paratubal cyst
Case 4
• A 54 y.o. G0 post-menopausal woman is referred to you by an NP for evaluation of a left ovarian cystic mass. The patient was experiencing some non-specific abdominal bloating several weeks ago which prompted the pelvic ultrasound. A 5 cm, unilocular, anechoic cyst with an echogenic mural nodule is described. Color Doppler imaging shows normal vascular flow. There is no free fluid in the pelvis. Her grandmother died from ovarian cancer.
What would you do next?

6/21/2013
11
Mural Nodule
What would you do next?
1. Repeat an ultrasound in 6-12 weeks
2. Refer to a gyn oncologist
3. Order a serum CA 125
4. Order a serum OVA1®
5. Perform a L/S oophorectomy
ACOG/SGO Referral Guidelines-Preoperative consultation with a gynecologic oncologist for one or
more of following criteria:
Premenopausal women1. CA 125 greater than 200 units/mL
2. Ascites
3. Evidence of abdominal or distant metastasis
4. Family history of breast or ovarian cancer (in a first-degree relative)
The revisions to the College guidelines proposed by Dearking include:
1) eliminating the family history of one or more first-degree relatives with ovarian or breast cancer
2) lowering the CA 125 threshold in premenopausal women to 67 units/mL.
ACOG/SGO Referral Guidelines-Preoperative consultation with a gynecologic oncologist for one or
more of following criteria:
Postmenopausal women (older than 50 yrs)
1. Elevated CA 125 (> 35 units/mL)
2. Nodular or fixed pelvic mass
3. Ascites
4. Evidence of abdominal or distant metastasis
5. Family history of ovarian or breast cancer (in a first-degree relative)
The revisions to the College guidelines proposed by Dearking include: 1) eliminating the family history of one or more first-degree relatives with ovarian or breast cancer
6/21/2013
12
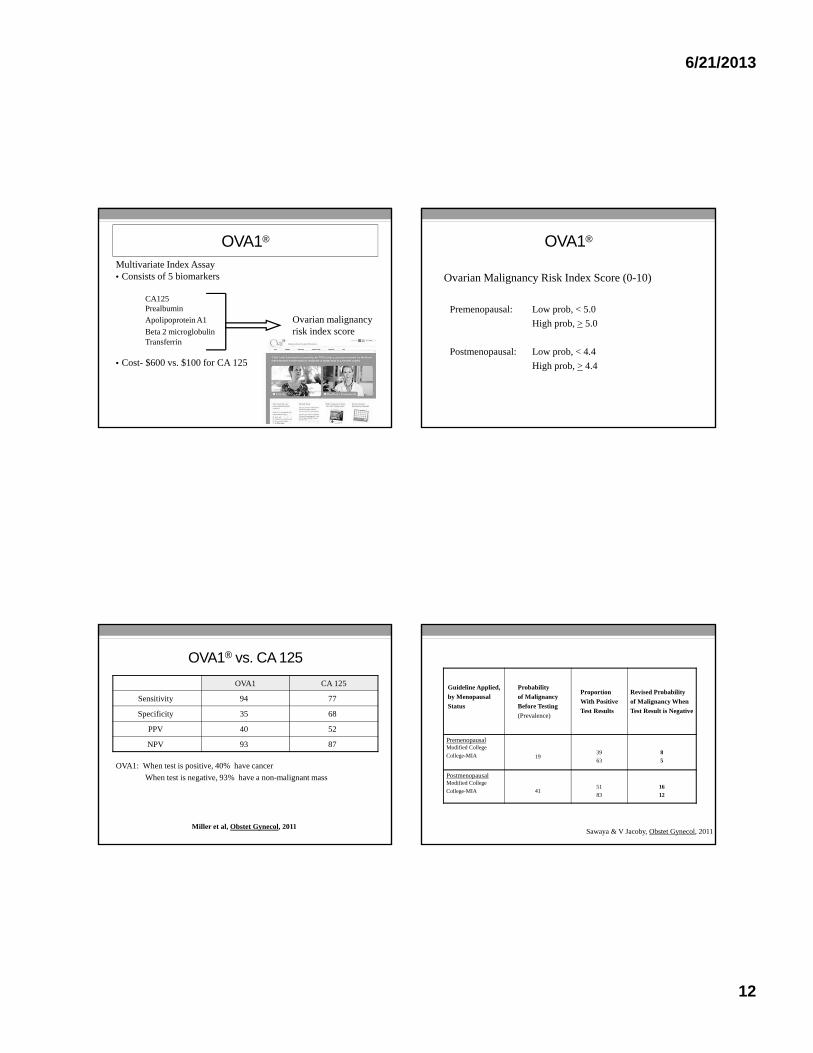
OVA1®
Multivariate Index Assay• Consists of 5 biomarkers
CA125Prealbumin
Apolipoprotein A1 Ovarian malignancyBeta 2 microglobulin risk index scoreTransferrin
• Cost- $600 vs. $100 for CA 125
OVA1®
Ovarian Malignancy Risk Index Score (0-10)
Premenopausal: Low prob, < 5.0
High prob, > 5.0
Postmenopausal: Low prob, < 4.4
High prob, > 4.4
OVA1® vs. CA 125
OVA1 CA 125
Sensitivity 94 77
Specificity 35 68
PPV 40 52
NPV 93 87
OVA1: When test is positive, 40% have cancer
When test is negative, 93% have a non-malignant mass
Miller et al, Obstet Gynecol, 2011
Guideline Applied,
by Menopausal
Status
Probability
of Malignancy
Before Testing
(Prevalence)
Proportion
With Positive
Test Results
Revised Probability
of Malignancy When
Test Result is Negative
Premenopausal Modified College
College-MIA 1939
63
8
5
Postmenopausal Modified College
College-MIA 4151
83
16
12
Sawaya & V Jacoby, Obstet Gynecol, 2011

6/21/2013
13
Case 4
• A 54 y.o. G0 post-menopausal woman is referred to you by an NP for evaluation of a left ovarian cystic mass. The patient was experiencing some non-specific abdominal bloating several weeks ago which prompted the pelvic ultrasound. A 5 cm, unilocular, anechoic cyst with an echogenic mural nodule is described. Color Doppler imaging shows normal vascular flow. There is no free fluid in the pelvis. Her grandmother died from ovarian cancer.
What would you do next?
What would you do next?
1. Repeat an ultrasound in 6-12 weeks
2. Refer to a gyn oncologist
3. Order a serum CA 125
4. Order a serum OVA1®
5. Perform a L/S oophorectomy
Recommendation
Women of average risk for ovarian cancer:
Do not offer screening
• ACOG, USPSTF, SGO, Canadian Task Force
Recommendation
Women with family history of Ov Ca but lowsuspicion for hereditary ovarian cancer
syndrome (BRCA, Lynch II):
Limited evidence for effectiveness of screening and potential for adverse effects of screening

6/21/2013
14
Recommendation
Women with high risk family history concerning for hereditary ovarian cancer syndrome:
Refer to Genetic counselor for discussion of BRCA mutation testing
SGO, National Comprehensive Cancer Network
In Conclusion…
The objectives of this presentation were to provide a….
• Reminder of Ovarian Cancer risk factors
• Evidence based review of Ovarian Cancer screening outcomes
• Clinically relevant examples of adnexal mass management
• Guidelines for referring patients to a gyn oncologist
• Balanced discussion of the new (heavily marketed) OVA1 test

Page 1
Cancer Screening 2013
Current Controversies in Lung, Colon, and Skin Cancer Screening
Jeffrey A. Tice, MD
Division of General Internal MedicineUniversity of California, San Francisco I have no conflicts of interest
Selected Controversies
• Lung Cancer Screening
– Does screening work?
– Chest x-ray?
– What about low dose CT?
• Colorectal Cancer
– What test and how often?
– Are there new screening options?
• Skin Cancer
– Should we screen?
Estimated New Cancer Cases* in the US in 2013
Page 2
Cancer Death Rates* Among Women, US,1930-2009
USPSTF
• Rigorous review of existing peer‐
reviewed evidence
–Ratings reflect the strength of the evidence on the harms and benefits of a preventive service• Task Force does not consider the costs of providing service or make recommendations for coverage
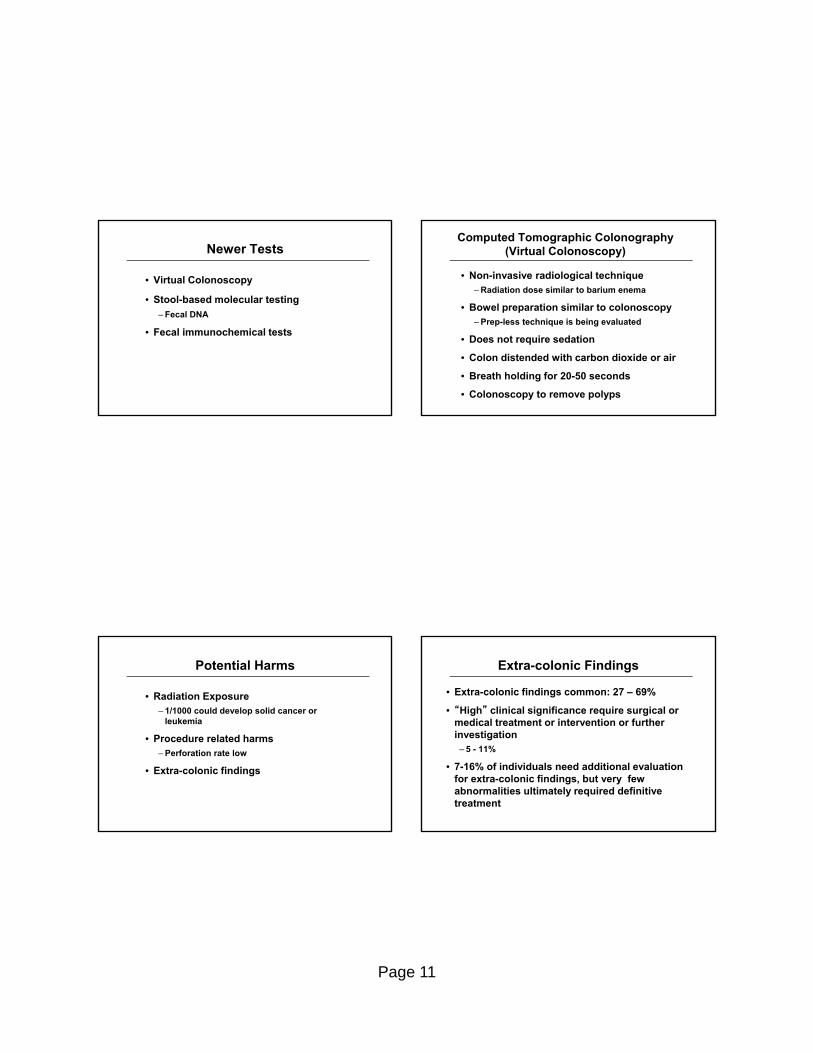
USPSTF Grades
Grade Evidence Recommendation
A High certainty of substantial net benefit Provide
B High certainty of moderate net benefitModerate certainty of moderate/substantial net benefit
Provide
C Moderate certainty that net benefit is small Selectively offer/provide
D No net benefit or harms outweigh benefits Do not provide
I Insufficient evidence regarding balance of benefits and harms
Lung Cancer Screening

Page 3
Question?
• Ms. Nicka Teen is a 69 year old woman with a 50 pack-year history of smoking and COPD. You have previously been unsuccessful in encouraging her to quit smoking. She comes in for a check-up, is worried about developing lung cancer and wants to know what test you think she should have. What do you recommend?
– Chest X ray
– Sputum cytology
– Spiral CT
– None of these tests
Lung Cancer Screening:Systematic Review of Chest X-rays
• 7 trials of lung cancer screening
• Frequent screening with chest x-rays was associated with an increase in mortality
– RR 1.11 (95% C.I. 1.00-1.23)
• No difference in chest X-ray plus cytology versus chest X-ray alone
Manser, Thorax, 2003
PLCO: Lung Cancer Screening
• PCLO randomly assigned 154,901 adults
aged 55 through 74 to annual CXR for 4
years vs. usual care
• Followed for 13 years
• Cumulative lung cancer mortality
– 14.0/10,000 py screening group vs. 14.2/10,000 py control group
–Rate ratio: 0.99 (95% CI 0.87‐1.22)
Oken MM. JAMA 2011;306:1865
Low Dose Spiral Computed Tomography
• Scans lung in < 20 seconds (single breath)
• No IV contrast
• More radiation exposure than CXR but less than conventional CT
• Can detect much smaller lesions than chest X-ray
Page 4
The National Lung Screening Trial (NLST)
53,454 participants randomized to CT or CXR
- Current or former heavy smokers: ≥ 30 pack-years
- Ages 55 to 74
- Annual CT scans x 3 years. 6.5 years follow-up
LDCT CXR∆ RR (95% CI)
Lung Cancer Deaths 356 44387 .80 (.73-.93)
Any death 1877 2000121 .93 (.86-.98)
Number needed to invite to screen
• NNI to prevent one lung cancer death in 6.5 years = 320
• NNI to prevent one death from any cause in 6.5 years = 218
Balanced by…
• 75,000 CT scans
• 18,146 positive tests
• 17,066 false positive tests
• 713 thoracotomy / mediastinoscopy
• 671 bronchoscopies
• 322 needle biopsies
• To prevent 87 deaths from lung cancer
NLST Harms
• False positives
– At least 1 positive test in 39% CT
• False positive results in 96% CT
• Possible over diagnosis
–Higher cancer incidence with CT
• 1060 vs. 941 cancers
• Rate ratio 1.13 (95% CI 1.03‐1.23)
• Radiation exposure
• Incidental findings

Page 5
Concern: Control = Chest x-ray
• Screening with CXR was ineffective in 30,341
subjects in the PLCO meeting NSLT criteria
– 30+ pack year, smoked within past 15 years
–Cumulative lung cancer mortality was 36.1/10,000 py screening group vs. 38.3/10,000 py controls• Rate ratio: 0.94 (0.81‐1.10)
• Reasonable to conclude that CT screening is
more effective than usual care
Health Policy not yet established
• ~ 94 million current or former smokers in the U.S.
• ~ 7 million meet NLST criteria
• Implementation issues
–Multidisciplinary teams
–Trained radiologist
• Expensive… $ $ $
Guidelines and recommendations
• Recommend for those meeting NLST entry criteria at specialized centers
–ACCP / ASCP / ATS
–ACS
–ALA
–NCCN
–AATS

Page 6
Guidelines and recommendations
• USPSTF recommendations
–Screening: “I” insufficient evidence (2004)
–Smoking cessation counseling: “A”(2009)• 85% of cancers among smokers attributed to smoking
Trends in Tobacco Use and Lung Cancer Death Rates* in the US
Trends in Cigarette Smoking, Adults 18 and Older, US, 1965-2011Trends in Cigarette Smoking* among Female High School Students,
US, 1991-2011

Page 7
Primary Prevention OfLung Cancer
• Smoking cessation
• Smoking cessation
• Smoking cessation
• Smoking cessation
• Smoking cessation
• Smoking cessation
• Smoking cessation!!!!!
Implications
• Smoking cessation
• Strict adherence to NLST entry criteria
– 55-74 years, 30+ pack years
• Use experienced centers / demonstration projects to ensure quality and effectiveness
Colorectal Cancer
Question?
• What do you most commonly recommend for colorectal cancer screening?
– Fecal occult blood test (FOBT)
– Sigmoidoscopy
– Colonoscopy
– Air contrast barium enema
– Virtual Colonoscopy
– Fecal DNA
– Fecal immunochemical Test (FIT)

Page 8
New Joint Guideline: ACS, ACR,…
• FOBT annually
• Fecal immunochemical test annually
• Flexible sigmoidoscopy every 5 years
• DCBE every 5 years
• CT colonography every 5 years
• Colonoscopy every 10 years
• Stool DNA testing (interval uncertain)
Levin, Gastroenterology, 2008
Joint Guideline Recommendation
• Clinicians should make patients aware of the full range of screening options
• Offer patients a choice between a screening test that is effective at both early cancer detection and cancer prevention through the detection and removal of polyps and a test that is primarily effective at cancer detection
• CRC prevention should be the primary goal of screening
USPSTF
• USPSTF: “A” recommendation (2008)
–Routine screening from age 50 until 75• Individualized decisions from 76 to 85
• No screening after 85
USPSTF Annals IM 2008
USPSTF (continued)
• USPSTF: “A” recommendation (2008)
–Acceptable modalities • Colonoscopy
• Fecal blood test– Fecal immunochemical test, high‐sensitivity hemoccult
• Flexible sigmoidoscopy
– Insufficient evidence for CT colonography, fecal DNA
USPSTF Annals IM 2008

Page 9
Colonoscopy
• American College of Gastroenterology
guidelines for colorectal cancer
screening (Rex DK. Am J Gastroenterol 2009;104:739)
–Colonoscopy… remains the preferred CRC screening strategy
Colonoscopy: RCTs in progress
• VA
– Colonoscopy versus fecal immunochemical test in reducing mortality from colorectal cancer
• Spain
– Colorectal cancer screening in average‐risk population: immunochemical fecal occult blood testing versus colonoscopy
• Netherlands
– Colonoscopy or colonography for screening
Flexible Sigmoidoscopy
• Flexible sigmoidoscopy reduces
colorectal cancer incidence by 21% and
colorectal cancer mortality by 26% (Schoen RE. NEJM 2012;366:25)
Flexible Sigmoidoscopy
• Prostate, Lung, Colorectal, and Ovarian
Cancer Screening Trial (PLCO)
–Randomly assigned 154,890 average‐risk adults, age 50 to 74, to either screening with flexible sigmoidoscopy (baseline, 3‐5 years) or usual care
–Median follow‐up 11.9 years

Page 10
Flexible Sigmoidoscopy
• Reduced CRC incidence
–Relative risk: 0.79 (95% CI 0.72‐0.85)
–Absolute risk reduction: 3.3/10,000 person years• Number needed to invite to screening (NNI): 285 (95% CI 210‐427)
Flexible Sigmoidoscopy
• Reduced CRC mortality
–Relative risk: 0.74 (95% CI 0.63‐0.87)
–Absolute risk reduction: 1.0/10,000 person years• NNI: 871 (95% CI 567‐1874)
–Mortality reduction limited to distal cancers
Flexible Sigmoidoscopy
• United Kingdom study showed one‐time
flex sig reduced CRC incidence by 23%
and mortality by 31% (Atkin WS. Lancet
2010;375:1624)
• Fewer primary care physicians now
recommend flex sig (Klabunde CN. Am J Prev Med
2009;37:8)
–78% (2000) to 26% (2007)
Flexible Sigmoidoscopy
• United Kingdom study showed one‐time
flex sig reduced CRC incidence by 23%
and mortality by 31% (Atkin WS. Lancet
2010;375:1624)
• Fewer primary care physicians now
recommend flex sig (Klabunde CN. Am J Prev Med
2009;37:8)
–78% (2000) to 26% (2007)
–Colonoscopy recommendations increased from 38% to 95%
Page 11
Newer Tests
• Virtual Colonoscopy
• Stool-based molecular testing
– Fecal DNA
• Fecal immunochemical tests
Computed Tomographic Colonography (Virtual Colonoscopy)
• Non-invasive radiological technique– Radiation dose similar to barium enema
• Bowel preparation similar to colonoscopy– Prep-less technique is being evaluated
• Does not require sedation
• Colon distended with carbon dioxide or air
• Breath holding for 20-50 seconds
• Colonoscopy to remove polyps
Potential Harms
• Radiation Exposure– 1/1000 could develop solid cancer or
leukemia
• Procedure related harms– Perforation rate low
• Extra-colonic findings
Extra-colonic Findings
• Extra-colonic findings common: 27 – 69%
• “High” clinical significance require surgical or medical treatment or intervention or further investigation
– 5 - 11%
• 7-16% of individuals need additional evaluation for extra-colonic findings, but very few abnormalities ultimately required definitive treatment

Page 12
Fecal DNA Testing
• PCR test for DNA mutations in the stool
• Potential advantages
– Non-invasive
– No preparation
– Detection along entire length of the colon
Fecal DNA Testing
• Screening test in multi-center study
• Fecal DNA test (23 mutations), FOBT, and colonoscopy
• 4482 average risk adults
• Fecal DNA detects more neoplasms than FOBT, but with more false positive results
• Expensive: $400 to $800 versus $3 to $40 for FOBT
Ahlquist, 2008
Fecal Immunochemical Testing (FIT)
• Uses labeled antibodies that attach to antigens of any human globin present in the stool
• Globin does not survive passage of the upper GI tract
• No dietary restrictions (easier than FOBT)
Fecal Immunochemical Testing
• FIT is more sensitive in detecting CRC and large adenomas (>1 cm) than FOBT
• FIT is a little less specific than FOBT

Page 13
Colorectal Cancer Screening
Fecal immunochemical test (FIT) more acceptable than colonoscopy (Quintero E. NEJM 2012;366:697)
Colorectal Cancer Screening
• Randomized screening trial in Spain of
biennial FIT vs. one‐time colonoscopy
53,302 subjects ages 50 to 69
• Primary outcome is CRC mortality after
10 years
Screening Outcomes
Quintero E. NEJM 2012;366:697
Colorectal Cancer Screening
• Recommending only colonoscopy
resulted in lower adherence (Inadomi JM. Arch
Intern Med 2012;172:575)
Page 14
Colorectal Cancer Screening
• Randomized trial offering colonoscopy,
FOBT, or choice of colonoscopy/FOBT
• 997 subjects ages 50 to 79
• 12‐month follow up
Screening Completion
Inadomi JM. Arch Intern Med 2012;172:575
How Are We Doing?
Year FOBT in past year
or ever scope in 10?
2002 54%
2004 57%
2006 61%
2008 64%
Rim, MMWR, 2011
Colorectal Cancer Screening: Conclusions
• Any screening is better than no screening for reducing colorectal cancer mortality
• Increase awareness of the importance of colorectal cancer screening
• Virtual colonoscopy and fecal DNA testing are included as options in the new joint guidelines but not in USPSTF guidelines

Page 15
Implications for Practice
Offer screening
Testing modalities Fecal immunochemical tests more
acceptable and accurate than Hemoccult II Flex sig no longer routinely performed Colonoscopy RCT ongoing CT colonography not reimbursed by
Medicare
Implications for Practice
• Recognize importance of patient
preferences
–“The best test is the one that gets done”
• Positive fecal blood tests must be
evaluated with diagnostic colonoscopy
Skin Cancer
The American Cancer Society Estimates
• > 1 million cases of basal and squamous cell cancers annually in the US
• ~ 68,720 melanomas and 8,650 deaths
• Melanoma rates are more than 10 times higher in Caucasians than in African Americans

Page 16
Skin Cancer Screening
• USPSTF recommendations
–Screening: “I” insufficient evidence (2009)
–UV radiation counseling: “B” (2012)• Counsel the young (ages 10‐24 years) who have fair skin about minimizing exposure to UV radiation to reduce risk for skin cancer
• Australia Cancer Network/ NZ Guidelines
– Identical
• Inspect moles for changes
• Remove suspicious moles
• Remove actinic keratoses and other precancerous lesions
Screening and Early Detection
– A Asymmetry: one portion of the mole does not match the other
– B Border: edges are irregular, notched, or blurred
– C Color: different shades of black or brown, patchy colors
– D Diameter: spot is 6 millimeters across, or growing larger
A B
C D
ABCD rule for melanoma
• Most common (75%)
• Usually slow growing
• Rarely metastasizes
• Head and arms
• May cause functional or cosmetic impairment
Basal cell carcinoma

Page 17
• Pink, pearly, translucent papules with prominent telangiectasia
• May ulcerate in center
• Uncommon subtypes
- Scar-like appearance
- Red macules
Basal cell appearance
(pictures of Basal Cell Carcinoma)
• Faster growing
• May metastasize (3 - 30%)
• May cause functional or cosmetic impairment
Squamous cell carcinoma
• Red nodule
• With or without ulceration
• On sun-exposed skin
• On traumatized skin
Squamous cell cancer: appearance

Page 18
(pictures of squamous cell cancer)
Sunburn Prevalence* in the Past Year, Adults 18 and Older, US, 2010
Prevalence of Behaviors that Protect against Ultraviolet Radiation Exposure, Adults 18 and Older, US, 2010
Three Things To Remember
•Nearly all skin cancers are preventable by limiting unprotected exposure to the sun•Most skin cancers can be treated successfully if detected early – even melanoma.•“Slip! Slop! Slap! Wrap!”
–Slip on a shirt– Slop on SPF 15+ sunscreen– Slap on a hat– Wrap on sunglasses

Page 19
Questions?Thank you!
PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN
1
Robert Baron MD, MS
PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN
Robert B. Baron MD MSProfessor and Associate Dean
UCSF School of Medicine
Declaration of full disclosure: No conflict of interest
Ford ES, NEJM, 2007
EXPLAINING THE DECREASE IN DEATHS FROM CHD
1980 to 2000:
• Death rate fell from:542.9 to 266.8 per 100K men 263.3 to 134.4 per 100K women
• 341,745 fewer deaths from CHD in 2000
Ford ES, NEJM, 2007
EXPLAINING THE DECREASE IN DEATHS FROM CHD
• 47% from CHD treatments, 44% from risk factor modification
• Reductions in cholesterol: 24%
Reductions in Major Coronary Events Relative to Placebo
Placebo-Controlled Statin Trials
simva 20-40 mg prava 40 mg prava 40 mg simva 40 mg prava 40 mg lova 80 mg
PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN
2
Robert Baron MD, MS
Remaining Major Coronary Events Relative to Placebo
Is there more we can do to identify and treat the
non-responders?
simva 20-40 mg prava 40 mg prava 40 mg simva 40 mg prava 40 mg lova 80 mg
Placebo-Controlled Statin Trials – Celebrating Successes but Forgetting the Majority?
Riskreduction
$$ Harm
The benefit from any given intervention is a function of: 1) The relative risk reduction conferred by the
intervention, and2) The native risk of the patient
A RISK-BASED APPROACH
Mosca, Circulation 2011
Overwhelming majority of recommendations are the same for women and for men
Aspirin use is a notable exception
But…”there may be gender differences in the magnitude of the relative and absolute potential benefits”
Prevention Of CVD in WomenA 40 year women, in good health. In for annual wellness visit. BMI, BP, diet and
exercise all at ideal. What blood tests will you order to screen her for a lipid disorder?
1. Total cholesterol
2. LDL cholesterol and HDL cholesterol
3. LDL, HDL, and hs-CRP
4. LDL, HDL, hs-CRP, and Lp(a)
5. No screening blood tests for lipids
PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN
3
Robert Baron MD, MS
USPSTF
USPSTF: Screening Recommendations
Men: age 35 and older, regardless of risk level
age 20 to 35, at increased risk
Women: age 20 and older at increased risk If not at increased risk, no recommendation (I)
Increased Risk:
tobacco use, diabetes, hypertension, obesity, and family history of premature CV disease.
Mosca, Circulation 2011
ACC/AHA CVD Risk: Ideal All of These
Total cholesterol <200 mg/dL (untreated)
BP <120/<80 mm Hg (untreated)
Fasting blood glucose <100 mg/dL (untreated)
Body mass index <25 kg/m2
Abstinence from smoking
Physical activity at goal for adults >20 y of age: 150 min/wk moderate intensity, 75 min/wk vigorous intensity, or combination
Healthy (DASH-like) diet
A 40 year women, in good health. In for annual wellness visit. BMI, diet and exercise all at ideal. What blood tests will you order
to screen her for a lipid disorder?
1. Total cholesterol
2. LDL cholesterol and HDL cholesterol
3. LDL, HDL, and hs-CRP
4. LDL, HDL, hs-CRP, and LP(a)
5. No screening blood tests for lipids
A 40 year women, in good health. Which of the following is the most effective
intervention for primary prevention of CVD?
1. Aspirin
2. Folic acid
3. Estrogen
4. Vitamin E, C and beta carotene
5. Oily fish twice per week
6. All are effective
7. None are effective

PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN
4
Robert Baron MD, MS
Ineffective Interventions in WomenACC/AHA 2011
Hormone therapy should not be used for the primary orsecondary prevention of CVD (Evidence A).
Antioxidant vitamin supplements (eg, vitamin E, C, andbeta carotene) should not be used for the primary orsecondary prevention of CVD (Evidence A).
Folic Acid, with or without B6 and B12 supplementation,should not be used for the primary or secondaryprevention of CVD (Evidence A).
Routine use of aspirin in healthy women <65 years ofage is not recommended to prevent MI (Evidence B) Cochrane Library, 2009
Omega 3 Fatty Acids: Meta-analysis
• 48 RCTs of 36,913 participants; 41 cohort trials
• No significant effect of omega 3 fats on mortality, CV events, or cancer
• Analysis of diet only trials: also no benefit
• No reason to advise people to stop rich sources of omega 3 fats, but better trials needed
ORIGEN, NEJM, 2012
ORIGEN Trial
RCT, 12,537 subjects; impaired FBS, IGT, or new diabetes, and high CV risk
900 mg n-3 fatty acids vs. placebo; 6.2 years
Results: No difference in CV outcomes9.1% vs. 9.3% (p=0.72)
A 40 year women, in good health. Which of the following is the most effective
intervention for primary prevention of CVD?
1. Aspirin
2. Folic acid
3. Estrogen
4. Vitamin E, C and beta carotene
5. Oily fish twice per week
6. All are effective
7. None are effective

PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN
5
Robert Baron MD, MS
63 yo woman; s/p MI
LDL 115
HDL 45
TG 160
63 yo woman; s/p MI
LDL 3.0 SIHDL 1.2 SITG 4.1 SI
mg/dl / 38.67 = SI (mmol/l)
The best next step in lipid management is:
1. Continue current therapy
2. Begin a statin to goal LDL <100
3. Begin a statin to goal LDL <70
4. Begin a statin plus ezetimibe to LDL goal <70
5. Begin niacin
LDL Goal and Cutpoints in Patients with CHD and CHD Risk Equivalents (10-Year Risk >20%)
100 mg/dL
(<100mg/dL:drug optional)
100 mg/dL
<100 mg/dL
Optional : <70
LDL Level at Which to Consider Drug Therapy
LDL Level at Which to Initiate DietLDL Goal
Adult Treatment Panel III, 2004

PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN
6
Robert Baron MD, MS
BaselineFeature
LDL (mg/dL)
<100
≥100 <130
≥130
ALL PATIENTS
Statin Placebo(10,269) (10,267)
285 360
670 881
1087 1365
2042 2606(19.9%) (25.4%)
0.4 0.6 0.8 1.0 1.2 1.4
24% reduction(p<0.00001)
Heart Protection Study: VascularEvents by Baseline LDL-C
Risk Ratio and 95% Cl
Statin better Statin
worse
No. Events
Larosa NEJM, 2005
TREATING TO NEW TARGETS (TNT)
• RCT of 10,001 patients with stable CHD; 35-75 yr
• LDL <130 mg/dl
• Atorvastatin 10 vs atorvastain 80
• Followed for 4.9 years
• Research question: safety and efficacy of lowering LDL below 100 mg/dl
TREATING TO NEW TARGETS (TNT)
LDL Event % Death % LFTs %Atorv 10 101 10.9 2.5 0.2
Atorv 80 77 8.7 2.0 1.2
p value <0.001 0.09
Lancet, 2010
SEARCH TRIAL
• RCT; 7 years; 10,064 patients with MI; • Funded by Merck• Simvastatin 80mg vs. 20mg
• Outcome: major vascular events (coronary death, MI, stroke, revascularization)
• Results: No difference (RR 0.94; CI 0.88 – 1.01)
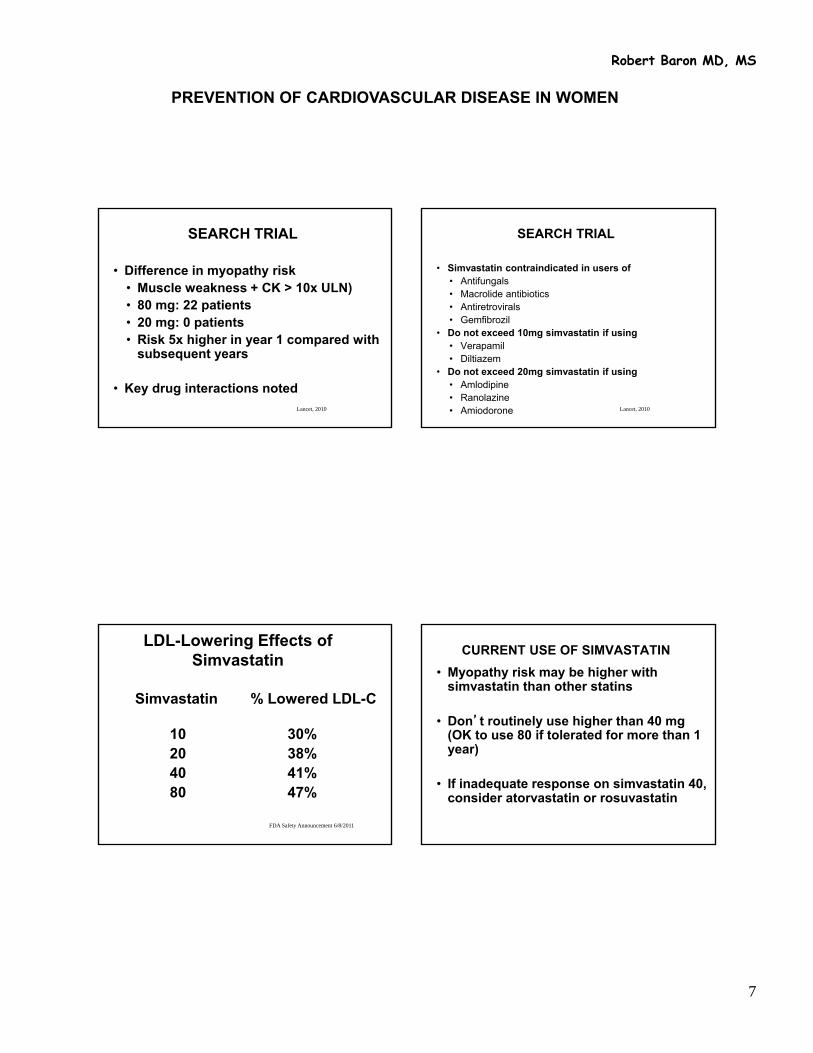
PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN
7
Robert Baron MD, MS
Lancet, 2010
SEARCH TRIAL
• Difference in myopathy risk• Muscle weakness + CK > 10x ULN)• 80 mg: 22 patients• 20 mg: 0 patients• Risk 5x higher in year 1 compared with
subsequent years
• Key drug interactions notedLancet, 2010
SEARCH TRIAL
• Simvastatin contraindicated in users of• Antifungals• Macrolide antibiotics• Antiretrovirals• Gemfibrozil
• Do not exceed 10mg simvastatin if using • Verapamil• Diltiazem
• Do not exceed 20mg simvastatin if using • Amlodipine• Ranolazine• Amiodorone
FDA Safety Announcement 6/8/2011
LDL-Lowering Effects of Simvastatin
Simvastatin % Lowered LDL-C
10 30%20 38%40 41%80 47%
CURRENT USE OF SIMVASTATIN
• Myopathy risk may be higher with simvastatin than other statins
• Don’t routinely use higher than 40 mg (OK to use 80 if tolerated for more than 1 year)
• If inadequate response on simvastatin 40, consider atorvastatin or rosuvastatin

PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN
8
Robert Baron MD, MS
Golomb, Arch Int Med 2012
STATINS AND FATIGUE
• Small RCT; 6 months; 1016 healthy patients
• Simvastatin 20mg vs pravastatin 40 vs placebo
• Outcome: self ratings of change in energy and fatigue with exertion on 5-point scale
• Results: • Statins worse than placebo• Simvastatin worse than pravastatin• Women more than men
The best next step in lipid management is:
1. Continue current therapy
2. Begin a statin to goal LDL <100
3. Begin a statin to goal LDL <70
4. Begin a statin plus ezetimibe to LDL goal <70
5. Begin niacin
63 yo woman; s/p MI. On atorvastatin 80.
LDL 95
HDL 40
TG 200
The best next step in lipid management is:
1. Continue current therapy
2. Switch to rosuvastatin
3. Add fenofibrate
4. Add fish oil
5. Add niacin
6. Add ezetimibe

PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN
9
Robert Baron MD, MS
Effects of Fibrates on Cardiovascular Outcomes
4 Recent meta-analyses
18 RCTs, 45,000 patients
Fibrate vs. Placebo and CVD Risk
OutcomeRelative
Risk 95% CI P Value
All-cause mortality 1.00 0.98-1.08 0.92
Cardiovascular death 0.97 0.88-1.07 0.59
Non-fatal coronary events 0.81 0.75-0.89 <0.0001
Total stroke 1.03 0.91-1.16 0.69
Jun et al. The Lancet 2010
ACCORD, NEJM 2010
Fenofibrate plus statin vs. statin alone: ACCORD
• RCT of 5518 patients with type 2 DM
Fenofibrate Placebo p
• CV events: 2.24 2.41 .32• Death 1.47 1.61 .33
• No difference in any secondary outcome
• Results do not support routine use of combination therapy in DM
Brukert, Atherosclerosis 2010
NIACIN META-ANALYSIS OF RCTS
• 11 RCTS
• Coronary Drug Project (1970s) only large RCT
• Others very small

PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN
10
Robert Baron MD, MS
Niacin Meta-Analysis: Summary of Results for Cardiovascular Events
27% lower risk of CVD events
Bruckert, Atherosclerosis 2010
37
?
Publication bias?
Brukert, Atherosclerosis 2010 NEJM, 2011
AIM-HIGH Trial
• RCT of 3,414 patients with established CVD
• Simvastatin (or simvastatin + ezetimibe) to keep LDL at 40 – 80 mg/dl (mean 71).
• HDL 35 mg/dl, TG 161 mg/dl
• Randomized to receive sustained-release niacin or placebo
NEJM, 2011
AIM-HIGH Trial
• Results: Study stopped early
– No reduction in cardiovascular events, MI and stroke
– Increase risk in ischemic stroke (28 vs 12)
Taylor NEJM, 2009
Extended-release Niacin vs. Ezetimibe
• RCT of 208 patients with CHD or CHD risk-equivalent on statin at goal LDL
• Niacin 2000 vs Ezetimibe 10• Outcome: carotid intima-media thickness
(IMT)
• Results: Niacin better– Reduction in IMT– Major cardiovascular events, 1% vs 5%
PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN
11
Robert Baron MD, MS
Summary Lipid-Lowering Drugs
• Statins are treatment of choice to decrease risk
• No evidence to support adding niacin or fibrates to statins
• If statin-intolerant, niacin may reduce CVD risk (weak evidence)
• Fibrates appear to lower MI risk, but no other CVD endpoints
• Ezetimibe: just say no
The best next step in lipid management is:
1. Continue current therapy
2. Switch to rosuvastatin
3. Add fenofibrate
4. Add fish oil
5. Add niacin
6. Add ezetimibe
63 yo woman, no risk factors
LDL 155HDL 55TG 160SBP 120Nonsmoker
The best next step in lipid management is:
1. Continue current therapy
2. Begin a statin
3. Begin fenofibrate
4. Begin a statin plus ezetimibe
5. Begin niacin
PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN
12
Robert Baron MD, MS
Truth About CVD Risk Prevention
Health professionals are not good at judging CV risk
Counting risk factors is a “blunt instrument”and often leads to misclassification
Calculate 10-year risk of hard CHD events (CHD death or non-fatal MI) using the Framingham Risk Score
Framingham Risk -Limitations
• Not accurate in patients under 30 or over 75
• Provide risk over 4-12 years only
• Relatively few patients with diabetes; no family history
BUT
• Good discrimination for future CHD events
• Validated in several populations and found to be relatively “transportable” for risk ordering but calibration varies
Examples of Proposed Novel Risk Markers
• C-reactive protein• Fibrinogen• vWf• Factor VII• Homocysteine• Lipoprotein a• LDL sub-fractions
• ST segment depression
• Heart rate variability
• Carotid Doppler
• Ankle-brachial index
• EBCT for coronary calcium
• Platelet activity
CRP AND Risk
CRP does not change overall predictive ability of Framingham
However, CRP (plus family history) may reclassify some patients (especially intermediate risk patients)

PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN
13
Robert Baron MD, MS
C-reactive protein (CRP)
Hard to directly integrate into the Framingham risk….
Rough calculations:
CRP in top third increases risk by
factor of 1.2-1.3
Average risk = x
Risk in top tertile = 1.3x
Risk in middle tertile = x
Risk in middle tertile = 0.7x Bonow RO, NEJM 2009
Coronary Calcium (CAC) and CV Prevention
Broad population-based strategy not warranted
CAC may reclassify intermediate risk patients
Unknown if findings lead to improved outcomes
63 yo woman, no risks
LDL 155HDL 55TG 160SBP 120Nonsmoker
10 yr risk: 2%… Therefore no medication recommended
The best next step in lipid management is:
1. Continue current therapy
2. Begin a statin
3. Begin fenofibrate
4. Begin a statin plus ezetimibe
5. Begin niacin (sustained release)

PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN
14
Robert Baron MD, MS
Mosca, Circulation 2011
Prevention of CVD Risk in Women: Aspirin
Aspirin (81–325 mg/d) in women with CHD unless contraindicated (Evidence A).
Aspirin in women >65 y of age (81 mg daily) if benefit for ischemic stroke and MI prevention is likely to outweigh risk of GI bleed and hemorrhagic stroke (Class IIa; Evidence B)
Aspirin may be reasonable for women <65 y of age for ischemic stroke prevention (Class IIb; Level of Evidence B).
CONCLUSIONS
Patients with CHD or CHD equivalent:
• Treat aggressively with statin independent of LDL level (to LDL <70 in most cases)
• Treat other risk factors aggressively as well, especially easy ones (HTN, Aspirin use)
• Treat elevated non-HDL cholesterol and low HDL
• Patients at high risk are undertreated. Maximize adherence and avoid clinical inertia
CONCLUSIONS
Patients without CHD:
• Assess lifetime CV risk with risk factors and 10-year CHD risk with Framingham Risk Score
• Novel markers (hsCRP, coronary calcium score) may be useful for further discrimination among those with intermediate risk
• Do a better job with what we have: HTN, ASA, smoking, weight, exercise, diet
• Engage patient in shared decision making, especially if risk <10%
CONCLUSIONS
Patients without CHD:
• Use medications at thresholds based on risk:
LDL goal LDL drug threshhold
High Risk (>20%) <100 (<70 optional) ≥100
Mod high risk (10-20%) <100 ≥130
Moderate risk (<10%) <100 ≥160
Low risk (no risk factors) <100 ≥190

PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN
15
Robert Baron MD, MS
CONCLUSIONS
Patients without CHD:
• Use medications at thresholds based on risk:
ASA STATIN
High Risk (>20%) YES YES
Mod high risk (10-20%) YES YES
Moderate risk (<10%) NO Occasional YES
Low risk (no risk factors)NO Usually NO

NEW DEVELOPMENTS IN HYPERTENSION
Eliseo J. Pérez-Stable, MD
Management of Hypertension in Women
Eliseo J. Pérez-Stable MD
Professor of Medicine
DGIM, Department of Medicine
July 1, 2013Declaration of full disclosure: No conflict of interest
(I have never been funded by a for-profit company)
Main Teaching Points TodaySet goal SBP and treat with drugs at
any age for SBP >160Goal SBP level is relative, not fixed
or there is nothing magical in 140/90Use the Framingham Risk Score to
assess overall CV risk in all patientsThiazides, ACE-I, ARB, and CCB are
similar–combinations in almost allCo-morbid condition and age
considerations in selecting meds
Current Population Status of Hypertension
• Prevalence is 29%; Blacks at 33.5%
• About 72.5% are treated and 53.5% are
uncontrolled (average >140/90)
• Latinos, Blacks, age 18-44 and ≥80,
<300% poverty, < college degree have
higher rates of uncontrolled BP
• Having any insurance, ≥2 visits, and
usual source of care = better controlMMWR 2012;61: 703-709
Racial Difference of Elevated SBP
• Reasons for Geographic and Racial
Differences in Stroke: 27,748 Black and
White, followed 4.5 y to 2011
• 715 incident strokes
• SBP 10 mm Hg: 8% increase for Whites and
24% for Blacks
• HR = 2.38 for stage 1 Htn, age 45-64 y
• SBP elevations have differential effects on
stroke incidence by raceHoward G, et al, JAMA Intern Med 2013; 173: 46-51
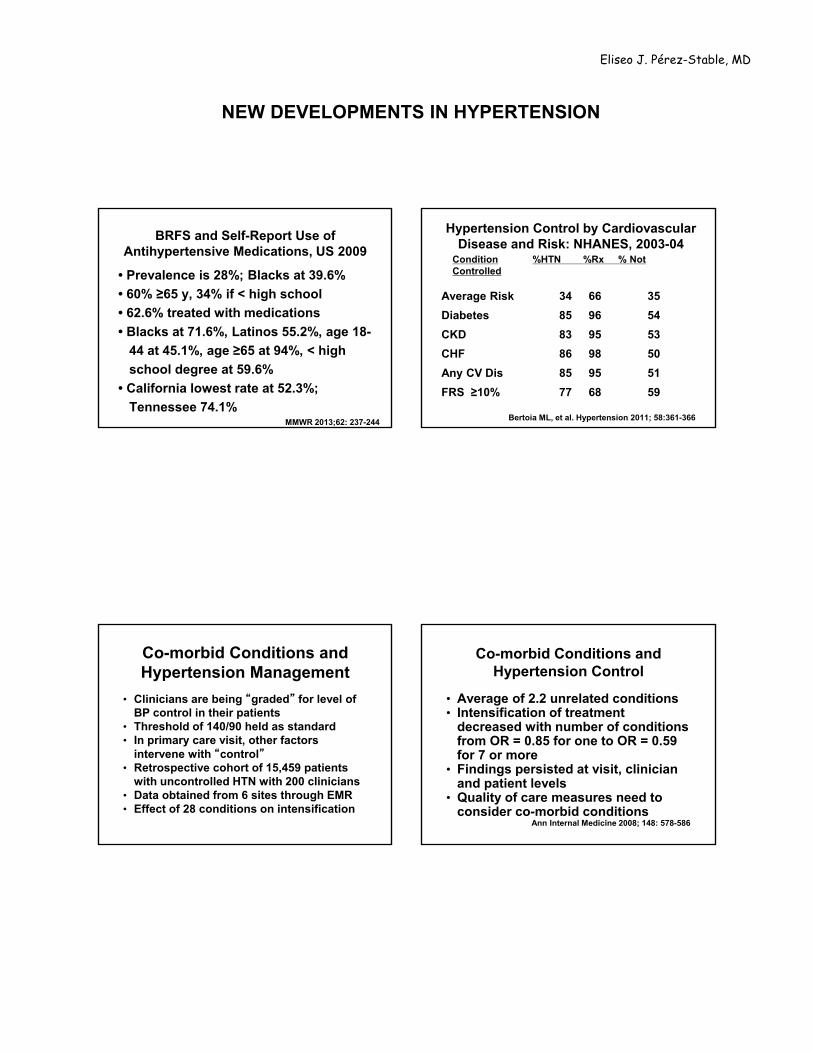
NEW DEVELOPMENTS IN HYPERTENSION
Eliseo J. Pérez-Stable, MD
BRFS and Self-Report Use of Antihypertensive Medications, US 2009
• Prevalence is 28%; Blacks at 39.6%
• 60% ≥65 y, 34% if < high school
• 62.6% treated with medications
• Blacks at 71.6%, Latinos 55.2%, age 18-
44 at 45.1%, age ≥65 at 94%, < high
school degree at 59.6%
• California lowest rate at 52.3%;
Tennessee 74.1%MMWR 2013;62: 237-244
Hypertension Control by Cardiovascular Disease and Risk: NHANES, 2003-04
Condition %HTN %Rx % Not Controlled
Average Risk 34 66 35
Diabetes 85 96 54
CKD 83 95 53
CHF 86 98 50
Any CV Dis 85 95 51
FRS ≥10% 77 68 59
Bertoia ML, et al. Hypertension 2011; 58:361-366
Co-morbid Conditions and Hypertension Management
• Clinicians are being “graded” for level of BP control in their patients
• Threshold of 140/90 held as standard• In primary care visit, other factors
intervene with “control”• Retrospective cohort of 15,459 patients
with uncontrolled HTN with 200 clinicians• Data obtained from 6 sites through EMR• Effect of 28 conditions on intensification
Co-morbid Conditions and Hypertension Control
• Average of 2.2 unrelated conditions• Intensification of treatment
decreased with number of conditions from OR = 0.85 for one to OR = 0.59 for 7 or more
• Findings persisted at visit, clinician and patient levels
• Quality of care measures need to consider co-morbid conditions
Ann Internal Medicine 2008; 148: 578-586

NEW DEVELOPMENTS IN HYPERTENSION
Eliseo J. Pérez-Stable, MD
Hypertension Treatment after 80 y
• No clinical trial showing clear benefit• Meta-analysis of 7 RCT, 1670 patients,
75% women showed a 3.3% absolute reduction in stroke (NNT = 30) and 2.1% reduction in CHF (NNT = 48)
• Borderline trend to increase deaths from any cause in treated group
• Observational data showed risk of death inversely related to BP level
Hypertension in the Very Elderly Trial (HYVET)
• 3845 patients ≥ 80 y • >160 mm Hg – goal of 150/80 mm Hg• Indapamide SR 1.5 mg vs. placebo• Added perindopril if needed• Follow up of 2 years• 60% women, age 83.6 y, BP = 173/91• 12% with CV disease, 7% diabetes,
64% already treated for hypertensionBeckett NS, NEJM 2008; 358: 1887-1898
HYVET Study ResultsBeckett NS, NEJM 2008; 358: 1887-1898
End Point Meds Placebo HR (95% CI)
Stroke 12.4 17.7 0.64 (0.46 -0.95)
CVA Death 6.5 10.7 0.55 (0.33 -0.93)
CHF 5.3 14.8 0.28 (0.17 -0.48)
CV Death 23.9 30.7 0.73 (0.55 -0.97)
Any Death 47.2 59.6 0.72 (0.59-0.88)
Conclusions and ImplicationsOffer BP Treatment at any
age!• Benefits appear at 1 year of Rx
• NNT = 20 to prevent one stroke
• NNT = 10 to prevent one CHF
• Not a specific drug effect
• Never too old to treat SBP > 160
• Goal does not have to be < 140

NEW DEVELOPMENTS IN HYPERTENSION
Eliseo J. Pérez-Stable, MD
Other Considerations in Elderly with Hypertension
• Canadian study of 301,591 newly treated older adults observed from 2000-2009
• 1463 incident hip fractures
• 43% increased risk during the first 45 days following treatment
• Evaluate co-morbidityButt D, Arch Intern Med 2012; 172: 1739-44
Gait Speed, Hypertension, and Mortality: NHANES
• 2340 persons, ≥ 65 y
• Walking speed over 6 m: faster = ≥0.8 m/s (n=1307)
• SBP ≥ 140 associated with mortality in faster gait speed (HR = 1.35, 95% CI 1.03-1.77)
• No association with slow gaitOdden MC, Arch Intern Med 2012; 172: 1162-68
Chronic Kidney Disease and Hypertension
• Continuous risk significant at SBP >120 and DBP >80. The lower the better?
• Detection with serum creatinine and urine albumin/creatinine ratio to identify CKD
• CKD identified patients should be treated with ACE/ARB and lower SBP
• Goal SBP is optimal in 130-140 mm Hg once CKD established
• BP control in 10,813 patients with CKD was only 13.2%; worse in early CKD
(Am J Med 2008; 121: 332-40)
SBP and Risk of Recurrent StrokeOvbiagele B, JAMA 2011; 306: 2137-44
• 20,330 patients ≥50 y with CVA < 120 da followed for 2.5 years, 695 centers
• Outcome: recurrent stroke any type• Predictors: SBP in mm Hg
– <120 8.0%120-<130 7.2%130 -<140 6.8% Optimal SBP
140 - <150 8.7%≥150 14.1%
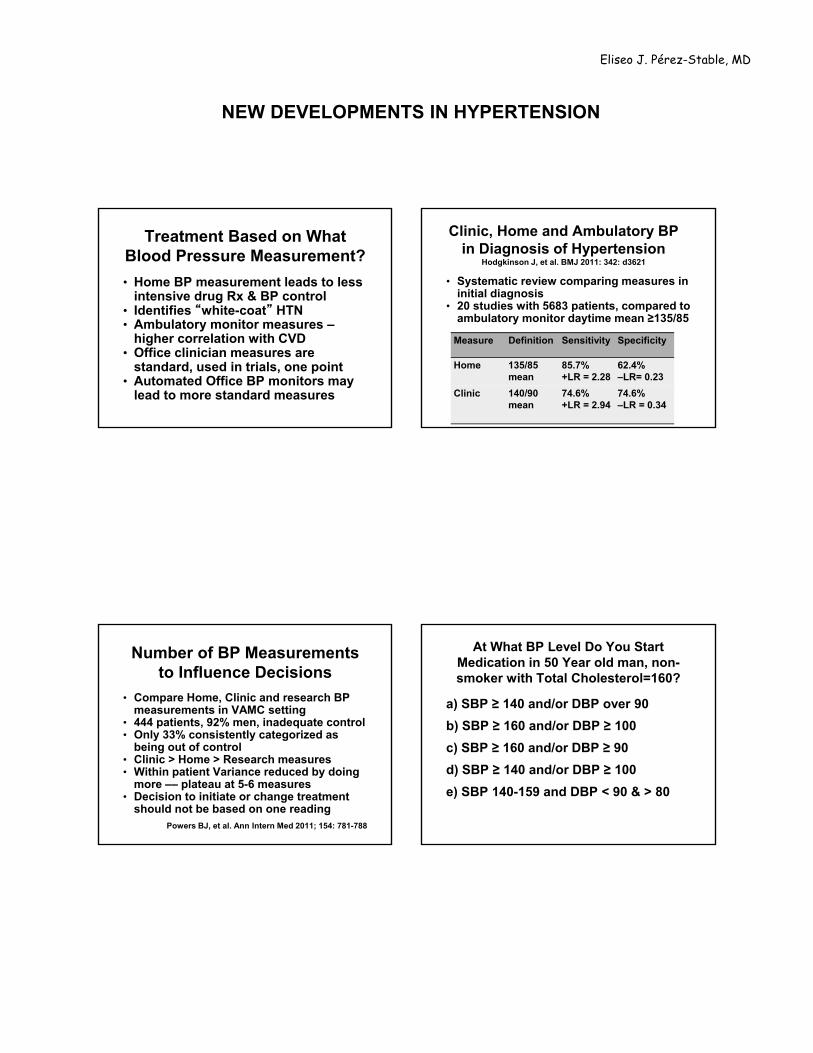
NEW DEVELOPMENTS IN HYPERTENSION
Eliseo J. Pérez-Stable, MD
Treatment Based on What Blood Pressure Measurement?
• Home BP measurement leads to less intensive drug Rx & BP control
• Identifies “white-coat” HTN• Ambulatory monitor measures –
higher correlation with CVD • Office clinician measures are
standard, used in trials, one point• Automated Office BP monitors may
lead to more standard measures
Clinic, Home and Ambulatory BP in Diagnosis of Hypertension
Hodgkinson J, et al. BMJ 2011: 342: d3621
• Systematic review comparing measures in initial diagnosis
• 20 studies with 5683 patients, compared to ambulatory monitor daytime mean ≥135/85
Measure Definition Sensitivity Specificity
Home 135/85 mean
85.7%+LR = 2.28
62.4%–LR= 0.23
Clinic 140/90 mean
74.6%+LR = 2.94
74.6%–LR = 0.34
Number of BP Measurements to Influence Decisions
• Compare Home, Clinic and research BP measurements in VAMC setting
• 444 patients, 92% men, inadequate control• Only 33% consistently categorized as
being out of control• Clinic > Home > Research measures• Within patient Variance reduced by doing
more –– plateau at 5-6 measures• Decision to initiate or change treatment
should not be based on one readingPowers BJ, et al. Ann Intern Med 2011; 154: 781-788
At What BP Level Do You Start Medication in 50 Year old man, non-smoker with Total Cholesterol=160?
a) SBP ≥ 140 and/or DBP over 90
b) SBP ≥ 160 and/or DBP ≥ 100
c) SBP ≥ 160 and/or DBP ≥ 90
d) SBP ≥ 140 and/or DBP ≥ 100
e) SBP 140-159 and DBP < 90 & > 80

NEW DEVELOPMENTS IN HYPERTENSION
Eliseo J. Pérez-Stable, MD
JNC 7 Classification of Blood Pressure
mm Hg SBP DBP
Normal (115) <120 and <80
Pre-hypertension 120-139 or 80-89
HypertensionStage 1 140-159 or 90-99Stage 2 ≥160 or ≥100
Risk of CVD doubles with each increment of 20/10 mm Hg – SBP more important risk factor
When to Treat Hypertension
• Lifestyle advice for all • Initial lifestyle for stage 1 HTN• Drug treatment for all with SBP > 160 • Drug treatment for all with CV co-
morbidity and SBP > 140 or DBP > 90• Drug treatment for all with DBP > 100• If lifestyle fails, drugs for DBP > 90• If lifestyle fails, drugs for SBP >140
Individual Lifestyle Modifications for Hypertension Control
• Weight loss if overweight: 5-20 mm Hg/10-kg weight loss
• Limit alcohol to ≤ 1 oz/day: 2-4 mm Hg• Reduce sodium intake to ≤100 meq/d
(2.4 g Na): 2-8 mm Hg in SBP• DASH Diet: 6 mm alone; 14 mm plus Na
• Physical activity 30 min/day: 4-9 mm Hg
• Habitual caffeine consumption not associated with risk of HTN
Drugs always better than lifestyle in
head-to head clinical comparisons
Better Living through chemistry

NEW DEVELOPMENTS IN HYPERTENSION
Eliseo J. Pérez-Stable, MD
Salt and Public Policy• Coronary Heart Disease Policy Model
to quantify benefits of 3 g salt/day reduction in US– average is 8-10 g/d
• Benefit through a reduction in SBP from 1-9 mm Hg in selected populations
• New cases of CHD decrease by 4.7 -8.3 and stroke by 2.4 to 3.9 /10,000
• Regulatory change leads to wide benefit and is cost-effective
Bibbins-Domingo K, et al. NEJM 2010
Benefits of Less Salt in Food• Compelling evidence associating
high sodium intake with higher SBP• Urine Na excretion shows J-shaped
curve with CV events• Higher urine K excretion lowers
stroke and SBP• Dispute regarding 24 hour data vs.
estimates• Ratio Na/K most important
O’Donnell MJ, et al JAMA 2011; 306: 2229-2238Yang Q, et al, Arch IM 2011; 171:1183-91
Stolarz-Skrzypek K, et al, JAMA 2011; 305: 1777-85
Initial Drug Treatment of Hypertension Based on JNC 7
Initial Drug Choices
Stage 1: Thiazides for mostStage 2: 2-drug combination for most – thiazides plus -blockers, ACE-I, ARB, CCB
Based on randomized controlled trials
60 Year Old Man, BP=160/96; lipids OK; Which treatment?
1) Thiazide diuretic 12.5 or 25 mg
2) Beta blocker of choice
3) Ace Inhibitor or ARB
4) Calcium Channel Blocker
5) Alpha-blocker/Other
6) Intensify lifestyle

NEW DEVELOPMENTS IN HYPERTENSION
Eliseo J. Pérez-Stable, MD
60 Year Old woman, BP=160/96, with Diabetes; which drug?
1) Thiazide diuretic 12.5 or 25 mg
2) Beta blocker of choice
3) Ace Inhibitor or ARB
4) Calcium Channel Blocker
5) ACE/ARB plus Diuretic
6) ACE/ARB plus CCB
Possible JNC 8 Recommendations
• Medication choice menu: Thiazides, ACE Inhibitor or ARB, Calcium Channel Blocker
• Beta blockers restricted to <60 years • Use urinary albumin to identify
patients with diabetes and CKD for ACE/ARB Rx
• Combination of ACE + CCB preferred over ACE + Hctz in highest risk
• Coordinate with pharmacists to enhance adherence
Compelling Indications for Drug Selection in Hypertension
• Low EF Heart Failure: BB, ACE-I or ARB, and aldosterone antagonist
• Post ant MI: Beta Blocker, ACE-I• CAD Risk: BB or just lower SBP• Diabetes with proteinuria: ACE-I, ARB• Renal Disease: ACE-I, ARB• Recurrent stroke prevention:
thiazide, ACE-I
NICE Guidance: Management of Hypertension
Krause T, et al, BMJ 2011; 343:d4891
• Guideline development in the UK• If BP 140/90 in office, use ambulatory
monitor to confirm • Estimate CV risk (FRS), evaluate for target
organ effects (LVH, CKD, retinopathy)• Treat stage 1 with meds only if target
organ damage, known CVD, diabetes, 10-year CV risk ≥ 20%
• Offer meds to all at any age with stage 2 (>155/95) independent of other effects

NEW DEVELOPMENTS IN HYPERTENSION
Eliseo J. Pérez-Stable, MD
Step 4
Summary of antihypertensive drug treatment
Aged over 55 years or black person of African or Caribbean family origin of any age
Aged under55 years
CCBA –ACE/AR
B
ACE/ARB + CCB
ACE/ARB + CCB + Thiazide
Resistant hypertension
A + C + D + consider further diuretic3, 4 or alpha‐ or
beta‐blocker5
Consider seeking expert advice
Step 1
Step 2
Step 3
Thiazide Diuretics
• Very effective for systolic BP• Do not increase sudden death• Most effective in LVH regression• Lipid effects are short lasting (1 y)• Hyperglycemia only in high doses• Still effective in early CKD• Erectile dysfunction in 20%• Adverse effects of low Na or K?
Chlorthalidone vs. HCTZPopulation-based Cohort Study
• 29,873 patients, >65 yrs, 59% women: 10 384 on chlorthalidone (CTD)
• Event rate: 3.2 /100 person-yrs CTD and 3.4/100 person-yrs on HCTZ; HR = 0.93 (95% CI 0.81-1.06)
• CTD led to more hospitalizations for low K (HR = 3.06; 95% CI 2.04-4.58) and low Na (HR = 1.68; 95% CI 1.24-2.28)
Dhalla IA, et al, Ann Intern Med 2013; 158:447-55
Chlorthalidone Treatment in Systolic Hypertension
• 2365 treated with CTD and 2371 with placebo in 4.5 y; RCT
• Outcomes determined at 22 years with national death index
• CV Death reduced by 11%, but no difference in all-cause mortality
• One month of treatment = 1 day life extension
Kostis JB, et al, JAMA 2011; 306: 2588-93

NEW DEVELOPMENTS IN HYPERTENSION
Eliseo J. Pérez-Stable, MD
Efficacy of HCTZ by Ambulatory Monitoring
Messerli FH, et al, JACC 2011; 57: 590-600
Medication Class Decrease in mm Hg
HCTZ: 12.5 -25 mg 6.5/4.5
HCTZ: 50 mg 12.0/5.4
ACE-I 12.9/7.7
ARB 13.3/7.8
CCB 11.0/8.1
Beta Blockers 11.2/8.5
Beta Blockers• Question benefit to prevent MI or
decrease all cause CAD mortality• Adverse effects limited: Do not cause
depression or sexual dysfunction• Glucose elevation with A1C increase
by 0.2% –– less with carvedilol• No lasting effect on lipids• Compelling evidence to use in systolic
HF to decrease mortality • Less efficacy in stroke prevention
among those older than 60 years
ACE–I or ARB• 30% reduction of ESRD (dialysis)
and/or of doubling of serum creatinine; optimal with GFR 30-60, proteinuria
• Not better tolerated than other drugs• Regression of LVH not more than
other drugs – SBP reduction• Elevates K+• Do not use in women < 50 y without
guaranteed contraception• Best choice in diabetes?• Infrequent need to combine the two
Renin Angiotensin System Antagonists and Mortality
• Heart failure with preserved EF• Swedish Heart Failure registry• 16,216 patients with EF ≥40%, age 75 y,
46% women; 12 453 treated with RAS antagonists
• Propensity score of all-cause mortality: • Matched cohort showed 1-year survival
was 77% vs. 72% with HR = 0.91 (95% CI 0.85-0.98); Overall in cohort: 86% vs. 69%; Dose effect observed
Lund LH, et al, JAMA 2012; 308: 2108-17

NEW DEVELOPMENTS IN HYPERTENSION
Eliseo J. Pérez-Stable, MD
Valsartan for Prevention of DM and CV Events in Patients with Pre-Diabetes
• 9306 patients, 50% women, with pre-DM and CV risk factors or disease
• Valsartan 160 mg or placebo plus lifestyle• Follow for 5 years, outcomes are new
diabetes and CV events• Diabetes: 33.1% vs. 36.8% (HR= 0.86; 0.80-
0.92)• No benefit on CV outcomes: 14.5% vs.
14.8%• DREAM Trial showed no benefit (ramipril)
The Navigator Study Group. NEJM 2010; 362: 1477-1490
Benazepril for CKD:Is it Ever Too Late to Try?
• 442 patients randomized to benazepril or placebo and followed for 3.4 years
• Creatinine 1.5 to 3: benazepril 20 mg (1)• Creatinine 3.1 to 5: benazepril vs. placebo• Outcomes: ESRD, 2X creatinine or death• 22% in group 1; 41% in group 2 on ACE
vs. 60% on placebo• Similar AE; not mediated by SBP
NEJM 2006; 131-140
Calcium Channel Blockers
• Effective in preventing CV events• Do not reverse atherosclerosis• No increase risk of cancer• Short acting CCB may be harmful • Effective in systolic hypertension• Better outcomes in latest trials
ACCOMPLISH Calcium Blockers combined with ACE
• Comparison of combinations: ACE-I + hctz vs. ACE-I + amlodipine for htn
• RCT, 11,506 patients, ≥ 65 y, 60% men, 83% White, 60% DM, BMI = 31
• Outcomes: CV death, MI, stroke, CAD hospitalization, resuscitation after cardiac arrest, CABG or PCI
• Follow-up 36 months• Funded by Novartis: USA and 4 N
EuropeJamerson K, NEJM 2008; 359:2417-28

NEW DEVELOPMENTS IN HYPERTENSION
Eliseo J. Pérez-Stable, MD
ACCOMPLISH Results
Primary Outcomes
Benazepril +AmlodipineN=5744
Benazepril + HCTZN=5762
Hazard Ratio (95% CI)
All Events 552 (9.6%) 679 (11.8%) 0.80 (0.72-0.90)
CV Death 107 (1.9%) 134 (2.3%) 0.80 (0.62-1.03)
All MI 125 (2.2%) 159 (2.8%) 0.78 (0.62-0.99)
All Strokes 112 (1.9%) 133 (2.3%) 0.84 (0.65-1.08)
Revasc procedure
334 (5.8%) 386 (6.7%) 0.86 (0.74-1.00)
ACCOMPLISH Conclusions
• Combination of CCB and ACE was superior to ACE/HCTZ
• BP differences of 1 mm only• Different populations may matter• Chlorthalidone vs. HCTZ?• Recommendation to change practice
in highest risk patients – ACE and CCB may have special benefits
What About Other Drugs?
• CNS sympatholytic: Clonidine plus• No reason to use methyldopa• Alpha-1 blockers: OK but inferior as
single drug and tachyphylaxis• Labetalol good 5th or 6th choice• Direct vasodilators - hydralazine or
minoxidil - need more diuretics• Peripheral adrenergic antagonists?
Final Take Home Points
Risk of CVD is linear to SBP level120-139/80-89 is “pre-hypertension”
and merits lifestyle modifications in all and may need drug treatment with co-morbidity of DM, CAD, CKDMost patients will need two or more
drugs to achieve goal SBPControl only occurs with motivated
patients who trust their clinician

6/21/2013
1
Preventing the Unintended: Update in Contraception
Jody Steinauer, MD, MASDept. Ob/Gyn & Reproductive SciencesUniversity of California, San Francisco
Disclosure Statement
I have nothing to disclose.
Are you familiar with the US Medical Eligibility Criteria for Contraception?
a. Yes
b. No
How comfortable would you be offering a nulliparous woman an IUD if she had a history of Chlamydia and no current infection?
a. Very comfortable
b. Somewhat comfortable
c. Uncomfortable

6/21/2013
2
Would you offer a 20 year‐old woman with migraine the combined oral contraceptive?
a. Yes
b. It depends
c. No
Objectives
To review contraceptive methods so that you can prioritize contraceptive counseling and provision in your practice
To be comfortable using CDC Medical Eligibility Criteria (MEC) to determine safety
Review basics, controversies, myths and new updates about contraceptive methods
Jane is a 27 year‐old woman taking combined oral contraceptive pills, who presents to your clinic for an annual examination. She reports having missed two periods. Her urine pregnancy test is positive.
6.4 Million U.S. Pregnancies Annually
52 % Intended
25 % UnintendedDespite method use
23 % UnintendedNo method used
Jones PSRH 2008 Mosher Vital Health Stat 2010
6/21/2013
3
Why did Jane get pregnant?
Jane ran out of pills last month. She tried to schedule an appointment, but because she was overdue for a pap smear the clinic staff couldn’t call in refills. Today was the first day she could get an appointment.
Provider Barriers to Contraception
• Clinical Visit
– BP check to initiate estrogen‐containing methods
– No pap smear or other examination
– Refill methods without seeing patient
• Remember birth control
– 48% using D or X rx counseled on contraception1
• Knowledge about contraindications
– US guidelines
Schwarz Ann Intern Med, 2007.
Case: US Guidelines
After Jane has completed her pregnancy she returns to you for contraceptive counseling. Jane has had migraine headaches since she was a teen. She has no aura and they have not changed with the combined pill.
Can she use the pill again?
Can my patient use this method?
1 Can use the method No restrictions
2 Can use the method Advantages generally outweigh theoretical or proven risks.
3 Should not use method unless no other method is appropriate
Theoretical or proven risks generally outweigh advantages
4 Should not use method Unacceptable health risk
US Medical Eligibility Criteria (MEC)
6/21/2013
4
Medical Condition
Birth Control Methods
MEC Category
Where do you find the US MEC?
U.S. Medical Eligibility Criteria forContraceptive Use (USMEC)
United States Medical Eligibility Criteria for Contraceptive Use http://www.cdc.gov/reproductivehealth/unintendedpregnancy/USMEC.htm
Migraine and Combined Hormonal Contraception (CHC)
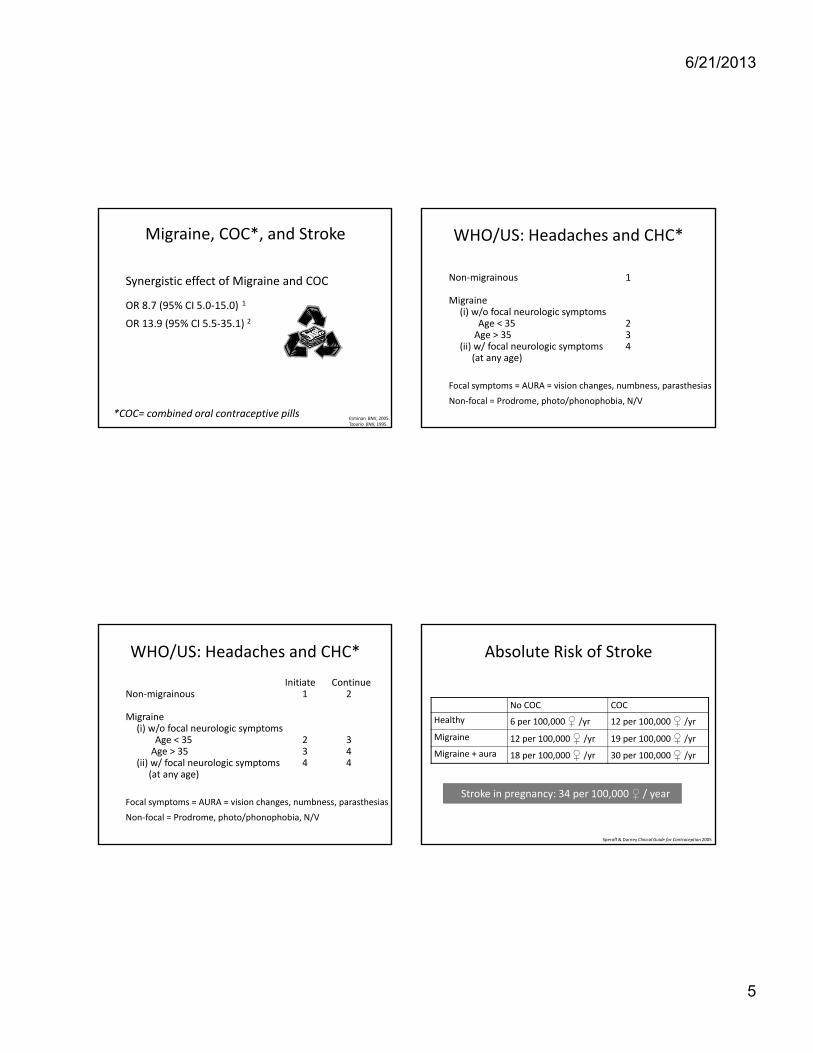
6/21/2013
5
Migraine, COC*, and Stroke
Synergistic effect of Migraine and COC
OR 8.7 (95% CI 5.0‐15.0) 1
OR 13.9 (95% CI 5.5‐35.1) 2
Etminan BMJ, 2005. Tzourio BMJ, 1995.
*COC= combined oral contraceptive pills
WHO/US: Headaches and CHC*
Non‐migrainous 1
Migraine(i) w/o focal neurologic symptoms
Age < 35 2Age > 35 3
(ii) w/ focal neurologic symptoms 4(at any age)
Focal symptoms = AURA = vision changes, numbness, parasthesias
Non‐focal = Prodrome, photo/phonophobia, N/V
WHO/US: Headaches and CHC*
Initiate ContinueNon‐migrainous 1 2
Migraine(i) w/o focal neurologic symptoms
Age < 35 2 3Age > 35 3 4
(ii) w/ focal neurologic symptoms 4 4(at any age)
Focal symptoms = AURA = vision changes, numbness, parasthesias
Non‐focal = Prodrome, photo/phonophobia, N/V
Absolute Risk of Stroke
No COC COC
Healthy 6 per 100,000 /yr 12 per 100,000 /yr
Migraine 12 per 100,000 /yr 19 per 100,000 /yr
Migraine + aura 18 per 100,000 /yr 30 per 100,000 /yr
Stroke in pregnancy: 34 per 100,000 / year
Speroff & Darney Clinical Guide for Contraception 2005
6/21/2013
6
Case: Counseling Issues
After reviewing the US and WHO MEC you decide Jane can use the pill again.
But is it the best method for her?
Safety Efficacy
Helping patients choose the best method
Patient Preference
Perfect use efficacyFrequency of intervention
ConvenienceSide effectsEfficacy
Non‐contraceptive benefitsFuture pregnancy plans
Always balance against the risk of pregnancy
How effective is the combined oral contraceptive for prevention of pregnancy?
Typical use ≠ Perfect use
Efficacy
How effective is the combined oral contraceptive for prevention of pregnancy?
8% failure rate in 1 year
How many pills, on average, do women forget to take each month (not including placebo)?
Typical use ≠ Perfect use
Efficacy

6/21/2013
7
0
1
2
3
4
5
6
1 2 3
Diary
EMD
Oral Contraceptives 2010: Missed Pills
Hou, Ob Gynecol, 2010
Mean Pills Missed
Cycle
← 5 pills
← admit 1
Contraceptive Method Use, U.S.*
0
5
10
15
20
25
30
35
40
Method
Mosher Vital Health Statistics, 2010Alan Guttmacher Institute, Facts In Brief, 2010.
6.6%
28%
*Among the 38 million women currentlyusing birth control
Most effective
EffectiveLeast effective
10 million = 800,000 pregnancies each year
Contraception Methods
Episodic Daily Weekly Monthly 3 Mo’s 3 yrs 5 yrs 10 yrs Permanent
Barrier
OCPs
Patch
Ring
DMPA(IM or SQ)
Progestin Implant
LNG-IUS
CopperIUD
BTLHysteroscopic
Vasectomy
Combined Hormonal Progestin Only IUC Sterilization
Least effective Most effective
EC
>99%94%92%<83%
Natural Family Planning
Contraceptive MethodFailure Rate
Perfect Use Typical Use
No Method 85% 85%
Periodic Abstinence
Standard Days Method®* 5% 12%
Ovulation Method 3% 22%
Symptothermal 2% 13‐20%
Two‐Day Method® 3% 14%
* Including Cycle Beads
National Center Health Statistics; Contraceptive Technology

6/21/2013
8
Barrier Methods
Contraceptive MethodFailure Rate
Perfect Use Typical Use
Withdrawal 4 % 18 %
Condoms 2 % 17 %
Cervical Cap (parous/nullip) 26%/9% 32%/16%
Sponge (parous/nulliparous) 20%/9% 32%/16%
Female Condoms 5 % 27 %
Diaphragm 6 % 16 %
National Center Health Statistics; Contraceptive Technology
Hormonal Methods
Contraceptive MethodFailure Rate
Perfect Use Typical Use
Combined Hormonal Pills <1 % 8 %
Progestin Only Pills <1 % 8 %
Transdermal Patch <1 % 8 %
Vaginal Ring <1 % 8 %
3‐Month Injection <1 % 3 %
Implants <1 % <1 %
Copper IUD/LNG IUS <1 % <1 %
National Center Health Statistics; Contraceptive Technology
http://www.fhi.org/nr/shared/enFHI/Resources/EffectivenessChart.pdf
Frequency of Intervention
• Permanent: sterilization
• Every 10 years: IUD
• Every 5 years: IUD
• Every 3 years: implant
• Every 3 Months: injection
• Monthly: vaginal ring
• Weekly: patch
• Daily: pill, NFP
• Episodic: barrier methods, NFPIncreasing efficacy
6/21/2013
9
Daily: Natural Family Planning
• Help women identify fertile days
– Fertility window 6‐8 days
– Failure rate 12‐22%
• Two‐day method®
– Simple, accurate method – quicker to learn
– Two questions
• Did I note secretions today?
• Did I note secretions yesterday?
• If yes to either, consider fertile
Natural Family Planning: Two‐day Method®
• Study of 450 women – 3,928 cycles
• Failure rates:
– 14% typical use
– 3% perfect use (no intercourse)
– 6% semi‐perfect (barriers or withdrawal)
– Half of pregnancies in first 3 months
• Mean fertile window 12 days
• High acceptability
Arevalo, Fertil Steril, 2004.
Daily: Combined Oral Contraceptives
• Estrogen + progestin
• Traditional prescription flawed
– Daily x 3 weeks / 1 week off
• Extended cycle may ↑efficacy
Baerwald, Contraception, 2004.
Extended Cycle: Shortened hormone‐free week
• 23, 24 or 26 days hormones + 2‐5 d placebo– Decreased ovarian activity at end of placebo
– Shorter withdrawal bleeds
– Similar breakthrough bleeding
– 3 FDA‐approved products in US
Spona Contraception, 1996 Bachman Contraception, 2004 Endrikat Contraception, 2001.

6/21/2013
10
Extended Cycle:Fewer hormone‐free weeks
• 12 weeks hormone/1 week off
• Ethinyl estradiol and levonorgestrel
– 84 days LNG 150 µg/EE 30 µg; 7 days placebo
– Decreased breakthrough bleeding over time
Anderson Contraception, 2003
Tricycle Breakthrough Bleeding/Spotting
Anderson FD, et al., Contraception, 2003.
Extended Cycle: Continuous Use
• Continuous for one year
– Increased spotting in first six months
– Median 1.5 days spotting in last trimester
• FDA‐approved: ethinyl estradiol and levonorgestrel
– 90 mcg levonorgestrel + 20 mcg EE
Miller Obstetrics and Gynecology, 2003. Kwiecen, Contraception, 2003. Foidart, Contraception, 2006.
Choosing a COC
• Estrogen dose– Low dose = < 50 mcg
• Progestin type– 1st‐generation: norethindrone– Second‐generation: levonorgestrel– Third‐generation: desogestrel– Drospirenone: spironolactone derivative
Kemmeren BMJ 2001; Lidegaard BMJ 2009
6/21/2013
11
VTE & oral progestin type
• Desogestrel and drosperinone OCPs may increase risk of VTE
• BUT. . . Absolute risk remains low
Non‐pregnant, no COCs: 4.4 per 10,000 ‐ yrs
Levonorgestrel COCs: 5.0 per 10,000 ‐ yrsDesogestrel COCs: 6.5 per 10,000 ‐ yrsDrosperinone COCs: 7.8 per 10,000 ‐ yrs
PREGNANCY: 29 per 10,000 ‐ yrs
Lidegaard 2009 BMJHeinemann 2007 Contraception
Choosing a COC
• Careful with very low‐dose estrogen –↑ bleeding• Monophasic fine• No clear benefit of drospirenone
– PMDD: fewer sxs 6 months – equivalent at 2 yr– Acne: Equivalent to other pills
30 or 35 mcg EE + 2nd generation progestinShortened or erased placebo week if possibleMonophasic
VanViet Cochrane 2006LaGuardia Contraception, 2003Freeman Womens Health 2001van Vloten Cutis 2002
Jane no longer wants to take a pill every day. She asks you about other birth control methods which she doesn’t have to think about as often.
What can you offer her?
Weekly
Monthly
3 months
3 years
5‐10 years
Daily:Progestin‐only Pills (POPs)
• 35 mcg norethindrone DAILY
– No hormone free interval!!
• Primary mechanism = cervical mucus thickening
• Requires punctual dosing
– If > 3 hours late, need back up x 48 hours

6/21/2013
12
Weekly: Patch
• Norelgestromin and EE
– 20mcg EE & 150mcg norelgestromin
• One patch a week for 3 weeks, then no x 1 wk• Few side effects – comparable to pills except:
– 20% skin irritation – 2% stopped method
– More breast discomfort and spotting in first 2 cyclesthan pills
– 3% detached –RCT 46% experience at least one detachment in one cycle• Prescribe replacement patch
CreininObstet Gynecol 2008
Monthly: Ring
• Ethinyl estradiol and etonogestrel– 15 mcg EE & 120 mcg desogestrel
• One ring each month:– Ring in x 3 wks– Ring out x 1 week
• Few side effects – comparable to pills except– Spotting: only 5% (significantly less in first month)
– Discharge: 1% stop method
– Discomfort: 2.5% stop method
– Expulsion: RCT: 20% expelled at least once during 3‐week period
Dieben Obstet Gynecol, 2002 CreininObstet Gynecol, 2008
Monthly: Extended Cycle Ring
• RCT of 561: 4wk, 8 wk, 12 wk, continuous:
– All regimens well‐tolerated
– Extended: ↓ bleeding days, spotting days
• Potential for use on a monthly basis
– Serum levels for 35 days
I instruct patients to remove ring the last 3‐4 days of the month if they want withdrawal bleed.
Miller Obstet Gynecol, 2005
Non‐oral HC and VTE
2 case‐control studies
• No association‐ new users
– OR=1.1 (CI 0.6–2.1) 1
• Association‐ all users
– OR=2.4 (CI 1.1‐5.5)2
Retro cohort, 9.4 m ‐yrs3
• Attributable risk:
– +7.6/10K (vs. non)
– +3.5/10K (vs. COC)
Retro cohort, 9.4 m ‐yrs3
• Attributable risk:
– +5.7/10K (vs. non)
– +1.5/10K (vs. COC)
• NNT (switch to COC):– 2000 ring users
– 1250 patch users
• No info on BMI, smoking, famhx
1. Jick SS 2007 Contraception2. Cole JA 2007 Obstet Gynecol3. Lidegaard 2012 BMJ

6/21/2013
13
EE Exposure with combined hormonal contraception
Van den Heuvel, Contraception 2005(*30 mcg EE COC)
AUC (pg/ml):
Patch = 37.7 + 5.6
COC = 22.7 + 2.8
Ring = 11.2 + 2.7
Every 3 months:Progestin Injection
• Medroxyprogesterone acetate 150 mg IM
– One injection every 12‐13 weeks
• Very effective
– Typical use failure = 3%
• Side effects:
– Delayed return to fertility (9‐10 months)
– Irregular bleeding, amenorrhea (50% at 1 yr)
– Weight gain (5 lbs at 1 year, 16 lbs at 5 yrs)
• SQ low‐dose (104 mg) version now available
Progestin Injection & BMD
• BMD decreases by 1‐2% per year
• FDA: limit to 2 yrs. in young women
– WHO & ACOG do not agree
– Bone loss reverses by 1 year after discontinuation.
– No evidence of increased fractures.
• No indication for DEXA
• Weigh risks against risk of pregnancy
Meier, J Clin EndocrinMetab, 2010. Scholes Arch Pediatr Adolesc Med, 2005.; Scholes, Epidemiology, 2002; ACOG 2008 Com Opin 415.
Progestin Injection: Delay
• Traditionally recommend caution after > 14 weeks from last DMPA injection
• WHO recommends 4‐week grace period
– Repeat up to 16 weeks

6/21/2013
14
Missed Hormonal Contraceptives: New Recommendations
• Guidelines for CHC and DMPA• For CHC:
– The hormone free interval (HFI) not > 7 days– In the 1st week
• Back‐up should be used after >1 missed dose until 7 days of use occur. Consider EC.
– In the 2nd and 3rd week• If < 3 days are missed, eliminate the next HFI• If > 3 days are missed, back‐up contraception and consideration of EC should be added
Soc Ob GYN of Canada, JOGC 2008; 219:1050‐62
Every 3 years:Single‐Rod Implant
• Etonogestrel 60mcg/day• New version replaced old in 2011
– Identical but with radiopaque rod– Easier‐to‐use inserter– Must complete FDA‐approvedtraining
• Efficacy > 99%• 1 year continuation: 75%‐90%
– Reasons for discontinuation: Bleeding ( up to 40%)
Blumenthal Eur J Contracept Reprod Health Care, 2008
Progestin Implant: Side Effects
• Bleeding: “Irregularly irregular” (40%)– Amenorrhea: 22%– 7% frequent: > 5 B‐S episodes in 90‐day period– 18% prolonged: at least 1 B‐S episode > 14 days– 20% have B‐S for >50 days in first 90‐day period– Generally NOT heavy
• Treatment of bleeding
Blumenthal Eur J Contracept Reprod Health Care, 2008 Mansour Eur J Contracept Reprod Health Care 2008.
Implant: Bleeding Treatment
Therapy Evidence?
1. COC x 21d/7d (3 mo) or Estrogen alone (0.5 mg estradiol x 21 d) (3 mo)
Minimal
2. Cyclic progestin (MPA 10bid) x 21d/7d (3mo)
Anecdotal
3. POP daily up to 3 mo Anecdotal
4. NSAIDs, COX‐2 inhibitors x 5‐10dTranexamic acid 500 bid x 5d
MinimalAnecdotal
Adapted from Mansour et al 2010, and 2011 Contraception
6/21/2013
15
Every 5‐10 Years: Intrauterine Devices (IUD, IUC, IUD, IUS)
Levonorgestrel Intrauterine System (LNG‐IUS)
• Levonorgestrel 20 mcg/day
• 0.1% failure (1 yr) 1.1% (7 yr)
Copper T 380A IUD
0.8% failure (1 yr) 1.2% failure (7 yr)
Lockhat Fertil Steril, 2005
Comparable to BTL failure rate of 1.8% /10 yrs
10 years
5 years
IUD Review
• Current IUDs do NOT cause PID!!!– Transient increased risk at time of insertion
– STI at time of insertion increases risk
– GC/CT screening can follow CDC guidelines
– Okay to screen on insertion day – treat if +
• Beyond time of insertion• Overall decreased risk with LNG IUS • No increased risk with Copper IUD
• Okay to treat for PID with IUD in place
Svensson L, et al. JAMA. 1984; Sivin I, et al. Contraception. 1991.Farley T, et al. Lancet. 1992; Hubacher, NEJM, 2003.
Routine GC/CT screening NOT necessary!
• Retrospective cohort, n=57,728 IUDs
• Evidence‐based STI screening, treat if + test
Sufrin et al In press, Obstet Gynecol
All women: Risk of PIDNon-screening = Screening
OR= 1.05 (0.78, 1.43)
Screened Women: Risk of PIDSame day = Pre-insertion
OR=.997 (.64, 1.54)
Overall PID risk = 0.54%
Women appropriately selected for non-screening
Most accurate screening time is day of insertionSame
results < 26 yo
IUC, Nulliparity & Infertility
• Nulliparity is not a contraindication
– May have increased pain with insertion
– May have increased risk of expulsion
• IUDs do NOT cause infertility
– Tubal factor 1° infertility is not associated with prior IUD use (OR=1)
Hubacher 2003 N Engl J Med

6/21/2013
16
Is Jane a candidate for an IUD?
Women of any reproductive age seeking
long‐term, highly effective contraception
Post‐pregnancy Intrauterine Contraception
2010 US MEC: Postpartum IUD Insertion
Postpartum (BF or non‐BF women) including post‐caesarean section
LNG‐IUD Cu‐IUD
<10 min after delivery of placenta
2 1
10 min after delivery of placenta to <4 wks
2 2
>4 wks 1 1
Puerperal sepsis 4 4
Why 10 minutes?Postpartum IUD Insertion
Chi Contraception 1985
9.5%
31.5%
37.3%
28.8%
0%
5%
10%
15%
20%
25%
30%
35%
40%
Ad
just
ed
Cu
mu
lati
veE
xpu
lsio
n R
ates
p<0.001 (≤10 minutes compared to all other groups)
6/21/2013
17
How do you do it?Post‐placental IUD Insertion
2
1
WHO and US Medical Eligibility Criteria: Post‐abortion
LNG‐IUC Cu‐IUC
1st trimester 1 1
2nd trimester 2 2
Immediate post‐septic abortion
4 4
Permanent: Tubal Sterilization
• Postpartum salpingectomy
• Silicone Band
(Yoon, Fallope)
• Filshie Clip
• Electrosurgical dessication – unipolar lowest failure
Failure risk 0.5‐1.8%Increases over time
Permanent:Hysteroscopic Tubal Sterilization
• Coils inserted into proximal tubes via hysteroscopy
– Induces scarring reaction in tubes
• Back‐up method x 3 mo, confirm w/ HSG
• Low failure rate (0.26% at 5 yrs)
• Non‐invasive
6/21/2013
18
Post‐exposure:Oral Emergency Contraception
Levonorgestrel 120 mg x 1, up to 5 days
Ulipristal Acetate• Selective progesterone receptor modulator
• Proposed mechanism:1
– Delay follicular rupture
• Will not harm existing pregnancy
• Dosing: 30mg, FDA‐approved up to 5 days
1. Brache 2010 Hum Reprod
Emergency Contraception: Ulipristal Acetate
Effectiveness:1,2
“non‐inferior” to LNG: 1.4% vs. 2.2%
Meta‐analysis of 3445 120 hrs: OR = .55 (.32‐.93)
24 hrs: OR = .35 (.11‐.93)
Side effects: Headache (20%), nausea (12%)
1. Glasier 2010 Lancet2. Creinin 2006 Obstet Gynecol
Alternatives to LNG EC & Ulipristal acetate?
• Copper IUD– VERY effective as EC up to 7 days!
– More effective than LNG EC
• Mifepristone (10, 25 or 50 mg)– More effective than LNG
• Yuzpe regimen– More side effects and less effective
Cheng 2008 Cochrane Database
Jane
You counsel Jane about the other options available, emphasizing those with high efficacy that require less intervention. She ends up choosing a highly effective IUD which you place that same day.
6/21/2013
19
Summary
• Unintended pregnancy remains a common problem in the US.
• We can minimize barriers to successful contraception.
• Consider including efficacy in your contraception counseling in addition to other priorities of the patient.
References
Many easily accessible resources exist to help solve contraception quandaries. . . .
www.arhp.org
www.cdc.gov
http://www.who.int/reproductivehealth/publications/family_planning
http://www.managingcontraception.com/
http://www.cochrane.org/
www.acog.org
UCSF Family Planning Consult Service(415) 443-6318
6/21/2013
20
Resources
• WHO and US Medical Eligibility Criteria for Contraceptive Use
– www.who.int
– www.cdc.gov
– www.reproductiveaccess.org
• A Pocket Guide to Managing Contraception
• UCSF Family Planning Consult Service
– (415) 443‐6318
Acknowledgments
Thanks to all who have shared slides!
– Carolyn Sufrin
– Mike Policar
– Phil Darney
– Sarah Prager

6/21/2013
1
Abortion: Patient-centered Counseling and Evidence-based Care
Jody Steinauer, MD, MAS
Dept. of Obstetrics, Gynecology & Reproductive Sciences
University of California, San Francisco
Disclosures
• I have no relevant financial disclosures.
Acknowledgements• Karen Meckstroth and Jen Kerns
Objectives
• Understand abortion global epidemiology• Understand abortion techniques
– Many skills transferable to non-abortion settings
• List the most common complications of uterine aspiration and medical abortion
Outline
• Abortion Epidemiology– US and international settings
• 1st-trimester Abortion– Manual vacuum aspiration– Medical abortion
• 2nd-trimester Abortion• Abortion Complications
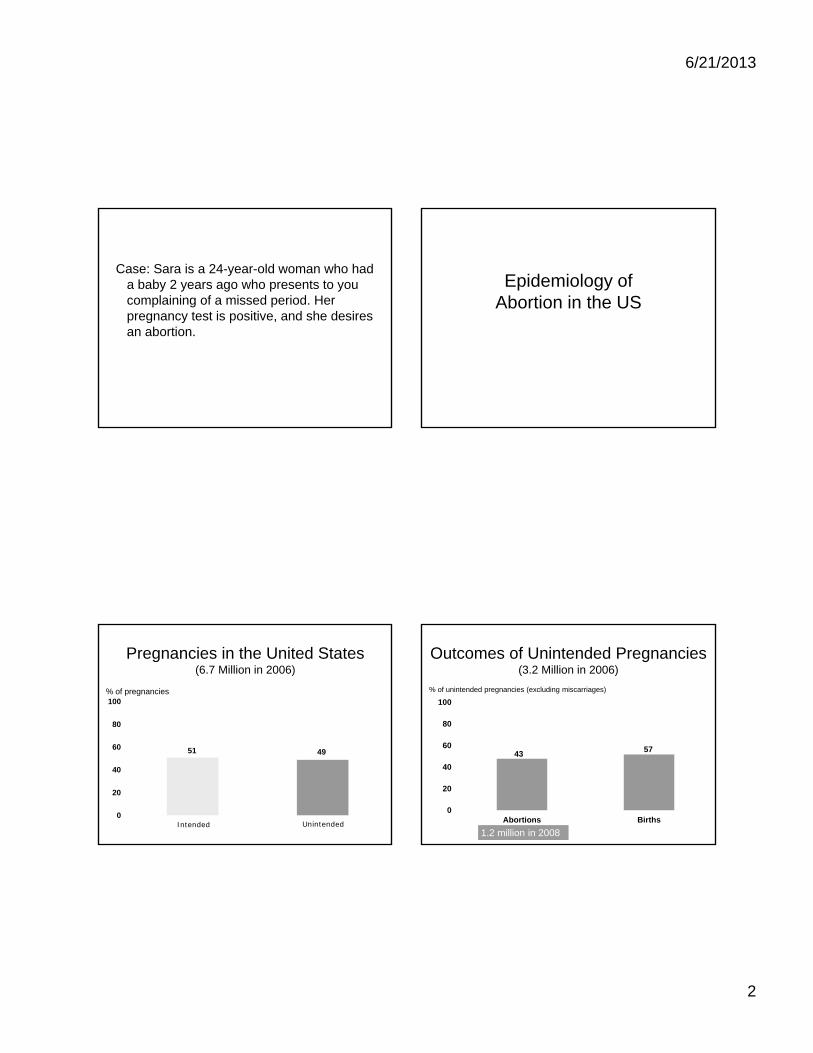
6/21/2013
2
Case: Sara is a 24-year-old woman who had a baby 2 years ago who presents to you complaining of a missed period. Her pregnancy test is positive, and she desires an abortion.
Epidemiology of Abortion in the US
Pregnancies in the United States (6.7 Million in 2006)
51 49
0
20
40
60
80
100
UnintendedIntended
% of pregnancies
Outcomes of Unintended Pregnancies(3.2 Million in 2006)
4357
0
20
40
60
80
100
Abortions Births
% of unintended pregnancies (excluding miscarriages)
1.2 million in 2008
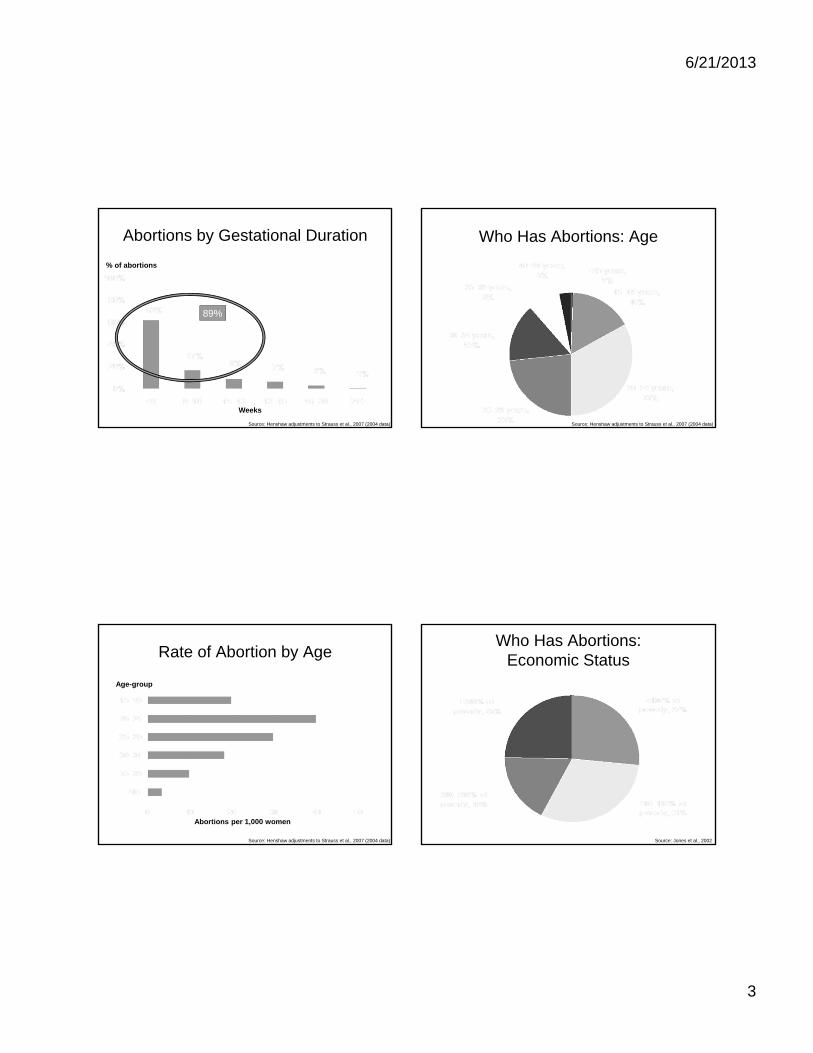
6/21/2013
3
Abortions by Gestational Duration
Source: Henshaw adjustments to Strauss et al., 2007 (2004 data)
Weeks
% of abortions
89%
Who Has Abortions: Age
Source: Henshaw adjustments to Strauss et al., 2007 (2004 data)
Rate of Abortion by Age
Abortions per 1,000 women
Age-group
Source: Henshaw adjustments to Strauss et al., 2007 (2004 data)
Who Has Abortions: Economic Status
Source: Jones et al., 2002
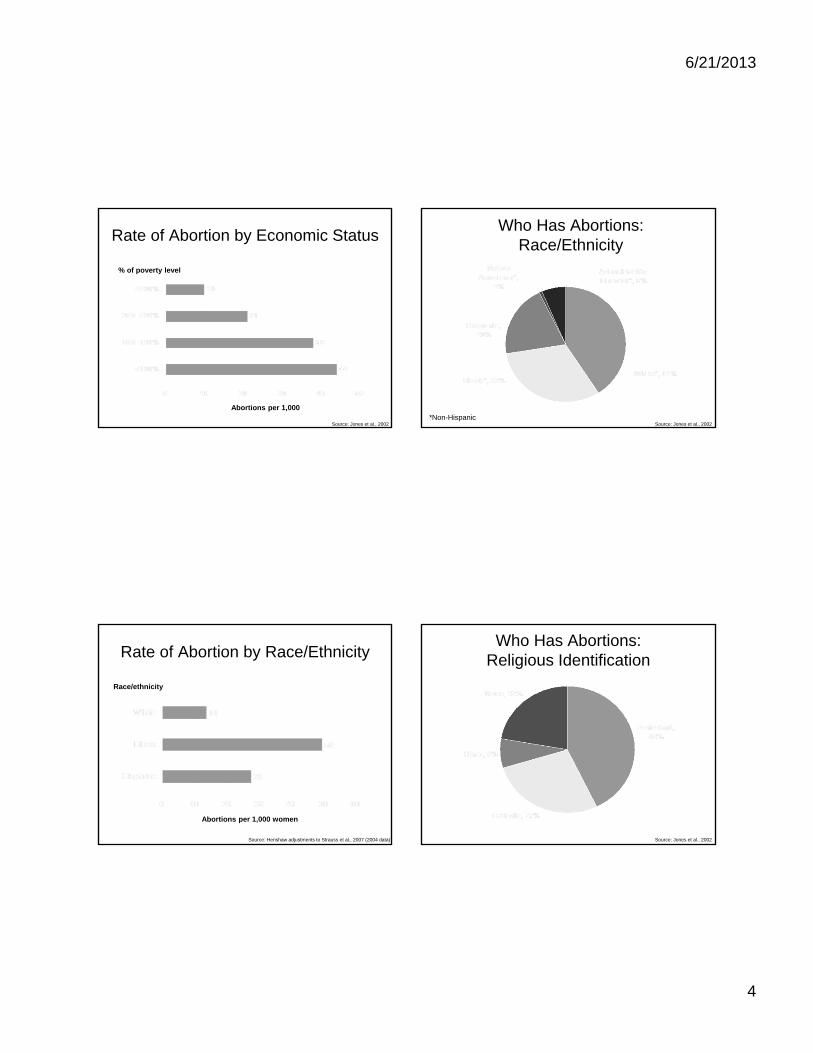
6/21/2013
4
Rate of Abortion by Economic Status
Source: Jones et al., 2002
% of poverty level
Abortions per 1,000
Who Has Abortions: Race/Ethnicity
Source: Jones et al., 2002*Non-Hispanic
Rate of Abortion by Race/Ethnicity
Race/ethnicity
Abortions per 1,000 women
Source: Henshaw adjustments to Strauss et al., 2007 (2004 data)
Who Has Abortions:Religious Identification
Source: Jones et al., 2002

6/21/2013
5
Who Has Abortions: Prior Pregnancies
Source: Jones et al., 2002
Global Epidemiology of Abortion
Abortion Worldwide
Millions of abortions
Source: Sedgh, 2007
Abortions per 1,000 women
U.S. Abortion Rate Higher Than in Many Other Industrialized Countries
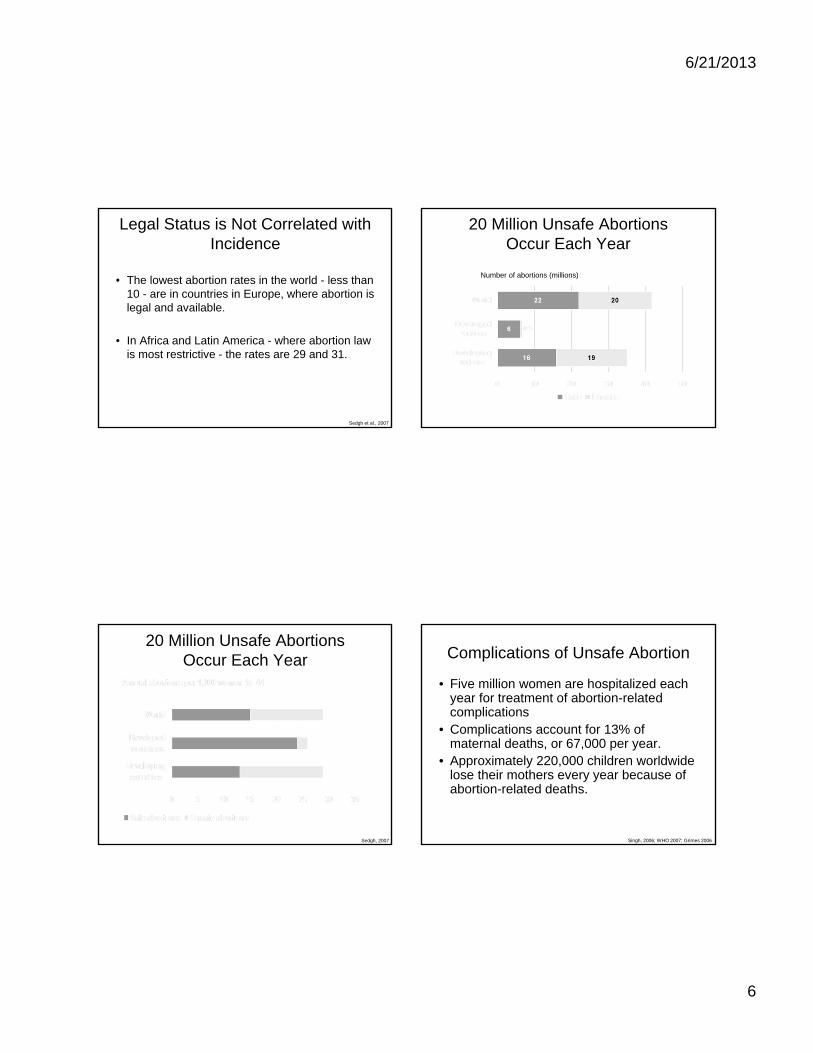
6/21/2013
6
Legal Status is Not Correlated with Incidence
• The lowest abortion rates in the world - less than 10 - are in countries in Europe, where abortion is legal and available.
• In Africa and Latin America - where abortion law is most restrictive - the rates are 29 and 31.
Sedgh et al., 2007
Number of abortions (millions)
20 Million Unsafe Abortions Occur Each Year
Sedgh, 2007
20 Million Unsafe Abortions Occur Each Year Complications of Unsafe Abortion
• Five million women are hospitalized each year for treatment of abortion-related complications
• Complications account for 13% of maternal deaths, or 67,000 per year.
• Approximately 220,000 children worldwide lose their mothers every year because of abortion-related deaths.
Singh, 2006; WHO 2007; Grimes 2006

6/21/2013
7
Deaths from Abortion Declined Immediately After Legalization Conclusions: Epidemiology
• Unintended pregnancy is common.
• We should be prepared to counsel women about pregnancy options.
• Abortion should be legal and safe.
Counseling Points
• What do you think/hope the results will be?
• Validate and Normalize
• Seek understanding– Can you say more about what you are feeling?
• Reframe– Use what you have learned from her
– What I hear you saying is that you are making this decision because you care about your children’s well-being
• If needed find someone to help
• www.faithaloud.org / www.yourbackline.org
Obligations to Patient
• Study of 1200 physicians in 2007• Would it be ethical to describe why the physician
objects to the requested procedure? – 63% yes
• Does the physician have obligation to present all options to patient, including information about the requested procedure? – 86% yes
• Does the physician have an obligation to refer?– 71% yes
Curlin, NEJM, 2007.

6/21/2013
8
Conscientious Refusal
• When clinicians claim a right to refuse to provide certain services, to refer patients, or to inform patients about their existing options.
• Widespread in area of reproductive medicine –pharmacists EC and contraception, IUI, life-threatening medical conditions and abortion
• Claim that to provide services would compromise the moral integrity of a provider or institution
Ethical Responsibilities
• Criteria for assessing conscientious refusal– Potential for imposition
• on patients who do not share their beliefs
– Effect on patient health
– Scientific integrity of the claim• EC, abortion and breast cancer
– Potential for discrimination • Fertility assistance in same-sex couples
ACOG Practice Bulletin
Responsibilities
• Prioritize patient’s well-being
• Provide accurate & unbiased information
• Provide potential patients with accurate and prior notice of their moral commitments, not use their authority to argue their position
• Refer in a timely manner
• Emergency – obligation to provide medically necessary services
ACOG Practice Bulletin
Abortion Safety
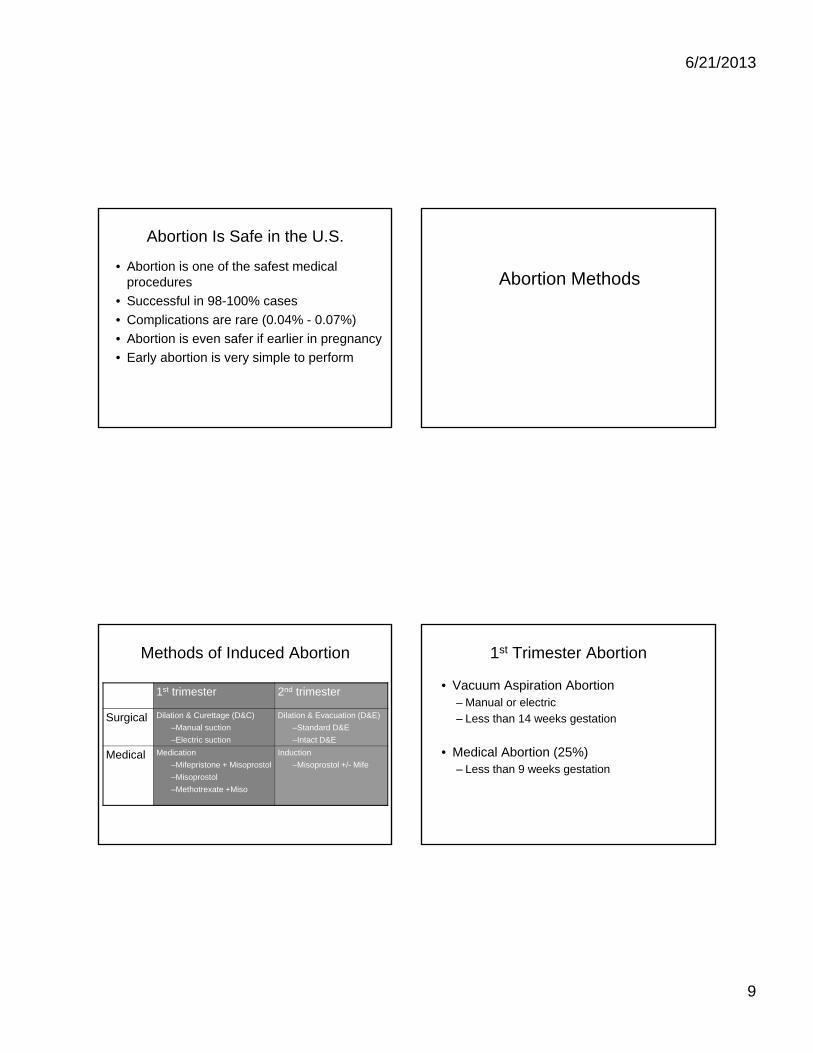
6/21/2013
9
Abortion Is Safe in the U.S.
• Abortion is one of the safest medical procedures
• Successful in 98-100% cases
• Complications are rare (0.04% - 0.07%)
• Abortion is even safer if earlier in pregnancy
• Early abortion is very simple to perform
Abortion Methods
Methods of Induced Abortion
1st trimester 2nd trimester
Surgical Dilation & Curettage (D&C)
–Manual suction
–Electric suction
Dilation & Evacuation (D&E)
–Standard D&E
–Intact D&E
Medical Medication
–Mifepristone + Misoprostol
–Misoprostol
–Methotrexate +Miso
Induction
–Misoprostol +/- Mife
1st Trimester Abortion
• Vacuum Aspiration Abortion – Manual or electric
– Less than 14 weeks gestation
• Medical Abortion (25%)– Less than 9 weeks gestation

6/21/2013
10
1st Trimester Surgical Abortion
• Counseling– Pregnancy options
– Procedural
– Contraception
• Preoperative Assessment• Analgesia and Anesthesia• Cervical Dilation• Aspiration• Recovery
Manual Vacuum Aspiration
• About 50% of U.S. abortion providers use MVAs1
• Usually without sharp curettage
• Must empty syringe during procedure with gestation > 7 or 8 wks
• Women appreciate less noise2,3,4
1. O’Connell, 2008, 2. Bird et al., 2001; 3. Edelman et al., 2001; 4. Dean et al 2003
First-Trimester Aspiration Abortion Surgical Abortion < 6 weeks
• Studies in 1970’s found increased rates of continuing pregnancy & complications < 6 wks
• Now new technology: sensitive urine pregnancy tests and transvaginal sonography
• May require more careful surveillance for equal success
• % of U.S. providers offering abortion at 4 weeks rose from 7% in 1993 to 40% in 2005 1
1. Jones 2008

6/21/2013
11
Cervical Block Decreases Pain
• 20 mL 1% buffered lidocaine
• Slow, deep injection at tenac + 4 sites
• Stratified by <8 weeks (early), 8-10 weeks (late)
Pain /100 BLOCK NO BLOCK
With block 49/58 24/35 p=.001
Dilation 34/51 75/83 p<.001
Aspiration 58/67 88/88 p<.001
Renner. Ob Gyn May 2012
Cervical & Uterine Nerves
Uterine fundusSympathetic nerves via: • infundibulopelvic pelvic
ligament utero-ovarian lig• inf hypogastric nerve through
uterosacral ligaments, T10 - L1
Lower uterus/cervixParasympathetic plexus lateral to
cervix, S2 - S4
Sensory nerves also found in uterine tissue
Tingaker. Repro bio & endoc 2006
Paracervical vs. intracervical
Superficial vs. deep injection
Cervical Injections
Hybrid
Cervical Block for Uterine Aspiration
1. Deep injections better than superficial (but hurt)
2. Larger volume of injection better (20ml vs. less)
3. Slow injection helps with block pain
4. Buffering lidocaine - less pain than not or bupiv
5. Routinely waiting more than a couple minutes after administering block unlikely to be helpful
6. Adding vasopressin decreases bleeding and possibly re-aspirationand increases amount ofblock that can be used
1 Wiebe et al. Am J Ob Gyn, 19922. Stubblefielf. Int J Gynecol Obstet 19893. Wiebe et al Int J Gynecol Obstet 19954. Wiebe et al. Am J Ob Gyn, 19925. Phair et al Am J Ob Gyn, 20026. Wiebe et al, Contraception. 2003

6/21/2013
12
Medical Abortion 1st Trimester Medical Abortion
• Counseling and assessment• Take mifepristone in office• Go home with pain medications• Six hours to three days later:
– Place misoprostol pills in vagina
– Over next 4 to 24 hours+ bleeding
• Return to clinic as early as 3 days later– New evidence – follow-up regimens
Medical Abortion
Worldwide
• Over 60% of outpatient abortions in several European countries
• Over 30 million worldwide
• Abortions occur earlier where MAB widely available
FDA-Approved vs. Evidenced-Based Regimens for Medical Abortion
FDA-Approved
• 600 mg Mifeprex PO given in the clinic
• Miso given orally
• 400 mcg misoprostol
• Miso 2 days later
• Miso given in the clinic
• Follow-up day 14
• Gestational limit 7 wks
Evidenced-Based
• 200 mg Mifeprex PO given in the clinic
• Miso vaginally/ buccally
• 800 mcg misoprostol
• Miso 6 hrs-3 days* later
• Pt takes at home
• Follow-up day 3 to 14
• Gestational limit 9 wks
*3 days studied to 8 wks gestation
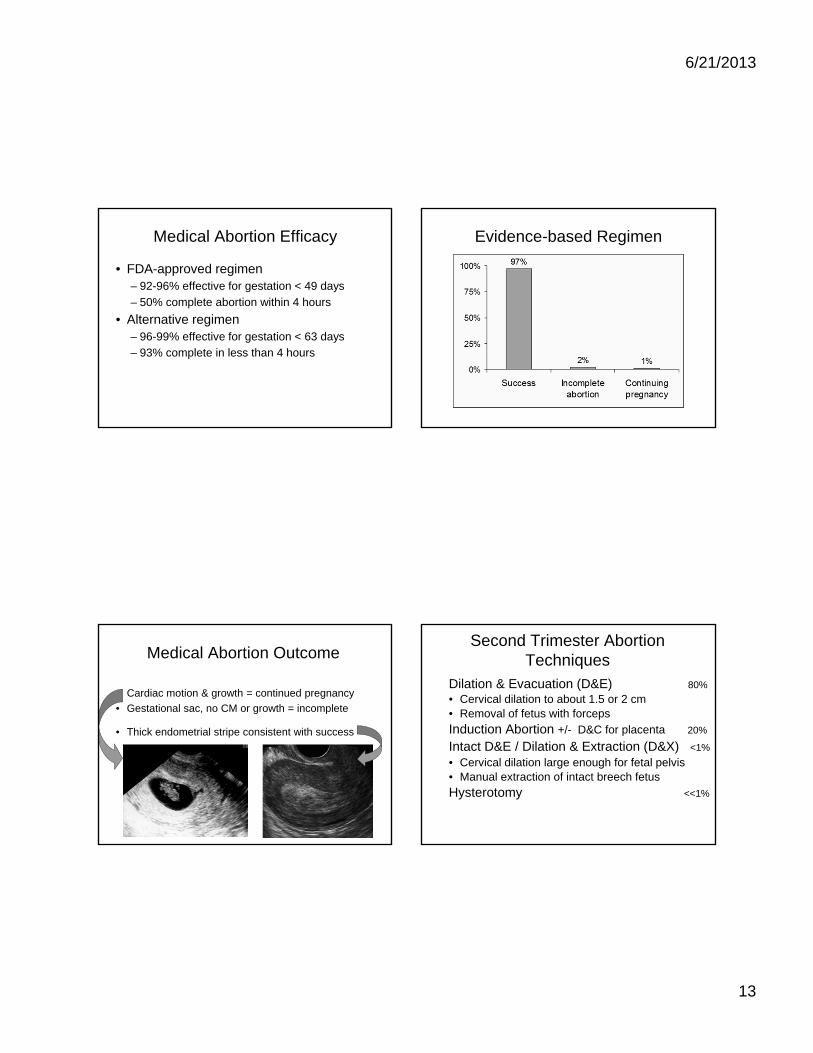
6/21/2013
13
Medical Abortion Efficacy
• FDA-approved regimen– 92-96% effective for gestation < 49 days
– 50% complete abortion within 4 hours
• Alternative regimen– 96-99% effective for gestation < 63 days
– 93% complete in less than 4 hours
Evidence-based Regimen
Medical Abortion Outcome
• Cardiac motion & growth = continued pregnancy
• Gestational sac, no CM or growth = incomplete
• Thick endometrial stripe consistent with success
Second Trimester Abortion Techniques
Dilation & Evacuation (D&E) 80%
• Cervical dilation to about 1.5 or 2 cm• Removal of fetus with forceps
Induction Abortion +/- D&C for placenta 20%
Intact D&E / Dilation & Extraction (D&X) <1%
• Cervical dilation large enough for fetal pelvis • Manual extraction of intact breech fetus
Hysterotomy <<1%

6/21/2013
14
Reasons for Delay in2nd-Trimester Patients
*statistically significant vs. early abortion patients, p<0.05
Difficulty in getting to our clinic 63%*Emotional factors 51%Initially referred to other clinic(s) 47%*Afraid 35%Didn’t suspect pregnancy 34%*Unsure of decision 30%*In denial about being pregnant 21%*Difficulty with Medi-Cal, money, insurance 20%*Difficulty figuring out where to go 20%*Unsupportive partner 19%
Drey E et al, Ob Gyn, 2006
Induction Abortion
• Misoprostol alone: > 90% of women abort within 48 hrs, mean interval of ~ 15 hrs
• Mifepristone + misoprostol: > 90% of women abort within 24 hrs, mean interval of ~ 6 hrs
• Osmotic dilators can shorten interval
1. Autry et al. Am J Ob Gyn, 20022. Ngai, Tang and Ho. Best Prac Res Clin Ob Gyn, 2002
Dilation & Extraction (D&X)(also “Intact D&E”)
• “Partial Birth Abortion,” named by anti-abortion groups, usually describes D&X
• Goal to minimize uterine instrumentation and/or deliver an intact fetus
• Cervical dilation usually requires 2 days
• Performed when:– Family desires autopsy or to see fetus intact
– Fetal anomaly: cystic hygroma, hydrocephalus
– Hemorrhage requires intervention with induction or Sab
Surgical Abortion: Cervical Ripening to Decrease Risk of
Cervical Laceration• SFP 2007
– Consider priming for all adolescents– All women over 12 to 14 weeks
• WHO 2003– Younger than 18 years old – Nulliparous over 9 weeks – All women over 12 weeks
• RCOG 2004– Younger than 18 years old– All women over 10 weeks

6/21/2013
15
Abortion Complications
An Abortion Is Safer the Earlier in Pregnancy It Is Performed
Sources: All births and abortions: CDC.gov; Abortion by gestation: Bartlett et al., 2004 (1988–1997 data)
Deaths per 100,000 abortions
Abortions by gestation
Causes of Abortion-Related Deaths
Source: Bartlett et al., 2004 (1988–1997 data)
% of abortion deaths (on average, 8 per year)
First-trimester Complications1st trimestermedical
1st trimestersurgical
Overall ---------------- 0.07% (major)
Hemorrhage 0.1 – 0.4% (transfusion) 0.01%
Infection 0.9% 0.1 – 0.4%
Perforation ---------------- 0.1%
Cervical laceration ----------------
Retained products 2 – 5%(~8% for 9wks)
0.3 – 2%
Peterson et al. Obstet Gynecol 1983 Hern et al. Obstet Gynecol 1984Ben-Ami et al. AJOG 2009 Autry et al. AJOG 2002Frick et al. Obstet Gynecol 2012 Paul et al. NAF Textbook 2009Hakim-Elahi et al. Obstet Gynecol 1990
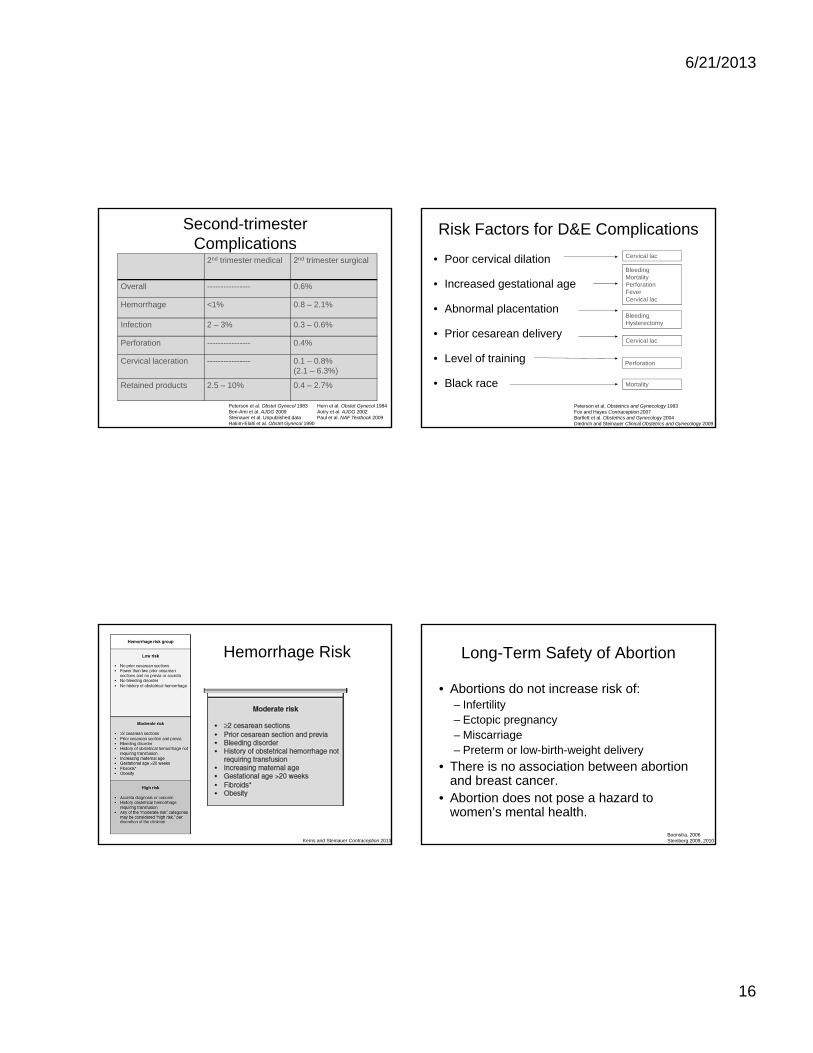
6/21/2013
16
Second-trimester Complications
2nd trimester medical 2nd trimester surgical
Overall ---------------- 0.6%
Hemorrhage <1% 0.8 – 2.1%
Infection 2 – 3% 0.3 – 0.6%
Perforation ---------------- 0.4%
Cervical laceration ---------------- 0.1 – 0.8% (2.1 – 6.3%)
Retained products 2.5 – 10% 0.4 – 2.7%
Peterson et al. Obstet Gynecol 1983 Hern et al. Obstet Gynecol 1984Ben-Ami et al. AJOG 2009 Autry et al. AJOG 2002Steinauer et al. Unpublished data Paul et al. NAF Textbook 2009Hakim-Elahi et al. Obstet Gynecol 1990
Risk Factors for D&E Complications
• Poor cervical dilation
• Increased gestational age
• Abnormal placentation
• Prior cesarean delivery
• Level of training
• Black race
Peterson et al. Obstetrics and Gynecology 1983Fox and Hayes Contraception 2007Bartlett et al. Obstetrics and Gynecology 2004Diedrich and Steinauer Clinical Obstetrics and Gynecology 2009
Cervical lac
BleedingMortality PerforationFeverCervical lac
Bleeding Hysterectomy
Mortality
Cervical lac
Perforation
Hemorrhage Risk
Kerns and Steinauer Contraception 2013
Long-Term Safety of Abortion
• Abortions do not increase risk of:– Infertility– Ectopic pregnancy– Miscarriage– Preterm or low-birth-weight delivery
• There is no association between abortion and breast cancer.
• Abortion does not pose a hazard to women’s mental health.
Boonstra, 2006Steinberg 2009, 2010
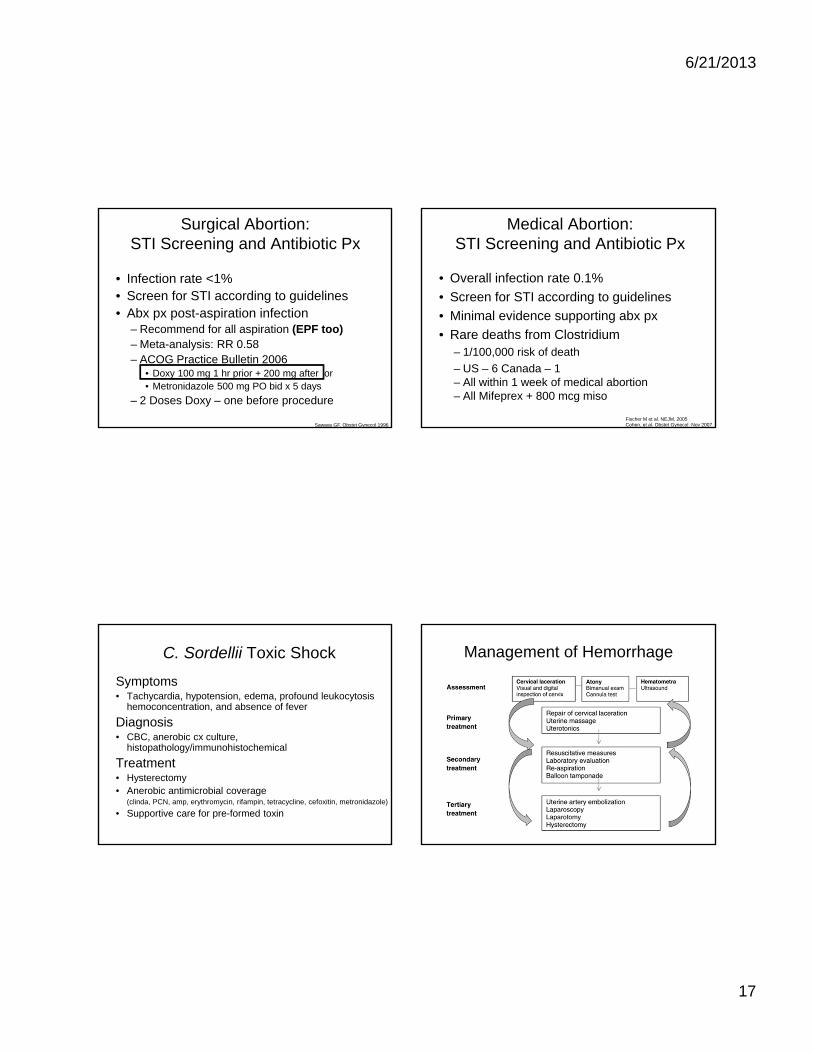
6/21/2013
17
Surgical Abortion: STI Screening and Antibiotic Px
• Infection rate <1%• Screen for STI according to guidelines• Abx px post-aspiration infection
– Recommend for all aspiration (EPF too)– Meta-analysis: RR 0.58– ACOG Practice Bulletin 2006
• Doxy 100 mg 1 hr prior + 200 mg after or• Metronidazole 500 mg PO bid x 5 days
– 2 Doses Doxy – one before procedure
Sawaya GF. Obstet Gynecol 1996
Medical Abortion: STI Screening and Antibiotic Px
• Overall infection rate 0.1%
• Screen for STI according to guidelines
• Minimal evidence supporting abx px
• Rare deaths from Clostridium– 1/100,000 risk of death
– US – 6 Canada – 1 – All within 1 week of medical abortion– All Mifeprex + 800 mcg miso
Fischer M et al. NEJM, 2005Cohen, et al. Obstet Gynecol Nov 2007
C. Sordellii Toxic Shock
Symptoms • Tachycardia, hypotension, edema, profound leukocytosis
hemoconcentration, and absence of fever
Diagnosis• CBC, anerobic cx culture,
histopathology/immunohistochemical
Treatment• Hysterectomy• Anerobic antimicrobial coverage
(clinda, PCN, amp, erythromycin, rifampin, tetracycline, cefoxitin, metronidazole)
• Supportive care for pre-formed toxin
Management of Hemorrhage

6/21/2013
18
Summary
• Abortions are common, safe, and most are early in the US.
• Abortion is safest and not more common when legal.
• Refer women as soon as possible for care.
• First-trimester uterine aspiration can be safely provided in outpatient setting.
• Antibiotics decrease infection after uterine aspiration.
Summary
• Early pregnancy loss
• Brief abortion update– Cervical preparation
– Medication abortion
Resources
• www.papayaworkshop.org
• Society of Family Planning guidelines
• www.yourbackline.org
• www.faithaloud.org
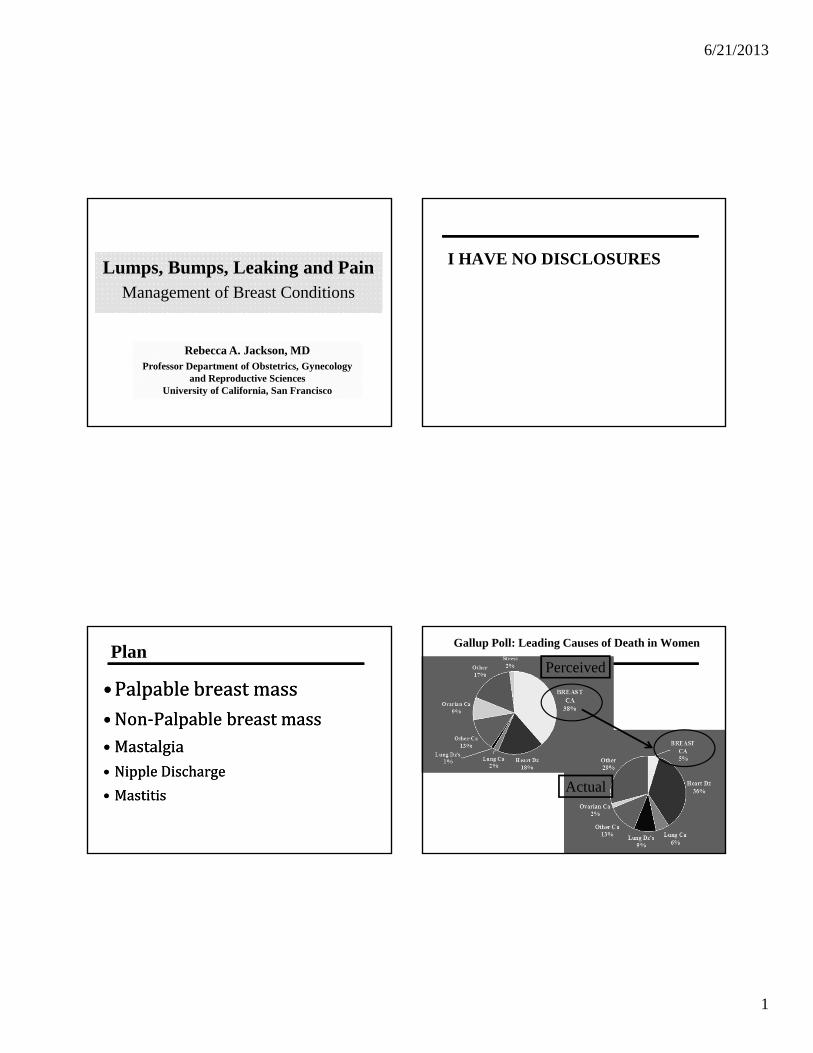
6/21/2013
1
Lumps, Bumps, Leaking and PainManagement of Breast Conditions
Rebecca A. Jackson, MDProfessor Department of Obstetrics, Gynecology
and Reproductive SciencesUniversity of California, San Francisco
I HAVE NO DISCLOSURES
Plan
•Palpablebreastmass•Non‐Palpablebreastmass• Mastalgia• NippleDischarge
• Mastitis
•Palpablebreastmass•Non‐Palpablebreastmass• Mastalgia• NippleDischarge
• Mastitis
Gallup Poll: Leading Causes of Death in Women
Gallup Poll
Perceived
Actual
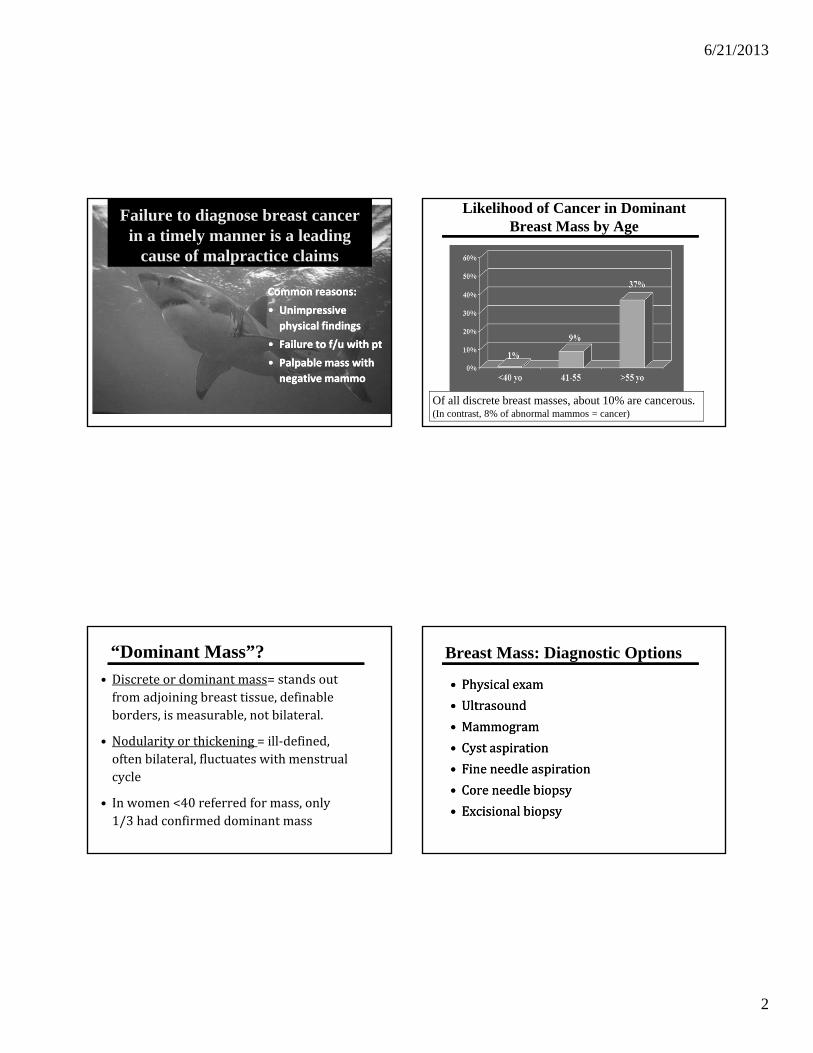
6/21/2013
2
Failure to diagnose breast cancer in a timely manner is a leading
cause of malpractice claims
Common reasons:
• Unimpressive
physical findings
• Failure to f/u with pt
• Palpable mass with
negative mammo
Common reasons:
• Unimpressive
physical findings
• Failure to f/u with pt
• Palpable mass with
negative mammo
Likelihood of Cancer in Dominant Breast Mass by Age
Of all discrete breast masses, about 10% are cancerous. (In contrast, 8% of abnormal mammos = cancer)
“Dominant Mass”?
• Discreteordominantmass=standsoutfromadjoiningbreasttissue,definableborders,ismeasurable,notbilateral.
• Nodularityorthickening=ill‐defined,oftenbilateral,fluctuateswithmenstrualcycle
• Inwomen<40referredformass,only1/3hadconfirmeddominantmass
Breast Mass: Diagnostic Options
• Physicalexam
• Ultrasound
• Mammogram
• Cystaspiration
• Fineneedleaspiration
• Coreneedlebiopsy
• Excisionalbiopsy
• Physicalexam
• Ultrasound
• Mammogram
• Cystaspiration
• Fineneedleaspiration
• Coreneedlebiopsy
• Excisionalbiopsy

6/21/2013
3
Question 1
A42yroldwomanwithnofamilyorpersonalhistoryofbreastcancerhasfoundabreastlump.Shedoesn’tknowhowlongithasbeenthere.Itisnotpainful.
Onexam,itisadiscretemass,2cm,relativelysmooth,mobileandnon‐tender.Shehasnoaxillarylymphadenopathy.
Whatisyournextstep?
A42yroldwomanwithnofamilyorpersonalhistoryofbreastcancerhasfoundabreastlump.Shedoesn’tknowhowlongithasbeenthere.Itisnotpainful.
Onexam,itisadiscretemass,2cm,relativelysmooth,mobileandnon‐tender.Shehasnoaxillarylymphadenopathy.
Whatisyournextstep?
Q1: Palpable mass in 42 yo
Nextstep(pickone)?
A. Nothingnow.Re‐examinein1‐2months
B. Ultrasound
C. Mammography
D. Officeaspiration
E. FNAB
F. Corebiopsy
Nextstep(pickone)?
A. Nothingnow.Re‐examinein1‐2months
B. Ultrasound
C. Mammography
D. Officeaspiration
E. FNAB
F. Corebiopsy
Q1b: Palpable mass in 42 yo
Amammographywaschosenandisnegative.Nextstep(pickone)?
A. Re‐examinein1‐2months
B. F/u1yearforannualexam
C. Ultrasound
D. Officeaspiration
E. FNAB
F. Corebiopsy
Amammographywaschosenandisnegative.Nextstep(pickone)?
A. Re‐examinein1‐2months
B. F/u1yearforannualexam
C. Ultrasound
D. Officeaspiration
E. FNAB
F. Corebiopsy
Q1c: Palpable mass in 42 yo
Anultrasoundwaschosenasthefirststep.Itshowsacysticmass.Nextstep?
A. Re‐examinein1‐2months
B. F/u1yearforannualexam
C. Officeaspiration
D. FNA
E. Corebiopsy
Anultrasoundwaschosenasthefirststep.Itshowsacysticmass.Nextstep?
A. Re‐examinein1‐2months
B. F/u1yearforannualexam
C. Officeaspiration
D. FNA
E. Corebiopsy

6/21/2013
4
Step 1: Palpable Breast Mass
• Determineifmassiscysticorsolid
• Simplecystsarebenignanddon’trequirefurtherevaluation
• 20‐25%ofpalpablemassesaresimplecysts,mostoccurringin40‐49yo’s
• Options?:Ultrasound,officeaspiration,FNA,coreneedlebiopsy
• Determineifmassiscysticorsolid
• Simplecystsarebenignanddon’trequirefurtherevaluation
• 20‐25%ofpalpablemassesaresimplecysts,mostoccurringin40‐49yo’s
• Options?:Ultrasound,officeaspiration,FNA,coreneedlebiopsy
Breast Exam
• Nethersensitive(50‐60%)norspecific(60‐90%)(evenwhendonebyexperts)
• Cannotreliablydistinguishcystfromsolid• Nonetheless,itisimportantfordeterminingifmassisdiscrete(vsnodularityorthickening),isanecessaryadjuncttomammogramandisrequiredforfollow‐upofmasses
• Performin2positions,methodical,spiralsorstrips
• Markmasspriortobiopsysootherscanfindit
• Nethersensitive(50‐60%)norspecific(60‐90%)(evenwhendonebyexperts)
• Cannotreliablydistinguishcystfromsolid• Nonetheless,itisimportantfordeterminingifmassisdiscrete(vsnodularityorthickening),isanecessaryadjuncttomammogramandisrequiredforfollow‐upofmasses
• Performin2positions,methodical,spiralsorstrips
• Markmasspriortobiopsysootherscanfindit
Ultrasound
• PrimaryUse:Classifymassascysticor
solid
• Guidanceforcystaspirationorbiopsy
• Adjuncttoevaluatesymmetricdensitiesdetectedbymammography
• Canbethefirsttestperformed&ifcystisconfirmed—theonlytestrequired
• PrimaryUse:Classifymassascysticor
solid
• Guidanceforcystaspirationorbiopsy
• Adjuncttoevaluatesymmetricdensitiesdetectedbymammography
• Canbethefirsttestperformed&ifcystisconfirmed—theonlytestrequired
Fibroadenoma Cancer
Well-circumscribed, superficial
Irregular, deep
Cyst
Anechoic, well-circumscribed,
Ultrasound is 98-100% accurate for diagnosis of simple cysts. However, for solid masses, it cannot reliably distinguish benign from malignant.
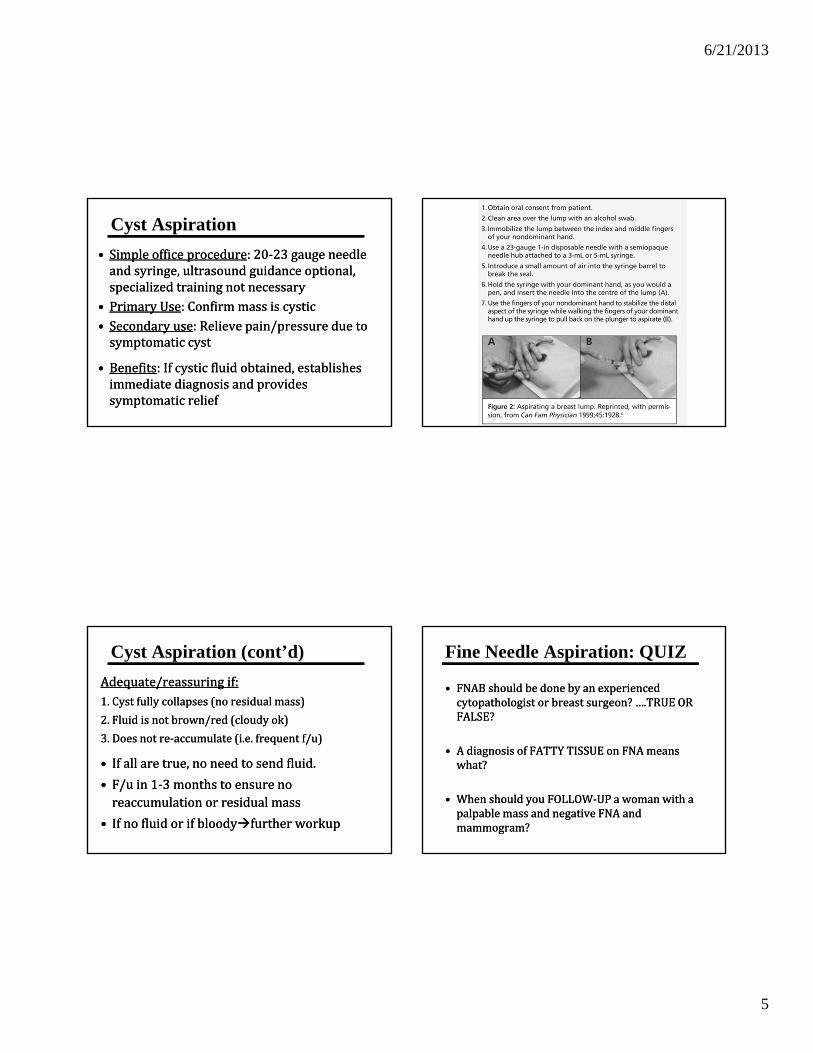
6/21/2013
5
Cyst Aspiration
• Simpleofficeprocedure:20‐23gaugeneedleandsyringe,ultrasoundguidanceoptional,specializedtrainingnotnecessary
• PrimaryUse:Confirmmassiscystic• Secondaryuse:Relievepain/pressureduetosymptomaticcyst
• Benefits:Ifcysticfluidobtained,establishesimmediatediagnosisandprovidessymptomaticrelief
• Simpleofficeprocedure:20‐23gaugeneedleandsyringe,ultrasoundguidanceoptional,specializedtrainingnotnecessary
• PrimaryUse:Confirmmassiscystic• Secondaryuse:Relievepain/pressureduetosymptomaticcyst
• Benefits:Ifcysticfluidobtained,establishesimmediatediagnosisandprovidessymptomaticrelief
Cyst Aspiration (cont’d)
Adequate/reassuringif:1.Cystfullycollapses(noresidualmass)
2.Fluidisnotbrown/red(cloudyok)
3.Doesnotre‐accumulate(i.e.frequentf/u)
• Ifallaretrue,noneedtosendfluid.
• F/uin1‐3monthstoensurenoreaccumulationorresidualmass
• Ifnofluidorifbloodyfurtherworkup
Adequate/reassuringif:1.Cystfullycollapses(noresidualmass)
2.Fluidisnotbrown/red(cloudyok)
3.Doesnotre‐accumulate(i.e.frequentf/u)
• Ifallaretrue,noneedtosendfluid.
• F/uin1‐3monthstoensurenoreaccumulationorresidualmass
• Ifnofluidorifbloodyfurtherworkup
Fine Needle Aspiration: QUIZ
• FNABshouldbedonebyanexperiencedcytopathologistorbreastsurgeon?….TRUEORFALSE?
• AdiagnosisofFATTYTISSUEonFNAmeanswhat?
• WhenshouldyouFOLLOW‐UPawomanwithapalpablemassandnegativeFNAandmammogram?
• FNABshouldbedonebyanexperiencedcytopathologistorbreastsurgeon?….TRUEORFALSE?
• AdiagnosisofFATTYTISSUEonFNAmeanswhat?
• WhenshouldyouFOLLOW‐UPawomanwithapalpablemassandnegativeFNAandmammogram?
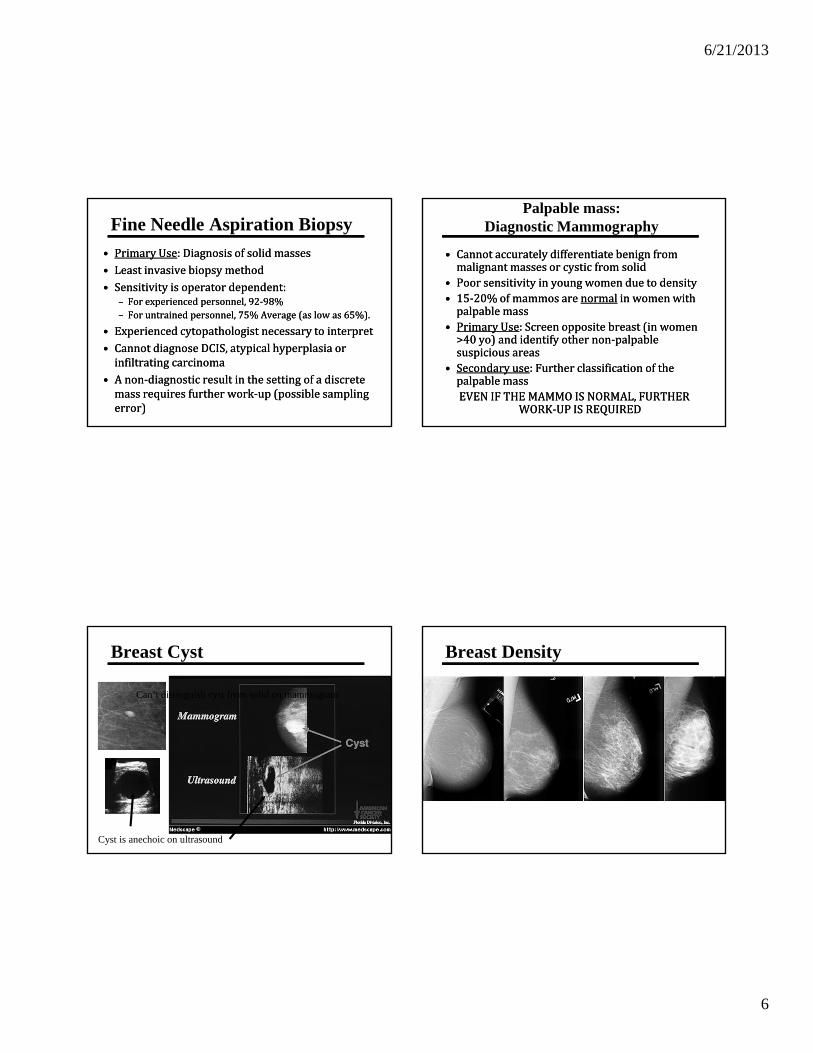
6/21/2013
6
Fine Needle Aspiration Biopsy
• PrimaryUse:Diagnosisofsolidmasses• Leastinvasivebiopsymethod• Sensitivityisoperatordependent:
– Forexperiencedpersonnel,92‐98%– Foruntrainedpersonnel,75%Average(aslowas65%).
• Experiencedcytopathologistnecessarytointerpret• CannotdiagnoseDCIS,atypicalhyperplasiaorinfiltratingcarcinoma
• Anon‐diagnosticresultinthesettingofadiscretemassrequiresfurtherwork‐up(possiblesamplingerror)
• PrimaryUse:Diagnosisofsolidmasses• Leastinvasivebiopsymethod• Sensitivityisoperatordependent:
– Forexperiencedpersonnel,92‐98%– Foruntrainedpersonnel,75%Average(aslowas65%).
• Experiencedcytopathologistnecessarytointerpret• CannotdiagnoseDCIS,atypicalhyperplasiaorinfiltratingcarcinoma
• Anon‐diagnosticresultinthesettingofadiscretemassrequiresfurtherwork‐up(possiblesamplingerror)
Palpable mass: Diagnostic Mammography
• Cannotaccuratelydifferentiatebenignfrommalignantmassesorcysticfromsolid
• Poorsensitivityinyoungwomenduetodensity• 15‐20%ofmammosarenormal inwomenwithpalpablemass
• PrimaryUse:Screenoppositebreast(inwomen>40yo)andidentifyothernon‐palpablesuspiciousareas
• Secondaryuse:FurtherclassificationofthepalpablemassEVENIFTHEMAMMOISNORMAL,FURTHER
WORK‐UPISREQUIRED
• Cannotaccuratelydifferentiatebenignfrommalignantmassesorcysticfromsolid
• Poorsensitivityinyoungwomenduetodensity• 15‐20%ofmammosarenormal inwomenwithpalpablemass
• PrimaryUse:Screenoppositebreast(inwomen>40yo)andidentifyothernon‐palpablesuspiciousareas
• Secondaryuse:FurtherclassificationofthepalpablemassEVENIFTHEMAMMOISNORMAL,FURTHER
WORK‐UPISREQUIRED
Breast Cyst
Cyst is anechoic on ultrasound
Can’t distinguish cyst from solid on mammogram
Breast Density
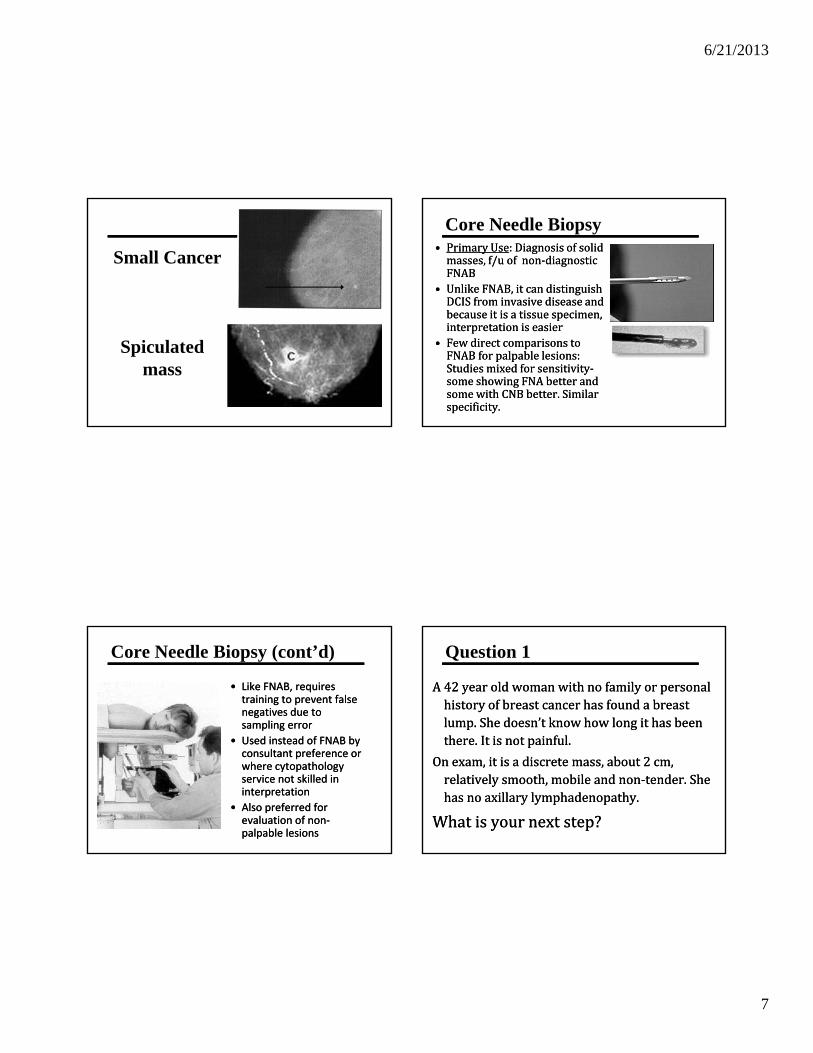
6/21/2013
7
Spiculated mass
Small Cancer
Core Needle Biopsy• PrimaryUse:Diagnosisofsolidmasses,f/uofnon‐diagnosticFNAB
• UnlikeFNAB,itcandistinguishDCISfrominvasivediseaseandbecauseitisatissuespecimen,interpretationiseasier
• FewdirectcomparisonstoFNABforpalpablelesions:Studiesmixedforsensitivity‐someshowingFNAbetterandsomewithCNBbetter.Similarspecificity.
• PrimaryUse:Diagnosisofsolidmasses,f/uofnon‐diagnosticFNAB
• UnlikeFNAB,itcandistinguishDCISfrominvasivediseaseandbecauseitisatissuespecimen,interpretationiseasier
• FewdirectcomparisonstoFNABforpalpablelesions:Studiesmixedforsensitivity‐someshowingFNAbetterandsomewithCNBbetter.Similarspecificity.
Core Needle Biopsy (cont’d)
• Like FNAB, requires training to prevent false negatives due to sampling error
• Used instead of FNAB by consultant preference or where cytopathology service not skilled in interpretation
• Also preferred for evaluation of non‐palpable lesions
• Like FNAB, requires training to prevent false negatives due to sampling error
• Used instead of FNAB by consultant preference or where cytopathology service not skilled in interpretation
• Also preferred for evaluation of non‐palpable lesions
Question 1
A42yearoldwomanwithnofamilyorpersonalhistoryofbreastcancer hasfoundabreastlump.Shedoesn’tknowhowlongithasbeenthere.Itisnotpainful.
Onexam,itisadiscretemass,about2cm,relativelysmooth,mobileandnon‐tender.Shehasnoaxillarylymphadenopathy.
Whatisyournextstep?
A42yearoldwomanwithnofamilyorpersonalhistoryofbreastcancer hasfoundabreastlump.Shedoesn’tknowhowlongithasbeenthere.Itisnotpainful.
Onexam,itisadiscretemass,about2cm,relativelysmooth,mobileandnon‐tender.Shehasnoaxillarylymphadenopathy.
Whatisyournextstep?
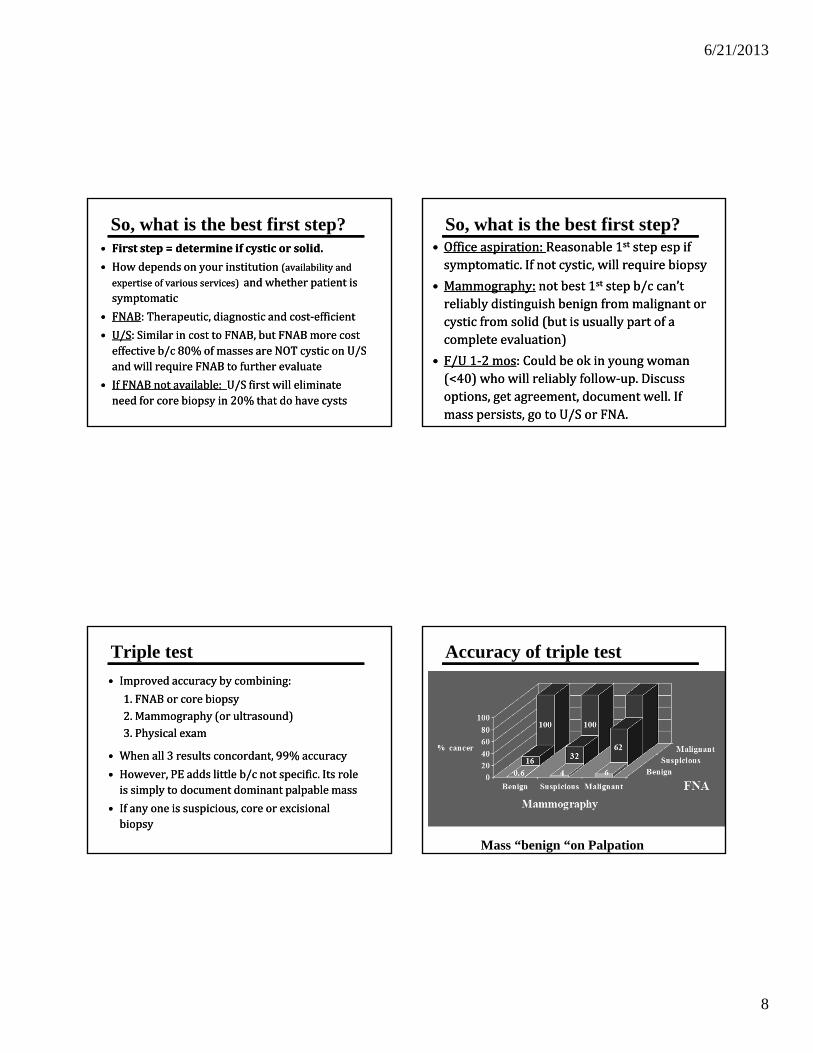
6/21/2013
8
So, what is the best first step?• Firststep=determineifcysticorsolid.
• Howdependsonyourinstitution(availabilityandexpertiseofvariousservices)andwhetherpatientissymptomatic
• FNAB:Therapeutic,diagnosticandcost‐efficient
• U/S:SimilarincosttoFNAB,butFNABmorecosteffectiveb/c80%ofmassesareNOTcysticonU/SandwillrequireFNABtofurtherevaluate
• IfFNABnotavailable:U/Sfirstwilleliminateneedforcorebiopsyin20%thatdohavecysts
• Firststep=determineifcysticorsolid.
• Howdependsonyourinstitution(availabilityandexpertiseofvariousservices)andwhetherpatientissymptomatic
• FNAB:Therapeutic,diagnosticandcost‐efficient
• U/S:SimilarincosttoFNAB,butFNABmorecosteffectiveb/c80%ofmassesareNOTcysticonU/SandwillrequireFNABtofurtherevaluate
• IfFNABnotavailable:U/Sfirstwilleliminateneedforcorebiopsyin20%thatdohavecysts
So, what is the best first step?• Officeaspiration:Reasonable1st stepespifsymptomatic.Ifnotcystic,willrequirebiopsy
• Mammography: notbest1st stepb/ccan’treliablydistinguishbenignfrommalignantorcysticfromsolid(butisusuallypartofacompleteevaluation)
• F/U1‐2mos:Couldbeokinyoungwoman(<40)whowillreliablyfollow‐up.Discussoptions,getagreement,documentwell.Ifmasspersists,gotoU/SorFNA.
• Officeaspiration:Reasonable1st stepespifsymptomatic.Ifnotcystic,willrequirebiopsy
• Mammography: notbest1st stepb/ccan’treliablydistinguishbenignfrommalignantorcysticfromsolid(butisusuallypartofacompleteevaluation)
• F/U1‐2mos:Couldbeokinyoungwoman(<40)whowillreliablyfollow‐up.Discussoptions,getagreement,documentwell.Ifmasspersists,gotoU/SorFNA.
Triple test
• Improvedaccuracybycombining:
1.FNABorcorebiopsy2.Mammography(orultrasound)3.Physicalexam
• Whenall3resultsconcordant,99%accuracy
• However,PEaddslittleb/cnotspecific.Itsroleissimplytodocumentdominantpalpablemass
• Ifanyoneissuspicious,coreorexcisionalbiopsy
• Improvedaccuracybycombining:
1.FNABorcorebiopsy2.Mammography(orultrasound)3.Physicalexam
• Whenall3resultsconcordant,99%accuracy
• However,PEaddslittleb/cnotspecific.Itsroleissimplytodocumentdominantpalpablemass
• Ifanyoneissuspicious,coreorexcisionalbiopsy
Accuracy of triple test
Mass “benign “on Palpation

6/21/2013
9
Step 2: for a cystic mass…
• Ifsymptomatic,aspirate• Ifdiagnosedbyultrasoundandnoaspirationisdone,f/u1year.
• Ifaspiratedandfluidisnotbloody,f/u1‐3monthstoensurenoresidualmassorre‐accumulation
• Foranypatient>40,alsogetmammoforscreening(>50recommend,>40shareddecision)
• Ifsymptomatic,aspirate• Ifdiagnosedbyultrasoundandnoaspirationisdone,f/u1year.
• Ifaspiratedandfluidisnotbloody,f/u1‐3monthstoensurenoresidualmassorre‐accumulation
• Foranypatient>40,alsogetmammoforscreening(>50recommend,>40shareddecision)
Step 2: for a solid mass
Biopsy (FNAorcoreneedlebiopsy)
PLUS
Mammogram (tofurthercharacterizemassandtoscreenrestofbreasts)
• Ifbotharenegative,f/u3‐6months
• Ifeitherisequivocalorresultsarenotconcordant,refertobreastsurgeonforfurtherevaluation
Biopsy (FNAorcoreneedlebiopsy)
PLUS
Mammogram (tofurthercharacterizemassandtoscreenrestofbreasts)
• Ifbotharenegative,f/u3‐6months
• Ifeitherisequivocalorresultsarenotconcordant,refertobreastsurgeonforfurtherevaluation
Ultrasound F/u instead of biopsy for solid mass?
• 2smallretrospectivecohortstudies—largestn=312withpalpablemass&U/S=“probablybenign”
• Mostlyyoungwomensolowpretestprobabilityofcancer(avgage34yo)
• Strictcriteriaforcallinglesion“probablybenign”
• 2of312werecancer.NPV=0.6%.
• Concludeoktonotbiopsyandfollowwithq6mou/sfor2yrs(simtof/uofbirads3mammo)
• Caution:retrospective
• 2smallretrospectivecohortstudies—largestn=312withpalpablemass&U/S=“probablybenign”
• Mostlyyoungwomensolowpretestprobabilityofcancer(avgage34yo)
• Strictcriteriaforcallinglesion“probablybenign”
• 2of312werecancer.NPV=0.6%.
• Concludeoktonotbiopsyandfollowwithq6mou/sfor2yrs(simtof/uofbirads3mammo)
• Caution:retrospectivePark, Acta Radiologica, 2008
How are we doing?
• Inastudyofwomenwithapalpablemassandnegativemammo,only57%receivedany subsequentevaluation.– Latinas,obeseanduninsuredlesslikelytohaveanysubsequentevaluation
• Arecentstudyofdelayindiagnosisfoundthemostcommonreasonwasinappropriatereassuranceofwomenwithalumpandnormalmammogram
• Inastudyofwomenwithapalpablemassandnegativemammo,only57%receivedany subsequentevaluation.– Latinas,obeseanduninsuredlesslikelytohaveanysubsequentevaluation
• Arecentstudyofdelayindiagnosisfoundthemostcommonreasonwasinappropriatereassuranceofwomenwithalumpandnormalmammogram
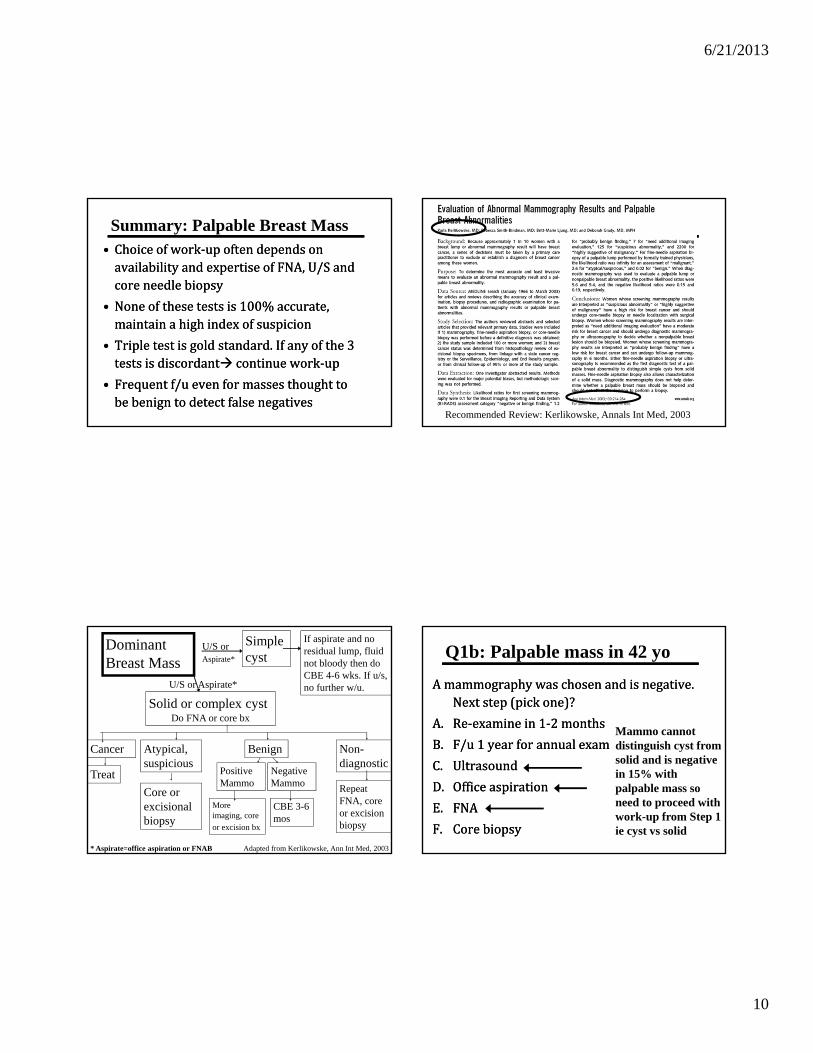
6/21/2013
10
Summary: Palpable Breast Mass• Choiceofwork‐upoftendependsonavailabilityandexpertiseofFNA,U/Sandcoreneedlebiopsy
• Noneofthesetestsis100%accurate,maintainahighindexofsuspicion
• Tripletestisgoldstandard.Ifanyofthe3testsisdiscordant continuework‐up
• Frequentf/uevenformassesthoughttobebenigntodetectfalsenegatives
• Choiceofwork‐upoftendependsonavailabilityandexpertiseofFNA,U/Sandcoreneedlebiopsy
• Noneofthesetestsis100%accurate,maintainahighindexofsuspicion
• Tripletestisgoldstandard.Ifanyofthe3testsisdiscordant continuework‐up
• Frequentf/uevenformassesthoughttobebenigntodetectfalsenegatives
Recommended Review: Kerlikowske, Annals Int Med, 2003
Dominant Breast Mass
U/S or Aspirate*
Solid or complex cystDo FNA or core bx
Simple cyst
If aspirate and no residual lump, fluid not bloody then do CBE 4-6 wks. If u/s, no further w/u.
BenignAtypical, suspicious
Cancer Non-diagnostic
Treat
Core or excisional biopsy
Repeat FNA, core or excision biopsy
Positive Mammo
Negative Mammo
CBE 3-6 mos
More imaging, core
or excision bx
U/S or Aspirate*
* Aspirate=office aspiration or FNAB Adapted from Kerlikowske, Ann Int Med, 2003
Q1b: Palpable mass in 42 yo
Amammographywaschosenandisnegative.Nextstep(pickone)?
A. Re‐examinein1‐2months
B. F/u1yearforannualexam
C. Ultrasound
D. Officeaspiration
E. FNA
F. Corebiopsy
Amammographywaschosenandisnegative.Nextstep(pickone)?
A. Re‐examinein1‐2months
B. F/u1yearforannualexam
C. Ultrasound
D. Officeaspiration
E. FNA
F. Corebiopsy
Mammo cannot distinguish cyst from solid and is negative in 15% with palpable mass so need to proceed with work-up from Step 1 ie cyst vs solid
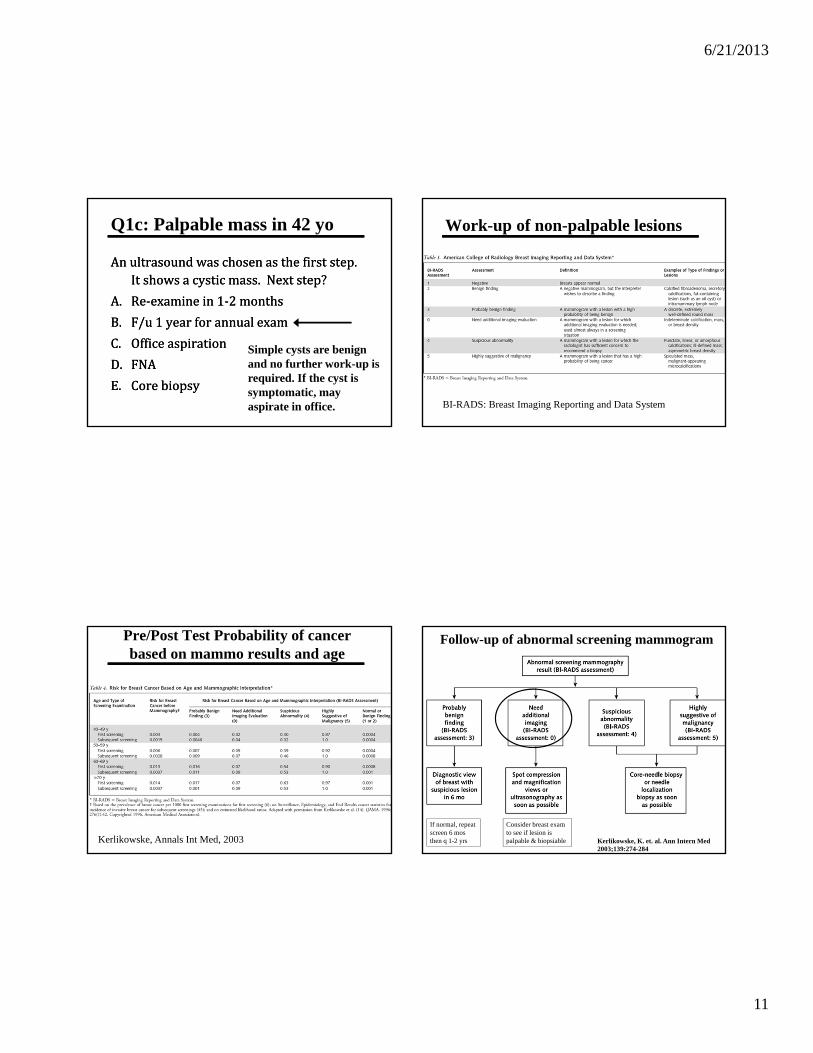
6/21/2013
11
Q1c: Palpable mass in 42 yo
Anultrasoundwaschosenasthefirststep.Itshowsacysticmass.Nextstep?
A. Re‐examinein1‐2months
B. F/u1yearforannualexam
C. Officeaspiration
D. FNA
E. Corebiopsy
Anultrasoundwaschosenasthefirststep.Itshowsacysticmass.Nextstep?
A. Re‐examinein1‐2months
B. F/u1yearforannualexam
C. Officeaspiration
D. FNA
E. Corebiopsy
Simple cysts are benign and no further work-up is required. If the cyst is symptomatic, may aspirate in office.
Work-up of non-palpable lesions
BI-RADS: Breast Imaging Reporting and Data System
Pre/Post Test Probability of cancer based on mammo results and age
Kerlikowske, Annals Int Med, 2003
Follow-up of abnormal screening mammogram
Kerlikowske, K. et. al. Ann Intern Med 2003;139:274-284
If normal, repeat screen 6 mos then q 1-2 yrs
Consider breast exam to see if lesion is palpable & biopsiable

6/21/2013
12
Breast Pain
• 2/3 -3/4 report it
• > 1/2 of breast visits
• Etiology unknown: not associated with prolactin,
estrogen or progesterone levels
• 2 types: cyclic & non-cyclic
• Both types chronic, relapsing especially if severe or early onset
• Severe breast pain interferes with sex (46%), activity (36%), social (13%), work (6%)
• 2/3 -3/4 report it
• > 1/2 of breast visits
• Etiology unknown: not associated with prolactin,
estrogen or progesterone levels
• 2 types: cyclic & non-cyclic
• Both types chronic, relapsing especially if severe or early onset
• Severe breast pain interferes with sex (46%), activity (36%), social (13%), work (6%)
Mastalgia: Treatment
• Work‐up:riskfactorevaluation,exam,
mammoif>40years
• DetermineeffectonQOL
• 60‐80%resolvespontaneously.
• Reassuranceoftensufficient
• Work‐up:riskfactorevaluation,exam,
mammoif>40years
• DetermineeffectonQOL
• 60‐80%resolvespontaneously.
• Reassuranceoftensufficient
Mastalgia: TreatmentProven in RCT’s:• NSAID’s (topical and oral) • Evening Primrose Oil • Iodine• Vitex agnus castus extract-
containing solution (VACS) • Gestrinone (N/A in US)• Progesterone vaginal cream• Bromocryptine• Danazol• Tamoxifen
Proven in RCT’s:• NSAID’s (topical and oral) • Evening Primrose Oil • Iodine• Vitex agnus castus extract-
containing solution (VACS) • Gestrinone (N/A in US)• Progesterone vaginal cream• Bromocryptine• Danazol• Tamoxifen
No benefit (per RCT’s, though many are small and likely underpowered)
• Caffeine restriction• Vitamin E• Vitamin B6• Diuretics• Provera • Soya protein• Isoflavones
No benefit (per RCT’s, though many are small and likely underpowered)
• Caffeine restriction• Vitamin E• Vitamin B6• Diuretics• Provera • Soya protein• Isoflavones
Other: Supportive, well fitting bra, bra at night, trigger point injections for localized pain, OCP’s—help some, make worse in others. If on OCP, try lower dose of Estradiol
Most effective but poorly tolerated
Possibly effective, 1000 mg bid-tid for 2-3 months
Topical diclofenac very effective
Topical NSAID for mastalgiaDiclofenac topical (Voltaren) q 8hr vs placebo cream. Randomized, double-blinded
Colac, Journal of the American College of Surgeons, April 2003
Very large decrease in pain score
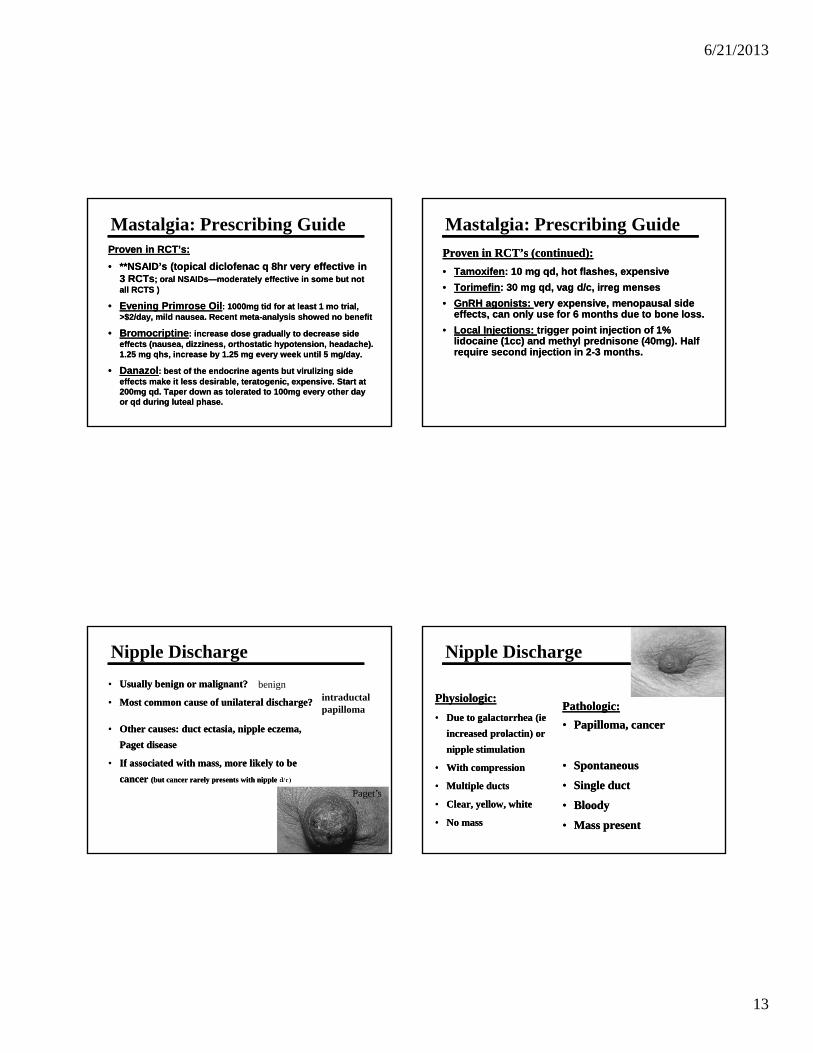
6/21/2013
13
Mastalgia: Prescribing GuideProven in RCT’s:
• **NSAID’s (topical diclofenac q 8hr very effective in 3 RCTs; oral NSAIDs—moderately effective in some but not all RCTS )
• Evening Primrose Oil: 1000mg tid for at least 1 mo trial, >$2/day, mild nausea. Recent meta-analysis showed no benefit
• Bromocriptine: increase dose gradually to decrease side effects (nausea, dizziness, orthostatic hypotension, headache). 1.25 mg qhs, increase by 1.25 mg every week until 5 mg/day.
• Danazol: best of the endocrine agents but virulizing side effects make it less desirable, teratogenic, expensive. Start at 200mg qd. Taper down as tolerated to 100mg every other day or qd during luteal phase.
Proven in RCT’s:
• **NSAID’s (topical diclofenac q 8hr very effective in 3 RCTs; oral NSAIDs—moderately effective in some but not all RCTS )
• Evening Primrose Oil: 1000mg tid for at least 1 mo trial, >$2/day, mild nausea. Recent meta-analysis showed no benefit
• Bromocriptine: increase dose gradually to decrease side effects (nausea, dizziness, orthostatic hypotension, headache). 1.25 mg qhs, increase by 1.25 mg every week until 5 mg/day.
• Danazol: best of the endocrine agents but virulizing side effects make it less desirable, teratogenic, expensive. Start at 200mg qd. Taper down as tolerated to 100mg every other day or qd during luteal phase.
Mastalgia: Prescribing Guide
Proven in RCT’s (continued):
• Tamoxifen: 10 mg qd, hot flashes, expensive
• Torimefin: 30 mg qd, vag d/c, irreg menses
• GnRH agonists: very expensive, menopausal side effects, can only use for 6 months due to bone loss.
• Local Injections: trigger point injection of 1% lidocaine (1cc) and methyl prednisone (40mg). Half require second injection in 2-3 months.
Proven in RCT’s (continued):
• Tamoxifen: 10 mg qd, hot flashes, expensive
• Torimefin: 30 mg qd, vag d/c, irreg menses
• GnRH agonists: very expensive, menopausal side effects, can only use for 6 months due to bone loss.
• Local Injections: trigger point injection of 1% lidocaine (1cc) and methyl prednisone (40mg). Half require second injection in 2-3 months.
Nipple Discharge
• Usually benign or malignant?
• Most common cause of unilateral discharge?
• Other causes: duct ectasia, nipple eczema,
Paget disease
• If associated with mass, more likely to be
cancer (but cancer rarely presents with nipple d/c)
• Usually benign or malignant?
• Most common cause of unilateral discharge?
• Other causes: duct ectasia, nipple eczema,
Paget disease
• If associated with mass, more likely to be
cancer (but cancer rarely presents with nipple d/c)
benignintraductal papilloma
Paget’s
Nipple Discharge
Physiologic:
• Due to galactorrhea (ie
increased prolactin) or
nipple stimulation
• With compression
• Multiple ducts
• Clear, yellow, white
• No mass
Physiologic:
• Due to galactorrhea (ie
increased prolactin) or
nipple stimulation
• With compression
• Multiple ducts
• Clear, yellow, white
• No mass
Pathologic:
• Papilloma, cancer
• Spontaneous
• Single duct
• Bloody
• Mass present
Pathologic:
• Papilloma, cancer
• Spontaneous
• Single duct
• Bloody
• Mass present
6/21/2013
14
Nipple Discharge: Diagnosis
Physiologic:
• History: running,
breast stimulation
• Prolactin, TSH
• Meds:
Psychotropics
Physiologic:
• History: running,
breast stimulation
• Prolactin, TSH
• Meds:
Psychotropics
Pathologic (Spont, unilat):
• Isolate involved duct
• Hemoccult to confirm blood, cytology not useful
• Mammography with retro-alveolar views
• Galactography controversial
• Surgery referral
Pathologic (Spont, unilat):
• Isolate involved duct
• Hemoccult to confirm blood, cytology not useful
• Mammography with retro-alveolar views
• Galactography controversial
• Surgery referral
Mastitis
• 2types:lactatingvsnon‐lactating
• Primaryvssecondary(cellulitis,folliculitis,hydradinitis,sebaceouscyst)
• 2types:lactatingvsnon‐lactating
• Primaryvssecondary(cellulitis,folliculitis,hydradinitis,sebaceouscyst)
Cellulitis
Lactational Mastitis
• Suspect in any breast-feeding woman with a fever and malaise
• Often wedge shaped redness over involved duct
• Staph, Strept—(community acquired MRSA becoming more common so do culture of milk)
• Suspect in any breast-feeding woman with a fever and malaise
• Often wedge shaped redness over involved duct
• Staph, Strept—(community acquired MRSA becoming more common so do culture of milk)
Non-Lactational Mastitis
• Difficult to treat
• Often chronic, recurrent
• Peri-areolar: young (avg 32), 90% are smokers, central pain, nipple retraction and discharge, often assoc with abscess
• Difficult to treat
• Often chronic, recurrent
• Peri-areolar: young (avg 32), 90% are smokers, central pain, nipple retraction and discharge, often assoc with abscess
• Peripheral: elderly, usually associated with underlying disease (diabetes) or trauma
• Gram negatives, staph, strept, anaerobes
• Peripheral: elderly, usually associated with underlying disease (diabetes) or trauma
• Gram negatives, staph, strept, anaerobes
6/21/2013
15
Mastitis Treatment
Lactational
• Increase feeding, warm compresses
• Keflex, Dicloxicillin
• IV if not better quickly
• Septra or Clinda for community acquired MRSA
Lactational
• Increase feeding, warm compresses
• Keflex, Dicloxicillin
• IV if not better quickly
• Septra or Clinda for community acquired MRSA
Non-Lacatational
• Include anaerobic coverage
• Clindamycin or Flagyl + Ancef or Nafcillin
Non-Lacatational
• Include anaerobic coverage
• Clindamycin or Flagyl + Ancef or Nafcillin
** Biopsy if recurrent or doesn’t resolve
Cancer can mimic mastitis
Inflammatory Cancer
Breast Abscess• Suspectif“lump”onexamorifmastitisnotrespondingtoabx
• Ultrasoundtoconfirm• Getculture• AspirationnowpreferredoverI&D
• Sometimesneedrepeatedaspirations
• I&Doftenassocwithpoorcosmeticresultorfistula
• Suspectif“lump”onexamorifmastitisnotrespondingtoabx
• Ultrasoundtoconfirm• Getculture• AspirationnowpreferredoverI&D
• Sometimesneedrepeatedaspirations
• I&Doftenassocwithpoorcosmeticresultorfistula

6/21/2013
1
Topics inPediatric & Adolescent Gynecology
No financial disclosures
No discussion of off label medications
Objectives Illustrate techniques for examining
children
Review common Pedi-Gyn conditions
Discuss etiology and treatment of AUB in adolescents
Normal Anatomy: baby
6/21/2013
2
Case 1
A 4 week old infant has a mass bulging at her introitus. She has no difficulty passing urine or stool.
The family’s medical insurance expires in 2 weeks…
What would you do?
A. Schedule hymenotomy in ORB. Aspirate fluid to decompress C. Reassure parents it will resolve
spontanouslyD. Check chromosomes
Case 2
A 4 yr old presents with a 6 wk history of vulvar erythema, itching and scant yellowish discharge on her underwear. Her parents are very concerned.
Vulvovaginitis
History
•Duration, color, odor, quantity, bleeding, itching, burning, dysuria, redness
Detailed description of symptomsDetailed description of symptoms
•Nylon tights, wet bathing suits, close fitting jeans
ClothingClothing
•Front to back wiping
Hygiene habitsHygiene habits
•Recent URI or GI illness
Systemic illnessSystemic illness
•Autoimmune, atopic dermatitis, eczema
Chronic illnessChronic illness
6/21/2013
3
Vulvovaginitis
MedicationsMedications
•Laundry detergents, bubble baths
SoapsSoaps
AllergiesAllergies
BedwettingBedwetting
PetsPets
Favorite play activitiesFavorite play activities
•Potential for sexual abuse
CaretakersCaretakers
History
Case 2
She is a healthy little girl without any systemic or dermatologic problems. She has no allergies and takes no medications. She is active in ballet and swimming.
Physical ExaminationGeneral Principles: Maximize exposure for visualization Minimize stress Win her confidence Give her a sense of control Never be forceful or hurried
Pediatric Genital Exam
Supine Frog Leg Position Knee Chest Position

6/21/2013
4
Supine labial separation method Supine labial traction technique
Supine labial traction technique Knee Chest Position

6/21/2013
5
DischargeDischarge
InflammationInflammation
TraumaTraumaStool
ContaminationStool
Contamination
ForeignBody
ForeignBody
What to look for:
Vulvovaginitis
Most common gynecologic problem for pre-pubertal girls
Accounts for at least half of all visits to pediatric gynecologists
Anxiety producing for parents
Why does it happen?
Vulvovaginitis
Contributing factors Suboptimal handwashing Tight, non-absorbent or wet clothing Topical irritants- bubble baths, detergents
Vulvovaginitis
Short distance between vagina and anus
Lack of vulvar fat pads
Small labia minora
Small hymenalopening prevents outflow of secretions
Anatomic Factors

6/21/2013
6
Vulvovaginitis
Physiologic factors
Lack of estrogen atrophic mucosaneutral pH
Minimal antibodies in secretions
Auto-inoculation eg. Strep URI
Vulvovaginitis
Etiology:
Non-Specific vs. Specific
Non-Specific Vulvovaginitis
75% of vulvovaginitis cases Vaginal culture identifies normal flora No infectious etiology found Clinically, less discharge and erythema
than in cases with infectious etiology
Non-Specific Vulvovaginitis
Treatment: Remove tight-fitting clothes and wet
bathing suits immediately after use Avoid bubble baths and strong detergents Cotton underwear Desotin, A&D ointment, other emollients Short course of a mild topical steroid to
reduce itching

6/21/2013
7
Case 3
A 5 yr old girl presents with a 2 month history of vulvar irritation and a pink, malodorous vaginal discharge. She has mild perineal itching. Her history is otherwise negative.
In frog leg position, the introitus and perineum are erythematous. A pink discharge is visible in the lower vagina.
Case 3
Vaginal gram stain and cultures show moderate PMN’s, RBC’s and abundant genital flora including E. coli.
Case 3
A 10 day course of amoxicillin resulted in modest improvement in the discharge
Symptoms and discharge recurred within 2 weeks
What would you do next?
Case 3
In addition to general measures such as good hygiene and mild soaps, What would you do next?
A. Retreat with Amoxicillin for 30 daysB. Change to a Cephalosporin C. Perform an exam under anesthesiaD. Apply topical estrogen cream
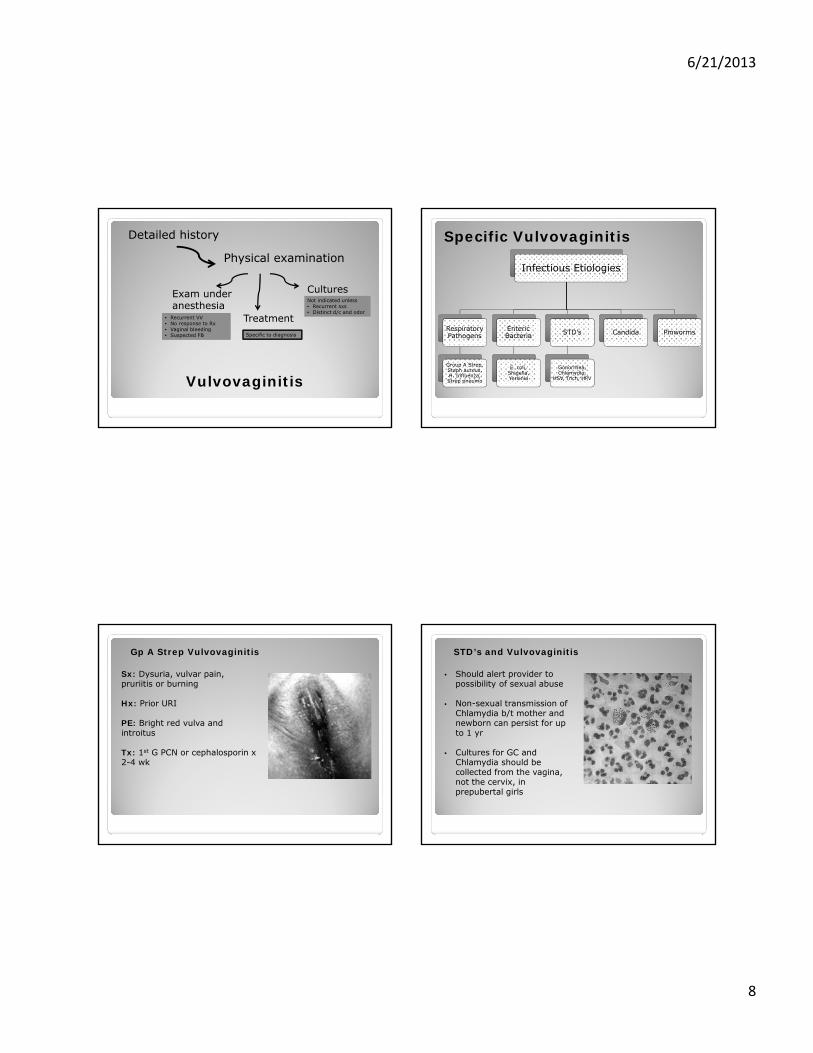
6/21/2013
8
Vulvovaginitis
Detailed history
Physical examination
CulturesExam under anesthesia
Treatment• Recurrent VV• No response to Rx• Vaginal bleeding• Suspected FB
Not indicated unless• Recurrent sxs• Distinct d/c and odor
Specific to diagnosis
Specific Vulvovaginitis
Infectious Etiologies
Respiratory Pathogens
Group A Strep, Staph aureus, H. Influenza, Strep pneumo
Enteric Bacteria
E. coli, Shigella, Yersinia
STD’s
Gonorrhea, Chlamydia,
HSV, Trich, HPV
Candida Pinworms
Gp A Strep Vulvovaginitis
Sx: Dysuria, vulvar pain, pruriitis or burning
Hx: Prior URI
PE: Bright red vulva and introitus
Tx: 1st G PCN or cephalosporin x 2-4 wk
STD’s and Vulvovaginitis
• Should alert provider to possibility of sexual abuse
• Non-sexual transmission of Chlamydia b/t mother and newborn can persist for up to 1 yr
• Cultures for GC and Chlamydia should be collected from the vagina, not the cervix, in prepubertal girls

6/21/2013
9
Candida Vulvovaginitis
Sx: Pruritis, thick white d/c
Hx: Rare in prepubertal girls unless recent Abx use, wearing diapers, diabetic or immunocompromisedCommon in pubertal girls
PE: Bright red vulva and satellite lesions
Tx: Topical antifungal
Pinworm (Enterobius vermicularis)
Sx: intense vulvar or perianal pruritis, esp at night
Hx: Siblings with similar sxs
PE: Scotch tape test in am, affix to slide, observe for eggs
Tx: Mebendazole 100 mg PO x 1
Specific Vulvovaginitis
Non-Infectious Etiologies
Foreign Body
Systemic Illness
Kawasaki disease Mononucleosis, Crohn’s disease
Vulvar Skin
Disease
Atopic dermatitis, Seborrhea,
Psoriasis, Lichen sclerosis
Trauma Misc
Draining pelvic
abscess, Ectopic ureter
Vaginal Foreign Body
Sx: Purulent, foul smelling, often bloody vaginal discharge
PE: Vulvovaginal erythema
Tx: EUA, vaginoscopy
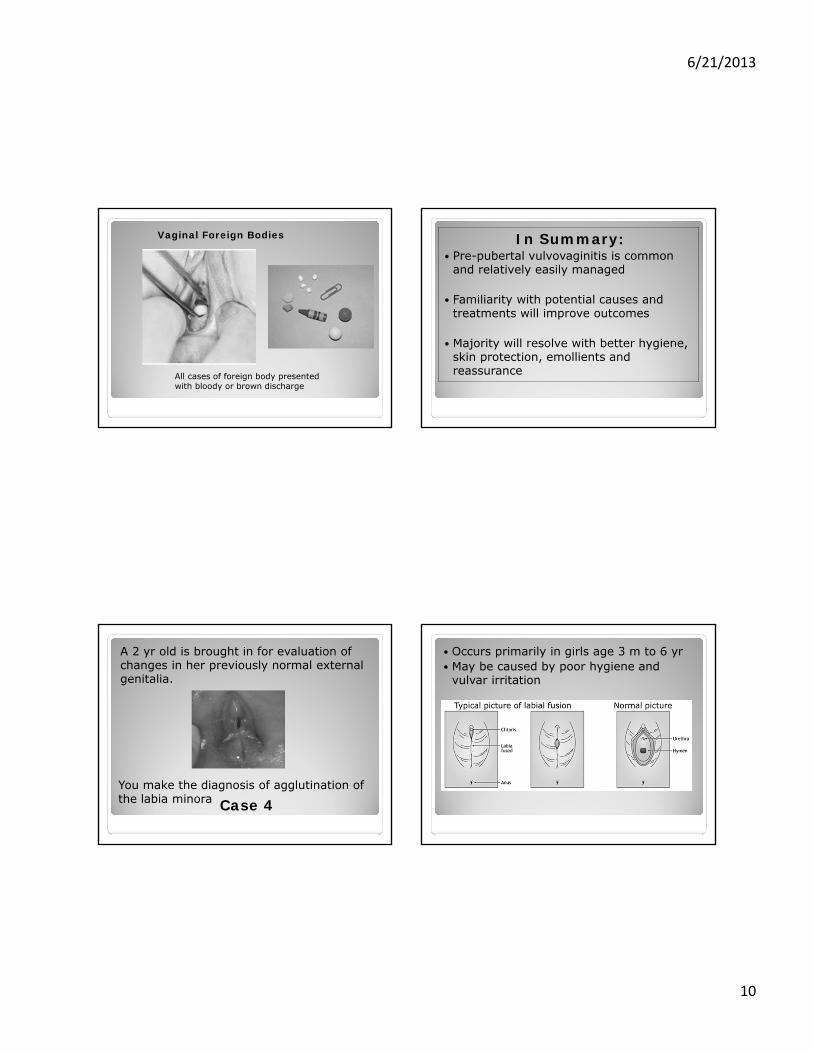
6/21/2013
10
Vaginal Foreign Bodies
All cases of foreign body presented with bloody or brown discharge
In Summary: Pre-pubertal vulvovaginitis is common
and relatively easily managed
Familiarity with potential causes and treatments will improve outcomes
Majority will resolve with better hygiene, skin protection, emollients and reassurance
Case 4
A 2 yr old is brought in for evaluation of changes in her previously normal external genitalia.
You make the diagnosis of agglutination of the labia minora
Occurs primarily in girls age 3 m to 6 yr May be caused by poor hygiene and
vulvar irritation

6/21/2013
11
Labial Agglutination
What would you recommend?A. Await spontaneous resolutionB. Apply topical estrogen cream x 6 wkC. Perform a manual separation in the officeD. Incise the adhesion in the OR
Labial Agglutination3 month old 9 month old
Teenagers and
Abnormal Uterine Bleeding
Case 5
A 15 yr old presents for evaluation of irregular cycles and prolonged, heavy bleeding. She had menarche at age 14 and has never had reg cycles. She runs track and has a BMI of 19. She denies sexual activity.

6/21/2013
12
AUB What is it? Irregular cycles Prolonged periods (> 7d) Heavy bleeding (1-2 pads/hr)
Who does it affect? Transcends ethnic and geographic boundaries
What is the impact of AUB? Adversely affects academic, athletic and social activities
Why do teens have AUB?
A. Underlying bleeding disordersB. Anovulatory cyclesC. Endocrine abnormalitiesD. Eating disorders
The Menstrual Cycle
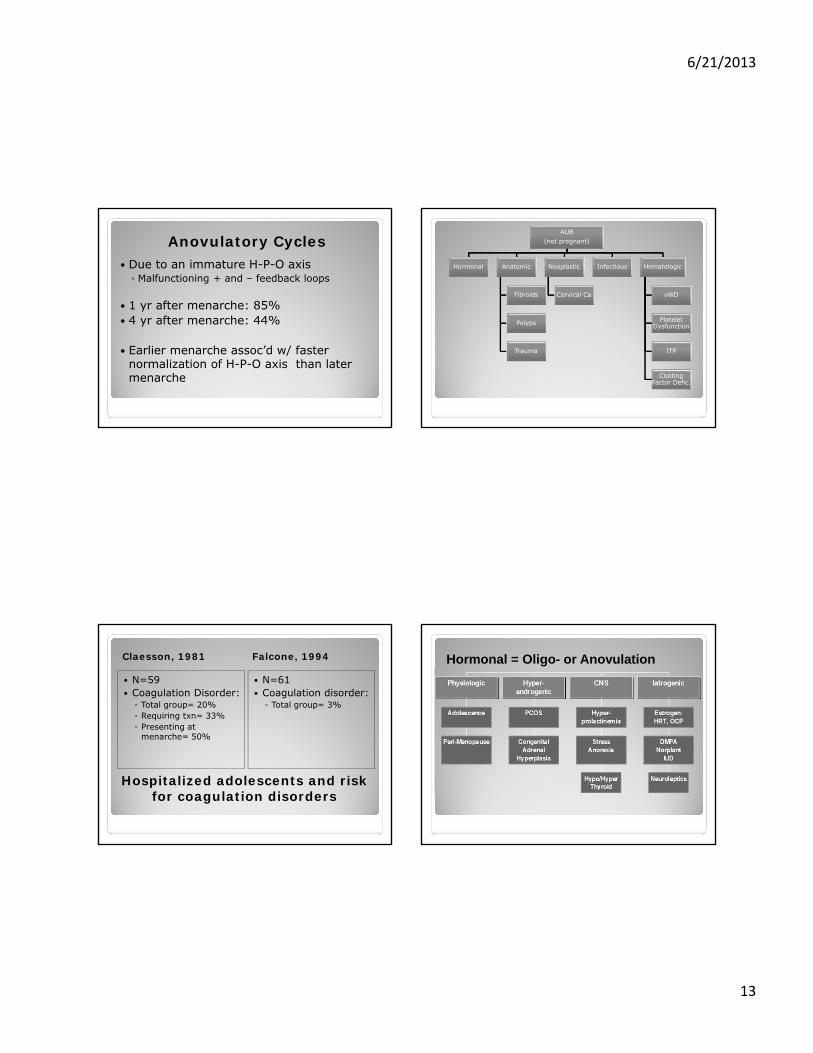
6/21/2013
13
Anovulatory Cycles Due to an immature H-P-O axis Malfunctioning + and – feedback loops
1 yr after menarche: 85% 4 yr after menarche: 44%
Earlier menarche assoc’d w/ faster normalization of H-P-O axis than later menarche
AUB(not pregnant)
Hormonal Anatomic
Fibroids
Polyps
Trauma
Neoplastic
Cervical Ca
Infectious Hematologic
vWD
Platelet Dysfunction
ITP
Clotting Factor Defic.
Hospitalized adolescents and risk for coagulation disorders
Claesson, 1981 Falcone, 1994
N=59 Coagulation Disorder: Total group= 20% Requiring txn= 33% Presenting at
menarche= 50%
N=61 Coagulation disorder: Total group= 3%
Hormonal = Oligo- or Anovulation
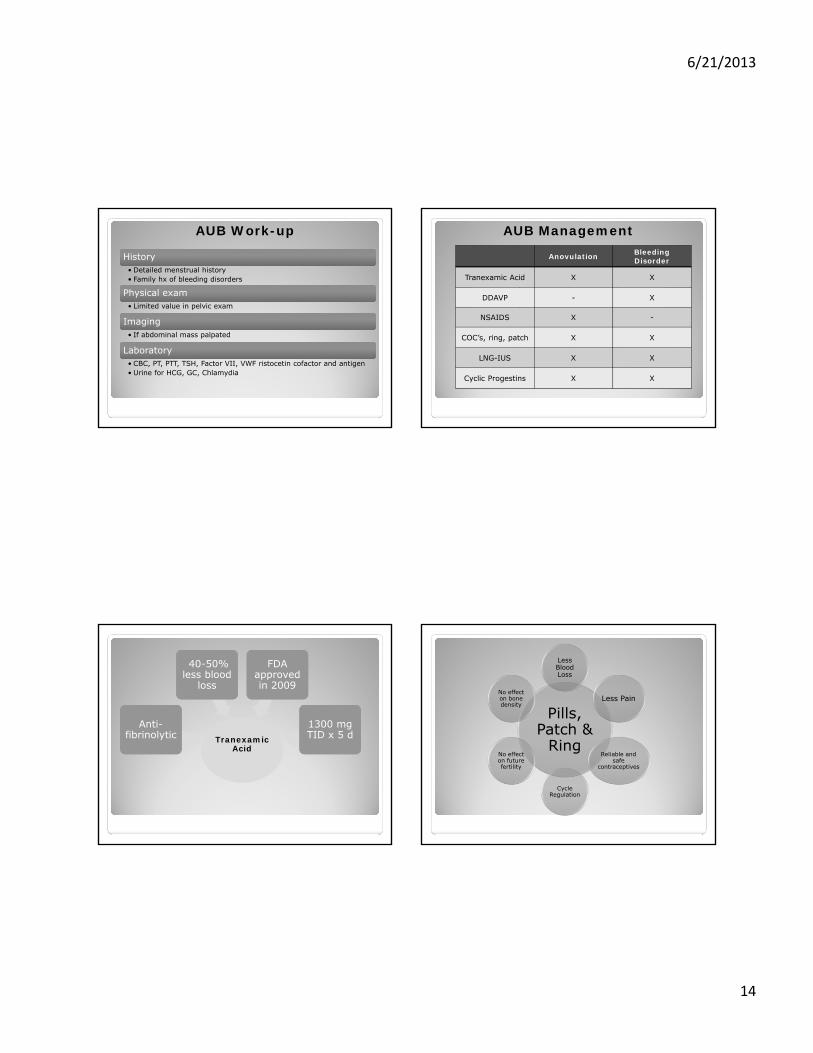
6/21/2013
14
AUB Work-up
HistoryHistory• Detailed menstrual history• Family hx of bleeding disorders
Physical examPhysical exam• Limited value in pelvic exam
ImagingImaging• If abdominal mass palpated
LaboratoryLaboratory• CBC, PT, PTT, TSH, Factor VII, VWF ristocetin cofactor and antigen• Urine for HCG, GC, Chlamydia
AUB Management
Anovulation Bleeding Disorder
Tranexamic Acid X X
DDAVP - X
NSAIDS X -
COC’s, ring, patch X X
LNG-IUS X X
Cyclic Progestins X X
TranexamicAcid
TranexamicAcid
Anti-fibrinolytic
Anti-fibrinolytic
40-50% less blood
loss
40-50% less blood
loss
FDA approved in 2009
FDA approved in 2009
1300 mg TID x 5 d1300 mg TID x 5 d
Pills, Patch &
Ring
Less Blood Loss
Less Pain
Reliable and safe
contraceptives
Cycle Regulation
No effect on future fertility
No effect on bone density

6/21/2013
15
Take home points:
Minimize emotional trauma and physical discomfort for children having a genital exam by knowing examination techniques and the appearance of normal anatomy
When necessary, examine under anesthesia
Take home points: Be familiar with common causes and
interventions for vulvovaginitis Remove vulvar irritants Improve hygiene Treat with organism-specific antimicrobials
Leave labial agglutination to resolve spontaneously Unless inability to void or recurrent UTI’s.
Take home points:
AUB in adolescents is common and almost always due to anovulatory cycles
Anticipate that parents may be reluctant to start teens on birth control pills
Remember bleeding disorders, especially in a teen who is hospitalized, transfused or presents during her first period
Thank You

6/21/2013
1
What’s That?Recognizing common gynecologic lesions
Alison F. Jacoby, MDUCSF
Objectives
Review normal features of the external genitalia, vagina and cervix
Recognize common abnormal findings such as herpes, molluscum and warts
Discuss diagnosis and management of various vulvovaginal conditions
Vulvar Bumps

6/21/2013
2
What is this?1. Condylomata
2. Hymenal tags
3. Vulvar papillomatosis
6/21/2013
3
What is this? 1. Condylomata
2. Vulvar papillomatosis
Pigmented Lesions

6/21/2013
4
What is this?
1. Benign
2. Malignant

6/21/2013
5
Which is concerning for melanoma?1. A2. B
A B
What is the diagnosis?1. Angiokeratomas
2. Nevi
3. Cavernous hemangioma
4. Melanoma

6/21/2013
6
Vulvar Papules & Ulcers

6/21/2013
7

6/21/2013
8
Vaginal and Vulvar Cysts

6/21/2013
9
6/21/2013
10

6/21/2013
11

6/21/2013
12
What is this?
1. Gartner’s duct cyst
2. Bartholin’s cyst
3. Inclusion cyst
4. Skene’s duct cyst
6/21/2013
13
Genital Growths
6/21/2013
14
Vulvar Skin Conditions

6/21/2013
15

6/21/2013
16

6/21/2013
17

6/21/2013
18
Other STD’s
6/21/2013
19

6/21/2013
20
Congenital Anomalies
6/21/2013
21
6/21/2013
22
Pediatric Lesions
How would you treat this?
1. Topical estrogen cream
2. Supportive care until menarche
3. Surgical separation
4. Manual separation
6/21/2013
23
Cervical Lesions
6/21/2013
24

6/21/2013
25

6/21/2013
26
What is this?1. Cervical cancer
2. Cervical ectropion
3. CIN I
Thank you and see you at the pool
Picture credits go to Mark Theisswww.UltimateChase.com
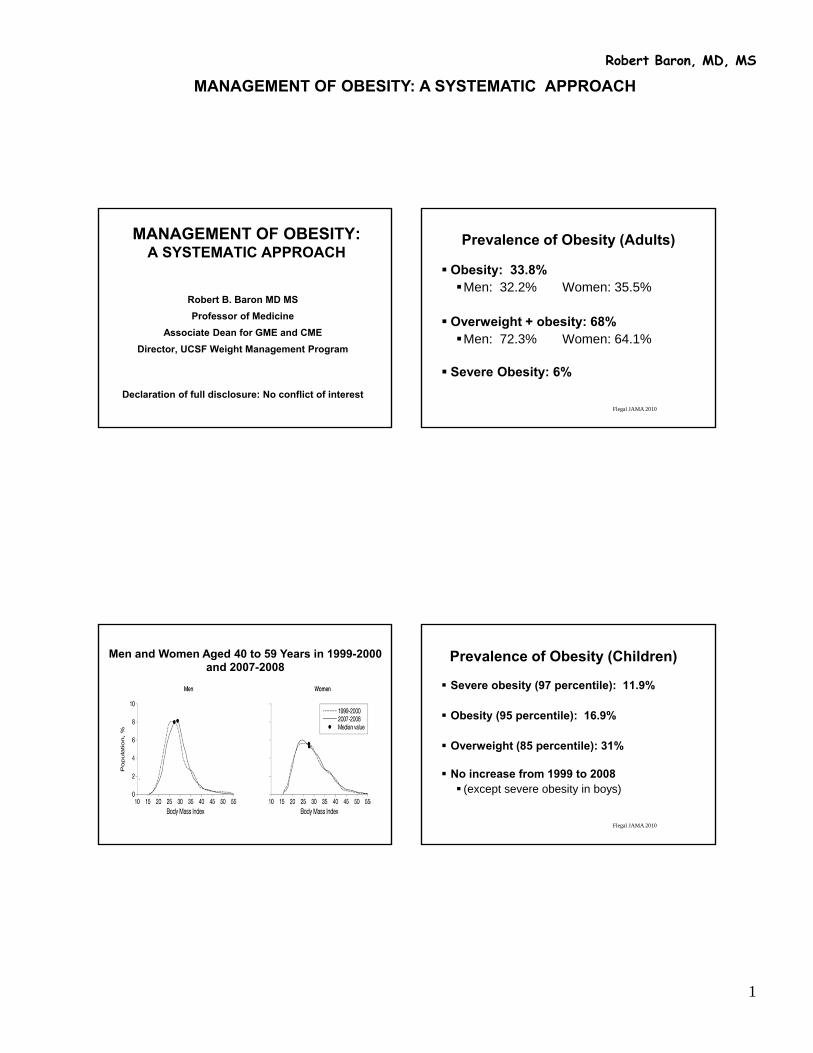
MANAGEMENT OF OBESITY: A SYSTEMATIC APPROACH
1
Robert Baron, MD, MS
MANAGEMENT OF OBESITY: A SYSTEMATIC APPROACH
Robert B. Baron MD MS
Professor of Medicine
Associate Dean for GME and CME
Director, UCSF Weight Management Program
Declaration of full disclosure: No conflict of interestFlegal JAMA 2010
Prevalence of Obesity (Adults)
Obesity: 33.8%Men: 32.2% Women: 35.5%
Overweight + obesity: 68% Men: 72.3% Women: 64.1%
Severe Obesity: 6%
.
Men and Women Aged 40 to 59 Years in 1999-2000 and 2007-2008
Flegal JAMA 2010
Prevalence of Obesity (Children)
Severe obesity (97 percentile): 11.9%
Obesity (95 percentile): 16.9%
Overweight (85 percentile): 31%
No increase from 1999 to 2008 (except severe obesity in boys)

MANAGEMENT OF OBESITY: A SYSTEMATIC APPROACH
2
Robert Baron, MD, MS
Copyright © 2012 American Medical Association. All rights reserved.
Prevalence of Obesity and Trends in Body Mass Index Among US Children and Adolescents, 1999-2010
JAMA. 2012;307(5):483-490
Flegal JAMA 2010
Obesity Disparities
Women, 40-59Black: 52%, Hispanic: 47%, Whites: 36%
TeensBlack: 29%, Hispanic: 17.5%, Whites: 14.5%
Mental illnessOverweight + obese: 83%
Obesity Trends* Among U.S. AdultsBRFSS, 2010
(*BMI ≥30, or ~ 30 lbs. overweight for 5’ 4” person)
No Data <10% 10%–14% 15%–19% 20%–24% 25%–29% ≥30%
For a 40 yo woman, with normal BP, lipids, and FBS which BMI is
associated with the lowest all-cause mortality?
1. 18
2. 24
3. 28
4. 34
5. 38

MANAGEMENT OF OBESITY: A SYSTEMATIC APPROACH
3
Robert Baron, MD, MS
CLASSIFICATION OF OVERWEIGHT AND OBESITY BY BMI
Obesity Class BMI (kg/m2)
Underweight <18.5
Normal 18.5 – 24.9
Overweight 25.0 – 29.9
Obesity I 30.0 – 34.9
II 35.0 – 39.9
Extreme Obesity III >40
Flegal, JAMA, 2005
BMI AND MORTALITY: Overall
Combined NHANES I, II, and III data set
BMI 25-59 y 60-69 y ≥70 y
<18.5 1.38 2.30 1.6918.5-<25 1.00 1.00 1.0025 to <30 0.83 0.95 0.9130 to <35 1.20 1.13 1.03≥35 1.83 1.63 1.17
Flegal, JAMA, 2013
MORTALITY AND OBESITY
Meta-analysis of 97 studies of 2.8M people, 270,000 deaths
BMI HRBelow 25 (Normal) 1.025-30 (Overweight) 0.94Above 30 (Obese) 1.18
***30-35 (Grade 1 Obesity) 0.95Above 35 (Grade 2/3 Obesity) 1.29
For a 40 yo woman, with normal BP, lipids, and FBS which BMI is
associated with the lowest all-cause mortality?
1. 18
2. 24
3. 28
4. 34
5. 38

MANAGEMENT OF OBESITY: A SYSTEMATIC APPROACH
4
Robert Baron, MD, MS
Epidemic of Inactivity
60% US adults don’t exercise regularly
25% are sedentary
Shaw, Cochrane, 2006
EXERCISE FOR OBESITY Meta-analysis of 43 RCTs: 3476 participants
• Exercise plus diet vs diet alone – -1.1 kg
• Increased intensity of exercise – -1.5 kg
• Exercise without weight loss– Reduced: BP, triglycerides, blood
sugar
Wei, JAMA 1999
FITNESS AND MORTALITYAerobics Center Longitudinal Study
CV death (RR)normal overweight obese
Fit 1.0 1.5 1.6Not fit 3.1 4.5 5.0
Total death (RR)normal overweight obese
Fit 1.0 1.1 1.1Not fit 2.2 2.5 3.1
25,714 men, 44 years old, 14 year observational study
Relative Risk* of Death According to Body Mass and Physical Activity
Body mass index (BMI)
25 – 29.9< 25 > 30
> 3.5 hours/week
1 – 3.4 hours/week
< 1 hour/week
Physical activity level
* RR’s adjusted for age, smoking status, family history, menopausal status, hormone use, and other factors
** Reference group = women with 3.5 or > hours/week of physical activity and BMI of 25 or less
Hu FB, et al. N Engl J Med 2004;351:2694
2.42
1.91
1.64
1.331.28
1.55
1.181.00
**

MANAGEMENT OF OBESITY: A SYSTEMATIC APPROACH
5
Robert Baron, MD, MS
Estimating Calorie Needs
To estimate calories for weight maintenance: If you are moderately active, multiply current
weight (pounds) x 15.
To estimate calories for weight loss: Subtract 500 calories to lose approximately 1.0
pound per week A pound of fat is about 3500 kcals
Dansinger, JAMA 2005
COMPARISON OF ATKINS, ORNISH, WEIGHT WATCHERS, AND ZONE
Intention to treat at 1 yearAtkins Ornish WW Zone
Wt Loss (kg) 2.1 3.3 3.0 3.2Completers (%) 53 50 65 65
Completers at 1 yearAtkins Ornish WW Zone
Wt Loss (kg) 3.9 6.6 4.6 4.9
160 patients, randomly assigned
Dansinger, JAMA, 2005
COMPARISON OF ATKINS, ORNISH, WEIGHT WATCHERS, AND ZONE
Weight loss associated with adherence, but not diet type
Each group: 25% lost 5%, 10% lost 10% of initial weight
Each diet reduced LDL/HDL by 10%
No significant effects on BP or glucose

MANAGEMENT OF OBESITY: A SYSTEMATIC APPROACH
6
Robert Baron, MD, MS
Sacks, NEJM, 2009
COMPARISON OF WEIGHT LOSS DIETS WITH DIFFERENT MACRONUTRIENTS
RCT of 811 patients, 4 diets: fat/protein/carbs20/15/65; 20/25/55; 40/15/45; 40/25/35
6 months: 6kg, 7% weight; at 2 years: completers lost 4kg; 15% lost 10% of weight
Results similar for: 15% pro v. 25% pro 20% fat v. 40% fat 35% carbs v. 65% carbs
Attendance highly correlated with weight loss; satiety, hunger, lipids, insulin all equal
Heterogeneity of Response to Weight Loss Diets: Insulin Resistance
Insulin sensitive: low carb and high carb both effective for weight loss
Insulin resistant: low carb more effective
Tsai and Wadden, Obesity, 2006
Very Low Calorie Diets (VLCD) vs Low Calorie Diets (LCD): Meta-analysis of 6 RCTs
• Trials with direct comparisons• Short-term: mean 12.7 weeks • Long-term: mean 1.9 years
Weight loss (as % of initial weight):short-term long-term
LCDs 9.7 5.0VLCDs 16.1 6.3
(p) (0.001) (0.2)
WEIGHT LOSS DIET BOTTOM LINE
• The type of diet does not really matter for weight loss.
• Sticking to the diet does matter
• Calories “trump” macronutrients
• But, select healthy, nutrient rich foods
MANAGEMENT OF OBESITY: A SYSTEMATIC APPROACH
7
Robert Baron, MD, MS
Weight Loss Diet Tips
• Ready to lose weight?
• Set realistic expectations.
• Choose diet that is easy to follow and compatible with lifestyle.
• Control portion size (plate method, etc).
• Vegetables, fruit and whole grains
• Maintaining the weight you lose is key.
BEHAVIORAL ASPECTS OF WEIGHT LOSS
Goal setting
Self-monitoring
Stimulus control
Cognitive skills
40 yo woman, BMI 36. Much to your surprise (and satisfaction),
she has lost 35 pounds. In order to maintain her new weight, her
lifelong daily calorie intake should be:
1. 2000 kcals
2 1800 kcals
3 1600 kcals
4. 1400 kcals
5. 1200 kcals

MANAGEMENT OF OBESITY: A SYSTEMATIC APPROACH
8
Robert Baron, MD, MS
Wing, Am J Clin Nutr, 2005
SUCCESSFUL WEIGHT LOSS MAINTENANCE
3000 subjects in National Weight Control Registry: 30-lb weight loss for 1-year
Average weight loss 33 kg (10 BMI units less), average weight maintenance 5.5 years
45 years old, 80% women, 97% Caucasian
46% overweight as child, 46% one parent obese, 27% both parents
SUCCESSFUL WEIGHT LOSS MAINTENANCE
• High levels of physical activity• Women 2545 kcal/week, men 3293 kcal/week • (1-hour moderate intensity per day• Only 9% report no physical activity
• Diet low in calories• 1381 kcal day• 4.87 meals or snacks/day• Fast food 0.74/week
• Regular self-monitoring of weight• 44% weigh once per day; 31% once per week
40 yo woman, BMI 36. Much to your surprise, she has lost 35
pounds. In order to maintain her new weight, her lifelong daily
calorie intake should be:
1. 2000 kcals
2 1800 kcals
3 1600 kcals
4. 1400 kcals
5. 1200 kcals

MANAGEMENT OF OBESITY: A SYSTEMATIC APPROACH
9
Robert Baron, MD, MS
In the last year, I have prescribed a medication for weight loss.
1. Yes
2 No
The medication I most commonly prescribe for weight loss is:
1. Phentermine2. Orlistat (Xenical™, Alli™)3. Buproprion (Wellbutrin™)4. Exenatide (Byetta™, Bydureon™)5. Phentermine/topiramate (Qsymia™)6. Other
The Neuroendocrinology of Energy Balance“LONG TERM” PHARMACOTHERAPY OF
OBESITYReview of all RCT’s more than 36 weeks published since 1960
Weight loss in excess of placebo:
% of initial kg’s
Phen-fen 11.0% 9.6 kg
Phentermine 8.1% 7.9 kg
Sibutramine 5.0% 4.3 kg
Orlistat 3.4% 3.4 kg
Dexfenfluramine 3.0% 2.5 Kg
Fluoxetine -0.4% -0.4 kg
Diethyproprion -1.5% -1.5 kg

MANAGEMENT OF OBESITY: A SYSTEMATIC APPROACH
10
Robert Baron, MD, MS
James, NEJM 2010
SIBUTRAMINE AND CARDIOVASCULAR OUTCOMES (SCOUT)
9804 patients, over 55, with CV disease or diabetes
Sibutramine vs. placebo, 3.4 year f/u
Outcomes MI, stroke, cardiac arrest, CV death
ResultsWeight: -1.7 kg BP: 1.2 vs 1.4 mm Hg Combined outcome: 11.4% vs. 10.0% (HR 1.16, p = 0.02) Nonfatal MI: 4.1% vs. 3.1% (HR 1.28; p = 0.02) Nonfatal Stroke: 2.6% vs 1.9% (HR 1.36; p = 0.03) Death: No differences
LORCASERIN
Selective serotonin 2C receptor agonist
RCT of 3,182 adults, 52 week study
45% vs. 55% drop-out (lorcaserin vs. placeb)
5.8±0.2 kg vs. 2.2±0.1 kg wt. loss
Frequent adverse events: headache, dizziness, and nausea
No increase in valvulopathy
Smith, NEJM, 2010
Weight Loss Medications: October, 2010
• Sibutramine (Meridia™): withdrawn by Abbott• Increased risk of stroke and MI
• Lorcaserin (selective serotonin receptor agonist, more specific than fenfluramine): not approved by FDA• Animals with increased mammary adenocarcinoma
• Phentermine/topiramate (Qnexa™): not approved by FDA• Psychiatric adverse events: sleep, anxiety depression:
21% vs 10% with placebo• Increased heart rate• Teratogenicity
Lorcaserin Update: May-June 2012
• FDA panel approved after new round of studies
• Industry sponsored study: 604 patients with type 2 diabetes• After 1 year, 3.1% more weight loss (criteria >5%)• 38% lost >5% weight vs. 16% on placebo
• Lingering uncertainty re breast tumors, valvular heart disease, psychiatric issues
• Approved June 2012. Trade name Belviq™

MANAGEMENT OF OBESITY: A SYSTEMATIC APPROACH
11
Robert Baron, MD, MS
Lorcaserin Update (Belviq™): June 2013
• Classified as Schedule IV controlled substance
• Available as of June 7, 2013
Phentermine/Topiramate Update: February-July 2012
• FDA panel approved 20:2
• Industry sponsored study: 4323 subjects• 9.3% weight loss• Increased heart rate, increased cleft lip
• Recommend post-market monitoring for CV risk and recommendation against use in pregnancy
• Company plans larger trial (16,000 subjects)
• Approved July 2012. Trade name Qsymia™
Phentermine/Topiramate (Qsymia™) Side Effects
• Paraesthesia, dizziness, dysgeusia, insomnia, constipation, dry mouth
• Fetal harm: cleft lip, cleft palate• Mood disorders: anxiety and depression• Suicidal thoughts or behavior• Acute angle glaucoma• Cognitive dysfunction: concentration memory,
language• Metabolic acidosis and renal failure• Hypoglycemia (in association with diabeyes meds)• Interactions with alcohol and sedatives
Prescribing Phentermine/Topiramate (Qysmia™)
• Two prescriptions: • 14 days on 3.75/23 and • 30 days on 7.5/46
• Need DEA #• Fax to certified pharmacy• Pharmacy will call patient• Drug delivered to patient’s home
• Local pharmacy availability soon
MANAGEMENT OF OBESITY: A SYSTEMATIC APPROACH
12
Robert Baron, MD, MS
OTHER INVESTIGATIONAL DRUGS
• Buproprion/naltrexone (Contrave™): Approved by FDA panel 12/10; rejected by FDA 2/11 (concern re heart attacks and CV risk.)
• Buproprion/zonisamide (Empatic™): Phase 3
• Exenatide (Byetta™), Liraglutide (Victoza™: Phase 2/3
• Pramlintide/metreleptin: Phase 2/3
• Cetilistat: Phase 3 in Japan
PRINCIPLES OF DRUG THERAPY
• NIH: BMI > 30 kg/m2 or 27 kg/m2 with co-morbidity (but in practice almost never)
• Motivated to begin structured exercise and low calorie diet
• Begin medications at completion of one month successful diet and exercise
• Continue medications only if additional weight loss achieved in first month with meds
Wouldn’t It Be Easier Just To Have Surgery ?
Definition BMINormal < 25Overweight 25-29.9Obese, class 1 30-34.9
Obese, class 2 35-39.9Obese, class 3 40+“Superobese” 60+
SURGERY
with co-morbidity
INDICATIONS FOR BARIATRIC SURGERY

MANAGEMENT OF OBESITY: A SYSTEMATIC APPROACH
13
Robert Baron, MD, MS
Types of Surgery
Restrictive• Horizontal Gastroplasties• Vertical Banded Gastroplasty (VGB)• Silastic Ring Vertical Gastroplasty (SRVG)• Adjustable Gastric Banding• Sleeve Gastrectomy
Malabsorptive• Jejunoileal Bypass (JIB)• Biliopancreatic Diversion (BPD)• Duodenal Switch• Long Limb Gastric Bypass
Restrictive with Malabsorptive Component• Roux-en-Y Gastric Bypass (RYGPB)
Restrictive and Mixed Procedures
VBG Adjustable Gastric Banding Roux-en-Y GB
Sleeve Gastrectomy
Years
Bariatric Surgery: Weight Change
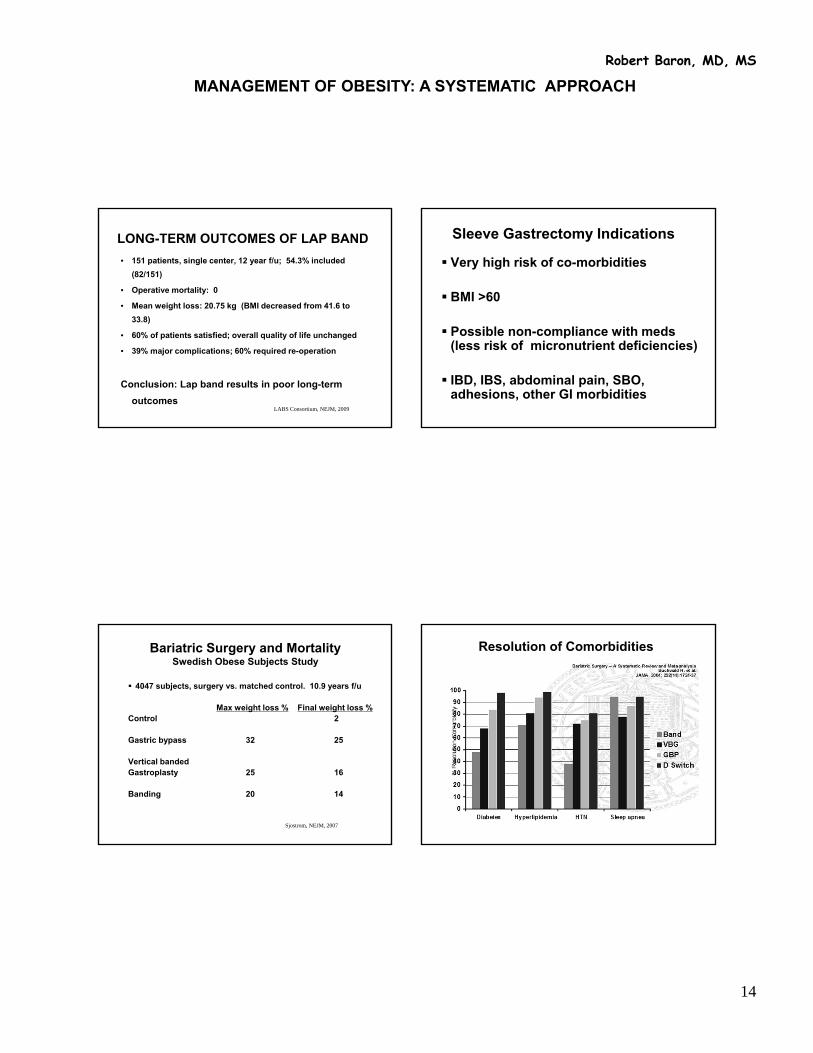
MANAGEMENT OF OBESITY: A SYSTEMATIC APPROACH
14
Robert Baron, MD, MS
LABS Consortium, NEJM, 2009
LONG-TERM OUTCOMES OF LAP BAND
• 151 patients, single center, 12 year f/u; 54.3% included
(82/151)
• Operative mortality: 0
• Mean weight loss: 20.75 kg (BMI decreased from 41.6 to
33.8)
• 60% of patients satisfied; overall quality of life unchanged
• 39% major complications; 60% required re-operation
Conclusion: Lap band results in poor long-term
outcomes
Sleeve Gastrectomy Indications
Very high risk of co-morbidities
BMI >60
Possible non-compliance with meds (less risk of micronutrient deficiencies)
IBD, IBS, abdominal pain, SBO, adhesions, other GI morbidities
Sjostrom, NEJM, 2007
Bariatric Surgery and MortalitySwedish Obese Subjects Study
4047 subjects, surgery vs. matched control. 10.9 years f/u
Max weight loss % Final weight loss %Control 2
Gastric bypass 32 25
Vertical banded Gastroplasty 25 16
Banding 20 14
Resolution of Comorbidities

MANAGEMENT OF OBESITY: A SYSTEMATIC APPROACH
15
Robert Baron, MD, MS
35 yo woman, BMI 42 in good health, asks about bariatric surgery. Her surgeon suggests a laporoscopic
roux-n-y. Her risk of mortality, DVT, reintervention, or prolonged hospital
stay is:
1. 1 in 200 2. 1 in 1003. 1 in 504. 1 in 255. 1 in 10
LABS Consortium, NEJM, 2009
BARIATRIC SURGERY OUTCOMES
• Ten sites, 4776 patients. 3/4 roux-en-y (87% lap); 1/4 lap band
• 30 Day overall mortality: 0.3%
-lap band 0.0%
-roux-en-y (lap) 0.2%
-roux-en-y (open) 2.1%
• Composite (death, DVT, reintervention, 30 + days in hosp): 4.1%
-lap band 1.0%
-roux-en-y (lap) 4.8%
-roux-en-y (open) 7.8%
35 yo woman, BMI 42 in good health, asks about bariatric surgery. Her surgeon suggests a laporoscopic
roux-n-y. Her risk of mortality, DVT, reintervention, or prolonged hospital
stay is:
1. 1 in 200 2. 1 in 1003. 1 in 504. 1 in 255. 1 in 10
57 yo woman, BMI 42 with diabetes, hypertension, and
creatinine 1.4 asks about bariatric surgery. Her risk of mortality 30
days post-op is
1. 1 in 200 2. 1 in 1003. 1 in 504. 1 in 255. 1 in 10
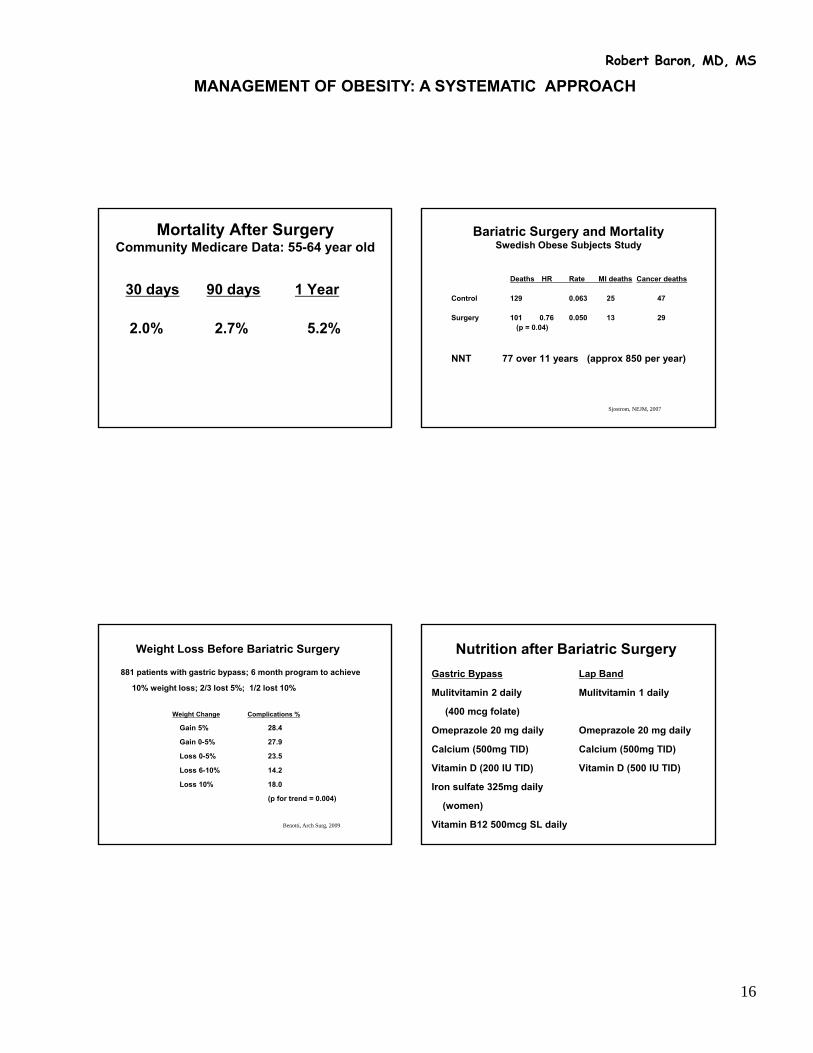
MANAGEMENT OF OBESITY: A SYSTEMATIC APPROACH
16
Robert Baron, MD, MS
Mortality After SurgeryCommunity Medicare Data: 55-64 year old
30 days 90 days 1 Year
2.0% 2.7% 5.2%
Sjostrom, NEJM, 2007
Bariatric Surgery and MortalitySwedish Obese Subjects Study
Deaths HR Rate MI deaths Cancer deaths
Control 129 0.063 25 47
Surgery 101 0.76 0.050 13 29(p = 0.04)
NNT 77 over 11 years (approx 850 per year)
Benotti, Arch Surg, 2009
Weight Loss Before Bariatric Surgery
881 patients with gastric bypass; 6 month program to achieve
10% weight loss; 2/3 lost 5%; 1/2 lost 10%
Weight Change Complications %
Gain 5% 28.4
Gain 0-5% 27.9
Loss 0-5% 23.5
Loss 6-10% 14.2
Loss 10% 18.0
(p for trend = 0.004)
Nutrition after Bariatric Surgery
Gastric Bypass Lap Band
Mulitvitamin 2 daily Mulitvitamin 1 daily
(400 mcg folate)
Omeprazole 20 mg daily Omeprazole 20 mg daily
Calcium (500mg TID) Calcium (500mg TID)
Vitamin D (200 IU TID) Vitamin D (500 IU TID)
Iron sulfate 325mg daily
(women)
Vitamin B12 500mcg SL daily
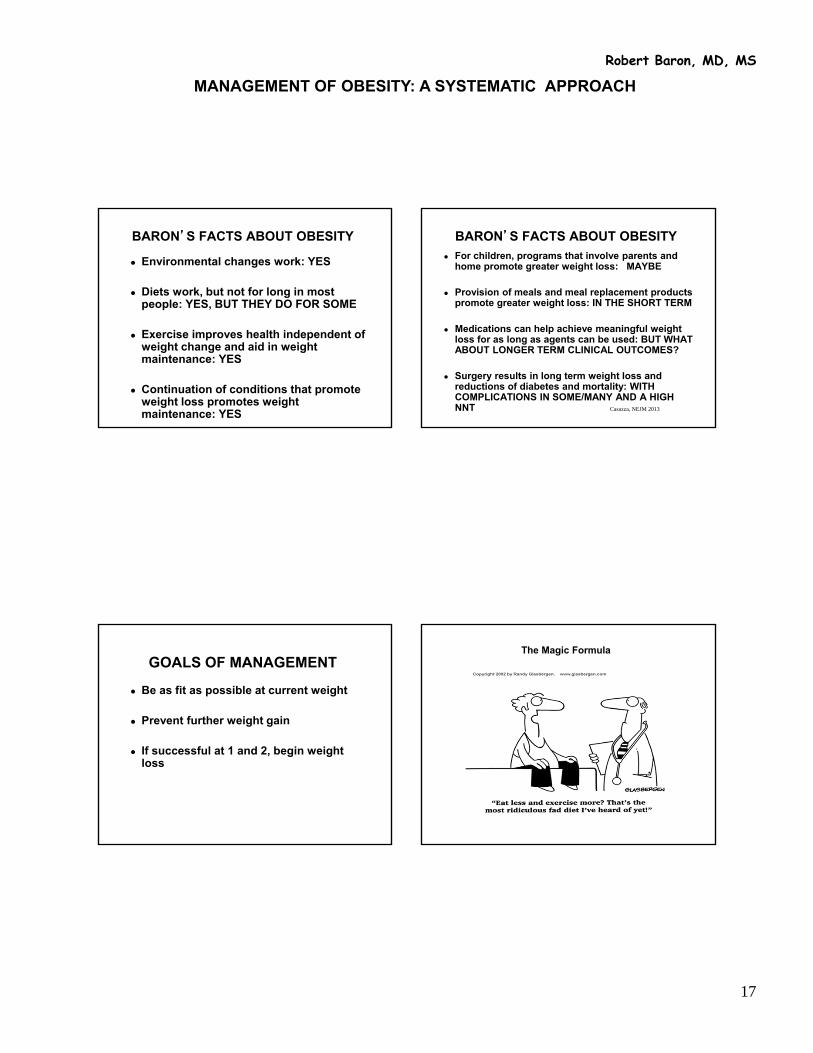
MANAGEMENT OF OBESITY: A SYSTEMATIC APPROACH
17
Robert Baron, MD, MS
BARON’S FACTS ABOUT OBESITY
Environmental changes work: YES
Diets work, but not for long in most people: YES, BUT THEY DO FOR SOME
Exercise improves health independent of weight change and aid in weight maintenance: YES
Continuation of conditions that promote weight loss promotes weight maintenance: YES
BARON’S FACTS ABOUT OBESITY
For children, programs that involve parents and home promote greater weight loss: MAYBE
Provision of meals and meal replacement products promote greater weight loss: IN THE SHORT TERM
Medications can help achieve meaningful weight loss for as long as agents can be used: BUT WHAT ABOUT LONGER TERM CLINICAL OUTCOMES?
Surgery results in long term weight loss and reductions of diabetes and mortality: WITH COMPLICATIONS IN SOME/MANY AND A HIGH NNT Casazza, NEJM 2013
GOALS OF MANAGEMENT
Be as fit as possible at current weight
Prevent further weight gain
If successful at 1 and 2, begin weight loss
The Magic Formula

Vaccinations for Adult and Adolescent Women
Eliseo J. Pérez-Stable, MDProfessor of MedicineDGIM, Department of Medicine
University of California, San Francisco
July 3, 2013Declaration of full disclosure: No conflict of interest
Vaccines Available in the US
Tetanus, Diptheria, Pertussis, Measles, Mumps, Rubella,
Varicella, HPV, Polio Meningococcus, Pneumococcus,
Influenza, Hepatitis B, Hepatitis A, H influenza, Rabies, Typhoid, Yellow Fever, Japanese
encephalitis, Typhoid
Effect of Full Use of Adult Immunizations
Deaths/yr. Efficacy Use Prev Deaths/yr
Influenza 36,000 70% 65% 18,000
Pneumonia 40,000 60% 60% 20,000
HBV 6,000 90% 30% 4,000
Tetanus-D < 25 99% 64% < 15
MMR < 30 95% varies < 30
Trends in Vaccine-Preventable Diseases Post Vaccine
• Measles and Rubella: 99.9% reduction (66 cases total and 1 case CRS in 2006)
• Tetanus: 93% reduction• Pertussis: 92% reduction (recent increase)• Hepatitis A: 87% reduction• Acute HBV: 80% reduction• Invasive pneumococcal disease: 34%
cases and 25% mortality reduction• Varicella: 85% reduction
Roush SW, et al. JAMA 2007; 298: 2155-63

Vaccination Coverage in US Adults by Age Groups, 2011
• HPV: 29.5% women 19-26 y• Td or TDaP past 10 years: 64.5% (19-49 y),
63.9% (50-64 y), 54.4% (≥65 y)
• Hepatitis A: 12.5% (19-49 y) and 20.1% for those who travel outside US
• HBV: 35.9% (19-49 y)
• Pneumococcal: 20.1% (19-64 y), 62.3% (≥65 y)
• Varicella: 15.8% ≥60 y• Health Care Staff: TDaP 26.8% and HBV
63.8%CDC, MMWR 2013; 62: 66-72
26 year old woman, immigrant from Guatemala with no records; says she got “usual shots”. What would you do?
10
1. Order tests for rubella, measles, and varicella antibodies before immunizing
2. Obtain detailed clinical history of possible childhood infections
3. Offer vaccines without tests given that immunization rate is low
4. Obtain medical record documentation or immunization card
5. Ask about possible social contacts before giving live viral vaccines
45 year old woman traveling to South Africa in May for 3 months and asks about need for vaccines. Besides advising her to check the CDC web site, are any of the following NOT needed?
10
1. Tetanus booster if more than 10 years from last dose
2. Influenza vaccine
3. Hepatitis A vaccine in two doses if not previously given or one dose if > 10 years
4. Hepatitis B series
5. Meningococcal C vaccine
70 year old man with diabetes and hypertension for routine visit. Which of the following do you recommend?
10
1. Tetanus booster with acellular pertussis – last Td was 3 years ago
2. Intra-nasal Influenza vaccine
3. Pneumococcal vaccine booster originally given at age 65
4. Zoster vaccine without checking antibodies
5. Zoster vaccine only if no prior shingles and with documented positive varicella Ab

Summary of Presentation
• Pertussis vaccine revisited
• Varicella Zoster Vaccine
• Influenza & Pneumonia vaccines
• Hepatitis A and B
• Measles, Mumps, Rubella
• Human Papilloma Virus vaccine
New Information from Today
• Pertussis vaccine for 65 y +• Varicella Zoster Vaccine at 50?• Pneumonia vaccine for asthma• Pneumococcal conjugate vaccine for
selected adults• Hepatitis B vaccine for persons with
diabetes• Human Papilloma Virus vaccine 2
doses may be good enough
PertussisTdap for Adults
Pertussis…not just for children anymore

Pertussis Vaccine•Original - whole cell vaccine
consisting of killed organisms•Acellular vaccine contains purified,
detoxified antigens•Childhood DTaP: diptheria toxoid,
tetanus toxoid, and acellular pertussis•Adult/adolescent Td and Tdap:
tetanus + reduced dose diptheria +/-reduced dose pertussis antigens
Tetanus and Diphtheria Toxoid +Acellular Pertussis Vaccine (Tdap)
• Available as of June 2005• Replace Td with Tdap in adolescents at
age 11 - 12 or give as single dose by 18 y • Tdap should replace Td in adults 18-64 y
as a one-time dose as part of primary series or as routine booster
• Administer to adults caring for children <1 year and all staff with direct patient contact at any age
• May be done at any timeCDC, Updated recommendations MMWR 2011; 60:13
Pertussis Vaccine – What’s the Evidence?
2781 subjects aged 15-65 randomized to reduced dose of acellular pertussis vaccine or hepatitis A “placebo”
Followed for 2.5 years
Based on primary pertussis definition (cough and positive culture/PCR), vaccine 92% effective
Ward JL et al. NEJM, 2005;353(13)
Varicella Zoster Virus VaccinePrevention of Chicken Pox
Disease and MortalityVaccine to Prevent Shingles
and Neuralgia
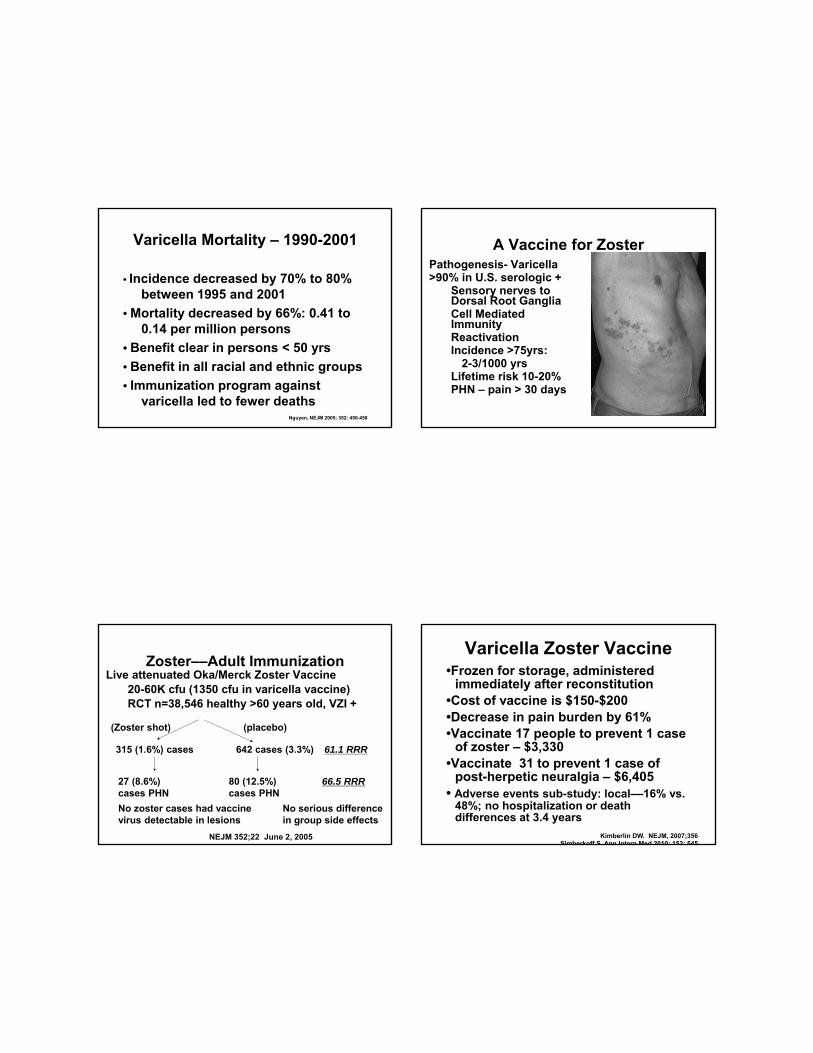
Varicella Mortality – 1990-2001
• Incidence decreased by 70% to 80% between 1995 and 2001
• Mortality decreased by 66%: 0.41 to 0.14 per million persons
• Benefit clear in persons < 50 yrs
• Benefit in all racial and ethnic groups
• Immunization program against varicella led to fewer deaths
Nguyen, NEJM 2005; 352: 450-458
A Vaccine for ZosterPathogenesis- Varicella>90% in U.S. serologic +
Sensory nerves to Dorsal Root GangliaCell Mediated ImmunityReactivationIncidence >75yrs:
2-3/1000 yrsLifetime risk 10-20%PHN – pain > 30 days
Zoster––Adult ImmunizationLive attenuated Oka/Merck Zoster Vaccine
20-60K cfu (1350 cfu in varicella vaccine)RCT n=38,546 healthy >60 years old, VZI +
(placebo)(Zoster shot)
315 (1.6%) cases 642 cases (3.3%) 61.1 RRR
27 (8.6%) cases PHN
80 (12.5%) cases PHN
66.5 RRR
No zoster cases had vaccine virus detectable in lesions
No serious difference in group side effects
NEJM 352;22 June 2, 2005
Varicella Zoster Vaccine•Frozen for storage, administered
immediately after reconstitution•Cost of vaccine is $150-$200•Decrease in pain burden by 61%•Vaccinate 17 people to prevent 1 case
of zoster – $3,330•Vaccinate 31 to prevent 1 case of
post-herpetic neuralgia – $6,405 • Adverse events sub-study: local––16% vs.
48%; no hospitalization or death differences at 3.4 years
Kimberlin DW. NEJM, 2007;356Simberkoff S, Ann Intern Med 2010; 152: 545

Barriers to Use of Zoster Vaccine
• National survey of primary care MDs
• 72% response: 301 GIM and 297 FM
• 49% stock and deliver in their office
• 36% refer to purchase and bring back
• 33% refer to a pharmacy for shot
• 88% recommend HZV; 41% strongly
• 45% aware Medicare part D covers
• Reimbursement issues–12% stoppedHurley L, et al. Ann Intern Med 2010; 152:555-560
Varicella Zoster Vaccine• Vaccinate once at age 60 • No need to check for evidence of
varicella immunity• FDA approved VZV for adults at age 50,
but CDC is not recommending• If high coverage with childhood
varicella vaccine, what happens to Zoster?
• Patients with previous shingles
Influenza and Pneumonia
Seasonal FluH1N1
Pneumococcal Vaccine
Adult Vaccines Did Not Precipitate Acute Cardiac Events or Strokes
• British study of 20,486 patients with MI and 19,063 cases of stroke
• No increase in risk of MI or stroke after vaccination against the flu, pneumococcal disease and tetanus
• There was an increased risk in the 3 days after a systemic respiratory infection–RR = 4.95 (4.43 a 5.53)
Smeeth, NEJM, 2004; 351: 2611-2618
Seasonal Influenza Vaccine:The Evidence to Support Use
RCT of 1952 healthy adults age 18-49 during 2007-2008 of Inactivated vs. live attenuated vaccine
•Absolute efficacy of inactivated vaccine was 73%
•Absolute efficacy of the live vaccine was 51%
Monto AS, et al. NEJM, 2009;361.
Influenza Vaccine Priority Recommendations
•Persons 50 years of age and older
•Residents of chronic care facilities
•Chronic cardiopulmonary disorders
•Chronic metabolic diseases, renal dysfunction, hemoglobinopathies, or immunosuppression requiring regular medical follow up
• Women who will be in 2nd or 3rd trimester of pregnancy
Universal Immunization Recommended
Seasonal Flu Vaccine for All Persons
Effectiveness of Influenza Vaccine(Nichol KL, et al. NEJM 2007; 357:1373-81)
• Pooled data, 18 cohorts from 1990-91 to 1999-2000
• 713,872 person-seasons of observations• 58% vaccinated; mean age 73; 43% men• High-risk conditions more prevalent by
among vaccinated (56% vs 46%)•27% (OR= 0.73; 0.68-0.77) reduction in
hospitalizations (all but 1 season)• 48% (OR=0.52; 0.50-0.55) reduction in risk
of death present in all seasons• 1 death prevented for every 302 flu shots!
Influenza Vaccine Points
• Flu vaccine for Health Care Workers helps patients: 17% vs. 10% mortality in study of SNF in Scotland
• Survey in 2011-12 of 2348 health care workers: 66.9% vaccinated (86% MDs)
• Decline in GBS cases from 0.17 to 0.04 per 100,000 coincided with stepped up food safety interventions and 28% decline in campylobacter infections
• 65% adults >65 vaccinated, 50% for Latinos and Blacks, more if MD contact
• Automatic orders work
Influenza A H1N1April 21, 2009: CDC
confirms 2 in CASegments from
previous swine influenza viruses
June 11, 2009: 30,000 cases across 74 countries
WHO issues phase 6 alert = official pandemic is now over!
Pneumococcus - BackgroundRisk factors for invasive disease
Age >65 or <2 yearsPeople with chronic illnessCrowding Chronic use of Proton Pump InhibitorsAntecedent respiratory infection and
recent antibioticSmokersAfrican Americans and American
Indians
Pneumococcal Vaccine Indications・ All persons older than 65 y –– 50 y?
・ Chronic cardiovascular disease
・ Chronic pulmonary disease + asthma
・ Diabetes mellitus, smokers
・ Cirrhosis, Alcoholism, CSF leaks
・ Functional or anatomic asplenia
・ HIV infection
・ Immunocompromised persons
MMWR1997; 46:1-24 (RR-8)

Pneumococcal vaccine Re-Vaccination: CDC
• Only one-time re-vaccination at 5 years recommended for:–no spleen - functional or anatomical–chronic kidney disease–immune suppressed conditions –chemotherapy with cancer drugs
• Persons at age 65 years if first dose was given ≥ 5 years before
• Otherwise--Re-vaccination not needed!
Efficacy of Pneumococcal Vaccine
• Randomized trials showed no decrease in death or bacteremia; 50% decrease in pneumonia
• Case control studies--60% to 70% protective efficacy for bacteremia
• CDC cohort analysis: 57% (95% CI= 45%-66%) protection, sustained over time
• Vaccine cost effective: saves money and lives even after including future costs
Pneumococcal Conjugate Vaccine
• Used for infants in the US since 2000• Cases of drug resistant Strep Pneumo
invasive disease decreased (cases /100,000)1999 2004
Penicillin resistant 6.3 2.7Muliple Abx resistant 4.1 1.7
• Decline of 50% among adults 65 years and older
NEJM 2006;354:1455-63
Recommendation of Pneumococcal Conjugate (PCV13) Vaccine in Adults
• More immunogenic, 3X more expensive• PCV13 first, followed by PPSV23 ≥ 8 weeks later• If already received PPSV23, give PCV13 ≥ 1 yr
later; boost once at 5 years if given < 65 y• Conditions: CSF leak, cochlear implant• Sickle cell disease, asplenia• HIVn infection, chronic renal failure, nephrotic
syndrome, leukemia, lymphoma, Hodgkin disease, myeloma, solid organ transplant, iatrogenic immunosuppression
CDC, MMWR 2012; 61: 8116-19
Hepatitis Vaccines
Prevention of Acute and Chronic Hepatitis and
Cancer!
Global Burden of Illness of Hepatitis B
• 2 billion persons with hepatitis B• 350 million chronic carriers• 1 million deaths per year• HBV vaccination programs have been
implemented in > 100 countries• Reduction of chronic infections and liver
cancer • Most of chronic infections are acquired
as children
Hepatitis B Vaccination• 2006: 13,200 acute cases, 1460 hospitalized,
47 deaths; 2007: 1815 deaths from chronic HBV
• Adults–target sexually active, health care workers, injection drug users, ESRD, diabetes < 60 y
• Needle exchange programs are effective
• Immunity = >10 U/ml anti-HBs
• Check post-vaccination serology 1-2 m after series in selected patients
• Universal vaccination is the goal
HBV Vaccination Protection• Antibody (HBsAb) levels decline to
undetectable by 6 yrs. in up to 50%
• Initial non-responders re-vaccinated with one more dose 15% to 25% respond three more doses 50% to 75% respond
• No documented case of symptomatic hepatitis in vaccine recipient with initial antibody response
• Long incubation of HBV allows triggering T cell memory
• Boosters are not routinely recommended

Hepatitis A Vaccination• Only 19.7% of adults 19 to 49 years with
chronic liver conditions have received 2 doses of hepatitis A vaccine
• Target: Injection drug usersPatients with chronic liver diseaseTravelers to high/intermediate risk areas in LMICHousehold contacts adoptees
Measles, Mumps, Rubella
Have you ever seen a case?
Status of MMR Diseases in 2006
Measles55 cases; no deathsGlobal: 242,000 deaths; 68% reduction from 2000
Mumps6584 cases; no deaths
Rubella11 cases; no deaths; 1 CRS
Measles, Mumps, Rubella Vaccine
•Use combined MMR vaccine in most people
•Born after 1957––limited exposure
•Documentation of vaccine receipt; Clinical diagnosis of disease––documented or Serologic evidence of immunity
•Health care workers a priority
•Non-infectious clinical syndromes
•No evidence for autism association
Human Papilloma Virus Vaccine
Cancer Prevention at its Best?
Human Papilloma Virus• HPV causes cervical cancer (90%+)• 50% of adults are infected with HPV• 13,000 cases of cervical cancer per year
in the US; 3700 deaths• High burden of disease in low and
middle income countries•HPV is not curable or treatable• $2 billion dollars to prevent up to 7000
cases of cervical cancer if vaccine is 100% effective
HPV Vaccine Efficacy
• Prevention of warts, persistent HPV infection, and HGSIL lesions
• Lag time to detect efficacy in prevention of cervical cancer will be 10 to 20 years
• CIN 2 or CIN 3: about 40% progress to cervical cancer
• Near 100% effective at decreasing HGSIL of cervix in published trials
• HPV 16/18 include about 70% of oncogenic HPV types but varies by country
HPV Vaccine Recommendations by CDC/ACIP and the ACS
• All girls at age 9 to 11 years or as adolescents (CDC)
• All Women 18 to 26 years (not ACS)• Give before onset of sexual activity• Not to be administered during
pregnancy• Boys at age 11-12; 13-26 if not done• Adverse effects: minor local
reactions, low-grade fever, fainting
• Cost is about $360 –– it is covered

HPV Vaccine Phase 3 Trials:Futures I and II
• HPV 16/18 + 6/11 vaccine• 12,167 and 5455 women age 15-26 y; 3
years follow up• Per-protocol analysis = no viral evidence of
infection by month 7• CIN grade 2 or 3 or cancer––Efficacy = 98%
(86 to 100)• Intention to treat efficacy = 44% (26–58) or
34% (15 to 49)• Efficacy for all CIN 2/3 or cancer was only
17% (1 to 31) or 20% (8 to 31)
HPV Vaccine Questions
• Duration of immunity unknown• Acceptability by parents?• Reassurance regarding safe sex?• Cover more oncogenic types?• Alter routine Pap screening?• Global Application?• 21% of women age 18-26 had
received HPV in 2010
HPV Vaccine In “Older” Women•Women aged 24-45 yrs, randomized,
placebo-controlled, double-blind study with no h/o genital warts or cervical disease
•3817 women received quadrivalent HPV vaccine vs. placebo – 3 doses
Outcome=disease/infection related to HPV 6, 11, 16, 18
Efficacy 90.5%, but ITT efficacy: 30.9%Munoz N, et al. Lancet, 2009;373
Immunogenicity of 2 Doses of HPV Vaccine in Adolescents
•Mean Ab levels to HPV-16 and 18• 830 women randomized; girls 9-13
y to either 2 or 3 doses; women 16-26 y received 3 doses
• Outcome = geometric mean titer of Ab; non-inferiority up to 36 months
• No significant difference in GMT
• Dobson S, et al. JAMA 2013; 309: 1793-1802

Patient Reminders for Immunizations
• Are effective: 5% to 20% absolute increase in 33 of 41 RCT
• Immunization rate: 42% vs. 27%
• Influenza, pneumococcal, tetanus
• All ages--children do better
• Academic > private or public clinic
• Telephone is most effective, costly
• Mailed postcards and auto-dials OK
Immunization Information Resources
CDC Travel Advisoryhttp://www.cdc.gov/travel/diseases.htm
National Immunization Programhttp://www.cdc.gov/nip/
National Vaccine Program Officehttp://www.cdc.gov/od/nvpo/
Immunization Action Coalitionhttp://www.immunize.org/
CURRENT ISSUES IN DIABETES MANAGEMENT
1
Robert Baron, MD, MS
CURRENT ISSUES IN DIABETES MANAGEMENT
Robert B. Baron MD MS
Professor and Associate Dean
UCSF School of Medicine
Declaration of full disclosure: No conflict of
interestADA Diabetes Care, 2013
Screening for Diabetes 2013
BMI ≥25 plus other risk factorsInactivity Low HDL or high TG
First degree relative PCOS
High-risk ethnicity Acanthosis nigricans
Gestational DM Hx CVD
HTN
Age 45
ADA Diabetes Care, 2013
Diagnosis of Diabetes 2013
A1C ≥ 6.5% (New, 2010)
FPG ≥ 126 mg/dl (7.0 mmol/L)
2-h plasma glucose ≥ 200 during OGTT
Symptoms and random plasma glucose ≥200 mg/dl (11.1 mmol/L)
Need two separate measurements
Advantages of HbA1c as a Diagnostic Test
Non fasting
Lower intra-individual variation
HbA1c: 2%
FPG: 6.5%
2 hour plasma glucose: 16-17%

CURRENT ISSUES IN DIABETES MANAGEMENT
2
Robert Baron, MD, MS
ADA Diabetes Care, 2013
Diagnosis of Pre-Diabetes 2013
A1C 5.7 – 6.4% (New, 2010)
FPG 100 - 125 mg/dl (5.6mmol/L - 6.9 mmol/L)
2-h plasma glucose 140 mg/dl – 199 mg/dl during OGTT (7.8mmol/L – 11.0 mmol/L)
ADA Diabetes Care, 2013
Risk of Pre-Diabetes 2013
Increased risk of progression to diabetes
44,203 individuals; 16 studies, 5.6 years
A1C 5.5 – 6.0: risk of DM 9 - 25%
A1C 6.0 – 6.5: risk of DM 25 – 50%
ADA Diabetes Care, 2013
Treatment of Pre-Diabetes 2013
Weight loss 7%; physical activity 150 min/week
Metformin (but only metformin) may be considered, especially for those with BMI >35, age <60, and women with history of gestational DM
ADA Diabetes Care, 2013
2013 Practice Guidelines: ASA
ASA: only in those at increased CV risk (10 year risk >10%. (Typically men over 50, women over 60 with other risk factors)
2009:
ASA: over age 40 and for those with other CHD risk factors

CURRENT ISSUES IN DIABETES MANAGEMENT
3
Robert Baron, MD, MS
ADA Diabetes Care, 2013
2013 Practice Guidelines: HTN and Lipids and Tobacco
BP: Goal less than 130 and less than 80
LDL: Goal less than 70 (with CVD); less than 100 (without CVD)
Don’t forget tobaccoACCORD, NEJM 2010
Intensive BP Control in Type 2 DM: ACCORD
• RCT of 4733 patients with type 2 DM • Compare BP less than 120 mm Hg vs 140
120 140 p• BP 119 133• CV events plus death 1.87% 2.09% .20 • Mortality 1.28% 1.19% .55• Stroke 0.32% 0.53% .01• Adverse events 3.3% 1.3% .001
In type 2 DM: treating to 120 mm Hg did not reduce therate of composite fatal and non-fatal CV events
Case 1
70 yo woman with type 2 diabetes, hypertension, and coronary heart disease (s/p MI in 2003).
Meds: Metformin, glipizide, aspirin, lisinopril, metoprolol, and simvastatin
Exam: BP 130/80, BMI 29 kg/m2
Normal exam
Case 1 Her glycemic goal should be:
1. HbA1c <6.0%
2. HbA1c <6.5%
3. HbA1c <7.0%
4. HbA1c <7.5%
5. HbA1c <8.0%
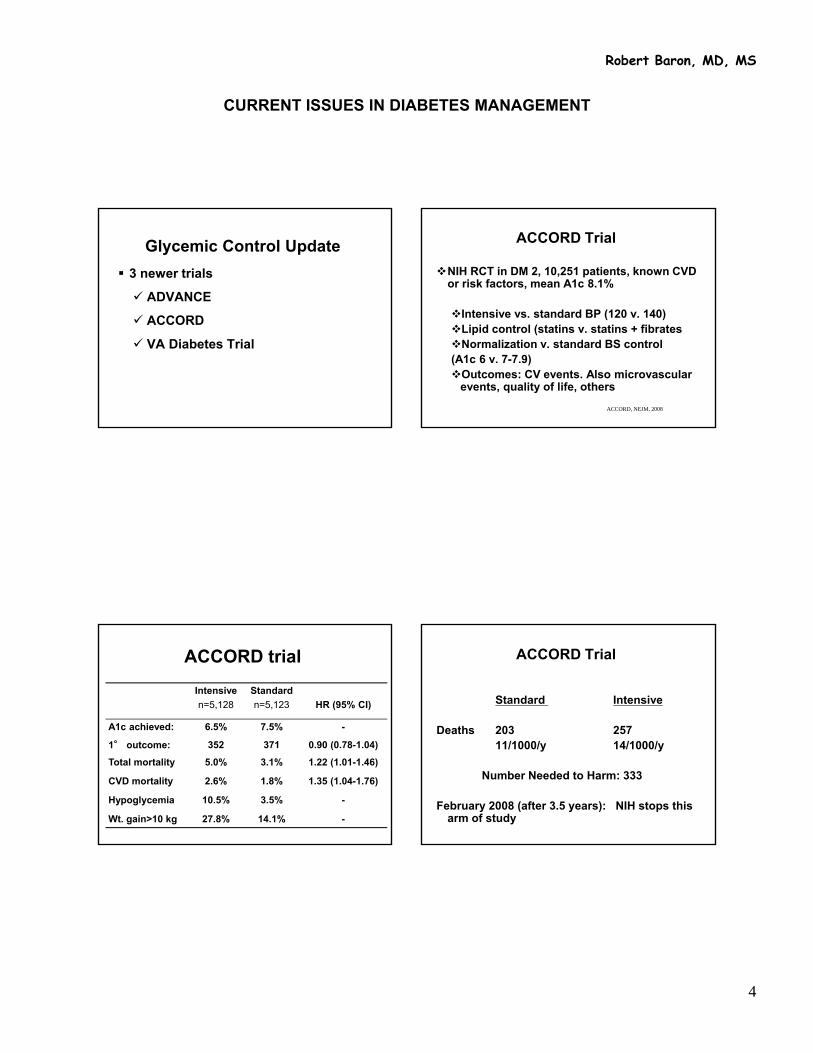
CURRENT ISSUES IN DIABETES MANAGEMENT
4
Robert Baron, MD, MS
Glycemic Control Update
3 newer trials
ADVANCE
ACCORD
VA Diabetes Trial
ACCORD, NEJM, 2008
ACCORD Trial
NIH RCT in DM 2, 10,251 patients, known CVD or risk factors, mean A1c 8.1%
Intensive vs. standard BP (120 v. 140)Lipid control (statins v. statins + fibratesNormalization v. standard BS control (A1c 6 v. 7-7.9)Outcomes: CV events. Also microvascular
events, quality of life, others
ACCORD trial
Intensive
n=5,128
Standard
n=5,123 HR (95% CI)
A1c achieved: 6.5% 7.5% -
1° outcome: 352 371 0.90 (0.78-1.04)
Total mortality 5.0% 3.1% 1.22 (1.01-1.46)
CVD mortality 2.6% 1.8% 1.35 (1.04-1.76)
Hypoglycemia 10.5% 3.5% -
Wt. gain>10 kg 27.8% 14.1% -
ACCORD Trial
Standard Intensive
Deaths 203 25711/1000/y 14/1000/y
Number Needed to Harm: 333
February 2008 (after 3.5 years): NIH stops this arm of study

CURRENT ISSUES IN DIABETES MANAGEMENT
5
Robert Baron, MD, MS
ACCORD, NEJM, 2011
ACCORD Trial5-Year Outcomes
Additional follow-up of 1.5 years
All subjects treated to HbA1c of 7-7.9% during this period
Results: Mortality still higher in intensive
group (7.6% vs 6.4%; HR 1.19)Boussageon, BMJ 2011
Outcome of Intensive Glucose Lowering in Type 2 DM
Meta-analysis of 13 RCTs in DM 2; 34,533 pts
RRAll cause mortality 1.04 (0.91 – 1.19CV death 1.11 (0.86 – 1.43)Non-fatal MI 0.85 (0.74 – 0.96)*Microalbuminuria 0.90 (0.85 – 0.96)*Severe hypoglycemia 2.33 (21.62 -3.36)*
* P <0.001
Boussageon, BMJ 2011
Outcome of Intensive Glucose Lowering in Type 2 DM
Over five year period:NNT to prevent one MI 117-150
NNT to prevent onemicroalbuminuria 32- 142
NNT to cause one episode of severe hypoglycemia 15-52
ORIGEN, NEJM, 2012
ORIGEN Trial
RCT, 12,537 subjects; impaired FBS, IGT, or new diabetes, and high CV risk
Mean FBS 131 mg/dl
Glargine to FBS <95 mg/dl; 6.2 years
Results: No difference in CV outcomes

CURRENT ISSUES IN DIABETES MANAGEMENT
6
Robert Baron, MD, MS
Glycemic Control Summary No consistent evidence that tight glycemic
control reduces risk of CVD in DM 2
Possible subgroups with benefit:
shorter diabetes duration, no CVD
Strong evidence to support decrease in microvascular disease outcomes with more intensive glucose control
More hypoglycemia and weight gain with more intensive regimens
ADA Diabetes Care, 2013
2013 Practice Guidelines: Glucose Control
Goal A1C ≤7 for most
Goal A1C <6.5 for some: short duration, long life expectancy, and no CVD
Goal less stringent (≤8) for history of hypoglycemia, limited life expectancy, mico or macrovascular complications, comorbid conditions, and those in whom the goal is difficult to attain
Critically Ill patients?Meta-analysis of 29 RCTs (n=8,432 patients)
Mortality Rates
Tight Usual RR (95% CI)
Overall 21.6% 23.3% 0.93 (0.85-1.03)
Very tight, ≤110 mg/dl 23.0% 25.2% 0.90 (0.77-10.4)
Moderate, <150 mg/dl 17.3% 18.0% 0.99 (0.83-1.18)
Medical ICU 26.9% 29.7% 0.92 (0.82-1.04)
Surgical ICU 8.8% 10.8% 0.88 (0.63-1.22)
Med-Surg ICU 26.1% 27.0% 0.95 (0.80-1.13)
Glycemic Control Summary
No consistent evidence that tight glucose control improves mortality in hospitalized patients.

CURRENT ISSUES IN DIABETES MANAGEMENT
7
Robert Baron, MD, MS
ADA Diabetes Care, 2013
2013 Practice Guidelines: Glucose Control in Hospital
Critically ill: Goal 140 - 180.
IV protocol
Non-critically ill: premeal <140 if can be done safely; random < 180. Less stringent if severe comorbidities
Scheduled subcu insulin with basal, nutritional, and correction components
Case 1 Her glycemic goal should be:
1. HbA1c <6.0%
2. HbA1c <6.5%
3. HbA1c <7.0%
4. HbA1c <7.5%
5. HbA1c <8.0%
In my practice, I have initiated:
1. Exenatide (Byetta™) or Liraglutide (Victoza™)
2. Sitagliptin (Januvia™) or Saxagliptin (Onglyza™)
3. Both exenatide and sitagliptin
4. Pramlintide (Symlin™)
5. All three of the above
6. None of the above
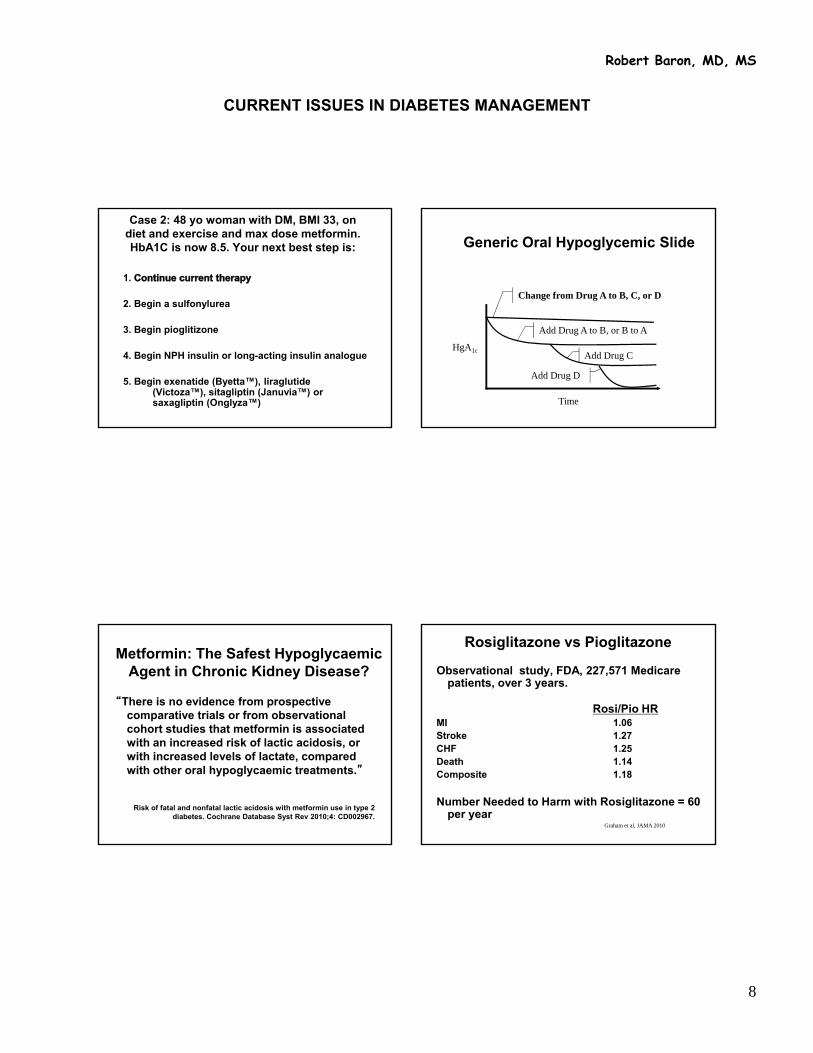
CURRENT ISSUES IN DIABETES MANAGEMENT
8
Robert Baron, MD, MS
Case 2: 48 yo woman with DM, BMI 33, on diet and exercise and max dose metformin. HbA1C is now 8.5. Your next best step is:
1.
2. Begin a sulfonylurea
3. Begin pioglitizone
4. Begin NPH insulin or long-acting insulin analogue
5. Begin exenatide (Byetta™), liraglutide(Victoza™), sitagliptin (Januvia™) or saxagliptin (Onglyza™)
Generic Oral Hypoglycemic Slide
HgA1c
Time
Change from Drug A to B, C, or D
Add Drug A to B, or B to A
Add Drug C
Add Drug D
Metformin: The Safest Hypoglycaemic Agent in Chronic Kidney Disease?
“There is no evidence from prospective comparative trials or from observational cohort studies that metformin is associated with an increased risk of lactic acidosis, or with increased levels of lactate, compared with other oral hypoglycaemic treatments.”
Risk of fatal and nonfatal lactic acidosis with metformin use in type 2 diabetes. Cochrane Database Syst Rev 2010;4: CD002967.
Graham et al, JAMA 2010
Rosiglitazone vs Pioglitazone
Observational study, FDA, 227,571 Medicare patients, over 3 years.
Rosi/Pio HRMI 1.06Stroke 1.27CHF 1.25Death 1.14Composite 1.18
Number Needed to Harm with Rosiglitazone = 60 per year

CURRENT ISSUES IN DIABETES MANAGEMENT
9
Robert Baron, MD, MS
Oral Agent “Failure”Why does this occur?
Changing HbA1c goals
Compliance, side effects
Wrong diagnosis (LADA--latent autoimmune diabetes in adults 10%)
Stress, diabetogenic medications
Postprandial hyperglycemia
Natural progression of the disease
Relative Contributions of Fasting and Postprandial Plasma Glucose to Total Glycemic Excursions as a Function of A1C
Monnier L et al. Diabetes Care. 2003;26:881-885.
0
20
60
80
2(7.3–8.4)
3(8.5–9.2)
4(9.3–10.2)
5(>10.2)
1(<7.3)
40
Co
ntr
ibu
tio
n (
%)
A1C (%) Quintiles
Postprandial hyperglycemia
Fasting hyperglycemia
Natural History of Type 2 Diabetes
050
100150200250
-10 -5 0 5 10 15 20 25 30
Years of Diabetes
Glucose(mg/dL)
Relative Function
(%)
Insulin Resistance
Insulin Level`Beta-cell failure
*IFG = impaired fasting glucose
50100150200250300350
Fasting Glucose
Post-meal Glucose
Obesity IFG* Diabetes Uncontrolled hyperglycemia
Natural History of Type 2 Diabetes
050
100150200250
50100150200250300350
-10 -5 0 5 10 15 20 25 30Years of Diabetes
Glucose(mg/dL)
Relative Function
(%)
Lifestyle SU
Insulin Resistance
Insulin Level
Fasting Glucose
Beta-cell failure
Post-meal Glucose
Insulin
Biguanide

CURRENT ISSUES IN DIABETES MANAGEMENT
10
Robert Baron, MD, MS
Insulin Plus Oral Agents
Introduction of insulin
– Bedtime
– Intermediate/Long-acting insulins
• NPH, glargine, levemir
• 10 units
– Self-monitoring of blood glucose (hypoglycemia education)
Insulin plus other oral agent combinations (maintain effect on insulin sensitivity)
When to go to > 1 shot per day HgA1c >7
Glucose in AM at goal but glucose before dinner >140
Options
Add premeal lispro/aspart
Add bid premixed insulin – 70/30, 75/25
Questions
Continue metformin
? Sulfonylurea, ? Thiazolidinedione (mostly not)
Function of Insulin in Regimens
Meal coverage (carbohydrates)
Basal insulin
Correction of high blood sugar
INCRETINS
Gut factors that promote insulin secretion in response to nutrients
Major incretins: GLP-1, CCK, GIP

CURRENT ISSUES IN DIABETES MANAGEMENT
11
Robert Baron, MD, MS
Oral Glucose Promotes More Insulin Release than IV
Glucose - Indicating a Role for Incretins
Incretin Drugs
GLP Agonists
– Exenatide
– Liraglutide
– Exenatide Lar
– Semaglutide
– Aliglutide
– Taspoglutide
– Lixsenatide
DPP IV Inhibitors
– Sitagliptin
– Saxagliptin
– Vildagliptin
– Alogliptin
– Linagliptin
– Dutogliptin
– Metogliptin
A1C (%) Effect (change from baseline)
Placebo BID 5 mcg exenatide BID 10 mcg exenatide BID
MET 0.1 -0.4 -0.8
SFU 0.1 -0.5 -0.9
MET+SFU 0.2 -0.6 -0.8
Changes in A1C from baseline vs placebo statistically significant

CURRENT ISSUES IN DIABETES MANAGEMENT
12
Robert Baron, MD, MS
Weight (change from baseline) & Hypoglycemia
Placebo BID
5 mcg exenatide BID 10 mcg exenatide BID
Weight (kg) -1.4 -3.1 -4.2
Hypoglycemia (%)
MET
SFU
MET + SFU
5.3
3.3
1.26
4.5
14.4
19.2
5.3
35.7
27.8
Open-label extension study to 90 weeks: persistence in weight loss and A1C
Side Effects
GI– Nausea (44% vs 18% with placebo); incidence
lessens over time; 3% dropout rate due to nausea
– Vomiting (13% vs 4%)– Diarrhea (13% vs 6%)
Headache (9% vs 6%)Hypoglycemia (see previous slide)
Improvements in HbA1C With Initial Co-administration of Sitagliptin and Metformin
Placebo
Sita 100 mg QD
Sita 50 mg BID + Met 500 mg BID
Sita 50 mg BID + Met 1000 mg BID
Met 1000 mg BID
Met 500 mg BID
* Placebo-subtracted LS mean change form baseline at Week 24.Sita=sitagliptin; Met=metformin.
-2.5
-2.0
-1.5
-1.0
-0.5
Hb
A1C
(%)* -0.8
-1.0
-1.3
-1.6
-2.1
Mean Baseline HbA1C = 8.8%
N=1091
Aschner P, et al. Oral presentation at the EASD 42nd Annual Meeting; 14-17 September 2006; Copenhagen.
Number of patients (%)
Sitagliptin Placebo
Monotherapy n = 443 n = 363
Nasopharyngitis 23 (5.2) 12 (3.3)
+ pioglitazone n = 175 n = 178
Upper resp. infection
11 (6.3) 6 (3.4)
Small increase in WBC – neutrophil count higher by 200 on Sitagliptin
No nausea or vomiting
No weight loss
Sitagliptin – adverse reactions
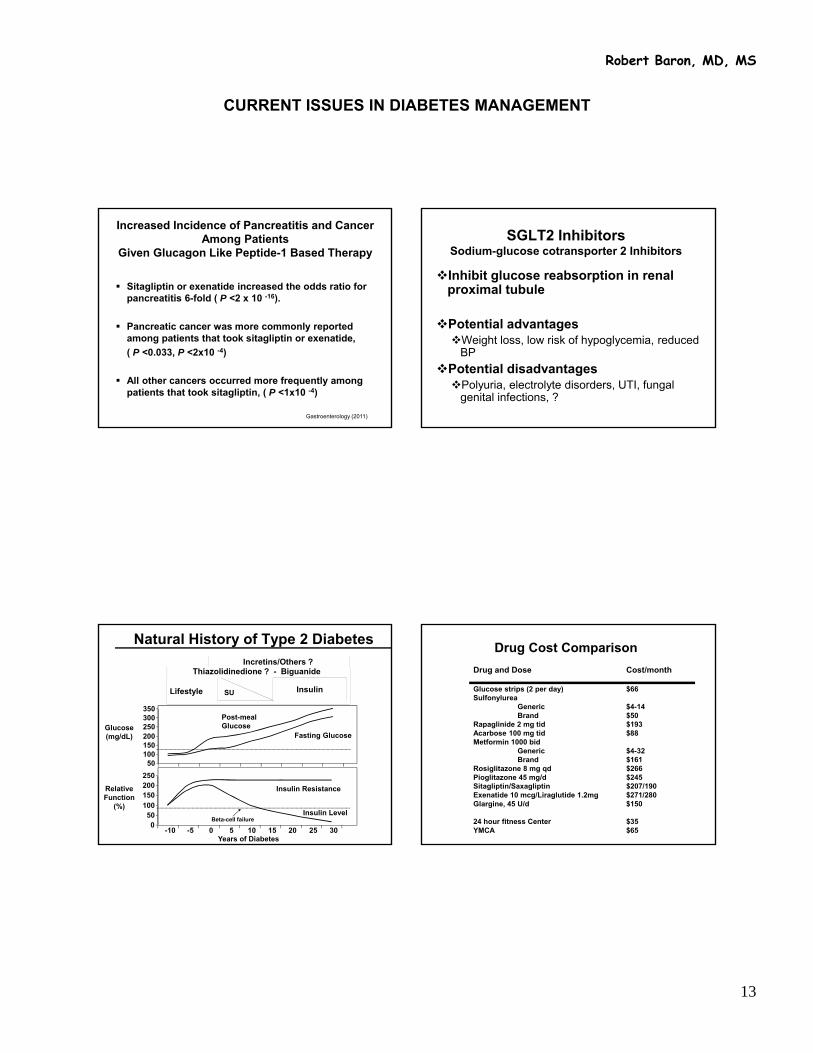
CURRENT ISSUES IN DIABETES MANAGEMENT
13
Robert Baron, MD, MS
Increased Incidence of Pancreatitis and Cancer Among Patients
Given Glucagon Like Peptide-1 Based Therapy
Sitagliptin or exenatide increased the odds ratio for pancreatitis 6-fold ( P <2 x 10 -16).
Pancreatic cancer was more commonly reported among patients that took sitagliptin or exenatide,
( P <0.033, P <2x10 -4)
All other cancers occurred more frequently among patients that took sitagliptin, ( P <1x10 -4)
Gastroenterology (2011)
SGLT2 InhibitorsSodium-glucose cotransporter 2 Inhibitors
Inhibit glucose reabsorption in renal proximal tubule
Potential advantagesWeight loss, low risk of hypoglycemia, reduced
BP
Potential disadvantagesPolyuria, electrolyte disorders, UTI, fungal
genital infections, ?
Natural History of Type 2 Diabetes
050
100150200250
50100150200250300350
-10 -5 0 5 10 15 20 25 30Years of Diabetes
Glucose(mg/dL)
Relative Function
(%)
Lifestyle SU
Insulin Resistance
Insulin Level
Fasting Glucose
Beta-cell failure
Post-meal Glucose
Insulin
Thiazolidinedione ? - Biguanide Incretins/Others ?
Drug Cost Comparison
Drug and Dose Cost/month
Glucose strips (2 per day) $66Sulfonylurea
Generic $4-14Brand $50
Rapaglinide 2 mg tid $193Acarbose 100 mg tid $88Metformin 1000 bid
Generic $4-32 Brand $161
Rosiglitazone 8 mg qd $266Pioglitazone 45 mg/d $245Sitagliptin/Saxagliptin $207/190Exenatide 10 mcg/Liraglutide 1.2mg $271/280Glargine, 45 U/d $150
24 hour fitness Center $35YMCA $65
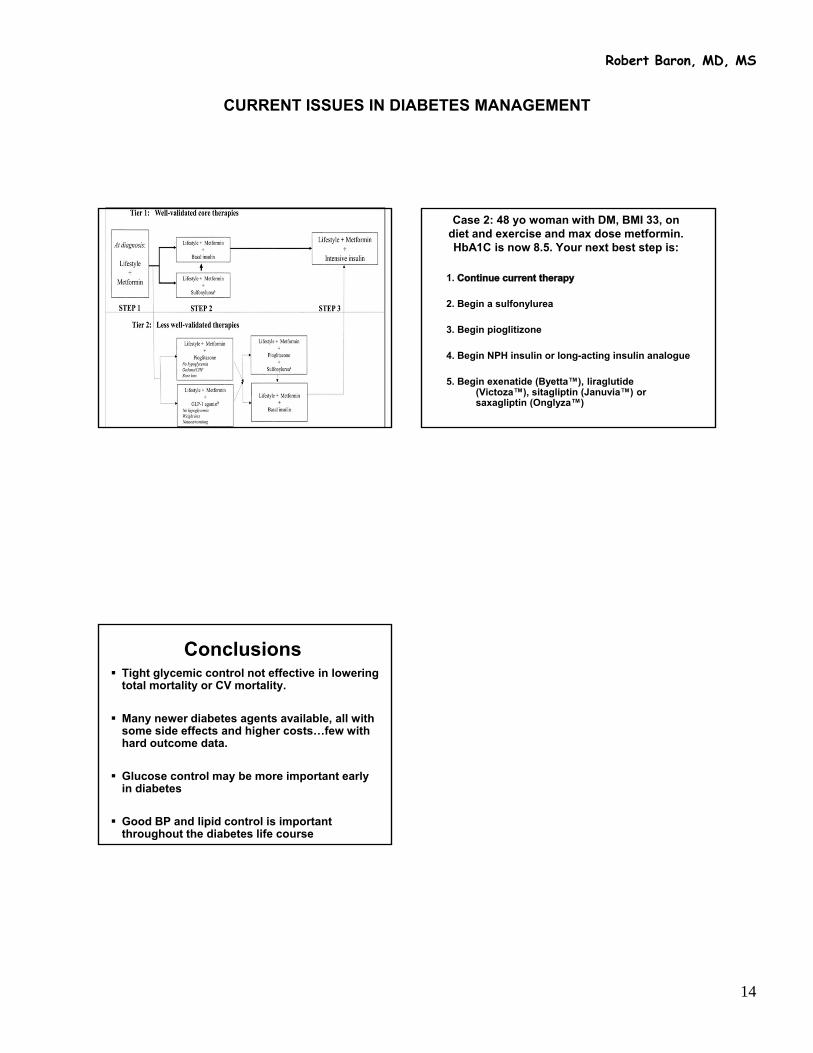
CURRENT ISSUES IN DIABETES MANAGEMENT
14
Robert Baron, MD, MS
Case 2: 48 yo woman with DM, BMI 33, on diet and exercise and max dose metformin. HbA1C is now 8.5. Your next best step is:
1.
2. Begin a sulfonylurea
3. Begin pioglitizone
4. Begin NPH insulin or long-acting insulin analogue
5. Begin exenatide (Byetta™), liraglutide(Victoza™), sitagliptin (Januvia™) or saxagliptin (Onglyza™)
Conclusions Tight glycemic control not effective in lowering
total mortality or CV mortality.
Many newer diabetes agents available, all with some side effects and higher costs…few with hard outcome data.
Glucose control may be more important early in diabetes
Good BP and lipid control is important throughout the diabetes life course
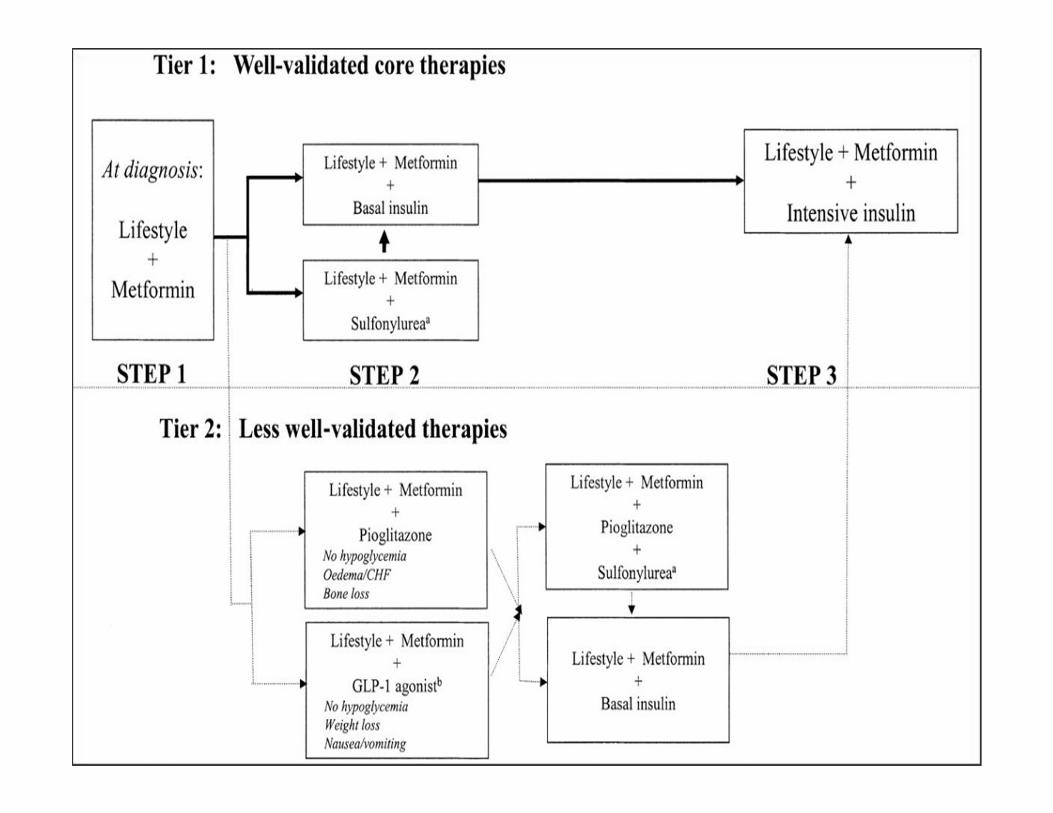

6/21/2013
1
Department of Medicine
Breast Cancer: Key issues for the non-oncologist
Essentials of Women’s HealthJeffrey A. Tice, MDAssociate Professor
July 2013
Department of Medicine
• I have no financial disclosures
• I developed and validated one of the models that will be discussed. I hold no patents and derive no financial benefit from the model.
2
Department of Medicine
OUTLINE• Risk Assessment
• Risk Reduction
• Screening
• Tests at Diagnosis
3
Department of Medicine
Case: Maria
• 35 yo white woman, has 2 children ages 1 and 4. She started menstruating at age 11 and took birth control pills from age 19 to 26.
• She recently had a biopsy for a breast lump which was benign (cyst)
• Her mother diagnosed BC at age 69
• She is an advertising executive and drinks 2-3 glasses of wine/night.

6/21/2013
2
Department of Medicine
Maria’s questions
• What is my risk for developing breast cancer?
• What can I do to lower my risk?
Department of Medicine
6
Risk Assessment
Department of Medicine
Why risk assessment?
• Breast cancer is most commonly diagnosed cancer in U.S. women
– 1 in 8-9 women will be diagnosed in her lifetime
• 2nd most common cause of cancer death in women
– >39,000 deaths in 2011
• Risk assessment tools are available
• Risk reduction is possible
Department of Medicine
Risk factors for breast cancer
• Strong– Age
– Breast density
– Atypical hyperplasia
– LCIS
– BRCA mutation
• Moderate– Family history
– Breast biopsy
– Race / ethnicity
– Hormone therapy
– Hormone levels (E2, T, IGF-1)
– Benign breast disease
• Weak– Age at first birth
– Menarche age
– Height, weight, BMI
– Bone mineral density
– NAF/Lavage
– SNPs
– Age of diagnosis for family history
– 2nd degree relatives
– Alcohol intake
– Diabetes
– Physical activity
– Breast feeding
– Menopause age
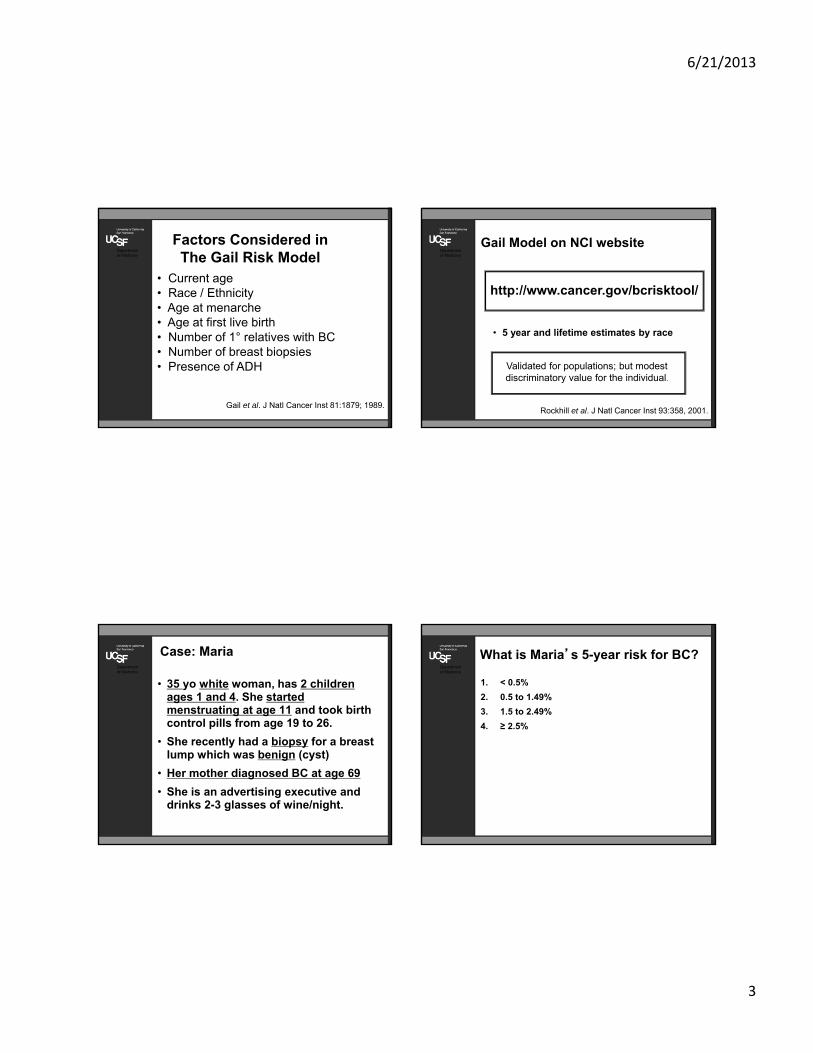
6/21/2013
3
Department of Medicine
Factors Considered inThe Gail Risk Model
• Current age• Race / Ethnicity • Age at menarche• Age at first live birth• Number of 1° relatives with BC • Number of breast biopsies• Presence of ADH
Gail et al. J Natl Cancer Inst 81:1879; 1989.
Department of Medicine
Gail Model on NCI website
• 5 year and lifetime estimates by race
Validated for populations; but modest discriminatory value for the individual.
Rockhill et al. J Natl Cancer Inst 93:358, 2001.
http://www.cancer.gov/bcrisktool/
Department of Medicine
Case: Maria
• 35 yo white woman, has 2 children ages 1 and 4. She started menstruating at age 11 and took birth control pills from age 19 to 26.
• She recently had a biopsy for a breast lump which was benign (cyst)
• Her mother diagnosed BC at age 69
• She is an advertising executive and drinks 2-3 glasses of wine/night.
Department of Medicine
What is Maria’s 5-year risk for BC?
1. < 0.5%
2. 0.5 to 1.49%
3. 1.5 to 2.49%
4. ≥ 2.5%
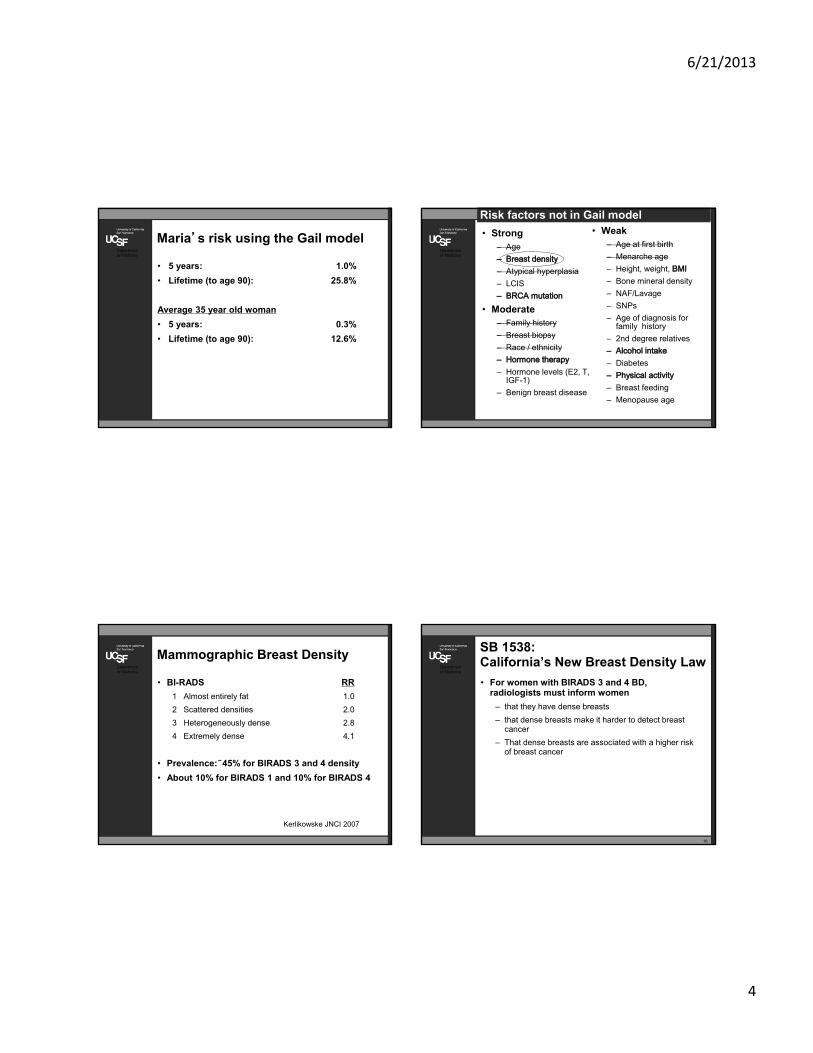
6/21/2013
4
Department of Medicine
Maria’s risk using the Gail model
• 5 years: 1.0%
• Lifetime (to age 90): 25.8%
Average 35 year old woman
• 5 years: 0.3%
• Lifetime (to age 90): 12.6%
Department of Medicine
Risk factors not in Gail model
• Strong– Age
– Atypical hyperplasia
– LCIS
• Moderate– Family history
– Breast biopsy
– Race / ethnicity
– Hormone levels (E2, T, IGF-1)
– Benign breast disease
• Weak– Age at first birth
– Menarche age
– Height, weight,
– Bone mineral density
– NAF/Lavage
– SNPs
– Age of diagnosis for family history
– 2nd degree relatives
– Diabetes
– Breast feeding
– Menopause age
Department of Medicine
Mammographic Breast Density
• BI-RADS RR
1 Almost entirely fat 1.0
2 Scattered densities 2.0
3 Heterogeneously dense 2.8
4 Extremely dense 4.1
• Prevalence: 45% for BIRADS 3 and 4 density
• About 10% for BIRADS 1 and 10% for BIRADS 4
Kerlikowske JNCI 2007
Department of Medicine
SB 1538: California’s New Breast Density Law
• For women with BIRADS 3 and 4 BD, radiologists must inform women
– that they have dense breasts
– that dense breasts make it harder to detect breast cancer
– That dense breasts are associated with a higher risk of breast cancer
16

6/21/2013
5
Department of Medicine
BCSC breast density model
• Age, race, BD, family history, breast biopsy
Tice, Annals IM, 2008.
https://tools.bcsc-scc.org/BC5yearRisk/
Department of Medicine
Maria’s 5-year risk comparing models
Gail Model 1.0%
BCSC Model
• Almost entirely fat .24%
• Scattered densities .50%
• Heterogeneously dense .77%
• Extremely dense 1.0%
(Average 35 yo woman’s 5 year risk is 0.3%)
Department of Medicine
19
Risk Reduction
Department of Medicine
Which of these will NOT decrease Maria’s risk for breast cancer?
1. Eating more fruits and vegetables
2. Brisk walking 30 minutes/day
3. Losing 10 kg (to BMI of 24 kg/m2)
4. Cutting back on alcohol

6/21/2013
6
Department of Medicine
Which of these will NOT decrease Maria’s risk for breast cancer?
1. Eating more fruits and vegetables
2. Brisk walking 30 minutes/day
3. Losing 10 kg (to BMI of 24 kg/m2)
4. Cutting back on alcohol
Department of Medicine
LIFESTYLE
22
Department of Medicine
No association with breast cancer
• Fruits & vegetables
– Smith-Warner, JAMA, 2001
– Pooled prospective studies
– 7377 cases in 351,825 women
• Carotenoids; Vitamins A, C, E
• Selenium
Mixed results on dietary fat intake – the jury is still out
Obesity
• Premenopausal – small decreased risk
• Postmenopausal – increased risk
Alcohol and breast cancer risk:Meta-analysis
0 10 20 30 40 50 60Total Alcohol Intake g/d
Mu
ltiv
aria
te R
elat
ive
Ris
k 2.52.0
1.5
1.0
0
Smith-Warner, 1998

6/21/2013
7
Department of Medicine
Exercise and risk of breast cancer
• Overall 25-30% decreased risk
• Greatest in thinner women
• Lifetime exercise matters
• Modest amounts: 1-3 hours brisk walking/week
0
0.2
0.4
0.6
0.8
1
1.2
0 ≤5 5 to10
>40
RR
MET-h/week
WHI Observational Cohort(n=74,171; 1780 cancers)
McTiernan, JAMA, 2003.
Department of Medicine
Hormone Therapy
Women’s Health Initiative
• E + P 1.24 (1.01-1.54) ITT
1.49 (as treated)
• E 0.77 (0.59-1.01)
• Survival curves do not separate until 3 years on treatment
• Risk is lower if started at least 5 years after menopause
• Risk dropped to baseline within 2 years of stopping therapy
Chlebowski, JAMA, 2003/2004; NEJM 2009
Department of Medicine
CHEMOPREVENTION
27
Department of Medicine
SERMs Reduce the Risk of Breast Cancer
6/21/2013
8
Department of Medicine
Adverse Events From Prevention Trials of Tamoxifen & Raloxifene
• DVT/PE: 1.9 (1.4-2.6)
• Endometrial cancer 2.4 (1.5-4.0)
• risk fatal stroke
• risk cataracts
• risk hot flashes
** Majority of adverse events in women ≥ 50 years
Fisher JNCI,1998; Cuzick Lancet, 2003; Barrett-Conner, NEJM, 2006.
Department of Medicine
• SERMS
– BCPT 1998:
• 5-yrs tamoxifen reduced risk of invasive breast ca 49% -- increased endometrial CA, VTE, cataracts
– STAR trial 2006:
• raloxifene equal to tamoxifen in reducing risk of invasive breast cancer –significantly less thromboembolism and cataracts
30
Department of Medicine
USPSTF Draft Recommendation
• “…clinicians engage in shared decision-making with women at increased risk of breast cancer regarding medications to reduce their risk. For women who are at increased risk for breast cancer and at low risk for adverse medication effects, clinicians should offer to prescribe risk-reducing medications such as tamoxifen or raloxifene.”
• “In general, women with an estimated 5-year breast cancer risk of 3% or greater are more likely to benefit from tamoxifen or raloxifene”
http://www.uspreventiveservicestaskforce.org/
31
Department of Medicine
SERM Risk Benefit Ratio LikelyTo Be Favorable For …
5 yr Gail
Age <50 >1.5 – >1.67%
Age >50no uterus >2.5%uterus intact >5.0%
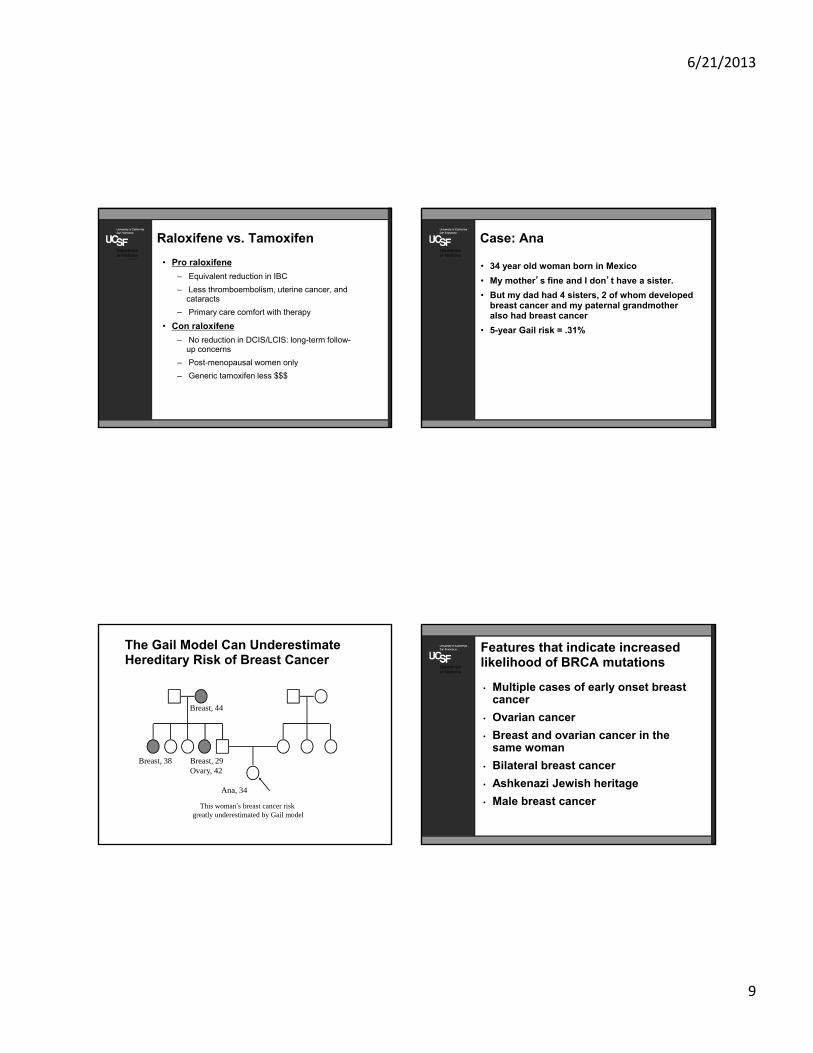
6/21/2013
9
Department of Medicine
Raloxifene vs. Tamoxifen
• Pro raloxifene
– Equivalent reduction in IBC
– Less thromboembolism, uterine cancer, and cataracts
– Primary care comfort with therapy
• Con raloxifene
– No reduction in DCIS/LCIS: long-term follow-up concerns
– Post-menopausal women only
– Generic tamoxifen less $$$
Department of Medicine
Case: Ana
• 34 year old woman born in Mexico
• My mother’s fine and I don’t have a sister.
• But my dad had 4 sisters, 2 of whom developed breast cancer and my paternal grandmother also had breast cancer
• 5-year Gail risk = .31%
The Gail Model Can Underestimate Hereditary Risk of Breast Cancer
This woman’s breast cancer risk greatly underestimated by Gail model
Breast, 44
Breast, 38 Breast, 29Ovary, 42
Ana, 34
Department of Medicine
Features that indicate increased likelihood of BRCA mutations
• Multiple cases of early onset breast cancer
• Ovarian cancer
• Breast and ovarian cancer in the same woman
• Bilateral breast cancer
• Ashkenazi Jewish heritage
• Male breast cancer

6/21/2013
10
BRCA1/2 Mutations Increase the Risk of Early-Onset Breast Cancer
Population Risk
Hereditary Risk
By age 50
2%
33%-50%
By age 70
7%
56%-87%
By age 40
10%-20%
0.5%
38
Department of Medicine
Surgical strategies for women with BRCA mutations
• Risk-reducing oophorectomy (RRSO)
– 50% reduction in breast cancer
• Risk-reducing mastectomy (RRM)
– 90% - 95% risk reduction
Rebbeck , NEJM 2002Kauf, NEJM 2002Rebbeck, JNCI 1999Rebbeck, JCO, 2004
Department of Medicine
40
Screening
6/21/2013
11
Department of Medicine
Screening controversies
• Covered by Dr. Rebecca Jackson Sunday evening
Department of Medicine
42
Tests at Diagnosis
Department of Medicine
Abnormal Mammogram
• Cumulative risk of false positive result: 49% after ten mammograms
Elmore et al NEJM 1998
• False positive rates highest for women in their 40’s and 50’s
Nelson et al Annals Int Med 2009
Department of Medicine
Case
• Your patient AH, a 56 yo woman, goes for her screening mammogram. A few days later, you get a call from the radiologist. The mammogram shows increased density and possibly a calcification on the right. The radiologist says they are reading it as a BIRADS 0 and the patient should get follow-up, could you please let her know?
6/21/2013
12
Department of Medicine
What kind of follow-up does this patient need next?
1. A repeat mammogram in 3-6 months
2. A mammogram at the usual screening interval
3. A diagnostic mammogram with spot-compression views
4. A referral to the breast surgeon/clinic for a biopsy
Department of Medicine
American College of Radiology BIRADS category (breast imaging reporting and data system)
Normal
1: negative routine follow-up
2: benign finding routine follow-up
Abnormal
0: indeterminate immediate follow-up
(spot-compression views +- u/s)
3: low chance malignancy (~2%) short interval follow-up
(3-6 months repeat mammo)
4: >2-95% chance malignancy (a: low; b: intermediate;
c: moderate) biopsy
5: ≥95% chance invasive malignancy biopsy
Department of Medicine
MQSA: Mammography Quality Standards Act
• Passed by U.S. Congress in 1992
• Mammography facility must send patient written report of her mammogram within 30 days of exam
• Report must be in words she can easily understand
• For BIRADS 4 or 5 results, facility expected to contact patient as soon as possible –‘expectation’ within 5 days
• If verbal contact, still need to send letter
47
www.fda.gov/Radiation-EmittingProducts/MammographyQualityStandardsActandProgram/ConsumerInformation/ucm113968.htm
Department of Medicine
Communication Matters• Adequate communication of abnormal
results improves receipt of appropriate follow-up
Poon et al, JGIM 2004
• Minority women report lower rates of adequate communication, and are less likely to know their abnormal mammogram results
Zapka et al, Prev Med 2004
• Women who received their results verbally (in person or over the telephone) more likely to know that their mammogram was abnormal
Karliner et al, JGIM 2005
48

6/21/2013
13
Department of Medicine
Delays in Diagnosis• 20-40% women undergoing breast ca
diagnosis experience delays to diagnosis or treatment
• Delay of ≥ 3 months (symptoms to treatment)associated with 12% lower 5-year survival
– Most of this attributable to later stage diseaseRichards et al, Lancet 1999
• African-American women are more likely to suffer delays than White women
Elmore et al, Med Care 2005
• Hospitals disproportionately serving non-English speaking and minority women have longer delays
Karliner et al, Med Care 2011
Department of Medicine
Causes of Delay• Mammogram Facility
– Resource issues
– Tracking systems
– Appointment access
• Communication
– Physician inaction (not contacting patient; not ordering follow-up tests)
– Inadequate communication of abnormal results and need for follow-up
– Language barriers
• Patient
– Patient inaction (lack of knowledge / understanding, fear, anxiety)
Department of Medicine
Case: Gwen
• You are seeing Gwen, a 50-year-old Chinese-American woman, for her routine annual exam. She tells you about a new lump she found in her breast, which you feel and find to be firm with regular borders.
• You send her for a diagnostic mammogram which shows an area of calcification BIRADS 4 and next she undergoes a core biopsy.
Department of Medicine
What Pathologic Staining Findings are Indicative of the Poorest Prognosis Tumor?
1. ER/PR positive staining
2. ER/PR and HER2Neu positive staining
3. ER/PR/Her2Neu negative staining
52
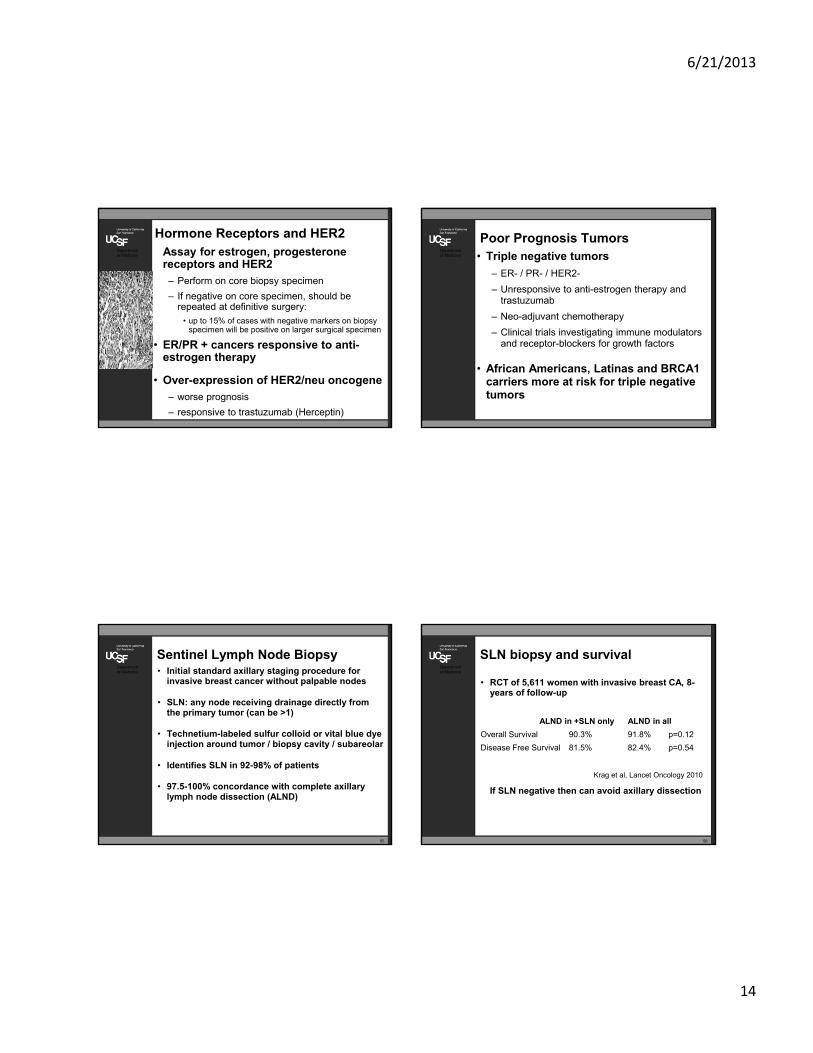
6/21/2013
14
Department of Medicine
Hormone Receptors and HER2Assay for estrogen, progesterone receptors and HER2
– Perform on core biopsy specimen
– If negative on core specimen, should be repeated at definitive surgery:
• up to 15% of cases with negative markers on biopsy specimen will be positive on larger surgical specimen
• ER/PR + cancers responsive to anti-estrogen therapy
• Over-expression of HER2/neu oncogene
– worse prognosis
– responsive to trastuzumab (Herceptin)
Department of Medicine
Poor Prognosis Tumors• Triple negative tumors
– ER- / PR- / HER2-
– Unresponsive to anti-estrogen therapy and trastuzumab
– Neo-adjuvant chemotherapy
– Clinical trials investigating immune modulators and receptor-blockers for growth factors
• African Americans, Latinas and BRCA1 carriers more at risk for triple negative tumors
Department of Medicine
Sentinel Lymph Node Biopsy• Initial standard axillary staging procedure for
invasive breast cancer without palpable nodes
• SLN: any node receiving drainage directly from the primary tumor (can be >1)
• Technetium-labeled sulfur colloid or vital blue dye injection around tumor / biopsy cavity / subareolar
• Identifies SLN in 92-98% of patients
• 97.5-100% concordance with complete axillary lymph node dissection (ALND)
55
Department of Medicine
SLN biopsy and survival
• RCT of 5,611 women with invasive breast CA, 8-years of follow-up
ALND in +SLN only ALND in all
Overall Survival 90.3% 91.8% p=0.12
Disease Free Survival 81.5% 82.4% p=0.54
If SLN negative then can avoid axillary dissection
56
Krag et al, Lancet Oncology 2010

6/21/2013
15
Department of Medicine
SLN and Survival
• If SLN positive – medical necessity of ALND is at question –
– RCT of no further axillary treatment vs. ALND– T1-T2 invasive breast cancer, no palpable adenopathy,
– 1-2 SLN with mets
– No difference in 5-year overall or disease free survival
– Only able to enroll half target (891/1900 women)
Giuliano et al, JAMA 2011
• When ALND required, standard: removal of at least 6-10 nodes (level I and II dissection, not radical dissection)
57
Department of Medicine
Gene Expression Profiling
• Goal: improve risk stratification in early stage breast cancer to better tailor use of chemotherapy
• Used to classify tumor according to recurrence risk and to predict response to chemotherapy
• Oncotype Dx best studied
– HR+, LN- <5cm tumors
– Recurrence risk low (<18) no benefit from chemo
– Recurrence risk high (>30) + benefit from chemo
• Ongoing RCTs using Oncotype Dx (TAILORx) and Mammaprint (MINDACT)
58
Department of Medicine
Metastatic Work-up**Mets are rare without symptoms**
• Physical exam: breasts, skin, lymph nodes, abdomen
• Diagnostic bilateral mammography; possible breast MRI
• CBC, LFTs
• Chest x-ray; possibly CT pre-radiation
• Staging CT – liver, pelvis, chest – and bone scan in stage III disease and above
Department of Medicine
Post-Treatment Survival
• 2,838 women Stage I-III treated w/ adjuvant or neo-adjuvant systemic therapy
• 1985-2001; disease free x 5 years
• Residual disease-free recurrence rate
– 10 years post-diagnosis 89%
– 15 years post-diagnosis 80%
• By stage residual risk of recurrence at 10 years
– Stage I 7%
– Stage II 11%
– Stage III 13%
Brewster et al JNCI, 2008

6/21/2013
16
Department of Medicine
Summary
Risk Reduction
• Lifestyle
– Exercise, weight loss or maintenance
– Minimize alcohol
– Avoid/stop HT
– Low fat diet?
• Consider tamoxifen or raloxifene for high risk women - risk/benefit
• Assess familial risk
– Refer to genetic counseling / high risk breast clinic
Department of Medicine
Summary
Tests at Diagnosis
• Delays in diagnosis are common after an abnormal mammogram
• Improved communication of abnormal results improves receipt of appropriate follow-up
• SLN biopsy can help avoid axillary dissection and results can help determine need for chemo
• Metastases are rare without symptoms
The good news:
If a woman survives 5-years, her 10-year survival is very good (Stage I-III)

NOTES
Presentation slides will not be used for this session.

NEW DEVELOPMENTS IN HYPERTENSION
Eliseo J. Pérez-Stable, MD
Common Problems in Older WomenUsing Geriatric Principles in Every Day Practice
Eliseo J. Pérez-Stable MD
Professor of Medicine
DGIM, Department of Medicine
July 3, 2013Declaration of full disclosure: No conflict of interest
Summary of TopicsShift of paradigm in caring for older
or frail patients: Geriatrics Principles
Medications overuse and avoidance
Recognition and management of Cognitive Impairment
Urinary Incontinence
Falls: Risk and prevention
Osteoarthritis
Main Teaching Points Today Geriatric Principles and Topics
• Focus on quality of life and not on quantity or prolongation
• Comorbidity: Multiple chronic diseases and symptoms
• Functional Status should be a vital sign• Cognitive Status affects all• Care across settings (Home/hospital/SNF)
and and Long term care options• Palliative Care and symptom management
NEW DEVELOPMENTS IN HYPERTENSION
Eliseo J. Pérez-Stable, MD
Comorbidity• Older persons with a major diagnosis
(such as heart failure) have other diseases as well
• Other diseases can have profound impact on clinical presentation, prognosis, optimal treatment, outcomes and management
• Dementia or Cognitive impairment is the big ticket item affecting all
Geriatrics Principles
Functional and Cognitive Status
• The holy grail of Geriatrics: The end outcome of all diseases.
• Diseases matter to the extent they impact functional status
• How do functional and cognitive status impact natural history and outcomes of the condition
• What is the impact of the condition on ADL, IADL, cognitive function?
ADL and IADL Status in All
• Activities of Daily Living: dress, transfer, toilet needs, bathing, feeding
•Patients in long-term care institutions almost always have ≥2 ADL limitations
• Instrumental Activities of Daily Living: manage own finances, transportation within community, shopping for food/clothing, preparation, use of phone or computer, housework, handle own meds

NEW DEVELOPMENTS IN HYPERTENSION
Eliseo J. Pérez-Stable, MD
Physical and Cognitive Function• Use of functional status measures in
clinical practice as routine practice
• Measurement of gait speed predicts falls risk and morbidity/mortality
• Get up and Go Test
• Evaluate cognitive status
• Establish decision-maker for goals of care and teach communication about issues
• Use functional status as a target of therapy: prevent ADL disability or delirium
Care Across Settings and Options for Long Term Care
•Care transitions often disastrous for elders
•Hospital-home; hospital-SNF; SNF-hospital
•Interventions to improve care transitions
•Long term care not just nursing homes
•Family caregivers
•Other informal care
•Assisted living
•Evaluate personal finances
Palliative Care and Symptom Management
• End of life care and hospice are underused for virtually any clinical problem
• Palliative Care is focused on improving symptoms, well being, and quality of life
• Should be present throughout the course of serious illness
• Focus on major sources of distress including patient perspective
How these Principles Apply to Patient with COPD as an Example
• Comorbidity
– How do conditions such as diabetes, dementia, depression impact outcomes of steroid treatment for exacerbations
• Function/Cognitive impairment
– As COPD progresses, what happens to ADL and IADL function. Does COPD increase risk for dementia?

NEW DEVELOPMENTS IN HYPERTENSION
Eliseo J. Pérez-Stable, MD
How these Principles Apply to Patient with COPD as an Example
• Transitions/Long Term Care
– How can we prevent readmission in persons with COPD and cognitive impairment
– Treatment of COPD in nursing homes• Palliative Care
– What are the most important sources of distress in older persons with COPD?
Medication Management
Appropriate Medication Management in Geriatrics Medicine
• 90% take medications every day and 46% take 5 or more
• 54% have more than one clinician prescribing and 35% use >1 pharmacy
• Over 50% of all prescribed drugs• Half do not take all medications as
prescribed• Up to 60% of outpatients have
medications considered suboptimal
Adverse Drug Effects are Common
• 25% of outpatient practices report• Abiut 10% to 17% of hospital
admissions are due to ADE• Increase in ADE is disproportionately
affecting elderly: 20% of all ADEs• Greatest predictor of ADE is the total
number of prescribed meds

NEW DEVELOPMENTS IN HYPERTENSION
Eliseo J. Pérez-Stable, MD
Beers Criteria 2012+www.americangeriatrics.org
• Goal to reduce inappropriate medications Beers meds linked to ADE, hospitalization, delirium, falls, GI bleed
• 53 classes of medications listed in 3 categories:
– Avoid regardless
– Inappropriate with certain diseases or syndromes
– Use with caution
New Beers Listed Meds to Avoid regardless or in some
• Megestrol: minimal benefit on appetite, weight but increase in embolic events
• Glyburide: Prolonged hypoglycemia• Spironolactone >25 mg: High K• Sliding scale insulin• Pioglitazone/rosiglitazone in heart failure• Acetyl cholinesterase inhibitors in
patients with syncope• SSRIs with falls or fractures• Histamine blockers in delirium/dementia
Cognitive Impairment
Cognitive Impairment Clinical Case
EM is a 67 year-old woman with a h/o high blood pressure. Brought in by husband who is reporting that patient’s personality has changed over the last year. She is becoming more suspicious, and at times talks and “doesn’t make sense”. She is paranoid about the neighbors.
NEW DEVELOPMENTS IN HYPERTENSION
Eliseo J. Pérez-Stable, MD
Prevalence Cognitive Impairment
• AD estimated prevalence 24.3 million world-wide in 2001
• Predicted rise to 42.3 million in 2020
• 81.1 million by 2040• Lifetime risk of
dementia after age 65 is 17-20%
• Costs $150 billion/yr
Ferri CP, et al. Lancet 2005; Simmons BB et al. AAFP 2011
Risk Factors for Cognitive Impairment
• Age• Down’s syndrome• Head trauma• Fewer years of formal education• Female sex• Family history of Alzheimer• Vascular Disease risk factors • Cerebrovascular events
Clinical Presentation of Dementia
• Cognitive changes• Personality changes• Changes in day-to-day functioning• Activities that require calculation or
planning first to be impaired• Psychiatric symptoms• Problem Behaviors• Dementia is under-diagnosed• Have a High index of suspicion• Ask caregivers, family and friends
Rapid Screening for Cognitive Impairment
• Routine screening not recommended• Use as indicated as diagnostic screen • Verbal Fluency Test: Sensitivity 88%;
specificity 96%; takes One minute• Ask patient to name as many animals as
possible in one minute
– 1 point/animal
– Score <15 suggestive of dementia
• Score <12 if 1-7 years of school
• Score <9 if no education
Simmons BB, et al. AAFP, 2011

NEW DEVELOPMENTS IN HYPERTENSION
Eliseo J. Pérez-Stable, MD
Mini-Cog: Three Item Recall and Clock Draw
• Ask the standard orientation questions
• Give three items to learn and repeat right away and then ask for recall after one minute
• Draw a clock
• Validated in multiple languages
• Sensitivity is 76%
• Specificity is 89%
Borson, JAGS, 2003
Definitions of Dementia
Clinical (DSM4) diagnostic criteria Memory impairment AND one or more:
Aphasia: language problems Apraxia: motor problems Agnosia: sensory problems Disturbance in executive functioning
Deficits impair social/occupational function, represent a decline from baseline, not due to delirium
Mild cognitive impairment: impairment does not affect function
Mini-Mental State Exam• Maximum score 30
Score <24 suggests cognitive impairment Decline of 4 points over 1-4 y significant
Scores inversely correlated with age; median score = 25 if age >80
Not as sensitive in people with higher levels of education; median score = 22 if 0-4 yr of educationhttp://www.angelfire.com/retro/michaelpoon168/mini_mental_state_examination_normative%20data.htm
MMSE is proprietaryCrum RM et al. JAMA, 1993;269(18); Holsinger T, et al. JAMA, 2007;297.
Montreal Cognitive Assessment
Maximum score is 30 points
>26 is normal
May be better at diagnosing mild cognitive impairment
Includes executive function testing
Better for use with patients with limited formal education
www.mocatest.org
Not proprietary

NEW DEVELOPMENTS IN HYPERTENSION
Eliseo J. Pérez-Stable, MD
Symptomatic Treatment of Memory Disturbance
Cholinesterase Inhibitors delay degradation of acetylcholine at the synaptic cleft
Indicated for mild-moderate Alzheimer’s
Donepezil (Aricept)--5-10mg/day Rivastigmine (Exelon)--6-12mg/day
Galantamine (Razadyne)--24-32mg/day or patch 4.6-9.5mg
May cause weight loss, nausea, vomiting, diarrhea, vivid dreams, AV Block, bradycardia
Clinical Significance of Long-term Donepezil Treatment
565 patients with mild-mod AD randomly assigned to donepezil 5mg or placebo for 12-week run-in; Followed up to 3 years
End points: Institutionalization or progression of disability (loss of ADLs): No difference in rates by treatment No difference in care costs, unpaid
caregiver time, behavioral/psychological symptoms AD2000 Collaborative Group, Lancet 2004;363.
Exercise and Dementia Prevention
• Meta-analysis: 33,816 non-demented patients followed prospectively
• Participants with high-level physical activity protected against cognitive decline (HR=0.62; 95% CI 0.54-0.7)
• Low-moderate exercise was also protective (HR 0.65; CI 0.57-0.75)
Sofi F et al. J Intern Med, 2011
β-Amyloid 42/40, Cognitive Reserve and Cognitive Decline
Yaffe K, et al. JAMA, 2011;305(3)

NEW DEVELOPMENTS IN HYPERTENSION
Eliseo J. Pérez-Stable, MD
Evaluation of Driving Risk in Dementia – Practice Parameter
• Patient at increased risk for unsafe driving:
– Caregiver rates patient’s driving ability as marginal or unsafe
– Pt has previous accidents or citations
– Pt has reduced driving mileage or self-reported situational avoidance
– MMSE score < 24
– Pt with aggressive/impulsive personality
– Report to DMV Iverson DJ, et al. Neurology, 2010;74.
Urinary Incontinence
70 year-old African American woman, for follow-up of hypertension, obesity, and pre-diabetes. Her weight has remained the same since her last visit 2 months ago. Her current medications are amlodipine and atorvastatin, although she’s been somewhat inconsistent in taking them in the past year. During your initial review of systems, she denies any complaints, but as you prepare to wrap up, she pulls out an authorization form for adult diapers for you to sign. On further questioning, she admits to experiencing involuntary urine leakage at least once or twice a week, for more than 5 years. When you ask her why she never brought this up before, she says, “I did not think there was anything you could do– I just had too many kids, and now I’m getting old.”
Which of the following statements about risk factors for UI in women are true?
(Choose ALL that apply)
A. Although UI can occur in young women, the prevalence of UI increases linearly with age
B. Both vaginal and C-section delivery increase the risk of UI in women
C. Obesity is a risk factor for UI, but weight loss does not usually improve UI
D. Diabetes is associated with an increased risk of UI in women, independent of obesity

NEW DEVELOPMENTS IN HYPERTENSION
Eliseo J. Pérez-Stable, MD
Prevalence of urinary incontinence in women across the age spectrum
Hannestad et al. J Clin Epidemiol, 2000; 53: 1150-1157.
The EPINCONT Study (N=27,000)
Changes in Lower Urinary Tract Function with Aging involuntary bladder muscle
contractions total capacity of the bladder bladder contractility and
urinary flow atrophy of urethral mucosal
epithelium
Over-activity of thedetrusor muscle
Sphincter deficiency &/orpelvic floor weakness
Urge incontinence(leakage from a sudden or
strong urge to urinate)
Stress incontinence(leakage associated with in abdominal pressure)
Pathophysiology of incontinence
Bladder outlet obstruction or detrusor weakness
Overflow incontinence(frequent or constant small-volume urine leakage)
Major mobility or cognitive impairment
Functional incontinence(inability to get to the toilet or recognize the need to void)
Distribution of stress, urge, and mixed UI in women across the age spectrum
Adapted from Hannestad et al. J Clin Epidemiol, 2000
The EPINCONT Study (N=27,000)

NEW DEVELOPMENTS IN HYPERTENSION
Eliseo J. Pérez-Stable, MD
Rortveit G, et al. NEJM. 2003;348:900-907.
Comparison Any UI Moderate or severe UI
C-section vs no delivery
1.7 (1.3-2.1) 1.6 (1.1-2.3)
Vaginal delivery vs no delivery
2.8 (2.5-3.2) 3.3 (2.7-4.0)
Vaginal delivery vs C-section
1.7 (1.2-2.1) 2.2 (1.5-3.1)
Adjusted odds ratios for UI by mode of delivery*
Vaginal and C-section delivery both increase risk of incontinence
*Adjusted for age, parity, years since last delivery, & BMI
Dose-response between body mass index and incontinence risk
Subak L, et al. Journal of Urology 2009; 182: S2-S7.
Any incontinence Severe
The impact of diabetes on urinary incontinence risk in women
• Diabetic women with 28% risk of any UI and 40% risk of severe UI in Nurses Health Study
• Risk of incident UI increased with increasing duration of diabetes
• Adjustment for age, parity, BMI, and medication use did not explain increased risk
• Possible mechanisms– damage to innervation of bladder & urethra, volume of urine
Behavioral treatment for Urgency Incontinence
• Pelvic floor muscle exercises
• Bladder training techniques
• Urge suppression techniques
NEW DEVELOPMENTS IN HYPERTENSION
Eliseo J. Pérez-Stable, MD
Pelvic floor muscle exercises
• Encourage patients to work up to holding contractions for 3+ seconds at a time
• Teach patients to distinguish between pelvic vsabdominal or buttock muscles
• Recommend repetitions on a set schedule (e.g., set of 10, 5 times/day)
Bladder training techniques
• Instruct patients to starting void every hour regardless of need to urinate
• Progressively increase the interval by 30 minute increments to reach 3-4 hours
• Recommend pelvic muscle contractions for urgency between voiding
Urge suppression techniques
When you feel the urge to urinate. . . .
- Stop, sit down, and take deep breaths- Imagine the urge peaking, then subsiding- Practice pelvic floor muscle exercises
Once you feel the urge is under control- Walk slowly to the bathroom and void
The traditional extended evaluation for incontinence in women
Clinical history
Urinalysis test
Voiding diary
Neurologic exam
Pelvic exam
Post void residual
Cough stress test
NEW DEVELOPMENTS IN HYPERTENSION
Eliseo J. Pérez-Stable, MD
Relationship of PVR to urinary symptoms in 1017 older women
Urinary symptom PVR <50
(N = 780)
PVR 50-99
(N = 95)
PVR 100-199
(N = 67)
PVR ≥200
(N = 45)
Urgency UI (weekly)
(N=312)
32% 30%) 25% 47%
Stress UI (weekly)
(N=351)
37% 32% 21% 44%
Daytime frequency
(N=299)
29% 38% 33% 27%
Nocturnal frequency
(N=305)
30% 36% 36% 38%
None of the above
(N=322)
34% 30% 30% 27%
Huang AJ, et al. Journal of the American Geriatrics Society, 2010
The 3 Incontinence Questions (3IQ)1.During the last 3 months, have you leaked urine, even a small amount? a. Yes; No → no further questions.2. During the last 3 months, have you leaked urine: a. When you were performing some physical activity such as coughing, sneezing, lifting or exercise? b. When you had the urge or the feeling that you needed to empty your bladder but you could not get to the toilet fast enough? c. Without any physical activity or a sense of urgency3. During the last 3 months, have you leaked urine most often:a. When you were performing some physical activity such as coughing, sneezing, lifting, or exercise? b. When you had the urge or the feeling that you needed to empty your bladder but you could not get to the toilet fast enough? c. Without any physical activity or without a sense of urgency? d. About equally as often with a physical activity and with urgency?
Diagnostic Aspects of Incontinence Study (DAISy)
Multi-center study of ambulatory women with weekly incontinence (N=301)
Exclusions: self-reported stroke or major neurologic condition, prolapse, urologic surgery
Compared diagnosis by 3IQ+urinalysis versus traditional extended evaluation
3IQ had sensitivity & specificity of 0.75 and 0.77 for urge UI, 0.86 and 0.60 for stress UI
BRIDGES clinical trial
Goal: evaluate efficacy and safety of pharmacologic therapy for urgency UI in women diagnosed by 3IQ
645 ambulatory women identified by the 3IQ randomized to pharmacologic therapy vs placebo
Moderate decrease in incontinence frequency over 12 weeks (average reduction of 1 episode per day)
No serious adverse events associated with pharmacologic therapy in this setting
Huang AJ, et al. American Journal of Obstetrics & Gynecology 2012

NEW DEVELOPMENTS IN HYPERTENSION
Eliseo J. Pérez-Stable, MD
Name Available forms
Instructions for use Cost
Immediate-release
Oxybutynin (Ditropan)
2.5 or 5 mg Start at 2.5 mg (1/2 pill) BIDAdjust to maximum of 5 mg QID
$
Tolterodine (Detrol)
1 or 2 mg Start at 2 mg BID, lower to 1 mg BID if poorly tolerated
$$$
Trospium (Santura)
20 mg Take 20 mg BID, lower to 20 mg QHS if poorly tolerated
$$$
Extended-release
Oxybutynin ER (Ditropan XL)
5, 10, or 15 mg
Start at 5 or 10 mg QD, increase to max of 30 mg QD
$
Tolterodine LA (Detrol LA)
2 or 4 mg Start at 4 mg QD, lower to 2 mg QD if poorly tolerated
$$$
Darifenacin (Enablex)
7.5 or15 mg Start at 7.5 mg QD, wait ≥2 weeks before increasing dose to 15 mg
$$$
Trospium XL (Santura)
60 mg Take 60 mg QD $$$
Solifenacin (Vesicare)
5 or 10 mg Start at 5 mg QD, increase to max of 10 mg QD as tolerated
$$$
Fesoterodine (Toviaz)
4 or 8 mg Start at 4 mg QD, increase to max of 8 mg as tolerated
$$$$
Tips on starting an anti-muscarinic medication for urge incontinence
• Avoid in patients with gastric retention, severely-decreased GI motility
• Contraindicated in narrow-angle glaucoma (consider possibility in elderly, farsighted, Asian)
• Start with a low dose (e.g., ½ pill of oxybutynin 5 mg twice daily), then increase as tolerated
• Discuss strategies for preventing or decreasing side effects (e.g., lozenges)
Risk and Prevention of Falls
Falls Burden in Older Adults
• 15,000 deaths, 475,000 hospitalizations, 1,360,000 ED Visits; Latinos have highest rate of falls
• Serious Falls-related Injuries:
– Hip fractures (55%): 20% mortality at 1 year
– Non-Hip fractures (21%)
– Traumatic Brain Hemorrhage (10%)
– Chest Injury (7%)

NEW DEVELOPMENTS IN HYPERTENSION
Eliseo J. Pérez-Stable, MD
Functional Consequences of Falls
• 60% report moderate activity restriction
• 33% require help with ADLs
• Increases risk of nursing home placement
• One-third develop fear of falling:
– Decreases physical and social activity
– Decreases self-reported health status
– Increased depression
LR of Risk Factors for Future Falls
• Fall in last year: 2.8 - 3.8
• Orthostatic hypotension –
• Visual acuity –2
• Gait and Balance 2
• Medications 1.7
• Assess Cognition 4 - 17
• Limitation in ADLs or IDLs: 2 - 4
Gait and Falls
• Gait abnormalities in 20% to 40% of persons >65 and over 50% if ≥ 85 y
• Gait speed predicts 10-year mortality• Assess normal, safe speed• In office tests: Gait balance test• Learn with physical therapy evaluation• Risk of multiple falls among >64 y from
California Health Interview Survey: Latinos 17%, Blacks 11%, Asians 8%, Whites 12%
Falls Recommendations USPSTF
• Exercise and physical therapy significantly reduces falls; the more the better: RR = 0.85 (0.78-0.92)
• Vitamin D supplementaion without calcium: RR = 0.83 (0.77-0.89)
• Vision correction shows no reduction• Multifactorial intervention seems to
reduce falls but not statistically significant
NEW DEVELOPMENTS IN HYPERTENSION
Eliseo J. Pérez-Stable, MD
Osteoarthritis
Radiographs: Two keys to ordering knee X-rays
• Minimum 2 views of every joint (AP and lateral)
• Knee has 2 articulations: want 2 views of each: 1. Patella – femur 2. Femur- tibia
• Weight-bearing views to evaluate for arthritis
• Arthritis is not painful if it’s not weight-bearing. Reproduce the painful situation to see the degree of cartilage loss.
Radiographic findings in osteoarthritis
1. Joint space narrowing
2. Sub-chondral sclerosis
3. Osteophytosis
4 components of non-operative treatment for knee osteoarthritis
• Patient education• Modules on exercise, healthy eating,
medications, surgical treatment• Identify goals and action plans Moderate
effect size on pain relief• Exercise: low-impact aerobic ––
significant pain relief• Weight loss: 5% body weight significant
functional improvement, unclear effect on pain

NEW DEVELOPMENTS IN HYPERTENSION
Eliseo J. Pérez-Stable, MD
Acupuncture in Treatment of Neck and Knee Pain
Mechanical Neck Pain• RCT in UK, 135 pts
age 18 to 80• Outcome: Pain 1 week
after treatment (visual analog)
• 8 sessions• 12% (3%-21%) better• 1 practitioner• Clinical significance?
AIM 2004; 141:911-919
• OA Knee• RCT, 570 pts age 65• 23 sessions; 26 wks• Pain and function
scores, SF-36, 6’-walk• Pain: –2.5 (–4.7 - –0.4)
at 26 wks• drop out in controls• Benefit shown–useful
adjunctive therapyAIM 2004; 141: 901-910
Medications for OA Pain control
• Glucosamine• APAP (≤ 3 g/day) or NSAID unless
contraindication • Significant reduction in pain compared to placebo• NSAIDs more effective than APAP but higher GI
risk –– Consider topical NSAIDs• Steroid injection: Significant short-term pain
relief for at least 3 weeks; No effect on function Max 4/year due to concern about cartilage
• Visco-supplementation: Evidence limited by publication bias; May provide longer term pain relief (5-13 weeks)

Page 1
Vitamins and Supplementsin Women’s Health
An Evidence-Based Approach
Jeffrey A. Tice, MD
Division of General Internal MedicineUniversity of California, San Francisco I HAVE NO CONFLICTS OF INTEREST
Nutrition in a Bottle?
?

Page 2
Vitamins / supplements to be covered
• Antioxidants
– Beta-carotene / Vitamin A
– Vitamin E
– Vitamin C
• Folic acid / B-vitamins and homocysteine lowering
• Vitamin D / Calcium
• Omega – 3 polyunsaturated fatty acids
What percentage of Americans regularly use vitamin supplements?
• 0 to 20%
• 21 to 40%
• 41 to 60%
• 61 to 80%
• 81 to 100%
Vitamin Use in the U.S.A.
• 52% of Americans and increasing
– More than doubled since 1970s
• $9.4 billion in 2009
• Reports from observational studies of diet are very popular with patients and are always in the news
Why are they so popular?
• Diseases of deficiency
– Vitamin C: Scurvy
– Vitamin D: Rickets
– Thiamine (B1): Beriberi
• More is better philosophy in America
– Super-size me!
• Self-efficacy / prevention / wellness
Page 3
Guiding Principle: Primum non nocere
When recommending a therapy to an otherwise healthy person (i.e. for disease prevention / wellness), you should have the highest level of evidence guiding your recommendation: randomized trials with patient-centered outcomes.
Why antioxidants?
• Laboratory and animal research show that antioxidants prevent the free radical damage that is associated with cancer, heart disease, and aging
• Antioxidants are provided by a healthy diet that includes a variety of fruits and vegetables
• Vitamins A, C, E, beta-carotene
ß Carotene and RetinolEfficacy Trial (CARET)
• Subjects
–18,314 smokers, former smokers, asbestos
–Age 45 - 74, mean 58. 34% women
–Enrolled 1985, Seattle
• Follow-up 4 years
• RCT ß-carotene 30 mg, Vit A 25000 IU
• Outcome: Lung CA, Death, CVD death
CARET Randomized Trial Results
> 18,000 participants followed for 4+ years on beta-carotene or placebo
Omenn, NEJM, 1996

Page 4
Vitamin E
• Factor X: a group of fat soluble compounds, the tocopherols
• Deficiency: Rare
• They are the primary fat soluble anti-oxidants
• US RDA 22 IU in men and women
Nurses’ Health Study (NHS)
• Subjects
–87,245 US Female Nurses
–No CHD, Stroke or Cancer
• Follow-up 8 years
• Outcome: Non fatal MI, CHD Death
Stampfer, NEJM, 1993
NHS Results for MI or CHD Death
Quintiles of Vitamin E Intake
1st 2nd 3rd 4th 5th
IU/d 2.8 4.2 5.9 17 208
RR 1.0 1.0 1.1 .74 .66
More is better: p-value for trend = 0.001
Stampfer, NEJM, 1993
Women’s Health Study
• 40,000 healthy women at least 45 years old
• 10+ years of follow-up
• Vitamin E 600 IU every other day
– No effect on cancer (RR 1.01)
– No significant benefit for major CVD events
Lee, JAMA, 2005.
Page 5
The answer!
• Meta-analysis of 47 high quality randomized trials of antioxidants
• 181,000 individuals
• 25,000 deaths
Bjelakovic, JAMA, 2007.
Death from any cause
• Vitamin A 16% increase
• Beta-carotene 7% increase
• Vitamin E 4% increase
• Vitamin C Trend towards increase (6%)
All p << 0.05 except vitamin C
Bottom line: actively discourage anti-oxidant useBjelakovic, JAMA, 2007.
Why?
• Postulated benefits of controlled oxidative damage (free radicals)
– Kill bacteria
– Eliminate damaged cells
Vitamin C…Brrrrr
• Marathon runners, skiers, soldiers on sub-arctic exercises
– 50% reduction in the incidence of colds
• General public
– No reduction in incidence
– 10% reduction in duration
Hemila, Chalker. Cochrane review, 2012.
Page 6
Vitamins, Homocysteine, and Heart Disease
Homocystinuria
• In-born error of metabolism (1962)
• Homocysteine levels in the blood: 100-400 µmol/L
• Normal homocysteine 8 to 12 µmol/L
• 1 in 150,000 live births
Homocystinuria: Clinical Features
• Premature cardiovascular disease
– 50% experience major event by age 30 years
• Connective tissue defects
– Osteoporosis
– Lens dislocation
• Cognitive deficits
Homocysteine and Risk of Death
Homocysteine RR
< 9 1.0
9-14.9 3.3
15-19.9 6.3
≥ 20 9.9 p<0.001
Nygard, NEJM, 1997

Page 7
Vitamins To Lower Homocysteine
• > 40 Randomized Clinical Trials
• Folic acid lowers homocysteine 25%
• Vitamin B12 lowers it an additional 7%
The Answer!
• Pooled meta-analysis of 8 large, high quality randomized trials
• 37,485 individuals
• 5,125 deaths
• 9,326 major vascular events
• 3,010 cancers
Clarke, Archives IM, 2010.
Folate / Homocysteine RCTs
• Homocysteine 25% decrease
• Death No effect: 1.02 (.97-1.08)
• CVD events No effect: 1.01 (.97-1.05)
• Cancer No effect: 1.05 (.98-1.13)
Folate does not prevent cancer or heart disease
Clarke, Archives IM, 2010.
Folate And Neural Tube Defects (NTD)
• 70% reduction in 2nd occurences
– 4 mg of folate
• 63% reduction in 1st occurrence
– 0.4 mg of folate
• Since flour fortification
– 46% reduction in NTD Meta-analysis, Blencowe, IJE, 2010.
Page 8
MULTIVITAMINSIn the news
Multivitamins…kill?
• Iowa Women’s Study
–38,772 women ages 55-69 followed 19 years
–MVI: RR death 1.06 (1.02-1.10)
–2.4% absolute increase in mortality• NNH = 42
–Observational!
Mursu, Archives IM, 2011
TO D OR NOT TO D...?That is the question!
Nutrient of the year!The sun is rising on Vitamin D
Sales increased 82% from 2008 to 2009

Page 9
Vitamin D
• Vitamin: prevents rickets in children
• Hormone: 1,25 dihydroxy-vitamin D
– Intestinal and renal absorption of calcium, phosphate
– Lowers PTH, prevents secondary hyperPTH
– Neuromuscular function
– Regulation of up to 10% of the human genome
Institute of Medicine Report
Panel reviewed 1000 studies on 25 health outcomes to updateprevious 1997 recommendations
Vitamin D:Adult Dietary Reference Intake* (U.S.)
• Age
• 1-70 years 600 IU / day
• > 70 years 800 IU / day
*Institute of Medicine, 2010: Sufficient to meet the needs of virtually all people.
Vitamin D Status: Levels of 25(OH)D
ng/mL nmol/L
Deficient < 12 < 30
Insufficient 12 – 20 30 - 50
Sufficient ≥ 20 ≥ 50
Potentially harmful ≥ 50 ≥ 125
(hypercalcemia, hyperphosphatemia)
1 ng/mL = 2.5 nmol/L

Page 10
Vitamin D levels in Americans
Prevalence of inadequate 25(OH) vitamin D among American women ≥14 years old by IOM definitions
< 12 ng/ml 10 to 12% At risk of deficiency
< 20 ng/ml 34 to 39% At risk of inadequacy
< 30 ng/ml ~80%
NHANES 2003-2006
Why so little D?
Vitamin D and Sunlight
• Most of the world relies on natural exposure to sunlight to maintain adequate levels
• Sunscreens of > 8 SPF can prevent synthesis
• Smog, smoke, window glass, even window screens can reduce synthesis
Sources of Vitamin D
400 IU/ tsp 100 IU/ 8 fl oz 20 IU/ egg yolk
400 IU/3oz 90 IU/ 8 fl oz 2700 IU/ serving
Treatment Of Low Vitamin D
• At risk for Deficiency (< 12 ng/ml)
– 50,000 IU of Vitamin D2 or D3 per week for 6-8 weeks and then 800-1000 IU per day
• Nutritional Insufficiency (< 20 ng/ml)
– 800-1000 IU per day
– Goal will be reached in 3 months
• Monitor at 3 months
• Tolerable upper limit for Vitamin D is 4000 units per day per IOM.
Page 11
Vitamin D supplements: Two forms
• Vitamin D2: ergocalciferol
• (milk fortification, U.S. supplements, plants)
• Vitamin D3: cholecalciferol
• (“natural”: sunlight, fatty fish)
Should we be recommending supplementsfor prevention?
Systematic Review for fracture prevention: Conflicting Results
• 25 RCTs of vitamin D with fracture outcomes
• Heterogeneity: Population
– Average age 53 to 85 years
– Nursing homes versus community
– Prior hip fracture versus no prior fractures
• Heterogeneity: Treatment
– 300 to 500,000 IU D2 or D3
– Daily to annually
– With or without calcium
Best Early Trial: Benefit!
• Chapuy NEJM 2002
– 3270 women in 180 nursing homes in France
– Daily 800 IU D3 + 1200 mg calcium versus placebo
– Hip fractures
• 5% versus 7%, p = 0.004
– Non-vertebral fracture
• 10% versus 13%, p < 0.001
Most Recent Trial: Harm!
• Sanders JAMA 2010: The VITAL D trial
– 2256 women ≥ 70 years in Australia with risk factors for hip fracture
– Annual 500,000 IU D3 without calcium. (~1400 IU/d)
– Falls: 15% increase with vitamin D (p = 0.03)
– Fractures: 26% increase (p = 0.047)
Page 12
Why The Variation?
• Significant contributors
– Calcium supplementation with vitamin D
• Not significant
– Age, sex, baseline vitamin D level
– Vitamin D type, dose, frequency
– Calcium for control group
** Note: All of the studies that included calcium
used daily dosing of vitamin D
Vitamin D and Fractures
• Daily vitamin D plus calcium reduces fracture risk
– 18% for hip fractures
– 14% for all fractures
• Greater absolute benefit in high risk groups
– Age > 70 years
– Prior fracture
– Low baseline intake
• Harms are uncommon, though recent concerns about calcium supplementation and heart disease
Harms of Vitamin D ± Calcium
• Slight excess of hypercalcemia, constipation
– Approximately 1% more in vitamin D group
• Significant increase in kidney stones over 7 years
– 2.5% versus 2.1% (HR 1.17, 95% CI 1.02 to 1.34) in WHI
• Non-significant trend towards fewer deaths
– In WHI: 63 fewer deaths, 68 more kidney stones
Vitamin D: The New Panacea
• Reduces the following diseases...
– Cancer (Colon, Breast, Prostate, Pancreatic, ...)
– Cardiovascular disease
– Multiple sclerosis, Type 1 DM, RA
– Influenza and URIs
– Chronic pain
– Total Mortality!

Page 13
Melamed, M. L. et al. Arch Intern Med 2008;168:1629-1637.
Serum 25-hydroxyvitamin D and all-cause mortality in13,331 NHANES 3 participants
Meta-analysis of D and Total Mortality
• 24 randomized trials, n = 88,097
– 87% female
– Median age 70
• Vitamin D alone did not affect mortality
• Vitamin D + calcium reduced total mortality 9% (95% CI 2% to 16%)
• NNT = 151 over 3 yearsRejnmark, JCEM, August 2012
Copyright restrictions may apply.
Ginde, A. A. et al. Arch Intern Med 2009;169:384-390.
Upper Respiratory Tract Infection By Serum 25-hydroxyvitamin D Level And Season
RCT: VIDARIS Trial, JAMA, October 2012
• 322 healthy adults in New Zealand
• 100,000 IU D3 monthly
• 18 months follow-up
25(OH) D URI incidence
Vitamin D 48 ng/mL 3.7 infections/person
Placebo 25 ng/mL 3.7 infections/person
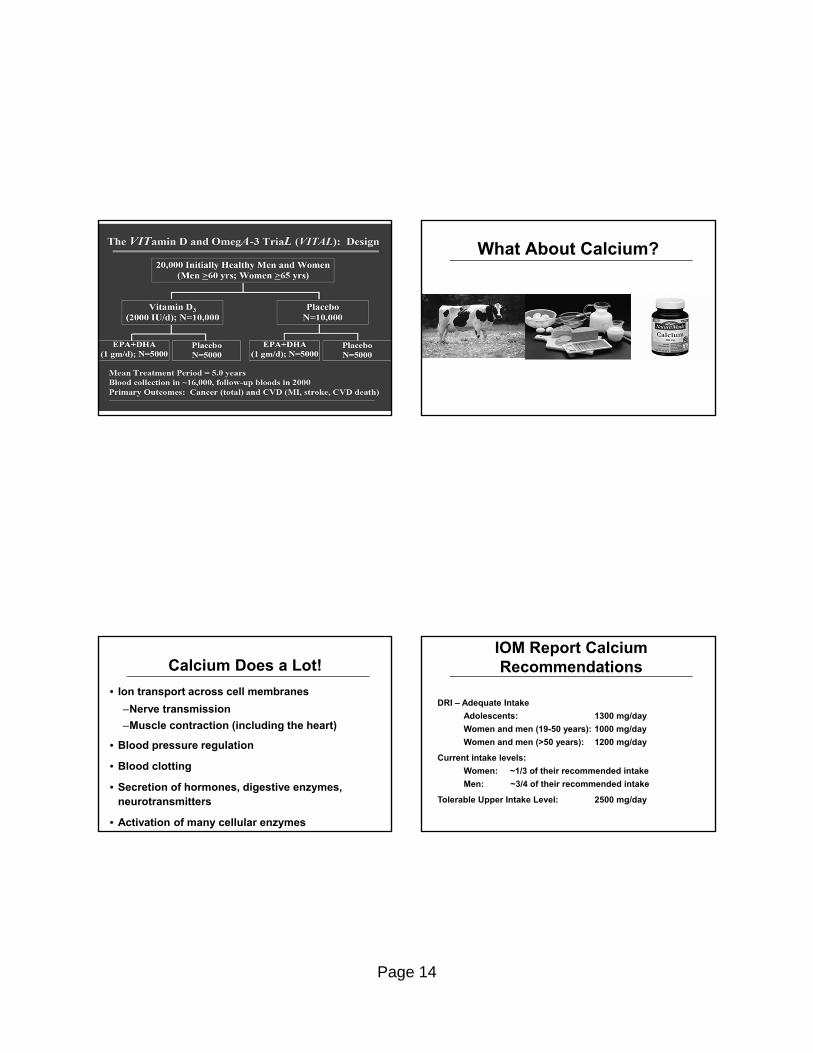
Page 14
What About Calcium?
Calcium Does a Lot!
• Ion transport across cell membranes
–Nerve transmission
–Muscle contraction (including the heart)
• Blood pressure regulation
• Blood clotting
• Secretion of hormones, digestive enzymes, neurotransmitters
• Activation of many cellular enzymes
IOM Report Calcium Recommendations
DRI – Adequate Intake
Adolescents: 1300 mg/day
Women and men (19-50 years): 1000 mg/day
Women and men (>50 years): 1200 mg/day
Current intake levels:
Women: ~1/3 of their recommended intake
Men: ~3/4 of their recommended intake
Tolerable Upper Intake Level: 2500 mg/day

Page 15
Yet Another Caveat
• 1000 mg calcium supplement may be too much: 24% increase MI (p=.004), 15% increase MI or Stroke (p=.009)
Vitamin D and Calcium Take Home Points
• Vitamin D insufficiency is common
• 25 OH vitamin D is a predictor of bone health in terms of fracture risk and risk of falls
• Target frail, older patients
• 800 IU of vitamin D3 per day is sufficient
– Ensure adequate calcium intake
• Testing is expensive and unnecessary
• Evidence is weak for other diseases
OMEGA 3 FATTY ACIDSA fishy story…
Epidemiology
• Sinclair 1944: CHD rare in Greenland Eskimos despite a high fat diet with few vegetables, fruits, or complex carbohydrates
Page 16
Omega-3 Fatty Acids: Observations
• Oily, cold water fish = best sources of Ω-3 fatty acids–EPA = eicosapentanoic acid–DHA = docosahexanoic acid
• People who consume fish rich in EPA and DHA have fewer fatal and non fatal CV events
• 1-2 servings/week fish associated with 36% less risk of CV death and 17% less total mortality
How Much Should I Consume?
American Heart Association 2003 Guidelines
• Healthy people:
–At least 2 servings of fish/week AND plant-based sources of Ω-3’s
• People with CAD:
–1 gram of EPA + DHA/day
Randomized trials of Ω-3s in heart disease
• GISSI-Prevention: Lancet 1999
– 11,323 patients within 3 months of MI
– 1 gram EPA + DHA
– 21% reduction total mortality
– 45% reduction in sudden death
• 2010: 5 studies. NEJM, Circ, JAMA, BMJ
– Not even a trend towards benefit for post-MI, CVD or atrial fibrillation
• Intubated with acute lung injury: JAMA 2011
– Harm: 3 extra days in ICU, trend - more death (p=0.054)
2012 Meta-analysis of RCTs
• 14 RCTs: 20,485 patients with CVD
• 0.4 to 4.8 g/day omega-3 fatty acids
• 1-5 years of follow-up, mean 2 years
• No significant reduction in
– All-cause mortality
– Sudden cardiac death
– Major cardiovascular events
Kwak, Archives IM, 2012

Page 17
Since meta-analysis
• ORIGIN trial: RCT in NEJM 6/11/12
– 12,536 patients with DM or high sugar
– 1 g daily of omega-3 x 6.2 years
– NO reduction in death, CVD events
• Risk and Prevention Trial: NEJM May 2013
– 12,513 patients at high risk for CVD
– 1 g daily of omega-3 x 5 years
– NO reduction in death, CVD events
Summary Omega-3 FA / Fish oil
• No benefit in modern era of medical therapy for vascular disease
• No significant harms: trend towards fewer deaths in most trials
We Evolved to Eat REAL Food
• When nutrients are isolated from whole foods, they don’t always act the same
≠
Dietary studies: Randomized
• RCT Mediterranean diet vs. low fat
– Spain, 7500 people, 5 years FU
– Enriched for olive oil or nuts
– 30% reduction in CVD events
• Recommend: fruits, vegetables, legumes, tomato sauce, fish, wine
• Discourage: sodas, sweets, pastries, red and processed meats.
Estruch, NEJM, 2013
Page 18
Dietary studies: Observational
• Adventist Health Study 2
–73,000 participants; 2570 deaths
–5.8 years follow-up
• Compare: vegans, pesco-; lacto-ovo-; and semi-vegetarians to non-vegetariants
• Outcome: lowest mortality in pesco-vegetarians and vegans (15-20%).
Orlich, JAMA IM, 2013
Summary
• Beta-carotene Discourage - harmful
• Vitamin E Discourage - harmful
• Folate For child-bearing age to prevent neural tube defects
• Vit D + calcium Older, frail patients to prevent fractures & falls
• Omega-3s No benefit
Michael Pollan’s Recommendations
• Eat real food
• Not too much
• Mostly plants
• Some fish
QUESTIONS?Thank you!
Page 19
If I Decide to Take a Supplement,How Can I Find a Quality Product?
Use Information from Independent Testing Laboratories
• ConsumerLab.com
Look for a “Seal of Approval” Learn As Much As You Can
• Office of Dietary Supplements http://ods.od.nih.gov
• Medline: CAM on PubMed
• Natural Standard database ($)
www.naturalstandard.com

Page 20
The final word
“Vitamins taken in excess of the dose required to prevent deficiency states have not improved our patients’ health and may harm them. We should recommend therapies to prevent disease in healthy patients only when randomized trials unequivocally demonstrate that net benefits outweigh net harms, and we should continue to emphasize the importance of a nutritious diet, regular physical activity, and no smoking as the best ways to optimize health.”
Tice, JA. Archives IM, 2010.
Observational studies: Healthy user effect
• Vitamin supplement users have healthier lifestyles:
– More educated
– More physically active
– More likely to eat a healthy diet
– Thinner
– Less likely to smoke
– Less likely to have diabetes
– Have lower blood pressure
Page 1
New Developments in Osteoporosis
Eliseo J. Pérez-Stable MDProfessor of Medicine
Division of General Internal MedicineDepartment of Medicine
July 4, 2013
Declaration of full disclosure: No conflict of interest
What’s New in Osteoporosis
• Absolute risk
• Under-recognition
• Poor medication adherence
• When to stop bisphosphonates
• New treatments
55 year old woman for routine visit, what do you ask and do about bone health?
A) Screening DxA of hip and spine
B) Screening DxA of hip only
C) Recommend calcium and vitamin D supplements
D) Ask about family history, alcohol, smoking, get BMI and check Vitamin D
E) Defer until age 60 or 65
What Would You Do? Mrs. C…
• 66 WF recently moved to Switzerland. No previous fracture. Sister had breast cancer, 3 drinks/d, healthy. No meds. Exam normal.
• About 5’7” and weighs 130
• Hip BMD T-score -2.2
• No contraindication to treatment
• What tests would you order? How would you manage her?

Page 2
Osteoporosis in a Nutshell
• What is it?
• Risk factors
• Evaluation
• Treatments–Efficacy of available agents–New side effects and clinical
implications
What is Osteoporosis?
• In adults, bone is constantly removed and replaced
• Osteoporosis is loss of mineral and structural integrity with resulting fragility
• Fractures common in older individuals
What About Trauma?
• Even non-osteoporotic bone will fracture with extreme trauma
• There is no threshold for skeletal fragility
• The weaker the bone the less trauma required to fracture…
Traditional Risk Factors for Fracture
• The Big Three: Older age, Postmenopausal woman, and Caucasian/East Asian race
• Other important risk factors- Family history of fracture- Low body weight (<127 lbs. in women) - Smoker, >3 drinks/d- Certain drugs (steroids, PPIs) and diseases- Previous fracture (especially hip or spine)
• Measurement of bone mineral density (BMD) strongly predicts fracture
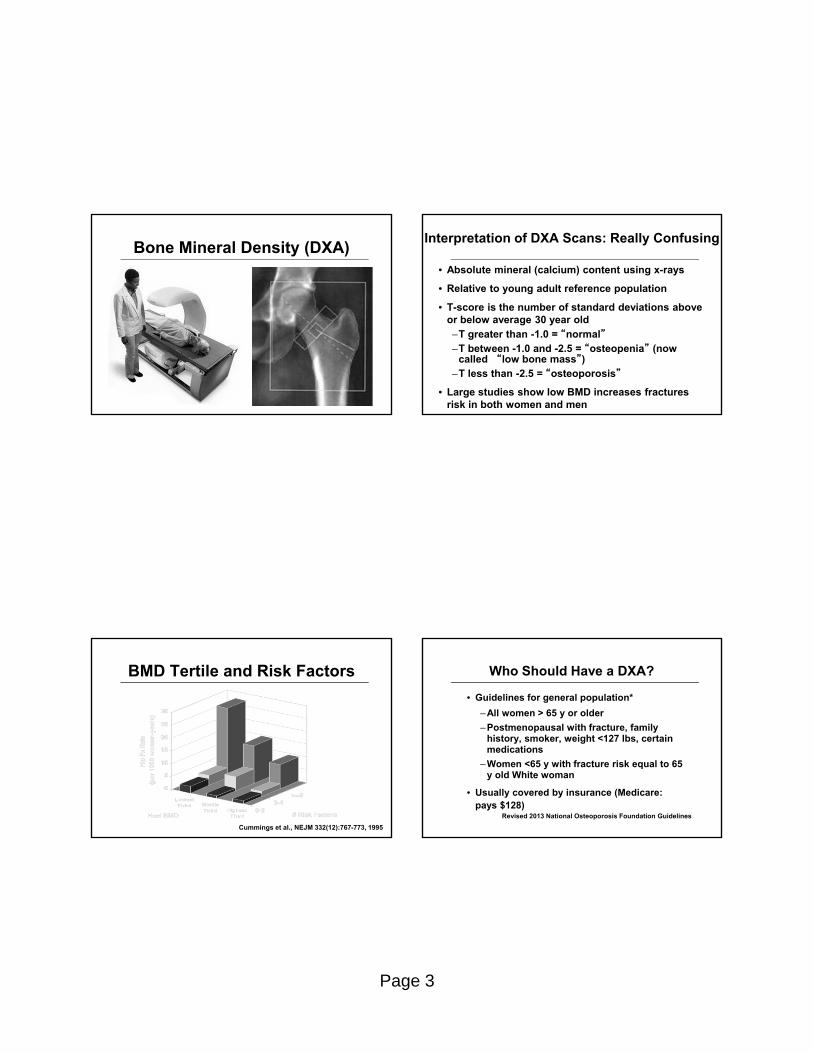
Page 3
Bone Mineral Density (DXA)Interpretation of DXA Scans: Really Confusing
• Absolute mineral (calcium) content using x-rays
• Relative to young adult reference population
• T-score is the number of standard deviations above or below average 30 year old–T greater than -1.0 = “normal”–T between -1.0 and -2.5 = “osteopenia” (now
called “low bone mass”)–T less than -2.5 = “osteoporosis”
• Large studies show low BMD increases fractures risk in both women and men
BMD Tertile and Risk Factors
Cummings et al., NEJM 332(12):767-773, 1995
Who Should Have a DXA?
• Guidelines for general population*
–All women > 65 y or older
–Postmenopausal with fracture, family history, smoker, weight <127 lbs, certain medications
–Women <65 y with fracture risk equal to 65 y old White woman
• Usually covered by insurance (Medicare: pays $128)
Revised 2013 National Osteoporosis Foundation Guidelines
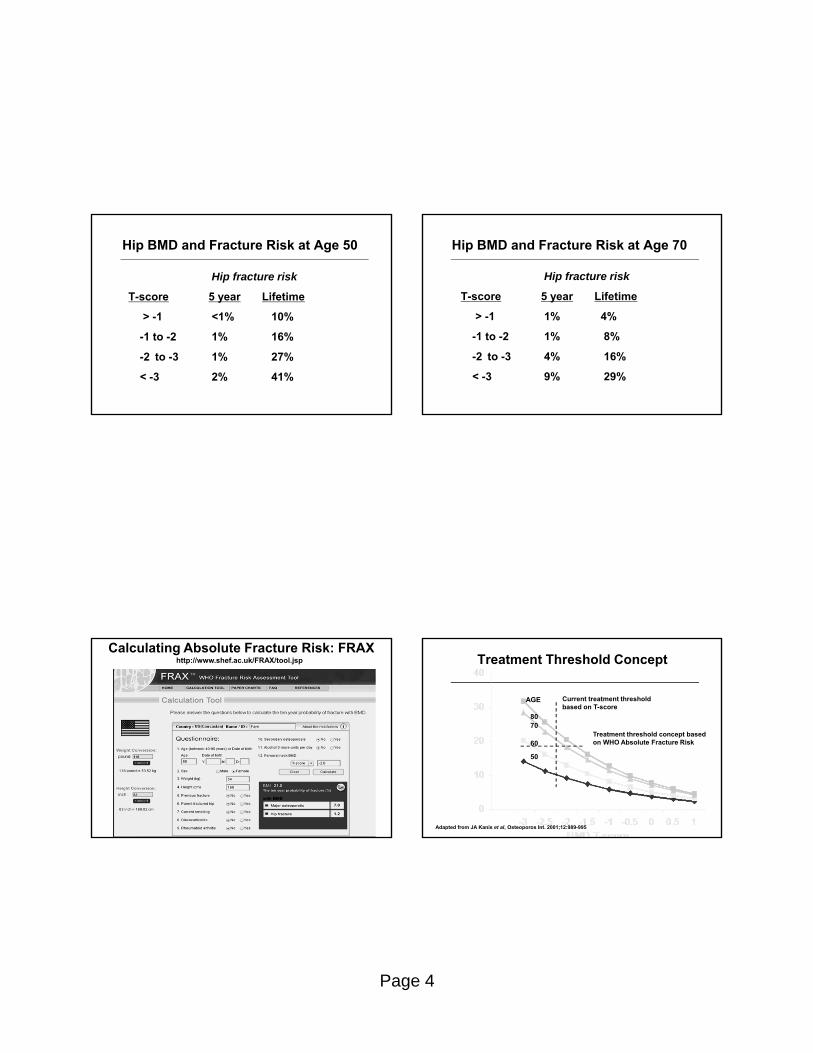
Page 4
Hip BMD and Fracture Risk at Age 50
Hip fracture risk
T-score 5 year Lifetime
> -1 <1% 10%
-1 to -2 1% 16%
-2 to -3 1% 27%
< -3 2% 41%
Hip BMD and Fracture Risk at Age 70
Hip fracture risk
T-score 5 year Lifetime
> -1 1% 4%
-1 to -2 1% 8%
-2 to -3 4% 16%
< -3 9% 29%
http://www.shef.ac.uk/FRAX/tool.jsp
Calculating Absolute Fracture Risk: FRAXTreatment Threshold Concept
80
AGE
70
60
50
Current treatment threshold based on T-score
Treatment threshold concept based on WHO Absolute Fracture Risk
Adapted from JA Kanis et al, Osteoporos Int. 2001;12:989-995

Page 5
What About Interval Screening?
• Recommendations of q 2 y as interval to measure change
• No evidence based guidelines
• 4597 women in Study of Osteoporosis Fractures: BMD baseline, 2, 6, 10, 16 y
• Estimated interval to transition from normal to low bone mass, to osteoporosis
Risk of Osteoporosis in 15 years by BMD Result at Age 65 (NEJM 2012; 366: 225-33)
BMD ResultFemoral Neck
Risk of Osteoporosis
Time to 10% BMD <–2.5
Normal > –1.0
0.8% 16.8 y
Mild OsteopeniaT = –1.01 to –1.49
4.6% 17.3 y
Moderate OsteopeniaT = –1.50 to –1.99
20.9% 4.7 y
Advanced OsteopeniaT = –2.00 to –2.49
62.3% 1.1 y
Implications for Screening
• BMD results of more than –1.49 at age 65 can defer repeat screening to age 80
• BMD results of–1.50 to –1.99 at age 65 can merits repeat screening BMD at 5 years
• BMD results –2.00 to –2.49 may need rescreening at 2 years
• Caution: 49% original SOF sample had osteoporosis
Gourlay ML, et al. NEJM 2012; 366: 225-33
Under Recognition of Osteoporosis
• Among women with fracture or BMD T < –2.5 only 20-30% are evaluated and treated!
• 12 months after hip fracture at the VA: 2% had DXA, 15% treated with appropriate drug
• Implications for providers: Ask about fracture history, note vertebral fractures, use chart reminders for DXA
Soloman, Mayo Clin Proc, 2005Shibli-Rahhal, Osteo Internat, 2011
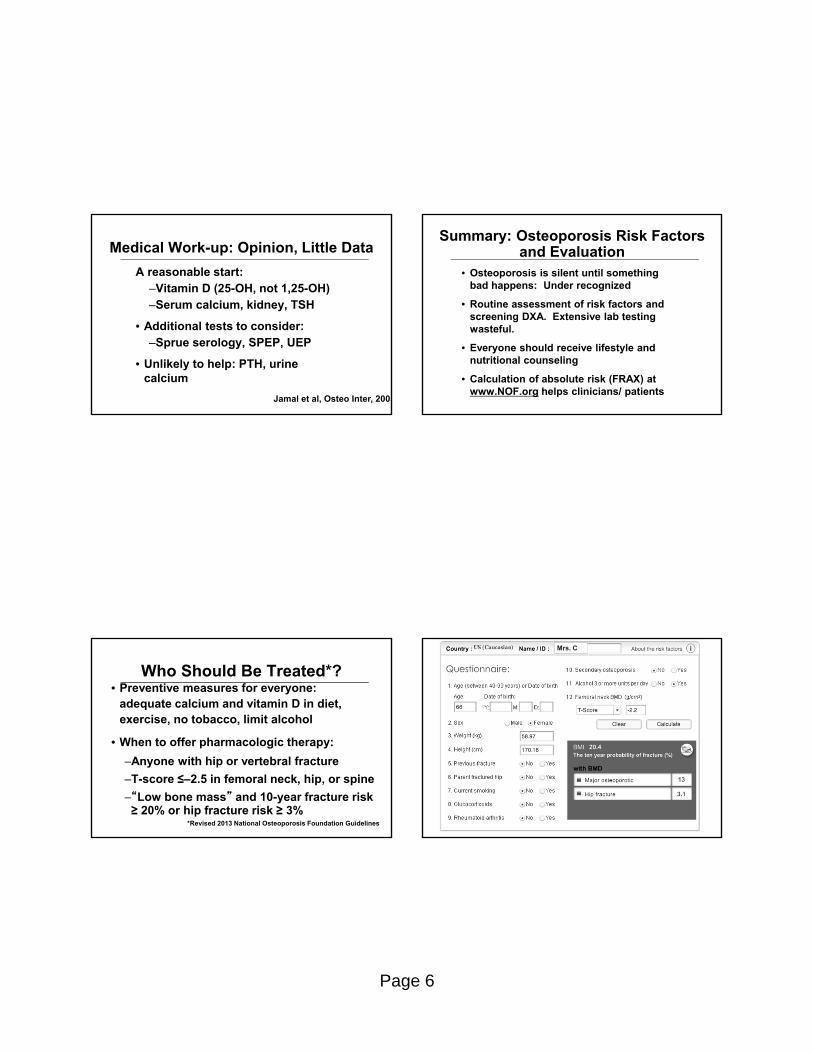
Page 6
Medical Work-up: Opinion, Little Data
A reasonable start:–Vitamin D (25-OH, not 1,25-OH) –Serum calcium, kidney, TSH
• Additional tests to consider:–Sprue serology, SPEP, UEP
• Unlikely to help: PTH, urine calcium
Jamal et al, Osteo Inter, 2005
Summary: Osteoporosis Risk Factors and Evaluation
• Osteoporosis is silent until something bad happens: Under recognized
• Routine assessment of risk factors and screening DXA. Extensive lab testing wasteful.
• Everyone should receive lifestyle and nutritional counseling
• Calculation of absolute risk (FRAX) at www.NOF.org helps clinicians/ patients
Who Should Be Treated*?• Preventive measures for everyone:
adequate calcium and vitamin D in diet, exercise, no tobacco, limit alcohol
• When to offer pharmacologic therapy:
–Anyone with hip or vertebral fracture
–T-score ≤–2.5 in femoral neck, hip, or spine
–“Low bone mass” and 10-year fracture risk ≥ 20% or hip fracture risk ≥ 3%
*Revised 2013 National Osteoporosis Foundation Guidelines
Mrs. C

Page 7
What Can Be Done To Prevent Osteoporosis?Non-pharmacologic Interventions
• Smoking cessation, avoid alcohol abuse
• Physical activity: modest transient effect on BMD but reduces fracture risk
• Conflicting data on hip protector pads (adherence is big problem)
• Calcium and vitamin D
Calcium and Vitamin D
• Chapuy, 1992– Elderly women in long-
term care– 30% decrease in hip
fracture
• Porthouse, 2005:
– Independent women >70 with 1+ risk factor
– No benefit on hip or other fractures
Chapuy, NEJM, 1992
• Pooled studies: 12% fewer fractures together, little benefit alone
News Flash: Calcium Kills!!!
• Pooled 15 calcium trials: cardiovascular events up 30% – Not 1° endpoint; trials with vitamin D excluded– Calcium + vitamin D in WHI did not increase risk
• Pool calcium + D trials? Similar but only after excluding those taking personal calcium supplements in WHI
• Little supporting scientific data – No effect on other surrogates (coronary calcium on CT)– Dietary calcium not implicated in German study
• The weight of the evidence is insufficient to conclude that calcium supplements cause adverse CV events
Bolland, BMJ, 2010, 2011Bockman, ASBMR, 2010

Page 8
How Much Is Enough for Skeletal Health? The Institute of Medicine
• Calcium– 1200 mg/d for women >50, men >70
• Vitamin D–Recommends daily intake 600-800 IU/d,
no more than 4,000/d–Recommends serum levels 20-50 ng/ml–Non-skeletal benefits not established,
harms minimized
IOM Report, 2010
US Preventive Task Force Recommendations
• Insufficient evidence to assess risks/benefits for daily supplementation with calcium >1000 mg/d and vitamin D3 400 IU
• Recommends against daily supplements of Vitamin D 400 IU or less and calcium 1000 mg or less to prevent fractures
• Vitamin D supplements effective in preventing fractures in ≥65 y at risk of falls
Moyer VA, USPTF, Ann Intern Med 2013; 691-6
Bisphosphonates• Bind to bone and prevent absorption and remodeling
–Resides in bone for decades
• Four approved agents: alendronate, risedronate, ibandronate, and zoledronic acid– No head-to-head fracture studies
• What we know: fracture risk reduced 30-50% if – Existing vertebral fracture OR– Low BMD (T-score < -2.5)
• May not be as useful if higher BMD (“osteopenia”)
Effect of Alendronate on Non-spine Fracture Depends on Baseline BMD
Baseline hip BMD
Overall
T < -2.5
T -2.0 – -2.5
T -1.5 – -2.0
0.1 1 10Relative Hazard (± 95% CI)
0.86 (0.73, 1.01)
0.69 (0.53, 0.88)
0.97 (0.72, 1.29)
1.06 (0.77, 1.46)
Cummings, Jama, 1998
Page 9
Risedronate HIP Study: Two Groups
Group 1
• 5445 age <80; hip BMD T-score < -3.0
• 39% decreased hip fracture risk
Group 2
• 3886 age >80; risk factors for hip fx
• No significant effect on hip fracture riskMcClung, NEJM, 2001
Adherence with Bisphosphonates is Poor
• Burdensome oral administration (fasting, remain upright for 30 minutes)
• Upset stomach and heartburn can occur
• 50-60% persistence after one year with daily dosing–Similar to other preventative tx–Multiple practice settings
• Likely better with weekly, monthly and yearly (intravenous) administration
Bisphosponates Once-a-week
• Identical effects on BMD
• Possibly fewer effects on esophagus
• No fracture trials
Schnitzer, Aging, 20
Alendronate: Daily vs. WeeklyAlendronate: Daily vs. Weekly
Does Dosing Interval Matter?
• Poor quality data:– Daily to weekly may improve compliance– Weekly to monthly may not
• Yearly dosing now available: zolendronate–Extremely potent bisphosphonate–3 year, multicenter controlled trial–7741 women 55-89, T-score <-2.5 or < -1
+ vertebral fracture–Zolendronate 5mg IV once/yr vs. placebo
Black et al, NEJM, 2007

Page 10
A New Side Effect of Potent Bisphosphonates? Osteonecrosis of the Jaw
• Associated with potent bisphosphonate use:
–94% treated with IV bisphosphonates
–4% of cases have OP, most have cancer
–60% caused by tooth extraction. Other risk factors unknown. Infection?
• Key points: extremely rare, early identification, conservative treatment
• Dental exam recommended before Rx, but no need to stop for dental procedures
Atypical Subtrochanteric Fractures?
• Rare case reports in long-term bisphosphonate users (and others)
• Transverse not spiral, cortical thickening, minimal trauma
• Often bilateral, preceding pain, abnormal x-ray or bone scan
• ASBMR Task Force (2011)
“Causation not established”“Risk factors uncertain”“Mechanism unknown”
How Long to Use Bisphosphonates?
• Prolonged use (decades) common
• Long half-life suggests that life-long treatment is not always necessary
• What happens when you stop?
• FIT Long-term Extension (FLEX) study– Women given ALN in FIT for 5 yr.– Randomized to ALN or PBO for 5 yr.
Black; Jama, 2006
Page 11
FLEX Change in Hip BMD: % Change from FIT Baseline
= Placebo= ALN (Pooled 5 mg and 10 mg groups)
0
1
2
3
4
5
6
F 0 F 1 F 2 F 3 F 4 FL 0 FL 1 FL 2 FL 3 FL 4 FL 5
Mea
n P
erc
ent
Ch
ang
e
Year
2%
Start of FLEX
P<0.001 ALN vs PBO
FIT FLEX
New Fractures During FLEX
ALN (N = 662) RR (95% CI)
3%
19%
2%
1.1 (0.5, 2.3)
1.0 (0.8, 1.4)
0.5 (0.2, 0.8)
3%Hip
20%Any
5%
PBO (N = 437)
10% 0.9 (0.6, 1.2)11%Any
Vertebral
Non-spine
Painful
FDA View of Long-term Bisphosphonate Use (Sept. 2011)
• Independent review of epidemiologic studies to date and all bisphosphonate trial data…
• After 5 years of treatment, fracture benefit less certain
• Regarding side effects
–Atypical fractures: “conflicting results…causality uncertain” “no agreement on effects of duration or cumulative dose”
–ONJ: “some evidence that risk increases after 4 yr.” “causality not established”
Discontinuation of Bisphosphonates After 3-5 Years?
• NOF recommendation for clinical reassessment after 3-5 years of use
• Driven by lack of non-spine fracture benefit after 5 yr and accumulating evidence of harm even if small risk
• No pharmacologic therapy should be considered indefinite
• Decisions need to be individualized

Page 12
Implications of Bisphosphonate Trials
• Bisphosphonates reduce risk of spine, hip and non-spine fracture in women with existing spine fracture or low BMD (T-score < -2.5)
• May not reduce risk of non-spine fracture in women without spine fracture or BMD < -2.5, even if at high risk.
• Intermittent dosing, even yearly, effective
• Best data of any approved treatment
• After 5 years of treatment, some may stop–BMD >-2.5 and no hip or vertebral fractures
Other Anti-resorptive Agents
• Less effective than bisphosphonates
–Calcitonin (poor quality studies)
–Raloxifene (prevents vertebral fractures only; use for breast cancer prevention)
• Hormone replacement: WHI benefits
• Denosumab (antibody to RANKL)
Women’s Health Initiative• RCT of ERT, PERT or PBO among women age
50-79, 10,739 with hysterectomy. Primary prevention
• PERT, ERT arms stopped after 5-7 years
– Follow-up 93% complete
• Fracture Endpoints: ERT vs. PBO
– Hip RR = 0.61 (0.41, 0.91)
– Non-spine RR = 0.70 (0.63, 0.79)
– CVD RR = 1.12 (1.01, 1.24 WHI Writing Group, Jama, 200
The Future: Anabolic AgentsNeer, NEJM, 2001
• Most treatments for osteoporosis inhibit bone resorption (and formation)
• Anabolic agents (anabolic steroids, fluoride, intermittent parathyroid hormone) stimulate formation
• Daily injections of PTH for 18 mo. reduces vertebral and non-spine fracture. No hip fracture data.
• Should be followed by bisphosphonate therapy
• Very expensive, daily self-administered injections...– Use with severe OP, when other agents have failed?

Page 13
Summary of Treatment
• Bisphosphonates: treatment of choice in selected individuals: Spine/hip fracture or T<-2.5. Benefit for others less clear.
• Duration of therapy? 3-5 years then off?
• Other agents available but expensive and unclear when to use
• New diagnostic tests and better treatments on the way…
Take Home Points• Absolute risk estimates help with decisions
• Aggressive screening and treatment = fewer fractures; start for all women by 65 yrs
• Interval screening defined by baseline BMD
• Identify those who have already have the disease!
• Bisphosphonates: treatment of choice– Use for spine/hip fracture or T< – 2.5– Adherence counseling. Intermittent dosing.– Duration of therapy? 5 years then off?
1
Abnormal Uterine Bleeding:Evaluation of Premenopausal Women
Vanessa Jacoby, MD, MASAssistant Professor
Ob, Gyn, & Reproductive SciencesUCSF
Objectives
• Define normal and abnormal menstrual bleeding
• Review differential diagnosis and evaluation for abnormal bleeding in premenopausal women
• Recommend guidelines for the use of endometrial biopsy
Normal Uterine Bleeding
Classically…
• Cycle length 21 to 35 days
• Menses 2-7 days
• Less than 80 cc per cycle
The Menstrual Cycle
2
Case 1
A 24 year old G0 presents with heavy irregular bleeding for 6 months. Her bleeding is every 15-35 days, lasts 4-15 days.
She has…
A. Menorrhagia
B. Dysfunctional uterine bleeding (DUB)
C. Menometrorrhagia
Classic Definitions
Excess Bleeding• Menorrhagia: heavy, regular timing• Metrorrhagia: light, frequent intervals• Menometrorrhagia: heavy, frequent, irregular• Polymenorrhea: regular, <24 days apart• Intermenstrual spotting: bleeding between menses
Decreased bleeding• Oligomenorrhea: bleeding >35 days apart
Dysfunctional Uterine Bleeding
• Excessive noncyclic bleeding not caused by anatomic lesion, medications, pregnancy or systemic disease
• Primarily due to anovulation
Challenges with Classic Definitions
• Data is from women in Minnesota, 1930s
• Lack of uniformity across clinical settings
Treloar EA, Boynton, Int J Fertil 1967
Hallberg L, Hogdahl AM et al, Acta Obstet Gynecol Scand 1966
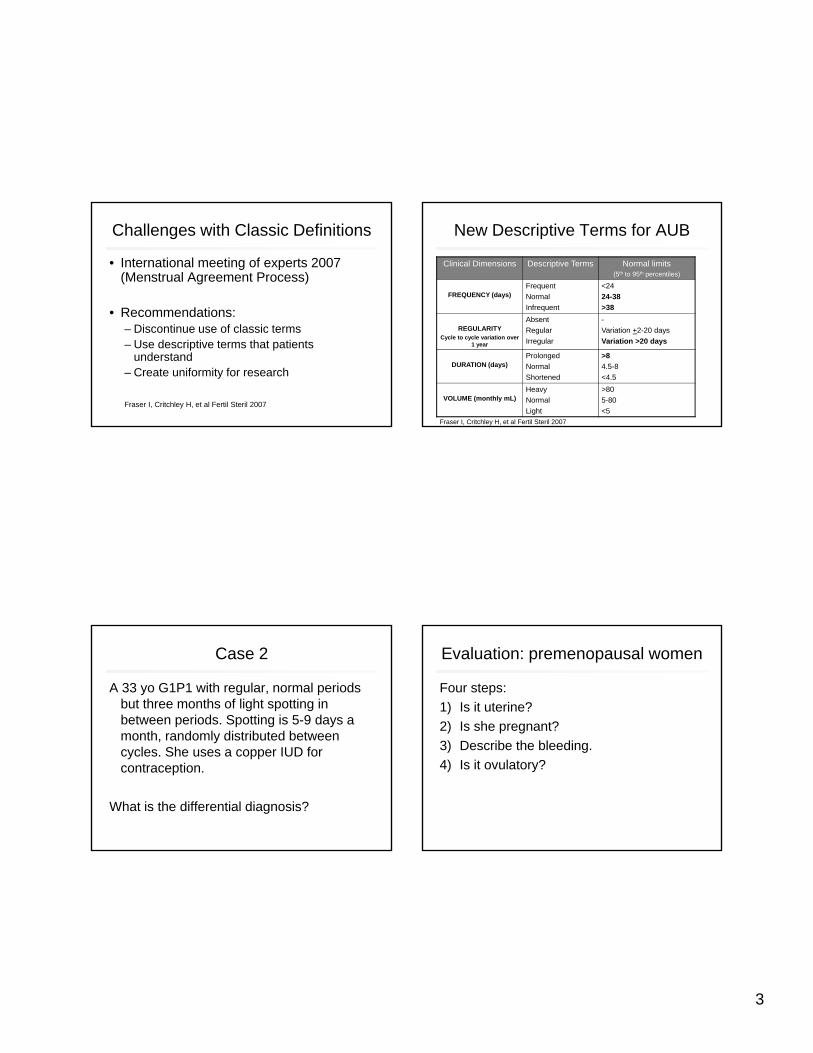
3
Challenges with Classic Definitions
• International meeting of experts 2007 (Menstrual Agreement Process)
• Recommendations:– Discontinue use of classic terms– Use descriptive terms that patients
understand– Create uniformity for research
Fraser I, Critchley H, et al Fertil Steril 2007
New Descriptive Terms for AUB
Clinical Dimensions Descriptive Terms Normal limits (5th to 95th percentiles)
FREQUENCY (days)Frequent
Normal
Infrequent
<24
24-38
>38
REGULARITY Cycle to cycle variation over
1 year
Absent
Regular
Irregular
-
Variation +2-20 days
Variation >20 days
DURATION (days)Prolonged
Normal
Shortened
>8
4.5-8
<4.5
VOLUME (monthly mL)Heavy
Normal
Light
>80
5-80
<5
Fraser I, Critchley H, et al Fertil Steril 2007
Case 2
A 33 yo G1P1 with regular, normal periods but three months of light spotting in between periods. Spotting is 5-9 days a month, randomly distributed between cycles. She uses a copper IUD for contraception.
What is the differential diagnosis?
Evaluation: premenopausal women
Four steps:
1) Is it uterine?
2) Is she pregnant?
3) Describe the bleeding.
4) Is it ovulatory?

4
FIGO Classification: PALM-COEIN
– Fraser I, Hilary OD, et al Fertil Steril 2007
Munro et al, Fertil Steril 2011;95:2204–8
Evaluation: premenopausal women
Four steps:
1) Is it uterine?• Detailed history to r/o GI/GU sources
• Exam to r/o obvious vulvar, vaginal, cervical lesions
• Up to date Pap smear
Case 2
During the pelvic exam, the patient is noted to have a 2cm cervical polyp which is removed in the office. She has full resolution of her bleeding at 6 week follow-up.
Evaluation: premenopausal women
Four steps:
1) Is it uterine?
2) Is she pregnant?Check pregnancy test in at-risk women
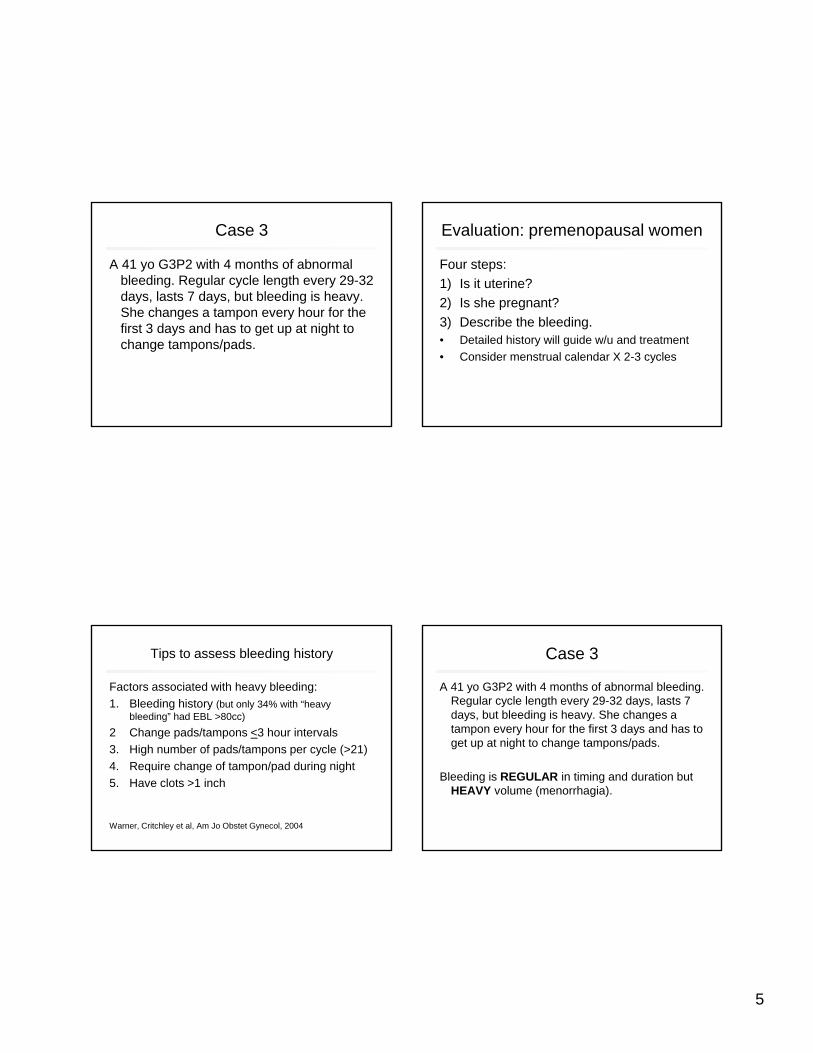
5
Case 3
A 41 yo G3P2 with 4 months of abnormal bleeding. Regular cycle length every 29-32 days, lasts 7 days, but bleeding is heavy. She changes a tampon every hour for the first 3 days and has to get up at night to change tampons/pads.
Evaluation: premenopausal women
Four steps:
1) Is it uterine?
2) Is she pregnant?
3) Describe the bleeding.• Detailed history will guide w/u and treatment
• Consider menstrual calendar X 2-3 cycles
Tips to assess bleeding history
Factors associated with heavy bleeding:
1. Bleeding history (but only 34% with “heavy bleeding” had EBL >80cc)
2 Change pads/tampons <3 hour intervals
3. High number of pads/tampons per cycle (>21)
4. Require change of tampon/pad during night
5. Have clots >1 inch
Warner, Critchley et al, Am Jo Obstet Gynecol, 2004
Case 3
A 41 yo G3P2 with 4 months of abnormal bleeding. Regular cycle length every 29-32 days, lasts 7 days, but bleeding is heavy. She changes a tampon every hour for the first 3 days and has to get up at night to change tampons/pads.
Bleeding is REGULAR in timing and duration but HEAVY volume (menorrhagia).
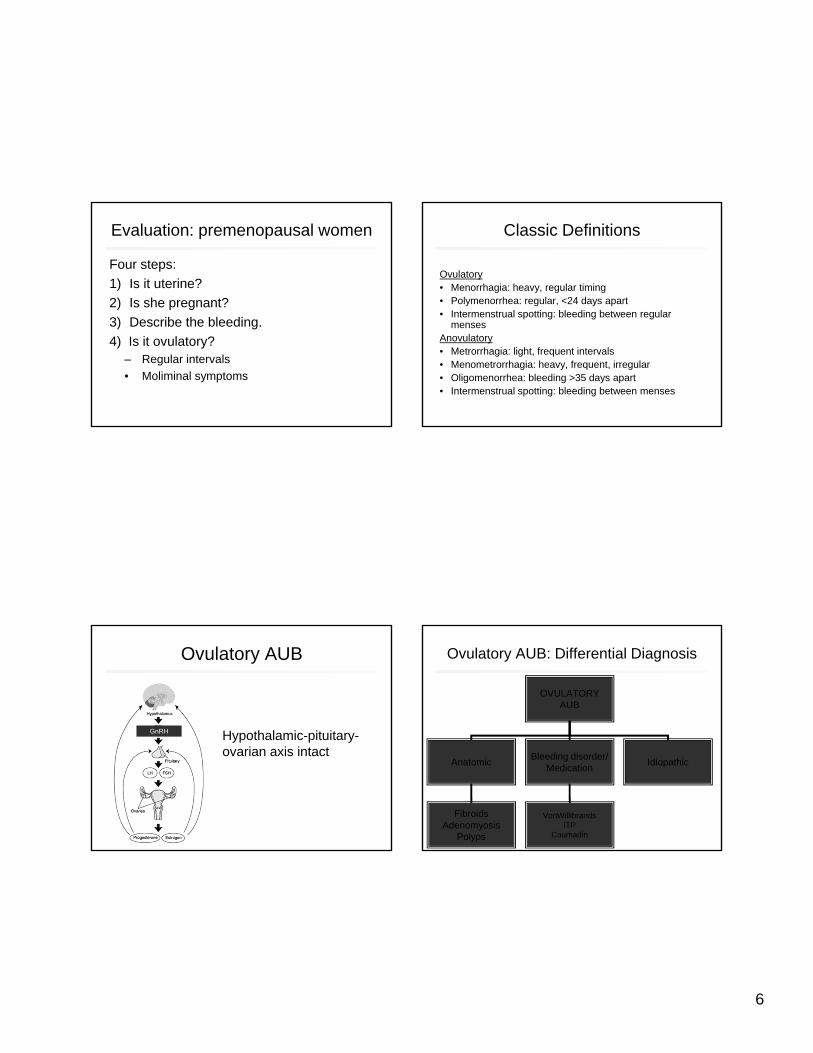
6
Evaluation: premenopausal women
Four steps:
1) Is it uterine?
2) Is she pregnant?
3) Describe the bleeding.
4) Is it ovulatory?– Regular intervals
• Moliminal symptoms
Classic Definitions
Ovulatory• Menorrhagia: heavy, regular timing• Polymenorrhea: regular, <24 days apart• Intermenstrual spotting: bleeding between regular
mensesAnovulatory• Metrorrhagia: light, frequent intervals • Menometrorrhagia: heavy, frequent, irregular • Oligomenorrhea: bleeding >35 days apart• Intermenstrual spotting: bleeding between menses
Ovulatory AUB
Hypothalamic-pituitary-ovarian axis intact
GnRH
Ovulatory AUB: Differential Diagnosis
OVULATORYAUB
AnatomicBleeding disorder/
MedicationIdiopathic
FibroidsAdenomyosis
Polyps
VonWillibrandsITP
Coumadin

7
Ovulatory AUB: History
• Medical comorbidities
• Medications
• Thyroid symptoms (see Thyroid slides)
• Disorder of hemostasis
– Heavy menses since menarche OR
– History of postpartum hemorrhage, bleeding with surgery/dental work OR
– 2 or more of the following---bruising >5cm or epistaxis 1-2/month, frequent gum bleeding, family history of bleeding
Kouides P, Conrad J, et al, Fertil Steril 2005
Ovulatory AUB: Physical exam
Fibroids Adenomyosis
Ovulatory AUB: Blood tests
• CBC, TSH
• Screen for disorders of hemostasis according to history or if pt plans major surgery
– PT, APTT
– VWF antigen, ristocetin cofactor, factor VIII
Kouides P, Conrad J, et al, Fertil Steril 2005
Ovulatory AUB: Imaging Options
• Pelvic ultrasound vs. MRI
• In 108 premenopausal women with ovulatory AUB scheduled for hysterectomy: *both performed well for fibroid detection
*MRI better for exact fibroid location
DETECTION OF FIBROIDS
Pelvic Ultrasound Pelvic MRI
Sensitivity (%) 99 99
Specificity (%) 91 86
Positive predictive value (%) 96 92
Negative predictive value (%)
97 97
Dueholm, et al, Am J Obstet Gynecol:2002
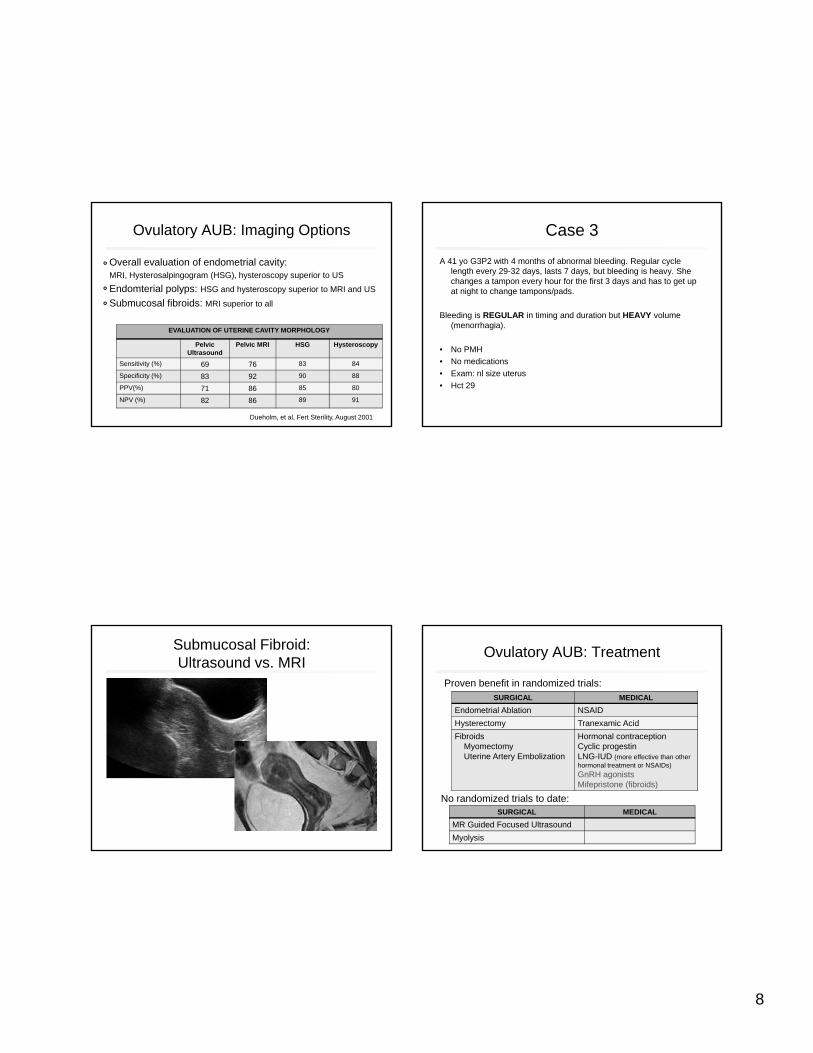
8
Ovulatory AUB: Imaging Options
Overall evaluation of endometrial cavity:MRI, Hysterosalpingogram (HSG), hysteroscopy superior to US
Endomterial polyps: HSG and hysteroscopy superior to MRI and US
Submucosal fibroids: MRI superior to all
EVALUATION OF UTERINE CAVITY MORPHOLOGY
Pelvic Ultrasound
Pelvic MRI HSG Hysteroscopy
Sensitivity (%) 69 76 83 84
Specificity (%) 83 92 90 88
PPV(%) 71 86 85 80
NPV (%) 82 86 89 91
Dueholm, et al, Fert Sterility, August 2001
Case 3
A 41 yo G3P2 with 4 months of abnormal bleeding. Regular cycle length every 29-32 days, lasts 7 days, but bleeding is heavy. She changes a tampon every hour for the first 3 days and has to get up at night to change tampons/pads.
Bleeding is REGULAR in timing and duration but HEAVY volume (menorrhagia).
• No PMH
• No medications
• Exam: nl size uterus
• Hct 29
Submucosal Fibroid: Ultrasound vs. MRI
Ovulatory AUB: Treatment
SURGICAL MEDICAL
Endometrial Ablation NSAID
Hysterectomy Tranexamic Acid
FibroidsMyomectomyUterine Artery Embolization
Hormonal contraceptionCyclic progestinLNG-IUD (more effective than other hormonal treatment or NSAIDs)
GnRH agonistsMifepristone (fibroids)
Proven benefit in randomized trials:
No randomized trials to date: SURGICAL MEDICAL
MR Guided Focused Ultrasound
Myolysis

9
Ovulatory AUB: Medicine vs. Surgery
In meta-analysis of 12 randomized trials (n=1,049 women):
-- 58% of “medical management” group had undergone surgery
within 2 years.
– Surgery (hysterectomy or endometrial ablation) decreased
bleeding more than oral medication.
– LNG-IUD comparable to surgery for improvement in quality of life.
Marjoribanks J, et al, Surgery versus medical therapy for heavy menstrual bleeding. Cochrane Database of Systematic Reviews 2006.
Case 4: Ovulatory bleeding
49 yo G2P2 with 5 months of heavy bleeding. Regular cycle length and duration, but heavy bleeding resulting in significant anemia with hct of 25%.
Does she need an endometrial biopsy?
1) Yes
2) No
Case 5: Anovulatory bleeding
38 yo G2P2 with 5 months of irregular bleeding. Bleeding is every 2-3 weeks, lasts 5-12 days, and heavy. Has to change tampon every 1-2 hours for the first few days.
Does she need an endometrial biopsy?1) Yes2) No
Endometrial Biopsy
Endometrial Cancer Facts
• 4th most common cancer in
women (2.5% lifetime risk)
• Average age 61 but 25%
occur pre-menopausally
• Rare to have cancer without abnormal bleeding
• Risk factors: unopposed estrogen (anovulation),
obesity, nulliparity, diabetes, hypertension

10
ACOG guideline
“…based on age alone, endometrial
assessment to exclude cancer is
indicated in any woman older than 35
years who is suspected of having
anovulatory uterine bleeding.”
ACOG guideline July 2012
“Endometrial sampling should be
performed in patients with AUB who are
>45 years as a first-line test.....and <45
years with a history of unopposed
estrogen exposure, failed medical
management, and persistent AUB”
ACOG Practice Bulletin, Number 128, July 2012
Normal Perimenopause
•12% suddenly stop menstruating
•18% have longer, heavier menses
•70% have short, irregular menses
Should we perform EMB on 88% of
perimenopausal women?
Treloar EA, Boynton, Int J Fertil 1967Hallberg L, Hogdahl AM et al, Acta Obstet Gynecol Scand 1966
Suggested guidelines for performingendometrial biopsy
Premenopausal, age >45 years:
– Heavy, irregular bleeding:
– Risk factors for cancer:
– Perimenopausal infrequent/scant bleeding:
– Regular bleeding pattern:
YES
YES
NO
NO
ACOG guideline: Level C evidence (not studies, consensus and expert opinion)
11
AUB: Thyroid disorders
HYPERthyroid HYPOthyroid
Frequency of abnormal cycles
21% 23%
Oligo/amenorrhea 63% 55%
Heavy bleeding 37% 30%
•Consider checking TSH in women with any type of AUB
•Check TSH/Free T4 if suspect hypothalmic/pituitary lesion to detect central hypothyroidism
Krassas, G, Fertil Steril 2000
Case 6: Anovulatory bleeding
A 24 yo G0 with 8 months abnormal bleeding. Bleeding is every 10-45 days, lasts 5-20 days, heavy for most days of bleeding. BMI 33.
Evaluation: premenopausal women
Four steps:1) Is it uterine? YES.2) Is she pregnant?
Upreg neg.3) Describe the bleeding.
Heavy, frequent, irregular, prolonged(menometrorragia)
3) Is it ovulatory? NO.
Anovulatory AUB: Differential Diagnosis
ANOVULATORYAUB
Estrogenic(excess bleeding)
Hypoestrogenic(decreased bleeding)

12
Anovulatory AUB: Differential Diagnosis
ANOVULATORYAUB
Estrogenic
Physiologic Hyperandrogenic
AdolescencePerimenopause
PCOS, CAH, Cushings
Systemic disease/Medications
Renal or liver diseaseChronic steroids
Anovulatory AUB: Differential Diagnosis
ANOVULATORYAUB
Hypoestrogenic
Hypothalamic(stress, anorexia,
mass lesion)Hyperprolactinemia
Ovarian Failure(Premature: POF)
Miscellaneous
Ovulatory, but irregular
• Infection
Usually light/frequent bleeding
• Endometrial hyperplasia/cancer
Usually heavy/frequent
Anovulatory, iatrogenic
– Use of hormonal contraception
Anovulatory AUB: History
History (Estrogenic)• Hirsutism, other androgen excess• Medications• Chronic diseaseHistory (Hypoestrogenic)• Galactorrhea• Hot flashes, other menopausal symptoms
Physical• BMI• Hirsutism• Acanthosis nigracans
13
Anovulatory AUB: Tests and Imaging
Labs• CBC• TSH• Prolactin
– for oligomenorrhea only
• FSH – For oligomenorrhea in <40 years with menopausal symptoms
and/or no other explanation of hypoestrogenism
Androgens for PCOS if no clinical manifestations (Be aware of accuracy of free testosterone assay in your clinic)
Consider EMBImaging• Not necessary unless abnormal exam or
does not respond to treatment
Case 6: Anovulatory bleeding
A 24 yo G0 with 8 months abnormal bleeding. Bleeding is every 10-4 days,
lasts 5-20 days, heavy for most days of bleeding. BMI 33.
• No PMH. No meds.
• Removes hair from upper lip and chin every 2 weeks.
• Exam: obese, coarse dark hair upper lip, uterus/adnexa not palpable.
• Labs: Hct 30. TSH wnl.
Case 6: Anovulatory bleeding
A 24 yo G0 with 8 months abnormal bleeding. Bleeding is every 10-14
days, lasts 5-20 days, heavy for most days of bleeding. BMI 33.
• No PMH. No meds.
• Removes hair from upper lip and chin every 2 weeks.
• Exam: obese, coarse dark hair upper lip, uterus/adnexa not palpable.
• Labs: Hct 30. TSH wnl.
Diagnosis: Polycystic ovarian syndrome
Treatment: Oral contraceptives to
*decrease bleeding
*prevent hyperplasia
*decrease hirsuitism
Anovulatory AUB: Treatment
SURGICAL MEDICAL
Endometrial AblationHysterectomy
Hormonal contraceptionCyclic progestinLNG-IUD (more effective than other hormonal treatment or NSAIDs)
For estrogenic anovulatory bleeding:
For hypoestrogenic anovulatory bleeding:
SURGICAL MEDICAL
Dopamine agonists for high prolactin
Estrogen/progestinreplacement or hormonal contraception for POI

14
Summary
• Distinguish ovulatory (regular) vs. anovulatory (irregular) bleeding
• If ovulatory, likely anatomic cause– Order pelvic imaging (ultrasound vs. MRI)
– Consider surgery for long term treatment
• If anovulatory, most likely estrogenic:– Consider endometrial biopsy
– Prevent endometrial hyperplasia with progestin

1
Workshop: Case Management of Abnormal Pap Smears and Colposcopies
Rebecca Jackson, MDProfessor
Obstetrics, Gynecology & Reproductive Sciences and Epidemiology & Biostatistics
I have no financial interests to disclose.
Case Based Problems
Emphasis on 2012 guidelines by ASCCP (American Society of Colposcopy and Cervical Pathology) and how they differ from last
Changes for <25yos Who needs colposcopy vs who can be
managed expectantly? Next steps after colposcopy Treatment options: cryotherapy, laser,
LEEP and cone biopsy Post-treatment surveillance
Recommended Guidelines
ASCCP guidelines 2012– For work-up of abnormal cytology and treatment of
CIN: (or just search ASCCP guidelines)http://www.asccp.org/Portals/9/docs/Updated%20ASCCP%20
Algorithms%204%2011%2013%20-%20PDF.pdf
Rationale behind guidelines: – ObstetGynecol: 2013; 121(4); 829–846
SFGH 2010 guidelines in your syllabus (developed by Dr. George Sawaya, very similar to ASCCP but not yet updated with the new 2013 recommendations)
2
$7.00
$9.99 $9.99
Laminated cards with tabs at top so can find the algorithm you need
Either enter pt info and it gives you the recommendation and assoc algorithm OR you can simply view the algorithms
Good news: most prior guidelines reaffirmed, easier to read, guidance for no ECC’s on pap & discordant co-test results
Bad news: even more complex than prior guidelines
What’s New (2012 ASCCP)
**Extend adolescent (age <21) management guidelines to women < age 25: there are now 2 pathways for most algorithms—One for<25 and one for >25
Less aggressive w/u of ASC-US How to manage discordant cotest results: (HPV+/PapNl;
HPV-/Pap ≥ ASC-US), unsatisfactory cytology and missing endocervical or t- zone cells
Post-colpo management now includes co-testing, even in <25 yo
Treat CIN1 on ECC as CIN1 (not as +ECC)
Histology Primer
Cervical intraepithelial neoplasia (CIN)Graded based on proportion of epithelium involved
CIN 1: indicates active HPV infection; treatment discouraged since spontaneous resolution is high
CIN 2: most are treated, but about 40% resolve over 6 month period; treatment may be deferred in young women
CIN 3: the most proximal cancer precursor, also known as carcinoma in situ always treat
Adenocarcinoma in situ (AIS): widely considered a cancer precursor always treat
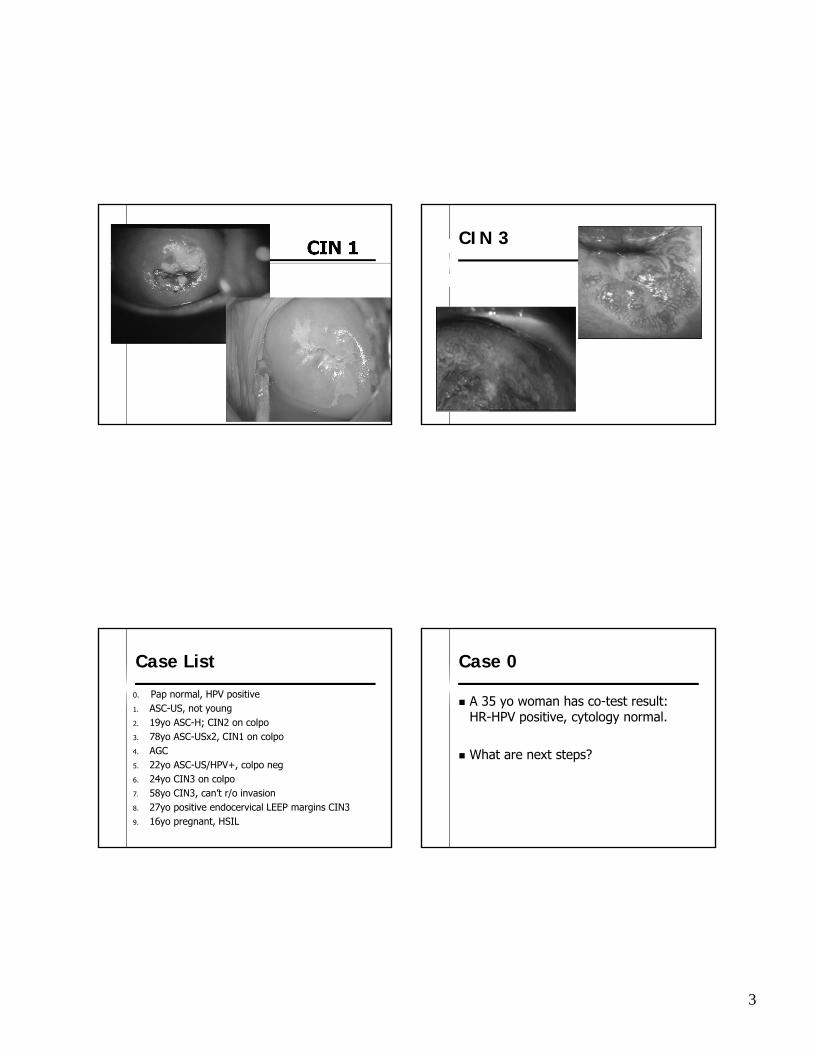
3
CIN 1 CIN 3
Case List
0. Pap normal, HPV positive1. ASC-US, not young2. 19yo ASC-H; CIN2 on colpo3. 78yo ASC-USx2, CIN1 on colpo4. AGC5. 22yo ASC-US/HPV+, colpo neg6. 24yo CIN3 on colpo7. 58yo CIN3, can’t r/o invasion8. 27yo positive endocervical LEEP margins CIN39. 16yo pregnant, HSIL
Case 0
A 35 yo woman has co-test result: HR-HPV positive, cytology normal.
What are next steps?
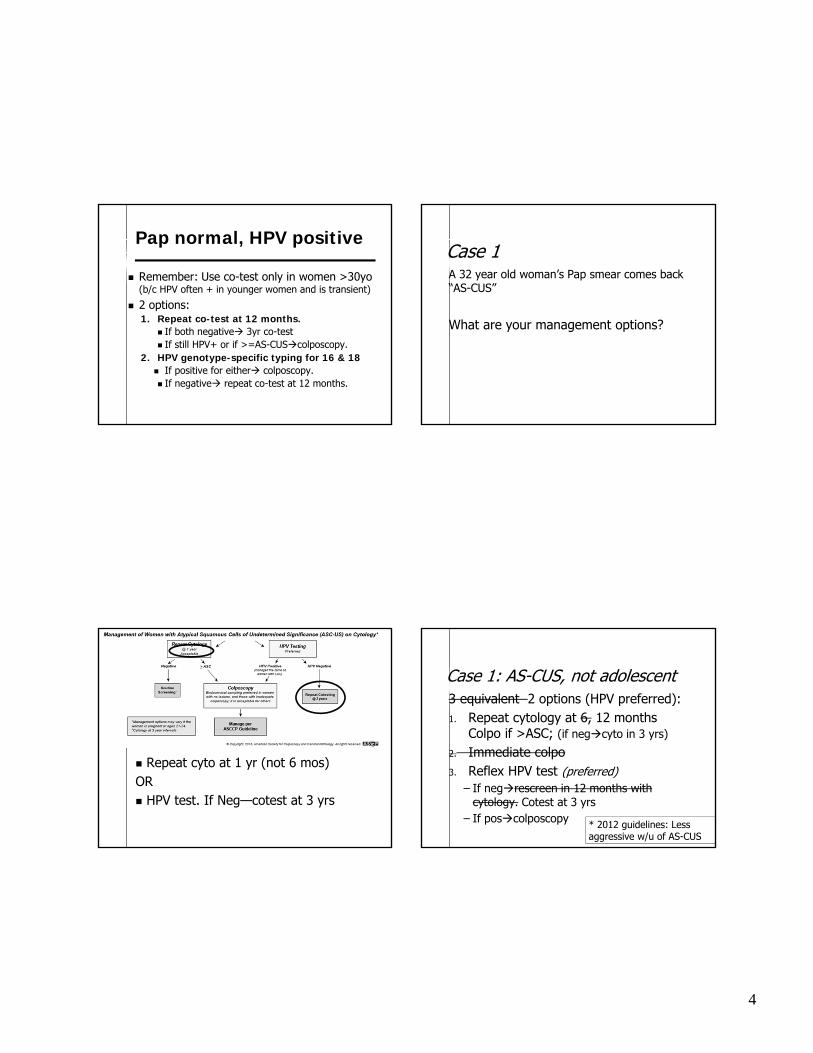
4
Pap normal, HPV positive
Remember: Use co-test only in women >30yo (b/c HPV often + in younger women and is transient)
2 options:1. Repeat co-test at 12 months.
If both negative 3yr co-test If still HPV+ or if >=AS-CUScolposcopy.
2. HPV genotype-specific typing for 16 & 18 If positive for either colposcopy. If negative repeat co-test at 12 months.
Case 1A 32 year old woman’s Pap smear comes back “AS-CUS”
What are your management options?
Repeat cyto at 1 yr (not 6 mos)OR HPV test. If Neg—cotest at 3 yrs
Case 1: AS-CUS, not adolescent3 equivalent 2 options (HPV preferred):1. Repeat cytology at 6, 12 months
Colpo if >ASC; (if negcyto in 3 yrs)
2. Immediate colpo3. Reflex HPV test (preferred)
– If negrescreen in 12 months with cytology. Cotest at 3 yrs
– If poscolposcopy * 2012 guidelines: Less aggressive w/u of AS-CUS
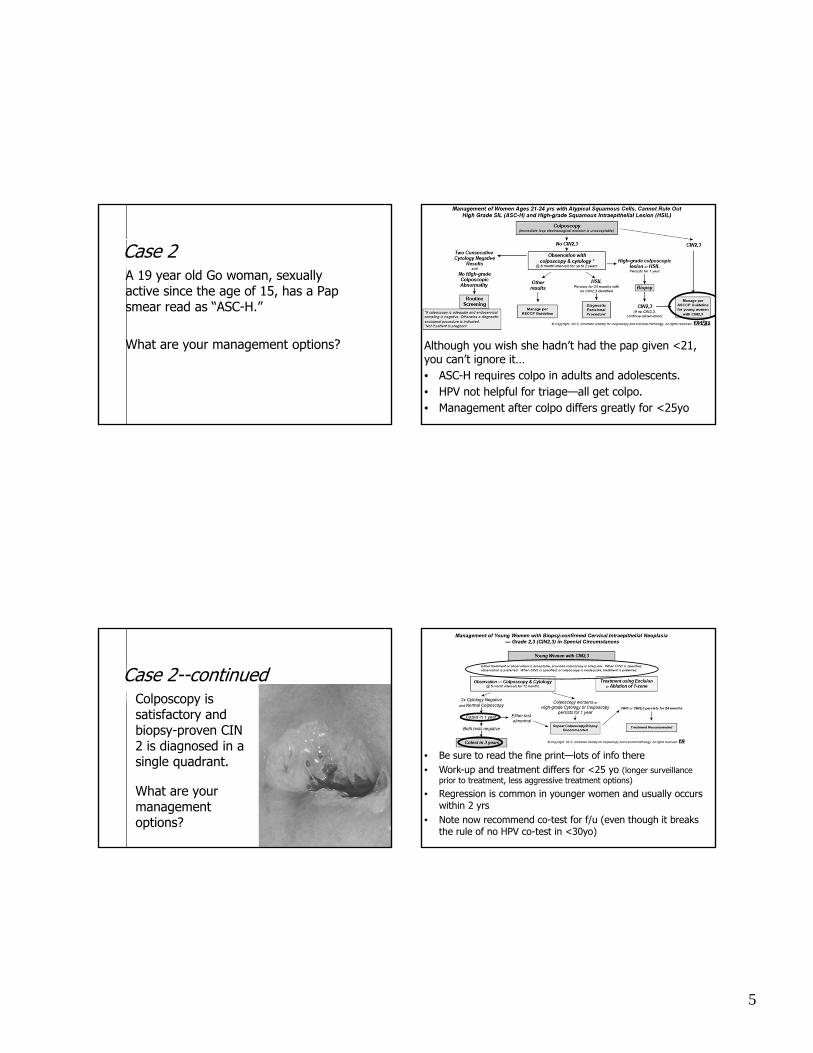
5
Case 2A 19 year old Go woman, sexually active since the age of 15, has a Pap smear read as “ASC-H.”
What are your management options? Although you wish she hadn’t had the pap given <21, you can’t ignore it…• ASC-H requires colpo in adults and adolescents. • HPV not helpful for triage—all get colpo.• Management after colpo differs greatly for <25yo
Case 2--continuedColposcopy is satisfactory and biopsy-proven CIN 2 is diagnosed in a single quadrant.
What are your management options?
• Be sure to read the fine print—lots of info there• Work-up and treatment differs for <25 yo (longer surveillance
prior to treatment, less aggressive treatment options)
• Regression is common in younger women and usually occurs within 2 yrs
• Note now recommend co-test for f/u (even though it breaks the rule of no HPV co-test in <30yo)
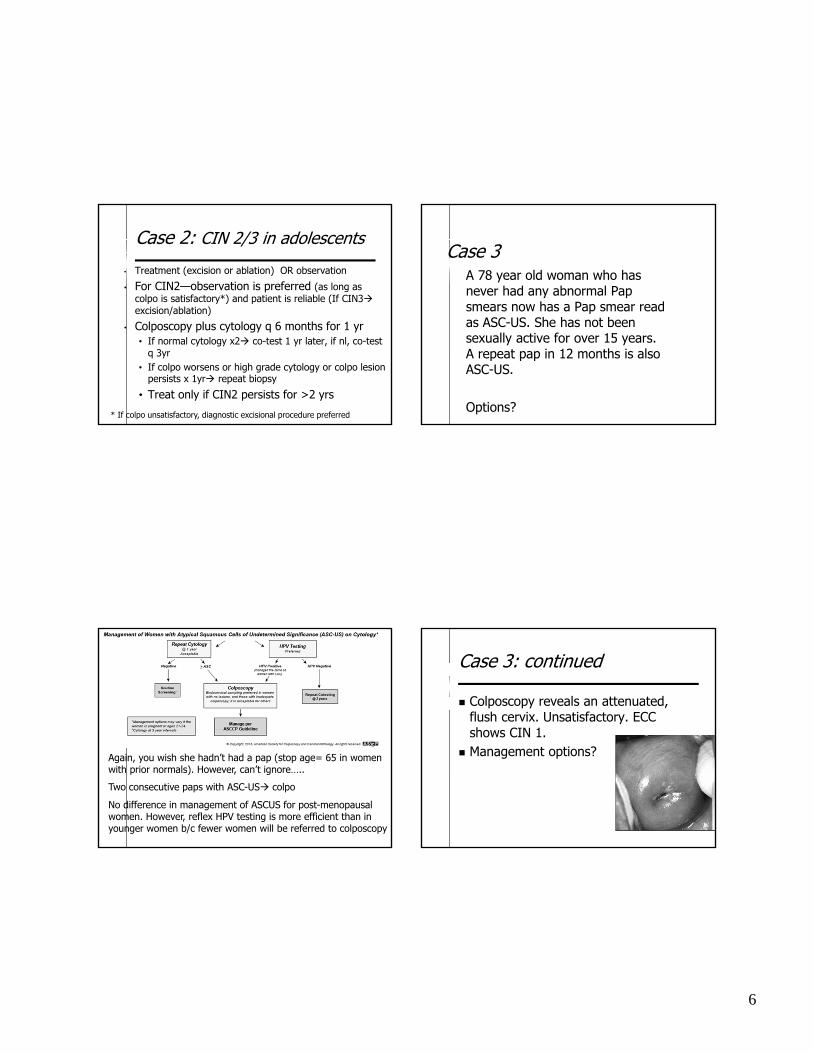
6
Case 2: CIN 2/3 in adolescents
• Treatment (excision or ablation) OR observation
• For CIN2—observation is preferred (as long as colpo is satisfactory*) and patient is reliable (If CIN3excision/ablation)
• Colposcopy plus cytology q 6 months for 1 yr• If normal cytology x2 co-test 1 yr later, if nl, co-test
q 3yr• If colpo worsens or high grade cytology or colpo lesion
persists x 1yr repeat biopsy
• Treat only if CIN2 persists for >2 yrs
* If colpo unsatisfactory, diagnostic excisional procedure preferred
Case 3A 78 year old woman who has never had any abnormal Pap smears now has a Pap smear read as ASC-US. She has not been sexually active for over 15 years. A repeat pap in 12 months is also ASC-US.
Options?
Again, you wish she hadn’t had a pap (stop age= 65 in women with prior normals). However, can’t ignore…..
Two consecutive paps with ASC-US colpo
No difference in management of ASCUS for post-menopausal women. However, reflex HPV testing is more efficient than in younger women b/c fewer women will be referred to colposcopy
Case 3: continued
Colposcopy reveals an attenuated, flush cervix. Unsatisfactory. ECC shows CIN 1.
Management options?
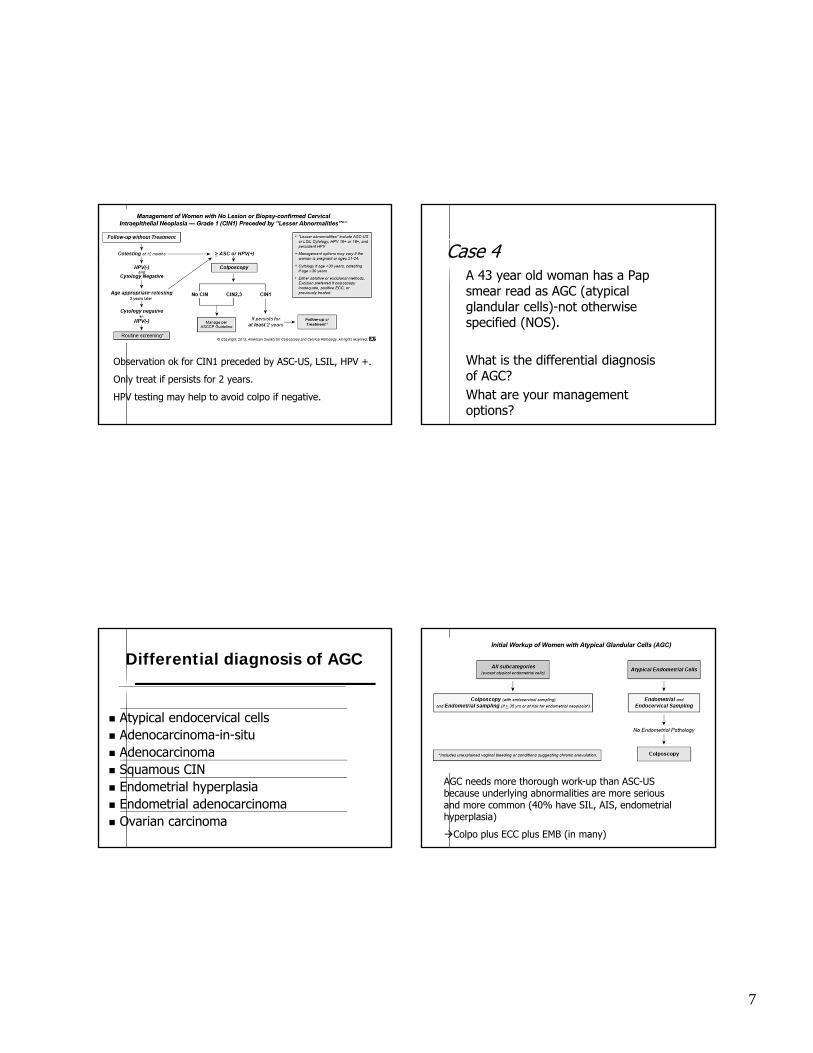
7
Observation ok for CIN1 preceded by ASC-US, LSIL, HPV +.
Only treat if persists for 2 years.
HPV testing may help to avoid colpo if negative.
Case 4A 43 year old woman has a Pap smear read as AGC (atypical glandular cells)-not otherwise specified (NOS).
What is the differential diagnosis of AGC?What are your management options?
Differential diagnosis of AGC
Atypical endocervical cells Adenocarcinoma-in-situ Adenocarcinoma Squamous CIN Endometrial hyperplasia Endometrial adenocarcinoma Ovarian carcinoma
AGC needs more thorough work-up than ASC-US because underlying abnormalities are more serious and more common (40% have SIL, AIS, endometrial hyperplasia)
Colpo plus ECC plus EMB (in many)
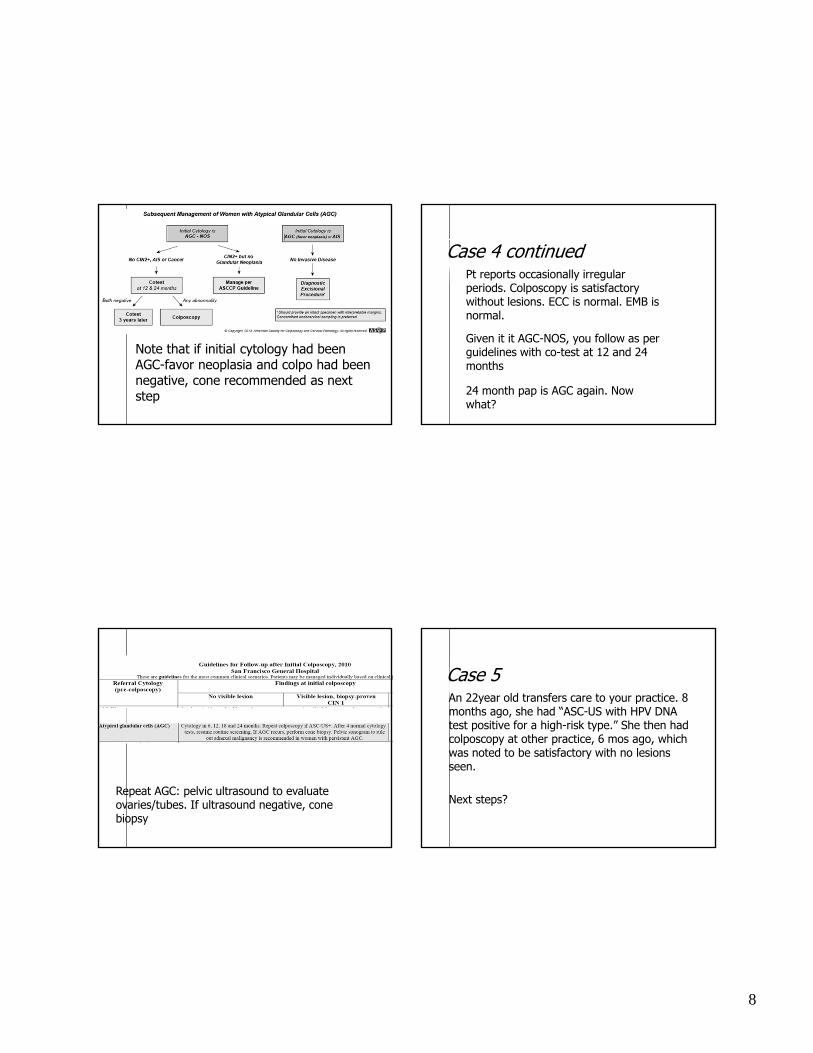
8
Note that if initial cytology had been AGC-favor neoplasia and colpo had been negative, cone recommended as next step
Case 4 continuedPt reports occasionally irregular periods. Colposcopy is satisfactory without lesions. ECC is normal. EMB is normal.
Given it it AGC-NOS, you follow as per guidelines with co-test at 12 and 24 months
24 month pap is AGC again. Now what?
Repeat AGC: pelvic ultrasound to evaluate ovaries/tubes. If ultrasound negative, cone biopsy
Case 5An 22year old transfers care to your practice. 8 months ago, she had “ASC-US with HPV DNA test positive for a high-risk type.” She then had colposcopy at other practice, 6 mos ago, which was noted to be satisfactory with no lesions seen.
Next steps?

9
Cytology preferred for f/u AS-CUS in young women (reflex HPV testing ok)
If HPV posrepeat cytology only at 12 mos (ie shouldn’t have had colpo)
What to do when pts receive testing that was not recommended per guidelines or who are lost to f/u after abn pap and then have repeat pap nl?
In general, act on most severe abnormality. EG, If 30yo had LSIL pap then lost to f/u and has repeat nl pap, still needs colpo
In this case, can follow per guidelines after nl colpo b/c f/u is essentially the same as if she hadn’t had colpo
Case 6A 24 yo G0 woman has biopsy-proven CIN 3, a satisfactory colposcopy and a negative endocervical curettage.
What are your management options? What if the ECC were positive?
Potential adverse effects of LEEP
Preterm delivery 70% Low birth weight 82% PPROM 169%
Lancet 2006 367:489-98
No randomized trials.
Perinatal mortality 187% Severe preterm delivery 178% Extreme low birthweight 186%
BMJ 2008 Sep 18;337
Potential adverse effects of cone biopsy
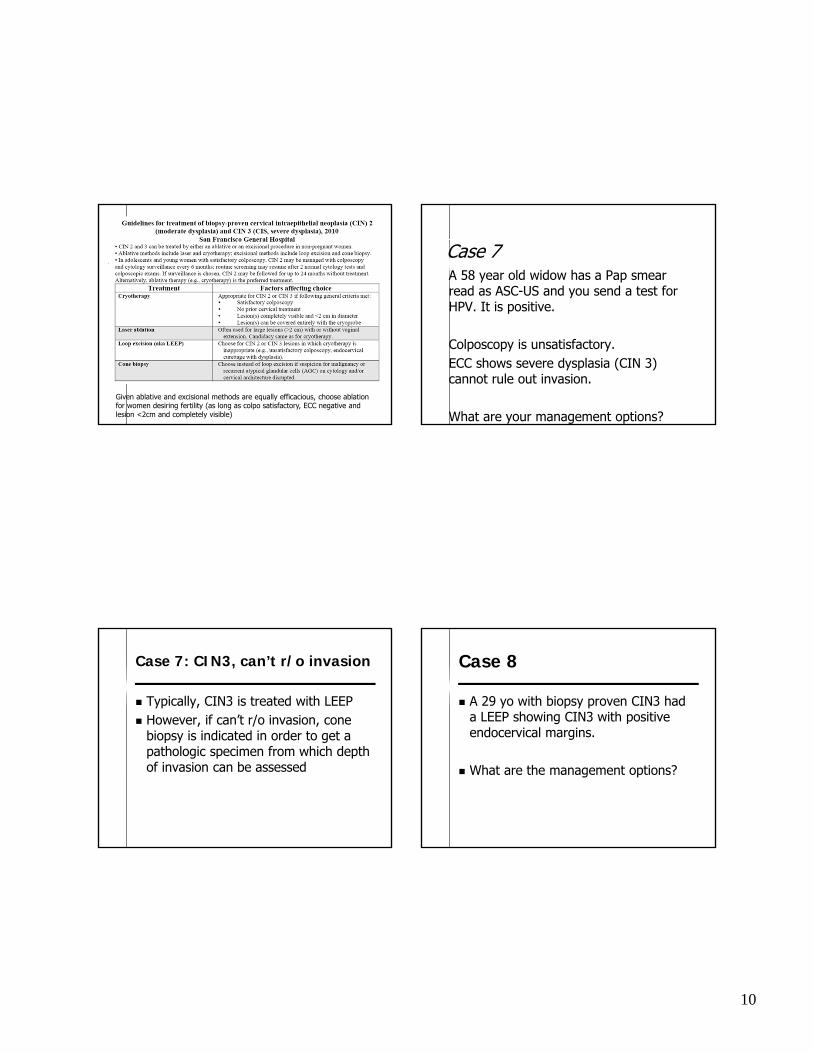
10
Given ablative and excisional methods are equally efficacious, choose ablation for women desiring fertility (as long as colpo satisfactory, ECC negative and lesion <2cm and completely visible)
Case 7A 58 year old widow has a Pap smear read as ASC-US and you send a test for HPV. It is positive.
Colposcopy is unsatisfactory.ECC shows severe dysplasia (CIN 3) cannot rule out invasion.
What are your management options?
Case 7: CIN3, can’t r/o invasion
Typically, CIN3 is treated with LEEP However, if can’t r/o invasion, cone
biopsy is indicated in order to get a pathologic specimen from which depth of invasion can be assessed
Case 8
A 29 yo with biopsy proven CIN3 had a LEEP showing CIN3 with positive endocervical margins.
What are the management options?
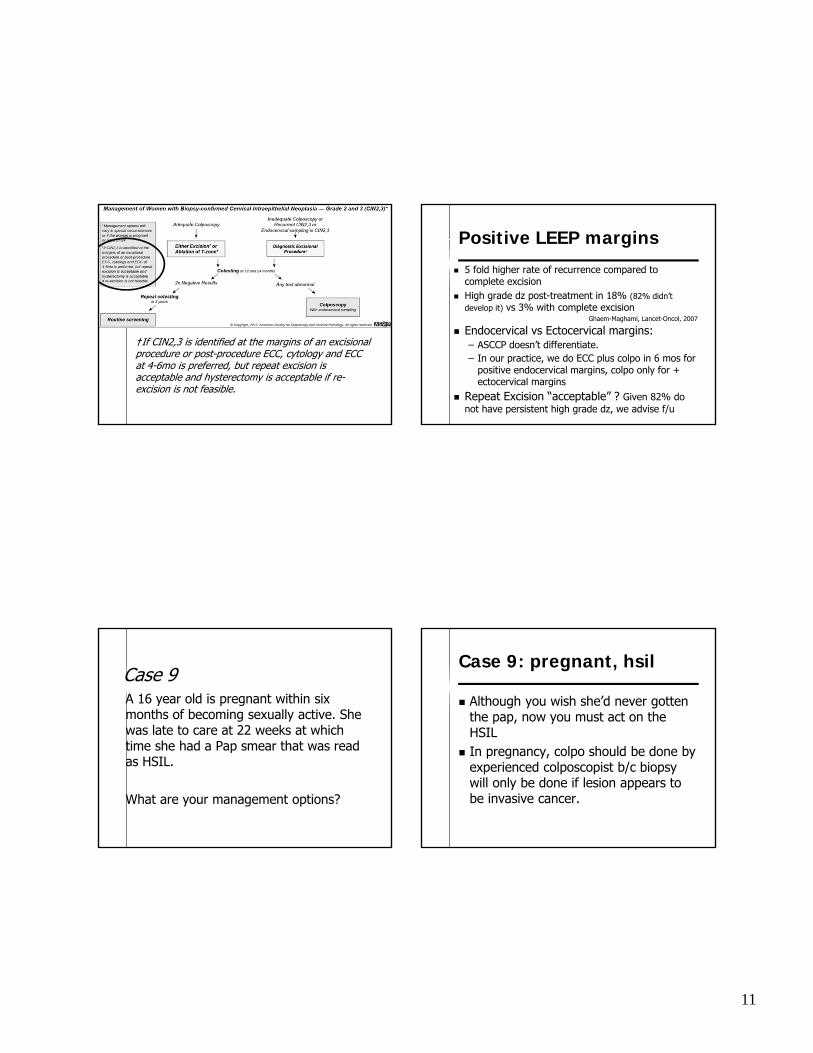
11
†If CIN2,3 is identified at the margins of an excisional procedure or post-procedure ECC, cytology and ECCat 4-6mo is preferred, but repeat excision is acceptable and hysterectomy is acceptable if re-excision is not feasible.
Positive LEEP margins
5 fold higher rate of recurrence compared to complete excision
High grade dz post-treatment in 18% (82% didn’t develop it) vs 3% with complete excision
Endocervical vs Ectocervical margins:– ASCCP doesn’t differentiate. – In our practice, we do ECC plus colpo in 6 mos for
positive endocervical margins, colpo only for + ectocervical margins
Repeat Excision “acceptable” ? Given 82% do not have persistent high grade dz, we advise f/u
Ghaem-Maghami, Lancet-Oncol, 2007
Case 9A 16 year old is pregnant within six months of becoming sexually active. She was late to care at 22 weeks at which time she had a Pap smear that was read as HSIL.
What are your management options?
Case 9: pregnant, hsil
Although you wish she’d never gotten the pap, now you must act on the HSIL
In pregnancy, colpo should be done by experienced colposcopist b/c biopsy will only be done if lesion appears to be invasive cancer.

12
General rules
Less is better for adolescents/<25yo (start screening later, space out surveillence, less aggressive treatment)
Don’t use HPV test in <30yo unless it is to follow colpo (possibly can decrease need for repeat colpo, if negative)
AGC is worse than ASC-US. Requires extensive work-up
Typically don’t need to treat CIN1 unless persists
Consider getting pap/path results re-read if discordant
Pearls
Make sure women have adequate education about HPV if HPV DNA testing is used
Involve women in decisions when uncertainty exists in guidelines
Stress smoking cessation Consider HIV testing for women with biopsy proven
dysplasia
Final Thoughts
Cervical cancer screening will never completely eliminate cervical cancer: must balance benefits (which occur rarely) and harms (which affect a large number of women)
Goal: optimal strategies aim to identify HPV-related abnormalities that are likely to progress to invasive cancers while avoiding treating lesions not destined to become cancerous
Additional summary from 2012 ASCCP guidelines

13
Unsatisfactory or Absent endocervical cells
Unsatisfactory cytology:– No HPV done or Neg HPV: repeat cytology 2-4 mos– Pos HPV: either repeat cyto 2-4 mos or colpo– 2 conseq unsats: colpo
Cytology Neg but absent/insuff EC/TZ:– <30yo: Routine screening (don’t’ do HPV)– >30yo, no HPV: Do HPV (pap 3 yr also ok)– >30, HPV neg: routine screening– > 30 HPV pos: co-test in one year
Excision vs ablation
Excision: – CIN2+ AND unsatisfactory colpo– ECC showing CIN2+– Recurrent cin2+– Negative colpo preceded by AIS, AGC-favor
neoplasia, HSIL papx2
Ablation:– Preferred in younger women (possibly less
chance of preterm delivery)– Lesion < 2 cm and completely visible

1- Sawaya & Smith-McCune, August 2010
Guidelines for Screening for Cervical Cancer and its Precursors, 2010 San Francisco General Hospital
These are guidelines for use of cervical cytology in asymptomatic women as a screening tool for cervical cancer and its precursors. Tests performed in symptomatic women should be evaluated in clinical context. Screening guidelines do not apply to women with prior treatment of high-grade cervical dysplasia (CIN 2 or CIN 3) or cervical cancer; see other aspects of this guideline for surveillance after treatment. Age to begin screening Age 21 years; avoid screening within 3 years of
becoming sexually active and in known virgins. Interval of screening Screen every 2 years with cytology. At or after age
30 years, women with 3+ prior consecutive, normal tests may be screened every 3 years.
Age to end screening Screening may end at or after age 65 years if 3+ consecutive, normal cytology tests have been documented within the prior 10 years and there is no history of treated CIN 2, CIN 3, AIS or cervical cancer.
Special populations Pregnant women Screen as above; do not screen within 3 years of
becoming sexually active. Women with HIV infection or
immunocompromised Annual screening after 2 normal cytology tests 6 months apart in the year following initial HIV diagnosis or immunocompromised state.
After total hysterectomy in women with no prior history of CIN 2 or CIN 3
Screening should not be performed.
After total hysterectomy in women with a prior history of CIN 2 or CIN 3
Annual cytology. After 3 consecutive, normal tests, screening may be performed every 3 years.
After diagnosis and treatment of cervical cancer
Surveillance as per gynecologic oncology protocols
CIN indicates cervical intraepithelial lesion.

2- Sawaya & Smith-McCune, August 2010
Guidelines for Initial Management of Abnormal Cervical Cytology, 2010 San Francisco General Hospital
Cytology Interpretation Action Common Benign Findings
Unsatisfactory Repeat cytology next available Satisfactory, but no endocervical cells Repeat cytology in 12 months Benign-appearing endometrial cells Pre-menopausal: No action. Post-menopausal: Endometrial biopsy.
Epithelial Cell Abnormalities Atypical squamous cells of
undetermined significance (ASC-US) Three different strategies may be adopted, but colposcopy is the least preferred: 1. Repeat cytology at 6 and 12 months. If ASC-US+, colposcopy. After 2 normal cytology tests, resume routine screening. 2. HPV testing for high-risk types. If positive, colposcopy. If negative, repeat cytology in one year; do not do HPV testing in women age 20 or less. 3. Colposcopy† If age 20 or less, repeat cytology at 12 months (colposcopy if ASC-H or HSIL+) and at 24 months (colposcopy if ASC-US+). If normal, resume routine screening. For pregnant women age 21+, repeat cytology at 6 months; if ASC-US+, colposcopy 6 weeks post-partum.
ASC, cannot exclude HSIL (ASC-H) Colposcopy† Low-grade SIL (LSIL) Colposcopy†
If age 20 or less, repeat cytology at 12 months (colposcopy if ASC-H or HSIL+) and at 24 months (colposcopy if ASC-US+). If normal, resume routine screening. For pregnant women age 21+, colposcopy may be deferred to 6 weeks post-partum. For post-menopausal women, LSIL may be managed identically to ASC-US.
High-grade SIL (HSIL) Colposcopy† Squamous cell carcinoma Colposcopy†
Glandular Cell Abnormalities Atypical glandular cells (AGC) • endocervical Colposcopy† with endocervical curettage (ECC) • endometrial Colposcopy† with ECC and EMB • not otherwise specified Colposcopy† with ECC; add EMB if abnormal bleeding, chronic
anovulation or age 35+ Adenocarcinoma in situ (AIS) Colposcopy† with ECC and EMB
Common Infections • shift in flora suggestive of bacterial
vaginosis (BV) Consider evaluation of and treatment for BV if symptomatic. Repeat cytology at appropriate screening interval.
• fungal organisms consistent with Candida.
Consider evaluation of and treatment for yeast vaginitis if symptomatic. Repeat cytology at appropriate screening interval.
• cellular changes consistent with herpes simplex virus (HSV)
Diagnostic of HSV. Finding may indicate other STIs. Repeat cytology at appropriate screening interval.
• Trichomonas vaginalis (TV) Consider evaluation of and treatment for TV if symptomatic. Finding may indicate other STIs. Repeat cytology at appropriate screening interval.
DEP indicates diagnostic excisional procedure (e.g., cone biopsy, loop excision). HSIL+ indicates HSIL, AGC, AIS and/or cancer. ASC-US + indicates ASC-US, ASC-H, LSIL and/or HSIL+. ECC indicates endocervical curettage. †ECC should be performed in all non-pregnant women with unsatisfactory colposcopy and in those with cytology interpreted as AGC, AIS and cancer. Vaginal colposcopy with Lugol’s solution should be performed in all women with no obvious lesion seen and cytology interpreted as HSIL, AGC, AIS or cancer. In pregnant women, ECC is contraindicated.
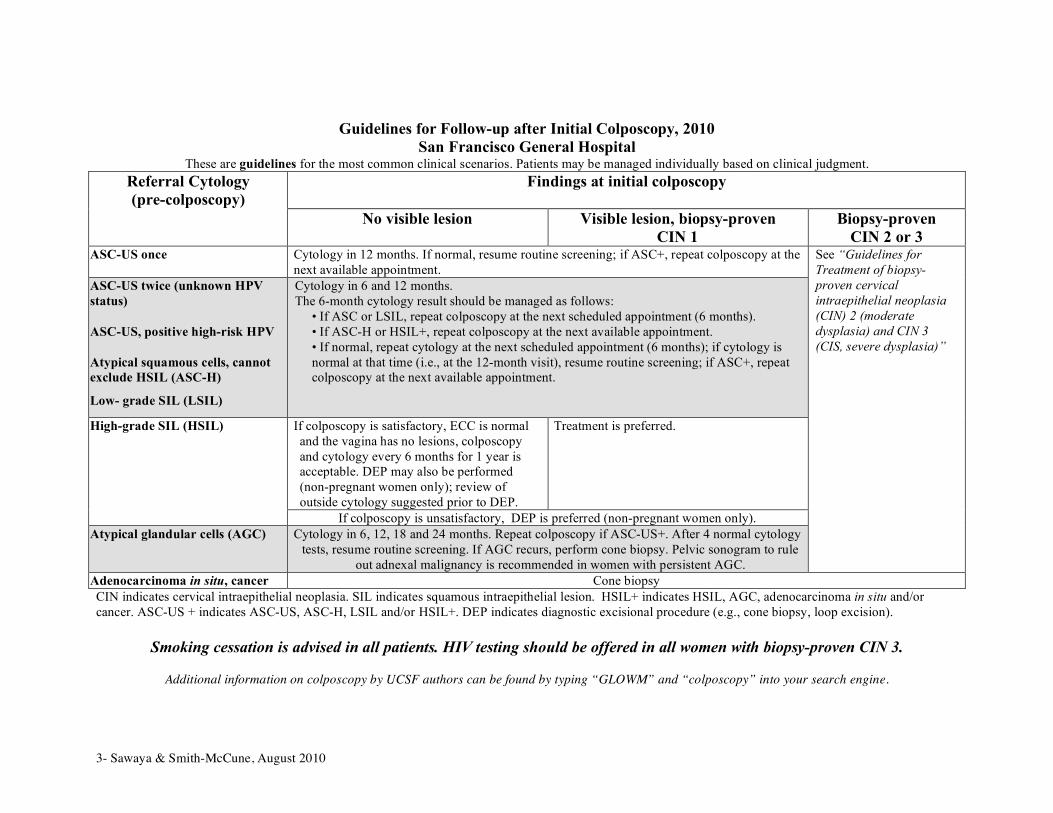
3- Sawaya & Smith-McCune, August 2010
Guidelines for Follow-up after Initial Colposcopy, 2010 San Francisco General Hospital
These are guidelines for the most common clinical scenarios. Patients may be managed individually based on clinical judgment. Referral Cytology (pre-colposcopy)
Findings at initial colposcopy
No visible lesion Visible lesion, biopsy-proven CIN 1
Biopsy-proven CIN 2 or 3
ASC-US once Cytology in 12 months. If normal, resume routine screening; if ASC+, repeat colposcopy at the next available appointment.
ASC-US twice (unknown HPV status)
ASC-US, positive high-risk HPV Atypical squamous cells, cannot exclude HSIL (ASC-H)
Low- grade SIL (LSIL)
Cytology in 6 and 12 months. The 6-month cytology result should be managed as follows:
• If ASC or LSIL, repeat colposcopy at the next scheduled appointment (6 months). • If ASC-H or HSIL+, repeat colposcopy at the next available appointment. • If normal, repeat cytology at the next scheduled appointment (6 months); if cytology is normal at that time (i.e., at the 12-month visit), resume routine screening; if ASC+, repeat colposcopy at the next available appointment.
If colposcopy is satisfactory, ECC is normal and the vagina has no lesions, colposcopy and cytology every 6 months for 1 year is acceptable. DEP may also be performed (non-pregnant women only); review of outside cytology suggested prior to DEP.
Treatment is preferred.
High-grade SIL (HSIL)
If colposcopy is unsatisfactory, DEP is preferred (non-pregnant women only). Atypical glandular cells (AGC) Cytology in 6, 12, 18 and 24 months. Repeat colposcopy if ASC-US+. After 4 normal cytology
tests, resume routine screening. If AGC recurs, perform cone biopsy. Pelvic sonogram to rule out adnexal malignancy is recommended in women with persistent AGC.
See “Guidelines for Treatment of biopsy-proven cervical intraepithelial neoplasia (CIN) 2 (moderate dysplasia) and CIN 3 (CIS, severe dysplasia)”
Adenocarcinoma in situ, cancer Cone biopsy CIN indicates cervical intraepithelial neoplasia. SIL indicates squamous intraepithelial lesion. HSIL+ indicates HSIL, AGC, adenocarcinoma in situ and/or cancer. ASC-US + indicates ASC-US, ASC-H, LSIL and/or HSIL+. DEP indicates diagnostic excisional procedure (e.g., cone biopsy, loop excision).
Smoking cessation is advised in all patients. HIV testing should be offered in all women with biopsy-proven CIN 3.
Additional information on colposcopy by UCSF authors can be found by typing “GLOWM” and “colposcopy” into your search engine.
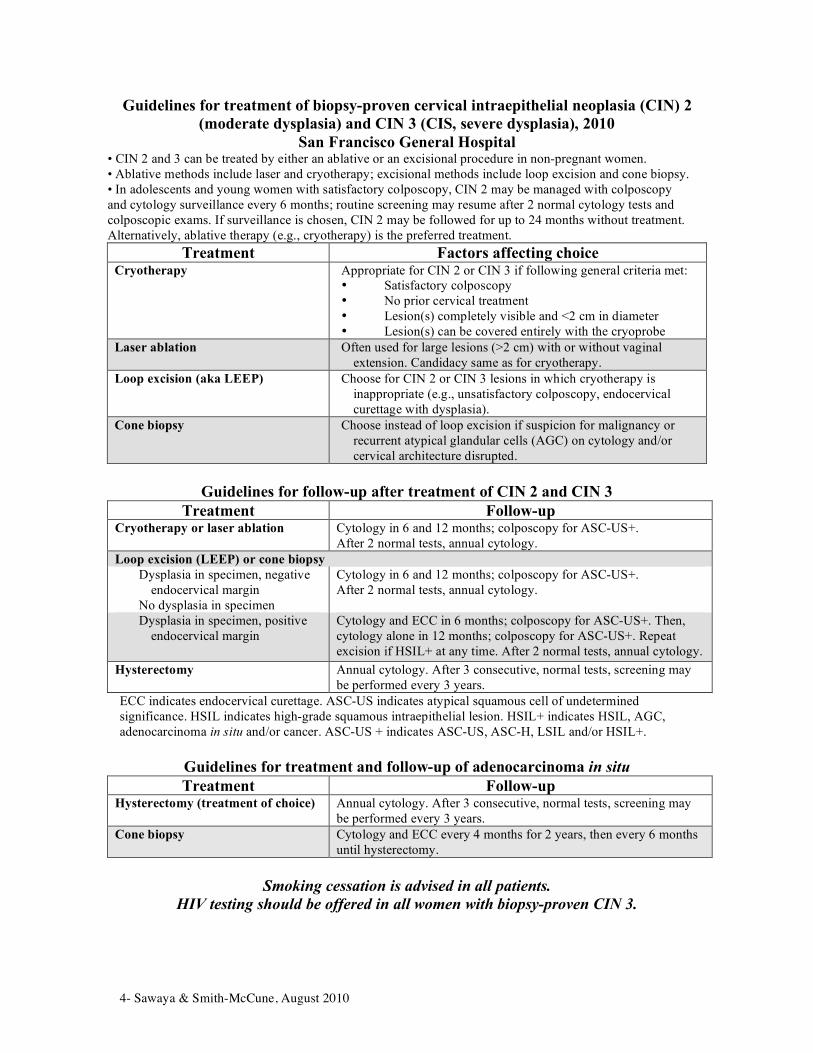
4- Sawaya & Smith-McCune, August 2010
Guidelines for treatment of biopsy-proven cervical intraepithelial neoplasia (CIN) 2 (moderate dysplasia) and CIN 3 (CIS, severe dysplasia), 2010
San Francisco General Hospital • CIN 2 and 3 can be treated by either an ablative or an excisional procedure in non-pregnant women. • Ablative methods include laser and cryotherapy; excisional methods include loop excision and cone biopsy. • In adolescents and young women with satisfactory colposcopy, CIN 2 may be managed with colposcopy and cytology surveillance every 6 months; routine screening may resume after 2 normal cytology tests and colposcopic exams. If surveillance is chosen, CIN 2 may be followed for up to 24 months without treatment. Alternatively, ablative therapy (e.g., cryotherapy) is the preferred treatment.
Treatment Factors affecting choice Cryotherapy
Appropriate for CIN 2 or CIN 3 if following general criteria met: • Satisfactory colposcopy • No prior cervical treatment • Lesion(s) completely visible and <2 cm in diameter • Lesion(s) can be covered entirely with the cryoprobe
Laser ablation Often used for large lesions (>2 cm) with or without vaginal extension. Candidacy same as for cryotherapy.
Loop excision (aka LEEP) Choose for CIN 2 or CIN 3 lesions in which cryotherapy is inappropriate (e.g., unsatisfactory colposcopy, endocervical curettage with dysplasia).
Cone biopsy Choose instead of loop excision if suspicion for malignancy or recurrent atypical glandular cells (AGC) on cytology and/or cervical architecture disrupted.
Guidelines for follow-up after treatment of CIN 2 and CIN 3
Treatment Follow-up Cryotherapy or laser ablation Cytology in 6 and 12 months; colposcopy for ASC-US+.
After 2 normal tests, annual cytology. Loop excision (LEEP) or cone biopsy
Dysplasia in specimen, negative endocervical margin
No dysplasia in specimen
Cytology in 6 and 12 months; colposcopy for ASC-US+. After 2 normal tests, annual cytology.
Dysplasia in specimen, positive endocervical margin
Cytology and ECC in 6 months; colposcopy for ASC-US+. Then, cytology alone in 12 months; colposcopy for ASC-US+. Repeat excision if HSIL+ at any time. After 2 normal tests, annual cytology.
Hysterectomy Annual cytology. After 3 consecutive, normal tests, screening may be performed every 3 years.
ECC indicates endocervical curettage. ASC-US indicates atypical squamous cell of undetermined significance. HSIL indicates high-grade squamous intraepithelial lesion. HSIL+ indicates HSIL, AGC, adenocarcinoma in situ and/or cancer. ASC-US + indicates ASC-US, ASC-H, LSIL and/or HSIL+.
Guidelines for treatment and follow-up of adenocarcinoma in situ Treatment Follow-up
Hysterectomy (treatment of choice) Annual cytology. After 3 consecutive, normal tests, screening may be performed every 3 years.
Cone biopsy Cytology and ECC every 4 months for 2 years, then every 6 months until hysterectomy.
Smoking cessation is advised in all patients.
HIV testing should be offered in all women with biopsy-proven CIN 3.

Page 1
Clinical Dilemmas in Genetic Testing
A Case-based Approach
Jeffrey A. Tice, MD
Division of General Internal MedicineUniversity of California, San Francisco I have no conflicts of interest
Definitions
• “Genetic Testing”
–Many types (full sequencing, single site, common mutations, chromosome analysis, etc.)
–Many tissues (tumors, blood, buccal mucosa)
–Not just a test, a process
–Specialty labs
• “Disease Predisposition”
–Risk is a complex issue, not “all or nothing”
–What to do with results?
4 possible cases
• Ivana Test: 24 year old, mother just diagnosed; aunt died of breast cancer “I just want the test”
• Cy Fibrosis: 28 year old with male infertility. His genetic testing for cystic fibrosis is prompting his wife to consider testing.
• Ima Clotter: Healthy 30 year old whose sister was found to carry “blood clotting genes” after several miscarriages. Not sure she wants to test, “How would it change things for me?”
• Dina Child: Healthy 36 year old woman who is pregnant and wants that new DNA test using her blood to tell her the sex of the fetus.
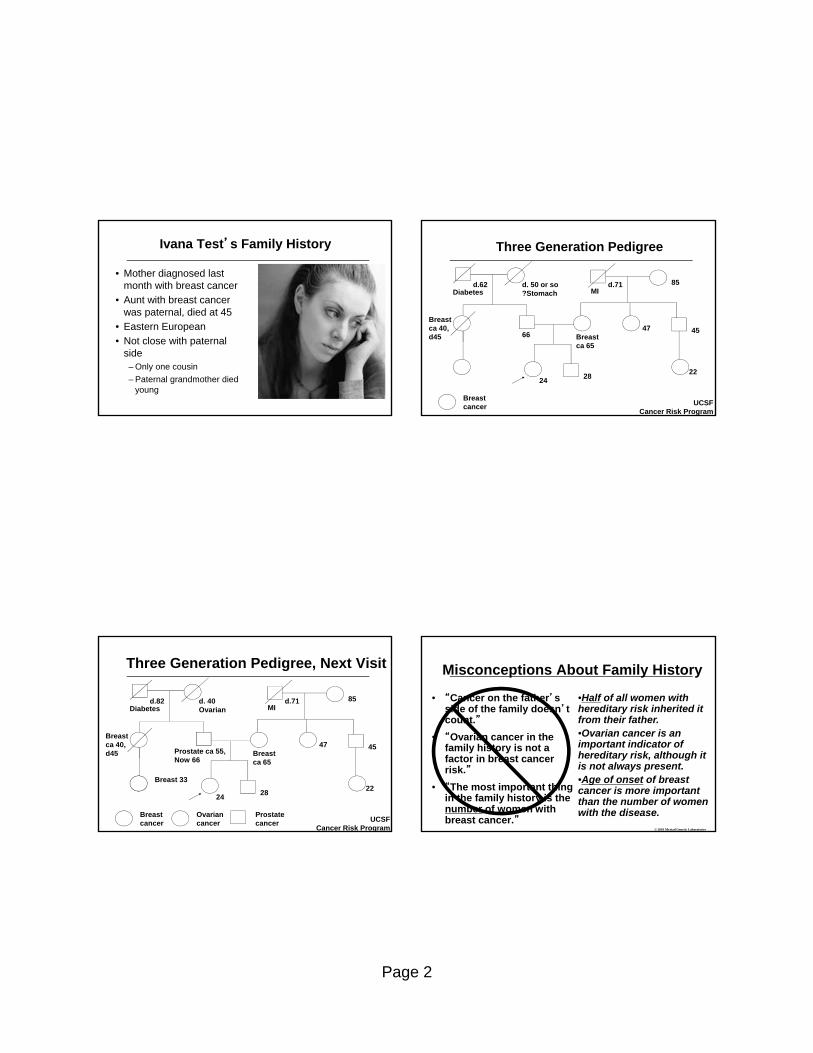
Page 2
Ivana Test’s Family History
• Mother diagnosed last month with breast cancer
• Aunt with breast cancer was paternal, died at 45
• Eastern European
• Not close with paternal side
– Only one cousin
– Paternal grandmother died young
Three Generation Pedigree
85MI
45
22
47Breastca 65
2824
66
Breast ca 40, d45
d. 50 or so?StomachDiabetes
Breast cancer UCSF
Cancer Risk Program
d.71d.62
Three Generation Pedigree, Next Visit
85MI
45
22
47Breastca 65
2824
Prostate ca 55, Now 66
Breast ca 40, d45
d. 40OvarianDiabetes
Breast cancer
Prostate cancer UCSF
Cancer Risk Program
d.71d.82
Breast 33
Ovarian cancer
• “Cancer on the father’s side of the family doesn’t count.”
• “Ovarian cancer in the family history is not a factor in breast cancer risk.”
• “The most important thing in the family history is the number of women with breast cancer.”
Misconceptions About Family History
•Half of all women with hereditary risk inherited it from their father.•Ovarian cancer is an important indicator of hereditary risk, although it is not always present.•Age of onset of breast cancer is more important than the number of women with the disease.
© 2001 Myriad Genetic Laboratories
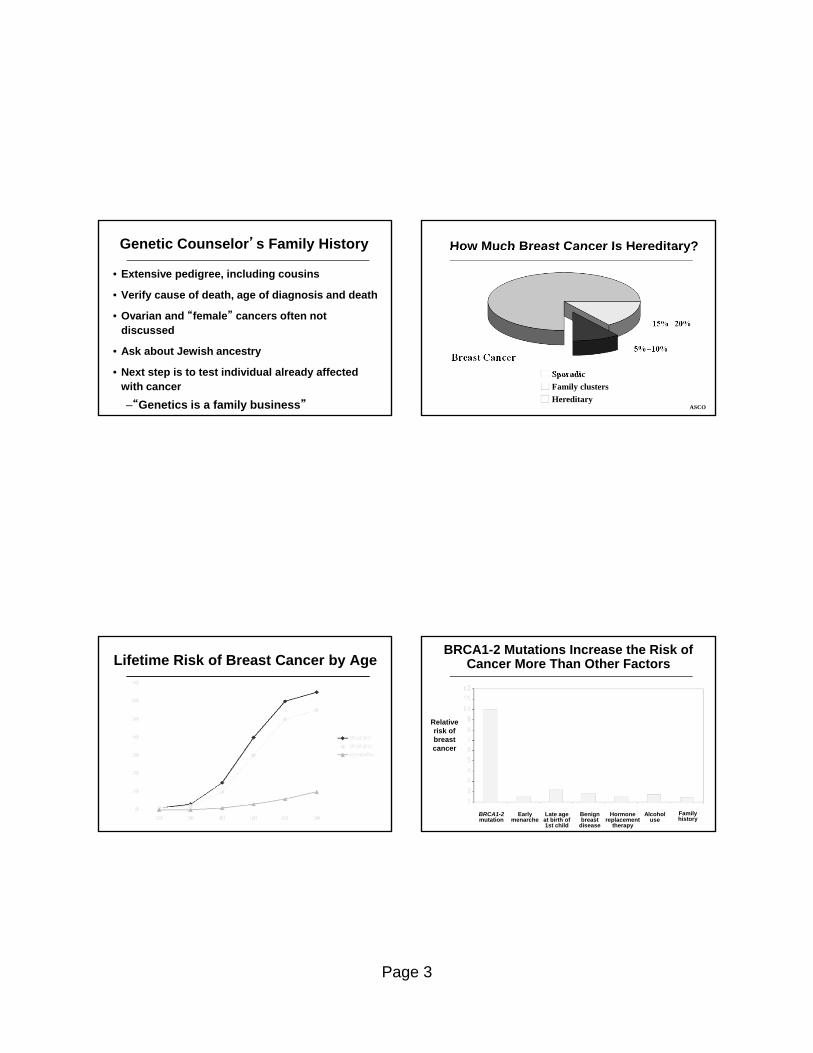
Page 3
Genetic Counselor’s Family History
• Extensive pedigree, including cousins
• Verify cause of death, age of diagnosis and death
• Ovarian and “female” cancers often not discussed
• Ask about Jewish ancestry
• Next step is to test individual already affected with cancer
–“Genetics is a family business” ASCO
How Much Breast Cancer Is Hereditary?
Sporadic
Family clusters
Hereditary
Breast Cancer5%–10%
15%20%
Lifetime Risk of Breast Cancer by AgeBRCA1-2 Mutations Increase the Risk of
Cancer More Than Other Factors
Relative risk of breast cancer
Family history
BRCA1-2mutation
Early menarche
Late age at birth of 1st child
Benign breast
disease
Hormone replacement
therapy
Alcohol use

Page 4
Cells have Two Copies of BRCA1
and BRCA2
BRCA2 BRCA1
Adapted from Tools for Understanding GeneticsNational Human Genome Research Institute
Office of Science Education and Outreachwww.nhgri.nih.gov/DIR/VIP
Each child has a 50% chance of inheriting an autosomal dominant disorder
Father withmutation on one chromosome
Autosomal Dominant Inheritance
BRCA 1 / 2 Associated Cancers:Lifetime Risk
Breast Cancer 12% 60-85%
Second Primary Breast <1% 40-50%
Ovarian Cancer 1.5%
BRCA1 - 20-40%
BRCA2 - 10-20%
General BRCA Population Population
Other cancers associated with BRCA2 mutations
Relative Risk*
• Melanoma 2.6
• Stomach 2.6
• Pancreatic 3.5
• Prostate 4.7
• Biliary tree 5.0
* Br Ca Linkage Consortium, JNCI 1999
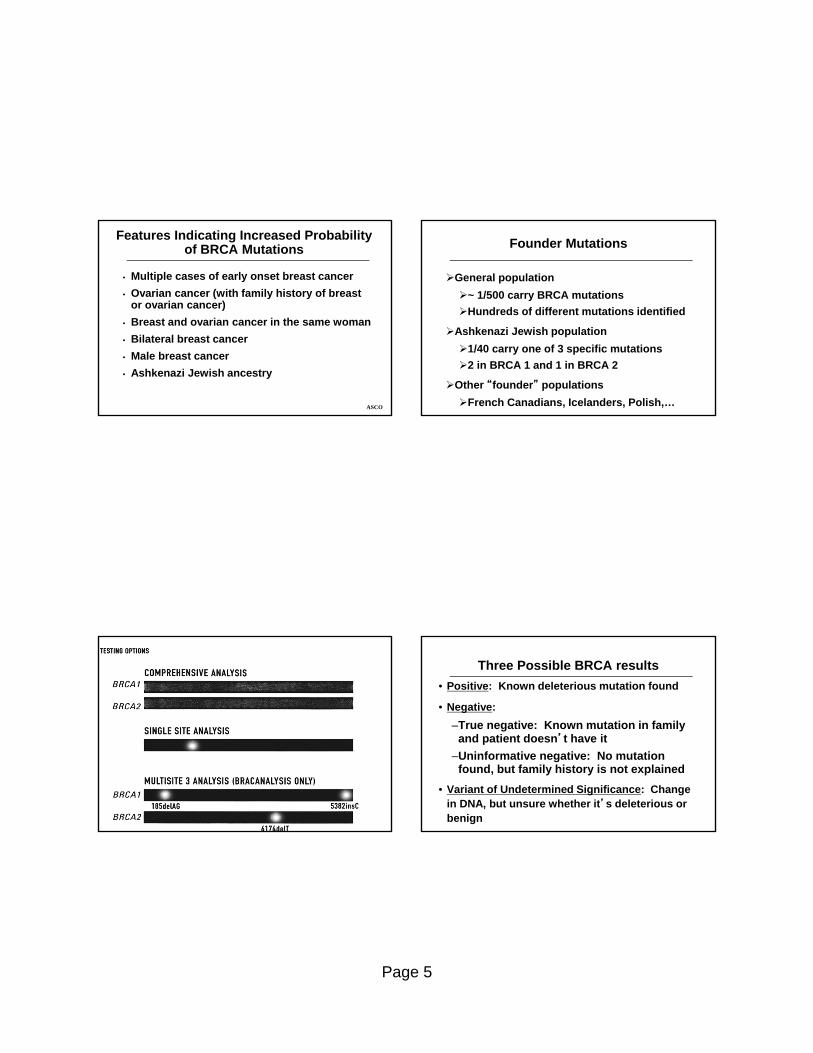
Page 5
ASCO
Features Indicating Increased Probability of BRCA Mutations
• Multiple cases of early onset breast cancer
• Ovarian cancer (with family history of breast or ovarian cancer)
• Breast and ovarian cancer in the same woman
• Bilateral breast cancer
• Male breast cancer
• Ashkenazi Jewish ancestry
Founder Mutations
General population
~ 1/500 carry BRCA mutations
Hundreds of different mutations identified
Ashkenazi Jewish population
1/40 carry one of 3 specific mutations
2 in BRCA 1 and 1 in BRCA 2
Other “founder” populations
French Canadians, Icelanders, Polish,…
Three Possible BRCA results
• Positive: Known deleterious mutation found
• Negative:
–True negative: Known mutation in family and patient doesn’t have it
–Uninformative negative: No mutation found, but family history is not explained
• Variant of Undetermined Significance: Change in DNA, but unsure whether it’s deleterious or benign

Page 6
How many “uninformative negatives” are really positive?
• 300 very high risk families with “uninformative negative”results AND 4 family members with breast or ovarian cancer
• 12% had duplications (repeated words), deletions (missing word), or rearrangements (misplaced word) in BRCA1 or BRCA2
• Unclear how common these “false negatives” are in the larger population receiving BRCA testing
Walsh, JAMA 2006
What are the Options for Carriers of Mutations?
Breast Cancer
Increased and earlier surveillance
Chemoprevention
Prophylactic Mastectomy-- 90% risk reduction
Ovarian Cancer
Trans-vaginal ultrasound and CA-125 q 6 mos
Birth control pills—50% risk reduction in 5 yrs
Risk Reducing Salpingo Oophrectomy (RRSO)
Insurance Questions • Will health insurance cover testing?
– Most cover if medically indicated: Pre-authorization
• Can health insurance plans increase premiums with a positive test?
– It is illegal to change or drop coverage based on a test result; not a pre-existing condition (HIPAA)
• Are there any protections against life insurance discrimination?
– Currently, no federal laws include life insurance
Ivana Test, Conclusion
• Ivana’s father tested positive for a mutation common in the Jewish population
– Men can carry mutations in BRCA1/2
– Start with an affected individual if possible
• Ivana then tested using the Jewish panel and was negative
– A negative result is only a “true negative” when there is a positive result in the family

Page 7
Cy Fibrosis’s History
• Infertility work-up showed azoospermia
• Congenital absence of vas defrens (1-2% of infertile men)
• Standard CF testing showed patient is a carrier of Delta F508
• He wants to use ICSI (intracytoplasmic sperm injection)
CF is Autosomal Recessive
Cystic Fibrosis Genetics
• CF is caused by mutations in a single large gene on chromosome 7 (codes CFTR protein)
• 250 kilobases, 1480 amino acid protein
• Wide phenotypic variation of disease
• 1998 consensus statement for screening– Family history of CF or partner’s family hx of CF
– Whites of European or AJ descent planning pregnancy or seeking prenatal care
Screen Cy’s wife? If so, how?
Ethnicity Incidence Carrier Frequency F508
White 1/3300 1/25 70%
Hispanic 1/8500 1/46 46%
AJ 1/29 30%
Black 1/15,300 1/65 48%
Native American
Zuni 1/3970 0%
Pueblo 1/1500 0%
Asian 1/32,100 1/90 30%

Page 8
Cy’s wife has a “variant”
• “Variants of Undetermined Significance” (VUS) occur in over 5% of whites receiving full sequence testing, 20-40% of non-whites
• Fetus: 1/4 chance of
–Carrying VUS
–Carrying Delta F508 mutation
–No mutation/no VUS
–Mutation + VUS
Cy Fibrosis’s Messages
• In any testing process, plan for “next step”
• Use genetic counselors to counsel and provide “informed consent”
• VUS are becoming more common
–Full sequence testing becoming more common
–Testing is becoming more accepted and available in non-white populations
Ima Clotter’s Family History
• Ima is G1P1, on birth control pills, and healthy.
• After 3 miscarriages, Ima’s older sister was found to have a “double defect”
• A third sister is currently pregnant.
• Feels it’s “opened Pandora’s Box” and wonders “How will it change my care if I test?”
What is a “double defect?”
Two inherited thrombophilias
Factor V Leiden , nucleotide 1691 transition from guanine to adenine results in Arg506Gln protein
Prothrombin 20210, guanine to adenine, untranslated
MTHFR variant (C677T)
Protein C deficiency
Protein S deficiency

Page 9
Risks of first venous thrombosis
Condition Relative Risk Annual Incidence
Normal 1.0 0.008
Hyperhomocysteinemia 2.5 0.02
(MTHFR C677T) 1.0
PT 20210 2.8 0.02
OCP’s 4.0 0.03
Factor V Leiden hetero 7.0 0.06
Plus OCPs 35 0.29
Factor V Leiden homo 80 0.5-1.0
Thromboembolism in Pregnant Women with Inherited Thrombophilias
Condition Probability per pregnancy
None 0.03%
Factor V Leiden 0.25%
PT 20210 0.5%
Factor V and PT 20210 4.6%
Anti-thrombin deficiency 0.4%
Gerhardt, NEJM 2000
Would testing change management?
• Indefinite anticoagulation recommended if
–2 or more spontaneous thromboses
–1 spontaneous thrombosis and-Antithrombin deficiency or antiphospholipid Ab -Life threatening or unusual site-”Double” or more defects
• Anticoagulate during pregnancy if
–Antithrombin deficiency or “double defect”
–Consider if personal or FH of thrombosis
Ima Clotter, Conclusion
• Ima is heterozygous for Factor V Leiden
– She stops OCPs
• Ima’s pregnant sister carries a “double defect”
– She is discussing anticoagulation with her OB
• Both defects are autosomal dominant
• Testing was fairly straightforward, as there were 2 genes with known mutations
Page 10
Fetal Aneuploidy Detection by Maternal Plasma DNA Sampling
Cell-free fetal DNA testing
Background
Trisomy 21(Down’s)
Trisomy 18(Edwards)
Trisomy 13(Patau)
• Most common chromosome abnormality
• Prevalence increases with maternal advancing age
• 5-10% survive to 1 year
• Severe intellectual disability
• 80% die in the first year
• Severe intellectual disability in survivors
Prenatal Testing is widely used to test for chromosomal abnormalities
Prenatal Diagnostic Testing
Noninvasive tests (screening)
• Maternal serum markers interpreted in the context of maternal age
• Nuchal translucency• Tests often used in
combination
Invasive tests (diagnostic)
• Chorionic Villus Sampling (CVS)
• Amniocentesis
ACOG recommends that pregnant women be offered screening and that all should have the option of diagnostic testing
Prenatal Diagnostic Testing
• Noninvasive tests are “screen positive” or “screen negative”
- Screen negative: risk of a baby with Down syndrome is less than a predetermined level (eg <1/500)
Individualized risk scores provided
- Screen positive: Patient is offered option of CVS or amniocentesis
• Invasive tests are diagnostic
- Fetal karyotyping
- CVS performed earlier than amniocentesis

Page 11
• Fetal blood found in the maternal circulation• Cell free nucleic acids more plentiful in maternal
circulation- Fetal DNA can be detected by 5th postmenstrual week- % increases with increasing gestational age
Cell-free Fetal DNA (cfDNA)
Massive Parallel Signature Sequencing (MPSS)
Directed Analysis(DANSR)
• Massive parallel sequencing random analysis of millions of cell free DNA fragments and assigns all free DNA fragments to specific chromosomes
• Number of chromosome counts compared to control values
• Directed DNA analysis selectively sequences relevant chromosomes
• Digital analysis of selected regions (DANSR)
• Uses fewer genetic fragments than MPSS
cfDNA: Potential Roles
Primary screening to replace current noninvasive tests
“Advanced”screening test
Potentially could reduce number of invasive tests and resulting loss of normal fetuses
Cannot replace diagnostic tests
Screening Test
Currently available cfDNA tests
Company LDT nameTrisomy identified Testing approach
T21(Down
Syndrome)
T18(Edwards
Syndrome)
T13(Patau
Syndrome)DANSR MPSS
AriosaDiagnostics
Harmony Prenatal Test
X X X X
Sequenom MaterniT21 X X X X
VerinataHealth
verifi prenataltest
X X X X
cfDNA: Evidence
• Eight studies evaluated cfDNa as screening for fetal aneuploidy
- 5 used MPSS
- 3 used DANSR
• Most studies were in high risk women
• Trisomies- All studies evaluated T21
- 6 studies evaluated T18
- 2 studies evaluated T13
• In all studies, true chromosome status was known

Page 12
cfDNA: Evidence
Palomaki, 2011; Palomaki, 2012;
Number of fetuses with abnormal karyotypes ranged from 39 to 283 in the largest study
Bianchi Study Palomaki Study
Aneuploid fetuses 221 283
Trisomy 21 89 212
Trisomy 18 36 59
Trisomy 13 14 12Other aneuploidies 82 None
MELISSA: cfDNA Multicenter Study
• 2,882 high risk women undergoing prenatal diagnostic procedures at 60 sites
• Nested case-control- All singleton pregnancies with any abnormal karyotype- Balanced number of randomly selected euploid
pregnancies
Bianchi, 2012
522 samples (221 abnormal karyotypes*)# cases Sensitivity Specificity
Trisomy 21 89 100%
100%Trisomy 18 36 97.2%
Trisomy 13 14 78.6%
*139 other aneuploidies
cfDNA Multicenter Validation Study
• Nested case control study in cohort of 4,664 high risk pregnancies
• 212 Down Syndrome and 1,484 matched euploidpregnancies
• 98.6% sensitivity for Down Syndrome
• 0.2% false positive rate
• Testing failed in 0.8% of pregnancies
Palomaki, 2011
NICE: Prospective Cohort Study
Multi-center cohort study: 3,228 participants all undergoing prenatal diagnostic procedure for any
reason
Norton, 2012
N=3,228Number of aneuploidy
casesSensitivity Specificity
Trisomy 21 81 100% 99.97%
Trisomy 18 38 97.4% 99.93%

Page 13
cfDNA: Comparative Studies
How does use of cfDNA compare with the established alternatives?
• Currently no direct evidence comparing cfDNA with established screening strategies for primary screening
• No studies have evaluated the potential role of cfDNAas a primary screening strategy
• To date studies have only evaluated high risk women using cfDNA as an advanced screening test
cfDNA: Clinical and Economic Model
• Used clinical data from MELISSA study
• Evaluated the impact of incorporating cfDNA into routine clinical care
- High risk women
- Advanced screening test
• 66% reduction in diagnostic induced miscarriages
• 38% more women receiving T21 diagnosis
• 1% overall reduction in prenatal screening and diagnostic costs
Garfield, 2012
Average risk women
• 2,049 women undergoing routine screening at 11-13 weeks gestation
• Fetal karyotyping in 86 cases
- Remainder considered phenotypically normal
• For all 8 cases of T21, the T21 Risk Score was >99%
• For 2 of the 3 cases of T18, the risk score was >99%
• cfDNA testing could not be performed on 4.9% of cases
cfDNA: Conclusions
• Promising new technology with high sensitivity and specificity for fetal aneuploidy when evaluated in high risk women
• To date, cfDNA has not been compared with current screening methods as an alternative to primary screening
• Currently no evidence to support use in average risk women

Page 14
To summarize…
Why consider testing for predisposition genes?
• To identify patients not at risk despite family history - reassurance
• To identify patients at very high risk of disease
• To allow high risk patients to consider increased screening and prevention
• To assist with prenatal counseling
• To allow patient to enter screening/ prevention trials
• To provide important health info to extended family
ASCO
A Multi-Step Process: Pretest Genetic Counseling
AssessPersonal and family medical historyRisk perception and motivation for testing
EducateBasic genetics and inheritanceGenotype/phenotype disparities and risk
DiscussRisks, benefits, and limitations of testing Test procedure Alternatives to testingManagement options
ASCO
A Multi-Step Process: Post-test Genetic Counseling
ReviewEducational concepts and family historyRisk and prior probabilities
DiscloseTest results Interpretation of results
DiscussPlans for prevention and treatmentSharing results with family membersPotentially testing other family members

6/24/2013
1
Chronic Pelvic Pain…..Relief for clinicians, and for patientsRebecca Jackson, MDProfessorObstetrics & GynecologyUniversity of California, San Francisco
DisclosuresI have no affiliation with any pharmaceutical companies, etc.
I will discuss off-label use of drugs.
2
The Challenge of CPPFrustrated (or desperate) patients want a definitive diagnosis and treatment right nowLack of clear national guidelinesLack of understanding of CPP among GYNs (and PCP’s)Lack of understanding among pain MDs of the pelvisHigh utilization of services often without improvement in patient pain or functioning
Goals of this lectureGive you hope (and skills necessary) that you can help many women with CPPConcentrate on interconnected, multi-factorial nature of CPPHow to create a therapeutic relationshipStepwise algorithm for diagnosis AND treatmentTreatment focus: trigger points, pelvic floor dysfunction, vulvodynia, neuropathic pain

6/24/2013
2
Syllabus NoteSyllabus includes slides that will not be addressed in lecture but are included for reference
These slides are marked with “REF”
Overview of CPP
Affects physical and sexual function, and emotional well-being Severely impacts quality of life
Multiple systems interact and contribute to the pathophysiology of CPP
In many cases a direct cause of CPP cannot be identified
Increased risk of a history of abuse, depression, and anxiety, which exacerbate painful symptoms
6
What CPP patients want1. Personalized care
2. To feel understood and taken seriously
3. Explanation of the cause
4. Reassurance
Set clear expectations Ask for her goals/concerns (and acknowledge them)
Set realistic expectations: 1. Improvement in pain/function; not pain free2. You will look for conditions that can be treated, but
even if can’t make clear diagnosis, you have options to help with pain
3. This will take awhile. Multiple visits. Multiple treatment modalities
4. If she wants relief, she will have to work at it. (PT, exercises etc)
5. Visits scheduled, not during flares6. Outline next steps, but don’t be pushed into an
immediate diagnosis7. You will partner with her throughout to help her
improve8. Pain contract for opiates (if necessary)
6/24/2013
3
Differential Diagnosis!
Gynecologic Urinary tract Mental health issues(cause increased pain)
Endometriosis* Interstitial cystitis* SomatizationAdenomyosis* Recurrent UTI Substance abusePost-PID syndrome Urethral diverticulum Physical and sexual abuse, PTSDVulvodynia, vulvar vestibulitis Chronic urethral syndrome Depression, Anxiety
Pelvic adhesions (maybe?) Neoplasia Musculoskeletal Pelvic congestion (maybe?) Radiation cystitis Pelvic floor myalgia*
Ovarian remnant syndrome Gastrointestinal tract Myofascial pain (trigger point neuralgia)*
Leiomyoma (pressure) Irritable bowel syndrome* HerniaEndosalpingiosis Chronic constipation Abnormal postureNeoplasia Inflammatory bowel disease Fibromyalgia
Fallopian tubal prolapse (post-hyst) Diverticular colitis Chronic abdominal wall pain
Tuberculous salpingitis Chronic intermittent bowel obstruction Neurologic
Benign cystic mesothelioma NeoplasiaNeuralgia of pelvic/pudendal nerves* (post-surgical or ob)
Postoperative peritoneal cysts Celiac disease Herniated discNeuropathic pain (diabetes)
* Most common
Mental Health Issues
GUGIGyn Musculoskeletal
Depression, anxiety, PTSD, IPV, h/o abuse: Exacerbate painful symptoms
Primary etiology of pain can be Gyn, GI, GU or M-S
Initial insult can cause musculoskeletal dysfunction that can persist after initial insult resolves, or can feedback and make primary visceral symptoms worse
It’s all connected
Musculoskeletal
Stepwise approach to Eval & Treatment
Step 1: Address Mental HealthTreat depression if present
Counseling if h/o abuse
Step 2: Eval and treat musculo-skel issues
Step 3: Choose possible diagnosis and treat empirically
Step 4: If not improved: Consider another diagnosis/trtment
Add other meds (TCA, gabapentin)
Re-address M-S issues: physical therapy if not yet tried Order of steps not important: Do in
whatever order makes sense for given patient
The CPP History & PENot just for getting to diagnosis but also….
Powerful therapeutic toolCareful history, close listening, thorough (but sensitive) PE build rapport, trustTherapeutic benefit from the telling of one’s story (therefore, use written history forms only as adjunct)Reflect back what you have heardDiscuss concerns, fears

6/24/2013
4
2
Chronic Pelvic Pain.Howard, Fred; MS, MD
Obstetrics & Gynecology. 101(3):594‐611, March 2003.
Particularly Important Questions to Ask of Women With Chronic Pelvic Pain
Point to it
Did anything happen that may have brought it on?
If intermitt: how long is each episode?
Relation to BM, voiding?
CPP: History Clues
Timing relative to menses, urination, BMMost endometriosis initially includes dysmenorrhea (may progress to continuous, non-cyclic pain)Quality of painSqueezing, cramps: visceralSharp, shooting, lancinating: somaticCyclic pain is usually gynecologic but both IBS and interstitial cystitis can be worsened with menses
What do you think is the cause?
CPP: HistoryUrinary symptoms
Dysuria, frequency, nocturia, incomplete voiding
Pain worse with full bladder?
GI symptoms
Dyschezia, nausea, diarrhea, constipation, mucus stools, hematochezia, melena
Pain relieved by bowel movements?
Musculoskeletal symptoms
LBP, joint pain, sciatica
Effect of movement on pain
CPP Physical Exam GoalsIdentify underlying pathologyReproduce painEstablish trust, minimize fearNot just a pelvic exam! Observe gait/posture, thorough exam of abdwall, pelvic floor muscles, vaginal introitus

6/24/2013
5
CPP: Before Leaving…Get More Information!!
Pain diary with menstrual calendar
Voiding diary
Bladder questionnaires
Medical record review
Back to the Stepwise approach
Step 1: Address Mental HealthTreat depression if present
Counseling if h/o abuse
Step 2: Eval and treat musculo-skel issues
Step 3: Choose possible diagnosis and treat empirically
Step 4: If not improved: Consider another diagnosis/trtment
Add other meds (TCA, gabapentin)
Re-address M-S issues: physical therapy if not yet tried Order of steps not important: Do in
whatever order makes sense for given patient
1. Address mental health issues
Pain has impact on quality of life and functional capacityWomen become isolated and have difficulty communicating needsRelationships become strainedPre-existing psych issues such as PTSDexacerbated by painAnxiety, depression, IPV, h/o of abuse are common act to exacerbate pain
Assess quality of life (REF) In the past month, how much has your pelvic pain kept
you from doing your usual activities such as self-care, work or recreation? (scale 1-5)
How much has your pelvic pain interfered with your quality of life?
How much have the treatments you have received for your pelvic pain improved your quality of life?
How do you cope with your pain?
How does your partner, family etc. respond when you are in pain?
20

6/24/2013
6
“Sensitive History”
IPV, h/o abuse, sexual functioning, depressionFrame it: remember, these pts may distrust medical system, think you are trying to say their pain is in their heads“I would like to ask you questions about the rest
of your life to help me understand how the pain is affecting you. This will help me know how best to treat you.”“I ask these questions of all my patients”
Emotional Health (REF)Screen for current or prior physical or sexual violence,
including events in childhood "At any time, has a partner hit, kicked, or otherwise hurt or threatened
you?" “Has your partner or a former partner every hit or hurt you? Has he or
she ever threatened to hurt you?” “Do you ever feel afraid of your partner?” Have you ever been forced to have sex when you didn’t want to?
Depression (12-35%) During the past month, have you been bothered by little interest or
pleasure in doing things?
During the past month, have you been bothered by feeling down or hopeless?”
Assess sexual functioning (68% have dysfunction) Desire, frequency, satisfaction, orgasm and discomfort
22
Treating Sexual Pain (REF)
Learn about your body Explore your pleasure spotsEducate your partnerConnect with your partner in sexual and non-sexual waysPrepare for sex: relax the PF muscles, use lubricants, take time for arousalReinvent your sex lifeAvoid painful activities
23
Heather Howard, PhD Sexual Rehab.org
1. Address mental health issues
SSRI for depression
Counseling (especially cognitive-behavioral therapy) for h/o abuse, difficulty coping with pain
Address sexual pain

6/24/2013
7
2. Evaluate and treat musculoskeletal issues
Myofascial Pelvic Pain Syndrome
28 muscles have direct attachments to the pelvis!
Inciting event: injury/trauma, visceral condition (IBS, EM, EC), referred pain from viscera, poor posture
Leads to: Short, tight, tender pelvic floor muscles and pain in pelvis, vagina, vulva, rectum, or bladder, or referred to thighs, buttocks, or lower abdomen.
Many experts believe that many, if not most, women with chronic pelvic pain have some degree of MPPS
Trigger points are the hallmark of myofascial pain
Even without classic trigger points, muscular pain prominent in many women with CPP (regardless of etiology)
Pelvic Floor Myalgia
FindingsPain is aching, throbbing, or heavinessLow back, sacral pain; can radiate to hip, thighOften worse with prolonged standingLevators are tense, tender on vaginal examManagementPelvic physical therapy and biofeedbackNeuropathic pain medications (gabapentin, TCAs)Vaginal or abdominal wall trigger point injectionsRelaxation therapy (breathing, visualization)Ice, heat (to the vagina!)
Carnett’s SignDifferentiates pain originating from the abdominal wall versus peritoneal cavity (Suleiman et al., 2001)
The patient raises her head and shoulders from the examination table while the provider palpates the tender area on the abdomen.
Positive Carnett’s sign: pain remains unchanged or increases when the abdominal muscles are tensed.
28

6/24/2013
8
Examining Pelvic Floor Muscles29
12-point Unimanual UnidigitVaginal Exam
Palpate in 4 quadrants x 3 depths Single fingerNO abdominal palpationJust beyond hymen12:00 urethra, 6:00 rectum3:00/9:00 obturator internusMid-vagina12:00 bladder base, 6:00 rectum3:00/9:00 puborectalisJust before cervix12:00 bladder, 6:00 rectum/cul-de-sac3:00/9:00 pubo/iliococcygeus
30
“Does this reproduce your pain?”
A couple patients1. 21 yo with CPP x 1.5 yr, band across her
lower abd, thinks it started with IUD placement. IUD removed 3 mos ago, no change. Of note, had leg injury and walks with cane
2. 51 yo with CPP many yrs, now w 10/10 flare. RLQ. s/p hyst (no relief), s/p l/s 1 yr ago—adhesions but o/w nl. Percoset with some relief. Thinks its due to ovarian cysts b/c had some on earlier u/s.
Both had….
Myofascial Trigger Points32
Trigger points are hyperirritable palpable nodules that are taut bands of muscle fibers (Tough et al., 2007)
When palpated the pain usually radiates to another location
Found in abdominal wall, perineum and pelvic floor locations
Abdominal wall and vagina share T10-12 dermatomes with pelvic organs: Pain from trigger points referred to pelvic organs
See also: Lavelle, E., Lavelle, W., & Smith, H. (2007). Myofascial trigger points. Anesthesiology Clinics, 25, 841-51.

6/24/2013
9
Trigger Point Injection Therapy Local anesthetic injection(s) directly into
trigger point (TP). Thought to interrupt pain pathway 93% success by 5th injection in abdomen (Kuan,
2006) Agent: Lidocaine 1%, Bupivicaine 0.25%, Plus /minus
triamcinolone 10mg (caution corticosteroids) Volume: 2 to 10 cc. (use 2 cc if multiple trigger point,
larger volume if only one. Beware lido toxicity—limit to <15-20 cc)
22 or 25 gauge needle, long enough to reach the TP. Find the TP with the needle: TP=maximal burning pain Weekly injections, stop if no relief at all. Continue if
any relief.
Best if combined with physical therapy
33
Intravaginaltrigger points can be accessed with trumpet pudendalneedle guide
Langford, Neurourology and UrodynamicsVolume 26, Issue 1, pages 59–62, January 2007
Botulinum toxinA few small studies of injections into levator ani show benefit
Consider it experimental
Risk of major side effects: urinary or fecal incontinence or retention
Another patient….25 yo with CPP and known endometriosis (l/s proven), much improved with continuous OCP but still w significant dysparunea and pain that affects her QOL.
She had….
6/24/2013
10
Myofascial pain treatment
Anti-inflammatories, ice to vagina, vulvaRefer patients to physical therapists specializing in pelvic floor muscle work (advanced training)Myofascial releaseBiofeedbackHome exercise programAbdominal breathing, rescue poses, stretching
exercises
37
See American Physical Therapy website for referrals
3. Choose possible diagnosis & treat empirically
These 5 diagnoses account for most known causes of CPP:1. IBS2. Interstitial Cystitis3. Endometriosis4. Adenomyosis5. Vulvodynia/vulvar vestibulitis
Pain or discomfort for 3 days/month in the prior 3 months with 2 or more of: Improvement with defecation Onset associated with a change in frequency of stool Onset associated with a change in appearance of stool
Symptoms lending support to diagnosis
>3 bm per day or <3 bm per week
Lumpy/hard or loose/watery stool, mucus passage
Urgency or incomplete emptying
Bloating or distension
Symptoms may be precipitated by meals or certain foods
Caveats: Can be worse with menses so don’t r/o if pain is cyclic
Irritable Bowel Syndrome(IBS)
Rome III Diagnostic Criteria
Treatment for IBS (REF) Dietary recommendations: Elimination diet
Fiber—Mainstay of treatment Eat at regular times
Watch dairy products
Drink plenty of fluids
Pain/gas/bloating: antispasmodic (dicyclomine, hyoscyamine)
Constipation: increased fiber and psyllium
Diarrhea: loperamide
Stress reduction
Exercise regularly
Antidepressants
Alosetron (diarrhea) or lubiprostone (constipation)
CAM: acupuncture, herbs, probiotics, hypnosis, peppermint oil
6/24/2013
11
Interstitial Cystitis (IC)Symptoms/Signs Urgency, frequency, nocturia, bladder painPain worse on filling bladder; better on voidingMay also have dyspareunia, urge incontinence Bladder tenderness + pelvic floor tenderness Absence of objective evidence of another disease that
could cause the symptoms
Diagnosis of IC: PUF Questionnaire (pain/urgency/freq)
Max score = 35 PPV 91% (vs. KCL sensitivity) if score > 20 Lowest threshold for diagnosis is score >12
Parsons CL et al. Urology 2002;59:329‐33 and 60:573‐8.PUF questionnaire avail online: search: “PUF Interstitial cysitis
Treatments for IC Start with:
Oral sodium pentosan polysulfate (PPS) 100mg TID (Elmiron)
Eliminate bladder irritants: acidic foods, artificial sweeteners, caffeine, tea, chocolate
Stop Smoking
Bladder training
Physical therapy, stretching
Refer to urogyn if not effective: Intravesical treatments Hydrodistension under general anesthesia: “mainstay of treatment”
Dimethylsulfoxide Q1-2wks x 4-8 times: remission not cure
BCG (Bacillus Calmette-Guerin) 6 weekly treatments TENS
Endometriosis (EM): Presentation
Classical EM occurs in a minority of patients
Dysmenorrhea
Dyspareunia
Perimenstrual tenesmus, diarrhea, dysuria, hematuria, sacral backache
Commonly, continuous CPP is the sole complaint (although
many will give h/o of significant dysmenorrhea)
Bimanual exam may show:
Uterosacral ligament nodularity, fixed uterine retroflexion
Stenotic cervical os, deviated cervix
Corpus and adnexal tenderness
Tender pelvic floor
Endometriosis (EM): Role of L/S
Conventional wisdom
EM requires a surgical diagnosis
Recent trend
Empirical diagnosis of women likely to have EM is safer and more cost-effective than laparoscopy
If history consistent and pain improved with either continuous hormonal methods or with GnRHagonist, assume endometriosis
Reserve laparoscopy to treat endometriosis in setting of infertility, desiring pregnancy (improved fertility rates after surgical trtment) and for endometriomas

6/24/2013
12
Endometriosis, empiric therapy
No
NSAID + Continuous OC x2‐3 mo
Improved?
Yes
Continue OC* GnRHa x2 mo
Pain Improved?#
YesComplete* 6‐9 mo No
Consider L/S, other diagnoses, Musc‐skeleval/trt
# Both pain score and functionality improve
*Or transition to DMPA, ?Implanon, LNG-IUS, (or OC)
Adenomyosis Presentation
Endometrial glands, stroma within myometriumSymptomsOnset usually in late 30s-40sNew onset dysmenorrhea; constant CPP possibleSometimes: dyspareuniaIrregular vaginal bleedingNo bowel or bladder symptoms unless EM’osisSignsUterus enlarged, “boggy” and tenderNo adnexal tenderness
Adenomyosis: Diagnosis/Treatment
DiagnosisPathologic diagnosis.
More recently, MRI being used. However, unclear clinical utility, can simply start empiric therapy.
Treatment: Ovarian suppression: OCs, Patch, DMPA, Implanon
Levonorgestrel IUD
If fail hysterectomy
Medical management often ineffective for controlling pain of adenomyosis. (works for bleeding)Unlike for other pelvic pain syndromes, hysterectomy for
adenomyosis is often curative b/c symptoms confined to uterus
VulvodyniaIncidence: 3-5% of reproductive age women
Risk Factors:Vulvovaginal infectionOC usePhysical, emotional or sexual traumaComorbid disorders:ICIBSFibromyalgia/Chronic Fatigue SyndromePsychosocial and sexual impairment
48

6/24/2013
13
Vulvodynia: Q Tip Test
Purpose: identify and map changes in sensation including allodyniaGently touch with a q-tipStart at the thigh and work down to perineum bilaterallyInclude clitoris and perianal areasProceed from labia majora to labia minora then the vestibule
49 Diagnosis of Vulvodynia & Vestibulodynia
Chronic Vulvar Pain
PENo visible findings
Erythema
Hyperalgesia
Allodynia
VulvodyniaGeneralized pain
Burning, stabbing, stinging, etc.
VestibulodyniaPain at vestibule only
Provoked
Burning
R/OInfectious,
inflammatory, neoplastic and
neurologic cause
Treat accordingly
50
Vulvar Vestibule51 Treatments: Vulvodynia & Vestibulodynia 52
• Behavioral: Avoidance of vulvar irritants, constipation, sitzbath bid followed by vaseline, Ice/cool for burning, after sex
• Meds: No meds clearly superior, may need to try several, Start with topical lidocaine or topical gabapentin 6%. 3 mos trial; Other meds: Oral TCA’s, Anticonvulsants, SSNRI’s, Opioids; Topical: estradiol cream (if atrophic), compounded antidepressants, anticonvulasants
• Pelvic floor therapy, biofeedback very important• Psychotherapy, CBT, Sex therapy• Nerve blocks, Nuerostimulation• Surgery? For generalized vulvodynia, surgery
contraindicated. For localized vestibulitis, vestibulectomyhas been shown effective

6/24/2013
14
4. If no improvementConsider another diagnosis/trtment
Add other meds (TCA, gabapentin)
Re-address M-S issues: physical therapy if not yet tried
When pain is a disease and not a symptomAfter 4-6 months, pain can become an illness, not just a symptom“Central Sensitization”= Maladaptation: “an
amplification of neural signaling within the central nervous system that elicits pain hypersensitivity”
Inciting event might have been treated, pain persistsTreatment focuses not on cure but on managing the pain
Treating Pain: Medications
Analgesics:NSAIDS (try at least 3)
Opioids (short course)
Topical anesthetics*
AntidepressantsTricyclics*
SSRI’s/SNRI’s*
Anticonvulsants gabapentin
pregabalin
Muscle relaxants
Vaginal preparations (valium, anti-depressant, anti-convulsant)
Refer to pain management
nerve blocks
neurotoxin: OnabotulinumtoxinA*
medication consult
55
*Off label use
Treatment of Neuropathic Pain
Mainly helpful in women with daily painClinical depression is presentSSRI (e.g., fluoxetine) or SNRI (e.g., venlafaxine)Advance to “primary care” dosing limitsClinical depression not prominentGabapentin 100-300 mg QHS, adv to 900 mg TIDTCA: nortriptyline 10 mg QHS, adv weekly to 50 mg
Sleep problemsHerbals, antihistaminesShort acting sleeping meds: e.g., zolpidem

6/24/2013
15
Integrative ApproachMind/body interventions: breathing exercises, imagery, MBSR, laughter yoga, etc.Movement therapies: yoga, Tai Chi, Feldenkrais, etc.Nutrition: anti-inflammatory diet/herbs, multivitamins, B complex, fish oil, calcium/magnesium, herbal tonicsAlternative providers: TCM, craniosacral, chiropractic, energy medicine, strain/counter strain, etc.
57
Take It HomeSpend time to establish trust
Set realistic goals with your patient: improved function vs. complete remission
Think beyond “making a diagnosis”
Manage the reactive depression that can make the perception of pain much worse
Pelvic floor dysfunction is common and perpetuates the pain cycle. Treat with pelvic PT plus/minus trigger point injections
If your first empiric therapy is ineffective, don’t give up. Revisit other diagnoses, depression and musculo-skeletal issues.
Build a community: physical therapist, pain consultant
What CPP patients want1. Personalized care
2. To feel understood and taken seriously
3. Explanation of the cause
4. Reassurance
Although we often can’t give them #3, we can explain the interconnectedness of pelvic organs, muscles and pain pathways.
Patients don’t really come to us because they are in pain, they come to us because they are suffering.Ling, APS Conference 2010
60

6/24/2013
16
Resources
International Pelvic Pain Society
National Vulvodynia Association
Endometriosis.org
Sexuality Information and Education Council of US
Interstitial Cystitis Association
Irritable Bowel Syndrome: see NIDDK/NIH
American Physical Therapy Association
American Chronic Pain Association
UCSF Chronic Pelvic Pain Clinic
61 ReferencesReferencesACOG Committee on Practice Bulletins--Gynecology
ACOG Practice Bulletin No. 51. Chronic pelvic pain. Obstet Gynecol. 2004 Mar;103(3):589-605
Jarrell F, et al. Consensus guidelines for the management of chronic pelvic pain J Obstet GynaecolCan. 2005;27(8):781-826.
Howard FM. Chronic pelvic pain. Ob Gynecol. 2003;101:594-611.
Abercrombie PD, Learman LA. Providing Holistic Care for Women with Chronic Pelvic Pain. J Obstet GynecolNeonatal Nurs. 2012 Aug 3. (Entire issue devoted to chronic pelvic pain)

6/24/2013
1
Why am I Bleeding?Management of 1st Trimester Bleeding
Alison Jacoby, MD
Dept. of Obstetrics, Gynecology & Reproductive Sciences
University of California, San Francisco
Disclosures
• I have no relevant financial disclosures.
• I will discuss off-label use of misoprostol.
Acknowledgements• Robin Wallace, Carolyn Sufrin, Jody
Steinauer and Meg Autry
Julie is a 23 year-old G1P0 at 6+5 by LMP with spotting x 1 day, no pain, β-HCG = 2672.
MSD = 25mm, no fetal pole
Objectives
1. Review early pregnancy loss
2. Review clinical, serum, and ultrasonographic diagnostic features
3. Compare management options– Discuss role of patient preferences
– Expectant, medical, surgical (office vs. OR)
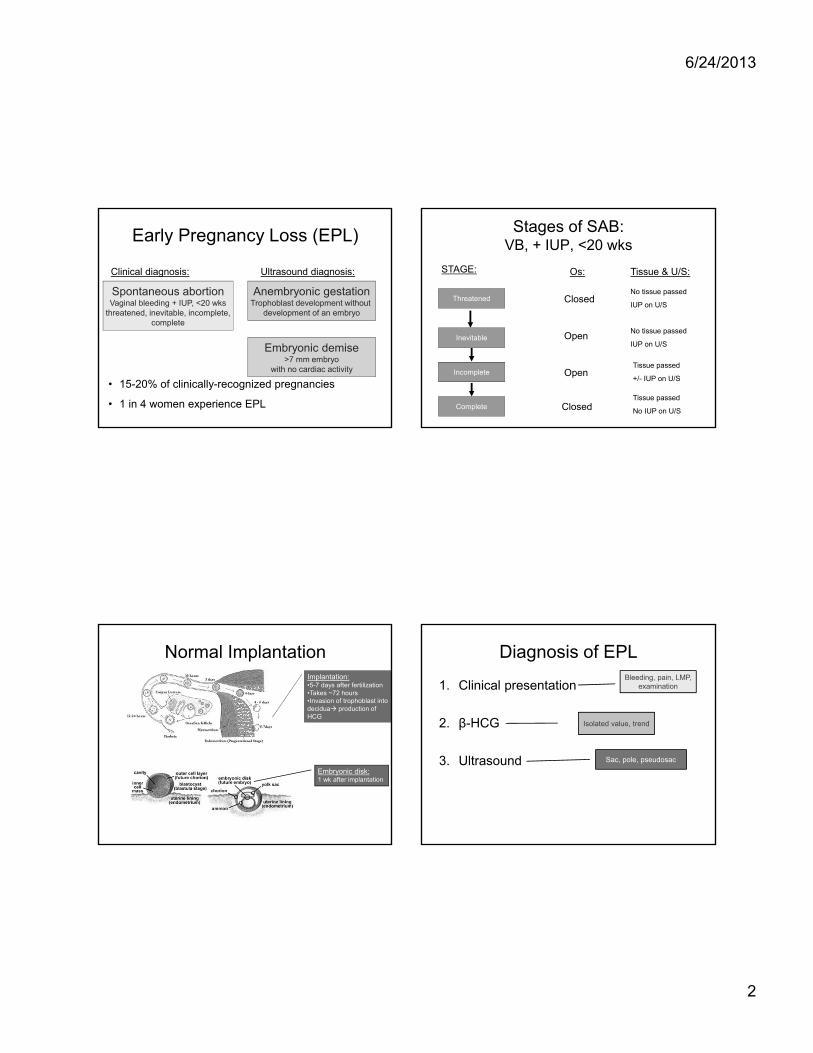
6/24/2013
2
Early Pregnancy Loss (EPL)
• 15-20% of clinically-recognized pregnancies
• 1 in 4 women experience EPL
Spontaneous abortionVaginal bleeding + IUP, <20 wks
threatened, inevitable, incomplete,complete
Embryonic demise>7 mm embryo
with no cardiac activity
Anembryonic gestationTrophoblast development without
development of an embryo
Clinical diagnosis: Ultrasound diagnosis:
Stages of SAB:VB, + IUP, <20 wks
Threatened
Inevitable
Incomplete
Complete
ClosedNo tissue passed
IUP on U/S
OpenNo tissue passed
IUP on U/S
Tissue passed
+/- IUP on U/S
Tissue passed
No IUP on U/S
Open
Closed
STAGE: Os: Tissue & U/S:
Normal ImplantationImplantation:•5-7 days after fertilization•Takes ~72 hours•Invasion of trophoblast into decidua production of HCG
Embryonic disk: 1 wk after implantation
Diagnosis of EPL
1. Clinical presentation
2. β-HCG
3. Ultrasound
Bleeding, pain, LMP, examination
Isolated value, trend
Sac, pole, pseudosac

6/24/2013
3
Beta Curves, Redefined
• Rate of increase depends on gestational age1
• 49 normal intrauterine pregnancies• Doubling time varies by gestational age
<5 wks: 1.5 d5-6 wks: 2 d>7 wks: 3d
1. Pittaway 1985 Fertil Steril & Am J Ob Gyn
Letting go of the “double in 48 hours” rule
Beta Curves, Redefined
• Early studies used 85% CI as lower limit1
– Retrospective study of 20 women
– Mean doubling time 2 days
– 66% increase in 48 hrs• Poor sensitivity and specificity in cohort:
– Of 12 ectopics – 17% normal rise
– Of 16 normal pregnancies - 18% abnormal rise
• Newer data - different median and mean 2
2. Barnhart 2004 Obstet Gynecol
1. Kadar 1981 Obstet Gynecol
Letting go of the “double in 48 hours” rule
• 287 women with pain or bleeding and +UPT– No IUP on U/S but eventually had normal IUP
– Initial β-HCG < 5000
• Ave GA by LMP = 38 days (range, 0-107)
• At least 2 β-HCG’s within 7 days
Barnhart 2004 Obstet Gynecol
Beta Curves, RedefinedLetting go of the “double in 48 hours” rule
β HCG Trends in Normal IUP
Barnhart 2004 Obstet Gynecol
99% of nl IUPs1 day rise ≥ 24%2 day rise ≥ 53%
Median rise:1 day= 50%
2 day =124%
Slowest expected increase for normal pregnancy = 53%

6/24/2013
4
Ultrasound & Early Pregnancy:Key Findings
Gestational sac
Yolk Sac
Embryonic Pole
Cardiac Activity
Double decidual signGrows ~ 1mm/day
Early circulatory system
Grows ~ 1mm/day
100bpm140 bpm
Ultrasound MilestonesWhen should you see it?
Abnormality
Gestational Sac Discriminatory Level
β = 1500-2000
Ectopic v. abnl IUP
Multiple gestation
Complete SAB
Yolk sac MSD>13-16mm (wait for fetal pole)
Fetal pole MSD >20mm Anembryonicgestation
Cardiac activity Fetal pole ≥ 5.3mm Embryonic demise
5mm cut off = 8.3% false +5.3mm cut off = 0 false +
(Abdallah et al 2011 [Oct] Ultrasound Obstet Gynecol)
Ultrasound Diagnosis of EPL:Anembryonic Gestation
Mean sac diameter >=21mm(20 mm = 0.5% false positive)AND no fetal pole
Growth?Cut off 0.6mm/day 90% specCut off 0.2mm/day 99% spec
1.4mm/week
Abdallah et al 2011 (Aug) Ultrasound Obstet Gynecol
ACR Appropriateness Criteria for First Trimester Bleeding
Failed pregnancy can be diagnosed by:
Mean sac diameter >= 25mm AND no embryo
Absence of cardiac activity in an embryo > 7mm in CRL
Barton et al 2013 (Jun) Ultrasound Quarterly
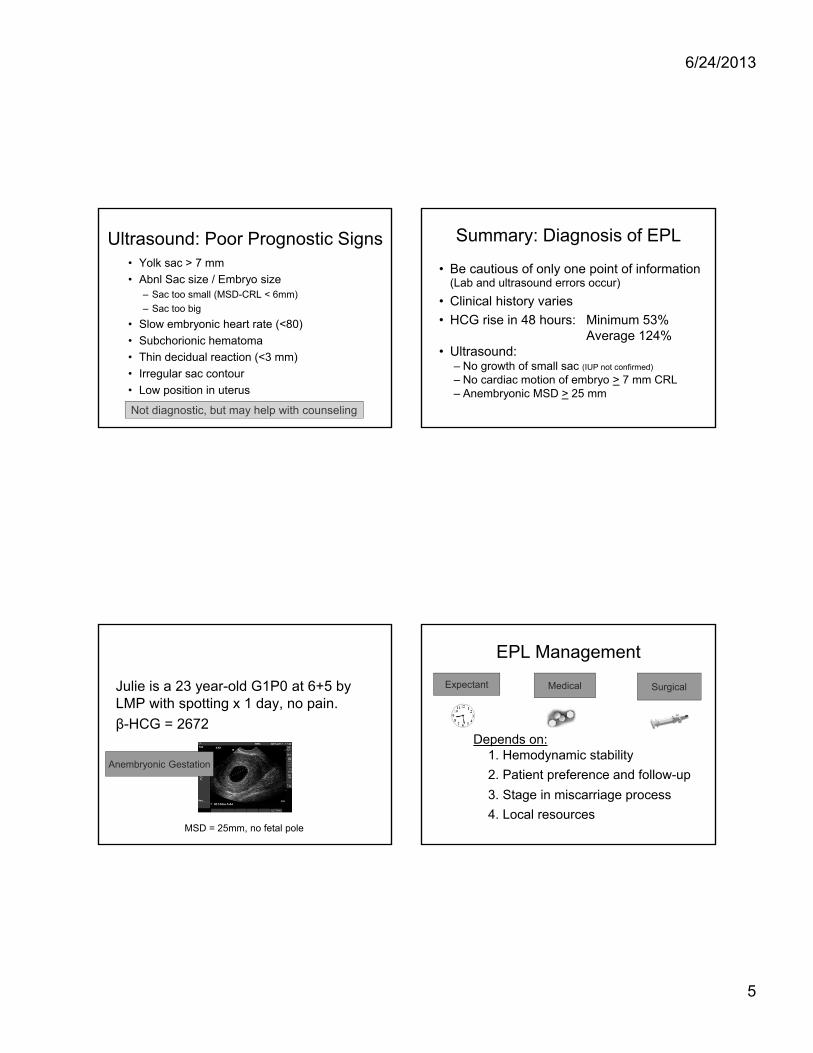
6/24/2013
5
Ultrasound: Poor Prognostic Signs• Yolk sac > 7 mm
• Abnl Sac size / Embryo size– Sac too small (MSD-CRL < 6mm)
– Sac too big
• Slow embryonic heart rate (<80)
• Subchorionic hematoma
• Thin decidual reaction (<3 mm)
• Irregular sac contour
• Low position in uterus
Not diagnostic, but may help with counseling
Summary: Diagnosis of EPL
• Be cautious of only one point of information(Lab and ultrasound errors occur)
• Clinical history varies
• HCG rise in 48 hours: Minimum 53%Average 124%
• Ultrasound:– No growth of small sac (IUP not confirmed)
– No cardiac motion of embryo > 7 mm CRL– Anembryonic MSD > 25 mm
Julie is a 23 year-old G1P0 at 6+5 by LMP with spotting x 1 day, no pain.
β-HCG = 2672
MSD = 25mm, no fetal pole
Anembryonic Gestation
EPL Management
Medical SurgicalExpectant
Depends on:1. Hemodynamic stability
2. Patient preference and follow-up
3. Stage in miscarriage process
4. Local resources
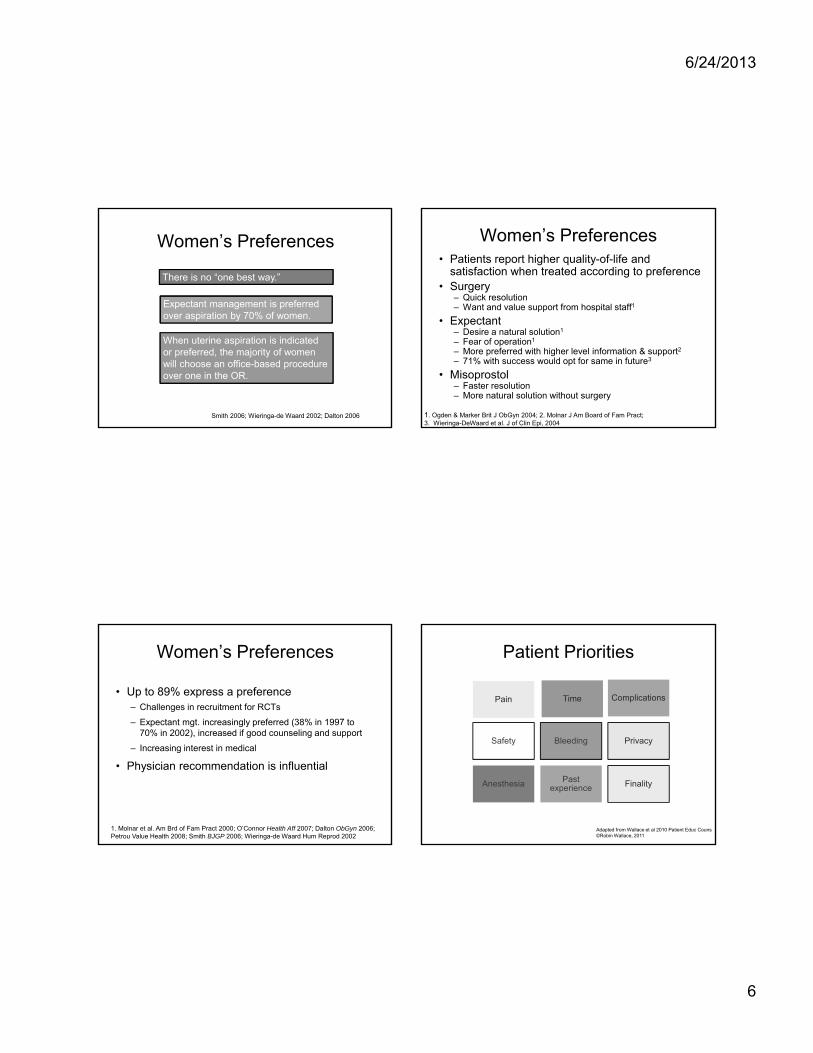
6/24/2013
6
Women’s Preferences
There is no “one best way.”
Expectant management is preferred over aspiration by 70% of women.
When uterine aspiration is indicated or preferred, the majority of women will choose an office-based procedure over one in the OR.
Smith 2006; Wieringa-de Waard 2002; Dalton 2006
Women’s Preferences• Patients report higher quality-of-life and
satisfaction when treated according to preference• Surgery
– Quick resolution – Want and value support from hospital staff1
• Expectant – Desire a natural solution1
– Fear of operation1
– More preferred with higher level information & support2– 71% with success would opt for same in future3
• Misoprostol– Faster resolution– More natural solution without surgery
1. Ogden & Marker Brit J ObGyn 2004; 2. Molnar J Am Board of Fam Pract;3. Wieringa-DeWaard et al. J of Clin Epi, 2004
Women’s Preferences
• Up to 89% express a preference– Challenges in recruitment for RCTs
– Expectant mgt. increasingly preferred (38% in 1997 to 70% in 2002), increased if good counseling and support
– Increasing interest in medical
• Physician recommendation is influential
1. Molnar et al. Am Brd of Fam Pract 2000; O’Connor Health Aff 2007; Dalton ObGyn 2006; Petrou Value Health 2008; Smith BJGP 2006; Wieringa-de Waard Hum Reprod 2002
Patient Priorities
Pain Time Complications
Safety Bleeding Privacy
Anesthesia Past experience Finality
Adapted from Wallace et al 2010 Patient Educ Couns©Robin Wallace, 2011
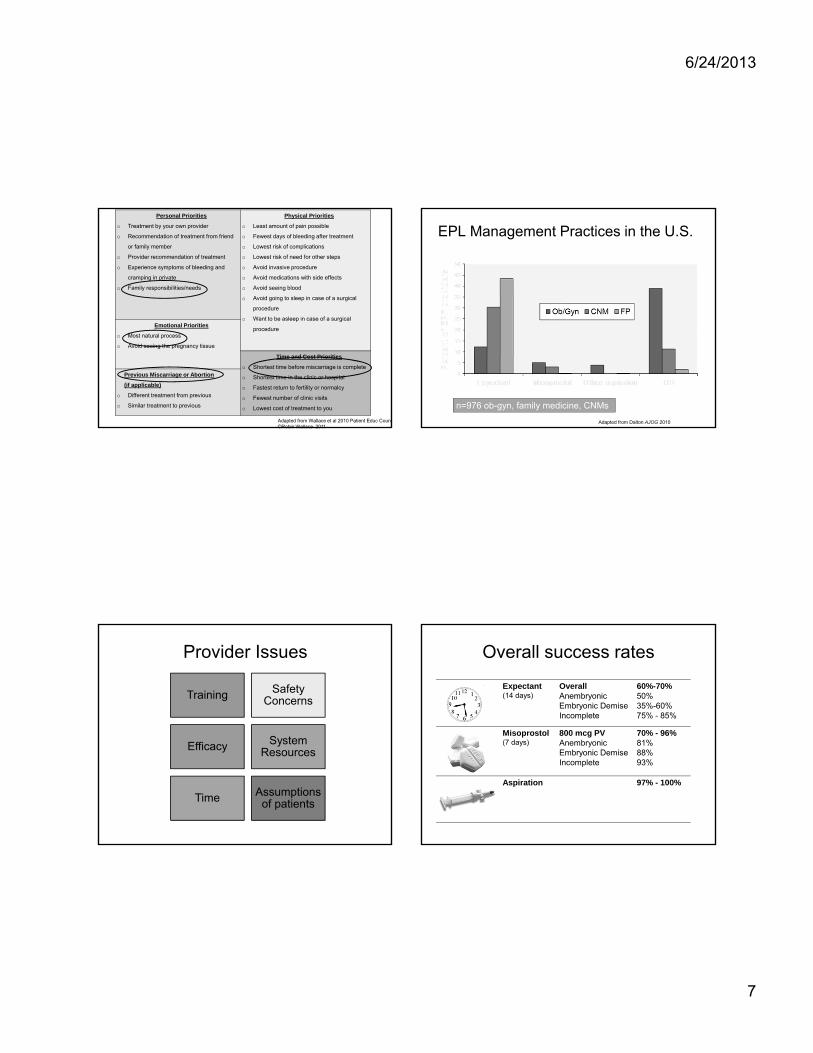
6/24/2013
7
Personal Priorities
o Treatment by your own provider
o Recommendation of treatment from friend
or family member
o Provider recommendation of treatment
o Experience symptoms of bleeding and
cramping in private
o Family responsibilities/needs
Physical Priorities
o Least amount of pain possible
o Fewest days of bleeding after treatment
o Lowest risk of complications
o Lowest risk of need for other steps
o Avoid invasive procedure
o Avoid medications with side effects
o Avoid seeing blood
o Avoid going to sleep in case of a surgical
procedure
o Want to be asleep in case of a surgical
procedureEmotional Priorities
o Most natural process
o Avoid seeing the pregnancy tissue
Time and Cost Priorities
o Shortest time before miscarriage is complete
o Shortest time in the clinic or hospital
o Fastest return to fertility or normalcy
o Fewest number of clinic visits
o Lowest cost of treatment to you
Previous Miscarriage or Abortion
(if applicable)
o Different treatment from previous
o Similar treatment to previous
Adapted from Wallace et al 2010 Patient Educ Couns©Robin Wallace, 2011
EPL Management Practices in the U.S.
Adapted from Dalton AJOG 2010
n=976 ob-gyn, family medicine, CNMs
Provider Issues
Training Safety Concerns
Efficacy System Resources
Time Assumptions of patients
Expectant (14 days)
OverallAnembryonicEmbryonic DemiseIncomplete
60%-70%50%35%-60%75% - 85%
Misoprostol(7 days)
800 mcg PVAnembryonicEmbryonic DemiseIncomplete
70% - 96%81%88%93%
Aspiration 97% - 100%
Overall success rates
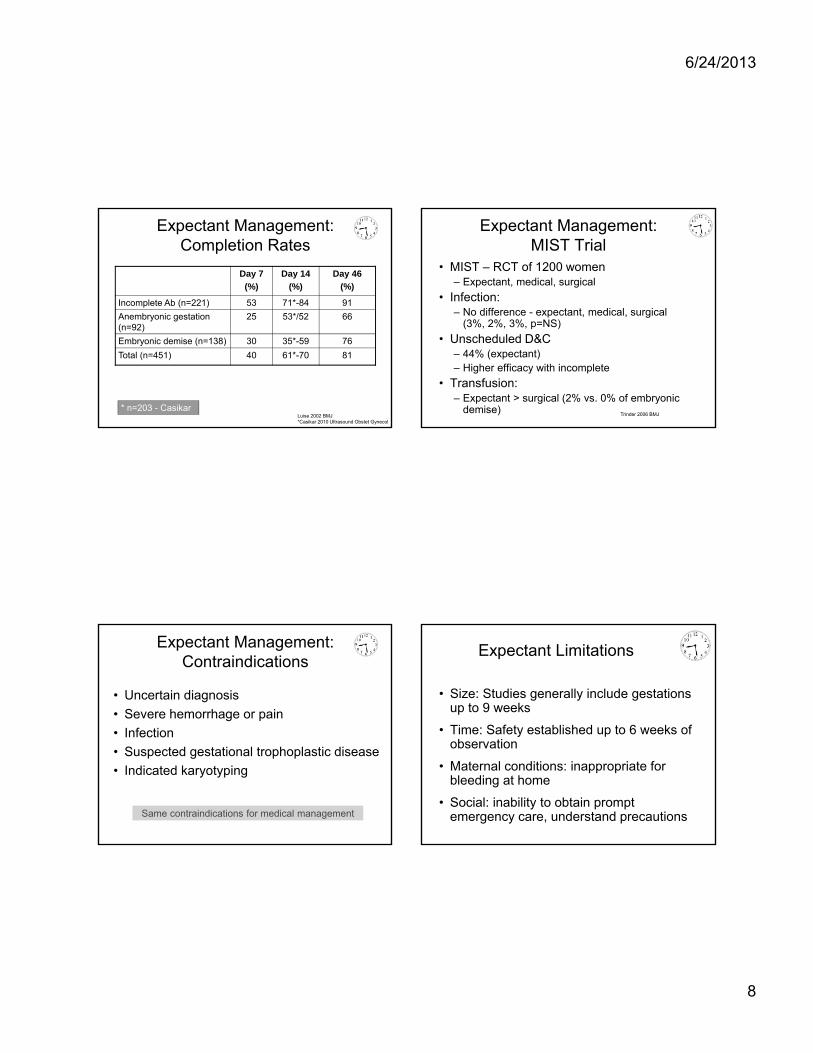
6/24/2013
8
Expectant Management: Completion Rates
Day 7
(%)
Day 14
(%)
Day 46
(%)
Incomplete Ab (n=221) 53 71*-84 91
Anembryonic gestation (n=92)
25 53*/52 66
Embryonic demise (n=138) 30 35*-59 76
Total (n=451) 40 61*-70 81
Luise 2002 BMJ*Casikar 2010 Ultrasound Obstet Gynecol
* n=203 - Casikar
Expectant Management:MIST Trial
• MIST – RCT of 1200 women– Expectant, medical, surgical
• Infection:– No difference - expectant, medical, surgical
(3%, 2%, 3%, p=NS)
• Unscheduled D&C– 44% (expectant)– Higher efficacy with incomplete
• Transfusion:– Expectant > surgical (2% vs. 0% of embryonic
demise)Trinder 2006 BMJ
Expectant Management: Contraindications
• Uncertain diagnosis
• Severe hemorrhage or pain
• Infection
• Suspected gestational trophoplastic disease
• Indicated karyotyping
Same contraindications for medical management
Expectant Limitations
• Size: Studies generally include gestations up to 9 weeks
• Time: Safety established up to 6 weeks of observation
• Maternal conditions: inappropriate for bleeding at home
• Social: inability to obtain prompt emergency care, understand precautions

6/24/2013
9
Medical Management of EPL
Advantages:• Avoidance of
anesthesia and surgery
• Faster completion of miscarriage compared to expectant
• Reduced emergency visits and D&C’S
Disadvantages• Pain and increased
analgesic requirements
• Increased duration of bleeding vs. surgical
• Gastrointestinal and systemic side effects
• Surgical management may still be necessary
Misoprostol• PGE1 analogue
• Tabs 100 mcg unscored, 200 mcg scored
• Inexpensive
• Rapidly absorbed PO, PV, PR, SL, buccal
• Common obstetrical uses: labor induction, medical abortion, PPH, cervical ripening
Misoprostol: Off-label Use
• FDA approved for prevention/txof gastric ulcers
• Once licensed, FDA doesnot regulate how used1
• Commonly practiced, often standard of care1
• Not experimental if based on sound scientific evidence2
1. Friedman, FDA Deputy Commissioner speech to U.S. House of Representatives 19962. Rayburn, Obstet Gynecol 1993
Physiologic Effects of Misoprostol
Uterine:
Cervical:
Gastrointestinal:
Systemic:
• Stimulates contractions
• Softens and primes cervix
• Prevents/treats ulcers • Nausea & vomiting • Diarrhea
• Fever, chills
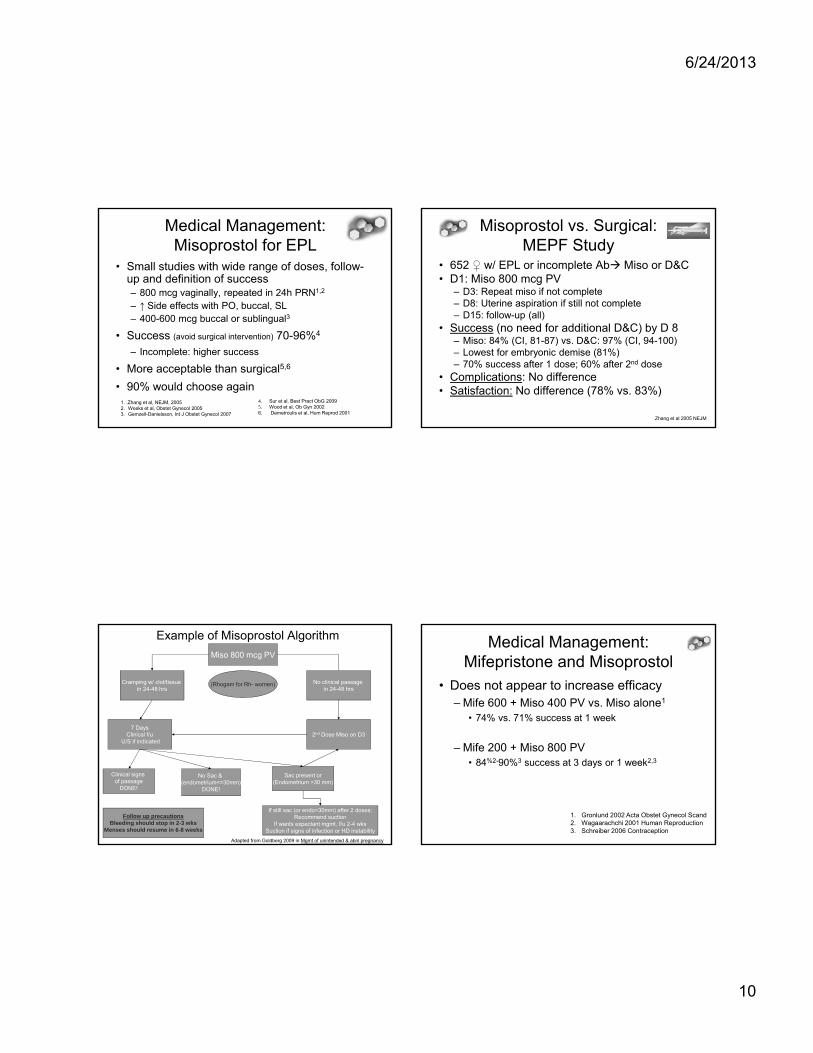
6/24/2013
10
Medical Management: Misoprostol for EPL
• Small studies with wide range of doses, follow-up and definition of success– 800 mcg vaginally, repeated in 24h PRN1,2
– ↑ Side effects with PO, buccal, SL– 400-600 mcg buccal or sublingual3
• Success (avoid surgical intervention) 70-96%4
– Incomplete: higher success
• More acceptable than surgical5,6
• 90% would choose again4. Sur et al. Best Pract ObG 20095. Wood et al, Ob Gyn 20026. Demetroulis et al, Hum Reprod 2001
1. .Zhang et al, NEJM, 20052. Weeks et al, Obstet Gynecol 20053. Gemzell-Danielsson, Int J Obstet Gynecol 2007
Misoprostol vs. Surgical: MEPF Study
• 652 w/ EPL or incomplete Ab Miso or D&C • D1: Miso 800 mcg PV
– D3: Repeat miso if not complete– D8: Uterine aspiration if still not complete– D15: follow-up (all)
• Success (no need for additional D&C) by D 8– Miso: 84% (CI, 81-87) vs. D&C: 97% (CI, 94-100)– Lowest for embryonic demise (81%)– 70% success after 1 dose; 60% after 2nd dose
• Complications: No difference • Satisfaction: No difference (78% vs. 83%)
Zhang et al 2005 NEJM
Example of Misoprostol Algorithm
Miso 800 mcg PV
Cramping w/ clot/tissue in 24-48 hrs
2nd Dose Miso on D37 Days
Clinical f/uU/S if indicated
Clinical signs of passage
DONE!
Sac present or(Endometrium >30 mm)
No Sac & (endometrium<=30mm)
DONE!
If still sac (or endo>30mm) after 2 doses:Recommend suction
If wants expectant mgmt, f/u 2-4 wksSuction if signs of infection or HD instability
Follow up precautionsBleeding should stop in 2-3 wks
Menses should resume in 6-8 weeks
No clinical passage in 24-48 hrs
(Rhogam for Rh- women)
Adapted from Goldberg 2009 in Mgmt of unintended & abnl pregnancy
Medical Management: Mifepristone and Misoprostol
• Does not appear to increase efficacy– Mife 600 + Miso 400 PV vs. Miso alone1
• 74% vs. 71% success at 1 week
– Mife 200 + Miso 800 PV• 84%2-90%3 success at 3 days or 1 week2,3
1. Gronlund 2002 Acta Obstet Gynecol Scand2. Wagaarachchi 2001 Human Reproduction3. Schreiber 2006 Contraception

6/24/2013
11
Surgical Management:Suction Curettage
• Safe, high efficacy (>95%)
• No need to do in Operating Room– Outpatient or ED setting – cost-effective
– Manual Uterine Aspiration / Manual Vacuum Aspiration
Used with 5-12 mm cannulaeCapacity 60 cc
Surgical Management:MUA/MVA
• Manual v. electric: no difference - complication (2.5% vs. 2.1%)1, pain, provider or pt. satisfaction2,3
• MUA in ER compared to EVA in OR:4
EVA in OR MUA in ER
Wait time (↓52%) 7.14 hrs 3.45 hrs
Procedure time 33 min 19 min
Total cost (↓ 41%) $1404 $827
1.Goldberg 2004 Ob Gyn; 2.Dean, Contraception 2003; 3. Edelman A. Ob Gyn 2001;184:1564; 4. Blumenthal 1992 IJOG; 5. Raush Fertil Steril 2012.
2012 study supports cost-effectiveness of outpatient MUA to OR-based UA5
Moving MUA out of OR
• Process described by U Michigan– Medical evidence review
– Review of hospital policy for office procedures
– Trained physicians, nurses, and MAs• Hands-on workshops
– Institution of privileging program
– Review experience of patients
– Review cost – gyn reimbursement same, lower institutional cost - $1965 v. $968
90% uterine aspirations are done in OR
Harris, AJOG, 2007.
Overall Success Rates
D&C: 97%-100%
Misoprostol (800 mcg pv) up to 81-96% success in 1 week
Expectant up to 70-85% in 2 wks

6/24/2013
12
Follow-up for Miscarriage
Confirm pregnancy passed:
• Surgical: done at time of aspiration
• Expectant & Medical– Symptoms, ultrasound or pregnancy test
– Phone call is an option
Other benefits of an office visit:– Emotional support
– Preconception counseling or contraception
– Recurrence risk – 2% after first SAB
The Patient – provider Interaction
•Affects patient choice and satisfaction
•One half of women would change their decision based on our recommendation
Molnar 2000
Support women in identifying their values in and priorities for management.
Be prepared to offer all options, including misoprostol and office-based uterine aspiration.
• Threatened Abortion– Keep the patient informed
• Provide reassurance, but avoid guarantees that “everything will be all right”
• Provide support through process
• What does the bleeding mean?– 50% ongoing pregnancy with closed os
– 85% ongoing pregnancy with viable IUP on u/s
– Up to 30% of normal pregnancies have VB
The Patient – provider Interaction• Remain silent after initial results or information
• Follow-up with open-ended questions & active listening
• Use neutral responses
• Determine how the woman feels about the pregnancy
• Normalize emotions
• Validate feelings rather than trying to change them
• Avoid opinions about what patient ‘‘should’’ do
• Encourage seeking emotional support from others
• Assure that you will be available to her through the process, and answer questions as they arise
Wallace, Patient Educ Couns, 2010.
The Patient – provider Interaction

6/24/2013
13
Key Points: Management
• Offer all 3 management options if stable– Know success rates when counseling patients– Patient preference plays a major role– Minimal difference in risk
• Need for surgical intervention should be based on clinical judgment
• Outpatient MUA is acceptable to women and cost-effective
6/21/2013
1
Caring for Challenging Patients in Women’s Health: Insights into Empathy and Professionalism
Jody Steinauer, MD, MAS
University of California, San Francisco
Statement of Disclosure
I do not have any relevant financial relationships with any commercial interests.
Jody Steinauer, MD, MAS
Obstetrics Service
A woman who had a planned home birth of a breech baby and now has retained placenta has just arrived in triage. As you go in to meet her the doula tries to keep you from talking directly to the patient.
Gynecologic Clinic
You are seeing a woman to give her results of her endometrial biopsy: endometrial cancer. As you discuss her basic treatment options she refuses your recommendation of surgery and shows you documents she found on the internet supporting her preference. She then asks dozens of questions.

6/21/2013
2
Primary Care Clinic
You are seeing a 24 year‐old woman who has had 2 prior abortions who visits your clinic for a pregnancy test. She is now pregnant again. She has not been using contraception and desires another abortion.
• Obstetrics
• Gynecology
• Primary Care
Would any of these patients frustrate you?
Objectives
1. To explore the “difficult” or “challenging” patient
2. To review the literature about judgment and bias
3. To gain practical skills for managing our feelings about patients, improving patient‐centered care, and preventing burnout
Professionalism in Medicine
• Respect, compassion, accountability, altruism
• Patient‐centered care
– Put aside personal values and self‐interest (self‐awareness) in order to prioritize the culture, family, and values of patients
• Challenges us to be empathetic, respectful, and compassionate toward patients, particularly during challenging encounters
ACGME Core Competencies
6/21/2013
3
Professionalism
• Respect, compassion, accountability, humanism, altruism
• Patient‐centered care– Put aside personal values and self‐interest (self‐awareness) in order to prioritize the culture, family, and values of patients
• Challenges us to be empathetic, respectful, and compassionate toward patients, particularly during challenging encounters
ACGME Core Competencies
Patient‐centered Care
Patient Physician
Focusing care on patient needs and preferences
Improved patient satisfaction, clinical outcomes
Little, BMJ, 2001; Luxford, Intl J Quality Health Care, 2011.
The “Difficult Patient” The “Difficult Patient”
The Textbook “Difficult Patient”
– The Angry patient
– The Silent Patient
– The Demanding Patient
– The "Yes, But" Patient
Feldman, Behavioral Medicine: A Guide for Clinical Practice, Third Edition, 2008.

6/21/2013
4
Patient Physician
The Textbook “Difficult Patient”
Angry FrustratedCalm
Elicit the patient’s reason for being angry.
Solicit the patient’s perspective.
Empathize with the patient’s experience.
Happy
High‐quality, patient‐centered care
The Actual “Difficult Patient”
Patient Physician
Actions
Behavior
Speak curtlySpend little timeAvoid patientBody languageComplain about her
FrustratedFrustrated
Low‐quality care
Fatigue, bad moodEmotional reactionWe don’t like herWe feel defensiveWe blame herWe judge her
The difficult patient– The Angry Patient
– The Silent Patient
– The Demanding Patient
– The "Yes, But" Patient
– The “No” Patient
– The Bad Patient
– The Needy Patient
– The Surprising Patient
The “Difficult Patient” The “NO” Patient
• Disagrees with us
• Does not adhere to medication or tx plan
• “Refuses” our recommendations
– Gynecology patient
• Does not trust us
• Has alternate beliefs about disease
– Obstetrics and gynecology patients
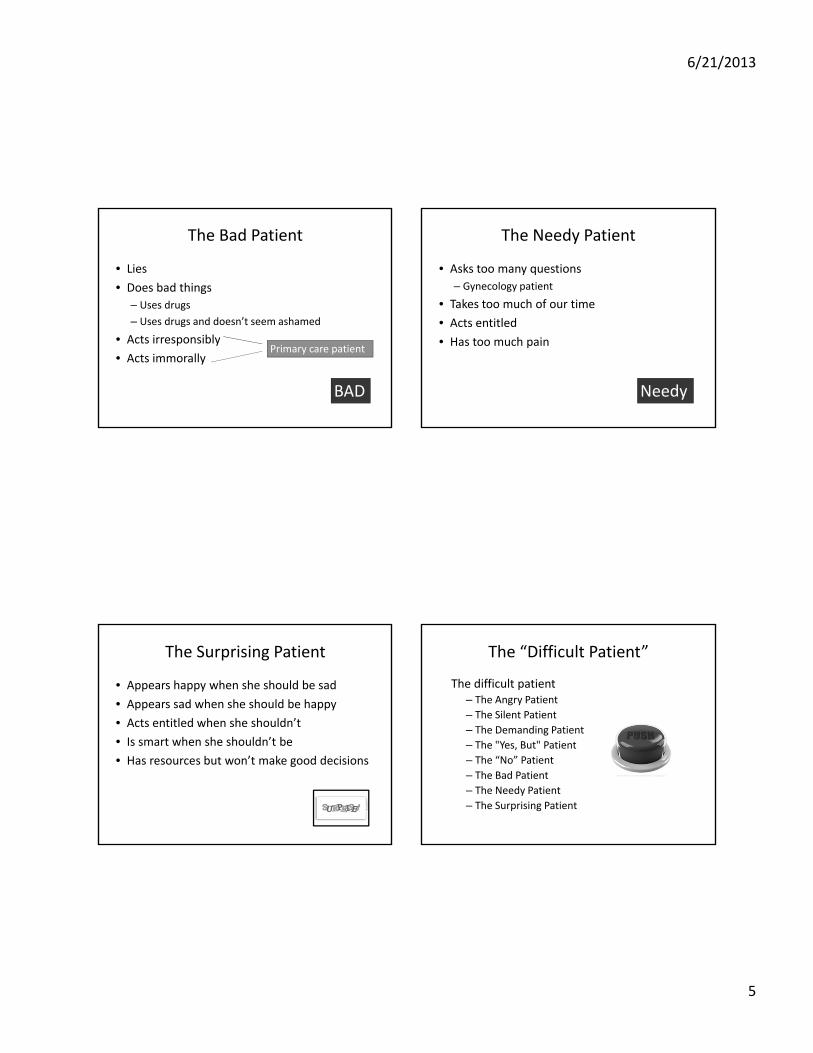
6/21/2013
5
The Bad Patient
• Lies
• Does bad things
– Uses drugs
– Uses drugs and doesn’t seem ashamed
• Acts irresponsibly
• Acts immorally
BAD
Primary care patient
The Needy Patient
• Asks too many questions
– Gynecology patient
• Takes too much of our time
• Acts entitled
• Has too much pain
Needy
The Surprising Patient
• Appears happy when she should be sad
• Appears sad when she should be happy
• Acts entitled when she shouldn’t
• Is smart when she shouldn’t be
• Has resources but won’t make good decisions
The “Difficult Patient”
The difficult patient– The Angry Patient
– The Silent Patient
– The Demanding Patient
– The "Yes, But" Patient
– The “No” Patient
– The Bad Patient
– The Needy Patient
– The Surprising Patient
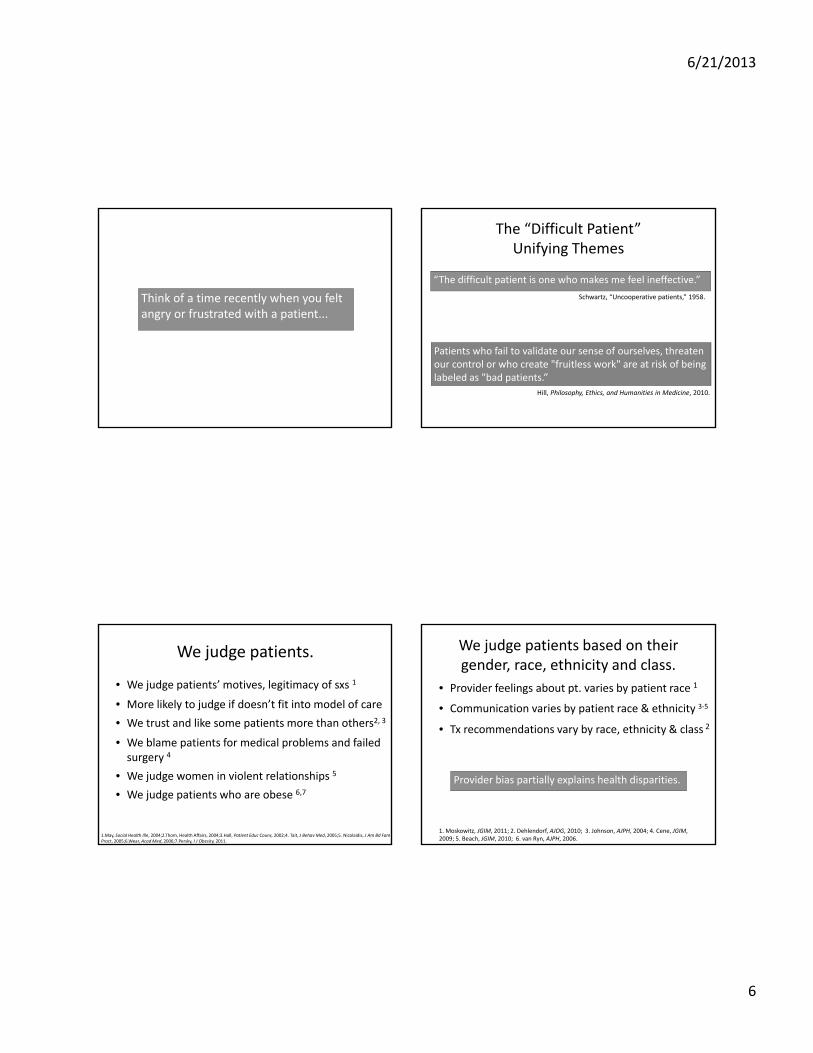
6/21/2013
6
Think of a time recently when you felt angry or frustrated with a patient...
The “Difficult Patient” Unifying Themes
“The difficult patient is one who makes me feel ineffective.”
Schwartz, “Uncooperative patients,” 1958.
Patients who fail to validate our sense of ourselves, threaten our control or who create "fruitless work" are at risk of being labeled as "bad patients.”
Hill, Philosophy, Ethics, and Humanities in Medicine, 2010.
We judge patients.
• We judge patients’ motives, legitimacy of sxs 1
• More likely to judge if doesn’t fit into model of care
• We trust and like some patients more than others2, 3
• We blame patients for medical problems and failed surgery 4
• We judge women in violent relationships 5
• We judge patients who are obese 6,7
1.May, Social Health Illn, 2004;2.Thom, Health Affairs, 2004;3.Hall, Patient Educ Couns, 2002;4. Tait, J BehavMed, 2005;5. Nicolaidis, J Am Bd FamPract, 2005;6.Wear, AcadMed, 2006;7.Persky, I J Obesity, 2011.
We judge patients based on their gender, race, ethnicity and class.
• Provider feelings about pt. varies by patient race 1
• Communication varies by patient race & ethnicity 3‐5
• Tx recommendations vary by race, ethnicity & class 2
1. Moskowitz, JGIM, 2011; 2. Dehlendorf, AJOG, 2010; 3. Johnson, AJPH, 2004; 4. Cene, JGIM, 2009; 5. Beach, JGIM, 2010; 6. van Ryn, AJPH, 2006.
Provider bias partially explains health disparities.
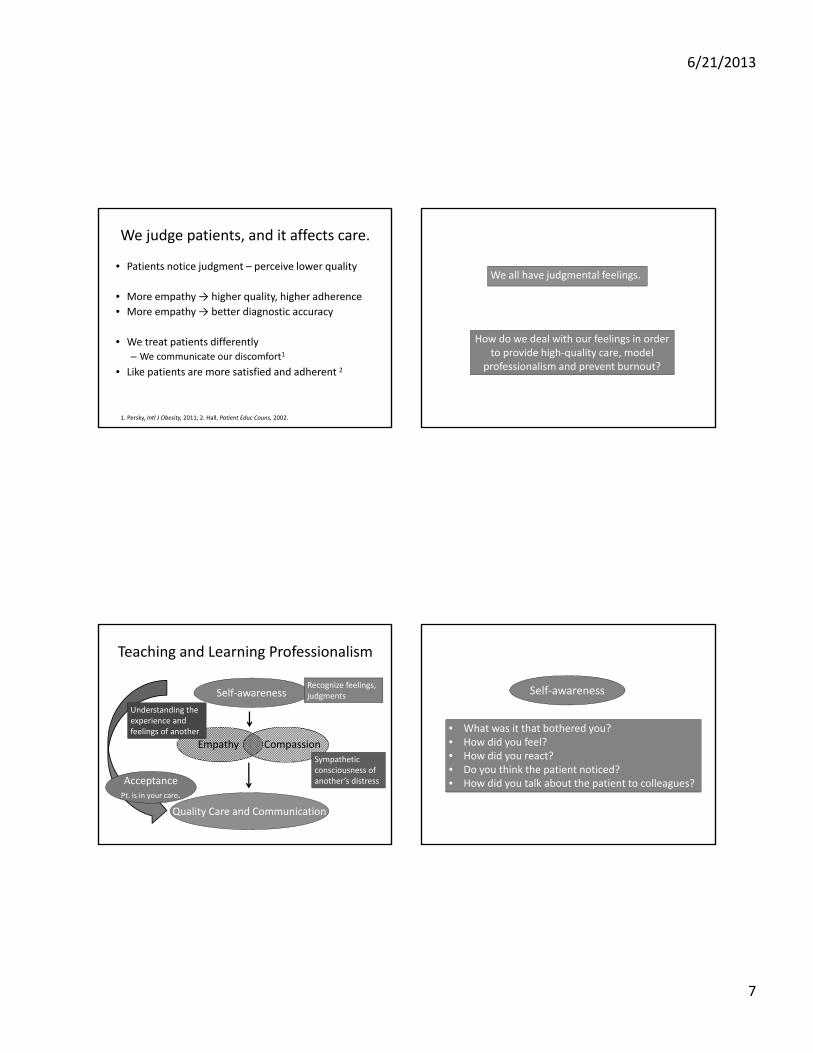
6/21/2013
7
We judge patients, and it affects care.
• Patients notice judgment – perceive lower quality
• More empathy → higher quality, higher adherence
• More empathy → better diagnostic accuracy
• We treat patients differently– We communicate our discomfort1
• Like patients are more satisfied and adherent 2
1. Persky, Intl J Obesity, 2011; 2. Hall, Patient Educ Couns, 2002.
We all have judgmental feelings.
How do we deal with our feelings in order to provide high‐quality care, model
professionalism and prevent burnout?
Teaching and Learning Professionalism
Self‐awareness
Quality Care and Communication
AcceptancePt. is in your care.
Empathy Compassion
Recognize feelings, judgments
Sympathetic consciousness of another’s distress
Understanding the experience and feelings of another • What was it that bothered you?
• How did you feel?• How did you react? • Do you think the patient noticed? • How did you talk about the patient to colleagues?
Self‐awareness

6/21/2013
8
Empathy
Compassion
• What do you think is going on with the patient?
• Even if you can’t put yourself in this person’s shoes, do you feel that she might be having a hard time?
Acceptance
• Can you accept that she is in your care? • How can you take care of yourself while taking care of her? • How can you care for her professionally?
Empathy
• Empathy is associated with positive outcomes– Increased dx accuracy, pt. participation, compliance, satisfaction, quality of life
Neumann, AcadMed, 2011; Shapiro, Phil Ethics Humanities, 2008.
Empathy
Empathy Decline
• Empathy is associated with positive outcomes– Increased dx accuracy, pt. participation, compliance, satisfaction, quality of life
• Empathy decreases in once trainees enterclinical practice– Increased vulnerability, distance themselves
– Increased responsibility
– Increased burnout
– Increasingly think of patients as “other”
Neumann, AcadMed, 2011; Shapiro, Phil Ethics Humanities, 2008.
Empathy
Teaching Professionalism through a Case‐based Workshop
• Faculty‐facilitated workshop with 8‐16 learners
• Workshop experience:– UCSF: >400 learners
• Medical students, ob‐gyn residents, faculty physicians, nurses and nurse practitioners students
– 20 other medical schools and residency programs
– 45 trained faculty in US
Professionalism, Empathy & Patient Care

6/21/2013
9
Professionalism, Empathy & Patient Care
Case‐based workshop– Part 1: Each learner introduces actual case
• Group selects one or two to talk through
• Self‐awareness → empathy → compassion → acceptance
– Part 2: Clinical cases• Family Planning
• Incarceration
• High‐risk obstetrics
• Substance use
1 hour
Part 1: Actual Cases
Tell us about a time recently when you felt angry or frustrated with a patient...
Teaching and Learning Professionalism
Self‐awareness
Quality Care and Communication
Acceptance
Empathy Compassion
How did it make you feel?
Was the patient having a hard time?
What was going on with the patient?
How can you take care of her?
Actual Cases
• Develop awareness of our reactions and buttons– Did patient notice and did it interfere with care?
• Consider theoretical and actual circumstances that contributed to patient’s behavior– Add to the library of potential reasons
– We have a list of good and bad reasons
– If patient acts apologetic or ashamed – we are nicer
– Notice how attached we can be to our expertise and model of medicine
• Discuss how we might act in future

6/21/2013
10
Part 2: Theoretical Cases
• Abortion ‐ perfect for practicing this framework
– Common in U.S. (1.2 million)
– We come to medicine with opinions
• Many judge women for not using birth control, having one (or more) abortion, presenting in the second trimester, or choosing abortion for specific circumstances.
Family Planning Case
A 24 year‐old woman who has had two abortions comes to you with an undesired pregnancy and wants an abortion.
Teaching and Learning Professionalism
Self‐awareness
Quality Care and Communication
Acceptance
Empathy Compassion
What upsets you about her having had many abortions? How does it make you feel?Why would someone have three
unintended pregnancies? What might be going on in her life?
Do you think she’s having a hard time? Can you feel for her?
How can you care for her professionally?
Strategies to Teach/Learn Empathy
• Mindfulness‐based Stress Reduction1
• Balint groups,2 support groups,3 self‐awareness training
• Reflection4 and narratives
• Home visits, service programs
• Perspective‐taking5 – put yourself in patient’s shoes
• Prioritizing empathy in clinical team discussions
• Unconscious bias literature – recommends approaching each patient with fresh perspective
• Our workshop – positive, qualitative outcomes
1. Krasner, JAMA, 2009; 2. Adams, AJOG, 2006; 3. Harris, Soc Science Med, 2011; 4. Learman, AJOG, 2008; 5. Blatt, AcadMed, 2010.

6/21/2013
11
Professionalism
• Respect, compassion, accountability, humanism, altruism
• Patient‐centered care– Put aside personal values and self‐interest (self‐awareness) in order to prioritize the culture, family, and values of patients
• Challenges us to be empathetic, respectful, and compassionate toward patients, particularly during challenging encounters.
ACGME Core Competencies
Conclusion
• Patients who challenge us offer an opportunity to develop empathy, compassion and self‐awareness.
• We must prioritize this dimension of patient care in our clinical settings.
• Feel free to use this schema!
Self‐awareness
CompassionEmpathy
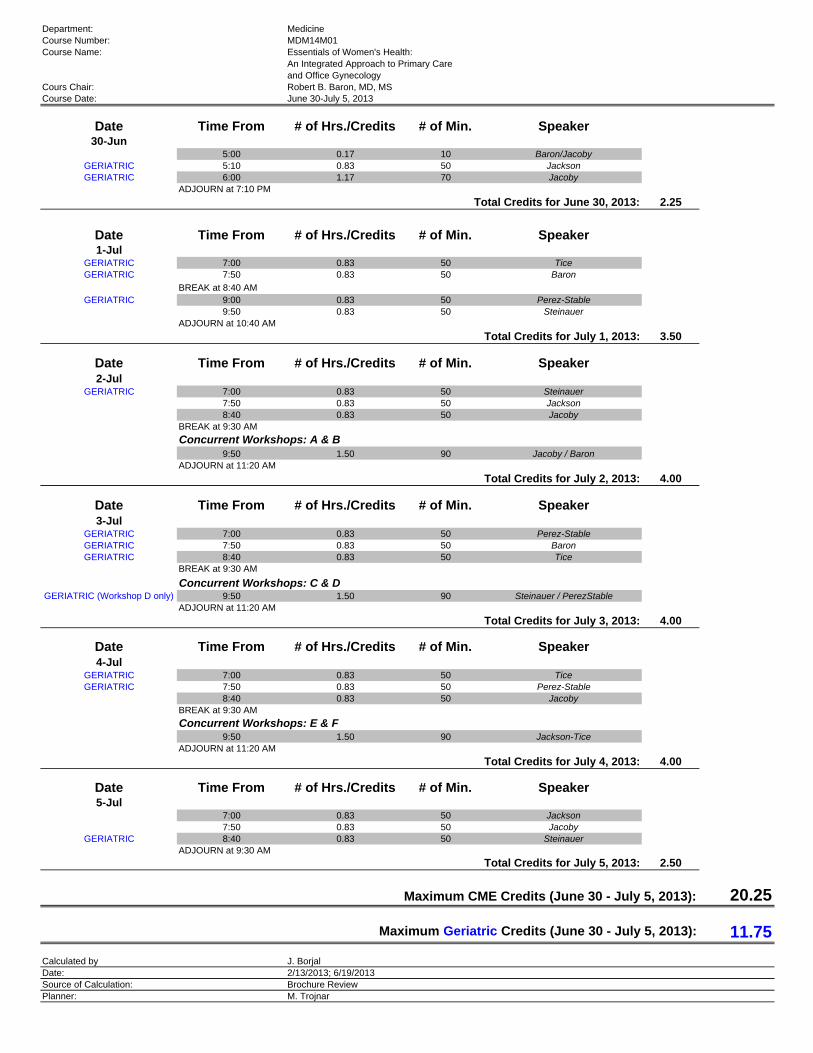
Department: MedicineCourse Number: MDM14M01Course Name: Essentials of Women's Health:
An Integrated Approach to Primary Careand Office Gynecology
Cours Chair: Robert B. Baron, MD, MSCourse Date: June 30-July 5, 2013
Date Time From # of Hrs./Credits # of Min. Speaker30-Jun
5:00 0.17 10 Baron/JacobyGERIATRIC 5:10 0.83 50 JacksonGERIATRIC 6:00 1.17 70 Jacoby
ADJOURN at 7:10 PM
Total Credits for June 30, 2013: 2.25
Date Time From # of Hrs./Credits # of Min. Speaker1-Jul
GERIATRIC 7:00 0.83 50 TiceGERIATRIC 7:50 0.83 50 Baron
BREAK at 8:40 AMGERIATRIC 9:00 0.83 50 Perez-Stable
9:50 0.83 50 SteinauerADJOURN at 10:40 AM
Total Credits for July 1, 2013: 3.50
Date Time From # of Hrs./Credits # of Min. Speaker2-Jul
GERIATRIC 7:00 0.83 50 Steinauer7:50 0.83 50 Jackson8:40 0.83 50 Jacoby
BREAK at 9:30 AM
Concurrent Workshops: A & B9:50 1.50 90 Jacoby / Baron
ADJOURN at 11:20 AM
Total Credits for July 2, 2013: 4.00
Date Time From # of Hrs./Credits # of Min. Speaker3-Jul
GERIATRIC 7:00 0.83 50 Perez-StableGERIATRIC 7:50 0.83 50 BaronGERIATRIC 8:40 0.83 50 Tice
BREAK at 9:30 AM
Concurrent Workshops: C & DGERIATRIC (Workshop D only) 9:50 1.50 90 Steinauer / PerezStable
ADJOURN at 11:20 AM
Total Credits for July 3, 2013: 4.00
Date Time From # of Hrs./Credits # of Min. Speaker4-Jul
GERIATRIC 7:00 0.83 50 TiceGERIATRIC 7:50 0.83 50 Perez-Stable
8:40 0.83 50 JacobyBREAK at 9:30 AM
Concurrent Workshops: E & F9:50 1.50 90 Jackson-Tice
ADJOURN at 11:20 AM
Total Credits for July 4, 2013: 4.00
Date Time From # of Hrs./Credits # of Min. Speaker5-Jul
7:00 0.83 50 Jackson7:50 0.83 50 Jacoby
GERIATRIC 8:40 0.83 50 SteinauerADJOURN at 9:30 AM
Total Credits for July 5, 2013: 2.50
Maximum CME Credits (June 30 - July 5, 2013): 20.25
Maximum Geriatric Credits (June 30 - July 5, 2013): 11.75
Calculated by J. BorjalDate: 2/13/2013; 6/19/2013Source of Calculation: Brochure ReviewPlanner: M. Trojnar