
Development and validation of the double duty caregiving scale
21
Résumé Conception et validation d’un instrument de mesure de la double tâche en matière de prestation des soins Catherine Ward-Griffin, Janice Keefe,Anne Martin-Matthews, Michael Kerr, Judith Belle Brown et Abram Oudshoorn Les auteurs ont mis au point un instrument de mesure qui vise à élargir les con- naissances sur la double tâche en matière de prestation des soins. Par double tâche, on entend la prestation de soins à des proches âgés par des professionnels de la santé qui exercent activement leur profession.L’étude présentée ici visait à vérifier les propriétés psychométriques de l’instrument en question. Les données ont été recueillies auprès d’un échantillon aléatoire de 187 infirmières autorisées de sexe féminin, qui occupent un emploi et dispensent aussi des soins à un proche âgé. Neuf facteurs contribuant à la double tâche ressortent de l’analyse exploratoire.On a relevé une corrélation moyenne entre les sous-échelles de mesure et les mesures normalisées sur la santé incluses dans l’étude. Également, on a constaté une forte corrélation négative entre l’interface vie privée – vie professionnelle en matière de prestation des soins (soit la mesure dans laquelle la frontière entre sphères professionnelle et personnelle s’efface), et le bien-être et la santé mentale. Ces résultats confirment le point de vue des auteurs sur les mesures nécessaires pour soutenir les personnes amenées à assumer une double tâche en matière de prestation des soins. Mots clés : prestation des soins, instrument de mesure CJNR 2009,Vol. 41 N o 3, 108 –128 108
Transcript of Development and validation of the double duty caregiving scale

Reacutesumeacute
Conception et validation drsquouninstrument de mesure de la double tacircche
en matiegravere de prestation des soins
CatherineWard-Griffin Janice KeefeAnne Martin-MatthewsMichael Kerr Judith Belle Brown et Abram Oudshoorn
Les auteurs ont mis au point un instrument de mesure qui vise agrave eacutelargir les con-naissances sur la double tacircche en matiegravere de prestation des soins Par doubletacircche on entend la prestation de soins agrave des proches acircgeacutes par des professionnelsde la santeacute qui exercent activement leur profession Lrsquoeacutetude preacutesenteacutee ici visait agraveveacuterifier les proprieacuteteacutes psychomeacutetriques de lrsquoinstrument en question Les donneacuteesont eacuteteacute recueillies aupregraves drsquoun eacutechantillon aleacuteatoire de 187 infirmiegraveres autoriseacuteesde sexe feacuteminin qui occupent un emploi et dispensent aussi des soins agrave unproche acircgeacute Neuf facteurs contribuant agrave la double tacircche ressortent de lrsquoanalyseexploratoire On a releveacute une correacutelation moyenne entre les sous-eacutechelles demesure et les mesures normaliseacutees sur la santeacute incluses dans lrsquoeacutetude Eacutegalementon a constateacute une forte correacutelation neacutegative entre lrsquointerface vie priveacutee ndash vieprofessionnelle en matiegravere de prestation des soins (soit la mesure dans laquelle lafrontiegravere entre sphegraveres professionnelle et personnelle srsquoefface) et le bien-ecirctre et lasanteacute mentale Ces reacutesultats confirment le point de vue des auteurs sur lesmesures neacutecessaires pour soutenir les personnes ameneacutees agrave assumer une doubletacircche en matiegravere de prestation des soins
Mots cleacutes prestation des soins instrument de mesure
CJNR 2009Vol 41 No 3 108ndash128
108
copyMcGill University School of Nursing 109
CJNR 2009Vol 41 No 3 108ndash128
Development andValidationof the Double DutyCaregiving Scale
CatherineWard-Griffin Janice KeefeAnne Martin-Matthews Michael Kerr
Judith Belle Brown and Abram Oudshoorn
In order to gain an understanding of double duty caregiving (DDC) definedhere as the provision of care to elderly relatives by practising health professionalsa DDC scale has been developedThis study tests the psychometric propertiesof the scale Survey data were collected from a random sample of 187 femaleregistered nurses who were employed and also provided care to elderly relativesNine factors contributing to DDC emerged from exploratory factor analysisThe DDC subscales were moderately correlated with the standardized healthmeasures included in the studyThe caregiving interface (degree of blurringbetween the professional and personal caregiving domains) was significantlynegatively correlated with well-being and mental healthThis result extends ourunderstanding of the supports needed by those providing DDC
Keywords caregiving instrument development feminist perspective work-family interface
As the Canadian population continues to age one of the challengesahead is the care of our most frail older citizens In 2002 more than 14million Canadians over 45 years of age combined paid employment withcare for elderly relatives (Fast 2005) Furthermore as the average age ofhealth professionals continues to rise in Canada (Canadian Institute ofHealth Information 2006) there is an increasing likelihood that healthprofessionals will be providing care to elderly relatives How health pro-fessionals balance their personal life such as caring for aging parents withtheir professional responsibilities has become a priority in humanresource planning amongst health-care organizations (Shields ampWilkins2005) Although the prevalence of double duty caregiving (DDC)defined here as the provision of care to elderly relatives by practisinghealth professionals is currently unknown previous research suggests that30 to 50 of the working population provides care to elderly relatives(Martin-Matthews 2000)Thus an understanding of DDC and how itinfluences the health and well-being of health professionals is particularlyimportant given the aging population the aging health-care workforceand the increasingly dire shortage of health-care providers (Keefe Leacutegareacute
amp Carriegravere 2007)To assist researchers interested in studying the socialsupport needed by providers of DDC we have developed a new mea-surement tool In this article we describe the conceptual basis initialdevelopment and psychometric validation of the Double DutyCaregiving Scale (DDCS) as well as discuss the implications for furtherresearch associated with social support for health providers caring forelderly relatives
Existing Knowledge
Although there are numerous scales measuring role strain role stress andcaregiver well-being (Lengacher amp Sellers 2003Tebb 1995Tebb Berg-Weger amp Rubio 2000) these do not adequately measure the phenome-non of DDC Caregiving has different meanings for different caregivergroups (Martin-Matthews 2000) and while role strain and caregiverburden may be common amongst employed family caregivers the expe-rience of simultaneous paid and unpaid caregiving and its impact on thehealth and well-being of caregivers may be obscured if a general tool isused Based on a critical feminist perspective our goal was to develop asensitive measure capable of capturing the unique caregiving experiencesof health professionals who also care for elderly relativesThe lack of attention to DDC is due in part to the tendency to treat
professional paid caregiving and personal unpaid caregiving as separatedomains (Ward-Griffin 2008)A critical feminist approach to caregivingexplores the connections of womenrsquos domestic labour with other formsof gendered caring work (Baines 2004Ungerson 1990Ward-Griffin ampMarshall 2003) and examines how the public and private domains areinterwoven and interdependent through the idea of reproduction andproduction (Pascall 1986) Double duty caregivers may be caughtbetween the public and private domains of caregiving in an ldquointermedi-ate domainrdquo (Stacey amp Davies 1983 cited in Mayall 1993) wherecomplex dimensions of location and social relations are brought togetherin caring workThe few studies that have looked at DDC report that most hospital
and community nurses experience high levels of stress associated withcaring for relatives of all ages (Ross Rideout amp Carson 1996) howevercaring for an elderly relative is positively correlated (r = 39 p lt 05)with health problems for female nurses only (Walters et al 1996) likelyreflecting a greater sense of obligation to care due to their professionalstatus within the health-care system (Ward-Griffin BrownVandervoortMcNair amp Dashnay 2005)Because women are more likely than men to care for an elderly rela-
tive (Armstrong ampArmstrong 2004) they are also at greatest risk for any
Ward-Griffin Keefe Martin-Matthews Kerr Brown and Oudshoorn
CJNR 2009Vol 41 No 3 110
negative effects of DDCThere is evidence that DDCs experience a senseof powerlessness and distress (Rutman 1996) and must make continualadjustments to achieve equilibrium in response to the demands placed onthem (Chen Feudtner Rhodes amp Green 2001 Guberman amp Maheu1999) although work-related knowledge can act as a buffer rather thanas an additional strain (Phillips Bernard amp Chittenden 2002)Ward-Griffin (2004) found that female community nurses caring for elderlyfamily members used a variety of coping strategies such as setting limitson the specific care they providedAlthough women in the health pro-fessions are often viewed as needing to develop coping strategies toaddress the stress of ldquobalancingrdquo or ldquojugglingrdquo two or more roles attemptsat setting limits often prove unsuccessful in dealing with the demands andtensions of family caregiving (Ward-Griffin 2004Ward-Griffin et al2005)The difficulty of demarcating boundaries between professional and
personal caregiving domains was particularly evident in our qualitativedescriptive study with 37 female nurses family physicians physiothera-pists and social workers who provided care to elderly relatives (Ward-Griffin et al 2005) Four dimensions of DDC were illuminatedExpectations Supports Negotiating Strategies and Caregiving InterfaceDespite using a variety of strategies for managing their DDC demandsmany of the participants experienced a blurring of boundaries betweentheir professional and personal caring workThis area of overlap was con-ceptualized as the caregiving interfaceThe extent of the interface variedfor each participant depending on the degree of expectation of familialcare and on the level of support available to manage multiple caregivingdemands From this study with female health professionals caring forelderly relatives we identified three prototypes of DDC based on thedegree of caregiving interface making it work working to manage and livingon the edge (see Figure 1)The women were able to make it work when theinterface between the professional and personal caregiving domains wasminimal they worked to manage when there was moderate overlap or blur-ring of their professional and personal caregiving boundaries and theylived on the edge when there was a high degree of overlap or interfacebetween their personal and professional domains of careIn our study the women tended over time to oscillate from one pro-
totype to another depending on their level of expectations supportnegotiating strategies and caregiving interface (Ward-Griffin et al 2005)In living on the edge the level of expectations to provide complex dailycare was exceedingly high Family and workplace supports were weak ornon-existent Some participants mostly nurses either took time off workto provide daily family care or provided professional care on their ldquodaysoff rdquo from family careAlthough setting limits and making connections
Development andValidation of the Double Duty Caregiving Scale
CJNR 2009Vol 41 No 3 111
Ward-Griffin Keefe Martin-Matthews Kerr Brown and Oudshoorn
CJNR 2009Vol 41 No 3 112
Figu
re1
Prototypesof
Dou
bleDutyCaregiving
SourceW
ard-Griffinetal(2005)
Makingitwork
Workingto
manage
Livingontheedge
ExpectationsLow
SupportsStrong
BoundariesConnected
CaregivinginterfaceSm
all
ExpectationsModerate
SupportsDiminishing
BoundariesBlurred
CaregivinginterfaceMedium
ExpectationsHigh
SupportsWeak
BoundariesEroded
CaregivinginterfaceLarge
Expectations
Support
Professional
care
Personal
care
Expectations
Support
Professional
care
Personal
care
Expectations
Support
were used to manage increasing caregiving demands with limited sup-ports many women experienced a dramatic blurring of their professionaland family caregiving boundaries characterized by tension exhaustionand a feeling of isolationThus female health professionals who providecare for elderly relatives especially those with limited tangible supportsmay experience ill health as a consequenceBuilding on the existing empirical knowledge described above and in
response to the need for further research on DDC the study had twoaimsThe first was to develop and validate a tool for measuring DDCwith a sample of female registered nurses capturing the variation withinthis populationThe second was to compare the health of DDCs andnon-DDCs
Development of the DDC Scale
The development of the DDCS (seeTable 1) began with an examinationof our previous qualitative interview data (Ward-Griffin et al 2005)Twoof the investigators (Ward-Griffin and Brown) reviewed the original tran-scripts looking for specific phrases and words that reflected the fourdimensions of DDC Expectations Supports Negotiating Strategies andCaregiving Interface Item development was refined at team meetingswhere all investigators generated an initial item pool (57 items) intendedto create four subscales to address the four dimensionsOne to two neg-atively worded items were included in each subscale to help decreaseresponse bias
Expectations
A total of 16 items were developed to address three proposed sources ofExpectations to provide care to an elderly relative expectations of self (9items) expectations of family (4 items) and expectations from within theprofession (3 items) Expectations of care include the expectations ofoneself to provide care as part of onersquos role in the family due to creden-tials and professional knowledge and skills Familial expectations maycome directly from the elderly recipient of care with hisher requests forassistance or may come from other family members Professional expec-tations may come from health professionals who are involved directly inthe care of the relative or from professional colleagues or friends who arenot involved directly professional expectations include those that may beheld by the DDCs themselves based on their credentials
Supports
Eight items were developed to assess Supports reflecting sources ofsupport from the personal (4 items) and professional (4 items) caregiving
Development andValidation of the Double Duty Caregiving Scale
CJNR 2009Vol 41 No 3 113
Ward-Griffin Keefe Martin-Matthews Kerr Brown and Oudshoorn
CJNR 2009Vol 41 No 3 114
Tabl
e1
Develop
men
tof
theDou
bleDutyCaregivingScale(D
DCS)
Dim
ensions
ofDDC
1Expectations
(expectations
tocarefor
elderlyrelatives)
2Supports
(supportsused
tomanagecaregiving)
3Negotiating
Strategies
(strategiesused
tonegotiatepersonal
professionalboundaries)
4Caregiving
Interface(CI)
(degreeofblurring
betweenprofessional
andpersonalcaregiving)
InitialItem
Pool
(n=57)
Self(9)
Family
(4)
Professional
(3)
Personal(4)
Professional
(4)
Settinglim
its(10)
Making
connections
(13)
CI(10)
Item
sDeleted
Based
on
CVIa
-1 -1 0 -1 -1 0 -3 -1
Provisional
DDCS
(n=49)
(8)
(3)
(3)
(3)
(3)
(10)
(10) (9)
Item
sDeleted
Based
onEFA
b
-5 -4 -5 -2
Revised
DDCS
Tool(n
=33)
Familial(5)
Professional(4)
Personal(3)
Professional(3)
Awarenessof
boundaries(3)
Active
resistance(3)
Making
connections(5)
Perceptionsof
CI(4)
Consequences
ofCI(3)
Sam
pleItem
s
Becauseofmyhealthcare
background
ndashIhavehigh
expectationsofmyselfto
providecaretomyrelative
Asacaregiverformyelderly
relativendashMyworkplace
supportsmetoprovidecareto
myrelative
BecauseIam
ahealthcare
providerwho
alsoprovidescare
tomyrelativendashIsetalim
itof
whattype
ofcareIwillprovide
myrelative
BecauseIam
ahealthcare
providerwho
alsoprovidescare
tomyrelativendashIfeellikeIam
caughtbetweentwoworlds
(professionaland
family)
aContentvalidity
indices
bExploratoryfactoranalyses
domains Double duty caregivers usually receive some degree of emo-tional informational and substantive support from family members andfriendsAlthough there are well-established instruments for measuringsocial support (Cohen Underwood amp Gottlieb 2000) the unique per-sonal and professional supports received within DDC may not be fullycaptured using a generic standard tool Often siblings spouses childrenor friends are also involved in the caregivingAdditionally many care-givers receive professional support this can include information orresources from onersquos workplace such as flexible work hours or access toemployee assistance programs
Negotiating Strategies
The third dimensionNegotiating Strategies addresses two main types ofstrategies Setting Limits and Making ConnectionsThese help DDCs tonegotiate their professional and personal boundaries thereby potentiallymoderating the negative impacts of the caregiving interface Double dutycaregivers set limits with respect to personal and professional expectationsconcerning the provision of familial care Setting Limits includes strate-gies for keeping the personal and professional caregiving domains sepa-rate and distinct while Making Connections examines the multipleinteractions that serve to bring the two domains closer together InSetting Limits (10 items) DDCs refuse to take on professional caregiv-ing tasks for family members or arrange for others to provide this careAs well DDCs increase their supports by Making Connections (13items)These include accessing health-care information or care for onersquosrelative using professional knowledge and connections to obtain care ornavigating the health-care system
Caregiving Interface
Ten items were developed to measure the caregiving interface (CI) orthe degree of blurring between the professional and personal caregivingdomains (intermediate domain)This dimension addresses the extent ofthe connections between elder caregiving and other forms of genderedcaring work (eg nursing)The CI encompasses both feelings about theblurring of roles and the psychological impact of these feelings Feelingsabout the blurring of roles can include being pulled in two differentdirections being unable to escape from the caregiving role and strugglingto separate caregiving at home from caregiving at workThe psycholog-ical impact of increasing blurring of boundaries can include stress thefeeling that onersquos caregiving is not being recognized and confusionregarding onersquos professional and personal roles
Development andValidation of the Double Duty Caregiving Scale
CJNR 2009Vol 41 No 3 115
ContentValidation of the DDC Scale
Because of the importance of preserving the inductively derived meaningof DDC in a quantitative instrument (Morris amp Field 1995) judgementsabout clarity internal consistency and initial content validity were madeby a panel of four DDCs representing the disciplines of nursing medi-cine physiotherapy and social work as used in our previous qualitativestudyThese content experts independently rated the relevance of theprovisional items on the DDCS using a four-point scale ranging from notrelevant to very relevant This review process facilitated a systematicapproach to item revision Raters also indicated whether the conceptualdomain of each subscale was adequately represented by the set of itemsAlthough consensus was reached for each of the four dimensions theexperts recommended clarification of certain items which were subse-quently reworded or deletedContent validity indices (CVI) for each item subscales and total scale
were calculated setting the criteria for item-level acceptance at 78 orhigher for three or more reviewers (Polit Beck amp Owen 2007)TheCVI ranged from 75 to 10 for all retained items (one item fell below78 but was retained because it measured a key conceptual aspect of theCI subscale recognition of professional status) Eight items were deleteddue to lack of clarity redundancy or a relatively low CVI thus reducingthe provisional DDCS from 57 items to 49The provisional DDCS was constructed using a five-point Likert scale
(1 = strongly disagree 5 = strongly agree) Prior to the analysis negativelyworded items were recoded so that for all items a higher score reflecteda higher degree of Expectations SupportsNegotiating Strategies andCaregiving InterfaceWithin each subscale the scores were calculated byaveraging the relevant individual item scores Data imputation for missingvalues was not used as non-response for the items was very lowThe sub-scales were developed for separate use of each dimension thus they werenot combined into a single overall DDCS score
Pilot Testing of the DDC Scale
Sampling
Following institutional ethics review board approval the 49-item provi-sional DDCS was administered to an age-stratified sample of femalenurses randomly selected from the registry list of the College of Nursesof Ontario Because previous research suggested that approximately onehalf of the working nurse population is likely to provide care to anelderly relative 800 female full-time (more than 30 hoursweek) regis-tered nurses 40 years of age or older were asked to complete a mailed
Ward-Griffin Keefe Martin-Matthews Kerr Brown and Oudshoorn
CJNR 2009Vol 41 No 3 116
survey packageThe aim was to have 200 eligible DDC respondentscomplete and return the package which consisted of (1) an informationletter (2) a short demographic questionnaire which also determined eli-gibility for the study (3) the provisional DDCS described above and(4) established comparative measures including theWomenrsquos Role StrainInventory (WRSI) (Lengacher amp Sellers 2003) the CaregiverWell-BeingScale (CWBS) (Tebb et al 2000) and Health Related Outcomes(Medical Outcomes Study Short-Form SF-12 version 20 acute form4-week recall)The time needed to complete the survey package wasestimated at between 30 and 45 minutes Each package contained amodest gift certificate as a token of appreciation Nurses not providingcare for an elderly relative or friend were asked to complete all question-naires except the DDCS the purpose being to generate data for com-paring DDC and non-DDC nursesOf the 800 questionnaires mailed 394 were returned of these eight
respondents did not meet the eligibility criteria (two male and six unem-ployed) six questionnaires were blank and three were returned to senderyielding a sample of 377 respondents (49 response rate)A total of 193respondents (51) were caring for an elderly relative (ie the DDCs) and184 (49) were not (ie the non-DDCs)Of the 193 respondents iden-tified as DDCs six left sections of the DDCS blank which led to a finalusable DDC sample of 187 a total sample size that is considered adequatefor instrument development analysis (Gable ampWolf 1993)
Reliability and ConstructValidity Analyses
Contingency table (chi square) analyses were performed on all categori-cal variables while independent sample t tests were used with all contin-uous variables when comparing DDCs and non-DDCsAppropriatemeasures of association were used to examine the relationship betweentheoretically relevant demographic variables (eg hours of employmentper week hours of caregiving per week) and the CIConstruct validity of the provisional 49-item tool was assessed at the
preliminary stage with a combination of exploratory factor analysis (EFA)using a principal components factor approach and assessment of scalereliability Even though our previous qualitative work and initial concep-tualization of DDC informed the construction of the provisional DDCSitems EFA was selected over confirmatory factor analysis (CFA) For theEFA initial factor extraction was based on eigenvalues greater than 100(Polit amp Beck 2008 p 488) Each subscale of the provisional DDCS wasthen subjected to varimax rotation to select the factor structure that bestrepresented the underlying relationship of the items within the fourdimensions (Expectations Supports Negotiating Strategies andCaregiver Interface)Although loadings with an absolute value of 040 or
Development andValidation of the Double Duty Caregiving Scale
CJNR 2009Vol 41 No 3 117
higher are often used as factor loading cut-off values (Carruth 1996)smaller values are acceptable if the item pool is large (Polit amp Beck 2008p 491) Cronbachrsquos alpha reliability coefficients were also used to deter-mine internal consistency among the items of the four subscales of theprovisional DDCS Based on these preliminary analyses a combinationof low inter-item correlations (lt 20) weak factor loadings (lt 35)andor poor conceptual clarity 16 of the original 49 items were removedfrom the provisional DDCS yielding a tool with a total of 33 items forthe remaining construct validity analysesWe also correlated each of the DDCS subscale scores with those of
theWRSI the CWBS and the SF-12v2TheWRSI is a previously vali-dated 44-item five-point Likert scale that measures role strain in femalenurses with multiple roles (Lengacher amp Sellers 2003) with high relia-bility coefficients for the total scale (086ndash095) and subscales of distress(074ndash091) enhancement (079ndash089) and support (065ndash087)Developed and validated byTebb et al (2000) the CWBS-ShortVersionis a 16-item five-point Likert scale that assesses activities and needs ofcaregivers (eight items for each subscale) Overall and for each subscale(Needs and Activities of Daily Living) the coefficient alpha was 094091 and 088 respectively Finally the SF-12v2 is a well-established toolthat measures the perceptions and activities of acute health and well-being It is a shortened version of the SF-36 which includes general andphysical health index scores as well as eight subscales (bodily pain generalhealth vitality social functioning physical functioning role limitationsdue to physical problems role limitations due to emotional problems andmental health)Ware KosinskiTurner-Bowker and Gandek (2002) reportinternal consistency reliability coefficients ranging from 066 to 090 Inthe present study internal consistency reliability coefficients for each ofthese established instruments were 091 (WRSI) 073 (CWBS-needs)078 (CWBS-activities) and 080 (SF-12v2)
Results
Sample
The sample comprised 193 DDCs (this figure includes six respondentswho failed to complete all items on the DDCS but completed thedemographic questionnaire) and 184 non-DDCs (see Table 2 for anoverview)The typical DDC was 520 years old (range = 41ndash65 SD =490) was married (742) held a diploma in nursing (679) had amean household income of $101778 (range = $12500ndash$300000 SD =$4409373) was employed part-time or full-time (968) with a meanof 390 hours worked per week (range 7ndash80 SD 786) had practisednursing for 25 years or more (676) and had at least one child (ranging
Ward-Griffin Keefe Martin-Matthews Kerr Brown and Oudshoorn
CJNR 2009Vol 41 No 3 118
in age from 2 to 32 years) living with her (65)The DDC respondentsprovided an average of 6 hours per week of care to one (53) or two(30) elderly relativesmostly parents (77) or parents-in-law (12) wholived nearbyThe typical non-DDC respondent was 515 years old (range= 41ndash65 SD = 585) was married (739) held a diploma in nursing(678) had a mean household income of $105618 (range = $35000ndash$770000 SD = 6700684) was employed part-time or full-time (989)with a mean of 408 hours worked per week (range = 22ndash80) had prac-tised nursing for 25 years or more (525) and had at least one child(ranging in age from 1 to 37 years) living with her (620)There wereno significant differences between DDCs and non-DDCs with respect toage household income and number of hours worked per week
Preliminary ConstructValidity Step 1
To facilitate a better understanding of the item contents of the new scaleprincipal components analysis was conducted on each of the four sub-scales of the Provisional DDCSAlthough each dimension was provi-sionally structured as a single subscale the results of our subsequent factoranalysis suggested that Negotiating Strategies should be split into twosubscales Setting Limits and Making Connections Nine factors wereidentified from our analyses (Table 3) which is consistent with our orig-inal conceptualization about the dimensionality of DDCTwo factorsemerged from Expectations (familial expectations and professional expec-tations) accounting for 63 of the variance Five items loaded on famil-ial expectations with loadings ranging from 058 to 087 Four itemsloaded on professional expectations with loadings ranging from 049 to089As expected this indicates that among DDCs there are both famil-ial and professional expectations to provide care to elderly relatives
Development andValidation of the Double Duty Caregiving Scale
CJNR 2009Vol 41 No 3 119
Table 2 Overview of Development andValidation of Double DutyCaregiving Scale (DDCS)
Initial Item Pool ContentValidity Pilot Testing
Qualitative Mailed SurveySource Interview Data Expert Panel (n = 800)
Sample 37 female DDCs 4 female DDCs 377 female DDCs15 registered nurses 1 registered nurse 193 DDCs9 social workers 1 social worker 184 non-DDCs7 physiotherapists 1 physiotherapist6 physicians 1 physician
NoteDDC = double duty caregiver
Ward-Griffin Keefe Martin-Matthews Kerr Brown and Oudshoorn
CJNR 2009Vol 41 No 3 120
Tabl
e3
Revised
DDCS(N
=18
7)
Number
Item
-Total
Cronbachrsquos
Factor
Factor
Subscale
Factors
ofItem
sMean
SDCorrelations
Alpha
Variance
Loading
Exp
ectation
s378
712
Familialexpectations
5040ndash073
080
058ndash087
Professionalexpectations
4030ndash056
069
049ndash089
Total
9028ndash066
083
625
Supp
orts
332
646
Personalsupports
3043ndash058
068
070ndash086
Professionalsupports
3024ndash062
065
035ndash091
Total
6031ndash052
071
617
SettingLim
its
311
678
Awarenessofboundaries
3041ndash059
067
061ndash087
Activeresistance
3033ndash061
065
068ndash084
Total
6034ndash058
071
629
Mak
ingCon
nections
389
677
Makingconnections
5042ndash069
075
465
060ndash076
CaregivingIn
terface
301
826
Perceptionsofinterface
4048ndash071
081
080ndash084
Consequencesofinterface
3053ndash077
083
080ndash084
Total
7044ndash074
085
703
Two factors emerged from Supports (personal supports and profes-sional supports) accounting for 62 of the variance and indicating theimportance of personal and professional supports to DDCs providingcare to elderly relativesThree items loaded on personal supports withloadings ranging from 070 to 086Three items loaded on professionalsupports with loadings ranging from 035 to 091Two factors labelled Awareness of Boundaries and Active Resistance
emerged from Setting Limits accounting for 63 of the varianceThreeitems loaded on Awareness of Boundaries with loadings ranging from061 to 087Three items loaded on Active Resistance with loadingsranging from 068 to 084 One factor was extracted from MakingConnections accounting for 47 of the variance Loadings for the fiveitems on Making Connections ranged from 060 to 076This suggeststhat DDCs are aware of the boundaries between their personal and pro-fessional caregiving and that in an attempt to negotiate these boundariesthey resist providing care to their elderly relative as well as making con-nections to increase their supportsTwo factors emerged from CIThese were labelled Perceptions of CI
and Consequences of CI accounting for 70 of the variance Four itemsloaded on Perceptions of CI with loadings ranging from 054 to 085and three items loaded on Consequences of CI with loadings rangingfrom 080 to 084These results indicate that DDCs both are aware ofand experience consequences of the blurring of boundaries between per-sonal and professional caregiving
Reliability
Inter-item correlations and internal consistency (reliability) were exam-ined for each of the subscales of the Revised DDCSOverall in the finalversion of the 33-item DDCS inter-item correlations ranged from 024to 077 (Table 3) Cronbachrsquos alpha reliability coefficients of the fiveDDC subscales ranged from 085 (CI) to 071 (Supports and SettingLimits)Moreover Cronbachrsquos alpha reliability coefficients of the subscalefactors ranged from 083 (CI-Consequences) to 065 (for both Supports-Professional and Setting Limits-Active Resistance)
ConstructValidity Step 2
Pearson correlations were conducted to assess construct validity betweeneach of the subscales within the DDCS andWRSICWBS and SF-12v2(physical) and SF-12v2 (mental) (Table 3) In line with the underlyingtheory driving the scale there were weak to moderate correlations in theexpected direction between the Revised DDCS subscales ofExpectations Supports Setting LimitsMaking Connections and CI andthe established measuresThe strongest significant correlations were
Development andValidation of the Double Duty Caregiving Scale
CJNR 2009Vol 41 No 3 121
Ward-Griffin Keefe Martin-Matthews Kerr Brown and Oudshoorn
CJNR 2009Vol 41 No 3 122
Tabl
e4
Correlation
BetweenRevised
DDC
Subscalesan
dEstab
lished
Measures
Setting
Making
Caregiving
Scale
Expectations
Supports
Lim
its
Connections
Interface
WRSI
ar
-34
41
09
04
-49
p000
000
240
625
000
CaregiverWell-Being
Scale
r-16
34
-05
-01
-29
Activitiesb
p03
00
48
89
00
CaregiverWell-Being
Scale
r-16
34
03
-03
-36
Needsc
p04
00
71
69
00
SF12
PhysicalIndexd
r06
14
-14
-03
-02
p42
06
06
69
78
SF12
MentalIndex
dr
-26
26
09
01
-39
p00
22
22
60
00
Expectations
ar
1-12
-07
38
55
p095
344
000
000
Supportsa
r-12
104
10
-26
p095
552
174
000
Strategiesndash
r1
01
-23
SettingLimits
ap
851
002
Strategiesndash
r1
18
MakingConnections
ap
013
CaregivingInterfacea
r1
p
aN=187
bN=174
cN=180
dN=176plt05(2-tailed)
plt01(2-tailed)
between CI andWRSI (r = -49 p lt 001) between Supports andWRSI(r = 041 p lt001) and between CI and SF-12v2 (mental) (r = -39 p lt001) Finally the CI of the DDCS was also negatively correlated withcaregiver well-being (r = -29 p lt 001 [activities] and r = -36 p lt001[needs])The strongest subscale inter-correlations (ie within the Revised
DDCS itself) were between Expectations and CI (r = 055 p lt 001) andbetween Expectations and Making Connections (r = 038 p lt 001) Inaddition there was a weak positive association between MakingConnections and CI (r = 018 p lt 05) and negative associationsbetween Supports and CI (r = -026 p lt 001) and between SettingLimits and CI (r = -23 p lt 001) None of the other DDCS subscaleinter-correlations were statistically significant (Table 4)
Contrasted Groups Approach
Although there were no significant differences between DDCs andnon-DDCs in their overall scores for theWRSI CWBS and SF-12v2(physical and mental scores) there were significant differences betweennon-DDCs (n = 67) and the DDC subgroup (n = 84) defined as livingon the edge (ie those scoring above the mean on the CI subscale) Poorerhealth was observed for the living on the edge DDCs on their overall SF-12v2 mental health index score (t = -276 p lt 05) and on four of theeight SF-12v2 subscales vitality (t = -237 p lt 05) social functioning(t = -291 p lt 01) role emotional (t = -306 p lt 05) and mental health(t = -227 p lt 05) Moreover there were significant differences withinthe DDC group between those who were living on the edge and thosewith lower CI scores for the following SF-12 subscales vitality (t = -20p lt 05) social functioning (t = -356 p lt 01) role emotional (t = -483p lt 01) and mental health (t = -398 p lt 05)The living on the edgegroup also had significantly lower well-being scores for the activities(t = -363 p lt 05) and needs (t = -447 p lt 05) subscales than theother DDC respondentsWhile not all results were statistically significantoverall there was an observed tendency for the living on the edge group ofDDCs to have the lowest health and well-being scores whereas the otherDDCs (eg making it work) with low CI scores tended to have slightlybetter health scores than the non-DDC group
Discussion
The main purpose of this study was to develop and test a tool intendedto advance our understanding of DDC using a random sample of regis-tered nurses providing care to elderly relatives
Development andValidation of the Double Duty Caregiving Scale
CJNR 2009Vol 41 No 3 123
The nine factors we identified were consistent with the theorized coreDDC dimensions of Expectations (Familial and Professional) Supports(Personal and Professional) Setting Limits (Awareness of BoundariesActive Resistance) Making Connections and Caregiving Interface(Perceptions and Consequences) which can yield important informationregarding how much variance is accounted for by the factors Howeveradditional analyses are required to establish the psychometric propertiesof the DDCS including test-retest reliability to assess construct stabilityBased on the EFA results a measurement model of DDC will be pro-posed and analyzed in a future study using CFA to enhance the psycho-metric validation of the DDCS For researchers looking for a shorterversion of the DDCS it is worth noting that based on the strength andconsistency of the overall findings the seven-item CI subscale could beused to determine the extent of DDC when survey respondent burdenis a key factor in instrument selection (ie when use of the full 33DDCS items is not possible) adding to the potential value of the DDCS
The positive correlation between Expectations and CI and the nega-tive correlation between Supports and CI and between Setting Limitsand CI are theoretically consistent with the conceptual model of DDCThat is if expectations are high both personally and professionally withrespect to caring for onersquos relatives there will be greater CI or blurringof boundaries Conversely if one has strong personal and professionalsupports it follows that a lower degree of CI will result Similarly whenone sets limits on caregiving then less blurring or a lower degree of CIshould result However the positive association between MakingConnections and Expectations was unexpected Perhaps high expecta-tions lead one to increase supports by making connections both person-ally and professionally to help meet these expectationsComparison of the SF-12 v2 scores for living on the edge DDCs and
non-DDCs revealed significant differences for SF-12v2 mental healthand specific SF-12v2 subscales of vitality social functioning role emo-tional and mental healthThese findings suggest that DDCs who expe-rience a high degree of blurring of their professional and personalboundaries are at greater risk for poor health than those health profes-sionals who do not care for elderly relatives or who do not experiencethis blurring In addition those DDCs who could be characterized asliving on the edge scored significantly higher on the same four SF-12 sub-scales than DDCs with lower CI scoresThis observed pattern suggeststwo possibilities there exists a threshold effect for the negative healtheffects of DDC or manageable exposure to DDC has a beneficial effectFurther exploration of these interesting findings is warrantedAlthough we conducted a systematic and comprehensive analysis to
assess the psychometric properties of a new scale further reliability and
Ward-Griffin Keefe Martin-Matthews Kerr Brown and Oudshoorn
CJNR 2009Vol 41 No 3 124
validity studies are needed Confirmatory validation studies with otherhealth-care provider populations such as family physicians social workersand physiotherapists are particularly important as these professionals havethe potential to be DDCs and their experiences as documented in ouroriginal qualitative study of DDC helped to formulate the theoreticalunderpinnings of the DDCS In addition research with these groups willadvance our understanding of how occupational health groups may differin terms of expectations supports negotiating strategies and degree ofCIAs the identification of health-advantage and health-risk factors isinfluenced by health and social environments the negotiating strategiescould also be examined through the use of qualitative methodologiessuch as in-depth interviews or focus groupsFinally research that draws linkages between professional and personal
caregiving has the added value of furthering knowledge about employedcaregiving specifically as it relates to the relationship between health out-comes and provision of familial care by health-care providersAlthoughthe convergence (and avoidance) of professional and personal caregivingboundaries is not a new issue in nursing and other health professions thenotion that it is the individualrsquos responsibility to negotiate this boundarytends to predominate (Ward-Griffin 2008)To that end further testingand refinement of the DDCS will be helpful in identifying areas whereDDCs may need specific or different types of support It is also impor-tant to understand how specific social supports shape the health experi-ences of DDCs as well as to investigate different types of social supportinterventions with DDCsThis information is particularly meaningfultoday with the intersection of three challenges an aging population anaging health-care workforce and a shortage of health professionals Suchknowledge could contribute to workplace and other health initiativesspearheaded by professional groups policy-makers and other key stake-holders interested in assessing and addressing the health effects of DDCIn summary the DDCS is a valid tool for the assessment of double
duty caregiving Such assessment is a crucial step in understanding theexperience of the blurring of personal and professional boundaries ofcaregiving among health professionalsA quantitative study of both maleand female DDCs could help us to understand the relationship betweencertain factors (ie gender health-care occupation) and the potentialhealth effects of DDCMoreover our finding that respondents with highCI scores (living on the edge) had significantly lower health and well-beingscores than DDC respondents with lower CI scores warrants furtherinvestigation to determine if one group of DDCs is at particular risk fordeveloping negative health effects Given the current climate of health-care reform in Canada developing a better understanding of DDC andits health effects is particularly relevant for policy-makers and others who
Development andValidation of the Double Duty Caregiving Scale
CJNR 2009Vol 41 No 3 125
are committed to developing health-promoting programs and policies forfamilial caregivers of the elderly Clearly now is the time to monitor theeffects of changing demographics both in the general population andwithin the health professions in order to develop appropriate and tar-geted strategies thereby creating and sustaining healthy work environ-ments and health-care workforcesWith further refinement the DDCSmay assist with these endeavours
References
Armstrong P amp ArmstrongH (2004)Thinking it throughWomenwork andcaring in the new millennium In K Grant CArmaratunga PArmstrongM BoscoeA Pederson amp KWillson (Eds)Caring forcaring aboutWomenhome care and unpaid caregiving (pp 5ndash44)Aurora ONGaramond
Baines D (2004) Seven kinds of work ndash only one paid Raced gendered andrestructured work in social servicesAtlantis 28(2) 19ndash28
Canadian Institute for Health Information (2006)Workforce trends of registerednurses in Canada 2005 Retrieved November 5 2006 fromhttpsecurecihicacihiwebproductsndb_worforce_trends_registered_nurses_canada_2005_epdf
CarruthA K (1996) Development and testing of the Caregiver ReciprocityScaleNursing Research 45(2) 92ndash97
Chen F Feudtner C Rhodes L amp Green L (2001) Role conflicts of physi-cians and their family members Rules but no rule bookWestern Journal ofMedicine 175(4) 236ndash239
Cohen S Underwood L G amp Gottlieb BH (Eds) (2000) Social support mea-surement and interventionA guide for health and social scientistsOxford OxfordUniversity Press
Fast J (2005)Hidden costsinvisible contributions report Reworking workThe experi-ence of employed caregivers of older adults Retrieved August 16 2007 fromwwwhecolualbertacahcic
Gable R ampWolfe M (1993) Instrument development 2nd ed Boston KluwerGubermanN amp Maheu P (1999) Combining employment and caregivingAn
intricate juggling actCanadian Journal on Aging 18(1) 84ndash106Keefe J Leacutegareacute J amp CarriegravereY (2007) Developing new strategies to support
future caregivers of older Canadians with disabilities Projections of need andtheir policy implicationsCanadian Public Policy 33 S65ndash80
Lengacher CA amp Sellers E (2003)TheWomenrsquos Role Strain Inventory InO L Strickland amp CDilorio (Eds)Measurement of nursing outcomes 2nd ed(pp 109ndash127) NewYork Springer
Martin-MatthewsA (2000) Intergenerational caregivingHow apocalyptic anddominant demography frame the questions and shape the answers In EMGee amp GGutman (Eds)The overselling of population agingApocalyptic demog-raphy intergenerational challenges and social policy (pp 64ndash79)Toronto OxfordUniversity Press
Ward-Griffin Keefe Martin-Matthews Kerr Brown and Oudshoorn
CJNR 2009Vol 41 No 3 126
Mayall B (1993) Keeping children healthy ndash the intermediate domain SocialScience and Medicine 36(1) 77ndash83
Morris JM amp Field PA (1995) Qualitative research methods for health profession-als 2nd ed London Sage
Pascall G (1986) Social policyA feminist analysis NewYorkTavistockPhillips J BernardM amp ChittendenM (2002) Juggling work and careThe expe-riences of older adults Bristol Policy Press
Polit D F amp Beck CT (2008)Nursing research Generating and assessing evidencefor nursing practice 8th ed Philadelphia LippincottWilliams ampWilkins
Polit D F amp Beck CT amp Owen SV (2007) Is the CVI an acceptable indica-tor of content validity Appraisal and recommendationsResearch in Nursingand Health 30 459ndash467
RossMM Rideout EM amp CarsonMM (1996) Nursesrsquo work Balancingpersonal and professional caregiving careers Canadian Journal of NursingResearch 26(4) 43ndash59
RutmanD (1996) Caregiving as womenrsquos workWomenrsquos experiences of pow-erfulness and powerlessness as caregiversQualitative Health Research 6(1) 90ndash111
ShieldsM ampWilkins K (2005)National Survey of theWork and Health of Nurses2005 Provincial profiles Ottawa Statistics CanadaRetrieved August 24 2007from httpwwwstatcancaenglishresearch11-621-MIE11-621-MIE2006052htm
StaceyM amp Davies C (1983)Division of labour in child health care Final report toSSRCCoventry Sociology Department University ofWarwick
Tebb S (1995)An aid to empowermentA caregiver well-being scaleHealth andSocialWork 20(2) 87ndash92
Tebb S Berg-WgerM amp Rubio DM (2000) CaregiverWell-Being Scale InDRoyse BAThyer D K Padgett ampT K Logan (Eds) Program evaluation3rd ed (pp 320ndash323) Pacific Grove CA BrooksCole
Ungerson C (1990) The language of care Crossing the boundaries InCUngerson (Ed)Gender and caringWork and welfare in Britain and Scandinavia(pp 8ndash33) NewYork Harvester
WaltersV LentonR French S Eyles JMayr J amp Newbold B (1996) Paidwork unpaid work and social supportA study of the health of male andfemale nurses Social Science and Medicine 43(11) 1627ndash1636
Ward-Griffin C (2004) Nurses as caregivers of elderly relatives Negotiatingpersonal and professional boundariesCJNR 36(1) 92ndash114
Ward-Griffin C (2008)Health professionals caring for aging relativesA profes-sional or personal issue In AMartin-Matthews amp J Phillips (Eds)Blurringthe boundariesAgeing at the intersection of work and home life (pp 1ndash20) NewYorkTaylor amp FrancisPsychology Press
Ward-Griffin C Brown JVandervoortA McNair S amp Dashnay I (2005)Double duty caregivingWomen in the health professionsCanadian Journalon Aging 24(4) 379ndash394
Ward-Griffin C amp MarshallV (2003) Reconceptualizing the relationshipbetween public and private eldercare Journal of Aging Studies 17 189ndash208
Development andValidation of the Double Duty Caregiving Scale
CJNR 2009Vol 41 No 3 127
Ware J E Kosinksi MTurner-Bowker L amp Gandek B (2002)How to scoreversion 2 of the SF-12 health survey Lincoln RIQuality Metric Inc
Acknowledgements
This study was funded by the Social Sciences and Humanities ResearchCouncil (Internal) and the Institute of Gender and Health CanadianInstitutes of Health ResearchThere are no conflicts of interest or financial disclosures
CatherineWard-Griffin RN PhD is ProfessorArthur Labatt Family School ofNursing University ofWestern Ontario London Canada Janice Keefe PhD isProfessor and Canada Research Chair in Aging and Caregiving Policy FamilyStudies and GerontologyMount SaintVincent University HalifaxNova ScotiaCanadaAnne Martin-Matthews PhD is Professor School of SocialWork andFamily Studies University of British ColumbiaVancouver Canada MichaelKerr PhD is Associate ProfessorArthur Labatt Family School of NursingUniversity ofWestern Ontario Judith Belle Brown PhD is Professor Departmentof Family Medicine University ofWestern OntarioAbram Oudshoorn RN is aPhD candidate in the Arthur Labatt Family School of Nursing University ofWestern Ontario
Ward-Griffin Keefe Martin-Matthews Kerr Brown and Oudshoorn
CJNR 2009Vol 41 No 3 128
copyMcGill University School of Nursing 109
CJNR 2009Vol 41 No 3 108ndash128
Development andValidationof the Double DutyCaregiving Scale
CatherineWard-Griffin Janice KeefeAnne Martin-Matthews Michael Kerr
Judith Belle Brown and Abram Oudshoorn
In order to gain an understanding of double duty caregiving (DDC) definedhere as the provision of care to elderly relatives by practising health professionalsa DDC scale has been developedThis study tests the psychometric propertiesof the scale Survey data were collected from a random sample of 187 femaleregistered nurses who were employed and also provided care to elderly relativesNine factors contributing to DDC emerged from exploratory factor analysisThe DDC subscales were moderately correlated with the standardized healthmeasures included in the studyThe caregiving interface (degree of blurringbetween the professional and personal caregiving domains) was significantlynegatively correlated with well-being and mental healthThis result extends ourunderstanding of the supports needed by those providing DDC
Keywords caregiving instrument development feminist perspective work-family interface
As the Canadian population continues to age one of the challengesahead is the care of our most frail older citizens In 2002 more than 14million Canadians over 45 years of age combined paid employment withcare for elderly relatives (Fast 2005) Furthermore as the average age ofhealth professionals continues to rise in Canada (Canadian Institute ofHealth Information 2006) there is an increasing likelihood that healthprofessionals will be providing care to elderly relatives How health pro-fessionals balance their personal life such as caring for aging parents withtheir professional responsibilities has become a priority in humanresource planning amongst health-care organizations (Shields ampWilkins2005) Although the prevalence of double duty caregiving (DDC)defined here as the provision of care to elderly relatives by practisinghealth professionals is currently unknown previous research suggests that30 to 50 of the working population provides care to elderly relatives(Martin-Matthews 2000)Thus an understanding of DDC and how itinfluences the health and well-being of health professionals is particularlyimportant given the aging population the aging health-care workforceand the increasingly dire shortage of health-care providers (Keefe Leacutegareacute
amp Carriegravere 2007)To assist researchers interested in studying the socialsupport needed by providers of DDC we have developed a new mea-surement tool In this article we describe the conceptual basis initialdevelopment and psychometric validation of the Double DutyCaregiving Scale (DDCS) as well as discuss the implications for furtherresearch associated with social support for health providers caring forelderly relatives
Existing Knowledge
Although there are numerous scales measuring role strain role stress andcaregiver well-being (Lengacher amp Sellers 2003Tebb 1995Tebb Berg-Weger amp Rubio 2000) these do not adequately measure the phenome-non of DDC Caregiving has different meanings for different caregivergroups (Martin-Matthews 2000) and while role strain and caregiverburden may be common amongst employed family caregivers the expe-rience of simultaneous paid and unpaid caregiving and its impact on thehealth and well-being of caregivers may be obscured if a general tool isused Based on a critical feminist perspective our goal was to develop asensitive measure capable of capturing the unique caregiving experiencesof health professionals who also care for elderly relativesThe lack of attention to DDC is due in part to the tendency to treat
professional paid caregiving and personal unpaid caregiving as separatedomains (Ward-Griffin 2008)A critical feminist approach to caregivingexplores the connections of womenrsquos domestic labour with other formsof gendered caring work (Baines 2004Ungerson 1990Ward-Griffin ampMarshall 2003) and examines how the public and private domains areinterwoven and interdependent through the idea of reproduction andproduction (Pascall 1986) Double duty caregivers may be caughtbetween the public and private domains of caregiving in an ldquointermedi-ate domainrdquo (Stacey amp Davies 1983 cited in Mayall 1993) wherecomplex dimensions of location and social relations are brought togetherin caring workThe few studies that have looked at DDC report that most hospital
and community nurses experience high levels of stress associated withcaring for relatives of all ages (Ross Rideout amp Carson 1996) howevercaring for an elderly relative is positively correlated (r = 39 p lt 05)with health problems for female nurses only (Walters et al 1996) likelyreflecting a greater sense of obligation to care due to their professionalstatus within the health-care system (Ward-Griffin BrownVandervoortMcNair amp Dashnay 2005)Because women are more likely than men to care for an elderly rela-
tive (Armstrong ampArmstrong 2004) they are also at greatest risk for any
Ward-Griffin Keefe Martin-Matthews Kerr Brown and Oudshoorn
CJNR 2009Vol 41 No 3 110
negative effects of DDCThere is evidence that DDCs experience a senseof powerlessness and distress (Rutman 1996) and must make continualadjustments to achieve equilibrium in response to the demands placed onthem (Chen Feudtner Rhodes amp Green 2001 Guberman amp Maheu1999) although work-related knowledge can act as a buffer rather thanas an additional strain (Phillips Bernard amp Chittenden 2002)Ward-Griffin (2004) found that female community nurses caring for elderlyfamily members used a variety of coping strategies such as setting limitson the specific care they providedAlthough women in the health pro-fessions are often viewed as needing to develop coping strategies toaddress the stress of ldquobalancingrdquo or ldquojugglingrdquo two or more roles attemptsat setting limits often prove unsuccessful in dealing with the demands andtensions of family caregiving (Ward-Griffin 2004Ward-Griffin et al2005)The difficulty of demarcating boundaries between professional and
personal caregiving domains was particularly evident in our qualitativedescriptive study with 37 female nurses family physicians physiothera-pists and social workers who provided care to elderly relatives (Ward-Griffin et al 2005) Four dimensions of DDC were illuminatedExpectations Supports Negotiating Strategies and Caregiving InterfaceDespite using a variety of strategies for managing their DDC demandsmany of the participants experienced a blurring of boundaries betweentheir professional and personal caring workThis area of overlap was con-ceptualized as the caregiving interfaceThe extent of the interface variedfor each participant depending on the degree of expectation of familialcare and on the level of support available to manage multiple caregivingdemands From this study with female health professionals caring forelderly relatives we identified three prototypes of DDC based on thedegree of caregiving interface making it work working to manage and livingon the edge (see Figure 1)The women were able to make it work when theinterface between the professional and personal caregiving domains wasminimal they worked to manage when there was moderate overlap or blur-ring of their professional and personal caregiving boundaries and theylived on the edge when there was a high degree of overlap or interfacebetween their personal and professional domains of careIn our study the women tended over time to oscillate from one pro-
totype to another depending on their level of expectations supportnegotiating strategies and caregiving interface (Ward-Griffin et al 2005)In living on the edge the level of expectations to provide complex dailycare was exceedingly high Family and workplace supports were weak ornon-existent Some participants mostly nurses either took time off workto provide daily family care or provided professional care on their ldquodaysoff rdquo from family careAlthough setting limits and making connections
Development andValidation of the Double Duty Caregiving Scale
CJNR 2009Vol 41 No 3 111
Ward-Griffin Keefe Martin-Matthews Kerr Brown and Oudshoorn
CJNR 2009Vol 41 No 3 112
Figu
re1
Prototypesof
Dou
bleDutyCaregiving
SourceW
ard-Griffinetal(2005)
Makingitwork
Workingto
manage
Livingontheedge
ExpectationsLow
SupportsStrong
BoundariesConnected
CaregivinginterfaceSm
all
ExpectationsModerate
SupportsDiminishing
BoundariesBlurred
CaregivinginterfaceMedium
ExpectationsHigh
SupportsWeak
BoundariesEroded
CaregivinginterfaceLarge
Expectations
Support
Professional
care
Personal
care
Expectations
Support
Professional
care
Personal
care
Expectations
Support
were used to manage increasing caregiving demands with limited sup-ports many women experienced a dramatic blurring of their professionaland family caregiving boundaries characterized by tension exhaustionand a feeling of isolationThus female health professionals who providecare for elderly relatives especially those with limited tangible supportsmay experience ill health as a consequenceBuilding on the existing empirical knowledge described above and in
response to the need for further research on DDC the study had twoaimsThe first was to develop and validate a tool for measuring DDCwith a sample of female registered nurses capturing the variation withinthis populationThe second was to compare the health of DDCs andnon-DDCs
Development of the DDC Scale
The development of the DDCS (seeTable 1) began with an examinationof our previous qualitative interview data (Ward-Griffin et al 2005)Twoof the investigators (Ward-Griffin and Brown) reviewed the original tran-scripts looking for specific phrases and words that reflected the fourdimensions of DDC Expectations Supports Negotiating Strategies andCaregiving Interface Item development was refined at team meetingswhere all investigators generated an initial item pool (57 items) intendedto create four subscales to address the four dimensionsOne to two neg-atively worded items were included in each subscale to help decreaseresponse bias
Expectations
A total of 16 items were developed to address three proposed sources ofExpectations to provide care to an elderly relative expectations of self (9items) expectations of family (4 items) and expectations from within theprofession (3 items) Expectations of care include the expectations ofoneself to provide care as part of onersquos role in the family due to creden-tials and professional knowledge and skills Familial expectations maycome directly from the elderly recipient of care with hisher requests forassistance or may come from other family members Professional expec-tations may come from health professionals who are involved directly inthe care of the relative or from professional colleagues or friends who arenot involved directly professional expectations include those that may beheld by the DDCs themselves based on their credentials
Supports
Eight items were developed to assess Supports reflecting sources ofsupport from the personal (4 items) and professional (4 items) caregiving
Development andValidation of the Double Duty Caregiving Scale
CJNR 2009Vol 41 No 3 113
Ward-Griffin Keefe Martin-Matthews Kerr Brown and Oudshoorn
CJNR 2009Vol 41 No 3 114
Tabl
e1
Develop
men
tof
theDou
bleDutyCaregivingScale(D
DCS)
Dim
ensions
ofDDC
1Expectations
(expectations
tocarefor
elderlyrelatives)
2Supports
(supportsused
tomanagecaregiving)
3Negotiating
Strategies
(strategiesused
tonegotiatepersonal
professionalboundaries)
4Caregiving
Interface(CI)
(degreeofblurring
betweenprofessional
andpersonalcaregiving)
InitialItem
Pool
(n=57)
Self(9)
Family
(4)
Professional
(3)
Personal(4)
Professional
(4)
Settinglim
its(10)
Making
connections
(13)
CI(10)
Item
sDeleted
Based
on
CVIa
-1 -1 0 -1 -1 0 -3 -1
Provisional
DDCS
(n=49)
(8)
(3)
(3)
(3)
(3)
(10)
(10) (9)
Item
sDeleted
Based
onEFA
b
-5 -4 -5 -2
Revised
DDCS
Tool(n
=33)
Familial(5)
Professional(4)
Personal(3)
Professional(3)
Awarenessof
boundaries(3)
Active
resistance(3)
Making
connections(5)
Perceptionsof
CI(4)
Consequences
ofCI(3)
Sam
pleItem
s
Becauseofmyhealthcare
background
ndashIhavehigh
expectationsofmyselfto
providecaretomyrelative
Asacaregiverformyelderly
relativendashMyworkplace
supportsmetoprovidecareto
myrelative
BecauseIam
ahealthcare
providerwho
alsoprovidescare
tomyrelativendashIsetalim
itof
whattype
ofcareIwillprovide
myrelative
BecauseIam
ahealthcare
providerwho
alsoprovidescare
tomyrelativendashIfeellikeIam
caughtbetweentwoworlds
(professionaland
family)
aContentvalidity
indices
bExploratoryfactoranalyses
domains Double duty caregivers usually receive some degree of emo-tional informational and substantive support from family members andfriendsAlthough there are well-established instruments for measuringsocial support (Cohen Underwood amp Gottlieb 2000) the unique per-sonal and professional supports received within DDC may not be fullycaptured using a generic standard tool Often siblings spouses childrenor friends are also involved in the caregivingAdditionally many care-givers receive professional support this can include information orresources from onersquos workplace such as flexible work hours or access toemployee assistance programs
Negotiating Strategies
The third dimensionNegotiating Strategies addresses two main types ofstrategies Setting Limits and Making ConnectionsThese help DDCs tonegotiate their professional and personal boundaries thereby potentiallymoderating the negative impacts of the caregiving interface Double dutycaregivers set limits with respect to personal and professional expectationsconcerning the provision of familial care Setting Limits includes strate-gies for keeping the personal and professional caregiving domains sepa-rate and distinct while Making Connections examines the multipleinteractions that serve to bring the two domains closer together InSetting Limits (10 items) DDCs refuse to take on professional caregiv-ing tasks for family members or arrange for others to provide this careAs well DDCs increase their supports by Making Connections (13items)These include accessing health-care information or care for onersquosrelative using professional knowledge and connections to obtain care ornavigating the health-care system
Caregiving Interface
Ten items were developed to measure the caregiving interface (CI) orthe degree of blurring between the professional and personal caregivingdomains (intermediate domain)This dimension addresses the extent ofthe connections between elder caregiving and other forms of genderedcaring work (eg nursing)The CI encompasses both feelings about theblurring of roles and the psychological impact of these feelings Feelingsabout the blurring of roles can include being pulled in two differentdirections being unable to escape from the caregiving role and strugglingto separate caregiving at home from caregiving at workThe psycholog-ical impact of increasing blurring of boundaries can include stress thefeeling that onersquos caregiving is not being recognized and confusionregarding onersquos professional and personal roles
Development andValidation of the Double Duty Caregiving Scale
CJNR 2009Vol 41 No 3 115
ContentValidation of the DDC Scale
Because of the importance of preserving the inductively derived meaningof DDC in a quantitative instrument (Morris amp Field 1995) judgementsabout clarity internal consistency and initial content validity were madeby a panel of four DDCs representing the disciplines of nursing medi-cine physiotherapy and social work as used in our previous qualitativestudyThese content experts independently rated the relevance of theprovisional items on the DDCS using a four-point scale ranging from notrelevant to very relevant This review process facilitated a systematicapproach to item revision Raters also indicated whether the conceptualdomain of each subscale was adequately represented by the set of itemsAlthough consensus was reached for each of the four dimensions theexperts recommended clarification of certain items which were subse-quently reworded or deletedContent validity indices (CVI) for each item subscales and total scale
were calculated setting the criteria for item-level acceptance at 78 orhigher for three or more reviewers (Polit Beck amp Owen 2007)TheCVI ranged from 75 to 10 for all retained items (one item fell below78 but was retained because it measured a key conceptual aspect of theCI subscale recognition of professional status) Eight items were deleteddue to lack of clarity redundancy or a relatively low CVI thus reducingthe provisional DDCS from 57 items to 49The provisional DDCS was constructed using a five-point Likert scale
(1 = strongly disagree 5 = strongly agree) Prior to the analysis negativelyworded items were recoded so that for all items a higher score reflecteda higher degree of Expectations SupportsNegotiating Strategies andCaregiving InterfaceWithin each subscale the scores were calculated byaveraging the relevant individual item scores Data imputation for missingvalues was not used as non-response for the items was very lowThe sub-scales were developed for separate use of each dimension thus they werenot combined into a single overall DDCS score
Pilot Testing of the DDC Scale
Sampling
Following institutional ethics review board approval the 49-item provi-sional DDCS was administered to an age-stratified sample of femalenurses randomly selected from the registry list of the College of Nursesof Ontario Because previous research suggested that approximately onehalf of the working nurse population is likely to provide care to anelderly relative 800 female full-time (more than 30 hoursweek) regis-tered nurses 40 years of age or older were asked to complete a mailed
Ward-Griffin Keefe Martin-Matthews Kerr Brown and Oudshoorn
CJNR 2009Vol 41 No 3 116
survey packageThe aim was to have 200 eligible DDC respondentscomplete and return the package which consisted of (1) an informationletter (2) a short demographic questionnaire which also determined eli-gibility for the study (3) the provisional DDCS described above and(4) established comparative measures including theWomenrsquos Role StrainInventory (WRSI) (Lengacher amp Sellers 2003) the CaregiverWell-BeingScale (CWBS) (Tebb et al 2000) and Health Related Outcomes(Medical Outcomes Study Short-Form SF-12 version 20 acute form4-week recall)The time needed to complete the survey package wasestimated at between 30 and 45 minutes Each package contained amodest gift certificate as a token of appreciation Nurses not providingcare for an elderly relative or friend were asked to complete all question-naires except the DDCS the purpose being to generate data for com-paring DDC and non-DDC nursesOf the 800 questionnaires mailed 394 were returned of these eight
respondents did not meet the eligibility criteria (two male and six unem-ployed) six questionnaires were blank and three were returned to senderyielding a sample of 377 respondents (49 response rate)A total of 193respondents (51) were caring for an elderly relative (ie the DDCs) and184 (49) were not (ie the non-DDCs)Of the 193 respondents iden-tified as DDCs six left sections of the DDCS blank which led to a finalusable DDC sample of 187 a total sample size that is considered adequatefor instrument development analysis (Gable ampWolf 1993)
Reliability and ConstructValidity Analyses
Contingency table (chi square) analyses were performed on all categori-cal variables while independent sample t tests were used with all contin-uous variables when comparing DDCs and non-DDCsAppropriatemeasures of association were used to examine the relationship betweentheoretically relevant demographic variables (eg hours of employmentper week hours of caregiving per week) and the CIConstruct validity of the provisional 49-item tool was assessed at the
preliminary stage with a combination of exploratory factor analysis (EFA)using a principal components factor approach and assessment of scalereliability Even though our previous qualitative work and initial concep-tualization of DDC informed the construction of the provisional DDCSitems EFA was selected over confirmatory factor analysis (CFA) For theEFA initial factor extraction was based on eigenvalues greater than 100(Polit amp Beck 2008 p 488) Each subscale of the provisional DDCS wasthen subjected to varimax rotation to select the factor structure that bestrepresented the underlying relationship of the items within the fourdimensions (Expectations Supports Negotiating Strategies andCaregiver Interface)Although loadings with an absolute value of 040 or
Development andValidation of the Double Duty Caregiving Scale
CJNR 2009Vol 41 No 3 117
higher are often used as factor loading cut-off values (Carruth 1996)smaller values are acceptable if the item pool is large (Polit amp Beck 2008p 491) Cronbachrsquos alpha reliability coefficients were also used to deter-mine internal consistency among the items of the four subscales of theprovisional DDCS Based on these preliminary analyses a combinationof low inter-item correlations (lt 20) weak factor loadings (lt 35)andor poor conceptual clarity 16 of the original 49 items were removedfrom the provisional DDCS yielding a tool with a total of 33 items forthe remaining construct validity analysesWe also correlated each of the DDCS subscale scores with those of
theWRSI the CWBS and the SF-12v2TheWRSI is a previously vali-dated 44-item five-point Likert scale that measures role strain in femalenurses with multiple roles (Lengacher amp Sellers 2003) with high relia-bility coefficients for the total scale (086ndash095) and subscales of distress(074ndash091) enhancement (079ndash089) and support (065ndash087)Developed and validated byTebb et al (2000) the CWBS-ShortVersionis a 16-item five-point Likert scale that assesses activities and needs ofcaregivers (eight items for each subscale) Overall and for each subscale(Needs and Activities of Daily Living) the coefficient alpha was 094091 and 088 respectively Finally the SF-12v2 is a well-established toolthat measures the perceptions and activities of acute health and well-being It is a shortened version of the SF-36 which includes general andphysical health index scores as well as eight subscales (bodily pain generalhealth vitality social functioning physical functioning role limitationsdue to physical problems role limitations due to emotional problems andmental health)Ware KosinskiTurner-Bowker and Gandek (2002) reportinternal consistency reliability coefficients ranging from 066 to 090 Inthe present study internal consistency reliability coefficients for each ofthese established instruments were 091 (WRSI) 073 (CWBS-needs)078 (CWBS-activities) and 080 (SF-12v2)
Results
Sample
The sample comprised 193 DDCs (this figure includes six respondentswho failed to complete all items on the DDCS but completed thedemographic questionnaire) and 184 non-DDCs (see Table 2 for anoverview)The typical DDC was 520 years old (range = 41ndash65 SD =490) was married (742) held a diploma in nursing (679) had amean household income of $101778 (range = $12500ndash$300000 SD =$4409373) was employed part-time or full-time (968) with a meanof 390 hours worked per week (range 7ndash80 SD 786) had practisednursing for 25 years or more (676) and had at least one child (ranging
Ward-Griffin Keefe Martin-Matthews Kerr Brown and Oudshoorn
CJNR 2009Vol 41 No 3 118
in age from 2 to 32 years) living with her (65)The DDC respondentsprovided an average of 6 hours per week of care to one (53) or two(30) elderly relativesmostly parents (77) or parents-in-law (12) wholived nearbyThe typical non-DDC respondent was 515 years old (range= 41ndash65 SD = 585) was married (739) held a diploma in nursing(678) had a mean household income of $105618 (range = $35000ndash$770000 SD = 6700684) was employed part-time or full-time (989)with a mean of 408 hours worked per week (range = 22ndash80) had prac-tised nursing for 25 years or more (525) and had at least one child(ranging in age from 1 to 37 years) living with her (620)There wereno significant differences between DDCs and non-DDCs with respect toage household income and number of hours worked per week
Preliminary ConstructValidity Step 1
To facilitate a better understanding of the item contents of the new scaleprincipal components analysis was conducted on each of the four sub-scales of the Provisional DDCSAlthough each dimension was provi-sionally structured as a single subscale the results of our subsequent factoranalysis suggested that Negotiating Strategies should be split into twosubscales Setting Limits and Making Connections Nine factors wereidentified from our analyses (Table 3) which is consistent with our orig-inal conceptualization about the dimensionality of DDCTwo factorsemerged from Expectations (familial expectations and professional expec-tations) accounting for 63 of the variance Five items loaded on famil-ial expectations with loadings ranging from 058 to 087 Four itemsloaded on professional expectations with loadings ranging from 049 to089As expected this indicates that among DDCs there are both famil-ial and professional expectations to provide care to elderly relatives
Development andValidation of the Double Duty Caregiving Scale
CJNR 2009Vol 41 No 3 119
Table 2 Overview of Development andValidation of Double DutyCaregiving Scale (DDCS)
Initial Item Pool ContentValidity Pilot Testing
Qualitative Mailed SurveySource Interview Data Expert Panel (n = 800)
Sample 37 female DDCs 4 female DDCs 377 female DDCs15 registered nurses 1 registered nurse 193 DDCs9 social workers 1 social worker 184 non-DDCs7 physiotherapists 1 physiotherapist6 physicians 1 physician
NoteDDC = double duty caregiver
Ward-Griffin Keefe Martin-Matthews Kerr Brown and Oudshoorn
CJNR 2009Vol 41 No 3 120
Tabl
e3
Revised
DDCS(N
=18
7)
Number
Item
-Total
Cronbachrsquos
Factor
Factor
Subscale
Factors
ofItem
sMean
SDCorrelations
Alpha
Variance
Loading
Exp
ectation
s378
712
Familialexpectations
5040ndash073
080
058ndash087
Professionalexpectations
4030ndash056
069
049ndash089
Total
9028ndash066
083
625
Supp
orts
332
646
Personalsupports
3043ndash058
068
070ndash086
Professionalsupports
3024ndash062
065
035ndash091
Total
6031ndash052
071
617
SettingLim
its
311
678
Awarenessofboundaries
3041ndash059
067
061ndash087
Activeresistance
3033ndash061
065
068ndash084
Total
6034ndash058
071
629
Mak
ingCon
nections
389
677
Makingconnections
5042ndash069
075
465
060ndash076
CaregivingIn
terface
301
826
Perceptionsofinterface
4048ndash071
081
080ndash084
Consequencesofinterface
3053ndash077
083
080ndash084
Total
7044ndash074
085
703
Two factors emerged from Supports (personal supports and profes-sional supports) accounting for 62 of the variance and indicating theimportance of personal and professional supports to DDCs providingcare to elderly relativesThree items loaded on personal supports withloadings ranging from 070 to 086Three items loaded on professionalsupports with loadings ranging from 035 to 091Two factors labelled Awareness of Boundaries and Active Resistance
emerged from Setting Limits accounting for 63 of the varianceThreeitems loaded on Awareness of Boundaries with loadings ranging from061 to 087Three items loaded on Active Resistance with loadingsranging from 068 to 084 One factor was extracted from MakingConnections accounting for 47 of the variance Loadings for the fiveitems on Making Connections ranged from 060 to 076This suggeststhat DDCs are aware of the boundaries between their personal and pro-fessional caregiving and that in an attempt to negotiate these boundariesthey resist providing care to their elderly relative as well as making con-nections to increase their supportsTwo factors emerged from CIThese were labelled Perceptions of CI
and Consequences of CI accounting for 70 of the variance Four itemsloaded on Perceptions of CI with loadings ranging from 054 to 085and three items loaded on Consequences of CI with loadings rangingfrom 080 to 084These results indicate that DDCs both are aware ofand experience consequences of the blurring of boundaries between per-sonal and professional caregiving
Reliability
Inter-item correlations and internal consistency (reliability) were exam-ined for each of the subscales of the Revised DDCSOverall in the finalversion of the 33-item DDCS inter-item correlations ranged from 024to 077 (Table 3) Cronbachrsquos alpha reliability coefficients of the fiveDDC subscales ranged from 085 (CI) to 071 (Supports and SettingLimits)Moreover Cronbachrsquos alpha reliability coefficients of the subscalefactors ranged from 083 (CI-Consequences) to 065 (for both Supports-Professional and Setting Limits-Active Resistance)
ConstructValidity Step 2
Pearson correlations were conducted to assess construct validity betweeneach of the subscales within the DDCS andWRSICWBS and SF-12v2(physical) and SF-12v2 (mental) (Table 3) In line with the underlyingtheory driving the scale there were weak to moderate correlations in theexpected direction between the Revised DDCS subscales ofExpectations Supports Setting LimitsMaking Connections and CI andthe established measuresThe strongest significant correlations were
Development andValidation of the Double Duty Caregiving Scale
CJNR 2009Vol 41 No 3 121
Ward-Griffin Keefe Martin-Matthews Kerr Brown and Oudshoorn
CJNR 2009Vol 41 No 3 122
Tabl
e4
Correlation
BetweenRevised
DDC
Subscalesan
dEstab
lished
Measures
Setting
Making
Caregiving
Scale
Expectations
Supports
Lim
its
Connections
Interface
WRSI
ar
-34
41
09
04
-49
p000
000
240
625
000
CaregiverWell-Being
Scale
r-16
34
-05
-01
-29
Activitiesb
p03
00
48
89
00
CaregiverWell-Being
Scale
r-16
34
03
-03
-36
Needsc
p04
00
71
69
00
SF12
PhysicalIndexd
r06
14
-14
-03
-02
p42
06
06
69
78
SF12
MentalIndex
dr
-26
26
09
01
-39
p00
22
22
60
00
Expectations
ar
1-12
-07
38
55
p095
344
000
000
Supportsa
r-12
104
10
-26
p095
552
174
000
Strategiesndash
r1
01
-23
SettingLimits
ap
851
002
Strategiesndash
r1
18
MakingConnections
ap
013
CaregivingInterfacea
r1
p
aN=187
bN=174
cN=180
dN=176plt05(2-tailed)
plt01(2-tailed)
between CI andWRSI (r = -49 p lt 001) between Supports andWRSI(r = 041 p lt001) and between CI and SF-12v2 (mental) (r = -39 p lt001) Finally the CI of the DDCS was also negatively correlated withcaregiver well-being (r = -29 p lt 001 [activities] and r = -36 p lt001[needs])The strongest subscale inter-correlations (ie within the Revised
DDCS itself) were between Expectations and CI (r = 055 p lt 001) andbetween Expectations and Making Connections (r = 038 p lt 001) Inaddition there was a weak positive association between MakingConnections and CI (r = 018 p lt 05) and negative associationsbetween Supports and CI (r = -026 p lt 001) and between SettingLimits and CI (r = -23 p lt 001) None of the other DDCS subscaleinter-correlations were statistically significant (Table 4)
Contrasted Groups Approach
Although there were no significant differences between DDCs andnon-DDCs in their overall scores for theWRSI CWBS and SF-12v2(physical and mental scores) there were significant differences betweennon-DDCs (n = 67) and the DDC subgroup (n = 84) defined as livingon the edge (ie those scoring above the mean on the CI subscale) Poorerhealth was observed for the living on the edge DDCs on their overall SF-12v2 mental health index score (t = -276 p lt 05) and on four of theeight SF-12v2 subscales vitality (t = -237 p lt 05) social functioning(t = -291 p lt 01) role emotional (t = -306 p lt 05) and mental health(t = -227 p lt 05) Moreover there were significant differences withinthe DDC group between those who were living on the edge and thosewith lower CI scores for the following SF-12 subscales vitality (t = -20p lt 05) social functioning (t = -356 p lt 01) role emotional (t = -483p lt 01) and mental health (t = -398 p lt 05)The living on the edgegroup also had significantly lower well-being scores for the activities(t = -363 p lt 05) and needs (t = -447 p lt 05) subscales than theother DDC respondentsWhile not all results were statistically significantoverall there was an observed tendency for the living on the edge group ofDDCs to have the lowest health and well-being scores whereas the otherDDCs (eg making it work) with low CI scores tended to have slightlybetter health scores than the non-DDC group
Discussion
The main purpose of this study was to develop and test a tool intendedto advance our understanding of DDC using a random sample of regis-tered nurses providing care to elderly relatives
Development andValidation of the Double Duty Caregiving Scale
CJNR 2009Vol 41 No 3 123
The nine factors we identified were consistent with the theorized coreDDC dimensions of Expectations (Familial and Professional) Supports(Personal and Professional) Setting Limits (Awareness of BoundariesActive Resistance) Making Connections and Caregiving Interface(Perceptions and Consequences) which can yield important informationregarding how much variance is accounted for by the factors Howeveradditional analyses are required to establish the psychometric propertiesof the DDCS including test-retest reliability to assess construct stabilityBased on the EFA results a measurement model of DDC will be pro-posed and analyzed in a future study using CFA to enhance the psycho-metric validation of the DDCS For researchers looking for a shorterversion of the DDCS it is worth noting that based on the strength andconsistency of the overall findings the seven-item CI subscale could beused to determine the extent of DDC when survey respondent burdenis a key factor in instrument selection (ie when use of the full 33DDCS items is not possible) adding to the potential value of the DDCS
The positive correlation between Expectations and CI and the nega-tive correlation between Supports and CI and between Setting Limitsand CI are theoretically consistent with the conceptual model of DDCThat is if expectations are high both personally and professionally withrespect to caring for onersquos relatives there will be greater CI or blurringof boundaries Conversely if one has strong personal and professionalsupports it follows that a lower degree of CI will result Similarly whenone sets limits on caregiving then less blurring or a lower degree of CIshould result However the positive association between MakingConnections and Expectations was unexpected Perhaps high expecta-tions lead one to increase supports by making connections both person-ally and professionally to help meet these expectationsComparison of the SF-12 v2 scores for living on the edge DDCs and
non-DDCs revealed significant differences for SF-12v2 mental healthand specific SF-12v2 subscales of vitality social functioning role emo-tional and mental healthThese findings suggest that DDCs who expe-rience a high degree of blurring of their professional and personalboundaries are at greater risk for poor health than those health profes-sionals who do not care for elderly relatives or who do not experiencethis blurring In addition those DDCs who could be characterized asliving on the edge scored significantly higher on the same four SF-12 sub-scales than DDCs with lower CI scoresThis observed pattern suggeststwo possibilities there exists a threshold effect for the negative healtheffects of DDC or manageable exposure to DDC has a beneficial effectFurther exploration of these interesting findings is warrantedAlthough we conducted a systematic and comprehensive analysis to
assess the psychometric properties of a new scale further reliability and
Ward-Griffin Keefe Martin-Matthews Kerr Brown and Oudshoorn
CJNR 2009Vol 41 No 3 124
validity studies are needed Confirmatory validation studies with otherhealth-care provider populations such as family physicians social workersand physiotherapists are particularly important as these professionals havethe potential to be DDCs and their experiences as documented in ouroriginal qualitative study of DDC helped to formulate the theoreticalunderpinnings of the DDCS In addition research with these groups willadvance our understanding of how occupational health groups may differin terms of expectations supports negotiating strategies and degree ofCIAs the identification of health-advantage and health-risk factors isinfluenced by health and social environments the negotiating strategiescould also be examined through the use of qualitative methodologiessuch as in-depth interviews or focus groupsFinally research that draws linkages between professional and personal
caregiving has the added value of furthering knowledge about employedcaregiving specifically as it relates to the relationship between health out-comes and provision of familial care by health-care providersAlthoughthe convergence (and avoidance) of professional and personal caregivingboundaries is not a new issue in nursing and other health professions thenotion that it is the individualrsquos responsibility to negotiate this boundarytends to predominate (Ward-Griffin 2008)To that end further testingand refinement of the DDCS will be helpful in identifying areas whereDDCs may need specific or different types of support It is also impor-tant to understand how specific social supports shape the health experi-ences of DDCs as well as to investigate different types of social supportinterventions with DDCsThis information is particularly meaningfultoday with the intersection of three challenges an aging population anaging health-care workforce and a shortage of health professionals Suchknowledge could contribute to workplace and other health initiativesspearheaded by professional groups policy-makers and other key stake-holders interested in assessing and addressing the health effects of DDCIn summary the DDCS is a valid tool for the assessment of double
duty caregiving Such assessment is a crucial step in understanding theexperience of the blurring of personal and professional boundaries ofcaregiving among health professionalsA quantitative study of both maleand female DDCs could help us to understand the relationship betweencertain factors (ie gender health-care occupation) and the potentialhealth effects of DDCMoreover our finding that respondents with highCI scores (living on the edge) had significantly lower health and well-beingscores than DDC respondents with lower CI scores warrants furtherinvestigation to determine if one group of DDCs is at particular risk fordeveloping negative health effects Given the current climate of health-care reform in Canada developing a better understanding of DDC andits health effects is particularly relevant for policy-makers and others who
Development andValidation of the Double Duty Caregiving Scale
CJNR 2009Vol 41 No 3 125
are committed to developing health-promoting programs and policies forfamilial caregivers of the elderly Clearly now is the time to monitor theeffects of changing demographics both in the general population andwithin the health professions in order to develop appropriate and tar-geted strategies thereby creating and sustaining healthy work environ-ments and health-care workforcesWith further refinement the DDCSmay assist with these endeavours
References
Armstrong P amp ArmstrongH (2004)Thinking it throughWomenwork andcaring in the new millennium In K Grant CArmaratunga PArmstrongM BoscoeA Pederson amp KWillson (Eds)Caring forcaring aboutWomenhome care and unpaid caregiving (pp 5ndash44)Aurora ONGaramond
Baines D (2004) Seven kinds of work ndash only one paid Raced gendered andrestructured work in social servicesAtlantis 28(2) 19ndash28
Canadian Institute for Health Information (2006)Workforce trends of registerednurses in Canada 2005 Retrieved November 5 2006 fromhttpsecurecihicacihiwebproductsndb_worforce_trends_registered_nurses_canada_2005_epdf
CarruthA K (1996) Development and testing of the Caregiver ReciprocityScaleNursing Research 45(2) 92ndash97
Chen F Feudtner C Rhodes L amp Green L (2001) Role conflicts of physi-cians and their family members Rules but no rule bookWestern Journal ofMedicine 175(4) 236ndash239
Cohen S Underwood L G amp Gottlieb BH (Eds) (2000) Social support mea-surement and interventionA guide for health and social scientistsOxford OxfordUniversity Press
Fast J (2005)Hidden costsinvisible contributions report Reworking workThe experi-ence of employed caregivers of older adults Retrieved August 16 2007 fromwwwhecolualbertacahcic
Gable R ampWolfe M (1993) Instrument development 2nd ed Boston KluwerGubermanN amp Maheu P (1999) Combining employment and caregivingAn
intricate juggling actCanadian Journal on Aging 18(1) 84ndash106Keefe J Leacutegareacute J amp CarriegravereY (2007) Developing new strategies to support
future caregivers of older Canadians with disabilities Projections of need andtheir policy implicationsCanadian Public Policy 33 S65ndash80
Lengacher CA amp Sellers E (2003)TheWomenrsquos Role Strain Inventory InO L Strickland amp CDilorio (Eds)Measurement of nursing outcomes 2nd ed(pp 109ndash127) NewYork Springer
Martin-MatthewsA (2000) Intergenerational caregivingHow apocalyptic anddominant demography frame the questions and shape the answers In EMGee amp GGutman (Eds)The overselling of population agingApocalyptic demog-raphy intergenerational challenges and social policy (pp 64ndash79)Toronto OxfordUniversity Press
Ward-Griffin Keefe Martin-Matthews Kerr Brown and Oudshoorn
CJNR 2009Vol 41 No 3 126
Mayall B (1993) Keeping children healthy ndash the intermediate domain SocialScience and Medicine 36(1) 77ndash83
Morris JM amp Field PA (1995) Qualitative research methods for health profession-als 2nd ed London Sage
Pascall G (1986) Social policyA feminist analysis NewYorkTavistockPhillips J BernardM amp ChittendenM (2002) Juggling work and careThe expe-riences of older adults Bristol Policy Press
Polit D F amp Beck CT (2008)Nursing research Generating and assessing evidencefor nursing practice 8th ed Philadelphia LippincottWilliams ampWilkins
Polit D F amp Beck CT amp Owen SV (2007) Is the CVI an acceptable indica-tor of content validity Appraisal and recommendationsResearch in Nursingand Health 30 459ndash467
RossMM Rideout EM amp CarsonMM (1996) Nursesrsquo work Balancingpersonal and professional caregiving careers Canadian Journal of NursingResearch 26(4) 43ndash59
RutmanD (1996) Caregiving as womenrsquos workWomenrsquos experiences of pow-erfulness and powerlessness as caregiversQualitative Health Research 6(1) 90ndash111
ShieldsM ampWilkins K (2005)National Survey of theWork and Health of Nurses2005 Provincial profiles Ottawa Statistics CanadaRetrieved August 24 2007from httpwwwstatcancaenglishresearch11-621-MIE11-621-MIE2006052htm
StaceyM amp Davies C (1983)Division of labour in child health care Final report toSSRCCoventry Sociology Department University ofWarwick
Tebb S (1995)An aid to empowermentA caregiver well-being scaleHealth andSocialWork 20(2) 87ndash92
Tebb S Berg-WgerM amp Rubio DM (2000) CaregiverWell-Being Scale InDRoyse BAThyer D K Padgett ampT K Logan (Eds) Program evaluation3rd ed (pp 320ndash323) Pacific Grove CA BrooksCole
Ungerson C (1990) The language of care Crossing the boundaries InCUngerson (Ed)Gender and caringWork and welfare in Britain and Scandinavia(pp 8ndash33) NewYork Harvester
WaltersV LentonR French S Eyles JMayr J amp Newbold B (1996) Paidwork unpaid work and social supportA study of the health of male andfemale nurses Social Science and Medicine 43(11) 1627ndash1636
Ward-Griffin C (2004) Nurses as caregivers of elderly relatives Negotiatingpersonal and professional boundariesCJNR 36(1) 92ndash114
Ward-Griffin C (2008)Health professionals caring for aging relativesA profes-sional or personal issue In AMartin-Matthews amp J Phillips (Eds)Blurringthe boundariesAgeing at the intersection of work and home life (pp 1ndash20) NewYorkTaylor amp FrancisPsychology Press
Ward-Griffin C Brown JVandervoortA McNair S amp Dashnay I (2005)Double duty caregivingWomen in the health professionsCanadian Journalon Aging 24(4) 379ndash394
Ward-Griffin C amp MarshallV (2003) Reconceptualizing the relationshipbetween public and private eldercare Journal of Aging Studies 17 189ndash208
Development andValidation of the Double Duty Caregiving Scale
CJNR 2009Vol 41 No 3 127
Ware J E Kosinksi MTurner-Bowker L amp Gandek B (2002)How to scoreversion 2 of the SF-12 health survey Lincoln RIQuality Metric Inc
Acknowledgements
This study was funded by the Social Sciences and Humanities ResearchCouncil (Internal) and the Institute of Gender and Health CanadianInstitutes of Health ResearchThere are no conflicts of interest or financial disclosures
CatherineWard-Griffin RN PhD is ProfessorArthur Labatt Family School ofNursing University ofWestern Ontario London Canada Janice Keefe PhD isProfessor and Canada Research Chair in Aging and Caregiving Policy FamilyStudies and GerontologyMount SaintVincent University HalifaxNova ScotiaCanadaAnne Martin-Matthews PhD is Professor School of SocialWork andFamily Studies University of British ColumbiaVancouver Canada MichaelKerr PhD is Associate ProfessorArthur Labatt Family School of NursingUniversity ofWestern Ontario Judith Belle Brown PhD is Professor Departmentof Family Medicine University ofWestern OntarioAbram Oudshoorn RN is aPhD candidate in the Arthur Labatt Family School of Nursing University ofWestern Ontario
Ward-Griffin Keefe Martin-Matthews Kerr Brown and Oudshoorn
CJNR 2009Vol 41 No 3 128

amp Carriegravere 2007)To assist researchers interested in studying the socialsupport needed by providers of DDC we have developed a new mea-surement tool In this article we describe the conceptual basis initialdevelopment and psychometric validation of the Double DutyCaregiving Scale (DDCS) as well as discuss the implications for furtherresearch associated with social support for health providers caring forelderly relatives
Existing Knowledge
Although there are numerous scales measuring role strain role stress andcaregiver well-being (Lengacher amp Sellers 2003Tebb 1995Tebb Berg-Weger amp Rubio 2000) these do not adequately measure the phenome-non of DDC Caregiving has different meanings for different caregivergroups (Martin-Matthews 2000) and while role strain and caregiverburden may be common amongst employed family caregivers the expe-rience of simultaneous paid and unpaid caregiving and its impact on thehealth and well-being of caregivers may be obscured if a general tool isused Based on a critical feminist perspective our goal was to develop asensitive measure capable of capturing the unique caregiving experiencesof health professionals who also care for elderly relativesThe lack of attention to DDC is due in part to the tendency to treat
professional paid caregiving and personal unpaid caregiving as separatedomains (Ward-Griffin 2008)A critical feminist approach to caregivingexplores the connections of womenrsquos domestic labour with other formsof gendered caring work (Baines 2004Ungerson 1990Ward-Griffin ampMarshall 2003) and examines how the public and private domains areinterwoven and interdependent through the idea of reproduction andproduction (Pascall 1986) Double duty caregivers may be caughtbetween the public and private domains of caregiving in an ldquointermedi-ate domainrdquo (Stacey amp Davies 1983 cited in Mayall 1993) wherecomplex dimensions of location and social relations are brought togetherin caring workThe few studies that have looked at DDC report that most hospital
and community nurses experience high levels of stress associated withcaring for relatives of all ages (Ross Rideout amp Carson 1996) howevercaring for an elderly relative is positively correlated (r = 39 p lt 05)with health problems for female nurses only (Walters et al 1996) likelyreflecting a greater sense of obligation to care due to their professionalstatus within the health-care system (Ward-Griffin BrownVandervoortMcNair amp Dashnay 2005)Because women are more likely than men to care for an elderly rela-
tive (Armstrong ampArmstrong 2004) they are also at greatest risk for any
Ward-Griffin Keefe Martin-Matthews Kerr Brown and Oudshoorn
CJNR 2009Vol 41 No 3 110
negative effects of DDCThere is evidence that DDCs experience a senseof powerlessness and distress (Rutman 1996) and must make continualadjustments to achieve equilibrium in response to the demands placed onthem (Chen Feudtner Rhodes amp Green 2001 Guberman amp Maheu1999) although work-related knowledge can act as a buffer rather thanas an additional strain (Phillips Bernard amp Chittenden 2002)Ward-Griffin (2004) found that female community nurses caring for elderlyfamily members used a variety of coping strategies such as setting limitson the specific care they providedAlthough women in the health pro-fessions are often viewed as needing to develop coping strategies toaddress the stress of ldquobalancingrdquo or ldquojugglingrdquo two or more roles attemptsat setting limits often prove unsuccessful in dealing with the demands andtensions of family caregiving (Ward-Griffin 2004Ward-Griffin et al2005)The difficulty of demarcating boundaries between professional and
personal caregiving domains was particularly evident in our qualitativedescriptive study with 37 female nurses family physicians physiothera-pists and social workers who provided care to elderly relatives (Ward-Griffin et al 2005) Four dimensions of DDC were illuminatedExpectations Supports Negotiating Strategies and Caregiving InterfaceDespite using a variety of strategies for managing their DDC demandsmany of the participants experienced a blurring of boundaries betweentheir professional and personal caring workThis area of overlap was con-ceptualized as the caregiving interfaceThe extent of the interface variedfor each participant depending on the degree of expectation of familialcare and on the level of support available to manage multiple caregivingdemands From this study with female health professionals caring forelderly relatives we identified three prototypes of DDC based on thedegree of caregiving interface making it work working to manage and livingon the edge (see Figure 1)The women were able to make it work when theinterface between the professional and personal caregiving domains wasminimal they worked to manage when there was moderate overlap or blur-ring of their professional and personal caregiving boundaries and theylived on the edge when there was a high degree of overlap or interfacebetween their personal and professional domains of careIn our study the women tended over time to oscillate from one pro-
totype to another depending on their level of expectations supportnegotiating strategies and caregiving interface (Ward-Griffin et al 2005)In living on the edge the level of expectations to provide complex dailycare was exceedingly high Family and workplace supports were weak ornon-existent Some participants mostly nurses either took time off workto provide daily family care or provided professional care on their ldquodaysoff rdquo from family careAlthough setting limits and making connections
Development andValidation of the Double Duty Caregiving Scale
CJNR 2009Vol 41 No 3 111
Ward-Griffin Keefe Martin-Matthews Kerr Brown and Oudshoorn
CJNR 2009Vol 41 No 3 112
Figu
re1
Prototypesof
Dou
bleDutyCaregiving
SourceW
ard-Griffinetal(2005)
Makingitwork
Workingto
manage
Livingontheedge
ExpectationsLow
SupportsStrong
BoundariesConnected
CaregivinginterfaceSm
all
ExpectationsModerate
SupportsDiminishing
BoundariesBlurred
CaregivinginterfaceMedium
ExpectationsHigh
SupportsWeak
BoundariesEroded
CaregivinginterfaceLarge
Expectations
Support
Professional
care
Personal
care
Expectations
Support
Professional
care
Personal
care
Expectations
Support
were used to manage increasing caregiving demands with limited sup-ports many women experienced a dramatic blurring of their professionaland family caregiving boundaries characterized by tension exhaustionand a feeling of isolationThus female health professionals who providecare for elderly relatives especially those with limited tangible supportsmay experience ill health as a consequenceBuilding on the existing empirical knowledge described above and in
response to the need for further research on DDC the study had twoaimsThe first was to develop and validate a tool for measuring DDCwith a sample of female registered nurses capturing the variation withinthis populationThe second was to compare the health of DDCs andnon-DDCs
Development of the DDC Scale
The development of the DDCS (seeTable 1) began with an examinationof our previous qualitative interview data (Ward-Griffin et al 2005)Twoof the investigators (Ward-Griffin and Brown) reviewed the original tran-scripts looking for specific phrases and words that reflected the fourdimensions of DDC Expectations Supports Negotiating Strategies andCaregiving Interface Item development was refined at team meetingswhere all investigators generated an initial item pool (57 items) intendedto create four subscales to address the four dimensionsOne to two neg-atively worded items were included in each subscale to help decreaseresponse bias
Expectations
A total of 16 items were developed to address three proposed sources ofExpectations to provide care to an elderly relative expectations of self (9items) expectations of family (4 items) and expectations from within theprofession (3 items) Expectations of care include the expectations ofoneself to provide care as part of onersquos role in the family due to creden-tials and professional knowledge and skills Familial expectations maycome directly from the elderly recipient of care with hisher requests forassistance or may come from other family members Professional expec-tations may come from health professionals who are involved directly inthe care of the relative or from professional colleagues or friends who arenot involved directly professional expectations include those that may beheld by the DDCs themselves based on their credentials
Supports
Eight items were developed to assess Supports reflecting sources ofsupport from the personal (4 items) and professional (4 items) caregiving
Development andValidation of the Double Duty Caregiving Scale
CJNR 2009Vol 41 No 3 113
Ward-Griffin Keefe Martin-Matthews Kerr Brown and Oudshoorn
CJNR 2009Vol 41 No 3 114
Tabl
e1
Develop
men
tof
theDou
bleDutyCaregivingScale(D
DCS)
Dim
ensions
ofDDC
1Expectations
(expectations
tocarefor
elderlyrelatives)
2Supports
(supportsused
tomanagecaregiving)
3Negotiating
Strategies
(strategiesused
tonegotiatepersonal
professionalboundaries)
4Caregiving
Interface(CI)
(degreeofblurring
betweenprofessional
andpersonalcaregiving)
InitialItem
Pool
(n=57)
Self(9)
Family
(4)
Professional
(3)
Personal(4)
Professional
(4)
Settinglim
its(10)
Making
connections
(13)
CI(10)
Item
sDeleted
Based
on
CVIa
-1 -1 0 -1 -1 0 -3 -1
Provisional
DDCS
(n=49)
(8)
(3)
(3)
(3)
(3)
(10)
(10) (9)
Item
sDeleted
Based
onEFA
b
-5 -4 -5 -2
Revised
DDCS
Tool(n
=33)
Familial(5)
Professional(4)
Personal(3)
Professional(3)
Awarenessof
boundaries(3)
Active
resistance(3)
Making
connections(5)
Perceptionsof
CI(4)
Consequences
ofCI(3)
Sam
pleItem
s
Becauseofmyhealthcare
background
ndashIhavehigh
expectationsofmyselfto
providecaretomyrelative
Asacaregiverformyelderly
relativendashMyworkplace
supportsmetoprovidecareto
myrelative
BecauseIam
ahealthcare
providerwho
alsoprovidescare
tomyrelativendashIsetalim
itof
whattype
ofcareIwillprovide
myrelative
BecauseIam
ahealthcare
providerwho
alsoprovidescare
tomyrelativendashIfeellikeIam
caughtbetweentwoworlds
(professionaland
family)
aContentvalidity
indices
bExploratoryfactoranalyses
domains Double duty caregivers usually receive some degree of emo-tional informational and substantive support from family members andfriendsAlthough there are well-established instruments for measuringsocial support (Cohen Underwood amp Gottlieb 2000) the unique per-sonal and professional supports received within DDC may not be fullycaptured using a generic standard tool Often siblings spouses childrenor friends are also involved in the caregivingAdditionally many care-givers receive professional support this can include information orresources from onersquos workplace such as flexible work hours or access toemployee assistance programs
Negotiating Strategies
The third dimensionNegotiating Strategies addresses two main types ofstrategies Setting Limits and Making ConnectionsThese help DDCs tonegotiate their professional and personal boundaries thereby potentiallymoderating the negative impacts of the caregiving interface Double dutycaregivers set limits with respect to personal and professional expectationsconcerning the provision of familial care Setting Limits includes strate-gies for keeping the personal and professional caregiving domains sepa-rate and distinct while Making Connections examines the multipleinteractions that serve to bring the two domains closer together InSetting Limits (10 items) DDCs refuse to take on professional caregiv-ing tasks for family members or arrange for others to provide this careAs well DDCs increase their supports by Making Connections (13items)These include accessing health-care information or care for onersquosrelative using professional knowledge and connections to obtain care ornavigating the health-care system
Caregiving Interface
Ten items were developed to measure the caregiving interface (CI) orthe degree of blurring between the professional and personal caregivingdomains (intermediate domain)This dimension addresses the extent ofthe connections between elder caregiving and other forms of genderedcaring work (eg nursing)The CI encompasses both feelings about theblurring of roles and the psychological impact of these feelings Feelingsabout the blurring of roles can include being pulled in two differentdirections being unable to escape from the caregiving role and strugglingto separate caregiving at home from caregiving at workThe psycholog-ical impact of increasing blurring of boundaries can include stress thefeeling that onersquos caregiving is not being recognized and confusionregarding onersquos professional and personal roles
Development andValidation of the Double Duty Caregiving Scale
CJNR 2009Vol 41 No 3 115
ContentValidation of the DDC Scale
Because of the importance of preserving the inductively derived meaningof DDC in a quantitative instrument (Morris amp Field 1995) judgementsabout clarity internal consistency and initial content validity were madeby a panel of four DDCs representing the disciplines of nursing medi-cine physiotherapy and social work as used in our previous qualitativestudyThese content experts independently rated the relevance of theprovisional items on the DDCS using a four-point scale ranging from notrelevant to very relevant This review process facilitated a systematicapproach to item revision Raters also indicated whether the conceptualdomain of each subscale was adequately represented by the set of itemsAlthough consensus was reached for each of the four dimensions theexperts recommended clarification of certain items which were subse-quently reworded or deletedContent validity indices (CVI) for each item subscales and total scale
were calculated setting the criteria for item-level acceptance at 78 orhigher for three or more reviewers (Polit Beck amp Owen 2007)TheCVI ranged from 75 to 10 for all retained items (one item fell below78 but was retained because it measured a key conceptual aspect of theCI subscale recognition of professional status) Eight items were deleteddue to lack of clarity redundancy or a relatively low CVI thus reducingthe provisional DDCS from 57 items to 49The provisional DDCS was constructed using a five-point Likert scale
(1 = strongly disagree 5 = strongly agree) Prior to the analysis negativelyworded items were recoded so that for all items a higher score reflecteda higher degree of Expectations SupportsNegotiating Strategies andCaregiving InterfaceWithin each subscale the scores were calculated byaveraging the relevant individual item scores Data imputation for missingvalues was not used as non-response for the items was very lowThe sub-scales were developed for separate use of each dimension thus they werenot combined into a single overall DDCS score
Pilot Testing of the DDC Scale
Sampling
Following institutional ethics review board approval the 49-item provi-sional DDCS was administered to an age-stratified sample of femalenurses randomly selected from the registry list of the College of Nursesof Ontario Because previous research suggested that approximately onehalf of the working nurse population is likely to provide care to anelderly relative 800 female full-time (more than 30 hoursweek) regis-tered nurses 40 years of age or older were asked to complete a mailed
Ward-Griffin Keefe Martin-Matthews Kerr Brown and Oudshoorn
CJNR 2009Vol 41 No 3 116
survey packageThe aim was to have 200 eligible DDC respondentscomplete and return the package which consisted of (1) an informationletter (2) a short demographic questionnaire which also determined eli-gibility for the study (3) the provisional DDCS described above and(4) established comparative measures including theWomenrsquos Role StrainInventory (WRSI) (Lengacher amp Sellers 2003) the CaregiverWell-BeingScale (CWBS) (Tebb et al 2000) and Health Related Outcomes(Medical Outcomes Study Short-Form SF-12 version 20 acute form4-week recall)The time needed to complete the survey package wasestimated at between 30 and 45 minutes Each package contained amodest gift certificate as a token of appreciation Nurses not providingcare for an elderly relative or friend were asked to complete all question-naires except the DDCS the purpose being to generate data for com-paring DDC and non-DDC nursesOf the 800 questionnaires mailed 394 were returned of these eight
respondents did not meet the eligibility criteria (two male and six unem-ployed) six questionnaires were blank and three were returned to senderyielding a sample of 377 respondents (49 response rate)A total of 193respondents (51) were caring for an elderly relative (ie the DDCs) and184 (49) were not (ie the non-DDCs)Of the 193 respondents iden-tified as DDCs six left sections of the DDCS blank which led to a finalusable DDC sample of 187 a total sample size that is considered adequatefor instrument development analysis (Gable ampWolf 1993)
Reliability and ConstructValidity Analyses
Contingency table (chi square) analyses were performed on all categori-cal variables while independent sample t tests were used with all contin-uous variables when comparing DDCs and non-DDCsAppropriatemeasures of association were used to examine the relationship betweentheoretically relevant demographic variables (eg hours of employmentper week hours of caregiving per week) and the CIConstruct validity of the provisional 49-item tool was assessed at the
preliminary stage with a combination of exploratory factor analysis (EFA)using a principal components factor approach and assessment of scalereliability Even though our previous qualitative work and initial concep-tualization of DDC informed the construction of the provisional DDCSitems EFA was selected over confirmatory factor analysis (CFA) For theEFA initial factor extraction was based on eigenvalues greater than 100(Polit amp Beck 2008 p 488) Each subscale of the provisional DDCS wasthen subjected to varimax rotation to select the factor structure that bestrepresented the underlying relationship of the items within the fourdimensions (Expectations Supports Negotiating Strategies andCaregiver Interface)Although loadings with an absolute value of 040 or
Development andValidation of the Double Duty Caregiving Scale
CJNR 2009Vol 41 No 3 117
higher are often used as factor loading cut-off values (Carruth 1996)smaller values are acceptable if the item pool is large (Polit amp Beck 2008p 491) Cronbachrsquos alpha reliability coefficients were also used to deter-mine internal consistency among the items of the four subscales of theprovisional DDCS Based on these preliminary analyses a combinationof low inter-item correlations (lt 20) weak factor loadings (lt 35)andor poor conceptual clarity 16 of the original 49 items were removedfrom the provisional DDCS yielding a tool with a total of 33 items forthe remaining construct validity analysesWe also correlated each of the DDCS subscale scores with those of
theWRSI the CWBS and the SF-12v2TheWRSI is a previously vali-dated 44-item five-point Likert scale that measures role strain in femalenurses with multiple roles (Lengacher amp Sellers 2003) with high relia-bility coefficients for the total scale (086ndash095) and subscales of distress(074ndash091) enhancement (079ndash089) and support (065ndash087)Developed and validated byTebb et al (2000) the CWBS-ShortVersionis a 16-item five-point Likert scale that assesses activities and needs ofcaregivers (eight items for each subscale) Overall and for each subscale(Needs and Activities of Daily Living) the coefficient alpha was 094091 and 088 respectively Finally the SF-12v2 is a well-established toolthat measures the perceptions and activities of acute health and well-being It is a shortened version of the SF-36 which includes general andphysical health index scores as well as eight subscales (bodily pain generalhealth vitality social functioning physical functioning role limitationsdue to physical problems role limitations due to emotional problems andmental health)Ware KosinskiTurner-Bowker and Gandek (2002) reportinternal consistency reliability coefficients ranging from 066 to 090 Inthe present study internal consistency reliability coefficients for each ofthese established instruments were 091 (WRSI) 073 (CWBS-needs)078 (CWBS-activities) and 080 (SF-12v2)
Results
Sample
The sample comprised 193 DDCs (this figure includes six respondentswho failed to complete all items on the DDCS but completed thedemographic questionnaire) and 184 non-DDCs (see Table 2 for anoverview)The typical DDC was 520 years old (range = 41ndash65 SD =490) was married (742) held a diploma in nursing (679) had amean household income of $101778 (range = $12500ndash$300000 SD =$4409373) was employed part-time or full-time (968) with a meanof 390 hours worked per week (range 7ndash80 SD 786) had practisednursing for 25 years or more (676) and had at least one child (ranging
Ward-Griffin Keefe Martin-Matthews Kerr Brown and Oudshoorn
CJNR 2009Vol 41 No 3 118
in age from 2 to 32 years) living with her (65)The DDC respondentsprovided an average of 6 hours per week of care to one (53) or two(30) elderly relativesmostly parents (77) or parents-in-law (12) wholived nearbyThe typical non-DDC respondent was 515 years old (range= 41ndash65 SD = 585) was married (739) held a diploma in nursing(678) had a mean household income of $105618 (range = $35000ndash$770000 SD = 6700684) was employed part-time or full-time (989)with a mean of 408 hours worked per week (range = 22ndash80) had prac-tised nursing for 25 years or more (525) and had at least one child(ranging in age from 1 to 37 years) living with her (620)There wereno significant differences between DDCs and non-DDCs with respect toage household income and number of hours worked per week
Preliminary ConstructValidity Step 1
To facilitate a better understanding of the item contents of the new scaleprincipal components analysis was conducted on each of the four sub-scales of the Provisional DDCSAlthough each dimension was provi-sionally structured as a single subscale the results of our subsequent factoranalysis suggested that Negotiating Strategies should be split into twosubscales Setting Limits and Making Connections Nine factors wereidentified from our analyses (Table 3) which is consistent with our orig-inal conceptualization about the dimensionality of DDCTwo factorsemerged from Expectations (familial expectations and professional expec-tations) accounting for 63 of the variance Five items loaded on famil-ial expectations with loadings ranging from 058 to 087 Four itemsloaded on professional expectations with loadings ranging from 049 to089As expected this indicates that among DDCs there are both famil-ial and professional expectations to provide care to elderly relatives
Development andValidation of the Double Duty Caregiving Scale
CJNR 2009Vol 41 No 3 119
Table 2 Overview of Development andValidation of Double DutyCaregiving Scale (DDCS)
Initial Item Pool ContentValidity Pilot Testing
Qualitative Mailed SurveySource Interview Data Expert Panel (n = 800)
Sample 37 female DDCs 4 female DDCs 377 female DDCs15 registered nurses 1 registered nurse 193 DDCs9 social workers 1 social worker 184 non-DDCs7 physiotherapists 1 physiotherapist6 physicians 1 physician
NoteDDC = double duty caregiver
Ward-Griffin Keefe Martin-Matthews Kerr Brown and Oudshoorn
CJNR 2009Vol 41 No 3 120
Tabl
e3
Revised
DDCS(N
=18
7)
Number
Item
-Total
Cronbachrsquos
Factor
Factor
Subscale
Factors
ofItem
sMean
SDCorrelations
Alpha
Variance
Loading
Exp
ectation
s378
712
Familialexpectations
5040ndash073
080
058ndash087
Professionalexpectations
4030ndash056
069
049ndash089
Total
9028ndash066
083
625
Supp
orts
332
646
Personalsupports
3043ndash058
068
070ndash086
Professionalsupports
3024ndash062
065
035ndash091
Total
6031ndash052
071
617
SettingLim
its
311
678
Awarenessofboundaries
3041ndash059
067
061ndash087
Activeresistance
3033ndash061
065
068ndash084
Total
6034ndash058
071
629
Mak
ingCon
nections
389
677
Makingconnections
5042ndash069
075
465
060ndash076
CaregivingIn
terface
301
826
Perceptionsofinterface
4048ndash071
081
080ndash084
Consequencesofinterface
3053ndash077
083
080ndash084
Total
7044ndash074
085
703
Two factors emerged from Supports (personal supports and profes-sional supports) accounting for 62 of the variance and indicating theimportance of personal and professional supports to DDCs providingcare to elderly relativesThree items loaded on personal supports withloadings ranging from 070 to 086Three items loaded on professionalsupports with loadings ranging from 035 to 091Two factors labelled Awareness of Boundaries and Active Resistance
emerged from Setting Limits accounting for 63 of the varianceThreeitems loaded on Awareness of Boundaries with loadings ranging from061 to 087Three items loaded on Active Resistance with loadingsranging from 068 to 084 One factor was extracted from MakingConnections accounting for 47 of the variance Loadings for the fiveitems on Making Connections ranged from 060 to 076This suggeststhat DDCs are aware of the boundaries between their personal and pro-fessional caregiving and that in an attempt to negotiate these boundariesthey resist providing care to their elderly relative as well as making con-nections to increase their supportsTwo factors emerged from CIThese were labelled Perceptions of CI
and Consequences of CI accounting for 70 of the variance Four itemsloaded on Perceptions of CI with loadings ranging from 054 to 085and three items loaded on Consequences of CI with loadings rangingfrom 080 to 084These results indicate that DDCs both are aware ofand experience consequences of the blurring of boundaries between per-sonal and professional caregiving
Reliability
Inter-item correlations and internal consistency (reliability) were exam-ined for each of the subscales of the Revised DDCSOverall in the finalversion of the 33-item DDCS inter-item correlations ranged from 024to 077 (Table 3) Cronbachrsquos alpha reliability coefficients of the fiveDDC subscales ranged from 085 (CI) to 071 (Supports and SettingLimits)Moreover Cronbachrsquos alpha reliability coefficients of the subscalefactors ranged from 083 (CI-Consequences) to 065 (for both Supports-Professional and Setting Limits-Active Resistance)
ConstructValidity Step 2
Pearson correlations were conducted to assess construct validity betweeneach of the subscales within the DDCS andWRSICWBS and SF-12v2(physical) and SF-12v2 (mental) (Table 3) In line with the underlyingtheory driving the scale there were weak to moderate correlations in theexpected direction between the Revised DDCS subscales ofExpectations Supports Setting LimitsMaking Connections and CI andthe established measuresThe strongest significant correlations were
Development andValidation of the Double Duty Caregiving Scale
CJNR 2009Vol 41 No 3 121
Ward-Griffin Keefe Martin-Matthews Kerr Brown and Oudshoorn
CJNR 2009Vol 41 No 3 122
Tabl
e4
Correlation
BetweenRevised
DDC
Subscalesan
dEstab
lished
Measures
Setting
Making
Caregiving
Scale
Expectations
Supports
Lim
its
Connections
Interface
WRSI
ar
-34
41
09
04
-49
p000
000
240
625
000
CaregiverWell-Being
Scale
r-16
34
-05
-01
-29
Activitiesb
p03
00
48
89
00
CaregiverWell-Being
Scale
r-16
34
03
-03
-36
Needsc
p04
00
71
69
00
SF12
PhysicalIndexd
r06
14
-14
-03
-02
p42
06
06
69
78
SF12
MentalIndex
dr
-26
26
09
01
-39
p00
22
22
60
00
Expectations
ar
1-12
-07
38
55
p095
344
000
000
Supportsa
r-12
104
10
-26
p095
552
174
000
Strategiesndash
r1
01
-23
SettingLimits
ap
851
002
Strategiesndash
r1
18
MakingConnections
ap
013
CaregivingInterfacea
r1
p
aN=187
bN=174
cN=180
dN=176plt05(2-tailed)
plt01(2-tailed)
between CI andWRSI (r = -49 p lt 001) between Supports andWRSI(r = 041 p lt001) and between CI and SF-12v2 (mental) (r = -39 p lt001) Finally the CI of the DDCS was also negatively correlated withcaregiver well-being (r = -29 p lt 001 [activities] and r = -36 p lt001[needs])The strongest subscale inter-correlations (ie within the Revised
DDCS itself) were between Expectations and CI (r = 055 p lt 001) andbetween Expectations and Making Connections (r = 038 p lt 001) Inaddition there was a weak positive association between MakingConnections and CI (r = 018 p lt 05) and negative associationsbetween Supports and CI (r = -026 p lt 001) and between SettingLimits and CI (r = -23 p lt 001) None of the other DDCS subscaleinter-correlations were statistically significant (Table 4)
Contrasted Groups Approach
Although there were no significant differences between DDCs andnon-DDCs in their overall scores for theWRSI CWBS and SF-12v2(physical and mental scores) there were significant differences betweennon-DDCs (n = 67) and the DDC subgroup (n = 84) defined as livingon the edge (ie those scoring above the mean on the CI subscale) Poorerhealth was observed for the living on the edge DDCs on their overall SF-12v2 mental health index score (t = -276 p lt 05) and on four of theeight SF-12v2 subscales vitality (t = -237 p lt 05) social functioning(t = -291 p lt 01) role emotional (t = -306 p lt 05) and mental health(t = -227 p lt 05) Moreover there were significant differences withinthe DDC group between those who were living on the edge and thosewith lower CI scores for the following SF-12 subscales vitality (t = -20p lt 05) social functioning (t = -356 p lt 01) role emotional (t = -483p lt 01) and mental health (t = -398 p lt 05)The living on the edgegroup also had significantly lower well-being scores for the activities(t = -363 p lt 05) and needs (t = -447 p lt 05) subscales than theother DDC respondentsWhile not all results were statistically significantoverall there was an observed tendency for the living on the edge group ofDDCs to have the lowest health and well-being scores whereas the otherDDCs (eg making it work) with low CI scores tended to have slightlybetter health scores than the non-DDC group
Discussion
The main purpose of this study was to develop and test a tool intendedto advance our understanding of DDC using a random sample of regis-tered nurses providing care to elderly relatives
Development andValidation of the Double Duty Caregiving Scale
CJNR 2009Vol 41 No 3 123
The nine factors we identified were consistent with the theorized coreDDC dimensions of Expectations (Familial and Professional) Supports(Personal and Professional) Setting Limits (Awareness of BoundariesActive Resistance) Making Connections and Caregiving Interface(Perceptions and Consequences) which can yield important informationregarding how much variance is accounted for by the factors Howeveradditional analyses are required to establish the psychometric propertiesof the DDCS including test-retest reliability to assess construct stabilityBased on the EFA results a measurement model of DDC will be pro-posed and analyzed in a future study using CFA to enhance the psycho-metric validation of the DDCS For researchers looking for a shorterversion of the DDCS it is worth noting that based on the strength andconsistency of the overall findings the seven-item CI subscale could beused to determine the extent of DDC when survey respondent burdenis a key factor in instrument selection (ie when use of the full 33DDCS items is not possible) adding to the potential value of the DDCS
The positive correlation between Expectations and CI and the nega-tive correlation between Supports and CI and between Setting Limitsand CI are theoretically consistent with the conceptual model of DDCThat is if expectations are high both personally and professionally withrespect to caring for onersquos relatives there will be greater CI or blurringof boundaries Conversely if one has strong personal and professionalsupports it follows that a lower degree of CI will result Similarly whenone sets limits on caregiving then less blurring or a lower degree of CIshould result However the positive association between MakingConnections and Expectations was unexpected Perhaps high expecta-tions lead one to increase supports by making connections both person-ally and professionally to help meet these expectationsComparison of the SF-12 v2 scores for living on the edge DDCs and
non-DDCs revealed significant differences for SF-12v2 mental healthand specific SF-12v2 subscales of vitality social functioning role emo-tional and mental healthThese findings suggest that DDCs who expe-rience a high degree of blurring of their professional and personalboundaries are at greater risk for poor health than those health profes-sionals who do not care for elderly relatives or who do not experiencethis blurring In addition those DDCs who could be characterized asliving on the edge scored significantly higher on the same four SF-12 sub-scales than DDCs with lower CI scoresThis observed pattern suggeststwo possibilities there exists a threshold effect for the negative healtheffects of DDC or manageable exposure to DDC has a beneficial effectFurther exploration of these interesting findings is warrantedAlthough we conducted a systematic and comprehensive analysis to
assess the psychometric properties of a new scale further reliability and
Ward-Griffin Keefe Martin-Matthews Kerr Brown and Oudshoorn
CJNR 2009Vol 41 No 3 124
validity studies are needed Confirmatory validation studies with otherhealth-care provider populations such as family physicians social workersand physiotherapists are particularly important as these professionals havethe potential to be DDCs and their experiences as documented in ouroriginal qualitative study of DDC helped to formulate the theoreticalunderpinnings of the DDCS In addition research with these groups willadvance our understanding of how occupational health groups may differin terms of expectations supports negotiating strategies and degree ofCIAs the identification of health-advantage and health-risk factors isinfluenced by health and social environments the negotiating strategiescould also be examined through the use of qualitative methodologiessuch as in-depth interviews or focus groupsFinally research that draws linkages between professional and personal
caregiving has the added value of furthering knowledge about employedcaregiving specifically as it relates to the relationship between health out-comes and provision of familial care by health-care providersAlthoughthe convergence (and avoidance) of professional and personal caregivingboundaries is not a new issue in nursing and other health professions thenotion that it is the individualrsquos responsibility to negotiate this boundarytends to predominate (Ward-Griffin 2008)To that end further testingand refinement of the DDCS will be helpful in identifying areas whereDDCs may need specific or different types of support It is also impor-tant to understand how specific social supports shape the health experi-ences of DDCs as well as to investigate different types of social supportinterventions with DDCsThis information is particularly meaningfultoday with the intersection of three challenges an aging population anaging health-care workforce and a shortage of health professionals Suchknowledge could contribute to workplace and other health initiativesspearheaded by professional groups policy-makers and other key stake-holders interested in assessing and addressing the health effects of DDCIn summary the DDCS is a valid tool for the assessment of double
duty caregiving Such assessment is a crucial step in understanding theexperience of the blurring of personal and professional boundaries ofcaregiving among health professionalsA quantitative study of both maleand female DDCs could help us to understand the relationship betweencertain factors (ie gender health-care occupation) and the potentialhealth effects of DDCMoreover our finding that respondents with highCI scores (living on the edge) had significantly lower health and well-beingscores than DDC respondents with lower CI scores warrants furtherinvestigation to determine if one group of DDCs is at particular risk fordeveloping negative health effects Given the current climate of health-care reform in Canada developing a better understanding of DDC andits health effects is particularly relevant for policy-makers and others who
Development andValidation of the Double Duty Caregiving Scale
CJNR 2009Vol 41 No 3 125
are committed to developing health-promoting programs and policies forfamilial caregivers of the elderly Clearly now is the time to monitor theeffects of changing demographics both in the general population andwithin the health professions in order to develop appropriate and tar-geted strategies thereby creating and sustaining healthy work environ-ments and health-care workforcesWith further refinement the DDCSmay assist with these endeavours
References
Armstrong P amp ArmstrongH (2004)Thinking it throughWomenwork andcaring in the new millennium In K Grant CArmaratunga PArmstrongM BoscoeA Pederson amp KWillson (Eds)Caring forcaring aboutWomenhome care and unpaid caregiving (pp 5ndash44)Aurora ONGaramond
Baines D (2004) Seven kinds of work ndash only one paid Raced gendered andrestructured work in social servicesAtlantis 28(2) 19ndash28
Canadian Institute for Health Information (2006)Workforce trends of registerednurses in Canada 2005 Retrieved November 5 2006 fromhttpsecurecihicacihiwebproductsndb_worforce_trends_registered_nurses_canada_2005_epdf
CarruthA K (1996) Development and testing of the Caregiver ReciprocityScaleNursing Research 45(2) 92ndash97
Chen F Feudtner C Rhodes L amp Green L (2001) Role conflicts of physi-cians and their family members Rules but no rule bookWestern Journal ofMedicine 175(4) 236ndash239
Cohen S Underwood L G amp Gottlieb BH (Eds) (2000) Social support mea-surement and interventionA guide for health and social scientistsOxford OxfordUniversity Press
Fast J (2005)Hidden costsinvisible contributions report Reworking workThe experi-ence of employed caregivers of older adults Retrieved August 16 2007 fromwwwhecolualbertacahcic
Gable R ampWolfe M (1993) Instrument development 2nd ed Boston KluwerGubermanN amp Maheu P (1999) Combining employment and caregivingAn
intricate juggling actCanadian Journal on Aging 18(1) 84ndash106Keefe J Leacutegareacute J amp CarriegravereY (2007) Developing new strategies to support
future caregivers of older Canadians with disabilities Projections of need andtheir policy implicationsCanadian Public Policy 33 S65ndash80
Lengacher CA amp Sellers E (2003)TheWomenrsquos Role Strain Inventory InO L Strickland amp CDilorio (Eds)Measurement of nursing outcomes 2nd ed(pp 109ndash127) NewYork Springer
Martin-MatthewsA (2000) Intergenerational caregivingHow apocalyptic anddominant demography frame the questions and shape the answers In EMGee amp GGutman (Eds)The overselling of population agingApocalyptic demog-raphy intergenerational challenges and social policy (pp 64ndash79)Toronto OxfordUniversity Press
Ward-Griffin Keefe Martin-Matthews Kerr Brown and Oudshoorn
CJNR 2009Vol 41 No 3 126
Mayall B (1993) Keeping children healthy ndash the intermediate domain SocialScience and Medicine 36(1) 77ndash83
Morris JM amp Field PA (1995) Qualitative research methods for health profession-als 2nd ed London Sage
Pascall G (1986) Social policyA feminist analysis NewYorkTavistockPhillips J BernardM amp ChittendenM (2002) Juggling work and careThe expe-riences of older adults Bristol Policy Press
Polit D F amp Beck CT (2008)Nursing research Generating and assessing evidencefor nursing practice 8th ed Philadelphia LippincottWilliams ampWilkins
Polit D F amp Beck CT amp Owen SV (2007) Is the CVI an acceptable indica-tor of content validity Appraisal and recommendationsResearch in Nursingand Health 30 459ndash467
RossMM Rideout EM amp CarsonMM (1996) Nursesrsquo work Balancingpersonal and professional caregiving careers Canadian Journal of NursingResearch 26(4) 43ndash59
RutmanD (1996) Caregiving as womenrsquos workWomenrsquos experiences of pow-erfulness and powerlessness as caregiversQualitative Health Research 6(1) 90ndash111
ShieldsM ampWilkins K (2005)National Survey of theWork and Health of Nurses2005 Provincial profiles Ottawa Statistics CanadaRetrieved August 24 2007from httpwwwstatcancaenglishresearch11-621-MIE11-621-MIE2006052htm
StaceyM amp Davies C (1983)Division of labour in child health care Final report toSSRCCoventry Sociology Department University ofWarwick
Tebb S (1995)An aid to empowermentA caregiver well-being scaleHealth andSocialWork 20(2) 87ndash92
Tebb S Berg-WgerM amp Rubio DM (2000) CaregiverWell-Being Scale InDRoyse BAThyer D K Padgett ampT K Logan (Eds) Program evaluation3rd ed (pp 320ndash323) Pacific Grove CA BrooksCole
Ungerson C (1990) The language of care Crossing the boundaries InCUngerson (Ed)Gender and caringWork and welfare in Britain and Scandinavia(pp 8ndash33) NewYork Harvester
WaltersV LentonR French S Eyles JMayr J amp Newbold B (1996) Paidwork unpaid work and social supportA study of the health of male andfemale nurses Social Science and Medicine 43(11) 1627ndash1636
Ward-Griffin C (2004) Nurses as caregivers of elderly relatives Negotiatingpersonal and professional boundariesCJNR 36(1) 92ndash114
Ward-Griffin C (2008)Health professionals caring for aging relativesA profes-sional or personal issue In AMartin-Matthews amp J Phillips (Eds)Blurringthe boundariesAgeing at the intersection of work and home life (pp 1ndash20) NewYorkTaylor amp FrancisPsychology Press
Ward-Griffin C Brown JVandervoortA McNair S amp Dashnay I (2005)Double duty caregivingWomen in the health professionsCanadian Journalon Aging 24(4) 379ndash394
Ward-Griffin C amp MarshallV (2003) Reconceptualizing the relationshipbetween public and private eldercare Journal of Aging Studies 17 189ndash208
Development andValidation of the Double Duty Caregiving Scale
CJNR 2009Vol 41 No 3 127
Ware J E Kosinksi MTurner-Bowker L amp Gandek B (2002)How to scoreversion 2 of the SF-12 health survey Lincoln RIQuality Metric Inc
Acknowledgements
This study was funded by the Social Sciences and Humanities ResearchCouncil (Internal) and the Institute of Gender and Health CanadianInstitutes of Health ResearchThere are no conflicts of interest or financial disclosures
CatherineWard-Griffin RN PhD is ProfessorArthur Labatt Family School ofNursing University ofWestern Ontario London Canada Janice Keefe PhD isProfessor and Canada Research Chair in Aging and Caregiving Policy FamilyStudies and GerontologyMount SaintVincent University HalifaxNova ScotiaCanadaAnne Martin-Matthews PhD is Professor School of SocialWork andFamily Studies University of British ColumbiaVancouver Canada MichaelKerr PhD is Associate ProfessorArthur Labatt Family School of NursingUniversity ofWestern Ontario Judith Belle Brown PhD is Professor Departmentof Family Medicine University ofWestern OntarioAbram Oudshoorn RN is aPhD candidate in the Arthur Labatt Family School of Nursing University ofWestern Ontario
Ward-Griffin Keefe Martin-Matthews Kerr Brown and Oudshoorn
CJNR 2009Vol 41 No 3 128
negative effects of DDCThere is evidence that DDCs experience a senseof powerlessness and distress (Rutman 1996) and must make continualadjustments to achieve equilibrium in response to the demands placed onthem (Chen Feudtner Rhodes amp Green 2001 Guberman amp Maheu1999) although work-related knowledge can act as a buffer rather thanas an additional strain (Phillips Bernard amp Chittenden 2002)Ward-Griffin (2004) found that female community nurses caring for elderlyfamily members used a variety of coping strategies such as setting limitson the specific care they providedAlthough women in the health pro-fessions are often viewed as needing to develop coping strategies toaddress the stress of ldquobalancingrdquo or ldquojugglingrdquo two or more roles attemptsat setting limits often prove unsuccessful in dealing with the demands andtensions of family caregiving (Ward-Griffin 2004Ward-Griffin et al2005)The difficulty of demarcating boundaries between professional and
personal caregiving domains was particularly evident in our qualitativedescriptive study with 37 female nurses family physicians physiothera-pists and social workers who provided care to elderly relatives (Ward-Griffin et al 2005) Four dimensions of DDC were illuminatedExpectations Supports Negotiating Strategies and Caregiving InterfaceDespite using a variety of strategies for managing their DDC demandsmany of the participants experienced a blurring of boundaries betweentheir professional and personal caring workThis area of overlap was con-ceptualized as the caregiving interfaceThe extent of the interface variedfor each participant depending on the degree of expectation of familialcare and on the level of support available to manage multiple caregivingdemands From this study with female health professionals caring forelderly relatives we identified three prototypes of DDC based on thedegree of caregiving interface making it work working to manage and livingon the edge (see Figure 1)The women were able to make it work when theinterface between the professional and personal caregiving domains wasminimal they worked to manage when there was moderate overlap or blur-ring of their professional and personal caregiving boundaries and theylived on the edge when there was a high degree of overlap or interfacebetween their personal and professional domains of careIn our study the women tended over time to oscillate from one pro-
totype to another depending on their level of expectations supportnegotiating strategies and caregiving interface (Ward-Griffin et al 2005)In living on the edge the level of expectations to provide complex dailycare was exceedingly high Family and workplace supports were weak ornon-existent Some participants mostly nurses either took time off workto provide daily family care or provided professional care on their ldquodaysoff rdquo from family careAlthough setting limits and making connections
Development andValidation of the Double Duty Caregiving Scale
CJNR 2009Vol 41 No 3 111
Ward-Griffin Keefe Martin-Matthews Kerr Brown and Oudshoorn
CJNR 2009Vol 41 No 3 112
Figu
re1
Prototypesof
Dou
bleDutyCaregiving
SourceW
ard-Griffinetal(2005)
Makingitwork
Workingto
manage
Livingontheedge
ExpectationsLow
SupportsStrong
BoundariesConnected
CaregivinginterfaceSm
all
ExpectationsModerate
SupportsDiminishing
BoundariesBlurred
CaregivinginterfaceMedium
ExpectationsHigh
SupportsWeak
BoundariesEroded
CaregivinginterfaceLarge
Expectations
Support
Professional
care
Personal
care
Expectations
Support
Professional
care
Personal
care
Expectations
Support
were used to manage increasing caregiving demands with limited sup-ports many women experienced a dramatic blurring of their professionaland family caregiving boundaries characterized by tension exhaustionand a feeling of isolationThus female health professionals who providecare for elderly relatives especially those with limited tangible supportsmay experience ill health as a consequenceBuilding on the existing empirical knowledge described above and in
response to the need for further research on DDC the study had twoaimsThe first was to develop and validate a tool for measuring DDCwith a sample of female registered nurses capturing the variation withinthis populationThe second was to compare the health of DDCs andnon-DDCs
Development of the DDC Scale
The development of the DDCS (seeTable 1) began with an examinationof our previous qualitative interview data (Ward-Griffin et al 2005)Twoof the investigators (Ward-Griffin and Brown) reviewed the original tran-scripts looking for specific phrases and words that reflected the fourdimensions of DDC Expectations Supports Negotiating Strategies andCaregiving Interface Item development was refined at team meetingswhere all investigators generated an initial item pool (57 items) intendedto create four subscales to address the four dimensionsOne to two neg-atively worded items were included in each subscale to help decreaseresponse bias
Expectations
A total of 16 items were developed to address three proposed sources ofExpectations to provide care to an elderly relative expectations of self (9items) expectations of family (4 items) and expectations from within theprofession (3 items) Expectations of care include the expectations ofoneself to provide care as part of onersquos role in the family due to creden-tials and professional knowledge and skills Familial expectations maycome directly from the elderly recipient of care with hisher requests forassistance or may come from other family members Professional expec-tations may come from health professionals who are involved directly inthe care of the relative or from professional colleagues or friends who arenot involved directly professional expectations include those that may beheld by the DDCs themselves based on their credentials
Supports
Eight items were developed to assess Supports reflecting sources ofsupport from the personal (4 items) and professional (4 items) caregiving
Development andValidation of the Double Duty Caregiving Scale
CJNR 2009Vol 41 No 3 113
Ward-Griffin Keefe Martin-Matthews Kerr Brown and Oudshoorn
CJNR 2009Vol 41 No 3 114
Tabl
e1
Develop
men
tof
theDou
bleDutyCaregivingScale(D
DCS)
Dim
ensions
ofDDC
1Expectations
(expectations
tocarefor
elderlyrelatives)
2Supports
(supportsused
tomanagecaregiving)
3Negotiating
Strategies
(strategiesused
tonegotiatepersonal
professionalboundaries)
4Caregiving
Interface(CI)
(degreeofblurring
betweenprofessional
andpersonalcaregiving)
InitialItem
Pool
(n=57)
Self(9)
Family
(4)
Professional
(3)
Personal(4)
Professional
(4)
Settinglim
its(10)
Making
connections
(13)
CI(10)
Item
sDeleted
Based
on
CVIa
-1 -1 0 -1 -1 0 -3 -1
Provisional
DDCS
(n=49)
(8)
(3)
(3)
(3)
(3)
(10)
(10) (9)
Item
sDeleted
Based
onEFA
b
-5 -4 -5 -2
Revised
DDCS
Tool(n
=33)
Familial(5)
Professional(4)
Personal(3)
Professional(3)
Awarenessof
boundaries(3)
Active
resistance(3)
Making
connections(5)
Perceptionsof
CI(4)
Consequences
ofCI(3)
Sam
pleItem
s
Becauseofmyhealthcare
background
ndashIhavehigh
expectationsofmyselfto
providecaretomyrelative
Asacaregiverformyelderly
relativendashMyworkplace
supportsmetoprovidecareto
myrelative
BecauseIam
ahealthcare
providerwho
alsoprovidescare
tomyrelativendashIsetalim
itof
whattype
ofcareIwillprovide
myrelative
BecauseIam
ahealthcare
providerwho
alsoprovidescare
tomyrelativendashIfeellikeIam
caughtbetweentwoworlds
(professionaland
family)
aContentvalidity
indices
bExploratoryfactoranalyses
domains Double duty caregivers usually receive some degree of emo-tional informational and substantive support from family members andfriendsAlthough there are well-established instruments for measuringsocial support (Cohen Underwood amp Gottlieb 2000) the unique per-sonal and professional supports received within DDC may not be fullycaptured using a generic standard tool Often siblings spouses childrenor friends are also involved in the caregivingAdditionally many care-givers receive professional support this can include information orresources from onersquos workplace such as flexible work hours or access toemployee assistance programs
Negotiating Strategies
The third dimensionNegotiating Strategies addresses two main types ofstrategies Setting Limits and Making ConnectionsThese help DDCs tonegotiate their professional and personal boundaries thereby potentiallymoderating the negative impacts of the caregiving interface Double dutycaregivers set limits with respect to personal and professional expectationsconcerning the provision of familial care Setting Limits includes strate-gies for keeping the personal and professional caregiving domains sepa-rate and distinct while Making Connections examines the multipleinteractions that serve to bring the two domains closer together InSetting Limits (10 items) DDCs refuse to take on professional caregiv-ing tasks for family members or arrange for others to provide this careAs well DDCs increase their supports by Making Connections (13items)These include accessing health-care information or care for onersquosrelative using professional knowledge and connections to obtain care ornavigating the health-care system
Caregiving Interface
Ten items were developed to measure the caregiving interface (CI) orthe degree of blurring between the professional and personal caregivingdomains (intermediate domain)This dimension addresses the extent ofthe connections between elder caregiving and other forms of genderedcaring work (eg nursing)The CI encompasses both feelings about theblurring of roles and the psychological impact of these feelings Feelingsabout the blurring of roles can include being pulled in two differentdirections being unable to escape from the caregiving role and strugglingto separate caregiving at home from caregiving at workThe psycholog-ical impact of increasing blurring of boundaries can include stress thefeeling that onersquos caregiving is not being recognized and confusionregarding onersquos professional and personal roles
Development andValidation of the Double Duty Caregiving Scale
CJNR 2009Vol 41 No 3 115
ContentValidation of the DDC Scale
Because of the importance of preserving the inductively derived meaningof DDC in a quantitative instrument (Morris amp Field 1995) judgementsabout clarity internal consistency and initial content validity were madeby a panel of four DDCs representing the disciplines of nursing medi-cine physiotherapy and social work as used in our previous qualitativestudyThese content experts independently rated the relevance of theprovisional items on the DDCS using a four-point scale ranging from notrelevant to very relevant This review process facilitated a systematicapproach to item revision Raters also indicated whether the conceptualdomain of each subscale was adequately represented by the set of itemsAlthough consensus was reached for each of the four dimensions theexperts recommended clarification of certain items which were subse-quently reworded or deletedContent validity indices (CVI) for each item subscales and total scale
were calculated setting the criteria for item-level acceptance at 78 orhigher for three or more reviewers (Polit Beck amp Owen 2007)TheCVI ranged from 75 to 10 for all retained items (one item fell below78 but was retained because it measured a key conceptual aspect of theCI subscale recognition of professional status) Eight items were deleteddue to lack of clarity redundancy or a relatively low CVI thus reducingthe provisional DDCS from 57 items to 49The provisional DDCS was constructed using a five-point Likert scale
(1 = strongly disagree 5 = strongly agree) Prior to the analysis negativelyworded items were recoded so that for all items a higher score reflecteda higher degree of Expectations SupportsNegotiating Strategies andCaregiving InterfaceWithin each subscale the scores were calculated byaveraging the relevant individual item scores Data imputation for missingvalues was not used as non-response for the items was very lowThe sub-scales were developed for separate use of each dimension thus they werenot combined into a single overall DDCS score
Pilot Testing of the DDC Scale
Sampling
Following institutional ethics review board approval the 49-item provi-sional DDCS was administered to an age-stratified sample of femalenurses randomly selected from the registry list of the College of Nursesof Ontario Because previous research suggested that approximately onehalf of the working nurse population is likely to provide care to anelderly relative 800 female full-time (more than 30 hoursweek) regis-tered nurses 40 years of age or older were asked to complete a mailed
Ward-Griffin Keefe Martin-Matthews Kerr Brown and Oudshoorn
CJNR 2009Vol 41 No 3 116
survey packageThe aim was to have 200 eligible DDC respondentscomplete and return the package which consisted of (1) an informationletter (2) a short demographic questionnaire which also determined eli-gibility for the study (3) the provisional DDCS described above and(4) established comparative measures including theWomenrsquos Role StrainInventory (WRSI) (Lengacher amp Sellers 2003) the CaregiverWell-BeingScale (CWBS) (Tebb et al 2000) and Health Related Outcomes(Medical Outcomes Study Short-Form SF-12 version 20 acute form4-week recall)The time needed to complete the survey package wasestimated at between 30 and 45 minutes Each package contained amodest gift certificate as a token of appreciation Nurses not providingcare for an elderly relative or friend were asked to complete all question-naires except the DDCS the purpose being to generate data for com-paring DDC and non-DDC nursesOf the 800 questionnaires mailed 394 were returned of these eight
respondents did not meet the eligibility criteria (two male and six unem-ployed) six questionnaires were blank and three were returned to senderyielding a sample of 377 respondents (49 response rate)A total of 193respondents (51) were caring for an elderly relative (ie the DDCs) and184 (49) were not (ie the non-DDCs)Of the 193 respondents iden-tified as DDCs six left sections of the DDCS blank which led to a finalusable DDC sample of 187 a total sample size that is considered adequatefor instrument development analysis (Gable ampWolf 1993)
Reliability and ConstructValidity Analyses
Contingency table (chi square) analyses were performed on all categori-cal variables while independent sample t tests were used with all contin-uous variables when comparing DDCs and non-DDCsAppropriatemeasures of association were used to examine the relationship betweentheoretically relevant demographic variables (eg hours of employmentper week hours of caregiving per week) and the CIConstruct validity of the provisional 49-item tool was assessed at the
preliminary stage with a combination of exploratory factor analysis (EFA)using a principal components factor approach and assessment of scalereliability Even though our previous qualitative work and initial concep-tualization of DDC informed the construction of the provisional DDCSitems EFA was selected over confirmatory factor analysis (CFA) For theEFA initial factor extraction was based on eigenvalues greater than 100(Polit amp Beck 2008 p 488) Each subscale of the provisional DDCS wasthen subjected to varimax rotation to select the factor structure that bestrepresented the underlying relationship of the items within the fourdimensions (Expectations Supports Negotiating Strategies andCaregiver Interface)Although loadings with an absolute value of 040 or
Development andValidation of the Double Duty Caregiving Scale
CJNR 2009Vol 41 No 3 117
higher are often used as factor loading cut-off values (Carruth 1996)smaller values are acceptable if the item pool is large (Polit amp Beck 2008p 491) Cronbachrsquos alpha reliability coefficients were also used to deter-mine internal consistency among the items of the four subscales of theprovisional DDCS Based on these preliminary analyses a combinationof low inter-item correlations (lt 20) weak factor loadings (lt 35)andor poor conceptual clarity 16 of the original 49 items were removedfrom the provisional DDCS yielding a tool with a total of 33 items forthe remaining construct validity analysesWe also correlated each of the DDCS subscale scores with those of
theWRSI the CWBS and the SF-12v2TheWRSI is a previously vali-dated 44-item five-point Likert scale that measures role strain in femalenurses with multiple roles (Lengacher amp Sellers 2003) with high relia-bility coefficients for the total scale (086ndash095) and subscales of distress(074ndash091) enhancement (079ndash089) and support (065ndash087)Developed and validated byTebb et al (2000) the CWBS-ShortVersionis a 16-item five-point Likert scale that assesses activities and needs ofcaregivers (eight items for each subscale) Overall and for each subscale(Needs and Activities of Daily Living) the coefficient alpha was 094091 and 088 respectively Finally the SF-12v2 is a well-established toolthat measures the perceptions and activities of acute health and well-being It is a shortened version of the SF-36 which includes general andphysical health index scores as well as eight subscales (bodily pain generalhealth vitality social functioning physical functioning role limitationsdue to physical problems role limitations due to emotional problems andmental health)Ware KosinskiTurner-Bowker and Gandek (2002) reportinternal consistency reliability coefficients ranging from 066 to 090 Inthe present study internal consistency reliability coefficients for each ofthese established instruments were 091 (WRSI) 073 (CWBS-needs)078 (CWBS-activities) and 080 (SF-12v2)
Results
Sample
The sample comprised 193 DDCs (this figure includes six respondentswho failed to complete all items on the DDCS but completed thedemographic questionnaire) and 184 non-DDCs (see Table 2 for anoverview)The typical DDC was 520 years old (range = 41ndash65 SD =490) was married (742) held a diploma in nursing (679) had amean household income of $101778 (range = $12500ndash$300000 SD =$4409373) was employed part-time or full-time (968) with a meanof 390 hours worked per week (range 7ndash80 SD 786) had practisednursing for 25 years or more (676) and had at least one child (ranging
Ward-Griffin Keefe Martin-Matthews Kerr Brown and Oudshoorn
CJNR 2009Vol 41 No 3 118
in age from 2 to 32 years) living with her (65)The DDC respondentsprovided an average of 6 hours per week of care to one (53) or two(30) elderly relativesmostly parents (77) or parents-in-law (12) wholived nearbyThe typical non-DDC respondent was 515 years old (range= 41ndash65 SD = 585) was married (739) held a diploma in nursing(678) had a mean household income of $105618 (range = $35000ndash$770000 SD = 6700684) was employed part-time or full-time (989)with a mean of 408 hours worked per week (range = 22ndash80) had prac-tised nursing for 25 years or more (525) and had at least one child(ranging in age from 1 to 37 years) living with her (620)There wereno significant differences between DDCs and non-DDCs with respect toage household income and number of hours worked per week
Preliminary ConstructValidity Step 1
To facilitate a better understanding of the item contents of the new scaleprincipal components analysis was conducted on each of the four sub-scales of the Provisional DDCSAlthough each dimension was provi-sionally structured as a single subscale the results of our subsequent factoranalysis suggested that Negotiating Strategies should be split into twosubscales Setting Limits and Making Connections Nine factors wereidentified from our analyses (Table 3) which is consistent with our orig-inal conceptualization about the dimensionality of DDCTwo factorsemerged from Expectations (familial expectations and professional expec-tations) accounting for 63 of the variance Five items loaded on famil-ial expectations with loadings ranging from 058 to 087 Four itemsloaded on professional expectations with loadings ranging from 049 to089As expected this indicates that among DDCs there are both famil-ial and professional expectations to provide care to elderly relatives
Development andValidation of the Double Duty Caregiving Scale
CJNR 2009Vol 41 No 3 119
Table 2 Overview of Development andValidation of Double DutyCaregiving Scale (DDCS)
Initial Item Pool ContentValidity Pilot Testing
Qualitative Mailed SurveySource Interview Data Expert Panel (n = 800)
Sample 37 female DDCs 4 female DDCs 377 female DDCs15 registered nurses 1 registered nurse 193 DDCs9 social workers 1 social worker 184 non-DDCs7 physiotherapists 1 physiotherapist6 physicians 1 physician
NoteDDC = double duty caregiver
Ward-Griffin Keefe Martin-Matthews Kerr Brown and Oudshoorn
CJNR 2009Vol 41 No 3 120
Tabl
e3
Revised
DDCS(N
=18
7)
Number
Item
-Total
Cronbachrsquos
Factor
Factor
Subscale
Factors
ofItem
sMean
SDCorrelations
Alpha
Variance
Loading
Exp
ectation
s378
712
Familialexpectations
5040ndash073
080
058ndash087
Professionalexpectations
4030ndash056
069
049ndash089
Total
9028ndash066
083
625
Supp
orts
332
646
Personalsupports
3043ndash058
068
070ndash086
Professionalsupports
3024ndash062
065
035ndash091
Total
6031ndash052
071
617
SettingLim
its
311
678
Awarenessofboundaries
3041ndash059
067
061ndash087
Activeresistance
3033ndash061
065
068ndash084
Total
6034ndash058
071
629
Mak
ingCon
nections
389
677
Makingconnections
5042ndash069
075
465
060ndash076
CaregivingIn
terface
301
826
Perceptionsofinterface
4048ndash071
081
080ndash084
Consequencesofinterface
3053ndash077
083
080ndash084
Total
7044ndash074
085
703
Two factors emerged from Supports (personal supports and profes-sional supports) accounting for 62 of the variance and indicating theimportance of personal and professional supports to DDCs providingcare to elderly relativesThree items loaded on personal supports withloadings ranging from 070 to 086Three items loaded on professionalsupports with loadings ranging from 035 to 091Two factors labelled Awareness of Boundaries and Active Resistance
emerged from Setting Limits accounting for 63 of the varianceThreeitems loaded on Awareness of Boundaries with loadings ranging from061 to 087Three items loaded on Active Resistance with loadingsranging from 068 to 084 One factor was extracted from MakingConnections accounting for 47 of the variance Loadings for the fiveitems on Making Connections ranged from 060 to 076This suggeststhat DDCs are aware of the boundaries between their personal and pro-fessional caregiving and that in an attempt to negotiate these boundariesthey resist providing care to their elderly relative as well as making con-nections to increase their supportsTwo factors emerged from CIThese were labelled Perceptions of CI
and Consequences of CI accounting for 70 of the variance Four itemsloaded on Perceptions of CI with loadings ranging from 054 to 085and three items loaded on Consequences of CI with loadings rangingfrom 080 to 084These results indicate that DDCs both are aware ofand experience consequences of the blurring of boundaries between per-sonal and professional caregiving
Reliability
Inter-item correlations and internal consistency (reliability) were exam-ined for each of the subscales of the Revised DDCSOverall in the finalversion of the 33-item DDCS inter-item correlations ranged from 024to 077 (Table 3) Cronbachrsquos alpha reliability coefficients of the fiveDDC subscales ranged from 085 (CI) to 071 (Supports and SettingLimits)Moreover Cronbachrsquos alpha reliability coefficients of the subscalefactors ranged from 083 (CI-Consequences) to 065 (for both Supports-Professional and Setting Limits-Active Resistance)
ConstructValidity Step 2
Pearson correlations were conducted to assess construct validity betweeneach of the subscales within the DDCS andWRSICWBS and SF-12v2(physical) and SF-12v2 (mental) (Table 3) In line with the underlyingtheory driving the scale there were weak to moderate correlations in theexpected direction between the Revised DDCS subscales ofExpectations Supports Setting LimitsMaking Connections and CI andthe established measuresThe strongest significant correlations were
Development andValidation of the Double Duty Caregiving Scale
CJNR 2009Vol 41 No 3 121
Ward-Griffin Keefe Martin-Matthews Kerr Brown and Oudshoorn
CJNR 2009Vol 41 No 3 122
Tabl
e4
Correlation
BetweenRevised
DDC
Subscalesan
dEstab
lished
Measures
Setting
Making
Caregiving
Scale
Expectations
Supports
Lim
its
Connections
Interface
WRSI
ar
-34
41
09
04
-49
p000
000
240
625
000
CaregiverWell-Being
Scale
r-16
34
-05
-01
-29
Activitiesb
p03
00
48
89
00
CaregiverWell-Being
Scale
r-16
34
03
-03
-36
Needsc
p04
00
71
69
00
SF12
PhysicalIndexd
r06
14
-14
-03
-02
p42
06
06
69
78
SF12
MentalIndex
dr
-26
26
09
01
-39
p00
22
22
60
00
Expectations
ar
1-12
-07
38
55
p095
344
000
000
Supportsa
r-12
104
10
-26
p095
552
174
000
Strategiesndash
r1
01
-23
SettingLimits
ap
851
002
Strategiesndash
r1
18
MakingConnections
ap
013
CaregivingInterfacea
r1
p
aN=187
bN=174
cN=180
dN=176plt05(2-tailed)
plt01(2-tailed)
between CI andWRSI (r = -49 p lt 001) between Supports andWRSI(r = 041 p lt001) and between CI and SF-12v2 (mental) (r = -39 p lt001) Finally the CI of the DDCS was also negatively correlated withcaregiver well-being (r = -29 p lt 001 [activities] and r = -36 p lt001[needs])The strongest subscale inter-correlations (ie within the Revised
DDCS itself) were between Expectations and CI (r = 055 p lt 001) andbetween Expectations and Making Connections (r = 038 p lt 001) Inaddition there was a weak positive association between MakingConnections and CI (r = 018 p lt 05) and negative associationsbetween Supports and CI (r = -026 p lt 001) and between SettingLimits and CI (r = -23 p lt 001) None of the other DDCS subscaleinter-correlations were statistically significant (Table 4)
Contrasted Groups Approach
Although there were no significant differences between DDCs andnon-DDCs in their overall scores for theWRSI CWBS and SF-12v2(physical and mental scores) there were significant differences betweennon-DDCs (n = 67) and the DDC subgroup (n = 84) defined as livingon the edge (ie those scoring above the mean on the CI subscale) Poorerhealth was observed for the living on the edge DDCs on their overall SF-12v2 mental health index score (t = -276 p lt 05) and on four of theeight SF-12v2 subscales vitality (t = -237 p lt 05) social functioning(t = -291 p lt 01) role emotional (t = -306 p lt 05) and mental health(t = -227 p lt 05) Moreover there were significant differences withinthe DDC group between those who were living on the edge and thosewith lower CI scores for the following SF-12 subscales vitality (t = -20p lt 05) social functioning (t = -356 p lt 01) role emotional (t = -483p lt 01) and mental health (t = -398 p lt 05)The living on the edgegroup also had significantly lower well-being scores for the activities(t = -363 p lt 05) and needs (t = -447 p lt 05) subscales than theother DDC respondentsWhile not all results were statistically significantoverall there was an observed tendency for the living on the edge group ofDDCs to have the lowest health and well-being scores whereas the otherDDCs (eg making it work) with low CI scores tended to have slightlybetter health scores than the non-DDC group
Discussion
The main purpose of this study was to develop and test a tool intendedto advance our understanding of DDC using a random sample of regis-tered nurses providing care to elderly relatives
Development andValidation of the Double Duty Caregiving Scale
CJNR 2009Vol 41 No 3 123
The nine factors we identified were consistent with the theorized coreDDC dimensions of Expectations (Familial and Professional) Supports(Personal and Professional) Setting Limits (Awareness of BoundariesActive Resistance) Making Connections and Caregiving Interface(Perceptions and Consequences) which can yield important informationregarding how much variance is accounted for by the factors Howeveradditional analyses are required to establish the psychometric propertiesof the DDCS including test-retest reliability to assess construct stabilityBased on the EFA results a measurement model of DDC will be pro-posed and analyzed in a future study using CFA to enhance the psycho-metric validation of the DDCS For researchers looking for a shorterversion of the DDCS it is worth noting that based on the strength andconsistency of the overall findings the seven-item CI subscale could beused to determine the extent of DDC when survey respondent burdenis a key factor in instrument selection (ie when use of the full 33DDCS items is not possible) adding to the potential value of the DDCS
The positive correlation between Expectations and CI and the nega-tive correlation between Supports and CI and between Setting Limitsand CI are theoretically consistent with the conceptual model of DDCThat is if expectations are high both personally and professionally withrespect to caring for onersquos relatives there will be greater CI or blurringof boundaries Conversely if one has strong personal and professionalsupports it follows that a lower degree of CI will result Similarly whenone sets limits on caregiving then less blurring or a lower degree of CIshould result However the positive association between MakingConnections and Expectations was unexpected Perhaps high expecta-tions lead one to increase supports by making connections both person-ally and professionally to help meet these expectationsComparison of the SF-12 v2 scores for living on the edge DDCs and
non-DDCs revealed significant differences for SF-12v2 mental healthand specific SF-12v2 subscales of vitality social functioning role emo-tional and mental healthThese findings suggest that DDCs who expe-rience a high degree of blurring of their professional and personalboundaries are at greater risk for poor health than those health profes-sionals who do not care for elderly relatives or who do not experiencethis blurring In addition those DDCs who could be characterized asliving on the edge scored significantly higher on the same four SF-12 sub-scales than DDCs with lower CI scoresThis observed pattern suggeststwo possibilities there exists a threshold effect for the negative healtheffects of DDC or manageable exposure to DDC has a beneficial effectFurther exploration of these interesting findings is warrantedAlthough we conducted a systematic and comprehensive analysis to
assess the psychometric properties of a new scale further reliability and
Ward-Griffin Keefe Martin-Matthews Kerr Brown and Oudshoorn
CJNR 2009Vol 41 No 3 124
validity studies are needed Confirmatory validation studies with otherhealth-care provider populations such as family physicians social workersand physiotherapists are particularly important as these professionals havethe potential to be DDCs and their experiences as documented in ouroriginal qualitative study of DDC helped to formulate the theoreticalunderpinnings of the DDCS In addition research with these groups willadvance our understanding of how occupational health groups may differin terms of expectations supports negotiating strategies and degree ofCIAs the identification of health-advantage and health-risk factors isinfluenced by health and social environments the negotiating strategiescould also be examined through the use of qualitative methodologiessuch as in-depth interviews or focus groupsFinally research that draws linkages between professional and personal
caregiving has the added value of furthering knowledge about employedcaregiving specifically as it relates to the relationship between health out-comes and provision of familial care by health-care providersAlthoughthe convergence (and avoidance) of professional and personal caregivingboundaries is not a new issue in nursing and other health professions thenotion that it is the individualrsquos responsibility to negotiate this boundarytends to predominate (Ward-Griffin 2008)To that end further testingand refinement of the DDCS will be helpful in identifying areas whereDDCs may need specific or different types of support It is also impor-tant to understand how specific social supports shape the health experi-ences of DDCs as well as to investigate different types of social supportinterventions with DDCsThis information is particularly meaningfultoday with the intersection of three challenges an aging population anaging health-care workforce and a shortage of health professionals Suchknowledge could contribute to workplace and other health initiativesspearheaded by professional groups policy-makers and other key stake-holders interested in assessing and addressing the health effects of DDCIn summary the DDCS is a valid tool for the assessment of double
duty caregiving Such assessment is a crucial step in understanding theexperience of the blurring of personal and professional boundaries ofcaregiving among health professionalsA quantitative study of both maleand female DDCs could help us to understand the relationship betweencertain factors (ie gender health-care occupation) and the potentialhealth effects of DDCMoreover our finding that respondents with highCI scores (living on the edge) had significantly lower health and well-beingscores than DDC respondents with lower CI scores warrants furtherinvestigation to determine if one group of DDCs is at particular risk fordeveloping negative health effects Given the current climate of health-care reform in Canada developing a better understanding of DDC andits health effects is particularly relevant for policy-makers and others who
Development andValidation of the Double Duty Caregiving Scale
CJNR 2009Vol 41 No 3 125
are committed to developing health-promoting programs and policies forfamilial caregivers of the elderly Clearly now is the time to monitor theeffects of changing demographics both in the general population andwithin the health professions in order to develop appropriate and tar-geted strategies thereby creating and sustaining healthy work environ-ments and health-care workforcesWith further refinement the DDCSmay assist with these endeavours
References
Armstrong P amp ArmstrongH (2004)Thinking it throughWomenwork andcaring in the new millennium In K Grant CArmaratunga PArmstrongM BoscoeA Pederson amp KWillson (Eds)Caring forcaring aboutWomenhome care and unpaid caregiving (pp 5ndash44)Aurora ONGaramond
Baines D (2004) Seven kinds of work ndash only one paid Raced gendered andrestructured work in social servicesAtlantis 28(2) 19ndash28
Canadian Institute for Health Information (2006)Workforce trends of registerednurses in Canada 2005 Retrieved November 5 2006 fromhttpsecurecihicacihiwebproductsndb_worforce_trends_registered_nurses_canada_2005_epdf
CarruthA K (1996) Development and testing of the Caregiver ReciprocityScaleNursing Research 45(2) 92ndash97
Chen F Feudtner C Rhodes L amp Green L (2001) Role conflicts of physi-cians and their family members Rules but no rule bookWestern Journal ofMedicine 175(4) 236ndash239
Cohen S Underwood L G amp Gottlieb BH (Eds) (2000) Social support mea-surement and interventionA guide for health and social scientistsOxford OxfordUniversity Press
Fast J (2005)Hidden costsinvisible contributions report Reworking workThe experi-ence of employed caregivers of older adults Retrieved August 16 2007 fromwwwhecolualbertacahcic
Gable R ampWolfe M (1993) Instrument development 2nd ed Boston KluwerGubermanN amp Maheu P (1999) Combining employment and caregivingAn
intricate juggling actCanadian Journal on Aging 18(1) 84ndash106Keefe J Leacutegareacute J amp CarriegravereY (2007) Developing new strategies to support
future caregivers of older Canadians with disabilities Projections of need andtheir policy implicationsCanadian Public Policy 33 S65ndash80
Lengacher CA amp Sellers E (2003)TheWomenrsquos Role Strain Inventory InO L Strickland amp CDilorio (Eds)Measurement of nursing outcomes 2nd ed(pp 109ndash127) NewYork Springer
Martin-MatthewsA (2000) Intergenerational caregivingHow apocalyptic anddominant demography frame the questions and shape the answers In EMGee amp GGutman (Eds)The overselling of population agingApocalyptic demog-raphy intergenerational challenges and social policy (pp 64ndash79)Toronto OxfordUniversity Press
Ward-Griffin Keefe Martin-Matthews Kerr Brown and Oudshoorn
CJNR 2009Vol 41 No 3 126
Mayall B (1993) Keeping children healthy ndash the intermediate domain SocialScience and Medicine 36(1) 77ndash83
Morris JM amp Field PA (1995) Qualitative research methods for health profession-als 2nd ed London Sage
Pascall G (1986) Social policyA feminist analysis NewYorkTavistockPhillips J BernardM amp ChittendenM (2002) Juggling work and careThe expe-riences of older adults Bristol Policy Press
Polit D F amp Beck CT (2008)Nursing research Generating and assessing evidencefor nursing practice 8th ed Philadelphia LippincottWilliams ampWilkins
Polit D F amp Beck CT amp Owen SV (2007) Is the CVI an acceptable indica-tor of content validity Appraisal and recommendationsResearch in Nursingand Health 30 459ndash467
RossMM Rideout EM amp CarsonMM (1996) Nursesrsquo work Balancingpersonal and professional caregiving careers Canadian Journal of NursingResearch 26(4) 43ndash59
RutmanD (1996) Caregiving as womenrsquos workWomenrsquos experiences of pow-erfulness and powerlessness as caregiversQualitative Health Research 6(1) 90ndash111
ShieldsM ampWilkins K (2005)National Survey of theWork and Health of Nurses2005 Provincial profiles Ottawa Statistics CanadaRetrieved August 24 2007from httpwwwstatcancaenglishresearch11-621-MIE11-621-MIE2006052htm
StaceyM amp Davies C (1983)Division of labour in child health care Final report toSSRCCoventry Sociology Department University ofWarwick
Tebb S (1995)An aid to empowermentA caregiver well-being scaleHealth andSocialWork 20(2) 87ndash92
Tebb S Berg-WgerM amp Rubio DM (2000) CaregiverWell-Being Scale InDRoyse BAThyer D K Padgett ampT K Logan (Eds) Program evaluation3rd ed (pp 320ndash323) Pacific Grove CA BrooksCole
Ungerson C (1990) The language of care Crossing the boundaries InCUngerson (Ed)Gender and caringWork and welfare in Britain and Scandinavia(pp 8ndash33) NewYork Harvester
WaltersV LentonR French S Eyles JMayr J amp Newbold B (1996) Paidwork unpaid work and social supportA study of the health of male andfemale nurses Social Science and Medicine 43(11) 1627ndash1636
Ward-Griffin C (2004) Nurses as caregivers of elderly relatives Negotiatingpersonal and professional boundariesCJNR 36(1) 92ndash114
Ward-Griffin C (2008)Health professionals caring for aging relativesA profes-sional or personal issue In AMartin-Matthews amp J Phillips (Eds)Blurringthe boundariesAgeing at the intersection of work and home life (pp 1ndash20) NewYorkTaylor amp FrancisPsychology Press
Ward-Griffin C Brown JVandervoortA McNair S amp Dashnay I (2005)Double duty caregivingWomen in the health professionsCanadian Journalon Aging 24(4) 379ndash394
Ward-Griffin C amp MarshallV (2003) Reconceptualizing the relationshipbetween public and private eldercare Journal of Aging Studies 17 189ndash208
Development andValidation of the Double Duty Caregiving Scale
CJNR 2009Vol 41 No 3 127
Ware J E Kosinksi MTurner-Bowker L amp Gandek B (2002)How to scoreversion 2 of the SF-12 health survey Lincoln RIQuality Metric Inc
Acknowledgements
This study was funded by the Social Sciences and Humanities ResearchCouncil (Internal) and the Institute of Gender and Health CanadianInstitutes of Health ResearchThere are no conflicts of interest or financial disclosures
CatherineWard-Griffin RN PhD is ProfessorArthur Labatt Family School ofNursing University ofWestern Ontario London Canada Janice Keefe PhD isProfessor and Canada Research Chair in Aging and Caregiving Policy FamilyStudies and GerontologyMount SaintVincent University HalifaxNova ScotiaCanadaAnne Martin-Matthews PhD is Professor School of SocialWork andFamily Studies University of British ColumbiaVancouver Canada MichaelKerr PhD is Associate ProfessorArthur Labatt Family School of NursingUniversity ofWestern Ontario Judith Belle Brown PhD is Professor Departmentof Family Medicine University ofWestern OntarioAbram Oudshoorn RN is aPhD candidate in the Arthur Labatt Family School of Nursing University ofWestern Ontario
Ward-Griffin Keefe Martin-Matthews Kerr Brown and Oudshoorn
CJNR 2009Vol 41 No 3 128
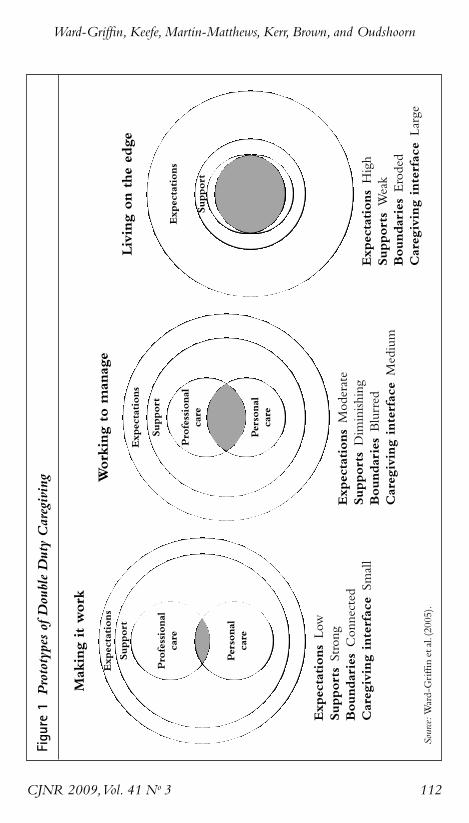
Ward-Griffin Keefe Martin-Matthews Kerr Brown and Oudshoorn
CJNR 2009Vol 41 No 3 112
Figu
re1
Prototypesof
Dou
bleDutyCaregiving
SourceW
ard-Griffinetal(2005)
Makingitwork
Workingto
manage
Livingontheedge
ExpectationsLow
SupportsStrong
BoundariesConnected
CaregivinginterfaceSm
all
ExpectationsModerate
SupportsDiminishing
BoundariesBlurred
CaregivinginterfaceMedium
ExpectationsHigh
SupportsWeak
BoundariesEroded
CaregivinginterfaceLarge
Expectations
Support
Professional
care
Personal
care
Expectations
Support
Professional
care
Personal
care
Expectations
Support
were used to manage increasing caregiving demands with limited sup-ports many women experienced a dramatic blurring of their professionaland family caregiving boundaries characterized by tension exhaustionand a feeling of isolationThus female health professionals who providecare for elderly relatives especially those with limited tangible supportsmay experience ill health as a consequenceBuilding on the existing empirical knowledge described above and in
response to the need for further research on DDC the study had twoaimsThe first was to develop and validate a tool for measuring DDCwith a sample of female registered nurses capturing the variation withinthis populationThe second was to compare the health of DDCs andnon-DDCs
Development of the DDC Scale
The development of the DDCS (seeTable 1) began with an examinationof our previous qualitative interview data (Ward-Griffin et al 2005)Twoof the investigators (Ward-Griffin and Brown) reviewed the original tran-scripts looking for specific phrases and words that reflected the fourdimensions of DDC Expectations Supports Negotiating Strategies andCaregiving Interface Item development was refined at team meetingswhere all investigators generated an initial item pool (57 items) intendedto create four subscales to address the four dimensionsOne to two neg-atively worded items were included in each subscale to help decreaseresponse bias
Expectations
A total of 16 items were developed to address three proposed sources ofExpectations to provide care to an elderly relative expectations of self (9items) expectations of family (4 items) and expectations from within theprofession (3 items) Expectations of care include the expectations ofoneself to provide care as part of onersquos role in the family due to creden-tials and professional knowledge and skills Familial expectations maycome directly from the elderly recipient of care with hisher requests forassistance or may come from other family members Professional expec-tations may come from health professionals who are involved directly inthe care of the relative or from professional colleagues or friends who arenot involved directly professional expectations include those that may beheld by the DDCs themselves based on their credentials
Supports
Eight items were developed to assess Supports reflecting sources ofsupport from the personal (4 items) and professional (4 items) caregiving
Development andValidation of the Double Duty Caregiving Scale
CJNR 2009Vol 41 No 3 113
Ward-Griffin Keefe Martin-Matthews Kerr Brown and Oudshoorn
CJNR 2009Vol 41 No 3 114
Tabl
e1
Develop
men
tof
theDou
bleDutyCaregivingScale(D
DCS)
Dim
ensions
ofDDC
1Expectations
(expectations
tocarefor
elderlyrelatives)
2Supports
(supportsused
tomanagecaregiving)
3Negotiating
Strategies
(strategiesused
tonegotiatepersonal
professionalboundaries)
4Caregiving
Interface(CI)
(degreeofblurring
betweenprofessional
andpersonalcaregiving)
InitialItem
Pool
(n=57)
Self(9)
Family
(4)
Professional
(3)
Personal(4)
Professional
(4)
Settinglim
its(10)
Making
connections
(13)
CI(10)
Item
sDeleted
Based
on
CVIa
-1 -1 0 -1 -1 0 -3 -1
Provisional
DDCS
(n=49)
(8)
(3)
(3)
(3)
(3)
(10)
(10) (9)
Item
sDeleted
Based
onEFA
b
-5 -4 -5 -2
Revised
DDCS
Tool(n
=33)
Familial(5)
Professional(4)
Personal(3)
Professional(3)
Awarenessof
boundaries(3)
Active
resistance(3)
Making
connections(5)
Perceptionsof
CI(4)
Consequences
ofCI(3)
Sam
pleItem
s
Becauseofmyhealthcare
background
ndashIhavehigh
expectationsofmyselfto
providecaretomyrelative
Asacaregiverformyelderly
relativendashMyworkplace
supportsmetoprovidecareto
myrelative
BecauseIam
ahealthcare
providerwho
alsoprovidescare
tomyrelativendashIsetalim
itof
whattype
ofcareIwillprovide
myrelative
BecauseIam
ahealthcare
providerwho
alsoprovidescare
tomyrelativendashIfeellikeIam
caughtbetweentwoworlds
(professionaland
family)
aContentvalidity
indices
bExploratoryfactoranalyses
domains Double duty caregivers usually receive some degree of emo-tional informational and substantive support from family members andfriendsAlthough there are well-established instruments for measuringsocial support (Cohen Underwood amp Gottlieb 2000) the unique per-sonal and professional supports received within DDC may not be fullycaptured using a generic standard tool Often siblings spouses childrenor friends are also involved in the caregivingAdditionally many care-givers receive professional support this can include information orresources from onersquos workplace such as flexible work hours or access toemployee assistance programs
Negotiating Strategies
The third dimensionNegotiating Strategies addresses two main types ofstrategies Setting Limits and Making ConnectionsThese help DDCs tonegotiate their professional and personal boundaries thereby potentiallymoderating the negative impacts of the caregiving interface Double dutycaregivers set limits with respect to personal and professional expectationsconcerning the provision of familial care Setting Limits includes strate-gies for keeping the personal and professional caregiving domains sepa-rate and distinct while Making Connections examines the multipleinteractions that serve to bring the two domains closer together InSetting Limits (10 items) DDCs refuse to take on professional caregiv-ing tasks for family members or arrange for others to provide this careAs well DDCs increase their supports by Making Connections (13items)These include accessing health-care information or care for onersquosrelative using professional knowledge and connections to obtain care ornavigating the health-care system
Caregiving Interface
Ten items were developed to measure the caregiving interface (CI) orthe degree of blurring between the professional and personal caregivingdomains (intermediate domain)This dimension addresses the extent ofthe connections between elder caregiving and other forms of genderedcaring work (eg nursing)The CI encompasses both feelings about theblurring of roles and the psychological impact of these feelings Feelingsabout the blurring of roles can include being pulled in two differentdirections being unable to escape from the caregiving role and strugglingto separate caregiving at home from caregiving at workThe psycholog-ical impact of increasing blurring of boundaries can include stress thefeeling that onersquos caregiving is not being recognized and confusionregarding onersquos professional and personal roles
Development andValidation of the Double Duty Caregiving Scale
CJNR 2009Vol 41 No 3 115
ContentValidation of the DDC Scale
Because of the importance of preserving the inductively derived meaningof DDC in a quantitative instrument (Morris amp Field 1995) judgementsabout clarity internal consistency and initial content validity were madeby a panel of four DDCs representing the disciplines of nursing medi-cine physiotherapy and social work as used in our previous qualitativestudyThese content experts independently rated the relevance of theprovisional items on the DDCS using a four-point scale ranging from notrelevant to very relevant This review process facilitated a systematicapproach to item revision Raters also indicated whether the conceptualdomain of each subscale was adequately represented by the set of itemsAlthough consensus was reached for each of the four dimensions theexperts recommended clarification of certain items which were subse-quently reworded or deletedContent validity indices (CVI) for each item subscales and total scale
were calculated setting the criteria for item-level acceptance at 78 orhigher for three or more reviewers (Polit Beck amp Owen 2007)TheCVI ranged from 75 to 10 for all retained items (one item fell below78 but was retained because it measured a key conceptual aspect of theCI subscale recognition of professional status) Eight items were deleteddue to lack of clarity redundancy or a relatively low CVI thus reducingthe provisional DDCS from 57 items to 49The provisional DDCS was constructed using a five-point Likert scale
(1 = strongly disagree 5 = strongly agree) Prior to the analysis negativelyworded items were recoded so that for all items a higher score reflecteda higher degree of Expectations SupportsNegotiating Strategies andCaregiving InterfaceWithin each subscale the scores were calculated byaveraging the relevant individual item scores Data imputation for missingvalues was not used as non-response for the items was very lowThe sub-scales were developed for separate use of each dimension thus they werenot combined into a single overall DDCS score
Pilot Testing of the DDC Scale
Sampling
Following institutional ethics review board approval the 49-item provi-sional DDCS was administered to an age-stratified sample of femalenurses randomly selected from the registry list of the College of Nursesof Ontario Because previous research suggested that approximately onehalf of the working nurse population is likely to provide care to anelderly relative 800 female full-time (more than 30 hoursweek) regis-tered nurses 40 years of age or older were asked to complete a mailed
Ward-Griffin Keefe Martin-Matthews Kerr Brown and Oudshoorn
CJNR 2009Vol 41 No 3 116
survey packageThe aim was to have 200 eligible DDC respondentscomplete and return the package which consisted of (1) an informationletter (2) a short demographic questionnaire which also determined eli-gibility for the study (3) the provisional DDCS described above and(4) established comparative measures including theWomenrsquos Role StrainInventory (WRSI) (Lengacher amp Sellers 2003) the CaregiverWell-BeingScale (CWBS) (Tebb et al 2000) and Health Related Outcomes(Medical Outcomes Study Short-Form SF-12 version 20 acute form4-week recall)The time needed to complete the survey package wasestimated at between 30 and 45 minutes Each package contained amodest gift certificate as a token of appreciation Nurses not providingcare for an elderly relative or friend were asked to complete all question-naires except the DDCS the purpose being to generate data for com-paring DDC and non-DDC nursesOf the 800 questionnaires mailed 394 were returned of these eight
respondents did not meet the eligibility criteria (two male and six unem-ployed) six questionnaires were blank and three were returned to senderyielding a sample of 377 respondents (49 response rate)A total of 193respondents (51) were caring for an elderly relative (ie the DDCs) and184 (49) were not (ie the non-DDCs)Of the 193 respondents iden-tified as DDCs six left sections of the DDCS blank which led to a finalusable DDC sample of 187 a total sample size that is considered adequatefor instrument development analysis (Gable ampWolf 1993)
Reliability and ConstructValidity Analyses
Contingency table (chi square) analyses were performed on all categori-cal variables while independent sample t tests were used with all contin-uous variables when comparing DDCs and non-DDCsAppropriatemeasures of association were used to examine the relationship betweentheoretically relevant demographic variables (eg hours of employmentper week hours of caregiving per week) and the CIConstruct validity of the provisional 49-item tool was assessed at the
preliminary stage with a combination of exploratory factor analysis (EFA)using a principal components factor approach and assessment of scalereliability Even though our previous qualitative work and initial concep-tualization of DDC informed the construction of the provisional DDCSitems EFA was selected over confirmatory factor analysis (CFA) For theEFA initial factor extraction was based on eigenvalues greater than 100(Polit amp Beck 2008 p 488) Each subscale of the provisional DDCS wasthen subjected to varimax rotation to select the factor structure that bestrepresented the underlying relationship of the items within the fourdimensions (Expectations Supports Negotiating Strategies andCaregiver Interface)Although loadings with an absolute value of 040 or
Development andValidation of the Double Duty Caregiving Scale
CJNR 2009Vol 41 No 3 117
higher are often used as factor loading cut-off values (Carruth 1996)smaller values are acceptable if the item pool is large (Polit amp Beck 2008p 491) Cronbachrsquos alpha reliability coefficients were also used to deter-mine internal consistency among the items of the four subscales of theprovisional DDCS Based on these preliminary analyses a combinationof low inter-item correlations (lt 20) weak factor loadings (lt 35)andor poor conceptual clarity 16 of the original 49 items were removedfrom the provisional DDCS yielding a tool with a total of 33 items forthe remaining construct validity analysesWe also correlated each of the DDCS subscale scores with those of
theWRSI the CWBS and the SF-12v2TheWRSI is a previously vali-dated 44-item five-point Likert scale that measures role strain in femalenurses with multiple roles (Lengacher amp Sellers 2003) with high relia-bility coefficients for the total scale (086ndash095) and subscales of distress(074ndash091) enhancement (079ndash089) and support (065ndash087)Developed and validated byTebb et al (2000) the CWBS-ShortVersionis a 16-item five-point Likert scale that assesses activities and needs ofcaregivers (eight items for each subscale) Overall and for each subscale(Needs and Activities of Daily Living) the coefficient alpha was 094091 and 088 respectively Finally the SF-12v2 is a well-established toolthat measures the perceptions and activities of acute health and well-being It is a shortened version of the SF-36 which includes general andphysical health index scores as well as eight subscales (bodily pain generalhealth vitality social functioning physical functioning role limitationsdue to physical problems role limitations due to emotional problems andmental health)Ware KosinskiTurner-Bowker and Gandek (2002) reportinternal consistency reliability coefficients ranging from 066 to 090 Inthe present study internal consistency reliability coefficients for each ofthese established instruments were 091 (WRSI) 073 (CWBS-needs)078 (CWBS-activities) and 080 (SF-12v2)
Results
Sample
The sample comprised 193 DDCs (this figure includes six respondentswho failed to complete all items on the DDCS but completed thedemographic questionnaire) and 184 non-DDCs (see Table 2 for anoverview)The typical DDC was 520 years old (range = 41ndash65 SD =490) was married (742) held a diploma in nursing (679) had amean household income of $101778 (range = $12500ndash$300000 SD =$4409373) was employed part-time or full-time (968) with a meanof 390 hours worked per week (range 7ndash80 SD 786) had practisednursing for 25 years or more (676) and had at least one child (ranging
Ward-Griffin Keefe Martin-Matthews Kerr Brown and Oudshoorn
CJNR 2009Vol 41 No 3 118
in age from 2 to 32 years) living with her (65)The DDC respondentsprovided an average of 6 hours per week of care to one (53) or two(30) elderly relativesmostly parents (77) or parents-in-law (12) wholived nearbyThe typical non-DDC respondent was 515 years old (range= 41ndash65 SD = 585) was married (739) held a diploma in nursing(678) had a mean household income of $105618 (range = $35000ndash$770000 SD = 6700684) was employed part-time or full-time (989)with a mean of 408 hours worked per week (range = 22ndash80) had prac-tised nursing for 25 years or more (525) and had at least one child(ranging in age from 1 to 37 years) living with her (620)There wereno significant differences between DDCs and non-DDCs with respect toage household income and number of hours worked per week
Preliminary ConstructValidity Step 1
To facilitate a better understanding of the item contents of the new scaleprincipal components analysis was conducted on each of the four sub-scales of the Provisional DDCSAlthough each dimension was provi-sionally structured as a single subscale the results of our subsequent factoranalysis suggested that Negotiating Strategies should be split into twosubscales Setting Limits and Making Connections Nine factors wereidentified from our analyses (Table 3) which is consistent with our orig-inal conceptualization about the dimensionality of DDCTwo factorsemerged from Expectations (familial expectations and professional expec-tations) accounting for 63 of the variance Five items loaded on famil-ial expectations with loadings ranging from 058 to 087 Four itemsloaded on professional expectations with loadings ranging from 049 to089As expected this indicates that among DDCs there are both famil-ial and professional expectations to provide care to elderly relatives
Development andValidation of the Double Duty Caregiving Scale
CJNR 2009Vol 41 No 3 119
Table 2 Overview of Development andValidation of Double DutyCaregiving Scale (DDCS)
Initial Item Pool ContentValidity Pilot Testing
Qualitative Mailed SurveySource Interview Data Expert Panel (n = 800)
Sample 37 female DDCs 4 female DDCs 377 female DDCs15 registered nurses 1 registered nurse 193 DDCs9 social workers 1 social worker 184 non-DDCs7 physiotherapists 1 physiotherapist6 physicians 1 physician
NoteDDC = double duty caregiver
Ward-Griffin Keefe Martin-Matthews Kerr Brown and Oudshoorn
CJNR 2009Vol 41 No 3 120
Tabl
e3
Revised
DDCS(N
=18
7)
Number
Item
-Total
Cronbachrsquos
Factor
Factor
Subscale
Factors
ofItem
sMean
SDCorrelations
Alpha
Variance
Loading
Exp
ectation
s378
712
Familialexpectations
5040ndash073
080
058ndash087
Professionalexpectations
4030ndash056
069
049ndash089
Total
9028ndash066
083
625
Supp
orts
332
646
Personalsupports
3043ndash058
068
070ndash086
Professionalsupports
3024ndash062
065
035ndash091
Total
6031ndash052
071
617
SettingLim
its
311
678
Awarenessofboundaries
3041ndash059
067
061ndash087
Activeresistance
3033ndash061
065
068ndash084
Total
6034ndash058
071
629
Mak
ingCon
nections
389
677
Makingconnections
5042ndash069
075
465
060ndash076
CaregivingIn
terface
301
826
Perceptionsofinterface
4048ndash071
081
080ndash084
Consequencesofinterface
3053ndash077
083
080ndash084
Total
7044ndash074
085
703
Two factors emerged from Supports (personal supports and profes-sional supports) accounting for 62 of the variance and indicating theimportance of personal and professional supports to DDCs providingcare to elderly relativesThree items loaded on personal supports withloadings ranging from 070 to 086Three items loaded on professionalsupports with loadings ranging from 035 to 091Two factors labelled Awareness of Boundaries and Active Resistance
emerged from Setting Limits accounting for 63 of the varianceThreeitems loaded on Awareness of Boundaries with loadings ranging from061 to 087Three items loaded on Active Resistance with loadingsranging from 068 to 084 One factor was extracted from MakingConnections accounting for 47 of the variance Loadings for the fiveitems on Making Connections ranged from 060 to 076This suggeststhat DDCs are aware of the boundaries between their personal and pro-fessional caregiving and that in an attempt to negotiate these boundariesthey resist providing care to their elderly relative as well as making con-nections to increase their supportsTwo factors emerged from CIThese were labelled Perceptions of CI
and Consequences of CI accounting for 70 of the variance Four itemsloaded on Perceptions of CI with loadings ranging from 054 to 085and three items loaded on Consequences of CI with loadings rangingfrom 080 to 084These results indicate that DDCs both are aware ofand experience consequences of the blurring of boundaries between per-sonal and professional caregiving
Reliability
Inter-item correlations and internal consistency (reliability) were exam-ined for each of the subscales of the Revised DDCSOverall in the finalversion of the 33-item DDCS inter-item correlations ranged from 024to 077 (Table 3) Cronbachrsquos alpha reliability coefficients of the fiveDDC subscales ranged from 085 (CI) to 071 (Supports and SettingLimits)Moreover Cronbachrsquos alpha reliability coefficients of the subscalefactors ranged from 083 (CI-Consequences) to 065 (for both Supports-Professional and Setting Limits-Active Resistance)
ConstructValidity Step 2
Pearson correlations were conducted to assess construct validity betweeneach of the subscales within the DDCS andWRSICWBS and SF-12v2(physical) and SF-12v2 (mental) (Table 3) In line with the underlyingtheory driving the scale there were weak to moderate correlations in theexpected direction between the Revised DDCS subscales ofExpectations Supports Setting LimitsMaking Connections and CI andthe established measuresThe strongest significant correlations were
Development andValidation of the Double Duty Caregiving Scale
CJNR 2009Vol 41 No 3 121
Ward-Griffin Keefe Martin-Matthews Kerr Brown and Oudshoorn
CJNR 2009Vol 41 No 3 122
Tabl
e4
Correlation
BetweenRevised
DDC
Subscalesan
dEstab
lished
Measures
Setting
Making
Caregiving
Scale
Expectations
Supports
Lim
its
Connections
Interface
WRSI
ar
-34
41
09
04
-49
p000
000
240
625
000
CaregiverWell-Being
Scale
r-16
34
-05
-01
-29
Activitiesb
p03
00
48
89
00
CaregiverWell-Being
Scale
r-16
34
03
-03
-36
Needsc
p04
00
71
69
00
SF12
PhysicalIndexd
r06
14
-14
-03
-02
p42
06
06
69
78
SF12
MentalIndex
dr
-26
26
09
01
-39
p00
22
22
60
00
Expectations
ar
1-12
-07
38
55
p095
344
000
000
Supportsa
r-12
104
10
-26
p095
552
174
000
Strategiesndash
r1
01
-23
SettingLimits
ap
851
002
Strategiesndash
r1
18
MakingConnections
ap
013
CaregivingInterfacea
r1
p
aN=187
bN=174
cN=180
dN=176plt05(2-tailed)
plt01(2-tailed)
between CI andWRSI (r = -49 p lt 001) between Supports andWRSI(r = 041 p lt001) and between CI and SF-12v2 (mental) (r = -39 p lt001) Finally the CI of the DDCS was also negatively correlated withcaregiver well-being (r = -29 p lt 001 [activities] and r = -36 p lt001[needs])The strongest subscale inter-correlations (ie within the Revised
DDCS itself) were between Expectations and CI (r = 055 p lt 001) andbetween Expectations and Making Connections (r = 038 p lt 001) Inaddition there was a weak positive association between MakingConnections and CI (r = 018 p lt 05) and negative associationsbetween Supports and CI (r = -026 p lt 001) and between SettingLimits and CI (r = -23 p lt 001) None of the other DDCS subscaleinter-correlations were statistically significant (Table 4)
Contrasted Groups Approach
Although there were no significant differences between DDCs andnon-DDCs in their overall scores for theWRSI CWBS and SF-12v2(physical and mental scores) there were significant differences betweennon-DDCs (n = 67) and the DDC subgroup (n = 84) defined as livingon the edge (ie those scoring above the mean on the CI subscale) Poorerhealth was observed for the living on the edge DDCs on their overall SF-12v2 mental health index score (t = -276 p lt 05) and on four of theeight SF-12v2 subscales vitality (t = -237 p lt 05) social functioning(t = -291 p lt 01) role emotional (t = -306 p lt 05) and mental health(t = -227 p lt 05) Moreover there were significant differences withinthe DDC group between those who were living on the edge and thosewith lower CI scores for the following SF-12 subscales vitality (t = -20p lt 05) social functioning (t = -356 p lt 01) role emotional (t = -483p lt 01) and mental health (t = -398 p lt 05)The living on the edgegroup also had significantly lower well-being scores for the activities(t = -363 p lt 05) and needs (t = -447 p lt 05) subscales than theother DDC respondentsWhile not all results were statistically significantoverall there was an observed tendency for the living on the edge group ofDDCs to have the lowest health and well-being scores whereas the otherDDCs (eg making it work) with low CI scores tended to have slightlybetter health scores than the non-DDC group
Discussion
The main purpose of this study was to develop and test a tool intendedto advance our understanding of DDC using a random sample of regis-tered nurses providing care to elderly relatives
Development andValidation of the Double Duty Caregiving Scale
CJNR 2009Vol 41 No 3 123
The nine factors we identified were consistent with the theorized coreDDC dimensions of Expectations (Familial and Professional) Supports(Personal and Professional) Setting Limits (Awareness of BoundariesActive Resistance) Making Connections and Caregiving Interface(Perceptions and Consequences) which can yield important informationregarding how much variance is accounted for by the factors Howeveradditional analyses are required to establish the psychometric propertiesof the DDCS including test-retest reliability to assess construct stabilityBased on the EFA results a measurement model of DDC will be pro-posed and analyzed in a future study using CFA to enhance the psycho-metric validation of the DDCS For researchers looking for a shorterversion of the DDCS it is worth noting that based on the strength andconsistency of the overall findings the seven-item CI subscale could beused to determine the extent of DDC when survey respondent burdenis a key factor in instrument selection (ie when use of the full 33DDCS items is not possible) adding to the potential value of the DDCS
The positive correlation between Expectations and CI and the nega-tive correlation between Supports and CI and between Setting Limitsand CI are theoretically consistent with the conceptual model of DDCThat is if expectations are high both personally and professionally withrespect to caring for onersquos relatives there will be greater CI or blurringof boundaries Conversely if one has strong personal and professionalsupports it follows that a lower degree of CI will result Similarly whenone sets limits on caregiving then less blurring or a lower degree of CIshould result However the positive association between MakingConnections and Expectations was unexpected Perhaps high expecta-tions lead one to increase supports by making connections both person-ally and professionally to help meet these expectationsComparison of the SF-12 v2 scores for living on the edge DDCs and
non-DDCs revealed significant differences for SF-12v2 mental healthand specific SF-12v2 subscales of vitality social functioning role emo-tional and mental healthThese findings suggest that DDCs who expe-rience a high degree of blurring of their professional and personalboundaries are at greater risk for poor health than those health profes-sionals who do not care for elderly relatives or who do not experiencethis blurring In addition those DDCs who could be characterized asliving on the edge scored significantly higher on the same four SF-12 sub-scales than DDCs with lower CI scoresThis observed pattern suggeststwo possibilities there exists a threshold effect for the negative healtheffects of DDC or manageable exposure to DDC has a beneficial effectFurther exploration of these interesting findings is warrantedAlthough we conducted a systematic and comprehensive analysis to
assess the psychometric properties of a new scale further reliability and
Ward-Griffin Keefe Martin-Matthews Kerr Brown and Oudshoorn
CJNR 2009Vol 41 No 3 124
validity studies are needed Confirmatory validation studies with otherhealth-care provider populations such as family physicians social workersand physiotherapists are particularly important as these professionals havethe potential to be DDCs and their experiences as documented in ouroriginal qualitative study of DDC helped to formulate the theoreticalunderpinnings of the DDCS In addition research with these groups willadvance our understanding of how occupational health groups may differin terms of expectations supports negotiating strategies and degree ofCIAs the identification of health-advantage and health-risk factors isinfluenced by health and social environments the negotiating strategiescould also be examined through the use of qualitative methodologiessuch as in-depth interviews or focus groupsFinally research that draws linkages between professional and personal
caregiving has the added value of furthering knowledge about employedcaregiving specifically as it relates to the relationship between health out-comes and provision of familial care by health-care providersAlthoughthe convergence (and avoidance) of professional and personal caregivingboundaries is not a new issue in nursing and other health professions thenotion that it is the individualrsquos responsibility to negotiate this boundarytends to predominate (Ward-Griffin 2008)To that end further testingand refinement of the DDCS will be helpful in identifying areas whereDDCs may need specific or different types of support It is also impor-tant to understand how specific social supports shape the health experi-ences of DDCs as well as to investigate different types of social supportinterventions with DDCsThis information is particularly meaningfultoday with the intersection of three challenges an aging population anaging health-care workforce and a shortage of health professionals Suchknowledge could contribute to workplace and other health initiativesspearheaded by professional groups policy-makers and other key stake-holders interested in assessing and addressing the health effects of DDCIn summary the DDCS is a valid tool for the assessment of double
duty caregiving Such assessment is a crucial step in understanding theexperience of the blurring of personal and professional boundaries ofcaregiving among health professionalsA quantitative study of both maleand female DDCs could help us to understand the relationship betweencertain factors (ie gender health-care occupation) and the potentialhealth effects of DDCMoreover our finding that respondents with highCI scores (living on the edge) had significantly lower health and well-beingscores than DDC respondents with lower CI scores warrants furtherinvestigation to determine if one group of DDCs is at particular risk fordeveloping negative health effects Given the current climate of health-care reform in Canada developing a better understanding of DDC andits health effects is particularly relevant for policy-makers and others who
Development andValidation of the Double Duty Caregiving Scale
CJNR 2009Vol 41 No 3 125
are committed to developing health-promoting programs and policies forfamilial caregivers of the elderly Clearly now is the time to monitor theeffects of changing demographics both in the general population andwithin the health professions in order to develop appropriate and tar-geted strategies thereby creating and sustaining healthy work environ-ments and health-care workforcesWith further refinement the DDCSmay assist with these endeavours
References
Armstrong P amp ArmstrongH (2004)Thinking it throughWomenwork andcaring in the new millennium In K Grant CArmaratunga PArmstrongM BoscoeA Pederson amp KWillson (Eds)Caring forcaring aboutWomenhome care and unpaid caregiving (pp 5ndash44)Aurora ONGaramond
Baines D (2004) Seven kinds of work ndash only one paid Raced gendered andrestructured work in social servicesAtlantis 28(2) 19ndash28
Canadian Institute for Health Information (2006)Workforce trends of registerednurses in Canada 2005 Retrieved November 5 2006 fromhttpsecurecihicacihiwebproductsndb_worforce_trends_registered_nurses_canada_2005_epdf
CarruthA K (1996) Development and testing of the Caregiver ReciprocityScaleNursing Research 45(2) 92ndash97
Chen F Feudtner C Rhodes L amp Green L (2001) Role conflicts of physi-cians and their family members Rules but no rule bookWestern Journal ofMedicine 175(4) 236ndash239
Cohen S Underwood L G amp Gottlieb BH (Eds) (2000) Social support mea-surement and interventionA guide for health and social scientistsOxford OxfordUniversity Press
Fast J (2005)Hidden costsinvisible contributions report Reworking workThe experi-ence of employed caregivers of older adults Retrieved August 16 2007 fromwwwhecolualbertacahcic
Gable R ampWolfe M (1993) Instrument development 2nd ed Boston KluwerGubermanN amp Maheu P (1999) Combining employment and caregivingAn
intricate juggling actCanadian Journal on Aging 18(1) 84ndash106Keefe J Leacutegareacute J amp CarriegravereY (2007) Developing new strategies to support
future caregivers of older Canadians with disabilities Projections of need andtheir policy implicationsCanadian Public Policy 33 S65ndash80
Lengacher CA amp Sellers E (2003)TheWomenrsquos Role Strain Inventory InO L Strickland amp CDilorio (Eds)Measurement of nursing outcomes 2nd ed(pp 109ndash127) NewYork Springer
Martin-MatthewsA (2000) Intergenerational caregivingHow apocalyptic anddominant demography frame the questions and shape the answers In EMGee amp GGutman (Eds)The overselling of population agingApocalyptic demog-raphy intergenerational challenges and social policy (pp 64ndash79)Toronto OxfordUniversity Press
Ward-Griffin Keefe Martin-Matthews Kerr Brown and Oudshoorn
CJNR 2009Vol 41 No 3 126
Mayall B (1993) Keeping children healthy ndash the intermediate domain SocialScience and Medicine 36(1) 77ndash83
Morris JM amp Field PA (1995) Qualitative research methods for health profession-als 2nd ed London Sage
Pascall G (1986) Social policyA feminist analysis NewYorkTavistockPhillips J BernardM amp ChittendenM (2002) Juggling work and careThe expe-riences of older adults Bristol Policy Press
Polit D F amp Beck CT (2008)Nursing research Generating and assessing evidencefor nursing practice 8th ed Philadelphia LippincottWilliams ampWilkins
Polit D F amp Beck CT amp Owen SV (2007) Is the CVI an acceptable indica-tor of content validity Appraisal and recommendationsResearch in Nursingand Health 30 459ndash467
RossMM Rideout EM amp CarsonMM (1996) Nursesrsquo work Balancingpersonal and professional caregiving careers Canadian Journal of NursingResearch 26(4) 43ndash59
RutmanD (1996) Caregiving as womenrsquos workWomenrsquos experiences of pow-erfulness and powerlessness as caregiversQualitative Health Research 6(1) 90ndash111
ShieldsM ampWilkins K (2005)National Survey of theWork and Health of Nurses2005 Provincial profiles Ottawa Statistics CanadaRetrieved August 24 2007from httpwwwstatcancaenglishresearch11-621-MIE11-621-MIE2006052htm
StaceyM amp Davies C (1983)Division of labour in child health care Final report toSSRCCoventry Sociology Department University ofWarwick
Tebb S (1995)An aid to empowermentA caregiver well-being scaleHealth andSocialWork 20(2) 87ndash92
Tebb S Berg-WgerM amp Rubio DM (2000) CaregiverWell-Being Scale InDRoyse BAThyer D K Padgett ampT K Logan (Eds) Program evaluation3rd ed (pp 320ndash323) Pacific Grove CA BrooksCole
Ungerson C (1990) The language of care Crossing the boundaries InCUngerson (Ed)Gender and caringWork and welfare in Britain and Scandinavia(pp 8ndash33) NewYork Harvester
WaltersV LentonR French S Eyles JMayr J amp Newbold B (1996) Paidwork unpaid work and social supportA study of the health of male andfemale nurses Social Science and Medicine 43(11) 1627ndash1636
Ward-Griffin C (2004) Nurses as caregivers of elderly relatives Negotiatingpersonal and professional boundariesCJNR 36(1) 92ndash114
Ward-Griffin C (2008)Health professionals caring for aging relativesA profes-sional or personal issue In AMartin-Matthews amp J Phillips (Eds)Blurringthe boundariesAgeing at the intersection of work and home life (pp 1ndash20) NewYorkTaylor amp FrancisPsychology Press
Ward-Griffin C Brown JVandervoortA McNair S amp Dashnay I (2005)Double duty caregivingWomen in the health professionsCanadian Journalon Aging 24(4) 379ndash394
Ward-Griffin C amp MarshallV (2003) Reconceptualizing the relationshipbetween public and private eldercare Journal of Aging Studies 17 189ndash208
Development andValidation of the Double Duty Caregiving Scale
CJNR 2009Vol 41 No 3 127
Ware J E Kosinksi MTurner-Bowker L amp Gandek B (2002)How to scoreversion 2 of the SF-12 health survey Lincoln RIQuality Metric Inc
Acknowledgements
This study was funded by the Social Sciences and Humanities ResearchCouncil (Internal) and the Institute of Gender and Health CanadianInstitutes of Health ResearchThere are no conflicts of interest or financial disclosures
CatherineWard-Griffin RN PhD is ProfessorArthur Labatt Family School ofNursing University ofWestern Ontario London Canada Janice Keefe PhD isProfessor and Canada Research Chair in Aging and Caregiving Policy FamilyStudies and GerontologyMount SaintVincent University HalifaxNova ScotiaCanadaAnne Martin-Matthews PhD is Professor School of SocialWork andFamily Studies University of British ColumbiaVancouver Canada MichaelKerr PhD is Associate ProfessorArthur Labatt Family School of NursingUniversity ofWestern Ontario Judith Belle Brown PhD is Professor Departmentof Family Medicine University ofWestern OntarioAbram Oudshoorn RN is aPhD candidate in the Arthur Labatt Family School of Nursing University ofWestern Ontario
Ward-Griffin Keefe Martin-Matthews Kerr Brown and Oudshoorn
CJNR 2009Vol 41 No 3 128
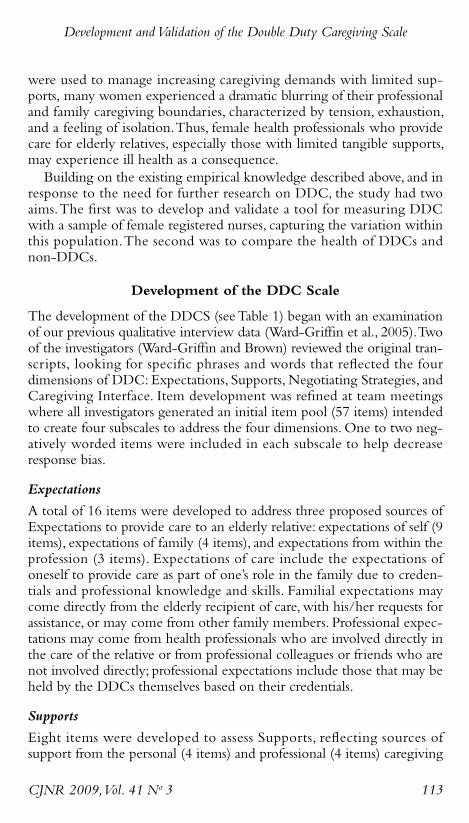
were used to manage increasing caregiving demands with limited sup-ports many women experienced a dramatic blurring of their professionaland family caregiving boundaries characterized by tension exhaustionand a feeling of isolationThus female health professionals who providecare for elderly relatives especially those with limited tangible supportsmay experience ill health as a consequenceBuilding on the existing empirical knowledge described above and in
response to the need for further research on DDC the study had twoaimsThe first was to develop and validate a tool for measuring DDCwith a sample of female registered nurses capturing the variation withinthis populationThe second was to compare the health of DDCs andnon-DDCs
Development of the DDC Scale
The development of the DDCS (seeTable 1) began with an examinationof our previous qualitative interview data (Ward-Griffin et al 2005)Twoof the investigators (Ward-Griffin and Brown) reviewed the original tran-scripts looking for specific phrases and words that reflected the fourdimensions of DDC Expectations Supports Negotiating Strategies andCaregiving Interface Item development was refined at team meetingswhere all investigators generated an initial item pool (57 items) intendedto create four subscales to address the four dimensionsOne to two neg-atively worded items were included in each subscale to help decreaseresponse bias
Expectations
A total of 16 items were developed to address three proposed sources ofExpectations to provide care to an elderly relative expectations of self (9items) expectations of family (4 items) and expectations from within theprofession (3 items) Expectations of care include the expectations ofoneself to provide care as part of onersquos role in the family due to creden-tials and professional knowledge and skills Familial expectations maycome directly from the elderly recipient of care with hisher requests forassistance or may come from other family members Professional expec-tations may come from health professionals who are involved directly inthe care of the relative or from professional colleagues or friends who arenot involved directly professional expectations include those that may beheld by the DDCs themselves based on their credentials
Supports
Eight items were developed to assess Supports reflecting sources ofsupport from the personal (4 items) and professional (4 items) caregiving
Development andValidation of the Double Duty Caregiving Scale
CJNR 2009Vol 41 No 3 113
Ward-Griffin Keefe Martin-Matthews Kerr Brown and Oudshoorn
CJNR 2009Vol 41 No 3 114
Tabl
e1
Develop
men
tof
theDou
bleDutyCaregivingScale(D
DCS)
Dim
ensions
ofDDC
1Expectations
(expectations
tocarefor
elderlyrelatives)
2Supports
(supportsused
tomanagecaregiving)
3Negotiating
Strategies
(strategiesused
tonegotiatepersonal
professionalboundaries)
4Caregiving
Interface(CI)
(degreeofblurring
betweenprofessional
andpersonalcaregiving)
InitialItem
Pool
(n=57)
Self(9)
Family
(4)
Professional
(3)
Personal(4)
Professional
(4)
Settinglim
its(10)
Making
connections
(13)
CI(10)
Item
sDeleted
Based
on
CVIa
-1 -1 0 -1 -1 0 -3 -1
Provisional
DDCS
(n=49)
(8)
(3)
(3)
(3)
(3)
(10)
(10) (9)
Item
sDeleted
Based
onEFA
b
-5 -4 -5 -2
Revised
DDCS
Tool(n
=33)
Familial(5)
Professional(4)
Personal(3)
Professional(3)
Awarenessof
boundaries(3)
Active
resistance(3)
Making
connections(5)
Perceptionsof
CI(4)
Consequences
ofCI(3)
Sam
pleItem
s
Becauseofmyhealthcare
background
ndashIhavehigh
expectationsofmyselfto
providecaretomyrelative
Asacaregiverformyelderly
relativendashMyworkplace
supportsmetoprovidecareto
myrelative
BecauseIam
ahealthcare
providerwho
alsoprovidescare
tomyrelativendashIsetalim
itof
whattype
ofcareIwillprovide
myrelative
BecauseIam
ahealthcare
providerwho
alsoprovidescare
tomyrelativendashIfeellikeIam
caughtbetweentwoworlds
(professionaland
family)
aContentvalidity
indices
bExploratoryfactoranalyses
domains Double duty caregivers usually receive some degree of emo-tional informational and substantive support from family members andfriendsAlthough there are well-established instruments for measuringsocial support (Cohen Underwood amp Gottlieb 2000) the unique per-sonal and professional supports received within DDC may not be fullycaptured using a generic standard tool Often siblings spouses childrenor friends are also involved in the caregivingAdditionally many care-givers receive professional support this can include information orresources from onersquos workplace such as flexible work hours or access toemployee assistance programs
Negotiating Strategies
The third dimensionNegotiating Strategies addresses two main types ofstrategies Setting Limits and Making ConnectionsThese help DDCs tonegotiate their professional and personal boundaries thereby potentiallymoderating the negative impacts of the caregiving interface Double dutycaregivers set limits with respect to personal and professional expectationsconcerning the provision of familial care Setting Limits includes strate-gies for keeping the personal and professional caregiving domains sepa-rate and distinct while Making Connections examines the multipleinteractions that serve to bring the two domains closer together InSetting Limits (10 items) DDCs refuse to take on professional caregiv-ing tasks for family members or arrange for others to provide this careAs well DDCs increase their supports by Making Connections (13items)These include accessing health-care information or care for onersquosrelative using professional knowledge and connections to obtain care ornavigating the health-care system
Caregiving Interface
Ten items were developed to measure the caregiving interface (CI) orthe degree of blurring between the professional and personal caregivingdomains (intermediate domain)This dimension addresses the extent ofthe connections between elder caregiving and other forms of genderedcaring work (eg nursing)The CI encompasses both feelings about theblurring of roles and the psychological impact of these feelings Feelingsabout the blurring of roles can include being pulled in two differentdirections being unable to escape from the caregiving role and strugglingto separate caregiving at home from caregiving at workThe psycholog-ical impact of increasing blurring of boundaries can include stress thefeeling that onersquos caregiving is not being recognized and confusionregarding onersquos professional and personal roles
Development andValidation of the Double Duty Caregiving Scale
CJNR 2009Vol 41 No 3 115
ContentValidation of the DDC Scale
Because of the importance of preserving the inductively derived meaningof DDC in a quantitative instrument (Morris amp Field 1995) judgementsabout clarity internal consistency and initial content validity were madeby a panel of four DDCs representing the disciplines of nursing medi-cine physiotherapy and social work as used in our previous qualitativestudyThese content experts independently rated the relevance of theprovisional items on the DDCS using a four-point scale ranging from notrelevant to very relevant This review process facilitated a systematicapproach to item revision Raters also indicated whether the conceptualdomain of each subscale was adequately represented by the set of itemsAlthough consensus was reached for each of the four dimensions theexperts recommended clarification of certain items which were subse-quently reworded or deletedContent validity indices (CVI) for each item subscales and total scale
were calculated setting the criteria for item-level acceptance at 78 orhigher for three or more reviewers (Polit Beck amp Owen 2007)TheCVI ranged from 75 to 10 for all retained items (one item fell below78 but was retained because it measured a key conceptual aspect of theCI subscale recognition of professional status) Eight items were deleteddue to lack of clarity redundancy or a relatively low CVI thus reducingthe provisional DDCS from 57 items to 49The provisional DDCS was constructed using a five-point Likert scale
(1 = strongly disagree 5 = strongly agree) Prior to the analysis negativelyworded items were recoded so that for all items a higher score reflecteda higher degree of Expectations SupportsNegotiating Strategies andCaregiving InterfaceWithin each subscale the scores were calculated byaveraging the relevant individual item scores Data imputation for missingvalues was not used as non-response for the items was very lowThe sub-scales were developed for separate use of each dimension thus they werenot combined into a single overall DDCS score
Pilot Testing of the DDC Scale
Sampling
Following institutional ethics review board approval the 49-item provi-sional DDCS was administered to an age-stratified sample of femalenurses randomly selected from the registry list of the College of Nursesof Ontario Because previous research suggested that approximately onehalf of the working nurse population is likely to provide care to anelderly relative 800 female full-time (more than 30 hoursweek) regis-tered nurses 40 years of age or older were asked to complete a mailed
Ward-Griffin Keefe Martin-Matthews Kerr Brown and Oudshoorn
CJNR 2009Vol 41 No 3 116
survey packageThe aim was to have 200 eligible DDC respondentscomplete and return the package which consisted of (1) an informationletter (2) a short demographic questionnaire which also determined eli-gibility for the study (3) the provisional DDCS described above and(4) established comparative measures including theWomenrsquos Role StrainInventory (WRSI) (Lengacher amp Sellers 2003) the CaregiverWell-BeingScale (CWBS) (Tebb et al 2000) and Health Related Outcomes(Medical Outcomes Study Short-Form SF-12 version 20 acute form4-week recall)The time needed to complete the survey package wasestimated at between 30 and 45 minutes Each package contained amodest gift certificate as a token of appreciation Nurses not providingcare for an elderly relative or friend were asked to complete all question-naires except the DDCS the purpose being to generate data for com-paring DDC and non-DDC nursesOf the 800 questionnaires mailed 394 were returned of these eight
respondents did not meet the eligibility criteria (two male and six unem-ployed) six questionnaires were blank and three were returned to senderyielding a sample of 377 respondents (49 response rate)A total of 193respondents (51) were caring for an elderly relative (ie the DDCs) and184 (49) were not (ie the non-DDCs)Of the 193 respondents iden-tified as DDCs six left sections of the DDCS blank which led to a finalusable DDC sample of 187 a total sample size that is considered adequatefor instrument development analysis (Gable ampWolf 1993)
Reliability and ConstructValidity Analyses
Contingency table (chi square) analyses were performed on all categori-cal variables while independent sample t tests were used with all contin-uous variables when comparing DDCs and non-DDCsAppropriatemeasures of association were used to examine the relationship betweentheoretically relevant demographic variables (eg hours of employmentper week hours of caregiving per week) and the CIConstruct validity of the provisional 49-item tool was assessed at the
preliminary stage with a combination of exploratory factor analysis (EFA)using a principal components factor approach and assessment of scalereliability Even though our previous qualitative work and initial concep-tualization of DDC informed the construction of the provisional DDCSitems EFA was selected over confirmatory factor analysis (CFA) For theEFA initial factor extraction was based on eigenvalues greater than 100(Polit amp Beck 2008 p 488) Each subscale of the provisional DDCS wasthen subjected to varimax rotation to select the factor structure that bestrepresented the underlying relationship of the items within the fourdimensions (Expectations Supports Negotiating Strategies andCaregiver Interface)Although loadings with an absolute value of 040 or
Development andValidation of the Double Duty Caregiving Scale
CJNR 2009Vol 41 No 3 117
higher are often used as factor loading cut-off values (Carruth 1996)smaller values are acceptable if the item pool is large (Polit amp Beck 2008p 491) Cronbachrsquos alpha reliability coefficients were also used to deter-mine internal consistency among the items of the four subscales of theprovisional DDCS Based on these preliminary analyses a combinationof low inter-item correlations (lt 20) weak factor loadings (lt 35)andor poor conceptual clarity 16 of the original 49 items were removedfrom the provisional DDCS yielding a tool with a total of 33 items forthe remaining construct validity analysesWe also correlated each of the DDCS subscale scores with those of
theWRSI the CWBS and the SF-12v2TheWRSI is a previously vali-dated 44-item five-point Likert scale that measures role strain in femalenurses with multiple roles (Lengacher amp Sellers 2003) with high relia-bility coefficients for the total scale (086ndash095) and subscales of distress(074ndash091) enhancement (079ndash089) and support (065ndash087)Developed and validated byTebb et al (2000) the CWBS-ShortVersionis a 16-item five-point Likert scale that assesses activities and needs ofcaregivers (eight items for each subscale) Overall and for each subscale(Needs and Activities of Daily Living) the coefficient alpha was 094091 and 088 respectively Finally the SF-12v2 is a well-established toolthat measures the perceptions and activities of acute health and well-being It is a shortened version of the SF-36 which includes general andphysical health index scores as well as eight subscales (bodily pain generalhealth vitality social functioning physical functioning role limitationsdue to physical problems role limitations due to emotional problems andmental health)Ware KosinskiTurner-Bowker and Gandek (2002) reportinternal consistency reliability coefficients ranging from 066 to 090 Inthe present study internal consistency reliability coefficients for each ofthese established instruments were 091 (WRSI) 073 (CWBS-needs)078 (CWBS-activities) and 080 (SF-12v2)
Results
Sample
The sample comprised 193 DDCs (this figure includes six respondentswho failed to complete all items on the DDCS but completed thedemographic questionnaire) and 184 non-DDCs (see Table 2 for anoverview)The typical DDC was 520 years old (range = 41ndash65 SD =490) was married (742) held a diploma in nursing (679) had amean household income of $101778 (range = $12500ndash$300000 SD =$4409373) was employed part-time or full-time (968) with a meanof 390 hours worked per week (range 7ndash80 SD 786) had practisednursing for 25 years or more (676) and had at least one child (ranging
Ward-Griffin Keefe Martin-Matthews Kerr Brown and Oudshoorn
CJNR 2009Vol 41 No 3 118
in age from 2 to 32 years) living with her (65)The DDC respondentsprovided an average of 6 hours per week of care to one (53) or two(30) elderly relativesmostly parents (77) or parents-in-law (12) wholived nearbyThe typical non-DDC respondent was 515 years old (range= 41ndash65 SD = 585) was married (739) held a diploma in nursing(678) had a mean household income of $105618 (range = $35000ndash$770000 SD = 6700684) was employed part-time or full-time (989)with a mean of 408 hours worked per week (range = 22ndash80) had prac-tised nursing for 25 years or more (525) and had at least one child(ranging in age from 1 to 37 years) living with her (620)There wereno significant differences between DDCs and non-DDCs with respect toage household income and number of hours worked per week
Preliminary ConstructValidity Step 1
To facilitate a better understanding of the item contents of the new scaleprincipal components analysis was conducted on each of the four sub-scales of the Provisional DDCSAlthough each dimension was provi-sionally structured as a single subscale the results of our subsequent factoranalysis suggested that Negotiating Strategies should be split into twosubscales Setting Limits and Making Connections Nine factors wereidentified from our analyses (Table 3) which is consistent with our orig-inal conceptualization about the dimensionality of DDCTwo factorsemerged from Expectations (familial expectations and professional expec-tations) accounting for 63 of the variance Five items loaded on famil-ial expectations with loadings ranging from 058 to 087 Four itemsloaded on professional expectations with loadings ranging from 049 to089As expected this indicates that among DDCs there are both famil-ial and professional expectations to provide care to elderly relatives
Development andValidation of the Double Duty Caregiving Scale
CJNR 2009Vol 41 No 3 119
Table 2 Overview of Development andValidation of Double DutyCaregiving Scale (DDCS)
Initial Item Pool ContentValidity Pilot Testing
Qualitative Mailed SurveySource Interview Data Expert Panel (n = 800)
Sample 37 female DDCs 4 female DDCs 377 female DDCs15 registered nurses 1 registered nurse 193 DDCs9 social workers 1 social worker 184 non-DDCs7 physiotherapists 1 physiotherapist6 physicians 1 physician
NoteDDC = double duty caregiver
Ward-Griffin Keefe Martin-Matthews Kerr Brown and Oudshoorn
CJNR 2009Vol 41 No 3 120
Tabl
e3
Revised
DDCS(N
=18
7)
Number
Item
-Total
Cronbachrsquos
Factor
Factor
Subscale
Factors
ofItem
sMean
SDCorrelations
Alpha
Variance
Loading
Exp
ectation
s378
712
Familialexpectations
5040ndash073
080
058ndash087
Professionalexpectations
4030ndash056
069
049ndash089
Total
9028ndash066
083
625
Supp
orts
332
646
Personalsupports
3043ndash058
068
070ndash086
Professionalsupports
3024ndash062
065
035ndash091
Total
6031ndash052
071
617
SettingLim
its
311
678
Awarenessofboundaries
3041ndash059
067
061ndash087
Activeresistance
3033ndash061
065
068ndash084
Total
6034ndash058
071
629
Mak
ingCon
nections
389
677
Makingconnections
5042ndash069
075
465
060ndash076
CaregivingIn
terface
301
826
Perceptionsofinterface
4048ndash071
081
080ndash084
Consequencesofinterface
3053ndash077
083
080ndash084
Total
7044ndash074
085
703
Two factors emerged from Supports (personal supports and profes-sional supports) accounting for 62 of the variance and indicating theimportance of personal and professional supports to DDCs providingcare to elderly relativesThree items loaded on personal supports withloadings ranging from 070 to 086Three items loaded on professionalsupports with loadings ranging from 035 to 091Two factors labelled Awareness of Boundaries and Active Resistance
emerged from Setting Limits accounting for 63 of the varianceThreeitems loaded on Awareness of Boundaries with loadings ranging from061 to 087Three items loaded on Active Resistance with loadingsranging from 068 to 084 One factor was extracted from MakingConnections accounting for 47 of the variance Loadings for the fiveitems on Making Connections ranged from 060 to 076This suggeststhat DDCs are aware of the boundaries between their personal and pro-fessional caregiving and that in an attempt to negotiate these boundariesthey resist providing care to their elderly relative as well as making con-nections to increase their supportsTwo factors emerged from CIThese were labelled Perceptions of CI
and Consequences of CI accounting for 70 of the variance Four itemsloaded on Perceptions of CI with loadings ranging from 054 to 085and three items loaded on Consequences of CI with loadings rangingfrom 080 to 084These results indicate that DDCs both are aware ofand experience consequences of the blurring of boundaries between per-sonal and professional caregiving
Reliability
Inter-item correlations and internal consistency (reliability) were exam-ined for each of the subscales of the Revised DDCSOverall in the finalversion of the 33-item DDCS inter-item correlations ranged from 024to 077 (Table 3) Cronbachrsquos alpha reliability coefficients of the fiveDDC subscales ranged from 085 (CI) to 071 (Supports and SettingLimits)Moreover Cronbachrsquos alpha reliability coefficients of the subscalefactors ranged from 083 (CI-Consequences) to 065 (for both Supports-Professional and Setting Limits-Active Resistance)
ConstructValidity Step 2
Pearson correlations were conducted to assess construct validity betweeneach of the subscales within the DDCS andWRSICWBS and SF-12v2(physical) and SF-12v2 (mental) (Table 3) In line with the underlyingtheory driving the scale there were weak to moderate correlations in theexpected direction between the Revised DDCS subscales ofExpectations Supports Setting LimitsMaking Connections and CI andthe established measuresThe strongest significant correlations were
Development andValidation of the Double Duty Caregiving Scale
CJNR 2009Vol 41 No 3 121
Ward-Griffin Keefe Martin-Matthews Kerr Brown and Oudshoorn
CJNR 2009Vol 41 No 3 122
Tabl
e4
Correlation
BetweenRevised
DDC
Subscalesan
dEstab
lished
Measures
Setting
Making
Caregiving
Scale
Expectations
Supports
Lim
its
Connections
Interface
WRSI
ar
-34
41
09
04
-49
p000
000
240
625
000
CaregiverWell-Being
Scale
r-16
34
-05
-01
-29
Activitiesb
p03
00
48
89
00
CaregiverWell-Being
Scale
r-16
34
03
-03
-36
Needsc
p04
00
71
69
00
SF12
PhysicalIndexd
r06
14
-14
-03
-02
p42
06
06
69
78
SF12
MentalIndex
dr
-26
26
09
01
-39
p00
22
22
60
00
Expectations
ar
1-12
-07
38
55
p095
344
000
000
Supportsa
r-12
104
10
-26
p095
552
174
000
Strategiesndash
r1
01
-23
SettingLimits
ap
851
002
Strategiesndash
r1
18
MakingConnections
ap
013
CaregivingInterfacea
r1
p
aN=187
bN=174
cN=180
dN=176plt05(2-tailed)
plt01(2-tailed)
between CI andWRSI (r = -49 p lt 001) between Supports andWRSI(r = 041 p lt001) and between CI and SF-12v2 (mental) (r = -39 p lt001) Finally the CI of the DDCS was also negatively correlated withcaregiver well-being (r = -29 p lt 001 [activities] and r = -36 p lt001[needs])The strongest subscale inter-correlations (ie within the Revised
DDCS itself) were between Expectations and CI (r = 055 p lt 001) andbetween Expectations and Making Connections (r = 038 p lt 001) Inaddition there was a weak positive association between MakingConnections and CI (r = 018 p lt 05) and negative associationsbetween Supports and CI (r = -026 p lt 001) and between SettingLimits and CI (r = -23 p lt 001) None of the other DDCS subscaleinter-correlations were statistically significant (Table 4)
Contrasted Groups Approach
Although there were no significant differences between DDCs andnon-DDCs in their overall scores for theWRSI CWBS and SF-12v2(physical and mental scores) there were significant differences betweennon-DDCs (n = 67) and the DDC subgroup (n = 84) defined as livingon the edge (ie those scoring above the mean on the CI subscale) Poorerhealth was observed for the living on the edge DDCs on their overall SF-12v2 mental health index score (t = -276 p lt 05) and on four of theeight SF-12v2 subscales vitality (t = -237 p lt 05) social functioning(t = -291 p lt 01) role emotional (t = -306 p lt 05) and mental health(t = -227 p lt 05) Moreover there were significant differences withinthe DDC group between those who were living on the edge and thosewith lower CI scores for the following SF-12 subscales vitality (t = -20p lt 05) social functioning (t = -356 p lt 01) role emotional (t = -483p lt 01) and mental health (t = -398 p lt 05)The living on the edgegroup also had significantly lower well-being scores for the activities(t = -363 p lt 05) and needs (t = -447 p lt 05) subscales than theother DDC respondentsWhile not all results were statistically significantoverall there was an observed tendency for the living on the edge group ofDDCs to have the lowest health and well-being scores whereas the otherDDCs (eg making it work) with low CI scores tended to have slightlybetter health scores than the non-DDC group
Discussion
The main purpose of this study was to develop and test a tool intendedto advance our understanding of DDC using a random sample of regis-tered nurses providing care to elderly relatives
Development andValidation of the Double Duty Caregiving Scale
CJNR 2009Vol 41 No 3 123
The nine factors we identified were consistent with the theorized coreDDC dimensions of Expectations (Familial and Professional) Supports(Personal and Professional) Setting Limits (Awareness of BoundariesActive Resistance) Making Connections and Caregiving Interface(Perceptions and Consequences) which can yield important informationregarding how much variance is accounted for by the factors Howeveradditional analyses are required to establish the psychometric propertiesof the DDCS including test-retest reliability to assess construct stabilityBased on the EFA results a measurement model of DDC will be pro-posed and analyzed in a future study using CFA to enhance the psycho-metric validation of the DDCS For researchers looking for a shorterversion of the DDCS it is worth noting that based on the strength andconsistency of the overall findings the seven-item CI subscale could beused to determine the extent of DDC when survey respondent burdenis a key factor in instrument selection (ie when use of the full 33DDCS items is not possible) adding to the potential value of the DDCS
The positive correlation between Expectations and CI and the nega-tive correlation between Supports and CI and between Setting Limitsand CI are theoretically consistent with the conceptual model of DDCThat is if expectations are high both personally and professionally withrespect to caring for onersquos relatives there will be greater CI or blurringof boundaries Conversely if one has strong personal and professionalsupports it follows that a lower degree of CI will result Similarly whenone sets limits on caregiving then less blurring or a lower degree of CIshould result However the positive association between MakingConnections and Expectations was unexpected Perhaps high expecta-tions lead one to increase supports by making connections both person-ally and professionally to help meet these expectationsComparison of the SF-12 v2 scores for living on the edge DDCs and
non-DDCs revealed significant differences for SF-12v2 mental healthand specific SF-12v2 subscales of vitality social functioning role emo-tional and mental healthThese findings suggest that DDCs who expe-rience a high degree of blurring of their professional and personalboundaries are at greater risk for poor health than those health profes-sionals who do not care for elderly relatives or who do not experiencethis blurring In addition those DDCs who could be characterized asliving on the edge scored significantly higher on the same four SF-12 sub-scales than DDCs with lower CI scoresThis observed pattern suggeststwo possibilities there exists a threshold effect for the negative healtheffects of DDC or manageable exposure to DDC has a beneficial effectFurther exploration of these interesting findings is warrantedAlthough we conducted a systematic and comprehensive analysis to
assess the psychometric properties of a new scale further reliability and
Ward-Griffin Keefe Martin-Matthews Kerr Brown and Oudshoorn
CJNR 2009Vol 41 No 3 124
validity studies are needed Confirmatory validation studies with otherhealth-care provider populations such as family physicians social workersand physiotherapists are particularly important as these professionals havethe potential to be DDCs and their experiences as documented in ouroriginal qualitative study of DDC helped to formulate the theoreticalunderpinnings of the DDCS In addition research with these groups willadvance our understanding of how occupational health groups may differin terms of expectations supports negotiating strategies and degree ofCIAs the identification of health-advantage and health-risk factors isinfluenced by health and social environments the negotiating strategiescould also be examined through the use of qualitative methodologiessuch as in-depth interviews or focus groupsFinally research that draws linkages between professional and personal
caregiving has the added value of furthering knowledge about employedcaregiving specifically as it relates to the relationship between health out-comes and provision of familial care by health-care providersAlthoughthe convergence (and avoidance) of professional and personal caregivingboundaries is not a new issue in nursing and other health professions thenotion that it is the individualrsquos responsibility to negotiate this boundarytends to predominate (Ward-Griffin 2008)To that end further testingand refinement of the DDCS will be helpful in identifying areas whereDDCs may need specific or different types of support It is also impor-tant to understand how specific social supports shape the health experi-ences of DDCs as well as to investigate different types of social supportinterventions with DDCsThis information is particularly meaningfultoday with the intersection of three challenges an aging population anaging health-care workforce and a shortage of health professionals Suchknowledge could contribute to workplace and other health initiativesspearheaded by professional groups policy-makers and other key stake-holders interested in assessing and addressing the health effects of DDCIn summary the DDCS is a valid tool for the assessment of double
duty caregiving Such assessment is a crucial step in understanding theexperience of the blurring of personal and professional boundaries ofcaregiving among health professionalsA quantitative study of both maleand female DDCs could help us to understand the relationship betweencertain factors (ie gender health-care occupation) and the potentialhealth effects of DDCMoreover our finding that respondents with highCI scores (living on the edge) had significantly lower health and well-beingscores than DDC respondents with lower CI scores warrants furtherinvestigation to determine if one group of DDCs is at particular risk fordeveloping negative health effects Given the current climate of health-care reform in Canada developing a better understanding of DDC andits health effects is particularly relevant for policy-makers and others who
Development andValidation of the Double Duty Caregiving Scale
CJNR 2009Vol 41 No 3 125
are committed to developing health-promoting programs and policies forfamilial caregivers of the elderly Clearly now is the time to monitor theeffects of changing demographics both in the general population andwithin the health professions in order to develop appropriate and tar-geted strategies thereby creating and sustaining healthy work environ-ments and health-care workforcesWith further refinement the DDCSmay assist with these endeavours
References
Armstrong P amp ArmstrongH (2004)Thinking it throughWomenwork andcaring in the new millennium In K Grant CArmaratunga PArmstrongM BoscoeA Pederson amp KWillson (Eds)Caring forcaring aboutWomenhome care and unpaid caregiving (pp 5ndash44)Aurora ONGaramond
Baines D (2004) Seven kinds of work ndash only one paid Raced gendered andrestructured work in social servicesAtlantis 28(2) 19ndash28
Canadian Institute for Health Information (2006)Workforce trends of registerednurses in Canada 2005 Retrieved November 5 2006 fromhttpsecurecihicacihiwebproductsndb_worforce_trends_registered_nurses_canada_2005_epdf
CarruthA K (1996) Development and testing of the Caregiver ReciprocityScaleNursing Research 45(2) 92ndash97
Chen F Feudtner C Rhodes L amp Green L (2001) Role conflicts of physi-cians and their family members Rules but no rule bookWestern Journal ofMedicine 175(4) 236ndash239
Cohen S Underwood L G amp Gottlieb BH (Eds) (2000) Social support mea-surement and interventionA guide for health and social scientistsOxford OxfordUniversity Press
Fast J (2005)Hidden costsinvisible contributions report Reworking workThe experi-ence of employed caregivers of older adults Retrieved August 16 2007 fromwwwhecolualbertacahcic
Gable R ampWolfe M (1993) Instrument development 2nd ed Boston KluwerGubermanN amp Maheu P (1999) Combining employment and caregivingAn
intricate juggling actCanadian Journal on Aging 18(1) 84ndash106Keefe J Leacutegareacute J amp CarriegravereY (2007) Developing new strategies to support
future caregivers of older Canadians with disabilities Projections of need andtheir policy implicationsCanadian Public Policy 33 S65ndash80
Lengacher CA amp Sellers E (2003)TheWomenrsquos Role Strain Inventory InO L Strickland amp CDilorio (Eds)Measurement of nursing outcomes 2nd ed(pp 109ndash127) NewYork Springer
Martin-MatthewsA (2000) Intergenerational caregivingHow apocalyptic anddominant demography frame the questions and shape the answers In EMGee amp GGutman (Eds)The overselling of population agingApocalyptic demog-raphy intergenerational challenges and social policy (pp 64ndash79)Toronto OxfordUniversity Press
Ward-Griffin Keefe Martin-Matthews Kerr Brown and Oudshoorn
CJNR 2009Vol 41 No 3 126
Mayall B (1993) Keeping children healthy ndash the intermediate domain SocialScience and Medicine 36(1) 77ndash83
Morris JM amp Field PA (1995) Qualitative research methods for health profession-als 2nd ed London Sage
Pascall G (1986) Social policyA feminist analysis NewYorkTavistockPhillips J BernardM amp ChittendenM (2002) Juggling work and careThe expe-riences of older adults Bristol Policy Press
Polit D F amp Beck CT (2008)Nursing research Generating and assessing evidencefor nursing practice 8th ed Philadelphia LippincottWilliams ampWilkins
Polit D F amp Beck CT amp Owen SV (2007) Is the CVI an acceptable indica-tor of content validity Appraisal and recommendationsResearch in Nursingand Health 30 459ndash467
RossMM Rideout EM amp CarsonMM (1996) Nursesrsquo work Balancingpersonal and professional caregiving careers Canadian Journal of NursingResearch 26(4) 43ndash59
RutmanD (1996) Caregiving as womenrsquos workWomenrsquos experiences of pow-erfulness and powerlessness as caregiversQualitative Health Research 6(1) 90ndash111
ShieldsM ampWilkins K (2005)National Survey of theWork and Health of Nurses2005 Provincial profiles Ottawa Statistics CanadaRetrieved August 24 2007from httpwwwstatcancaenglishresearch11-621-MIE11-621-MIE2006052htm
StaceyM amp Davies C (1983)Division of labour in child health care Final report toSSRCCoventry Sociology Department University ofWarwick
Tebb S (1995)An aid to empowermentA caregiver well-being scaleHealth andSocialWork 20(2) 87ndash92
Tebb S Berg-WgerM amp Rubio DM (2000) CaregiverWell-Being Scale InDRoyse BAThyer D K Padgett ampT K Logan (Eds) Program evaluation3rd ed (pp 320ndash323) Pacific Grove CA BrooksCole
Ungerson C (1990) The language of care Crossing the boundaries InCUngerson (Ed)Gender and caringWork and welfare in Britain and Scandinavia(pp 8ndash33) NewYork Harvester
WaltersV LentonR French S Eyles JMayr J amp Newbold B (1996) Paidwork unpaid work and social supportA study of the health of male andfemale nurses Social Science and Medicine 43(11) 1627ndash1636
Ward-Griffin C (2004) Nurses as caregivers of elderly relatives Negotiatingpersonal and professional boundariesCJNR 36(1) 92ndash114
Ward-Griffin C (2008)Health professionals caring for aging relativesA profes-sional or personal issue In AMartin-Matthews amp J Phillips (Eds)Blurringthe boundariesAgeing at the intersection of work and home life (pp 1ndash20) NewYorkTaylor amp FrancisPsychology Press
Ward-Griffin C Brown JVandervoortA McNair S amp Dashnay I (2005)Double duty caregivingWomen in the health professionsCanadian Journalon Aging 24(4) 379ndash394
Ward-Griffin C amp MarshallV (2003) Reconceptualizing the relationshipbetween public and private eldercare Journal of Aging Studies 17 189ndash208
Development andValidation of the Double Duty Caregiving Scale
CJNR 2009Vol 41 No 3 127
Ware J E Kosinksi MTurner-Bowker L amp Gandek B (2002)How to scoreversion 2 of the SF-12 health survey Lincoln RIQuality Metric Inc
Acknowledgements
This study was funded by the Social Sciences and Humanities ResearchCouncil (Internal) and the Institute of Gender and Health CanadianInstitutes of Health ResearchThere are no conflicts of interest or financial disclosures
CatherineWard-Griffin RN PhD is ProfessorArthur Labatt Family School ofNursing University ofWestern Ontario London Canada Janice Keefe PhD isProfessor and Canada Research Chair in Aging and Caregiving Policy FamilyStudies and GerontologyMount SaintVincent University HalifaxNova ScotiaCanadaAnne Martin-Matthews PhD is Professor School of SocialWork andFamily Studies University of British ColumbiaVancouver Canada MichaelKerr PhD is Associate ProfessorArthur Labatt Family School of NursingUniversity ofWestern Ontario Judith Belle Brown PhD is Professor Departmentof Family Medicine University ofWestern OntarioAbram Oudshoorn RN is aPhD candidate in the Arthur Labatt Family School of Nursing University ofWestern Ontario
Ward-Griffin Keefe Martin-Matthews Kerr Brown and Oudshoorn
CJNR 2009Vol 41 No 3 128
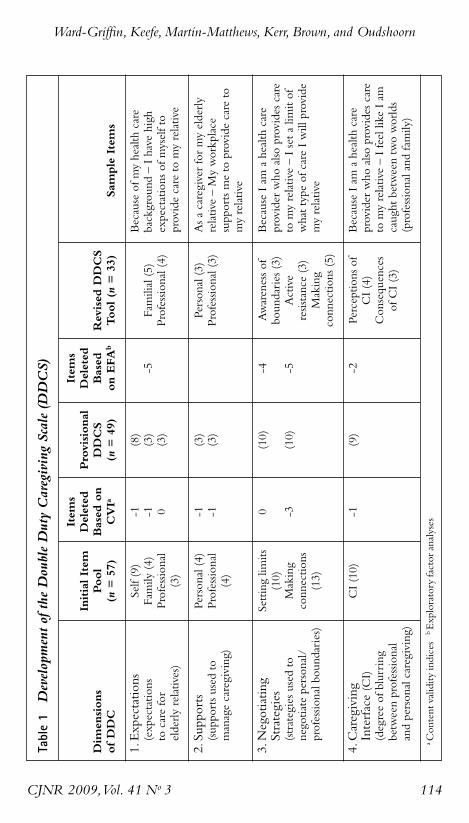
Ward-Griffin Keefe Martin-Matthews Kerr Brown and Oudshoorn
CJNR 2009Vol 41 No 3 114
Tabl
e1
Develop
men
tof
theDou
bleDutyCaregivingScale(D
DCS)
Dim
ensions
ofDDC
1Expectations
(expectations
tocarefor
elderlyrelatives)
2Supports
(supportsused
tomanagecaregiving)
3Negotiating
Strategies
(strategiesused
tonegotiatepersonal
professionalboundaries)
4Caregiving
Interface(CI)
(degreeofblurring
betweenprofessional
andpersonalcaregiving)
InitialItem
Pool
(n=57)
Self(9)
Family
(4)
Professional
(3)
Personal(4)
Professional
(4)
Settinglim
its(10)
Making
connections
(13)
CI(10)
Item
sDeleted
Based
on
CVIa
-1 -1 0 -1 -1 0 -3 -1
Provisional
DDCS
(n=49)
(8)
(3)
(3)
(3)
(3)
(10)
(10) (9)
Item
sDeleted
Based
onEFA
b
-5 -4 -5 -2
Revised
DDCS
Tool(n
=33)
Familial(5)
Professional(4)
Personal(3)
Professional(3)
Awarenessof
boundaries(3)
Active
resistance(3)
Making
connections(5)
Perceptionsof
CI(4)
Consequences
ofCI(3)
Sam
pleItem
s
Becauseofmyhealthcare
background
ndashIhavehigh
expectationsofmyselfto
providecaretomyrelative
Asacaregiverformyelderly
relativendashMyworkplace
supportsmetoprovidecareto
myrelative
BecauseIam
ahealthcare
providerwho
alsoprovidescare
tomyrelativendashIsetalim
itof
whattype
ofcareIwillprovide
myrelative
BecauseIam
ahealthcare
providerwho
alsoprovidescare
tomyrelativendashIfeellikeIam
caughtbetweentwoworlds
(professionaland
family)
aContentvalidity
indices
bExploratoryfactoranalyses
domains Double duty caregivers usually receive some degree of emo-tional informational and substantive support from family members andfriendsAlthough there are well-established instruments for measuringsocial support (Cohen Underwood amp Gottlieb 2000) the unique per-sonal and professional supports received within DDC may not be fullycaptured using a generic standard tool Often siblings spouses childrenor friends are also involved in the caregivingAdditionally many care-givers receive professional support this can include information orresources from onersquos workplace such as flexible work hours or access toemployee assistance programs
Negotiating Strategies
The third dimensionNegotiating Strategies addresses two main types ofstrategies Setting Limits and Making ConnectionsThese help DDCs tonegotiate their professional and personal boundaries thereby potentiallymoderating the negative impacts of the caregiving interface Double dutycaregivers set limits with respect to personal and professional expectationsconcerning the provision of familial care Setting Limits includes strate-gies for keeping the personal and professional caregiving domains sepa-rate and distinct while Making Connections examines the multipleinteractions that serve to bring the two domains closer together InSetting Limits (10 items) DDCs refuse to take on professional caregiv-ing tasks for family members or arrange for others to provide this careAs well DDCs increase their supports by Making Connections (13items)These include accessing health-care information or care for onersquosrelative using professional knowledge and connections to obtain care ornavigating the health-care system
Caregiving Interface
Ten items were developed to measure the caregiving interface (CI) orthe degree of blurring between the professional and personal caregivingdomains (intermediate domain)This dimension addresses the extent ofthe connections between elder caregiving and other forms of genderedcaring work (eg nursing)The CI encompasses both feelings about theblurring of roles and the psychological impact of these feelings Feelingsabout the blurring of roles can include being pulled in two differentdirections being unable to escape from the caregiving role and strugglingto separate caregiving at home from caregiving at workThe psycholog-ical impact of increasing blurring of boundaries can include stress thefeeling that onersquos caregiving is not being recognized and confusionregarding onersquos professional and personal roles
Development andValidation of the Double Duty Caregiving Scale
CJNR 2009Vol 41 No 3 115
ContentValidation of the DDC Scale
Because of the importance of preserving the inductively derived meaningof DDC in a quantitative instrument (Morris amp Field 1995) judgementsabout clarity internal consistency and initial content validity were madeby a panel of four DDCs representing the disciplines of nursing medi-cine physiotherapy and social work as used in our previous qualitativestudyThese content experts independently rated the relevance of theprovisional items on the DDCS using a four-point scale ranging from notrelevant to very relevant This review process facilitated a systematicapproach to item revision Raters also indicated whether the conceptualdomain of each subscale was adequately represented by the set of itemsAlthough consensus was reached for each of the four dimensions theexperts recommended clarification of certain items which were subse-quently reworded or deletedContent validity indices (CVI) for each item subscales and total scale
were calculated setting the criteria for item-level acceptance at 78 orhigher for three or more reviewers (Polit Beck amp Owen 2007)TheCVI ranged from 75 to 10 for all retained items (one item fell below78 but was retained because it measured a key conceptual aspect of theCI subscale recognition of professional status) Eight items were deleteddue to lack of clarity redundancy or a relatively low CVI thus reducingthe provisional DDCS from 57 items to 49The provisional DDCS was constructed using a five-point Likert scale
(1 = strongly disagree 5 = strongly agree) Prior to the analysis negativelyworded items were recoded so that for all items a higher score reflecteda higher degree of Expectations SupportsNegotiating Strategies andCaregiving InterfaceWithin each subscale the scores were calculated byaveraging the relevant individual item scores Data imputation for missingvalues was not used as non-response for the items was very lowThe sub-scales were developed for separate use of each dimension thus they werenot combined into a single overall DDCS score
Pilot Testing of the DDC Scale
Sampling
Following institutional ethics review board approval the 49-item provi-sional DDCS was administered to an age-stratified sample of femalenurses randomly selected from the registry list of the College of Nursesof Ontario Because previous research suggested that approximately onehalf of the working nurse population is likely to provide care to anelderly relative 800 female full-time (more than 30 hoursweek) regis-tered nurses 40 years of age or older were asked to complete a mailed
Ward-Griffin Keefe Martin-Matthews Kerr Brown and Oudshoorn
CJNR 2009Vol 41 No 3 116
survey packageThe aim was to have 200 eligible DDC respondentscomplete and return the package which consisted of (1) an informationletter (2) a short demographic questionnaire which also determined eli-gibility for the study (3) the provisional DDCS described above and(4) established comparative measures including theWomenrsquos Role StrainInventory (WRSI) (Lengacher amp Sellers 2003) the CaregiverWell-BeingScale (CWBS) (Tebb et al 2000) and Health Related Outcomes(Medical Outcomes Study Short-Form SF-12 version 20 acute form4-week recall)The time needed to complete the survey package wasestimated at between 30 and 45 minutes Each package contained amodest gift certificate as a token of appreciation Nurses not providingcare for an elderly relative or friend were asked to complete all question-naires except the DDCS the purpose being to generate data for com-paring DDC and non-DDC nursesOf the 800 questionnaires mailed 394 were returned of these eight
respondents did not meet the eligibility criteria (two male and six unem-ployed) six questionnaires were blank and three were returned to senderyielding a sample of 377 respondents (49 response rate)A total of 193respondents (51) were caring for an elderly relative (ie the DDCs) and184 (49) were not (ie the non-DDCs)Of the 193 respondents iden-tified as DDCs six left sections of the DDCS blank which led to a finalusable DDC sample of 187 a total sample size that is considered adequatefor instrument development analysis (Gable ampWolf 1993)
Reliability and ConstructValidity Analyses
Contingency table (chi square) analyses were performed on all categori-cal variables while independent sample t tests were used with all contin-uous variables when comparing DDCs and non-DDCsAppropriatemeasures of association were used to examine the relationship betweentheoretically relevant demographic variables (eg hours of employmentper week hours of caregiving per week) and the CIConstruct validity of the provisional 49-item tool was assessed at the
preliminary stage with a combination of exploratory factor analysis (EFA)using a principal components factor approach and assessment of scalereliability Even though our previous qualitative work and initial concep-tualization of DDC informed the construction of the provisional DDCSitems EFA was selected over confirmatory factor analysis (CFA) For theEFA initial factor extraction was based on eigenvalues greater than 100(Polit amp Beck 2008 p 488) Each subscale of the provisional DDCS wasthen subjected to varimax rotation to select the factor structure that bestrepresented the underlying relationship of the items within the fourdimensions (Expectations Supports Negotiating Strategies andCaregiver Interface)Although loadings with an absolute value of 040 or
Development andValidation of the Double Duty Caregiving Scale
CJNR 2009Vol 41 No 3 117
higher are often used as factor loading cut-off values (Carruth 1996)smaller values are acceptable if the item pool is large (Polit amp Beck 2008p 491) Cronbachrsquos alpha reliability coefficients were also used to deter-mine internal consistency among the items of the four subscales of theprovisional DDCS Based on these preliminary analyses a combinationof low inter-item correlations (lt 20) weak factor loadings (lt 35)andor poor conceptual clarity 16 of the original 49 items were removedfrom the provisional DDCS yielding a tool with a total of 33 items forthe remaining construct validity analysesWe also correlated each of the DDCS subscale scores with those of
theWRSI the CWBS and the SF-12v2TheWRSI is a previously vali-dated 44-item five-point Likert scale that measures role strain in femalenurses with multiple roles (Lengacher amp Sellers 2003) with high relia-bility coefficients for the total scale (086ndash095) and subscales of distress(074ndash091) enhancement (079ndash089) and support (065ndash087)Developed and validated byTebb et al (2000) the CWBS-ShortVersionis a 16-item five-point Likert scale that assesses activities and needs ofcaregivers (eight items for each subscale) Overall and for each subscale(Needs and Activities of Daily Living) the coefficient alpha was 094091 and 088 respectively Finally the SF-12v2 is a well-established toolthat measures the perceptions and activities of acute health and well-being It is a shortened version of the SF-36 which includes general andphysical health index scores as well as eight subscales (bodily pain generalhealth vitality social functioning physical functioning role limitationsdue to physical problems role limitations due to emotional problems andmental health)Ware KosinskiTurner-Bowker and Gandek (2002) reportinternal consistency reliability coefficients ranging from 066 to 090 Inthe present study internal consistency reliability coefficients for each ofthese established instruments were 091 (WRSI) 073 (CWBS-needs)078 (CWBS-activities) and 080 (SF-12v2)
Results
Sample
The sample comprised 193 DDCs (this figure includes six respondentswho failed to complete all items on the DDCS but completed thedemographic questionnaire) and 184 non-DDCs (see Table 2 for anoverview)The typical DDC was 520 years old (range = 41ndash65 SD =490) was married (742) held a diploma in nursing (679) had amean household income of $101778 (range = $12500ndash$300000 SD =$4409373) was employed part-time or full-time (968) with a meanof 390 hours worked per week (range 7ndash80 SD 786) had practisednursing for 25 years or more (676) and had at least one child (ranging
Ward-Griffin Keefe Martin-Matthews Kerr Brown and Oudshoorn
CJNR 2009Vol 41 No 3 118
in age from 2 to 32 years) living with her (65)The DDC respondentsprovided an average of 6 hours per week of care to one (53) or two(30) elderly relativesmostly parents (77) or parents-in-law (12) wholived nearbyThe typical non-DDC respondent was 515 years old (range= 41ndash65 SD = 585) was married (739) held a diploma in nursing(678) had a mean household income of $105618 (range = $35000ndash$770000 SD = 6700684) was employed part-time or full-time (989)with a mean of 408 hours worked per week (range = 22ndash80) had prac-tised nursing for 25 years or more (525) and had at least one child(ranging in age from 1 to 37 years) living with her (620)There wereno significant differences between DDCs and non-DDCs with respect toage household income and number of hours worked per week
Preliminary ConstructValidity Step 1
To facilitate a better understanding of the item contents of the new scaleprincipal components analysis was conducted on each of the four sub-scales of the Provisional DDCSAlthough each dimension was provi-sionally structured as a single subscale the results of our subsequent factoranalysis suggested that Negotiating Strategies should be split into twosubscales Setting Limits and Making Connections Nine factors wereidentified from our analyses (Table 3) which is consistent with our orig-inal conceptualization about the dimensionality of DDCTwo factorsemerged from Expectations (familial expectations and professional expec-tations) accounting for 63 of the variance Five items loaded on famil-ial expectations with loadings ranging from 058 to 087 Four itemsloaded on professional expectations with loadings ranging from 049 to089As expected this indicates that among DDCs there are both famil-ial and professional expectations to provide care to elderly relatives
Development andValidation of the Double Duty Caregiving Scale
CJNR 2009Vol 41 No 3 119
Table 2 Overview of Development andValidation of Double DutyCaregiving Scale (DDCS)
Initial Item Pool ContentValidity Pilot Testing
Qualitative Mailed SurveySource Interview Data Expert Panel (n = 800)
Sample 37 female DDCs 4 female DDCs 377 female DDCs15 registered nurses 1 registered nurse 193 DDCs9 social workers 1 social worker 184 non-DDCs7 physiotherapists 1 physiotherapist6 physicians 1 physician
NoteDDC = double duty caregiver
Ward-Griffin Keefe Martin-Matthews Kerr Brown and Oudshoorn
CJNR 2009Vol 41 No 3 120
Tabl
e3
Revised
DDCS(N
=18
7)
Number
Item
-Total
Cronbachrsquos
Factor
Factor
Subscale
Factors
ofItem
sMean
SDCorrelations
Alpha
Variance
Loading
Exp
ectation
s378
712
Familialexpectations
5040ndash073
080
058ndash087
Professionalexpectations
4030ndash056
069
049ndash089
Total
9028ndash066
083
625
Supp
orts
332
646
Personalsupports
3043ndash058
068
070ndash086
Professionalsupports
3024ndash062
065
035ndash091
Total
6031ndash052
071
617
SettingLim
its
311
678
Awarenessofboundaries
3041ndash059
067
061ndash087
Activeresistance
3033ndash061
065
068ndash084
Total
6034ndash058
071
629
Mak
ingCon
nections
389
677
Makingconnections
5042ndash069
075
465
060ndash076
CaregivingIn
terface
301
826
Perceptionsofinterface
4048ndash071
081
080ndash084
Consequencesofinterface
3053ndash077
083
080ndash084
Total
7044ndash074
085
703
Two factors emerged from Supports (personal supports and profes-sional supports) accounting for 62 of the variance and indicating theimportance of personal and professional supports to DDCs providingcare to elderly relativesThree items loaded on personal supports withloadings ranging from 070 to 086Three items loaded on professionalsupports with loadings ranging from 035 to 091Two factors labelled Awareness of Boundaries and Active Resistance
emerged from Setting Limits accounting for 63 of the varianceThreeitems loaded on Awareness of Boundaries with loadings ranging from061 to 087Three items loaded on Active Resistance with loadingsranging from 068 to 084 One factor was extracted from MakingConnections accounting for 47 of the variance Loadings for the fiveitems on Making Connections ranged from 060 to 076This suggeststhat DDCs are aware of the boundaries between their personal and pro-fessional caregiving and that in an attempt to negotiate these boundariesthey resist providing care to their elderly relative as well as making con-nections to increase their supportsTwo factors emerged from CIThese were labelled Perceptions of CI
and Consequences of CI accounting for 70 of the variance Four itemsloaded on Perceptions of CI with loadings ranging from 054 to 085and three items loaded on Consequences of CI with loadings rangingfrom 080 to 084These results indicate that DDCs both are aware ofand experience consequences of the blurring of boundaries between per-sonal and professional caregiving
Reliability
Inter-item correlations and internal consistency (reliability) were exam-ined for each of the subscales of the Revised DDCSOverall in the finalversion of the 33-item DDCS inter-item correlations ranged from 024to 077 (Table 3) Cronbachrsquos alpha reliability coefficients of the fiveDDC subscales ranged from 085 (CI) to 071 (Supports and SettingLimits)Moreover Cronbachrsquos alpha reliability coefficients of the subscalefactors ranged from 083 (CI-Consequences) to 065 (for both Supports-Professional and Setting Limits-Active Resistance)
ConstructValidity Step 2
Pearson correlations were conducted to assess construct validity betweeneach of the subscales within the DDCS andWRSICWBS and SF-12v2(physical) and SF-12v2 (mental) (Table 3) In line with the underlyingtheory driving the scale there were weak to moderate correlations in theexpected direction between the Revised DDCS subscales ofExpectations Supports Setting LimitsMaking Connections and CI andthe established measuresThe strongest significant correlations were
Development andValidation of the Double Duty Caregiving Scale
CJNR 2009Vol 41 No 3 121
Ward-Griffin Keefe Martin-Matthews Kerr Brown and Oudshoorn
CJNR 2009Vol 41 No 3 122
Tabl
e4
Correlation
BetweenRevised
DDC
Subscalesan
dEstab
lished
Measures
Setting
Making
Caregiving
Scale
Expectations
Supports
Lim
its
Connections
Interface
WRSI
ar
-34
41
09
04
-49
p000
000
240
625
000
CaregiverWell-Being
Scale
r-16
34
-05
-01
-29
Activitiesb
p03
00
48
89
00
CaregiverWell-Being
Scale
r-16
34
03
-03
-36
Needsc
p04
00
71
69
00
SF12
PhysicalIndexd
r06
14
-14
-03
-02
p42
06
06
69
78
SF12
MentalIndex
dr
-26
26
09
01
-39
p00
22
22
60
00
Expectations
ar
1-12
-07
38
55
p095
344
000
000
Supportsa
r-12
104
10
-26
p095
552
174
000
Strategiesndash
r1
01
-23
SettingLimits
ap
851
002
Strategiesndash
r1
18
MakingConnections
ap
013
CaregivingInterfacea
r1
p
aN=187
bN=174
cN=180
dN=176plt05(2-tailed)
plt01(2-tailed)
between CI andWRSI (r = -49 p lt 001) between Supports andWRSI(r = 041 p lt001) and between CI and SF-12v2 (mental) (r = -39 p lt001) Finally the CI of the DDCS was also negatively correlated withcaregiver well-being (r = -29 p lt 001 [activities] and r = -36 p lt001[needs])The strongest subscale inter-correlations (ie within the Revised
DDCS itself) were between Expectations and CI (r = 055 p lt 001) andbetween Expectations and Making Connections (r = 038 p lt 001) Inaddition there was a weak positive association between MakingConnections and CI (r = 018 p lt 05) and negative associationsbetween Supports and CI (r = -026 p lt 001) and between SettingLimits and CI (r = -23 p lt 001) None of the other DDCS subscaleinter-correlations were statistically significant (Table 4)
Contrasted Groups Approach
Although there were no significant differences between DDCs andnon-DDCs in their overall scores for theWRSI CWBS and SF-12v2(physical and mental scores) there were significant differences betweennon-DDCs (n = 67) and the DDC subgroup (n = 84) defined as livingon the edge (ie those scoring above the mean on the CI subscale) Poorerhealth was observed for the living on the edge DDCs on their overall SF-12v2 mental health index score (t = -276 p lt 05) and on four of theeight SF-12v2 subscales vitality (t = -237 p lt 05) social functioning(t = -291 p lt 01) role emotional (t = -306 p lt 05) and mental health(t = -227 p lt 05) Moreover there were significant differences withinthe DDC group between those who were living on the edge and thosewith lower CI scores for the following SF-12 subscales vitality (t = -20p lt 05) social functioning (t = -356 p lt 01) role emotional (t = -483p lt 01) and mental health (t = -398 p lt 05)The living on the edgegroup also had significantly lower well-being scores for the activities(t = -363 p lt 05) and needs (t = -447 p lt 05) subscales than theother DDC respondentsWhile not all results were statistically significantoverall there was an observed tendency for the living on the edge group ofDDCs to have the lowest health and well-being scores whereas the otherDDCs (eg making it work) with low CI scores tended to have slightlybetter health scores than the non-DDC group
Discussion
The main purpose of this study was to develop and test a tool intendedto advance our understanding of DDC using a random sample of regis-tered nurses providing care to elderly relatives
Development andValidation of the Double Duty Caregiving Scale
CJNR 2009Vol 41 No 3 123
The nine factors we identified were consistent with the theorized coreDDC dimensions of Expectations (Familial and Professional) Supports(Personal and Professional) Setting Limits (Awareness of BoundariesActive Resistance) Making Connections and Caregiving Interface(Perceptions and Consequences) which can yield important informationregarding how much variance is accounted for by the factors Howeveradditional analyses are required to establish the psychometric propertiesof the DDCS including test-retest reliability to assess construct stabilityBased on the EFA results a measurement model of DDC will be pro-posed and analyzed in a future study using CFA to enhance the psycho-metric validation of the DDCS For researchers looking for a shorterversion of the DDCS it is worth noting that based on the strength andconsistency of the overall findings the seven-item CI subscale could beused to determine the extent of DDC when survey respondent burdenis a key factor in instrument selection (ie when use of the full 33DDCS items is not possible) adding to the potential value of the DDCS
The positive correlation between Expectations and CI and the nega-tive correlation between Supports and CI and between Setting Limitsand CI are theoretically consistent with the conceptual model of DDCThat is if expectations are high both personally and professionally withrespect to caring for onersquos relatives there will be greater CI or blurringof boundaries Conversely if one has strong personal and professionalsupports it follows that a lower degree of CI will result Similarly whenone sets limits on caregiving then less blurring or a lower degree of CIshould result However the positive association between MakingConnections and Expectations was unexpected Perhaps high expecta-tions lead one to increase supports by making connections both person-ally and professionally to help meet these expectationsComparison of the SF-12 v2 scores for living on the edge DDCs and
non-DDCs revealed significant differences for SF-12v2 mental healthand specific SF-12v2 subscales of vitality social functioning role emo-tional and mental healthThese findings suggest that DDCs who expe-rience a high degree of blurring of their professional and personalboundaries are at greater risk for poor health than those health profes-sionals who do not care for elderly relatives or who do not experiencethis blurring In addition those DDCs who could be characterized asliving on the edge scored significantly higher on the same four SF-12 sub-scales than DDCs with lower CI scoresThis observed pattern suggeststwo possibilities there exists a threshold effect for the negative healtheffects of DDC or manageable exposure to DDC has a beneficial effectFurther exploration of these interesting findings is warrantedAlthough we conducted a systematic and comprehensive analysis to
assess the psychometric properties of a new scale further reliability and
Ward-Griffin Keefe Martin-Matthews Kerr Brown and Oudshoorn
CJNR 2009Vol 41 No 3 124
validity studies are needed Confirmatory validation studies with otherhealth-care provider populations such as family physicians social workersand physiotherapists are particularly important as these professionals havethe potential to be DDCs and their experiences as documented in ouroriginal qualitative study of DDC helped to formulate the theoreticalunderpinnings of the DDCS In addition research with these groups willadvance our understanding of how occupational health groups may differin terms of expectations supports negotiating strategies and degree ofCIAs the identification of health-advantage and health-risk factors isinfluenced by health and social environments the negotiating strategiescould also be examined through the use of qualitative methodologiessuch as in-depth interviews or focus groupsFinally research that draws linkages between professional and personal
caregiving has the added value of furthering knowledge about employedcaregiving specifically as it relates to the relationship between health out-comes and provision of familial care by health-care providersAlthoughthe convergence (and avoidance) of professional and personal caregivingboundaries is not a new issue in nursing and other health professions thenotion that it is the individualrsquos responsibility to negotiate this boundarytends to predominate (Ward-Griffin 2008)To that end further testingand refinement of the DDCS will be helpful in identifying areas whereDDCs may need specific or different types of support It is also impor-tant to understand how specific social supports shape the health experi-ences of DDCs as well as to investigate different types of social supportinterventions with DDCsThis information is particularly meaningfultoday with the intersection of three challenges an aging population anaging health-care workforce and a shortage of health professionals Suchknowledge could contribute to workplace and other health initiativesspearheaded by professional groups policy-makers and other key stake-holders interested in assessing and addressing the health effects of DDCIn summary the DDCS is a valid tool for the assessment of double
duty caregiving Such assessment is a crucial step in understanding theexperience of the blurring of personal and professional boundaries ofcaregiving among health professionalsA quantitative study of both maleand female DDCs could help us to understand the relationship betweencertain factors (ie gender health-care occupation) and the potentialhealth effects of DDCMoreover our finding that respondents with highCI scores (living on the edge) had significantly lower health and well-beingscores than DDC respondents with lower CI scores warrants furtherinvestigation to determine if one group of DDCs is at particular risk fordeveloping negative health effects Given the current climate of health-care reform in Canada developing a better understanding of DDC andits health effects is particularly relevant for policy-makers and others who
Development andValidation of the Double Duty Caregiving Scale
CJNR 2009Vol 41 No 3 125
are committed to developing health-promoting programs and policies forfamilial caregivers of the elderly Clearly now is the time to monitor theeffects of changing demographics both in the general population andwithin the health professions in order to develop appropriate and tar-geted strategies thereby creating and sustaining healthy work environ-ments and health-care workforcesWith further refinement the DDCSmay assist with these endeavours
References
Armstrong P amp ArmstrongH (2004)Thinking it throughWomenwork andcaring in the new millennium In K Grant CArmaratunga PArmstrongM BoscoeA Pederson amp KWillson (Eds)Caring forcaring aboutWomenhome care and unpaid caregiving (pp 5ndash44)Aurora ONGaramond
Baines D (2004) Seven kinds of work ndash only one paid Raced gendered andrestructured work in social servicesAtlantis 28(2) 19ndash28
Canadian Institute for Health Information (2006)Workforce trends of registerednurses in Canada 2005 Retrieved November 5 2006 fromhttpsecurecihicacihiwebproductsndb_worforce_trends_registered_nurses_canada_2005_epdf
CarruthA K (1996) Development and testing of the Caregiver ReciprocityScaleNursing Research 45(2) 92ndash97
Chen F Feudtner C Rhodes L amp Green L (2001) Role conflicts of physi-cians and their family members Rules but no rule bookWestern Journal ofMedicine 175(4) 236ndash239
Cohen S Underwood L G amp Gottlieb BH (Eds) (2000) Social support mea-surement and interventionA guide for health and social scientistsOxford OxfordUniversity Press
Fast J (2005)Hidden costsinvisible contributions report Reworking workThe experi-ence of employed caregivers of older adults Retrieved August 16 2007 fromwwwhecolualbertacahcic
Gable R ampWolfe M (1993) Instrument development 2nd ed Boston KluwerGubermanN amp Maheu P (1999) Combining employment and caregivingAn
intricate juggling actCanadian Journal on Aging 18(1) 84ndash106Keefe J Leacutegareacute J amp CarriegravereY (2007) Developing new strategies to support
future caregivers of older Canadians with disabilities Projections of need andtheir policy implicationsCanadian Public Policy 33 S65ndash80
Lengacher CA amp Sellers E (2003)TheWomenrsquos Role Strain Inventory InO L Strickland amp CDilorio (Eds)Measurement of nursing outcomes 2nd ed(pp 109ndash127) NewYork Springer
Martin-MatthewsA (2000) Intergenerational caregivingHow apocalyptic anddominant demography frame the questions and shape the answers In EMGee amp GGutman (Eds)The overselling of population agingApocalyptic demog-raphy intergenerational challenges and social policy (pp 64ndash79)Toronto OxfordUniversity Press
Ward-Griffin Keefe Martin-Matthews Kerr Brown and Oudshoorn
CJNR 2009Vol 41 No 3 126
Mayall B (1993) Keeping children healthy ndash the intermediate domain SocialScience and Medicine 36(1) 77ndash83
Morris JM amp Field PA (1995) Qualitative research methods for health profession-als 2nd ed London Sage
Pascall G (1986) Social policyA feminist analysis NewYorkTavistockPhillips J BernardM amp ChittendenM (2002) Juggling work and careThe expe-riences of older adults Bristol Policy Press
Polit D F amp Beck CT (2008)Nursing research Generating and assessing evidencefor nursing practice 8th ed Philadelphia LippincottWilliams ampWilkins
Polit D F amp Beck CT amp Owen SV (2007) Is the CVI an acceptable indica-tor of content validity Appraisal and recommendationsResearch in Nursingand Health 30 459ndash467
RossMM Rideout EM amp CarsonMM (1996) Nursesrsquo work Balancingpersonal and professional caregiving careers Canadian Journal of NursingResearch 26(4) 43ndash59
RutmanD (1996) Caregiving as womenrsquos workWomenrsquos experiences of pow-erfulness and powerlessness as caregiversQualitative Health Research 6(1) 90ndash111
ShieldsM ampWilkins K (2005)National Survey of theWork and Health of Nurses2005 Provincial profiles Ottawa Statistics CanadaRetrieved August 24 2007from httpwwwstatcancaenglishresearch11-621-MIE11-621-MIE2006052htm
StaceyM amp Davies C (1983)Division of labour in child health care Final report toSSRCCoventry Sociology Department University ofWarwick
Tebb S (1995)An aid to empowermentA caregiver well-being scaleHealth andSocialWork 20(2) 87ndash92
Tebb S Berg-WgerM amp Rubio DM (2000) CaregiverWell-Being Scale InDRoyse BAThyer D K Padgett ampT K Logan (Eds) Program evaluation3rd ed (pp 320ndash323) Pacific Grove CA BrooksCole
Ungerson C (1990) The language of care Crossing the boundaries InCUngerson (Ed)Gender and caringWork and welfare in Britain and Scandinavia(pp 8ndash33) NewYork Harvester
WaltersV LentonR French S Eyles JMayr J amp Newbold B (1996) Paidwork unpaid work and social supportA study of the health of male andfemale nurses Social Science and Medicine 43(11) 1627ndash1636
Ward-Griffin C (2004) Nurses as caregivers of elderly relatives Negotiatingpersonal and professional boundariesCJNR 36(1) 92ndash114
Ward-Griffin C (2008)Health professionals caring for aging relativesA profes-sional or personal issue In AMartin-Matthews amp J Phillips (Eds)Blurringthe boundariesAgeing at the intersection of work and home life (pp 1ndash20) NewYorkTaylor amp FrancisPsychology Press
Ward-Griffin C Brown JVandervoortA McNair S amp Dashnay I (2005)Double duty caregivingWomen in the health professionsCanadian Journalon Aging 24(4) 379ndash394
Ward-Griffin C amp MarshallV (2003) Reconceptualizing the relationshipbetween public and private eldercare Journal of Aging Studies 17 189ndash208
Development andValidation of the Double Duty Caregiving Scale
CJNR 2009Vol 41 No 3 127
Ware J E Kosinksi MTurner-Bowker L amp Gandek B (2002)How to scoreversion 2 of the SF-12 health survey Lincoln RIQuality Metric Inc
Acknowledgements
This study was funded by the Social Sciences and Humanities ResearchCouncil (Internal) and the Institute of Gender and Health CanadianInstitutes of Health ResearchThere are no conflicts of interest or financial disclosures
CatherineWard-Griffin RN PhD is ProfessorArthur Labatt Family School ofNursing University ofWestern Ontario London Canada Janice Keefe PhD isProfessor and Canada Research Chair in Aging and Caregiving Policy FamilyStudies and GerontologyMount SaintVincent University HalifaxNova ScotiaCanadaAnne Martin-Matthews PhD is Professor School of SocialWork andFamily Studies University of British ColumbiaVancouver Canada MichaelKerr PhD is Associate ProfessorArthur Labatt Family School of NursingUniversity ofWestern Ontario Judith Belle Brown PhD is Professor Departmentof Family Medicine University ofWestern OntarioAbram Oudshoorn RN is aPhD candidate in the Arthur Labatt Family School of Nursing University ofWestern Ontario
Ward-Griffin Keefe Martin-Matthews Kerr Brown and Oudshoorn
CJNR 2009Vol 41 No 3 128
domains Double duty caregivers usually receive some degree of emo-tional informational and substantive support from family members andfriendsAlthough there are well-established instruments for measuringsocial support (Cohen Underwood amp Gottlieb 2000) the unique per-sonal and professional supports received within DDC may not be fullycaptured using a generic standard tool Often siblings spouses childrenor friends are also involved in the caregivingAdditionally many care-givers receive professional support this can include information orresources from onersquos workplace such as flexible work hours or access toemployee assistance programs
Negotiating Strategies
The third dimensionNegotiating Strategies addresses two main types ofstrategies Setting Limits and Making ConnectionsThese help DDCs tonegotiate their professional and personal boundaries thereby potentiallymoderating the negative impacts of the caregiving interface Double dutycaregivers set limits with respect to personal and professional expectationsconcerning the provision of familial care Setting Limits includes strate-gies for keeping the personal and professional caregiving domains sepa-rate and distinct while Making Connections examines the multipleinteractions that serve to bring the two domains closer together InSetting Limits (10 items) DDCs refuse to take on professional caregiv-ing tasks for family members or arrange for others to provide this careAs well DDCs increase their supports by Making Connections (13items)These include accessing health-care information or care for onersquosrelative using professional knowledge and connections to obtain care ornavigating the health-care system
Caregiving Interface
Ten items were developed to measure the caregiving interface (CI) orthe degree of blurring between the professional and personal caregivingdomains (intermediate domain)This dimension addresses the extent ofthe connections between elder caregiving and other forms of genderedcaring work (eg nursing)The CI encompasses both feelings about theblurring of roles and the psychological impact of these feelings Feelingsabout the blurring of roles can include being pulled in two differentdirections being unable to escape from the caregiving role and strugglingto separate caregiving at home from caregiving at workThe psycholog-ical impact of increasing blurring of boundaries can include stress thefeeling that onersquos caregiving is not being recognized and confusionregarding onersquos professional and personal roles
Development andValidation of the Double Duty Caregiving Scale
CJNR 2009Vol 41 No 3 115
ContentValidation of the DDC Scale
Because of the importance of preserving the inductively derived meaningof DDC in a quantitative instrument (Morris amp Field 1995) judgementsabout clarity internal consistency and initial content validity were madeby a panel of four DDCs representing the disciplines of nursing medi-cine physiotherapy and social work as used in our previous qualitativestudyThese content experts independently rated the relevance of theprovisional items on the DDCS using a four-point scale ranging from notrelevant to very relevant This review process facilitated a systematicapproach to item revision Raters also indicated whether the conceptualdomain of each subscale was adequately represented by the set of itemsAlthough consensus was reached for each of the four dimensions theexperts recommended clarification of certain items which were subse-quently reworded or deletedContent validity indices (CVI) for each item subscales and total scale
were calculated setting the criteria for item-level acceptance at 78 orhigher for three or more reviewers (Polit Beck amp Owen 2007)TheCVI ranged from 75 to 10 for all retained items (one item fell below78 but was retained because it measured a key conceptual aspect of theCI subscale recognition of professional status) Eight items were deleteddue to lack of clarity redundancy or a relatively low CVI thus reducingthe provisional DDCS from 57 items to 49The provisional DDCS was constructed using a five-point Likert scale
(1 = strongly disagree 5 = strongly agree) Prior to the analysis negativelyworded items were recoded so that for all items a higher score reflecteda higher degree of Expectations SupportsNegotiating Strategies andCaregiving InterfaceWithin each subscale the scores were calculated byaveraging the relevant individual item scores Data imputation for missingvalues was not used as non-response for the items was very lowThe sub-scales were developed for separate use of each dimension thus they werenot combined into a single overall DDCS score
Pilot Testing of the DDC Scale
Sampling
Following institutional ethics review board approval the 49-item provi-sional DDCS was administered to an age-stratified sample of femalenurses randomly selected from the registry list of the College of Nursesof Ontario Because previous research suggested that approximately onehalf of the working nurse population is likely to provide care to anelderly relative 800 female full-time (more than 30 hoursweek) regis-tered nurses 40 years of age or older were asked to complete a mailed
Ward-Griffin Keefe Martin-Matthews Kerr Brown and Oudshoorn
CJNR 2009Vol 41 No 3 116
survey packageThe aim was to have 200 eligible DDC respondentscomplete and return the package which consisted of (1) an informationletter (2) a short demographic questionnaire which also determined eli-gibility for the study (3) the provisional DDCS described above and(4) established comparative measures including theWomenrsquos Role StrainInventory (WRSI) (Lengacher amp Sellers 2003) the CaregiverWell-BeingScale (CWBS) (Tebb et al 2000) and Health Related Outcomes(Medical Outcomes Study Short-Form SF-12 version 20 acute form4-week recall)The time needed to complete the survey package wasestimated at between 30 and 45 minutes Each package contained amodest gift certificate as a token of appreciation Nurses not providingcare for an elderly relative or friend were asked to complete all question-naires except the DDCS the purpose being to generate data for com-paring DDC and non-DDC nursesOf the 800 questionnaires mailed 394 were returned of these eight
respondents did not meet the eligibility criteria (two male and six unem-ployed) six questionnaires were blank and three were returned to senderyielding a sample of 377 respondents (49 response rate)A total of 193respondents (51) were caring for an elderly relative (ie the DDCs) and184 (49) were not (ie the non-DDCs)Of the 193 respondents iden-tified as DDCs six left sections of the DDCS blank which led to a finalusable DDC sample of 187 a total sample size that is considered adequatefor instrument development analysis (Gable ampWolf 1993)
Reliability and ConstructValidity Analyses
Contingency table (chi square) analyses were performed on all categori-cal variables while independent sample t tests were used with all contin-uous variables when comparing DDCs and non-DDCsAppropriatemeasures of association were used to examine the relationship betweentheoretically relevant demographic variables (eg hours of employmentper week hours of caregiving per week) and the CIConstruct validity of the provisional 49-item tool was assessed at the
preliminary stage with a combination of exploratory factor analysis (EFA)using a principal components factor approach and assessment of scalereliability Even though our previous qualitative work and initial concep-tualization of DDC informed the construction of the provisional DDCSitems EFA was selected over confirmatory factor analysis (CFA) For theEFA initial factor extraction was based on eigenvalues greater than 100(Polit amp Beck 2008 p 488) Each subscale of the provisional DDCS wasthen subjected to varimax rotation to select the factor structure that bestrepresented the underlying relationship of the items within the fourdimensions (Expectations Supports Negotiating Strategies andCaregiver Interface)Although loadings with an absolute value of 040 or
Development andValidation of the Double Duty Caregiving Scale
CJNR 2009Vol 41 No 3 117
higher are often used as factor loading cut-off values (Carruth 1996)smaller values are acceptable if the item pool is large (Polit amp Beck 2008p 491) Cronbachrsquos alpha reliability coefficients were also used to deter-mine internal consistency among the items of the four subscales of theprovisional DDCS Based on these preliminary analyses a combinationof low inter-item correlations (lt 20) weak factor loadings (lt 35)andor poor conceptual clarity 16 of the original 49 items were removedfrom the provisional DDCS yielding a tool with a total of 33 items forthe remaining construct validity analysesWe also correlated each of the DDCS subscale scores with those of
theWRSI the CWBS and the SF-12v2TheWRSI is a previously vali-dated 44-item five-point Likert scale that measures role strain in femalenurses with multiple roles (Lengacher amp Sellers 2003) with high relia-bility coefficients for the total scale (086ndash095) and subscales of distress(074ndash091) enhancement (079ndash089) and support (065ndash087)Developed and validated byTebb et al (2000) the CWBS-ShortVersionis a 16-item five-point Likert scale that assesses activities and needs ofcaregivers (eight items for each subscale) Overall and for each subscale(Needs and Activities of Daily Living) the coefficient alpha was 094091 and 088 respectively Finally the SF-12v2 is a well-established toolthat measures the perceptions and activities of acute health and well-being It is a shortened version of the SF-36 which includes general andphysical health index scores as well as eight subscales (bodily pain generalhealth vitality social functioning physical functioning role limitationsdue to physical problems role limitations due to emotional problems andmental health)Ware KosinskiTurner-Bowker and Gandek (2002) reportinternal consistency reliability coefficients ranging from 066 to 090 Inthe present study internal consistency reliability coefficients for each ofthese established instruments were 091 (WRSI) 073 (CWBS-needs)078 (CWBS-activities) and 080 (SF-12v2)
Results
Sample
The sample comprised 193 DDCs (this figure includes six respondentswho failed to complete all items on the DDCS but completed thedemographic questionnaire) and 184 non-DDCs (see Table 2 for anoverview)The typical DDC was 520 years old (range = 41ndash65 SD =490) was married (742) held a diploma in nursing (679) had amean household income of $101778 (range = $12500ndash$300000 SD =$4409373) was employed part-time or full-time (968) with a meanof 390 hours worked per week (range 7ndash80 SD 786) had practisednursing for 25 years or more (676) and had at least one child (ranging
Ward-Griffin Keefe Martin-Matthews Kerr Brown and Oudshoorn
CJNR 2009Vol 41 No 3 118
in age from 2 to 32 years) living with her (65)The DDC respondentsprovided an average of 6 hours per week of care to one (53) or two(30) elderly relativesmostly parents (77) or parents-in-law (12) wholived nearbyThe typical non-DDC respondent was 515 years old (range= 41ndash65 SD = 585) was married (739) held a diploma in nursing(678) had a mean household income of $105618 (range = $35000ndash$770000 SD = 6700684) was employed part-time or full-time (989)with a mean of 408 hours worked per week (range = 22ndash80) had prac-tised nursing for 25 years or more (525) and had at least one child(ranging in age from 1 to 37 years) living with her (620)There wereno significant differences between DDCs and non-DDCs with respect toage household income and number of hours worked per week
Preliminary ConstructValidity Step 1
To facilitate a better understanding of the item contents of the new scaleprincipal components analysis was conducted on each of the four sub-scales of the Provisional DDCSAlthough each dimension was provi-sionally structured as a single subscale the results of our subsequent factoranalysis suggested that Negotiating Strategies should be split into twosubscales Setting Limits and Making Connections Nine factors wereidentified from our analyses (Table 3) which is consistent with our orig-inal conceptualization about the dimensionality of DDCTwo factorsemerged from Expectations (familial expectations and professional expec-tations) accounting for 63 of the variance Five items loaded on famil-ial expectations with loadings ranging from 058 to 087 Four itemsloaded on professional expectations with loadings ranging from 049 to089As expected this indicates that among DDCs there are both famil-ial and professional expectations to provide care to elderly relatives
Development andValidation of the Double Duty Caregiving Scale
CJNR 2009Vol 41 No 3 119
Table 2 Overview of Development andValidation of Double DutyCaregiving Scale (DDCS)
Initial Item Pool ContentValidity Pilot Testing
Qualitative Mailed SurveySource Interview Data Expert Panel (n = 800)
Sample 37 female DDCs 4 female DDCs 377 female DDCs15 registered nurses 1 registered nurse 193 DDCs9 social workers 1 social worker 184 non-DDCs7 physiotherapists 1 physiotherapist6 physicians 1 physician
NoteDDC = double duty caregiver
Ward-Griffin Keefe Martin-Matthews Kerr Brown and Oudshoorn
CJNR 2009Vol 41 No 3 120
Tabl
e3
Revised
DDCS(N
=18
7)
Number
Item
-Total
Cronbachrsquos
Factor
Factor
Subscale
Factors
ofItem
sMean
SDCorrelations
Alpha
Variance
Loading
Exp
ectation
s378
712
Familialexpectations
5040ndash073
080
058ndash087
Professionalexpectations
4030ndash056
069
049ndash089
Total
9028ndash066
083
625
Supp
orts
332
646
Personalsupports
3043ndash058
068
070ndash086
Professionalsupports
3024ndash062
065
035ndash091
Total
6031ndash052
071
617
SettingLim
its
311
678
Awarenessofboundaries
3041ndash059
067
061ndash087
Activeresistance
3033ndash061
065
068ndash084
Total
6034ndash058
071
629
Mak
ingCon
nections
389
677
Makingconnections
5042ndash069
075
465
060ndash076
CaregivingIn
terface
301
826
Perceptionsofinterface
4048ndash071
081
080ndash084
Consequencesofinterface
3053ndash077
083
080ndash084
Total
7044ndash074
085
703
Two factors emerged from Supports (personal supports and profes-sional supports) accounting for 62 of the variance and indicating theimportance of personal and professional supports to DDCs providingcare to elderly relativesThree items loaded on personal supports withloadings ranging from 070 to 086Three items loaded on professionalsupports with loadings ranging from 035 to 091Two factors labelled Awareness of Boundaries and Active Resistance
emerged from Setting Limits accounting for 63 of the varianceThreeitems loaded on Awareness of Boundaries with loadings ranging from061 to 087Three items loaded on Active Resistance with loadingsranging from 068 to 084 One factor was extracted from MakingConnections accounting for 47 of the variance Loadings for the fiveitems on Making Connections ranged from 060 to 076This suggeststhat DDCs are aware of the boundaries between their personal and pro-fessional caregiving and that in an attempt to negotiate these boundariesthey resist providing care to their elderly relative as well as making con-nections to increase their supportsTwo factors emerged from CIThese were labelled Perceptions of CI
and Consequences of CI accounting for 70 of the variance Four itemsloaded on Perceptions of CI with loadings ranging from 054 to 085and three items loaded on Consequences of CI with loadings rangingfrom 080 to 084These results indicate that DDCs both are aware ofand experience consequences of the blurring of boundaries between per-sonal and professional caregiving
Reliability
Inter-item correlations and internal consistency (reliability) were exam-ined for each of the subscales of the Revised DDCSOverall in the finalversion of the 33-item DDCS inter-item correlations ranged from 024to 077 (Table 3) Cronbachrsquos alpha reliability coefficients of the fiveDDC subscales ranged from 085 (CI) to 071 (Supports and SettingLimits)Moreover Cronbachrsquos alpha reliability coefficients of the subscalefactors ranged from 083 (CI-Consequences) to 065 (for both Supports-Professional and Setting Limits-Active Resistance)
ConstructValidity Step 2
Pearson correlations were conducted to assess construct validity betweeneach of the subscales within the DDCS andWRSICWBS and SF-12v2(physical) and SF-12v2 (mental) (Table 3) In line with the underlyingtheory driving the scale there were weak to moderate correlations in theexpected direction between the Revised DDCS subscales ofExpectations Supports Setting LimitsMaking Connections and CI andthe established measuresThe strongest significant correlations were
Development andValidation of the Double Duty Caregiving Scale
CJNR 2009Vol 41 No 3 121
Ward-Griffin Keefe Martin-Matthews Kerr Brown and Oudshoorn
CJNR 2009Vol 41 No 3 122
Tabl
e4
Correlation
BetweenRevised
DDC
Subscalesan
dEstab
lished
Measures
Setting
Making
Caregiving
Scale
Expectations
Supports
Lim
its
Connections
Interface
WRSI
ar
-34
41
09
04
-49
p000
000
240
625
000
CaregiverWell-Being
Scale
r-16
34
-05
-01
-29
Activitiesb
p03
00
48
89
00
CaregiverWell-Being
Scale
r-16
34
03
-03
-36
Needsc
p04
00
71
69
00
SF12
PhysicalIndexd
r06
14
-14
-03
-02
p42
06
06
69
78
SF12
MentalIndex
dr
-26
26
09
01
-39
p00
22
22
60
00
Expectations
ar
1-12
-07
38
55
p095
344
000
000
Supportsa
r-12
104
10
-26
p095
552
174
000
Strategiesndash
r1
01
-23
SettingLimits
ap
851
002
Strategiesndash
r1
18
MakingConnections
ap
013
CaregivingInterfacea
r1
p
aN=187
bN=174
cN=180
dN=176plt05(2-tailed)
plt01(2-tailed)
between CI andWRSI (r = -49 p lt 001) between Supports andWRSI(r = 041 p lt001) and between CI and SF-12v2 (mental) (r = -39 p lt001) Finally the CI of the DDCS was also negatively correlated withcaregiver well-being (r = -29 p lt 001 [activities] and r = -36 p lt001[needs])The strongest subscale inter-correlations (ie within the Revised
DDCS itself) were between Expectations and CI (r = 055 p lt 001) andbetween Expectations and Making Connections (r = 038 p lt 001) Inaddition there was a weak positive association between MakingConnections and CI (r = 018 p lt 05) and negative associationsbetween Supports and CI (r = -026 p lt 001) and between SettingLimits and CI (r = -23 p lt 001) None of the other DDCS subscaleinter-correlations were statistically significant (Table 4)
Contrasted Groups Approach
Although there were no significant differences between DDCs andnon-DDCs in their overall scores for theWRSI CWBS and SF-12v2(physical and mental scores) there were significant differences betweennon-DDCs (n = 67) and the DDC subgroup (n = 84) defined as livingon the edge (ie those scoring above the mean on the CI subscale) Poorerhealth was observed for the living on the edge DDCs on their overall SF-12v2 mental health index score (t = -276 p lt 05) and on four of theeight SF-12v2 subscales vitality (t = -237 p lt 05) social functioning(t = -291 p lt 01) role emotional (t = -306 p lt 05) and mental health(t = -227 p lt 05) Moreover there were significant differences withinthe DDC group between those who were living on the edge and thosewith lower CI scores for the following SF-12 subscales vitality (t = -20p lt 05) social functioning (t = -356 p lt 01) role emotional (t = -483p lt 01) and mental health (t = -398 p lt 05)The living on the edgegroup also had significantly lower well-being scores for the activities(t = -363 p lt 05) and needs (t = -447 p lt 05) subscales than theother DDC respondentsWhile not all results were statistically significantoverall there was an observed tendency for the living on the edge group ofDDCs to have the lowest health and well-being scores whereas the otherDDCs (eg making it work) with low CI scores tended to have slightlybetter health scores than the non-DDC group
Discussion
The main purpose of this study was to develop and test a tool intendedto advance our understanding of DDC using a random sample of regis-tered nurses providing care to elderly relatives
Development andValidation of the Double Duty Caregiving Scale
CJNR 2009Vol 41 No 3 123
The nine factors we identified were consistent with the theorized coreDDC dimensions of Expectations (Familial and Professional) Supports(Personal and Professional) Setting Limits (Awareness of BoundariesActive Resistance) Making Connections and Caregiving Interface(Perceptions and Consequences) which can yield important informationregarding how much variance is accounted for by the factors Howeveradditional analyses are required to establish the psychometric propertiesof the DDCS including test-retest reliability to assess construct stabilityBased on the EFA results a measurement model of DDC will be pro-posed and analyzed in a future study using CFA to enhance the psycho-metric validation of the DDCS For researchers looking for a shorterversion of the DDCS it is worth noting that based on the strength andconsistency of the overall findings the seven-item CI subscale could beused to determine the extent of DDC when survey respondent burdenis a key factor in instrument selection (ie when use of the full 33DDCS items is not possible) adding to the potential value of the DDCS
The positive correlation between Expectations and CI and the nega-tive correlation between Supports and CI and between Setting Limitsand CI are theoretically consistent with the conceptual model of DDCThat is if expectations are high both personally and professionally withrespect to caring for onersquos relatives there will be greater CI or blurringof boundaries Conversely if one has strong personal and professionalsupports it follows that a lower degree of CI will result Similarly whenone sets limits on caregiving then less blurring or a lower degree of CIshould result However the positive association between MakingConnections and Expectations was unexpected Perhaps high expecta-tions lead one to increase supports by making connections both person-ally and professionally to help meet these expectationsComparison of the SF-12 v2 scores for living on the edge DDCs and
non-DDCs revealed significant differences for SF-12v2 mental healthand specific SF-12v2 subscales of vitality social functioning role emo-tional and mental healthThese findings suggest that DDCs who expe-rience a high degree of blurring of their professional and personalboundaries are at greater risk for poor health than those health profes-sionals who do not care for elderly relatives or who do not experiencethis blurring In addition those DDCs who could be characterized asliving on the edge scored significantly higher on the same four SF-12 sub-scales than DDCs with lower CI scoresThis observed pattern suggeststwo possibilities there exists a threshold effect for the negative healtheffects of DDC or manageable exposure to DDC has a beneficial effectFurther exploration of these interesting findings is warrantedAlthough we conducted a systematic and comprehensive analysis to
assess the psychometric properties of a new scale further reliability and
Ward-Griffin Keefe Martin-Matthews Kerr Brown and Oudshoorn
CJNR 2009Vol 41 No 3 124
validity studies are needed Confirmatory validation studies with otherhealth-care provider populations such as family physicians social workersand physiotherapists are particularly important as these professionals havethe potential to be DDCs and their experiences as documented in ouroriginal qualitative study of DDC helped to formulate the theoreticalunderpinnings of the DDCS In addition research with these groups willadvance our understanding of how occupational health groups may differin terms of expectations supports negotiating strategies and degree ofCIAs the identification of health-advantage and health-risk factors isinfluenced by health and social environments the negotiating strategiescould also be examined through the use of qualitative methodologiessuch as in-depth interviews or focus groupsFinally research that draws linkages between professional and personal
caregiving has the added value of furthering knowledge about employedcaregiving specifically as it relates to the relationship between health out-comes and provision of familial care by health-care providersAlthoughthe convergence (and avoidance) of professional and personal caregivingboundaries is not a new issue in nursing and other health professions thenotion that it is the individualrsquos responsibility to negotiate this boundarytends to predominate (Ward-Griffin 2008)To that end further testingand refinement of the DDCS will be helpful in identifying areas whereDDCs may need specific or different types of support It is also impor-tant to understand how specific social supports shape the health experi-ences of DDCs as well as to investigate different types of social supportinterventions with DDCsThis information is particularly meaningfultoday with the intersection of three challenges an aging population anaging health-care workforce and a shortage of health professionals Suchknowledge could contribute to workplace and other health initiativesspearheaded by professional groups policy-makers and other key stake-holders interested in assessing and addressing the health effects of DDCIn summary the DDCS is a valid tool for the assessment of double
duty caregiving Such assessment is a crucial step in understanding theexperience of the blurring of personal and professional boundaries ofcaregiving among health professionalsA quantitative study of both maleand female DDCs could help us to understand the relationship betweencertain factors (ie gender health-care occupation) and the potentialhealth effects of DDCMoreover our finding that respondents with highCI scores (living on the edge) had significantly lower health and well-beingscores than DDC respondents with lower CI scores warrants furtherinvestigation to determine if one group of DDCs is at particular risk fordeveloping negative health effects Given the current climate of health-care reform in Canada developing a better understanding of DDC andits health effects is particularly relevant for policy-makers and others who
Development andValidation of the Double Duty Caregiving Scale
CJNR 2009Vol 41 No 3 125
are committed to developing health-promoting programs and policies forfamilial caregivers of the elderly Clearly now is the time to monitor theeffects of changing demographics both in the general population andwithin the health professions in order to develop appropriate and tar-geted strategies thereby creating and sustaining healthy work environ-ments and health-care workforcesWith further refinement the DDCSmay assist with these endeavours
References
Armstrong P amp ArmstrongH (2004)Thinking it throughWomenwork andcaring in the new millennium In K Grant CArmaratunga PArmstrongM BoscoeA Pederson amp KWillson (Eds)Caring forcaring aboutWomenhome care and unpaid caregiving (pp 5ndash44)Aurora ONGaramond
Baines D (2004) Seven kinds of work ndash only one paid Raced gendered andrestructured work in social servicesAtlantis 28(2) 19ndash28
Canadian Institute for Health Information (2006)Workforce trends of registerednurses in Canada 2005 Retrieved November 5 2006 fromhttpsecurecihicacihiwebproductsndb_worforce_trends_registered_nurses_canada_2005_epdf
CarruthA K (1996) Development and testing of the Caregiver ReciprocityScaleNursing Research 45(2) 92ndash97
Chen F Feudtner C Rhodes L amp Green L (2001) Role conflicts of physi-cians and their family members Rules but no rule bookWestern Journal ofMedicine 175(4) 236ndash239
Cohen S Underwood L G amp Gottlieb BH (Eds) (2000) Social support mea-surement and interventionA guide for health and social scientistsOxford OxfordUniversity Press
Fast J (2005)Hidden costsinvisible contributions report Reworking workThe experi-ence of employed caregivers of older adults Retrieved August 16 2007 fromwwwhecolualbertacahcic
Gable R ampWolfe M (1993) Instrument development 2nd ed Boston KluwerGubermanN amp Maheu P (1999) Combining employment and caregivingAn
intricate juggling actCanadian Journal on Aging 18(1) 84ndash106Keefe J Leacutegareacute J amp CarriegravereY (2007) Developing new strategies to support
future caregivers of older Canadians with disabilities Projections of need andtheir policy implicationsCanadian Public Policy 33 S65ndash80
Lengacher CA amp Sellers E (2003)TheWomenrsquos Role Strain Inventory InO L Strickland amp CDilorio (Eds)Measurement of nursing outcomes 2nd ed(pp 109ndash127) NewYork Springer
Martin-MatthewsA (2000) Intergenerational caregivingHow apocalyptic anddominant demography frame the questions and shape the answers In EMGee amp GGutman (Eds)The overselling of population agingApocalyptic demog-raphy intergenerational challenges and social policy (pp 64ndash79)Toronto OxfordUniversity Press
Ward-Griffin Keefe Martin-Matthews Kerr Brown and Oudshoorn
CJNR 2009Vol 41 No 3 126
Mayall B (1993) Keeping children healthy ndash the intermediate domain SocialScience and Medicine 36(1) 77ndash83
Morris JM amp Field PA (1995) Qualitative research methods for health profession-als 2nd ed London Sage
Pascall G (1986) Social policyA feminist analysis NewYorkTavistockPhillips J BernardM amp ChittendenM (2002) Juggling work and careThe expe-riences of older adults Bristol Policy Press
Polit D F amp Beck CT (2008)Nursing research Generating and assessing evidencefor nursing practice 8th ed Philadelphia LippincottWilliams ampWilkins
Polit D F amp Beck CT amp Owen SV (2007) Is the CVI an acceptable indica-tor of content validity Appraisal and recommendationsResearch in Nursingand Health 30 459ndash467
RossMM Rideout EM amp CarsonMM (1996) Nursesrsquo work Balancingpersonal and professional caregiving careers Canadian Journal of NursingResearch 26(4) 43ndash59
RutmanD (1996) Caregiving as womenrsquos workWomenrsquos experiences of pow-erfulness and powerlessness as caregiversQualitative Health Research 6(1) 90ndash111
ShieldsM ampWilkins K (2005)National Survey of theWork and Health of Nurses2005 Provincial profiles Ottawa Statistics CanadaRetrieved August 24 2007from httpwwwstatcancaenglishresearch11-621-MIE11-621-MIE2006052htm
StaceyM amp Davies C (1983)Division of labour in child health care Final report toSSRCCoventry Sociology Department University ofWarwick
Tebb S (1995)An aid to empowermentA caregiver well-being scaleHealth andSocialWork 20(2) 87ndash92
Tebb S Berg-WgerM amp Rubio DM (2000) CaregiverWell-Being Scale InDRoyse BAThyer D K Padgett ampT K Logan (Eds) Program evaluation3rd ed (pp 320ndash323) Pacific Grove CA BrooksCole
Ungerson C (1990) The language of care Crossing the boundaries InCUngerson (Ed)Gender and caringWork and welfare in Britain and Scandinavia(pp 8ndash33) NewYork Harvester
WaltersV LentonR French S Eyles JMayr J amp Newbold B (1996) Paidwork unpaid work and social supportA study of the health of male andfemale nurses Social Science and Medicine 43(11) 1627ndash1636
Ward-Griffin C (2004) Nurses as caregivers of elderly relatives Negotiatingpersonal and professional boundariesCJNR 36(1) 92ndash114
Ward-Griffin C (2008)Health professionals caring for aging relativesA profes-sional or personal issue In AMartin-Matthews amp J Phillips (Eds)Blurringthe boundariesAgeing at the intersection of work and home life (pp 1ndash20) NewYorkTaylor amp FrancisPsychology Press
Ward-Griffin C Brown JVandervoortA McNair S amp Dashnay I (2005)Double duty caregivingWomen in the health professionsCanadian Journalon Aging 24(4) 379ndash394
Ward-Griffin C amp MarshallV (2003) Reconceptualizing the relationshipbetween public and private eldercare Journal of Aging Studies 17 189ndash208
Development andValidation of the Double Duty Caregiving Scale
CJNR 2009Vol 41 No 3 127
Ware J E Kosinksi MTurner-Bowker L amp Gandek B (2002)How to scoreversion 2 of the SF-12 health survey Lincoln RIQuality Metric Inc
Acknowledgements
This study was funded by the Social Sciences and Humanities ResearchCouncil (Internal) and the Institute of Gender and Health CanadianInstitutes of Health ResearchThere are no conflicts of interest or financial disclosures
CatherineWard-Griffin RN PhD is ProfessorArthur Labatt Family School ofNursing University ofWestern Ontario London Canada Janice Keefe PhD isProfessor and Canada Research Chair in Aging and Caregiving Policy FamilyStudies and GerontologyMount SaintVincent University HalifaxNova ScotiaCanadaAnne Martin-Matthews PhD is Professor School of SocialWork andFamily Studies University of British ColumbiaVancouver Canada MichaelKerr PhD is Associate ProfessorArthur Labatt Family School of NursingUniversity ofWestern Ontario Judith Belle Brown PhD is Professor Departmentof Family Medicine University ofWestern OntarioAbram Oudshoorn RN is aPhD candidate in the Arthur Labatt Family School of Nursing University ofWestern Ontario
Ward-Griffin Keefe Martin-Matthews Kerr Brown and Oudshoorn
CJNR 2009Vol 41 No 3 128
ContentValidation of the DDC Scale
Because of the importance of preserving the inductively derived meaningof DDC in a quantitative instrument (Morris amp Field 1995) judgementsabout clarity internal consistency and initial content validity were madeby a panel of four DDCs representing the disciplines of nursing medi-cine physiotherapy and social work as used in our previous qualitativestudyThese content experts independently rated the relevance of theprovisional items on the DDCS using a four-point scale ranging from notrelevant to very relevant This review process facilitated a systematicapproach to item revision Raters also indicated whether the conceptualdomain of each subscale was adequately represented by the set of itemsAlthough consensus was reached for each of the four dimensions theexperts recommended clarification of certain items which were subse-quently reworded or deletedContent validity indices (CVI) for each item subscales and total scale
were calculated setting the criteria for item-level acceptance at 78 orhigher for three or more reviewers (Polit Beck amp Owen 2007)TheCVI ranged from 75 to 10 for all retained items (one item fell below78 but was retained because it measured a key conceptual aspect of theCI subscale recognition of professional status) Eight items were deleteddue to lack of clarity redundancy or a relatively low CVI thus reducingthe provisional DDCS from 57 items to 49The provisional DDCS was constructed using a five-point Likert scale
(1 = strongly disagree 5 = strongly agree) Prior to the analysis negativelyworded items were recoded so that for all items a higher score reflecteda higher degree of Expectations SupportsNegotiating Strategies andCaregiving InterfaceWithin each subscale the scores were calculated byaveraging the relevant individual item scores Data imputation for missingvalues was not used as non-response for the items was very lowThe sub-scales were developed for separate use of each dimension thus they werenot combined into a single overall DDCS score
Pilot Testing of the DDC Scale
Sampling
Following institutional ethics review board approval the 49-item provi-sional DDCS was administered to an age-stratified sample of femalenurses randomly selected from the registry list of the College of Nursesof Ontario Because previous research suggested that approximately onehalf of the working nurse population is likely to provide care to anelderly relative 800 female full-time (more than 30 hoursweek) regis-tered nurses 40 years of age or older were asked to complete a mailed
Ward-Griffin Keefe Martin-Matthews Kerr Brown and Oudshoorn
CJNR 2009Vol 41 No 3 116
survey packageThe aim was to have 200 eligible DDC respondentscomplete and return the package which consisted of (1) an informationletter (2) a short demographic questionnaire which also determined eli-gibility for the study (3) the provisional DDCS described above and(4) established comparative measures including theWomenrsquos Role StrainInventory (WRSI) (Lengacher amp Sellers 2003) the CaregiverWell-BeingScale (CWBS) (Tebb et al 2000) and Health Related Outcomes(Medical Outcomes Study Short-Form SF-12 version 20 acute form4-week recall)The time needed to complete the survey package wasestimated at between 30 and 45 minutes Each package contained amodest gift certificate as a token of appreciation Nurses not providingcare for an elderly relative or friend were asked to complete all question-naires except the DDCS the purpose being to generate data for com-paring DDC and non-DDC nursesOf the 800 questionnaires mailed 394 were returned of these eight
respondents did not meet the eligibility criteria (two male and six unem-ployed) six questionnaires were blank and three were returned to senderyielding a sample of 377 respondents (49 response rate)A total of 193respondents (51) were caring for an elderly relative (ie the DDCs) and184 (49) were not (ie the non-DDCs)Of the 193 respondents iden-tified as DDCs six left sections of the DDCS blank which led to a finalusable DDC sample of 187 a total sample size that is considered adequatefor instrument development analysis (Gable ampWolf 1993)
Reliability and ConstructValidity Analyses
Contingency table (chi square) analyses were performed on all categori-cal variables while independent sample t tests were used with all contin-uous variables when comparing DDCs and non-DDCsAppropriatemeasures of association were used to examine the relationship betweentheoretically relevant demographic variables (eg hours of employmentper week hours of caregiving per week) and the CIConstruct validity of the provisional 49-item tool was assessed at the
preliminary stage with a combination of exploratory factor analysis (EFA)using a principal components factor approach and assessment of scalereliability Even though our previous qualitative work and initial concep-tualization of DDC informed the construction of the provisional DDCSitems EFA was selected over confirmatory factor analysis (CFA) For theEFA initial factor extraction was based on eigenvalues greater than 100(Polit amp Beck 2008 p 488) Each subscale of the provisional DDCS wasthen subjected to varimax rotation to select the factor structure that bestrepresented the underlying relationship of the items within the fourdimensions (Expectations Supports Negotiating Strategies andCaregiver Interface)Although loadings with an absolute value of 040 or
Development andValidation of the Double Duty Caregiving Scale
CJNR 2009Vol 41 No 3 117
higher are often used as factor loading cut-off values (Carruth 1996)smaller values are acceptable if the item pool is large (Polit amp Beck 2008p 491) Cronbachrsquos alpha reliability coefficients were also used to deter-mine internal consistency among the items of the four subscales of theprovisional DDCS Based on these preliminary analyses a combinationof low inter-item correlations (lt 20) weak factor loadings (lt 35)andor poor conceptual clarity 16 of the original 49 items were removedfrom the provisional DDCS yielding a tool with a total of 33 items forthe remaining construct validity analysesWe also correlated each of the DDCS subscale scores with those of
theWRSI the CWBS and the SF-12v2TheWRSI is a previously vali-dated 44-item five-point Likert scale that measures role strain in femalenurses with multiple roles (Lengacher amp Sellers 2003) with high relia-bility coefficients for the total scale (086ndash095) and subscales of distress(074ndash091) enhancement (079ndash089) and support (065ndash087)Developed and validated byTebb et al (2000) the CWBS-ShortVersionis a 16-item five-point Likert scale that assesses activities and needs ofcaregivers (eight items for each subscale) Overall and for each subscale(Needs and Activities of Daily Living) the coefficient alpha was 094091 and 088 respectively Finally the SF-12v2 is a well-established toolthat measures the perceptions and activities of acute health and well-being It is a shortened version of the SF-36 which includes general andphysical health index scores as well as eight subscales (bodily pain generalhealth vitality social functioning physical functioning role limitationsdue to physical problems role limitations due to emotional problems andmental health)Ware KosinskiTurner-Bowker and Gandek (2002) reportinternal consistency reliability coefficients ranging from 066 to 090 Inthe present study internal consistency reliability coefficients for each ofthese established instruments were 091 (WRSI) 073 (CWBS-needs)078 (CWBS-activities) and 080 (SF-12v2)
Results
Sample
The sample comprised 193 DDCs (this figure includes six respondentswho failed to complete all items on the DDCS but completed thedemographic questionnaire) and 184 non-DDCs (see Table 2 for anoverview)The typical DDC was 520 years old (range = 41ndash65 SD =490) was married (742) held a diploma in nursing (679) had amean household income of $101778 (range = $12500ndash$300000 SD =$4409373) was employed part-time or full-time (968) with a meanof 390 hours worked per week (range 7ndash80 SD 786) had practisednursing for 25 years or more (676) and had at least one child (ranging
Ward-Griffin Keefe Martin-Matthews Kerr Brown and Oudshoorn
CJNR 2009Vol 41 No 3 118
in age from 2 to 32 years) living with her (65)The DDC respondentsprovided an average of 6 hours per week of care to one (53) or two(30) elderly relativesmostly parents (77) or parents-in-law (12) wholived nearbyThe typical non-DDC respondent was 515 years old (range= 41ndash65 SD = 585) was married (739) held a diploma in nursing(678) had a mean household income of $105618 (range = $35000ndash$770000 SD = 6700684) was employed part-time or full-time (989)with a mean of 408 hours worked per week (range = 22ndash80) had prac-tised nursing for 25 years or more (525) and had at least one child(ranging in age from 1 to 37 years) living with her (620)There wereno significant differences between DDCs and non-DDCs with respect toage household income and number of hours worked per week
Preliminary ConstructValidity Step 1
To facilitate a better understanding of the item contents of the new scaleprincipal components analysis was conducted on each of the four sub-scales of the Provisional DDCSAlthough each dimension was provi-sionally structured as a single subscale the results of our subsequent factoranalysis suggested that Negotiating Strategies should be split into twosubscales Setting Limits and Making Connections Nine factors wereidentified from our analyses (Table 3) which is consistent with our orig-inal conceptualization about the dimensionality of DDCTwo factorsemerged from Expectations (familial expectations and professional expec-tations) accounting for 63 of the variance Five items loaded on famil-ial expectations with loadings ranging from 058 to 087 Four itemsloaded on professional expectations with loadings ranging from 049 to089As expected this indicates that among DDCs there are both famil-ial and professional expectations to provide care to elderly relatives
Development andValidation of the Double Duty Caregiving Scale
CJNR 2009Vol 41 No 3 119
Table 2 Overview of Development andValidation of Double DutyCaregiving Scale (DDCS)
Initial Item Pool ContentValidity Pilot Testing
Qualitative Mailed SurveySource Interview Data Expert Panel (n = 800)
Sample 37 female DDCs 4 female DDCs 377 female DDCs15 registered nurses 1 registered nurse 193 DDCs9 social workers 1 social worker 184 non-DDCs7 physiotherapists 1 physiotherapist6 physicians 1 physician
NoteDDC = double duty caregiver
Ward-Griffin Keefe Martin-Matthews Kerr Brown and Oudshoorn
CJNR 2009Vol 41 No 3 120
Tabl
e3
Revised
DDCS(N
=18
7)
Number
Item
-Total
Cronbachrsquos
Factor
Factor
Subscale
Factors
ofItem
sMean
SDCorrelations
Alpha
Variance
Loading
Exp
ectation
s378
712
Familialexpectations
5040ndash073
080
058ndash087
Professionalexpectations
4030ndash056
069
049ndash089
Total
9028ndash066
083
625
Supp
orts
332
646
Personalsupports
3043ndash058
068
070ndash086
Professionalsupports
3024ndash062
065
035ndash091
Total
6031ndash052
071
617
SettingLim
its
311
678
Awarenessofboundaries
3041ndash059
067
061ndash087
Activeresistance
3033ndash061
065
068ndash084
Total
6034ndash058
071
629
Mak
ingCon
nections
389
677
Makingconnections
5042ndash069
075
465
060ndash076
CaregivingIn
terface
301
826
Perceptionsofinterface
4048ndash071
081
080ndash084
Consequencesofinterface
3053ndash077
083
080ndash084
Total
7044ndash074
085
703
Two factors emerged from Supports (personal supports and profes-sional supports) accounting for 62 of the variance and indicating theimportance of personal and professional supports to DDCs providingcare to elderly relativesThree items loaded on personal supports withloadings ranging from 070 to 086Three items loaded on professionalsupports with loadings ranging from 035 to 091Two factors labelled Awareness of Boundaries and Active Resistance
emerged from Setting Limits accounting for 63 of the varianceThreeitems loaded on Awareness of Boundaries with loadings ranging from061 to 087Three items loaded on Active Resistance with loadingsranging from 068 to 084 One factor was extracted from MakingConnections accounting for 47 of the variance Loadings for the fiveitems on Making Connections ranged from 060 to 076This suggeststhat DDCs are aware of the boundaries between their personal and pro-fessional caregiving and that in an attempt to negotiate these boundariesthey resist providing care to their elderly relative as well as making con-nections to increase their supportsTwo factors emerged from CIThese were labelled Perceptions of CI
and Consequences of CI accounting for 70 of the variance Four itemsloaded on Perceptions of CI with loadings ranging from 054 to 085and three items loaded on Consequences of CI with loadings rangingfrom 080 to 084These results indicate that DDCs both are aware ofand experience consequences of the blurring of boundaries between per-sonal and professional caregiving
Reliability
Inter-item correlations and internal consistency (reliability) were exam-ined for each of the subscales of the Revised DDCSOverall in the finalversion of the 33-item DDCS inter-item correlations ranged from 024to 077 (Table 3) Cronbachrsquos alpha reliability coefficients of the fiveDDC subscales ranged from 085 (CI) to 071 (Supports and SettingLimits)Moreover Cronbachrsquos alpha reliability coefficients of the subscalefactors ranged from 083 (CI-Consequences) to 065 (for both Supports-Professional and Setting Limits-Active Resistance)
ConstructValidity Step 2
Pearson correlations were conducted to assess construct validity betweeneach of the subscales within the DDCS andWRSICWBS and SF-12v2(physical) and SF-12v2 (mental) (Table 3) In line with the underlyingtheory driving the scale there were weak to moderate correlations in theexpected direction between the Revised DDCS subscales ofExpectations Supports Setting LimitsMaking Connections and CI andthe established measuresThe strongest significant correlations were
Development andValidation of the Double Duty Caregiving Scale
CJNR 2009Vol 41 No 3 121
Ward-Griffin Keefe Martin-Matthews Kerr Brown and Oudshoorn
CJNR 2009Vol 41 No 3 122
Tabl
e4
Correlation
BetweenRevised
DDC
Subscalesan
dEstab
lished
Measures
Setting
Making
Caregiving
Scale
Expectations
Supports
Lim
its
Connections
Interface
WRSI
ar
-34
41
09
04
-49
p000
000
240
625
000
CaregiverWell-Being
Scale
r-16
34
-05
-01
-29
Activitiesb
p03
00
48
89
00
CaregiverWell-Being
Scale
r-16
34
03
-03
-36
Needsc
p04
00
71
69
00
SF12
PhysicalIndexd
r06
14
-14
-03
-02
p42
06
06
69
78
SF12
MentalIndex
dr
-26
26
09
01
-39
p00
22
22
60
00
Expectations
ar
1-12
-07
38
55
p095
344
000
000
Supportsa
r-12
104
10
-26
p095
552
174
000
Strategiesndash
r1
01
-23
SettingLimits
ap
851
002
Strategiesndash
r1
18
MakingConnections
ap
013
CaregivingInterfacea
r1
p
aN=187
bN=174
cN=180
dN=176plt05(2-tailed)
plt01(2-tailed)
between CI andWRSI (r = -49 p lt 001) between Supports andWRSI(r = 041 p lt001) and between CI and SF-12v2 (mental) (r = -39 p lt001) Finally the CI of the DDCS was also negatively correlated withcaregiver well-being (r = -29 p lt 001 [activities] and r = -36 p lt001[needs])The strongest subscale inter-correlations (ie within the Revised
DDCS itself) were between Expectations and CI (r = 055 p lt 001) andbetween Expectations and Making Connections (r = 038 p lt 001) Inaddition there was a weak positive association between MakingConnections and CI (r = 018 p lt 05) and negative associationsbetween Supports and CI (r = -026 p lt 001) and between SettingLimits and CI (r = -23 p lt 001) None of the other DDCS subscaleinter-correlations were statistically significant (Table 4)
Contrasted Groups Approach
Although there were no significant differences between DDCs andnon-DDCs in their overall scores for theWRSI CWBS and SF-12v2(physical and mental scores) there were significant differences betweennon-DDCs (n = 67) and the DDC subgroup (n = 84) defined as livingon the edge (ie those scoring above the mean on the CI subscale) Poorerhealth was observed for the living on the edge DDCs on their overall SF-12v2 mental health index score (t = -276 p lt 05) and on four of theeight SF-12v2 subscales vitality (t = -237 p lt 05) social functioning(t = -291 p lt 01) role emotional (t = -306 p lt 05) and mental health(t = -227 p lt 05) Moreover there were significant differences withinthe DDC group between those who were living on the edge and thosewith lower CI scores for the following SF-12 subscales vitality (t = -20p lt 05) social functioning (t = -356 p lt 01) role emotional (t = -483p lt 01) and mental health (t = -398 p lt 05)The living on the edgegroup also had significantly lower well-being scores for the activities(t = -363 p lt 05) and needs (t = -447 p lt 05) subscales than theother DDC respondentsWhile not all results were statistically significantoverall there was an observed tendency for the living on the edge group ofDDCs to have the lowest health and well-being scores whereas the otherDDCs (eg making it work) with low CI scores tended to have slightlybetter health scores than the non-DDC group
Discussion
The main purpose of this study was to develop and test a tool intendedto advance our understanding of DDC using a random sample of regis-tered nurses providing care to elderly relatives
Development andValidation of the Double Duty Caregiving Scale
CJNR 2009Vol 41 No 3 123
The nine factors we identified were consistent with the theorized coreDDC dimensions of Expectations (Familial and Professional) Supports(Personal and Professional) Setting Limits (Awareness of BoundariesActive Resistance) Making Connections and Caregiving Interface(Perceptions and Consequences) which can yield important informationregarding how much variance is accounted for by the factors Howeveradditional analyses are required to establish the psychometric propertiesof the DDCS including test-retest reliability to assess construct stabilityBased on the EFA results a measurement model of DDC will be pro-posed and analyzed in a future study using CFA to enhance the psycho-metric validation of the DDCS For researchers looking for a shorterversion of the DDCS it is worth noting that based on the strength andconsistency of the overall findings the seven-item CI subscale could beused to determine the extent of DDC when survey respondent burdenis a key factor in instrument selection (ie when use of the full 33DDCS items is not possible) adding to the potential value of the DDCS
The positive correlation between Expectations and CI and the nega-tive correlation between Supports and CI and between Setting Limitsand CI are theoretically consistent with the conceptual model of DDCThat is if expectations are high both personally and professionally withrespect to caring for onersquos relatives there will be greater CI or blurringof boundaries Conversely if one has strong personal and professionalsupports it follows that a lower degree of CI will result Similarly whenone sets limits on caregiving then less blurring or a lower degree of CIshould result However the positive association between MakingConnections and Expectations was unexpected Perhaps high expecta-tions lead one to increase supports by making connections both person-ally and professionally to help meet these expectationsComparison of the SF-12 v2 scores for living on the edge DDCs and
non-DDCs revealed significant differences for SF-12v2 mental healthand specific SF-12v2 subscales of vitality social functioning role emo-tional and mental healthThese findings suggest that DDCs who expe-rience a high degree of blurring of their professional and personalboundaries are at greater risk for poor health than those health profes-sionals who do not care for elderly relatives or who do not experiencethis blurring In addition those DDCs who could be characterized asliving on the edge scored significantly higher on the same four SF-12 sub-scales than DDCs with lower CI scoresThis observed pattern suggeststwo possibilities there exists a threshold effect for the negative healtheffects of DDC or manageable exposure to DDC has a beneficial effectFurther exploration of these interesting findings is warrantedAlthough we conducted a systematic and comprehensive analysis to
assess the psychometric properties of a new scale further reliability and
Ward-Griffin Keefe Martin-Matthews Kerr Brown and Oudshoorn
CJNR 2009Vol 41 No 3 124
validity studies are needed Confirmatory validation studies with otherhealth-care provider populations such as family physicians social workersand physiotherapists are particularly important as these professionals havethe potential to be DDCs and their experiences as documented in ouroriginal qualitative study of DDC helped to formulate the theoreticalunderpinnings of the DDCS In addition research with these groups willadvance our understanding of how occupational health groups may differin terms of expectations supports negotiating strategies and degree ofCIAs the identification of health-advantage and health-risk factors isinfluenced by health and social environments the negotiating strategiescould also be examined through the use of qualitative methodologiessuch as in-depth interviews or focus groupsFinally research that draws linkages between professional and personal
caregiving has the added value of furthering knowledge about employedcaregiving specifically as it relates to the relationship between health out-comes and provision of familial care by health-care providersAlthoughthe convergence (and avoidance) of professional and personal caregivingboundaries is not a new issue in nursing and other health professions thenotion that it is the individualrsquos responsibility to negotiate this boundarytends to predominate (Ward-Griffin 2008)To that end further testingand refinement of the DDCS will be helpful in identifying areas whereDDCs may need specific or different types of support It is also impor-tant to understand how specific social supports shape the health experi-ences of DDCs as well as to investigate different types of social supportinterventions with DDCsThis information is particularly meaningfultoday with the intersection of three challenges an aging population anaging health-care workforce and a shortage of health professionals Suchknowledge could contribute to workplace and other health initiativesspearheaded by professional groups policy-makers and other key stake-holders interested in assessing and addressing the health effects of DDCIn summary the DDCS is a valid tool for the assessment of double
duty caregiving Such assessment is a crucial step in understanding theexperience of the blurring of personal and professional boundaries ofcaregiving among health professionalsA quantitative study of both maleand female DDCs could help us to understand the relationship betweencertain factors (ie gender health-care occupation) and the potentialhealth effects of DDCMoreover our finding that respondents with highCI scores (living on the edge) had significantly lower health and well-beingscores than DDC respondents with lower CI scores warrants furtherinvestigation to determine if one group of DDCs is at particular risk fordeveloping negative health effects Given the current climate of health-care reform in Canada developing a better understanding of DDC andits health effects is particularly relevant for policy-makers and others who
Development andValidation of the Double Duty Caregiving Scale
CJNR 2009Vol 41 No 3 125
are committed to developing health-promoting programs and policies forfamilial caregivers of the elderly Clearly now is the time to monitor theeffects of changing demographics both in the general population andwithin the health professions in order to develop appropriate and tar-geted strategies thereby creating and sustaining healthy work environ-ments and health-care workforcesWith further refinement the DDCSmay assist with these endeavours
References
Armstrong P amp ArmstrongH (2004)Thinking it throughWomenwork andcaring in the new millennium In K Grant CArmaratunga PArmstrongM BoscoeA Pederson amp KWillson (Eds)Caring forcaring aboutWomenhome care and unpaid caregiving (pp 5ndash44)Aurora ONGaramond
Baines D (2004) Seven kinds of work ndash only one paid Raced gendered andrestructured work in social servicesAtlantis 28(2) 19ndash28
Canadian Institute for Health Information (2006)Workforce trends of registerednurses in Canada 2005 Retrieved November 5 2006 fromhttpsecurecihicacihiwebproductsndb_worforce_trends_registered_nurses_canada_2005_epdf
CarruthA K (1996) Development and testing of the Caregiver ReciprocityScaleNursing Research 45(2) 92ndash97
Chen F Feudtner C Rhodes L amp Green L (2001) Role conflicts of physi-cians and their family members Rules but no rule bookWestern Journal ofMedicine 175(4) 236ndash239
Cohen S Underwood L G amp Gottlieb BH (Eds) (2000) Social support mea-surement and interventionA guide for health and social scientistsOxford OxfordUniversity Press
Fast J (2005)Hidden costsinvisible contributions report Reworking workThe experi-ence of employed caregivers of older adults Retrieved August 16 2007 fromwwwhecolualbertacahcic
Gable R ampWolfe M (1993) Instrument development 2nd ed Boston KluwerGubermanN amp Maheu P (1999) Combining employment and caregivingAn
intricate juggling actCanadian Journal on Aging 18(1) 84ndash106Keefe J Leacutegareacute J amp CarriegravereY (2007) Developing new strategies to support
future caregivers of older Canadians with disabilities Projections of need andtheir policy implicationsCanadian Public Policy 33 S65ndash80
Lengacher CA amp Sellers E (2003)TheWomenrsquos Role Strain Inventory InO L Strickland amp CDilorio (Eds)Measurement of nursing outcomes 2nd ed(pp 109ndash127) NewYork Springer
Martin-MatthewsA (2000) Intergenerational caregivingHow apocalyptic anddominant demography frame the questions and shape the answers In EMGee amp GGutman (Eds)The overselling of population agingApocalyptic demog-raphy intergenerational challenges and social policy (pp 64ndash79)Toronto OxfordUniversity Press
Ward-Griffin Keefe Martin-Matthews Kerr Brown and Oudshoorn
CJNR 2009Vol 41 No 3 126
Mayall B (1993) Keeping children healthy ndash the intermediate domain SocialScience and Medicine 36(1) 77ndash83
Morris JM amp Field PA (1995) Qualitative research methods for health profession-als 2nd ed London Sage
Pascall G (1986) Social policyA feminist analysis NewYorkTavistockPhillips J BernardM amp ChittendenM (2002) Juggling work and careThe expe-riences of older adults Bristol Policy Press
Polit D F amp Beck CT (2008)Nursing research Generating and assessing evidencefor nursing practice 8th ed Philadelphia LippincottWilliams ampWilkins
Polit D F amp Beck CT amp Owen SV (2007) Is the CVI an acceptable indica-tor of content validity Appraisal and recommendationsResearch in Nursingand Health 30 459ndash467
RossMM Rideout EM amp CarsonMM (1996) Nursesrsquo work Balancingpersonal and professional caregiving careers Canadian Journal of NursingResearch 26(4) 43ndash59
RutmanD (1996) Caregiving as womenrsquos workWomenrsquos experiences of pow-erfulness and powerlessness as caregiversQualitative Health Research 6(1) 90ndash111
ShieldsM ampWilkins K (2005)National Survey of theWork and Health of Nurses2005 Provincial profiles Ottawa Statistics CanadaRetrieved August 24 2007from httpwwwstatcancaenglishresearch11-621-MIE11-621-MIE2006052htm
StaceyM amp Davies C (1983)Division of labour in child health care Final report toSSRCCoventry Sociology Department University ofWarwick
Tebb S (1995)An aid to empowermentA caregiver well-being scaleHealth andSocialWork 20(2) 87ndash92
Tebb S Berg-WgerM amp Rubio DM (2000) CaregiverWell-Being Scale InDRoyse BAThyer D K Padgett ampT K Logan (Eds) Program evaluation3rd ed (pp 320ndash323) Pacific Grove CA BrooksCole
Ungerson C (1990) The language of care Crossing the boundaries InCUngerson (Ed)Gender and caringWork and welfare in Britain and Scandinavia(pp 8ndash33) NewYork Harvester
WaltersV LentonR French S Eyles JMayr J amp Newbold B (1996) Paidwork unpaid work and social supportA study of the health of male andfemale nurses Social Science and Medicine 43(11) 1627ndash1636
Ward-Griffin C (2004) Nurses as caregivers of elderly relatives Negotiatingpersonal and professional boundariesCJNR 36(1) 92ndash114
Ward-Griffin C (2008)Health professionals caring for aging relativesA profes-sional or personal issue In AMartin-Matthews amp J Phillips (Eds)Blurringthe boundariesAgeing at the intersection of work and home life (pp 1ndash20) NewYorkTaylor amp FrancisPsychology Press
Ward-Griffin C Brown JVandervoortA McNair S amp Dashnay I (2005)Double duty caregivingWomen in the health professionsCanadian Journalon Aging 24(4) 379ndash394
Ward-Griffin C amp MarshallV (2003) Reconceptualizing the relationshipbetween public and private eldercare Journal of Aging Studies 17 189ndash208
Development andValidation of the Double Duty Caregiving Scale
CJNR 2009Vol 41 No 3 127
Ware J E Kosinksi MTurner-Bowker L amp Gandek B (2002)How to scoreversion 2 of the SF-12 health survey Lincoln RIQuality Metric Inc
Acknowledgements
This study was funded by the Social Sciences and Humanities ResearchCouncil (Internal) and the Institute of Gender and Health CanadianInstitutes of Health ResearchThere are no conflicts of interest or financial disclosures
CatherineWard-Griffin RN PhD is ProfessorArthur Labatt Family School ofNursing University ofWestern Ontario London Canada Janice Keefe PhD isProfessor and Canada Research Chair in Aging and Caregiving Policy FamilyStudies and GerontologyMount SaintVincent University HalifaxNova ScotiaCanadaAnne Martin-Matthews PhD is Professor School of SocialWork andFamily Studies University of British ColumbiaVancouver Canada MichaelKerr PhD is Associate ProfessorArthur Labatt Family School of NursingUniversity ofWestern Ontario Judith Belle Brown PhD is Professor Departmentof Family Medicine University ofWestern OntarioAbram Oudshoorn RN is aPhD candidate in the Arthur Labatt Family School of Nursing University ofWestern Ontario
Ward-Griffin Keefe Martin-Matthews Kerr Brown and Oudshoorn
CJNR 2009Vol 41 No 3 128

survey packageThe aim was to have 200 eligible DDC respondentscomplete and return the package which consisted of (1) an informationletter (2) a short demographic questionnaire which also determined eli-gibility for the study (3) the provisional DDCS described above and(4) established comparative measures including theWomenrsquos Role StrainInventory (WRSI) (Lengacher amp Sellers 2003) the CaregiverWell-BeingScale (CWBS) (Tebb et al 2000) and Health Related Outcomes(Medical Outcomes Study Short-Form SF-12 version 20 acute form4-week recall)The time needed to complete the survey package wasestimated at between 30 and 45 minutes Each package contained amodest gift certificate as a token of appreciation Nurses not providingcare for an elderly relative or friend were asked to complete all question-naires except the DDCS the purpose being to generate data for com-paring DDC and non-DDC nursesOf the 800 questionnaires mailed 394 were returned of these eight
respondents did not meet the eligibility criteria (two male and six unem-ployed) six questionnaires were blank and three were returned to senderyielding a sample of 377 respondents (49 response rate)A total of 193respondents (51) were caring for an elderly relative (ie the DDCs) and184 (49) were not (ie the non-DDCs)Of the 193 respondents iden-tified as DDCs six left sections of the DDCS blank which led to a finalusable DDC sample of 187 a total sample size that is considered adequatefor instrument development analysis (Gable ampWolf 1993)
Reliability and ConstructValidity Analyses
Contingency table (chi square) analyses were performed on all categori-cal variables while independent sample t tests were used with all contin-uous variables when comparing DDCs and non-DDCsAppropriatemeasures of association were used to examine the relationship betweentheoretically relevant demographic variables (eg hours of employmentper week hours of caregiving per week) and the CIConstruct validity of the provisional 49-item tool was assessed at the
preliminary stage with a combination of exploratory factor analysis (EFA)using a principal components factor approach and assessment of scalereliability Even though our previous qualitative work and initial concep-tualization of DDC informed the construction of the provisional DDCSitems EFA was selected over confirmatory factor analysis (CFA) For theEFA initial factor extraction was based on eigenvalues greater than 100(Polit amp Beck 2008 p 488) Each subscale of the provisional DDCS wasthen subjected to varimax rotation to select the factor structure that bestrepresented the underlying relationship of the items within the fourdimensions (Expectations Supports Negotiating Strategies andCaregiver Interface)Although loadings with an absolute value of 040 or
Development andValidation of the Double Duty Caregiving Scale
CJNR 2009Vol 41 No 3 117
higher are often used as factor loading cut-off values (Carruth 1996)smaller values are acceptable if the item pool is large (Polit amp Beck 2008p 491) Cronbachrsquos alpha reliability coefficients were also used to deter-mine internal consistency among the items of the four subscales of theprovisional DDCS Based on these preliminary analyses a combinationof low inter-item correlations (lt 20) weak factor loadings (lt 35)andor poor conceptual clarity 16 of the original 49 items were removedfrom the provisional DDCS yielding a tool with a total of 33 items forthe remaining construct validity analysesWe also correlated each of the DDCS subscale scores with those of
theWRSI the CWBS and the SF-12v2TheWRSI is a previously vali-dated 44-item five-point Likert scale that measures role strain in femalenurses with multiple roles (Lengacher amp Sellers 2003) with high relia-bility coefficients for the total scale (086ndash095) and subscales of distress(074ndash091) enhancement (079ndash089) and support (065ndash087)Developed and validated byTebb et al (2000) the CWBS-ShortVersionis a 16-item five-point Likert scale that assesses activities and needs ofcaregivers (eight items for each subscale) Overall and for each subscale(Needs and Activities of Daily Living) the coefficient alpha was 094091 and 088 respectively Finally the SF-12v2 is a well-established toolthat measures the perceptions and activities of acute health and well-being It is a shortened version of the SF-36 which includes general andphysical health index scores as well as eight subscales (bodily pain generalhealth vitality social functioning physical functioning role limitationsdue to physical problems role limitations due to emotional problems andmental health)Ware KosinskiTurner-Bowker and Gandek (2002) reportinternal consistency reliability coefficients ranging from 066 to 090 Inthe present study internal consistency reliability coefficients for each ofthese established instruments were 091 (WRSI) 073 (CWBS-needs)078 (CWBS-activities) and 080 (SF-12v2)
Results
Sample
The sample comprised 193 DDCs (this figure includes six respondentswho failed to complete all items on the DDCS but completed thedemographic questionnaire) and 184 non-DDCs (see Table 2 for anoverview)The typical DDC was 520 years old (range = 41ndash65 SD =490) was married (742) held a diploma in nursing (679) had amean household income of $101778 (range = $12500ndash$300000 SD =$4409373) was employed part-time or full-time (968) with a meanof 390 hours worked per week (range 7ndash80 SD 786) had practisednursing for 25 years or more (676) and had at least one child (ranging
Ward-Griffin Keefe Martin-Matthews Kerr Brown and Oudshoorn
CJNR 2009Vol 41 No 3 118
in age from 2 to 32 years) living with her (65)The DDC respondentsprovided an average of 6 hours per week of care to one (53) or two(30) elderly relativesmostly parents (77) or parents-in-law (12) wholived nearbyThe typical non-DDC respondent was 515 years old (range= 41ndash65 SD = 585) was married (739) held a diploma in nursing(678) had a mean household income of $105618 (range = $35000ndash$770000 SD = 6700684) was employed part-time or full-time (989)with a mean of 408 hours worked per week (range = 22ndash80) had prac-tised nursing for 25 years or more (525) and had at least one child(ranging in age from 1 to 37 years) living with her (620)There wereno significant differences between DDCs and non-DDCs with respect toage household income and number of hours worked per week
Preliminary ConstructValidity Step 1
To facilitate a better understanding of the item contents of the new scaleprincipal components analysis was conducted on each of the four sub-scales of the Provisional DDCSAlthough each dimension was provi-sionally structured as a single subscale the results of our subsequent factoranalysis suggested that Negotiating Strategies should be split into twosubscales Setting Limits and Making Connections Nine factors wereidentified from our analyses (Table 3) which is consistent with our orig-inal conceptualization about the dimensionality of DDCTwo factorsemerged from Expectations (familial expectations and professional expec-tations) accounting for 63 of the variance Five items loaded on famil-ial expectations with loadings ranging from 058 to 087 Four itemsloaded on professional expectations with loadings ranging from 049 to089As expected this indicates that among DDCs there are both famil-ial and professional expectations to provide care to elderly relatives
Development andValidation of the Double Duty Caregiving Scale
CJNR 2009Vol 41 No 3 119
Table 2 Overview of Development andValidation of Double DutyCaregiving Scale (DDCS)
Initial Item Pool ContentValidity Pilot Testing
Qualitative Mailed SurveySource Interview Data Expert Panel (n = 800)
Sample 37 female DDCs 4 female DDCs 377 female DDCs15 registered nurses 1 registered nurse 193 DDCs9 social workers 1 social worker 184 non-DDCs7 physiotherapists 1 physiotherapist6 physicians 1 physician
NoteDDC = double duty caregiver
Ward-Griffin Keefe Martin-Matthews Kerr Brown and Oudshoorn
CJNR 2009Vol 41 No 3 120
Tabl
e3
Revised
DDCS(N
=18
7)
Number
Item
-Total
Cronbachrsquos
Factor
Factor
Subscale
Factors
ofItem
sMean
SDCorrelations
Alpha
Variance
Loading
Exp
ectation
s378
712
Familialexpectations
5040ndash073
080
058ndash087
Professionalexpectations
4030ndash056
069
049ndash089
Total
9028ndash066
083
625
Supp
orts
332
646
Personalsupports
3043ndash058
068
070ndash086
Professionalsupports
3024ndash062
065
035ndash091
Total
6031ndash052
071
617
SettingLim
its
311
678
Awarenessofboundaries
3041ndash059
067
061ndash087
Activeresistance
3033ndash061
065
068ndash084
Total
6034ndash058
071
629
Mak
ingCon
nections
389
677
Makingconnections
5042ndash069
075
465
060ndash076
CaregivingIn
terface
301
826
Perceptionsofinterface
4048ndash071
081
080ndash084
Consequencesofinterface
3053ndash077
083
080ndash084
Total
7044ndash074
085
703
Two factors emerged from Supports (personal supports and profes-sional supports) accounting for 62 of the variance and indicating theimportance of personal and professional supports to DDCs providingcare to elderly relativesThree items loaded on personal supports withloadings ranging from 070 to 086Three items loaded on professionalsupports with loadings ranging from 035 to 091Two factors labelled Awareness of Boundaries and Active Resistance
emerged from Setting Limits accounting for 63 of the varianceThreeitems loaded on Awareness of Boundaries with loadings ranging from061 to 087Three items loaded on Active Resistance with loadingsranging from 068 to 084 One factor was extracted from MakingConnections accounting for 47 of the variance Loadings for the fiveitems on Making Connections ranged from 060 to 076This suggeststhat DDCs are aware of the boundaries between their personal and pro-fessional caregiving and that in an attempt to negotiate these boundariesthey resist providing care to their elderly relative as well as making con-nections to increase their supportsTwo factors emerged from CIThese were labelled Perceptions of CI
and Consequences of CI accounting for 70 of the variance Four itemsloaded on Perceptions of CI with loadings ranging from 054 to 085and three items loaded on Consequences of CI with loadings rangingfrom 080 to 084These results indicate that DDCs both are aware ofand experience consequences of the blurring of boundaries between per-sonal and professional caregiving
Reliability
Inter-item correlations and internal consistency (reliability) were exam-ined for each of the subscales of the Revised DDCSOverall in the finalversion of the 33-item DDCS inter-item correlations ranged from 024to 077 (Table 3) Cronbachrsquos alpha reliability coefficients of the fiveDDC subscales ranged from 085 (CI) to 071 (Supports and SettingLimits)Moreover Cronbachrsquos alpha reliability coefficients of the subscalefactors ranged from 083 (CI-Consequences) to 065 (for both Supports-Professional and Setting Limits-Active Resistance)
ConstructValidity Step 2
Pearson correlations were conducted to assess construct validity betweeneach of the subscales within the DDCS andWRSICWBS and SF-12v2(physical) and SF-12v2 (mental) (Table 3) In line with the underlyingtheory driving the scale there were weak to moderate correlations in theexpected direction between the Revised DDCS subscales ofExpectations Supports Setting LimitsMaking Connections and CI andthe established measuresThe strongest significant correlations were
Development andValidation of the Double Duty Caregiving Scale
CJNR 2009Vol 41 No 3 121
Ward-Griffin Keefe Martin-Matthews Kerr Brown and Oudshoorn
CJNR 2009Vol 41 No 3 122
Tabl
e4
Correlation
BetweenRevised
DDC
Subscalesan
dEstab
lished
Measures
Setting
Making
Caregiving
Scale
Expectations
Supports
Lim
its
Connections
Interface
WRSI
ar
-34
41
09
04
-49
p000
000
240
625
000
CaregiverWell-Being
Scale
r-16
34
-05
-01
-29
Activitiesb
p03
00
48
89
00
CaregiverWell-Being
Scale
r-16
34
03
-03
-36
Needsc
p04
00
71
69
00
SF12
PhysicalIndexd
r06
14
-14
-03
-02
p42
06
06
69
78
SF12
MentalIndex
dr
-26
26
09
01
-39
p00
22
22
60
00
Expectations
ar
1-12
-07
38
55
p095
344
000
000
Supportsa
r-12
104
10
-26
p095
552
174
000
Strategiesndash
r1
01
-23
SettingLimits
ap
851
002
Strategiesndash
r1
18
MakingConnections
ap
013
CaregivingInterfacea
r1
p
aN=187
bN=174
cN=180
dN=176plt05(2-tailed)
plt01(2-tailed)
between CI andWRSI (r = -49 p lt 001) between Supports andWRSI(r = 041 p lt001) and between CI and SF-12v2 (mental) (r = -39 p lt001) Finally the CI of the DDCS was also negatively correlated withcaregiver well-being (r = -29 p lt 001 [activities] and r = -36 p lt001[needs])The strongest subscale inter-correlations (ie within the Revised
DDCS itself) were between Expectations and CI (r = 055 p lt 001) andbetween Expectations and Making Connections (r = 038 p lt 001) Inaddition there was a weak positive association between MakingConnections and CI (r = 018 p lt 05) and negative associationsbetween Supports and CI (r = -026 p lt 001) and between SettingLimits and CI (r = -23 p lt 001) None of the other DDCS subscaleinter-correlations were statistically significant (Table 4)
Contrasted Groups Approach
Although there were no significant differences between DDCs andnon-DDCs in their overall scores for theWRSI CWBS and SF-12v2(physical and mental scores) there were significant differences betweennon-DDCs (n = 67) and the DDC subgroup (n = 84) defined as livingon the edge (ie those scoring above the mean on the CI subscale) Poorerhealth was observed for the living on the edge DDCs on their overall SF-12v2 mental health index score (t = -276 p lt 05) and on four of theeight SF-12v2 subscales vitality (t = -237 p lt 05) social functioning(t = -291 p lt 01) role emotional (t = -306 p lt 05) and mental health(t = -227 p lt 05) Moreover there were significant differences withinthe DDC group between those who were living on the edge and thosewith lower CI scores for the following SF-12 subscales vitality (t = -20p lt 05) social functioning (t = -356 p lt 01) role emotional (t = -483p lt 01) and mental health (t = -398 p lt 05)The living on the edgegroup also had significantly lower well-being scores for the activities(t = -363 p lt 05) and needs (t = -447 p lt 05) subscales than theother DDC respondentsWhile not all results were statistically significantoverall there was an observed tendency for the living on the edge group ofDDCs to have the lowest health and well-being scores whereas the otherDDCs (eg making it work) with low CI scores tended to have slightlybetter health scores than the non-DDC group
Discussion
The main purpose of this study was to develop and test a tool intendedto advance our understanding of DDC using a random sample of regis-tered nurses providing care to elderly relatives
Development andValidation of the Double Duty Caregiving Scale
CJNR 2009Vol 41 No 3 123
The nine factors we identified were consistent with the theorized coreDDC dimensions of Expectations (Familial and Professional) Supports(Personal and Professional) Setting Limits (Awareness of BoundariesActive Resistance) Making Connections and Caregiving Interface(Perceptions and Consequences) which can yield important informationregarding how much variance is accounted for by the factors Howeveradditional analyses are required to establish the psychometric propertiesof the DDCS including test-retest reliability to assess construct stabilityBased on the EFA results a measurement model of DDC will be pro-posed and analyzed in a future study using CFA to enhance the psycho-metric validation of the DDCS For researchers looking for a shorterversion of the DDCS it is worth noting that based on the strength andconsistency of the overall findings the seven-item CI subscale could beused to determine the extent of DDC when survey respondent burdenis a key factor in instrument selection (ie when use of the full 33DDCS items is not possible) adding to the potential value of the DDCS
The positive correlation between Expectations and CI and the nega-tive correlation between Supports and CI and between Setting Limitsand CI are theoretically consistent with the conceptual model of DDCThat is if expectations are high both personally and professionally withrespect to caring for onersquos relatives there will be greater CI or blurringof boundaries Conversely if one has strong personal and professionalsupports it follows that a lower degree of CI will result Similarly whenone sets limits on caregiving then less blurring or a lower degree of CIshould result However the positive association between MakingConnections and Expectations was unexpected Perhaps high expecta-tions lead one to increase supports by making connections both person-ally and professionally to help meet these expectationsComparison of the SF-12 v2 scores for living on the edge DDCs and
non-DDCs revealed significant differences for SF-12v2 mental healthand specific SF-12v2 subscales of vitality social functioning role emo-tional and mental healthThese findings suggest that DDCs who expe-rience a high degree of blurring of their professional and personalboundaries are at greater risk for poor health than those health profes-sionals who do not care for elderly relatives or who do not experiencethis blurring In addition those DDCs who could be characterized asliving on the edge scored significantly higher on the same four SF-12 sub-scales than DDCs with lower CI scoresThis observed pattern suggeststwo possibilities there exists a threshold effect for the negative healtheffects of DDC or manageable exposure to DDC has a beneficial effectFurther exploration of these interesting findings is warrantedAlthough we conducted a systematic and comprehensive analysis to
assess the psychometric properties of a new scale further reliability and
Ward-Griffin Keefe Martin-Matthews Kerr Brown and Oudshoorn
CJNR 2009Vol 41 No 3 124
validity studies are needed Confirmatory validation studies with otherhealth-care provider populations such as family physicians social workersand physiotherapists are particularly important as these professionals havethe potential to be DDCs and their experiences as documented in ouroriginal qualitative study of DDC helped to formulate the theoreticalunderpinnings of the DDCS In addition research with these groups willadvance our understanding of how occupational health groups may differin terms of expectations supports negotiating strategies and degree ofCIAs the identification of health-advantage and health-risk factors isinfluenced by health and social environments the negotiating strategiescould also be examined through the use of qualitative methodologiessuch as in-depth interviews or focus groupsFinally research that draws linkages between professional and personal
caregiving has the added value of furthering knowledge about employedcaregiving specifically as it relates to the relationship between health out-comes and provision of familial care by health-care providersAlthoughthe convergence (and avoidance) of professional and personal caregivingboundaries is not a new issue in nursing and other health professions thenotion that it is the individualrsquos responsibility to negotiate this boundarytends to predominate (Ward-Griffin 2008)To that end further testingand refinement of the DDCS will be helpful in identifying areas whereDDCs may need specific or different types of support It is also impor-tant to understand how specific social supports shape the health experi-ences of DDCs as well as to investigate different types of social supportinterventions with DDCsThis information is particularly meaningfultoday with the intersection of three challenges an aging population anaging health-care workforce and a shortage of health professionals Suchknowledge could contribute to workplace and other health initiativesspearheaded by professional groups policy-makers and other key stake-holders interested in assessing and addressing the health effects of DDCIn summary the DDCS is a valid tool for the assessment of double
duty caregiving Such assessment is a crucial step in understanding theexperience of the blurring of personal and professional boundaries ofcaregiving among health professionalsA quantitative study of both maleand female DDCs could help us to understand the relationship betweencertain factors (ie gender health-care occupation) and the potentialhealth effects of DDCMoreover our finding that respondents with highCI scores (living on the edge) had significantly lower health and well-beingscores than DDC respondents with lower CI scores warrants furtherinvestigation to determine if one group of DDCs is at particular risk fordeveloping negative health effects Given the current climate of health-care reform in Canada developing a better understanding of DDC andits health effects is particularly relevant for policy-makers and others who
Development andValidation of the Double Duty Caregiving Scale
CJNR 2009Vol 41 No 3 125
are committed to developing health-promoting programs and policies forfamilial caregivers of the elderly Clearly now is the time to monitor theeffects of changing demographics both in the general population andwithin the health professions in order to develop appropriate and tar-geted strategies thereby creating and sustaining healthy work environ-ments and health-care workforcesWith further refinement the DDCSmay assist with these endeavours
References
Armstrong P amp ArmstrongH (2004)Thinking it throughWomenwork andcaring in the new millennium In K Grant CArmaratunga PArmstrongM BoscoeA Pederson amp KWillson (Eds)Caring forcaring aboutWomenhome care and unpaid caregiving (pp 5ndash44)Aurora ONGaramond
Baines D (2004) Seven kinds of work ndash only one paid Raced gendered andrestructured work in social servicesAtlantis 28(2) 19ndash28
Canadian Institute for Health Information (2006)Workforce trends of registerednurses in Canada 2005 Retrieved November 5 2006 fromhttpsecurecihicacihiwebproductsndb_worforce_trends_registered_nurses_canada_2005_epdf
CarruthA K (1996) Development and testing of the Caregiver ReciprocityScaleNursing Research 45(2) 92ndash97
Chen F Feudtner C Rhodes L amp Green L (2001) Role conflicts of physi-cians and their family members Rules but no rule bookWestern Journal ofMedicine 175(4) 236ndash239
Cohen S Underwood L G amp Gottlieb BH (Eds) (2000) Social support mea-surement and interventionA guide for health and social scientistsOxford OxfordUniversity Press
Fast J (2005)Hidden costsinvisible contributions report Reworking workThe experi-ence of employed caregivers of older adults Retrieved August 16 2007 fromwwwhecolualbertacahcic
Gable R ampWolfe M (1993) Instrument development 2nd ed Boston KluwerGubermanN amp Maheu P (1999) Combining employment and caregivingAn
intricate juggling actCanadian Journal on Aging 18(1) 84ndash106Keefe J Leacutegareacute J amp CarriegravereY (2007) Developing new strategies to support
future caregivers of older Canadians with disabilities Projections of need andtheir policy implicationsCanadian Public Policy 33 S65ndash80
Lengacher CA amp Sellers E (2003)TheWomenrsquos Role Strain Inventory InO L Strickland amp CDilorio (Eds)Measurement of nursing outcomes 2nd ed(pp 109ndash127) NewYork Springer
Martin-MatthewsA (2000) Intergenerational caregivingHow apocalyptic anddominant demography frame the questions and shape the answers In EMGee amp GGutman (Eds)The overselling of population agingApocalyptic demog-raphy intergenerational challenges and social policy (pp 64ndash79)Toronto OxfordUniversity Press
Ward-Griffin Keefe Martin-Matthews Kerr Brown and Oudshoorn
CJNR 2009Vol 41 No 3 126
Mayall B (1993) Keeping children healthy ndash the intermediate domain SocialScience and Medicine 36(1) 77ndash83
Morris JM amp Field PA (1995) Qualitative research methods for health profession-als 2nd ed London Sage
Pascall G (1986) Social policyA feminist analysis NewYorkTavistockPhillips J BernardM amp ChittendenM (2002) Juggling work and careThe expe-riences of older adults Bristol Policy Press
Polit D F amp Beck CT (2008)Nursing research Generating and assessing evidencefor nursing practice 8th ed Philadelphia LippincottWilliams ampWilkins
Polit D F amp Beck CT amp Owen SV (2007) Is the CVI an acceptable indica-tor of content validity Appraisal and recommendationsResearch in Nursingand Health 30 459ndash467
RossMM Rideout EM amp CarsonMM (1996) Nursesrsquo work Balancingpersonal and professional caregiving careers Canadian Journal of NursingResearch 26(4) 43ndash59
RutmanD (1996) Caregiving as womenrsquos workWomenrsquos experiences of pow-erfulness and powerlessness as caregiversQualitative Health Research 6(1) 90ndash111
ShieldsM ampWilkins K (2005)National Survey of theWork and Health of Nurses2005 Provincial profiles Ottawa Statistics CanadaRetrieved August 24 2007from httpwwwstatcancaenglishresearch11-621-MIE11-621-MIE2006052htm
StaceyM amp Davies C (1983)Division of labour in child health care Final report toSSRCCoventry Sociology Department University ofWarwick
Tebb S (1995)An aid to empowermentA caregiver well-being scaleHealth andSocialWork 20(2) 87ndash92
Tebb S Berg-WgerM amp Rubio DM (2000) CaregiverWell-Being Scale InDRoyse BAThyer D K Padgett ampT K Logan (Eds) Program evaluation3rd ed (pp 320ndash323) Pacific Grove CA BrooksCole
Ungerson C (1990) The language of care Crossing the boundaries InCUngerson (Ed)Gender and caringWork and welfare in Britain and Scandinavia(pp 8ndash33) NewYork Harvester
WaltersV LentonR French S Eyles JMayr J amp Newbold B (1996) Paidwork unpaid work and social supportA study of the health of male andfemale nurses Social Science and Medicine 43(11) 1627ndash1636
Ward-Griffin C (2004) Nurses as caregivers of elderly relatives Negotiatingpersonal and professional boundariesCJNR 36(1) 92ndash114
Ward-Griffin C (2008)Health professionals caring for aging relativesA profes-sional or personal issue In AMartin-Matthews amp J Phillips (Eds)Blurringthe boundariesAgeing at the intersection of work and home life (pp 1ndash20) NewYorkTaylor amp FrancisPsychology Press
Ward-Griffin C Brown JVandervoortA McNair S amp Dashnay I (2005)Double duty caregivingWomen in the health professionsCanadian Journalon Aging 24(4) 379ndash394
Ward-Griffin C amp MarshallV (2003) Reconceptualizing the relationshipbetween public and private eldercare Journal of Aging Studies 17 189ndash208
Development andValidation of the Double Duty Caregiving Scale
CJNR 2009Vol 41 No 3 127
Ware J E Kosinksi MTurner-Bowker L amp Gandek B (2002)How to scoreversion 2 of the SF-12 health survey Lincoln RIQuality Metric Inc
Acknowledgements
This study was funded by the Social Sciences and Humanities ResearchCouncil (Internal) and the Institute of Gender and Health CanadianInstitutes of Health ResearchThere are no conflicts of interest or financial disclosures
CatherineWard-Griffin RN PhD is ProfessorArthur Labatt Family School ofNursing University ofWestern Ontario London Canada Janice Keefe PhD isProfessor and Canada Research Chair in Aging and Caregiving Policy FamilyStudies and GerontologyMount SaintVincent University HalifaxNova ScotiaCanadaAnne Martin-Matthews PhD is Professor School of SocialWork andFamily Studies University of British ColumbiaVancouver Canada MichaelKerr PhD is Associate ProfessorArthur Labatt Family School of NursingUniversity ofWestern Ontario Judith Belle Brown PhD is Professor Departmentof Family Medicine University ofWestern OntarioAbram Oudshoorn RN is aPhD candidate in the Arthur Labatt Family School of Nursing University ofWestern Ontario
Ward-Griffin Keefe Martin-Matthews Kerr Brown and Oudshoorn
CJNR 2009Vol 41 No 3 128

higher are often used as factor loading cut-off values (Carruth 1996)smaller values are acceptable if the item pool is large (Polit amp Beck 2008p 491) Cronbachrsquos alpha reliability coefficients were also used to deter-mine internal consistency among the items of the four subscales of theprovisional DDCS Based on these preliminary analyses a combinationof low inter-item correlations (lt 20) weak factor loadings (lt 35)andor poor conceptual clarity 16 of the original 49 items were removedfrom the provisional DDCS yielding a tool with a total of 33 items forthe remaining construct validity analysesWe also correlated each of the DDCS subscale scores with those of
theWRSI the CWBS and the SF-12v2TheWRSI is a previously vali-dated 44-item five-point Likert scale that measures role strain in femalenurses with multiple roles (Lengacher amp Sellers 2003) with high relia-bility coefficients for the total scale (086ndash095) and subscales of distress(074ndash091) enhancement (079ndash089) and support (065ndash087)Developed and validated byTebb et al (2000) the CWBS-ShortVersionis a 16-item five-point Likert scale that assesses activities and needs ofcaregivers (eight items for each subscale) Overall and for each subscale(Needs and Activities of Daily Living) the coefficient alpha was 094091 and 088 respectively Finally the SF-12v2 is a well-established toolthat measures the perceptions and activities of acute health and well-being It is a shortened version of the SF-36 which includes general andphysical health index scores as well as eight subscales (bodily pain generalhealth vitality social functioning physical functioning role limitationsdue to physical problems role limitations due to emotional problems andmental health)Ware KosinskiTurner-Bowker and Gandek (2002) reportinternal consistency reliability coefficients ranging from 066 to 090 Inthe present study internal consistency reliability coefficients for each ofthese established instruments were 091 (WRSI) 073 (CWBS-needs)078 (CWBS-activities) and 080 (SF-12v2)
Results
Sample
The sample comprised 193 DDCs (this figure includes six respondentswho failed to complete all items on the DDCS but completed thedemographic questionnaire) and 184 non-DDCs (see Table 2 for anoverview)The typical DDC was 520 years old (range = 41ndash65 SD =490) was married (742) held a diploma in nursing (679) had amean household income of $101778 (range = $12500ndash$300000 SD =$4409373) was employed part-time or full-time (968) with a meanof 390 hours worked per week (range 7ndash80 SD 786) had practisednursing for 25 years or more (676) and had at least one child (ranging
Ward-Griffin Keefe Martin-Matthews Kerr Brown and Oudshoorn
CJNR 2009Vol 41 No 3 118
in age from 2 to 32 years) living with her (65)The DDC respondentsprovided an average of 6 hours per week of care to one (53) or two(30) elderly relativesmostly parents (77) or parents-in-law (12) wholived nearbyThe typical non-DDC respondent was 515 years old (range= 41ndash65 SD = 585) was married (739) held a diploma in nursing(678) had a mean household income of $105618 (range = $35000ndash$770000 SD = 6700684) was employed part-time or full-time (989)with a mean of 408 hours worked per week (range = 22ndash80) had prac-tised nursing for 25 years or more (525) and had at least one child(ranging in age from 1 to 37 years) living with her (620)There wereno significant differences between DDCs and non-DDCs with respect toage household income and number of hours worked per week
Preliminary ConstructValidity Step 1
To facilitate a better understanding of the item contents of the new scaleprincipal components analysis was conducted on each of the four sub-scales of the Provisional DDCSAlthough each dimension was provi-sionally structured as a single subscale the results of our subsequent factoranalysis suggested that Negotiating Strategies should be split into twosubscales Setting Limits and Making Connections Nine factors wereidentified from our analyses (Table 3) which is consistent with our orig-inal conceptualization about the dimensionality of DDCTwo factorsemerged from Expectations (familial expectations and professional expec-tations) accounting for 63 of the variance Five items loaded on famil-ial expectations with loadings ranging from 058 to 087 Four itemsloaded on professional expectations with loadings ranging from 049 to089As expected this indicates that among DDCs there are both famil-ial and professional expectations to provide care to elderly relatives
Development andValidation of the Double Duty Caregiving Scale
CJNR 2009Vol 41 No 3 119
Table 2 Overview of Development andValidation of Double DutyCaregiving Scale (DDCS)
Initial Item Pool ContentValidity Pilot Testing
Qualitative Mailed SurveySource Interview Data Expert Panel (n = 800)
Sample 37 female DDCs 4 female DDCs 377 female DDCs15 registered nurses 1 registered nurse 193 DDCs9 social workers 1 social worker 184 non-DDCs7 physiotherapists 1 physiotherapist6 physicians 1 physician
NoteDDC = double duty caregiver
Ward-Griffin Keefe Martin-Matthews Kerr Brown and Oudshoorn
CJNR 2009Vol 41 No 3 120
Tabl
e3
Revised
DDCS(N
=18
7)
Number
Item
-Total
Cronbachrsquos
Factor
Factor
Subscale
Factors
ofItem
sMean
SDCorrelations
Alpha
Variance
Loading
Exp
ectation
s378
712
Familialexpectations
5040ndash073
080
058ndash087
Professionalexpectations
4030ndash056
069
049ndash089
Total
9028ndash066
083
625
Supp
orts
332
646
Personalsupports
3043ndash058
068
070ndash086
Professionalsupports
3024ndash062
065
035ndash091
Total
6031ndash052
071
617
SettingLim
its
311
678
Awarenessofboundaries
3041ndash059
067
061ndash087
Activeresistance
3033ndash061
065
068ndash084
Total
6034ndash058
071
629
Mak
ingCon
nections
389
677
Makingconnections
5042ndash069
075
465
060ndash076
CaregivingIn
terface
301
826
Perceptionsofinterface
4048ndash071
081
080ndash084
Consequencesofinterface
3053ndash077
083
080ndash084
Total
7044ndash074
085
703
Two factors emerged from Supports (personal supports and profes-sional supports) accounting for 62 of the variance and indicating theimportance of personal and professional supports to DDCs providingcare to elderly relativesThree items loaded on personal supports withloadings ranging from 070 to 086Three items loaded on professionalsupports with loadings ranging from 035 to 091Two factors labelled Awareness of Boundaries and Active Resistance
emerged from Setting Limits accounting for 63 of the varianceThreeitems loaded on Awareness of Boundaries with loadings ranging from061 to 087Three items loaded on Active Resistance with loadingsranging from 068 to 084 One factor was extracted from MakingConnections accounting for 47 of the variance Loadings for the fiveitems on Making Connections ranged from 060 to 076This suggeststhat DDCs are aware of the boundaries between their personal and pro-fessional caregiving and that in an attempt to negotiate these boundariesthey resist providing care to their elderly relative as well as making con-nections to increase their supportsTwo factors emerged from CIThese were labelled Perceptions of CI
and Consequences of CI accounting for 70 of the variance Four itemsloaded on Perceptions of CI with loadings ranging from 054 to 085and three items loaded on Consequences of CI with loadings rangingfrom 080 to 084These results indicate that DDCs both are aware ofand experience consequences of the blurring of boundaries between per-sonal and professional caregiving
Reliability
Inter-item correlations and internal consistency (reliability) were exam-ined for each of the subscales of the Revised DDCSOverall in the finalversion of the 33-item DDCS inter-item correlations ranged from 024to 077 (Table 3) Cronbachrsquos alpha reliability coefficients of the fiveDDC subscales ranged from 085 (CI) to 071 (Supports and SettingLimits)Moreover Cronbachrsquos alpha reliability coefficients of the subscalefactors ranged from 083 (CI-Consequences) to 065 (for both Supports-Professional and Setting Limits-Active Resistance)
ConstructValidity Step 2
Pearson correlations were conducted to assess construct validity betweeneach of the subscales within the DDCS andWRSICWBS and SF-12v2(physical) and SF-12v2 (mental) (Table 3) In line with the underlyingtheory driving the scale there were weak to moderate correlations in theexpected direction between the Revised DDCS subscales ofExpectations Supports Setting LimitsMaking Connections and CI andthe established measuresThe strongest significant correlations were
Development andValidation of the Double Duty Caregiving Scale
CJNR 2009Vol 41 No 3 121
Ward-Griffin Keefe Martin-Matthews Kerr Brown and Oudshoorn
CJNR 2009Vol 41 No 3 122
Tabl
e4
Correlation
BetweenRevised
DDC
Subscalesan
dEstab
lished
Measures
Setting
Making
Caregiving
Scale
Expectations
Supports
Lim
its
Connections
Interface
WRSI
ar
-34
41
09
04
-49
p000
000
240
625
000
CaregiverWell-Being
Scale
r-16
34
-05
-01
-29
Activitiesb
p03
00
48
89
00
CaregiverWell-Being
Scale
r-16
34
03
-03
-36
Needsc
p04
00
71
69
00
SF12
PhysicalIndexd
r06
14
-14
-03
-02
p42
06
06
69
78
SF12
MentalIndex
dr
-26
26
09
01
-39
p00
22
22
60
00
Expectations
ar
1-12
-07
38
55
p095
344
000
000
Supportsa
r-12
104
10
-26
p095
552
174
000
Strategiesndash
r1
01
-23
SettingLimits
ap
851
002
Strategiesndash
r1
18
MakingConnections
ap
013
CaregivingInterfacea
r1
p
aN=187
bN=174
cN=180
dN=176plt05(2-tailed)
plt01(2-tailed)
between CI andWRSI (r = -49 p lt 001) between Supports andWRSI(r = 041 p lt001) and between CI and SF-12v2 (mental) (r = -39 p lt001) Finally the CI of the DDCS was also negatively correlated withcaregiver well-being (r = -29 p lt 001 [activities] and r = -36 p lt001[needs])The strongest subscale inter-correlations (ie within the Revised
DDCS itself) were between Expectations and CI (r = 055 p lt 001) andbetween Expectations and Making Connections (r = 038 p lt 001) Inaddition there was a weak positive association between MakingConnections and CI (r = 018 p lt 05) and negative associationsbetween Supports and CI (r = -026 p lt 001) and between SettingLimits and CI (r = -23 p lt 001) None of the other DDCS subscaleinter-correlations were statistically significant (Table 4)
Contrasted Groups Approach
Although there were no significant differences between DDCs andnon-DDCs in their overall scores for theWRSI CWBS and SF-12v2(physical and mental scores) there were significant differences betweennon-DDCs (n = 67) and the DDC subgroup (n = 84) defined as livingon the edge (ie those scoring above the mean on the CI subscale) Poorerhealth was observed for the living on the edge DDCs on their overall SF-12v2 mental health index score (t = -276 p lt 05) and on four of theeight SF-12v2 subscales vitality (t = -237 p lt 05) social functioning(t = -291 p lt 01) role emotional (t = -306 p lt 05) and mental health(t = -227 p lt 05) Moreover there were significant differences withinthe DDC group between those who were living on the edge and thosewith lower CI scores for the following SF-12 subscales vitality (t = -20p lt 05) social functioning (t = -356 p lt 01) role emotional (t = -483p lt 01) and mental health (t = -398 p lt 05)The living on the edgegroup also had significantly lower well-being scores for the activities(t = -363 p lt 05) and needs (t = -447 p lt 05) subscales than theother DDC respondentsWhile not all results were statistically significantoverall there was an observed tendency for the living on the edge group ofDDCs to have the lowest health and well-being scores whereas the otherDDCs (eg making it work) with low CI scores tended to have slightlybetter health scores than the non-DDC group
Discussion
The main purpose of this study was to develop and test a tool intendedto advance our understanding of DDC using a random sample of regis-tered nurses providing care to elderly relatives
Development andValidation of the Double Duty Caregiving Scale
CJNR 2009Vol 41 No 3 123
The nine factors we identified were consistent with the theorized coreDDC dimensions of Expectations (Familial and Professional) Supports(Personal and Professional) Setting Limits (Awareness of BoundariesActive Resistance) Making Connections and Caregiving Interface(Perceptions and Consequences) which can yield important informationregarding how much variance is accounted for by the factors Howeveradditional analyses are required to establish the psychometric propertiesof the DDCS including test-retest reliability to assess construct stabilityBased on the EFA results a measurement model of DDC will be pro-posed and analyzed in a future study using CFA to enhance the psycho-metric validation of the DDCS For researchers looking for a shorterversion of the DDCS it is worth noting that based on the strength andconsistency of the overall findings the seven-item CI subscale could beused to determine the extent of DDC when survey respondent burdenis a key factor in instrument selection (ie when use of the full 33DDCS items is not possible) adding to the potential value of the DDCS
The positive correlation between Expectations and CI and the nega-tive correlation between Supports and CI and between Setting Limitsand CI are theoretically consistent with the conceptual model of DDCThat is if expectations are high both personally and professionally withrespect to caring for onersquos relatives there will be greater CI or blurringof boundaries Conversely if one has strong personal and professionalsupports it follows that a lower degree of CI will result Similarly whenone sets limits on caregiving then less blurring or a lower degree of CIshould result However the positive association between MakingConnections and Expectations was unexpected Perhaps high expecta-tions lead one to increase supports by making connections both person-ally and professionally to help meet these expectationsComparison of the SF-12 v2 scores for living on the edge DDCs and
non-DDCs revealed significant differences for SF-12v2 mental healthand specific SF-12v2 subscales of vitality social functioning role emo-tional and mental healthThese findings suggest that DDCs who expe-rience a high degree of blurring of their professional and personalboundaries are at greater risk for poor health than those health profes-sionals who do not care for elderly relatives or who do not experiencethis blurring In addition those DDCs who could be characterized asliving on the edge scored significantly higher on the same four SF-12 sub-scales than DDCs with lower CI scoresThis observed pattern suggeststwo possibilities there exists a threshold effect for the negative healtheffects of DDC or manageable exposure to DDC has a beneficial effectFurther exploration of these interesting findings is warrantedAlthough we conducted a systematic and comprehensive analysis to
assess the psychometric properties of a new scale further reliability and
Ward-Griffin Keefe Martin-Matthews Kerr Brown and Oudshoorn
CJNR 2009Vol 41 No 3 124
validity studies are needed Confirmatory validation studies with otherhealth-care provider populations such as family physicians social workersand physiotherapists are particularly important as these professionals havethe potential to be DDCs and their experiences as documented in ouroriginal qualitative study of DDC helped to formulate the theoreticalunderpinnings of the DDCS In addition research with these groups willadvance our understanding of how occupational health groups may differin terms of expectations supports negotiating strategies and degree ofCIAs the identification of health-advantage and health-risk factors isinfluenced by health and social environments the negotiating strategiescould also be examined through the use of qualitative methodologiessuch as in-depth interviews or focus groupsFinally research that draws linkages between professional and personal
caregiving has the added value of furthering knowledge about employedcaregiving specifically as it relates to the relationship between health out-comes and provision of familial care by health-care providersAlthoughthe convergence (and avoidance) of professional and personal caregivingboundaries is not a new issue in nursing and other health professions thenotion that it is the individualrsquos responsibility to negotiate this boundarytends to predominate (Ward-Griffin 2008)To that end further testingand refinement of the DDCS will be helpful in identifying areas whereDDCs may need specific or different types of support It is also impor-tant to understand how specific social supports shape the health experi-ences of DDCs as well as to investigate different types of social supportinterventions with DDCsThis information is particularly meaningfultoday with the intersection of three challenges an aging population anaging health-care workforce and a shortage of health professionals Suchknowledge could contribute to workplace and other health initiativesspearheaded by professional groups policy-makers and other key stake-holders interested in assessing and addressing the health effects of DDCIn summary the DDCS is a valid tool for the assessment of double
duty caregiving Such assessment is a crucial step in understanding theexperience of the blurring of personal and professional boundaries ofcaregiving among health professionalsA quantitative study of both maleand female DDCs could help us to understand the relationship betweencertain factors (ie gender health-care occupation) and the potentialhealth effects of DDCMoreover our finding that respondents with highCI scores (living on the edge) had significantly lower health and well-beingscores than DDC respondents with lower CI scores warrants furtherinvestigation to determine if one group of DDCs is at particular risk fordeveloping negative health effects Given the current climate of health-care reform in Canada developing a better understanding of DDC andits health effects is particularly relevant for policy-makers and others who
Development andValidation of the Double Duty Caregiving Scale
CJNR 2009Vol 41 No 3 125
are committed to developing health-promoting programs and policies forfamilial caregivers of the elderly Clearly now is the time to monitor theeffects of changing demographics both in the general population andwithin the health professions in order to develop appropriate and tar-geted strategies thereby creating and sustaining healthy work environ-ments and health-care workforcesWith further refinement the DDCSmay assist with these endeavours
References
Armstrong P amp ArmstrongH (2004)Thinking it throughWomenwork andcaring in the new millennium In K Grant CArmaratunga PArmstrongM BoscoeA Pederson amp KWillson (Eds)Caring forcaring aboutWomenhome care and unpaid caregiving (pp 5ndash44)Aurora ONGaramond
Baines D (2004) Seven kinds of work ndash only one paid Raced gendered andrestructured work in social servicesAtlantis 28(2) 19ndash28
Canadian Institute for Health Information (2006)Workforce trends of registerednurses in Canada 2005 Retrieved November 5 2006 fromhttpsecurecihicacihiwebproductsndb_worforce_trends_registered_nurses_canada_2005_epdf
CarruthA K (1996) Development and testing of the Caregiver ReciprocityScaleNursing Research 45(2) 92ndash97
Chen F Feudtner C Rhodes L amp Green L (2001) Role conflicts of physi-cians and their family members Rules but no rule bookWestern Journal ofMedicine 175(4) 236ndash239
Cohen S Underwood L G amp Gottlieb BH (Eds) (2000) Social support mea-surement and interventionA guide for health and social scientistsOxford OxfordUniversity Press
Fast J (2005)Hidden costsinvisible contributions report Reworking workThe experi-ence of employed caregivers of older adults Retrieved August 16 2007 fromwwwhecolualbertacahcic
Gable R ampWolfe M (1993) Instrument development 2nd ed Boston KluwerGubermanN amp Maheu P (1999) Combining employment and caregivingAn
intricate juggling actCanadian Journal on Aging 18(1) 84ndash106Keefe J Leacutegareacute J amp CarriegravereY (2007) Developing new strategies to support
future caregivers of older Canadians with disabilities Projections of need andtheir policy implicationsCanadian Public Policy 33 S65ndash80
Lengacher CA amp Sellers E (2003)TheWomenrsquos Role Strain Inventory InO L Strickland amp CDilorio (Eds)Measurement of nursing outcomes 2nd ed(pp 109ndash127) NewYork Springer
Martin-MatthewsA (2000) Intergenerational caregivingHow apocalyptic anddominant demography frame the questions and shape the answers In EMGee amp GGutman (Eds)The overselling of population agingApocalyptic demog-raphy intergenerational challenges and social policy (pp 64ndash79)Toronto OxfordUniversity Press
Ward-Griffin Keefe Martin-Matthews Kerr Brown and Oudshoorn
CJNR 2009Vol 41 No 3 126
Mayall B (1993) Keeping children healthy ndash the intermediate domain SocialScience and Medicine 36(1) 77ndash83
Morris JM amp Field PA (1995) Qualitative research methods for health profession-als 2nd ed London Sage
Pascall G (1986) Social policyA feminist analysis NewYorkTavistockPhillips J BernardM amp ChittendenM (2002) Juggling work and careThe expe-riences of older adults Bristol Policy Press
Polit D F amp Beck CT (2008)Nursing research Generating and assessing evidencefor nursing practice 8th ed Philadelphia LippincottWilliams ampWilkins
Polit D F amp Beck CT amp Owen SV (2007) Is the CVI an acceptable indica-tor of content validity Appraisal and recommendationsResearch in Nursingand Health 30 459ndash467
RossMM Rideout EM amp CarsonMM (1996) Nursesrsquo work Balancingpersonal and professional caregiving careers Canadian Journal of NursingResearch 26(4) 43ndash59
RutmanD (1996) Caregiving as womenrsquos workWomenrsquos experiences of pow-erfulness and powerlessness as caregiversQualitative Health Research 6(1) 90ndash111
ShieldsM ampWilkins K (2005)National Survey of theWork and Health of Nurses2005 Provincial profiles Ottawa Statistics CanadaRetrieved August 24 2007from httpwwwstatcancaenglishresearch11-621-MIE11-621-MIE2006052htm
StaceyM amp Davies C (1983)Division of labour in child health care Final report toSSRCCoventry Sociology Department University ofWarwick
Tebb S (1995)An aid to empowermentA caregiver well-being scaleHealth andSocialWork 20(2) 87ndash92
Tebb S Berg-WgerM amp Rubio DM (2000) CaregiverWell-Being Scale InDRoyse BAThyer D K Padgett ampT K Logan (Eds) Program evaluation3rd ed (pp 320ndash323) Pacific Grove CA BrooksCole
Ungerson C (1990) The language of care Crossing the boundaries InCUngerson (Ed)Gender and caringWork and welfare in Britain and Scandinavia(pp 8ndash33) NewYork Harvester
WaltersV LentonR French S Eyles JMayr J amp Newbold B (1996) Paidwork unpaid work and social supportA study of the health of male andfemale nurses Social Science and Medicine 43(11) 1627ndash1636
Ward-Griffin C (2004) Nurses as caregivers of elderly relatives Negotiatingpersonal and professional boundariesCJNR 36(1) 92ndash114
Ward-Griffin C (2008)Health professionals caring for aging relativesA profes-sional or personal issue In AMartin-Matthews amp J Phillips (Eds)Blurringthe boundariesAgeing at the intersection of work and home life (pp 1ndash20) NewYorkTaylor amp FrancisPsychology Press
Ward-Griffin C Brown JVandervoortA McNair S amp Dashnay I (2005)Double duty caregivingWomen in the health professionsCanadian Journalon Aging 24(4) 379ndash394
Ward-Griffin C amp MarshallV (2003) Reconceptualizing the relationshipbetween public and private eldercare Journal of Aging Studies 17 189ndash208
Development andValidation of the Double Duty Caregiving Scale
CJNR 2009Vol 41 No 3 127
Ware J E Kosinksi MTurner-Bowker L amp Gandek B (2002)How to scoreversion 2 of the SF-12 health survey Lincoln RIQuality Metric Inc
Acknowledgements
This study was funded by the Social Sciences and Humanities ResearchCouncil (Internal) and the Institute of Gender and Health CanadianInstitutes of Health ResearchThere are no conflicts of interest or financial disclosures
CatherineWard-Griffin RN PhD is ProfessorArthur Labatt Family School ofNursing University ofWestern Ontario London Canada Janice Keefe PhD isProfessor and Canada Research Chair in Aging and Caregiving Policy FamilyStudies and GerontologyMount SaintVincent University HalifaxNova ScotiaCanadaAnne Martin-Matthews PhD is Professor School of SocialWork andFamily Studies University of British ColumbiaVancouver Canada MichaelKerr PhD is Associate ProfessorArthur Labatt Family School of NursingUniversity ofWestern Ontario Judith Belle Brown PhD is Professor Departmentof Family Medicine University ofWestern OntarioAbram Oudshoorn RN is aPhD candidate in the Arthur Labatt Family School of Nursing University ofWestern Ontario
Ward-Griffin Keefe Martin-Matthews Kerr Brown and Oudshoorn
CJNR 2009Vol 41 No 3 128

in age from 2 to 32 years) living with her (65)The DDC respondentsprovided an average of 6 hours per week of care to one (53) or two(30) elderly relativesmostly parents (77) or parents-in-law (12) wholived nearbyThe typical non-DDC respondent was 515 years old (range= 41ndash65 SD = 585) was married (739) held a diploma in nursing(678) had a mean household income of $105618 (range = $35000ndash$770000 SD = 6700684) was employed part-time or full-time (989)with a mean of 408 hours worked per week (range = 22ndash80) had prac-tised nursing for 25 years or more (525) and had at least one child(ranging in age from 1 to 37 years) living with her (620)There wereno significant differences between DDCs and non-DDCs with respect toage household income and number of hours worked per week
Preliminary ConstructValidity Step 1
To facilitate a better understanding of the item contents of the new scaleprincipal components analysis was conducted on each of the four sub-scales of the Provisional DDCSAlthough each dimension was provi-sionally structured as a single subscale the results of our subsequent factoranalysis suggested that Negotiating Strategies should be split into twosubscales Setting Limits and Making Connections Nine factors wereidentified from our analyses (Table 3) which is consistent with our orig-inal conceptualization about the dimensionality of DDCTwo factorsemerged from Expectations (familial expectations and professional expec-tations) accounting for 63 of the variance Five items loaded on famil-ial expectations with loadings ranging from 058 to 087 Four itemsloaded on professional expectations with loadings ranging from 049 to089As expected this indicates that among DDCs there are both famil-ial and professional expectations to provide care to elderly relatives
Development andValidation of the Double Duty Caregiving Scale
CJNR 2009Vol 41 No 3 119
Table 2 Overview of Development andValidation of Double DutyCaregiving Scale (DDCS)
Initial Item Pool ContentValidity Pilot Testing
Qualitative Mailed SurveySource Interview Data Expert Panel (n = 800)
Sample 37 female DDCs 4 female DDCs 377 female DDCs15 registered nurses 1 registered nurse 193 DDCs9 social workers 1 social worker 184 non-DDCs7 physiotherapists 1 physiotherapist6 physicians 1 physician
NoteDDC = double duty caregiver
Ward-Griffin Keefe Martin-Matthews Kerr Brown and Oudshoorn
CJNR 2009Vol 41 No 3 120
Tabl
e3
Revised
DDCS(N
=18
7)
Number
Item
-Total
Cronbachrsquos
Factor
Factor
Subscale
Factors
ofItem
sMean
SDCorrelations
Alpha
Variance
Loading
Exp
ectation
s378
712
Familialexpectations
5040ndash073
080
058ndash087
Professionalexpectations
4030ndash056
069
049ndash089
Total
9028ndash066
083
625
Supp
orts
332
646
Personalsupports
3043ndash058
068
070ndash086
Professionalsupports
3024ndash062
065
035ndash091
Total
6031ndash052
071
617
SettingLim
its
311
678
Awarenessofboundaries
3041ndash059
067
061ndash087
Activeresistance
3033ndash061
065
068ndash084
Total
6034ndash058
071
629
Mak
ingCon
nections
389
677
Makingconnections
5042ndash069
075
465
060ndash076
CaregivingIn
terface
301
826
Perceptionsofinterface
4048ndash071
081
080ndash084
Consequencesofinterface
3053ndash077
083
080ndash084
Total
7044ndash074
085
703
Two factors emerged from Supports (personal supports and profes-sional supports) accounting for 62 of the variance and indicating theimportance of personal and professional supports to DDCs providingcare to elderly relativesThree items loaded on personal supports withloadings ranging from 070 to 086Three items loaded on professionalsupports with loadings ranging from 035 to 091Two factors labelled Awareness of Boundaries and Active Resistance
emerged from Setting Limits accounting for 63 of the varianceThreeitems loaded on Awareness of Boundaries with loadings ranging from061 to 087Three items loaded on Active Resistance with loadingsranging from 068 to 084 One factor was extracted from MakingConnections accounting for 47 of the variance Loadings for the fiveitems on Making Connections ranged from 060 to 076This suggeststhat DDCs are aware of the boundaries between their personal and pro-fessional caregiving and that in an attempt to negotiate these boundariesthey resist providing care to their elderly relative as well as making con-nections to increase their supportsTwo factors emerged from CIThese were labelled Perceptions of CI
and Consequences of CI accounting for 70 of the variance Four itemsloaded on Perceptions of CI with loadings ranging from 054 to 085and three items loaded on Consequences of CI with loadings rangingfrom 080 to 084These results indicate that DDCs both are aware ofand experience consequences of the blurring of boundaries between per-sonal and professional caregiving
Reliability
Inter-item correlations and internal consistency (reliability) were exam-ined for each of the subscales of the Revised DDCSOverall in the finalversion of the 33-item DDCS inter-item correlations ranged from 024to 077 (Table 3) Cronbachrsquos alpha reliability coefficients of the fiveDDC subscales ranged from 085 (CI) to 071 (Supports and SettingLimits)Moreover Cronbachrsquos alpha reliability coefficients of the subscalefactors ranged from 083 (CI-Consequences) to 065 (for both Supports-Professional and Setting Limits-Active Resistance)
ConstructValidity Step 2
Pearson correlations were conducted to assess construct validity betweeneach of the subscales within the DDCS andWRSICWBS and SF-12v2(physical) and SF-12v2 (mental) (Table 3) In line with the underlyingtheory driving the scale there were weak to moderate correlations in theexpected direction between the Revised DDCS subscales ofExpectations Supports Setting LimitsMaking Connections and CI andthe established measuresThe strongest significant correlations were
Development andValidation of the Double Duty Caregiving Scale
CJNR 2009Vol 41 No 3 121
Ward-Griffin Keefe Martin-Matthews Kerr Brown and Oudshoorn
CJNR 2009Vol 41 No 3 122
Tabl
e4
Correlation
BetweenRevised
DDC
Subscalesan
dEstab
lished
Measures
Setting
Making
Caregiving
Scale
Expectations
Supports
Lim
its
Connections
Interface
WRSI
ar
-34
41
09
04
-49
p000
000
240
625
000
CaregiverWell-Being
Scale
r-16
34
-05
-01
-29
Activitiesb
p03
00
48
89
00
CaregiverWell-Being
Scale
r-16
34
03
-03
-36
Needsc
p04
00
71
69
00
SF12
PhysicalIndexd
r06
14
-14
-03
-02
p42
06
06
69
78
SF12
MentalIndex
dr
-26
26
09
01
-39
p00
22
22
60
00
Expectations
ar
1-12
-07
38
55
p095
344
000
000
Supportsa
r-12
104
10
-26
p095
552
174
000
Strategiesndash
r1
01
-23
SettingLimits
ap
851
002
Strategiesndash
r1
18
MakingConnections
ap
013
CaregivingInterfacea
r1
p
aN=187
bN=174
cN=180
dN=176plt05(2-tailed)
plt01(2-tailed)
between CI andWRSI (r = -49 p lt 001) between Supports andWRSI(r = 041 p lt001) and between CI and SF-12v2 (mental) (r = -39 p lt001) Finally the CI of the DDCS was also negatively correlated withcaregiver well-being (r = -29 p lt 001 [activities] and r = -36 p lt001[needs])The strongest subscale inter-correlations (ie within the Revised
DDCS itself) were between Expectations and CI (r = 055 p lt 001) andbetween Expectations and Making Connections (r = 038 p lt 001) Inaddition there was a weak positive association between MakingConnections and CI (r = 018 p lt 05) and negative associationsbetween Supports and CI (r = -026 p lt 001) and between SettingLimits and CI (r = -23 p lt 001) None of the other DDCS subscaleinter-correlations were statistically significant (Table 4)
Contrasted Groups Approach
Although there were no significant differences between DDCs andnon-DDCs in their overall scores for theWRSI CWBS and SF-12v2(physical and mental scores) there were significant differences betweennon-DDCs (n = 67) and the DDC subgroup (n = 84) defined as livingon the edge (ie those scoring above the mean on the CI subscale) Poorerhealth was observed for the living on the edge DDCs on their overall SF-12v2 mental health index score (t = -276 p lt 05) and on four of theeight SF-12v2 subscales vitality (t = -237 p lt 05) social functioning(t = -291 p lt 01) role emotional (t = -306 p lt 05) and mental health(t = -227 p lt 05) Moreover there were significant differences withinthe DDC group between those who were living on the edge and thosewith lower CI scores for the following SF-12 subscales vitality (t = -20p lt 05) social functioning (t = -356 p lt 01) role emotional (t = -483p lt 01) and mental health (t = -398 p lt 05)The living on the edgegroup also had significantly lower well-being scores for the activities(t = -363 p lt 05) and needs (t = -447 p lt 05) subscales than theother DDC respondentsWhile not all results were statistically significantoverall there was an observed tendency for the living on the edge group ofDDCs to have the lowest health and well-being scores whereas the otherDDCs (eg making it work) with low CI scores tended to have slightlybetter health scores than the non-DDC group
Discussion
The main purpose of this study was to develop and test a tool intendedto advance our understanding of DDC using a random sample of regis-tered nurses providing care to elderly relatives
Development andValidation of the Double Duty Caregiving Scale
CJNR 2009Vol 41 No 3 123
The nine factors we identified were consistent with the theorized coreDDC dimensions of Expectations (Familial and Professional) Supports(Personal and Professional) Setting Limits (Awareness of BoundariesActive Resistance) Making Connections and Caregiving Interface(Perceptions and Consequences) which can yield important informationregarding how much variance is accounted for by the factors Howeveradditional analyses are required to establish the psychometric propertiesof the DDCS including test-retest reliability to assess construct stabilityBased on the EFA results a measurement model of DDC will be pro-posed and analyzed in a future study using CFA to enhance the psycho-metric validation of the DDCS For researchers looking for a shorterversion of the DDCS it is worth noting that based on the strength andconsistency of the overall findings the seven-item CI subscale could beused to determine the extent of DDC when survey respondent burdenis a key factor in instrument selection (ie when use of the full 33DDCS items is not possible) adding to the potential value of the DDCS
The positive correlation between Expectations and CI and the nega-tive correlation between Supports and CI and between Setting Limitsand CI are theoretically consistent with the conceptual model of DDCThat is if expectations are high both personally and professionally withrespect to caring for onersquos relatives there will be greater CI or blurringof boundaries Conversely if one has strong personal and professionalsupports it follows that a lower degree of CI will result Similarly whenone sets limits on caregiving then less blurring or a lower degree of CIshould result However the positive association between MakingConnections and Expectations was unexpected Perhaps high expecta-tions lead one to increase supports by making connections both person-ally and professionally to help meet these expectationsComparison of the SF-12 v2 scores for living on the edge DDCs and
non-DDCs revealed significant differences for SF-12v2 mental healthand specific SF-12v2 subscales of vitality social functioning role emo-tional and mental healthThese findings suggest that DDCs who expe-rience a high degree of blurring of their professional and personalboundaries are at greater risk for poor health than those health profes-sionals who do not care for elderly relatives or who do not experiencethis blurring In addition those DDCs who could be characterized asliving on the edge scored significantly higher on the same four SF-12 sub-scales than DDCs with lower CI scoresThis observed pattern suggeststwo possibilities there exists a threshold effect for the negative healtheffects of DDC or manageable exposure to DDC has a beneficial effectFurther exploration of these interesting findings is warrantedAlthough we conducted a systematic and comprehensive analysis to
assess the psychometric properties of a new scale further reliability and
Ward-Griffin Keefe Martin-Matthews Kerr Brown and Oudshoorn
CJNR 2009Vol 41 No 3 124
validity studies are needed Confirmatory validation studies with otherhealth-care provider populations such as family physicians social workersand physiotherapists are particularly important as these professionals havethe potential to be DDCs and their experiences as documented in ouroriginal qualitative study of DDC helped to formulate the theoreticalunderpinnings of the DDCS In addition research with these groups willadvance our understanding of how occupational health groups may differin terms of expectations supports negotiating strategies and degree ofCIAs the identification of health-advantage and health-risk factors isinfluenced by health and social environments the negotiating strategiescould also be examined through the use of qualitative methodologiessuch as in-depth interviews or focus groupsFinally research that draws linkages between professional and personal
caregiving has the added value of furthering knowledge about employedcaregiving specifically as it relates to the relationship between health out-comes and provision of familial care by health-care providersAlthoughthe convergence (and avoidance) of professional and personal caregivingboundaries is not a new issue in nursing and other health professions thenotion that it is the individualrsquos responsibility to negotiate this boundarytends to predominate (Ward-Griffin 2008)To that end further testingand refinement of the DDCS will be helpful in identifying areas whereDDCs may need specific or different types of support It is also impor-tant to understand how specific social supports shape the health experi-ences of DDCs as well as to investigate different types of social supportinterventions with DDCsThis information is particularly meaningfultoday with the intersection of three challenges an aging population anaging health-care workforce and a shortage of health professionals Suchknowledge could contribute to workplace and other health initiativesspearheaded by professional groups policy-makers and other key stake-holders interested in assessing and addressing the health effects of DDCIn summary the DDCS is a valid tool for the assessment of double
duty caregiving Such assessment is a crucial step in understanding theexperience of the blurring of personal and professional boundaries ofcaregiving among health professionalsA quantitative study of both maleand female DDCs could help us to understand the relationship betweencertain factors (ie gender health-care occupation) and the potentialhealth effects of DDCMoreover our finding that respondents with highCI scores (living on the edge) had significantly lower health and well-beingscores than DDC respondents with lower CI scores warrants furtherinvestigation to determine if one group of DDCs is at particular risk fordeveloping negative health effects Given the current climate of health-care reform in Canada developing a better understanding of DDC andits health effects is particularly relevant for policy-makers and others who
Development andValidation of the Double Duty Caregiving Scale
CJNR 2009Vol 41 No 3 125
are committed to developing health-promoting programs and policies forfamilial caregivers of the elderly Clearly now is the time to monitor theeffects of changing demographics both in the general population andwithin the health professions in order to develop appropriate and tar-geted strategies thereby creating and sustaining healthy work environ-ments and health-care workforcesWith further refinement the DDCSmay assist with these endeavours
References
Armstrong P amp ArmstrongH (2004)Thinking it throughWomenwork andcaring in the new millennium In K Grant CArmaratunga PArmstrongM BoscoeA Pederson amp KWillson (Eds)Caring forcaring aboutWomenhome care and unpaid caregiving (pp 5ndash44)Aurora ONGaramond
Baines D (2004) Seven kinds of work ndash only one paid Raced gendered andrestructured work in social servicesAtlantis 28(2) 19ndash28
Canadian Institute for Health Information (2006)Workforce trends of registerednurses in Canada 2005 Retrieved November 5 2006 fromhttpsecurecihicacihiwebproductsndb_worforce_trends_registered_nurses_canada_2005_epdf
CarruthA K (1996) Development and testing of the Caregiver ReciprocityScaleNursing Research 45(2) 92ndash97
Chen F Feudtner C Rhodes L amp Green L (2001) Role conflicts of physi-cians and their family members Rules but no rule bookWestern Journal ofMedicine 175(4) 236ndash239
Cohen S Underwood L G amp Gottlieb BH (Eds) (2000) Social support mea-surement and interventionA guide for health and social scientistsOxford OxfordUniversity Press
Fast J (2005)Hidden costsinvisible contributions report Reworking workThe experi-ence of employed caregivers of older adults Retrieved August 16 2007 fromwwwhecolualbertacahcic
Gable R ampWolfe M (1993) Instrument development 2nd ed Boston KluwerGubermanN amp Maheu P (1999) Combining employment and caregivingAn
intricate juggling actCanadian Journal on Aging 18(1) 84ndash106Keefe J Leacutegareacute J amp CarriegravereY (2007) Developing new strategies to support
future caregivers of older Canadians with disabilities Projections of need andtheir policy implicationsCanadian Public Policy 33 S65ndash80
Lengacher CA amp Sellers E (2003)TheWomenrsquos Role Strain Inventory InO L Strickland amp CDilorio (Eds)Measurement of nursing outcomes 2nd ed(pp 109ndash127) NewYork Springer
Martin-MatthewsA (2000) Intergenerational caregivingHow apocalyptic anddominant demography frame the questions and shape the answers In EMGee amp GGutman (Eds)The overselling of population agingApocalyptic demog-raphy intergenerational challenges and social policy (pp 64ndash79)Toronto OxfordUniversity Press
Ward-Griffin Keefe Martin-Matthews Kerr Brown and Oudshoorn
CJNR 2009Vol 41 No 3 126
Mayall B (1993) Keeping children healthy ndash the intermediate domain SocialScience and Medicine 36(1) 77ndash83
Morris JM amp Field PA (1995) Qualitative research methods for health profession-als 2nd ed London Sage
Pascall G (1986) Social policyA feminist analysis NewYorkTavistockPhillips J BernardM amp ChittendenM (2002) Juggling work and careThe expe-riences of older adults Bristol Policy Press
Polit D F amp Beck CT (2008)Nursing research Generating and assessing evidencefor nursing practice 8th ed Philadelphia LippincottWilliams ampWilkins
Polit D F amp Beck CT amp Owen SV (2007) Is the CVI an acceptable indica-tor of content validity Appraisal and recommendationsResearch in Nursingand Health 30 459ndash467
RossMM Rideout EM amp CarsonMM (1996) Nursesrsquo work Balancingpersonal and professional caregiving careers Canadian Journal of NursingResearch 26(4) 43ndash59
RutmanD (1996) Caregiving as womenrsquos workWomenrsquos experiences of pow-erfulness and powerlessness as caregiversQualitative Health Research 6(1) 90ndash111
ShieldsM ampWilkins K (2005)National Survey of theWork and Health of Nurses2005 Provincial profiles Ottawa Statistics CanadaRetrieved August 24 2007from httpwwwstatcancaenglishresearch11-621-MIE11-621-MIE2006052htm
StaceyM amp Davies C (1983)Division of labour in child health care Final report toSSRCCoventry Sociology Department University ofWarwick
Tebb S (1995)An aid to empowermentA caregiver well-being scaleHealth andSocialWork 20(2) 87ndash92
Tebb S Berg-WgerM amp Rubio DM (2000) CaregiverWell-Being Scale InDRoyse BAThyer D K Padgett ampT K Logan (Eds) Program evaluation3rd ed (pp 320ndash323) Pacific Grove CA BrooksCole
Ungerson C (1990) The language of care Crossing the boundaries InCUngerson (Ed)Gender and caringWork and welfare in Britain and Scandinavia(pp 8ndash33) NewYork Harvester
WaltersV LentonR French S Eyles JMayr J amp Newbold B (1996) Paidwork unpaid work and social supportA study of the health of male andfemale nurses Social Science and Medicine 43(11) 1627ndash1636
Ward-Griffin C (2004) Nurses as caregivers of elderly relatives Negotiatingpersonal and professional boundariesCJNR 36(1) 92ndash114
Ward-Griffin C (2008)Health professionals caring for aging relativesA profes-sional or personal issue In AMartin-Matthews amp J Phillips (Eds)Blurringthe boundariesAgeing at the intersection of work and home life (pp 1ndash20) NewYorkTaylor amp FrancisPsychology Press
Ward-Griffin C Brown JVandervoortA McNair S amp Dashnay I (2005)Double duty caregivingWomen in the health professionsCanadian Journalon Aging 24(4) 379ndash394
Ward-Griffin C amp MarshallV (2003) Reconceptualizing the relationshipbetween public and private eldercare Journal of Aging Studies 17 189ndash208
Development andValidation of the Double Duty Caregiving Scale
CJNR 2009Vol 41 No 3 127
Ware J E Kosinksi MTurner-Bowker L amp Gandek B (2002)How to scoreversion 2 of the SF-12 health survey Lincoln RIQuality Metric Inc
Acknowledgements
This study was funded by the Social Sciences and Humanities ResearchCouncil (Internal) and the Institute of Gender and Health CanadianInstitutes of Health ResearchThere are no conflicts of interest or financial disclosures
CatherineWard-Griffin RN PhD is ProfessorArthur Labatt Family School ofNursing University ofWestern Ontario London Canada Janice Keefe PhD isProfessor and Canada Research Chair in Aging and Caregiving Policy FamilyStudies and GerontologyMount SaintVincent University HalifaxNova ScotiaCanadaAnne Martin-Matthews PhD is Professor School of SocialWork andFamily Studies University of British ColumbiaVancouver Canada MichaelKerr PhD is Associate ProfessorArthur Labatt Family School of NursingUniversity ofWestern Ontario Judith Belle Brown PhD is Professor Departmentof Family Medicine University ofWestern OntarioAbram Oudshoorn RN is aPhD candidate in the Arthur Labatt Family School of Nursing University ofWestern Ontario
Ward-Griffin Keefe Martin-Matthews Kerr Brown and Oudshoorn
CJNR 2009Vol 41 No 3 128

Ward-Griffin Keefe Martin-Matthews Kerr Brown and Oudshoorn
CJNR 2009Vol 41 No 3 120
Tabl
e3
Revised
DDCS(N
=18
7)
Number
Item
-Total
Cronbachrsquos
Factor
Factor
Subscale
Factors
ofItem
sMean
SDCorrelations
Alpha
Variance
Loading
Exp
ectation
s378
712
Familialexpectations
5040ndash073
080
058ndash087
Professionalexpectations
4030ndash056
069
049ndash089
Total
9028ndash066
083
625
Supp
orts
332
646
Personalsupports
3043ndash058
068
070ndash086
Professionalsupports
3024ndash062
065
035ndash091
Total
6031ndash052
071
617
SettingLim
its
311
678
Awarenessofboundaries
3041ndash059
067
061ndash087
Activeresistance
3033ndash061
065
068ndash084
Total
6034ndash058
071
629
Mak
ingCon
nections
389
677
Makingconnections
5042ndash069
075
465
060ndash076
CaregivingIn
terface
301
826
Perceptionsofinterface
4048ndash071
081
080ndash084
Consequencesofinterface
3053ndash077
083
080ndash084
Total
7044ndash074
085
703
Two factors emerged from Supports (personal supports and profes-sional supports) accounting for 62 of the variance and indicating theimportance of personal and professional supports to DDCs providingcare to elderly relativesThree items loaded on personal supports withloadings ranging from 070 to 086Three items loaded on professionalsupports with loadings ranging from 035 to 091Two factors labelled Awareness of Boundaries and Active Resistance
emerged from Setting Limits accounting for 63 of the varianceThreeitems loaded on Awareness of Boundaries with loadings ranging from061 to 087Three items loaded on Active Resistance with loadingsranging from 068 to 084 One factor was extracted from MakingConnections accounting for 47 of the variance Loadings for the fiveitems on Making Connections ranged from 060 to 076This suggeststhat DDCs are aware of the boundaries between their personal and pro-fessional caregiving and that in an attempt to negotiate these boundariesthey resist providing care to their elderly relative as well as making con-nections to increase their supportsTwo factors emerged from CIThese were labelled Perceptions of CI
and Consequences of CI accounting for 70 of the variance Four itemsloaded on Perceptions of CI with loadings ranging from 054 to 085and three items loaded on Consequences of CI with loadings rangingfrom 080 to 084These results indicate that DDCs both are aware ofand experience consequences of the blurring of boundaries between per-sonal and professional caregiving
Reliability
Inter-item correlations and internal consistency (reliability) were exam-ined for each of the subscales of the Revised DDCSOverall in the finalversion of the 33-item DDCS inter-item correlations ranged from 024to 077 (Table 3) Cronbachrsquos alpha reliability coefficients of the fiveDDC subscales ranged from 085 (CI) to 071 (Supports and SettingLimits)Moreover Cronbachrsquos alpha reliability coefficients of the subscalefactors ranged from 083 (CI-Consequences) to 065 (for both Supports-Professional and Setting Limits-Active Resistance)
ConstructValidity Step 2
Pearson correlations were conducted to assess construct validity betweeneach of the subscales within the DDCS andWRSICWBS and SF-12v2(physical) and SF-12v2 (mental) (Table 3) In line with the underlyingtheory driving the scale there were weak to moderate correlations in theexpected direction between the Revised DDCS subscales ofExpectations Supports Setting LimitsMaking Connections and CI andthe established measuresThe strongest significant correlations were
Development andValidation of the Double Duty Caregiving Scale
CJNR 2009Vol 41 No 3 121
Ward-Griffin Keefe Martin-Matthews Kerr Brown and Oudshoorn
CJNR 2009Vol 41 No 3 122
Tabl
e4
Correlation
BetweenRevised
DDC
Subscalesan
dEstab
lished
Measures
Setting
Making
Caregiving
Scale
Expectations
Supports
Lim
its
Connections
Interface
WRSI
ar
-34
41
09
04
-49
p000
000
240
625
000
CaregiverWell-Being
Scale
r-16
34
-05
-01
-29
Activitiesb
p03
00
48
89
00
CaregiverWell-Being
Scale
r-16
34
03
-03
-36
Needsc
p04
00
71
69
00
SF12
PhysicalIndexd
r06
14
-14
-03
-02
p42
06
06
69
78
SF12
MentalIndex
dr
-26
26
09
01
-39
p00
22
22
60
00
Expectations
ar
1-12
-07
38
55
p095
344
000
000
Supportsa
r-12
104
10
-26
p095
552
174
000
Strategiesndash
r1
01
-23
SettingLimits
ap
851
002
Strategiesndash
r1
18
MakingConnections
ap
013
CaregivingInterfacea
r1
p
aN=187
bN=174
cN=180
dN=176plt05(2-tailed)
plt01(2-tailed)
between CI andWRSI (r = -49 p lt 001) between Supports andWRSI(r = 041 p lt001) and between CI and SF-12v2 (mental) (r = -39 p lt001) Finally the CI of the DDCS was also negatively correlated withcaregiver well-being (r = -29 p lt 001 [activities] and r = -36 p lt001[needs])The strongest subscale inter-correlations (ie within the Revised
DDCS itself) were between Expectations and CI (r = 055 p lt 001) andbetween Expectations and Making Connections (r = 038 p lt 001) Inaddition there was a weak positive association between MakingConnections and CI (r = 018 p lt 05) and negative associationsbetween Supports and CI (r = -026 p lt 001) and between SettingLimits and CI (r = -23 p lt 001) None of the other DDCS subscaleinter-correlations were statistically significant (Table 4)
Contrasted Groups Approach
Although there were no significant differences between DDCs andnon-DDCs in their overall scores for theWRSI CWBS and SF-12v2(physical and mental scores) there were significant differences betweennon-DDCs (n = 67) and the DDC subgroup (n = 84) defined as livingon the edge (ie those scoring above the mean on the CI subscale) Poorerhealth was observed for the living on the edge DDCs on their overall SF-12v2 mental health index score (t = -276 p lt 05) and on four of theeight SF-12v2 subscales vitality (t = -237 p lt 05) social functioning(t = -291 p lt 01) role emotional (t = -306 p lt 05) and mental health(t = -227 p lt 05) Moreover there were significant differences withinthe DDC group between those who were living on the edge and thosewith lower CI scores for the following SF-12 subscales vitality (t = -20p lt 05) social functioning (t = -356 p lt 01) role emotional (t = -483p lt 01) and mental health (t = -398 p lt 05)The living on the edgegroup also had significantly lower well-being scores for the activities(t = -363 p lt 05) and needs (t = -447 p lt 05) subscales than theother DDC respondentsWhile not all results were statistically significantoverall there was an observed tendency for the living on the edge group ofDDCs to have the lowest health and well-being scores whereas the otherDDCs (eg making it work) with low CI scores tended to have slightlybetter health scores than the non-DDC group
Discussion
The main purpose of this study was to develop and test a tool intendedto advance our understanding of DDC using a random sample of regis-tered nurses providing care to elderly relatives
Development andValidation of the Double Duty Caregiving Scale
CJNR 2009Vol 41 No 3 123
The nine factors we identified were consistent with the theorized coreDDC dimensions of Expectations (Familial and Professional) Supports(Personal and Professional) Setting Limits (Awareness of BoundariesActive Resistance) Making Connections and Caregiving Interface(Perceptions and Consequences) which can yield important informationregarding how much variance is accounted for by the factors Howeveradditional analyses are required to establish the psychometric propertiesof the DDCS including test-retest reliability to assess construct stabilityBased on the EFA results a measurement model of DDC will be pro-posed and analyzed in a future study using CFA to enhance the psycho-metric validation of the DDCS For researchers looking for a shorterversion of the DDCS it is worth noting that based on the strength andconsistency of the overall findings the seven-item CI subscale could beused to determine the extent of DDC when survey respondent burdenis a key factor in instrument selection (ie when use of the full 33DDCS items is not possible) adding to the potential value of the DDCS
The positive correlation between Expectations and CI and the nega-tive correlation between Supports and CI and between Setting Limitsand CI are theoretically consistent with the conceptual model of DDCThat is if expectations are high both personally and professionally withrespect to caring for onersquos relatives there will be greater CI or blurringof boundaries Conversely if one has strong personal and professionalsupports it follows that a lower degree of CI will result Similarly whenone sets limits on caregiving then less blurring or a lower degree of CIshould result However the positive association between MakingConnections and Expectations was unexpected Perhaps high expecta-tions lead one to increase supports by making connections both person-ally and professionally to help meet these expectationsComparison of the SF-12 v2 scores for living on the edge DDCs and
non-DDCs revealed significant differences for SF-12v2 mental healthand specific SF-12v2 subscales of vitality social functioning role emo-tional and mental healthThese findings suggest that DDCs who expe-rience a high degree of blurring of their professional and personalboundaries are at greater risk for poor health than those health profes-sionals who do not care for elderly relatives or who do not experiencethis blurring In addition those DDCs who could be characterized asliving on the edge scored significantly higher on the same four SF-12 sub-scales than DDCs with lower CI scoresThis observed pattern suggeststwo possibilities there exists a threshold effect for the negative healtheffects of DDC or manageable exposure to DDC has a beneficial effectFurther exploration of these interesting findings is warrantedAlthough we conducted a systematic and comprehensive analysis to
assess the psychometric properties of a new scale further reliability and
Ward-Griffin Keefe Martin-Matthews Kerr Brown and Oudshoorn
CJNR 2009Vol 41 No 3 124
validity studies are needed Confirmatory validation studies with otherhealth-care provider populations such as family physicians social workersand physiotherapists are particularly important as these professionals havethe potential to be DDCs and their experiences as documented in ouroriginal qualitative study of DDC helped to formulate the theoreticalunderpinnings of the DDCS In addition research with these groups willadvance our understanding of how occupational health groups may differin terms of expectations supports negotiating strategies and degree ofCIAs the identification of health-advantage and health-risk factors isinfluenced by health and social environments the negotiating strategiescould also be examined through the use of qualitative methodologiessuch as in-depth interviews or focus groupsFinally research that draws linkages between professional and personal
caregiving has the added value of furthering knowledge about employedcaregiving specifically as it relates to the relationship between health out-comes and provision of familial care by health-care providersAlthoughthe convergence (and avoidance) of professional and personal caregivingboundaries is not a new issue in nursing and other health professions thenotion that it is the individualrsquos responsibility to negotiate this boundarytends to predominate (Ward-Griffin 2008)To that end further testingand refinement of the DDCS will be helpful in identifying areas whereDDCs may need specific or different types of support It is also impor-tant to understand how specific social supports shape the health experi-ences of DDCs as well as to investigate different types of social supportinterventions with DDCsThis information is particularly meaningfultoday with the intersection of three challenges an aging population anaging health-care workforce and a shortage of health professionals Suchknowledge could contribute to workplace and other health initiativesspearheaded by professional groups policy-makers and other key stake-holders interested in assessing and addressing the health effects of DDCIn summary the DDCS is a valid tool for the assessment of double
duty caregiving Such assessment is a crucial step in understanding theexperience of the blurring of personal and professional boundaries ofcaregiving among health professionalsA quantitative study of both maleand female DDCs could help us to understand the relationship betweencertain factors (ie gender health-care occupation) and the potentialhealth effects of DDCMoreover our finding that respondents with highCI scores (living on the edge) had significantly lower health and well-beingscores than DDC respondents with lower CI scores warrants furtherinvestigation to determine if one group of DDCs is at particular risk fordeveloping negative health effects Given the current climate of health-care reform in Canada developing a better understanding of DDC andits health effects is particularly relevant for policy-makers and others who
Development andValidation of the Double Duty Caregiving Scale
CJNR 2009Vol 41 No 3 125
are committed to developing health-promoting programs and policies forfamilial caregivers of the elderly Clearly now is the time to monitor theeffects of changing demographics both in the general population andwithin the health professions in order to develop appropriate and tar-geted strategies thereby creating and sustaining healthy work environ-ments and health-care workforcesWith further refinement the DDCSmay assist with these endeavours
References
Armstrong P amp ArmstrongH (2004)Thinking it throughWomenwork andcaring in the new millennium In K Grant CArmaratunga PArmstrongM BoscoeA Pederson amp KWillson (Eds)Caring forcaring aboutWomenhome care and unpaid caregiving (pp 5ndash44)Aurora ONGaramond
Baines D (2004) Seven kinds of work ndash only one paid Raced gendered andrestructured work in social servicesAtlantis 28(2) 19ndash28
Canadian Institute for Health Information (2006)Workforce trends of registerednurses in Canada 2005 Retrieved November 5 2006 fromhttpsecurecihicacihiwebproductsndb_worforce_trends_registered_nurses_canada_2005_epdf
CarruthA K (1996) Development and testing of the Caregiver ReciprocityScaleNursing Research 45(2) 92ndash97
Chen F Feudtner C Rhodes L amp Green L (2001) Role conflicts of physi-cians and their family members Rules but no rule bookWestern Journal ofMedicine 175(4) 236ndash239
Cohen S Underwood L G amp Gottlieb BH (Eds) (2000) Social support mea-surement and interventionA guide for health and social scientistsOxford OxfordUniversity Press
Fast J (2005)Hidden costsinvisible contributions report Reworking workThe experi-ence of employed caregivers of older adults Retrieved August 16 2007 fromwwwhecolualbertacahcic
Gable R ampWolfe M (1993) Instrument development 2nd ed Boston KluwerGubermanN amp Maheu P (1999) Combining employment and caregivingAn
intricate juggling actCanadian Journal on Aging 18(1) 84ndash106Keefe J Leacutegareacute J amp CarriegravereY (2007) Developing new strategies to support
future caregivers of older Canadians with disabilities Projections of need andtheir policy implicationsCanadian Public Policy 33 S65ndash80
Lengacher CA amp Sellers E (2003)TheWomenrsquos Role Strain Inventory InO L Strickland amp CDilorio (Eds)Measurement of nursing outcomes 2nd ed(pp 109ndash127) NewYork Springer
Martin-MatthewsA (2000) Intergenerational caregivingHow apocalyptic anddominant demography frame the questions and shape the answers In EMGee amp GGutman (Eds)The overselling of population agingApocalyptic demog-raphy intergenerational challenges and social policy (pp 64ndash79)Toronto OxfordUniversity Press
Ward-Griffin Keefe Martin-Matthews Kerr Brown and Oudshoorn
CJNR 2009Vol 41 No 3 126
Mayall B (1993) Keeping children healthy ndash the intermediate domain SocialScience and Medicine 36(1) 77ndash83
Morris JM amp Field PA (1995) Qualitative research methods for health profession-als 2nd ed London Sage
Pascall G (1986) Social policyA feminist analysis NewYorkTavistockPhillips J BernardM amp ChittendenM (2002) Juggling work and careThe expe-riences of older adults Bristol Policy Press
Polit D F amp Beck CT (2008)Nursing research Generating and assessing evidencefor nursing practice 8th ed Philadelphia LippincottWilliams ampWilkins
Polit D F amp Beck CT amp Owen SV (2007) Is the CVI an acceptable indica-tor of content validity Appraisal and recommendationsResearch in Nursingand Health 30 459ndash467
RossMM Rideout EM amp CarsonMM (1996) Nursesrsquo work Balancingpersonal and professional caregiving careers Canadian Journal of NursingResearch 26(4) 43ndash59
RutmanD (1996) Caregiving as womenrsquos workWomenrsquos experiences of pow-erfulness and powerlessness as caregiversQualitative Health Research 6(1) 90ndash111
ShieldsM ampWilkins K (2005)National Survey of theWork and Health of Nurses2005 Provincial profiles Ottawa Statistics CanadaRetrieved August 24 2007from httpwwwstatcancaenglishresearch11-621-MIE11-621-MIE2006052htm
StaceyM amp Davies C (1983)Division of labour in child health care Final report toSSRCCoventry Sociology Department University ofWarwick
Tebb S (1995)An aid to empowermentA caregiver well-being scaleHealth andSocialWork 20(2) 87ndash92
Tebb S Berg-WgerM amp Rubio DM (2000) CaregiverWell-Being Scale InDRoyse BAThyer D K Padgett ampT K Logan (Eds) Program evaluation3rd ed (pp 320ndash323) Pacific Grove CA BrooksCole
Ungerson C (1990) The language of care Crossing the boundaries InCUngerson (Ed)Gender and caringWork and welfare in Britain and Scandinavia(pp 8ndash33) NewYork Harvester
WaltersV LentonR French S Eyles JMayr J amp Newbold B (1996) Paidwork unpaid work and social supportA study of the health of male andfemale nurses Social Science and Medicine 43(11) 1627ndash1636
Ward-Griffin C (2004) Nurses as caregivers of elderly relatives Negotiatingpersonal and professional boundariesCJNR 36(1) 92ndash114
Ward-Griffin C (2008)Health professionals caring for aging relativesA profes-sional or personal issue In AMartin-Matthews amp J Phillips (Eds)Blurringthe boundariesAgeing at the intersection of work and home life (pp 1ndash20) NewYorkTaylor amp FrancisPsychology Press
Ward-Griffin C Brown JVandervoortA McNair S amp Dashnay I (2005)Double duty caregivingWomen in the health professionsCanadian Journalon Aging 24(4) 379ndash394
Ward-Griffin C amp MarshallV (2003) Reconceptualizing the relationshipbetween public and private eldercare Journal of Aging Studies 17 189ndash208
Development andValidation of the Double Duty Caregiving Scale
CJNR 2009Vol 41 No 3 127
Ware J E Kosinksi MTurner-Bowker L amp Gandek B (2002)How to scoreversion 2 of the SF-12 health survey Lincoln RIQuality Metric Inc
Acknowledgements
This study was funded by the Social Sciences and Humanities ResearchCouncil (Internal) and the Institute of Gender and Health CanadianInstitutes of Health ResearchThere are no conflicts of interest or financial disclosures
CatherineWard-Griffin RN PhD is ProfessorArthur Labatt Family School ofNursing University ofWestern Ontario London Canada Janice Keefe PhD isProfessor and Canada Research Chair in Aging and Caregiving Policy FamilyStudies and GerontologyMount SaintVincent University HalifaxNova ScotiaCanadaAnne Martin-Matthews PhD is Professor School of SocialWork andFamily Studies University of British ColumbiaVancouver Canada MichaelKerr PhD is Associate ProfessorArthur Labatt Family School of NursingUniversity ofWestern Ontario Judith Belle Brown PhD is Professor Departmentof Family Medicine University ofWestern OntarioAbram Oudshoorn RN is aPhD candidate in the Arthur Labatt Family School of Nursing University ofWestern Ontario
Ward-Griffin Keefe Martin-Matthews Kerr Brown and Oudshoorn
CJNR 2009Vol 41 No 3 128
Two factors emerged from Supports (personal supports and profes-sional supports) accounting for 62 of the variance and indicating theimportance of personal and professional supports to DDCs providingcare to elderly relativesThree items loaded on personal supports withloadings ranging from 070 to 086Three items loaded on professionalsupports with loadings ranging from 035 to 091Two factors labelled Awareness of Boundaries and Active Resistance
emerged from Setting Limits accounting for 63 of the varianceThreeitems loaded on Awareness of Boundaries with loadings ranging from061 to 087Three items loaded on Active Resistance with loadingsranging from 068 to 084 One factor was extracted from MakingConnections accounting for 47 of the variance Loadings for the fiveitems on Making Connections ranged from 060 to 076This suggeststhat DDCs are aware of the boundaries between their personal and pro-fessional caregiving and that in an attempt to negotiate these boundariesthey resist providing care to their elderly relative as well as making con-nections to increase their supportsTwo factors emerged from CIThese were labelled Perceptions of CI
and Consequences of CI accounting for 70 of the variance Four itemsloaded on Perceptions of CI with loadings ranging from 054 to 085and three items loaded on Consequences of CI with loadings rangingfrom 080 to 084These results indicate that DDCs both are aware ofand experience consequences of the blurring of boundaries between per-sonal and professional caregiving
Reliability
Inter-item correlations and internal consistency (reliability) were exam-ined for each of the subscales of the Revised DDCSOverall in the finalversion of the 33-item DDCS inter-item correlations ranged from 024to 077 (Table 3) Cronbachrsquos alpha reliability coefficients of the fiveDDC subscales ranged from 085 (CI) to 071 (Supports and SettingLimits)Moreover Cronbachrsquos alpha reliability coefficients of the subscalefactors ranged from 083 (CI-Consequences) to 065 (for both Supports-Professional and Setting Limits-Active Resistance)
ConstructValidity Step 2
Pearson correlations were conducted to assess construct validity betweeneach of the subscales within the DDCS andWRSICWBS and SF-12v2(physical) and SF-12v2 (mental) (Table 3) In line with the underlyingtheory driving the scale there were weak to moderate correlations in theexpected direction between the Revised DDCS subscales ofExpectations Supports Setting LimitsMaking Connections and CI andthe established measuresThe strongest significant correlations were
Development andValidation of the Double Duty Caregiving Scale
CJNR 2009Vol 41 No 3 121
Ward-Griffin Keefe Martin-Matthews Kerr Brown and Oudshoorn
CJNR 2009Vol 41 No 3 122
Tabl
e4
Correlation
BetweenRevised
DDC
Subscalesan
dEstab
lished
Measures
Setting
Making
Caregiving
Scale
Expectations
Supports
Lim
its
Connections
Interface
WRSI
ar
-34
41
09
04
-49
p000
000
240
625
000
CaregiverWell-Being
Scale
r-16
34
-05
-01
-29
Activitiesb
p03
00
48
89
00
CaregiverWell-Being
Scale
r-16
34
03
-03
-36
Needsc
p04
00
71
69
00
SF12
PhysicalIndexd
r06
14
-14
-03
-02
p42
06
06
69
78
SF12
MentalIndex
dr
-26
26
09
01
-39
p00
22
22
60
00
Expectations
ar
1-12
-07
38
55
p095
344
000
000
Supportsa
r-12
104
10
-26
p095
552
174
000
Strategiesndash
r1
01
-23
SettingLimits
ap
851
002
Strategiesndash
r1
18
MakingConnections
ap
013
CaregivingInterfacea
r1
p
aN=187
bN=174
cN=180
dN=176plt05(2-tailed)
plt01(2-tailed)
between CI andWRSI (r = -49 p lt 001) between Supports andWRSI(r = 041 p lt001) and between CI and SF-12v2 (mental) (r = -39 p lt001) Finally the CI of the DDCS was also negatively correlated withcaregiver well-being (r = -29 p lt 001 [activities] and r = -36 p lt001[needs])The strongest subscale inter-correlations (ie within the Revised
DDCS itself) were between Expectations and CI (r = 055 p lt 001) andbetween Expectations and Making Connections (r = 038 p lt 001) Inaddition there was a weak positive association between MakingConnections and CI (r = 018 p lt 05) and negative associationsbetween Supports and CI (r = -026 p lt 001) and between SettingLimits and CI (r = -23 p lt 001) None of the other DDCS subscaleinter-correlations were statistically significant (Table 4)
Contrasted Groups Approach
Although there were no significant differences between DDCs andnon-DDCs in their overall scores for theWRSI CWBS and SF-12v2(physical and mental scores) there were significant differences betweennon-DDCs (n = 67) and the DDC subgroup (n = 84) defined as livingon the edge (ie those scoring above the mean on the CI subscale) Poorerhealth was observed for the living on the edge DDCs on their overall SF-12v2 mental health index score (t = -276 p lt 05) and on four of theeight SF-12v2 subscales vitality (t = -237 p lt 05) social functioning(t = -291 p lt 01) role emotional (t = -306 p lt 05) and mental health(t = -227 p lt 05) Moreover there were significant differences withinthe DDC group between those who were living on the edge and thosewith lower CI scores for the following SF-12 subscales vitality (t = -20p lt 05) social functioning (t = -356 p lt 01) role emotional (t = -483p lt 01) and mental health (t = -398 p lt 05)The living on the edgegroup also had significantly lower well-being scores for the activities(t = -363 p lt 05) and needs (t = -447 p lt 05) subscales than theother DDC respondentsWhile not all results were statistically significantoverall there was an observed tendency for the living on the edge group ofDDCs to have the lowest health and well-being scores whereas the otherDDCs (eg making it work) with low CI scores tended to have slightlybetter health scores than the non-DDC group
Discussion
The main purpose of this study was to develop and test a tool intendedto advance our understanding of DDC using a random sample of regis-tered nurses providing care to elderly relatives
Development andValidation of the Double Duty Caregiving Scale
CJNR 2009Vol 41 No 3 123
The nine factors we identified were consistent with the theorized coreDDC dimensions of Expectations (Familial and Professional) Supports(Personal and Professional) Setting Limits (Awareness of BoundariesActive Resistance) Making Connections and Caregiving Interface(Perceptions and Consequences) which can yield important informationregarding how much variance is accounted for by the factors Howeveradditional analyses are required to establish the psychometric propertiesof the DDCS including test-retest reliability to assess construct stabilityBased on the EFA results a measurement model of DDC will be pro-posed and analyzed in a future study using CFA to enhance the psycho-metric validation of the DDCS For researchers looking for a shorterversion of the DDCS it is worth noting that based on the strength andconsistency of the overall findings the seven-item CI subscale could beused to determine the extent of DDC when survey respondent burdenis a key factor in instrument selection (ie when use of the full 33DDCS items is not possible) adding to the potential value of the DDCS
The positive correlation between Expectations and CI and the nega-tive correlation between Supports and CI and between Setting Limitsand CI are theoretically consistent with the conceptual model of DDCThat is if expectations are high both personally and professionally withrespect to caring for onersquos relatives there will be greater CI or blurringof boundaries Conversely if one has strong personal and professionalsupports it follows that a lower degree of CI will result Similarly whenone sets limits on caregiving then less blurring or a lower degree of CIshould result However the positive association between MakingConnections and Expectations was unexpected Perhaps high expecta-tions lead one to increase supports by making connections both person-ally and professionally to help meet these expectationsComparison of the SF-12 v2 scores for living on the edge DDCs and
non-DDCs revealed significant differences for SF-12v2 mental healthand specific SF-12v2 subscales of vitality social functioning role emo-tional and mental healthThese findings suggest that DDCs who expe-rience a high degree of blurring of their professional and personalboundaries are at greater risk for poor health than those health profes-sionals who do not care for elderly relatives or who do not experiencethis blurring In addition those DDCs who could be characterized asliving on the edge scored significantly higher on the same four SF-12 sub-scales than DDCs with lower CI scoresThis observed pattern suggeststwo possibilities there exists a threshold effect for the negative healtheffects of DDC or manageable exposure to DDC has a beneficial effectFurther exploration of these interesting findings is warrantedAlthough we conducted a systematic and comprehensive analysis to
assess the psychometric properties of a new scale further reliability and
Ward-Griffin Keefe Martin-Matthews Kerr Brown and Oudshoorn
CJNR 2009Vol 41 No 3 124
validity studies are needed Confirmatory validation studies with otherhealth-care provider populations such as family physicians social workersand physiotherapists are particularly important as these professionals havethe potential to be DDCs and their experiences as documented in ouroriginal qualitative study of DDC helped to formulate the theoreticalunderpinnings of the DDCS In addition research with these groups willadvance our understanding of how occupational health groups may differin terms of expectations supports negotiating strategies and degree ofCIAs the identification of health-advantage and health-risk factors isinfluenced by health and social environments the negotiating strategiescould also be examined through the use of qualitative methodologiessuch as in-depth interviews or focus groupsFinally research that draws linkages between professional and personal
caregiving has the added value of furthering knowledge about employedcaregiving specifically as it relates to the relationship between health out-comes and provision of familial care by health-care providersAlthoughthe convergence (and avoidance) of professional and personal caregivingboundaries is not a new issue in nursing and other health professions thenotion that it is the individualrsquos responsibility to negotiate this boundarytends to predominate (Ward-Griffin 2008)To that end further testingand refinement of the DDCS will be helpful in identifying areas whereDDCs may need specific or different types of support It is also impor-tant to understand how specific social supports shape the health experi-ences of DDCs as well as to investigate different types of social supportinterventions with DDCsThis information is particularly meaningfultoday with the intersection of three challenges an aging population anaging health-care workforce and a shortage of health professionals Suchknowledge could contribute to workplace and other health initiativesspearheaded by professional groups policy-makers and other key stake-holders interested in assessing and addressing the health effects of DDCIn summary the DDCS is a valid tool for the assessment of double
duty caregiving Such assessment is a crucial step in understanding theexperience of the blurring of personal and professional boundaries ofcaregiving among health professionalsA quantitative study of both maleand female DDCs could help us to understand the relationship betweencertain factors (ie gender health-care occupation) and the potentialhealth effects of DDCMoreover our finding that respondents with highCI scores (living on the edge) had significantly lower health and well-beingscores than DDC respondents with lower CI scores warrants furtherinvestigation to determine if one group of DDCs is at particular risk fordeveloping negative health effects Given the current climate of health-care reform in Canada developing a better understanding of DDC andits health effects is particularly relevant for policy-makers and others who
Development andValidation of the Double Duty Caregiving Scale
CJNR 2009Vol 41 No 3 125
are committed to developing health-promoting programs and policies forfamilial caregivers of the elderly Clearly now is the time to monitor theeffects of changing demographics both in the general population andwithin the health professions in order to develop appropriate and tar-geted strategies thereby creating and sustaining healthy work environ-ments and health-care workforcesWith further refinement the DDCSmay assist with these endeavours
References
Armstrong P amp ArmstrongH (2004)Thinking it throughWomenwork andcaring in the new millennium In K Grant CArmaratunga PArmstrongM BoscoeA Pederson amp KWillson (Eds)Caring forcaring aboutWomenhome care and unpaid caregiving (pp 5ndash44)Aurora ONGaramond
Baines D (2004) Seven kinds of work ndash only one paid Raced gendered andrestructured work in social servicesAtlantis 28(2) 19ndash28
Canadian Institute for Health Information (2006)Workforce trends of registerednurses in Canada 2005 Retrieved November 5 2006 fromhttpsecurecihicacihiwebproductsndb_worforce_trends_registered_nurses_canada_2005_epdf
CarruthA K (1996) Development and testing of the Caregiver ReciprocityScaleNursing Research 45(2) 92ndash97
Chen F Feudtner C Rhodes L amp Green L (2001) Role conflicts of physi-cians and their family members Rules but no rule bookWestern Journal ofMedicine 175(4) 236ndash239
Cohen S Underwood L G amp Gottlieb BH (Eds) (2000) Social support mea-surement and interventionA guide for health and social scientistsOxford OxfordUniversity Press
Fast J (2005)Hidden costsinvisible contributions report Reworking workThe experi-ence of employed caregivers of older adults Retrieved August 16 2007 fromwwwhecolualbertacahcic
Gable R ampWolfe M (1993) Instrument development 2nd ed Boston KluwerGubermanN amp Maheu P (1999) Combining employment and caregivingAn
intricate juggling actCanadian Journal on Aging 18(1) 84ndash106Keefe J Leacutegareacute J amp CarriegravereY (2007) Developing new strategies to support
future caregivers of older Canadians with disabilities Projections of need andtheir policy implicationsCanadian Public Policy 33 S65ndash80
Lengacher CA amp Sellers E (2003)TheWomenrsquos Role Strain Inventory InO L Strickland amp CDilorio (Eds)Measurement of nursing outcomes 2nd ed(pp 109ndash127) NewYork Springer
Martin-MatthewsA (2000) Intergenerational caregivingHow apocalyptic anddominant demography frame the questions and shape the answers In EMGee amp GGutman (Eds)The overselling of population agingApocalyptic demog-raphy intergenerational challenges and social policy (pp 64ndash79)Toronto OxfordUniversity Press
Ward-Griffin Keefe Martin-Matthews Kerr Brown and Oudshoorn
CJNR 2009Vol 41 No 3 126
Mayall B (1993) Keeping children healthy ndash the intermediate domain SocialScience and Medicine 36(1) 77ndash83
Morris JM amp Field PA (1995) Qualitative research methods for health profession-als 2nd ed London Sage
Pascall G (1986) Social policyA feminist analysis NewYorkTavistockPhillips J BernardM amp ChittendenM (2002) Juggling work and careThe expe-riences of older adults Bristol Policy Press
Polit D F amp Beck CT (2008)Nursing research Generating and assessing evidencefor nursing practice 8th ed Philadelphia LippincottWilliams ampWilkins
Polit D F amp Beck CT amp Owen SV (2007) Is the CVI an acceptable indica-tor of content validity Appraisal and recommendationsResearch in Nursingand Health 30 459ndash467
RossMM Rideout EM amp CarsonMM (1996) Nursesrsquo work Balancingpersonal and professional caregiving careers Canadian Journal of NursingResearch 26(4) 43ndash59
RutmanD (1996) Caregiving as womenrsquos workWomenrsquos experiences of pow-erfulness and powerlessness as caregiversQualitative Health Research 6(1) 90ndash111
ShieldsM ampWilkins K (2005)National Survey of theWork and Health of Nurses2005 Provincial profiles Ottawa Statistics CanadaRetrieved August 24 2007from httpwwwstatcancaenglishresearch11-621-MIE11-621-MIE2006052htm
StaceyM amp Davies C (1983)Division of labour in child health care Final report toSSRCCoventry Sociology Department University ofWarwick
Tebb S (1995)An aid to empowermentA caregiver well-being scaleHealth andSocialWork 20(2) 87ndash92
Tebb S Berg-WgerM amp Rubio DM (2000) CaregiverWell-Being Scale InDRoyse BAThyer D K Padgett ampT K Logan (Eds) Program evaluation3rd ed (pp 320ndash323) Pacific Grove CA BrooksCole
Ungerson C (1990) The language of care Crossing the boundaries InCUngerson (Ed)Gender and caringWork and welfare in Britain and Scandinavia(pp 8ndash33) NewYork Harvester
WaltersV LentonR French S Eyles JMayr J amp Newbold B (1996) Paidwork unpaid work and social supportA study of the health of male andfemale nurses Social Science and Medicine 43(11) 1627ndash1636
Ward-Griffin C (2004) Nurses as caregivers of elderly relatives Negotiatingpersonal and professional boundariesCJNR 36(1) 92ndash114
Ward-Griffin C (2008)Health professionals caring for aging relativesA profes-sional or personal issue In AMartin-Matthews amp J Phillips (Eds)Blurringthe boundariesAgeing at the intersection of work and home life (pp 1ndash20) NewYorkTaylor amp FrancisPsychology Press
Ward-Griffin C Brown JVandervoortA McNair S amp Dashnay I (2005)Double duty caregivingWomen in the health professionsCanadian Journalon Aging 24(4) 379ndash394
Ward-Griffin C amp MarshallV (2003) Reconceptualizing the relationshipbetween public and private eldercare Journal of Aging Studies 17 189ndash208
Development andValidation of the Double Duty Caregiving Scale
CJNR 2009Vol 41 No 3 127
Ware J E Kosinksi MTurner-Bowker L amp Gandek B (2002)How to scoreversion 2 of the SF-12 health survey Lincoln RIQuality Metric Inc
Acknowledgements
This study was funded by the Social Sciences and Humanities ResearchCouncil (Internal) and the Institute of Gender and Health CanadianInstitutes of Health ResearchThere are no conflicts of interest or financial disclosures
CatherineWard-Griffin RN PhD is ProfessorArthur Labatt Family School ofNursing University ofWestern Ontario London Canada Janice Keefe PhD isProfessor and Canada Research Chair in Aging and Caregiving Policy FamilyStudies and GerontologyMount SaintVincent University HalifaxNova ScotiaCanadaAnne Martin-Matthews PhD is Professor School of SocialWork andFamily Studies University of British ColumbiaVancouver Canada MichaelKerr PhD is Associate ProfessorArthur Labatt Family School of NursingUniversity ofWestern Ontario Judith Belle Brown PhD is Professor Departmentof Family Medicine University ofWestern OntarioAbram Oudshoorn RN is aPhD candidate in the Arthur Labatt Family School of Nursing University ofWestern Ontario
Ward-Griffin Keefe Martin-Matthews Kerr Brown and Oudshoorn
CJNR 2009Vol 41 No 3 128
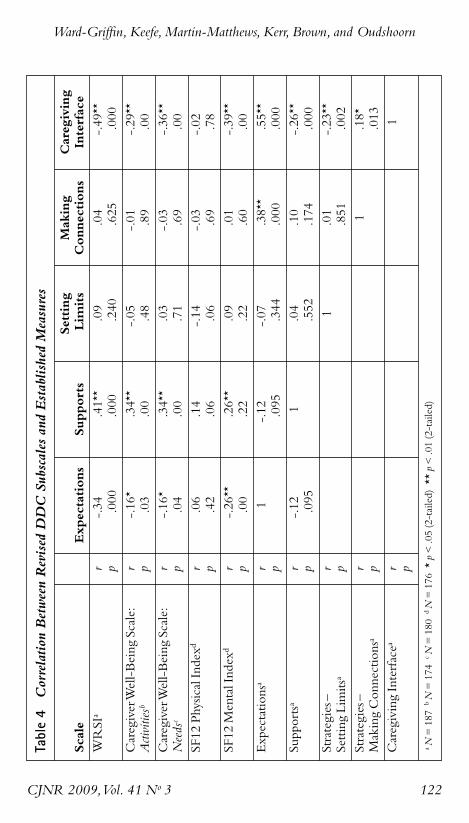
Ward-Griffin Keefe Martin-Matthews Kerr Brown and Oudshoorn
CJNR 2009Vol 41 No 3 122
Tabl
e4
Correlation
BetweenRevised
DDC
Subscalesan
dEstab
lished
Measures
Setting
Making
Caregiving
Scale
Expectations
Supports
Lim
its
Connections
Interface
WRSI
ar
-34
41
09
04
-49
p000
000
240
625
000
CaregiverWell-Being
Scale
r-16
34
-05
-01
-29
Activitiesb
p03
00
48
89
00
CaregiverWell-Being
Scale
r-16
34
03
-03
-36
Needsc
p04
00
71
69
00
SF12
PhysicalIndexd
r06
14
-14
-03
-02
p42
06
06
69
78
SF12
MentalIndex
dr
-26
26
09
01
-39
p00
22
22
60
00
Expectations
ar
1-12
-07
38
55
p095
344
000
000
Supportsa
r-12
104
10
-26
p095
552
174
000
Strategiesndash
r1
01
-23
SettingLimits
ap
851
002
Strategiesndash
r1
18
MakingConnections
ap
013
CaregivingInterfacea
r1
p
aN=187
bN=174
cN=180
dN=176plt05(2-tailed)
plt01(2-tailed)
between CI andWRSI (r = -49 p lt 001) between Supports andWRSI(r = 041 p lt001) and between CI and SF-12v2 (mental) (r = -39 p lt001) Finally the CI of the DDCS was also negatively correlated withcaregiver well-being (r = -29 p lt 001 [activities] and r = -36 p lt001[needs])The strongest subscale inter-correlations (ie within the Revised
DDCS itself) were between Expectations and CI (r = 055 p lt 001) andbetween Expectations and Making Connections (r = 038 p lt 001) Inaddition there was a weak positive association between MakingConnections and CI (r = 018 p lt 05) and negative associationsbetween Supports and CI (r = -026 p lt 001) and between SettingLimits and CI (r = -23 p lt 001) None of the other DDCS subscaleinter-correlations were statistically significant (Table 4)
Contrasted Groups Approach
Although there were no significant differences between DDCs andnon-DDCs in their overall scores for theWRSI CWBS and SF-12v2(physical and mental scores) there were significant differences betweennon-DDCs (n = 67) and the DDC subgroup (n = 84) defined as livingon the edge (ie those scoring above the mean on the CI subscale) Poorerhealth was observed for the living on the edge DDCs on their overall SF-12v2 mental health index score (t = -276 p lt 05) and on four of theeight SF-12v2 subscales vitality (t = -237 p lt 05) social functioning(t = -291 p lt 01) role emotional (t = -306 p lt 05) and mental health(t = -227 p lt 05) Moreover there were significant differences withinthe DDC group between those who were living on the edge and thosewith lower CI scores for the following SF-12 subscales vitality (t = -20p lt 05) social functioning (t = -356 p lt 01) role emotional (t = -483p lt 01) and mental health (t = -398 p lt 05)The living on the edgegroup also had significantly lower well-being scores for the activities(t = -363 p lt 05) and needs (t = -447 p lt 05) subscales than theother DDC respondentsWhile not all results were statistically significantoverall there was an observed tendency for the living on the edge group ofDDCs to have the lowest health and well-being scores whereas the otherDDCs (eg making it work) with low CI scores tended to have slightlybetter health scores than the non-DDC group
Discussion
The main purpose of this study was to develop and test a tool intendedto advance our understanding of DDC using a random sample of regis-tered nurses providing care to elderly relatives
Development andValidation of the Double Duty Caregiving Scale
CJNR 2009Vol 41 No 3 123
The nine factors we identified were consistent with the theorized coreDDC dimensions of Expectations (Familial and Professional) Supports(Personal and Professional) Setting Limits (Awareness of BoundariesActive Resistance) Making Connections and Caregiving Interface(Perceptions and Consequences) which can yield important informationregarding how much variance is accounted for by the factors Howeveradditional analyses are required to establish the psychometric propertiesof the DDCS including test-retest reliability to assess construct stabilityBased on the EFA results a measurement model of DDC will be pro-posed and analyzed in a future study using CFA to enhance the psycho-metric validation of the DDCS For researchers looking for a shorterversion of the DDCS it is worth noting that based on the strength andconsistency of the overall findings the seven-item CI subscale could beused to determine the extent of DDC when survey respondent burdenis a key factor in instrument selection (ie when use of the full 33DDCS items is not possible) adding to the potential value of the DDCS
The positive correlation between Expectations and CI and the nega-tive correlation between Supports and CI and between Setting Limitsand CI are theoretically consistent with the conceptual model of DDCThat is if expectations are high both personally and professionally withrespect to caring for onersquos relatives there will be greater CI or blurringof boundaries Conversely if one has strong personal and professionalsupports it follows that a lower degree of CI will result Similarly whenone sets limits on caregiving then less blurring or a lower degree of CIshould result However the positive association between MakingConnections and Expectations was unexpected Perhaps high expecta-tions lead one to increase supports by making connections both person-ally and professionally to help meet these expectationsComparison of the SF-12 v2 scores for living on the edge DDCs and
non-DDCs revealed significant differences for SF-12v2 mental healthand specific SF-12v2 subscales of vitality social functioning role emo-tional and mental healthThese findings suggest that DDCs who expe-rience a high degree of blurring of their professional and personalboundaries are at greater risk for poor health than those health profes-sionals who do not care for elderly relatives or who do not experiencethis blurring In addition those DDCs who could be characterized asliving on the edge scored significantly higher on the same four SF-12 sub-scales than DDCs with lower CI scoresThis observed pattern suggeststwo possibilities there exists a threshold effect for the negative healtheffects of DDC or manageable exposure to DDC has a beneficial effectFurther exploration of these interesting findings is warrantedAlthough we conducted a systematic and comprehensive analysis to
assess the psychometric properties of a new scale further reliability and
Ward-Griffin Keefe Martin-Matthews Kerr Brown and Oudshoorn
CJNR 2009Vol 41 No 3 124
validity studies are needed Confirmatory validation studies with otherhealth-care provider populations such as family physicians social workersand physiotherapists are particularly important as these professionals havethe potential to be DDCs and their experiences as documented in ouroriginal qualitative study of DDC helped to formulate the theoreticalunderpinnings of the DDCS In addition research with these groups willadvance our understanding of how occupational health groups may differin terms of expectations supports negotiating strategies and degree ofCIAs the identification of health-advantage and health-risk factors isinfluenced by health and social environments the negotiating strategiescould also be examined through the use of qualitative methodologiessuch as in-depth interviews or focus groupsFinally research that draws linkages between professional and personal
caregiving has the added value of furthering knowledge about employedcaregiving specifically as it relates to the relationship between health out-comes and provision of familial care by health-care providersAlthoughthe convergence (and avoidance) of professional and personal caregivingboundaries is not a new issue in nursing and other health professions thenotion that it is the individualrsquos responsibility to negotiate this boundarytends to predominate (Ward-Griffin 2008)To that end further testingand refinement of the DDCS will be helpful in identifying areas whereDDCs may need specific or different types of support It is also impor-tant to understand how specific social supports shape the health experi-ences of DDCs as well as to investigate different types of social supportinterventions with DDCsThis information is particularly meaningfultoday with the intersection of three challenges an aging population anaging health-care workforce and a shortage of health professionals Suchknowledge could contribute to workplace and other health initiativesspearheaded by professional groups policy-makers and other key stake-holders interested in assessing and addressing the health effects of DDCIn summary the DDCS is a valid tool for the assessment of double
duty caregiving Such assessment is a crucial step in understanding theexperience of the blurring of personal and professional boundaries ofcaregiving among health professionalsA quantitative study of both maleand female DDCs could help us to understand the relationship betweencertain factors (ie gender health-care occupation) and the potentialhealth effects of DDCMoreover our finding that respondents with highCI scores (living on the edge) had significantly lower health and well-beingscores than DDC respondents with lower CI scores warrants furtherinvestigation to determine if one group of DDCs is at particular risk fordeveloping negative health effects Given the current climate of health-care reform in Canada developing a better understanding of DDC andits health effects is particularly relevant for policy-makers and others who
Development andValidation of the Double Duty Caregiving Scale
CJNR 2009Vol 41 No 3 125
are committed to developing health-promoting programs and policies forfamilial caregivers of the elderly Clearly now is the time to monitor theeffects of changing demographics both in the general population andwithin the health professions in order to develop appropriate and tar-geted strategies thereby creating and sustaining healthy work environ-ments and health-care workforcesWith further refinement the DDCSmay assist with these endeavours
References
Armstrong P amp ArmstrongH (2004)Thinking it throughWomenwork andcaring in the new millennium In K Grant CArmaratunga PArmstrongM BoscoeA Pederson amp KWillson (Eds)Caring forcaring aboutWomenhome care and unpaid caregiving (pp 5ndash44)Aurora ONGaramond
Baines D (2004) Seven kinds of work ndash only one paid Raced gendered andrestructured work in social servicesAtlantis 28(2) 19ndash28
Canadian Institute for Health Information (2006)Workforce trends of registerednurses in Canada 2005 Retrieved November 5 2006 fromhttpsecurecihicacihiwebproductsndb_worforce_trends_registered_nurses_canada_2005_epdf
CarruthA K (1996) Development and testing of the Caregiver ReciprocityScaleNursing Research 45(2) 92ndash97
Chen F Feudtner C Rhodes L amp Green L (2001) Role conflicts of physi-cians and their family members Rules but no rule bookWestern Journal ofMedicine 175(4) 236ndash239
Cohen S Underwood L G amp Gottlieb BH (Eds) (2000) Social support mea-surement and interventionA guide for health and social scientistsOxford OxfordUniversity Press
Fast J (2005)Hidden costsinvisible contributions report Reworking workThe experi-ence of employed caregivers of older adults Retrieved August 16 2007 fromwwwhecolualbertacahcic
Gable R ampWolfe M (1993) Instrument development 2nd ed Boston KluwerGubermanN amp Maheu P (1999) Combining employment and caregivingAn
intricate juggling actCanadian Journal on Aging 18(1) 84ndash106Keefe J Leacutegareacute J amp CarriegravereY (2007) Developing new strategies to support
future caregivers of older Canadians with disabilities Projections of need andtheir policy implicationsCanadian Public Policy 33 S65ndash80
Lengacher CA amp Sellers E (2003)TheWomenrsquos Role Strain Inventory InO L Strickland amp CDilorio (Eds)Measurement of nursing outcomes 2nd ed(pp 109ndash127) NewYork Springer
Martin-MatthewsA (2000) Intergenerational caregivingHow apocalyptic anddominant demography frame the questions and shape the answers In EMGee amp GGutman (Eds)The overselling of population agingApocalyptic demog-raphy intergenerational challenges and social policy (pp 64ndash79)Toronto OxfordUniversity Press
Ward-Griffin Keefe Martin-Matthews Kerr Brown and Oudshoorn
CJNR 2009Vol 41 No 3 126
Mayall B (1993) Keeping children healthy ndash the intermediate domain SocialScience and Medicine 36(1) 77ndash83
Morris JM amp Field PA (1995) Qualitative research methods for health profession-als 2nd ed London Sage
Pascall G (1986) Social policyA feminist analysis NewYorkTavistockPhillips J BernardM amp ChittendenM (2002) Juggling work and careThe expe-riences of older adults Bristol Policy Press
Polit D F amp Beck CT (2008)Nursing research Generating and assessing evidencefor nursing practice 8th ed Philadelphia LippincottWilliams ampWilkins
Polit D F amp Beck CT amp Owen SV (2007) Is the CVI an acceptable indica-tor of content validity Appraisal and recommendationsResearch in Nursingand Health 30 459ndash467
RossMM Rideout EM amp CarsonMM (1996) Nursesrsquo work Balancingpersonal and professional caregiving careers Canadian Journal of NursingResearch 26(4) 43ndash59
RutmanD (1996) Caregiving as womenrsquos workWomenrsquos experiences of pow-erfulness and powerlessness as caregiversQualitative Health Research 6(1) 90ndash111
ShieldsM ampWilkins K (2005)National Survey of theWork and Health of Nurses2005 Provincial profiles Ottawa Statistics CanadaRetrieved August 24 2007from httpwwwstatcancaenglishresearch11-621-MIE11-621-MIE2006052htm
StaceyM amp Davies C (1983)Division of labour in child health care Final report toSSRCCoventry Sociology Department University ofWarwick
Tebb S (1995)An aid to empowermentA caregiver well-being scaleHealth andSocialWork 20(2) 87ndash92
Tebb S Berg-WgerM amp Rubio DM (2000) CaregiverWell-Being Scale InDRoyse BAThyer D K Padgett ampT K Logan (Eds) Program evaluation3rd ed (pp 320ndash323) Pacific Grove CA BrooksCole
Ungerson C (1990) The language of care Crossing the boundaries InCUngerson (Ed)Gender and caringWork and welfare in Britain and Scandinavia(pp 8ndash33) NewYork Harvester
WaltersV LentonR French S Eyles JMayr J amp Newbold B (1996) Paidwork unpaid work and social supportA study of the health of male andfemale nurses Social Science and Medicine 43(11) 1627ndash1636
Ward-Griffin C (2004) Nurses as caregivers of elderly relatives Negotiatingpersonal and professional boundariesCJNR 36(1) 92ndash114
Ward-Griffin C (2008)Health professionals caring for aging relativesA profes-sional or personal issue In AMartin-Matthews amp J Phillips (Eds)Blurringthe boundariesAgeing at the intersection of work and home life (pp 1ndash20) NewYorkTaylor amp FrancisPsychology Press
Ward-Griffin C Brown JVandervoortA McNair S amp Dashnay I (2005)Double duty caregivingWomen in the health professionsCanadian Journalon Aging 24(4) 379ndash394
Ward-Griffin C amp MarshallV (2003) Reconceptualizing the relationshipbetween public and private eldercare Journal of Aging Studies 17 189ndash208
Development andValidation of the Double Duty Caregiving Scale
CJNR 2009Vol 41 No 3 127
Ware J E Kosinksi MTurner-Bowker L amp Gandek B (2002)How to scoreversion 2 of the SF-12 health survey Lincoln RIQuality Metric Inc
Acknowledgements
This study was funded by the Social Sciences and Humanities ResearchCouncil (Internal) and the Institute of Gender and Health CanadianInstitutes of Health ResearchThere are no conflicts of interest or financial disclosures
CatherineWard-Griffin RN PhD is ProfessorArthur Labatt Family School ofNursing University ofWestern Ontario London Canada Janice Keefe PhD isProfessor and Canada Research Chair in Aging and Caregiving Policy FamilyStudies and GerontologyMount SaintVincent University HalifaxNova ScotiaCanadaAnne Martin-Matthews PhD is Professor School of SocialWork andFamily Studies University of British ColumbiaVancouver Canada MichaelKerr PhD is Associate ProfessorArthur Labatt Family School of NursingUniversity ofWestern Ontario Judith Belle Brown PhD is Professor Departmentof Family Medicine University ofWestern OntarioAbram Oudshoorn RN is aPhD candidate in the Arthur Labatt Family School of Nursing University ofWestern Ontario
Ward-Griffin Keefe Martin-Matthews Kerr Brown and Oudshoorn
CJNR 2009Vol 41 No 3 128
between CI andWRSI (r = -49 p lt 001) between Supports andWRSI(r = 041 p lt001) and between CI and SF-12v2 (mental) (r = -39 p lt001) Finally the CI of the DDCS was also negatively correlated withcaregiver well-being (r = -29 p lt 001 [activities] and r = -36 p lt001[needs])The strongest subscale inter-correlations (ie within the Revised
DDCS itself) were between Expectations and CI (r = 055 p lt 001) andbetween Expectations and Making Connections (r = 038 p lt 001) Inaddition there was a weak positive association between MakingConnections and CI (r = 018 p lt 05) and negative associationsbetween Supports and CI (r = -026 p lt 001) and between SettingLimits and CI (r = -23 p lt 001) None of the other DDCS subscaleinter-correlations were statistically significant (Table 4)
Contrasted Groups Approach
Although there were no significant differences between DDCs andnon-DDCs in their overall scores for theWRSI CWBS and SF-12v2(physical and mental scores) there were significant differences betweennon-DDCs (n = 67) and the DDC subgroup (n = 84) defined as livingon the edge (ie those scoring above the mean on the CI subscale) Poorerhealth was observed for the living on the edge DDCs on their overall SF-12v2 mental health index score (t = -276 p lt 05) and on four of theeight SF-12v2 subscales vitality (t = -237 p lt 05) social functioning(t = -291 p lt 01) role emotional (t = -306 p lt 05) and mental health(t = -227 p lt 05) Moreover there were significant differences withinthe DDC group between those who were living on the edge and thosewith lower CI scores for the following SF-12 subscales vitality (t = -20p lt 05) social functioning (t = -356 p lt 01) role emotional (t = -483p lt 01) and mental health (t = -398 p lt 05)The living on the edgegroup also had significantly lower well-being scores for the activities(t = -363 p lt 05) and needs (t = -447 p lt 05) subscales than theother DDC respondentsWhile not all results were statistically significantoverall there was an observed tendency for the living on the edge group ofDDCs to have the lowest health and well-being scores whereas the otherDDCs (eg making it work) with low CI scores tended to have slightlybetter health scores than the non-DDC group
Discussion
The main purpose of this study was to develop and test a tool intendedto advance our understanding of DDC using a random sample of regis-tered nurses providing care to elderly relatives
Development andValidation of the Double Duty Caregiving Scale
CJNR 2009Vol 41 No 3 123
The nine factors we identified were consistent with the theorized coreDDC dimensions of Expectations (Familial and Professional) Supports(Personal and Professional) Setting Limits (Awareness of BoundariesActive Resistance) Making Connections and Caregiving Interface(Perceptions and Consequences) which can yield important informationregarding how much variance is accounted for by the factors Howeveradditional analyses are required to establish the psychometric propertiesof the DDCS including test-retest reliability to assess construct stabilityBased on the EFA results a measurement model of DDC will be pro-posed and analyzed in a future study using CFA to enhance the psycho-metric validation of the DDCS For researchers looking for a shorterversion of the DDCS it is worth noting that based on the strength andconsistency of the overall findings the seven-item CI subscale could beused to determine the extent of DDC when survey respondent burdenis a key factor in instrument selection (ie when use of the full 33DDCS items is not possible) adding to the potential value of the DDCS
The positive correlation between Expectations and CI and the nega-tive correlation between Supports and CI and between Setting Limitsand CI are theoretically consistent with the conceptual model of DDCThat is if expectations are high both personally and professionally withrespect to caring for onersquos relatives there will be greater CI or blurringof boundaries Conversely if one has strong personal and professionalsupports it follows that a lower degree of CI will result Similarly whenone sets limits on caregiving then less blurring or a lower degree of CIshould result However the positive association between MakingConnections and Expectations was unexpected Perhaps high expecta-tions lead one to increase supports by making connections both person-ally and professionally to help meet these expectationsComparison of the SF-12 v2 scores for living on the edge DDCs and
non-DDCs revealed significant differences for SF-12v2 mental healthand specific SF-12v2 subscales of vitality social functioning role emo-tional and mental healthThese findings suggest that DDCs who expe-rience a high degree of blurring of their professional and personalboundaries are at greater risk for poor health than those health profes-sionals who do not care for elderly relatives or who do not experiencethis blurring In addition those DDCs who could be characterized asliving on the edge scored significantly higher on the same four SF-12 sub-scales than DDCs with lower CI scoresThis observed pattern suggeststwo possibilities there exists a threshold effect for the negative healtheffects of DDC or manageable exposure to DDC has a beneficial effectFurther exploration of these interesting findings is warrantedAlthough we conducted a systematic and comprehensive analysis to
assess the psychometric properties of a new scale further reliability and
Ward-Griffin Keefe Martin-Matthews Kerr Brown and Oudshoorn
CJNR 2009Vol 41 No 3 124
validity studies are needed Confirmatory validation studies with otherhealth-care provider populations such as family physicians social workersand physiotherapists are particularly important as these professionals havethe potential to be DDCs and their experiences as documented in ouroriginal qualitative study of DDC helped to formulate the theoreticalunderpinnings of the DDCS In addition research with these groups willadvance our understanding of how occupational health groups may differin terms of expectations supports negotiating strategies and degree ofCIAs the identification of health-advantage and health-risk factors isinfluenced by health and social environments the negotiating strategiescould also be examined through the use of qualitative methodologiessuch as in-depth interviews or focus groupsFinally research that draws linkages between professional and personal
caregiving has the added value of furthering knowledge about employedcaregiving specifically as it relates to the relationship between health out-comes and provision of familial care by health-care providersAlthoughthe convergence (and avoidance) of professional and personal caregivingboundaries is not a new issue in nursing and other health professions thenotion that it is the individualrsquos responsibility to negotiate this boundarytends to predominate (Ward-Griffin 2008)To that end further testingand refinement of the DDCS will be helpful in identifying areas whereDDCs may need specific or different types of support It is also impor-tant to understand how specific social supports shape the health experi-ences of DDCs as well as to investigate different types of social supportinterventions with DDCsThis information is particularly meaningfultoday with the intersection of three challenges an aging population anaging health-care workforce and a shortage of health professionals Suchknowledge could contribute to workplace and other health initiativesspearheaded by professional groups policy-makers and other key stake-holders interested in assessing and addressing the health effects of DDCIn summary the DDCS is a valid tool for the assessment of double
duty caregiving Such assessment is a crucial step in understanding theexperience of the blurring of personal and professional boundaries ofcaregiving among health professionalsA quantitative study of both maleand female DDCs could help us to understand the relationship betweencertain factors (ie gender health-care occupation) and the potentialhealth effects of DDCMoreover our finding that respondents with highCI scores (living on the edge) had significantly lower health and well-beingscores than DDC respondents with lower CI scores warrants furtherinvestigation to determine if one group of DDCs is at particular risk fordeveloping negative health effects Given the current climate of health-care reform in Canada developing a better understanding of DDC andits health effects is particularly relevant for policy-makers and others who
Development andValidation of the Double Duty Caregiving Scale
CJNR 2009Vol 41 No 3 125
are committed to developing health-promoting programs and policies forfamilial caregivers of the elderly Clearly now is the time to monitor theeffects of changing demographics both in the general population andwithin the health professions in order to develop appropriate and tar-geted strategies thereby creating and sustaining healthy work environ-ments and health-care workforcesWith further refinement the DDCSmay assist with these endeavours
References
Armstrong P amp ArmstrongH (2004)Thinking it throughWomenwork andcaring in the new millennium In K Grant CArmaratunga PArmstrongM BoscoeA Pederson amp KWillson (Eds)Caring forcaring aboutWomenhome care and unpaid caregiving (pp 5ndash44)Aurora ONGaramond
Baines D (2004) Seven kinds of work ndash only one paid Raced gendered andrestructured work in social servicesAtlantis 28(2) 19ndash28
Canadian Institute for Health Information (2006)Workforce trends of registerednurses in Canada 2005 Retrieved November 5 2006 fromhttpsecurecihicacihiwebproductsndb_worforce_trends_registered_nurses_canada_2005_epdf
CarruthA K (1996) Development and testing of the Caregiver ReciprocityScaleNursing Research 45(2) 92ndash97
Chen F Feudtner C Rhodes L amp Green L (2001) Role conflicts of physi-cians and their family members Rules but no rule bookWestern Journal ofMedicine 175(4) 236ndash239
Cohen S Underwood L G amp Gottlieb BH (Eds) (2000) Social support mea-surement and interventionA guide for health and social scientistsOxford OxfordUniversity Press
Fast J (2005)Hidden costsinvisible contributions report Reworking workThe experi-ence of employed caregivers of older adults Retrieved August 16 2007 fromwwwhecolualbertacahcic
Gable R ampWolfe M (1993) Instrument development 2nd ed Boston KluwerGubermanN amp Maheu P (1999) Combining employment and caregivingAn
intricate juggling actCanadian Journal on Aging 18(1) 84ndash106Keefe J Leacutegareacute J amp CarriegravereY (2007) Developing new strategies to support
future caregivers of older Canadians with disabilities Projections of need andtheir policy implicationsCanadian Public Policy 33 S65ndash80
Lengacher CA amp Sellers E (2003)TheWomenrsquos Role Strain Inventory InO L Strickland amp CDilorio (Eds)Measurement of nursing outcomes 2nd ed(pp 109ndash127) NewYork Springer
Martin-MatthewsA (2000) Intergenerational caregivingHow apocalyptic anddominant demography frame the questions and shape the answers In EMGee amp GGutman (Eds)The overselling of population agingApocalyptic demog-raphy intergenerational challenges and social policy (pp 64ndash79)Toronto OxfordUniversity Press
Ward-Griffin Keefe Martin-Matthews Kerr Brown and Oudshoorn
CJNR 2009Vol 41 No 3 126
Mayall B (1993) Keeping children healthy ndash the intermediate domain SocialScience and Medicine 36(1) 77ndash83
Morris JM amp Field PA (1995) Qualitative research methods for health profession-als 2nd ed London Sage
Pascall G (1986) Social policyA feminist analysis NewYorkTavistockPhillips J BernardM amp ChittendenM (2002) Juggling work and careThe expe-riences of older adults Bristol Policy Press
Polit D F amp Beck CT (2008)Nursing research Generating and assessing evidencefor nursing practice 8th ed Philadelphia LippincottWilliams ampWilkins
Polit D F amp Beck CT amp Owen SV (2007) Is the CVI an acceptable indica-tor of content validity Appraisal and recommendationsResearch in Nursingand Health 30 459ndash467
RossMM Rideout EM amp CarsonMM (1996) Nursesrsquo work Balancingpersonal and professional caregiving careers Canadian Journal of NursingResearch 26(4) 43ndash59
RutmanD (1996) Caregiving as womenrsquos workWomenrsquos experiences of pow-erfulness and powerlessness as caregiversQualitative Health Research 6(1) 90ndash111
ShieldsM ampWilkins K (2005)National Survey of theWork and Health of Nurses2005 Provincial profiles Ottawa Statistics CanadaRetrieved August 24 2007from httpwwwstatcancaenglishresearch11-621-MIE11-621-MIE2006052htm
StaceyM amp Davies C (1983)Division of labour in child health care Final report toSSRCCoventry Sociology Department University ofWarwick
Tebb S (1995)An aid to empowermentA caregiver well-being scaleHealth andSocialWork 20(2) 87ndash92
Tebb S Berg-WgerM amp Rubio DM (2000) CaregiverWell-Being Scale InDRoyse BAThyer D K Padgett ampT K Logan (Eds) Program evaluation3rd ed (pp 320ndash323) Pacific Grove CA BrooksCole
Ungerson C (1990) The language of care Crossing the boundaries InCUngerson (Ed)Gender and caringWork and welfare in Britain and Scandinavia(pp 8ndash33) NewYork Harvester
WaltersV LentonR French S Eyles JMayr J amp Newbold B (1996) Paidwork unpaid work and social supportA study of the health of male andfemale nurses Social Science and Medicine 43(11) 1627ndash1636
Ward-Griffin C (2004) Nurses as caregivers of elderly relatives Negotiatingpersonal and professional boundariesCJNR 36(1) 92ndash114
Ward-Griffin C (2008)Health professionals caring for aging relativesA profes-sional or personal issue In AMartin-Matthews amp J Phillips (Eds)Blurringthe boundariesAgeing at the intersection of work and home life (pp 1ndash20) NewYorkTaylor amp FrancisPsychology Press
Ward-Griffin C Brown JVandervoortA McNair S amp Dashnay I (2005)Double duty caregivingWomen in the health professionsCanadian Journalon Aging 24(4) 379ndash394
Ward-Griffin C amp MarshallV (2003) Reconceptualizing the relationshipbetween public and private eldercare Journal of Aging Studies 17 189ndash208
Development andValidation of the Double Duty Caregiving Scale
CJNR 2009Vol 41 No 3 127
Ware J E Kosinksi MTurner-Bowker L amp Gandek B (2002)How to scoreversion 2 of the SF-12 health survey Lincoln RIQuality Metric Inc
Acknowledgements
This study was funded by the Social Sciences and Humanities ResearchCouncil (Internal) and the Institute of Gender and Health CanadianInstitutes of Health ResearchThere are no conflicts of interest or financial disclosures
CatherineWard-Griffin RN PhD is ProfessorArthur Labatt Family School ofNursing University ofWestern Ontario London Canada Janice Keefe PhD isProfessor and Canada Research Chair in Aging and Caregiving Policy FamilyStudies and GerontologyMount SaintVincent University HalifaxNova ScotiaCanadaAnne Martin-Matthews PhD is Professor School of SocialWork andFamily Studies University of British ColumbiaVancouver Canada MichaelKerr PhD is Associate ProfessorArthur Labatt Family School of NursingUniversity ofWestern Ontario Judith Belle Brown PhD is Professor Departmentof Family Medicine University ofWestern OntarioAbram Oudshoorn RN is aPhD candidate in the Arthur Labatt Family School of Nursing University ofWestern Ontario
Ward-Griffin Keefe Martin-Matthews Kerr Brown and Oudshoorn
CJNR 2009Vol 41 No 3 128

The nine factors we identified were consistent with the theorized coreDDC dimensions of Expectations (Familial and Professional) Supports(Personal and Professional) Setting Limits (Awareness of BoundariesActive Resistance) Making Connections and Caregiving Interface(Perceptions and Consequences) which can yield important informationregarding how much variance is accounted for by the factors Howeveradditional analyses are required to establish the psychometric propertiesof the DDCS including test-retest reliability to assess construct stabilityBased on the EFA results a measurement model of DDC will be pro-posed and analyzed in a future study using CFA to enhance the psycho-metric validation of the DDCS For researchers looking for a shorterversion of the DDCS it is worth noting that based on the strength andconsistency of the overall findings the seven-item CI subscale could beused to determine the extent of DDC when survey respondent burdenis a key factor in instrument selection (ie when use of the full 33DDCS items is not possible) adding to the potential value of the DDCS
The positive correlation between Expectations and CI and the nega-tive correlation between Supports and CI and between Setting Limitsand CI are theoretically consistent with the conceptual model of DDCThat is if expectations are high both personally and professionally withrespect to caring for onersquos relatives there will be greater CI or blurringof boundaries Conversely if one has strong personal and professionalsupports it follows that a lower degree of CI will result Similarly whenone sets limits on caregiving then less blurring or a lower degree of CIshould result However the positive association between MakingConnections and Expectations was unexpected Perhaps high expecta-tions lead one to increase supports by making connections both person-ally and professionally to help meet these expectationsComparison of the SF-12 v2 scores for living on the edge DDCs and
non-DDCs revealed significant differences for SF-12v2 mental healthand specific SF-12v2 subscales of vitality social functioning role emo-tional and mental healthThese findings suggest that DDCs who expe-rience a high degree of blurring of their professional and personalboundaries are at greater risk for poor health than those health profes-sionals who do not care for elderly relatives or who do not experiencethis blurring In addition those DDCs who could be characterized asliving on the edge scored significantly higher on the same four SF-12 sub-scales than DDCs with lower CI scoresThis observed pattern suggeststwo possibilities there exists a threshold effect for the negative healtheffects of DDC or manageable exposure to DDC has a beneficial effectFurther exploration of these interesting findings is warrantedAlthough we conducted a systematic and comprehensive analysis to
assess the psychometric properties of a new scale further reliability and
Ward-Griffin Keefe Martin-Matthews Kerr Brown and Oudshoorn
CJNR 2009Vol 41 No 3 124
validity studies are needed Confirmatory validation studies with otherhealth-care provider populations such as family physicians social workersand physiotherapists are particularly important as these professionals havethe potential to be DDCs and their experiences as documented in ouroriginal qualitative study of DDC helped to formulate the theoreticalunderpinnings of the DDCS In addition research with these groups willadvance our understanding of how occupational health groups may differin terms of expectations supports negotiating strategies and degree ofCIAs the identification of health-advantage and health-risk factors isinfluenced by health and social environments the negotiating strategiescould also be examined through the use of qualitative methodologiessuch as in-depth interviews or focus groupsFinally research that draws linkages between professional and personal
caregiving has the added value of furthering knowledge about employedcaregiving specifically as it relates to the relationship between health out-comes and provision of familial care by health-care providersAlthoughthe convergence (and avoidance) of professional and personal caregivingboundaries is not a new issue in nursing and other health professions thenotion that it is the individualrsquos responsibility to negotiate this boundarytends to predominate (Ward-Griffin 2008)To that end further testingand refinement of the DDCS will be helpful in identifying areas whereDDCs may need specific or different types of support It is also impor-tant to understand how specific social supports shape the health experi-ences of DDCs as well as to investigate different types of social supportinterventions with DDCsThis information is particularly meaningfultoday with the intersection of three challenges an aging population anaging health-care workforce and a shortage of health professionals Suchknowledge could contribute to workplace and other health initiativesspearheaded by professional groups policy-makers and other key stake-holders interested in assessing and addressing the health effects of DDCIn summary the DDCS is a valid tool for the assessment of double
duty caregiving Such assessment is a crucial step in understanding theexperience of the blurring of personal and professional boundaries ofcaregiving among health professionalsA quantitative study of both maleand female DDCs could help us to understand the relationship betweencertain factors (ie gender health-care occupation) and the potentialhealth effects of DDCMoreover our finding that respondents with highCI scores (living on the edge) had significantly lower health and well-beingscores than DDC respondents with lower CI scores warrants furtherinvestigation to determine if one group of DDCs is at particular risk fordeveloping negative health effects Given the current climate of health-care reform in Canada developing a better understanding of DDC andits health effects is particularly relevant for policy-makers and others who
Development andValidation of the Double Duty Caregiving Scale
CJNR 2009Vol 41 No 3 125
are committed to developing health-promoting programs and policies forfamilial caregivers of the elderly Clearly now is the time to monitor theeffects of changing demographics both in the general population andwithin the health professions in order to develop appropriate and tar-geted strategies thereby creating and sustaining healthy work environ-ments and health-care workforcesWith further refinement the DDCSmay assist with these endeavours
References
Armstrong P amp ArmstrongH (2004)Thinking it throughWomenwork andcaring in the new millennium In K Grant CArmaratunga PArmstrongM BoscoeA Pederson amp KWillson (Eds)Caring forcaring aboutWomenhome care and unpaid caregiving (pp 5ndash44)Aurora ONGaramond
Baines D (2004) Seven kinds of work ndash only one paid Raced gendered andrestructured work in social servicesAtlantis 28(2) 19ndash28
Canadian Institute for Health Information (2006)Workforce trends of registerednurses in Canada 2005 Retrieved November 5 2006 fromhttpsecurecihicacihiwebproductsndb_worforce_trends_registered_nurses_canada_2005_epdf
CarruthA K (1996) Development and testing of the Caregiver ReciprocityScaleNursing Research 45(2) 92ndash97
Chen F Feudtner C Rhodes L amp Green L (2001) Role conflicts of physi-cians and their family members Rules but no rule bookWestern Journal ofMedicine 175(4) 236ndash239
Cohen S Underwood L G amp Gottlieb BH (Eds) (2000) Social support mea-surement and interventionA guide for health and social scientistsOxford OxfordUniversity Press
Fast J (2005)Hidden costsinvisible contributions report Reworking workThe experi-ence of employed caregivers of older adults Retrieved August 16 2007 fromwwwhecolualbertacahcic
Gable R ampWolfe M (1993) Instrument development 2nd ed Boston KluwerGubermanN amp Maheu P (1999) Combining employment and caregivingAn
intricate juggling actCanadian Journal on Aging 18(1) 84ndash106Keefe J Leacutegareacute J amp CarriegravereY (2007) Developing new strategies to support
future caregivers of older Canadians with disabilities Projections of need andtheir policy implicationsCanadian Public Policy 33 S65ndash80
Lengacher CA amp Sellers E (2003)TheWomenrsquos Role Strain Inventory InO L Strickland amp CDilorio (Eds)Measurement of nursing outcomes 2nd ed(pp 109ndash127) NewYork Springer
Martin-MatthewsA (2000) Intergenerational caregivingHow apocalyptic anddominant demography frame the questions and shape the answers In EMGee amp GGutman (Eds)The overselling of population agingApocalyptic demog-raphy intergenerational challenges and social policy (pp 64ndash79)Toronto OxfordUniversity Press
Ward-Griffin Keefe Martin-Matthews Kerr Brown and Oudshoorn
CJNR 2009Vol 41 No 3 126
Mayall B (1993) Keeping children healthy ndash the intermediate domain SocialScience and Medicine 36(1) 77ndash83
Morris JM amp Field PA (1995) Qualitative research methods for health profession-als 2nd ed London Sage
Pascall G (1986) Social policyA feminist analysis NewYorkTavistockPhillips J BernardM amp ChittendenM (2002) Juggling work and careThe expe-riences of older adults Bristol Policy Press
Polit D F amp Beck CT (2008)Nursing research Generating and assessing evidencefor nursing practice 8th ed Philadelphia LippincottWilliams ampWilkins
Polit D F amp Beck CT amp Owen SV (2007) Is the CVI an acceptable indica-tor of content validity Appraisal and recommendationsResearch in Nursingand Health 30 459ndash467
RossMM Rideout EM amp CarsonMM (1996) Nursesrsquo work Balancingpersonal and professional caregiving careers Canadian Journal of NursingResearch 26(4) 43ndash59
RutmanD (1996) Caregiving as womenrsquos workWomenrsquos experiences of pow-erfulness and powerlessness as caregiversQualitative Health Research 6(1) 90ndash111
ShieldsM ampWilkins K (2005)National Survey of theWork and Health of Nurses2005 Provincial profiles Ottawa Statistics CanadaRetrieved August 24 2007from httpwwwstatcancaenglishresearch11-621-MIE11-621-MIE2006052htm
StaceyM amp Davies C (1983)Division of labour in child health care Final report toSSRCCoventry Sociology Department University ofWarwick
Tebb S (1995)An aid to empowermentA caregiver well-being scaleHealth andSocialWork 20(2) 87ndash92
Tebb S Berg-WgerM amp Rubio DM (2000) CaregiverWell-Being Scale InDRoyse BAThyer D K Padgett ampT K Logan (Eds) Program evaluation3rd ed (pp 320ndash323) Pacific Grove CA BrooksCole
Ungerson C (1990) The language of care Crossing the boundaries InCUngerson (Ed)Gender and caringWork and welfare in Britain and Scandinavia(pp 8ndash33) NewYork Harvester
WaltersV LentonR French S Eyles JMayr J amp Newbold B (1996) Paidwork unpaid work and social supportA study of the health of male andfemale nurses Social Science and Medicine 43(11) 1627ndash1636
Ward-Griffin C (2004) Nurses as caregivers of elderly relatives Negotiatingpersonal and professional boundariesCJNR 36(1) 92ndash114
Ward-Griffin C (2008)Health professionals caring for aging relativesA profes-sional or personal issue In AMartin-Matthews amp J Phillips (Eds)Blurringthe boundariesAgeing at the intersection of work and home life (pp 1ndash20) NewYorkTaylor amp FrancisPsychology Press
Ward-Griffin C Brown JVandervoortA McNair S amp Dashnay I (2005)Double duty caregivingWomen in the health professionsCanadian Journalon Aging 24(4) 379ndash394
Ward-Griffin C amp MarshallV (2003) Reconceptualizing the relationshipbetween public and private eldercare Journal of Aging Studies 17 189ndash208
Development andValidation of the Double Duty Caregiving Scale
CJNR 2009Vol 41 No 3 127
Ware J E Kosinksi MTurner-Bowker L amp Gandek B (2002)How to scoreversion 2 of the SF-12 health survey Lincoln RIQuality Metric Inc
Acknowledgements
This study was funded by the Social Sciences and Humanities ResearchCouncil (Internal) and the Institute of Gender and Health CanadianInstitutes of Health ResearchThere are no conflicts of interest or financial disclosures
CatherineWard-Griffin RN PhD is ProfessorArthur Labatt Family School ofNursing University ofWestern Ontario London Canada Janice Keefe PhD isProfessor and Canada Research Chair in Aging and Caregiving Policy FamilyStudies and GerontologyMount SaintVincent University HalifaxNova ScotiaCanadaAnne Martin-Matthews PhD is Professor School of SocialWork andFamily Studies University of British ColumbiaVancouver Canada MichaelKerr PhD is Associate ProfessorArthur Labatt Family School of NursingUniversity ofWestern Ontario Judith Belle Brown PhD is Professor Departmentof Family Medicine University ofWestern OntarioAbram Oudshoorn RN is aPhD candidate in the Arthur Labatt Family School of Nursing University ofWestern Ontario
Ward-Griffin Keefe Martin-Matthews Kerr Brown and Oudshoorn
CJNR 2009Vol 41 No 3 128

validity studies are needed Confirmatory validation studies with otherhealth-care provider populations such as family physicians social workersand physiotherapists are particularly important as these professionals havethe potential to be DDCs and their experiences as documented in ouroriginal qualitative study of DDC helped to formulate the theoreticalunderpinnings of the DDCS In addition research with these groups willadvance our understanding of how occupational health groups may differin terms of expectations supports negotiating strategies and degree ofCIAs the identification of health-advantage and health-risk factors isinfluenced by health and social environments the negotiating strategiescould also be examined through the use of qualitative methodologiessuch as in-depth interviews or focus groupsFinally research that draws linkages between professional and personal
caregiving has the added value of furthering knowledge about employedcaregiving specifically as it relates to the relationship between health out-comes and provision of familial care by health-care providersAlthoughthe convergence (and avoidance) of professional and personal caregivingboundaries is not a new issue in nursing and other health professions thenotion that it is the individualrsquos responsibility to negotiate this boundarytends to predominate (Ward-Griffin 2008)To that end further testingand refinement of the DDCS will be helpful in identifying areas whereDDCs may need specific or different types of support It is also impor-tant to understand how specific social supports shape the health experi-ences of DDCs as well as to investigate different types of social supportinterventions with DDCsThis information is particularly meaningfultoday with the intersection of three challenges an aging population anaging health-care workforce and a shortage of health professionals Suchknowledge could contribute to workplace and other health initiativesspearheaded by professional groups policy-makers and other key stake-holders interested in assessing and addressing the health effects of DDCIn summary the DDCS is a valid tool for the assessment of double
duty caregiving Such assessment is a crucial step in understanding theexperience of the blurring of personal and professional boundaries ofcaregiving among health professionalsA quantitative study of both maleand female DDCs could help us to understand the relationship betweencertain factors (ie gender health-care occupation) and the potentialhealth effects of DDCMoreover our finding that respondents with highCI scores (living on the edge) had significantly lower health and well-beingscores than DDC respondents with lower CI scores warrants furtherinvestigation to determine if one group of DDCs is at particular risk fordeveloping negative health effects Given the current climate of health-care reform in Canada developing a better understanding of DDC andits health effects is particularly relevant for policy-makers and others who
Development andValidation of the Double Duty Caregiving Scale
CJNR 2009Vol 41 No 3 125
are committed to developing health-promoting programs and policies forfamilial caregivers of the elderly Clearly now is the time to monitor theeffects of changing demographics both in the general population andwithin the health professions in order to develop appropriate and tar-geted strategies thereby creating and sustaining healthy work environ-ments and health-care workforcesWith further refinement the DDCSmay assist with these endeavours
References
Armstrong P amp ArmstrongH (2004)Thinking it throughWomenwork andcaring in the new millennium In K Grant CArmaratunga PArmstrongM BoscoeA Pederson amp KWillson (Eds)Caring forcaring aboutWomenhome care and unpaid caregiving (pp 5ndash44)Aurora ONGaramond
Baines D (2004) Seven kinds of work ndash only one paid Raced gendered andrestructured work in social servicesAtlantis 28(2) 19ndash28
Canadian Institute for Health Information (2006)Workforce trends of registerednurses in Canada 2005 Retrieved November 5 2006 fromhttpsecurecihicacihiwebproductsndb_worforce_trends_registered_nurses_canada_2005_epdf
CarruthA K (1996) Development and testing of the Caregiver ReciprocityScaleNursing Research 45(2) 92ndash97
Chen F Feudtner C Rhodes L amp Green L (2001) Role conflicts of physi-cians and their family members Rules but no rule bookWestern Journal ofMedicine 175(4) 236ndash239
Cohen S Underwood L G amp Gottlieb BH (Eds) (2000) Social support mea-surement and interventionA guide for health and social scientistsOxford OxfordUniversity Press
Fast J (2005)Hidden costsinvisible contributions report Reworking workThe experi-ence of employed caregivers of older adults Retrieved August 16 2007 fromwwwhecolualbertacahcic
Gable R ampWolfe M (1993) Instrument development 2nd ed Boston KluwerGubermanN amp Maheu P (1999) Combining employment and caregivingAn
intricate juggling actCanadian Journal on Aging 18(1) 84ndash106Keefe J Leacutegareacute J amp CarriegravereY (2007) Developing new strategies to support
future caregivers of older Canadians with disabilities Projections of need andtheir policy implicationsCanadian Public Policy 33 S65ndash80
Lengacher CA amp Sellers E (2003)TheWomenrsquos Role Strain Inventory InO L Strickland amp CDilorio (Eds)Measurement of nursing outcomes 2nd ed(pp 109ndash127) NewYork Springer
Martin-MatthewsA (2000) Intergenerational caregivingHow apocalyptic anddominant demography frame the questions and shape the answers In EMGee amp GGutman (Eds)The overselling of population agingApocalyptic demog-raphy intergenerational challenges and social policy (pp 64ndash79)Toronto OxfordUniversity Press
Ward-Griffin Keefe Martin-Matthews Kerr Brown and Oudshoorn
CJNR 2009Vol 41 No 3 126
Mayall B (1993) Keeping children healthy ndash the intermediate domain SocialScience and Medicine 36(1) 77ndash83
Morris JM amp Field PA (1995) Qualitative research methods for health profession-als 2nd ed London Sage
Pascall G (1986) Social policyA feminist analysis NewYorkTavistockPhillips J BernardM amp ChittendenM (2002) Juggling work and careThe expe-riences of older adults Bristol Policy Press
Polit D F amp Beck CT (2008)Nursing research Generating and assessing evidencefor nursing practice 8th ed Philadelphia LippincottWilliams ampWilkins
Polit D F amp Beck CT amp Owen SV (2007) Is the CVI an acceptable indica-tor of content validity Appraisal and recommendationsResearch in Nursingand Health 30 459ndash467
RossMM Rideout EM amp CarsonMM (1996) Nursesrsquo work Balancingpersonal and professional caregiving careers Canadian Journal of NursingResearch 26(4) 43ndash59
RutmanD (1996) Caregiving as womenrsquos workWomenrsquos experiences of pow-erfulness and powerlessness as caregiversQualitative Health Research 6(1) 90ndash111
ShieldsM ampWilkins K (2005)National Survey of theWork and Health of Nurses2005 Provincial profiles Ottawa Statistics CanadaRetrieved August 24 2007from httpwwwstatcancaenglishresearch11-621-MIE11-621-MIE2006052htm
StaceyM amp Davies C (1983)Division of labour in child health care Final report toSSRCCoventry Sociology Department University ofWarwick
Tebb S (1995)An aid to empowermentA caregiver well-being scaleHealth andSocialWork 20(2) 87ndash92
Tebb S Berg-WgerM amp Rubio DM (2000) CaregiverWell-Being Scale InDRoyse BAThyer D K Padgett ampT K Logan (Eds) Program evaluation3rd ed (pp 320ndash323) Pacific Grove CA BrooksCole
Ungerson C (1990) The language of care Crossing the boundaries InCUngerson (Ed)Gender and caringWork and welfare in Britain and Scandinavia(pp 8ndash33) NewYork Harvester
WaltersV LentonR French S Eyles JMayr J amp Newbold B (1996) Paidwork unpaid work and social supportA study of the health of male andfemale nurses Social Science and Medicine 43(11) 1627ndash1636
Ward-Griffin C (2004) Nurses as caregivers of elderly relatives Negotiatingpersonal and professional boundariesCJNR 36(1) 92ndash114
Ward-Griffin C (2008)Health professionals caring for aging relativesA profes-sional or personal issue In AMartin-Matthews amp J Phillips (Eds)Blurringthe boundariesAgeing at the intersection of work and home life (pp 1ndash20) NewYorkTaylor amp FrancisPsychology Press
Ward-Griffin C Brown JVandervoortA McNair S amp Dashnay I (2005)Double duty caregivingWomen in the health professionsCanadian Journalon Aging 24(4) 379ndash394
Ward-Griffin C amp MarshallV (2003) Reconceptualizing the relationshipbetween public and private eldercare Journal of Aging Studies 17 189ndash208
Development andValidation of the Double Duty Caregiving Scale
CJNR 2009Vol 41 No 3 127
Ware J E Kosinksi MTurner-Bowker L amp Gandek B (2002)How to scoreversion 2 of the SF-12 health survey Lincoln RIQuality Metric Inc
Acknowledgements
This study was funded by the Social Sciences and Humanities ResearchCouncil (Internal) and the Institute of Gender and Health CanadianInstitutes of Health ResearchThere are no conflicts of interest or financial disclosures
CatherineWard-Griffin RN PhD is ProfessorArthur Labatt Family School ofNursing University ofWestern Ontario London Canada Janice Keefe PhD isProfessor and Canada Research Chair in Aging and Caregiving Policy FamilyStudies and GerontologyMount SaintVincent University HalifaxNova ScotiaCanadaAnne Martin-Matthews PhD is Professor School of SocialWork andFamily Studies University of British ColumbiaVancouver Canada MichaelKerr PhD is Associate ProfessorArthur Labatt Family School of NursingUniversity ofWestern Ontario Judith Belle Brown PhD is Professor Departmentof Family Medicine University ofWestern OntarioAbram Oudshoorn RN is aPhD candidate in the Arthur Labatt Family School of Nursing University ofWestern Ontario
Ward-Griffin Keefe Martin-Matthews Kerr Brown and Oudshoorn
CJNR 2009Vol 41 No 3 128
are committed to developing health-promoting programs and policies forfamilial caregivers of the elderly Clearly now is the time to monitor theeffects of changing demographics both in the general population andwithin the health professions in order to develop appropriate and tar-geted strategies thereby creating and sustaining healthy work environ-ments and health-care workforcesWith further refinement the DDCSmay assist with these endeavours
References
Armstrong P amp ArmstrongH (2004)Thinking it throughWomenwork andcaring in the new millennium In K Grant CArmaratunga PArmstrongM BoscoeA Pederson amp KWillson (Eds)Caring forcaring aboutWomenhome care and unpaid caregiving (pp 5ndash44)Aurora ONGaramond
Baines D (2004) Seven kinds of work ndash only one paid Raced gendered andrestructured work in social servicesAtlantis 28(2) 19ndash28
Canadian Institute for Health Information (2006)Workforce trends of registerednurses in Canada 2005 Retrieved November 5 2006 fromhttpsecurecihicacihiwebproductsndb_worforce_trends_registered_nurses_canada_2005_epdf
CarruthA K (1996) Development and testing of the Caregiver ReciprocityScaleNursing Research 45(2) 92ndash97
Chen F Feudtner C Rhodes L amp Green L (2001) Role conflicts of physi-cians and their family members Rules but no rule bookWestern Journal ofMedicine 175(4) 236ndash239
Cohen S Underwood L G amp Gottlieb BH (Eds) (2000) Social support mea-surement and interventionA guide for health and social scientistsOxford OxfordUniversity Press
Fast J (2005)Hidden costsinvisible contributions report Reworking workThe experi-ence of employed caregivers of older adults Retrieved August 16 2007 fromwwwhecolualbertacahcic
Gable R ampWolfe M (1993) Instrument development 2nd ed Boston KluwerGubermanN amp Maheu P (1999) Combining employment and caregivingAn
intricate juggling actCanadian Journal on Aging 18(1) 84ndash106Keefe J Leacutegareacute J amp CarriegravereY (2007) Developing new strategies to support
future caregivers of older Canadians with disabilities Projections of need andtheir policy implicationsCanadian Public Policy 33 S65ndash80
Lengacher CA amp Sellers E (2003)TheWomenrsquos Role Strain Inventory InO L Strickland amp CDilorio (Eds)Measurement of nursing outcomes 2nd ed(pp 109ndash127) NewYork Springer
Martin-MatthewsA (2000) Intergenerational caregivingHow apocalyptic anddominant demography frame the questions and shape the answers In EMGee amp GGutman (Eds)The overselling of population agingApocalyptic demog-raphy intergenerational challenges and social policy (pp 64ndash79)Toronto OxfordUniversity Press
Ward-Griffin Keefe Martin-Matthews Kerr Brown and Oudshoorn
CJNR 2009Vol 41 No 3 126
Mayall B (1993) Keeping children healthy ndash the intermediate domain SocialScience and Medicine 36(1) 77ndash83
Morris JM amp Field PA (1995) Qualitative research methods for health profession-als 2nd ed London Sage
Pascall G (1986) Social policyA feminist analysis NewYorkTavistockPhillips J BernardM amp ChittendenM (2002) Juggling work and careThe expe-riences of older adults Bristol Policy Press
Polit D F amp Beck CT (2008)Nursing research Generating and assessing evidencefor nursing practice 8th ed Philadelphia LippincottWilliams ampWilkins
Polit D F amp Beck CT amp Owen SV (2007) Is the CVI an acceptable indica-tor of content validity Appraisal and recommendationsResearch in Nursingand Health 30 459ndash467
RossMM Rideout EM amp CarsonMM (1996) Nursesrsquo work Balancingpersonal and professional caregiving careers Canadian Journal of NursingResearch 26(4) 43ndash59
RutmanD (1996) Caregiving as womenrsquos workWomenrsquos experiences of pow-erfulness and powerlessness as caregiversQualitative Health Research 6(1) 90ndash111
ShieldsM ampWilkins K (2005)National Survey of theWork and Health of Nurses2005 Provincial profiles Ottawa Statistics CanadaRetrieved August 24 2007from httpwwwstatcancaenglishresearch11-621-MIE11-621-MIE2006052htm
StaceyM amp Davies C (1983)Division of labour in child health care Final report toSSRCCoventry Sociology Department University ofWarwick
Tebb S (1995)An aid to empowermentA caregiver well-being scaleHealth andSocialWork 20(2) 87ndash92
Tebb S Berg-WgerM amp Rubio DM (2000) CaregiverWell-Being Scale InDRoyse BAThyer D K Padgett ampT K Logan (Eds) Program evaluation3rd ed (pp 320ndash323) Pacific Grove CA BrooksCole
Ungerson C (1990) The language of care Crossing the boundaries InCUngerson (Ed)Gender and caringWork and welfare in Britain and Scandinavia(pp 8ndash33) NewYork Harvester
WaltersV LentonR French S Eyles JMayr J amp Newbold B (1996) Paidwork unpaid work and social supportA study of the health of male andfemale nurses Social Science and Medicine 43(11) 1627ndash1636
Ward-Griffin C (2004) Nurses as caregivers of elderly relatives Negotiatingpersonal and professional boundariesCJNR 36(1) 92ndash114
Ward-Griffin C (2008)Health professionals caring for aging relativesA profes-sional or personal issue In AMartin-Matthews amp J Phillips (Eds)Blurringthe boundariesAgeing at the intersection of work and home life (pp 1ndash20) NewYorkTaylor amp FrancisPsychology Press
Ward-Griffin C Brown JVandervoortA McNair S amp Dashnay I (2005)Double duty caregivingWomen in the health professionsCanadian Journalon Aging 24(4) 379ndash394
Ward-Griffin C amp MarshallV (2003) Reconceptualizing the relationshipbetween public and private eldercare Journal of Aging Studies 17 189ndash208
Development andValidation of the Double Duty Caregiving Scale
CJNR 2009Vol 41 No 3 127
Ware J E Kosinksi MTurner-Bowker L amp Gandek B (2002)How to scoreversion 2 of the SF-12 health survey Lincoln RIQuality Metric Inc
Acknowledgements
This study was funded by the Social Sciences and Humanities ResearchCouncil (Internal) and the Institute of Gender and Health CanadianInstitutes of Health ResearchThere are no conflicts of interest or financial disclosures
CatherineWard-Griffin RN PhD is ProfessorArthur Labatt Family School ofNursing University ofWestern Ontario London Canada Janice Keefe PhD isProfessor and Canada Research Chair in Aging and Caregiving Policy FamilyStudies and GerontologyMount SaintVincent University HalifaxNova ScotiaCanadaAnne Martin-Matthews PhD is Professor School of SocialWork andFamily Studies University of British ColumbiaVancouver Canada MichaelKerr PhD is Associate ProfessorArthur Labatt Family School of NursingUniversity ofWestern Ontario Judith Belle Brown PhD is Professor Departmentof Family Medicine University ofWestern OntarioAbram Oudshoorn RN is aPhD candidate in the Arthur Labatt Family School of Nursing University ofWestern Ontario
Ward-Griffin Keefe Martin-Matthews Kerr Brown and Oudshoorn
CJNR 2009Vol 41 No 3 128

Mayall B (1993) Keeping children healthy ndash the intermediate domain SocialScience and Medicine 36(1) 77ndash83
Morris JM amp Field PA (1995) Qualitative research methods for health profession-als 2nd ed London Sage
Pascall G (1986) Social policyA feminist analysis NewYorkTavistockPhillips J BernardM amp ChittendenM (2002) Juggling work and careThe expe-riences of older adults Bristol Policy Press
Polit D F amp Beck CT (2008)Nursing research Generating and assessing evidencefor nursing practice 8th ed Philadelphia LippincottWilliams ampWilkins
Polit D F amp Beck CT amp Owen SV (2007) Is the CVI an acceptable indica-tor of content validity Appraisal and recommendationsResearch in Nursingand Health 30 459ndash467
RossMM Rideout EM amp CarsonMM (1996) Nursesrsquo work Balancingpersonal and professional caregiving careers Canadian Journal of NursingResearch 26(4) 43ndash59
RutmanD (1996) Caregiving as womenrsquos workWomenrsquos experiences of pow-erfulness and powerlessness as caregiversQualitative Health Research 6(1) 90ndash111
ShieldsM ampWilkins K (2005)National Survey of theWork and Health of Nurses2005 Provincial profiles Ottawa Statistics CanadaRetrieved August 24 2007from httpwwwstatcancaenglishresearch11-621-MIE11-621-MIE2006052htm
StaceyM amp Davies C (1983)Division of labour in child health care Final report toSSRCCoventry Sociology Department University ofWarwick
Tebb S (1995)An aid to empowermentA caregiver well-being scaleHealth andSocialWork 20(2) 87ndash92
Tebb S Berg-WgerM amp Rubio DM (2000) CaregiverWell-Being Scale InDRoyse BAThyer D K Padgett ampT K Logan (Eds) Program evaluation3rd ed (pp 320ndash323) Pacific Grove CA BrooksCole
Ungerson C (1990) The language of care Crossing the boundaries InCUngerson (Ed)Gender and caringWork and welfare in Britain and Scandinavia(pp 8ndash33) NewYork Harvester
WaltersV LentonR French S Eyles JMayr J amp Newbold B (1996) Paidwork unpaid work and social supportA study of the health of male andfemale nurses Social Science and Medicine 43(11) 1627ndash1636
Ward-Griffin C (2004) Nurses as caregivers of elderly relatives Negotiatingpersonal and professional boundariesCJNR 36(1) 92ndash114
Ward-Griffin C (2008)Health professionals caring for aging relativesA profes-sional or personal issue In AMartin-Matthews amp J Phillips (Eds)Blurringthe boundariesAgeing at the intersection of work and home life (pp 1ndash20) NewYorkTaylor amp FrancisPsychology Press
Ward-Griffin C Brown JVandervoortA McNair S amp Dashnay I (2005)Double duty caregivingWomen in the health professionsCanadian Journalon Aging 24(4) 379ndash394
Ward-Griffin C amp MarshallV (2003) Reconceptualizing the relationshipbetween public and private eldercare Journal of Aging Studies 17 189ndash208
Development andValidation of the Double Duty Caregiving Scale
CJNR 2009Vol 41 No 3 127
Ware J E Kosinksi MTurner-Bowker L amp Gandek B (2002)How to scoreversion 2 of the SF-12 health survey Lincoln RIQuality Metric Inc
Acknowledgements
This study was funded by the Social Sciences and Humanities ResearchCouncil (Internal) and the Institute of Gender and Health CanadianInstitutes of Health ResearchThere are no conflicts of interest or financial disclosures
CatherineWard-Griffin RN PhD is ProfessorArthur Labatt Family School ofNursing University ofWestern Ontario London Canada Janice Keefe PhD isProfessor and Canada Research Chair in Aging and Caregiving Policy FamilyStudies and GerontologyMount SaintVincent University HalifaxNova ScotiaCanadaAnne Martin-Matthews PhD is Professor School of SocialWork andFamily Studies University of British ColumbiaVancouver Canada MichaelKerr PhD is Associate ProfessorArthur Labatt Family School of NursingUniversity ofWestern Ontario Judith Belle Brown PhD is Professor Departmentof Family Medicine University ofWestern OntarioAbram Oudshoorn RN is aPhD candidate in the Arthur Labatt Family School of Nursing University ofWestern Ontario
Ward-Griffin Keefe Martin-Matthews Kerr Brown and Oudshoorn
CJNR 2009Vol 41 No 3 128

Ware J E Kosinksi MTurner-Bowker L amp Gandek B (2002)How to scoreversion 2 of the SF-12 health survey Lincoln RIQuality Metric Inc
Acknowledgements
This study was funded by the Social Sciences and Humanities ResearchCouncil (Internal) and the Institute of Gender and Health CanadianInstitutes of Health ResearchThere are no conflicts of interest or financial disclosures
CatherineWard-Griffin RN PhD is ProfessorArthur Labatt Family School ofNursing University ofWestern Ontario London Canada Janice Keefe PhD isProfessor and Canada Research Chair in Aging and Caregiving Policy FamilyStudies and GerontologyMount SaintVincent University HalifaxNova ScotiaCanadaAnne Martin-Matthews PhD is Professor School of SocialWork andFamily Studies University of British ColumbiaVancouver Canada MichaelKerr PhD is Associate ProfessorArthur Labatt Family School of NursingUniversity ofWestern Ontario Judith Belle Brown PhD is Professor Departmentof Family Medicine University ofWestern OntarioAbram Oudshoorn RN is aPhD candidate in the Arthur Labatt Family School of Nursing University ofWestern Ontario
Ward-Griffin Keefe Martin-Matthews Kerr Brown and Oudshoorn
CJNR 2009Vol 41 No 3 128




















