
Development and validation of a nomogram based on clinical factors and standard laboratory tests for...
11
Copyright © Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited. Development and validation of a nomogram based on clinical factors and standard laboratory tests for prediction of clinically significant liver fibrosis in chronic hepatitis C virus infection Elisabetta Sagrini a , Ilaria Ardoino c , Giuseppe Marano c , Alice Gianstefani a , Alessandra Orlandini e , Giada Sebastiani f , Gabriele Donati g , Alessandro Cucchetti b , Guido Pelosi e , Carlo Ferrari e , Alfredo Alberti f , Elia Biganzoli c,d , Fabio Piscaglia a and Luigi Bolondi a Objectives Staging liver fibrosis in chronic viral hepatitis C (HCV) patients is essential for prompting surveillance and treatment. The aim of this study was to develop a nomogram, on the basis of simple clinical and laboratory variables, to predict three clinically significant stages of fibrosis (nil–mild, moderate, advanced/cirrhosis), using histology as reference, and to compare its performance with that of FibroTest, a widely used noninvasive fibrosis score. Materials and methods Nomograms are graphical representations of a mathematical formula, used as predictive tools. The study retrospectively recruited 406 HCV patients undergoing liver biopsy. Nomogram was developed in a training set of 252 patients and tested in a validation set of 154 patients. Histology was staged according to the Metavir system. Fibrosis stages were subgrouped as follows: advanced fibrosis/cirrhosis (F3/F4, 24%), nil–mild (F0/F1, 36%), and moderate (F2, 40%). Age at biopsy, aspartate aminotransferase, c-glutamyl transpeptidase, albumin, platelet count, and prothrombin activity formed the basis for the so-called Fibro-Nomogram, which, in one graphical representation, estimates probability for different stages of fibrosis. Results Areas under the receiver-operating characteristic curves for advanced fibrosis/cirrhosis were similar for training (0.86) and validation sets (0.87). For nil–mild fibrosis, area under the receiver-operating characteristics were 0.81 and 0.79. Compared with FibroTest, Fibro-Nomogram performed slightly better at predicting severe fibrosis (F3/F4) with positive likelihood ratio (LR +) 5.07 (95% confidence interval 3.08–8.37) versus LR + 3.82 (95% confidence interval 2.56–5.71) for FibroTest. For nil–mild fibrosis, the two tests showed limited but comparable performances. Conclusion In HCV patients, Fibro-Nomogram, an inexpensive and readily available predictive tool, could enable clinicians to interpret patients’ profile, concurrently stratifying patients into three clinically relevant probability categories with good overall performance. Eur J Gastroenterol Hepatol 00:000–000 c 2013 Wolters Kluwer Health | Lippincott Williams & Wilkins. European Journal of Gastroenterology & Hepatology 2013, 00:000–000 Keywords: chronic viral hepatitis C, clinical decision making, liver fibrosis prediction, nomogram a Department of Digestive Diseases and Internal Medicine, Division of Internal Medicine, b Division of Surgery and Liver Transplantation, S. Orsola-Malpighi University and General Hospital, Bologna, c Department of Clinical Sciences and Community Health, University of Milan, d Unit of Medical Statistics, Biometry and Bioinformatics, Fondazione IRCCS National Cancer Institute Milan, Milan, e Unit of Infectious Diseases and Hepatology, University Hospital, Parma, f Venetian Institute of Molecular Medicine (VIMM), University of Padova, Padova and g Division of Internal Medicine, Ospedale di Rimini, Rimini, Italy Correspondence to Elisabetta Sagrini, MD, Department of Digestive Diseases and Internal Medicine, Division of Internal Medicine, S. Orsola-Malpighi University and General Hospital, Via Albertoni 15, 40138 Bologna, Italy Tel: + 39 051 6362582/ + 39 051 6362542; fax: + 39 051 6362725; e-mail: [email protected] Received 2 February 2013 Accepted 4 June 2013 Introduction Among patients with chronic hepatitis C virus (HCV) infection, which is a leading cause of chronic liver disease, the prevalence of bridging fibrosis/cirrhosis depends on the population considered and the presence of cofactors, ranging from 10% in those with persistently normal aminotransferase levels up to 27–35% in patients with persistently high aminotransferase levels [1–4]. Accurate staging of disease is crucial for predicting the natural history of an individual patient’s disease and the need for antiviral therapy, expensive and with relevant side effects. The extent of liver fibrosis is a predictor of treatment response [5–7], whereas the higher the stage of fibrosis, the higher the risk of developing complica- tions: hepatocellular carcinoma, portal hypertension, and liver failure [8]. Recently, several new noninvasive liver fibrosis markers have been developed, led by the desire to overcome the limits of biopsy (complications, sampling errors, hardly repeatable in the midterm). Original article 1 0954-691X c 2013 Wolters Kluwer Health | Lippincott Williams & Wilkins DOI: 10.1097/MEG.0b013e328363e29d
Transcript of Development and validation of a nomogram based on clinical factors and standard laboratory tests for...

Copyright © Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
Development and validation of a nomogram based on clinicalfactors and standard laboratory tests for prediction ofclinically significant liver fibrosis in chronic hepatitis C virusinfectionElisabetta Sagrinia, Ilaria Ardoinoc, Giuseppe Maranoc, Alice Gianstefania,Alessandra Orlandinie, Giada Sebastianif, Gabriele Donatig,Alessandro Cucchettib, Guido Pelosie, Carlo Ferrarie, Alfredo Albertif,Elia Biganzolic,d, Fabio Piscagliaa and Luigi Bolondia
Objectives Staging liver fibrosis in chronic viral hepatitis
C (HCV) patients is essential for prompting surveillance
and treatment. The aim of this study was to develop a
nomogram, on the basis of simple clinical and laboratory
variables, to predict three clinically significant stages of
fibrosis (nil–mild, moderate, advanced/cirrhosis), using
histology as reference, and to compare its performance
with that of FibroTest, a widely used noninvasive fibrosis
score.
Materials and methods Nomograms are graphical
representations of a mathematical formula, used as
predictive tools. The study retrospectively recruited 406
HCV patients undergoing liver biopsy. Nomogram was
developed in a training set of 252 patients and tested
in a validation set of 154 patients. Histology was staged
according to the Metavir system. Fibrosis stages were
subgrouped as follows: advanced fibrosis/cirrhosis
(F3/F4, 24%), nil–mild (F0/F1, 36%), and moderate (F2,
40%). Age at biopsy, aspartate aminotransferase,
c-glutamyl transpeptidase, albumin, platelet count, and
prothrombin activity formed the basis for the so-called
Fibro-Nomogram, which, in one graphical representation,
estimates probability for different stages of fibrosis.
Results Areas under the receiver-operating characteristic
curves for advanced fibrosis/cirrhosis were similar for
training (0.86) and validation sets (0.87). For nil–mild
fibrosis, area under the receiver-operating characteristics
were 0.81 and 0.79. Compared with FibroTest,
Fibro-Nomogram performed slightly better at predicting
severe fibrosis (F3/F4) with positive likelihood ratio (LR +)
5.07 (95% confidence interval 3.08–8.37) versus LR + 3.82
(95% confidence interval 2.56–5.71) for FibroTest. For
nil–mild fibrosis, the two tests showed limited but
comparable performances.
Conclusion In HCV patients, Fibro-Nomogram, an
inexpensive and readily available predictive tool, could
enable clinicians to interpret patients’ profile, concurrently
stratifying patients into three clinically relevant probability
categories with good overall performance. Eur J
Gastroenterol Hepatol 00:000–000 �c 2013 Wolters Kluwer
Health | Lippincott Williams & Wilkins.
European Journal of Gastroenterology & Hepatology 2013, 00:000–000
Keywords: chronic viral hepatitis C, clinical decision making, liver fibrosisprediction, nomogram
aDepartment of Digestive Diseases and Internal Medicine, Division of InternalMedicine, bDivision of Surgery and Liver Transplantation, S. Orsola-MalpighiUniversity and General Hospital, Bologna, cDepartment of Clinical Sciencesand Community Health, University of Milan, dUnit of Medical Statistics, Biometryand Bioinformatics, Fondazione IRCCS National Cancer Institute Milan, Milan,eUnit of Infectious Diseases and Hepatology, University Hospital, Parma,fVenetian Institute of Molecular Medicine (VIMM), University of Padova, Padovaand gDivision of Internal Medicine, Ospedale di Rimini, Rimini, Italy
Correspondence to Elisabetta Sagrini, MD, Department of Digestive Diseasesand Internal Medicine, Division of Internal Medicine, S. Orsola-Malpighi Universityand General Hospital, Via Albertoni 15, 40138 Bologna, ItalyTel: + 39 051 6362582/ + 39 051 6362542; fax: + 39 051 6362725;e-mail: [email protected]
Received 2 February 2013 Accepted 4 June 2013
IntroductionAmong patients with chronic hepatitis C virus (HCV)
infection, which is a leading cause of chronic liver disease,
the prevalence of bridging fibrosis/cirrhosis depends on
the population considered and the presence of cofactors,
ranging from 10% in those with persistently normal
aminotransferase levels up to 27–35% in patients with
persistently high aminotransferase levels [1–4].
Accurate staging of disease is crucial for predicting the
natural history of an individual patient’s disease and the
need for antiviral therapy, expensive and with relevant
side effects. The extent of liver fibrosis is a predictor of
treatment response [5–7], whereas the higher the stage
of fibrosis, the higher the risk of developing complica-
tions: hepatocellular carcinoma, portal hypertension, and
liver failure [8].
Recently, several new noninvasive liver fibrosis markers
have been developed, led by the desire to overcome the
limits of biopsy (complications, sampling errors, hardly
repeatable in the midterm).
Original article 1
0954-691X �c 2013 Wolters Kluwer Health | Lippincott Williams & Wilkins DOI: 10.1097/MEG.0b013e328363e29d

Copyright © Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
According to the latest EASL guidelines for the manage-
ment of HCV infection [4], noninvasive serum markers
can be used for the detection of significant liver fibrosis
(MetavirZ 2), taking into consideration that a combina-
tion of serum markers plus transient elastography [9] can
improve the accuracy of prediction. Liver biopsy is still
needed to resolve uncertainty and is considered as the
reference method to assess the grade of inflammation and
stage of fibrosis.
Most studies on noninvasive predictors of disease stage in
chronic hepatitis C grouped the patients grossly into
either nil–mild fibrosis versus moderate–severe fibrosis or
cirrhosis, or distinguished severe fibrosis/cirrhosis from all
other stages [10–13]. Severe fibrosis identifies high-risk
patients in whom an antiviral therapy and periodic follow-
up are highly recommended, whereas lower stages of
fibrosis describe lower-risk patients, in whom a ‘wait and
see’ policy could be considered, according to the patients’
age and desire.
This categorization into two risk groups includes a highly
heterogeneous population, thus leaving a large proportion
of patients undetermined.
A classification into three groups (nil–mild vs. moderate
vs. severe fibrosis/cirrhosis), with narrowed categories,
would leave a lower proportion of patients unclassified.
The primary aim of this study was to develop a predictive
model, consisting of routinely available laboratory tests, to
predict the above-mentioned subgroups of fibrosis, nil–
mild versus moderate versus severe fibrosis/cirrhosis, in
HCV-infected patients, using liver histology as reference.
The predictive model was validated on an external cohort
and the results compared with those of FibroTest, a
widely used and validated noninvasive score of liver
fibrosis [12].
The predictive model involved the development of a
nomogram to support clinicians in the assessment of the
probability of their patients having no–mild, moderate, or
advanced fibrosis, directly at the bedside, without the
need for complex formulae.
Model-based nomograms are graphical devices, often
favored because of their ease of use, that allow bedside
prediction with ‘paper and ruler’. We are not aware of any
studies that sought to develop a nomogram for fibrosis
prediction in the setting of HCV infection.
Materials and methodsStudy population and data collection
Four hundred and forty four patients with chronic HCV
infection who underwent liver biopsy between 1998 and
2006 were collected consecutively at three Medical Units
of Northern Italy, while being evaluated for antiviral
treatment. The inclusion criteria of this retrospective
study were chronic HCV infection, confirmed by positive
anti-HCV antibodies and HCV-RNA PCR assays in
serum, and compensated stage of disease (Child–Pugh
A5). Patients with clear signs of decompensated disease
such as hepatic encephalopathy and esophageal varices, or
insufficient liver tissue for staging fibrosis in bioptic
specimen, according to accepted recommendations (ade-
quate biopsy fragments should have a length > 1.5 cm and
contain Z 10 portal spaces), or incomplete laboratory
tests, were excluded from the study. Coexisting liver
diseases (alcohol, hepatitis B virus infection, primary
biliary cirrhosis, autoimmune hepatitis, hemochromato-
sis) were reasonably excluded by history and laboratory
data.
The total population comprised 230 patients recruited
from Parma Hospital, 40 patients from Rimini Hospital,
and 174 patients from Padova Medical Center. The study
was approved by the Institutional Review Boards of the
participating centers.
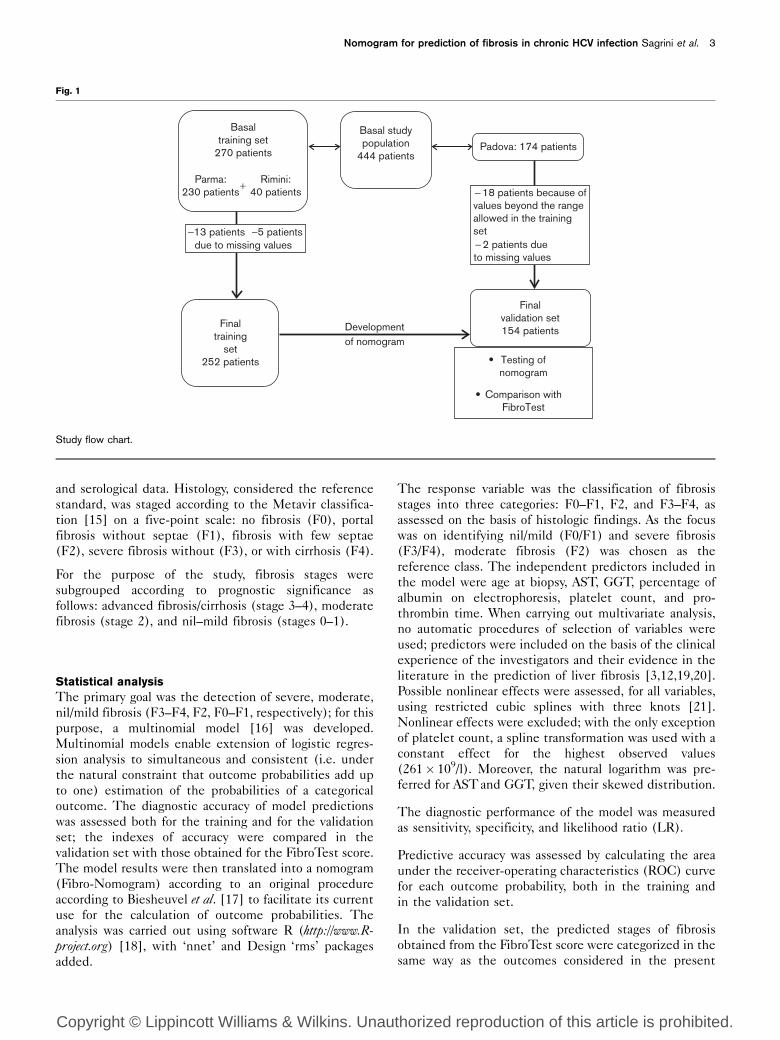
The patients were divided into two sets: patients from
Parma and Rimini constituted the training set, including
252 patients after exclusion of 13 patients from Parma
and 5 from Rimini because of incomplete data. The
validation set included 154 of 174 patients from Padova.
Two patients were excluded because of incomplete data;
18 patients were excluded as some covariates presented
values beyond the range allowed in the training set to
avoid extrapolation in the assessment of the prediction
tool [14] (Fig. 1). Patients from Padova were part of a
previous study for whom FibroTest results were available.
Therefore, data emerging from the present study could
be immediately assessed against the FibroTest [12],
calculated from the patented formula on the basis of
g-glutamyl transpeptidase (GGT), haptoglobin, a2-
macroglobulin, bilirubin, and apolipoprotein A1 (http://www.biopredictive.com). The use of a validation strategy in
the development of the predictive tool, resorting to an
external group, would reinforce the results obtained. The
development of the predictive model was followed by the
creation of a nomogram (called Fibro-Nomogram).
The analysis of the accuracy of the FibroTest in the
present series and the comparison with our predictive
model were carried out in a second independent step
after building the model on the training set and testing
on the validation set.
Sex and age at biopsy were recorded. Laboratory data
were collected within 1 month of biopsy. Requested
data were aspartate aminotransferase (AST), alanine
aminotransferase (ALT), platelet count, GGT, alkaline
phosphatase, prothrombin time, total serum protein,
percentage of albumin, total bilirubin, total cholesterol,
creatinine, white blood cells, and hemoglobin.
An ultrasound-guided liver biopsy was obtained for each
patient. Liver biopsy specimens were assessed in
each center at the time of biopsy blinded to clinical
2 European Journal of Gastroenterology & Hepatology 2013, Vol 00 No 00
Copyright © Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
and serological data. Histology, considered the reference
standard, was staged according to the Metavir classifica-
tion [15] on a five-point scale: no fibrosis (F0), portal
fibrosis without septae (F1), fibrosis with few septae
(F2), severe fibrosis without (F3), or with cirrhosis (F4).
For the purpose of the study, fibrosis stages were
subgrouped according to prognostic significance as
follows: advanced fibrosis/cirrhosis (stage 3–4), moderate
fibrosis (stage 2), and nil–mild fibrosis (stages 0–1).
Statistical analysis
The primary goal was the detection of severe, moderate,
nil/mild fibrosis (F3–F4, F2, F0–F1, respectively); for this
purpose, a multinomial model [16] was developed.
Multinomial models enable extension of logistic regres-
sion analysis to simultaneous and consistent (i.e. under
the natural constraint that outcome probabilities add up
to one) estimation of the probabilities of a categorical
outcome. The diagnostic accuracy of model predictions
was assessed both for the training and for the validation
set; the indexes of accuracy were compared in the
validation set with those obtained for the FibroTest score.
The model results were then translated into a nomogram
(Fibro-Nomogram) according to an original procedure
according to Biesheuvel et al. [17] to facilitate its current
use for the calculation of outcome probabilities. The
analysis was carried out using software R (http://www.R-project.org) [18], with ‘nnet’ and Design ‘rms’ packages
added.
The response variable was the classification of fibrosis
stages into three categories: F0–F1, F2, and F3–F4, as
assessed on the basis of histologic findings. As the focus
was on identifying nil/mild (F0/F1) and severe fibrosis
(F3/F4), moderate fibrosis (F2) was chosen as the
reference class. The independent predictors included in
the model were age at biopsy, AST, GGT, percentage of
albumin on electrophoresis, platelet count, and pro-
thrombin time. When carrying out multivariate analysis,
no automatic procedures of selection of variables were
used; predictors were included on the basis of the clinical
experience of the investigators and their evidence in the
literature in the prediction of liver fibrosis [3,12,19,20].
Possible nonlinear effects were assessed, for all variables,
using restricted cubic splines with three knots [21].
Nonlinear effects were excluded; with the only exception
of platelet count, a spline transformation was used with a
constant effect for the highest observed values
(261� 109/l). Moreover, the natural logarithm was pre-
ferred for AST and GGT, given their skewed distribution.
The diagnostic performance of the model was measured
as sensitivity, specificity, and likelihood ratio (LR).
Predictive accuracy was assessed by calculating the area
under the receiver-operating characteristics (ROC) curve
for each outcome probability, both in the training and
in the validation set.
In the validation set, the predicted stages of fibrosis
obtained from the FibroTest score were categorized in the
same way as the outcomes considered in the present
Fig. 1
Basaltraining set
270 patients
Finaltraining
set252 patients
Developmentof nomogram
−13 patientsdue to missing values
−5 patients
Comparison withFibroTest
Testing ofnomogram
Finalvalidation set154 patients
Padova: 174 patients
− 2 patients dueto missing values
− 18 patients because ofvalues beyond the rangeallowed in the trainingset
Basal studypopulation
444 patients
Rimini:40 patients
Parma:230 patients
+
Study flow chart.
Nomogram for prediction of fibrosis in chronic HCV infection Sagrini et al. 3

Copyright © Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
work. The 95% confidence intervals (CIs) for the area
under the ROC curve were based on the DeLong
method [22].
Fibro-Nomogram
Nomogram is a two-dimensional diagram designed to
compute a mathematical function graphically. Nomo-
grams constitute attractive user-friendly interfaces used
to calculate predictions of clinical outcomes, without
resorting to complex formulas or web access.
We present an original diagram for calculating predictions
of polytomous outcomes. The diagram calculates the
probability of each outcome category. Specifically, prob-
abilities of severe fibrosis (F3–F4), or no–mild fibrosis
(F0–F1) are first obtained, and then the probability of F2
can be calculated as their complement to one. The
prediction diagram is divided into two parts: the two
nomograms at the top (Fig. 2a and b) compute the values
of the two distinct model predictors (i.e. linear combina-
tions of the independent variables included in the
model), associated with a specific patient’s covariate
profile. The axis length of covariates is proportional to the
prognostic impact of variables. The values obtained are
translated into the diagram at the bottom to obtain the
probability of the outcome of interest (Fig. 2c).
How to use Fibro-Nomogram
The nomogram is used by first locating a patient’s
position on each predictor variable scale (Fig. 2a and b).
Each scale position has corresponding prognostic points
(top axis). In the top panels, the values of the linear
predictors (LPs) for severe fibrosis (LP.Sev) and no or
mild fibrosis are computed (LP.Mild): the values of each
predictor are located in the corresponding axes, and then
a line straight upward to the points axis determines how
many points the patient receives for each predictor. The
sum of the points obtained for each predictor is placed on
the total point axis. A line straight down to the bottom
axis will find the value of the LP. The curves depicted in
the diagram (Fig. 2c) represent the probability of the
outcome of interest for different values of LP. For severe
fibrosis, the labels LP* and LP indicate LP.Sev and
LP.Mild, respectively; for no–mild fibrosis, LP* corre-
sponds to LP.Mild and LP to LP.Sev.
To facilitate understanding of nomogram use, please see
the example described in Fig. 2.
ResultsPatient characteristics at the time of biopsy and fibrosis
stages are reported in Table 1.
The nomogram (Fibro-Nomogram) derived from the
multinomial model enabling the calculation of the three
outcome probabilities, (a) nil–mild, (b) moderate, or (c)
advanced fibrosis/cirrhosis, is shown in Fig. 2. In the
Fibro-Nomogram represented in Fig. 2a and b, because
of the negligible influence of some variables in predicting
specific outcomes, not all the variables included in the
multinomial model are graphically represented. The
Fibro-Nomogram actually provides adjusted probabilities
for reference values (i.e. the median) of the predictors
not shown, which closely approximate the unadjusted
probabilities both in the training and in the testing
populations.
The ROC curves for each outcome probability shown
in Figs 3–5 are explained further below.
Prediction of severe fibrosis
From a clinical standpoint, severe fibrosis (F3, F4)
preludes a stage at which complications of chronic liver
disease may already occur. On this basis, we considered it
important to have a predictive approach able to confirm
with accuracy this condition to take clinical decisions
(antiviral treatment, ultrasound surveillance, endoscopic
screening for esophageal varices). When this outcome is
considered, the statistical model results showed a good
discrimination performance with an area under the ROC
curve of 0.86 (CI 0.80–0.92) in the training set. The same
value (0.87 CI 0.80–0.93) was maintained in the
validation set, showing an intrinsic robust performance
of the predictive model in terms of outcome discrimina-
tion.
Choosing the point on the ROC curve corresponding to
the best cutoff (the black dot superimposed on the ROC
curve in Fig. 3), the model predicted severe fibrosis with
a sensitivity of 72% and a specificity of 86% in the training
set. In the validation set, the same cutoff yielded
a sensitivity of 68% and a specificity of 87%.
Prediction of nil–mild fibrosis
From a clinical standpoint, the other situation which the
authors considered relevant for clinical management was
to know whether a patient with chronic HCV has no or
mild fibrosis. At this stage, no complications of the
disease are expected and treatment is not compelling, to
be decided according to the patients’ age and desire. In
this case, our model enabled correct identification of
patients with nil–mild fibrosis with an area under the
ROC curve of 0.81 (CI 0.75–0.86) for the training set and
0.79 (CI 0.71–0.86) for the validation set (Fig. 5).
Choosing the point on the ROC curve corresponding to
the best cutoff (the black dot superimposed on the ROC
curve in Fig. 5) in the training set, the sensitivity and
specificity for nil–mild fibrosis were 77% and 70%,
respectively. In the validation set, the same cutoff
yielded a sensitivity of 82% and a specificity of 60%.
Prediction of moderate fibrosis
The main limitation of the proposed model is its
weakness in the correct identification of patients with
moderate fibrosis against the two extreme situations:
4 European Journal of Gastroenterology & Hepatology 2013, Vol 00 No 00

Copyright © Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
Fig. 2
Points0
75
320
50
60
340
0 50 100
0.025 0.1
0.1 0.2 0.5 1 2 4 6 13.50.05
0.25 0.5 1 2 3 7
150 200 250 300 350
160 80 50 30 20 10 7 5
65 70 75 80 85 90 95 105 115 125
60 70 80 90 100 120 140 160 180 250
260 200 160 120 80 60 50 40 30 20
65 55 45 35 25
10 20 30 40 50 60 70 80 90 100 0
20
20
200
70
0 20
0.025
0.05 0.1 0.2 0.5 1 2 4 9.75 38.75 97
0.1 0.25 0.5 1 2 5 10 20 50
40 60 80 100 120 140 160 180 200 220 240
66 62 58 54 50 46 42
170 150 130120110100 90 80 70 60 50
30 50 80 120 200 320
30 40 50 60 70
10 20 30 40 50 60 70 80 90 100(a) (b)
Age
AST
Platelet
Points
Age
AST
Platelet
Albumin%
Total points
Linear predictor
LP.severe
Total points
Linear predictor
LP.mild
1.0(c)LP = 0LP = 1
LP = 5
LP = 15
LP = 16LP = 18
LP = 20
LP = 25
LP = 30
LP = 35
LP = 40LP = 45
LP = 50
LP = 60
LP = 70LP = 80
LP = 90LP = 100
0.9
0.8
0.7
0.6
0.5
Pre
dict
ed p
roba
bilit
y
0.4
0.3
0.2
0.1
0.0
0 10 20 30LP∗
40 50 60
Prothrombin time
γ-Glutamyltranspeptidase
(a–c) Fibro-Nomogram for the prediction of Metavir fibrosis stages. The following steps are a guide on how to calculate outcome probabilities. Here,a case of a chronic hepatitis C virus-infected patient, a 52-year-old man, aspartate aminotransferase (AST) 150 IU/l, platelet count 158�103/ml,prothrombin time 80%, g-glutamyl transpeptidase 250 IU/l, and serum albumin 55%, is presented. He contributes 22 points for his age both in (a)and (b); this is determined by drawing a vertical line between the point of value 52 on the age axis and the points scale above. The point values for allclinical predictor variables are determined in the same manner and summed up to a total value, which is plotted on the total point axis (third from thebottom). Then, a vertical line is drawn from the total point axis straight to the linear predictor (LP) axis. He is thus assigned 147 total points(respectively 22 + 28 + 70 + 23 + 4) for predicting mild fibrosis. His total points correspond to almost 0.2 read on the LP.Mild axis. Following thesame instructions, total points of 127 (22 + 40 + 25 + 40) are obtained on the nomogram in (b) for the prediction of severe fibrosis, whichcorresponds to a LP.Sev of about 3. Let us translate the results in (c). For the prediction of severe fibrosis, let the labels LP* and LP indicate LP.Sevand LP.Mild, respectively. For the prediction of no–mild fibrosis, let LP* be LP.Mild and LP be LP.Sev. Now locate LP* (= LP.Sev of 3) on the abscissaand draw a line straight upward to find the intersection with the curve corresponding to LP value (= LP.Mild of 0.2). We obtain a probability of severefibrosis between the first two curves of high, which is about 0.58 projected on the Y-axis. The second probability of mild fibrosis can be read locatingLP.Mild on the X-axis very near the origin and is about 0.12, which is a rather negligible value. The probability of moderate fibrosis will be 0.3[(1) – (0.58) – (0.12)]. The diagram should not appear confusing when in (c) very low values are considered on the abscissa: prediction generallyresults in practically null probability. Consistent with Fibro-Nomogram outcome, the above patient had a fibrosis stage F3 on liver biopsy.
Nomogram for prediction of fibrosis in chronic HCV infection Sagrini et al. 5

Copyright © Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
Table 1 Clinical and laboratory features of the training and the validation seta
Training set Validation set
Parma (n = 217) Rimini (n = 35) Total (n = 252) Padova (n = 154)
Stage [n (%)]0 0 (0.00) 9 (25.71) 9 (3.57) 5 (3.25)1 82 (37.79) 10 (28.57) 92 (36.51) 40 (25.97)2 79 (36.41) 8 (22.86) 87 (34.52) 75 (48.70)3 40 (18.43) 6 (17.14) 46 (18.25) 17 (11.04)4 16 (7.37) 2 (5.71) 18 (7.14) 17 (11.04)
Sex (male) [n (%)] 117 (53.92) 28 (80.00) 145 (57.54) 85 (55.19)Other characteristics [mean (SD)]
Age at biopsy (years) 51.34 (11.62) 41.80 (9.21) 50.01 (11.78) 48.32 (12.15)AST (UI/l) 81 (61.9) 64.5 (49.8) 78.7 (60.5) 67 (42.2)ALT (UI/l) 128.2 (103) 99.2 (84.7) 124.1 (101.1) 106.4 (77.5)GGT (UI/l) 52.6 (44.3) 75.8 (63.7) 55.8 (47.8) 56.5 (53.1)Alkaline phosphatase (UI/l) 77 (38.1) 201.7 (78.1) 94.3 (62.8) 79.9 (28.2)Total bilirubin (mg/dl) 0.92 (0.36) 0.85 (0.25) 0.91 (0.35) 0.70 (0.30)Total protein (g/dl) 7.27 (0.62) 7.57 (0.49) 7.31 (0.62) 7.62 (0.50)Percentage of albumin 58.4 (4.1) 54.9 (4.6) 57.9 (4.3) 55.1 (3.9)Platelet count (103/ml) 194 (65) 179 (49) 192 (63) 215 (62)Prothrombin time (%) 98.8 (12.9) 88.5 (10.1) 97.3 (13.0) 90.9 (11.3)Total cholesterol (mg/dl) 173.2 (38) 168.9 (26.3) 172.6 (36.6) 172.3 (33)
ALT, alanine aminotransferase; AST, aspartate aminotransferase; GGT, g-glutamyl transpeptidase.aData are presented as total counts and percentages or as means and SDs.
Fig. 3
1−specificity
Severe fibrosis/cirrhosis
(F3 − F4)
LR+
LR−
AUC
Specificity
Sensitivity
Training TestingFibroTest
(Testing)
80.00% (71.96 − 86.18)
3.82 (2.56 − 5.71)
0.29 (0.16 − 0.54)
0.867 (0.803 − 0.931)
0.37 (0.23 − 0.61)
5.07 (3.08 − 8.37)
86.67% (79.44 − 91.62)
67.65% (50.84 − 80.87)71.88% (59.87 − 81.41)
85.64% (79.91 − 89.94)
5.00 (3.44 − 7.29)
0.33 (0.22 − 0.49)
0.859 (0.803 − 0.915)
76.47% (60.00 − 87.56)
1−specificity
1.0 F3 − F4
Training
0.8
0.6
0.4Sen
sitiv
ity
0.2
0.0
0.0 0.2 0.4 0.6 0.8 1.0
1.0 F3 − F4
Validation
0.8
0.6
0.4
0.2
0.0
0.0 0.2 0.4 0.6 0.8 1.0
Cut-off: 0.3068Sensitivity: 0.7188Specificity: 0.8564AUC: 0.8590 AUC: 0.8672
Accuracy of Fibro-Nomogram in predicting severe fibrosis stages (F3–F4). The empty circle in the validation set graph represents FibroTestperformance on the same subgroup of patients. Black dots along the receiver-operating characteristic (ROC) curve represent the ‘best’ cutoff(the point closest to the left corner of the curve) for which sensitivity, specificity, positive, and negative likelihood ratios (LRs) can be calculated.
6 European Journal of Gastroenterology & Hepatology 2013, Vol 00 No 00

Copyright © Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
actually, in such a case, the area under the ROC curve was
0.70 (CI 0.63–0.76), with a 68% sensitivity and a 67%
specificity in the training set, whereas the area under the
ROC curve for the validation set was 0.59 (CI 0.50–0.68),
with a sensitivity and a specificity of 51 and 56%,
respectively (Fig. 4).
Comparison of performance of the newly constructed
model with that of FibroTest
The Fibro-Nomogram allows evaluation of how likely the
fibrosis stage is according to specific covariate patterns.
To facilitate the comparison of our predictive model with
the FibroTest, the sensitivity and specificity for the
outcomes considered were calculated. Results were
combined with the ROC curves obtained from the
validation series (the empty circle in the second panel
of Figs 3–5). The points representing FibroTest were
superimposed with the ROC curve, showing substantially
comparable results between the two models in predicting
no–mild fibrosis (F0/F1) and in confirming severe fibrosis
(F3/F4). The FibroTest performed slightly better at
predicting intermediate fibrosis. Different choices are
available to identify a ‘best cutoff ’ on the ROC curve:
a typical option is to consider the point closest to the left
corner of the curve. When this cutoff is considered, the
LR + and LR – can be calculated to improve the
comparison with the FibroTest.
Albeit neither of the test shows optimal performance
(and their use cannot be recommended instead of the
biopsy), the main result suggests that the novel Fibro-
Nomogram, with a LR + 5.07 (95% CI 3.08–8.37) in the
prediction of F3/F4 fibrosis versus LR + 3.82 (95% CI
2.56–5.71) for FibroTest, can strengthen the confirmation
of severe fibrosis, with a possible improvement over
FibroTest performances despite wide CIs.
In terms of the diagnosis of the absence of fibrosis (i.e. for
the exclusion of fibrosis), Fibro-Nomogram (LR – 0.30,
Fig. 4
1−specificity
Training TestingFibroTest
(testing)
Moderate fibrosis
(F2)
Sensitivity 67.82% (57.43 − 76.70)
55.70% (44.73 − 66.13)
1.41 (0.83 − 1.58)
0.89 (0.65 − 1.20)
0.592 (0.501 − 0.682)
50.67% (39.60 − 61.67)
2.23 (1.41 − 3.53)
0.66 (0.52 − 0.85)
78.48% (68.21 − 86.11)
48.00% (37.07 − 59.13)
2.03 (1.57 − 2.64)
0.48 (0.35 − 0.67)
0.695 (0.629 − 0.762)
66.67% (59.17 − 73.41)
LR+
LR−
AUC
Specificity
1−specificity
1.0 F2
TrainingS
ensi
tivity
Validation
0.8
0.6
0.4
0.2
0.0
0.0 0.2 0.4 0.6 0.8 1.0
1.0 F2
0.8
0.6
0.4
0.2
0.0
0.0 0.2 0.4 0.6 0.8 1.0
Cut-off: 0.3838Sensitivity: 0.6782Specificity: 0.6667AUC: 0.6954 AUC: 0.5917
Accuracy of Fibro-Nomogram in predicting moderate fibrosis stage (F2). Empty circle in the validation set graph represents FibroTest performance onthe same subgroup of patients. Black dots along the receiver-operating characteristic (ROC) curve represent the ‘best’ cut-off (the point closest tothe left corner of the curve) for which sensitivity, specificity, positive, and negative likelihood ratios (LRs) can be calculated.
Nomogram for prediction of fibrosis in chronic HCV infection Sagrini et al. 7

Copyright © Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
95% CI 0.16–0.57) and FibroTest (LR – 0.48, 95% CI
0.33–0.71) showed limited but comparable performances.
DiscussionSeveral attempts have been made to overcome the need
for liver biopsy in the assessment of liver fibrosis. The
limitations of liver biopsy are invasiveness, morbidity,
costs, sampling errors, and interintraobserver variations,
producing around 20% false-negative cases for cirrhosis in
comparison with the real gold standard (whole liver) and
overlapping of intermediate stages [23]. The error in liver
biopsy itself makes it impossible to achieve an accuracy of
100% for any invasive test. As Mehta et al. [24] have
shown, an area under the ROC curve of more than 0.90
cannot be achieved even for a perfect marker, even in
a most favorable scenario.
Literature reports a distinction between patented and
nonpatented biochemical/clinical markers or morphologi-
cal methods such as elastography (ultrasound-based or
magnetic resonance elastography) or acoustic radiation
force imaging [9,25,26] to noninvasively assess liver
fibrosis [12,27,28]. Patented ones have been approved
by French authorities for first assessment of fibrosis in
HCV patients [29]. Patented methods are expensive, but
show better performances, in particular the FibroTest and
fibrometer, which incorporate direct markers of fibro-
sis [30].
Almost all available noninvasive tests have reported good
diagnostic accuracy, with area under the ROC around 0.80
for the prediction of significant fibrosis [31,32], but no
test accurate enough to reliably predict the single stage of
fibrosis. Simpler tests, such as APRI or Forns’ [10,11],
which provide cut-off values, have high accuracy when
results are at one end of the test spectrum, but leave a
proportion of patients undetermined, because of the gray
zone between proposed cutoffs. Most studies grouped
the patients essentially into nil–mild fibrosis versus
significant fibrosis/cirrhosis or distinguished severe fibrosis/
Fig. 5
Training TestingFibroTest(testing)
Nil−mild fibrosis
(F0 − F1)
Sensitivity 77.23% (68.14 − 84.32) 82.22% (68.67 − 90.71) 62.22% (47.63 − 74.89)
78.90% (70.32 − 85.51)
2.95 (1.95 − 4.47)
0.48 (0.33 − 0.71)
59.63% (50.25 − 68.36)
2.04 (1.54 − 2.69)
0.30 (0.16 − 0.57)
0.789 (0.714 − 0.864)
70.20% (62.48 − 76.92)
2.59 (1.98 − 3.39)
0.32 (0.22 − 0.47)
0.805 (0.751 − 0.858)
LR+
LR−
AUC
Specificity
1−specificity1−specificity
1.0
TrainingS
ensi
tivity
Validation
F0–F1F0 − F1
0.8
0.6
0.4
0.2
0.0
0.0 0.2 0.4 0.6 0.8 1.0
1.0
0.8
0.6
0.4
0.2
0.0
0.0 0.2 0.4 0.6 0.8 1.0
Cut-off: 0.4144Sensitivity: 0.7822Specificity: 0.7020AUC: 0.8045 AUC: 0.7890
Accuracy of Fibro-Nomogram in predicting the nil–mild fibrosis stage (F0–F1). Empty circle in the validation set graph represents FibroTestperformance on the same subgroup of patients. Black dots along the receiver-operating characteristic (ROC) curve represent the ‘best’ cut-off(the point closest to the left corner of the curve) for which sensitivity, specificity, positive, and negative likelihood ratios (LRs) can be calculated.
8 European Journal of Gastroenterology & Hepatology 2013, Vol 00 No 00

Copyright © Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
cirrhosis from all others. Indeed, noninvasive markers have
been shown to be able to accurately predict these two
extreme stages of fibrosis, for whom the need for therapy
and follow-up are quite established, as for example,
transient elastography and biomarkers such as APRI and
FibroTest perform similarly well in predicting severe fibrosis
in chronic HCV patients [33], whereas transient elasto-
graphy performs better in predicting cirrhosis than lesser
degree of fibrosis [34], with a reported area under the ROC
0.94–0.95 [35].
In our opinion, the use of a simple classification of
patients as with or without significant fibrosis (FZ 2) is
too broad for any accurate prognostic information (having
F2 or rather F4 implies a completely different prognosis
over the midterm either in the overall survival and
response to treatment). Similarly, having or not having
cirrhosis is also too broad as this may include either nil
fibrosis or severe fibrosis.
From a practical and clinical point of view, grouping
together patients with moderate (F2) and severe fibrosis
(F3) or cirrhosis (F4) does not help much, as the
prognosis and management may be different in F2 and
F3/F4 patients. At variance, if a test is aimed only at
excluding severe fibrosis, thus classifying patients into
one group including F0, F1, and F2 fibrosis, the clinical
benefit is again limited.
Therefore, we attempted to create a model with more
accurate prognostic information in terms of narrower
categories. On this basis, the study population was
evaluated not just simply as patients with or without
significant fibrosis (Metavir FZ 2) or cirrhosis, but by
subgrouping patients into three categories, F0–F1, F2,
and F3–F4, and developed a model to predict these three
clinical endpoints.
The model obtained an area under the ROC curve for
advanced fibrosis (FZ 3) equal to 0.86 and 0.87 in the
training and the validation set, respectively, and 0.81 and
0.79 in the prediction of nil–mild fibrosis (F0–F1),
corresponding to an intrinsic robust performance in terms
of outcome discrimination, especially helpful in con-
firmation of the extreme types of fibrosis stages.
One limitation of the model appears to be a poor
performance in correctly predicting the presence of
moderate fibrosis (F2). Among the variables entered in
the model, none seems to specifically characterize an
intermediate stage of the disease.
Indeed, this is a main limitation not only of our approach
but of almost all noninvasive tools to assess disease stages.
Namely, a considerable overlap between contiguous
stages of intermediate fibrosis occurs and any tool is
poorly able to discriminate the exact stage. Moreover, this
is not only a limitation of noninvasive tools but of biopsy
itself, given the small specimen often obtainable by
biopsy not well representative of the entire liver.
Furthermore, it is important to outline that the nomo-
gram is not a pure and absolute classification rule: it
provides the likelihood that a patient, given his/her
biomarker profile, belongs to a distinct outcome category.
Another purpose of the present work was to introduce
nomograms, original alternative tools to current noninvasive
fibrosis tests, available at the bedside. Nomograms are user-
friendly interfaces providing a measure of evidence of the
outcome of interest; they may be helpful for physicians in
validating their own judgments. These predictive tools are
being used in several medical fields such as oncology, in
which they are mainly used to predict outcomes or to stage
cancers [36]. They allow immediate assessment of the
impact of each prognostic factor for the specific outcomes,
which can be read on the length of single axis, thus
providing a sensible advantage over the so-called black-box
approaches. The interpretation of predictions is left to
practitioners also on the basis of patient profiles.
Here, an original nomogram (Fibro-Nomogram) was
developed for first-line evaluation of liver fibrosis. It
was based on clinical and laboratory data, routinely
available in patients affected by chronic HCV infection,
without any additional cost.
Comparisons between the results of Fibro-Nomogram and
FibroTest, on the validation set, were performed in the
second part of the study.
FibroTest has been validated widely in the HCV
population, with good performances globally, and is a
patented test for the diagnosis of liver fibrosis in adult
patients with untreated HCV. In the original paper,
Fibrotest obtained high positive and negative predictive
values for the diagnosis of clinically significant fibrosis
(FZ 2) and of cirrhosis or severe fibrosis (F3–F4).
On the validation set, both Fibro-Nomogram and
FibroTest showed substantially concordant results in the
prediction of extreme degrees of fibrosis. To facilitate the
comparison, as the prevalence of liver fibrosis stages is a
factor of variability in assessing the diagnostic value of a
fibrosis marker [37], attention has been focused on the
results with LRs. LRs can be less influenced by the
differences in the prevalence of diagnosis with respect to
predictive values (LR around 1 contribute scarce
significance to the post-test probability, LR around 2–5
mild increase, LR between 5 and 10 moderate increase,
and LR >10 large increase. For negative LR, less than the
unity, the smaller the LR, the greater the reduction in
post-test probability in excluding the diagnosis) [38]. In
the prediction of severe fibrosis, the model performed
slightly better than FibroTest, considering the higher
positive LR, although with a wide CI. Thus, our model
allowed to estimate simultaneously the probability
Nomogram for prediction of fibrosis in chronic HCV infection Sagrini et al. 9

Copyright © Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
of each outcome category (under the natural constraint,
these probabilities sum up to 1). If it is likely that a
patient does not have severe fibrosis, at the same time, it
is possible to derive the probability that he/she has
moderate or nil–mild fibrosis. If the latter probability is
high, a noninvasive procedure may be considered
sufficient. Vice versa, biopsy might be recommended for
a more precise assessment for patients initially predicted
to have no nil–mild fibrosis or advanced fibrosis, which
represent cases of uncertainty, when we concurrently
obtain from the nomogram similar probability values for
all three clinical outcomes. There is widespread con-
sensus that the use of a noninvasive test (serum
biomarkers or elastography) would be helpful if evidence
for cirrhosis or minimal to no fibrosis is indicated by these
tests. Should the results of noninvasive testing be
indeterminate, in our case when the ‘probability pattern’
is uncertain, then more prediction tools such as liver
biopsy would be relevant for stage confirmation.
Our predictive model was constructed on the basis of
simple laboratory values. We chose variables whose
association with the outcome of interest is biologically
plausible; age [3], GGT [12], AST [19], platelet
count [20], and serum albumin, routine biochemical
markers of liver disease, fulfilled this criterion as all of
them are known predictors of liver fibrosis.
The retrospective nature of this study and the collection
of data from different medical units did not allow for the
possibility to control for a series of confounding variables
that could have influenced the performance of the model.
A limitation could be the choice of variables, especially
AST and GGT, whose results may differ from day to day
because of transient fluctuations in hepatitis activity.
Fibro-Nomogram is a novel approach that could be used to
stratify patients with chronic HCV infection into three
clinically relevant probability categories. It showed good
overall performance, validated in an external cohort of
patients, especially in the confirmation of both extreme
stages of fibrosis. It was found to be comparable with
FibroTest results, but inexpensive and readily available.
These former issues should also be considered for countries
in which FibroTest or more expensive imaging is not
available. Moreover, the model could concurrently predict
the likelihood of different stages of fibrosis, at the same
time, at the bedside. We underline that nomograms are not
decision rules and like almost all proposed scores are
unlikely to entirely replace liver biopsy. From a clinical
standpoint, in a multimodality approach, the application of a
nomogram could help clinicians interpret patients’ profile.
AcknowledgementsThe analysis of data has been possible thanks to free
collaboration with ‘Unita di Statistica Medica, Biometria
e Bioinformatica – Fondazione IRCCS Istituto Nazionale
Tumori’ (Milan).
Elisabetta Sagrini, Alice Gianstefani, and Alessandra
Orlandini participated in collecting data and conception
and design of the study. Fabio Piscaglia, Elisabetta
Sagrini, and Alessandro Cucchetti participated in the
conception and design of the study. Elisabetta Sagrini,
Fabio Piscaglia, Ilaria Ardoino, Giuseppe Marano, and Elia
Biganzoli participated in drafting of the article. Ilaria
Ardoino, Giuseppe Marano, and Elia Biganzoli analyzed
data and carried out statistical analysis. Gabriele Donati,
Alessandro Cucchetti, Guido Pelosi, Alessandra Orlandini,
Carlo Ferrari, Alfredo Alberti, and Giada Sebastiani
provided pool of patients. All authors read and approved
the final manuscript.
Conflicts of interest
There are no conflicts of interest.
References1 Benvegnu L, Gios M, Boccato S, Alberti A. Natural history of compensated
viral cirrhosis: a prospective study on the incidence and hierarchy of majorcomplications. Gut 2004; 53:744–749.
2 Ikeda Y, Shimada M, Hasegawa H, Gion T, Kajiyama K, Shirabe K, et al.Prognosis of hepatocellular carcinoma with diabetes mellitus after hepaticresection. Hepatology 1998; 27:1567–1571.
3 Poynard T, Bedossa P, Opolon P. Natural history of liver fibrosis progressionin patients with chronic hepatitis C. The OBSVIRC, METAVIR, CLINIVIR,and DOSVIRC groups. Lancet 1997; 349:825–832.
4 Craxı A, Pawlotsky JM, Wedemeyer H, Bjoro K, Flisiak R, Forns X, et al. EASLClinical Practice Guidelines: management of hepatitis C virus infection.J Hepatol 2011; 55:245–264.
5 Davis GL, Lau JY. Factors predictive of a beneficial response to therapyof hepatitis C. Hepatology 1997; 26:122S–127S.
6 Marcellin P, Asselah T, Boyer N. Fibrosis and disease progression inhepatitis C. Hepatology 2002; 36:S47–S56.
7 Strader DB, Wright T, Thomas DL, Seeff LB. Diagnosis, management, andtreatment of hepatitis C. Hepatology 2004; 39:1147–1171.
8 Yano M, Kumada H, Kage M, Ikeda M, Shimamatsu K, Inoue O, et al. Thelong-term pathological evolution of chronic hepatitis C. Hepatology 1996;23:1334–1340.
9 Friedrich-Rust M, Ong MF, Martens S, Sarrazin C, Bojunga J, Zezem S, et al.Performance of transient elastography for the staging of liver fibrosis:a meta-analysis. Gastroenterology 2008; 134:960–974.
10 Wai CT, Greenson JK, Fontana RJ, Kalbfleisch JD, Marrero JA,Conjeevaram HS, et al. A simple noninvasive index can predict bothsignificant fibrosis and cirrhosis in patients with chronic hepatitis C.Hepatology 2003; 38:518–526.
11 Forns X, Ampurdanes S, Llovet JM, Aponte J, Quinto L, Martinez-Bauer E,et al. Identification of chronic hepatitis C patients without hepatic fibrosis bya simple predictive model. Hepatology 2002; 36:986–992.
12 Imbert-Bismut F, Ratziu V, Pieroni L, Charlotte F, Benhamou Y, Poynard T.Biochemical markers of liver fibrosis in patients with hepatitis C virusinfection: a prospective study. Lancet 2001; 357:1069–1075.
13 Vallet-Pichard A, Mallet V, Nalpas B, Verkarre V, Nalpas A, Dhalluin-Venier V,et al. FIB-4: an inexpensive and accurate marker of fibrosis in HCV infection.Comparison with liver biopsy and FibroTest. Hepatology 2007; 46:32–36.
14 Miller ME, Hui SL. Validation techniques for logistic regression model. StatMed 1991; 10:1213–1226.
15 Bedossa P, Poynard T. An algorithm for the grading of activity in chronichepatitis C. The METAVIR Cooperative Study Group. Hepatology 1996;24:289–293.
16 Venables WN, Ripley BD. Modern applied statistics with S. 4th ed. NewYork: Springer; 2002.
17 Biesheuvel CJ, Vergouwe Y, Steyerberg EW, Grobbee DE, Moons KG.Polytomous logistic regression analysis could be applied more often indiagnostic research. J Clin Epidemiol 2008; 61:125–134.
18 R Development Core Team. R: a language and environment for statisticalcomputing. Vienna, Austria: R Foundation for Statistical Computing; 2009.
19 Okuda M, Li K, Beard MR, Showalter LA, Scholle F, Lemon SM,Weinman SA. Mitochondrial injury, oxidative stress, and antioxidant gene
10 European Journal of Gastroenterology & Hepatology 2013, Vol 00 No 00

Copyright © Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
expression are induced by hepatitis C virus core protein. Gastroenterology2002; 122:366–375.
20 Adinolfi LE, Giordano MG, Andreana A, Tripodi MF, Utili R, Cesaro G, et al.Hepatic fibrosis plays a central role in the pathogenesis ofthrombocytopenia in patients with chronic viral hepatitis. Br J Haematol2001; 113:590–595.
21 Harrell FE Jr. Regression modelling strategies: with application to linearmodels, logistic regression, and survival analysis. New York: Springer; 2001.
22 Pepe M. The statistical evaluation of medical tests for classification andprediction. Oxford: Oxford University Press; 2003.
23 Bedossa P, Dargere D, Paradis V. Sampling variability of liver fibrosis inchronic hepatitis C. Hepatology 2003; 38:1449–1457.
24 Mehta SH, Lau B, Afdhal NH, Thomas DL. Exceeding the limits of liverhistology markers. J Hepatol 2009; 50:36–41.
25 Huwart L, Sempoux C, Vicaut E, Salameh N, Annet L, Danse E, et al.Magnetic resonance elastography for the noninvasive staging of liverfibrosis. Gastroenterology 2008; 135:32–40.
26 Piscaglia F, Salvatore V, Di Donato R, D’Onofrio M, Gualandi S, Gallotti A,et al. Accuracy of VirtualTouch Acoustic Radiation Force Impulse (ARFI)imaging for the diagnosis of cirrhosis during liver ultrasonography.Ultraschall Med 2011; 32:167–175.
27 Cales P, Oberti F, Michalak S, Hubert-Fouchard I, Rousselet MC, Konate A,et al. A novel panel of blood markers to assess the degree of liver fibrosis.Hepatology 2005; 42:1373–1381.
28 Adams LA, Bulsara M, Rossi E, DeBoer B, Speers D, George J, et al.Hepascore: an accurate validated predictor of liver fibrosis in chronichepatitis C infection. Clin Chem 2005; 51:1867–1873.
29 Haute Autorite de Sante. Non invasive methods for the evolution of hepaticfibrosis/cirrhosis: an update. Available at: http://www.has-sante.fr[Accessed 2 December 2012]; 2008.
30 Leroy V, Halfon P, Bacq Y, Boursier J, Rousselet MC, Bourliere M, et al.Diagnostic accuracy, reproducibility and robustness of fibrosis blood tests inchronic hepatitis C: a meta-analysis with individual data. Clin Biochem2008; 41:1368–1376.
31 Leroy V, Hilleret MN, Sturm N, Trocme C, Renversez JC, Faure P, et al.Prospective comparison of six non-invasive scores for the diagnosis of liverfibrosis in chronic hepatitis C. J Hepatol 2007; 46:775–782.
32 Parkes J, Guha IN, Roderick P, Rosenberg W. Performance of serummarker panels for liver fibrosis in chronic hepatitis C. J Hepatol 2006;44:462–474.
33 Castera L, Vergniol J, Foucher J, Le Bail B, Chanteloup E, Haaser M, et al.Prospective comparison of transient elastography, FibroTest, APRI, and liverbiopsy for the assessment of fibrosis in chronic hepatitis C.Gastroenterology 2005; 128:343–350.
34 Shaheen AA, Wan AF, Myers RP. FibroTest and FibroScan for the predictionof hepatitis C-related fibrosis: a systematic review of diagnostic testaccuracy. Am J Gastroenterol 2007; 102:2589–2600.
35 Friedrich-Rust M, Ong MF, Martens S, Sarrazin C, Bojunga J, Zeuzem S,et al. Performance of transient elastography for the staging of liver fibrosis:a meta-analysis. Gastroenterology 2008; 134:960–974.
36 Kattan MW, Yu C, Salomon L, Vora K, Touijer K, Guillonneau B. Developmentand validation of preoperative nomogram for disease recurrence within 5years after laparoscopic radical prostatectomy for prostate cancer. Urology2011; 77:396–401.
37 Poynard T, Halfon P, Castera L, Munteanu M, Imbert-Bismut F, Ratziu V, et al.Standardization of ROC curve areas for diagnostic evaluation of liver fibrosismarkers based on prevalences of fibrosis stages. Clin Chem 2007;53:1615–1622.
38 Grimes DA, Schulz KF. Refining clinical diagnosis with likelihood ratios.Lancet 2005; 365:1500–1505.
Nomogram for prediction of fibrosis in chronic HCV infection Sagrini et al. 11




















