
Developing practice in breastfeeding
17
© 2006 The Authors. Journal compilation © 2006 Blackwell Publishing Ltd. Maternal and Child Nutrition, 2, pp. 245–261 245 Blackwell Publishing LtdOxford, UKMCNMaternal and Child Nutrition1740-8695© 2006 The Authors. Journal compilation © 2006 Blackwell Publishing Ltd 200624245261Original ArticleDeveloping practice in breastfeedingM.J. Renfrew et al. Correspondence: Mary J. Renfrew, Mother and Infant Research Unit, Department of Health Sciences, University of York, Heslington, York YO10 5DD, UK. E-mail: [email protected] Original Article Developing practice in breastfeeding Mary J. Renfrew * , Gill Herbert † , Louise M. Wallace ‡ , Helen Spiby * and Alison McFadden * * Mother and Infant Research Unit, Department of Health Sciences, University of York, Heslington, York YO10 5DD, UK, † Gill Herbert, Consultancy and Development Ltd, 20 Wood Lane, Newsome, Huddersfield HD4 6QG, UK, and ‡ Health Services Research Centre, Coventry University, Priory Street, Coventry CV1 5FB, UK Abstract This paper reports on an approach to practice development in breastfeeding as part of a national programme of work to address inequalities in maternal and child nutrition. The production and dissemination of evidence and guidelines is necessary but not sufficient on its own to effect change in practice, particularly when dealing with complex public health issues. In the case of breastfeeding, review evidence and national guidance have shown that multifaceted changes are essential if policy aspirations are to be realized. The objectives of the programme described here were to (1) inform and enable practice development in breastfeeding in low-income areas; (2) evaluate the impact of approaches used; and (3) develop robust approaches and appropriate material for use nationally. A conceptual framework was established, and a six-stage process is outlined. The recruitment of four sentinel sites across whole health economies, involving pro- fessionals and the voluntary sector, was an essential component of the programme. The strength of the model is that it provides a structured, cross-sectoral approach to practice development in public health. A key challenge is to identify whose responsibility it is to resource practice development when a number of disciplines and sectors are involved. This question needs to be addressed if public health guidance is to be of sustained benefit. Keywords: breastfeeding, practice development, evidence-based practice, public health guid- ance, multi-sectoral working, cross-sectoral working, service user involvement. Introduction and context Despite the proven public health benefits of breast- feeding (e.g. Howie et al . 1990; British Paediatric Association 1994; Wilson et al . 1998; Kramer et al . 2001; Quigley et al . 2006) and recent policy aspirations (e.g. DH 2002a, 2004a; WHO 2003), breastfeeding is not a high priority for health service organizations in the UK, and many practitioners, even those in key roles, are ill-prepared to promote and support breast- feeding (Abbott et al . 2006; Dykes 2006; McFadden et al . 2006; Renfrew et al . 2006; Wallace & Kosmala- Anderson 2006; Wallace & Kosmala-Anderson in press). Published literature suggests that this not only is a problem for the UK, but reflects a wider interna- tional problem in developed countries (Dykes 2006).
-
Upload
independent -
Category
Documents
-
view
1 -
download
0
Transcript of Developing practice in breastfeeding

copy 2006 The Authors Journal compilation copy 2006 Blackwell Publishing Ltd
Maternal and Child Nutrition
2
pp 245ndash261
245
Blackwell Publishing LtdOxford UKMCNMaternal and Child Nutrition1740-8695copy 2006 The Authors Journal compilation copy 2006 Blackwell Publishing Ltd
2006
24245261Original Article
Developing practice in breastfeeding
MJ Renfrew
et al
Correspondence Mary J Renfrew Mother and Infant Research
Unit Department of Health Sciences University of York
Heslington York YO10 5DD UK E-mail mjr505yorkacuk
Original Article
Developing practice in breastfeeding
Mary J Renfrew
Gill Herbert
dagger
Louise M Wallace
Dagger
Helen Spiby
and Alison McFadden
Mother and Infant Research Unit Department of Health Sciences University of York Heslington York YO10 5DD UK
dagger
Gill Herbert Consultancy and Development Ltd 20 Wood Lane Newsome Huddersfield HD4 6QG UK and
Dagger
Health Services Research Centre Coventry University Priory Street Coventry CV1 5FB UK
Abstract
This paper reports on an approach to practice development in breastfeeding as part of a nationalprogramme of work to address inequalities in maternal and child nutrition The production anddissemination of evidence and guidelines is necessary but not sufficient on its own to effectchange in practice particularly when dealing with complex public health issues In the case ofbreastfeeding review evidence and national guidance have shown that multifaceted changesare essential if policy aspirations are to be realized The objectives of the programme describedhere were to (1) inform and enable practice development in breastfeeding in low-income areas(2) evaluate the impact of approaches used and (3) develop robust approaches and appropriatematerial for use nationally A conceptual framework was established and a six-stage process isoutlined The recruitment of four sentinel sites across whole health economies involving pro-fessionals and the voluntary sector was an essential component of the programme The strengthof the model is that it provides a structured cross-sectoral approach to practice developmentin public health A key challenge is to identify whose responsibility it is to resource practicedevelopment when a number of disciplines and sectors are involved This question needs to beaddressed if public health guidance is to be of sustained benefit
Keywords
breastfeeding practice development evidence-based practice public health guid-
ance multi-sectoral working cross-sectoral working service user involvement
Introduction and context
Despite the proven public health benefits of breast-feeding (eg Howie
et al
1990 British PaediatricAssociation 1994 Wilson
et al
1998 Kramer
et al
2001 Quigley
et al
2006) and recent policy aspirations
(eg DH 2002a 2004a WHO 2003) breastfeeding isnot a high priority for health service organizations inthe UK and many practitioners even those in keyroles are ill-prepared to promote and support breast-feeding (Abbott
et al
2006 Dykes 2006 McFadden
et al
2006 Renfrew
et al
2006 Wallace amp Kosmala-Anderson 2006 Wallace amp Kosmala-Anderson inpress) Published literature suggests that this not onlyis a problem for the UK but reflects a wider interna-tional problem in developed countries (Dykes 2006)
246
MJ Renfrew
et al
copy 2006 The Authors Journal compilation copy 2006 Blackwell Publishing Ltd
Maternal and Child Nutrition
2
pp 245ndash261
At the same time evidence does exist that caninform practice and policy (eg Fairbank
et al
2000Sikorski
et al
2004 Renfrew
et al
2005a) andnational and international guidelines on public healthinterventions based on that evidence has been pub-lished (EU 2004 Dyson
et al
2006) Many of thoseinterventions are not however in mainstream prac-tice and the lack of staff training and educationsuggests that it will be difficult to change thatsituation
In late 2004 we were commissioned to conducta national programme of practice development inbreastfeeding Our group involved a multidisci-plinary multi-sectoral consortium of academicshealth professionals practice developers profes-sional organizations the voluntary sector and rep-resentatives of service users The main aim of thework was lsquoto address inequalities in health byimproving maternal and child nutritionrsquo Breast-feeding was the first priority for what was seen asa 3-year programme of work The first stage was thelearning needs assessment programme described inthe other papers in this journal issue (Renfrew
et al
2006) and the second stage was to conduct thepractice development programme Structuralchanges in the funding organization howeverresulted in practice development falling outside oftheir remit and support being withdrawn before theprogramme could be implemented
In this paper we describe what the national pro-gramme aimed to address and the approach devel-oped to achieve practice change We describe theconceptual framework the planning and the earlydevelopment stage to inform the work of othersand encourage investment in such programmes inthe future
From evidence to practice and policy development
In the past two decades there have been significantadvances in the conduct of systematic reviews anddevelopment of evidence-based guidance (Chalmersamp Altman 1995 Sackett
et al
1996 Gray
et al
1997NICE 2004) Effective ways of moving beyond thatstage to create real change however are less well
developed and it is clear that traditional dissemina-tion by publication in learned journals and formalguidance (NICE 2005) is far from being enough Someof the stages needed to create practice and policychange have been examined in studies and reviews(eg Oxman
et al
1995 Moulding
et al
1999 NHSCRD 1999 Grimshaw
et al
2004 Greenhalgh
et al
2005) These include starting with an organizationallsquodiagnostic analysisrsquo to identify the main barriers toadherence and developing a coherent theoretical baseto make multifaceted interventions more effectiveWidespread diffusion of innovations will then beneeded to incorporate an understanding of currentevidence and issues to build on and move from thatpoint to create change (Greenhalgh
et al
2005)Working with single staff groups is insufficient Anessential component has been shown to be a focus ona framework of organizational and inter-organiza-tional systems and cultural change (Oxman
et al
1995Moulding
et al
1999 NHS CRD 1999 Grimshaw
et al
2004)
Moving from studies of doing this to making ithappen in practice in large-scale systems is a chal-lenging process which can be termed lsquopracticedevelopmentrsquo Practice development should enablethe introduction and diffusion of identified behav-iours and activities that have been demonstrated tobe beneficial or to achieve good outcomes and itshould challenge areas which are demonstrated bythe evidence to be detrimental or harmful ensuringthat bad practice is eliminated and poor practiceaddressed This will require the ability of practitio-ners to change how they provide care commission-ers to question their priorities and managers to re-examine the systems for which they are responsibleSuch action may require a reassessment of beliefsand attitudes changes to communication and othersystems and a fundamental and planned restructur-ing of the way people and systems work We arguethat the identification of effective ways of encour-aging this organizational change is as important asthe review of existing practice in formal clinicalactivity Without sustained change in the practicesof clinical and managerial staff to improve out-comes and health the evidence available howeverstrong is impotent
Developing practice in breastfeeding
247
copy 2006 The Authors Journal compilation copy 2006 Blackwell Publishing Ltd
Maternal and Child Nutrition
2
pp 245ndash261
Practice development can have the added benefitof informing the research agenda by identifying ques-tions which need investigation to inform the nextstage of development The iterative interdependenceof testing and questioning different approaches canstrengthen otherwise disconnected parts of the sys-tem making much better links between researchpractice and policy developments
Practice development and public health
Relatively simple organizational change may beenough when creating some kinds of evidence-basedpractice change For example the introduction of asingle new clinical treatment or its withdrawal frompractice may require active dissemination of inf-ormation to relevant staff groups a monitoringsystem and support for staff through the period oftransition
In the field of public health any changes are likelyto be more complex Sustained change may requirethe introduction of a new kind of practitioner a shiftin the balance of responsibilities between profes-sional groups increased cross-sectoral cooperationdevelopment of completely new skills changed orga-nizational priorities and intervention on an inter-agency basis across the health and social serviceseducation voluntary services and local politicalforums to influence the wider societyrsquos attitudes andbehaviour The learning of members of the public andtheir access to evidence-based is a vital aspect of pub-lic health This may involve not only improvements informal education of professionals but use of accessi-ble and user-friendly key messages to inform the pop-ulation whose health or whose childrenrsquos health canbe affected Use of social marketing and other mediacampaign methods integration of positive images inpopular press and entertainment provision of learn-ing opportunities and events and other ways of influ-encing day-to-day learning by all those likely to beaffected are just as important as changing the way inwhich professionals work Such complex change mayinvolve influencing aspects of public policy such asenvironmental and employment issues and requirecompetition with market forces changing what peo-ple buy and the products they use
Promoting and supporting breastfeeding is anexcellent example of the challenges to be faced in thisfield Systematic reviews (Fairbank
et al
2000Sikorski
et al
2004 Renfrew
et al
2005a) nationaland international guidelines (EU 2004 Dyson
et al
2006) and our learning needs assessment which is anexample of high-level national lsquodiagnostic analysisrsquo(Grimshaw
et al
2004 Renfrew
et al
2006) have allshown that multifaceted changes are needed if realchange is to occur There are parallels with publichealth interventions for tobacco control and obesityprevention and treatment If policy aspirations forpublic health are to be realized practice developmentwill be essential (WHO 2003 DH 2004b)
Practice development in reality
Regardless of what is known about the need for struc-tured and sustained approaches to changing practiceorganizational response to new evidence and guid-ance seems currently to rely more on individualsrsquointerests and less on planned and structured change(Audit Commission 2000 Coote
et al
2004) Furtherlsquopractice developmentrsquo is a term that is interpretedinconsistently In the past two decades or so lsquopracticedevelopmentrsquo nurses and midwives have beeninvolved in activities as disparate as audit guidelinedevelopment training in specific clinical skills or inmore general organizational support in ensuringattendance at appropriate training events
lsquoPractice developmentrsquo staff often find themselvesworking in isolation from colleagues in other disci-plines and indeed from senior colleagues in the orga-nization who have control of some of the levers forchange While there are examples of positive practicedevelopment working between midwifery and healthvisiting colleagues (eg Dominey
et al
2002) suchcollaboration is more likely to be achieved throughinformal networking and shared commitment ratherthan the proactive whole systems approach neededAs a result health service experience of lsquopracticedevelopmentrsquo is of a patchy often unstructuredapproach led by one discipline even by one individ-ual usually a nurse or midwife
Unsworth (2000) suggests that the key characteris-tics of practice development in nursing include using
248
MJ Renfrew
et al
copy 2006 The Authors Journal compilation copy 2006 Blackwell Publishing Ltd
Maternal and Child Nutrition
2
pp 245ndash261
new approaches that lead to direct and quantifiableimprovements in services such changes occur as aresponse to problems or needs and contribute to theprovision of effective services However there hasbeen little systematic exploration of practice develop-ment within midwifery posts although individualmaternity settings have been able to apply for accred-itation as practice development units (McSherry ampMcFadden 2001)
In other fields there are examples of practicedevelopment being led by task forces or developmentagencies linked to particular policy drivers for exam-ple the Change Agents Team at the Department ofHealth in relation to Older Peoplesrsquo policies (DH2002b) and the Adoption Taskforce (DfES 2000)While using existing evidence to inform practicechange such groups also use many different interven-tions and learning models to address major changeThis approach can tackle the interdisciplinary andinter-agency agendas which are needed in manyareas of public health to achieve positive change
Breastfeeding and practice development
A recent systematic review of interventions promot-ing the duration of breastfeeding revealed a dearth ofliterature in the fields of training and education ofhealthcare professionals and breastfeeding counsel-lors and of evidence-based practice or practice devel-opment initiatives (Renfrew
et al
2005a) Thisincludes the absence of high-quality evidence aboutways of preparing practitioners to deliver care to sup-port health policy initiatives Only one study of arelevant evidence-based practice initiative was iden-tified (Grant
et al
2000)Some 79 practice development initiatives in breast-
feeding were funded by the Department of Health inEngland over the period 1999ndash2002 (Dykes 2003)These included establishing breastfeeding supportcentres education for health professionals develop-ment of the role of healthcare assistants in supportingbreastfeeding developing peer support involvingbreastfeeding counsellors and developing services forvulnerable groups such as adolescent womenAlthough preliminary evaluation suggests that thesewere successful formal evaluations were limited
There is also no evidence of a coordinated strategyand funding to support mainstream implementationof practice change such as described above in otherfields so many of these initiatives have since beendiscontinued or have remained as isolated initiativesSuch use of short-term funding without clear strategiesfor creating sustainable change to mainstream prac-tice or integrate learning into future service develop-ment seems to be reflected in other areas across theNational Health Service (NHS) in England and Wales
Like practice development posts more widelyinfant feeding or breastfeeding development postshave a range of remits including providing skilledexpertise in addressing serious breastfeeding prob-lems developing guidelines supporting worktowards achieving accreditation with UNICEF UKBaby Friendly Initiative (BFI) providing educa-tional support to colleagues in developing theirbreastfeeding expertise educating mothers on tech-niques and developing positive attitudes to breast-feeding and other aspects of breast care Manyindividuals in such posts work in relative isolation(Abbott
et al
2006) and are expected to fulfil theirbreastfeeding or infant feeding remit in addition toother midwifery or health visiting workload andresponsibilities This is true even of the nationalnetwork of infant feeding coordinators in Englandwhere coordinators often carry out the work inaddition to their existing duties Development postsare normally restricted to the maternity service thatfunds them often not even having a remit outsideof their own discipline They are unlikely to be ableto support breastfeeding across different sectorswithin the whole health economy in the way thatwe have identified as necessary (Renfrew
et al
2006Wallace amp Jardine 2006)
Unusually three local authority health scrutinieshave recently taken a multi-sectoral approach toexamining how a range of agencies not just localmaternity and community health services canremove barriers to breastfeeding and improve directhealthcare provision to support breastfeedingwomen (Richards 2003 Thomas 2006 Wallace ampJardine 2006) All of these contain recommenda-tions for health services education the voluntarysector trainers of healthcare staff local employers
Developing practice in breastfeeding
249
copy 2006 The Authors Journal compilation copy 2006 Blackwell Publishing Ltd
Maternal and Child Nutrition
2
pp 245ndash261
and lsquoownersrsquo of public spaces as well as the councilsthemselves Inter-sectoral strategic planning led bypublic health where there has also been a sharedinterest in seeking a health economy-wide approachto UNICEF UK BFI status has resulted in moreinter-sectoral practitioner learning networks andshared resources for training staff in breastfeedingsupport (Wallace amp Jardine 2006) The extent towhich this innovative approach is effective and sus-tainable in the longer term is unknown
Breastfeeding development projects
Our approach to practice development drew on thelessons learned from much of the literature summa-rized above Three previous evidence-based prac-tice developments in breastfeeding also directlyinformed our thinking The Breastfeeding in LeedsConsortium was a cross-sectoral partnership thataimed to increase breastfeeding rates by raising theprofile of breastfeeding locally providing educa-tional events and bringing together those withshared interests in supporting breastfeedingwomen As part of that work a Department ofHealth-funded initiative supported a project (Spiby
et al
2002) in which two experienced lay breastfeed-ing counsellors worked to increase evidence-basedsupport to breastfeeding They contributed to edu-cation for undergraduate and registered healthcarepractitioners from a range of disciplines workedwith practitioners providing direct care to womenand provided a range of community developmentactivities The model used in this project was oneof providing evidence-based information forwomen and their families to use rather than atraditional advice-based approach Evaluation ofthis initiative was overwhelmingly positive The layrole was considered compatible rather than conflict-ing with that of healthcare professionals The psy-chosocial perspectives of breastfeeding used by thecounsellors were adopted widely replacing the tra-ditional health lsquobenefits of breastfeeding approachrsquo
Two further developments arose from this suc-cessful preliminary work One project worked tosupport breastfeeding across the health economy inLeeds with a special emphasis on working with
women and families from low-income groups(Spiby
et al
2005) Using the combination of a laycounsellor with a midwife with a specialist breast-feeding background the project delivered multidis-ciplinary and multi-sectoral training using bothhealth and social perspectives It supported the lsquorolloutrsquo of the acute Trustrsquos infant feeding policy andits adoption in the majority of local primary careservices and it demonstrated that collaborativeworking between healthcare professionals andbreastfeeding counsellors can succeed Problemswere also identified some groups of healthcare pro-fessionals are more difficult to engage than otherscross-boundary and inter-sectoral working was stillrelatively new for some health service staff andprotection of professional roles was clearly identi-fied as a problem While support for the initiativehad been identified at a senior level within boththe acute and primary care sectors that support wasnot evident in practice and senior-level projectchampions were not clearly identifiable
A third project included work with local SureStart partnerships in the Leeds and Bradford areasThis delivered staff training helped to establishsupport groups for breastfeeding women initiatedchanges that would reinforce positive messagesabout breastfeeding on Sure Start premises advisedon resources and policies developed support mech-anisms for women in disadvantaged communitiesand developed provided and evaluated a firstcohort of peer support training for women from theSure Start areas The lessons learned from thatwork included the importance of early engagementacross all relevant sectors and disciplines findingout about local needs from local communities theneed to reduce organizational barriers boundariesand tensions and the opportunities that multidisci-plinary education brings This work has now beenincorporated into mainstream practice in the city(Spiby
et al
2005)All three developments were successful in
increasing the number of practitioners women andfamilies receiving evidence-based support withbreastfeeding (Spiby
et al
2005) All includedtrained breastfeeding counsellors as key sources ofsupport and development work and breastfeeding
250
MJ Renfrew
et al
copy 2006 The Authors Journal compilation copy 2006 Blackwell Publishing Ltd
Maternal and Child Nutrition
2
pp 245ndash261
rates in the city including the low-income communi-ties served on discharge from hospital increasedfrom around 45 in early 2002 to 51 in late 2004(St James University Hospital Breastfeeding Statis-tics) All were influential in informing our thinkingaround the conceptual framework and in planningthe structures for the national practice developmentwork described here
Aims and methods
The overall aim of our practice development workwas to address inequalities in health by improvingmaternal and child nutrition The objectives of theprogramme were to (1) inform and enable practicedevelopment in breastfeeding in a number of low-income areas (2) evaluate the impact of approachesused and (3) develop robust approaches and appro-priate material for use across the country in futureyears
Core team
A core team was formed to plan this work The teamincluded the following backgrounds knowledge ofthe evidence base and relevant research methods andcritique in general the development of evidence-based guidance the education of health professionalsat pre- and post-registration levels information tech-nology (IT) and web-based communication skillsknowledge of breastfeeding from public health andclinical perspectives senior NHS managementchange management and practice development in theNHS and related sectors and strategic planning andleadership
National network
At a very early stage a national network was estab-lished with the aim of informing and supporting thework Partners in this network included
bull
academic partners
to ensure that the evidence basewas soundbull
professional bodies
including relevant Royal Col-leges and professional organizations representing thewide range of practitioner groups likely to be
involved to inform the development plans to sup-port dissemination of information to provide con-tacts and communication systems and to enhance thelegitimacy of the workbull
NHS partners
including clinical practitioners withrelevant clinical skills representatives of a StrategicHealth Authority a Public Health Observatory (Pub-lic Health Observatories are funded by the Dep-artment of Health to strengthen the availability anduse of health information at a local level in the UK)NHS Direct (NHS Direct is an online and telephonehealth information enquiry service for the publichttpwwwnhsdirectnhsukindexasp) RDLearning(RDLearning is a web-based national resource ofaccredited health-related education courses httpwwwrdlearningorguk) and primary care researchnetworks to inform practice development plans tooffer communication networks and skills in routinedata collection and analysis and to support the iden-tification of key contacts andbull
representatives of consumer groups voluntary
organizations and non-government organizations
toensure that we were able to benefit from their expe-rience of providing services and gaining user per-spectives to inform the practice development plansand offer communication networks
Links were also made with relevant governmentdepartments and professional advice was taken oncommunication strategies
We developed the system to be flexible and respon-sive with two-way communication systems and fre-quent dialogue with commissioners and partners aswe recognized that the source of funding for this workwas a government agency and that government prior-ities can shift and change over time
Conceptual framework and programme development
A conceptual framework for the project was estab-lished based on the literature and our practice devel-opment experience in breastfeeding (describedabove) and other fields including developing learningnetworks in other areas of practice (eg Herbert ampLake 2005) It was finalized through discussions
Developing practice in breastfeeding
251
copy 2006 The Authors Journal compilation copy 2006 Blackwell Publishing Ltd
Maternal and Child Nutrition
2
pp 245ndash261
among the core team and input from network part-ners This framework then informed all decisions andplans Key elements of the framework included anevidence-based approach multi-sectoral and multi-disciplinary working service userconsumer involve-ment mainstreaming and sustainable systems aparticipatory approach to consultation and communi-cation and embedded evaluation Specific elementsof this approach are shown in Box 1
Based on the conceptual framework a six-stageprocess was developed (Fig 1) Following assessmentof the literature on effective interventions a diagnos-tic analysis of the field was planned to include alearning needs assessment (as reported in this issueof the journal) and a general assessment of the readi-ness of the field to undertake this work (Stage 1) Thiswas followed by a synthesis of those two stages yield-ing an analysis of the problem and potential solutions
Box 1
Elements of conceptual framework
Evidence-based approach
All proposed interventions will be based on a rigorous assessment of the published literature togetherwith practitioner and user views of that evidence base
An eclectic mix of approaches and models will be drawn on based on evidence of lsquowhat worksrsquo indifferent communities
Multi-sectoral and multidisciplinary working including service userconsumer perspectives
Health professionals other relevant professionals from social and education sectors community and layworkers usersconsumers and their families will all have a role in informing and delivering the ongoingprogramme of work
Mainstreaming and sustainable systems
The programme will work to mainstream maternal and child nutrition into all relevant work pro-grammes of other agencies and organizations to avoid a sense of being lsquoinitiative-basedrsquo and to createsustainable change
Existing networks and resources will be used wherever possible to ensure an embedded approach topractice development and to create new systems only when necessary
Solid foundations will be built for long-lasting change and to avoid a lsquodash for growthrsquo
Participatory approach to consultation and communication
All collaborative work will be based on a democratic and participative approach where all constituenciesof interest have an equal voice at all stages regardless of seniority or background
Work will address all levels of the organization ie from senior-level policymakers through regionaland local levels to practitioners in the field and service usersconsumers and their families and willinclude approaches at the level of the individual organization service and community
Embedded evaluation
All approaches used will be evaluated and findings from these evaluations will be synthesized andwidely disseminated to stakeholders including policymakers and professional leaders and other appro-priate audiences
252
MJ Renfrew
et al
copy 2006 The Authors Journal compilation copy 2006 Blackwell Publishing Ltd
Maternal and Child Nutrition
2
pp 245ndash261
Fig
1
Prac
tice
deve
lopm
ent
cycl
e N
HS
Nat
iona
l Hea
lth S
ervi
ce N
GO
non
-gov
ernm
enta
l org
aniz
atio
n
Pre
curs
ors
Sys
tem
atic
re
view
s an
d gu
idan
ce
Oth
er
reli
able
so
urce
s of
ev
iden
ce
bull E
xam
ine
syst
ems
Map
ping
and
di
agno
stic
an
alys
is
bull Id
enti
fica
tion
of
rele
vant
grou
ps
bull L
earn
ing
need
s m
easu
rem
ent
bull A
sses
smen
t of
educ
atio
n pr
ovis
ion
bull D
evel
opm
ent
oppo
rtun
itie
s
Ove
rvie
w a
ndsy
nthe
sis
of
curr
ent
prob
lem
s an
d so
luti
ons
Pla
nnin
g
Net
wor
k de
velo
pmen
t e
gbull
NH
Sbull
Pro
fess
iona
l or
gani
zati
ons
bull N
GO
s bull
Cro
ss-s
ecto
ral
Too
l dev
elop
men
t e
gbull
Dis
tanc
e le
arni
ng
bull T
oolk
its
Cap
acit
y bu
ildi
ng
syst
ems
bull In
divi
dual
bull
Org
aniz
atio
nal
bull S
ervi
ce
bull C
omm
unit
y
Pla
n to
add
ress
ca
paci
ty
buil
ding
and
chan
ge
man
agem
ent a
tdi
ffer
ent l
evel
s an
d in
dif
fere
nt
sect
ors
Cap
acit
y bu
ildi
ng a
ndde
velo
pmen
t
Mea
sure
men
t an
dm
onit
orin
g
Indi
vidu
al le
vel
eg
bull Fa
ce-t
o-fa
ce
educ
atio
n bull
Tw
inni
ng
budd
ying
bull
Dis
tanc
e le
arni
ng
Sys
tem
atic
da
ta c
olle
ctio
n an
d an
alys
is ndash
qual
itat
ive
and
quan
tita
tive
Org
aniz
atio
n an
dse
rvic
e le
vel
eg
bull C
ham
pion
s fo
r ch
ange
bull
Act
ion
lear
ning
se
ts
bull D
emon
stra
tion
pr
ojec
ts
bull Jo
int p
lann
ing
Wor
ksho
pob
serv
atio
n an
d cr
oss-
or
gani
zati
onal
au
dits
Sel
f-ev
alua
tion
an
d be
nchm
arki
ng
netw
orks
Com
mun
ity
leve
l e
gbull
Mul
ti-a
genc
y w
orki
ng
bull C
omm
unit
y re
sour
ces
rese
arch
bull A
ctio
n
Act
ion
rese
arch
and
le
arni
ng s
ets
Pol
icy
impe
rati
ves
Pri
orit
y se
ttin
g an
d
plan
for
di
agno
stic
an
alys
is
Rep
ort o
n m
easu
rem
ent
and
mon
itor
ing
Developing practice in breastfeeding
253
copy 2006 The Authors Journal compilation copy 2006 Blackwell Publishing Ltd
Maternal and Child Nutrition
2
pp 245ndash261
(Stage 2) Stage 3 involved developing relevant net-works tools for education and training evaluationmethods and capacity building systems at individualorganizational service and community levels Follow-ing this a plan to conduct the work would be finalized(Stage 4) implemented (Stage 5) and evaluated Theprocess was intended to be iterative alternatingbetween phases of information appraisal and plan-ning to identify the next stages of development activ-ity and evaluation of the impact to inform futureplanning Stage 6 included finalization of qualitativeand quantitative measurement and monitoring sys-tems that would feedback through all stages of theprocess
It was envisaged that this model would allow effec-tive structures and processes to be identified for usein other aspects of public health practice
Due to changes in funding the programme wasdiscontinued during Stage 3 although in fact somepreliminary work had already been carried out on theplan
Engagement with practitioners
Developing a national programme of change anddevelopment is an ambitious goal A cost-effectiveapproach to engagement had to be developed both tostay within budget and that could roll out acrossEngland and Wales Learning from the successfulLeeds partnership work described above it wasplanned to recruit a series of sentinel sites where wecould test out a range of approaches to maximizelearning and cost-effectiveness as well as respond toideas from the field Work in those sites wouldbecome a model for national developments inform-ing material for education training and assessmentsupported by communications at different levelsthrough our established national network The use ofsentinel sites also allowed for the development ofapproaches sensitive to varying local contexts so pro-viding alternatives and examples to inform nationalimplementation
The first stage in that process was to recruit rele-vant sentinel sites Sites were conceived as includingthe whole health economy in a locality and had tomeet specific criteria These are detailed in Box 2
Four sites were identified and agreed to join thefirst wave of sentinel sites Each site engaged andplanned the programme of work differently Forexample one site had already worked with membersof the core team and were keen to take existing workfurther In the few months in which we worked withthem they put into place a system for the accuratemonitoring of breastfeeding rates and created anextensive network of individuals at a range of seniorlevels from different sectors including Primary CareTrusts (PCTs) Strategic Health Authority the acuteTrust Sure Start and the local authority Benefits thesites have seen even since the work stopped haveincluded
bull improved communication across relevant disci-plines and sectorsbull the observation that the practice developmentwork lsquokept breastfeeding on everyonersquos agendarsquobull the work was used to support a business case for acoordinator for BFI planningbull in one sentinel site the primary care and acutematernity services have formed a health economy-wide breastfeeding strategy groupbull in another a joint primary care and maternity ser-vices group has been establishedbull two sites are taking forward systems for collect-ing breastfeeding data which have been used toprovide feedback to staff each monthbull a new approach to training all staff in one siteincluded commissioning the local university todevelop a self-study workbook and then to test itseffectiveness using an objective skills assessment toolandbull in one site a successful peer support programmewas rolled out throughout Sure Start programmes
A key part of the work in the sentinel sites was tosupport the learning needs assessment (McFadden
et al
2006) Although the sites were at an early stageof engagement this was conducted very successfullyand rapidly as sites supported the identification andinvolvement of practitioners Many assisted with sur-vey distribution and in return received a report ofthe training needs identified for their staff The nexttest was the running of fieldwork meetings and
254
MJ Renfrew
et al
copy 2006 The Authors Journal compilation copy 2006 Blackwell Publishing Ltd
Maternal and Child Nutrition
2
pp 245ndash261
workshops to finalize guidance based on researchevidence as part of a related programme of workThe aim of this work was to take the results of aseries of systematic reviews (which gave informationon lsquowhat works from research evidencersquo) and consultwith practitioners managers and users on lsquowhatreally works in practicersquo (Dyson
et al
2006) Thenewly established sentinel site system supported thiswork by offering venues for meetings providing listsof eligible participants and enabling and encourag-ing staff to attend (Renfrew
et al
2005b) The finalstage of this guidance work was a series of majorworkshops with over 30 participants in each repre-senting a lsquodiagonal slicersquo through the whole healtheconomy from field-level practitioners includingpeer support workers to managers and planners andincluding the range of relevant disciplines as well as
the voluntary sector Concerns around the realitiesand influences on practice and key issues for practi-tioners and managers in developing good practicewere discussed as well as organizational and struc-tural barriers to change Participants were encour-aged to discuss not only practices that need to beintroduced but also those that need to be aban-doned thereby potentially saving time and resourcesand to identify actual or potential barriers to imple-menting change (Renfrew
et al
2005b) These facili-tated groups examined the ability of the service torespond to identified gaps and made recommenda-tions for improvements to the system They feddirectly into the final stages of the development ofNational Institute for Health and Clinical Excellence(NICE) public health recommendations for breast-feeding offering participants the satisfaction of
Box 2
Sentinel site criteriaSentinel sites were expected to
bull Have a deprivation profile that demonstrated a substantial proportion of low-income groups and adiverse ethnic profile and serve contrasting areas (eg urban rural)
bull Offer a range of services for children and women with an interest in nutrition
bull Be able to include the whole health economy in a locality (or at least agree to working across allrelevant sectors)
bull Provide a key contact personpeople who would act to facilitate communication and broker agree-ments with different parts of the health economy and managers who were supportive of the plannedwork willing to support and enable staff participation
bull In the first instance sites would be those where contact already existed with members of our coreteam Future sites would be brought in once any initial problems with the approach had been identifiedand addressed
In return for their involvement in the work it was recognized that the sentinel sites would benefit in arange of ways including
bull Support for staff development and learning through access to programme staff and expertise involve-ment in and learning from a regular newsletter and attendance at an annual leading-edge conferenceon maternal and child nutrition
bull Developing links with other sites and sharing good practice and problem solving
bull The opportunity to help to develop national practice resulting in a raised profile for their work andtheir staff
bull Early access to emerging evidence in the field of maternal and child nutrition
Developing practice in breastfeeding
255
copy 2006 The Authors Journal compilation copy 2006 Blackwell Publishing Ltd
Maternal and Child Nutrition
2
pp 245ndash261
knowing that their input would make a difference(Dyson
et al
2006) These workshops also tested outthe use of language the conceptual understanding ofparticipants in relation to the evidence reviews andgathered intelligence on what approaches to imple-mentation of practice development may be mosteffective They also provided an opportunity for dis-cussion debate and deliberation about the meaningof the evidence Participants reported this to be veryuseful in assisting their understanding of the evi-dence and in considering how best to change theirown and their colleaguesrsquo practice in response to itand as an important contribution to practice devel-opment in their own locality (McFadden
et al
2005)The input of representatives of service users was ofcritical importance
It was planned that once the guidance was final-ized each participating site would be in a strong posi-tion to act on it Not only would they feel someownership but they would also have staff from alllevels and sectors in their health economy who hadspent time discussing the issues with colleagues andwith service user representatives They would haveaccess to specific local information about localitiesand groups that needed to be prioritized creatingchange was therefore brought several stages closerAt the end of each workshop email and telephonecontact details were exchanged among the workshopparticipants many of whom had never met beforedespite working in related parts of the same systemto support closer local networking The opportunityto consult with national experts in the network alsoacted as a variant on educational outreach which hasbeen shown to be moderately successful in guidelineimplementation (NHS CRD 1999) The impact ofsuch exchanges in increasing opportunities for net-work support is virtually impossible to evaluate for-mally but there was confidence in those whoparticipated at these events that positive changewould result and that the evidence would be moreeffectively used in the future as a consequence
Interactive conference
The other main activity was a conference on maternaland child nutrition to which all partners ndash academic
professional NHS and userconsumer ndash and stafffrom sentinel sites were invited Commissioners ofthe work were invited as were staff from key govern-ment departments with an interest in nutrition childhealth Sure Start nursing and midwifery and ine-qualities in health Around 90 participants took partin a day which included presentations participativeworking and active networking A report of the dayis available at httpwwwyorkacukresmcncccon-ferenceReporthtm Feedback was strongly positiveand the impact of networking with others in similarsituations and between those working in local andnational organizations was especially valued It wasplanned that this would be an annual event
Had we been able to continue the practice devel-opment programme we planned to use the follow-ing approaches
Establishing learning networks
We planned to identify appropriate learning net-works for different constituencies which wouldenable communication among staff from differentsectors as well as communication with programmestaff Activities were planned to include
bull Staff working at strategic and senior managementlevels would be supported and appropriate informa-tion provided to allow them to create cross-systemchanges Senior-level lsquochampions for changersquo wouldbe identified These would be used in a range of waysthose wishing to be involved in learning networkswould be supported to do sobull Learning sets would be established This wouldenable focused exchange between stakeholders onhow best to make use of the evidence in practice andhow to influence mainstream practice across locali-ties Through feedback loops we planned to developlearningeducation material to be made availablethrough web-based routes to wider constituenciesbull Peer supporters and trained breastfeeding counsel-lors are key groups in regard to breastfeeding promo-tion and support We planned to include them inlearning sets They have much to offer health profes-sionals in coming to understand the needs of womenand families and indeed the evidence suggests thattheir involvement in advisory work and peer support
256
MJ Renfrew
et al
copy 2006 The Authors Journal compilation copy 2006 Blackwell Publishing Ltd
Maternal and Child Nutrition
2
pp 245ndash261
enhances and strengthens the impact of informationand evidence-based guidance possibly more thanthat of health professionalsrsquo practice Our experiencedescribed above has identified a valuable contribu-tion from lay breastfeeding counsellors into educa-tion and training provision
Educational approaches
The breadth of constituencies that the programmeneeded to reach was to be reflected in the range ofeducational approaches required For some profes-sions continuing professional development (CPD)time is factored in regularly to the job plan in a rollingprogramme of group education with routine sessionalwork suspended for other groups CPD is a self-verified individual activity that can be achievedthrough a range of methods including distance learn-ing We hoped to reach directly a broad group ofwomen as well as professionals through some of theroutes developed A range of materials was thereforeplanned to address all needs Materials would bedeveloped for web-based access CD-ROM access andon paper These were to include
bull Toolkits to promote and support breastfeeding tomonitor breastfeeding rates and on practice develop-ment and changebull Distance learning modules providing accreditedlearning opportunities at a range of levelsbull An email and telephone-based service to putindividuals and organizations in touch with otherswho can support and advise them supported byRDLearning a national web-based resourcebull Learning material that could be directly dissemi-nated through the Internet to a wide audiencebull Buddy systems and mentoring for practice devel-opment and public health strategic development inbreastfeeding and use of cascade systemsbull Summaries of approaches to dissemination andpromotion of information that have proved to be suc-cessful and of practice change programmes that havebeen evaluated as having a positive impact on initia-tion and duration of breastfeedingbull Through NHS Direct we planned to reach the gen-eral public Information could be provided to informthe development of new algorithms that could be
used by staff taking enquiries from breastfeedingwomen We planned also to provide information thatcould be used on the NHS Direct website which isaccessed directly by women and families as well ashealth professionalsbull Other material to reach the general public wouldbe developed We aimed to have informative paperspublished in womenrsquos and familiesrsquo magazines and inthe general media on a regular basis A professionalwriter was one of our partners her role was to informand advise us about reaching women directly
Discussion
The work described in this paper was a structuredcross-sectoral approach to practice development inpublic health As a result of funding problems a fullevaluation could not be conducted and our contribu-tion to the knowledge base on practice change inpublic health is limited Lessons were learned how-ever and feedback was gained from participants atdifferent stages of the process We received strongsupport for our approach and the willingness of localand national partners to engage actively in the pro-gramme testifies to its potential
Lessons learned
There is increasing emphasis in public health andhealth policy on the need for good partnership work-ing and integration across disciplines professionsorganizations and localities as shown in the recentWhite Paper from the Department of Health (DH2006) and in the Children Act (2004) Prevention ofill health and promotion of well-being featurestrongly in these and other policy documents with arecognition that this cannot be achieved without fullengagement at strategic and operational levels withthose who use or depend on public-sector services Itwas clear at every stage of this process that engage-ment was needed across the whole health economyIt is only in working with all the relevant layers andpartnerships of professionals that we can hope for thefull impact of evidence to be realized Traditionalapproaches however only disseminate evidence tointerest groups in isolation Our use of lsquodiagonal slicersquo
Developing practice in breastfeeding 257
copy 2006 The Authors Journal compilation copy 2006 Blackwell Publishing Ltd Maternal and Child Nutrition 2 pp 245ndash261
workshops in which staff at all levels and across allsectors were engaged and including representativesof service users and the voluntary sector enabledmuch greater understanding of the consequences ofparticular activity or behaviour in other parts of thesystem and allowed creative and informed challengesto assumptions and prejudices This laid good foun-dations for whole systems approaches to introducingdriving and implementing new approaches whichcould lead to positive health outcomes It proved avery positive learning experience for all thoseinvolved
Practice change needs to involve the whole rangeof health professionals involved in work directly withpregnant women and new mothers to ensure coordi-nated working and consistent messages Despiteactive support from relevant Royal Colleges and sev-eral strongly supportive individuals engagement bydoctors was noticeably less compared with otherhealth professions This supports the findings of otherwork (eg Smale et al 2006) This really matters in afield such as breastfeeding where paediatriciansobstetricians general practitioners and public healthphysicians have an important role to play Futurework will need to address this
Key constituents in practice development in breast-feeding include mothers and potential mothersgrandmothers and men We had strong support andinvolvement from service users and user groups butengaging men proved to be difficult To reach thepublic good-quality easily accessible information isneeded perhaps the developing DiPEX module onbreastfeeding will contribute to this (httpwwwdipexorgDesktopDefaultaspx) Recent gov-ernment policy directives acknowledge the potentialcontribution that incorporating patient and serviceuser experience into service provision can bring (egDH 2006) Recent developments in the approach tolong-term conditions management have introducedthe Expert Patient Programme which enables peoplewith disabilities to take much more effective controlover the management and treatment of their disease(DH 2004c 2006) There is perhaps potential for theparallel development of an lsquoExpert Mothers Pro-grammersquo to have similar positive impact in relation tonutrition and health
Service user involvement is actively encouraged ininforming research and practice (Hanley et al 2004)Breastfeeding and maternity care as a whole have along-standing history of the active engagement of ser-vice users Volunteer counsellors and supporterstrained and accredited by their own voluntary orga-nizations have filled the gap left by the health ser-vices They have taken the initiative in setting uptelephone support services training and supervisingpeer supporters and contributing to the education ofhealth professionals (Smale et al 2006) In our cur-rent and previous practice development work thecontribution of service users and voluntary groupswent much further than simply offering advice andinformation They took an active role in planning thework and in some cases delivering education andservices Our experience was that lay workers havean essential role in developing services and they areable to advise at a strategic level as well as participat-ing in service delivery They are able to see throughthe organizational barriers that often constrain pro-fessionals and can see solutions that will work formothers and families From our experience we wouldadvise that others explore ways of actively engaginglay workers adequately remunerated in the deliveryof health care and in the education of healthprofessionals
The fundamental importance of multidisciplinaryand multi-professional working was also apparent inthe way in which the core team worked and in thesupport gained from the network of partners Atevery stage we had expertise and support availableto us as well as an effective communication systemand network Practice change in public health needsto be led and informed by those who know the topicarea and who have the wide range of skills neededto convince many different kinds of professionals thatthe work is worthwhile and achievable
Another positive contribution was the synergy ofthis programme with the evidence base The sameteam had also been responsible for systematicreviews of the field (eg Fairbank et al 2000Protheroe et al 2003 Sikorski et al 2004 Renfrewet al 2005a) and the approach was grounded in thisevidence which was at the same time being devel-oped into national guidance The interaction between
258 MJ Renfrew et al
copy 2006 The Authors Journal compilation copy 2006 Blackwell Publishing Ltd Maternal and Child Nutrition 2 pp 245ndash261
these elements should not be underestimated part-ners and sentinel sites were able to inform the guid-ance and up-to-date knowledge of the evidence basehelped strengthen the practice development work
The sentinel site system was proving to be asuccessful lsquowin-winrsquo situation for all involved Itprovided a test bed for ideas it was a source ofinformation and debate and the programme gaineda richness and diversity of input that would be hardto match At the same time it offered the sitesengagement in leading-edge work an increased pro-file and high-quality staff development Although itwas not formally evaluated all involved were con-vinced that it was a very cost-effective system theprogramme could conduct work at speed and to ahigh quality and governance issues were streamlinedThe system was very flexible and could adapt to thedifferent circumstances of each site It would havebeen able to accommodate future service and educa-tion developments such as Childrenrsquos Centres Trustreorganization and inter-professional educationOver time we could have expanded to include othersectors and practitioners such as retailers and child-minders Had the programme continued future siteswould have been identified and material developedfor national use based on our learning in the originalfour sites
Major challenges
Throughout the programme getting breastfeedingrecognized as a priority was difficult This has beenthe case for many years despite its fundamental con-tribution to public health in the short and long termit has only recently been included in national publichealth policy statements PCT targets and monitoringAs we found in the learning needs assessment andother work breastfeeding services are often seen asthe remit of enthusiastic individuals discussed interms reminiscent of lsquoreligious zealotryrsquo (Smale et al2006) rather than as a part of the mainstream ofhealth provision Creating real change in theapproach to breastfeeding in the health service willrequire it to be seen as a priority for senior managersand commissioners Our experience has demon-strated that it is possible to engage such senior people
in this work and that discussion and debate with theirown colleagues can have an impact on their thinking
A key area of practice development that canimpact on breastfeeding duration is working withmothers to sustain breastfeeding while going back towork and the ways that public health strategy andpractice can influence employers to provide breast-feeding-friendly maternity policies and facilities(Kosmala-Anderson amp Wallace in press) We did nothave an impact on this area but it was clear that itwas an area that needed to be addressed One goodplace to start would be with the employment condi-tions for NHS employees themselves this would havethe dual advantage of improving conditions for thelargest female workforce in the country while alsoproviding a model of good practice for others
Although the aim of this work was to address ine-qualities in health it is clear that reaching the hard-to-reach remains challenging We did see signs of suc-cess for example Sure Start schemes were making adifference in some areas but ensuring that all vulner-able women receive the support and care they needis still a distant goal whether they are teenagers asy-lum seekers or simply women who live in areas wherebottle feeding has been endemic for generations
Finally there is a debate to be had on whoseresponsibility it is to create such change The work ofresearchers is seen to be complete when their studyis finished and disseminated through publication andconference presentation Systematic reviewers takeon a responsibility to make the results of a wide rangeof studies available through publication but not toengage with what services might do with those find-ings Those responsible for guidance are responsiblefor developing and publishing that work and somealso take responsibility for lsquoimplementationrsquo (egNICE 2005) But where does responsibility rest forpractice development which requires a deep engage-ment with the practice setting and with those affectedby the issues raised by the evidence Lack of invest-ment at the national level in formal evaluation ofprogrammes of change limits the available evidencebase and detracts from our achieving a better under-standing of what actually works in relation to thesemore complex health issues funding for the lsquoRrsquoaspects of research and development is more com-
Developing practice in breastfeeding 259
copy 2006 The Authors Journal compilation copy 2006 Blackwell Publishing Ltd Maternal and Child Nutrition 2 pp 245ndash261
mon than for the lsquoDrsquo (NHS Executive 1997) Thewithdrawal of funding to this programme part waythrough its cycle was regretted by our commissionersit was evident that practice development was nolonger their remit given their changed circumstancesIt is however not clear that responsibility now restswith any particular agency Is development work forindividual health service organizations themselves totake on Is this work that should be led by nationalprogrammes supported by public-sector funding orshould it rely on other sources of support If so fromwhere will it be resourced and how will cross-sectoraland multidisciplinary developments be addressedThere are also questions about who will lead thiswork when a number of professional disciplines areinvolved and where the client interface spans bothprimary and acute care healthcare settings social ser-vices and other development agencies These ques-tions will become more pressing as guidancecontinues to be produced especially in public health
Acknowledgements
We would like to thank all participants from sentinelsites and our consortium of academic professionalNHS and consumer partners and the two anonymousreferees who reviewed the manuscript This work wascommissioned by the former Health DevelopmentAgency and subsequently funded by NICE
References
Abbott S Renfrew MJ amp McFadden A (2006) lsquoInformalrsquo learning to support breastfeeding local problems and opportunities Maternal and Child Nutrition 2 232ndash238
Audit Commission (2000) United They Stand Coordinating Care for Elderly Patients with Hip Fracture Audit Com-mission London
British Paediatric Association (1994) Statement of the stand-ing committee on nutrition is breastfeeding beneficial in the UK Archive of Diseases in Childhood 71 376ndash380
Chalmers I amp Altman DG (eds) (1995) Systematic Reviews BMJ Publishing Group London
Children Act (2004) Available at httpwwwopsigovukactsacts200420040031htm (accessed 21 March 2006)
Coote A Allen J amp Woodhead D (2004) Finding out What Works Building Knowledge about Complex Community-Based Initiatives Kingrsquos Fund London
DfES (2000) Adoption and Permanence Taskforce Available at httpwwwdfesgovukadoptionadoptionreformstaskforceshtml (accessed 29 March 2006)
DH (2002a) Improvement Expansion and Reform The Next 3 Years Priorities and Planning Framework 2003ndash2006 Department of Health London
DH (2002b) The Health and Social Care Change Agent Team Available at httpwwwchangeagentteamorguk (accessed 29 March 2006)
DH (2004a) National Service Framework for Children Young People and Maternity Services Stationery Office London
DH (2004b) Choosing Health Making Healthy Choices Eas-ier Stationery Office London
DH (2004c) Self Care ndash A Real Choice Self Care Support ndash A Practical Option Stationery Office London
DH (2006) Our Health Our Care Our Say A New Direction for Community Services Stationery Office London
Dominey M Archibald A Edgecombe D Lawrence J amp Thomson L (2002) Breastfeeding and drug misuse Mak-ing an informed choice Year 3 Practice project In Infant Feeding Initiative A Report Evaluating the Breastfeeding Practice Projects 1999ndash2002 (ed F Dykes 2003) p 64 Department of Health London
Dykes F (2003) Infant Feeding Initiative A Report Evaluat-ing the Breastfeeding Practice Projects 1999ndash2002 Depart-ment of Health London
Dykes F (2006) The education of health practitioners sup-porting breastfeeding women time for critical reflection Maternal and Child Nutrition 2 204ndash216
Dyson L Renfrew MJ McFadden A McCormick F Herbert G amp Thomas J (2006) Promotion of Breastfeed-ing Initiation and Duration Evidence into Practice Brief-ing National Institute for Health and Clinical Excellence London httpwwwniceorgukdown-loadaspxo=346169 (accessed 26 July 2006)
EU (2004) Project on Promotion of Breastfeeding in Europe Protection Promotion and Support of Breastfeeding A Blueprint for Action European Commission Directorate Public Health and Risk Assessment Luxembourg
Fairbank L OrsquoMeara S Renfrew MJ Woolridge M Sowden AJ amp Lister-Sharp D (2000) A systematic review to evaluate the effectiveness of interventions to promote the initiation of breastfeeding Health Technol-ogy Assessment 4 1ndash171
Grant J Fletcher M amp Warwick C (2000) The South Thames Evidence Based Practice (STEP) Project Sup-porting Breastfeeding Women South Bank University London
Greenhalgh T Robert G Bate P Mcfarlane F amp Kyriakidou O (2005) Diffusion of Innovations in Health Service Organisations A Systematic Literature Review Blackwell Publishing Limited Oxford
260 MJ Renfrew et al
copy 2006 The Authors Journal compilation copy 2006 Blackwell Publishing Ltd Maternal and Child Nutrition 2 pp 245ndash261
Grimshaw JM Thomas RE MacLennan G Fraser C Ramsay CR Vale L et al (2004) Effectiveness and efficiency of guideline dissemination and implementation strategies Health Technology Assessment 8 indashxi 1ndash72
Hanley B Bradburn J Barnes M Evans C Goodare H Kelson M et al (2004) Involving the Public in NHS Pub-lic Health and Social Care Research Briefing Notes for Researchers INVOLVE Department of Health London
Herbert G amp Lake G (2005) Making connections Effective development of the intermediate tier Journal of Inte-grated Care 13 35ndash42
Howie PW Forsyth JS Ogston SA Clark A amp Florey CD (1990) Protective effect of breastfeeding against infection British Medical Journal 300 11ndash16
Kosmala-Anderson J amp Wallace LM (in press) Breastfeed-ing works the role of employers in supporting women who wish to breastfeed and work in four organizations in England Journal of Public Health (in press)
Kramer M Chalmers B Hodnett H Sevovskaya Z Dzikovich I Shapiro S et al (2001) Promotion of breast-feeding intervention trial (PROBIT) Journal of the American Medical Association 285 413ndash420
McFadden A Renfrew MJ Dyson L McCormick F Herbert G amp Thomas J (2005) Effective Active Briefing on the Initiation and Duration of Breastfeeding Fieldwork Report National Institute for Health and Clinical Excel-lence London
McFadden A Renfrew MJ Dykes F amp Burt S (2006) Assessing learning needs for breastfeeding setting the scene Maternal and Child Nutrition 2 196ndash203
McSherry R amp McFadden A (2001) Practice Development Accreditation Assessment Maternity Services Darlington Memorial Hospital South Durham Healthcare NHS Trust Final Report University of Teesside Middlesbrough
Moulding NT Silagy CA amp Weller DP (1999) A frame-work for effective management of change in clinical prac-tice dissemination and implementation of clinical practice guidelines Quality in Health Care 8 177ndash183
Gray JA Haynes RB Sackett DL Cook DJ amp Guyatt GH (1997) Transferring evidence from research into practice 3 Developing evidence-based clinical policy Evidence-Based Medicine 2 36ndash38
NHS Centre for Reviews and Dissemination (CRD) (1999) Getting evidence into practice Effective Health Care 5 1ndash16
NHS Executive (1997) RampD in Primary Care National Working Group Report (Mant Report) Stationery Office London
NICE (2004) The Guideline Development Process National Institute for Health and Clinical Excellence London
NICE (2005) Putting NICE Guidance into Practice National Institute for Health and Clinical Excellence London
Oxman AD Thomson MA Davis DA amp Haynes RB (1995) No magic bullets a systematic review of 102 trials of interventions to improve professional practice Canadian Medical Association Journal 153 1423ndash1431
Protheroe L Dyson L Renfrew MJ Bull J amp Mulvihill C (2003) The Effectiveness of Public Health Interventions to Promote the Initiation of Breastfeeding Evidence Briefing Health Development Agency London
Quigley MA Cumberland P Cowden JM amp Rodrigues LC (2006) How protective is breast feeding against diar-rhoeal disease in infants in 1990s England A case control study Archives of Disease in Childhood 91 245ndash250
Renfrew MJ Dyson L Wallace L DrsquoSouza L McCormick FM amp Spiby H (2005a) The Effectiveness of Health Interventions to Promote the Duration of Breast-feeding Systematic Review 1st edn National Institute for Health and Clinical Excellence London
Renfrew MJ Dyson L McFadden A McCormick F Herbert G amp Thomas J (2005b) Effective Active Briefing on the Initiation and Duration of Breastfeeding Technical Report National Institute for Health and Clinical Excel-lence London
Renfrew MJ McFadden A Dykes F Wallace L Abbott S Burt S et al (2006) Addressing the learning deficit in breastfeeding strategies for change Maternal and Child Nutrition 2 239ndash244
Richards D (2003) Childrenrsquos Nutrition ndash Mothers Who Wish to Breast-Feed Birmingham City Council Available at httpwwwbirmingahmgovukscrutiny (accessed 27 July 2006)
Sackett DL Rosenberg WMC Gray JAM Haynes RB amp Richardson WS (1996) Evidence-based medicine what it is and what it isnrsquot British Medical Journal 312 71ndash72
Sikorski J Renfrew MJ Pindoria S amp Wade A (2004) Support for breastfeeding mothers (Cochrane Review) The Cochrane Database of Systematic Reviews Issue 2 John Wiley amp Sons Ltd Chichester
Smale M Renfrew MJ Marshall JL amp Spiby H (2006) Turning policy into practice more difficult that it seems The case of breastfeeding education Maternal and Child Nutrition 2 103ndash113
Spiby H Ker R DrsquoSouza L amp Renfrew MJ (2002) Intro-ducing a Consumer-Practitioner into breastfeeding prac-tice Year 2 In Infant Feeding Initiative A Report Evaluating the Breastfeeding Practice Projects 1999ndash2002 (ed F Dykes 2003) p 44 Department of Health London
Spiby H Wallis S Stone C amp Renfrew MJ (2005) Support-ing and Promoting Breastfeeding in Leeds Final Report to December 2004 Report to Leeds PCTs Children and Families Modernisation Team Leeds
Thomas C (2006) Darlington ndash A Breastfeeding Friendly Town Darlington Borough Council Darlington
Developing practice in breastfeeding 261
copy 2006 The Authors Journal compilation copy 2006 Blackwell Publishing Ltd Maternal and Child Nutrition 2 pp 245ndash261
Unsworth J (2000) Practice development a concept analy-sis Journal of Nursing Management 8 317ndash326
Wallace LM amp Jardine J (2006) A Health Scrutiny of Ser-vices to Support the Initiation and Duration of Breastfeed-ing in Coventry and Warwickshire Coventry and Warwickshire County Councils Coventry
Wallace L amp Kosmala-Anderson J (2006) A training needs survey of doctorsrsquo breastfeeding support skills in England Maternal and Child Nutrition 2 217ndash231
Wallace L amp Kosmala-Anderson J (in press) Training needs survey of midwives health visitors and voluntary sector
breastfeeding support staff in England Maternal and Child Nutrition (in press)
WHO (2003) Global Strategy for Infant and Young Child Feeding World Health Organization Geneva
Wilson AC Forsyth JS Green SA Irvine L Hau C amp Howie PW (1998) Relation of infant diet to childhood health seven year follow up of a cohort of children in Dundee infant feeding study British Medical Journal 316 21ndash25

246
MJ Renfrew
et al
copy 2006 The Authors Journal compilation copy 2006 Blackwell Publishing Ltd
Maternal and Child Nutrition
2
pp 245ndash261
At the same time evidence does exist that caninform practice and policy (eg Fairbank
et al
2000Sikorski
et al
2004 Renfrew
et al
2005a) andnational and international guidelines on public healthinterventions based on that evidence has been pub-lished (EU 2004 Dyson
et al
2006) Many of thoseinterventions are not however in mainstream prac-tice and the lack of staff training and educationsuggests that it will be difficult to change thatsituation
In late 2004 we were commissioned to conducta national programme of practice development inbreastfeeding Our group involved a multidisci-plinary multi-sectoral consortium of academicshealth professionals practice developers profes-sional organizations the voluntary sector and rep-resentatives of service users The main aim of thework was lsquoto address inequalities in health byimproving maternal and child nutritionrsquo Breast-feeding was the first priority for what was seen asa 3-year programme of work The first stage was thelearning needs assessment programme described inthe other papers in this journal issue (Renfrew
et al
2006) and the second stage was to conduct thepractice development programme Structuralchanges in the funding organization howeverresulted in practice development falling outside oftheir remit and support being withdrawn before theprogramme could be implemented
In this paper we describe what the national pro-gramme aimed to address and the approach devel-oped to achieve practice change We describe theconceptual framework the planning and the earlydevelopment stage to inform the work of othersand encourage investment in such programmes inthe future
From evidence to practice and policy development
In the past two decades there have been significantadvances in the conduct of systematic reviews anddevelopment of evidence-based guidance (Chalmersamp Altman 1995 Sackett
et al
1996 Gray
et al
1997NICE 2004) Effective ways of moving beyond thatstage to create real change however are less well
developed and it is clear that traditional dissemina-tion by publication in learned journals and formalguidance (NICE 2005) is far from being enough Someof the stages needed to create practice and policychange have been examined in studies and reviews(eg Oxman
et al
1995 Moulding
et al
1999 NHSCRD 1999 Grimshaw
et al
2004 Greenhalgh
et al
2005) These include starting with an organizationallsquodiagnostic analysisrsquo to identify the main barriers toadherence and developing a coherent theoretical baseto make multifaceted interventions more effectiveWidespread diffusion of innovations will then beneeded to incorporate an understanding of currentevidence and issues to build on and move from thatpoint to create change (Greenhalgh
et al
2005)Working with single staff groups is insufficient Anessential component has been shown to be a focus ona framework of organizational and inter-organiza-tional systems and cultural change (Oxman
et al
1995Moulding
et al
1999 NHS CRD 1999 Grimshaw
et al
2004)
Moving from studies of doing this to making ithappen in practice in large-scale systems is a chal-lenging process which can be termed lsquopracticedevelopmentrsquo Practice development should enablethe introduction and diffusion of identified behav-iours and activities that have been demonstrated tobe beneficial or to achieve good outcomes and itshould challenge areas which are demonstrated bythe evidence to be detrimental or harmful ensuringthat bad practice is eliminated and poor practiceaddressed This will require the ability of practitio-ners to change how they provide care commission-ers to question their priorities and managers to re-examine the systems for which they are responsibleSuch action may require a reassessment of beliefsand attitudes changes to communication and othersystems and a fundamental and planned restructur-ing of the way people and systems work We arguethat the identification of effective ways of encour-aging this organizational change is as important asthe review of existing practice in formal clinicalactivity Without sustained change in the practicesof clinical and managerial staff to improve out-comes and health the evidence available howeverstrong is impotent
Developing practice in breastfeeding
247
copy 2006 The Authors Journal compilation copy 2006 Blackwell Publishing Ltd
Maternal and Child Nutrition
2
pp 245ndash261
Practice development can have the added benefitof informing the research agenda by identifying ques-tions which need investigation to inform the nextstage of development The iterative interdependenceof testing and questioning different approaches canstrengthen otherwise disconnected parts of the sys-tem making much better links between researchpractice and policy developments
Practice development and public health
Relatively simple organizational change may beenough when creating some kinds of evidence-basedpractice change For example the introduction of asingle new clinical treatment or its withdrawal frompractice may require active dissemination of inf-ormation to relevant staff groups a monitoringsystem and support for staff through the period oftransition
In the field of public health any changes are likelyto be more complex Sustained change may requirethe introduction of a new kind of practitioner a shiftin the balance of responsibilities between profes-sional groups increased cross-sectoral cooperationdevelopment of completely new skills changed orga-nizational priorities and intervention on an inter-agency basis across the health and social serviceseducation voluntary services and local politicalforums to influence the wider societyrsquos attitudes andbehaviour The learning of members of the public andtheir access to evidence-based is a vital aspect of pub-lic health This may involve not only improvements informal education of professionals but use of accessi-ble and user-friendly key messages to inform the pop-ulation whose health or whose childrenrsquos health canbe affected Use of social marketing and other mediacampaign methods integration of positive images inpopular press and entertainment provision of learn-ing opportunities and events and other ways of influ-encing day-to-day learning by all those likely to beaffected are just as important as changing the way inwhich professionals work Such complex change mayinvolve influencing aspects of public policy such asenvironmental and employment issues and requirecompetition with market forces changing what peo-ple buy and the products they use
Promoting and supporting breastfeeding is anexcellent example of the challenges to be faced in thisfield Systematic reviews (Fairbank
et al
2000Sikorski
et al
2004 Renfrew
et al
2005a) nationaland international guidelines (EU 2004 Dyson
et al
2006) and our learning needs assessment which is anexample of high-level national lsquodiagnostic analysisrsquo(Grimshaw
et al
2004 Renfrew
et al
2006) have allshown that multifaceted changes are needed if realchange is to occur There are parallels with publichealth interventions for tobacco control and obesityprevention and treatment If policy aspirations forpublic health are to be realized practice developmentwill be essential (WHO 2003 DH 2004b)
Practice development in reality
Regardless of what is known about the need for struc-tured and sustained approaches to changing practiceorganizational response to new evidence and guid-ance seems currently to rely more on individualsrsquointerests and less on planned and structured change(Audit Commission 2000 Coote
et al
2004) Furtherlsquopractice developmentrsquo is a term that is interpretedinconsistently In the past two decades or so lsquopracticedevelopmentrsquo nurses and midwives have beeninvolved in activities as disparate as audit guidelinedevelopment training in specific clinical skills or inmore general organizational support in ensuringattendance at appropriate training events
lsquoPractice developmentrsquo staff often find themselvesworking in isolation from colleagues in other disci-plines and indeed from senior colleagues in the orga-nization who have control of some of the levers forchange While there are examples of positive practicedevelopment working between midwifery and healthvisiting colleagues (eg Dominey
et al
2002) suchcollaboration is more likely to be achieved throughinformal networking and shared commitment ratherthan the proactive whole systems approach neededAs a result health service experience of lsquopracticedevelopmentrsquo is of a patchy often unstructuredapproach led by one discipline even by one individ-ual usually a nurse or midwife
Unsworth (2000) suggests that the key characteris-tics of practice development in nursing include using
248
MJ Renfrew
et al
copy 2006 The Authors Journal compilation copy 2006 Blackwell Publishing Ltd
Maternal and Child Nutrition
2
pp 245ndash261
new approaches that lead to direct and quantifiableimprovements in services such changes occur as aresponse to problems or needs and contribute to theprovision of effective services However there hasbeen little systematic exploration of practice develop-ment within midwifery posts although individualmaternity settings have been able to apply for accred-itation as practice development units (McSherry ampMcFadden 2001)
In other fields there are examples of practicedevelopment being led by task forces or developmentagencies linked to particular policy drivers for exam-ple the Change Agents Team at the Department ofHealth in relation to Older Peoplesrsquo policies (DH2002b) and the Adoption Taskforce (DfES 2000)While using existing evidence to inform practicechange such groups also use many different interven-tions and learning models to address major changeThis approach can tackle the interdisciplinary andinter-agency agendas which are needed in manyareas of public health to achieve positive change
Breastfeeding and practice development
A recent systematic review of interventions promot-ing the duration of breastfeeding revealed a dearth ofliterature in the fields of training and education ofhealthcare professionals and breastfeeding counsel-lors and of evidence-based practice or practice devel-opment initiatives (Renfrew
et al
2005a) Thisincludes the absence of high-quality evidence aboutways of preparing practitioners to deliver care to sup-port health policy initiatives Only one study of arelevant evidence-based practice initiative was iden-tified (Grant
et al
2000)Some 79 practice development initiatives in breast-
feeding were funded by the Department of Health inEngland over the period 1999ndash2002 (Dykes 2003)These included establishing breastfeeding supportcentres education for health professionals develop-ment of the role of healthcare assistants in supportingbreastfeeding developing peer support involvingbreastfeeding counsellors and developing services forvulnerable groups such as adolescent womenAlthough preliminary evaluation suggests that thesewere successful formal evaluations were limited
There is also no evidence of a coordinated strategyand funding to support mainstream implementationof practice change such as described above in otherfields so many of these initiatives have since beendiscontinued or have remained as isolated initiativesSuch use of short-term funding without clear strategiesfor creating sustainable change to mainstream prac-tice or integrate learning into future service develop-ment seems to be reflected in other areas across theNational Health Service (NHS) in England and Wales
Like practice development posts more widelyinfant feeding or breastfeeding development postshave a range of remits including providing skilledexpertise in addressing serious breastfeeding prob-lems developing guidelines supporting worktowards achieving accreditation with UNICEF UKBaby Friendly Initiative (BFI) providing educa-tional support to colleagues in developing theirbreastfeeding expertise educating mothers on tech-niques and developing positive attitudes to breast-feeding and other aspects of breast care Manyindividuals in such posts work in relative isolation(Abbott
et al
2006) and are expected to fulfil theirbreastfeeding or infant feeding remit in addition toother midwifery or health visiting workload andresponsibilities This is true even of the nationalnetwork of infant feeding coordinators in Englandwhere coordinators often carry out the work inaddition to their existing duties Development postsare normally restricted to the maternity service thatfunds them often not even having a remit outsideof their own discipline They are unlikely to be ableto support breastfeeding across different sectorswithin the whole health economy in the way thatwe have identified as necessary (Renfrew
et al
2006Wallace amp Jardine 2006)
Unusually three local authority health scrutinieshave recently taken a multi-sectoral approach toexamining how a range of agencies not just localmaternity and community health services canremove barriers to breastfeeding and improve directhealthcare provision to support breastfeedingwomen (Richards 2003 Thomas 2006 Wallace ampJardine 2006) All of these contain recommenda-tions for health services education the voluntarysector trainers of healthcare staff local employers
Developing practice in breastfeeding
249
copy 2006 The Authors Journal compilation copy 2006 Blackwell Publishing Ltd
Maternal and Child Nutrition
2
pp 245ndash261
and lsquoownersrsquo of public spaces as well as the councilsthemselves Inter-sectoral strategic planning led bypublic health where there has also been a sharedinterest in seeking a health economy-wide approachto UNICEF UK BFI status has resulted in moreinter-sectoral practitioner learning networks andshared resources for training staff in breastfeedingsupport (Wallace amp Jardine 2006) The extent towhich this innovative approach is effective and sus-tainable in the longer term is unknown
Breastfeeding development projects
Our approach to practice development drew on thelessons learned from much of the literature summa-rized above Three previous evidence-based prac-tice developments in breastfeeding also directlyinformed our thinking The Breastfeeding in LeedsConsortium was a cross-sectoral partnership thataimed to increase breastfeeding rates by raising theprofile of breastfeeding locally providing educa-tional events and bringing together those withshared interests in supporting breastfeedingwomen As part of that work a Department ofHealth-funded initiative supported a project (Spiby
et al
2002) in which two experienced lay breastfeed-ing counsellors worked to increase evidence-basedsupport to breastfeeding They contributed to edu-cation for undergraduate and registered healthcarepractitioners from a range of disciplines workedwith practitioners providing direct care to womenand provided a range of community developmentactivities The model used in this project was oneof providing evidence-based information forwomen and their families to use rather than atraditional advice-based approach Evaluation ofthis initiative was overwhelmingly positive The layrole was considered compatible rather than conflict-ing with that of healthcare professionals The psy-chosocial perspectives of breastfeeding used by thecounsellors were adopted widely replacing the tra-ditional health lsquobenefits of breastfeeding approachrsquo
Two further developments arose from this suc-cessful preliminary work One project worked tosupport breastfeeding across the health economy inLeeds with a special emphasis on working with
women and families from low-income groups(Spiby
et al
2005) Using the combination of a laycounsellor with a midwife with a specialist breast-feeding background the project delivered multidis-ciplinary and multi-sectoral training using bothhealth and social perspectives It supported the lsquorolloutrsquo of the acute Trustrsquos infant feeding policy andits adoption in the majority of local primary careservices and it demonstrated that collaborativeworking between healthcare professionals andbreastfeeding counsellors can succeed Problemswere also identified some groups of healthcare pro-fessionals are more difficult to engage than otherscross-boundary and inter-sectoral working was stillrelatively new for some health service staff andprotection of professional roles was clearly identi-fied as a problem While support for the initiativehad been identified at a senior level within boththe acute and primary care sectors that support wasnot evident in practice and senior-level projectchampions were not clearly identifiable
A third project included work with local SureStart partnerships in the Leeds and Bradford areasThis delivered staff training helped to establishsupport groups for breastfeeding women initiatedchanges that would reinforce positive messagesabout breastfeeding on Sure Start premises advisedon resources and policies developed support mech-anisms for women in disadvantaged communitiesand developed provided and evaluated a firstcohort of peer support training for women from theSure Start areas The lessons learned from thatwork included the importance of early engagementacross all relevant sectors and disciplines findingout about local needs from local communities theneed to reduce organizational barriers boundariesand tensions and the opportunities that multidisci-plinary education brings This work has now beenincorporated into mainstream practice in the city(Spiby
et al
2005)All three developments were successful in
increasing the number of practitioners women andfamilies receiving evidence-based support withbreastfeeding (Spiby
et al
2005) All includedtrained breastfeeding counsellors as key sources ofsupport and development work and breastfeeding
250
MJ Renfrew
et al
copy 2006 The Authors Journal compilation copy 2006 Blackwell Publishing Ltd
Maternal and Child Nutrition
2
pp 245ndash261
rates in the city including the low-income communi-ties served on discharge from hospital increasedfrom around 45 in early 2002 to 51 in late 2004(St James University Hospital Breastfeeding Statis-tics) All were influential in informing our thinkingaround the conceptual framework and in planningthe structures for the national practice developmentwork described here
Aims and methods
The overall aim of our practice development workwas to address inequalities in health by improvingmaternal and child nutrition The objectives of theprogramme were to (1) inform and enable practicedevelopment in breastfeeding in a number of low-income areas (2) evaluate the impact of approachesused and (3) develop robust approaches and appro-priate material for use across the country in futureyears
Core team
A core team was formed to plan this work The teamincluded the following backgrounds knowledge ofthe evidence base and relevant research methods andcritique in general the development of evidence-based guidance the education of health professionalsat pre- and post-registration levels information tech-nology (IT) and web-based communication skillsknowledge of breastfeeding from public health andclinical perspectives senior NHS managementchange management and practice development in theNHS and related sectors and strategic planning andleadership
National network
At a very early stage a national network was estab-lished with the aim of informing and supporting thework Partners in this network included
bull
academic partners
to ensure that the evidence basewas soundbull
professional bodies
including relevant Royal Col-leges and professional organizations representing thewide range of practitioner groups likely to be
involved to inform the development plans to sup-port dissemination of information to provide con-tacts and communication systems and to enhance thelegitimacy of the workbull
NHS partners
including clinical practitioners withrelevant clinical skills representatives of a StrategicHealth Authority a Public Health Observatory (Pub-lic Health Observatories are funded by the Dep-artment of Health to strengthen the availability anduse of health information at a local level in the UK)NHS Direct (NHS Direct is an online and telephonehealth information enquiry service for the publichttpwwwnhsdirectnhsukindexasp) RDLearning(RDLearning is a web-based national resource ofaccredited health-related education courses httpwwwrdlearningorguk) and primary care researchnetworks to inform practice development plans tooffer communication networks and skills in routinedata collection and analysis and to support the iden-tification of key contacts andbull
representatives of consumer groups voluntary
organizations and non-government organizations
toensure that we were able to benefit from their expe-rience of providing services and gaining user per-spectives to inform the practice development plansand offer communication networks
Links were also made with relevant governmentdepartments and professional advice was taken oncommunication strategies
We developed the system to be flexible and respon-sive with two-way communication systems and fre-quent dialogue with commissioners and partners aswe recognized that the source of funding for this workwas a government agency and that government prior-ities can shift and change over time
Conceptual framework and programme development
A conceptual framework for the project was estab-lished based on the literature and our practice devel-opment experience in breastfeeding (describedabove) and other fields including developing learningnetworks in other areas of practice (eg Herbert ampLake 2005) It was finalized through discussions
Developing practice in breastfeeding
251
copy 2006 The Authors Journal compilation copy 2006 Blackwell Publishing Ltd
Maternal and Child Nutrition
2
pp 245ndash261
among the core team and input from network part-ners This framework then informed all decisions andplans Key elements of the framework included anevidence-based approach multi-sectoral and multi-disciplinary working service userconsumer involve-ment mainstreaming and sustainable systems aparticipatory approach to consultation and communi-cation and embedded evaluation Specific elementsof this approach are shown in Box 1
Based on the conceptual framework a six-stageprocess was developed (Fig 1) Following assessmentof the literature on effective interventions a diagnos-tic analysis of the field was planned to include alearning needs assessment (as reported in this issueof the journal) and a general assessment of the readi-ness of the field to undertake this work (Stage 1) Thiswas followed by a synthesis of those two stages yield-ing an analysis of the problem and potential solutions
Box 1
Elements of conceptual framework
Evidence-based approach
All proposed interventions will be based on a rigorous assessment of the published literature togetherwith practitioner and user views of that evidence base
An eclectic mix of approaches and models will be drawn on based on evidence of lsquowhat worksrsquo indifferent communities
Multi-sectoral and multidisciplinary working including service userconsumer perspectives
Health professionals other relevant professionals from social and education sectors community and layworkers usersconsumers and their families will all have a role in informing and delivering the ongoingprogramme of work
Mainstreaming and sustainable systems
The programme will work to mainstream maternal and child nutrition into all relevant work pro-grammes of other agencies and organizations to avoid a sense of being lsquoinitiative-basedrsquo and to createsustainable change
Existing networks and resources will be used wherever possible to ensure an embedded approach topractice development and to create new systems only when necessary
Solid foundations will be built for long-lasting change and to avoid a lsquodash for growthrsquo
Participatory approach to consultation and communication
All collaborative work will be based on a democratic and participative approach where all constituenciesof interest have an equal voice at all stages regardless of seniority or background
Work will address all levels of the organization ie from senior-level policymakers through regionaland local levels to practitioners in the field and service usersconsumers and their families and willinclude approaches at the level of the individual organization service and community
Embedded evaluation
All approaches used will be evaluated and findings from these evaluations will be synthesized andwidely disseminated to stakeholders including policymakers and professional leaders and other appro-priate audiences
252
MJ Renfrew
et al
copy 2006 The Authors Journal compilation copy 2006 Blackwell Publishing Ltd
Maternal and Child Nutrition
2
pp 245ndash261
Fig
1
Prac
tice
deve
lopm
ent
cycl
e N
HS
Nat
iona
l Hea
lth S
ervi
ce N
GO
non
-gov
ernm
enta
l org
aniz
atio
n
Pre
curs
ors
Sys
tem
atic
re
view
s an
d gu
idan
ce
Oth
er
reli
able
so
urce
s of
ev
iden
ce
bull E
xam
ine
syst
ems
Map
ping
and
di
agno
stic
an
alys
is
bull Id
enti
fica
tion
of
rele
vant
grou
ps
bull L
earn
ing
need
s m
easu
rem
ent
bull A
sses
smen
t of
educ
atio
n pr
ovis
ion
bull D
evel
opm
ent
oppo
rtun
itie
s
Ove
rvie
w a
ndsy
nthe
sis
of
curr
ent
prob
lem
s an
d so
luti
ons
Pla
nnin
g
Net
wor
k de
velo
pmen
t e
gbull
NH
Sbull
Pro
fess
iona
l or
gani
zati
ons
bull N
GO
s bull
Cro
ss-s
ecto
ral
Too
l dev
elop
men
t e
gbull
Dis
tanc
e le
arni
ng
bull T
oolk
its
Cap
acit
y bu
ildi
ng
syst
ems
bull In
divi
dual
bull
Org
aniz
atio
nal
bull S
ervi
ce
bull C
omm
unit
y
Pla
n to
add
ress
ca
paci
ty
buil
ding
and
chan
ge
man
agem
ent a
tdi
ffer
ent l
evel
s an
d in
dif
fere
nt
sect
ors
Cap
acit
y bu
ildi
ng a
ndde
velo
pmen
t
Mea
sure
men
t an
dm
onit
orin
g
Indi
vidu
al le
vel
eg
bull Fa
ce-t
o-fa
ce
educ
atio
n bull
Tw
inni
ng
budd
ying
bull
Dis
tanc
e le
arni
ng
Sys
tem
atic
da
ta c
olle
ctio
n an
d an
alys
is ndash
qual
itat
ive
and
quan
tita
tive
Org
aniz
atio
n an
dse
rvic
e le
vel
eg
bull C
ham
pion
s fo
r ch
ange
bull
Act
ion
lear
ning
se
ts
bull D
emon
stra
tion
pr
ojec
ts
bull Jo
int p
lann
ing
Wor
ksho
pob
serv
atio
n an
d cr
oss-
or
gani
zati
onal
au
dits
Sel
f-ev
alua
tion
an
d be
nchm
arki
ng
netw
orks
Com
mun
ity
leve
l e
gbull
Mul
ti-a
genc
y w
orki
ng
bull C
omm
unit
y re
sour
ces
rese
arch
bull A
ctio
n
Act
ion
rese
arch
and
le
arni
ng s
ets
Pol
icy
impe
rati
ves
Pri
orit
y se
ttin
g an
d
plan
for
di
agno
stic
an
alys
is
Rep
ort o
n m
easu
rem
ent
and
mon
itor
ing
Developing practice in breastfeeding
253
copy 2006 The Authors Journal compilation copy 2006 Blackwell Publishing Ltd
Maternal and Child Nutrition
2
pp 245ndash261
(Stage 2) Stage 3 involved developing relevant net-works tools for education and training evaluationmethods and capacity building systems at individualorganizational service and community levels Follow-ing this a plan to conduct the work would be finalized(Stage 4) implemented (Stage 5) and evaluated Theprocess was intended to be iterative alternatingbetween phases of information appraisal and plan-ning to identify the next stages of development activ-ity and evaluation of the impact to inform futureplanning Stage 6 included finalization of qualitativeand quantitative measurement and monitoring sys-tems that would feedback through all stages of theprocess
It was envisaged that this model would allow effec-tive structures and processes to be identified for usein other aspects of public health practice
Due to changes in funding the programme wasdiscontinued during Stage 3 although in fact somepreliminary work had already been carried out on theplan
Engagement with practitioners
Developing a national programme of change anddevelopment is an ambitious goal A cost-effectiveapproach to engagement had to be developed both tostay within budget and that could roll out acrossEngland and Wales Learning from the successfulLeeds partnership work described above it wasplanned to recruit a series of sentinel sites where wecould test out a range of approaches to maximizelearning and cost-effectiveness as well as respond toideas from the field Work in those sites wouldbecome a model for national developments inform-ing material for education training and assessmentsupported by communications at different levelsthrough our established national network The use ofsentinel sites also allowed for the development ofapproaches sensitive to varying local contexts so pro-viding alternatives and examples to inform nationalimplementation
The first stage in that process was to recruit rele-vant sentinel sites Sites were conceived as includingthe whole health economy in a locality and had tomeet specific criteria These are detailed in Box 2
Four sites were identified and agreed to join thefirst wave of sentinel sites Each site engaged andplanned the programme of work differently Forexample one site had already worked with membersof the core team and were keen to take existing workfurther In the few months in which we worked withthem they put into place a system for the accuratemonitoring of breastfeeding rates and created anextensive network of individuals at a range of seniorlevels from different sectors including Primary CareTrusts (PCTs) Strategic Health Authority the acuteTrust Sure Start and the local authority Benefits thesites have seen even since the work stopped haveincluded
bull improved communication across relevant disci-plines and sectorsbull the observation that the practice developmentwork lsquokept breastfeeding on everyonersquos agendarsquobull the work was used to support a business case for acoordinator for BFI planningbull in one sentinel site the primary care and acutematernity services have formed a health economy-wide breastfeeding strategy groupbull in another a joint primary care and maternity ser-vices group has been establishedbull two sites are taking forward systems for collect-ing breastfeeding data which have been used toprovide feedback to staff each monthbull a new approach to training all staff in one siteincluded commissioning the local university todevelop a self-study workbook and then to test itseffectiveness using an objective skills assessment toolandbull in one site a successful peer support programmewas rolled out throughout Sure Start programmes
A key part of the work in the sentinel sites was tosupport the learning needs assessment (McFadden
et al
2006) Although the sites were at an early stageof engagement this was conducted very successfullyand rapidly as sites supported the identification andinvolvement of practitioners Many assisted with sur-vey distribution and in return received a report ofthe training needs identified for their staff The nexttest was the running of fieldwork meetings and
254
MJ Renfrew
et al
copy 2006 The Authors Journal compilation copy 2006 Blackwell Publishing Ltd
Maternal and Child Nutrition
2
pp 245ndash261
workshops to finalize guidance based on researchevidence as part of a related programme of workThe aim of this work was to take the results of aseries of systematic reviews (which gave informationon lsquowhat works from research evidencersquo) and consultwith practitioners managers and users on lsquowhatreally works in practicersquo (Dyson
et al
2006) Thenewly established sentinel site system supported thiswork by offering venues for meetings providing listsof eligible participants and enabling and encourag-ing staff to attend (Renfrew
et al
2005b) The finalstage of this guidance work was a series of majorworkshops with over 30 participants in each repre-senting a lsquodiagonal slicersquo through the whole healtheconomy from field-level practitioners includingpeer support workers to managers and planners andincluding the range of relevant disciplines as well as
the voluntary sector Concerns around the realitiesand influences on practice and key issues for practi-tioners and managers in developing good practicewere discussed as well as organizational and struc-tural barriers to change Participants were encour-aged to discuss not only practices that need to beintroduced but also those that need to be aban-doned thereby potentially saving time and resourcesand to identify actual or potential barriers to imple-menting change (Renfrew
et al
2005b) These facili-tated groups examined the ability of the service torespond to identified gaps and made recommenda-tions for improvements to the system They feddirectly into the final stages of the development ofNational Institute for Health and Clinical Excellence(NICE) public health recommendations for breast-feeding offering participants the satisfaction of
Box 2
Sentinel site criteriaSentinel sites were expected to
bull Have a deprivation profile that demonstrated a substantial proportion of low-income groups and adiverse ethnic profile and serve contrasting areas (eg urban rural)
bull Offer a range of services for children and women with an interest in nutrition
bull Be able to include the whole health economy in a locality (or at least agree to working across allrelevant sectors)
bull Provide a key contact personpeople who would act to facilitate communication and broker agree-ments with different parts of the health economy and managers who were supportive of the plannedwork willing to support and enable staff participation
bull In the first instance sites would be those where contact already existed with members of our coreteam Future sites would be brought in once any initial problems with the approach had been identifiedand addressed
In return for their involvement in the work it was recognized that the sentinel sites would benefit in arange of ways including
bull Support for staff development and learning through access to programme staff and expertise involve-ment in and learning from a regular newsletter and attendance at an annual leading-edge conferenceon maternal and child nutrition
bull Developing links with other sites and sharing good practice and problem solving
bull The opportunity to help to develop national practice resulting in a raised profile for their work andtheir staff
bull Early access to emerging evidence in the field of maternal and child nutrition
Developing practice in breastfeeding
255
copy 2006 The Authors Journal compilation copy 2006 Blackwell Publishing Ltd
Maternal and Child Nutrition
2
pp 245ndash261
knowing that their input would make a difference(Dyson
et al
2006) These workshops also tested outthe use of language the conceptual understanding ofparticipants in relation to the evidence reviews andgathered intelligence on what approaches to imple-mentation of practice development may be mosteffective They also provided an opportunity for dis-cussion debate and deliberation about the meaningof the evidence Participants reported this to be veryuseful in assisting their understanding of the evi-dence and in considering how best to change theirown and their colleaguesrsquo practice in response to itand as an important contribution to practice devel-opment in their own locality (McFadden
et al
2005)The input of representatives of service users was ofcritical importance
It was planned that once the guidance was final-ized each participating site would be in a strong posi-tion to act on it Not only would they feel someownership but they would also have staff from alllevels and sectors in their health economy who hadspent time discussing the issues with colleagues andwith service user representatives They would haveaccess to specific local information about localitiesand groups that needed to be prioritized creatingchange was therefore brought several stages closerAt the end of each workshop email and telephonecontact details were exchanged among the workshopparticipants many of whom had never met beforedespite working in related parts of the same systemto support closer local networking The opportunityto consult with national experts in the network alsoacted as a variant on educational outreach which hasbeen shown to be moderately successful in guidelineimplementation (NHS CRD 1999) The impact ofsuch exchanges in increasing opportunities for net-work support is virtually impossible to evaluate for-mally but there was confidence in those whoparticipated at these events that positive changewould result and that the evidence would be moreeffectively used in the future as a consequence
Interactive conference
The other main activity was a conference on maternaland child nutrition to which all partners ndash academic
professional NHS and userconsumer ndash and stafffrom sentinel sites were invited Commissioners ofthe work were invited as were staff from key govern-ment departments with an interest in nutrition childhealth Sure Start nursing and midwifery and ine-qualities in health Around 90 participants took partin a day which included presentations participativeworking and active networking A report of the dayis available at httpwwwyorkacukresmcncccon-ferenceReporthtm Feedback was strongly positiveand the impact of networking with others in similarsituations and between those working in local andnational organizations was especially valued It wasplanned that this would be an annual event
Had we been able to continue the practice devel-opment programme we planned to use the follow-ing approaches
Establishing learning networks
We planned to identify appropriate learning net-works for different constituencies which wouldenable communication among staff from differentsectors as well as communication with programmestaff Activities were planned to include
bull Staff working at strategic and senior managementlevels would be supported and appropriate informa-tion provided to allow them to create cross-systemchanges Senior-level lsquochampions for changersquo wouldbe identified These would be used in a range of waysthose wishing to be involved in learning networkswould be supported to do sobull Learning sets would be established This wouldenable focused exchange between stakeholders onhow best to make use of the evidence in practice andhow to influence mainstream practice across locali-ties Through feedback loops we planned to developlearningeducation material to be made availablethrough web-based routes to wider constituenciesbull Peer supporters and trained breastfeeding counsel-lors are key groups in regard to breastfeeding promo-tion and support We planned to include them inlearning sets They have much to offer health profes-sionals in coming to understand the needs of womenand families and indeed the evidence suggests thattheir involvement in advisory work and peer support
256
MJ Renfrew
et al
copy 2006 The Authors Journal compilation copy 2006 Blackwell Publishing Ltd
Maternal and Child Nutrition
2
pp 245ndash261
enhances and strengthens the impact of informationand evidence-based guidance possibly more thanthat of health professionalsrsquo practice Our experiencedescribed above has identified a valuable contribu-tion from lay breastfeeding counsellors into educa-tion and training provision
Educational approaches
The breadth of constituencies that the programmeneeded to reach was to be reflected in the range ofeducational approaches required For some profes-sions continuing professional development (CPD)time is factored in regularly to the job plan in a rollingprogramme of group education with routine sessionalwork suspended for other groups CPD is a self-verified individual activity that can be achievedthrough a range of methods including distance learn-ing We hoped to reach directly a broad group ofwomen as well as professionals through some of theroutes developed A range of materials was thereforeplanned to address all needs Materials would bedeveloped for web-based access CD-ROM access andon paper These were to include
bull Toolkits to promote and support breastfeeding tomonitor breastfeeding rates and on practice develop-ment and changebull Distance learning modules providing accreditedlearning opportunities at a range of levelsbull An email and telephone-based service to putindividuals and organizations in touch with otherswho can support and advise them supported byRDLearning a national web-based resourcebull Learning material that could be directly dissemi-nated through the Internet to a wide audiencebull Buddy systems and mentoring for practice devel-opment and public health strategic development inbreastfeeding and use of cascade systemsbull Summaries of approaches to dissemination andpromotion of information that have proved to be suc-cessful and of practice change programmes that havebeen evaluated as having a positive impact on initia-tion and duration of breastfeedingbull Through NHS Direct we planned to reach the gen-eral public Information could be provided to informthe development of new algorithms that could be
used by staff taking enquiries from breastfeedingwomen We planned also to provide information thatcould be used on the NHS Direct website which isaccessed directly by women and families as well ashealth professionalsbull Other material to reach the general public wouldbe developed We aimed to have informative paperspublished in womenrsquos and familiesrsquo magazines and inthe general media on a regular basis A professionalwriter was one of our partners her role was to informand advise us about reaching women directly
Discussion
The work described in this paper was a structuredcross-sectoral approach to practice development inpublic health As a result of funding problems a fullevaluation could not be conducted and our contribu-tion to the knowledge base on practice change inpublic health is limited Lessons were learned how-ever and feedback was gained from participants atdifferent stages of the process We received strongsupport for our approach and the willingness of localand national partners to engage actively in the pro-gramme testifies to its potential
Lessons learned
There is increasing emphasis in public health andhealth policy on the need for good partnership work-ing and integration across disciplines professionsorganizations and localities as shown in the recentWhite Paper from the Department of Health (DH2006) and in the Children Act (2004) Prevention ofill health and promotion of well-being featurestrongly in these and other policy documents with arecognition that this cannot be achieved without fullengagement at strategic and operational levels withthose who use or depend on public-sector services Itwas clear at every stage of this process that engage-ment was needed across the whole health economyIt is only in working with all the relevant layers andpartnerships of professionals that we can hope for thefull impact of evidence to be realized Traditionalapproaches however only disseminate evidence tointerest groups in isolation Our use of lsquodiagonal slicersquo
Developing practice in breastfeeding 257
copy 2006 The Authors Journal compilation copy 2006 Blackwell Publishing Ltd Maternal and Child Nutrition 2 pp 245ndash261
workshops in which staff at all levels and across allsectors were engaged and including representativesof service users and the voluntary sector enabledmuch greater understanding of the consequences ofparticular activity or behaviour in other parts of thesystem and allowed creative and informed challengesto assumptions and prejudices This laid good foun-dations for whole systems approaches to introducingdriving and implementing new approaches whichcould lead to positive health outcomes It proved avery positive learning experience for all thoseinvolved
Practice change needs to involve the whole rangeof health professionals involved in work directly withpregnant women and new mothers to ensure coordi-nated working and consistent messages Despiteactive support from relevant Royal Colleges and sev-eral strongly supportive individuals engagement bydoctors was noticeably less compared with otherhealth professions This supports the findings of otherwork (eg Smale et al 2006) This really matters in afield such as breastfeeding where paediatriciansobstetricians general practitioners and public healthphysicians have an important role to play Futurework will need to address this
Key constituents in practice development in breast-feeding include mothers and potential mothersgrandmothers and men We had strong support andinvolvement from service users and user groups butengaging men proved to be difficult To reach thepublic good-quality easily accessible information isneeded perhaps the developing DiPEX module onbreastfeeding will contribute to this (httpwwwdipexorgDesktopDefaultaspx) Recent gov-ernment policy directives acknowledge the potentialcontribution that incorporating patient and serviceuser experience into service provision can bring (egDH 2006) Recent developments in the approach tolong-term conditions management have introducedthe Expert Patient Programme which enables peoplewith disabilities to take much more effective controlover the management and treatment of their disease(DH 2004c 2006) There is perhaps potential for theparallel development of an lsquoExpert Mothers Pro-grammersquo to have similar positive impact in relation tonutrition and health
Service user involvement is actively encouraged ininforming research and practice (Hanley et al 2004)Breastfeeding and maternity care as a whole have along-standing history of the active engagement of ser-vice users Volunteer counsellors and supporterstrained and accredited by their own voluntary orga-nizations have filled the gap left by the health ser-vices They have taken the initiative in setting uptelephone support services training and supervisingpeer supporters and contributing to the education ofhealth professionals (Smale et al 2006) In our cur-rent and previous practice development work thecontribution of service users and voluntary groupswent much further than simply offering advice andinformation They took an active role in planning thework and in some cases delivering education andservices Our experience was that lay workers havean essential role in developing services and they areable to advise at a strategic level as well as participat-ing in service delivery They are able to see throughthe organizational barriers that often constrain pro-fessionals and can see solutions that will work formothers and families From our experience we wouldadvise that others explore ways of actively engaginglay workers adequately remunerated in the deliveryof health care and in the education of healthprofessionals
The fundamental importance of multidisciplinaryand multi-professional working was also apparent inthe way in which the core team worked and in thesupport gained from the network of partners Atevery stage we had expertise and support availableto us as well as an effective communication systemand network Practice change in public health needsto be led and informed by those who know the topicarea and who have the wide range of skills neededto convince many different kinds of professionals thatthe work is worthwhile and achievable
Another positive contribution was the synergy ofthis programme with the evidence base The sameteam had also been responsible for systematicreviews of the field (eg Fairbank et al 2000Protheroe et al 2003 Sikorski et al 2004 Renfrewet al 2005a) and the approach was grounded in thisevidence which was at the same time being devel-oped into national guidance The interaction between
258 MJ Renfrew et al
copy 2006 The Authors Journal compilation copy 2006 Blackwell Publishing Ltd Maternal and Child Nutrition 2 pp 245ndash261
these elements should not be underestimated part-ners and sentinel sites were able to inform the guid-ance and up-to-date knowledge of the evidence basehelped strengthen the practice development work
The sentinel site system was proving to be asuccessful lsquowin-winrsquo situation for all involved Itprovided a test bed for ideas it was a source ofinformation and debate and the programme gaineda richness and diversity of input that would be hardto match At the same time it offered the sitesengagement in leading-edge work an increased pro-file and high-quality staff development Although itwas not formally evaluated all involved were con-vinced that it was a very cost-effective system theprogramme could conduct work at speed and to ahigh quality and governance issues were streamlinedThe system was very flexible and could adapt to thedifferent circumstances of each site It would havebeen able to accommodate future service and educa-tion developments such as Childrenrsquos Centres Trustreorganization and inter-professional educationOver time we could have expanded to include othersectors and practitioners such as retailers and child-minders Had the programme continued future siteswould have been identified and material developedfor national use based on our learning in the originalfour sites
Major challenges
Throughout the programme getting breastfeedingrecognized as a priority was difficult This has beenthe case for many years despite its fundamental con-tribution to public health in the short and long termit has only recently been included in national publichealth policy statements PCT targets and monitoringAs we found in the learning needs assessment andother work breastfeeding services are often seen asthe remit of enthusiastic individuals discussed interms reminiscent of lsquoreligious zealotryrsquo (Smale et al2006) rather than as a part of the mainstream ofhealth provision Creating real change in theapproach to breastfeeding in the health service willrequire it to be seen as a priority for senior managersand commissioners Our experience has demon-strated that it is possible to engage such senior people
in this work and that discussion and debate with theirown colleagues can have an impact on their thinking
A key area of practice development that canimpact on breastfeeding duration is working withmothers to sustain breastfeeding while going back towork and the ways that public health strategy andpractice can influence employers to provide breast-feeding-friendly maternity policies and facilities(Kosmala-Anderson amp Wallace in press) We did nothave an impact on this area but it was clear that itwas an area that needed to be addressed One goodplace to start would be with the employment condi-tions for NHS employees themselves this would havethe dual advantage of improving conditions for thelargest female workforce in the country while alsoproviding a model of good practice for others
Although the aim of this work was to address ine-qualities in health it is clear that reaching the hard-to-reach remains challenging We did see signs of suc-cess for example Sure Start schemes were making adifference in some areas but ensuring that all vulner-able women receive the support and care they needis still a distant goal whether they are teenagers asy-lum seekers or simply women who live in areas wherebottle feeding has been endemic for generations
Finally there is a debate to be had on whoseresponsibility it is to create such change The work ofresearchers is seen to be complete when their studyis finished and disseminated through publication andconference presentation Systematic reviewers takeon a responsibility to make the results of a wide rangeof studies available through publication but not toengage with what services might do with those find-ings Those responsible for guidance are responsiblefor developing and publishing that work and somealso take responsibility for lsquoimplementationrsquo (egNICE 2005) But where does responsibility rest forpractice development which requires a deep engage-ment with the practice setting and with those affectedby the issues raised by the evidence Lack of invest-ment at the national level in formal evaluation ofprogrammes of change limits the available evidencebase and detracts from our achieving a better under-standing of what actually works in relation to thesemore complex health issues funding for the lsquoRrsquoaspects of research and development is more com-
Developing practice in breastfeeding 259
copy 2006 The Authors Journal compilation copy 2006 Blackwell Publishing Ltd Maternal and Child Nutrition 2 pp 245ndash261
mon than for the lsquoDrsquo (NHS Executive 1997) Thewithdrawal of funding to this programme part waythrough its cycle was regretted by our commissionersit was evident that practice development was nolonger their remit given their changed circumstancesIt is however not clear that responsibility now restswith any particular agency Is development work forindividual health service organizations themselves totake on Is this work that should be led by nationalprogrammes supported by public-sector funding orshould it rely on other sources of support If so fromwhere will it be resourced and how will cross-sectoraland multidisciplinary developments be addressedThere are also questions about who will lead thiswork when a number of professional disciplines areinvolved and where the client interface spans bothprimary and acute care healthcare settings social ser-vices and other development agencies These ques-tions will become more pressing as guidancecontinues to be produced especially in public health
Acknowledgements
We would like to thank all participants from sentinelsites and our consortium of academic professionalNHS and consumer partners and the two anonymousreferees who reviewed the manuscript This work wascommissioned by the former Health DevelopmentAgency and subsequently funded by NICE
References
Abbott S Renfrew MJ amp McFadden A (2006) lsquoInformalrsquo learning to support breastfeeding local problems and opportunities Maternal and Child Nutrition 2 232ndash238
Audit Commission (2000) United They Stand Coordinating Care for Elderly Patients with Hip Fracture Audit Com-mission London
British Paediatric Association (1994) Statement of the stand-ing committee on nutrition is breastfeeding beneficial in the UK Archive of Diseases in Childhood 71 376ndash380
Chalmers I amp Altman DG (eds) (1995) Systematic Reviews BMJ Publishing Group London
Children Act (2004) Available at httpwwwopsigovukactsacts200420040031htm (accessed 21 March 2006)
Coote A Allen J amp Woodhead D (2004) Finding out What Works Building Knowledge about Complex Community-Based Initiatives Kingrsquos Fund London
DfES (2000) Adoption and Permanence Taskforce Available at httpwwwdfesgovukadoptionadoptionreformstaskforceshtml (accessed 29 March 2006)
DH (2002a) Improvement Expansion and Reform The Next 3 Years Priorities and Planning Framework 2003ndash2006 Department of Health London
DH (2002b) The Health and Social Care Change Agent Team Available at httpwwwchangeagentteamorguk (accessed 29 March 2006)
DH (2004a) National Service Framework for Children Young People and Maternity Services Stationery Office London
DH (2004b) Choosing Health Making Healthy Choices Eas-ier Stationery Office London
DH (2004c) Self Care ndash A Real Choice Self Care Support ndash A Practical Option Stationery Office London
DH (2006) Our Health Our Care Our Say A New Direction for Community Services Stationery Office London
Dominey M Archibald A Edgecombe D Lawrence J amp Thomson L (2002) Breastfeeding and drug misuse Mak-ing an informed choice Year 3 Practice project In Infant Feeding Initiative A Report Evaluating the Breastfeeding Practice Projects 1999ndash2002 (ed F Dykes 2003) p 64 Department of Health London
Dykes F (2003) Infant Feeding Initiative A Report Evaluat-ing the Breastfeeding Practice Projects 1999ndash2002 Depart-ment of Health London
Dykes F (2006) The education of health practitioners sup-porting breastfeeding women time for critical reflection Maternal and Child Nutrition 2 204ndash216
Dyson L Renfrew MJ McFadden A McCormick F Herbert G amp Thomas J (2006) Promotion of Breastfeed-ing Initiation and Duration Evidence into Practice Brief-ing National Institute for Health and Clinical Excellence London httpwwwniceorgukdown-loadaspxo=346169 (accessed 26 July 2006)
EU (2004) Project on Promotion of Breastfeeding in Europe Protection Promotion and Support of Breastfeeding A Blueprint for Action European Commission Directorate Public Health and Risk Assessment Luxembourg
Fairbank L OrsquoMeara S Renfrew MJ Woolridge M Sowden AJ amp Lister-Sharp D (2000) A systematic review to evaluate the effectiveness of interventions to promote the initiation of breastfeeding Health Technol-ogy Assessment 4 1ndash171
Grant J Fletcher M amp Warwick C (2000) The South Thames Evidence Based Practice (STEP) Project Sup-porting Breastfeeding Women South Bank University London
Greenhalgh T Robert G Bate P Mcfarlane F amp Kyriakidou O (2005) Diffusion of Innovations in Health Service Organisations A Systematic Literature Review Blackwell Publishing Limited Oxford
260 MJ Renfrew et al
copy 2006 The Authors Journal compilation copy 2006 Blackwell Publishing Ltd Maternal and Child Nutrition 2 pp 245ndash261
Grimshaw JM Thomas RE MacLennan G Fraser C Ramsay CR Vale L et al (2004) Effectiveness and efficiency of guideline dissemination and implementation strategies Health Technology Assessment 8 indashxi 1ndash72
Hanley B Bradburn J Barnes M Evans C Goodare H Kelson M et al (2004) Involving the Public in NHS Pub-lic Health and Social Care Research Briefing Notes for Researchers INVOLVE Department of Health London
Herbert G amp Lake G (2005) Making connections Effective development of the intermediate tier Journal of Inte-grated Care 13 35ndash42
Howie PW Forsyth JS Ogston SA Clark A amp Florey CD (1990) Protective effect of breastfeeding against infection British Medical Journal 300 11ndash16
Kosmala-Anderson J amp Wallace LM (in press) Breastfeed-ing works the role of employers in supporting women who wish to breastfeed and work in four organizations in England Journal of Public Health (in press)
Kramer M Chalmers B Hodnett H Sevovskaya Z Dzikovich I Shapiro S et al (2001) Promotion of breast-feeding intervention trial (PROBIT) Journal of the American Medical Association 285 413ndash420
McFadden A Renfrew MJ Dyson L McCormick F Herbert G amp Thomas J (2005) Effective Active Briefing on the Initiation and Duration of Breastfeeding Fieldwork Report National Institute for Health and Clinical Excel-lence London
McFadden A Renfrew MJ Dykes F amp Burt S (2006) Assessing learning needs for breastfeeding setting the scene Maternal and Child Nutrition 2 196ndash203
McSherry R amp McFadden A (2001) Practice Development Accreditation Assessment Maternity Services Darlington Memorial Hospital South Durham Healthcare NHS Trust Final Report University of Teesside Middlesbrough
Moulding NT Silagy CA amp Weller DP (1999) A frame-work for effective management of change in clinical prac-tice dissemination and implementation of clinical practice guidelines Quality in Health Care 8 177ndash183
Gray JA Haynes RB Sackett DL Cook DJ amp Guyatt GH (1997) Transferring evidence from research into practice 3 Developing evidence-based clinical policy Evidence-Based Medicine 2 36ndash38
NHS Centre for Reviews and Dissemination (CRD) (1999) Getting evidence into practice Effective Health Care 5 1ndash16
NHS Executive (1997) RampD in Primary Care National Working Group Report (Mant Report) Stationery Office London
NICE (2004) The Guideline Development Process National Institute for Health and Clinical Excellence London
NICE (2005) Putting NICE Guidance into Practice National Institute for Health and Clinical Excellence London
Oxman AD Thomson MA Davis DA amp Haynes RB (1995) No magic bullets a systematic review of 102 trials of interventions to improve professional practice Canadian Medical Association Journal 153 1423ndash1431
Protheroe L Dyson L Renfrew MJ Bull J amp Mulvihill C (2003) The Effectiveness of Public Health Interventions to Promote the Initiation of Breastfeeding Evidence Briefing Health Development Agency London
Quigley MA Cumberland P Cowden JM amp Rodrigues LC (2006) How protective is breast feeding against diar-rhoeal disease in infants in 1990s England A case control study Archives of Disease in Childhood 91 245ndash250
Renfrew MJ Dyson L Wallace L DrsquoSouza L McCormick FM amp Spiby H (2005a) The Effectiveness of Health Interventions to Promote the Duration of Breast-feeding Systematic Review 1st edn National Institute for Health and Clinical Excellence London
Renfrew MJ Dyson L McFadden A McCormick F Herbert G amp Thomas J (2005b) Effective Active Briefing on the Initiation and Duration of Breastfeeding Technical Report National Institute for Health and Clinical Excel-lence London
Renfrew MJ McFadden A Dykes F Wallace L Abbott S Burt S et al (2006) Addressing the learning deficit in breastfeeding strategies for change Maternal and Child Nutrition 2 239ndash244
Richards D (2003) Childrenrsquos Nutrition ndash Mothers Who Wish to Breast-Feed Birmingham City Council Available at httpwwwbirmingahmgovukscrutiny (accessed 27 July 2006)
Sackett DL Rosenberg WMC Gray JAM Haynes RB amp Richardson WS (1996) Evidence-based medicine what it is and what it isnrsquot British Medical Journal 312 71ndash72
Sikorski J Renfrew MJ Pindoria S amp Wade A (2004) Support for breastfeeding mothers (Cochrane Review) The Cochrane Database of Systematic Reviews Issue 2 John Wiley amp Sons Ltd Chichester
Smale M Renfrew MJ Marshall JL amp Spiby H (2006) Turning policy into practice more difficult that it seems The case of breastfeeding education Maternal and Child Nutrition 2 103ndash113
Spiby H Ker R DrsquoSouza L amp Renfrew MJ (2002) Intro-ducing a Consumer-Practitioner into breastfeeding prac-tice Year 2 In Infant Feeding Initiative A Report Evaluating the Breastfeeding Practice Projects 1999ndash2002 (ed F Dykes 2003) p 44 Department of Health London
Spiby H Wallis S Stone C amp Renfrew MJ (2005) Support-ing and Promoting Breastfeeding in Leeds Final Report to December 2004 Report to Leeds PCTs Children and Families Modernisation Team Leeds
Thomas C (2006) Darlington ndash A Breastfeeding Friendly Town Darlington Borough Council Darlington
Developing practice in breastfeeding 261
copy 2006 The Authors Journal compilation copy 2006 Blackwell Publishing Ltd Maternal and Child Nutrition 2 pp 245ndash261
Unsworth J (2000) Practice development a concept analy-sis Journal of Nursing Management 8 317ndash326
Wallace LM amp Jardine J (2006) A Health Scrutiny of Ser-vices to Support the Initiation and Duration of Breastfeed-ing in Coventry and Warwickshire Coventry and Warwickshire County Councils Coventry
Wallace L amp Kosmala-Anderson J (2006) A training needs survey of doctorsrsquo breastfeeding support skills in England Maternal and Child Nutrition 2 217ndash231
Wallace L amp Kosmala-Anderson J (in press) Training needs survey of midwives health visitors and voluntary sector
breastfeeding support staff in England Maternal and Child Nutrition (in press)
WHO (2003) Global Strategy for Infant and Young Child Feeding World Health Organization Geneva
Wilson AC Forsyth JS Green SA Irvine L Hau C amp Howie PW (1998) Relation of infant diet to childhood health seven year follow up of a cohort of children in Dundee infant feeding study British Medical Journal 316 21ndash25

Developing practice in breastfeeding
247
copy 2006 The Authors Journal compilation copy 2006 Blackwell Publishing Ltd
Maternal and Child Nutrition
2
pp 245ndash261
Practice development can have the added benefitof informing the research agenda by identifying ques-tions which need investigation to inform the nextstage of development The iterative interdependenceof testing and questioning different approaches canstrengthen otherwise disconnected parts of the sys-tem making much better links between researchpractice and policy developments
Practice development and public health
Relatively simple organizational change may beenough when creating some kinds of evidence-basedpractice change For example the introduction of asingle new clinical treatment or its withdrawal frompractice may require active dissemination of inf-ormation to relevant staff groups a monitoringsystem and support for staff through the period oftransition
In the field of public health any changes are likelyto be more complex Sustained change may requirethe introduction of a new kind of practitioner a shiftin the balance of responsibilities between profes-sional groups increased cross-sectoral cooperationdevelopment of completely new skills changed orga-nizational priorities and intervention on an inter-agency basis across the health and social serviceseducation voluntary services and local politicalforums to influence the wider societyrsquos attitudes andbehaviour The learning of members of the public andtheir access to evidence-based is a vital aspect of pub-lic health This may involve not only improvements informal education of professionals but use of accessi-ble and user-friendly key messages to inform the pop-ulation whose health or whose childrenrsquos health canbe affected Use of social marketing and other mediacampaign methods integration of positive images inpopular press and entertainment provision of learn-ing opportunities and events and other ways of influ-encing day-to-day learning by all those likely to beaffected are just as important as changing the way inwhich professionals work Such complex change mayinvolve influencing aspects of public policy such asenvironmental and employment issues and requirecompetition with market forces changing what peo-ple buy and the products they use
Promoting and supporting breastfeeding is anexcellent example of the challenges to be faced in thisfield Systematic reviews (Fairbank
et al
2000Sikorski
et al
2004 Renfrew
et al
2005a) nationaland international guidelines (EU 2004 Dyson
et al
2006) and our learning needs assessment which is anexample of high-level national lsquodiagnostic analysisrsquo(Grimshaw
et al
2004 Renfrew
et al
2006) have allshown that multifaceted changes are needed if realchange is to occur There are parallels with publichealth interventions for tobacco control and obesityprevention and treatment If policy aspirations forpublic health are to be realized practice developmentwill be essential (WHO 2003 DH 2004b)
Practice development in reality
Regardless of what is known about the need for struc-tured and sustained approaches to changing practiceorganizational response to new evidence and guid-ance seems currently to rely more on individualsrsquointerests and less on planned and structured change(Audit Commission 2000 Coote
et al
2004) Furtherlsquopractice developmentrsquo is a term that is interpretedinconsistently In the past two decades or so lsquopracticedevelopmentrsquo nurses and midwives have beeninvolved in activities as disparate as audit guidelinedevelopment training in specific clinical skills or inmore general organizational support in ensuringattendance at appropriate training events
lsquoPractice developmentrsquo staff often find themselvesworking in isolation from colleagues in other disci-plines and indeed from senior colleagues in the orga-nization who have control of some of the levers forchange While there are examples of positive practicedevelopment working between midwifery and healthvisiting colleagues (eg Dominey
et al
2002) suchcollaboration is more likely to be achieved throughinformal networking and shared commitment ratherthan the proactive whole systems approach neededAs a result health service experience of lsquopracticedevelopmentrsquo is of a patchy often unstructuredapproach led by one discipline even by one individ-ual usually a nurse or midwife
Unsworth (2000) suggests that the key characteris-tics of practice development in nursing include using
248
MJ Renfrew
et al
copy 2006 The Authors Journal compilation copy 2006 Blackwell Publishing Ltd
Maternal and Child Nutrition
2
pp 245ndash261
new approaches that lead to direct and quantifiableimprovements in services such changes occur as aresponse to problems or needs and contribute to theprovision of effective services However there hasbeen little systematic exploration of practice develop-ment within midwifery posts although individualmaternity settings have been able to apply for accred-itation as practice development units (McSherry ampMcFadden 2001)
In other fields there are examples of practicedevelopment being led by task forces or developmentagencies linked to particular policy drivers for exam-ple the Change Agents Team at the Department ofHealth in relation to Older Peoplesrsquo policies (DH2002b) and the Adoption Taskforce (DfES 2000)While using existing evidence to inform practicechange such groups also use many different interven-tions and learning models to address major changeThis approach can tackle the interdisciplinary andinter-agency agendas which are needed in manyareas of public health to achieve positive change
Breastfeeding and practice development
A recent systematic review of interventions promot-ing the duration of breastfeeding revealed a dearth ofliterature in the fields of training and education ofhealthcare professionals and breastfeeding counsel-lors and of evidence-based practice or practice devel-opment initiatives (Renfrew
et al
2005a) Thisincludes the absence of high-quality evidence aboutways of preparing practitioners to deliver care to sup-port health policy initiatives Only one study of arelevant evidence-based practice initiative was iden-tified (Grant
et al
2000)Some 79 practice development initiatives in breast-
feeding were funded by the Department of Health inEngland over the period 1999ndash2002 (Dykes 2003)These included establishing breastfeeding supportcentres education for health professionals develop-ment of the role of healthcare assistants in supportingbreastfeeding developing peer support involvingbreastfeeding counsellors and developing services forvulnerable groups such as adolescent womenAlthough preliminary evaluation suggests that thesewere successful formal evaluations were limited
There is also no evidence of a coordinated strategyand funding to support mainstream implementationof practice change such as described above in otherfields so many of these initiatives have since beendiscontinued or have remained as isolated initiativesSuch use of short-term funding without clear strategiesfor creating sustainable change to mainstream prac-tice or integrate learning into future service develop-ment seems to be reflected in other areas across theNational Health Service (NHS) in England and Wales
Like practice development posts more widelyinfant feeding or breastfeeding development postshave a range of remits including providing skilledexpertise in addressing serious breastfeeding prob-lems developing guidelines supporting worktowards achieving accreditation with UNICEF UKBaby Friendly Initiative (BFI) providing educa-tional support to colleagues in developing theirbreastfeeding expertise educating mothers on tech-niques and developing positive attitudes to breast-feeding and other aspects of breast care Manyindividuals in such posts work in relative isolation(Abbott
et al
2006) and are expected to fulfil theirbreastfeeding or infant feeding remit in addition toother midwifery or health visiting workload andresponsibilities This is true even of the nationalnetwork of infant feeding coordinators in Englandwhere coordinators often carry out the work inaddition to their existing duties Development postsare normally restricted to the maternity service thatfunds them often not even having a remit outsideof their own discipline They are unlikely to be ableto support breastfeeding across different sectorswithin the whole health economy in the way thatwe have identified as necessary (Renfrew
et al
2006Wallace amp Jardine 2006)
Unusually three local authority health scrutinieshave recently taken a multi-sectoral approach toexamining how a range of agencies not just localmaternity and community health services canremove barriers to breastfeeding and improve directhealthcare provision to support breastfeedingwomen (Richards 2003 Thomas 2006 Wallace ampJardine 2006) All of these contain recommenda-tions for health services education the voluntarysector trainers of healthcare staff local employers
Developing practice in breastfeeding
249
copy 2006 The Authors Journal compilation copy 2006 Blackwell Publishing Ltd
Maternal and Child Nutrition
2
pp 245ndash261
and lsquoownersrsquo of public spaces as well as the councilsthemselves Inter-sectoral strategic planning led bypublic health where there has also been a sharedinterest in seeking a health economy-wide approachto UNICEF UK BFI status has resulted in moreinter-sectoral practitioner learning networks andshared resources for training staff in breastfeedingsupport (Wallace amp Jardine 2006) The extent towhich this innovative approach is effective and sus-tainable in the longer term is unknown
Breastfeeding development projects
Our approach to practice development drew on thelessons learned from much of the literature summa-rized above Three previous evidence-based prac-tice developments in breastfeeding also directlyinformed our thinking The Breastfeeding in LeedsConsortium was a cross-sectoral partnership thataimed to increase breastfeeding rates by raising theprofile of breastfeeding locally providing educa-tional events and bringing together those withshared interests in supporting breastfeedingwomen As part of that work a Department ofHealth-funded initiative supported a project (Spiby
et al
2002) in which two experienced lay breastfeed-ing counsellors worked to increase evidence-basedsupport to breastfeeding They contributed to edu-cation for undergraduate and registered healthcarepractitioners from a range of disciplines workedwith practitioners providing direct care to womenand provided a range of community developmentactivities The model used in this project was oneof providing evidence-based information forwomen and their families to use rather than atraditional advice-based approach Evaluation ofthis initiative was overwhelmingly positive The layrole was considered compatible rather than conflict-ing with that of healthcare professionals The psy-chosocial perspectives of breastfeeding used by thecounsellors were adopted widely replacing the tra-ditional health lsquobenefits of breastfeeding approachrsquo
Two further developments arose from this suc-cessful preliminary work One project worked tosupport breastfeeding across the health economy inLeeds with a special emphasis on working with
women and families from low-income groups(Spiby
et al
2005) Using the combination of a laycounsellor with a midwife with a specialist breast-feeding background the project delivered multidis-ciplinary and multi-sectoral training using bothhealth and social perspectives It supported the lsquorolloutrsquo of the acute Trustrsquos infant feeding policy andits adoption in the majority of local primary careservices and it demonstrated that collaborativeworking between healthcare professionals andbreastfeeding counsellors can succeed Problemswere also identified some groups of healthcare pro-fessionals are more difficult to engage than otherscross-boundary and inter-sectoral working was stillrelatively new for some health service staff andprotection of professional roles was clearly identi-fied as a problem While support for the initiativehad been identified at a senior level within boththe acute and primary care sectors that support wasnot evident in practice and senior-level projectchampions were not clearly identifiable
A third project included work with local SureStart partnerships in the Leeds and Bradford areasThis delivered staff training helped to establishsupport groups for breastfeeding women initiatedchanges that would reinforce positive messagesabout breastfeeding on Sure Start premises advisedon resources and policies developed support mech-anisms for women in disadvantaged communitiesand developed provided and evaluated a firstcohort of peer support training for women from theSure Start areas The lessons learned from thatwork included the importance of early engagementacross all relevant sectors and disciplines findingout about local needs from local communities theneed to reduce organizational barriers boundariesand tensions and the opportunities that multidisci-plinary education brings This work has now beenincorporated into mainstream practice in the city(Spiby
et al
2005)All three developments were successful in
increasing the number of practitioners women andfamilies receiving evidence-based support withbreastfeeding (Spiby
et al
2005) All includedtrained breastfeeding counsellors as key sources ofsupport and development work and breastfeeding
250
MJ Renfrew
et al
copy 2006 The Authors Journal compilation copy 2006 Blackwell Publishing Ltd
Maternal and Child Nutrition
2
pp 245ndash261
rates in the city including the low-income communi-ties served on discharge from hospital increasedfrom around 45 in early 2002 to 51 in late 2004(St James University Hospital Breastfeeding Statis-tics) All were influential in informing our thinkingaround the conceptual framework and in planningthe structures for the national practice developmentwork described here
Aims and methods
The overall aim of our practice development workwas to address inequalities in health by improvingmaternal and child nutrition The objectives of theprogramme were to (1) inform and enable practicedevelopment in breastfeeding in a number of low-income areas (2) evaluate the impact of approachesused and (3) develop robust approaches and appro-priate material for use across the country in futureyears
Core team
A core team was formed to plan this work The teamincluded the following backgrounds knowledge ofthe evidence base and relevant research methods andcritique in general the development of evidence-based guidance the education of health professionalsat pre- and post-registration levels information tech-nology (IT) and web-based communication skillsknowledge of breastfeeding from public health andclinical perspectives senior NHS managementchange management and practice development in theNHS and related sectors and strategic planning andleadership
National network
At a very early stage a national network was estab-lished with the aim of informing and supporting thework Partners in this network included
bull
academic partners
to ensure that the evidence basewas soundbull
professional bodies
including relevant Royal Col-leges and professional organizations representing thewide range of practitioner groups likely to be
involved to inform the development plans to sup-port dissemination of information to provide con-tacts and communication systems and to enhance thelegitimacy of the workbull
NHS partners
including clinical practitioners withrelevant clinical skills representatives of a StrategicHealth Authority a Public Health Observatory (Pub-lic Health Observatories are funded by the Dep-artment of Health to strengthen the availability anduse of health information at a local level in the UK)NHS Direct (NHS Direct is an online and telephonehealth information enquiry service for the publichttpwwwnhsdirectnhsukindexasp) RDLearning(RDLearning is a web-based national resource ofaccredited health-related education courses httpwwwrdlearningorguk) and primary care researchnetworks to inform practice development plans tooffer communication networks and skills in routinedata collection and analysis and to support the iden-tification of key contacts andbull
representatives of consumer groups voluntary
organizations and non-government organizations
toensure that we were able to benefit from their expe-rience of providing services and gaining user per-spectives to inform the practice development plansand offer communication networks
Links were also made with relevant governmentdepartments and professional advice was taken oncommunication strategies
We developed the system to be flexible and respon-sive with two-way communication systems and fre-quent dialogue with commissioners and partners aswe recognized that the source of funding for this workwas a government agency and that government prior-ities can shift and change over time
Conceptual framework and programme development
A conceptual framework for the project was estab-lished based on the literature and our practice devel-opment experience in breastfeeding (describedabove) and other fields including developing learningnetworks in other areas of practice (eg Herbert ampLake 2005) It was finalized through discussions
Developing practice in breastfeeding
251
copy 2006 The Authors Journal compilation copy 2006 Blackwell Publishing Ltd
Maternal and Child Nutrition
2
pp 245ndash261
among the core team and input from network part-ners This framework then informed all decisions andplans Key elements of the framework included anevidence-based approach multi-sectoral and multi-disciplinary working service userconsumer involve-ment mainstreaming and sustainable systems aparticipatory approach to consultation and communi-cation and embedded evaluation Specific elementsof this approach are shown in Box 1
Based on the conceptual framework a six-stageprocess was developed (Fig 1) Following assessmentof the literature on effective interventions a diagnos-tic analysis of the field was planned to include alearning needs assessment (as reported in this issueof the journal) and a general assessment of the readi-ness of the field to undertake this work (Stage 1) Thiswas followed by a synthesis of those two stages yield-ing an analysis of the problem and potential solutions
Box 1
Elements of conceptual framework
Evidence-based approach
All proposed interventions will be based on a rigorous assessment of the published literature togetherwith practitioner and user views of that evidence base
An eclectic mix of approaches and models will be drawn on based on evidence of lsquowhat worksrsquo indifferent communities
Multi-sectoral and multidisciplinary working including service userconsumer perspectives
Health professionals other relevant professionals from social and education sectors community and layworkers usersconsumers and their families will all have a role in informing and delivering the ongoingprogramme of work
Mainstreaming and sustainable systems
The programme will work to mainstream maternal and child nutrition into all relevant work pro-grammes of other agencies and organizations to avoid a sense of being lsquoinitiative-basedrsquo and to createsustainable change
Existing networks and resources will be used wherever possible to ensure an embedded approach topractice development and to create new systems only when necessary
Solid foundations will be built for long-lasting change and to avoid a lsquodash for growthrsquo
Participatory approach to consultation and communication
All collaborative work will be based on a democratic and participative approach where all constituenciesof interest have an equal voice at all stages regardless of seniority or background
Work will address all levels of the organization ie from senior-level policymakers through regionaland local levels to practitioners in the field and service usersconsumers and their families and willinclude approaches at the level of the individual organization service and community
Embedded evaluation
All approaches used will be evaluated and findings from these evaluations will be synthesized andwidely disseminated to stakeholders including policymakers and professional leaders and other appro-priate audiences
252
MJ Renfrew
et al
copy 2006 The Authors Journal compilation copy 2006 Blackwell Publishing Ltd
Maternal and Child Nutrition
2
pp 245ndash261
Fig
1
Prac
tice
deve
lopm
ent
cycl
e N
HS
Nat
iona
l Hea
lth S
ervi
ce N
GO
non
-gov
ernm
enta
l org
aniz
atio
n
Pre
curs
ors
Sys
tem
atic
re
view
s an
d gu
idan
ce
Oth
er
reli
able
so
urce
s of
ev
iden
ce
bull E
xam
ine
syst
ems
Map
ping
and
di
agno
stic
an
alys
is
bull Id
enti
fica
tion
of
rele
vant
grou
ps
bull L
earn
ing
need
s m
easu
rem
ent
bull A
sses
smen
t of
educ
atio
n pr
ovis
ion
bull D
evel
opm
ent
oppo
rtun
itie
s
Ove
rvie
w a
ndsy
nthe
sis
of
curr
ent
prob
lem
s an
d so
luti
ons
Pla
nnin
g
Net
wor
k de
velo
pmen
t e
gbull
NH
Sbull
Pro
fess
iona
l or
gani
zati
ons
bull N
GO
s bull
Cro
ss-s
ecto
ral
Too
l dev
elop
men
t e
gbull
Dis
tanc
e le
arni
ng
bull T
oolk
its
Cap
acit
y bu
ildi
ng
syst
ems
bull In
divi
dual
bull
Org
aniz
atio
nal
bull S
ervi
ce
bull C
omm
unit
y
Pla
n to
add
ress
ca
paci
ty
buil
ding
and
chan
ge
man
agem
ent a
tdi
ffer
ent l
evel
s an
d in
dif
fere
nt
sect
ors
Cap
acit
y bu
ildi
ng a
ndde
velo
pmen
t
Mea
sure
men
t an
dm
onit
orin
g
Indi
vidu
al le
vel
eg
bull Fa
ce-t
o-fa
ce
educ
atio
n bull
Tw
inni
ng
budd
ying
bull
Dis
tanc
e le
arni
ng
Sys
tem
atic
da
ta c
olle
ctio
n an
d an
alys
is ndash
qual
itat
ive
and
quan
tita
tive
Org
aniz
atio
n an
dse
rvic
e le
vel
eg
bull C
ham
pion
s fo
r ch
ange
bull
Act
ion
lear
ning
se
ts
bull D
emon
stra
tion
pr
ojec
ts
bull Jo
int p
lann
ing
Wor
ksho
pob
serv
atio
n an
d cr
oss-
or
gani
zati
onal
au
dits
Sel
f-ev
alua
tion
an
d be
nchm
arki
ng
netw
orks
Com
mun
ity
leve
l e
gbull
Mul
ti-a
genc
y w
orki
ng
bull C
omm
unit
y re
sour
ces
rese
arch
bull A
ctio
n
Act
ion
rese
arch
and
le
arni
ng s
ets
Pol
icy
impe
rati
ves
Pri
orit
y se
ttin
g an
d
plan
for
di
agno
stic
an
alys
is
Rep
ort o
n m
easu
rem
ent
and
mon
itor
ing
Developing practice in breastfeeding
253
copy 2006 The Authors Journal compilation copy 2006 Blackwell Publishing Ltd
Maternal and Child Nutrition
2
pp 245ndash261
(Stage 2) Stage 3 involved developing relevant net-works tools for education and training evaluationmethods and capacity building systems at individualorganizational service and community levels Follow-ing this a plan to conduct the work would be finalized(Stage 4) implemented (Stage 5) and evaluated Theprocess was intended to be iterative alternatingbetween phases of information appraisal and plan-ning to identify the next stages of development activ-ity and evaluation of the impact to inform futureplanning Stage 6 included finalization of qualitativeand quantitative measurement and monitoring sys-tems that would feedback through all stages of theprocess
It was envisaged that this model would allow effec-tive structures and processes to be identified for usein other aspects of public health practice
Due to changes in funding the programme wasdiscontinued during Stage 3 although in fact somepreliminary work had already been carried out on theplan
Engagement with practitioners
Developing a national programme of change anddevelopment is an ambitious goal A cost-effectiveapproach to engagement had to be developed both tostay within budget and that could roll out acrossEngland and Wales Learning from the successfulLeeds partnership work described above it wasplanned to recruit a series of sentinel sites where wecould test out a range of approaches to maximizelearning and cost-effectiveness as well as respond toideas from the field Work in those sites wouldbecome a model for national developments inform-ing material for education training and assessmentsupported by communications at different levelsthrough our established national network The use ofsentinel sites also allowed for the development ofapproaches sensitive to varying local contexts so pro-viding alternatives and examples to inform nationalimplementation
The first stage in that process was to recruit rele-vant sentinel sites Sites were conceived as includingthe whole health economy in a locality and had tomeet specific criteria These are detailed in Box 2
Four sites were identified and agreed to join thefirst wave of sentinel sites Each site engaged andplanned the programme of work differently Forexample one site had already worked with membersof the core team and were keen to take existing workfurther In the few months in which we worked withthem they put into place a system for the accuratemonitoring of breastfeeding rates and created anextensive network of individuals at a range of seniorlevels from different sectors including Primary CareTrusts (PCTs) Strategic Health Authority the acuteTrust Sure Start and the local authority Benefits thesites have seen even since the work stopped haveincluded
bull improved communication across relevant disci-plines and sectorsbull the observation that the practice developmentwork lsquokept breastfeeding on everyonersquos agendarsquobull the work was used to support a business case for acoordinator for BFI planningbull in one sentinel site the primary care and acutematernity services have formed a health economy-wide breastfeeding strategy groupbull in another a joint primary care and maternity ser-vices group has been establishedbull two sites are taking forward systems for collect-ing breastfeeding data which have been used toprovide feedback to staff each monthbull a new approach to training all staff in one siteincluded commissioning the local university todevelop a self-study workbook and then to test itseffectiveness using an objective skills assessment toolandbull in one site a successful peer support programmewas rolled out throughout Sure Start programmes
A key part of the work in the sentinel sites was tosupport the learning needs assessment (McFadden
et al
2006) Although the sites were at an early stageof engagement this was conducted very successfullyand rapidly as sites supported the identification andinvolvement of practitioners Many assisted with sur-vey distribution and in return received a report ofthe training needs identified for their staff The nexttest was the running of fieldwork meetings and
254
MJ Renfrew
et al
copy 2006 The Authors Journal compilation copy 2006 Blackwell Publishing Ltd
Maternal and Child Nutrition
2
pp 245ndash261
workshops to finalize guidance based on researchevidence as part of a related programme of workThe aim of this work was to take the results of aseries of systematic reviews (which gave informationon lsquowhat works from research evidencersquo) and consultwith practitioners managers and users on lsquowhatreally works in practicersquo (Dyson
et al
2006) Thenewly established sentinel site system supported thiswork by offering venues for meetings providing listsof eligible participants and enabling and encourag-ing staff to attend (Renfrew
et al
2005b) The finalstage of this guidance work was a series of majorworkshops with over 30 participants in each repre-senting a lsquodiagonal slicersquo through the whole healtheconomy from field-level practitioners includingpeer support workers to managers and planners andincluding the range of relevant disciplines as well as
the voluntary sector Concerns around the realitiesand influences on practice and key issues for practi-tioners and managers in developing good practicewere discussed as well as organizational and struc-tural barriers to change Participants were encour-aged to discuss not only practices that need to beintroduced but also those that need to be aban-doned thereby potentially saving time and resourcesand to identify actual or potential barriers to imple-menting change (Renfrew
et al
2005b) These facili-tated groups examined the ability of the service torespond to identified gaps and made recommenda-tions for improvements to the system They feddirectly into the final stages of the development ofNational Institute for Health and Clinical Excellence(NICE) public health recommendations for breast-feeding offering participants the satisfaction of
Box 2
Sentinel site criteriaSentinel sites were expected to
bull Have a deprivation profile that demonstrated a substantial proportion of low-income groups and adiverse ethnic profile and serve contrasting areas (eg urban rural)
bull Offer a range of services for children and women with an interest in nutrition
bull Be able to include the whole health economy in a locality (or at least agree to working across allrelevant sectors)
bull Provide a key contact personpeople who would act to facilitate communication and broker agree-ments with different parts of the health economy and managers who were supportive of the plannedwork willing to support and enable staff participation
bull In the first instance sites would be those where contact already existed with members of our coreteam Future sites would be brought in once any initial problems with the approach had been identifiedand addressed
In return for their involvement in the work it was recognized that the sentinel sites would benefit in arange of ways including
bull Support for staff development and learning through access to programme staff and expertise involve-ment in and learning from a regular newsletter and attendance at an annual leading-edge conferenceon maternal and child nutrition
bull Developing links with other sites and sharing good practice and problem solving
bull The opportunity to help to develop national practice resulting in a raised profile for their work andtheir staff
bull Early access to emerging evidence in the field of maternal and child nutrition
Developing practice in breastfeeding
255
copy 2006 The Authors Journal compilation copy 2006 Blackwell Publishing Ltd
Maternal and Child Nutrition
2
pp 245ndash261
knowing that their input would make a difference(Dyson
et al
2006) These workshops also tested outthe use of language the conceptual understanding ofparticipants in relation to the evidence reviews andgathered intelligence on what approaches to imple-mentation of practice development may be mosteffective They also provided an opportunity for dis-cussion debate and deliberation about the meaningof the evidence Participants reported this to be veryuseful in assisting their understanding of the evi-dence and in considering how best to change theirown and their colleaguesrsquo practice in response to itand as an important contribution to practice devel-opment in their own locality (McFadden
et al
2005)The input of representatives of service users was ofcritical importance
It was planned that once the guidance was final-ized each participating site would be in a strong posi-tion to act on it Not only would they feel someownership but they would also have staff from alllevels and sectors in their health economy who hadspent time discussing the issues with colleagues andwith service user representatives They would haveaccess to specific local information about localitiesand groups that needed to be prioritized creatingchange was therefore brought several stages closerAt the end of each workshop email and telephonecontact details were exchanged among the workshopparticipants many of whom had never met beforedespite working in related parts of the same systemto support closer local networking The opportunityto consult with national experts in the network alsoacted as a variant on educational outreach which hasbeen shown to be moderately successful in guidelineimplementation (NHS CRD 1999) The impact ofsuch exchanges in increasing opportunities for net-work support is virtually impossible to evaluate for-mally but there was confidence in those whoparticipated at these events that positive changewould result and that the evidence would be moreeffectively used in the future as a consequence
Interactive conference
The other main activity was a conference on maternaland child nutrition to which all partners ndash academic
professional NHS and userconsumer ndash and stafffrom sentinel sites were invited Commissioners ofthe work were invited as were staff from key govern-ment departments with an interest in nutrition childhealth Sure Start nursing and midwifery and ine-qualities in health Around 90 participants took partin a day which included presentations participativeworking and active networking A report of the dayis available at httpwwwyorkacukresmcncccon-ferenceReporthtm Feedback was strongly positiveand the impact of networking with others in similarsituations and between those working in local andnational organizations was especially valued It wasplanned that this would be an annual event
Had we been able to continue the practice devel-opment programme we planned to use the follow-ing approaches
Establishing learning networks
We planned to identify appropriate learning net-works for different constituencies which wouldenable communication among staff from differentsectors as well as communication with programmestaff Activities were planned to include
bull Staff working at strategic and senior managementlevels would be supported and appropriate informa-tion provided to allow them to create cross-systemchanges Senior-level lsquochampions for changersquo wouldbe identified These would be used in a range of waysthose wishing to be involved in learning networkswould be supported to do sobull Learning sets would be established This wouldenable focused exchange between stakeholders onhow best to make use of the evidence in practice andhow to influence mainstream practice across locali-ties Through feedback loops we planned to developlearningeducation material to be made availablethrough web-based routes to wider constituenciesbull Peer supporters and trained breastfeeding counsel-lors are key groups in regard to breastfeeding promo-tion and support We planned to include them inlearning sets They have much to offer health profes-sionals in coming to understand the needs of womenand families and indeed the evidence suggests thattheir involvement in advisory work and peer support
256
MJ Renfrew
et al
copy 2006 The Authors Journal compilation copy 2006 Blackwell Publishing Ltd
Maternal and Child Nutrition
2
pp 245ndash261
enhances and strengthens the impact of informationand evidence-based guidance possibly more thanthat of health professionalsrsquo practice Our experiencedescribed above has identified a valuable contribu-tion from lay breastfeeding counsellors into educa-tion and training provision
Educational approaches
The breadth of constituencies that the programmeneeded to reach was to be reflected in the range ofeducational approaches required For some profes-sions continuing professional development (CPD)time is factored in regularly to the job plan in a rollingprogramme of group education with routine sessionalwork suspended for other groups CPD is a self-verified individual activity that can be achievedthrough a range of methods including distance learn-ing We hoped to reach directly a broad group ofwomen as well as professionals through some of theroutes developed A range of materials was thereforeplanned to address all needs Materials would bedeveloped for web-based access CD-ROM access andon paper These were to include
bull Toolkits to promote and support breastfeeding tomonitor breastfeeding rates and on practice develop-ment and changebull Distance learning modules providing accreditedlearning opportunities at a range of levelsbull An email and telephone-based service to putindividuals and organizations in touch with otherswho can support and advise them supported byRDLearning a national web-based resourcebull Learning material that could be directly dissemi-nated through the Internet to a wide audiencebull Buddy systems and mentoring for practice devel-opment and public health strategic development inbreastfeeding and use of cascade systemsbull Summaries of approaches to dissemination andpromotion of information that have proved to be suc-cessful and of practice change programmes that havebeen evaluated as having a positive impact on initia-tion and duration of breastfeedingbull Through NHS Direct we planned to reach the gen-eral public Information could be provided to informthe development of new algorithms that could be
used by staff taking enquiries from breastfeedingwomen We planned also to provide information thatcould be used on the NHS Direct website which isaccessed directly by women and families as well ashealth professionalsbull Other material to reach the general public wouldbe developed We aimed to have informative paperspublished in womenrsquos and familiesrsquo magazines and inthe general media on a regular basis A professionalwriter was one of our partners her role was to informand advise us about reaching women directly
Discussion
The work described in this paper was a structuredcross-sectoral approach to practice development inpublic health As a result of funding problems a fullevaluation could not be conducted and our contribu-tion to the knowledge base on practice change inpublic health is limited Lessons were learned how-ever and feedback was gained from participants atdifferent stages of the process We received strongsupport for our approach and the willingness of localand national partners to engage actively in the pro-gramme testifies to its potential
Lessons learned
There is increasing emphasis in public health andhealth policy on the need for good partnership work-ing and integration across disciplines professionsorganizations and localities as shown in the recentWhite Paper from the Department of Health (DH2006) and in the Children Act (2004) Prevention ofill health and promotion of well-being featurestrongly in these and other policy documents with arecognition that this cannot be achieved without fullengagement at strategic and operational levels withthose who use or depend on public-sector services Itwas clear at every stage of this process that engage-ment was needed across the whole health economyIt is only in working with all the relevant layers andpartnerships of professionals that we can hope for thefull impact of evidence to be realized Traditionalapproaches however only disseminate evidence tointerest groups in isolation Our use of lsquodiagonal slicersquo
Developing practice in breastfeeding 257
copy 2006 The Authors Journal compilation copy 2006 Blackwell Publishing Ltd Maternal and Child Nutrition 2 pp 245ndash261
workshops in which staff at all levels and across allsectors were engaged and including representativesof service users and the voluntary sector enabledmuch greater understanding of the consequences ofparticular activity or behaviour in other parts of thesystem and allowed creative and informed challengesto assumptions and prejudices This laid good foun-dations for whole systems approaches to introducingdriving and implementing new approaches whichcould lead to positive health outcomes It proved avery positive learning experience for all thoseinvolved
Practice change needs to involve the whole rangeof health professionals involved in work directly withpregnant women and new mothers to ensure coordi-nated working and consistent messages Despiteactive support from relevant Royal Colleges and sev-eral strongly supportive individuals engagement bydoctors was noticeably less compared with otherhealth professions This supports the findings of otherwork (eg Smale et al 2006) This really matters in afield such as breastfeeding where paediatriciansobstetricians general practitioners and public healthphysicians have an important role to play Futurework will need to address this
Key constituents in practice development in breast-feeding include mothers and potential mothersgrandmothers and men We had strong support andinvolvement from service users and user groups butengaging men proved to be difficult To reach thepublic good-quality easily accessible information isneeded perhaps the developing DiPEX module onbreastfeeding will contribute to this (httpwwwdipexorgDesktopDefaultaspx) Recent gov-ernment policy directives acknowledge the potentialcontribution that incorporating patient and serviceuser experience into service provision can bring (egDH 2006) Recent developments in the approach tolong-term conditions management have introducedthe Expert Patient Programme which enables peoplewith disabilities to take much more effective controlover the management and treatment of their disease(DH 2004c 2006) There is perhaps potential for theparallel development of an lsquoExpert Mothers Pro-grammersquo to have similar positive impact in relation tonutrition and health
Service user involvement is actively encouraged ininforming research and practice (Hanley et al 2004)Breastfeeding and maternity care as a whole have along-standing history of the active engagement of ser-vice users Volunteer counsellors and supporterstrained and accredited by their own voluntary orga-nizations have filled the gap left by the health ser-vices They have taken the initiative in setting uptelephone support services training and supervisingpeer supporters and contributing to the education ofhealth professionals (Smale et al 2006) In our cur-rent and previous practice development work thecontribution of service users and voluntary groupswent much further than simply offering advice andinformation They took an active role in planning thework and in some cases delivering education andservices Our experience was that lay workers havean essential role in developing services and they areable to advise at a strategic level as well as participat-ing in service delivery They are able to see throughthe organizational barriers that often constrain pro-fessionals and can see solutions that will work formothers and families From our experience we wouldadvise that others explore ways of actively engaginglay workers adequately remunerated in the deliveryof health care and in the education of healthprofessionals
The fundamental importance of multidisciplinaryand multi-professional working was also apparent inthe way in which the core team worked and in thesupport gained from the network of partners Atevery stage we had expertise and support availableto us as well as an effective communication systemand network Practice change in public health needsto be led and informed by those who know the topicarea and who have the wide range of skills neededto convince many different kinds of professionals thatthe work is worthwhile and achievable
Another positive contribution was the synergy ofthis programme with the evidence base The sameteam had also been responsible for systematicreviews of the field (eg Fairbank et al 2000Protheroe et al 2003 Sikorski et al 2004 Renfrewet al 2005a) and the approach was grounded in thisevidence which was at the same time being devel-oped into national guidance The interaction between
258 MJ Renfrew et al
copy 2006 The Authors Journal compilation copy 2006 Blackwell Publishing Ltd Maternal and Child Nutrition 2 pp 245ndash261
these elements should not be underestimated part-ners and sentinel sites were able to inform the guid-ance and up-to-date knowledge of the evidence basehelped strengthen the practice development work
The sentinel site system was proving to be asuccessful lsquowin-winrsquo situation for all involved Itprovided a test bed for ideas it was a source ofinformation and debate and the programme gaineda richness and diversity of input that would be hardto match At the same time it offered the sitesengagement in leading-edge work an increased pro-file and high-quality staff development Although itwas not formally evaluated all involved were con-vinced that it was a very cost-effective system theprogramme could conduct work at speed and to ahigh quality and governance issues were streamlinedThe system was very flexible and could adapt to thedifferent circumstances of each site It would havebeen able to accommodate future service and educa-tion developments such as Childrenrsquos Centres Trustreorganization and inter-professional educationOver time we could have expanded to include othersectors and practitioners such as retailers and child-minders Had the programme continued future siteswould have been identified and material developedfor national use based on our learning in the originalfour sites
Major challenges
Throughout the programme getting breastfeedingrecognized as a priority was difficult This has beenthe case for many years despite its fundamental con-tribution to public health in the short and long termit has only recently been included in national publichealth policy statements PCT targets and monitoringAs we found in the learning needs assessment andother work breastfeeding services are often seen asthe remit of enthusiastic individuals discussed interms reminiscent of lsquoreligious zealotryrsquo (Smale et al2006) rather than as a part of the mainstream ofhealth provision Creating real change in theapproach to breastfeeding in the health service willrequire it to be seen as a priority for senior managersand commissioners Our experience has demon-strated that it is possible to engage such senior people
in this work and that discussion and debate with theirown colleagues can have an impact on their thinking
A key area of practice development that canimpact on breastfeeding duration is working withmothers to sustain breastfeeding while going back towork and the ways that public health strategy andpractice can influence employers to provide breast-feeding-friendly maternity policies and facilities(Kosmala-Anderson amp Wallace in press) We did nothave an impact on this area but it was clear that itwas an area that needed to be addressed One goodplace to start would be with the employment condi-tions for NHS employees themselves this would havethe dual advantage of improving conditions for thelargest female workforce in the country while alsoproviding a model of good practice for others
Although the aim of this work was to address ine-qualities in health it is clear that reaching the hard-to-reach remains challenging We did see signs of suc-cess for example Sure Start schemes were making adifference in some areas but ensuring that all vulner-able women receive the support and care they needis still a distant goal whether they are teenagers asy-lum seekers or simply women who live in areas wherebottle feeding has been endemic for generations
Finally there is a debate to be had on whoseresponsibility it is to create such change The work ofresearchers is seen to be complete when their studyis finished and disseminated through publication andconference presentation Systematic reviewers takeon a responsibility to make the results of a wide rangeof studies available through publication but not toengage with what services might do with those find-ings Those responsible for guidance are responsiblefor developing and publishing that work and somealso take responsibility for lsquoimplementationrsquo (egNICE 2005) But where does responsibility rest forpractice development which requires a deep engage-ment with the practice setting and with those affectedby the issues raised by the evidence Lack of invest-ment at the national level in formal evaluation ofprogrammes of change limits the available evidencebase and detracts from our achieving a better under-standing of what actually works in relation to thesemore complex health issues funding for the lsquoRrsquoaspects of research and development is more com-
Developing practice in breastfeeding 259
copy 2006 The Authors Journal compilation copy 2006 Blackwell Publishing Ltd Maternal and Child Nutrition 2 pp 245ndash261
mon than for the lsquoDrsquo (NHS Executive 1997) Thewithdrawal of funding to this programme part waythrough its cycle was regretted by our commissionersit was evident that practice development was nolonger their remit given their changed circumstancesIt is however not clear that responsibility now restswith any particular agency Is development work forindividual health service organizations themselves totake on Is this work that should be led by nationalprogrammes supported by public-sector funding orshould it rely on other sources of support If so fromwhere will it be resourced and how will cross-sectoraland multidisciplinary developments be addressedThere are also questions about who will lead thiswork when a number of professional disciplines areinvolved and where the client interface spans bothprimary and acute care healthcare settings social ser-vices and other development agencies These ques-tions will become more pressing as guidancecontinues to be produced especially in public health
Acknowledgements
We would like to thank all participants from sentinelsites and our consortium of academic professionalNHS and consumer partners and the two anonymousreferees who reviewed the manuscript This work wascommissioned by the former Health DevelopmentAgency and subsequently funded by NICE
References
Abbott S Renfrew MJ amp McFadden A (2006) lsquoInformalrsquo learning to support breastfeeding local problems and opportunities Maternal and Child Nutrition 2 232ndash238
Audit Commission (2000) United They Stand Coordinating Care for Elderly Patients with Hip Fracture Audit Com-mission London
British Paediatric Association (1994) Statement of the stand-ing committee on nutrition is breastfeeding beneficial in the UK Archive of Diseases in Childhood 71 376ndash380
Chalmers I amp Altman DG (eds) (1995) Systematic Reviews BMJ Publishing Group London
Children Act (2004) Available at httpwwwopsigovukactsacts200420040031htm (accessed 21 March 2006)
Coote A Allen J amp Woodhead D (2004) Finding out What Works Building Knowledge about Complex Community-Based Initiatives Kingrsquos Fund London
DfES (2000) Adoption and Permanence Taskforce Available at httpwwwdfesgovukadoptionadoptionreformstaskforceshtml (accessed 29 March 2006)
DH (2002a) Improvement Expansion and Reform The Next 3 Years Priorities and Planning Framework 2003ndash2006 Department of Health London
DH (2002b) The Health and Social Care Change Agent Team Available at httpwwwchangeagentteamorguk (accessed 29 March 2006)
DH (2004a) National Service Framework for Children Young People and Maternity Services Stationery Office London
DH (2004b) Choosing Health Making Healthy Choices Eas-ier Stationery Office London
DH (2004c) Self Care ndash A Real Choice Self Care Support ndash A Practical Option Stationery Office London
DH (2006) Our Health Our Care Our Say A New Direction for Community Services Stationery Office London
Dominey M Archibald A Edgecombe D Lawrence J amp Thomson L (2002) Breastfeeding and drug misuse Mak-ing an informed choice Year 3 Practice project In Infant Feeding Initiative A Report Evaluating the Breastfeeding Practice Projects 1999ndash2002 (ed F Dykes 2003) p 64 Department of Health London
Dykes F (2003) Infant Feeding Initiative A Report Evaluat-ing the Breastfeeding Practice Projects 1999ndash2002 Depart-ment of Health London
Dykes F (2006) The education of health practitioners sup-porting breastfeeding women time for critical reflection Maternal and Child Nutrition 2 204ndash216
Dyson L Renfrew MJ McFadden A McCormick F Herbert G amp Thomas J (2006) Promotion of Breastfeed-ing Initiation and Duration Evidence into Practice Brief-ing National Institute for Health and Clinical Excellence London httpwwwniceorgukdown-loadaspxo=346169 (accessed 26 July 2006)
EU (2004) Project on Promotion of Breastfeeding in Europe Protection Promotion and Support of Breastfeeding A Blueprint for Action European Commission Directorate Public Health and Risk Assessment Luxembourg
Fairbank L OrsquoMeara S Renfrew MJ Woolridge M Sowden AJ amp Lister-Sharp D (2000) A systematic review to evaluate the effectiveness of interventions to promote the initiation of breastfeeding Health Technol-ogy Assessment 4 1ndash171
Grant J Fletcher M amp Warwick C (2000) The South Thames Evidence Based Practice (STEP) Project Sup-porting Breastfeeding Women South Bank University London
Greenhalgh T Robert G Bate P Mcfarlane F amp Kyriakidou O (2005) Diffusion of Innovations in Health Service Organisations A Systematic Literature Review Blackwell Publishing Limited Oxford
260 MJ Renfrew et al
copy 2006 The Authors Journal compilation copy 2006 Blackwell Publishing Ltd Maternal and Child Nutrition 2 pp 245ndash261
Grimshaw JM Thomas RE MacLennan G Fraser C Ramsay CR Vale L et al (2004) Effectiveness and efficiency of guideline dissemination and implementation strategies Health Technology Assessment 8 indashxi 1ndash72
Hanley B Bradburn J Barnes M Evans C Goodare H Kelson M et al (2004) Involving the Public in NHS Pub-lic Health and Social Care Research Briefing Notes for Researchers INVOLVE Department of Health London
Herbert G amp Lake G (2005) Making connections Effective development of the intermediate tier Journal of Inte-grated Care 13 35ndash42
Howie PW Forsyth JS Ogston SA Clark A amp Florey CD (1990) Protective effect of breastfeeding against infection British Medical Journal 300 11ndash16
Kosmala-Anderson J amp Wallace LM (in press) Breastfeed-ing works the role of employers in supporting women who wish to breastfeed and work in four organizations in England Journal of Public Health (in press)
Kramer M Chalmers B Hodnett H Sevovskaya Z Dzikovich I Shapiro S et al (2001) Promotion of breast-feeding intervention trial (PROBIT) Journal of the American Medical Association 285 413ndash420
McFadden A Renfrew MJ Dyson L McCormick F Herbert G amp Thomas J (2005) Effective Active Briefing on the Initiation and Duration of Breastfeeding Fieldwork Report National Institute for Health and Clinical Excel-lence London
McFadden A Renfrew MJ Dykes F amp Burt S (2006) Assessing learning needs for breastfeeding setting the scene Maternal and Child Nutrition 2 196ndash203
McSherry R amp McFadden A (2001) Practice Development Accreditation Assessment Maternity Services Darlington Memorial Hospital South Durham Healthcare NHS Trust Final Report University of Teesside Middlesbrough
Moulding NT Silagy CA amp Weller DP (1999) A frame-work for effective management of change in clinical prac-tice dissemination and implementation of clinical practice guidelines Quality in Health Care 8 177ndash183
Gray JA Haynes RB Sackett DL Cook DJ amp Guyatt GH (1997) Transferring evidence from research into practice 3 Developing evidence-based clinical policy Evidence-Based Medicine 2 36ndash38
NHS Centre for Reviews and Dissemination (CRD) (1999) Getting evidence into practice Effective Health Care 5 1ndash16
NHS Executive (1997) RampD in Primary Care National Working Group Report (Mant Report) Stationery Office London
NICE (2004) The Guideline Development Process National Institute for Health and Clinical Excellence London
NICE (2005) Putting NICE Guidance into Practice National Institute for Health and Clinical Excellence London
Oxman AD Thomson MA Davis DA amp Haynes RB (1995) No magic bullets a systematic review of 102 trials of interventions to improve professional practice Canadian Medical Association Journal 153 1423ndash1431
Protheroe L Dyson L Renfrew MJ Bull J amp Mulvihill C (2003) The Effectiveness of Public Health Interventions to Promote the Initiation of Breastfeeding Evidence Briefing Health Development Agency London
Quigley MA Cumberland P Cowden JM amp Rodrigues LC (2006) How protective is breast feeding against diar-rhoeal disease in infants in 1990s England A case control study Archives of Disease in Childhood 91 245ndash250
Renfrew MJ Dyson L Wallace L DrsquoSouza L McCormick FM amp Spiby H (2005a) The Effectiveness of Health Interventions to Promote the Duration of Breast-feeding Systematic Review 1st edn National Institute for Health and Clinical Excellence London
Renfrew MJ Dyson L McFadden A McCormick F Herbert G amp Thomas J (2005b) Effective Active Briefing on the Initiation and Duration of Breastfeeding Technical Report National Institute for Health and Clinical Excel-lence London
Renfrew MJ McFadden A Dykes F Wallace L Abbott S Burt S et al (2006) Addressing the learning deficit in breastfeeding strategies for change Maternal and Child Nutrition 2 239ndash244
Richards D (2003) Childrenrsquos Nutrition ndash Mothers Who Wish to Breast-Feed Birmingham City Council Available at httpwwwbirmingahmgovukscrutiny (accessed 27 July 2006)
Sackett DL Rosenberg WMC Gray JAM Haynes RB amp Richardson WS (1996) Evidence-based medicine what it is and what it isnrsquot British Medical Journal 312 71ndash72
Sikorski J Renfrew MJ Pindoria S amp Wade A (2004) Support for breastfeeding mothers (Cochrane Review) The Cochrane Database of Systematic Reviews Issue 2 John Wiley amp Sons Ltd Chichester
Smale M Renfrew MJ Marshall JL amp Spiby H (2006) Turning policy into practice more difficult that it seems The case of breastfeeding education Maternal and Child Nutrition 2 103ndash113
Spiby H Ker R DrsquoSouza L amp Renfrew MJ (2002) Intro-ducing a Consumer-Practitioner into breastfeeding prac-tice Year 2 In Infant Feeding Initiative A Report Evaluating the Breastfeeding Practice Projects 1999ndash2002 (ed F Dykes 2003) p 44 Department of Health London
Spiby H Wallis S Stone C amp Renfrew MJ (2005) Support-ing and Promoting Breastfeeding in Leeds Final Report to December 2004 Report to Leeds PCTs Children and Families Modernisation Team Leeds
Thomas C (2006) Darlington ndash A Breastfeeding Friendly Town Darlington Borough Council Darlington
Developing practice in breastfeeding 261
copy 2006 The Authors Journal compilation copy 2006 Blackwell Publishing Ltd Maternal and Child Nutrition 2 pp 245ndash261
Unsworth J (2000) Practice development a concept analy-sis Journal of Nursing Management 8 317ndash326
Wallace LM amp Jardine J (2006) A Health Scrutiny of Ser-vices to Support the Initiation and Duration of Breastfeed-ing in Coventry and Warwickshire Coventry and Warwickshire County Councils Coventry
Wallace L amp Kosmala-Anderson J (2006) A training needs survey of doctorsrsquo breastfeeding support skills in England Maternal and Child Nutrition 2 217ndash231
Wallace L amp Kosmala-Anderson J (in press) Training needs survey of midwives health visitors and voluntary sector
breastfeeding support staff in England Maternal and Child Nutrition (in press)
WHO (2003) Global Strategy for Infant and Young Child Feeding World Health Organization Geneva
Wilson AC Forsyth JS Green SA Irvine L Hau C amp Howie PW (1998) Relation of infant diet to childhood health seven year follow up of a cohort of children in Dundee infant feeding study British Medical Journal 316 21ndash25

248
MJ Renfrew
et al
copy 2006 The Authors Journal compilation copy 2006 Blackwell Publishing Ltd
Maternal and Child Nutrition
2
pp 245ndash261
new approaches that lead to direct and quantifiableimprovements in services such changes occur as aresponse to problems or needs and contribute to theprovision of effective services However there hasbeen little systematic exploration of practice develop-ment within midwifery posts although individualmaternity settings have been able to apply for accred-itation as practice development units (McSherry ampMcFadden 2001)
In other fields there are examples of practicedevelopment being led by task forces or developmentagencies linked to particular policy drivers for exam-ple the Change Agents Team at the Department ofHealth in relation to Older Peoplesrsquo policies (DH2002b) and the Adoption Taskforce (DfES 2000)While using existing evidence to inform practicechange such groups also use many different interven-tions and learning models to address major changeThis approach can tackle the interdisciplinary andinter-agency agendas which are needed in manyareas of public health to achieve positive change
Breastfeeding and practice development
A recent systematic review of interventions promot-ing the duration of breastfeeding revealed a dearth ofliterature in the fields of training and education ofhealthcare professionals and breastfeeding counsel-lors and of evidence-based practice or practice devel-opment initiatives (Renfrew
et al
2005a) Thisincludes the absence of high-quality evidence aboutways of preparing practitioners to deliver care to sup-port health policy initiatives Only one study of arelevant evidence-based practice initiative was iden-tified (Grant
et al
2000)Some 79 practice development initiatives in breast-
feeding were funded by the Department of Health inEngland over the period 1999ndash2002 (Dykes 2003)These included establishing breastfeeding supportcentres education for health professionals develop-ment of the role of healthcare assistants in supportingbreastfeeding developing peer support involvingbreastfeeding counsellors and developing services forvulnerable groups such as adolescent womenAlthough preliminary evaluation suggests that thesewere successful formal evaluations were limited
There is also no evidence of a coordinated strategyand funding to support mainstream implementationof practice change such as described above in otherfields so many of these initiatives have since beendiscontinued or have remained as isolated initiativesSuch use of short-term funding without clear strategiesfor creating sustainable change to mainstream prac-tice or integrate learning into future service develop-ment seems to be reflected in other areas across theNational Health Service (NHS) in England and Wales
Like practice development posts more widelyinfant feeding or breastfeeding development postshave a range of remits including providing skilledexpertise in addressing serious breastfeeding prob-lems developing guidelines supporting worktowards achieving accreditation with UNICEF UKBaby Friendly Initiative (BFI) providing educa-tional support to colleagues in developing theirbreastfeeding expertise educating mothers on tech-niques and developing positive attitudes to breast-feeding and other aspects of breast care Manyindividuals in such posts work in relative isolation(Abbott
et al
2006) and are expected to fulfil theirbreastfeeding or infant feeding remit in addition toother midwifery or health visiting workload andresponsibilities This is true even of the nationalnetwork of infant feeding coordinators in Englandwhere coordinators often carry out the work inaddition to their existing duties Development postsare normally restricted to the maternity service thatfunds them often not even having a remit outsideof their own discipline They are unlikely to be ableto support breastfeeding across different sectorswithin the whole health economy in the way thatwe have identified as necessary (Renfrew
et al
2006Wallace amp Jardine 2006)
Unusually three local authority health scrutinieshave recently taken a multi-sectoral approach toexamining how a range of agencies not just localmaternity and community health services canremove barriers to breastfeeding and improve directhealthcare provision to support breastfeedingwomen (Richards 2003 Thomas 2006 Wallace ampJardine 2006) All of these contain recommenda-tions for health services education the voluntarysector trainers of healthcare staff local employers
Developing practice in breastfeeding
249
copy 2006 The Authors Journal compilation copy 2006 Blackwell Publishing Ltd
Maternal and Child Nutrition
2
pp 245ndash261
and lsquoownersrsquo of public spaces as well as the councilsthemselves Inter-sectoral strategic planning led bypublic health where there has also been a sharedinterest in seeking a health economy-wide approachto UNICEF UK BFI status has resulted in moreinter-sectoral practitioner learning networks andshared resources for training staff in breastfeedingsupport (Wallace amp Jardine 2006) The extent towhich this innovative approach is effective and sus-tainable in the longer term is unknown
Breastfeeding development projects
Our approach to practice development drew on thelessons learned from much of the literature summa-rized above Three previous evidence-based prac-tice developments in breastfeeding also directlyinformed our thinking The Breastfeeding in LeedsConsortium was a cross-sectoral partnership thataimed to increase breastfeeding rates by raising theprofile of breastfeeding locally providing educa-tional events and bringing together those withshared interests in supporting breastfeedingwomen As part of that work a Department ofHealth-funded initiative supported a project (Spiby
et al
2002) in which two experienced lay breastfeed-ing counsellors worked to increase evidence-basedsupport to breastfeeding They contributed to edu-cation for undergraduate and registered healthcarepractitioners from a range of disciplines workedwith practitioners providing direct care to womenand provided a range of community developmentactivities The model used in this project was oneof providing evidence-based information forwomen and their families to use rather than atraditional advice-based approach Evaluation ofthis initiative was overwhelmingly positive The layrole was considered compatible rather than conflict-ing with that of healthcare professionals The psy-chosocial perspectives of breastfeeding used by thecounsellors were adopted widely replacing the tra-ditional health lsquobenefits of breastfeeding approachrsquo
Two further developments arose from this suc-cessful preliminary work One project worked tosupport breastfeeding across the health economy inLeeds with a special emphasis on working with
women and families from low-income groups(Spiby
et al
2005) Using the combination of a laycounsellor with a midwife with a specialist breast-feeding background the project delivered multidis-ciplinary and multi-sectoral training using bothhealth and social perspectives It supported the lsquorolloutrsquo of the acute Trustrsquos infant feeding policy andits adoption in the majority of local primary careservices and it demonstrated that collaborativeworking between healthcare professionals andbreastfeeding counsellors can succeed Problemswere also identified some groups of healthcare pro-fessionals are more difficult to engage than otherscross-boundary and inter-sectoral working was stillrelatively new for some health service staff andprotection of professional roles was clearly identi-fied as a problem While support for the initiativehad been identified at a senior level within boththe acute and primary care sectors that support wasnot evident in practice and senior-level projectchampions were not clearly identifiable
A third project included work with local SureStart partnerships in the Leeds and Bradford areasThis delivered staff training helped to establishsupport groups for breastfeeding women initiatedchanges that would reinforce positive messagesabout breastfeeding on Sure Start premises advisedon resources and policies developed support mech-anisms for women in disadvantaged communitiesand developed provided and evaluated a firstcohort of peer support training for women from theSure Start areas The lessons learned from thatwork included the importance of early engagementacross all relevant sectors and disciplines findingout about local needs from local communities theneed to reduce organizational barriers boundariesand tensions and the opportunities that multidisci-plinary education brings This work has now beenincorporated into mainstream practice in the city(Spiby
et al
2005)All three developments were successful in
increasing the number of practitioners women andfamilies receiving evidence-based support withbreastfeeding (Spiby
et al
2005) All includedtrained breastfeeding counsellors as key sources ofsupport and development work and breastfeeding
250
MJ Renfrew
et al
copy 2006 The Authors Journal compilation copy 2006 Blackwell Publishing Ltd
Maternal and Child Nutrition
2
pp 245ndash261
rates in the city including the low-income communi-ties served on discharge from hospital increasedfrom around 45 in early 2002 to 51 in late 2004(St James University Hospital Breastfeeding Statis-tics) All were influential in informing our thinkingaround the conceptual framework and in planningthe structures for the national practice developmentwork described here
Aims and methods
The overall aim of our practice development workwas to address inequalities in health by improvingmaternal and child nutrition The objectives of theprogramme were to (1) inform and enable practicedevelopment in breastfeeding in a number of low-income areas (2) evaluate the impact of approachesused and (3) develop robust approaches and appro-priate material for use across the country in futureyears
Core team
A core team was formed to plan this work The teamincluded the following backgrounds knowledge ofthe evidence base and relevant research methods andcritique in general the development of evidence-based guidance the education of health professionalsat pre- and post-registration levels information tech-nology (IT) and web-based communication skillsknowledge of breastfeeding from public health andclinical perspectives senior NHS managementchange management and practice development in theNHS and related sectors and strategic planning andleadership
National network
At a very early stage a national network was estab-lished with the aim of informing and supporting thework Partners in this network included
bull
academic partners
to ensure that the evidence basewas soundbull
professional bodies
including relevant Royal Col-leges and professional organizations representing thewide range of practitioner groups likely to be
involved to inform the development plans to sup-port dissemination of information to provide con-tacts and communication systems and to enhance thelegitimacy of the workbull
NHS partners
including clinical practitioners withrelevant clinical skills representatives of a StrategicHealth Authority a Public Health Observatory (Pub-lic Health Observatories are funded by the Dep-artment of Health to strengthen the availability anduse of health information at a local level in the UK)NHS Direct (NHS Direct is an online and telephonehealth information enquiry service for the publichttpwwwnhsdirectnhsukindexasp) RDLearning(RDLearning is a web-based national resource ofaccredited health-related education courses httpwwwrdlearningorguk) and primary care researchnetworks to inform practice development plans tooffer communication networks and skills in routinedata collection and analysis and to support the iden-tification of key contacts andbull
representatives of consumer groups voluntary
organizations and non-government organizations
toensure that we were able to benefit from their expe-rience of providing services and gaining user per-spectives to inform the practice development plansand offer communication networks
Links were also made with relevant governmentdepartments and professional advice was taken oncommunication strategies
We developed the system to be flexible and respon-sive with two-way communication systems and fre-quent dialogue with commissioners and partners aswe recognized that the source of funding for this workwas a government agency and that government prior-ities can shift and change over time
Conceptual framework and programme development
A conceptual framework for the project was estab-lished based on the literature and our practice devel-opment experience in breastfeeding (describedabove) and other fields including developing learningnetworks in other areas of practice (eg Herbert ampLake 2005) It was finalized through discussions
Developing practice in breastfeeding
251
copy 2006 The Authors Journal compilation copy 2006 Blackwell Publishing Ltd
Maternal and Child Nutrition
2
pp 245ndash261
among the core team and input from network part-ners This framework then informed all decisions andplans Key elements of the framework included anevidence-based approach multi-sectoral and multi-disciplinary working service userconsumer involve-ment mainstreaming and sustainable systems aparticipatory approach to consultation and communi-cation and embedded evaluation Specific elementsof this approach are shown in Box 1
Based on the conceptual framework a six-stageprocess was developed (Fig 1) Following assessmentof the literature on effective interventions a diagnos-tic analysis of the field was planned to include alearning needs assessment (as reported in this issueof the journal) and a general assessment of the readi-ness of the field to undertake this work (Stage 1) Thiswas followed by a synthesis of those two stages yield-ing an analysis of the problem and potential solutions
Box 1
Elements of conceptual framework
Evidence-based approach
All proposed interventions will be based on a rigorous assessment of the published literature togetherwith practitioner and user views of that evidence base
An eclectic mix of approaches and models will be drawn on based on evidence of lsquowhat worksrsquo indifferent communities
Multi-sectoral and multidisciplinary working including service userconsumer perspectives
Health professionals other relevant professionals from social and education sectors community and layworkers usersconsumers and their families will all have a role in informing and delivering the ongoingprogramme of work
Mainstreaming and sustainable systems
The programme will work to mainstream maternal and child nutrition into all relevant work pro-grammes of other agencies and organizations to avoid a sense of being lsquoinitiative-basedrsquo and to createsustainable change
Existing networks and resources will be used wherever possible to ensure an embedded approach topractice development and to create new systems only when necessary
Solid foundations will be built for long-lasting change and to avoid a lsquodash for growthrsquo
Participatory approach to consultation and communication
All collaborative work will be based on a democratic and participative approach where all constituenciesof interest have an equal voice at all stages regardless of seniority or background
Work will address all levels of the organization ie from senior-level policymakers through regionaland local levels to practitioners in the field and service usersconsumers and their families and willinclude approaches at the level of the individual organization service and community
Embedded evaluation
All approaches used will be evaluated and findings from these evaluations will be synthesized andwidely disseminated to stakeholders including policymakers and professional leaders and other appro-priate audiences
252
MJ Renfrew
et al
copy 2006 The Authors Journal compilation copy 2006 Blackwell Publishing Ltd
Maternal and Child Nutrition
2
pp 245ndash261
Fig
1
Prac
tice
deve
lopm
ent
cycl
e N
HS
Nat
iona
l Hea
lth S
ervi
ce N
GO
non
-gov
ernm
enta
l org
aniz
atio
n
Pre
curs
ors
Sys
tem
atic
re
view
s an
d gu
idan
ce
Oth
er
reli
able
so
urce
s of
ev
iden
ce
bull E
xam
ine
syst
ems
Map
ping
and
di
agno
stic
an
alys
is
bull Id
enti
fica
tion
of
rele
vant
grou
ps
bull L
earn
ing
need
s m
easu
rem
ent
bull A
sses
smen
t of
educ
atio
n pr
ovis
ion
bull D
evel
opm
ent
oppo
rtun
itie
s
Ove
rvie
w a
ndsy
nthe
sis
of
curr
ent
prob
lem
s an
d so
luti
ons
Pla
nnin
g
Net
wor
k de
velo
pmen
t e
gbull
NH
Sbull
Pro
fess
iona
l or
gani
zati
ons
bull N
GO
s bull
Cro
ss-s
ecto
ral
Too
l dev
elop
men
t e
gbull
Dis
tanc
e le
arni
ng
bull T
oolk
its
Cap
acit
y bu
ildi
ng
syst
ems
bull In
divi
dual
bull
Org
aniz
atio
nal
bull S
ervi
ce
bull C
omm
unit
y
Pla
n to
add
ress
ca
paci
ty
buil
ding
and
chan
ge
man
agem
ent a
tdi
ffer
ent l
evel
s an
d in
dif
fere
nt
sect
ors
Cap
acit
y bu
ildi
ng a
ndde
velo
pmen
t
Mea
sure
men
t an
dm
onit
orin
g
Indi
vidu
al le
vel
eg
bull Fa
ce-t
o-fa
ce
educ
atio
n bull
Tw
inni
ng
budd
ying
bull
Dis
tanc
e le
arni
ng
Sys
tem
atic
da
ta c
olle
ctio
n an
d an
alys
is ndash
qual
itat
ive
and
quan
tita
tive
Org
aniz
atio
n an
dse
rvic
e le
vel
eg
bull C
ham
pion
s fo
r ch
ange
bull
Act
ion
lear
ning
se
ts
bull D
emon
stra
tion
pr
ojec
ts
bull Jo
int p
lann
ing
Wor
ksho
pob
serv
atio
n an
d cr
oss-
or
gani
zati
onal
au
dits
Sel
f-ev
alua
tion
an
d be
nchm
arki
ng
netw
orks
Com
mun
ity
leve
l e
gbull
Mul
ti-a
genc
y w
orki
ng
bull C
omm
unit
y re
sour
ces
rese
arch
bull A
ctio
n
Act
ion
rese
arch
and
le
arni
ng s
ets
Pol
icy
impe
rati
ves
Pri
orit
y se
ttin
g an
d
plan
for
di
agno
stic
an
alys
is
Rep
ort o
n m
easu
rem
ent
and
mon
itor
ing
Developing practice in breastfeeding
253
copy 2006 The Authors Journal compilation copy 2006 Blackwell Publishing Ltd
Maternal and Child Nutrition
2
pp 245ndash261
(Stage 2) Stage 3 involved developing relevant net-works tools for education and training evaluationmethods and capacity building systems at individualorganizational service and community levels Follow-ing this a plan to conduct the work would be finalized(Stage 4) implemented (Stage 5) and evaluated Theprocess was intended to be iterative alternatingbetween phases of information appraisal and plan-ning to identify the next stages of development activ-ity and evaluation of the impact to inform futureplanning Stage 6 included finalization of qualitativeand quantitative measurement and monitoring sys-tems that would feedback through all stages of theprocess
It was envisaged that this model would allow effec-tive structures and processes to be identified for usein other aspects of public health practice
Due to changes in funding the programme wasdiscontinued during Stage 3 although in fact somepreliminary work had already been carried out on theplan
Engagement with practitioners
Developing a national programme of change anddevelopment is an ambitious goal A cost-effectiveapproach to engagement had to be developed both tostay within budget and that could roll out acrossEngland and Wales Learning from the successfulLeeds partnership work described above it wasplanned to recruit a series of sentinel sites where wecould test out a range of approaches to maximizelearning and cost-effectiveness as well as respond toideas from the field Work in those sites wouldbecome a model for national developments inform-ing material for education training and assessmentsupported by communications at different levelsthrough our established national network The use ofsentinel sites also allowed for the development ofapproaches sensitive to varying local contexts so pro-viding alternatives and examples to inform nationalimplementation
The first stage in that process was to recruit rele-vant sentinel sites Sites were conceived as includingthe whole health economy in a locality and had tomeet specific criteria These are detailed in Box 2
Four sites were identified and agreed to join thefirst wave of sentinel sites Each site engaged andplanned the programme of work differently Forexample one site had already worked with membersof the core team and were keen to take existing workfurther In the few months in which we worked withthem they put into place a system for the accuratemonitoring of breastfeeding rates and created anextensive network of individuals at a range of seniorlevels from different sectors including Primary CareTrusts (PCTs) Strategic Health Authority the acuteTrust Sure Start and the local authority Benefits thesites have seen even since the work stopped haveincluded
bull improved communication across relevant disci-plines and sectorsbull the observation that the practice developmentwork lsquokept breastfeeding on everyonersquos agendarsquobull the work was used to support a business case for acoordinator for BFI planningbull in one sentinel site the primary care and acutematernity services have formed a health economy-wide breastfeeding strategy groupbull in another a joint primary care and maternity ser-vices group has been establishedbull two sites are taking forward systems for collect-ing breastfeeding data which have been used toprovide feedback to staff each monthbull a new approach to training all staff in one siteincluded commissioning the local university todevelop a self-study workbook and then to test itseffectiveness using an objective skills assessment toolandbull in one site a successful peer support programmewas rolled out throughout Sure Start programmes
A key part of the work in the sentinel sites was tosupport the learning needs assessment (McFadden
et al
2006) Although the sites were at an early stageof engagement this was conducted very successfullyand rapidly as sites supported the identification andinvolvement of practitioners Many assisted with sur-vey distribution and in return received a report ofthe training needs identified for their staff The nexttest was the running of fieldwork meetings and
254
MJ Renfrew
et al
copy 2006 The Authors Journal compilation copy 2006 Blackwell Publishing Ltd
Maternal and Child Nutrition
2
pp 245ndash261
workshops to finalize guidance based on researchevidence as part of a related programme of workThe aim of this work was to take the results of aseries of systematic reviews (which gave informationon lsquowhat works from research evidencersquo) and consultwith practitioners managers and users on lsquowhatreally works in practicersquo (Dyson
et al
2006) Thenewly established sentinel site system supported thiswork by offering venues for meetings providing listsof eligible participants and enabling and encourag-ing staff to attend (Renfrew
et al
2005b) The finalstage of this guidance work was a series of majorworkshops with over 30 participants in each repre-senting a lsquodiagonal slicersquo through the whole healtheconomy from field-level practitioners includingpeer support workers to managers and planners andincluding the range of relevant disciplines as well as
the voluntary sector Concerns around the realitiesand influences on practice and key issues for practi-tioners and managers in developing good practicewere discussed as well as organizational and struc-tural barriers to change Participants were encour-aged to discuss not only practices that need to beintroduced but also those that need to be aban-doned thereby potentially saving time and resourcesand to identify actual or potential barriers to imple-menting change (Renfrew
et al
2005b) These facili-tated groups examined the ability of the service torespond to identified gaps and made recommenda-tions for improvements to the system They feddirectly into the final stages of the development ofNational Institute for Health and Clinical Excellence(NICE) public health recommendations for breast-feeding offering participants the satisfaction of
Box 2
Sentinel site criteriaSentinel sites were expected to
bull Have a deprivation profile that demonstrated a substantial proportion of low-income groups and adiverse ethnic profile and serve contrasting areas (eg urban rural)
bull Offer a range of services for children and women with an interest in nutrition
bull Be able to include the whole health economy in a locality (or at least agree to working across allrelevant sectors)
bull Provide a key contact personpeople who would act to facilitate communication and broker agree-ments with different parts of the health economy and managers who were supportive of the plannedwork willing to support and enable staff participation
bull In the first instance sites would be those where contact already existed with members of our coreteam Future sites would be brought in once any initial problems with the approach had been identifiedand addressed
In return for their involvement in the work it was recognized that the sentinel sites would benefit in arange of ways including
bull Support for staff development and learning through access to programme staff and expertise involve-ment in and learning from a regular newsletter and attendance at an annual leading-edge conferenceon maternal and child nutrition
bull Developing links with other sites and sharing good practice and problem solving
bull The opportunity to help to develop national practice resulting in a raised profile for their work andtheir staff
bull Early access to emerging evidence in the field of maternal and child nutrition
Developing practice in breastfeeding
255
copy 2006 The Authors Journal compilation copy 2006 Blackwell Publishing Ltd
Maternal and Child Nutrition
2
pp 245ndash261
knowing that their input would make a difference(Dyson
et al
2006) These workshops also tested outthe use of language the conceptual understanding ofparticipants in relation to the evidence reviews andgathered intelligence on what approaches to imple-mentation of practice development may be mosteffective They also provided an opportunity for dis-cussion debate and deliberation about the meaningof the evidence Participants reported this to be veryuseful in assisting their understanding of the evi-dence and in considering how best to change theirown and their colleaguesrsquo practice in response to itand as an important contribution to practice devel-opment in their own locality (McFadden
et al
2005)The input of representatives of service users was ofcritical importance
It was planned that once the guidance was final-ized each participating site would be in a strong posi-tion to act on it Not only would they feel someownership but they would also have staff from alllevels and sectors in their health economy who hadspent time discussing the issues with colleagues andwith service user representatives They would haveaccess to specific local information about localitiesand groups that needed to be prioritized creatingchange was therefore brought several stages closerAt the end of each workshop email and telephonecontact details were exchanged among the workshopparticipants many of whom had never met beforedespite working in related parts of the same systemto support closer local networking The opportunityto consult with national experts in the network alsoacted as a variant on educational outreach which hasbeen shown to be moderately successful in guidelineimplementation (NHS CRD 1999) The impact ofsuch exchanges in increasing opportunities for net-work support is virtually impossible to evaluate for-mally but there was confidence in those whoparticipated at these events that positive changewould result and that the evidence would be moreeffectively used in the future as a consequence
Interactive conference
The other main activity was a conference on maternaland child nutrition to which all partners ndash academic
professional NHS and userconsumer ndash and stafffrom sentinel sites were invited Commissioners ofthe work were invited as were staff from key govern-ment departments with an interest in nutrition childhealth Sure Start nursing and midwifery and ine-qualities in health Around 90 participants took partin a day which included presentations participativeworking and active networking A report of the dayis available at httpwwwyorkacukresmcncccon-ferenceReporthtm Feedback was strongly positiveand the impact of networking with others in similarsituations and between those working in local andnational organizations was especially valued It wasplanned that this would be an annual event
Had we been able to continue the practice devel-opment programme we planned to use the follow-ing approaches
Establishing learning networks
We planned to identify appropriate learning net-works for different constituencies which wouldenable communication among staff from differentsectors as well as communication with programmestaff Activities were planned to include
bull Staff working at strategic and senior managementlevels would be supported and appropriate informa-tion provided to allow them to create cross-systemchanges Senior-level lsquochampions for changersquo wouldbe identified These would be used in a range of waysthose wishing to be involved in learning networkswould be supported to do sobull Learning sets would be established This wouldenable focused exchange between stakeholders onhow best to make use of the evidence in practice andhow to influence mainstream practice across locali-ties Through feedback loops we planned to developlearningeducation material to be made availablethrough web-based routes to wider constituenciesbull Peer supporters and trained breastfeeding counsel-lors are key groups in regard to breastfeeding promo-tion and support We planned to include them inlearning sets They have much to offer health profes-sionals in coming to understand the needs of womenand families and indeed the evidence suggests thattheir involvement in advisory work and peer support
256
MJ Renfrew
et al
copy 2006 The Authors Journal compilation copy 2006 Blackwell Publishing Ltd
Maternal and Child Nutrition
2
pp 245ndash261
enhances and strengthens the impact of informationand evidence-based guidance possibly more thanthat of health professionalsrsquo practice Our experiencedescribed above has identified a valuable contribu-tion from lay breastfeeding counsellors into educa-tion and training provision
Educational approaches
The breadth of constituencies that the programmeneeded to reach was to be reflected in the range ofeducational approaches required For some profes-sions continuing professional development (CPD)time is factored in regularly to the job plan in a rollingprogramme of group education with routine sessionalwork suspended for other groups CPD is a self-verified individual activity that can be achievedthrough a range of methods including distance learn-ing We hoped to reach directly a broad group ofwomen as well as professionals through some of theroutes developed A range of materials was thereforeplanned to address all needs Materials would bedeveloped for web-based access CD-ROM access andon paper These were to include
bull Toolkits to promote and support breastfeeding tomonitor breastfeeding rates and on practice develop-ment and changebull Distance learning modules providing accreditedlearning opportunities at a range of levelsbull An email and telephone-based service to putindividuals and organizations in touch with otherswho can support and advise them supported byRDLearning a national web-based resourcebull Learning material that could be directly dissemi-nated through the Internet to a wide audiencebull Buddy systems and mentoring for practice devel-opment and public health strategic development inbreastfeeding and use of cascade systemsbull Summaries of approaches to dissemination andpromotion of information that have proved to be suc-cessful and of practice change programmes that havebeen evaluated as having a positive impact on initia-tion and duration of breastfeedingbull Through NHS Direct we planned to reach the gen-eral public Information could be provided to informthe development of new algorithms that could be
used by staff taking enquiries from breastfeedingwomen We planned also to provide information thatcould be used on the NHS Direct website which isaccessed directly by women and families as well ashealth professionalsbull Other material to reach the general public wouldbe developed We aimed to have informative paperspublished in womenrsquos and familiesrsquo magazines and inthe general media on a regular basis A professionalwriter was one of our partners her role was to informand advise us about reaching women directly
Discussion
The work described in this paper was a structuredcross-sectoral approach to practice development inpublic health As a result of funding problems a fullevaluation could not be conducted and our contribu-tion to the knowledge base on practice change inpublic health is limited Lessons were learned how-ever and feedback was gained from participants atdifferent stages of the process We received strongsupport for our approach and the willingness of localand national partners to engage actively in the pro-gramme testifies to its potential
Lessons learned
There is increasing emphasis in public health andhealth policy on the need for good partnership work-ing and integration across disciplines professionsorganizations and localities as shown in the recentWhite Paper from the Department of Health (DH2006) and in the Children Act (2004) Prevention ofill health and promotion of well-being featurestrongly in these and other policy documents with arecognition that this cannot be achieved without fullengagement at strategic and operational levels withthose who use or depend on public-sector services Itwas clear at every stage of this process that engage-ment was needed across the whole health economyIt is only in working with all the relevant layers andpartnerships of professionals that we can hope for thefull impact of evidence to be realized Traditionalapproaches however only disseminate evidence tointerest groups in isolation Our use of lsquodiagonal slicersquo
Developing practice in breastfeeding 257
copy 2006 The Authors Journal compilation copy 2006 Blackwell Publishing Ltd Maternal and Child Nutrition 2 pp 245ndash261
workshops in which staff at all levels and across allsectors were engaged and including representativesof service users and the voluntary sector enabledmuch greater understanding of the consequences ofparticular activity or behaviour in other parts of thesystem and allowed creative and informed challengesto assumptions and prejudices This laid good foun-dations for whole systems approaches to introducingdriving and implementing new approaches whichcould lead to positive health outcomes It proved avery positive learning experience for all thoseinvolved
Practice change needs to involve the whole rangeof health professionals involved in work directly withpregnant women and new mothers to ensure coordi-nated working and consistent messages Despiteactive support from relevant Royal Colleges and sev-eral strongly supportive individuals engagement bydoctors was noticeably less compared with otherhealth professions This supports the findings of otherwork (eg Smale et al 2006) This really matters in afield such as breastfeeding where paediatriciansobstetricians general practitioners and public healthphysicians have an important role to play Futurework will need to address this
Key constituents in practice development in breast-feeding include mothers and potential mothersgrandmothers and men We had strong support andinvolvement from service users and user groups butengaging men proved to be difficult To reach thepublic good-quality easily accessible information isneeded perhaps the developing DiPEX module onbreastfeeding will contribute to this (httpwwwdipexorgDesktopDefaultaspx) Recent gov-ernment policy directives acknowledge the potentialcontribution that incorporating patient and serviceuser experience into service provision can bring (egDH 2006) Recent developments in the approach tolong-term conditions management have introducedthe Expert Patient Programme which enables peoplewith disabilities to take much more effective controlover the management and treatment of their disease(DH 2004c 2006) There is perhaps potential for theparallel development of an lsquoExpert Mothers Pro-grammersquo to have similar positive impact in relation tonutrition and health
Service user involvement is actively encouraged ininforming research and practice (Hanley et al 2004)Breastfeeding and maternity care as a whole have along-standing history of the active engagement of ser-vice users Volunteer counsellors and supporterstrained and accredited by their own voluntary orga-nizations have filled the gap left by the health ser-vices They have taken the initiative in setting uptelephone support services training and supervisingpeer supporters and contributing to the education ofhealth professionals (Smale et al 2006) In our cur-rent and previous practice development work thecontribution of service users and voluntary groupswent much further than simply offering advice andinformation They took an active role in planning thework and in some cases delivering education andservices Our experience was that lay workers havean essential role in developing services and they areable to advise at a strategic level as well as participat-ing in service delivery They are able to see throughthe organizational barriers that often constrain pro-fessionals and can see solutions that will work formothers and families From our experience we wouldadvise that others explore ways of actively engaginglay workers adequately remunerated in the deliveryof health care and in the education of healthprofessionals
The fundamental importance of multidisciplinaryand multi-professional working was also apparent inthe way in which the core team worked and in thesupport gained from the network of partners Atevery stage we had expertise and support availableto us as well as an effective communication systemand network Practice change in public health needsto be led and informed by those who know the topicarea and who have the wide range of skills neededto convince many different kinds of professionals thatthe work is worthwhile and achievable
Another positive contribution was the synergy ofthis programme with the evidence base The sameteam had also been responsible for systematicreviews of the field (eg Fairbank et al 2000Protheroe et al 2003 Sikorski et al 2004 Renfrewet al 2005a) and the approach was grounded in thisevidence which was at the same time being devel-oped into national guidance The interaction between
258 MJ Renfrew et al
copy 2006 The Authors Journal compilation copy 2006 Blackwell Publishing Ltd Maternal and Child Nutrition 2 pp 245ndash261
these elements should not be underestimated part-ners and sentinel sites were able to inform the guid-ance and up-to-date knowledge of the evidence basehelped strengthen the practice development work
The sentinel site system was proving to be asuccessful lsquowin-winrsquo situation for all involved Itprovided a test bed for ideas it was a source ofinformation and debate and the programme gaineda richness and diversity of input that would be hardto match At the same time it offered the sitesengagement in leading-edge work an increased pro-file and high-quality staff development Although itwas not formally evaluated all involved were con-vinced that it was a very cost-effective system theprogramme could conduct work at speed and to ahigh quality and governance issues were streamlinedThe system was very flexible and could adapt to thedifferent circumstances of each site It would havebeen able to accommodate future service and educa-tion developments such as Childrenrsquos Centres Trustreorganization and inter-professional educationOver time we could have expanded to include othersectors and practitioners such as retailers and child-minders Had the programme continued future siteswould have been identified and material developedfor national use based on our learning in the originalfour sites
Major challenges
Throughout the programme getting breastfeedingrecognized as a priority was difficult This has beenthe case for many years despite its fundamental con-tribution to public health in the short and long termit has only recently been included in national publichealth policy statements PCT targets and monitoringAs we found in the learning needs assessment andother work breastfeeding services are often seen asthe remit of enthusiastic individuals discussed interms reminiscent of lsquoreligious zealotryrsquo (Smale et al2006) rather than as a part of the mainstream ofhealth provision Creating real change in theapproach to breastfeeding in the health service willrequire it to be seen as a priority for senior managersand commissioners Our experience has demon-strated that it is possible to engage such senior people
in this work and that discussion and debate with theirown colleagues can have an impact on their thinking
A key area of practice development that canimpact on breastfeeding duration is working withmothers to sustain breastfeeding while going back towork and the ways that public health strategy andpractice can influence employers to provide breast-feeding-friendly maternity policies and facilities(Kosmala-Anderson amp Wallace in press) We did nothave an impact on this area but it was clear that itwas an area that needed to be addressed One goodplace to start would be with the employment condi-tions for NHS employees themselves this would havethe dual advantage of improving conditions for thelargest female workforce in the country while alsoproviding a model of good practice for others
Although the aim of this work was to address ine-qualities in health it is clear that reaching the hard-to-reach remains challenging We did see signs of suc-cess for example Sure Start schemes were making adifference in some areas but ensuring that all vulner-able women receive the support and care they needis still a distant goal whether they are teenagers asy-lum seekers or simply women who live in areas wherebottle feeding has been endemic for generations
Finally there is a debate to be had on whoseresponsibility it is to create such change The work ofresearchers is seen to be complete when their studyis finished and disseminated through publication andconference presentation Systematic reviewers takeon a responsibility to make the results of a wide rangeof studies available through publication but not toengage with what services might do with those find-ings Those responsible for guidance are responsiblefor developing and publishing that work and somealso take responsibility for lsquoimplementationrsquo (egNICE 2005) But where does responsibility rest forpractice development which requires a deep engage-ment with the practice setting and with those affectedby the issues raised by the evidence Lack of invest-ment at the national level in formal evaluation ofprogrammes of change limits the available evidencebase and detracts from our achieving a better under-standing of what actually works in relation to thesemore complex health issues funding for the lsquoRrsquoaspects of research and development is more com-
Developing practice in breastfeeding 259
copy 2006 The Authors Journal compilation copy 2006 Blackwell Publishing Ltd Maternal and Child Nutrition 2 pp 245ndash261
mon than for the lsquoDrsquo (NHS Executive 1997) Thewithdrawal of funding to this programme part waythrough its cycle was regretted by our commissionersit was evident that practice development was nolonger their remit given their changed circumstancesIt is however not clear that responsibility now restswith any particular agency Is development work forindividual health service organizations themselves totake on Is this work that should be led by nationalprogrammes supported by public-sector funding orshould it rely on other sources of support If so fromwhere will it be resourced and how will cross-sectoraland multidisciplinary developments be addressedThere are also questions about who will lead thiswork when a number of professional disciplines areinvolved and where the client interface spans bothprimary and acute care healthcare settings social ser-vices and other development agencies These ques-tions will become more pressing as guidancecontinues to be produced especially in public health
Acknowledgements
We would like to thank all participants from sentinelsites and our consortium of academic professionalNHS and consumer partners and the two anonymousreferees who reviewed the manuscript This work wascommissioned by the former Health DevelopmentAgency and subsequently funded by NICE
References
Abbott S Renfrew MJ amp McFadden A (2006) lsquoInformalrsquo learning to support breastfeeding local problems and opportunities Maternal and Child Nutrition 2 232ndash238
Audit Commission (2000) United They Stand Coordinating Care for Elderly Patients with Hip Fracture Audit Com-mission London
British Paediatric Association (1994) Statement of the stand-ing committee on nutrition is breastfeeding beneficial in the UK Archive of Diseases in Childhood 71 376ndash380
Chalmers I amp Altman DG (eds) (1995) Systematic Reviews BMJ Publishing Group London
Children Act (2004) Available at httpwwwopsigovukactsacts200420040031htm (accessed 21 March 2006)
Coote A Allen J amp Woodhead D (2004) Finding out What Works Building Knowledge about Complex Community-Based Initiatives Kingrsquos Fund London
DfES (2000) Adoption and Permanence Taskforce Available at httpwwwdfesgovukadoptionadoptionreformstaskforceshtml (accessed 29 March 2006)
DH (2002a) Improvement Expansion and Reform The Next 3 Years Priorities and Planning Framework 2003ndash2006 Department of Health London
DH (2002b) The Health and Social Care Change Agent Team Available at httpwwwchangeagentteamorguk (accessed 29 March 2006)
DH (2004a) National Service Framework for Children Young People and Maternity Services Stationery Office London
DH (2004b) Choosing Health Making Healthy Choices Eas-ier Stationery Office London
DH (2004c) Self Care ndash A Real Choice Self Care Support ndash A Practical Option Stationery Office London
DH (2006) Our Health Our Care Our Say A New Direction for Community Services Stationery Office London
Dominey M Archibald A Edgecombe D Lawrence J amp Thomson L (2002) Breastfeeding and drug misuse Mak-ing an informed choice Year 3 Practice project In Infant Feeding Initiative A Report Evaluating the Breastfeeding Practice Projects 1999ndash2002 (ed F Dykes 2003) p 64 Department of Health London
Dykes F (2003) Infant Feeding Initiative A Report Evaluat-ing the Breastfeeding Practice Projects 1999ndash2002 Depart-ment of Health London
Dykes F (2006) The education of health practitioners sup-porting breastfeeding women time for critical reflection Maternal and Child Nutrition 2 204ndash216
Dyson L Renfrew MJ McFadden A McCormick F Herbert G amp Thomas J (2006) Promotion of Breastfeed-ing Initiation and Duration Evidence into Practice Brief-ing National Institute for Health and Clinical Excellence London httpwwwniceorgukdown-loadaspxo=346169 (accessed 26 July 2006)
EU (2004) Project on Promotion of Breastfeeding in Europe Protection Promotion and Support of Breastfeeding A Blueprint for Action European Commission Directorate Public Health and Risk Assessment Luxembourg
Fairbank L OrsquoMeara S Renfrew MJ Woolridge M Sowden AJ amp Lister-Sharp D (2000) A systematic review to evaluate the effectiveness of interventions to promote the initiation of breastfeeding Health Technol-ogy Assessment 4 1ndash171
Grant J Fletcher M amp Warwick C (2000) The South Thames Evidence Based Practice (STEP) Project Sup-porting Breastfeeding Women South Bank University London
Greenhalgh T Robert G Bate P Mcfarlane F amp Kyriakidou O (2005) Diffusion of Innovations in Health Service Organisations A Systematic Literature Review Blackwell Publishing Limited Oxford
260 MJ Renfrew et al
copy 2006 The Authors Journal compilation copy 2006 Blackwell Publishing Ltd Maternal and Child Nutrition 2 pp 245ndash261
Grimshaw JM Thomas RE MacLennan G Fraser C Ramsay CR Vale L et al (2004) Effectiveness and efficiency of guideline dissemination and implementation strategies Health Technology Assessment 8 indashxi 1ndash72
Hanley B Bradburn J Barnes M Evans C Goodare H Kelson M et al (2004) Involving the Public in NHS Pub-lic Health and Social Care Research Briefing Notes for Researchers INVOLVE Department of Health London
Herbert G amp Lake G (2005) Making connections Effective development of the intermediate tier Journal of Inte-grated Care 13 35ndash42
Howie PW Forsyth JS Ogston SA Clark A amp Florey CD (1990) Protective effect of breastfeeding against infection British Medical Journal 300 11ndash16
Kosmala-Anderson J amp Wallace LM (in press) Breastfeed-ing works the role of employers in supporting women who wish to breastfeed and work in four organizations in England Journal of Public Health (in press)
Kramer M Chalmers B Hodnett H Sevovskaya Z Dzikovich I Shapiro S et al (2001) Promotion of breast-feeding intervention trial (PROBIT) Journal of the American Medical Association 285 413ndash420
McFadden A Renfrew MJ Dyson L McCormick F Herbert G amp Thomas J (2005) Effective Active Briefing on the Initiation and Duration of Breastfeeding Fieldwork Report National Institute for Health and Clinical Excel-lence London
McFadden A Renfrew MJ Dykes F amp Burt S (2006) Assessing learning needs for breastfeeding setting the scene Maternal and Child Nutrition 2 196ndash203
McSherry R amp McFadden A (2001) Practice Development Accreditation Assessment Maternity Services Darlington Memorial Hospital South Durham Healthcare NHS Trust Final Report University of Teesside Middlesbrough
Moulding NT Silagy CA amp Weller DP (1999) A frame-work for effective management of change in clinical prac-tice dissemination and implementation of clinical practice guidelines Quality in Health Care 8 177ndash183
Gray JA Haynes RB Sackett DL Cook DJ amp Guyatt GH (1997) Transferring evidence from research into practice 3 Developing evidence-based clinical policy Evidence-Based Medicine 2 36ndash38
NHS Centre for Reviews and Dissemination (CRD) (1999) Getting evidence into practice Effective Health Care 5 1ndash16
NHS Executive (1997) RampD in Primary Care National Working Group Report (Mant Report) Stationery Office London
NICE (2004) The Guideline Development Process National Institute for Health and Clinical Excellence London
NICE (2005) Putting NICE Guidance into Practice National Institute for Health and Clinical Excellence London
Oxman AD Thomson MA Davis DA amp Haynes RB (1995) No magic bullets a systematic review of 102 trials of interventions to improve professional practice Canadian Medical Association Journal 153 1423ndash1431
Protheroe L Dyson L Renfrew MJ Bull J amp Mulvihill C (2003) The Effectiveness of Public Health Interventions to Promote the Initiation of Breastfeeding Evidence Briefing Health Development Agency London
Quigley MA Cumberland P Cowden JM amp Rodrigues LC (2006) How protective is breast feeding against diar-rhoeal disease in infants in 1990s England A case control study Archives of Disease in Childhood 91 245ndash250
Renfrew MJ Dyson L Wallace L DrsquoSouza L McCormick FM amp Spiby H (2005a) The Effectiveness of Health Interventions to Promote the Duration of Breast-feeding Systematic Review 1st edn National Institute for Health and Clinical Excellence London
Renfrew MJ Dyson L McFadden A McCormick F Herbert G amp Thomas J (2005b) Effective Active Briefing on the Initiation and Duration of Breastfeeding Technical Report National Institute for Health and Clinical Excel-lence London
Renfrew MJ McFadden A Dykes F Wallace L Abbott S Burt S et al (2006) Addressing the learning deficit in breastfeeding strategies for change Maternal and Child Nutrition 2 239ndash244
Richards D (2003) Childrenrsquos Nutrition ndash Mothers Who Wish to Breast-Feed Birmingham City Council Available at httpwwwbirmingahmgovukscrutiny (accessed 27 July 2006)
Sackett DL Rosenberg WMC Gray JAM Haynes RB amp Richardson WS (1996) Evidence-based medicine what it is and what it isnrsquot British Medical Journal 312 71ndash72
Sikorski J Renfrew MJ Pindoria S amp Wade A (2004) Support for breastfeeding mothers (Cochrane Review) The Cochrane Database of Systematic Reviews Issue 2 John Wiley amp Sons Ltd Chichester
Smale M Renfrew MJ Marshall JL amp Spiby H (2006) Turning policy into practice more difficult that it seems The case of breastfeeding education Maternal and Child Nutrition 2 103ndash113
Spiby H Ker R DrsquoSouza L amp Renfrew MJ (2002) Intro-ducing a Consumer-Practitioner into breastfeeding prac-tice Year 2 In Infant Feeding Initiative A Report Evaluating the Breastfeeding Practice Projects 1999ndash2002 (ed F Dykes 2003) p 44 Department of Health London
Spiby H Wallis S Stone C amp Renfrew MJ (2005) Support-ing and Promoting Breastfeeding in Leeds Final Report to December 2004 Report to Leeds PCTs Children and Families Modernisation Team Leeds
Thomas C (2006) Darlington ndash A Breastfeeding Friendly Town Darlington Borough Council Darlington
Developing practice in breastfeeding 261
copy 2006 The Authors Journal compilation copy 2006 Blackwell Publishing Ltd Maternal and Child Nutrition 2 pp 245ndash261
Unsworth J (2000) Practice development a concept analy-sis Journal of Nursing Management 8 317ndash326
Wallace LM amp Jardine J (2006) A Health Scrutiny of Ser-vices to Support the Initiation and Duration of Breastfeed-ing in Coventry and Warwickshire Coventry and Warwickshire County Councils Coventry
Wallace L amp Kosmala-Anderson J (2006) A training needs survey of doctorsrsquo breastfeeding support skills in England Maternal and Child Nutrition 2 217ndash231
Wallace L amp Kosmala-Anderson J (in press) Training needs survey of midwives health visitors and voluntary sector
breastfeeding support staff in England Maternal and Child Nutrition (in press)
WHO (2003) Global Strategy for Infant and Young Child Feeding World Health Organization Geneva
Wilson AC Forsyth JS Green SA Irvine L Hau C amp Howie PW (1998) Relation of infant diet to childhood health seven year follow up of a cohort of children in Dundee infant feeding study British Medical Journal 316 21ndash25

Developing practice in breastfeeding
249
copy 2006 The Authors Journal compilation copy 2006 Blackwell Publishing Ltd
Maternal and Child Nutrition
2
pp 245ndash261
and lsquoownersrsquo of public spaces as well as the councilsthemselves Inter-sectoral strategic planning led bypublic health where there has also been a sharedinterest in seeking a health economy-wide approachto UNICEF UK BFI status has resulted in moreinter-sectoral practitioner learning networks andshared resources for training staff in breastfeedingsupport (Wallace amp Jardine 2006) The extent towhich this innovative approach is effective and sus-tainable in the longer term is unknown
Breastfeeding development projects
Our approach to practice development drew on thelessons learned from much of the literature summa-rized above Three previous evidence-based prac-tice developments in breastfeeding also directlyinformed our thinking The Breastfeeding in LeedsConsortium was a cross-sectoral partnership thataimed to increase breastfeeding rates by raising theprofile of breastfeeding locally providing educa-tional events and bringing together those withshared interests in supporting breastfeedingwomen As part of that work a Department ofHealth-funded initiative supported a project (Spiby
et al
2002) in which two experienced lay breastfeed-ing counsellors worked to increase evidence-basedsupport to breastfeeding They contributed to edu-cation for undergraduate and registered healthcarepractitioners from a range of disciplines workedwith practitioners providing direct care to womenand provided a range of community developmentactivities The model used in this project was oneof providing evidence-based information forwomen and their families to use rather than atraditional advice-based approach Evaluation ofthis initiative was overwhelmingly positive The layrole was considered compatible rather than conflict-ing with that of healthcare professionals The psy-chosocial perspectives of breastfeeding used by thecounsellors were adopted widely replacing the tra-ditional health lsquobenefits of breastfeeding approachrsquo
Two further developments arose from this suc-cessful preliminary work One project worked tosupport breastfeeding across the health economy inLeeds with a special emphasis on working with
women and families from low-income groups(Spiby
et al
2005) Using the combination of a laycounsellor with a midwife with a specialist breast-feeding background the project delivered multidis-ciplinary and multi-sectoral training using bothhealth and social perspectives It supported the lsquorolloutrsquo of the acute Trustrsquos infant feeding policy andits adoption in the majority of local primary careservices and it demonstrated that collaborativeworking between healthcare professionals andbreastfeeding counsellors can succeed Problemswere also identified some groups of healthcare pro-fessionals are more difficult to engage than otherscross-boundary and inter-sectoral working was stillrelatively new for some health service staff andprotection of professional roles was clearly identi-fied as a problem While support for the initiativehad been identified at a senior level within boththe acute and primary care sectors that support wasnot evident in practice and senior-level projectchampions were not clearly identifiable
A third project included work with local SureStart partnerships in the Leeds and Bradford areasThis delivered staff training helped to establishsupport groups for breastfeeding women initiatedchanges that would reinforce positive messagesabout breastfeeding on Sure Start premises advisedon resources and policies developed support mech-anisms for women in disadvantaged communitiesand developed provided and evaluated a firstcohort of peer support training for women from theSure Start areas The lessons learned from thatwork included the importance of early engagementacross all relevant sectors and disciplines findingout about local needs from local communities theneed to reduce organizational barriers boundariesand tensions and the opportunities that multidisci-plinary education brings This work has now beenincorporated into mainstream practice in the city(Spiby
et al
2005)All three developments were successful in
increasing the number of practitioners women andfamilies receiving evidence-based support withbreastfeeding (Spiby
et al
2005) All includedtrained breastfeeding counsellors as key sources ofsupport and development work and breastfeeding
250
MJ Renfrew
et al
copy 2006 The Authors Journal compilation copy 2006 Blackwell Publishing Ltd
Maternal and Child Nutrition
2
pp 245ndash261
rates in the city including the low-income communi-ties served on discharge from hospital increasedfrom around 45 in early 2002 to 51 in late 2004(St James University Hospital Breastfeeding Statis-tics) All were influential in informing our thinkingaround the conceptual framework and in planningthe structures for the national practice developmentwork described here
Aims and methods
The overall aim of our practice development workwas to address inequalities in health by improvingmaternal and child nutrition The objectives of theprogramme were to (1) inform and enable practicedevelopment in breastfeeding in a number of low-income areas (2) evaluate the impact of approachesused and (3) develop robust approaches and appro-priate material for use across the country in futureyears
Core team
A core team was formed to plan this work The teamincluded the following backgrounds knowledge ofthe evidence base and relevant research methods andcritique in general the development of evidence-based guidance the education of health professionalsat pre- and post-registration levels information tech-nology (IT) and web-based communication skillsknowledge of breastfeeding from public health andclinical perspectives senior NHS managementchange management and practice development in theNHS and related sectors and strategic planning andleadership
National network
At a very early stage a national network was estab-lished with the aim of informing and supporting thework Partners in this network included
bull
academic partners
to ensure that the evidence basewas soundbull
professional bodies
including relevant Royal Col-leges and professional organizations representing thewide range of practitioner groups likely to be
involved to inform the development plans to sup-port dissemination of information to provide con-tacts and communication systems and to enhance thelegitimacy of the workbull
NHS partners
including clinical practitioners withrelevant clinical skills representatives of a StrategicHealth Authority a Public Health Observatory (Pub-lic Health Observatories are funded by the Dep-artment of Health to strengthen the availability anduse of health information at a local level in the UK)NHS Direct (NHS Direct is an online and telephonehealth information enquiry service for the publichttpwwwnhsdirectnhsukindexasp) RDLearning(RDLearning is a web-based national resource ofaccredited health-related education courses httpwwwrdlearningorguk) and primary care researchnetworks to inform practice development plans tooffer communication networks and skills in routinedata collection and analysis and to support the iden-tification of key contacts andbull
representatives of consumer groups voluntary
organizations and non-government organizations
toensure that we were able to benefit from their expe-rience of providing services and gaining user per-spectives to inform the practice development plansand offer communication networks
Links were also made with relevant governmentdepartments and professional advice was taken oncommunication strategies
We developed the system to be flexible and respon-sive with two-way communication systems and fre-quent dialogue with commissioners and partners aswe recognized that the source of funding for this workwas a government agency and that government prior-ities can shift and change over time
Conceptual framework and programme development
A conceptual framework for the project was estab-lished based on the literature and our practice devel-opment experience in breastfeeding (describedabove) and other fields including developing learningnetworks in other areas of practice (eg Herbert ampLake 2005) It was finalized through discussions
Developing practice in breastfeeding
251
copy 2006 The Authors Journal compilation copy 2006 Blackwell Publishing Ltd
Maternal and Child Nutrition
2
pp 245ndash261
among the core team and input from network part-ners This framework then informed all decisions andplans Key elements of the framework included anevidence-based approach multi-sectoral and multi-disciplinary working service userconsumer involve-ment mainstreaming and sustainable systems aparticipatory approach to consultation and communi-cation and embedded evaluation Specific elementsof this approach are shown in Box 1
Based on the conceptual framework a six-stageprocess was developed (Fig 1) Following assessmentof the literature on effective interventions a diagnos-tic analysis of the field was planned to include alearning needs assessment (as reported in this issueof the journal) and a general assessment of the readi-ness of the field to undertake this work (Stage 1) Thiswas followed by a synthesis of those two stages yield-ing an analysis of the problem and potential solutions
Box 1
Elements of conceptual framework
Evidence-based approach
All proposed interventions will be based on a rigorous assessment of the published literature togetherwith practitioner and user views of that evidence base
An eclectic mix of approaches and models will be drawn on based on evidence of lsquowhat worksrsquo indifferent communities
Multi-sectoral and multidisciplinary working including service userconsumer perspectives
Health professionals other relevant professionals from social and education sectors community and layworkers usersconsumers and their families will all have a role in informing and delivering the ongoingprogramme of work
Mainstreaming and sustainable systems
The programme will work to mainstream maternal and child nutrition into all relevant work pro-grammes of other agencies and organizations to avoid a sense of being lsquoinitiative-basedrsquo and to createsustainable change
Existing networks and resources will be used wherever possible to ensure an embedded approach topractice development and to create new systems only when necessary
Solid foundations will be built for long-lasting change and to avoid a lsquodash for growthrsquo
Participatory approach to consultation and communication
All collaborative work will be based on a democratic and participative approach where all constituenciesof interest have an equal voice at all stages regardless of seniority or background
Work will address all levels of the organization ie from senior-level policymakers through regionaland local levels to practitioners in the field and service usersconsumers and their families and willinclude approaches at the level of the individual organization service and community
Embedded evaluation
All approaches used will be evaluated and findings from these evaluations will be synthesized andwidely disseminated to stakeholders including policymakers and professional leaders and other appro-priate audiences
252
MJ Renfrew
et al
copy 2006 The Authors Journal compilation copy 2006 Blackwell Publishing Ltd
Maternal and Child Nutrition
2
pp 245ndash261
Fig
1
Prac
tice
deve
lopm
ent
cycl
e N
HS
Nat
iona
l Hea
lth S
ervi
ce N
GO
non
-gov
ernm
enta
l org
aniz
atio
n
Pre
curs
ors
Sys
tem
atic
re
view
s an
d gu
idan
ce
Oth
er
reli
able
so
urce
s of
ev
iden
ce
bull E
xam
ine
syst
ems
Map
ping
and
di
agno
stic
an
alys
is
bull Id
enti
fica
tion
of
rele
vant
grou
ps
bull L
earn
ing
need
s m
easu
rem
ent
bull A
sses
smen
t of
educ
atio
n pr
ovis
ion
bull D
evel
opm
ent
oppo
rtun
itie
s
Ove
rvie
w a
ndsy
nthe
sis
of
curr
ent
prob
lem
s an
d so
luti
ons
Pla
nnin
g
Net
wor
k de
velo
pmen
t e
gbull
NH
Sbull
Pro
fess
iona
l or
gani
zati
ons
bull N
GO
s bull
Cro
ss-s
ecto
ral
Too
l dev
elop
men
t e
gbull
Dis
tanc
e le
arni
ng
bull T
oolk
its
Cap
acit
y bu
ildi
ng
syst
ems
bull In
divi
dual
bull
Org
aniz
atio
nal
bull S
ervi
ce
bull C
omm
unit
y
Pla
n to
add
ress
ca
paci
ty
buil
ding
and
chan
ge
man
agem
ent a
tdi
ffer
ent l
evel
s an
d in
dif
fere
nt
sect
ors
Cap
acit
y bu
ildi
ng a
ndde
velo
pmen
t
Mea
sure
men
t an
dm
onit
orin
g
Indi
vidu
al le
vel
eg
bull Fa
ce-t
o-fa
ce
educ
atio
n bull
Tw
inni
ng
budd
ying
bull
Dis
tanc
e le
arni
ng
Sys
tem
atic
da
ta c
olle
ctio
n an
d an
alys
is ndash
qual
itat
ive
and
quan
tita
tive
Org
aniz
atio
n an
dse
rvic
e le
vel
eg
bull C
ham
pion
s fo
r ch
ange
bull
Act
ion
lear
ning
se
ts
bull D
emon
stra
tion
pr
ojec
ts
bull Jo
int p
lann
ing
Wor
ksho
pob
serv
atio
n an
d cr
oss-
or
gani
zati
onal
au
dits
Sel
f-ev
alua
tion
an
d be
nchm
arki
ng
netw
orks
Com
mun
ity
leve
l e
gbull
Mul
ti-a
genc
y w
orki
ng
bull C
omm
unit
y re
sour
ces
rese
arch
bull A
ctio
n
Act
ion
rese
arch
and
le
arni
ng s
ets
Pol
icy
impe
rati
ves
Pri
orit
y se
ttin
g an
d
plan
for
di
agno
stic
an
alys
is
Rep
ort o
n m
easu
rem
ent
and
mon
itor
ing
Developing practice in breastfeeding
253
copy 2006 The Authors Journal compilation copy 2006 Blackwell Publishing Ltd
Maternal and Child Nutrition
2
pp 245ndash261
(Stage 2) Stage 3 involved developing relevant net-works tools for education and training evaluationmethods and capacity building systems at individualorganizational service and community levels Follow-ing this a plan to conduct the work would be finalized(Stage 4) implemented (Stage 5) and evaluated Theprocess was intended to be iterative alternatingbetween phases of information appraisal and plan-ning to identify the next stages of development activ-ity and evaluation of the impact to inform futureplanning Stage 6 included finalization of qualitativeand quantitative measurement and monitoring sys-tems that would feedback through all stages of theprocess
It was envisaged that this model would allow effec-tive structures and processes to be identified for usein other aspects of public health practice
Due to changes in funding the programme wasdiscontinued during Stage 3 although in fact somepreliminary work had already been carried out on theplan
Engagement with practitioners
Developing a national programme of change anddevelopment is an ambitious goal A cost-effectiveapproach to engagement had to be developed both tostay within budget and that could roll out acrossEngland and Wales Learning from the successfulLeeds partnership work described above it wasplanned to recruit a series of sentinel sites where wecould test out a range of approaches to maximizelearning and cost-effectiveness as well as respond toideas from the field Work in those sites wouldbecome a model for national developments inform-ing material for education training and assessmentsupported by communications at different levelsthrough our established national network The use ofsentinel sites also allowed for the development ofapproaches sensitive to varying local contexts so pro-viding alternatives and examples to inform nationalimplementation
The first stage in that process was to recruit rele-vant sentinel sites Sites were conceived as includingthe whole health economy in a locality and had tomeet specific criteria These are detailed in Box 2
Four sites were identified and agreed to join thefirst wave of sentinel sites Each site engaged andplanned the programme of work differently Forexample one site had already worked with membersof the core team and were keen to take existing workfurther In the few months in which we worked withthem they put into place a system for the accuratemonitoring of breastfeeding rates and created anextensive network of individuals at a range of seniorlevels from different sectors including Primary CareTrusts (PCTs) Strategic Health Authority the acuteTrust Sure Start and the local authority Benefits thesites have seen even since the work stopped haveincluded
bull improved communication across relevant disci-plines and sectorsbull the observation that the practice developmentwork lsquokept breastfeeding on everyonersquos agendarsquobull the work was used to support a business case for acoordinator for BFI planningbull in one sentinel site the primary care and acutematernity services have formed a health economy-wide breastfeeding strategy groupbull in another a joint primary care and maternity ser-vices group has been establishedbull two sites are taking forward systems for collect-ing breastfeeding data which have been used toprovide feedback to staff each monthbull a new approach to training all staff in one siteincluded commissioning the local university todevelop a self-study workbook and then to test itseffectiveness using an objective skills assessment toolandbull in one site a successful peer support programmewas rolled out throughout Sure Start programmes
A key part of the work in the sentinel sites was tosupport the learning needs assessment (McFadden
et al
2006) Although the sites were at an early stageof engagement this was conducted very successfullyand rapidly as sites supported the identification andinvolvement of practitioners Many assisted with sur-vey distribution and in return received a report ofthe training needs identified for their staff The nexttest was the running of fieldwork meetings and
254
MJ Renfrew
et al
copy 2006 The Authors Journal compilation copy 2006 Blackwell Publishing Ltd
Maternal and Child Nutrition
2
pp 245ndash261
workshops to finalize guidance based on researchevidence as part of a related programme of workThe aim of this work was to take the results of aseries of systematic reviews (which gave informationon lsquowhat works from research evidencersquo) and consultwith practitioners managers and users on lsquowhatreally works in practicersquo (Dyson
et al
2006) Thenewly established sentinel site system supported thiswork by offering venues for meetings providing listsof eligible participants and enabling and encourag-ing staff to attend (Renfrew
et al
2005b) The finalstage of this guidance work was a series of majorworkshops with over 30 participants in each repre-senting a lsquodiagonal slicersquo through the whole healtheconomy from field-level practitioners includingpeer support workers to managers and planners andincluding the range of relevant disciplines as well as
the voluntary sector Concerns around the realitiesand influences on practice and key issues for practi-tioners and managers in developing good practicewere discussed as well as organizational and struc-tural barriers to change Participants were encour-aged to discuss not only practices that need to beintroduced but also those that need to be aban-doned thereby potentially saving time and resourcesand to identify actual or potential barriers to imple-menting change (Renfrew
et al
2005b) These facili-tated groups examined the ability of the service torespond to identified gaps and made recommenda-tions for improvements to the system They feddirectly into the final stages of the development ofNational Institute for Health and Clinical Excellence(NICE) public health recommendations for breast-feeding offering participants the satisfaction of
Box 2
Sentinel site criteriaSentinel sites were expected to
bull Have a deprivation profile that demonstrated a substantial proportion of low-income groups and adiverse ethnic profile and serve contrasting areas (eg urban rural)
bull Offer a range of services for children and women with an interest in nutrition
bull Be able to include the whole health economy in a locality (or at least agree to working across allrelevant sectors)
bull Provide a key contact personpeople who would act to facilitate communication and broker agree-ments with different parts of the health economy and managers who were supportive of the plannedwork willing to support and enable staff participation
bull In the first instance sites would be those where contact already existed with members of our coreteam Future sites would be brought in once any initial problems with the approach had been identifiedand addressed
In return for their involvement in the work it was recognized that the sentinel sites would benefit in arange of ways including
bull Support for staff development and learning through access to programme staff and expertise involve-ment in and learning from a regular newsletter and attendance at an annual leading-edge conferenceon maternal and child nutrition
bull Developing links with other sites and sharing good practice and problem solving
bull The opportunity to help to develop national practice resulting in a raised profile for their work andtheir staff
bull Early access to emerging evidence in the field of maternal and child nutrition
Developing practice in breastfeeding
255
copy 2006 The Authors Journal compilation copy 2006 Blackwell Publishing Ltd
Maternal and Child Nutrition
2
pp 245ndash261
knowing that their input would make a difference(Dyson
et al
2006) These workshops also tested outthe use of language the conceptual understanding ofparticipants in relation to the evidence reviews andgathered intelligence on what approaches to imple-mentation of practice development may be mosteffective They also provided an opportunity for dis-cussion debate and deliberation about the meaningof the evidence Participants reported this to be veryuseful in assisting their understanding of the evi-dence and in considering how best to change theirown and their colleaguesrsquo practice in response to itand as an important contribution to practice devel-opment in their own locality (McFadden
et al
2005)The input of representatives of service users was ofcritical importance
It was planned that once the guidance was final-ized each participating site would be in a strong posi-tion to act on it Not only would they feel someownership but they would also have staff from alllevels and sectors in their health economy who hadspent time discussing the issues with colleagues andwith service user representatives They would haveaccess to specific local information about localitiesand groups that needed to be prioritized creatingchange was therefore brought several stages closerAt the end of each workshop email and telephonecontact details were exchanged among the workshopparticipants many of whom had never met beforedespite working in related parts of the same systemto support closer local networking The opportunityto consult with national experts in the network alsoacted as a variant on educational outreach which hasbeen shown to be moderately successful in guidelineimplementation (NHS CRD 1999) The impact ofsuch exchanges in increasing opportunities for net-work support is virtually impossible to evaluate for-mally but there was confidence in those whoparticipated at these events that positive changewould result and that the evidence would be moreeffectively used in the future as a consequence
Interactive conference
The other main activity was a conference on maternaland child nutrition to which all partners ndash academic
professional NHS and userconsumer ndash and stafffrom sentinel sites were invited Commissioners ofthe work were invited as were staff from key govern-ment departments with an interest in nutrition childhealth Sure Start nursing and midwifery and ine-qualities in health Around 90 participants took partin a day which included presentations participativeworking and active networking A report of the dayis available at httpwwwyorkacukresmcncccon-ferenceReporthtm Feedback was strongly positiveand the impact of networking with others in similarsituations and between those working in local andnational organizations was especially valued It wasplanned that this would be an annual event
Had we been able to continue the practice devel-opment programme we planned to use the follow-ing approaches
Establishing learning networks
We planned to identify appropriate learning net-works for different constituencies which wouldenable communication among staff from differentsectors as well as communication with programmestaff Activities were planned to include
bull Staff working at strategic and senior managementlevels would be supported and appropriate informa-tion provided to allow them to create cross-systemchanges Senior-level lsquochampions for changersquo wouldbe identified These would be used in a range of waysthose wishing to be involved in learning networkswould be supported to do sobull Learning sets would be established This wouldenable focused exchange between stakeholders onhow best to make use of the evidence in practice andhow to influence mainstream practice across locali-ties Through feedback loops we planned to developlearningeducation material to be made availablethrough web-based routes to wider constituenciesbull Peer supporters and trained breastfeeding counsel-lors are key groups in regard to breastfeeding promo-tion and support We planned to include them inlearning sets They have much to offer health profes-sionals in coming to understand the needs of womenand families and indeed the evidence suggests thattheir involvement in advisory work and peer support
256
MJ Renfrew
et al
copy 2006 The Authors Journal compilation copy 2006 Blackwell Publishing Ltd
Maternal and Child Nutrition
2
pp 245ndash261
enhances and strengthens the impact of informationand evidence-based guidance possibly more thanthat of health professionalsrsquo practice Our experiencedescribed above has identified a valuable contribu-tion from lay breastfeeding counsellors into educa-tion and training provision
Educational approaches
The breadth of constituencies that the programmeneeded to reach was to be reflected in the range ofeducational approaches required For some profes-sions continuing professional development (CPD)time is factored in regularly to the job plan in a rollingprogramme of group education with routine sessionalwork suspended for other groups CPD is a self-verified individual activity that can be achievedthrough a range of methods including distance learn-ing We hoped to reach directly a broad group ofwomen as well as professionals through some of theroutes developed A range of materials was thereforeplanned to address all needs Materials would bedeveloped for web-based access CD-ROM access andon paper These were to include
bull Toolkits to promote and support breastfeeding tomonitor breastfeeding rates and on practice develop-ment and changebull Distance learning modules providing accreditedlearning opportunities at a range of levelsbull An email and telephone-based service to putindividuals and organizations in touch with otherswho can support and advise them supported byRDLearning a national web-based resourcebull Learning material that could be directly dissemi-nated through the Internet to a wide audiencebull Buddy systems and mentoring for practice devel-opment and public health strategic development inbreastfeeding and use of cascade systemsbull Summaries of approaches to dissemination andpromotion of information that have proved to be suc-cessful and of practice change programmes that havebeen evaluated as having a positive impact on initia-tion and duration of breastfeedingbull Through NHS Direct we planned to reach the gen-eral public Information could be provided to informthe development of new algorithms that could be
used by staff taking enquiries from breastfeedingwomen We planned also to provide information thatcould be used on the NHS Direct website which isaccessed directly by women and families as well ashealth professionalsbull Other material to reach the general public wouldbe developed We aimed to have informative paperspublished in womenrsquos and familiesrsquo magazines and inthe general media on a regular basis A professionalwriter was one of our partners her role was to informand advise us about reaching women directly
Discussion
The work described in this paper was a structuredcross-sectoral approach to practice development inpublic health As a result of funding problems a fullevaluation could not be conducted and our contribu-tion to the knowledge base on practice change inpublic health is limited Lessons were learned how-ever and feedback was gained from participants atdifferent stages of the process We received strongsupport for our approach and the willingness of localand national partners to engage actively in the pro-gramme testifies to its potential
Lessons learned
There is increasing emphasis in public health andhealth policy on the need for good partnership work-ing and integration across disciplines professionsorganizations and localities as shown in the recentWhite Paper from the Department of Health (DH2006) and in the Children Act (2004) Prevention ofill health and promotion of well-being featurestrongly in these and other policy documents with arecognition that this cannot be achieved without fullengagement at strategic and operational levels withthose who use or depend on public-sector services Itwas clear at every stage of this process that engage-ment was needed across the whole health economyIt is only in working with all the relevant layers andpartnerships of professionals that we can hope for thefull impact of evidence to be realized Traditionalapproaches however only disseminate evidence tointerest groups in isolation Our use of lsquodiagonal slicersquo
Developing practice in breastfeeding 257
copy 2006 The Authors Journal compilation copy 2006 Blackwell Publishing Ltd Maternal and Child Nutrition 2 pp 245ndash261
workshops in which staff at all levels and across allsectors were engaged and including representativesof service users and the voluntary sector enabledmuch greater understanding of the consequences ofparticular activity or behaviour in other parts of thesystem and allowed creative and informed challengesto assumptions and prejudices This laid good foun-dations for whole systems approaches to introducingdriving and implementing new approaches whichcould lead to positive health outcomes It proved avery positive learning experience for all thoseinvolved
Practice change needs to involve the whole rangeof health professionals involved in work directly withpregnant women and new mothers to ensure coordi-nated working and consistent messages Despiteactive support from relevant Royal Colleges and sev-eral strongly supportive individuals engagement bydoctors was noticeably less compared with otherhealth professions This supports the findings of otherwork (eg Smale et al 2006) This really matters in afield such as breastfeeding where paediatriciansobstetricians general practitioners and public healthphysicians have an important role to play Futurework will need to address this
Key constituents in practice development in breast-feeding include mothers and potential mothersgrandmothers and men We had strong support andinvolvement from service users and user groups butengaging men proved to be difficult To reach thepublic good-quality easily accessible information isneeded perhaps the developing DiPEX module onbreastfeeding will contribute to this (httpwwwdipexorgDesktopDefaultaspx) Recent gov-ernment policy directives acknowledge the potentialcontribution that incorporating patient and serviceuser experience into service provision can bring (egDH 2006) Recent developments in the approach tolong-term conditions management have introducedthe Expert Patient Programme which enables peoplewith disabilities to take much more effective controlover the management and treatment of their disease(DH 2004c 2006) There is perhaps potential for theparallel development of an lsquoExpert Mothers Pro-grammersquo to have similar positive impact in relation tonutrition and health
Service user involvement is actively encouraged ininforming research and practice (Hanley et al 2004)Breastfeeding and maternity care as a whole have along-standing history of the active engagement of ser-vice users Volunteer counsellors and supporterstrained and accredited by their own voluntary orga-nizations have filled the gap left by the health ser-vices They have taken the initiative in setting uptelephone support services training and supervisingpeer supporters and contributing to the education ofhealth professionals (Smale et al 2006) In our cur-rent and previous practice development work thecontribution of service users and voluntary groupswent much further than simply offering advice andinformation They took an active role in planning thework and in some cases delivering education andservices Our experience was that lay workers havean essential role in developing services and they areable to advise at a strategic level as well as participat-ing in service delivery They are able to see throughthe organizational barriers that often constrain pro-fessionals and can see solutions that will work formothers and families From our experience we wouldadvise that others explore ways of actively engaginglay workers adequately remunerated in the deliveryof health care and in the education of healthprofessionals
The fundamental importance of multidisciplinaryand multi-professional working was also apparent inthe way in which the core team worked and in thesupport gained from the network of partners Atevery stage we had expertise and support availableto us as well as an effective communication systemand network Practice change in public health needsto be led and informed by those who know the topicarea and who have the wide range of skills neededto convince many different kinds of professionals thatthe work is worthwhile and achievable
Another positive contribution was the synergy ofthis programme with the evidence base The sameteam had also been responsible for systematicreviews of the field (eg Fairbank et al 2000Protheroe et al 2003 Sikorski et al 2004 Renfrewet al 2005a) and the approach was grounded in thisevidence which was at the same time being devel-oped into national guidance The interaction between
258 MJ Renfrew et al
copy 2006 The Authors Journal compilation copy 2006 Blackwell Publishing Ltd Maternal and Child Nutrition 2 pp 245ndash261
these elements should not be underestimated part-ners and sentinel sites were able to inform the guid-ance and up-to-date knowledge of the evidence basehelped strengthen the practice development work
The sentinel site system was proving to be asuccessful lsquowin-winrsquo situation for all involved Itprovided a test bed for ideas it was a source ofinformation and debate and the programme gaineda richness and diversity of input that would be hardto match At the same time it offered the sitesengagement in leading-edge work an increased pro-file and high-quality staff development Although itwas not formally evaluated all involved were con-vinced that it was a very cost-effective system theprogramme could conduct work at speed and to ahigh quality and governance issues were streamlinedThe system was very flexible and could adapt to thedifferent circumstances of each site It would havebeen able to accommodate future service and educa-tion developments such as Childrenrsquos Centres Trustreorganization and inter-professional educationOver time we could have expanded to include othersectors and practitioners such as retailers and child-minders Had the programme continued future siteswould have been identified and material developedfor national use based on our learning in the originalfour sites
Major challenges
Throughout the programme getting breastfeedingrecognized as a priority was difficult This has beenthe case for many years despite its fundamental con-tribution to public health in the short and long termit has only recently been included in national publichealth policy statements PCT targets and monitoringAs we found in the learning needs assessment andother work breastfeeding services are often seen asthe remit of enthusiastic individuals discussed interms reminiscent of lsquoreligious zealotryrsquo (Smale et al2006) rather than as a part of the mainstream ofhealth provision Creating real change in theapproach to breastfeeding in the health service willrequire it to be seen as a priority for senior managersand commissioners Our experience has demon-strated that it is possible to engage such senior people
in this work and that discussion and debate with theirown colleagues can have an impact on their thinking
A key area of practice development that canimpact on breastfeeding duration is working withmothers to sustain breastfeeding while going back towork and the ways that public health strategy andpractice can influence employers to provide breast-feeding-friendly maternity policies and facilities(Kosmala-Anderson amp Wallace in press) We did nothave an impact on this area but it was clear that itwas an area that needed to be addressed One goodplace to start would be with the employment condi-tions for NHS employees themselves this would havethe dual advantage of improving conditions for thelargest female workforce in the country while alsoproviding a model of good practice for others
Although the aim of this work was to address ine-qualities in health it is clear that reaching the hard-to-reach remains challenging We did see signs of suc-cess for example Sure Start schemes were making adifference in some areas but ensuring that all vulner-able women receive the support and care they needis still a distant goal whether they are teenagers asy-lum seekers or simply women who live in areas wherebottle feeding has been endemic for generations
Finally there is a debate to be had on whoseresponsibility it is to create such change The work ofresearchers is seen to be complete when their studyis finished and disseminated through publication andconference presentation Systematic reviewers takeon a responsibility to make the results of a wide rangeof studies available through publication but not toengage with what services might do with those find-ings Those responsible for guidance are responsiblefor developing and publishing that work and somealso take responsibility for lsquoimplementationrsquo (egNICE 2005) But where does responsibility rest forpractice development which requires a deep engage-ment with the practice setting and with those affectedby the issues raised by the evidence Lack of invest-ment at the national level in formal evaluation ofprogrammes of change limits the available evidencebase and detracts from our achieving a better under-standing of what actually works in relation to thesemore complex health issues funding for the lsquoRrsquoaspects of research and development is more com-
Developing practice in breastfeeding 259
copy 2006 The Authors Journal compilation copy 2006 Blackwell Publishing Ltd Maternal and Child Nutrition 2 pp 245ndash261
mon than for the lsquoDrsquo (NHS Executive 1997) Thewithdrawal of funding to this programme part waythrough its cycle was regretted by our commissionersit was evident that practice development was nolonger their remit given their changed circumstancesIt is however not clear that responsibility now restswith any particular agency Is development work forindividual health service organizations themselves totake on Is this work that should be led by nationalprogrammes supported by public-sector funding orshould it rely on other sources of support If so fromwhere will it be resourced and how will cross-sectoraland multidisciplinary developments be addressedThere are also questions about who will lead thiswork when a number of professional disciplines areinvolved and where the client interface spans bothprimary and acute care healthcare settings social ser-vices and other development agencies These ques-tions will become more pressing as guidancecontinues to be produced especially in public health
Acknowledgements
We would like to thank all participants from sentinelsites and our consortium of academic professionalNHS and consumer partners and the two anonymousreferees who reviewed the manuscript This work wascommissioned by the former Health DevelopmentAgency and subsequently funded by NICE
References
Abbott S Renfrew MJ amp McFadden A (2006) lsquoInformalrsquo learning to support breastfeeding local problems and opportunities Maternal and Child Nutrition 2 232ndash238
Audit Commission (2000) United They Stand Coordinating Care for Elderly Patients with Hip Fracture Audit Com-mission London
British Paediatric Association (1994) Statement of the stand-ing committee on nutrition is breastfeeding beneficial in the UK Archive of Diseases in Childhood 71 376ndash380
Chalmers I amp Altman DG (eds) (1995) Systematic Reviews BMJ Publishing Group London
Children Act (2004) Available at httpwwwopsigovukactsacts200420040031htm (accessed 21 March 2006)
Coote A Allen J amp Woodhead D (2004) Finding out What Works Building Knowledge about Complex Community-Based Initiatives Kingrsquos Fund London
DfES (2000) Adoption and Permanence Taskforce Available at httpwwwdfesgovukadoptionadoptionreformstaskforceshtml (accessed 29 March 2006)
DH (2002a) Improvement Expansion and Reform The Next 3 Years Priorities and Planning Framework 2003ndash2006 Department of Health London
DH (2002b) The Health and Social Care Change Agent Team Available at httpwwwchangeagentteamorguk (accessed 29 March 2006)
DH (2004a) National Service Framework for Children Young People and Maternity Services Stationery Office London
DH (2004b) Choosing Health Making Healthy Choices Eas-ier Stationery Office London
DH (2004c) Self Care ndash A Real Choice Self Care Support ndash A Practical Option Stationery Office London
DH (2006) Our Health Our Care Our Say A New Direction for Community Services Stationery Office London
Dominey M Archibald A Edgecombe D Lawrence J amp Thomson L (2002) Breastfeeding and drug misuse Mak-ing an informed choice Year 3 Practice project In Infant Feeding Initiative A Report Evaluating the Breastfeeding Practice Projects 1999ndash2002 (ed F Dykes 2003) p 64 Department of Health London
Dykes F (2003) Infant Feeding Initiative A Report Evaluat-ing the Breastfeeding Practice Projects 1999ndash2002 Depart-ment of Health London
Dykes F (2006) The education of health practitioners sup-porting breastfeeding women time for critical reflection Maternal and Child Nutrition 2 204ndash216
Dyson L Renfrew MJ McFadden A McCormick F Herbert G amp Thomas J (2006) Promotion of Breastfeed-ing Initiation and Duration Evidence into Practice Brief-ing National Institute for Health and Clinical Excellence London httpwwwniceorgukdown-loadaspxo=346169 (accessed 26 July 2006)
EU (2004) Project on Promotion of Breastfeeding in Europe Protection Promotion and Support of Breastfeeding A Blueprint for Action European Commission Directorate Public Health and Risk Assessment Luxembourg
Fairbank L OrsquoMeara S Renfrew MJ Woolridge M Sowden AJ amp Lister-Sharp D (2000) A systematic review to evaluate the effectiveness of interventions to promote the initiation of breastfeeding Health Technol-ogy Assessment 4 1ndash171
Grant J Fletcher M amp Warwick C (2000) The South Thames Evidence Based Practice (STEP) Project Sup-porting Breastfeeding Women South Bank University London
Greenhalgh T Robert G Bate P Mcfarlane F amp Kyriakidou O (2005) Diffusion of Innovations in Health Service Organisations A Systematic Literature Review Blackwell Publishing Limited Oxford
260 MJ Renfrew et al
copy 2006 The Authors Journal compilation copy 2006 Blackwell Publishing Ltd Maternal and Child Nutrition 2 pp 245ndash261
Grimshaw JM Thomas RE MacLennan G Fraser C Ramsay CR Vale L et al (2004) Effectiveness and efficiency of guideline dissemination and implementation strategies Health Technology Assessment 8 indashxi 1ndash72
Hanley B Bradburn J Barnes M Evans C Goodare H Kelson M et al (2004) Involving the Public in NHS Pub-lic Health and Social Care Research Briefing Notes for Researchers INVOLVE Department of Health London
Herbert G amp Lake G (2005) Making connections Effective development of the intermediate tier Journal of Inte-grated Care 13 35ndash42
Howie PW Forsyth JS Ogston SA Clark A amp Florey CD (1990) Protective effect of breastfeeding against infection British Medical Journal 300 11ndash16
Kosmala-Anderson J amp Wallace LM (in press) Breastfeed-ing works the role of employers in supporting women who wish to breastfeed and work in four organizations in England Journal of Public Health (in press)
Kramer M Chalmers B Hodnett H Sevovskaya Z Dzikovich I Shapiro S et al (2001) Promotion of breast-feeding intervention trial (PROBIT) Journal of the American Medical Association 285 413ndash420
McFadden A Renfrew MJ Dyson L McCormick F Herbert G amp Thomas J (2005) Effective Active Briefing on the Initiation and Duration of Breastfeeding Fieldwork Report National Institute for Health and Clinical Excel-lence London
McFadden A Renfrew MJ Dykes F amp Burt S (2006) Assessing learning needs for breastfeeding setting the scene Maternal and Child Nutrition 2 196ndash203
McSherry R amp McFadden A (2001) Practice Development Accreditation Assessment Maternity Services Darlington Memorial Hospital South Durham Healthcare NHS Trust Final Report University of Teesside Middlesbrough
Moulding NT Silagy CA amp Weller DP (1999) A frame-work for effective management of change in clinical prac-tice dissemination and implementation of clinical practice guidelines Quality in Health Care 8 177ndash183
Gray JA Haynes RB Sackett DL Cook DJ amp Guyatt GH (1997) Transferring evidence from research into practice 3 Developing evidence-based clinical policy Evidence-Based Medicine 2 36ndash38
NHS Centre for Reviews and Dissemination (CRD) (1999) Getting evidence into practice Effective Health Care 5 1ndash16
NHS Executive (1997) RampD in Primary Care National Working Group Report (Mant Report) Stationery Office London
NICE (2004) The Guideline Development Process National Institute for Health and Clinical Excellence London
NICE (2005) Putting NICE Guidance into Practice National Institute for Health and Clinical Excellence London
Oxman AD Thomson MA Davis DA amp Haynes RB (1995) No magic bullets a systematic review of 102 trials of interventions to improve professional practice Canadian Medical Association Journal 153 1423ndash1431
Protheroe L Dyson L Renfrew MJ Bull J amp Mulvihill C (2003) The Effectiveness of Public Health Interventions to Promote the Initiation of Breastfeeding Evidence Briefing Health Development Agency London
Quigley MA Cumberland P Cowden JM amp Rodrigues LC (2006) How protective is breast feeding against diar-rhoeal disease in infants in 1990s England A case control study Archives of Disease in Childhood 91 245ndash250
Renfrew MJ Dyson L Wallace L DrsquoSouza L McCormick FM amp Spiby H (2005a) The Effectiveness of Health Interventions to Promote the Duration of Breast-feeding Systematic Review 1st edn National Institute for Health and Clinical Excellence London
Renfrew MJ Dyson L McFadden A McCormick F Herbert G amp Thomas J (2005b) Effective Active Briefing on the Initiation and Duration of Breastfeeding Technical Report National Institute for Health and Clinical Excel-lence London
Renfrew MJ McFadden A Dykes F Wallace L Abbott S Burt S et al (2006) Addressing the learning deficit in breastfeeding strategies for change Maternal and Child Nutrition 2 239ndash244
Richards D (2003) Childrenrsquos Nutrition ndash Mothers Who Wish to Breast-Feed Birmingham City Council Available at httpwwwbirmingahmgovukscrutiny (accessed 27 July 2006)
Sackett DL Rosenberg WMC Gray JAM Haynes RB amp Richardson WS (1996) Evidence-based medicine what it is and what it isnrsquot British Medical Journal 312 71ndash72
Sikorski J Renfrew MJ Pindoria S amp Wade A (2004) Support for breastfeeding mothers (Cochrane Review) The Cochrane Database of Systematic Reviews Issue 2 John Wiley amp Sons Ltd Chichester
Smale M Renfrew MJ Marshall JL amp Spiby H (2006) Turning policy into practice more difficult that it seems The case of breastfeeding education Maternal and Child Nutrition 2 103ndash113
Spiby H Ker R DrsquoSouza L amp Renfrew MJ (2002) Intro-ducing a Consumer-Practitioner into breastfeeding prac-tice Year 2 In Infant Feeding Initiative A Report Evaluating the Breastfeeding Practice Projects 1999ndash2002 (ed F Dykes 2003) p 44 Department of Health London
Spiby H Wallis S Stone C amp Renfrew MJ (2005) Support-ing and Promoting Breastfeeding in Leeds Final Report to December 2004 Report to Leeds PCTs Children and Families Modernisation Team Leeds
Thomas C (2006) Darlington ndash A Breastfeeding Friendly Town Darlington Borough Council Darlington
Developing practice in breastfeeding 261
copy 2006 The Authors Journal compilation copy 2006 Blackwell Publishing Ltd Maternal and Child Nutrition 2 pp 245ndash261
Unsworth J (2000) Practice development a concept analy-sis Journal of Nursing Management 8 317ndash326
Wallace LM amp Jardine J (2006) A Health Scrutiny of Ser-vices to Support the Initiation and Duration of Breastfeed-ing in Coventry and Warwickshire Coventry and Warwickshire County Councils Coventry
Wallace L amp Kosmala-Anderson J (2006) A training needs survey of doctorsrsquo breastfeeding support skills in England Maternal and Child Nutrition 2 217ndash231
Wallace L amp Kosmala-Anderson J (in press) Training needs survey of midwives health visitors and voluntary sector
breastfeeding support staff in England Maternal and Child Nutrition (in press)
WHO (2003) Global Strategy for Infant and Young Child Feeding World Health Organization Geneva
Wilson AC Forsyth JS Green SA Irvine L Hau C amp Howie PW (1998) Relation of infant diet to childhood health seven year follow up of a cohort of children in Dundee infant feeding study British Medical Journal 316 21ndash25

250
MJ Renfrew
et al
copy 2006 The Authors Journal compilation copy 2006 Blackwell Publishing Ltd
Maternal and Child Nutrition
2
pp 245ndash261
rates in the city including the low-income communi-ties served on discharge from hospital increasedfrom around 45 in early 2002 to 51 in late 2004(St James University Hospital Breastfeeding Statis-tics) All were influential in informing our thinkingaround the conceptual framework and in planningthe structures for the national practice developmentwork described here
Aims and methods
The overall aim of our practice development workwas to address inequalities in health by improvingmaternal and child nutrition The objectives of theprogramme were to (1) inform and enable practicedevelopment in breastfeeding in a number of low-income areas (2) evaluate the impact of approachesused and (3) develop robust approaches and appro-priate material for use across the country in futureyears
Core team
A core team was formed to plan this work The teamincluded the following backgrounds knowledge ofthe evidence base and relevant research methods andcritique in general the development of evidence-based guidance the education of health professionalsat pre- and post-registration levels information tech-nology (IT) and web-based communication skillsknowledge of breastfeeding from public health andclinical perspectives senior NHS managementchange management and practice development in theNHS and related sectors and strategic planning andleadership
National network
At a very early stage a national network was estab-lished with the aim of informing and supporting thework Partners in this network included
bull
academic partners
to ensure that the evidence basewas soundbull
professional bodies
including relevant Royal Col-leges and professional organizations representing thewide range of practitioner groups likely to be
involved to inform the development plans to sup-port dissemination of information to provide con-tacts and communication systems and to enhance thelegitimacy of the workbull
NHS partners
including clinical practitioners withrelevant clinical skills representatives of a StrategicHealth Authority a Public Health Observatory (Pub-lic Health Observatories are funded by the Dep-artment of Health to strengthen the availability anduse of health information at a local level in the UK)NHS Direct (NHS Direct is an online and telephonehealth information enquiry service for the publichttpwwwnhsdirectnhsukindexasp) RDLearning(RDLearning is a web-based national resource ofaccredited health-related education courses httpwwwrdlearningorguk) and primary care researchnetworks to inform practice development plans tooffer communication networks and skills in routinedata collection and analysis and to support the iden-tification of key contacts andbull
representatives of consumer groups voluntary
organizations and non-government organizations
toensure that we were able to benefit from their expe-rience of providing services and gaining user per-spectives to inform the practice development plansand offer communication networks
Links were also made with relevant governmentdepartments and professional advice was taken oncommunication strategies
We developed the system to be flexible and respon-sive with two-way communication systems and fre-quent dialogue with commissioners and partners aswe recognized that the source of funding for this workwas a government agency and that government prior-ities can shift and change over time
Conceptual framework and programme development
A conceptual framework for the project was estab-lished based on the literature and our practice devel-opment experience in breastfeeding (describedabove) and other fields including developing learningnetworks in other areas of practice (eg Herbert ampLake 2005) It was finalized through discussions
Developing practice in breastfeeding
251
copy 2006 The Authors Journal compilation copy 2006 Blackwell Publishing Ltd
Maternal and Child Nutrition
2
pp 245ndash261
among the core team and input from network part-ners This framework then informed all decisions andplans Key elements of the framework included anevidence-based approach multi-sectoral and multi-disciplinary working service userconsumer involve-ment mainstreaming and sustainable systems aparticipatory approach to consultation and communi-cation and embedded evaluation Specific elementsof this approach are shown in Box 1
Based on the conceptual framework a six-stageprocess was developed (Fig 1) Following assessmentof the literature on effective interventions a diagnos-tic analysis of the field was planned to include alearning needs assessment (as reported in this issueof the journal) and a general assessment of the readi-ness of the field to undertake this work (Stage 1) Thiswas followed by a synthesis of those two stages yield-ing an analysis of the problem and potential solutions
Box 1
Elements of conceptual framework
Evidence-based approach
All proposed interventions will be based on a rigorous assessment of the published literature togetherwith practitioner and user views of that evidence base
An eclectic mix of approaches and models will be drawn on based on evidence of lsquowhat worksrsquo indifferent communities
Multi-sectoral and multidisciplinary working including service userconsumer perspectives
Health professionals other relevant professionals from social and education sectors community and layworkers usersconsumers and their families will all have a role in informing and delivering the ongoingprogramme of work
Mainstreaming and sustainable systems
The programme will work to mainstream maternal and child nutrition into all relevant work pro-grammes of other agencies and organizations to avoid a sense of being lsquoinitiative-basedrsquo and to createsustainable change
Existing networks and resources will be used wherever possible to ensure an embedded approach topractice development and to create new systems only when necessary
Solid foundations will be built for long-lasting change and to avoid a lsquodash for growthrsquo
Participatory approach to consultation and communication
All collaborative work will be based on a democratic and participative approach where all constituenciesof interest have an equal voice at all stages regardless of seniority or background
Work will address all levels of the organization ie from senior-level policymakers through regionaland local levels to practitioners in the field and service usersconsumers and their families and willinclude approaches at the level of the individual organization service and community
Embedded evaluation
All approaches used will be evaluated and findings from these evaluations will be synthesized andwidely disseminated to stakeholders including policymakers and professional leaders and other appro-priate audiences
252
MJ Renfrew
et al
copy 2006 The Authors Journal compilation copy 2006 Blackwell Publishing Ltd
Maternal and Child Nutrition
2
pp 245ndash261
Fig
1
Prac
tice
deve
lopm
ent
cycl
e N
HS
Nat
iona
l Hea
lth S
ervi
ce N
GO
non
-gov
ernm
enta
l org
aniz
atio
n
Pre
curs
ors
Sys
tem
atic
re
view
s an
d gu
idan
ce
Oth
er
reli
able
so
urce
s of
ev
iden
ce
bull E
xam
ine
syst
ems
Map
ping
and
di
agno
stic
an
alys
is
bull Id
enti
fica
tion
of
rele
vant
grou
ps
bull L
earn
ing
need
s m
easu
rem
ent
bull A
sses
smen
t of
educ
atio
n pr
ovis
ion
bull D
evel
opm
ent
oppo
rtun
itie
s
Ove
rvie
w a
ndsy
nthe
sis
of
curr
ent
prob
lem
s an
d so
luti
ons
Pla
nnin
g
Net
wor
k de
velo
pmen
t e
gbull
NH
Sbull
Pro
fess
iona
l or
gani
zati
ons
bull N
GO
s bull
Cro
ss-s
ecto
ral
Too
l dev
elop
men
t e
gbull
Dis
tanc
e le
arni
ng
bull T
oolk
its
Cap
acit
y bu
ildi
ng
syst
ems
bull In
divi
dual
bull
Org
aniz
atio
nal
bull S
ervi
ce
bull C
omm
unit
y
Pla
n to
add
ress
ca
paci
ty
buil
ding
and
chan
ge
man
agem
ent a
tdi
ffer
ent l
evel
s an
d in
dif
fere
nt
sect
ors
Cap
acit
y bu
ildi
ng a
ndde
velo
pmen
t
Mea
sure
men
t an
dm
onit
orin
g
Indi
vidu
al le
vel
eg
bull Fa
ce-t
o-fa
ce
educ
atio
n bull
Tw
inni
ng
budd
ying
bull
Dis
tanc
e le
arni
ng
Sys
tem
atic
da
ta c
olle
ctio
n an
d an
alys
is ndash
qual
itat
ive
and
quan
tita
tive
Org
aniz
atio
n an
dse
rvic
e le
vel
eg
bull C
ham
pion
s fo
r ch
ange
bull
Act
ion
lear
ning
se
ts
bull D
emon
stra
tion
pr
ojec
ts
bull Jo
int p
lann
ing
Wor
ksho
pob
serv
atio
n an
d cr
oss-
or
gani
zati
onal
au
dits
Sel
f-ev
alua
tion
an
d be
nchm
arki
ng
netw
orks
Com
mun
ity
leve
l e
gbull
Mul
ti-a
genc
y w
orki
ng
bull C
omm
unit
y re
sour
ces
rese
arch
bull A
ctio
n
Act
ion
rese
arch
and
le
arni
ng s
ets
Pol
icy
impe
rati
ves
Pri
orit
y se
ttin
g an
d
plan
for
di
agno
stic
an
alys
is
Rep
ort o
n m
easu
rem
ent
and
mon
itor
ing
Developing practice in breastfeeding
253
copy 2006 The Authors Journal compilation copy 2006 Blackwell Publishing Ltd
Maternal and Child Nutrition
2
pp 245ndash261
(Stage 2) Stage 3 involved developing relevant net-works tools for education and training evaluationmethods and capacity building systems at individualorganizational service and community levels Follow-ing this a plan to conduct the work would be finalized(Stage 4) implemented (Stage 5) and evaluated Theprocess was intended to be iterative alternatingbetween phases of information appraisal and plan-ning to identify the next stages of development activ-ity and evaluation of the impact to inform futureplanning Stage 6 included finalization of qualitativeand quantitative measurement and monitoring sys-tems that would feedback through all stages of theprocess
It was envisaged that this model would allow effec-tive structures and processes to be identified for usein other aspects of public health practice
Due to changes in funding the programme wasdiscontinued during Stage 3 although in fact somepreliminary work had already been carried out on theplan
Engagement with practitioners
Developing a national programme of change anddevelopment is an ambitious goal A cost-effectiveapproach to engagement had to be developed both tostay within budget and that could roll out acrossEngland and Wales Learning from the successfulLeeds partnership work described above it wasplanned to recruit a series of sentinel sites where wecould test out a range of approaches to maximizelearning and cost-effectiveness as well as respond toideas from the field Work in those sites wouldbecome a model for national developments inform-ing material for education training and assessmentsupported by communications at different levelsthrough our established national network The use ofsentinel sites also allowed for the development ofapproaches sensitive to varying local contexts so pro-viding alternatives and examples to inform nationalimplementation
The first stage in that process was to recruit rele-vant sentinel sites Sites were conceived as includingthe whole health economy in a locality and had tomeet specific criteria These are detailed in Box 2
Four sites were identified and agreed to join thefirst wave of sentinel sites Each site engaged andplanned the programme of work differently Forexample one site had already worked with membersof the core team and were keen to take existing workfurther In the few months in which we worked withthem they put into place a system for the accuratemonitoring of breastfeeding rates and created anextensive network of individuals at a range of seniorlevels from different sectors including Primary CareTrusts (PCTs) Strategic Health Authority the acuteTrust Sure Start and the local authority Benefits thesites have seen even since the work stopped haveincluded
bull improved communication across relevant disci-plines and sectorsbull the observation that the practice developmentwork lsquokept breastfeeding on everyonersquos agendarsquobull the work was used to support a business case for acoordinator for BFI planningbull in one sentinel site the primary care and acutematernity services have formed a health economy-wide breastfeeding strategy groupbull in another a joint primary care and maternity ser-vices group has been establishedbull two sites are taking forward systems for collect-ing breastfeeding data which have been used toprovide feedback to staff each monthbull a new approach to training all staff in one siteincluded commissioning the local university todevelop a self-study workbook and then to test itseffectiveness using an objective skills assessment toolandbull in one site a successful peer support programmewas rolled out throughout Sure Start programmes
A key part of the work in the sentinel sites was tosupport the learning needs assessment (McFadden
et al
2006) Although the sites were at an early stageof engagement this was conducted very successfullyand rapidly as sites supported the identification andinvolvement of practitioners Many assisted with sur-vey distribution and in return received a report ofthe training needs identified for their staff The nexttest was the running of fieldwork meetings and
254
MJ Renfrew
et al
copy 2006 The Authors Journal compilation copy 2006 Blackwell Publishing Ltd
Maternal and Child Nutrition
2
pp 245ndash261
workshops to finalize guidance based on researchevidence as part of a related programme of workThe aim of this work was to take the results of aseries of systematic reviews (which gave informationon lsquowhat works from research evidencersquo) and consultwith practitioners managers and users on lsquowhatreally works in practicersquo (Dyson
et al
2006) Thenewly established sentinel site system supported thiswork by offering venues for meetings providing listsof eligible participants and enabling and encourag-ing staff to attend (Renfrew
et al
2005b) The finalstage of this guidance work was a series of majorworkshops with over 30 participants in each repre-senting a lsquodiagonal slicersquo through the whole healtheconomy from field-level practitioners includingpeer support workers to managers and planners andincluding the range of relevant disciplines as well as
the voluntary sector Concerns around the realitiesand influences on practice and key issues for practi-tioners and managers in developing good practicewere discussed as well as organizational and struc-tural barriers to change Participants were encour-aged to discuss not only practices that need to beintroduced but also those that need to be aban-doned thereby potentially saving time and resourcesand to identify actual or potential barriers to imple-menting change (Renfrew
et al
2005b) These facili-tated groups examined the ability of the service torespond to identified gaps and made recommenda-tions for improvements to the system They feddirectly into the final stages of the development ofNational Institute for Health and Clinical Excellence(NICE) public health recommendations for breast-feeding offering participants the satisfaction of
Box 2
Sentinel site criteriaSentinel sites were expected to
bull Have a deprivation profile that demonstrated a substantial proportion of low-income groups and adiverse ethnic profile and serve contrasting areas (eg urban rural)
bull Offer a range of services for children and women with an interest in nutrition
bull Be able to include the whole health economy in a locality (or at least agree to working across allrelevant sectors)
bull Provide a key contact personpeople who would act to facilitate communication and broker agree-ments with different parts of the health economy and managers who were supportive of the plannedwork willing to support and enable staff participation
bull In the first instance sites would be those where contact already existed with members of our coreteam Future sites would be brought in once any initial problems with the approach had been identifiedand addressed
In return for their involvement in the work it was recognized that the sentinel sites would benefit in arange of ways including
bull Support for staff development and learning through access to programme staff and expertise involve-ment in and learning from a regular newsletter and attendance at an annual leading-edge conferenceon maternal and child nutrition
bull Developing links with other sites and sharing good practice and problem solving
bull The opportunity to help to develop national practice resulting in a raised profile for their work andtheir staff
bull Early access to emerging evidence in the field of maternal and child nutrition
Developing practice in breastfeeding
255
copy 2006 The Authors Journal compilation copy 2006 Blackwell Publishing Ltd
Maternal and Child Nutrition
2
pp 245ndash261
knowing that their input would make a difference(Dyson
et al
2006) These workshops also tested outthe use of language the conceptual understanding ofparticipants in relation to the evidence reviews andgathered intelligence on what approaches to imple-mentation of practice development may be mosteffective They also provided an opportunity for dis-cussion debate and deliberation about the meaningof the evidence Participants reported this to be veryuseful in assisting their understanding of the evi-dence and in considering how best to change theirown and their colleaguesrsquo practice in response to itand as an important contribution to practice devel-opment in their own locality (McFadden
et al
2005)The input of representatives of service users was ofcritical importance
It was planned that once the guidance was final-ized each participating site would be in a strong posi-tion to act on it Not only would they feel someownership but they would also have staff from alllevels and sectors in their health economy who hadspent time discussing the issues with colleagues andwith service user representatives They would haveaccess to specific local information about localitiesand groups that needed to be prioritized creatingchange was therefore brought several stages closerAt the end of each workshop email and telephonecontact details were exchanged among the workshopparticipants many of whom had never met beforedespite working in related parts of the same systemto support closer local networking The opportunityto consult with national experts in the network alsoacted as a variant on educational outreach which hasbeen shown to be moderately successful in guidelineimplementation (NHS CRD 1999) The impact ofsuch exchanges in increasing opportunities for net-work support is virtually impossible to evaluate for-mally but there was confidence in those whoparticipated at these events that positive changewould result and that the evidence would be moreeffectively used in the future as a consequence
Interactive conference
The other main activity was a conference on maternaland child nutrition to which all partners ndash academic
professional NHS and userconsumer ndash and stafffrom sentinel sites were invited Commissioners ofthe work were invited as were staff from key govern-ment departments with an interest in nutrition childhealth Sure Start nursing and midwifery and ine-qualities in health Around 90 participants took partin a day which included presentations participativeworking and active networking A report of the dayis available at httpwwwyorkacukresmcncccon-ferenceReporthtm Feedback was strongly positiveand the impact of networking with others in similarsituations and between those working in local andnational organizations was especially valued It wasplanned that this would be an annual event
Had we been able to continue the practice devel-opment programme we planned to use the follow-ing approaches
Establishing learning networks
We planned to identify appropriate learning net-works for different constituencies which wouldenable communication among staff from differentsectors as well as communication with programmestaff Activities were planned to include
bull Staff working at strategic and senior managementlevels would be supported and appropriate informa-tion provided to allow them to create cross-systemchanges Senior-level lsquochampions for changersquo wouldbe identified These would be used in a range of waysthose wishing to be involved in learning networkswould be supported to do sobull Learning sets would be established This wouldenable focused exchange between stakeholders onhow best to make use of the evidence in practice andhow to influence mainstream practice across locali-ties Through feedback loops we planned to developlearningeducation material to be made availablethrough web-based routes to wider constituenciesbull Peer supporters and trained breastfeeding counsel-lors are key groups in regard to breastfeeding promo-tion and support We planned to include them inlearning sets They have much to offer health profes-sionals in coming to understand the needs of womenand families and indeed the evidence suggests thattheir involvement in advisory work and peer support
256
MJ Renfrew
et al
copy 2006 The Authors Journal compilation copy 2006 Blackwell Publishing Ltd
Maternal and Child Nutrition
2
pp 245ndash261
enhances and strengthens the impact of informationand evidence-based guidance possibly more thanthat of health professionalsrsquo practice Our experiencedescribed above has identified a valuable contribu-tion from lay breastfeeding counsellors into educa-tion and training provision
Educational approaches
The breadth of constituencies that the programmeneeded to reach was to be reflected in the range ofeducational approaches required For some profes-sions continuing professional development (CPD)time is factored in regularly to the job plan in a rollingprogramme of group education with routine sessionalwork suspended for other groups CPD is a self-verified individual activity that can be achievedthrough a range of methods including distance learn-ing We hoped to reach directly a broad group ofwomen as well as professionals through some of theroutes developed A range of materials was thereforeplanned to address all needs Materials would bedeveloped for web-based access CD-ROM access andon paper These were to include
bull Toolkits to promote and support breastfeeding tomonitor breastfeeding rates and on practice develop-ment and changebull Distance learning modules providing accreditedlearning opportunities at a range of levelsbull An email and telephone-based service to putindividuals and organizations in touch with otherswho can support and advise them supported byRDLearning a national web-based resourcebull Learning material that could be directly dissemi-nated through the Internet to a wide audiencebull Buddy systems and mentoring for practice devel-opment and public health strategic development inbreastfeeding and use of cascade systemsbull Summaries of approaches to dissemination andpromotion of information that have proved to be suc-cessful and of practice change programmes that havebeen evaluated as having a positive impact on initia-tion and duration of breastfeedingbull Through NHS Direct we planned to reach the gen-eral public Information could be provided to informthe development of new algorithms that could be
used by staff taking enquiries from breastfeedingwomen We planned also to provide information thatcould be used on the NHS Direct website which isaccessed directly by women and families as well ashealth professionalsbull Other material to reach the general public wouldbe developed We aimed to have informative paperspublished in womenrsquos and familiesrsquo magazines and inthe general media on a regular basis A professionalwriter was one of our partners her role was to informand advise us about reaching women directly
Discussion
The work described in this paper was a structuredcross-sectoral approach to practice development inpublic health As a result of funding problems a fullevaluation could not be conducted and our contribu-tion to the knowledge base on practice change inpublic health is limited Lessons were learned how-ever and feedback was gained from participants atdifferent stages of the process We received strongsupport for our approach and the willingness of localand national partners to engage actively in the pro-gramme testifies to its potential
Lessons learned
There is increasing emphasis in public health andhealth policy on the need for good partnership work-ing and integration across disciplines professionsorganizations and localities as shown in the recentWhite Paper from the Department of Health (DH2006) and in the Children Act (2004) Prevention ofill health and promotion of well-being featurestrongly in these and other policy documents with arecognition that this cannot be achieved without fullengagement at strategic and operational levels withthose who use or depend on public-sector services Itwas clear at every stage of this process that engage-ment was needed across the whole health economyIt is only in working with all the relevant layers andpartnerships of professionals that we can hope for thefull impact of evidence to be realized Traditionalapproaches however only disseminate evidence tointerest groups in isolation Our use of lsquodiagonal slicersquo
Developing practice in breastfeeding 257
copy 2006 The Authors Journal compilation copy 2006 Blackwell Publishing Ltd Maternal and Child Nutrition 2 pp 245ndash261
workshops in which staff at all levels and across allsectors were engaged and including representativesof service users and the voluntary sector enabledmuch greater understanding of the consequences ofparticular activity or behaviour in other parts of thesystem and allowed creative and informed challengesto assumptions and prejudices This laid good foun-dations for whole systems approaches to introducingdriving and implementing new approaches whichcould lead to positive health outcomes It proved avery positive learning experience for all thoseinvolved
Practice change needs to involve the whole rangeof health professionals involved in work directly withpregnant women and new mothers to ensure coordi-nated working and consistent messages Despiteactive support from relevant Royal Colleges and sev-eral strongly supportive individuals engagement bydoctors was noticeably less compared with otherhealth professions This supports the findings of otherwork (eg Smale et al 2006) This really matters in afield such as breastfeeding where paediatriciansobstetricians general practitioners and public healthphysicians have an important role to play Futurework will need to address this
Key constituents in practice development in breast-feeding include mothers and potential mothersgrandmothers and men We had strong support andinvolvement from service users and user groups butengaging men proved to be difficult To reach thepublic good-quality easily accessible information isneeded perhaps the developing DiPEX module onbreastfeeding will contribute to this (httpwwwdipexorgDesktopDefaultaspx) Recent gov-ernment policy directives acknowledge the potentialcontribution that incorporating patient and serviceuser experience into service provision can bring (egDH 2006) Recent developments in the approach tolong-term conditions management have introducedthe Expert Patient Programme which enables peoplewith disabilities to take much more effective controlover the management and treatment of their disease(DH 2004c 2006) There is perhaps potential for theparallel development of an lsquoExpert Mothers Pro-grammersquo to have similar positive impact in relation tonutrition and health
Service user involvement is actively encouraged ininforming research and practice (Hanley et al 2004)Breastfeeding and maternity care as a whole have along-standing history of the active engagement of ser-vice users Volunteer counsellors and supporterstrained and accredited by their own voluntary orga-nizations have filled the gap left by the health ser-vices They have taken the initiative in setting uptelephone support services training and supervisingpeer supporters and contributing to the education ofhealth professionals (Smale et al 2006) In our cur-rent and previous practice development work thecontribution of service users and voluntary groupswent much further than simply offering advice andinformation They took an active role in planning thework and in some cases delivering education andservices Our experience was that lay workers havean essential role in developing services and they areable to advise at a strategic level as well as participat-ing in service delivery They are able to see throughthe organizational barriers that often constrain pro-fessionals and can see solutions that will work formothers and families From our experience we wouldadvise that others explore ways of actively engaginglay workers adequately remunerated in the deliveryof health care and in the education of healthprofessionals
The fundamental importance of multidisciplinaryand multi-professional working was also apparent inthe way in which the core team worked and in thesupport gained from the network of partners Atevery stage we had expertise and support availableto us as well as an effective communication systemand network Practice change in public health needsto be led and informed by those who know the topicarea and who have the wide range of skills neededto convince many different kinds of professionals thatthe work is worthwhile and achievable
Another positive contribution was the synergy ofthis programme with the evidence base The sameteam had also been responsible for systematicreviews of the field (eg Fairbank et al 2000Protheroe et al 2003 Sikorski et al 2004 Renfrewet al 2005a) and the approach was grounded in thisevidence which was at the same time being devel-oped into national guidance The interaction between
258 MJ Renfrew et al
copy 2006 The Authors Journal compilation copy 2006 Blackwell Publishing Ltd Maternal and Child Nutrition 2 pp 245ndash261
these elements should not be underestimated part-ners and sentinel sites were able to inform the guid-ance and up-to-date knowledge of the evidence basehelped strengthen the practice development work
The sentinel site system was proving to be asuccessful lsquowin-winrsquo situation for all involved Itprovided a test bed for ideas it was a source ofinformation and debate and the programme gaineda richness and diversity of input that would be hardto match At the same time it offered the sitesengagement in leading-edge work an increased pro-file and high-quality staff development Although itwas not formally evaluated all involved were con-vinced that it was a very cost-effective system theprogramme could conduct work at speed and to ahigh quality and governance issues were streamlinedThe system was very flexible and could adapt to thedifferent circumstances of each site It would havebeen able to accommodate future service and educa-tion developments such as Childrenrsquos Centres Trustreorganization and inter-professional educationOver time we could have expanded to include othersectors and practitioners such as retailers and child-minders Had the programme continued future siteswould have been identified and material developedfor national use based on our learning in the originalfour sites
Major challenges
Throughout the programme getting breastfeedingrecognized as a priority was difficult This has beenthe case for many years despite its fundamental con-tribution to public health in the short and long termit has only recently been included in national publichealth policy statements PCT targets and monitoringAs we found in the learning needs assessment andother work breastfeeding services are often seen asthe remit of enthusiastic individuals discussed interms reminiscent of lsquoreligious zealotryrsquo (Smale et al2006) rather than as a part of the mainstream ofhealth provision Creating real change in theapproach to breastfeeding in the health service willrequire it to be seen as a priority for senior managersand commissioners Our experience has demon-strated that it is possible to engage such senior people
in this work and that discussion and debate with theirown colleagues can have an impact on their thinking
A key area of practice development that canimpact on breastfeeding duration is working withmothers to sustain breastfeeding while going back towork and the ways that public health strategy andpractice can influence employers to provide breast-feeding-friendly maternity policies and facilities(Kosmala-Anderson amp Wallace in press) We did nothave an impact on this area but it was clear that itwas an area that needed to be addressed One goodplace to start would be with the employment condi-tions for NHS employees themselves this would havethe dual advantage of improving conditions for thelargest female workforce in the country while alsoproviding a model of good practice for others
Although the aim of this work was to address ine-qualities in health it is clear that reaching the hard-to-reach remains challenging We did see signs of suc-cess for example Sure Start schemes were making adifference in some areas but ensuring that all vulner-able women receive the support and care they needis still a distant goal whether they are teenagers asy-lum seekers or simply women who live in areas wherebottle feeding has been endemic for generations
Finally there is a debate to be had on whoseresponsibility it is to create such change The work ofresearchers is seen to be complete when their studyis finished and disseminated through publication andconference presentation Systematic reviewers takeon a responsibility to make the results of a wide rangeof studies available through publication but not toengage with what services might do with those find-ings Those responsible for guidance are responsiblefor developing and publishing that work and somealso take responsibility for lsquoimplementationrsquo (egNICE 2005) But where does responsibility rest forpractice development which requires a deep engage-ment with the practice setting and with those affectedby the issues raised by the evidence Lack of invest-ment at the national level in formal evaluation ofprogrammes of change limits the available evidencebase and detracts from our achieving a better under-standing of what actually works in relation to thesemore complex health issues funding for the lsquoRrsquoaspects of research and development is more com-
Developing practice in breastfeeding 259
copy 2006 The Authors Journal compilation copy 2006 Blackwell Publishing Ltd Maternal and Child Nutrition 2 pp 245ndash261
mon than for the lsquoDrsquo (NHS Executive 1997) Thewithdrawal of funding to this programme part waythrough its cycle was regretted by our commissionersit was evident that practice development was nolonger their remit given their changed circumstancesIt is however not clear that responsibility now restswith any particular agency Is development work forindividual health service organizations themselves totake on Is this work that should be led by nationalprogrammes supported by public-sector funding orshould it rely on other sources of support If so fromwhere will it be resourced and how will cross-sectoraland multidisciplinary developments be addressedThere are also questions about who will lead thiswork when a number of professional disciplines areinvolved and where the client interface spans bothprimary and acute care healthcare settings social ser-vices and other development agencies These ques-tions will become more pressing as guidancecontinues to be produced especially in public health
Acknowledgements
We would like to thank all participants from sentinelsites and our consortium of academic professionalNHS and consumer partners and the two anonymousreferees who reviewed the manuscript This work wascommissioned by the former Health DevelopmentAgency and subsequently funded by NICE
References
Abbott S Renfrew MJ amp McFadden A (2006) lsquoInformalrsquo learning to support breastfeeding local problems and opportunities Maternal and Child Nutrition 2 232ndash238
Audit Commission (2000) United They Stand Coordinating Care for Elderly Patients with Hip Fracture Audit Com-mission London
British Paediatric Association (1994) Statement of the stand-ing committee on nutrition is breastfeeding beneficial in the UK Archive of Diseases in Childhood 71 376ndash380
Chalmers I amp Altman DG (eds) (1995) Systematic Reviews BMJ Publishing Group London
Children Act (2004) Available at httpwwwopsigovukactsacts200420040031htm (accessed 21 March 2006)
Coote A Allen J amp Woodhead D (2004) Finding out What Works Building Knowledge about Complex Community-Based Initiatives Kingrsquos Fund London
DfES (2000) Adoption and Permanence Taskforce Available at httpwwwdfesgovukadoptionadoptionreformstaskforceshtml (accessed 29 March 2006)
DH (2002a) Improvement Expansion and Reform The Next 3 Years Priorities and Planning Framework 2003ndash2006 Department of Health London
DH (2002b) The Health and Social Care Change Agent Team Available at httpwwwchangeagentteamorguk (accessed 29 March 2006)
DH (2004a) National Service Framework for Children Young People and Maternity Services Stationery Office London
DH (2004b) Choosing Health Making Healthy Choices Eas-ier Stationery Office London
DH (2004c) Self Care ndash A Real Choice Self Care Support ndash A Practical Option Stationery Office London
DH (2006) Our Health Our Care Our Say A New Direction for Community Services Stationery Office London
Dominey M Archibald A Edgecombe D Lawrence J amp Thomson L (2002) Breastfeeding and drug misuse Mak-ing an informed choice Year 3 Practice project In Infant Feeding Initiative A Report Evaluating the Breastfeeding Practice Projects 1999ndash2002 (ed F Dykes 2003) p 64 Department of Health London
Dykes F (2003) Infant Feeding Initiative A Report Evaluat-ing the Breastfeeding Practice Projects 1999ndash2002 Depart-ment of Health London
Dykes F (2006) The education of health practitioners sup-porting breastfeeding women time for critical reflection Maternal and Child Nutrition 2 204ndash216
Dyson L Renfrew MJ McFadden A McCormick F Herbert G amp Thomas J (2006) Promotion of Breastfeed-ing Initiation and Duration Evidence into Practice Brief-ing National Institute for Health and Clinical Excellence London httpwwwniceorgukdown-loadaspxo=346169 (accessed 26 July 2006)
EU (2004) Project on Promotion of Breastfeeding in Europe Protection Promotion and Support of Breastfeeding A Blueprint for Action European Commission Directorate Public Health and Risk Assessment Luxembourg
Fairbank L OrsquoMeara S Renfrew MJ Woolridge M Sowden AJ amp Lister-Sharp D (2000) A systematic review to evaluate the effectiveness of interventions to promote the initiation of breastfeeding Health Technol-ogy Assessment 4 1ndash171
Grant J Fletcher M amp Warwick C (2000) The South Thames Evidence Based Practice (STEP) Project Sup-porting Breastfeeding Women South Bank University London
Greenhalgh T Robert G Bate P Mcfarlane F amp Kyriakidou O (2005) Diffusion of Innovations in Health Service Organisations A Systematic Literature Review Blackwell Publishing Limited Oxford
260 MJ Renfrew et al
copy 2006 The Authors Journal compilation copy 2006 Blackwell Publishing Ltd Maternal and Child Nutrition 2 pp 245ndash261
Grimshaw JM Thomas RE MacLennan G Fraser C Ramsay CR Vale L et al (2004) Effectiveness and efficiency of guideline dissemination and implementation strategies Health Technology Assessment 8 indashxi 1ndash72
Hanley B Bradburn J Barnes M Evans C Goodare H Kelson M et al (2004) Involving the Public in NHS Pub-lic Health and Social Care Research Briefing Notes for Researchers INVOLVE Department of Health London
Herbert G amp Lake G (2005) Making connections Effective development of the intermediate tier Journal of Inte-grated Care 13 35ndash42
Howie PW Forsyth JS Ogston SA Clark A amp Florey CD (1990) Protective effect of breastfeeding against infection British Medical Journal 300 11ndash16
Kosmala-Anderson J amp Wallace LM (in press) Breastfeed-ing works the role of employers in supporting women who wish to breastfeed and work in four organizations in England Journal of Public Health (in press)
Kramer M Chalmers B Hodnett H Sevovskaya Z Dzikovich I Shapiro S et al (2001) Promotion of breast-feeding intervention trial (PROBIT) Journal of the American Medical Association 285 413ndash420
McFadden A Renfrew MJ Dyson L McCormick F Herbert G amp Thomas J (2005) Effective Active Briefing on the Initiation and Duration of Breastfeeding Fieldwork Report National Institute for Health and Clinical Excel-lence London
McFadden A Renfrew MJ Dykes F amp Burt S (2006) Assessing learning needs for breastfeeding setting the scene Maternal and Child Nutrition 2 196ndash203
McSherry R amp McFadden A (2001) Practice Development Accreditation Assessment Maternity Services Darlington Memorial Hospital South Durham Healthcare NHS Trust Final Report University of Teesside Middlesbrough
Moulding NT Silagy CA amp Weller DP (1999) A frame-work for effective management of change in clinical prac-tice dissemination and implementation of clinical practice guidelines Quality in Health Care 8 177ndash183
Gray JA Haynes RB Sackett DL Cook DJ amp Guyatt GH (1997) Transferring evidence from research into practice 3 Developing evidence-based clinical policy Evidence-Based Medicine 2 36ndash38
NHS Centre for Reviews and Dissemination (CRD) (1999) Getting evidence into practice Effective Health Care 5 1ndash16
NHS Executive (1997) RampD in Primary Care National Working Group Report (Mant Report) Stationery Office London
NICE (2004) The Guideline Development Process National Institute for Health and Clinical Excellence London
NICE (2005) Putting NICE Guidance into Practice National Institute for Health and Clinical Excellence London
Oxman AD Thomson MA Davis DA amp Haynes RB (1995) No magic bullets a systematic review of 102 trials of interventions to improve professional practice Canadian Medical Association Journal 153 1423ndash1431
Protheroe L Dyson L Renfrew MJ Bull J amp Mulvihill C (2003) The Effectiveness of Public Health Interventions to Promote the Initiation of Breastfeeding Evidence Briefing Health Development Agency London
Quigley MA Cumberland P Cowden JM amp Rodrigues LC (2006) How protective is breast feeding against diar-rhoeal disease in infants in 1990s England A case control study Archives of Disease in Childhood 91 245ndash250
Renfrew MJ Dyson L Wallace L DrsquoSouza L McCormick FM amp Spiby H (2005a) The Effectiveness of Health Interventions to Promote the Duration of Breast-feeding Systematic Review 1st edn National Institute for Health and Clinical Excellence London
Renfrew MJ Dyson L McFadden A McCormick F Herbert G amp Thomas J (2005b) Effective Active Briefing on the Initiation and Duration of Breastfeeding Technical Report National Institute for Health and Clinical Excel-lence London
Renfrew MJ McFadden A Dykes F Wallace L Abbott S Burt S et al (2006) Addressing the learning deficit in breastfeeding strategies for change Maternal and Child Nutrition 2 239ndash244
Richards D (2003) Childrenrsquos Nutrition ndash Mothers Who Wish to Breast-Feed Birmingham City Council Available at httpwwwbirmingahmgovukscrutiny (accessed 27 July 2006)
Sackett DL Rosenberg WMC Gray JAM Haynes RB amp Richardson WS (1996) Evidence-based medicine what it is and what it isnrsquot British Medical Journal 312 71ndash72
Sikorski J Renfrew MJ Pindoria S amp Wade A (2004) Support for breastfeeding mothers (Cochrane Review) The Cochrane Database of Systematic Reviews Issue 2 John Wiley amp Sons Ltd Chichester
Smale M Renfrew MJ Marshall JL amp Spiby H (2006) Turning policy into practice more difficult that it seems The case of breastfeeding education Maternal and Child Nutrition 2 103ndash113
Spiby H Ker R DrsquoSouza L amp Renfrew MJ (2002) Intro-ducing a Consumer-Practitioner into breastfeeding prac-tice Year 2 In Infant Feeding Initiative A Report Evaluating the Breastfeeding Practice Projects 1999ndash2002 (ed F Dykes 2003) p 44 Department of Health London
Spiby H Wallis S Stone C amp Renfrew MJ (2005) Support-ing and Promoting Breastfeeding in Leeds Final Report to December 2004 Report to Leeds PCTs Children and Families Modernisation Team Leeds
Thomas C (2006) Darlington ndash A Breastfeeding Friendly Town Darlington Borough Council Darlington
Developing practice in breastfeeding 261
copy 2006 The Authors Journal compilation copy 2006 Blackwell Publishing Ltd Maternal and Child Nutrition 2 pp 245ndash261
Unsworth J (2000) Practice development a concept analy-sis Journal of Nursing Management 8 317ndash326
Wallace LM amp Jardine J (2006) A Health Scrutiny of Ser-vices to Support the Initiation and Duration of Breastfeed-ing in Coventry and Warwickshire Coventry and Warwickshire County Councils Coventry
Wallace L amp Kosmala-Anderson J (2006) A training needs survey of doctorsrsquo breastfeeding support skills in England Maternal and Child Nutrition 2 217ndash231
Wallace L amp Kosmala-Anderson J (in press) Training needs survey of midwives health visitors and voluntary sector
breastfeeding support staff in England Maternal and Child Nutrition (in press)
WHO (2003) Global Strategy for Infant and Young Child Feeding World Health Organization Geneva
Wilson AC Forsyth JS Green SA Irvine L Hau C amp Howie PW (1998) Relation of infant diet to childhood health seven year follow up of a cohort of children in Dundee infant feeding study British Medical Journal 316 21ndash25
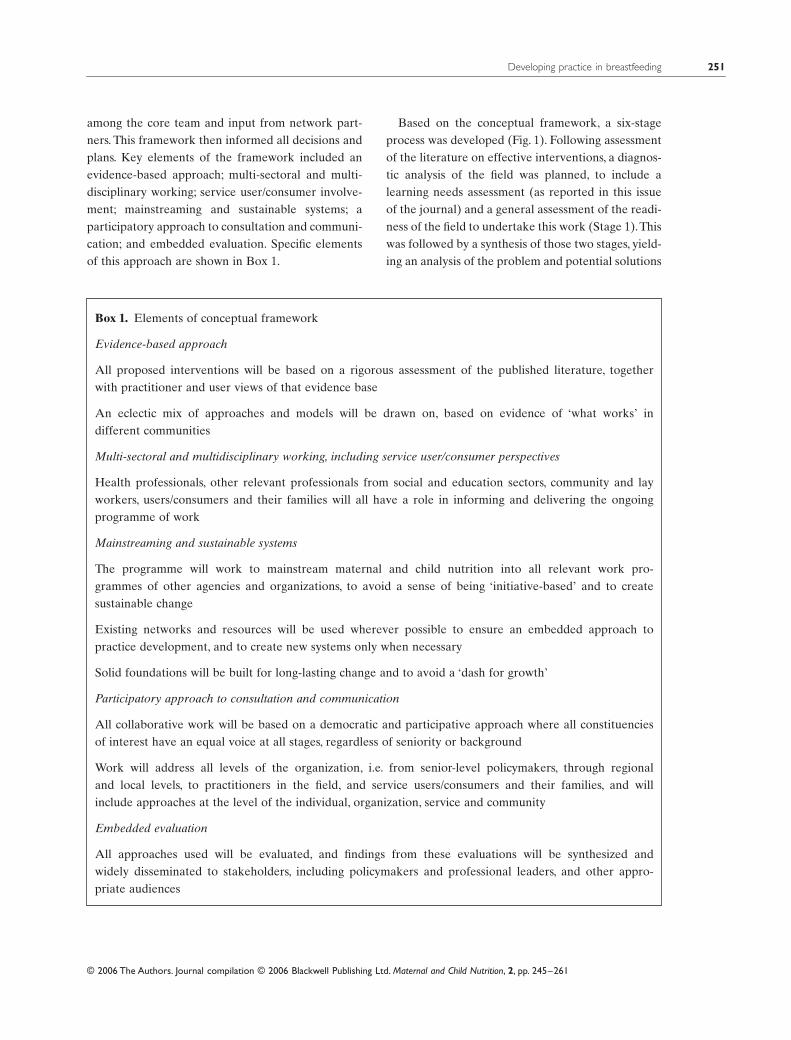
Developing practice in breastfeeding
251
copy 2006 The Authors Journal compilation copy 2006 Blackwell Publishing Ltd
Maternal and Child Nutrition
2
pp 245ndash261
among the core team and input from network part-ners This framework then informed all decisions andplans Key elements of the framework included anevidence-based approach multi-sectoral and multi-disciplinary working service userconsumer involve-ment mainstreaming and sustainable systems aparticipatory approach to consultation and communi-cation and embedded evaluation Specific elementsof this approach are shown in Box 1
Based on the conceptual framework a six-stageprocess was developed (Fig 1) Following assessmentof the literature on effective interventions a diagnos-tic analysis of the field was planned to include alearning needs assessment (as reported in this issueof the journal) and a general assessment of the readi-ness of the field to undertake this work (Stage 1) Thiswas followed by a synthesis of those two stages yield-ing an analysis of the problem and potential solutions
Box 1
Elements of conceptual framework
Evidence-based approach
All proposed interventions will be based on a rigorous assessment of the published literature togetherwith practitioner and user views of that evidence base
An eclectic mix of approaches and models will be drawn on based on evidence of lsquowhat worksrsquo indifferent communities
Multi-sectoral and multidisciplinary working including service userconsumer perspectives
Health professionals other relevant professionals from social and education sectors community and layworkers usersconsumers and their families will all have a role in informing and delivering the ongoingprogramme of work
Mainstreaming and sustainable systems
The programme will work to mainstream maternal and child nutrition into all relevant work pro-grammes of other agencies and organizations to avoid a sense of being lsquoinitiative-basedrsquo and to createsustainable change
Existing networks and resources will be used wherever possible to ensure an embedded approach topractice development and to create new systems only when necessary
Solid foundations will be built for long-lasting change and to avoid a lsquodash for growthrsquo
Participatory approach to consultation and communication
All collaborative work will be based on a democratic and participative approach where all constituenciesof interest have an equal voice at all stages regardless of seniority or background
Work will address all levels of the organization ie from senior-level policymakers through regionaland local levels to practitioners in the field and service usersconsumers and their families and willinclude approaches at the level of the individual organization service and community
Embedded evaluation
All approaches used will be evaluated and findings from these evaluations will be synthesized andwidely disseminated to stakeholders including policymakers and professional leaders and other appro-priate audiences
252
MJ Renfrew
et al
copy 2006 The Authors Journal compilation copy 2006 Blackwell Publishing Ltd
Maternal and Child Nutrition
2
pp 245ndash261
Fig
1
Prac
tice
deve
lopm
ent
cycl
e N
HS
Nat
iona
l Hea
lth S
ervi
ce N
GO
non
-gov
ernm
enta
l org
aniz
atio
n
Pre
curs
ors
Sys
tem
atic
re
view
s an
d gu
idan
ce
Oth
er
reli
able
so
urce
s of
ev
iden
ce
bull E
xam
ine
syst
ems
Map
ping
and
di
agno
stic
an
alys
is
bull Id
enti
fica
tion
of
rele
vant
grou
ps
bull L
earn
ing
need
s m
easu
rem
ent
bull A
sses
smen
t of
educ
atio
n pr
ovis
ion
bull D
evel
opm
ent
oppo
rtun
itie
s
Ove
rvie
w a
ndsy
nthe
sis
of
curr
ent
prob
lem
s an
d so
luti
ons
Pla
nnin
g
Net
wor
k de
velo
pmen
t e
gbull
NH
Sbull
Pro
fess
iona
l or
gani
zati
ons
bull N
GO
s bull
Cro
ss-s
ecto
ral
Too
l dev
elop
men
t e
gbull
Dis
tanc
e le
arni
ng
bull T
oolk
its
Cap
acit
y bu
ildi
ng
syst
ems
bull In
divi
dual
bull
Org
aniz
atio
nal
bull S
ervi
ce
bull C
omm
unit
y
Pla
n to
add
ress
ca
paci
ty
buil
ding
and
chan
ge
man
agem
ent a
tdi
ffer
ent l
evel
s an
d in
dif
fere
nt
sect
ors
Cap
acit
y bu
ildi
ng a
ndde
velo
pmen
t
Mea
sure
men
t an
dm
onit
orin
g
Indi
vidu
al le
vel
eg
bull Fa
ce-t
o-fa
ce
educ
atio
n bull
Tw
inni
ng
budd
ying
bull
Dis
tanc
e le
arni
ng
Sys
tem
atic
da
ta c
olle
ctio
n an
d an
alys
is ndash
qual
itat
ive
and
quan
tita
tive
Org
aniz
atio
n an
dse
rvic
e le
vel
eg
bull C
ham
pion
s fo
r ch
ange
bull
Act
ion
lear
ning
se
ts
bull D
emon
stra
tion
pr
ojec
ts
bull Jo
int p
lann
ing
Wor
ksho
pob
serv
atio
n an
d cr
oss-
or
gani
zati
onal
au
dits
Sel
f-ev
alua
tion
an
d be
nchm
arki
ng
netw
orks
Com
mun
ity
leve
l e
gbull
Mul
ti-a
genc
y w
orki
ng
bull C
omm
unit
y re
sour
ces
rese
arch
bull A
ctio
n
Act
ion
rese
arch
and
le
arni
ng s
ets
Pol
icy
impe
rati
ves
Pri
orit
y se
ttin
g an
d
plan
for
di
agno
stic
an
alys
is
Rep
ort o
n m
easu
rem
ent
and
mon
itor
ing
Developing practice in breastfeeding
253
copy 2006 The Authors Journal compilation copy 2006 Blackwell Publishing Ltd
Maternal and Child Nutrition
2
pp 245ndash261
(Stage 2) Stage 3 involved developing relevant net-works tools for education and training evaluationmethods and capacity building systems at individualorganizational service and community levels Follow-ing this a plan to conduct the work would be finalized(Stage 4) implemented (Stage 5) and evaluated Theprocess was intended to be iterative alternatingbetween phases of information appraisal and plan-ning to identify the next stages of development activ-ity and evaluation of the impact to inform futureplanning Stage 6 included finalization of qualitativeand quantitative measurement and monitoring sys-tems that would feedback through all stages of theprocess
It was envisaged that this model would allow effec-tive structures and processes to be identified for usein other aspects of public health practice
Due to changes in funding the programme wasdiscontinued during Stage 3 although in fact somepreliminary work had already been carried out on theplan
Engagement with practitioners
Developing a national programme of change anddevelopment is an ambitious goal A cost-effectiveapproach to engagement had to be developed both tostay within budget and that could roll out acrossEngland and Wales Learning from the successfulLeeds partnership work described above it wasplanned to recruit a series of sentinel sites where wecould test out a range of approaches to maximizelearning and cost-effectiveness as well as respond toideas from the field Work in those sites wouldbecome a model for national developments inform-ing material for education training and assessmentsupported by communications at different levelsthrough our established national network The use ofsentinel sites also allowed for the development ofapproaches sensitive to varying local contexts so pro-viding alternatives and examples to inform nationalimplementation
The first stage in that process was to recruit rele-vant sentinel sites Sites were conceived as includingthe whole health economy in a locality and had tomeet specific criteria These are detailed in Box 2
Four sites were identified and agreed to join thefirst wave of sentinel sites Each site engaged andplanned the programme of work differently Forexample one site had already worked with membersof the core team and were keen to take existing workfurther In the few months in which we worked withthem they put into place a system for the accuratemonitoring of breastfeeding rates and created anextensive network of individuals at a range of seniorlevels from different sectors including Primary CareTrusts (PCTs) Strategic Health Authority the acuteTrust Sure Start and the local authority Benefits thesites have seen even since the work stopped haveincluded
bull improved communication across relevant disci-plines and sectorsbull the observation that the practice developmentwork lsquokept breastfeeding on everyonersquos agendarsquobull the work was used to support a business case for acoordinator for BFI planningbull in one sentinel site the primary care and acutematernity services have formed a health economy-wide breastfeeding strategy groupbull in another a joint primary care and maternity ser-vices group has been establishedbull two sites are taking forward systems for collect-ing breastfeeding data which have been used toprovide feedback to staff each monthbull a new approach to training all staff in one siteincluded commissioning the local university todevelop a self-study workbook and then to test itseffectiveness using an objective skills assessment toolandbull in one site a successful peer support programmewas rolled out throughout Sure Start programmes
A key part of the work in the sentinel sites was tosupport the learning needs assessment (McFadden
et al
2006) Although the sites were at an early stageof engagement this was conducted very successfullyand rapidly as sites supported the identification andinvolvement of practitioners Many assisted with sur-vey distribution and in return received a report ofthe training needs identified for their staff The nexttest was the running of fieldwork meetings and
254
MJ Renfrew
et al
copy 2006 The Authors Journal compilation copy 2006 Blackwell Publishing Ltd
Maternal and Child Nutrition
2
pp 245ndash261
workshops to finalize guidance based on researchevidence as part of a related programme of workThe aim of this work was to take the results of aseries of systematic reviews (which gave informationon lsquowhat works from research evidencersquo) and consultwith practitioners managers and users on lsquowhatreally works in practicersquo (Dyson
et al
2006) Thenewly established sentinel site system supported thiswork by offering venues for meetings providing listsof eligible participants and enabling and encourag-ing staff to attend (Renfrew
et al
2005b) The finalstage of this guidance work was a series of majorworkshops with over 30 participants in each repre-senting a lsquodiagonal slicersquo through the whole healtheconomy from field-level practitioners includingpeer support workers to managers and planners andincluding the range of relevant disciplines as well as
the voluntary sector Concerns around the realitiesand influences on practice and key issues for practi-tioners and managers in developing good practicewere discussed as well as organizational and struc-tural barriers to change Participants were encour-aged to discuss not only practices that need to beintroduced but also those that need to be aban-doned thereby potentially saving time and resourcesand to identify actual or potential barriers to imple-menting change (Renfrew
et al
2005b) These facili-tated groups examined the ability of the service torespond to identified gaps and made recommenda-tions for improvements to the system They feddirectly into the final stages of the development ofNational Institute for Health and Clinical Excellence(NICE) public health recommendations for breast-feeding offering participants the satisfaction of
Box 2
Sentinel site criteriaSentinel sites were expected to
bull Have a deprivation profile that demonstrated a substantial proportion of low-income groups and adiverse ethnic profile and serve contrasting areas (eg urban rural)
bull Offer a range of services for children and women with an interest in nutrition
bull Be able to include the whole health economy in a locality (or at least agree to working across allrelevant sectors)
bull Provide a key contact personpeople who would act to facilitate communication and broker agree-ments with different parts of the health economy and managers who were supportive of the plannedwork willing to support and enable staff participation
bull In the first instance sites would be those where contact already existed with members of our coreteam Future sites would be brought in once any initial problems with the approach had been identifiedand addressed
In return for their involvement in the work it was recognized that the sentinel sites would benefit in arange of ways including
bull Support for staff development and learning through access to programme staff and expertise involve-ment in and learning from a regular newsletter and attendance at an annual leading-edge conferenceon maternal and child nutrition
bull Developing links with other sites and sharing good practice and problem solving
bull The opportunity to help to develop national practice resulting in a raised profile for their work andtheir staff
bull Early access to emerging evidence in the field of maternal and child nutrition
Developing practice in breastfeeding
255
copy 2006 The Authors Journal compilation copy 2006 Blackwell Publishing Ltd
Maternal and Child Nutrition
2
pp 245ndash261
knowing that their input would make a difference(Dyson
et al
2006) These workshops also tested outthe use of language the conceptual understanding ofparticipants in relation to the evidence reviews andgathered intelligence on what approaches to imple-mentation of practice development may be mosteffective They also provided an opportunity for dis-cussion debate and deliberation about the meaningof the evidence Participants reported this to be veryuseful in assisting their understanding of the evi-dence and in considering how best to change theirown and their colleaguesrsquo practice in response to itand as an important contribution to practice devel-opment in their own locality (McFadden
et al
2005)The input of representatives of service users was ofcritical importance
It was planned that once the guidance was final-ized each participating site would be in a strong posi-tion to act on it Not only would they feel someownership but they would also have staff from alllevels and sectors in their health economy who hadspent time discussing the issues with colleagues andwith service user representatives They would haveaccess to specific local information about localitiesand groups that needed to be prioritized creatingchange was therefore brought several stages closerAt the end of each workshop email and telephonecontact details were exchanged among the workshopparticipants many of whom had never met beforedespite working in related parts of the same systemto support closer local networking The opportunityto consult with national experts in the network alsoacted as a variant on educational outreach which hasbeen shown to be moderately successful in guidelineimplementation (NHS CRD 1999) The impact ofsuch exchanges in increasing opportunities for net-work support is virtually impossible to evaluate for-mally but there was confidence in those whoparticipated at these events that positive changewould result and that the evidence would be moreeffectively used in the future as a consequence
Interactive conference
The other main activity was a conference on maternaland child nutrition to which all partners ndash academic
professional NHS and userconsumer ndash and stafffrom sentinel sites were invited Commissioners ofthe work were invited as were staff from key govern-ment departments with an interest in nutrition childhealth Sure Start nursing and midwifery and ine-qualities in health Around 90 participants took partin a day which included presentations participativeworking and active networking A report of the dayis available at httpwwwyorkacukresmcncccon-ferenceReporthtm Feedback was strongly positiveand the impact of networking with others in similarsituations and between those working in local andnational organizations was especially valued It wasplanned that this would be an annual event
Had we been able to continue the practice devel-opment programme we planned to use the follow-ing approaches
Establishing learning networks
We planned to identify appropriate learning net-works for different constituencies which wouldenable communication among staff from differentsectors as well as communication with programmestaff Activities were planned to include
bull Staff working at strategic and senior managementlevels would be supported and appropriate informa-tion provided to allow them to create cross-systemchanges Senior-level lsquochampions for changersquo wouldbe identified These would be used in a range of waysthose wishing to be involved in learning networkswould be supported to do sobull Learning sets would be established This wouldenable focused exchange between stakeholders onhow best to make use of the evidence in practice andhow to influence mainstream practice across locali-ties Through feedback loops we planned to developlearningeducation material to be made availablethrough web-based routes to wider constituenciesbull Peer supporters and trained breastfeeding counsel-lors are key groups in regard to breastfeeding promo-tion and support We planned to include them inlearning sets They have much to offer health profes-sionals in coming to understand the needs of womenand families and indeed the evidence suggests thattheir involvement in advisory work and peer support
256
MJ Renfrew
et al
copy 2006 The Authors Journal compilation copy 2006 Blackwell Publishing Ltd
Maternal and Child Nutrition
2
pp 245ndash261
enhances and strengthens the impact of informationand evidence-based guidance possibly more thanthat of health professionalsrsquo practice Our experiencedescribed above has identified a valuable contribu-tion from lay breastfeeding counsellors into educa-tion and training provision
Educational approaches
The breadth of constituencies that the programmeneeded to reach was to be reflected in the range ofeducational approaches required For some profes-sions continuing professional development (CPD)time is factored in regularly to the job plan in a rollingprogramme of group education with routine sessionalwork suspended for other groups CPD is a self-verified individual activity that can be achievedthrough a range of methods including distance learn-ing We hoped to reach directly a broad group ofwomen as well as professionals through some of theroutes developed A range of materials was thereforeplanned to address all needs Materials would bedeveloped for web-based access CD-ROM access andon paper These were to include
bull Toolkits to promote and support breastfeeding tomonitor breastfeeding rates and on practice develop-ment and changebull Distance learning modules providing accreditedlearning opportunities at a range of levelsbull An email and telephone-based service to putindividuals and organizations in touch with otherswho can support and advise them supported byRDLearning a national web-based resourcebull Learning material that could be directly dissemi-nated through the Internet to a wide audiencebull Buddy systems and mentoring for practice devel-opment and public health strategic development inbreastfeeding and use of cascade systemsbull Summaries of approaches to dissemination andpromotion of information that have proved to be suc-cessful and of practice change programmes that havebeen evaluated as having a positive impact on initia-tion and duration of breastfeedingbull Through NHS Direct we planned to reach the gen-eral public Information could be provided to informthe development of new algorithms that could be
used by staff taking enquiries from breastfeedingwomen We planned also to provide information thatcould be used on the NHS Direct website which isaccessed directly by women and families as well ashealth professionalsbull Other material to reach the general public wouldbe developed We aimed to have informative paperspublished in womenrsquos and familiesrsquo magazines and inthe general media on a regular basis A professionalwriter was one of our partners her role was to informand advise us about reaching women directly
Discussion
The work described in this paper was a structuredcross-sectoral approach to practice development inpublic health As a result of funding problems a fullevaluation could not be conducted and our contribu-tion to the knowledge base on practice change inpublic health is limited Lessons were learned how-ever and feedback was gained from participants atdifferent stages of the process We received strongsupport for our approach and the willingness of localand national partners to engage actively in the pro-gramme testifies to its potential
Lessons learned
There is increasing emphasis in public health andhealth policy on the need for good partnership work-ing and integration across disciplines professionsorganizations and localities as shown in the recentWhite Paper from the Department of Health (DH2006) and in the Children Act (2004) Prevention ofill health and promotion of well-being featurestrongly in these and other policy documents with arecognition that this cannot be achieved without fullengagement at strategic and operational levels withthose who use or depend on public-sector services Itwas clear at every stage of this process that engage-ment was needed across the whole health economyIt is only in working with all the relevant layers andpartnerships of professionals that we can hope for thefull impact of evidence to be realized Traditionalapproaches however only disseminate evidence tointerest groups in isolation Our use of lsquodiagonal slicersquo
Developing practice in breastfeeding 257
copy 2006 The Authors Journal compilation copy 2006 Blackwell Publishing Ltd Maternal and Child Nutrition 2 pp 245ndash261
workshops in which staff at all levels and across allsectors were engaged and including representativesof service users and the voluntary sector enabledmuch greater understanding of the consequences ofparticular activity or behaviour in other parts of thesystem and allowed creative and informed challengesto assumptions and prejudices This laid good foun-dations for whole systems approaches to introducingdriving and implementing new approaches whichcould lead to positive health outcomes It proved avery positive learning experience for all thoseinvolved
Practice change needs to involve the whole rangeof health professionals involved in work directly withpregnant women and new mothers to ensure coordi-nated working and consistent messages Despiteactive support from relevant Royal Colleges and sev-eral strongly supportive individuals engagement bydoctors was noticeably less compared with otherhealth professions This supports the findings of otherwork (eg Smale et al 2006) This really matters in afield such as breastfeeding where paediatriciansobstetricians general practitioners and public healthphysicians have an important role to play Futurework will need to address this
Key constituents in practice development in breast-feeding include mothers and potential mothersgrandmothers and men We had strong support andinvolvement from service users and user groups butengaging men proved to be difficult To reach thepublic good-quality easily accessible information isneeded perhaps the developing DiPEX module onbreastfeeding will contribute to this (httpwwwdipexorgDesktopDefaultaspx) Recent gov-ernment policy directives acknowledge the potentialcontribution that incorporating patient and serviceuser experience into service provision can bring (egDH 2006) Recent developments in the approach tolong-term conditions management have introducedthe Expert Patient Programme which enables peoplewith disabilities to take much more effective controlover the management and treatment of their disease(DH 2004c 2006) There is perhaps potential for theparallel development of an lsquoExpert Mothers Pro-grammersquo to have similar positive impact in relation tonutrition and health
Service user involvement is actively encouraged ininforming research and practice (Hanley et al 2004)Breastfeeding and maternity care as a whole have along-standing history of the active engagement of ser-vice users Volunteer counsellors and supporterstrained and accredited by their own voluntary orga-nizations have filled the gap left by the health ser-vices They have taken the initiative in setting uptelephone support services training and supervisingpeer supporters and contributing to the education ofhealth professionals (Smale et al 2006) In our cur-rent and previous practice development work thecontribution of service users and voluntary groupswent much further than simply offering advice andinformation They took an active role in planning thework and in some cases delivering education andservices Our experience was that lay workers havean essential role in developing services and they areable to advise at a strategic level as well as participat-ing in service delivery They are able to see throughthe organizational barriers that often constrain pro-fessionals and can see solutions that will work formothers and families From our experience we wouldadvise that others explore ways of actively engaginglay workers adequately remunerated in the deliveryof health care and in the education of healthprofessionals
The fundamental importance of multidisciplinaryand multi-professional working was also apparent inthe way in which the core team worked and in thesupport gained from the network of partners Atevery stage we had expertise and support availableto us as well as an effective communication systemand network Practice change in public health needsto be led and informed by those who know the topicarea and who have the wide range of skills neededto convince many different kinds of professionals thatthe work is worthwhile and achievable
Another positive contribution was the synergy ofthis programme with the evidence base The sameteam had also been responsible for systematicreviews of the field (eg Fairbank et al 2000Protheroe et al 2003 Sikorski et al 2004 Renfrewet al 2005a) and the approach was grounded in thisevidence which was at the same time being devel-oped into national guidance The interaction between
258 MJ Renfrew et al
copy 2006 The Authors Journal compilation copy 2006 Blackwell Publishing Ltd Maternal and Child Nutrition 2 pp 245ndash261
these elements should not be underestimated part-ners and sentinel sites were able to inform the guid-ance and up-to-date knowledge of the evidence basehelped strengthen the practice development work
The sentinel site system was proving to be asuccessful lsquowin-winrsquo situation for all involved Itprovided a test bed for ideas it was a source ofinformation and debate and the programme gaineda richness and diversity of input that would be hardto match At the same time it offered the sitesengagement in leading-edge work an increased pro-file and high-quality staff development Although itwas not formally evaluated all involved were con-vinced that it was a very cost-effective system theprogramme could conduct work at speed and to ahigh quality and governance issues were streamlinedThe system was very flexible and could adapt to thedifferent circumstances of each site It would havebeen able to accommodate future service and educa-tion developments such as Childrenrsquos Centres Trustreorganization and inter-professional educationOver time we could have expanded to include othersectors and practitioners such as retailers and child-minders Had the programme continued future siteswould have been identified and material developedfor national use based on our learning in the originalfour sites
Major challenges
Throughout the programme getting breastfeedingrecognized as a priority was difficult This has beenthe case for many years despite its fundamental con-tribution to public health in the short and long termit has only recently been included in national publichealth policy statements PCT targets and monitoringAs we found in the learning needs assessment andother work breastfeeding services are often seen asthe remit of enthusiastic individuals discussed interms reminiscent of lsquoreligious zealotryrsquo (Smale et al2006) rather than as a part of the mainstream ofhealth provision Creating real change in theapproach to breastfeeding in the health service willrequire it to be seen as a priority for senior managersand commissioners Our experience has demon-strated that it is possible to engage such senior people
in this work and that discussion and debate with theirown colleagues can have an impact on their thinking
A key area of practice development that canimpact on breastfeeding duration is working withmothers to sustain breastfeeding while going back towork and the ways that public health strategy andpractice can influence employers to provide breast-feeding-friendly maternity policies and facilities(Kosmala-Anderson amp Wallace in press) We did nothave an impact on this area but it was clear that itwas an area that needed to be addressed One goodplace to start would be with the employment condi-tions for NHS employees themselves this would havethe dual advantage of improving conditions for thelargest female workforce in the country while alsoproviding a model of good practice for others
Although the aim of this work was to address ine-qualities in health it is clear that reaching the hard-to-reach remains challenging We did see signs of suc-cess for example Sure Start schemes were making adifference in some areas but ensuring that all vulner-able women receive the support and care they needis still a distant goal whether they are teenagers asy-lum seekers or simply women who live in areas wherebottle feeding has been endemic for generations
Finally there is a debate to be had on whoseresponsibility it is to create such change The work ofresearchers is seen to be complete when their studyis finished and disseminated through publication andconference presentation Systematic reviewers takeon a responsibility to make the results of a wide rangeof studies available through publication but not toengage with what services might do with those find-ings Those responsible for guidance are responsiblefor developing and publishing that work and somealso take responsibility for lsquoimplementationrsquo (egNICE 2005) But where does responsibility rest forpractice development which requires a deep engage-ment with the practice setting and with those affectedby the issues raised by the evidence Lack of invest-ment at the national level in formal evaluation ofprogrammes of change limits the available evidencebase and detracts from our achieving a better under-standing of what actually works in relation to thesemore complex health issues funding for the lsquoRrsquoaspects of research and development is more com-
Developing practice in breastfeeding 259
copy 2006 The Authors Journal compilation copy 2006 Blackwell Publishing Ltd Maternal and Child Nutrition 2 pp 245ndash261
mon than for the lsquoDrsquo (NHS Executive 1997) Thewithdrawal of funding to this programme part waythrough its cycle was regretted by our commissionersit was evident that practice development was nolonger their remit given their changed circumstancesIt is however not clear that responsibility now restswith any particular agency Is development work forindividual health service organizations themselves totake on Is this work that should be led by nationalprogrammes supported by public-sector funding orshould it rely on other sources of support If so fromwhere will it be resourced and how will cross-sectoraland multidisciplinary developments be addressedThere are also questions about who will lead thiswork when a number of professional disciplines areinvolved and where the client interface spans bothprimary and acute care healthcare settings social ser-vices and other development agencies These ques-tions will become more pressing as guidancecontinues to be produced especially in public health
Acknowledgements
We would like to thank all participants from sentinelsites and our consortium of academic professionalNHS and consumer partners and the two anonymousreferees who reviewed the manuscript This work wascommissioned by the former Health DevelopmentAgency and subsequently funded by NICE
References
Abbott S Renfrew MJ amp McFadden A (2006) lsquoInformalrsquo learning to support breastfeeding local problems and opportunities Maternal and Child Nutrition 2 232ndash238
Audit Commission (2000) United They Stand Coordinating Care for Elderly Patients with Hip Fracture Audit Com-mission London
British Paediatric Association (1994) Statement of the stand-ing committee on nutrition is breastfeeding beneficial in the UK Archive of Diseases in Childhood 71 376ndash380
Chalmers I amp Altman DG (eds) (1995) Systematic Reviews BMJ Publishing Group London
Children Act (2004) Available at httpwwwopsigovukactsacts200420040031htm (accessed 21 March 2006)
Coote A Allen J amp Woodhead D (2004) Finding out What Works Building Knowledge about Complex Community-Based Initiatives Kingrsquos Fund London
DfES (2000) Adoption and Permanence Taskforce Available at httpwwwdfesgovukadoptionadoptionreformstaskforceshtml (accessed 29 March 2006)
DH (2002a) Improvement Expansion and Reform The Next 3 Years Priorities and Planning Framework 2003ndash2006 Department of Health London
DH (2002b) The Health and Social Care Change Agent Team Available at httpwwwchangeagentteamorguk (accessed 29 March 2006)
DH (2004a) National Service Framework for Children Young People and Maternity Services Stationery Office London
DH (2004b) Choosing Health Making Healthy Choices Eas-ier Stationery Office London
DH (2004c) Self Care ndash A Real Choice Self Care Support ndash A Practical Option Stationery Office London
DH (2006) Our Health Our Care Our Say A New Direction for Community Services Stationery Office London
Dominey M Archibald A Edgecombe D Lawrence J amp Thomson L (2002) Breastfeeding and drug misuse Mak-ing an informed choice Year 3 Practice project In Infant Feeding Initiative A Report Evaluating the Breastfeeding Practice Projects 1999ndash2002 (ed F Dykes 2003) p 64 Department of Health London
Dykes F (2003) Infant Feeding Initiative A Report Evaluat-ing the Breastfeeding Practice Projects 1999ndash2002 Depart-ment of Health London
Dykes F (2006) The education of health practitioners sup-porting breastfeeding women time for critical reflection Maternal and Child Nutrition 2 204ndash216
Dyson L Renfrew MJ McFadden A McCormick F Herbert G amp Thomas J (2006) Promotion of Breastfeed-ing Initiation and Duration Evidence into Practice Brief-ing National Institute for Health and Clinical Excellence London httpwwwniceorgukdown-loadaspxo=346169 (accessed 26 July 2006)
EU (2004) Project on Promotion of Breastfeeding in Europe Protection Promotion and Support of Breastfeeding A Blueprint for Action European Commission Directorate Public Health and Risk Assessment Luxembourg
Fairbank L OrsquoMeara S Renfrew MJ Woolridge M Sowden AJ amp Lister-Sharp D (2000) A systematic review to evaluate the effectiveness of interventions to promote the initiation of breastfeeding Health Technol-ogy Assessment 4 1ndash171
Grant J Fletcher M amp Warwick C (2000) The South Thames Evidence Based Practice (STEP) Project Sup-porting Breastfeeding Women South Bank University London
Greenhalgh T Robert G Bate P Mcfarlane F amp Kyriakidou O (2005) Diffusion of Innovations in Health Service Organisations A Systematic Literature Review Blackwell Publishing Limited Oxford
260 MJ Renfrew et al
copy 2006 The Authors Journal compilation copy 2006 Blackwell Publishing Ltd Maternal and Child Nutrition 2 pp 245ndash261
Grimshaw JM Thomas RE MacLennan G Fraser C Ramsay CR Vale L et al (2004) Effectiveness and efficiency of guideline dissemination and implementation strategies Health Technology Assessment 8 indashxi 1ndash72
Hanley B Bradburn J Barnes M Evans C Goodare H Kelson M et al (2004) Involving the Public in NHS Pub-lic Health and Social Care Research Briefing Notes for Researchers INVOLVE Department of Health London
Herbert G amp Lake G (2005) Making connections Effective development of the intermediate tier Journal of Inte-grated Care 13 35ndash42
Howie PW Forsyth JS Ogston SA Clark A amp Florey CD (1990) Protective effect of breastfeeding against infection British Medical Journal 300 11ndash16
Kosmala-Anderson J amp Wallace LM (in press) Breastfeed-ing works the role of employers in supporting women who wish to breastfeed and work in four organizations in England Journal of Public Health (in press)
Kramer M Chalmers B Hodnett H Sevovskaya Z Dzikovich I Shapiro S et al (2001) Promotion of breast-feeding intervention trial (PROBIT) Journal of the American Medical Association 285 413ndash420
McFadden A Renfrew MJ Dyson L McCormick F Herbert G amp Thomas J (2005) Effective Active Briefing on the Initiation and Duration of Breastfeeding Fieldwork Report National Institute for Health and Clinical Excel-lence London
McFadden A Renfrew MJ Dykes F amp Burt S (2006) Assessing learning needs for breastfeeding setting the scene Maternal and Child Nutrition 2 196ndash203
McSherry R amp McFadden A (2001) Practice Development Accreditation Assessment Maternity Services Darlington Memorial Hospital South Durham Healthcare NHS Trust Final Report University of Teesside Middlesbrough
Moulding NT Silagy CA amp Weller DP (1999) A frame-work for effective management of change in clinical prac-tice dissemination and implementation of clinical practice guidelines Quality in Health Care 8 177ndash183
Gray JA Haynes RB Sackett DL Cook DJ amp Guyatt GH (1997) Transferring evidence from research into practice 3 Developing evidence-based clinical policy Evidence-Based Medicine 2 36ndash38
NHS Centre for Reviews and Dissemination (CRD) (1999) Getting evidence into practice Effective Health Care 5 1ndash16
NHS Executive (1997) RampD in Primary Care National Working Group Report (Mant Report) Stationery Office London
NICE (2004) The Guideline Development Process National Institute for Health and Clinical Excellence London
NICE (2005) Putting NICE Guidance into Practice National Institute for Health and Clinical Excellence London
Oxman AD Thomson MA Davis DA amp Haynes RB (1995) No magic bullets a systematic review of 102 trials of interventions to improve professional practice Canadian Medical Association Journal 153 1423ndash1431
Protheroe L Dyson L Renfrew MJ Bull J amp Mulvihill C (2003) The Effectiveness of Public Health Interventions to Promote the Initiation of Breastfeeding Evidence Briefing Health Development Agency London
Quigley MA Cumberland P Cowden JM amp Rodrigues LC (2006) How protective is breast feeding against diar-rhoeal disease in infants in 1990s England A case control study Archives of Disease in Childhood 91 245ndash250
Renfrew MJ Dyson L Wallace L DrsquoSouza L McCormick FM amp Spiby H (2005a) The Effectiveness of Health Interventions to Promote the Duration of Breast-feeding Systematic Review 1st edn National Institute for Health and Clinical Excellence London
Renfrew MJ Dyson L McFadden A McCormick F Herbert G amp Thomas J (2005b) Effective Active Briefing on the Initiation and Duration of Breastfeeding Technical Report National Institute for Health and Clinical Excel-lence London
Renfrew MJ McFadden A Dykes F Wallace L Abbott S Burt S et al (2006) Addressing the learning deficit in breastfeeding strategies for change Maternal and Child Nutrition 2 239ndash244
Richards D (2003) Childrenrsquos Nutrition ndash Mothers Who Wish to Breast-Feed Birmingham City Council Available at httpwwwbirmingahmgovukscrutiny (accessed 27 July 2006)
Sackett DL Rosenberg WMC Gray JAM Haynes RB amp Richardson WS (1996) Evidence-based medicine what it is and what it isnrsquot British Medical Journal 312 71ndash72
Sikorski J Renfrew MJ Pindoria S amp Wade A (2004) Support for breastfeeding mothers (Cochrane Review) The Cochrane Database of Systematic Reviews Issue 2 John Wiley amp Sons Ltd Chichester
Smale M Renfrew MJ Marshall JL amp Spiby H (2006) Turning policy into practice more difficult that it seems The case of breastfeeding education Maternal and Child Nutrition 2 103ndash113
Spiby H Ker R DrsquoSouza L amp Renfrew MJ (2002) Intro-ducing a Consumer-Practitioner into breastfeeding prac-tice Year 2 In Infant Feeding Initiative A Report Evaluating the Breastfeeding Practice Projects 1999ndash2002 (ed F Dykes 2003) p 44 Department of Health London
Spiby H Wallis S Stone C amp Renfrew MJ (2005) Support-ing and Promoting Breastfeeding in Leeds Final Report to December 2004 Report to Leeds PCTs Children and Families Modernisation Team Leeds
Thomas C (2006) Darlington ndash A Breastfeeding Friendly Town Darlington Borough Council Darlington
Developing practice in breastfeeding 261
copy 2006 The Authors Journal compilation copy 2006 Blackwell Publishing Ltd Maternal and Child Nutrition 2 pp 245ndash261
Unsworth J (2000) Practice development a concept analy-sis Journal of Nursing Management 8 317ndash326
Wallace LM amp Jardine J (2006) A Health Scrutiny of Ser-vices to Support the Initiation and Duration of Breastfeed-ing in Coventry and Warwickshire Coventry and Warwickshire County Councils Coventry
Wallace L amp Kosmala-Anderson J (2006) A training needs survey of doctorsrsquo breastfeeding support skills in England Maternal and Child Nutrition 2 217ndash231
Wallace L amp Kosmala-Anderson J (in press) Training needs survey of midwives health visitors and voluntary sector
breastfeeding support staff in England Maternal and Child Nutrition (in press)
WHO (2003) Global Strategy for Infant and Young Child Feeding World Health Organization Geneva
Wilson AC Forsyth JS Green SA Irvine L Hau C amp Howie PW (1998) Relation of infant diet to childhood health seven year follow up of a cohort of children in Dundee infant feeding study British Medical Journal 316 21ndash25
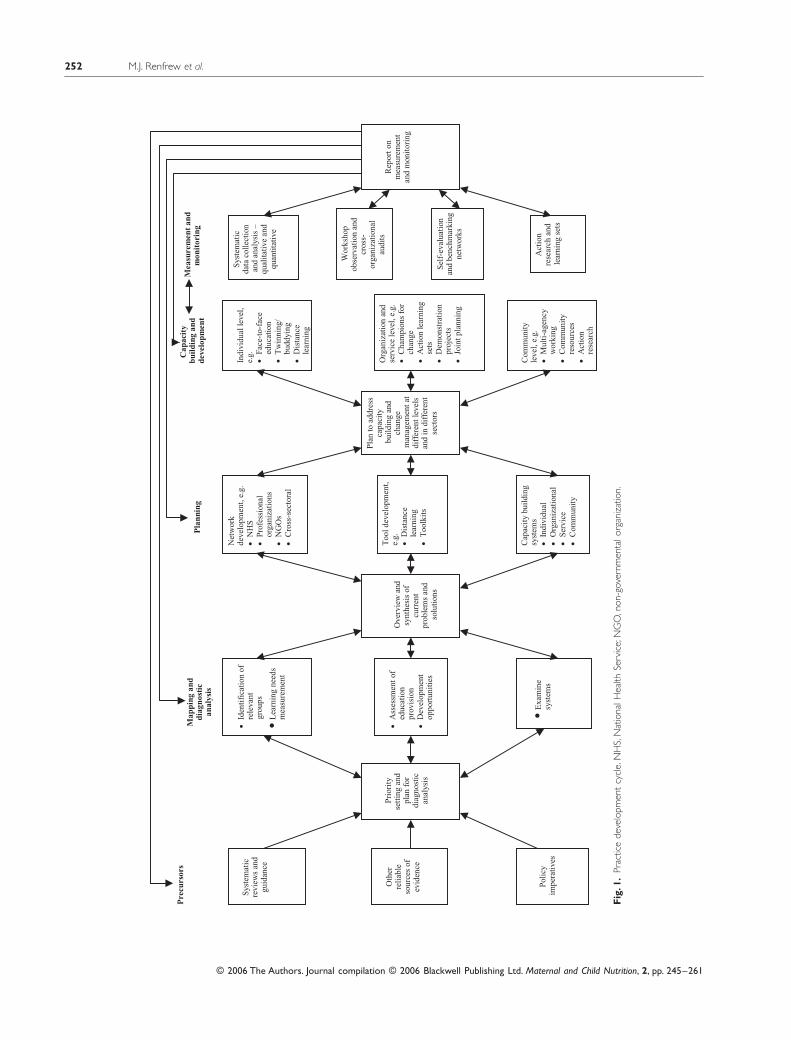
252
MJ Renfrew
et al
copy 2006 The Authors Journal compilation copy 2006 Blackwell Publishing Ltd
Maternal and Child Nutrition
2
pp 245ndash261
Fig
1
Prac
tice
deve
lopm
ent
cycl
e N
HS
Nat
iona
l Hea
lth S
ervi
ce N
GO
non
-gov
ernm
enta
l org
aniz
atio
n
Pre
curs
ors
Sys
tem
atic
re
view
s an
d gu
idan
ce
Oth
er
reli
able
so
urce
s of
ev
iden
ce
bull E
xam
ine
syst
ems
Map
ping
and
di
agno
stic
an
alys
is
bull Id
enti
fica
tion
of
rele
vant
grou
ps
bull L
earn
ing
need
s m
easu
rem
ent
bull A
sses
smen
t of
educ
atio
n pr
ovis
ion
bull D
evel
opm
ent
oppo
rtun
itie
s
Ove
rvie
w a
ndsy
nthe
sis
of
curr
ent
prob
lem
s an
d so
luti
ons
Pla
nnin
g
Net
wor
k de
velo
pmen
t e
gbull
NH
Sbull
Pro
fess
iona
l or
gani
zati
ons
bull N
GO
s bull
Cro
ss-s
ecto
ral
Too
l dev
elop
men
t e
gbull
Dis
tanc
e le
arni
ng
bull T
oolk
its
Cap
acit
y bu
ildi
ng
syst
ems
bull In
divi
dual
bull
Org
aniz
atio
nal
bull S
ervi
ce
bull C
omm
unit
y
Pla
n to
add
ress
ca
paci
ty
buil
ding
and
chan
ge
man
agem
ent a
tdi
ffer
ent l
evel
s an
d in
dif
fere
nt
sect
ors
Cap
acit
y bu
ildi
ng a
ndde
velo
pmen
t
Mea
sure
men
t an
dm
onit
orin
g
Indi
vidu
al le
vel
eg
bull Fa
ce-t
o-fa
ce
educ
atio
n bull
Tw
inni
ng
budd
ying
bull
Dis
tanc
e le
arni
ng
Sys
tem
atic
da
ta c
olle
ctio
n an
d an
alys
is ndash
qual
itat
ive
and
quan
tita
tive
Org
aniz
atio
n an
dse
rvic
e le
vel
eg
bull C
ham
pion
s fo
r ch
ange
bull
Act
ion
lear
ning
se
ts
bull D
emon
stra
tion
pr
ojec
ts
bull Jo
int p
lann
ing
Wor
ksho
pob
serv
atio
n an
d cr
oss-
or
gani
zati
onal
au
dits
Sel
f-ev
alua
tion
an
d be
nchm
arki
ng
netw
orks
Com
mun
ity
leve
l e
gbull
Mul
ti-a
genc
y w
orki
ng
bull C
omm
unit
y re
sour
ces
rese
arch
bull A
ctio
n
Act
ion
rese
arch
and
le
arni
ng s
ets
Pol
icy
impe
rati
ves
Pri
orit
y se
ttin
g an
d
plan
for
di
agno
stic
an
alys
is
Rep
ort o
n m
easu
rem
ent
and
mon
itor
ing
Developing practice in breastfeeding
253
copy 2006 The Authors Journal compilation copy 2006 Blackwell Publishing Ltd
Maternal and Child Nutrition
2
pp 245ndash261
(Stage 2) Stage 3 involved developing relevant net-works tools for education and training evaluationmethods and capacity building systems at individualorganizational service and community levels Follow-ing this a plan to conduct the work would be finalized(Stage 4) implemented (Stage 5) and evaluated Theprocess was intended to be iterative alternatingbetween phases of information appraisal and plan-ning to identify the next stages of development activ-ity and evaluation of the impact to inform futureplanning Stage 6 included finalization of qualitativeand quantitative measurement and monitoring sys-tems that would feedback through all stages of theprocess
It was envisaged that this model would allow effec-tive structures and processes to be identified for usein other aspects of public health practice
Due to changes in funding the programme wasdiscontinued during Stage 3 although in fact somepreliminary work had already been carried out on theplan
Engagement with practitioners
Developing a national programme of change anddevelopment is an ambitious goal A cost-effectiveapproach to engagement had to be developed both tostay within budget and that could roll out acrossEngland and Wales Learning from the successfulLeeds partnership work described above it wasplanned to recruit a series of sentinel sites where wecould test out a range of approaches to maximizelearning and cost-effectiveness as well as respond toideas from the field Work in those sites wouldbecome a model for national developments inform-ing material for education training and assessmentsupported by communications at different levelsthrough our established national network The use ofsentinel sites also allowed for the development ofapproaches sensitive to varying local contexts so pro-viding alternatives and examples to inform nationalimplementation
The first stage in that process was to recruit rele-vant sentinel sites Sites were conceived as includingthe whole health economy in a locality and had tomeet specific criteria These are detailed in Box 2
Four sites were identified and agreed to join thefirst wave of sentinel sites Each site engaged andplanned the programme of work differently Forexample one site had already worked with membersof the core team and were keen to take existing workfurther In the few months in which we worked withthem they put into place a system for the accuratemonitoring of breastfeeding rates and created anextensive network of individuals at a range of seniorlevels from different sectors including Primary CareTrusts (PCTs) Strategic Health Authority the acuteTrust Sure Start and the local authority Benefits thesites have seen even since the work stopped haveincluded
bull improved communication across relevant disci-plines and sectorsbull the observation that the practice developmentwork lsquokept breastfeeding on everyonersquos agendarsquobull the work was used to support a business case for acoordinator for BFI planningbull in one sentinel site the primary care and acutematernity services have formed a health economy-wide breastfeeding strategy groupbull in another a joint primary care and maternity ser-vices group has been establishedbull two sites are taking forward systems for collect-ing breastfeeding data which have been used toprovide feedback to staff each monthbull a new approach to training all staff in one siteincluded commissioning the local university todevelop a self-study workbook and then to test itseffectiveness using an objective skills assessment toolandbull in one site a successful peer support programmewas rolled out throughout Sure Start programmes
A key part of the work in the sentinel sites was tosupport the learning needs assessment (McFadden
et al
2006) Although the sites were at an early stageof engagement this was conducted very successfullyand rapidly as sites supported the identification andinvolvement of practitioners Many assisted with sur-vey distribution and in return received a report ofthe training needs identified for their staff The nexttest was the running of fieldwork meetings and
254
MJ Renfrew
et al
copy 2006 The Authors Journal compilation copy 2006 Blackwell Publishing Ltd
Maternal and Child Nutrition
2
pp 245ndash261
workshops to finalize guidance based on researchevidence as part of a related programme of workThe aim of this work was to take the results of aseries of systematic reviews (which gave informationon lsquowhat works from research evidencersquo) and consultwith practitioners managers and users on lsquowhatreally works in practicersquo (Dyson
et al
2006) Thenewly established sentinel site system supported thiswork by offering venues for meetings providing listsof eligible participants and enabling and encourag-ing staff to attend (Renfrew
et al
2005b) The finalstage of this guidance work was a series of majorworkshops with over 30 participants in each repre-senting a lsquodiagonal slicersquo through the whole healtheconomy from field-level practitioners includingpeer support workers to managers and planners andincluding the range of relevant disciplines as well as
the voluntary sector Concerns around the realitiesand influences on practice and key issues for practi-tioners and managers in developing good practicewere discussed as well as organizational and struc-tural barriers to change Participants were encour-aged to discuss not only practices that need to beintroduced but also those that need to be aban-doned thereby potentially saving time and resourcesand to identify actual or potential barriers to imple-menting change (Renfrew
et al
2005b) These facili-tated groups examined the ability of the service torespond to identified gaps and made recommenda-tions for improvements to the system They feddirectly into the final stages of the development ofNational Institute for Health and Clinical Excellence(NICE) public health recommendations for breast-feeding offering participants the satisfaction of
Box 2
Sentinel site criteriaSentinel sites were expected to
bull Have a deprivation profile that demonstrated a substantial proportion of low-income groups and adiverse ethnic profile and serve contrasting areas (eg urban rural)
bull Offer a range of services for children and women with an interest in nutrition
bull Be able to include the whole health economy in a locality (or at least agree to working across allrelevant sectors)
bull Provide a key contact personpeople who would act to facilitate communication and broker agree-ments with different parts of the health economy and managers who were supportive of the plannedwork willing to support and enable staff participation
bull In the first instance sites would be those where contact already existed with members of our coreteam Future sites would be brought in once any initial problems with the approach had been identifiedand addressed
In return for their involvement in the work it was recognized that the sentinel sites would benefit in arange of ways including
bull Support for staff development and learning through access to programme staff and expertise involve-ment in and learning from a regular newsletter and attendance at an annual leading-edge conferenceon maternal and child nutrition
bull Developing links with other sites and sharing good practice and problem solving
bull The opportunity to help to develop national practice resulting in a raised profile for their work andtheir staff
bull Early access to emerging evidence in the field of maternal and child nutrition
Developing practice in breastfeeding
255
copy 2006 The Authors Journal compilation copy 2006 Blackwell Publishing Ltd
Maternal and Child Nutrition
2
pp 245ndash261
knowing that their input would make a difference(Dyson
et al
2006) These workshops also tested outthe use of language the conceptual understanding ofparticipants in relation to the evidence reviews andgathered intelligence on what approaches to imple-mentation of practice development may be mosteffective They also provided an opportunity for dis-cussion debate and deliberation about the meaningof the evidence Participants reported this to be veryuseful in assisting their understanding of the evi-dence and in considering how best to change theirown and their colleaguesrsquo practice in response to itand as an important contribution to practice devel-opment in their own locality (McFadden
et al
2005)The input of representatives of service users was ofcritical importance
It was planned that once the guidance was final-ized each participating site would be in a strong posi-tion to act on it Not only would they feel someownership but they would also have staff from alllevels and sectors in their health economy who hadspent time discussing the issues with colleagues andwith service user representatives They would haveaccess to specific local information about localitiesand groups that needed to be prioritized creatingchange was therefore brought several stages closerAt the end of each workshop email and telephonecontact details were exchanged among the workshopparticipants many of whom had never met beforedespite working in related parts of the same systemto support closer local networking The opportunityto consult with national experts in the network alsoacted as a variant on educational outreach which hasbeen shown to be moderately successful in guidelineimplementation (NHS CRD 1999) The impact ofsuch exchanges in increasing opportunities for net-work support is virtually impossible to evaluate for-mally but there was confidence in those whoparticipated at these events that positive changewould result and that the evidence would be moreeffectively used in the future as a consequence
Interactive conference
The other main activity was a conference on maternaland child nutrition to which all partners ndash academic
professional NHS and userconsumer ndash and stafffrom sentinel sites were invited Commissioners ofthe work were invited as were staff from key govern-ment departments with an interest in nutrition childhealth Sure Start nursing and midwifery and ine-qualities in health Around 90 participants took partin a day which included presentations participativeworking and active networking A report of the dayis available at httpwwwyorkacukresmcncccon-ferenceReporthtm Feedback was strongly positiveand the impact of networking with others in similarsituations and between those working in local andnational organizations was especially valued It wasplanned that this would be an annual event
Had we been able to continue the practice devel-opment programme we planned to use the follow-ing approaches
Establishing learning networks
We planned to identify appropriate learning net-works for different constituencies which wouldenable communication among staff from differentsectors as well as communication with programmestaff Activities were planned to include
bull Staff working at strategic and senior managementlevels would be supported and appropriate informa-tion provided to allow them to create cross-systemchanges Senior-level lsquochampions for changersquo wouldbe identified These would be used in a range of waysthose wishing to be involved in learning networkswould be supported to do sobull Learning sets would be established This wouldenable focused exchange between stakeholders onhow best to make use of the evidence in practice andhow to influence mainstream practice across locali-ties Through feedback loops we planned to developlearningeducation material to be made availablethrough web-based routes to wider constituenciesbull Peer supporters and trained breastfeeding counsel-lors are key groups in regard to breastfeeding promo-tion and support We planned to include them inlearning sets They have much to offer health profes-sionals in coming to understand the needs of womenand families and indeed the evidence suggests thattheir involvement in advisory work and peer support
256
MJ Renfrew
et al
copy 2006 The Authors Journal compilation copy 2006 Blackwell Publishing Ltd
Maternal and Child Nutrition
2
pp 245ndash261
enhances and strengthens the impact of informationand evidence-based guidance possibly more thanthat of health professionalsrsquo practice Our experiencedescribed above has identified a valuable contribu-tion from lay breastfeeding counsellors into educa-tion and training provision
Educational approaches
The breadth of constituencies that the programmeneeded to reach was to be reflected in the range ofeducational approaches required For some profes-sions continuing professional development (CPD)time is factored in regularly to the job plan in a rollingprogramme of group education with routine sessionalwork suspended for other groups CPD is a self-verified individual activity that can be achievedthrough a range of methods including distance learn-ing We hoped to reach directly a broad group ofwomen as well as professionals through some of theroutes developed A range of materials was thereforeplanned to address all needs Materials would bedeveloped for web-based access CD-ROM access andon paper These were to include
bull Toolkits to promote and support breastfeeding tomonitor breastfeeding rates and on practice develop-ment and changebull Distance learning modules providing accreditedlearning opportunities at a range of levelsbull An email and telephone-based service to putindividuals and organizations in touch with otherswho can support and advise them supported byRDLearning a national web-based resourcebull Learning material that could be directly dissemi-nated through the Internet to a wide audiencebull Buddy systems and mentoring for practice devel-opment and public health strategic development inbreastfeeding and use of cascade systemsbull Summaries of approaches to dissemination andpromotion of information that have proved to be suc-cessful and of practice change programmes that havebeen evaluated as having a positive impact on initia-tion and duration of breastfeedingbull Through NHS Direct we planned to reach the gen-eral public Information could be provided to informthe development of new algorithms that could be
used by staff taking enquiries from breastfeedingwomen We planned also to provide information thatcould be used on the NHS Direct website which isaccessed directly by women and families as well ashealth professionalsbull Other material to reach the general public wouldbe developed We aimed to have informative paperspublished in womenrsquos and familiesrsquo magazines and inthe general media on a regular basis A professionalwriter was one of our partners her role was to informand advise us about reaching women directly
Discussion
The work described in this paper was a structuredcross-sectoral approach to practice development inpublic health As a result of funding problems a fullevaluation could not be conducted and our contribu-tion to the knowledge base on practice change inpublic health is limited Lessons were learned how-ever and feedback was gained from participants atdifferent stages of the process We received strongsupport for our approach and the willingness of localand national partners to engage actively in the pro-gramme testifies to its potential
Lessons learned
There is increasing emphasis in public health andhealth policy on the need for good partnership work-ing and integration across disciplines professionsorganizations and localities as shown in the recentWhite Paper from the Department of Health (DH2006) and in the Children Act (2004) Prevention ofill health and promotion of well-being featurestrongly in these and other policy documents with arecognition that this cannot be achieved without fullengagement at strategic and operational levels withthose who use or depend on public-sector services Itwas clear at every stage of this process that engage-ment was needed across the whole health economyIt is only in working with all the relevant layers andpartnerships of professionals that we can hope for thefull impact of evidence to be realized Traditionalapproaches however only disseminate evidence tointerest groups in isolation Our use of lsquodiagonal slicersquo
Developing practice in breastfeeding 257
copy 2006 The Authors Journal compilation copy 2006 Blackwell Publishing Ltd Maternal and Child Nutrition 2 pp 245ndash261
workshops in which staff at all levels and across allsectors were engaged and including representativesof service users and the voluntary sector enabledmuch greater understanding of the consequences ofparticular activity or behaviour in other parts of thesystem and allowed creative and informed challengesto assumptions and prejudices This laid good foun-dations for whole systems approaches to introducingdriving and implementing new approaches whichcould lead to positive health outcomes It proved avery positive learning experience for all thoseinvolved
Practice change needs to involve the whole rangeof health professionals involved in work directly withpregnant women and new mothers to ensure coordi-nated working and consistent messages Despiteactive support from relevant Royal Colleges and sev-eral strongly supportive individuals engagement bydoctors was noticeably less compared with otherhealth professions This supports the findings of otherwork (eg Smale et al 2006) This really matters in afield such as breastfeeding where paediatriciansobstetricians general practitioners and public healthphysicians have an important role to play Futurework will need to address this
Key constituents in practice development in breast-feeding include mothers and potential mothersgrandmothers and men We had strong support andinvolvement from service users and user groups butengaging men proved to be difficult To reach thepublic good-quality easily accessible information isneeded perhaps the developing DiPEX module onbreastfeeding will contribute to this (httpwwwdipexorgDesktopDefaultaspx) Recent gov-ernment policy directives acknowledge the potentialcontribution that incorporating patient and serviceuser experience into service provision can bring (egDH 2006) Recent developments in the approach tolong-term conditions management have introducedthe Expert Patient Programme which enables peoplewith disabilities to take much more effective controlover the management and treatment of their disease(DH 2004c 2006) There is perhaps potential for theparallel development of an lsquoExpert Mothers Pro-grammersquo to have similar positive impact in relation tonutrition and health
Service user involvement is actively encouraged ininforming research and practice (Hanley et al 2004)Breastfeeding and maternity care as a whole have along-standing history of the active engagement of ser-vice users Volunteer counsellors and supporterstrained and accredited by their own voluntary orga-nizations have filled the gap left by the health ser-vices They have taken the initiative in setting uptelephone support services training and supervisingpeer supporters and contributing to the education ofhealth professionals (Smale et al 2006) In our cur-rent and previous practice development work thecontribution of service users and voluntary groupswent much further than simply offering advice andinformation They took an active role in planning thework and in some cases delivering education andservices Our experience was that lay workers havean essential role in developing services and they areable to advise at a strategic level as well as participat-ing in service delivery They are able to see throughthe organizational barriers that often constrain pro-fessionals and can see solutions that will work formothers and families From our experience we wouldadvise that others explore ways of actively engaginglay workers adequately remunerated in the deliveryof health care and in the education of healthprofessionals
The fundamental importance of multidisciplinaryand multi-professional working was also apparent inthe way in which the core team worked and in thesupport gained from the network of partners Atevery stage we had expertise and support availableto us as well as an effective communication systemand network Practice change in public health needsto be led and informed by those who know the topicarea and who have the wide range of skills neededto convince many different kinds of professionals thatthe work is worthwhile and achievable
Another positive contribution was the synergy ofthis programme with the evidence base The sameteam had also been responsible for systematicreviews of the field (eg Fairbank et al 2000Protheroe et al 2003 Sikorski et al 2004 Renfrewet al 2005a) and the approach was grounded in thisevidence which was at the same time being devel-oped into national guidance The interaction between
258 MJ Renfrew et al
copy 2006 The Authors Journal compilation copy 2006 Blackwell Publishing Ltd Maternal and Child Nutrition 2 pp 245ndash261
these elements should not be underestimated part-ners and sentinel sites were able to inform the guid-ance and up-to-date knowledge of the evidence basehelped strengthen the practice development work
The sentinel site system was proving to be asuccessful lsquowin-winrsquo situation for all involved Itprovided a test bed for ideas it was a source ofinformation and debate and the programme gaineda richness and diversity of input that would be hardto match At the same time it offered the sitesengagement in leading-edge work an increased pro-file and high-quality staff development Although itwas not formally evaluated all involved were con-vinced that it was a very cost-effective system theprogramme could conduct work at speed and to ahigh quality and governance issues were streamlinedThe system was very flexible and could adapt to thedifferent circumstances of each site It would havebeen able to accommodate future service and educa-tion developments such as Childrenrsquos Centres Trustreorganization and inter-professional educationOver time we could have expanded to include othersectors and practitioners such as retailers and child-minders Had the programme continued future siteswould have been identified and material developedfor national use based on our learning in the originalfour sites
Major challenges
Throughout the programme getting breastfeedingrecognized as a priority was difficult This has beenthe case for many years despite its fundamental con-tribution to public health in the short and long termit has only recently been included in national publichealth policy statements PCT targets and monitoringAs we found in the learning needs assessment andother work breastfeeding services are often seen asthe remit of enthusiastic individuals discussed interms reminiscent of lsquoreligious zealotryrsquo (Smale et al2006) rather than as a part of the mainstream ofhealth provision Creating real change in theapproach to breastfeeding in the health service willrequire it to be seen as a priority for senior managersand commissioners Our experience has demon-strated that it is possible to engage such senior people
in this work and that discussion and debate with theirown colleagues can have an impact on their thinking
A key area of practice development that canimpact on breastfeeding duration is working withmothers to sustain breastfeeding while going back towork and the ways that public health strategy andpractice can influence employers to provide breast-feeding-friendly maternity policies and facilities(Kosmala-Anderson amp Wallace in press) We did nothave an impact on this area but it was clear that itwas an area that needed to be addressed One goodplace to start would be with the employment condi-tions for NHS employees themselves this would havethe dual advantage of improving conditions for thelargest female workforce in the country while alsoproviding a model of good practice for others
Although the aim of this work was to address ine-qualities in health it is clear that reaching the hard-to-reach remains challenging We did see signs of suc-cess for example Sure Start schemes were making adifference in some areas but ensuring that all vulner-able women receive the support and care they needis still a distant goal whether they are teenagers asy-lum seekers or simply women who live in areas wherebottle feeding has been endemic for generations
Finally there is a debate to be had on whoseresponsibility it is to create such change The work ofresearchers is seen to be complete when their studyis finished and disseminated through publication andconference presentation Systematic reviewers takeon a responsibility to make the results of a wide rangeof studies available through publication but not toengage with what services might do with those find-ings Those responsible for guidance are responsiblefor developing and publishing that work and somealso take responsibility for lsquoimplementationrsquo (egNICE 2005) But where does responsibility rest forpractice development which requires a deep engage-ment with the practice setting and with those affectedby the issues raised by the evidence Lack of invest-ment at the national level in formal evaluation ofprogrammes of change limits the available evidencebase and detracts from our achieving a better under-standing of what actually works in relation to thesemore complex health issues funding for the lsquoRrsquoaspects of research and development is more com-
Developing practice in breastfeeding 259
copy 2006 The Authors Journal compilation copy 2006 Blackwell Publishing Ltd Maternal and Child Nutrition 2 pp 245ndash261
mon than for the lsquoDrsquo (NHS Executive 1997) Thewithdrawal of funding to this programme part waythrough its cycle was regretted by our commissionersit was evident that practice development was nolonger their remit given their changed circumstancesIt is however not clear that responsibility now restswith any particular agency Is development work forindividual health service organizations themselves totake on Is this work that should be led by nationalprogrammes supported by public-sector funding orshould it rely on other sources of support If so fromwhere will it be resourced and how will cross-sectoraland multidisciplinary developments be addressedThere are also questions about who will lead thiswork when a number of professional disciplines areinvolved and where the client interface spans bothprimary and acute care healthcare settings social ser-vices and other development agencies These ques-tions will become more pressing as guidancecontinues to be produced especially in public health
Acknowledgements
We would like to thank all participants from sentinelsites and our consortium of academic professionalNHS and consumer partners and the two anonymousreferees who reviewed the manuscript This work wascommissioned by the former Health DevelopmentAgency and subsequently funded by NICE
References
Abbott S Renfrew MJ amp McFadden A (2006) lsquoInformalrsquo learning to support breastfeeding local problems and opportunities Maternal and Child Nutrition 2 232ndash238
Audit Commission (2000) United They Stand Coordinating Care for Elderly Patients with Hip Fracture Audit Com-mission London
British Paediatric Association (1994) Statement of the stand-ing committee on nutrition is breastfeeding beneficial in the UK Archive of Diseases in Childhood 71 376ndash380
Chalmers I amp Altman DG (eds) (1995) Systematic Reviews BMJ Publishing Group London
Children Act (2004) Available at httpwwwopsigovukactsacts200420040031htm (accessed 21 March 2006)
Coote A Allen J amp Woodhead D (2004) Finding out What Works Building Knowledge about Complex Community-Based Initiatives Kingrsquos Fund London
DfES (2000) Adoption and Permanence Taskforce Available at httpwwwdfesgovukadoptionadoptionreformstaskforceshtml (accessed 29 March 2006)
DH (2002a) Improvement Expansion and Reform The Next 3 Years Priorities and Planning Framework 2003ndash2006 Department of Health London
DH (2002b) The Health and Social Care Change Agent Team Available at httpwwwchangeagentteamorguk (accessed 29 March 2006)
DH (2004a) National Service Framework for Children Young People and Maternity Services Stationery Office London
DH (2004b) Choosing Health Making Healthy Choices Eas-ier Stationery Office London
DH (2004c) Self Care ndash A Real Choice Self Care Support ndash A Practical Option Stationery Office London
DH (2006) Our Health Our Care Our Say A New Direction for Community Services Stationery Office London
Dominey M Archibald A Edgecombe D Lawrence J amp Thomson L (2002) Breastfeeding and drug misuse Mak-ing an informed choice Year 3 Practice project In Infant Feeding Initiative A Report Evaluating the Breastfeeding Practice Projects 1999ndash2002 (ed F Dykes 2003) p 64 Department of Health London
Dykes F (2003) Infant Feeding Initiative A Report Evaluat-ing the Breastfeeding Practice Projects 1999ndash2002 Depart-ment of Health London
Dykes F (2006) The education of health practitioners sup-porting breastfeeding women time for critical reflection Maternal and Child Nutrition 2 204ndash216
Dyson L Renfrew MJ McFadden A McCormick F Herbert G amp Thomas J (2006) Promotion of Breastfeed-ing Initiation and Duration Evidence into Practice Brief-ing National Institute for Health and Clinical Excellence London httpwwwniceorgukdown-loadaspxo=346169 (accessed 26 July 2006)
EU (2004) Project on Promotion of Breastfeeding in Europe Protection Promotion and Support of Breastfeeding A Blueprint for Action European Commission Directorate Public Health and Risk Assessment Luxembourg
Fairbank L OrsquoMeara S Renfrew MJ Woolridge M Sowden AJ amp Lister-Sharp D (2000) A systematic review to evaluate the effectiveness of interventions to promote the initiation of breastfeeding Health Technol-ogy Assessment 4 1ndash171
Grant J Fletcher M amp Warwick C (2000) The South Thames Evidence Based Practice (STEP) Project Sup-porting Breastfeeding Women South Bank University London
Greenhalgh T Robert G Bate P Mcfarlane F amp Kyriakidou O (2005) Diffusion of Innovations in Health Service Organisations A Systematic Literature Review Blackwell Publishing Limited Oxford
260 MJ Renfrew et al
copy 2006 The Authors Journal compilation copy 2006 Blackwell Publishing Ltd Maternal and Child Nutrition 2 pp 245ndash261
Grimshaw JM Thomas RE MacLennan G Fraser C Ramsay CR Vale L et al (2004) Effectiveness and efficiency of guideline dissemination and implementation strategies Health Technology Assessment 8 indashxi 1ndash72
Hanley B Bradburn J Barnes M Evans C Goodare H Kelson M et al (2004) Involving the Public in NHS Pub-lic Health and Social Care Research Briefing Notes for Researchers INVOLVE Department of Health London
Herbert G amp Lake G (2005) Making connections Effective development of the intermediate tier Journal of Inte-grated Care 13 35ndash42
Howie PW Forsyth JS Ogston SA Clark A amp Florey CD (1990) Protective effect of breastfeeding against infection British Medical Journal 300 11ndash16
Kosmala-Anderson J amp Wallace LM (in press) Breastfeed-ing works the role of employers in supporting women who wish to breastfeed and work in four organizations in England Journal of Public Health (in press)
Kramer M Chalmers B Hodnett H Sevovskaya Z Dzikovich I Shapiro S et al (2001) Promotion of breast-feeding intervention trial (PROBIT) Journal of the American Medical Association 285 413ndash420
McFadden A Renfrew MJ Dyson L McCormick F Herbert G amp Thomas J (2005) Effective Active Briefing on the Initiation and Duration of Breastfeeding Fieldwork Report National Institute for Health and Clinical Excel-lence London
McFadden A Renfrew MJ Dykes F amp Burt S (2006) Assessing learning needs for breastfeeding setting the scene Maternal and Child Nutrition 2 196ndash203
McSherry R amp McFadden A (2001) Practice Development Accreditation Assessment Maternity Services Darlington Memorial Hospital South Durham Healthcare NHS Trust Final Report University of Teesside Middlesbrough
Moulding NT Silagy CA amp Weller DP (1999) A frame-work for effective management of change in clinical prac-tice dissemination and implementation of clinical practice guidelines Quality in Health Care 8 177ndash183
Gray JA Haynes RB Sackett DL Cook DJ amp Guyatt GH (1997) Transferring evidence from research into practice 3 Developing evidence-based clinical policy Evidence-Based Medicine 2 36ndash38
NHS Centre for Reviews and Dissemination (CRD) (1999) Getting evidence into practice Effective Health Care 5 1ndash16
NHS Executive (1997) RampD in Primary Care National Working Group Report (Mant Report) Stationery Office London
NICE (2004) The Guideline Development Process National Institute for Health and Clinical Excellence London
NICE (2005) Putting NICE Guidance into Practice National Institute for Health and Clinical Excellence London
Oxman AD Thomson MA Davis DA amp Haynes RB (1995) No magic bullets a systematic review of 102 trials of interventions to improve professional practice Canadian Medical Association Journal 153 1423ndash1431
Protheroe L Dyson L Renfrew MJ Bull J amp Mulvihill C (2003) The Effectiveness of Public Health Interventions to Promote the Initiation of Breastfeeding Evidence Briefing Health Development Agency London
Quigley MA Cumberland P Cowden JM amp Rodrigues LC (2006) How protective is breast feeding against diar-rhoeal disease in infants in 1990s England A case control study Archives of Disease in Childhood 91 245ndash250
Renfrew MJ Dyson L Wallace L DrsquoSouza L McCormick FM amp Spiby H (2005a) The Effectiveness of Health Interventions to Promote the Duration of Breast-feeding Systematic Review 1st edn National Institute for Health and Clinical Excellence London
Renfrew MJ Dyson L McFadden A McCormick F Herbert G amp Thomas J (2005b) Effective Active Briefing on the Initiation and Duration of Breastfeeding Technical Report National Institute for Health and Clinical Excel-lence London
Renfrew MJ McFadden A Dykes F Wallace L Abbott S Burt S et al (2006) Addressing the learning deficit in breastfeeding strategies for change Maternal and Child Nutrition 2 239ndash244
Richards D (2003) Childrenrsquos Nutrition ndash Mothers Who Wish to Breast-Feed Birmingham City Council Available at httpwwwbirmingahmgovukscrutiny (accessed 27 July 2006)
Sackett DL Rosenberg WMC Gray JAM Haynes RB amp Richardson WS (1996) Evidence-based medicine what it is and what it isnrsquot British Medical Journal 312 71ndash72
Sikorski J Renfrew MJ Pindoria S amp Wade A (2004) Support for breastfeeding mothers (Cochrane Review) The Cochrane Database of Systematic Reviews Issue 2 John Wiley amp Sons Ltd Chichester
Smale M Renfrew MJ Marshall JL amp Spiby H (2006) Turning policy into practice more difficult that it seems The case of breastfeeding education Maternal and Child Nutrition 2 103ndash113
Spiby H Ker R DrsquoSouza L amp Renfrew MJ (2002) Intro-ducing a Consumer-Practitioner into breastfeeding prac-tice Year 2 In Infant Feeding Initiative A Report Evaluating the Breastfeeding Practice Projects 1999ndash2002 (ed F Dykes 2003) p 44 Department of Health London
Spiby H Wallis S Stone C amp Renfrew MJ (2005) Support-ing and Promoting Breastfeeding in Leeds Final Report to December 2004 Report to Leeds PCTs Children and Families Modernisation Team Leeds
Thomas C (2006) Darlington ndash A Breastfeeding Friendly Town Darlington Borough Council Darlington
Developing practice in breastfeeding 261
copy 2006 The Authors Journal compilation copy 2006 Blackwell Publishing Ltd Maternal and Child Nutrition 2 pp 245ndash261
Unsworth J (2000) Practice development a concept analy-sis Journal of Nursing Management 8 317ndash326
Wallace LM amp Jardine J (2006) A Health Scrutiny of Ser-vices to Support the Initiation and Duration of Breastfeed-ing in Coventry and Warwickshire Coventry and Warwickshire County Councils Coventry
Wallace L amp Kosmala-Anderson J (2006) A training needs survey of doctorsrsquo breastfeeding support skills in England Maternal and Child Nutrition 2 217ndash231
Wallace L amp Kosmala-Anderson J (in press) Training needs survey of midwives health visitors and voluntary sector
breastfeeding support staff in England Maternal and Child Nutrition (in press)
WHO (2003) Global Strategy for Infant and Young Child Feeding World Health Organization Geneva
Wilson AC Forsyth JS Green SA Irvine L Hau C amp Howie PW (1998) Relation of infant diet to childhood health seven year follow up of a cohort of children in Dundee infant feeding study British Medical Journal 316 21ndash25

Developing practice in breastfeeding
253
copy 2006 The Authors Journal compilation copy 2006 Blackwell Publishing Ltd
Maternal and Child Nutrition
2
pp 245ndash261
(Stage 2) Stage 3 involved developing relevant net-works tools for education and training evaluationmethods and capacity building systems at individualorganizational service and community levels Follow-ing this a plan to conduct the work would be finalized(Stage 4) implemented (Stage 5) and evaluated Theprocess was intended to be iterative alternatingbetween phases of information appraisal and plan-ning to identify the next stages of development activ-ity and evaluation of the impact to inform futureplanning Stage 6 included finalization of qualitativeand quantitative measurement and monitoring sys-tems that would feedback through all stages of theprocess
It was envisaged that this model would allow effec-tive structures and processes to be identified for usein other aspects of public health practice
Due to changes in funding the programme wasdiscontinued during Stage 3 although in fact somepreliminary work had already been carried out on theplan
Engagement with practitioners
Developing a national programme of change anddevelopment is an ambitious goal A cost-effectiveapproach to engagement had to be developed both tostay within budget and that could roll out acrossEngland and Wales Learning from the successfulLeeds partnership work described above it wasplanned to recruit a series of sentinel sites where wecould test out a range of approaches to maximizelearning and cost-effectiveness as well as respond toideas from the field Work in those sites wouldbecome a model for national developments inform-ing material for education training and assessmentsupported by communications at different levelsthrough our established national network The use ofsentinel sites also allowed for the development ofapproaches sensitive to varying local contexts so pro-viding alternatives and examples to inform nationalimplementation
The first stage in that process was to recruit rele-vant sentinel sites Sites were conceived as includingthe whole health economy in a locality and had tomeet specific criteria These are detailed in Box 2
Four sites were identified and agreed to join thefirst wave of sentinel sites Each site engaged andplanned the programme of work differently Forexample one site had already worked with membersof the core team and were keen to take existing workfurther In the few months in which we worked withthem they put into place a system for the accuratemonitoring of breastfeeding rates and created anextensive network of individuals at a range of seniorlevels from different sectors including Primary CareTrusts (PCTs) Strategic Health Authority the acuteTrust Sure Start and the local authority Benefits thesites have seen even since the work stopped haveincluded
bull improved communication across relevant disci-plines and sectorsbull the observation that the practice developmentwork lsquokept breastfeeding on everyonersquos agendarsquobull the work was used to support a business case for acoordinator for BFI planningbull in one sentinel site the primary care and acutematernity services have formed a health economy-wide breastfeeding strategy groupbull in another a joint primary care and maternity ser-vices group has been establishedbull two sites are taking forward systems for collect-ing breastfeeding data which have been used toprovide feedback to staff each monthbull a new approach to training all staff in one siteincluded commissioning the local university todevelop a self-study workbook and then to test itseffectiveness using an objective skills assessment toolandbull in one site a successful peer support programmewas rolled out throughout Sure Start programmes
A key part of the work in the sentinel sites was tosupport the learning needs assessment (McFadden
et al
2006) Although the sites were at an early stageof engagement this was conducted very successfullyand rapidly as sites supported the identification andinvolvement of practitioners Many assisted with sur-vey distribution and in return received a report ofthe training needs identified for their staff The nexttest was the running of fieldwork meetings and
254
MJ Renfrew
et al
copy 2006 The Authors Journal compilation copy 2006 Blackwell Publishing Ltd
Maternal and Child Nutrition
2
pp 245ndash261
workshops to finalize guidance based on researchevidence as part of a related programme of workThe aim of this work was to take the results of aseries of systematic reviews (which gave informationon lsquowhat works from research evidencersquo) and consultwith practitioners managers and users on lsquowhatreally works in practicersquo (Dyson
et al
2006) Thenewly established sentinel site system supported thiswork by offering venues for meetings providing listsof eligible participants and enabling and encourag-ing staff to attend (Renfrew
et al
2005b) The finalstage of this guidance work was a series of majorworkshops with over 30 participants in each repre-senting a lsquodiagonal slicersquo through the whole healtheconomy from field-level practitioners includingpeer support workers to managers and planners andincluding the range of relevant disciplines as well as
the voluntary sector Concerns around the realitiesand influences on practice and key issues for practi-tioners and managers in developing good practicewere discussed as well as organizational and struc-tural barriers to change Participants were encour-aged to discuss not only practices that need to beintroduced but also those that need to be aban-doned thereby potentially saving time and resourcesand to identify actual or potential barriers to imple-menting change (Renfrew
et al
2005b) These facili-tated groups examined the ability of the service torespond to identified gaps and made recommenda-tions for improvements to the system They feddirectly into the final stages of the development ofNational Institute for Health and Clinical Excellence(NICE) public health recommendations for breast-feeding offering participants the satisfaction of
Box 2
Sentinel site criteriaSentinel sites were expected to
bull Have a deprivation profile that demonstrated a substantial proportion of low-income groups and adiverse ethnic profile and serve contrasting areas (eg urban rural)
bull Offer a range of services for children and women with an interest in nutrition
bull Be able to include the whole health economy in a locality (or at least agree to working across allrelevant sectors)
bull Provide a key contact personpeople who would act to facilitate communication and broker agree-ments with different parts of the health economy and managers who were supportive of the plannedwork willing to support and enable staff participation
bull In the first instance sites would be those where contact already existed with members of our coreteam Future sites would be brought in once any initial problems with the approach had been identifiedand addressed
In return for their involvement in the work it was recognized that the sentinel sites would benefit in arange of ways including
bull Support for staff development and learning through access to programme staff and expertise involve-ment in and learning from a regular newsletter and attendance at an annual leading-edge conferenceon maternal and child nutrition
bull Developing links with other sites and sharing good practice and problem solving
bull The opportunity to help to develop national practice resulting in a raised profile for their work andtheir staff
bull Early access to emerging evidence in the field of maternal and child nutrition
Developing practice in breastfeeding
255
copy 2006 The Authors Journal compilation copy 2006 Blackwell Publishing Ltd
Maternal and Child Nutrition
2
pp 245ndash261
knowing that their input would make a difference(Dyson
et al
2006) These workshops also tested outthe use of language the conceptual understanding ofparticipants in relation to the evidence reviews andgathered intelligence on what approaches to imple-mentation of practice development may be mosteffective They also provided an opportunity for dis-cussion debate and deliberation about the meaningof the evidence Participants reported this to be veryuseful in assisting their understanding of the evi-dence and in considering how best to change theirown and their colleaguesrsquo practice in response to itand as an important contribution to practice devel-opment in their own locality (McFadden
et al
2005)The input of representatives of service users was ofcritical importance
It was planned that once the guidance was final-ized each participating site would be in a strong posi-tion to act on it Not only would they feel someownership but they would also have staff from alllevels and sectors in their health economy who hadspent time discussing the issues with colleagues andwith service user representatives They would haveaccess to specific local information about localitiesand groups that needed to be prioritized creatingchange was therefore brought several stages closerAt the end of each workshop email and telephonecontact details were exchanged among the workshopparticipants many of whom had never met beforedespite working in related parts of the same systemto support closer local networking The opportunityto consult with national experts in the network alsoacted as a variant on educational outreach which hasbeen shown to be moderately successful in guidelineimplementation (NHS CRD 1999) The impact ofsuch exchanges in increasing opportunities for net-work support is virtually impossible to evaluate for-mally but there was confidence in those whoparticipated at these events that positive changewould result and that the evidence would be moreeffectively used in the future as a consequence
Interactive conference
The other main activity was a conference on maternaland child nutrition to which all partners ndash academic
professional NHS and userconsumer ndash and stafffrom sentinel sites were invited Commissioners ofthe work were invited as were staff from key govern-ment departments with an interest in nutrition childhealth Sure Start nursing and midwifery and ine-qualities in health Around 90 participants took partin a day which included presentations participativeworking and active networking A report of the dayis available at httpwwwyorkacukresmcncccon-ferenceReporthtm Feedback was strongly positiveand the impact of networking with others in similarsituations and between those working in local andnational organizations was especially valued It wasplanned that this would be an annual event
Had we been able to continue the practice devel-opment programme we planned to use the follow-ing approaches
Establishing learning networks
We planned to identify appropriate learning net-works for different constituencies which wouldenable communication among staff from differentsectors as well as communication with programmestaff Activities were planned to include
bull Staff working at strategic and senior managementlevels would be supported and appropriate informa-tion provided to allow them to create cross-systemchanges Senior-level lsquochampions for changersquo wouldbe identified These would be used in a range of waysthose wishing to be involved in learning networkswould be supported to do sobull Learning sets would be established This wouldenable focused exchange between stakeholders onhow best to make use of the evidence in practice andhow to influence mainstream practice across locali-ties Through feedback loops we planned to developlearningeducation material to be made availablethrough web-based routes to wider constituenciesbull Peer supporters and trained breastfeeding counsel-lors are key groups in regard to breastfeeding promo-tion and support We planned to include them inlearning sets They have much to offer health profes-sionals in coming to understand the needs of womenand families and indeed the evidence suggests thattheir involvement in advisory work and peer support
256
MJ Renfrew
et al
copy 2006 The Authors Journal compilation copy 2006 Blackwell Publishing Ltd
Maternal and Child Nutrition
2
pp 245ndash261
enhances and strengthens the impact of informationand evidence-based guidance possibly more thanthat of health professionalsrsquo practice Our experiencedescribed above has identified a valuable contribu-tion from lay breastfeeding counsellors into educa-tion and training provision
Educational approaches
The breadth of constituencies that the programmeneeded to reach was to be reflected in the range ofeducational approaches required For some profes-sions continuing professional development (CPD)time is factored in regularly to the job plan in a rollingprogramme of group education with routine sessionalwork suspended for other groups CPD is a self-verified individual activity that can be achievedthrough a range of methods including distance learn-ing We hoped to reach directly a broad group ofwomen as well as professionals through some of theroutes developed A range of materials was thereforeplanned to address all needs Materials would bedeveloped for web-based access CD-ROM access andon paper These were to include
bull Toolkits to promote and support breastfeeding tomonitor breastfeeding rates and on practice develop-ment and changebull Distance learning modules providing accreditedlearning opportunities at a range of levelsbull An email and telephone-based service to putindividuals and organizations in touch with otherswho can support and advise them supported byRDLearning a national web-based resourcebull Learning material that could be directly dissemi-nated through the Internet to a wide audiencebull Buddy systems and mentoring for practice devel-opment and public health strategic development inbreastfeeding and use of cascade systemsbull Summaries of approaches to dissemination andpromotion of information that have proved to be suc-cessful and of practice change programmes that havebeen evaluated as having a positive impact on initia-tion and duration of breastfeedingbull Through NHS Direct we planned to reach the gen-eral public Information could be provided to informthe development of new algorithms that could be
used by staff taking enquiries from breastfeedingwomen We planned also to provide information thatcould be used on the NHS Direct website which isaccessed directly by women and families as well ashealth professionalsbull Other material to reach the general public wouldbe developed We aimed to have informative paperspublished in womenrsquos and familiesrsquo magazines and inthe general media on a regular basis A professionalwriter was one of our partners her role was to informand advise us about reaching women directly
Discussion
The work described in this paper was a structuredcross-sectoral approach to practice development inpublic health As a result of funding problems a fullevaluation could not be conducted and our contribu-tion to the knowledge base on practice change inpublic health is limited Lessons were learned how-ever and feedback was gained from participants atdifferent stages of the process We received strongsupport for our approach and the willingness of localand national partners to engage actively in the pro-gramme testifies to its potential
Lessons learned
There is increasing emphasis in public health andhealth policy on the need for good partnership work-ing and integration across disciplines professionsorganizations and localities as shown in the recentWhite Paper from the Department of Health (DH2006) and in the Children Act (2004) Prevention ofill health and promotion of well-being featurestrongly in these and other policy documents with arecognition that this cannot be achieved without fullengagement at strategic and operational levels withthose who use or depend on public-sector services Itwas clear at every stage of this process that engage-ment was needed across the whole health economyIt is only in working with all the relevant layers andpartnerships of professionals that we can hope for thefull impact of evidence to be realized Traditionalapproaches however only disseminate evidence tointerest groups in isolation Our use of lsquodiagonal slicersquo
Developing practice in breastfeeding 257
copy 2006 The Authors Journal compilation copy 2006 Blackwell Publishing Ltd Maternal and Child Nutrition 2 pp 245ndash261
workshops in which staff at all levels and across allsectors were engaged and including representativesof service users and the voluntary sector enabledmuch greater understanding of the consequences ofparticular activity or behaviour in other parts of thesystem and allowed creative and informed challengesto assumptions and prejudices This laid good foun-dations for whole systems approaches to introducingdriving and implementing new approaches whichcould lead to positive health outcomes It proved avery positive learning experience for all thoseinvolved
Practice change needs to involve the whole rangeof health professionals involved in work directly withpregnant women and new mothers to ensure coordi-nated working and consistent messages Despiteactive support from relevant Royal Colleges and sev-eral strongly supportive individuals engagement bydoctors was noticeably less compared with otherhealth professions This supports the findings of otherwork (eg Smale et al 2006) This really matters in afield such as breastfeeding where paediatriciansobstetricians general practitioners and public healthphysicians have an important role to play Futurework will need to address this
Key constituents in practice development in breast-feeding include mothers and potential mothersgrandmothers and men We had strong support andinvolvement from service users and user groups butengaging men proved to be difficult To reach thepublic good-quality easily accessible information isneeded perhaps the developing DiPEX module onbreastfeeding will contribute to this (httpwwwdipexorgDesktopDefaultaspx) Recent gov-ernment policy directives acknowledge the potentialcontribution that incorporating patient and serviceuser experience into service provision can bring (egDH 2006) Recent developments in the approach tolong-term conditions management have introducedthe Expert Patient Programme which enables peoplewith disabilities to take much more effective controlover the management and treatment of their disease(DH 2004c 2006) There is perhaps potential for theparallel development of an lsquoExpert Mothers Pro-grammersquo to have similar positive impact in relation tonutrition and health
Service user involvement is actively encouraged ininforming research and practice (Hanley et al 2004)Breastfeeding and maternity care as a whole have along-standing history of the active engagement of ser-vice users Volunteer counsellors and supporterstrained and accredited by their own voluntary orga-nizations have filled the gap left by the health ser-vices They have taken the initiative in setting uptelephone support services training and supervisingpeer supporters and contributing to the education ofhealth professionals (Smale et al 2006) In our cur-rent and previous practice development work thecontribution of service users and voluntary groupswent much further than simply offering advice andinformation They took an active role in planning thework and in some cases delivering education andservices Our experience was that lay workers havean essential role in developing services and they areable to advise at a strategic level as well as participat-ing in service delivery They are able to see throughthe organizational barriers that often constrain pro-fessionals and can see solutions that will work formothers and families From our experience we wouldadvise that others explore ways of actively engaginglay workers adequately remunerated in the deliveryof health care and in the education of healthprofessionals
The fundamental importance of multidisciplinaryand multi-professional working was also apparent inthe way in which the core team worked and in thesupport gained from the network of partners Atevery stage we had expertise and support availableto us as well as an effective communication systemand network Practice change in public health needsto be led and informed by those who know the topicarea and who have the wide range of skills neededto convince many different kinds of professionals thatthe work is worthwhile and achievable
Another positive contribution was the synergy ofthis programme with the evidence base The sameteam had also been responsible for systematicreviews of the field (eg Fairbank et al 2000Protheroe et al 2003 Sikorski et al 2004 Renfrewet al 2005a) and the approach was grounded in thisevidence which was at the same time being devel-oped into national guidance The interaction between
258 MJ Renfrew et al
copy 2006 The Authors Journal compilation copy 2006 Blackwell Publishing Ltd Maternal and Child Nutrition 2 pp 245ndash261
these elements should not be underestimated part-ners and sentinel sites were able to inform the guid-ance and up-to-date knowledge of the evidence basehelped strengthen the practice development work
The sentinel site system was proving to be asuccessful lsquowin-winrsquo situation for all involved Itprovided a test bed for ideas it was a source ofinformation and debate and the programme gaineda richness and diversity of input that would be hardto match At the same time it offered the sitesengagement in leading-edge work an increased pro-file and high-quality staff development Although itwas not formally evaluated all involved were con-vinced that it was a very cost-effective system theprogramme could conduct work at speed and to ahigh quality and governance issues were streamlinedThe system was very flexible and could adapt to thedifferent circumstances of each site It would havebeen able to accommodate future service and educa-tion developments such as Childrenrsquos Centres Trustreorganization and inter-professional educationOver time we could have expanded to include othersectors and practitioners such as retailers and child-minders Had the programme continued future siteswould have been identified and material developedfor national use based on our learning in the originalfour sites
Major challenges
Throughout the programme getting breastfeedingrecognized as a priority was difficult This has beenthe case for many years despite its fundamental con-tribution to public health in the short and long termit has only recently been included in national publichealth policy statements PCT targets and monitoringAs we found in the learning needs assessment andother work breastfeeding services are often seen asthe remit of enthusiastic individuals discussed interms reminiscent of lsquoreligious zealotryrsquo (Smale et al2006) rather than as a part of the mainstream ofhealth provision Creating real change in theapproach to breastfeeding in the health service willrequire it to be seen as a priority for senior managersand commissioners Our experience has demon-strated that it is possible to engage such senior people
in this work and that discussion and debate with theirown colleagues can have an impact on their thinking
A key area of practice development that canimpact on breastfeeding duration is working withmothers to sustain breastfeeding while going back towork and the ways that public health strategy andpractice can influence employers to provide breast-feeding-friendly maternity policies and facilities(Kosmala-Anderson amp Wallace in press) We did nothave an impact on this area but it was clear that itwas an area that needed to be addressed One goodplace to start would be with the employment condi-tions for NHS employees themselves this would havethe dual advantage of improving conditions for thelargest female workforce in the country while alsoproviding a model of good practice for others
Although the aim of this work was to address ine-qualities in health it is clear that reaching the hard-to-reach remains challenging We did see signs of suc-cess for example Sure Start schemes were making adifference in some areas but ensuring that all vulner-able women receive the support and care they needis still a distant goal whether they are teenagers asy-lum seekers or simply women who live in areas wherebottle feeding has been endemic for generations
Finally there is a debate to be had on whoseresponsibility it is to create such change The work ofresearchers is seen to be complete when their studyis finished and disseminated through publication andconference presentation Systematic reviewers takeon a responsibility to make the results of a wide rangeof studies available through publication but not toengage with what services might do with those find-ings Those responsible for guidance are responsiblefor developing and publishing that work and somealso take responsibility for lsquoimplementationrsquo (egNICE 2005) But where does responsibility rest forpractice development which requires a deep engage-ment with the practice setting and with those affectedby the issues raised by the evidence Lack of invest-ment at the national level in formal evaluation ofprogrammes of change limits the available evidencebase and detracts from our achieving a better under-standing of what actually works in relation to thesemore complex health issues funding for the lsquoRrsquoaspects of research and development is more com-
Developing practice in breastfeeding 259
copy 2006 The Authors Journal compilation copy 2006 Blackwell Publishing Ltd Maternal and Child Nutrition 2 pp 245ndash261
mon than for the lsquoDrsquo (NHS Executive 1997) Thewithdrawal of funding to this programme part waythrough its cycle was regretted by our commissionersit was evident that practice development was nolonger their remit given their changed circumstancesIt is however not clear that responsibility now restswith any particular agency Is development work forindividual health service organizations themselves totake on Is this work that should be led by nationalprogrammes supported by public-sector funding orshould it rely on other sources of support If so fromwhere will it be resourced and how will cross-sectoraland multidisciplinary developments be addressedThere are also questions about who will lead thiswork when a number of professional disciplines areinvolved and where the client interface spans bothprimary and acute care healthcare settings social ser-vices and other development agencies These ques-tions will become more pressing as guidancecontinues to be produced especially in public health
Acknowledgements
We would like to thank all participants from sentinelsites and our consortium of academic professionalNHS and consumer partners and the two anonymousreferees who reviewed the manuscript This work wascommissioned by the former Health DevelopmentAgency and subsequently funded by NICE
References
Abbott S Renfrew MJ amp McFadden A (2006) lsquoInformalrsquo learning to support breastfeeding local problems and opportunities Maternal and Child Nutrition 2 232ndash238
Audit Commission (2000) United They Stand Coordinating Care for Elderly Patients with Hip Fracture Audit Com-mission London
British Paediatric Association (1994) Statement of the stand-ing committee on nutrition is breastfeeding beneficial in the UK Archive of Diseases in Childhood 71 376ndash380
Chalmers I amp Altman DG (eds) (1995) Systematic Reviews BMJ Publishing Group London
Children Act (2004) Available at httpwwwopsigovukactsacts200420040031htm (accessed 21 March 2006)
Coote A Allen J amp Woodhead D (2004) Finding out What Works Building Knowledge about Complex Community-Based Initiatives Kingrsquos Fund London
DfES (2000) Adoption and Permanence Taskforce Available at httpwwwdfesgovukadoptionadoptionreformstaskforceshtml (accessed 29 March 2006)
DH (2002a) Improvement Expansion and Reform The Next 3 Years Priorities and Planning Framework 2003ndash2006 Department of Health London
DH (2002b) The Health and Social Care Change Agent Team Available at httpwwwchangeagentteamorguk (accessed 29 March 2006)
DH (2004a) National Service Framework for Children Young People and Maternity Services Stationery Office London
DH (2004b) Choosing Health Making Healthy Choices Eas-ier Stationery Office London
DH (2004c) Self Care ndash A Real Choice Self Care Support ndash A Practical Option Stationery Office London
DH (2006) Our Health Our Care Our Say A New Direction for Community Services Stationery Office London
Dominey M Archibald A Edgecombe D Lawrence J amp Thomson L (2002) Breastfeeding and drug misuse Mak-ing an informed choice Year 3 Practice project In Infant Feeding Initiative A Report Evaluating the Breastfeeding Practice Projects 1999ndash2002 (ed F Dykes 2003) p 64 Department of Health London
Dykes F (2003) Infant Feeding Initiative A Report Evaluat-ing the Breastfeeding Practice Projects 1999ndash2002 Depart-ment of Health London
Dykes F (2006) The education of health practitioners sup-porting breastfeeding women time for critical reflection Maternal and Child Nutrition 2 204ndash216
Dyson L Renfrew MJ McFadden A McCormick F Herbert G amp Thomas J (2006) Promotion of Breastfeed-ing Initiation and Duration Evidence into Practice Brief-ing National Institute for Health and Clinical Excellence London httpwwwniceorgukdown-loadaspxo=346169 (accessed 26 July 2006)
EU (2004) Project on Promotion of Breastfeeding in Europe Protection Promotion and Support of Breastfeeding A Blueprint for Action European Commission Directorate Public Health and Risk Assessment Luxembourg
Fairbank L OrsquoMeara S Renfrew MJ Woolridge M Sowden AJ amp Lister-Sharp D (2000) A systematic review to evaluate the effectiveness of interventions to promote the initiation of breastfeeding Health Technol-ogy Assessment 4 1ndash171
Grant J Fletcher M amp Warwick C (2000) The South Thames Evidence Based Practice (STEP) Project Sup-porting Breastfeeding Women South Bank University London
Greenhalgh T Robert G Bate P Mcfarlane F amp Kyriakidou O (2005) Diffusion of Innovations in Health Service Organisations A Systematic Literature Review Blackwell Publishing Limited Oxford
260 MJ Renfrew et al
copy 2006 The Authors Journal compilation copy 2006 Blackwell Publishing Ltd Maternal and Child Nutrition 2 pp 245ndash261
Grimshaw JM Thomas RE MacLennan G Fraser C Ramsay CR Vale L et al (2004) Effectiveness and efficiency of guideline dissemination and implementation strategies Health Technology Assessment 8 indashxi 1ndash72
Hanley B Bradburn J Barnes M Evans C Goodare H Kelson M et al (2004) Involving the Public in NHS Pub-lic Health and Social Care Research Briefing Notes for Researchers INVOLVE Department of Health London
Herbert G amp Lake G (2005) Making connections Effective development of the intermediate tier Journal of Inte-grated Care 13 35ndash42
Howie PW Forsyth JS Ogston SA Clark A amp Florey CD (1990) Protective effect of breastfeeding against infection British Medical Journal 300 11ndash16
Kosmala-Anderson J amp Wallace LM (in press) Breastfeed-ing works the role of employers in supporting women who wish to breastfeed and work in four organizations in England Journal of Public Health (in press)
Kramer M Chalmers B Hodnett H Sevovskaya Z Dzikovich I Shapiro S et al (2001) Promotion of breast-feeding intervention trial (PROBIT) Journal of the American Medical Association 285 413ndash420
McFadden A Renfrew MJ Dyson L McCormick F Herbert G amp Thomas J (2005) Effective Active Briefing on the Initiation and Duration of Breastfeeding Fieldwork Report National Institute for Health and Clinical Excel-lence London
McFadden A Renfrew MJ Dykes F amp Burt S (2006) Assessing learning needs for breastfeeding setting the scene Maternal and Child Nutrition 2 196ndash203
McSherry R amp McFadden A (2001) Practice Development Accreditation Assessment Maternity Services Darlington Memorial Hospital South Durham Healthcare NHS Trust Final Report University of Teesside Middlesbrough
Moulding NT Silagy CA amp Weller DP (1999) A frame-work for effective management of change in clinical prac-tice dissemination and implementation of clinical practice guidelines Quality in Health Care 8 177ndash183
Gray JA Haynes RB Sackett DL Cook DJ amp Guyatt GH (1997) Transferring evidence from research into practice 3 Developing evidence-based clinical policy Evidence-Based Medicine 2 36ndash38
NHS Centre for Reviews and Dissemination (CRD) (1999) Getting evidence into practice Effective Health Care 5 1ndash16
NHS Executive (1997) RampD in Primary Care National Working Group Report (Mant Report) Stationery Office London
NICE (2004) The Guideline Development Process National Institute for Health and Clinical Excellence London
NICE (2005) Putting NICE Guidance into Practice National Institute for Health and Clinical Excellence London
Oxman AD Thomson MA Davis DA amp Haynes RB (1995) No magic bullets a systematic review of 102 trials of interventions to improve professional practice Canadian Medical Association Journal 153 1423ndash1431
Protheroe L Dyson L Renfrew MJ Bull J amp Mulvihill C (2003) The Effectiveness of Public Health Interventions to Promote the Initiation of Breastfeeding Evidence Briefing Health Development Agency London
Quigley MA Cumberland P Cowden JM amp Rodrigues LC (2006) How protective is breast feeding against diar-rhoeal disease in infants in 1990s England A case control study Archives of Disease in Childhood 91 245ndash250
Renfrew MJ Dyson L Wallace L DrsquoSouza L McCormick FM amp Spiby H (2005a) The Effectiveness of Health Interventions to Promote the Duration of Breast-feeding Systematic Review 1st edn National Institute for Health and Clinical Excellence London
Renfrew MJ Dyson L McFadden A McCormick F Herbert G amp Thomas J (2005b) Effective Active Briefing on the Initiation and Duration of Breastfeeding Technical Report National Institute for Health and Clinical Excel-lence London
Renfrew MJ McFadden A Dykes F Wallace L Abbott S Burt S et al (2006) Addressing the learning deficit in breastfeeding strategies for change Maternal and Child Nutrition 2 239ndash244
Richards D (2003) Childrenrsquos Nutrition ndash Mothers Who Wish to Breast-Feed Birmingham City Council Available at httpwwwbirmingahmgovukscrutiny (accessed 27 July 2006)
Sackett DL Rosenberg WMC Gray JAM Haynes RB amp Richardson WS (1996) Evidence-based medicine what it is and what it isnrsquot British Medical Journal 312 71ndash72
Sikorski J Renfrew MJ Pindoria S amp Wade A (2004) Support for breastfeeding mothers (Cochrane Review) The Cochrane Database of Systematic Reviews Issue 2 John Wiley amp Sons Ltd Chichester
Smale M Renfrew MJ Marshall JL amp Spiby H (2006) Turning policy into practice more difficult that it seems The case of breastfeeding education Maternal and Child Nutrition 2 103ndash113
Spiby H Ker R DrsquoSouza L amp Renfrew MJ (2002) Intro-ducing a Consumer-Practitioner into breastfeeding prac-tice Year 2 In Infant Feeding Initiative A Report Evaluating the Breastfeeding Practice Projects 1999ndash2002 (ed F Dykes 2003) p 44 Department of Health London
Spiby H Wallis S Stone C amp Renfrew MJ (2005) Support-ing and Promoting Breastfeeding in Leeds Final Report to December 2004 Report to Leeds PCTs Children and Families Modernisation Team Leeds
Thomas C (2006) Darlington ndash A Breastfeeding Friendly Town Darlington Borough Council Darlington
Developing practice in breastfeeding 261
copy 2006 The Authors Journal compilation copy 2006 Blackwell Publishing Ltd Maternal and Child Nutrition 2 pp 245ndash261
Unsworth J (2000) Practice development a concept analy-sis Journal of Nursing Management 8 317ndash326
Wallace LM amp Jardine J (2006) A Health Scrutiny of Ser-vices to Support the Initiation and Duration of Breastfeed-ing in Coventry and Warwickshire Coventry and Warwickshire County Councils Coventry
Wallace L amp Kosmala-Anderson J (2006) A training needs survey of doctorsrsquo breastfeeding support skills in England Maternal and Child Nutrition 2 217ndash231
Wallace L amp Kosmala-Anderson J (in press) Training needs survey of midwives health visitors and voluntary sector
breastfeeding support staff in England Maternal and Child Nutrition (in press)
WHO (2003) Global Strategy for Infant and Young Child Feeding World Health Organization Geneva
Wilson AC Forsyth JS Green SA Irvine L Hau C amp Howie PW (1998) Relation of infant diet to childhood health seven year follow up of a cohort of children in Dundee infant feeding study British Medical Journal 316 21ndash25

254
MJ Renfrew
et al
copy 2006 The Authors Journal compilation copy 2006 Blackwell Publishing Ltd
Maternal and Child Nutrition
2
pp 245ndash261
workshops to finalize guidance based on researchevidence as part of a related programme of workThe aim of this work was to take the results of aseries of systematic reviews (which gave informationon lsquowhat works from research evidencersquo) and consultwith practitioners managers and users on lsquowhatreally works in practicersquo (Dyson
et al
2006) Thenewly established sentinel site system supported thiswork by offering venues for meetings providing listsof eligible participants and enabling and encourag-ing staff to attend (Renfrew
et al
2005b) The finalstage of this guidance work was a series of majorworkshops with over 30 participants in each repre-senting a lsquodiagonal slicersquo through the whole healtheconomy from field-level practitioners includingpeer support workers to managers and planners andincluding the range of relevant disciplines as well as
the voluntary sector Concerns around the realitiesand influences on practice and key issues for practi-tioners and managers in developing good practicewere discussed as well as organizational and struc-tural barriers to change Participants were encour-aged to discuss not only practices that need to beintroduced but also those that need to be aban-doned thereby potentially saving time and resourcesand to identify actual or potential barriers to imple-menting change (Renfrew
et al
2005b) These facili-tated groups examined the ability of the service torespond to identified gaps and made recommenda-tions for improvements to the system They feddirectly into the final stages of the development ofNational Institute for Health and Clinical Excellence(NICE) public health recommendations for breast-feeding offering participants the satisfaction of
Box 2
Sentinel site criteriaSentinel sites were expected to
bull Have a deprivation profile that demonstrated a substantial proportion of low-income groups and adiverse ethnic profile and serve contrasting areas (eg urban rural)
bull Offer a range of services for children and women with an interest in nutrition
bull Be able to include the whole health economy in a locality (or at least agree to working across allrelevant sectors)
bull Provide a key contact personpeople who would act to facilitate communication and broker agree-ments with different parts of the health economy and managers who were supportive of the plannedwork willing to support and enable staff participation
bull In the first instance sites would be those where contact already existed with members of our coreteam Future sites would be brought in once any initial problems with the approach had been identifiedand addressed
In return for their involvement in the work it was recognized that the sentinel sites would benefit in arange of ways including
bull Support for staff development and learning through access to programme staff and expertise involve-ment in and learning from a regular newsletter and attendance at an annual leading-edge conferenceon maternal and child nutrition
bull Developing links with other sites and sharing good practice and problem solving
bull The opportunity to help to develop national practice resulting in a raised profile for their work andtheir staff
bull Early access to emerging evidence in the field of maternal and child nutrition
Developing practice in breastfeeding
255
copy 2006 The Authors Journal compilation copy 2006 Blackwell Publishing Ltd
Maternal and Child Nutrition
2
pp 245ndash261
knowing that their input would make a difference(Dyson
et al
2006) These workshops also tested outthe use of language the conceptual understanding ofparticipants in relation to the evidence reviews andgathered intelligence on what approaches to imple-mentation of practice development may be mosteffective They also provided an opportunity for dis-cussion debate and deliberation about the meaningof the evidence Participants reported this to be veryuseful in assisting their understanding of the evi-dence and in considering how best to change theirown and their colleaguesrsquo practice in response to itand as an important contribution to practice devel-opment in their own locality (McFadden
et al
2005)The input of representatives of service users was ofcritical importance
It was planned that once the guidance was final-ized each participating site would be in a strong posi-tion to act on it Not only would they feel someownership but they would also have staff from alllevels and sectors in their health economy who hadspent time discussing the issues with colleagues andwith service user representatives They would haveaccess to specific local information about localitiesand groups that needed to be prioritized creatingchange was therefore brought several stages closerAt the end of each workshop email and telephonecontact details were exchanged among the workshopparticipants many of whom had never met beforedespite working in related parts of the same systemto support closer local networking The opportunityto consult with national experts in the network alsoacted as a variant on educational outreach which hasbeen shown to be moderately successful in guidelineimplementation (NHS CRD 1999) The impact ofsuch exchanges in increasing opportunities for net-work support is virtually impossible to evaluate for-mally but there was confidence in those whoparticipated at these events that positive changewould result and that the evidence would be moreeffectively used in the future as a consequence
Interactive conference
The other main activity was a conference on maternaland child nutrition to which all partners ndash academic
professional NHS and userconsumer ndash and stafffrom sentinel sites were invited Commissioners ofthe work were invited as were staff from key govern-ment departments with an interest in nutrition childhealth Sure Start nursing and midwifery and ine-qualities in health Around 90 participants took partin a day which included presentations participativeworking and active networking A report of the dayis available at httpwwwyorkacukresmcncccon-ferenceReporthtm Feedback was strongly positiveand the impact of networking with others in similarsituations and between those working in local andnational organizations was especially valued It wasplanned that this would be an annual event
Had we been able to continue the practice devel-opment programme we planned to use the follow-ing approaches
Establishing learning networks
We planned to identify appropriate learning net-works for different constituencies which wouldenable communication among staff from differentsectors as well as communication with programmestaff Activities were planned to include
bull Staff working at strategic and senior managementlevels would be supported and appropriate informa-tion provided to allow them to create cross-systemchanges Senior-level lsquochampions for changersquo wouldbe identified These would be used in a range of waysthose wishing to be involved in learning networkswould be supported to do sobull Learning sets would be established This wouldenable focused exchange between stakeholders onhow best to make use of the evidence in practice andhow to influence mainstream practice across locali-ties Through feedback loops we planned to developlearningeducation material to be made availablethrough web-based routes to wider constituenciesbull Peer supporters and trained breastfeeding counsel-lors are key groups in regard to breastfeeding promo-tion and support We planned to include them inlearning sets They have much to offer health profes-sionals in coming to understand the needs of womenand families and indeed the evidence suggests thattheir involvement in advisory work and peer support
256
MJ Renfrew
et al
copy 2006 The Authors Journal compilation copy 2006 Blackwell Publishing Ltd
Maternal and Child Nutrition
2
pp 245ndash261
enhances and strengthens the impact of informationand evidence-based guidance possibly more thanthat of health professionalsrsquo practice Our experiencedescribed above has identified a valuable contribu-tion from lay breastfeeding counsellors into educa-tion and training provision
Educational approaches
The breadth of constituencies that the programmeneeded to reach was to be reflected in the range ofeducational approaches required For some profes-sions continuing professional development (CPD)time is factored in regularly to the job plan in a rollingprogramme of group education with routine sessionalwork suspended for other groups CPD is a self-verified individual activity that can be achievedthrough a range of methods including distance learn-ing We hoped to reach directly a broad group ofwomen as well as professionals through some of theroutes developed A range of materials was thereforeplanned to address all needs Materials would bedeveloped for web-based access CD-ROM access andon paper These were to include
bull Toolkits to promote and support breastfeeding tomonitor breastfeeding rates and on practice develop-ment and changebull Distance learning modules providing accreditedlearning opportunities at a range of levelsbull An email and telephone-based service to putindividuals and organizations in touch with otherswho can support and advise them supported byRDLearning a national web-based resourcebull Learning material that could be directly dissemi-nated through the Internet to a wide audiencebull Buddy systems and mentoring for practice devel-opment and public health strategic development inbreastfeeding and use of cascade systemsbull Summaries of approaches to dissemination andpromotion of information that have proved to be suc-cessful and of practice change programmes that havebeen evaluated as having a positive impact on initia-tion and duration of breastfeedingbull Through NHS Direct we planned to reach the gen-eral public Information could be provided to informthe development of new algorithms that could be
used by staff taking enquiries from breastfeedingwomen We planned also to provide information thatcould be used on the NHS Direct website which isaccessed directly by women and families as well ashealth professionalsbull Other material to reach the general public wouldbe developed We aimed to have informative paperspublished in womenrsquos and familiesrsquo magazines and inthe general media on a regular basis A professionalwriter was one of our partners her role was to informand advise us about reaching women directly
Discussion
The work described in this paper was a structuredcross-sectoral approach to practice development inpublic health As a result of funding problems a fullevaluation could not be conducted and our contribu-tion to the knowledge base on practice change inpublic health is limited Lessons were learned how-ever and feedback was gained from participants atdifferent stages of the process We received strongsupport for our approach and the willingness of localand national partners to engage actively in the pro-gramme testifies to its potential
Lessons learned
There is increasing emphasis in public health andhealth policy on the need for good partnership work-ing and integration across disciplines professionsorganizations and localities as shown in the recentWhite Paper from the Department of Health (DH2006) and in the Children Act (2004) Prevention ofill health and promotion of well-being featurestrongly in these and other policy documents with arecognition that this cannot be achieved without fullengagement at strategic and operational levels withthose who use or depend on public-sector services Itwas clear at every stage of this process that engage-ment was needed across the whole health economyIt is only in working with all the relevant layers andpartnerships of professionals that we can hope for thefull impact of evidence to be realized Traditionalapproaches however only disseminate evidence tointerest groups in isolation Our use of lsquodiagonal slicersquo
Developing practice in breastfeeding 257
copy 2006 The Authors Journal compilation copy 2006 Blackwell Publishing Ltd Maternal and Child Nutrition 2 pp 245ndash261
workshops in which staff at all levels and across allsectors were engaged and including representativesof service users and the voluntary sector enabledmuch greater understanding of the consequences ofparticular activity or behaviour in other parts of thesystem and allowed creative and informed challengesto assumptions and prejudices This laid good foun-dations for whole systems approaches to introducingdriving and implementing new approaches whichcould lead to positive health outcomes It proved avery positive learning experience for all thoseinvolved
Practice change needs to involve the whole rangeof health professionals involved in work directly withpregnant women and new mothers to ensure coordi-nated working and consistent messages Despiteactive support from relevant Royal Colleges and sev-eral strongly supportive individuals engagement bydoctors was noticeably less compared with otherhealth professions This supports the findings of otherwork (eg Smale et al 2006) This really matters in afield such as breastfeeding where paediatriciansobstetricians general practitioners and public healthphysicians have an important role to play Futurework will need to address this
Key constituents in practice development in breast-feeding include mothers and potential mothersgrandmothers and men We had strong support andinvolvement from service users and user groups butengaging men proved to be difficult To reach thepublic good-quality easily accessible information isneeded perhaps the developing DiPEX module onbreastfeeding will contribute to this (httpwwwdipexorgDesktopDefaultaspx) Recent gov-ernment policy directives acknowledge the potentialcontribution that incorporating patient and serviceuser experience into service provision can bring (egDH 2006) Recent developments in the approach tolong-term conditions management have introducedthe Expert Patient Programme which enables peoplewith disabilities to take much more effective controlover the management and treatment of their disease(DH 2004c 2006) There is perhaps potential for theparallel development of an lsquoExpert Mothers Pro-grammersquo to have similar positive impact in relation tonutrition and health
Service user involvement is actively encouraged ininforming research and practice (Hanley et al 2004)Breastfeeding and maternity care as a whole have along-standing history of the active engagement of ser-vice users Volunteer counsellors and supporterstrained and accredited by their own voluntary orga-nizations have filled the gap left by the health ser-vices They have taken the initiative in setting uptelephone support services training and supervisingpeer supporters and contributing to the education ofhealth professionals (Smale et al 2006) In our cur-rent and previous practice development work thecontribution of service users and voluntary groupswent much further than simply offering advice andinformation They took an active role in planning thework and in some cases delivering education andservices Our experience was that lay workers havean essential role in developing services and they areable to advise at a strategic level as well as participat-ing in service delivery They are able to see throughthe organizational barriers that often constrain pro-fessionals and can see solutions that will work formothers and families From our experience we wouldadvise that others explore ways of actively engaginglay workers adequately remunerated in the deliveryof health care and in the education of healthprofessionals
The fundamental importance of multidisciplinaryand multi-professional working was also apparent inthe way in which the core team worked and in thesupport gained from the network of partners Atevery stage we had expertise and support availableto us as well as an effective communication systemand network Practice change in public health needsto be led and informed by those who know the topicarea and who have the wide range of skills neededto convince many different kinds of professionals thatthe work is worthwhile and achievable
Another positive contribution was the synergy ofthis programme with the evidence base The sameteam had also been responsible for systematicreviews of the field (eg Fairbank et al 2000Protheroe et al 2003 Sikorski et al 2004 Renfrewet al 2005a) and the approach was grounded in thisevidence which was at the same time being devel-oped into national guidance The interaction between
258 MJ Renfrew et al
copy 2006 The Authors Journal compilation copy 2006 Blackwell Publishing Ltd Maternal and Child Nutrition 2 pp 245ndash261
these elements should not be underestimated part-ners and sentinel sites were able to inform the guid-ance and up-to-date knowledge of the evidence basehelped strengthen the practice development work
The sentinel site system was proving to be asuccessful lsquowin-winrsquo situation for all involved Itprovided a test bed for ideas it was a source ofinformation and debate and the programme gaineda richness and diversity of input that would be hardto match At the same time it offered the sitesengagement in leading-edge work an increased pro-file and high-quality staff development Although itwas not formally evaluated all involved were con-vinced that it was a very cost-effective system theprogramme could conduct work at speed and to ahigh quality and governance issues were streamlinedThe system was very flexible and could adapt to thedifferent circumstances of each site It would havebeen able to accommodate future service and educa-tion developments such as Childrenrsquos Centres Trustreorganization and inter-professional educationOver time we could have expanded to include othersectors and practitioners such as retailers and child-minders Had the programme continued future siteswould have been identified and material developedfor national use based on our learning in the originalfour sites
Major challenges
Throughout the programme getting breastfeedingrecognized as a priority was difficult This has beenthe case for many years despite its fundamental con-tribution to public health in the short and long termit has only recently been included in national publichealth policy statements PCT targets and monitoringAs we found in the learning needs assessment andother work breastfeeding services are often seen asthe remit of enthusiastic individuals discussed interms reminiscent of lsquoreligious zealotryrsquo (Smale et al2006) rather than as a part of the mainstream ofhealth provision Creating real change in theapproach to breastfeeding in the health service willrequire it to be seen as a priority for senior managersand commissioners Our experience has demon-strated that it is possible to engage such senior people
in this work and that discussion and debate with theirown colleagues can have an impact on their thinking
A key area of practice development that canimpact on breastfeeding duration is working withmothers to sustain breastfeeding while going back towork and the ways that public health strategy andpractice can influence employers to provide breast-feeding-friendly maternity policies and facilities(Kosmala-Anderson amp Wallace in press) We did nothave an impact on this area but it was clear that itwas an area that needed to be addressed One goodplace to start would be with the employment condi-tions for NHS employees themselves this would havethe dual advantage of improving conditions for thelargest female workforce in the country while alsoproviding a model of good practice for others
Although the aim of this work was to address ine-qualities in health it is clear that reaching the hard-to-reach remains challenging We did see signs of suc-cess for example Sure Start schemes were making adifference in some areas but ensuring that all vulner-able women receive the support and care they needis still a distant goal whether they are teenagers asy-lum seekers or simply women who live in areas wherebottle feeding has been endemic for generations
Finally there is a debate to be had on whoseresponsibility it is to create such change The work ofresearchers is seen to be complete when their studyis finished and disseminated through publication andconference presentation Systematic reviewers takeon a responsibility to make the results of a wide rangeof studies available through publication but not toengage with what services might do with those find-ings Those responsible for guidance are responsiblefor developing and publishing that work and somealso take responsibility for lsquoimplementationrsquo (egNICE 2005) But where does responsibility rest forpractice development which requires a deep engage-ment with the practice setting and with those affectedby the issues raised by the evidence Lack of invest-ment at the national level in formal evaluation ofprogrammes of change limits the available evidencebase and detracts from our achieving a better under-standing of what actually works in relation to thesemore complex health issues funding for the lsquoRrsquoaspects of research and development is more com-
Developing practice in breastfeeding 259
copy 2006 The Authors Journal compilation copy 2006 Blackwell Publishing Ltd Maternal and Child Nutrition 2 pp 245ndash261
mon than for the lsquoDrsquo (NHS Executive 1997) Thewithdrawal of funding to this programme part waythrough its cycle was regretted by our commissionersit was evident that practice development was nolonger their remit given their changed circumstancesIt is however not clear that responsibility now restswith any particular agency Is development work forindividual health service organizations themselves totake on Is this work that should be led by nationalprogrammes supported by public-sector funding orshould it rely on other sources of support If so fromwhere will it be resourced and how will cross-sectoraland multidisciplinary developments be addressedThere are also questions about who will lead thiswork when a number of professional disciplines areinvolved and where the client interface spans bothprimary and acute care healthcare settings social ser-vices and other development agencies These ques-tions will become more pressing as guidancecontinues to be produced especially in public health
Acknowledgements
We would like to thank all participants from sentinelsites and our consortium of academic professionalNHS and consumer partners and the two anonymousreferees who reviewed the manuscript This work wascommissioned by the former Health DevelopmentAgency and subsequently funded by NICE
References
Abbott S Renfrew MJ amp McFadden A (2006) lsquoInformalrsquo learning to support breastfeeding local problems and opportunities Maternal and Child Nutrition 2 232ndash238
Audit Commission (2000) United They Stand Coordinating Care for Elderly Patients with Hip Fracture Audit Com-mission London
British Paediatric Association (1994) Statement of the stand-ing committee on nutrition is breastfeeding beneficial in the UK Archive of Diseases in Childhood 71 376ndash380
Chalmers I amp Altman DG (eds) (1995) Systematic Reviews BMJ Publishing Group London
Children Act (2004) Available at httpwwwopsigovukactsacts200420040031htm (accessed 21 March 2006)
Coote A Allen J amp Woodhead D (2004) Finding out What Works Building Knowledge about Complex Community-Based Initiatives Kingrsquos Fund London
DfES (2000) Adoption and Permanence Taskforce Available at httpwwwdfesgovukadoptionadoptionreformstaskforceshtml (accessed 29 March 2006)
DH (2002a) Improvement Expansion and Reform The Next 3 Years Priorities and Planning Framework 2003ndash2006 Department of Health London
DH (2002b) The Health and Social Care Change Agent Team Available at httpwwwchangeagentteamorguk (accessed 29 March 2006)
DH (2004a) National Service Framework for Children Young People and Maternity Services Stationery Office London
DH (2004b) Choosing Health Making Healthy Choices Eas-ier Stationery Office London
DH (2004c) Self Care ndash A Real Choice Self Care Support ndash A Practical Option Stationery Office London
DH (2006) Our Health Our Care Our Say A New Direction for Community Services Stationery Office London
Dominey M Archibald A Edgecombe D Lawrence J amp Thomson L (2002) Breastfeeding and drug misuse Mak-ing an informed choice Year 3 Practice project In Infant Feeding Initiative A Report Evaluating the Breastfeeding Practice Projects 1999ndash2002 (ed F Dykes 2003) p 64 Department of Health London
Dykes F (2003) Infant Feeding Initiative A Report Evaluat-ing the Breastfeeding Practice Projects 1999ndash2002 Depart-ment of Health London
Dykes F (2006) The education of health practitioners sup-porting breastfeeding women time for critical reflection Maternal and Child Nutrition 2 204ndash216
Dyson L Renfrew MJ McFadden A McCormick F Herbert G amp Thomas J (2006) Promotion of Breastfeed-ing Initiation and Duration Evidence into Practice Brief-ing National Institute for Health and Clinical Excellence London httpwwwniceorgukdown-loadaspxo=346169 (accessed 26 July 2006)
EU (2004) Project on Promotion of Breastfeeding in Europe Protection Promotion and Support of Breastfeeding A Blueprint for Action European Commission Directorate Public Health and Risk Assessment Luxembourg
Fairbank L OrsquoMeara S Renfrew MJ Woolridge M Sowden AJ amp Lister-Sharp D (2000) A systematic review to evaluate the effectiveness of interventions to promote the initiation of breastfeeding Health Technol-ogy Assessment 4 1ndash171
Grant J Fletcher M amp Warwick C (2000) The South Thames Evidence Based Practice (STEP) Project Sup-porting Breastfeeding Women South Bank University London
Greenhalgh T Robert G Bate P Mcfarlane F amp Kyriakidou O (2005) Diffusion of Innovations in Health Service Organisations A Systematic Literature Review Blackwell Publishing Limited Oxford
260 MJ Renfrew et al
copy 2006 The Authors Journal compilation copy 2006 Blackwell Publishing Ltd Maternal and Child Nutrition 2 pp 245ndash261
Grimshaw JM Thomas RE MacLennan G Fraser C Ramsay CR Vale L et al (2004) Effectiveness and efficiency of guideline dissemination and implementation strategies Health Technology Assessment 8 indashxi 1ndash72
Hanley B Bradburn J Barnes M Evans C Goodare H Kelson M et al (2004) Involving the Public in NHS Pub-lic Health and Social Care Research Briefing Notes for Researchers INVOLVE Department of Health London
Herbert G amp Lake G (2005) Making connections Effective development of the intermediate tier Journal of Inte-grated Care 13 35ndash42
Howie PW Forsyth JS Ogston SA Clark A amp Florey CD (1990) Protective effect of breastfeeding against infection British Medical Journal 300 11ndash16
Kosmala-Anderson J amp Wallace LM (in press) Breastfeed-ing works the role of employers in supporting women who wish to breastfeed and work in four organizations in England Journal of Public Health (in press)
Kramer M Chalmers B Hodnett H Sevovskaya Z Dzikovich I Shapiro S et al (2001) Promotion of breast-feeding intervention trial (PROBIT) Journal of the American Medical Association 285 413ndash420
McFadden A Renfrew MJ Dyson L McCormick F Herbert G amp Thomas J (2005) Effective Active Briefing on the Initiation and Duration of Breastfeeding Fieldwork Report National Institute for Health and Clinical Excel-lence London
McFadden A Renfrew MJ Dykes F amp Burt S (2006) Assessing learning needs for breastfeeding setting the scene Maternal and Child Nutrition 2 196ndash203
McSherry R amp McFadden A (2001) Practice Development Accreditation Assessment Maternity Services Darlington Memorial Hospital South Durham Healthcare NHS Trust Final Report University of Teesside Middlesbrough
Moulding NT Silagy CA amp Weller DP (1999) A frame-work for effective management of change in clinical prac-tice dissemination and implementation of clinical practice guidelines Quality in Health Care 8 177ndash183
Gray JA Haynes RB Sackett DL Cook DJ amp Guyatt GH (1997) Transferring evidence from research into practice 3 Developing evidence-based clinical policy Evidence-Based Medicine 2 36ndash38
NHS Centre for Reviews and Dissemination (CRD) (1999) Getting evidence into practice Effective Health Care 5 1ndash16
NHS Executive (1997) RampD in Primary Care National Working Group Report (Mant Report) Stationery Office London
NICE (2004) The Guideline Development Process National Institute for Health and Clinical Excellence London
NICE (2005) Putting NICE Guidance into Practice National Institute for Health and Clinical Excellence London
Oxman AD Thomson MA Davis DA amp Haynes RB (1995) No magic bullets a systematic review of 102 trials of interventions to improve professional practice Canadian Medical Association Journal 153 1423ndash1431
Protheroe L Dyson L Renfrew MJ Bull J amp Mulvihill C (2003) The Effectiveness of Public Health Interventions to Promote the Initiation of Breastfeeding Evidence Briefing Health Development Agency London
Quigley MA Cumberland P Cowden JM amp Rodrigues LC (2006) How protective is breast feeding against diar-rhoeal disease in infants in 1990s England A case control study Archives of Disease in Childhood 91 245ndash250
Renfrew MJ Dyson L Wallace L DrsquoSouza L McCormick FM amp Spiby H (2005a) The Effectiveness of Health Interventions to Promote the Duration of Breast-feeding Systematic Review 1st edn National Institute for Health and Clinical Excellence London
Renfrew MJ Dyson L McFadden A McCormick F Herbert G amp Thomas J (2005b) Effective Active Briefing on the Initiation and Duration of Breastfeeding Technical Report National Institute for Health and Clinical Excel-lence London
Renfrew MJ McFadden A Dykes F Wallace L Abbott S Burt S et al (2006) Addressing the learning deficit in breastfeeding strategies for change Maternal and Child Nutrition 2 239ndash244
Richards D (2003) Childrenrsquos Nutrition ndash Mothers Who Wish to Breast-Feed Birmingham City Council Available at httpwwwbirmingahmgovukscrutiny (accessed 27 July 2006)
Sackett DL Rosenberg WMC Gray JAM Haynes RB amp Richardson WS (1996) Evidence-based medicine what it is and what it isnrsquot British Medical Journal 312 71ndash72
Sikorski J Renfrew MJ Pindoria S amp Wade A (2004) Support for breastfeeding mothers (Cochrane Review) The Cochrane Database of Systematic Reviews Issue 2 John Wiley amp Sons Ltd Chichester
Smale M Renfrew MJ Marshall JL amp Spiby H (2006) Turning policy into practice more difficult that it seems The case of breastfeeding education Maternal and Child Nutrition 2 103ndash113
Spiby H Ker R DrsquoSouza L amp Renfrew MJ (2002) Intro-ducing a Consumer-Practitioner into breastfeeding prac-tice Year 2 In Infant Feeding Initiative A Report Evaluating the Breastfeeding Practice Projects 1999ndash2002 (ed F Dykes 2003) p 44 Department of Health London
Spiby H Wallis S Stone C amp Renfrew MJ (2005) Support-ing and Promoting Breastfeeding in Leeds Final Report to December 2004 Report to Leeds PCTs Children and Families Modernisation Team Leeds
Thomas C (2006) Darlington ndash A Breastfeeding Friendly Town Darlington Borough Council Darlington
Developing practice in breastfeeding 261
copy 2006 The Authors Journal compilation copy 2006 Blackwell Publishing Ltd Maternal and Child Nutrition 2 pp 245ndash261
Unsworth J (2000) Practice development a concept analy-sis Journal of Nursing Management 8 317ndash326
Wallace LM amp Jardine J (2006) A Health Scrutiny of Ser-vices to Support the Initiation and Duration of Breastfeed-ing in Coventry and Warwickshire Coventry and Warwickshire County Councils Coventry
Wallace L amp Kosmala-Anderson J (2006) A training needs survey of doctorsrsquo breastfeeding support skills in England Maternal and Child Nutrition 2 217ndash231
Wallace L amp Kosmala-Anderson J (in press) Training needs survey of midwives health visitors and voluntary sector
breastfeeding support staff in England Maternal and Child Nutrition (in press)
WHO (2003) Global Strategy for Infant and Young Child Feeding World Health Organization Geneva
Wilson AC Forsyth JS Green SA Irvine L Hau C amp Howie PW (1998) Relation of infant diet to childhood health seven year follow up of a cohort of children in Dundee infant feeding study British Medical Journal 316 21ndash25

Developing practice in breastfeeding
255
copy 2006 The Authors Journal compilation copy 2006 Blackwell Publishing Ltd
Maternal and Child Nutrition
2
pp 245ndash261
knowing that their input would make a difference(Dyson
et al
2006) These workshops also tested outthe use of language the conceptual understanding ofparticipants in relation to the evidence reviews andgathered intelligence on what approaches to imple-mentation of practice development may be mosteffective They also provided an opportunity for dis-cussion debate and deliberation about the meaningof the evidence Participants reported this to be veryuseful in assisting their understanding of the evi-dence and in considering how best to change theirown and their colleaguesrsquo practice in response to itand as an important contribution to practice devel-opment in their own locality (McFadden
et al
2005)The input of representatives of service users was ofcritical importance
It was planned that once the guidance was final-ized each participating site would be in a strong posi-tion to act on it Not only would they feel someownership but they would also have staff from alllevels and sectors in their health economy who hadspent time discussing the issues with colleagues andwith service user representatives They would haveaccess to specific local information about localitiesand groups that needed to be prioritized creatingchange was therefore brought several stages closerAt the end of each workshop email and telephonecontact details were exchanged among the workshopparticipants many of whom had never met beforedespite working in related parts of the same systemto support closer local networking The opportunityto consult with national experts in the network alsoacted as a variant on educational outreach which hasbeen shown to be moderately successful in guidelineimplementation (NHS CRD 1999) The impact ofsuch exchanges in increasing opportunities for net-work support is virtually impossible to evaluate for-mally but there was confidence in those whoparticipated at these events that positive changewould result and that the evidence would be moreeffectively used in the future as a consequence
Interactive conference
The other main activity was a conference on maternaland child nutrition to which all partners ndash academic
professional NHS and userconsumer ndash and stafffrom sentinel sites were invited Commissioners ofthe work were invited as were staff from key govern-ment departments with an interest in nutrition childhealth Sure Start nursing and midwifery and ine-qualities in health Around 90 participants took partin a day which included presentations participativeworking and active networking A report of the dayis available at httpwwwyorkacukresmcncccon-ferenceReporthtm Feedback was strongly positiveand the impact of networking with others in similarsituations and between those working in local andnational organizations was especially valued It wasplanned that this would be an annual event
Had we been able to continue the practice devel-opment programme we planned to use the follow-ing approaches
Establishing learning networks
We planned to identify appropriate learning net-works for different constituencies which wouldenable communication among staff from differentsectors as well as communication with programmestaff Activities were planned to include
bull Staff working at strategic and senior managementlevels would be supported and appropriate informa-tion provided to allow them to create cross-systemchanges Senior-level lsquochampions for changersquo wouldbe identified These would be used in a range of waysthose wishing to be involved in learning networkswould be supported to do sobull Learning sets would be established This wouldenable focused exchange between stakeholders onhow best to make use of the evidence in practice andhow to influence mainstream practice across locali-ties Through feedback loops we planned to developlearningeducation material to be made availablethrough web-based routes to wider constituenciesbull Peer supporters and trained breastfeeding counsel-lors are key groups in regard to breastfeeding promo-tion and support We planned to include them inlearning sets They have much to offer health profes-sionals in coming to understand the needs of womenand families and indeed the evidence suggests thattheir involvement in advisory work and peer support
256
MJ Renfrew
et al
copy 2006 The Authors Journal compilation copy 2006 Blackwell Publishing Ltd
Maternal and Child Nutrition
2
pp 245ndash261
enhances and strengthens the impact of informationand evidence-based guidance possibly more thanthat of health professionalsrsquo practice Our experiencedescribed above has identified a valuable contribu-tion from lay breastfeeding counsellors into educa-tion and training provision
Educational approaches
The breadth of constituencies that the programmeneeded to reach was to be reflected in the range ofeducational approaches required For some profes-sions continuing professional development (CPD)time is factored in regularly to the job plan in a rollingprogramme of group education with routine sessionalwork suspended for other groups CPD is a self-verified individual activity that can be achievedthrough a range of methods including distance learn-ing We hoped to reach directly a broad group ofwomen as well as professionals through some of theroutes developed A range of materials was thereforeplanned to address all needs Materials would bedeveloped for web-based access CD-ROM access andon paper These were to include
bull Toolkits to promote and support breastfeeding tomonitor breastfeeding rates and on practice develop-ment and changebull Distance learning modules providing accreditedlearning opportunities at a range of levelsbull An email and telephone-based service to putindividuals and organizations in touch with otherswho can support and advise them supported byRDLearning a national web-based resourcebull Learning material that could be directly dissemi-nated through the Internet to a wide audiencebull Buddy systems and mentoring for practice devel-opment and public health strategic development inbreastfeeding and use of cascade systemsbull Summaries of approaches to dissemination andpromotion of information that have proved to be suc-cessful and of practice change programmes that havebeen evaluated as having a positive impact on initia-tion and duration of breastfeedingbull Through NHS Direct we planned to reach the gen-eral public Information could be provided to informthe development of new algorithms that could be
used by staff taking enquiries from breastfeedingwomen We planned also to provide information thatcould be used on the NHS Direct website which isaccessed directly by women and families as well ashealth professionalsbull Other material to reach the general public wouldbe developed We aimed to have informative paperspublished in womenrsquos and familiesrsquo magazines and inthe general media on a regular basis A professionalwriter was one of our partners her role was to informand advise us about reaching women directly
Discussion
The work described in this paper was a structuredcross-sectoral approach to practice development inpublic health As a result of funding problems a fullevaluation could not be conducted and our contribu-tion to the knowledge base on practice change inpublic health is limited Lessons were learned how-ever and feedback was gained from participants atdifferent stages of the process We received strongsupport for our approach and the willingness of localand national partners to engage actively in the pro-gramme testifies to its potential
Lessons learned
There is increasing emphasis in public health andhealth policy on the need for good partnership work-ing and integration across disciplines professionsorganizations and localities as shown in the recentWhite Paper from the Department of Health (DH2006) and in the Children Act (2004) Prevention ofill health and promotion of well-being featurestrongly in these and other policy documents with arecognition that this cannot be achieved without fullengagement at strategic and operational levels withthose who use or depend on public-sector services Itwas clear at every stage of this process that engage-ment was needed across the whole health economyIt is only in working with all the relevant layers andpartnerships of professionals that we can hope for thefull impact of evidence to be realized Traditionalapproaches however only disseminate evidence tointerest groups in isolation Our use of lsquodiagonal slicersquo
Developing practice in breastfeeding 257
copy 2006 The Authors Journal compilation copy 2006 Blackwell Publishing Ltd Maternal and Child Nutrition 2 pp 245ndash261
workshops in which staff at all levels and across allsectors were engaged and including representativesof service users and the voluntary sector enabledmuch greater understanding of the consequences ofparticular activity or behaviour in other parts of thesystem and allowed creative and informed challengesto assumptions and prejudices This laid good foun-dations for whole systems approaches to introducingdriving and implementing new approaches whichcould lead to positive health outcomes It proved avery positive learning experience for all thoseinvolved
Practice change needs to involve the whole rangeof health professionals involved in work directly withpregnant women and new mothers to ensure coordi-nated working and consistent messages Despiteactive support from relevant Royal Colleges and sev-eral strongly supportive individuals engagement bydoctors was noticeably less compared with otherhealth professions This supports the findings of otherwork (eg Smale et al 2006) This really matters in afield such as breastfeeding where paediatriciansobstetricians general practitioners and public healthphysicians have an important role to play Futurework will need to address this
Key constituents in practice development in breast-feeding include mothers and potential mothersgrandmothers and men We had strong support andinvolvement from service users and user groups butengaging men proved to be difficult To reach thepublic good-quality easily accessible information isneeded perhaps the developing DiPEX module onbreastfeeding will contribute to this (httpwwwdipexorgDesktopDefaultaspx) Recent gov-ernment policy directives acknowledge the potentialcontribution that incorporating patient and serviceuser experience into service provision can bring (egDH 2006) Recent developments in the approach tolong-term conditions management have introducedthe Expert Patient Programme which enables peoplewith disabilities to take much more effective controlover the management and treatment of their disease(DH 2004c 2006) There is perhaps potential for theparallel development of an lsquoExpert Mothers Pro-grammersquo to have similar positive impact in relation tonutrition and health
Service user involvement is actively encouraged ininforming research and practice (Hanley et al 2004)Breastfeeding and maternity care as a whole have along-standing history of the active engagement of ser-vice users Volunteer counsellors and supporterstrained and accredited by their own voluntary orga-nizations have filled the gap left by the health ser-vices They have taken the initiative in setting uptelephone support services training and supervisingpeer supporters and contributing to the education ofhealth professionals (Smale et al 2006) In our cur-rent and previous practice development work thecontribution of service users and voluntary groupswent much further than simply offering advice andinformation They took an active role in planning thework and in some cases delivering education andservices Our experience was that lay workers havean essential role in developing services and they areable to advise at a strategic level as well as participat-ing in service delivery They are able to see throughthe organizational barriers that often constrain pro-fessionals and can see solutions that will work formothers and families From our experience we wouldadvise that others explore ways of actively engaginglay workers adequately remunerated in the deliveryof health care and in the education of healthprofessionals
The fundamental importance of multidisciplinaryand multi-professional working was also apparent inthe way in which the core team worked and in thesupport gained from the network of partners Atevery stage we had expertise and support availableto us as well as an effective communication systemand network Practice change in public health needsto be led and informed by those who know the topicarea and who have the wide range of skills neededto convince many different kinds of professionals thatthe work is worthwhile and achievable
Another positive contribution was the synergy ofthis programme with the evidence base The sameteam had also been responsible for systematicreviews of the field (eg Fairbank et al 2000Protheroe et al 2003 Sikorski et al 2004 Renfrewet al 2005a) and the approach was grounded in thisevidence which was at the same time being devel-oped into national guidance The interaction between
258 MJ Renfrew et al
copy 2006 The Authors Journal compilation copy 2006 Blackwell Publishing Ltd Maternal and Child Nutrition 2 pp 245ndash261
these elements should not be underestimated part-ners and sentinel sites were able to inform the guid-ance and up-to-date knowledge of the evidence basehelped strengthen the practice development work
The sentinel site system was proving to be asuccessful lsquowin-winrsquo situation for all involved Itprovided a test bed for ideas it was a source ofinformation and debate and the programme gaineda richness and diversity of input that would be hardto match At the same time it offered the sitesengagement in leading-edge work an increased pro-file and high-quality staff development Although itwas not formally evaluated all involved were con-vinced that it was a very cost-effective system theprogramme could conduct work at speed and to ahigh quality and governance issues were streamlinedThe system was very flexible and could adapt to thedifferent circumstances of each site It would havebeen able to accommodate future service and educa-tion developments such as Childrenrsquos Centres Trustreorganization and inter-professional educationOver time we could have expanded to include othersectors and practitioners such as retailers and child-minders Had the programme continued future siteswould have been identified and material developedfor national use based on our learning in the originalfour sites
Major challenges
Throughout the programme getting breastfeedingrecognized as a priority was difficult This has beenthe case for many years despite its fundamental con-tribution to public health in the short and long termit has only recently been included in national publichealth policy statements PCT targets and monitoringAs we found in the learning needs assessment andother work breastfeeding services are often seen asthe remit of enthusiastic individuals discussed interms reminiscent of lsquoreligious zealotryrsquo (Smale et al2006) rather than as a part of the mainstream ofhealth provision Creating real change in theapproach to breastfeeding in the health service willrequire it to be seen as a priority for senior managersand commissioners Our experience has demon-strated that it is possible to engage such senior people
in this work and that discussion and debate with theirown colleagues can have an impact on their thinking
A key area of practice development that canimpact on breastfeeding duration is working withmothers to sustain breastfeeding while going back towork and the ways that public health strategy andpractice can influence employers to provide breast-feeding-friendly maternity policies and facilities(Kosmala-Anderson amp Wallace in press) We did nothave an impact on this area but it was clear that itwas an area that needed to be addressed One goodplace to start would be with the employment condi-tions for NHS employees themselves this would havethe dual advantage of improving conditions for thelargest female workforce in the country while alsoproviding a model of good practice for others
Although the aim of this work was to address ine-qualities in health it is clear that reaching the hard-to-reach remains challenging We did see signs of suc-cess for example Sure Start schemes were making adifference in some areas but ensuring that all vulner-able women receive the support and care they needis still a distant goal whether they are teenagers asy-lum seekers or simply women who live in areas wherebottle feeding has been endemic for generations
Finally there is a debate to be had on whoseresponsibility it is to create such change The work ofresearchers is seen to be complete when their studyis finished and disseminated through publication andconference presentation Systematic reviewers takeon a responsibility to make the results of a wide rangeof studies available through publication but not toengage with what services might do with those find-ings Those responsible for guidance are responsiblefor developing and publishing that work and somealso take responsibility for lsquoimplementationrsquo (egNICE 2005) But where does responsibility rest forpractice development which requires a deep engage-ment with the practice setting and with those affectedby the issues raised by the evidence Lack of invest-ment at the national level in formal evaluation ofprogrammes of change limits the available evidencebase and detracts from our achieving a better under-standing of what actually works in relation to thesemore complex health issues funding for the lsquoRrsquoaspects of research and development is more com-
Developing practice in breastfeeding 259
copy 2006 The Authors Journal compilation copy 2006 Blackwell Publishing Ltd Maternal and Child Nutrition 2 pp 245ndash261
mon than for the lsquoDrsquo (NHS Executive 1997) Thewithdrawal of funding to this programme part waythrough its cycle was regretted by our commissionersit was evident that practice development was nolonger their remit given their changed circumstancesIt is however not clear that responsibility now restswith any particular agency Is development work forindividual health service organizations themselves totake on Is this work that should be led by nationalprogrammes supported by public-sector funding orshould it rely on other sources of support If so fromwhere will it be resourced and how will cross-sectoraland multidisciplinary developments be addressedThere are also questions about who will lead thiswork when a number of professional disciplines areinvolved and where the client interface spans bothprimary and acute care healthcare settings social ser-vices and other development agencies These ques-tions will become more pressing as guidancecontinues to be produced especially in public health
Acknowledgements
We would like to thank all participants from sentinelsites and our consortium of academic professionalNHS and consumer partners and the two anonymousreferees who reviewed the manuscript This work wascommissioned by the former Health DevelopmentAgency and subsequently funded by NICE
References
Abbott S Renfrew MJ amp McFadden A (2006) lsquoInformalrsquo learning to support breastfeeding local problems and opportunities Maternal and Child Nutrition 2 232ndash238
Audit Commission (2000) United They Stand Coordinating Care for Elderly Patients with Hip Fracture Audit Com-mission London
British Paediatric Association (1994) Statement of the stand-ing committee on nutrition is breastfeeding beneficial in the UK Archive of Diseases in Childhood 71 376ndash380
Chalmers I amp Altman DG (eds) (1995) Systematic Reviews BMJ Publishing Group London
Children Act (2004) Available at httpwwwopsigovukactsacts200420040031htm (accessed 21 March 2006)
Coote A Allen J amp Woodhead D (2004) Finding out What Works Building Knowledge about Complex Community-Based Initiatives Kingrsquos Fund London
DfES (2000) Adoption and Permanence Taskforce Available at httpwwwdfesgovukadoptionadoptionreformstaskforceshtml (accessed 29 March 2006)
DH (2002a) Improvement Expansion and Reform The Next 3 Years Priorities and Planning Framework 2003ndash2006 Department of Health London
DH (2002b) The Health and Social Care Change Agent Team Available at httpwwwchangeagentteamorguk (accessed 29 March 2006)
DH (2004a) National Service Framework for Children Young People and Maternity Services Stationery Office London
DH (2004b) Choosing Health Making Healthy Choices Eas-ier Stationery Office London
DH (2004c) Self Care ndash A Real Choice Self Care Support ndash A Practical Option Stationery Office London
DH (2006) Our Health Our Care Our Say A New Direction for Community Services Stationery Office London
Dominey M Archibald A Edgecombe D Lawrence J amp Thomson L (2002) Breastfeeding and drug misuse Mak-ing an informed choice Year 3 Practice project In Infant Feeding Initiative A Report Evaluating the Breastfeeding Practice Projects 1999ndash2002 (ed F Dykes 2003) p 64 Department of Health London
Dykes F (2003) Infant Feeding Initiative A Report Evaluat-ing the Breastfeeding Practice Projects 1999ndash2002 Depart-ment of Health London
Dykes F (2006) The education of health practitioners sup-porting breastfeeding women time for critical reflection Maternal and Child Nutrition 2 204ndash216
Dyson L Renfrew MJ McFadden A McCormick F Herbert G amp Thomas J (2006) Promotion of Breastfeed-ing Initiation and Duration Evidence into Practice Brief-ing National Institute for Health and Clinical Excellence London httpwwwniceorgukdown-loadaspxo=346169 (accessed 26 July 2006)
EU (2004) Project on Promotion of Breastfeeding in Europe Protection Promotion and Support of Breastfeeding A Blueprint for Action European Commission Directorate Public Health and Risk Assessment Luxembourg
Fairbank L OrsquoMeara S Renfrew MJ Woolridge M Sowden AJ amp Lister-Sharp D (2000) A systematic review to evaluate the effectiveness of interventions to promote the initiation of breastfeeding Health Technol-ogy Assessment 4 1ndash171
Grant J Fletcher M amp Warwick C (2000) The South Thames Evidence Based Practice (STEP) Project Sup-porting Breastfeeding Women South Bank University London
Greenhalgh T Robert G Bate P Mcfarlane F amp Kyriakidou O (2005) Diffusion of Innovations in Health Service Organisations A Systematic Literature Review Blackwell Publishing Limited Oxford
260 MJ Renfrew et al
copy 2006 The Authors Journal compilation copy 2006 Blackwell Publishing Ltd Maternal and Child Nutrition 2 pp 245ndash261
Grimshaw JM Thomas RE MacLennan G Fraser C Ramsay CR Vale L et al (2004) Effectiveness and efficiency of guideline dissemination and implementation strategies Health Technology Assessment 8 indashxi 1ndash72
Hanley B Bradburn J Barnes M Evans C Goodare H Kelson M et al (2004) Involving the Public in NHS Pub-lic Health and Social Care Research Briefing Notes for Researchers INVOLVE Department of Health London
Herbert G amp Lake G (2005) Making connections Effective development of the intermediate tier Journal of Inte-grated Care 13 35ndash42
Howie PW Forsyth JS Ogston SA Clark A amp Florey CD (1990) Protective effect of breastfeeding against infection British Medical Journal 300 11ndash16
Kosmala-Anderson J amp Wallace LM (in press) Breastfeed-ing works the role of employers in supporting women who wish to breastfeed and work in four organizations in England Journal of Public Health (in press)
Kramer M Chalmers B Hodnett H Sevovskaya Z Dzikovich I Shapiro S et al (2001) Promotion of breast-feeding intervention trial (PROBIT) Journal of the American Medical Association 285 413ndash420
McFadden A Renfrew MJ Dyson L McCormick F Herbert G amp Thomas J (2005) Effective Active Briefing on the Initiation and Duration of Breastfeeding Fieldwork Report National Institute for Health and Clinical Excel-lence London
McFadden A Renfrew MJ Dykes F amp Burt S (2006) Assessing learning needs for breastfeeding setting the scene Maternal and Child Nutrition 2 196ndash203
McSherry R amp McFadden A (2001) Practice Development Accreditation Assessment Maternity Services Darlington Memorial Hospital South Durham Healthcare NHS Trust Final Report University of Teesside Middlesbrough
Moulding NT Silagy CA amp Weller DP (1999) A frame-work for effective management of change in clinical prac-tice dissemination and implementation of clinical practice guidelines Quality in Health Care 8 177ndash183
Gray JA Haynes RB Sackett DL Cook DJ amp Guyatt GH (1997) Transferring evidence from research into practice 3 Developing evidence-based clinical policy Evidence-Based Medicine 2 36ndash38
NHS Centre for Reviews and Dissemination (CRD) (1999) Getting evidence into practice Effective Health Care 5 1ndash16
NHS Executive (1997) RampD in Primary Care National Working Group Report (Mant Report) Stationery Office London
NICE (2004) The Guideline Development Process National Institute for Health and Clinical Excellence London
NICE (2005) Putting NICE Guidance into Practice National Institute for Health and Clinical Excellence London
Oxman AD Thomson MA Davis DA amp Haynes RB (1995) No magic bullets a systematic review of 102 trials of interventions to improve professional practice Canadian Medical Association Journal 153 1423ndash1431
Protheroe L Dyson L Renfrew MJ Bull J amp Mulvihill C (2003) The Effectiveness of Public Health Interventions to Promote the Initiation of Breastfeeding Evidence Briefing Health Development Agency London
Quigley MA Cumberland P Cowden JM amp Rodrigues LC (2006) How protective is breast feeding against diar-rhoeal disease in infants in 1990s England A case control study Archives of Disease in Childhood 91 245ndash250
Renfrew MJ Dyson L Wallace L DrsquoSouza L McCormick FM amp Spiby H (2005a) The Effectiveness of Health Interventions to Promote the Duration of Breast-feeding Systematic Review 1st edn National Institute for Health and Clinical Excellence London
Renfrew MJ Dyson L McFadden A McCormick F Herbert G amp Thomas J (2005b) Effective Active Briefing on the Initiation and Duration of Breastfeeding Technical Report National Institute for Health and Clinical Excel-lence London
Renfrew MJ McFadden A Dykes F Wallace L Abbott S Burt S et al (2006) Addressing the learning deficit in breastfeeding strategies for change Maternal and Child Nutrition 2 239ndash244
Richards D (2003) Childrenrsquos Nutrition ndash Mothers Who Wish to Breast-Feed Birmingham City Council Available at httpwwwbirmingahmgovukscrutiny (accessed 27 July 2006)
Sackett DL Rosenberg WMC Gray JAM Haynes RB amp Richardson WS (1996) Evidence-based medicine what it is and what it isnrsquot British Medical Journal 312 71ndash72
Sikorski J Renfrew MJ Pindoria S amp Wade A (2004) Support for breastfeeding mothers (Cochrane Review) The Cochrane Database of Systematic Reviews Issue 2 John Wiley amp Sons Ltd Chichester
Smale M Renfrew MJ Marshall JL amp Spiby H (2006) Turning policy into practice more difficult that it seems The case of breastfeeding education Maternal and Child Nutrition 2 103ndash113
Spiby H Ker R DrsquoSouza L amp Renfrew MJ (2002) Intro-ducing a Consumer-Practitioner into breastfeeding prac-tice Year 2 In Infant Feeding Initiative A Report Evaluating the Breastfeeding Practice Projects 1999ndash2002 (ed F Dykes 2003) p 44 Department of Health London
Spiby H Wallis S Stone C amp Renfrew MJ (2005) Support-ing and Promoting Breastfeeding in Leeds Final Report to December 2004 Report to Leeds PCTs Children and Families Modernisation Team Leeds
Thomas C (2006) Darlington ndash A Breastfeeding Friendly Town Darlington Borough Council Darlington
Developing practice in breastfeeding 261
copy 2006 The Authors Journal compilation copy 2006 Blackwell Publishing Ltd Maternal and Child Nutrition 2 pp 245ndash261
Unsworth J (2000) Practice development a concept analy-sis Journal of Nursing Management 8 317ndash326
Wallace LM amp Jardine J (2006) A Health Scrutiny of Ser-vices to Support the Initiation and Duration of Breastfeed-ing in Coventry and Warwickshire Coventry and Warwickshire County Councils Coventry
Wallace L amp Kosmala-Anderson J (2006) A training needs survey of doctorsrsquo breastfeeding support skills in England Maternal and Child Nutrition 2 217ndash231
Wallace L amp Kosmala-Anderson J (in press) Training needs survey of midwives health visitors and voluntary sector
breastfeeding support staff in England Maternal and Child Nutrition (in press)
WHO (2003) Global Strategy for Infant and Young Child Feeding World Health Organization Geneva
Wilson AC Forsyth JS Green SA Irvine L Hau C amp Howie PW (1998) Relation of infant diet to childhood health seven year follow up of a cohort of children in Dundee infant feeding study British Medical Journal 316 21ndash25

256
MJ Renfrew
et al
copy 2006 The Authors Journal compilation copy 2006 Blackwell Publishing Ltd
Maternal and Child Nutrition
2
pp 245ndash261
enhances and strengthens the impact of informationand evidence-based guidance possibly more thanthat of health professionalsrsquo practice Our experiencedescribed above has identified a valuable contribu-tion from lay breastfeeding counsellors into educa-tion and training provision
Educational approaches
The breadth of constituencies that the programmeneeded to reach was to be reflected in the range ofeducational approaches required For some profes-sions continuing professional development (CPD)time is factored in regularly to the job plan in a rollingprogramme of group education with routine sessionalwork suspended for other groups CPD is a self-verified individual activity that can be achievedthrough a range of methods including distance learn-ing We hoped to reach directly a broad group ofwomen as well as professionals through some of theroutes developed A range of materials was thereforeplanned to address all needs Materials would bedeveloped for web-based access CD-ROM access andon paper These were to include
bull Toolkits to promote and support breastfeeding tomonitor breastfeeding rates and on practice develop-ment and changebull Distance learning modules providing accreditedlearning opportunities at a range of levelsbull An email and telephone-based service to putindividuals and organizations in touch with otherswho can support and advise them supported byRDLearning a national web-based resourcebull Learning material that could be directly dissemi-nated through the Internet to a wide audiencebull Buddy systems and mentoring for practice devel-opment and public health strategic development inbreastfeeding and use of cascade systemsbull Summaries of approaches to dissemination andpromotion of information that have proved to be suc-cessful and of practice change programmes that havebeen evaluated as having a positive impact on initia-tion and duration of breastfeedingbull Through NHS Direct we planned to reach the gen-eral public Information could be provided to informthe development of new algorithms that could be
used by staff taking enquiries from breastfeedingwomen We planned also to provide information thatcould be used on the NHS Direct website which isaccessed directly by women and families as well ashealth professionalsbull Other material to reach the general public wouldbe developed We aimed to have informative paperspublished in womenrsquos and familiesrsquo magazines and inthe general media on a regular basis A professionalwriter was one of our partners her role was to informand advise us about reaching women directly
Discussion
The work described in this paper was a structuredcross-sectoral approach to practice development inpublic health As a result of funding problems a fullevaluation could not be conducted and our contribu-tion to the knowledge base on practice change inpublic health is limited Lessons were learned how-ever and feedback was gained from participants atdifferent stages of the process We received strongsupport for our approach and the willingness of localand national partners to engage actively in the pro-gramme testifies to its potential
Lessons learned
There is increasing emphasis in public health andhealth policy on the need for good partnership work-ing and integration across disciplines professionsorganizations and localities as shown in the recentWhite Paper from the Department of Health (DH2006) and in the Children Act (2004) Prevention ofill health and promotion of well-being featurestrongly in these and other policy documents with arecognition that this cannot be achieved without fullengagement at strategic and operational levels withthose who use or depend on public-sector services Itwas clear at every stage of this process that engage-ment was needed across the whole health economyIt is only in working with all the relevant layers andpartnerships of professionals that we can hope for thefull impact of evidence to be realized Traditionalapproaches however only disseminate evidence tointerest groups in isolation Our use of lsquodiagonal slicersquo
Developing practice in breastfeeding 257
copy 2006 The Authors Journal compilation copy 2006 Blackwell Publishing Ltd Maternal and Child Nutrition 2 pp 245ndash261
workshops in which staff at all levels and across allsectors were engaged and including representativesof service users and the voluntary sector enabledmuch greater understanding of the consequences ofparticular activity or behaviour in other parts of thesystem and allowed creative and informed challengesto assumptions and prejudices This laid good foun-dations for whole systems approaches to introducingdriving and implementing new approaches whichcould lead to positive health outcomes It proved avery positive learning experience for all thoseinvolved
Practice change needs to involve the whole rangeof health professionals involved in work directly withpregnant women and new mothers to ensure coordi-nated working and consistent messages Despiteactive support from relevant Royal Colleges and sev-eral strongly supportive individuals engagement bydoctors was noticeably less compared with otherhealth professions This supports the findings of otherwork (eg Smale et al 2006) This really matters in afield such as breastfeeding where paediatriciansobstetricians general practitioners and public healthphysicians have an important role to play Futurework will need to address this
Key constituents in practice development in breast-feeding include mothers and potential mothersgrandmothers and men We had strong support andinvolvement from service users and user groups butengaging men proved to be difficult To reach thepublic good-quality easily accessible information isneeded perhaps the developing DiPEX module onbreastfeeding will contribute to this (httpwwwdipexorgDesktopDefaultaspx) Recent gov-ernment policy directives acknowledge the potentialcontribution that incorporating patient and serviceuser experience into service provision can bring (egDH 2006) Recent developments in the approach tolong-term conditions management have introducedthe Expert Patient Programme which enables peoplewith disabilities to take much more effective controlover the management and treatment of their disease(DH 2004c 2006) There is perhaps potential for theparallel development of an lsquoExpert Mothers Pro-grammersquo to have similar positive impact in relation tonutrition and health
Service user involvement is actively encouraged ininforming research and practice (Hanley et al 2004)Breastfeeding and maternity care as a whole have along-standing history of the active engagement of ser-vice users Volunteer counsellors and supporterstrained and accredited by their own voluntary orga-nizations have filled the gap left by the health ser-vices They have taken the initiative in setting uptelephone support services training and supervisingpeer supporters and contributing to the education ofhealth professionals (Smale et al 2006) In our cur-rent and previous practice development work thecontribution of service users and voluntary groupswent much further than simply offering advice andinformation They took an active role in planning thework and in some cases delivering education andservices Our experience was that lay workers havean essential role in developing services and they areable to advise at a strategic level as well as participat-ing in service delivery They are able to see throughthe organizational barriers that often constrain pro-fessionals and can see solutions that will work formothers and families From our experience we wouldadvise that others explore ways of actively engaginglay workers adequately remunerated in the deliveryof health care and in the education of healthprofessionals
The fundamental importance of multidisciplinaryand multi-professional working was also apparent inthe way in which the core team worked and in thesupport gained from the network of partners Atevery stage we had expertise and support availableto us as well as an effective communication systemand network Practice change in public health needsto be led and informed by those who know the topicarea and who have the wide range of skills neededto convince many different kinds of professionals thatthe work is worthwhile and achievable
Another positive contribution was the synergy ofthis programme with the evidence base The sameteam had also been responsible for systematicreviews of the field (eg Fairbank et al 2000Protheroe et al 2003 Sikorski et al 2004 Renfrewet al 2005a) and the approach was grounded in thisevidence which was at the same time being devel-oped into national guidance The interaction between
258 MJ Renfrew et al
copy 2006 The Authors Journal compilation copy 2006 Blackwell Publishing Ltd Maternal and Child Nutrition 2 pp 245ndash261
these elements should not be underestimated part-ners and sentinel sites were able to inform the guid-ance and up-to-date knowledge of the evidence basehelped strengthen the practice development work
The sentinel site system was proving to be asuccessful lsquowin-winrsquo situation for all involved Itprovided a test bed for ideas it was a source ofinformation and debate and the programme gaineda richness and diversity of input that would be hardto match At the same time it offered the sitesengagement in leading-edge work an increased pro-file and high-quality staff development Although itwas not formally evaluated all involved were con-vinced that it was a very cost-effective system theprogramme could conduct work at speed and to ahigh quality and governance issues were streamlinedThe system was very flexible and could adapt to thedifferent circumstances of each site It would havebeen able to accommodate future service and educa-tion developments such as Childrenrsquos Centres Trustreorganization and inter-professional educationOver time we could have expanded to include othersectors and practitioners such as retailers and child-minders Had the programme continued future siteswould have been identified and material developedfor national use based on our learning in the originalfour sites
Major challenges
Throughout the programme getting breastfeedingrecognized as a priority was difficult This has beenthe case for many years despite its fundamental con-tribution to public health in the short and long termit has only recently been included in national publichealth policy statements PCT targets and monitoringAs we found in the learning needs assessment andother work breastfeeding services are often seen asthe remit of enthusiastic individuals discussed interms reminiscent of lsquoreligious zealotryrsquo (Smale et al2006) rather than as a part of the mainstream ofhealth provision Creating real change in theapproach to breastfeeding in the health service willrequire it to be seen as a priority for senior managersand commissioners Our experience has demon-strated that it is possible to engage such senior people
in this work and that discussion and debate with theirown colleagues can have an impact on their thinking
A key area of practice development that canimpact on breastfeeding duration is working withmothers to sustain breastfeeding while going back towork and the ways that public health strategy andpractice can influence employers to provide breast-feeding-friendly maternity policies and facilities(Kosmala-Anderson amp Wallace in press) We did nothave an impact on this area but it was clear that itwas an area that needed to be addressed One goodplace to start would be with the employment condi-tions for NHS employees themselves this would havethe dual advantage of improving conditions for thelargest female workforce in the country while alsoproviding a model of good practice for others
Although the aim of this work was to address ine-qualities in health it is clear that reaching the hard-to-reach remains challenging We did see signs of suc-cess for example Sure Start schemes were making adifference in some areas but ensuring that all vulner-able women receive the support and care they needis still a distant goal whether they are teenagers asy-lum seekers or simply women who live in areas wherebottle feeding has been endemic for generations
Finally there is a debate to be had on whoseresponsibility it is to create such change The work ofresearchers is seen to be complete when their studyis finished and disseminated through publication andconference presentation Systematic reviewers takeon a responsibility to make the results of a wide rangeof studies available through publication but not toengage with what services might do with those find-ings Those responsible for guidance are responsiblefor developing and publishing that work and somealso take responsibility for lsquoimplementationrsquo (egNICE 2005) But where does responsibility rest forpractice development which requires a deep engage-ment with the practice setting and with those affectedby the issues raised by the evidence Lack of invest-ment at the national level in formal evaluation ofprogrammes of change limits the available evidencebase and detracts from our achieving a better under-standing of what actually works in relation to thesemore complex health issues funding for the lsquoRrsquoaspects of research and development is more com-
Developing practice in breastfeeding 259
copy 2006 The Authors Journal compilation copy 2006 Blackwell Publishing Ltd Maternal and Child Nutrition 2 pp 245ndash261
mon than for the lsquoDrsquo (NHS Executive 1997) Thewithdrawal of funding to this programme part waythrough its cycle was regretted by our commissionersit was evident that practice development was nolonger their remit given their changed circumstancesIt is however not clear that responsibility now restswith any particular agency Is development work forindividual health service organizations themselves totake on Is this work that should be led by nationalprogrammes supported by public-sector funding orshould it rely on other sources of support If so fromwhere will it be resourced and how will cross-sectoraland multidisciplinary developments be addressedThere are also questions about who will lead thiswork when a number of professional disciplines areinvolved and where the client interface spans bothprimary and acute care healthcare settings social ser-vices and other development agencies These ques-tions will become more pressing as guidancecontinues to be produced especially in public health
Acknowledgements
We would like to thank all participants from sentinelsites and our consortium of academic professionalNHS and consumer partners and the two anonymousreferees who reviewed the manuscript This work wascommissioned by the former Health DevelopmentAgency and subsequently funded by NICE
References
Abbott S Renfrew MJ amp McFadden A (2006) lsquoInformalrsquo learning to support breastfeeding local problems and opportunities Maternal and Child Nutrition 2 232ndash238
Audit Commission (2000) United They Stand Coordinating Care for Elderly Patients with Hip Fracture Audit Com-mission London
British Paediatric Association (1994) Statement of the stand-ing committee on nutrition is breastfeeding beneficial in the UK Archive of Diseases in Childhood 71 376ndash380
Chalmers I amp Altman DG (eds) (1995) Systematic Reviews BMJ Publishing Group London
Children Act (2004) Available at httpwwwopsigovukactsacts200420040031htm (accessed 21 March 2006)
Coote A Allen J amp Woodhead D (2004) Finding out What Works Building Knowledge about Complex Community-Based Initiatives Kingrsquos Fund London
DfES (2000) Adoption and Permanence Taskforce Available at httpwwwdfesgovukadoptionadoptionreformstaskforceshtml (accessed 29 March 2006)
DH (2002a) Improvement Expansion and Reform The Next 3 Years Priorities and Planning Framework 2003ndash2006 Department of Health London
DH (2002b) The Health and Social Care Change Agent Team Available at httpwwwchangeagentteamorguk (accessed 29 March 2006)
DH (2004a) National Service Framework for Children Young People and Maternity Services Stationery Office London
DH (2004b) Choosing Health Making Healthy Choices Eas-ier Stationery Office London
DH (2004c) Self Care ndash A Real Choice Self Care Support ndash A Practical Option Stationery Office London
DH (2006) Our Health Our Care Our Say A New Direction for Community Services Stationery Office London
Dominey M Archibald A Edgecombe D Lawrence J amp Thomson L (2002) Breastfeeding and drug misuse Mak-ing an informed choice Year 3 Practice project In Infant Feeding Initiative A Report Evaluating the Breastfeeding Practice Projects 1999ndash2002 (ed F Dykes 2003) p 64 Department of Health London
Dykes F (2003) Infant Feeding Initiative A Report Evaluat-ing the Breastfeeding Practice Projects 1999ndash2002 Depart-ment of Health London
Dykes F (2006) The education of health practitioners sup-porting breastfeeding women time for critical reflection Maternal and Child Nutrition 2 204ndash216
Dyson L Renfrew MJ McFadden A McCormick F Herbert G amp Thomas J (2006) Promotion of Breastfeed-ing Initiation and Duration Evidence into Practice Brief-ing National Institute for Health and Clinical Excellence London httpwwwniceorgukdown-loadaspxo=346169 (accessed 26 July 2006)
EU (2004) Project on Promotion of Breastfeeding in Europe Protection Promotion and Support of Breastfeeding A Blueprint for Action European Commission Directorate Public Health and Risk Assessment Luxembourg
Fairbank L OrsquoMeara S Renfrew MJ Woolridge M Sowden AJ amp Lister-Sharp D (2000) A systematic review to evaluate the effectiveness of interventions to promote the initiation of breastfeeding Health Technol-ogy Assessment 4 1ndash171
Grant J Fletcher M amp Warwick C (2000) The South Thames Evidence Based Practice (STEP) Project Sup-porting Breastfeeding Women South Bank University London
Greenhalgh T Robert G Bate P Mcfarlane F amp Kyriakidou O (2005) Diffusion of Innovations in Health Service Organisations A Systematic Literature Review Blackwell Publishing Limited Oxford
260 MJ Renfrew et al
copy 2006 The Authors Journal compilation copy 2006 Blackwell Publishing Ltd Maternal and Child Nutrition 2 pp 245ndash261
Grimshaw JM Thomas RE MacLennan G Fraser C Ramsay CR Vale L et al (2004) Effectiveness and efficiency of guideline dissemination and implementation strategies Health Technology Assessment 8 indashxi 1ndash72
Hanley B Bradburn J Barnes M Evans C Goodare H Kelson M et al (2004) Involving the Public in NHS Pub-lic Health and Social Care Research Briefing Notes for Researchers INVOLVE Department of Health London
Herbert G amp Lake G (2005) Making connections Effective development of the intermediate tier Journal of Inte-grated Care 13 35ndash42
Howie PW Forsyth JS Ogston SA Clark A amp Florey CD (1990) Protective effect of breastfeeding against infection British Medical Journal 300 11ndash16
Kosmala-Anderson J amp Wallace LM (in press) Breastfeed-ing works the role of employers in supporting women who wish to breastfeed and work in four organizations in England Journal of Public Health (in press)
Kramer M Chalmers B Hodnett H Sevovskaya Z Dzikovich I Shapiro S et al (2001) Promotion of breast-feeding intervention trial (PROBIT) Journal of the American Medical Association 285 413ndash420
McFadden A Renfrew MJ Dyson L McCormick F Herbert G amp Thomas J (2005) Effective Active Briefing on the Initiation and Duration of Breastfeeding Fieldwork Report National Institute for Health and Clinical Excel-lence London
McFadden A Renfrew MJ Dykes F amp Burt S (2006) Assessing learning needs for breastfeeding setting the scene Maternal and Child Nutrition 2 196ndash203
McSherry R amp McFadden A (2001) Practice Development Accreditation Assessment Maternity Services Darlington Memorial Hospital South Durham Healthcare NHS Trust Final Report University of Teesside Middlesbrough
Moulding NT Silagy CA amp Weller DP (1999) A frame-work for effective management of change in clinical prac-tice dissemination and implementation of clinical practice guidelines Quality in Health Care 8 177ndash183
Gray JA Haynes RB Sackett DL Cook DJ amp Guyatt GH (1997) Transferring evidence from research into practice 3 Developing evidence-based clinical policy Evidence-Based Medicine 2 36ndash38
NHS Centre for Reviews and Dissemination (CRD) (1999) Getting evidence into practice Effective Health Care 5 1ndash16
NHS Executive (1997) RampD in Primary Care National Working Group Report (Mant Report) Stationery Office London
NICE (2004) The Guideline Development Process National Institute for Health and Clinical Excellence London
NICE (2005) Putting NICE Guidance into Practice National Institute for Health and Clinical Excellence London
Oxman AD Thomson MA Davis DA amp Haynes RB (1995) No magic bullets a systematic review of 102 trials of interventions to improve professional practice Canadian Medical Association Journal 153 1423ndash1431
Protheroe L Dyson L Renfrew MJ Bull J amp Mulvihill C (2003) The Effectiveness of Public Health Interventions to Promote the Initiation of Breastfeeding Evidence Briefing Health Development Agency London
Quigley MA Cumberland P Cowden JM amp Rodrigues LC (2006) How protective is breast feeding against diar-rhoeal disease in infants in 1990s England A case control study Archives of Disease in Childhood 91 245ndash250
Renfrew MJ Dyson L Wallace L DrsquoSouza L McCormick FM amp Spiby H (2005a) The Effectiveness of Health Interventions to Promote the Duration of Breast-feeding Systematic Review 1st edn National Institute for Health and Clinical Excellence London
Renfrew MJ Dyson L McFadden A McCormick F Herbert G amp Thomas J (2005b) Effective Active Briefing on the Initiation and Duration of Breastfeeding Technical Report National Institute for Health and Clinical Excel-lence London
Renfrew MJ McFadden A Dykes F Wallace L Abbott S Burt S et al (2006) Addressing the learning deficit in breastfeeding strategies for change Maternal and Child Nutrition 2 239ndash244
Richards D (2003) Childrenrsquos Nutrition ndash Mothers Who Wish to Breast-Feed Birmingham City Council Available at httpwwwbirmingahmgovukscrutiny (accessed 27 July 2006)
Sackett DL Rosenberg WMC Gray JAM Haynes RB amp Richardson WS (1996) Evidence-based medicine what it is and what it isnrsquot British Medical Journal 312 71ndash72
Sikorski J Renfrew MJ Pindoria S amp Wade A (2004) Support for breastfeeding mothers (Cochrane Review) The Cochrane Database of Systematic Reviews Issue 2 John Wiley amp Sons Ltd Chichester
Smale M Renfrew MJ Marshall JL amp Spiby H (2006) Turning policy into practice more difficult that it seems The case of breastfeeding education Maternal and Child Nutrition 2 103ndash113
Spiby H Ker R DrsquoSouza L amp Renfrew MJ (2002) Intro-ducing a Consumer-Practitioner into breastfeeding prac-tice Year 2 In Infant Feeding Initiative A Report Evaluating the Breastfeeding Practice Projects 1999ndash2002 (ed F Dykes 2003) p 44 Department of Health London
Spiby H Wallis S Stone C amp Renfrew MJ (2005) Support-ing and Promoting Breastfeeding in Leeds Final Report to December 2004 Report to Leeds PCTs Children and Families Modernisation Team Leeds
Thomas C (2006) Darlington ndash A Breastfeeding Friendly Town Darlington Borough Council Darlington
Developing practice in breastfeeding 261
copy 2006 The Authors Journal compilation copy 2006 Blackwell Publishing Ltd Maternal and Child Nutrition 2 pp 245ndash261
Unsworth J (2000) Practice development a concept analy-sis Journal of Nursing Management 8 317ndash326
Wallace LM amp Jardine J (2006) A Health Scrutiny of Ser-vices to Support the Initiation and Duration of Breastfeed-ing in Coventry and Warwickshire Coventry and Warwickshire County Councils Coventry
Wallace L amp Kosmala-Anderson J (2006) A training needs survey of doctorsrsquo breastfeeding support skills in England Maternal and Child Nutrition 2 217ndash231
Wallace L amp Kosmala-Anderson J (in press) Training needs survey of midwives health visitors and voluntary sector
breastfeeding support staff in England Maternal and Child Nutrition (in press)
WHO (2003) Global Strategy for Infant and Young Child Feeding World Health Organization Geneva
Wilson AC Forsyth JS Green SA Irvine L Hau C amp Howie PW (1998) Relation of infant diet to childhood health seven year follow up of a cohort of children in Dundee infant feeding study British Medical Journal 316 21ndash25

Developing practice in breastfeeding 257
copy 2006 The Authors Journal compilation copy 2006 Blackwell Publishing Ltd Maternal and Child Nutrition 2 pp 245ndash261
workshops in which staff at all levels and across allsectors were engaged and including representativesof service users and the voluntary sector enabledmuch greater understanding of the consequences ofparticular activity or behaviour in other parts of thesystem and allowed creative and informed challengesto assumptions and prejudices This laid good foun-dations for whole systems approaches to introducingdriving and implementing new approaches whichcould lead to positive health outcomes It proved avery positive learning experience for all thoseinvolved
Practice change needs to involve the whole rangeof health professionals involved in work directly withpregnant women and new mothers to ensure coordi-nated working and consistent messages Despiteactive support from relevant Royal Colleges and sev-eral strongly supportive individuals engagement bydoctors was noticeably less compared with otherhealth professions This supports the findings of otherwork (eg Smale et al 2006) This really matters in afield such as breastfeeding where paediatriciansobstetricians general practitioners and public healthphysicians have an important role to play Futurework will need to address this
Key constituents in practice development in breast-feeding include mothers and potential mothersgrandmothers and men We had strong support andinvolvement from service users and user groups butengaging men proved to be difficult To reach thepublic good-quality easily accessible information isneeded perhaps the developing DiPEX module onbreastfeeding will contribute to this (httpwwwdipexorgDesktopDefaultaspx) Recent gov-ernment policy directives acknowledge the potentialcontribution that incorporating patient and serviceuser experience into service provision can bring (egDH 2006) Recent developments in the approach tolong-term conditions management have introducedthe Expert Patient Programme which enables peoplewith disabilities to take much more effective controlover the management and treatment of their disease(DH 2004c 2006) There is perhaps potential for theparallel development of an lsquoExpert Mothers Pro-grammersquo to have similar positive impact in relation tonutrition and health
Service user involvement is actively encouraged ininforming research and practice (Hanley et al 2004)Breastfeeding and maternity care as a whole have along-standing history of the active engagement of ser-vice users Volunteer counsellors and supporterstrained and accredited by their own voluntary orga-nizations have filled the gap left by the health ser-vices They have taken the initiative in setting uptelephone support services training and supervisingpeer supporters and contributing to the education ofhealth professionals (Smale et al 2006) In our cur-rent and previous practice development work thecontribution of service users and voluntary groupswent much further than simply offering advice andinformation They took an active role in planning thework and in some cases delivering education andservices Our experience was that lay workers havean essential role in developing services and they areable to advise at a strategic level as well as participat-ing in service delivery They are able to see throughthe organizational barriers that often constrain pro-fessionals and can see solutions that will work formothers and families From our experience we wouldadvise that others explore ways of actively engaginglay workers adequately remunerated in the deliveryof health care and in the education of healthprofessionals
The fundamental importance of multidisciplinaryand multi-professional working was also apparent inthe way in which the core team worked and in thesupport gained from the network of partners Atevery stage we had expertise and support availableto us as well as an effective communication systemand network Practice change in public health needsto be led and informed by those who know the topicarea and who have the wide range of skills neededto convince many different kinds of professionals thatthe work is worthwhile and achievable
Another positive contribution was the synergy ofthis programme with the evidence base The sameteam had also been responsible for systematicreviews of the field (eg Fairbank et al 2000Protheroe et al 2003 Sikorski et al 2004 Renfrewet al 2005a) and the approach was grounded in thisevidence which was at the same time being devel-oped into national guidance The interaction between
258 MJ Renfrew et al
copy 2006 The Authors Journal compilation copy 2006 Blackwell Publishing Ltd Maternal and Child Nutrition 2 pp 245ndash261
these elements should not be underestimated part-ners and sentinel sites were able to inform the guid-ance and up-to-date knowledge of the evidence basehelped strengthen the practice development work
The sentinel site system was proving to be asuccessful lsquowin-winrsquo situation for all involved Itprovided a test bed for ideas it was a source ofinformation and debate and the programme gaineda richness and diversity of input that would be hardto match At the same time it offered the sitesengagement in leading-edge work an increased pro-file and high-quality staff development Although itwas not formally evaluated all involved were con-vinced that it was a very cost-effective system theprogramme could conduct work at speed and to ahigh quality and governance issues were streamlinedThe system was very flexible and could adapt to thedifferent circumstances of each site It would havebeen able to accommodate future service and educa-tion developments such as Childrenrsquos Centres Trustreorganization and inter-professional educationOver time we could have expanded to include othersectors and practitioners such as retailers and child-minders Had the programme continued future siteswould have been identified and material developedfor national use based on our learning in the originalfour sites
Major challenges
Throughout the programme getting breastfeedingrecognized as a priority was difficult This has beenthe case for many years despite its fundamental con-tribution to public health in the short and long termit has only recently been included in national publichealth policy statements PCT targets and monitoringAs we found in the learning needs assessment andother work breastfeeding services are often seen asthe remit of enthusiastic individuals discussed interms reminiscent of lsquoreligious zealotryrsquo (Smale et al2006) rather than as a part of the mainstream ofhealth provision Creating real change in theapproach to breastfeeding in the health service willrequire it to be seen as a priority for senior managersand commissioners Our experience has demon-strated that it is possible to engage such senior people
in this work and that discussion and debate with theirown colleagues can have an impact on their thinking
A key area of practice development that canimpact on breastfeeding duration is working withmothers to sustain breastfeeding while going back towork and the ways that public health strategy andpractice can influence employers to provide breast-feeding-friendly maternity policies and facilities(Kosmala-Anderson amp Wallace in press) We did nothave an impact on this area but it was clear that itwas an area that needed to be addressed One goodplace to start would be with the employment condi-tions for NHS employees themselves this would havethe dual advantage of improving conditions for thelargest female workforce in the country while alsoproviding a model of good practice for others
Although the aim of this work was to address ine-qualities in health it is clear that reaching the hard-to-reach remains challenging We did see signs of suc-cess for example Sure Start schemes were making adifference in some areas but ensuring that all vulner-able women receive the support and care they needis still a distant goal whether they are teenagers asy-lum seekers or simply women who live in areas wherebottle feeding has been endemic for generations
Finally there is a debate to be had on whoseresponsibility it is to create such change The work ofresearchers is seen to be complete when their studyis finished and disseminated through publication andconference presentation Systematic reviewers takeon a responsibility to make the results of a wide rangeof studies available through publication but not toengage with what services might do with those find-ings Those responsible for guidance are responsiblefor developing and publishing that work and somealso take responsibility for lsquoimplementationrsquo (egNICE 2005) But where does responsibility rest forpractice development which requires a deep engage-ment with the practice setting and with those affectedby the issues raised by the evidence Lack of invest-ment at the national level in formal evaluation ofprogrammes of change limits the available evidencebase and detracts from our achieving a better under-standing of what actually works in relation to thesemore complex health issues funding for the lsquoRrsquoaspects of research and development is more com-
Developing practice in breastfeeding 259
copy 2006 The Authors Journal compilation copy 2006 Blackwell Publishing Ltd Maternal and Child Nutrition 2 pp 245ndash261
mon than for the lsquoDrsquo (NHS Executive 1997) Thewithdrawal of funding to this programme part waythrough its cycle was regretted by our commissionersit was evident that practice development was nolonger their remit given their changed circumstancesIt is however not clear that responsibility now restswith any particular agency Is development work forindividual health service organizations themselves totake on Is this work that should be led by nationalprogrammes supported by public-sector funding orshould it rely on other sources of support If so fromwhere will it be resourced and how will cross-sectoraland multidisciplinary developments be addressedThere are also questions about who will lead thiswork when a number of professional disciplines areinvolved and where the client interface spans bothprimary and acute care healthcare settings social ser-vices and other development agencies These ques-tions will become more pressing as guidancecontinues to be produced especially in public health
Acknowledgements
We would like to thank all participants from sentinelsites and our consortium of academic professionalNHS and consumer partners and the two anonymousreferees who reviewed the manuscript This work wascommissioned by the former Health DevelopmentAgency and subsequently funded by NICE
References
Abbott S Renfrew MJ amp McFadden A (2006) lsquoInformalrsquo learning to support breastfeeding local problems and opportunities Maternal and Child Nutrition 2 232ndash238
Audit Commission (2000) United They Stand Coordinating Care for Elderly Patients with Hip Fracture Audit Com-mission London
British Paediatric Association (1994) Statement of the stand-ing committee on nutrition is breastfeeding beneficial in the UK Archive of Diseases in Childhood 71 376ndash380
Chalmers I amp Altman DG (eds) (1995) Systematic Reviews BMJ Publishing Group London
Children Act (2004) Available at httpwwwopsigovukactsacts200420040031htm (accessed 21 March 2006)
Coote A Allen J amp Woodhead D (2004) Finding out What Works Building Knowledge about Complex Community-Based Initiatives Kingrsquos Fund London
DfES (2000) Adoption and Permanence Taskforce Available at httpwwwdfesgovukadoptionadoptionreformstaskforceshtml (accessed 29 March 2006)
DH (2002a) Improvement Expansion and Reform The Next 3 Years Priorities and Planning Framework 2003ndash2006 Department of Health London
DH (2002b) The Health and Social Care Change Agent Team Available at httpwwwchangeagentteamorguk (accessed 29 March 2006)
DH (2004a) National Service Framework for Children Young People and Maternity Services Stationery Office London
DH (2004b) Choosing Health Making Healthy Choices Eas-ier Stationery Office London
DH (2004c) Self Care ndash A Real Choice Self Care Support ndash A Practical Option Stationery Office London
DH (2006) Our Health Our Care Our Say A New Direction for Community Services Stationery Office London
Dominey M Archibald A Edgecombe D Lawrence J amp Thomson L (2002) Breastfeeding and drug misuse Mak-ing an informed choice Year 3 Practice project In Infant Feeding Initiative A Report Evaluating the Breastfeeding Practice Projects 1999ndash2002 (ed F Dykes 2003) p 64 Department of Health London
Dykes F (2003) Infant Feeding Initiative A Report Evaluat-ing the Breastfeeding Practice Projects 1999ndash2002 Depart-ment of Health London
Dykes F (2006) The education of health practitioners sup-porting breastfeeding women time for critical reflection Maternal and Child Nutrition 2 204ndash216
Dyson L Renfrew MJ McFadden A McCormick F Herbert G amp Thomas J (2006) Promotion of Breastfeed-ing Initiation and Duration Evidence into Practice Brief-ing National Institute for Health and Clinical Excellence London httpwwwniceorgukdown-loadaspxo=346169 (accessed 26 July 2006)
EU (2004) Project on Promotion of Breastfeeding in Europe Protection Promotion and Support of Breastfeeding A Blueprint for Action European Commission Directorate Public Health and Risk Assessment Luxembourg
Fairbank L OrsquoMeara S Renfrew MJ Woolridge M Sowden AJ amp Lister-Sharp D (2000) A systematic review to evaluate the effectiveness of interventions to promote the initiation of breastfeeding Health Technol-ogy Assessment 4 1ndash171
Grant J Fletcher M amp Warwick C (2000) The South Thames Evidence Based Practice (STEP) Project Sup-porting Breastfeeding Women South Bank University London
Greenhalgh T Robert G Bate P Mcfarlane F amp Kyriakidou O (2005) Diffusion of Innovations in Health Service Organisations A Systematic Literature Review Blackwell Publishing Limited Oxford
260 MJ Renfrew et al
copy 2006 The Authors Journal compilation copy 2006 Blackwell Publishing Ltd Maternal and Child Nutrition 2 pp 245ndash261
Grimshaw JM Thomas RE MacLennan G Fraser C Ramsay CR Vale L et al (2004) Effectiveness and efficiency of guideline dissemination and implementation strategies Health Technology Assessment 8 indashxi 1ndash72
Hanley B Bradburn J Barnes M Evans C Goodare H Kelson M et al (2004) Involving the Public in NHS Pub-lic Health and Social Care Research Briefing Notes for Researchers INVOLVE Department of Health London
Herbert G amp Lake G (2005) Making connections Effective development of the intermediate tier Journal of Inte-grated Care 13 35ndash42
Howie PW Forsyth JS Ogston SA Clark A amp Florey CD (1990) Protective effect of breastfeeding against infection British Medical Journal 300 11ndash16
Kosmala-Anderson J amp Wallace LM (in press) Breastfeed-ing works the role of employers in supporting women who wish to breastfeed and work in four organizations in England Journal of Public Health (in press)
Kramer M Chalmers B Hodnett H Sevovskaya Z Dzikovich I Shapiro S et al (2001) Promotion of breast-feeding intervention trial (PROBIT) Journal of the American Medical Association 285 413ndash420
McFadden A Renfrew MJ Dyson L McCormick F Herbert G amp Thomas J (2005) Effective Active Briefing on the Initiation and Duration of Breastfeeding Fieldwork Report National Institute for Health and Clinical Excel-lence London
McFadden A Renfrew MJ Dykes F amp Burt S (2006) Assessing learning needs for breastfeeding setting the scene Maternal and Child Nutrition 2 196ndash203
McSherry R amp McFadden A (2001) Practice Development Accreditation Assessment Maternity Services Darlington Memorial Hospital South Durham Healthcare NHS Trust Final Report University of Teesside Middlesbrough
Moulding NT Silagy CA amp Weller DP (1999) A frame-work for effective management of change in clinical prac-tice dissemination and implementation of clinical practice guidelines Quality in Health Care 8 177ndash183
Gray JA Haynes RB Sackett DL Cook DJ amp Guyatt GH (1997) Transferring evidence from research into practice 3 Developing evidence-based clinical policy Evidence-Based Medicine 2 36ndash38
NHS Centre for Reviews and Dissemination (CRD) (1999) Getting evidence into practice Effective Health Care 5 1ndash16
NHS Executive (1997) RampD in Primary Care National Working Group Report (Mant Report) Stationery Office London
NICE (2004) The Guideline Development Process National Institute for Health and Clinical Excellence London
NICE (2005) Putting NICE Guidance into Practice National Institute for Health and Clinical Excellence London
Oxman AD Thomson MA Davis DA amp Haynes RB (1995) No magic bullets a systematic review of 102 trials of interventions to improve professional practice Canadian Medical Association Journal 153 1423ndash1431
Protheroe L Dyson L Renfrew MJ Bull J amp Mulvihill C (2003) The Effectiveness of Public Health Interventions to Promote the Initiation of Breastfeeding Evidence Briefing Health Development Agency London
Quigley MA Cumberland P Cowden JM amp Rodrigues LC (2006) How protective is breast feeding against diar-rhoeal disease in infants in 1990s England A case control study Archives of Disease in Childhood 91 245ndash250
Renfrew MJ Dyson L Wallace L DrsquoSouza L McCormick FM amp Spiby H (2005a) The Effectiveness of Health Interventions to Promote the Duration of Breast-feeding Systematic Review 1st edn National Institute for Health and Clinical Excellence London
Renfrew MJ Dyson L McFadden A McCormick F Herbert G amp Thomas J (2005b) Effective Active Briefing on the Initiation and Duration of Breastfeeding Technical Report National Institute for Health and Clinical Excel-lence London
Renfrew MJ McFadden A Dykes F Wallace L Abbott S Burt S et al (2006) Addressing the learning deficit in breastfeeding strategies for change Maternal and Child Nutrition 2 239ndash244
Richards D (2003) Childrenrsquos Nutrition ndash Mothers Who Wish to Breast-Feed Birmingham City Council Available at httpwwwbirmingahmgovukscrutiny (accessed 27 July 2006)
Sackett DL Rosenberg WMC Gray JAM Haynes RB amp Richardson WS (1996) Evidence-based medicine what it is and what it isnrsquot British Medical Journal 312 71ndash72
Sikorski J Renfrew MJ Pindoria S amp Wade A (2004) Support for breastfeeding mothers (Cochrane Review) The Cochrane Database of Systematic Reviews Issue 2 John Wiley amp Sons Ltd Chichester
Smale M Renfrew MJ Marshall JL amp Spiby H (2006) Turning policy into practice more difficult that it seems The case of breastfeeding education Maternal and Child Nutrition 2 103ndash113
Spiby H Ker R DrsquoSouza L amp Renfrew MJ (2002) Intro-ducing a Consumer-Practitioner into breastfeeding prac-tice Year 2 In Infant Feeding Initiative A Report Evaluating the Breastfeeding Practice Projects 1999ndash2002 (ed F Dykes 2003) p 44 Department of Health London
Spiby H Wallis S Stone C amp Renfrew MJ (2005) Support-ing and Promoting Breastfeeding in Leeds Final Report to December 2004 Report to Leeds PCTs Children and Families Modernisation Team Leeds
Thomas C (2006) Darlington ndash A Breastfeeding Friendly Town Darlington Borough Council Darlington
Developing practice in breastfeeding 261
copy 2006 The Authors Journal compilation copy 2006 Blackwell Publishing Ltd Maternal and Child Nutrition 2 pp 245ndash261
Unsworth J (2000) Practice development a concept analy-sis Journal of Nursing Management 8 317ndash326
Wallace LM amp Jardine J (2006) A Health Scrutiny of Ser-vices to Support the Initiation and Duration of Breastfeed-ing in Coventry and Warwickshire Coventry and Warwickshire County Councils Coventry
Wallace L amp Kosmala-Anderson J (2006) A training needs survey of doctorsrsquo breastfeeding support skills in England Maternal and Child Nutrition 2 217ndash231
Wallace L amp Kosmala-Anderson J (in press) Training needs survey of midwives health visitors and voluntary sector
breastfeeding support staff in England Maternal and Child Nutrition (in press)
WHO (2003) Global Strategy for Infant and Young Child Feeding World Health Organization Geneva
Wilson AC Forsyth JS Green SA Irvine L Hau C amp Howie PW (1998) Relation of infant diet to childhood health seven year follow up of a cohort of children in Dundee infant feeding study British Medical Journal 316 21ndash25

258 MJ Renfrew et al
copy 2006 The Authors Journal compilation copy 2006 Blackwell Publishing Ltd Maternal and Child Nutrition 2 pp 245ndash261
these elements should not be underestimated part-ners and sentinel sites were able to inform the guid-ance and up-to-date knowledge of the evidence basehelped strengthen the practice development work
The sentinel site system was proving to be asuccessful lsquowin-winrsquo situation for all involved Itprovided a test bed for ideas it was a source ofinformation and debate and the programme gaineda richness and diversity of input that would be hardto match At the same time it offered the sitesengagement in leading-edge work an increased pro-file and high-quality staff development Although itwas not formally evaluated all involved were con-vinced that it was a very cost-effective system theprogramme could conduct work at speed and to ahigh quality and governance issues were streamlinedThe system was very flexible and could adapt to thedifferent circumstances of each site It would havebeen able to accommodate future service and educa-tion developments such as Childrenrsquos Centres Trustreorganization and inter-professional educationOver time we could have expanded to include othersectors and practitioners such as retailers and child-minders Had the programme continued future siteswould have been identified and material developedfor national use based on our learning in the originalfour sites
Major challenges
Throughout the programme getting breastfeedingrecognized as a priority was difficult This has beenthe case for many years despite its fundamental con-tribution to public health in the short and long termit has only recently been included in national publichealth policy statements PCT targets and monitoringAs we found in the learning needs assessment andother work breastfeeding services are often seen asthe remit of enthusiastic individuals discussed interms reminiscent of lsquoreligious zealotryrsquo (Smale et al2006) rather than as a part of the mainstream ofhealth provision Creating real change in theapproach to breastfeeding in the health service willrequire it to be seen as a priority for senior managersand commissioners Our experience has demon-strated that it is possible to engage such senior people
in this work and that discussion and debate with theirown colleagues can have an impact on their thinking
A key area of practice development that canimpact on breastfeeding duration is working withmothers to sustain breastfeeding while going back towork and the ways that public health strategy andpractice can influence employers to provide breast-feeding-friendly maternity policies and facilities(Kosmala-Anderson amp Wallace in press) We did nothave an impact on this area but it was clear that itwas an area that needed to be addressed One goodplace to start would be with the employment condi-tions for NHS employees themselves this would havethe dual advantage of improving conditions for thelargest female workforce in the country while alsoproviding a model of good practice for others
Although the aim of this work was to address ine-qualities in health it is clear that reaching the hard-to-reach remains challenging We did see signs of suc-cess for example Sure Start schemes were making adifference in some areas but ensuring that all vulner-able women receive the support and care they needis still a distant goal whether they are teenagers asy-lum seekers or simply women who live in areas wherebottle feeding has been endemic for generations
Finally there is a debate to be had on whoseresponsibility it is to create such change The work ofresearchers is seen to be complete when their studyis finished and disseminated through publication andconference presentation Systematic reviewers takeon a responsibility to make the results of a wide rangeof studies available through publication but not toengage with what services might do with those find-ings Those responsible for guidance are responsiblefor developing and publishing that work and somealso take responsibility for lsquoimplementationrsquo (egNICE 2005) But where does responsibility rest forpractice development which requires a deep engage-ment with the practice setting and with those affectedby the issues raised by the evidence Lack of invest-ment at the national level in formal evaluation ofprogrammes of change limits the available evidencebase and detracts from our achieving a better under-standing of what actually works in relation to thesemore complex health issues funding for the lsquoRrsquoaspects of research and development is more com-
Developing practice in breastfeeding 259
copy 2006 The Authors Journal compilation copy 2006 Blackwell Publishing Ltd Maternal and Child Nutrition 2 pp 245ndash261
mon than for the lsquoDrsquo (NHS Executive 1997) Thewithdrawal of funding to this programme part waythrough its cycle was regretted by our commissionersit was evident that practice development was nolonger their remit given their changed circumstancesIt is however not clear that responsibility now restswith any particular agency Is development work forindividual health service organizations themselves totake on Is this work that should be led by nationalprogrammes supported by public-sector funding orshould it rely on other sources of support If so fromwhere will it be resourced and how will cross-sectoraland multidisciplinary developments be addressedThere are also questions about who will lead thiswork when a number of professional disciplines areinvolved and where the client interface spans bothprimary and acute care healthcare settings social ser-vices and other development agencies These ques-tions will become more pressing as guidancecontinues to be produced especially in public health
Acknowledgements
We would like to thank all participants from sentinelsites and our consortium of academic professionalNHS and consumer partners and the two anonymousreferees who reviewed the manuscript This work wascommissioned by the former Health DevelopmentAgency and subsequently funded by NICE
References
Abbott S Renfrew MJ amp McFadden A (2006) lsquoInformalrsquo learning to support breastfeeding local problems and opportunities Maternal and Child Nutrition 2 232ndash238
Audit Commission (2000) United They Stand Coordinating Care for Elderly Patients with Hip Fracture Audit Com-mission London
British Paediatric Association (1994) Statement of the stand-ing committee on nutrition is breastfeeding beneficial in the UK Archive of Diseases in Childhood 71 376ndash380
Chalmers I amp Altman DG (eds) (1995) Systematic Reviews BMJ Publishing Group London
Children Act (2004) Available at httpwwwopsigovukactsacts200420040031htm (accessed 21 March 2006)
Coote A Allen J amp Woodhead D (2004) Finding out What Works Building Knowledge about Complex Community-Based Initiatives Kingrsquos Fund London
DfES (2000) Adoption and Permanence Taskforce Available at httpwwwdfesgovukadoptionadoptionreformstaskforceshtml (accessed 29 March 2006)
DH (2002a) Improvement Expansion and Reform The Next 3 Years Priorities and Planning Framework 2003ndash2006 Department of Health London
DH (2002b) The Health and Social Care Change Agent Team Available at httpwwwchangeagentteamorguk (accessed 29 March 2006)
DH (2004a) National Service Framework for Children Young People and Maternity Services Stationery Office London
DH (2004b) Choosing Health Making Healthy Choices Eas-ier Stationery Office London
DH (2004c) Self Care ndash A Real Choice Self Care Support ndash A Practical Option Stationery Office London
DH (2006) Our Health Our Care Our Say A New Direction for Community Services Stationery Office London
Dominey M Archibald A Edgecombe D Lawrence J amp Thomson L (2002) Breastfeeding and drug misuse Mak-ing an informed choice Year 3 Practice project In Infant Feeding Initiative A Report Evaluating the Breastfeeding Practice Projects 1999ndash2002 (ed F Dykes 2003) p 64 Department of Health London
Dykes F (2003) Infant Feeding Initiative A Report Evaluat-ing the Breastfeeding Practice Projects 1999ndash2002 Depart-ment of Health London
Dykes F (2006) The education of health practitioners sup-porting breastfeeding women time for critical reflection Maternal and Child Nutrition 2 204ndash216
Dyson L Renfrew MJ McFadden A McCormick F Herbert G amp Thomas J (2006) Promotion of Breastfeed-ing Initiation and Duration Evidence into Practice Brief-ing National Institute for Health and Clinical Excellence London httpwwwniceorgukdown-loadaspxo=346169 (accessed 26 July 2006)
EU (2004) Project on Promotion of Breastfeeding in Europe Protection Promotion and Support of Breastfeeding A Blueprint for Action European Commission Directorate Public Health and Risk Assessment Luxembourg
Fairbank L OrsquoMeara S Renfrew MJ Woolridge M Sowden AJ amp Lister-Sharp D (2000) A systematic review to evaluate the effectiveness of interventions to promote the initiation of breastfeeding Health Technol-ogy Assessment 4 1ndash171
Grant J Fletcher M amp Warwick C (2000) The South Thames Evidence Based Practice (STEP) Project Sup-porting Breastfeeding Women South Bank University London
Greenhalgh T Robert G Bate P Mcfarlane F amp Kyriakidou O (2005) Diffusion of Innovations in Health Service Organisations A Systematic Literature Review Blackwell Publishing Limited Oxford
260 MJ Renfrew et al
copy 2006 The Authors Journal compilation copy 2006 Blackwell Publishing Ltd Maternal and Child Nutrition 2 pp 245ndash261
Grimshaw JM Thomas RE MacLennan G Fraser C Ramsay CR Vale L et al (2004) Effectiveness and efficiency of guideline dissemination and implementation strategies Health Technology Assessment 8 indashxi 1ndash72
Hanley B Bradburn J Barnes M Evans C Goodare H Kelson M et al (2004) Involving the Public in NHS Pub-lic Health and Social Care Research Briefing Notes for Researchers INVOLVE Department of Health London
Herbert G amp Lake G (2005) Making connections Effective development of the intermediate tier Journal of Inte-grated Care 13 35ndash42
Howie PW Forsyth JS Ogston SA Clark A amp Florey CD (1990) Protective effect of breastfeeding against infection British Medical Journal 300 11ndash16
Kosmala-Anderson J amp Wallace LM (in press) Breastfeed-ing works the role of employers in supporting women who wish to breastfeed and work in four organizations in England Journal of Public Health (in press)
Kramer M Chalmers B Hodnett H Sevovskaya Z Dzikovich I Shapiro S et al (2001) Promotion of breast-feeding intervention trial (PROBIT) Journal of the American Medical Association 285 413ndash420
McFadden A Renfrew MJ Dyson L McCormick F Herbert G amp Thomas J (2005) Effective Active Briefing on the Initiation and Duration of Breastfeeding Fieldwork Report National Institute for Health and Clinical Excel-lence London
McFadden A Renfrew MJ Dykes F amp Burt S (2006) Assessing learning needs for breastfeeding setting the scene Maternal and Child Nutrition 2 196ndash203
McSherry R amp McFadden A (2001) Practice Development Accreditation Assessment Maternity Services Darlington Memorial Hospital South Durham Healthcare NHS Trust Final Report University of Teesside Middlesbrough
Moulding NT Silagy CA amp Weller DP (1999) A frame-work for effective management of change in clinical prac-tice dissemination and implementation of clinical practice guidelines Quality in Health Care 8 177ndash183
Gray JA Haynes RB Sackett DL Cook DJ amp Guyatt GH (1997) Transferring evidence from research into practice 3 Developing evidence-based clinical policy Evidence-Based Medicine 2 36ndash38
NHS Centre for Reviews and Dissemination (CRD) (1999) Getting evidence into practice Effective Health Care 5 1ndash16
NHS Executive (1997) RampD in Primary Care National Working Group Report (Mant Report) Stationery Office London
NICE (2004) The Guideline Development Process National Institute for Health and Clinical Excellence London
NICE (2005) Putting NICE Guidance into Practice National Institute for Health and Clinical Excellence London
Oxman AD Thomson MA Davis DA amp Haynes RB (1995) No magic bullets a systematic review of 102 trials of interventions to improve professional practice Canadian Medical Association Journal 153 1423ndash1431
Protheroe L Dyson L Renfrew MJ Bull J amp Mulvihill C (2003) The Effectiveness of Public Health Interventions to Promote the Initiation of Breastfeeding Evidence Briefing Health Development Agency London
Quigley MA Cumberland P Cowden JM amp Rodrigues LC (2006) How protective is breast feeding against diar-rhoeal disease in infants in 1990s England A case control study Archives of Disease in Childhood 91 245ndash250
Renfrew MJ Dyson L Wallace L DrsquoSouza L McCormick FM amp Spiby H (2005a) The Effectiveness of Health Interventions to Promote the Duration of Breast-feeding Systematic Review 1st edn National Institute for Health and Clinical Excellence London
Renfrew MJ Dyson L McFadden A McCormick F Herbert G amp Thomas J (2005b) Effective Active Briefing on the Initiation and Duration of Breastfeeding Technical Report National Institute for Health and Clinical Excel-lence London
Renfrew MJ McFadden A Dykes F Wallace L Abbott S Burt S et al (2006) Addressing the learning deficit in breastfeeding strategies for change Maternal and Child Nutrition 2 239ndash244
Richards D (2003) Childrenrsquos Nutrition ndash Mothers Who Wish to Breast-Feed Birmingham City Council Available at httpwwwbirmingahmgovukscrutiny (accessed 27 July 2006)
Sackett DL Rosenberg WMC Gray JAM Haynes RB amp Richardson WS (1996) Evidence-based medicine what it is and what it isnrsquot British Medical Journal 312 71ndash72
Sikorski J Renfrew MJ Pindoria S amp Wade A (2004) Support for breastfeeding mothers (Cochrane Review) The Cochrane Database of Systematic Reviews Issue 2 John Wiley amp Sons Ltd Chichester
Smale M Renfrew MJ Marshall JL amp Spiby H (2006) Turning policy into practice more difficult that it seems The case of breastfeeding education Maternal and Child Nutrition 2 103ndash113
Spiby H Ker R DrsquoSouza L amp Renfrew MJ (2002) Intro-ducing a Consumer-Practitioner into breastfeeding prac-tice Year 2 In Infant Feeding Initiative A Report Evaluating the Breastfeeding Practice Projects 1999ndash2002 (ed F Dykes 2003) p 44 Department of Health London
Spiby H Wallis S Stone C amp Renfrew MJ (2005) Support-ing and Promoting Breastfeeding in Leeds Final Report to December 2004 Report to Leeds PCTs Children and Families Modernisation Team Leeds
Thomas C (2006) Darlington ndash A Breastfeeding Friendly Town Darlington Borough Council Darlington
Developing practice in breastfeeding 261
copy 2006 The Authors Journal compilation copy 2006 Blackwell Publishing Ltd Maternal and Child Nutrition 2 pp 245ndash261
Unsworth J (2000) Practice development a concept analy-sis Journal of Nursing Management 8 317ndash326
Wallace LM amp Jardine J (2006) A Health Scrutiny of Ser-vices to Support the Initiation and Duration of Breastfeed-ing in Coventry and Warwickshire Coventry and Warwickshire County Councils Coventry
Wallace L amp Kosmala-Anderson J (2006) A training needs survey of doctorsrsquo breastfeeding support skills in England Maternal and Child Nutrition 2 217ndash231
Wallace L amp Kosmala-Anderson J (in press) Training needs survey of midwives health visitors and voluntary sector
breastfeeding support staff in England Maternal and Child Nutrition (in press)
WHO (2003) Global Strategy for Infant and Young Child Feeding World Health Organization Geneva
Wilson AC Forsyth JS Green SA Irvine L Hau C amp Howie PW (1998) Relation of infant diet to childhood health seven year follow up of a cohort of children in Dundee infant feeding study British Medical Journal 316 21ndash25

Developing practice in breastfeeding 259
copy 2006 The Authors Journal compilation copy 2006 Blackwell Publishing Ltd Maternal and Child Nutrition 2 pp 245ndash261
mon than for the lsquoDrsquo (NHS Executive 1997) Thewithdrawal of funding to this programme part waythrough its cycle was regretted by our commissionersit was evident that practice development was nolonger their remit given their changed circumstancesIt is however not clear that responsibility now restswith any particular agency Is development work forindividual health service organizations themselves totake on Is this work that should be led by nationalprogrammes supported by public-sector funding orshould it rely on other sources of support If so fromwhere will it be resourced and how will cross-sectoraland multidisciplinary developments be addressedThere are also questions about who will lead thiswork when a number of professional disciplines areinvolved and where the client interface spans bothprimary and acute care healthcare settings social ser-vices and other development agencies These ques-tions will become more pressing as guidancecontinues to be produced especially in public health
Acknowledgements
We would like to thank all participants from sentinelsites and our consortium of academic professionalNHS and consumer partners and the two anonymousreferees who reviewed the manuscript This work wascommissioned by the former Health DevelopmentAgency and subsequently funded by NICE
References
Abbott S Renfrew MJ amp McFadden A (2006) lsquoInformalrsquo learning to support breastfeeding local problems and opportunities Maternal and Child Nutrition 2 232ndash238
Audit Commission (2000) United They Stand Coordinating Care for Elderly Patients with Hip Fracture Audit Com-mission London
British Paediatric Association (1994) Statement of the stand-ing committee on nutrition is breastfeeding beneficial in the UK Archive of Diseases in Childhood 71 376ndash380
Chalmers I amp Altman DG (eds) (1995) Systematic Reviews BMJ Publishing Group London
Children Act (2004) Available at httpwwwopsigovukactsacts200420040031htm (accessed 21 March 2006)
Coote A Allen J amp Woodhead D (2004) Finding out What Works Building Knowledge about Complex Community-Based Initiatives Kingrsquos Fund London
DfES (2000) Adoption and Permanence Taskforce Available at httpwwwdfesgovukadoptionadoptionreformstaskforceshtml (accessed 29 March 2006)
DH (2002a) Improvement Expansion and Reform The Next 3 Years Priorities and Planning Framework 2003ndash2006 Department of Health London
DH (2002b) The Health and Social Care Change Agent Team Available at httpwwwchangeagentteamorguk (accessed 29 March 2006)
DH (2004a) National Service Framework for Children Young People and Maternity Services Stationery Office London
DH (2004b) Choosing Health Making Healthy Choices Eas-ier Stationery Office London
DH (2004c) Self Care ndash A Real Choice Self Care Support ndash A Practical Option Stationery Office London
DH (2006) Our Health Our Care Our Say A New Direction for Community Services Stationery Office London
Dominey M Archibald A Edgecombe D Lawrence J amp Thomson L (2002) Breastfeeding and drug misuse Mak-ing an informed choice Year 3 Practice project In Infant Feeding Initiative A Report Evaluating the Breastfeeding Practice Projects 1999ndash2002 (ed F Dykes 2003) p 64 Department of Health London
Dykes F (2003) Infant Feeding Initiative A Report Evaluat-ing the Breastfeeding Practice Projects 1999ndash2002 Depart-ment of Health London
Dykes F (2006) The education of health practitioners sup-porting breastfeeding women time for critical reflection Maternal and Child Nutrition 2 204ndash216
Dyson L Renfrew MJ McFadden A McCormick F Herbert G amp Thomas J (2006) Promotion of Breastfeed-ing Initiation and Duration Evidence into Practice Brief-ing National Institute for Health and Clinical Excellence London httpwwwniceorgukdown-loadaspxo=346169 (accessed 26 July 2006)
EU (2004) Project on Promotion of Breastfeeding in Europe Protection Promotion and Support of Breastfeeding A Blueprint for Action European Commission Directorate Public Health and Risk Assessment Luxembourg
Fairbank L OrsquoMeara S Renfrew MJ Woolridge M Sowden AJ amp Lister-Sharp D (2000) A systematic review to evaluate the effectiveness of interventions to promote the initiation of breastfeeding Health Technol-ogy Assessment 4 1ndash171
Grant J Fletcher M amp Warwick C (2000) The South Thames Evidence Based Practice (STEP) Project Sup-porting Breastfeeding Women South Bank University London
Greenhalgh T Robert G Bate P Mcfarlane F amp Kyriakidou O (2005) Diffusion of Innovations in Health Service Organisations A Systematic Literature Review Blackwell Publishing Limited Oxford
260 MJ Renfrew et al
copy 2006 The Authors Journal compilation copy 2006 Blackwell Publishing Ltd Maternal and Child Nutrition 2 pp 245ndash261
Grimshaw JM Thomas RE MacLennan G Fraser C Ramsay CR Vale L et al (2004) Effectiveness and efficiency of guideline dissemination and implementation strategies Health Technology Assessment 8 indashxi 1ndash72
Hanley B Bradburn J Barnes M Evans C Goodare H Kelson M et al (2004) Involving the Public in NHS Pub-lic Health and Social Care Research Briefing Notes for Researchers INVOLVE Department of Health London
Herbert G amp Lake G (2005) Making connections Effective development of the intermediate tier Journal of Inte-grated Care 13 35ndash42
Howie PW Forsyth JS Ogston SA Clark A amp Florey CD (1990) Protective effect of breastfeeding against infection British Medical Journal 300 11ndash16
Kosmala-Anderson J amp Wallace LM (in press) Breastfeed-ing works the role of employers in supporting women who wish to breastfeed and work in four organizations in England Journal of Public Health (in press)
Kramer M Chalmers B Hodnett H Sevovskaya Z Dzikovich I Shapiro S et al (2001) Promotion of breast-feeding intervention trial (PROBIT) Journal of the American Medical Association 285 413ndash420
McFadden A Renfrew MJ Dyson L McCormick F Herbert G amp Thomas J (2005) Effective Active Briefing on the Initiation and Duration of Breastfeeding Fieldwork Report National Institute for Health and Clinical Excel-lence London
McFadden A Renfrew MJ Dykes F amp Burt S (2006) Assessing learning needs for breastfeeding setting the scene Maternal and Child Nutrition 2 196ndash203
McSherry R amp McFadden A (2001) Practice Development Accreditation Assessment Maternity Services Darlington Memorial Hospital South Durham Healthcare NHS Trust Final Report University of Teesside Middlesbrough
Moulding NT Silagy CA amp Weller DP (1999) A frame-work for effective management of change in clinical prac-tice dissemination and implementation of clinical practice guidelines Quality in Health Care 8 177ndash183
Gray JA Haynes RB Sackett DL Cook DJ amp Guyatt GH (1997) Transferring evidence from research into practice 3 Developing evidence-based clinical policy Evidence-Based Medicine 2 36ndash38
NHS Centre for Reviews and Dissemination (CRD) (1999) Getting evidence into practice Effective Health Care 5 1ndash16
NHS Executive (1997) RampD in Primary Care National Working Group Report (Mant Report) Stationery Office London
NICE (2004) The Guideline Development Process National Institute for Health and Clinical Excellence London
NICE (2005) Putting NICE Guidance into Practice National Institute for Health and Clinical Excellence London
Oxman AD Thomson MA Davis DA amp Haynes RB (1995) No magic bullets a systematic review of 102 trials of interventions to improve professional practice Canadian Medical Association Journal 153 1423ndash1431
Protheroe L Dyson L Renfrew MJ Bull J amp Mulvihill C (2003) The Effectiveness of Public Health Interventions to Promote the Initiation of Breastfeeding Evidence Briefing Health Development Agency London
Quigley MA Cumberland P Cowden JM amp Rodrigues LC (2006) How protective is breast feeding against diar-rhoeal disease in infants in 1990s England A case control study Archives of Disease in Childhood 91 245ndash250
Renfrew MJ Dyson L Wallace L DrsquoSouza L McCormick FM amp Spiby H (2005a) The Effectiveness of Health Interventions to Promote the Duration of Breast-feeding Systematic Review 1st edn National Institute for Health and Clinical Excellence London
Renfrew MJ Dyson L McFadden A McCormick F Herbert G amp Thomas J (2005b) Effective Active Briefing on the Initiation and Duration of Breastfeeding Technical Report National Institute for Health and Clinical Excel-lence London
Renfrew MJ McFadden A Dykes F Wallace L Abbott S Burt S et al (2006) Addressing the learning deficit in breastfeeding strategies for change Maternal and Child Nutrition 2 239ndash244
Richards D (2003) Childrenrsquos Nutrition ndash Mothers Who Wish to Breast-Feed Birmingham City Council Available at httpwwwbirmingahmgovukscrutiny (accessed 27 July 2006)
Sackett DL Rosenberg WMC Gray JAM Haynes RB amp Richardson WS (1996) Evidence-based medicine what it is and what it isnrsquot British Medical Journal 312 71ndash72
Sikorski J Renfrew MJ Pindoria S amp Wade A (2004) Support for breastfeeding mothers (Cochrane Review) The Cochrane Database of Systematic Reviews Issue 2 John Wiley amp Sons Ltd Chichester
Smale M Renfrew MJ Marshall JL amp Spiby H (2006) Turning policy into practice more difficult that it seems The case of breastfeeding education Maternal and Child Nutrition 2 103ndash113
Spiby H Ker R DrsquoSouza L amp Renfrew MJ (2002) Intro-ducing a Consumer-Practitioner into breastfeeding prac-tice Year 2 In Infant Feeding Initiative A Report Evaluating the Breastfeeding Practice Projects 1999ndash2002 (ed F Dykes 2003) p 44 Department of Health London
Spiby H Wallis S Stone C amp Renfrew MJ (2005) Support-ing and Promoting Breastfeeding in Leeds Final Report to December 2004 Report to Leeds PCTs Children and Families Modernisation Team Leeds
Thomas C (2006) Darlington ndash A Breastfeeding Friendly Town Darlington Borough Council Darlington
Developing practice in breastfeeding 261
copy 2006 The Authors Journal compilation copy 2006 Blackwell Publishing Ltd Maternal and Child Nutrition 2 pp 245ndash261
Unsworth J (2000) Practice development a concept analy-sis Journal of Nursing Management 8 317ndash326
Wallace LM amp Jardine J (2006) A Health Scrutiny of Ser-vices to Support the Initiation and Duration of Breastfeed-ing in Coventry and Warwickshire Coventry and Warwickshire County Councils Coventry
Wallace L amp Kosmala-Anderson J (2006) A training needs survey of doctorsrsquo breastfeeding support skills in England Maternal and Child Nutrition 2 217ndash231
Wallace L amp Kosmala-Anderson J (in press) Training needs survey of midwives health visitors and voluntary sector
breastfeeding support staff in England Maternal and Child Nutrition (in press)
WHO (2003) Global Strategy for Infant and Young Child Feeding World Health Organization Geneva
Wilson AC Forsyth JS Green SA Irvine L Hau C amp Howie PW (1998) Relation of infant diet to childhood health seven year follow up of a cohort of children in Dundee infant feeding study British Medical Journal 316 21ndash25

260 MJ Renfrew et al
copy 2006 The Authors Journal compilation copy 2006 Blackwell Publishing Ltd Maternal and Child Nutrition 2 pp 245ndash261
Grimshaw JM Thomas RE MacLennan G Fraser C Ramsay CR Vale L et al (2004) Effectiveness and efficiency of guideline dissemination and implementation strategies Health Technology Assessment 8 indashxi 1ndash72
Hanley B Bradburn J Barnes M Evans C Goodare H Kelson M et al (2004) Involving the Public in NHS Pub-lic Health and Social Care Research Briefing Notes for Researchers INVOLVE Department of Health London
Herbert G amp Lake G (2005) Making connections Effective development of the intermediate tier Journal of Inte-grated Care 13 35ndash42
Howie PW Forsyth JS Ogston SA Clark A amp Florey CD (1990) Protective effect of breastfeeding against infection British Medical Journal 300 11ndash16
Kosmala-Anderson J amp Wallace LM (in press) Breastfeed-ing works the role of employers in supporting women who wish to breastfeed and work in four organizations in England Journal of Public Health (in press)
Kramer M Chalmers B Hodnett H Sevovskaya Z Dzikovich I Shapiro S et al (2001) Promotion of breast-feeding intervention trial (PROBIT) Journal of the American Medical Association 285 413ndash420
McFadden A Renfrew MJ Dyson L McCormick F Herbert G amp Thomas J (2005) Effective Active Briefing on the Initiation and Duration of Breastfeeding Fieldwork Report National Institute for Health and Clinical Excel-lence London
McFadden A Renfrew MJ Dykes F amp Burt S (2006) Assessing learning needs for breastfeeding setting the scene Maternal and Child Nutrition 2 196ndash203
McSherry R amp McFadden A (2001) Practice Development Accreditation Assessment Maternity Services Darlington Memorial Hospital South Durham Healthcare NHS Trust Final Report University of Teesside Middlesbrough
Moulding NT Silagy CA amp Weller DP (1999) A frame-work for effective management of change in clinical prac-tice dissemination and implementation of clinical practice guidelines Quality in Health Care 8 177ndash183
Gray JA Haynes RB Sackett DL Cook DJ amp Guyatt GH (1997) Transferring evidence from research into practice 3 Developing evidence-based clinical policy Evidence-Based Medicine 2 36ndash38
NHS Centre for Reviews and Dissemination (CRD) (1999) Getting evidence into practice Effective Health Care 5 1ndash16
NHS Executive (1997) RampD in Primary Care National Working Group Report (Mant Report) Stationery Office London
NICE (2004) The Guideline Development Process National Institute for Health and Clinical Excellence London
NICE (2005) Putting NICE Guidance into Practice National Institute for Health and Clinical Excellence London
Oxman AD Thomson MA Davis DA amp Haynes RB (1995) No magic bullets a systematic review of 102 trials of interventions to improve professional practice Canadian Medical Association Journal 153 1423ndash1431
Protheroe L Dyson L Renfrew MJ Bull J amp Mulvihill C (2003) The Effectiveness of Public Health Interventions to Promote the Initiation of Breastfeeding Evidence Briefing Health Development Agency London
Quigley MA Cumberland P Cowden JM amp Rodrigues LC (2006) How protective is breast feeding against diar-rhoeal disease in infants in 1990s England A case control study Archives of Disease in Childhood 91 245ndash250
Renfrew MJ Dyson L Wallace L DrsquoSouza L McCormick FM amp Spiby H (2005a) The Effectiveness of Health Interventions to Promote the Duration of Breast-feeding Systematic Review 1st edn National Institute for Health and Clinical Excellence London
Renfrew MJ Dyson L McFadden A McCormick F Herbert G amp Thomas J (2005b) Effective Active Briefing on the Initiation and Duration of Breastfeeding Technical Report National Institute for Health and Clinical Excel-lence London
Renfrew MJ McFadden A Dykes F Wallace L Abbott S Burt S et al (2006) Addressing the learning deficit in breastfeeding strategies for change Maternal and Child Nutrition 2 239ndash244
Richards D (2003) Childrenrsquos Nutrition ndash Mothers Who Wish to Breast-Feed Birmingham City Council Available at httpwwwbirmingahmgovukscrutiny (accessed 27 July 2006)
Sackett DL Rosenberg WMC Gray JAM Haynes RB amp Richardson WS (1996) Evidence-based medicine what it is and what it isnrsquot British Medical Journal 312 71ndash72
Sikorski J Renfrew MJ Pindoria S amp Wade A (2004) Support for breastfeeding mothers (Cochrane Review) The Cochrane Database of Systematic Reviews Issue 2 John Wiley amp Sons Ltd Chichester
Smale M Renfrew MJ Marshall JL amp Spiby H (2006) Turning policy into practice more difficult that it seems The case of breastfeeding education Maternal and Child Nutrition 2 103ndash113
Spiby H Ker R DrsquoSouza L amp Renfrew MJ (2002) Intro-ducing a Consumer-Practitioner into breastfeeding prac-tice Year 2 In Infant Feeding Initiative A Report Evaluating the Breastfeeding Practice Projects 1999ndash2002 (ed F Dykes 2003) p 44 Department of Health London
Spiby H Wallis S Stone C amp Renfrew MJ (2005) Support-ing and Promoting Breastfeeding in Leeds Final Report to December 2004 Report to Leeds PCTs Children and Families Modernisation Team Leeds
Thomas C (2006) Darlington ndash A Breastfeeding Friendly Town Darlington Borough Council Darlington
Developing practice in breastfeeding 261
copy 2006 The Authors Journal compilation copy 2006 Blackwell Publishing Ltd Maternal and Child Nutrition 2 pp 245ndash261
Unsworth J (2000) Practice development a concept analy-sis Journal of Nursing Management 8 317ndash326
Wallace LM amp Jardine J (2006) A Health Scrutiny of Ser-vices to Support the Initiation and Duration of Breastfeed-ing in Coventry and Warwickshire Coventry and Warwickshire County Councils Coventry
Wallace L amp Kosmala-Anderson J (2006) A training needs survey of doctorsrsquo breastfeeding support skills in England Maternal and Child Nutrition 2 217ndash231
Wallace L amp Kosmala-Anderson J (in press) Training needs survey of midwives health visitors and voluntary sector
breastfeeding support staff in England Maternal and Child Nutrition (in press)
WHO (2003) Global Strategy for Infant and Young Child Feeding World Health Organization Geneva
Wilson AC Forsyth JS Green SA Irvine L Hau C amp Howie PW (1998) Relation of infant diet to childhood health seven year follow up of a cohort of children in Dundee infant feeding study British Medical Journal 316 21ndash25

Developing practice in breastfeeding 261
copy 2006 The Authors Journal compilation copy 2006 Blackwell Publishing Ltd Maternal and Child Nutrition 2 pp 245ndash261
Unsworth J (2000) Practice development a concept analy-sis Journal of Nursing Management 8 317ndash326
Wallace LM amp Jardine J (2006) A Health Scrutiny of Ser-vices to Support the Initiation and Duration of Breastfeed-ing in Coventry and Warwickshire Coventry and Warwickshire County Councils Coventry
Wallace L amp Kosmala-Anderson J (2006) A training needs survey of doctorsrsquo breastfeeding support skills in England Maternal and Child Nutrition 2 217ndash231
Wallace L amp Kosmala-Anderson J (in press) Training needs survey of midwives health visitors and voluntary sector
breastfeeding support staff in England Maternal and Child Nutrition (in press)
WHO (2003) Global Strategy for Infant and Young Child Feeding World Health Organization Geneva
Wilson AC Forsyth JS Green SA Irvine L Hau C amp Howie PW (1998) Relation of infant diet to childhood health seven year follow up of a cohort of children in Dundee infant feeding study British Medical Journal 316 21ndash25




















