Detection of immunoglobulin heavy chain gene rearrangement by polymerase chain reaction in chronic...
7
Detection of Immunoglobulin Heavy Chain Gene Rearrangement by Polymerase Chain Reaction in Chronic Active Gastritis Associated With Helicobacter pylori ERIC D. HSI, MD, JOEL K. GREENSON, MD, TIMOTHY P. SINGLETON, MD, JAVED SIDDIQUI, MS, BERTRAM SCHNITZER, MD, AND CHARLES W. ROSS, MD Chronic active gastritis associated with Helicobacter pylori (CAG- Hp) has been linked to the pathogenesis of gastric B-cell lymphomas of mueosa-associated lymphoid tissue (MALT). To determine whether monoclonal lymphoid populations are present in CAG-Hp and histological predictors of monoclonality exist, the authors exam- ined 46 endoscopic biopsies from 41 patients with CAG-Hp. The authors scored gastric biopsies for the presence of lymphoepithelial lesions (l~El.s), intensity of lymphoid infiltrate, presence of lymphoid aggregates and germinal centers, coexpression of CD43 (Leu 22) on B cells, and cytoplasmic immunoglobulin light chain restriction in formalin-fixed, paraffin-embedded tissues. DNA extracts from these routinely processed tissues were analyzed for immtmoglobulin heavy chain (IgH) gene rearrangement by polymerase chain reaction (PCR). Histological features, immtmophenotype, gene rearrangement status, and clinical information were correlated. Six of the 46 biopsies (13%) from six of 41 patients (15%) showed a monoclonal PCR pattern. Monoclonal PCR patterns correlated with the presence of LELs (P < .015) but not with intensity of lymphoid infiltrate, presence of germinal centers, or presence of lymphoid aggregates. LFI.~ corre- lated with germinal centers (P < .003) and intensity of infiltrate (P < .0001). None of the eases showed cytoplasmic light chain restriction nor coexpression of CD43 on B cells by immunohistochemistry. Clini- cal follow-up was available in all six patients whose gastric biopsies had a monoclonal PCR pattern (median, 58 months; range, 1 to 66 months) and 33 of the 35 patients with biopsies showing a polyclonal PCR pattern (median, 41 months; range 0.1 to 63 months). No patient developed gastric lymphoma. Monoclonallty of lymphoid cells was detected by IgH PCR in 13% of patients with CAG-Hp. Although the authors cannot exclude the possibility that some patients with monoclonal gastric lymphoid infiltrates may eventually develop overt lymphoma, no histological, immunophenotypic, nor clinical evidence of lymphoma was noted at presentation or on clinical follow-up. Given the high incidence of CAG-Hp in the general population and the relatively low incidence of gastric MALT lymphoma, clinicopathologic correlation is needed when interpreting tests for donallty in this setting. The presence of clonal IgH gene rearrangement in CAG-Hp supports the hypothesis that H pylor/is involved in the pathogenesis of low grade gastric B-cell MALT lymphomas. HuM PATHOL 27:290-- 296. Copyright © 1996 by W.B. Saunders Company Key words: Helicobacter pylori, gastritis, immunoglobulin gene re- arrangement, polymerase chain reaction, non-Hodgkln's lymphoma. Abbreviations: CAG-Hp, chronic active gastritis associated with Helicobacter pylori; MALT, mucosa-associated lymphoid tissue; I.EI., lymphoepithelial lesions; PCR, polymerase chain reaction; DAB, 3,3 '- diaminobenzidine tetrahydrochioride. Helicobacterpylori infects nearly one half the world's population] This bacterium is recognized as a cause of chronic active gastritis (CAG-Hp) and is thought to play a causative role in peptic ulcer disease.2 H pylori has also been implicated in causing type B atrophic gastritis and thus may play an important role in gastric carcino- genesis.~-5 Recently, some investigators have postulated that CAG-Hp may also play a role in the pathogenesis of gastric low grade B-cell lymphoma of mucosa-associated lymphoid tissue (MALT). ~8 Subsequent studies seem to support this hypothesis. In fact, some investigators advocate the treatment of low-stage, low-grade B-cell gastric lymphoma of MALT with antibiotics directed against H pylori. 9 lz Because H pylori may be involved in the pathogenesis of gastric lymphoma, the authors hypothesized that small monoclonal B-cell populations might exist in CAG-Hp. The polymerase chain reaction (PCR) can detect immunoglobulin heavy chain gene rearrangements with a sensitivity comparable with Southern blot meth- ods. 13 Furthermore, PCR is applicable to small clinical samples including archival (fixed) tissue extracts. The authors used this technique to study 46 gastric endo- scopic biopsies of CAG-Hp to determine whether mono- clonal B-cell populations may be detected in this benign process. The authors then correlated these findings with histological features, immunophenotype in paraf- fin-embedded tissues, and clinical follow-up. MATERIALS AND METHODS Case Selection All cases coded as H pyl0r/ gastritis between March 1, 1989, and October 1, 1990, were retrieved from the files of the University of Michigan Department of Pathology. Cases were reviewed by EDH and JKG to confirm the diagnosis of CAG-Hp. No cases had the histological features of MALT lymphoma. From the Department of Pathology, the University of Michigan, Ann Arbor, MI. Accepted for publication October 25, 1995. Address correspondence and reprint requests to Charles W. Ross, MD, Department of Pathology, University of Michigan, 1301 Cather- ine St, Ann Arbor, MI 481094)602. Copyright © 1996 by W.B. Saunders Company 0046-8177/96/2703-000955.00/0 Histological Examination Hematoxylin-eosin-stained tissue sections were reviewed for density of lymphoid infiltrate (scored 1 = slight; 2 = moderate; and 3 = severe); activity (degree of intraepithelial neutrophilic infiltrate: 1 = slight; 2 = moderate; and 3 = severe); presence or absence of lymphoepithelial lesions 290
-
Upload
independent -
Category
Documents
-
view
1 -
download
0
Transcript of Detection of immunoglobulin heavy chain gene rearrangement by polymerase chain reaction in chronic...

Detection of Immunoglobulin Heavy Chain Gene Rearrangement by Polymerase Chain Reaction in Chronic Active Gastritis Associated With Helicobacter pylori ERIC D. HSI, MD, JOEL K. GREENSON, MD, TIMOTHY P. SINGLETON, MD, JAVED SIDDIQUI, MS, BERTRAM SCHNITZER, MD, AND CHARLES W. ROSS, MD
Chronic active gastritis associated with Helicobacter pylori (CAG- Hp) has been linked to the pathogenesis of gastric B-cell lymphomas of mueosa-associated lymphoid tissue (MALT). To determine whether monoclonal lymphoid populations are present in CAG-Hp and histological predictors of monoclonality exist, the authors exam- ined 46 endoscopic biopsies from 41 patients with CAG-Hp. The authors scored gastric biopsies for the presence of lymphoepithelial lesions (l~El.s), intensity of lymphoid infiltrate, presence of lymphoid aggregates and germinal centers, coexpression of CD43 (Leu 22) on B cells, and cytoplasmic immunoglobulin light chain restriction in formalin-fixed, paraffin-embedded tissues. DNA extracts from these routinely processed tissues were analyzed for immtmoglobulin heavy chain (IgH) gene rearrangement by polymerase chain reaction (PCR). Histological features, immtmophenotype, gene rearrangement status, and clinical information were correlated. Six of the 46 biopsies (13%) from six of 41 patients (15%) showed a monoclonal PCR pattern. Monoclonal PCR patterns correlated with the presence of LELs (P < .015) but not with intensity of lymphoid infiltrate, presence of germinal centers, or presence of lymphoid aggregates. LFI.~ corre- lated with germinal centers (P < .003) and intensity of infiltrate (P < .0001). None of the eases showed cytoplasmic light chain restriction nor coexpression of CD43 on B cells by immunohistochemistry. Clini- cal follow-up was available in all six patients whose gastric biopsies
had a monoclonal PCR pattern (median, 58 months; range, 1 to 66 months) and 33 of the 35 patients with biopsies showing a polyclonal PCR pattern (median, 41 months; range 0.1 to 63 months). No patient developed gastric lymphoma. Monoclonallty of lymphoid cells was detected by IgH PCR in 13% of patients with CAG-Hp. Although the authors cannot exclude the possibility that some patients with monoclonal gastric lymphoid infiltrates may eventually develop overt lymphoma, no histological, immunophenotypic, nor clinical evidence of lymphoma was noted at presentation or on clinical follow-up. Given the high incidence of CAG-Hp in the general population and the relatively low incidence of gastric MALT lymphoma, clinicopathologic correlation is needed when interpreting tests for donallty in this setting. The presence of clonal IgH gene rearrangement in CAG-Hp supports the hypothesis that H pylor/is involved in the pathogenesis of low grade gastric B-cell MALT lymphomas. HuM PATHOL 27:290-- 296. Copyright © 1996 by W.B. Saunders Company
Key words: Helicobacter pylori, gastritis, immunoglobulin gene re- arrangement, polymerase chain reaction, non-Hodgkln's lymphoma.
Abbreviations: CAG-Hp, chronic active gastritis associated with Helicobacter pylori; MALT, mucosa-associated lymphoid tissue; I.EI., lymphoepithelial lesions; PCR, polymerase chain reaction; DAB, 3,3 '- diaminobenzidine tetrahydrochioride.
Helicobacterpylori infects nearly one half the world's population] This bacterium is recognized as a cause of chronic active gastritis (CAG-Hp) and is thought to play a causative role in peptic ulcer disease. 2 H pylori has also been implicated in causing type B atrophic gastritis and thus may play an important role in gastric carcino- genesis. ~-5 Recently, some investigators have postulated that CAG-Hp may also play a role in the pathogenesis of gastric low grade B-cell lymphoma of mucosa-associated lymphoid tissue (MALT). ~8 Subsequent studies seem to support this hypothesis. In fact, some investigators advocate the treatment of low-stage, low-grade B-cell gastric lymphoma of MALT with antibiotics directed against H pylori. 9 lz Because H pylori may be involved in the pathogenesis of gastric lymphoma, the authors hypothesized that small monoclonal B-cell populations might exist in CAG-Hp.
The polymerase chain reaction (PCR) can detect immunoglobulin heavy chain gene rearrangements
with a sensitivity comparable with Southern blot meth- ods. 13 Furthermore, PCR is applicable to small clinical samples including archival (fixed) tissue extracts. The authors used this technique to study 46 gastric endo- scopic biopsies of CAG-Hp to determine whether mono- clonal B-cell populations may be detected in this benign process. The authors then correlated these findings with histological features, immunophenotype in paraf- fin-embedded tissues, and clinical follow-up.
MATERIALS AND METHODS
Case Selection
All cases coded as H pyl0r/ gastritis between March 1, 1989, and October 1, 1990, were retrieved f rom the files of the University o f Michigan Depar tment o f Pathology. Cases were reviewed by EDH and JKG to conf i rm the diagnosis of CAG-Hp. No cases had the histological features of MALT lymphoma.
From the Department of Pathology, the University of Michigan, Ann Arbor, MI. Accepted for publication October 25, 1995.
Address correspondence and reprint requests to Charles W. Ross, MD, Department of Pathology, University of Michigan, 1301 Cather- ine St, Ann Arbor, MI 481094)602.
Copyright © 1996 by W.B. Saunders Company 0046-8177/96/2703-000955.00/0
Histological Examination
Hematoxyl in-eos in-s ta ined tissue sections were reviewed for density o f lymphoid infiltrate (scored 1 = slight; 2 = moderate; and 3 = severe); activity (degree of intraepithelial neutrophi l ic infiltrate: 1 = slight; 2 = moderate; and 3 = severe); presence or absence of lymphoepithel ial lesions
290

IGH GENE REARRANGEMENT IN H pylofi GASTRITIS (Hsi et al)
(LELs); presence or absence of lymphoid aggregates without germinal centers; presence or absence of follicles with germi- nal centers; and presence or absence of Dutcher bodies. LELs were defined as clusters of three or more lymphocytes in glandular epithelium. Hq6 Specimens were reviewed in a blinded fashion regarding other study data.
Immunoh is tochemis t r y
Formalin-fixed, paraffin-embedded tissues were deparaf- finized in xylene, dehydrated with alcohol and then stained with the following antibodies: L26 (CD20, 1:500 titer; DAKO Corporation, Carpinteria, CA), Leu 22 (CD43, 1:100; Becton Dickinson, San Jose, CA), peroxidase-conjugated rabbit poly- clonal anti-K (1:20, DAKO), or peroxidase-conjugated rabbit polyclonal anti-k (1:20, DAKO). Four cases were stained also with A6 (CD45RO, 1:50; Zymed Laboratories, Inc, San Fran- cisco, CA) to help identify T cells. For L26, anti-K and anti- k, the slides were pretreated for antigen retrieval by microwav- ing for 15 minutes at full power inside a pressure cooker (Tender Cooker; Nordic Ware, Minneapolis, MN) in a 1,000- W microwave (Frigidaire, Cleveland, OH) in 10 mmol /L ci- trate buffer (pH 6.0), followed by 20 minutes of cooling. Staining with the monoclonal antibodies was performed using an automated stainer (Ventana 320; Ventana Medical Systems, Inc, Tucson, AZ), and a Ventana DAB Detection Kit. Briefly, the kit has the following reagents to be added in sequential steps (36°C): inhibitor for endogenous peroxidase, primary antibody for 32 minutes, biotinylated secondary antibody, avi- din-biotin complex with horseradish peroxidase, 3,3'-diami- nobenzidine tetrahydrochloride (DAB) /hydrogen peroxide, and copper enhancer. The peroxidase-conjugated polyclonal antibodies were detected by incubating the deparaffinized microwaved tissues with the following sequence of reagents (room temperature): 3% hydrogen peroxide/methanol for 20 minutes, suppressor goat serum (1:20) for 10 minutes, primary antiserum for 1 hour, and 0.4 g /L DAB with 60 rag/ L hydrogen peroxide in phosphate-buffered saline (pH 7,15) tbr 10 minutes. The slides were counterstained with hematox- ylin and reviewed (by EDH and TPS) for coexpression of CD43 on CD20-positive B cells, identification of LELs, and light chain restriction. CD43 coexpression on B cells is indica- tive of lymphoma, and cytoplasmic immunoglobulin light
1719 chain restriction is evidence of monoclonality. -
DNA Extract ion
Four-micron tissue sections were prepared on plain glass slides and were transferred with a disposable razor blade to 100 #L of xylene in a 1.7-mL nonsiliconized microcentrifuge tube. An equal volume of 100% ethanol was added, and the samples were pelleted (10 minutes in a countertop microcen- trifuge), dried under vacuum, and digested overnight with 200 ng /#L proteinase K (Boehringer Mannheim, Indianapo- lis, IN) in 100 #L of 50 mmol /L TRIS pH 8.3 at 37°C. Samples were then boiled for 8 minutes, placed on ice, and centrifuged for 5 minutes to pellet out debris. DNA extraction was per- formed in batches of five to 10 specimens.
Polymerase Cha in Reac t ion
Seminested PCR was performed using primers FR3A and LJH (round 1), and FR3A and VLJH (round 2). 2°'21 Briefly, the round 1 reaction contained 20 to 30 #L of template DNA extract, 250 ng each of FR3A and LJH primers, 0.2 mmol /L of each dNTP, and 1.5 units of Taq polymerase (Boehringer Mannheim) in the PCR buffer of McCarthy e t a l , 22 with a total volume of 50 #L per reaction for both rounds of amplifica-
M 1 2 3 4 5 6 7 8
118 bp )~
72bp )~
Direction of migration
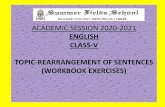
FIGURE 1. Sensitivity study of IgH PCR assay. Raji cell line DNA diluted in reactive tonsillar DNA. Ethidium bromide stained 8% PAGE gel visualized under UV light. Lane M, marker: (1) 100% Raji cell line DNA, (2) 50%, (3) 10%, (4) 5%, (5) 2%, (6) 1%, (7) 0.1%, and (8) 0,01%. A monoclonal population is detectable at the 2% level.
Lion. Reactions were performed in duplicate with separate aliquots of DNA extract using an automated thermocycler (Perkin Elmer, Norwalk, CT). First-round amplification was performed for 30 cycles of 94°C denaturation for 2 minutes, 55°C annealing for 2 minutes, and 72°C extension for 2 min- utes, ending with a final extension at 72°C for 10 minutes. A 1-#L aliquot of first-round product was used as the template DNA for round 2. Twenty cycles of amplification were per- formed in round 2, using the same reaction conditions as in round 1, except that the VLJH primer was substituted for the LJH primer.
Ten microliters of the final PCR product was analyzed using 8% polyacrylamide gel electrophoresis and was visual- ized by ethidium bromide staining. A monoclonal pattern was defined as one or two reproducible, dominant bands in the expected size range of 80 to 120 base pairs. Positive and nega- tive controls were Raji cell line DNA and water, respectively.
To determine the sensitivity of detecting a monoclonal population in a polyclonal background, the authors per- formed a dilutional assay in which Raji cell line DNA was progressively diluted with tonsillar DNA and subjected to PCR for immunoglobulin heavy chain (IgH) gene rearrangement as earlier. The authors were able to detect a monoclonal band at a dilution of 2% Raft cell line DNA to reactive tonsillar DNA (Fig 1).
Cl in ica l Fol low-Up
Information regarding patient clinical status was ob- tained from chart review and communication with referring physicians.
Stat ist ical Analysis
Statistical analysis was performed using Fisher's exact test- ing for nominal features and the Mann-Whitney U statistic for ordinal features.
RESULTS
Cl in ica l D a t a
Forty-six endoscop ic biopsies f rom 41 patients (24 men; 17 women) were inc luded in the study. Patients r a n g e d in age f rom 32 to 89 years (mean, 57 years; median , 55 years). Endoscop ic reports were available for all patients. Indicat ions for endoscopy at t ime of biopsy inc luded dyspepsia (13 patients) , abdomina l pain (six patients) , b loa t ing /gas (four patients), nausea and vomit ing ( three patients) , history o f pept ic ulcer disease ( three patients), atypical chest pain (two pa- tients), dysphagia (two patients) , evidence o f gastroin-
291

HUMAN PATHOLOGY VoLume 27, No. 3 (March 1996)
testinal hemorrhage (two patients), previous biopsy sus- picious for gastric adenocarcinoma (one patient), weight loss and diarrhea (one patient), intractable hic- cups (one patient), evaluation for carcinoid tumor (one patient), evaluation for Zollinger-Ellison syndrome (one patient), and evaluation for a possible gastric mass (one patient). Endoscopic findings included ulcer or erosion (19 patients), erythema (nine patients), atro- phy (two patients), "possible mass" (one patient), and normal mucosa (10 patients). The patient with the en- doscopic "possible mass" was later found to have a gastric leiomyosarcoma. Clinical follow-up was available in 39 patients with a median of 46 months (range, 0.13 to 66 months; mean, 36 months). For patients with biopsies that were monoclonal by IgH PCR, the median follow-up was 58 months (range, 1 to 66 months; mean, 42 months). For patients with biopsies that were poly- clonal by IgH PCR, the median follow-up was 41 months (range, 0.13 to 63 months; mean, 35 months). Two of the patients in the study died with no evidence of lymphoma at 4 days and 1 month after endoscopy. None of the patients was found to have gastric lymphoma in the follow-up period.
Histopathoiogy
The mononuclear infiltrate consisted of small lym- phocytes with round nuclei and plasma cells, but rare or no centrocyte-like cells. The infiltrate was either slight (32 biopsies) or moderate (14 biopsies). Neutro- philic infiltrate (activity) was present in all biopsies and was slight in 26 biopsies, moderate in 14, and severe in 6. Ulcers were present in three biopsy specimens, and intestinal metaplasia was seen in 11. LELs were present in 15 of the biopsies, lymphoid aggregates in 33, and follicles with germinal centers in 16. All biopsies with LELs had one or two LELs with the exception of patient no. 2, who had five LELs in two biopsy pieces. The LELs in all patients were small and nondestructive. Dutcher bodies were not seen in any of the specimens. Of the six specimens defined as monoclonal by PCR, five had LELs, three had moderate lymphoid infiltrates, two had intestinal metaplasia, and all six had either lymphoid aggregates or germinal centers. Figure 2 shows the his- topathology of a specimen with a monoclonal PCR pat- tern. Of the 40 polyclonal specimens, LELs were found in 10, moderate lymphoid infiltrates in 11, foci of intes- tinal metaplasia in nine, and lymphoid aggregates or germinal centers in 31.
Immunohistochemistry
The lamina propria contained a superficial layer of plasma cells, which was polytypic in all specimens. Lymphoid aggregates and germinal centers were lo- cated near the base of the mucosa and were B lineage. None of the specimens showed unequivocal coexpres- sion of CD43 on B cells. LEL lymphocytes phenotyped as B lineage, when present in stained sections. Art exam- ple of an LEL stained with L26 (CD20) is shown in Fig 2.
Polymerase Chain React ion
PCR of the DNA extracts showed a polyclonal smear or "ladder" of multiple bands in 40 of the 46 specimens. Six specimens from six different patients showed either one or two reproducible bands discern- ible above the background, indicating a clonal lymphoid population. PCR amplicons from each of these patient specimens were of distinctly different sizes. Figure 3 shows examples of two specimens with polyclonal patterns and one specimen with a single re- producible dominant band, indicative of a clonal lymphoid population. Figure 4 shows a composite of three additional specimens interpreted as having clonal patterns. A summary of histological and clinical features associated with these biopsies is presented in Table 1.
Statistics
Monoclonal PCR pattern correlated with the pres- ence of LELs (P < .015), but not with the presence of germinal centers (P = .163) or lymphoid aggregates (P = .660), using Fisher's exact test. LELs, however, were associated with the presence of germinal centers (P < .003). Intensity of the lymphoid infiltrate correlated with the presence of LELs (P < .0001) but did not correlate with monoclonal PCR pattern (P = .379), us- ing the Mann-Whitney U statistic.
DISCUSSION
The authors chose to study cases of CAG-Hp be- cause of its proposed relationship to low grade B-cell lymphoma of MALT. Some investigators hypothesize that H py/on" gastritis stimulates the formation of an "acquired MALT," which, as a result of a deregulated immune response, becomes neoplastic in a minority of cases. 912 The authors found that small clonal popula- tions of lymphoid ceils were detectable in some cases of CAG-Hp and that lymphoepithelial lesions (LELs) were significantly associated with detection of these clones.
In the 46 biopsies examined in this study, six were found to have a detectable monoclonal lymphoid popu- lation. Histologically, these specimens were diagnostic of CAG-Hp and did not represent lymphoma. Low grade gastric B-cell MALT lymphoma is characterized by a dense lymphoid infiltrate composed of small lym- phocytes with slightly irregular nuclear contours and abundant pale cytoplasm, termed centrocyte-like cells by Isaacson and colleagues 14'16'23'24 or monocytoid B cells/ marginal zone cells by others. 15'25 These cells have the propensity to invade gastric pit and glandular epithe- lium to form prominent destructive LELs and may colo- nize germinal centers. An overlying superficial plas- macytosis may be present and may be monoclonal in some specimens. The specimens in this study are distin- guished from MALT lymphoma on the basis of the fol- lowing features: lack of dense lymphoid infiltrate, rare to absent centrocyte-like cells, rarity of the small nonde- structive LELs, absence of Dutcher bodies, absence of immunophenotypic abnormalities, and no clinical evi-
292

IGH GENE REARRANGEMENT IN H pylori GASTRITIS (Hsi et al)
FIGURE 2. Case no. 2. Chronic active gastritis with H, pylofi organisms. (A) Low magnification shows a mild inflammatory infiltrate, a lymphoid follicle and foci of intestinal metaplasia. (Hematoxylin-eosin stain; original magnification x50.) (B) Higher magnification shows an isolated lymphoepithelial le- sion. (Hematoxylin-eosin stain; original magnification ×400.) (C) Immunoperoxidase stain for CD20 (L26) demonstrating B-cell phenotype of lymphocytes within a lymphoepithelial lesion. (Original magnification ×400.)
dence of lymphoma. The authors cannot exclude the possibility that some of these patients may develop lymphoma in the future.
Several investigators have reported the successful use o f IgH PCR in endoscopic biopsies to show clonality in gastric lymphomas, a3'26'27 The primers used in this study are commonly used and amplify 65% to 90% of cases that are clonal by Southern blot techniques. 22'2s-s3 The sensitivity of PCR has been shown by other groups,
as well as by us, to be on the order of 2% to 5% clonal B cells in a polyclonal background, similar to Southern blot methods. ~3'22 Some may argue that our monoclonal cases may represent false positives because relatively few lymphoid cells are analyzed. Wan et a134 directly ad- dressed this problem in a dilutional study and found false-positive rnonoclonal bands only when the number of PCR "targets" (cell equivalents) was reduced to an
118 bp ~"
72bp ~-
M A B C D E F (-) +
I Direction of migrat ion
FIGURE 3. Examples of polyclonal and monoclonal patterns, duplicate samples. Ethidium bromide stained 8% PAGE gel visu- alized under ultraviolet light. M, marker. (A and B) Case no. 8; (C and D) case no. 40; (E and F) case no. 2. Lanes A to D show a polyclonal pattern, whereas lanes E and F demonstrate a reproducible single dominant band.
M A B C + (-)
1i8bp ~"
72 bp )~
Direction of migration
FIGURE 4. Examples of monoclonal patterns. Ethidium bro- mide stained 8% polyacrylamide gel-electrophoresis visualized under ultraviolet light. M, marker. (A) Case no. 5; (B) case no. 4; (C) case no. 1; +, Raji cell line positive control; - , negative control, no DNA template.
293

HUMAN PATHOLOGY Volume 27, No. 3 (March 1996)
TABLE 1. Summary of Clinical, Histological, andMolecular Genetic Data
Case Age Infiltrate Lymphoid Germinal Mo of No. (yr) Sex PCR Results LEL Intensity* Aggregates Centers Act iv i ty-~ Follow-Up Follow-Up
1 84 2 38 3 57 4 42 5 43 6 72 7 57 8 78 9 48
10 50 11 36 12a 68 12b 68 12c 68 12d 67 13 52 14 45 15 55 16 56 17 51 18a 89 18b 89 19 34 20 41 M 21 65 M 22 77 F 23 63 F 24a 50 M 24b 50 M 25 76 F 26 87 F 27 54 F 28 41 M 29 64 F 30 66 M 31 32 F 32 82 F 33 46 M 34 62 F 35 52 M 36 39 M 37 62 M 38 39 M 39 72 M 40 56 F 41 44 F
M Monoclonal F Monoclonal M Monoclonal M Monoclonal M Monoclonal F Monoclonal M Pol zclonal M Pol mlonal F Pol ~clonal F Pol rclonal M Pol lclonal M Pol tclonal M Pol zclonal M Pol lclonal M Pol zclonal M Pol rclonal M Pol lclonal F Pol ~clonal M Pol lclonal M Pol rclonal F Pol rclonal F Pol Tclonal M Pol lclonal
Pol rclonal Pot rclonal Pol ,clonal Pol rclonal Pot rclonal Pot ,clonal Pol' ,clonal Pol rclonal Pol ,clonal Pol ~clonal Pol" ,clonal Pol' ,clonal Pol' ,clonal Pol' ,clonal Pol' 'clonal Pol' 'clonal Pol" ,clonal Pol' 'clonal Pol' 'clonal Pol' 'clonal Polyclonal Polyclonal Polyclonal
No 1 Yes No 1 1 DNEL Yes 1 No Yes 1 5 ANEL Yes 1 Yes Yes 2 65 ANEL Yes 2 Yes Yes 1 53 ANEL Yes 2 Yes No 2 63 ANEL Yes 2 Yes Yes 1 66 ANEL No 1 No No 1 0 None No 1 No No 1 0.13 DNEL No 1 No No 1 20 ANEL No 1 No No 2 33 ANEL No 1 No No 1 36 ANEL No 1 No No 3 46 ANEL No 1 Yes No 1 46 ANEL No 1 Yes No 1 46 ANEL No 1 Yes No 1 49 ANEL No 1 No No 2 52 ANEL No 1 No No 1 54 ANEL No 1 Yes No 2 1 ANEL No 1 Yes No 1 4 ANEL No 1 Yes No 1 11 ANEL No 1 Yes No 2 ' 16 ANEL No 1 No Yes 3 14 ANEL No I Yes No 1 20 ANEL No 1 Yes No 1 46 ANEL No 1 Yes No 1 48 ANEL No 1 Yes No 1 51 ANEL No 1 Yes No 2 51 ANEL No 1 Yes No 1 54 ANEL No 1 Yes Yes 1 52 ANEL No 1 Yes No 3 63 ANEL No 1 No Yes 2 0 None No 1 No Yes 1 51 ANEL No 1 Yes Yes 3 12 ANEL No 1 Yes Yes 1 48 ANEL No 2 No No 1 62 ANEL No 2 Yes No 2 25 ANEL Yes 1 Yes No 2 3 ANEL Yes 2 Yes No 2 35 ANEL Yes 2 Yes No 2 41 ANEL Yes 2 Yes No 1 46 ANEL Yes 2 Yes Yes 3 14 ANEL Yes 2 Yes Yes 1 16 ANEL Yes 2 Yes Yes 2 36 ANEL Yes 2 Yes Yes 3 46 ANEL Yes 2 Yes Yes 1 48 ANEL Yes 2 Yes Yes 2 54 ANEL
Abbreviations: PCR, polymerase chain reaction; LEL, lymphoepithelial evidence of lymphoma.
* Infiltrate intensity: 1 = mild, 2 = moderate, and 3 = severe. t Activity: 1 = mild, 2 = moderate, and 3 = severe.
lesions; ANEL, alive, no evidence of lymphoma; DNEL, dead, no
average of six per sample. By contrast, our monoclonal specimens contained lymphoid aggregates or germinal centers with many B cells. Furthermore, no correlation existed between the intensity of the lymphoid infiltrate and monoclonality by PCR in these specimens. The different monoclonal patterns in different patients' bi- opsies excludes contamination as a source for false-posi- tive results. Actually, it is possible that additional cases in this study might contain monoclonal lymphoid popu- lations because the consensus primers used in this study are not capable of detecting all possible IgH gene rear- rangements. 22,a5,36
The authors are aware of two studies that have peripherally addressed the question of whether gastritis
may contain monoclonal B-cell populations. Using the same primers as in this study, Sukpanichnant et a127 analyzed seven specimens with "gastritis" for IgH gene rearrangement by PCR; none contained a detectable monoclonal lymphoid population. An abstract by Woth-
37 erspoon et al repor ted PCR detection of a monoclonal population of lymphoid cells in two of 58 specimens with H pylori gastritis.
The experience of other investigators, 1°'11 and the findings of the present study, suggest that molecular techniques may detect a small monoclonal population of lymphoid cells in the absence of clinical or histologi- cal evidence of lymphoma. Monoclonal lymphoid popu- lations have been described in conditions that do not
294

IGH GENE REARRANGEMENT IN H pylofi GASTRITIS (Hsi et al)
necessarily behave in a malignant fashion, such as lymphomatoid papulosis, myoepithelial sialadenitis, and posttransplant lyrnphoproliferative disorder. 38-43 Conversely, gene rearrangement studies may be poly- clonal in the presence of histological evidence of dis- ease, possibly because of sampling error, problems with primer specificity, or other technical limitations. 44 The authors conclude that a diagnosis of gastric low grade B-cell MALT lymphoma should not be based solely on the finding of a monoclonal gene rearrangement by PCR.
In summary, the authors found a monoclonal pat- tern by IgH PCR in six of 46 biopsies of CAG-Hp. None of the study patients had histological, immunopheno- typic, or clinical evidence of lymphoma at presentation or on follow-up. From a practical standpoint, the au- thors emphasize the need for clinicopathologic correla- tion when interpreting molecular diagnostic studies for clonality. The finding of a monoclonal immunoglobu- fin gene rearrangement does not necessarily connote B-cell malignancy. From a theoretical standpoint, the presence of B-cell monoclones in CAG-Hp specimens supports the hypothesis that Hpylori is involved in the pathogenesis of low-grade lymphoma of MALT.
Acknowledgment. The authors acknowledge T. S. Frank, MD, for technical assistance and Char Fegan for secretarial assistance.
REFERENCES
1. Marshall BJ: Helicobacterpylori:A primer for 1994. Gastroenter- ology 1:241-247, 1993
2. Blaser MJ: Helicobacterpyloriand the pathogenesis ofgastrodu- odenal inflammation. J Infect Dis 161:626-633, 1990
3. Nomura A, Stemmermann GN, Chyou PH, et al: HeIicobacter py/0r/infections and gastric carcinoma among Japanese Americans in Hawaii. N EnglJ Med 325:1132-1136, 1991
4. ParsonnetJ, Freidman GD, Vandersteen DP, et al: Helicobacter py/0r/ infection and the risk of gastric carcinoma. N Engl J Med 326:1127-1131, 1991
5. Correa P, Haenszel W, Cuello C, et al: Gastric precancerous process in a high risk population: Cohort follow-up. Cancer Res 50:4737-4740, 1990
6. Wotherspoon AC, Ortiz-Hidalgo C, Falzon M, et al: Helicobacter py/ori-associated gastritis and primary B-cell lymphoma. Lancet 338:1175-1176, 1991
7. Dogliani C, Wotherspoon A, Moschini A, et al: High incidence of primary gastric lymphoma in northeastern Italy. Lancet 339:834- 835, 1992
8. Isaacson PG, Spencer J: Is gastric lymphoma an infectious disease? HUM PATHOL 24:569-570, 1993
9. Hussell T, Isaacson PG, Crabtree JE, et al: The response of cells from low grade B-cell lymphomas of mucosa-associated lymphoid tissue to Helicobacterpylori. Lancet 342:571-574, 1993
10. Wotherspoon AC, Doglioni C, Diss TC, et al: Regression of primary low-grade B-cell gastric lymphoma of mucosa-associated lymphoid tissue type after eradication of Helicobacter pylori. Lancet 342:575-577, 1993
11. Wotherspoon AC, Doglioni C, de Boni M, et al: Antibiotic treatment for lowgrade gastric MALT lymphoma. Lancet 343:1503, 1994
12. Greiner A, Marx A, Heesmann J, et al: Idiotype identity in a MALT-type lymphoma and B cells in Helicobacter pylori associated chronic gastritis. Lab Invest 70:572-578, 1994
13. Algara P, Martinez P, Sanchez L, et al: The detection of B- cell monoclonal populations by polymerase chain reaction: Accuracy
of approach and application in gastric endoscopic biopsy specimens. HUM PATHOL 24:1184-1188, 1993
14. Isaacson PG, Spencer J, Finn T: Primary B~ell gastric lymphoma. HuM PATHOL 17:72-82, 1986
15. Zukerberg LR, FerryJA, Southern JF, et al: Lymphoid infil- trates of the stomach: Evaluation of histologic criteria for the diagno- sis of low-grade gastric lymphoma on endoscopic biopsy specimens. Am J Surg Pathol 14:1087-1099, 1990
16. Isaacson P, Wright DH: Extranodal malignant lymphoma arising from mucosa-associated lymphoid tissue. Cancer 53:2515- 2524, 1984
17. Picker LJ, Weiss LM, Medeiros LJ, et al: Immunophenotypic criteria for the diagnosis of non-Hodgkin's lymphoma. Am J Pathol 128:181-201, 1987
18. Ngan B, Picker LJ, Medeiros LJ, et al: Immunophenotypic diagnosis of non-Hodgkin's lymphoma in paraffin sections. AmJ Clin Pathol 91:579-583, 1989
19. Gelb AB, Rouse RV, Dorfman RF, et al: Detection of immu- nophenotypic abnormalities in paraffin-embedded B-lineage non- Hodgkin's lymphoma. Am J Clin Pathol 102:825-834, 1994
20. Wan JH, Trainor KJ, Brisco MJ, et al: Monoclonality in B cell lymphoma detected in paraffin wax embedded sections using the polymerase chain reaction. J Clin Pathol 43:888-890, 1990
21. Brisco MJ, Tan LW, Orsborn AM, et al: Development of a highly sensitive assay, based on the polymerase chain reaction, for rare B-lymphocyte clones in a polyclonal population. BrJ Haematol 75:163-167, 1990
22. McCarthy KP, SloaneJP, Wiedemann LM: Rapid method for distinguishing clonal fi'om polyclonal B cell populations in surgical biopsy specimens. J Clin Pathol 43:429-432, 1990
23. Isaacson PG, Spencer J: Malignant lymphoma of mucosa- associated lymphoid tissue. Histopathology 11:445-462, 1987
24. Myhre MJ, Isaacson PG: Primary B-cell gastric lymphoma: A reassessment of its histogenesis. J Pathol 152:1-11, 1987
25. Harris NL,Jaffe ES, Stein H, et al: A revised European-Ameri- can classification of lymphoid neoplasms: A proposal from the Inter- national Lymphoma Study Group. Blood 84:1361-1392, 1994
26. Pan LX, Diss TC, Peng HZ, et al: Clonality analysis of defined B-cell populations in archival tissue sections using microdissection and the polymerase chain reaction. Histopathology 24:323-327, 1994
27. Snkpanichnant S, Vnencak-Jones CL, McCurley TL: Determi- nation of B-cell clonality in paraffin-embedded endoscopic biopsy specimens of abnormal lymphocytic infiltrates and gastrointestinal lymphoma by polymerase chain reaction. Am J Clin Pathol 102:229- 305, 1994
28. Reed TJ, Reid A, Wallberg K, et al: Determination of B-cell clonality in paraffin-embedded lymph nodes using the polymerase chain reaction. Diagn Mol Pathol 2:42-49, 1993
29. Inghirami G, Szabolcs MJ, Yee HT, et al: Detection of immu- noglobulin gene rearrangement of B cell non-Hodgkin's lymphomas and leukemias in fresh, unfixed and formalin-fixed, paraffin-embed- ded tissue by polymerase chain reaction. Lab Invest 68:746-757, 1993
30. Ramasamy I, Brisco M, Morley A: Improved PCR method for detecting monoclonal immunoglobulin heavy chain rearrangement in B cell neoplasms. J Clin Pathol 45:770-775, 1992
31. Deane M, McCarthy KP, Wiedermann KM, et al: An im- proved method for detection of B-lymphoid clonality by the polymer- ase chain reaction. Leukemia 5:726-730, 1991
32. Segal GH, Wittwer CT, Fishleder AJ, et al: Identification of monoclonal B-cell populations by rapid cycle polymerase chain reac- tion: A practical screening method for the detection of immunoglob- ulin gene rearrangements. A m J Pathol 141:1291-1297, 1992
33. Deane M, Norton JD: Immunoglobulin gene "fingerprint- ing": An approach to analysis of B lymphoid clonality in lymphopro- liferative disorders. BrJ Haematol 77:274-281, 1991
34. WanJH, Sykes PJ, Orell SR, et al: Rapid method for detecting monoclonality in B cell lyrnphoma in lymph node aspirates using the polymerase chain reaction. J Clin Pathol 45:420-423, 1992
35. Deane M, Norton JD: Detection of immunoglobulin gene rearrangement in B-cell neoplasias by polymerase chain reaction gene amplification. Leuk Lymphoma 5:9-22, 1991
36. Diss TC, Peng H, Wotherspoon AC, et al: Detection ofmono- clonality in low-grade B-cell lymphomas using the polymerase chain reaction is dependent on primer selection and lymphoma type. J Pathol 169:291-295, 1993
295

HUMAN PATHOLOGY Volume 27, No. 3 (March 1996)
37. Wotherspoon AC, Diss TC, Pan L, et al: Diagnosis of low grade MALT lyanphoma in gastric biopsies: Histology, PCR or both? J Pathol 173:151A, 1994
38. Nalesnik MA, Jaffe R, Starzl TE, et al: The pathology of posttran splant lymphoproliferafive disorders occurring in the setting of cyclosporine A-prednisone immunosuppression. Am J Pathol 133:173-192, 1988
39. Locker J, Nalesnick M: Molecular genetic analysis of lymphoid tumors arising after organ transplantation. Am J Pathol 135:977-987, 1989
40. Cleary ML, Warnke R, Sklar J: Monoclonality of lymphopro- liferative lesions in cardiac-transplant recipients: Clonal analysis based on immunoglobulin gene rearrangements. N Engl J Med 310:47% 482, 1984
41. Weiss LM, Wood GS, Trela M, et al: Clonal T-cell popula- tions in lymphomatoid papulosis: Evidence of a lymphoprolifera- tive origin for a clinically benign disease. N Engl J Med 315:475- 479, 1986
42. Hsi ED, Siddiqui J, Alkan S, et al: Analysis of immunoglobu- lin heavy chain gene rearrangement in myoepithelial sialadenitis by polymerase chain reaction. Mod Pathol 7:111A, 1994
43. Fishleder A, Tubbs R, Hesse B, et al: Uniform detection of immunoglobulin-gene rearrangement in benign lymphoepithelial lesions. N EnglJ Med 316:1118-1121, 1987
44. Weber DM, Dimopoulos MA, Anandu DP, et al: Regression of gastric lymphoma of mucosa-associated lymphoid tissue with antibi- otic therapy for Helicobacter pylori. Gastroenterology 107:1835-1838, 1994
996