
Depression in adolescents: Feasibility, efficacy, and neural ...
167
Department of Child and Adolescent Psychiatry and Psychotherapy, University of Ulm Prof. Dr. Jörg M. Fegert (Department Head) Depression in adolescents: Feasibility, efficacy, and neural correlates of a brief group psychotherapeutic treatment, along with insights on epidemiology, symptoms, and diagnostics Thesis presented to the Faculty of Engineering, Computer Science and Psychology Ulm University for the degree of Doctor of Philosophy Joana Franziska Straub Freiburg 2015
-
Upload
khangminh22 -
Category
Documents
-
view
3 -
download
0
Transcript of Depression in adolescents: Feasibility, efficacy, and neural ...
Department of Child and Adolescent Psychiatry and Psychotherapy, University of Ulm
Prof. Dr. Jörg M. Fegert (Department Head)
Depression in adolescents: Feasibility, efficacy, and neural
correlates of a brief group psychotherapeutic treatment, along with
insights on epidemiology, symptoms, and diagnostics
Thesis presented to the
Faculty of Engineering, Computer Science and Psychology
Ulm University
for the degree of Doctor of Philosophy
Joana Franziska Straub
Freiburg
2015
I
Acting dean:
Prof. Dr. T. Seufert
1. Representative:
Prof. Dr. M.G. Kölch
2. Representative:
Prof. Dr. Dr. M. Holtmann
Day of disputation: 12th November 2015
II
Acknowledgements
I would like to thank…
… Prof. Dr. Michael Kölch, who gave me the opportunity to explore different research
topics, fostered my scientific interests, and supervised and supported me during my
years as a PhD student.
… Prof. Dr. Birgit Abler, Dr. Paul Plener and Dr. Nina Spröber who spent a great amount
of time and effort to support, encourage, and improve my work. Thank you for this
intensive mentoring.
… Prof. Dr. Ferdinand Keller and Prof. Dr. Georg Grön, for their statistical and technical
support and for sharing helpful ideas on research questions.
… my colleagues Martina Bonenberger and Rebecca Groschwitz, for always lending me
an ear and for laughing together.
… my colleagues in the fMRI lab.
… the research assistants who helped me with data acquisition and literature searches.
… all patients and subjects who agreed to participate in the studies.
… Prof. Dr. Michael Kölch and Prof. Dr. Dr. Martin Holtmann for reviewing this
dissertation.
… my partner, my friends, and my whole family for their constant support during the
time I worked on this thesis.
Without you, this thesis would not have been possible. Thank you!
III
IV
Table of Contents
Abstract ...................................................................................................................................... X
German Summary/Zusammenfassung ..................................................................................... XII
1. General Introduction ........................................................................................................... 1
1.1. Epidemiology of depressive disorders in adolescents .................................................... 1
1.2. Classification of symptoms .............................................................................................. 3
1.3. Instruments for diagnosing depression in adolescents .................................................. 4
1.4. Aetiology.......................................................................................................................... 7
1.4.1. Psychological and social factors .................................................................................. 8
1.4.2. Biological factors .......................................................................................................... 9
1.4.2.1. Genetics, sex, neurotransmitters and structural brain differences......................... 9
1.4.2.2. Brain development and development of psychiatric disorders ............................ 10
1.4.2.3. Functional differences in brain imaging in adolescents with depression.............. 12
1.5. Pharmacological and psychotherapeutic treatment of depression in adolescents ..... 13
1.5.1. Guidelines for the treatment of depression in minors .............................................. 13
1.5.2. Efficacy of psychotherapeutic treatment .................................................................. 14
1.6. Treatment programs for depression ............................................................................. 14
1.6.1. Individual treatment programs available in English-speaking countries .................. 15
1.6.2. International group treatment programs .................................................................. 17
1.6.3. Treatment programs available in Germany .............................................................. 18
1.6.4. Duration of treatment ............................................................................................... 19
1.6.5. Development of a brief CBT-G called MICHI ............................................................. 20
1.7. Neural correlates of depression treatment .................................................................. 21
1.7.1. Neural correlates of pharmacological treatment ...................................................... 21
1.7.2. Neural correlates of psychotherapeutic treatment .................................................. 21
V
1.7.3. Neural correlates of depression treatment in children and adolescents ................. 24
1.7.4. Paradigm for assessing neuronal correlates of depression treatment ..................... 24
2. Aims and research questions of the present work ........................................................... 25
3. Results ............................................................................................................................... 30
3.1. Changes in prevalence rates of ICD-10 F3 diagnoses in the inpatient setting .............. 30
3.2. Association between symptoms of depression plus mania and suicidal behavior ...... 30
3.3. Convergence of CDRS-R scores with a mild depressive episode according to ICD-10.. 31
3.4. Agreement between BDI-II and CDRS-R in assessing depression in minors ................. 32
3.5. Literature review on psychotherapeutic group treatment for depressed minors ....... 33
3.6. Pilot study on feasibility and acceptance of MICHI in adolescent inpatients ............... 34
3.7. Pilot study on feasibility and acceptance of MICHI in adolescent outpatients ............ 35
3.8. RCT for the assessment of efficacy of MICHI in depressed adolescent outpatients .... 36
3.9. Neural correlates of successful psychotherapy of depression in adolescents ............. 38
4. General discussion ............................................................................................................ 40
4.1 Limitations ..................................................................................................................... 49
4.2 Conclusions and perspectives ....................................................................................... 52
5 References ........................................................................................................................ 56
6 Original research articles .................................................................................................. 74
6.1 Treatment of mental diseases in children in German hospitals: analysis of frequencies
in the years 2003 to 2012. ........................................................................................................ 74
6.2 Suicidal behavior in German adolescents: prevalence and association with depressive
and manic symptoms ............................................................................................................... 81
6.3 Convergence of children's depression rating scale-revised scores and clinical diagnosis
in rating adolescent depressive symptomatology ................................................................... 89
6.4 Agreement between self-report and clinician’s assessment in depressed adolescents,
using the example of BDI-II and CDRS-R .................................................................................. 93
VI
6.5 Psychotherapeutic treatment of children and adolescents with depression. Review of
the literature on cognitive-behavioral and interpersonal group therapies ........................... 104
6.6 Innovations in Practice: MICHI, a brief cognitive-behavioural group therapy for
adolescents with depression - a pilot study of feasibility in an inpatient setting ................. 114
6.7 A brief cognitive-behavioural group therapy programme for the treatment of
depression in adolescent outpatients: a pilot study .............................................................. 119
6.8 MICHI – a brief, manualized cognitive behavioural group therapy for the treatment of
depression in adolescents: randomized controlled trial. ....................................................... 130
6.9 Neural correlates of successful psychotherapy of depression in adolescents ........... 141
7 Curriculum Vitae ............................................................................................................. 150
8 Scientific articles published in peer-reviewed journals .................................................. 151
VII
List of Tables
Table 1 Questionnaires and structured interviews for the assessment of depression in
adolescents ................................................................................................................................. 5
Table 2 Meta-analyses about the efficacy of psychotherapies of depressed children and
adolescents ............................................................................................................................... 15
Table 3 German-language therapy programs for the treatment of depressed minors ........... 19
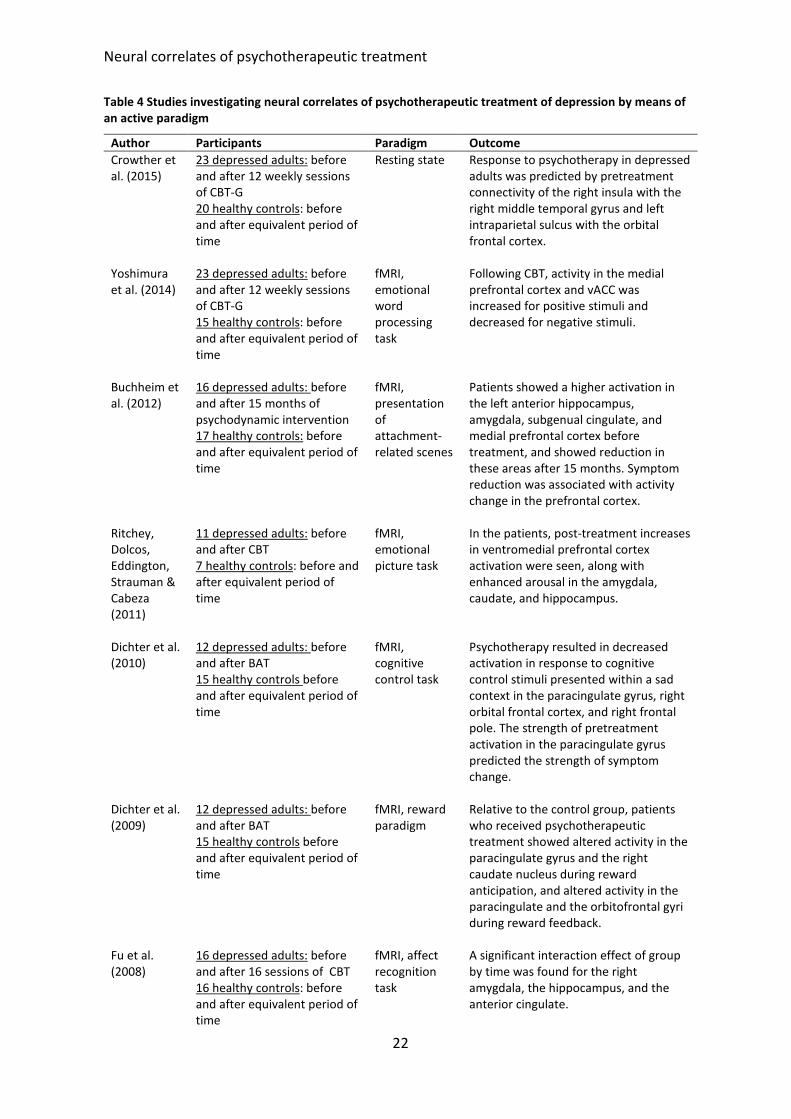
Table 4 Studies investigating neural correlates of psychotherapeutic treatment of depression
by means of an active paradigm .............................................................................................. 22
List of Figures
Figure 1 Neurobiological model demonstrating that bottom-up processes develop faster
than top-down processes in adolescents (modified after Casey et al. 2008) .......................... 11
VIII
Abbreviations
ACC anterior cingulate cortex
BAT behavioural activation therapy
BDI-II Beck Depression Inventory-Revision
CAR cortisol awakening response
CBT cognitive behavioural psychotherapy
CBT-G group cognitive behavioural therapy
CDRS-R Children’s Depression Rating Scale-Revised
CWD-A Coping With Depression course for Adolescents
DSM Diagnostic and Statistical Manual of Mental Disorders
fMRI functional Magnetic Resonance Imaging
ICD International Classification System of Diseases
IPT interpersonal psychotherapy
IPT-A interpersonal psychotherapy for depressed adolescents
MDD major depressive disorder
MICHI Manualized Intervention to Cope with depressive symptoms, Help strengthen
resources and Improve emotion regulation
PASCET Primary and Secondary Control Enhancement Training
PAT-I Depressed adolescent patients (PAT) assigned to the intervention group (I)
PAT-W Depressed adolescent patients (PAT) assigned to the wait-list control group (W)
RCT randomized controlled trial
sgACC subgenual anterior cingulate cortex
SSRI selective serotonin reuptake inhibitor
TAU psychiatric treatment as usual
vACC ventral anterior cingulate cortex
WHO World Health Organization
WL wait list

IX
X
Abstract
At the time the present research was started, the treatment of depression in adolescents in
Germany was only addressed by a small number of structured intervention programs.
However, none of these combined the advantages of a cognitive behavioural treatment that
is brief, is applied in a group setting, is intended to treat all levels of severities of depression,
and has been evaluated with respect to acceptance, feasibility, and efficacy. Furthermore, no
investigations had been done on neural correlates of psychotherapeutic treatment of
depression in adolescents. To address all these issues, we developed a brief cognitive-
behavioural group psychotherapy for depressed adolescents titled “Manualized Intervention
to Cope with depressive symptoms, Help strengthen resources and Improve emotion
regulation” (MICHI). In two pilot studies, one conducted in inpatients and the other in
outpatients, MICHI was shown to be feasible and accepted, and to reveal first trends of
efficacy. In a subsequent randomized controlled trial, depressed adolescent patients were
assigned to either an intervention group that received MICHI (PAT-I) or a wait-list control
group that received treatment as usual (PAT-W). Results indicated a significant interaction
effect between groups (PAT-I/PAT-W) and time-points of measurement (pre/post), with small
to moderate effect sizes seen in reduction of depressive symptoms.
Neural correlates of the psychotherapeutic interventions were investigated using
functional Magnetic Resonance Imaging (fMRI). In the PAT-I group, pre-to-post symptom
changes were found to be significantly associated with changes in activity in the subgenual
anterior cingulate cortex (sgACC), the amygdala, and the hippocampus, all brain areas that are
closely associated with depression. Post hoc analyses revealed a significant interaction effect
between groups (PAT-I/PAT-W) and time points of measurement (pre/post) for the bilateral
sgACC, the left amygdala, and the left hippocampus. Additionally, bilateral sgACC activity
before treatment correlated significantly with subsequent pre-to-post symptom improvement
in PAT-I.
Further analyses were aimed at acquiring new insights into the epidemiology,
symptoms, and diagnostics of affective disorders in adolescents, as follows: 1) An examination
of trends in inpatient treatment in Germany for depressive disorders in adolescents between
2003 and 2012 found that admissions increased over this period, which highlights the need
for fast and efficacious help. A frequent reason for referral to inpatient treatment is acute
suicidality, whose underlying contributing factors are still not fully understood in minors.

XI
2) Results of our study indicated that symptoms of mania have a predictive value when it
comes to suicidality, even after controlling for depression scores. This underscores the need
for valid diagnostic instruments for the assessment of mental health symptoms. 3) For the
assessment of depression in minors, the structured interview most frequently used in clinical
and research contexts is the Children‘s Depression Rating Scale-Revised (CDRS-R). Up to now,
it was not known how the sum scores in the CDRS-R are associated with severity of depression
as assessed by the International Classification System of Diseases (ICD-10), which is important
for recognizing depressive disorders and being able to refer patients for proper treatments.
Our study determined a cut-off score of 36 on the CDRS-R to be indicative of a mild to moderate
depressive episode. 4) Another frequently used diagnostic self-report instrument is the Beck
Depression Inventory-Revision (BDI-II), but it was unclear how similar this is to the CDRS-R for
measuring symptoms of depression in minors. Accordingly, the two instruments were
compared, and were found to correlate highly in scores, specifically on the symptom level,
with the item of suicidality having the highest correlation.
XII
German Summary/Zusammenfassung
Zu dem Zeitpunkt, als die vorliegende Arbeit begonnen wurde, lagen in Deutschland drei
Therapieprogramme zur Behandlung von Depressionen bei Jugendlichen vor, wobei keines
von ihnen die Vorteile einer Gruppen-, Kurzzeit- und kognitiven Verhaltenstherapie
kombinierte. Außerdem wurde keines von ihnen für alle Schweregrade der Depression
konzipiert. Darüber hinaus wurde keines dieser Programme hinsichtlich Akzeptanz,
Machbarkeit und Effektivität hin untersucht. Weiterhin gibt es keine Studie, die die neuronale
Gehirnaktivität von depressiven Jugendlichen, die entweder psychotherapeutisch behandelt
wurden, oder Behandlung der Regelversorgung erhielten, verglich. Unter Berücksichtigung all
dieser Aspekte entwickelten wir eine kognitiv behaviorale Gruppen-Kurzzeitintervention
“Manualized Intervention to Cope with depressive symptoms, Help strengthen resources and
Improve emotion regulation” (MICHI). In zwei Pilot-Studien mit depressiven Jugendlichen, die
sowohl stationär als auch ambulant behandelt wurden, wies MICHI eine hohe Akzeptanz,
Machbarkeit und erste Hinweise auf Wirksamkeit auf. Im Zuge einer Effektivitäts-Studie
wurden depressive jugendliche Patienten entweder der Interventionsgruppe (PAT-I), die
MICHI erhielt, oder der Wartelistenkontrollgruppe (PAT-W), die Behandlung der
psychiatrischen Regelversorgung erhielt, randomisiert zugeordnet. Die Ergebnisse lieferten
Hinweise auf einen signifikanten Interaktionseffekt zwischen Gruppenzugehörigkeit (PAT-
I/PAT-W) und Messzeitpunkten (pre/post) mit kleinen bis moderaten Effektstärken
hinsichtlich Reduktion der depressiven Symptomatik.
Weiterhin gingen in PAT-I Veränderungen der neuronalen Aktivität (gemessen anhand
funktioneller Magnetresonanztomographie (fMRT)) im subgenualen anterioren Cingulum
(sgACC), der Amygdala und dem Hippocampus, Areale die eng mit Depressionen assoziiert
sind, mit prä-post-test Symptomveränderungen einher. Post hoc Analysen ergaben einen
signifikanten Interaktionseffekt zwischen Gruppenzugehörigkeit (PAT-I/PAT-W) und
Messzeitpunkten (prä/post) im bilateralen sgACC, der linken Amygdala, und dem linken
Hippocampus. Außerdem korrelierte die bilaterale sgACC Aktivität vor Therapie signifikant mit
dem anschließenden Ansprechen auf die Therapie in PAT-I.
Weitere Studien verfolgten das Ziel neue Einblicke in die Epidemiologie, Symptomatik
und Diagnostik von affektiven Störungen bei Jugendlichen zu erlangen: 1) Eine Untersuchung
welche Anzahlen, der wegen depressiven Episoden im stationären Setting behandelten
Jugendlichen zwischen 2003 und 2012 in Deutschland verglich, ergab einen Anstieg über die
XIII
Zeit hinweg was wiederum die Notwendigkeit einer schnellen und wirksamen Behandlung
unterstreicht. Ein häufiger Grund für eine stationäre Aufnahme ist akute Suizidalität deren
zugrunde liegende Faktoren bei Jugendlichen immer noch unzureichend untersucht sind. 2)
Das Ergebnis unserer Studie weist darauf hin, dass Manie-Symptome mit erhöhter Suizidalität
einhergehen, auch nachdem für Depressionswerte kontrolliert wurde. Dies wiederum
unterstreicht die Notwendigkeit valider diagnostischer Instrumente zur Erfassung psychischer
Störungen. Für die Erfassung depressiver Symptome bei Minderjährigen, eignet sich das sehr
häufig angewandte klinische Interview „Children‘s Depression Rating Scale-Revised“ (CDRS-R).
3) Bisher gab es jedoch keine Anhaltspunkte dahingehend, welcher Summenwert der
deutschen Version der CDRS-R welchem Schweregrad einer depressiven Episode nach ICD-10
(Internationales Klassifikationssystem für psychische Störungen) entspricht, was wiederum
wichtig wäre um depressive Störungen erkennen und um die entsprechende Behandlung in
die Wege leiten zu können. Unsere Studie zeigte erstmals, dass ein Summenwert von 36 einer
leichten bis mittelgradig depressiven Episode entspricht. 4) Ein weiterhin häufig eingesetztes
Fragebogeninstrument ist das Beck Depressionsinventar-Revision (BDI-II) aber es ist unklar
wie ähnlich beide Instrumente depressive Symptome bei Minderjährigen messen. Um diese
Lücke zu schließen wurden beide Instrumente miteinander verglichen, wobei sich hohe
Korrelationen zeigten, besonders auf Symptomebene. Dabei korrelierte das Item Suizidalität
am höchsten.
General Introduction
1
1. General Introduction
1.1. Epidemiology of depressive disorders in adolescents
With respect to age of onset of depression, first episodes are sometimes seen in childhood
but more commonly in early or middle adolescence (Groen & Petermann, 2008). Individuals
who meet the criteria for a major depressive disorder for the first time in adolescence
(Fombonne, Woster, Cooper, Harrington & Rutter, 2001) are at higher risk (62.4%) for
recurrence in adulthood. Studies have found a wide variation in the duration of depressive
episodes, with a mean length of approximately eight months (Mehler-Wex, 2008). However,
Patton et al. (2014) found that if episodes of depression in adolescents last longer than six
months, symptoms often persist until adulthood, which highlights the need for prompt and
effective treatments during adolescence that keep episodes as short as possible.
In German children of elementary school age, lifetime prevalence rates of depressive
disorders are assumed to range from 1% to 2%, with an equal distribution between the sexes;
however, this may differ from the prevalence rates in other countries (Groen & Petermann,
2008). In adolescents aged 13 to 18 years, the prevalence rate of depressive episodes that
last from 1 to 12 months is 5.6% (Costello, Erkanli & Angold, 2006), with the rate in this age
group being higher for girls (5.9%) than for boys (4.6%). Based on the findings of 17
European studies, the prevalence rates of depression in adults range from 3.1% to 10.1%
(median: 6.9%) (Wittchen & Jacobi, 2005). As adolescents get older, their overall prevalence
rates of depression become more and more comparable to those of adults.
According to the World Health Organization (WHO), depression is expected to be the
most frequent disorder in industrialized countries by 2030 (Allianz Deutschland, 2011) and a
comparison of prevalence rates of depression in adults between 2004 and 2008 revealed an
increase of 23%. However, little research exists on whether prevalence rates of depressive
disorders in minors rose within this time frame as well. In one meta-analysis, which included
all studies that had used structured interviews to assess depressive disorders in children and
adolescents born between 1965 and 1996, Costello et al. (2006) found no evidence for an
increasing prevalence of depressive disorder over this time period. However, two other
studies looked at whether there were changes over time in the prevalence rates for the
broader concept of emotional problems, comprising questions about sorrows, sadness,
Epidemiology of depressive disorders in adolescents
2
reduced self-esteem, and anxiety. One study of three British birth cohorts born in 1974,
1986, and 1999 found a trend-wise increase in emotional problems (Collishaw, Maughan,
Goodman & Pickles, 2004), and a German study that assessed psychopathological problems
in children and adolescents at two time points, 2003–2006 and 2009–2012, found a slight
increase of emotional problems in the age group of 11- to 17-year-olds (Hoelling et al., 2014).
Thus, while prevalence rates for depressive disorders in children and adolescents did not
change over time, prevalence rates for emotional problems did.
Despite the finding of no increase in prevalence rates for depression, the number of
antidepressants being prescribed for children and adolescents has been increasing (Zito et
al., 2003); specifically, prescriptions for selective serotonin reuptake inhibitors (SSRIs) and
hypericum (Fegert, Koelch, Zito, Glaeske & Janhsen, 2006). Furthermore, in Germany, it has
been found that outpatient treatment diagnoses of depressive disorders in children and
adolescents under the age of 15 years rose about 16% from 2005 to 2008 (Annuss et al.,
2010). These increases in pharmaceutical treatment and outpatient treatment might reflect
increased help-seeking behaviour, improved diagnostic skills at the primary care level, more
openness to seeking help, or an improved health supply in general (Hegerl, 2013). To date,
there exists one study of Holtmann et al. (2010) that examined national trends in the rates
of inpatients between 2000 and 2007. Results indicate increased rates of inpatients up to 19
years that were diagnosed with depressive disorder. However following our knowledge
newer studies are missing. Inpatient treatment is especially relevant for severely affected
minors suffering from an acute crisis (e.g., acute suicidality) whose very low psychosocial
functioning level might prevent them from attending school, and for those whose
symptomatology is closely related to family dysfunction.
In summary, prevalence rates for depressive disorders increase from childhood to
adolescence, reaching levels in older adolescents that are similar to those seen in adults.
Despite no increase in the overall prevalence of depressive disorders, increases have been
seen in the numbers of both psychopharmacological prescriptions and of outpatients being
treated for depressive disorders. However there are newer studies missing about whether
those rising numbers of out- and inpatients are still rising. The high relapse rate in adulthood
in individuals whose first depressive episode occurred during adolescence highlights the
need for more studies investigating effective treatments in this age group.
Classification of symptoms
3
1.2. Classification of symptoms
In about 40% of cases, depression is accompanied by one or more co-morbidities (Essau,
Conradt & Petermann, 2000) such as anxiety disorders, eating disorders, substance abuse,
and attention deficit hyperactivity disorder (ADHD) (Bettge et al., 2008). In children and
adolescents, depression is also often accompanied by problems such as irritable mood, loss
of interest in school, and decline in academic performance (Mehler-Wex, 2012). Taken
together, all those aspects affect family and school life as well as personal relationships.
Given the nature and associated risks of depression, the Global Burden of Disease Study of
the WHO (Vos, Flaxman, Naghavi, Lozano & Michaud, 2012) has identified it as one of the
most debilitating disorders worldwide.
A depressive disorder may be diagnosed using either the Diagnostic and Statistical
Manual of Mental Disorders (DSM) or the International Classification System of Diseases
(ICD). Both specify that symptoms must last at least two weeks, but they differ in that DSM-
5 (American Psychiatric Association, 2013) says only that at least five symptoms must be
fulfilled in order for a diagnosis of a major depression to be made, while ICD-10 specifies the
fulfilment of four, six, or eight symptoms for the diagnosis of mild, moderate, or severe
depressive disorder, respectively (Remschmidt, Schmidt & Poustka, 2009). The only change
from DSM-IV (American Psychiatric Association, 1994) to DSM-5 (American Psychiatric
Association, 2013) has been removal of the previously exclusion criterion of depressive
symptoms lasting less than two months following the death of a loved one. Therefore,
assessment instruments referring to previous classification systems for diagnosing a
depressive disorder can still be applied.
In both the ICD-10 (Remschmidt, et al., 2009) and the DSM-5 (American Psychiatric
Association, 2013), the main symptoms of a depressive episode are low mood, reduced
energy, and decreased activity. Other common symptoms include reduction in the capacity
for enjoyment, interest, concentration, marked tiredness, sleep disturbance, diminished
appetite, feelings of guilt or worthlessness, and (in ICD-10 only) reduced self-esteem. Other
symptoms of depressive disorders are elevated levels of suicidal ideation, suicidal behaviour,
and completed suicide (Nock et al., 2013); the last being among the most common causes of
death in European adolescents (Wilkinson, Kelvin, Roberts, Dubicka & Goodyer, 2011).
Among US adolescents, lifetime prevalence rates for suicidal ideation, plans, and attempts
have been found to be 12.1%, 4.0%, and 4.1%, respectively (Nock et al., 2013); while in
Instruments for diagnosing depression in adolescents
4
Germany, more than a third of adolescents have reported having had suicidal ideation at
some point (Donath, Graessel, Baier & Hillemacher, 2013; Plener, Kapusta, Fegert & Keller,
2009). Suicidal ideation and attempts are seen more frequently in females (Kokkevi, Rotsika,
Arapaki & Richardson, 2012), but completed suicide is more frequent in males (Värnik et al.,
2009).
The category of affective disorders (F3) in ICD-10 also includes bipolar disorders,
which are characterized by alternating depressive and (hypo-) mania episodes, and have a
prevalence rate of 2.1% among 15- to 18-year-olds (Kozloff et al., 2010). In about 9 out of 10
adolescents, bipolar disorders start with a depressive episode and about 10% of depressed
adolescents develop a (hypo-) mania episode within ten years (Birkle & Holtmann, 2014).
Like depressive disorder, bipolar disorder has been shown to be associated with elevated
levels of suicidal behaviour (Allison, Roeger, Martin & Keeves, 2001; Brent et al., 1993),
especially in the case of an early onset (Van Meter, Moreira & Youngstrom, 2011). The
criteria for bipolar disorder have been found to be fulfilled at least once by 9.1% of those
reporting lifetime suicidal ideation, by 13.2% of those reporting a lifetime suicide attempt
(Nock et al., 2013), and by 17.9% of those who actually committed suicide (Brent et al., 1993).
However, there is little knowledge about whether the extent for suicide risk is higher in
adolescents with symptoms of both mania and depression compared to those with
depressive symptoms alone.
In sum, the two classification systems use similar symptoms for diagnosing a
depressive disorder, but the ICD-10 allows the classification of episodes into different levels
of severity. Suicidal ideation is a devastating symptom of depression, with a high prevalence
rate in the general adolescent population and an even higher one in the depressed
adolescent population. Accordingly, better understanding is needed of predictors for suicide
in adolescents, including whether symptoms of mania in addition to those of depression
predict suicidal ideation and behaviours more strongly than do depressive symptoms alone.
1.3. Instruments for diagnosing depression in adolescents
As a foundation for determining the most suitable treatment, diagnostic instruments that
can appropriately detect the presence and severity of a depressive episode are necessary. In
Germany, the guidelines for the treatment of depression in adults (Deutsche Gesellschaft für
Psychiatrie Psychotherapie und Nervenheilkunde, 2009) state that questionnaires should be
Instruments for diagnosing depression in adolescents
5
used for the early detection of depressive symptoms, and that the nature of the symptoms
as well as their severity and duration should be explored by means of structured interviews
in order to make a valid diagnosis. The level of recommendation for this is “B”, meaning
that the recommendation is based on knowledge derived from non–randomized controlled
trials (RCT). Following the German guidelines for the treatment of depression in children
and adolescents issued by the “Deutsche Gesellschaft für Kinder- und Jugendpsychiatrie
Psychosomatik und Psychotherapie” (2013) clinical assessment and diagnosis should only be
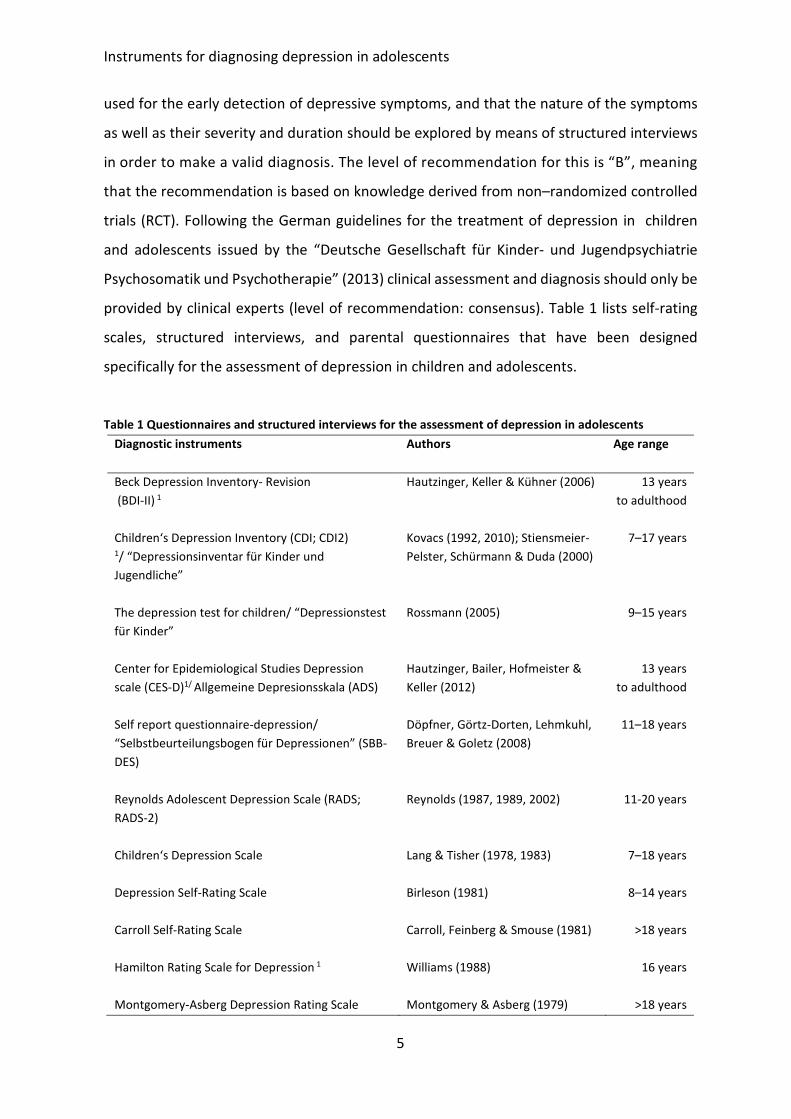
provided by clinical experts (level of recommendation: consensus). Table 1 lists self-rating
scales, structured interviews, and parental questionnaires that have been designed
specifically for the assessment of depression in children and adolescents.
Table 1 Questionnaires and structured interviews for the assessment of depression in adolescents
Diagnostic instruments
Authors Age range
Beck Depression Inventory- Revision
(BDI-II) 1
Hautzinger, Keller & Kühner (2006) 13 years
to adulthood
Children‘s Depression Inventory (CDI; CDI2) 1/ “Depressionsinventar für Kinder und
Jugendliche”
Kovacs (1992, 2010); Stiensmeier-
Pelster, Schürmann & Duda (2000)
7–17 years
The depression test for children/ “Depressionstest
für Kinder”
Rossmann (2005) 9–15 years
Center for Epidemiological Studies Depression
scale (CES-D)1/ Allgemeine Depresionsskala (ADS)
Hautzinger, Bailer, Hofmeister &
Keller (2012)
13 years
to adulthood
Self report questionnaire-depression/
“Selbstbeurteilungsbogen für Depressionen” (SBB-
DES)
Döpfner, Görtz-Dorten, Lehmkuhl,
Breuer & Goletz (2008)
11–18 years
Reynolds Adolescent Depression Scale (RADS;
RADS-2)
Reynolds (1987, 1989, 2002) 11-20 years
Children‘s Depression Scale Lang & Tisher (1978, 1983)
7–18 years
Depression Self-Rating Scale
Birleson (1981) 8–14 years
Carroll Self-Rating Scale Carroll, Feinberg & Smouse (1981)
>18 years
Hamilton Rating Scale for Depression 1
Williams (1988) 16 years
Montgomery-Asberg Depression Rating Scale Montgomery & Asberg (1979) >18 years
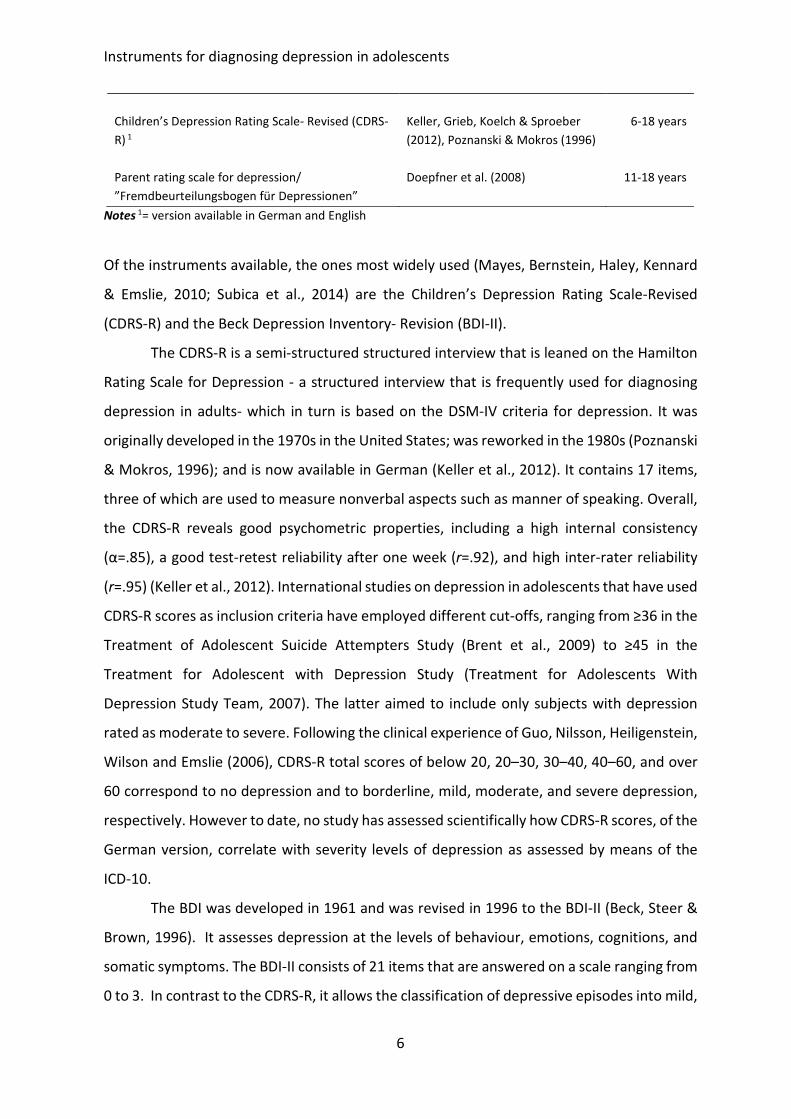
Instruments for diagnosing depression in adolescents
6
Children’s Depression Rating Scale- Revised (CDRS-
R) 1
Keller, Grieb, Koelch & Sproeber
(2012), Poznanski & Mokros (1996)
6-18 years
Parent rating scale for depression/
”Fremdbeurteilungsbogen für Depressionen”
Doepfner et al. (2008) 11-18 years
Notes 1= version available in German and English
Of the instruments available, the ones most widely used (Mayes, Bernstein, Haley, Kennard
& Emslie, 2010; Subica et al., 2014) are the Children’s Depression Rating Scale-Revised
(CDRS-R) and the Beck Depression Inventory- Revision (BDI-II).
The CDRS-R is a semi-structured structured interview that is leaned on the Hamilton
Rating Scale for Depression - a structured interview that is frequently used for diagnosing
depression in adults- which in turn is based on the DSM-IV criteria for depression. It was
originally developed in the 1970s in the United States; was reworked in the 1980s (Poznanski
& Mokros, 1996); and is now available in German (Keller et al., 2012). It contains 17 items,
three of which are used to measure nonverbal aspects such as manner of speaking. Overall,
the CDRS-R reveals good psychometric properties, including a high internal consistency
(α=.85), a good test-retest reliability after one week (r=.92), and high inter-rater reliability
(r=.95) (Keller et al., 2012). International studies on depression in adolescents that have used
CDRS-R scores as inclusion criteria have employed different cut-offs, ranging from ≥36 in the
Treatment of Adolescent Suicide Attempters Study (Brent et al., 2009) to ≥45 in the
Treatment for Adolescent with Depression Study (Treatment for Adolescents With
Depression Study Team, 2007). The latter aimed to include only subjects with depression
rated as moderate to severe. Following the clinical experience of Guo, Nilsson, Heiligenstein,
Wilson and Emslie (2006), CDRS-R total scores of below 20, 20–30, 30–40, 40–60, and over
60 correspond to no depression and to borderline, mild, moderate, and severe depression,
respectively. However to date, no study has assessed scientifically how CDRS-R scores, of the
German version, correlate with severity levels of depression as assessed by means of the
ICD-10.
The BDI was developed in 1961 and was revised in 1996 to the BDI-II (Beck, Steer &
Brown, 1996). It assesses depression at the levels of behaviour, emotions, cognitions, and
somatic symptoms. The BDI-II consists of 21 items that are answered on a scale ranging from
0 to 3. In contrast to the CDRS-R, it allows the classification of depressive episodes into mild,
Aetiology
7
moderate, and severe. Its internal consistency has been found to range between .89 and .94
in a psychiatric sample and between .84 and .91 in a non-psychiatric sample; and test-re-test
reliability and validity are high in both the original English version (Beck et al., 1996) and the
German version (Hautzinger et al., 2006).
Self-rating and clinician rating instruments each have advantages and disadvantages
(for an overview, see Stieglitz, 2008), and it remains unclear how similarly they assess
particular symptoms of depression. A study that correlated the sum scores of the CDRS-R
and the BDI-II in a healthy school sample and a clinical psychiatric population (Keller et al.,
2012) found correlation coefficients of .70 and .74, respectively. Correlation between CDRS-
R and BDI-II within HIV-positive adolescents in Malavi was moderately (r=.42, p<.001) (Kim
et al., 2014). These instruments have not yet however been compared within a population
comprising depressed adolescents only. Most of the studies that compared self-ratings and
clinician ratings have focused on correlations at the level of sum scores rather than at the
level of subscales or items. The one study that analysed the concordance of the self-report
and structured interview versions of the Inventory for Depressive Symptomatology (Rush et
al., 1986) found that items that assessed somatic aspects of depression correlated more
highly than did those that assessed depressive mood (Corruble, Legrand, Zvenigorowski,
Duret & Guelfi, 1999). Particularly with respect to the exploration of sensitive subjects such
as suicidality, it is important for both clinicians and researchers to know how well the
answers to self-administered and clinician-administered scales correlate, and whether one
instrument can be replaced by the other.
Taken together, there exist many diagnostic instruments for the assessment of
depressive disorders in children and adolescents, of which the BDI-II and CDRS-R are the
most frequently applied in both clinical practice and research. However, the CDRS-R data do
not provide information about the severity level of a depressive episode according to ICD-
10, and it is unclear how much overlap there is between the information on depressive
symptoms that is collected from structured interviews vs. self-report questionnaires.
1.4. Aetiology
The fact that depressive disorders arise in heterogeneous ways can be attributed to an
interplay of multiple causes such as psychological, social and biological factors.
Psychological and social factors
8
1.4.1. Psychological and social factors
Several psychological models have been formulated to explain the development and
persistence of depressive disorders. Beck’s cognitive theory (Beck, 1976) combines the
concepts of dysfunctional cognitive schemata, negative cognitive triad, and cognitive errors.
Dysfunctional cognitive schemata influence the selection and interpretation of incoming
data in a biased, negative way. The cognitive triad comprises a negative view about oneself,
the world, and the future. Cognitive errors include over-generalization, arbitrary
conclusions, and cognitive biases such as maximization (overestimation of failure and
punishment) and minimization (underestimation of winning and positive reinforcement),
both of which are closely connected to the reward system (Elliott, Sahakian, Herrod, Robbins
& Paykel, 1997).
Seligman’s learned helplessness theory (Seligman, 1975) suggests that an individual
who repeatedly experiences negative situations might come to believe that life is
uncontrollable, which could lead to the development of dysfunctional cognitions such as
attributing negative situations stably, internally, and globally.
According to Lewinsohn and Graf (1973), depressive symptoms arise in response to a
reduction in positive reinforcements. Reasons for this reduction could include withdrawing
from others, demonstrating behaviours (such as inadequate social skills) that are sanctioned
rather than reinforced positively, becoming less able to enjoy positive experiences, or
becoming more prone to focus on negative ones.
In addition, certain negative life circumstances such as sexual abuse, low
socioeconomic status (McLeod & Shanahan, 1996), difficult family relationships and parental
divorce (Gilman, Kawachi, Fitzmaurice & Buka, 2003), and non-sexual abuse or neglect
(Widom, DuMont & Czaja, 2007) are risk factors for depression. In one study of depressed
adolescents, 77% of participants mentioned that their depressive episodes were reactions
to typical adolescent experiences such as break-ups and difficulties with parents or friends
(Essau et al., 2000). In addition, chronic stress, such as that due to long-term emotional and
physical neglect, is predictive for the later development of mental health symptoms (Essex,
Klein & Kalin, 2002). Conversely, social supports such as caring parents are shown to be a
protective factor that can prevent the occurrence of depressive disorders (Kaufman et al.,
2004).
Biological factors
9
In summary, when it comes to the development of cognitive behavioural psychotherapies,
the main elements of successful treatment consist of helping the patient learn how to
recognize and alter dysfunctional cognitions, integrate positive experiences and activities
into daily life, and improve the ability to handle stressors and negative life experiences.
Another important factor is the involvement in the therapy process of a supportive person,
such as a family member or a friend, whom the patient trusts.
1.4.2. Biological factors
The focus in this section is on neuronal aspects of depression; other biological aspects are
touched on only briefly.
1.4.2.1. Genetics, sex, neurotransmitters and structural brain differences
Studies that have looked for associations between environmental aspects and genetic
factors of depression have found them in 80% of cases (Dunn et al., 2011). Depressive
disorders in childhood and adolescence have a genetic component, with heritability of
youth-onset depression ranging from 30% to 80% (Rice, Harold & Thapar, 2002). In many
cases, depression in children of depressed parents can be explained by the interplay
between a short allele form of the serotonin transporter gene 5-HTTLPR and stressful life
events (Eley et al., 2004). Furthermore, a significant three-way interaction in predicting
depression in children has been found between 5-HTTLPR, the Met allele of brain-derived
neurotropic factor, and a history of maltreatment (Kaufman et al., 2006). However, there are
still studies missing that found a robust relationship between specific candidate genes or
genomes and depression (Shyn et al., 2011; Sullivan et al., 2009).
Variables such as personality traits have been suggested as potential moderators on
genetic influences. Some attention has been focused on the behavioural activation system,
which regulates approach and appetitive motivation and is related to sensitivity of reward
(Gruber et al., 2013). An altered reward system in turn has been proposed as a candidate
endophenotype of depression, as it is a risk characteristic that is likely to be heritable, is
present regardless of illness state, and is predictive for the onset of depression (Forbes &
Dahl, 2012).
With respect to sex effects, a longitudinal study found that the risk for developing a
depressive disorder after tanner stage III is higher in girls than in boys (Angold, Costello &
Brain development and development of psychiatric disorders
10
Worthman, 1998), which could be explained by an imbalance of androgens and oestrogens.
Furthermore, one study related the cortisol awakening response (CAR; increase of cortisol
levels in the first half hour after waking), of late adolescents with the subsequent
development of major depressive disorder (MDD). They found that higher baseline CAR was
associated with an increased risk of developing MDD highlighting the role of a dysregulated
hypothalamic pituitary adrenal axis when it comes to the development of depression (Adam
et al., 2010).
In a meta-analysis of structural brain abnormalities that have been associated with
MDD, Bora, Harrison, Davey, Yuecel & Pantelis (2012) found volume reductions in the
prefrontal cortex, the anterior cingulate cortex, the caudate nucleus, and the putamen. They
additionally found reports that the subgenual anterior cingulate cortex (sgACC) and the
orbitofrontal cortices were smaller in patients who were being treated with antidepressants
than in patients who were medication naïve. In a meta-analysis of 143 studies, Kempton et
al. (2011) found that MDD is associated with larger lateral ventricles, greater volume of
cerebrospinal fluid, and smaller volumes of the basal ganglia, thalamus, hippocampus,
frontal lobe, orbitofrontal cortex, and gyrus rectus. In a longitudinal study of 86 adolescents
without a history of depressive disorders who had been scanned during their early and mid-
adolescence, Whittle et al. (2014) found that 30 subjects later experienced a depressive
episode, with a relationship seen between the development of depression and volumetric
changes in the hippocampus, amygdala, and putamen.
1.4.2.2. Brain development and development of psychiatric disorders
Investigating neural correlates of psychiatric disorders in a younger population can help with
understanding the neurobiological origin and course of such disorders, as it avoids the
confounds, that are often present in adults, such as long-term use of psychotropic
medications and recurrent or chronic course of the illnesses (Cullen, 2012). Furthermore, the
adolescent brain is in a state of transition in which developmental plasticity enables constant
adaptation to the environment. On the one hand, such plasticity may account for the
increase in several psychiatric disorders during this vulnerable period in life (Crews, He &
Hodge, 2007), but on the other hand it enables the investigation of therapeutic interventions
during a very sensitive phase of brain development (Davey, Yücel & Allen, 2008; Giedd et al.,
2009).
Brain development and development of psychiatric disorders
11
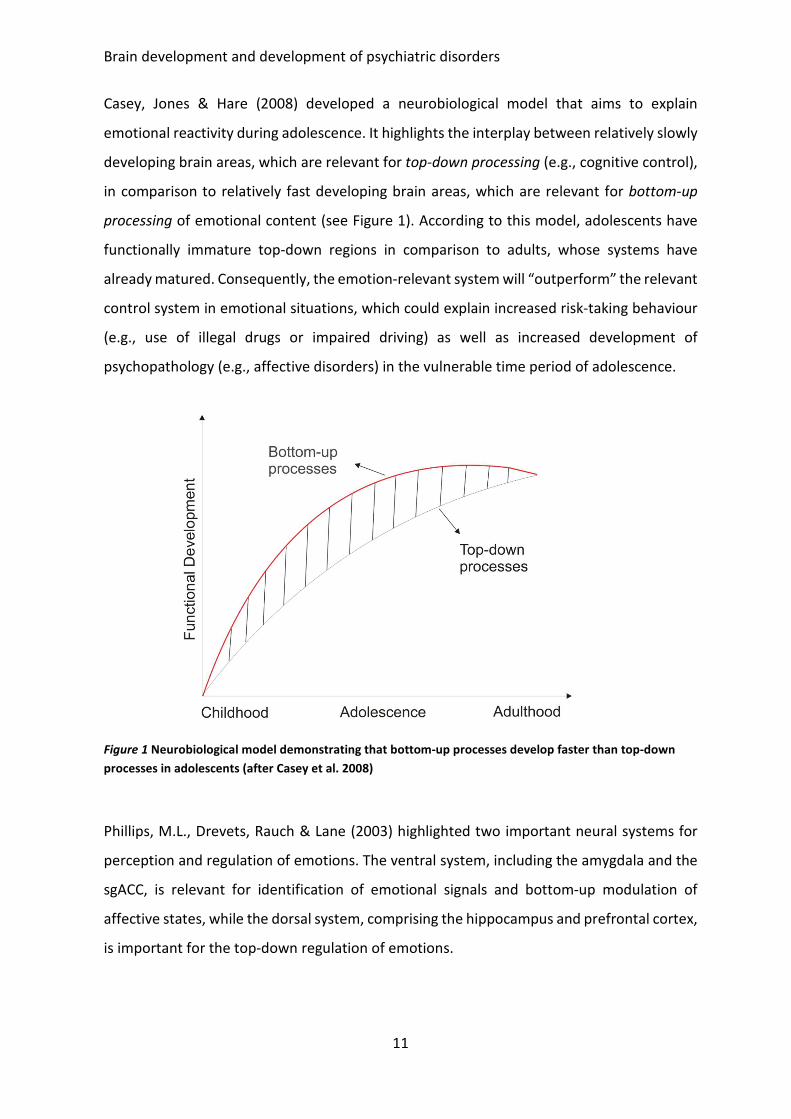
Casey, Jones & Hare (2008) developed a neurobiological model that aims to explain
emotional reactivity during adolescence. It highlights the interplay between relatively slowly
developing brain areas, which are relevant for top-down processing (e.g., cognitive control),
in comparison to relatively fast developing brain areas, which are relevant for bottom-up
processing of emotional content (see Figure 1). According to this model, adolescents have
functionally immature top-down regions in comparison to adults, whose systems have
already matured. Consequently, the emotion-relevant system will “outperform” the relevant
control system in emotional situations, which could explain increased risk-taking behaviour
(e.g., use of illegal drugs or impaired driving) as well as increased development of
psychopathology (e.g., affective disorders) in the vulnerable time period of adolescence.
Figure 1 Neurobiological model demonstrating that bottom-up processes develop faster than top-down
processes in adolescents (after Casey et al. 2008)
Phillips, M.L., Drevets, Rauch & Lane (2003) highlighted two important neural systems for
perception and regulation of emotions. The ventral system, including the amygdala and the
sgACC, is relevant for identification of emotional signals and bottom-up modulation of
affective states, while the dorsal system, comprising the hippocampus and prefrontal cortex,
is important for the top-down regulation of emotions.
Functional differences in brain imaging in adolescents with depression
12
1.4.2.3. Functional differences in brain imaging in adolescents with depression
Kerestes, Davey, Stephanou, Whittle & Harrison (2014) reviewed 28 functional magnetic
resonance imaging (fMRI) studies conducted in adolescents aged 13 to 18 years and in young
adults aged 19 to 25 years, focusing on imaging domains such as emotion processing,
cognitive control, affective cognition, reward processing, and resting-state functional
connectivity. Concerning those studies, an elevated activity was found in the amygdala, the
anterior cingulate cortex (ACC) (including the sgACC), and frontal brain areas such as the
ventro-medial prefrontal cortex and orbitofrontal cortex. In studies that examined
depression in adolescents using a reward paradigm, elevated activity in the ventral striatum
was seen as well (Davey, Allen, Harrison & Yuecel, 2011; Forbes et al., 2006; Forbes et al.,
2009; Forbes et al., 2010; Olino et al., 2011; Shad, Bidesi, Chen, Ernst & Rao, 2011).
In the following those brain regions will be considered more closely: when depressed
patients are compared with healthy controls, altered activity in the amygdala is seen in both
adults (Almeida, Versace, Hassel, Kupfer & Phillips, 2010; Arnone et al., 2012; Fu et al., 2004;
Godlewska, Norbury, Selvaraj, Cowen & Harmer, 2012; Mingtian et al., 2012; Rosenblau et
al., 2012; Sheline et al., 2001) and adolescents (Roberson-Nay et al., 2006; Yang et al., 2010).
Several studies in adults have identified increased signal activity in the sgACC in depressed
patients in comparison to healthy controls (Baeken et al., 2010; Gotlib et al., 2005; Kumari
et al., 2003); and Liotti et al. (2000) showed that the generation of sadness in healthy women
by reading autobiographical memory scripts, led to a heightened signal activity in the sgACC.
Yang et al. (2009) found an elevated neural signal in the sgACC in depressed adolescents in
comparison to a healthy control group during the performance of a stop signal task. Other
researchers have found increased connectivity between the sgACC and the
dorsomedial/dorsolateral frontal cortex (Davey, Harrison, Yuecel & Allen, 2012) as well as
elevated activity between the sgACC and the insula/amygdala (Connolly et al., 2013). Masten
et al. (2011) examined the relationship between sgACC activity during peer rejection and
subsequent increases in depressive symptoms, and found that a heightened activity in sgACC
during the exclusion phase was associated with elevated depression scores a year later.
Furthermore, depressed adolescents, in comparison to healthy controls, demonstrated a
decreased neural signal in the right hippocampus during a motivated attention task
(Chantiluke et al., 2012) and an increased signal during an emotional picture task (R. Tao et
al., 2012).
Pharmacological and psychotherapeutic treatment of depression in adolescents
13
In sum, several biological factors including genes, sex, neurotransmitters, and structural
brain differences have been identified to contribute to the development of depressive
disorders. Investigating neural correlates of psychiatric disorders and their treatment early
in life is of great interest; first, because elevated levels of neuroplasticity might enable rapid
changes in response to treatment, and second, because the adolescent brain is not yet
affected by factors such as long-term pharmacological treatment or a chronic course of the
disorder, as is often the case with adults. Neurobiological models explain the increasing
incidence of affective disorders in adolescents by the fast maturation of brain areas that are
relevant with respect to bottom-up processes, such as the amygdala and sgACC, in contrast
to slowly maturing top-down processes involving brain areas such as the hippocampus and
prefrontal cortex. Those brain areas also showed altered activity in comparisons between
healthy and depressed adolescents.
1.5. Pharmacological and psychotherapeutic treatment of depression in adolescents
1.5.1. Guidelines for the treatment of depression in minors
In Germany, the guidelines for the treatment of depression in adults (Deutsche Gesellschaft
für Psychiatrie Psychotherapie und Nervenheilkunde, 2009) state that patients with mild to
moderate depression should receive either psychotherapy or pharmacological treatment,
while those with severe depression should be treated with a combination of both (level of
recommendation is “A”, meaning that the recommendation is based on knowledge derived
from either a meta-analysis, a systematic review including RCTs, or an RCT). With respect to
the German guidelines for the treatment of depression in children and adolescents issued
by the “Deutsche Gesellschaft für Kinder- und Jugendpsychiatrie Psychosomatik und
Psychotherapie” (2013) older children and adolescents should be treated with either
psychotherapy, the antidepressant drug fluoxetine, or a combination of both. Due to
possible negative side effects of drug treatment, psychotherapy should be favoured (level of
recommendation: B). In case of mild to moderate depressive symptoms, psychotherapy
should be the first-line treatment, and in case of severely depressive symptoms, a
combination of psychotherapeutic and pharmacological treatment should be applied (level
of recommendation: consensus).
Efficacy of psychotherapeutic treatment
14
Contrasting guidelines for adults and youngsters reveals that that guidelines for adults are
based on levels of recommendation A and B while those for children and adolescents are
based on the less certain levels of recommendation B and consensus. This highlights the
need for further scientific studies on depression in children and adolescents.
1.5.2. Efficacy of psychotherapeutic treatment
Earlier meta-analyses that compared cognitive behavioural therapy (CBT) with control
treatments such as relaxation training found large effect sizes in favour of CBT (Harrington,
Whittaker, Shoebridge & Campbell, 1998; Lewinsohn & Clarke, 1999; Reinecke, Ryan &
DuBois, 1998). More recent meta-analyses, which applied firmer inclusion criteria, have
found effect sizes ranging from small to large. Nine meta-analyses that have been published
since 2000, seven of which included both children and adolescents and two of which
included adolescents only, are summarized in Table 2. The mean number of included studies
per meta-analysis was 20.55 (SD=9.15), and all included only studies in which a
psychotherapeutic intervention, usually CBT or interpersonal psychotherapy (IPT), was
compared to an active, inactive, or wait list control group. For those that reported effect
sizes, the mean effect size was 0.58 (SD=.30) (Erford et al., 2011; Klein, Jacobs & Reinecke,
2007; McDermut, Miller & Brown, 2001; Michael & Crowley, 2002; Weisz, McCarty & Valeri,
2006).
1.6. Treatment programs for depression
Many of the manualized CBT programs that have been conceptualized for children and
adolescents are concerned with the prevention of depression (Essau & Conradt, 2003; Horn,
2004; Poessel & Horn, 2004; Shochet, Holland & Whitefield, 1997) rather than its treatment.
The following section focuses on 1) just those programs concerned with treatment, and 2)
different types of CBT and of Interpersonal Psychotherapy for Depressed Adolescents (IPT-
A) treatments, as both these formats have been shown to be effective (level of
recommendation B).
Individual treatment programs available in English-speaking countries
15
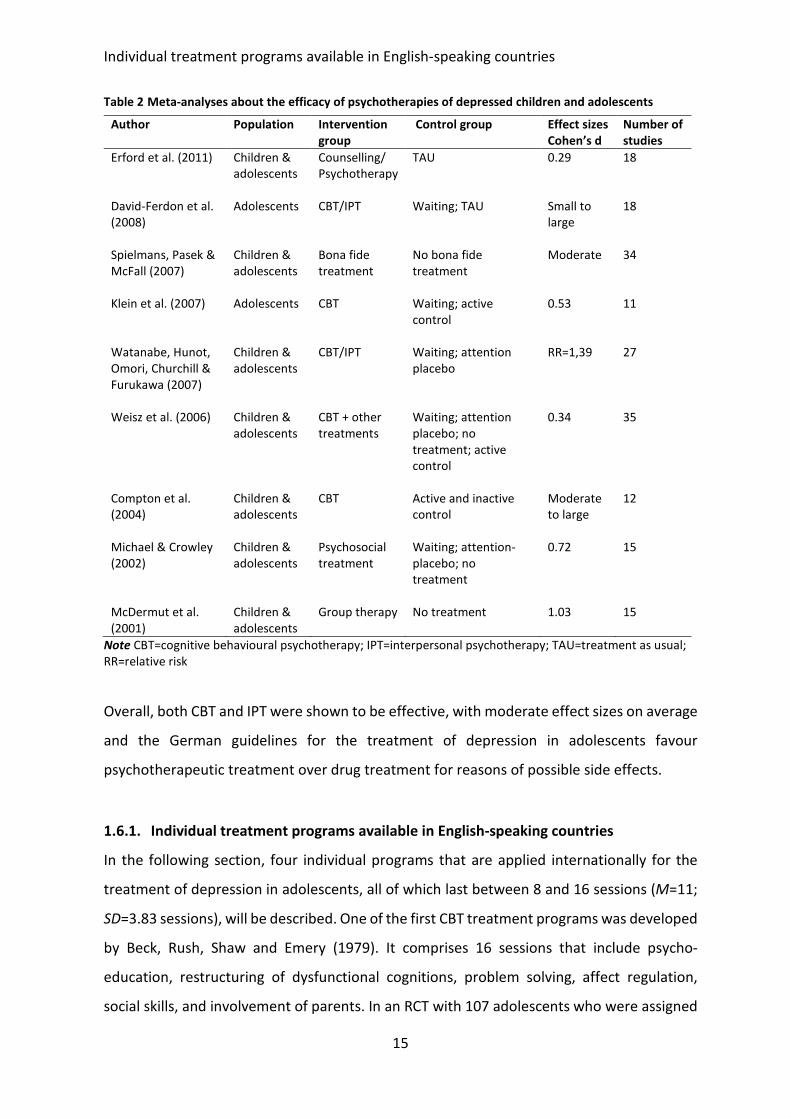
Table 2 Meta-analyses about the efficacy of psychotherapies of depressed children and adolescents
Note CBT=cognitive behavioural psychotherapy; IPT=interpersonal psychotherapy; TAU=treatment as usual;
RR=relative risk
Overall, both CBT and IPT were shown to be effective, with moderate effect sizes on average
and the German guidelines for the treatment of depression in adolescents favour
psychotherapeutic treatment over drug treatment for reasons of possible side effects.
1.6.1. Individual treatment programs available in English-speaking countries
In the following section, four individual programs that are applied internationally for the
treatment of depression in adolescents, all of which last between 8 and 16 sessions (M=11;
SD=3.83 sessions), will be described. One of the first CBT treatment programs was developed
by Beck, Rush, Shaw and Emery (1979). It comprises 16 sessions that include psycho-
education, restructuring of dysfunctional cognitions, problem solving, affect regulation,
social skills, and involvement of parents. In an RCT with 107 adolescents who were assigned
Author Population Intervention
group
Control group Effect sizes
Cohen’s d
Number of
studies
Erford et al. (2011) Children &
adolescents
Counselling/
Psychotherapy
TAU 0.29 18
David-Ferdon et al.
(2008)
Adolescents CBT/IPT
Waiting; TAU Small to
large
18
Spielmans, Pasek &
McFall (2007)
Children &
adolescents
Bona fide
treatment
No bona fide
treatment
Moderate 34
Klein et al. (2007) Adolescents CBT Waiting; active
control
0.53 11
Watanabe, Hunot,
Omori, Churchill &
Furukawa (2007)
Children &
adolescents
CBT/IPT Waiting; attention
placebo
RR=1,39 27
Weisz et al. (2006) Children &
adolescents
CBT + other
treatments
Waiting; attention
placebo; no
treatment; active
control
0.34 35
Compton et al.
(2004)
Children &
adolescents
CBT Active and inactive
control
Moderate
to large
12
Michael & Crowley
(2002)
Children &
adolescents
Psychosocial
treatment
Waiting; attention-
placebo; no
treatment
0.72 15
McDermut et al.
(2001)
Children &
adolescents
Group therapy No treatment 1.03 15
Individual treatment programs available in English-speaking countries
16
to either individual CBT, nondirective supportive therapy, or systemic behaviour family
therapy, CBT was found to be more effective than the other active control interventions
(Brent et al., 1997).
A CBT program called Primary and Secondary Control Enhancement Training
(PASCET) comprises eight sessions of 50 minutes each (Weisz, Thurber, Sweeney, Proffitt &
LeGagnoux, 1997). PASCET was built on the two-process model of perceived control and
coping: primary control involves coping by making objective conditions fit one’s wishes (e.g.,
peer relationships), while secondary control involves coping by adapting oneself to
conditions that cannot be altered. Weisz et al. (2009) randomly assigned 57 children and
adolescents aged 8 to 15 years to either PASCET or treatment as usual (TAU). Participants in
both groups improved significantly, but there was no difference in improvement between
the groups. However, compared with TAU, subjects in the PASCET group needed fewer
sessions to reach levels of recovery and were less likely to require additional services; also,
sessions were less costly.
Vostanis and Harrington (1994) developed an individual treatment program
consisting of eight 45-minute sessions. The aims of this program are to help children and
adolescents to improve their recognition and naming of different emotions, to change
negative cognitions, and to extend social skills. Efficacy was investigated in two studies.
Vostanis, Feehan, Grattan & Bickerton (1996) compared CBT with a non-focused
intervention in 56 children. At the end of the treatment (average of six sessions), 87% of the
CBT group and 75% of the control group no longer fulfilled criteria for a depressive disorder,
with no superiority of CBT over the non-focused intervention. Wood, Harrington and Moore
(1996) randomly assigned outpatients aged 9 to 17 years to either the depression treatment
program or relaxation training. A total of 48 participants completed the trial. The treatment
group was significantly more likely to improve than the control group, with a moderate effect
size of .73. These results were only found in the patient ratings, and did not reach significance
in the parental ratings.
IPT-A is a brief, specified psychotherapy that can be applied in either a group or an
individual setting. It lasts for 12 weeks, and addresses common adolescent developmental
issues such as separation from parents, interpersonal relationships, and peer pressure. To
test efficacy of the treatment, Mufson, Weissman, Moreau and Garfinkel (1999) randomly
assigned 24 participants to an IPT-A treatment group and 24 to a clinical monitoring group.
International group treatment programs
17
Significant group differences were found post-treatment in favour of the treatment group.
In a further study, Mufson, Pollack, Olfson, Weissman and Hoagwood (2004) investigated
whether IPT-A would be effective in a school-based mental health setting, by randomly
assigning 63 depressed students to either IPT-A or TAU delivered by school-based health
clinicians. Results indicated that participants treated with IPT-A showed greater symptom
reduction compared to those who received TAU. Tang, Jou, Ko, Huang and Yen (2009)
randomly assigned 73 depressed adolescents aged 12 to 18 years to either IPT-A or TAU, and
found significantly higher reduction of depression scores in the IPT-A group.
In another study, IPT-A and CBT were compared with each other and with a wait list
group (WL) (Rossello & Bernal, 1999). The CBT program was based on the cognitive-
behavioural model developed by Muñoz and Miranda (1986), which was originally developed
as a group intervention for adults and was adapted for the individual treatment of
adolescents. It consists of 12 one-hour individual therapy sessions, and is based on the
concepts of cognitive behavioural therapy and rational-emotive therapy, aiming to identify
thoughts and actions that influence depressive feelings. Results of the study that compared
IPT-A, CBT, and WL indicated that both active treatment forms led to significantly reduced
depressive symptoms when compared to the WL condition, but there were no differences
on depression scores between IPT and CBT.
Taken together CBT was shown to be superior to active control treatment in two
studies and comparable to TAU in two further studies. Also IPT-A was shown to be superior
to clinical monitoring and TAU in two studies.
1.6.2. International group treatment programs
In a review of the efficacy of group cognitive behavioural therapy (CBT-G) for the treatment
of unipolar depressive disorder in adults, Oei and Dingle (2008) reported small (d=0.1) to
large (d=2.87) effect sizes, with a mean effect size of d=1.1. In a review of CBT-G versus
individual CBT, McDermut, Miller and Brown (2001) found a comparable mean effect size of
d=1.02 (average effect size of 1.27 for CBT-G; 1.49 for individual CBT). The difference was
not significant, indicating that CBT-G is comparable to individual CBT. As CBT-G can be
delivered to multiple participants with a minimum amount of time and staff, it offers
advantages with respect to both research and treatment (Oei & Dingle, 2008) .
Treatment programs available in Germany
18
1.6.3. Treatment programs available in Germany
Besides of the treatment program we developed (see section 1.6.5) there existed three
programs for the treatment of depressed children and adolescents between the ages of 8
and 21 years in the German language; two of which are conceptualized for group therapy
and one for individual therapy (see Table 3). The number of sessions in these programs
ranges from 8 to 17 (M=11.66; SD=4.73), while the session durations range from 45 to 100
minutes (M=78.33; SD=29.30). Both of the group therapy programs are derived from the
English-language program “Coping with depression course for adolescents” (CWD-A). One of
them, titled “Stimmungsprobleme bewältigen”(Dealing with mood problems), focuses on
psycho-education, relaxation, cognitive restructuring, problem-solving, and social skills (Ihle
& Herrle, 2011). The other, “Kognitive Verhaltenstherapie bei Kindern und Jugendlichen”
(Cognitive behavioral therapy in children and adolescents) (Abel & Hautzinger, 2013) focuses
on psycho-education, positive activation, cognitive restructuring, social skills, and parent
sessions. The third program, which provides individual treatment, is derived from the
program developed by Vostanis and Harrington (1994) (see section 1.6.1) and was translated
into German by Jans, Warnke, and Remschmidt (Harrington, 2001).
None of these three German-adapted programs has been evaluated in an RCT. Pilot
studies were conducted on the “Stimmungsprobleme bewältigen” program, with the results
summarized by Straub, Keller, Sproeber, Koelch und Plener (2014). The “Kognitive
Verhaltenstherapie bei Kindern und Jugendlichen” (Harrington, 2001) program was
evaluated in a pre-post-follow-up test design that enrolled 33 depressed adolescent in- and
outpatients. Results indicated a significant reduction of depressive symptoms in the pre-
post-test comparison, based on both self-ratings and parent ratings, with medium to large
effect sizes, and the results were still robust at a follow-up test six months later. The
individual program has only been evaluated in the English-language studies described above
(see Section 1.6.1).

Duration of treatment
19
Table 3 German-language therapy programs for the treatment of depressed minors
German version of English Original Age range Setting Number and duration of
sessions
„Kognitive Verhaltenstherapie bei
depressiven Kindern und Jugendlichen“
8-17 years Individual
setting
8 sessions of 45 minutes
each
“Stimmungsprobleme bewältigen” 16-21 years Group setting 10 sessions of 90
minutes each
„Kognitive Verhaltenstherapie bei Kindern
und Jugendlichen“
12-18 years Group setting 17 sessions of 90–120
minutes each
1.6.4. Duration of treatment
The duration of therapeutic treatment plays an important role when it comes to
conceptualization of psychotherapy, and is also of interest from an economic point of view.
Two models of the dose-effect relationship of psychotherapeutic treatment exist. In the
good enough level model, Barkham et al. (2006; 1996) found session-to-session
improvement to be more or less linear, assuming that symptoms improve until the patient
reaches a good enough level, at which point the patient and/or therapist stops treatment or
focuses on other psychotherapeutic aims. The model of negative acceleration (Howard,
Kopta, Krause & Orlinsky, 1986) states that symptom improvement after psychotherapeutic
treatment is a negatively accelerated function of treatment length, in which 30% of patients
improve after two sessions, 41% after four sessions, 53% after eight sessions, 63% after 13
sessions, and 83% after 52 sessions. Lambert, Hansen, and Finch (2001) found that 50% of
patients showed significant symptom reduction after only 7 sessions and 75% after 14
sessions. Supporting the negative acceleration model, Barkham et al. (1996) randomly
assigned depressed patients to either 8 or 16 sessions of time-limited psychotherapy (CBT
or IPT). For most of the outcome parameters, the eight-session group showed greater
symptom reduction at the end of treatment (after eight sessions) than did patients in the 16-
session group at mid-treatment (after eighth session). It seems that symptom change occurs
faster when tighter time restrictions are imposed. Supporting the model of negative
acceleration, the meta-analytic review of Harrington et al. (1998) demonstrated that a
quarter of depressed adolescents remit following relatively short psychosocial interventions
of 8 to 12 weekly sessions, while Goodyer et al. (2007) showed that 21% of adolescents with
Development of a brief CBT-G called MICHI
20
moderate to severe depressive symptoms improve after a brief psychosocial intervention
(M=3 sessions). In a recent meta-regression analysis Cuijpers, Huibers, Ebert and Koole
(2013) looked at the relationship between number of sessions, frequency, and intensity of
depression therapy and treatment efficacy in adults. They found that the number of weekly
sessions rather than duration of treatment was associated with larger effect sizes. An
increase from one to two sessions per week increased the effect size, with g=.45. Those
findings highlight the advantages of interventions that are brief and intensive.
In summary, the good enough level model assumes a linear relationship between
sessions and treatment response, while the negative acceleration model assumes greater
improvement within earlier over later sessions which was supported by several studies. To
our knowledge, there exists no treatment program that combines the potential advantages
of all the following: 1) based on CBT, 2) brief, 3) intense, 4) delivered via group therapy and
5) for all severities of depression. Furthermore, none of the programs available in Germany
for the treatment of depression in adolescents has been evaluated with respect to efficacy
by means of an RCT. The program described in the following section was designed to address
all of these issues.
1.6.5. Development of a brief CBT-G called MICHI
Based on what we viewed as gaps in the treatment options currently available, we developed
a program titled MICHI, which stands for “Manualized Intervention to Cope with depressive
symptoms, Help strengthen resources and Improve emotion regulation” (Sproeber, Straub,
Fegert & Koelch, 2012). MICHI encompasses five weekly sessions of approximately 75
minutes each, plus one booster session that is held five weeks after the last regular session.
Participants are depressed adolescents between 13 and 18 years of age. Four to six
participants are enrolled in a group, which is led by two trainers. Patients receive a handout
at each session, and trainers are provided with a manual to ensure adherence to the
procedures. Contents of the sessions include psycho-education, behavioural activation,
cognitive restructuring, enhancement of self-esteem, skills for improved problem solving,
and emotion regulation. Participants are asked to bring a trusted person (e.g., parent, sibling,
or friend) to the fifth session in order for this individual to be trained on how to help the
patient to prevent relapse. Unlike other programs, MICHI also teaches skills on how to deal
with acute crises such as elevated levels of suicidal ideation. Furthermore, it is the only
Neural correlates of depression treatment
21
program available in Germany for the treatment of depression in adolescents that has been
tested in two pilot studies as well as in an RCT (see Section 3.6 to 3.8).
1.7. Neural correlates of depression treatment
RCTs looking at evaluating treatment efficacy have traditionally assessed improvements in
depressive symptoms, using questionnaires or structured interviews. New approaches in
research are additionally evaluating treatment effects by assessing altered neuronal activity
and attempting to identify biomarkers for illness severity and improvement as well.
1.7.1. Neural correlates of pharmacological treatment
A wide range of studies has shown activity levels in the amygdala, the subgenual parts of the
ACC, the hippocampus, and the prefrontal cortex to be elevated in depressed individuals in
comparison to healthy controls (see Section 1.4.2.3). Several studies have found (Rosenblau
et al., 2012) elevated activity in the amygdala of depressed adults to normalize (Godlewska
et al., 2012) and to match that of a healthy control group (Rosenblau et al., 2012; Sheline,
2000) following treatment with antidepressants. Similarly, a significant reduction of sgACC
activity was seen after six weeks of paroxetine (Kennedy et al., 2001) or eight weeks of
fluoxetine (Mayberg et al., 2000); a significant reduction of hippocampal activity was seen
after six weeks of paroxetine (Kennedy et al., 2001) and eight weeks of fluoxetin (Fu et al.,
2007); and other studies have found altered activity in the prefrontal cortex following
treatment with medication (Goldapple et al., 2004; H. Tao et al., 2013).
1.7.2. Neural correlates of psychotherapeutic treatment
To date, ten neuroimaging studies have investigated neural changes before and after
psychotherapeutic treatment in depressed adults, using active paradigms, involving either
processing emotional stimuli, cognitive control, or processing of reward, or resting state (see
Table 4). However, there have been no studies investigating neural correlates of
psychotherapy of depression in adolescents.
Neural correlates of psychotherapeutic treatment
22
Table 4 Studies investigating neural correlates of psychotherapeutic treatment of depression by means of
an active paradigm
Author Participants Paradigm Outcome
Crowther et
al. (2015)
23 depressed adults: before
and after 12 weekly sessions
of CBT-G
20 healthy controls: before
and after equivalent period of
time
Resting state Response to psychotherapy in depressed
adults was predicted by pretreatment
connectivity of the right insula with the
right middle temporal gyrus and left
intraparietal sulcus with the orbital
frontal cortex.
Yoshimura
et al. (2014)
23 depressed adults: before
and after 12 weekly sessions
of CBT-G
15 healthy controls: before
and after equivalent period of
time
fMRI,
emotional
word
processing
task
Following CBT, activity in the medial
prefrontal cortex and vACC was
increased for positive stimuli and
decreased for negative stimuli.
Buchheim et
al. (2012)
16 depressed adults: before
and after 15 months of
psychodynamic intervention
17 healthy controls: before
and after equivalent period of
time
fMRI,
presentation
of
attachment-
related scenes
Patients showed a higher activation in
the left anterior hippocampus,
amygdala, subgenual cingulate, and
medial prefrontal cortex before
treatment, and showed reduction in
these areas after 15 months. Symptom
reduction was associated with activity
change in the prefrontal cortex.
Ritchey,
Dolcos,
Eddington,
Strauman &
Cabeza
(2011)
11 depressed adults: before
and after CBT
7 healthy controls: before and
after equivalent period of
time
fMRI,
emotional
picture task
In the patients, post-treatment increases
in ventromedial prefrontal cortex
activation were seen, along with
enhanced arousal in the amygdala,
caudate, and hippocampus.
Dichter et al.
(2010)
12 depressed adults: before
and after BAT
15 healthy controls before
and after equivalent period of
time
fMRI,
cognitive
control task
Psychotherapy resulted in decreased
activation in response to cognitive
control stimuli presented within a sad
context in the paracingulate gyrus, right
orbital frontal cortex, and right frontal
pole. The strength of pretreatment
activation in the paracingulate gyrus
predicted the strength of symptom
change.
Dichter et al.
(2009)
12 depressed adults: before
and after BAT
15 healthy controls before
and after equivalent period of
time
fMRI, reward
paradigm
Relative to the control group, patients
who received psychotherapeutic
treatment showed altered activity in the
paracingulate gyrus and the right
caudate nucleus during reward
anticipation, and altered activity in the
paracingulate and the orbitofrontal gyri
during reward feedback.
Fu et al.
(2008)
16 depressed adults: before
and after 16 sessions of CBT
16 healthy controls: before
and after equivalent period of
time
fMRI, affect
recognition
task
A significant interaction effect of group
by time was found for the right
amygdala, the hippocampus, and the
anterior cingulate.
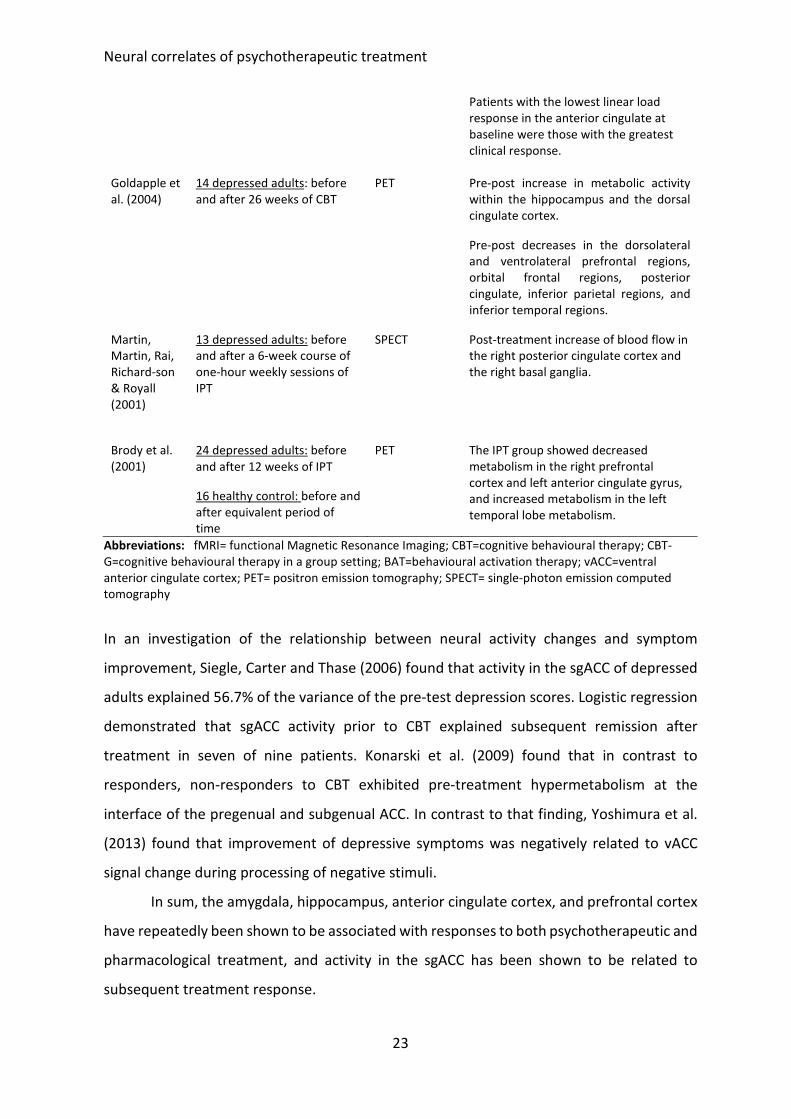
Neural correlates of psychotherapeutic treatment
23
Patients with the lowest linear load
response in the anterior cingulate at
baseline were those with the greatest
clinical response.
Goldapple et
al. (2004)
14 depressed adults: before
and after 26 weeks of CBT
PET Pre-post increase in metabolic activity
within the hippocampus and the dorsal
cingulate cortex.
Pre-post decreases in the dorsolateral
and ventrolateral prefrontal regions,
orbital frontal regions, posterior
cingulate, inferior parietal regions, and
inferior temporal regions.
Martin,
Martin, Rai,
Richard-son
& Royall
(2001)
13 depressed adults: before
and after a 6-week course of
one-hour weekly sessions of
IPT
SPECT Post-treatment increase of blood flow in
the right posterior cingulate cortex and
the right basal ganglia.
Brody et al.
(2001)
24 depressed adults: before
and after 12 weeks of IPT
16 healthy control: before and
after equivalent period of
time
PET The IPT group showed decreased
metabolism in the right prefrontal
cortex and left anterior cingulate gyrus,
and increased metabolism in the left
temporal lobe metabolism.
Abbreviations: fMRI= functional Magnetic Resonance Imaging; CBT=cognitive behavioural therapy; CBT-
G=cognitive behavioural therapy in a group setting; BAT=behavioural activation therapy; vACC=ventral
anterior cingulate cortex; PET= positron emission tomography; SPECT= single-photon emission computed
tomography
In an investigation of the relationship between neural activity changes and symptom
improvement, Siegle, Carter and Thase (2006) found that activity in the sgACC of depressed
adults explained 56.7% of the variance of the pre-test depression scores. Logistic regression
demonstrated that sgACC activity prior to CBT explained subsequent remission after
treatment in seven of nine patients. Konarski et al. (2009) found that in contrast to
responders, non-responders to CBT exhibited pre-treatment hypermetabolism at the
interface of the pregenual and subgenual ACC. In contrast to that finding, Yoshimura et al.
(2013) found that improvement of depressive symptoms was negatively related to vACC
signal change during processing of negative stimuli.
In sum, the amygdala, hippocampus, anterior cingulate cortex, and prefrontal cortex
have repeatedly been shown to be associated with responses to both psychotherapeutic and
pharmacological treatment, and activity in the sgACC has been shown to be related to
subsequent treatment response.
Neural correlates of depression treatment in children and adolescents
24
1.7.3. Neural correlates of depression treatment in children and adolescents
To date, only one study has examined the effects of therapy and a further study the effects
of medical treatment on depression-relevant brain areas in children and adolescents. Forbes
et al. (2010) examined reward-related brain functioning in adolescents with depression
before (but not after) treatment with either CBT alone or CBT plus SSRI. Pre-treatment
striatal activity was associated to symptom improvement in both forms of treatment. Tao et
al. (2012) compared brain activation prior to and after eight weeks of treatment with
fluoxetine, and found that formerly elevated activity levels in the sgACC and amygdala
normalized to levels of a healthy control group after treatment.
Taken together all of the psychotherapeutic studies and most of the pharmacological
studies have been done in adults and no controlled study has investigated psychotherapeutic
effects on neural substrates of depression in children and adolescents.
1.7.4. Paradigm for assessing neuronal correlates of depression treatment
Depressive symptomatology has been found to be associated with dysfunctional reward
processing, and may therefore be attributed to the same underlying neural mechanisms
(Forbes & Dahl, 2005; Olino et al., 2013). Some brain areas, such as the amygdala, are
relevant for both the processing of emotions and reward (Gabriel, Burhans & Kashef, 2003).
Deep brain stimulation to the sgACC, a brain region involved in reward processing, has been
shown to help adults with severe chronic depression (Schlaepfer et al., 2008). Furthermore,
pre-CBT activation of the ventral striatum by means of a reward task was shown to predict
symptom improvement after therapy in adolescents (Forbes et al., 2010). The hippocampus
has also been reliably shown in animal, lesion, and imaging studies to be important with
respect to processing of rewards (Haber & Knutson, 2010).
Reward paradigms have been demonstrated to be suitable for investigating
depressive symptoms in adolescents, but have rarely been investigated for the assessment
of psychotherapeutic treatment effects. The paradigm we chose for assessing the effects of
CBT was a monetary incentive task, which can be used irrespective of cultural and social
background and with a good test-re-test reliability (Abler, Hahlbrock, Unrath, Groen &
Kassubek, 2009).
Aims and research questions of the present work
25
2. Aims and research questions of the present work
As described in Section 1, compared to the literature for the adult population, there is
limited understanding about depressive disorders in minors with respect to prevalence,
diagnostic standards for the assessment of symptoms, efficacy of psychotherapy treatments,
and underlying neural correlates of treatment effects. This thesis aims to close some of these
gaps.
While the prevalence rate of depressive disorders in minors has remained fairly
constant, the number of antidepressant prescriptions and the number of individuals
receiving outpatient treatment for depression have been increasing (Annuss et al., 2010; Zito
et al., 2003). So far, there is a lack of recent studies that assessed whether the number of
depressed adolescent patients referred for inpatient treatment has increased within the last
years. To analyse trends of referrals for inpatient treatment, we looked at the number of F3
diagnoses (the ICD-10 classification of affective disorders) that were collected from children
and adolescents who were admitted for inpatient treatment in Germany between the years
2003 and 2012.
A frequent reason for referral to inpatient treatment for a depressive disorder is that
this disorder is often accompanied by additional problems such as missing school and
elevated levels of suicidal ideation and planning (Mehler-Wex, 2012). Diagnoses classified as
F3 include not only depression but also bipolar disorders, which have been shown to be
highly associated with elevated levels of suicidality (Allison et al., 2001). However, to our
knowledge, no previous study has looked at whether symptoms of mania apart from those
of depression predict symptoms of suicidality in adolescents.
The most frequently used instruments for diagnosing depression, and in doing so also
the symptom of suicidality, are the CDRS-R and the BDI-II (Mayes et al., 2010; Subica et al.,
2014). Some international RCTs on depressed adolescents have restricted enrolment to
subjects with a CDRS-R score >45 (Treatment for Adolescents With Depression Study Team,
2007), which indicates a severity level of moderate to severe. In our treatment study, to
avoid a positive bias, we wished to include subjects with mild depression as well. No study
has yet assessed which level of severity of depression, as diagnosed using ICD-10,
corresponds to which score on the German version of the CDRS-R. However, according to
the work of Guo et al. (2006), who based their ratings on clinical estimations rather than
Aims and research questions of the present work
26
structured interviews, a total score between 30 and 40 on the English version of the CDRS-R
indicates depression of mild severity.
According to the German guidelines, questionnaires can be used as screening tools,
and a diagnosis should then be verified by means of a structured interview (Deutsche
Gesellschaft für Kinder- und Jugendpsychiatrie Psychosomatik und Psychotherapie, 2013).
However, there is a lack of knowledge of how similarly these two types of instruments
measure the construct of depression in minors. Previous studies found high correlations at
the sum score level, but no studies have compared ratings at the subscale and item levels.
To address this, we compared the BDI-II and CDRS-R on all three levels.
Diagnostic instruments are necessary for validly and reliably detecting depressive
symptoms and determining their severity, so that, depending on the severity level of
depression, suitable treatment options can then be recommended. According to the German
guidelines for depression treatment in minors, psychotherapeutic interventions, specifically
CBT and IPT, are recommended for the treatment of depressive episodes of mild or
moderate severity, and a combination of pharmacological and psychotherapeutic
interventions is recommended for the treatment of severe episodes. Further, previous
studies have shown that interventions that are brief and that are applied in a group setting
can be effective. A literature search revealed that the therapy program options available in
the German mental health system for the treatment of depression in adolescents do not
include any that possess all the following features: 1) brief, 2) based on CBT, 3) provided as
group therapy, 4) directed at patients with any severity of depression, and 5) had been
evaluated in an RCT.
Those considerations led to the development of MICHI, described in Section 1.6.5.
This program integrates the advantages named above. An important aspect to keep in mind
in the development of new treatment programs is that some studies have found that suicidal
ideation may initially increase during psychotherapeutic treatment, especially in adolescents
and young adults (Simon & Savarino, 2007); thus, it is important to first evaluate a new
program in the protected environment of an inpatient setting before evaluating it in the
outpatient setting. Therefore, the first pilot study was conducted with inpatients, and
focused on determining feasibility, acceptance, and first trends of efficacy concerning
depression scores and effects on suicidality. In a next step, we conducted a second pilot
study in outpatients, using feedback from the first set of participants and trainers to re-work
Aims and research questions of the present work
27
some aspects of the therapy program. In a further step, the efficacy of the program was
assessed in an RCT in which depressed adolescent outpatients were randomly assigned to
either an intervention group that received MICHI or to a waiting control group that received
TAU.
Responses to both psychotherapeutic and pharmacological treatment have been
repeatedly shown to be associated with activity changes in the amygdala, hippocampus,
ACC, and prefrontal cortex; and activity in the sgACC has been shown to be related to
subsequent treatment response. However, no study to date had investigated neural
correlates in adolescents of pre-to-post psychotherapeutic treatment in comparison to pre-
to-post TAU.
Summary of minor hypotheses with respect to new insights on epidemiology, symptoms,
and diagnostic instruments of depression in adolescents:
H1: It was expected that the number of children and adolescents being referred for
inpatient treatment due to a diagnosis of depressive disorder has increased over
a time period of ten years (1st scientific article of Plener, Straub, Fegert & Keller,
2015).
H2: It was expected that both suicidal ideation and behaviour are predicted by mania
symptoms, above the symptoms of depression (2nd scientific article of Straub,
Keller, Sproeber, Koelch & Plener, 2015).
H3: It was expected that a total CDRS-R score of between 30 and 40 would indicate
depression of mild severity (3rd scientific article of Plener, Grieb, Sproeber,
Straub, Schneider, Keller & Koelch, 2012).
H4: It was expected that a high correlation would be found between the CDRS-R and
the BDI-II at the sum score level. With respect to the subscale level, it was
expected that higher correlations would be found between those subscales that
assess more objective aspects of depression (e.g., somatic aspects) than between
those that assess subjective aspects (e.g., depressive mood); while at the item
level, it was expected that the highest correlations would be found between
Aims and research questions of the present work
28
those items that assess similar rather than divergent aspects of depression (4th
scientific article of Straub, Plener, Koelch, & Keller, 2014).
Summary of major aims and hypothesis with respect to feasibility, efficacy and neuronal
correlates of the MICHI program:
Before developing a new therapy program, it is necessary to have a full understanding of
existing therapy programs and their appropriate effectiveness and efficacy.
Aim: To review current literature on cognitive behavioural and interpersonal group
therapy programs for the treatment of depression in adolescents, and to
summarize the results of studies (5th scientific article of Straub, Nicolaus, Plener,
Sproeber & Koelch, 2014).
H5: In a pilot study with depressed adolescent inpatients, it was expected that MICHI
would be found to be feasible, accepted, and to reveal first trends of efficacy (6th
scientific article of Straub, Koelch, Fegert, Plener, Gonzalez-Aracil, Voit &
Sproeber, 2013).
H6: In a pilot study with depressed adolescent outpatients, it was expected that
MICHI would be found to be feasible, accepted, and to reveal trends of efficacy
(7th scientific article of Straub, Sproeber, Plener, Fegert, Bonenberger & Koelch,
2014).
H7: It was expected that a significant interaction effect would be seen between time
points of measurement (pre/post) and group (patients who received MICHI vs.
patients in the wait-list control group who received TAU), with a greater
improvement in symptoms seen in the intervention group (8th scientific article
of Straub, Plener, Keller, Fegert, Sproeber & Koelch, accepted).

Aims and research questions of the present work
29
H8: It was expected that symptom changes in the MICHI group would be
accompanied by activity changes in depression-relevant brain areas such as the
amygdala, sgACC, hippocampus and frontal cortex which would not be seen in
the TAU group. Furthermore, it was expected that pre-treatment sgACC activity
would correlate with subsequent pre-post symptom changes (9th scientific
article of Straub, Plener, Sproeber, Sprenger, Koelch, Groen & Abler, 2015).
Results
30
3. Results
3.1. Changes in prevalence rates of ICD-10 F3 diagnoses in the inpatient setting
Plener, P.L., Straub, J., Fegert, J.M. & Keller, F. (2015). Treatment of mental diseases in
children in German hospitals: analysis of frequencies in the years 2003 to 2012.
Nervenheilkunde, 34, 18-23.
Introduction: Prevalence rates for depressive disorders remained stable between 1965 and
1996. However, the number of minors being treated in the outpatient setting, increased
between 2005 and 2008 as did the numbers of those receiving pharmaceutical treatment.
Furthermore, numbers of minors, being referred to the inpatient setting due to F3 diagnoses,
increased as well between 2000 and 2007. However, there is a lack of newer studies that
analysed whether numbers of F3 diagnoses are still increasing in the in- and outpatient
setting.
Methods: This study analysed the prevalence of F diagnoses according to ICD-10 in minors
up to 15 years of age from all German psychiatric hospitals between 2003 and 2012. Changes
over the years were assessed by means of linear regression analyses.
Results: A significant increase was seen in most diagnostic groups, including affective
disorders (the F3 category in ICD-10). The only diagnostic groups that showed stable or
decreasing rates of hospital treatments in the ten-year time frame were organic (F0),
schizophrenic (F2), and personality and behavioural disorders (F6).
Conclusion: The reasons for increasing prevalence rates might be an increased attention paid
to psychiatric disorders in the general population; furthermore, higher numbers of inpatients
might be traced back on shorter durations of stay in psychiatric hospitals, which in turn might
be explained by improvement of treatments.
3.2. Association between symptoms of depression plus mania and suicidal behavior
Straub, J., Keller, F., Sproeber, N., Koelch, M.G. & Plener, P.L. (2015). Suicidal behavior in
German adolescents: prevalence and association with depressive and manic symptoms.
Zeitschrift für Kinder- und Jugendpsychiatrie und Psychotherapie, 43(1), 39-45.
Convergence of CDRS-R scores with a mild depressive episode according to ICD-10
31
Introduction: With respect to affective disorders (the F3 category in ICD-10) in minors,
bipolar disorders are less prevalent than depressive disorders. However, an early onset of
bipolar disorder coincides with an elevated risk for suicide. The aim of this article was to
investigate whether mania symptoms, above symptoms of depression, predict suicidal
ideation and attempts.
Methods: A total of 1,117 adolescents from 13 German schools (mean age = 14.83; SD=.63)
completed questionnaires for the assessment of depression symptoms (Centre for
Epidemiological Studies Depression Scale), mania symptoms (nine questions for the
assessment of mania symptoms according to DSM-IV), and lifetime suicidal behaviour (Self-
Harm Behaviour Questionnaire). Logistic regression with a block-wise entry method was
applied to analyse the predictive value of mania and depression symptoms on suicidal
ideation and attempts.
Results: Results indicated that 39.4% of the girls and 23.1% of the boys reported lifetime
suicidal thoughts; 7.1% of the girls and 3.9% of the boys reported a lifetime history of suicide
attempts; 18.7% of the overall sample reported having experienced elevated symptoms of
depression; and 9% reported having had elevated levels of mania symptoms during the past
week. Elevated depression and mania scores were associated with lifetime suicidal ideation
and suicide attempts. Regression analyses revealed that elevated levels of mania symptoms,
above symptoms of depression, explained the occurrence of suicidal ideation. Furthermore,
mania symptoms, above symptoms of depression and age, predicted suicide attempts.
Conclusion: It can be concluded that bipolar symptoms heighten the possibility for suicidal
behaviour, which should alert clinicians.
3.3. Convergence of CDRS-R scores with a mild depressive episode according to ICD-10
Plener, P.L., Grieb, J., Sproeber, N., Straub, J., Schneider, A., Keller, F. & Koelch, M.G. (2012).
Convergence of Children's Depression Rating Scale-Revised scores and clinical diagnosis in
rating adolescent depressive symptomatology. Mental Illness, 4(e7), 29-31.
Introduction: Until now, no study had related the dimensional scores of the German version
of the CDRS-R to the categorical diagnoses (mild, moderate, or severe depressive episode)
of the ICD-10.
Agreement between BDI-II and CDRS-R in assessing depression in minors
32
Methods: Clinicians were asked to watch a videotape showing a structured interview with
an adolescent girl being asked about depressive symptoms. They were split into two groups,
with one group asked to rate the girl’s depressive symptoms using the CDRS-R and the other
to make a clinical diagnosis by means of the ICD-10.
Results: A raw score in the CDRS-R between 35 and 40 was found to be indicative for a mild
to moderate depressive episode according to ICD-10; specifically, a raw score of greater than
36 points was an indicator for a clinical diagnosis of a mild to moderate depression in nearly
two-thirds of the ratings.
Conclusion: Different studies found a CDRS-R score of 40 to indicate a depressive
symptomatology. Differences might be traced back on different classification systems applied
(DSM-IV/5 versus ICD-10).
3.4. Agreement between BDI-II and CDRS-R in assessing depression in minors
Straub, J., Plener, P.L., Koelch, M.G. & Keller, F. (2014). Agreement between self-report and
clinician’s assessment in depressed adolescents, using the example of BDI-II and CDRS-R.
Zeitschrift für Kinder- und Jugendpsychiatrie und Psychotherapie, 42(4), 243-252.
Introduction: Previous studies have demonstrated a high concordance between a patient’s
self-report of depression and the clinician’s assessment. However, few studies have focused
on the concordance at the sum-score level, the subscale level, and the single-item level in a
psychiatric adolescent sample. The influence of additional variables (age, sex, IQ, treatment
modality) on correlational strength and on whether an individual under- or overestimates
his/her symptomatology was assessed as well.
Methods: For correlational analyses, BDI-II and CDRS-R scores were collected from 105
adolescents (M=15.94 years; SD=1.63) within one week.
Results: At the sum-score level, there was a high correlation between the self-reports and
the clinicians’ assessments (r=.67, p<.001). At the subscale level, contrary to previous
studies, items assessing somatic contents did not have a higher concordance (r=.53), even if
they appeared more objective, than did items assessing cognitive and affective contents
(r=.54). At the symptom level, the correlation between items assessing similar contents was
moderate to large. The highest concordance was shown for the item that assessed suicidal
ideation (r=.57, p<.001). Additional variables had no influence on the strength of correlation
Literature review on psychotherapeutic group treatment for depressed minors
33
between self-reports and structured interview assessments. However, self-reports that
tended to overestimate symptomatology in comparison to the clinician’s rating were seen
more with outpatients than with inpatients, and more with patients with a high IQ than those
with a low IQ.
Conclusions: The high correlation between self-report and structured interview
assessments, especially with respect to the assessment of suicidality, indicates that
questionnaires can deliver first important information about symptoms of depression,
comparable to asking for them directly. As the correlation between both instruments is high
but not perfect, both instruments have rather complementary character but one instrument
shouldn’t be replaced by the other.
3.5. Literature review on psychotherapeutic group treatment for depressed minors
Straub, J., Nicolaus, L., Plener, P.L., Sproeber, N. & Koelch, M.G. (2014). Psychotherapeutic
treatment of children and adolescents with depression: review of the literature on cognitive-
behavioral and interpersonal group therapies. Der Psychotherapeut, 59, 7-15.
Introduction: According to the German guidelines for the treatment of depression in
adolescents, individuals who are mildly to moderately depressed should receive
psychotherapeutic treatment, while those who are severely depressed should receive a
combination of pharmaceutical and psychotherapeutic treatment. With respect to
psychotherapy, guidelines recommend CBT or IPT. According to the results of a meta-
analysis, effect sizes are comparable between the individual setting and the group setting.
Methods: Of 280 hits in a literature search that were reviewed for titles and abstracts, 46
full texts were read and 25 studies were finally included into the review.
Results: Most of the studies investigated the efficacy of CBT, two investigated the efficacy of
IPT, and two investigated a combination of these. The duration of psychotherapeutic
treatment varied from five sessions of 75–90 minutes each to 16 sessions of 90–120 minutes
each. Only three studies analyzed the effectiveness of treatment programs in Germany, and
two of these referred to the same population. Concerning studies that aimed to identify the
efficacy of English-speaking treatment programs, 16 out of 25 studies were RCTs, and five
were pilot studies. In 12 studies, the control group was a wait-list, while in four studies it was
Pilot study on feasibility and acceptance of MICHI in adolescent inpatients
34
TAU or an unspecific treatment. For English-language CBT group therapies, effect sizes
ranged from .02 to 1.34.
Conclusions: In most of the studies, post-test depression scores were significantly lower in
the intervention group than in the control group. However, in two studies, reduction of
depression scores was comparably between the groups. In both those cases, the control
group had received TAU, and it needs to be analysed in future studies whether the specific
treatment is comparable or superior to TAU.
3.6. Pilot study on feasibility and acceptance of MICHI in adolescent inpatients
Straub, J., Koelch, M.G., Fegert, J.M., Plener, P.L., Gonzalez-Aracil, I., Voit, A. & Sproeber, N.
(2013). Innovations in Practice: MICHI, a brief cognitive-behavioural group therapy for
adolescents with depression - a pilot study of feasibility in an inpatient setting. Child and
Adolescent Mental Health, 18(4), 247-250.
Introduction: In a first step, MICHI was studied with respect to feasibility and first trends of
effectiveness with depressed adolescent inpatients. The inpatient setting was chosen for
ethical reasons, as MICHI had not been evaluated before and because depression is
frequently accompanied by elevated levels of suicidality, especially at the beginning of a
treatment.
Methods: Nine depressed adolescent inpatients with a mean age of 16.33 years (SD=1.92)
were enrolled. Inclusion criteria included age between 13 and 18 years, IQ score ≥85, a raw-
summary score ≥36 on the CDRS-R, and a diagnosis of a mild, moderate, or severe depressive
episode. Co-morbid diagnoses were allowed except for a current diagnosis of a bipolar
disorder, schizophrenia, and substance abuse. Antidepressant medication was allowed, but
had to be stabilised three weeks prior to the start and during participation in the program.
The treatment comprised four sessions of 90 minutes each. Feasibility was assessed by
means of participants’ attendance at the sessions and evaluations by the trainers.
Acceptance of the training program and evaluation of its contents were assessed by means
of a process evaluation questionnaire (1=not true to 5=true). One question assessed the
global evaluation of the program (1=very bad to 10=very good). To assess trends of
Pilot study on feasibility and acceptance of MICHI in adolescent outpatients
35
effectiveness, the CDRS-R was assessed both before and after treatment. Suicidal ideation
was assessed by means of Item 13 of the CDRS-R.
Results: With respect to feasibility, the overall attendance rate was fair. The trainers stated
that the treatment manual was well-structured but that sessions were too long to guarantee
fully concentrated participation. With respect to contents, participants rated “emergency
plan for acute crises” as being the most helpful and “relaxation techniques” as being the
least helpful. The global evaluation revealed that participants rated MICHI as being positive
and effective overall (M=7.22; SD=1.79). Pre-post-test comparisons delivered a significant
reduction of CDRS-R depressive scores (z=-2.66; p=.008) and suicidality.
Discussion: Attendance was fair, but could be improved by the establishment of a
reinforcement system in future groups. In a further step, the treatment manual was
reworked, sessions were shortened to 75 minutes, and the contents of sessions were
reorganised, resulting in a final number of five regular sessions. The content on “relaxation
techniques” was removed from the program. The improvements seen with respect to
depressive scores and suicidality were promising, and were comparable with the results of
other studies. The findings were limited with respect to the small number of participants and
to the facts that some patients were receiving medication, that the inpatient setting could
influence results as well, and that no randomized controlled trial was applied.
3.7. Pilot study on feasibility and acceptance of MICHI in adolescent outpatients
Straub, J., Sproeber, N., Plener, P.L., Fegert, J.M., Bonenberger, M. & Koelch, M.G. (2014). A
brief cognitive-behavioural group therapy program for the treatment of depression in
adolescent outpatients: a pilot study. Child and adolescent psychiatry and mental health,
8(9), doi:10.1186/1753-2000-8-9.
Introduction: Before evaluating MICHI in a randomized controlled trial, we decided to
evaluate its feasibility and preliminary data on effectiveness in a second pilot study, this time
with outpatients. This was done for several reasons. First, the contents of the treatment
program had been reordered following comments of the trainers in the first pilot study,
ending up with fewer sessions and some content deleted. Second, having demonstrated fair
attendance in the inpatient setting, we wanted to test whether the same would be true in
RCT for the assessment of efficacy of MICHI in depressed adolescent outpatients
36
the outpatient setting. Third, as we were including individuals who were diagnosed with a
severe depressive episode, which is associated with a lowered psychosocial functioning level,
we wanted to test whether it would be feasible to apply MICHI in an outpatient setting as
well.
Methods: Fifteen outpatients (11 females) with a mean age of 16.42 years (SD=1.43) were
enrolled. Inclusion and exclusion criteria were the same as in the first pilot study (see Section
3.6). MICHI comprised five regular sessions and one booster session, each lasting between
75 and 90 minutes. Feasibility of the program was assessed by means of attendance rate,
participants’ and trainers’ feedback, and fidelity of implementation. Acceptance of MICHI
and evaluation of its contents were assessed by means of a process evaluation questionnaire
(1=not true to 5=true) and one question that assessed the global evaluation of the program
(1=very bad to 10=very good). To assess trends of efficacy, the CDRS-R, the BDI-II, and Item
13 of the CDRS-R were assessed before and after treatment. Furthermore parents filled out
a questionnaire about depression scores of their children.
Results: The mean attendance rate was 5.33 out of six sessions (88.83%), and adherence to
the treatment manual by the trainers was 93%. Participants reported that they liked being
in a group and would recommend the program to others, but doubted that the contents
learned would be helpful in school or family life. The overall satisfaction rating with the
program was 7.21 (SD=1.89). Depression scores were significantly reduced pre-to-post
treatment (CDRS-R: F(1,12)=11.76, p<.01; BDI-II: F(1,32)=11.19, p<.01), as was suicidal
ideation (F(1,33)=4.25, p<.05). However, reduction of depression scores in adolescents was
not found in parental ratings.
Conclusion: As the results indicated good feasibility and positive response to treatment, we
decided to next test the efficacy of MICHI in an RCT.
3.8. RCT for the assessment of efficacy of MICHI in depressed adolescent outpatients
Straub, J., Plener, P.L., Keller, F., Fegert, J.M., Spröber, N. & Kölch, M.G. (accepted). MICHI -
a brief, manualized cognitive behavioural group therapy for the treatment of depression in
adolescents: randomized controlled trial. Kindheit & Entwicklung.
RCT for the assessment of efficacy of MICHI in depressed adolescent outpatients
37
Introduction: According to current German guidelines, CBT is one of the first-line
interventions for the treatment of depression in minors. Therapy programs for the treatment
of depression in adolescents are sparse in Germany, and none has been evaluated in an RCT
with a German sample so far. To close this gap, the following study evaluated treatment
efficacy of MICHI, a brief group CBT program.
Methods: Inclusion and exclusion criteria were the same as in the first and second pilot study
(see Sections 3.6 and 3.7). MICHI comprised five regular sessions and one booster session,
each lasting 75 minutes (SD=9.57) on average. Adherence to the treatment manual by the
trainers was 98.24%. Thirty-eight depressed adolescents (30 females), mean age 15.86 years
(SD=1.70), were randomly assigned to MICHI (PAT-I) or TAU (PAT-W). Instruments for the
assessment of efficacy were the CDRS-R and the BDI-II.
Results: MICHI participants attended a mean of 5.39 (SD=.70) sessions (89.84%). Symptom
scores of depression declined in both treatment groups. Interaction effects for time points
of measurement (pre/post) and group (PAT-I/PAT-G) were significant with respect to the
CDRS-R (F(1,33)=6.01, p=.02, dcorrected =.75) and the BDI-II (F(1,33)=4.35, p=.04, dcorrected =.39).
Suicidal ideation and behaviour declined in PAT-I. However the interaction effect between
group (PAT-I/PAT-W) and time point of measurement (pre/post) was not significant
(F(1,33)=.66, p=.42). Excluding medicated patients from the analyses did not change the
results.
Discussion: The results indicated that treatment with MICHI was efficacious compared to
TAU. Effect sizes in this study were comparable to effect sizes found for treatment programs
that are applied in English-speaking countries. However, in comparison to those programs,
MICHI includes only half the number of sessions. Limitations of the present study are the
imbalanced sex ratio of the study population, which limits the generalization to the male
population. While pharmaceutical treatment had to be stable five weeks prior to start and
during the study, it could have biased the results (3 participants were taking Fluoxetine). The
PAT-W group received only 1.74 sessions with a child-and adolescent psychiatrist, which is
not comparable to the intensity of sessions that the PAT-I group received. However, in our
opinion, this reflects TAU in a child- and adolescent psychiatric context.
Neural correlates of successful psychotherapy of depression in adolescents
38
3.9. Neural correlates of successful psychotherapy of depression in adolescents
Straub, J., Plener, P.L., Koelch, M.G., Sproeber, N., Sprenger, L., Groen, G. & Abler, B.
(accepted). Neural correlates of successful psychotherapy of depression in adolescents.
Journal of Affective Disorders.
Introduction: Investigating neural correlates of depression in adolescents may help in
adapting therapies to the characteristics and needs of this population. Furthermore,
investigating brain activities early in life bypasses the confounding effects of long-term
medical treatment or structural changes resulting from a chronic disorder. Both adults and
adolescents with depression have been demonstrated to differ from healthy peers with
respect to brain activity in the sgACC, amygdala, hippocampus, and frontal cortex. Pre-to-
post activity changes in those brain regions were shown to be accompanied with pre-to-post
symptom reductions following therapeutic treatment in adults and pharmacological
treatment in adolescents and adults. Studies in adolescents are sparse, and changes of
neural activity before and after psychotherapy await empirical investigation. As depressed
patients tend to overestimate failure and punishment and underestimate success and
positive reinforcement, thus demonstrating a dysfunctional reward processing, we used a
reward paradigm to assess neural changes according to treatment. In previous studies, this
paradigm was shown to reliably activate relevant brain areas.
Methods: A total of 22 medication-naïve adolescents diagnosed with a major depressive
disorder were assigned to either PAT-W (N=12) or PAT-I (N=10). Eight participants in the PAT-
W group participated in MICHI after waiting, resulting in a total of 18 patients who ultimately
received MICHI (PAT-I complete; N=18). Pre-to-post activity changes in relevant regions of
interest (sgACC, amygdalda, hippocampus) were analysed, along with symptom changes
assessed by means of the BDI-II and CDRS-R. Interaction effects between group (PAT-I/PAT-
W) and time points of measurement (pre/post) were calculated. Furthermore, pre-to-post
signal chances and pre-signal activity in the sgACC were correlated with pre-to-post
symptom changes.
Results: Clinical assessments revealed significant interaction effects with respect to
depressive symptoms. In PAT-I but not in PAT-W, significant symptom reductions were
accompanied by significant signal changes in the left amygdala, left hippocampus, and right
Neural correlates of successful psychotherapy of depression in adolescents
39
sgACC, revealing significant interaction effects. Results indicated high correlations between
pre-to-post signal reduction in the sgACC, and pre-to-post symptom reduction following BDI-
II. Furthermore, bilateral sgACC activity prior to treatment predicted subsequent pre-to-post
symptom reduction significantly.
Discussion: Two brain systems are relevant when it comes to depressive disorder: the ventral
system, including the amygdala and sgACC, which is important for the identification of
emotional stimuli and bottom-up triggering of affective states; and the dorsal system,
including the hippocampus, which is important for the top-down regulation of emotional
states. A positive correlation between baseline sgACC activity and reduction of depression
scores was shown in previous studies, highlighting the importance of the sgACC in the
function of a biomarker.
General discussion
40
4. General discussion
While prevalence rates of depressive disorders in adolescents were relatively stable between
1965 and 1995 (Costello et al., 2006), the numbers of prescriptions for psychotropic
medications and patients being treated in the outpatient setting have increased between
2005 and 2008 (Annuss et al., 2010). Our research determined that the number of F3
(affective disorders) diagnoses of the ICD-10 (classification of mental and behavioral
disorders) in adolescent inpatients rose in Germany within 2003 and 2012, as expected,
despite a total decline of inpatients. One reason could be increased capacities within the
inpatient setting. However, the number of available beds in child and adolescent psychiatric
treatment centres declined from 8316 beds in 1991 to 5460 beds in 2010. At the same time,
bed occupancy rate increased only slightly from 83.7% in 1991 to 91.7% in 2010 (Boelt &
Graf, 2012). A second reason could be that due to a shorter duration of stay, more patients
can be treated within a comparable time frame than could be treated previously. This
assumption is in line with the finding that minors in 1991 stayed a mean number of 124.7
days and minors in 2010 a mean number of only 39.0 days in the child and adolescent
psychiatric treatment centres (Boelt & Graf, 2012). One explanation for shorter stays could
be that treatments are more efficacious than in earlier times
(Bundespsychotherapeutenkammer, 2014). In contrast to that assumption, Figueroa,
Harman and Engberg (2004) postulated that a reduced length of stay might be related to an
increased risk of readmission, wherefore increasing numbers wouldn’t reflect a “real” rise in
prevalence rates. Elevated readmissions might be especially high in depressed adolescents
due to elevated rates of recurrence of depressive disorders (Fombonne et al. 2001). Third,
there might be an increased awareness and recognition of symptoms of depression and
realization that depression is a prevalent and devastating disorder (Hegerl, 2013) which in
turn increases help seeking behaviour (Coppens et al., 2013). If this would be the reason, it
would make sense to train community facilitators to improve identification of depressive
disorders in minors, as has been previously done in adults (Coppens et al., 2014).
One of the symptoms of depression, which often leads to referral to an inpatient
treatment facility, is suicidality, and there is need to identify factors that are associated with
this very serious behaviour. In our study (Straub, Keller, Sproeber, Koelch & Plener, 2015) we
were able to show that symptoms of mania, above symptoms of depression, were able to
predict whether a student reported suicidal ideations and suicide attempts. Concerning
General discussion
41
suicide attempts, one more predictor was suicidal ideation. Nock et al. (2009) similarly found
a diagnosis of a bipolar disorder to be one of the best predictors for unplanned suicide
attempts; however, in the case of suicidal ideation, the authors found the best predictor to
be symptoms of depression only. Also differing from our results are those of Resch, Parzer,
and Brunner (2008), who found age to be a predictor for both suicidal ideation and suicide
attempts. One reason for that finding could be that Resch et al. (2008) included adolescents
with a broader age range (11 to 17 years) than we did (14 to 17 years). Our study points to
the added value of exploring symptoms of mania in addition to those of depression when
assessing suicidal behaviour in adolescents; an aspect that is often neglected in children and
adolescents, due to the low prevalence rate (Kozloff et al., 2010) of bipolar symptoms within
this age group. The highest prevalence rate for suicide attempts in our study was found in
adolescents who reported both elevated symptoms of mania and depression within the
previous week. This might support findings in adults that revealed elevated numbers of
suicide attempts within mixed episodes (Hawton, Sutton, Haw, Sinclair & Harriss, 2005).
The international gold standard for the structured assessment of depressive
symptoms in children and adolescents, as well as for measuring changes in these symptoms,
is the CDRS-R (Subica et al., 2014). As criteria for diagnosing depression have not changed
essentially from DSM-IV to DSM-5, existing diagnostic instruments can further be applied
without any changes. In our study, we found a CDRS-R score of ≥ 36 to indicate a mild to
moderate depressive episode following ICD-10 which conforms to our expectations.
However, a score of 36 is slightly lower than the score of 40 found by others (Mayes, et al.,
2010) which needs to be interpreted in the light of different classification systems: a
diagnosis of a major depressive episode based on DSM-IV specifies that the patient has
experienced five or more depressive symptoms over a two-week period, whereas a diagnosis
based on ICD-10 allows differentiation into mild and moderate if four or six symptoms,
respectively, are evidenced. Following the clinical work of Guo et al. (2006), a score of 36
would correspond more to a mild rather than mild to moderate depressive episode. This
might be explained by different versions of the CDRS-R (English versus German) as well as by
potential cultural differences when it comes to rating psychiatric symptoms such as those of
a depressive disorder (Alcantara & Gone, 2014).
The BDI-II is a further frequently used instrument for screening symptoms of
depression in adolescents and adults. Nevertheless, it was still unclear as to what extent the
General discussion
42
BDI-II and the CDRS-R scores were correlating and measuring symptoms in a similar way. We
identified a correlation coefficient of .67 (p<.001) which is high as expected before. However,
it is slightly but not significantly, lower than the correlation coefficients found in other
studies with healthy or clinically but not exclusively depressed patients (Keller et al., 2012).
There are two potential reasons for this. First, our time points of assessment with the two
instruments ranged from the same day up to one week apart, whereas other studies
assessed them on the same day only. However, the correlation coefficient was .73 in our
study when assessments were done on the same day. This coefficient was slightly, but not
significantly, higher than .67. Secondly, the BDI-II and CDRS-R were mostly assessed at the
start of treatment; and Dorz, Borgherini, Conforti, Scarso and Magni (2004) have shown that
the concordance between self-ratings and clinician ratings is poorer in the acute phase of
treatment than shortly before discharge. Following Dunlop et al. (2011), the increased
concordance over time could be explained through (1) a better shared understanding of
symptomatology, (2) a reduction in disorder-specific falsification due to improvement of
symptoms, and (3) increasing trust on the part of patient in the therapist, which enables
speaking about inner feelings more openly. With respect to correlations on the subscale
levels, we did not find a higher correlation for subscales that assessed more objective aspects
of depression than for those that assessed more subjective ones as hypothesized. This
finding differs from that of Corruble et al. (1999), who found objective subscales to correlate
more highly and could possibly be explained by methodological aspects since, unlike us,
Corruble et al. (1999) applied a structured interview and a questionnaire with identical
questions. Another possible explanation however, is that adolescents speak more openly
about their inner feelings than do adults, which needs to be investigated in future studies.
With respect to correlations at the item level, we found that items correlated highest when
they assessed comparable contents as we expected before, and our correlation coefficients
were similar to those found in adult studies (Keller, Ruppe, Stieglitz & Wolfersdorf, 1997).
Our finding that the item “suicidal behaviour” correlated the highest and the items
“depressive mood” and “concentration problems” the lowest was also reported by Corruble
et al. (1999). The high correlation of the item of suicidal behaviour in particular, highlights
the opportunity to apply the BDI-II for the screening and assessment of changes in suicidal
behaviour. Taken together, the correlation between self-report and structured interview
General discussion
43
assessments is high, but there is still some unexplained variance. Therefore one instrument
shouldn’t be replaced by the other.
The most recommended form of treatment for children and adolescents with mild to
moderate depressive episodes is psychotherapy, either CBT or IPT, while for those with
severe depression the recommended treatment is psychotherapy in combination with
pharmacological treatment. A review of the literature revealed that despite all the known
advantages of a brief group CBT intervention for depressed adolescents, no such program
was available in Germany. Furthermore, none of the existing German programs, aimed at
depressed adolescents, had been evaluated for efficacy. MICHI was designed to fill this gap.
Since we wished to include subjects with severe depression, which is often
accompanied by both an elevated risk for suicidal behaviour and a lowered level of
psychosocial functioning, we first evaluated the program in the safer and more structured
environment of an inpatient setting. As the results found MICHI to be feasible, well accepted,
and to lead to a significant reduction of depressive symptoms and suicidal ideation, we next
evaluated it in outpatients, after applying some revisions based on feedback of participants
and trainers from the first pilot study. Again, findings were positive. In a final step, MICHI
was tested in an RCT with outpatients, with the result of significant interaction effects (group
by time points), with small to moderate effect sizes.
In the first pilot study, that was designed to evaluate feasibility and acceptance of
MICHI in depressed adolescent inpatients, average attendance was 3.3 sessions out of four
regular sessions (82.50%), which is considered as fair. In the second pilot, and the RCT, which
both consisted of six sessions conducted in an outpatient setting, a reinforcement system
was implemented in an attempt to improve attendance. In the reinforcement system
patients received a voucher at the end of the study if they participated in all sessions. In
these studies, average attendance of patients in the sessions was 5.33 (88.83%) and 5.39
(89.84%), respectively which was slightly higher than the rate in the inpatient study.
However, attendance rates were expected to be higher due to the addition of a
reinforcement system. It needs to be taken into account that depressive disorders are often
accompanied by a low level of psychosocial functioning which might make it even more
difficult for outpatients to make it to sessions. Furthermore, reinforcements might work less
in depressed patients than in patients with different mental health problems, due to a
reduced sensitivity for reward (Elliott et al., 1997).
General discussion
44
With respect to the group setting, results of the process questionnaire indicated, that
participants liked being together with other adolescents and would furthermore recommend
the program to others. One reason for this could be that depressed adolescents, in
comparison to non-depressed, have fewer contacts with peers and more social deficits,
resulting in a higher probability of being socially rejected (Prinstein, Borelli, Cheah & Simon,
2005). A protected group therapy setting with like-minded peers might raise the opportunity
for positive social experiences and social contacts. Participants also shared that they felt well
understood by and comfortable with the trainers. A positive therapeutic alliance has been
shown to be a nonspecific, but very important, factor that could partly explain symptom
improvement as well (Martin, Garske & Davis, 2000).
In both pilot studies of MICHI, participants rated the transference of content learned
in the program to family life as not being very helpful, expressed doubt that family members
would be able to help them with their problems in the future, and did not feel that including
them in the program was helpful. One reason could be that during adolescence children
increasingly detach from their parents while same-aged peers become more and more
important which was also reflected in session 5, in which only one-third of the participants
brought a parent while the others brought a friend or sibling instead. A second reason could
be that inclusion of family members during only a single session might not be enough to
address all skills necessary and maybe the addition of cognitive family therapy sessions might
have improved results (Poessel & Hautzinger, 2006).
The therapeutic contents of the MICHI-program were evaluated positively overall in
both pilot studies. Specifically, participants of the first pilot study rated “development of an
emergency plan” as very helpful, highlighting the need for concrete guidelines on how to
behave in case of acute crisis, an element that has been neglected in some other treatment
programs. However, they evaluated “relaxation techniques” as being less helpful, which is
consistent with the findings of Mattejat et al. (2010) who stated that relaxation techniques
are of little help in patients with depression, as patients start to ruminate and focusing on
their sad feelings during relaxation. Based on this feedback, relaxation techniques were
eliminated from the program.
Concerning fidelity of implementation with respect to the trainers, there was an
increase in adherence to the treatment manual from the second pilot (93%) to the
randomized controlled study (98.24%). This may have been due to continuous supervision,
General discussion
45
to the detailed instructions provided in the treatment manual, and to increasing familiarity
by the trainers with the program’s contents. Treatment adherence was comparable to the
one of other manualized treatment programs ranging from 80% to 94% (Gaynor & Lawrence,
2002; Kahn, Kehle, Jenson & Clark, 1990; Listug-Lunde, Vogeltanz-Holm & Collins, 2013;
Rossello, Bernal & Rivera-Medina, 2008).
Pre-post-test comparisons of the first pilot study as well as both pre-post and follow-
up analyses of the second pilot study indicated significant improvements of depressive
symptoms, with effect sizes ranging from small (for self-ratings) to moderate (for structured
interview assessments). The remission rate in the intervention group (with remission defined
as a CDRS-R score <36) was 42% in the second pilot study and 47.37% in the RCT, which is
comparable to the rates of 45.2% and 56.0% reported by others (Ihle, Jahn, Spieß & Herrle,
2002; Ihle & Jahnke, 2003), who had evaluated the German version of the group treatment
program CWD-A in a pre-post-test design. These rates are also comparable to those of 39–
62% that have been reported in international studies that aimed to evaluate CBT therapies
for the treatment of depressed adolescents (Kahn et al., 1990; Rohde, Clarke, Mace,
Jorgensen & Seeley, 2004; Rossello et al., 2008). However, this comparison needs to be
interpreted with caution, as the definition of reliable remission differs between studies.
With respect to the RCT study, pre-to-post depressive symptoms decreased in both
the intervention and the waiting control group, however the decrease was greater in the
intervention group. One possible explanation is that the control group also received
treatment, and another is the high rate of spontaneous remission that is often seen in
depressive disorders in childhood and adolescence (Whiteford et al., 2013). The interaction
effects (group by time points of measurement) were significant with respect to both the
CDRS-R with moderate effect sizes (dcorrected=.75) and the BDI-II, with small effect sizes
(dcorrected=.39). As MICHI is the first program for the treatment of depression in adolescents
that has been evaluated by means of an RCT in a German sample; its efficacy can only be
compared to international programs at this time. The therapy program of Harrington (2001),
which is conceptualized for individual treatment, was found by Wood et al. (1996) with an
effect size of .73, while effect sizes of the group treatment program CWD-A were found to
range between .02 (Clarke et al., 2002) and 1.34 (Kahn et al., 1990), depending on the control
group. This needs to be interpreted in conjunction with the fact that MICHI is two to four
times shorter than other treatment programs (Abel & Hautzinger, 2013; Ihle & Herrle, 2011).
General discussion
46
Furthermore, our results are in line with the result of the meta-analysis of Cuijpers et al.
(2013), which reported a weak relationship between efficacy and duration of treatment but
a strong one between efficacy and weekly intensity of therapy. This finding also supports the
dose effects model which states that 41% of the patients improve after four
psychotherapeutic sessions and 53% after eight (Howard et al., 1986). Supporting this model,
Stulz, Lutz, Leach, Luco and Barkham (2007), working with two groups of highly impaired
clients, found that one group improved strongly (d=2.23) within the first sessions of
psychotherapy (<14 sessions). The other group however, improved slowly within the first
sessions (<14; d=.30) and also slowly during the remainder of the treatment, despite long
treatment durations (98% had >14 sessions). Taken together it appears as if there are two
categories, fast and slow responders. Based on those findings, one recommendation could
be that all patients start with a brief but intense psychotherapeutic treatment; and for those
who do not respond, a change in treatment (e.g. initiation of pharmacological treatment)
should be considered as recommended by the NICE guidelines (National Collaborating
Centre for Mental Health, 2005).
In consideration to parental reports in the pilot studies of MICHI, there was no
significant pre-post-test effect. These results are comparable to those of Weisz et al. (2006),
who doubted that parents are good informants with respect to affective symptoms of their
children.
In both MICHI pilot studies and the RCT, suicidal ideation declined significantly from
pre to post. Concerning participants of all three studies, 53.10% revealed moderate to severe
suicidal ideation before and only 21.72% after treatment on average. Given that in a study
of healthy European adolescents aged 14 to 16 years (Resch et al., 2010), 17% of females
and 8.3% of males reported having had suicidal ideation within the last two weeks, the
percentage of adolescents with post-intervention suicidal ideation in our sample was
comparable to that seen in non-clinical populations. We also found a significant decline of
pre-to-post suicidal ideation in the RCT, with a non-significant interaction effect between
group and time points of measurement. Others (Brunstein-Klomek & Stanley, 2007; Kapusta,
Fegert, Haring & Plener, 2013) have found comparable effects: a reduction of suicidal
ideation after psychosocial treatment that was strong but not significantly different from the
active control group.
General discussion
47
Besides feasibility and efficacy of MICHI, we also studied neural correlates of effective
psychotherapeutic treatment of adolescent depression. Reduction in clinical symptoms was
found to be accompanied by significant changes in brain activation in the left amygdala, left
hippocampus, and right sgACC revealing significant interaction effects between group (PAT-
I/PAT-W) and time points of measurement (pre/post). Furthermore pre-to-post signal
changes in the sgACC correlated highly with pre-to-post symptom changes in the BDI-II and
pre-treatment sgACC activity was able to predict subsequent treatment response. Change of
activity in the amygdala pre-to-post treatment is in line with one of the few studies on neural
effects of psychotherapy in adults. Fu et al. (2008) for example showed that activity of the
amygdala changed in parallel with symptom improvement following a short, but clinically
successful, psychotherapy. The amygdala was thereby confirmed as an important brain
structure for the identification of emotional states as well as for bottom-up modulation of
affective states (A. G. Phillips, Ahn & Howland, 2003).
Our findings were furthermore consistent with those reported in depressed adults
after a pharmacological intervention, which included a significant reduction in hippocampus
activity after treatment with paroxetine over six weeks (Kennedy et al., 2001), with
fluoxetine over eight weeks (Fu et al., 2007), and after CBT (Fu et al., 2008), with significant
interaction effects seen between group and time points of measurement. A conflicting
finding was that of Goldapple et al. (2004) who found a relative increase in metabolic activity
in the hippocampus following CBT where our results pointed towards a decrease; however,
different findings can possibly be explained by the application of different paradigms. As the
hippocampus is a region that contributes to emotional memory (Tahmasian et al., 2013), in
which cognitive processes are integrated, and which can be biased by emotional input, it has
been suggested that it contributes to executive functions, including effortful regulation of
affective states (M. L. Phillips et al., 2003), which in turn may be particularly sensitive to
cognitive interventions. Changes in hippocampal activation following psychotherapy may
reflect the ability of psychotherapy to modulate activation in key nodes of networks
mediating top-down processes.
The ACC plays a critical role in the expression and modulation of emotion (Papez,
1995) and in the regulation of limbic activity (Mayberg, 2003). The sgACC has been shown to
be important for the identification as well as bottom-up modulation of affective states (M.
L. Phillips et al., 2003). Activation of the sgACC has consistently been related to the clinical
General discussion
48
response to different antidepressant treatments, including SSRIs in both adults (Mayberg et
al., 2000) and adolescents (R. Tao et al., 2012), to electroconvulsive therapy, to repetitive
transcranial magnetic stimulation, and to ablative surgery (Mayberg et al., 2005), which
highlights its role as a key structure in depression. Also, with respect to psychotherapeutic
treatment effects, Yoshimura et al. (2013) found activity in the vACC to be increased for
positive stimuli and decreased for negative stimuli after CBT in depressed adult patients.
In our study, relatively increased pre-treatment activity in the sgACC was associated
with subsequent treatment response, a finding that has also been shown for
pharmacological treatment response in other studies (Fu et al., 2004; Goldapple et al., 2004;
Kennedy et al., 2001; Mayberg et al., 2000). In support of our results, Yoshimura et al. (2013)
found a negative correlation between signal change in the vACC and improvement of
depressive symptoms. In contrast, Konarski et al. (2009) found that non-responders, in
comparison to responders, exhibited pre-treatment hypermetabolism in the sgACC; and
Siegle et al. (2006) reported a significant association between reduced pre-treatment sgACC
activity and subsequent treatment response. Different findings could be explained by the
different paradigms applied; for example, Siegle et al. had focused on negative stimuli (-
activity), while we focused on the contrast between positive and negative stimuli ((+ activity)
– (- activity) = (+ activity)).
The named brain areas above were shown to be modulated by pharmacological
treatment in depressed patients (Arnone et al., 2012, Godlewska et al., 2012, Sheline et al.,
2001) however revealed similar effects in healthy subjects after placebo as well (Abler et al.,
2011; Macoveanu, 2014). Therefore there is some ambiguity about its underlying factors
(symptom, improvement and/or medication). In agreement with one of the rare studies on
neural effects of psychotherapeutic treatment in adults (Fu et al., 2008), we were able to
show that activity in the amygdala, sgACC and hippocampus changed in line with symptom
improvement after a clinically efficacious psychotherapy, but not in the depressed waitlist
control group. As our subjects were naïve to pharmacological treatment, present results
support the notion that neural activity changes are most likely related to treatment success
in general rather than to specific pharmacological treatment effects.
Studies that have mainly investigated both pharmacological (Fu et al., 2008;
Goldapple et al., 2004; R. Tao et al., 2012) and psychotherapeutic treatment effects (Brody
et al., 2001; Goldapple et al., 2004; Ritchey et al., 2011) in adults, have found altered pre-
General discussion
49
to-post treatment activity changes in the prefrontal cortex, but we were not able to replicate
those findings. One explanation could be that all studies listed above used either an
emotional picture/emotional word or a resting state paradigm. It might be assumed that
these paradigms are better suited to map activation changes in the prefrontal cortex, as this
brain region is associated with self-referential or other-referential processing of emotional
stimuli (Yoshimura et al., 2009), as, for example, a reward paradigm. However, one study
that used a reward paradigm in adults to assess signal changes before and after an average
of 11 sessions of BAT (Dichter et al., 2009) also revealed functional changes in the
orbitofrontal gyrus.
A second explanation could be that, as most of the above-mentioned studies were
done in adults, it could be hypothesized that signal changes in the prefrontal cortex might
be more difficult to detect in adolescents due to heterogeneous states of maturation (Casey
et al., 2008). Contrarily, Tao et al. (2012) found treatment effects with fluoxetine within the
orbitofrontal cortex in adolescents as well who were of a comparable age range (11–18
years) to those in our study (13–18 years).
Thirdly, a reason for diverse findings could lay in different reward paradigms applied.
Dichter et al. (2009) for example used the “Wheel of Fortune” reward paradigm which might
be better suited for the illustration of psychotherapeutic treatment effects, with respect to
prefrontal cortex areas, than the reward paradigm that we applied. However, Abler, Erk &
Walter (2007), who also applied a monetary incentive delayed task, found activity reduced
in the inferior frontal cortex after dopaminergic medication but not placebo, indicating that
this task is well suited to display treatment effects as well.
Fourth, activity changes in the studies of both Tao et al. (2012) and Dichter et al.
(2009) occurred after eight weeks of fluoxetine and 11 weeks of BAT, respectively. It could
be assumed that due to the brevity (only five weeks) of the psychotherapeutic treatment
MICHI, effects might be detectable sooner within subcortical brain areas than within cortical
ones, as changes might occur more quickly in regions that are relevant for bottom-up than
for top-down processing.
4.1 Limitations
In the study that looked at increasing numbers of F diagnoses in the inpatient setting from
2003 to 2012, the main diagnoses might rather be based on the judgement of the clinician
General discussion
50
than on standardized instruments (e.g., structured interviews). Furthermore different
classification systems (DSM or ICD) might have been used, influencing results as well.
Therefore, the quality of routine data from health systems may have some weakness
concerning validity of diagnoses (Dolle, Schulte-Koerne, von Hofacker, Izat & Allgaier, 2012).
With respect to the study that assessed the relationship between depression/mania
symptoms and lifetime suicidality, we cannot draw conclusions about the relationship
between bipolar disorder and suicidality directly. This is because we assessed symptoms of
mania and depression over the previous week by means of questionnaires in a cross-
sectional design, which neither measured the required time frame following ICD-10 (e.g.,
two weeks for depressive disorders), nor allowed us to obtain information about the course
of the episode (e.g., whether episodes of depression and mania were altered). Furthermore,
questionnaires instead of structured interviews were used, which might hamper validity of
diagnoses.
Concerning the study that looked at convergence between CDRS-R and clinical
diagnosis, results are limited due to the small sample size of raters as well as the great
diversity of professions within each group. Furthermore not all of them were trained in the
execution of the CDRS-R beforehand. It would also have been beneficial to conduct the same
procedure with more than one videotaped structured interview displaying different types of
severity of depressive disorder.
In the study that compared symptoms of depression on the sum score, subscale and
item level, assessed by means of the CDRS-R and BDI-II, both instruments were
conceptualized for the assessment of depression but they are not identical with respect to
item content and wording. Furthermore, instruments were not assessed on the same day,
but within one week and mostly directly after referral to the child and adolescent psychiatry.
Those aspects could have potentially affected correlational strength. With respect to third
variables, we only focused on age, sex, IQ, and treatment setting.
Both pilot studies primarily aimed to reveal information about acceptance and
feasibility of MICHI. However, findings concerning pre-to-post symptom improvement in
both pilot studies of MICHI must be interpreted with caution. The small number of
participants and the absence of a waiting control group, and of a randomized group
assignment, hampers conclusions about treatment efficacy. In the first pilot study, a further
limitation is the inability to separate effects of MICHI from the inpatient treatment setting.
General discussion
51
Another limitation, that affects both pilot studies and the RCT, is the inclusion of participants
taking antidepressant medications. We attempted to reduce this impact by including only
individuals whose regimen had been stable for three to five weeks prior to the start and
during the study. The inclusion of patients who are not medication-naïve was chosen as it
presents a naturalistic setting which is closer to a clinical real-life situation. Furthermore, the
instruments that were applied for the assessment of the contents of MICHI were
conceptualized by our own team under supervision however, they were not checked for
psychometric properties beforehand.
With regard to the RCT and fMRI study, the treatment received during the waiting
period by the control group comprised about two half-hour appointments with a
psychologist or psychiatrist. This cannot be put on the same level as an active control group,
as TAU was comparatively less intense than MICHI and was not applied in a standardized
manner. However, in our opinion this procedure reflects TAU reality in a German child and
adolescent psychiatry.
With respect to the fMRI study, we compared pre-to-post effects of PAT-I (N=10) with
pre-to-post effects of PAT-W (N=12). Due to small sample sizes, we were forced to include
all participants who received the intervention after waiting for within-group analyses.
Therefore, of the 18 subjects included in the pre-post-follow-up-test analyses, eight had
been assigned to the waiting control group prior to receiving the intervention. Potentially
the symptoms of these 8 participants may have improved during the waiting period through
spontaneous recovery (Whiteford, et al., 2013), which is not ideal with respect to scientific
standards. However, those participants of the waiting group who were later admitted to
participate in psychotherapy did not differ in CDRS-R raw sum scores from participants
randomly assigned to the immediate intervention group (PAT-I).
Two further aspects that affected all four previous studies, aimed to evaluate MICHI
and its neural correlates, were 1) a skewed gender recruitment (females=75%, males=25%),
which limits generalizability to males; and 2) inclusion of participants with co-morbid
disorders. On the one hand, both of these aspects could affect efficacy, but on the other,
they reflect treatment reality. A final factor is that patients were permitted to speak to the
trainer individually after a therapeutic or diagnostic session in case of an acute crisis. This
opportunity was used only a few times, but could still have influenced outcomes. This issue
was discussed beforehand and was found to be a necessary supplement for ethical reasons.
General discussion
52
4.2 Conclusions and perspectives
Rates of depressive disorders in minors remained stable between 1965 and 1996 however
numbers of emotional problems in 11 to 17 year olds rose between 2003-2006 and 2009-
2012. Furthermore, the number of pharmacological and outpatient treatments increased. In
line with those findings, we showed that inpatient treatment for F3 diagnoses rose as well
even after controlling for decrease of the total numbers of patients. Future studies, assessing
the course of the number of patients being treated in the inpatient setting, should ensure
that diagnoses are assessed by standardized diagnostic instruments (e.g. structured
interviews). Furthermore, studies should identify reasons for the increasing numbers of
inpatients (e.g. increased awareness for depressive symptoms in minors in both, the
population and primary health care). Furthermore, more recent meta-analyses are needed
about the course of prevalence rates of depressive disorders in Germany referring to the last
ten years. However there are two barriers in doing so: first of all, clinicians apply different
coding practices and use different classification systems (DSM, ICD). Second, alterations of
existing classification systems (e.g. from DSM-IV to DSM-5) also affect prevalence rates. (e.g.,
some children, that would have been diagnosed with depressive disorder according to DSM-
IV might now be diagnosed with disruptive mood dysregulation disorder following DSM-5
(Plener, Witt, Straub & Fegert, 2013)).
Considering symptoms of mania in addition to those of depression and their
association with suicidality, we were able to show that suicidal ideation was best predicted
by symptoms of depression, and above that by symptoms of mania, while suicide attempts
were best predicted by symptoms of depression and above that by symptoms of mania and
age. This points to the added value of specifically exploring symptoms of mania in addition
to those of depression (both symptoms of the ICD-10 chapter F3 “affective disorders”) when
assessing suicidal behaviour in adolescents. Prospectively, it would be interesting to assess
the relationship between bipolar disorders (diagnoses should be done by means of
structured interviews) and suicidal behaviour in a longitudinal design. Additionally, it should
be analysed also in minors whether suicide attempts rather occur during depressive or mixed
episodes than during episodes of mania, as was shown in adults (Hawton et al., 2005).
Our study, the first to assess the concordance between the clinical diagnoses of a
depressive episode following ICD-10 and CDRS-R scores of the German version, found a
CDRS-R value of greater than 36 to be indicative of a mild depressive episode. As most of the

General discussion
53
literature on the CDRS-R refers to samples in the United States, which compared interview
raw scores to diagnostic criteria of major depression following DSM-IV, there is a need for
further studies on convergence of CDRS-R scores and diagnoses according to ICD-10,
especially with its classification into moderate and severe depressive episodes. In doing so,
future studies should involve larger sample sizes of clinical experts rating interviews with a
wider range of videotaped structured interviews displaying various severities of depressive
disorders.
Sum scores of the BDI-II and CDRS-R correlated highly but not completely, indicating
that they measure similar, but not identical aspects of depression. On the item level, items
with related content, such as those dealing with suicidal ideation, were found to correlate
higher than did less related ones. On the subscale level, subscales measuring more objective
aspects of depression did not correlate higher than subscales measuring more subjective
aspects not supporting the finding of Corruble et al. (1999). Further studies should assess
whether this finding can be attributed to the assumption that adolescents tend to speak
more openly about their inner feelings than do adults where subscales measuring objective
and subjective contents were comparable. Dunlop et al. (2011) reported that in adults the
discrepancy between self-report and clinical assessment is higher at the beginning of
treatment than at the end. Therefore, it would be interesting to calculate concordance of
self-report questionnaires and structured interviews at both the beginning and end of
treatment, and to compare both values to see whether this assumption is also true for
adolescents. Further studies should identify factors that affect correlational strength such as
level of knowledge about symptoms of depression or shame with respect to answering
questions about depression openly in a structured interview.
The longer the duration of a depressive episode, the higher the chances for relapses
in adulthood. This highlights the need for brief and effective treatments of depression at its
beginnings. Prior to the development of MICHI, the only programs available in Germany for
the treatment of depressed adolescents lasted an average of 12 sessions and were
conceptualized for the treatment of mild to moderate depression; furthermore, none had
been evaluated in a randomized controlled design. To close this gap we developed a brief
cognitive behavioural group psychotherapy called MICHI. It was assessed in a step-wise
manner (inpatient pilot study, then outpatient pilot study, then outpatient RCT) and shown
to be feasible, accepted, and efficacious. The small to moderate effect sizes found for MICHI
General discussion
54
are comparable to those found for English-language CBT programs which last two to four
times longer than MICHI supporting the dose-effect model of negative acceleration (Howard,
et al., 1986). However, future studies should aim to identify characteristics of patients who
might profit from shorter lasting treatments and characteristics of patients who might profit
from longer lasting treatments. Besides that, forthcoming studies should investigate MICHI
in a multicentre study, comparing the treatment arm with a more active waiting control
group and adding follow-up measurements up to six to 12 months after termination of
psychotherapy, to investigate long-term effects. The further addition of cognitive
behavioural family therapy components (Poessel & Hautzinger, 2006) might possibly be
helpful, and needs to be explored in future studies. As the goal of integrating family or friends
into the program was to prevent relapse, which would more likely be necessary sometime
in the future rather than right after completion of the program, this aspect should be
evaluated in the long-term rather than the short-term. Furthermore, psychosocial
functioning level could be chosen as one more outcome parameter besides depression
scores.
As prevalence rates of depression are rising from childhood to adolescence, there is
a strong need to improve our knowledge about the underlying processes of depression
during this vulnerable period. Studying the neurobiology of depression in adolescents allows
us to avoid confounds that exist in studies with adults with respect to long-term medication,
neural changes due to relapses, or chronic course of the disorder. Worldwide, this is the first
study that has investigated neural correlates of successful psychotherapeutic treatment of
depression in adolescents as compared to a waiting group. Activation of the amygdala,
hippocampus, and sgACC, three areas that are commonly reported as relevant in depression,
were found to change with amelioration of depressive symptoms compared to those who
received only minimal wait-list treatment. Pre-treatment activity in the sgACC was related
to subsequent treatment response. The amygdala, sgACC and hippocampus were shown to
be relevant with respect to processing of negative stimuli, of ruminative thoughts and of
biased memory for negative stimuli in individuals with depression (Disner, Breevers, Haigh
& Beck, 2011) – aspects that seem to have been successfully tackled by CBT. More globally,
the amygdala and sgACC are important brain structures for the identification and bottom-up
modulation of affective states, while the hippocampus is more important for top-down
regulation. Therefore, our study supports models suggesting that dysfunctional neural
General discussion
55
mechanisms of emotion regulation in depression can be targeted by psychotherapy, at least
in the early stages of the illness, and may therefore constitute a state rather than a trait
marker. In future studies, neural correlates should be investigated with a larger sample size,
and it would be interesting to see whether effects remain stable in the long-term. In addition,
brief interventions should be compared with longer lasting therapies to reveal information
about how many sessions are needed to find neural correlates of successful treatment in the
prefrontal cortex as well. Furthermore, it would be interesting to compare neural correlates
of pharmacological versus psychotherapeutic treatment in adolescents as well. As functional
connectivity was shown to give valuable information about whether a subject was clinically
depressed or not (Craddock, Holtzheimer, Hu & Mayberg, 2009), future studies should
investigate functional connectivity and its changes as potential biomarkers and putative
treatment effects.
A proper diagnosis of depression requires a valid and reliable assessment, which is provided
by the German version of the CDRS-R. Furthermore, it is necessary to understand underlying
factors of suicidality to improve prevention of suicidal events – often reasons for referral to
the inpatient setting. Elevated rates of minors, being treated because of mood disorders in
the out- and inpatient setting, highlight the need for fast, available, and efficacious
treatments. MICHI is the first therapy program whose efficacy has been shown on both the
psychometric and neural levels. Our finding of a strong correlation between individual
expressions of brain activation and subsequent treatment response may be one more step
towards being able to identify certain bio-types to aid in the decision as to which form of
treatment is the most suitable for a given individual. The finding that a brief but intense
program can be helpful when it comes to treating depression in adolescents carries several
advantages. First, brief interventions in comparison to longer-lasting ones can reduce
barriers of psychotherapeutic health care utilization, as they can be more easily integrated
into daily lives. Second, the fact that the effects of a brief intervention are comparable to a
longer-lasting psychotherapy has both economic and political advantages. Based on the
present findings, and taking into account long waiting periods for psychotherapeutic
treatments in Germany on the one hand and strong need for treatments on the other, a brief
intervention could serve as a first-line treatment, reserving longer-lasting psychotherapies
or pharmacological treatment for those who fail to respond.
References
56
5 References
Abel, U. & Hautzinger, M. (2013). Kognitive Verhaltenstherapie bei Depressionen im Kindes-
und Jugendalter. Heidelberg: Springer
Abler, B., Erk, S. & Walter, H. (2007). Human reward system activation is modulated by a
single dose of olanzapine in healthy subjects in an event-related, double-blind,
placebo-controlled fMRI study. Psychopharmacology, 191, 823-833.
Abler, B., Hahlbrock, R., Unrath, A., Groen, G. & Kassubek, J. (2009). At-risk for pathological
gambling: imaging neural reward processing under chronic dopamine agonists. Brain:
A Journal of Neurology, 132, 2396-2402.
Abler, B., Seeringer, A., Hartmann, A., Gron, G., Metzger, C., Walter, M. & Stingl, J. (2011).
Neural correlates of antidepressant-related sexual dysfunction: a placebo-controlled
fMRI study on healthy males under subchronic paroxetine and bupropion.
Neuropsychopharmacology, 36(9), 1837-1847. doi: 10.1038/npp.2011.66npp201166
[pii]
Adam, E. K., Doane, L. D., Zinbarg, R. E., Mineka, S., Craske, M. G. & Griffith, J. W. (2010).
Prospective prediction of major depressive disorder from cortisol awakening
responses in adolescence. Psychoneuroendocrinology, 35(6), 921-931.
Alcantara, C. & Gone, J. P. (2014). Multicultural issues in the clinical interview and diagnostic
process. In F. T. Leong, L. Comas-Diaz, G. C. Nagayama Hall, V. C. McLoyd & J. E.
Trimble (Eds.), APA handbook of multicultural psychology (Vol. 2). Washington DC:
American Psychological Associations.
Allianz Deutschland, A. G., Rheinisch Westfälisches Institut für Wirtschaftsforschung (RWI),
(2011). Depression- Wie die Krankheit unserer Seele belastet. Retrieved 22.05.2015,
from http://www.rwi-essen.de/media/content/pages/publikationen/sonstige/
Allianz-Report-Depression.pdf
Allison, S., Roeger, L., Martin, G. & Keeves, J. (2001). Gender differences in the relationship
between depression and suicidal ideation in young adolescents. Australian and New
Zealand Journal of Psychiatry, 35, 498-503.
Almeida, J. R., Versace, A., Hassel, S., Kupfer, D. J. & Phillips, M. L. (2010). Elevated amygdala
activity to sad facial expressions: a state marker of bipolar but not unipolar
depression. Biological Psychiatry, 67(5), 414-421.
doi: http://dx.doi.org/10.1016/j.biopsych.2009.09.027
American Psychiatric Association (1994). Diagnostic and Statistical Manual of Mental
Disorder (Fourth ed.). Washington, DC.
American Psychiatric Association (2013). Diagnostic and Statistical Manual of Mental
Disorders (Fifth ed.). Airlington, VA: American Psychiatric Publishing.
Angold, A., Costello, E. & Worthman, C. (1998). Puberty and depression: the roles of age,
pubertal status and pubertal timing. Psychological Medicine, 28(1), 51-61.
References
57
Annuss, R., Budde, S., Hollederer, A., Puteanus, U., Simon, K. & Werse, W. (2010). Seelische
Gesundheit von Kindern und Jugendlichen in Nordrhein-Westfalen. In Landesinstitut
für Gesundheit und Arbeit des Landes Nordrhein-Westfalen (Ed.). Duesseldorf.
Arnone, D., McKie, S., Elliott, R., Thomas, E. J., Downey, D., Juhasz, G., . . . Anderson, I. M.
(2012). Increased amygdala responses to sad but not fearful faces in major
depression: relation to mood state and pharmacological treatment. The American
Journal of Psychiatry, 169(8), 841-850.
doi: http://dx.doi.org/10.1176/appi.ajp.2012.11121774
Baeken, C., van Schuerbeek, P., de Raedt, R., Ramsey, N. F., Bossuyt, A., de Mey, J., . . .
Luypaert, R. (2010). Reduced left subgenual anterior cingulate cortical activity during
withdrawal-related emotions in melancholic depressed female patients. Journal of
Affective Disorders, 127(1-3), 326-331.
doi: http://dx.doi.org/10.1016/j.jad.2010.05.013
Barkham, M., Connell, J., Stiles, W. B., Miles, J. N., Margison, F., Evans, C. & Mellor-Clark, J.
(2006). Dose-effect relations and responsive regulation of treatment duration: the
good enough level. Journal of Consulting and Clinical Psychology, 74(1), 160-167.
Barkham, M., Rees, A., Stiles, W. B., Shapiro, D. A., Hardy, G. E. & Reynolds, S. (1996). Dose-
effect relations in time-limited psychotherapy for depression. Journal of Consulting
and Clinical Psychology, 64(5), 927-935.
Beck, A. T. (1976). Depression: clinical, experimental and theoretical aspects. New York:
Harper & Row.
Beck, A. T., Rush, A. J., Shaw, B. F. & Emery, G. (1979). Cognitive therapy of depression. New
York: Guilford Press.
Beck, A. T., Steer, R. A. & Brown, G. K. (1996). Beck Depression Inventory - Second Edition.
San Antonio: The Psychological Corporation.
Bettge, S., Wille, N., Barkmann, C., Schulte-Markwort, M., Ravens-Sieberer, U. & the Bella
study group (2008). Depressive symptoms of children and adolescents in a German
representative sample: results of the BELLA study. European Child and Adolescent
Psychiatry, 17, 71-81. doi: 10.1007/s00787-008-1008-x
Birkle, S. & Holtmann, M. (2014). Bipolare Depression im Kindes- und Jugendalter. Praxis der
Kinderpsychologie und Kinderpsychiatrie, 63, 219-236.
Birleson, P. (1981). The validity of depressive disorder in childhood and the development of
a self-rating scale: a research report. Journal of Child Psychology and Psychiatry, 22,
73-88.
Boelt, U. & Graf, T. (2012). 20 Jahre Krankenhausstatistik. Statistisches Bundesamt,
Wirtschaft und Statistik. Retrieved 22.05.2015, from
https://www.destatis.de/DE/Publikationen/WirtschaftStatistik/Gesundheitswesen/
20JahreKrankenhausstatistik.pdf?__blob=publicationFile
Bora, E., Harrison, B. J., Davey, C. G., Yuecel, M. & Pantelis, C. (2012). Meta-analysis of
volumetric abnormalities in cortico-striatal-pallidal-thalamic circuits in major
depressive disorder. Psychological Medicine, 42(4), 671-681.
References
58
Brent, D. A., Greenhill, L. L., Compton, S., Emslie, G., Wells, K., Walkup, J. T., . . . Turner, J. B.
(2009). The Treatment of Adolescent Suicide Attempters study (TASA): predictors of
suicidal events in an open treatment trial. Journal of American Academy of Child &
Adolescent Psychiatry, 48(10), 987-996. doi: 10.1097/CHI.0b013e3181b5dbe4
Brent, D. A., Holder, D., Kolko, D., Birmaher, B., Baugher, M., Roth, C., . . . Johnson, B. A.
(1997). A clinical psychotherapy trial for adolescent depression comparing cognitive,
family, and supportive therapy. Archives of General Psychiatry, 54(9), 877-885.
Brent, D. A., Perper, J. A., Moritz, G., Allman, C., Friend, A., Roth, C., . . . Baugher, M. (1993).
Psychiatric risk factors for adolescent suicide: a case-control study. Journal of the
American Academy of Child & Adolescent Psychiatry, 32(3), 521-529.
Brody, A. L., Saxena, S., Stoessel, P., Gillies, L. A., Fairbanks, L. A., Alborzian, S., . . . Baxter, L.
R. (2001). Regional brain metabolic changes in patients with major depression
treated with either paroxetine or interpersonal therapy: preliminary findings.
Archives of General Psychiatry, 58(7), 631-640.
doi: http://dx.doi.org/10.1001/archpsyc.58.7.631
Brunstein-Klomek, A. & Stanley, B. (2007). Psychosocial treatment of depression and
suicidality in adolescents. CNS Spectrums, 12(2), 135-144.
Buchheim, A., Viviani, R., Kessler, H., Kaechele, H., Cierpka, M., Roth, G., . . . Taubner, S.
(2012). Changes in prefrontal-limbic function in major depression after 15 months of
long-term psychotherapy. PlosOne, 7(3). doi: e33745
BundesPsychotherapeutenKammer. BPtK-Studie zur stationären Versorgung psychisch
kranker Menschen: Ergebnisse einer Befragung der in Krankenhäuser angestellten
Psychotherapeuten 2014. Retrieved 14.08.2014, from
www.bptk.de/uploads/media/20140626_BPtK-Studie_zur_stationären_Versorgung
_psychisch_kranker_Menschen.pdf
Carroll, B. J., Feinberg, M. & Smouse, P. E. (1981). The Carroll Rating Scale for Depression. I.
Development, reliability and validation. British Journal of Psychiatry, 138, 194-200.
Casey, B. J., Jones, R. M. & Hare, T. A. (2008). The adolescent brain. Annals of the New York
Academy of Sciences, 1124, 111-126.
Chantiluke, K., Halari, R., Simic, M., Pariante, C. M., Papadopoulos, A., Giampietro, V. &
Rubia, K. (2012). Fronto-striato-cerebellar dysregulation in adolescents with
depression during motivated attention. Biological Psychiatry, 71(1), 59-67.
doi: http://dx.doi.org/10.1016/j.biopsych.2011.09.005
Clarke, G. N., Hornbrook, M., Lynch, F., Polen, M., Gale, J., O´Connor, E., . . . Debar, L. (2002).
Group cognitive-behavioral treatment for depressed adolescent offspring of
depressed parents in a health maintenance organization. Journal of the American
Academy of Child and Adolescent Psychiatry, 41(3), 305-313.
Clarke, G. N., Lewinsohn, P. M. & Hops, H. (1990). Leader's manual for adolescent groups:
adolescent coping with depression course. Eugene: Castalia Publishing Company.
Collishaw, S., Maughan, B., Goodman, R. & Pickles, A. (2004). Time trends in adolescent
mental health. Journal of Child Psychology and Psychiatry, 45(8), 1350-1362.
References
59
Compton, S. N., March, J. S., Brent, D., Albano, A. M., Weersing, R. & Curry, J. (2004).
Cognitive-behavioral psychotherapy for anxiety and depressive disorders in children
and adolescents: an evidence-based medicine review. Journal of American Academy
of Child & Adolescent Psychiatry, 43(8), 930-959.
Connolly, C. G., Wu, J., Ho, T. C., Hoeft, F., Wolkowitz, O., Eisendrath, S., . . . Yang, T. T. (2013).
Resting-state functional connectivity of subgenual anterior cingulate cortex in
depressed adolescents. Biological Psychiatry, 74(12).
doi: http://dx.doi.org/10.1016/j.biopsych.2013.05.036
Coppens, E., van Audenhoven, C., Iddi, S., Arensman, E., Gottlebe, K., Koburger, N., . . .
Hegerl, U. (2014). Effectiveness of comunity facilitator training in improving
knowledge, attitudes, and confidence in relation to depression and suicidal behavior:
results of the OSPI-Europe intervention in four European countries. Journal of
Affective Disorders, 165, 142-150.
Coppens, E., van Audenhoven, C., Scheerder, G., Arensman, E., Coffey, C., Costa, S., . . .
Hegerl, U. (2013). Public attitudes toward depression and help-seeking in four
European countries baseline survey prior to the OPSI-Europe intervention. Journal of
Affective Disorders, 150, 320-329.
Corruble, E., Legrand, J. M., Zvenigorowski, H., Duret, C. & Guelfi, J. D. (1999). Concordance
between self-report and clinicians' assessment of depression. Journal of Psychiatric
Research, 33, 457-465.
Costello, E., Erkanli, A. & Angold, A. (2006). Is there an epidemic of child or adolescent
depression? Journal of Child Psychology and Psychiatry, 47(12), 1263-1271.
Craddock, R. C., Holtzheimer, P. E., Hu, X. P. & Mayberg, H. S. (2009). Disease state prediction
from resting state functional connectivity. Journal of Magnetic Resonance in
Medicine, 62(6), 1619-1628.
Crews, F., He, J. & Hodge, C. (2007). Adolescent cortical development: a critical period of
vulnerability for addiction. Pharmacology, Biochemistry and Behavior, 86(2), 189-
199.
Crowther, A., Smoski, M.J., Minkel, J., Moore, T., Gibbs, D., Petty, C., Bizzell, J., Schiller, C.E.,
Sideris, J., Carls, H. & Dichter, G. (2015) Resting-state connectivity predictors of
response to psychotherapy in major depressive disorder.
Neuropsychopharmacology, 1-15. doi. 10.1038/npp.2015.12
Cuijpers, P., Huibers, M., Ebert, D. D. & Koole, S. L. (2013). How much psychotherapy is
needed to treat depression? A metaregression analysis. Journal of Affective
Disorders, 149, 1-13.
Cullen, K. R. (2012). Imaging adolescent depression treatment. The American Journal of
Psychiatry, 169(4), 348-350.
Davey, C. G., Harrison, B. J., Yuecel, M. & Allen, N. B. (2012). Regionally specific alterations
in functional connectivity of the anterior cingulate cortex in major depressive
disorder. Psychological Medicine, 42(10), 2071-2081.
doi: http://dx.doi.org/10.1017/S0033291712000323
References
60
Davey, C. G., Allen, N. B., Harrison, B. J. & Yuecel, M. (2011). Increased amygdala response
to positive social feedback in young people with major depressive disorder. Biological
Psychiatry, 69(8), 734-741.
Davey, C. G., Yuecel, M. & Allen, N. B. (2008). The emergence of depression in adolescence:
development of the prefrontal cortex and representation of reward. Neuroscience
and Biobehavioral Reviews, 32, 1-19.
David-Ferdon, C. & Kaslow, N. J. (2008). Evidence-based psychosocial treatments for child
and adolescent depression. Journal of Clinical Child and Adolescent Psychology, 37(1),
62-104.
Deutsche Gesellschaft für Kinder- und Jugendpsychiatrie Psychosomatik und Psychotherapie
(2013). Behandlung von depressiven Störungen bei Kindern und Jugendlichen.
Retrieved 22.05.2015, from http://www.awmf.org/uploads/tx_szleitlinien/028-
043l_S3_Depressive_St%C3%B6rungen_bei_Kindern_Jugendlichen_2013-07.pdf
Deutsche Gesellschaft für Psychiatrie Psychotherapie und Nervenheilkunde (2009). S3-
Leitlinie/Nationale Versorgungsleitlinie unipolare Depression. Berlin. Retrieved
22.05.2015, from http://www.awmf.org/uploads/tx_szleitlinien/nvl-
005l_S3_Unipolare_Depression_2012-01_01.pdf
Dichter, G. S., Felder, J. N. & Smoski, M. J. (2010). The effects of brief behavioral activation
therapy for depression on cognitive control in affective contexts: an fMRI
investigation. Journal of Affective Disorders, 126, 236-244.
Dichter, G. S., Felder, J. N., Petty, C., Bizzell, J., Ernst, M. & Smoski, M. J. (2009). The effects
of psychotherapy on neural responses to rewards in major depression. Biological
Psychiatry, 66, 886-897.
Disner S. G., Breevers, C. G., Haigh, E. A. & Beck, A. T. (2011). Neural mechanisms of the
cognitive model of depression. Nature Reviews, 12, 467-477.
Doepfner, M., Goertz-Dorten, A., Lehmkuhl, G., Breuer, B. & Goletz, H. (2008). Diagnostik-
System für psychische Stoerungen nach ICD-10 und DSM-IV fuer Kinder und
Jugendliche-II. Mannheim: Huber.
Dolle, K., Schulte-Koerne, G., von Hofacker, N., Izat, Y. & Allgaier, A.-K. (2012).
Übereinstimmung von klinischer Diagnose, strukturierten Interviews und
Selbstbeurteilungsfragebögen bei Depression im Kindes- und Jugendalter. Zeitschrift
für Kinder- und Jugendpsychiatrie und Psychotherapie, 40(6), 405-414.
Donath, C., Graessel, E., Baier, D. & Hillemacher, T. (2013). The prevalence of suicidal
thoughts and attempts in a representative sample of German adolescents. Paper
presented at the XIV International Congress of the International Federation of
Psychiatric Epidemiology, Leipzig.
Dorz, S., Borgherini, G., Conforti, D., Scarso, C. & Magni, G. (2004). Comparison of self-rated
and clinician-rated measures of depressive symptoms: a naturalistic study.
Psychology and Psychotherapy: Theory, Research and Practice, 77, 353-361.
Dunlop, B. W., Li, T., Kornstein, S. G., Friedman, E. S., Rothschild, A. J., Pedersen, R., . . .
Trivedi, M. H. (2011). Concordance between clinician and patient ratings as
References
61
predictors of response, remission, and recurrence in major depressive dirsorder.
Journal of Psychiatric Research, 45, 96-103.
Dunn, E. C., Uddin, M., Subramanian, S. V., Smoller, J. W., Galea, S. & Koenen, K. C. (2011).
Research Review: gene-environment interaction research in youth depression -
systematic review with recommendations for future research. Journal of Child
Psychology and Psychiatry, 52(12), 1223-1238.
Eley, T. C., Sugden, K., Corsico, A., Gregory, A. M., Sham, P., McGuffin, P., . . . Craig, I. W.
(2004). Gene-environment interaction analysis of serotonin system markers with
adolescent depression. Molecular Psychiatry, 9(10), 908-915.
Elliott, R., Sahakian, B. J., Herrod, J. J., Robbins, T. W. & Paykel, E. S. (1997). Abnormal
response to negative feedback in unipolar depression: evidence for a diagnosis
specific impairment. Journal of Neurology, Neurosurgery, and Psychiatry, 63, 74-82.
Erford, B. T., Erford, B. M., Lattanzi, G., Weller, J., Schein, H., Wolf, E., . . . Peacock, E. (2011).
Counseling outcoms from 1990 to 2008 for school-age youth with depression: a meta
analysis. Journal of Counseling and Development, 89(4), 439-457.
Essau, C. A. & Conradt, C. (2003). Trainingsprogramm zur Prävention von Angst und
Depression: Freunde für Kinder. Muenchen: Reinhardt.
Essau, C. A., Conradt, J. & Petermann, F. (2000). Frequency, comorbidity, and psychosocial
impairment of depressive disorders in adolescents. Journal of Adolescent Research,
15(4), 470-481.
Essex, M. J., Klein, M. H. & Kalin, N. H. (2002). Maternal stress beginning in infancy may
sensitize children to later stress exposure: effects on cortisol and behavior. Biological
Psychiatry, 52, 776-784.
Fegert, J. M., Koelch, M., Zito, J. M., Glaeske, G. & Janhsen, K. (2006). Antidepressant use in
children and adolescents in Germany. Journal of Child and Adolescent
Psychopharmacology, 16, 197-206.
Figueroa, R., Harman, J. & Engberg, J. (2004). Use of claims data to examine the impact of
length of inpatient psychiatric stay on readmission rate. Psychiatric Services, 55, 560-
565.
Fombonne, E., Woster, G., Cooper, V., Harrington, R. & Rutter, M. (2001). The Maudsley long-
term follow-up of child and adolescent depression: 1. Psychiatric outcomes in
adulthood. The British Journal of Psychiatry, 179(3), 210-217.
doi: 10.1192/bjp.179.3.210
Forbes, E. E. & Dahl, R. E. (2012). Altered reward function in adolescent depression: what,
when and how? Journal of Child Psychology and Psychiatry, 53(1), 3-15.
Forbes, E. E., Olino, T. M., Ryan, N. D., Birmaher, B., Axelson, D., Moyles, D. L. & Dahl, R. E.
(2010). Reward-related brain function as a predictor of treatment response in
adolescents with major depressive disorder. Cognitive Affective Behaviour
Neuroscience, 10(1), 107-118.
Forbes, E. E., Hairi, A. R., Martin, S. L., Silk, J. S., Moyles, D. L. & Fisher, P. M. (2009). Altered
striatal activation predicting real-world positive affect in adolescent major depressive
disorder. American Journal of Psychiatry, 166, 64-73.
References
62
Forbes, E. E., May, J. C., Siegle, G. J., Ladouceur, C. D., Ryan, N. D., Carter, C. S., . . . Dahl, R. E.
(2006). Reward-related decision-making in pediatric major depressive disorder: an
fMRI study. Child Psychology & Psychiatry & Allied Disciplines, 47(10), 1031-1040.
doi: http://dx.doi.org/10.1111/j.1469-7610.2006.01673.x
Forbes, E. E. & Dahl, R. E. (2005). Neural systems of positive affect: relevance to
understanding child and adolescent depression? Development and psychopathology,
17, 827-850.
Fu, C. H., Williams, S. C., Cleare, A. J., Scott, J., Mitterschiffthaler, M. T., Walsh, N. D., . . .
Murray, R. M. (2008). Neural responses to sad facial expressions in major depression
following cognitive behavioral therapy. Biological Psychiatry, 64(6), 505-512.
Fu, C. H., Williams, S. C., Brammer, M. J., Suckling, J., Kim, J., Cleare, A. J., . . . Bullmore, E. T.
(2007). Neural responses to happy facial expressions in major depression following
antidepressant treatment. The American Journal of Psychiatry, 164(4), 599-607.
doi: http://dx.doi.org/10.1176/appi.ajp.164.4.599
Fu, C. H., Williams, C. R., A.J., C., Brammer, M. J., Walsh, N. D., Kim, J., . . . Bullmore, E. T.
(2004). Attenuation of the neural response to sad faces on major depression by
antidepressant treatment. Archives of General Psychiatry, 61(9), 877-889.
Gabriel, M., Burhans, L. & Kashef, A. (2003). Consideration of a unified model of amygdalar
associative functions. Annual of New York Academy of Sciences, 985, 206-217.
Gaynor, S. T. & Lawrence, P. S. (2002). Complementing CBT for depressed adolescents with
learning through in vivo Experience (LIVE): conceptual analysis, treatment
description, and feasibility study. Behavioral and Cognitive Psychotherapy (30), 79-
101.
Giedd, J. N., Lalonde, F. M., Celano, M. J., White, S. L., Wallace, G. L., Lee, N. R. & Lenroot, R.
K. (2009). Anatomical brain magnetic resonance imaging of typically developing
children and adolescents. Journal of the American Academy of Child & Adolescent
Psychiatry, 48(5), 465-470.
Gilman, S. E., Kawachi, I., Fitzmaurice, G. M. & Buka, S. L. (2003). Family disruption in
childhood and risk of adult depression. American Journal of Psychiatry, 160(5), 939-
946.
Godlewska, B. R., Norbury, R., Selvaraj, S., Cowen, P. J. & Harmer, C. J. (2012). Short-term
SSRI treatment normalises amygdala hyperactivity in depressed patients.
Psychological Medicine, 42(12), 2609-2617.
doi: http://dx.doi.org/10.1017/S0033291712000591
Goldapple, K., Segal, Z., Garson, C., Lau, M., Bieling, P., Kennedy, S. & Mayberg, H. (2004).
Modulation of cortical-limbic pathways in major depression: treatment-specific
effects of cognitive behavior therapy. Archives of General Psychiatry, 61(1), 34-41.
doi: http://dx.doi.org/10.1001/archpsyc.61.1.34
Goodyer, I. M., Dubicka, B., Wilkinson, P., Kelvin, R., Roberts, C., Byford, S., . . . Harrington,
R. (2007). Selective serotonin reuptake inhibitors (SSRIs) and routine specialist care
with and without cognitive behavior therapy in adolescents with major depression:
randomised controlled trial. British Medical Journal, 335(7611), 142-150.
References
63
Gotlib, I. H., Sivers, H., Gabrieli, J. D., Whitfield-Gabrieli, S., Goldin, P., Minor, K. L. & Canli, T.
(2005). Subgenual anterior cingulate activation to valenced emotional stimuli in
major depression. Neuroreport, 16(16), 1731-1734.
doi: http://dx.doi.org/10.1097/01.wnr.0000183901.70030.82
Groen, G. & Petermann, F. (2008). Was wirkt in der Therapie von Depression bei Kindern und
Jugendlichen wirklich? Kindheit und Entwicklung, 17(4), 243-251.
Gruber, J., Gilbert, K. E., Youngstrom, E., Kogos Youngstrom, J., Feeny, N. C. & Findling, R. L.
(2013). Reward dysregulation and mood symptoms in an adolescent outpatient
sample. Journal of Abnormal Psychology. doi:10.1007/s10802-013-9746-8
Guo, Y., Nilsson, M. E., Heiligenstein, J., Wilson, M. G. & Emslie, G. (2006). An exploratory
factor analysis of the Children's Depression Rating Scale- Revised. Journal of Child and
Adolescent Psychopharmacology, 16(4), 482-491.
Haber, S. N. & Knutson, B. (2010). The reward circuit: linking primate anatomy and human
imaging. Neuropsychopharmacology Reviews, 35, 4-26.
Harrington, R. (2001). Kognitive Verhaltenstherapie bei depressiven Kindern und
Jugendlichen. Göppingen: Hogrefe.
Harrington, R., Whittaker, J., Shoebridge, P. & Campbell, F. (1998). Systematic review of
efficacy of cognitive behavior therapies in childhood and adolescent depressive
disorder. British Medical Journal, 316, 1559-1563.
Hautzinger, M., Bailer, M., Hofmeister, D. & Keller, F. (2012). Allgemeine Depressionsskalen
(ADS). Testhandbuch (2., erweiterte Auflage). Göttingen: Hogrefe.
Hautzinger, M., Keller, F. & Kuehner, C. (2006). Beck Depressions Inventar Revision (BDI-II).
Frankfurt/M.: Harcourt Test Services.
Hawton, K., Sutton, L., Haw, C., Sinclair, J. & Harriss, L. (2005). Suicide and attempted suicide
in bipolar disorder: a systematic review of risk factors. Journal of Clinical Psychiatry
66(6), 693-704.
Hegerl, U., Rummel-Kluge, C., Värnik, A., Arensman, E. & Koburger, N. (2013). Alliance against
depression - a community based approach to target depression and to prevent
suicidal behaviour. Neuroscience and Biobehavioral Reviews, 37, 2404-2409.
Hoelling, H., Schlack, R., Petermann, F., Ravens-Sieberer, U., Mauzz, E. & KiGGS Study Group.
(2014). Psychische Auffaelligkeiten und psychosoziale Beeintraechtigungen bei
Kindern und Jugendlichen im Alter von 3 bis 17 Jahren in Deutschland-Praevalenz und
zeitliche Trends zu 2 Erhebungszeitpunkten (2003-2006 und 2009-2012).
Bundegesundheitsblatt, 57, 807-819.
Holtman, M., Duketis, E., Poustka, L., Zepf, F.D. & Boelte, S. (2010). Bipolar disorder in
children and adolescents in Germany: national trends in the rates of inpatients, 2000-
2007. Bipolar Disorders, 12, 155-163.
Horn, A. B. (2004). Depressionspraevention durch Foerderung der Emotionsregulation:
Expressives Schreiben für Jugendliche (Vol. 7). Berlin: Logos.
Howard, K. I., Kopta, S. M., Krause, M. S. & Orlinsky, D. E. (1986). The dose-effect relationship
in psychotherapy. American Psychologist, 41(2), 159-164.
References
64
Ihle, W. & Herrle, J. (2011). Stimmungsprobleme bewaeltigen. Ein kognitiv-
verhaltenstherapeutisches Gruppenprogramm zur Praevention, Behandlung und
Rueckfallprophylaxe depressiver Stoerungen im Jugendalter nach Clarke, Lewinsohn
und Hops. Manual für Kursleiter (Vol. 2). Tuebingen: dgvt-Verlag.
Ihle, W. & Jahnke, D. (2003). Wirkt ein psychoedukatives kognitiv-verhaltenstherapeutisches
Gruppenprogramm auch bei depressiven Jugendlichen mit komorbiden Stoerungen?
Verhaltenstherapie und Verhaltensmedizin, 24(4), 513-528.
Ihle, W., Jahn, D., Spieß, L. & Herrle, J. (2002). Evaluation eines kognitiv-
verhaltenstherapeutischen Gruppenprogramms für depressive Jugendliche und
junge Erwachsene. Kindheit und Entwicklung, 11(4), 238-246.
Kahn, J. S., Kehle, T. J., Jenson, W. R. & Clark, E. (1990). Comparison of cognitive-behavioral,
relaxation, and self-modeling interventions for depression among middle-school
students. School Psychology Review, 19(2), 196-211.
Kapusta, N. D., Fegert, J. M., Haring, C. & Plener, P. L. (2013). Psychotherapeutische
Interventionen bei suizidalen Jugendlichen. Psychotherapeut, 59, 16-23.
Kaufman, J., Yang, B., Douglas-Palumberi, H., Grasso, D., Lipschitz, D., Houshyar, S., . . .
Gelernter, J. (2006). Brain-derived neurotrophic factor-5-HTTLPR gene interactions
and environmental modifiers of depression in children. Biological Psychiatry, 59(8),
673-680.
Kaufman, J., Yang, B. Z., Douglas-Palumberi, H., Houshyar, S., Lipschitz, D. & Krystal, J. H.
(2004). Social supports and serotonin transporter gene moderate depression in
maltreated children. Proceedings of the National Academy of Sciences of the United
States of America, 101, 17316-17321.
Keller, F., Grieb, J., Koelch, M. & Sproeber, N. (2012). CDRS-R Children’s Depression Rating
Scale – Revised by E. O. Poznanski and H. B. Mokros: Deutsche Version. Goettingen:
Hogrefe.
Keller, F., Ruppe, A., Stieglitz, R. D. & Wolfersdorf, M. (1997). Korrelationen zwischen Selbst-
und Fremdbeurteilung von Depressivität auf der Symptomebene. In M. Wolfersdorf
(Ed.), Depressionsstationen/ Stationaere Depressionsbehandlung (pp. 139-143).
Berlin: Springer.
Kempton, M. J., Salvador, Z., Munafo, M. R., Geddes, J. R., Simmons, A., Frangou, S. &
Williams, S. C. (2011). Structural neuroimaging studies in major depressive disorder.
Archives of General Psychiatry, 68(7), 675-690.
Kennedy, S. H., Evans, K. R., Krueger, S., Mayberg, H. S., Meyer, J. H., McCann, S., . . .
Vaccarino, F. J. (2001). Changes in regional brain glucose metabolism measured with
positron emission tomography after paroxetine treatment of major depression. The
American Journal of Psychiatry, 158(6), 899-905.
doi: http://dx.doi.org/10.1176/appi.ajp.158.6.899
Kerestes, R., Davey, C. G., Stephanou, K., Whittle, S. & Harrison, B. J. (2014). Functional brain
imaging studies of youth depression: a systematic review. NeuroImage: Clinical, 4,
209-231.
References
65
Kim, M. H., Mazenga, A. C., Devandra, A., Ahmed, S., Kazembe, P. N., Xiaoying, Y., . . . Sharp,
C. (2014). Prevalence of depression and validation of the Beck Depression Inventory-
II and the Children's Depression Inventory-Short amongst HIV-positive adolescents in
Malawi. Journal of the International AIDS Society, 17(18965), 1-8.
Klein, J. B., Jacobs, R. H. & Reinecke, M. A. (2007). Cognitive-behavioral therapy for
adolescent depression: a meta-analytic investigation of changes in effect-size
estimates. Journal of American Academy of Child & Adolescent Psychiatry, 46(11),
1403-1413.
Kokkevi, A., Rotsika, V., Arapaki, A. & Richardson, C. (2012). Adolescents' self-reported
suicide attempts, self-harm thoughts and their correlates across 17 European
countries. Child Psychology & Psychiatry & Allied Disciplines, 53(4), 381-389.
doi: http://dx.doi.org/10.1111/j.1469-7610.2011.02457.x
Konarski, J. Z., Kennedy, S. H., Segal, Z. V., Lau, M. A., Bieling, P. J., McIntyre, R. S. & Mayberg,
H. S. (2009). Predictors of nonresponse to cognitive behavioural therapy or
venlafaxine using glucose metabolism in major depressive disorder. Journal of
Psychiatry & Neuroscience, 34(3), 175-180.
Kovacs, M. (2010). Children's Depression Inventory (CDI). New York: Multi-health Systems
Incorporation.
Kovacs, M. (1992). The Children's Depression Inventory. North Tonawanda (New York):
Mental Health Systems.
Kozloff, N., Cheung, A. H., Schaffer, A., Cairney, J., Dewa, C. S., Veldhuizen, S., . . . Levitt, A. J.
(2010). Bipolar disorder among adolescents and young adults: results from an
epidemiological sample. Journal of Affective Disorders, 125, 350-354.
Kumari, V., Mitterschiffthaler, M. T., Teasdale, J. D., Malhi, G. S., Brown, R. G., Giampietro,
V., . . . Sharma, T. (2003). Neural abnormalities during cognitive generation of affect
in treatment-resistant depression. Biological Psychiatry, 54(8), 777-791.
doi: http://dx.doi.org/10.1016/S0006-3223%2802%2901785-7
Lambert, M. J., Hansen, N. B. & Finch, A. E. (2001). Patient-focused research: using patient
outcome data to enhance treatment effects. Journal of Consulting and Clinical
Psychology, 69(2), 159-172.
Lang, M. & Tisher, M. (1983). Childrens Depression Scale: Second Research Edition.
Melbourne: The Australian Council for Educational Research Limited.
Lang, M. & Tisher, M. (1978). Childrens Depression Scale: Research Edition. Melbourne: The
Australian Council for Educational Research Limited.
Lewinsohn, P. M. & Clarke, G. N. (1999). Psychosocial treatments for adolescent depression.
Clinical Psychology Review, 19(3), 329-342.
Lewinsohn, P. M. & Graf, M. (1973). Pleasant activities and depression. Journal of Consulting
and Clinical Psychology, 41, 261-268.
Liotti, M., Mayberg, H. S., Brannan, S. K., McGinnis, S., Jerabek, P. & Fox, P. T. (2000).
Differential limbic-cortical correlates of sadness and anxiety in healthy subjects:
implications for affective disorders. Biological Psychiatry, 48(1), 30-42.
doi: http://dx.doi.org/10.1016/S0006-3223%2800%2900874-X
References
66
Listug-Lunde, L., Vogeltanz-Holm, N. & Collins, J. (2013). A cognitive-behavioral treatment
for depression in rural American indian middle school students. American Indian and
Alaska Native Mental Health Research, 20(1), 16-34.
Macoveanu, J. (2014). Serotonergic modulation of reward and punishment: evidence from
pharmacological fMRI studies. Brain research, 1556, 19-27.
Martin, S. D., Martin, E., Rai, S. S., Richardson, M. A., & Royall, R. (2001). Brain blood flow
changes in depressed patients treated with interpersonal psychotherapy or
venlafaxine hydrochloride: preliminary findings. Archives of General Psychiatry,
58(7), 641-648. doi: http://dx.doi.org/10.1001/archpsyc.58.7.641
Martin, D. J., Garske, J. P. & Davis, K. (2000). Relation of the therapeutic alliance with
outcome and other variables: a meta-analytic review. Journal of Consulting and
Clinical Psychology, 68(3), 438-450.
Masten, C. L., Eisenberger, N. I., Borofsky, L. A., McNealy, K., Pfeifer, J. H. & Dapretto, M.
(2011). Subgenual anterior cingulate responses to peer rejection: a marker of
adolescents' risk for depression. Development and psychopathology, 23(1), 283-292.
doi: http://dx.doi.org/10.1017/S0954579410000799
Mattejat, F. (2010). Verhaltenstherapie mit Kindern und Jugendlichen und ihren Familien
(Vol. 4). München: CIP-Medien.
Mayberg, H. S., Lozano, A. M., Voon, V., McNeely, H. E., Seminowicz, D., Hamani, C., . . .
Kennedy, S. H. (2005). Deep brain stimulation for treatment-resistant depression.
Neuron, 45, 651-660.
Mayberg, H. S. (2003). Modulating dysfunctional limbic-cortical circuits in depression:
towards development of brain-based algorithms for diagnosis and optimised
treatment. British Medical Bulletin, 65(1), 193-207.
Mayberg, H. S., Brannan, S. K., Tekell, J. L., Silva, J. A., Mahurin, R. K., McGinnis, S. & Jerabek,
P. A. (2000). Regional metabolic effects of fluoxetine in major depression: serial
changes and relationship to clinical response. Biological Psychiatry, 48(8), 830-843.
doi: http://dx.doi.org/10.1016/S0006-3223%2800%2901036-2
Mayes, T. L., Bernstein, I. H., Haley, C. L., Kennard, B. D. & Emslie, G. J. (2010). Psychometric
Properties of the Children's Depression Rating Scale-Revised in Adolescents. Journal
of Child and Adolescent Psychopharmacology, 20(6), 513-516.
McDermut, W., Miller, I. & Brown, R. (2001). The efficacy of group psychotherapy for
depression: a meta-analysis and review of the emprirical research. Clinical
Psychology: Science and Practice, 8(1), 98-116.
McLeod, J. D. & Shanahan, M. J. (1996). Trajectories of poverty and children's mental health.
Journal of Health and Social Behavior, 37, 207-220.
Mehler-Wex, C. (2012). Entwicklungspsychiatrische Aspekte depressiver Stoerungen.
Nervenheilkunde, 31(7-8), 515-523.
Mehler-Wex, C. (2008). Psychotherapieverfahren. Depressive Stoerungen (pp. 100-114).
Heidelberg: Springer.
Michael, K. D. & Crowley, S. L. (2002). How effective are treatments for child and adolescent
depression? A meta-analytic review. Clinical Psychology Review(22), 247-269.
References
67
Mingtian, Z., Shuqiao, Y., Xiongzhao, Z., Jinyao, Y., Xueling, Z., Xiang, W., . . . Wei, W. (2012).
Elevated amygdala activity to negative faces in young adults with early onset major
depressive disorder. Psychiatry Research: Neuroimaging, 201(2), 107-112.
doi: http://dx.doi.org/10.1016/j.pscychresns.2011.06.003
Montgomery, S. A. & Asberg, M. (1979). A new depression scale desgined to be sensitive to
change. British Journal of Psychiatry, 134, 382-389.
Mufson, L. H., Pollack, D. P., Olfson, M., Weissman, M. M. & Hoagwood, K. (2004).
Effectiveness research: transporting interpersonal psychotherapy for depressed
adolescents (IPT-A) from the lab to school-based health clinics. Clinical Child and
Family Psychology Review, 7(4), 251-261.
Mufson, L., Weissman, M. M., Moreau, D. & Garfinkel, R. (1999). Efficacy of interpersonal
psychotherapy for depressed adolescents. Archives of General Psychiatry, 56, 573-
579.
Munoz, R. F. & Miranda, J. (1986). Group therapy for cognitive-behavioral treatment of
depression. San Francisco General Hospital: Depression Clinic.
National Collaborating Centre for Mental Health (2005). Depression in children and young
people: identification and management in primary, community and secondary care,
in National Clinical Practice Guideline Number 28.
Nock, M. K., Green, J. G., Hwang, I., McLaughlin, K. A., Sampson, N. A., Zaslavsky, A. M. &
Kessler, R. C. (2013). Prevalence, correlates, and treatment of lifetime suicidal
behavior among adolescents. Archives of General Psychiatry, 70(3), 300-310.
doi: 10.1001/2012.jamapsychiatry.55
Nock, M. K., Hwang, I., Sampson, N., Kessler, R. C., Angermeyer, M., Beautrais, A., . . .
Williams, D. R. (2009). Cross-national analysis of the associations among mental
disorders and suicide behavior: findings from the WHO World Health Survey. PLoS
Medicine, 6(8), 1-17.
Oei, T. & Dingle, G. (2008). The effectiveness of group cognitive behavior therapy for unipolar
depressive disorders. Journal of Affective Disorders, 107, 5-21.
Olino, T. M., McMakin, D. L., Morgan, J. K., Silk, J. S., Birmaher, B., Axelson, D. A., . . . Forbes,
E. E. (2013). Reduced reward anticipation in youth at high-risk for unipolar
depression: a preliminary study. Developmental Cognitive Neuroscience, 8, 55-64.
doi: http://dx.doi.org/10.1016/j.dcn.2013.11.005
Olino, T. M., McMakin, D. L., Dahl, R. E., Ryan, N. D., Silk, J. S., Birmaher, B., . . . Forbes, E. E.
(2011). "I won, but I'm not getting my hopes up": depression moderates the
relationship of outcomes and reward anticipation. Psychiatry Research, 194(3), 393-
394.
Papez, J. W. (1995). A proposed mechanism of emotion. Journal of Neuropsychiatry, 38(4),
725-743.
Patton, G. C., Coffey, C., Romaniuk, H., Mackinnon, A., Carlin, J. B., Degenhardt, L., . . . Moran,
P. (2014). The prognosis of common mental disorders in adolescents: a 14-year
prospective cohort study. The Lancet, 383(9926), 1404-1411.
References
68
Phillips, A. G., Ahn, S. & Howland, J. G. (2003). Amygdalar control of the mesocorticolimbic
dopamine system: parallel pathways to motivated behavior. Neuroscience and
Biobehavioral Reviews, 27, 543-554.
Phillips, M. L., Drevets, W. C., Rauch, S. L. & Lane, R. (2003). Neurobiology of emotion
perception I: the neural basis of normal emotion perception. Society of Biological
Psychiatry, 54, 504-514.
Plener, P.L., Straub, J., Fegert, J.M. & Keller, F. (2015). Treatment of mental diseases in
children in German hospitals: analysis of frequencies in the years 2003 to 2012.
Nervenheilkunde, 34, 18-23.
Plener, P.L., Grieb, J., Sproeber, N., Straub, J., Schneider, A., Keller, F. & Koelch, M.G. (2012).
Convergence of children's depression rating scale-revised scores and clinical
diagnosis in rating adolescent depressive symptomatology. Mental Illness, 4(e7), 29-
31.
Plener, P. L., Kapusta, N. D., Fegert, J. M. & Keller, F. (2009). Suizidalität in einer deutschen
Schulstichprobe. Suizidprophylaxe, 36, 181-185.
Poessel, P. & Hautzinger, M. (2006). Effects of pharmaco- and psychotherapeutic
interventions in depression among children and adolescents. Zeitschrift für Kinder-
und Jugendpsychiatrie und Psychotherapie, 34(4), 243-255.
Poessel, P. & Horn, A. B. (2004). Trainingsprogramm zur Praevention von Depressionen bei
Jugendlichen: Lust an realistischer Sicht & Leichtigkeit im sozialen Alltag. Goeppingen:
Hogrefe.
Poznanski, E. O. & Mokros, H. B. (1996). Children's Depression Rating Scale, Revised (CDRS-
R): Manual. Los Angeles: Western Psychological Services.
Prinstein, M. J., Borelli, J. L., Cheah, C. S. & Simon, V. A. (2005). Adolescent girl's interpersonal
vulnerability to depressive symptoms: a longitudinal examination of reassurance-
seeking and peer relationships. Journal of Abnormal Psychology, 114(4), 676-688.
Reinecke, M. A., Ryan, N. E. & DuBois, D. L. (1998). Cognitive-behavioral therapy of
depression and depressive symptoms during adolescence: a review and meta-
analysis. Journal of the American Academy of Child & Adolescent Psychiatry, 37(1),
26-34.
Remschmidt, H., Schmidt, M. & Poustka, F. (2009). Multiaxiales Klassifikationsschema für
psychische Störungen des Kindes- und Jugendalters nach ICD-10 der WHO (Vol. 5).
Bern: Verlag Hans Huber.
Resch, F., Brunner, R., Kaess, M., Parzer, P., Klug, K., Fischer, G., . . . Lenzen, C. (2010). SEYLE
Ergebnisbericht
Resch, F., Parzer, P. & Brunner, R. (2008). Self-mutilation and suicidal behaviour in children
and adolescents: prevalence and psychosocial correlates, results of the BELLA study.
Journal of European Child and Adolescent Psychiatry, 17 (Suppl 1), 92-98.
Reynolds, W. M. (2002). Reynolds Adolescent Depression Scale: Professional manual (2nd
ed.). Odessa, FL: Psychological Assessment Resources, Inc.
Reynolds, W. M. (1989). Reynolds Child Depression Scale Odessa (Florida): Psychological
Assessment Resources
References
69
Reynolds, W. M. (1987). Reynolds Adolescent Depression Scale Professional Manual. Odessa
(Florida): Psychological Assessment Resources.
Rice, F., Harold, G. & Thapar, A. (2002). The genetic aetiology of childhood depression: a
review. Journal of Child Psychology and Psychiatry, 43(1), 65-79.
Ritchey, M., Dolcos, F., Eddington, K. M., Strauman, T. J. & Cabeza, R. (2011). Neural
correlates of emotional processing in depression: changes with cognitive behavioral
therapy and predictors of treatment response. Journal of Psychiatric Research, 45(5),
577-587.
Roberson-Nay, R., McClure, E. B., Monk, C. S., Nelson, E. E., Guyer, A. E., Fromm, S. J., . . .
Pine, D. S. (2006). Increased amygdala activity during successful memory encoding in
adolescent major depressive disorder: an fMRI study. Biological Psychiatry, 60(9),
966-973. doi: http://dx.doi.org/10.1016/j.biopsych.2006.02.018
Rohde, P., Clarke, G. N., Mace, D. E., Jorgensen, J. S. & Seeley, J. R. (2004). An
efficacy/effectiveness study of cognitive-behavioral treatment for adolescents with
comorbid major depression and conduct disorder. Journal of American Academy of
Child & Adolescent Psychiatry, 43(6), 660-668.
Rosenblau, G., Sterzer, P., Stoy, M., Park, S., Friedel, E., Heinz, A., . . . Stroehle, A. (2012).
Functional neuroanatomy of emotion processing in major depressive disorder is
altered after successful antidepressant therapy. Journal of Psychopharmacology,
26(11), 1424-1433. doi: http://dx.doi.org/10.1177/0269881112450779
Rossello, J., Bernal, G. & Rivera-Medina, C. (2008). Individual and group CBT and IPT for
Puerto Rican adolescents with depressive symptoms. Cultural Diversity and Ethnic
Minority Psychology, 14(3), 234-245.
Rossello, J. & Bernal, G. (1999). The efficacy of cognitive-behavioral and interpersonal
treatments for depression in Puerto Rican adolescents. Journal of Consulting and
Clinical Psychology, 67(5), 734-745.
Rossmann, P. (2005). Depressionstest für Kinder (DTK) - Manual (2 Aufl.). Bern: Huber.
Rush, A. J., Giles, D. E., Schlesser, M. A., Fulton, C. L., Wiessenburger, J. & Burns, C. (1986).
The inventory for depressive symptomatology (IDS): Preliminary findings. Psychiatry
Research, 18, 65-87.
Schlaepfer, T. E., Frick, C., Zobel, A., Maier, W., Heuser, L., Bajbouj, M., . . . Hasdemir, M.
(2008). Vagus nerve stimulation for depression: efficacy and safety in a European
study. Psychological Medicine, 38(5), 651-661. doi: 10.1017/S0033291707001924
Seligman, M. E. (1975). Helplessness: on depression, development, and death. New York: W
H Freeman/Times Books/ Henry Holt & Co.
Shad, M. U., Bidesi, A. P., Chen, L., Ernst, M. & Rao, U. (2011). Neurobiology of decision
making in depressed adolescents: a functional magnetic resonance imaging study.
Journal of the American Academy of Child Psychiatry, 50(6), 612-621.
doi: http://dx.doi.org/10.1016/j.jaac.2011.03.011
Sheline, Y. I., Barch, D. M., Donnelly, J. M., Ollinger, J. M., Snyder, A. Z. & Mintun, M. A.
(2001). Increased amygdala response to masked emotional faces in depressed
References
70
subjects resolves with antidepressant treatment: an fMRI study. Biological
Psychiatry, 50(9), 651-658.
doi: http://dx.doi.org/10.1016/S0006-3223%2801%2901263-X
Sheline, Y. I. (2000). 3D MRI studies of neuroanatomic changes in unipolar major depression:
the role of stress and medical comorbidity. Society of Biological Psychiatry, 48(8),
791-800.
Shochet, I. M., Holland, D. & Whitefield, K. (1997). Resourceful adolescent program:
participant’s manual. Brisbane: Griffith University.
Shyn, S. I., Shi, J., Kraft, J. B., Potash, J. B., Knowles, J. A., Weissman, M. M., . . . Hamilton, S.
P. (2011). Novel loci for major depression identified by genome-wide association
study of Sequenced Treatment Alternatives to Relieve Depression and meta-analysis
of three studies. Molecular Psychiatry, 16(2), 202-215.
doi: http://www.nature.com/mp/journal/v16/n2/suppinfo/mp2009125s1.html
Siegle, G. J., Thompson, W. K., Collier, A., Berman, S. R., Feldmiller, J., Thase, M. E. &
Friedman, E. S. (2012). Toward clinically useful neuroimaging in depression
treatment: prognostic utility of subgenual cingulate activity for determining
depression outcome in cognitive therapy across studies, scanners, and patient
characteristics. Archives of General Psychiatry, 69(9), 913-924.
Siegle, G. J., Carter, C. S. & Thase, M. E. (2006). Use of fMRI to predict recovery from unipolar
depression with cognitive behavior therapy. The American Journal of Psychiatry,
163(4), 735-738.
Simon, G. E. & Savarino, J. (2007). Suicide attempts among patients starting depression
treatment with medications or psychotherapy. The American Journal of Psychiatry,
164, 1029-1034.
Spielmans, G. I., Pasek, L. F. & McFall, J. P. (2007). What are the active ingredients in cognitive
and behavioral psychotherapy for anxious and depressed children? A meta-analytic
review. Clinical Psychological Review, 27(5), 642-654.
Sproeber, N., Straub, J., Fegert, J. M. & Koelch, M. G. (2012). Depression im Jugendalter:
MICHI - Manual für die Gruppentherapie. Weinheim: Beltz.
Stieglitz, R. D. (2008). Diagnostik und Klassifikation in der Psychiatrie. Stuttgart: Kohlhammer.
Stiensmeier-Pelster, J., Schuermann, M. & Duda, K. (2000). Depressionsinventar fuer Kinder
und Jugendliche (Vol. 2. berarbeitete und neu normierte Auflage). Goettingen:
Hogrefe.
Straub, J., Plener, P.L., Sproeber, N., Sprenger, L., Koelch, M.G., Groen, G. & Abler, B. (2015).
Neural correlates of successful psychotherapy of depression in adolescents. Journal
of Affective Disorders, 183, 239-246.
Straub, J., Plener, P.L., Keller, F., Fegert, J.M., Sproeber, N. & Koelch, M.G. (accepted). MICHI
– a brief, manualized cognitive behavioural group therapy for the treatment of
depression in adolescents: randomized controlled trial. Kindheit & Entwicklung.
Straub, J., Keller, F., Sproeber, N., Koelch, M.G. & Plener, P.L. (2015). Suicidal behavior in
German adolescents: prevalence and association with depressive and manic
References
71
symptoms. Zeitschrift für Kinder- und Jugendpsychiatrie und Psychotherapie, 43(1),
39-45.
Straub, J., Plener, P.L., Koelch, M.G. & Keller, F. (2014). Agreement between self-report and
clinician’s assessment in depressed adolescents, using the example of BDI-II and
CDRS-R. Zeitschrift für Kinder- und Jugendpsychiatrie und Psychotherapie, 42(4), 243-
252.
Straub, J., Nicolaus, L., Plener, P.L., Sproeber, N. & Koelch, M.G. (2014). Psychotherapeutic
treatment of children and adolescents with depression. Review of the literature on
cognitive-behavioral and interpersonal group therapies. Der Psychotherapeut, 59, 7-
15.
Straub, J., Sproeber, N., Plener, P.L., Fegert, J.M., Bonenberger, M. & Koelch, M.G. (2014). A
brief cognitive-behavioural group therapy programme for the treatment of
depression in adolescent outpatients: a pilot study. Child and adolescent psychiatry
and mental health, 8(9), doi:10.1186/1753-2000-8-9
Straub, J., Koelch, M.G., Fegert, J.M., Plener, P.L., Gonzalez-Aracil, I., Voit, A. & Sproeber, N.
(2013). Innovations in Practice: MICHI, a brief cognitive-behavioural group therapy
for adolescents with depression - a pilot study of feasibility in an inpatient setting.
Child and Adolescent Mental Health, 18(4), 247-250.
Stulz, N., Lutz, W., Leach, C., Lucock, M. & Barkham, M. (2007). Shapes of early change in
psychotherapy under routine outpatient conditions. Journal of Consulting and
Clinical Psychology, 75(6), 864-874.
Subica, A. M., Fowler, J. C., Elhai, J. D., Frueh, B. C., Sharp, C., Kelly, E. L. & Allen, J. G. (2014).
Factor structure and diagnostic validity of the Beck Depression Inventory-II with adult
clinical inpatients: comparison to a gold-standard diagnostic interview. Psychological
Assessment, 26(4), 1106-1115.
Sullivan, P. F., de Geus, E. J., Willemsen, G., James, M. R., Smit, J. H., Zandbelt, T., . . . Penninx,
B. W. (2009). Genome-wide association for major depressive disorder: a possible role
for the presynaptic protein piccolo. Molecular Psychiatry, 14(4), 359-375.
Tahmasian, M., Knight, D. C., Manoliu, A., Schwerthoeffer, D., Scherr, M., Meng, C., . . . Sorg,
C. (2013). Aberrant intrinsic connectivity of hippocampus and amygdala overlap in
the fronto-insular and dorsomedial-prefrontal cortex in major depressive disorder.
Frontiers in Human Neuroscience, 7(639), 1-10. doi: 10.3389/fnhum.2013.00639
Tang, T. C., Jou, S. H., Ko, C. H., Huang, S. Y. & Yen, C. F. (2009). Randomized study of school-
based intensive interpersonal psychotherapy for depressed adolescents with suicidal
risk and parasuicide behaviors. Psychiatry and clinical neuroscience, 63, 463-470.
Tao, H., Guo, S., Ge, T., Kendrick, K. M., Xue, Z., Liu, Z. & Feng, J. (2013). Depression uncouples
brain hate circuit. Molecular Psychiatry, 18(1), 101-111.
doi: http://dx.doi.org/10.1038/mp.2011.127
Tao, R., Calley, C. S., Hart, J., Mayes, T. L., Nakonezny, P. A., Lu, H., . . . Emslie, G. J. (2012).
Brain activity in adolescent major depressive disorder before and after fluoxetine
treatment. The American Journal of Psychiatry, 169(4), 381-388.
References
72
Treatment for Adolescents With Depression Study Team (2007). The Treatment for
Adolescents with Depression Study (TADS): long-term effectiveness and safety
outcomes. Archives of General Psychiatry, 64(10), 1132-1144.
Van Meter, A. R., Moreira, A. L. R. & Youngstrom, E. A. (2011). Meta-analysis of epidemiologic
studies of pediatric bipolar disorder. Journal of Clinical Psychiatry, 72(9), 1250-1256.
Värnik, A., Kõlves, K., Allik, J., Arensman, E., Aromaa, E., van Audenhove, C., . . . Hegerl, U.
(2009). Gender issues in suicide rates, trends and methods among youths aged 15–
24 in 15 European countries. Journal of Affective Disorders, 113(3), 216-226.
doi: http://dx.doi.org/10.1016/j.jad.2008.06.004
Vos, T., Flaxman, A. D., Naghavi, M., Lozano, R. & Michaud, C. (2012). Years lived with
disability (YLDs) for 1160 sequelae of 289 diseases and injuries 1990-2010: a
systematic analysis for the Global Burden of Disease Study 2010. Lancet, 380(9859),
2163-2196.
Vostanis, P., Feehan, C., Grattan, E. & Bickerton, W. (1996). Treatment for children and
adolescents with depression: lessons from a controlled trial. Clinical Child Psychology
and Psychiatry, 1(2), 199-212.
Vostanis, P. & Harrington, R. (1994). Cognitive-behavioural treatment of depressive
disorders in child psychiatric patients: rationale and description of a treatment
package. European Child and Adolescent Psychiatry, 3, 111-1213.
Watanabe, N., Hunot, V., Omori, I., Churchill, R. & Furukawa, T. (2007). Psychotherapy for
depression among children and adolescents: a systematic review. Acta Psychiatrica
Scandinavica, 116(2), 84-95.
Weisz, J. R., Southam-Gerow, M. A., Gordis, E. B., Connor-Smith, J. K., Chu, B. C., Langer, D.
A., . . . Weiss, B. (2009). Cognitive–behavioral therapy versus usual clinical care for
youth depression: an initial test of transportability to community clinics and
clinicians. Journal of Consulting and Clinical Psychology, 77(3), 383-396.
doi: 10.1037/a0013877
Weisz, J. R., McCarty, C. & Valeri, S. (2006). Effects of psychotherapy in children and
adolescents: a meta-analysis. Psychological Bulletin, 132(1), 132-149.
Weisz, J. R., Thurber, C. A., Sweeney, L., Proffitt, V. D. & LeGagnoux, G. L. (1997). Brief
treatment of mild-to-moderate child depression using primary and secondary control
enhancement training. Journal of Consulting and Clinical Psychology, 65(4), 703-707.
Whiteford, H., Harris, M., McKeon, G., Baxter, A., Pennell, C., Barendregt, J. & Wang, J.
(2013). Estimating remission from untreated major depression: a systematic review
and meta-analysis. Psychological Medicine, 43(8), 1569-1585.
Whittle, S., Lichter, R., Dennison, M., Vijayakumar, N., Schwartz, O., Byrne, M. L., . . . Allen,
N. B. (2014). Structural brain development and depression onset during adolescence:
a prospective longitudinal study. The American Journal of Psychiatry, 171(5), 564-
571.
Widom, C. S., DuMont, K. & Czaja, S. J. (2007). A prospective investigation of major
depressive disorder and comorbidity in abused and neglected children grown up.
Archives of General Psychiatry, 64(1), 49-56. doi: 10.1001/archpsyc.64.1.49
References
73
Wilkinson, P., Kelvin, R., Roberts, C., Dubicka, B. & Goodyer, I. (2011). Clinical and
psychosocial predictors of suicide attempts and nonsuicidal self-injury in the
adolescent depression antidepressants and psychotherapy trial (ADAPT). American
Journal of Psychiatry, 168(5), 495-501.
Williams, J. B. (1988). A structured interview guide for the Hamilton Depression Scale.
Archives of General Psychiatry, 45, 742-747.
Wittchen, H. U. & Jacobi, F. (2005). Size and burden of mental disorders in Europe-a critical
review and appraisal of 27 studies. European Neuropsychopharmacology, 15, 357-
376.
Wood, A., Harrington, R. & Moore, A. (1996). Controlled trial of a brief cognitive-behavioural
intervention in adolescent patients with depressive disorders. Journal of Child
Psychology and Psychiatry, 37(6), 737-746. doi: 10.1111/j.1469-7610.1996.tb01466.x
Yang, T. T., Simmons, A. N., Matthews, S. C., Tapert, S. F., Frank, G. K., Max, J. E., . . . Paulus,
M. P. (2010). Adolescents with major depression demonstrate increased amygdala
activation. Journal of the American Academy of Child Psychiatry, 49(1), 42-51.
doi: http://dx.doi.org/10.1097/00004583-201001000-00008
Yang, T. T., Simmons, A. N., Matthews, S. C., Tapert, S. F., Frank, G. K., Bischoff-Grethe, A., . .
. Paulus, M. P. (2009). Depressed adolescents demonstrate greater subgenual
anterior cingulate activity. Neuroreport, 20(4), 440-444.
doi: http://dx.doi.org/10.1097/WNR.0b013e3283262e10
Yoshimura, S., Okamoto, Y., Onoda, K., Matsunaga, M., Okada, G., Kunisato, Y., . . . Yamawaki,
S. (2014). Cognitive behavioral therapy for depression changes medial prefrontal and
ventral anterior cingulate cortex activity associated with self-referential processing.
Social Cognitive and Affective Neuroscience, 9, 487-493. doi: 10.1093/scan/nst009
Yoshimura, S., Okamoto, Y., Onoda, K., Matsunaga, M., Okada, G., Kunisato, Y., . . . Yamawaki,
S. (2013). Cognitive behavioral therapy for depression changes medial prefrontal and
ventral anterior cingulate cortex activity associated with self-referential processing.
Social Cognitive and Affective Neuroscience. doi: 10.1093/scan/nst009
Yoshimura, S., Ueda, K., Suzuki, S., Onoda, K., Okamoto, Y. & Yamawaki, S. (2009). Self-
referential processing of negative stimuli within the ventral anterior cingulate gyrus
and right amygdala. Brain and cognition, 69(1), 218-225.
Zito, J. M., Safer, D. J., dosReis, S., Gardner, J. F., Magder, L., Soeken, K., . . . Riddle, M. A.
(2003). Psychotropic practice patterns for youth: a 10-year perspective. Archives of
Pediatric Adolescent Medicine, 157, 17-25.
Original research articles
74
6 Original research articles
6.1 Treatment of mental diseases in children in German hospitals: analysis of frequencies
in the years 2003 to 2012.
Main authors‘ contributions to the article:
P.L. Plener and F. Keller managed data acquisition, executed statistical analyses, and
interpreted statistical outcomes. P.L. Plener wrote the manuscript, integrated remarks of the
co-authors, and revised the manuscript according to reviewer’s comments.
Contribution of J. Straub to the article:
J. Straub researched literature and wrote parts of the manuscript. She and her co-author
helped with revising the manuscript according to the reviewer’s comments.
Reference
Plener, P.L., Straub, J., Fegert, J.M. & Keller, F. (2015). Treatment of mental diseases in
children in German hospitals: analysis of frequencies in the years 2003 to 2012.
Nervenheilkunde, 34, 18-23.
Reprinted from Nervenheilkunde, 34, Plener, P.L., Straub, J., Fegert, J.M. & Keller, F.
Treatment of mental diseases in children in German hospitals: analysis of frequencies in the
years 2003 to 2012, 18-23, Copyright (2015), with permission from Schattauer.

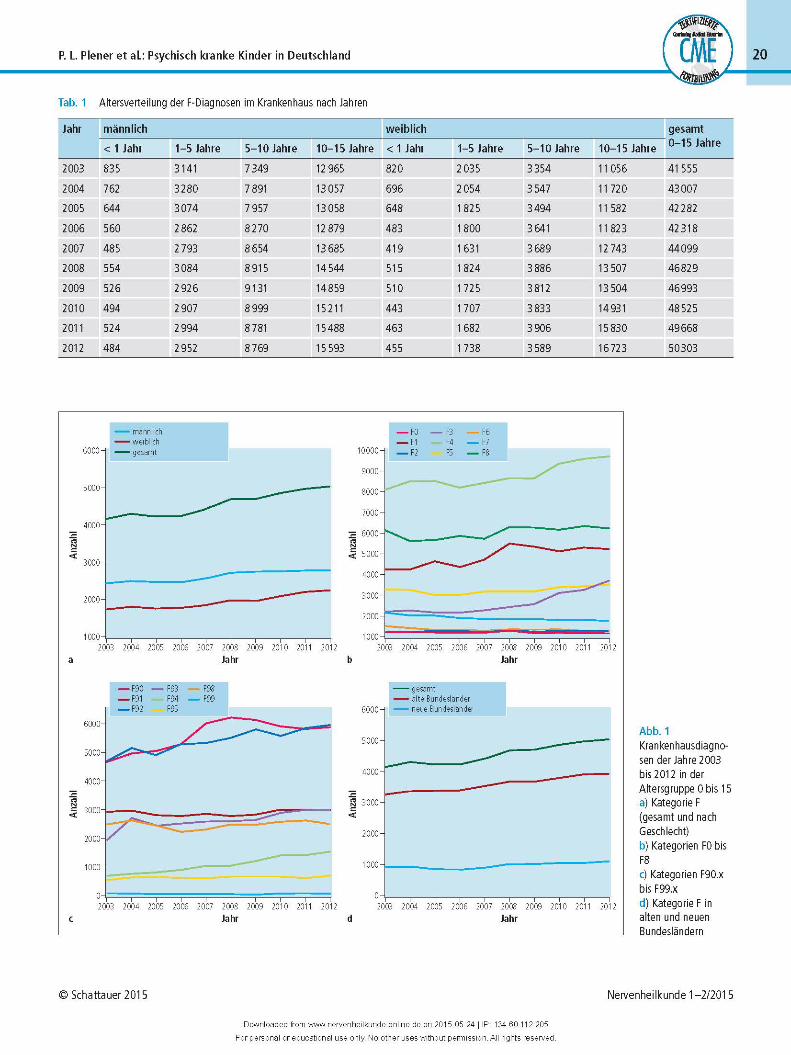
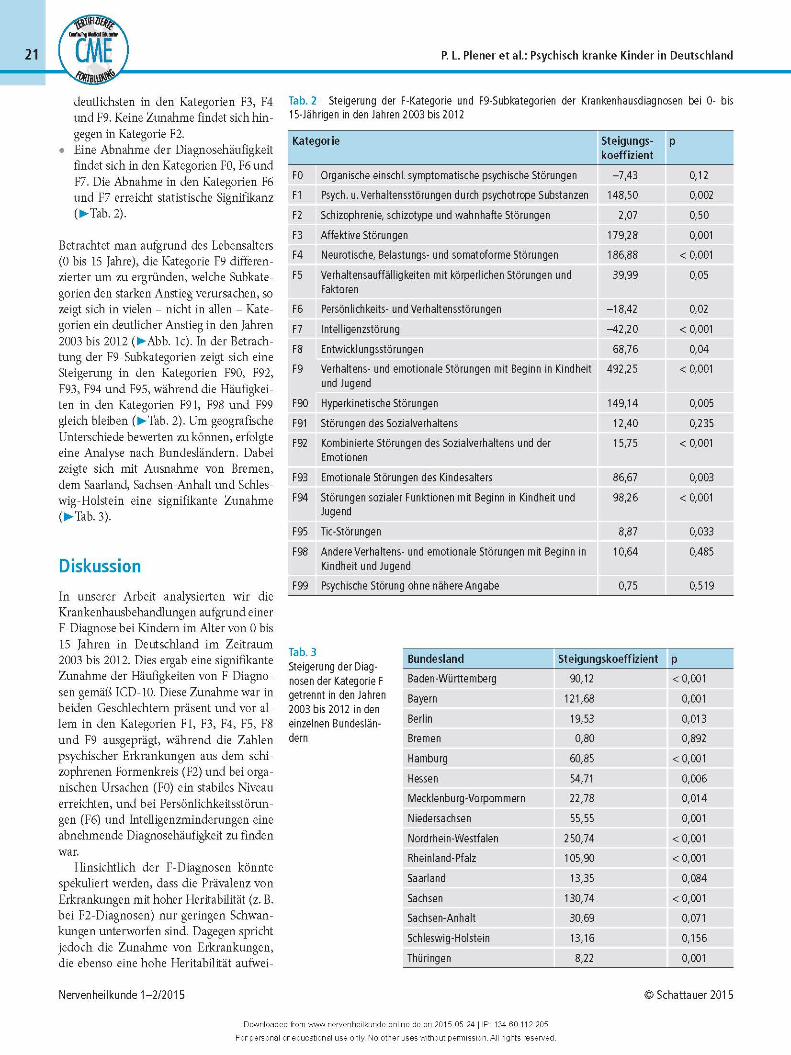


Suicidal behavior in German adolescents: prevalence and association with depressive and
manic symptoms
81
6.2 Suicidal behavior in German adolescents: prevalence and association with depressive
and manic symptoms
J. Straub‘s contribution to the article:
J. Straub generated the data matrix, did data input, executed statistical analyses, and
interpreted statistical outcomes. She researched literature, wrote the manuscript,
integrated remarks of the co-authors, revised the manuscript according to reviewer’s
comments, and created figures and tables.
Co-authors’ contributions to the article:
F. Keller assisted in statistical analyses. P.L. Plener conceptualised the study, coordinated its
procedure, and did data acquisition. All co-authors reviewed the draft and gave constructive
remarks.
Reference
Straub, J., Keller, F., Sproeber, N., Koelch, M.G. & Plener, P.L. (2015). Suicidal behavior in
German adolescents: prevalence and association with depressive and manic symptoms.
Zeitschrift für Kinder- und Jugendpsychiatrie und Psychotherapie, 43(1), 39-45.
Reprinted from Zeitschrift für Kinder- und Jugendpsychiatrie und Psychotherapie, 43 (1),
Straub, J., Keller, F., Sproeber, N., Koelch, M.G. & Plener, P.L., Suicidal behavior in German
adolescents: prevalence and association with depressive and manic symptoms, 39-45,
Copyright (2015), with permission from Huber.
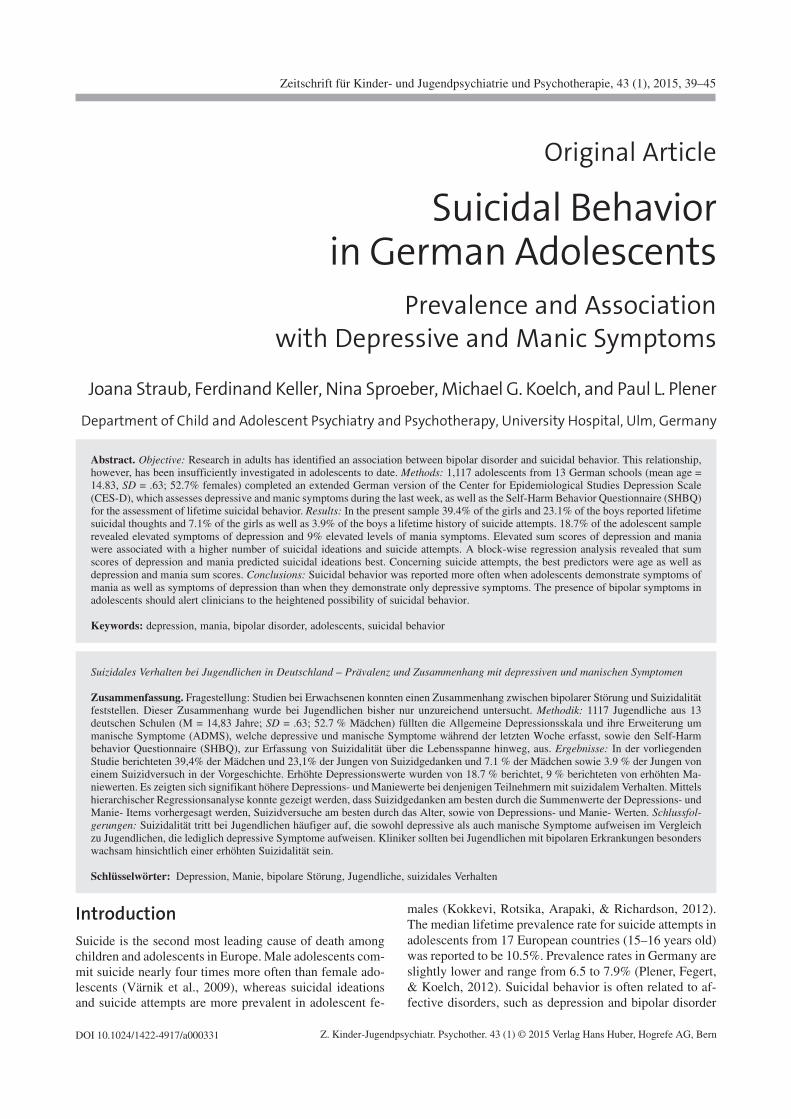
J. Straub et al.: Suicidal Behavior in German AdolescentsZ. Kinder-Jugendpsychiatr. Psychother. 43 (1) © 2015 Verlag Hans Huber, Hogrefe AG, Bern
Original Article
Suicidal Behaviorin German Adolescents
Prevalence and Associationwith Depressive and Manic Symptoms
Joana Straub, Ferdinand Keller, Nina Sproeber, Michael G. Koelch, and Paul L. Plener
Department of Child and Adolescent Psychiatry and Psychotherapy, University Hospital, Ulm, Germany
Zeitschrift für Kinder- und Jugendpsychiatrie und Psychotherapie, 43 (1), 2015, 39–45
DOI 10.1024/1422-4917/a000331
Abstract. Objective: Research in adults has identified an association between bipolar disorder and suicidal behavior. This relationship,however, has been insufficiently investigated in adolescents to date. Methods: 1,117 adolescents from 13 German schools (mean age =14.83, SD = .63; 52.7% females) completed an extended German version of the Center for Epidemiological Studies Depression Scale(CES-D), which assesses depressive and manic symptoms during the last week, as well as the Self-Harm Behavior Questionnaire (SHBQ)for the assessment of lifetime suicidal behavior. Results: In the present sample 39.4% of the girls and 23.1% of the boys reported lifetimesuicidal thoughts and 7.1% of the girls as well as 3.9% of the boys a lifetime history of suicide attempts. 18.7% of the adolescent samplerevealed elevated symptoms of depression and 9% elevated levels of mania symptoms. Elevated sum scores of depression and maniawere associated with a higher number of suicidal ideations and suicide attempts. A block-wise regression analysis revealed that sumscores of depression and mania predicted suicidal ideations best. Concerning suicide attempts, the best predictors were age as well asdepression and mania sum scores. Conclusions: Suicidal behavior was reported more often when adolescents demonstrate symptoms ofmania as well as symptoms of depression than when they demonstrate only depressive symptoms. The presence of bipolar symptoms inadolescents should alert clinicians to the heightened possibility of suicidal behavior.
Keywords: depression, mania, bipolar disorder, adolescents, suicidal behavior
Suizidales Verhalten bei Jugendlichen in Deutschland – Prävalenz und Zusammenhang mit depressiven und manischen Symptomen
Zusammenfassung. Fragestellung: Studien bei Erwachsenen konnten einen Zusammenhang zwischen bipolarer Störung und Suizidalitätfeststellen. Dieser Zusammenhang wurde bei Jugendlichen bisher nur unzureichend untersucht. Methodik: 1117 Jugendliche aus 13deutschen Schulen (M = 14,83 Jahre; SD = .63; 52.7 % Mädchen) füllten die Allgemeine Depressionsskala und ihre Erweiterung ummanische Symptome (ADMS), welche depressive und manische Symptome während der letzten Woche erfasst, sowie den Self-Harmbehavior Questionnaire (SHBQ), zur Erfassung von Suizidalität über die Lebensspanne hinweg, aus. Ergebnisse: In der vorliegendenStudie berichteten 39,4% der Mädchen und 23,1% der Jungen von Suizidgedanken und 7.1 % der Mädchen sowie 3.9 % der Jungen voneinem Suizidversuch in der Vorgeschichte. Erhöhte Depressionswerte wurden von 18.7 % berichtet, 9 % berichteten von erhöhten Ma-niewerten. Es zeigten sich signifikant höhere Depressions- und Maniewerte bei denjenigen Teilnehmern mit suizidalem Verhalten. Mittelshierarchischer Regressionsanalyse konnte gezeigt werden, dass Suizidgedanken am besten durch die Summenwerte der Depressions- undManie- Items vorhergesagt werden, Suizidversuche am besten durch das Alter, sowie von Depressions- und Manie- Werten. Schlussfol-gerungen: Suizidalität tritt bei Jugendlichen häufiger auf, die sowohl depressive als auch manische Symptome aufweisen im Vergleichzu Jugendlichen, die lediglich depressive Symptome aufweisen. Kliniker sollten bei Jugendlichen mit bipolaren Erkrankungen besonderswachsam hinsichtlich einer erhöhten Suizidalität sein.
Schlüsselwörter: Depression, Manie, bipolare Störung, Jugendliche, suizidales Verhalten
IntroductionSuicide is the second most leading cause of death amongchildren and adolescents in Europe. Male adolescents com-mit suicide nearly four times more often than female ado-lescents (Värnik et al., 2009), whereas suicidal ideationsand suicide attempts are more prevalent in adolescent fe-
males (Kokkevi, Rotsika, Arapaki, & Richardson, 2012).The median lifetime prevalence rate for suicide attempts inadolescents from 17 European countries (15–16 years old)was reported to be 10.5%. Prevalence rates in Germany areslightly lower and range from 6.5 to 7.9% (Plener, Fegert,& Koelch, 2012). Suicidal behavior is often related to af-fective disorders, such as depression and bipolar disorder
Z. Kinder-Jugendpsychiatr. Psychother. 43 (1) © 2015 Verlag Hans Huber, Hogrefe AG, Bern

(Allison, Roeger, Martin, & Keeves, 2001; Brent et al.,1993). Bipolar disorder emerges in prepubescent childrenand adolescents, demonstrating a lifetime prevalence of2.1% among 15–18-year-olds (Kozloff et al., 2010). Earlyonset of bipolar disorder coincides with a negative long-term prognosis for comorbid diagnoses and an elevated riskfor suicide (Azorin et al., 2010; Van Meter, Moreira, &Youngstrom, 2011). In a large study with adolescents fromthe United States, Nock et al. (2013) demonstrated that56.8% of adolescent suicide ideators suffered from majordepressive disorder (MDD) or dysthymia and 9.1% frombipolar disorders. Furthermore, 75.7% of suicide attempt-ers suffered from MDD or dysthymia and 13.2% of bipolardisorder. Lifetime prevalence rate for at least one suicideattempt of adolescents suffering from bipolar disorders ofother studies, range from 32% (Goldstein et al., 2005) to44% (Lewinsohn, Seeley, & Klein, 2003), and retrospec-tive analysis of adolescent suicide completers revealed that46.3% fulfilled criteria for lifetime diagnoses of MDD and17.9% for bipolar spectrum disorder (Brent et al., 1993).
Evidence providing population-based numbers for theGerman population is scarce, so that there is still a need forcomparable studies from Germany. The present studyaimed to explore (1) the prevalence rate of suicidal behav-ior, (2) depressive and manic symptoms in a German ado-lescent school sample, and (3) the relationship between de-pressive/manic symptoms and suicidal behavior. We werealso interested to discover (4) whether depressive/manicsymptoms predict suicidal behavior and (5) whether certaingroups of symptoms of the mania scale predict suicidal be-havior better than others.
Methods
Participants
Adolescents from the ninth grades (N = 1.117) of 13schools in southern Germany participated in an anonymousassessment. The adolescents were between the age of 14and 17 (M = 14.83; SD = .63); 52.7% were female and47.3% male. With regard to three different types of second-ary schools that are available in Germany, 469 (42%) wereattending a Gymnasium, 492 (44%) a Realschule, and 156(14%) a Hauptschule. Written informed consents, both bythe students and their caregivers, were obtained before datacollection, and approval was given by the regional council,the local education authority, and the principals of theschools. The study was approved by the IRB of the Uni-versity of Ulm. Due to regulations of the school authorities,no data could be obtained from nonparticipating students.
Diagnostic Instruments
The Centre for Epidemiological Studies Depression Scale(CES-D) (Radloff, 1977) is a frequently used instrument
for the assessment of depressive symptoms in the generalpopulation. It has been translated into the German versionAllgemeine Depressionsskala (ADS; Hautzinger, Bailer,Hofmeister & Keller, 2012; Hautzinger & Bailer, 1993),which consists of 20 items assessing depressive symptomsduring the previous week (item values range from 0–3),with an internal consistency of .85 (Meyer & Hautzinger,2001). A score above 22 indicates an elevated risk of de-pression (Hautzinger et al., 2012) and Cronbach’s α of thepresent sample was .87.
The ADS has been extended using nine questions (for itemcontent of the mania subscale see Table 1; item valuesrange from 0–3) to cover DSM-IV criteria for a hypoma-nia/mania episode (internal consistency of .64) by Meyerand Hautzinger (2001). Examples for items are “During thelast week I was unusually happy, aroused or hyped up” and“During the last week I was extremely active and busy withlots of things.” In our study Cronbach’s α was .65 for themania subscale. No cutoff has been established for the ma-nia subscale so far, but mean scores equal and above 12 (85percentile) (Meyer & Hautzinger, 2001) can be interpretedas elevated values or sub threshold values.
Suicidal behavior was assessed by means of the Self-Harm Behavior Questionnaire (SHBQ) (Gutierrez, Osman,Barrios & Kopper, 2001), which is a 34-item questionnaireassessing lifetime self-harm behavior, suicidal ideations,and attempts. The German version demonstrated a high in-ternal consistency (Cronbach’s α = .87–.96), good interrat-er reliability (r = .87) and satisfying test–retest reliability(3 days: r = .65). Furthermore concordance with a differentself-report questionnaire that assesses self-harm as well,was good (K = .63, ICC = .79) providing evidence for con-vergent validity. Correlations between clinician rating andSHBQ however was low (K = .22, ICC = .34) (Fliege et
Table 1Correlation of mania items of the modified ADS and sui-cidal ideations and suicide attempts of the SHBQ
Items Suicidalideations
Suicideattempts
21 Elevated mood (EMIS) .07* .06
22 Thoughts are racing (IDCA) .23*** .17***
23 Irritability (IDCA) .31*** .18***
24 Increase in goal-directed activity (EMIS) –.06 –.02
25 Distractibility (IDCA) .29*** .12***
26 Decreased need for sleep .03 .07*
27 More talkative than normal .13*** .05
28 Inflated self-esteem or grandiosity (EMIS) .08* .06
29 Psychomotor agitation .21*** .09**
IDCA .37*** .21***
EMIS .03 .04
Note. *p < .05, **p < .01, ***p < .001. Factor attributions in paren-theses: IDCA = irritability and disturbed cognitive abilities; EMIS =elevated mood and inflated self-esteem.
40 J. Straub et al.: Suicidal Behavior in German Adolescents
Z. Kinder-Jugendpsychiatr. Psychother. 43 (1) © 2015 Verlag Hans Huber, Hogrefe AG, Bern

al., 2006). Muehlenkamp, Cowles, and Gutierrez (2010)demonstrated that the four-factor structure of the SHBQ isrobust, and convergent validity was moderate. The ques-tions used for the assessment of suicidal behavior were,“Have you ever attempted suicide?” and “Have you everthought about committing suicide?”
Factors of the Mania Subscale
To determine factors of the mania subscale the scree-testand parallel analysis criteria were applied, and calculationswere done using O’Connor (2000)’s program. This wasdone to better understand which groups of items are espe-cially suitable to predict suicidal behavior.
A factor analysis of the mania subscale revealed eigen-values of 2.45 and 1.30; all other values were < 1. Accord-ing to the parallel-analysis criterion, the random value ofthe second eigenvalue was 1.13 (95%), which was exceed-ed by the second eigenvalue. Thus, it was assumed that themania subscale compasses two factors: The first factor in-cludes items 22, 23, and 25 and can be summarized as “ir-ritability and disturbed cognitive abilities” (IDCA); thesecond factor includes items 21, 24, and 28 (see Table 1 foritems) and can be best described as “elevated mood andinflated self-esteem” (EMIS). The remaining three itemshad similar loadings on both factors and could not be at-tributed clearly.
Statistical Methods
Differences between scores of depression and mania itemsin students reporting suicidal ideations or suicide attemptsand in those who didn’t as well as age effects on depressionand manic symptoms were calculated by means of t-tests,and associations were calculated by means of the Pearsoncorrelation coefficient. Differences between age groupsconcerning suicidal behavior were calculated by means ofχ² test. Furthermore, we ran a logistic regression withblock-wise entry method. In a first block we entered thecovariates age and sex. In a second block we entered the
depression sum score. In a third block we either entered themania sum score or both mania factors EMIS and IDCAinstead. Statistical analyses were performed using PASWstatistics 18 and SAS 9.3 software.
Results
Prevalence of Suicidal Behavior
Suicidal ideations in the past were reported by 31.8% of theadolescents. Split according to sex, 39.4% of the girls and23.1% of boys reported previous suicidal thoughts. Further-more, a total of 5.6% (7.1% of the girls and 3.9% of the boys)reported having attempted suicide in the past. 1.7% reportedsuicide attempts within the last year, which constituted 34.5%of all attempts. Of those who reported suicide attempts in thepast, 73.3% also reported having had prior suicidal ideations.Of those who reported suicidal ideations, 13.3% reported sui-cide attempts as well, whereas only 2.3% reported suicideattempts without having had any previous suicidal ideations.The number of suicide attempts (χ² (2) = 16.12, p = .001)increased by age especially between the age of 15 and 16 (seeTable 2), and suicidal ideations rose as well by age albeit notsignificantly (χ² (2) = 4.77, p = .09).
Mania and Depression Scores
The prevalence rate for elevated symptoms of depressionamounted to 18.7% (27% of the girls and 9.5% of boys) inthe present sample and the mean value of the depressionsubscale was 15.02 (SD = 9.54). The latter was significant-ly higher in girls (M = 17.86, SD = 9.92) than in boys (M= 11.82, SD = 7.96; t(1070) = 11.10, p < .001). Betweenthe age of 14 (M = 14.08, SD = 9.16) and 15 (M = 15.05,SD = 9.48) depression scores were comparable (t(968) =–1.52, p = .13). In comparisons of adolescents of 14 and16 years (M = 17.26, SD = 10.55) of age (t(410) = –2.90,p = .004) as well as 15 and 16 years of age, depressionscores differed significantly (t(752) = –2.12, p = .04).
Table 2Prevalence rates for elevated depression and mania symptoms as well as suicidal ideations and attempts for boys andgirls between 14 and 16 years of age
Age of 14 (N = 321) Age of 15 (N = 679) Age of 16 (N = 102)
Prevalencerate
Prevalencerate girls
Prevalencerate boys
Prevalencerate
Prevalencerate girls
Prevalencerate boys
Prevalencerate
Prevalencerate girls
Prevalencerate boys
Depression 18.1% 27.3% 7.4% 18% 25.1% 10.2% 25.5% 38.2% 10.6%
Mania 7.5% 8.7% 6.0% 9.1% 8.8% 9.5% 14.7% 12.7% 17.0%
Suicidal ideations 27.6% 34.3% 19.7% 33.0% 40.1% 24.9% 38.5% 51%
Suicide attempts 3.8% 5.3% 2.0% 5.0% 6.1% 3.8% 14.0% 17% 10.6%
Note. N = number of participants; prevalence rates split per sex were calculated in relation to their particular sex e.g., 27.3% of 14-year-old girlsin relation to all 14-year-old girls had elevated depression scores. Scores above 22 in the ADS indicate an elevated risk for depression. Scoresabove 12 in the extended version of the ADS indicate elevated hypomania/mania symptoms.
J. Straub et al.: Suicidal Behavior in German Adolescents 41
Z. Kinder-Jugendpsychiatr. Psychother. 43 (1) © 2015 Verlag Hans Huber, Hogrefe AG, Bern
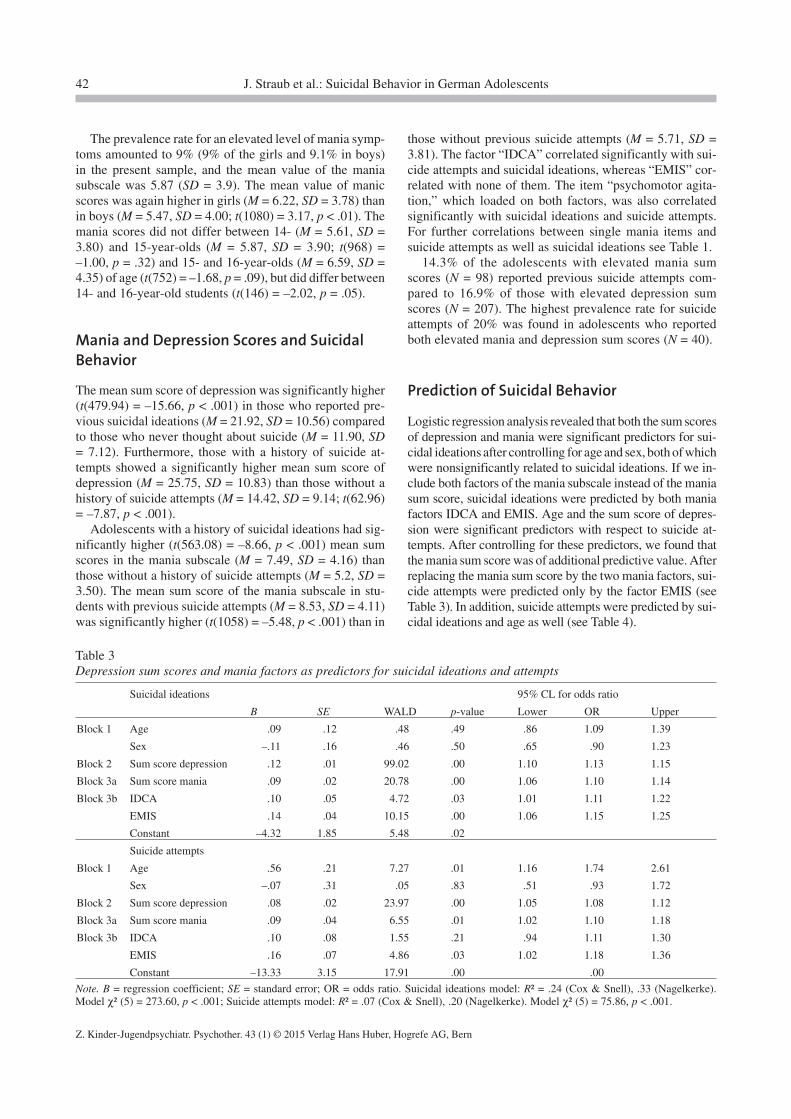
The prevalence rate for an elevated level of mania symp-toms amounted to 9% (9% of the girls and 9.1% in boys)in the present sample, and the mean value of the maniasubscale was 5.87 (SD = 3.9). The mean value of manicscores was again higher in girls (M = 6.22, SD = 3.78) thanin boys (M = 5.47, SD = 4.00; t(1080) = 3.17, p < .01). Themania scores did not differ between 14- (M = 5.61, SD =3.80) and 15-year-olds (M = 5.87, SD = 3.90; t(968) =–1.00, p = .32) and 15- and 16-year-olds (M = 6.59, SD =4.35) of age (t(752) = –1.68, p = .09), but did differ between14- and 16-year-old students (t(146) = –2.02, p = .05).
Mania and Depression Scores and SuicidalBehavior
The mean sum score of depression was significantly higher(t(479.94) = –15.66, p < .001) in those who reported pre-vious suicidal ideations (M = 21.92, SD = 10.56) comparedto those who never thought about suicide (M = 11.90, SD= 7.12). Furthermore, those with a history of suicide at-tempts showed a significantly higher mean sum score ofdepression (M = 25.75, SD = 10.83) than those without ahistory of suicide attempts (M = 14.42, SD = 9.14; t(62.96)= –7.87, p < .001).
Adolescents with a history of suicidal ideations had sig-nificantly higher (t(563.08) = –8.66, p < .001) mean sumscores in the mania subscale (M = 7.49, SD = 4.16) thanthose without a history of suicide attempts (M = 5.2, SD =3.50). The mean sum score of the mania subscale in stu-dents with previous suicide attempts (M = 8.53, SD = 4.11)was significantly higher (t(1058) = –5.48, p < .001) than in
those without previous suicide attempts (M = 5.71, SD =3.81). The factor “IDCA” correlated significantly with sui-cide attempts and suicidal ideations, whereas “EMIS” cor-related with none of them. The item “psychomotor agita-tion,” which loaded on both factors, was also correlatedsignificantly with suicidal ideations and suicide attempts.For further correlations between single mania items andsuicide attempts as well as suicidal ideations see Table 1.
14.3% of the adolescents with elevated mania sumscores (N = 98) reported previous suicide attempts com-pared to 16.9% of those with elevated depression sumscores (N = 207). The highest prevalence rate for suicideattempts of 20% was found in adolescents who reportedboth elevated mania and depression sum scores (N = 40).
Prediction of Suicidal Behavior
Logistic regression analysis revealed that both the sum scoresof depression and mania were significant predictors for sui-cidal ideations after controlling for age and sex, both of whichwere nonsignificantly related to suicidal ideations. If we in-clude both factors of the mania subscale instead of the maniasum score, suicidal ideations were predicted by both maniafactors IDCA and EMIS. Age and the sum score of depres-sion were significant predictors with respect to suicide at-tempts. After controlling for these predictors, we found thatthe mania sum score was of additional predictive value. Afterreplacing the mania sum score by the two mania factors, sui-cide attempts were predicted only by the factor EMIS (seeTable 3). In addition, suicide attempts were predicted by sui-cidal ideations and age as well (see Table 4).
Table 3Depression sum scores and mania factors as predictors for suicidal ideations and attempts
Suicidal ideations 95% CL for odds ratio
B SE WALD p-value Lower OR Upper
Block 1 Age .09 .12 .48 .49 .86 1.09 1.39
Sex –.11 .16 .46 .50 .65 .90 1.23
Block 2 Sum score depression .12 .01 99.02 .00 1.10 1.13 1.15
Block 3a Sum score mania .09 .02 20.78 .00 1.06 1.10 1.14
Block 3b IDCA .10 .05 4.72 .03 1.01 1.11 1.22
EMIS .14 .04 10.15 .00 1.06 1.15 1.25
Constant –4.32 1.85 5.48 .02
Suicide attempts
Block 1 Age .56 .21 7.27 .01 1.16 1.74 2.61
Sex –.07 .31 .05 .83 .51 .93 1.72
Block 2 Sum score depression .08 .02 23.97 .00 1.05 1.08 1.12
Block 3a Sum score mania .09 .04 6.55 .01 1.02 1.10 1.18
Block 3b IDCA .10 .08 1.55 .21 .94 1.11 1.30
EMIS .16 .07 4.86 .03 1.02 1.18 1.36
Constant –13.33 3.15 17.91 .00 .00
Note. B = regression coefficient; SE = standard error; OR = odds ratio. Suicidal ideations model: R² = .24 (Cox & Snell), .33 (Nagelkerke).Model χ² (5) = 273.60, p < .001; Suicide attempts model: R² = .07 (Cox & Snell), .20 (Nagelkerke). Model χ² (5) = 75.86, p < .001.
42 J. Straub et al.: Suicidal Behavior in German Adolescents
Z. Kinder-Jugendpsychiatr. Psychother. 43 (1) © 2015 Verlag Hans Huber, Hogrefe AG, Bern
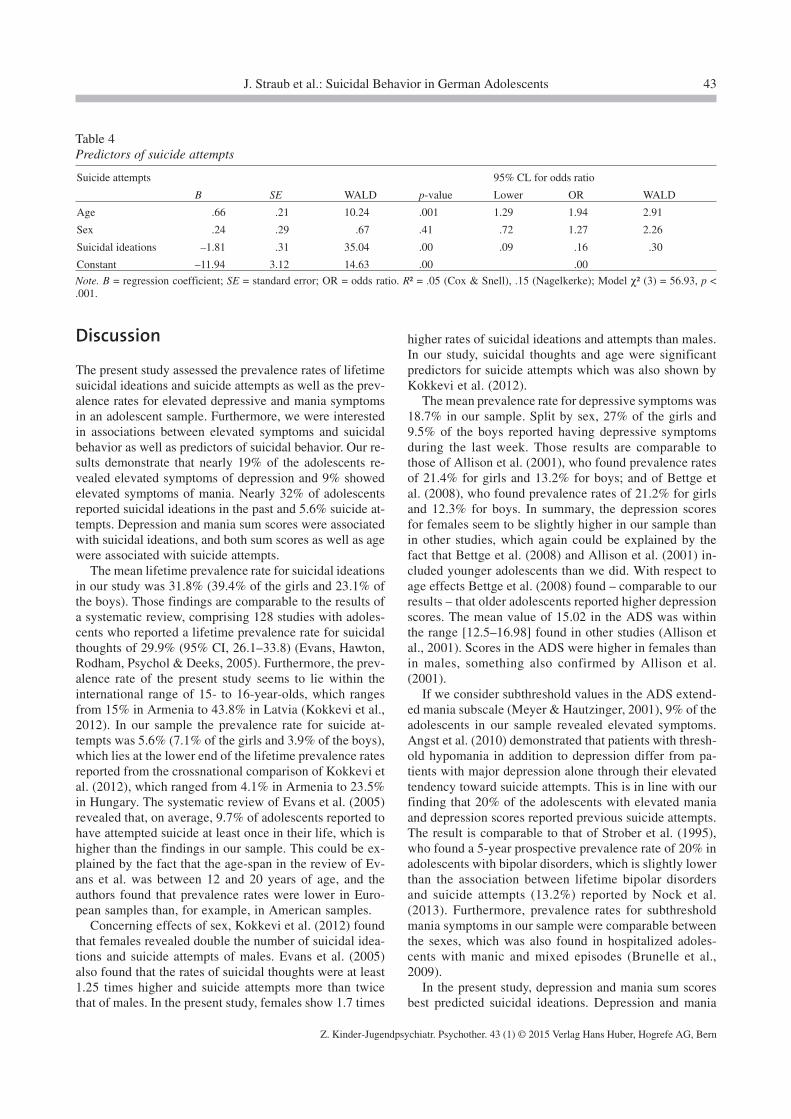
Discussion
The present study assessed the prevalence rates of lifetimesuicidal ideations and suicide attempts as well as the prev-alence rates for elevated depressive and mania symptomsin an adolescent sample. Furthermore, we were interestedin associations between elevated symptoms and suicidalbehavior as well as predictors of suicidal behavior. Our re-sults demonstrate that nearly 19% of the adolescents re-vealed elevated symptoms of depression and 9% showedelevated symptoms of mania. Nearly 32% of adolescentsreported suicidal ideations in the past and 5.6% suicide at-tempts. Depression and mania sum scores were associatedwith suicidal ideations, and both sum scores as well as agewere associated with suicide attempts.
The mean lifetime prevalence rate for suicidal ideationsin our study was 31.8% (39.4% of the girls and 23.1% ofthe boys). Those findings are comparable to the results ofa systematic review, comprising 128 studies with adoles-cents who reported a lifetime prevalence rate for suicidalthoughts of 29.9% (95% CI, 26.1–33.8) (Evans, Hawton,Rodham, Psychol & Deeks, 2005). Furthermore, the prev-alence rate of the present study seems to lie within theinternational range of 15- to 16-year-olds, which rangesfrom 15% in Armenia to 43.8% in Latvia (Kokkevi et al.,2012). In our sample the prevalence rate for suicide at-tempts was 5.6% (7.1% of the girls and 3.9% of the boys),which lies at the lower end of the lifetime prevalence ratesreported from the crossnational comparison of Kokkevi etal. (2012), which ranged from 4.1% in Armenia to 23.5%in Hungary. The systematic review of Evans et al. (2005)revealed that, on average, 9.7% of adolescents reported tohave attempted suicide at least once in their life, which ishigher than the findings in our sample. This could be ex-plained by the fact that the age-span in the review of Ev-ans et al. was between 12 and 20 years of age, and theauthors found that prevalence rates were lower in Euro-pean samples than, for example, in American samples.
Concerning effects of sex, Kokkevi et al. (2012) foundthat females revealed double the number of suicidal idea-tions and suicide attempts of males. Evans et al. (2005)also found that the rates of suicidal thoughts were at least1.25 times higher and suicide attempts more than twicethat of males. In the present study, females show 1.7 times
higher rates of suicidal ideations and attempts than males.In our study, suicidal thoughts and age were significantpredictors for suicide attempts which was also shown byKokkevi et al. (2012).
The mean prevalence rate for depressive symptoms was18.7% in our sample. Split by sex, 27% of the girls and9.5% of the boys reported having depressive symptomsduring the last week. Those results are comparable tothose of Allison et al. (2001), who found prevalence ratesof 21.4% for girls and 13.2% for boys; and of Bettge etal. (2008), who found prevalence rates of 21.2% for girlsand 12.3% for boys. In summary, the depression scoresfor females seem to be slightly higher in our sample thanin other studies, which again could be explained by thefact that Bettge et al. (2008) and Allison et al. (2001) in-cluded younger adolescents than we did. With respect toage effects Bettge et al. (2008) found – comparable to ourresults – that older adolescents reported higher depressionscores. The mean value of 15.02 in the ADS was withinthe range [12.5–16.98] found in other studies (Allison etal., 2001). Scores in the ADS were higher in females thanin males, something also confirmed by Allison et al.(2001).
If we consider subthreshold values in the ADS extend-ed mania subscale (Meyer & Hautzinger, 2001), 9% of theadolescents in our sample revealed elevated symptoms.Angst et al. (2010) demonstrated that patients with thresh-old hypomania in addition to depression differ from pa-tients with major depression alone through their elevatedtendency toward suicide attempts. This is in line with ourfinding that 20% of the adolescents with elevated maniaand depression scores reported previous suicide attempts.The result is comparable to that of Strober et al. (1995),who found a 5-year prospective prevalence rate of 20% inadolescents with bipolar disorders, which is slightly lowerthan the association between lifetime bipolar disordersand suicide attempts (13.2%) reported by Nock et al.(2013). Furthermore, prevalence rates for subthresholdmania symptoms in our sample were comparable betweenthe sexes, which was also found in hospitalized adoles-cents with manic and mixed episodes (Brunelle et al.,2009).
In the present study, depression and mania sum scoresbest predicted suicidal ideations. Depression and mania
Table 4Predictors of suicide attempts
Suicide attempts 95% CL for odds ratio
B SE WALD p-value Lower OR WALD
Age .66 .21 10.24 .001 1.29 1.94 2.91
Sex .24 .29 .67 .41 .72 1.27 2.26
Suicidal ideations –1.81 .31 35.04 .00 .09 .16 .30
Constant –11.94 3.12 14.63 .00 .00
Note. B = regression coefficient; SE = standard error; OR = odds ratio. R² = .05 (Cox & Snell), .15 (Nagelkerke); Model χ² (3) = 56.93, p <.001.
J. Straub et al.: Suicidal Behavior in German Adolescents 43
Z. Kinder-Jugendpsychiatr. Psychother. 43 (1) © 2015 Verlag Hans Huber, Hogrefe AG, Bern

sum scores as well as age predicted suicide attempts. Thoseresults show a different picture than in the study of Nockand colleagues (2009), who stated that depression alone isthe best predictor for suicidal ideations and bipolar disorderis one of the best predictors for unplanned suicide attempts.Contrary to our findings, Resch et al. (2008) found age ef-fects on both suicidal ideations and attempts. One explana-tion for the different outcomes could be the large age-spanranging from 11 to 17 years.
Under closer consideration of the mania symptoms, sui-cidal ideations were significantly predicted by both maniafactors of the extended version of the ADS, whereas sui-cide attempts were predicted only by the mania-factor “el-evated mood and inflated self-esteem (EMIS).” This maybe attributed to a heightened frustration because of the dis-crepancy between an initial highly positive state, which isoften followed by a subsequent depressive phase.
Our study has several limitations that need to be con-sidered. The extended version of the ADS assesses symp-toms of depression and mania occurring during the pre-ceding week. Therefore, memory bias is expected to beweak. But we didn’t collect information about the courseof manic, depressed, or mixed symptoms and whether ep-isodes alternate. Therefore, a further limitation is thecross-sectional design, because we related momentarymood to previous suicidal ideations and attempts. Furtherstudies should use a longitudinal design to investigate de-pressive and manic symptoms in the context of suicidalideation and attempts. In addition, self-reports instead ofclinical interviews were used to assess depressive andmanic symptoms. Furthermore, we defined depressionand mania sum scores as predictor variables for suicidalideations and attempts, although the causality is not clear.In addition, it remains unsolved whether mania symptomsin adolescents are clearly distinguishable from ADHD anddepressive disorders in adolescents, an aspect frequentlydiscussed in the literature (Meyer & Hautzinger, 2001;Meyer, Koßmann-Boehm, & Schlottke, 2004). Finally, itneeds to be pointed out that explained variance in regres-sion analysis as well as correlation coefficients weresmall. Furthermore, the mania factor “EMIS” was insig-nificantly correlated but still a significant predictor forsuicidal ideations and suicide attempts in the combinationwith other predictors in the regression analyses.
This study points to the added value of specifically ex-ploring symptoms of mania in addition to symptoms ofdepression when assessing suicidal behavior in adoles-cents – an aspect often neglected in children and adoles-cents because of its low prevalence rate. If we take a moredetailed look at the mania scale, the factor EMIS, whichdescribes elevated mood and inflated self-esteem, be-comes a significant predictor for suicidal ideations andsuicide attempts and the factor IDCA, which describes ir-ritability and disturbed cognitive abilities for suicidalideations. The clinician should also be alerted when pa-tients demonstrate psychomotor agitation as this item wasalso significantly associated with suicidal behavior.
References
Allison, S., Roeger, L., Martin, G., & Keeves, J. (2001). Genderdifferences in the relationship between depression and suicidalideation in young adolescents. Australian and New ZealandJournal of Psychiatry, 35, 498–503.
Angst, J., Cui, L., Swendsen, J., Rothen, S., Cravchik, A., Kessler,R. C., & Merikangas, K. (2010). Major depressive disorderwith subthreshold bipolarity in the National Comorbidity Sur-vey Replication. American Journal of Psychiatry, 167,1194–1201.
Azorin, J. M., Kaladjian, A., Besnier, N., Adida, M., Hantouche,E., Lancrenon, S., & Akiskal, H. (2010). Suicidal behaviourin a French cohort of major depressive patients: Characteristicsof attempters and nonattempters. Journal of Affective Disor-ders, 123, 87–94.
Bettge, S., Wille, N., Barkmann, C., Schulte-Markwort, M., Ra-vens, S., & the B. s. g. (2008). Depressive symptoms of chil-dren and adolescents in a German representative sample: Re-sults of the BELLA study. European Child & AdolescentPsychiatry, 17, 71–81.
Brent, D. A., Perper, J. A., Moritz, G., Allman, C., Friend, A.,Roth, C., . . . Baugher, M. (1993). Psychiatric risk factors foradolescent suicide: A case-control study. Journal of the Amer-ican Academy of Child & Adolescent Psychiatry, 32, 521–529.
Brunelle, J., Consoli, A., Tanguy, M.-L., Huynh, C., Périsse, D.,Deniau, E., . . . Cohen, D. (2009). Phenomenology, sociode-mographic factors and outcome upon discharge of manic andmixed episodes in hospitalized adolescents: A chart review.European Child & Adolescent Psychiatry, 18, 185–193.
Evans, E., Hawton, K., Rodham, K., Psychol, C., & Deeks, J.(2005). The prevalence of suicidal phenomena in adolescents:A systematic review of population-based studies. Suicide andLife-Threatening Behavior, 35, 239–250.
Fliege, H., Kocalevent, R. D., Walter, O. B., Beck, S., Gratz, K. L.,Gutierrez, P. M., Klapp, B. F. (2006). Three assessment toolsfor deliberate self-harm and suicide behavior: Evaluation andpsychopathological correlates. Journal of Psychosomatic Re-search, 61, 113–121.
Goldstein, T. R., Birmaher, B., Axelson, D., Ryan, N. D., Strober,M. A., Gill, M. K., . . . Keller, M. (2005). History of suicideattempts in pediatric bipolar disorder: Factors associated withincreased risk. Bipolar Disorders, 7, 525–535.
Gutierrez, P. M., Osman, A., Barrios, F. X., & Kopper, B. A.(2001). Development and initial validation of the Self-HarmBehavior Questionnaire. Journal of Personality Assessment,77, 475–490.
Hautzinger, M., & Bailer, M. (1993). Allgemeine Depressionsska-la (ADS) [CES-D Center for Epidemiological Studies Depres-sion Scale]. Göttingen: Beltz Test GmbH.
Hautzinger, M., Bailer, B., Hofmeister, D., & Keller, F. (2012).ADS Allgemeine Depressionsskala, 2. Auflage [CES-D Centerfor Epidemiological Studies Depression Scale, 2nd ed.]. Göt-tingen: Hogrefe.
Kokkevi, A., Rotsika, V., Arapaki, A., & Richardson, C. (2012).Adolescents’ self-reported suicide attempts, self-harm thoughtsand their correlates across 17 European countries. Child Psychol-ogy and Psychiatry and Allied Disciplines, 53, 381–389.
Kozloff, N., Cheung, A. H., Schaffer, A., Cairney, J., Dewa, C. S.,Veldhuizen, S., . . . Levitt, A. J. (2010). Bipolar disorder among
44 J. Straub et al.: Suicidal Behavior in German Adolescents
Z. Kinder-Jugendpsychiatr. Psychother. 43 (1) © 2015 Verlag Hans Huber, Hogrefe AG, Bern
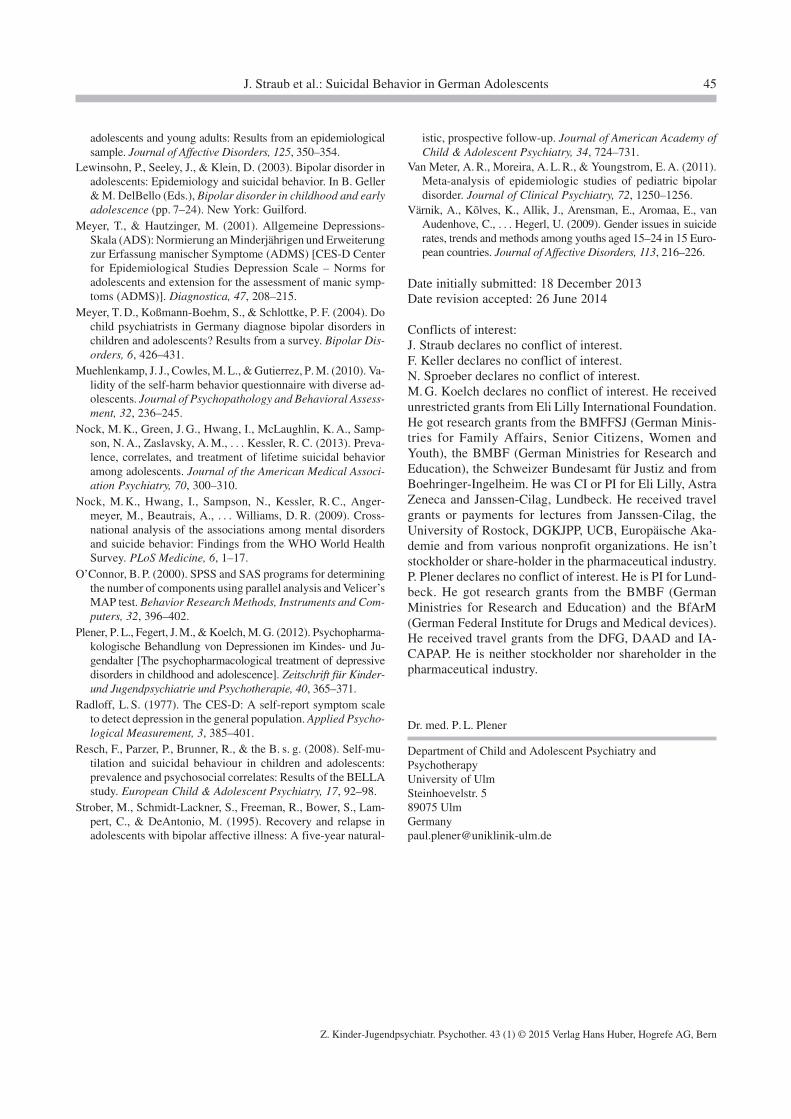
adolescents and young adults: Results from an epidemiologicalsample. Journal of Affective Disorders, 125, 350–354.
Lewinsohn, P., Seeley, J., & Klein, D. (2003). Bipolar disorder inadolescents: Epidemiology and suicidal behavior. In B. Geller& M. DelBello (Eds.), Bipolar disorder in childhood and earlyadolescence (pp. 7–24). New York: Guilford.
Meyer, T., & Hautzinger, M. (2001). Allgemeine Depressions-Skala (ADS): Normierung an Minderjährigen und Erweiterungzur Erfassung manischer Symptome (ADMS) [CES-D Centerfor Epidemiological Studies Depression Scale – Norms foradolescents and extension for the assessment of manic symp-toms (ADMS)]. Diagnostica, 47, 208–215.
Meyer, T. D., Koßmann-Boehm, S., & Schlottke, P. F. (2004). Dochild psychiatrists in Germany diagnose bipolar disorders inchildren and adolescents? Results from a survey. Bipolar Dis-orders, 6, 426–431.
Muehlenkamp, J. J., Cowles, M. L., & Gutierrez, P. M. (2010). Va-lidity of the self-harm behavior questionnaire with diverse ad-olescents. Journal of Psychopathology and Behavioral Assess-ment, 32, 236–245.
Nock, M. K., Green, J. G., Hwang, I., McLaughlin, K. A., Samp-son, N. A., Zaslavsky, A. M., . . . Kessler, R. C. (2013). Preva-lence, correlates, and treatment of lifetime suicidal behavioramong adolescents. Journal of the American Medical Associ-ation Psychiatry, 70, 300–310.
Nock, M. K., Hwang, I., Sampson, N., Kessler, R. C., Anger-meyer, M., Beautrais, A., . . . Williams, D. R. (2009). Cross-national analysis of the associations among mental disordersand suicide behavior: Findings from the WHO World HealthSurvey. PLoS Medicine, 6, 1–17.
O’Connor, B. P. (2000). SPSS and SAS programs for determiningthe number of components using parallel analysis and Velicer’sMAP test. Behavior Research Methods, Instruments and Com-puters, 32, 396–402.
Plener, P. L., Fegert, J. M., & Koelch, M. G. (2012). Psychopharma-kologische Behandlung von Depressionen im Kindes- und Ju-gendalter [The psychopharmacological treatment of depressivedisorders in childhood and adolescence]. Zeitschrift für Kinder-und Jugendpsychiatrie und Psychotherapie, 40, 365–371.
Radloff, L. S. (1977). The CES-D: A self-report symptom scaleto detect depression in the general population. Applied Psycho-logical Measurement, 3, 385–401.
Resch, F., Parzer, P., Brunner, R., & the B. s. g. (2008). Self-mu-tilation and suicidal behaviour in children and adolescents:prevalence and psychosocial correlates: Results of the BELLAstudy. European Child & Adolescent Psychiatry, 17, 92–98.
Strober, M., Schmidt-Lackner, S., Freeman, R., Bower, S., Lam-pert, C., & DeAntonio, M. (1995). Recovery and relapse inadolescents with bipolar affective illness: A five-year natural-
istic, prospective follow-up. Journal of American Academy ofChild & Adolescent Psychiatry, 34, 724–731.
Van Meter, A. R., Moreira, A. L. R., & Youngstrom, E. A. (2011).Meta-analysis of epidemiologic studies of pediatric bipolardisorder. Journal of Clinical Psychiatry, 72, 1250–1256.
Värnik, A., Kõlves, K., Allik, J., Arensman, E., Aromaa, E., vanAudenhove, C., . . . Hegerl, U. (2009). Gender issues in suiciderates, trends and methods among youths aged 15–24 in 15 Euro-pean countries. Journal of Affective Disorders, 113, 216–226.
Date initially submitted: 18 December 2013Date revision accepted: 26 June 2014
Conflicts of interest:J. Straub declares no conflict of interest.F. Keller declares no conflict of interest.N. Sproeber declares no conflict of interest.M. G. Koelch declares no conflict of interest. He receivedunrestricted grants from Eli Lilly International Foundation.He got research grants from the BMFFSJ (German Minis-tries for Family Affairs, Senior Citizens, Women andYouth), the BMBF (German Ministries for Research andEducation), the Schweizer Bundesamt für Justiz and fromBoehringer-Ingelheim. He was CI or PI for Eli Lilly, AstraZeneca and Janssen-Cilag, Lundbeck. He received travelgrants or payments for lectures from Janssen-Cilag, theUniversity of Rostock, DGKJPP, UCB, Europäische Aka-demie and from various nonprofit organizations. He isn’tstockholder or share-holder in the pharmaceutical industry.P. Plener declares no conflict of interest. He is PI for Lund-beck. He got research grants from the BMBF (GermanMinistries for Research and Education) and the BfArM(German Federal Institute for Drugs and Medical devices).He received travel grants from the DFG, DAAD and IA-CAPAP. He is neither stockholder nor shareholder in thepharmaceutical industry.
Dr. med. P. L. Plener
Department of Child and Adolescent Psychiatry andPsychotherapyUniversity of UlmSteinhoevelstr. 589075 [email protected]
J. Straub et al.: Suicidal Behavior in German Adolescents 45
Z. Kinder-Jugendpsychiatr. Psychother. 43 (1) © 2015 Verlag Hans Huber, Hogrefe AG, Bern

Convergence of children's depression rating scale-revised scores and clinical diagnosis in
rating adolescent depressive symptomatology
89
6.3 Convergence of children's depression rating scale-revised scores and clinical diagnosis
in rating adolescent depressive symptomatology
Main authors’ contributions to the article:
P.L. Plener together with M.G. Koelch conceptualized the study, coordinated the study
procedure, recruited the study participants, scheduled diagnostic appointments, and
controlled return of diagnostic instruments. P.L. Plener managed data input, executed
statistical analyses and interpreted statistical outcomes. He researched literature, wrote the
manuscript, integrated remarks of the co-authors, and revised the manuscript according to
reviewer’s comments.
Contributions of J. Straub and co-authors to the article:
We helped drafting and reviewing the manuscript and helped with revising the manuscript
according to the reviewer’s comments.
Reference
Plener, P.L., Grieb, J., Sproeber, N., Straub, J., Schneider, A., Keller, F. & Koelch, M.G. (2012).
Convergence of children's depression rating scale-revised scores and clinical diagnosis in
rating adolescent depressive symptomatology. Mental Illness, 4(e7), 29-31 (open access
Journal).

[Mental Illness 2012; 4:e7] [page 29]
Convergence of children’sdepression rating scale-revisedscores and clinical diagnosis in rating adolescent depressivesymptomatologyPaul L. Plener, Jasmin Grieb, NinaSpröber, Joana Straub, AlexanderSchneider, Ferdinand Keller, Michael G.Kölch Department of Child and AdolescentPsychiatry and Psychotherapy, Universityof Ulm, Germany
Abstract
The Children’s Depression Rating Scale-Revised (CDRS-R) is a widely used instrumentfor research on depression in minors. A rawscore of ≥40 has often been used as indicatorof depressive symptomatology. As a validatedGerman version of the CDRS-R has recentlybecame available, we assessed CDRS-R rawsummary scores of a video taped interview ses-sion in two different rater groups and com-pared them with clinical ratings ofInternational Classification of Diseases (ICD-10) depression diagnosis as observed by athird independent group. We found that for theGerman version a raw score between 35 and 40is indicative for mild depressive symptomatol-ogy as described by the ICD-10. CDRS-R scoresshow potential clinical applicability to deductlevels of depression.
Introduction
The Children’s Depression Rating Scale-Revised (CDRS-R)1 is nowadays one of themost frequently used instruments for theassessment of depressive symptomatology inminors in the context of clinical trials. It wasoriginally intended as rating scale for the agegroup from 6 to 12 years, but is also widelyused in adolescents.2 The CDRS-R is a clini-cian administered 17-item interview, withitem ratings between 1 (=no difficulties) and5 or 1 and 7(=clinically significant difficulties)(adding up to a total score between 17 to 113).It has been proposed, that a score of ≥40 indi-cates depressive symptomatology, whereas ascore ≤28 was often used as indicative ofremission within trials.2 Good psychometricproperties have been reported from the agegroup between 6 and 12 years (with an inter-nal consistency of Cronbach’s α=0.85) as wellas convergent validity with global depressionrating (r=0.92).1 In a placebo controlled treat-
ment study of 96 children (8-11 years) with flu-oxetine, a Cronbach’s α of 0.86 was reportedfor the CDRS, as well as a correlation with theMontgomery-Asberg Depression Scale(MADRS)3 at baseline (r=0.51) and after the 9weeks of the trial (r=0.85).4 Only recently, psy-chometric properties have been established ina sample of 145 adolescents with an age rangebetween 12 and 18 years.2 The authors report-ed an excellent internal consistency ofCronbach’s α ranging between 0.79 and 0.92for their three assessment waves (screening,baseline and exit). At the screening visit, theCDRS-R total score was significantly correlat-ed with an major depressive disorder (MDD)diagnosis obtained from the Kiddie-Schedulefor Affective Disorders and Schizophrenia (K-SADS)5 (r=0.64; P<0.01). CDRS-R total scoreswere highly correlated with the Clinical GlobalImpression-Severity (CGI-S) at each of thethree waves of the study (r=0.87, 0.80 and0.93; P<0.01). Recently a German version ofthe CDRS-R was applied in 60 child and adoles-cent psychiatric inpatients (age range: 7.5-17.9 years),6 demonstrating good psychometricproperties (internal consistency: Cronbach’sα=0.90) with high correlation with the Beck’sDepression Inventory II (German version byHautzinger et al., 2006) 7 in a subsample of 35adolescents (r=0.79, P<0.001). In addition, theGerman version of the CDRS-R was also vali-dated in a German child and adolescent (6.6 to17.9 years) school population (n=275), show-ing good internal consistency (Cronbach’sα=0.86) as well, with a mean CDRS-R rawscore of 25.18 (SD=7.96, range: 17-60).8
As up to now most of the literature availableon the CDRS-R refers to US samples, thuscomparing raw scores with Diagnostic and sta-tistical manual of mental disorders, 4th ed,(DSM-IV) criteria for MDD, so far to ourknowledge no study is available that comparedCDRS-R scores with the clinical impressionleading to International Classification ofDiseases-10 diagnosis. As DSM-IV andInternational Classification of Diseases-10(ICD-10) diagnostic criteria differ slightly, noinformation is available on how far CDRS-Rscores offer information about the level ofdepressive symptomatology (mild, moderate orsevere) of depressive episodes as defined bythe ICD-10 (diagnosis of F32.0, F32.1 and F32.2respectively). This is of relevance for estab-lishing cut-off scores for future studies aimingto address mild to moderate forms of depres-sive symptomatology as defined in the ICD-10and as treatment recommendations refer tothe severity of depression, which is hardlyassessed by assessment tools in clinical rou-tine care.9
The aim of this study was to explore the con-vergence between raw scores of the CDRS-Rand clinical diagnosis according to ICD-10.
Materials and Methods
The study consisted of two phases: in thefirst phase, we established a standardizationfor a video sample of an CDRS-R interview,conducted by a child and adolescent psy-chotherapist and clinical psychologist at PhDlevel with an adolescent female inpatient, 15years of age. The patient gave informed assentto use the video sample for research purpose tobe played to a clinical audience, writteninformed consent was obtained from the care-givers. The video was played to 22 mentalhealth professionals (psychologists and childand adolescent psychiatrists) to establish astandardized raw score. Ratings rangedbetween 29 and 58, with a mean raw score of39.05 (SD=7.30) and a median of 37. Theinternal consistency was good (Cronbachs α=0.82). In a second phase, the same videosample was played to an audience (n=32) withmixed clinical experience background (seeTable 1 for details). The audience was random-ized in two groups before the video sample wasplayed with one group performing a CDRS-Rrating and one group coming up with a clinicaldiagnosis according to ICD-10. CDRS-R andICD-10 criteria were handed out to the mem-
Mental Illness 2012; volume 4:e7
Correspondence: Paul L. Plener, Department ofChild and Adolescent Psychiatry andPsychotherapy, University of Ulm, Steinhoevelstr.5, 89075 Ulm, Germany. Tel. +49.0731.61765.E-mail:[email protected]
Key words: CDRS-R, children, adolescents,depression.
Contributions: PLP, JG conception of design,analysis of data, drafting and revising of paper,final approval; NS, JS, AS, conception of design,revising of paper, final approval; FK, MGK, con-ception of design, analysis of data, revising ofpaper, final approval.
Conflict of interest: Plener PL, Grieb J, Spröber N,Straub J, Schneider A, Keller F have no conflictsto disclose; Michael G. Kölch was an investigatorin clinical trials of Eli Lilly, Astra Zeneca and J&J.He received research grants from: EliLillyInternational Foundation, German Ministry forResearch.
Received for publication: 31 May 2011.Accepted for publication: 21 March 2012.
This work is licensed under a Creative CommonsAttribution NonCommercial 3.0 License (CC BY-NC 3.0).
©Copyright P.L. Plener et al., 2012Licensee PAGEPress, ItalyMental Illness 2012; 4:e7doi:10.4081/mi.2012.e7
[page 30] [Mental Illness 2012; 4:e7]
bers of the group accordingly. Furthermore allparticipants were asked to rate on the ClincialGlobal Impression-Severity scale (CGI-S)between 1 (not at all ill) and 7 (extremely ill).
Results
All participants handed back their CDRS-Rscores (n=18) or their ICD-10 diagnosis(n=14) respectively. Clinical experienceranged between 0 and 12 years (mean: 3.05years, SD: 4.07). 10 out of 32 participants werefamiliar with the CDRS-R.
CDRS-R mean raw score was 36.61 (SD:5.07; range: 28-46; median: 35.5). The internalconsistency was still satisfactory (Cronbachs α=0.71), but lower than in the first sample andprobably weakened by the two items withoutvariance. Several items show medium to highvalues, while others were rated close to 1 andtwo items (item 4 and 7) were consistentlyrated with 1 (details on the CDRS-R items areprovided in Table 2). Years of clinical experi-ence were not significantly correlated withCDRS-R scores (Spearman’s ρ=-0.26, n.s.).
CGI-S mean score was 2.96 (SD: 1.0; range:1-5), with years of clinical experience notbeing significantly correlated with CGI-S score(Spearman’s ρ=-0.02, n.s.). CGI-S score wascorrelated with CDRS-R raw score(Spearman’s ρ=0.55, P=0.04).
Clinical ICD-10 diagnosis was rated by 14participants and coded accordingly (0=no diag-nosis of depression, 1=mild, 2=moderate,3=severe depression). Out of the group, whorated clinically according to ICD-10, 5 partici-pants (35.7%) rated no depression, 7 rated thecase as mild depression (50%) and 2 (14.3%)rated it as moderate depression, with a meanscore of 0.77 (SD=0.73; range: 0-2) beingbelow the level of mild depression. CGI-S scorewas significantly correlated with severity ofICD-10 diagnosis (Spearman’s ρ=0.59,P=0.03). Years of experience were not corre-
lated with ICD-10 diagnostic level (Spearman’sρ=0.34, n.s.)
Discussion
We conducted a study on CDRS-R raw scoresin relation to ICD-10 clinical diagnosis ofdepression to provide a comparison how clini-cal estimation of mild to moderate depressionis correlated with scores of this frequentlyused assessment instruments. So far, a CDRS-R score of ≥40 was used as an indicator fordepression in relation to DSM-IV MDD in sev-eral studies.2 As the distinction between mild,moderate and severe depression according toICD-10 in relation to CDRS-R scores has so farnot been established, we sought to determinea comparison based on a standardized videotape of an adolescent being interviewed usingthe CDRS-R. The mean raw scores of CDRS-Rratings of two independent rater groups werecomparable (39.05 vs. 36.61 respectively), withthe median scores even more closely compara-ble (37 vs 35.5). We found, that a CDRS-R rawscore of approximately 37 points, was an indi-cator for a clinically derived diagnosis of mildto moderate depression in nearly 2/3 of theraters. The mean ratings for clinical diagnosiswere slightly below the level of a mild depres-sive episode. We also sought for a diversegroup of raters, finding, that the level of clini-cal experience did not affect the rating of thevideo tape. Based on our findings we wouldsuggest, that a CDRS-R raw score bandbetween 35 and 40 should be taken as indica-tive of mild to moderate depression accordingto the ICD-10. This may be of use to inform fur-ther studies using the CDRS-R as measure ofdepressive symptomatology. Limitationsinclude the small size of the rater sample aswell as the diversity of the group. However, theCDRS-R ratings were comparable to the rat-ings found in the previous group that was usedto establish standardization of the video sam-
ple. As CDRS-R scores and ICD-10 diagnosiswere not rated by the same persons, it is notpossible to correlate these measures directly.We chose this approach to allow the raters tofully concentrate on their respective task.Another limitation is the use of only one inter-view, which was rated. It would be interestingto compare the CDRS-R based on more inter-views. However, given the small size of therater group, this approach didn’t deem to befeasible. Despite the abovementioned limita-tions, this is the first study to try to bridge thegap between scores as measured by a scientif-ically highly relevant research instrument andclinical diagnosis.
References
1. Poznanski E, Mokros H. Children’sDepression Rating Scale-Revised (CDRS-R). Los Angeles: WPS; 1996.
2. Mayes TL, Bernstein IH, Haley CL, et al.Psychometric properties of the Children’sDepression Rating Scale-Revised in ado-lescents. J Child Adolesc Psychopharmacol2010;20:513-6.
3. Montgomery SA, Äsberg M. A new depres-sion scale designed to be sensitive tochange. Br J Psychiatry 1979;134:382-9.
4. Jain S, Carmody T, Trivedi MH, et al. A psy-chometric evaluation of the CDRS andMADRS in assessing depressive symptomsin children. J Am Acad Child Adolesc
Article
Table 1. Professions and years of experience of the participants in the rating experiment.CDRS-R, Children’s Depression Rating Scale-Revised; ICD-10, InternationalClassification of Diseases -10.
Profession n Years of Rating Rating experience CDRS-R ICD-10
Medical student (8-11th term) 10 0 4 6Psychologist 2 0-10 1 1
Child and Adolescent psychiatry resident 3 0-2 2 1Pedagogues 2 1-4 1 1
Psychotherapists in training 9 0-10 6 3Licensed psychotherapist 2 6 1 1
Music therapist 2 5-9 2 0Child and Adolescent Psychiatry Consultant 2 5-12 1 1
Table 2. Descriptives of CDRS items andsum score. CDRS-R, Children’s Depres -sion Rating Scale-Revised.
Item mean SD
CDRS-R 1 1.39 0.98CDRS-R 2 1.61 0.61
CDRS-R 3 5.22 1.17CDRS-R 4 1 0
CDRS-R 5 1.61 0.7CDRS-R 6 1.06 0.24
CDRS-R 7 1 0CDRS-R 8 2.56 0.78
CDRS-R 9 1.06 0.24CDRS-R 10 1.39 0.5
CDRS-R 11 2.94 0.87CDRS-R 12 2.89 1.18
CDRS-R 13 3.33 0.69CDRS-R 14 3 0.91
CDRS-R 15 2.5 0.79CDRS-R 16 1.72 0.67
CDRS-R 17 2.33 0.49CDRS sum score 36.61 5.07

[Mental Illness 2012; 4:e7] [page 31]
Psychiatry 2007;46:1204-12.5. Kaufman J, Birmaher B, Brent DA, et al.
K-SADS-PL. J Am Acad Child AdolescPsychiatry 2000;39:1208.
6. Keller F, Grieb J, Ernst M, et al. Children’sDepression Rating Scale-Revised (CDRS-R): development of a German version andpsychometric properties in a clinical sam-ple. Z Kinder Jugendpsychiatr Psychother2011;39:179-85. [Article in German].
7. Hautzinger M, Keller F, Kühner C. BDI-II.Beck-depressions-inventar revision –manual. Frankfurt: Harcourt Test Services;2006.
8. Kölch M, Fegert JM, Keller F, et al.Children’s Depression Rating Scale-Revised (CDRS-R): development of aGerman Version. Poster #14217 presentedat the 57th Annual meeting of theAmerican Academy of Child and
Adolescent Psychiatry, NYC, 2010.
9. National Institute for Clinical Excellence,
Depression in children and young people.
The British Psychological Society.
Available from: http://www.nice.org.uk/
nicemedia/pdf/cg028fullguideline.pdf.
2005.
Article
Agreement between self-report and clinician’s assessment in depressed adolescents, using
the example of BDI-II and CDRS-R
93
6.4 Agreement between self-report and clinician’s assessment in depressed adolescents,
using the example of BDI-II and CDRS-R
Contribution of J. Straub to the article:
J. Straub made decisions on the experimental design and conceptualized the study. She
coordinated the study procedure, recruited study participants, and scheduled diagnostic
appointments. She partially executed the diagnostic assessments. She generated the data
matrix, did data input, executed statistical analyses, and interpreted statistical outcomes.
She researched literature, wrote the manuscript, integrated remarks of the co-authors,
revised the manuscript according to reviewer’s comments, and created figures and tables.
Co-authors’ contributions to the article:
F. Keller made decision on the experimental design and conceptualized the study. He helped
with statistical analyses, interpreting the data, and writing and revising the manuscript
according to the reviewer’s comments. P.L. Plener and M.G. Koelch reviewed the draft and
gave constructive remarks. They helped with revising the manuscript according to the
reviewer’s comments.
Reference
Straub, J., Plener, P.L., Koelch, M.G. & Keller, F. (2014). Agreement between self-report and
clinician’s assessment in depressed adolescents, using the example of BDI-II and CDRS-R.
Zeitschrift für Kinder- und Jugendpsychiatrie und Psychotherapie, 42(4), 243-252.
Reprinted from Zeitschrift für Kinder- und Jugendpsychiatrie und Psychotherapie, 42(4),
Straub, J., Plener, P.L., Koelch, M.G. & Keller, F., Agreement between self-report and
clinician’s assessment in depressed adolescents, using the example of BDI-II and CDRS-R,
243-252, Copyright (2014), with permission from Huber.
J. Straub et al.: Selbst- und Klinikerurteil über depressive Symptomatik bei Jugendlich enZ. Kinder-Jugendpsychiatr. Psychother. 42 (4) © 2014 Verlag Hans Huber, Hogrefe AG, Bern
Originalarbeit
Konkordanz zwischen Selbst- undKlinikerurteil hinsichtlich depressiver
Symptomatik bei Jugendlichen amBeispiel von BDI-II und CDRS-R
Joana Straub1, Paul L. Plener1, Michael Koelch1.2 und Ferdinand Keller1
1Klinik für Kinder- und Jugendpsychiatrie- und Psychotherapie, Universitätsklinikum Ulm2Kliniken für Kinder- und Jugendpsychiatrie, Psychotherapie und Psychosomatik,
Vivantes Netzwerk für Gesundheit GmbH, Berlin
Zeitschrift für Kinder- und Jugendpsychiatrie und Psychotherapie, 42 (4), 2014, 243–252
DOI 10.1024/1422-4917/a000297
Zusammenfassung. Fragestellung: Vorhergehende Studien zeigen eine hohe Übereinstimmung von Selbst- und Klinikerurteil bei derErfassung von Depressivität. Die Übereinstimmung auf Summen-, Subskalen- und Einzelitemebene wurde aber bisher nicht bei einerpsychiatrischen jugendlichen Stichprobe untersucht. Der Einfluss von Drittvariablen, wie Alter, Geschlecht, IQ und Behandlungssettingwurde bei Jugendlichen bisher unzureichend überprüft. Methodik: Untersucht wurden 105 depressive Jugendliche (mittleres Alter =15.94) bei welchen innerhalb einer Woche das BDI-II und CDRS-R durchgeführt wurde. Korrelationsanalysen erfolgten auf Ebene derSummenwerte, Subskalen und Einzelitems. Ergebnisse: Es zeigte sich eine hohe Korrelation zwischen Selbst- und Klinikerurteil (r =.67). Auf Subskalen-Ebene zeigten Items, die somatische Inhalte erfassen, keine höhere Konkordanz als Subskalen, die kognitive oderaffektive Inhalte messen. Auf Symptom-Ebene zeigte sich die höchste Übereinstimmung bei dem Item Selbstmordgedanken. Drittva-riablen hatten keinen signifikanten Einfluss auf die Höhe der Korrelation aber Jugendliche mit einem eher hohen IQ und ambulantBehandelte neigten zur relativen Überschätzung ihrer Symptomatik. Schlussfolgerungen: Die Gesamtkorrelation war hoch und unter-schied sich nicht von Ergebnissen vergleichbarer Korrelationsstudien. Die höchste Übereinstimmung bei dem Item «Selbstmordgedan-ken» spricht für die gute Erfassbarkeit von Suizidalität auch im Klinikerurteil. Der Fragebogen kann somit deutliche Hinweise auf dasVorliegen einer Depression liefern, jedoch sollte trotz hoher Korrelationen nicht ein Verfahren durch ein anderes ersetzt werden.
Schlüsselwörter: Übereinstimmung von Selbst- und Fremdurteil, depressive Jugendliche, Korrelation auf Sunmmenwerts-, Subskalen-und Einzelitemebene
Abstract. Agreement between self-report and clinician’s assessment in depressed adolescents, using the example of BDI-II and CDRS-R
Objectives: Preceding studies demonstrated a high agreement between self-report and clinician’s assessment of depression. The concord-ance on the level of sum scores, subscales, and single items, however, has yet to be investigated in a psychiatric adolescent sample. Also,the influence of additional variables such as age, sex, and IQ has been insufficiently studied in adolescents. Methods: Scores on the BDI-IIand CDRS-R, assessed within 1 week, were collected from 105 adolescents (mean age = 15.94 years). Analyses of correlation were doneon levels of sum scores, subscales, and single items. Results: There was a high correlation between self-report and clinician’s assessment(r = .67). At the level of subscales, items assessing somatic contents demonstrated no higher agreement than did items assessing cognitiveand affective contents. The highest agreement at the symptom level was shown for the item assessing suicidal ideations. Additionalvariables had no significant influence on concordance. Adolescents with a high IQ and outpatient adolescents tended to overestimatetheir symptoms. Conclusions: The overall correlation was high and did not differ from results of comparable studies of correlations. Thehighest congruence was shown for the item assessing suicidal ideations, which underlines the accurate assessment of suicidality byclinicians as well. In summary, questionnaires can provide information about the existence of a depressive disorder, although one diag-nostic instrument should not be replaced by the other despite a high correlation.
Keywords: Beck Depression Inventory – BDI-II, Children’s Depression Rating Scale, Revised (CDRS-R), concordance between self-report and clinician’s assessment, depressive adolescents, correlations
Z. Kinder-Jugendpsychiatr. Psychother. 42 (4) © 2014 Verlag Hans Huber, Hogrefe AG, Bern
Persönliches Autorenexemplar (e-Sonderdruck)

Einleitung
In der Allgemeinbevölkerung der Jugendlichen zwischen12 und 18 Jahren erfüllen 2.5 % der männlichen und 3.7 %der weiblichen Jugendlichen die Kriterien einer depressi-ven Episode, welche in bis zu zwei Dritteln der Fälle miteiner komorbiden Störung einhergeht (Hoffmann, Peter-mann, Glaeske & Bachmann, 2012), häufig einen chroni-schen Verlauf zeigt und nicht zuletzt, wegen des häufig auf-tretenden Symptoms der Suizidalität, ein sehr ernstzuneh-mendes Störungsbild darstellt (Plener, Fegert & Kölch,2012; Saluja et al., 2004). Eine frühe Intervention setztauch eine spezifische und sensitive Diagnostik voraus. ImErwachsenenbereich gibt es eine Vielzahl an Diagnostikin-strumenten mit guten psychometrischen Eigenschaften, dieteilweise auch für Jugendliche validiert wurden, wie dasBeck Depressions Inventar in der revidierten Fassung(BDI-II; Besier, Goldbeck & Keller, 2008; Osman, Kopper,Barrios, Gutierrez & Bagge, 2004). Allerdings unterschei-det sich die Symptomatik von Kindern und Jugendlichenin manchen Bereichen von Erwachsenen (z. B. Vorkom-men erhöhter Reizbarkeit und somatischer Beschwerden;Jantzer, Parzer, Lehmkuhl & Resch, 2012; Mehler-Wex,2012), weshalb die Diagnostikinstrumente, die für Erwach-sene konzipiert wurden, nicht generell auf Kinder und Ju-gendliche übertragen werden können. Mittlerweile existie-ren mehrere Selbstbeurteilungsinstrumente (Fragebögenaus Sicht der Jugendlichen) und Fremdbeurteilungsinstru-mente (Fragebögen und Interviews aus Sicht des klinischenInterviewers) die für die Erfassung von Depressionen beiJugendlichen konzipiert wurden. Einige davon werden imFolgenden beispielhaft aufgeführt. Weiterhin gibt es äqui-valente Fragebögen, die die Depression des Jugendlichenaus dessen Sicht und aus der Sicht der Eltern erfassen, zumBeispiel der Selbstbeurteilungsbogen SBB-DES und derentsprechende Elternbogen FBB-DES (Döpfner, Görtz-Dorten, Lehmkuhl, Breuer & Goletz, 2008).
Neben diesen spezifischen Instrumenten sind noch kli-nische Interviews zu nennen, welche die Diagnosestellungpsychischer Störungen im Allgemeinen – darunter auchDepressionen – ermöglichen: Kiddie-Sads Present and life-time version (K-SADS-PL; Kaufman, Birmaher & Brent,1997); diagnostisches Interview bei psychischen Störun-gen im Kindes- und Jugendalter (Kinder-Dips; Schneider,Unnewehr & Margraf, 2009).
Selbst- und Fremdbeurteilungsverfahren haben diverseVor- und Nachteile (für einen Überblick s. Stieglitz, 2008),aber zentral bleibt die Frage inwiefern beide Arten von In-strumenten die jeweiligen Symptome der Depression ähn-lich oder sogar gleich abbilden. Über die uns bekanntenStudien hinweg liegen die Korrelationskoeffizienten zwi-schen Selbst- und Klinikerinstrumenten bei depressiven Ju-gendlichen zwischen .46 und .80. Shain, Naylor und Alessi(1990) verglichen die Children’s Depression Rating Scale– Revised (CDRS-R; Poznanski & Mokros, 1996) mit demChildren’s Depression Inventory (CDI; Kovacs, 1981,
1992) sowie die CDRS-R mit der Reynolds Adolescent De-pression Scale, second Edition (RADS-2; Reynolds, 1987,1989) und ermittelten Korrelationen von .78 und .77. Wei-terhin verglichen sie die Hamilton Depression-Scale(HAMD; Williams, 1988) mit dem CDI sowie das HAMDmit der RADS und zeigten Korrelationen von .72 und .73.Keller, Grieb, Koelch und Sproeber (2012) korrelierten dieCDRS-R bei Kindern mit dem Depressionsinventar fürKinder und Jugendliche (DIKJ; Stiensmeier-Pelster, Schür-mann & Duda, 2000) sowohl bei einer Schulstichprobe alsauch bei einer klinischen Stichprobe (r = .69 und .80). DieKorrelation zwischen CDRS-R und BDI-II bei einer ju-gendlichen Schulstichprobe und einer jugendlichen klini-schen Stichprobe zeigte Korrelationskoeffizienten von .70und .74. Die klinische Stichprobe war in beiden Fällen je-doch nicht homogen depressiv. Den hohen Korrelationenzwischen Selbst- und Fremdbeurteilungsinstrumenten stehtein eher niedriger Korrelationskoeffizient von .46 gegen-über (Robbins, Alessi, Colfer & Yanchyshyn, 1985), derbei dem Vergleich der HAMD und der Carroll Self-RatingScale (CRS; Carroll, Feinberg & Smouse, 1981) ermitteltwurde.
Dolle, Schulte-Körne, Hofacker, Izat und Allgaier(2012) untersuchten bei einer depressiven Kinder- und Ju-gendlichenstichprobe die Übereinstimmung von Selbstbe-urteilungsfragebögen (DIKJ, ADS) und klinischem Inter-view (Kinder-Dips). Bei Kindern, die über dem Cut-Off imDIKJ lagen, wurde bei nur 75 % eine depressive Episodediagnostiziert. Bei Jugendlichen, die über dem Cut-Off desADS-K lagen, sogar nur in 55 % der Fälle. Die Autorenschlussfolgern, dass Selbstbeurteilungsfragebögen zwargute Hilfsmittel seien, aber allein keine Diagnosestellungerlaubten. Lauth et al. (2010) verglichen Diagnosen des K-SADS, welches sowohl mit Eltern als auch Jugendlichendurchgeführt wurde, mit Ergebnissen des CDI. Sie fandeneine Korrelation von .47 zwischen erfüllten DSM-IV (Saß,Wittchen, Zaudig & Houben, 2003) Depressionskriterienund dem CDI Wert.
Die meisten Studien beschränken sich auf eine Korrelationdes Gesamtsummenwerts der jeweiligen Instrumente und nurwenige Studien gehen auf den Zusammenhang auf Symp-tomebene ein. Corruble, Legrand, Zvenigorowski, Duret undGuelfi (1999) untersuchten bei Erwachsenen die zwei Versio-nen (Selbst- und Fremdbeurteilung) des Inventars für depres-sive Symptomatik (IDS; Rush et al., 1986; Rush, Hiser &Giles, 1987) auf Itemebene und fanden, dass der Item-Inhaltsich auf die Höhe der Konkordanz auswirkt: Items, die sichauf somatische Inhalte bezogen, zeigten eine höhere Überein-stimmung als Items, die die Stimmung erfassten. Studien, diesich der Frage von Übereinstimmungen auf Item- oder Sub-skalenebene bei depressiven Kindern und Jugendlichen wid-men, stehen noch aus.
Weiterhin könnten sich Drittvariablen, wie die Art derDepression oder das Vorliegen einer komorbiden psychi-schen Störung, auf den Zusammenhang zwischen Selbst-und Klinikerurteil auswirken (Corruble et al., 1999; Dorz,Borgherini, Conforti, Scarso & Magni, 2004). Bezüglich
244 J. Straub et al.: Selbst- und Klinikerurteil über depressive Symptomatik bei Jugendlichen
Z. Kinder-Jugendpsychiatr. Psychother. 42 (4) © 2014 Verlag Hans Huber, Hogrefe AG, Bern
Persönliches Autorenexemplar (e-Sonderdruck)

des Einflusses demographischer Eigenschaften auf dieÜbereinstimmung von Selbst- und Klinikerurteil gibt eswidersprüchliche Ergebnisse: Corruble et al. (1999) fandenbei einer erwachsenen depressiven Stichprobe (Durch-schnittsalter: 41.7 Jahre) keinen Einfluss von Geschlecht,Alter, Dauer und Schweregrad der Symptomatik auf denoben genannten Zusammenhang. Allerdings zeigten Shainet al. (1990) bei einer jugendlichen Stichprobe (Durch-schnittsalter: 14.9 Jahre) einen Geschlechtereffekt, wobeider Zusammenhang zwischen Selbst- und Klinikerurteilbei Mädchen höher war als bei Jungen. Die oben aufge-führten Aspekte wurden bisher im kinder- und jugendpsy-chiatrischen Bereich nicht ausreichend erforscht.
Die vorliegende Studie untersucht bezüglich zweier häu-fig eingesetzter Verfahren zur Verlaufs- und Schweregrad-messung bei depressiven Jugendlichen, dem BDI-II, alsSelbstbeurteilungsinstrument, und der CDRS-R, als semi-strukturiertes klinisches Interview, ob sich erstens eine ähn-lich hohe Gesamtkorrelation von CDRS-R und BDI-II beieiner Stichprobe von depressiven Jugendlichen wie in ver-gleichbaren Studien finden lässt. Zweitens soll die Überein-stimmung von Selbst- und Klinikerurteil auf Subskalen-Ebe-ne untersucht werden unter Berücksichtigung der fünfCDRS-R Faktoren nach Guo, Nilsson, Heiligenstein, Wilsonund Emslie (2006) und der zwei üblicherweise unterschiede-nen BDI-II Faktoren «somatisch-affektiv» und «kognitiv»(vgl. zum Beispiel Keller, Hautzinger & Kühner, 2008). DieErwartung ist, dass der Faktor somatisch-affektiv des BDI-IIam höchsten mit dem CDRS-R Faktor körperliche Be-schwerden korreliert, angelehnt an die Ergebnisse von Cor-ruble et al. (1999). Drittens sollen die beiden Instrumente aufSymptom-Ebene verglichen werden mit der Annahme, dassinhaltlich ähnliche Items höher miteinander korrelieren alsinhaltlich weniger ähnliche. Viertens soll der Einfluss von inder Klinik routinemäßig erhobenen Drittvariablen, nämlichGeschlecht, Vorliegen einer komorbiden Störung, Höhe desIQs und Art der aktuellen Behandlung, hinsichtlich der Höhedes Zusammenhangs und fünftens hinsichtlich der Richtungder Diskrepanz (relative Über- und Unterschätzung der
Symptomatik aus Sicht des depressiven Jugendlichen) zwi-schen Selbst- und Klinikerurteil untersucht werden. In An-lehnung an die Studie von Shain et al. (1990) erwarten wirhinsichtlich der Höhe des Zusammenhangs, dass Mädcheneine stärkere Übereinstimmung zeigen als Jungen. Hinsicht-lich der Diskrepanz, könnte in Anlehnung an Ergebnisse derwenigen Studien mit Erwachsenen (Dunlop et al. 2011; Dorzet al. 2004) postuliert werden, dass Alter und Geschlecht vonBedeutung sind.
Methoden
Teilnehmer
Die Datenerhebung fand zwischen 06/2008 und 06/2013 inder Klinik für Kinder- und Jugendpsychiatrie und Psycho-therapie des Universitätsklinikums Ulm statt. Innerhalbdieses Zeitraums wurden sowohl CDRS-R als auch BDI-IIbei 212 Jugendlichen, die zwischen 13 und 19 Jahren altwaren, im Zuge der Routine-Eingangsdiagnostik durchge-führt. Wenn möglich werden CDRS-R und BDI-II am sel-ben Tag erhoben, was jedoch häufig nicht praktikabel ist,so dass mitunter einige Tage Differenz zwischen den Erhe-bungszeitpunkten liegen. Nach Abwägung zwischen aus-reichend großer Stichprobenzahl und geringer Änderungder depressiven Symptomatik zwischen den Erhebungs-zeitpunkten haben wir uns für eine maximale Differenz voneiner Woche entschieden. Damit konnten 132 Jugendlicheeingeschlossen werden, wobei gemäß Klinikerurteil bei105 Jugendlichen eine Depressionsdiagnose nach ICD-10(Remschmidt, Schmidt & Poustka, 2009) vergeben wurde(vgl. Tabelle 1, in der die ICD-10 Kategorien zur Schwereder Depression aufgeführt sind). Auf diese Stichprobe be-zieht sich die vorliegende Studie. Die Erhebung fand zu-meist zu Beginn der individuellen Behandlung statt – alsobevor weitere Behandlungsschritte wie Medikation oderPsychotherapie initiiert wurden.
Tabelle 1Depressionsdiagnosen und Komorbiditäten der Teilnehmer laut ICD-10
Depressive Störung Komorbide Störungen
F32.0 Leichte depressive Episode (N = 25)F32.1 Mittelgradig depressive Episode (N = 56)F32.2 Schwere depressive Episode (N = 11)F32.3 Schwere depressive Episode mit psychot. Sympt. (N = 2)F33.0 Rez. depressive Störung (leichte Episode) (N = 3)F33.1 Rez. depressive Störung (mittelgradige Episode) (N = 1)F33.2 Rez. depressive Störung (schwere Episode) (N = 1)F33.3 Rez. depressive Störung (schwere Episode mit psychot.Sympt.) (N = 1)F92.0 SSV mit depressiver Störung (N = 5)
F40 Phobische Störung (N = 15)F43 Reaktion auf schwere Belastungen (N = 6)F50 Essstörung (N = 6)F90 Hyperkinetische Störung (N = 6)F41 Andere Angststörungen (N = 3)F60 Persönlichkeitsstörung (N = 3)F93 Emotionale Störung d. Kindesalters (N = 3)F42 Zwangsstörung (N = 2)F98 Andere Störungen Beginn in Kindheit (N = 2)F10 Akute Alkoholintoxikation (N = 1)F45 Somatoforme Störung (N = 1)F55 Missbrauch von Substanzen (N = 1)F63 Abnorme Gewohnheiten (N = 1)F91 Störung des Sozialverhaltens (N = 1)
Anmerkungen: N = Anzahl; SSV = Störung des Sozialverhaltens; rez. = rezidivierend.
J. Straub et al.: Selbst- und Klinikerurteil über depressive Symptomatik bei Jugendlichen 245
Z. Kinder-Jugendpsychiatr. Psychother. 42 (4) © 2014 Verlag Hans Huber, Hogrefe AG, Bern
Persönliches Autorenexemplar (e-Sonderdruck)

Von den 105 Jugendlichen waren77 (73.31 %) weiblich und28 (26.66 %) männlich. Die Altersspanne reichte von 12.51 bis18.97 Jahren (M ± SD = 15.94 ± 1.63). 88 befanden sich inambulanter und 17 in stationärer Behandlung. Von ihnen be-suchten 15.7 % die Mittelschule, 34.5 % die Realschule,32.2 % das Gymnasium und 17.6 % befanden sich in einemAusbildungsverhältnis. Der IQ reichte von 73 bis 129 (M ± SD= 103.51 ± 10.85). Über die Hälfte der Teilnehmer (48.57 %)erfüllte die Kriterien für eine komorbide Störung (Tab. 1).
Instrumente
Die Durchführung des CDRS-R Interviews erfolgte durchfünf klinische Psychologen, die zuvor an einem von JS durch-geführten Training zur Anwendung des Interviews teilge-nommen hatten. Die Interviewer wurden regelmäßig bei derDurchführung der CDRS-R von den Autoren MK und JSsupervidiert. Die psychiatrische(n) Diagnose(n) wurde an-hand der ICD-10 im Rahmen der Routinediagnostik von Ärzten und Psychologen der Klinik gestellt, die nicht identischwaren mit den CDRS-R Interviewern bis auf etwa zehn Pro-zent bei denen die Diagnostik durch die gleiche Person er-folgte. Die Diagnostik wurde zu Beginn der ambulanten Be-handlung/des stationären Aufenthalts durchgeführt.
Intellektuelle Fähigkeiten wurde mit dem HamburgWechsler Intelligenztest für Kinder vierte Edition (HAWIKIV; Petermann & Petermann, 2008), dem Wechsler Intelli-genztest für Erwachsene (WIE; Aster, Neubauer & Horn,2006) oder dem Prüfsystem für Schul- und Bildungsbera-tung für 6. bis 13. Klassen (Horn, 2004) erhoben. Die Wahldes Verfahrens hing vom Alter der Patienten und der Mög-lichkeit, ob sie im Gruppensetting durchführbar waren, ab.
Bei der CDRS-R handelt es sich um ein semi-struktu-riertes klinisches Interview, das auf den DSM-IV Kriterienzur Erfassung von Depressionen beruht und in Anlehnungan die HAM-D entwickelt wurde. Die CDRS-R wurde ur-sprünglich in den 70er-Jahren im amerikanischenSprachraum entwickelt, in den 80er-Jahren überarbeitet(Poznanski & Mokros, 1996) und ist seit 2012 auch alsdeutsche Version erhältlich (Keller et al., 2012). Sie bestehtaus insgesamt 17 Items, wovon 3 Items nonverbale Symp-tome, wie beispielsweise den mimischen Ausdruck, erfas-sen. Insgesamt konnten gute psychometrische Eigenschaf-ten wie eine hohe interne Konsistenz (α = 0.85), guteTrennschärfekoeffizienten für die einzelnen Items sowieeine gute Test-Retest Reliabilität nach einer Woche (r =.92) sowie Interrater-Reliabilität (r = .95) belegt werden(Keller et al., 2012).
Das Beck Depressions Inventar (BDI) wurde 1961 zur Er-fassung von Depressionen entwickelt und 1996 von der Ar-beitsgruppe um Beck revidiert, was zur Entwicklung desBDI-II führte (Beck, Steer & Brown, 1996). Es ist eines dermeist eingesetzten Selbstbeurteilungsinstrumente bei Ju-gendlichen (Myers & Winters, 2002), obwohl auch Kritik ander Verständlichkeit einzelner Items insbesondere für jüngereJugendliche geübt wurde (Osman et al. 2004). Es erfasst De-
pression auf der Verhaltens-, Gefühls-, kognitiven und soma-tischen Ebene und besteht aus 21 Items, die jeweils auf einerSkala von 0–3 beantwortet werden. In psychiatrischen Stich-proben lag die interne Konsistenz im Bereich von .89 ≤ α ≤.94 und in nichtklinischen Stichproben im Bereich von .84 ≤α ≤ .91. Test-Retest Reliabilität und Validität sind ebenfallssowohl in dem englischen Original (Beck et al., 1996) alsauch in der deutschen Fassung (Hautzinger, Keller & Kühner,2006) als hoch zu berichten. Bei der Analyse auf Subskalen-Ebene orientierten wir uns an den CDRS-R Faktoren nachGuo et al. (2006): Der erste Faktor «beobachtete depressiveStimmung» ist gekennzeichnet durch die Items 15, 16, 17, derzweite Faktor «Anhedonie» durch die Items 2, 3, der dritteFaktor «Gedanken an den Tod» durch die Items 12, 13, dervierte Faktor «somatische Symptome» durch die Items 1, 4,6, 7 und der fünfte Faktor «berichtete depressive Stimmung»durch die Items 10, 11, 14 (Items s. Tab. 4). Bei den BDI-IIFaktoren orientierten wir uns an Keller et al. (2008): DemBDI-II Faktor «kognitiv» sind die Items «Pessimismus»,«Versagensgefühle», «Schuldgefühle», «Bestrafungsgefüh-le», «Selbstablehnung», «Selbstvorwürfe», «Selbstmordge-danken» und «Wertlosigkeit» zuzuordnen. Alle übrigenItems bilden den BDI-II Faktor «somatisch-affektiv».
Statistische Analysen
Zunächst wurden die BDI-II und CDRS-R Summenwertemittels des Kolmogorov-Smirnov Tests auf Normalität ge-prüft. Nachdem gezeigt werden konnte, dass von einer Nor-malverteilung ausgegangen werden kann, wurden Korrela-tionen nach Pearson berechnet. Gruppenvergleiche wurdenmittels t-Test bzw. mittels χ²-Test (bei Häufigkeitstabellen)vorgenommen. Signifikanztests zum Vergleich der Korrela-tionskoeffizienten zwischen verschiedenen Subgruppen er-folgten mittels z-Tests (Bortz, 2005). In Anlehnung an Dorzet al. (2004) und Dunlop et al. (2011) wurde außerdem derGrad der Diskrepanz zwischen BDI-II und CDRS-R be-stimmt. Dazu wurden die Summenwerte beider Verfahrenjeweils standardisiert auf M = 0 und SD = 1. Anschließendwurde der standardisierte CDRS-R-Wert vom standardisier-ten BDI-II-Wert abgezogen. Negative Diskrepanzwerte be-deuten also relative Unterschätzung (BDI-II-Wert ist relativgeringer als CDRS-R-Wert), positive Diskrepanzwerte rela-tive Überschätzung. Analog Dorz et al. (2004) wurden dieJugendlichen noch klassifiziert in Unterschätzer, wenn Disk-repanz < –1.0, und in Überschätzer, wenn Diskrepanz > 1; dieübrigen Jugendlichen wurden als konkordant bezeichnet.
Ergebnisse
Durchschnittlich hatten die Jugendlichen im BDI-II einenMittelwert von 24.76 (SD = 11.87) und in der CDRS-Reinen Mittelwert von 51.63 (SD = 13.99). Mädchen wiesen
246 J. Straub et al.: Selbst- und Klinikerurteil über depressive Symptomatik bei Jugendlichen
Z. Kinder-Jugendpsychiatr. Psychother. 42 (4) © 2014 Verlag Hans Huber, Hogrefe AG, Bern
Persönliches Autorenexemplar (e-Sonderdruck)
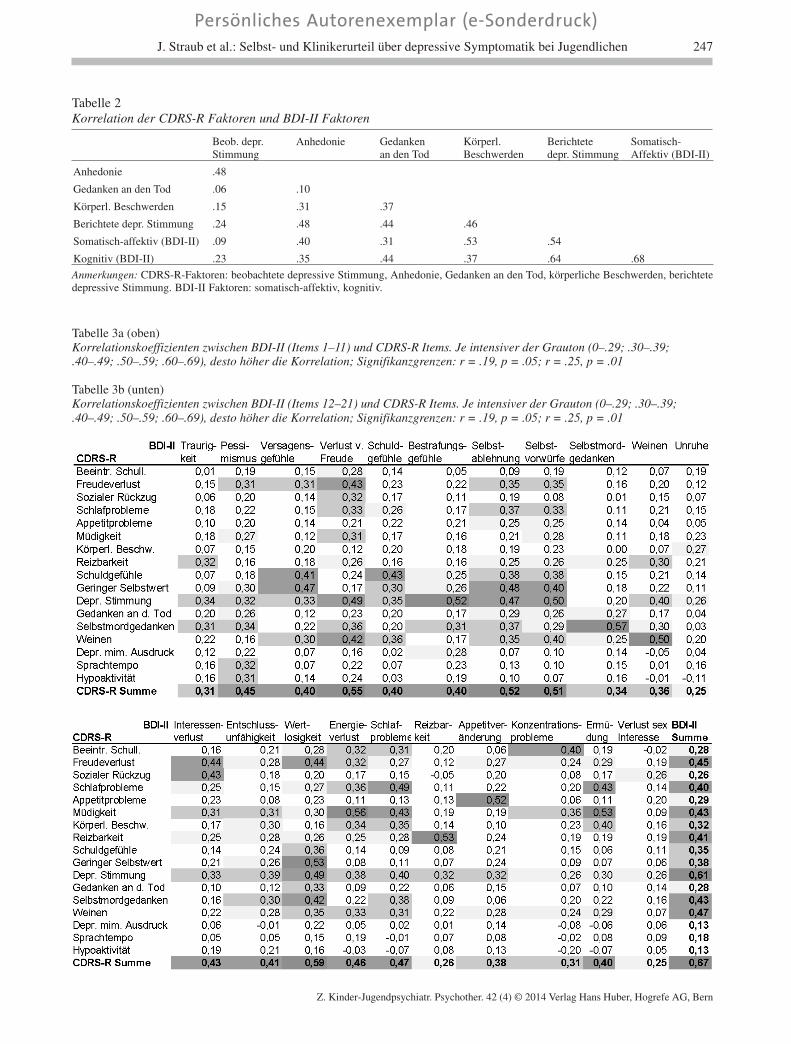
Tabelle 2Korrelation der CDRS-R Faktoren und BDI-II Faktoren
Beob. depr.Stimmung
Anhedonie Gedankenan den Tod
Körperl.Beschwerden
Berichtetedepr. Stimmung
Somatisch-Affektiv (BDI-II)
Anhedonie .48
Gedanken an den Tod .06 .10
Körperl. Beschwerden .15 .31 .37
Berichtete depr. Stimmung .24 .48 .44 .46
Somatisch-affektiv (BDI-II) .09 .40 .31 .53 .54
Kognitiv (BDI-II) .23 .35 .44 .37 .64 .68
Anmerkungen: CDRS-R-Faktoren: beobachtete depressive Stimmung, Anhedonie, Gedanken an den Tod, körperliche Beschwerden, berichtetedepressive Stimmung. BDI-II Faktoren: somatisch-affektiv, kognitiv.
Tabelle 3a (oben)Korrelationskoeffizienten zwischen BDI-II (Items 1–11) und CDRS-R Items. Je intensiver der Grauton (0–.29; .30–.39;.40–.49; .50–.59; .60–.69), desto höher die Korrelation; Signifikanzgrenzen: r = .19, p = .05; r = .25, p = .01
Tabelle 3b (unten)Korrelationskoeffizienten zwischen BDI-II (Items 12–21) und CDRS-R Items. Je intensiver der Grauton (0–.29; .30–.39;.40–.49; .50–.59; .60–.69), desto höher die Korrelation; Signifikanzgrenzen: r = .19, p = .05; r = .25, p = .01
J. Straub et al.: Selbst- und Klinikerurteil über depressive Symptomatik bei Jugendlichen 247
Z. Kinder-Jugendpsychiatr. Psychother. 42 (4) © 2014 Verlag Hans Huber, Hogrefe AG, Bern
Persönliches Autorenexemplar (e-Sonderdruck)

sowohl in der CDRS-R (M = 53.52; SD = 14.56) einensignifikant höheren Mittelwert auf als Jungen (M = 46.43;SD = 10.87), t(103) = 2.35, p = .02, als auch im BDI-II (M= 26.64; SD = 11.56) gegenüber den Jungen (M = 19.61;SD = 11.36), t(103) = 2.77, p = .007. Über alle depressivenJugendlichen wurde ein hoher Zusammenhang zwischendem Selbst- und Fremdbeurteilungsinstrument gefunden (r= .67, p < .001). Bei einer nach zeitlichem Abstand unter-schiedenen Auswertung zeigte sich, dass bei näher beiein-ander liegenden Erhebungszeitpunkten auch die Korrela-tion etwas höher ausfiel. Wurden CDRS-R und BDI-II amgleichen Tag erhoben (N = 71), zeigte sich eine Korrelationvon .73. Diese unterschied sich allerdings nicht signifikantvon der Korrelation, bei der die Messzeitpunkte bis zu einerWoche auseinander lagen (z = –1.43, p = .15).
Es zeigt sich, dass die inhaltlich ähnlichen Faktoren «so-matisch-affektiv» und «körperliche Beschwerden» hochmiteinander korrelierten, aber nicht höher als andere, wiezum Beispiel die Faktoren «kognitiv» und «berichtete de-pressive Stimmung» (siehe Tab. 2). Die Korrelationen derCDRS-R und BDI-II Items miteinander sind in Tabelle 3abgebildet. Einzelne CDRS-R Items wie «depressive Stim-mung» korrelieren mittel bis hoch mit vielen BDI-II Items.Andere CDRS-R Items wie «körperliche Beschwerden»korrelieren spezifischer. Umgekehrt gibt es auch BDI-IIItems, die sehr spezifisch mit CDRS-R Items korrelierenz. B. «Reizbarkeit». Betrachtet man nur die inhaltlich ver-
gleichbaren CDRS-R und BDI-II Items, so ergeben sichdurchweg signifikante, zumeist mittlere Korrelationskoef-fizienten (p < .001) (Tab. 4). Die höchste Korrelation zeigtesich zwischen dem CDRS-R und BDI-II Item zur Erfas-sung von Selbstmordgedanken. In einigen Fällen korrelier-ten CDRS-R Items höher mit inhaltlich weniger nahe lie-genden BDI-II Items, wie zum Beispiel das CDRS-R Item«depressive Stimmung» welches am Höchsten mit demBDI-II Item «Bestrafungsgefühle» korreliert. Von 11 in-haltlich äquivalenten CDRS-R und BDI-II Items korrelie-ren acht tatsächlich auch am höchsten miteinander.
Bei näherer Betrachtung von Drittvariablen in ihrer Aus-wirkung auf die Höhe der Zusammenhänge, fand sich beigetrennter Auswertung nach Geschlecht bei weiblichenTeilnehmern zwischen Selbst- und Fremdbeurteilungsin-strument eine höhere, aber nicht signifikant höhere Korre-lation (r = .67, p < .001) als bei männlichen Teilnehmern(r = .60, p < .01; z = –.54, p = .59). Weiterhin zeigten Pa-tienten, die eine komorbide Störung aufwiesen, eine gerin-gere, aber nicht signifikant geringere Übereinstimmungzwischen Selbst- und Klinikerurteil (r = .58, p < .001) alsPatienten ohne komorbide Störung (r = .73, p < .001; z =–1.29, p = .19). Es konnten weiterhin keine Unterschiedehinsichtlich der Übereinstimmung zwischen stationären (r= .67, p < .01) und ambulanten Patienten (r = .68, p < .001)gefunden werden (z = .10, p = .92). Jugendliche mit einemIQ unter 100 zeigten eine niedrigere Übereinstimmung (r
Tabelle 4Korrelation zwischen CDRS-R und BDI-II bei inhaltlich passenden Items und am höchsten korrelierte Items
CDRS-R Item Inhaltlich passendes BDI-II Item r BDI-II Item mit höchster Korrelation r
1) Beeinträchtigte Schulleistung/Konzentrationsprobleme
19) Konzentrationsschwierigkeiten .40**
2) Schwierigkeiten sich zu freuen 4) Verlust von Freude .43** 14) Wertlosigkeit .44**
3) Sozialer Rückzug – 12) Interessenverlust .43**
4) Schlafprobleme 16) Veränderung der Schlafgewohnheiten .49**
5) Appetitprobleme 18) Veränderungen des Appetits .52**
6) ausgeprägte Müdigkeit 20) Ermüdung oder Erschöpfung .53** 15) Energieverlust .56**
7) Körperliche Beschwerden – 20) Ermüdung .40**
8) Reizbarkeit 17) Reizbarkeit .53**
9) ausgeprägte Schuldgefühle 5) Schuldgefühle .43**
10) Geringes Selbstwertgefühl 7) Selbstablehnung .48**
14) Wertlosigkeit .53**
11) Depressive Stimmung 1) Traurigkeit .34** 6) Bestrafungsgefühle .52**
12) Gedanken an den Tod – 14) Wertlosigkeit .33**
13) Selbstmordgedanken 9) Selbstmordgedanken .57**
14) Ausgeprägtes Weinen 10) Weinen .50**
15) depressiver mimischer Ausdruck – 6) Bestrafungsgefühle .28*
16) Sprachtempo – 2) Pessimismus .32*
17) Hypoaktivität – 2) Pessimismus .31*
Anmerkungen: **p < .001, *p < .01. In Spalte 1 und 2 sind die inhaltlich am ähnlichsten CDRS-R und BDI-II Items aufgeführt, in Spalte 3 dieKorrelation dieser Items. Grau schattiert sind diese dann, wenn die beiden ähnlichsten CDRS-R und BDI-II Items auch am höchsten miteinanderkorrelieren. Korrelieren diese beiden nicht am höchsten, ist in Spalte 4 das BDI-II Item aufgeführt, das stattdessen am höchsten mit demjeweiligen CDRS-R Item korreliert und der jeweilige Korrelationskoeffizient ist in Spalte 5 abgebildet.
248 J. Straub et al.: Selbst- und Klinikerurteil über depressive Symptomatik bei Jugendlichen
Z. Kinder-Jugendpsychiatr. Psychother. 42 (4) © 2014 Verlag Hans Huber, Hogrefe AG, Bern
Persönliches Autorenexemplar (e-Sonderdruck)

= .55, p < .001) als diejenigen mit einem IQ größer 100 (r= .67, p < .001), auch hier erwies sich der Unterschied alsnicht signifikant, (z = –.86, p = .39).
Die Analyse der Diskrepanzwerte ergab zehn Unter-schätzer (d. h. Jugendliche schätzen ihre Symptomatik imBDI-II relativ geringer ein als der Interviewer in derCDRS-R) und zehn Überschätzer (d. h. Jugendliche schät-zen ihre Symptomatik im BDI-II relativ höher ein als derInterviewer in der CDRS-R); 85 Jugendliche waren kon-kordant. Eine Häufigkeitsauszählung mit den VariablenGeschlecht, ambulante vs. stationäre Behandlung und Ko-morbidität ergab in keiner der drei Variablen einen signifi-kanten Zusammenhang mit den drei Konkordanzkatego-rien. Auch eine Zusammenfassung der Unterschätzer undder Überschätzer in eine einzige Gruppe von Diskordantenergab keine signifikante Beziehung zu den drei Variablen.Verzichtet man auf die (informationsreduzierende) Katego-risierung in Unter- und Überschätzer und verwendet dieDiskrepanzwerte als quantitative Variable, ergibt sich wei-terhin kein Unterschied bei Geschlecht und Komorbidität.In der Behandlungsform zeigt sich jedoch ein signifikanterMittelwertsunterschied, wonach die stationär Behandelteneher in Richtung Unterschätzung tendierten (ambulante: M= 0.08; SD = 0.75; stationäre: M = –0.43; SD = 0.99), t(103)= 2.43, p = .02). Außerdem bestehen Zusammenhänge zwi-schen Diskrepanzwert und Intelligenz sowie Alter. DieKorrelation zur Intelligenz beträgt r = .27; p = .01 (N = 89),d. h. höhere Intelligenz ist mit relativer Überschätzung as-soziiert. Zum Alter ergibt sich eine tendenziell signifikanteKorrelation von r = –.18, (p = .06), d. h. ältere Jugendlicheweisen eher eine Unterschätzung auf. Zur weiteren Analy-se dieser Beziehungen wurden die Korrelationen zu denabsoluten Diskrepanzwerten bestimmt (= absolute Abwei-chung von Null, was den Grad der Diskrepanz unabhängigvon der Richtung widerspiegelt). Sowohl in der Korrela-tion zu Intelligenz wie auch zum Alter ergaben sich keinesignifikanten Korrelationen (r = .00 bzw. r = –.04), d. h. dieRichtung spielt eine Rolle.
Diskussion
In der vorliegenden Studie wurde der Zusammenhang zwi-schen Selbst- und Klinikerurteil anhand des BDI-II und derCDRS-R bei depressiven Jugendlichen auf Summen-, Sub-skalen- und Einzelitemebene untersucht. Bisherige Stu-dien, die die Übereinstimmung zwischen Selbst- und Kli-nikerurteil bei depressiven Jugendlichen untersuchten, fan-den Korrelationskoeffizienten bis zu .80. Auch wenn dieKorrelation der vorliegenden Studie im direkten Vergleichnicht ganz so hoch ausfällt, zeigt sich kein signifikanterUnterschied zu den bisherigen Studien (z-Werte zwischen–.17 und –1.19). Einflussfaktoren, die sich negativ auf dieHöhe des Zusammenhangs zwischen Selbst- und Kliniker-urteil ausgewirkt haben könnten, sind vielfältig: Zum einenkönnte der Erhebungszeitraum, der bis zu einer Woche be-
trägt und innerhalb dessen sich bereits eine Symptomver-änderung eingestellt haben könnte, von Einfluss sein. Einweiterer Einflussfaktor könnte darin bestehen, dass die di-agnostischen Instrumente meist zu Beginn der ambulantenoder stationären Behandlung durchgeführt wurden. VonDorz et al. (2004) wurde berichtet, dass die Konkordanzzwischen Selbst- und Klinikerurteil in der Akutphaseschlechter sei als in der Remissionsphase. Diese Verringe-rung der Diskrepanz über die Behandlungsphase hinwegfanden auch Dunlop et al. (2011), insbesondere bei Frauen,die in der Akutphase ihre Symptomatik eher überschätzten.Da unsere Studie vor Einleitung einer Behandlung durch-geführt wurde, ist nach dem Ergebnis von Dunlop et al.(2011) zu vermuten, dass die Diskrepanz zu diesem Zeit-punkt maximal ist und sich im Verlauf eher verringert.Letzteres begründen Dunlop et al. (2011) folgendermaßen:1) im Verlauf der Behandlung entsteht ein wachsendes ge-meinsames Verständnis für die sprachlichen Beschreibun-gen der Symptome, 2) der Patient entwickelt eine bessereKonzentrationsfähigkeit aufgrund einer Besserung derSymptomatik, 3) mit der Besserung der Symptomatikkommt es zu einer geringeren stimmungsbedingten Verzer-rung der Symptomeinschätzung der vergangenen Wocheund 4) es kommt zu einem vermehrten Öffnen des Patien-ten gegenüber dem Kliniker aufgrund des besser werden-den «rapports».
Die Subskalen des CDRS-R Faktors «körperliche Be-schwerden» und des BDI-II Faktors «somatisch-affektiv»zeigten eine hohe Korrelation, welche sich aber nicht un-terschied von Korrelationen anderer Faktoren wie demCDRS-R Faktor «berichtete depressive Stimmung» unddem BDI-II Faktor «kognitiv». Dies ist nicht in Einklangmit den Ergebnissen von Corruble et al. (1999), welche beiErwachsenen einen höheren Zusammenhang von Items, diesich auf somatische Inhalte bezogen, als bei Items die sichauf die Stimmung bezogen, fanden. Die Autoren erklärtenihre Ergebnisse damit, dass innerpsychische, subjektiveVorgänge für den Diagnostiker weniger zugänglich und da-mit schwerer einschätzbar seien als eher objektive körper-liche Symptome. Nachdem diese Ergebnisse bei den Ju-gendlichen nicht zu finden waren, bleiben zum einen me-thodische Unterschiede zur Erklärung, z. B. Itemebene beiCorruble et al. (1999) und Sub-Faktoren in unserem Fall,oder Jugendliche unterscheiden sich in der Wahrnehmungoder Verbalisierung ihrer affektiven Zustände von Erwach-senen, was aber näher untersucht werden müsste. Kritischzu sehen ist auch die Faktorenzusammenstellung von Guoet al. (2006), deren Faktoren teilweise nur auf zwei oderdrei Items beruhen. In der faktorenanalytischen Literaturwird dies allgemein als zu niedrig angesehen (Reise, Moore& Haviland, 2010), und auch in der eigenen Faktorenana-lyse der CDRS-R Daten ergaben sich nur zwei Faktoren:ein Faktor mit den im Interview erfragten Items (1–14) undein Faktor, der die drei auf Beobachtung beruhenden Items(15–17) umfasst (Keller et al. 2012). Neuere faktorenana-lytische Modelle dürften die Daten zudem besser beschrei-ben, insbesondere ein sogenanntes «bifactor model», bei
J. Straub et al.: Selbst- und Klinikerurteil über depressive Symptomatik bei Jugendlichen 249
Z. Kinder-Jugendpsychiatr. Psychother. 42 (4) © 2014 Verlag Hans Huber, Hogrefe AG, Bern
Persönliches Autorenexemplar (e-Sonderdruck)

dem alle Items auf einem Generalfaktor laden und einzelneItems gleichzeitig noch spezifische Faktoren bilden können(vgl. Reise et al., 2010), wie es inzwischen auch für dasBDI-II diskutiert wird (Brouwer, Meijer & Zevalkink2013).
Korrelationen auf Einzelitemebene bei inhaltlich ver-gleichbaren Items ergaben moderate bis hohe Korrelations-koeffizienten. Diese Ergebnisse sind vergleichbar mit denKorrelationskoeffizienten von Keller, Ruppe, Stieglitz &Wolfersdorf (1997) beim Vergleich der HAMD mit demBDI bei Erwachsenen (Korrelationskoeffizienten lagenzwischen .35 und .61). In der vorliegenden Arbeit korre-lierten die Items «Selbstmordgedanken», «Selbstwertge-fühl», «Reizbarkeit» und «ausgeprägte Müdigkeit» amhöchsten. Dieses Ergebnis repliziert teilweise das Ergebnisder Studie von Corruble et al. (1999), die den höchsten Zu-sammenhang bei den Items «Selbstmordgedanken», «Ap-petit- und Schlafprobleme» und «körperliche Probleme»fanden. Am geringsten korrelierten die Items «depressiveStimmung» und «Konzentrationsprobleme», was ebenso inder Studie von Corruble et al. (1999) berichtet wurde. Zu-sammenfassend kann festgehalten werden, dass inhaltlichähnliche Items üblicherweise am höchsten korrelierten. In-teressanterweise fanden sich keine durchgängig mittel-ho-hen Korrelationen zwischen den Items, was man aufgrundder hohen internen Konsistenz beider Instrumente und derTatsache, dass beide dasselbe Konstrukt messen, hätte er-warten können.
Die Untersuchung von Drittvariablen zeigte, dass wederdas Geschlecht, das Vorliegen einer komorbiden Störung,der IQ noch die Art der Behandlung einen direkten signi-fikanten Einfluss auf die Höhe des Zusammenhangs aus-übten. Ersteres steht im Widerspruch zu dem Ergebnis vonShain et al. (1990), die einen höheren Zusammenhang beiMädchen als bei Jungen feststellten, aber repliziert das Er-gebnis von Corruble et al. (1999), welche bei Erwachsenenkeinen geschlechtsspezifischen Einfluss fanden. Bei derUnterteilung in Unter- und Überschätzer ergaben sich je-doch Beziehungen zur Behandlungsform (ambulant Be-handelte tendieren eher zu relativer Überschätzung als sta-tionär Behandelte) und zur Intelligenz (höhere Intelligenzist eher mit einer relativen Überschätzung der Symptoma-tik verbunden); tendenziell ergibt sich auch eine negativeKorrelation zum Alter. Auch Stavrakaki, Vargo, Robertsund Boodoosingh (1987) fanden, dass ältere Jugendlicheund stationäre Patienten relativ zum Klinikerurteil ihreSymptomatik eher unterschätzten und jüngere Patienten imambulanten Setting eher überschätzten. Die Autoren füh-ren diese Unterschiedlichkeit auf den möglichen Einflussvon sozialer Erwünschtheit zurück. Weitere Einflussfakto-ren bleiben zu diskutieren, z. B. Relativierung der eigenenSymptomatik durch den Vergleich mit anderen stationärenPatienten im Sinne des sozialen Vergleichs.
Als Limitationen der vorliegenden Studie sind zu nen-nen, dass zum einen der Zeitpunkt der Erhebung der beidenDiagnostikinstrumente bis zu einer Woche auseinander lag.Außerdem ist nicht auszuschließen, dass die Erhebung
durch die Interviewer, trotz vorhergehender Schulung, ei-nen (weitgehend) unsystematischen Beurteilerfehler auf-weist, der sich auf die Höhe der Zusammenhänge auswir-ken könnte. Methodisch ist zu den Klassifizierungen vonUnter- und Überschätzern gemäß Dorz et al. (2004) bzw.Dunlop et al. (2011) noch anzumerken, dass eine solcheVorgehensweise immer einen gewissen Prozentsatz dieserPersonen «generieren» muss, da wegen der z-Transforma-tion sowohl in der CDRS-R als auch im BDI-II ca. 16 %unterhalb bzw. oberhalb einer Standardabweichung liegenmüssen. Für die Differenz der beiden z-Werte gilt dies zwarnicht mehr direkt, aber unter der gewählten Vorgehenswei-se ergeben sich in allen drei Studien jeweils ca. 10–15 %Unter- und Überschätzer. Anstatt dieses stichprobenabhän-gigen Ansatzes wären andere Lösungen, bei denen z. B.absolute Größenordnungen wie etwa Diskrepanzen inSchweregradkategorien der Depression Verwendung fin-den, eventuell besser. Solche Einstufungen sind aberschwierig zu begründen und auch ihnen haftet dann einegewisse Willkür an, weshalb darauf verzichtet wurde.
Weitere Studien sollten andere mögliche Einflussfakto-ren auf den Zusammenhang von Selbst- und Klinikerurtei-len näher untersuchen um weiterführende Aussagen überdie Übereinstimmungsvalidität treffen zu können. Außer-dem könnte untersucht werden, ob sich eine geringereDiskrepanz zwischen Selbst- und Klinikerurteil im Verlaufder Behandlung auch bei Jugendlichen einstellt, und ur-sächliche Faktoren dafür untersucht werden.
Insgesamt weisen die Ergebnisse auf eine hohe Korrela-tion zwischen Selbsturteil (BDI-II) und Klinikerurteil(CDRS-R) hin. Dennoch kann nicht davon ausgegangenwerden, dass das Interview durch den Fragebogen komplettersetzbar ist, da Fragebögen anfälliger für Verfälschungs-tendenzen und Urteilsfehler sind. Zudem sind sie wenigeränderungssensitiv und weniger geeignet für die Differen-zierung zwischen unterschiedlichen Schweregraden psy-chischer Phänomene (Stieglitz, 2008). Eine hohe Korrela-tion bedeutet außerdem nicht, dass die Einschätzungen na-hezu deckungsgleich sind, im Gegenteil bleibt immer nochviel Varianz unerklärt. Der Fragebogen kann jedoch deut-liche Hinweise auf das Vorliegen einer Depression liefernbeziehungsweise zum Ausschluss einer depressiven Episo-de dienen (Dolle et al., 2012) und ist daher auf Grund seinerzeitökonomischen Durchführung in Kliniken und Praxenals Routine-Eingangsdiagnostik empfehlenswert.
Literatur
Aster, M., Neubauer, A. & Horn, R. (2006). Wechsler Intelligenz-test für Erwachsene. Frankfurt: Harcourt Test Services.
Beck, A. T., Steer, R. A. & Brown, G. K. (1996). Beck DepressionInventory Manual (2nd ed.). San Antonio, TX: The Psycho-logical Corporation.
Besier, T., Goldbeck, L. & Keller, F. (2008). Psychometrische Gü-tekriterien des Beck-Depressions-Inventars II (BDI II) bei ju-
250 J. Straub et al.: Selbst- und Klinikerurteil über depressive Symptomatik bei Jugendlichen
Z. Kinder-Jugendpsychiatr. Psychother. 42 (4) © 2014 Verlag Hans Huber, Hogrefe AG, Bern
Persönliches Autorenexemplar (e-Sonderdruck)
gendpsychiatrischen Patienten. Psychotherapie, Psychosoma-tik, Medizinische Psychologie, 58, 63–68.
Bortz, J. (2005). Statistik für Human- und Sozialwissenschaftler(6. Aufl.). Heidelberg: Springer-Verlag.
Brouwer, D., Meijer, R. R. & Zevalkink, J. (2013). On the factorstructure of the Beck Depression Inventory-II: G is the key.Psychological Assessment 25, 136–145.
Carroll, B. J., Feinberg, M. & Smouse, P. E. (1981). The CarrollRating Scale for Depression. Development: Reliability and va-lidation. British Journal of Psychiatry, 138, 194–200.
Corruble, E., Legrand, J. M., Zvenigorowski, H., Duret, C. &Guelfi, J. D. (1999). Concordance between self-report and cli-nicians’ assessment of depression. Journal of Psychiatric Re-search, 33, 457–465.
Dolle, K., Schulte-Körne, G., v Hofacker, N., Izat, Y. & Allgaier,A. K. (2012). Übereinstimmung von klinischer Diagnose,strukturierten Interviews und Selbstbeurteilungsfragebögenbei Depressionen im Kindes- und Jugendalter. Zeitschrift fürKinder- und Jugendpsychiatrie und Psychotherapie, 40,405–414.
Döpfner, M., Görtz-Dorten, A., Lehmkuhl, G., Breuer, B. & Go-letz, H. (2008). Diagnostik-System für psychische Störungennach ICD-10 und DSM-IV für Kinder und Jugendliche-II.Mannheim: Huber.
Dorz, S., Borgherini, G., Conforti, D., Scarso, C. & Magni, G.(2004). Comparison of self-rated and clinician-rated measuresof depressive symptoms: A naturalistic study. Psychology andPsychotherapy: Theory, Research and Practice, 77, 353–361.
Dunlop, B. W., Li, T., Kornstein, S. G., Friedman, E. S., Roth-schild, A. J., Pedersen, R. . . . Trivedi, M. H. (2011). Concord-ance between clinician and patient ratings as predictors of re-sponse, remission and recurrence in major depressive disorder.Journal of Psychiatric Research, 45, 96–103.
Guo, Y., Nilsson, M. E., Heiligenstein, J., Wilson, M. G. & Emslie,G. (2006). An exploratory factor analysis of the Children’s De-pression Rating Scale – revised. Journal of Child and Adoles-cent Psychopharmacology, 16, 482–491.
Hautzinger, M., Keller, F. & Kühner, C. (2006). BDI-II Beck De-pressions-Inventar Revision. Frankfurt am Main: HarcourtTest Services.
Hoffmann, F., Petermann, F., Glaeske, G. & Bachmann, C.(2012). Prevalence and comorbidities of adolescent depressionin Germany. Zeitschrift für Kinder- und Jugendpsychiatrie undPsychotherapie, 40, 399–404.
Horn, W. (2004). Prüfsystem für Schul- und Bildungsberatung für6. bis 13. Klassen. Göttingen: Hogrefe
Jantzer, V., Parzer, P., Lehmkuhl, U. & Resch, F. (2012). NeuereEntwicklungen zur Diagnostik psychischer Störungen im Ju-gendalter. Kindheit und Entwicklung, 21, 198–207.
Kaufman, J., Birmaher, B. & Brent, D. (1997). Schedule for Af-fective Disorders and Schizophrenia for School-Age Children– Present and Lifetime Version (K-SADS-PL): Initial reliabil-ity and validity data. Journal of the American Academy ofChild & Adolescent Psychiatry, 36, 980–988.
Keller, F., Grieb, J., Koelch, M. & Sproeber, N. (2012). CDRS-RChildren’s Depression Rating Scale – Revised by E. O. Poz-nanski and H. B. Mokros: Deutsche Version. Göttingen: Ho-grefe.
Keller, F., Hautzinger, M. & Kühner, C. (2008). Zur faktoriellenStruktur des deutschsprachigen BDI-II. Zeitschrift für Klini-sche Psychologie und Psychotherapie, 37, 245–254.
Keller, F., Ruppe, A., Stieglitz, R. D. & Wolfersdorf, M. (1997).Korrelationen zwischen Selbst- und Fremdbeurteilung vonDepressivität auf der Symptomebene. In M. Wolfersdorf(Ed.), Depressionsstationen/Stationäre Depressionsbehandlung(pp. 139–143). Berlin: Springer-Verlag.
Kovacs, M. (1981). Rating scales to assess depression in school-aged children. Acta Paedopsychiatrica, 46, 305–315.
Kovacs, M. (1992). The Children’s Depression Inventory. NorthTonawanda, NY: Mental Health Systems.
Lauth, B., Arnkelsson, G. B., Magnusson, P., Skarphedinsson,G. A., Ferrari, P. & Petursson, H. (2010). Validity of K-SADS-PL (Schedule for Affective Disorders and Schizophrenia forSchool-Age Children – Present and Lifetime Version) depres-sion diagnoses in an adolescent clinical population. NordicJournal of Psychiatry, 64, 409 – 420.
Mehler-Wex, C. (2012). Entwicklungspsychiatrische Aspekte de-pressiver Störungen. Nervenheilkunde, 31, 515–523.
Myers, K. & Winters, N. C. (2002). Ten-year review of ratingscales. II: Scales for internalizing disorders. Journal of Amer-ican Academy of Child & Adolescent Psychiatry, 41, 634–659.
Osman, A., Kopper, B. A., Barrios, F., Gutierrez, P. M. & Bagge,C. L. (2004). Reliability and validity of the Beck DepressionInventory-II with adolescent psychiatric inpatients. Psycho-logical Assessment, 16, 120–132.
Petermann, F. & Petermann, U. (2008). Hamburg-Wechsler-Intel-ligenztest für Kinder-IV. Mannheim: Huber.
Plener, P. L., Fegert, J. M., Kölch, M. G. (2012). Psychopharma-kologische Behandlung von Depressionen im Kindes – undJugendalter: Entwicklung und Standards seit der «Black Box»Warnung. Zeitschrift für Kinder- und Jugendpsychiatrie undPsychotherapie, 40, 365–371.
Poznanski, E. O. & Mokros, H. B. (1996). Children’s DepressionRating Scale, Revised (CDRS-R): Manual. Los Angeles, CA:Western Psychological Services.
Reise, S. P., Moore, T. M. & Haviland, M. G. (2010). Bifactor mo-dels and rotations: Exploring the extent to which multidimen-sional data yield univocal scale scores. Journal of PersonalityAssessment, 92, 544–559.
Remschmidt, H., Schmidt, M. & Poustka, F. (2009). MultiaxialesKlassifikationsschema für psychische Störungen des Kindes-und Jugendalters nach ICD-10 der WHO. Bern: Huber.
Reynolds, W. M. (1987). Reynolds Adolescent Depression ScaleProfessional Manual. Odessa, FL: Psychological AssessmentResources.
Reynolds, W. M. (1989). Reynolds Child Depression Scale. Odes-sa, FL: Psychological Assessment Resources.
Robbins, D. R., Alessi, N. E., Colfer, M. V. & Yanchyshyn, G. W.(1985). Use of the Hamilton Rating Scale for Depression andthe Carroll Self-Rating Scale in Adolescents. Psychiatry Re-search, 14, 123–129.
Rush, A. J., Giles, D. E., Schlesser, M. A., Fulton, C. L., Wiessen-burger, J. & Burns, C. (1986). The Inventory for DepressiveSymptomatology (IDS): Preliminary findings. Psychiatry Re-search, 18, 65–87.
Rush, A. J., Hiser, W. & Giles, D. E. (1987). A comparison ofself-reported vs clinician-rated symptoms in depression. Jour-nal of Clinical Psychiatry, 48, 246–248.
Saluja, G., Iachan, R., Scheidt, P. C., Overpeck, M. D., Sun, W. &Giedd, J. N. (2004). Prevalence of and risk factors for depres-sive symptoms among young adolescents. Archives of Pediat-rics & Adolescent Medicine, 158, 760–765.
J. Straub et al.: Selbst- und Klinikerurteil über depressive Symptomatik bei Jugendlichen 251
Z. Kinder-Jugendpsychiatr. Psychother. 42 (4) © 2014 Verlag Hans Huber, Hogrefe AG, Bern
Persönliches Autorenexemplar (e-Sonderdruck)

Saß, H., Wittchen, H. U., Zaudig, M. & Houben, I. (2003). Diag-nostisches und Statistisches Manual Psychischer Störungen.Textrevision DSM-IV-TR. Göttingen: Hogrefe.
Schneider, S., Unnewehr, S. & Margraf, J. (2009). Kinder DIPS-Diagnostisches Interview bei psychischen Störungen im Kin-des- und Jugendalter (2. Aufl.). Heidelberg: Springer-Verlag.
Shain, B. N., Naylor, M. & Alessi, N. (1990). Comparison of self-rated and clinician-rated measures of depression in adoles-cents. American Journal of Psychiatry, 147, 793–795.
Stavrakaki, C., Vargo, B., Roberts, V. & Boodoosingh, L. (1987).Concordance among sources of information for ratings of an-xiety and depression in children. Journal of the AmericanAcademy of Child and Adolescents Psychiatry, 26, 733–737.
Stieglitz, R. D. (2008). Diagnostik und Klassifikation in der Psy-chiatrie. Stuttgart: Kohlhammer.
Stiensmeier-Pelster, J., Schürmann, M. & Duda, K. (2000). De-pressions-Inventar für Kinder und Jugendliche (DIKJ). Hand-anweisung (2. Aufl.). Göttingen: Hogrefe.
Williams, J. B. W. (1988). A structured interview guide for theHamilton Depression Scale. Archives of General Psychiatry,45, 742–747.
Manuskripteingang 20. September 2013Nach Revision angenommen 20. Dezember 2013
Interessenkonflikte– J. Straub hat keine Interessenkonflikte.– M. G. Kölch hat keine Interessenkonflikte. Er erhält
Subventionen von der internationalen Eli Lilly Stiftung.Er erhielt Forschungssubventionen des DMFFSJ (Bun-desministerium für Familien, Senioren, Frauen und Ju-gend), der BMBF (Bundesministerium für Bildung und
Forschung), des Schweizer Bundesamtes für Justiz undvon Boehringer Ingelheim. Er war Cl oder PI für EliLilly, Astra Zeneca und Janssen-Cilag, Lundbeck. Er er-hielt Reisezuschüsse für Vorträge von Janssen-Cilag, derUniversität von Rostock, DGKJPP, UCB, EuropäischeAkademie und gemeinnützigen Organisationen. Er istkein Aktieninhaber oder Aktionär in der pharmazeuti-schen Industrie.
– P. Plener hat keine Interessenkonflikte. Er ist PI fürLundbeck. Er erhielt Forschungssubventionen vomBMBF (Bundesministerium für Bildung und For-schung) und BfArM (Bundesinstitut für Arzneimittelund Medizinprodukte). Er erhielt Reisezuschüsse vonDFG, DAAF und IACAPAP. Er ist kein Aktieninhaberoder Aktionär in der pharmazeutischen Industrie.
– F. Keller hat keine Interessenkonflikte. Er ist der (Mit-)Herausgeber der deutschen Versionen des Beck Depres-sions-Inventars – zweite Edition (BDI–II) und derChildren’s Depression Rating Scale Revised (CDRS-R)und erhält dafür Lizenzgebühren.
Joana Straub, M.sc.
Klinik für Kinder- und Jugendpsychiatrie- und PsychotherapieUniversitätsklinikum UlmSteinhövelstraße 589075 [email protected]
252 J. Straub et al.: Selbst- und Klinikerurteil über depressive Symptomatik bei Jugendlichen
Z. Kinder-Jugendpsychiatr. Psychother. 42 (4) © 2014 Verlag Hans Huber, Hogrefe AG, Bern
Persönliches Autorenexemplar (e-Sonderdruck)

Psychotherapeutic treatment of children and adolescents with depression. Review of the
literature on cognitive-behavioral and interpersonal group therapies
104
6.5 Psychotherapeutic treatment of children and adolescents with depression. Review of
the literature on cognitive-behavioral and interpersonal group therapies
Contribution of Joana Straub to the article:
J. Straub researched literature, wrote the manuscript, integrated remarks of the co-authors,
revised the manuscript according to reviewer’s comments, and created tables.
Co-authors’ contributions to the article:
L. Nicolaus helped with literature research and creating tables. P.L. Plener, N. Sproeber, M.G.
Koelch reviewed the draft and gave constructive remarks. They helped with revising the
manuscript according to the reviewer’s comments.
Reference
Straub, J., Nicolaus, L., Plener, P.L., Sproeber, N. & Koelch, M.G. (2014). Psychotherapeutic
treatment of children and adolescents with depression. Review of the literature on cognitive-
behavioral and interpersonal group therapies. Der Psychotherapeut, 59, 7-15.
Reprinted from der Psychotherapeut, 59, Straub, J., Nicolaus, L., Plener, P.L., Sproeber, N. &
Koelch, M.G., Psychotherapeutic treatment of children and adolescents with depression.
Review of the literature on cognitive-behavioral and interpersonal group therapies, 7-15,
Copyright (2014), with permission from Springer.
Joana Straub1 · Leonie Nicolaus1 · Paul L. Plener1 · Nina Spröber1 · Michael Kölch1, 2
1 Klinik für Kinder- und Jugendpsychiatrie und Psychotherapie, Universität Ulm2 Vivantes Kliniken für Kinder- und Jugendpsychiatrie, Psychotherapie und Psychosomatik, Berlin
Psychotherapeutische Behandlung von depressiven Kindern und Jugendlichen
Literaturübersicht zu kognitiv-behavioralen und interpersonellen Gruppentherapieverfahren
Depressionen beginnen oft im Kin-des- und Jugendalter und persistie-ren in vielen Fällen bis ins Erwachse-nenalter. Sie gehen häufig mit einem erhöhten Suizidrisiko einher, und der Suizid stellt die zweithäufigste Todes-ursache bei Jugendlichen in Europa dar. Dies unterstreicht die Wichtigkeit einer frühzeitigen und wirkungsvol-len Intervention.
Hintergund
Die Prävalenz für depressive Störungen in der Allgemeinbevölkerung beträgt 4,7% bei männlichen und 9,7% bei weiblichen Jugendlichen (Bettge et al. 2008). Depres-sionen gehen häufig mit komorbiden Stö-rungen und einem erhöhten Suizidrisiko einher (Saluja et al. 2004). Vor allem das Suizidrisiko ist alarmierend in Anbetracht der Tatsache, dass der Suizid die zweithäu-figste Todesursache bei Jugendlichen in Europa darstellt (Steele u. Doey 2007). Die aufgeführten Aspekte legen die Notwen-digkeit einer schnellen und wirkungsvol-len Behandlung nahe. Die aktuellen Leit-linien der Arbeitsgemeinschaft der Wis-senschaftlichen Medizinischen Fachge-sellschaften (AWMF, Deutsche Gesell-schaft für Kinder- und Jugendpsychiat-rie u. Psychosomatik und Psychothera-pie 2013) empfehlen, dass depressive Kin-der und Jugendliche eine kognitiv-verhal-tenstherapeutische Therapie (KVT), eine interpersonelle Psychotherapie für Ado-
leszente (IPT-A), das Medikament Fluo-xetin oder eine Kombination aus KVT und Fluoxetin erhalten sollten. Hierbei ist zunächst der Psychotherapie Vorrang zu gewähren.
Hinsichtlich der Wirksamkeit findet sich zwischen kognitiv-verhaltensthera-peutischen Einzel- und Gruppenthera-pieverfahren kein Unterschied (Weisz et al. 2006). Gruppentherapien mit einigen Vorteilen einher: Sie sind ökonomischer, ermöglichen verkürzte Wartezeiten, die Teilnehmer unterstützen sich gegensei-tig, geben einander Rückmeldung, und der Gruppenprozess wirkt darüber hin-aus einer Stigmatisierung entgegen (Oei u. Dingle 2008).
In der vorliegenden systematischen Li-teraturübersicht werden die publizierten Studien zur Wirksamkeit von kognitiv-verhaltenstherapeutischen und interper-sonellen Gruppentherapien bei der Be-handlung von depressiven Kindern und Jugendlichen dargestellt. Die am häufigs-ten bei der Behandlung von Depressionen im Kindes- und Jugendalter eingesetzten englischen und deutschen Gruppenthera-pieprogramme werden in übersichtlicher Form erläutert.
Systematische Literaturrecherche
Die systematische Literaturrecherche mit-hilfe der Datenbanken PsycInfo, Pubmed und Psyndex mit den Suchbegriffen: „cog-
nitive behav* group therapy“ or „interper-sonal therapy“ and „adolesc*“ or „child*“ and „depression“ or „affective disorders“ ergab 1547 Treffer (PsycInfo: 1366, Pub-med: 142, Psyndex: 39). Daraufhin wur-den die Treffer von PsycInfo nochmals auf Vorkommen der letzten 2 Suchbegriffe im Abstract hin gefiltert (PsycInfo: 99). Die Titel und – im Bedarfsfall – die Abs-tracts der verbliebenen 280 Beiträge wur-den bezüglich der Relevanz der Inhalte für den Review begutachtet, woraufhin 46 Publikationen im Volltext durchge-sehen wurden. Zusätzlich wurden Über-sichtsarbeiten (Butler et al. 2006; Clarke u. Lewinsohn 1989; Compton et al. 2004; Cox et al. 2013; Cuijpers et al. 2009; Curry 2001; Klein et al. 2007; Kühner 2003; Le-winsohn u. Clarke 1999; Maag u. Swearer 2005; Marcotte 1997; Reinecke et al. 1998; Watanabe et al. 2007; Weisz et al. 2006) und die in diesen Reviews beschriebene Literatur, sofern nicht bereits durch die Li-teratursuche identifiziert, begutachtet.
In die vorliegende Übersicht wurden nur Originalarbeiten unter Berücksichti-gung folgender Parameter aufgenommen:FPublikationen in einer Zeitschrift mit
„Peer-review“-Verfahren (keine Dis-sertationen oder Buchbeiträge),
FVerwendung standardisierter Instru-mente bzw. klinischer Interviews zur Erfassung von Depressionen,
FVorliegen einer Depressionsdiagno-se [ermittelt anhand der International Statistical Classification of Diseases
Psychotherapeut 2013 DOI 10.1007/s00278-013-1026-0© Springer-Verlag Berlin Heidelberg 2013
1Psychotherapeut 2013 |
Schwerpunkt: Adoleszenzpsychiatrie und -psychotherapie – Übersichten

and Related Health Problems (ICD), des Diagnostic and Statistical Manual of Mental Disorders (DSM) oder der erreichten „Cut-off “-Werte in rele-vanten Fragebogen oder Interviews],
FStudienpopulation: Kinder oder Ju-gendliche/junge Erwachsene,
FPublikationsdatum: 01.01.1980–30.09.2013,
FStudien mit Fokus auf die Behand-lung und nicht Prävention depressiver Störungen und
FUntersuchung entweder kognitiv-ver-haltenstherapeutischer oder interper-soneller Gruppentherapieverfahren.
Die Berücksichtigung der Einschlusskri-terien bei der Aufnahme der ausgewähl-ten Beiträge wurde von 2 unabhängigen Beurteilern überprüft. Außerdem wurde die Übereinstimmung von Treffern mit aktuellen Reviews und Metaanalysen zu interpersonellen und kognitiv-behaviora-len Therapiestudien zur Behandlung von Depressionen überprüft.
Unter Berücksichtigung der oben ge-nannten Kriterien konnten schlussend-lich 25 Studien aufgenommen werden (.Tab. 1, 2, 3). Davon bezogen sich je-weils 2 Studien auf die gleiche Stichpro-be; deshalb werden sie in einer Zeile auf-geführt.
Ergebnisse
Die meisten Studien untersuchten die Wirksamkeit von kognitiv-behavioraler Gruppentherapie (.Tab. 1), 2 Studien untersuchten die interpersonelle Thera-pie (.Tab. 2) und 2 eine Mischung aus beiden Verfahren (.Tab. 1, 2). Die Länge der Therapien variierte deutlich von einer 5-wöchigen Therapiedauer mit jeweils einer Sitzung/Woche á 90 min (.Tab. 3) bis hin zu einer 16-wöchigen Therapie-dauer mit jeweils einer Sitzung/Woche á 90–120 min (.Tab. 2).
Es gab lediglich 3 Studien, die die Wirksamkeit von Depressionsgruppen-therapien im deutschen Sprachraum untersuchten, wobei sich 2 davon auf die-selbe Stichprobe bezogen (.Tab. 3). Sie-ben Studien fokussierten sich auf Kinder und 18 Studien auf Jugendliche und junge Erwachsene. Neun Programme wurden in Schulen, 14 im ambulanten Setting, eines im stationären Setting und eines online durchgeführt.
Die 4 am häufigsten eingesetzten dia-gnostischen Verfahren waren das „Child Depression Inventory“ (CDI), „Beck De-
pression Inventory“ (BDI), die „Hamil-ton Depression Rating Scale“ (HDRS) und „Children’s Depression Rating Sca-le-Revised“ (CDRS-R; Reihenfolge nach Verwendungshäufigkeit). Von allen Stu-dien waren 16 randomisierte kontrollier-te Studien, 4 mit Interventions- und Kon-trollgruppe, aber unklarer Zuordnung und 5 Pilotstudien. Zehn Studien ver-glichen eine Interventionsgruppe, und 7 verglichen 2 Interventionsgruppen mit der Kontrollgruppe. Drei Studien ver-glichen aktive Behandlungen miteinan-der. Als Kontrolle diente in den meis-ten Fällen eine Wartelistenkontrollgrup-pe (n=12) und in jeweils 2 Studien „treat-ment as usual“ (TAU) oder unspezifische Intervention.
Gruppentherapieverfahren
Im folgenden Abschnitt werden die bei-den gängigsten englischsprachigen ko-gnitiv-verhaltenstherapeutischen Grup-pentherapieverfahren, anschließend die interpersonelle Gruppentherapie für Ju-gendliche und die 2 deutschen kognitiv-verhaltenstherapeutischen Gruppenthe-rapieverfahren skizziert.
Lewinsohn und Clarkes’s Adolescent Coping with Depression Course (CWD-A; Clarke et al. 1990) umfasst 16 wöchent-liche Sitzungen á 2 h und ist für Grup-pengrößen von bis zu 10 Jugendlichen zwischen 14 und 18 Jahren ausgelegt. Die konkreten Therapieinhalte sind in .Infobox 1 aufgeführt. Der CWD-A wurde in randomisierten kontrollierten Studien untersucht und hat sich in allen bis auf 2 Studien (Clarke et al. 2002; Lis-tug-Lunde et al. 2013) den Kontrollbedin-gungen gegenüber als überlegen erwie-sen. In einer deutschen Metaanalyse wur-den insgesamt 24 deutsch- und englisch-sprachige Studien, die „Coping with De-pression“ (CWD) bei Jugendlichen und Erwachsenen im Einzel- und Gruppen-Setting untersuchten, mit dem Ergebnis einer hohen Effektstärke (ES =1,45) ein-bezogen. Die Behandlungseffekte blieben dabei mittelfristig stabil (Kühner 2003). In einer holländischen Metaanalyse wur-de abermals die Effektstärke von CWD für 18 randomisierte kontrollierte Studien, in denen CWD zur Behandlung von De-pressionen bei Jugendlichen und Erwach-
Infobox 2
Taking ActionFPsychoedukationFDefinition von TherapiezielenFErkennen des Fortschritts in Richtung
ZielerreichungFTraining von „Coping“-FertigkeitenFProblemlösetrainingFKognitive UmstrukturierungFAufbau eines positiven Selbstwerts
Infobox 3
Stimmungsprobleme bewältigenFPsychoedukationFSelbstbeobachtungFVerhaltensaktivierungFEntspannungstrainingFSoziales KompetenztrainingFKognitive UmstrukturierungFFörderung der Problemlösefähigkeiten
Infobox 4
Manualized Intervention to Cope with Depressive SymptomsFPsychoedukationFSelbstbeobachtungFKognitive UmstrukturierungFFörderung der ProblemlösefähigkeitenFVerhaltensaktivierungFUmgang mit Krisen
Infobox 1
Elemente des Programms Coping with Depression Course for AdolescentsFSelbstbeobachtungFTraining sozialer FertigkeitenFErhöhung angenehmer AktivitätenFVerringerung depressiver GedankenFErlernen von Konfliktlösestrategien
Mögliche VariantenFElterntrainingFAuffrischungssitzungen
2 | Psychotherapeut 2013
Schwerpunkt: Adoleszenzpsychiatrie und -psychotherapie – Übersichten

senen eingesetzt wurde, untersucht. Die Autoren fanden allerdings nur eine mitt-lere Effektstärke (ES =0,28; Cuijpers et al. 2009).
Die Effektstärken der Studien, in de-nen die Wirksamkeit von CWD-A im Gruppen-Setting untersucht wurde, reich-ten von 0,02–1,34. Die höchste Effektstär-ke zeigte sich beim Vergleich von CWD-A zur Kontrollgruppe (ES =1,34; Kahn u. Kehle 1990); keine Effekte fanden sich bei dem Vergleich von CWD-A (plus TAU) mit TAU (Clarke et al. 2002; Listug-Lun-de et al. 2013). In 2 Studien wurde die al-leinige Teilnahme an CWD-A mit der Teilnahme an CWD-A und zusätzlichem Elterntraining verglichen. Beide Grup-pen unterschieden sich nicht voneinan-der, woraus zu schlussfolgern ist, dass der Einbezug von Eltern vermutlich keinen zusätzlichen Beitrag zur Genesung der Jugendlichen leistet. In einer Studie wur-de online CWD-A mit Wartelistenkont-rollgruppe mit dem Ergebnis einer hohen Effektstärke verglichen (Van der Zanden et al. 2012).
Die Selbstkontrolltherapie „Taking Ac-tion“ (Stark et al. 2004; Stark et al. 1996) wird in Schulen für 2 bis 5 Schüler/Grup-pe angeboten und umfasst 20 Gruppen-sitzungen und 2 Einzelsitzungen über eine Dauer von insgesamt 11 Wochen (.Infobox 2). Das Programm basiert auf dem Modell der Selbstkontrolle, bei dem die Jugendlichen individuelle „Coping“-Fertigkeiten erwerben, und zielt auf eine Verbesserung des Selbstmanagements, der sozialen Fertigkeiten, der Selbstbe-hauptung, der Entspannung und auf ko-gnitive Umstrukturierung ab. Außerdem finden Eltern- und Lehrersitzungen statt, in denen die Bezugspersonen lernen, die Kinder bei der Verringerung von Konflik-ten sowie bei der Identifikation und Ver-änderung negativer Gedanken zu unter-stützen. Die konkreten Therapieinhalte sind in .Infobox 2 aufgeführt. Die Ef-fektstärken der Selbstkontrolltherapie „ta-king action“ beliefen sich von keinem Ef-fekt im direkten Prä-post-Vergleich (De Cuyper et al. 2004) bis hin zu 1,49 (Rey-nolds u. Coats 1986) – einem starken Ef-fekt – beim Vergleich von Interventions-gruppe mit Wartelistenkontrollgruppe.
Mufson’s interpersonale Psychotherapie für depressive Jugendliche (IPT-A; Muf-
son et al. 1993) wurde eigentlich als Ein-zeltherapie konzipiert, kann aber auch in Gruppen angewendet werden. Sie um-fasst 3 Behandlungsphasen mit jeweils 4 Sitzungen zu jeweils einer Stunde. In
der ersten Phase werden gemeinsam von Patient und Therapeut 1 oder 2 Problem-bereiche definiert (z. B. Trauer; interper-sonale Defizite), die Rolle des Patienten und die des Therapeuten geklärt und ein
Zusammenfassung · Abstract
Psychotherapeut 2013 · [jvn]:[afp]–[alp] DOI 10.1007/s00278-013-1026-0© Springer-Verlag Berlin Heidelberg 2013
Joana Straub · Leonie Nicolaus · Paul L. Plener · Nina Spröber · Michael KölchPsychotherapeutische Behandlung von depressiven Kindern und Jugendlichen. Literaturübersicht zu kognitiv-behavioralen und interpersonellen Gruppentherapieverfahren
ZusammenfassungHintergrund. Depression beschreibt eine psychische Störung mit stark beeinträchti-genden Symptomen (z. B. erhöhte Suizida-lität), die auch im Kindes- und Jugendalter eine hohe Prävalenzrate aufweist und häufig einen chronischen Verlauf zeigt. Sowohl die kognitive Verhaltenstherapie (KVT) als auch die interpersonelle Therapie stellen derzeit nach diversen Leitlinien die Therapien der ersten Wahl dar.Ziel der Arbeit. Die aktuelle Studienlage be-züglich kognitiv-verhaltenstherapeutischer und interpersoneller Gruppentherapiever-fahren zur Behandlung von Depressionen im Kindes- und Jugendalter sollte dargestellt werden. Die gängigsten Therapieprogramme werden in übersichtlicher Form erläutert.Material und Methode. Die Literaturre-cherche (PsycInfo, Psyndex, Pubmed) liefer-te 280 Treffer. Nach Durchsicht der Titel und Abstracts konnten 25 Studien in die vorlie-gende Arbeit aufgenommen werden.
Ergebnisse. Wirksamkeitsnachweise existie-ren v. a. für englischsprachige kognitiv-ver-haltenstherapeutische Gruppentherapiepro-gramme (Effektstärken zwischen 0,02 und 1,34) und nur wenige für die interpersonelle Gruppentherapie. Für den deutschen Sprach-raum liegen wenige Studien zu kognitiv-ver-haltenstherapeutischen Gruppentherapien und gemäß dem Wissen der Autoren keine zur interpersonellen Gruppentherapie vor.Schlussfolgerung. Die Wirksamkeit von Gruppentherapieverfahren zur Behandlung von depressiven Kindern und Jugendlichen sollte v. a. im deutschsprachigen Raum wei-terführend untersucht werden.
SchlüsselwörterWirksamkeit der Behandlung · Datensammlung · Deutsch · Englisch · Depression
Psychotherapeutic treatment of children and adolescents with depression. Review of the literature on cognitive-behavioral and interpersonal group therapies
AbstractBackground. Depression is a psychiatric dis-order with debilitating symptoms (e.g. sui-cidal behavior) with a high prevalence rate even in children and adolescents and the dis-order shows a chronic course in many cas-es. According to psychiatric guidelines, cog-nitive behavioral therapy and interperson-al therapy are the psychotherapeutic meth-ods of choice.Aim. This article gives an overview of the current studies on cognitive behavioral and interpersonal group therapy programs for the treatment of depression in children and ad-olescents as well as a short illustration of the most prevalent therapy programs.Material and methods. A literature research (PsycInfo, Psyndex, Pubmed) revealed 280 hits. After a review of all titles and abstracts 25 studies were included in this study.
Results. Efficacy studies mainly exist for cog-nitive behavioral group therapy programs (ef-fect sizes ranged from 0.02 to 1.34) from Eng-lish-speaking countries. There are only a few German programs available. With respect to interpersonal group therapies there are on-ly few articles published in English and to the best of our knowledge none in German.Conclusion. There is a great need for further studies that investigate the efficacy of group therapies for the treatment of depression in children and adolescents especially in Ger-man-speaking countries.
KeywordsTreatment efficacy · Data collection · German · English · Depression
3Psychotherapeut 2013 |
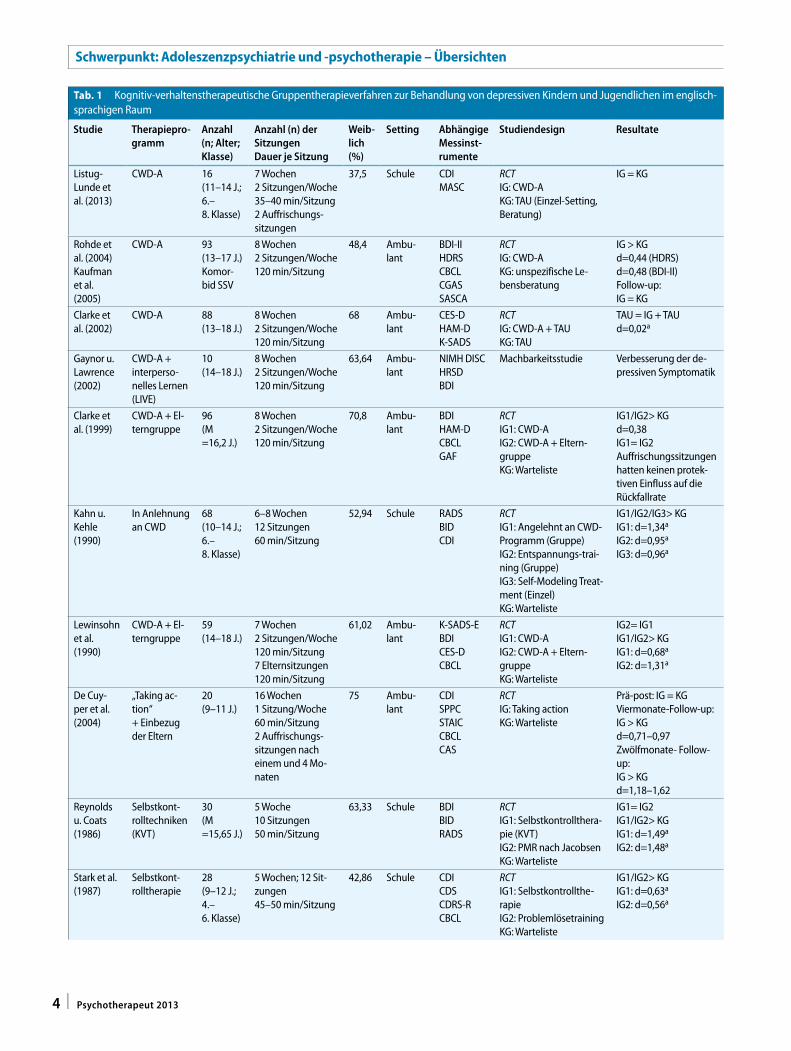
Tab. 1 Kognitiv-verhaltenstherapeutische Gruppentherapieverfahren zur Behandlung von depressiven Kindern und Jugendlichen im englisch-sprachigen Raum
Studie Therapiepro-gramm
Anzahl (n; Alter; Klasse)
Anzahl (n) der SitzungenDauer je Sitzung
Weib-lich (%)
Setting Abhängige Messinst-rumente
Studiendesign Resultate
Listug-Lunde et al. (2013)
CWD-A 16(11–14 J.;6.–8. Klasse)
7 Wochen2 Sitzungen/Woche35–40 min/Sitzung2 Auffrischungs-sitzungen
37,5 Schule CDIMASC
RCTIG: CWD-AKG: TAU (Einzel-Setting, Beratung)
IG = KG
Rohde et al. (2004)Kaufman et al. (2005)
CWD-A 93(13–17 J.)Komor-bid SSV
8 Wochen2 Sitzungen/Woche120 min/Sitzung
48,4 Ambu-lant
BDI-IIHDRSCBCLCGASSASCA
RCTIG: CWD-AKG: unspezifische Le-bensberatung
IG > KGd=0,44 (HDRS)d=0,48 (BDI-II)Follow-up:IG = KG
Clarke et al. (2002)
CWD-A 88(13–18 J.)
8 Wochen2 Sitzungen/Woche120 min/Sitzung
68 Ambu-lant
CES-DHAM-DK-SADS
RCTIG: CWD-A + TAUKG: TAU
TAU = IG + TAUd=0,02a
Gaynor u. Lawrence (2002)
CWD-A + interperso-nelles Lernen (LIVE)
10(14–18 J.)
8 Wochen2 Sitzungen/Woche120 min/Sitzung
63,64 Ambu-lant
NIMH DISCHRSDBDI
Machbarkeitsstudie Verbesserung der de-pressiven Symptomatik
Clarke et al. (1999)
CWD-A + El-terngruppe
96(M =16,2 J.)
8 Wochen2 Sitzungen/Woche120 min/Sitzung
70,8 Ambu-lant
BDIHAM-DCBCLGAF
RCTIG1: CWD-AIG2: CWD-A + Eltern-gruppeKG: Warteliste
IG1/IG2> KGd=0,38IG1= IG2Auffrischungssitzungen hatten keinen protek-tiven Einfluss auf die Rückfallrate
Kahn u. Kehle (1990)
In Anlehnung an CWD
68(10–14 J.;6.–8. Klasse)
6–8 Wochen12 Sitzungen60 min/Sitzung
52,94 Schule RADSBIDCDI
RCTIG1: Angelehnt an CWD-Programm (Gruppe)IG2: Entspannungs-trai-ning (Gruppe)IG3: Self-Modeling Treat-ment (Einzel)KG: Warteliste
IG1/IG2/IG3> KGIG1: d=1,34a
IG2: d=0,95a
IG3: d=0,96a
Lewinsohn et al. (1990)
CWD-A + El-terngruppe
59(14–18 J.)
7 Wochen2 Sitzungen/Woche120 min/Sitzung7 Elternsitzungen120 min/Sitzung
61,02 Ambu-lant
K-SADS-EBDICES-DCBCL
RCTIG1: CWD-AIG2: CWD-A + Eltern-gruppeKG: Warteliste
IG2= IG1IG1/IG2> KGIG1: d=0,68a
IG2: d=1,31a
De Cuy-per et al. (2004)
„Taking ac-tion“+ Einbezug der Eltern
20(9–11 J.)
16 Wochen1 Sitzung/Woche60 min/Sitzung2 Auffrischungs-sitzungen nach einem und 4 Mo-naten
75 Ambu-lant
CDISPPCSTAICCBCLCAS
RCTIG: Taking actionKG: Warteliste
Prä-post: IG = KGViermonate-Follow-up:IG > KGd=0,71–0,97Zwölfmonate- Follow-up:IG > KGd=1,18–1,62
Reynolds u. Coats (1986)
Selbstkont-rolltechniken (KVT)
30(M =15,65 J.)
5 Woche10 Sitzungen50 min/Sitzung
63,33 Schule BDIBIDRADS
RCTIG1: Selbstkontrollthera-pie (KVT)IG2: PMR nach JacobsenKG: Warteliste
IG1= IG2IG1/IG2> KGIG1: d=1,49a
IG2: d=1,48a
Stark et al. (1987)
Selbstkont-rolltherapie
28(9–12 J.;4.–6. Klasse)
5 Wochen; 12 Sit-zungen45–50 min/Sitzung
42,86 Schule CDICDSCDRS-RCBCL
RCTIG1: Selbstkontrollthe-rapieIG2: ProblemlösetrainingKG: Warteliste
IG1/IG2> KGIG1: d=0,63a
IG2: d=0,56a
4 | Psychotherapeut 2013
Schwerpunkt: Adoleszenzpsychiatrie und -psychotherapie – Übersichten
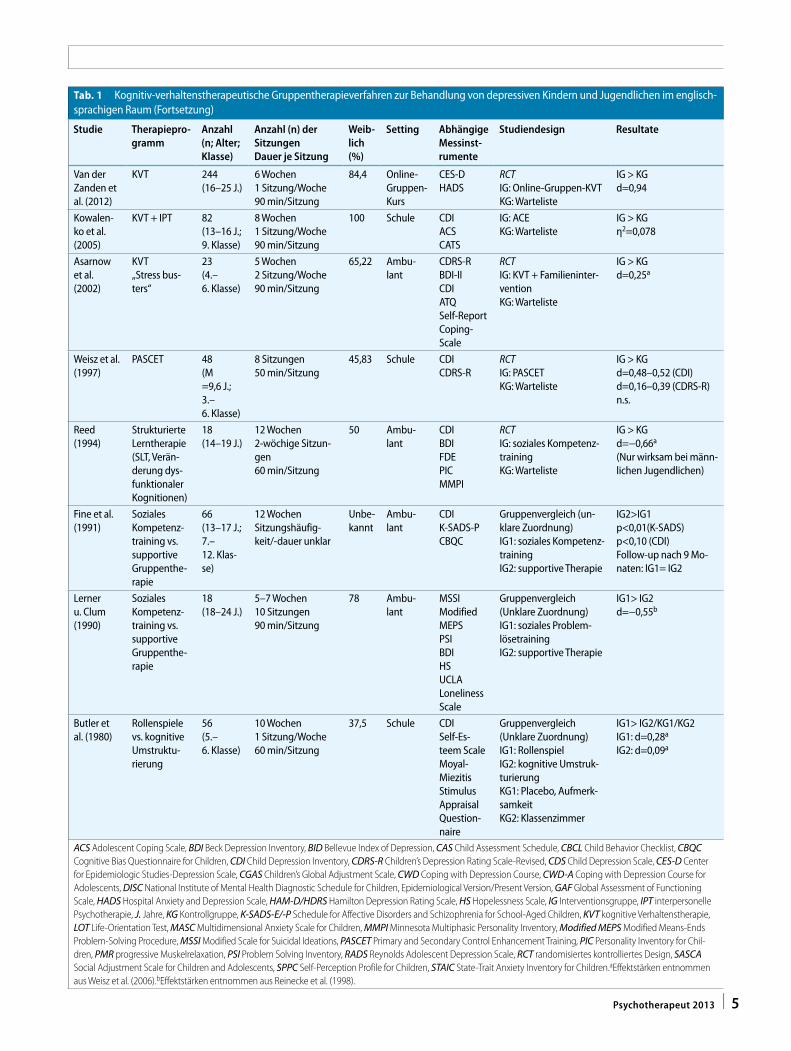
Tab. 1 Kognitiv-verhaltenstherapeutische Gruppentherapieverfahren zur Behandlung von depressiven Kindern und Jugendlichen im englisch-sprachigen Raum (Fortsetzung)
Studie Therapiepro-gramm
Anzahl (n; Alter; Klasse)
Anzahl (n) der SitzungenDauer je Sitzung
Weib-lich (%)
Setting Abhängige Messinst-rumente
Studiendesign Resultate
Van der Zanden et al. (2012)
KVT 244(16–25 J.)
6 Wochen1 Sitzung/Woche90 min/Sitzung
84,4 Online-Gruppen-Kurs
CES-DHADS
RCTIG: Online-Gruppen-KVTKG: Warteliste
IG > KGd=0,94
Kowalen-ko et al. (2005)
KVT + IPT 82(13–16 J.;9. Klasse)
8 Wochen1 Sitzung/Woche90 min/Sitzung
100 Schule CDIACSCATS
IG: ACEKG: Warteliste
IG > KGη2=0,078
Asarnow et al. (2002)
KVT„Stress bus-ters“
23(4.–6. Klasse)
5 Wochen2 Sitzung/Woche90 min/Sitzung
65,22 Ambu-lant
CDRS-RBDI-IICDIATQSelf-Report Coping-Scale
RCTIG: KVT + Familieninter-ventionKG: Warteliste
IG > KGd=0,25a
Weisz et al. (1997)
PASCET 48(M =9,6 J.;3.–6. Klasse)
8 Sitzungen50 min/Sitzung
45,83 Schule CDICDRS-R
RCTIG: PASCETKG: Warteliste
IG > KGd=0,48–0,52 (CDI)d=0,16–0,39 (CDRS-R) n.s.
Reed (1994)
Strukturierte Lerntherapie (SLT, Verän-derung dys-funktionaler Kognitionen)
18(14–19 J.)
12 Wochen2-wöchige Sitzun-gen60 min/Sitzung
50 Ambu-lant
CDIBDIFDEPICMMPI
RCTIG: soziales Kompetenz-trainingKG: Warteliste
IG > KGd=−0,66a
(Nur wirksam bei männ-lichen Jugendlichen)
Fine et al. (1991)
Soziales Kompetenz-training vs. supportive Gruppenthe-rapie
66(13–17 J.;7.–12. Klas-se)
12 WochenSitzungshäufig-keit/-dauer unklar
Unbe-kannt
Ambu-lant
CDIK-SADS-PCBQC
Gruppenvergleich (un-klare Zuordnung)IG1: soziales Kompetenz-trainingIG2: supportive Therapie
IG2>IG1p<0,01(K-SADS)p<0,10 (CDI)Follow-up nach 9 Mo-naten: IG1= IG2
Lerner u. Clum (1990)
Soziales Kompetenz-training vs. supportive Gruppenthe-rapie
18(18–24 J.)
5–7 Wochen10 Sitzungen90 min/Sitzung
78 Ambu-lant
MSSIModified MEPSPSIBDIHSUCLA Loneliness Scale
Gruppenvergleich(Unklare Zuordnung)IG1: soziales Problem-lösetrainingIG2: supportive Therapie
IG1> IG2d=−0,55b
Butler et al. (1980)
Rollenspiele vs. kognitive Umstruktu-rierung
56(5.–6. Klasse)
10 Wochen1 Sitzung/Woche60 min/Sitzung
37,5 Schule CDISelf-Es-teem ScaleMoyal-Miezitis Stimulus Appraisal Question-naire
Gruppenvergleich(Unklare Zuordnung)IG1: RollenspielIG2: kognitive Umstruk-turierungKG1: Placebo, Aufmerk-samkeitKG2: Klassenzimmer
IG1> IG2/KG1/KG2IG1: d=0,28a
IG2: d=0,09a
ACS Adolescent Coping Scale, BDI Beck Depression Inventory, BID Bellevue Index of Depression, CAS Child Assessment Schedule, CBCL Child Behavior Checklist, CBQC Cognitive Bias Questionnaire for Children, CDI Child Depression Inventory, CDRS-R Children’s Depression Rating Scale-Revised, CDS Child Depression Scale, CES-D Center for Epidemiologic Studies-Depression Scale, CGAS Children’s Global Adjustment Scale, CWD Coping with Depression Course, CWD-A Coping with Depression Course for Adolescents, DISC National Institute of Mental Health Diagnostic Schedule for Children, Epidemiological Version/Present Version, GAF Global Assessment of Functioning Scale, HADS Hospital Anxiety and Depression Scale, HAM-D/HDRS Hamilton Depression Rating Scale, HS Hopelessness Scale, IG Interventionsgruppe, IPT interpersonelle Psychotherapie, J. Jahre, KG Kontrollgruppe, K-SADS-E/-P Schedule for Affective Disorders and Schizophrenia for School-Aged Children, KVT kognitive Verhaltenstherapie, LOT Life-Orientation Test, MASC Multidimensional Anxiety Scale for Children, MMPI Minnesota Multiphasic Personality Inventory, Modified MEPS Modified Means-Ends Problem-Solving Procedure, MSSI Modified Scale for Suicidal Ideations, PASCET Primary and Secondary Control Enhancement Training, PIC Personality Inventory for Chil-dren, PMR progressive Muskelrelaxation, PSI Problem Solving Inventory, RADS Reynolds Adolescent Depression Scale, RCT randomisiertes kontrolliertes Design, SASCA Social Adjustment Scale for Children and Adolescents, SPPC Self-Perception Profile for Children, STAIC State-Trait Anxiety Inventory for Children.aEffektstärken entnommen aus Weisz et al. (2006).bEffektstärken entnommen aus Reinecke et al. (1998).
5Psychotherapeut 2013 |
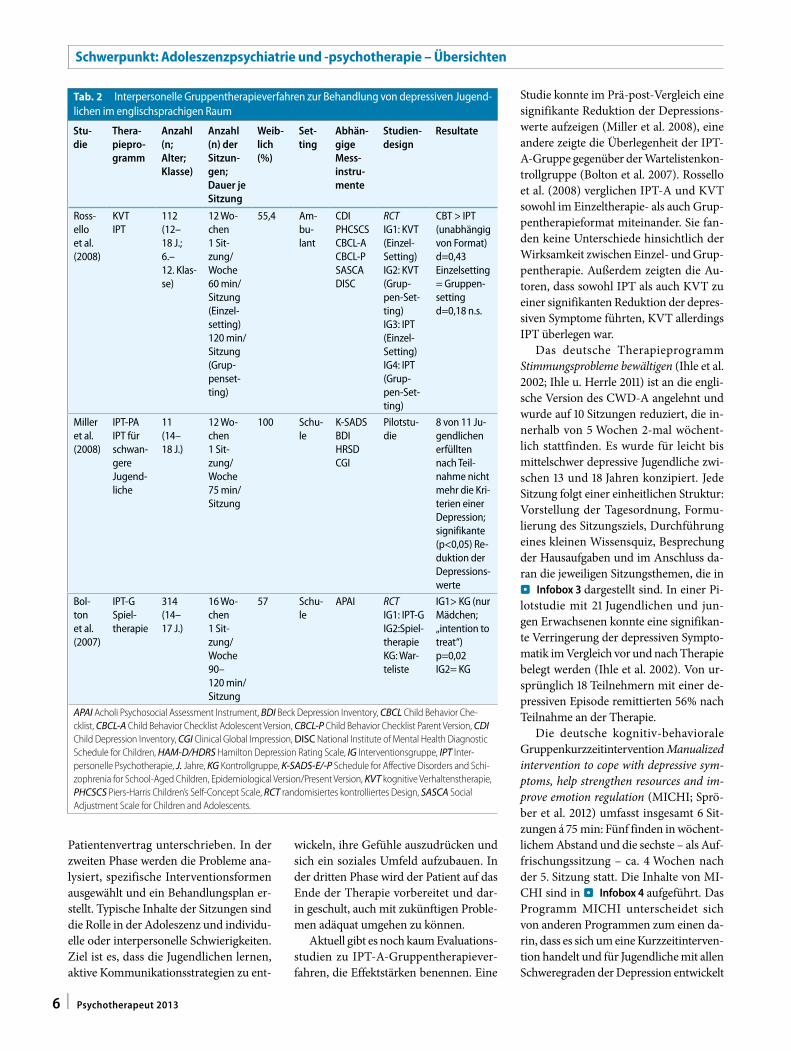
Patientenvertrag unterschrieben. In der zweiten Phase werden die Probleme ana-lysiert, spezifische Interventionsformen ausgewählt und ein Behandlungsplan er-stellt. Typische Inhalte der Sitzungen sind die Rolle in der Adoleszenz und individu-elle oder interpersonelle Schwierigkeiten. Ziel ist es, dass die Jugendlichen lernen, aktive Kommunikationsstrategien zu ent-
wickeln, ihre Gefühle auszudrücken und sich ein soziales Umfeld aufzubauen. In der dritten Phase wird der Patient auf das Ende der Therapie vorbereitet und dar-in geschult, auch mit zukünftigen Proble-men adäquat umgehen zu können.
Aktuell gibt es noch kaum Evaluations-studien zu IPT-A-Gruppentherapiever-fahren, die Effektstärken benennen. Eine
Studie konnte im Prä-post-Vergleich eine signifikante Reduktion der Depressions-werte aufzeigen (Miller et al. 2008), eine andere zeigte die Überlegenheit der IPT-A-Gruppe gegenüber der Wartelistenkon-trollgruppe (Bolton et al. 2007). Rossello et al. (2008) verglichen IPT-A und KVT sowohl im Einzeltherapie- als auch Grup-pentherapieformat miteinander. Sie fan-den keine Unterschiede hinsichtlich der Wirksamkeit zwischen Einzel- und Grup-pentherapie. Außerdem zeigten die Au-toren, dass sowohl IPT als auch KVT zu einer signifikanten Reduktion der depres-siven Symptome führten, KVT allerdings IPT überlegen war.
Das deutsche Therapieprogramm Stimmungsprobleme bewältigen (Ihle et al. 2002; Ihle u. Herrle 2011) ist an die engli-sche Version des CWD-A angelehnt und wurde auf 10 Sitzungen reduziert, die in-nerhalb von 5 Wochen 2-mal wöchent-lich stattfinden. Es wurde für leicht bis mittelschwer depressive Jugendliche zwi-schen 13 und 18 Jahren konzipiert. Jede Sitzung folgt einer einheitlichen Struktur: Vorstellung der Tagesordnung, Formu-lierung des Sitzungsziels, Durchführung eines kleinen Wissensquiz, Besprechung der Hausaufgaben und im Anschluss da-ran die jeweiligen Sitzungsthemen, die in .Infobox 3 dargestellt sind. In einer Pi-lotstudie mit 21 Jugendlichen und jun-gen Erwachsenen konnte eine signifikan-te Verringerung der depressiven Sympto-matik im Vergleich vor und nach Therapie belegt werden (Ihle et al. 2002). Von ur-sprünglich 18 Teilnehmern mit einer de-pressiven Episode remittierten 56% nach Teilnahme an der Therapie.
Die deutsche kognitiv-behaviorale Gruppenkurzzeitintervention Manualized intervention to cope with depressive sym-ptoms, help strengthen resources and im-prove emotion regulation (MICHI; Sprö-ber et al. 2012) umfasst insgesamt 6 Sit-zungen á 75 min: Fünf finden in wöchent-lichem Abstand und die sechste – als Auf-frischungssitzung – ca. 4 Wochen nach der 5. Sitzung statt. Die Inhalte von MI-CHI sind in .Infobox 4 aufgeführt. Das Programm MICHI unterscheidet sich von anderen Programmen zum einen da-rin, dass es sich um eine Kurzzeitinterven-tion handelt und für Jugendliche mit allen Schweregraden der Depression entwickelt
Tab. 2 Interpersonelle Gruppentherapieverfahren zur Behandlung von depressiven Jugend-lichen im englischsprachigen Raum
Stu-die
Thera-piepro-gramm
Anzahl (n; Alter; Klasse)
Anzahl (n) der Sitzun-gen; Dauer je Sitzung
Weib-lich (%)
Set-ting
Abhän-gige Mess-instru-mente
Studien-design
Resultate
Ross-ello et al. (2008)
KVTIPT
112(12–18 J.;6.–12. Klas-se)
12 Wo-chen1 Sit-zung/Woche60 min/Sitzung (Einzel-setting)120 min/Sitzung (Grup-penset-ting)
55,4 Am-bu-lant
CDIPHCSCSCBCL-ACBCL-PSASCADISC
RCTIG1: KVT (Einzel-Setting)IG2: KVT (Grup-pen-Set-ting)IG3: IPT (Einzel-Setting)IG4: IPT (Grup-pen-Set-ting)
CBT > IPT (unabhängig von Format)d=0,43Einzelsetting = Gruppen-settingd=0,18 n.s.
Miller et al. (2008)
IPT-PAIPT für schwan-gere Jugend-liche
11(14–18 J.)
12 Wo-chen1 Sit-zung/Woche75 min/Sitzung
100 Schu-le
K-SADSBDIHRSDCGI
Pilotstu-die
8 von 11 Ju-gendlichen erfüllten nach Teil-nahme nicht mehr die Kri-terien einer Depression; signifikante (p<0,05) Re-duktion der Depressions-werte
Bol-ton et al. (2007)
IPT-GSpiel-therapie
314(14–17 J.)
16 Wo-chen1 Sit-zung/Woche90–120 min/Sitzung
57 Schu-le
APAI RCTIG1: IPT-GIG2:Spiel-therapieKG: War-teliste
IG1> KG (nur Mädchen; „intention to treat“)p=0,02IG2= KG
APAI Acholi Psychosocial Assessment Instrument, BDI Beck Depression Inventory, CBCL Child Behavior Che-cklist, CBCL-A Child Behavior Checklist Adolescent Version, CBCL-P Child Behavior Checklist Parent Version, CDI Child Depression Inventory, CGI Clinical Global Impression, DISC National Institute of Mental Health Diagnostic Schedule for Children, HAM-D/HDRS Hamilton Depression Rating Scale, IG Interventionsgruppe, IPT Inter-personelle Psychotherapie, J. Jahre, KG Kontrollgruppe, K-SADS-E/-P Schedule for Affective Disorders and Schi-zophrenia for School-Aged Children, Epidemiological Version/Present Version, KVT kognitive Verhaltenstherapie, PHCSCS Piers-Harris Children’s Self-Concept Scale, RCT randomisiertes kontrolliertes Design, SASCA Social Adjustment Scale for Children and Adolescents.
6 | Psychotherapeut 2013
Schwerpunkt: Adoleszenzpsychiatrie und -psychotherapie – Übersichten
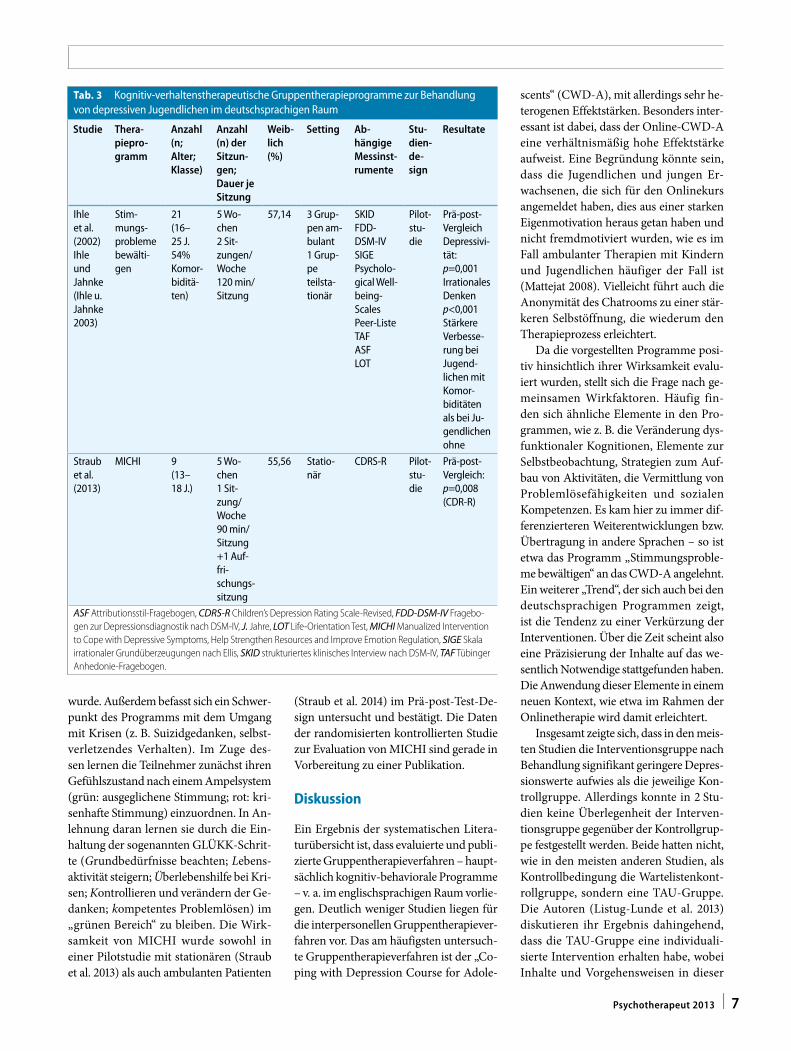
wurde. Außerdem befasst sich ein Schwer-punkt des Programms mit dem Umgang mit Krisen (z. B. Suizidgedanken, selbst-verletzendes Verhalten). Im Zuge des-sen lernen die Teilnehmer zunächst ihren Gefühlszustand nach einem Ampelsystem (grün: ausgeglichene Stimmung; rot: kri-senhafte Stimmung) einzuordnen. In An-lehnung daran lernen sie durch die Ein-haltung der sogenannten GLÜKK-Schrit-te (Grundbedürfnisse beachten; Lebens-aktivität steigern; Überlebenshilfe bei Kri-sen; Kontrollieren und verändern der Ge-danken; kompetentes Problemlösen) im „grünen Bereich“ zu bleiben. Die Wirk-samkeit von MICHI wurde sowohl in einer Pilotstudie mit stationären (Straub et al. 2013) als auch ambulanten Patienten
(Straub et al. 2014) im Prä-post-Test-De-sign untersucht und bestätigt. Die Daten der randomisierten kontrollierten Studie zur Evaluation von MICHI sind gerade in Vorbereitung zu einer Publikation.
Diskussion
Ein Ergebnis der systematischen Litera-turübersicht ist, dass evaluierte und publi-zierte Gruppentherapieverfahren – haupt-sächlich kognitiv-behaviorale Programme – v. a. im englischsprachigen Raum vorlie-gen. Deutlich weniger Studien liegen für die interpersonellen Gruppentherapiever-fahren vor. Das am häufigsten untersuch-te Gruppentherapieverfahren ist der „Co-ping with Depression Course for Adole-
scents“ (CWD-A), mit allerdings sehr he-terogenen Effektstärken. Besonders inter-essant ist dabei, dass der Online-CWD-A eine verhältnismäßig hohe Effektstärke aufweist. Eine Begründung könnte sein, dass die Jugendlichen und jungen Er-wachsenen, die sich für den Onlinekurs angemeldet haben, dies aus einer starken Eigenmotivation heraus getan haben und nicht fremdmotiviert wurden, wie es im Fall ambulanter Therapien mit Kindern und Jugendlichen häufiger der Fall ist (Mattejat 2008). Vielleicht führt auch die Anonymität des Chatrooms zu einer stär-keren Selbstöffnung, die wiederum den Therapieprozess erleichtert.
Da die vorgestellten Programme posi-tiv hinsichtlich ihrer Wirksamkeit evalu-iert wurden, stellt sich die Frage nach ge-meinsamen Wirkfaktoren. Häufig fin-den sich ähnliche Elemente in den Pro-grammen, wie z. B. die Veränderung dys-funktionaler Kognitionen, Elemente zur Selbstbeobachtung, Strategien zum Auf-bau von Aktivitäten, die Vermittlung von Problemlösefähigkeiten und sozialen Kompetenzen. Es kam hier zu immer dif-ferenzierteren Weiterentwicklungen bzw. Übertragung in andere Sprachen – so ist etwa das Programm „Stimmungsproble-me bewältigen“ an das CWD-A angelehnt. Ein weiterer „Trend“, der sich auch bei den deutschsprachigen Programmen zeigt, ist die Tendenz zu einer Verkürzung der Interventionen. Über die Zeit scheint also eine Präzisierung der Inhalte auf das we-sentlich Notwendige stattgefunden haben. Die Anwendung dieser Elemente in einem neuen Kontext, wie etwa im Rahmen der Onlinetherapie wird damit erleichtert.
Insgesamt zeigte sich, dass in den meis-ten Studien die Interventionsgruppe nach Behandlung signifikant geringere Depres-sionswerte aufwies als die jeweilige Kon-trollgruppe. Allerdings konnte in 2 Stu-dien keine Überlegenheit der Interven-tionsgruppe gegenüber der Kontrollgrup-pe festgestellt werden. Beide hatten nicht, wie in den meisten anderen Studien, als Kontrollbedingung die Wartelistenkont-rollgruppe, sondern eine TAU-Gruppe. Die Autoren (Listug-Lunde et al. 2013) diskutieren ihr Ergebnis dahingehend, dass die TAU-Gruppe eine individuali-sierte Intervention erhalten habe, wobei Inhalte und Vorgehensweisen in dieser
Tab. 3 Kognitiv-verhaltenstherapeutische Gruppentherapieprogramme zur Behandlung von depressiven Jugendlichen im deutschsprachigen Raum
Studie Thera-piepro-gramm
Anzahl (n; Alter; Klasse)
Anzahl (n) der Sitzun-gen; Dauer je Sitzung
Weib-lich (%)
Setting Ab-hängige Messinst-rumente
Stu-dien-de-sign
Resultate
Ihle et al. (2002)Ihle und Jahnke (Ihle u. Jahnke 2003)
Stim-mungs-probleme bewälti-gen
21(16–25 J.54% Komor-biditä-ten)
5 Wo-chen2 Sit-zungen/Woche120 min/Sitzung
57,14 3 Grup-pen am-bulant1 Grup-pe teilsta-tionär
SKIDFDD-DSM-IVSIGEPsycholo-gical Well-being-ScalesPeer-ListeTAFASFLOT
Pilot-stu-die
Prä-post-VergleichDepressivi-tät:p=0,001Irrationales Denkenp<0,001Stärkere Verbesse-rung bei Jugend-lichen mit Komor-biditäten als bei Ju-gendlichen ohne
Straub et al. (2013)
MICHI 9(13–18 J.)
5 Wo-chen1 Sit-zung/Woche90 min/Sitzung+1 Auf-fri-schungs-sitzung
55,56 Statio-när
CDRS-R Pilot-stu-die
Prä-post-Vergleich:p=0,008 (CDR-R)
ASF Attributionsstil-Fragebogen, CDRS-R Children’s Depression Rating Scale-Revised, FDD-DSM-IV Fragebo-gen zur Depressionsdiagnostik nach DSM-IV, J. Jahre, LOT Life-Orientation Test, MICHI Manualized Intervention to Cope with Depressive Symptoms, Help Strengthen Resources and Improve Emotion Regulation, SIGE Skala irrationaler Grundüberzeugungen nach Ellis, SKID strukturiertes klinisches Interview nach DSM-IV, TAF Tübinger Anhedonie-Fragebogen.
7Psychotherapeut 2013 |

Behandlung nicht erfasst worden seien. So kann es sich dabei auch um eine Interven-tion ähnlich einer Depressionseinzelthe-rapie gehandelt haben, was die vergleich-baren Effekte erklären würde. Die Auto-ren der zweiten Studie (Clarke et al. 2002) begründeten ihr Ergebnis damit, dass ihre Stichprobe (depressive Jugendliche mit mindestens einem depressiven Elternteil) von anderen depressiven Stichproben ab-weiche (betroffene Jugendliche sprächen schlechter auf Therapie an); dies erkläre, warum die Ergebnisse der TAU-Gruppe nicht signifikant von der Interventions-gruppe abwichen.
Im deutschsprachigen Raum gibt es bislang nur 2 Gruppentherapiepro-gramme zur Behandlung von Depressi-onen im Jugendalter, die bisher lediglich in Pilotstudien untersucht wurden. Dabei beinhalten beide deutschen Programme ähnliche therapeutische Inhalte wie Psy-choedukation, Selbstbeobachtung, kogni-tive Umstrukturierung, Förderung der Problemlösefähigkeiten und Verhaltens-aktivierung (Infoboxen 3 und 4). Sie un-terscheiden sich allerdings dahingehend, dass „Stimmungsprobleme bewältigen“ Elemente wie soziales Kompetenztrai-ning, Entspannung und Selbstinstrukti-onstechniken aufgreift und „MICHI“ ei-nen Fokus auf die Verhinderung der Ent-stehung sowie die Bewältigung von Kri-sen richtet und halb so zeitintensiv ist wie „Stimmungsprobleme bewältigen“.
Von Kaslow u. Thompson (1998) wur-den 4 Kriterien zur Abschätzung der Ef-fektivität einer therapeutischen Interven-tion vorgeschlagen: Manualisierung, de-taillierte Stichprobenbeschreibung, Test der Therapie im randomisierten kont-rollierten Design und Nachweis der Ef-fektivität durch mindestens 2 unabhängi-ge Forschergruppen. Legt man diese Kri-terien an die oben genannten Studien an, wird deutlich, welchen hohen Wirkungs-grad kognitiv-behaviorale Gruppenthe-rapieprogramme in der Behandlung de-pressiver Störungen bei Jugendlichen ha-ben. Die deutsche Studienlage zur Effekti-vität von Gruppentherapieverfahren und die Studienlage zu interpersoneller Psy-chotherapie sind hingegen als unbefriedi-gend zu bezeichnen, denkt man an die ho-he Prävalenz dieses Störungsbilds im Ju-gendalter sowie die mehrfach nachgewie-
sene Effektivität dieser Verfahren v. a. im Einzel-Setting.
Sowohl für Jugendliche (Weisz et al. 2006) als auch Erwachsene (McDermut et al. 2001) konnte festgestellt werden, dass sich die kognitiv-verhaltenstherapeuti-sche Gruppentherapie hinsichtlich ihrer Effektivität nicht von der kognitiv-verhal-tenstherapeutischen Einzeltherapie unter-scheidet. Das Gruppentherapieformat geht allerdings mit deutlichen Zeit- und Kostenersparnissen einher, was die Emp-fehlung nahelegt, die kognitiv-verhaltens-therapeutische Gruppentherapie als erstes Mittel der Depressionsbehandlung einzu-setzen. Zeigt diese nicht die gewünschte Wirkung, kann stufenweise eine Einzel-therapie oder Medikation folgen (McDer-mut et al. 2001). Erste Ergebnisse weisen darauf hin, dass die kognitiv-verhaltens-therapeutische Gruppenpsychothera-pie auch online gute Erfolge erzielt. Dies kann sicherlich in Anbetracht der häufig komorbid zu Depressionen auftretenden sozialen Phobie (Ranta et al. 2009) eine geeignete Alternative zu Gruppenthe-rapien in vivo darstellen. Diese Aspekte sollten bei zukünftigen Forschungsvorha-ben aufgegriffen werden. Da viele depres-sive Jugendliche medikamentös behan-delt werden, wäre es weiterführend wich-tig zu untersuchen, inwiefern sich eine zu-sätzliche Behandlung mit kognitiv-verhal-tenstherapeutischer Einzelpsychotherapie oder eine zusätzliche Behandlung mit ko-gnitiv-verhaltenstherapeutischer Grup-pentherapie in ihrer Wirksamkeit aus-wirkt (Dubicka et al. 2010).
Fazit für die Praxis
Die Effektivität von Gruppentherapiepro-grammen mit kognitiv-verhaltensthera-peutischer oder interpersoneller Orien-tierung zur Therapie depressiver Jugend-licher konnte für den englischsprachi-gen Raum in den letzten Jahren mehr-fach bestätigt werden. Im deutschspra-chigen Raum gibt es bis dato nur weni-ge Studien, die die Effektivität von kogni-tiv-verhaltenstherapeutischen und inter-personellen Gruppentherapieverfah-ren zur Behandlung von depressiven Kin-dern und Jugendlichen, untersucht ha-ben. Gruppentherapieprogramme stel-len eine zeit- und kosteneffiziente The-
rapieform dar, mithilfe derer die Warte-zeiten auf Psychotherapieplätze verkürzt werden könnte. Die meisten Programme beinhalten Elemente wie Veränderung dysfunktionaler Kognitionen, Selbstbe-obachtung, Aufbau von Aktivitäten, Pro-blemlösestrategien und sozialen Kom-petenzen.
Korrespondenzadresse
Joana StraubKlinik für Kinder- und Jugendpsychiatrie und Psychotherapie, Universität UlmSteinhövelstr. 5, 89075 [email protected]
Einhaltung ethischer Richtlinien
Interessenkonflikte. Nina Spröber, Joana Straub und Michael Kölch sind Autoren des Therapiemanu-als Depression im Jugendalter: MICHI – Manual für die Gruppentherapie. Joana Straub, Nina Spröber und Leonie Nicolaus haben keine (weiteren) Interessenkon-flikte. Michael Kölch hat keine (weiteren) Interessen-konflikte. Er erhält Subventionen von der internatio-nalen Eli Lilly Stiftung. Er erhielt Forschungssubventio-nen des DMFFSJ (Bundesministerium für Familien, Se-nioren, Frauen und Jugend), dem BMBF (Bundesmi-nisterium für Bildung und Forschung), dem Schwei-zer Bundesamt für Justiz und von Boehringer Ingel-heim. Er war CI oder PI für Eli Lilly, Astra Zeneca und Janssen-Cilag, Lundbeck. Er erhielt Reisezuschüsse für Vorträge von Janssen-Cilag, der Universität von Ros-tock, DGKJPP, UCB, Europäische Akademie und ge-meinnützigen Organisationen. Er ist kein Aktieninha-ber oder Aktionär in der pharmazeutischen Industrie. Paul L. Plener benennt keine Interessenkonflikte in Be-zug auf die vorliegende Publikation. In den vergange-nen 5 Jahren erhielt er Förderung durch das BfArM, das BMBF, das Ministerium für Wissenschaft, Forschung und Kunst Baden Württemberg, die Stiftung für ambu-lante Kinder- und Jugendpsychiatrie, den DAAD, die IACAPAP sowie Lundbeck pharmaceuticals. Alle im vor-liegenden Manuskript beschriebenen Untersuchun-gen am Menschen wurden mit Zustimmung der zu-ständigen Ethikkommission, im Einklang mit nationa-lem Recht sowie gemäß der Deklaration von Helsin-ki von 1975 (in der aktuellen, überarbeiteten Fassung) durchgeführt. Von allen beteiligten Patienten liegt eine Einverständniserklärung vor.
Literatur
Asarnow JR, Scott CV, Mintz J (2002) A combined cog-nitive–behavioral family education intervention for depression in children: a treatment develop-ment study. Cogn Ther Res 26:221–229
Bettge S, Wille N, Barkmann C et al (2008) Depressi-ve symptoms of children and adolescents in a Ger-man representative sample: results of the BEL-LA study. Eur Child Adolesc Psychiatry 17:71–81. doi:10.1007/s00787-008-1008-x
Bolton P, Bass J, Betancourt T et al (2007) Interventions for depression symptoms among adolescent survi-vors of war and displacement in northern Uganda: a randomized controlled trial. JAMA 298:519–527
8 | Psychotherapeut 2013
Schwerpunkt: Adoleszenzpsychiatrie und -psychotherapie – Übersichten
Butler AC, Chapman JE, Forman EM, Beck AT (2006) The empirical status of cognitive-behavioral the-rapy: a review of meta-analyses. Clin Psychol Rev 26:17–31
Butler L, Miezitis S, Friedman R, Cole E (1980) The effect of two school-based intervention programs on de-pressive symptoms in preadolescents. Am Educ Res J 17:111–119
Clarke GN, Hornbrook M, Lynch F et al (2002) Group cognitive-behavioral treatment for depressed ado-lescent offspring of depressed parents in a health maintenance organization. J Am Acad Child Ado-lesc Psychiatry 41:305–313
Clarke GN, Rohde P, Lewinsohn PM et al (1999) Cogni-tive-behavioral treatment of adolescent depres-sion: efficacy of acute group treatment and boos-ter sessions. J Am Acad Child Adolesc Psychiatry 38:272–279
Clarke G, Lewinsohn P (1989) The coping with depres-sion course: a group psychoeducational interventi-on for unipolar depression. Behav Change 6:54–69
Clarke GN, Lewinsohn PM, Hops H (1990) Leader’s ma-nual for adolescent groups. Adolescent coping with depression course. Castalia, Eugene
Compton SN, March JS, Brent D et al (2004) Cognitive-behavioral psychotherapy for anxiety and depres-sive disorders in children and adolescents: an evi-dence-based medicine review. J Am Acad Child Adolesc Psychiatry 43:930–959
Cox GR, Callahan P, Churchill R et al (2013) Psycho-logical therapies versus antidepressant medi-cation, alone and in combination for depressi-on in children and adolescents (Review). Cochra-ne Database Syst Rev 11. doi:10.1002/14651858.CD008324.pub2
Cuijpers P, Munoz RF, Clarke GN, Lewinsohn PM (2009) Psychoeducational treatment and prevention of depression: the „coping with depression course“ thirty years later. Clin Psychol Rev 29:449–458
Curry JF (2001) Specific psychotherapies for child-hood and adolescent depression. Biol Psychiatry 49:1091–1100
De Cuyper S, Timbremont B, Braet C et al (2004) Trea-ting depressive symptoms in schoolchildren. Eur Child Adolesc Psychiatry 13:105–114
Deutsche Gesellschaft für Kinder- und Jugendpsych-iatrie, Psychosomatik und Psychotherapie (2013) AWMF Leitlinien zur Behandlung von depressiven Störungen bei Kindern und Jugendlichen. http://www.awmf.org/leitlinien/detail/ll/028-043.html. Zugegriffen: 08. Nov. 2013
Dubicka B, Elvins R, Roberts C et al (2010) Combined treatment with cognitive-behavioural therapy in adolescent depression: meta-analysis. Br J Psychia-try 197:433–440
Fine S, Forth A, Gilbert M, Haley G (1991) Group thera-py for adolescent depressive disorder: a compari-son of social skills and therapeutic support. J Am Acad Child Adolesc Psychiatry 30:79–85
Gaynor ST, Lawrence PS (2002) Complementing CBT for depressed adolescents with learning through in vivo experience (LIVE): conceptual analysis, tre-atment description, and feasibility study. Behav Cogn Psychother 30:79–101
Ihle W, Jahnke D (2003) Wirkt ein psychoedukatives ko-gnitiv-verhaltenstherapeutisches Gruppenpro-gramm auch bei depressiven Jugendlichen mit ko-morbiden Störungen? Verhaltensther Verhaltens-med 24:513–528
Ihle W, Jahnke D, Spieß L, Herrle J (2002) Evaluation eines kognitiv-verhaltenstherapeutischen Grup-penprogramms für depressive Jugendliche und junge Erwachsene. Kindh Entwickl 11:238–246
Ihle W, Herrle J (2011) Stimmungsprobleme bewälti-gen. Ein kognitiv-verhaltenstherapeutisches Grup-penprogramm zur Prävention, Behandlung und Rückfallprophylaxe depressiver Störungen im Ju-gendalter nach Clarke, Lewinsohn und Hops. Ma-nual für Kursleiter. dgvt-Verlag, Tübingen
Kahn JS, Kehle TJ (1990) Comparison of cognitive-be-havioral, relaxation, and self-modeling interventi-ons for depression. School Psychol Rev 19:196–211
Kaslow NJ, Thompson MP (1998) Applying the crite-ria for empirically supported treatments to studies of psychosocial interventions for child and ado-lescent depression. J Clin Child Adolesc Psychol 27:146–155
Kaufman NK, Rohde P, Seeley JR et al (2005) Potential mediators of cognitive-behavioral therapy for ado-lescents with comorbid major depression and con-duct disorder. J Consult Clin Psychol 73:38–46
Klein JB, Jacobs RH, Reinecke MA (2007) Cognitive-be-havioral therapy for adolescent depression: a me-ta-analytic investigation of changes in effect-si-ze estimates. J Am Acad Child Adolesc Psychiatry 46:1403–1413
Kowalenko N, Rapee RM, Simmons J et al (2005) Short-term effectiveness of a school-based early inter-vention program for adolescent depression. Clin Child Psychol Psychiatry 10:493–507
Kühner C (2003) Das Gruppenprogramm „Depression bewältigen“ und seine Varianten – eine aktuali-siert Metaanalyse. Verhaltenstherapie 13:254–262
Lerner MS, Clum GA (1990) Treatment of suicide idea-tors: a problem-solving approach. Behav Ther 21:403–411
Lewinsohn PM, Clarke GN (1999) Psychosocial treat-ments for adolescent depression. Clin Psychol Rev 19:329–342
Lewinsohn PM, Clarke GN, Hops H, Andrews J (1990) Cognitive-behavioral treatment for depressed adolescents. Behav Ther 21:385–401
Listug-Lunde L, Vogeltanz-Holm N, Collins J (2013) A cognitive-behavioral treatment for depression in rural American Indian middle school students. Am Indian Alsk Native Ment Health Res 20:16–34
Maag JW, Swearer SM (2005) Cognitive-behavioral in-terventions for depression: review and implicati-ons for school personnel. Behav Disord 30:259–276
Marcotte D (1997) Treating depression in adolescence: a review of the effectiveness of cognitive-behavio-ral treatments. J Youth Adolesc 26:273–283
Mattejat F (2008) Grundlagen einer integrativen und entwicklungsorientierten Kinder- und Jugendli-chentherapie. In: Remschmidt H, Mattejat F, Warn-ke F (Hrsg) Therapie psychischer Störungen bei Kindern und Jugendlichen. Thieme, Stuttgart
McDermut W, Miller I, Brown R (2001) The efficacy of group psychotherapy for depression: a meta-ana-lysis and review of empirical research. Clin Psy-chol 8:98–116
Miller L, Gur M, Shanok A, Weissman M (2008) Inter-personal psychotherapy with pregnant adole-scents: two pilot studies. Child Psychol Psychiatry 49:733–742
Mufson L, Moreau D, Weissmann MM, Klerman GL (Hrsg) (1993) Interpersonal psychotherapy for de-pressed adolescents. Guilford Press, New York
Oei T, Dingle G (2008) The effectiveness of group cog-nitive behavior therapy for unipolar depressive di-sorders. J Affect Disord 107:5–21
Ranta K, Kaltiala-Heino R, Pelkonen M, Marttunen M (2009) Associations between peer victimization, self-reported depression and social phobia among adolescents: the role of comorbidity. J Adolesc 32:77–93
Reed MK (1994) Social skills training to reduce depres-sion in adolescents. Adolescence 29(114):293–302
Reinecke MA, Ryan NE, Dubois DL (1998) Cognitive-behavioral therapy of depression and depressi-ve symptoms during adolescence: a review and meta-analysis. J Am Acad Child Adolesc Psychia-try 37:26–34
Reynolds WM, Coats KI (1986) A comparison of cogni-tive-behavioral therapy and relaxation training for the treatment of depression in adolescents. J Con-sul Clin Psychol 54:653–660
Rohde P, Clarke GN, Mace DE et al (2004) An efficacy/effectiveness study of cognitive-behavioral tre-atment for adolescents with comorbid major de-pression and conduct disorder. J Am Acad Child Adolesc Psychiatry 43:660–668
Rossello J, Bernal G, Rivera-Medina C (2008) Individu-al and group CBT and IPT for Puerto Rican adole-scents with depressive symptoms. Cultur Divers Ethnic Minor Psychol 14:234–245
Saluja G, Iachan R, Scheidt PC et al (2004) Prevalen-ce of and risk factors for depressive symptoms among young adolescents. Arch Pediatr Adolesc Med 158:760–765
Spröber N, Straub J, Fegert J, Kölch M (2012) Depres-sion im Jugendalter: MICHI- Manual für die Grup-pentherapie. Beltz, Weinheim
Stark KD, Simpson J, Schnoebelen S et al (Hrsg) (2004) Therapist’s manual for ACTION. Workbook Publi-shing, Ardmore
Stark KD, Reynolds WM, Kaslow NJ (1987) A compa-rison of the relative efficacy of self-control thera-py and a behavioral problem-solving therapy for depression in children. J Abnorm Child Psychol 15:91–113
Stark K, Kendall P, McCarthy M et al (1996) Taking AC-TION: a workbook for overcoming depression. Workbook publishing, Ardmore
Steele MM, Doey T (2007) Suicidal behaviour in chil-dren and adolescents. part 1: etiology and risk fac-tors. Can J Psychiatry 52:21–33
Straub J, Koelch M, Fegert J et al (2013) Innovations in practice: MICHI, a brief cognitive-behavioural group therapy for adolescents with depression – a pilot study of feasibility in an inpatient setting. CAMH 18:247–250
Straub J, Sproeber N, Plener PL et al (2014) Treatment of adolescent outpatients with depression by me-ans of a brief cognitive-behavioural group therapy programme: results of a pilot study. Child Adolesc Psychiatry Ment Health (eingereicht)
Tucker M, Oei TP (2007) Is group more cost effecti-ve than individual cognitive behavior therapy? The evidence is not solid yet. Behav Cogn Psycho-ther 35:77–91
Van der Zanden R, Kramer J, Gerrits R, Cuijpers P (2012) Effectiveness of an online group course for depres-sion in adolescents and young adults: a randomi-zed trial. J Med Internet Res 14:e86. doi:10.2196/jmir.2033
Watanabe N, Hunot V, Omori IM et al (2007) Psycho-therapy for depression among children and ado-lescents: a systematic review. Acta Psychiatr Scand 116:84–95
Weisz JR, Thurber CA, Sweeney L et al (1997) Brief tre-atment of mild-to-moderate child depression using primary and secondary control enhance-ment training. J Consult Clin Psychol 65:703–707
Weisz JR, McCarty C, Valeri S (2006) Effects of psy-chotherapy for depression in children and adole-scents: a meta-analysis. Psychol Bull 132:132–149
9Psychotherapeut 2013 |

Innovations in Practice: MICHI, a brief cognitive-behavioural group therapy for adolescents
with depression - a pilot study of feasibility in an inpatient setting
114
6.6 Innovations in Practice: MICHI, a brief cognitive-behavioural group therapy for
adolescents with depression - a pilot study of feasibility in an inpatient setting
Contribution of J. Straub to the article:
J. Straub coordinated the study procedure, recruited participants, assessed suicidal ideation
and behaviour on a weekly basis, and scheduled diagnostic as well as psychotherapeutic
appointments. She controlled the return of questionnaires and executed diagnostic
assessments that didn’t have to be done by an independent evaluator (e.g. IQ
measurements). She executed weekly group therapy sessions. She did data acquisition, data
input, executed statistical analyses, and interpreted statistical outcomes. She researched
literature, wrote the manuscript, integrated remarks of the co-authors, revised the
manuscript according to reviewer’s comments, and created figures and tables.
Co-authors’ contributions to the article:
Gonzalez-Aracil, I. and Voit, A. made decisions on the experimental design and
conceptualized the study under supervision. They held weekly group therapy sessions,
configured diagnostic instruments, and, under supervision, developed a diagnostic
instrument for the assessment of acceptance. They helped with data acquisition and
generation of the data matrix. They reviewed the draft and gave constructive remarks. N.
Sproeber and M.G. Koelch supervised decisions on the experimental design and
conceptualized the study. They supervised the conduction of weekly group therapy sessions
as well as the configuration of diagnostic instruments. They reviewed the draft and gave
constructive remarks and helped with revising the manuscript according to the reviewer’s
comments. P.L. Plener and J.M. Fegert reviewed the draft and gave constructive remarks.
Reference
Straub, J., Koelch, M.G., Fegert, J.M., Plener, P.L., Gonzalez-Aracil, I., Voit, A. & Sproeber, N.
(2013). Innovations in Practice: MICHI, a brief cognitive-behavioural group therapy for
adolescents with depression - a pilot study of feasibility in an inpatient setting. Child and
Adolescent Mental Health, 18(4), 247-250.
Reprinted from Child and Adolescent Mental Health, 18(4), Straub, J., Koelch, M.G., Fegert,
J.M., Plener, P.L., Gonzalez-Aracil, I., Voit, A. & Sproeber, N., Innovations in Practice: MICHI,
a brief cognitive-behavioural group therapy for adolescents with depression - a pilot study
of feasibility in an inpatient setting, 247-250, Copyright (2013), with permission from Wiley.
Innovations in Practice: MICHI, a briefcognitive-behavioural group therapy foradolescents with depression – a pilot study offeasibility in an inpatient setting
Joana Straub1, Michael Koelch2, Joerg Fegert1, Paul Plener1, Inma Gonzalez-Aracil1, Anja Voit1 & Nina Sproeber1
1Kinder- und Jugendpsychiatrie des Universitatsklinikums Ulm, Steinhovelstraße 5, Ulm, 89075, Germany. E-mail:[email protected] Klinikum im Friedrichshain, Landsberger Allee, Kinder- und Jugendpsychiatrie, Berlin, Germany
Background: Group therapy is an economic intervention, allowing for fast access, for the treatment of severaldepressed adolescents simultaneously; evaluated manualised programs, however, are scarce. Method: Ninedepressive adolescent inpatients (M = 16.33 years; SD = 1.92) participated between October 2009 and March2010 in a brief manualised group therapy programme (MICHI), which was evaluated with respect to feasibilityand trends of efficacy. Results: MICHI demonstrated good feasibility, was positively evaluated by the partici-pants by means of an evaluation questionnaire ranging from 1 (very bad) to 10 (very good) (M = 7.22;SD = 1.79), and showed significant reduction of depressive symptoms (z = �2.66, p = .008) assessed by meansof a clinical interview. Conclusions: Feasibility of MICHI was demonstrated and larger trials for efficacy willfollow.
Key Practitioner Message:
• MICHI uniquely combines the factors of a cognitive-behavioural, brief and group psychotherapy, as all thosefactors on their own have been proven to be effective in the treatment of depression in adolescents
• MICHI was carried out with nine mildly to severely depressed inpatient adolescents and demonstrated good fea-sibility
• The pretest and posttest comparison demonstrated significant reduction in depression scores and reduced sui-cidal ideation
• Due to its brevity as well as the group format, MICHI allows fast access and treatment of several patients at thesame time, reserving long-term treatment for patients who fail to respond
Keywords: Depression; adolescents; brief psychotherapy; cognitive-behavioural group intervention
Introduction
About 18% of adolescents have experienced symptomsof depression at least once in their lives. Untreateddepression increases the risk for concomitant disorders,a chronic course of the disorder and numerous negativeeffects (Saluja et al., 2004). This fact highlights the needfor timely intervention for depressed adolescents (Clarkeet al., 2009). As cost efficacy is a worldwide issue inhealthcare systems, and availability of individual ther-apy is often restricted for several reasons, new forms ofinterventions that are effective, fast and economical areneeded.
Recent meta-analyses investigating behaviouralpsychotherapy (CBT) for the treatment of depressiondemonstrate a positive indication for efficacy (Weisz,McCarty, & Valeri, 2006). Considering the duration oftherapy, Goodyer et al. (2007) showed that afterparticipation in a brief psychosocial intervention in an
individual setting (M = three sessions), 21% of themoderately to severely depressed adolescents improved.Furthermore, the results of an eight-session manualisedtraining programme for groups of children with mild tomoderate depressive symptoms demonstrate thatchildhood depressive symptoms can be significantlyreduced, with CDRS-R (Children’s Depression RatingScale-Revised) (Poznanski & Mokros, 1996) scoresdeclining three times more in the treatment group (12points) than in the control group (Weisz, Thurber,Sweeney, Proffitt, & LeGagnoux,1997). Considering thetherapy setting, results of a meta-analysis reported amean effect size of 0.38 for group CBT (GCBT) and 0.37for individual treatment, demonstrating no significantdifferences between the therapy settings (Weisz et al.,2006).
To our knowledge, there is no study investigating anintervention that combines all those factors and thatmight result in a brief GCBT for the treatment of mildly
© 2012 The Authors. Child and Adolescent Mental Health. © 2012 Association for Child and Adolescent Mental Health.Published by John Wiley & Sons Ltd, 9600 Garsington Road, Oxford OX4 2DQ, UK and 350 Main St, Malden, MA 02148, USA
Child and Adolescent Mental Health 18, No. 4, 2013, pp. 247–250 doi:10.1111/j.1475-3588.2012.00678.x

to severely depressed adolescents; one that also lendsitself to standardisation in the form of a manual andcould be delivered to a large number of participants witha minimal amount of time and staff, and which wouldtherefore offer an ideal option for research and treatmentof depression (Oei & Dingle, 2008). The aim of our studywas to examine the feasibility of the brief (four-session)GCBT ‘Manualised Intervention to Cope with depressivesymptoms, Help strengthen resources, and Improveemotion regulation’ (MICHI, Japanese for ‘the way’) formildly to severely depressed adolescents. Suicidality wasassessed in this pilot study as well as first trends in effi-cacy with respect to reduction in depressive symptoms.
Method
ProcedureIn Germany, there are prevention group programs for adoles-cents with depression, but so far no evaluated brief (four ses-sions) cognitive-behavioural group therapy programs for mildlyto severely depressed adolescents. Therefore, little is knownabout group processes that might occur when working withdepressed adolescents. According to the treatment of adolescentsuicide attempters study (TASA), about half of the suicidalevents occurred within the first four weeks of treatment (Brentet al., 2009). Furthermore, suicidality has a contagious effect,particularly among adolescents (Gould, Wallenstein, Kleinman,O’Carroll, & Mercy, 1990), possibly leading to a heightened riskwithin groups (e.g. by talking with each other about suicidalideations). Because of the low psychosocial functioning ofdepressed adolescents, that could make attendance at regulartherapy difficult, participation can be better guaranteed in aninpatient setting. With respect to those aspects, the aim to givepatients the best support possible, and for ethical reasons, feasi-bility and efficacy of MICHI was evaluated at first in a protectedinpatient setting, between October 2009 and March 2010.
To qualify for inclusion in the study, participants wererequired to satisfy all the following criteria: aged between 13and 18 years, an IQ �85, a raw-summary score �36 in theCDRS-R and a diagnosis of a mild, moderate or severe majordepressive episode. Most comorbid diagnoses and antidepres-sant medications were allowed, as long as the diagnosis of amajor depression was prevailing and medication had beenstabilised for at least three weeks prior to the start. Participantswith the diagnosis of bipolar disorder, schizophrenia andsubstance abuse had to be excluded from the study as thosedisorders render a different form of prevailing treatment. Fur-ther exclusion criteria are the initiation of drug treatment orpsychotherapy while participating inMICHI.
The training programme was finally applied in two consecu-tive groups with weekly sessions lasting seven weeks in total(including the diagnostic process). The study was approved bythe IRB of the University of Ulm. Participants were informedabout the goals and course of therapy, the voluntary nature oftheir participation and confidentiality with regard to their data.Informed consent documents had to be signed by participantsand their parents.
InterventionEach session takes 90 min and includes in-session activitiesand reviews of the weekly homework. The sessions are built on aselection of methods used in clinical work and proven to be suc-cessful in the treatment of depression in youths. On the basis ofthe review of Bachmann, Bachmann, Rief, and Mattejat (2008),effective content for the treatment of depression in minors suchas ‘psycho education’, ‘activities to feel more comfortable’,‘challenging negative thinking’, ‘relaxation techniques’, ‘prob-lem-solving’ and ‘involving parents and friends’ were included.Besides that, an ‘emergency plan for acute crisis’was added.
The therapists were trained psychologists with a Master’sdegree, each with prior GCBT experience with adolescents. Theywere initially trained and supervised weekly during the inter-vention by a fully licensed psychotherapist. Sessions were vid-eotaped for supervision.
ParticipantsThe sample consists of nine depressed adolescents(M = 16.43 years; five girls) who had been referred for inpatienttreatment due to primary diagnoses of major depressive disor-der (MDD). Four of them received outpatient psychiatric treat-ment before hospitalisation. Four participants fulfilled criteriafor comorbid disorders, which were assessed by means of astandardised interview. Five were treated with antidepressants(see Table 1).
MeasuresFeasibility was assessed through the participants’ attendancein the training and the training evaluation of the trainers (openquestion). The acceptance of the training programme and theevaluation of the contents of MICHI by the participants wasaccomplished by means of a process evaluation questionnaire,ranging from 1 (not true) to 5 (true) (mean values �3.5 indicatepositive evaluation; mean values �2.5 indicate negative evalua-tion) as well as one global question assessing the evaluation ofthe whole training programme, ranging from 1 (very bad) to 10(very good) (Likert scale). To assess the criteria for MDD as wellas the improvement of depression, participants were inter-viewed by a clinical psychologist using the CDRS-R before andafter participation in MICHI. The CDRS-R is a semistructured,clinician-rated interview inquiring about symptoms of depres-sion in children and adolescents. Suicidal ideation wasassessed by means of item 13 of the CDRS-R. Pre- and posttestdifferences were analysed by means of the Wilcoxon signed-rank test (PASW statistics 18).
Results
Feasibility of MICHIFour of nine adolescents participated in each session,with four participants missing one session and oneparticipant missing two sessions, demonstrating fairattendance overall. Both trainers evaluated the manualas well-structured, that a lead time of about 30 min persession was sufficient and that it was fun to conductMICHI. They also made proposals for the improvement of
Table 1. Demographics of the inpatients
Age IQ Main diagnosis Comorbid disorders Medication
M = 16.43 years M = 99.75 F32.0Mild depressiveepisode (N = 1)
F42 Obsessive-compulsivedisorder (N = 1)
Antidepressants (N = 5)
SD = 1.68 [13; 00–18; 06] SD = 10.06 [87–116] F32.1Moderate depressiveepisode (N = 5)
F90.1 Hyperkinetic conductdisorder (N = 1)
Second generationantipsychotics (N = 2)
F32.2 Severe depressiveepisode (N = 2)
F43.1 Posttraumatic stressdisorder (N = 1)
F33.1 Recurrent depressiveepisode (N = 1)
F40.1 Social phobia (N = 1)
© 2012 The Authors. Child and Adolescent Mental Health © 2012 Association for Child and Adolescent Mental Health.
248 Joana Straub et al. Child Adolesc Ment Health 2013; 18(4): 247–50

the manual and stated that the second session was toooverloaded and that 90 min per session is too long toguarantee concentrated participation. The global evalu-ation revealed that adolescents rated the training pro-gramme as positive and effective overall (M = 7.22;SD = 1.79). The results of the evaluation questionnaireare demonstrated in Table 2.
Of the contents applied in MICHI, participants rateddevelopment of an ‘emergency plan for acute crisis’(M = 3.6) as helpful and positive, and ‘relaxation tech-niques’ (M = 2.1) as less helpful. All other elements wererated rather neutrally.
Efficacy of MICHIA positive trend, with regard to the reduction in depres-sion symptoms before and after participation in MICHI,was indicated by comparison of the CDRS-R pretest(M = 56.22; SD = 9.28) and posttest (M = 48.11;SD = 8.34), which demonstrated positive efficacy(z = �2.66, p = .008). With regard to suicidality, six ofnine patients demonstrated none to mild and threepatients demonstrated moderate to severe suicidal idea-tion before participation in MICHI. At the end of theprogramme, eight of nine patients demonstrated none tomild and only one patient demonstrated moderate tosevere suicidal ideation. Therefore, we observed areduction in suicidality in the pretest and posttestcomparison.
Discussion
The aim of this pilot study was the evaluation offeasibility of a newly developed, brief, manualised cogni-tive-behavioural group therapy for the treatment ofdepression in adolescents. Considering feasibility, theattendance of the participants was fair and could beimproved by the establishment of a reinforcement sys-tem in future applications. In response to feedback fromthe trainers, sessions will be shortened to 60–75 mineach and the contents of session two will be reorganised,resulting in five regular sessions. Furthermore, adoles-cents evaluated the whole training programme posi-tively. However, they doubted that the things learntwould help them with their family life or leisure time.
This needs to be interpreted with an eye on the inpatientsetting, which itself hampers transfer to daily life.
The content of ‘relaxation techniques’ was evaluatedas less helpful, a finding supported by Petermann(2010), who recently stated that an acute depressive epi-sode is a contraindication for relaxation techniques.Furthermore, participants rated the unique element‘emergency plan for acute crisis’ as very helpful, demon-strating the need for concrete steps about how to behaveshould a crisis arise.
Regarding the efficacy of MICHI, CDRS-R scoresdeclined significantly with a total drop of 8.11 points,slightly less than the reduction found by Weisz et al.(1997), still delivering promising results for furtherinvestigation. Furthermore, suicidal ideation wasreduced after participation in MICHI, which allows theexecution of MICHI in an ambulant setting as long as thetrainers are experienced in the clarification and han-dling of suicidal ideations. Due to the contagious effect ofsuicidality, it is very important that clients are notallowed to discuss suicidal thoughts or past behaviourwithin the group or outside the sessions, but they cantalk with the therapists individually.
Findings with regard to efficacy have several limita-tions. First, the number of participants is very small.Second, six of nine patients received medication. Wetried to overcome that by including only patients whosemedication was stabilised three weeks prior to thestart, but who still demonstrated symptoms of depres-sion. Third, the inpatient setting can influence theresults. Fourth, the absence of a control group or fol-low-up assessment allows only weak conclusions aboutefficacy and none about long-term effects. Therefore, inthis study, we can only speak of trends in efficacy butin a follow-up study, MICHI will be investigated with alarger sample in a controlled outpatient setting, andusing a longitudinal design.
As cognitive behaviour therapy is normally an expen-sive intervention, taking up to 16 sessions, our followingresults indicate a strong case for using a brief cognitive-behavioural intervention as the first line of treatment,and reserving long-term CBT for those patients who failto respond (Harrington, Whittaker, Shoebridge, &Campbell, 1998).
Acknowledgements
Funding of this study was provided by a grant of the Baden-Wuerttemberg Ministry of Education and Research and the‘Transregio Kompetenzzentrum KJP’. Those grants have nofurther role in the study design; in the collection, analysis andinterpretation of data; in the writing of the report; and in thedecision to submit themanuscript for publication.
All authors have declared that they have no competing orpotential conflicts of interest.
References
Bachmann, M., Bachmann, C., Rief, W., & Mattejat, F. (2008).Wirksamkeit psychiatrischer und psychotherapeutischerBehandlungen bei psychischen Störungen von Kindern undJugendlichen. Zeitschrift für Kinder- und Jugendpsychiatrieund Psychotherapie, 36, 309–320.
Brent, D.A., Greenhill, L.L., Compton, S., Emslie, G., Wells, K.,Walkup, J.T., ... & Turner, J.B. (2009). The treatment ofadolescent suicide attempters study (TASA): Predictors of
Table 2. Evaluation of MICHI (mean values �3.5 indicate positiveevaluation; mean values �2.5 indicate negative evaluation)
Items of the process evaluation questionnaire Mean value
Structure of the training programme 4Comprehensibility of the contents 4.22Importance of the contents 4.11Feeling comfortable in learning with others 3.78Feeling comfortable within the group 3.56Feeling comfortable with the trainers 4.11Feeling well understood by the trainers 4.11Estimation that MICHI could help otherdepressed adolescents, too
3.56
Estimation that MICHI would help themtomanage their problems
1.89
Estimation that the things learned inMICHIwould help themwithin their family life
2.22
Estimation that the things learned inMICHIwould help themwithin their leisure time
2.11
© 2012 The Authors. Child and Adolescent Mental Health © 2012 Association for Child and Adolescent Mental Health.
doi:10.1111/j.1475-3588.2012.00678.x Brief CBT for adolescents with depression 249

suicidal events in an open treamtent trial. Journal of theAmerican Academy of Child and Adolescent Psychiatry, 48,987–996.
Clarke, G.N., Hornbrook, M., Lynch, F., Polen, M., Gale, J.,Beardslee, W., ... & Seeley, J. (2009). A randomized trial of agroup cognitive intervention for preventing depression in ado-lescent offspring of depressed parents. Archives of GeneralPsychiatry, 58, 1127–1134.
Goodyer, I., Dubicka, B., Wilkinson, P., Kelvin, R., Roberts, C.,Byford, S., ... & Harrington, R. (2007). Selective serotonin re-uptake inhibitors (SSRIs) and routine specialist care with andwithout cognitive behavior therapy in adolescents with majordepression: randomised controlled trial. British MedicalJournal, 335, 142–150.
Gould, M.S., Wallenstein, S., Kleinman, M.H., O’Carroll, P., &Mercy, J. (1990). Suicide clusters: An examination of age-spe-cific effects. American Journal of Public Health, 80, 211–212.
Harrington, R., Whittaker, J., Shoebridge, P., & Campbell, F.(1998). Systematic review of efficacy of cognitive behaviortherapies in childhood and adolescent depressive disorder.British Medical Journal, 316, 1559–1563.
Oei, T., & Dingle, G. (2008). The efficacy of group cognitivebehavior therapy for unipolar depressive disorders. Journal ofAffective Disorders, 107, 5–21.
Petermann, U. (2010). Entspannungsverfahren. In F. Mattejat(Ed.), Lehrbuch der Psychotherapie: Verhaltenstherapie mitKindern, Jugendlichen und ihren Familien (Vol. 4).München: CIP-Medien.
Poznanski, E.O., & Mokros, H.B. (1996). Children’s depressionrating scale revised (CDRS-R): Manual. Los Angeles: WesternPsychological Services.
Saluja, G., Iachan, R., Scheidt, P., Overpeck, M., Sun, W., &Giedd, J. (2004). Prevalence of and risk factors for depressivesymptoms among young adolescents. Archives of Pediatricsand Adolescent Medicine, 158, 760–765.
Weisz, J., McCarty, C., & Valeri, S. (2006). Effects ofpsychotherapy in children and adolescents: A meta-analysis.Psychological Bulletin, 132, 132–149.
Weisz, J., Thurber, C., Sweeney, L., Proffitt, V., & LeGagnoux,G. (1997). Brief treatment of mild to moderate child depres-sion using primary and secondary control enhancementtraining. Journal of Consulting and Clinical Psychology, 65,703–707.
Accepted for publication: 14 May 2012Published online: 21 July 2012
© 2012 The Authors. Child and Adolescent Mental Health © 2012 Association for Child and Adolescent Mental Health.
250 Joana Straub et al. Child Adolesc Ment Health 2013; 18(4): 247–50

A brief cognitive-behavioural group therapy programme for the treatment of depression in
adolescent outpatients: a pilot study
119
6.7 A brief cognitive-behavioural group therapy programme for the treatment of
depression in adolescent outpatients: a pilot study
Contribution of J. Straub to the article:
J. Straub coordinated the study procedure and recruited participants. She executed weekly
group therapy sessions, assessed suicidal ideation and behaviour on a weekly basis, and
scheduled diagnostic as well as psychotherapeutic appointments. She controlled the return
of questionnaires and executed diagnostic assessments that didn’t have to be done by an
independent evaluator (e.g. IQ measurements). She did data acquisition, generated the data
matrix, did data input, executed statistical analyses, and interpreted statistical outcomes.
She researched literature, wrote the manuscript, integrated remarks of the co-authors,
revised the manuscript according to reviewer’s comments, and created figures and tables.
Co-authors’ contributions to the article:
M. Bonenberger was co-therapist in weekly group therapy sessions, helped with data
acquisition, reviewed the draft and gave constructive remarks. N. Sproeber and M.G. Koelch
supervised decisions on the experimental design and conceptualized and coordinated the
study. They supervised the conduction of weekly group therapy sessions. They reviewed the
draft and gave constructive remarks and helped with revising the manuscript according to
the reviewer’s comments. P.L. Plener and J.M. Fegert reviewed the draft and gave
constructive remarks.
Reference
Straub, J., Sproeber, N., Plener, P.L., Fegert, J.M., Bonenberger, M. & Koelch, M.G. (2014). A
brief cognitive-behavioural group therapy programme for the treatment of depression in
adolescent outpatients: a pilot study. Child and adolescent psychiatry and mental health,
8(9), 1-10 (open access Journal).
Straub et al. Child and Adolescent Psychiatry and Mental Health 2014, 8:9http://www.capmh.com/content/8/1/9
RESEARCH Open Access
A brief cognitive-behavioural group therapyprogramme for the treatment of depression inadolescent outpatients: a pilot studyJoana Straub1*, Nina Sproeber1, Paul L Plener1, Joerg M Fegert1, Martina Bonenberger1 and Michael G Koelch1,2
Abstract
Background: The goal of this pilot study was to examine the feasibility and clinical outcomes of a brief (6-session)group therapy programme in adolescent outpatients with depression. The programme had previously beenassessed in in-patients, with positive results.
Methods: A total of 15 outpatients aged 13 to 18 years took part in the programme between October 2010 andMay 2011, in 3 separate groups of 4–6 participants each. The outcomes measured were feasibility of theprogramme, as assessed by attendance rate, user feedback, fidelity of implementation, and response to treatment,as assessed by pre- and post-intervention measurement of depressive symptoms, quality of life, and suicidalideation.
Results: The programme demonstrated good feasibility, with a mean attendance rate of 5.33 out of 6 sessions, amean rating by participants on overall satisfaction with the programme of 7.21 out of 10 (SD = 1.89), and a 93%concurrence between the contents of the sessions and the contents of the treatment manual. Compared tobaseline scores, depressive symptoms at follow-up test were significantly reduced, as assessed by the Children’sDepression Rating Scale Revised (F(1, 12) = 11.76, p < .01) and the Beck Depression Inventory Revision (F(1, 32) =11.19, p < .01); quality of life improved, as assessed by the Inventory of Quality of Life (F(1, 31) = 5.27, p < .05); andsuicidal ideation was reduced. No significant changes were seen on the measures of the Parent Rating Scale forDepression and the Clinical Global Impression scale.
Conclusions: Based on the results of this pilot study, it is feasible to further assess this brief outpatient treatmentprogramme in a randomized controlled trial without further modifications.
BackgroundThe rate of depressive disorders in German adolescentsaged 11–17 years is reported to be 4.7% for males and9.7% for females [1]. Up to two-thirds of depressed ado-lescents suffer from co-morbid disorders [2], and depres-sion is often associated with poor health behaviours andsocial challenges as well as with an elevated risk forsuicide [3]. Suicide is the second most common cause ofdeath for adolescents in Europe [4]. Given the natureand associated risks of depression, the Global Burden ofDisease Study of the World Health Organization [5] has
* Correspondence: [email protected] of Child and Adolescent Psychiatry and Psychotherapy,University Hospital, Ulm, GermanyFull list of author information is available at the end of the article
© 2014 Straub et al.; licensee BioMed CentralCommons Attribution License (http://creativecreproduction in any medium, provided the orDedication waiver (http://creativecommons.orunless otherwise stated.
identified it as one of the most prevalent and debilitatingdisorders worldwide.Several authors have looked at factors that might
affect the effectiveness of therapies for children and ad-olescents with depression. In a meta-analysis of cogni-tive behavioural therapy (CBT) treatments, Weisz et al.[6] found a mean effect size (comparable to Cohen’s d)of .34. Group therapy was found to have several ad-vantages over individual therapy, as follows: the groupprocess can positively affect recovery, group memberscan learn from each other and give each other feedback,there is less stigmatisation, and the process may bemore economical. A disadvantage, however, is that indi-viduals with social anxiety or introversion may not re-ceive as much attention as other participants [7]. In arecent meta-regression analysis looking at treatments
Ltd. This is an Open Access article distributed under the terms of the Creativeommons.org/licenses/by/2.0), which permits unrestricted use, distribution, andiginal work is properly credited. The Creative Commons Public Domaing/publicdomain/zero/1.0/) applies to the data made available in this article,

Straub et al. Child and Adolescent Psychiatry and Mental Health 2014, 8:9 Page 2 of 10http://www.capmh.com/content/8/1/9
for depression in adults, Cuijpers et al. [8] found thatmore sessions per week led to a larger effect size whileevery additional week of therapy reduced the effect size,which suggests there may be advantages to interven-tions that are short and intensive. Goodyer et al. [9]found that about one-fifth of depressed adolescentsresponded to a brief initial intervention (mean of 3 ses-sions). Brief therapies have the advantage that theyallow for faster access to treatment and can be offeredas a first-line treatment, reserving longer therapies forindividuals who fail to respond.There are currently six cognitive behavioural therapy
programmes available in Germany to depressed adoles-cents: three for the prevention of depression and three fortreatment [10-15]. Of the treatment programmes, one isthe German version of the Adolescent Coping With De-pression Course (CWD-A), which consists of ten 2-hoursessions [12]; one provides individual treatment sessions[11]; and one is primarily for the treatment of perform-ance problems that may affect symptoms of depression[14]. However, none of these options combines the poten-tial advantages described above of an intervention thatuses CBT, is brief, and is delivered via group therapy. Thisarticle describes a brief (6-session) manualised programmethat was developed to fill this gap. The programme is ti-tled “Manualised Intervention to Cope with depressivesymptoms, Help strengthen resources, and Improve emo-tion regulation”, or MICHI, which is Japanese for “TheWay” [16].For safety reasons, as depression increases the risk for
suicidal behaviour, the MICHI programme was first eval-uated in in-patients [17]. The results of that initial pilotstudy, which was conducted in 9 adolescents (meanage = 16.33 years), showed good compliance in terms ofthe mean number of sessions attended (4.33 out of 5),positive user feedback on the programme content andthe group leaders, improvement in symptoms of depres-sion (CDRS-R: z = −2.66; p = .008), and reduction ofsuicidal ideation. Based on participants’ feedback, wechanged several aspects of the programme, includingreordering of the therapeutic contents, deleting somecontent such as relaxation techniques, and adding anextra session.
Objectives of the pilot studyBefore evaluating MICHI in a randomized controlledtrial, we chose to conduct a second pilot study, this timein out-patients. Overall reasons for conducting pilotstudies are to test the feasibility of a process, and to ob-tain preliminary data on the response to treatment [18].Feasibility was here defined through three measures.The first was attendance, since as depression goes handin hand with a lowered level of psychosocial functioning,participants might be expected to miss some sessions. A
participation rate of five out of six sessions (79%) wasdefined as acceptable [19]. The second measure was useracceptance, for which we designed a questionnaire thatasked participants how favourably they viewed variouselements of the programme. The third feasibility meas-ure was fidelity of implementation; i.e., how closely thepsychologists who conducted the sessions were adheringto the treatment protocol defined in the MICHI treat-ment manual. Fidelity rates for manualised treatmentstypically range between 80% and 94% [20-23], so we de-fined anything within this range as being acceptable.With respect to response to treatment, efficacy wasassessed by administering diagnostic tests of depressionpre- post-intervention and follow-up and looking to seeif scores were reduced following treatment. Safety wasassessed through pre- post-intervention and follow-upmeasurement of suicidal ideation, which is a frequentsymptom of depression. Since one of the goals of MICHIis to educate patients on how to deal with acute crisesand prevent suicidal behaviour, we hypothesized thatsuicidal ideation would be reduced after participation.
MethodsPopulationThe pilot study was carried out in 3 separate groups of 4to 6 participants each, with the first group starting inOctober 2010, the second in February 2011, and the thirdin March 2011. Recruitment was done by asking cliniciansof local outpatient child and adolescent psychiatry andother local outpatient mental health institutions to referany suitable patients to attend an information meetingheld by the MICHI group leaders. Individuals who ex-pressed interest following this meeting were scheduled fora screening visit, and those found eligible were enrolled inthe next available group. Participants had to be aged be-tween 13 and 18 years and to have an IQ of at least 80, araw summary score on the Children’s Depression RatingScale Revised (CDRS-R) [24] of at least 36 [25], and adiagnosis of a mild, moderate, or severe major depressiveepisode according to ICD-10 criteria [26]. In order for thesample to be representative of a naturalistic population, itwas decided to not exclude difficult-to-treat patients [27].Thus, co-morbid diagnoses were permitted as long assymptoms of depression were the main cause of the pa-tient seeking medical support; and antidepressant medica-tion was permitted provided it was stable for at least5 weeks prior to study start and during the study. Individ-uals with a diagnosis of bipolar disorder, schizophrenia, orsevere substance abuse were excluded, as these disordersrequire a different form of treatment and could be disrup-tive to the group process. Finally, participants and theirparents/guardians had to agree to not to initiate any newdrug treatment or new form of psychotherapy while par-ticipating in MICHI.

Straub et al. Child and Adolescent Psychiatry and Mental Health 2014, 8:9 Page 3 of 10http://www.capmh.com/content/8/1/9
The study was approved by the IRB of the Universityof Ulm, Germany, and informed consent was providedby participants and their parents or guardians.
Study designAs described in its treatment manual [16], MICHI is a CBTtreatment that combines a number of therapeutic com-ponents widely acknowledged to represent the standardof care [28, 29]. All sessions included (1) psycho-education,(2) cognitive restructuring with the aim of reducingrumination [30], (3) behavioural activation, (4) resourceactivation, (5) enhancement of self-esteem, (6) problem-solving skills, (7) emotion regulation, (8) management ofacute crises, and (9) prevention of relapse.The programme included 5 weekly visits of 75 to 90 mi-
nutes in length, plus a “booster” session held 5.5 weeksafter the last regular visit. An overview of the content andactivities of the sessions is shown in Table 1. Each sessionincluded a review of what had been covered the previousweek, provision of new information, therapist-assistedpractice, homework for the coming week, assessment ofmood using the Beck Depression Inventory–Revision(BDI-II) questionnaire [31], and the opportunity to talk tothe therapist individually after the session in cases of acutecrisis. Item 9 of the BDI-II, which asks about suicidal be-haviour, was checked at every session, and if a participantreported current suicidal ideation, the programme super-visor was to be consulted in order to conduct a risk assess-ment and to decide if hospitalization was necessary. ForSession 5, each participant was asked to bring along a“person of trust”, either a family member or a friend, whowould attend the session and be trained on how to sup-port the patient to help prevent relapse as well as on step-wise problem solving.The sessions were conducted according to the detailed
instructions provided in the MICHI treatment manual,and were led by two of the manual’s co-authors (JS andMB) who are psychologists with master’s degrees andprior group CBT experience with adolescents. Bothleaders were equally involved, and had predefined tasks toensure that the same intervention was provided at all threeMICHI groups. The group leaders were supervised by themanual’s main author and licensed psychotherapist (NS).The study design is presented in Figure 1. Assessments
were carried out prior to Session 1 (pre-intervention),following Session 5 (post-intervention), and between 1and 2.5 weeks after the booster session (follow-up). Eachof the 3 assessment periods spanned 10 days, to allowfor evaluation of all participants in the group.
Diagnostic instrumentsScreening measures included administration of the KiddieSchedule for Affective Disorders and Schizophrenia,Present and Lifetime Version (K-SADS-PL) [32] to assess
psychiatric disorders, and one of the following tests to as-sess intelligence: either the Wechsler Intelligence Scale forChildren–Fourth Edition (WISC IV) [33], the WechslerAdult Intelligence Scale (WAIS) [34], or the testing systemfor educational counselling (PSB) [35].The primary outcomes for assessment of MICHI were:
1) feasibility of the programme, as assessed by attendancerate, user acceptance, and fidelity of implementation, and2) preliminary data on the response to treatment assessedby the change in depressive symptoms, as measured bythe CDRS-R total score. Attendance was defined as thepercentage of sessions for which participants showed up.User acceptance was determined by having participantsanonymously complete an ad hoc evaluation form con-taining 21 statements (α = .92 in the present sample) thatwere rated on a scale of 1 (not true) to 5 (true) plus oneglobal question regarding overall satisfaction with theprogramme, rated on a scale of 1 (very poor) to 10 (verygood). To determine fidelity of implementation, all ses-sions were videotaped, and 25% were randomly selectedand viewed by an independent clinician to see if the re-quired elements in the MICHI treatment manual were be-ing implemented. A 57-item checklist was employed inthe rating, with each item scored as either present orabsent. The CDRS-R is a semi-structured clinician-ratedinterview, consisting of 17 questions, which asks aboutsymptoms of depression over the last 2 weeks [24]. Ascore of 36 or greater indicates evidence of clinically rele-vant symptoms of depression [25]. The interview hasshown a high internal consistency in previous studies withlarger sample sizes (α = .90) [36] and α = .79 in the presentsample). The German version of the CDRS-R was used inthis study [37].The independent evaluators who per-formed the interview were blinded to the time points ofmeasurement.The secondary outcomes were changes in depression
as measured by other instruments, changes in suicidalideation, and changes in other measures of mentalhealth. Two instruments were used for assessing depres-sion over the last 2 weeks, one administered to the pa-tient and the other to the parent/guardian: the BDI-II[31], which consists of 21 items (α = .95 in the presentsample), and the Parent Rating Scale for Depression(FBB-DES), which is part of the diagnostic system formental disorders in childhood and adolescence (DIS-YPS-II) [38] and is based on the international classifica-tion systems ICD-10 and DSM-IV (29 items; α = .89 inthe present sample). Suicidal ideation was assessed byItem 13 of the CDRS-R (asking for suicidal ideationsand suicide attempts). The question is answered using a7-item scale ranging from “none to mild” (never thoughtabout suicide or thought about it very seldom) to “mod-erate to severe” (thought about or attempted suicidewithin the last month). Other instruments used were the

Table 1 Contents of MICHI sessions
Sessionnumber
Contents Exercises
Session 1 • Get to know each other • Postcards with different emotional motifs were displayed, and participants wereencouraged to choose one that represented their depression best
• Psychoeducation about symptoms ofdepression • Related to the postcards, each participant was asked to tell his/her symptoms, and group
leaders highlighted typical symptoms of depression
• Homework: participants were asked to
- Think about individual possible causes for their depressive symptoms
- Conduct a positive activity each day and to evaluate how it affects their mood
- Bring an object to the next session that represents something they are good at/proud of(e.g., football)
Session 2 • Resource activation • Participants showed the object they brought that represented something they were goodat/ proud of
• Input about relationship betweenthoughts, behaviour, and feelings
• Participants were asked to name additional strengths and resources
• Psychoeducation a bout causationsof depression
• Psychoeducation about causation of depression (e.g., neurotransmitters, genetics, stressors)
• Homework: participants were asked to
- Focus on a positive and negative moment each day and to note down their behaviour,thoughts, and feelings in each moment
- Note down compliments they receive or positive moments that happen to them in a diary
Session 3 • Enhancement of self-esteem • Participants threw each other a ball, and each time they caught the ball they were askedto name a certain individual strength
• Increase of behavioural activation• Participants were invited to write each other compliments in their diaries
• Psychoeducation about dysfunctionalcognitions
• Input about the importance of positive self-esteem
• Input about how errors in reasoning, e.g., dichotomous thinking, negatively influenceshow one feels
Session 4 • Repetition of contents • Participants listened to an audiotaped interview with a depressed girl who talked abouther symptoms, and were asked to give her advice about what she could do to feel better,taking into account what they learned in MICHI so far• Management of acute crises
• Emotion regulation • Discussion and input about how to behave in case of crises (e.g., suicidal ideation)• Restructuring of dysfunctional cognitions • Identification of helpful skills
• Input about how to recognize negative thoughts and how to turn them into positive ones
Session 5 • Problem-solving skills prevention ofrelapse
• Participants learned how to solve problems in a theoretical stepwise manner; afterwards,they watched a video about a girl who is being bullied, and were asked how they wouldsolve a problem like the one of the protagonist, taking into account the stepwise mannerof problem-solving they learned before
• Participants brought a person of trust
• Conversation about how persons of trust can support participants in the future to preventrelapse
Boostersession 6
• Recapitulation of contents of MICHI • Contents of MICHI were repeated by means of a quiz
• Each participant was asked to recapitulate his/her mood since the last session of MICHI
• In case they found themselves in a depressed mood, they were asked whether they wereable to apply elements of MICHI to prevent themselves from relapse
• Participants were given a written case report of a depressed boy and were asked to advisehim what he could do to feel better with reference to the contents learned in MICHI
Straub et al. Child and Adolescent Psychiatry and Mental Health 2014, 8:9 Page 4 of 10http://www.capmh.com/content/8/1/9
Inventory for the Assessment of Quality of Life inChildren and Adolescents (IQLC) [39], which consists of 7items (α = .59 in the present sample) and assesses qualityof life in the past week; the Clinical Global Impression
(CGI) [40], which consists of 1 item and assesses severityof symptoms over the past week; and the Health of theNation Outcome Scales for Children and Adolescents(HoNOSCA) [41], which consists of 13 items (α = .74 in
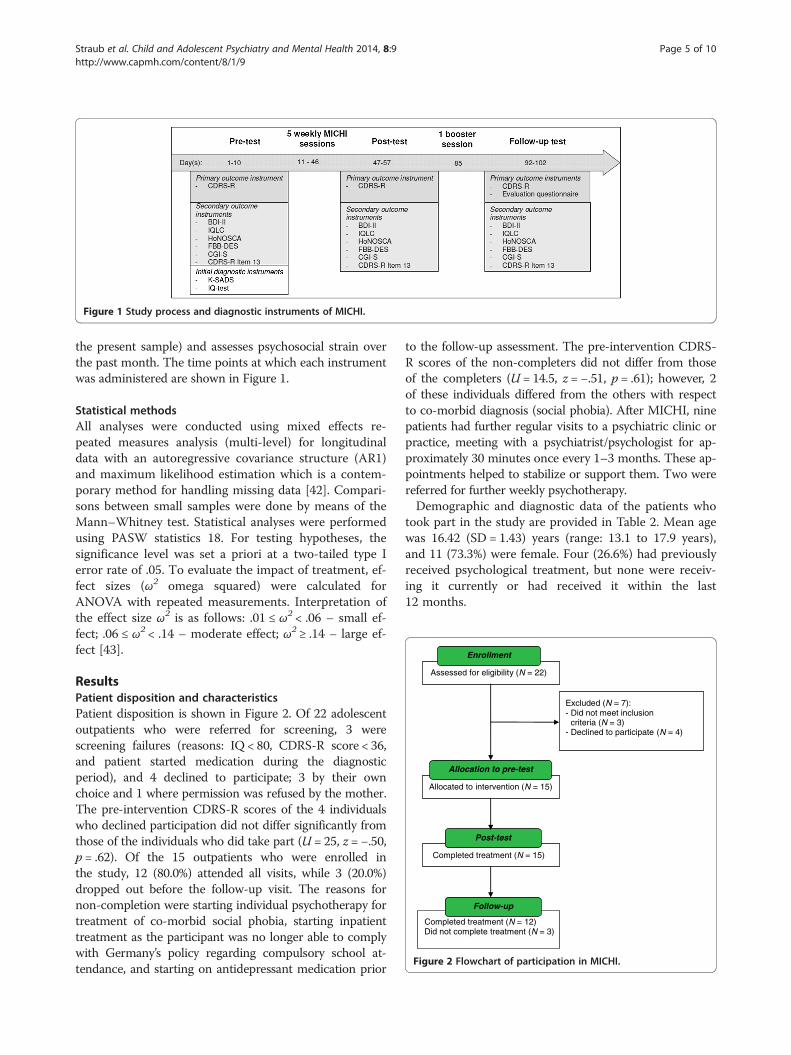
Figure 1 Study process and diagnostic instruments of MICHI.
Completed treatment (N = 12)Did not complete treatment (N = 3)
Completed treatment (N = 15)
Allocated to intervention (N = 15)
Assessed for eligibility (N = 22)
Excluded (N = 7):- Did not meet inclusion
criteria (N = 3)- Declined to participate (N = 4)
Allocation to pre-test
Post-test
Enrollment
Follow-up
Figure 2 Flowchart of participation in MICHI.
Straub et al. Child and Adolescent Psychiatry and Mental Health 2014, 8:9 Page 5 of 10http://www.capmh.com/content/8/1/9
the present sample) and assesses psychosocial strain overthe past month. The time points at which each instrumentwas administered are shown in Figure 1.
Statistical methodsAll analyses were conducted using mixed effects re-peated measures analysis (multi-level) for longitudinaldata with an autoregressive covariance structure (AR1)and maximum likelihood estimation which is a contem-porary method for handling missing data [42]. Compari-sons between small samples were done by means of theMann–Whitney test. Statistical analyses were performedusing PASW statistics 18. For testing hypotheses, thesignificance level was set a priori at a two-tailed type Ierror rate of .05. To evaluate the impact of treatment, ef-fect sizes (ω2 omega squared) were calculated forANOVA with repeated measurements. Interpretation ofthe effect size ω2 is as follows: .01 ≤ ω2 < .06 – small ef-fect; .06 ≤ ω2 < .14 – moderate effect; ω2 ≥ .14 – large ef-fect [43].
ResultsPatient disposition and characteristicsPatient disposition is shown in Figure 2. Of 22 adolescentoutpatients who were referred for screening, 3 werescreening failures (reasons: IQ < 80, CDRS-R score < 36,and patient started medication during the diagnosticperiod), and 4 declined to participate; 3 by their ownchoice and 1 where permission was refused by the mother.The pre-intervention CDRS-R scores of the 4 individualswho declined participation did not differ significantly fromthose of the individuals who did take part (U = 25, z = −.50,p = .62). Of the 15 outpatients who were enrolled inthe study, 12 (80.0%) attended all visits, while 3 (20.0%)dropped out before the follow-up visit. The reasons fornon-completion were starting individual psychotherapy fortreatment of co-morbid social phobia, starting inpatienttreatment as the participant was no longer able to complywith Germany’s policy regarding compulsory school at-tendance, and starting on antidepressant medication prior
to the follow-up assessment. The pre-intervention CDRS-R scores of the non-completers did not differ from thoseof the completers (U = 14.5, z = −.51, p = .61); however, 2of these individuals differed from the others with respectto co-morbid diagnosis (social phobia). After MICHI, ninepatients had further regular visits to a psychiatric clinic orpractice, meeting with a psychiatrist/psychologist for ap-proximately 30 minutes once every 1–3 months. These ap-pointments helped to stabilize or support them. Two werereferred for further weekly psychotherapy.Demographic and diagnostic data of the patients who
took part in the study are provided in Table 2. Mean agewas 16.42 (SD = 1.43) years (range: 13.1 to 17.9 years),and 11 (73.3%) were female. Four (26.6%) had previouslyreceived psychological treatment, but none were receiv-ing it currently or had received it within the last12 months.
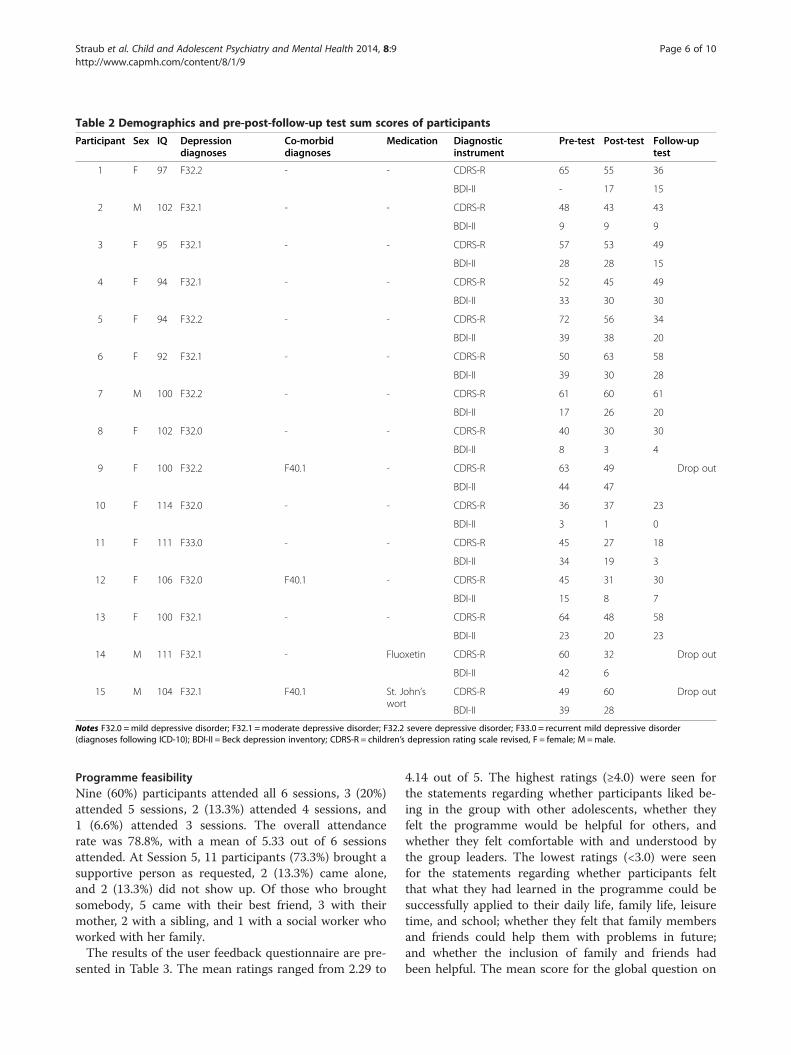
Table 2 Demographics and pre-post-follow-up test sum scores of participants
Participant Sex IQ Depressiondiagnoses
Co-morbiddiagnoses
Medication Diagnosticinstrument
Pre-test Post-test Follow-uptest
1 F 97 F32.2 - - CDRS-R 65 55 36
BDI-II - 17 15
2 M 102 F32.1 - - CDRS-R 48 43 43
BDI-II 9 9 9
3 F 95 F32.1 - - CDRS-R 57 53 49
BDI-II 28 28 15
4 F 94 F32.1 - - CDRS-R 52 45 49
BDI-II 33 30 30
5 F 94 F32.2 - - CDRS-R 72 56 34
BDI-II 39 38 20
6 F 92 F32.1 - - CDRS-R 50 63 58
BDI-II 39 30 28
7 M 100 F32.2 - - CDRS-R 61 60 61
BDI-II 17 26 20
8 F 102 F32.0 - - CDRS-R 40 30 30
BDI-II 8 3 4
9 F 100 F32.2 F40.1 - CDRS-R 63 49 Drop out
BDI-II 44 47
10 F 114 F32.0 - - CDRS-R 36 37 23
BDI-II 3 1 0
11 F 111 F33.0 - - CDRS-R 45 27 18
BDI-II 34 19 3
12 F 106 F32.0 F40.1 - CDRS-R 45 31 30
BDI-II 15 8 7
13 F 100 F32.1 - - CDRS-R 64 48 58
BDI-II 23 20 23
14 M 111 F32.1 - Fluoxetin CDRS-R 60 32 Drop out
BDI-II 42 6
15 M 104 F32.1 F40.1 St. John’swort
CDRS-R 49 60 Drop out
BDI-II 39 28
Notes F32.0 =mild depressive disorder; F32.1 =moderate depressive disorder; F32.2 severe depressive disorder; F33.0 = recurrent mild depressive disorder(diagnoses following ICD-10); BDI-II = Beck depression inventory; CDRS-R = children’s depression rating scale revised, F = female; M =male.
Straub et al. Child and Adolescent Psychiatry and Mental Health 2014, 8:9 Page 6 of 10http://www.capmh.com/content/8/1/9
Programme feasibilityNine (60%) participants attended all 6 sessions, 3 (20%)attended 5 sessions, 2 (13.3%) attended 4 sessions, and1 (6.6%) attended 3 sessions. The overall attendancerate was 78.8%, with a mean of 5.33 out of 6 sessionsattended. At Session 5, 11 participants (73.3%) brought asupportive person as requested, 2 (13.3%) came alone,and 2 (13.3%) did not show up. Of those who broughtsomebody, 5 came with their best friend, 3 with theirmother, 2 with a sibling, and 1 with a social worker whoworked with her family.The results of the user feedback questionnaire are pre-
sented in Table 3. The mean ratings ranged from 2.29 to
4.14 out of 5. The highest ratings (≥4.0) were seen forthe statements regarding whether participants liked be-ing in the group with other adolescents, whether theyfelt the programme would be helpful for others, andwhether they felt comfortable with and understood bythe group leaders. The lowest ratings (<3.0) were seenfor the statements regarding whether participants feltthat what they had learned in the programme could besuccessfully applied to their daily life, family life, leisuretime, and school; whether they felt that family membersand friends could help them with problems in future;and whether the inclusion of family and friends hadbeen helpful. The mean score for the global question on
Table 3 Evaluation questionnaire for the assessment ofacceptance
Item Meanrating
I like learning with other adolescents 4.14
I expect the training to be helpful to other adolescents aswell
4.07
I felt comfortable with the trainers 4.00
I felt well understood by the trainers 4.00
Advice of the trainers was helpful to me 3.93
I felt comfortable within the group 3.59
The exercises in the training were helpful 3.50
It is helpful to learn with other adolescents 3.43
I expect that the things I learned will help me in the future 3.29
The amount of homework was helpful 3.14
The homework in general was helpful 3.14
I liked the inclusion of family and friends 3.14
I would participate again in a training like MICHI 3.14
I expect to be able to implement the things I learned inthe future
3.07
The transfer of the things learned in the homework to dailylife was successful
2.93
The things learned were helpful in my leisure time 2.86
I expect that family and friends can help me with myproblems in the future
2.79
The inclusion of family and friends was helpful 2.64
The things learned were helpful to me in school/vocationaltraining
2.57
The things learned were helpful in my family life 2.29
Notes Evaluation questionnaire of MICHI (answers range from 1 to 5; thehigher the number, the stronger the agreement).
Table 4 Results of diagnostic instruments
M SD N F dfM dfR p ω2
Primary outcome
CDRS-R
Pre-test 53.80 12.24 15
Post-test 45.93 12.11 15
Follow-up 40.75 14.39 12 11.76 1 11.92 .005** .11
Secondary outcomes
BDI-II
Pre-test 26.64 14.00 14
Post-test 20.67 13.45 15
Follow-up 14.50 9.98 12 11.19 1 31.97 .002** .01
IQLC
Pre-test 20.60 3.85 15
Post-test 19.13 4.03 15
Follow-up 18.42 4.19 12 5.27 1 30.57 .03* .03
HoNOSCA
Pre-test 13.60 5.88 15
Post-test 13.14 6.02 14
Follow-up 9.25 5.14 12 4.54 1 36.92 .04* .04
FBB-DES
Pre-test 21.93 14.18 15
Post-test 23.31 12.30 13
Follow-up 17.11 7.90 9 .94 1 27.02 .34 .01
CGI-S
Pre-test 4.00 1.07 15
Post-test 4.00 1.00 15
Follow-up 3.33 1.56 12 2.11 1 14.37 .17 .01
Notes * p < .05, ** p < .01; high mean values demonstrate a higher symptomseverity; Explanation of abbreviations: M =mean; SD = standard deviation; N =number of participants; dfM = degrees of freedom for the effect of the model;dfR = degrees of freedom for the residuals of the model; effect sizes wereanalysed according to ANOVA with repeated measurements; ω2 = omegasquared effect size; Interpretation of the effect size ω2: .01 ≤ω2 < .06 – smalleffect; .06 ≤ω2 < .15 – moderate effect; ω2 ≥ .15 – large effect.
Straub et al. Child and Adolescent Psychiatry and Mental Health 2014, 8:9 Page 7 of 10http://www.capmh.com/content/8/1/9
overall satisfaction with the program was 7.21 (SD =1.89) out of 10.With respect to fidelity to the MICHI treatment manual,
based on the findings of the independent clinician whorated videotapes of randomly selected sessions, there wasa 93% concurrence between the manualised treatment andwhat was delivered.
Response to treatmentThe total CDRS-R scores decreased significantly frompre-intervention to follow-up assessment (F (1, 12) =11.76, p < .01), and 5 (42%) of the 12 participants whocompleted the follow-up assessment no longer met thecriteria for clinically significant depression (CDRS-Rscore < 36). Scores also decreased significantly for theBDI-II (F (1, 32) = 11.19, p < .01) and the HoNOSCA(F (1, 37) = 4.54, p < .05) and increased significantly forthe IQLC (F (1, 31) = 5.27, p < .05). No significant changeswere seen on the FBB-DES and the CGI. See Table 4. Fur-thermore Figure 3 demonstrates the course of the BDI-II
assessments per session. Results revealed a decline ofsymptom severity from session two onwards.With respect to suicidal ideation, pre-intervention, just
4 (26.7%) participants had a response of “none to mild”on Item 13 of the CDRS-R while 11 (73.3%) had a re-sponse of “moderate to severe”. Post Session 5, thesenumbers were 10 (67%) and 5 (33%), respectively; and atfollow-up, they had further improved to 10 (80.0%) and 2(20.0%), respectively. The change from pre-intervention tofollow-up was statistically significant (F (1, 32.81) = 4.25,p < .05).
DiscussionThe aim of this pilot study was to assess a brief cognitivebehavioural group therapy programme in adolescent out-
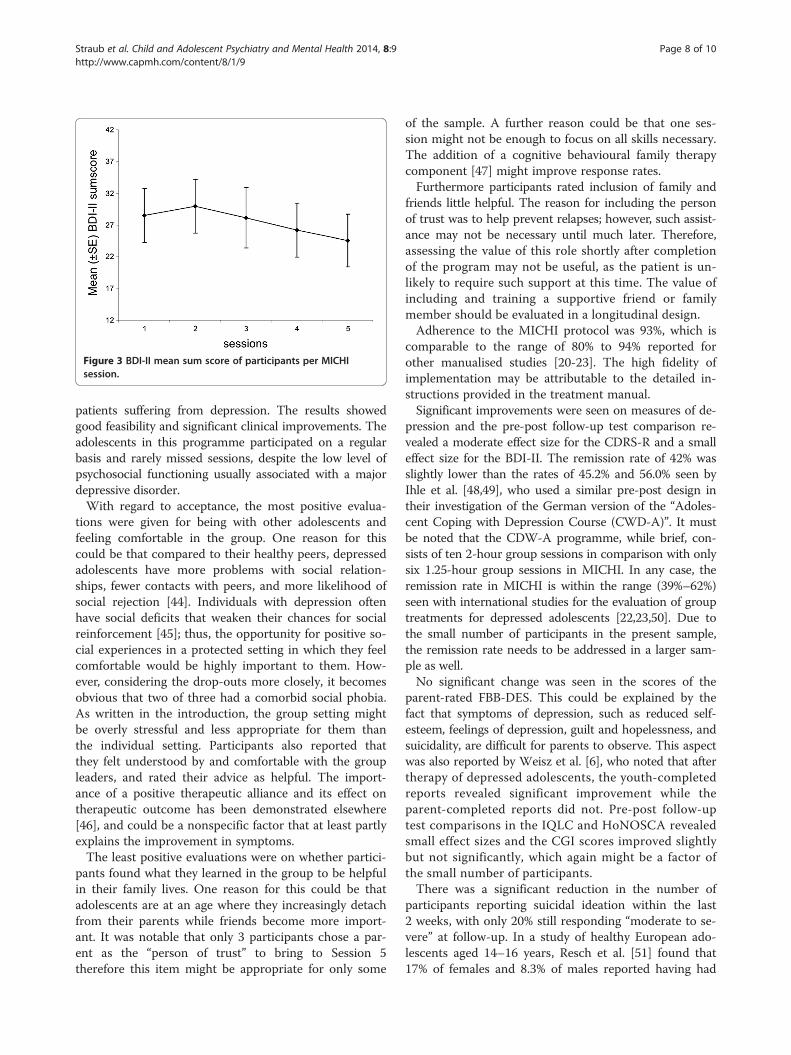
Figure 3 BDI-II mean sum score of participants per MICHIsession.
Straub et al. Child and Adolescent Psychiatry and Mental Health 2014, 8:9 Page 8 of 10http://www.capmh.com/content/8/1/9
patients suffering from depression. The results showedgood feasibility and significant clinical improvements. Theadolescents in this programme participated on a regularbasis and rarely missed sessions, despite the low level ofpsychosocial functioning usually associated with a majordepressive disorder.With regard to acceptance, the most positive evalua-
tions were given for being with other adolescents andfeeling comfortable in the group. One reason for thiscould be that compared to their healthy peers, depressedadolescents have more problems with social relation-ships, fewer contacts with peers, and more likelihood ofsocial rejection [44]. Individuals with depression oftenhave social deficits that weaken their chances for socialreinforcement [45]; thus, the opportunity for positive so-cial experiences in a protected setting in which they feelcomfortable would be highly important to them. How-ever, considering the drop-outs more closely, it becomesobvious that two of three had a comorbid social phobia.As written in the introduction, the group setting mightbe overly stressful and less appropriate for them thanthe individual setting. Participants also reported thatthey felt understood by and comfortable with the groupleaders, and rated their advice as helpful. The import-ance of a positive therapeutic alliance and its effect ontherapeutic outcome has been demonstrated elsewhere[46], and could be a nonspecific factor that at least partlyexplains the improvement in symptoms.The least positive evaluations were on whether partici-
pants found what they learned in the group to be helpfulin their family lives. One reason for this could be thatadolescents are at an age where they increasingly detachfrom their parents while friends become more import-ant. It was notable that only 3 participants chose a par-ent as the “person of trust” to bring to Session 5therefore this item might be appropriate for only some
of the sample. A further reason could be that one ses-sion might not be enough to focus on all skills necessary.The addition of a cognitive behavioural family therapycomponent [47] might improve response rates.Furthermore participants rated inclusion of family and
friends little helpful. The reason for including the personof trust was to help prevent relapses; however, such assist-ance may not be necessary until much later. Therefore,assessing the value of this role shortly after completionof the program may not be useful, as the patient is un-likely to require such support at this time. The value ofincluding and training a supportive friend or familymember should be evaluated in a longitudinal design.Adherence to the MICHI protocol was 93%, which is
comparable to the range of 80% to 94% reported forother manualised studies [20-23]. The high fidelity ofimplementation may be attributable to the detailed in-structions provided in the treatment manual.Significant improvements were seen on measures of de-
pression and the pre-post follow-up test comparison re-vealed a moderate effect size for the CDRS-R and a smalleffect size for the BDI-II. The remission rate of 42% wasslightly lower than the rates of 45.2% and 56.0% seen byIhle et al. [48,49], who used a similar pre-post design intheir investigation of the German version of the “Adoles-cent Coping with Depression Course (CWD-A)”. It mustbe noted that the CDW-A programme, while brief, con-sists of ten 2-hour group sessions in comparison with onlysix 1.25-hour group sessions in MICHI. In any case, theremission rate in MICHI is within the range (39%–62%)seen with international studies for the evaluation of grouptreatments for depressed adolescents [22,23,50]. Due tothe small number of participants in the present sample,the remission rate needs to be addressed in a larger sam-ple as well.No significant change was seen in the scores of the
parent-rated FBB-DES. This could be explained by thefact that symptoms of depression, such as reduced self-esteem, feelings of depression, guilt and hopelessness, andsuicidality, are difficult for parents to observe. This aspectwas also reported by Weisz et al. [6], who noted that aftertherapy of depressed adolescents, the youth-completedreports revealed significant improvement while theparent-completed reports did not. Pre-post follow-uptest comparisons in the IQLC and HoNOSCA revealedsmall effect sizes and the CGI scores improved slightlybut not significantly, which again might be a factor ofthe small number of participants.There was a significant reduction in the number of
participants reporting suicidal ideation within the last2 weeks, with only 20% still responding “moderate to se-vere” at follow-up. In a study of healthy European ado-lescents aged 14–16 years, Resch et al. [51] found that17% of females and 8.3% of males reported having had

Straub et al. Child and Adolescent Psychiatry and Mental Health 2014, 8:9 Page 9 of 10http://www.capmh.com/content/8/1/9
suicidal thoughts within the last 2 weeks, as assessed bythe Paykel Scale [52]. Thus, the percentage of adoles-cents with suicidal ideation seen in our sample follow-up-intervention is not much larger than that seen in anon-clinical population of the same age. This finding ofa reduction of suicidal thoughts following outpatienttreatment is important, as suicidality in adolescents is amajor public health problem due to its frequency, likeli-hood for recurrence, increased risk for completed sui-cide, and health costs [53].A comparison of the results of this pilot study with
the earlier pilot study of MICHI in in-patients [17] re-vealed no difference in feasibility and a nearly identicalimprovement in pre-post CDRS-R scores. With respectto suicidal ideation, the out-patients showed a higherpercentage of moderate to severe suicidal ideation pre-intervention than did the in-patients. Post-intervention,reduction of suicidal ideation was comparable betweenboth samples.Some limitations of this pilot study must be recognized.
These include a small sample size; the absence of a controlgroup, which allows for only weak conclusions about effi-cacy; a small cronbach’s alpha of the IQLC, which mightbe due to a small number of items and stronger changesin some items than others, and the inclusion of partici-pants who were receiving medication for depression. Weattempted to reduce the impact of medication by includ-ing only patients whose regimen was stable for five weeksprior to the start of and during therapy. Furthermore weincluded participants with co-morbid disorders that couldinfluence results. It is possible that permitting patients tospeak to a group leader individually following a session incase of an acute crisis could have influenced results; how-ever, this opportunity was used only few times. This issuewas discussed before the start of the programme, and wasfelt to be a necessary supplement for ethical reasons andbecause it reflects practical reality.
ConclusionsThe results of this pilot study revealed a reduction in de-pression and suicidal ideation and an improvement ofquality of life in adolescent outpatients following participa-tion in a brief manualised CBT group therapy programme.Overall, the findings support the feasibility of proceedingwith an investigation of the MICHI programme using alarger sample size in a randomized controlled trial design.If the findings are borne out in a controlled trial, this ap-proach could come to be considered a first-line treatmentfor adolescents with depression, reserving longer-lastingtherapies or medical treatment only for those who fail torespond.
Competing interestsAll authors declare no conflict of interests.
Authors’ contributionsPLP is PI in a study for Lundbeck. He has received research grants from theBMBF (German Ministries for Research and Education) and the BfArM (GermanFederal Institute for Drugs and Medical Devices) and the state foundation(Landesstiftung) Baden-Wuerttemberg. He has received travel grants from theDFG, DAAD and IACAPAP. He is not a shareholder in the pharmaceuticalindustry. JS managed the literature searches, acquisition of data, and analysisand interpretation of data, and was the primary author of the article. NSdeveloped the MICHI training manual and designed the study. PLP aided in theliterature search. MB conducted group therapy sessions and helped withacquisition of data. MGK supervised and coordinated the study. All authorscontributed to the manuscript and approved the final version. JMF has receivedresearch funding in the last 5 years from EU, DFG, BMG, BMBF, BMFSFJ, severalstate ministries of social affairs, State Foundation BaWue, VolkswagenFoundation, European Academy, Gregorian University, Vatican, RAZ, CJD, Eli Lillyresearch foundation, Janssen-Cilag (J&J), Medice, Celltech/UCB. Furthermore, hehas received travel grants, honoraria, and sponsoring for conferences andmedical educational purposes from DFG, AACAP, NIMH/NIH, EU, the Vatican,Goethe Institute, Pro Helvetia, Astra, Aventis, Bayer, Bristol-MS, Celltech/ UCB,Janssen-Cilag (J&J), Lilly, Medice, Novartis, Pfizer, Ratiopharm, Sanofi-Synthelabo,Shire, VfA, Generikaverband, several universities and professional associations,and German federal and state ministries. MGK has received unrestricted grantsfrom Eli Lilly International Foundation. He has received research grants from theBMFFSJ (German Ministries for Family Affairs, Senior Citizens, Women andYouth), the BMBF (German Ministries for Research and Education), theSchweizerBundesamt fuer Justiz, and BoehringerIngelheim. He has been a CI orPI for Eli Lilly, Astra Zeneca, and Janssen-Cilag, Lundbeck. He has received travelgrants or payments for lectures from Janssen-Cilag, the University of Rostock,DGKJPP, UCB, EuropaeischeAkademie and from various non-profit organizations.He is not a shareholder in the pharmaceutical industry.
Author details1Department of Child and Adolescent Psychiatry and Psychotherapy,University Hospital, Ulm, Germany. 2Department of Child and AdolescentPsychiatry, Psychotherapy and Psychosomatics, Vivantes Hospitals, Berlin,Germany.
Received: 8 October 2013 Accepted: 11 March 2014Published: 22 March 2014
References1. Bettge S, Wille N, Barkmann C, Schulte-Markwort M, Ravens-Sieberer U, the
BELLA study group: Depressive symptoms of children and adolescents ina German representative sample: results of the BELLA study. Eur ChildAdolesc Psychiatry 2008, 17:71–81.
2. Essau CA, Conradt J, Petermann F: Frequency, comorbidity, andpsychosocial impairment of depressive disorders in adolescents.J Adolesc Res 2000, 15(4):470–481.
3. Saluja G, Iachan R, Scheidt P, Overpeck M, Sun W, Giedd J: Prevalence ofand risk factors for depressive symptoms among young adolescents.Arch Pediatr Adolesc Med 2004, 158:760–765.
4. Wilkinson P, Levin R, Roberts C, Dubicka B, Goodyer I: Clinical andpsychosocial predictors of suicide attempts and nonsuicidal self-injury inthe adolescent depression antidepressants and psychotherapy trial(ADAPT). Am J Psychiatry 2011, 168(5):495–501.
5. Vos T, Flaxman AD, Naghavi M, Lozano R, Michaud C, Ezzati M, Shibuya K,Salomon JA, Abdalla S, Aboyans V, Abraham J, Ackerman I, Aggarwal R, Ahn YS,Ali MK, AlMazroa MA, Alvarado M, Anderson HR, Anderson LM, Andrews KG,Atkinson C, Baddour LM, Bahalim AN, Barker-Collo S, Barrero LH, Bartels DH,Basáñez MG, Baxter A, Bell ML, Benjamin EJ, et al: Years lived with disability (YLDs)for 1160 sequelae of 289 diseases and injuries 1990–2010: a systematic analysisfor the Global Burden of Disease Study 2010. Lancet 2012, 380:2163–2196.
6. Weisz J, McCarty C, Valeri S: Effects of psychotherapy for depression inchildren and adolescents: A meta-analysis. Psychol Bull 2006, 132(1):132–149.
7. Oei T, Dingle G: The effectiveness of group cognitive behavior therapyfor unipolar depressive disorders. J Affect Disord 2008, 107:5–21.
8. Cuijpers P, Huibers M, Ebert D, Koole S, Andersson G: How muchpsychotherapy is needed to treat depression? A metaregression analysis2013. J Affect Disord 2013, 149:1–13.
9. Goodyer IM, Dubicka B, Wilkinson P, Kelvin R, Roberts C, Byford S, Breen S,Ford C, Barrett B, Leech A, Rothwell J, White L, Harrington R: A randomized
Straub et al. Child and Adolescent Psychiatry and Mental Health 2014, 8:9 Page 10 of 10http://www.capmh.com/content/8/1/9
controlled trial of cognitive behaviour therapy in adolescents with majordepression treated by selective serotonin reuptake inhibitors. TheADAPT trial. Health Technol Assess 2008, 12(14):1–80.
10. Barrett P, Webster H, Turner C: FREUNDE fuer Kinder. Gruppenleitermanual.Trainingsprogramm zur Praevention von Angst und Depression. Muenchen:Reinhardt; 2003.
11. Harrington R: Kognitive Verhaltenstherapie bei depressiven Kindern undJugendlichen. Goeppingen: Hogrefe; 2001.
12. Ihle W, Herrle J: Stimmungsprobleme bewaeltigen. Ein kognitiv-verhaltenstherapeutisches Gruppenprogramm zur Praevention, Behandlung undRueckfallprophylaxe depressiver Stoerungen im Jugendalter nach Clarke,Lewinsohn und Hops. Manual fuer Kursleiter, Vol. 2. Tuebingen: dgvt-Verlag; 2011.
13. Poessel P, Horn AB, Seemann S, Hautzinger M: LARS & LISA: Lust anrealistischer Sicht und Leichtigkeit im sozialen Alltag: Trainingsprogramm zurPraevention von Depressionen bei Jugendlichen. Goettingen: Hogrefe; 2004.
14. Walter D, Doepfner M: Leistungsprobleme im Jugendalter. SELBST-Therapieprogramm fuer Jugendliche mit Selbstwert-, Leistungs- undBeziehungsstoerungen, Vol. 2. Goettingen: Hogrefe; 2009.
15. Junge J, Neumer SP, Manz R, Margraf J: Gesundheit und Optimismus. GO!Trainingsprogramm fuer Jugendliche. Weinheim: Beltz; 2002.
16. Sproeber N, Straub J, Fegert J, Koelch M: Depression im Jugendalter: MICHI-Manual fuer die Gruppentherapie. Weinheim: Beltz; 2012.
17. Straub J, Koelch M, Plener P, Fegert J, Gonzales I, Prestel A, Sproeber N:Innovations in Practice: MICHI, a brief cognitive-behavioural grouptherapy for adolescents with depression - a pilot study of feasibility inan inpatient setting. Child Adolesc Mental Health 2013, 18(4):247–50.
18. Thabane L, Ma J, Chu R, Cheng J, Ismaila A, Rios L, LP R, Thabane M,Giangregorio L, Goldsmith CH: A tutorial on pilot studies: The what, whyand how. BMC Med Res Methodol 2010, 10(1):1–10.
19. Green JM, Wood AJ, Kerfoot MJ, Trainor G, Roberts C, Rothwell J, WoodhamA, Ayodeji E, Barrett B, Byford S, Harrington R: Group therapy foradolescents with repeated self harm: Randomised controlled trial witheconomic evaluation. Br Med J 2011, 342:d682.
20. Listug-Lunde L, Vogeltanz-Holm N, Collins J: A cognitive-behavioraltreatment for depression in rural American Indian middle schoolstudents. Am Indian Alsk Native Ment Health Res 2013, 20(1):16–34.
21. Gaynor ST, Lawrence PS: Complementing CBT for depressed adolescents withlearning through in vivo experience (LIVE): Conceptual analysis, treatmentdescription, and feasibility study. Behav Cognit Psychother 2002, 30:79–101.
22. Rossello J, Bernal G, Rivera-Medina C: Individual and group CBT and IPT forPuerto Rican adolescents with depressive symptoms. Cult Divers EthnicMinor Psychol 2008, 14(3):234–45.
23. Kahn JS, Kehle TJ: Comparison of cognitive-behavioral, relaxation, andself-modeling interventions for depression. School Psychol Rev 1990, 19(2):196.
24. Poznanski EO, Mokros HB: Children's Depression Rating Scale Revised (CDRS-R):Manual. Los Angeles: Western Psychological Services; 1996.
25. Plener LP, Grieb J, Sproeber N, Straub J, Schneider A, Keller F, Koelch MG:Convergence of children's depression rating scale-revised scores andclinical diagnosis in rating adolescent depressive symptomatology.Mental Ilness 2012, 4(e7):29–31.
26. Remschmidt H, Schmidt M, Poustka F: Multiaxiales Klassifikationsschema fuerpsychische Stoerungen des Kindes- und Jugendalters nach ICD-10 oder WHO.Bern: Verlag Hans Huber; 2009.
27. Schindler AC, Hiller W, Witthoeft M: Benchmarking of cognitive-behavioraltherapy for depression in efficacy and effectiveness studies- How doexclusion criteria affect treatment outcome? Psychother Res 2011, 21(6):644–657.
28. Bachmann M, Bachmann C, Rief W, Mattejat F: Wirksamkeit psychiatrischerund psychotherapeutischer Behandlungen bei psychischen Stoerungenvon Kindern und Jugendlichen. Z Kinder Jugendpsychiatr Psychother 2008,36(5):309–320.
29. McCarty C, Weisz J: Effects of Psychotherapy for depression in children andadolescents: what we can (and can't) learn from meta-analysis andcomponent profiling. J Am Acad Child Adolesc Psychiatry 2007, 46(7):879–886.
30. Wilkinson PO, Goodyer IM: The effects of cognitive-behavioural therapyon mood-related ruminative response style in depressed adolescents.Child Adolesc Psychiatry Mental Health 2008, 2(3):1–10.
31. Hautzinger M, Keller F, Kuehner C: BDI-II Beck Depressions-Inventar Revision.Frankfurt am Main: Harcourt Test Services; 2006.
32. Kaufman J, Birmaher B, Brent D: Schedule for affective disorders andschizophrenia for school-age children- present and lifetime version
(K-SADS-PL): Initial reliability and validity data. J Am Acad Child AdolescPsychiatry 1997, 36:980–988.
33. Petermann F, Petermann U: Wechsler Intelligence Scale for Children. 4thedition. Frankfurt am Main: Pearson Assessment & Information GmbH; 2011.
34. Aster M, Neubauer A, Horn R: Wechsler Intelligenztest fuer Erwachsene.Frankfurt: Harcourt Test Services; 2006.
35. Horn W: Pruefsystem fuer Schul- und Bildungsberatung fuer 6. bis 13. Klassen.Goettingen: Hogrefe; 2004.
36. Keller F, Grieb J, Ernst M, Sproeber N, Fegert JM, Koelch M: Children'sDepression Rating Scale - Revised (CDRS-R): Development of a Germanversion and psychometric properties in a clinical sample. Z KinderJugendpsychiatr Psychother 2011, 39:179–185.
37. Keller F, Grieb J, Koelch M, Sproeber N: CDRS-R: Children's Depression RatingScale Revised. Goettingen: Hogrefe; 2012.
38. Doepfner M, Goertz-Dorten A, Lehmkuhl G, Breuer B, Goletz H: Diagnostik-System fuer psychische Stoerungen nach ICD-10 und DSM-IV fuer Kinder undJugendliche-II. Mannheim: Huber; 2008.
39. Mattejat F, Remschmidt H: ILK Inventar zur Erfassung der Lebensqualitaet beiKindern und Jugendlichen. Ratingbogen fuer Kinder, Jugendliche und Eltern.Bern: Verlag Hans Huber; 2006.
40. National Institute of Mental Health: CGI Clinical Global Impressions. Edited byGuy WE. Rockville Maryland: ECDEU Assessment for psychopharmacology.
41. Honosca-Team: NoNOSCA-Health of Nation Outcome Scales for Childrenand Adolescents. 2009. http://www.psychologie.zhaw.ch/de/psychologie/forschung/psychotherapie/diagnostik/honosca.html.
42. Bortz J: Statistik fuer Human- und Sozialwissenschaftler. Heidelberg: VerlagSpringer; 2005.
43. Kirk RE: Practical significance: A concept whose time has come.Educ Psychol Meas 1996, 56(5):746–69.
44. Prinstein MJ, Borelli JL, Cheah CSL, Simon VA: Adolescent girl'sinterpersonal vulnerability to depressive symptoms: A longitudinalexamination of reassurance-seeking and peer relationships.J Abnorm Psychol 2005, 114(4):676–688.
45. Perren S, Alsaker D: Depressive symptoms from kindergarten to earlyschool age: longitudinal associations with social skills deficits and peervictimization. Child Adolesc Psychiatry Mental Health 2009, 3(28):1–10.
46. Martin DJ, Garske JP, Davis K: Relation of the therapeutic alliance withoutcome and other variables: a meta-analytic review. J Consult ClinPsychol 2000, 68(3):438–450.
47. Poessel P, Hautzinger M: Effects of pharmaco- and psychotherapeuticinterventions in depression among children and adolescents. Zeitschriftfuer Kinder- und Jugendpsychiatrie und Psychotherapie 2006, 34(4):243–55.
48. Ihle W, Jahnke D:Wirkt ein pychoedukatives kognitiv-verhaltenstherapeutischesGruppenprogramm auch bei depressiven Jugendlichen mit komorbidenStoerungen? Verhaltenstherapie und Verhaltensmedizin 2003, 24(4):513–528.
49. Ihle W, Jahnke D, Spiess L, Herrle J: Evaluation eines kognitiv-verhaltenstherapeutischen Gruppenprogramms fuer depressiveJugendliche und junge Erwachsene. Kindheit und Entwicklung 2002,11(4):238–246.
50. Rohde P, Clarke GN, Mace DE, Jorgensen JS, Seeley JR: An efficacy/effectiveness study of cognitive-behavioral treatment for adolescentswith comorbid major depression and conduct disorder. J Am Acad ChildAdolescPsychiatry 2004, 43(6):660–8.
51. Resch F, Brunner R, Kaess M, Parzer P, Klug K, Fischer G, Frisch J, Schoenbach N,Schirmer J, Lenzen C: SEYLE Ergebnisbericht. 2010. http://www.jugendschutz-niedersachsen.de/wordpress/wp-content/uploads/2010/10/SEYLE-Ergebnisbericht.pdf.
52. Paykel ES, Myers JK, Lindenthal JJ, Tanner J: Suicidal feelings in the generalpopulation: A prevalence study. Br J Psychiatry 1974, 124:460–469.
53. Brent DA, Greenhill LL, Compton S, Emslie G, Wells K, Walkup JT, Vitiello B,Bukstein O, Stanley B, Posner K, Kennard BD, Cwik MF, Wagner A, Coffey B,March JS, Riddle M, Goldstein T, Curry J, Barnett S, Capasso L, Zelazny J,Hughes J, Shen S, Gugga S, Turner JB: The treatment of adolescent suicideattempters study (TASA): Predictors of suicidal events in an opentreatment trial. J Am Acad Child Adolesc Psychiatry 2009, 48(10):987–996.
doi:10.1186/1753-2000-8-9Cite this article as: Straub et al.: A brief cognitive-behavioural grouptherapy programme for the treatment of depression in adolescentoutpatients: a pilot study. Child and Adolescent Psychiatry and MentalHealth 2014 8:9.

MICHI – a brief, manualized cognitive behavioural group therapy for the treatment of
depression in adolescents: randomized controlled trial.
130
6.8 MICHI – a brief, manualized cognitive behavioural group therapy for the treatment of
depression in adolescents: randomized controlled trial.
Contribution of J. Straub to the article:
J. Straub coordinated the study procedure and recruited participants. She executed weekly
group therapy sessions, assessed suicidal ideation and behaviour on a weekly basis, and
scheduled diagnostic as well as psychotherapeutic appointments. She controlled the return
of questionnaires and executed diagnostic assessments that didn’t have to be done by an
independent evaluator (e.g. IQ measurements). She did data acquisition, generated the data
matrix, did data input, executed statistical analyses, and interpreted statistical outcomes.
She researched literature, wrote the manuscript, integrated remarks of the co-authors,
revised the manuscript according to reviewer’s comments, and created figures and tables.
Co-author’s contribution to the article:
N. Sproeber and M.G. Koelch supervised decisions on the experimental design and
conceptualized the study. They supervised the conduction of weekly group therapy sessions.
They reviewed the draft and gave constructive remarks and helped with revising the
manuscript according to the reviewer’s comments. F. Keller helped with statistical analyses.
P.L. Plener, F. Keller and J.M. Fegert reviewed the draft and gave constructive remarks.
Reference
Straub, J., Plener, P.L., Keller, F., Fegert, J.M., Sproeber, N. & Koelch, M.G. (accepted). MICHI
– a brief, manualized cognitive behavioural group therapy for the treatment of depression
in adolescents: randomized controlled trial. Kindheit & Entwicklung.
Reprinted from Kindheit & Entwicklung, Straub, J., Plener, P.L., Keller, F., Fegert, J.M.,
Sproeber, N. & Koelch, M.G. MICHI – a brief, manualized cognitive behavioural group therapy
for the treatment of depression in adolescents: randomized controlled trial, Copyright
(2015), with permission from Hogrefe.
MICHI – eine Gruppen-Kurzzeitpsychotherapie zurBehandlung von Depressionen bei Jugendlichen
Eine Randomisierte kontrollierte Studie
Joana Straub, Paul L. Plener, Ferdinand Keller, Jörg M. Fegert, Nina Spröberund Michael G. Kölch
Klinik für Kinder- und Jugendpsychiatrie/-psychotherapie des Universitätsklinikums Ulm
Zusammenfassung. Kognitive Verhaltenstherapie (KVT) gilt als Mittel der Wahl bei der Behandlung von Depressionen im Jugendalterwobei bis dato noch kein deutsches Behandlungsmanual in einem randomisierten, kontrollierten Design untersucht wurde. 38 depressiveJugendliche (M=15,86, SD=�1,70 Jahre alt; 78,9% weiblich) wurden randomisiert entweder der Kontrollgruppe (KG), die Behandlungwie ublich erhielt (TAU), oder Interventionsgruppe (IG), welche an einer ambulanten Gruppen-Kurzzeit-KVT (MICHI-Manual) teil-nahm, zugeordnet. Als Effektivitatsmaße dienten die CDRS-R und das BDI-II. Die Interaktion aus Gruppe und Messzeitpunkt warsowohl fur die CDRS-R (p=,02), mit einer mittleren Effektstarke (dkorr=,75), als auch fur den BDI-II (p=,04), mit einer kleinenEffektstarke (dkorr=,39), signifikant. Die Gruppen-Kurzzeit-KVT entsprechend dem MICHI Manual ist verglichen mit TAU wirksam.Schlusselworter: depressive Episode, Jugendliche, kognitiv-behaviorale Psychotherapie, Gruppentherapie MICHI
MICHI – A Brief, Manualized Cognitive Behavioral Group Therapy for the Treatment of Depression in Adolescents: A RandomizedControlled Trial
Abstract. Cognitive behavioral psychotherapy (CBT) is one of the first choices for the treatment of depression in adolescents but to dateno German treatment program has been evaluated in a randomized controlled trial. The study comprised 38 depressed adolescents (M =15.86; SD =�1.70 years old; 78.9% girls) who were randomly assigned to a control group (CG), a group that received treatment as usual(TAU), or an intervention group (IG) that participated in a brief outpatient group CBT called MICHI. To determine treatment efficacy,changes in the CDRS-R and BDI-II scores before and after TAU or CBT were collected and compared between groups. The interactioneffects, of groups and time points, were significant (p = .02) for the CDRS-R, with a moderate effect size (dkorr = .75), and for the BDI-II (p= .04), with a small effect size (dkorr = .39). The results of the present study reveal that a brief CBT, in a group format, was significantlymore effective than TAU.Keywords: depressive episode, adolescents, cognitive behavioral psychotherapy, group therapy
Im Grundschulalter wird die Lebenszeitpravalenz, fur dieEntwicklung einer depressiven Episode, auf 1– 2% beigleicher Geschlechterverteilung geschatzt (Groen & Pe-termann, 2008). Im Jugendalter liegt die Pravalenz furdepressive Storungen (laut Meta-Analyse unter Beruck-sichtigung verschiedener Diagnostik-Zeitraume) bei 5,6%(Costello, Erkanli & Angold, 2006) und Madchen sind mit9,7 % (Punktpravalenz) doppelt so haufig betroffen wieJungen mit 4,7 % (Bettge et al., 2008). Neben dem Sym-ptom der Suizidalitat, immerhin die zweithaufigste To-desursache im Jugendalter (Wilkinson, Kelvin, Roberts,Dubicka & Goodyer, 2011), besteht die hohe Gefahr eineschronischen Verlaufs dieses Storungsbildes (Park &Goodyer, 2000). Insbesondere bei Jugendlichen, derenEpisode in der Adoleszenz langer als sechs Monate an-dauerte, persistiert die depressive Symptomatik haufig bis
in das Erwachsenenalter (Patton et al., 2014). Daraus re-sultiert die Notwendigkeit einer effektiven, zielfuhrendenBehandlung bereits im Jugendalter, um die entsprechendeDauer der Episode so kurz wie moglich zu halten.
Die Deutsche Leitlinie zur Behandlung von depressi-ven Storungen bei Kindern und Jugendlichen (2013)empfiehlt, dass bei alteren Kindern und Jugendlichen mitleichter bis mittelgradiger depressiver Episode der Psy-chotherapie Vorrang zu geben sei und dabei entweder einekognitiv-verhaltenstherapeutische (KVT) oder interper-sonelle Psychotherapie (IPT) zum Einsatz kommen solle(Evidenzgrad A). Da bisher kaum deutsche Behand-lungsprogramme untersucht wurden, davon keines imrandomisiert kontrollierten Design (Deutsche Gesell-schaft fur Kinder- und Jugendpsychiatrie, 2013), basierendiese Empfehlungen primar auf Meta-Analysen, welcheenglischsprachige Wirksamkeitsstudien zur Therapie vonDepressionen bei Kindern und Jugendlichen berucksich-
Nina Sprober und Michael G. Kolch teilen sich die Letztautoren-schaft.
Kindheit und Entwicklung, 24 (3), 189 – 198 � Hogrefe Verlag, Gottingen 2015
DOI: 10.1026/0942-5403/a000175
Persönliches Autorenexemplar (e-Sonderdruck)Persönliches Autorenexemplar (e-Sonderdruck)Persönliches Autorenexemplar (e-Sonderdruck)Persönliches Autorenexemplar (e-Sonderdruck)Persönliches Autorenexemplar (e-Sonderdruck)

tigen. Seit dem Jahr 2000 wurden diesbezuglich neunMeta-Analysen veroffentlicht (Compton et al., 2004;David-Ferdon & Kaslow, 2008; Erford et al., 2011; Klein,Jacobs & Reinecke, 2007; McDermut, Miller & Brown,2001; Michael & Crowley, 2002; Spielmans, Pasek &McFall, 2007; Watanabe, Hunot, Omori, Churchill &Furukawa, 2007; Weisz, McCarty & Valeri, 2006), dieeine psychotherapeutische Intervention, zumeist KVT undIPT, mit einer aktiven, inaktiven oder Wartelisten-Kon-trollgruppe verglichen. Je Meta-Analyse wurden gemittelt20,56 (SD=9,15) Studien eingeschlossen. Die Effekt-starken lagen zwischen 0,29 (Erford et al., 2011) und 1,03(McDermut et al., 2001) mit einer mittleren Effektstarkevon 0,58 (SD=0,30), wobei nicht alle Studien eine Ef-fektstarke berichteten (Erford et al., 2011; Klein et al.,2007; McDermut et al., 2001; Michael & Crowley, 2002;Weisz et al., 2006) (fur einen Uberblick zu aktuellen Meta-Analysen s. auch Groen & Petermann, 2012).
Auf Deutsch liegt fur die Behandlung im Einzelsettingdas Manual „kognitive Verhaltenstherapie bei depressivenKindern und Jugendlichen“ vor (Dauer: 8 Sitzungen a45 Minuten), das aber nicht in der deutschen Fassung eva-luiert wurde (Harrington, 2001). Es wurde bisher in zweienglischsprachigen Studien, mit einer Effektstarke von 0,73gegenuber einer Entspannungsgruppe, evaluiert (Wood,Harrington & Moore, 1996) und zeigte keine Uberlegenheitgegenuber einer unspezifischen Intervention (Vostanis, Fee-han, Grattan & Bickerton, 1996). Weiterhin existieren imDeutschen zwei Behandlungsprogramme, die an die eng-lischsprachige Gruppentherapie „Coping with depressioncourse for adolescents“ (CWD-A) angelehnt sind. CWD-Awurde im englischen Sprachraum vielfach hinsichtlichWirksamkeit uberpruft (fur eine Ubersicht s. Straub, Nico-laus, Plener, Sprober & Kolch, 2014). Im deutschenSprachraum wurde das Programm „Stimmungsproblemebewaltigen“ (Dauer: 10 Sitzungen a 90 Minuten) (Ihle &Herrle, 2011) in einer pra-post Pilotstudie mit 16 bis25 Jahrigen evaluiert und fuhrte zu einer signifikanten Ver-besserung der depressiven Symptomatik und des irrationalenDenkens (Ihle, Jahn, Spieß & Herrle, 2002; Ihle & Jahnke,2003). Das Programm „kognitive Verhaltenstherapie beiKindern und Jugendlichen“ (Dauer: 17 Sitzungen a 90–120 Minuten) (Abel & Hautzinger, 2013) wurde in einer pra-post-follow-up Studie mit 33 depressiven Jugendlichen un-tersucht und wies im Patienten- als auch Elternurteil signi-fikante Verbesserungen mit mittleren bis hohen Effektstarkenauf. Insgesamt dauern die Gruppentherapieprogrammedemnach zwischen 10 und 17 Sitzungen a 90–120 Minuten.
Bezuglich des Verhaltnisses zwischen Anzahl Thera-piestunden und deren Wirksamkeit gibt es zwei bekannteModelle (Zaunmuller & Lutz, 2012): Das Good EnoughLevel (GEL)-Modell (Barkham et al., 1996) beschreibteine lineare Verbesserung zwischen Anzahl Sitzungen undVerbesserung der Symptomatik bis schlussendlich einzufriedenstellendes Niveau erreicht ist. Das Aufwand-Wirkungs-Modell (Howard, Kopta, Krause & Orlinsky,
1986) hingegen beschreibt eine besonders große Veran-derung in fruhen Therapiephasen welche im Verlauf ehernachlasst und es konnte gezeigt werden, dass sich dieSymptomatik bei 50 % der Patienten bereits nach 8 Sit-zungen besserte. Auch Harrington et al. (1998) konntenzeigen, dass ein Viertel der depressiven Jugendlichenbereits nach acht bis zwolf wochentlichen Sitzungen re-mittiert waren. Weisz et al. (1997) fanden heraus, dass sichdie depressive Symptomatik nach bereits acht Sitzungendreimal mehr in der Interventions- als in der Kontroll-gruppe reduzierte und in der Studie von Goodyer et al.(2008) besserte sich die depressive Symptomatik bei 21 %der mittelgradig bis schwer depressiven Jugendlichenbereits nach durchschnittlich drei Sitzungen. Unter Be-rucksichtigung des Aufwand-Wirkungs-Modells wurde diemanualisierte kognitiv-behaviorale Gruppen-Kurzzeitin-tervention namens MICHI (Manualized Intervention toCope with depressive symptoms, Help strengthen res-sources and Improve emotion regulation) (Sprober,Straub, Fegert & Kolch, 2012) entwickelt. Das Manualbeinhaltet u. a. Elemente aus den Bereichen Psychoedu-kation, kognitive Umstrukturierung, Verhaltens- undRessourcenaktivierung, Problemlosen sowie Krisenma-nagement. In ersten Pilotstudien konnte gezeigt werden,dass MICHI sowohl im stationaren als auch ambulantenSetting gut durchfuhrbar war und von den Jugendlichenpositiv aufgenommen wurde. Außerdem zeigte sich inbeiden Studien eine signifikante Reduktion der depressi-ven Symptomatik im pra-post Vergleich (Straub et al.,2013; Straub, Sproeber et al., 2014). Die folgende Studieuntersucht primar, ob depressive Jugendliche, die eineTherapie entsprechend des MICHI Manuals erhalten, einesignifikant starkere Reduktion der depressiven Symptomezeigen, als Jugendliche, die Behandlung der Regelver-sorgung („Treatment As Usual“-TAU) erhalten. Als se-kundare Zielgroße wird untersucht, ob die Symptomre-duktion in der Interventionsgruppe uber die Beendigungder Therapie hinaus uber einen Zeitraum von funf Wochenstabil bleibt.
Methoden
Prozedere
Die Rekrutierung erfolgte durch Mitarbeiter niedergelas-sener Kinder- und jugendpsychiatrischer und -psycho-therapeutischer Praxen sowie in der Ambulanz der Klinikfur Kinder- und Jugendpsychiatrie und Psychotherapiedes Universitatsklinikums Ulm. Diese wurden gebetenihren Patienten, sobald sie bei diesen eine depressiveSymptomatik feststellten, den Besuch eines MICHI In-formationsgesprachs nahe zu legen. Jugendliche, die beieinem solchen Informationstermin einen Rohwert>13 imBeck Depression Inventar Revision (BDI-II) (Beck, Steer& Brown, 1996; Hautzinger, Keller & Kuhner, 2006)aufwiesen, wurden wiederum zu einem ersten Diagnos-
190 Joana Straub et al.
Persönliches Autorenexemplar (e-Sonderdruck)Persönliches Autorenexemplar (e-Sonderdruck)Persönliches Autorenexemplar (e-Sonderdruck)Persönliches Autorenexemplar (e-Sonderdruck)Persönliches Autorenexemplar (e-Sonderdruck)

tiktermin eingeladen bei welchem das Vorliegen gegen-wartiger psychischer Storungen mittels klinischem Inter-view, sowie eine Erfassung des Intelligenzniveaus vor-genommen wurde.
Die randomisierte kontrollierte Studie wurde in funfDurchgangen von September 2011 bis Oktober 2013durchgefuhrt. Je Durchgang wurden ca. acht depressiveJugendliche randomisiert entweder der Interventions-gruppe (IG) oder der Kontrollgruppe (KG) zugeordnet.Anschließend folgte jeweils ein funfwochiger Zeitraum,in welchem die IG wochentlich eine Sitzung MICHI unddie KG TAU erhielt. Dann folgte eine post-Diagnostik unddie IG erhielt funfeinhalb Wochen nach der funftenMICHI-Sitzung eine Auffrischungssitzung. Funf Wochennach der post-Diagnostik nahm die Interventionsgruppean der Nachuntersuchungs-Diagnostik teil.
Aus ethischen Grunden wurde in beiden Gruppen einemogliche Verschlechterung der Symptomatik und Suizida-litat erfasst: Der BDI-II wurde von den Jugendlichen der IGnach jeder Sitzung erhoben, bei den Jugendlichen der TAUGruppe wochentlich. Wurde Item 9 des BDI-II, welchesakute Suizidalitat erfragt, mit 2 („ich mochte mich amliebsten umbringen“) oder hoher angegeben, wurde der Ju-gendliche umgehend kontaktiert und zu einem Gespracheingeladen bzw. es erfolgte nach der Sitzung ein Einzelge-sprach, um die Schwere und Akuitat der Suizidalitat und dasnotwendige weitere klinische Prozedere klaren zu konnen.
Die Studie wurde von der Ethikkommission der Uni-versitat Ulm begutachtet, und Teilnehmer und ihre Sor-geberechtigten wurden vor Studienbeginn uber die Stu-dienteilnahme mundlich wie schriftlich informiert undunterzeichneten anschließend die Einverstandniserkla-rung fur die Studienteilnahme. Aus ethischen Grundenbestand fur die Jugendlichen der KG die Moglichkeit, imAnschluss an den Wartezeitraum mit TAU ebenso anMICHI teilzunehmen.
Teilnehmer
Einschlusskriterien waren ein Alter zwischen 13 und 18Jahren, ein IQ großer 80, die Diagnose einer leichten, mit-telgradigen oder schweren depressiven Episode nach klini-schem diagnostischen Interview „Kiddie Schedule for Af-fective Disorders and Schizophrenia, Present and LifetimeVersion (K-SADS-PL)“ (Kaufman, Birmaher & Brent,1997) sowie ein Summenwert � 36 in der Children’s De-pression Rating Scale Revised (CDRS-R) (Keller, Grieb,Koelch & Sproeber, 2012; Poznanski & Mokros, 1996) wieer auch z.B. in der „The Treatment of Adolescent SuicideAttempters study (TASA)“- Studie herangezogen wurde(Brent et al., 2009). Acht Jugendliche wiesen einen CDRS-RWert <36 auf, wovon vier zudem nicht die Kriterien einerdepressiven Episode im K-SADS-PL erfullten, und konntendaher nicht in die Studie eingeschlossen werden (s. Abbil-
dung 1). Um eine fur den klinischen Alltag moglichst re-prasentative Stichprobe zu erhalten, wurden auch Jugendli-che mit komorbiden Storungen eingeschlossen, die depres-sive Storung (ICD F32, F33) sollte allerdings im Vorder-grund stehen und die vorrangige Storung sein, weshalbkinder- und jugendpsychiatrische/-psychotherapeutischeHilfe aufgesucht wurde. Jugendliche, die gegenwartig dieKriterien einer bipolaren Storung, Schizophrenie oderSuchterkrankung erfullten, wurden nicht in die Studie ein-geschlossen, da bei diesen Storungsbildern eine andere Be-handlung vorranging indiziert ist. Einnahme von Medikationwurde erlaubt, insofern diese mindestens funf Wochen vorTherapiebeginn begonnen wurde und es keine Anderung inder Dosierung wahrend der Studienteilnahme gab. Sowohldie Teilnehmer als auch ihre Erziehungsberechtigten wurdengebeten, eine etwaige Anderung der Medikation oder denBeginn einer anderweitigen Psychotherapie mitzuteilen, daihre Daten dann nicht in die Studie einbezogen werdenkonnten, dies jedoch nicht zu einem Ausschluss aus derTherapie fuhren wurde. Fur die Teilnehmer der IG galt dar-uber hinaus, dass sie mindestens vier von sechs Sitzungen(67%) besuchen mussten, da ihre Werte ansonsten als Drop-outs in die Analysen eingingen.
Interventionen
Grundlegende Behandlungselemente von MICHI sind:(1) Psychoedukation, (2) kognitive Umstrukturierung, (3)Verhaltensaktivierung, (4) Ressourcenaktivierung, (5)Steigerung des Selbstwertgefuhls, (6) schrittweises Pro-blemlosen, (7) Emotionsregulation, (8) Krisenmanage-ment (9) und Ruckfallprophylaxe (fur einen Uberblickuber die konkreten Sitzungsinhalte s. Sprober et al., 2012).Die funf Sitzungen plus eine Auffrischungssitzung wur-den in Kleingruppen von 4 –6 Teilnehmern abgehalten.Die funf Sitzungen dauerten zwischen 65 –90 Minuten(M=74,78; SD=9,57) und wurden von zwei Co-Autorendes Manuals, beides klinische Psychologinnen, durchge-fuhrt. Um eine bestmogliche Behandlungsintegritat zuerreichen, arbeiteten die Therapeuten nach Trainer-Ma-nual (Sprober et al., 2012) und erhielten zudem eineCheckliste mit den jeweiligen Sitzungsinhalten. Außer-dem wurden sie in der Durchfuhrung der Sitzungen vorabgeschult und wochentlich von der Entwicklerin des Ma-nuals supervidiert. Zur Erfassung der Behandlungsinte-gritat wurden alle Sitzungen auf Video aufgezeichnet,25 % der Sitzungen randomisiert ausgewahlt (N=15) undanhand einer Checkliste, von einer klinischen Psycholo-gin, die unabhangig von der Studien- und Therapie-durchfuhrung war, auf Durchfuhrungs-Integritat hinuberpruft. Diese betrug 98,24 % in der vorliegenden Stu-die.
Jugendliche der KG erhielten kinder- und jugend-psychiatrische Regelversorgung, welche fur den Warte-kontrollgruppenzeitraum aus 1,74 (SD=1,35) Terminen
MICHI – eine Gruppen-Kurzzeitpsychotherapie zur Behandlung von Depressionen bei Jugendlichen 191Persönliches Autorenexemplar (e-Sonderdruck)Persönliches Autorenexemplar (e-Sonderdruck)Persönliches Autorenexemplar (e-Sonderdruck)Persönliches Autorenexemplar (e-Sonderdruck)Persönliches Autorenexemplar (e-Sonderdruck)

bei einem Kinder-und Jugendpsychiater/–psychothera-peuten bestanden. Termine dauerten jeweils ca. 30 Mi-nuten in welchen zunachst die aktuelle Symptomatik,besondere Vorkommnisse und weiterhin depressionsspe-zifische Inhalte wie Aktivierung und Etablierung festerTagesstrukturen thematisiert wurden.
Erhebungsinstrumente
Zu Beginn wurde das K-SADS-PL (Kaufman et al., 1997)durchgefuhrt, um das Vorliegen aktueller psychischerStorungen erfassen bzw. den Schweregrad der depressi-ven Episode feststellen zu konnen. Intelligenz wurde inAbhangigkeit von Alter, und der Moglichkeit einerGruppentestung, durch verschiedene Verfahren erfasst(Aster, Neubauer & Horn, 2006; Horn, 2004; Petermann& Petermann, 2008).
Die Auspragung der depressiven Symptomatik, uber dieletzten zwei Wochen hinweg, wurden mittels CDRS-R(Keller et al., 2012) und BDI-II (Hautzinger et al., 2006)erfasst. Die Durchfuhrung fand bei der pra-Messung, post-Messung und im Falle der IG auch bei der Nachuntersuchungstatt. Beim CDRS-R handelt es sich um ein semi-struktu-riertes klinisches Interview welches von fur die Gruppen-zugehorigkeit (IG, KG) verblindeten, klinischen Psycholo-gen durchgefuhrt wurde. Ein Wert von�36 liefert Hinweiseauf eine klinisch bedeutsame Symptomatik (Plener et al.,2012). Sowohl die CDRS-R (a=,85) (Keller et al., 2011) alsauch das BDI-II weisen eine gute interne Konsistenz(,89�a�,94) (Beck et al., 1996; Hautzinger et al., 2006) auf.Um eine Veranderung der Suizidalitat erfassen zu konnen,wurde das CDRS-R Item 13 im klinischen Interview her-angezogen, welches eine Einstufung der Suizidalitat in„keine bis leichte“ sowie „moderate bis schwere“ Suizidalitatuber die letzten zwei Wochen ermoglicht.
Stichprobengröße
Die Stichprobengroße wurde vorab anhand von Power-Analysen bestimmt. Dabei wurde von einer Teststarke 1-b�,80, einem Risiko fur Fehler 1. Art a=,05 und einererwarteten mittleren Effektstarke von d=,50 ausgegan-gen. Es wurde eine Mindestteilnehmerzahl von N=34 (17Teilnehmer pro Gruppe) festgelegt.
Randomisierung
Die Randomisierung erfolgte anhand des computerge-stutzten Programms „minim“ (Evans, Day & Royston,1990) durch eine von der Studie unabhangigen Person, umeinen Selektionsbias auszuschließen. Dabei wurde dererste Teilnehmer zufallig zugeordnet und bei der Zutei-lung aller weiteren Teilnehmer die Verteilung anhand
festgelegter Merkmale in der Reihenfolge Alter, Ge-schlecht und Schweregrad vom Programm berucksichtigt.
Statistisches Vorgehen
Der pra-post Vergleich von IG und KG wurde anhand vonhierarchischen linearen Modellen (HLM) mit einemmixed effects Modell durchgefuhrt, wobei der Achsen-abschnitt (intercept) als random angenommen wurde (vgl.z.B. Singer, 1998). Erganzende Einzelvergleiche vonquantitativen pra-post bzw. post-follow-up Stichproben-merkmalen erfolgten anhand von ANOVA mit Messwie-derholung. Um den Effekt der Behandlung bestimmen zukonnen, wurden Effektstarken nach Cohen berechnet,welche fur die unterschiedlichen Ausgangswerte der je-weiligen Gruppe korrigiert wurden (Klauer, 2001). Wertevon Drop-outs gingen bei der Durchfuhrung des HLM alsfehlende Werte und bei der ANOVA mit Messwiederho-lung als „last observation carried forward“ (LOCF) ein.Statistische Analysen wurden anhand SPSS 21 durchge-fuhrt. Bei der Hypothesentestung wurde eine zweiseitigeTyp I Fehlerrate von ,05 angenommen.
Resultate
Charakteristika der Teilnehmer
38 Jugendliche erfullten die Einschlusskriterien undwurden randomisiert der IG oder KG zugeordnet.Durchschnittlich besuchten die Teilnehmer der IG 5,39(SD=,70) Sitzungen von sechs. In der KG erhielten dieJugendlichen durchschnittlich 1,74 (SD=1,35) Terminewahrend des funfwochigen Kontrollzeitraums. ZweiTeilnehmer der KG und ein Teilnehmer der IG verstießengegen das Studienprotokoll von pra nach post (Anderungder stabilen Medikationseinnahme; Beginn einer Psy-chotherapie) und zwei Teilnehmer der IG gegen das Stu-dienprotokoll von post zur Nachuntersuchung (Anderungder stabilen Medikationseinnahme) (s. Abb. 1).
Nach Studienteilnahme gaben 13 der 19 Jugendlichender IG an, weiterhin sozialpsychiatrisch angebunden zubleiben und zwei der Jugendlichen gaben an, eine wo-chentliche Psychotherapie beginnen zu wollen.
Die Gruppen unterschieden sich nicht hinsichtlich Alter,Geschlecht und IQ. Auch die Anzahl an Jugendlichen mitMigrationshintergrund sowie Jugendliche, bei denen imVerlauf akute Suizidalitat abgeklart werden musste, unter-schied sich kaum. In der KG waren mehr Gymnasiasten unddie Verteilung der Depressions-Schweregrade etwas ausge-wogener verteilt wobei sich der Schweregrad, gemessenanhand des CDRS-R, beider Gruppen nicht unterschied (s.Tab. 1).
192 Joana Straub et al.
Persönliches Autorenexemplar (e-Sonderdruck)Persönliches Autorenexemplar (e-Sonderdruck)Persönliches Autorenexemplar (e-Sonderdruck)Persönliches Autorenexemplar (e-Sonderdruck)Persönliches Autorenexemplar (e-Sonderdruck)
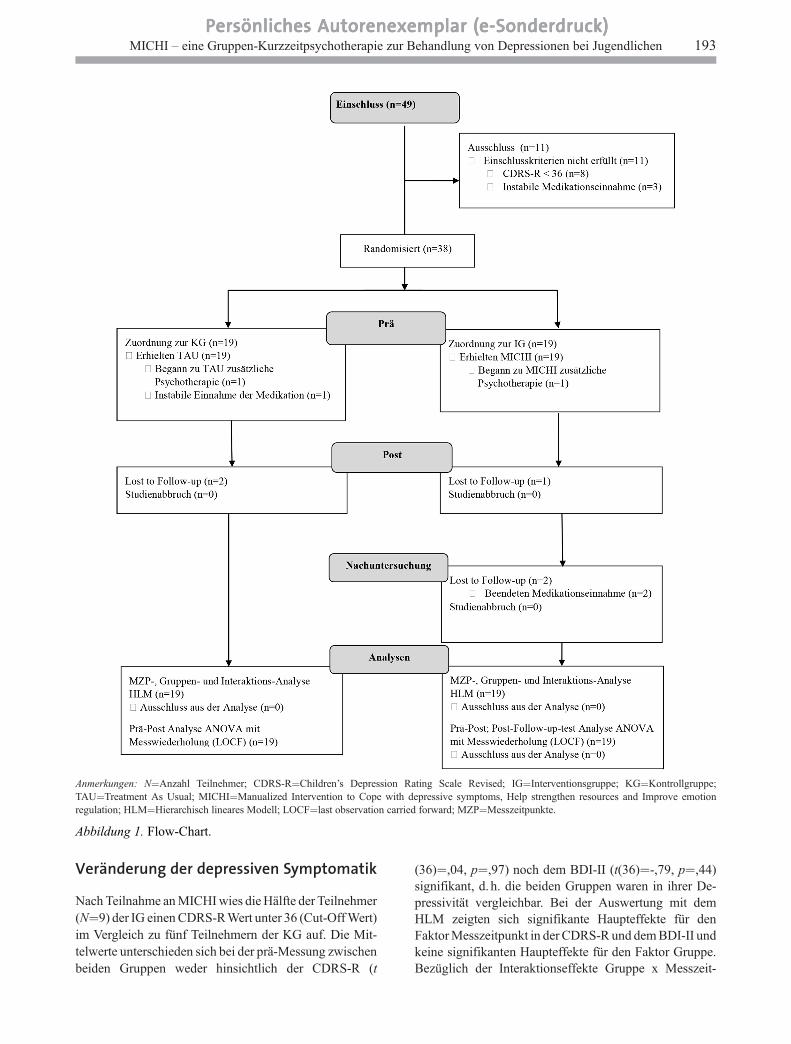
Veränderung der depressiven Symptomatik
Nach Teilnahme an MICHI wies die Halfte der Teilnehmer(N=9) der IG einen CDRS-RWert unter 36 (Cut-Off Wert)im Vergleich zu funf Teilnehmern der KG auf. Die Mit-telwerte unterschieden sich bei der pra-Messung zwischenbeiden Gruppen weder hinsichtlich der CDRS-R (t
(36)=,04, p=,97) noch dem BDI-II (t(36)=-,79, p=,44)signifikant, d. h. die beiden Gruppen waren in ihrer De-pressivitat vergleichbar. Bei der Auswertung mit demHLM zeigten sich signifikante Haupteffekte fur denFaktor Messzeitpunkt in der CDRS-R und dem BDI-II undkeine signifikanten Haupteffekte fur den Faktor Gruppe.Bezuglich der Interaktionseffekte Gruppe x Messzeit-
Anmerkungen: N=Anzahl Teilnehmer; CDRS-R=Children’s Depression Rating Scale Revised; IG=Interventionsgruppe; KG=Kontrollgruppe;TAU=Treatment As Usual; MICHI=Manualized Intervention to Cope with depressive symptoms, Help strengthen resources and Improve emotionregulation; HLM=Hierarchisch lineares Modell; LOCF=last observation carried forward; MZP=Messzeitpunkte.
Abbildung 1. Flow-Chart.
MICHI – eine Gruppen-Kurzzeitpsychotherapie zur Behandlung von Depressionen bei Jugendlichen 193Persönliches Autorenexemplar (e-Sonderdruck)Persönliches Autorenexemplar (e-Sonderdruck)Persönliches Autorenexemplar (e-Sonderdruck)Persönliches Autorenexemplar (e-Sonderdruck)Persönliches Autorenexemplar (e-Sonderdruck)
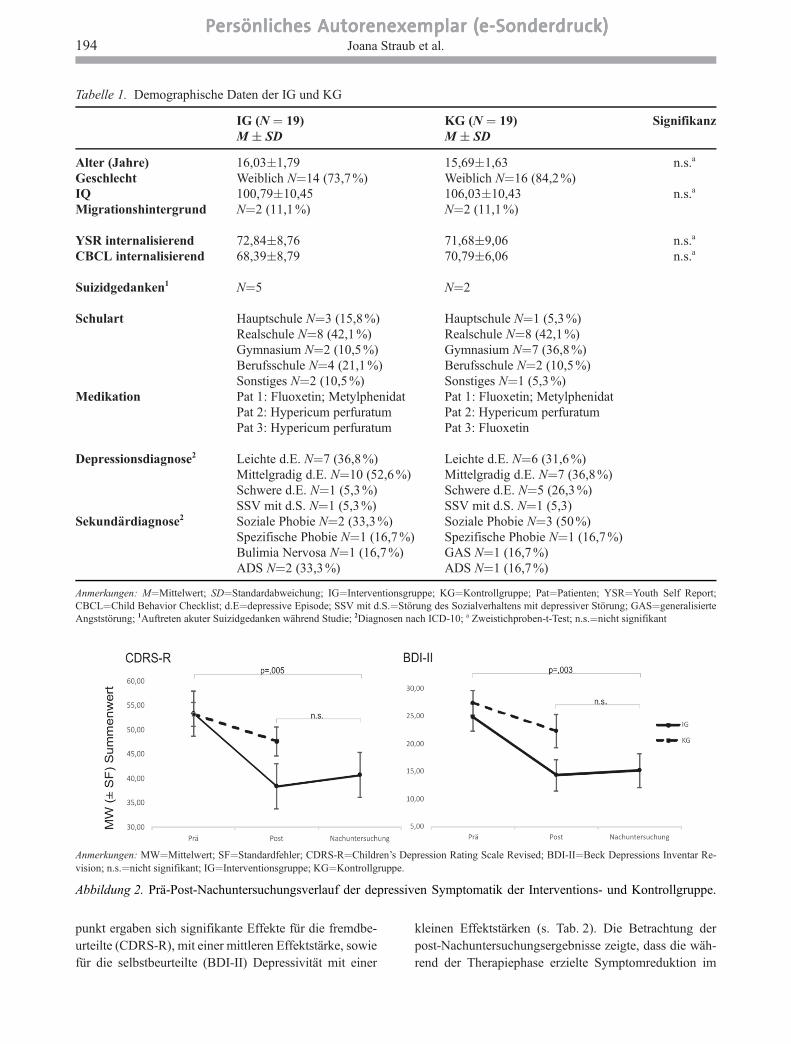
punkt ergaben sich signifikante Effekte fur die fremdbe-
urteilte (CDRS-R), mit einer mittleren Effektstarke, sowiefur die selbstbeurteilte (BDI-II) Depressivitat mit einer
kleinen Effektstarken (s. Tab. 2). Die Betrachtung der
post-Nachuntersuchungsergebnisse zeigte, dass die wah-rend der Therapiephase erzielte Symptomreduktion im
Tabelle 1. Demographische Daten der IG und KG
IG (N = 19)M � SD
KG (N = 19)M � SD
Signifikanz
Alter (Jahre) 16,03�1,79 15,69�1,63 n.s.a
Geschlecht Weiblich N=14 (73,7 %) Weiblich N=16 (84,2 %)IQ 100,79�10,45 106,03�10,43 n.s.a
Migrationshintergrund N=2 (11,1 %) N=2 (11,1 %)
YSR internalisierend 72,84�8,76 71,68�9,06 n.s.a
CBCL internalisierend 68,39�8,79 70,79�6,06 n.s.a
Suizidgedanken1 N=5 N=2
Schulart Hauptschule N=3 (15,8 %)Realschule N=8 (42,1 %)Gymnasium N=2 (10,5 %)Berufsschule N=4 (21,1 %)Sonstiges N=2 (10,5 %)
Hauptschule N=1 (5,3 %)Realschule N=8 (42,1 %)Gymnasium N=7 (36,8 %)Berufsschule N=2 (10,5 %)Sonstiges N=1 (5,3 %)
Medikation Pat 1: Fluoxetin; MetylphenidatPat 2: Hypericum perfuratumPat 3: Hypericum perfuratum
Pat 1: Fluoxetin; MetylphenidatPat 2: Hypericum perfuratumPat 3: Fluoxetin
Depressionsdiagnose2 Leichte d.E. N=7 (36,8 %)Mittelgradig d.E. N=10 (52,6 %)Schwere d.E. N=1 (5,3 %)SSV mit d.S. N=1 (5,3%)
Leichte d.E. N=6 (31,6 %)Mittelgradig d.E. N=7 (36,8 %)Schwere d.E. N=5 (26,3 %)SSV mit d.S. N=1 (5,3)
Sekundardiagnose2 Soziale Phobie N=2 (33,3 %)Spezifische Phobie N=1 (16,7 %)Bulimia Nervosa N=1 (16,7 %)ADS N=2 (33,3 %)
Soziale Phobie N=3 (50 %)Spezifische Phobie N=1 (16,7 %)GAS N=1 (16,7 %)ADS N=1 (16,7 %)
Anmerkungen: M=Mittelwert; SD=Standardabweichung; IG=Interventionsgruppe; KG=Kontrollgruppe; Pat=Patienten; YSR=Youth Self Report;CBCL=Child Behavior Checklist; d.E=depressive Episode; SSV mit d.S.=Storung des Sozialverhaltens mit depressiver Storung; GAS=generalisierteAngststorung; 1Auftreten akuter Suizidgedanken wahrend Studie; 2Diagnosen nach ICD-10; a Zweistichproben-t-Test; n.s.=nicht signifikant
Anmerkungen: MW=Mittelwert; SF=Standardfehler; CDRS-R=Children’s Depression Rating Scale Revised; BDI-II=Beck Depressions Inventar Re-vision; n.s.=nicht signifikant; IG=Interventionsgruppe; KG=Kontrollgruppe.
Abbildung 2. Pra-Post-Nachuntersuchungsverlauf der depressiven Symptomatik der Interventions- und Kontrollgruppe.
194 Joana Straub et al.
Persönliches Autorenexemplar (e-Sonderdruck)Persönliches Autorenexemplar (e-Sonderdruck)Persönliches Autorenexemplar (e-Sonderdruck)Persönliches Autorenexemplar (e-Sonderdruck)Persönliches Autorenexemplar (e-Sonderdruck)
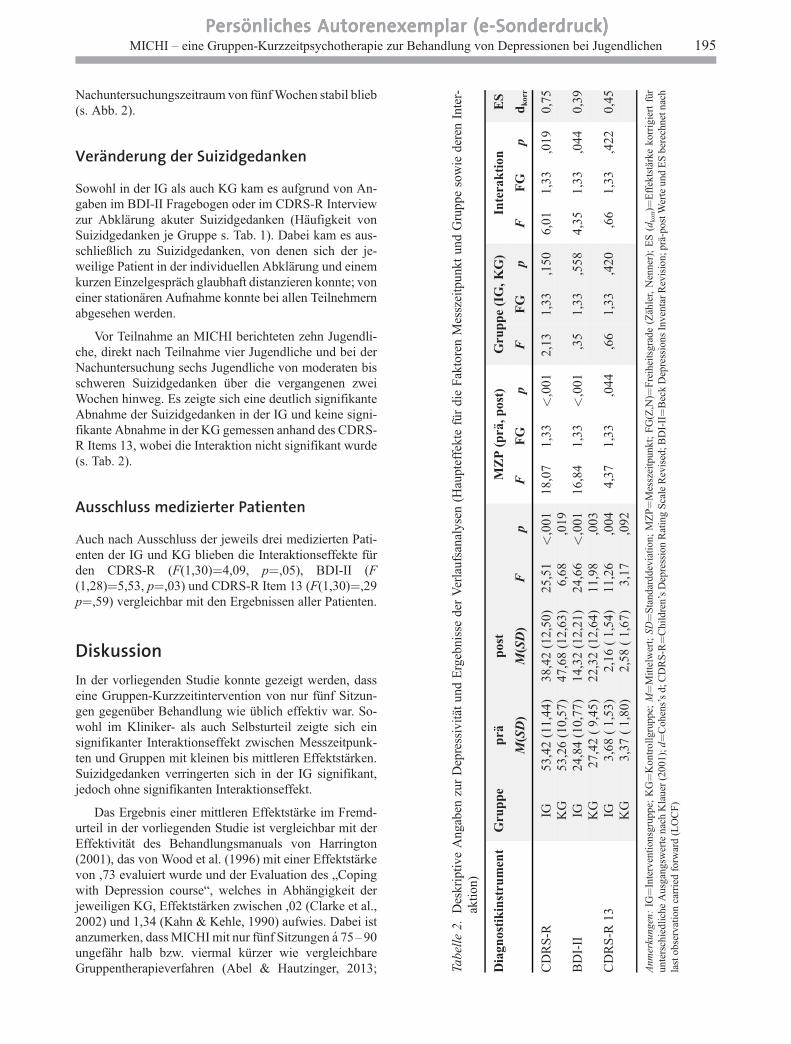
Nachuntersuchungszeitraum von funf Wochen stabil blieb(s. Abb. 2).
Veränderung der Suizidgedanken
Sowohl in der IG als auch KG kam es aufgrund von An-gaben im BDI-II Fragebogen oder im CDRS-R Interviewzur Abklarung akuter Suizidgedanken (Haufigkeit vonSuizidgedanken je Gruppe s. Tab. 1). Dabei kam es aus-schließlich zu Suizidgedanken, von denen sich der je-weilige Patient in der individuellen Abklarung und einemkurzen Einzelgesprach glaubhaft distanzieren konnte; voneiner stationaren Aufnahme konnte bei allen Teilnehmernabgesehen werden.
Vor Teilnahme an MICHI berichteten zehn Jugendli-che, direkt nach Teilnahme vier Jugendliche und bei derNachuntersuchung sechs Jugendliche von moderaten bisschweren Suizidgedanken uber die vergangenen zweiWochen hinweg. Es zeigte sich eine deutlich signifikanteAbnahme der Suizidgedanken in der IG und keine signi-fikante Abnahme in der KG gemessen anhand des CDRS-R Items 13, wobei die Interaktion nicht signifikant wurde(s. Tab. 2).
Ausschluss medizierter Patienten
Auch nach Ausschluss der jeweils drei medizierten Pati-enten der IG und KG blieben die Interaktionseffekte furden CDRS-R (F(1,30)=4,09, p=,05), BDI-II (F(1,28)=5,53, p=,03) und CDRS-R Item 13 (F(1,30)=,29p=,59) vergleichbar mit den Ergebnissen aller Patienten.
Diskussion
In der vorliegenden Studie konnte gezeigt werden, dasseine Gruppen-Kurzzeitintervention von nur funf Sitzun-gen gegenuber Behandlung wie ublich effektiv war. So-wohl im Kliniker- als auch Selbsturteil zeigte sich einsignifikanter Interaktionseffekt zwischen Messzeitpunk-ten und Gruppen mit kleinen bis mittleren Effektstarken.Suizidgedanken verringerten sich in der IG signifikant,jedoch ohne signifikanten Interaktionseffekt.
Das Ergebnis einer mittleren Effektstarke im Fremd-urteil in der vorliegenden Studie ist vergleichbar mit derEffektivitat des Behandlungsmanuals von Harrington(2001), das von Wood et al. (1996) mit einer Effektstarkevon ,73 evaluiert wurde und der Evaluation des „Copingwith Depression course“, welches in Abhangigkeit derjeweiligen KG, Effektstarken zwischen ,02 (Clarke et al.,2002) und 1,34 (Kahn & Kehle, 1990) aufwies. Dabei istanzumerken, dass MICHI mit nur funf Sitzungen a 75–90ungefahr halb bzw. viermal kurzer wie vergleichbareGruppentherapieverfahren (Abel & Hautzinger, 2013; Ta
bell
e2.
Des
krip
tive
Ang
aben
zur
Dep
ress
ivit
atun
dE
rgeb
niss
ede
rV
erla
ufsa
naly
sen
(Hau
ptef
fekt
efu
rdi
eF
akto
ren
Mes
szei
tpun
ktun
dG
rupp
eso
wie
dere
nIn
ter-
akti
on)
Dia
gnos
tik
inst
rum
ent
Gru
pp
ep
rap
ost
MZ
P(p
ra,p
ost)
Gru
pp
e(I
G,K
G)
Inte
rak
tion
ES
M(S
D)
M(S
D)
Fp
FF
Gp
FF
Gp
FF
Gp
dk
orr
CD
RS
-RIG
53,4
2(1
1,44
)38
,42
(12,
50)
25,5
1<
,001
18,0
71,
33<
,001
2,13
1,33
,150
6,01
1,33
,019
0,75
KG
53,2
6(1
0,57
)47
,68
(12,
63)
6,68
,019
BD
I-II
IG24
,84
(10,
77)
14,3
2(1
2,21
)24
,66
<,0
0116
,84
1,33
<,0
01,3
51,
33,5
584,
351,
33,0
440,
39K
G27
,42
(9,
45)
22,3
2(1
2,64
)11
,98
,003
CD
RS
-R13
IG3,
68(
1,53
)2,
16(
1,54
)11
,26
,004
4,37
1,33
,044
,66
1,33
,420
,66
1,33
,422
0,45
KG
3,37
(1,
80)
2,58
(1,
67)
3,17
,092
Anm
erku
ngen
:IG
=In
terv
enti
onsg
rupp
e;K
G=
Kon
trol
lgru
ppe;
M=
Mit
telw
ert;
SD=
Sta
ndar
ddev
iati
on;
MZ
P=
Mes
szei
tpun
kt;
FG
(Z,N
)=F
reih
eits
grad
e(Z
ahle
r,N
enne
r);
ES
(dko
rr)=
Eff
ekts
tark
eko
rrig
iert
fur
unte
rsch
iedl
iche
Aus
gang
swer
tena
chK
laue
r(2
001)
;d=
Coh
ens’
sd;
CD
RS
-R=
Chi
ldre
n’s
Dep
ress
ion
Rat
ing
Sca
leR
evis
ed;B
DI-
II=
Bec
kD
epre
ssio
nsIn
vent
arR
evis
ion;
pra-
post
Wer
teun
dE
Sbe
rech
netn
ach
last
obse
rvat
ion
carr
ied
forw
ard
(LO
CF
)
MICHI – eine Gruppen-Kurzzeitpsychotherapie zur Behandlung von Depressionen bei Jugendlichen 195Persönliches Autorenexemplar (e-Sonderdruck)Persönliches Autorenexemplar (e-Sonderdruck)Persönliches Autorenexemplar (e-Sonderdruck)Persönliches Autorenexemplar (e-Sonderdruck)Persönliches Autorenexemplar (e-Sonderdruck)

Ihle & Herrle, 2011) ist. Dieses Ergebnis ist in Einklangmit den Ergebnissen der Meta-Analyse von Cuijpers undKollegen (2013) in welcher die Autoren nur einen kleinenZusammenhang zwischen der Gesamtanzahl an Sitzungenbzw. Dauer der Therapie, jedoch einen starken Zusam-menhang zwischen der wochentlichen Intensitat bzw.Anzahl an Sitzungen und Wirksamkeit der Behandlungfanden.
Daruber hinaus bleibt zu diskutieren, warum sich auchin der KG Depressionswerte im Verlauf signifikant ver-ringerten. Dies lasst sich zum einen durch die Tatsache,dass auch die KG Behandlung wie ublich erhielt, sowiezum anderen durch eine hohe Spontanremissionsrate de-pressiver Storungen im Kindes- und Jugendalter (White-ford et al. 2012) erklaren.
Weiterhin zeigte sich keine signifikante Interaktionhinsichtlich Suizidgedanken. Dies konnte durch die Ab-klarung akuter Suizidalitat sowie gegebenenfalls direktstattfindender Krisenintervention, welche aus ethischenGrunden in beiden Gruppen erfolgte, erklart werden,sowie durch die Tatsache, dass ein einzelnes Item wenigerTeststarke aufweist als ein Summenscore. In Ubersichts-arbeiten (Brunstein Klomek & Stanley, 2007; Kapusta,Fegert, Haring & Plener, 2013) wird deutlich, dass sichSuizidalitat zwar haufig nach Teilnahme an einer psy-chosozialen Intervention bessert, sich diese Besserungallerdings nicht im Vergleich zu einer aktiven KG auf-rechterhalten lasst.
Ein Vorteil einer Gruppen-Kurzzeitintervention ist si-cherlich – verglichen mit langerdauernden Interventionen– der geringe zeitliche Aufwand fur Patienten. Damitkonnte auch die Inanspruchnahmeschwelle fur eine The-rapie sinken. Aus okonomischer bzw. gesundheitspoliti-scher Sicht ist das Ergebnis, dass eine Kurzzeitinterven-tion vergleichbare Effekte zeigt wie eine langer andau-ernde Psychotherapie, ebenfalls interessant. Hinsichtlicheiner umfassenden Therapiestrategie bei der Behandlungdepressiver Storungen im Jugendalter ist eine kurze In-tervention, bei der ausreichende Effekte nachweisbar sind,notig: entsprechend kann bei einem Nichtansprechen eineAnderung der Behandlung, z. B. eine medikamentoseTherapie, erfolgen, wie es auch die britische NICE-Gu-ideline empfiehlt (National Collaborating Centre forMental Health).
Limitationen der vorliegenden Studie sind zum einender geringe Anteil an mannlichen Teilnehmern, was dieGeneralisierbarkeit der Daten auf das mannliche Ge-schlecht einschrankt. Dabei ist allerdings anzumerken,dass die Geschlechterverteilung in der vorliegenden Stu-die vergleichbar mit der Pravalenz depressiver Storungenbeider Geschlechter ist. Weiterhin wurden in der vorlie-genden Studie teilweise medizierte Patienten einge-schlossen, wobei sich die Ergebnisse, bei Ausschluss dermedizierten Patienten, kaum anderten. Auch wenn sichdie CDRS-R Rohwerte beider Gruppen zu Beginn nicht
unterschieden, wies die KG einen hoheren Anteil an Ju-gendlichen mit schweren depressiven Episoden auf (er-fasst anhand des K-SADS-PL). Daruber hinaus erhielt dieKG durchschnittlich 1,74 Termine in der kinder- und ju-gendpsychiatrischen Versorgung, wobei die Kriterien fureine objektive Vergleichsgruppe, im strengen Sinne derempirischen Wirksamkeitsforschung, nicht erfullt waren.Nichtsdestotrotz bildet dieses Vorgehen aus unserer Sichtdie kinder- und jugendpsychiatrische Praxis am besten ab.In der Studie wurde ein primares Zielkriterium gewahlt,welches die depressive Symptomatik fokussiert. Moglichware es weitere Aspekte, wie das psychosoziale Funkti-onsniveau heranzuziehen, was in weiteren Studien anzu-streben ware.
In weiterfuhrenden Studien sollte die Wirksamkeit vonMICHI gegenuber einer Kontrollintervention im Langs-schnittdesign mit einer spateren Nachuntersuchung (z.B.nach sechs Monaten) erfasst werden, um das langfristigeAnhalten des Effekts uberprufen zu konnen. Weiterhinware es sinnvoll, die Wirksamkeit von MICHI in einergroßer angelegten multizentrischen Studie, gegebenen-falls auch im Vergleich zu einer medikamentos behan-delten Vergleichsgruppe, zu untersuchen.
Literatur
Abel, U. & Hautzinger, M. (2013). Kognitive Verhaltenstherapiebei Depressionen im Kindes- und Jugendalter. Heidelberg:Springer
Aster, M., Neubauer, A. & Horn, R. (Hrsg.). (2006). WechslerIntelligenztest fur Erwachsene. Frankfurt: Pearson Assess-ment.
Barkham, M., Rees, A., Stiles, W. B., Shapiro, D. A., Hardy, G.E. & Reynolds, S. (1996). Dose-effect relations in time-li-mited psychotherapy for depression. Journal of Consultingand Clinical Psychology, 64, 927–935.
Beck, A. T., Steer, R. A. & Brown, G. K. (1996). Beck Depres-sion Inventory – Second Edition. Manual. San Antonio: ThePsychological Corporation.
Bettge, S., Wille, N., Barkmann, C., Schulte-Markwort, M.,Ravens-Sieberer, U. & the Bella study group (2008). De-pressive symptoms of children and adolescents in a Germanrepresentative sample: Results of the BELLA study. Euro-pean Child and Adolescent Psychiatry, 17, 71–81.
Brent, D. A., Greenhill, L. L., Compton, S., Emslie, G., Wells,K., Walkup, J. T. et al. (2009). The Treatment of AdolescentSuicide Attempters study (TASA): Predictors of suicidalevents in an open treatment trial. Journal of AmericanAcademy of Child and Adolescent Psychiatry, 48, 987–996.
Brunstein Klomek, A. & Stanley, B. (2007). Psychosocialtreatment of depression and suicidality in adolescents. CNSSpectrums, 12, 135 –144.
Clarke, G. N., Hornbrook, M., Lynch, F., Polen, M., Gale, J.,O’Connor, E. et al. (2002). Group cognitive-behavioraltreatment for depressed adolescent offspring of depressedparents in a health maintenance organization. Journal ofAmerican Academy of Child and Adolescent Psychiatry, 41,305 –313.
196 Joana Straub et al.
Persönliches Autorenexemplar (e-Sonderdruck)Persönliches Autorenexemplar (e-Sonderdruck)Persönliches Autorenexemplar (e-Sonderdruck)Persönliches Autorenexemplar (e-Sonderdruck)Persönliches Autorenexemplar (e-Sonderdruck)
Compton, S. N., March, J. S., Brent, D., Albano, A. M., Weer-sing, R. & Curry, J. (2004). Cognitive-behavioral psycho-therapy for anxiety and depressive disorders in children andadolescents: An evidence-based medicine review. Journal ofAmerican Academy of Child and Adolescent Psychiatry, 43,930 –959.
Costello, E., Erkanli, A. & Angold, A. (2006). Is there an epi-demic of child or adolescent depression? Journal of ChildPsychology and Psychiatry, 47, 1263–1271.
Cuijpers, P., Huibers, M., Ebert, D. D. & Koole, S. L. (2013).How much psychotherapy is needed to treat depression? Ametaregression analysis. Journal of Affective Disorders, 149,1–13.
David-Ferdon, C. & Kaslow, N. J. (2008). Evidence-basedpsychosocial treatments for child and adolescent depression.Journal of Child and Adolescent Psychology, 37, 62–104.
Deutsche Gesellschaft fur Kinder- und Jugendpsychiatrie Psy-chosomatik und Psychotherapie. (2013). Behandlung vondepressiven Storungen bei Kindern und Jugendlichen: Evi-denz- und konsensbasierte Leitlinie. Zugriff am 21.03.2015.Verfugbar unter http://www.awmf.org/leitlinien/detail/ll/028 –043.html
Erford, B. T., Erford, B. M., Lattanzi, G., Weller, J., Schein, H.,Wolf, E. et al. (2011). Counseling Outcomes From 1990 to2008 for School-Age Youth With Depression: A Meta-Analysis. Journal of Counseling and Development, 89, 439 –457.
Evans, S., Day, S. & Royston, P. (1990). MINIM: A programmeof randomising patients to groups in clinical trials by themethod of minimisation. Version 1.5. London: HospitalMedical School.
Goodyer, I. M., Dubicka, B., Wilkinson, P., Kelvin, R., Roberts,C., Byford, S. et al. (2008). A randomized controlled trial ofcognitive behaviour therapy in adolescents with major de-pression treated by selective serotonin reuptake inhibitors.The ADAPT trial. Health Technology Assessment, 12.
Groen, G. & Petermann, F. (2008). Was wirkt in der Therapie vonDepression bei Kindern und Jugendlichen wirklich? Kind-heit und Entwicklung, 17, 243 –251.
Groen, G. & Petermann, F. (2012). Kognitive Verhaltenstherapiebei Depressionen im Kindes- und Jugendalter. Kindheit undEntwicklung, 40, 373 –384.
Harrington, R. (2001). Kognitive Verhaltenstherapie bei de-pressiven Kindern und Jugendlichen. Gottingen: Hogrefe.
Harrington, R., Whittaker, J., Shoebridge, P. & Campbell, F.(1998). Systematic review of efficacy of cognitive behaviortherapies in childhood and adolescent depressive disorder.British Medical Journal, 316, 1559–1563.
Hautzinger, M., Keller, F. & Kuhner, C. (2006). BDI-II BeckDepressions-Inventar Revision. Frankfurt a. Main: PearsonAssessment.
Horn, W. (2004). Prufsystem fur Schul- und Bildungsberatungfur 6. bis 13. Klassen. Gottingen: Hogrefe.
Howard, K. I., Kopta, S., Krause, M. S. & Orlinsky, D. E. (1986).The dose-effect relationship in psychotherapy. AmericanPsychologist, 41, 159 –164.
Ihle, W. & Herrle, J. (2011). Stimmungsprobleme bewaltigen.Ein kognitiv-verhaltenstherapeutisches Gruppenprogrammzur Pravention, Behandlung und Ruckfallprophylaxe de-pressiver Storungen im Jugendalter nach Clarke, Lewinsohnund Hops. Manual fur Kursleiter (2. Aufl.). Tubingen: dgvt-Verlag.
Ihle, W., Jahn, D., Spieß, L. & Herrle, J. (2002). Evaluation eineskognitiv-verhaltenstherapeutischen Gruppenprogramms furdepressive Jugendliche und junge Erwachsene. Kindheit undEntwicklung, 11, 238 –246.
Ihle, W., & Jahnke, D. (2003). Wirkt ein psychoedukatives ko-gnitiv-verhaltenstherapeutisches Gruppenprogramm auchbei depressiven Jugendlichen mit komorbiden Storungen?Verhaltenstherapie und Verhaltensmedizin, 24, 513 –528.
Kahn, J. S., & Kehle, T. J. (1990). Comparison of cognitive-behavioral, relaxation, and self-modeling interventions fordepression. School Psychology Review, 19, 196.
Kapusta, N. D., Fegert, J. M., Haring, C. & Plener, P. L. (2013).Psychotherapeutische Interventionen bei suizidalen Ju-gendlichen. Psychotherapeut, 59, 16 –23.
Kaufman, J., Birmaher, B. & Brent, D. (1997). Schedule forAffective Disorders and Schizophrenia for School-AgeChildren- Present and Lifetime Version (K-SADS-PL): In-itial reliability and validity data. Journal of the AmericanAcademy of Child and Adolescent Psychiatry, 36, 980–988.
Keller, F., Grieb, J., Ernst, M., Sprober, N., Fegert, J. M. &Kolch, M. G. (2011). Children’s Depression Rating Scale –Revised (CDRS-R): Entwicklung einer deutschen Versionund psychometrische Gutekriterien in einer klinischenStichprobe. Zeitschrift fur Kinder- und Jugendpsychiatrieund Psychotherapie, 39, 179– 185.
Keller, F., Grieb, J., Koelch, M. G., & Sproeber, N. (2012).CDRS-R Children’s Depression Rating Scale – Revised by E.O. Poznanski and H. B. Mokros: Deutsche Version. Gottin-gen: Hogrefe.
Klauer, K. J. (2001). Handbuch kognitives Training. Gottingen:Hogrefe.
Klein, J., Jacobs, R. H. & Reinecke, M. A. (2007). Cognitive-behavioral therapy for adolescent depression: A meta-ana-lytic investigation of changes in effect-size estimates. Jour-nal of the American Academy of Child and AdolescentPsychiatry, 46, 1403–1413.
McDermut, W., Miller, I. & Brown, R. (2001). The efficacy ofgroup psychotherapy for depression: A meta-analysis andreview of emprirical research. Clinical Psychology: Scienceand Practice, 8, 98–116.
Michael, K. & Crowley, S. (2002). How effective are treatmentsfor child and adolescent depression? A meta-analytic review.Clinical Psychology Review, 22, 247 –269.
National Collaborating Centre for Mental Health. Depression inChildren and Young People. Identification and Managementin Primary Community and Secondary Care. London: TheBritish Psychological Society & The Royal College ofPsychiatrists.
Park, R. J. & Goodyer, I. M. (2000). Clinical guidelines fordepressive disorders in childhood and adolescence. Euro-pean Child & Adolescent Psychiatry, 9, 147–161.
Patton, G. C., Coffey, C., Romaniuk, H., Mackinnon, A., Carlin,J. B., Degenhardt, L. et al. (2014). The prognosis of commonmental disorders in adolescents: A 14-year prospective co-hort study. The Lancet, 383, 1404– 1411.
Petermann, F. & Petermann, U. (Hrsg.). (2008). Hamburg-Wechsler-Intelligenztest fur Kinder-IV (HAWIK-IV). Bern:Huber.
Plener, P. L., Grieb, J., Sprober, N., Straub, J., Schneider, A.,Keller, F. et al. (2012). Convergence of children’s depressionrating scale-revised scores and clinical diagnosis in ratingadolescent depressive symptomatology. Mental Illness, 4(e7), 29 –31.
MICHI – eine Gruppen-Kurzzeitpsychotherapie zur Behandlung von Depressionen bei Jugendlichen 197Persönliches Autorenexemplar (e-Sonderdruck)Persönliches Autorenexemplar (e-Sonderdruck)Persönliches Autorenexemplar (e-Sonderdruck)Persönliches Autorenexemplar (e-Sonderdruck)Persönliches Autorenexemplar (e-Sonderdruck)

Poznanski, E. O. & Mokros, H. B. (1996). Children’s DepressionRating Scale, Revised (CDRS-R): Manual. Los Angeles:Western Psychological Services.
Spielmans, G. I., Pasek, L. F. & McFall, J. P. (2007). What are theactive ingredients in cognitive and behavioral psychotherapyfor anxious and depressed children? A meta-analytic review.Clinical Psychological Review, 27, 642 –654.
Sprober, N., Straub, J., Fegert, J. & Kolch, M. (2012). Depres-sion im Jugendalter: MICHI – Manual fur die Gruppen-therapie. Weinheim: Beltz.
Straub, J., Koelch, M. G., Fegert, J. M., Plener, P. L., Gonzalez-Aracil, I., Voit, A. et al. (2013). Innovations in practice:MICHI, a brief cognitive-behavioural group therapy foradolescents with depression – a pilot study of feasibility in aninpatient setting. Child and Adolescent Mental Health, 18,247 –250.
Straub, J., Nicolaus, L., Plener, P. L., Sprober, N. & Kolch, N.(2014). Psychotherapeutische Behandlung von depressivenKindern und Jugendlichen. Literaturubersicht zu kognitiv-behavioralen und interpersonellen Gruppentherapieverfah-ren. Psychotherapeut, 59, 7–15.
Straub, J., Sproeber, N., Plener, P. L., Fegert, J. M., Bonenberger,M. & Koelch, M. G. (2014). A brief cognitive-behaviouralgroup therapy programme for the treatment of depression inadolescent outpatients: A pilot study. Child and AdolescentPsychiatry and Mental Health, 8, 1–10.
Vostanis, P., Feehan, C., Grattan, E. & Bickerton, W. (1996).Treatment for children and adolescents with depression:Lessons from a controlled trial. Clinical Child Psychologyand Psychiatry, 1, 199 –212.
Watanabe, N., Hunot, V., Omori, I., Churchill, R. & Furukawa, T.(2007). Psychotherapy for depression among children and
adolescents: A systematic review. Acta Psychiatrica Scan-dinavica, 116, 84 –95.
Weisz, J. R., Thurber, C., Sweeney, L., Proffitt, V. & LeGagnoux,G. (1997). Brief treatment of mild to moderate child de-pression using primary and secondary control enhancementtraining. Journal of Consulting and Clinical Psychology, 65,703 –707.
Weisz, J. R., McCarty, C. & Valeri, S. (2006). Effects of psy-chotherapy for depression in children and adolescents: Ameta-analysis. Psychological Bulletin, 132, 132 –149.
Wilkinson, P., Kelvin, R., Roberts, C., Dubicka, B. & Goodyer, I.(2011). Clinical and psychosocial predictors of suicide at-tempts and nonsuicidal self-injury in the adolescent depres-sion antidepressants and psychotherapy trial (ADAPT).American Journal of Psychiatry, 168, 495 –501.
Wood, A., Harrington, R. & Moore, A. (1996). Controlled trial ofa brief cognitive-behavioural intervention in adolescent pa-tients with depressive disorders. Journal of Child Psycho-logy and Psychiatry, 37, 737 –746.
Joana Straub, M.Sc. Psych.Dr. Paul L. PlenerProf. Dr. Ferdinand KellerProf. Dr. Jorg M. FegertDr. Nina SproberProf. Dr. Michael G. Kolch
Universitatsklinik UlmKlinik fur Kinder- und Jugendpsychiatrie/-psychotherapieSteinhovelstraße 589075 UlmE-Mail: [email protected]
198 Joana Straub et al.
Persönliches Autorenexemplar (e-Sonderdruck)Persönliches Autorenexemplar (e-Sonderdruck)Persönliches Autorenexemplar (e-Sonderdruck)Persönliches Autorenexemplar (e-Sonderdruck)Persönliches Autorenexemplar (e-Sonderdruck)

Neural correlates of successful psychotherapy of depression in adolescents
141
6.9 Neural correlates of successful psychotherapy of depression in adolescents
Contribution of J. Straub to the article:
J. Straub coordinated the study procedure and recruited participants. She executed weekly
group therapy sessions, assessed suicidal ideation and behaviour in the patients on a weekly
basis, and scheduled diagnostic as well as psychotherapeutic appointments. She controlled
the return of questionnaires and executed diagnostic assessments that did not have to be
done by an independent evaluator (e.g. IQ measurements). With the technical assistance of
K. Braendle and E.-J. Sim she executed fMRI scans. She performed data acquisition,
generation of the data matrix, data input and execution of statistical analyses regarding
clinical, behavioural, and fMRI data. She interpreted statistical and neuroimaging outcomes.
She researched literature, wrote the manuscript, integrated remarks of the co-authors,
revised the manuscript according to reviewer’s comments, and created figures and tables.
Co-authors’ contributions to the article:
B. Abler made decisions on the experimental design, conceptualized the study, and
supervised the writing of the proposal for the ethical committee. She supervised the
coordination of study procedures, fMRI measurements, configuration of diagnostic
instruments, pre-processing of fMRI data, and higher level analyses by means of SPM. She
provided literature, supervised and helped with writing the manuscript, as well as integrating
the remarks of co-authors and reviewers comments. P.L. Plener helped conceptualize the
study, provided literature and made constructive remarks on the manuscript. N. Sproeber
helped conceptualize the study, helped with coordinating the study procedure and the
configuration of diagnostic instruments, and supervised the weekly group psychotherapy. L.
Sprenger helped conceptualize the study, wrote the proposal for the ethical committee,
reviewed the draft, and gave constructive remarks. M. Koelch decided on experimental
design and conceptualisation of the study, helped coordinate study procedure, reviewed the
draft, and gave constructive remarks. G. Groen supported study conceptualisation and
higher level analyses of functional brain imaging data by means of SPM. He helped with
writing the manuscript as well as integrating the remarks of co-authors and reviewer’s
comments.
Reference
Straub, J., Plener, P.L., Sproeber, N., Sprenger, L., Koelch, M.G., Groen, G. & Abler, B.
(accepted). Neural correlates of successful psychotherapy of depression in adolescents.
Journal of Affective Disorders, doi.10.1016/j.jad.2015.05.020
Reprinted from Journal of Affective Disorders, Straub, J., Plener, P.L., Sproeber, N., Sprenger,
L., Koelch, M.G., Groen, G. & Abler, B. Neural correlates of successful psychotherapy of
depression in adolescents, Copyright (2015), with permission from Elsevier.
Author's personal copy
Research report
Neural correlates of successful psychotherapyof depression in adolescents
J. Straub a,n, P.L. Plener a, N. Sproeber a, L. Sprenger c, M.G. Koelch a, G. Groen b, B. Abler b
a Department of Child and Adolescent Psychiatry and Psychotherapy, University Hospital Ulm, Germanyb Department of Psychiatry and Psychotherapy III, University Hospital Ulm, Germanyc Department of Child and Adolescent Psychiatry, Psychosomatics and Psychotherapy, Philipps-University Marburg, Germany
a r t i c l e i n f o
Article history:Received 13 January 2015Received in revised form8 May 2015Accepted 8 May 2015Available online 18 May 2015
Keywords:AdolescentsDepressionCBTGroup psychotherapyfMRIReward
a b s t r a c t
Background: While major effort has been put in investigating neural correlates of depression and itstreatment in adults, less is known about the effects of psychotherapy in adolescents. Given theconcordance of the ventral striatum, amygdala, hippocampus and the subgenual anterior cingulatecortex (sgACC) as correlates of depression and their involvement in reward processing, we usedfunctional magnetic resonance imaging (fMRI) during performance of a monetary reward task in anintervention versus waitlist-control design to investigate the clinical and neural effects of cognitivebehavioral group therapy (CBT-G).Methods: 22 medication naïve adolescents with major depressive disorder were scanned before and afterfive sessions of CBT-G (PAT-I), or before and after five weeks of waiting (PAT-W). Changes in symptomscales were analyzed along with neural activation changes within the amygdala, hippocampus, sgACCand ventral striatum regions of interest (ROI).Results: Psychometric assessments and ROI activation remained unchanged in PAT-W. In PAT-I,significant reduction in clinical symptoms accompanied significant changes in brain activation withinthe left amygdala, left hippocampus and bilateral sgACC. In line with previous findings in adults, pre-to-post-activation changes in the bilateral sgACC correlated with pre-to-post and pre-to-follow-upsymptom improvement, and individual expressions of sgACC activation before treatment were relatedto pre-to-follow-up therapeutic success.Limitations: Future studies should include larger sample sizes.Conclusions: Successful group psychotherapy of depression in adolescents was related to signal changesin brain regions previously demonstrated to be reliably linked with successful, particularly pharmaco-logical treatment in adults.
& 2015 Elsevier B.V. All rights reserved.
1. Introduction
Given the increased risk for the development of affective disordersin youth (Duggal et al., 2001), with a raising number of incidents (Ryanet al., 1992), and the risk for relapses in adulthood (Patton et al., 2014)effective therapies for depressed adolescents are needed (Jonssonet al., 2011). Understanding the neural correlates of adolescentdepression may assist in better shaping of therapies to the specialcharacteristics and needs of this particular group of patients. Further-more, investigating the neural correlates of psychiatric disorders inadolescents offers the opportunity to research a disorder at anearly stage, thus bypassing otherwise relevant effects of previous
medication and/or by changes in neural processing due to a chroniccourse of the disorder like in studies with adults (Cullen, 2012).
Research on regional brain activity modulated by depressionshowed a particularly consistent pattern of involvement of theamygdala, hippocampus, subgenual anterior cingulate cortex(sgACC), and ventral striatum for both adults and adolescents(Arnone et al., 2012, Forbes et al., 2009, Fu et al., 2008, Godlewskaet al., 2012, Goldapple et al., 2004, Gotlib et al., 2005, Hall et al.,2014, Kennedy et al., 2001, Mayberg et al., 2000, Sheline et al.,2001, Yang et al., 2010). In adults, pre-to-post-comparisons of theeffect of antidepressant medication reliably showed a reduction ofamygdala reactivity (Arnone et al., 2012, Godlewska et al., 2012,Sheline et al., 2001). Likewise, pharmacological pre-to-post-modulation of activations of the hippocampus and sgACC has beenrepeatedly reported, although the direction of activity changes wasless consistent as compared to results for the amygdala (Kennedy
Contents lists available at ScienceDirect
journal homepage: www.elsevier.com/locate/jad
Journal of Affective Disorders
http://dx.doi.org/10.1016/j.jad.2015.05.0200165-0327/& 2015 Elsevier B.V. All rights reserved.
n Corresponding author. Tel.: þ49 731 500 62630; fax: þ49 731 500 61602.E-mail address: [email protected] (J. Straub).
Journal of Affective Disorders 183 (2015) 239–246
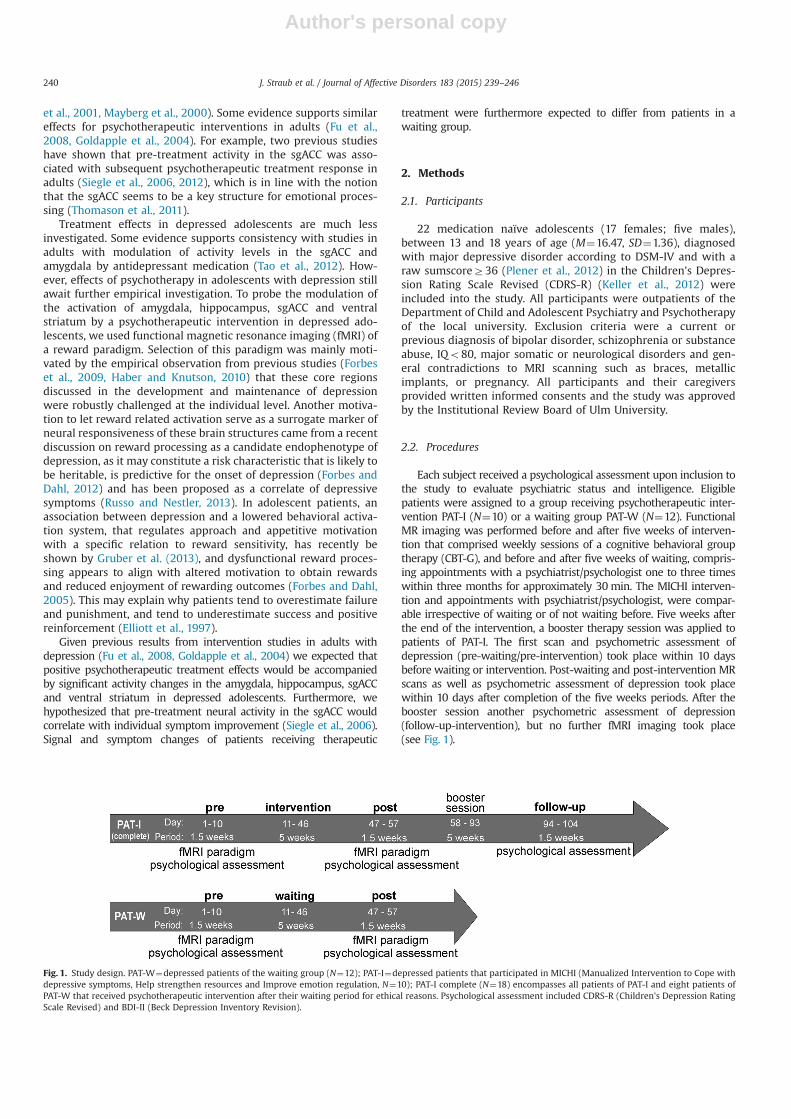
Author's personal copy
et al., 2001, Mayberg et al., 2000). Some evidence supports similareffects for psychotherapeutic interventions in adults (Fu et al.,2008, Goldapple et al., 2004). For example, two previous studieshave shown that pre-treatment activity in the sgACC was asso-ciated with subsequent psychotherapeutic treatment response inadults (Siegle et al., 2006, 2012), which is in line with the notionthat the sgACC seems to be a key structure for emotional proces-sing (Thomason et al., 2011).
Treatment effects in depressed adolescents are much lessinvestigated. Some evidence supports consistency with studies inadults with modulation of activity levels in the sgACC andamygdala by antidepressant medication (Tao et al., 2012). How-ever, effects of psychotherapy in adolescents with depression stillawait further empirical investigation. To probe the modulation ofthe activation of amygdala, hippocampus, sgACC and ventralstriatum by a psychotherapeutic intervention in depressed ado-lescents, we used functional magnetic resonance imaging (fMRI) ofa reward paradigm. Selection of this paradigm was mainly moti-vated by the empirical observation from previous studies (Forbeset al., 2009, Haber and Knutson, 2010) that these core regionsdiscussed in the development and maintenance of depressionwere robustly challenged at the individual level. Another motiva-tion to let reward related activation serve as a surrogate marker ofneural responsiveness of these brain structures came from a recentdiscussion on reward processing as a candidate endophenotype ofdepression, as it may constitute a risk characteristic that is likely tobe heritable, is predictive for the onset of depression (Forbes andDahl, 2012) and has been proposed as a correlate of depressivesymptoms (Russo and Nestler, 2013). In adolescent patients, anassociation between depression and a lowered behavioral activa-tion system, that regulates approach and appetitive motivationwith a specific relation to reward sensitivity, has recently beshown by Gruber et al. (2013), and dysfunctional reward proces-sing appears to align with altered motivation to obtain rewardsand reduced enjoyment of rewarding outcomes (Forbes and Dahl,2005). This may explain why patients tend to overestimate failureand punishment, and tend to underestimate success and positivereinforcement (Elliott et al., 1997).
Given previous results from intervention studies in adults withdepression (Fu et al., 2008, Goldapple et al., 2004) we expected thatpositive psychotherapeutic treatment effects would be accompaniedby significant activity changes in the amygdala, hippocampus, sgACCand ventral striatum in depressed adolescents. Furthermore, wehypothesized that pre-treatment neural activity in the sgACC wouldcorrelate with individual symptom improvement (Siegle et al., 2006).Signal and symptom changes of patients receiving therapeutic
treatment were furthermore expected to differ from patients in awaiting group.
2. Methods
2.1. Participants
22 medication naïve adolescents (17 females; five males),between 13 and 18 years of age (M¼16.47, SD¼1.36), diagnosedwith major depressive disorder according to DSM-IV and with araw sumscoreZ36 (Plener et al., 2012) in the Children's Depres-sion Rating Scale Revised (CDRS-R) (Keller et al., 2012) wereincluded into the study. All participants were outpatients of theDepartment of Child and Adolescent Psychiatry and Psychotherapyof the local university. Exclusion criteria were a current orprevious diagnosis of bipolar disorder, schizophrenia or substanceabuse, IQo80, major somatic or neurological disorders and gen-eral contradictions to MRI scanning such as braces, metallicimplants, or pregnancy. All participants and their caregiversprovided written informed consents and the study was approvedby the Institutional Review Board of Ulm University.
2.2. Procedures
Each subject received a psychological assessment upon inclusion tothe study to evaluate psychiatric status and intelligence. Eligiblepatients were assigned to a group receiving psychotherapeutic inter-vention PAT-I (N¼10) or a waiting group PAT-W (N¼12). FunctionalMR imaging was performed before and after five weeks of interven-tion that comprised weekly sessions of a cognitive behavioral grouptherapy (CBT-G), and before and after five weeks of waiting, compris-ing appointments with a psychiatrist/psychologist one to three timeswithin three months for approximately 30 min. The MICHI interven-tion and appointments with psychiatrist/psychologist, were compar-able irrespective of waiting or of not waiting before. Five weeks afterthe end of the intervention, a booster therapy session was applied topatients of PAT-I. The first scan and psychometric assessment ofdepression (pre-waiting/pre-intervention) took place within 10 daysbefore waiting or intervention. Post-waiting and post-intervention MRscans as well as psychometric assessment of depression took placewithin 10 days after completion of the five weeks periods. After thebooster session another psychometric assessment of depression(follow-up-intervention), but no further fMRI imaging took place(see Fig. 1).
Fig. 1. Study design. PAT-W¼depressed patients of the waiting group (N¼12); PAT-I¼depressed patients that participated in MICHI (Manualized Intervention to Cope withdepressive symptoms, Help strengthen resources and Improve emotion regulation, N¼10); PAT-I complete (N¼18) encompasses all patients of PAT-I and eight patients ofPAT-W that received psychotherapeutic intervention after their waiting period for ethical reasons. Psychological assessment included CDRS-R (Children's Depression RatingScale Revised) and BDI-II (Beck Depression Inventory Revision).
J. Straub et al. / Journal of Affective Disorders 183 (2015) 239–246240

Author's personal copy
Eight of the 12 participants initially assigned to PAT-W were alsoallowed to participate in the intervention after waiting for ethicalreasons. Together with PAT-I (N¼10), a total of 18 subjects receivedthe intervention (PAT-I complete). All subjects in PAT-I completereceived the same treatment irrespective of having been assigneddirectly to PAT-I or to the waiting group before the intervention.Associations between individual symptom improvement and subse-quent changes of neural activity were calculated within the PAT-Icomplete group. Longitudinal effects (pre-to-post, post-to-follow-upand pre-to-follow-up therapy) were assessed in the PAT-I and PAT-Wgroups.
The mean pre-test CDRS-R score was 56.11 (SD¼9.11) for PAT-Icomplete. Mean pre-test CDRS-R score (M¼56.70, SD¼11.28) forPAT-I (N¼10) was numerically comparable, and did not differ fromthe mean pre-test CDRS-R score (M¼54.92, SD¼11.40, t(20)¼0.37,po0.72) of the PAT-W group.
Additional analyses revealed, that post-waiting scores of PAT-W, before consecutive admission to MICHI (N¼8), did not differsignificantly from pre-intervention scores of PAT-I (N¼10), withneither respect to CDRS-R (t(16)¼0.67, po0.51) nor BDI-II (t(16)¼0.47, po0.47).
Furthermore, no differences were found with respect to age,sex, IQ, smoking behavior and diagnoses between the PAT-W andboth representations of PAT-I (see Table 1).
2.3. Psychotherapeutic treatment
Participants of PAT-I were assigned to groups of four to sixpatients who received weekly sessions (75–90 min) over fiveconsecutive weeks, as well as one booster session according to arecently evaluated CBT-G programme: “Manualized Interventionto Cope with depressive symptoms, Help strengthen resources andImprove emotion regulation (MICHI)” (Sproeber et al., 2012). Thetreatment manual combines therapeutic elements that are wellacknowledged as representing the standard of care in the treat-ment of adolescent depression including psycho-education, cog-nitive restructuring, behavioral activation, orientation towardresources, enhancement of self-esteem, problem-solving skills,
emotion regulation, management of acute crises, and preventionof relapse. Results with respect to acceptance, feasibility andefficacy are reported elsewhere (Straub et al., 2013, 2014). Twoclinical psychologists experienced in the administration of cogni-tive behavioral group therapies provided the treatment. On aver-age, patients of the intervention group participated in four of thefive treatment sessions (M¼4.4; SD¼0.7; range: 3–5).
2.4. Psychological assessment
Before inclusion into the study the psychiatric status was assessedby means of the Kiddie Schedule for Affective Disorders and Schizo-phrenia, Present and Lifetime Version (K-SADS-PL) (Kaufman et al.,1997), and intelligence was assessed by means of either the WechslerIntelligence Scale for Children-Fourth Edition (WISC IV), WechslerAdult Intelligence Scale (WAIS) or the testing system for educationalcounseling (PSB). The choice of the intelligence test depended on ageof participants and whether it was possible to arrange a groupassessment or not. Upon each fMRI scan (pre-post-waiting and pre-post-intervention) and at follow-up, the change in depressive symp-tomswas assessed bymeans of the CDRS-R (Keller et al., 2012) and theBeck Depression Inventory Revision (BDI-II) (Beck et al., 1996,Hautzinger et al., 2006) capturing symptoms during the past twoweeks. Diagnostics were done by trained clinical psychologists notinvolved in the interventional aspect of the study and blinded forgroup assignment.
Within each group, one-sample t-tests were computed to testwhether pre-to-post-intervention or pre-to-post-waiting differ-ences were different from zero to infer significant symptomchange over time. Within the PAT-I complete group, a one-sample t-test was also computed to test on differences from zeroregarding pre-to-post, pre-to-follow-up, and post-to-follow-up. Toinfer the significance of treatment effects, pre-to-post-clinicalsymptom changes were propagated to two-sample t-tests testingon significant interactions of group (PAT-I/PAT-W) and time (pre/post). Statistical analyses were performed using Statistical Packagefor the Social Sciences 21 (SPSS 21, IBM, Armonk, NY, USA).
Table 1Demographics and behavioral data for PAT-I (N¼10), PAT-W (N¼12) and PAT-I complete (N¼18). The latter compasses all patients of PAT-I (N¼10) and eight patients of PAT-W that received psychotherapeutic intervention after their waiting period for ethical reasons.
PAT-I complete (N¼18) PAT-I (N¼10) PAT-W (N¼12) Signifi-cance
M7SD M7SD M7SD
Age (years) 16.6671.37 16.3971.58 16.5471.21 n.s.a
Gender 15 females (83.3%) 8 females (80%) 9 females (75%)Handednessb 17 righthanded (94.4%) 10 righthanded (100%) 10 righthanded (83.3%)IQ 97.8177.29 100.0078.72 99.6777.55 n.s. a
Depression subtypesc Depressive disorder, mild (N¼3); moderate(N¼11); severe (N¼4)
Depressive disorder, mild (N¼2);moderate (N¼7); severe (N¼1)
Depressive disorder, mild (N¼4); moderate(N¼5); severe (N¼3)
Secondary diagnosisc Social phobia (N¼4); specific phobia (N¼1);socialized conduct disorder (N¼1);
Social phobia (N¼2); attention deficitwithout hyperactivity (N¼1)
Social phobia (N¼2); specific phobia (N¼1);socialized conduct disorder (N¼1)
Attention deficit without hyperactivity(N¼1)
Lifetime history ofpsychotherapy/medicationd
Psychotherapy (N¼2), Methylphenidate(N¼4)
Psychotherapy (N¼1),Methylphenidate (N¼3)
Psychotherapy (N¼2), Methylphenidate(N¼1)
Smoker 7 ( 38.9%) 5 (50%) 3 (25%)
Notes : n.s.¼not significant.a Independent sample t-test; significances were calculated between PAT-I (N¼10) and PAT-W (N¼12).b Edinburgh Handedness Inventory.c Diagnosis according to DSM-IV/ICD-10d psychological treatment and previous medical treatment relate to time periods where adolescents were initially treated outside the Department for Child and
Adolescent Psychiatry and Psychotherapy without success or with very limited success only.
J. Straub et al. / Journal of Affective Disorders 183 (2015) 239–246 241

Author's personal copy
2.5. fMRI paradigm
We used a well-established monetary incentive task (Ableret al., 2006, 2009) with parametric variation of probabilities(0%, 25%, 50%, 75%, 100%) to win a fixed amount of money (1€).Compared to our previous studies with adults, we had to adapt amaximum amount of money to win in line with the guidelines ofthe ethical committee of Ulm University that suggest limitedmonetary compensation for adolescent study participants.Furthermore adolescents received reward in form of vouchersinstead of bank transfers. Otherwise all technical parameters ofthe functional challenge were the same as in our previous studies.After an expectation period, subjects had to correctly react with abutton press to one of two different symbols. In reacting correctlythey preserved themselves the previously announced chance towin one Euro. Feedback (outcome) followed the targets disap-pearance and notified subjects about the amount of money (1€ –
win trial or 0€ – lose trial) they won in the trial.
2.6. fMRI acquisition
A 3.0T MR scanner (Siemens MAGNETOM Allegra, Erlangen, Ger-many) was used to perform T1 anatomical imaging (1�1�1mm3
voxels) and fMRI similar to previous experiments. Functional time serieswere recorded using a T2n-sensitive gradient echo sequence measuringchanges in BOLD-contrast. As in our previous studies with adults on theAllegra (Abler et al., 2006, 2007, 2009), we used slightly shortened echotime (TE), reduced slice thickness, and a tilt steeper than the usual AC–PC orientation to minimize the risk of signal loss or distortions in thesebrain regions. 23 transversal slices were acquired with an image size of64�64 pixels. Slice thickness was 3mmwith 0.75mm gap resulting invoxel sizes of 3�3�3.75mm3. Images were centered on basalstructures of the brain including subcortical regions of interest (limbicstructures and prefrontal regions). 401 volumes were obtained duringeach session at a repetition time (TR) of 1500ms and echo time (TE) of35ms.
2.7. fMRI analysis
Image processing and statistical analysis were carried out usingStatistical Parametric Mapping (SPM 8, Wellcome Trust Centre forNeuroimaging, London, UK). Preprocessing of individual functionaltime series included slice timing, realignment to correct formotion artifacts, spatial normalization via the segmentation tool-box into standard MNI space, and smoothing with an 8 mmFWHM Gaussian kernel. Intrinsic autocorrelations were accountedfor by first-order autocorrelation modeling and low frequencydrifts were removed via high pass filtering.
For individual first level analysis, we defined five regressors forthe five different types of reward expectation (exp. 0%, 25%, 50%,75%, 100%) and eight regressors for the outcome phases dependingon reward expectation (0–100%) and actual outcome (win/loss) atdifferent probabilities (Abler et al., 2009). According to their actualdurations, trials were modeled as timely extended events andconvolved with the hemodynamic response function. The sixrealignment parameters modeling residual motion were alsoadded to the individual models.
2.8. Region of interest (ROI) definition
For ROI definition we used anatomical ROIs and peak voxelcoordinates from two prior studies on adolescent depression withcharacteristic results. For the sgACC the MNI-coordinates x/y/z¼75/25/�10 (Davey et al., 2012) and for the hippocampus thecoordinates x/y/z¼�18/�12/�16 (van Eijndhoven et al., 2013),were used as starting points. We then defined spheres around
these maxima with radius r¼6 mm for the left sgACC ROI andr¼10 mm for the left hippocampus ROI. The resulting ROIs werethen mirrored to the opposite hemisphere to obtain the rightsgACC ROI and the right hippocampus ROI. The amygdala ROIswere defined using the standard masks provided by the WFU PickAtlas for SPM (http://fmri.wfubmc.edu/software/PickAtlas), andthe nucleus accumbens ROIs were defined using the masksprovided by the Harvard-Oxford cortical and subcortical structuralatlases (www.cma.mgh.harvard.edu/fsl_atlas.html).
The estimated mean fMRI signal averaged across all voxels ofeach ROI in each subject was then extracted separately for win andloss outcomes and the differential activation signal of win minusloss trials was computed. Afterwards, pre-to-post-differenceswithin each group (PAT-W and PAT-I complete) were testedagainst zero to assess significance on changes over time. As whatwould be denoted as primary outcome in classic pharmacologicaltreatment studies, relationships between individual fMRI pre-to-post-signal changes and pre-to-post as well as pre-to-follow-upsymptom score changes were tested on significance by computingcorrelation coefficients for the sgACC ROIs in the PAT-I completesample with 18 participants. Furthermore, to infer significance oftreatment effects, directed two-sample t-tests were computedtesting on significant interactions of group (PAT-W/PAT-I) andtime (pre-/post) in areas with significant win/lose differences.Since greater effects were expected a priori in PAT-I then PAT-W,we tested unidirectionally.
In the sense of a secondary outcome, fMRI signals from the pre-test sgACC ROIs of PAT-I complete were correlated with the pre-to-follow-up changes in symptom scores to assess the predictivevalue of the imaging results.
3. Results
3.1. Clinical assessments
Within group analyses revealed significant pre-to-post-reductionsin the CDRS-R (t(17)¼�3.65, p¼0.001) and BDI-II (t(17)¼�3.25,p¼0.003) for PAT-I complete (N¼18). These symptom improvementsremained stable from pre-to-follow-up assed by means of CDRS-R(t(17)¼�3.91, po0.001) and BDI-II (t(17)¼�4.35, po0.001), how-ever with no further significant improvements between post andfollow-up in CDRS-R (t(17)¼�0.78, p¼0.57) and BDI-II (t(17)¼�1.67,p¼0.71). Pre-to-post-changes within PAT-W were not significant (seeTable 2). Two-sample t-tests, to assess interaction effects betweengroup (PAT-W/PAT-I) and time (pre/post), were significant for bothrating scales, BDI-II and CDRS-R, indicating significant treatmenteffects of the intervention against waiting (see Table 2).
3.2. fMRI data analysis
A whole brain analyses across all patients prior to waiting orintervention (N¼22) was computed to assess pre-test (beforeintervention or waiting) main effects of the task. Focussing onthe outcome phase, we set up a contrast to compare activationbetween win minus lose trials. The whole brain analysis wasthresholded at po0.001 at the voxel level, with an extent thresh-old of 60 contiguously significant voxels per cluster to obtainclusters significant at po0.05, family-wise corrected for multiplecomparisons. We observed reliable activation within the ventralstriatum, amygdala, hippocampus and sgACC (see Fig. 2) as well asin regions of the reward system i.e. pregenual cingulate cortex andlateral prefrontal cortex, additionally.
Results of pre-to-post-differences of averaged signals per eachROI in PAT-I complete showed significant pre-to-post-signalreductions in the bilateral amygdala, bilateral hippocampus and
J. Straub et al. / Journal of Affective Disorders 183 (2015) 239–246242
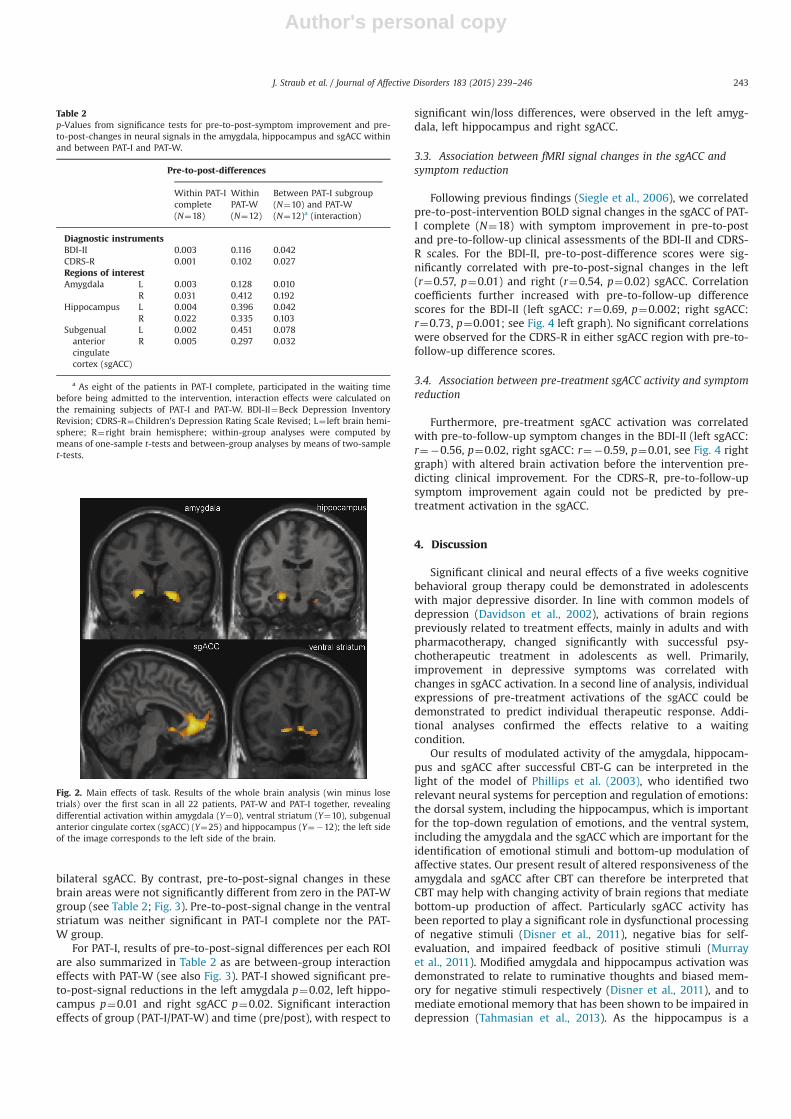
Author's personal copy
bilateral sgACC. By contrast, pre-to-post-signal changes in thesebrain areas were not significantly different from zero in the PAT-Wgroup (see Table 2; Fig. 3). Pre-to-post-signal change in the ventralstriatum was neither significant in PAT-I complete nor the PAT-W group.
For PAT-I, results of pre-to-post-signal differences per each ROIare also summarized in Table 2 as are between-group interactioneffects with PAT-W (see also Fig. 3). PAT-I showed significant pre-to-post-signal reductions in the left amygdala p¼0.02, left hippo-campus p¼0.01 and right sgACC p¼0.02. Significant interactioneffects of group (PAT-I/PAT-W) and time (pre/post), with respect to
significant win/loss differences, were observed in the left amyg-dala, left hippocampus and right sgACC.
3.3. Association between fMRI signal changes in the sgACC andsymptom reduction
Following previous findings (Siegle et al., 2006), we correlatedpre-to-post-intervention BOLD signal changes in the sgACC of PAT-I complete (N¼18) with symptom improvement in pre-to-postand pre-to-follow-up clinical assessments of the BDI-II and CDRS-R scales. For the BDI-II, pre-to-post-difference scores were sig-nificantly correlated with pre-to-post-signal changes in the left(r¼0.57, p¼0.01) and right (r¼0.54, p¼0.02) sgACC. Correlationcoefficients further increased with pre-to-follow-up differencescores for the BDI-II (left sgACC: r¼0.69, p¼0.002; right sgACC:r¼0.73, p¼0.001; see Fig. 4 left graph). No significant correlationswere observed for the CDRS-R in either sgACC region with pre-to-follow-up difference scores.
3.4. Association between pre-treatment sgACC activity and symptomreduction
Furthermore, pre-treatment sgACC activation was correlatedwith pre-to-follow-up symptom changes in the BDI-II (left sgACC:r¼�0.56, p¼0.02, right sgACC: r¼�0.59, p¼0.01, see Fig. 4 rightgraph) with altered brain activation before the intervention pre-dicting clinical improvement. For the CDRS-R, pre-to-follow-upsymptom improvement again could not be predicted by pre-treatment activation in the sgACC.
4. Discussion
Significant clinical and neural effects of a five weeks cognitivebehavioral group therapy could be demonstrated in adolescentswith major depressive disorder. In line with common models ofdepression (Davidson et al., 2002), activations of brain regionspreviously related to treatment effects, mainly in adults and withpharmacotherapy, changed significantly with successful psy-chotherapeutic treatment in adolescents as well. Primarily,improvement in depressive symptoms was correlated withchanges in sgACC activation. In a second line of analysis, individualexpressions of pre-treatment activations of the sgACC could bedemonstrated to predict individual therapeutic response. Addi-tional analyses confirmed the effects relative to a waitingcondition.
Our results of modulated activity of the amygdala, hippocam-pus and sgACC after successful CBT-G can be interpreted in thelight of the model of Phillips et al. (2003), who identified tworelevant neural systems for perception and regulation of emotions:the dorsal system, including the hippocampus, which is importantfor the top-down regulation of emotions, and the ventral system,including the amygdala and the sgACC which are important for theidentification of emotional stimuli and bottom-up modulation ofaffective states. Our present result of altered responsiveness of theamygdala and sgACC after CBT can therefore be interpreted thatCBT may help with changing activity of brain regions that mediatebottom-up production of affect. Particularly sgACC activity hasbeen reported to play a significant role in dysfunctional processingof negative stimuli (Disner et al., 2011), negative bias for self-evaluation, and impaired feedback of positive stimuli (Murrayet al., 2011). Modified amygdala and hippocampus activation wasdemonstrated to relate to ruminative thoughts and biased mem-ory for negative stimuli respectively (Disner et al., 2011), and tomediate emotional memory that has been shown to be impaired indepression (Tahmasian et al., 2013). As the hippocampus is a
Table 2p-Values from significance tests for pre-to-post-symptom improvement and pre-to-post-changes in neural signals in the amygdala, hippocampus and sgACC withinand between PAT-I and PAT-W.
Pre-to-post-differences
Within PAT-Icomplete(N¼18)
WithinPAT-W(N¼12)
Between PAT-I subgroup(N¼10) and PAT-W(N¼12)a (interaction)
Diagnostic instrumentsBDI-II 0.003 0.116 0.042CDRS-R 0.001 0.102 0.027Regions of interestAmygdala L 0.003 0.128 0.010
R 0.031 0.412 0.192Hippocampus L 0.004 0.396 0.042
R 0.022 0.335 0.103Subgenualanteriorcingulatecortex (sgACC)
L 0.002 0.451 0.078R 0.005 0.297 0.032
a As eight of the patients in PAT-I complete, participated in the waiting timebefore being admitted to the intervention, interaction effects were calculated onthe remaining subjects of PAT-I and PAT-W. BDI-II¼Beck Depression InventoryRevision; CDRS-R¼Children's Depression Rating Scale Revised; L¼ left brain hemi-sphere; R¼right brain hemisphere; within-group analyses were computed bymeans of one-sample t-tests and between-group analyses by means of two-samplet-tests.
Fig. 2. Main effects of task. Results of the whole brain analysis (win minus losetrials) over the first scan in all 22 patients, PAT-W and PAT-I together, revealingdifferential activation within amygdala (Y¼0), ventral striatum (Y¼10), subgenualanterior cingulate cortex (sgACC) (Y¼25) and hippocampus (Y¼�12); the left sideof the image corresponds to the left side of the brain.
J. Straub et al. / Journal of Affective Disorders 183 (2015) 239–246 243
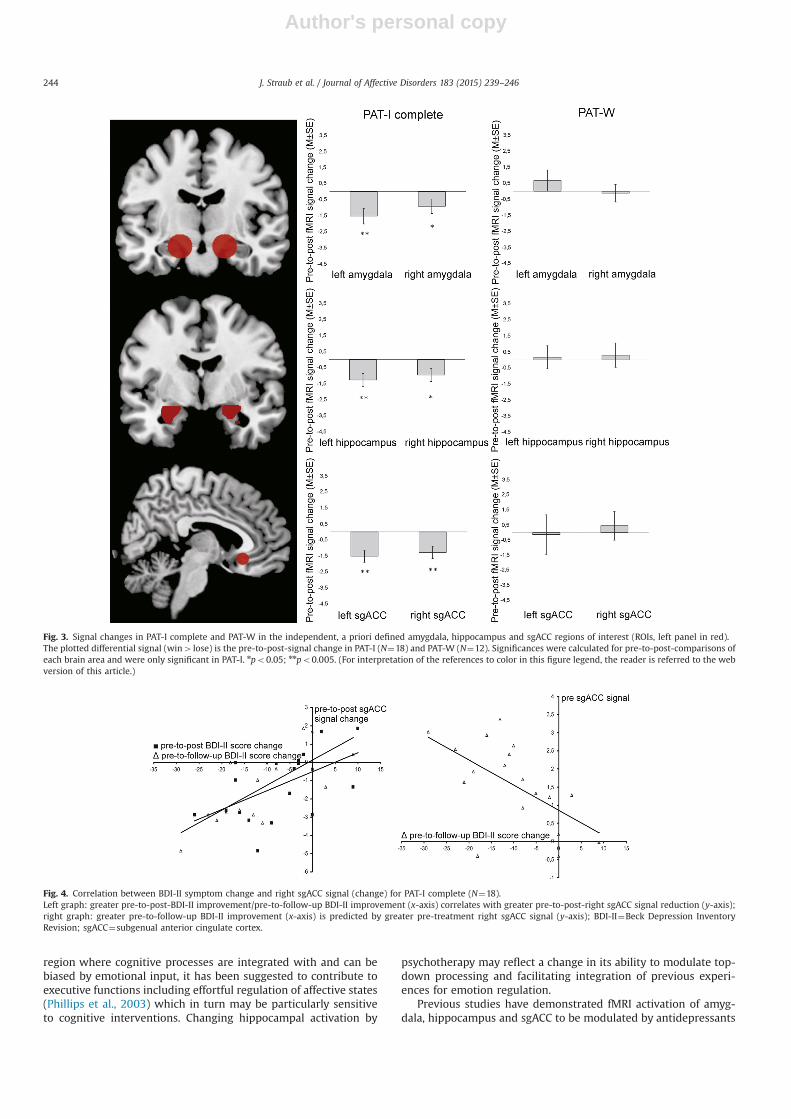
Author's personal copy
region where cognitive processes are integrated with and can bebiased by emotional input, it has been suggested to contribute toexecutive functions including effortful regulation of affective states(Phillips et al., 2003) which in turn may be particularly sensitiveto cognitive interventions. Changing hippocampal activation by
psychotherapy may reflect a change in its ability to modulate top-down processing and facilitating integration of previous experi-ences for emotion regulation.
Previous studies have demonstrated fMRI activation of amyg-dala, hippocampus and sgACC to be modulated by antidepressants
Fig. 3. Signal changes in PAT-I complete and PAT-W in the independent, a priori defined amygdala, hippocampus and sgACC regions of interest (ROIs, left panel in red).The plotted differential signal (win4 lose) is the pre-to-post-signal change in PAT-I (N¼18) and PAT-W (N¼12). Significances were calculated for pre-to-post-comparisons ofeach brain area and were only significant in PAT-I. npo0.05; nnpo0.005. (For interpretation of the references to color in this figure legend, the reader is referred to the webversion of this article.)
Fig. 4. Correlation between BDI-II symptom change and right sgACC signal (change) for PAT-I complete (N¼18).Left graph: greater pre-to-post-BDI-II improvement/pre-to-follow-up BDI-II improvement (x-axis) correlates with greater pre-to-post-right sgACC signal reduction (y-axis);right graph: greater pre-to-follow-up BDI-II improvement (x-axis) is predicted by greater pre-treatment right sgACC signal (y-axis); BDI-II¼Beck Depression InventoryRevision; sgACC¼subgenual anterior cingulate cortex.
J. Straub et al. / Journal of Affective Disorders 183 (2015) 239–246244

Author's personal copy
in depressed patients (Arnone et al., 2012, Godlewska et al., 2012,Sheline et al., 2001). However, antidepressants in healthy subjectshave been associated with similar effects (Abler et al., 2011,Macoveanu, 2014), which shows that changes in brain activationupon antidepressant treatment are ambiguous with respect to theunderlying factors (symptom, improvement and/or medication). Inline with one of the few studies on neural effects of psychotherapy,although in adults (Fu et al., 2008), in the present study we showthat activity of the amygdala, sgACC and hippocampus changed inalignment with symptom improvement upon clinically successfulpsychotherapy. As our subjects were naïve to pharmacologicaltreatment, present results therefore support the notion that neuralactivity changes most likely relate to treatment success rather thanto pharmacological treatment. Here, our findings may close a gap.
Also consistent with previous studies is our finding of a strongcorrelation between symptom improvement and activity in the sgACC,which was also reported by Fu et al. (2008) and Siegle et al. (2006,2012) for adult samples, Fu et al. (2008) found a significant relation-ship with linear load–response activity in the dorsal anterior cingulateregion in patients who showed greater improvement with CBT. Siegleet al. (2006) reported a significant association between reducedpretreatment activity in the sgACC and subsequent treatmentresponse. In our study relatively increased pretreatment activity inthe sgACC was associated with subsequent treatment response. WhileSiegle et al. (2006) focused on activation related to negative emotionalstimuli, we investigated activation related to positive (win) versusnegative (loss) stimuli.
In contrast to Yang et al. (2009) and Fu et al. (2008), whodemonstrated associations between signal change and treatmentresponse as assessed by means of clinical interviews, we found thatthe self-report scales were better predictors of clinical changes. Similarto the results reported by Siegle et al. (2006) our findings support theassumption that subjective impression may better reflect changesin brain activation than outer appearance assessed by externalobservation.
To our knowledge the present study is the first that investi-gated neural effects of psychotherapy in adolescents in a waitlistcontrol design. Allowing eight participants from the waiting listcondition to participate in the intervention after waiting, was donefor ethical reasons and adaptive to clinical circumstances but notideal with respect to scientific standards. Future studies shouldtake this issue into account by enrolling larger sample sizes as wasactually possible. This would also overcome the present limitationof a skewed gender recruitment, limiting generalizability to malepatients. Besides that, future studies should try to evaluate theideal dose of CBT by investigating programs with greater orsmaller session numbers and, additional follow-up fMRI measure-ments up to six to twelve months after termination of psychother-apy to investigate long-term effects. As functional connectivitywas shown to predict whether a subject was clinically depressedor healthy (Craddock et al., 2009), future studies should alsoconsider to investigate functional connectivity and changesthereof as potential biomarkers of putative treatment effects.
We demonstrate a distinct neural signature of successful grouppsychotherapy in adolescents with depression compared to ado-lescents who waited with minimal treatment. Activation of theamygdala, hippocampus and sgACC, commonly reported as rele-vant in depression (Arnone et al., 2012, Fu et al., 2007, 2008,Godlewska et al., 2012, Gotlib et al., 2005, Kumari et al., 2003,Rosenblau et al., 2012, Sheline et al., 2001, Yang et al., 2010),changed with amelioration of depressive symptoms. Our studysupports models suggesting that dysfunctional neural mechanismsof emotion regulation in depression can be reached by psychother-apy, at least in the early stages of the illness and may thereforeconstitute a state rather than a trait marker. As chronic courses ofdepression clearly have shown to modulate neural activity in the
long run and to leave neural scars even in remission (Elliott et al.,2012), this emphasizes the potential impact of interventions asearly in the course of the illness as possible. Our finding of ratherstrong correlations between individual expressions of brain acti-vation predicting individual therapeutic response may inspirefurther research on individualized therapies.
Role of funding sourceFinancial support received for this work: University of Ulm.
Conflict of interestJ. Straub report no biomedical financial interests or potential conflicts of interest.P.L. Plener report no biomedical financial interests or potential conflicts of
interest. He received research grants from the BMBF (German Ministries forResearch and Education) and the BfArM (German Federal Institute for Drugs andMedical devices) as well as He serves as PI in a clinical study for Lundbeck. Hereceived travel grants from the DFG, DAAD and IACAPAP. He is not stockholder orshare-holder in the pharmaceutical industry.
N. Sproeber report no biomedical financial interests or potential conflicts of interest.L. Sprenger report no biomedical financial interests or potential conflicts of interest.M.G. Koelch report no biomedical financial interests or potential conflicts of
interest. He got research grants from the BMFFSJ (German Ministries for FamilyAffairs, Senior Citizens, Women and Youth), the BMBF (German Ministries forResearch and Education), the Schweizer Bundesamt für Justiz and from BoehringerIngelheim. He was CI or PI for Eli Lilly, Astra Zeneca and Janssen-Cilag, Lundbeck,Pascoe. He is not stockholder or share-holder in the pharmaceutical industry.
G. Groen report no biomedical financial interests or potential conflicts of interest.B. Abler report no biomedical financial interests or potential conflicts of interest.
AcknowledgmentsWe thank all patients for their participation in the study.
References
Abler, B., Seeringer, A., Hartmann, A., Groen, G., Metzger, C., Walter, M., Stingl, J.,2011. Neural correlates of antidepressant-related sexual dysfunction: aplacebo-controlled fMRI study on healthy males under subchronic paroxetineand bupropion. Neuropsychopharmacology 36, 1837–1847.
Abler, B., Hahlbrock, R., Unrath, A., Groen, G., Kassubek, J., 2009. At-risk forpathological gambling: imaging neural reward processing under chronicdopamine agonists. Brain: J. Neurol. 132, 2396–2402.
Abler, B., Erk, S., Walter, H., 2007. Human reward system activation is modulated bya single dose of olanzapine in healthy subjects in an event-related, double-blind, placebo-controlled fMRI study. Psychopharmacology 191, 823–833.
Abler, B., Walter, H., Erk, S., Kammerer, H., Spitzer, M., 2006. Prediction error as alinear function of reward probability is coded in human nucleus accumbens.NeuroImage 31, 790–795.
Arnone, D., McKie, S., Elliott, R., Thomas, E.J., Downey, D., Juhasz, G., Williams, S.R.,Deakin, J.F., Anderson, I.M., 2012. Increased amygdala responses to sad but notfearful faces in major depression: relation to mood state and pharmacologicaltreatment. Am. J. Psychiatry 169, 841–850.
Beck, A.T., Steer, R.A., Brown, G.K., 1996. Beck Depression Inventory Second EditionManual. The Psychological Corporation, San Antonio.
Craddock, R.C., Holtzheimer, P.E., Hu, X.P., Mayberg, H.S., 2009. Disease stateprediction from resting state functional connectivity. J. Magn. Reson. Med. 62,1619–1628.
Cullen, K.R., 2012. Imaging adolescent depression treatment. Am. J. Psychiatry 169,348–350.
Davey, C.G., Harrison, B.J., Yuecel, M., Allen, N.B., 2012. Regionally specific altera-tions in functional connectivity of the anterior cingulate cortex in majordepressive disorder. Psychol. Med. 42, 2071–2081.
Davidson, R.J., Pizzagalli, D., Nitschke, J.B., Putnam, K., 2002. Depression: perspec-tives from affective neuroscience. Annu. Rev. Psychol. 53, 545–574.
Disner, S.G., Beevers, C.G., Haigh, E.A., Beck, A.T., 2011. Neural mechanisms of thecognitive model of depression. Nat. Rev. Neurosci. 12, 467–677.
Duggal, S., Carlson, E.A., Sroufe, L.A., Egeland, B., 2001. Depressive symptomatologyin childhood and adolescence. Dev. Psychopathol. 13, 143–164.
Elliott, R., Lythe, K., Lee, R., 2012. Reduced medial prefrontal responses to socialinteraction images in remitted depression. Arch. Gen. Psychiatry 69, 37–45.
Elliott, R., Sahakian, B.J., Herrod, J.J., Robbins, T.W., Paykel, E.S., 1997. Abnormalresponse to negative feedback in unipolar depression: evidence for a diagnosisspecific impairment. J. Neurol., Neurosurg., Psychiatry 63, 74–82.
Forbes, E.E., Dahl, R.E., 2012. Altered reward function in adolescent depression:what, when and how? J. Child Psychol. Psychiatry 53, 3–15.
Forbes, E.E., Hairi, A.R., Martin, S.L., Silk, J.S., Moyles, D.L., Fisher, P.M., 2009. Alteredstriatal activation predicting real-world positive affect in adolescent majordepressive disorder. Am. J. Psychiatry 166, 64–73.
J. Straub et al. / Journal of Affective Disorders 183 (2015) 239–246 245
Author's personal copy
Forbes, E.E., Dahl, R.E., 2005. Neural systems of positive affect: relevance tounderstanding child and adolescent depression? Dev. Psychopathol. 17,827–850.
Fu, C.H., Williams, S.C., Cleare, A.J., Scott, J., Mitterschiffthaler, M.T., Walsh, N.D.,Donaldson, C., Suckling, J., Andrew, C., Steiner, H., Murray, R.M., 2008. Neuralresponses to sad facial expressions in major depression following cognitivebehavioral therapy. Biol. Psychiatry 64, 505–512.
Fu, C.H., Williams, S.C., Brammer, M., Suckling, J., Kim, J., Cleare, A.J., Walsh, N.D.,Mitterschiffthaler, M.T., Andrew, C.M., Pich, E.M., Bullmore, E.T., 2007. Neuralresponses to happy facial expressions in major depression following antide-pressant treatment. Am. J. Psychiatry 164, 599–607.
Godlewska, B.R., Norbury, R., Selvaraj, S., Cowen, P.J., Harmer, C.J., 2012. Short-termSSRI treatment normalises amygdala hyperactivity in depressed patients.Psychol. Med. 42, 2609–2617.
Goldapple, K., Segal, Z., Garson, C., Lau, M., Bieling, P., Kennedy, S., Mayberg, H.,2004. Modulation of cortical–limbic pathways in major depression: treatment-specific effects of cognitive behavior therapy. Arch. Gen. Psychiatry 61, 34–41.
Gotlib, I.H., Sivers, H., Gabrieli, J.D.E., Whitfield-Gabrieli, S., Goldin, P., Minor, K.L.,Canli, T., 2005. Subgenual anterior cingulate activation to valenced emotionalstimuli in major depression. NeuroReport: Int. J. Rapid Commun. Res. Neurosci.16, 1731–1734.
Gruber, J., Gilbert, K.E., Youngstrom, E., Youngstrom, J.K., Feeny, N.C., Findling, R.L.,2013. Reward dysregulation and mood symptoms in an adolescent outpatientsample. J. Abnorm. Child Psychol. 41, 1053–1065.
Haber, S.N., Knutson, B., 2010. The reward circuit: linking primate anatomy andhuman imaging. Neuropsychopharmacol. Rev. 35, 4–26.
Hall, L.M.J., Klimes-Dougan, B., Hunt, R.H., Thomas, K.M., Houri, A., Noack, E., Cullen,K.R., 2014. An fMRI study of emotional face processing in adolescent majordepression. J. Affect. Disord. 168, 44–50.
Hautzinger, M., Keller, F., Kühner, C., 2006. BDI-II Beck Depressions-InventarRevision. Harcourt Test Services, Frankfurt am Main.
Jonsson, U., Bohman, H., von Knorring, L., Olsson, G., Paaren, A., von Knorring, A.-L.,2011. Mental health outcome of long-term and episodic adolescent depression:15-year follow-up of a community sample. J. Affect. Disord. 130, 395–404.
Kaufman, J., Birmaher, B., Brent, D., 1997. Schedule for affective disorders and schizo-phrenia for school-age children – Present and lifetime version (K-SADS-PL): initialreliability and validity data. J. Am. Acad. Child Adolesc. Psychiatry 36, 980–988.
Keller, F., Grieb, J., Koelch, M.G., Sproeber, N., 2012. CDRS-R Children's DepressionRating Scale – Revised by E.O. Poznanski and H.B. Mokros: German version.Hogrefe, Goettingen.
Kennedy, S.H., Evans, K.R., Krueger, S., Mayberg, H.S., Meyer, J.H., McCann, S.,Arifuzzman, A.I., Houle, S., Vaccarino, F.J., 2001. Changes in regional brainglucose metabolism measured with positron emission tomography afterparoxetine treatment of major depression. Am. J. Psychiatry 158, 899–905.
Kumari, V., Mitterschiffthaler, M.T., Teasdale, J.D., Malhi, G.S., Brown, R.G., Giampie-tro, V., Brammer, M.J., Poon, L., Simmons, A., Williams, S.C., Checkley, S.A.,Sharma, T., 2003. Neural abnormalities during cognitive generation of affect intreatment-resistant depression. Biol. Psychiatry 54, 777–791.
Mayberg, H.S., Brannan, S.K., Tekell, J.L., Silva, J.A., Mahurin, R.K., McGinnis, S.,Jerabek, P.A., 2000. Regional metabolic effects of fluoxetine in major depres-sion: serial changes and relationship to clinical response. Biol. Psychiatry 48,830–843.
Macoveanu, J., 2014. Serotonergic modulation of reward and punishment: evidencefrom pharmacological fMRI studies. Brain Res. 1556, 19–27.
Murray, E.A., Wise, S.P., Drevets, D.C., 2011. Localization of dysfunction in majordepressive disorder: prefrontal cortex and amygdala. Biol. Psychiatry 69 (12),e43–e54.
Patton, G.C., Coffey, C., Romaniuk, H., Mackinnon, A., Carlin, J.B., Degenhardt, L.,Olsson, C.A., Moran, P., 2014. The prognosis of common mental disorders inadolescents: a 14-year prospective cohort study. Lancet 383, 1404–1411.
Phillips, M.L., Drevets, W.C., Rauch, S.L., Lane, R., 2003. Neurobiology of emotionperception I: the neural basis of normal emotion perception. Soc. Biol.Psychiatry 54, 504–514.
Plener, P.L., Grieb, J., Sproeber, N., Straub, J., Schneider, A., Keller, F., Koelch, M.G.,2012. Convergence of children's depression rating scale-revised scores andclinical diagnosis in rating adolescent depressive symptomatology. Ment. Illn. 4,29–31.
Rosenblau, G., Sterzer, P., Stoy, M., Park, S., Friedel, E., Heinz, A., Pilhatsch, M., Bauer, M.,Stroehle, A., 2012. Functional neuroanatomy of emotion processing in majordepressive disorder is altered after successful antidepressant therapy. J. Psycho-pharmacol. 26, 1424–1433.
Russo, S.J., Nestler, E.J., 2013. The brain reward circuitry in mood disorders. Nat. Rev.Neurosci. 14, 609–625.
Ryan, N.D., Williamson, D.E., Iyengar, S., Orvaschel, H., Reich, T., Dahl, R., Puig-Antich, J., 1992. A secular increase in child and adolescent onset affectivedisorder. J. Am. Acad. Child Adolesc. Psychiatry 31, 600–605.
Sheline, Y.I., Barch, D.M., Donnelly, J.M., Ollinger, J.M., Snyder, A.Z., Mintun, M.A.,2001. Increased amygdala response to masked emotional faces in depressedsubjects resolves with antidepressant treatment: an fMRI study. Biol. Psychiatry50, 651–658.
Siegle, G.J., Carter, C.S., Thase, M.E., 2006. Use of fMRI to predict recovery fromunipolar depression with cognitive behavior therapy. Am. J. Psychiatry 163,735–738.
Siegle, G.J., Thompson, W.K., Collier, A., Berman, S.R., Feldmiller, J., Thase, M.E.,Friedman, E.S., 2012. Toward clinically useful neuroimaging in depressiontreatment: prognostic utility of subgenual cingulate activity for determiningdepression outcome in cognitive therapy across studies, scanners, and patientcharacteristics. Arch. Gen. Psychiatry 69, 913–924.
Sproeber, N., Straub, J., Fegert, J., Koelch, M., 2012. Depression im Jugendalter:MICHI - Manual für die Gruppentherapie. Beltz, Weinheim.
Straub, J., Koelch, M.G., Fegert, J.M., Plener, P.L., Gonzalez-Aracil, I., Voit, A.,Sproeber, N., 2013. Innovations in practice: MICHI, a brief cognitive–behavioralgroup therapy for adolescents with depression – a pilot study of feasibility in aninpatient setting. Child Adolesc. Ment. Health 18, 247–250.
Straub, J., Sproeber, N., Plener, P.L., Fegert, J.M., Bonenberger, M., Koelch, M.G., 2014.A brief cognitive–behavioural group therapy programme for the treatment ofdepression in adolescent outpatients: a pilot study. Child Adolesc. PsychiatryMent. Health 8, 1–10.
Tahmasian, M., Knight, D.C., Manoliu, A., Schwerthoeffer, D., Scherr, M., Meng, C.,Shao, J., Peters, H., Doll, A., Khazaie, H., Drzezga, A., Baeuml, J., Zimmer, C.,Foerstl, H., Wohlschlaeger, A.M., Riedl, V., Sorg, C., 2013. Aberrant intrinsicconnectivity of hippocampus and amygdala overlap in the fronto-insular anddorsomedial-prefrontal cortex in major depressive disorder. Front. Hum.Neurosci. 7, 1–10.
Tao, R., Calley, C.S., Hart, J., Mayes, T.L., Nakonezny, P.A., Lu, H., Kennard, B.D.,Tamminga, C.A., Emslie, G.J., 2012. Brain activity in adolescent major depressivedisorder before and after fluoxetine treatment. Am. J. Psychiatry 169, 381–388.
Thomason, M.E., Hamilton, J.P., Gotlib, I.H., 2011. Stress-induced activation of theHPA axis predicts connectivity between subgenual cingulate and saliencenetwork during rest in adolescents. J. Child Psychol. Psychiatry 52, 1026–1034.
van Eijndhoven, P., van Wingen, G., Fernandez, G., Rijpkema, M., Pop-Purceleanu,M., Verkes, R.J., Buitelaar, J., Tendolkar, I., 2013. Neural basis of recollection infirst-episode major depression. Hum. Brain Mapp. 34, 283–294.
Yang, T.T., Simmons, A.N., Matthews, S.C., Tapert, S.F., Frank, G.K., Max, J.E., Bischoff-Grethe, A., Lansing, A.E., Brown, G., Strigo, I.A., Wu, J., Paulus, M.P., 2010.Adolescents with major depression demonstrate increased amygdala activation.J. Am. Acad. Child Adoelesc. Psychiatry 49, 42–49.
Yang, T.T., Simmons, A.N., Matthews, S.C., Tapert, S.F., Frank, G.K., Bischoff-Grethe, A.,Lansing, A.E., Wu, J., Brown, G.G., Paulus, M.P., 2009. Depressed adolescentsdemonstrate greater subgenual anterior cingulate activity. NeuroReport 20,440–444.
J. Straub et al. / Journal of Affective Disorders 183 (2015) 239–246246
Curriculum Vitae
150
7 Curriculum Vitae
Persönliche Daten
Name Straub
Vorname Joana
Staatsangehörigkeit deutsch
Werdegang
05/2015 Leitende Psychologin der Klinik für Kinder- und Jugendpsychiatrie/
Psychotherapie des Universitätsklinikums Ulm 11/2014 Stipendium des Deutschen Akademischen Austausch Dienstes zur
Durchführung einer Kongressreise
seit 10/2010 Wissenschaftliche Mitarbeiterin mit dem Ziel der Promotion
10/2010 - 05/2014
Ausbildung mit dem Abschluss der Approbation zur Kinder- und
Jugendlichenpsychotherapeutin, Ulm
10/2008 – 07/2010
Master in Psychologie, Universität Konstanz
Scientific articles published in peer-reviewed journals
151
8 Scientific articles published in peer-reviewed journals
Straub, J., Plener, P.L., Sproeber, N., Sprenger, L., Koelch, M.G., Groen, G. & Abler, B. (2015).
Neural correlates of successful psychotherapy of depression in adolescents. Journal of
Affective Disorders, 183, 239-246.
Straub, J., Plener, P.L., Keller, F., Fegert, J.M., Sproeber, N. & Koelch, M.G. (accepted). MICHI
– a brief, manualized cognitive behavioural group therapy for the treatment of depression
in adolescents: randomized controlled trial. Kindheit & Entwicklung.
Straub, J., Keller, F., Sproeber, N., Koelch, M.G. & Plener, P.L. (2015). Suicidal behavior in
German adolescents: prevalence and association with depressive and manic symptoms.
Zeitschrift für Kinder- und Jugendpsychiatrie und Psychotherapie, 43(1), 39-45.
Straub, J., Plener, P.L., Koelch, M.G. & Keller, F. (2014). Agreement between self-report and
clinician’s assessment in depressed adolescents, using the example of BDI-II and CDRS-R.
Zeitschrift für Kinder- und Jugendpsychiatrie und Psychotherapie, 42(4), 243-252.
Straub, J., Nicolaus, L., Plener, P.L., Sproeber, N. & Koelch, M.G. (2014). Psychotherapeutic
treatment of children and adolescents with depression. Review of the literature on cognitive-
behavioral and interpersonal group therapies. Der Psychotherapeut, 59, 7-15.
Straub, J., Sproeber, N., Plener, P.L., Fegert, J.M., Bonenberger, M. & Koelch, M.G. (2014). A
brief cognitive-behavioural group therapy programme for the treatment of depression in
adolescent outpatients: a pilot study. Child and adolescent psychiatry and mental health,
8(9), doi:10.1186/1753-2000-8-9
Straub, J., Koelch, M.G., Fegert, J.M., Plener, P.L., Gonzalez-Aracil, I., Voit, A. & Sproeber, N.
(2013). Innovations in Practice: MICHI, a brief cognitive-behavioural group therapy for
adolescents with depression - a pilot study of feasibility in an inpatient setting. Child and
Adolescent Mental Health, 18(4), 247-250.
Articles as a co-author:
Plener, P.L., Straub, J., Fegert, J.M. & Keller, F. (2015). Treatment of mental diseases in
children in German hospitals: analysis of frequencies in the years 2003 to 2012.
Nervenheilkunde, 34, 18-23.
Plener, P.L., Witt, A., Straub, J. & Fegert, J.M. (2013). Disruptive Mood Dysregulation
Disorder. Kinder- und Jugendmedizin, 13, 313 – 388.
Plener, P.L., Grieb, J., Sproeber, N., Straub, J., Schneider, A., Keller, F. & Koelch, M.G. (2012).
Convergence of children's depression rating scale-revised scores and clinical diagnosis in
rating adolescent depressive symptomatology. Mental Illness, 4(e7), 29-31.
Scientific articles published in peer-reviewed journals
152
Plener, P.L., Straub, J., Kapusta, N.D., Fegert, J.M. & Sproeber, N. (2012). Assessment of
suicidal ideation in adolescents: comparison of two instruments. Praxis der
Kinderpsychologie und Kinderpsychiatrie, 61, 4-15.
Book:
Sproeber, N., Straub, J., Fegert, J.M., & Koelch, M.G. (2012). Depression im Jugendalter:
MICHI- Manual für die Gruppentherapie. Weinheim: Beltz.
Contributions to conventions:
Symposia:
Straub, J., Plener, P.L., Sproeber, N., Koelch, M.G., Groen, G. & Abler, B. (March, 2015).
Neural correlates of successful psychotherapy of depression in adolescents. 34. Kongress der
Deutschen Gesellschaft für Kinder- und Jugendpsychiatrie, Psychosomatik und
Psychotherapie (DGKJP), München.
Straub, J., Plener, P.L., Sproeber, N., Koelch, M.G., Groen, G. & Abler, B. (August, 2014).
Effects of a psychotherapy for the treatment of depressed adolescents, on neural substrates
(fMRI). 21st World Congress of the International Association for Child and Adolescent
Psychiatry and Allied Professions (IACAPAP), Durban, South Africa.
Straub, J., Plener, P.L., Sproeber, N., Koelch, M.G., Groen, G. & Abler, B. (December, 2013).
Zusammenhang von neuronalen Korrelaten (fMRT) und Effekten einer psychothera-
peutischen Gruppenintervention bei Jugendlichen mit depressiver Symptomatik. XX.
wissenschaftliche Tagung des Arbeitskreis Biologische Kinder- und Jugendpsychiatrie,
Psychosomatik und Psychotherapie, Köln.
Straub, J., Sproeber, N., Bonenberger, M., Plener, P.L., Fegert, J.M. & Koelch, M.G. (July,
2013). Evaluation of a manualised, psychosocial intervention programme for depressed
adolescents: pilot study results of outpatients and inpatients. The 15th international congress
of the European Society for Child and Adolescent Psychiatry (ESCAP), Dublin.
Straub, J., Sproeber, N., Plener, P.L., Fegert, J.M. & Koelch, M.G. (March, 2013). MICHI –
Evaluation eines manualisierten, psychosozialen Interventionsprogramms für Jugendliche
mit depressiven Symptomen in einer Pilotstudie. 33. Kongress der Deutschen Gesellschaft für
Kinder- und Jugendpsychiatrie, Psychosomatik und Psychotherapie (DGKJP), Rostock.
Keller, F. & Straub, J. (March, 2013). Die deutsche Version des CDRS-R: Faktorielle Struktur
und Korrelation zur selbstberichteten Depressivität. Vortrag auf dem 33. Kongress der
deutschen Gesellschaft für Kinder- und Jugendpsychiatrie, Psychosomatik und
Psychotherapie (DGKJP), Rostock.
Scientific articles published in peer-reviewed journals
153
Poster presentations:
Straub, J., Plener, P.L., Keller, F., Fegert, J.M., Sproeber, N. & Koelch, M.G. (November,
2014). Randomisierte, kontrollierte Studie zur Erfassung der Wirksamkeit einer
manualisierten, kognitiv-behavioralen Gruppen-Kurzzeitpsychotherapie zur Behandlung von
Depressionen bei Jugendlichen. Kongress der Deutschen Gesellschaft für Psychiatrie und
Psychotherapie, Psychosomatik und Nervenheilkunde (DGPPN), Berlin.
Sosic-Vasic, Z., Abler, B., Groen, G., Sproeber, N., Sprenger, L., Koelch, M.G., Plener, P.L. &
Straub, J. (November, 2014). Baseline brain perfusion following a five-week CBT group
intervention in adolescents with major depression disorder. Deutsche Gesellschaft für
Psychiatrie und Psychotherapie, Psychosomatik und Nervenheilkunde (DGPPN), Berlin.
Straub, J., Plener, P.L., Sproeber, N., Sprenger, L., Koelch, M.G., Kammer, T., Groen, G. &
Abler, B. (November, 2014). Neural correlates of successful psychotherapy of depression in
adolescents. Society for Neuroscience, Washington DC, United States of America.
Koelch, M.G., Straub, J., Plener, P.L., Sproeber, N., & Abler, B. (October, 2014). Neural
correlates of successful psychotherapy of depression in adolescents. American Academy of
Child and Adolescent Psychiatry’s 61st Annual Meeting, San Diego.
Straub, J., Plener, P.L., Sproeber, N., Sprenger, L., Koelch, M.G., Groen, G. & Abler, B. (June,
2014). Neural correlates of successful psychotherapy of depression in adolescents. Congress
of Human Brain Mapping (HBM), Hamburg.
Straub, J., Plener, P.L., Sproeber, N., Koelch, M.G. & Abler, B. (November, 2013).
Untersuchung von Therapieeffekten auf die cerebrale Aktivität des Belohnungssystems
mittels funktioneller Magnetresonanztomographie (fMRT) bei Jugendlichen mit depressiver
Symptomatik. Kongress der Deutschen Gesellschaft für Psychiatrie und Psychotherapie,
Psychosomatik und Nervenheilkunde (DGPPN), Berlin.




















