
Depression and Incident Alzheimer Disease: The Impact of Disease Severity
11
Depression and Incident Alzheimer Disease: The Impact of Disease Severity Patricia Gracia-García, M.D., Ph.D., Concepción de-la-Cámara, M.D., Ph.D., Javier Santabárbara, M.Stat., Raúl Lopez-Anton, Ph.D., Miguel Angel Quintanilla, M.D., Ph.D., Tirso Ventura, M.D., Ph.D., Guillermo Marcos, M.D., Ph.D., Antonio Campayo, M.D., Pedro Saz, M.D., Ph.D., Constantine Lyketsos, M.D., M.H.S., Antonio Lobo, M.D., Ph.D. Objectives: To test the hypothesis that clinically significant depression (particularly severe depression) increases the risk of Alzheimer's disease (AD). Methods: A longi- tudinal, three-wave epidemiologic study was implemented in a sample of individuals aged 55 years and older (n ¼ 4,803) followed up at 2.5 years and 4.5 years. This was a population-based cohort drawn from the Zaragoza Dementia and Depression (ZARADEMP) Project, in Zaragoza, Spain. Participants included individuals cogni- tively intact at baseline (n ¼ 3,864). The main outcome measures were depression as assessed by using the diagnostic interview Geriatric Mental State- Automated Geri- atric Examination for Computer Assisted Taxonomy package; and AD diagnosed by a panel of research psychiatrists according to Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition, criteria. The Fine and Gray multivariate regression model was used in the analysis, accounting for mortality. Results: At baseline, clin- ically significant depression was diagnosed in 452 participants (11.7%); of these, 16.4% had severe depression. Seventy incident cases of AD were found at follow-up. Compared with nondepressed individuals, the incidence rate of AD was significantly higher in the severely depressed subjects (incidence rate ratio: 3.59 [95% confidence interval: 1.30e9.94]). A consistent, significant association was observed between severe depression at baseline and incident AD in the multivariate model (hazard ratio: 4.30 [95% CI: 1.39e13.33]). Untreated depression was associated with incident AD in the unadjusted model; however, in the final model, this association was attenuated and nonsignificant. Conclusions: Severe depression increases the risk of AD, even after controlling for the competing risk of death. (Am J Geriatr Psychiatry 2013; -:-e-) Received October 9, 2012; revised February 5, 2013; accepted February 15, 2013. From the Psychiatry Service, Hospital Clínico Universitario (CDC, MAQ, AC, AL), Zaragoza, Spain; Department of Medicine and Psychiatry, Universidad de Zaragoza (PG-G, CDC, TV, AC, PS, AL), Zaragoza, Spain; Centro de Investigación Biom edica en Red de Salud Mental (CIBERSAM), Ministry of Science and Innovation (CDC, JS, RL-A,GM, AC, PS, AL), Madrid, Spain; Instituto Aragon es de Ciencias de la Salud (I+CS) (CDC, AC, AL), Zaragoza, Spain; Department of Preventive Medicine and Public Health, Universidad de Zaragoza (JS, GM), Zaragoza, Spain; Department of Psychology and Sociology, Universidad de Zaragoza (RL-A), Zaragoza, Spain; Psychiatry Service, Hospital Universitario Miguel Servet (TV), Zaragoza, Spain; Medical Records Service, Hospital Clínico Universitario (GM), Zaragoza, Spain; and Johns Hopkins University, Johns Hopkins Bayview Medical Center (CL), Baltimore, Maryland. Send correspondence and reprint requests to Antonio Lobo, M.D., Ph.D., Servicio de Psiquiatría, Hospital Clínico Universitario, Planta 3, Avd. San Juan Bosco, 15, 50009 Zaragoza, Spain. e-mail: [email protected] Ó 2013 American Association for Geriatric Psychiatry http://dx.doi.org/10.1016/j.jagp.2013.02.011 Am J Geriatr Psychiatry -:-, - 2013 1
-
Upload
independent -
Category
Documents
-
view
1 -
download
0
Transcript of Depression and Incident Alzheimer Disease: The Impact of Disease Severity

Depression and Incident AlzheimerDisease: The Impact of Disease Severity
Patricia Gracia-García, M.D., Ph.D., Concepción de-la-Cámara, M.D., Ph.D.,Javier Santabárbara, M.Stat., Raúl Lopez-Anton, Ph.D.,
Miguel Angel Quintanilla, M.D., Ph.D., Tirso Ventura, M.D., Ph.D.,Guillermo Marcos, M.D., Ph.D., Antonio Campayo, M.D., Pedro Saz, M.D., Ph.D.,
Constantine Lyketsos, M.D., M.H.S., Antonio Lobo, M.D., Ph.D.
Received Octobe(CDC, MAQ, ACZaragoza, SpainRL-A,GM, AC, PPreventive MediUniversidad de ZRecords Service,Center (CL), BaltClínico Universi
� 2013 Amehttp://dx.d
Am J Geriatr Ps
Objectives: To test the hypothesis that clinically significant depression (particularly
severe depression) increases the risk of Alzheimer's disease (AD). Methods: A longi-
tudinal, three-wave epidemiologic study was implemented in a sample of individuals
aged 55 years and older (n ¼ 4,803) followed up at 2.5 years and 4.5 years. This was
a population-based cohort drawn from the Zaragoza Dementia and Depression
(ZARADEMP) Project, in Zaragoza, Spain. Participants included individuals cogni-
tively intact at baseline (n ¼ 3,864). The main outcome measures were depression as
assessed by using the diagnostic interview Geriatric Mental State- Automated Geri-
atric Examination for Computer Assisted Taxonomy package; and AD diagnosed by
a panel of research psychiatrists according to Diagnostic and Statistical Manual ofMental Disorders, Fourth Edition, criteria. The Fine and Gray multivariate regression
model was used in the analysis, accounting for mortality. Results: At baseline, clin-ically significant depression was diagnosed in 452 participants (11.7%); of these,
16.4% had severe depression. Seventy incident cases of AD were found at follow-up.
Compared with nondepressed individuals, the incidence rate of AD was significantly
higher in the severely depressed subjects (incidence rate ratio: 3.59 [95% confidence
interval: 1.30e9.94]). A consistent, significant association was observed between
severe depression at baseline and incident AD in the multivariate model (hazard
ratio: 4.30 [95% CI: 1.39e13.33]). Untreated depression was associated with incident
AD in the unadjusted model; however, in the final model, this association was
attenuated and nonsignificant. Conclusions: Severe depression increases the risk of
AD, even after controlling for the competing risk of death. (Am J Geriatr Psychiatry2013; -:-e-)
r 9, 2012; revised February 5, 2013; accepted February 15, 2013. From the Psychiatry Service, Hospital Clínico Universitario, AL), Zaragoza, Spain; Department of Medicine and Psychiatry, Universidad de Zaragoza (PG-G, CDC, TV, AC, PS, AL),; Centro de Investigación Biom�edica en Red de Salud Mental (CIBERSAM), Ministry of Science and Innovation (CDC, JS,S, AL), Madrid, Spain; Instituto Aragon�es de Ciencias de la Salud (I+CS) (CDC, AC, AL), Zaragoza, Spain; Department ofcine and Public Health, Universidad de Zaragoza (JS, GM), Zaragoza, Spain; Department of Psychology and Sociology,aragoza (RL-A), Zaragoza, Spain; Psychiatry Service, Hospital Universitario Miguel Servet (TV), Zaragoza, Spain; MedicalHospital Clínico Universitario (GM), Zaragoza, Spain; and Johns Hopkins University, Johns Hopkins Bayview Medicalimore, Maryland. Send correspondence and reprint requests to Antonio Lobo, M.D., Ph.D., Servicio de Psiquiatría, Hospitaltario, Planta 3, Avd. San Juan Bosco, 15, 50009 Zaragoza, Spain. e-mail: [email protected] Association for Geriatric Psychiatryoi.org/10.1016/j.jagp.2013.02.011
ychiatry -:-, - 2013 1

2
Depression and Incident Alzheimer’s Disease
Key Words: Risk factor, depression, Alzheimer’s disease, incidence
he epidemic nature of both Alzheimer disease
T(AD) and depression in the elderly poses majorpublic health problems,1,2 and the complex relation-ships between the two conditions have been empha-sized.3 The most consistent risk factors for dementiaand AD are age1 and apoliprotein E genotype.4 Poten-tially modifiable risk factors have also been reported,such as vascular risk factors5 and possibly dietary andlifestyle factors6 or low educational background.7,8Several reports have also suggested that depression isa risk factor for AD,9e11 and a meta-analysis estimatedan odds ratio of 1.90 (95% confidence interval (CI):1.55e2.33).12 However, some studies found no associ-ation between these conditions,13,14 and some authorshave suggested that depressive symptoms may be anearly manifestation rather than a risk factor for AD.15
These inconsistencies reflect variation in severalfactors, such as length of observation, rate of follow-up participation, potentially modifying variablescontrolled for, and/or the approach to assessment ofboth depression and AD.9 Furthermore, most previousstudies on the association between depression and ADused nonoptimalmethods to assess depression, such assymptom-based scales,9,10,13,14,16,17 and therefore donot provide enough information on a relevant clinicalsubject such as treatable depression.
Few studies have assessed whether characteristicsof depression affect the risk of AD, and those thathave, produced rather unexpected results. Fuhreret al.16 reported an increased risk of AD in treated, asopposed to untreated, depression. Becker et al.14
found that persistent depression did not increase therisk for AD, and aDutch study found an increased riskof AD only in those with a history of early-onsetdepression.13 Because clinically significant, severedepression reportedly increases the risk of all-causedementia,18,19 it is important to examine for associa-tion specifically with AD. Furthermore, some studiesreporting a positive association between depressivesymptoms and AD show a linear increase of risk withthe number of symptoms.9,11
In light of inconclusive evidence, we tested thehypothesis that clinically significant depression
(severe depression in particular) increases the risk ofAD by studying a general population cohort.Depression and AD were diagnosed according tostandardized clinical criteria. As death may preventthe occurrence of AD in the aged population,a competing risk regression model was used, which isa novelmethod in this area of research. In addition, weexamined the effect of the following characteristics ofdepression as predictors of AD: first-ever depression,persistent depression, and untreated depression.
METHODS
Design Overview and Study Population
The sample for the current study was drawnfrom the Zaragoza Dementia and Depression(ZARADEMP) Project,7,20 a longitudinal three-waveepidemiologic study, conducted in Zaragoza, Spain,that estimated the incidence and risk factors fordementia and depression, as well as their link togeneral medical morbidity, in the adult populationaged 55 years or older. The Declaration of Helsinkiprinciples of written informed consent, privacy, andconfidentiality have been maintained throughout theproject. The ethics committee of the University ofZaragoza and the Fondo de Investigación Sanitariaapproved the project according to Spanish law.
A random sample of community-dwelling elderlysubjects, stratified with proportional allocation byage and gender, was drawn from the 1991 census.Sample size was driven by the project’s main objec-tive, which was to study risk factors for incidentdementia, taking in account information on attritionfrom a previous Zaragoza study.8 At enrollment, therefusal rate was 20.5%; 4,803 individuals were ulti-mately interviewed at baseline (Wave I, 1994). Indi-viduals with all-cause dementia were excluded fromfollow-up evaluations (Wave II, 1997; Wave III, 1999).To include in the follow-up cohort only cognitivelyintact individuals, stringent criteria were applied.Subjects with “subsyndromal” dementia (defined in
Am J Geriatr Psychiatry -:-, - 2013
Gracia-García et al.
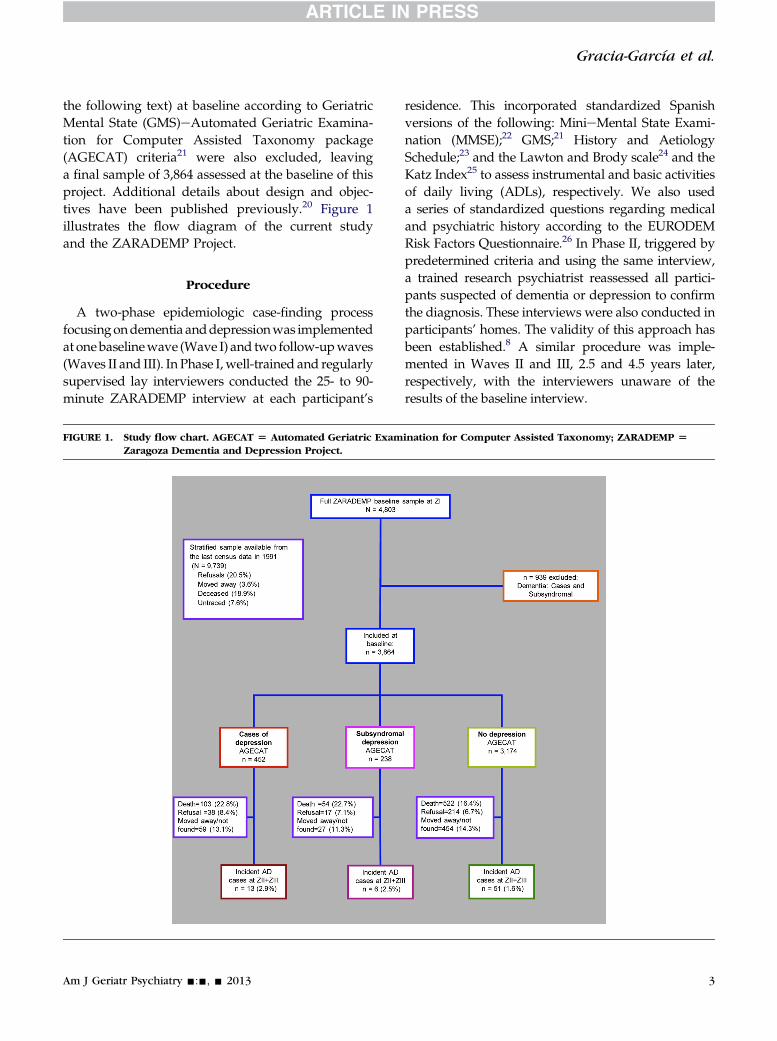
the following text) at baseline according to GeriatricMental State (GMS)eAutomated Geriatric Examina-tion for Computer Assisted Taxonomy package(AGECAT) criteria21 were also excluded, leavinga final sample of 3,864 assessed at the baseline of thisproject. Additional details about design and objec-tives have been published previously.20 Figure 1illustrates the flow diagram of the current studyand the ZARADEMP Project.
Procedure
A two-phase epidemiologic case-finding processfocusingondementia anddepressionwas implementedat onebaselinewave (Wave I) and two follow-upwaves(Waves II and III). In Phase I,well-trained and regularlysupervised lay interviewers conducted the 25- to 90-minute ZARADEMP interview at each participant’s
FIGURE 1. Study flow chart. AGECAT [ Automated Geriatric ExamZaragoza Dementia and Depression Project.
Am J Geriatr Psychiatry -:-, - 2013
residence. This incorporated standardized Spanishversions of the following: MinieMental State Exami-nation (MMSE);22 GMS;21 History and AetiologySchedule;23 and the Lawton and Brody scale24 and theKatz Index25 to assess instrumental and basic activitiesof daily living (ADLs), respectively. We also useda series of standardized questions regarding medicaland psychiatric history according to the EURODEMRisk Factors Questionnaire.26 In Phase II, triggered bypredetermined criteria and using the same interview,a trained research psychiatrist reassessed all partici-pants suspected of dementia or depression to confirmthe diagnosis. These interviews were also conducted inparticipants’ homes. The validity of this approach hasbeen established.8 A similar procedure was imple-mented in Waves II and III, 2.5 and 4.5 years later,respectively, with the interviewers unaware of theresults of the baseline interview.
ination for Computer Assisted Taxonomy; ZARADEMP [
3

TABLE 1. Characteristics of Participants at Baseline Accordingto Depression Status
NoDepression(n [ 3,174)
SubsyndromalDepression(n [ 238)
Depression(n [ 452)
Age, years 71.5 (8.9) 73.6 (9.3)a 73.5 (9.4)b
Female 1,576 (49.7) 168 (70.6)a 359 (79.4)b,c
EducationPrimary school 2,346 (74.5) 185 (77.7) 359 (80.3)High school orhigher
578 (19.0) 33 (13.9) 46 (10.3)a
MMSE 27.5 (2.4) 27 (2.0)a 26.6 (2.8)b,c
DisabilityBasic ADLs 159 (5) 30 (12.6)a 61 (13.5)b
Instrumental ADLs 313 (9.9) 37 (15.6)a 104 (23.2)b,c
Vascular risk factorsHypertension 1,974 (67.5) 146 (68.2) 299 (69.7)Diabetes 358 (11.4) 40 (17.1)a 73 (16.2)b
Vascular disease 339 (11.0) 33 (14.3)a 64 (15.0)b
Notes:Data are given asmean (standarddeviation) or number (%).ADLs ¼ activities of daily living; MMSE ¼ MinieMental State
Examination.aSignificant differences (p <0.05) between “subsyndromal
depression” and “no cases” of depression in either t (df ¼ 3,410)test or c2 (df ¼ 1) test.
bSignificant differences (p <0.05) between “cases” of depressionand “no cases” of depression in either t (df ¼ 3,624) test or c2
(df ¼ 1) test.cSignificant differences (p <0.05) between “cases” of depression
and “subsyndromal depression” in either t (df ¼ 688) test or c2
(df ¼ 1) test.
Depression and Incident Alzheimer’s Disease
Clinical Measurements
The diagnosis of depression was based on thestaged GMS-AGECAT approach. This is a validapproach for the detection of “depression requiringclinical attention” in community samples.2 Aftersymptom assessment (Stage I), a diagnosis ofdepression emerged from Stage II. In this stage,a computer program compares syndrome clusters(e.g., dementia, depression, anxiety) to reach a finaldiagnosis, recorded as either a diagnostic “sub-syndromal” (confidence levels 1 and 2) or a diagnostic“case” (confidence levels �3). AGECAT “caseness”implies the “desirability of intervention.”2,27 Further-more, “cases” of depression are classified as “severedepression” (which includes melancholic symptoms)and “nonsevere depression.” Subsyndromal in thissystem implies that the psychopathologic symptomsare not severe enough to merit an intervention.Information from the History and Aetiology Schedulewas used to define onset of depression, and use ofantidepressant treatment (classified according to theAnatomical Therapeutic Chemical Classificationsystem28 codes N06A* and/or N06C1A). Depressionwas defined as persistent if it was present at baselineand the first follow-up evaluation (Wave II).
For the diagnosis of dementia, assessments werecomplemented by medical reports and laboratorydata, that most people in Spain keep at home. Outsidecaregivers were interviewedwhen the participant wasconsidered to be unreliable (in “cases” of dementiaand approximately 10% of subsyndromal dementia).Participants were considered “probable cases” on thebasis of a GMS threshold “global” score (1/2) and/orMMSE (23/24) standard cutoff points. The Hachinskiscale29 and a neurologic examination were used in thediagnostic process to differentiate AD from othercauses of dementia (e.g., vascular dementia). Thevalidity of this process has been established previ-ously.8 Identified cases of dementia were presented toa panel of 4 research psychiatrists who made the finaldiagnosis. Variables in the ZARADEMP interviewwere operationalized to conform to the Diagnostic andStatistical Manual of Mental Disorders, Fourth Edition,criteria used to diagnose cases; for a diagnosis of“incident” dementia and “type of dementia” (AD,other), agreement by at least three of the four psychi-atrists was required. To document the accuracy of thepanel diagnosis of dementia, individuals considered
4
to be cases of AD by the panel were invited fora hospital diagnostic evaluation, which includedneuroimaging and a complete neuropsychologicaldiagnostic battery; National Institute of Neurologicaland Communicative Diseases and Stroke/Alz-heimer’s Disease and Related Disorders Associationcriteria30 were then used to diagnose AD. Only 15subjects diagnosed as having AD by the panel ofresearch psychiatrists accepted the invitation, and thediagnosis of AD was confirmed in 13 (86.7%).7
Potential confounders assessed at baseline includeddemographic variables, MMSE score, functionaldisability, and vascular risk factors or diseases. Thevariable “education” was categorized into threelevels: none, primary school, and secondary school orhigher. The Katz Index (basic ADLs)25 and theLawton and Brody Scale (instrumental ADLs) 24 weredichotomized, distinguishing between some disability(disability for at least one ADL) and no disability. Thepresence of vascular risk factors (hypertension, dia-betes) and/or diseases was based on the medicalhistory obtained by using the EURODEMRisk Factors
Am J Geriatr Psychiatry -:-, - 2013
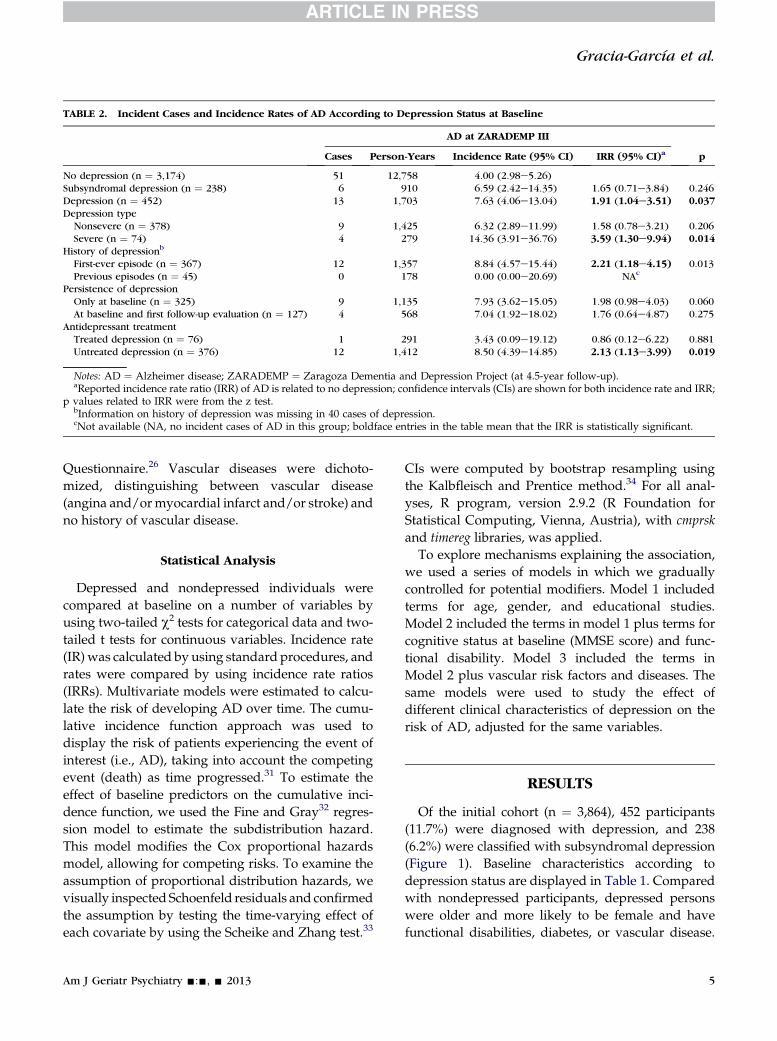
TABLE 2. Incident Cases and Incidence Rates of AD According to Depression Status at Baseline
AD at ZARADEMP III
pCases Person-Years Incidence Rate (95% CI) IRR (95% CI)a
No depression (n ¼ 3,174) 51 12,758 4.00 (2.98e5.26)Subsyndromal depression (n ¼ 238) 6 910 6.59 (2.42e14.35) 1.65 (0.71e3.84) 0.246Depression (n ¼ 452) 13 1,703 7.63 (4.06e13.04) 1.91 (1.04e3.51) 0.037Depression type
Nonsevere (n ¼ 378) 9 1,425 6.32 (2.89e11.99) 1.58 (0.78e3.21) 0.206Severe (n ¼ 74) 4 279 14.36 (3.91e36.76) 3.59 (1.30e9.94) 0.014
History of depressionb
First-ever episode (n ¼ 367) 12 1,357 8.84 (4.57e15.44) 2.21 (1.18e4.15) 0.013Previous episodes (n ¼ 45) 0 178 0.00 (0.00e20.69) NAc
Persistence of depressionOnly at baseline (n ¼ 325) 9 1,135 7.93 (3.62e15.05) 1.98 (0.98e4.03) 0.060At baseline and first follow-up evaluation (n ¼ 127) 4 568 7.04 (1.92e18.02) 1.76 (0.64e4.87) 0.275
Antidepressant treatmentTreated depression (n ¼ 76) 1 291 3.43 (0.09e19.12) 0.86 (0.12e6.22) 0.881Untreated depression (n ¼ 376) 12 1,412 8.50 (4.39e14.85) 2.13 (1.13e3.99) 0.019
Notes: AD ¼ Alzheimer disease; ZARADEMP ¼ Zaragoza Dementia and Depression Project (at 4.5-year follow-up).aReported incidence rate ratio (IRR) of AD is related to no depression; confidence intervals (CIs) are shown for both incidence rate and IRR;
p values related to IRR were from the z test.bInformation on history of depression was missing in 40 cases of depression.cNot available (NA, no incident cases of AD in this group; boldface entries in the table mean that the IRR is statistically significant.
Gracia-García et al.
Questionnaire.26 Vascular diseases were dichoto-mized, distinguishing between vascular disease(angina and/ormyocardial infarct and/or stroke) andno history of vascular disease.
Statistical Analysis
Depressed and nondepressed individuals werecompared at baseline on a number of variables byusing two-tailed c2 tests for categorical data and two-tailed t tests for continuous variables. Incidence rate(IR) was calculated by using standard procedures, andrates were compared by using incidence rate ratios(IRRs). Multivariate models were estimated to calcu-late the risk of developing AD over time. The cumu-lative incidence function approach was used todisplay the risk of patients experiencing the event ofinterest (i.e., AD), taking into account the competingevent (death) as time progressed.31 To estimate theeffect of baseline predictors on the cumulative inci-dence function, we used the Fine and Gray32 regres-sion model to estimate the subdistribution hazard.This model modifies the Cox proportional hazardsmodel, allowing for competing risks. To examine theassumption of proportional distribution hazards, wevisually inspected Schoenfeld residuals and confirmedthe assumption by testing the time-varying effect ofeach covariate by using the Scheike and Zhang test.33
Am J Geriatr Psychiatry -:-, - 2013
CIs were computed by bootstrap resampling usingthe Kalbfleisch and Prentice method.34 For all anal-yses, R program, version 2.9.2 (R Foundation forStatistical Computing, Vienna, Austria), with cmprskand timereg libraries, was applied.
To explore mechanisms explaining the association,we used a series of models in which we graduallycontrolled for potential modifiers. Model 1 includedterms for age, gender, and educational studies.Model 2 included the terms in model 1 plus terms forcognitive status at baseline (MMSE score) and func-tional disability. Model 3 included the terms inModel 2 plus vascular risk factors and diseases. Thesame models were used to study the effect ofdifferent clinical characteristics of depression on therisk of AD, adjusted for the same variables.
RESULTS
Of the initial cohort (n ¼ 3,864), 452 participants(11.7%) were diagnosed with depression, and 238(6.2%) were classified with subsyndromal depression(Figure 1). Baseline characteristics according todepression status are displayed in Table 1. Comparedwith nondepressed participants, depressed personswere older and more likely to be female and havefunctional disabilities, diabetes, or vascular disease.
5

TABLE 3. Risk of Alzheimer Disease in Clinical Significant Depression According to Characteristics of Depression
Model 0 Model 1 Model 2 Model 3
HR 95% CI p HR 95% CI p HR 95% CI p HR 95% CI p
Depressiona 1.82 0.97e3.42 0.062 1.22 0.65e2.32 0.540 1.13 0.58e2.18 0.710 1.11 0.57e2.15 0.750Subsyndromal depressiona 1.68 0.72e3.92 0.230 1.14 0.48e2.67 0.770 1.21 0.50e2.91 0.700 1.23 0.50e3.02 0.640Type of depressionSevere depressiona 3.63 1.32e9.96 0.013 4.08 1.44e11.53 0.008 4.07 1.34e12.34 0.013 4.30 1.39e13.33 0.011Nonsevere depressiona 1.46 0.69e3.08 0.320 0.91 0.43e1.93 0.800 0.83 0.38e1.81 0.640 0.81 0.37e1.76 0.590
History of depressionFirst-ever episodea 2.09 1.09e4.02 0.027 1.32 0.67e2.58 0.420 1.20 0.59e2.41 0.620 1.20 0.60e2.40 0.610Previous episodesa NAb NAb NAb NAb
Persistence of depressionDepression at baseline and first follow-up evaluationa 1.78 0.84e3.75 0.130 1.15 0.55e2.49 0.710 1.03 0.48e2.22 0.940 1.02 0.47e2.21 0.960Depression only at baselinea 2.13 0.77e5.91 0.150 1.55 0.54e4.51 0.420 1.54 0.52e4.58 0.440 1.53 0.54e4.39 0.420
Antidepressant treatmentUntreated depressiona 2.04 1.06e3.92 0.033 1.23 0.63e2.40 0.540 1.13 0.57e2.26 0.730 1.51 0.21e10.98 0.740Treated depressiona 1.02 0.14e7.44 0.990 1.66 0.22e12.42 0.620 1.51 0.20e11.19 0.690 1.12 0.56e2.23 0.680
Notes: Fine and Gray regression model, hazard ratios (HR), confidence intervals (CIs), and p values based on “normal approximation” of Wald c2 test with 1 df are shown for allvariables analyzed.
aReported risk of AD is related to no depression; boldface entries in the table mean that the HR is statistically significant; Model 0: bivariate analysis; Model 1: included terms forage, gender, and educational studies; Model 2: included the terms in model 1 plus terms for cognitive status at baseline (MinieMental State Examination score) and functionaldisability; Model 3: included the terms in model 2 plus vascular risk factors and diseases. Vascular disease includes history of angina and/or myocardial infarction and/or stroke.
bNot available (NA; no incident cases of AD were found in the group of depressed subjects with previous episodes of depression).
6Am
JGeriatr
Psych
iatry-:-,-
2013
Depressio
nandIncid
entAlzheim
er’sDise
ase

Gracia-García et al.
Depressed participants were less educated and per-formed worse cognitively. Compared with subjectswith subsyndromal depression, depressed partici-pants were more likely to be female and performworse cognitively.
Among those classified as depressed, 16.4% atbaseline (n ¼ 74) had severe depression; 9.9% (n ¼ 45)had history of depression, and 16.8% (n ¼ 76) weretaking antidepressant medication. At the first wavefollow-up (Wave II), 28.1% (n ¼ 127) continued to bedepressed (persistent depression) (Table 2). Seventyincident cases of AD were found at Wave II (n ¼3,237 interviewed) and Wave III (n ¼ 2,403). Person-years of follow-up are also shown. Mean (standarddeviation) age of incident cases of AD when diag-nosed was 86.5 (6.9) years. At baseline, as expected,mean age of individuals who eventually developedAD (83.7 [7.1] years) was higher than in the subjectswho did not develop AD (70.0 [7.8] years), thedifferences being statistically significant (t ¼ 14.58,df ¼ 3,862, p <0.001). Thirteen (18.6%) of all the casesof dementia occurred in individuals with depressionat baseline. When compared with the IR of ADamong the nondepressed participants, the IR washigher in subsyndromal depression and was almostdouble and significantly higher in cases of depression(IRR: 1.91 [95% CI: 1.04e3.51]).
Table 2 also shows that, compared with thenondepressed subjects, the IR of AD was high amongcases of nonsevere depression but was particularlyhigh among the severe cases (IRR: 3.59 [95% CI:1.30e9.94]). When compared with their counterparts,the IR of AD was higher among the cases of first-everdepression, nonpersistent depression, or untreateddepression, but the differences were not statisticallysignificant. However, when compared with thenondepressed subjects, the IR was significantlyhigher among the cases of both first-ever depressionand untreated depression.
In the Fine and Gray multivariate regressionmodel, the association between clinically significantdepression at baseline and incident AD was close tostatistical significance in the unadjusted model butwas attenuated in multivariate models (Table 3).However, and contrary to nonsevere depression,a consistent, significant association was observedbetween severe depression at baseline and incidentAD (in Model 3, hazard ratio [HR]: 4.30 [95% CI:1.39e13.33]).
Am J Geriatr Psychiatry -:-, - 2013
Table 3 also shows HRs for the development of ADin relation to other characteristics of depression. In theunadjusted model, both first-ever depression anduntreated depression were significantly associatedwith AD. However, in the final multivariate model,these associations were attenuated. Persistent depres-sion was not associated with AD.
CONCLUSIONS
This 5-year longitudinal study of community-dwelling adults aged 55 years or older supports thehypothesis that clinically significant, severe depres-sion increases the risk of AD. The IR of AD wasalmost double in subjects with clinically significant,overall depression when compared with the nonde-pressed subjects and was almost four times higher incases of severe depression. Although the IR was alsohigher in cases of nonsevere depression, the differ-ences were not statistically significant. It is conceiv-able that age at baseline has influenced the results,because we have shown, as expected, that mean ageof individuals who eventually developed AD wassignificantly higher than in the subjects who did notdevelop AD. Similarly, cognitive status at baselinemight have influenced the results: we observed thatthe mean MMSE score at baseline for subjectsdeveloping AD (24.6 [2.2]) was also significantlylower than in subjects nondemented at follow-up(27.7 [2.6]; t ¼ 9.91; df ¼ 3,862; p <0.001). However,and importantly, when controlling in the Fine andGray regression model for age and MMSE at base-line, as well as for other accepted risk factors of ADsuch as gender, educational level, functionaldisability, and vascular risk factors, and contrary tononsevere depression, severe depression was associ-ated with an increased risk of AD (HR: 4.30 [95% CI:1.39e13.33]). Furthermore, in support of the impactof depression severity on the increased risk of AD,subjects with severe depression (mean age: 71.1 [8.1]years) were significantly younger at baseline thansubjects with nonsevere depression (mean age: 74.1[9.5] years; t ¼ 2.54; df ¼ 450; p ¼ 0.011). However,the increased risk was only observed in the severelydepressed subjects.
It might be argued that only 4 cases of severedepression developed AD but, in fact, 74 such caseswere followed up, amounting to 279 person-years.
7

Depression and Incident Alzheimer’s Disease
Furthermore, and contrary to previous similarstudies, this may be the first report using a competingrisk model in studying depression as a risk factor forAD. Traditional models (e.g., Kaplan-Meier and Coxregression) do not take into account competing risksand may overestimate the risk of the disease (AD) inthe presence of high rates of mortality, because deathprevents the occurrence of the event of interest. Inview of the expected high mortality in the elderly, thecompeting risk approach to accurately determiningdisease risk for individuals in this age group ispreferred.35 This approach is particularly relevant instudying the outcome of depression in the elderly,because depression in this age group has beenassociated with increased mortality36 as previouslyreported in this same population.37
Some recent reports have documented the associ-ation between depression and all-cause dementia,38,39
and some found a specific association for severeforms of depression.18,19 However, these reports didnot specifically address the association with AD.Although the relationship between depression andAD has been addressed previously, most studiesused symptom-based scales and different thresholdlevels to identify depression, and the results wereinconsistent. Devanand et al.11 documented anincreased risk of AD for depression measured withthe Hamilton Depression Rating Scale, and similarresults were reported by Wilson et al.9 Saczynskiet al.10 and Li et al.40 using the Center for Epidemi-ologic Studies Depression Scale. In contrast, Beckeret al.14 found no significant association when usingthis same scale, and both Fuhrer et al.16 and DalForno et al.17 used the same instrument and foundthat the increased risk of AD was limited to men.
According to the AGECAT diagnostic criteria ofdepression, this study has advantages over previousstudies, as “caseness” implies the “desirability ofintervention.”2 A previous, 4.5-year follow-up studyin Zaragoza37 supports using this system in theassessment of community elderly because it was ableto predict mortality. Although agreement betweenAGECAT and DSM criteria for depression is onlymoderate,27 cases of depression considered to be“severe” according toAGECAT criteriamaybe similarto those considered “major” by some investigators.41
Geerlings et al.42 found an association betweendepression documented with GMS-AGECAT criteriaand incident AD, but this finding was limited to
8
individuals with >8 years of education (odds ratio:5.31). The relevance of our findings should beemphasized: most elderly living in the community incountries such as Spain have lower educationallevels.43 Furthermore, Geerlings et al. limited theiranalysis of AGECAT data to “syndrome clusters,”emerging from phase I of the computer program.Therefore, they could not complete the differentialdiagnosis emerging from phase II in AGECAT, as wedid, and could not differentiate between “severe” and“nonsevere” depression.
In relation to characteristics of depression, andsimilar to previous authors,14 we found no associationbetween persistent depression and AD. In untreateddepression, we did find a significantly increased IR ofAD; the risk of AD was also increased in the bivariatemodel. Although the strength and significance of thisassociation were attenuated after adjustment, itsdirection was maintained. Contrary to Fuhrer et al.16
we found no association between depression treatedwith antidepressants and risk of AD. Other studies inthe literature did not find that antidepressant intakemodified the association between depression anddementia.19 Nevertheless, sparse antidepressant uselimits statistical power and precludes definitiveconclusions.37
Regarding first-ever depression, we also founda significantly increased IR of AD, and a trend for anincreased risk of AD. Panza et al.15 concluded intheir review that first-ever depression in late life isassociated with incident AD. Very recently, Li et al.40
reported this association in late-onset depression, andargued with others that depression might bea prodrome of AD rather than a risk factor.15
However, this theory is controversial, as severalsupport the idea that depression increases the risk ofAD.10,12,19 Our findings support the notion ofincreased risk as opposed to prodrome for thefollowing reasons. First, to minimize the possibility ofincluding in the cohort individuals with cognitivedeficits at baseline, we excluded all those with verymild deficits (“subsyndromal” dementia). Further-more, cognitive status at baselinewas controlled in theanalysis. Second, it might be argued that individualswith nonsevere depression were in fact incipient,prodromal cases of AD.44 However, “severe”depression, but not its milder counterpart, was asso-ciated with AD. Finally, the specificity of the findingsupports the real risk interpretation, because incident
Am J Geriatr Psychiatry -:-, - 2013

Gracia-García et al.
AD, but not incident dementia, was associated withdepression in this study (data not shown). To explainthe findings supporting an increased risk of AD, wetend to favor the “brain reserve” and/or “cognitivereserve” hypothesis as the final common pathway,suggested by authors such as Butters et al.45: depres-sion might alter the reserve through different mecha-nisms, both biological and psychosocial.
Our study has several strengths, such as use ofa representative population sample, including insti-tutionalized individuals; longitudinal design; highsensitivity and specificity of case finding, withinstruments validated within the study; and inclu-sion of actual mortality data in the Fine and Graymodel to study depression as a risk factor for AD.
Although this study follows state-of-the-art epide-miologic approaches in psychiatry, some limitationsmust be noted, including the limited number ofsubjects with severe depression who developed AD.There was significant attrition from sampling toenrollment. However, the attrition rate was expectedby design,8,20 and we previously argued that ourinvestigation is comparable to several other two-stage epidemiologic studies.20 Another limitation isthat we do not have data on apolipoprotein E andthat the hospital-based diagnosis was not completedin all cases of dementia. In fact, in 2 cases (13.3% ofcases considered to be AD by the panel of psychia-trists), the final, hospital-based diagnosis was “mixeddementia” (AD type and vascular dementia type).We trust this does not importantly affect the mainconclusions, particularly given that we controlled forvascular risk factors in the association found betweendepression and incident AD.
In studying risk of AD, few reports assessed theeffect of characteristics of depression,13,14,40 and nonesimultaneously studied several characteristics ofdepression, as we did here. However, some of thesubgroups of depressionwere small, and therefore thestatistical power to detect small differences was weak.
In conclusion, clinically significant, severe depres-sion increased the risk of AD in these study subjects,even after controlling for the competing risk of death.This finding, as well as the finding that untreateddepression might be associated with incident AD,may stimulate studies about the effect of treatingdepression in relation to the risk of AD.
Am J Geriatr Psychiatry -:-, - 2013
This research was supported by grants from the Fondode Investigación Sanitaria, Instituto de Salud Carlos III,Spanish Ministry of Health, Madrid, Spain (grants 94/1562, 97/1321E, 98/0103, 01/0255, 03/0815, 06/0617,and G03/128) and Pfizer Foundation, Madrid, Spain.Dr. Lyketsos was supported by grant P50AG005146 to theJohns Hopkins Alzheimer’s Disease Research Center.
The authors acknowledge the contribution of the layinterviewers, senior medical students, and members of theZARADEMP Workgroup who participated in the study.
Disclosures: Dr. Gracia-García has received grantsupport from Janssen, AstraZeneca, and the Ilustre Colegiode M�edicos de Zaragoza; honorarium from AstraZenecaand Lilly; and received travel support from Lilly, Almirall,Lundbeck, Rovi, Pfizer, and Janssen. Dr. de-la-Cámara hasreceived financial support to attend scientific meetingsfrom Janssen-Cilag, Almirall, Eli Lilly, Lundbeck, Rovi,Esteve, Novartis, and AstraZeneca. Dr. Quintanilla hasbeen funded for acting as an associated researcher byJanssen-Cilag and has received travel support from Lund-beck. Dr. Ventura has received grant support from Fondode Investigación Sanitaria; Ministry of Sciences andInnovation, Spain and the Banco de Instrumentos ofCIBERSAM; he has received travel support from Pfizerand Lumbeck. Dr. Campayo has received grant support(research or European Accreditation Council forContinuing Medical Education) from Fondo de Inves-tigación Sanitaria and Rovi, and literature or travelsupport from Pfizer and sanofi-aventis. Dr. Lyketsos hasreceived grant support (research or continuing medicaleducation) from the National Institute of Mental Health,National Institute on Aging, Associated Jewish Federationof Baltimore, Weinberg Foundation, Forest, Glaxo-SmithKline, Eisai, Pfizer, AstraZeneca, Lilly, Ortho-McNeil, Bristol-Myers Squibb, Novartis, NationalFootball League, Elan, and Functional NeuromodulationInc.; has been a consultant or advisor to AstraZeneca,GlaxoSmithKline, Eisai, Novartis, Forest, Supernus,Adlyfe, Takeda, Wyeth, Lundbeck, Merz, Lilly, Pfizer,Genentech, Elan, NFL Players Association, NFL BenefitsOffice, Avanir, Zinfandel; and has received honorarium ortravel support from Pfizer, Forest, GlaxoSmithKline, andHealth Monitor. Dr. Lobo had a consultancy with Janssenand has received honorarium or travel support from EliLilly and Bial. None of these activities is related to thecurrent project. The other authors report no financialrelationships with commercial interest.
9

Depression and Incident Alzheimer’s Disease
References
1. Galik EM, Rabins P, Lyketsos CG: Dementia, in PsychosomaticMedicine. Edited by Blumenfield M, Strain JJ. Philadelphia, PA,Lippincott Williams & Wilkins, 2006, pp 513e535
2. Copeland JR, Beekman AT, Braam AW, et al: Depression amongolder people in Europe: the EURODEP studies. World Psychiatry2004; 3:45e49
3. Meyers BS, Bruce ML: The depression-dementia conundrum:integrating clinical and epidemiological perspectives. Arch GenPsychiatry 1998; 55:1082e1083
4. Farrer LA, Cupples LA, Haines JL, et al: Effects of age, sex, andethnicity on the association between apolipoprotein E genotypeand Alzheimer disease. A meta-analysis. APOE and AlzheimerDisease Meta Analysis Consortium. JAMA 1997; 278:1349e1356
5. Mielke MM, Rosenberg PB, Tschanz J, et al: Vascular factorspredict rate of progression in Alzheimer disease. Neurology 2007;69:1850e1858
6. Daviglus ML, Bell CC, Berrettini W, et al: National Institutes ofHealth State-of-the-Science Conference statement: preventingAlzheimer disease and cognitive decline. Ann Intern Med 2010;153:176e181
7. Lobo A, Lopez-Anton R, Santabarbara J, et al: Incidence and life-time risk of dementia and Alzheimer’s disease in a southernEuropean population. Acta Psychiatr Scand 2011; 124:372e383
8. Lobo A, Saz P, Marcos G, et al: The prevalence of dementia anddepression in the elderly community in a southern Europeanpopulation. The Zaragoza Study. Arch Gen Psychiatry 1995; 52:497e506
9. Wilson RS, Barnes LL, Mendes de Leon CF, et al: Depressivesymptoms, cognitive decline, and risk of AD in older persons.Neurology 2002; 59:364e370
10. Saczynski JS, Beiser A, Seshadri S, et al: Depressive symptoms andrisk of dementia: the Framingham Heart Study. Neurology 2010;75:35e41
11. Devanand DP, Sano M, Tang MX, et al: Depressed mood and theincidence of Alzheimer’s disease in the elderly living in thecommunity. Arch Gen Psychiatry 1996; 53:175e182
12. Ownby RL, Crocco E, Acevedo A, et al: Depression and risk forAlzheimer disease: systematic review, meta-analysis, and meta-regression analysis. Arch Gen Psychiatry 2006; 63:530e538
13. Geerlings MI, den Heijer T, Koudstaal PJ, et al: History of depres-sion, depressive symptoms, and medial temporal lobe atrophy andthe risk of Alzheimer disease. Neurology 2008; 70:1258e1264
14. Becker JT, Chang YF, Lopez OL, et al: Depressed mood is nota risk factor for incident dementia in a community-based cohort.Am J Geriatr Psychiatry 2009; 17:653e663
15. Panza F, Frisardi V, Capurso C, et al: Late-life depression, mildcognitive impairment, and dementia: possible continuum? Am JGeriatr Psychiatry 2010; 18:98e116
16. Fuhrer R, Dufouil C, Dartigues JF: Exploring sex differences inthe relationship between depressive symptoms and dementiaincidence: prospective results from the PAQUID Study. J AmGeriatr Soc 2003; 51:1055e1063
17. Dal FornoG, PalermoMT,Donohue JE, et al: Depressive symptoms,sex, and risk forAlzheimer’s disease.AnnNeurol 2005; 57:381e387
18. Palsson S, Aevarsson O, Skoog I: Depression, cerebral atrophy,cognitive performance and incidence of dementia. Populationstudy of 85-year-olds. Br J Psychiatry 1999; 174:249e253
19. Chen R, Hu Z, Wei L, et al: Severity of depression and risk forsubsequent dementia: cohort studies in China and the UK. Br JPsychiatry 2008; 193:373e377
10
20. Lobo A, Saz P, Día JL, et al; the ZARADEMP Workgroup: TheZARADEMP Project on the incidence, prevalence and risk factorsof dementia (and depression) in the elderly community. II.Methods and first results. Eur J Psychiatry 2005; 19:40e54
21. Copeland JR, Dewey ME, Griffiths-Jones HM: A computerizedpsychiatric diagnostic system and case nomenclature for elderlysubjects: GMS and AGECAT. Psychol Med 1986; 16:89e99
22. Folstein MF, Folstein SE, McHugh PR: Mini-Mental State: a prac-tical method for grading the cognitive state of patients for theclinician. J Psychiatr Res 1975; 12:189e198
23. Dewey ME, Copeland JR: Diagnosis of dementia from the historyand aetiology schedule. Int J Geriatr Psychiatry 2001; 16:912e917
24. Lawton MP, Brody EM: Assessment of older people: self-maintaining and instrumental activities of daily living. Gerontol-ogist 1969; 9:179e186
25. Katz S, Ford AB, Moskowitz RW, et al: Studies of illness in theaged. The index of ADL: a standardized measure of biological andpsychosocial function. JAMA 1963; 185:914e919
26. Launer LJ, Brayne C, Breteler MM: Epidemiologic approach to thestudy of dementing diseases: a nested case-control study inEuropean incidence studies of dementia. Neuroepidemiology1992; 11(suppl 1):S114eS148
27. Schaub RT, Linden M, Copeland JR: A comparison of GMS-A/AGECAT, DSM-III-R for dementia and depression, includingsubthreshold depression (SD)—results from the Berlin AgingStudy (BASE). Int J Geriatr Psychiatry 2003; 18:109e117
28. WHO Collaborating Centre for Drug Statistics Methodology.Guidelines for ATC Classification and DDD Assignment, 2012.Oslo, World Health Organization, 2011
29. Hachinski VC, Iliff LD, Zilhka E, et al: Cerebral blood flow indementia. Arch Neurol 1975; 32:632e637
30. McKhann G, Drachman D, Folstein M, et al: Clinical diagnosis ofAlzheimer’s disease: report of the NINCDS-ADRDA Work Groupunder the auspices of Department of Health and Human ServicesTask Force on Alzheimer’s Disease. Neurology 1984; 34:939e944
31. Putter H, FioccoM, Geskus RB: Tutorial in biostatistics: competingrisks and multi-state models. Stat Med 2007; 26:2389e2430
32. Fine JP, Gray RJ: A proportional hazards model for the sub-distribution of competing risk. J Am Stat Assoc 1999; 94:496e509
33. Scheike TH, Zhang MJ: Flexible competing risks regressionmodeling and goodness-of-fit. Lifetime Data Anal 2008; 14:464e483
34. Kalbfleisch JD, Prentice RL: The Statistical Analysis of FailureTime Data. New York, NY, John Wiley & Sons Inc., 1980
35. Berry SD, Ngo L, Samelson EJ, et al: Competing risk of death: animportant consideration in studies of older adults. J Am GeriatrSoc 2010; 58:783e787
36. Sharma VK, Copeland JR, Dewey ME, et al: Outcome of thedepressed elderly living in the community in Liverpool: a 5-yearfollow-up. Psychol Med 1998; 28:1329e1337
37. De-la-Cámara C, Saz P, Lopez-Anton R, et al: Depression in theelderly community: II Outcome in a 4.5 years follow-up. Eur JPsychiatry 2008; 22:141e150
38. Byers AL, Covinsky KE, Barnes DE, et al: Dysthymia and depres-sion increase risk of dementia and mortality among olderveterans. Am J Geriatr Psychiatry 2012; 20:664e672
39. Köhler S, van Boxtel M, Jolles J, et al: Depressive symptoms andrisk for dementia: a 9-year follow-up of the Maastricht AgingStudy. Am J Geriatr Psychiatry 2011; 19:902e905
Am J Geriatr Psychiatry -:-, - 2013

Gracia-García et al.
40. Li G, Wang LY, Shofer JB, et al: Temporal relationship betweendepression and dementia: findings from a large community-based15-year follow-up study. Arch Gen Psychiatry 2011; 68:970e977
41. Penninx BW, Geerlings SW, Deeg DJ, et al: Minor and majordepression and the risk of death in older persons. Arch GenPsychiatry 1999; 56:889e895
42. Geerlings MI, Schmand B, Braam AW, et al: Depressive symptomsand risk of Alzheimer’s disease in more highly educated olderpeople. J Am Geriatr Soc 2000; 48:1092e1097
Am J Geriatr Psychiatry -:-, - 2013
43. Instituto Nacional de Estadística. INEbase: Demografía y pobla-ción; Cifras de población y Censos demográficos. http://www.ine.es/inebmenu/mnu_cifraspob.htm. Accessed October 1, 2012
44. Forsell Y, Jorm AF, Winblad B: Variation in psychiatric and behav-ioural symptomsat different stagesofdementia:data fromphysicians’examinations and informants’ reports. Dementia 1993; 4:282e286
45. Butters MA, Young JB, Lopez O, et al: Pathways linking late-lifedepression to persistent cognitive impairment and dementia.Dialogues Clin Neurosci 2008; 10:345e357
11




















