Cultivable anaerobic microbiota of severe early childhood caries
Upload
khangminh22Category
view
1download
0
Umeå University Odontological Dissertations, No 115
Dental caries and background factors in children with heart disease
Linda Rosén
Department of Odontology
Umeå University
Umeå 2011

Responsible publisher under swedish law: the Dean of the Medical Faculty
© 2011 Linda Rosén
ISBN: 978-91-7459-139-2
ISSN: 0345-7532
E-version available at http://umu.diva-portal.org/
Printed by: Print & Media
Umeå, Sweden 2011

If you want to study yourself — look into the hearts of other people.
If you want to study other people — look into your own heart.
Quote from Friedrich von Schiller

1
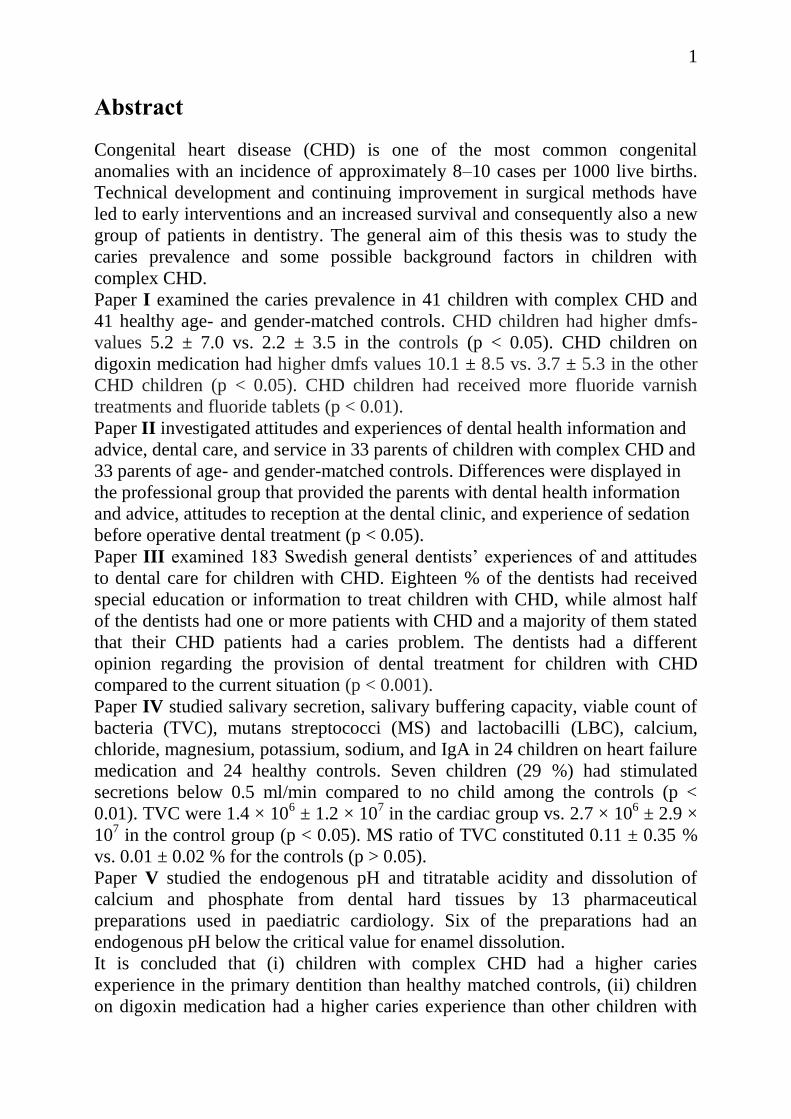
Abstract
Congenital heart disease (CHD) is one of the most common congenital
anomalies with an incidence of approximately 8–10 cases per 1000 live births.
Technical development and continuing improvement in surgical methods have
led to early interventions and an increased survival and consequently also a new
group of patients in dentistry. The general aim of this thesis was to study the
caries prevalence and some possible background factors in children with
complex CHD.
Paper I examined the caries prevalence in 41 children with complex CHD and
41 healthy age- and gender-matched controls. CHD children had higher dmfs-
values 5.2 ± 7.0 vs. 2.2 ± 3.5 in the controls (p < 0.05). CHD children on
digoxin medication had higher dmfs values 10.1 ± 8.5 vs. 3.7 ± 5.3 in the other
CHD children (p < 0.05). CHD children had received more fluoride varnish
treatments and fluoride tablets (p < 0.01).
Paper II investigated attitudes and experiences of dental health information and
advice, dental care, and service in 33 parents of children with complex CHD and
33 parents of age- and gender-matched controls. Differences were displayed in
the professional group that provided the parents with dental health information
and advice, attitudes to reception at the dental clinic, and experience of sedation
before operative dental treatment (p < 0.05).
Paper III examined 183 Swedish general dentists’ experiences of and attitudes
to dental care for children with CHD. Eighteen % of the dentists had received
special education or information to treat children with CHD, while almost half
of the dentists had one or more patients with CHD and a majority of them stated
that their CHD patients had a caries problem. The dentists had a different
opinion regarding the provision of dental treatment for children with CHD
compared to the current situation (p < 0.001).
Paper IV studied salivary secretion, salivary buffering capacity, viable count of
bacteria (TVC), mutans streptococci (MS) and lactobacilli (LBC), calcium,
chloride, magnesium, potassium, sodium, and IgA in 24 children on heart failure
medication and 24 healthy controls. Seven children (29 %) had stimulated
secretions below 0.5 ml/min compared to no child among the controls (p <
0.01). TVC were 1.4 × 106 ± 1.2 × 10
7 in the cardiac group vs. 2.7 × 10
6 ± 2.9 ×
107 in the control group (p < 0.05). MS ratio of TVC constituted 0.11 ± 0.35 %
vs. 0.01 ± 0.02 % for the controls (p > 0.05).
Paper V studied the endogenous pH and titratable acidity and dissolution of
calcium and phosphate from dental hard tissues by 13 pharmaceutical
preparations used in paediatric cardiology. Six of the preparations had an
endogenous pH below the critical value for enamel dissolution.
It is concluded that (i) children with complex CHD had a higher caries
experience in the primary dentition than healthy matched controls, (ii) children
on digoxin medication had a higher caries experience than other children with

2
complex CHD, (iii) children with complex CHD had received more caries
prevention than healthy controls, (iv) parents of children with complex CHD
were less satisfied with the reception and care they received than parents of
healthy children, (v) general dentists had a different opinion regarding the
provision of dental treatment to children with CHD compared to the current
situation (vi) children on heart failure medication can have a low saliva
secretion, (vii) pharmaceutical preparations used on long-term basis in paediatric
cardiology may pose a hazardous threat to dental hard tissues due to their
acidity.
Key words: attitudes, caries, children, dental care, heart disease, medication,
saliva

3
Contents
Abstract ........................................................................................................................... 1
Papers .............................................................................................................................. 5
Thesis at a glance ............................................................................................................ 6
Abbreviations .................................................................................................................. 8
Introduction ..................................................................................................................... 9
Signs and symptoms of heart disease ........................................................................ 11
Treatment of CHD ..................................................................................................... 11
Saliva ......................................................................................................................... 13
Dental caries .............................................................................................................. 15
Oral effects of pharmacotherapy ............................................................................... 19
Aims of the Thesis ........................................................................................................ 22
Materials........................................................................................................................ 23
Study designs ............................................................................................................. 23
Study and control groups........................................................................................... 23
Methods ......................................................................................................................... 26
Diagnosis, medication, and blood pressure ............................................................... 26
Caries registration (I) ................................................................................................ 26
Caries prevention (I) .................................................................................................. 26
Attitudes and experiences (II, III) ............................................................................. 27
Saliva (IV) ................................................................................................................. 27
Effects on dental hard tissues caused by medication (V) .......................................... 30
Ethical approval ......................................................................................................... 31
Ethical considerations ............................................................................................... 31
Statistical analyses ..................................................................................................... 31
Results ........................................................................................................................... 33
Discussion ..................................................................................................................... 38
Material and Methodological considerations ............................................................ 38
Evaluation of results .................................................................................................. 41
Clinical perspectives ................................................................................................. 47
Conclusions ................................................................................................................... 49
Populärvetenskaplig sammanfattning ........................................................................... 50
Acknowledgements ....................................................................................................... 51
References ..................................................................................................................... 53
APPENDIX I. Questionnaires Paper II ......................................................................... 59
APPENDIX II. Questionnaire paper III ........................................................................ 64

4

5
Papers
This thesis is based on the following original papers, which will be referred to
by their Roman numerals:
I. Stecksén-Blicks C, Rydberg A, Nyman L, Asplund S, Svanberg C.
Dental caries experience in children with congenital heart disease: a
case-control study. International Journal of Paediatric Dentistry 2004;
14: 94-100.
II. Grahn K, Wikström S, Nyman L, Rydberg A, Stecksén-Blicks C.
Attitudes about dental care among parents whose children suffer from
complex congenital heart disease: a case-control study. International
Journal of Paediatric Dentistry 2006; 16: 231-238.
III. Rosén L, Stecksén-Blicks C. Experience of dental care for children
with congenital heart disease among Swedish dentists. Swedish Dental
Journal 2007; 31: 85-90.
IV. Rosén L, Rydberg A, Sjöström I, Stecksén-Blicks C. Saliva profiles in
children using heart failure medication: a pilot study. European
Archives of Paediatric Dentistry 2010; 11: 187-191.
V. Rosén L, Rydberg A, Sjöström I, Lundgren T, Stecksén-Blicks C.
Acidity and in vitro effects on dental hard tissues of medicines used in
paediatric cardiology. Submitted.
The original papers are reprinted with kind permission from the publishers.

6
Thesis at a glance
Aims Material and Methods
I To study the caries prevalence in children
with complex CHD and compare with a
healthy age- and
gender-matched control group.
Each group comprised 41 children. Data were
collected from medical and dental records.
II To study attitudes and experiences of
parents of children with complex CHD with
respect to dental health information and
advice, dental care, and service and compare
with data from a healthy age- and gender-
matched control group.
Each group comprised parents of 33 children.
Data were collected with a questionnaire.
III To study experiences of and attitudes to
dental care for children with CHD among
Swedish general dentists.
General dentists from 2 Swedish counties
participated (n = 183). Data were collected with a
questionnaire.
IV To study saliva profiles in children on heart
failure medication and compare them with
healthy age- and gender-matched controls.
Each group comprised 24 children. Stimulated
saliva was collected. Salivary secretion rate,
buffering capacity, total viable count (TVC),
mutans streptococci (MS), lactobacilli (LBC),
calcium, chloride, magnesium, potassium,
sodium, and salivary IgA were determined.
V To study the endogenous pH, titratable
acidity, and dissolution of calcium and
phosphate from dental hard tissues by
pharmaceutical preparations used regularly
and on long-term basis in paediatric
cardiology.
Thirteen pharmaceutical preparations were
selected and the titratable acidity and the
dissolution of calcium and phosphate after
immersion of tooth specimens were quantified
for medicines with an endogenous pH below 5.5.

7
R
Results Conclusions
The dmfs-values were higher in the CHD group
(5.2 ± 7.0 vs. 2.2 ± 3.5, p < 0.05) while DMFS-
values not were different 0.9 ± 1.9 vs. 0.3 ± 0.6 (p
> 0.05). Children on digoxin medication had higher
dmfs values 10.1 ± 8.5 vs. 3.7 ± 5.3 (p < 0.05).
CHD children had received more fluoride varnish
treatments and fluoride tablets (p < 0.01).
Swedish children with complex CHD had more
caries in the primary dentition than healthy age-
and gender-matched controls in spite of
intensive preventive efforts.
A closer cooperation between paediatric
cardiology and paediatric dentistry is needed.
Differences were displayed in the professional
group that provided the parents with dental health
information and advice (p < 0.01) and attitudes to
reception at the dental clinic (p < 0.05). Parents of
children who were patients at a specialist clinic for
paediatric dentistry were more satisfied with the
reception compared to those who were patients in
the general dental practice (p < 0.01).
Parental attitudes to reception in the dental
service differed, and parents of healthy children
scored the reception at the dental clinic better
than parents of children with complex CHD. It
is suggested that children with complex CHD
should receive dental care in clinics for
paediatric dentistry particularly at early ages.
A minority of the dentists had received special
education to treat children with CHD. Almost half
of them had one or more patients with CHD. A
majority stated that their CHD patients had a caries
problem. The dentists had a different opinion
regarding the provision of dental treatment to
children with CHD compared to the current
situation (p < 0.001).
Data indicates that the Swedish dentists are
unsettled and insecure in the dental treatment of
children with CHD. Close cooperation between
specialists in paediatric dentistry, dentists with
special training, and general dentists is essential.
Twenty-nine % of the children on heart failure
medication had secretions below 0.5 ml/min
compared to no child in the control group (p <
0.01). TVC were lower in the cardiac group
compared to the control group (p < 0.05). MS ratio
of TVC constituted 0.11 ± 0.35 % vs. 0.01 ± 0.02
% for the controls (p > 0.05).
Children on heart failure medication can have a
low saliva secretion.
The pH of the pharmaceutical preparations varied
between 3.03 and 9.02 and 6 had an endogenous
pH below 5.5. The highest dissolved calcium and
phosphate from the tooth specimens was displayed
by captopril (12.5 mg) tablet water solution and by
the acetylsalicylic acid (75 mg) tablet water
solution.
Some pharmaceutical preparations used on a
long-term basis in paediatric cardiology may
pose a hazardous threat to dental hard tissues
due to their acidity.

8
Abbreviations
ACE Angiotensin-converting enzyme
ANOVA Analysis of variance
AS Aortic stenosis
ASD Atrial septal defect
BAO Blood agar oral plates
CFU Colony forming units
CHD Congenital heart disease
CoA Coarctation of the aorta
DCM Dilated cardiomyopathy
dmfs/DMFS Decayed, missed, filled surfaces for
primary/permanent teeth
ECC Early childhood caries
LBC Lactobacilli
LCC Late childhood caries
MS Mutans streptococci
PDA Patent ductus arteriosus
PDS Public dental service
PS Pulmonary stenosis
SWS Stimulated whole saliva
TGA Transposition of the great arteries
TOF Tetralogy of Fallot
TVC Total viable count
UWS Unstimulated whole saliva
VSD Ventricle septal defect

9
Introduction
The human heart develops between the 8th and the 12
th gestational week. A dis-
turbance in this process may result in an anomaly—a congenital heart disease
(CHD). CHD is one of the most common congenital anomalies in children, with
a mean incidence of approximately 8–10 cases per 1000 live births (1-4). Chil-
dren with complex anomalies constitute approximately one-third of all children
with CHD (3). Technical development and continuing improvement in surgical
methods have led to early interventions and an increased survival of children
with CHD (5). A majority of children with significant heart disease are today
subjected to successful surgery, but those children with very complex heart dis-
eases are often surgically palliated and not completely corrected (6, 7). The
aetiology behind cardiac developmental disturbances are in a majority of cases
unknown, but risk factors like maternal diseases and infections like diabetes,
rubella, HIV, and alcoholism have been suggested (4, 8). Many CHDs result
from genetic and environmental interactions rather than mendelian inheritance
(9). The CHD may occur individually as a single diagnosis, which is seen in a
majority of cases, or as a part of a syndrome or genetic malformation, e.g.
Down’s syndrome, Noonan’s syndrome, Turner’s syndrome, 22q11, and trisomy
18. Approximately 40 % of children with Down’s syndrome and a majority of
children with Noonan’s syndrome and trisomy 18 are affected with CHD (10,
11). Besides the group of congenital anomalies, heart disease in childhood may
also be caused by various kinds of cardiomyopathies leading to heart failure and
the need of anti-congestive medication (12).
CHD is the comprehensive term for congenital cardiac anomalies.
The most common anomalies can be divided into the sub-groups: left-right
shunts, obstructive heart diseases, and cyanotic congenital anomalies. The most
common diagnoses are listed in Table 1, and the frequency distributions of the
most common congenital cardiac diagnoses in live births are listed in Table 2.

10
Table 1. The most common cardiac diagnoses divided in sub-groups.
Left-right shunt Ventricle septal defect (VSD)
Atrial septal defect (ASD)
Patent ductus arteriosus (PDA)
Atrioventricular septal defect (AVSD)
Obstructive heart disease Coarctation of the aorta (CoA)
Aortic stenosis (AS)
Pulmonary stenosis (PS)
Cyanotic vitia Transposition of the great arteries (TGA)
Tetralogy of Fallot (TOF)
Table 2. Distribution of the most common congenital cardiac diagnoses in live
births according to the National Board of Health and Welfare (1).
Cardiac anomaly (%)
Ventricle septal defect (VSD) 20–30
Patent ductus arteriosus (PDA) 10–12
Atrial septal defect (ASD) 8–10
Pulmonary stenosis (PS) 8–10
Tetralogy of Fallot (TOF) 5–10
Coarctation of the aorta (CoA) 5–8
Atrioventricular septal defect (AVSD) 4–5
Transposition of the great arteries (TGA) 3–7
Aortic stenosis (AS) 3–5
Hypoplastic left heart syndrome (HLHS) 2–5

11
Signs and symptoms of heart disease
The main symptoms of CHD are cyanosis and/or heart failure. In cyanosis, de-
oxygenated blood is mixed with oxygenated blood or an increased amount of
blood goes to the pulmonary circulation. Low saturation in tissues and organs
may lead to acidosis, and this may cause an impaired heart function and heart
failure (4, 9).
Heart failure occurs either due to an increased blood flow to the
pulmonary circulation or due to a deteriorated ventricle, which fails to keep the
pumping function. Blood will accumulate in the lungs, and breathing will be
affected. The clinical signs are rapid breathing and an increased heart rate
(tachypnea and tachycardia), feeding problems, and inadequate weight gain. The
first signs of heart failure are often observed during the child’s first 3 months of
life.
Treatment of CHD
Pharmacological treatment
If left untreated, CHD is the single greatest cause of death during the neonatal
period after full-time pregnancies in the industrialized part of the world (4,9).
The medication is often complex in children with complex CHD, and the most
common pharmaceutical preparations used in paediatric cardiology can be found
in Table 3. Diuretics are the first treatment of choice in heart failure, decreasing
total blood volume and thereby diminishing the volume load of the heart. In
heart failure, medical treatment with angiotensin-converting enzyme (ACE)
inhibitors and/or cardiac glycosides, such as digitalis, can also be indicated.
ACE inhibitors inhibit the formation of angiotensin II, and as a result of this, the
peripheral resistance is decreasing both preload and afterload. Digitalis prepara-
tions reduce the heart rate and increase the contractility of the heart. Beta-
blockers are used in management of cardiac arrhythmias and may be indicated
as adjuncts to standard therapy in heart failure. Anticoagulants, as warfarin,

12
stops blood from clotting and antiplatelet drugs, such as acetylsalicylic acid,
decrease platelet aggregation formation. They are used in prevention of
thrombotic events in cardiovascular disease.
In duct-dependant anomalies, like in pulmonary atresia or hypo-
plastic left heart syndrome, it is of decisive importance that the ductus arteriosus
remains open, otherwise the child will die. In the late 1970’s, it was found that
prostaglandin keeps the ductus arteriosus open, and this finding has a key role in
the dramatically improved results of paediatric heart surgery. By giving
prostaglandin infusions, the child can be stabilized and transported to surgery
under considerably better circumstances.
Table 3. Pharmaceutical preparations used in paediatric cardiology.
Medicine Generic substances
ACE inhibitors enalapril
captopril
Diuretics spironolactone
furosemide
Beta-blockers metoprolol
propranolol
Cardiac glycosides digoxin
Anti-coagulants warfarin
Anti-platelet drugs acetylsalicylic acid

13
Surgical treatment
In 1938, the first paediatric heart surgery was performed. In 1953, the heart-lung
machine was used for the first time, and during 1970, the pacemaker and heart
transplantations on newborns were introduced in paediatric cardiology. In the
1980’s, catheter treatments of several CHD became possible. The use of
prostaglandin on duct dependent anomalies, as described earlier, taken together
with the development of the diagnostic instrument echocardiography, contrib-
uted to an increased survival rate of children subjected to paediatric heart
surgery. Figure 1 shows that the mortality rate decreased in children subjected to
open heart surgery in Sweden. Today surgery is successful for the majority of
children born with complex CHD (9). The median age of children subjected to
heart surgery is today below 2 years of age (4).
Fig. 1. Thirty-day mortality rate in children subjected to open heart surgery,
1988–2006 (data received from the National Board of Health and Welfare).
Saliva
To maintain a normal physiology in the oral cavity, an adequate salivary pro-
duction is of great importance. Saliva is produced by the 3 major pairs of
0
2
4
6
8
10
12
1988
1989
1990
1991
1992
1993
1994
1995
1996
1997
1998
1999
2000
2001
2002
2003
2004
2005
2006
Mo
rtal
ity
rate
(%
)
Year

14
salivary glands, namely, parotid, submandibular, and sublingual as well as by
numerous minor salivary glands, namely, buccal, lingual, labial, and palatinal, in
a total volume of 0.5–1.0 litre per day. The salivary glands seem to be fully de-
veloped at the age of 15, and the salivary flow rate increases with age and girls
have lower rates than boys (13). The saliva produced by the different gland
types has a characteristic composition, and the composition of the saliva has a
diurnal variation (14) and is affected by input stimuli (15). Saliva contains
inorganic components like calcium and phosphate and organic components like
proteins, carbohydrates, immunoglobulins, and enzymes. In the oral cavity, the
saliva from the salivary glands mixes with mucus from the nasal cavity and
pharynx, epithelial cells, and millions of microorganisms, and this mix is in the
literature referred to as whole saliva (14).
The salivary glands have a dual innervation with nerve fibres from
both sympathetic and parasympathetic nervous system. In general,
parasympathetic stimulation increases salivation, while sympathetic stimulation
produces more viscous saliva and therefore appears to depress salivation (14).
Pharmacotherapy is probably the most common cause of impaired salivary
secretion.
The saliva plays an important role in the complex oral ecosystem,
and several factors of great importance for maintaining oral health are present in
the saliva (16). One important objective of saliva in the defence against caries is
to neutralize acids in plaque, and an impaired salivary flow will result in an in-
creased risk of developing caries. Saliva acts as a lubricant for the oral tissues
and it facilitates swallowing and speech. Further, saliva contributes in the initial
step of digestive break down (14, 17). With its buffering capacity, saliva
protects the oral cavity against damaging pH changes. By several anti-microbial
components, such as immunoglobulins, the saliva also constitutes a barrier for
bacteria and viruses not to permeate the mucous membrane. Several types of
immunoglobulins are present in saliva, such as IgG, IgM, and IgA, of which the

15
secretory IgA (sIgA) is predominant (18). sIgA is produced by plasma cells
located in the connective tissues and is translocated through the duct cells of the
major and minor salivary glands (19, 20). Salivary IgA against mutans strepto-
cocci (MS) can be found in a majority of children over 3 years of age and the
amount increases with the length of exposure (18, 21).
Dental caries
Dental caries is defined as ‘a dynamic process taking place in the tooth bacterial
biofilm (plaque), which results in a disturbance of equilibrium between tooth
substance and the surrounding plaque fluid and finally results in a loss of
minerals from the tooth surface’ (22). Dental caries is one of the most prevalent
chronic and infectious diseases in man. Susceptibility to caries remains through-
out life, and it is the primary cause of oral pain and tooth loss in both the pri-
mary and the permanent dentition. The disease may be reversed if arrested in
time, but without proper care caries may progress until the tooth is destroyed
(23). Caries in young children may be divided into early childhood caries (ECC)
and late childhood caries (LCC) (24). Several studies have shown a close
relationship between caries in the primary dentition and caries in the permanent
dentition (25-28). The main assignment for paediatric dentistry is thus to
endeavour that dental caries never get established in the primary dentition.
Pathogenesis of dental caries
Dental caries develops in the interplay between acid-producing bacteria, e.g.
mutans streptococci (MS) and lactobacilli (LBC), dietary sugars that the bacteria
can metabolise, and several host or personal factors like teeth and saliva (23,
29). The most cariogenic group of bacteria present in the oral cavity is MS (30).
An increase in the proportion of acidogenic bacteria such as MS and LBC in the
oral biofilm has been shown to be associated with dental caries (31). Cariogenic
plaques normally contain high numbers of these bacteria and the acidogenic
16
potential is extensive. A shift in the composition of dental plaque towards
acidogenic bacteria occurs as an effect of environmental changes. Such changes
may occur due to reduced salivary flow, high and frequent intake of sucrose,
impaired oral hygiene or combinations of these factors (32-35). The low pH
generated from acids changes homeostasis in the microbial community in the
dental plaque and a selection towards bacteria with a capacity to induce caries
will take place. The acids produced by the cariogenic bacteria will cause a drop
in pH below the critical value where demineralisation of enamel occurs (pH ≤
5.5) (36). If the demineralization proceeds, cavitations in the tooth will be a fact.
On the other hand, if minerals in the saliva, like fluoride, calcium, and phos-
phate diffuse into the tooth, remineralisation occurs and the enamel turns more
acid-resistant. Remineralisation occurs frequently, especially when the biofilm
pH is restored by saliva, which acts as a buffer (36).
Risk factors
A potential risk factor is a variable associated with an increased risk of disease
or infection. The exposure must be established before the outcome and prospec-
tive studies are necessary to demonstrate risk factors, and they imply causality
(37). Low salivary secretion and high numbers of acid producing oral bacteria
are well-known risk factors for caries development. Risk factors for dental caries
may vary over time and are strongly affected by lifestyle and behavioural factors
that may expose the individual to risk factors. Poor oral hygiene habits, poor
dietary habits, and frequent use of medicines that contain sugar, are acidic,
and/or are xerogenic are examples of behavioural factors that may lead to an
increased caries risk (23).

17
Epidemiology
Several studies have reported the caries prevalence in Swedish children. Two
studies from 2006 and 2007 showed that 6–7 % of 2-year-old children have
caries (38, 39). Decreasing caries prevalence has been demonstrated in Swedish
children (40, 41). Caries prevalence and background factors were studied in a
series of cross-sectional studies from the northern part of Sweden in 4-year-olds
from 1967 to 2007. These studies showed a decreasing caries frequency over the
years, but it is also clear that caries is still a common problem in the primary
dentition (42). Many chronic diseases in childhood have been associated with
poor oral health (43). A number of studies have been carried out on the caries
prevalence in children with CHD (44-53) of which only five have been con-
trolled studies (44, 46-48, 52). Published studies on caries in children with heart
disease are presented in Table 4. In the controlled studies published between
1978 and 2008 from Australia and UK the severity of CHD and outcome
measures varies but the studies indicate more untreated caries, treatment need
and/or a higher caries prevalence compared to healthy children.
In Sweden, the caries distribution in children today is skewed, and
susceptible individuals like children with immigrant background (42) and some
medically compromised children (54-56) have more caries than non-immigrants
and healthy children. When this thesis was planned, little was known about the
caries prevalence in the increasing group of children with CHD in Sweden
where all children are offered organised dental care free of charge from an early
age.

18
Table 4. Published studies on caries in children with heart disease. Reference
number in parenthesis.
Author, year Country n Age Caries/age group
Berger, 1978 (44) Australia CHD=57
Ctr=57
8-10 Cyanotic CHD had higher
dt, DT and MT
Urquhart and
Blinkhorn, 1990
(45)
UK CHD=134 4-12 4-6 7-9 10-12
dmft DMFT DMFT
3.3 3.3 5.0
Pollard and Curzon,
1992 (46)
UK
Cardiac=100
Ctr=100
2-16 2-4 5-9 5-9 10-16
dmft dmft DMFT DMFT
1.8 4.3 * 0.6 1.8
1.6 2.8 0.5 1.6
Hallett et al, 1992
(47)
Australia
CHD=39
Ctr=33
2-15
1-15
dmft DMFT
4.2 * 0.9
2.3 0.6
Franco et al, 1996
(48)
UK
CHD=60
Ctr=60
2-16 dmft DMFT
3.7±3.2 2.7±3.4
3.9±3.2 2.0±2.9
untreated caries CHD=52 % *
Ctr=32 %
Hayes and Fasules,
2001 (49)
USA Children
scheduled for
cardiac
surgery=209
≥ 6
months
29 % with caries
Da Silva et al, 2002
(50)
Brazil Children with
risk of
IE=104
2-17 dmft DMFT
2.6±3.0 4.0±4.1
Balmer and
Bu´Lock, 2003 (51)
UK Children with
risk of IE=38
2-16 39 % with untreated caries
Tasioula et al, 2008
(52)
UK
CHD=76
Ctr=47
2-15
dmft DMFT Care index
1.6±3.0 0.8±1.4 10 % *
1.8±3.6 0.4±1.2 3 %
Rai et al, 2009 (53) India CHD=170 1-16 42 % with caries
* Statistically significant difference, IE=infective endocarditis

19
Caries prevention
The dental care for Swedish children has had a preventive approach for more
than 40 years with start in an early age of the child. The concept with an early
prevention start is based on the thought that initially children’s teeth are healthy
and that the dental health of the preschool child is important since it has a strong
influence on the future dental health (25-28). The beneficial development of the
dental health of preschool children during the 1970’s has been ascribed to the
introduction of early dental health information to parents and an increased use of
fluorides (57). Fluoride plays an important role in caries prevention (58, 59) and
stimulates self healing of minor cavities by reducing the demineralisation
process and promoting the remineralisation process (60). Further, fluoride also
affects the metabolism in caries-associated bacteria (61). The effect of fluoride
strongly depends on the frequency of administration. Fluoride toothpaste is
considered as the most cost-effective homecare measure (58), and semi-annual
fluoride varnish applications, as the best professional method for infants at risk
(62). In a group of special-needs children, the beneficial effect of daily fluorides
was demonstrated, and it was shown that both fluoride tablets and fluoride liquid
could prevent ECC in children with cleft lip and/or palate (63). In Sweden, basic
caries prevention in healthy individuals consists of tooth brushing twice a day
with fluoride toothpaste. In individuals with an increased risk for caries, like
some medically compromised patients (43, 54-56), additional fluoride may be
indicated and is suggested to be administered based on individual needs and
compliance (24).
Oral effects of pharmacotherapy
It is known that children with very complex CHD frequently require regular
long-term medication (7), but the knowledge of oral health effects caused by
long-term medication in medically compromised children is sparse (64). Many
pharmaceutical preparations used on a long-term basis may have a low pH, high

20
acidity, and contain sugar (65, 66). A strong correlation between xerostomia and
pharmacological treatment has been shown (67), and a number of drugs have
been listed as xerogenic (68). These drugs include those with a direct damage to
salivary glands such as cytotoxic drugs, drugs with anticholinergic activity,
drugs which deplete fluid as diuretics, and drugs acting on sympathetic system
like antihypertensive drugs (69). Only a few clinical studies have been carried
out on the outcome of salivary function with antihypertensive drugs, and the
outcome is not clear-cut (70). In healthy men, the effects of β-adrenoceptor
antagonists, such as atenolol and propranolol, on saliva flow and composition
was tested and no effect on saliva secretion was found; however, there was a
reduction in total salivary protein (71) and hypertensive patients increased their
salivary secretion during withdrawal of β1-selective drug metoprolol (72). Treat-
ment with the ACE inhibitor captopril increased the secretion rates for unstimu-
lated and paraffin-chewing stimulated whole saliva and for parotid secretion. No
alterations in the composition of saliva were observed (73). Thiazide diuretics
significantly reduced salivary secretion in 34 healthy adult volunteers (74).
To maintain chemical stability, control tonicity, and physiological
compatibility in medicines, acids are frequently used as buffering agents (64).
Fermentable sugars such as sucrose can also be added in paediatric medicines to
disguise their unpleasant taste and thereby facilitate compliance. Sugars in
medicines may, however, cause a pH drop in the oral biofilm as a result of their
fermentation in acid-producing bacteria (23, 43), and acids in medicines may
help to prolong the pH drop after a sugar challenge. Pharmacotherapy may
therefore, beside the effects on salivary secretion, also act directly on the dental
hard tissues with dental caries and/or erosive lesions as possible outcomes as a
result of their content of acids and fermentable sugars (66, 68, 75, 76). Dental
erosion is a multifactorial condition, defined as the ‘dissolution of the tooth by
acids when the surrounding aqueous phase is unsaturated with respect to tooth
mineral’ (77). Minerals in dental hard tissue are dominated by calcium and

21
phosphate mainly organised in hydroxyapatite crystals with a critical pH value
of 5.5 (36). Any substance with an endogenous pH below this value may cause
ionic dissolution of the hard tissue with caries and erosion as possible outcomes
(78). The causes behind the development of dental erosion are often divided into
either extrinsic or intrinsic factors. Extrinsic factors are factors like acidic food-
stuffs and medications. Intrinsic factors may be diseases and consequences of
diseases where acidic contents of the stomach reach the oral cavity and thereby
pose a threat to the oral health (79).

22
Aims of the Thesis
General aim
The general aim of this thesis was to investigate the caries prevalence in
children with complex CHD and potential background factors.
Specific aims
The specific aims of this thesis were to:
Study the caries prevalence in children with complex CHD and compare
with healthy age- and gender-matched children.
Study the attitudes and experiences of parents whose children have
complex CHD with respect to dental health information and advice, dental
care and service, and to compare the results with data from a healthy age-
and gender-matched control group.
Study the experience of and attitudes to dental care for children with CHD
among Swedish general dentists.
Study the secretion and composition of saliva in children on heart failure
medication, and to compare with saliva from healthy age- and gender-
matched controls.
Study the endogenous pH, titratable acidity, and dissolution of calcium
and phosphate from dental hard tissue by medicines used regularly and on
long-term basis in paediatric cardiology.

23
Materials
Study designs
• Study I, II and IV: Cross-sectional case-control design.
• Study III: Descriptive cohort study.
• Study V: In vitro study.
Study and control groups
Table 5. Number of invited, consented, gender distribution, and mean age.
Equal numbers and gender in study and control groups.
Study Invited Consented Boys Girls Mean age, range
(yrs)
I 43 41 25 16 6.5 (2–11)
II 38 33 20 13 9.4 (3–13)
IV 37 24 11 13 12.0 (6–19)
Paper I
All surviving children with CHD, complexity grading II and III, born between
1991 and 2000 and living in the county of Västerbotten were selected from the
Paediatric Cardiology Outpatient Clinic at University Hospital in the city of
Umeå, Sweden and invited to take part in the study (n = 43). Children with other
serious medical diagnoses and children with learning difficulties were excluded.
For each CHD, a healthy child with the same date of birth and gender was
selected. The first child in the population register who met the inclusion criteria
was included in the control group. Informed consent was received from the
parents of 95 % of the selected groups, which resulted in 41 children in each

24
group. The mean age of the children was 6.5 years, and there were 25 boys and
16 girls.
Paper II
Parents of all children with CHD between 3 and 13 years of age, complexity
grading II and III, without other chronic diseases, learning difficulties, or
syndromes registered in the Paediatric Cardiology Outpatient Clinic at
University Hospital in the city of Umeå were invited (n = 38). The parents of 2
children with CHD did not consent. For each child in the study group, a child of
the same gender and date of birth was selected from the population register for
the county of Västerbotten. Approximately 50 % of the parents replied to the
first questionnaire. After reminders 10 participants did not reply, and they were
exchanged with the parents of the next child with the same birth date and gender
in the population register. In spite of this, there were 3 non-respondents. To
match the controls, the parents of 3 children with CHD were excluded. The final
material thus consisted of 33 pairs of parents.
Paper III
All general dentists employed in the Public Dental Health Service and all private
dentists listed with dentistry for children in the county of Västerbotten (n = 145)
in the north of Sweden and all general dentists employed in the Public Dental
Health Service in the county of Uppsala (n = 100) in the middle of Sweden were
invited to participate in the study. All specialists were excluded from the invita-
tion. The final material consisted of 183 dentists (75 %) of which 40% were
males and 60 % were females. Seventy-two % of the dentists had their dental
degree 16 years ago or earlier, and 10 %, six years earlier or less.

25
Paper IV
All children with CHD complexity grading II and III, or dilated
cardiomyopathies (DCM), 5 years or older, medicating with ACE inhibitors
and/or diuretics, and attending the Paediatric Cardiology Clinics at the
University Hospital in the city of Umeå or at the Karolinska University Hospital,
Stockholm, Sweden, were invited to take part in the study (n = 37). Children
with other chronic diseases, learning difficulties or syndromes were not invited.
Each child in the study group who fulfilled the criteria for inclusion and con-
sented to participate was asked to bring along a friend, healthy, with the same
age and gender, to the saliva-sampling occasion. The final material consisted of
pairs of 24 children (65 %). Three cases were 1 year younger or older than their
control.
Paper V
Thirteen medicines commonly used in paediatric cardiology were selected. For
quantification of dissolution of calcium and phosphate, tooth specimens were
prepared from the central corona of extracted primary canines with no cracks in
enamel.

26
Methods
Diagnosis, medication, and blood pressure
Data on diagnosis, medication, and blood pressure in the study groups were ex-
tracted from the records at the Paediatric Cardiology Clinics at the University
Hospital in Umeå and at the Karolinska University Hospital, Stockholm,
Sweden. Data extraction was performed by an experienced paediatric
cardiologist.
Caries registration (I)
For both groups of children, copies of their dental records and bitewing radio-
graphs were collected from the dental clinic where the child received dental
treatment. Data on decayed, missing, filled, and carious surfaces (dmfs/DMFS)
were collected from the records, while data on posterior approximal caries were
collected from bitewing radiographs. The examiner was blinded to group when
reading the bitewing radiographs. All initial (in the enamel) and manifest (in the
dentine) caries lesions on approximal surfaces in posterior teeth, i.e. primary
molars in the primary dentition and first permanent molars, were included in the
dmfs/DMFS values. A primary molar that had been extracted due to caries was
counted as 3 missing surfaces in the dmfs values.
Caries prevention (I)
Data on the number of occasions the child had been treated with fluoride varnish
and professional polishing was noted from the dental records, as well as the
number of prescriptions of fluoride tablets.

27
Attitudes and experiences (II, III)
Paper II
A questionnaire with 20 questions was used for both groups of children.
Thirteen of the questions concerned dental health information and dental care
and service. Both groups were also asked 7 questions about dental health of the
child and his/her parents, the children’s and parents’ expectations before visits to
the dental clinic, and the educational level of the parents. In the questionnaire to
the parents of the children with CHD, 4 specific questions were added, con-
cerning if the child with CHD had siblings, the differences in dental health in-
formation compared to healthy siblings, parents’ knowledge about antibiotic
prophylaxis, and where they had received this information.
Paper III
The invited dentists were sent written information about the purpose of the study
and were asked to fill in a questionnaire. The questions were pre-tested in a
group of experienced clinicians, and a few changes were performed in the
questionnaire before data collection. The questionnaire had 18 questions con-
cerning the dentists’ experiences and attitudes to dental care for children with
CHD as well as the dentists’ age, gender, and year of graduation. Two reminders
were sent out to non-responders.
Saliva (IV)
Saliva sampling
Stimulated whole saliva (SWS) was collected before lunchtime, and the partici-
pants were asked to refrain from all eating, drinking, and tooth brushing at least
1 hour before sampling. Age, general health, and medication were checked for
the accompanying control.
SWS was collected by chewing on a standardised lump of paraffin.
Instructions were given to chew for 1 minute and thereafter to spit out or

28
swallow any saliva produced. The subject was then asked to chew paraffin for 5
minutes and to collect all saliva that was produced in a test tube. The saliva
samples were assessed for salivary secretion rate (ml/min), buffering capacity,
electrolyte concentration, salivary IgA, total viable counts (TVC), and caries-
associated bacteria, namely, MS and LBC. The secretion rate and buffering
capacity were determined at the sampling occasion, and the samples were then
transported to the laboratory at the department of Paediatric dentistry at Umeå
University for cultivation of oral bacteria. Saliva for assessment of electrolyte
concentrations and salivary IgA was stored frozen until the sampling was
finalized.
Assessment of stimulated saliva secretion rate and buffering capacity
The volume of the produced saliva was immediately measured and the secretion
rate was calculated (ml/min). A drop of saliva from the test tube was applied to a
Dentobuff Strip test pad (Orion Diagnostica Oy, Espoo, Finland) and the colour
of the pH pad was read and compared with the manufacturer’s colour chart.
Cultivation of bacteria
After sampling, the saliva samples were serially diluted in a potassium
phosphate buffer with NaCl to obtain 0, 40, 800, and 8000 times dilutions. MS
were cultivated on selective (MSB) agar (Difco Mitis Salivarius Agar, Becton,
Dickinson and Company, USA) and LBC were cultivated on Man, Rogosa,
Shape (MRS) agar (Merck, Germany). TVC were cultivated on blood agar oral
plates (BAO). All plates were incubated aerobically in 37 ˚C in 5 % CO2 for 48
hours and then examined under a light microscope to verify the colony forming
units (CFU). The total number of CFU in saliva was calculated as CFU/ml of
saliva.

29
Determination of the salivary composition of electrolytes
The saliva samples were diluted 1:1 with MQ-distillated water and centrifuged
at 13200 rpm for 10 minutes and then stored frozen (-20 ˚C) until all samples
were collected. All analyses of the electrolytes were performed in the same
session. Calcium and magnesium were measured by atomic absorption with an
acetylene flame, with a standard curve in the range of 0.8–1.5 mM total calcium
and 0.05–0.21 mM total magnesium. Sodium and potassium concentrations were
measured in the same way at 589.6 nm and 769.9 nm respectively, with a
standard curve in the range of 4–40 mM total sodium and 14–26 mM total
potassium. Chloride was measured indirectly by precipitation of silver at 328.1
nm, with a standard curve in the range of 9–34 mM total chloride. Phosphate
was determined spectrophotometrically at 700 nm with a standard curve in the
range of 2.2–5.7 mM total phosphate.
Determination of salivary IgA
The saliva for determination of salivary IgA was diluted, centrifuged, and stored
frozen as saliva for determination of electrolytes. As a standard preparation, a
purified human colostral IgA Sigma no 1-3755 was used. The salivary IgA
concentrations were calculated by reference to this standard. As a primary anti-
body, an affinity purified anti-human IgA α (alpha chain specific) from goat was
used, and as a secondary antibody, a peroxidased conjugated affinity purified
goat anti-human IgA α (alpha chain specific) was used. The analyses were per-
formed in triplets on Elisa plates, leaving the first wells as blanks. The IgA con-
centrations were determined spectrophotometrically at 490 nm, providing a
mean value for the sample in mg/l.

30
Effects on dental hard tissues caused by medication (V)
Medicines, sample preparation, and pH measurement
Of the 13 selected medicines, there were solid tablets (n = 7), capsules (n = 2),
and mixtures (n = 4). Citric acid (10 mM) was used as control. Tablets were
crushed in a mortar and dissolved in 10 ml of distilled water. For liquid medi-
cines, a 10 ml sample was taken. The endogenous pH values of the water solu-
tions of tablets or liquid medicines were measured with a pH meter.
Titration
Each medicine sample was titrated by adding 0.01 ml aliquots of a NaOH
solution (0.1 M) by using a titrator. The pH value achieved for each 0.01 ml
NaOH added was read with the pH meter and recorded. The titration was per-
formed until a pH value of 7.0 was reached. Samples with an endogenous pH
value > 5.5 were not titrated.
Loss of calcium and phosphate after immersion of dental hard tissue in
medicines
For medicines with a pH below 5.5, the dissolution of calcium and phosphate
after immersion of tooth specimens were quantified. Specimens were prepared
from the central corona of extracted primary canines with no cracks in enamel.
The teeth were embedded in Epofix (Struers, Ballerup, Denmark) and 3 hori-
zontal slices (thickness 80 µm) were cut from each tooth under water-cooling.
Prior to the experiment, the tooth specimens were pre-treated with immersion in
1 mM CaHPO4 + 1 mM F overnight in room temperature. Tablets were crushed
in a mortar, diluted in 2 ml MQ-water and rocked overnight in room tempera-
ture. Calcium and phosphate were analyzed as in Paper IV. First, the baseline
calcium and phosphate content of medicine solutions were measured in 100 µl
of each sample. Thereafter, 500 µl of each medicine solution was transferred
into cell cultivation chambers, and 2 chambers were filled with each medicine.

31
One tooth disc was put into each chamber and the plate was placed in 37 ˚C.
One hundred µl were collected from each chamber after 30 minutes of immer-
sion and analysed. The mean of 2 samples for each medicine was calculated.
Ethical approval
The protocols of studies I and II were approved by the Research Ethics
Committee of the Faculty of Medicine and Odontology at Umeå University and
IV was approved by the Regional Ethical Review Board at Umeå University.
For Paper V prior to the extractions for orthodontic reasons the patients and their
parents were informed about that the teeth should be used for research purposes
and consent were obtained. For paper III no ethical approval was applied for.
Ethical considerations
Informed consent from all the participating children and their parents was ob-
tained before the start of clinical studies in Paper I, II, and IV. The parents were
informed that participation was voluntarily, and any time the study could be
terminated, and the CHD group termination could be performed without harm to
the doctor-patient relation. As families with children with serious heart diseases
face heavy demands due to their surgery, medication, recurrent illness, and
occasional nutritional problems, the added burden the participation in these
studies constituted were carefully considered when the studies were planned. As
the caries problem constitute a considerably add to their burden the potential
medical benefits of these studies were considered to outweigh encroach in their
privacy.
Statistical analyses
All data were processed with the SPSS (versions 11.0-17.0, SPSS Inc., Chicago,
IL, USA).The following statistical analyses were performed: Paper I—One-way

32
analysis of variance (ANOVA) was used to compare the differences between
groups, and Spearman’s rank correlation was used to explore the relationship
between dental caries and selected variables. Chi-Square test was used to test the
differences between groups in the use of fluoride tablets. Paper II—Fischer’s
exact test (2-sided) was used to test the differences in standardised answers
between the 2 groups. Paper III—Chi-Square test was used to test the
differences between groups. Paper IV—Continuous data were analysed by
ANOVA, and categorical data, by chi-square test. In paper V, only descriptive
data were presented. In all statistical analyses, a p-value of less than 0.05 was
considered statistically significant.

33
Results
Paper I
Data for dmfs and DMFS are given in Table 6. All dmfs indices were
statistically significantly higher in the CHD group (p < 0.05), while no
statistically significant differences could be displayed for any of the DMFS
indices (p > 0.05). The number of months the child had been on digoxin
medication and the dmfs value had a statistically significant positive correlation
(r = 0.368, p < 0.05). Ten of the children in the CHD group had been on digoxin
medication between 6 and 87 months. This sub-group had a statistically
significant higher mean dmfs value compared to those children in the CHD
group who did not medicate with digoxin (10.1 ± 8.5 vs. 3.7 ± 5.3, p < 0.05).
The children in the CHD group had achieved statistically significant more
treatments with fluoride varnish and prescriptions of fluoride tablets compared
to the control group. The mean number of treatments with fluoride varnish was
3.8 ± 4.0 for children in the CHD group compared to 1.8 ± 2.2 in the control
group (p < 0.01). Fifty-two % of the children in the CHD group had been
prescribed fluoride tablets on one or more occasions compared to 17 % in the
control group (p < 0.01). There was a significant positive correlation between
the numbers of fluoride varnish treatments and the dmfs value of the child (r =
0.411, p < 0.01).

34
Table 6. dmfs and DMFS in the CHD group and the control group.
n CHD Control p
dmfstot
41
5.2 ± 7.0
2.2 ± 3.5
<0.05
dmfsdentine
41 4.7 ± 6.3 2.1 ± 3.4 <0.05
dmfsapproxtot *
41 3.4 ± 4.0 1.5 ± 2.8 <0.05
dmfsapproxintit *
DMFStot
41
26
0.5 ± 1.0
0.9 ± 1.9
0.1 ± 0.3
0.3 ± 0.6
<0.05
>0.05
DMFSdentine
26 0.6 ± 1.7 0.3 ± 0.6 >0.05
DMFSapproxtot *
26 0.1 ± 0.7 0.1 ± 0.2 >0.05
DMFSapproxintit *
26 0.1 ± 0.7 0.0 ± 0.0 >0.05
* approximal surfaces in canines, premolars, and molars
Paper II
Statistically significant differences were displayed in the professional group that
provided the parents with dental health information and advice, attitudes to re-
ception at the dental clinic, and experience of sedation before operative dental
treatment (p < 0.05). Parents of children with CHD who were patients at a
specialist clinic for paediatric dentistry scored the reception at the dental clinic
higher than those who were patients in general dental practice. This difference
was statistically significant (p < 0.01). No statistically significant differences in
educational level or parental experience of dental health were noted between the
2 groups (Table 7), (p > 0.05).

35
Table 7. Educational level and reported dental health in parents of the CHD
children and controls.
CHD
%
Control
%
p
Educational level of the mother
9 years
12 years
University/college
12
52
36
3
53
44
0.481
Educational level of the father
9 years
12 years
University/college
13
64
23
7
53
40
0.223
Dental health of the mother
No problems
Some problems
Large problems
61
30
9
63
25
12
0.872
Dental health of the father
No problems
Some problems
Large problems
76
24
0
63
31
6
0.400
Paper III
One-fifth of the dentists stated that they had received special education or in-
formation, except the graduate training, to treat children with CHD. Almost half
of the dentists had one or more patients with CHD, and a majority of these stated
that their CHD patients had a caries problem. Only 34 % knew that some of the
medicines used by CHD patients could increase the risk for caries. One-third of
the dentists (33 %) reported that the level of dental care for children with CHD
did not differ compared to healthy children at their clinic, and 42 % of the den-
tists reported that more caries prevention were given compared to healthy
children. Seven % of the dentists reported that shorter recall intervals were given
to children with CHD, while 16 % gave the answer that they did not know.

36
Statistically significant differences were displayed between the answers to the
questions ‘who in the dental team perform the major part of dental care for
children with CHD’ and ‘what is your opinion on who should perform the major
part of the dental care for this group of children’ (p < 0.001). Among dentists
whose clinical time mainly was used for dentistry for children, it was more
common to treat children with CHD than for dentists with less time with
dentistry for children (p < 0.001).
Paper IV
Seven of the children (29 %) on anti-congestive medication had secretion rates
below 0.5 ml/min compared to no child in the control group (p < 0.01), (Fig 2).
Four cases had the same secretion rate as a control with the same age. There
were no statistically significant differences concerning mean salivary secretion
rate, buffering capacity, calcium, chloride, magnesium, phosphate, potassium,
sodium, or salivary IgA concentrations (p > 0.05). TVC differed statistically
significantly between the 2 groups, 1.4 × 106 ± 1.2 × 10
7 in the CHD group vs.
2.7 × 106 ± 2.9 × 10
7 in the control group (p < 0.05). The MS levels were 5.2 ×
104 ± 1.5 × 10
5 in the cardiac group vs. 8.1 × 10
3 ± 1.3 × 10
4 in the control group
(p > 0.05), and the MS ratio of TVC constituted 0.11 ± 0.35 % compared to 0.01
± 0.02 % for the control group (p > 0.05).

37
Fig. 2. Stimulated salivary secretion rate by age in children with heart disease on
heart failure medication and healthy age- and gender-matched controls. Filled
circles show cases, unfilled circles show controls.
Paper V
The endogenous pH values varied between 3.03 and 9.02 of the 13 medicines
that were studied. Six of these (46 %) had an endogenous pH below the critical
pH of 5.5. The lowest pH was recorded for the captopril 12.5 mg tablet water
solution, while the propranolol hydrochloride mixture displayed the highest ti-
tratable acidity. The highest dissolved calcium and phosphate from the tooth
specimens was displayed for the captopril (12.5 mg) tablet water solution 1.9
mM and 1.1 mM, respectively, and with the acetylsalicylic acid (75 mg) tablet
water solution, 1.6 mM calcium and 0.7 mM phosphate were dissolved.
age
17,51512,5107,5
secre
tio
n m
l/m
in
4,00
3,00
2,00
1,00
0,00

38
Discussion
Material and Methodological considerations
Study designs and study groups
For the studies in Paper I, II, and IV in this thesis, a case-control study design
was chosen. Case-control studies can be used to study risk factors by compari-
sons of individuals who have a condition (the cases) with patients who do not
have the condition but are otherwise similar (the controls) (80). Data for each
case-control pair are assessed and are then aggregated. Case-control studies are
relatively inexpensive and can be carried out by small teams or individual re-
searchers in single facilities in a way that more structured experimental studies
often cannot be. They have pointed to a number of important discoveries, but the
hierarchical level of scientific evidence is considered to be relatively low be-
cause of the retrospective exposure, non-randomized nature, and often blinding
not is possible. The shortcomings in the case-control design can be overcome by
cohort study design were exposed and non-exposed are compared. Cohort
studies are however often not possible for practical reasons when the disease is
rare.
Study III examined the experience of dental care for children with
CHD among Swedish general dentists using a descriptive cross-sectional design.
Cross-sectional studies performed with convenience samples cannot be
generalized to the entire population. However, they can identify risk indicators
of those parameters that are significantly associated with the condition being
investigated. One benefit of cross-sectional studies is that they are considered to
be hypothesis-generating (80).
Using plaque pH measurements (81) in Paper V could have given in-
formation of the in vivo effects of medication. This experiment was considered,
but due to the added burden, the participation would have implied for this medi-
cally comprised group, we decided to give up the idea. As the composition of
teeth is variable, due to genetic influences, environmental conditions, and post-
39
eruptive maturation and dentin sclerosis, such differences may lead to large
variations in their response under acidic challenges. The in vitro design that
made it possible to pre-treat the tooth specimens, with immersion in a calcium
phosphate medium, helped to increase the standardization of the specimens.
Clinical decision making should ideally be based on powered high-
quality studies. Using a multicenter approach in Paper I could have made it pos-
sible to include more individuals. As the study group in Paper I included all
children with complex CHD in the area who fulfilled the inclusion criteria, ex-
cept 2 whose families did not give consent to their child to participate, a multi-
center approach was not considered. It is possible however, that the caries
experience in the permanent dentition also would have reached a statistically
significant difference with increased numbers. In Paper II, among the 38 invited
parents, there were only 2 who did not give consent. To match the controls,
parents of 3 children with CHD were excluded. In Paper IV, a multicenter
approach was used for increasing power and significance, as children who ful-
filled inclusion criteria in the county of Västerbotten was limited. In Paper III,
75 % of the invited dentists responded, and the non-responding rate is
considered acceptable for a study based on a questionnaire (82).
Caries registration
Caries were assessed from recordings in dental records and bitewing radiographs
in the Public Dental Service (PDS). Ideally, the same examiner would have ex-
amined all the children in both groups to remove the effects of variation in caries
diagnosis between different examiners. As the children had many medical
contacts already, it was considered unethical to add to their burden. The study
was, therefore, performed on data that had already been collected at the dental
clinics, despite the disadvantages of this procedure. Partly to reduce the effect of
variation in caries diagnoses, all data on posterior approximal caries were col-
lected by one of the authors from bitewing radiographs for both groups of

40
children. In order to increase the level of evidence, all reading of bitewing
radiographs were performed blinded to the examiner, and initial caries were an-
alysed separately.
Saliva collection, cultivation of bacteria, and analysis of saliva
Measurement and analysis of saliva is non-invasive, fast, and cost-effective
diagnostic tool. The salivary secretion rate varies during the day and is affected
by temperature, fluid balance, state of health, frame of mind, and medication.
Hence, the collection of saliva should be standardized so that the results can be
comparable with those from other clinical investigations (14, 20). To meet this,
all saliva samples in study IV were collected before lunchtime and the partici-
pants were asked to refrain from eating, drinking, and tooth brushing 90 minutes
before sampling.
Saliva may be collected as whole saliva or as selectively collected
secretion from specific salivary glands. In the clinic, whole saliva secretion
often is used to asses salivary flow rate, and buffer capacity. Whole saliva can
be collected as unstimulated whole saliva (UWS) or stimulated whole saliva
(SWS). The total volume of saliva collected is expressed as ml/min. An UWS
rate less than 0.1 ml/min is considered a risk value (20). A SWS of 1–3 ml/min
is considered normal and 0.7 ml/min and below is considered a risk value for
caries (83). For schoolchildren, a cut-off of less than 0.5 ml/min is considered
low with regard to caries risk (24).
Questionnaires
There are several methods available to collect qualitative data such as attitudes
and experiences, for example, questionnaires and interviews. Both strategies for
data collection have strengths and shortcomings. The questionnaire can be dis-
tributed in groups or geographic areas and the method is proportionately cost-
effective. Standardized questions can be formulated, that is, all questions and

41
responding-alternatives are presented in the same way for every respondent. The
strengths with interviews on the other hand are that the questions can be formu-
lated in a more detailed way, there is a possibility to ask follow-up questions,
and the non-responding rate is often lower in interviews compared to
questionnaires.
When designing a questionnaire, great effort has to be made when
formulating the questions. The questions should be unambiguous, not leading,
and formulated in a language suited to the target group. The questionnaire
should be followed by a prepaid envelope and a letter. Two reminders are
considered normal (82, 84).
Evaluation of results
In Papers I, II and IV a null-hypothesis was tested and could be rejected for
some of the primary outcome measures as caries experience, attitudes and
experiences of dental care and saliva secretion.
Paper I shows that caries is a common oral health problem in
Swedish children with complex CHD, especially at early ages, and it confirms
findings from studies with different study designs, inclusion criterias, outcome
measures and from countries with differing dental care system (44-53). The
difference in caries prevalence between Swedish children with CHD and healthy
controls was larger than that shown in a British study with a similar design as
ours (48), which only showed more untreated caries in children with CHD. The
high caries frequency is not acceptable and calls for strategies for disease
control.
Due to the great progress in surgical techniques and intensive care
for infants with CHD, the number of surviving children is increasing (1). Groups
of medically compromised children such as immuno-compromised from disease
and/or therapy and children with complex CHD have an increased risk of

42
developing systemic complications from dental infections, which may prove
fatal (43). Poor dental health gives an increased risk of dental bacteraemia that
may lead to infective endocarditis, and healthy teeth may decrease this risk.
Dentists are advised to provide antibiotic prophylaxis against endocarditis in
many of the children with complex CHD, before invasive dental procedures (1).
Healthy teeth among CHD children may contribute to a decrease in the use of
antibiotics for dental/oral infections. Healthy teeth also decrease the need of
general anaesthesia and tooth extractions, which may be more complicated in
complex CHD because of the increased medical risks with general anaesthesia
and the risk of prolonged bleeding amongst children on anti-coagulants and anti-
platelets. Siahi-Benlarbi et al (85) assumed that high levels of oral Candida,
which are associated with caries (86-88), and its descending/resorption through
the gastrointestinal tract may lead to serologic Candida accumulation or
candidiasis. Therefore, a healthy oral cavity (especially before and after heart
transplantation) is an important precondition to prevent Candida infections since
these infections are opportunistic and when the immune system is depressed an
acute infection may occur. Of major significance is also the fact that untreated
caries can be a contraindication for heart surgery and as patients with more
complex anomalies often require several surgical interventions, it is particularly
important that scheduled surgery does not have to be postponed because of
dental disease.
The dental care for children in Sweden is organized by the county
councils and is free of charge. The parents can choose between dental care for
their children organized within the PDS or by private clinics. Around 90 % of
the dental care for children in Sweden is provided within the PDS. The dental
care system offers all children a comprehensive dental care between the ages of
3 and 19 years. The care has a strong preventive approach from an early age,
and all parents are offered dental health information when the child is between
1- and 2-years-old. A common clinical experience in children with CHD is that
43
their parents do not attend this early dental health information and, thus, they do
not benefit from early oral health promotion to the same extent as most
individuals. Paper I showed that children with complex CHD had received more
caries prevention than the healthy controls, and there was a positive correlation
between the caries prevalence and number of fluoride varnish treatments, but the
care had been offered when caries already had become a problem.
Socio-economic factors of the family and the oral health of the care-
taker are closely associated with the oral health and the oral health habits of the
child (89). No differences in educational level of the parents or in their dental
health could be detected between parents of the cases and their controls in Paper
ІІ. Based on this finding, there must be other reasons that explain the increased
caries experience in children with complex CHD.
Saliva plays a key role in the biological interaction between many
medical conditions and oral health related either directly, as in 22q11 and ecto-
dermal dysplasia, with a reduced salivary secretion (90, 91) or due to effects of
pharmacological treatment (92, 93). Medication-induced xerostomia has been
considered as a caries-risk factor in CHD children (94). Paper IV showed that
reduced salivary secretion could be a caries-risk factor in children on heart
failure medication. It is therefore possible that some participants had a reduced
salivary flow in Paper I and this may contribute to the explanation of the high
caries experience in children with complex CHD. Use of antibiotics during early
childhood has been associated with higher MS levels in children aged 5 to 12
years (95), and it is a clinical experience that antibiotics are used more fre-
quently among children with heart disease than healthy children but higher MS
levels has not been shown earlier (48, 96) or in Paper IV. Paper IV showed that
MS constituted a non-significantly higher proportion of the TVC in the study
group and this fit into the theory that a differentiation towards aciduric
microorganisms in the oral ecology precedes dental caries (34).

44
A novel finding was the strong correlation between digoxin
medication and caries experience in Paper I. Sucrose is added to the syrup to
disguise unpleasant taste and thereby facilitate compliance. Sucrose-containing
medicines are often given together with diuretics that can reduce salivary
secretion (68), which add to the cariogenic challenge. Sugars in medicines cause
a pH drop in the oral biofilm as a result of their fermentation in acid-producing
bacteria (23, 43). Additionally, acids in medicines may help to prolong the pH
drop after a sugar challenge. The clinical effects of the low pH, titratable acidity,
and effect on dental hard tissues shown in Paper V can only be speculated on as
data were obtained in vitro. It is, however, clear that some pharmaceutical
preparations commonly used in paediatric cardiology in Sweden have a low
endogenous pH and a potential to dissolve dental hard tissues. The erosive
potential depends on the intimate interplay between chemical factors like
endogenous pH and titratable acidity; biological factors such as the properties of
the saliva; and behavioural factors like oral hygiene, vomiting, and frequency of
medication (97). If this finding is taken together with the fact that these
medicines may be given together with Lanoxin® (digoxin), which contains
sucrose and some of the patients suffer from medication-induced xerostomia, it
is clear that medication may pose a hazardous threat to the oral health in
children with complex CHD. These findings support the hypothesis that both
caries and erosions are possible outcomes in connection with the regular use of
pharmaceutical preparations (97). An assessment of the prevalence of erosions
was not the within the aim of this thesis, however. In a study on the erosive
potential of 97 medicines used regularly and long term by children, 57 % had an
endogenous pH below 5.5, and those used for the cardiovascular system had the
lowest mean endogenous pH, and it was 4.05 (98). Further, Neves et al (75) con-
cluded that several paediatric medicines showed high sugar concentration, pH
values below the critical value, and high titratable acidity values, all of which
increase the medicines' cariogenic and erosive potentials.

45
Ersin et al (99) studied oral and dental manifestations of young
asthmatics in relation to medication, severity, and duration of the condition. The
results of their study supported the hypothesis that factors related to asthmatic
condition and/or medication might increase the risk of caries due to the lower
salivary flow rate and pH in asthmatics. In addition, the duration of medication
and the duration of illness were shown to be risk factors for caries development
in asthmatic children. The authors concluded that asthmatic patients especially
in the younger age groups should receive intensive preventive care, including
oral hygiene instruction, dietary advice, and regular topical fluoride treatments.
Stensson et al (56) investigated preschool children with asthma and found a
higher caries frequency among asthmatic children. They pointed to the
importance of developing preventive dental programs for preschool children
with asthma and of developing collaboration between dental and medical care-
givers in relation to children with asthma. This is also applicable for children
with complex CHD.
Being born with a heart anomaly may, depending on the severity of
the CHD, cause a dramatic start in life for the affected child and the family.
Surgery may be performed directly after birth or within the first year of life and
be followed by several complementary surgeries. Multiple medications and long
periods of hospitalisation with frequent contacts with medical staff become the
part of everyday life to families with children affected with complex CHD.
Feeding problems are often seen during the first years of life. Vomiting is
common and to compensate for this, feeds are frequent and night meals are often
necessary to maintain energy intake at an acceptable level. Infections often last
for longer periods than in healthy children, with an increased need for drinking,
sometimes at night, when salivary protection is low (4). Brain injury is the most
significant complication of surgery for CHD (100). Neurodevelopmental out-
come, however, is influenced mostly by genetic co-morbidity and preoperative
neurological status (101). A systematic review of psychological adjustment and

46
quality of life after open-heart surgery for congenital heart disease concluded
that children with more severe heart defects, or those in need of future surgical
interventions and children with neurodevelopmental impairment are at particular
risk for maladjustment (102). It is clear that children with complex CHD,
particularly at early ages, should be considered as a group with special needs in
dentistry (103-105).
Paper III showed that parents of children with complex CHD did not
have the same satisfaction with the reception they received in dental care than
the healthy controls. Children with CHD had received sedation before operative
dental treatment significantly more often than healthy children, reflecting a
higher need of operative dental treatment. The CHD group had also received
more caries prevention (Paper I). Lowry et al (106) compared dental attitudes
knowledge and health practice between a CHD group and a matched control
group and found that 18 % of the children with CHD had not received dental
care. In a study on the provision of dental care for medically compromised
children, it was shown that dental practitioners had treated patients with CHD in
0 to 5 sessions in the past 5 years with an average of 2 patients for each
practitioner (107). Only 37 % felt confident in providing dental treatment for
children with cardiac disease, while 80 % of the respondents stated they would
benefit from further regular training. Jowet and Cabot (108) noted that many
dentists were not confident in treating children with CHD, which is in coherence
with data in Paper III that indicated that Swedish dentists are unsettled and
insecure in the dental treatment of children with heart disease. As the PDS does
not differ significantly from county to county, the results of the study are
considered applicable to Sweden in general. The findings should, however, be
generalized to the whole group of children with CHD as it was considered
difficult for the dentists to classify their CHD patients due to limited information
on medical background facts. This lack of experience regarding these children’s
medical conditions and pharmacological regimes is a cause of concern and

47
suggests a need for specialist dental care for these children. These data also
support the need for further education about dental treatment for groups of
medically compromised children (109).
The transition into adulthood has been a significant clinical concern
as the survival rate for adolescents with CHD increases. There is a continued
need to support and counsel adolescents to maintain their health-promoting
behaviour. Health promotion counselling for adolescents with CHD should
encourage improving lifestyle habits, including adequate physical exercise and
good oral hygiene (110).
Clinical perspectives
Except for the replacement of sucrose in Lanoxin® with a non-cariogenic
sweetener, factors that can be changed in a more health-promoting direction in
children with complex CHD are oral hygiene habits, fluoride exposure, and
sugar consumption.
In the clinical management of children with complex CHD, high-
caries-risk children should be identified as early as possible, which is possible if
a close cooperation between the paediatric cardiologist and paediatric dentist is
established. Early preventive care should be adjusted to the special needs of
children with CHD and an individual preventive program should be
implemented during the first year of life (49). This regime is supported by Gussy
et al who in their review on caries in early childhood found evidence that
potentially effective interventions should occur in the first 2 years of life of the
child at risk (27). An interdisciplinary approach integrating the professional
knowledge and skills may help to improve the results for the individual patient
(43, 107, 111, 112).
The paediatrician should facilitate referral to dental services and
emphasize the importance of good oral health. For high-caries-risk groups, it is
recommended that regular dental care is offered within clinics for specialized

48
paediatric dentistry (103, 104). Together with parents, a plan for dental care
should be established, and the responsibilities for dental care and for families
should be made clear. Individual need of antibiotics for prophylaxis for infective
endocarditis at invasive dental treatments should also be determined (1). Short
recall intervals should be offered until the caries-risk factors are eliminated.
Children on medication with sugar-containing syrups should be given extra
attention, and salivary secretion should be assessed in children on heart failure
medication. Tooth brushing using fluoridated toothpaste should be encouraged.
Based on individual needs, additional fluoride may be indicated and is suggested
to be administered based on caries risk and compliance (24). Parents should be
advised to avoid added sugar at meals. Today, there is poor knowledge of the
early feeding practice in children with CHD. We will obtain knowledge from a
running prospective study of dietary habits and colonisation of the oral
microflora from an early age in children with complex CHD.
A continuous issue for improving the oral health is the
accomplishment of education and training for both dental and medical health
care providers about oral health problems and their prevention in this new group
of patients (109, 113).

49
Conclusions
Children with complex CHD had a higher caries experience than healthy
age- and gender-matched controls.
Children with complex CHD on digoxin medication had a higher caries
experience than other children with complex CHD.
Children with complex CHD had received more caries prevention than
healthy controls.
Parents of children with complex CHD were less satisfied with the
reception and care they received in the dental service compared with the
parents of healthy children.
Swedish dentists had a different opinion regarding the provision of dental
treatment to children with CHD compared to the current situation.
Children on heart failure medication can have a low saliva secretion.
Some pharmaceutical preparations used on long-term basis in paediatric
cardiology may pose a hazardous threat to dental hard tissues due to their
acidity.

50
Populärvetenskaplig sammanfattning
Medfödda hjärtfel (CHD) är en av de vanligaste utvecklingsanomalierna hos barn och
förekommer hos ca 8-10 per 1000 levande födda barn. Med anledning av stora
framsteg inom barnkardiologin de senaste decennierna så överlever idag allt fler barn
som föds med komplexa CHD. Detta har inneburit att barn med CHD blivit en ny och
växande patientgrupp även inom tandvården. Den övergripande målsättningen med
denna avhandling var att kartlägga kariesförekomsten och potentiella
bakgrundsfaktorer hos barn med komplexa CHD.
I delarbete I undersöktes kariesförekomsten hos 41 barn med komplexa
CHD och en kontrollgrupp av friska ålders- och könsmatchade barn. Barnen med
komplexa CHD hade en ökad kariesförekomst i mjölktandsbettet. Barn med CHD som
medicinerade med digoxin hade en högre kariesförekomst än de hjärtbarn som inte
använde denna medicin. Barnen med CHD hade fått mer kariesprofylax i tandvården
än friska barn.
I delarbete II studerades föräldrars attityder till och erfarenheter av
omhändertagande av barn med CHD i tandvården. Trettiotre föräldrar till barn med
komplexa CHD jämfördes mot en matchad grupp av föräldrar till friska barn. Föräldrar
till friska barn var mer nöjda med omhändertagandet och bemötandet inom tandvården
än föräldrar till barn med CHD. Studien rekommenderar att barn med komplexa CHD
erhåller sin tandvård hos specialistkliniker för barntandvård särskilt de första
levnadsåren.
I delarbete III studerades attityder till och erfarenheter av tandvård för
barn med CHD bland 183 allmäntandläkare. En minoritet av de tillfrågade tandläkarna
hade erhållit någon kompletterande utbildning av tandvård för barn med CHD. Cirka
50 % av tandläkarna hade en eller flera patienter med CHD och majoriteten av dessa
hade noterat en ökad kariesförekomst hos dessa barn. Studien visade att tandvård för
barn med CHD utförs till största del av tandsköterskor, tandhygienister och
allmäntandläkare vilket avvek från tandläkarnas önskemål om hur tandvården skall
organiseras för barn med CHD.
Många barn med komplexa CHD måste medicinera över lång tid och vissa
mediciner kan minska salivflödet och därigenom bidra till att karies utvecklas.
Salivens egenskaper studerades hos 24 barn som hade hjärtsviktsmedicinering i
delarbete IV och jämfördes mot saliv från en frisk kontrollgrupp. Salivens
sekretionshastighet, buffringskapacitet, bakteriehalter samt elektrolytnivåer
undersöktes. Tjugonio % av barnen med hjärtsviktsmedicinering hade låg
salivsekretion jämfört med inget barn i kontrollgruppen. En slutsats är att barn med
hjärtsviktsmedicinering kan ha låg salivsekretion och det kan vara en riskfaktor för att
utveckla karies.
I delarbete V studerades 13 av de mest använda medicinerna vid CHD
med avseende på pH, buffring samt förmåga till att lösa mineral från tandvävnad. Sex
av medicinerna hade ett pH-värde som kan vara skadligt för tandsubstans. Det
konkluderades att några av de vanligast förekommande medicinerna inom svensk
barnkardiologi kan utgöra ett hot mot tandvävnad på grund av surhetsgraden och
förmågan att lösa ut mineral.

51
Acknowledgements
First I would like to express my sincere gratitude to all children and parents who
have participated in the studies. Further, I am so grateful to all you who have
helped and supported me and made it possible to for me to complete my thesis.
In particular, I would like to thank:
Associate Professor Christina Stecksén-Blicks, my principal supervisor, co-
author and Head of the Division of Paediatric Dentistry, Umeå University, for
introducing me to the field of scientific research. Thank you for generously
sharing your vast scientific knowledge and your never ending inspiration, your
endless support and for always believing in me. I am so grateful for having you
by my side during this journey and I am looking forward to further
collaboration.
Associate Professor Annika Rydberg, my co-supervisor and co-author for
introducing me to and guiding me in the world of paediatric cardiology. Thank
you for your great expertise, good advice, valuable comments and the
enthusiasm you bring me every time we meet.
Technical assistant Inger Sjöström, co-author in papers IV and V and my
supervisor in the laboratory. Without your outstanding advice and assistance
with the laboratory management this would not have been possible.
Sofia Asplund, Kristin Grahn, Charlotta Svanberg and Sara Wikström, co-
authors, for your cooperation with the data collection in Paper I and II.
Hjördis Olsson for excellent help and support with administrative problems and
academic logistics.
Staff at the Paediatric Cardiology Clinics at the University Hospital, Umeå and
at the Karolinska University Hospital, Stockholm, Sweden, for helpful
assistance. You do a tremendous job for all children with CHD.
Colleagues and workmates at the Department of Paediatric Dentistry in Uppsala,
Umeå and at Eastmaninstitutet, Stockholm, for support, encouragement and
friendship.

52
Margaret Grindefjord, Head of the Department of Paediatric Dentistry,
Eastmaninstitutet, Stockholm, for making it possible for me to finish my PhD-
studies studies within the scope of my work and for always being so supportive.
Dental nurses Lena Lif and Barbro Enocson, Eastmaninstitutet, Stockholm, for
your assistance in the data collection, encouragement and never-ending
positivism.
Leila Aghababa, my dear friend, colleague and the best of roommates. Thank
you for interesting discussions, tremendous support and delicious lunches.
My family and friends for great support, patience and encouragement.
Signe and Ingrid, my beloved little daughters. Thank you for brighten up my
day with all your laughter, hugs and sweet kisses.
Fredrik. Thank you for your never ending love, your great encouragement,
support and interest in my work. I love you.
These studies were supported by grants from the Swedish Heart-Children’s
Association (Hjärtebarnsfonden), the Patent Revenue Found for Dental
Prophylaxis and the County Council of Uppsala, Sweden.

53
References
1. The National Board of Health and Welfare (Socialstyrelsen). Nationella riktlinjer för
hjärtsjukvård 2008 (In Swedish). Socialstyrelsens publikationer, artikelnummer 2008-
102-7. 2008.
2. Cameron AC, Widmer RP, eds. Handbook of Pediatric Dentistry. Third ed.
Philadelphia: Mosby 2008.
3. Hoffman JI, Kaplan S. The incidence of congenital heart disease. J Am Coll Cardiol
2002;39:1890-900.
4. Sunnegårdh J. Barnkardiologi - en översikt. First ed. Lund: Studentlitteratur; 2000.
5. Bhat AH, Sahn DJ. Congenital heart disease never goes away, even when it has been
'treated': the adult with congenital heart disease. Curr Opin Pediatr 2004;16:500-7.
6. Rosenkranz ER. Surgery for congenital heart disease. Curr Opin Cardiol 1993;8:262-
75.
7. Reybrouck T, Vangesselen S, Gewillig M. Impaired chronotropic response to exercise
in children with repaired cyanotic congenital heart disease. Acta Cardiol 2009;64:723-
7.
8. Burd L, Deal E, Rios R, Adickes E, Wynne J, Klug MG. Congenital heart defects and
fetal alcohol spectrum disorders. Congenit Heart Dis 2007;2:250-5.
9. Allen HD, Driscoll DJ, Shaddy RE, Feltes TF. Moss and Adams' Heart Disease in
Infants, Children, and Adolescents. Philadelphia: Lippincott Williams & Wilkins;
2008.
10. Vis JC, Duffels MG, Winter MM, Weijerman ME, Cobben JM, Huisman SA, et al.
Down syndrome: a cardiovascular perspective. J Intellect Disabil Res 2009;53:419-25.
11. van der Burgt I. Noonan syndrome. Orphanet J Rare Dis 2007;2:4.
12. Richardson P, McKenna W, Bristow M, Maisch B, Mautner B, O'Connell J, et al.
Report of the 1995 World Health Organization/International Society and Federation of
Cardiology Task Force on the Definition and Classification of cardiomyopathies.
Circulation 1996;93:841-2.
13. Crossner CG. Salivary flow rate in children and adolescents. Swed Dent J 1984;8:271-
6.
14. Wong DT. Salivary Diagnostics. Singapore: Wiley-Blackwell; 2008.
15. Dawes C. Physiological factors affecting salivary flow rate, oral sugar clearance, and
the sensation of dry mouth in man. J Dent Res 1987;66 Spec No:648-53.
16. Lagerlof F, Oliveby A. Caries-protective factors in saliva. Adv Dent Res 1994;8:229-
38.
17. Dowd FJ. Saliva and dental caries. Dent Clin North Am 1999;43:579-97.
18. Lenander-Lumikari M, Loimaranta V. Saliva and dental caries. Adv Dent Res
2000;14:40-7.
19. Tappuni AR, Challacombe SJ. A comparison of salivary immunoglobulin A (IgA) and
IgA subclass concentrations in predentate and dentate children and adults. Oral
Microbiol Immunol 1994;9:142-5.
20. Humphrey SP, Williamson RT. A review of saliva: normal composition, flow, and
function. J Prosthet Dent 2001;85:162-9.
54
21. Smith DJ, Taubman MA. Ontogeny of immunity to oral microbiota in humans. Crit
Rev Oral Biol Med 1992;3:109-33.
22. Tylstrup A, Fejerskov O, eds. Textbook of Clinical Cariology. Copenhagen:
Munksgaard; 1999.
23. Selwitz RH, Ismail AI, Pitts NB. Dental caries. Lancet 2007;369:51-9.
24. Koch G, Poulsen S, eds. Pediatric Dentistry A Clinical Approach. Second ed. West
Sussex: Wiley-Blackwell; 2009.
25. Alm A, Wendt LK, Koch G, Birkhed D. Prevalence of approximal caries in posterior
teeth in 15-year-old Swedish teenagers in relation to their caries experience at 3 years
of age. Caries Res 2007;41:392-8.
26. Alm A, Wendt LK, Koch G, Birkhed D. Oral hygiene and parent-related factors
during early childhood in relation to approximal caries at 15 years of age. Caries Res
2008;42:28-36.
27. Gussy MG, Waters EG, Walsh O, Kilpatrick NM. Early childhood caries: current
evidence for aetiology and prevention. J Paediatr Child Health 2006;42:37-43.
28. Skeie MS, Raadal M, Strand GV, Espelid I. The relationship between caries in the
primary dentition at 5 years of age and permanent dentition at 10 years of age - a
longitudinal study. Int J Paediatr Dent 2006;16:152-60.
29. Hara AT, Zero DT. The caries environment: saliva, pellicle, diet, and hard tissue
ultrastructure. Dent Clin North Am 2010;54:455-67.
30. de Soet JJ, van Loveren C, Lammens AJ, Pavicic MJ, Homburg CH, ten Cate JM, et
al. Differences in cariogenicity between fresh isolates of Streptococcus sobrinus and
Streptococcus mutans. Caries Res 1991;25:116-22.
31. Marsh PD. Microbiologic aspects of dental plaque and dental caries. Dent Clin North
Am 1999;43:599-614, v-vi.
32. Bradshaw DJ, Marsh PD. Analysis of pH-driven disruption of oral microbial
communities in vitro. Caries Res 1998;32:456-62.
33. Sbordone L, Bortolaia C. Oral microbial biofilms and plaque-related diseases:
microbial communities and their role in the shift from oral health to disease. Clin Oral
Investig 2003;7:181-8.
34. Marsh PD. Dental plaque as a biofilm and a microbial community - implications for
health and disease. BMC Oral Health 2006;6 Suppl 1:S14.
35. Marsh PD. Microbiology of dental plaque biofilms and their role in oral health and
caries. Dent Clin North Am 2010;54:441-54.
36. Fejerskov O, Kidd E, eds. Dental Caries. The disease and its clinical management.
First ed. Copenhagen: Blackwell Munksggard; 2003.
37. Burt BA. Concepts of risk in dental public health. Community Dent Oral Epidemiol
2005;33:240-7.
38. Bankel M, Eriksson UC, Robertson A, Kohler B. Caries and associated factors in a
group of Swedish children 2- 3 years of age. Swed Dent J 2006;30:137-46.
39. Stecksen-Blicks C, Holgerson PL, Twetman S. Caries risk profiles in two-year-old
children from northern Sweden. Oral Health Prev Dent 2007;5:215-21.
40. Hugoson A, Koch G, Helkimo AN, Lundin SA. Caries prevalence and distribution in
individuals aged 3-20 years in Jonkoping, Sweden, over a 30-year period (1973-2003).
Int J Paediatr Dent 2008;18:18-26.

55
41. The National Board of Health and Welfare (Socialstyrelsen). Karies hos barn och
ungdomar. En lägesrapport för år 2008 (in Swedish). Socialstyrelsens publikationer,
artikelnummer: 2010-3-5. 2008.
42. Stecksen-Blicks C, Kieri C, Nyman JE, Pilebro C, Borssen E. Caries prevalence and
background factors in Swedish 4-year-old children - a 40-year perspective. Int J
Paediatr Dent 2008;18:317-24.
43. Foster H, Fitzgerald J. Dental disease in children with chronic illness. Arch Dis Child
2005;90:703-8.
44. Berger EN. Attitudes and preventive dental health behaviour in children with
congenital cardiac disease. Aust Dent J 1978;23:87-90.
45. Urquhart AP, Blinkhorn AS. The dental health of children with congenital cardiac
disease. Scott Med J 1990;35:166-8.
46. Pollard MA, Curzon ME. Dental health and salivary Streptococcus mutans levels in a
group of children with heart defects. Int J Paediatr Dent 1992;2:81-5.
47. Hallett KB, Radford DJ, Seow WK. Oral health of children with congenital cardiac
diseases: a controlled study. Pediatr Dent 1992;14:224-30.
48. Franco E, Saunders CP, Roberts GJ, Suwanprasit A. Dental disease, caries related
microflora and salivary IgA of children with severe congenital cardiac disease: an
epidemiological and oral microbial survey. Pediatr Dent 1996;18:228-35.
49. Hayes PA, Fasules J. Dental screening of pediatric cardiac surgical patients. ASDC J
Dent Child 2001;68:255-8, 28-9.
50. da Silva DB, Souza IP, Cunha MC. Knowledge, attitudes and status of oral health in
children at risk for infective endocarditis. Int J Paediatr Dent 2002;12:124-31.
51. Balmer R, Bu'Lock FA. The experiences with oral health and dental prevention of
children with congenital heart disease. Cardiol Young 2003;13:439-43.
52. Tasioula V, Balmer R, Parsons J. Dental health and treatment in a group of children
with congenital heart disease. Pediatr Dent 2008;30:323-8.
53. Rai K, Supriya S, Hegde AM. Oral health status of children with congenital heart
disease and the awareness, attitude and knowledge of their parents. J Clin Pediatr Dent
2009;33:315-8.
54. Engvall M, Sjogreen L, Kjellberg H, Robertson A, Sundell S, Kiliaridis S. Oral health
in children and adolescents with myotonic dystrophy. Eur J Oral Sci 2007;115:192-7.
55. Blomqvist M, Holmberg K, Fernell E, Ek U, Dahllof G. Oral health, dental anxiety,
and behavior management problems in children with attention deficit hyperactivity
disorder. Eur J Oral Sci 2006;114:385-90.
56. Stensson M, Wendt LK, Koch G, Oldaeus G, Birkhed D. Oral health in preschool
children with asthma. Int J Paediatr Dent 2008;18:243-50.
57. Stecksen-Blicks C, Holm AK, Mayanagi H. Dental caries in Swedish 4-year-old
children. Changes between 1967 and 1987. Swed Dent J 1989;13:39-44.
58. SBU. Att förebygga karies. En systematisk litteraturöversikt. SBU-rapport nr 161 (In
Swedish). Göteborg: Swedish Council on Technology Assessment in Health Care;
2002.
59. Twetman S. Caries prevention with fluoride toothpaste in children: an update. Eur
Arch Paediatr Dent 2009;10:162-7.

56
60. Ten Cate JM. Fluorides in caries prevention and control: empiricism or science. Caries
Res 2004;38:254-7.
61. van Loveren C, Hoogenkamp MA, Deng DM, ten Cate JM. Effects of different kinds
of fluorides on enolase and ATPase activity of a fluoride-sensitive and fluoride-
resistant Streptococcus mutans strain. Caries Res 2008;42:429-34.
62. Twetman S. Prevention of early childhood caries (ECC)--review of literature
published 1998-2007. Eur Arch Paediatr Dent 2008;9:12-8.
63. Lin YT, Tsai CL. Comparative anti-caries effects of tablet and liquid fluorides in cleft
children. J Clin Dent 2000;11:104-6.
64. Nunn JH, Ng SK, Sharkey I, Coulthard M. The dental implications of chronic use of
acidic medicines in medically compromised children. Pharm World Sci 2001;23:118-
9.
65. O'Sullivan EA, Curzon ME. Salivary factors affecting dental erosion in children.
Caries Res 2000;34:82-7.
66. Pomarico L, Czauski G, Portela MB, de Souza IP, Kneipp L, de Araujo Soares RM, et
al. Cariogenic and erosive potential of the medication used by HIV-infected children:
pH and sugar concentration. Community Dent Health 2008;25:170-2.
67. Nederfors T, Isaksson R, Mornstad H, Dahlof C. Prevalence of perceived symptoms of
dry mouth in an adult Swedish population--relation to age, sex and pharmacotherapy.
Community Dent Oral Epidemiol 1997;25:211-6.
68. Sreebny LM, Schwartz SS. A reference guide to drugs and dry mouth. Gerodontology
1986;5:75-99.
69. Scully C, Felix DH. Oral medicine -- update for the dental practitioner: dry mouth and
disorders of salivation. Br Dent J 2005;199:423-7.
70. Streckfus CF. Salivary function and hypertension: a review of the literature and a case
report. J Am Dent Assoc 1995;126:1012-7.
71. Nederfors T, Dahlof C, Twetman S. Effects of the beta-adrenoceptor antagonists
atenolol and propranolol on human unstimulated whole saliva flow rate and protein
composition. Scand J Dent Res 1994;102:235-7.
72. Nederfors T, Dahlof C. Effects on salivary flow rate and composition of withdrawal of
and re-exposure to the beta 1-selective antagonist metoprolol in a hypertensive patient
population. Eur J Oral Sci 1996;104:262-8.
73. Nederfors T, Dahlof C, Ericsson T, Twetman S. Effects of the antihypertensive drug
captopril on human salivary secretion rate and composition. Eur J Oral Sci
1995;103:351-4.
74. Nederfors T, Twetman S, Dahlof C. Effects of the thiazide diuretic
bendroflumethiazide on salivary flow rate and composition. Scand J Dent Res
1989;97:520-7.
75. Neves BG, Farah A, Lucas E, de Sousa VP, Maia LC. Are paediatric medicines risk
factors for dental caries and dental erosion? Community Dent Health 2010;27:46-51.
76. Valinoti AC, Da Silva Pierro VS, Da Silva EM, Maia LC. In vitro alterations in dental
enamel exposed to acidic medicines. Int J Paediatr Dent 2010:Oct 21. doi:
10.1111/j.365-263X.2010.01104.x. [Epub ahead of print].
77. Larsen MJ. Chemical events during tooth dissolution. J Dent Res 1990;69 Spec
No:575-80; discussion 634-6.

57
78. Meurman JH, ten Cate JM. Pathogenesis and modifying factors of dental erosion. Eur
J Oral Sci 1996;104:199-206.
79. Johansson AK. Dental Erosion. Tandläkartidningen 2004;97:57-61.
80. Wang JJ, Attia J. Study designs in epidemiology and levels of evidence. Am J
Ophthalmol 2010;149:367-70.
81. Lingstrom P, Imfeld T, Birkhed D. Comparison of three different methods for
measurement of plaque-pH in humans after consumption of soft bread and potato
chips. J Dent Res 1993;72:865-70.
82. Sudman S, Bradburn N. Asking questions: A practical guide to questionnaire design.
San Fransisco: Jossey-Bass; 1982.
83. Ericsson Y, Hardwick L. Individual diagnosis, prognosis and counselling for caries
prevention. Caries Res 1978;12 Suppl 1:94-102.
84. Ejlertsson G. Enkäten i praktiken. Lund: Studentlitteratur; 1996.
85. Siahi-Benlarbi R, Nies SM, Sziegoleit A, Bauer J, Schranz D, Wetzel WE. Caries-,
Candida- and Candida antigen/antibody frequency in children after heart
transplantation and children with congenital heart disease. Pediatr Transplant
2010;14:715-21.
86. de Carvalho FG, Silva DS, Hebling J, Spolidorio LC, Spolidorio DM. Presence of
mutans streptococci and Candida spp. in dental plaque/dentine of carious teeth and
early childhood caries. Arch Oral Biol 2006;51:1024-8.
87. Ollila PS, Larmas MA. Long-term predictive value of salivary microbial diagnostic
tests in children. Eur Arch Paediatr Dent 2008;9:25-30.
88. Klinke T, Kneist S, de Soet JJ, Kuhlisch E, Mauersberger S, Forster A, et al. Acid
production by oral strains of Candida albicans and lactobacilli. Caries Res 2009;43:83-
91.
89. Meurman PK, Pienihakkinen K. Factors Associated with Caries Increment: A
Longitudinal Study from 18 Months to 5 Years of Age. Caries Res 2010;44:519-24.
90. Klingberg G, Lingstrom P, Oskarsdottir S, Friman V, Bohman E, Carlen A. Caries-
related saliva properties in individuals with 22q11 deletion syndrome. Oral Surg Oral
Med Oral Pathol Oral Radiol Endod 2007;103:497-504.
91. Bergendal B, Norderyd J, Bagesund M, Holst A. Signs and symptoms from
ectodermal organs in young Swedish individuals with oligodontia. Int J Paediatr Dent
2006;16:320-6.
92. Moore PA, Guggenheimer J. Medication-induced hyposalivation: etiology, diagnosis,
and treatment. Compend Contin Educ Dent 2008;29:50-5.
93. Maupome G, Shulman JD, Medina-Solis CE, Ladeinde O. Is there a relationship
between asthma and dental caries?: a critical review of the literature. J Am Dent Assoc
2010;141:1061-74.
94. da Fonseca MA, Evans M, Teske D, Thikkurissy S, Amini H. The impact of oral
health on the quality of life of young patients with congenital cardiac disease. Cardiol
Young 2009;19:252-6.
95. Dasanayake AP, Roseman JM, Caufield PW, Butts JT. Distribution and determinants
of mutans streptococci among African-American children and association with
selected variables. Pediatr Dent 1995;17:192-8.
96. Torres MC, Ramos ME, Coelho TL, Harari S. Salivary Streptococcus mutans and
Lactobacillus sp levels in cardiac children. J Clin Pediatr Dent 2001;26:103-9.

58
97. Lussi A, Jaeggi T. Erosion--diagnosis and risk factors. Clin Oral Investig 2008;12
Suppl 1:S5-13.
98. Maguire A, Baqir W, Nunn JH. Are sugars-free medicines more erosive than sugars-
containing medicines? An in vitro study of paediatric medicines with prolonged oral
clearance used regularly and long-term by children. Int J Paediatr Dent 2007;17:231-8.
99. Ersin NK, Gulen F, Eronat N, Cogulu D, Demir E, Tanac R, et al. Oral and dental
manifestations of young asthmatics related to medication, severity and duration of
condition. Pediatr Int 2006;48:549-54.
100. Snookes SH, Gunn JK, Eldridge BJ, Donath SM, Hunt RW, Galea MP, et al. A
systematic review of motor and cognitive outcomes after early surgery for congenital
heart disease. Pediatrics 2010;125:e818-27.
101. Knirsch W, Zingg W, Bernet V, Balmer C, Dimitropoulos A, Pretre R, et al.
Determinants of body weight gain and association with neurodevelopmental outcome
in infants operated for congenital heart disease. Interact Cardiovasc Thorac Surg
2010;10:377-82.
102. Latal B, Helfricht S, Fischer JE, Bauersfeld U, Landolt MA. Psychological adjustment
and quality of life in children and adolescents following open-heart surgery for
congenital heart disease: a systematic review. BMC Pediatr 2009;9:6.
103. Svenska Pedodontiföreningen. Prioriteringar och patientsäkerhet i tandvård för barn
och ungdomar (In Swedish). 2008: http://www.spf.nu/vardprogram/sarskildvard.asp.
104. Dahllof G, Hallström U, Klingberg G, Koch G, Lundin SA, Mejare I, et al. Dentistry
for children and adolenscents in Sweden: A mission statement from the Swedish
sociesty for pediatric dentistry. Tandläkartidningen 2001;93:38-41.
105. FitzGerald K, Fleming P, Franklin O. Dental health and management for children with
congenital heart disease. Prim Dent Care 2010;17:21-5.
106. Lowry LY, Evans DJ, Lowry RJ, Welbury RR. Under-registration for dental care of
children with heart defects in the north-east of England: a comparative study. Prim
Dent Care 1996;3:68-70.
107. Parry JA, Khan FA. Provision of dental care for medically compromised children in
the UK by General Dental Practitioners. Int J Paediatr Dent 2000;10:322-7.
108. Jowett NI, Cabot LB. Patients with cardiac disease: considerations for the dental
practitioner. Br Dent J 2000;189:297-302.
109. Krause M, Vainio L, Zwetchkenbaum S, Inglehart MR. Dental education about
patients with special needs: a survey of U.S. and Canadian dental schools. J Dent Educ
2010;74:1179-89.
110. Chen CW, Chen YC, Chen MY, Wang JK, Su WJ, Wang HL. Health-promoting
behavior of adolescents with congenital heart disease. J Adolesc Health 2007;41:602-
9.
111. Rogers JP, Stewart PR, Stapleton JV, Hribar DL, Adams P, Gale AE. An
interdisciplinary approach to the management of complex medical and dental
conditions. Aust Dent J 2000;45:270-6.
112. Krol DM. Children's oral health and the role of the pediatrician. Curr Opin Pediatr
2010:Sep 30. doi: 10.1097/MOP.0b013e3283402e3b. [Epub ahead of print].
113. Kagihara LE, Niederhauser VP, Stark M. Assessment, management, and prevention of
early childhood caries. J Am Acad Nurse Pract 2009;21:1-10.

59
APPENDIX I. Questionnaires Paper II
CHD
Dental health information and advice Describe the dental health information and advice. The
information has been Very good
Good
Neither good nor poor
Poor
Very poor
The quantity of information has been Sufficient
Neither sufficient nor
insufficient
Insufficient
Does your child have siblings? Yes
No
Did you notice differences in dental health information
compared to your child’s healthy siblings? Yes, more extensive
Yes, more adjusted to existing
needs
No
Don´t know
When did you receive information and advice on oral
health? When the child was < 6 months
6 months – 1 year
1-3 years
> 3 years
From where did you receive the information and advice? Physician
Dentist
Dental hygienist
Found information on my own
Other source
Is it possible to follow the current advice? Yes, completely
Yes, partly
No, I am doubtful
No, not at all
Have you been informed that your child needs antibiotic
prophylaxis before invasive dental treatment? Yes
No
From where did you first receive information about
antibiotic prophylaxis? Physician
Dentist
Dental hygienist
Found information on my own
Other source
Does the current dental health information need to be
changed? Yes, a lot
Yes, some
No, not in need of change
No opinion

60
Dental care and service Describe the reception at the dental clinic Excellent
Satisfactory
Decent
Poor
Very poor
Are enough time provided during appointments at the
dental clinic? Yes, definitely
Yes, partially
Probably not
No, not at all
Have sedatives or general anesthesia been used for your
child? Never
1-2 occasions
3-4 occasions
>4 occasions
What was your experience of sedatives or general
anesthesia Excellent
Satisfactory
Decent
Poor
Very poor
Was local anesthesia used when teeth were filled? Always
Often
Sometimes
Never
Don´t know
What was your experience with respect to the
competence of the dental staff Very good
Good
Varying
Bad
Very bad
Do you believe the control intervals were adjusted to
meet the needs of your child? Gaps were to long
Sufficient
Too close
Don´t know
Children and parents
How would you describe your child’s dental health? No problems
Some problems
Large problems
How do you experience your child´s expectations before
a visit to the dental clinic? Positive
Neither positive nor negative
Negative
Don´t know
Does you or the other parent experience discomfort
before your own visits at the dental clinic? Always
Sometimes
Never
Don´t know

61
Dental health of mother No problems
Some problems
Large problems
Educational level of mother Nine years
12 years
University/college
Dental health of father No problems
Some problems
Large problems
Educational level of father Nine years
12 years
University/college
Your comments

62
Controls
Dental health information and advice Describe the information you received regarding oral
health care. The information has been Very good
Good
Neither good nor poor
Poor
Very poor
The quantity of information has been Sufficient
Neither sufficient nor
insufficient
Insufficient
When did you first receive information and advice on
oral health? When the child was < 6 months
6 months – 1 year
1-3 years
> 3 years
From where did you receive the information and advice? Physician
Dentist
Dental hygienist
Found information on my own
Other source
Is it possible to follow the current advice? Yes, completely
Yes, partly
No, I am doubtful
No, not at all
Does the current dental health information need to be
changed? Yes, a lot
Yes, some
No, not in need of change
No opinion
Dental care and service
Describe the reception at the dental clinic Excellent
Satisfactory
Decent
Poor
Very poor
Are enough time provided during the appointments at
the dental clinic? Yes, definitely
Yes, partially
Probably not
No, not at all
Have sedatives or general anesthesia been used for your
child? Never
1-2 occasions
3-4 occasions
>4 occasions
What was your experience of sedatives or general
anesthesia Excellent
Satisfactory
Decent
Poor
Very poor

63
Was local anesthesia used when teeth were filled? Always
Often
Sometimes
Never
Don´t know
What is your experience with respect to the competence
of the dental staff Very good
Good
Varying
Bad
Very bad
Do you believe the control intervals were adjusted to
meet the needs of your child? Gaps were to long
Sufficient
Too close
Don´t know
Children and parents
How would you describe your child’s dental health? No problems
Some problems
Large problems
How do you experience your child´s expectations before
a visit to the dental clinic? Positive
Neither positive nor negative
Negative
Don´t know
Does you or the other parent experience discomfort
before your own visits at the dental clinic? Always
Sometimes
Never
Don´t know
Dental health of mother No problems
Some problems
Large problems
Educational level of mother Nine years
12 years
University/college
Dental health of father No problems
Some problems
Large problems
Educational level of father Nine years
12 years
University/college
Your comments

64
APPENDIX II. Questionnaire Paper III
1. How much of your clinical time do you practice dentistry
for children? 0 %
0-24 %
25-49 %
50-74 %
75-100 %
2. Have you received any education/information regarding
dental care of children with heart disease except that during
the graduate training?
Yes
No
I don´t know
3. Has any of your child patients a heart disease? Yes, one or several
No, no one
I don´t know
I don´t treat children
If response alternative 2-4 in question 3, please go to question
12
4. Do you know the child’s/children’s heart diagnosis? Yes
No
5. Do you know if the any of the child/children has any heart
medication? Yes
No
6. Has your child patient/s with heart disease display a caries
experience? Yes
No
I don´t know
7. Do you know the name/s of the child’s/children’s
physician/s? Yes
No
8. Have you been in contact with the child’s/children’s
physician/s? Yes
No
If no please go to question 11
9. If yes in question 8, what was your opinion of the
cooperation? Positive
Negative
Neither positive nor negative
10. What is your experience on providing dental treatment for
children with heart disease? More than one alternative may be
chosen.
No special difficulties
Odontological difficulties
Medical difficulties
Insecurity regarding the
child´s medical condition
11. How is the dental treatment and care of children with heart
disease arranged in your clinic? The same as for healthy
children
More caries prevention
Longer visits
Shorter recall intervals
No opinion
12. Do you know if any of the pharmaceutical preparations
taken by children with heart disease can increase the caries
risk?
Yes
No
No opinion

65
13. Have you received clear cut information regarding which
heart diagnoses that should be provided with antibiotic
prophylaxis before invasive dental treatment?
Yes
No
No opinion
14. Who in the dental team perform the major part of dental
care for children with heart disease? Dental nurse
Dental hygienist
General dentists
Dentists with special training
Specialists in paediatric
dentistry
15. What is your opinion on who in the dental team that
should perform the major part of the dental care for this group
of children?
Dental nurse
Dental hygienist
General dentists
Dentists with special training
Specialists in paediatric
dentistry
16. Your gender? Male
Female
17. Year of your dental graduation?
18. University?
Your comments
Copyright © 2022 FDOKUMEN