Dengue Shock Sindrome
22
J Emerg Trauma Shock. 2011 Jan-Mar; 4(1): 120–127. doi: 10.4103/0974-2700.76835 PMCID: PMC3097561 Dengue shock Senaka Rajapakse Author information ► Article notes ► Copyright and License information ► This article has been cited by other articles in PMC. INTRODUCTION Infection with dengue virus imperils about 20 million people every year in tropical and subtropical countries.[1 ] The mortality rate is around 1–2%. The spectrum of disease manifestations is wide, ranging from asymptomatic or mild infection, through varying degrees of thrombocytopenia and vascular leakage that is typical of dengue hemorrhagic fever (DHF), to a severe shock syndrome and multiorgan failure.[2 ] Multiple organs can be affected: liver damage, rhabdomyolysis, myocardial depression, and various neurologic and ophthalmologic manifestations have been reported.[2 ] The case fatality of severe dengue in Asian countries is around 0.5–3.5%.[3 ] CASE REPORT A 49-year-old woman was admitted to hospital with fever for 5 days. She had no significant previous medical history. Her main symptoms were body aches, headache, loss of appetite, vomiting, and high fever. On day 5 of the illness, a full blood count showed a platelet count of 45,000 mm 3. She was admitted to the ICU. On admission, she was conscious and alert, but was restless and looked ill. She had a diffuse cutaneous blanching erythema. Her pulse rate was 120 beats per minute and blood pressure 130/80mmHg, with a postural drop of 20 mmHg. The heart sounds were normal. Her respiratory rate was 28/min, and her lungs were clear. Her abdomen was soft, with no free fluid; epigastric and right hypochondrial tenderness was present. She was neurologically normal. Her electrocardiogram (ECG) was normal,
Transcript of Dengue Shock Sindrome
J Emerg Trauma Shock. 2011 Jan-Mar; 4(1): 120–127.
doi: 10.4103/0974-2700.76835
PMCID: PMC3097561
Dengue shockSenaka Rajapakse
Author information ► Article notes ► Copyright and License information ►
This article has been cited by other articles in PMC.
INTRODUCTION
Infection with dengue virus imperils about 20 million people every year in tropical and subtropical countries.[1] The mortality rate is around 1–2%. The spectrum of disease manifestations is wide, ranging from asymptomatic or mild infection, through varying degrees of thrombocytopenia and vascular leakage that is typical of dengue hemorrhagic fever (DHF), to a severe shock syndrome and multiorgan failure.[2] Multiple organs can be affected: liver damage, rhabdomyolysis, myocardial depression, and various neurologic and ophthalmologic manifestations have been reported.[2] The case fatality of severedengue in Asian countries is around 0.5–3.5%.[3]
CASE REPORT
A 49-year-old woman was admitted to hospital with fever for 5 days. She had no significant previous medical history. Her main symptoms were body aches, headache, loss of appetite, vomiting, and high fever. On day 5 of the illness, a full blood count showed a platelet count of 45,000 mm3. She was admitted to the ICU. On admission, she was conscious and alert, but was restless and looked ill. She had a diffuse cutaneous blanching erythema. Her pulse rate was 120 beats per minute and blood pressure 130/80mmHg, with a postural drop of 20 mmHg. The heart sounds were normal. Her respiratory rate was 28/min, and her lungs were clear. Her abdomen was soft, with no free fluid; epigastric and right hypochondrial tenderness was present. She was neurologically normal. Her electrocardiogram (ECG) was normal,
apart from sinus tachycardia. DHF was the likely clinical diagnosis. Intravenous (IV) Hartmann solution 2 ml/kg/h was commenced in view of the postural drop in blood pressure. She became hypotensive 4 h after admission, with blood pressure falling to 70/40 mmHg, and her heart rate increased to 140/min. Arepeat ECG showed diffuse T wave inversions. An urgent echocardiogram showed global hypokinesia, with an ejection fraction of 40%. Based on a clinical diagnosis of dengue shock syndrome (DSS) plus myocarditis, dobutamine and noradrenaline infusions were started. Repeat platelet count was 22,000mm3 and the hematocrit 48%. Fluids were given with caution, and fresh frozen plasma (FFP) and platelet transfusion was commenced. She then had coffee grounds aspirate through the nasogastric tube andwas therefore started on omeprazole 80 mg bolus followed by 8 mg/h infusion. She remained in intractable shock, with no response to inotropes or intravenous hydrocortisone, and requiredventilation due to worsening pulmonary edema. Her ECG now showed widespread T wave inversions with first-degree heart block. She progressively deteriorated, became anuric, and developed adult respiratory distress syndrome (ARDS). She also developed completeheart block, for which a temporary pacemaker was inserted. Although rate control was achieved, her blood pressure remained low on maximum inotropes. She was started on IV immunoglobulins 0.4 mg/kg by infusion. Her condition continued to deteriorate, and blood pressure became unrecordable. External cardiac massage alone seemed to raise the blood pressure to recordable levels. Repeat echocardiogram showed a dilated, globally hypokinetic heart, and it appeared that the myocardium was not responding to inotropes at all. She died in asystole shortly afterwards, 15 h after admission. Investigation results received after the patient’s death showed positive IgM and IgG antibodies to dengue.Dengue PCR was also positive. All bacterial cultures were negative. Serum cortisol levels were normal.
PATHOGENESIS OF SHOCK IN DSS
Dengue viruses are transmitted to humans by infected mosquitoes, mainly Aedes aegypti and Aedes albopictus.[2] There are four serotypes of the dengue virus: types 1, 2, 3, and 4. Although referred to
as serotypes, these have actually been identified as four different species belonging to the family Flaviviridae and genus Flavivirus. Infection with the dengue virus has a wide range of manifestations. Many infections are asymptomatic. Symptomatic dengue results in two defined syndromes: dengue fever (DF) and DHF/DSS. While DF is a simple, self-limiting febrile illness, DHFis a severe and potentially life-threatening condition. DHF/DSS is characterized by thrombocytopenia, with the resultant hemorrhagic manifestations; in addition, there is increased vascular permeability, resulting in depleted intravascular volumeand shock. Severe, profound shock is known to occur in extreme cases and is associated with high mortality.
Two theories have been proposed to explain the pathophysiology ofDHF/DSS.[4] According to one theory, DHF/DSS is caused by more virulent strains of the dengue virus. The other theory suggests that DHF/DSS results from abnormal and exaggerated host immune responses – in particular, the production of dengue virus cross-reactive antibodies – which augments the infection. In primary infection with the dengue virus, cross-reactive antibodies that lack neutralizing activity are produced. During secondary infection by a different serotype, the dengue virus and non-neutralizing antibodies form virus–antibody complexes. The Fc portion of these antibodies bind to FcγRI- and FcγRII-bearing cells, resulting in an increased number of cells being infected by the dengue virus.[5] This phenomenon is known as antibody-dependent enhancement and is believed to play an important part in the pathogenesis of shock.[5–8]
Patients with severe dengue die of progressively worsening shock and multiorgan failure. The exact mechanism of this phenomenon isnot fully understood although it is thought that increased vascular permeability occurs largely due to malfunction of vascular endothelial cells induced by cytokines or chemical mediators,[9] as also occurs in severe sepsis. It appears that a Th1 response occurs in the first few days of dengue infection; this later switches over to a Th2 response, which correlates withthe development of shock.[10] TNF-α, interleukin (IL)-2, IL-6, and IFN-γ levels are highest in the first 3 days of illness, whereas IL-10, IL-5, and IL-4 tend to appear later.[10] IL-2 and
IFN-γ are Th1-type cytokines, while IL-5 and IL-4 are Th2-type cytokines. Dengue virus–infected monocytes and endothelial cells have been shown to produce multiple cytokines, including TNF-α.[11,12] In the presence of enhancing antibodies, monocytes infected with dengue virus produce TNF-α. TNF-α has been shown toinduce plasma leakage in vitro.[13] Basophils and mast cells infected with dengue virus produce IL-1 and IL-6, while IFN-γ, IL-2, and TNF-α are also produced by virus-specific T lymphocytesupon activation.[12,14] Lymphocytes infected with the dengue virus produce IFN-α and IFN-γ,[15] IFN-α levels are higher in patients with DHF, though there is no difference in its levels indifferent grades of DHF.[16] IFN-γ levels are no different in patients with DF and DHF.[15] The precise role played by interferon in the pathogenesis of dengue shock is unclear. The cytokines TNF-α,[17] IL-6,[10,18,19] IL-8,[19] IL-13,[10,20] IL-18,[10,20] and cytotoxic factor[10] are significantly elevated inDHF as compared with DF. Levels of IL-13,[10] IL-18,[10] and IL-8[21] correlate positively with increasing grades of DHF. On the other hand, IL-12 levels are high in uncomplicated DF, but low indengue-induced shock.[20] Levels of transforming growth factor-β (an inhibitor of Th1- and enhancer of Th2-type cytokines) correlate with severity of disease and show an inverse relationship with IL-12 levels. Complement activation is a constant finding in DHF. Higher complement levels correlate with increasing disease severity.[4,22] The dengue virus is also knownto infect endothelial cells and cause direct damage through apoptosis;[23] nonetheless, it is believed that endothelial activation occurs predominantly through an indirect mechanism.[13] Increased endothelial cell expression of VCAM-1 and ICAM-1 occurs, and TNF-α is a key intermediary in this process.[13] Dengue infections are associated with reduced numbers of CD4+ T-cells, CD8+ T-cells, and natural killer cells.[24] Levels of these cells are lowest at the point when the fever settles and the onset of shock takes place, and increase subsequently. B-cellnumbers are not affected.
CLINICAL FEATURES OF DENGUE ILLNESS PROGRESSING TO SHOCK
Dengue infection should be considered when patients who live in areas where dengue is prevalent present with a febrile illness together with hemorrhagic manifestations or features of shock. The WHO case definitions for dengue shock are shown in Box 1. Dengue infection begins as a febrile illness; the fever is accompanied by constitutional symptoms and a characteristic flushing of the skin. Intermittent high-grade fever accompanied by chills and rigors is a feature. Vomiting, headache, myalgia, epigastric discomfort, and abdominal pain are common, and patients often feel quite ill.[25] The fever lasts 2–7 days and is followed by a fall in temperature; complications of dengue often take place at this point. Patients who remain ill, despite their temperature returning to normal, are more likely to developshock. Shock generally occurs on day 3–4 of the illness.[26] Thrombocytopenia is a characteristic finding. Platelet counts below 100,000/mm3 together with a rise in the hematocrit define DHF. In the classical shock syndrome, increased vascular permeability results in third space fluid loss, leading to pleural effusions, pericardial effusions, ascites, non-cardiogenic pulmonary edema and, subsequently, hypotension. Righthypochondrial pain occurs similar to that seen in cholecystitis; acalculous cholecystitis is a characteristic feature of DHF.[27] Myocarditis is a well-known complication[28] and although often mild it can result in heart block and can be severe enough to result in progressive and intractable acute heart failure with global hypokinesia and acute cardiac dilatation.[28–30] Lactic acidosis, which occurs[31] as a result of the sluggish circulation, possibly contributes to myocardial depression in severe cases. Acute hepatic derangement can occur though fulminant liver failure is rare.[4] Acute renal failure is usually secondary to hypotension in shock syndrome and is associated with increased mortality.[32] Death is usually due to severe hemorrhage or intractable shock with multiorgan failure.Box 1: WHO case definitions for dengue shock[1]
Features of dengue hemorrhagic fever
Fever, or history of acute fever, lasting 2–7 days, occasionally biphasic
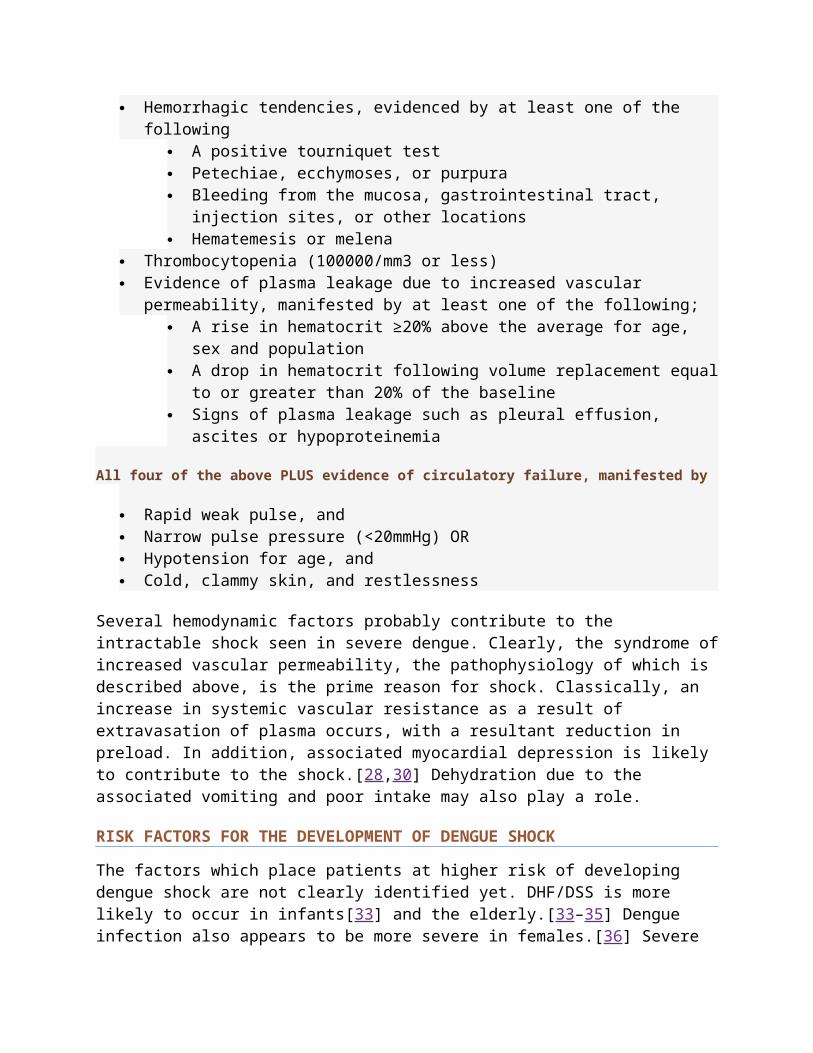
Hemorrhagic tendencies, evidenced by at least one of the following
A positive tourniquet test Petechiae, ecchymoses, or purpura Bleeding from the mucosa, gastrointestinal tract,
injection sites, or other locations Hematemesis or melena
Thrombocytopenia (100000/mm3 or less) Evidence of plasma leakage due to increased vascular
permeability, manifested by at least one of the following; A rise in hematocrit ≥20% above the average for age,
sex and population A drop in hematocrit following volume replacement equal
to or greater than 20% of the baseline Signs of plasma leakage such as pleural effusion,
ascites or hypoproteinemia
All four of the above PLUS evidence of circulatory failure, manifested by
Rapid weak pulse, and Narrow pulse pressure (<20mmHg) OR Hypotension for age, and Cold, clammy skin, and restlessness
Several hemodynamic factors probably contribute to the intractable shock seen in severe dengue. Clearly, the syndrome ofincreased vascular permeability, the pathophysiology of which is described above, is the prime reason for shock. Classically, an increase in systemic vascular resistance as a result of extravasation of plasma occurs, with a resultant reduction in preload. In addition, associated myocardial depression is likely to contribute to the shock.[28,30] Dehydration due to the associated vomiting and poor intake may also play a role.
RISK FACTORS FOR THE DEVELOPMENT OF DENGUE SHOCK
The factors which place patients at higher risk of developing dengue shock are not clearly identified yet. DHF/DSS is more likely to occur in infants[33] and the elderly.[33–35] Dengue infection also appears to be more severe in females.[36] Severe
dengue is more likely to occur in patients with chronic illness such as diabetes mellitus or asthma.[37,38] Although malnutritionpredisposes to many infectious diseases it does not appear to increase the likelihood of severe dengue.[39] The serotype of theinfecting virus may influence the severity of dengue; DEN-1 infection, followed by DEN-2 infection, has been reported to be associated with worse outcome.[40] There is some evidence that genetic susceptibility (ethnic variation,[41] HLA typing,[42] etc.) may play a role in the development of dengue shock, but this has not been studied thoroughly.
DIAGNOSIS
The WHO guidelines on dengue have clearly defined criteria for the diagnosis of dengue shock [Box 1].[1] Confirmation of dengue infection is by serology or detection of dengue viral material inblood by RT-PCR. Dengue-specific IgG and IgM ELISA is widely used.[43] The test is relatively inexpensive, and becomes positive for IgM antibodies on or after day 5 of the fever. IgM ELISA has a sensitivity of 83.9–98.4% and a specificity of 100%.[44] The presence of IgG antibodies indicates previous infection;hence, the presence of both IgG and IgM antibodies suggest the possibility of a secondary infection, although this has not been validated in clinical studies. Cordeiro et al.[45] proposed a two-dimensional classifier to differentiate primary and secondary dengue infection based on dengue IgM ELISA and the number of dayssince the onset of symptoms; the method showed over 90% specificity and sensitivity. Serotyping can also be done using ELISA.[46] RT-PCR for dengue viral material can help to diagnose the illness early, before antibodies become positive; the method,although relatively expensive, is very sensitive and allows for serotyping.[47] While these tests are used for diagnosis of dengue infection, they do not accurately predict which patients are likely to develop dengue shock. The association between high antibody titers or high viral load and the clinical manifestations of dengue has not been studied. No other biochemical investigations are available to predict which patients will develop shock, which is largely a clinical diagnosis. Hemoconcentration and dropping platelet counts herald
the onset of shock. Extravasation of fluid due to vascular leakage can be detected radiologically (chest radiography for pleural effusions, echocardiography for pericardial effusions, ultrasonography for ascites). The presence of fluid around the gall bladder, together with thickening of the gallbladder wall, has been shown to be associated with shock.[27,48] None of these features, however, predict the development of severe shock syndrome or mortality. Patients with shock do, however, show a variety of metabolic derangements, including lactic acidosis, elevated transaminases, and rising serum creatinine and blood urea. Pulse oximetry and arterial blood gas analysis showing hypoxia may indicate the development of pulmonary edema, which may be cardiogenic or non-cardiogenic. Electrocardiography is useful in identifying early myocarditis (T wave and ST segment changes are seen).[28] Echocardiography is the main investigationused to diagnose myocardial dysfunction and should be done early when impending shock is suspected. The place of cardiac troponinsin diagnosing myocarditis has not been evaluated.
MANAGEMENT
The WHO has issued guidelines for the management of DSS.[1] Much of the evidence on therapeutic measures in dengue are from children, and evidence from adults is lacking [Table 1]. Close monitoring is required as shock can develop rapidly, and transferto an ICU is indicated. The patient should be kept under close observation. Pulse, blood pressure, and respiration should be monitored–continuously if possible or at least every 15 min. Oxygen saturation should be monitored using a pulse oximeter, andoxygen should be given by face mask. Two wide-bore cannulae should be inserted for venous access. Blood should be drawn for grouping and cross-matching, blood urea, serum electrolytes, liver function tests, full blood count, prothrombin time, and c-reactive protein. Paracetamol may be used to control the fever.
Table 1Evidence base for key interventions in dengue shock
The only known effective treatment in DSS is timely and aggressive fluid resuscitation. No trials have been conducted comparing the use of intravenous fluids vs placebo due to obviousethical considerations. Fluids used for volume expansion include normal saline, Ringer lactate, 5% glucose diluted 1:2 or 1:1 in normal saline, plasma, plasma substitutes, or 5% albumin. There is no evidence that colloids are superior to crystalloids for resuscitation. Three studies conducted in Vietnam have compared the use of crystalloids and colloids. Dung et al.[49] compared four IV fluid regimens (Ringer lactate, normal saline, 3% gelatin, and dextran 70) in 50 children aged 5–15 years with dengue shock; no difference was seen in the occurrence or duration of shock between the groups. No difference was seen between the fluid requirements of crystalloids or colloids. All patients recovered. However, this study was thought to be underpowered to detect a difference between the two groups. Ngo et al.[50] conducted a larger study comparing the same fluid regimens in 230 children aged 1–15 years. The study included a larger proportion of patients with more severe grades of DHF. Although a trend towards benefit with colloids over crystalloids was shown, a clear difference between the four regimens was not demonstrated. Subgroup analysis showed that more severely ill patients may benefit from early administration of colloids. Wills et al.[51] compared three fluid regimens (Ringer lactate, dextran 70, and 6% hydroxyethyl starch) in 512 children aged 2–15years with dengue shock. The authors stratified the study population into two groups; moderate shock (pulse pressure >10 and <20 mmHg) and severe shock (pulse pressure <10 mmHg). Patients with moderate shock (n = 383) were randomized to receiveRinger lactate, dextran, or starch and those in severe shock (n =
129) were randomized to receive dextran or starch. No statistically significant differences were seen in either severity group in the requirement for colloid subsequent to the initial episode of shock, in the volumes of rescue colloid, in total parenteral fluid administered, or in the number of days in the hospital. The authors concluded that treatment with colloids did not provide any benefit over treatment with Ringer lactate inpatients with moderate shock. In patients with severe shock, no clear benefit with either starch or dextran was demonstrated. Despite the fact that there is no evidence to support the use of colloids in patients with severe shock, the authors felt that it would be unethical to compare colloids to crystalloids in such patients since it is generally accepted that colloids are needed in cases of severe shock.
The ideal dose of fluids has not been studied in clinical trials,and recommendations are based on practices in centers that have treated large numbers of cases. In the case of shock, fluids should be administered as a rapid (over less than 20 min) intravenous bolus of 10–20 ml/kg body weight. If shock persists, and the hematocrit is rising, plasma, plasma substitutes, or albumin should be given as a rapid bolus and repeated if necessary to a total dose or 20–30 ml/kg of colloid. If shock persists, and particularly if the hematocrit decreases, fresh whole-blood transfusion may be required (10 ml/kg). With appropriate use of fluid resuscitation in DSS, mortality rates have been shown to be <0.2%. It is important to reduce the IV fluids once the patient is recovering, as overhydration can result in intravascular fluid overload once the vascular permeability reverses with recovery.
Platelet transfusions are usually given to patients who develop serious hemorrhagic manifestations or have very low platelet counts, although the exact platelet count at which platelets should be given has not been defined. Transfused platelets survive only for a very short period in patients with shock syndrome.[52] The degree of elevation of circulating platelets after transfusion varies directly with the amount of platelets transfused and inversely with the degree of shock. Blood transfusion is required in patients with severe hemorrhage. There
is some evidence of benefit with fresh frozen plasma transfusion in increasing the platelet counts,[53] although the effect of plasma transfusion in dengue shock has not been studied in a controlled clinical trial.
The WHO guidelines for the management of dengue do not discuss the role of corticosteroids. While corticosteroids have various immunosuppressant effects, evidence of beneficial effects of corticosteroids on the deranged immunological mechanisms in dengue is very limited. In patients with ARDS, high-dose corticosteroids have been shown to reduce the levels of the cytokines TNF-α, interleukin (IL)-1β, IL-6, and IL-8.[55] However, Medin et al.[54] demonstrated that no reduction was seen in IL-8 after treatment with dexamethasone in patients with dengue. No other studies have examined the effects of corticosteroids on the cytokine cascade. Clinical trials of corticosteroids have been inconclusive so far and for the most part have been underpowered and lacking in methodological quality.[56–63] Some of the early studies demonstrated possible beneficial effects of corticosteroids in dengue shock. Min et al.,[56] in a randomized controlled study of children with DSS treated with hydrocortisone, demonstrated a statistically significant mortality benefit with corticosteroids in children aged 8 years and over, although this benefit was not seen in younger children. Futrakul et al.[57] reported a series of 22 children with shock syndrome who were treated with pulsed methylprednisolone therapy vs saline and plasma replacement. Nineout of 11 children in the corticosteroid-treated group survived, while in the group treated with saline and plasma replacement, all died. Significant hemodynamic improvement was seen in the nine survivors after administration of methylprednisolone. This study was non-blinded and non-randomized. However, subsequent studies of corticosteroids in dengue have all failed to show any benefit either in terms of survival or hemodynamic improvement,[58–62] and a Cochrane review on the subject concluded that therewas no evidence of benefit in using corticosteroids in DSS.[64] It must be noted that the previous studies have been small: the total number of patients in all the randomized controlled studieswas 284. Of three other non-randomized studies, one study showed
no benefit, one study showed a survival benefit, and one very small study showed hemodynamic improvement, including apparent improvement in plasma leakage. All these studies were underpowered, were conducted a long time ago, and have only studied children. There is no evidence from clinical trials regarding the effect of corticosteroids in adults.
Replacement doses of corticosteroids are thought to improve mortality and duration of shock in patients with septic shock whoshowed a blunted adrenocortical response to the ACTH stimulation test.[65] Cortisol levels are low in a subgroup of patients with septic shock, and a blunted cortisol response to ACTH stimulationis associated with poor prognosis.[66] In contrast, cortisol levels are high in DHF during both the acute and convalescent phases.[67] A correlation between cortisol levels and prognosis in dengue has not been studied. Although some clinicians use steroids in treatment,[68] there is currently no clear evidence to justify the use of corticosteroids in the treatment of DSS. There is a clear need for adequately powered, randomized, double-blind, placebo-controlled clinical trials in both children and adults to fully evaluate the possible benefit or lack of benefit of corticosteroids in dengue infection.
Similar to corticosteroids, the place of IV immunoglobulins (IVIG) is also not mentioned in the WHO guidelines on the management of dengue. Theoretically, the immunomodulatory effectsof IVIG can be postulated to have effects on the dengue virus–induced cytokine cascade.[69,70] IVIG selectively triggers the production of IL-1 receptor antagonist (IL-1ra),[70] and also prevents the generation of the complement membrane attack complex(C5b-9) and subsequent complement-mediated tissue damage.[69] There is limited evidence that IVIG is beneficial in the treatment of septic shock in neonates,[71] and a meta-analysis has demonstrated an overall reduction in mortality in adults withsevere sepsis/septic shock.[72]
Ostranoff et al.[73] reported a series of five patients in Brazil with dengue and severe thrombocytopenia who were treated with IVIG (500 mg/kg/ day infusions over 3 h for 5 days). Clinical improvement, together with improvement in platelet count, was
seen in these patients. The only published randomized controlled trial investigating the effect of IVIG on thrombocytopenia showedno benefit;[74] IVIG seemed to have no effect on platelet counts.Seriously ill patients with hemorrhage or shock were excluded from that study and hence the possible effects of IVIG on DSS were not studied. One important conclusion was that IVIG was safe, no significant side effects being encountered during the trial. Alejandria[75] discusses an unpublished randomized controlled trial conducted in the Philippines that compared treatment with IVIG vs placebo in children with DSS. This study showed a significant mortality reduction with IVIG treatment. Overall, however, there is currently insufficient evidence to make any recommendation regarding the use of IVIG in dengue shock.[76]
Carbazochrome sodium sulfonate (AC-17) is a hemostatic drug with a capillary-stabilizing action. It has been shown to reduce the vascular hyperpermeability induced by vasoactive substances through an agonist-induced inhibition of phosphoinositide hydrolysis.[77] Its effect in DSS has been investigated in a randomized clinical trial (RCT), conducted in 95 Thai children.[78] The primary outcome measure was the prevention of capillary leakage as evidenced by the presence of pleural effusion, and thesecondary outcome was the prevention of shock. No evidence of benefit in either outcome measures was seen with treatment of DSSwith AC-17, although the study was underpowered to detect a potential treatment benefit.
An RCT compared the use of nasal continuous positive airway pressure (NCPAP) vs oxygen by mask in patients with DSS and acuterespiratory failure.[79] The study was conducted in 37 Vietnamesechildren. The primary outcome measure was a PaO2>80 mmHg after 30min. Although the study was small, NCPAP effectively decreased hypoxemia and reduced the number of children requiring intubationand ventilation. Thus, NCPAP appears to be an effective treatmentin acute respiratory failure associated with DSS.
The role of different inotropic and vasopressor agents in dengue shock has not been investigated in clinical trials. Vasopressor drugs such as noradrenaline and dopamine are indicated in shock
that is unresponsive to fluids but no clinical trials are available on their use in dengue. In the case of cardiac dysfunction, it is appropriate to use cardiac inotropic drugs such as dobutamine or adrenaline in combination with a vasopressor although, again, no evidence is available.
CONCLUSION
DSS is a dangerous condition that can rapidly progress to death. Diagnosis is based largely on clinical grounds. No specific therapy has yet been proven to be of value, and the mainstay of management continues to be careful fluid resuscitation. While no definite benefit has been shown of colloids over crystalloids, colloids will continue to have a place in the management of severe shock, pending further research. The role of corticosteroids and immunoglobulins in dengue shock is clearly anarea for future research. Much of the recommendations are based on research done in children, and management protocols for adultsare based on extrapolation of these findings. Further research onthe management of dengue shock in adults is clearly needed.
FootnotesSource of Support: Nil
Conflict of Interest: None declared.
REFERENCES1. 2nd Edition. World Health Organization; 19977. Dengue haemorrhagic fever: diagnosis, treatment, prevention and control.
2. Halstead SB. Dengue. Lancet. 2007;370:1644–52. [PubMed]
3. Halstead SB. Is there an inapparent dengue explosion? Lancet. 1999;353:1100–1. [PubMed]
4. Kurane I. Dengue hemorrhagic fever with special emphasis on immunopathogenesis. Comp Immunol Microbiol Infect Dis. 2007;30:329–40. [PubMed]
5. Littaua R, Kurane I, Ennis FA. Human IgG Fc receptor II mediates antibody-dependent enhancement of dengue virus infection. J Immunol. 1990;144:3183–6. [PubMed]
6. Mady BJ, Erbe DV, Kurane I, Fanger MW, Ennis FA. Antibody-dependent enhancement of dengue virus infection mediated by bispecific antibodies against cell surface molecules other than Fc gamma receptors. Antibody-dependent enhancement of dengue virus infection mediated by bispecific antibodies against cell surface molecules other than Fc gamma receptors. 1991;147:3139–44. [PubMed]
7. Halstead SB, Venkateshan CN, Gentry MK, Larsen LK. Heterogeneity of infection enhancement of dengue 2 strains by monoclonal antibodies. J Immunol. 1984;132:1529–32. [PubMed]
8. Morens DM. Antibody-dependent enhancement of infection and thepathogenesis of viral disease. Clin Infect Dis. 1994;19:500–12. [PubMed]
9. Basu A, Chaturvedi UC. Vascular endothelium: the battlefield of dengue viruses. FEMS Immunol Med Microbiol. 2008;53:287–99. [PubMed]
10. Chaturvedi UC, Agarwal R, Elbishbishi EA, Mustafa AS. Cytokine cascade in dengue hemorrhagic fever: implications for pathogenesis. FEMS Immunol Med Microbiol. 2000;28:183–8. [PubMed]
11. Kurane I, Ennis FE. Immunity and immunopathology in dengue virus infections. Semin Immunol.1992;4:121–7. [PubMed]
12. Green S, Rothman A. Immunopathological mechanisms in dengue and dengue hemorrhagic fever. Curr Opin Infect Dis. 2006;19:429–36. [PubMed]
13. Anderson R, Wang S, Osiowy C, Issekutz AC. Activation of endothelial cells via antibody-enhanced dengue virus infection ofperipheral blood monocytes. J Virol. 1997;71:4226–32. [PMC free article][PubMed]
14. King CA, Anderson R, Marshall JS. Dengue virus selectively induces human mast cell chemokine production. J Virol. 2002;76:8408–19. [PMC free article] [PubMed]
15. Kurane I, Meager A, Ennis FA. Induction of interferon alpha and gamma from human lymphocytes by dengue virus-infected cells. J Gen Virol. 1986;67:1653–61. [PubMed]
16. Kurane I, Innis BL, Nimmannitya S, Nisalak A, Meager A, EnnisFA. High levels of interferon alpha in the sera of children with dengue virus infection. Am J Trop Med Hyg. 1993;48:222–9. [PubMed]
17. Vitarana T, de Silva H, Withana N, Gunasekera C. Elevated tumour necrosis factor in dengue fever and dengue haemorrhagic fever. Ceylon Med J. 1991;36:63–5. [PubMed]
18. Juffrie M, Meer GM, Hack CE, Haasnoot K, Sutaryo, Veerman AJ,et al. Inflammatory mediators in dengue virus infection in children: interleukin-6 and its relation to C-reactive protein and secretory phospholipase A2. Am J Trop Med Hyg. 2001;65:70–5. [PubMed]
19. Huang YH, Lei HY, Liu HS, Lin YS, Liu CC, Yeh TM. Dengue virus infects human endothelial cells and induces IL-6 and IL-8 production. Am J Trop Med Hyg. 2000;63:71–5. [PubMed]
20. Mustafa AS, Elbishbishi EA, Agarwal R, Chaturvedi UC. Elevated levels of interleukin-13 and IL-18 in patients with dengue hemorrhagic fever. FEMS Immunol Med Microbiol. 2001;30:229–33. [PubMed]
21. Raghupathy R, Chaturvedi UC, Al-Sayer H, Elbishbishi EA, Agarwal R, Nagar R, et al. Elevated levels of IL-8 in dengue hemorrhagic fever. J Med Virol. 1998;56:280–5. [PubMed]
22. Malasit P. Complement and dengue haemorrhagic fever/shock syndrome. Southeast Asian J Trop Med Public Health. 1987;18:316–20. [PubMed]
23. Avirutnan P, Malasit P, Seliger B, Bhakdi S, Husmann M. Dengue virus infection of human endothelial cells leads to chemokine production, complement activation, and apoptosis. J Immunol. 1998;161:6338–46.[PubMed]
24. Sarasombath S, Suvatte V, Homchampa P. Kinetics of lymphocytesubpopulations in dengue hemorrhagic fever/dengue shock syndrome. Southeast Asian J Trop Med Public Health. 1988;19:649–56.[PubMed]
25. Narayanan M, Aravind MA, Thilothammal N, Prema R, Sargunam CS, Ramamurty N. Dengue fever epidemic in Chennai-a study of clinical profile and outcome. Indian Pediatr. 2002;39:1027–33. [PubMed]
26. uzmán MG, Alvarez M, Rodríguez R, Rosario D, Vázquez S, Vald s L, et al. Fatal dengue hemorrhagic fever in Cuba, 1997. Int J Infect Dis. 1999;3:130–5. [PubMed]
27. Wu KL, Changchien CS, Kuo CM, Chuah SK, Lu SN, Eng HL, et al.Dengue fever with acute acalculous cholecystitis. Am J Trop Med Hyg. 2003;68:657–60. [PubMed]
28. Wali JP, Biswas A, Chandra S, Malhotra A, Aggarwal P, Handa R, et al. Cardiac involvement in Dengue Haemorrhagic Fever. Int JCardiol. 1998;64:31–6. [PubMed]
29. Kabra SK, Juneja R, Madhulika, Jain Y, Singhal T, Dar L, et al. Myocardial dysfunction in children with dengue haemorrhagic fever. Natl Med J India. 1998;11:59–61. [PubMed]
30. Khongphatthanayothin A, Lertsapcharoen P, SupachokchaiwattanaP, La-Orkhun V, Khumtonvong A, Boonlarptaveechoke C, et al. Myocardial depression in dengue hemorrhagic fever: prevalence andclinical description. Pediatr Crit Care Med. 2007;8:524–9. [PubMed]
31. Nimmannitya S, Thisyakorn U, Hemsrichart V. Dengue haemorrhagic fever with unusual manifestations.Southeast Asian J Trop Med Public Health. 1987;18:398–406. [PubMed]
32. Kuo MC, Lu PL, Chang JM, Lin MY, Tsai JJ, Chen YH, et al. Impact of renal failure on the outcome of dengue viral infection. Clin J Am Soc Nephrol. 2008;3:1350–6. [PMC free article] [PubMed]
33. Guzmán MG, Kouri G, Bravo J, Valdes L, Vazquez S, Halstead SB, et al. Effect of age on outcome of secondary dengue 2 infections. Int J Infect Dis. 2002;6:118–24. [PubMed]
34. Guzmán MG, Kourí G. Dengue: an update. Lancet Infect Dis. 2002;2:33–42. [PubMed]
35. Malavige GN, Velathanthiri VG, Wijewickrama ES, Fernando S, Jayaratne SD, Aaskov J, et al. Patterns of disease among adults hospitalized with dengue infections. QJM. 2006;99:299–305. [PubMed]
36. Kabra SK, Jain Y, Pandey RM, Madhulika, Singhal T, Tripathi P, et al. Dengue haemorrhagic fever in children in the 1996 Delhiepidemic. Trans R Soc Trop Med Hyg. 1999;93:294–8. [PubMed]
37. Bravo JR, Guzmán MG, Kouri GP. Why dengue haemorrhagic fever in Cuba? 1. Individual risk factors for dengue haemorrhagic fever/dengue shock syndrome (DHF/DSS) Trans R Soc Trop Med Hyg.1987;81:816–20. [PubMed]
38. Cunha RV, Schatzmayr HG, Miagostovich MP, Barbosa AM, Paiva FG, Miranda RM, et al. Dengue epidemic in the State of Rio Grandedo Norte, Brazil, in 1997. Trans R Soc Trop Med Hyg. 1999;93:247–9.[PubMed]
39. Thisyakorn U, Nimmannitya S. Nutritional status of children with dengue hemorrhagic fever. Clin Infect Dis. 1993;16:295–7. [PubMed]
40. Guzmán MG, Kouri GP, Bravo J, Soler M, Vazquez S, Morier L. Dengue hemorrhagic fever in Cuba, 1981: a retrospective seroepidemiologic study. Am J Trop Med Hyg. 1990;42:179–84. [PubMed]
41. Halstead SB, Streit TG, Lafontant JG, Putvatana R, Russell K,Sun W, et al. Haiti: absence of dengue hemorrhagic fever despite hyperendemic dengue virus transmission. Am J Trop Med Hyg. 2001;65:180–3.[PubMed]
42. Loke H, Bethell DB, Phuong CX, Dung M, Schneider J, White NJ,et al. Strong HLA class I-restricted T cell responses in dengue hemorrhagic fever: a double-edged sword? J Infect Dis. 2001;184:1369–73.[PubMed]
43. Guzmán MG, Kourí G. Dengue diagnosis, advances and challenges. Int J Infect Dis. 2004;8:69–80.[PubMed]
44. Guzman MG, Kouri G, Soler M, Bravo J, Rodríguez de La Vega A,Vazquez S, et al. Dengue 2 virus enhancement in asthmatic and non
asthmatic individual. Mem Inst Oswaldo Cruz. 1992;87:559–564.[PubMed]
45. Cordeiro MT, Braga-Neto U, Nogueira RM, Marques ET., Jr Reliable classifier to differentiate primary and secondary acute dengue infection based on IgG ELISA. PLoS One. 2009;4:4945. [PMC free article][PubMed]
46. Nawa M, Ichikawa Y, Inouye S. Serotyping of dengue viruses byan enzyme-linked immunosorbent assay. Jpn J Med Sci Biol. 1985;38:217–21. [PubMed]
47. De Paula SO, Fonseca BA. Dengue: a review of the laboratory tests a clinician must know to achieve a correct diagnosis. Braz J Infect Dis. 2004;8:390–8. [PubMed]
48. Méndez A, González G. Dengue haemorrhagic fever in children: ten years of clinical experience.Biomedica. 2003;23:180–93. [PubMed]
49. Dung NM, Day NP, Tam DT, Loan HT, Chau HT, Minh LN, et al. Fluid replacement in dengue shock syndrome: a randomized, double-blind comparison of four intravenous-fluid regimens. Clin Infect Dis.1999;29:787–94. [PubMed]
50. Ngo NT, Cao XT, Kneen R, Wills B, Nguyen VM, Nguyen TQ, et al. Acute management of dengue shock syndrome: a randomized double-blind comparison of 4 intravenous fluid regimens in the first hour.Clin Infect Dis. 2001;32:204–13. [PubMed]
51. Wills BA, Nguyen MD, Ha TL, Dong TH, Tran TN, Le TT, et al. Comparison of three fluid solutions for resuscitation in dengue shock syndrome. N Engl J Med. 2005;353:877–89. [PubMed]
52. Isarangkura P, Tuchinda S. The behavior of transfused platelets in dengue hemorrhagic fever. Southeast Asian J Trop MedPublic Health. 1993;24:222–4. [PubMed]
53. Sellahewa KH, Samaraweera N, Thusita KP, Fernando JL. Is fresh frozen plasma effective for thrombocytopenia in adults withdengue fever? A prospective randomised double blind controlled study.Ceylon Med J. 2008;53:36–40. [PubMed]
54. Medin CL, Rothman AL. Cell type-specific mechanisms of interleukin-8 induction by dengue virus and differential responseto drug treatment. J Infect Dis. 2006;193:1070–7. [PubMed]
55. Meduri GU, Headley AS, Golden E, Carson SJ, Umberger RA, Kelso T, et al. Effect of prolonged methylprednisolone therapy inunresolving acute respiratory distress syndrome: a randomized controlled trial.JAM. 1998;280:159–65. [PubMed]
56. Min M, U T, Aye M, Shwe TN, Swe T, et al. Hydrocortisone in the management of dengue shock syndrome. Southeast Asian J Trop Med Public Health. 1975;6:573–9. [PubMed]
57. Futrakul P, Vasanauthana S, Poshyachinda M, Mitrakul C, Cherdboonchart V, Kanthirat V. Pulse therapy in severe form of dengue shock syndrome. J Med Assoc Thai. 1981;64:485–91. [PubMed]
58. Sumarmo, Talogo W, Asrin A, Isnuhandojo B, Sahudi A. Failure of hydrocortisone to affect outcome in dengue shock syndrome. Pediatrics. 1982;69:45–9. [PubMed]
59. Futrakul P, Poshyachinda M, Mitrakul C, Kwakpetoon S, Unchumchoke P, Teranaparin C, et al. Hemodynamic response to high-dose methyl prednisolone and mannitol in severe dengue-shockpatients unresponsive to fluid replacement. Southeast Asian J Trop Med Public Health. 1987;18:373–9. [PubMed]
60. Pongpanich B, Bhanchet P, Phanichyakarn P, Valyasevi A. Studies on dengue hemorrhagic fever.Clinical study: an evaluationof steroids as a treatment. J Med Assoc Thai. 1973;56:6–14. [PubMed]
61. Tassniyom S, Vasanawathana S, Chirawatkul A, Rojanasuphot S. Failure of high-dose methylprednisolone in established dengue shock syndrome: a placebo-controlled, double-blind study.Pediatrics. 1993;92:111–5. [PubMed]
62. Sumarmo The role of steroids in dengue shock syndrome. Southeast Asian J Trop Med Public Health.1987;18:383–9. [PubMed]
63. Rajapakse S. Corticosteroids in the treatment of dengue illness. Trans R Soc Trop Med Hyg.2009;103:122–6. [PubMed]
64. Panpanich R, Sornchai P, Kanjanaratanakorn K. Corticosteroidsfor treating dengue shock syndrome.Cochrane Database Syst Rev. 2006;3:CD003488. [PubMed]
65. Annane D, Bellissant E, Bollaert PE, Briegel J, Confalonieri M, De Gaudio R, et al. Corticosteroids in the treatment of severesepsis and septic shock in adults: a systematic review. JAMA. 2009;301:2362–75.[PubMed]
66. Annane D, Sébille V, Troché G, Raphaël JC, Gajdos P, Bellissant E. A 3-level prognostic classification in septic shockbased on cortisol levels and cortisol response to corticotropin. JAMA. 2000;283:1038–45.[PubMed]
67. Myo-Khin, Soe-Thein, Thein-Thein-Myint, Than-Nu-Swe, Tin-Tin-Saw, Muya-Than Serum cortisol levels in children with dengue haemorrhagic fever. J Trop Pediatr. 1995;41:295–7. [PubMed]
68. Kularatne SA. Survey on the management of dengue infection inSri Lanka: opinions of physicians and pediatricians. Southeast Asian J Trop Med Public Health. 2005;36:1198–200. [PubMed]
69. Sibéril S, Elluru S, Negi VS, Ephrem A, Misra N, Delignat S, et al. Intravenous immunoglobulin in autoimmune and inflammatory diseases: more than mere transfer of antibodies. Transfus Apher Sci.2007;37:103–7. [PubMed]
70. Andersson U, Björk L, Skansén-Saphir U, Andersson J. Pooled human IgG modulates cytokine production in lymphocytes and monocytes. Immunol Rev. 1994;139:21–42. [PubMed]
71. El-Nawawy A, El-Kinany H, Hamdy El-Sayed M, Boshra N. Intravenous polyclonal immunoglobulin administration to sepsis syndrome patients: a prospective study in a pediatric intensive care unit. J Trop Pediatr. 2005;51:271–8. [PubMed]
72. Laupland KB, Kirkpatrick AW, Delaney A. Polyclonal intravenous immunoglobulin for the treatment of severe sepsis andseptic shock in critically ill adults: a systematic review and meta-analysis. Crit Care Med.2007;12:2686–92. [PubMed]
73. Ostronoff M, Ostronoff F, Florêncio R, Florêncio M, DominguesMC, Calixto R, et al. Serious thrombocytopenia due to dengue
hemorrhagic fever treated with high dosages of immunoglobulin. Clin Infect Dis. 2003;36:1623–4. [PubMed]
74. Dimaano EM, Saito M, Honda S, Miranda EA, Alonzo MT, Valerio MD, et al. Lack of efficacy of high-dose intravenous immunoglobulin treatment of severe thrombocytopenia in patients with secondary dengue virus infection. Am J Trop Med Hyg. 2007;77:1135–8. [PubMed]
75. Alejandria M. Dengue fever. Clin Evid. 2005:887–95. [PubMed]
76. Rajapakse S. Intravenous immunoglobulins in the treatment of dengue illness. Trans R Soc Trop Med Hyg. 2009;103:867–70. [PubMed]
77. Sendo T, Itoh Y, Aki K, Oka M, Oishi R. Carbazochrome sodium sulfonate (AC-17) reverses endothelial barrier dysfunction through inhibition of phosphatidylinositol hydrolysis in culturedporcine endothelial cells. Naunyn Schmiedebergs Arch Pharmacol. 2003;368:175–80. [PubMed]
78. Tassniyom S, Vasanawathana S, Dhiensiri T, Nisalak A, Chirawatkul A. Failure of carbazochrome sodium sulfonate (AC-17) to prevent dengue vascular permeability or shock: a randomized, controlled trial. J Pediatr. 1997;131:525–8. [PubMed]
79. Cam BV, Tuan DT, Fonsmark L, Poulsen A, Tien NM, Tuan HM, Heegaard ED. Randomized comparison of oxygen mask treatment vs. nasal continuous positive airway pressure in dengue shock syndrome with acute respiratory failure. J Trop Pediatr. 2002;48:335–9. [PubMed]
Articles from Journal of Emergencies, Trauma, and Shock are provided herecourtesy of Medknow Publications
Sumber: http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3097561/