
Deletion of p16 and p15 genes In schistosomiasis-associated bladder cancer (SABC
11
Clinica Chimica Acta 300 (2000) 159–169 www.elsevier.com / locate / clinchim Deletion of p16 and p15 genes In schistosomiasis- associated bladder cancer (SABC) * Sanaa Eissa , R. Ali-Labib, A. Khalifa Oncology Diagnostic Unit, Biochemistry department, Ain Sharns Faculty of Medicine, Abbassia, Cairo, Egypt Received 6 September 1999; received in revised form 11 May 2000; accepted 15 May 2000 Abstract Alterations of p16 and p15 genes have been reported in cancer cell lines and in certain malignant neoplasm. These genes are designated as candidate tumor suppressor genes because they encode proteins that function as negative cell cycle regulators at G -S checkpoint. One 1 hundred and sixty eight tumor tissue, 20 schistosomal tissue, and 50 normal tissue samples were examined. The status of p16 and p15 genes in these tissues was determined by the polymerase chain reaction and by sequencing the DNA fragments produced during PCR. In addition, the expression of p16 and p15 proteins was examined by Western blot analysis. p16 and p15 genes were detected in all normal and schistosomal tissues. Deletion of both p16 and p15 genes was observed in 72 and 36 bladder tumors, respectively. Twenty eight of the 72 cases that exhibited p16 deletions also displayed deletions of p15. Only eight cases showed loss of the p15 gene while retaining p16 gene, and p16 deletion with apparently intact p15 gene was identified in 44 cases. The present analysis also reveals that deletion in the two genes are associated with low-stage, low grade bladder cancer, schistosomiasis-associated bladder cancer (SABC) and squamous cell carcinoma type (SCC). No point mutations were identified in either gene. The expression of p16 and p15 proteins was undetectable in 75 and 38 bladder tumors, respectively, by Western blot analysis. Alteration of the p16 and p15 genes appears to be an early event in bladder cancer which occurs more frequently in SABC and SCC, and may play an important role in the development of schistosomal bladder cancer. 2000 Elsevier Science B.V. All rights reserved. Keywords: Cyclin dependent kinase inhibitors; Tumor suppressor gene; p15; p16; Bladder cancer; SCC; Schistosomiasis. *Corresponding author. Fax: 1 202-28-59-928. E-mail address: sanaa [email protected] (S. Eissa). ] 0009-8981 / 00 / $ – see front matter 2000 Elsevier Science B.V. All rights reserved. PII: S0009-8981(00)00317-X
-
Upload
independent -
Category
Documents
-
view
3 -
download
0
Transcript of Deletion of p16 and p15 genes In schistosomiasis-associated bladder cancer (SABC

Clinica Chimica Acta 300 (2000) 159–169www.elsevier.com/ locate /clinchim
Deletion of p16 and p15 genes In schistosomiasis-associated bladder cancer (SABC)
*Sanaa Eissa , R. Ali-Labib, A. Khalifa
Oncology Diagnostic Unit, Biochemistry department, Ain Sharns Faculty of Medicine, Abbassia, Cairo,Egypt
Received 6 September 1999; received in revised form 11 May 2000; accepted 15 May 2000
Abstract
Alterations of p16 and p15 genes have been reported in cancer cell lines and in certainmalignant neoplasm. These genes are designated as candidate tumor suppressor genes becausethey encode proteins that function as negative cell cycle regulators at G -S checkpoint. One1
hundred and sixty eight tumor tissue, 20 schistosomal tissue, and 50 normal tissue samples wereexamined. The status of p16 and p15 genes in these tissues was determined by the polymerasechain reaction and by sequencing the DNA fragments produced during PCR. In addition, theexpression of p16 and p15 proteins was examined by Western blot analysis. p16 and p15 geneswere detected in all normal and schistosomal tissues. Deletion of both p16 and p15 genes wasobserved in 72 and 36 bladder tumors, respectively. Twenty eight of the 72 cases that exhibitedp16 deletions also displayed deletions of p15. Only eight cases showed loss of the p15 gene whileretaining p16 gene, and p16 deletion with apparently intact p15 gene was identified in 44 cases.The present analysis also reveals that deletion in the two genes are associated with low-stage, lowgrade bladder cancer, schistosomiasis-associated bladder cancer (SABC) and squamous cellcarcinoma type (SCC). No point mutations were identified in either gene. The expression of p16and p15 proteins was undetectable in 75 and 38 bladder tumors, respectively, by Western blotanalysis. Alteration of the p16 and p15 genes appears to be an early event in bladder cancer whichoccurs more frequently in SABC and SCC, and may play an important role in the development ofschistosomal bladder cancer. 2000 Elsevier Science B.V. All rights reserved.
Keywords: Cyclin dependent kinase inhibitors; Tumor suppressor gene; p15; p16; Bladder cancer;SCC; Schistosomiasis.
*Corresponding author. Fax: 1 202-28-59-928.E-mail address: sanaa [email protected] (S. Eissa).
]
0009-8981/00/$ – see front matter 2000 Elsevier Science B.V. All rights reserved.PI I : S0009-8981( 00 )00317-X

160 S. Eissa et al. / Clinica Chimica Acta 300 (2000) 159 –169
1. Introduction
p16 and p15 genes, located in the 9p21 region, and the encoded proteins, p16and p15, regulate cell proliferation during the G phase of the cell cycle by1
inhibiting the activity of the cyclin D/cyclin-dependent kinase 4 (CDK4)complex [1]. The latter catalyzes the phosphorylation of retinoblastoma (pRB),which releases transcription factors such as E2F correlated with the passagethrough the G checkpoint and results in G to S cell cycle progression [2,3].1 1
Thus, p16 and p15 are thought to be a part of the regulatory feedback circuitwith cyclin D/CDK4 and pRB at the G checkpoint pathway.1
Several studies [4–7] have revealed that homozygous deletion of the p16 andp15 genes is frequent in most cell lines screened and that such deletions arecommon in certain cancers. In addition, point mutations in the p16 gene havebeen identified in several types of neoplasms [8–13], including transitional cellcarcinomas of the urinary bladder [11–13]. The present study was undertaken tobetter delineate the frequency and potential clinical relevance (i.e., associationswith tumor stages and/or grade) of p16 and p15 gene alterations in a well-characterized cohort of human primary urinary bladder tumors includingtransitional cell carcinoma (TCC) and squamous cell carcinoma (SCC), schis-tosomiasis associated and non schistosomiasis associated types.
2. Materials and methods
2.1. Tissue and patient characteristics
The tumors analyzed were obtained from transurethral resections or radicalcystectomy samples from 168 patients affected with bladder cancer. Demo-graphic data on this cohort may be summarized as follows: 134 patients weremales and 34 were females, and the median patient age was 65 years. Tumorstaging was classified according to the TNM system [14] as follows: Thirteen Ta(papillary superficial noninvasive tumors), 45 T1 (lesions invading the laminapropria), and 110 T2 to T4 (T2 1 , muscle-invasive lesions). Tumor grading(World Health Organization System) was available for 164 patients. Twelvetumors were classified as low grade (grade 1), 96 as intermediate grade (grade2), and 56 as high grade (grade 3). Normal tissues were also obtained from 50patients from a tumor-free area of the same bladder specimen. Twenty sampleswere obtained from patients with urinary schistosomiasis. All specimens werestored at 2 708C. Representative hematoxylin-eosin stained sections of eachfrozen block were examined microscopically to confirm the presence of tumor,and only lesions with more than 50% neoplastic cells were included in the study.

S. Eissa et al. / Clinica Chimica Acta 300 (2000) 159 –169 161
2.2. Polymerase chain reaction (PCR)
Tumor tissues were digested with proteinase K, and high molecular weightgenomic DNA was extracted by the phenol–chloroform method [15] andsubjected to polymerase chain reaction (PCR) using slight modification of themethod described [16] PCR was performed on 50 ng each of genomic DNAextracted from the human bladder tissue and from human placental DNAincluded as positive control.
For amplification of p15, primers p15 (2) F and p15 (2) R were used toamplify a 430 bp product from exon 2 of the p15 gene, as described previously[6], Table 1. The reaction mix consisted of 67 mmol / l Tris pH 8.8, 16.6 mmol / lammonium sulphate, 6 mmol / l magnesium chloride, 10 mmol / l b-mercap-toethanol, 6% (V/V) dimethylsulphoxide (DMSO), 1.25 mmol / l dNTPs, 1mmol / l of each oligonucleotide primer and 5 U of Ampli Taq. The PCR cyclingconditions were denaturation for 2 min at 958C followed by 35 cycles ofdenaturation at 958C for 30 s, reannealing at 668C for 1 min and extension at708C for 1 min, with a final extension at 708C for 5 min.
For amplification of p16, primers were chosen that span an intron–exonboundary of the human (p16) gene and amplify a 167 bp product by PCR [5],Table 1. The reaction mix consisted of 10 mmol / l Tris pH 8.3, 50 mmol / lpotassium chloride, 0.2 mmol / l dNTPs, 2.5 mmol / l magnesium chloride, 0.15mmol / l of each oligonucleotide primer and 1U Ampli Taq. Cycling conditionswere denaturation at 958C for 30 s and extension at 728C for 10 min. In all caseswhere a negative results was obtained, the reaction was repeated.
PCR products from individual experiments were run on 2% agarose gels andvisualized with UV light after staining with ethidium bromide.
2.3. Direct sequence analysis
The samples were isolated and run on 2% agarose gels and purified using a
Table 1Oligonucleotide sequences
Gene Primer Position Sequence
p15 p15(2) F Forward 59-CCTTAAATGGCTCCACCTGC-39
p15(2) R Reverse 59-CGTTGGCAGCCTTCATCG-39
p16 p16f Forward 59-GGAAATTGGAAACTGGAAGC-39
P16r Reverse 59-CTGCCCATCATCATGACCTG-39
162 S. Eissa et al. / Clinica Chimica Acta 300 (2000) 159 –169
Geneclean II kit (Bio 101 Corp., La Jolla, CA) in preparation for sequencing.The sequencing reaction was performed by means of the dideoxy method [17]using the termination mixture supplied with the Circum Vent Thermal CycleSequencing Kit (New England Biolab, Beverly, MA). Following the manufactur-er’s instructions, 35 cycles of amplification were performed in a thermal cycler
32Pwith the addition of (g- ) ATP to the samples. PCR products were electrophor-esed on 8% polyacrylamide–7 mol / l urea gels for 2–3 h at 1800 volts. The gelswere dried and exposed to X-ray film without intensifying screens at 2 708Covernight.
2.4. Preparation of cell lysates
All steps of sample preparation was devised in our laboratory. Tissues werehomogenized and lysed on ice in an extraction buffer: 10 mmol / l HEPES buffer(pH 7.5; containing 10 mmol / l K EDTA, 50 mmol / l NaCl, 5 mmol / l2
benzarnidine, 10 mg/ l Triton X-100, 10 mmol / l 2-mercaptoethanol, 0.39 mmol /l PMSF, and 5 mg/ l aprotenin) and processed as previously described [18] Aftercentrifugation at 20 000 3 g for 20 min at 48C the supernatant was frozen at2 808C.
2.5. Detection of p16 and p15 by WB technique
Western blots were performed according to Sambrook et al. [19] and adaptedby us as follows. Lysates were spun down, and the supernatant fluid wasquantified using Bradford method [20]. Then, 100 mg of total protein per lanewere ran on a 15% sodium dodecyl sulfate–polyacrylamide gel electrophoresis(SDS–PAGE) gel for p15 and p16, followed by electrophoretic transfer tonitrocellulose membranes. P16 and p15 were probed with anti-p16 and anti-p15monoclonal antibodies (Santa Cruz Biotechnology, California, USA) at adilution of 1:100 at room temperature for 1 h, and horseradish peroxidase-conjugated antimouse immunoglobulin G (IgG) antibody was used for visualiza-tion of positive bands.
3. Results
Using the specific p16 primers, the expected 167 bp-sized single product wasamplified by PCR from human placental DNA (included as positive control) andwith DNA from 96 out of the 168 bladder carcinoma samples. The specific p15
S. Eissa et al. / Clinica Chimica Acta 300 (2000) 159 –169 163
primers amplified the expected single 430 bp product from the control humanplacental DNA and from 132 bladder carcinoma samples. Deletion of p16 andp15 genes was not observed in either normal nor schistosomal bladder tissues.However, deletion of the p16 gene was observed in 72 bladder tumors. Twentyeight of the 72 cases that exhibited p16 deletions also displayed deletions of p15.Only 8 cases showed loss of the p15 gene while retaining p16 gene and p16deletion with apparently intact p15 gene was identified in 44 cases, Table 2, Fig.1.
Expression of p16 and p15 protein was undetectable in 75 and 38 of 168bladder tumors by WB analysis, Fig, 2.
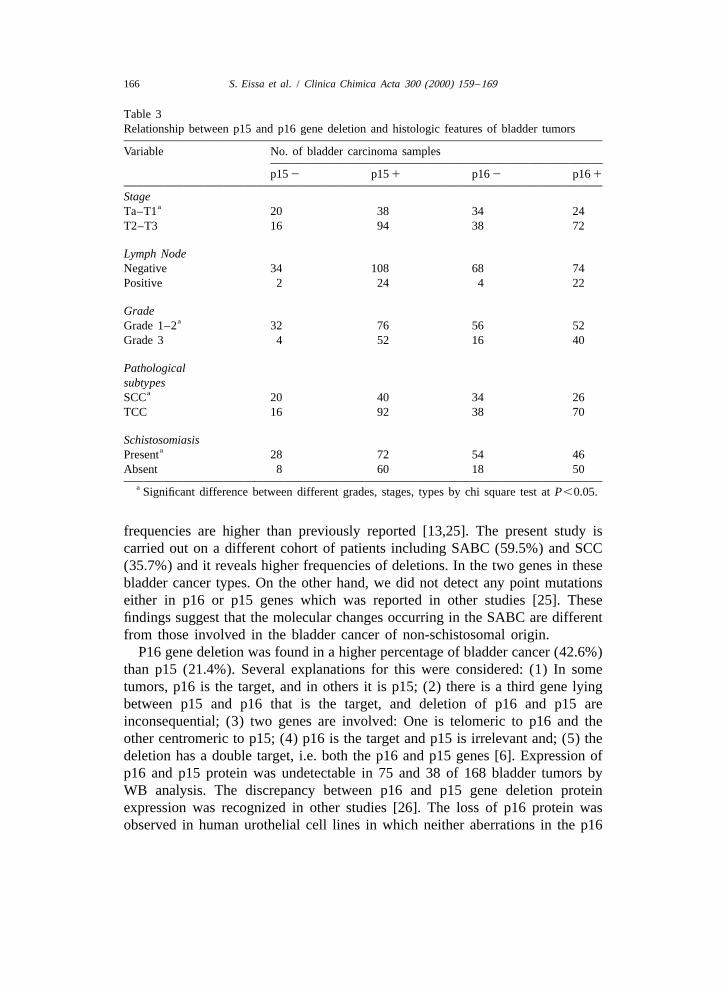
A statistically significant association was observed between p16 gene deletionand the tumor of lower stage, Table 3. While 58.6% (34/58) of superficialtumors showed p16 deletions, only 34.5% (38/110) of invasive lesions werealtered, in addition, a significant association was found between low tumorsgrade and p16 deletions: 51.9% (56/108) of low and intermediate grade tumorshad p16 deletions; such alterations were detected in 28.6% (16/56) of highgrade lesions. Similarly, p15 deletions were statistically associated with tumorsof lower stage, whereas 34.5% (20/58) of superficial tumors showed thesealterations. We also observed an association between p15 gene deletion andtumor grade [grade 1 and grade 2:29.6% (32/108); and grade 3:7.1% (4/56).The overall frequencies of p16 and p15 gene deletions for the cohort of bladdertumors analyzed was 42.9% (72/168) and 21.4% (36/168), respectively.
A statistically significant association was observed between p16, p15 genedeletions and squamous cell carcinoma type of bladder cancer. While 56.7%(34/60) and 33.3% (20/60) of SCC showed p16 and p15 gene deletions,respectively; only 38.8% (38/108) and 14.8% (16/106) showed these deletionsin TCC type. Similarly, p16 and p15 gene deletion were significantly associatedwith schistosomiasis (SABC, p16: 54% (54/100) and p15: 28% (28/100);non-SABC, p16: 26.5%(18/68) and p15: 11.8% (8/68), Table 3
Screening for point mutations by sequence analysis revealed no specificgenetic alterations.
Table 2Relationship between p15 and p16 gene deletion in bladder tumors.
Parameter Bladder carcinoma samples (no. 168)
p16 gene status p16 1 ve p16 2 veSamples no. 96 72p15 gene status p15 1 ve p15 2 ve p15 1 ve p15 2 veSamples no. 88 8 44 28
164 S. Eissa et al. / Clinica Chimica Acta 300 (2000) 159 –169
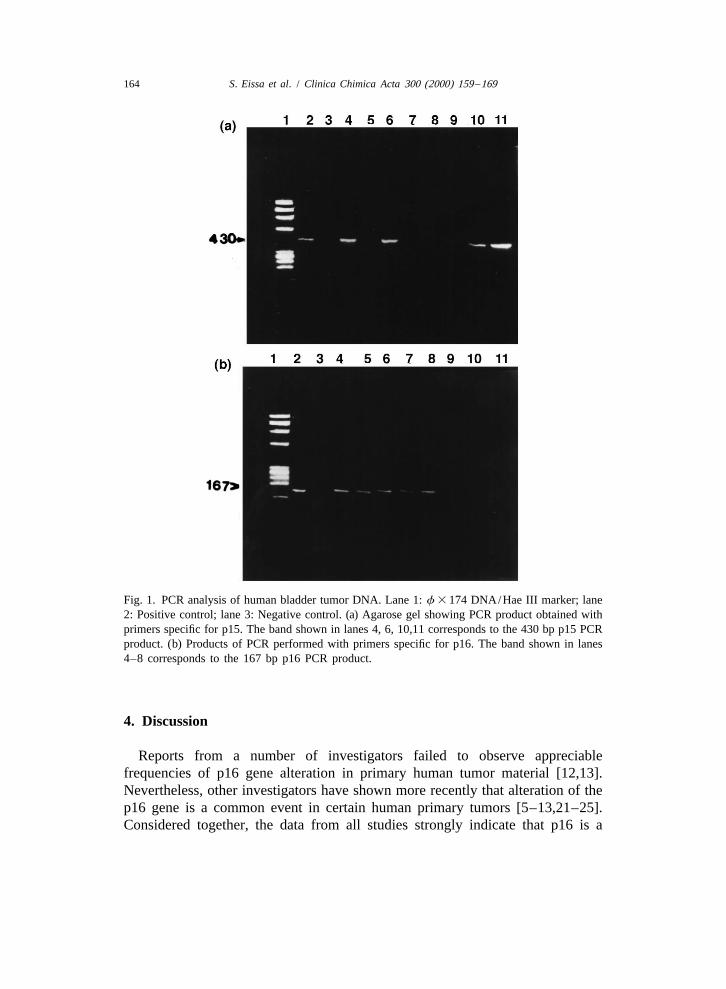
Fig. 1. PCR analysis of human bladder tumor DNA. Lane 1: f 3 174 DNA/Hae III marker; lane2: Positive control; lane 3: Negative control. (a) Agarose gel showing PCR product obtained withprimers specific for p15. The band shown in lanes 4, 6, 10,11 corresponds to the 430 bp p15 PCRproduct. (b) Products of PCR performed with primers specific for p16. The band shown in lanes4–8 corresponds to the 167 bp p16 PCR product.
4. Discussion
Reports from a number of investigators failed to observe appreciablefrequencies of p16 gene alteration in primary human tumor material [12,13].Nevertheless, other investigators have shown more recently that alteration of thep16 gene is a common event in certain human primary tumors [5–13,21–25].Considered together, the data from all studies strongly indicate that p16 is a
S. Eissa et al. / Clinica Chimica Acta 300 (2000) 159 –169 165
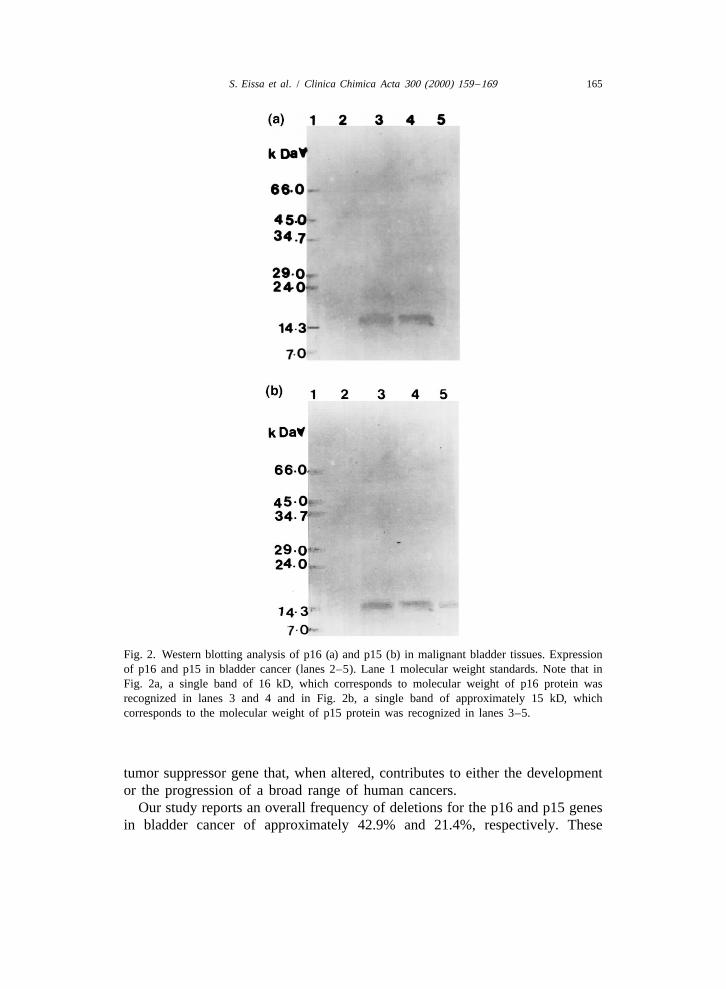
Fig. 2. Western blotting analysis of p16 (a) and p15 (b) in malignant bladder tissues. Expressionof p16 and p15 in bladder cancer (lanes 2–5). Lane 1 molecular weight standards. Note that inFig. 2a, a single band of 16 kD, which corresponds to molecular weight of p16 protein wasrecognized in lanes 3 and 4 and in Fig. 2b, a single band of approximately 15 kD, whichcorresponds to the molecular weight of p15 protein was recognized in lanes 3–5.
tumor suppressor gene that, when altered, contributes to either the developmentor the progression of a broad range of human cancers.
Our study reports an overall frequency of deletions for the p16 and p15 genesin bladder cancer of approximately 42.9% and 21.4%, respectively. These
166 S. Eissa et al. / Clinica Chimica Acta 300 (2000) 159 –169
Table 3Relationship between p15 and p16 gene deletion and histologic features of bladder tumors
Variable No. of bladder carcinoma samples
p15 2 p15 1 p16 2 p16 1
StageaTa–T1 20 38 34 24
T2–T3 16 94 38 72
Lymph NodeNegative 34 108 68 74Positive 2 24 4 22
GradeaGrade 1–2 32 76 56 52
Grade 3 4 52 16 40
Pathologicalsubtypes
aSCC 20 40 34 26TCC 16 92 38 70
SchistosomiasisaPresent 28 72 54 46
Absent 8 60 18 50a Significant difference between different grades, stages, types by chi square test at P,0.05.
frequencies are higher than previously reported [13,25]. The present study iscarried out on a different cohort of patients including SABC (59.5%) and SCC(35.7%) and it reveals higher frequencies of deletions. In the two genes in thesebladder cancer types. On the other hand, we did not detect any point mutationseither in p16 or p15 genes which was reported in other studies [25]. Thesefindings suggest that the molecular changes occurring in the SABC are differentfrom those involved in the bladder cancer of non-schistosomal origin.
P16 gene deletion was found in a higher percentage of bladder cancer (42.6%)than p15 (21.4%). Several explanations for this were considered: (1) In sometumors, p16 is the target, and in others it is p15; (2) there is a third gene lyingbetween p15 and p16 that is the target, and deletion of p16 and p15 areinconsequential; (3) two genes are involved: One is telomeric to p16 and theother centromeric to p15; (4) p16 is the target and p15 is irrelevant and; (5) thedeletion has a double target, i.e. both the p16 and p15 genes [6]. Expression ofp16 and p15 protein was undetectable in 75 and 38 of 168 bladder tumors byWB analysis. The discrepancy between p16 and p15 gene deletion proteinexpression was recognized in other studies [26]. The loss of p16 protein wasobserved in human urothelial cell lines in which neither aberrations in the p16

S. Eissa et al. / Clinica Chimica Acta 300 (2000) 159 –169 167
coding regions nor loss of p16 in RNA were detected. These findings may beconsistent with the possibility of posttranscriptional regulation of p16 levels[27]. The present analysis also reveals that deletion in the two genes areassociated with low-stage, low grade bladder cancer confirming previousfindings [25] and suggesting that the loss of p16 and p15 genes may be an earlyevent in bladder carcinogenesins. Conclusively, our data indicate consistentassociation of p16 and p15 gene deletion with SABC, low stage and low gradebladder cancer suggesting that a determination of pl6 and p15 gene status maybe useful both diagnostically and prognostically in the evaluation of patientsaffected by bladder cancer, particularly those associated with schistosoimasis.
The role of p15 and p16 as negative regulators of the cell cycle in the SABcarcinogenesis is yet to be resolved and further investigations are warranted tounderstand the participation of p15 and p16 in SAB carcinogenesis and possiblecooperative and cumulative effects between p15 and p16 and other tumorsuppressor genes in transforming normal cells into the malignant phenotypeduring schistosomiasis.
Acknowledgements
The authors thank Professor Malak Kotb, Director of Immunology, SurgeryDepartment, University of Tennessee, Memphis, USA, for her kind support. Wealso acknowledge the pathological section of Oncology Diagnostic Unit forproviding us with samples with their histopathological evaluation.
References
[1] Serrano M, Hannon GJ, Beach D. A new regulatory motif in cell-cycle control causingspecific inhibitor of cyclin D/CDK4. Nature 1993;366:704–7.
[2] Schulze A, Zerfass K, Spitkovsky D, Hengiein B, Jansen DP. Activation of the E2FINK4transcription factor by cyclin Dl is blocked by P16 the putative tumor supressor gene
MTS. Oncogene 1994;9:3475–82.[3] Serrano M, Gomez LE, Depinho RA, Beach D, Bar SD. Inhibition of rasinduced proliferation
INK4and cellular transformation by P16 . Science 1995;297:249–52.[4] Kamb A, Gruis NA, Weaver-Feldhaus J, Liu Q, Harshan K, Tavtigian SV. A cell cycle
regulator potentially involved in genesis of many tumor types. Science 1994;264:436–40.[5] Nobori T, Miura K, Wu DJ, Lois A, Takabayashi K, Carson DA. Deletions of the
cyclin-dependent kinase-4 inhibitor gene in multiple human cancers. Nature 1994;368:753–6.[6] Jen J, Harper JW, Bigner SH, Bigner DD, Papadopulos N, Markowitz S, Willson JKV, Kinzer
KW, Vogel Stein B. Deletion of p16 and p15 genes in brain tumors. Cancer Res1994;54:6353–8.
168 S. Eissa et al. / Clinica Chimica Acta 300 (2000) 159 –169
[7] Washimi O, Nagatake M, Osada H, Ueda R, Koshikawa T, Seki T. In vivo occurrence of p16(MTSI) and p15 (MTS2) alterations preferentially in non-small cell lung cancers. Cancer Res1995;55:514–7.
[8] Mori T, Miura K, Aoki T, Nishihira T, Mon S, Nakamura Y. Frequent somatic mutation ofthe MTS/CDK4I (multiple tumor suppressor /cyclin-dependent kinase 4 inhibitor) gene inesophageal squamous cell carcinoma. Cancer Res 1994;54:3396–7.
[9] Caldas C, Hahn SA, de Costa LT, Redston MS, Schutte M, Seymour AB. Frequent somaticmutations and homozygous deletions of the p16 (MTSI) gene in pancreatic adenocar-cinomna. Nat Genet 1994;8:27–32.
[10] Hussussian CJ, Struewing JP, Goldstein AM, Higgins PA, Ally DS, Sheahan MID. Gennlinep16 mutations in familial melanoma. Nat Genet 1994;8:15–21.
[11] Kamb A, Liu Q, Harshman K, Tavtigian S, Cordon-cardo C, Skolnick MH. Rates of p16(MTSI) mutations in primary tumors with 9p loss. Science 1994;265:416–7.
[12] Cairns P, Merlo A, Lee DJ, Schwab D, Eby Y. Rates of p16 (MTSI) mutations in primarytumors with 9p loss. Science 1994;265:415–6.
[13] Spruck III CH, Gonzalez-Zulueta M, Shibata A, Simoneau AR, Lin ME, Gonzales F. P16gene in uncultured tumors. Nature 1994;370:183–4.
[14] American Joint Committee on Cancer. In: Beahrs OH, Henson DE, Fluter RV et al., editors,Manual for staging of cancer, 4th ed, Philadelphia: Lippincott, 1992.
[15] Jackson DP, Hayden JD, Quirke P. Extraction of nucleic acid from fresh and archivalmaterial. In: McPherson MJ, Quirke P, Taor GR, editors, PCR: A practical approach, OxfordUniversity Press, 1991, pp. 29–49.
[16] Southgate J, Proffitt J, Roberts P, Smith B, Selby P. Loss of cyclin-dependent kinase inhibitorgenes and chromosome 9 karyotypic abnormalities in human bladder cancer cell lines. Br JCancer 1995;12:1214–8.
[17] Sanger F, Nicklen S, Coulson A. DNA sequencing with chain-teminating inhibitors. ProcNatl Acad Sci USA 1977;74:5463–7.
[18] Bissa S, Seada LS. Quantitation of bcl-2 protein in bladder cancer tissue by enzymeimmunoassay: comparison with Western blot and immunohistochemistry. Clin Chem1998;44:1423–9.
[19] Samnbrook J, Fritsch EF, Maniatis T. In: 2nd ed, Molecular clonning. Laboratory manual,Vol. 18, Cold spring Harbor: Laboratory press, 1989, pp. 42–59.
[20] Bradford MM. A rapid and sensitive method for quantitation of microgram quantities ofprotein utilizing the principle of protein dye binding. Anal Bioch 1976;72:248–51.
[21] Schmidt BE, Ichimura K, Reifenberger G, Collins P. CDKN2 (p16/MTSI) gene deletion orCDK4 amplification occurs in the majority of glioblastomnas. Cancer Res 1994;54:6321–4.
[22] Walker DG, Duan W, Popovic BA, Kaye AH, Tomnlinson FH, Lavin M. Homozygousdeletions of the multiple tumor suppressor gene 1 in the progression of human astrocytomas.Cancer Res 1995;55:20–3.
[23] Gruis NA, Weaver-Feldhaus J, Liu Q, Frye C, Eeles R, Orlow I. Genetic evidence inmelanoma and bladder cancers that p16 and p53 function in separate pathways of tumorsuppression. Am J Pathol 1995;146:1199–206.
[24] Sarkis AS, Dalbagni G, Cordon-Cardo C, Melamed J, Zhang ZF, Sheinfeld J. Association ofp53 nuclear overexpression and tumor progression in carcinoma in situ of the bladder. J Urol1994;152:388–92.
[25] Orlow I, Lacombe L, Hannan GJ, Serrano M, Pellicer I, Dalbagni G, Reuter VB, Zhang Z-F,Beach D, Cardon-Cardo C. Deletion of the p16 and p15 Genes in Human Bladder Tumors. JNatl Cancer instit 1995;87:1524–9.

S. Eissa et al. / Clinica Chimica Acta 300 (2000) 159 –169 169
[26] Tsuzuki T, Tsunoda S, Sakaki T, Konishi N, Hiasa Y, Nakarnura M. Alterations ofRetinoblastoma, p513, p16(CDKN2), and p15 Genes in Human Astrocytomas. Cancer1996;78:287–93.
[27] Yeager T, Stadler W, Belair C, Puthenveettil J, Olopade O, Rezuikoff C. Increased P16 levelsRBcorrelate with P alterations in human urothelial cells. Cancer Res 1995;55:493–7.




















