Reference Model 3.0 Geospatial Data Infrastructure (GDI) North-Rhine-Westfalia
Upload
khangminh22Category
view
1download
0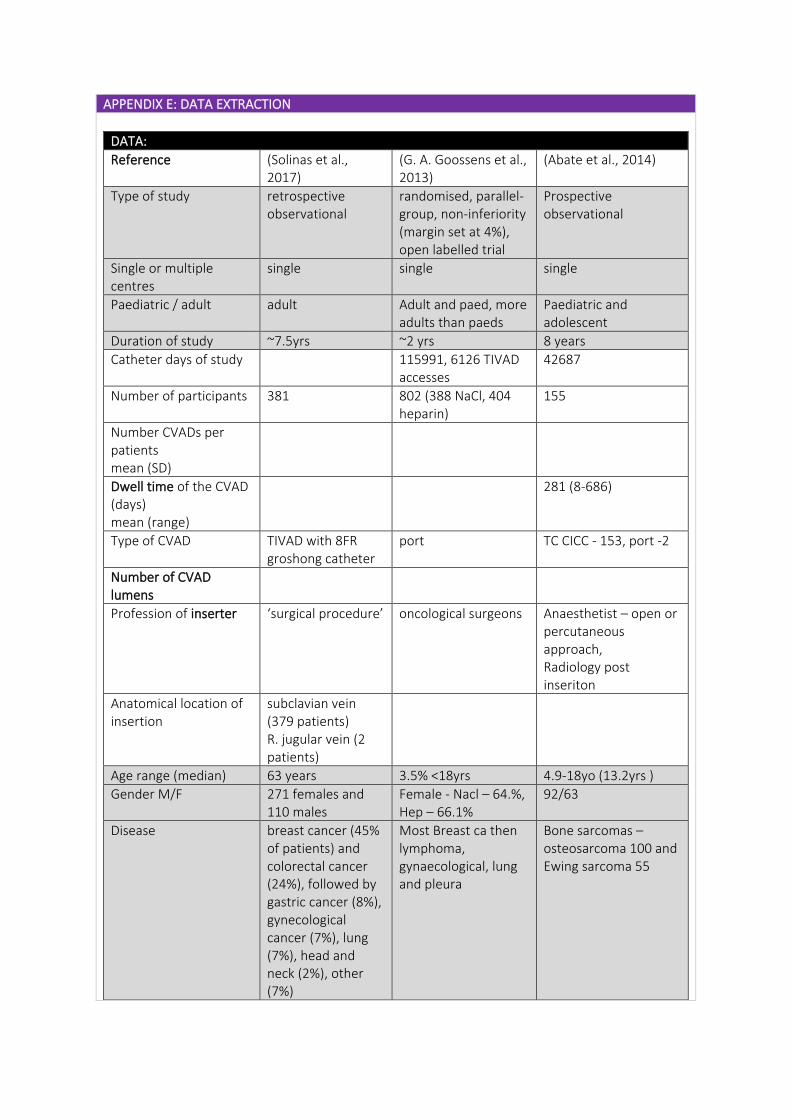
APPENDIX E: DATA EXTRACTION
DATA:
Reference (Solinas et al., 2017)
(G. A. Goossens et al., 2013)
(Abate et al., 2014)
Type of study retrospective observational
randomised, parallel-group, non-inferiority (margin set at 4%), open labelled trial
Prospective observational
Single or multiple centres
single single single
Paediatric / adult adult Adult and paed, more adults than paeds
Paediatric and adolescent
Duration of study ~7.5yrs ~2 yrs 8 years
Catheter days of study 115991, 6126 TIVAD accesses
42687
Number of participants 381 802 (388 NaCl, 404 heparin)
155
Number CVADs per patients mean (SD)
Dwell time of the CVAD (days) mean (range)
281 (8-686)
Type of CVAD TIVAD with 8FR groshong catheter
port TC CICC - 153, port -2
Number of CVAD lumens
Profession of inserter ‘surgical procedure’ oncological surgeons Anaesthetist – open or percutaneous approach, Radiology post inseriton
Anatomical location of insertion
subclavian vein (379 patients) R. jugular vein (2 patients)
Age range (median) 63 years 3.5% <18yrs 4.9-18yo (13.2yrs )
Gender M/F 271 females and 110 males
Female - Nacl – 64.%, Hep – 66.1%
92/63
Disease breast cancer (45% of patients) and colorectal cancer (24%), followed by gastric cancer (8%), gynecological cancer (7%), lung (7%), head and neck (2%), other (7%)
Most Breast ca then lymphoma, gynaecological, lung and pleura
Bone sarcomas – osteosarcoma 100 and Ewing sarcoma 55
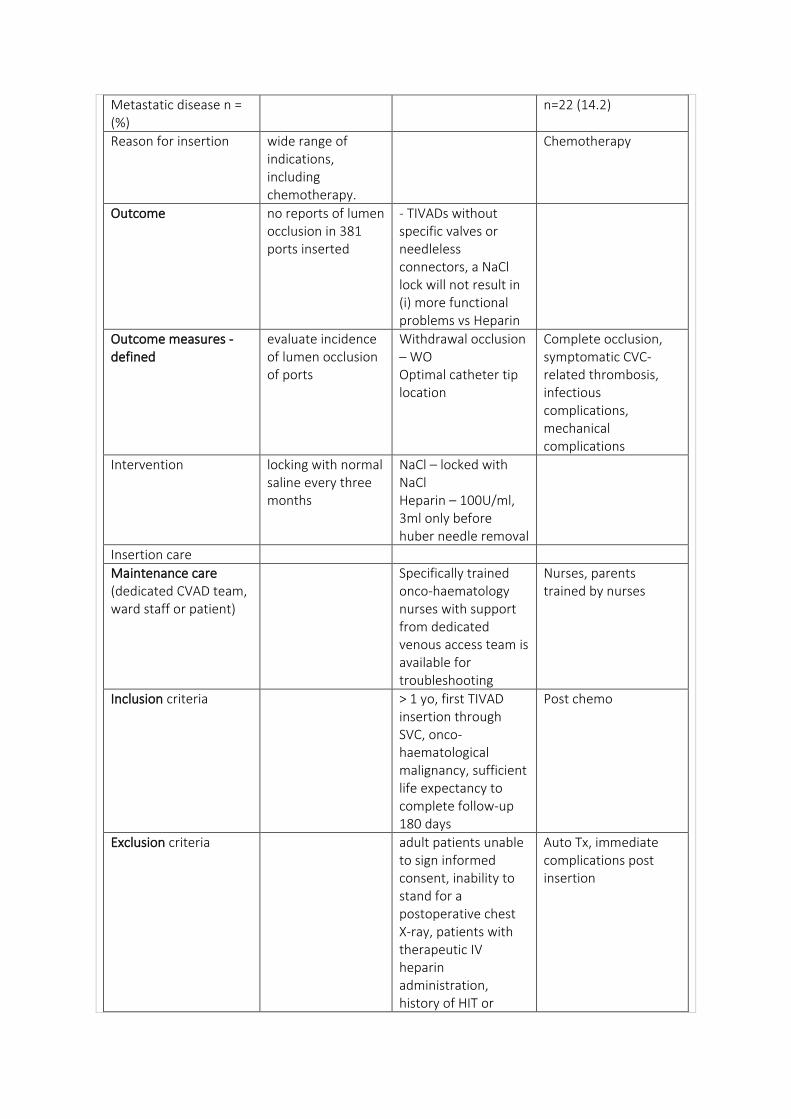
Metastatic disease n = (%)
n=22 (14.2)
Reason for insertion wide range of indications, including chemotherapy.
Chemotherapy
Outcome no reports of lumen occlusion in 381 ports inserted
- TIVADs without specific valves or needleless connectors, a NaCl lock will not result in (i) more functional problems vs Heparin
Outcome measures - defined
evaluate incidence of lumen occlusion of ports
Withdrawal occlusion – WO Optimal catheter tip location
Complete occlusion, symptomatic CVC-related thrombosis, infectious complications, mechanical complications
Intervention locking with normal saline every three months
NaCl – locked with NaCl Heparin – 100U/ml, 3ml only before huber needle removal
Insertion care
Maintenance care (dedicated CVAD team, ward staff or patient)
Specifically trained onco-haematology nurses with support from dedicated venous access team is available for troubleshooting
Nurses, parents trained by nurses
Inclusion criteria > 1 yo, first TIVAD insertion through SVC, onco-haematological malignancy, sufficient life expectancy to complete follow-up 180 days
Post chemo
Exclusion criteria adult patients unable to sign informed consent, inability to stand for a postoperative chest X-ray, patients with therapeutic IV heparin administration, history of HIT or
Auto Tx, immediate complications post insertion
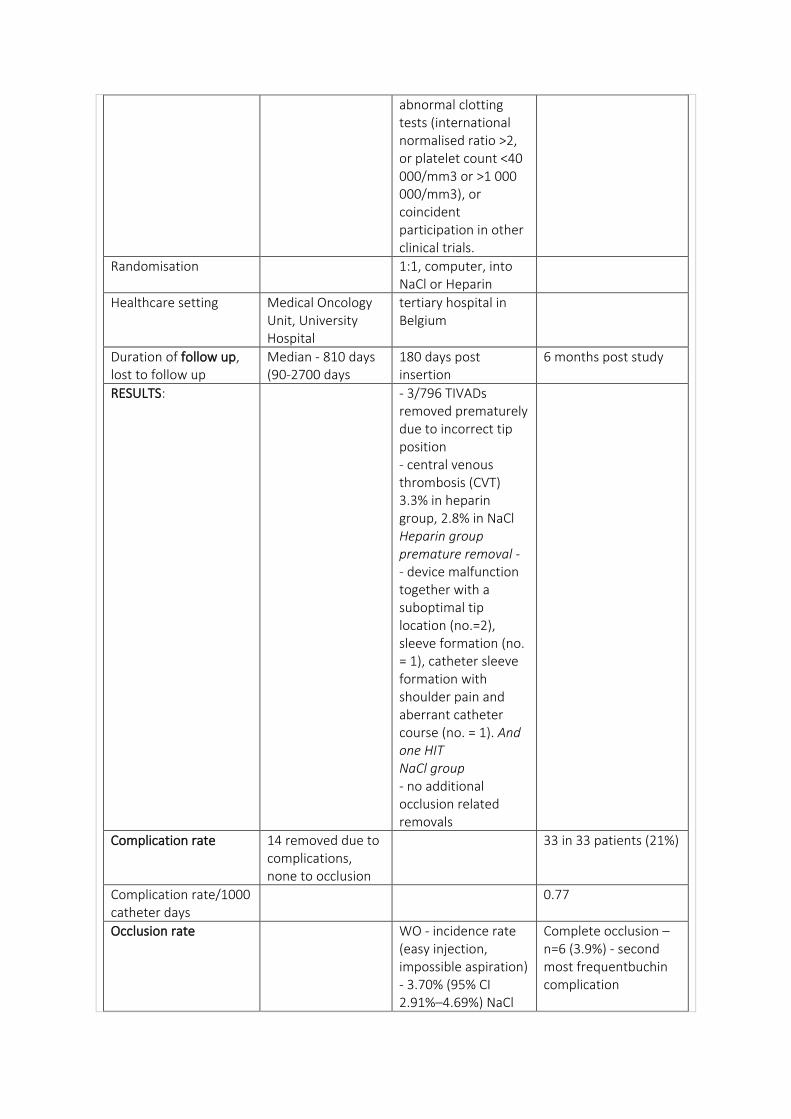
abnormal clotting tests (international normalised ratio >2, or platelet count <40 000/mm3 or >1 000 000/mm3), or coincident participation in other clinical trials.
Randomisation 1:1, computer, into NaCl or Heparin
Healthcare setting Medical Oncology Unit, University Hospital
tertiary hospital in Belgium
Duration of follow up, lost to follow up
Median - 810 days (90-2700 days
180 days post insertion
6 months post study
RESULTS: - 3/796 TIVADs removed prematurely due to incorrect tip position - central venous thrombosis (CVT) 3.3% in heparin group, 2.8% in NaCl Heparin group premature removal - - device malfunction together with a suboptimal tip location (no.=2), sleeve formation (no. = 1), catheter sleeve formation with shoulder pain and aberrant catheter course (no. = 1). And one HIT NaCl group - no additional occlusion related removals
Complication rate 14 removed due to complications, none to occlusion
33 in 33 patients (21%)
Complication rate/1000 catheter days
0.77
Occlusion rate WO - incidence rate (easy injection, impossible aspiration) - 3.70% (95% CI 2.91%–4.69%) NaCl
Complete occlusion – n=6 (3.9%) - second most frequentbuchin complication
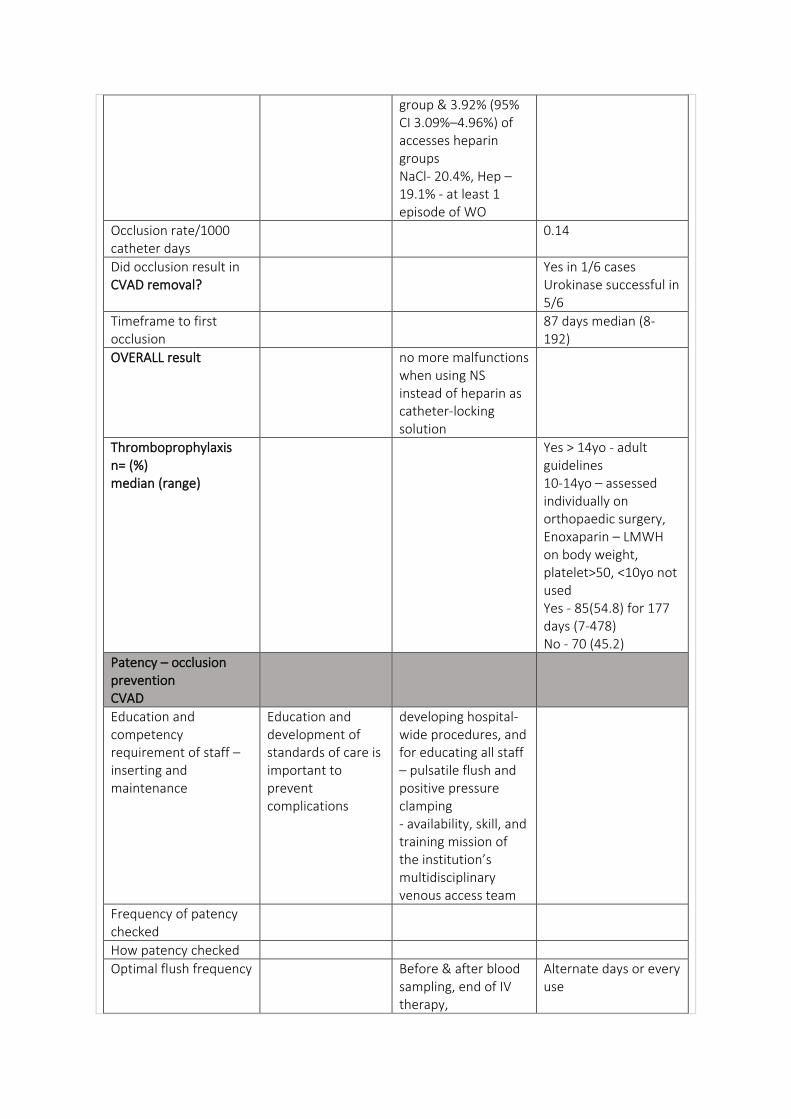
group & 3.92% (95% CI 3.09%–4.96%) of accesses heparin groups NaCl- 20.4%, Hep – 19.1% - at least 1 episode of WO
Occlusion rate/1000 catheter days
0.14
Did occlusion result in CVAD removal?
Yes in 1/6 cases Urokinase successful in 5/6
Timeframe to first occlusion
87 days median (8-192)
OVERALL result no more malfunctions when using NS instead of heparin as catheter-locking solution
Thromboprophylaxis n= (%) median (range)
Yes > 14yo - adult guidelines 10-14yo – assessed individually on orthopaedic surgery, Enoxaparin – LMWH on body weight, platelet>50, <10yo not used Yes - 85(54.8) for 177 days (7-478) No - 70 (45.2)
Patency – occlusion prevention CVAD
Education and competency requirement of staff – inserting and maintenance
Education and development of standards of care is important to prevent complications
developing hospital-wide procedures, and for educating all staff – pulsatile flush and positive pressure clamping - availability, skill, and training mission of the institution’s multidisciplinary venous access team
Frequency of patency checked
How patency checked
Optimal flush frequency
Before & after blood sampling, end of IV therapy,
Alternate days or every use
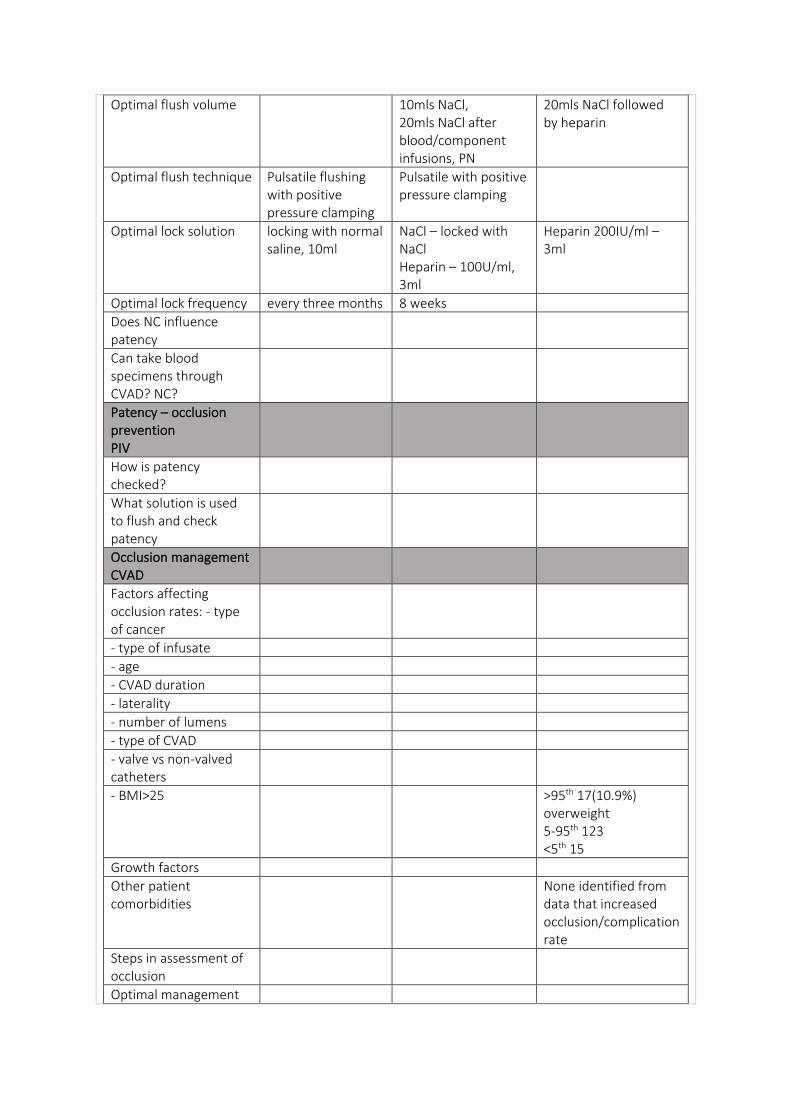
Optimal flush volume 10mls NaCl, 20mls NaCl after blood/component infusions, PN
20mls NaCl followed by heparin
Optimal flush technique Pulsatile flushing with positive pressure clamping
Pulsatile with positive pressure clamping
Optimal lock solution locking with normal saline, 10ml
NaCl – locked with NaCl Heparin – 100U/ml, 3ml
Heparin 200IU/ml – 3ml
Optimal lock frequency every three months 8 weeks
Does NC influence patency
Can take blood specimens through CVAD? NC?
Patency – occlusion prevention PIV
How is patency checked?
What solution is used to flush and check patency
Occlusion management CVAD
Factors affecting occlusion rates: - type of cancer
- type of infusate
- age
- CVAD duration
- laterality
- number of lumens
- type of CVAD
- valve vs non-valved catheters
- BMI>25 >95th 17(10.9%) overweight 5-95th 123 <5th 15
Growth factors
Other patient comorbidities
None identified from data that increased occlusion/complication rate
Steps in assessment of occlusion
Optimal management
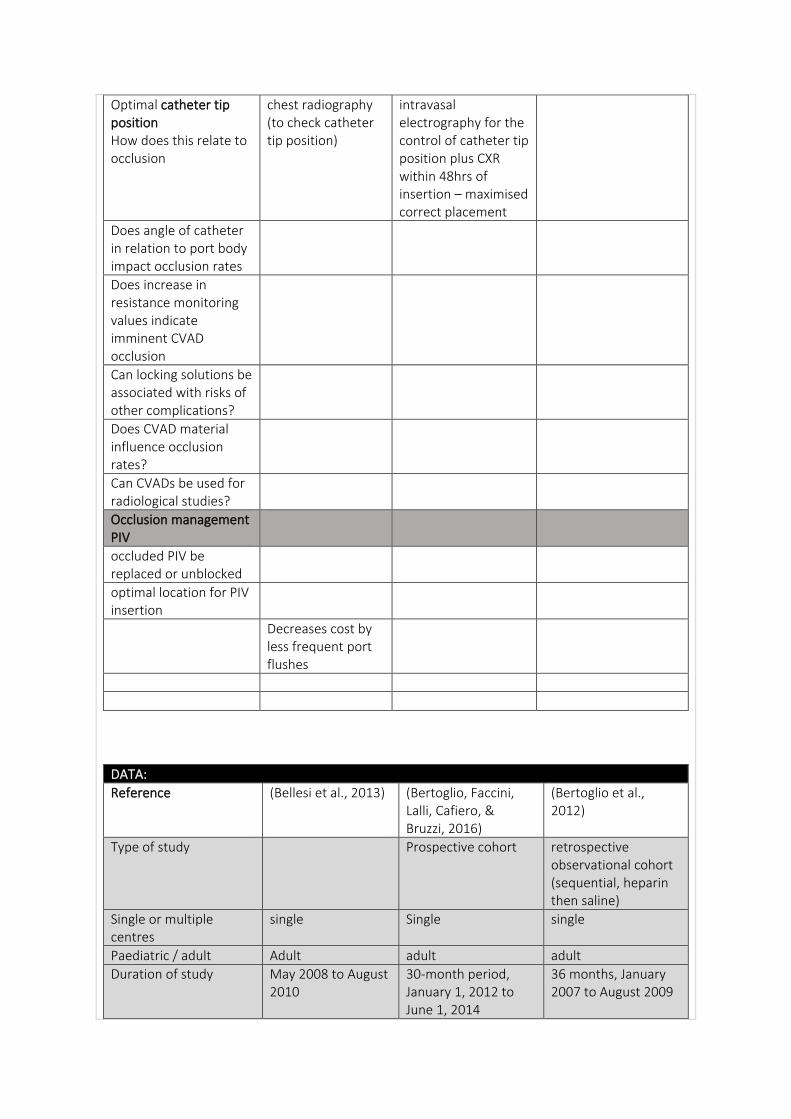
Optimal catheter tip position How does this relate to occlusion
chest radiography (to check catheter tip position)
intravasal electrography for the control of catheter tip position plus CXR within 48hrs of insertion – maximised correct placement
Does angle of catheter in relation to port body impact occlusion rates
Does increase in resistance monitoring values indicate imminent CVAD occlusion
Can locking solutions be associated with risks of other complications?
Does CVAD material influence occlusion rates?
Can CVADs be used for radiological studies?
Occlusion management PIV
occluded PIV be replaced or unblocked
optimal location for PIV insertion
Decreases cost by less frequent port flushes
DATA:
Reference (Bellesi et al., 2013) (Bertoglio, Faccini, Lalli, Cafiero, & Bruzzi, 2016)
(Bertoglio et al., 2012)
Type of study Prospective cohort retrospective observational cohort (sequential, heparin then saline)
Single or multiple centres
single Single single
Paediatric / adult Adult adult adult
Duration of study May 2008 to August 2010
30-month period, January 1, 2012 to June 1, 2014
36 months, January 2007 to August 2009
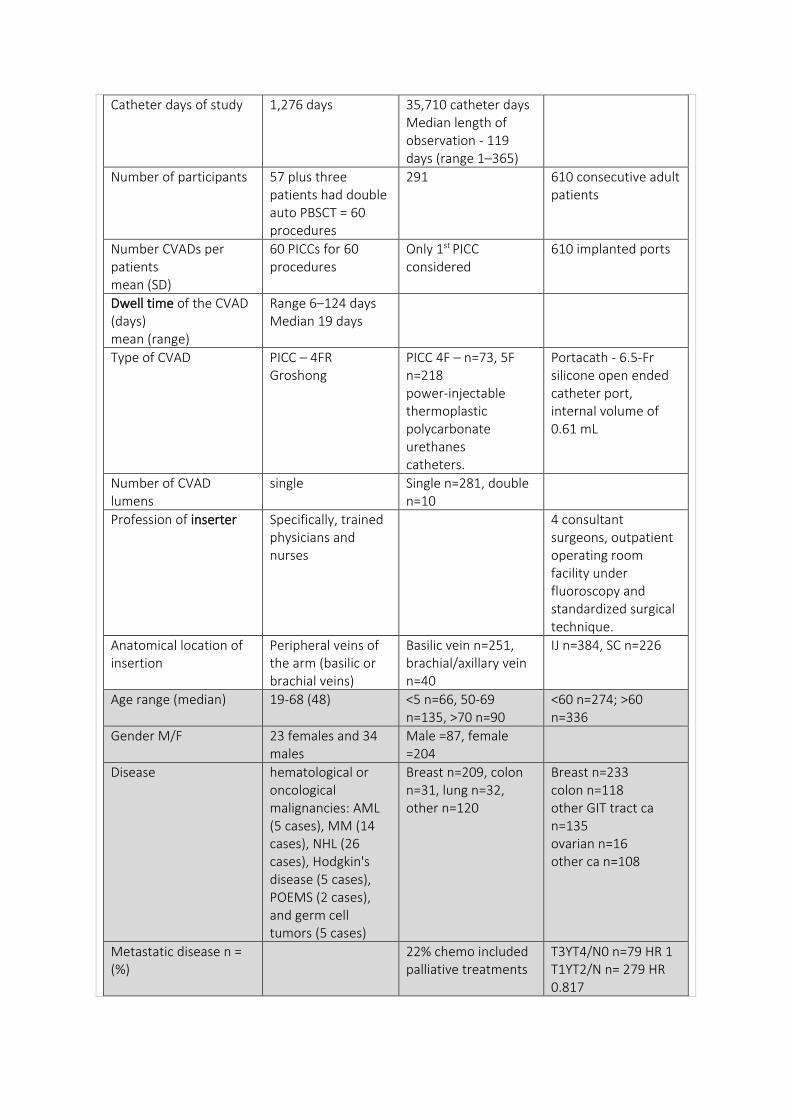
Catheter days of study 1,276 days 35,710 catheter days Median length of observation - 119 days (range 1–365)
Number of participants 57 plus three patients had double auto PBSCT = 60 procedures
291 610 consecutive adult patients
Number CVADs per patients mean (SD)
60 PICCs for 60 procedures
Only 1st PICC considered
610 implanted ports
Dwell time of the CVAD (days) mean (range)
Range 6–124 days Median 19 days
Type of CVAD PICC – 4FR Groshong
PICC 4F – n=73, 5F n=218 power-injectable thermoplastic polycarbonate urethanes catheters.
Portacath - 6.5-Fr silicone open ended catheter port, internal volume of 0.61 mL
Number of CVAD lumens
single Single n=281, double n=10
Profession of inserter Specifically, trained physicians and nurses
4 consultant surgeons, outpatient operating room facility under fluoroscopy and standardized surgical technique.
Anatomical location of insertion
Peripheral veins of the arm (basilic or brachial veins)
Basilic vein n=251, brachial/axillary vein n=40
IJ n=384, SC n=226
Age range (median) 19-68 (48) <5 n=66, 50-69 n=135, >70 n=90
<60 n=274; >60 n=336
Gender M/F 23 females and 34 males
Male =87, female =204
Disease hematological or oncological malignancies: AML (5 cases), MM (14 cases), NHL (26 cases), Hodgkin's disease (5 cases), POEMS (2 cases), and germ cell tumors (5 cases)
Breast n=209, colon n=31, lung n=32, other n=120
Breast n=233 colon n=118 other GIT tract ca n=135 ovarian n=16 other ca n=108
Metastatic disease n = (%)
22% chemo included palliative treatments
T3YT4/N0 n=79 HR 1 T1YT2/N n= 279 HR 0.817
IV stage/M+ n=252 HR 1.943
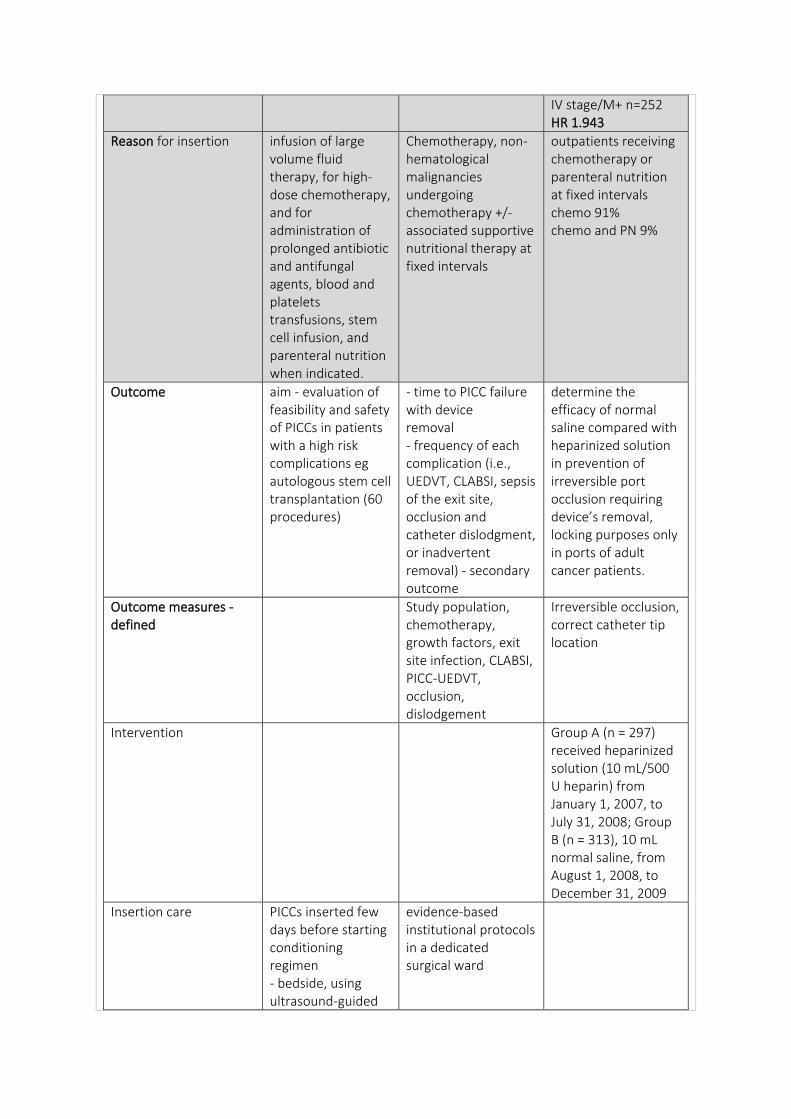
Reason for insertion infusion of large volume fluid therapy, for high-dose chemotherapy, and for administration of prolonged antibiotic and antifungal agents, blood and platelets transfusions, stem cell infusion, and parenteral nutrition when indicated.
Chemotherapy, non-hematological malignancies undergoing chemotherapy +/- associated supportive nutritional therapy at fixed intervals
outpatients receiving chemotherapy or parenteral nutrition at fixed intervals chemo 91% chemo and PN 9%
Outcome aim - evaluation of feasibility and safety of PICCs in patients with a high risk complications eg autologous stem cell transplantation (60 procedures)
- time to PICC failure with device removal - frequency of each complication (i.e., UEDVT, CLABSI, sepsis of the exit site, occlusion and catheter dislodgment, or inadvertent removal) - secondary outcome
determine the efficacy of normal saline compared with heparinized solution in prevention of irreversible port occlusion requiring device’s removal, locking purposes only in ports of adult cancer patients.
Outcome measures - defined
Study population, chemotherapy, growth factors, exit site infection, CLABSI, PICC-UEDVT, occlusion, dislodgement
Irreversible occlusion, correct catheter tip location
Intervention Group A (n = 297) received heparinized solution (10 mL/500 U heparin) from January 1, 2007, to July 31, 2008; Group B (n = 313), 10 mL normal saline, from August 1, 2008, to December 31, 2009
Insertion care PICCs inserted few days before starting conditioning regimen - bedside, using ultrasound-guided
evidence-based institutional protocols in a dedicated surgical ward
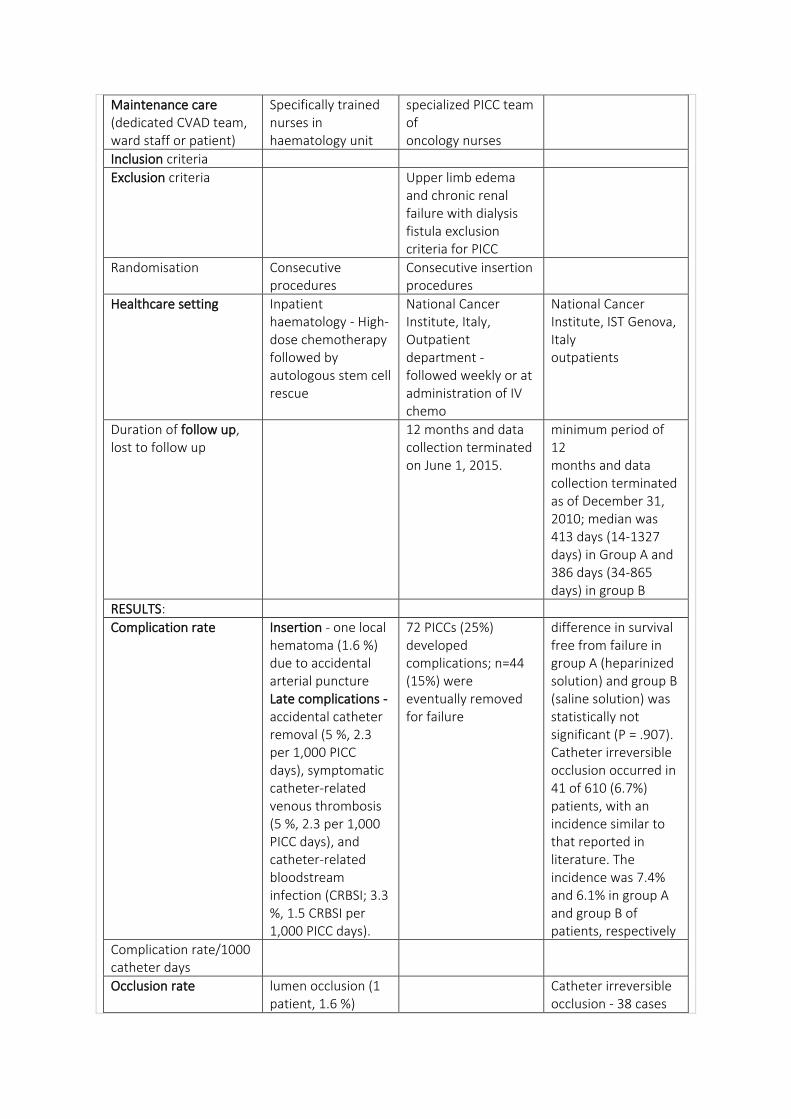
Maintenance care (dedicated CVAD team, ward staff or patient)
Specifically trained nurses in haematology unit
specialized PICC team of oncology nurses
Inclusion criteria
Exclusion criteria Upper limb edema and chronic renal failure with dialysis fistula exclusion criteria for PICC
Randomisation Consecutive procedures
Consecutive insertion procedures
Healthcare setting Inpatient haematology - High-dose chemotherapy followed by autologous stem cell rescue
National Cancer Institute, Italy, Outpatient department - followed weekly or at administration of IV chemo
National Cancer Institute, IST Genova, Italy outpatients
Duration of follow up, lost to follow up
12 months and data collection terminated on June 1, 2015.
minimum period of 12 months and data collection terminated as of December 31, 2010; median was 413 days (14-1327 days) in Group A and 386 days (34-865 days) in group B
RESULTS:
Complication rate Insertion - one local hematoma (1.6 %) due to accidental arterial puncture Late complications - accidental catheter removal (5 %, 2.3 per 1,000 PICC days), symptomatic catheter-related venous thrombosis (5 %, 2.3 per 1,000 PICC days), and catheter-related bloodstream infection (CRBSI; 3.3 %, 1.5 CRBSI per 1,000 PICC days).
72 PICCs (25%) developed complications; n=44 (15%) were eventually removed for failure
difference in survival free from failure in group A (heparinized solution) and group B (saline solution) was statistically not significant (P = .907). Catheter irreversible occlusion occurred in 41 of 610 (6.7%) patients, with an incidence similar to that reported in literature. The incidence was 7.4% and 6.1% in group A and group B of patients, respectively
Complication rate/1000 catheter days
Occlusion rate lumen occlusion (1 patient, 1.6 %)
Catheter irreversible occlusion - 38 cases
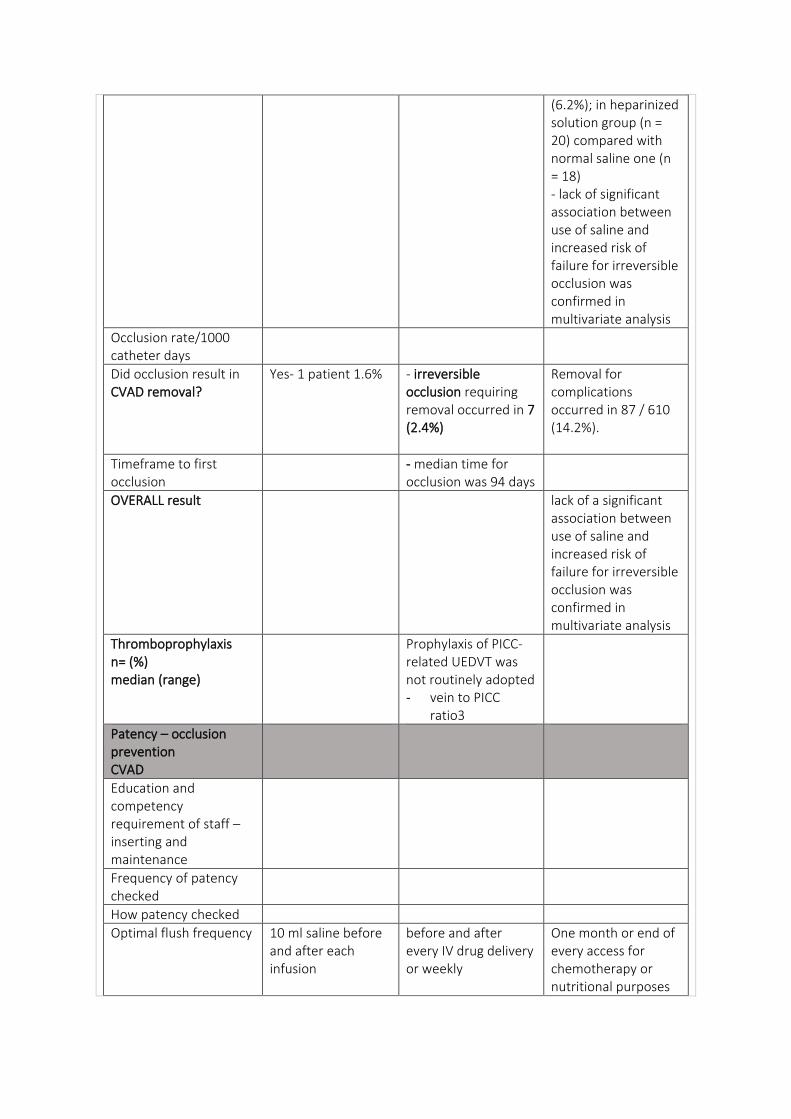
(6.2%); in heparinized solution group (n = 20) compared with normal saline one (n = 18) - lack of significant association between use of saline and increased risk of failure for irreversible occlusion was confirmed in multivariate analysis
Occlusion rate/1000 catheter days
Did occlusion result in CVAD removal?
Yes- 1 patient 1.6% - irreversible occlusion requiring removal occurred in 7 (2.4%)
Removal for complications occurred in 87 / 610 (14.2%).
Timeframe to first occlusion
- median time for occlusion was 94 days
OVERALL result lack of a significant association between use of saline and increased risk of failure for irreversible occlusion was confirmed in multivariate analysis
Thromboprophylaxis n= (%) median (range)
Prophylaxis of PICC-related UEDVT was not routinely adopted - vein to PICC
ratio3
Patency – occlusion prevention CVAD
Education and competency requirement of staff – inserting and maintenance
Frequency of patency checked
How patency checked
Optimal flush frequency 10 ml saline before and after each infusion
before and after every IV drug delivery or weekly
One month or end of every access for chemotherapy or nutritional purposes
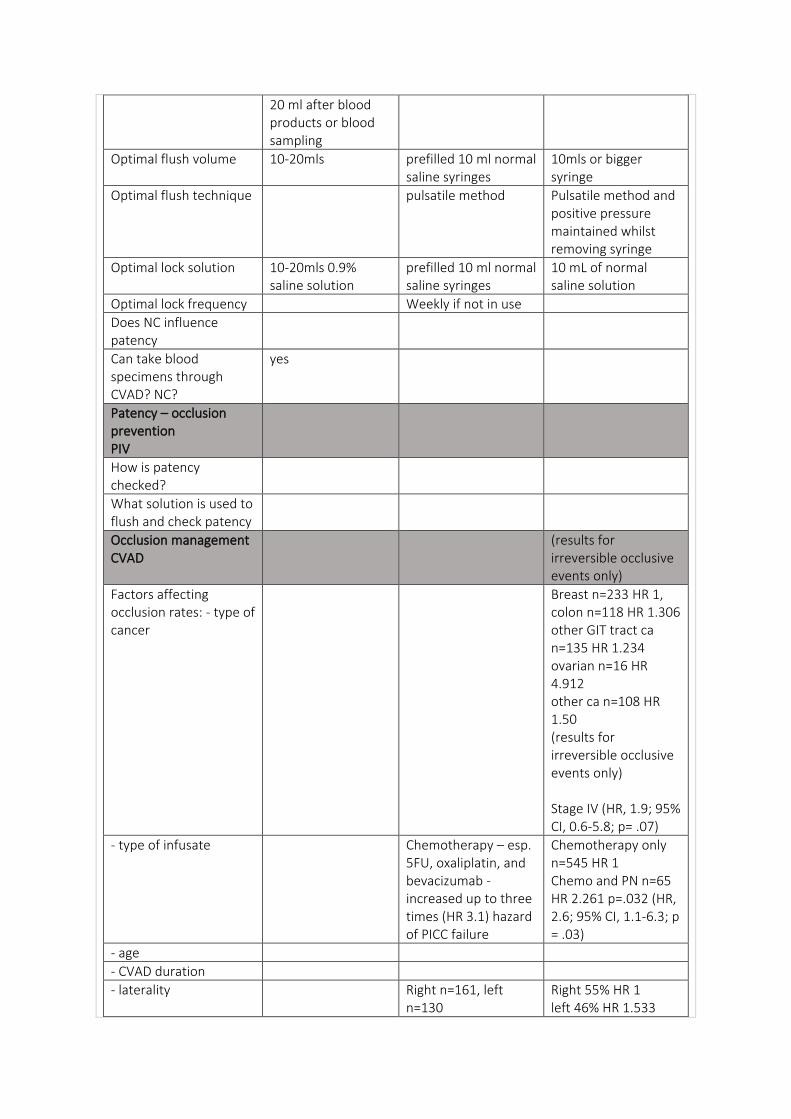
20 ml after blood products or blood sampling
Optimal flush volume 10-20mls
prefilled 10 ml normal saline syringes
10mls or bigger syringe
Optimal flush technique pulsatile method Pulsatile method and positive pressure maintained whilst removing syringe
Optimal lock solution 10-20mls 0.9% saline solution
prefilled 10 ml normal saline syringes
10 mL of normal saline solution
Optimal lock frequency Weekly if not in use
Does NC influence patency
Can take blood specimens through CVAD? NC?
yes
Patency – occlusion prevention PIV
How is patency checked?
What solution is used to flush and check patency
Occlusion management CVAD
(results for irreversible occlusive events only)
Factors affecting occlusion rates: - type of cancer
Breast n=233 HR 1, colon n=118 HR 1.306 other GIT tract ca n=135 HR 1.234 ovarian n=16 HR 4.912 other ca n=108 HR 1.50 (results for irreversible occlusive events only) Stage IV (HR, 1.9; 95% CI, 0.6-5.8; p= .07)
- type of infusate Chemotherapy – esp. 5FU, oxaliplatin, and bevacizumab - increased up to three times (HR 3.1) hazard of PICC failure
Chemotherapy only n=545 HR 1 Chemo and PN n=65 HR 2.261 p=.032 (HR, 2.6; 95% CI, 1.1-6.3; p = .03)
- age
- CVAD duration
- laterality Right n=161, left n=130
Right 55% HR 1 left 46% HR 1.533
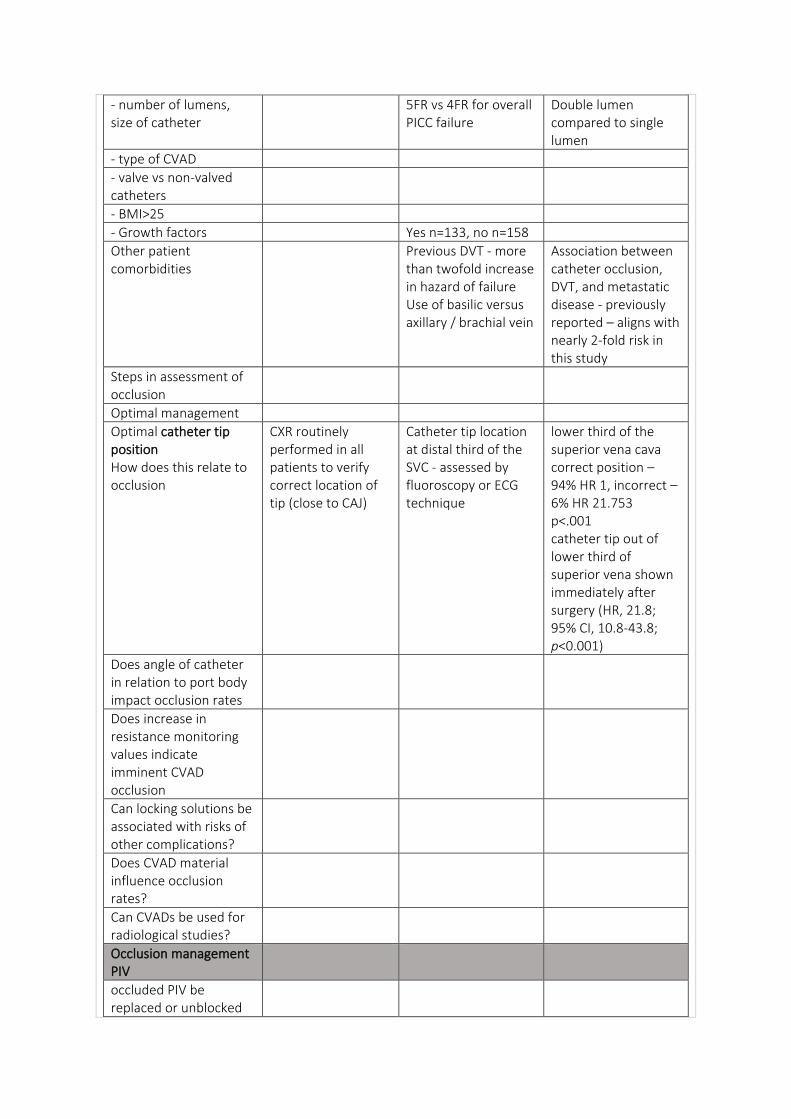
- number of lumens, size of catheter
5FR vs 4FR for overall PICC failure
Double lumen compared to single lumen
- type of CVAD
- valve vs non-valved catheters
- BMI>25
- Growth factors Yes n=133, no n=158
Other patient comorbidities
Previous DVT - more than twofold increase in hazard of failure Use of basilic versus axillary / brachial vein
Association between catheter occlusion, DVT, and metastatic disease - previously reported – aligns with nearly 2-fold risk in this study
Steps in assessment of occlusion
Optimal management
Optimal catheter tip position How does this relate to occlusion
CXR routinely performed in all patients to verify correct location of tip (close to CAJ)
Catheter tip location at distal third of the SVC - assessed by fluoroscopy or ECG technique
lower third of the superior vena cava correct position – 94% HR 1, incorrect – 6% HR 21.753 p<.001 catheter tip out of lower third of superior vena shown immediately after surgery (HR, 21.8; 95% CI, 10.8-43.8; p<0.001)
Does angle of catheter in relation to port body impact occlusion rates
Does increase in resistance monitoring values indicate imminent CVAD occlusion
Can locking solutions be associated with risks of other complications?
Does CVAD material influence occlusion rates?
Can CVADs be used for radiological studies?
Occlusion management PIV
occluded PIV be replaced or unblocked
optimal location for PIV insertion
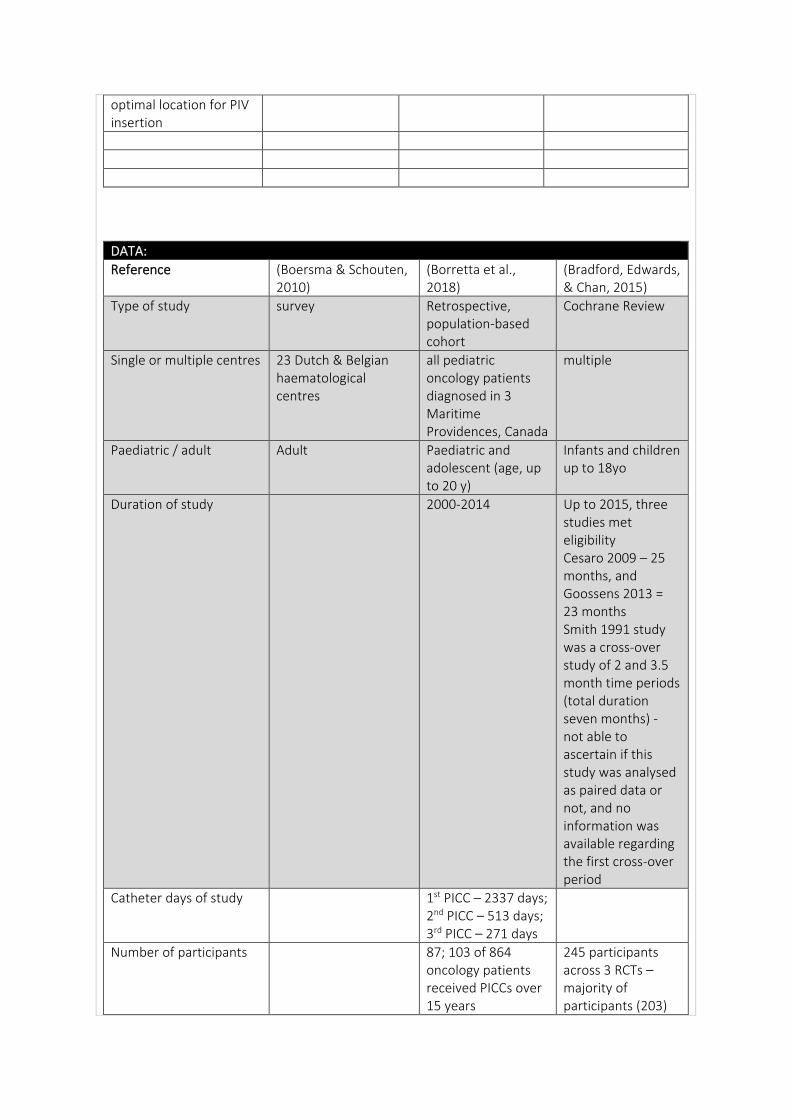
DATA:
Reference (Boersma & Schouten, 2010)
(Borretta et al., 2018)
(Bradford, Edwards, & Chan, 2015)
Type of study survey Retrospective, population-based cohort
Cochrane Review
Single or multiple centres 23 Dutch & Belgian haematological centres
all pediatric oncology patients diagnosed in 3 Maritime Providences, Canada
multiple
Paediatric / adult Adult Paediatric and adolescent (age, up to 20 y)
Infants and children up to 18yo
Duration of study 2000-2014 Up to 2015, three studies met eligibility Cesaro 2009 – 25 months, and Goossens 2013 = 23 months Smith 1991 study was a cross-over study of 2 and 3.5 month time periods (total duration seven months) - not able to ascertain if this study was analysed as paired data or not, and no information was available regarding the first cross-over period
Catheter days of study 1st PICC – 2337 days; 2nd PICC – 513 days; 3rd PICC – 271 days
Number of participants 87; 103 of 864 oncology patients received PICCs over 15 years
245 participants across 3 RCTs – majority of participants (203)
coming from Cesaro 2009
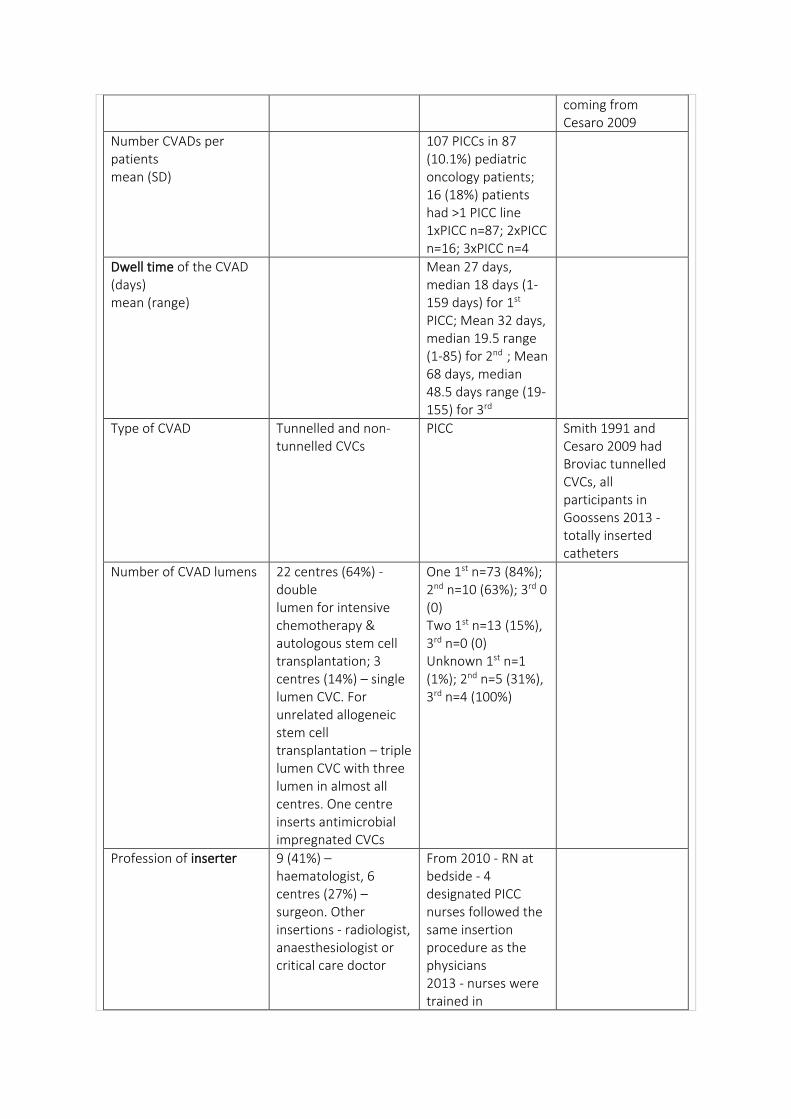
Number CVADs per patients mean (SD)
107 PICCs in 87 (10.1%) pediatric oncology patients; 16 (18%) patients had >1 PICC line 1xPICC n=87; 2xPICC n=16; 3xPICC n=4
Dwell time of the CVAD (days) mean (range)
Mean 27 days, median 18 days (1-159 days) for 1st PICC; Mean 32 days, median 19.5 range (1-85) for 2nd ; Mean 68 days, median 48.5 days range (19-155) for 3rd
Type of CVAD Tunnelled and non-tunnelled CVCs
PICC Smith 1991 and Cesaro 2009 had Broviac tunnelled CVCs, all participants in Goossens 2013 - totally inserted catheters
Number of CVAD lumens 22 centres (64%) - double lumen for intensive chemotherapy & autologous stem cell transplantation; 3 centres (14%) – single lumen CVC. For unrelated allogeneic stem cell transplantation – triple lumen CVC with three lumen in almost all centres. One centre inserts antimicrobial impregnated CVCs
One 1st n=73 (84%); 2nd n=10 (63%); 3rd 0 (0) Two 1st n=13 (15%), 3rd n=0 (0) Unknown 1st n=1 (1%); 2nd n=5 (31%), 3rd n=4 (100%)
Profession of inserter 9 (41%) – haematologist, 6 centres (27%) – surgeon. Other insertions - radiologist, anaesthesiologist or critical care doctor
From 2010 - RN at bedside - 4 designated PICC nurses followed the same insertion procedure as the physicians 2013 - nurses were trained in
ultrasound guided PICC insertions using a modified Seldinger technique. All patients CXR
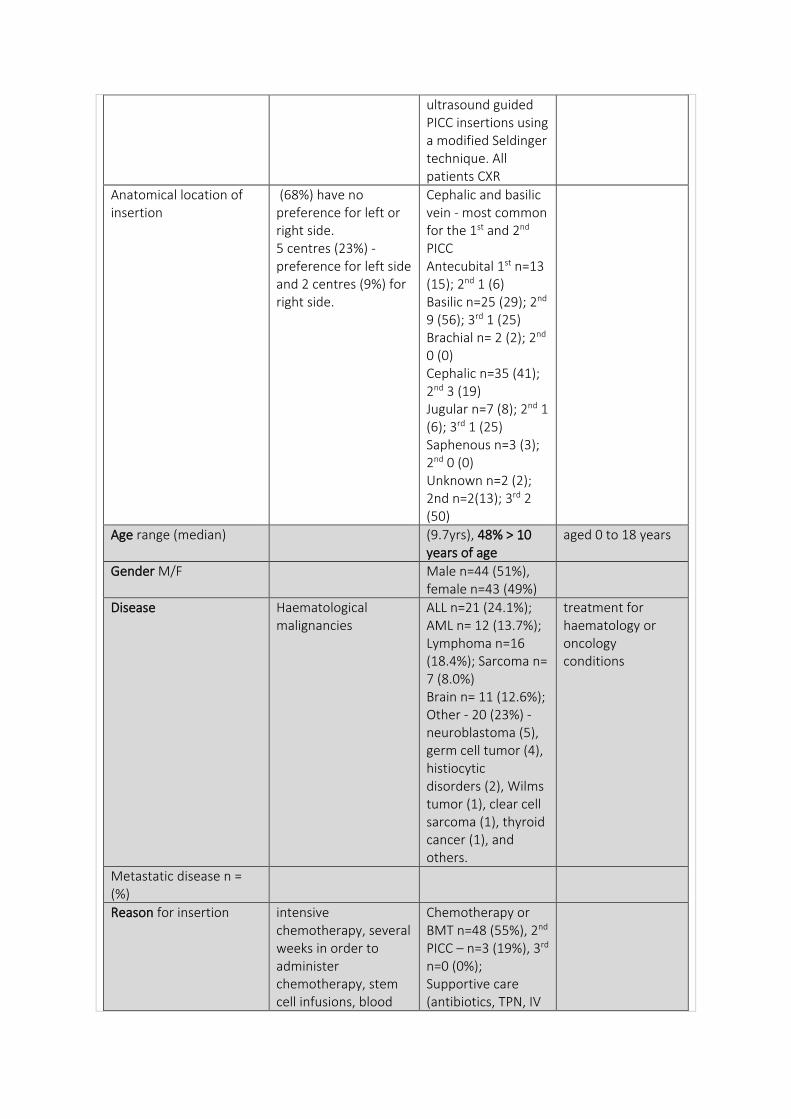
Anatomical location of insertion
(68%) have no preference for left or right side. 5 centres (23%) - preference for left side and 2 centres (9%) for right side.
Cephalic and basilic vein - most common for the 1st and 2nd PICC Antecubital 1st n=13 (15); 2nd 1 (6) Basilic n=25 (29); 2nd 9 (56); 3rd 1 (25) Brachial n= 2 (2); 2nd 0 (0) Cephalic n=35 (41); 2nd 3 (19) Jugular n=7 (8); 2nd 1 (6); 3rd 1 (25) Saphenous n=3 (3); 2nd 0 (0) Unknown n=2 (2); 2nd n=2(13); 3rd 2 (50)
Age range (median) (9.7yrs), 48% > 10 years of age
aged 0 to 18 years
Gender M/F Male n=44 (51%), female n=43 (49%)
Disease Haematological malignancies
ALL n=21 (24.1%); AML n= 12 (13.7%); Lymphoma n=16 (18.4%); Sarcoma n= 7 (8.0%) Brain n= 11 (12.6%); Other - 20 (23%) - neuroblastoma (5), germ cell tumor (4), histiocytic disorders (2), Wilms tumor (1), clear cell sarcoma (1), thyroid cancer (1), and others.
treatment for haematology or oncology conditions
Metastatic disease n = (%)
Reason for insertion intensive chemotherapy, several weeks in order to administer chemotherapy, stem cell infusions, blood
Chemotherapy or BMT n=48 (55%), 2nd PICC – n=3 (19%), 3rd n=0 (0%); Supportive care (antibiotics, TPN, IV
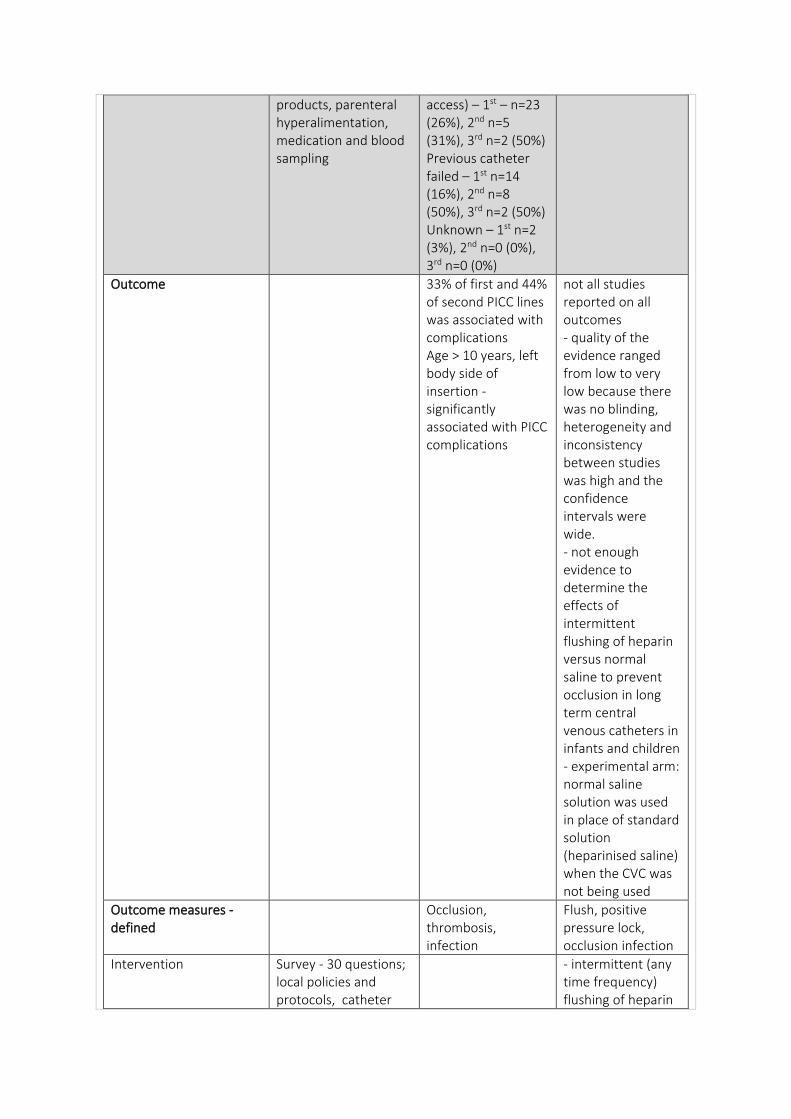
products, parenteral hyperalimentation, medication and blood sampling
access) – 1st – n=23 (26%), 2nd n=5 (31%), 3rd n=2 (50%) Previous catheter failed – 1st n=14 (16%), 2nd n=8 (50%), 3rd n=2 (50%) Unknown – 1st n=2 (3%), 2nd n=0 (0%), 3rd n=0 (0%)
Outcome 33% of first and 44% of second PICC lines was associated with complications Age > 10 years, left body side of insertion - significantly associated with PICC complications
not all studies reported on all outcomes - quality of the evidence ranged from low to very low because there was no blinding, heterogeneity and inconsistency between studies was high and the confidence intervals were wide. - not enough evidence to determine the effects of intermittent flushing of heparin versus normal saline to prevent occlusion in long term central venous catheters in infants and children - experimental arm: normal saline solution was used in place of standard solution (heparinised saline) when the CVC was not being used
Outcome measures - defined
Occlusion, thrombosis, infection
Flush, positive pressure lock, occlusion infection
Intervention Survey - 30 questions; local policies and protocols, catheter
- intermittent (any time frequency) flushing of heparin
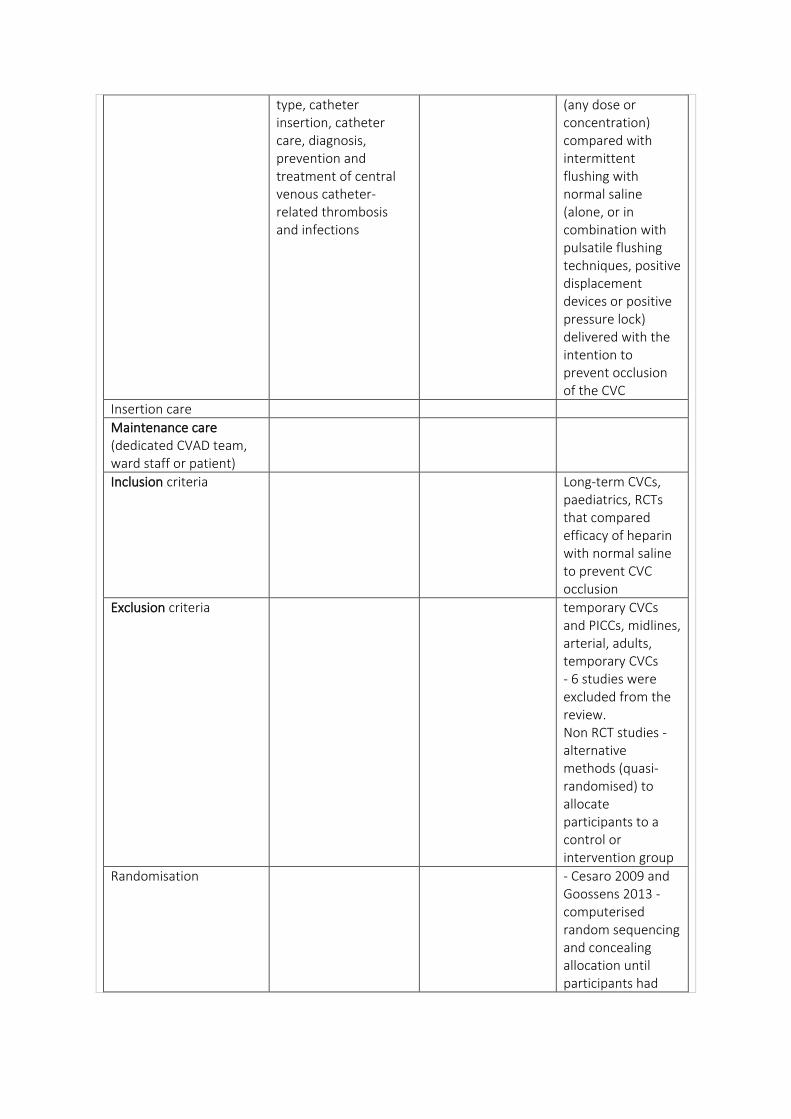
type, catheter insertion, catheter care, diagnosis, prevention and treatment of central venous catheter-related thrombosis and infections
(any dose or concentration) compared with intermittent flushing with normal saline (alone, or in combination with pulsatile flushing techniques, positive displacement devices or positive pressure lock) delivered with the intention to prevent occlusion of the CVC
Insertion care
Maintenance care (dedicated CVAD team, ward staff or patient)
Inclusion criteria Long-term CVCs, paediatrics, RCTs that compared efficacy of heparin with normal saline to prevent CVC occlusion
Exclusion criteria temporary CVCs and PICCs, midlines, arterial, adults, temporary CVCs - 6 studies were excluded from the review. Non RCT studies - alternative methods (quasi-randomised) to allocate participants to a control or intervention group
Randomisation - Cesaro 2009 and Goossens 2013 - computerised random sequencing and concealing allocation until participants had
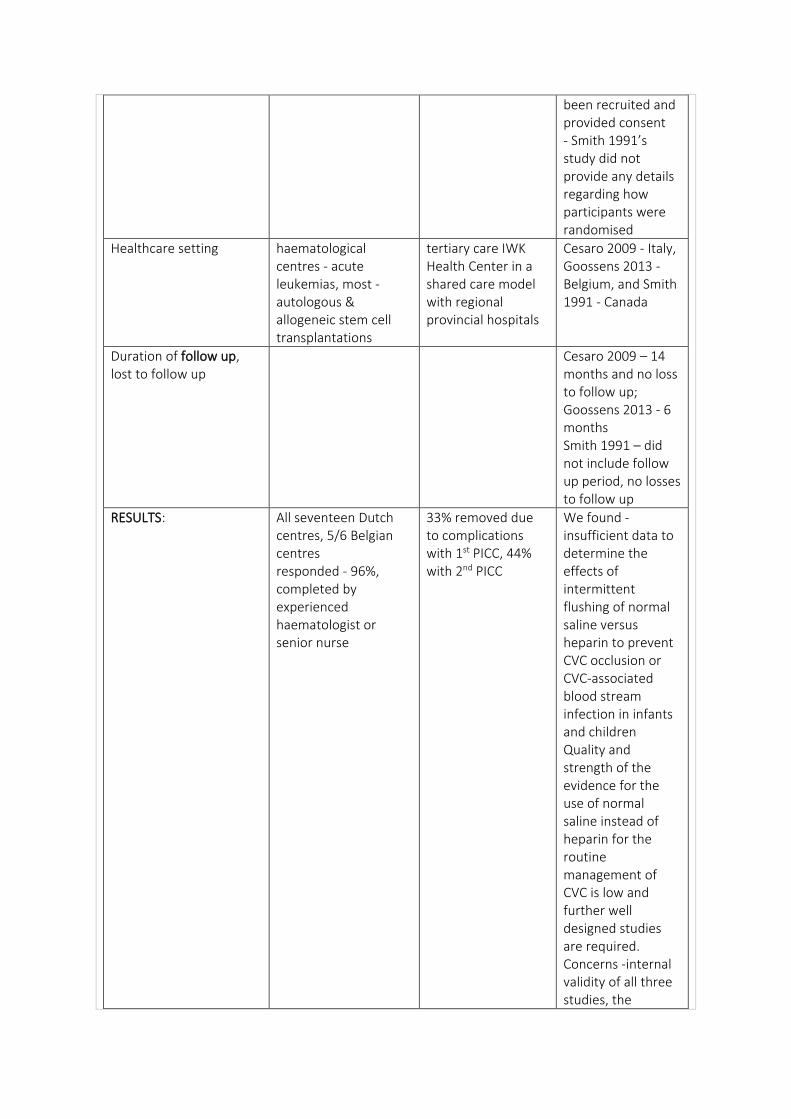
been recruited and provided consent - Smith 1991’s study did not provide any details regarding how participants were randomised
Healthcare setting haematological centres - acute leukemias, most -autologous & allogeneic stem cell transplantations
tertiary care IWK Health Center in a shared care model with regional provincial hospitals
Cesaro 2009 - Italy, Goossens 2013 - Belgium, and Smith 1991 - Canada
Duration of follow up, lost to follow up
Cesaro 2009 – 14 months and no loss to follow up; Goossens 2013 - 6 months Smith 1991 – did not include follow up period, no losses to follow up
RESULTS: All seventeen Dutch centres, 5/6 Belgian centres responded - 96%, completed by experienced haematologist or senior nurse
33% removed due to complications with 1st PICC, 44% with 2nd PICC
We found - insufficient data to determine the effects of intermittent flushing of normal saline versus heparin to prevent CVC occlusion or CVC-associated blood stream infection in infants and children Quality and strength of the evidence for the use of normal saline instead of heparin for the routine management of CVC is low and further well designed studies are required. Concerns -internal validity of all three studies, the
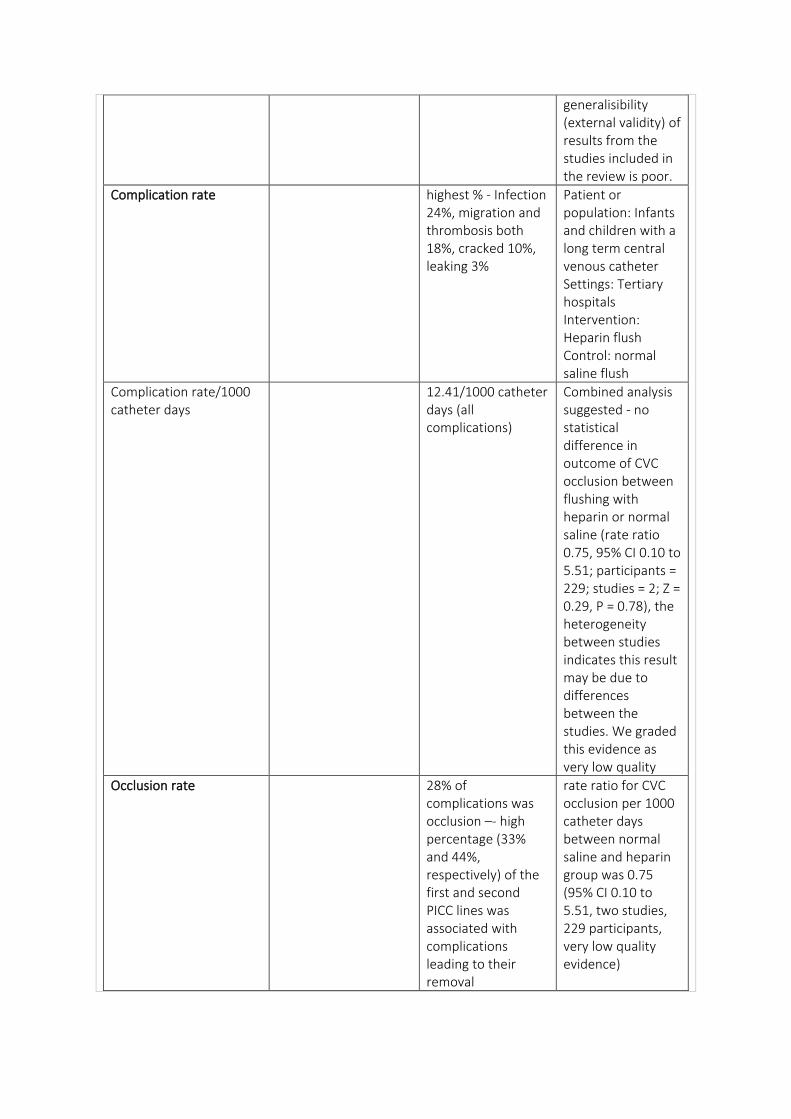
generalisibility (external validity) of results from the studies included in the review is poor.
Complication rate highest % - Infection 24%, migration and thrombosis both 18%, cracked 10%, leaking 3%
Patient or population: Infants and children with a long term central venous catheter Settings: Tertiary hospitals Intervention: Heparin flush Control: normal saline flush
Complication rate/1000 catheter days
12.41/1000 catheter days (all complications)
Combined analysis suggested - no statistical difference in outcome of CVC occlusion between flushing with heparin or normal saline (rate ratio 0.75, 95% CI 0.10 to 5.51; participants = 229; studies = 2; Z = 0.29, P = 0.78), the heterogeneity between studies indicates this result may be due to differences between the studies. We graded this evidence as very low quality
Occlusion rate 28% of complications was occlusion –- high percentage (33% and 44%, respectively) of the first and second PICC lines was associated with complications leading to their removal
rate ratio for CVC occlusion per 1000 catheter days between normal saline and heparin group was 0.75 (95% CI 0.10 to 5.51, two studies, 229 participants, very low quality evidence)
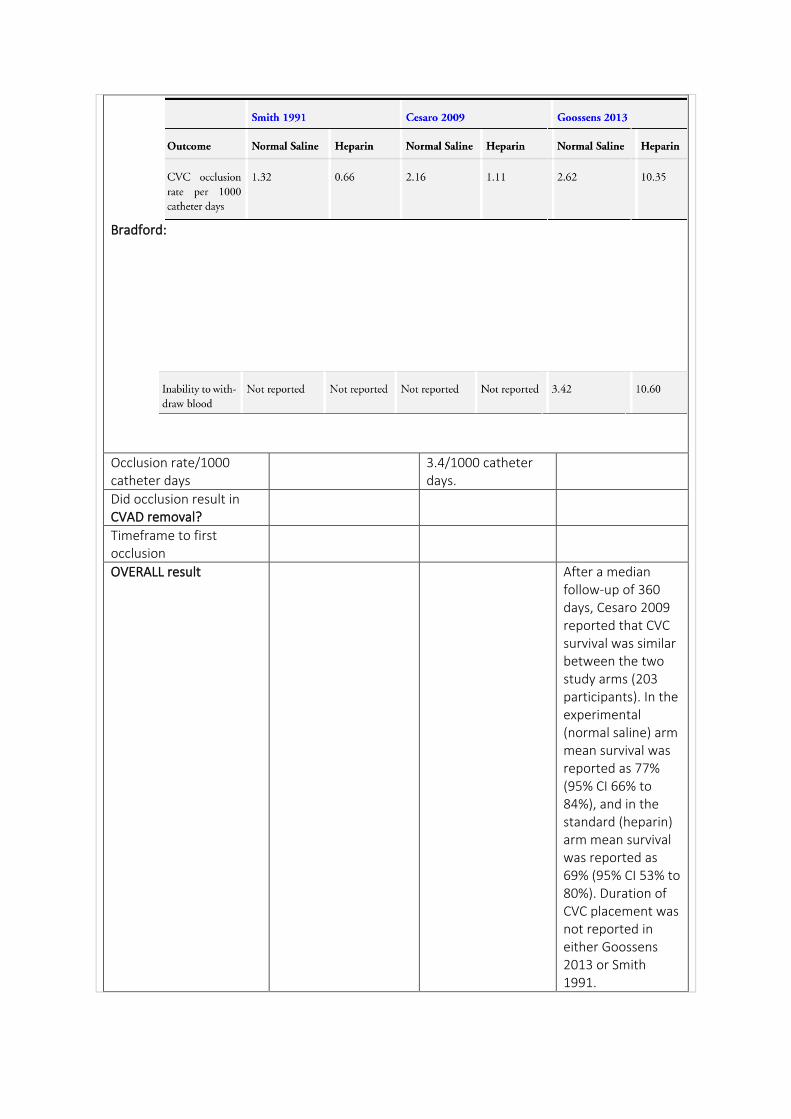
Bradford:
Occlusion rate/1000 catheter days
3.4/1000 catheter days.
Did occlusion result in CVAD removal?
Timeframe to first occlusion
OVERALL result After a median follow-up of 360 days, Cesaro 2009 reported that CVC survival was similar between the two study arms (203 participants). In the experimental (normal saline) arm mean survival was reported as 77% (95% CI 66% to 84%), and in the standard (heparin) arm mean survival was reported as 69% (95% CI 53% to 80%). Duration of CVC placement was not reported in either Goossens 2013 or Smith 1991.
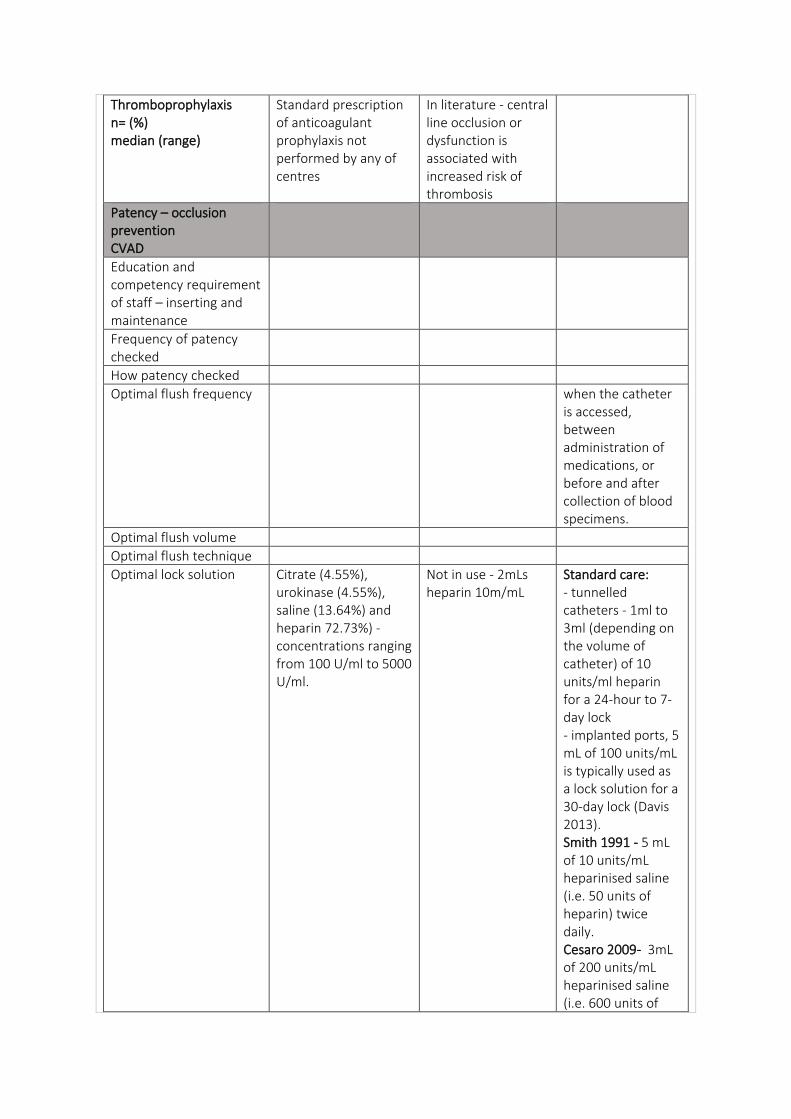
Thromboprophylaxis n= (%) median (range)
Standard prescription of anticoagulant prophylaxis not performed by any of centres
In literature - central line occlusion or dysfunction is associated with increased risk of thrombosis
Patency – occlusion prevention CVAD
Education and competency requirement of staff – inserting and maintenance
Frequency of patency checked
How patency checked
Optimal flush frequency when the catheter is accessed, between administration of medications, or before and after collection of blood specimens.
Optimal flush volume
Optimal flush technique
Optimal lock solution Citrate (4.55%), urokinase (4.55%), saline (13.64%) and heparin 72.73%) - concentrations ranging from 100 U/ml to 5000 U/ml.
Not in use - 2mLs heparin 10m/mL
Standard care: - tunnelled catheters - 1ml to 3ml (depending on the volume of catheter) of 10 units/ml heparin for a 24-hour to 7-day lock - implanted ports, 5 mL of 100 units/mL is typically used as a lock solution for a 30-day lock (Davis 2013). Smith 1991 - 5 mL of 10 units/mL heparinised saline (i.e. 50 units of heparin) twice daily. Cesaro 2009- 3mL of 200 units/mL heparinised saline (i.e. 600 units of
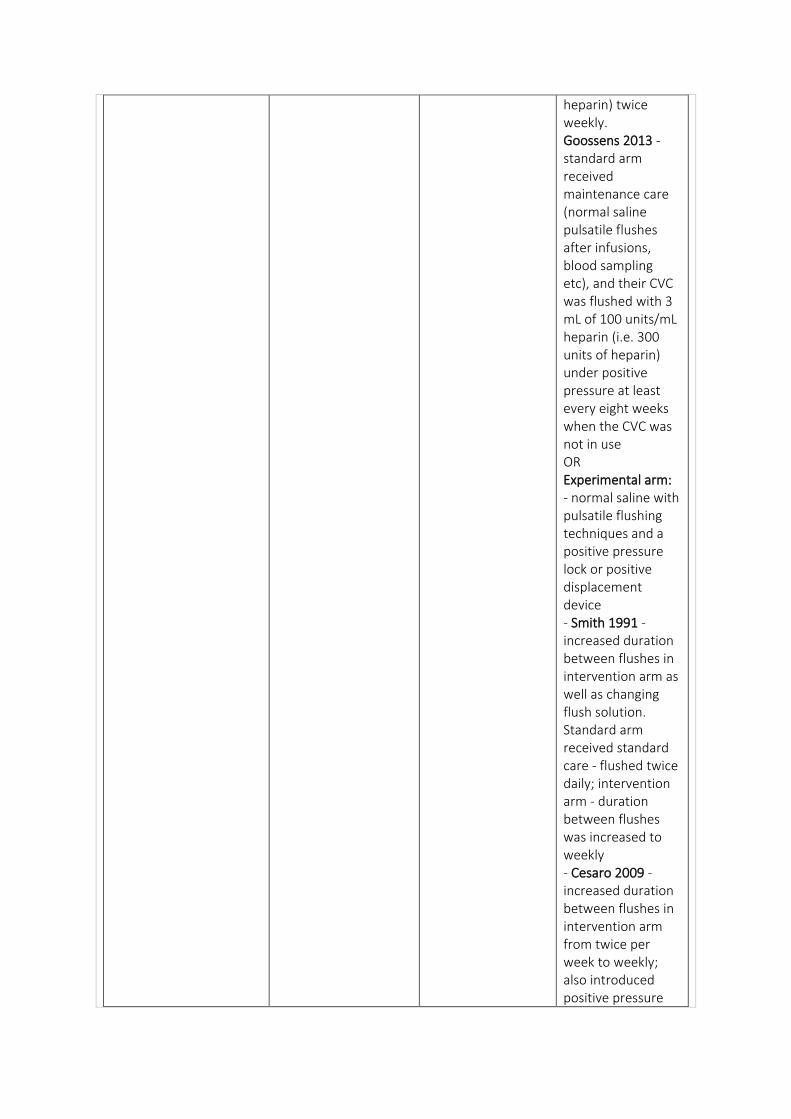
heparin) twice weekly. Goossens 2013 - standard arm received maintenance care (normal saline pulsatile flushes after infusions, blood sampling etc), and their CVC was flushed with 3 mL of 100 units/mL heparin (i.e. 300 units of heparin) under positive pressure at least every eight weeks when the CVC was not in use OR Experimental arm: - normal saline with pulsatile flushing techniques and a positive pressure lock or positive displacement device - Smith 1991 - increased duration between flushes in intervention arm as well as changing flush solution. Standard arm received standard care - flushed twice daily; intervention arm - duration between flushes was increased to weekly - Cesaro 2009 - increased duration between flushes in intervention arm from twice per week to weekly; also introduced positive pressure
cap into intervention arm. These changes confound the interventions, so it is not possible to associate outcomes with use of solution alone - Goossens 2013 - only study where the only difference between the intervention and standard arm was the use of normal saline (experimental) or heparin (standard) solution to flush the CVC under positive pressure.
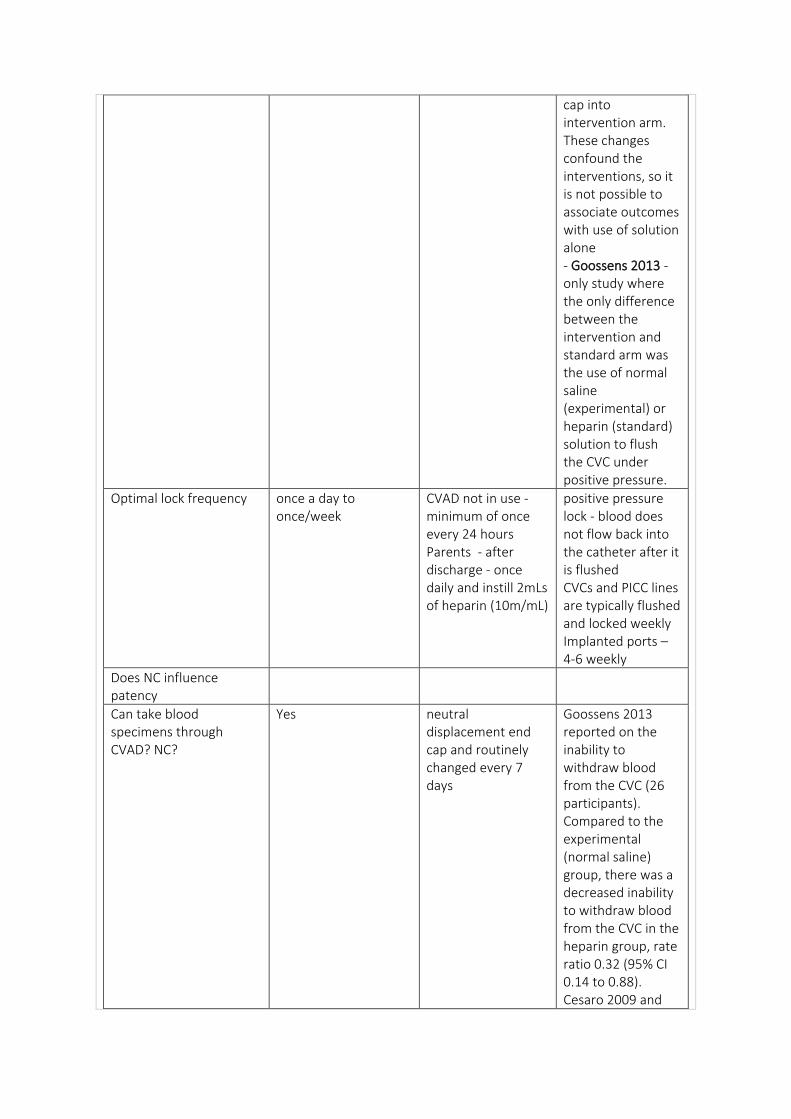
Optimal lock frequency once a day to once/week
CVAD not in use - minimum of once every 24 hours Parents - after discharge - once daily and instill 2mLs of heparin (10m/mL)
positive pressure lock - blood does not flow back into the catheter after it is flushed CVCs and PICC lines are typically flushed and locked weekly Implanted ports – 4-6 weekly
Does NC influence patency
Can take blood specimens through CVAD? NC?
Yes neutral displacement end cap and routinely changed every 7 days
Goossens 2013 reported on the inability to withdraw blood from the CVC (26 participants). Compared to the experimental (normal saline) group, there was a decreased inability to withdraw blood from the CVC in the heparin group, rate ratio 0.32 (95% CI 0.14 to 0.88). Cesaro 2009 and
Smith 1991 did not report on the (in)ability to withdraw blood from the CVC.
Patency – occlusion prevention PIV
How is patency checked?
What solution is used to flush and check patency
Occlusion management CVAD
Factors affecting occlusion rates: - type of cancer
- type of infusate
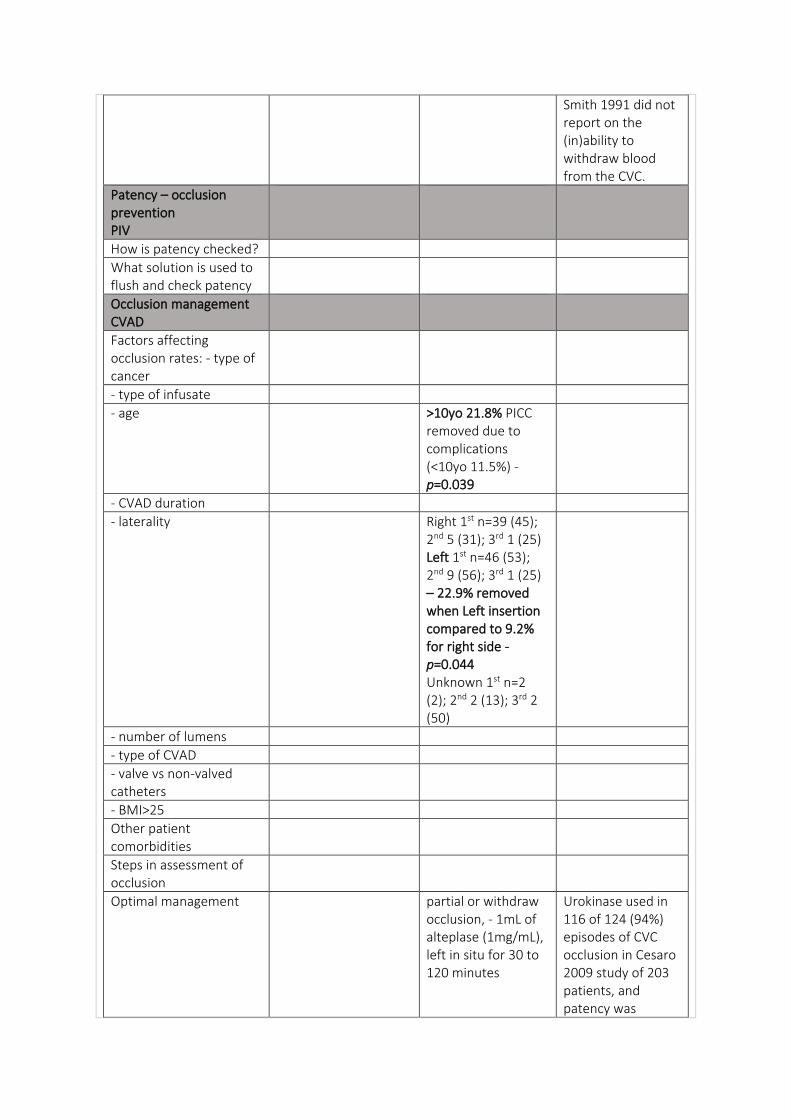
- age >10yo 21.8% PICC removed due to complications (<10yo 11.5%) - p=0.039
- CVAD duration
- laterality Right 1st n=39 (45); 2nd 5 (31); 3rd 1 (25) Left 1st n=46 (53); 2nd 9 (56); 3rd 1 (25) – 22.9% removed when Left insertion compared to 9.2% for right side - p=0.044 Unknown 1st n=2 (2); 2nd 2 (13); 3rd 2 (50)
- number of lumens
- type of CVAD
- valve vs non-valved catheters
- BMI>25
Other patient comorbidities
Steps in assessment of occlusion
Optimal management partial or withdraw occlusion, - 1mL of alteplase (1mg/mL), left in situ for 30 to 120 minutes
Urokinase used in 116 of 124 (94%) episodes of CVC occlusion in Cesaro 2009 study of 203 patients, and patency was
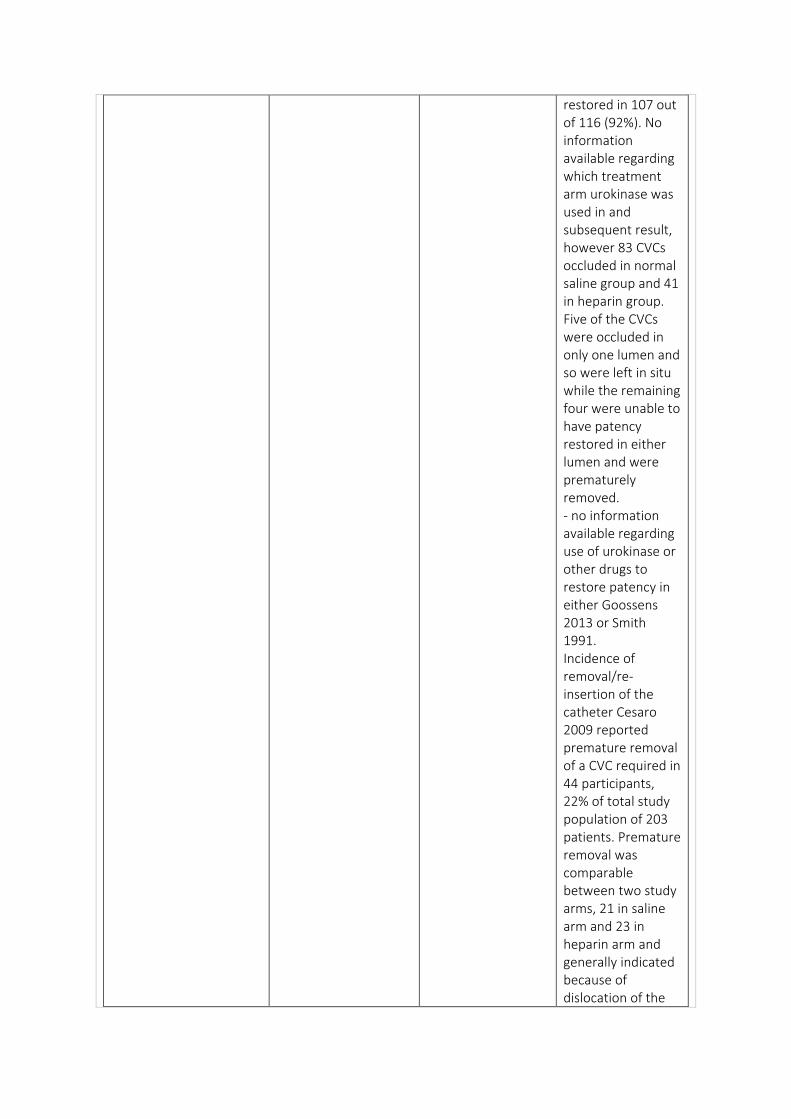
restored in 107 out of 116 (92%). No information available regarding which treatment arm urokinase was used in and subsequent result, however 83 CVCs occluded in normal saline group and 41 in heparin group. Five of the CVCs were occluded in only one lumen and so were left in situ while the remaining four were unable to have patency restored in either lumen and were prematurely removed. - no information available regarding use of urokinase or other drugs to restore patency in either Goossens 2013 or Smith 1991. Incidence of removal/re-insertion of the catheter Cesaro 2009 reported premature removal of a CVC required in 44 participants, 22% of total study population of 203 patients. Premature removal was comparable between two study arms, 21 in saline arm and 23 in heparin arm and generally indicated because of dislocation of the
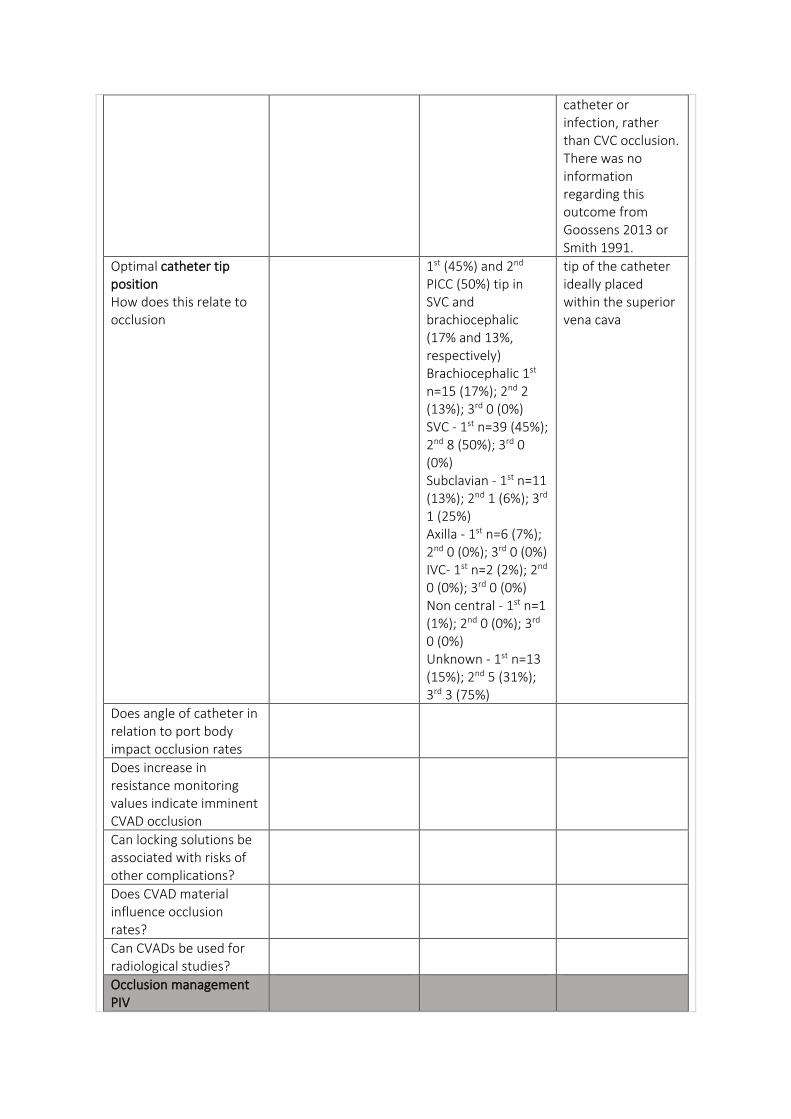
catheter or infection, rather than CVC occlusion. There was no information regarding this outcome from Goossens 2013 or Smith 1991.
Optimal catheter tip position How does this relate to occlusion
1st (45%) and 2nd PICC (50%) tip in SVC and brachiocephalic (17% and 13%, respectively) Brachiocephalic 1st n=15 (17%); 2nd 2 (13%); 3rd 0 (0%) SVC - 1st n=39 (45%); 2nd 8 (50%); 3rd 0 (0%) Subclavian - 1st n=11 (13%); 2nd 1 (6%); 3rd 1 (25%) Axilla - 1st n=6 (7%); 2nd 0 (0%); 3rd 0 (0%) IVC- 1st n=2 (2%); 2nd 0 (0%); 3rd 0 (0%) Non central - 1st n=1 (1%); 2nd 0 (0%); 3rd 0 (0%) Unknown - 1st n=13 (15%); 2nd 5 (31%); 3rd 3 (75%)
tip of the catheter ideally placed within the superior vena cava
Does angle of catheter in relation to port body impact occlusion rates
Does increase in resistance monitoring values indicate imminent CVAD occlusion
Can locking solutions be associated with risks of other complications?
Does CVAD material influence occlusion rates?
Can CVADs be used for radiological studies?
Occlusion management PIV
occluded PIV be replaced or unblocked
optimal location for PIV insertion
DATA:
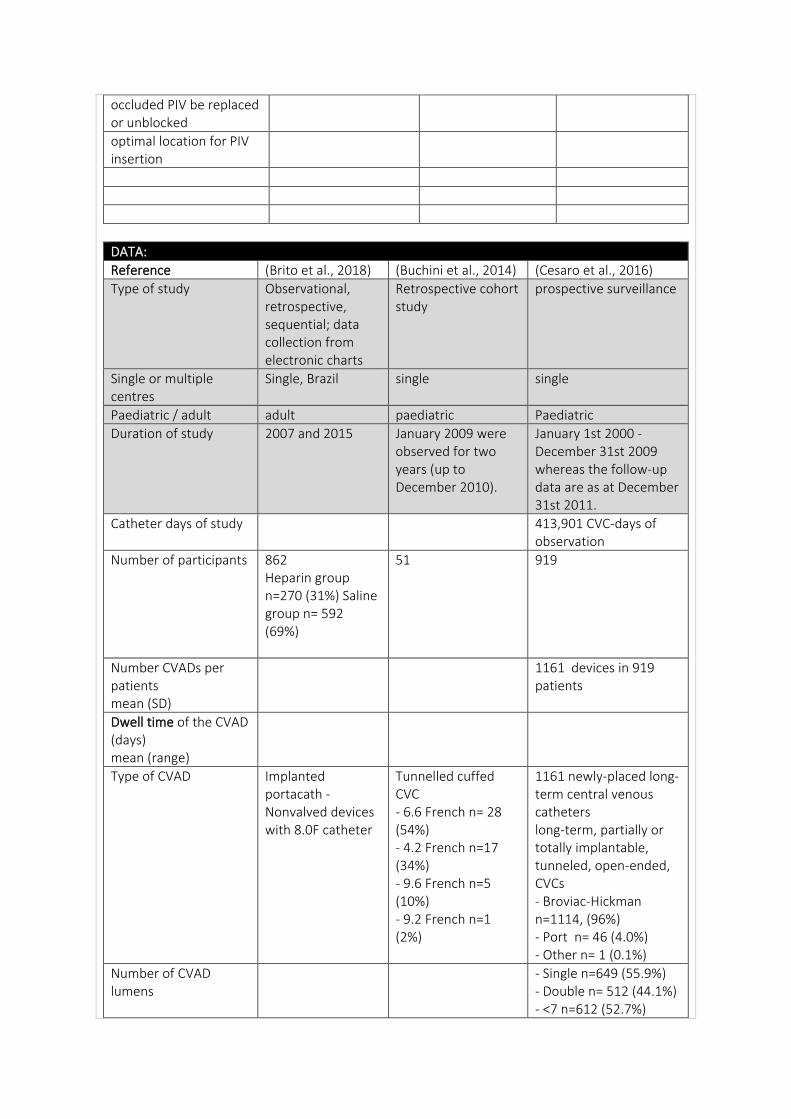
Reference (Brito et al., 2018) (Buchini et al., 2014) (Cesaro et al., 2016)
Type of study Observational, retrospective, sequential; data collection from electronic charts
Retrospective cohort study
prospective surveillance
Single or multiple centres
Single, Brazil single single
Paediatric / adult adult paediatric Paediatric
Duration of study 2007 and 2015 January 2009 were observed for two years (up to December 2010).
January 1st 2000 - December 31st 2009 whereas the follow-up data are as at December 31st 2011.
Catheter days of study 413,901 CVC-days of observation
Number of participants 862 Heparin group n=270 (31%) Saline group n= 592 (69%)
51 919
Number CVADs per patients mean (SD)
1161 devices in 919 patients
Dwell time of the CVAD (days) mean (range)
Type of CVAD Implanted portacath - Nonvalved devices with 8.0F catheter
Tunnelled cuffed CVC - 6.6 French n= 28 (54%) - 4.2 French n=17 (34%) - 9.6 French n=5 (10%) - 9.2 French n=1 (2%)
1161 newly-placed long-term central venous catheters long-term, partially or totally implantable, tunneled, open-ended, CVCs - Broviac-Hickman n=1114, (96%) - Port n= 46 (4.0%) - Other n= 1 (0.1%)
Number of CVAD lumens
- Single n=649 (55.9%) - Double n= 512 (44.1%) - <7 n=612 (52.7%)
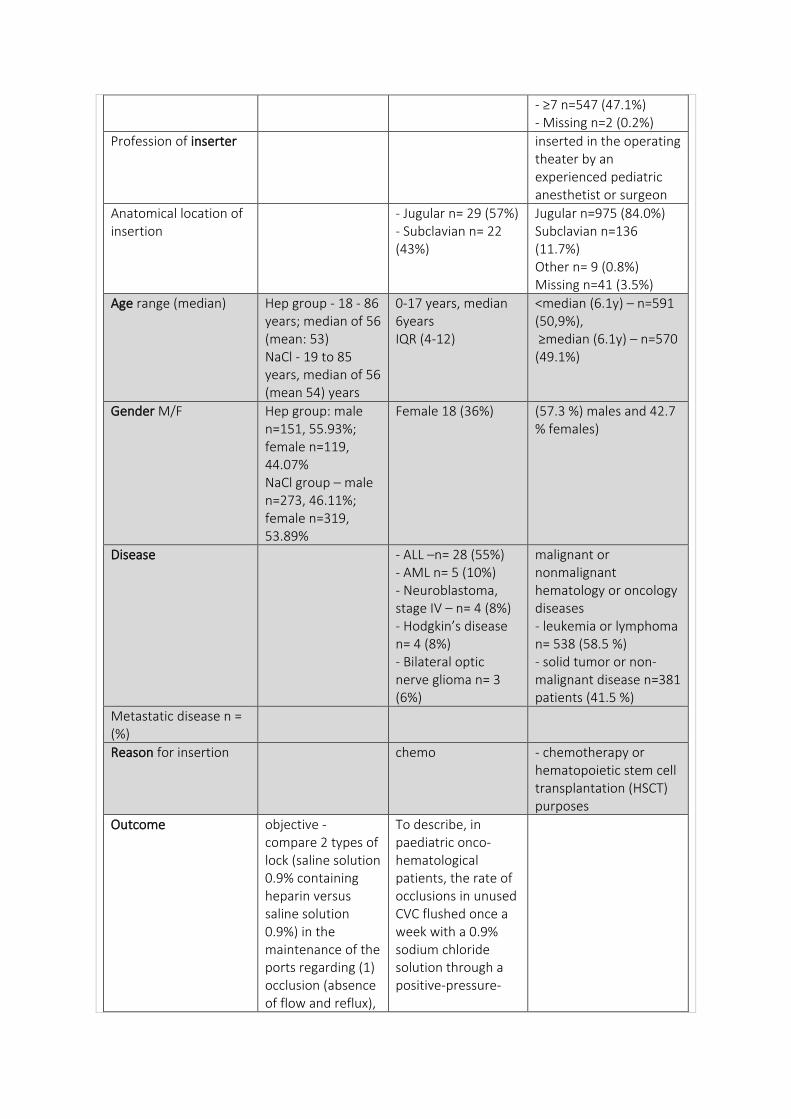
- ≥7 n=547 (47.1%) - Missing n=2 (0.2%)
Profession of inserter inserted in the operating theater by an experienced pediatric anesthetist or surgeon
Anatomical location of insertion
- Jugular n= 29 (57%) - Subclavian n= 22 (43%)
Jugular n=975 (84.0%) Subclavian n=136 (11.7%) Other n= 9 (0.8%) Missing n=41 (3.5%)
Age range (median) Hep group - 18 - 86 years; median of 56 (mean: 53) NaCl - 19 to 85 years, median of 56 (mean 54) years
0-17 years, median 6years IQR (4-12)
<median (6.1y) – n=591 (50,9%), ≥median (6.1y) – n=570 (49.1%)
Gender M/F Hep group: male n=151, 55.93%; female n=119, 44.07% NaCl group – male n=273, 46.11%; female n=319, 53.89%
Female 18 (36%) (57.3 %) males and 42.7 % females)
Disease - ALL –n= 28 (55%) - AML n= 5 (10%) - Neuroblastoma, stage IV – n= 4 (8%) - Hodgkin’s disease n= 4 (8%) - Bilateral optic nerve glioma n= 3 (6%)
malignant or nonmalignant hematology or oncology diseases - leukemia or lymphoma n= 538 (58.5 %) - solid tumor or non-malignant disease n=381 patients (41.5 %)
Metastatic disease n = (%)
Reason for insertion chemo - chemotherapy or hematopoietic stem cell transplantation (HSCT) purposes
Outcome objective - compare 2 types of lock (saline solution 0.9% containing heparin versus saline solution 0.9%) in the maintenance of the ports regarding (1) occlusion (absence of flow and reflux),
To describe, in paediatric onco-hematological patients, the rate of occlusions in unused CVC flushed once a week with a 0.9% sodium chloride solution through a positive-pressure-
(2) reflux dysfunction (normal flow without reflux), and (3) flow dysfunction (abnormal flow and abnormal reflux).
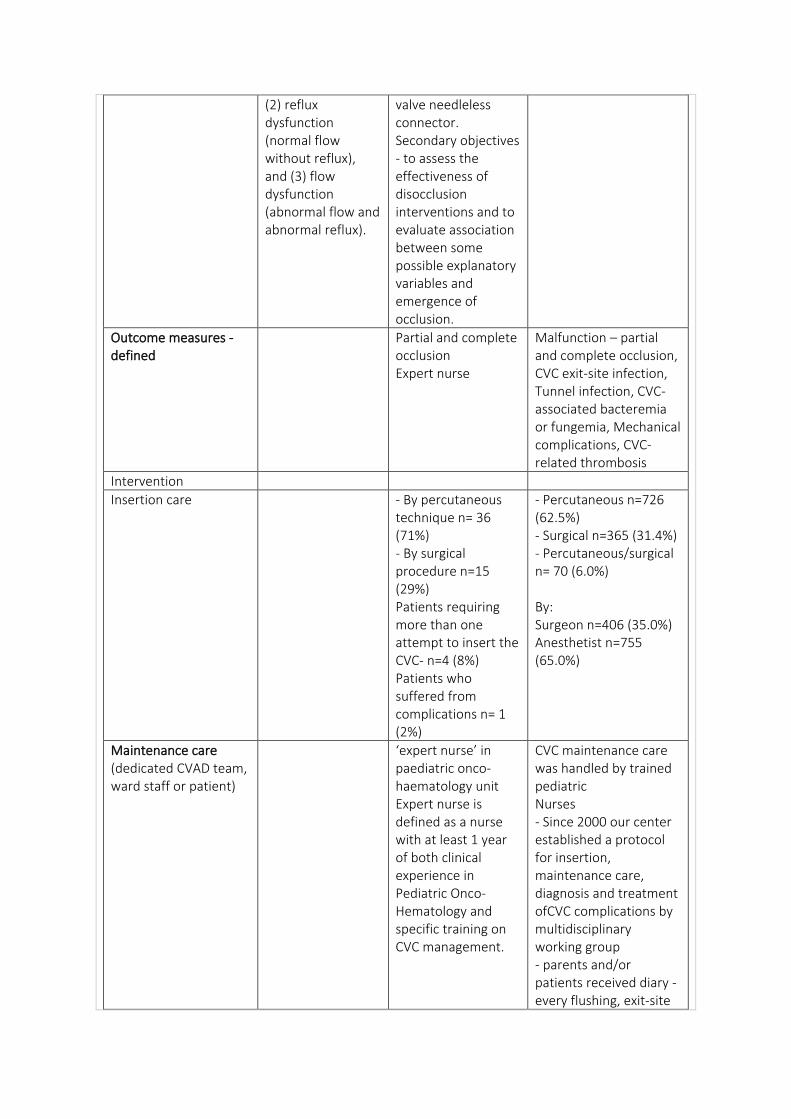
valve needleless connector. Secondary objectives - to assess the effectiveness of disocclusion interventions and to evaluate association between some possible explanatory variables and emergence of occlusion.
Outcome measures - defined
Partial and complete occlusion Expert nurse
Malfunction – partial and complete occlusion, CVC exit-site infection, Tunnel infection, CVC-associated bacteremia or fungemia, Mechanical complications, CVC-related thrombosis
Intervention
Insertion care - By percutaneous technique n= 36 (71%) - By surgical procedure n=15 (29%) Patients requiring more than one attempt to insert the CVC- n=4 (8%) Patients who suffered from complications n= 1 (2%)
- Percutaneous n=726 (62.5%) - Surgical n=365 (31.4%) - Percutaneous/surgical n= 70 (6.0%) By: Surgeon n=406 (35.0%) Anesthetist n=755 (65.0%)
Maintenance care (dedicated CVAD team, ward staff or patient)
‘expert nurse’ in paediatric onco-haematology unit Expert nurse is defined as a nurse with at least 1 year of both clinical experience in Pediatric Onco-Hematology and specific training on CVC management.
CVC maintenance care was handled by trained pediatric Nurses - Since 2000 our center established a protocol for insertion, maintenance care, diagnosis and treatment ofCVC complications by multidisciplinary working group - parents and/or patients received diary - every flushing, exit-site
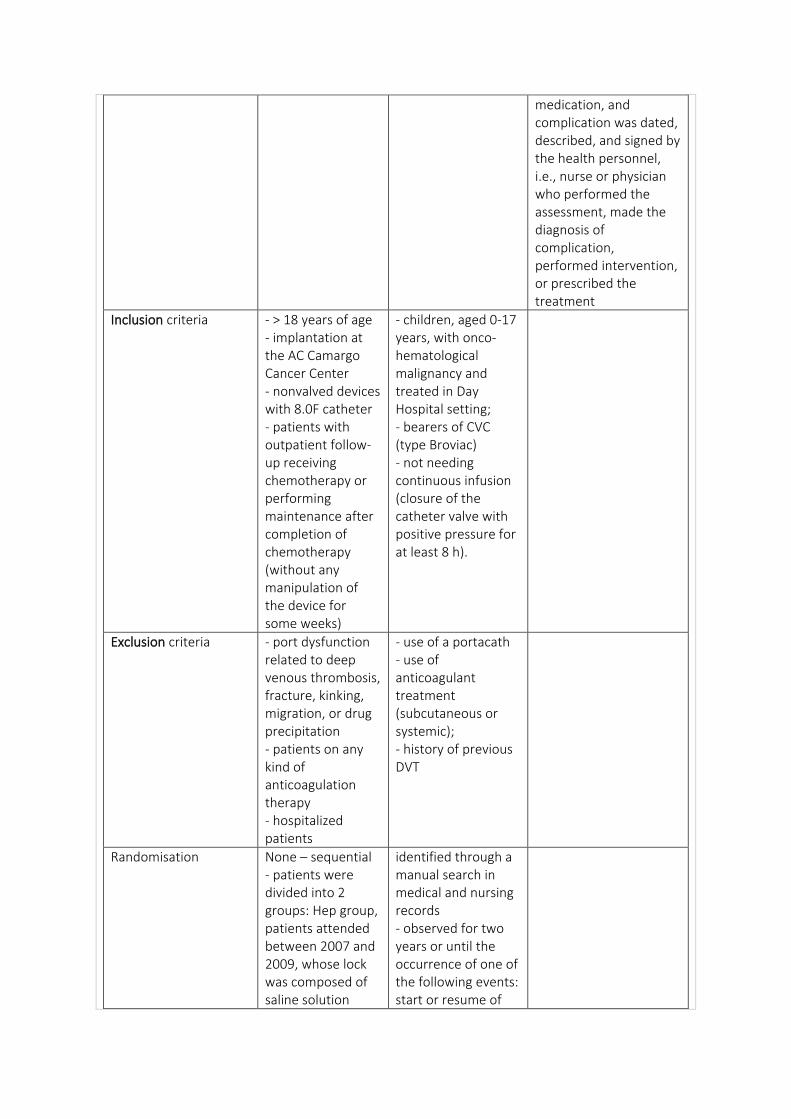
medication, and complication was dated, described, and signed by the health personnel, i.e., nurse or physician who performed the assessment, made the diagnosis of complication, performed intervention, or prescribed the treatment
Inclusion criteria - > 18 years of age - implantation at the AC Camargo Cancer Center - nonvalved devices with 8.0F catheter - patients with outpatient follow-up receiving chemotherapy or performing maintenance after completion of chemotherapy (without any manipulation of the device for some weeks)
- children, aged 0-17 years, with onco-hematological malignancy and treated in Day Hospital setting; - bearers of CVC (type Broviac) - not needing continuous infusion (closure of the catheter valve with positive pressure for at least 8 h).
Exclusion criteria - port dysfunction related to deep venous thrombosis, fracture, kinking, migration, or drug precipitation - patients on any kind of anticoagulation therapy - hospitalized patients
- use of a portacath - use of anticoagulant treatment (subcutaneous or systemic); - history of previous DVT
Randomisation None – sequential - patients were divided into 2 groups: Hep group, patients attended between 2007 and 2009, whose lock was composed of saline solution
identified through a manual search in medical and nursing records - observed for two years or until the occurrence of one of the following events: start or resume of
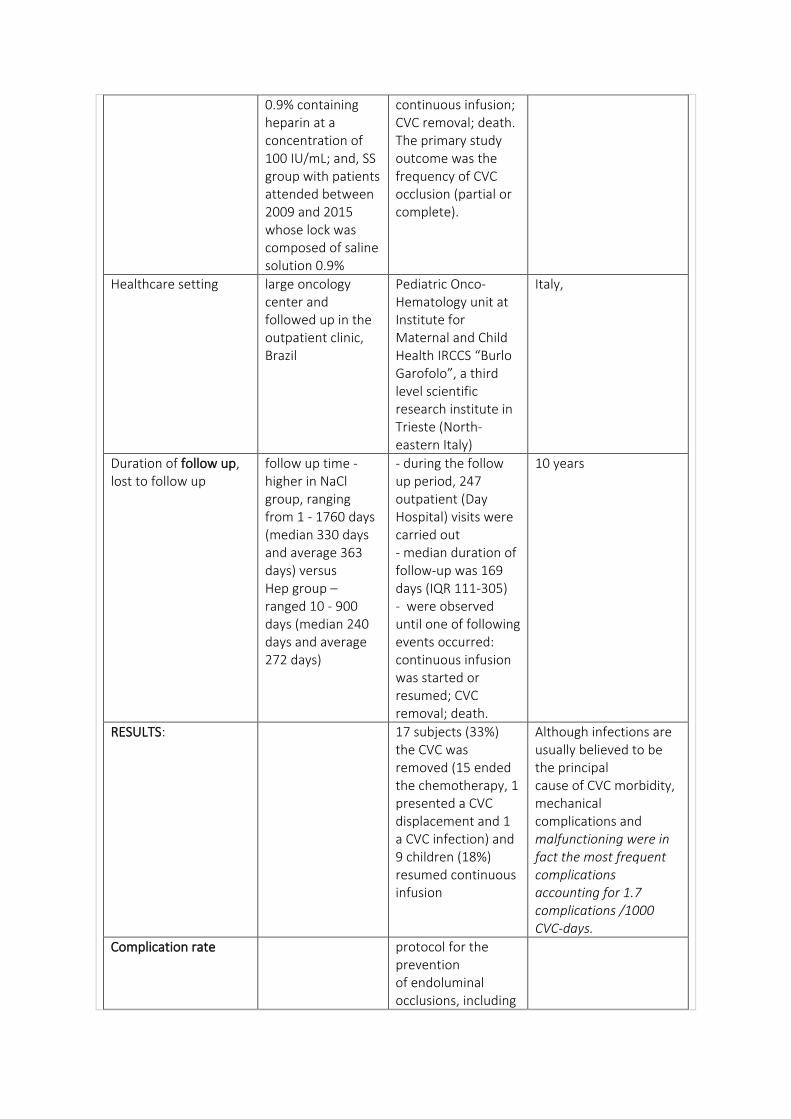
0.9% containing heparin at a concentration of 100 IU/mL; and, SS group with patients attended between 2009 and 2015 whose lock was composed of saline solution 0.9%
continuous infusion; CVC removal; death. The primary study outcome was the frequency of CVC occlusion (partial or complete).
Healthcare setting large oncology center and followed up in the outpatient clinic, Brazil
Pediatric Onco-Hematology unit at Institute for Maternal and Child Health IRCCS “Burlo Garofolo”, a third level scientific research institute in Trieste (North-eastern Italy)
Italy,
Duration of follow up, lost to follow up
follow up time - higher in NaCl group, ranging from 1 - 1760 days (median 330 days and average 363 days) versus Hep group – ranged 10 - 900 days (median 240 days and average 272 days)
- during the follow up period, 247 outpatient (Day Hospital) visits were carried out - median duration of follow-up was 169 days (IQR 111-305) - were observed until one of following events occurred: continuous infusion was started or resumed; CVC removal; death.
10 years
RESULTS: 17 subjects (33%) the CVC was removed (15 ended the chemotherapy, 1 presented a CVC displacement and 1 a CVC infection) and 9 children (18%) resumed continuous infusion
Although infections are usually believed to be the principal cause of CVC morbidity, mechanical complications and malfunctioning were in fact the most frequent complications accounting for 1.7 complications /1000 CVC-days.
Complication rate protocol for the prevention of endoluminal occlusions, including
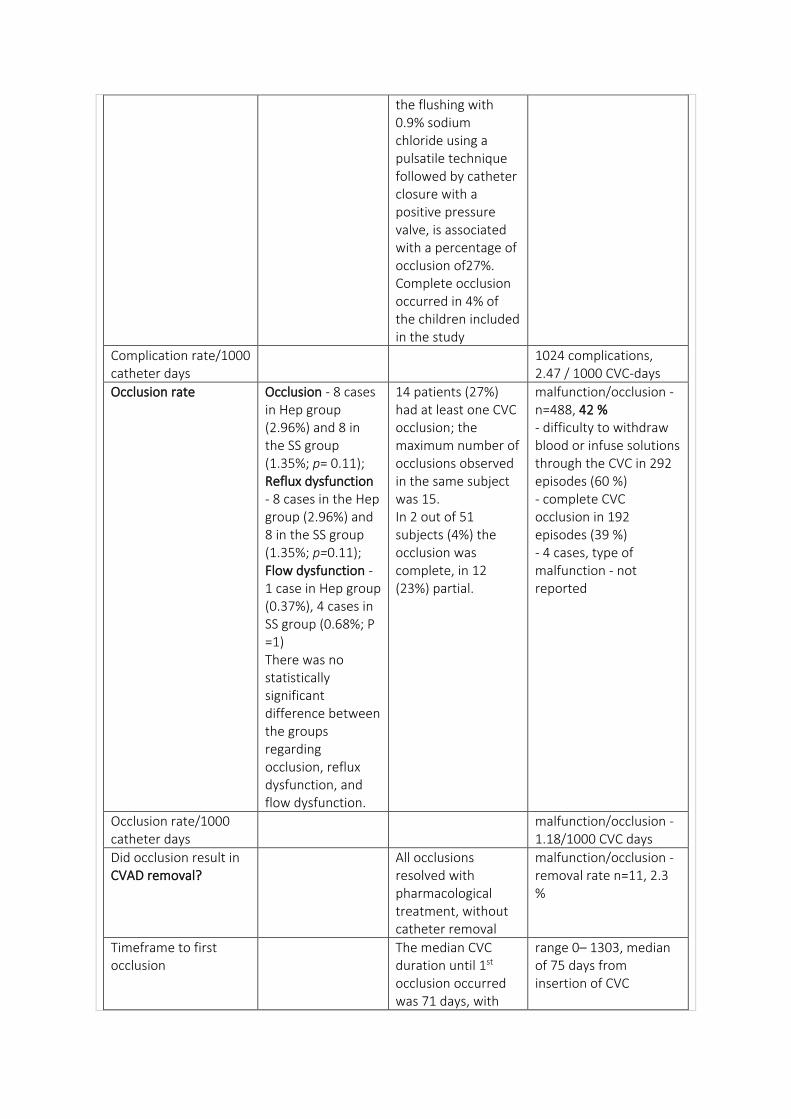
the flushing with 0.9% sodium chloride using a pulsatile technique followed by catheter closure with a positive pressure valve, is associated with a percentage of occlusion of27%. Complete occlusion occurred in 4% of the children included in the study
Complication rate/1000 catheter days
1024 complications, 2.47 / 1000 CVC-days
Occlusion rate Occlusion - 8 cases in Hep group (2.96%) and 8 in the SS group (1.35%; p= 0.11); Reflux dysfunction - 8 cases in the Hep group (2.96%) and 8 in the SS group (1.35%; p=0.11); Flow dysfunction - 1 case in Hep group (0.37%), 4 cases in SS group (0.68%; P =1) There was no statistically significant difference between the groups regarding occlusion, reflux dysfunction, and flow dysfunction.
14 patients (27%) had at least one CVC occlusion; the maximum number of occlusions observed in the same subject was 15. In 2 out of 51 subjects (4%) the occlusion was complete, in 12 (23%) partial.
malfunction/occlusion - n=488, 42 % - difficulty to withdraw blood or infuse solutions through the CVC in 292 episodes (60 %) - complete CVC occlusion in 192 episodes (39 %) - 4 cases, type of malfunction - not reported
Occlusion rate/1000 catheter days
malfunction/occlusion - 1.18/1000 CVC days
Did occlusion result in CVAD removal?
All occlusions resolved with pharmacological treatment, without catheter removal
malfunction/occlusion - removal rate n=11, 2.3 %
Timeframe to first occlusion
The median CVC duration until 1st occlusion occurred was 71 days, with
range 0– 1303, median of 75 days from insertion of CVC
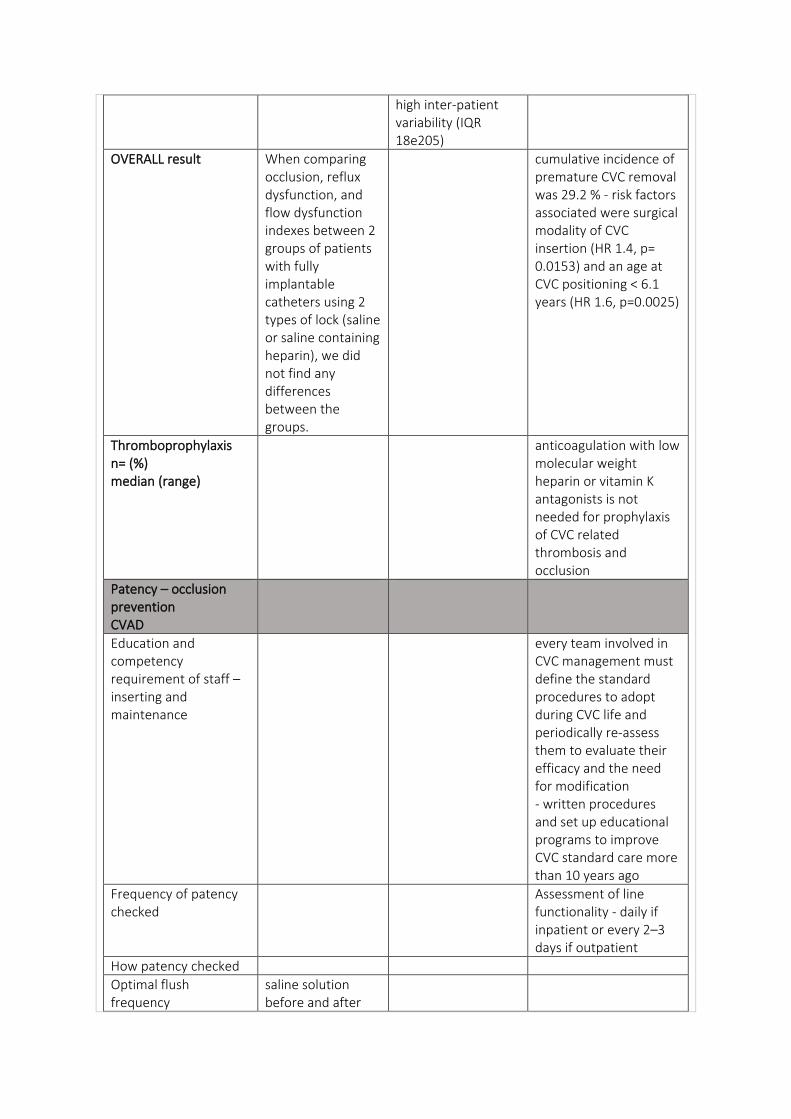
high inter-patient variability (IQR 18e205)
OVERALL result When comparing occlusion, reflux dysfunction, and flow dysfunction indexes between 2 groups of patients with fully implantable catheters using 2 types of lock (saline or saline containing heparin), we did not find any differences between the groups.
cumulative incidence of premature CVC removal was 29.2 % - risk factors associated were surgical modality of CVC insertion (HR 1.4, p= 0.0153) and an age at CVC positioning < 6.1 years (HR 1.6, p=0.0025)
Thromboprophylaxis n= (%) median (range)
anticoagulation with low molecular weight heparin or vitamin K antagonists is not needed for prophylaxis of CVC related thrombosis and occlusion
Patency – occlusion prevention CVAD
Education and competency requirement of staff – inserting and maintenance
every team involved in CVC management must define the standard procedures to adopt during CVC life and periodically re-assess them to evaluate their efficacy and the need for modification - written procedures and set up educational programs to improve CVC standard care more than 10 years ago
Frequency of patency checked
Assessment of line functionality - daily if inpatient or every 2–3 days if outpatient
How patency checked
Optimal flush frequency
saline solution before and after
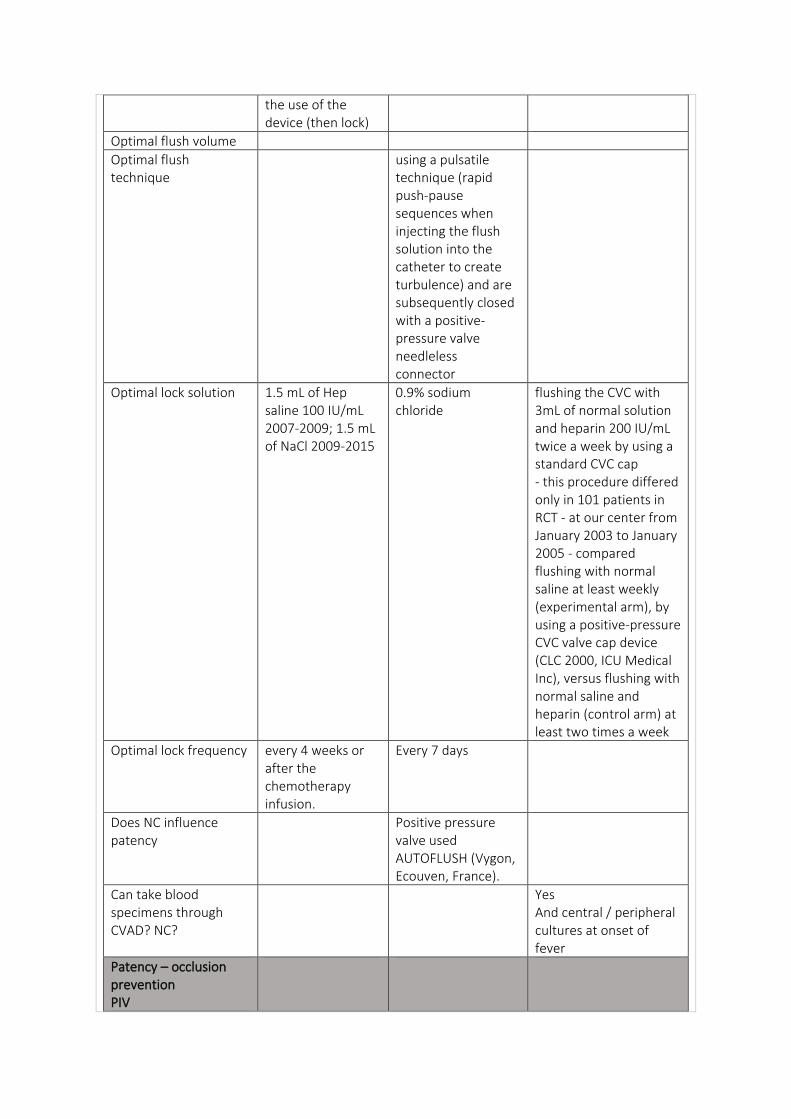
the use of the device (then lock)
Optimal flush volume
Optimal flush technique
using a pulsatile technique (rapid push-pause sequences when injecting the flush solution into the catheter to create turbulence) and are subsequently closed with a positive-pressure valve needleless connector
Optimal lock solution 1.5 mL of Hep saline 100 IU/mL 2007-2009; 1.5 mL of NaCl 2009-2015
0.9% sodium chloride
flushing the CVC with 3mL of normal solution and heparin 200 IU/mL twice a week by using a standard CVC cap - this procedure differed only in 101 patients in RCT - at our center from January 2003 to January 2005 - compared flushing with normal saline at least weekly (experimental arm), by using a positive-pressure CVC valve cap device (CLC 2000, ICU Medical Inc), versus flushing with normal saline and heparin (control arm) at least two times a week
Optimal lock frequency every 4 weeks or after the chemotherapy infusion.
Every 7 days
Does NC influence patency
Positive pressure valve used AUTOFLUSH (Vygon, Ecouven, France).
Can take blood specimens through CVAD? NC?
Yes And central / peripheral cultures at onset of fever
Patency – occlusion prevention PIV
How is patency checked?
What solution is used to flush and check patency
Occlusion management CVAD
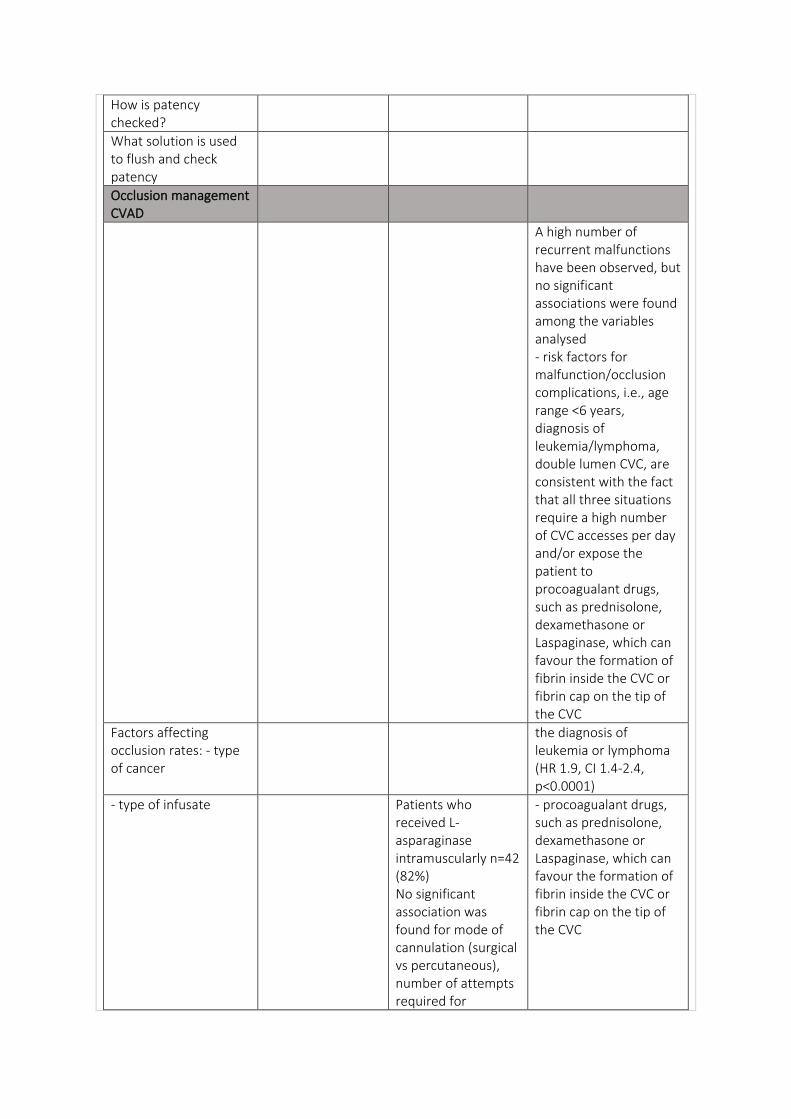
A high number of recurrent malfunctions have been observed, but no significant associations were found among the variables analysed - risk factors for malfunction/occlusion complications, i.e., age range <6 years, diagnosis of leukemia/lymphoma, double lumen CVC, are consistent with the fact that all three situations require a high number of CVC accesses per day and/or expose the patient to procoagualant drugs, such as prednisolone, dexamethasone or Laspaginase, which can favour the formation of fibrin inside the CVC or fibrin cap on the tip of the CVC
Factors affecting occlusion rates: - type of cancer
the diagnosis of leukemia or lymphoma (HR 1.9, CI 1.4-2.4, p<0.0001)
- type of infusate Patients who received L-asparaginase intramuscularly n=42 (82%) No significant association was found for mode of cannulation (surgical vs percutaneous), number of attempts required for
- procoagualant drugs, such as prednisolone, dexamethasone or Laspaginase, which can favour the formation of fibrin inside the CVC or fibrin cap on the tip of the CVC
insertion (more than one vs one), vein cannulated (jugular vs subclavian vein), laterality of cannulation (right vs left side) and administration of Lasparaginase.
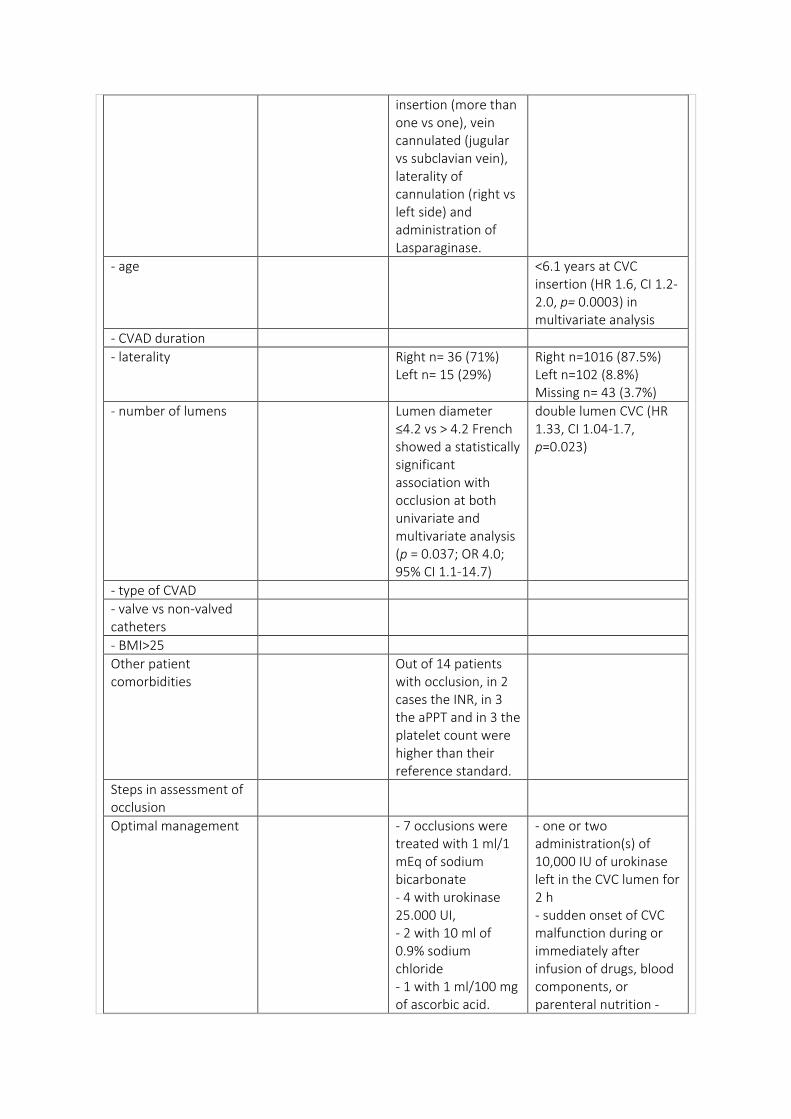
- age <6.1 years at CVC insertion (HR 1.6, CI 1.2-2.0, p= 0.0003) in multivariate analysis
- CVAD duration
- laterality Right n= 36 (71%) Left n= 15 (29%)
Right n=1016 (87.5%) Left n=102 (8.8%) Missing n= 43 (3.7%)
- number of lumens Lumen diameter ≤4.2 vs > 4.2 French showed a statistically significant association with occlusion at both univariate and multivariate analysis (p = 0.037; OR 4.0; 95% CI 1.1-14.7)
double lumen CVC (HR 1.33, CI 1.04-1.7, p=0.023)
- type of CVAD
- valve vs non-valved catheters
- BMI>25
Other patient comorbidities
Out of 14 patients with occlusion, in 2 cases the INR, in 3 the aPPT and in 3 the platelet count were higher than their reference standard.
Steps in assessment of occlusion
Optimal management - 7 occlusions were treated with 1 ml/1 mEq of sodium bicarbonate - 4 with urokinase 25.000 UI, - 2 with 10 ml of 0.9% sodium chloride - 1 with 1 ml/100 mg of ascorbic acid.
- one or two administration(s) of 10,000 IU of urokinase left in the CVC lumen for 2 h - sudden onset of CVC malfunction during or immediately after infusion of drugs, blood components, or parenteral nutrition -
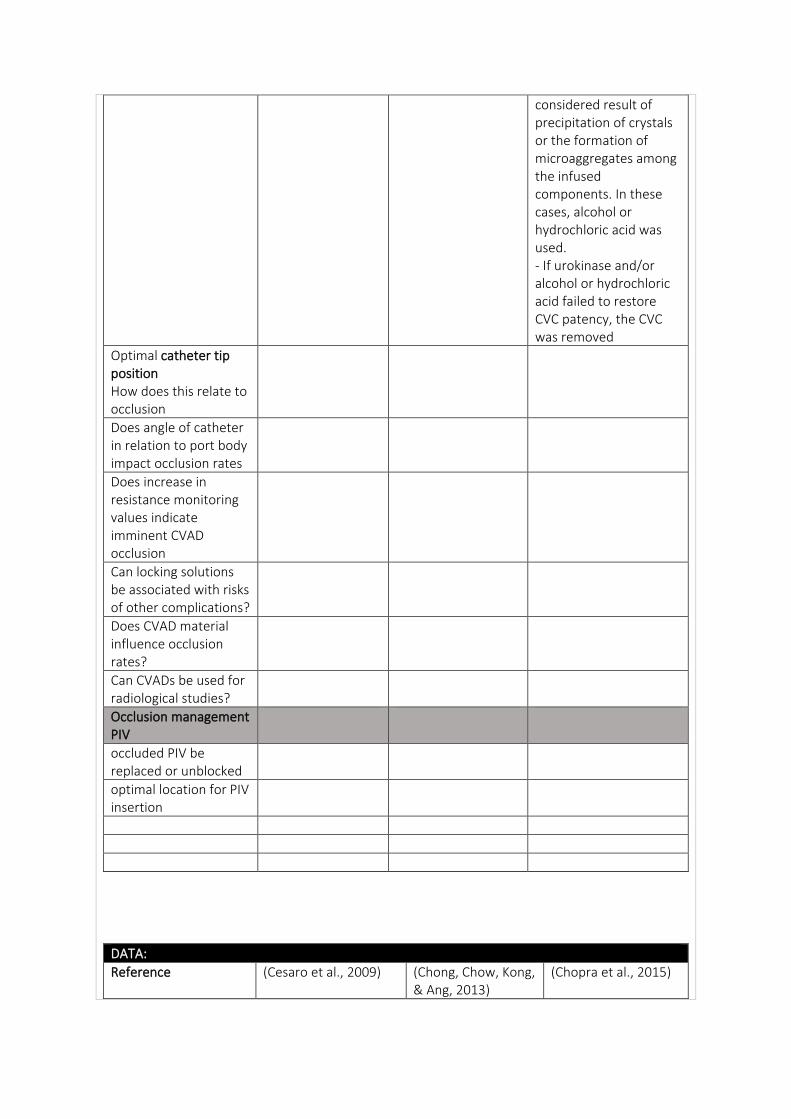
considered result of precipitation of crystals or the formation of microaggregates among the infused components. In these cases, alcohol or hydrochloric acid was used. - If urokinase and/or alcohol or hydrochloric acid failed to restore CVC patency, the CVC was removed
Optimal catheter tip position How does this relate to occlusion
Does angle of catheter in relation to port body impact occlusion rates
Does increase in resistance monitoring values indicate imminent CVAD occlusion
Can locking solutions be associated with risks of other complications?
Does CVAD material influence occlusion rates?
Can CVADs be used for radiological studies?
Occlusion management PIV
occluded PIV be replaced or unblocked
optimal location for PIV insertion
DATA:
Reference (Cesaro et al., 2009) (Chong, Chow, Kong, & Ang, 2013)
(Chopra et al., 2015)
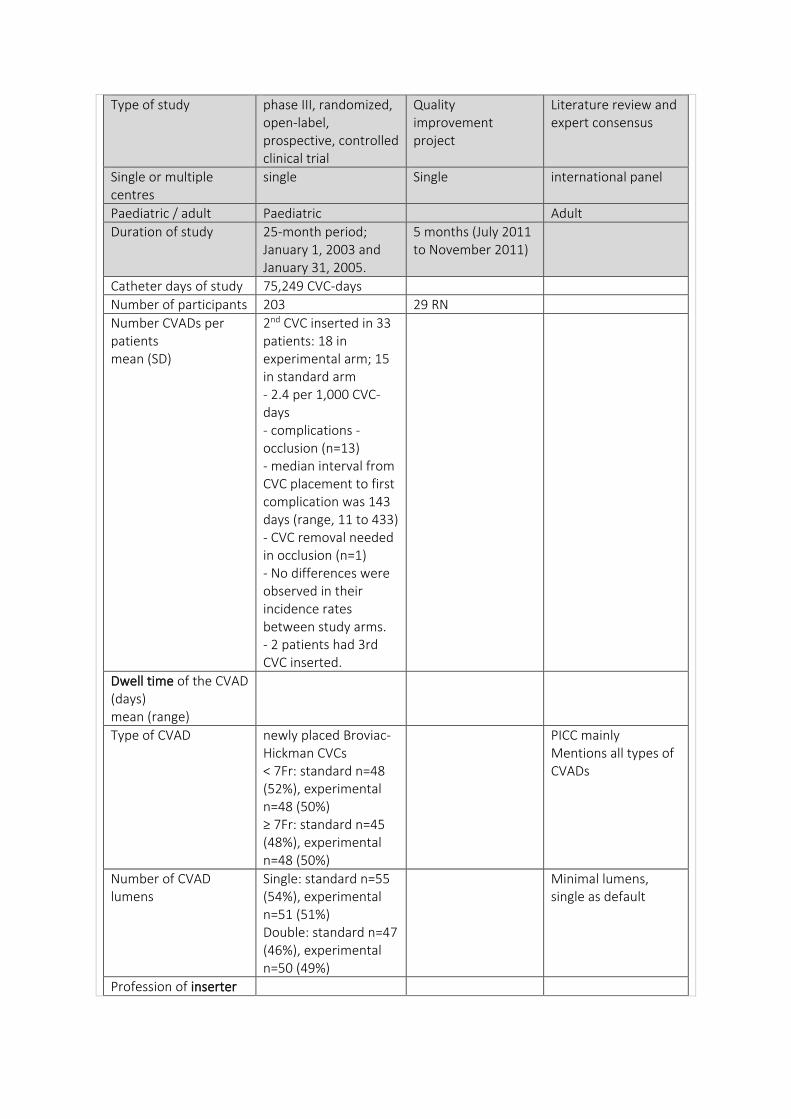
Type of study phase III, randomized, open-label, prospective, controlled clinical trial
Quality improvement project
Literature review and expert consensus
Single or multiple centres
single Single international panel
Paediatric / adult Paediatric Adult
Duration of study 25-month period; January 1, 2003 and January 31, 2005.
5 months (July 2011 to November 2011)
Catheter days of study 75,249 CVC-days
Number of participants 203 29 RN
Number CVADs per patients mean (SD)
2nd CVC inserted in 33 patients: 18 in experimental arm; 15 in standard arm - 2.4 per 1,000 CVC-days - complications - occlusion (n=13) - median interval from CVC placement to first complication was 143 days (range, 11 to 433) - CVC removal needed in occlusion (n=1) - No differences were observed in their incidence rates between study arms. - 2 patients had 3rd CVC inserted.
Dwell time of the CVAD (days) mean (range)
Type of CVAD newly placed Broviac-Hickman CVCs < 7Fr: standard n=48 (52%), experimental n=48 (50%) ≥ 7Fr: standard n=45 (48%), experimental n=48 (50%)
PICC mainly Mentions all types of CVADs
Number of CVAD lumens
Single: standard n=55 (54%), experimental n=51 (51%) Double: standard n=47 (46%), experimental n=50 (49%)
Minimal lumens, single as default
Profession of inserter
Anatomical location of insertion
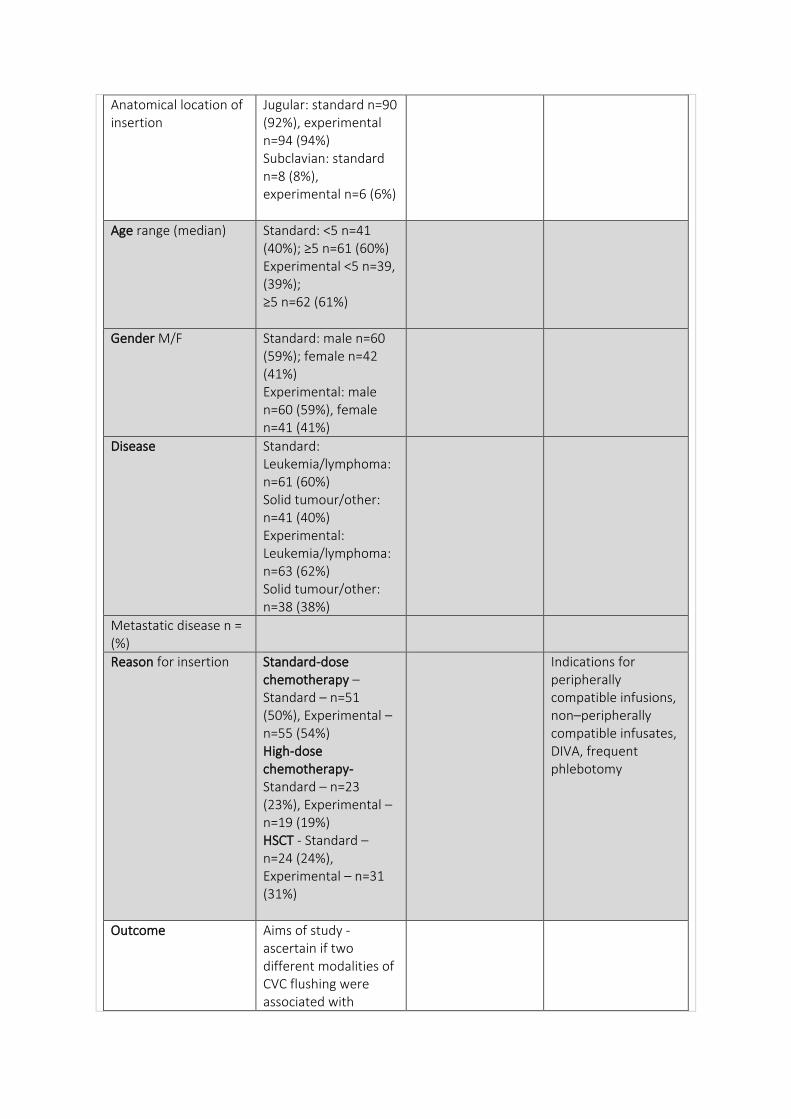
Jugular: standard n=90 (92%), experimental n=94 (94%) Subclavian: standard n=8 (8%), experimental n=6 (6%)
Age range (median) Standard: <5 n=41 (40%); ≥5 n=61 (60%) Experimental <5 n=39, (39%); ≥5 n=62 (61%)
Gender M/F Standard: male n=60 (59%); female n=42 (41%) Experimental: male n=60 (59%), female n=41 (41%)
Disease Standard: Leukemia/lymphoma: n=61 (60%) Solid tumour/other: n=41 (40%) Experimental: Leukemia/lymphoma: n=63 (62%) Solid tumour/other: n=38 (38%)
Metastatic disease n = (%)
Reason for insertion Standard-dose chemotherapy – Standard – n=51 (50%), Experimental – n=55 (54%) High-dose chemotherapy- Standard – n=23 (23%), Experimental – n=19 (19%) HSCT - Standard – n=24 (24%), Experimental – n=31 (31%)
Indications for peripherally compatible infusions, non–peripherally compatible infusates, DIVA, frequent phlebotomy
Outcome Aims of study - ascertain if two different modalities of CVC flushing were associated with
significantly different CVC complication rates (primary aim) and/or different CVC survival rates (secondary aim)
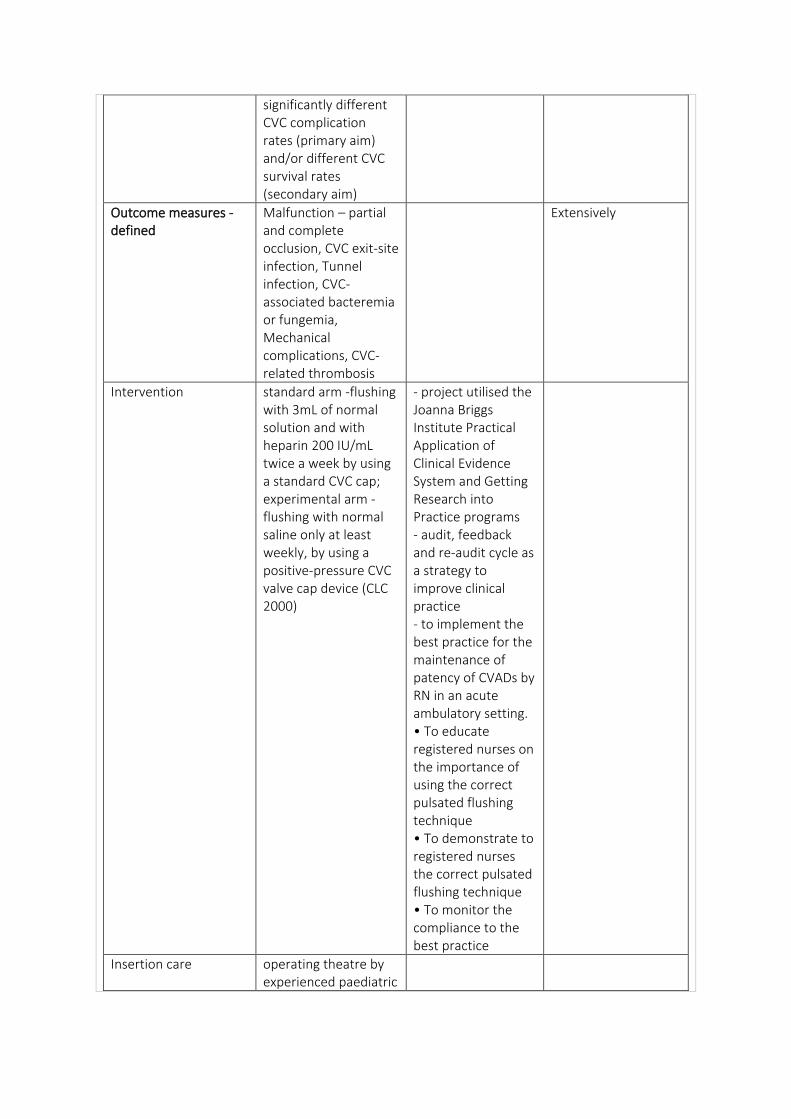
Outcome measures - defined
Malfunction – partial and complete occlusion, CVC exit-site infection, Tunnel infection, CVC-associated bacteremia or fungemia, Mechanical complications, CVC-related thrombosis
Extensively
Intervention standard arm -flushing with 3mL of normal solution and with heparin 200 IU/mL twice a week by using a standard CVC cap; experimental arm - flushing with normal saline only at least weekly, by using a positive-pressure CVC valve cap device (CLC 2000)
- project utilised the Joanna Briggs Institute Practical Application of Clinical Evidence System and Getting Research into Practice programs - audit, feedback and re-audit cycle as a strategy to improve clinical practice - to implement the best practice for the maintenance of patency of CVADs by RN in an acute ambulatory setting. • To educate registered nurses on the importance of using the correct pulsated flushing technique • To demonstrate to registered nurses the correct pulsated flushing technique • To monitor the compliance to the best practice
Insertion care operating theatre by experienced paediatric
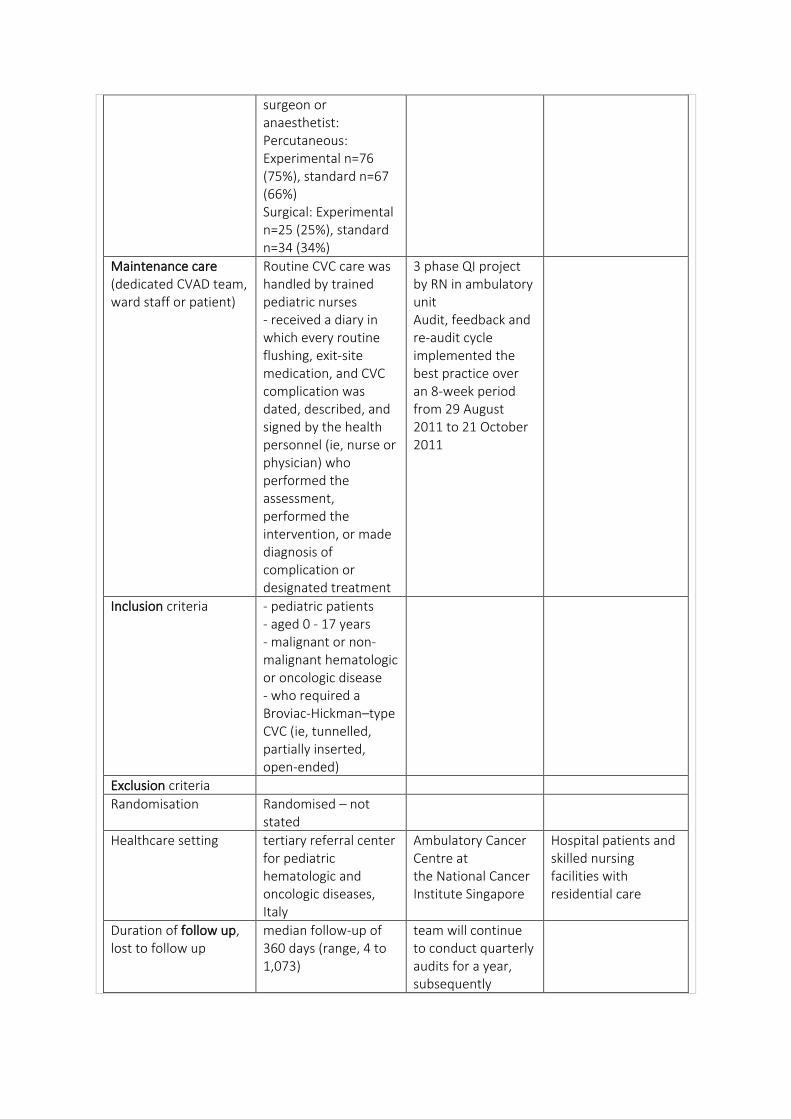
surgeon or anaesthetist: Percutaneous: Experimental n=76 (75%), standard n=67 (66%) Surgical: Experimental n=25 (25%), standard n=34 (34%)
Maintenance care (dedicated CVAD team, ward staff or patient)
Routine CVC care was handled by trained pediatric nurses - received a diary in which every routine flushing, exit-site medication, and CVC complication was dated, described, and signed by the health personnel (ie, nurse or physician) who performed the assessment, performed the intervention, or made diagnosis of complication or designated treatment
3 phase QI project by RN in ambulatory unit Audit, feedback and re-audit cycle implemented the best practice over an 8-week period from 29 August 2011 to 21 October 2011
Inclusion criteria - pediatric patients - aged 0 - 17 years - malignant or non-malignant hematologic or oncologic disease - who required a Broviac-Hickman–type CVC (ie, tunnelled, partially inserted, open-ended)
Exclusion criteria
Randomisation Randomised – not stated
Healthcare setting tertiary referral center for pediatric hematologic and oncologic diseases, Italy
Ambulatory Cancer Centre at the National Cancer Institute Singapore
Hospital patients and skilled nursing facilities with residential care
Duration of follow up, lost to follow up
median follow-up of 360 days (range, 4 to 1,073)
team will continue to conduct quarterly audits for a year, subsequently
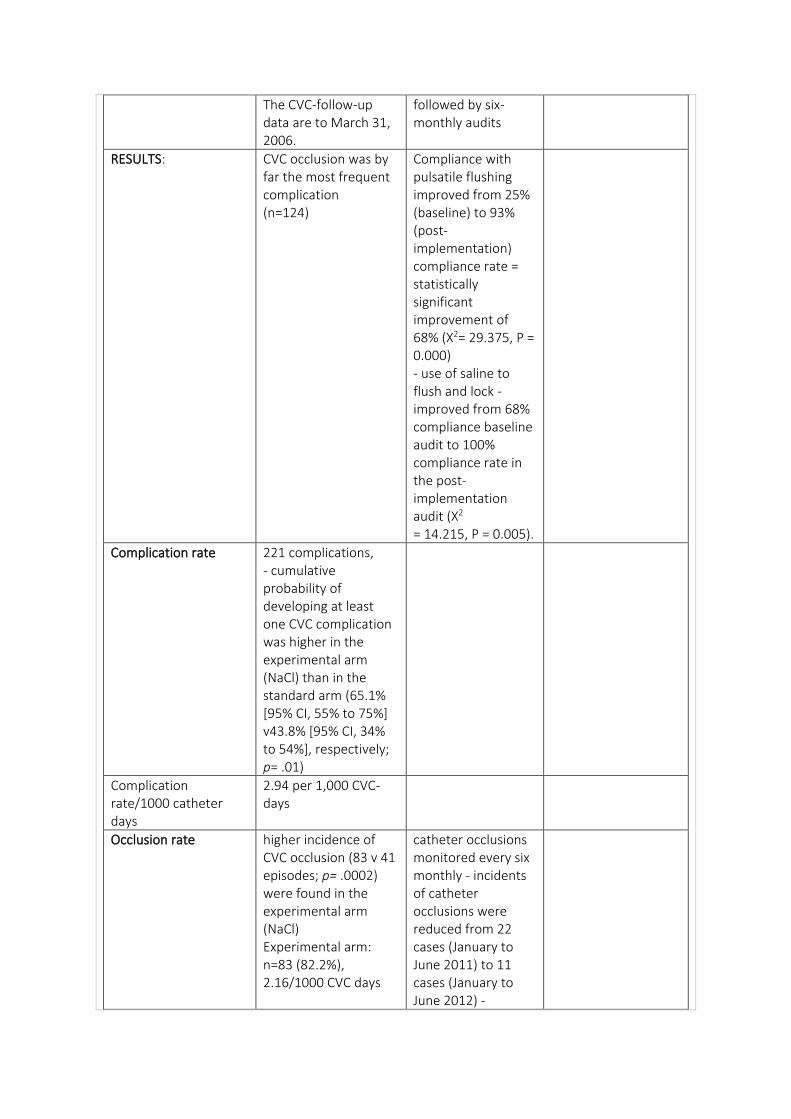
The CVC-follow-up data are to March 31, 2006.
followed by six-monthly audits
RESULTS: CVC occlusion was by far the most frequent complication (n=124)
Compliance with pulsatile flushing improved from 25% (baseline) to 93% (post-implementation) compliance rate = statistically significant improvement of 68% (X2= 29.375, P = 0.000) - use of saline to flush and lock - improved from 68% compliance baseline audit to 100% compliance rate in the post-implementation audit (X2 = 14.215, P = 0.005).
Complication rate 221 complications, - cumulative probability of developing at least one CVC complication was higher in the experimental arm (NaCl) than in the standard arm (65.1% [95% CI, 55% to 75%] v43.8% [95% CI, 34% to 54%], respectively; p= .01)
Complication rate/1000 catheter days
2.94 per 1,000 CVC-days
Occlusion rate higher incidence of CVC occlusion (83 v 41 episodes; p= .0002) were found in the experimental arm (NaCl) Experimental arm: n=83 (82.2%), 2.16/1000 CVC days
catheter occlusions monitored every six monthly - incidents of catheter occlusions were reduced from 22 cases (January to June 2011) to 11 cases (January to June 2012) -
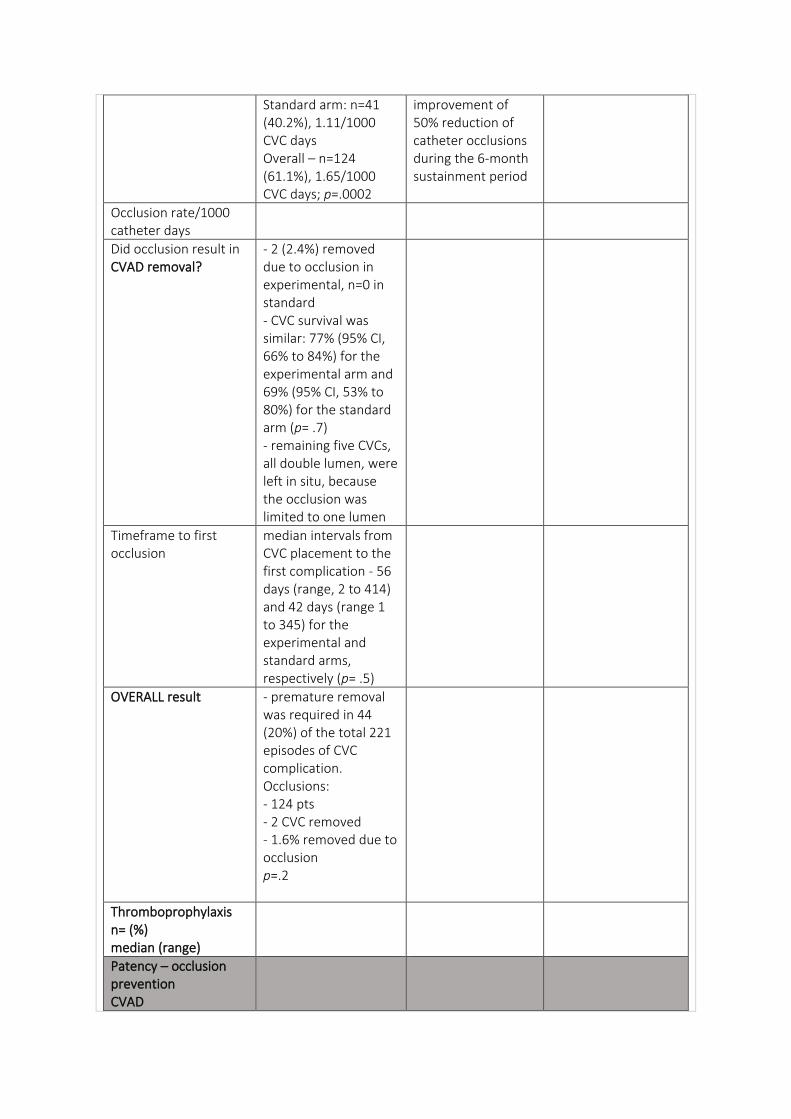
Standard arm: n=41 (40.2%), 1.11/1000 CVC days Overall – n=124 (61.1%), 1.65/1000 CVC days; p=.0002
improvement of 50% reduction of catheter occlusions during the 6-month sustainment period
Occlusion rate/1000 catheter days
Did occlusion result in CVAD removal?
- 2 (2.4%) removed due to occlusion in experimental, n=0 in standard - CVC survival was similar: 77% (95% CI, 66% to 84%) for the experimental arm and 69% (95% CI, 53% to 80%) for the standard arm (p= .7) - remaining five CVCs, all double lumen, were left in situ, because the occlusion was limited to one lumen
Timeframe to first occlusion
median intervals from CVC placement to the first complication - 56 days (range, 2 to 414) and 42 days (range 1 to 345) for the experimental and standard arms, respectively (p= .5)
OVERALL result - premature removal was required in 44 (20%) of the total 221 episodes of CVC complication. Occlusions: - 124 pts - 2 CVC removed - 1.6% removed due to occlusion p=.2
Thromboprophylaxis n= (%) median (range)
Patency – occlusion prevention CVAD
Education and competency requirement of staff – inserting and maintenance
Frequency of patency checked
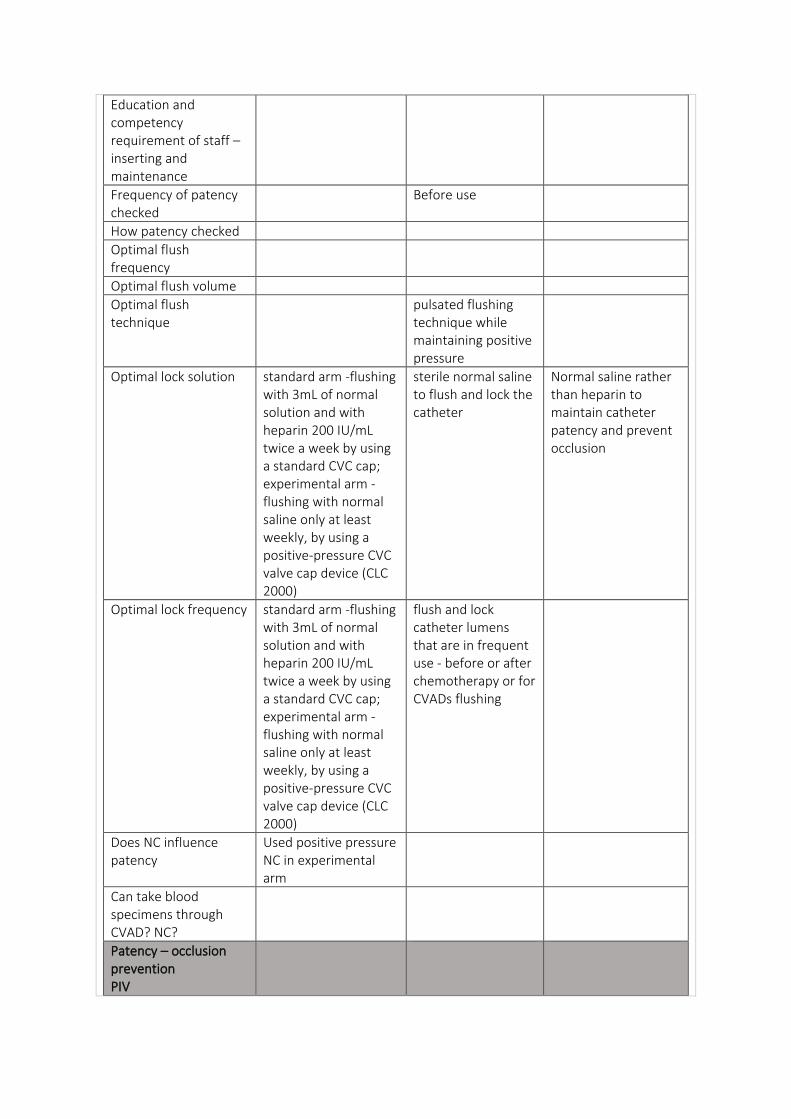
Before use
How patency checked
Optimal flush frequency
Optimal flush volume
Optimal flush technique
pulsated flushing technique while maintaining positive pressure
Optimal lock solution standard arm -flushing with 3mL of normal solution and with heparin 200 IU/mL twice a week by using a standard CVC cap; experimental arm - flushing with normal saline only at least weekly, by using a positive-pressure CVC valve cap device (CLC 2000)
sterile normal saline to flush and lock the catheter
Normal saline rather than heparin to maintain catheter patency and prevent occlusion
Optimal lock frequency standard arm -flushing with 3mL of normal solution and with heparin 200 IU/mL twice a week by using a standard CVC cap; experimental arm - flushing with normal saline only at least weekly, by using a positive-pressure CVC valve cap device (CLC 2000)
flush and lock catheter lumens that are in frequent use - before or after chemotherapy or for CVADs flushing
Does NC influence patency
Used positive pressure NC in experimental arm
Can take blood specimens through CVAD? NC?
Patency – occlusion prevention PIV
How is patency checked?
What solution is used to flush and check patency
Occlusion management CVAD
Factors affecting occlusion rates: - type of cancer
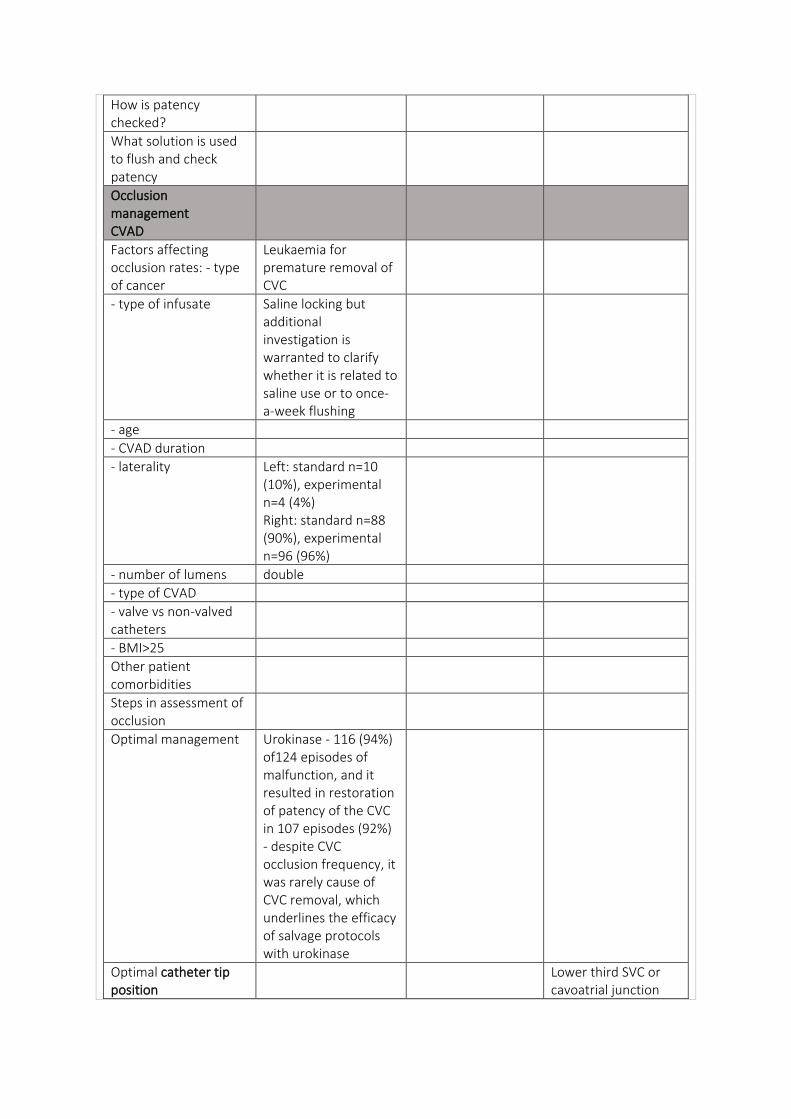
Leukaemia for premature removal of CVC
- type of infusate Saline locking but additional investigation is warranted to clarify whether it is related to saline use or to once-a-week flushing
- age
- CVAD duration
- laterality Left: standard n=10 (10%), experimental n=4 (4%) Right: standard n=88 (90%), experimental n=96 (96%)
- number of lumens double
- type of CVAD
- valve vs non-valved catheters
- BMI>25
Other patient comorbidities
Steps in assessment of occlusion
Optimal management Urokinase - 116 (94%) of124 episodes of malfunction, and it resulted in restoration of patency of the CVC in 107 episodes (92%) - despite CVC occlusion frequency, it was rarely cause of CVC removal, which underlines the efficacy of salvage protocols with urokinase
Optimal catheter tip position
Lower third SVC or cavoatrial junction
How does this relate to occlusion
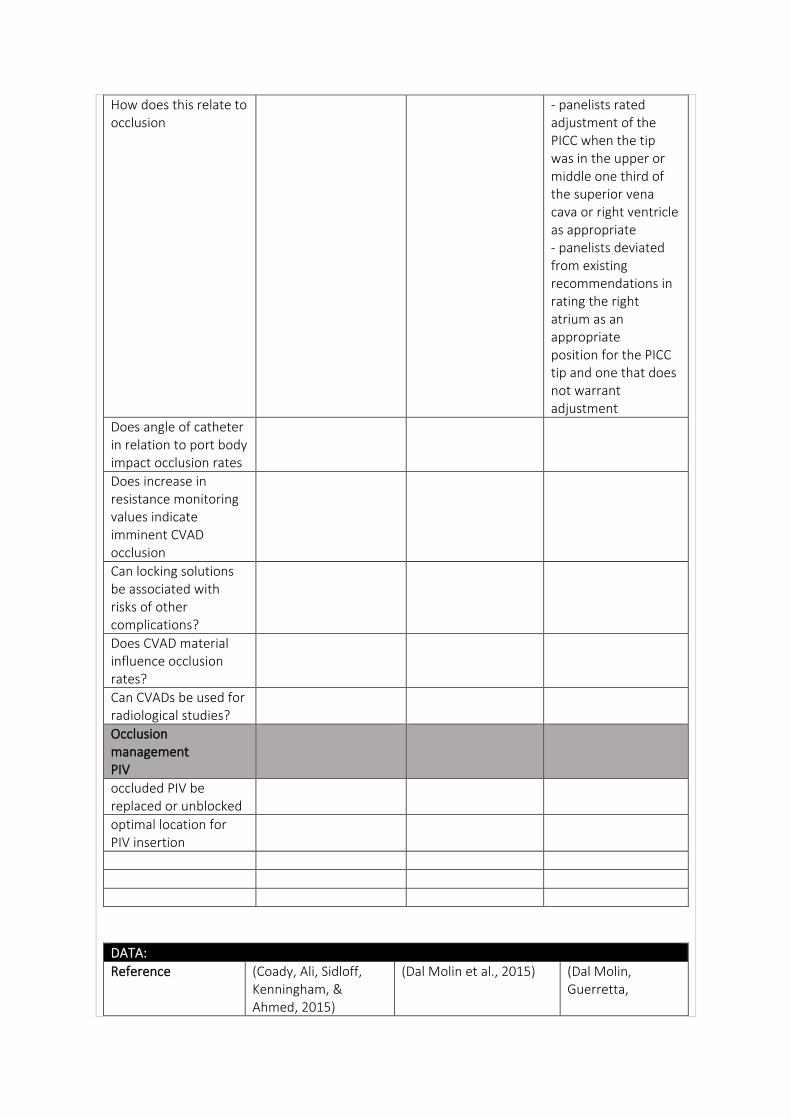
- panelists rated adjustment of the PICC when the tip was in the upper or middle one third of the superior vena cava or right ventricle as appropriate - panelists deviated from existing recommendations in rating the right atrium as an appropriate position for the PICC tip and one that does not warrant adjustment
Does angle of catheter in relation to port body impact occlusion rates
Does increase in resistance monitoring values indicate imminent CVAD occlusion
Can locking solutions be associated with risks of other complications?
Does CVAD material influence occlusion rates?
Can CVADs be used for radiological studies?
Occlusion management PIV
occluded PIV be replaced or unblocked
optimal location for PIV insertion
DATA:
Reference (Coady, Ali, Sidloff, Kenningham, & Ahmed, 2015)
(Dal Molin et al., 2015) (Dal Molin, Guerretta,
Mazzufero, & Rasero, 2009)
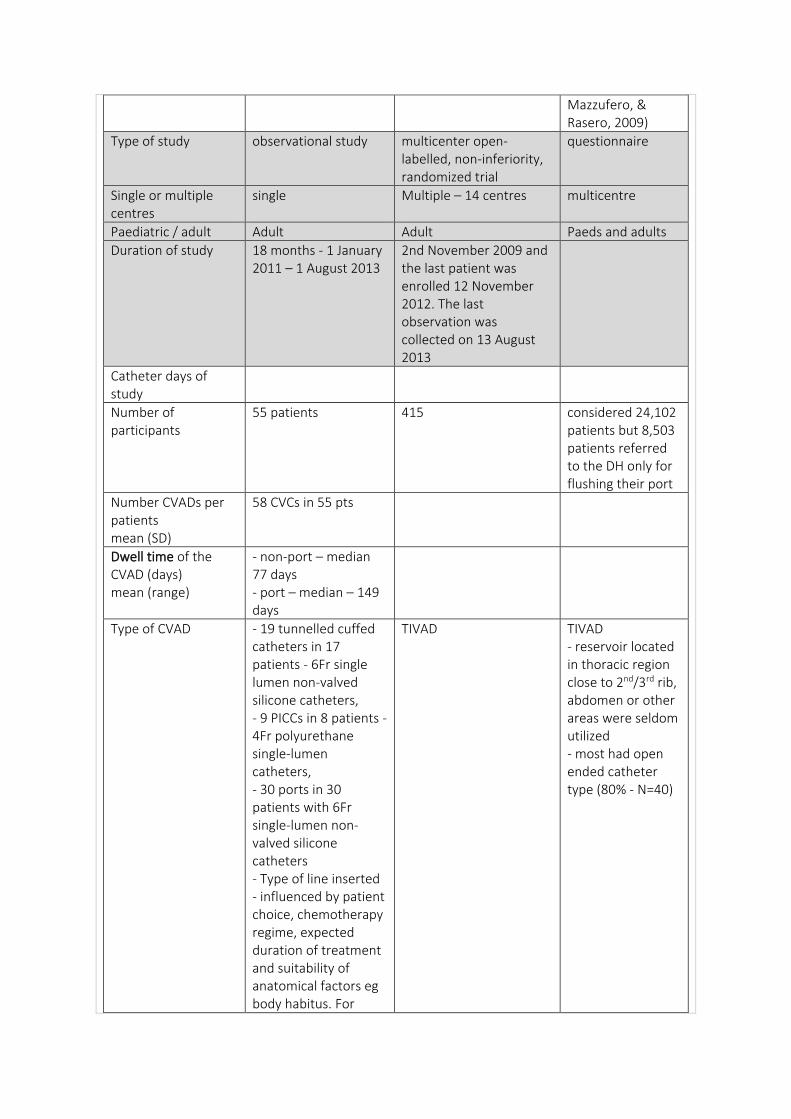
Type of study observational study multicenter open-labelled, non-inferiority, randomized trial
questionnaire
Single or multiple centres
single Multiple – 14 centres multicentre
Paediatric / adult Adult Adult Paeds and adults
Duration of study 18 months - 1 January 2011 – 1 August 2013
2nd November 2009 and the last patient was enrolled 12 November 2012. The last observation was collected on 13 August 2013
Catheter days of study
Number of participants
55 patients 415 considered 24,102 patients but 8,503 patients referred to the DH only for flushing their port
Number CVADs per patients mean (SD)
58 CVCs in 55 pts
Dwell time of the CVAD (days) mean (range)
- non-port – median 77 days - port – median – 149 days
Type of CVAD - 19 tunnelled cuffed catheters in 17 patients - 6Fr single lumen non-valved silicone catheters, - 9 PICCs in 8 patients - 4Fr polyurethane single-lumen catheters, - 30 ports in 30 patients with 6Fr single-lumen non-valved silicone catheters - Type of line inserted - influenced by patient choice, chemotherapy regime, expected duration of treatment and suitability of anatomical factors eg body habitus. For
TIVAD TIVAD - reservoir located in thoracic region close to 2nd/3rd rib, abdomen or other areas were seldom utilized - most had open ended catheter type (80% - N=40)
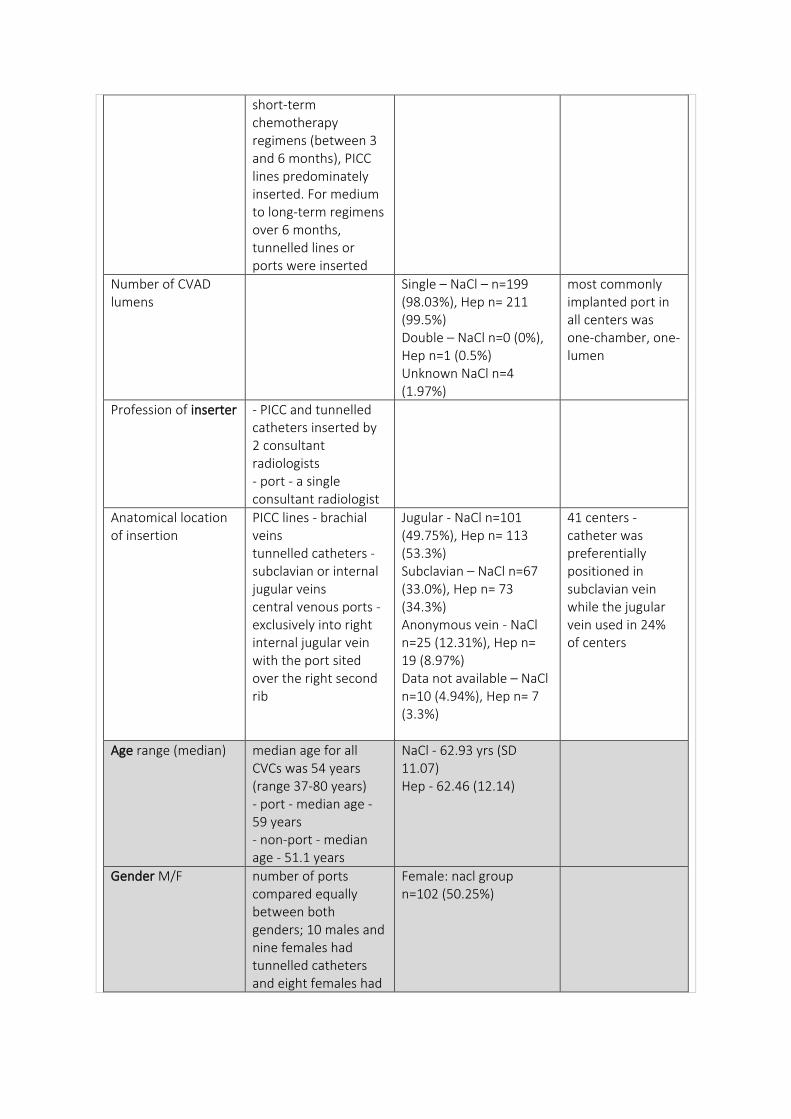
short-term chemotherapy regimens (between 3 and 6 months), PICC lines predominately inserted. For medium to long-term regimens over 6 months, tunnelled lines or ports were inserted
Number of CVAD lumens
Single – NaCl – n=199 (98.03%), Hep n= 211 (99.5%) Double – NaCl n=0 (0%), Hep n=1 (0.5%) Unknown NaCl n=4 (1.97%)
most commonly implanted port in all centers was one-chamber, one-lumen
Profession of inserter - PICC and tunnelled catheters inserted by 2 consultant radiologists - port - a single consultant radiologist
Anatomical location of insertion
PICC lines - brachial veins tunnelled catheters - subclavian or internal jugular veins central venous ports - exclusively into right internal jugular vein with the port sited over the right second rib
Jugular - NaCl n=101 (49.75%), Hep n= 113 (53.3%) Subclavian – NaCl n=67 (33.0%), Hep n= 73 (34.3%) Anonymous vein - NaCl n=25 (12.31%), Hep n= 19 (8.97%) Data not available – NaCl n=10 (4.94%), Hep n= 7 (3.3%)
41 centers - catheter was preferentially positioned in subclavian vein while the jugular vein used in 24% of centers
Age range (median) median age for all CVCs was 54 years (range 37-80 years) - port - median age - 59 years - non-port - median age - 51.1 years
NaCl - 62.93 yrs (SD 11.07) Hep - 62.46 (12.14)
Gender M/F number of ports compared equally between both genders; 10 males and nine females had tunnelled catheters and eight females had
Female: nacl group n=102 (50.25%)
nine PICC lines inserted
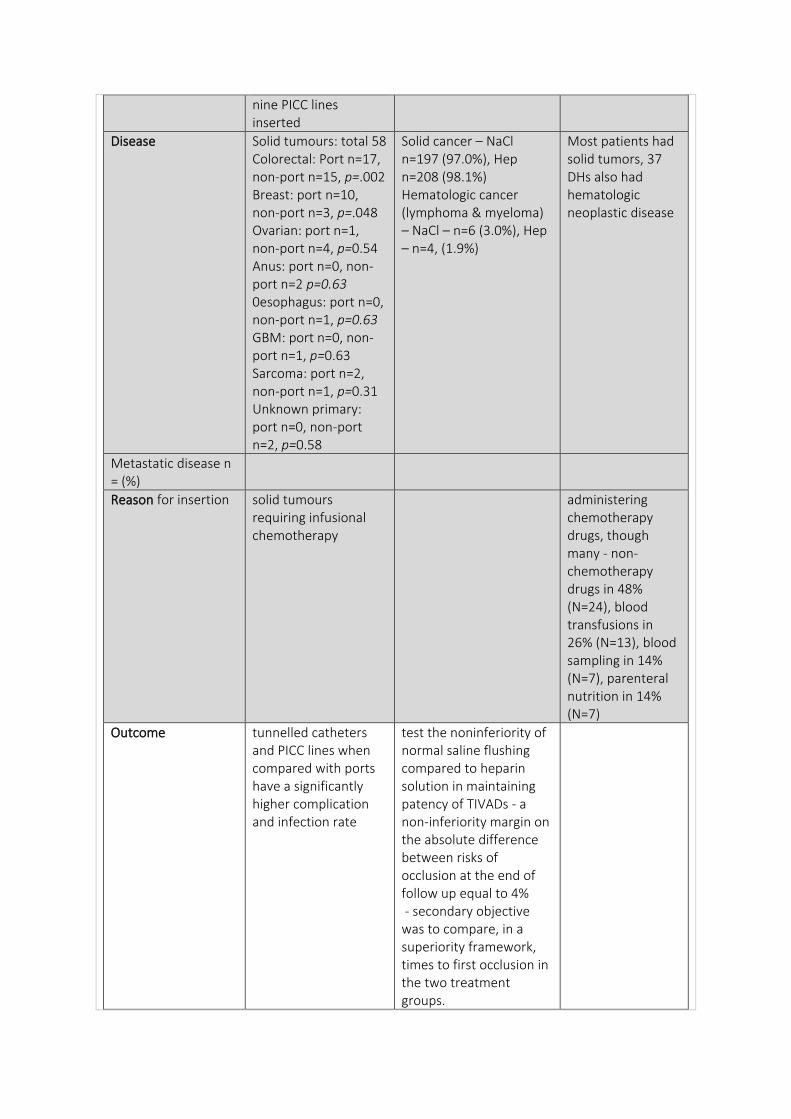
Disease Solid tumours: total 58 Colorectal: Port n=17, non-port n=15, p=.002 Breast: port n=10, non-port n=3, p=.048 Ovarian: port n=1, non-port n=4, p=0.54 Anus: port n=0, non-port n=2 p=0.63 0esophagus: port n=0, non-port n=1, p=0.63 GBM: port n=0, non-port n=1, p=0.63 Sarcoma: port n=2, non-port n=1, p=0.31 Unknown primary: port n=0, non-port n=2, p=0.58
Solid cancer – NaCl n=197 (97.0%), Hep n=208 (98.1%) Hematologic cancer (lymphoma & myeloma) – NaCl – n=6 (3.0%), Hep – n=4, (1.9%)
Most patients had solid tumors, 37 DHs also had hematologic neoplastic disease
Metastatic disease n = (%)
Reason for insertion solid tumours requiring infusional chemotherapy
administering chemotherapy drugs, though many - non-chemotherapy drugs in 48% (N=24), blood transfusions in 26% (N=13), blood sampling in 14% (N=7), parenteral nutrition in 14% (N=7)
Outcome tunnelled catheters and PICC lines when compared with ports have a significantly higher complication and infection rate
test the noninferiority of normal saline flushing compared to heparin solution in maintaining patency of TIVADs - a non-inferiority margin on the absolute difference between risks of occlusion at the end of follow up equal to 4% - secondary objective was to compare, in a superiority framework, times to first occlusion in the two treatment groups.
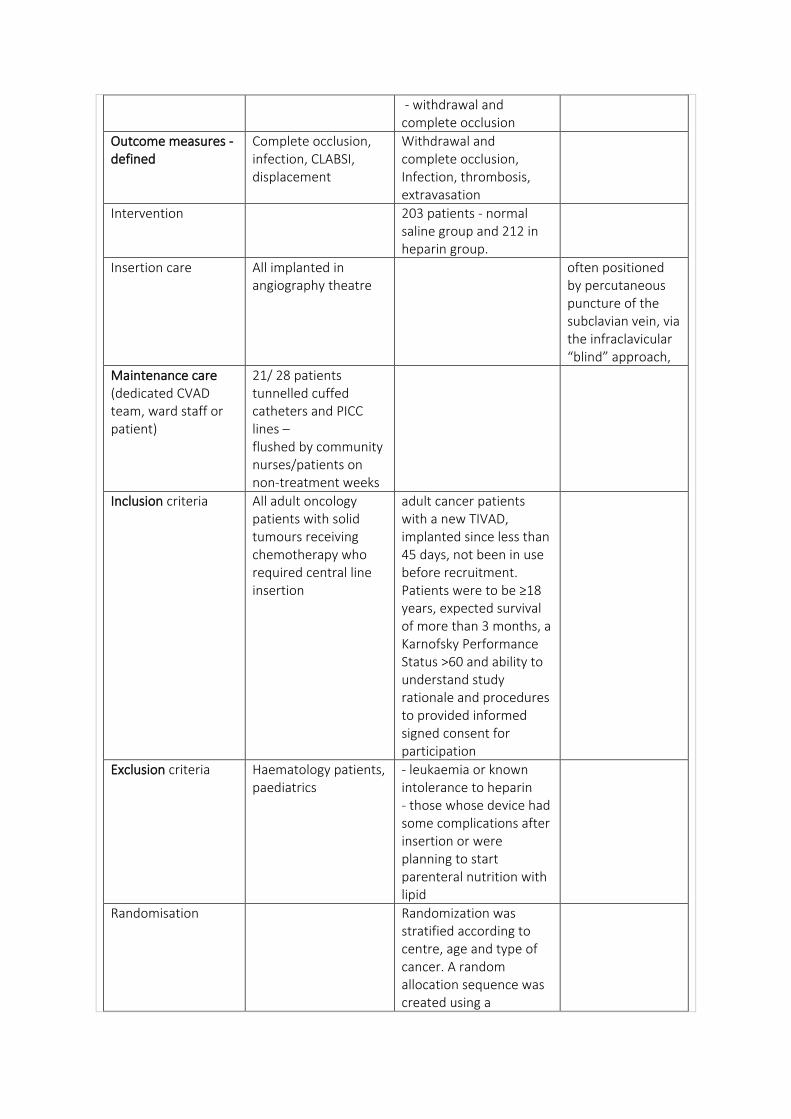
- withdrawal and complete occlusion
Outcome measures - defined
Complete occlusion, infection, CLABSI, displacement
Withdrawal and complete occlusion, Infection, thrombosis, extravasation
Intervention 203 patients - normal saline group and 212 in heparin group.
Insertion care All implanted in angiography theatre
often positioned by percutaneous puncture of the subclavian vein, via the infraclavicular “blind” approach,
Maintenance care (dedicated CVAD team, ward staff or patient)
21/ 28 patients tunnelled cuffed catheters and PICC lines – flushed by community nurses/patients on non-treatment weeks
Inclusion criteria All adult oncology patients with solid tumours receiving chemotherapy who required central line insertion
adult cancer patients with a new TIVAD, implanted since less than 45 days, not been in use before recruitment. Patients were to be ≥18 years, expected survival of more than 3 months, a Karnofsky Performance Status >60 and ability to understand study rationale and procedures to provided informed signed consent for participation
Exclusion criteria Haematology patients, paediatrics
- leukaemia or known intolerance to heparin - those whose device had some complications after insertion or were planning to start parenteral nutrition with lipid
Randomisation Randomization was stratified according to centre, age and type of cancer. A random allocation sequence was created using a
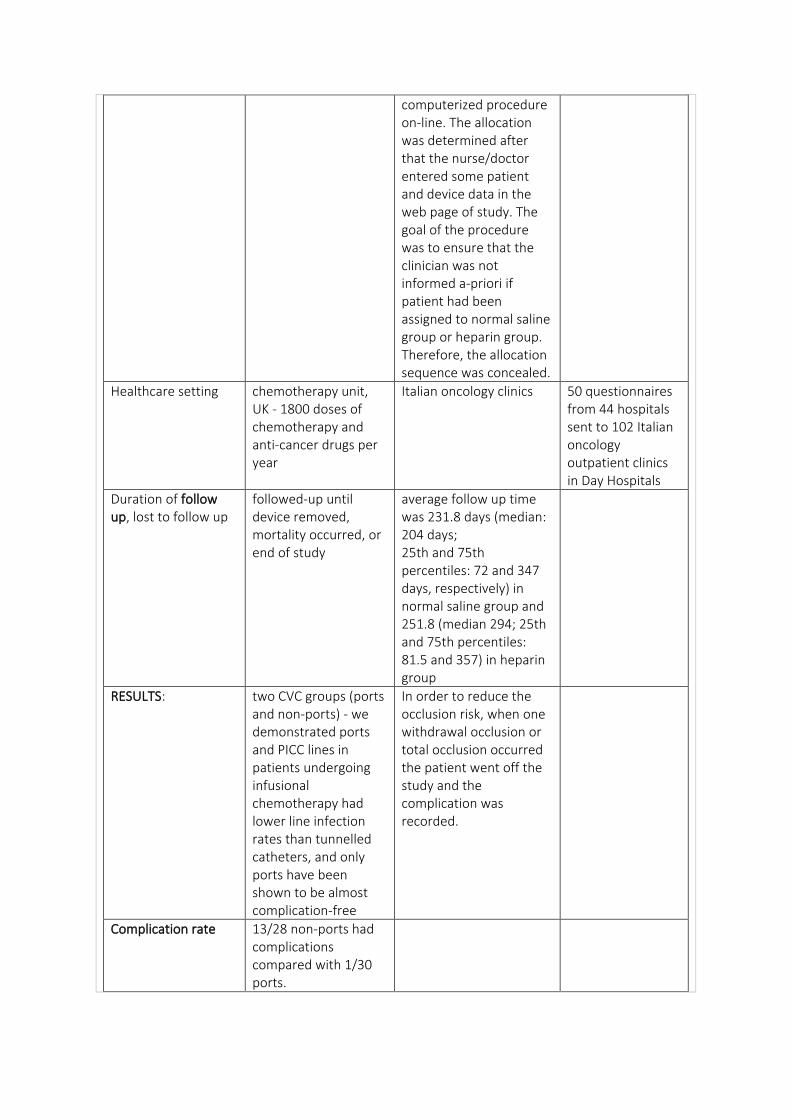
computerized procedure on-line. The allocation was determined after that the nurse/doctor entered some patient and device data in the web page of study. The goal of the procedure was to ensure that the clinician was not informed a-priori if patient had been assigned to normal saline group or heparin group. Therefore, the allocation sequence was concealed.
Healthcare setting chemotherapy unit, UK - 1800 doses of chemotherapy and anti-cancer drugs per year
Italian oncology clinics 50 questionnaires from 44 hospitals sent to 102 Italian oncology outpatient clinics in Day Hospitals
Duration of follow up, lost to follow up
followed-up until device removed, mortality occurred, or end of study
average follow up time was 231.8 days (median: 204 days; 25th and 75th percentiles: 72 and 347 days, respectively) in normal saline group and 251.8 (median 294; 25th and 75th percentiles: 81.5 and 357) in heparin group
RESULTS: two CVC groups (ports and non-ports) - we demonstrated ports and PICC lines in patients undergoing infusional chemotherapy had lower line infection rates than tunnelled catheters, and only ports have been shown to be almost complication-free
In order to reduce the occlusion risk, when one withdrawal occlusion or total occlusion occurred the patient went off the study and the complication was recorded.
Complication rate 13/28 non-ports had complications compared with 1/30 ports.
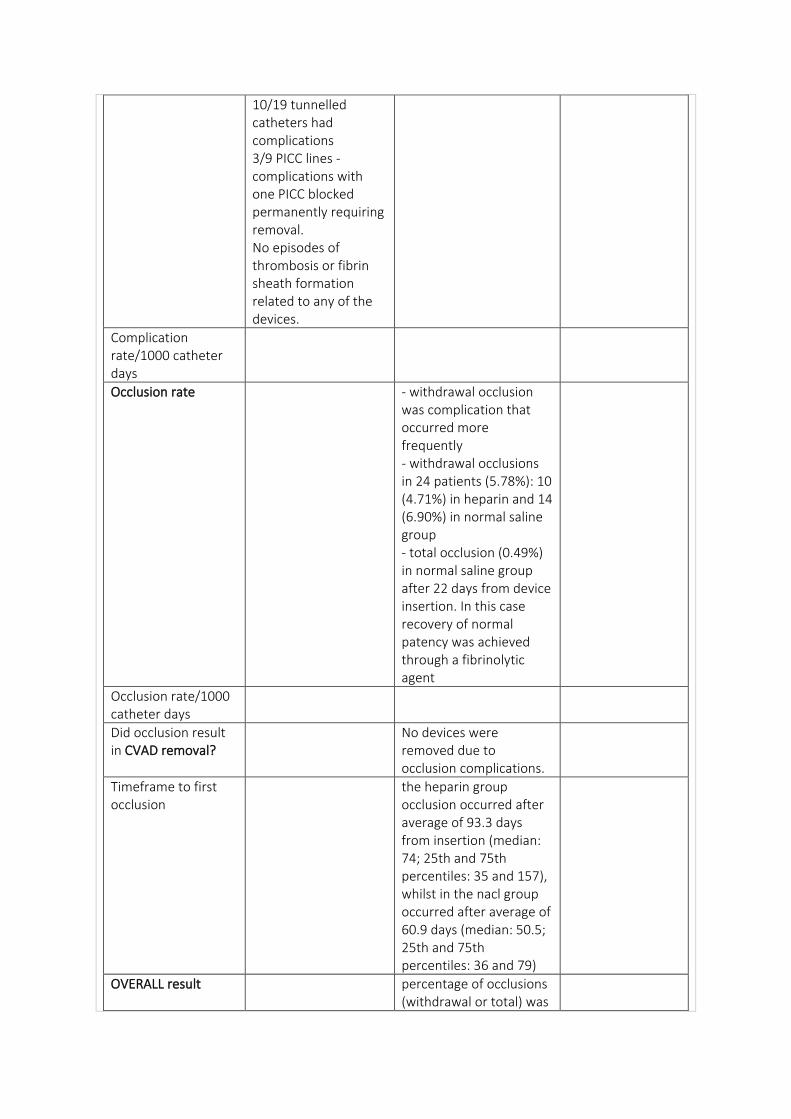
10/19 tunnelled catheters had complications 3/9 PICC lines - complications with one PICC blocked permanently requiring removal. No episodes of thrombosis or fibrin sheath formation related to any of the devices.
Complication rate/1000 catheter days
Occlusion rate - withdrawal occlusion was complication that occurred more frequently - withdrawal occlusions in 24 patients (5.78%): 10 (4.71%) in heparin and 14 (6.90%) in normal saline group - total occlusion (0.49%) in normal saline group after 22 days from device insertion. In this case recovery of normal patency was achieved through a fibrinolytic agent
Occlusion rate/1000 catheter days
Did occlusion result in CVAD removal?
No devices were removed due to occlusion complications.
Timeframe to first occlusion
the heparin group occlusion occurred after average of 93.3 days from insertion (median: 74; 25th and 75th percentiles: 35 and 157), whilst in the nacl group occurred after average of 60.9 days (median: 50.5; 25th and 75th percentiles: 36 and 79)
OVERALL result percentage of occlusions (withdrawal or total) was
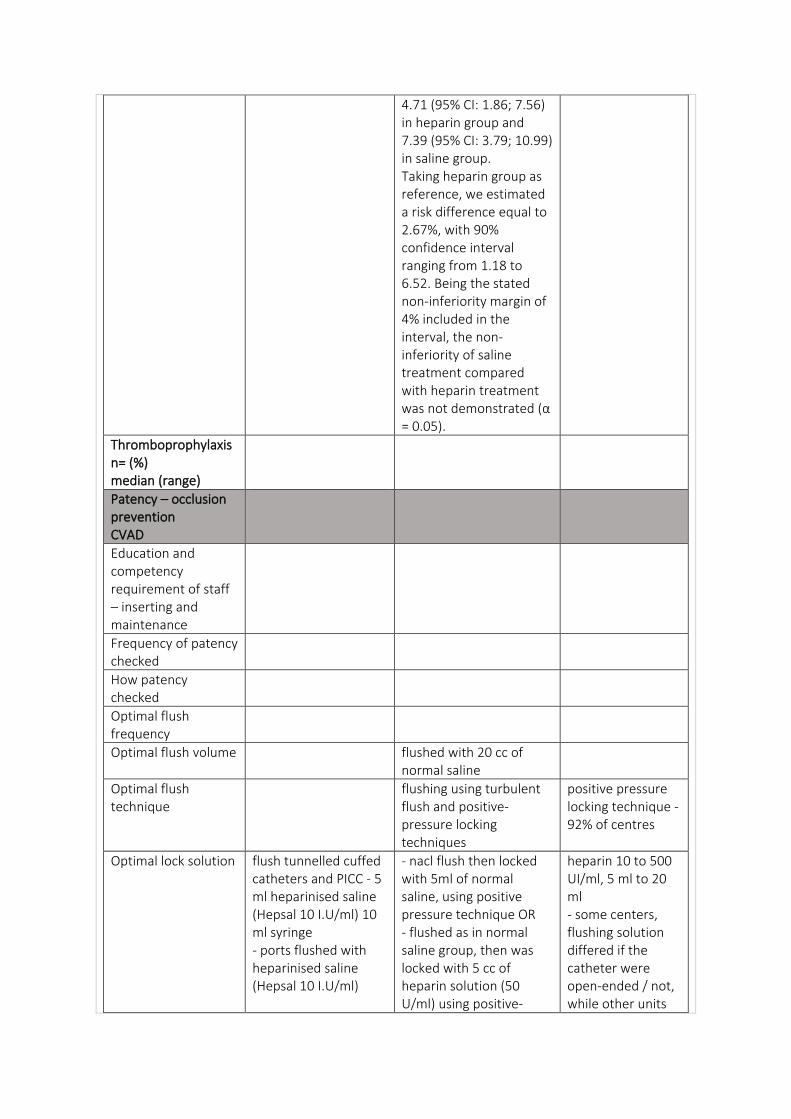
4.71 (95% CI: 1.86; 7.56) in heparin group and 7.39 (95% CI: 3.79; 10.99) in saline group. Taking heparin group as reference, we estimated a risk difference equal to 2.67%, with 90% confidence interval ranging from 1.18 to 6.52. Being the stated non-inferiority margin of 4% included in the interval, the non-inferiority of saline treatment compared with heparin treatment was not demonstrated (α = 0.05).
Thromboprophylaxis n= (%) median (range)
Patency – occlusion prevention CVAD
Education and competency requirement of staff – inserting and maintenance
Frequency of patency checked
How patency checked
Optimal flush frequency
Optimal flush volume flushed with 20 cc of normal saline
Optimal flush technique
flushing using turbulent flush and positive-pressure locking techniques
positive pressure locking technique - 92% of centres
Optimal lock solution flush tunnelled cuffed catheters and PICC - 5 ml heparinised saline (Hepsal 10 I.U/ml) 10 ml syringe - ports flushed with heparinised saline (Hepsal 10 I.U/ml)
- nacl flush then locked with 5ml of normal saline, using positive pressure technique OR - flushed as in normal saline group, then was locked with 5 cc of heparin solution (50 U/ml) using positive-
heparin 10 to 500 UI/ml, 5 ml to 20 ml - some centers, flushing solution differed if the catheter were open-ended / not, while other units
pressure technique
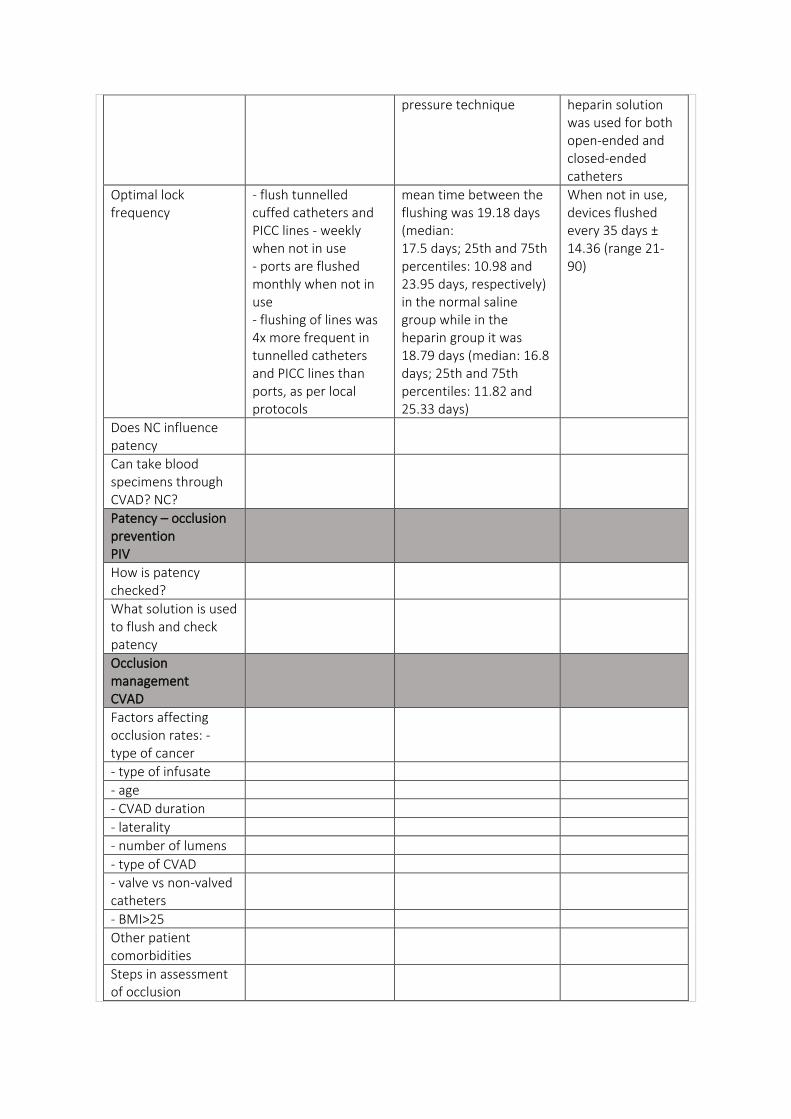
heparin solution was used for both open-ended and closed-ended catheters
Optimal lock frequency
- flush tunnelled cuffed catheters and PICC lines - weekly when not in use - ports are flushed monthly when not in use - flushing of lines was 4x more frequent in tunnelled catheters and PICC lines than ports, as per local protocols
mean time between the flushing was 19.18 days (median: 17.5 days; 25th and 75th percentiles: 10.98 and 23.95 days, respectively) in the normal saline group while in the heparin group it was 18.79 days (median: 16.8 days; 25th and 75th percentiles: 11.82 and 25.33 days)
When not in use, devices flushed every 35 days ± 14.36 (range 21-90)
Does NC influence patency
Can take blood specimens through CVAD? NC?
Patency – occlusion prevention PIV
How is patency checked?
What solution is used to flush and check patency
Occlusion management CVAD
Factors affecting occlusion rates: - type of cancer
- type of infusate
- age
- CVAD duration
- laterality
- number of lumens
- type of CVAD
- valve vs non-valved catheters
- BMI>25
Other patient comorbidities
Steps in assessment of occlusion
Optimal management
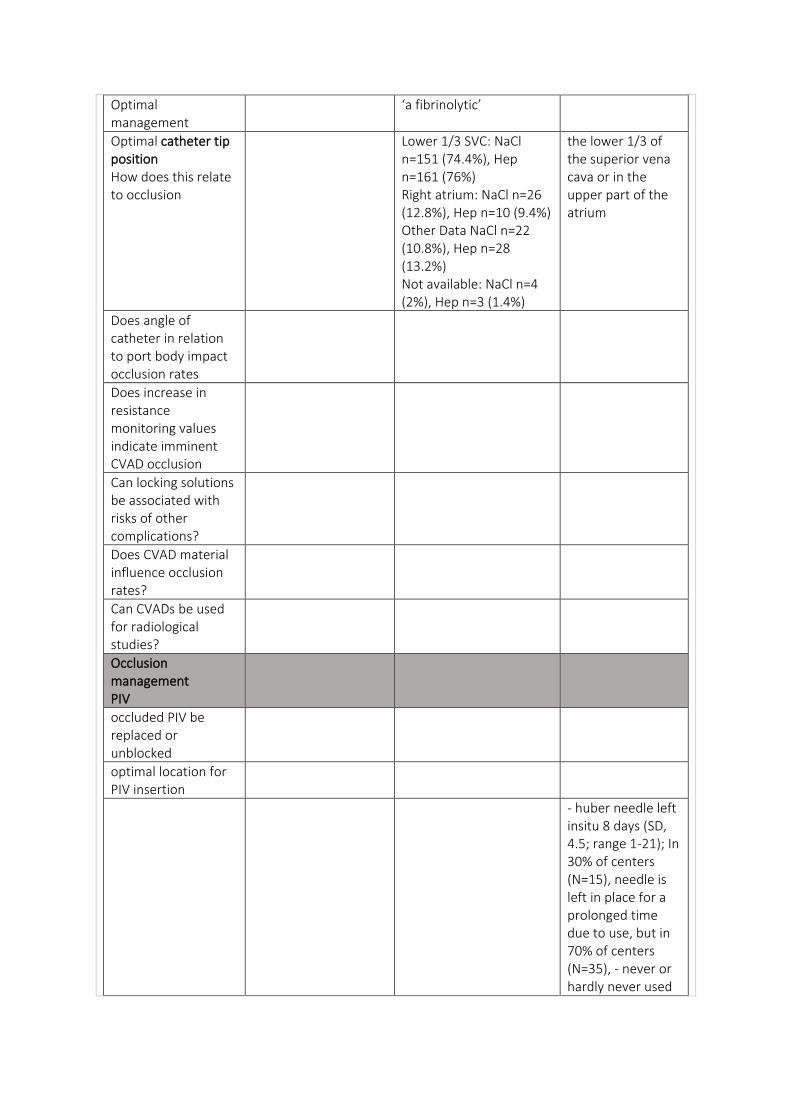
‘a fibrinolytic’
Optimal catheter tip position How does this relate to occlusion
Lower 1/3 SVC: NaCl n=151 (74.4%), Hep n=161 (76%) Right atrium: NaCl n=26 (12.8%), Hep n=10 (9.4%) Other Data NaCl n=22 (10.8%), Hep n=28 (13.2%) Not available: NaCl n=4 (2%), Hep n=3 (1.4%)
the lower 1/3 of the superior vena cava or in the upper part of the atrium
Does angle of catheter in relation to port body impact occlusion rates
Does increase in resistance monitoring values indicate imminent CVAD occlusion
Can locking solutions be associated with risks of other complications?
Does CVAD material influence occlusion rates?
Can CVADs be used for radiological studies?
Occlusion management PIV
occluded PIV be replaced or unblocked
optimal location for PIV insertion
- huber needle left insitu 8 days (SD, 4.5; range 1-21); In 30% of centers (N=15), needle is left in place for a prolonged time due to use, but in 70% of centers (N=35), - never or hardly never used
- 10ml syringes most used, 10% used smaller syringes
DATA:
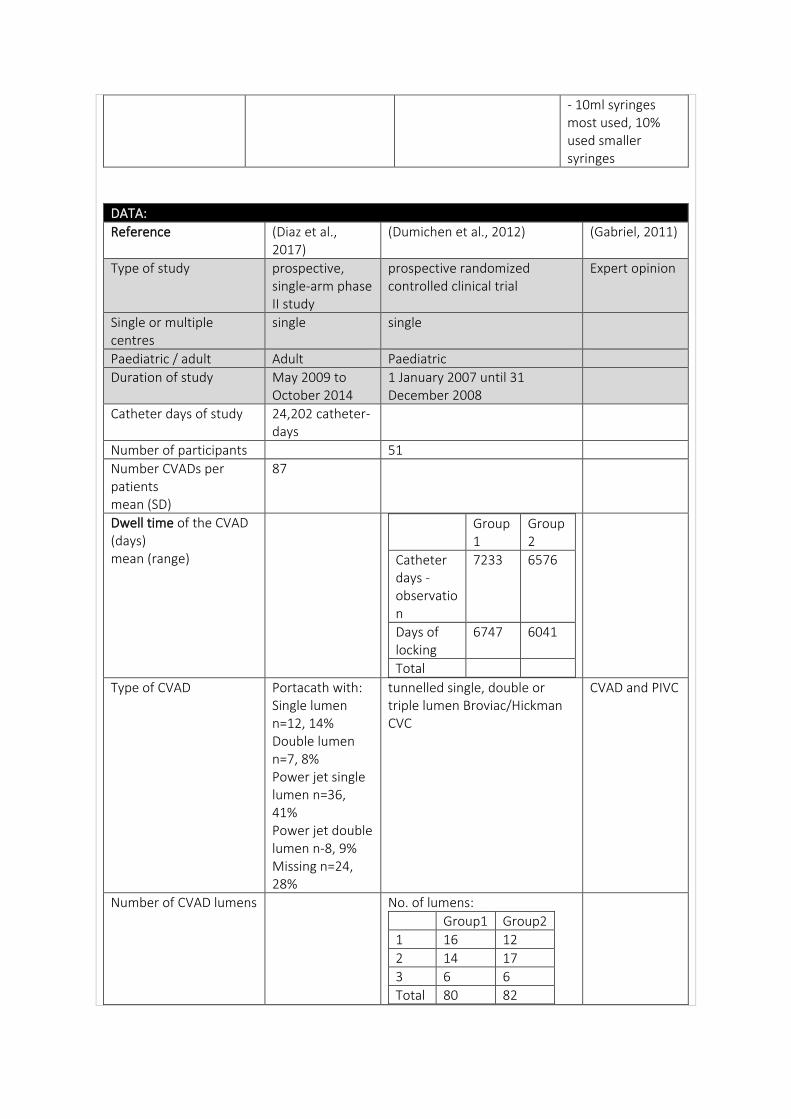
Reference (Diaz et al., 2017)
(Dumichen et al., 2012) (Gabriel, 2011)
Type of study prospective, single-arm phase II study
prospective randomized controlled clinical trial
Expert opinion
Single or multiple centres
single single
Paediatric / adult Adult Paediatric
Duration of study May 2009 to October 2014
1 January 2007 until 31 December 2008
Catheter days of study 24,202 catheter-days
Number of participants 51
Number CVADs per patients mean (SD)
87
Dwell time of the CVAD (days) mean (range)
Group1
Group2
Catheter days - observation
7233 6576
Days of locking
6747 6041
Total
Type of CVAD Portacath with: Single lumen n=12, 14% Double lumen n=7, 8% Power jet single lumen n=36, 41% Power jet double lumen n-8, 9% Missing n=24, 28%
tunnelled single, double or triple lumen Broviac/Hickman CVC
CVAD and PIVC
Number of CVAD lumens No. of lumens:
Group1 Group2
1 16 12
2 14 17
3 6 6
Total 80 82
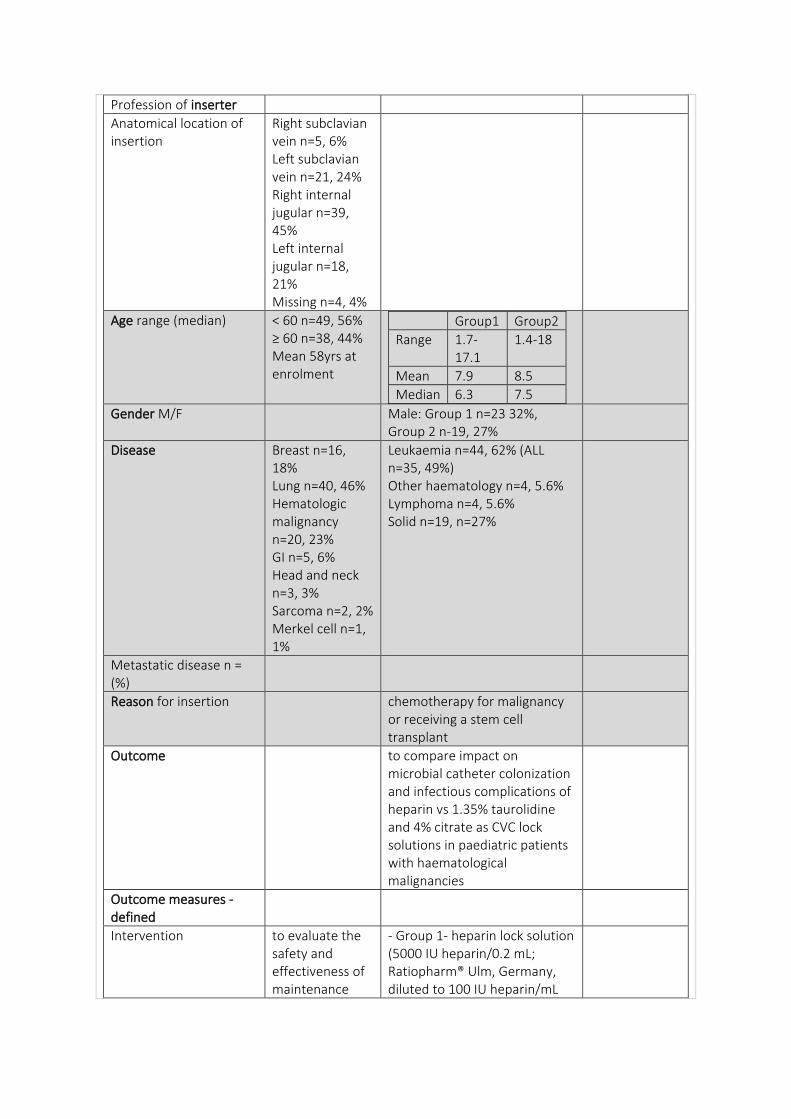
Profession of inserter
Anatomical location of insertion
Right subclavian vein n=5, 6% Left subclavian vein n=21, 24% Right internal jugular n=39, 45% Left internal jugular n=18, 21% Missing n=4, 4%
Age range (median) < 60 n=49, 56% ≥ 60 n=38, 44% Mean 58yrs at enrolment
Group1 Group2
Range 1.7-17.1
1.4-18
Mean 7.9 8.5
Median 6.3 7.5
Gender M/F Male: Group 1 n=23 32%, Group 2 n-19, 27%
Disease Breast n=16, 18% Lung n=40, 46% Hematologic malignancy n=20, 23% GI n=5, 6% Head and neck n=3, 3% Sarcoma n=2, 2% Merkel cell n=1, 1%
Leukaemia n=44, 62% (ALL n=35, 49%) Other haematology n=4, 5.6% Lymphoma n=4, 5.6% Solid n=19, n=27%
Metastatic disease n = (%)
Reason for insertion chemotherapy for malignancy or receiving a stem cell transplant
Outcome to compare impact on microbial catheter colonization and infectious complications of heparin vs 1.35% taurolidine and 4% citrate as CVC lock solutions in paediatric patients with haematological malignancies
Outcome measures - defined
Intervention to evaluate the safety and effectiveness of maintenance
- Group 1- heparin lock solution (5000 IU heparin/0.2 mL; Ratiopharm® Ulm, Germany, diluted to 100 IU heparin/mL
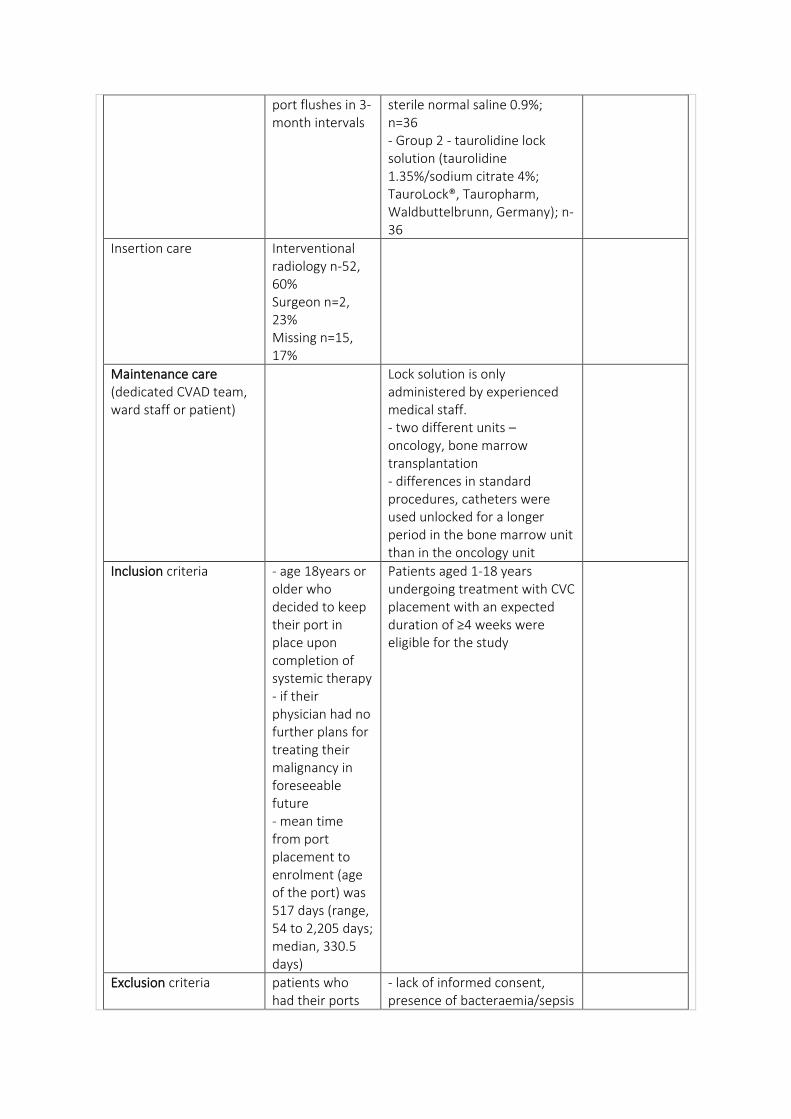
port flushes in 3-month intervals
sterile normal saline 0.9%; n=36 - Group 2 - taurolidine lock solution (taurolidine 1.35%/sodium citrate 4%; TauroLock®, Tauropharm, Waldbuttelbrunn, Germany); n-36
Insertion care Interventional radiology n-52, 60% Surgeon n=2, 23% Missing n=15, 17%
Maintenance care (dedicated CVAD team, ward staff or patient)
Lock solution is only administered by experienced medical staff. - two different units – oncology, bone marrow transplantation - differences in standard procedures, catheters were used unlocked for a longer period in the bone marrow unit than in the oncology unit
Inclusion criteria - age 18years or older who decided to keep their port in place upon completion of systemic therapy - if their physician had no further plans for treating their malignancy in foreseeable future - mean time from port placement to enrolment (age of the port) was 517 days (range, 54 to 2,205 days; median, 330.5 days)
Patients aged 1-18 years undergoing treatment with CVC placement with an expected duration of ≥4 weeks were eligible for the study
Exclusion criteria patients who had their ports
- lack of informed consent, presence of bacteraemia/sepsis
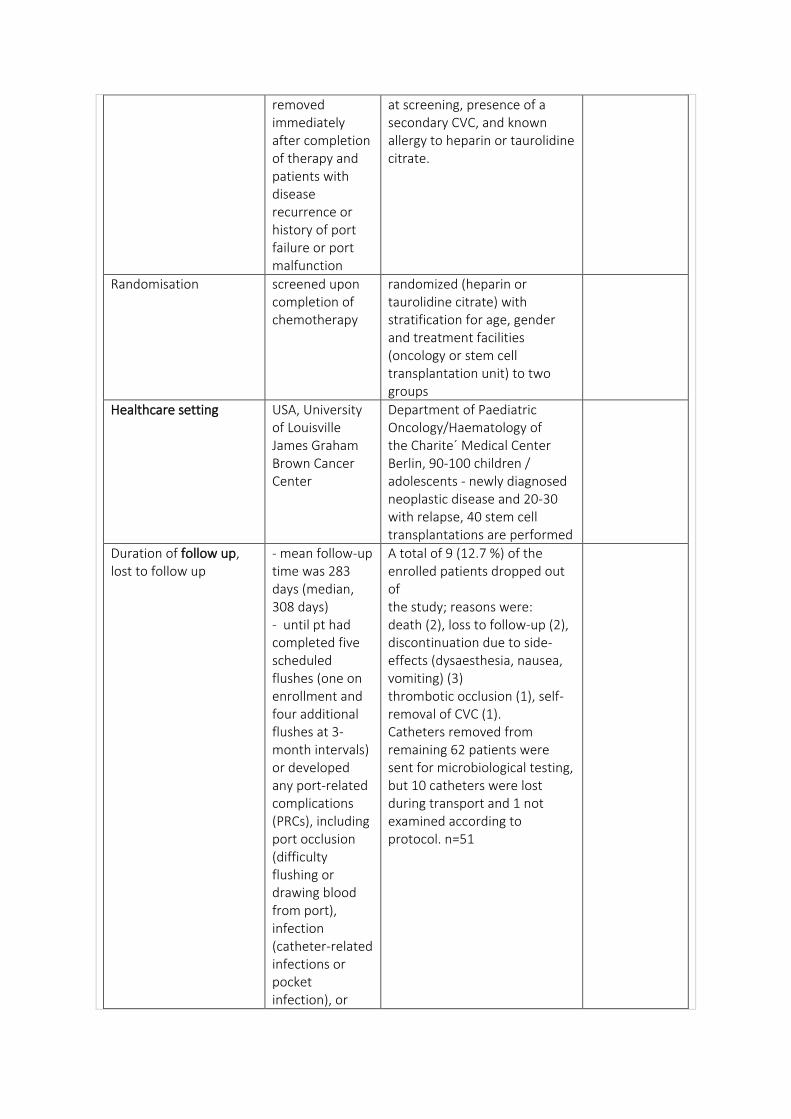
removed immediately after completion of therapy and patients with disease recurrence or history of port failure or port malfunction
at screening, presence of a secondary CVC, and known allergy to heparin or taurolidine citrate.
Randomisation screened upon completion of chemotherapy
randomized (heparin or taurolidine citrate) with stratification for age, gender and treatment facilities (oncology or stem cell transplantation unit) to two groups
Healthcare setting USA, University of Louisville James Graham Brown Cancer Center
Department of Paediatric Oncology/Haematology of the Charite´ Medical Center Berlin, 90-100 children / adolescents - newly diagnosed neoplastic disease and 20-30 with relapse, 40 stem cell transplantations are performed
Duration of follow up, lost to follow up
- mean follow-up time was 283 days (median, 308 days) - until pt had completed five scheduled flushes (one on enrollment and four additional flushes at 3-month intervals) or developed any port-related complications (PRCs), including port occlusion (difficulty flushing or drawing blood from port), infection (catheter-related infections or pocket infection), or
A total of 9 (12.7 %) of the enrolled patients dropped out of the study; reasons were: death (2), loss to follow-up (2), discontinuation due to side-effects (dysaesthesia, nausea, vomiting) (3) thrombotic occlusion (1), self-removal of CVC (1). Catheters removed from remaining 62 patients were sent for microbiological testing, but 10 catheters were lost during transport and 1 not examined according to protocol. n=51
symptomatic thrombosis - n=38 observed for 12 months, remainder < 12 mths
RESULTS:
Complication rate - 10 complications occurred in 10 patients (11.49%; 95% CI, 4.85% to 18.14%; 0.414/1,000 catheter-days); all occlusions and all <60yo - 4 patients (4.6%; 95% CI, 0.40% to 8.80%; 0.17/1,000 catheter days) underwent port revision under fluoroscopic guidance: 2 developed a fibrin sheath in the tip of the catheter; 1 of them underwent fibrin stripping - 1 patient had short catheter that possibly caused saccular aneurysm in superior vena cava, and port was removed.
Complication rate/1000 catheter days
Occlusion rate Catheter occlusion due to suspected thrombosis was diagnosed in 11 patients - thrombus formation was confirmed in 5 patients (2 in the heparin, 3 in the taurolidine citrate group)
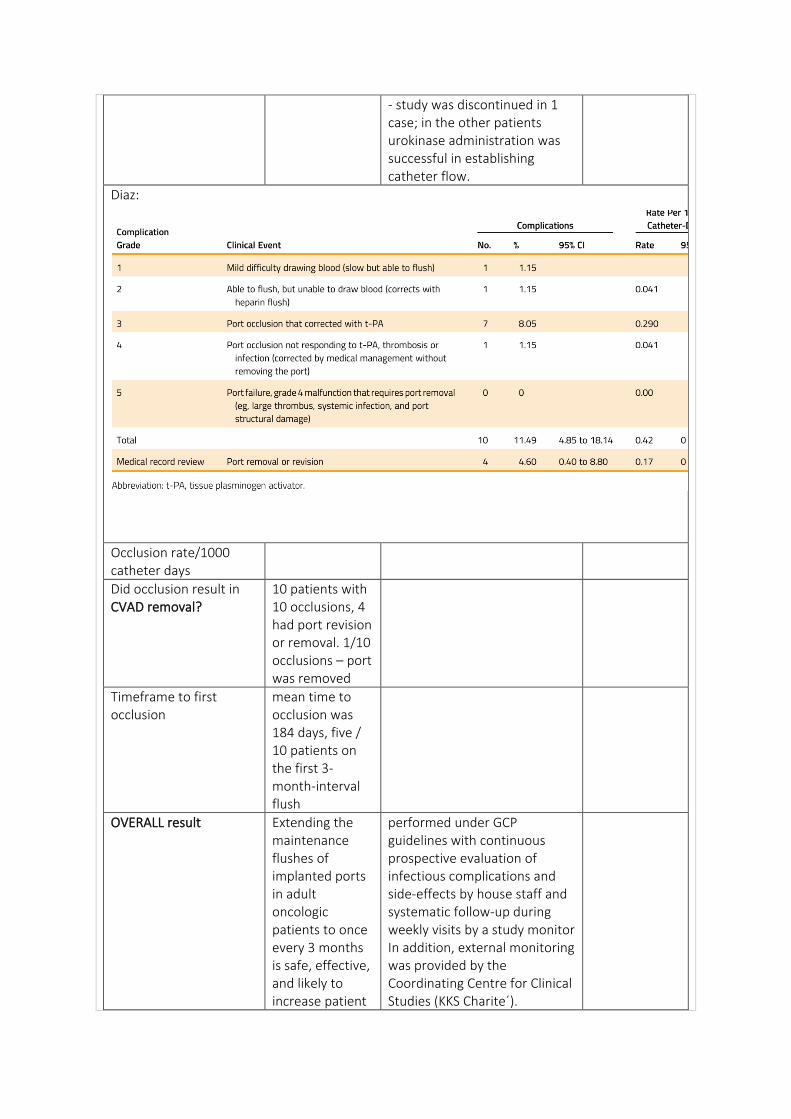
- study was discontinued in 1 case; in the other patients urokinase administration was successful in establishing catheter flow.
Diaz:
Occlusion rate/1000 catheter days
Did occlusion result in CVAD removal?
10 patients with 10 occlusions, 4 had port revision or removal. 1/10 occlusions – port was removed
Timeframe to first occlusion
mean time to occlusion was 184 days, five / 10 patients on the first 3-month-interval flush
OVERALL result Extending the maintenance flushes of implanted ports in adult oncologic patients to once every 3 months is safe, effective, and likely to increase patient
performed under GCP guidelines with continuous prospective evaluation of infectious complications and side-effects by house staff and systematic follow-up during weekly visits by a study monitor In addition, external monitoring was provided by the Coordinating Centre for Clinical Studies (KKS Charite´).
adherence and satisfaction while decreasing the associated cost
Thromboprophylaxis n= (%) median (range)
No n=67 Yes n=20, 23%
Patency – occlusion prevention CVAD
Education and competency requirement of staff – inserting and maintenance
Frequency of patency checked
How patency checked
Optimal flush frequency 3 monthly when not on treatment followed by lock
Optimal flush volume 10ml
Optimal flush technique Pulsatile flush with positive pressure clamping
Optimal lock solution 5 mL of heparin flush (100 units/mL)
group 1 - heparin lock solution (5000 IU heparin/0.2 mL; diluted to 100 IU heparin/mL sterile normal saline 0.9%); group 2, taurolidine lock solution (taurolidine 1.35%/sodium citrate 4%) All catheters were tagged with piece of colour tape to indicate group assignment
Heparin / sodium chloride– variance exists ports - monthly basis using heparinised sodium chloride
Optimal lock frequency locked with the appropriate filling volume. Lock solution was removed by aspiration without flushing
Does NC influence patency
Can take blood specimens through CVAD? NC?
Yes Yes – flush asap after
Patency – occlusion prevention PIV
How is patency checked?
What solution is used to flush and check patency
Occlusion management CVAD
Factors affecting occlusion rates: - type of cancer
- type of infusate
- age
- CVAD duration
- laterality
- number of lumens
- type of CVAD
- valve vs non-valved catheters
- BMI>25
Other patient comorbidities
Steps in assessment of occlusion
Intraluminal (thrombotic, drug/ infusate precipitation) or extraluminal (fibrin tail, fibrin sheath, mural, pressure applied externally to tissue overlying the VAD in a blood vessel)
Optimal management tissue plasminogen activator (t-PA; 2 mg/2 mL) was used if no blood return - repeated three times if necessary at 20- to 30-minute intervals - complications documented and graded on a scale of 1 – 5; grade 0, normal function; grade 1, mild difficulty drawing blood (slowbut able to flush); grade 2, able to flush but unable to draw blood (corrected
urokinase - pharmacist should be consulted re agents available to help dissolve precipitation - 0.1% hydrochloric acid – specific antibiotic occlusions (Bravery 1999) - 7% (sic) alcohol - occlusions resulting from lipids (Dougherty 2006) - thrombotic or fibrin - can perform a cathetergram
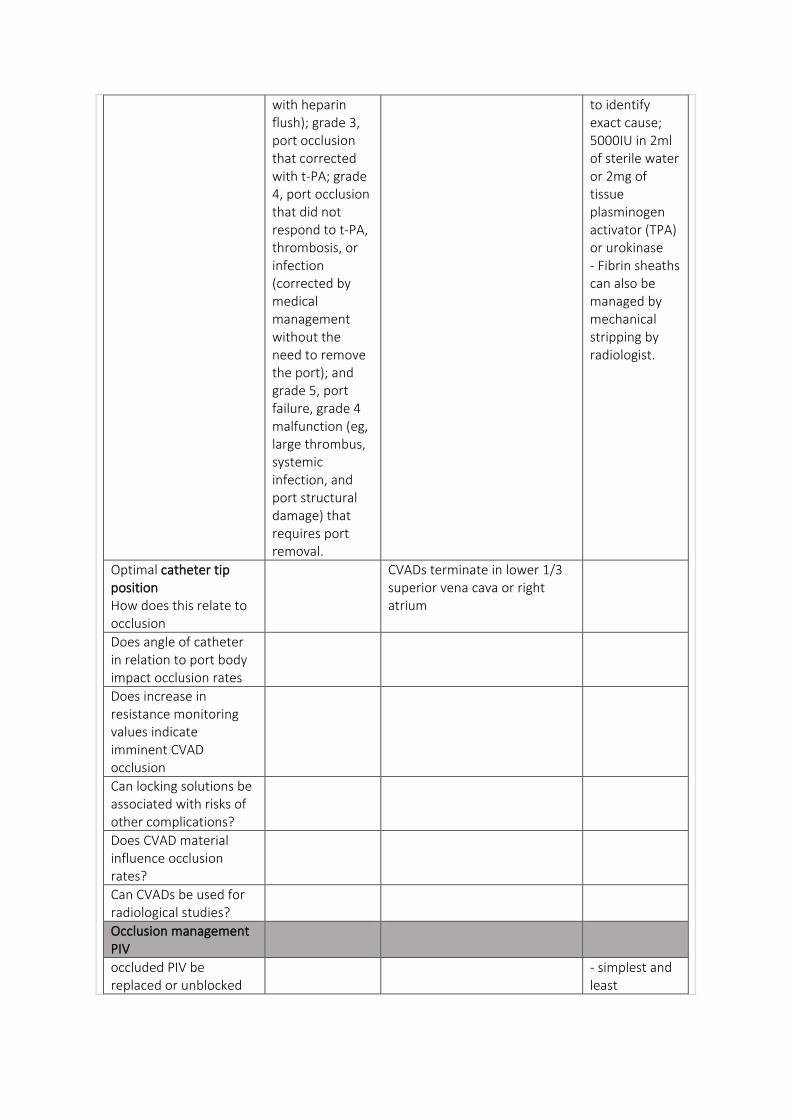
with heparin flush); grade 3, port occlusion that corrected with t-PA; grade 4, port occlusion that did not respond to t-PA, thrombosis, or infection (corrected by medical management without the need to remove the port); and grade 5, port failure, grade 4 malfunction (eg, large thrombus, systemic infection, and port structural damage) that requires port removal.
to identify exact cause; 5000IU in 2ml of sterile water or 2mg of tissue plasminogen activator (TPA) or urokinase - Fibrin sheaths can also be managed by mechanical stripping by radiologist.
Optimal catheter tip position How does this relate to occlusion
CVADs terminate in lower 1/3 superior vena cava or right atrium
Does angle of catheter in relation to port body impact occlusion rates
Does increase in resistance monitoring values indicate imminent CVAD occlusion
Can locking solutions be associated with risks of other complications?
Does CVAD material influence occlusion rates?
Can CVADs be used for radiological studies?
Occlusion management PIV
occluded PIV be replaced or unblocked
- simplest and least
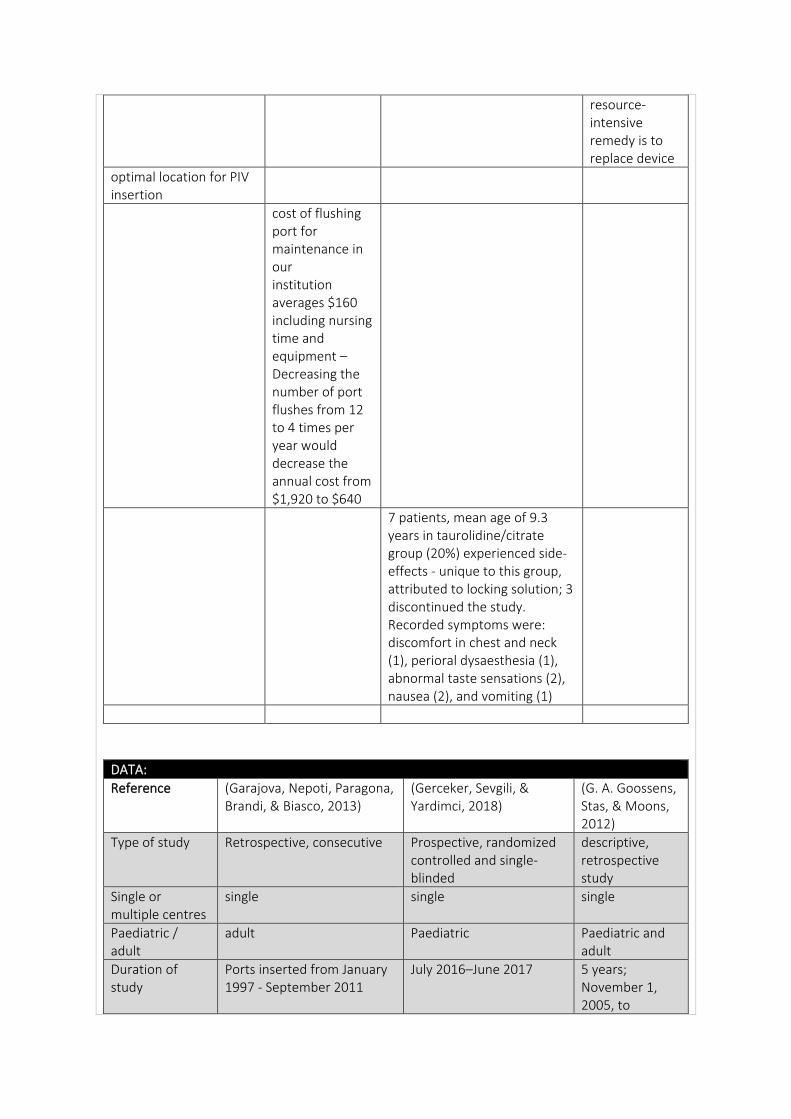
resource-intensive remedy is to replace device
optimal location for PIV insertion
cost of flushing port for maintenance in our institution averages $160 including nursing time and equipment – Decreasing the number of port flushes from 12 to 4 times per year would decrease the annual cost from $1,920 to $640
7 patients, mean age of 9.3 years in taurolidine/citrate group (20%) experienced side-effects - unique to this group, attributed to locking solution; 3 discontinued the study. Recorded symptoms were: discomfort in chest and neck (1), perioral dysaesthesia (1), abnormal taste sensations (2), nausea (2), and vomiting (1)
DATA:
Reference (Garajova, Nepoti, Paragona, Brandi, & Biasco, 2013)
(Gerceker, Sevgili, & Yardimci, 2018)
(G. A. Goossens, Stas, & Moons, 2012)
Type of study Retrospective, consecutive Prospective, randomized controlled and single-blinded
descriptive, retrospective study
Single or multiple centres
single single single
Paediatric / adult
adult Paediatric Paediatric and adult
Duration of study
Ports inserted from January 1997 - September 2011
July 2016–June 2017 5 years; November 1, 2005, to
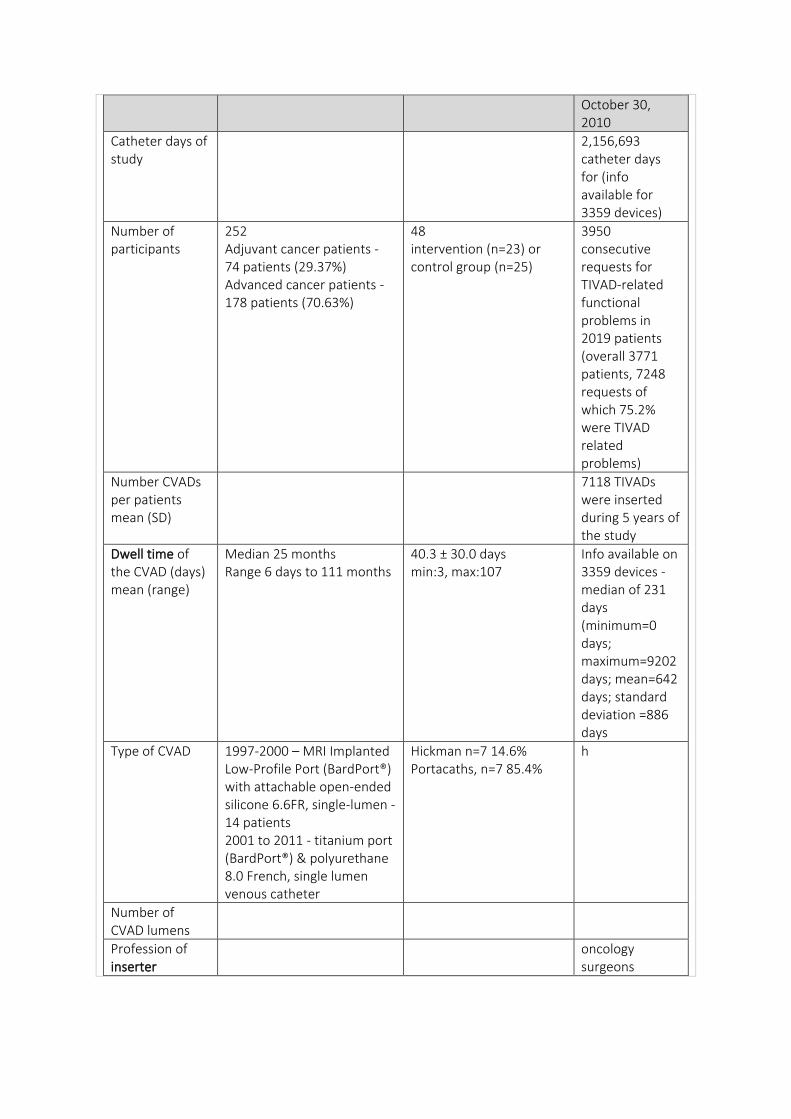
October 30, 2010
Catheter days of study
2,156,693 catheter days for (info available for 3359 devices)
Number of participants
252 Adjuvant cancer patients - 74 patients (29.37%) Advanced cancer patients - 178 patients (70.63%)
48 intervention (n=23) or control group (n=25)
3950 consecutive requests for TIVAD-related functional problems in 2019 patients (overall 3771 patients, 7248 requests of which 75.2% were TIVAD related problems)
Number CVADs per patients mean (SD)
7118 TIVADs were inserted during 5 years of the study
Dwell time of the CVAD (days) mean (range)
Median 25 months Range 6 days to 111 months
40.3 ± 30.0 days min:3, max:107
Info available on 3359 devices - median of 231 days (minimum=0 days; maximum=9202 days; mean=642 days; standard deviation =886 days
Type of CVAD 1997-2000 – MRI Implanted Low-Profile Port (BardPort®) with attachable open-ended silicone 6.6FR, single-lumen - 14 patients 2001 to 2011 - titanium port (BardPort®) & polyurethane 8.0 French, single lumen venous catheter
Hickman n=7 14.6% Portacaths, n=7 85.4%
h
Number of CVAD lumens
Profession of inserter
oncology surgeons
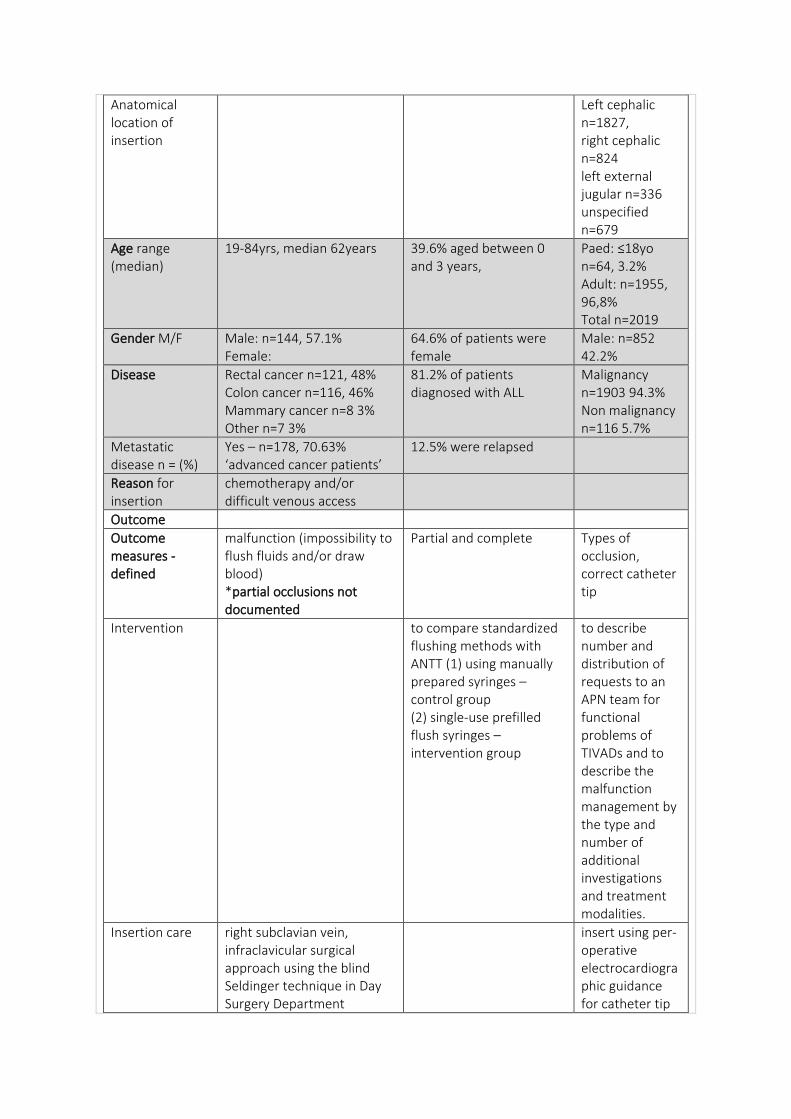
Anatomical location of insertion
Left cephalic n=1827, right cephalic n=824 left external jugular n=336 unspecified n=679
Age range (median)
19-84yrs, median 62years 39.6% aged between 0 and 3 years,
Paed: ≤18yo n=64, 3.2% Adult: n=1955, 96,8% Total n=2019
Gender M/F Male: n=144, 57.1% Female:
64.6% of patients were female
Male: n=852 42.2%
Disease Rectal cancer n=121, 48% Colon cancer n=116, 46% Mammary cancer n=8 3% Other n=7 3%
81.2% of patients diagnosed with ALL
Malignancy n=1903 94.3% Non malignancy n=116 5.7%
Metastatic disease n = (%)
Yes – n=178, 70.63% ‘advanced cancer patients’
12.5% were relapsed
Reason for insertion
chemotherapy and/or difficult venous access
Outcome
Outcome measures - defined
malfunction (impossibility to flush fluids and/or draw blood) *partial occlusions not documented
Partial and complete Types of occlusion, correct catheter tip
Intervention to compare standardized flushing methods with ANTT (1) using manually prepared syringes – control group (2) single-use prefilled flush syringes – intervention group
to describe number and distribution of requests to an APN team for functional problems of TIVADs and to describe the malfunction management by the type and number of additional investigations and treatment modalities.
Insertion care right subclavian vein, infraclavicular surgical approach using the blind Seldinger technique in Day Surgery Department
insert using per-operative electrocardiographic guidance for catheter tip
positioning in operating theatre
Maintenance care (dedicated CVAD team, ward staff or patient)
nurses working in onco-hematology wards - very skilled in caring and maintaining TIVADs and are trained to initiate measures to restore patency supported by five specialized nurses of the APN team and two oncology surgeons
Inclusion criteria
Exclusion criteria
Randomisation Gpower statistical program calculated the required sample size as 21 children in each group, 42 children in total at significance level of 0.05, 80% power, and large effect size. 48 patients who met the inclusion criteria were included
Healthcare setting
University hospital, Bologna Italy
Ege University Pediatric Hemato-oncology Unit - 17 beds, hemato-oncological malignancies, and majority - pediatric acute leukemia.
University Hospitals Leuven (UHL), Belgium,
Duration of follow up, lost to follow up
Catheter indwelling-time was calculated from insertion date to 1. 30 September 2011, 2. date of the patient’s death 3. date of catheter failure or 4. date of last visit
35 requests (0.9%), information on injection and/or aspiration abilities was not specified Missing data for 591 patients
RESULTS:
Complication rate
Adjuvant group: n=11, 14.86% incl. hypersensitivity reaction to heparin (1
highest number of requests (66.9%, n=2642)
patient, 1.35% - after 52 months of maintenance,), malfunction (1 patient, 0.39%) Advanced cancer group: n=11, 6.1% incl. malfunction (1 patient, 0.56%)
concerned ‘easy injection, but impossible blood aspiration’ - second highest (10.6%; n=416) was ‘impossible injection and aspiration’
Complication rate/1000 catheter days
Occlusion rate malfunction (1 patient, 0.39%)
Intervention
Control
Yes
n=2 8.7% n=5, 20%
Total (both groups) n=7, 14.6%
All occlusions occurred in ports
Malfunctions were accountable for 72.2% (n=3950) of all TIVAD-related problems requests - largest malfunction categories– injection was easy but blood aspiration was difficult or impossible (72.2% of all malfunctions)
Occlusion rate/1000 catheter days
1.9/1000 catheter days – intervention group 5.6/1000 per catheter-days- control group
Did occlusion result in CVAD removal?
All complications - Adjuvant patients n=4, 5.4% advanced cancer patients n=7, 3.9%
zero In 175 (4.4%) requests, TIVAD removal/exchange was advised. In 141 (80.6%) of these cases, malfunction was associated with suboptimal position or malposition of catheter tip, or with another complication
Timeframe to first occlusion
Adjuvant
Advanced
Median
0 7
Range 0-52 28d-24mth
OVERALL result using ANTT and pulsatile flushing with 10 mL NaCl once a day according to the literature compared manually prepared and single use pre-filled flush syringes - no difference of occlusion, however, statistically significant difference was found in CLABSI
Thromboprophylaxis n= (%) median (range)
Patency – occlusion prevention CVAD
Education and competency requirement of staff – inserting and maintenance
Flushing training for nurses - necessity, frequency, quality, and size of syringes to be used, ANTT and pulsatile flushing technique
Frequency of patency checked
How patency checked
Optimal flush frequency
flush of 10 ml of NS is used soon after accessing port, and prior to / after each blood sampling, at the end of each infusion therapy session - after packed cells or parenteral nutrition, 20 ml of NS is flushed
Optimal flush volume
Optimal flush technique
Pulsatile technique, 10ml syringe using 0.9% NaCl
10 ml of normal saline (NS) using pulsated flush method using a positive-pressure clamp technique
Optimal lock solution
heparinised saline (50 UI/5 ml) after each use
10 mL to avoid fibrin leftovers in the catheter lumen in cases such as blood draw and blood transfusion
3 ml heparinized saline (100 IU/ml) lock
Optimal lock frequency
heparin lock was changed every 30–40 days
Once/day prior to Huber needle removal and every 6 - 8 weeks with 10 ml of NS followed by a 3 ml heparinized saline lock (100 IU/ml).
Does NC influence patency
Can take blood specimens through CVAD? NC?
Patency – occlusion prevention PIV
How is patency checked?
What solution is used to flush and check patency
Occlusion management CVAD
Factors affecting occlusion rates: - type of cancer
statistically significant difference - any type of complications in adjuvant vs. advanced cancer patients (p = 0.04)
- type of infusate
At time of occlusion – 14.3% (n=1) of the patients had received TPN and 28.6% (n=2) had continuous infusion
- age
- CVAD duration
- laterality Left n=2624 right n=1314
- number of lumens
- type of CVAD
- valve vs non-valved catheters
- BMI>25
Other patient comorbidities
Reported elsewhere of DVT later in life due to frequent occlusions Journeycake, J.M., Buchanan, G.R., 2006. Catheter-related deep venous thrombosis and other catheter complications in children with cancer. J. Clin. Oncol. 24 (28), 4575–4580.
Steps in assessment of occlusion
Optimal management
urokinase - APN-team advises CXR as 1st investigation in malfunction management, a linogram only in limited cases to further detect the cause of malfunction - thrombolytics - in 41 (1.8%) cases, two study drugs were evaluated: alfimeprase (n=9) (Moll et al., 2006) and microplasmin (n=32) (Verhamme et al., 2009). In all other cases, urokinase 100,000 IU - lock or instillation consisted of 3 ml
(15,000 IU) and continuous infusion of 40,000 IU urokinase) was administered - thrombolytics given in 2332 (59.0%) requests for help for malfunction. lock was preferred method and applied in 1214 (52.1%) cases - Instillations were done in 754 (32.3%) cases. In 111 (14.7%) of these instillations, more than one instillation (with a maximum of 7) per call for help were used in an attempt to resolve the malfunction. - assume more effective thrombolytic treatment can be achieved with continuous infusion (40,000 IU over 1 hour) than with instillation or lock due to the short circulating half-life (two minutes) of urokinase - 0.7% of all requests involving malfunctions, products for dissolving drug
precipitates or lipid debris. In all but one case, these products were administered as a lock: sodium hydroxide 0.1 meq/L (n=13); ethanol 70% (n= 8); sodium bicarbonate 1 mg/ml (n= 4); and hydrochloric acid 0.1 M (n= 2) - we now substitute sodium hydroxide 0.1 meq/L to ethanol 70% when we suspect that a malfunction is caused by a combination of fibrin and lipid deposits (Bader et al., 2007). - line-o-grams: in total, in 4.9% (n=192) of requests a linogram was available. - top 3 of malfunction problems which led to linogram was difficult injection in combination (1) with impossible aspiration (11.9%), (2) with easy aspiration (8.1%) and (3) with difficult aspiration (7.8%).
- Proportionally, sleeve formation was found more frequently in case of aspiration problems (while injection was easy or difficult). - radiological findings - sleeve formation in 40.6% (n=78); a normal contrast jet in 26.0% (n= 50); a CTT in 7.8% (n=15); and a combination of sleeve and a CTT in 7.3% (n=14)
Optimal catheter tip position How does this relate to occlusion
After the device implantation, all patients had a chest radiographs to evaluate the correct position and perioperative complications
- catheters inserted through the SVC system- in the vicinity of the lower one-third of the SVC, near the juncture with the right atrium (RA) - catheters from the inferior vena cava system - at the level of the transition between the inferior vena cava and RA - devices inserted through the SVC, tip locations in the deep RA or the upper two-thirds of the SVC were considered suboptimal and tips located outside the SVC or RA were considered as
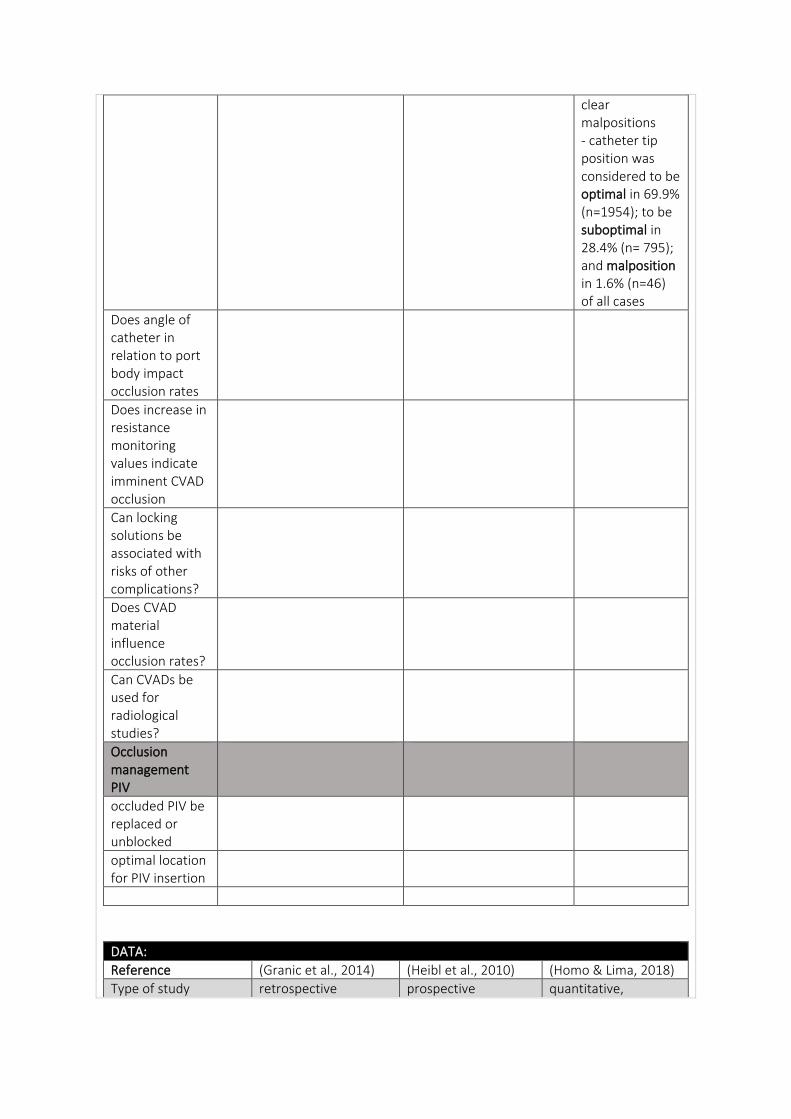
clear malpositions - catheter tip position was considered to be optimal in 69.9% (n=1954); to be suboptimal in 28.4% (n= 795); and malposition in 1.6% (n=46) of all cases
Does angle of catheter in relation to port body impact occlusion rates
Does increase in resistance monitoring values indicate imminent CVAD occlusion
Can locking solutions be associated with risks of other complications?
Does CVAD material influence occlusion rates?
Can CVADs be used for radiological studies?
Occlusion management PIV
occluded PIV be replaced or unblocked
optimal location for PIV insertion
DATA:
Reference (Granic et al., 2014) (Heibl et al., 2010) (Homo & Lima, 2018)
Type of study retrospective prospective quantitative,
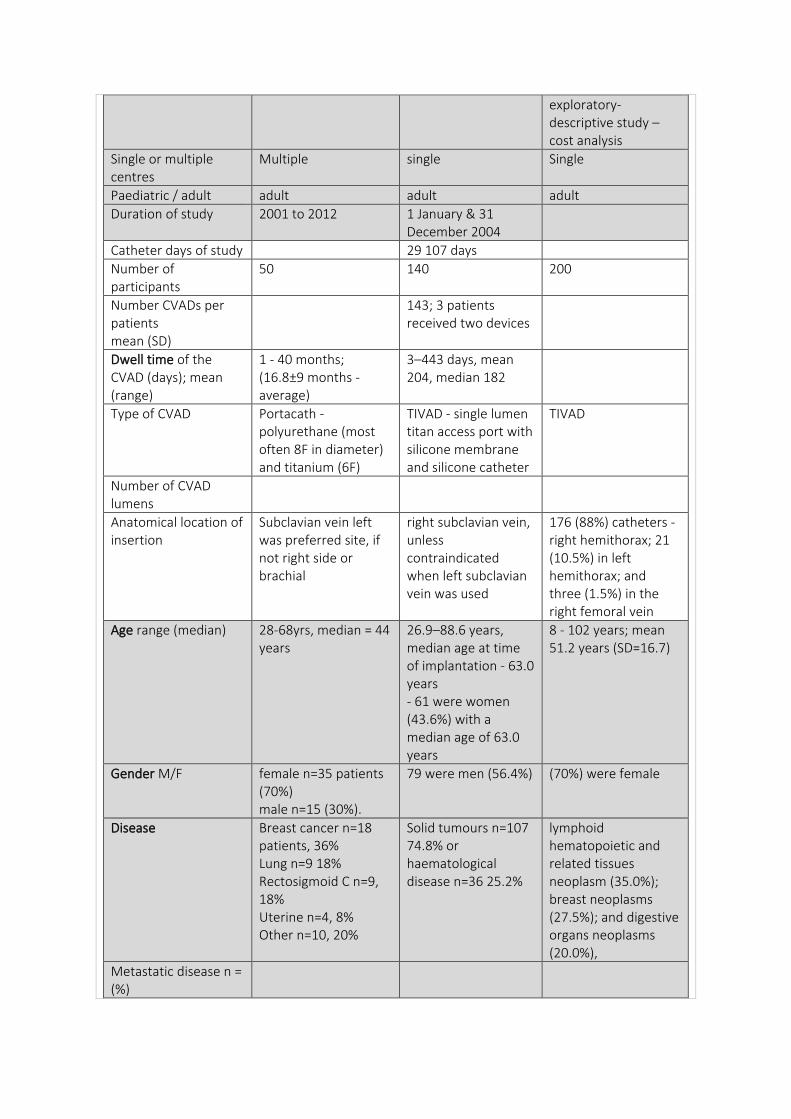
exploratory-descriptive study – cost analysis
Single or multiple centres
Multiple single Single
Paediatric / adult adult adult adult
Duration of study 2001 to 2012 1 January & 31 December 2004
Catheter days of study 29 107 days
Number of participants
50 140 200
Number CVADs per patients mean (SD)
143; 3 patients received two devices
Dwell time of the CVAD (days); mean (range)
1 - 40 months; (16.8±9 months - average)
3–443 days, mean 204, median 182
Type of CVAD Portacath - polyurethane (most often 8F in diameter) and titanium (6F)
TIVAD - single lumen titan access port with silicone membrane and silicone catheter
TIVAD
Number of CVAD lumens
Anatomical location of insertion
Subclavian vein left was preferred site, if not right side or brachial
right subclavian vein, unless contraindicated when left subclavian vein was used
176 (88%) catheters - right hemithorax; 21 (10.5%) in left hemithorax; and three (1.5%) in the right femoral vein
Age range (median) 28-68yrs, median = 44 years
26.9–88.6 years, median age at time of implantation - 63.0 years - 61 were women (43.6%) with a median age of 63.0 years
8 - 102 years; mean 51.2 years (SD=16.7)
Gender M/F female n=35 patients (70%) male n=15 (30%).
79 were men (56.4%) (70%) were female
Disease Breast cancer n=18 patients, 36% Lung n=9 18% Rectosigmoid C n=9, 18% Uterine n=4, 8% Other n=10, 20%
Solid tumours n=107 74.8% or haematological disease n=36 25.2%
lymphoid hematopoietic and related tissues neoplasm (35.0%); breast neoplasms (27.5%); and digestive organs neoplasms (20.0%),
Metastatic disease n = (%)
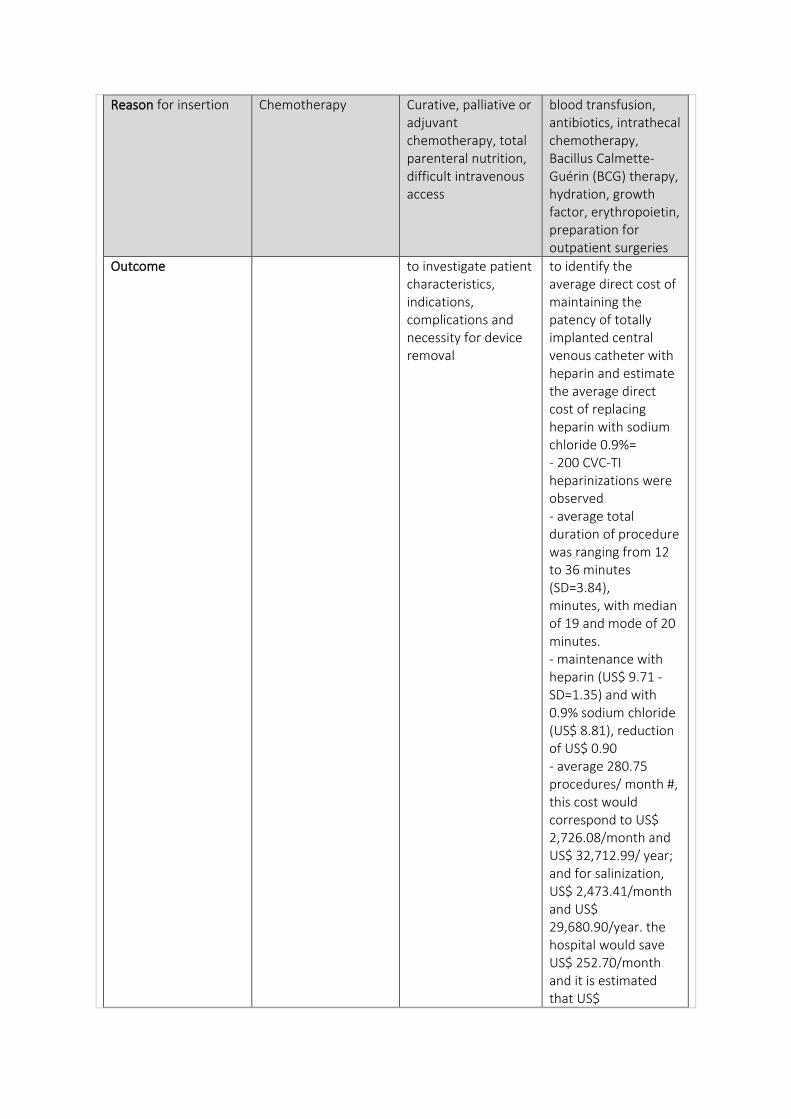
Reason for insertion Chemotherapy Curative, palliative or adjuvant chemotherapy, total parenteral nutrition, difficult intravenous access
blood transfusion, antibiotics, intrathecal chemotherapy, Bacillus Calmette-Guérin (BCG) therapy, hydration, growth factor, erythropoietin, preparation for outpatient surgeries
Outcome to investigate patient characteristics, indications, complications and necessity for device removal
to identify the average direct cost of maintaining the patency of totally implanted central venous catheter with heparin and estimate the average direct cost of replacing heparin with sodium chloride 0.9%= - 200 CVC-TI heparinizations were observed - average total duration of procedure was ranging from 12 to 36 minutes (SD=3.84), minutes, with median of 19 and mode of 20 minutes. - maintenance with heparin (US$ 9.71 - SD=1.35) and with 0.9% sodium chloride (US$ 8.81), reduction of US$ 0.90 - average 280.75 procedures/ month #, this cost would correspond to US$ 2,726.08/month and US$ 32,712.99/ year; and for salinization, US$ 2,473.41/month and US$ 29,680.90/year. the hospital would save US$ 252.70/month and it is estimated that US$
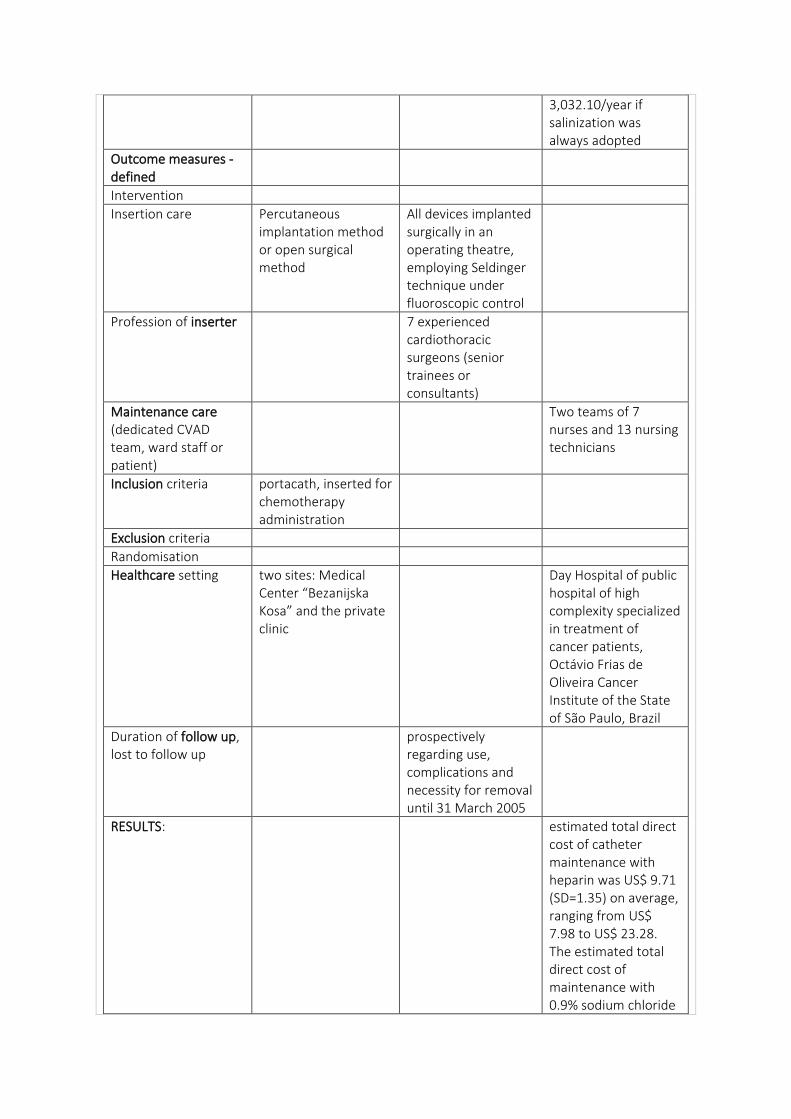
3,032.10/year if salinization was always adopted
Outcome measures - defined
Intervention
Insertion care Percutaneous implantation method or open surgical method
All devices implanted surgically in an operating theatre, employing Seldinger technique under fluoroscopic control
Profession of inserter 7 experienced cardiothoracic surgeons (senior trainees or consultants)
Maintenance care (dedicated CVAD team, ward staff or patient)
Two teams of 7 nurses and 13 nursing technicians
Inclusion criteria portacath, inserted for chemotherapy administration
Exclusion criteria
Randomisation
Healthcare setting two sites: Medical Center “Bezanijska Kosa” and the private clinic
Day Hospital of public hospital of high complexity specialized in treatment of cancer patients, Octávio Frias de Oliveira Cancer Institute of the State of São Paulo, Brazil
Duration of follow up, lost to follow up
prospectively regarding use, complications and necessity for removal until 31 March 2005
RESULTS: estimated total direct cost of catheter maintenance with heparin was US$ 9.71 (SD=1.35) on average, ranging from US$ 7.98 to US$ 23.28. The estimated total direct cost of maintenance with 0.9% sodium chloride
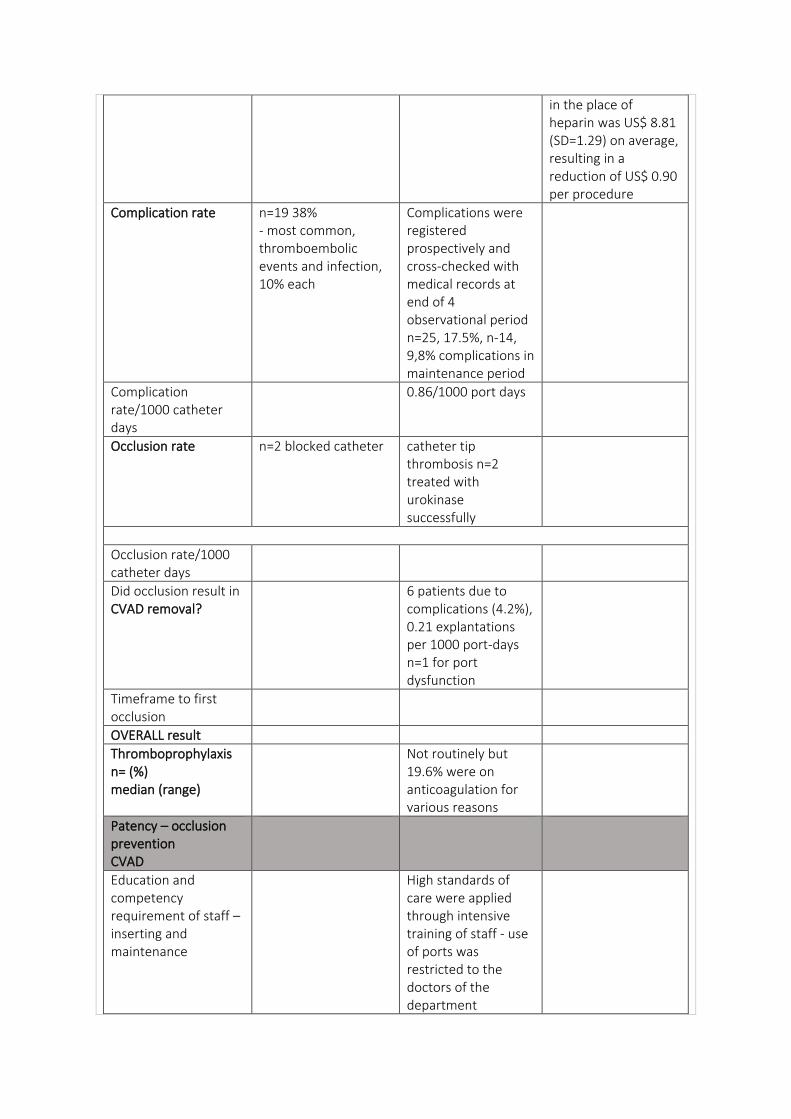
in the place of heparin was US$ 8.81 (SD=1.29) on average, resulting in a reduction of US$ 0.90 per procedure
Complication rate n=19 38% - most common, thromboembolic events and infection, 10% each
Complications were registered prospectively and cross-checked with medical records at end of 4 observational period n=25, 17.5%, n-14, 9,8% complications in maintenance period
Complication rate/1000 catheter days
0.86/1000 port days
Occlusion rate n=2 blocked catheter catheter tip thrombosis n=2 treated with urokinase successfully
Occlusion rate/1000 catheter days
Did occlusion result in CVAD removal?
6 patients due to complications (4.2%), 0.21 explantations per 1000 port-days n=1 for port dysfunction
Timeframe to first occlusion
OVERALL result
Thromboprophylaxis n= (%) median (range)
Not routinely but 19.6% were on anticoagulation for various reasons
Patency – occlusion prevention CVAD
Education and competency requirement of staff – inserting and maintenance
High standards of care were applied through intensive training of staff - use of ports was restricted to the doctors of the department
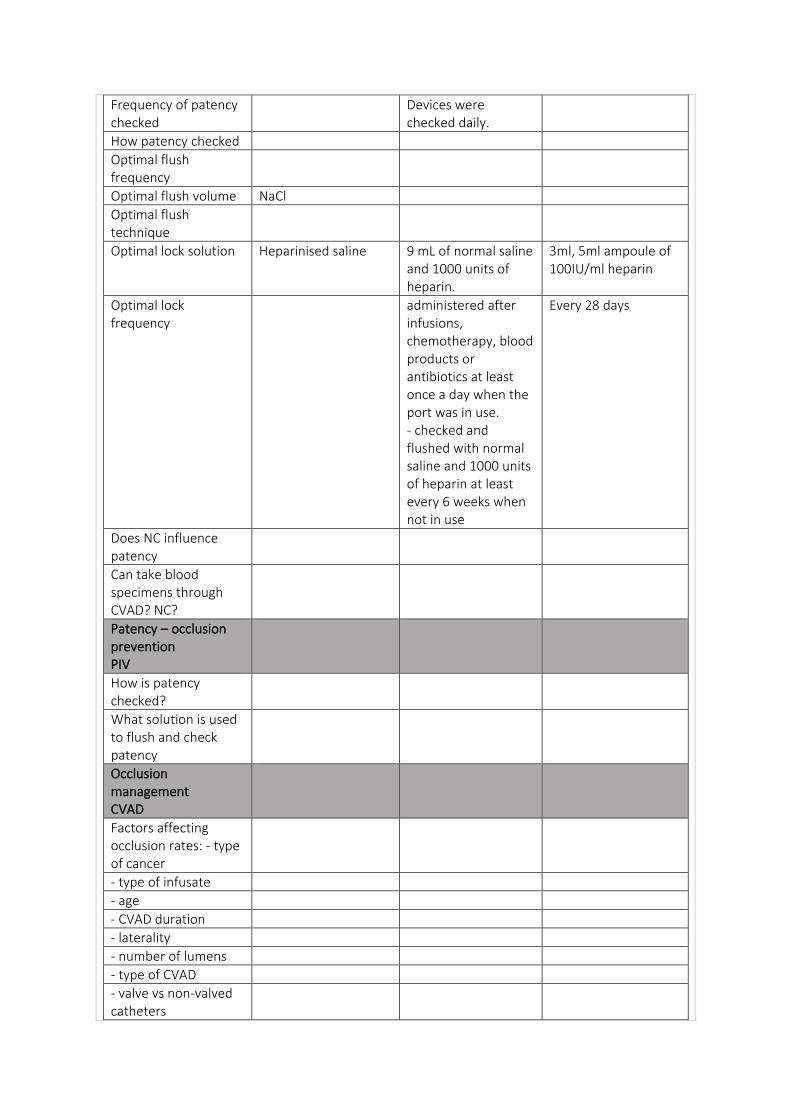
Frequency of patency checked
Devices were checked daily.
How patency checked
Optimal flush frequency
Optimal flush volume NaCl
Optimal flush technique
Optimal lock solution Heparinised saline 9 mL of normal saline and 1000 units of heparin.
3ml, 5ml ampoule of 100IU/ml heparin
Optimal lock frequency
administered after infusions, chemotherapy, blood products or antibiotics at least once a day when the port was in use. - checked and flushed with normal saline and 1000 units of heparin at least every 6 weeks when not in use
Every 28 days
Does NC influence patency
Can take blood specimens through CVAD? NC?
Patency – occlusion prevention PIV
How is patency checked?
What solution is used to flush and check patency
Occlusion management CVAD
Factors affecting occlusion rates: - type of cancer
- type of infusate
- age
- CVAD duration
- laterality
- number of lumens
- type of CVAD
- valve vs non-valved catheters
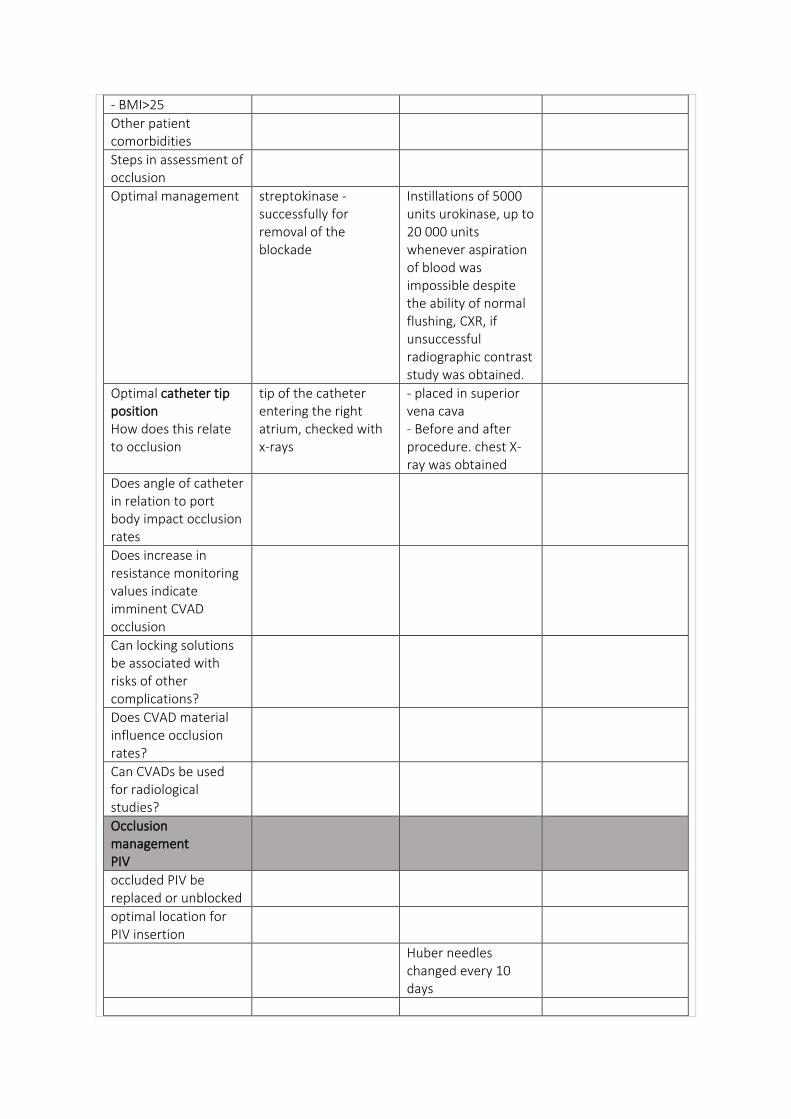
- BMI>25
Other patient comorbidities
Steps in assessment of occlusion
Optimal management streptokinase - successfully for removal of the blockade
Instillations of 5000 units urokinase, up to 20 000 units whenever aspiration of blood was impossible despite the ability of normal flushing, CXR, if unsuccessful radiographic contrast study was obtained.
Optimal catheter tip position How does this relate to occlusion
tip of the catheter entering the right atrium, checked with x-rays
- placed in superior vena cava - Before and after procedure. chest X-ray was obtained
Does angle of catheter in relation to port body impact occlusion rates
Does increase in resistance monitoring values indicate imminent CVAD occlusion
Can locking solutions be associated with risks of other complications?
Does CVAD material influence occlusion rates?
Can CVADs be used for radiological studies?
Occlusion management PIV
occluded PIV be replaced or unblocked
optimal location for PIV insertion
Huber needles changed every 10 days
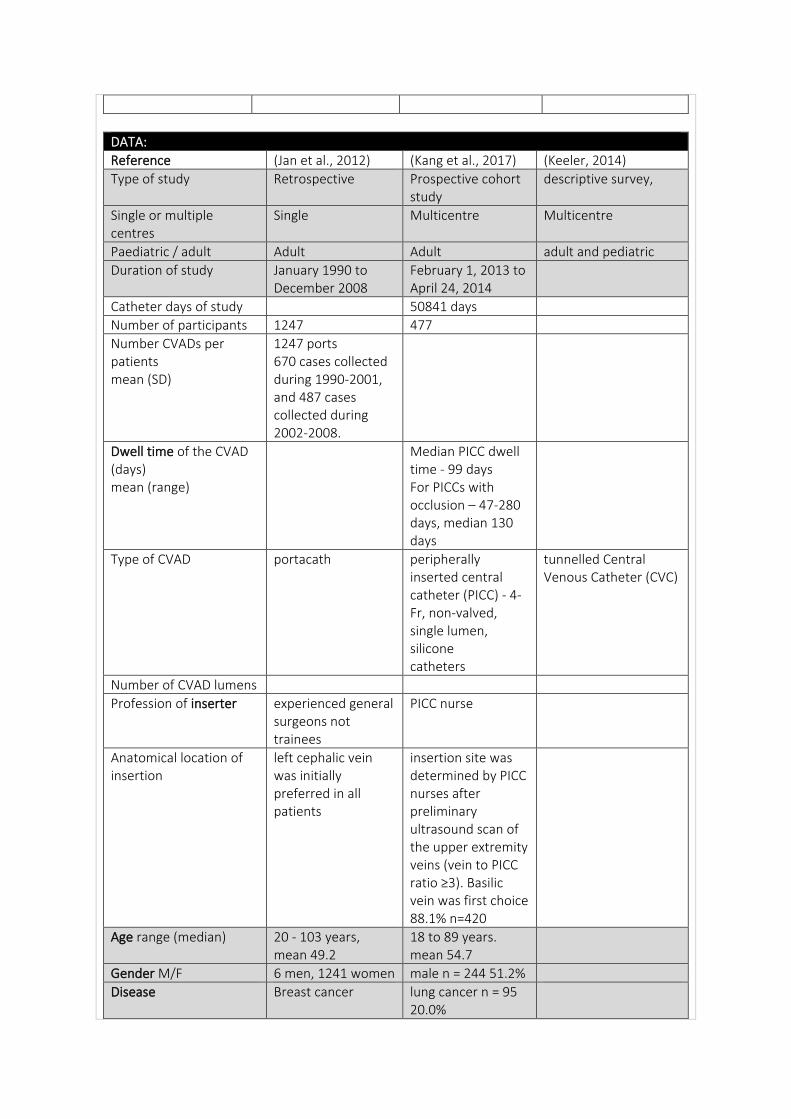
DATA:
Reference (Jan et al., 2012) (Kang et al., 2017) (Keeler, 2014)
Type of study Retrospective Prospective cohort study
descriptive survey,
Single or multiple centres
Single Multicentre Multicentre
Paediatric / adult Adult Adult adult and pediatric
Duration of study January 1990 to December 2008
February 1, 2013 to April 24, 2014
Catheter days of study 50841 days
Number of participants 1247 477
Number CVADs per patients mean (SD)
1247 ports 670 cases collected during 1990-2001, and 487 cases collected during 2002-2008.
Dwell time of the CVAD (days) mean (range)
Median PICC dwell time - 99 days For PICCs with occlusion – 47-280 days, median 130 days
Type of CVAD portacath peripherally inserted central catheter (PICC) - 4-Fr, non-valved, single lumen, silicone catheters
tunnelled Central Venous Catheter (CVC)
Number of CVAD lumens
Profession of inserter experienced general surgeons not trainees
PICC nurse
Anatomical location of insertion
left cephalic vein was initially preferred in all patients
insertion site was determined by PICC nurses after preliminary ultrasound scan of the upper extremity veins (vein to PICC ratio ≥3). Basilic vein was first choice 88.1% n=420
Age range (median) 20 - 103 years, mean 49.2
18 to 89 years. mean 54.7
Gender M/F 6 men, 1241 women male n = 244 51.2%
Disease Breast cancer lung cancer n = 95 20.0%
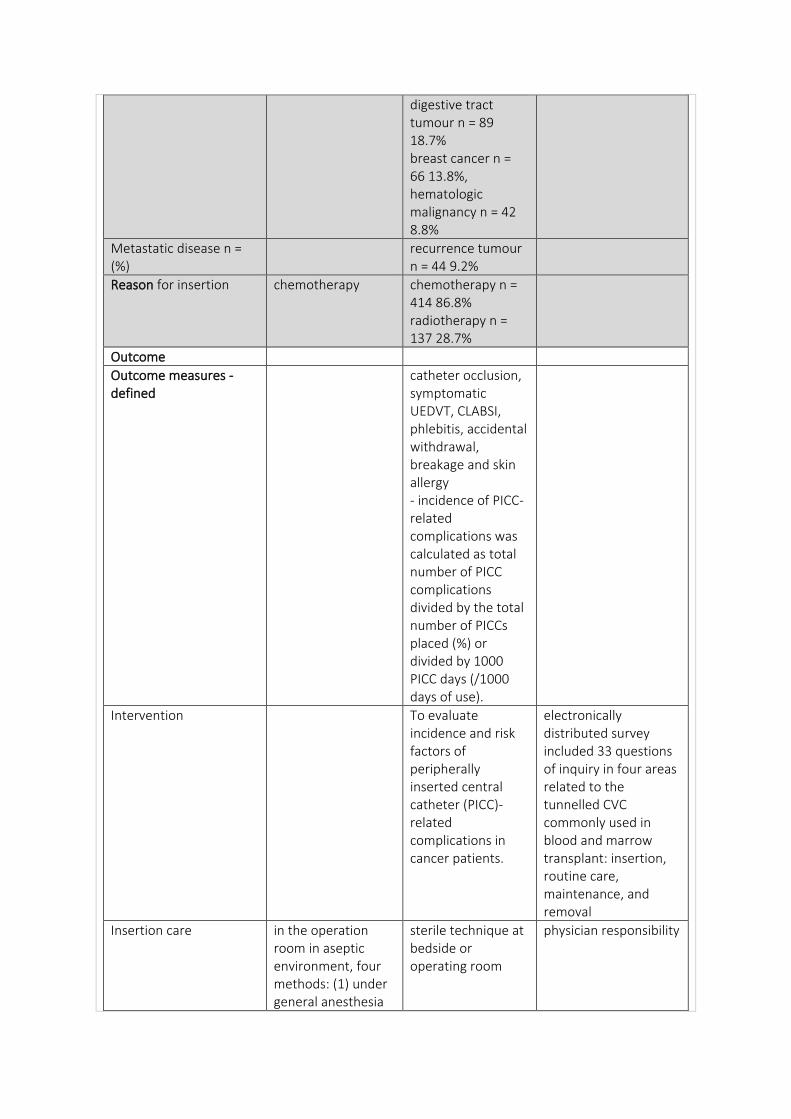
digestive tract tumour n = 89 18.7% breast cancer n = 66 13.8%, hematologic malignancy n = 42 8.8%
Metastatic disease n = (%)
recurrence tumour n = 44 9.2%
Reason for insertion chemotherapy chemotherapy n = 414 86.8% radiotherapy n = 137 28.7%
Outcome
Outcome measures - defined
catheter occlusion, symptomatic UEDVT, CLABSI, phlebitis, accidental withdrawal, breakage and skin allergy - incidence of PICC-related complications was calculated as total number of PICC complications divided by the total number of PICCs placed (%) or divided by 1000 PICC days (/1000 days of use).
Intervention To evaluate incidence and risk factors of peripherally inserted central catheter (PICC)-related complications in cancer patients.
electronically distributed survey included 33 questions of inquiry in four areas related to the tunnelled CVC commonly used in blood and marrow transplant: insertion, routine care, maintenance, and removal
Insertion care in the operation room in aseptic environment, four methods: (1) under general anesthesia
sterile technique at bedside or operating room
physician responsibility
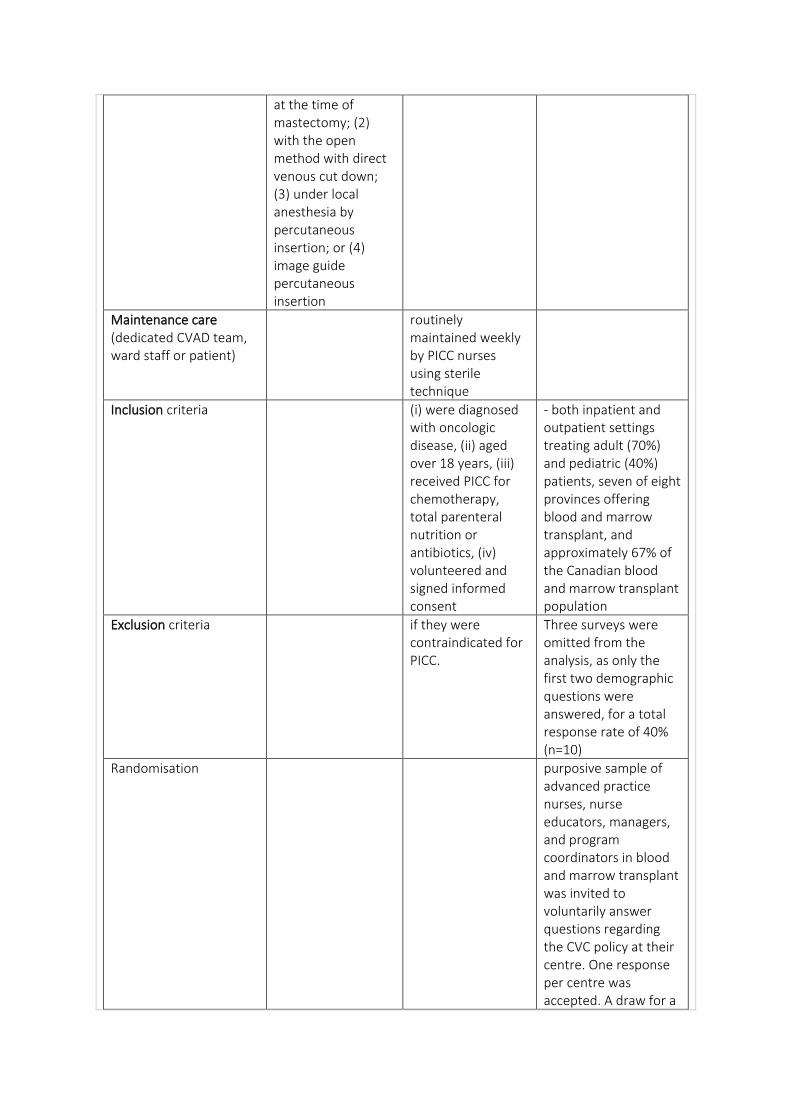
at the time of mastectomy; (2) with the open method with direct venous cut down; (3) under local anesthesia by percutaneous insertion; or (4) image guide percutaneous insertion
Maintenance care (dedicated CVAD team, ward staff or patient)
routinely maintained weekly by PICC nurses using sterile technique
Inclusion criteria (i) were diagnosed with oncologic disease, (ii) aged over 18 years, (iii) received PICC for chemotherapy, total parenteral nutrition or antibiotics, (iv) volunteered and signed informed consent
- both inpatient and outpatient settings treating adult (70%) and pediatric (40%) patients, seven of eight provinces offering blood and marrow transplant, and approximately 67% of the Canadian blood and marrow transplant population
Exclusion criteria if they were contraindicated for PICC.
Three surveys were omitted from the analysis, as only the first two demographic questions were answered, for a total response rate of 40% (n=10)
Randomisation purposive sample of advanced practice nurses, nurse educators, managers, and program coordinators in blood and marrow transplant was invited to voluntarily answer questions regarding the CVC policy at their centre. One response per centre was accepted. A draw for a
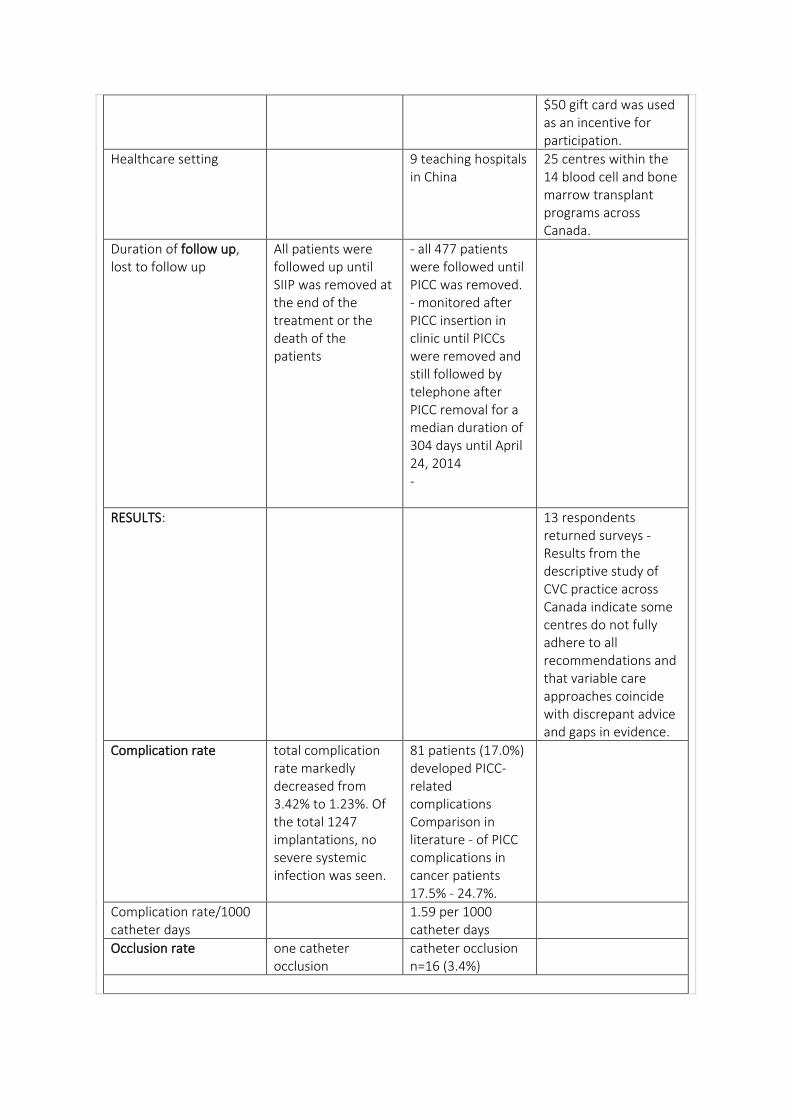
$50 gift card was used as an incentive for participation.
Healthcare setting 9 teaching hospitals in China
25 centres within the 14 blood cell and bone marrow transplant programs across Canada.
Duration of follow up, lost to follow up
All patients were followed up until SIIP was removed at the end of the treatment or the death of the patients
- all 477 patients were followed until PICC was removed. - monitored after PICC insertion in clinic until PICCs were removed and still followed by telephone after PICC removal for a median duration of 304 days until April 24, 2014 -
RESULTS: 13 respondents returned surveys - Results from the descriptive study of CVC practice across Canada indicate some centres do not fully adhere to all recommendations and that variable care approaches coincide with discrepant advice and gaps in evidence.
Complication rate total complication rate markedly decreased from 3.42% to 1.23%. Of the total 1247 implantations, no severe systemic infection was seen.
81 patients (17.0%) developed PICC-related complications Comparison in literature - of PICC complications in cancer patients 17.5% - 24.7%.
Complication rate/1000 catheter days
1.59 per 1000 catheter days
Occlusion rate one catheter occlusion
catheter occlusion n=16 (3.4%)
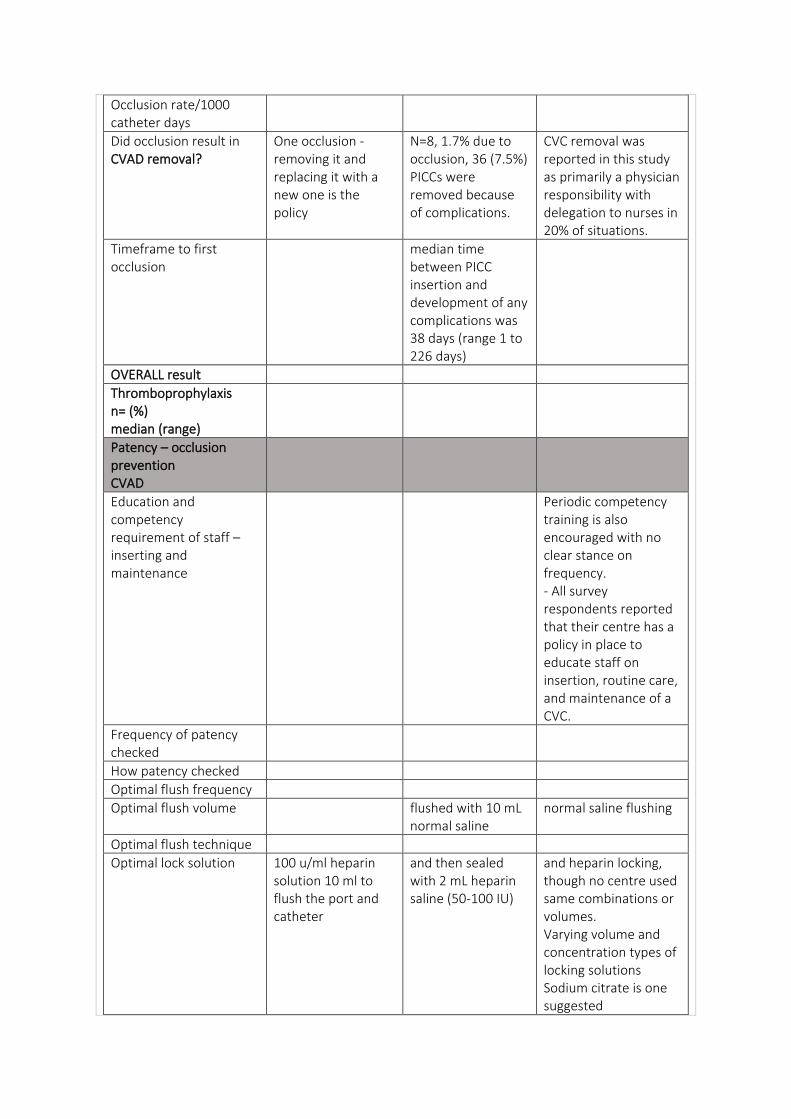
Occlusion rate/1000 catheter days
Did occlusion result in CVAD removal?
One occlusion - removing it and replacing it with a new one is the policy
N=8, 1.7% due to occlusion, 36 (7.5%) PICCs were removed because of complications.
CVC removal was reported in this study as primarily a physician responsibility with delegation to nurses in 20% of situations.
Timeframe to first occlusion
median time between PICC insertion and development of any complications was 38 days (range 1 to 226 days)
OVERALL result
Thromboprophylaxis n= (%) median (range)
Patency – occlusion prevention CVAD
Education and competency requirement of staff – inserting and maintenance
Periodic competency training is also encouraged with no clear stance on frequency. - All survey respondents reported that their centre has a policy in place to educate staff on insertion, routine care, and maintenance of a CVC.
Frequency of patency checked
How patency checked
Optimal flush frequency
Optimal flush volume flushed with 10 mL normal saline
normal saline flushing
Optimal flush technique
Optimal lock solution 100 u/ml heparin solution 10 ml to flush the port and catheter
and then sealed with 2 mL heparin saline (50-100 IU)
and heparin locking, though no centre used same combinations or volumes. Varying volume and concentration types of locking solutions Sodium citrate is one suggested
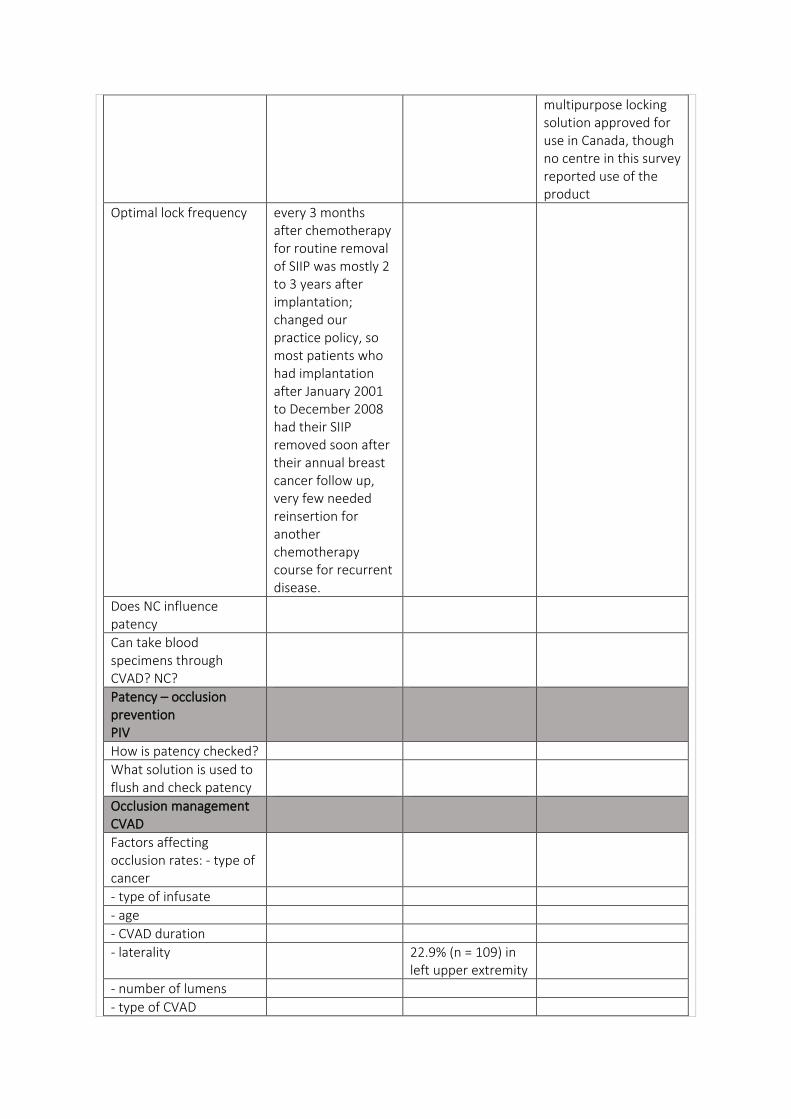
multipurpose locking solution approved for use in Canada, though no centre in this survey reported use of the product
Optimal lock frequency every 3 months after chemotherapy for routine removal of SIIP was mostly 2 to 3 years after implantation; changed our practice policy, so most patients who had implantation after January 2001 to December 2008 had their SIIP removed soon after their annual breast cancer follow up, very few needed reinsertion for another chemotherapy course for recurrent disease.
Does NC influence patency
Can take blood specimens through CVAD? NC?
Patency – occlusion prevention PIV
How is patency checked?
What solution is used to flush and check patency
Occlusion management CVAD
Factors affecting occlusion rates: - type of cancer
- type of infusate
- age
- CVAD duration
- laterality 22.9% (n = 109) in left upper extremity
- number of lumens
- type of CVAD
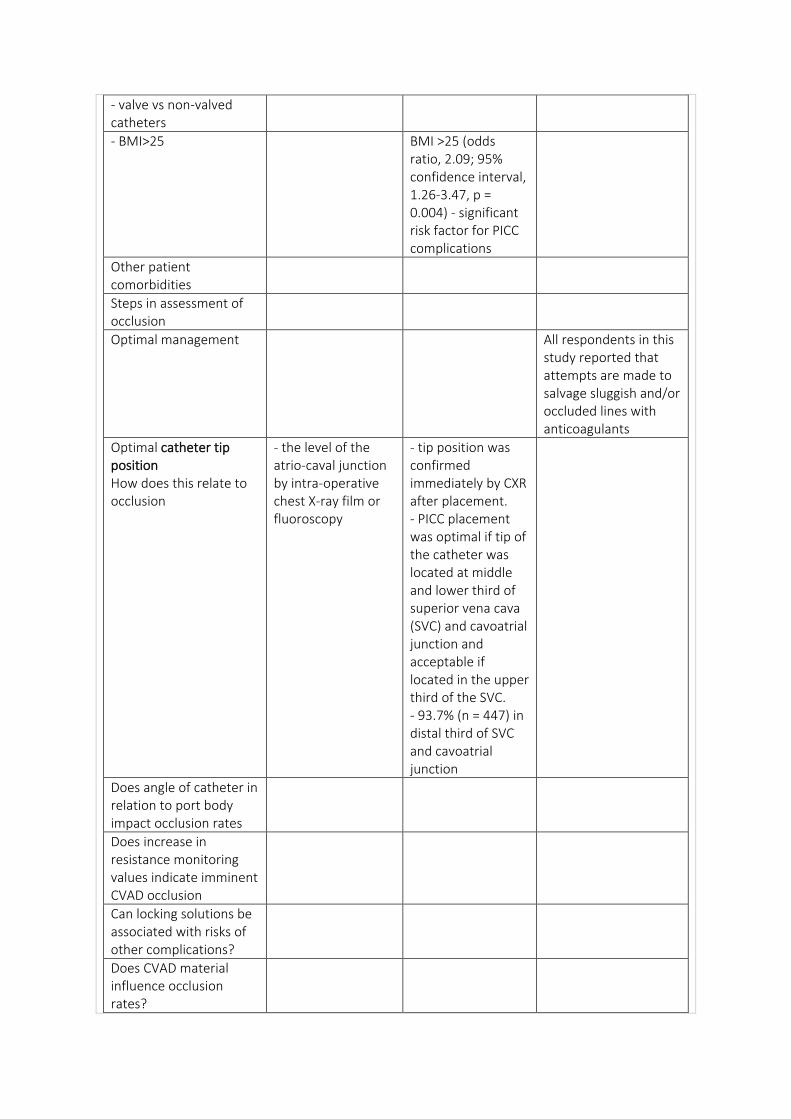
- valve vs non-valved catheters
- BMI>25 BMI >25 (odds ratio, 2.09; 95% confidence interval, 1.26-3.47, p = 0.004) - significant risk factor for PICC complications
Other patient comorbidities
Steps in assessment of occlusion
Optimal management All respondents in this study reported that attempts are made to salvage sluggish and/or occluded lines with anticoagulants
Optimal catheter tip position How does this relate to occlusion
- the level of the atrio-caval junction by intra-operative chest X-ray film or fluoroscopy
- tip position was confirmed immediately by CXR after placement. - PICC placement was optimal if tip of the catheter was located at middle and lower third of superior vena cava (SVC) and cavoatrial junction and acceptable if located in the upper third of the SVC. - 93.7% (n = 447) in distal third of SVC and cavoatrial junction
Does angle of catheter in relation to port body impact occlusion rates
Does increase in resistance monitoring values indicate imminent CVAD occlusion
Can locking solutions be associated with risks of other complications?
Does CVAD material influence occlusion rates?
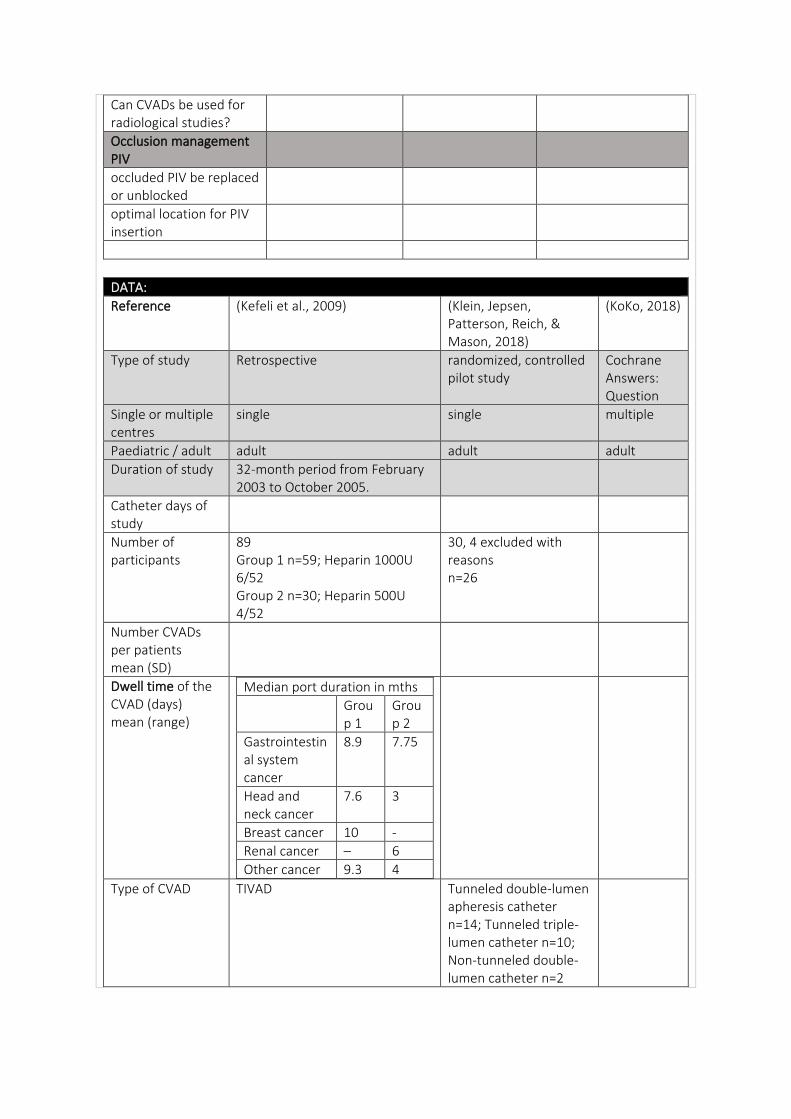
Can CVADs be used for radiological studies?
Occlusion management PIV
occluded PIV be replaced or unblocked
optimal location for PIV insertion
DATA:
Reference (Kefeli et al., 2009) (Klein, Jepsen, Patterson, Reich, & Mason, 2018)
(KoKo, 2018)
Type of study Retrospective randomized, controlled pilot study
Cochrane Answers: Question
Single or multiple centres
single single multiple
Paediatric / adult adult adult adult
Duration of study 32-month period from February 2003 to October 2005.
Catheter days of study
Number of participants
89 Group 1 n=59; Heparin 1000U 6/52 Group 2 n=30; Heparin 500U 4/52
30, 4 excluded with reasons n=26
Number CVADs per patients mean (SD)
Dwell time of the CVAD (days) mean (range)
Median port duration in mths
Group 1
Group 2
Gastrointestinal system cancer
8.9
7.75
Head and neck cancer
7.6 3
Breast cancer 10 -
Renal cancer – 6
Other cancer 9.3 4
Type of CVAD TIVAD Tunneled double-lumen apheresis catheter n=14; Tunneled triple-lumen catheter n=10; Non-tunneled double-lumen catheter n=2
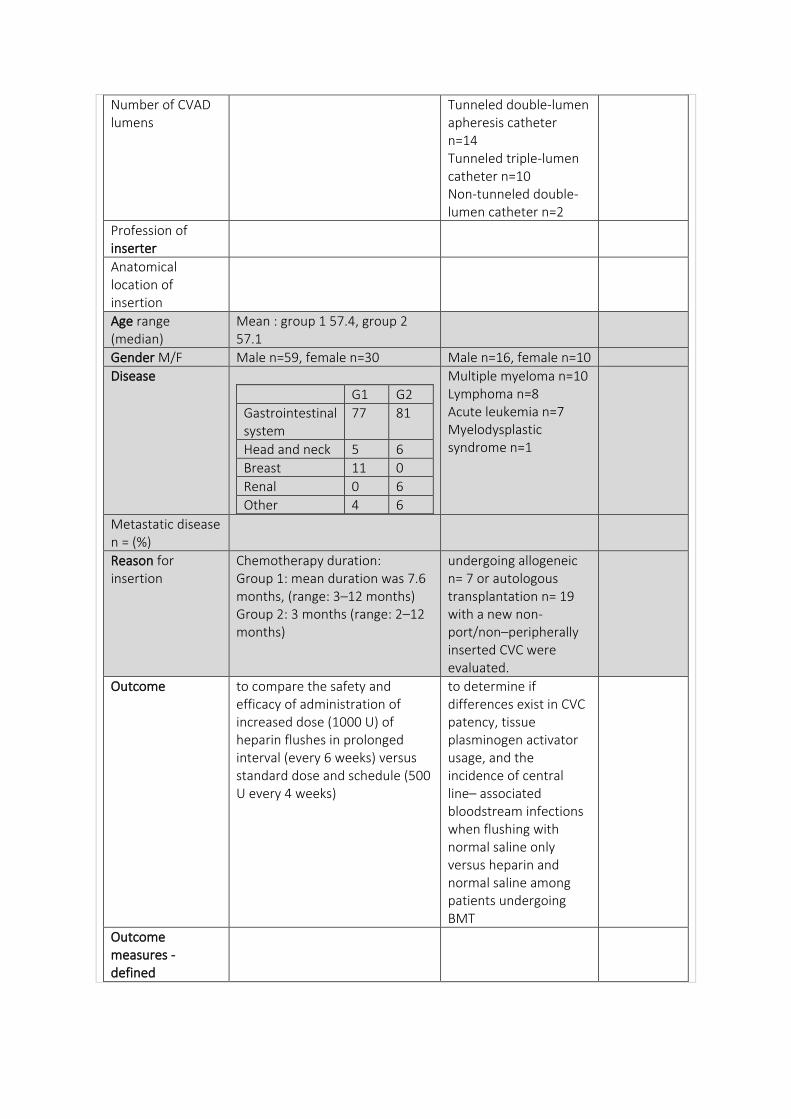
Number of CVAD lumens
Tunneled double-lumen apheresis catheter n=14 Tunneled triple-lumen catheter n=10 Non-tunneled double-lumen catheter n=2
Profession of inserter
Anatomical location of insertion
Age range (median)
Mean : group 1 57.4, group 2 57.1
Gender M/F Male n=59, female n=30 Male n=16, female n=10
Disease
G1 G2
Gastrointestinal system
77
81
Head and neck 5 6
Breast 11 0
Renal 0 6
Other 4 6
Multiple myeloma n=10 Lymphoma n=8 Acute leukemia n=7 Myelodysplastic syndrome n=1
Metastatic disease n = (%)
Reason for insertion
Chemotherapy duration: Group 1: mean duration was 7.6 months, (range: 3–12 months) Group 2: 3 months (range: 2–12 months)
undergoing allogeneic n= 7 or autologous transplantation n= 19 with a new non-port/non–peripherally inserted CVC were evaluated.
Outcome to compare the safety and efficacy of administration of increased dose (1000 U) of heparin flushes in prolonged interval (every 6 weeks) versus standard dose and schedule (500 U every 4 weeks)
to determine if differences exist in CVC patency, tissue plasminogen activator usage, and the incidence of central line– associated bloodstream infections when flushing with normal saline only versus heparin and normal saline among patients undergoing BMT
Outcome measures - defined
Intervention During active chemotherapy, all patients received 500 U of heparin flushes. After completing chemotherapy: Group 1: 59 patients received 1000 U of heparin flushes in 3 ml of normal saline in every 6 weeks Group 2: 30 patients administered 500 U of heparin in 3.5 ml of normal saline in every 4 weeks
Insertion care
Maintenance care (dedicated CVAD team, ward staff or patient)
received regular port care by same group of trained oncology nurses according to clinic’s standard regulations
Inclusion criteria Solid tumours - undergoing BMT and had newly placed central lines, including tunneled double-lumen apheresis catheters, tunneled triple-lumen catheters, and non-tunneled double-lumen catheters, that had been placed at the Moffitt Cancer Center.
Adults with central venous catheters inserted for a range of conditions (chronic kidney disease [2 RCTs], cancer [2 RCTs], in intensive care [ICU] for respiratory disorders [1 RCT] or for a range of disorders [4 RCTs], or not reported [2 RCTs])
Exclusion criteria - patients taking oral anticoagulants or patients having contraindications for heparin usage
- peripherally inserted central lines, implanted ports, and lines placed at an outside facility. - if patient was readmitted to a unit other than the BMT unit, or if a patient was transferred from the BMT unit to another unit, such as the
intensive care unit, the patient no longer qualified to participate in the research study.
Randomisation convenience sample; assigned to groups using block randomization of six blocks to receive either standard of care or normal saline–only flushing. 15 in each group
Healthcare setting 36-bed BMT unit and outpatient BMT treatment center at H. Lee Moffitt Cancer Center and Research Institute, Tampa, Florida USA
Duration of follow up, lost to follow up
followed regularly for clinical signs of thrombosis and central venous port-related infections for at least 3 months.
remained in the study for 90 days post-transplantation or until CVC line was removed
RESULTS:
Complication rate no clinically documented port-related infection or thrombosis has been found among these two groups. Also, none of the devices were removed during this time
Complication rate/1000 catheter days
Occlusion rate rates of line problems were similar between flushing with heparin and normal saline (8.8%) and with normal saline (8.5%) (p = 0.88) These rates did not change at the patient level (p = 0.95).
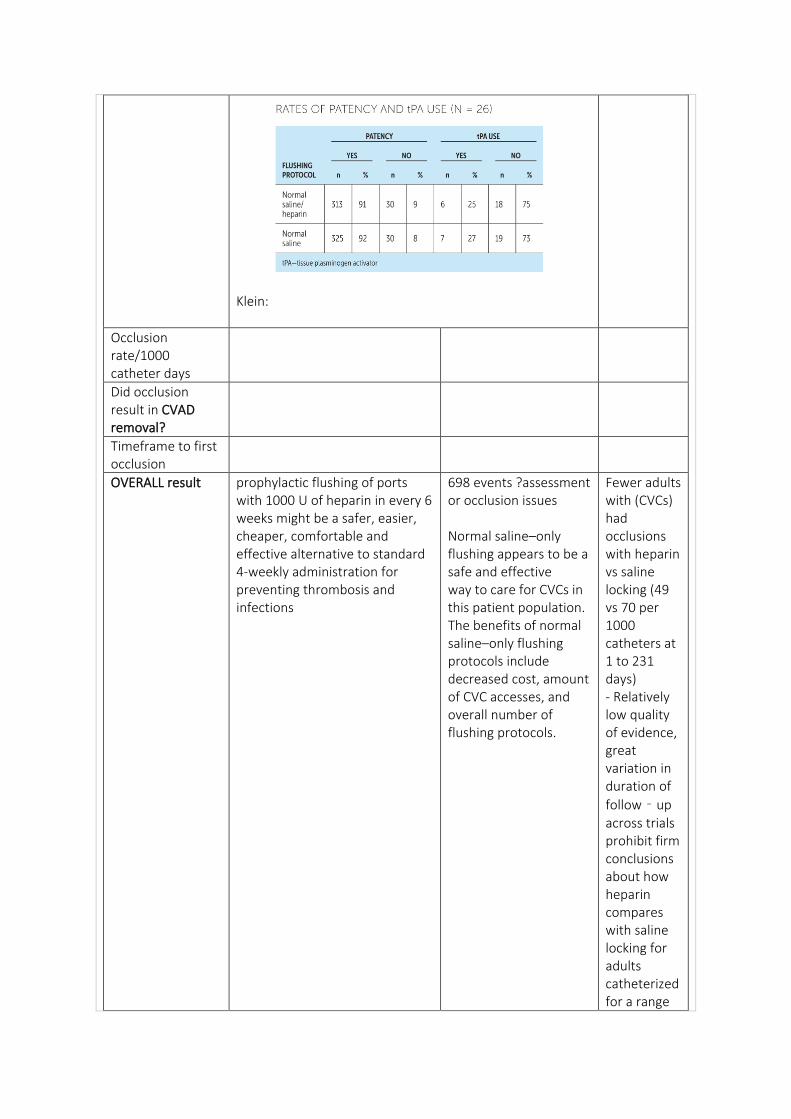
Klein:
Occlusion rate/1000 catheter days
Did occlusion result in CVAD removal?
Timeframe to first occlusion
OVERALL result prophylactic flushing of ports with 1000 U of heparin in every 6 weeks might be a safer, easier, cheaper, comfortable and effective alternative to standard 4-weekly administration for preventing thrombosis and infections
698 events ?assessment or occlusion issues Normal saline–only flushing appears to be a safe and effective way to care for CVCs in this patient population. The benefits of normal saline–only flushing protocols include decreased cost, amount of CVC accesses, and overall number of flushing protocols.
Fewer adults with (CVCs) had occlusions with heparin vs saline locking (49 vs 70 per 1000 catheters at 1 to 231 days) - Relatively low quality of evidence, great variation in duration of
follow‐up across trials prohibit firm conclusions about how heparin compares with saline locking for adults catheterized for a range
of conditions - The quality of evidence was moderate for hemorrhage from any site and
CVC‐related thrombosis outcomes and was low for all other outcomes. No trials assessed allergic reactions to heparin.
Thromboprophylaxis n= (%) median (range)
Patency – occlusion prevention CVAD
Education and competency requirement of staff – inserting and maintenance
ability to minimize and accurately recognize catheter-related problems requires adequate [etrt of nurses and physicians because their inexperience has been documented to be the factor that is most frequently related to catheter complications.
Education was provided to the inpatient and outpatient nursing staff through huddles (informal meetings) and one-on-one education.
Frequency of patency checked
line patency was documented once per shift (twice daily). Outpatient nursing staff documented patency after each line access.
How patency checked
Optimal flush frequency
Optimal flush volume
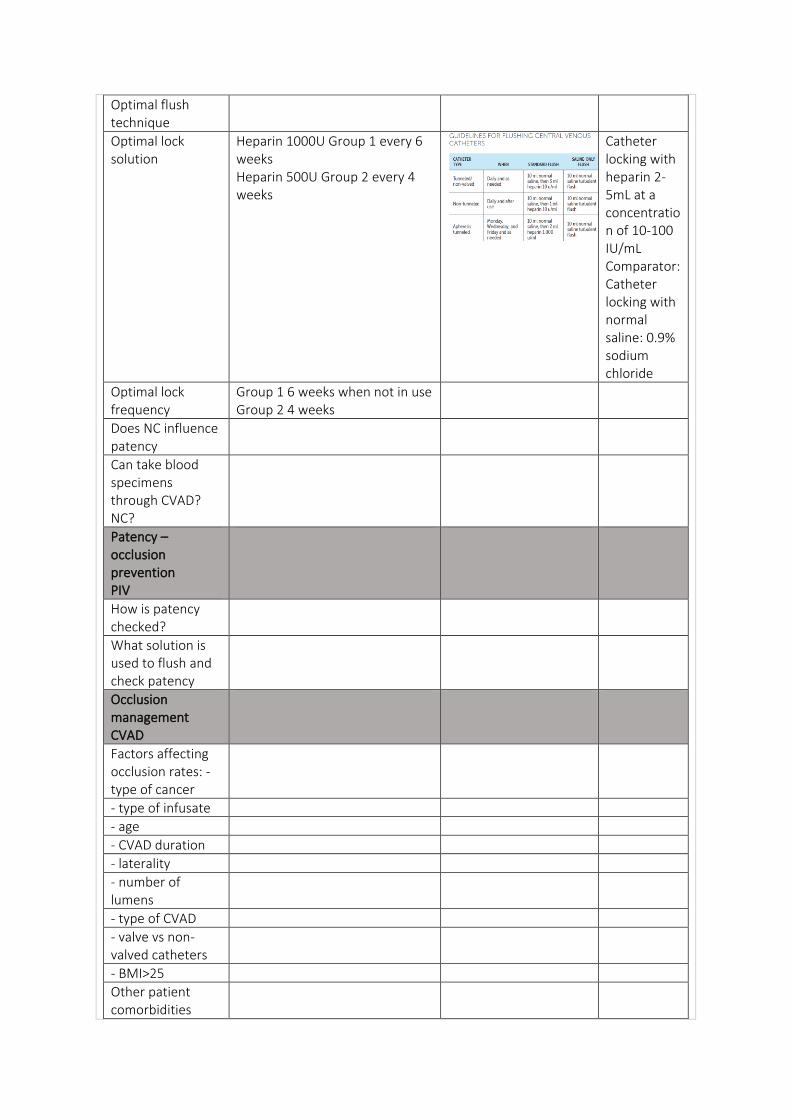
Optimal flush technique
Optimal lock solution
Heparin 1000U Group 1 every 6 weeks Heparin 500U Group 2 every 4 weeks
Catheter locking with heparin 2‐5mL at a concentration of 10‐100 IU/mL Comparator: Catheter locking with normal saline: 0.9% sodium chloride
Optimal lock frequency
Group 1 6 weeks when not in use Group 2 4 weeks
Does NC influence patency
Can take blood specimens through CVAD? NC?
Patency – occlusion prevention PIV
How is patency checked?
What solution is used to flush and check patency
Occlusion management CVAD
Factors affecting occlusion rates: - type of cancer
- type of infusate
- age
- CVAD duration
- laterality
- number of lumens
- type of CVAD
- valve vs non-valved catheters
- BMI>25
Other patient comorbidities
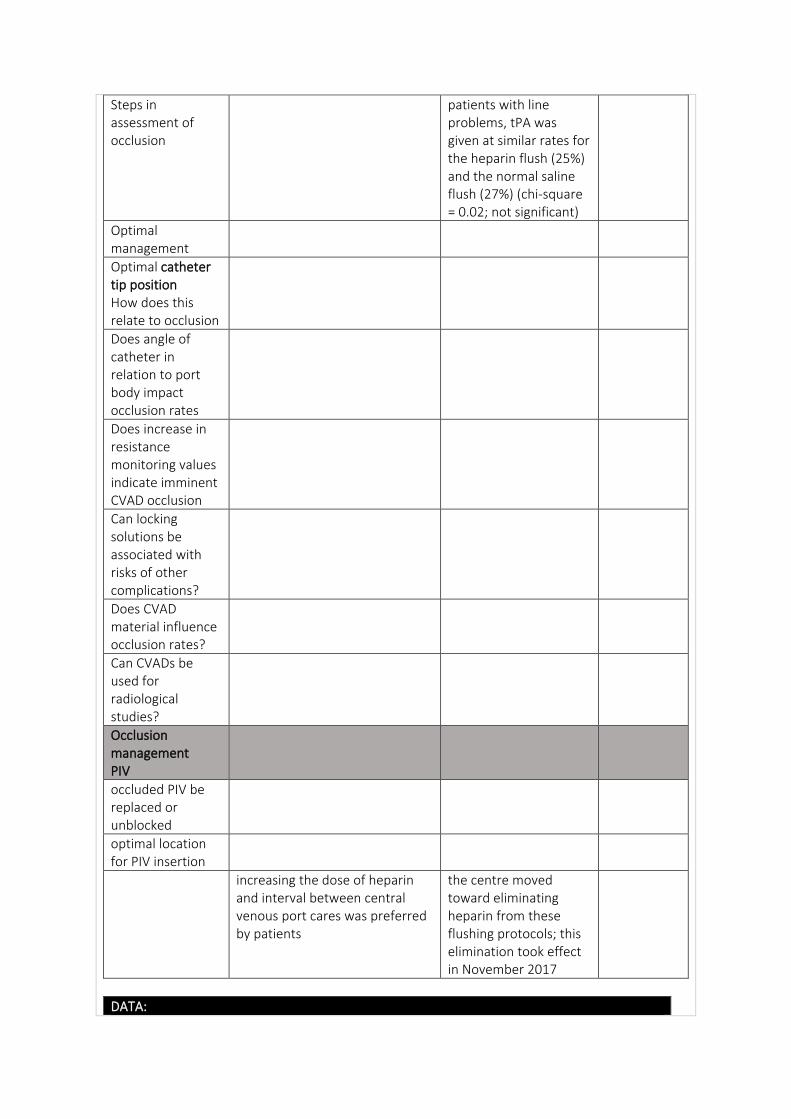
Steps in assessment of occlusion
patients with line problems, tPA was given at similar rates for the heparin flush (25%) and the normal saline flush (27%) (chi-square = 0.02; not significant)
Optimal management
Optimal catheter tip position How does this relate to occlusion
Does angle of catheter in relation to port body impact occlusion rates
Does increase in resistance monitoring values indicate imminent CVAD occlusion
Can locking solutions be associated with risks of other complications?
Does CVAD material influence occlusion rates?
Can CVADs be used for radiological studies?
Occlusion management PIV
occluded PIV be replaced or unblocked
optimal location for PIV insertion
increasing the dose of heparin and interval between central venous port cares was preferred by patients
the centre moved toward eliminating heparin from these flushing protocols; this elimination took effect in November 2017
DATA:
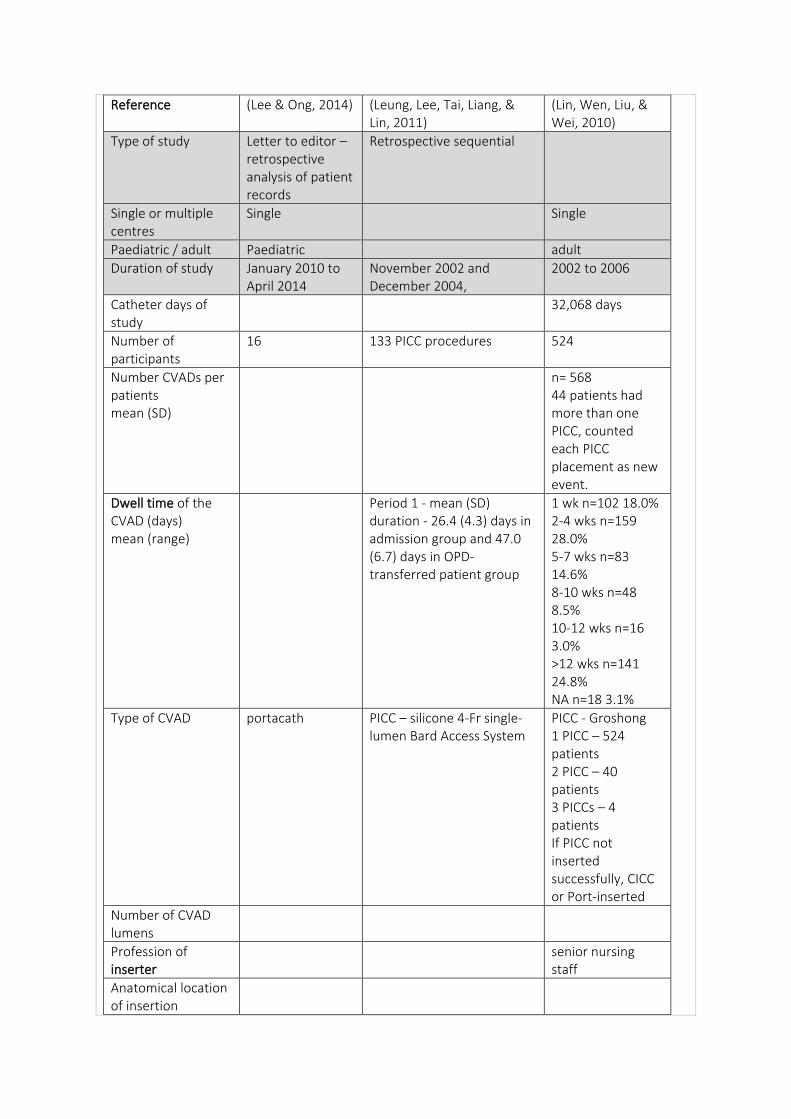
Reference (Lee & Ong, 2014) (Leung, Lee, Tai, Liang, & Lin, 2011)
(Lin, Wen, Liu, & Wei, 2010)
Type of study Letter to editor – retrospective analysis of patient records
Retrospective sequential
Single or multiple centres
Single Single
Paediatric / adult Paediatric adult
Duration of study January 2010 to April 2014
November 2002 and December 2004,
2002 to 2006
Catheter days of study
32,068 days
Number of participants
16 133 PICC procedures 524
Number CVADs per patients mean (SD)
n= 568 44 patients had more than one PICC, counted each PICC placement as new event.
Dwell time of the CVAD (days) mean (range)
Period 1 - mean (SD) duration - 26.4 (4.3) days in admission group and 47.0 (6.7) days in OPD-transferred patient group
1 wk n=102 18.0% 2-4 wks n=159 28.0% 5-7 wks n=83 14.6% 8-10 wks n=48 8.5% 10-12 wks n=16 3.0% >12 wks n=141 24.8% NA n=18 3.1%
Type of CVAD portacath PICC – silicone 4-Fr single-lumen Bard Access System
PICC - Groshong 1 PICC – 524 patients 2 PICC – 40 patients 3 PICCs – 4 patients If PICC not inserted successfully, CICC or Port-inserted
Number of CVAD lumens
Profession of inserter
senior nursing staff
Anatomical location of insertion
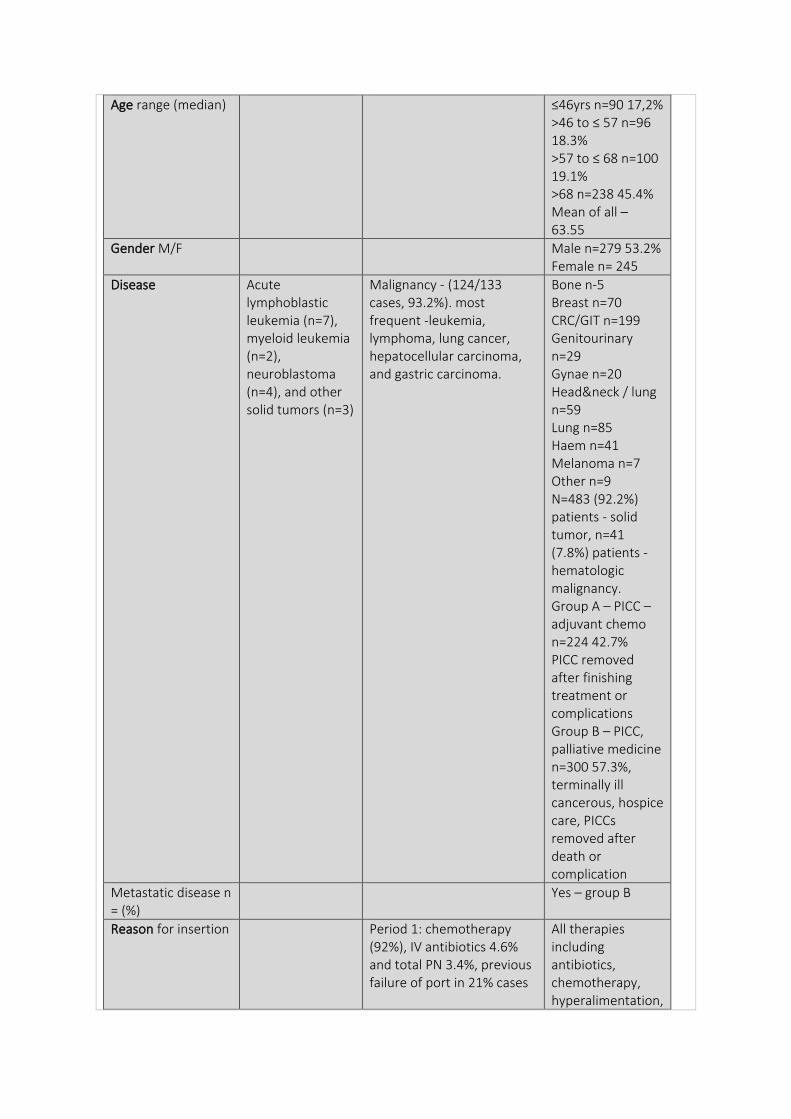
Age range (median) ≤46yrs n=90 17,2% >46 to ≤ 57 n=96 18.3% >57 to ≤ 68 n=100 19.1% >68 n=238 45.4% Mean of all – 63.55
Gender M/F Male n=279 53.2% Female n= 245
Disease Acute lymphoblastic leukemia (n=7), myeloid leukemia (n=2), neuroblastoma (n=4), and other solid tumors (n=3)
Malignancy - (124/133 cases, 93.2%). most frequent -leukemia, lymphoma, lung cancer, hepatocellular carcinoma, and gastric carcinoma.
Bone n-5 Breast n=70 CRC/GIT n=199 Genitourinary n=29 Gynae n=20 Head&neck / lung n=59 Lung n=85 Haem n=41 Melanoma n=7 Other n=9 N=483 (92.2%) patients - solid tumor, n=41 (7.8%) patients - hematologic malignancy. Group A – PICC – adjuvant chemo n=224 42.7% PICC removed after finishing treatment or complications Group B – PICC, palliative medicine n=300 57.3%, terminally ill cancerous, hospice care, PICCs removed after death or complication
Metastatic disease n = (%)
Yes – group B
Reason for insertion Period 1: chemotherapy (92%), IV antibiotics 4.6% and total PN 3.4%, previous failure of port in 21% cases
All therapies including antibiotics, chemotherapy, hyperalimentation,
blood component transfusion, and other medications were allowed via the PICC.
Outcome - to evaluate most important factors causing failure of PICCs by comparing 2 periods of retrospectively studied cases before and after implemented nursing care improvements - outcomes of PICC insertions (?overall line survival) significantly improved from 33.8% in the first period to 64.3% in the second period (odds ratio, 3.53)
Outcome measures - defined
occlusion self-care ability – high or low to care for PICC post insertion
“Successful completion” “Premature extubation” dislodgment, phlebitis, occlusion, or infection according to guidelines from the Centers for Disease Control and Prevention
Intervention 2 periods - cases before n=133 and after nursing care improvements n=143 - comprehensive educational guidelines for post-PICC manipulation
Insertion care fluoroscopic guidance in Diagnostic Radiology
Bedside, Seldingerʼs technique with standard aseptic precautions, percutaneous entrance into an antecubital vein.
Maintenance care (dedicated CVAD
- patient’s family member or intensive care nurse perform PICC flushing -
Trained nurses
team, ward staff or patient)
findings reflect the presence of discriminative medical care quality among different socioeconomic classes - self care ability - patient’s capability of performing self-cleaning, redressing the insertion area, and flushing the PICC on his or her own - - special care by ICU nurse for low level of self-care ability before being accepted to receive a PICC in the second review period, there was no significant difference between patients with low and those with high levels of self-care ability in terms of the PICC success rate, in contrast to period 1
- patient requests for PICC removal were one of the reasons during both periods, the development of a PICC care easier to maintain than current designs, is also mandatory
Inclusion criteria had complete admission notes from the OPD, and the same patient has only 1 PICC placement during the study period
Exclusion criteria
Randomisation Convenience sample, complete OPD records
Healthcare setting Children’s Haematology and Cancer Centre, Mount Elizabeth Hospital, Singapore
Taiwan, Taipei Medical University Hospital
Executive Yuan Hsin-Chu Hospital, 714-bed metropolitan teaching hospital
Duration of follow up, lost to follow up
RESULTS:
Complication rate first part of study - unacceptably high failure rate
N=123 21.6% Death n=288 50.8% End treatment n=130 22.9% Unplanned n=120 21.1% Pt request n=3 0.5% NA n=11 1.9% Keep n=16 2.8%
Complication rate/1000 catheter days
3.8/1000 catheter days
Occlusion rate 26 occasions involving 16 children in which port access was done after 8 weeks of catheter flush-lock On 24 (92.3%) occasions, the port remained patent.
Period 1: n=9 6.7% November 2002 to December 2004 Period 2: n=4 down to 2.8% Odds ratio 0.40 p=0.029 January 2005 to December 2008
Palliative pts – n=41 Adjuvant pts n=34 p=0.4876 Adjuvant chemo = occlusion most in week 6 n=26 Palliative medicine – most occlusion in week 6 n=25
Occlusion rate/1000 catheter days
two (7.7%) occasions of catheter occlusion - 0.34/1,000 port-days. 1. male 5.5 years, returned for salvage treatment with relapsed neuroblastoma, port last flush-locked 304 days ago. Catheter patency was restored after locking with urokinase (6,000 units in 1 ml). 2. 16.5-year male, AML, on follow-up for labs, port last flush-locked 390 days previously,
disease recurrence unlikely, the port removed next day with no attempt to restore patency.
Did occlusion result in CVAD removal?
Timeframe to first occlusion
OVERALL result
Thromboprophylaxis n= (%) median (range)
Patency – occlusion prevention CVAD
Education and competency requirement of staff – inserting and maintenance
Education re nursing practice to confront the complications of post-PICC insertion in the first 24 hours (bleeding, oozing, ecchymosis, and a persistent pain sensation at the insertion site) and from then on (mechanical phlebitis, infection, cellulitis, thrombophlebitis, an occluded catheter, catheter migration, air embolism, and pain during infusion).
Frequency of patency checked
How patency checked
Optimal flush frequency
Optimal flush volume
Optimal flush technique
Optimal lock solution
Heparin saline 10U/ml using positive pressure technique
2 - 10 mL of a dilute heparin solution (5,000 units/mL), to prevent blood from plugging the catheter
Saline (Groshong)
Optimal lock frequency
No routine maintenance flush-lock is practiced until the port is next
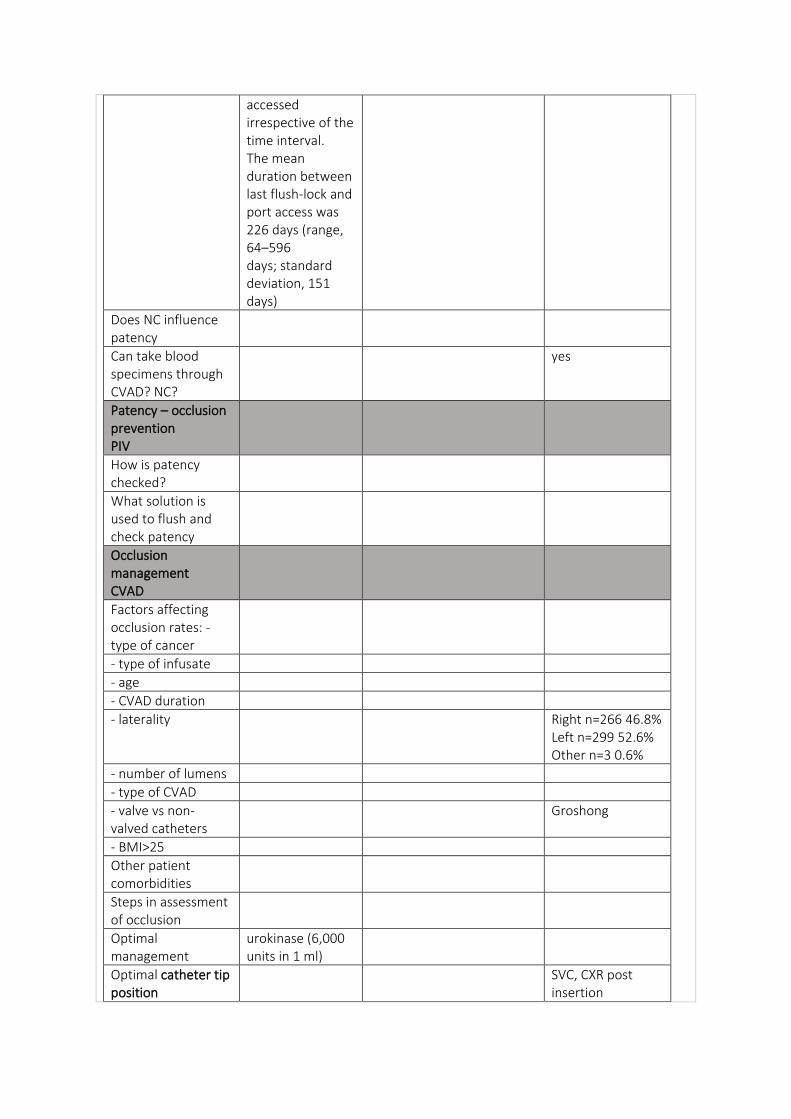
accessed irrespective of the time interval. The mean duration between last flush-lock and port access was 226 days (range, 64–596 days; standard deviation, 151 days)
Does NC influence patency
Can take blood specimens through CVAD? NC?
yes
Patency – occlusion prevention PIV
How is patency checked?
What solution is used to flush and check patency
Occlusion management CVAD
Factors affecting occlusion rates: - type of cancer
- type of infusate
- age
- CVAD duration
- laterality Right n=266 46.8% Left n=299 52.6% Other n=3 0.6%
- number of lumens
- type of CVAD
- valve vs non-valved catheters
Groshong
- BMI>25
Other patient comorbidities
Steps in assessment of occlusion
Optimal management
urokinase (6,000 units in 1 ml)
Optimal catheter tip position
SVC, CXR post insertion
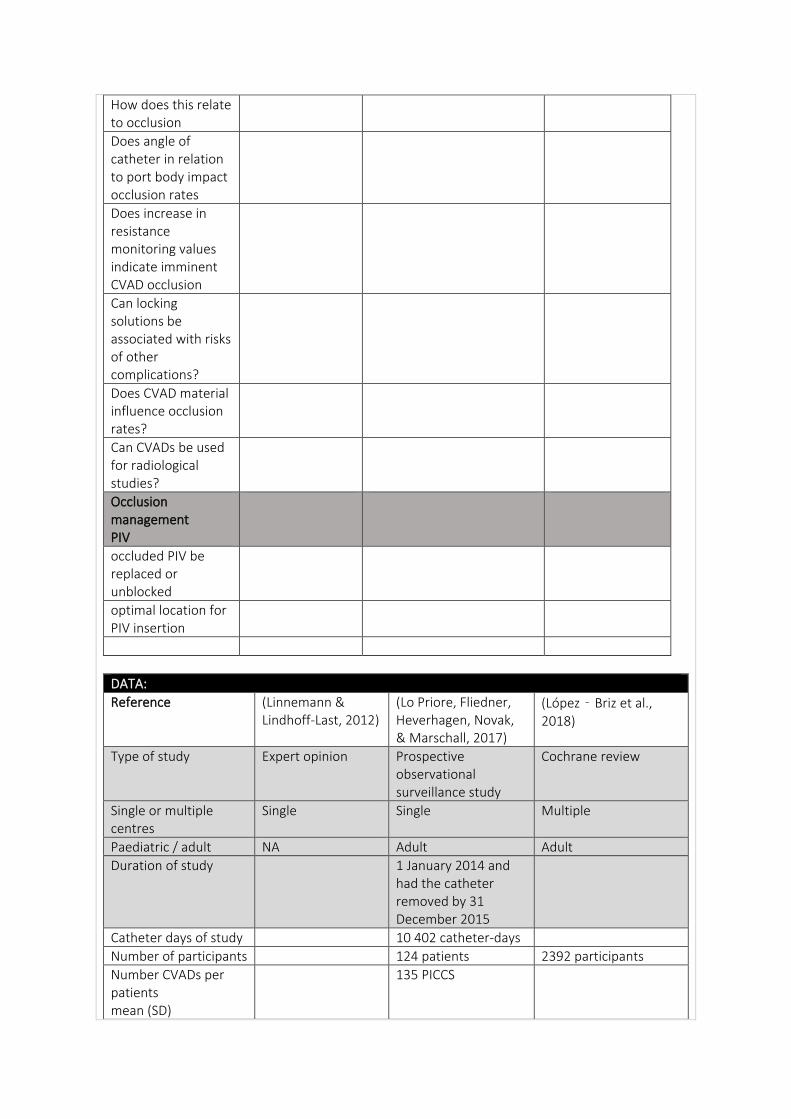
How does this relate to occlusion
Does angle of catheter in relation to port body impact occlusion rates
Does increase in resistance monitoring values indicate imminent CVAD occlusion
Can locking solutions be associated with risks of other complications?
Does CVAD material influence occlusion rates?
Can CVADs be used for radiological studies?
Occlusion management PIV
occluded PIV be replaced or unblocked
optimal location for PIV insertion
DATA:
Reference (Linnemann & Lindhoff-Last, 2012)
(Lo Priore, Fliedner, Heverhagen, Novak, & Marschall, 2017)
(López‐Briz et al., 2018)
Type of study Expert opinion Prospective observational surveillance study
Cochrane review
Single or multiple centres
Single Single Multiple
Paediatric / adult NA Adult Adult
Duration of study 1 January 2014 and had the catheter removed by 31 December 2015
Catheter days of study 10 402 catheter-days
Number of participants 124 patients 2392 participants
Number CVADs per patients mean (SD)
135 PICCS
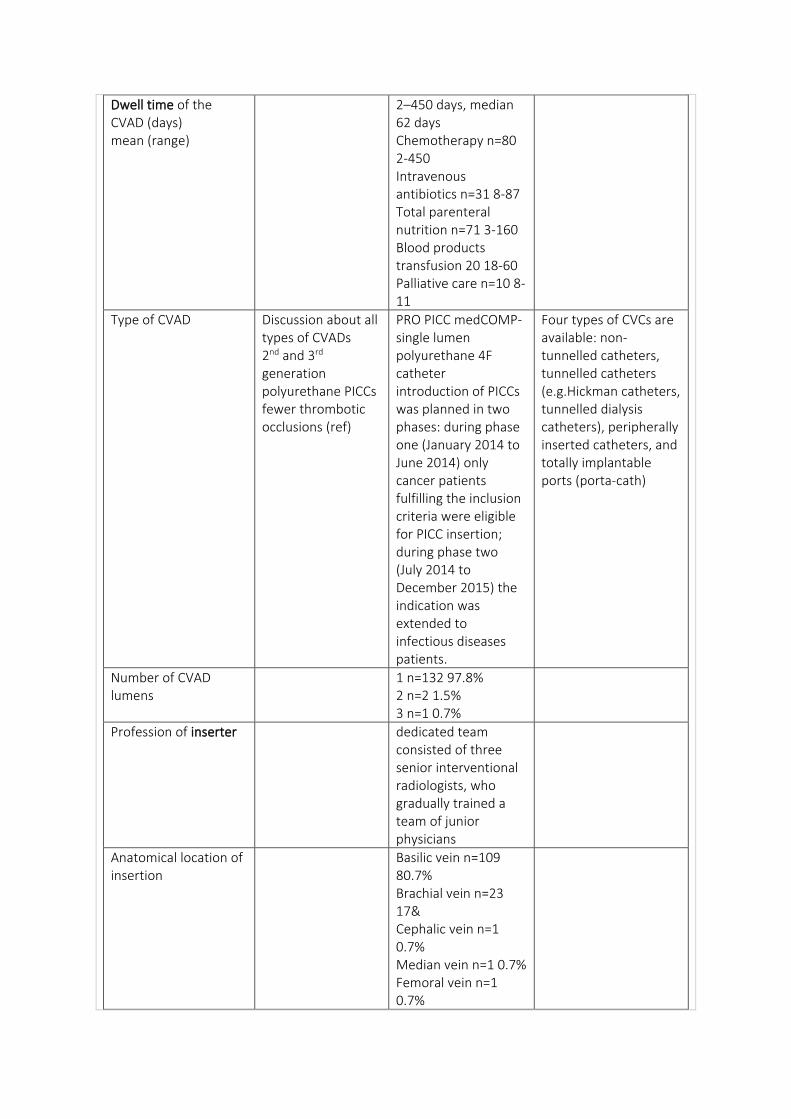
Dwell time of the CVAD (days) mean (range)
2–450 days, median 62 days Chemotherapy n=80 2-450 Intravenous antibiotics n=31 8-87 Total parenteral nutrition n=71 3-160 Blood products transfusion 20 18-60 Palliative care n=10 8-11
Type of CVAD Discussion about all types of CVADs 2nd and 3rd generation polyurethane PICCs fewer thrombotic occlusions (ref)
PRO PICC medCOMP- single lumen polyurethane 4F catheter introduction of PICCs was planned in two phases: during phase one (January 2014 to June 2014) only cancer patients fulfilling the inclusion criteria were eligible for PICC insertion; during phase two (July 2014 to December 2015) the indication was extended to infectious diseases patients.
Four types of CVCs are available: non-tunnelled catheters, tunnelled catheters (e.g.Hickman catheters, tunnelled dialysis catheters), peripherally inserted catheters, and totally implantable ports (porta-cath)
Number of CVAD lumens
1 n=132 97.8% 2 n=2 1.5% 3 n=1 0.7%
Profession of inserter dedicated team consisted of three senior interventional radiologists, who gradually trained a team of junior physicians
Anatomical location of insertion
Basilic vein n=109 80.7% Brachial vein n=23 17& Cephalic vein n=1 0.7% Median vein n=1 0.7% Femoral vein n=1 0.7%
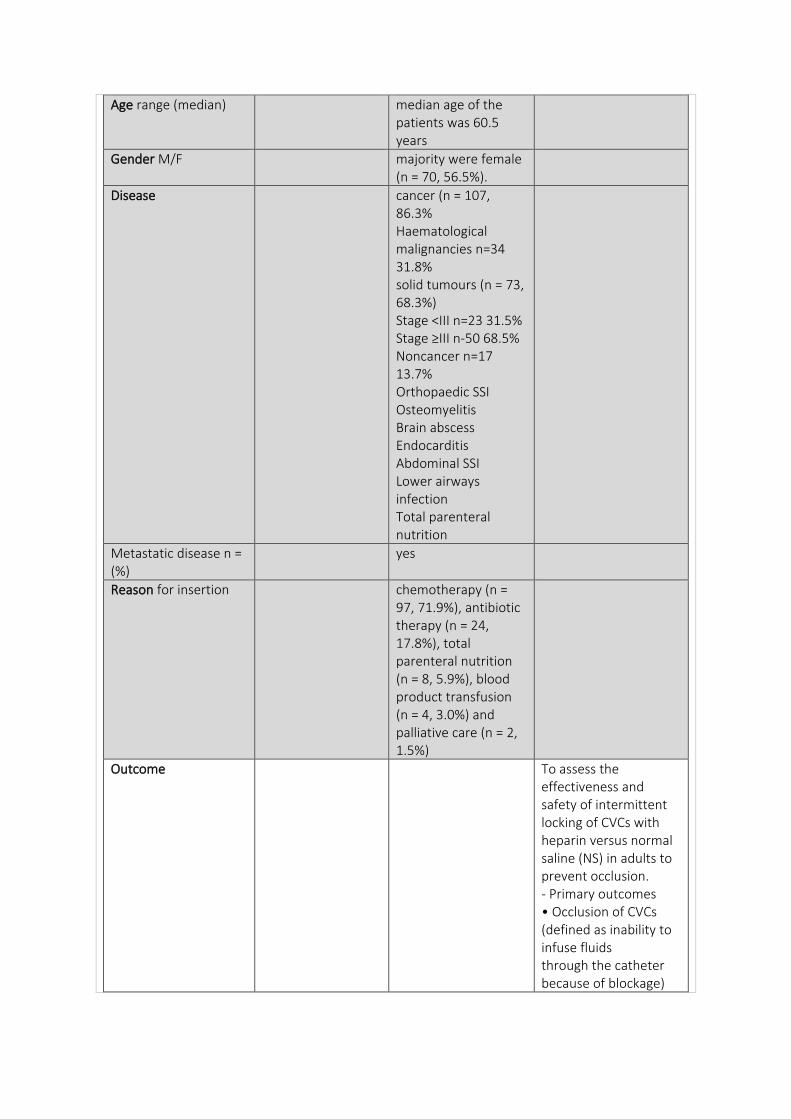
Age range (median) median age of the patients was 60.5 years
Gender M/F majority were female (n = 70, 56.5%).
Disease cancer (n = 107, 86.3% Haematological malignancies n=34 31.8% solid tumours (n = 73, 68.3%) Stage <III n=23 31.5% Stage ≥III n-50 68.5% Noncancer n=17 13.7% Orthopaedic SSI Osteomyelitis Brain abscess Endocarditis Abdominal SSI Lower airways infection Total parenteral nutrition
Metastatic disease n = (%)
yes
Reason for insertion chemotherapy (n = 97, 71.9%), antibiotic therapy (n = 24, 17.8%), total parenteral nutrition (n = 8, 5.9%), blood product transfusion (n = 4, 3.0%) and palliative care (n = 2, 1.5%)
Outcome To assess the effectiveness and safety of intermittent locking of CVCs with heparin versus normal saline (NS) in adults to prevent occlusion. - Primary outcomes • Occlusion of CVCs (defined as inability to infuse fluids through the catheter because of blockage)
• Duration (in days) of catheter patency
Outcome measures - defined
- complete occlusion Infection (primary outcome) - secondary endpoint: catheter related-venous thrombosis, catheter tip migration, catheter occlusion and mechanical complications (catheter rupture, haemothorax, pneumothorax, cardiac tamponade or arrhythmia)
Intervention new interdisciplinary project to introduce PICCs in an academic hospital, with an embedded interdisciplinary surveillance programme for both infectious and noninfectious outcomes
5 new studies, 6 prior n=11,
Insertion care selection of the insertion site and vein to cannulate was based on patient preference and vascular anatomy. Veins were cannulated under sonographic guidance; subsequent catheter insertion and tip localisation were evaluated under fluoroscopic guidance.
Maintenance care (dedicated CVAD team, ward staff or patient)
Only trained personnel were allowed to manipulate the catheters.
Inclusion criteria All patients requiring intravenous therapy
We included randomised controlled
for more than 7 days primarily in the outpatient setting, according to the decision of the treating oncologist or infectious diseases specialist, were eligible for inclusion.
trials in adults ≥ 18 years of age with a CVC that compared intermittent locking with heparin at any concentration versus NS. We applied no restriction on language.
Exclusion criteria studies on infants and children, PIVC, arterial
Randomisation
Healthcare setting 950-bed academic hospital (Bern University Hospital, Switzerland)
Duration of follow up, lost to follow up
- ambulatory and in-hospital care. Of the 124 patients, 62 (50%) were hospitalised for at least 24 hours during the observation period. Fifty-five patients (44.4%) were managed in the outpatient setting only and seven were managed solely as inpatients (5.6%). None of the patients were hospitalised in an ICU. - manual review of each patient’s electronic medical record, from the catheter booklet and by contacting both the hospital-based and home care nursing teams.
follow-up (1 to 251.8 days),
RESULTS: unit of analysis used (participant, catheter, line access).
Complication rate N=46 10 episodes of catheter tip migration occurred in 10 patients, and resulted
in PICC removal in 7 cases.
Complication rate/1000 catheter days
4.5 per 1000 catheter-days
Occlusion rate 14-36% within 1-2 years (ref) PICCs>CVCs 27.2% vs 9.6% p=0.001 (ref)
(n = 7) - most frequent complication was catheter flow dysfunction (not related to the above-cited complications) and occurred in 22 separate episodes. - 18 of 22 cases the flow could be successfully re-established by use of alteplase lock. - 1 case, the catheter removed owing to irreversible occlusion - 3 remaining cases the flow dysfunction spontaneously resolved without further intervention.
Only one study used line access as the unit of analysis (Goosens 2013). This study included 6137 observations and showed no differences in the number of occlusions between heparin and NS locking (RR1.08, 95%CI 0.84 to 1.40). We judged the quality of evidence to be moderate.
Occlusion rate/1000 catheter days
0.68/1000 catheter days for catheter occlusion
Did occlusion result in CVAD removal?
17 catheters (12.6%) were removed because of any complication N=1 for occlusion 0.7%
Timeframe to first occlusion
OVERALL result - Very low-quality evidence suggests that in adults, intermittent locking of CVCs with heparin may result in fewer occlusions than intermittent locking with NS. Low-quality evidence suggests that heparin has little or no effect on catheter patency.
- fewer occlusions with heparin than with NS (risk ratio (RR) 0.70, 95% confidence interval (CI) 0.51 to 0.95; P = 0.02; 1672 participants; 1025 catheters from 10 studies; I² = 14%) and provided very low-quality evidence. - When the unit of analysis was the participant or catheter - show no difference in this outcome between heparin and NS groups (mean difference (MD) 0.44, 95% CI -0.10 to 0.99; P = 0.11 Quality of evidence- low - When the unit of analysis was the participant detected no clear differences between heparin and NS groups (MD 0.66, 95% CI -0.66 to 1.97; I² = 0%; P = 0.33; Analysis 4.1). We judged the quality of evidence to be low. - Only one study used line access as the unit of analysis - showed no differences in the number of occlusions between heparin and NS locking (RR1.08, 95%CI 0.84 to 1.40) - quality of evidence to be moderate. SUMMARY - no clear differences in the duration of catheter patency (mean difference (MD) 0.44 days, 95% CI -0.10 to 0.99; P = 0.11; 1036 participants; 752
catheters; six studies; low-quality evidence) - very low quality of the evidence, we are uncertain whether intermittent locking with heparin results in fewer occlusions than intermittent locking with NS. Low-quality evidence suggests that heparin may have little or no effect on catheter patency. - Despite results suggesting no differences in safety, it is probable that a high proportion of patients could be at increased risk with heparin use - The quality of evidence for the main outcome (all occlusions of CVC) was very low.
Thromboprophylaxis n= (%) median (range)
antithrombotic prophylaxis was not routinely administered.
Patency – occlusion prevention CVAD
Education and competency requirement of staff – inserting and maintenance
Educational sessions were offered to hospital-based (infection prevention team and vascular access team) and community-based (home care nurse) nursing services under the lead of a nurse practitioner - establishment of evidence-based guidelines for introduction of new vascular access highlights the importance of implementation
science in promoting the integration of evidence-based findings into daily clinical practice.
Frequency of patency checked
How patency checked
Optimal flush frequency
‘regular’ flushing important for prevention of occlusion
Optimal flush volume
Optimal flush technique
flushed by exerting intermittent pressure with a 0.9% saline solution before and after each use.
Optimal lock solution Saline or UFH equally efficient, Evidence for rt-PA for haemodialysis catheters, urokinase as well – meta analysis – these are expensive alternatives
heparin solution (200 IU); home team used different lock – trisodium citrate prefilled syringes (Dura Lock®, medComp®, Harleysville, PA, USA),
variation in heparin concentrations (10 to 5000 IU/mL)
Optimal lock frequency Port – once a month, or less frequent
Following use,
Does NC influence patency
Homecare used different needleless device (NeutraClear®,
Can take blood specimens through CVAD? NC?
Patency – occlusion prevention PIV
How is patency checked?
What solution is used to flush and check patency
Occlusion management CVAD
Factors affecting occlusion rates: - type of cancer
Cancers due to hypercoagulable state esp ovaries,
brain and pancreas (ref)
- type of infusate L’asparaginase, thalidomide, lenalidomide, - DVT rate (ref)
- age
- CVAD duration
- laterality Left side > right 5 fold increase in DVT (ref)
Left n=101 74.8% Right n=34 25.2%
- number of lumens Triple lumen higher incidence of thrombotic complications (ref)
- type of CVAD
- valve vs non-valved catheters
- BMI>25 25.3 (16-52)
Other patient comorbidities
Steps in assessment of occlusion
Optimal management Mechanical causes ruled out, then precipitation of drugs or PN. Majority are thrombotic cause. Contrast study helpful to determine what type of thrombotic causes. UFH first for partial occlusions, complete – urokinase and rt-PA
Optimal catheter tip position How does this relate to occlusion
Malposition important risk factor for DVT – 7-fold risk from lower to upper half of SVC
tips terminate in the inferior third of the vena cava at the junction with the right atrium.
tip that lies within the proximal third of the superior vena cava, the right atrium, or the inferior vena cava.
Does angle of catheter in relation to port body impact occlusion rates
Does increase in resistance monitoring values indicate imminent CVAD occlusion
Can locking solutions be associated with risks of other complications?
Does CVAD material influence occlusion rates?
Can CVADs be used for radiological studies?
Occlusion management PIV
occluded PIV be replaced or unblocked
optimal location for PIV insertion
Implications for practice Very low-quality evidence suggests that in adults, central venous catheters that are intermittently locked with heparin result in fewer occlusions than catheters locked with normal saline (NS). Low quality evidence suggests that heparin may have little or no effect on duration of catheter patency. We found no evidence of an increased effect with increasing concentrations of heparin and no evidence of differences in the relative safety of the two methods of intermittent locking when central venous catheter (CVC)-related sepsis, mortality, or haemorrhage was considered, although the trials combined are not powered to detect rare adverse events such as heparin-induced
thrombocytopaenia. To sum up, we are uncertain about the effects of heparin compared to NS, and review findings should be interpreted with caution. - Occlusions and adverse events must be the focus of future trials, and we suggest at least one month of follow-up
DATA:
Reference (Malec, Cooper, Rudolph, Michaels, & Ragni, 2018)
(Mason, Ferrall, Boyington, & Reich, 2014)
(Mathur, Mott, Collins, & Schlueter, 2019)
Type of study Pilot study- PN for short bowel syndrome Effectiveness
Cross-sectional exploratory survey - oncology nurses re different troubleshooting techniques for clearing occluded central venous access devices (CVADs)
Retrospective chart review
Single or multiple centres
Single Multiple single
Paediatric / adult Paediatrics Nurse survey adult
Duration of study December 2015 to September 2016
Catheter days of study
Number of participants
8 224 nurses participated in the study (less than 5% response rate 2-41 years being a nurse 2-35 yrs in oncology
10
Number CVADs per patients mean (SD)
7/8 had more than 1 line; 1-6 lines As a group, they underwent CVAD replacement/reinsertion with a median number of life time CVADs of 6.5 (IQR 3–14), and median of 2
93 extracorporeal photopheresis procedures in 10 patients was perform - Other than flushes, the lines were not accessed between ECP procedures
CVAD re insertions in the 6 months before study (IQR 1.8–3.3)
Dwell time of the CVAD (days) mean (range)
Type of CVAD tc-CICC Double lumen 13.5FR (n=2) to 14.5FR (n=8) Equistream Long-Term Hemodialysis Catheters
Number of CVAD lumens
2
Profession of inserter
Anatomical location of insertion
R. IJ 90%
Age range (median) 1.4-11.9, median age 4.4 years
23-74yrs, average 51 years
Gender M/F 4 boys, 4 girls 6 male, 4 female
Disease
Metastatic disease n = (%)
Reason for insertion Long-term PN bronchiolitis obliterans syndrome following lung transplant (5 patients), graft vs host disease following hematopoietic stem cell transplant (4 patients), and Sezary syndrome (1 patient)
Outcome
Outcome measures - defined
No issues Some issues Significant issues
Intervention to examine efficacy of weekly rtPA lock therapy in prevention of line-associated venous thrombosis - secondary aims were to study the impact of rtPA lock therapy in prevention of CVAD-associated line infection, rates of hospitalization, and minimization of need
Prior to embarking on main study, pilot study undertaken to evaluate (a) ease of completing online survey, (b) clarity of instructions, and (c) data collection process n=26 - 14 questions using the ordered category responses extremely, very, moderately, slightly, and not at all
catheter malfunction rates using recombinant tissue plasminogen activator (rt-PA) vs heparin for locking CVC between apheresis procedures were compared. - 1000 U/mL heparin or 2 mg rt-PA was used as the locking solution. -
for CVAD replacement.
- TTQ further explored nursing CVAD management with the following items: (a) referral of troubleshooting to another healthcare professional (five-level ordered category response), (b) identification of other types of healthcare professionals who may receive referrals (open ended), (c) frequency of dye studies obtained (five-level ordered category response), and (d) a request for additional comments (open ended). Seven demographic questions about nursing experience and work setting appeared at the end of the questionnaire. No personal identifying information was requested.
Insertion care placed by interventional radiology
Maintenance care (dedicated CVAD team, ward staff or patient)
initial lock therapy was performed by the subjects’ nurse with the subject’s parent/caregiver present to observe the instillation of rtPA and demonstration of subsequent rtPA aspiration from the line. - If a subject remained hospitalized for >1 week, rtPA lock therapy was administered by the inpatient nurse,
educating parents/providers. For subjects discharged <1 week after admission, education was provided to ensure parent/caregiver comfort with the study procedure.
Inclusion criteria Inclusion criteria included diagnosis of SBS, requirement for CVAD for long-term total parenteral nutrition (TPN) administration, age <18 years, insertion of new CVAD, and ability to be enrolled and initiate rtPA lock therapy within 48 hours of CVAD placement
(a) more than five years of oncology experience, (b) primary specialty of biotherapy or chemotherapy and outpatient infusion, and (c) registered a U.S. mailing address with permission for it to be distributed.
Exclusion criteria platelet count <50,000, presence of active CVAD-related infection defined as positive blood culture with 48 hours before CVAD insertion, concomitant use of therapeutic anticoagulant, and active internal or external bleeding
Procedures where interval since the last procedure was less than 5 days were excluded because these procedures would not have been expected to benefit from rt-PA locks
Randomisation Convenience sample – subjects were identified when they presented to the hospital due to need for CVAD insertion
Healthcare setting Children’s Hospital of Pittsburgh of University of Pittsburgh Medical Center.
DeGowin Blood Center, University of Iowa Healthcare (UIHC)
Duration of follow up, lost to follow up
Subjects were followed for a total of 24 weeks after enrolment
- 2 subjects did not complete the 24 weeks; 1 subject withdrew from the study due to parental preference to not continue use of weekly rtPA and 1 subject changed institutions and was lost due to follow-up; the remaining subjects completed the full study course.
RESULTS:
Complication rate Based on analysis of this limited data set, outcomes from use of rt-PA CVC lock for lines used for a series of apheresis procedures with >5 days interval between procedures not found to be statistically different as compared to using heparin lock. The results also suggest that heparin may increase a patient’s odds of having CVC flow rate problems compared to rt-PA, but this would need to be evaluated in a larger sample to draw definitive conclusions. - the problems encountered with apheresis flow rates did not correlate well with the length of time between locks, for either heparin or rt-PA - we changed our standard practice to lock CVCs with 1000 U/mL heparin if the
next apheresis procedure is anticipated in ≤7 days, and lock with 2 mg rt-PA per lumen if the interval is expected to be 8 to 28 days.
Complication rate/1000 catheter days
Occlusion rate
Occlusion rate/1000 catheter days
Did occlusion result in CVAD removal?
2 patients had removals due to line occlusion 1 patient with partial line malfunction (inability to obtain a blood draw) required an additional dose of rtPA to restore line patency and function. 1 patient had line malfunction (inability to obtain a blood return and flushing of the catheter with resistance), which necessitated line replacement; no other subjects had issues with line malfunction while on study.
Timeframe to first occlusion
OVERALL result study intervention demonstrated use of rtPA lock therapy was feasible however with no adverse events suggesting that rtPA lock therapy should be investigated in a larger cohort of patients with SBS.
67 % nurses reported a technique not expected to yield results (e.g., instill heparin and wait). About 25% of nurses mentioned using a contraindicated technique, such as flushing rapidly against resistance.
n %
HEPARIN
Significant issues
9 13
Some issues
24
34
No issues 37
53
rtPA
Significant issues
3 13
Some issues
4 17
No issues 16
70
There was c) - no association between the length of time the lock was in place prior to the procedure and the degree of line-related issues, either for heparin lock or rt-PA lock
Thromboprophylaxis n= (%) median (range)
Patency – occlusion prevention CVAD
Education and competency requirement of staff – inserting and maintenance
Participants represent an experienced and educated group, with 63% educated at a bachelor’s level or higher and almost 96% certified—with the majority (84%) holding certification in oncology
Frequency of patency checked
How patency checked
Optimal flush frequency
Optimal flush volume both lumens were flushed with 10 mL NS
Optimal flush technique
Optimal lock solution rtPA/alteplase (Cathflo) 2 mg/2 mL, or 110% of the volume of the catheter lumen if <2 mL, administered locally in a volume to fill the lumen (dead space) of the CVAD, During days when rtPA was not administered,
- either 2 mL of 1000 U/mL heparin or 2 mg rtPA in 2.2 mL sterile water per lumen - per protocol, heparin locks were changed a minimum of once per week, whereas rt-PA locks could be left in place for up to 4 weeks.
participants received heparin 10 U/mL flush according to the subject’s existing line care instructions and standard of care.
- 4 patients had line locks with heparin initially, and then transitioned to rt-PA locks, and 6 patients had line locks entirely with heparin during the study period.
Optimal lock frequency
once weekly for a total of 24 weeks. rtPA was given as ‘‘lock therapy’’ in that it dwelled within the catheter of the CVAD for a specified duration of time and was subsequently removed aspirated; Dwell times of rtPA were until the next access (a minimum of 4 hours and maximum of 10 hours) as determined by the patient’s existing TPN schedule
70 procedures used heparin locks and 23 used rt-PA locks. The average interval between procedures was 12 days (range 5-67 days). The average interval between procedures when heparin locks (changed at least weekly) was 9 days (range 5-33 days), and when rt-PA locks were used was also 9 days (range 5-67 days). There were three instances where the interval between procedures exceeded the protocol limit for a rt-PA lock of 28 days due to patient scheduling issues. In each of these cases, the lock was not changed in the interval (33, 34, and 67 days), and the line worked well for the subsequent procedure.
Does NC influence patency
Can take blood specimens through CVAD? NC?
Patency – occlusion prevention PIV
How is patency checked?
What solution is used to flush and check patency
Occlusion management CVAD
Factors affecting occlusion rates: - type of cancer
- type of infusate
- age
- CVAD duration
- laterality
- number of lumens
- type of CVAD
- valve vs non-valved catheters
- BMI>25
Other patient comorbidities
Steps in assessment of occlusion
Optimal management All nurses ask pt to alter position - instilling a thrombolytic agent to be the most effective technique, followed by these noninvasive techniques: (a) ask patient to lie down, (b) use back-and-forth technique to flush, and (c) ask patient to take deep breaths - No associations were found between techniques and years in oncology nursing, work setting, certification, or academic degree - other medications used, 28 nurses answered and the majority (n = 11) used IV saline. - Two nurses listed using thrombolytic agents longer than
recommended (i.e., three hours then repeat the next day, if needed, for 24 hours); two reported using dexamethasone to confirm IV placement; and three listed a plan for future maintenance, including increasing heparin flush to 1,000 units (n = 2) and using low-dose warfarin (n = 1) if the problem persisted. Almost all respondents (n = 208) referred patients to another healthcare provider. The majority of referrals were to radiology (n = 119), another nurse (n = 58), or the surgeon or radiologist who placed the line (n = 39).
Optimal catheter tip position How does this relate to occlusion
Does angle of catheter in relation to port body impact occlusion rates
Does increase in resistance monitoring values indicate imminent CVAD occlusion
Can locking solutions be associated with risks of other complications?
Does CVAD material influence occlusion rates?
Can CVADs be used for radiological studies?
Occlusion management PIV
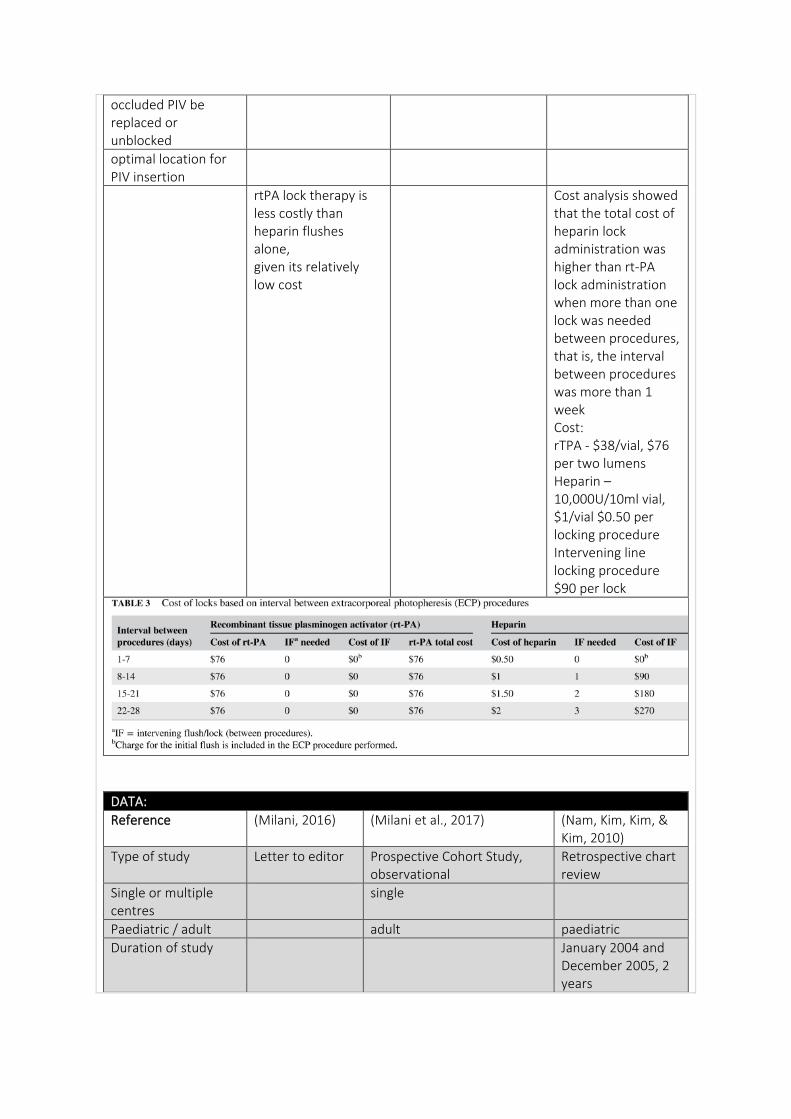
occluded PIV be replaced or unblocked
optimal location for PIV insertion
rtPA lock therapy is less costly than heparin flushes alone, given its relatively low cost
Cost analysis showed that the total cost of heparin lock administration was higher than rt-PA lock administration when more than one lock was needed between procedures, that is, the interval between procedures was more than 1 week Cost: rTPA - $38/vial, $76 per two lumens Heparin – 10,000U/10ml vial, $1/vial $0.50 per locking procedure Intervening line locking procedure $90 per lock
DATA:
Reference (Milani, 2016) (Milani et al., 2017) (Nam, Kim, Kim, & Kim, 2010)
Type of study Letter to editor Prospective Cohort Study, observational
Retrospective chart review
Single or multiple centres
single
Paediatric / adult adult paediatric
Duration of study January 2004 and December 2005, 2 years
Catheter days of study
Number of participants
218, 20 excluded N=198 For 4111 observations
225
Number CVADs per patients mean (SD)
235 ports 1 port n=224 2 ports – n=9 3 ports n=2
Dwell time of the CVAD (days) mean (range)
- mean maintenance period was 724.8+/- 500.6 days (range: 17–2,124).
Type of CVAD portacath TIVAD - 5.8 Fr single-lumen Port-A-Caths (SIMS, Deltec) were used in 169 cases, 9.6 Fr single-lumen Port-A-Caths (Bard, Inc., Salt Lake City) in 63, and other types of TIAPs in 6 - ports implanted into almost all pediatric hematology–oncology patients with the exception of those who require medications that are not given usually or required to be given through a central vein and those who are scheduled for bone marrow transplantation.
Number of CVAD lumens
Profession of inserter
Anatomical location of insertion
N (%)
R. external jugular vein n=178 cases (74.8%); R. IJ n=34 (14.3%), the L. external jugular vein n=20 (8.4%); L. IJ n= 6 (2.5%).
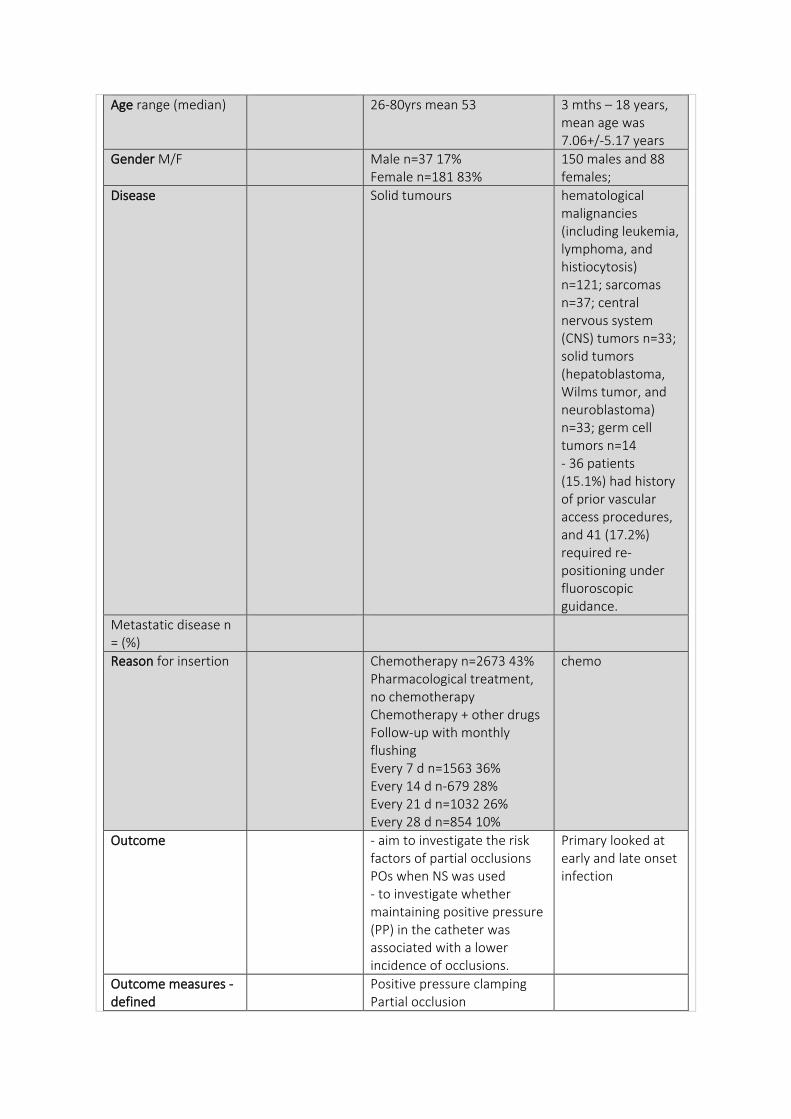
Age range (median) 26-80yrs mean 53 3 mths – 18 years, mean age was 7.06+/-5.17 years
Gender M/F Male n=37 17% Female n=181 83%
150 males and 88 females;
Disease Solid tumours hematological malignancies (including leukemia, lymphoma, and histiocytosis) n=121; sarcomas n=37; central nervous system (CNS) tumors n=33; solid tumors (hepatoblastoma, Wilms tumor, and neuroblastoma) n=33; germ cell tumors n=14 - 36 patients (15.1%) had history of prior vascular access procedures, and 41 (17.2%) required re-positioning under fluoroscopic guidance.
Metastatic disease n = (%)
Reason for insertion Chemotherapy n=2673 43% Pharmacological treatment, no chemotherapy Chemotherapy + other drugs Follow-up with monthly flushing Every 7 d n=1563 36% Every 14 d n-679 28% Every 21 d n=1032 26% Every 28 d n=854 10%
chemo
Outcome - aim to investigate the risk factors of partial occlusions POs when NS was used - to investigate whether maintaining positive pressure (PP) in the catheter was associated with a lower incidence of occlusions.
Primary looked at early and late onset infection
Outcome measures - defined
Positive pressure clamping Partial occlusion
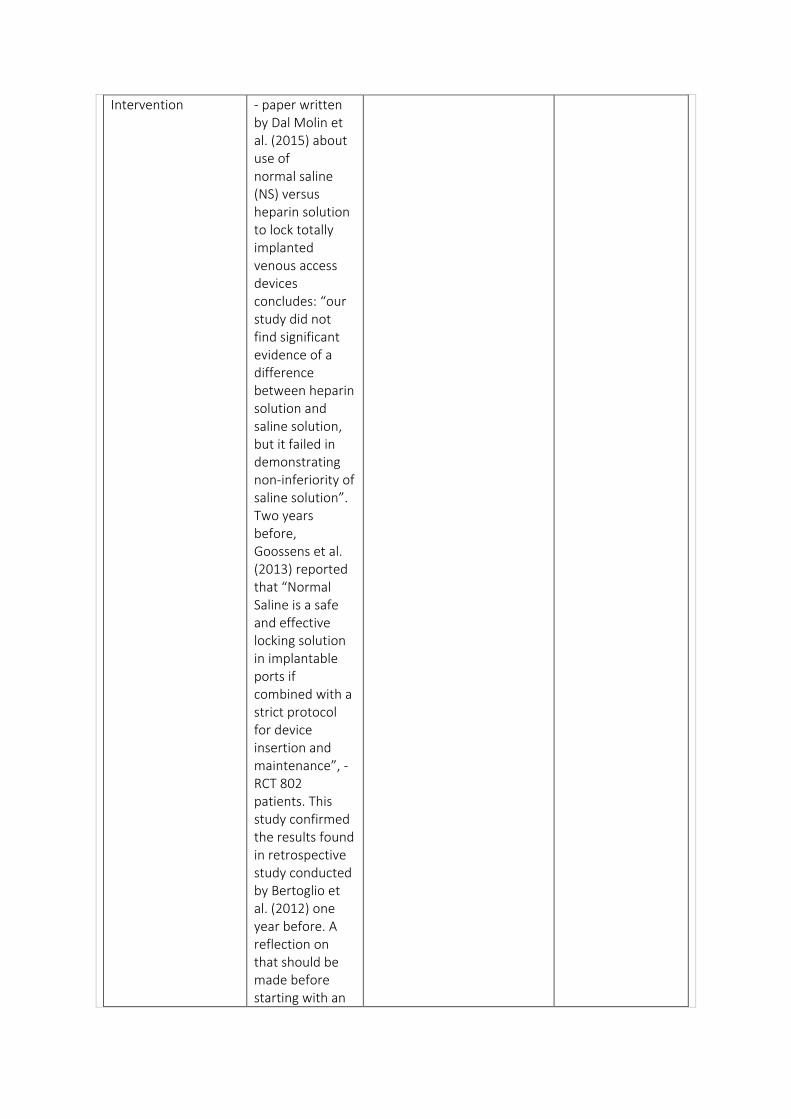
Intervention - paper written by Dal Molin et al. (2015) about use of normal saline (NS) versus heparin solution to lock totally implanted venous access devices concludes: “our study did not find significant evidence of a difference between heparin solution and saline solution, but it failed in demonstrating non-inferiority of saline solution”. Two years before, Goossens et al. (2013) reported that “Normal Saline is a safe and effective locking solution in implantable ports if combined with a strict protocol for device insertion and maintenance”, - RCT 802 patients. This study confirmed the results found in retrospective study conducted by Bertoglio et al. (2012) one year before. A reflection on that should be made before starting with an
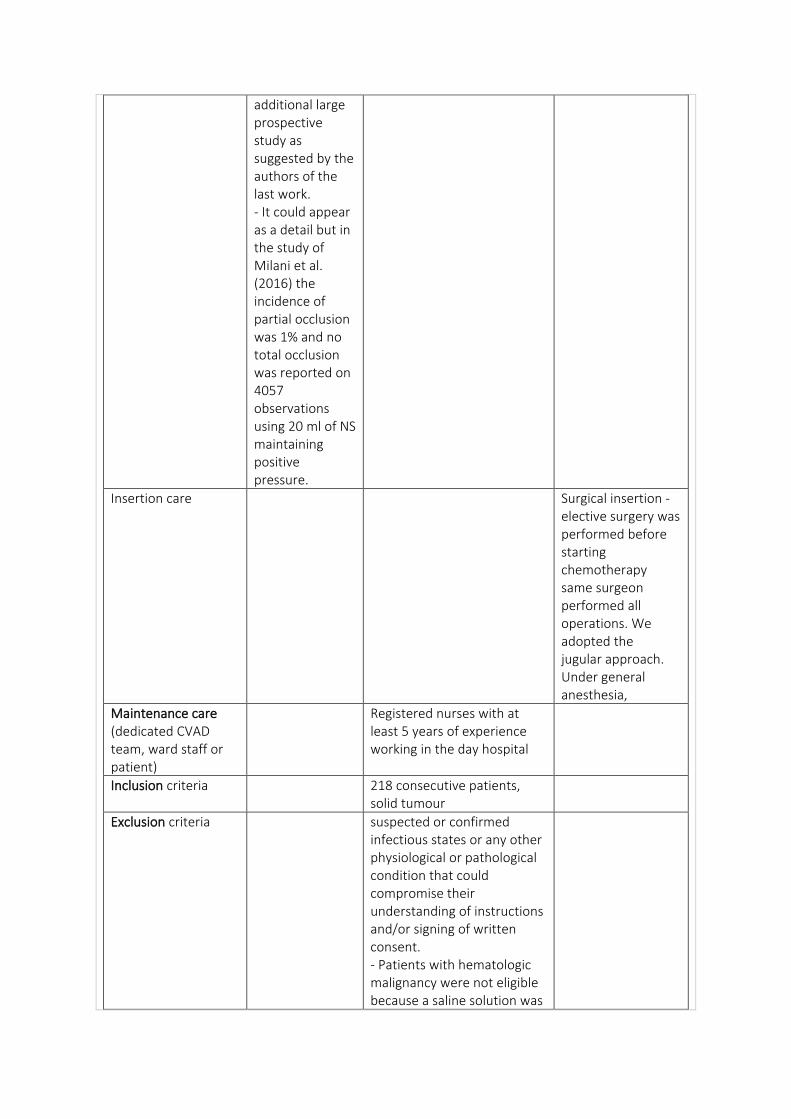
additional large prospective study as suggested by the authors of the last work. - It could appear as a detail but in the study of Milani et al. (2016) the incidence of partial occlusion was 1% and no total occlusion was reported on 4057 observations using 20 ml of NS maintaining positive pressure.
Insertion care Surgical insertion - elective surgery was performed before starting chemotherapy same surgeon performed all operations. We adopted the jugular approach. Under general anesthesia,
Maintenance care (dedicated CVAD team, ward staff or patient)
Registered nurses with at least 5 years of experience working in the day hospital
Inclusion criteria 218 consecutive patients, solid tumour
Exclusion criteria suspected or confirmed infectious states or any other physiological or pathological condition that could compromise their understanding of instructions and/or signing of written consent. - Patients with hematologic malignancy were not eligible because a saline solution was
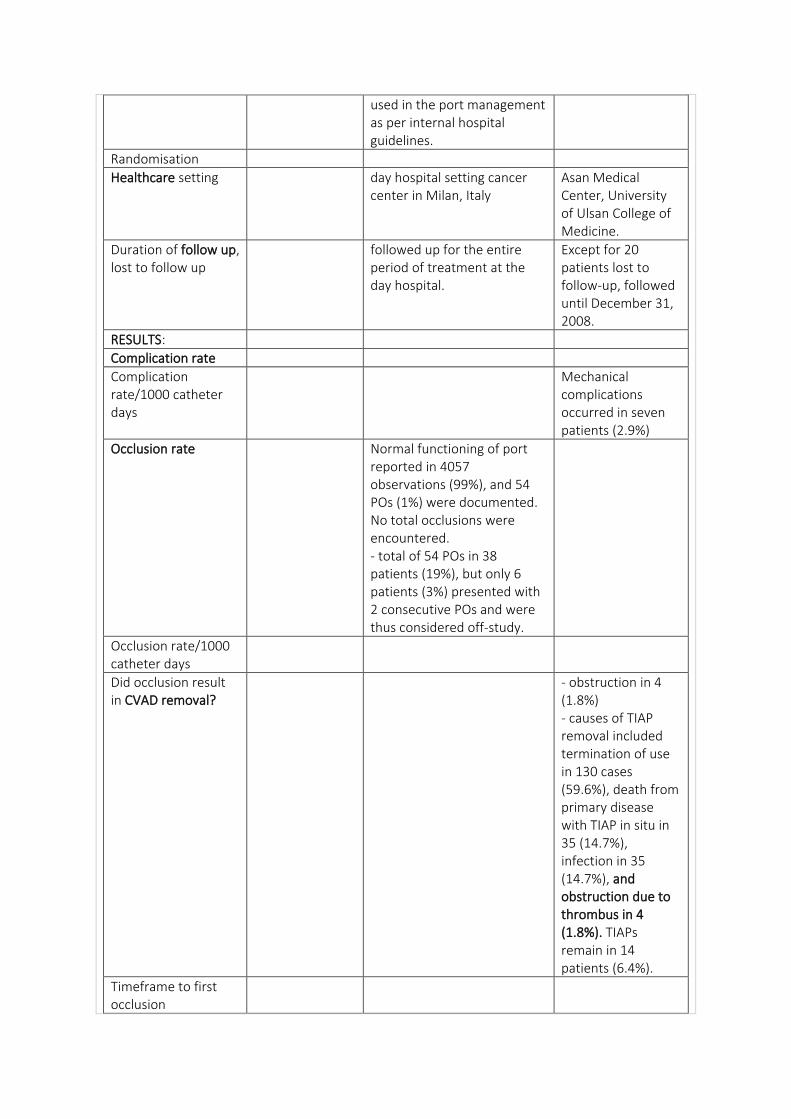
used in the port management as per internal hospital guidelines.
Randomisation
Healthcare setting day hospital setting cancer center in Milan, Italy
Asan Medical Center, University of Ulsan College of Medicine.
Duration of follow up, lost to follow up
followed up for the entire period of treatment at the day hospital.
Except for 20 patients lost to follow-up, followed until December 31, 2008.
RESULTS:
Complication rate
Complication rate/1000 catheter days
Mechanical complications occurred in seven patients (2.9%)
Occlusion rate Normal functioning of port reported in 4057 observations (99%), and 54 POs (1%) were documented. No total occlusions were encountered. - total of 54 POs in 38 patients (19%), but only 6 patients (3%) presented with 2 consecutive POs and were thus considered off-study.
Occlusion rate/1000 catheter days
Did occlusion result in CVAD removal?
- obstruction in 4 (1.8%) - causes of TIAP removal included termination of use in 130 cases (59.6%), death from primary disease with TIAP in situ in 35 (14.7%), infection in 35 (14.7%), and obstruction due to thrombus in 4 (1.8%). TIAPs remain in 14 patients (6.4%).
Timeframe to first occlusion
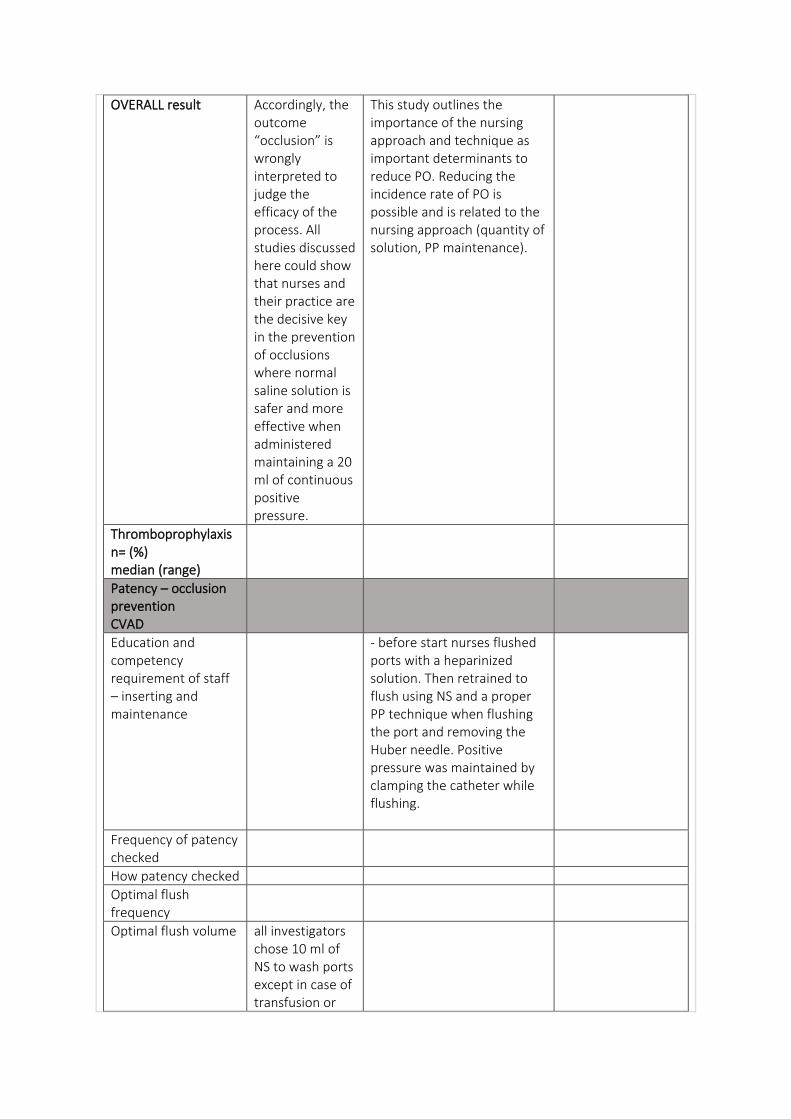
OVERALL result Accordingly, the outcome “occlusion” is wrongly interpreted to judge the efficacy of the process. All studies discussed here could show that nurses and their practice are the decisive key in the prevention of occlusions where normal saline solution is safer and more effective when administered maintaining a 20 ml of continuous positive pressure.
This study outlines the importance of the nursing approach and technique as important determinants to reduce PO. Reducing the incidence rate of PO is possible and is related to the nursing approach (quantity of solution, PP maintenance).
Thromboprophylaxis n= (%) median (range)
Patency – occlusion prevention CVAD
Education and competency requirement of staff – inserting and maintenance
- before start nurses flushed ports with a heparinized solution. Then retrained to flush using NS and a proper PP technique when flushing the port and removing the Huber needle. Positive pressure was maintained by clamping the catheter while flushing.
Frequency of patency checked
How patency checked
Optimal flush frequency
Optimal flush volume all investigators chose 10 ml of NS to wash ports except in case of transfusion or
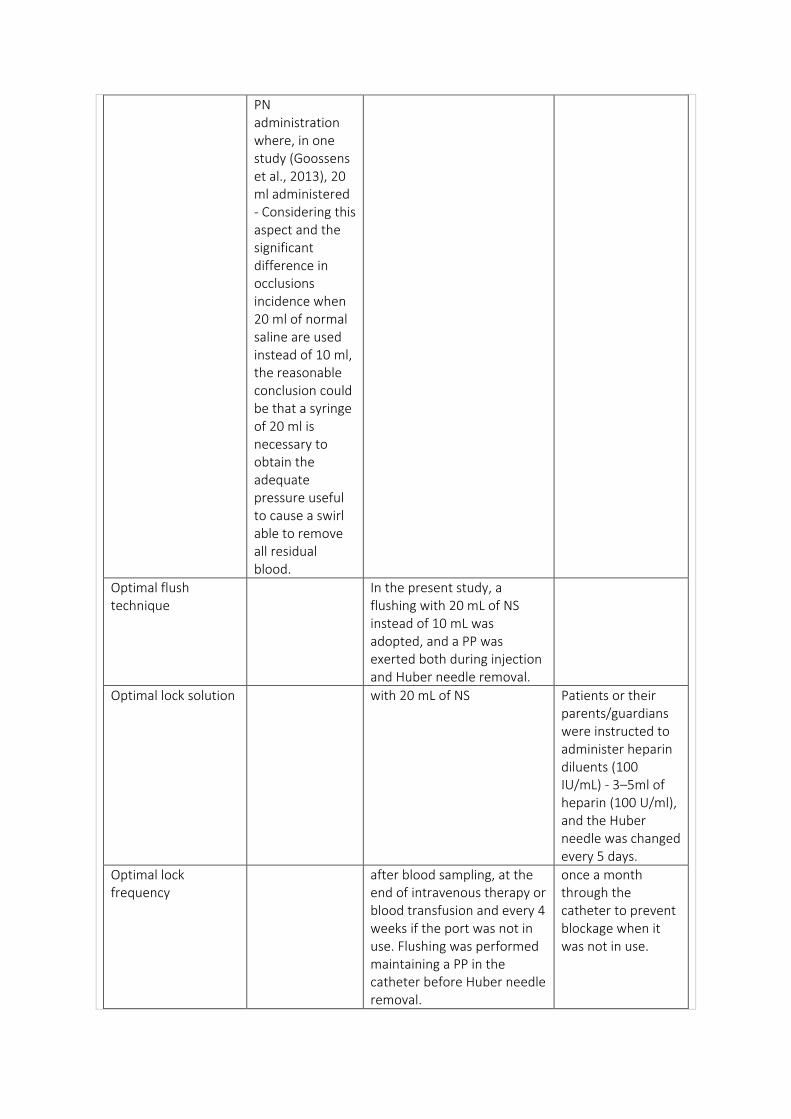
PN administration where, in one study (Goossens et al., 2013), 20 ml administered - Considering this aspect and the significant difference in occlusions incidence when 20 ml of normal saline are used instead of 10 ml, the reasonable conclusion could be that a syringe of 20 ml is necessary to obtain the adequate pressure useful to cause a swirl able to remove all residual blood.
Optimal flush technique
In the present study, a flushing with 20 mL of NS instead of 10 mL was adopted, and a PP was exerted both during injection and Huber needle removal.
Optimal lock solution with 20 mL of NS Patients or their parents/guardians were instructed to administer heparin diluents (100 IU/mL) - 3–5ml of heparin (100 U/ml), and the Huber needle was changed every 5 days.
Optimal lock frequency
after blood sampling, at the end of intravenous therapy or blood transfusion and every 4 weeks if the port was not in use. Flushing was performed maintaining a PP in the catheter before Huber needle removal.
once a month through the catheter to prevent blockage when it was not in use.
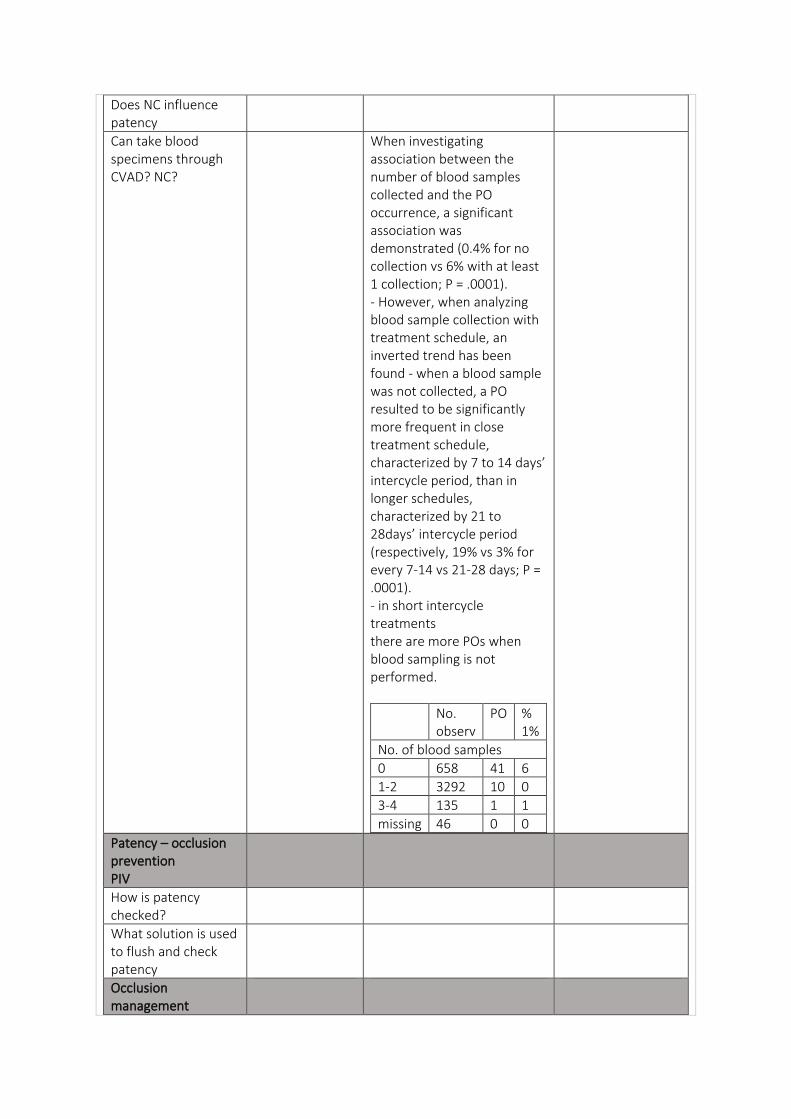
Does NC influence patency
Can take blood specimens through CVAD? NC?
When investigating association between the number of blood samples collected and the PO occurrence, a significant association was demonstrated (0.4% for no collection vs 6% with at least 1 collection; P = .0001). - However, when analyzing blood sample collection with treatment schedule, an inverted trend has been found - when a blood sample was not collected, a PO resulted to be significantly more frequent in close treatment schedule, characterized by 7 to 14 days’ intercycle period, than in longer schedules, characterized by 21 to 28days’ intercycle period (respectively, 19% vs 3% for every 7-14 vs 21-28 days; P = .0001). - in short intercycle treatments there are more POs when blood sampling is not performed.
No. observ
PO % 1%
No. of blood samples
0 658 41 6
1-2 3292 10 0
3-4 135 1 1
missing 46 0 0
Patency – occlusion prevention PIV
How is patency checked?
What solution is used to flush and check patency
Occlusion management
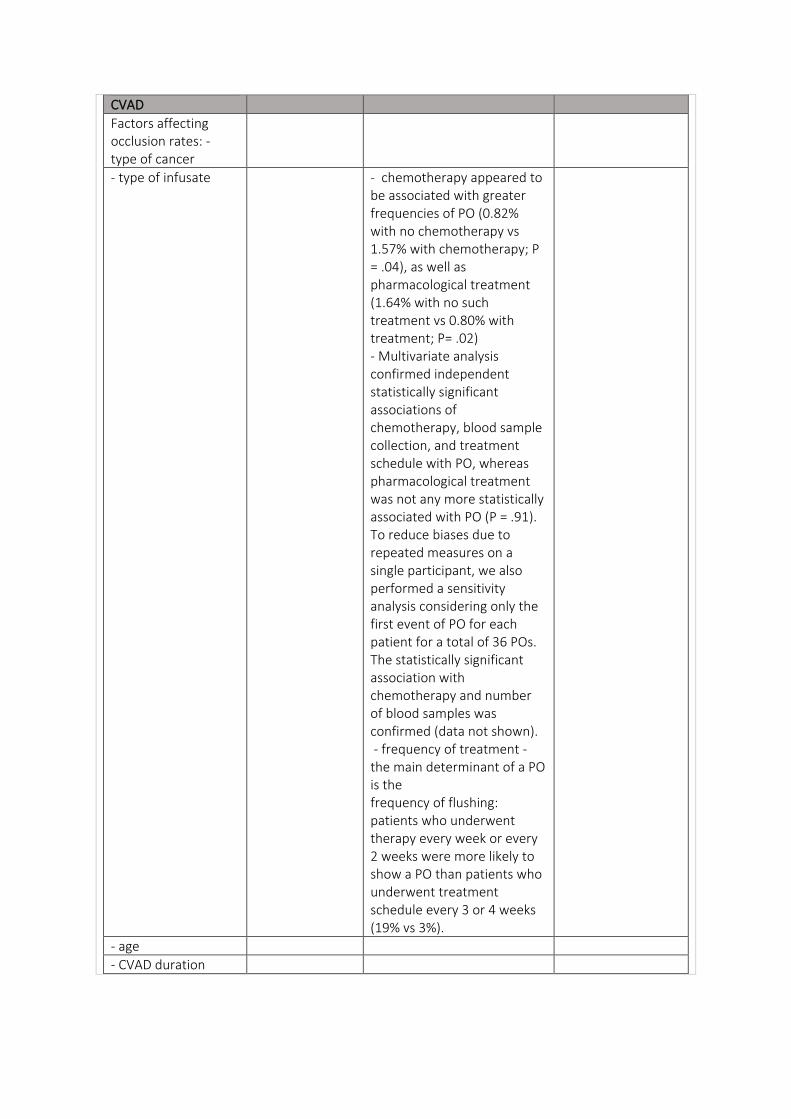
CVAD
Factors affecting occlusion rates: - type of cancer
- type of infusate - chemotherapy appeared to be associated with greater frequencies of PO (0.82% with no chemotherapy vs 1.57% with chemotherapy; P = .04), as well as pharmacological treatment (1.64% with no such treatment vs 0.80% with treatment; P= .02) - Multivariate analysis confirmed independent statistically significant associations of chemotherapy, blood sample collection, and treatment schedule with PO, whereas pharmacological treatment was not any more statistically associated with PO (P = .91). To reduce biases due to repeated measures on a single participant, we also performed a sensitivity analysis considering only the first event of PO for each patient for a total of 36 POs. The statistically significant association with chemotherapy and number of blood samples was confirmed (data not shown). - frequency of treatment - the main determinant of a PO is the frequency of flushing: patients who underwent therapy every week or every 2 weeks were more likely to show a PO than patients who underwent treatment schedule every 3 or 4 weeks (19% vs 3%).
- age
- CVAD duration
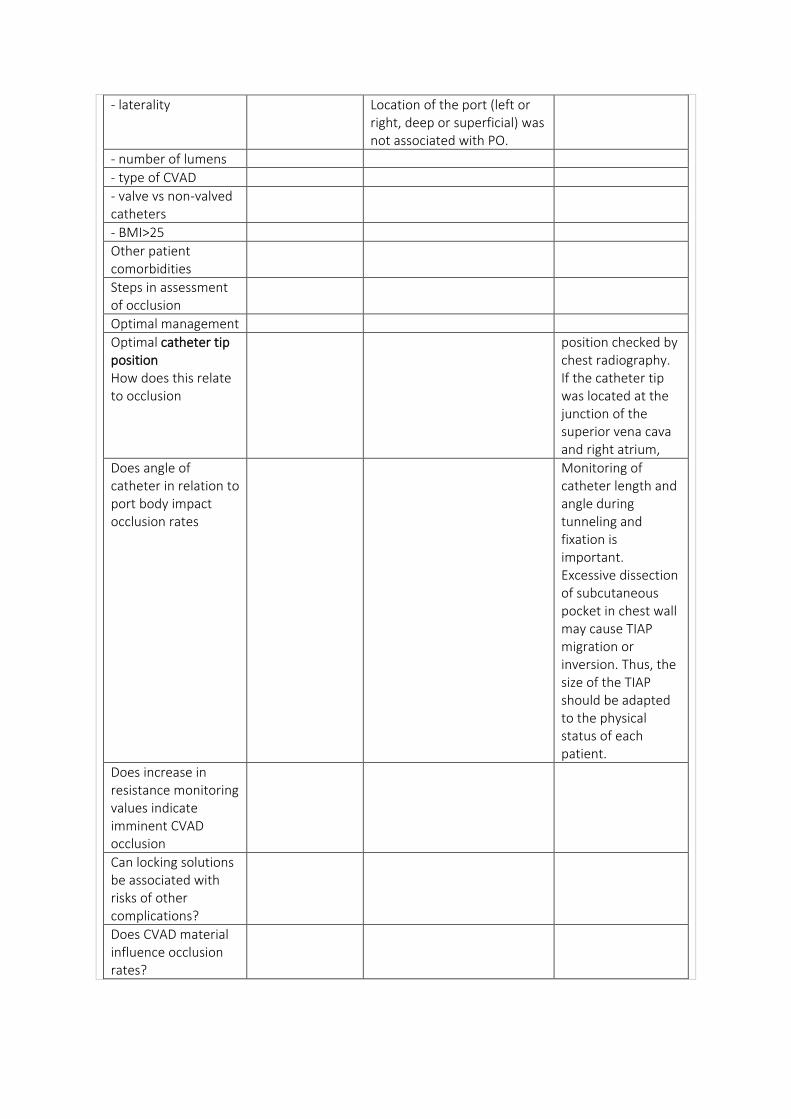
- laterality Location of the port (left or right, deep or superficial) was not associated with PO.
- number of lumens
- type of CVAD
- valve vs non-valved catheters
- BMI>25
Other patient comorbidities
Steps in assessment of occlusion
Optimal management
Optimal catheter tip position How does this relate to occlusion
position checked by chest radiography. If the catheter tip was located at the junction of the superior vena cava and right atrium,
Does angle of catheter in relation to port body impact occlusion rates
Monitoring of catheter length and angle during tunneling and fixation is important. Excessive dissection of subcutaneous pocket in chest wall may cause TIAP migration or inversion. Thus, the size of the TIAP should be adapted to the physical status of each patient.
Does increase in resistance monitoring values indicate imminent CVAD occlusion
Can locking solutions be associated with risks of other complications?
Does CVAD material influence occlusion rates?
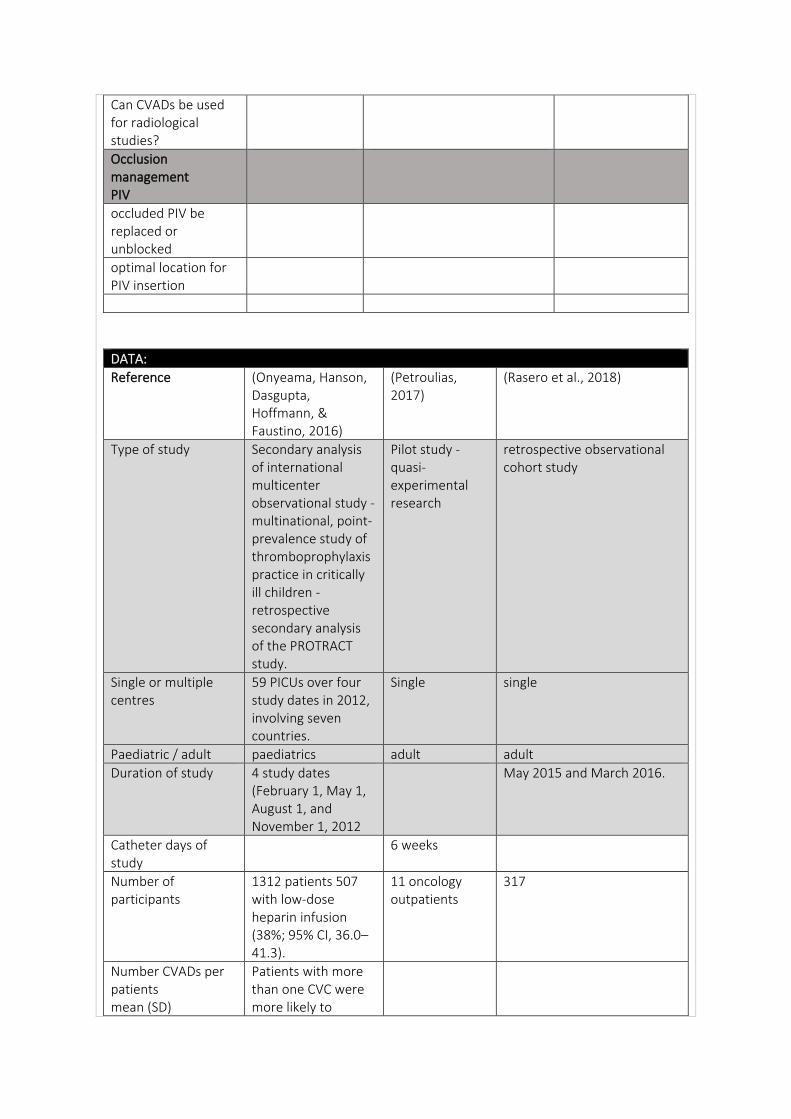
Can CVADs be used for radiological studies?
Occlusion management PIV
occluded PIV be replaced or unblocked
optimal location for PIV insertion
DATA:
Reference (Onyeama, Hanson, Dasgupta, Hoffmann, & Faustino, 2016)
(Petroulias, 2017)
(Rasero et al., 2018)
Type of study Secondary analysis of international multicenter observational study - multinational, point-prevalence study of thromboprophylaxis practice in critically ill children - retrospective secondary analysis of the PROTRACT study.
Pilot study - quasi-experimental research
retrospective observational cohort study
Single or multiple centres
59 PICUs over four study dates in 2012, involving seven countries.
Single single
Paediatric / adult paediatrics adult adult
Duration of study 4 study dates (February 1, May 1, August 1, and November 1, 2012
May 2015 and March 2016.
Catheter days of study
6 weeks
Number of participants
1312 patients 507 with low-dose heparin infusion (38%; 95% CI, 36.0–41.3).
11 oncology outpatients
317
Number CVADs per patients mean (SD)
Patients with more than one CVC were more likely to
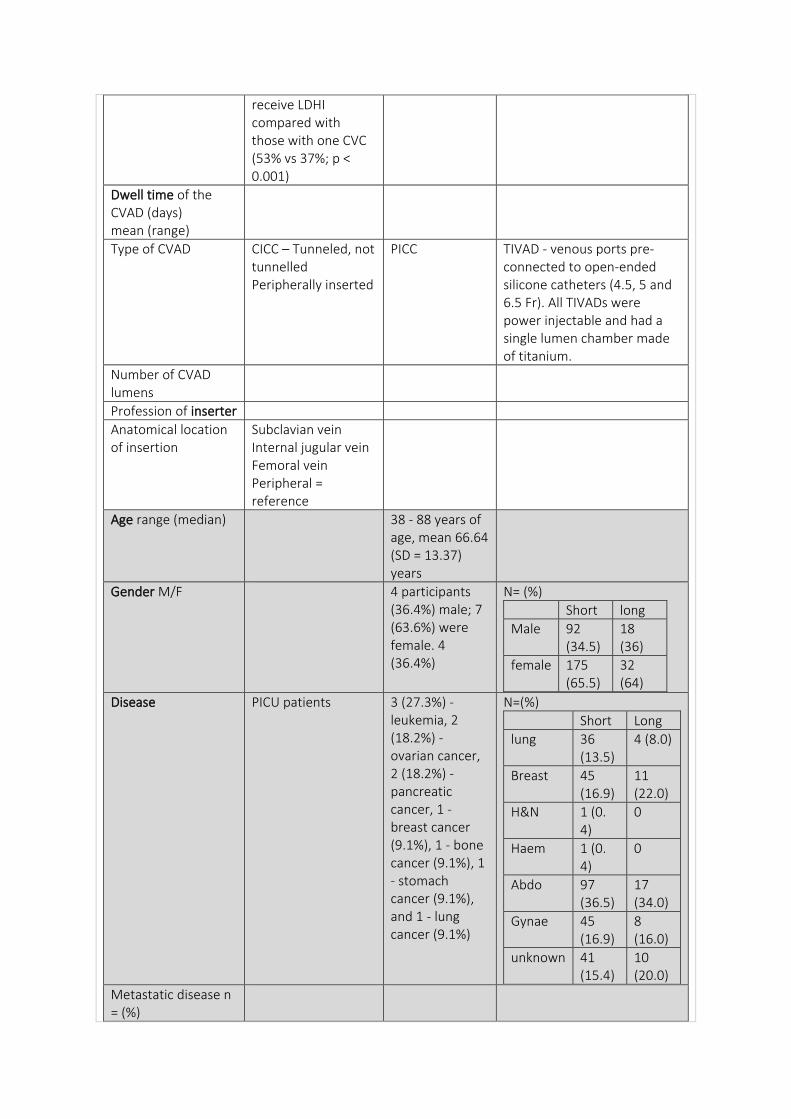
receive LDHI compared with those with one CVC (53% vs 37%; p < 0.001)
Dwell time of the CVAD (days) mean (range)
Type of CVAD CICC – Tunneled, not tunnelled Peripherally inserted
PICC TIVAD - venous ports pre-connected to open-ended silicone catheters (4.5, 5 and 6.5 Fr). All TIVADs were power injectable and had a single lumen chamber made of titanium.
Number of CVAD lumens
Profession of inserter
Anatomical location of insertion
Subclavian vein Internal jugular vein Femoral vein Peripheral = reference
Age range (median) 38 - 88 years of age, mean 66.64 (SD = 13.37) years
Gender M/F 4 participants (36.4%) male; 7 (63.6%) were female. 4 (36.4%)
N= (%)
Short long
Male 92 (34.5)
18 (36)
female 175 (65.5)
32 (64)
Disease PICU patients 3 (27.3%) - leukemia, 2 (18.2%) - ovarian cancer, 2 (18.2%) - pancreatic cancer, 1 - breast cancer (9.1%), 1 - bone cancer (9.1%), 1 - stomach cancer (9.1%), and 1 - lung cancer (9.1%)
N=(%)
Short Long
lung 36 (13.5)
4 (8.0)
Breast 45 (16.9)
11 (22.0)
H&N 1 (0. 4)
0
Haem 1 (0. 4)
0
Abdo 97 (36.5)
17 (34.0)
Gynae 45 (16.9)
8 (16.0)
unknown 41 (15.4)
10 (20.0)
Metastatic disease n = (%)
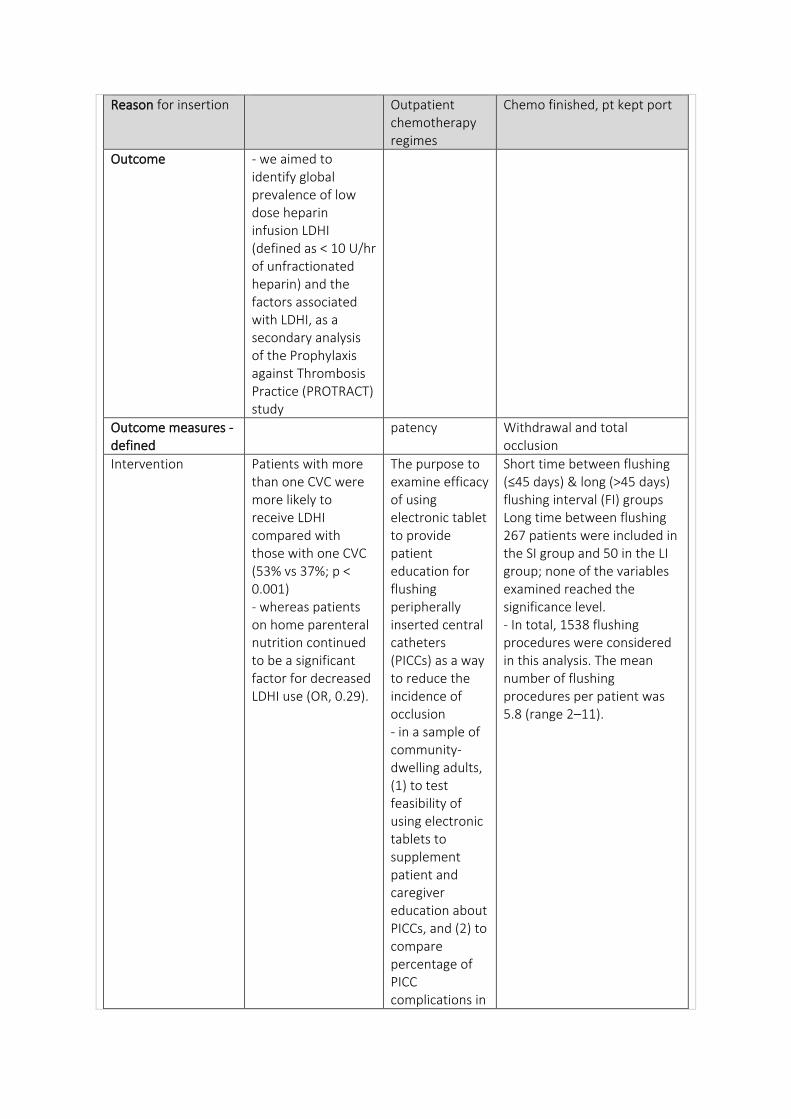
Reason for insertion Outpatient chemotherapy regimes
Chemo finished, pt kept port
Outcome - we aimed to identify global prevalence of low dose heparin infusion LDHI (defined as < 10 U/hr of unfractionated heparin) and the factors associated with LDHI, as a secondary analysis of the Prophylaxis against Thrombosis Practice (PROTRACT) study
Outcome measures - defined
patency Withdrawal and total occlusion
Intervention Patients with more than one CVC were more likely to receive LDHI compared with those with one CVC (53% vs 37%; p < 0.001) - whereas patients on home parenteral nutrition continued to be a significant factor for decreased LDHI use (OR, 0.29).
The purpose to examine efficacy of using electronic tablet to provide patient education for flushing peripherally inserted central catheters (PICCs) as a way to reduce the incidence of occlusion - in a sample of community-dwelling adults, (1) to test feasibility of using electronic tablets to supplement patient and caregiver education about PICCs, and (2) to compare percentage of PICC complications in
Short time between flushing (≤45 days) & long (>45 days) flushing interval (FI) groups Long time between flushing 267 patients were included in the SI group and 50 in the LI group; none of the variables examined reached the significance level. - In total, 1538 flushing procedures were considered in this analysis. The mean number of flushing procedures per patient was 5.8 (range 2–11).
intervention group with national percentage rates for patients and caregivers who were educated using the standard method of education.
Insertion care
Maintenance care (dedicated CVAD team, ward staff or patient)
Patients and caregivers need to learn and demonstrate appropriate techniques to prevent catheter occlusion to ensure safe and effective self-management.
Inclusion criteria Children less than 18 years old with a central venous catheter who were admitted to a participating unit and enrolled in the completed Prophylaxis against Thrombosis Practice study were included.
- 18 years of age or older, not pregnant, and diagnosed with cancer. Participants had to understand and communicate in English and be cognitively alert. All participants familiar with electronic devices (eg, laptop computers, smartphones, electronic tablets) and were able to use the Internet to navigate the FaceTime application.
adult patient with cancer (age≥18 years old); having a TIVAD in place that was not in use, and was being flushed to maintain it; and having received at least two flushing procedures during the period of the study.
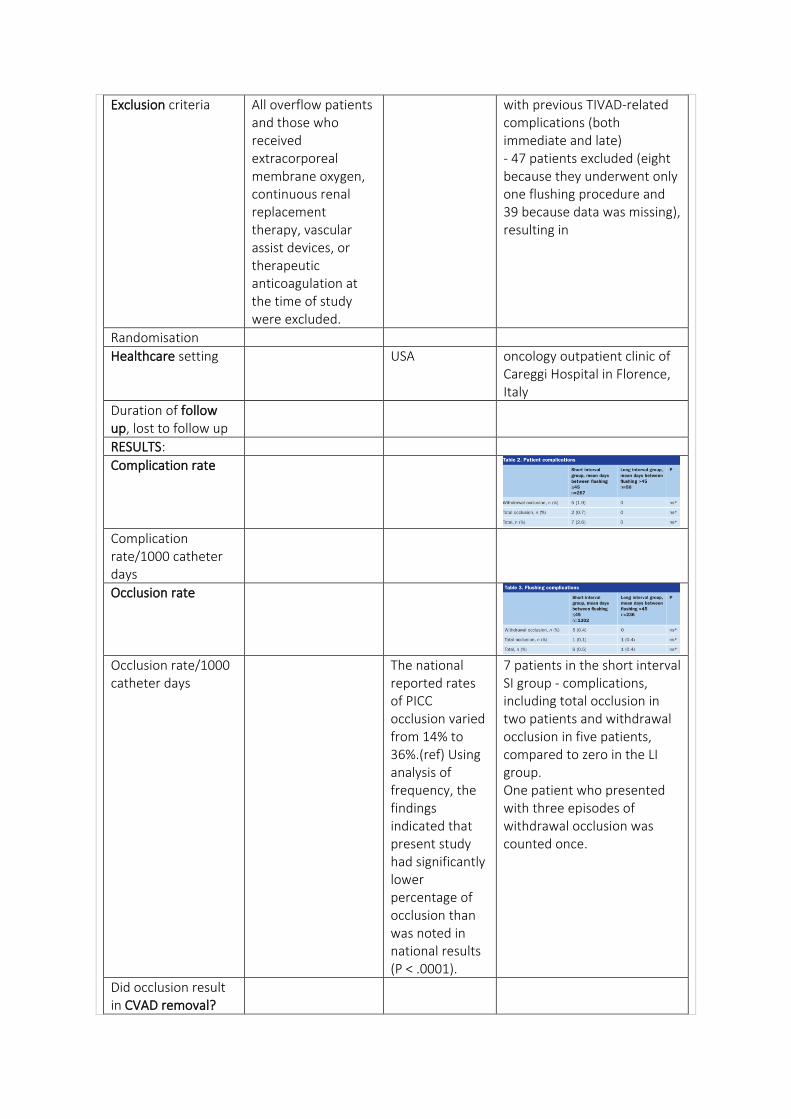
Exclusion criteria All overflow patients and those who received extracorporeal membrane oxygen, continuous renal replacement therapy, vascular assist devices, or therapeutic anticoagulation at the time of study were excluded.
with previous TIVAD-related complications (both immediate and late) - 47 patients excluded (eight because they underwent only one flushing procedure and 39 because data was missing), resulting in
Randomisation
Healthcare setting USA oncology outpatient clinic of Careggi Hospital in Florence, Italy
Duration of follow up, lost to follow up
RESULTS:
Complication rate
Complication rate/1000 catheter days
Occlusion rate
Occlusion rate/1000 catheter days
The national reported rates of PICC occlusion varied from 14% to 36%.(ref) Using analysis of frequency, the findings indicated that present study had significantly lower percentage of occlusion than was noted in national results (P < .0001).
7 patients in the short interval SI group - complications, including total occlusion in two patients and withdrawal occlusion in five patients, compared to zero in the LI group. One patient who presented with three episodes of withdrawal occlusion was counted once.
Did occlusion result in CVAD removal?
Timeframe to first occlusion
OVERALL result Patient, central venous catheter, and hospital factors are associated with the use of low-dose heparin infusion in critically ill children. - multivariable analysis - most patient comorbidities, including chronic disease and thrombosis history, did not impact LDHI use, whereas hospital and geographic factors retained significance. Conclusion: LDHI remains a common method for the maintenance of CVC patency in critically ill children despite the lack of substantial data supporting its efficacy. In our analysis of the PROTRACT study, we showed that LDHI use has global prevalence, as 38% of patients with CVCs in this study received LDHI. Various patient, hospital, and CVC factors are associated with LDHI use.
The patients in the present study did not experience any occlusions during the 6 weeks of the intervention.
Results from the current analysis, which included a sizeable number of patients and procedures, indicated that FIs longer than 45 days did not result in a greater amount of catheter-related adverse events than more frequent FIs (≤45 days). - results indicated that there were no differences between the long and short interval group in terms of rate of complications when considering the number of patients and procedures
Thromboprophylaxis n= (%) median (range)
Patency – occlusion prevention
CVAD
Education and competency requirement of staff – inserting and maintenance
Using electronic tablet to detail the steps required to flush their PICCs could help patients master the process better than receiving the standard method of patient education. The standard method of education consists of an infusion nurse demonstrating how to flush the PICC and providing the patient with a printed handout describing the steps. Therefore, the intervention for this project was an initial face-to-face session for the patient with an infusion nurse, as well as coaching via FaceTime (Apple, Cupertino, CA) by means of an electronic tablet and access to a video that outlined the 10 steps of flushing - Patients or caregivers were asked to demonstrate their ability to
Good nursing practice can help maintain TIVAD function
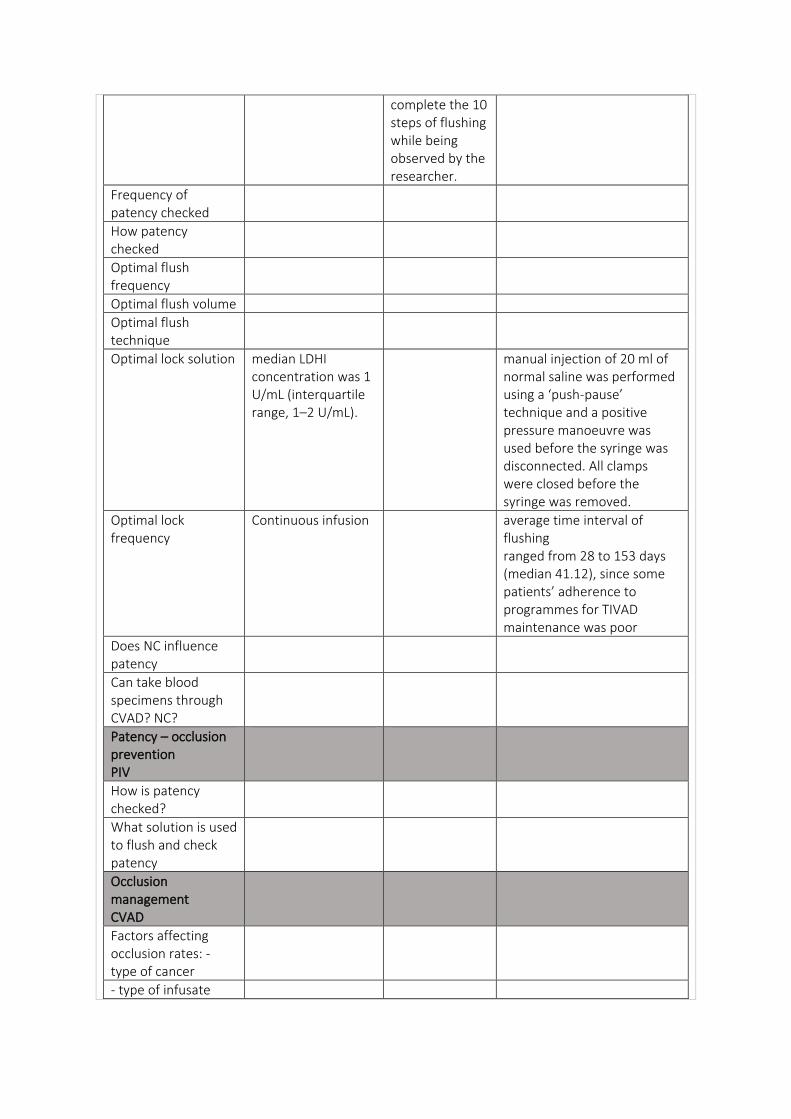
complete the 10 steps of flushing while being observed by the researcher.
Frequency of patency checked
How patency checked
Optimal flush frequency
Optimal flush volume
Optimal flush technique
Optimal lock solution median LDHI concentration was 1 U/mL (interquartile range, 1–2 U/mL).
manual injection of 20 ml of normal saline was performed using a ‘push-pause’ technique and a positive pressure manoeuvre was used before the syringe was disconnected. All clamps were closed before the syringe was removed.
Optimal lock frequency
Continuous infusion average time interval of flushing ranged from 28 to 153 days (median 41.12), since some patients’ adherence to programmes for TIVAD maintenance was poor
Does NC influence patency
Can take blood specimens through CVAD? NC?
Patency – occlusion prevention PIV
How is patency checked?
What solution is used to flush and check patency
Occlusion management CVAD
Factors affecting occlusion rates: - type of cancer
- type of infusate
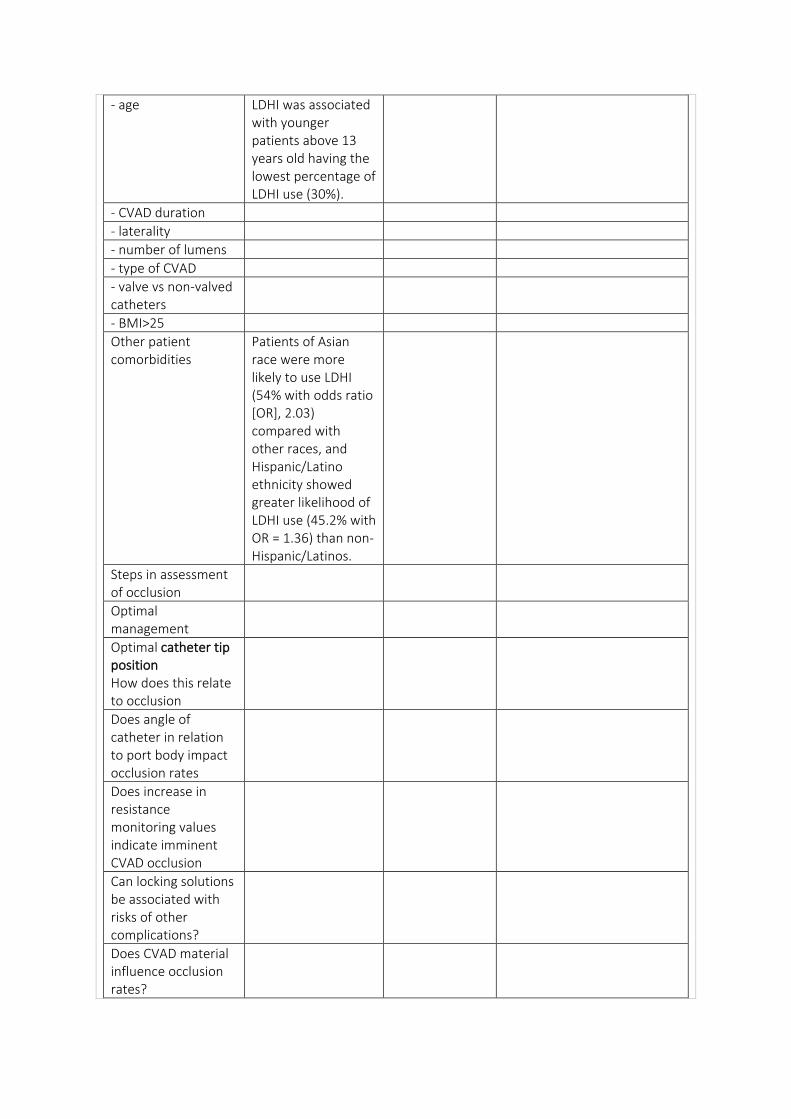
- age LDHI was associated with younger patients above 13 years old having the lowest percentage of LDHI use (30%).
- CVAD duration
- laterality
- number of lumens
- type of CVAD
- valve vs non-valved catheters
- BMI>25
Other patient comorbidities
Patients of Asian race were more likely to use LDHI (54% with odds ratio [OR], 2.03) compared with other races, and Hispanic/Latino ethnicity showed greater likelihood of LDHI use (45.2% with OR = 1.36) than non-Hispanic/Latinos.
Steps in assessment of occlusion
Optimal management
Optimal catheter tip position How does this relate to occlusion
Does angle of catheter in relation to port body impact occlusion rates
Does increase in resistance monitoring values indicate imminent CVAD occlusion
Can locking solutions be associated with risks of other complications?
Does CVAD material influence occlusion rates?
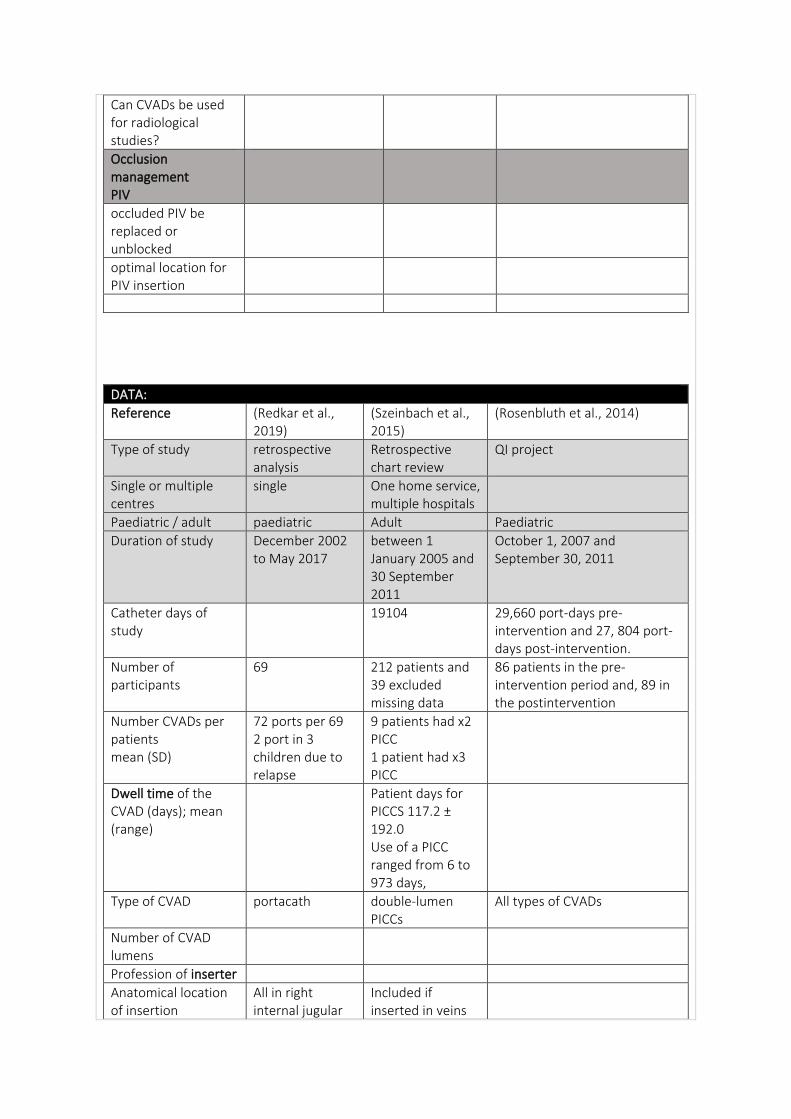
Can CVADs be used for radiological studies?
Occlusion management PIV
occluded PIV be replaced or unblocked
optimal location for PIV insertion
DATA:
Reference (Redkar et al., 2019)
(Szeinbach et al., 2015)
(Rosenbluth et al., 2014)
Type of study retrospective analysis
Retrospective chart review
QI project
Single or multiple centres
single One home service, multiple hospitals
Paediatric / adult paediatric Adult Paediatric
Duration of study December 2002 to May 2017
between 1 January 2005 and 30 September 2011
October 1, 2007 and September 30, 2011
Catheter days of study
19104 29,660 port-days pre-intervention and 27, 804 port-days post-intervention.
Number of participants
69 212 patients and 39 excluded missing data
86 patients in the pre-intervention period and, 89 in the postintervention
Number CVADs per patients mean (SD)
72 ports per 69 2 port in 3 children due to relapse
9 patients had x2 PICC 1 patient had x3 PICC
Dwell time of the CVAD (days); mean (range)
Patient days for PICCS 117.2 ± 192.0 Use of a PICC ranged from 6 to 973 days,
Type of CVAD portacath double-lumen PICCs
All types of CVADs
Number of CVAD lumens
Profession of inserter
Anatomical location of insertion
All in right internal jugular
Included if inserted in veins
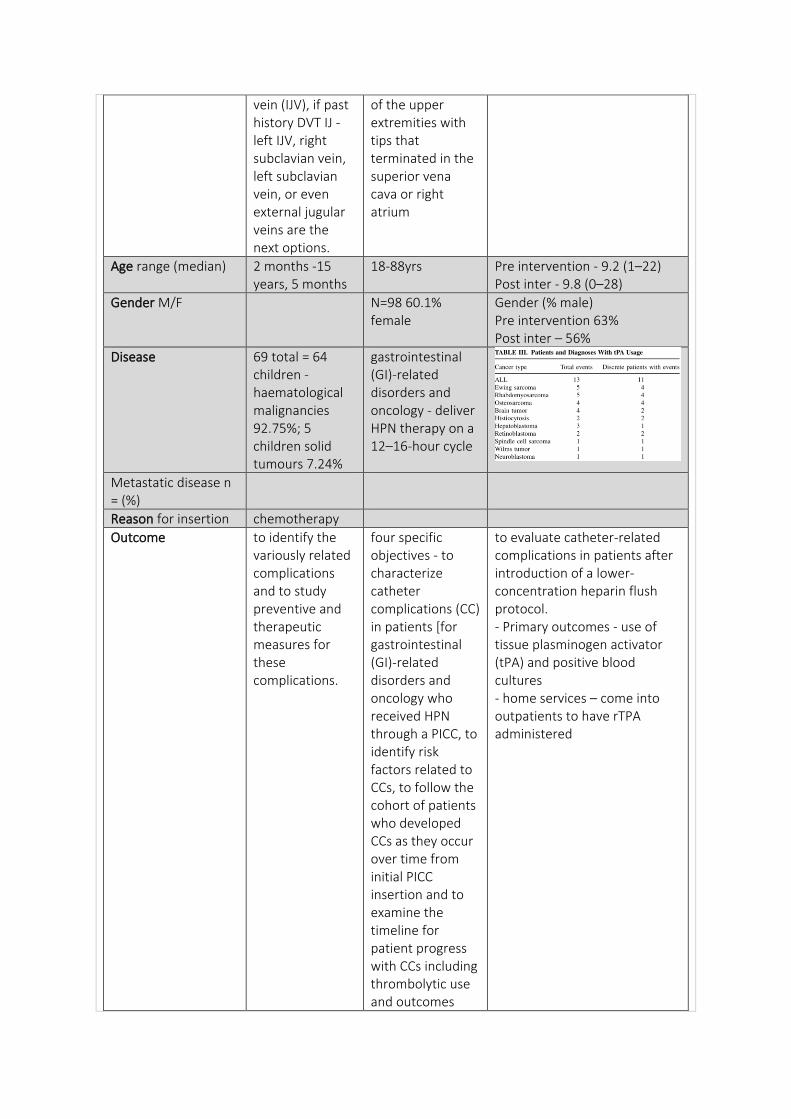
vein (IJV), if past history DVT IJ - left IJV, right subclavian vein, left subclavian vein, or even external jugular veins are the next options.
of the upper extremities with tips that terminated in the superior vena cava or right atrium
Age range (median) 2 months -15 years, 5 months
18-88yrs Pre intervention - 9.2 (1–22) Post inter - 9.8 (0–28)
Gender M/F N=98 60.1% female
Gender (% male) Pre intervention 63% Post inter – 56%
Disease 69 total = 64 children - haematological malignancies 92.75%; 5 children solid tumours 7.24%
gastrointestinal (GI)-related disorders and oncology - deliver HPN therapy on a 12–16-hour cycle
Metastatic disease n = (%)
Reason for insertion chemotherapy
Outcome to identify the variously related complications and to study preventive and therapeutic measures for these complications.
four specific objectives - to characterize catheter complications (CC) in patients [for gastrointestinal (GI)-related disorders and oncology who received HPN through a PICC, to identify risk factors related to CCs, to follow the cohort of patients who developed CCs as they occur over time from initial PICC insertion and to examine the timeline for patient progress with CCs including thrombolytic use and outcomes
to evaluate catheter-related complications in patients after introduction of a lower-concentration heparin flush protocol. - Primary outcomes - use of tissue plasminogen activator (tPA) and positive blood cultures - home services – come into outpatients to have rTPA administered
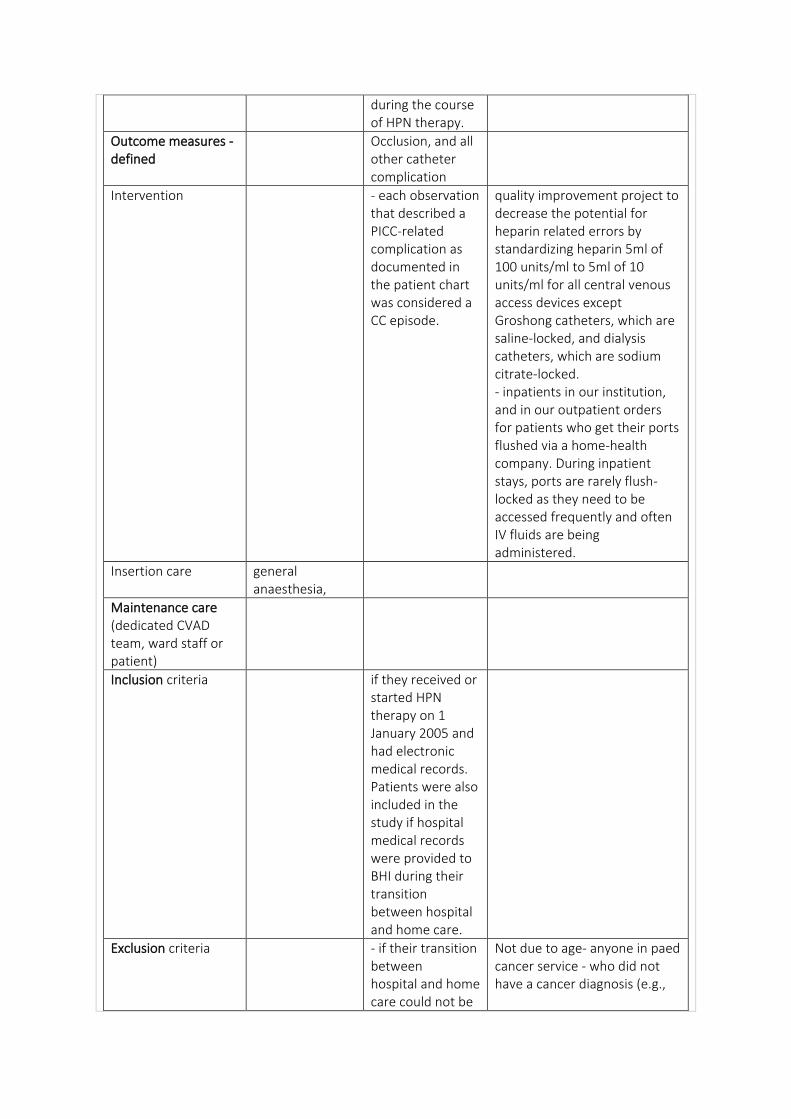
during the course of HPN therapy.
Outcome measures - defined
Occlusion, and all other catheter complication
Intervention - each observation that described a PICC-related complication as documented in the patient chart was considered a CC episode.
quality improvement project to decrease the potential for heparin related errors by standardizing heparin 5ml of 100 units/ml to 5ml of 10 units/ml for all central venous access devices except Groshong catheters, which are saline-locked, and dialysis catheters, which are sodium citrate-locked. - inpatients in our institution, and in our outpatient orders for patients who get their ports flushed via a home-health company. During inpatient stays, ports are rarely flush-locked as they need to be accessed frequently and often IV fluids are being administered.
Insertion care general anaesthesia,
Maintenance care (dedicated CVAD team, ward staff or patient)
Inclusion criteria if they received or started HPN therapy on 1 January 2005 and had electronic medical records. Patients were also included in the study if hospital medical records were provided to BHI during their transition between hospital and home care.
Exclusion criteria - if their transition between hospital and home care could not be
Not due to age- anyone in paed cancer service - who did not have a cancer diagnosis (e.g.,
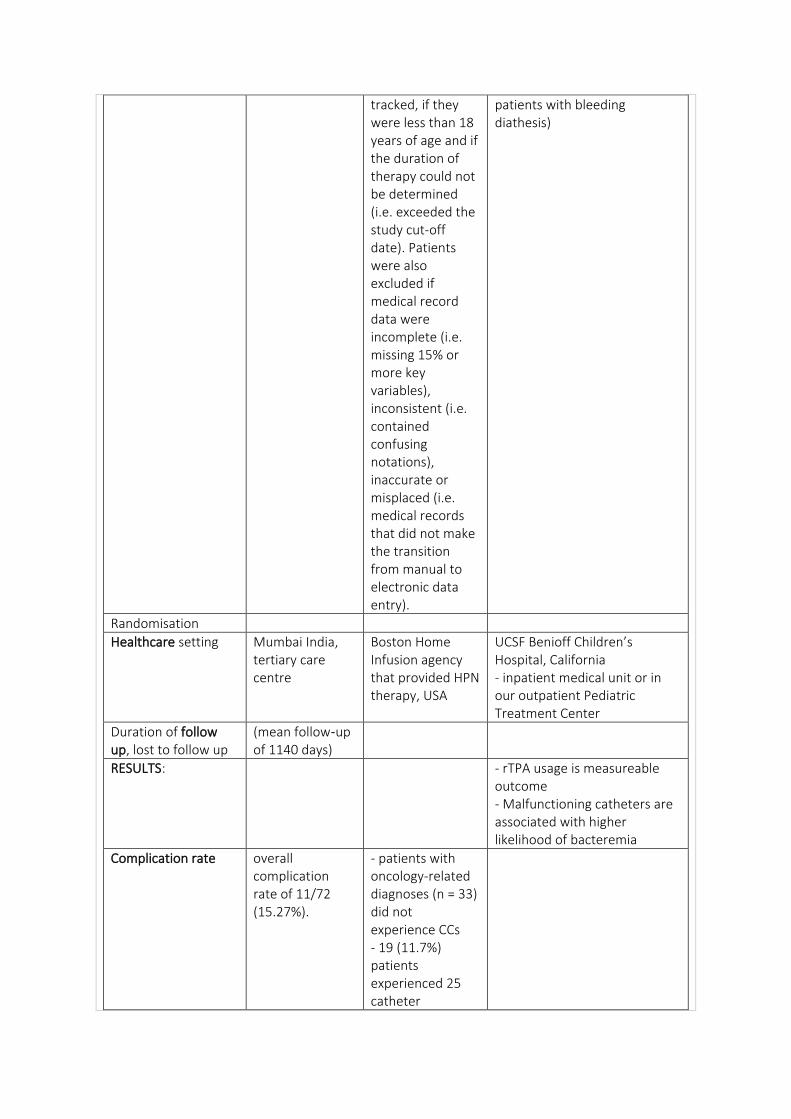
tracked, if they were less than 18 years of age and if the duration of therapy could not be determined (i.e. exceeded the study cut-off date). Patients were also excluded if medical record data were incomplete (i.e. missing 15% or more key variables), inconsistent (i.e. contained confusing notations), inaccurate or misplaced (i.e. medical records that did not make the transition from manual to electronic data entry).
patients with bleeding diathesis)
Randomisation
Healthcare setting Mumbai India, tertiary care centre
Boston Home Infusion agency that provided HPN therapy, USA
UCSF Benioff Children’s Hospital, California - inpatient medical unit or in our outpatient Pediatric Treatment Center
Duration of follow up, lost to follow up
(mean follow‑up of 1140 days)
RESULTS: - rTPA usage is measureable outcome - Malfunctioning catheters are associated with higher likelihood of bacteremia
Complication rate overall complication rate of 11/72 (15.27%).
- patients with oncology-related diagnoses (n = 33) did not experience CCs - 19 (11.7%) patients experienced 25 catheter
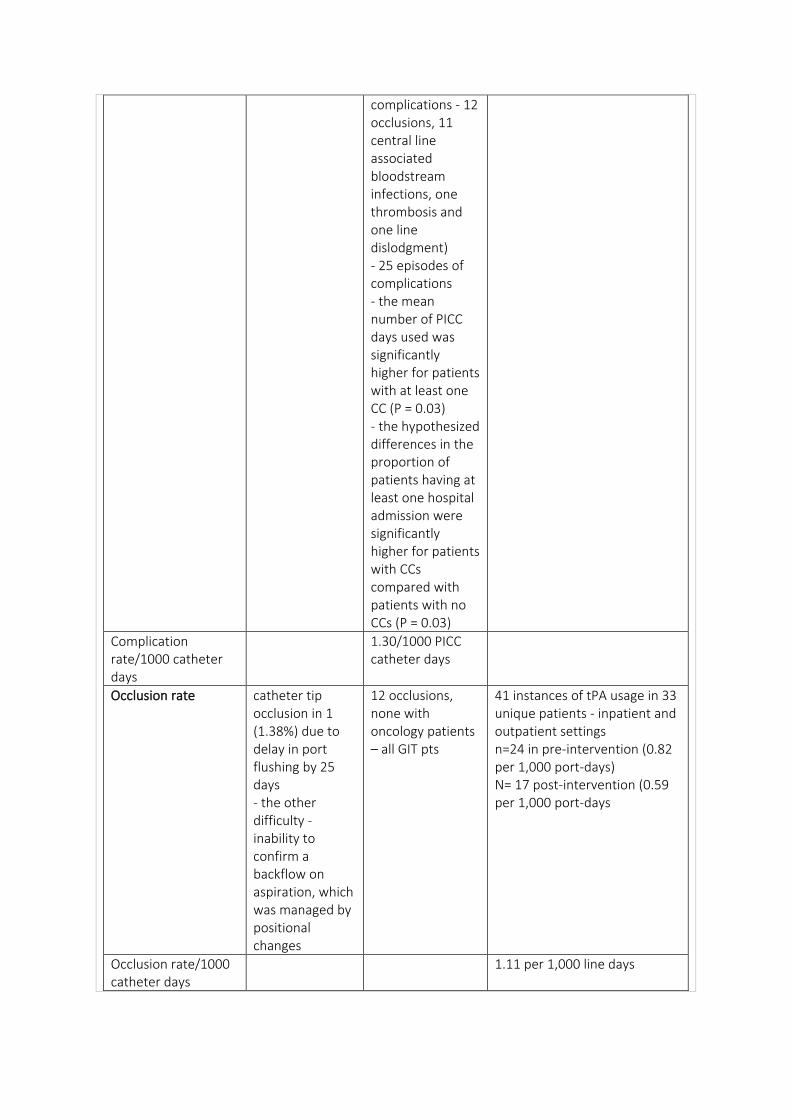
complications - 12 occlusions, 11 central line associated bloodstream infections, one thrombosis and one line dislodgment) - 25 episodes of complications - the mean number of PICC days used was significantly higher for patients with at least one CC (P = 0.03) - the hypothesized differences in the proportion of patients having at least one hospital admission were significantly higher for patients with CCs compared with patients with no CCs (P = 0.03)
Complication rate/1000 catheter days
1.30/1000 PICC catheter days
Occlusion rate catheter tip occlusion in 1 (1.38%) due to delay in port flushing by 25 days - the other difficulty - inability to confirm a backflow on aspiration, which was managed by positional changes
12 occlusions, none with oncology patients – all GIT pts
41 instances of tPA usage in 33 unique patients - inpatient and outpatient settings n=24 in pre-intervention (0.82 per 1,000 port-days) N= 17 post-intervention (0.59 per 1,000 port-days
Occlusion rate/1000 catheter days
1.11 per 1,000 line days
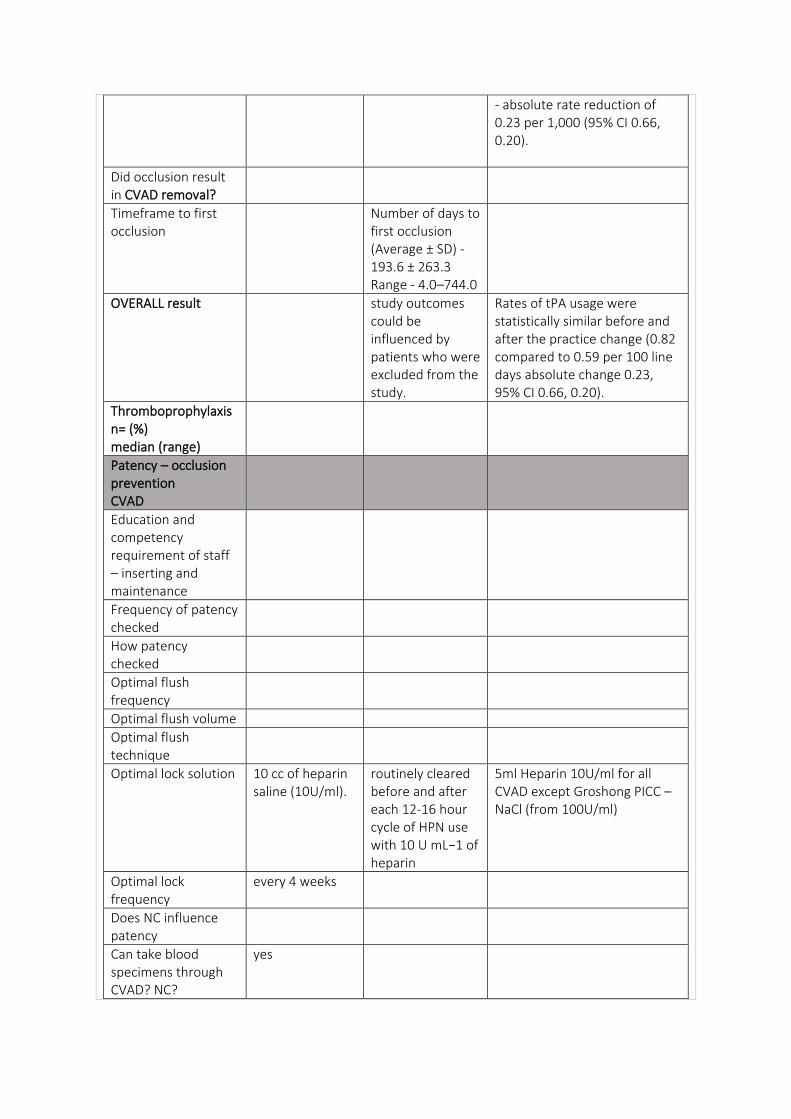
- absolute rate reduction of 0.23 per 1,000 (95% CI 0.66, 0.20).
Did occlusion result in CVAD removal?
Timeframe to first occlusion
Number of days to first occlusion (Average ± SD) - 193.6 ± 263.3 Range - 4.0–744.0
OVERALL result study outcomes could be influenced by patients who were excluded from the study.
Rates of tPA usage were statistically similar before and after the practice change (0.82 compared to 0.59 per 100 line days absolute change 0.23, 95% CI 0.66, 0.20).
Thromboprophylaxis n= (%) median (range)
Patency – occlusion prevention CVAD
Education and competency requirement of staff – inserting and maintenance
Frequency of patency checked
How patency checked
Optimal flush frequency
Optimal flush volume
Optimal flush technique
Optimal lock solution 10 cc of heparin saline (10U/ml).
routinely cleared before and after each 12-16 hour cycle of HPN use with 10 U mL−1 of heparin
5ml Heparin 10U/ml for all CVAD except Groshong PICC – NaCl (from 100U/ml)
Optimal lock frequency
every 4 weeks
Does NC influence patency
Can take blood specimens through CVAD? NC?
yes
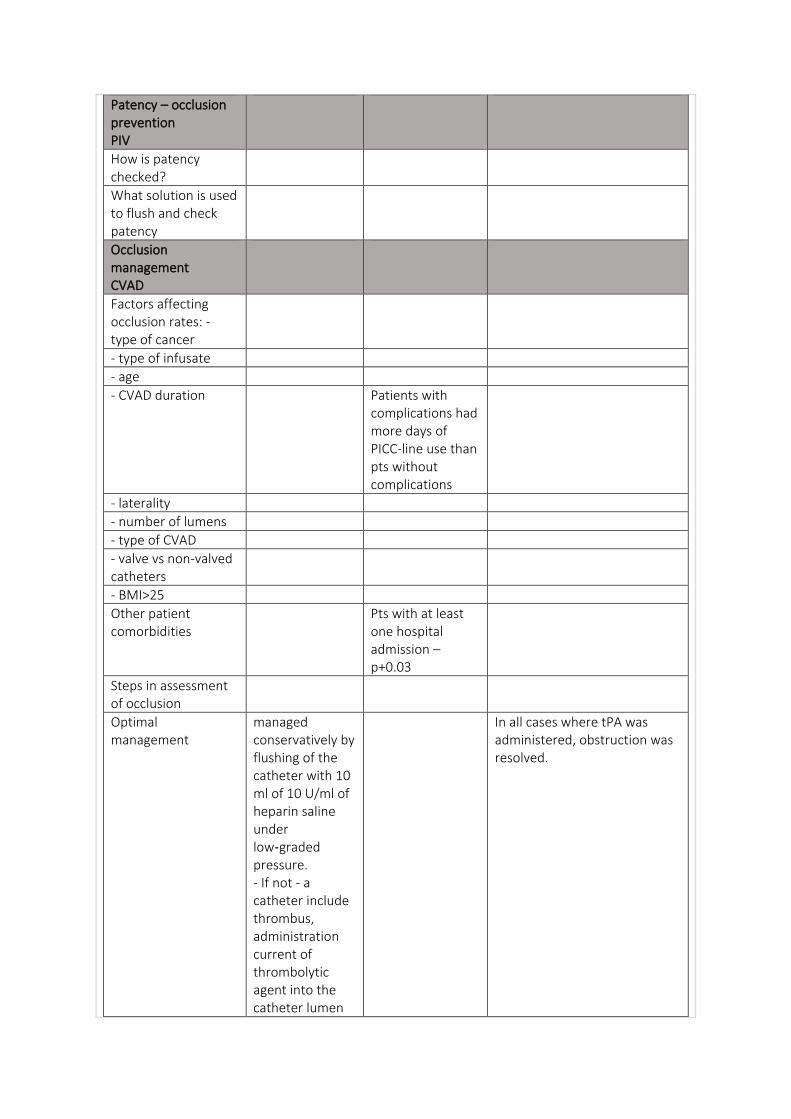
Patency – occlusion prevention PIV
How is patency checked?
What solution is used to flush and check patency
Occlusion management CVAD
Factors affecting occlusion rates: - type of cancer
- type of infusate
- age
- CVAD duration Patients with complications had more days of PICC-line use than pts without complications
- laterality
- number of lumens
- type of CVAD
- valve vs non-valved catheters
- BMI>25
Other patient comorbidities
Pts with at least one hospital admission – p+0.03
Steps in assessment of occlusion
Optimal management
managed conservatively by flushing of the catheter with 10 ml of 10 U/ml of heparin saline under low‑graded pressure. - If not - a catheter include thrombus, administration current of thrombolytic agent into the catheter lumen
In all cases where tPA was administered, obstruction was resolved.
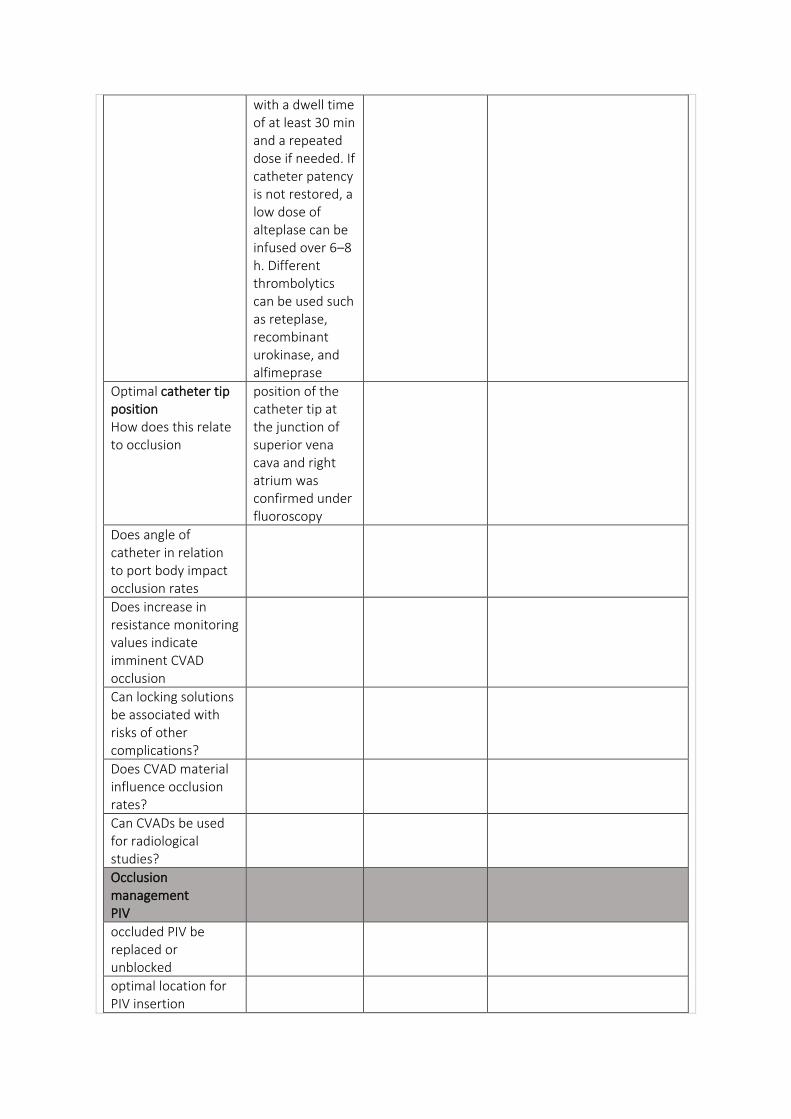
with a dwell time of at least 30 min and a repeated dose if needed. If catheter patency is not restored, a low dose of alteplase can be infused over 6–8 h. Different thrombolytics can be used such as reteplase, recombinant urokinase, and alfimeprase
Optimal catheter tip position How does this relate to occlusion
position of the catheter tip at the junction of superior vena cava and right atrium was confirmed under fluoroscopy
Does angle of catheter in relation to port body impact occlusion rates
Does increase in resistance monitoring values indicate imminent CVAD occlusion
Can locking solutions be associated with risks of other complications?
Does CVAD material influence occlusion rates?
Can CVADs be used for radiological studies?
Occlusion management PIV
occluded PIV be replaced or unblocked
optimal location for PIV insertion
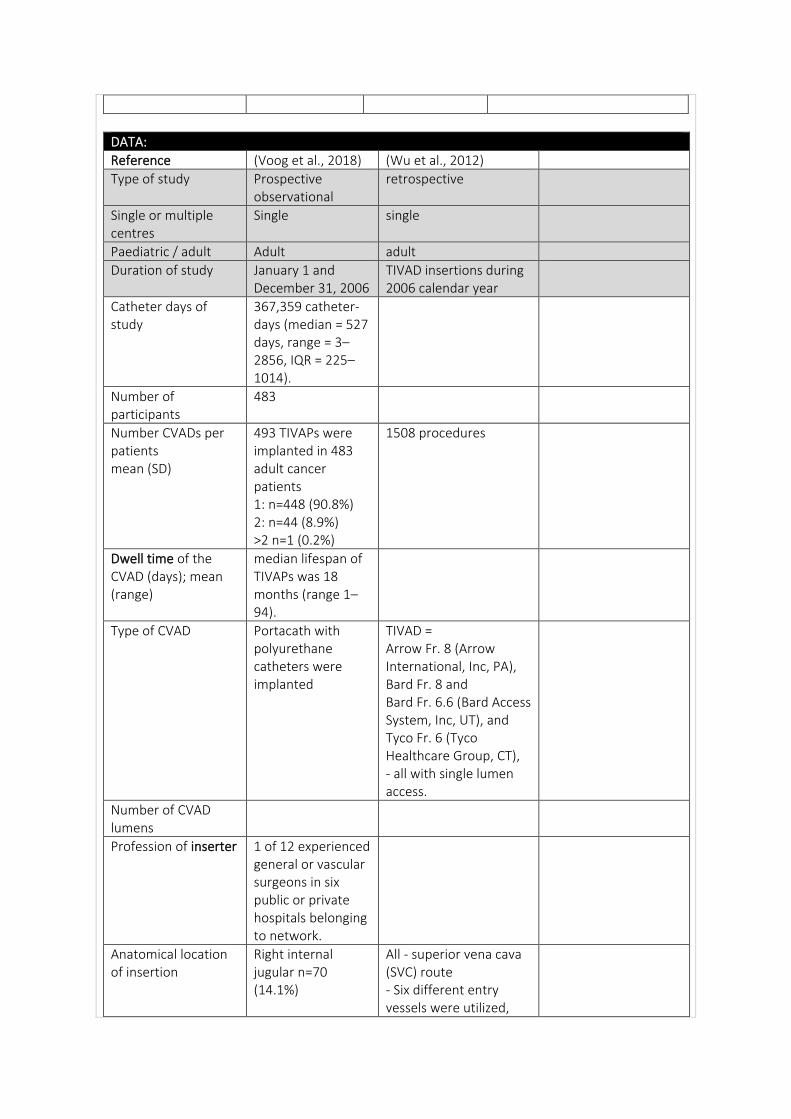
DATA:
Reference (Voog et al., 2018) (Wu et al., 2012)
Type of study Prospective observational
retrospective
Single or multiple centres
Single single
Paediatric / adult Adult adult
Duration of study January 1 and December 31, 2006
TIVAD insertions during 2006 calendar year
Catheter days of study
367,359 catheter-days (median = 527 days, range = 3–2856, IQR = 225–1014).
Number of participants
483
Number CVADs per patients mean (SD)
493 TIVAPs were implanted in 483 adult cancer patients 1: n=448 (90.8%) 2: n=44 (8.9%) >2 n=1 (0.2%)
1508 procedures
Dwell time of the CVAD (days); mean (range)
median lifespan of TIVAPs was 18 months (range 1–94).
Type of CVAD Portacath with polyurethane catheters were implanted
TIVAD = Arrow Fr. 8 (Arrow International, Inc, PA), Bard Fr. 8 and Bard Fr. 6.6 (Bard Access System, Inc, UT), and Tyco Fr. 6 (Tyco Healthcare Group, CT), - all with single lumen access.
Number of CVAD lumens
Profession of inserter 1 of 12 experienced general or vascular surgeons in six public or private hospitals belonging to network.
Anatomical location of insertion
Right internal jugular n=70 (14.1%)
All - superior vena cava (SVC) route - Six different entry vessels were utilized,
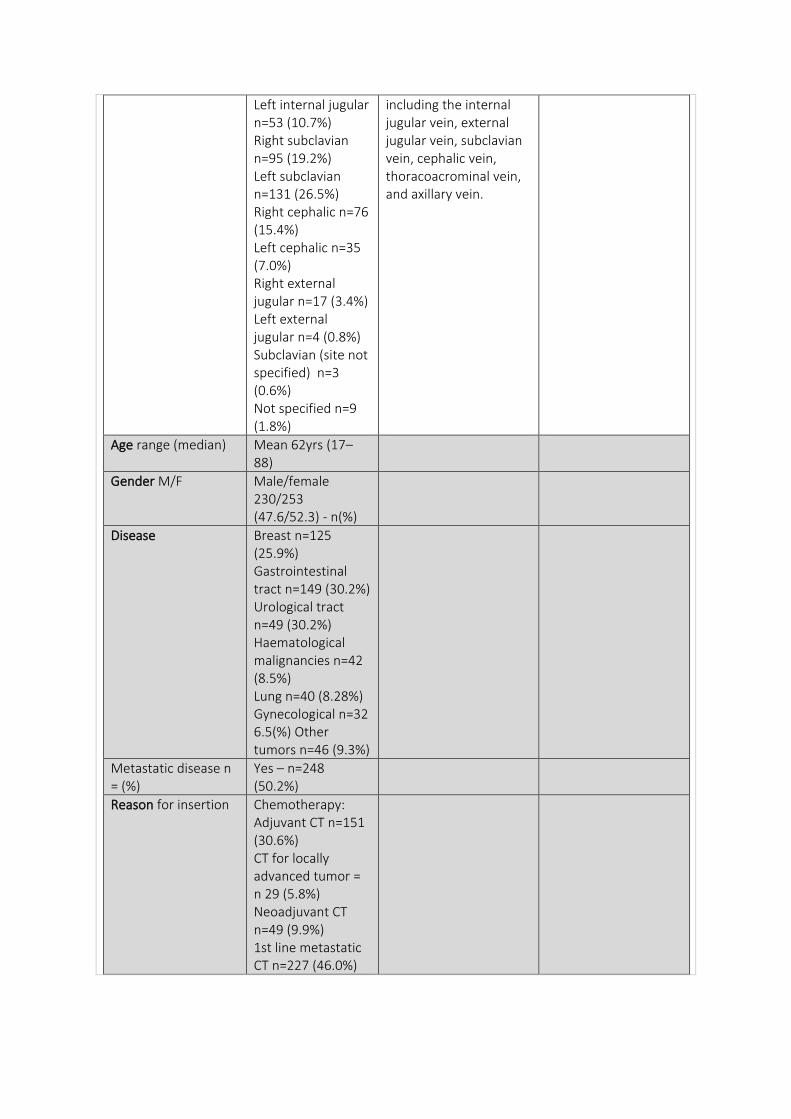
Left internal jugular n=53 (10.7%) Right subclavian n=95 (19.2%) Left subclavian n=131 (26.5%) Right cephalic n=76 (15.4%) Left cephalic n=35 (7.0%) Right external jugular n=17 (3.4%) Left external jugular n=4 (0.8%) Subclavian (site not specified) n=3 (0.6%) Not specified n=9 (1.8%)
including the internal jugular vein, external jugular vein, subclavian vein, cephalic vein, thoracoacrominal vein, and axillary vein.
Age range (median) Mean 62yrs (17–88)
Gender M/F Male/female 230/253 (47.6/52.3) - n(%)
Disease Breast n=125 (25.9%) Gastrointestinal tract n=149 (30.2%) Urological tract n=49 (30.2%) Haematological malignancies n=42 (8.5%) Lung n=40 (8.28%) Gynecological n=32 6.5(%) Other tumors n=46 (9.3%)
Metastatic disease n = (%)
Yes – n=248 (50.2%)
Reason for insertion Chemotherapy: Adjuvant CT n=151 (30.6%) CT for locally advanced tumor = n 29 (5.8%) Neoadjuvant CT n=49 (9.9%) 1st line metastatic CT n=227 (46.0%)
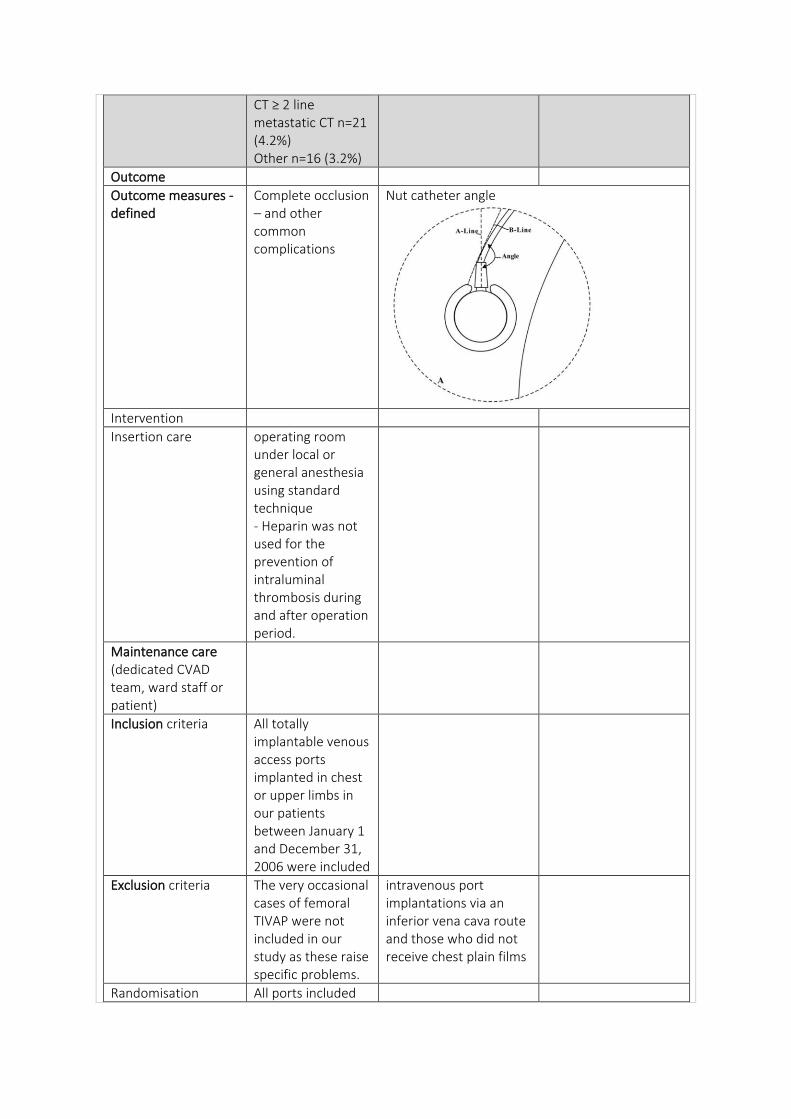
CT ≥ 2 line metastatic CT n=21 (4.2%) Other n=16 (3.2%)
Outcome
Outcome measures - defined
Complete occlusion – and other common complications
Nut catheter angle
Intervention
Insertion care operating room under local or general anesthesia using standard technique - Heparin was not used for the prevention of intraluminal thrombosis during and after operation period.
Maintenance care (dedicated CVAD team, ward staff or patient)
Inclusion criteria All totally implantable venous access ports implanted in chest or upper limbs in our patients between January 1 and December 31, 2006 were included
Exclusion criteria The very occasional cases of femoral TIVAP were not included in our study as these raise specific problems.
intravenous port implantations via an inferior vena cava route and those who did not receive chest plain films
Randomisation All ports included
Healthcare setting cancer center - Clinique Victor Hugo, Institut Inter-régional de Cancérologie, Le Mans, France
Chang Gung Memorial Hospital Taiwan
Duration of follow up, lost to follow up
until the removal of the device, the patient’s death, or until December 31, 2013 - Median patient follow-up was 30 months (range 1–94) and median follow-up ofthe TIVAPs was 18 months (range 1–94),
followed up until June 30, 2010 - patients still alive, the last outpatient follow-up date was considered as the end point. For the remaining patients, the date of death or discharge against advice were considered as the end points. - Patients undergoing chemotherapy were followed up every 2 weeks to check the ports, and patients not undergoing chemotherapy were followed up every month
RESULTS:
Complication rate 87 complications; 62 (71.3%) occurred during the first year after implantation
44 procedures (26 men and 18 women) were performed to resolve catheter malfunctions, compared to 1463 procedures (860 men and 633 women) without malfunctions performed for port implantation and revision.
Complication rate/1000 catheter days
0.237/1000 catheter-days, 95% Poisson exact CI, 0.190 to 0.292
Occlusion rate Non-functional TIVAD n=1, 1.1% - no cases of catheter occlusion without venous thrombosis
44 procedures (26 men and 18 women) were performed to resolve catheter malfunctions - 25 patients presented with straight malfunctions - difficulty with blood withdrawal
and normal saline irrigation. 1/25 retrospectively identified to have a clotted catheter and tight stay suture on chest plain film. - other 19 cases with complicated malfunctions of the intravenous ports were found to have coexisting catheter kinking, fracture, migration, and infection. - nearly half of the patients (20 of 44) received a Bard Fr. 8 intravenous valve-tip port. - The Nut-Catheter Angle was the only significant risk factor for the prediction of catheter malfunction (P = 0.001). negative ˆa-coefficient of −0.02 was found, indicating that a sharper angle was associated with a greater risk of malfunction (odds ratio = 0.98; 95% confidence interval = 0.97–0.99). - a smaller Nut-Catheter Angle was found to be a possible risk factor of catheter malfunction.
Occlusion rate/1000 catheter days
Did occlusion result in CVAD removal?
N=41, 27.5% complications resulted in removal Nonfunctional TIVAD n=1 0.6%
Timeframe to first occlusion
median time to occurrence of any complications was 128 days (range 6 to 2533)
- 49 (56%) complications occurred within 6 months, 13 (15%) between 6 and 12 months (62 (74.7%) within a year), and only 25 (29%) after 1 year.
OVERALL result a smaller Nut-Catheter Angle had a greater risk for catheter malfunction - causes a sharp catheter contour and mechanical compression of the catheter, possibly leading to the catheter becoming compromised and presenting as intermittent back flow in withdrawal tests - Catheter impingement caused by inadequate pocket creation and port implantation lead to compromised catheter lumen and difficulty flushing - suggests that malfunction could be prevented by adequate pocket creation and by establishing a smooth route between the catheter and port.
Thromboprophylaxis n= (%) median (range)
16.36% on some type of anticoagulant 35 patients (7.2%) were receiving Vitamin K antagonists, 34 (7%) were receiving platelet antiaggregants, 9 (1.8%) were receiving preventative dose low molecular weight heparin (LMWH) (1.8%),
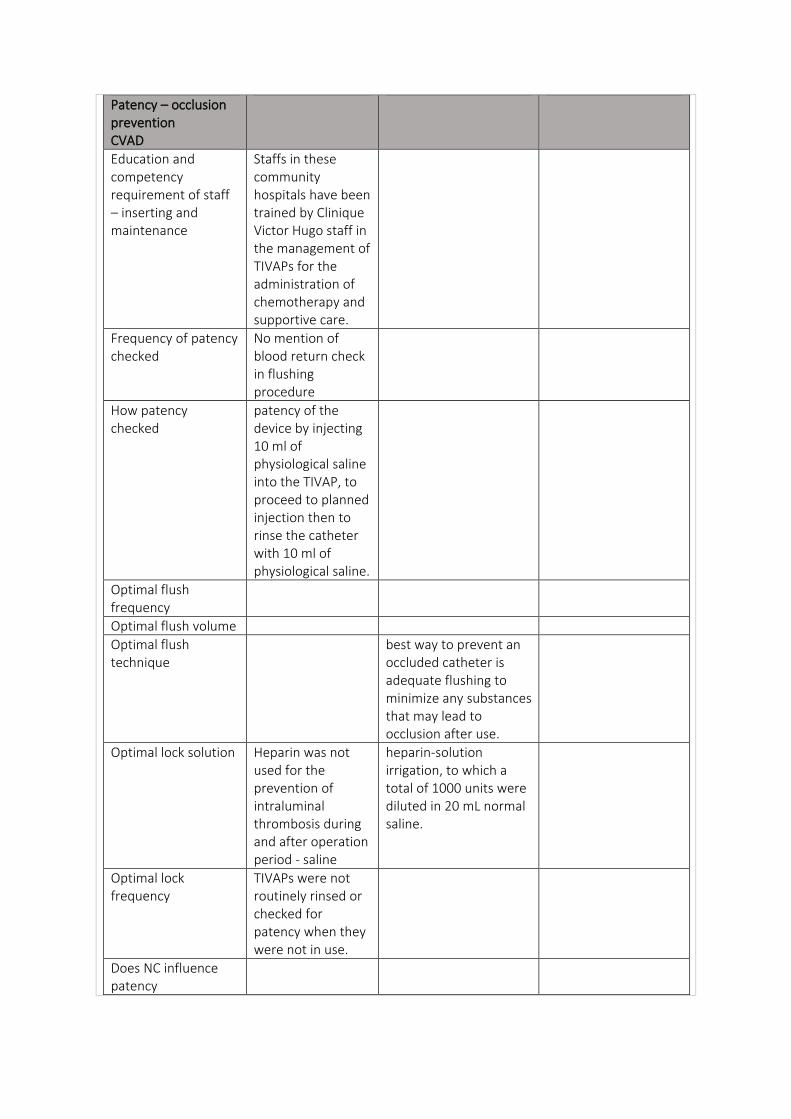
Patency – occlusion prevention CVAD
Education and competency requirement of staff – inserting and maintenance
Staffs in these community hospitals have been trained by Clinique Victor Hugo staff in the management of TIVAPs for the administration of chemotherapy and supportive care.
Frequency of patency checked
No mention of blood return check in flushing procedure
How patency checked
patency of the device by injecting 10 ml of physiological saline into the TIVAP, to proceed to planned injection then to rinse the catheter with 10 ml of physiological saline.
Optimal flush frequency
Optimal flush volume
Optimal flush technique
best way to prevent an occluded catheter is adequate flushing to minimize any substances that may lead to occlusion after use.
Optimal lock solution Heparin was not used for the prevention of intraluminal thrombosis during and after operation period - saline
heparin-solution irrigation, to which a total of 1000 units were diluted in 20 mL normal saline.
Optimal lock frequency
TIVAPs were not routinely rinsed or checked for patency when they were not in use.
Does NC influence patency
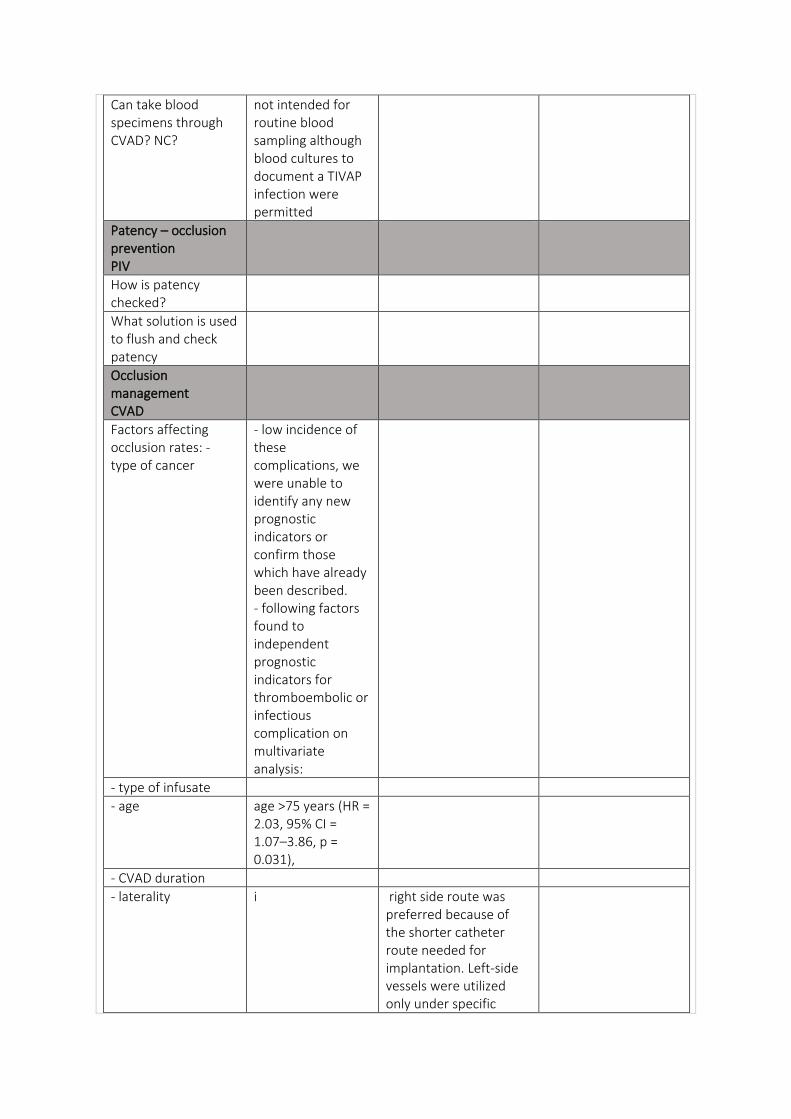
Can take blood specimens through CVAD? NC?
not intended for routine blood sampling although blood cultures to document a TIVAP infection were permitted
Patency – occlusion prevention PIV
How is patency checked?
What solution is used to flush and check patency
Occlusion management CVAD
Factors affecting occlusion rates: - type of cancer
- low incidence of these complications, we were unable to identify any new prognostic indicators or confirm those which have already been described. - following factors found to independent prognostic indicators for thromboembolic or infectious complication on multivariate analysis:
- type of infusate
- age age >75 years (HR = 2.03, 95% CI = 1.07–3.86, p = 0.031),
- CVAD duration
- laterality i right side route was preferred because of the shorter catheter route needed for implantation. Left-side vessels were utilized only under specific
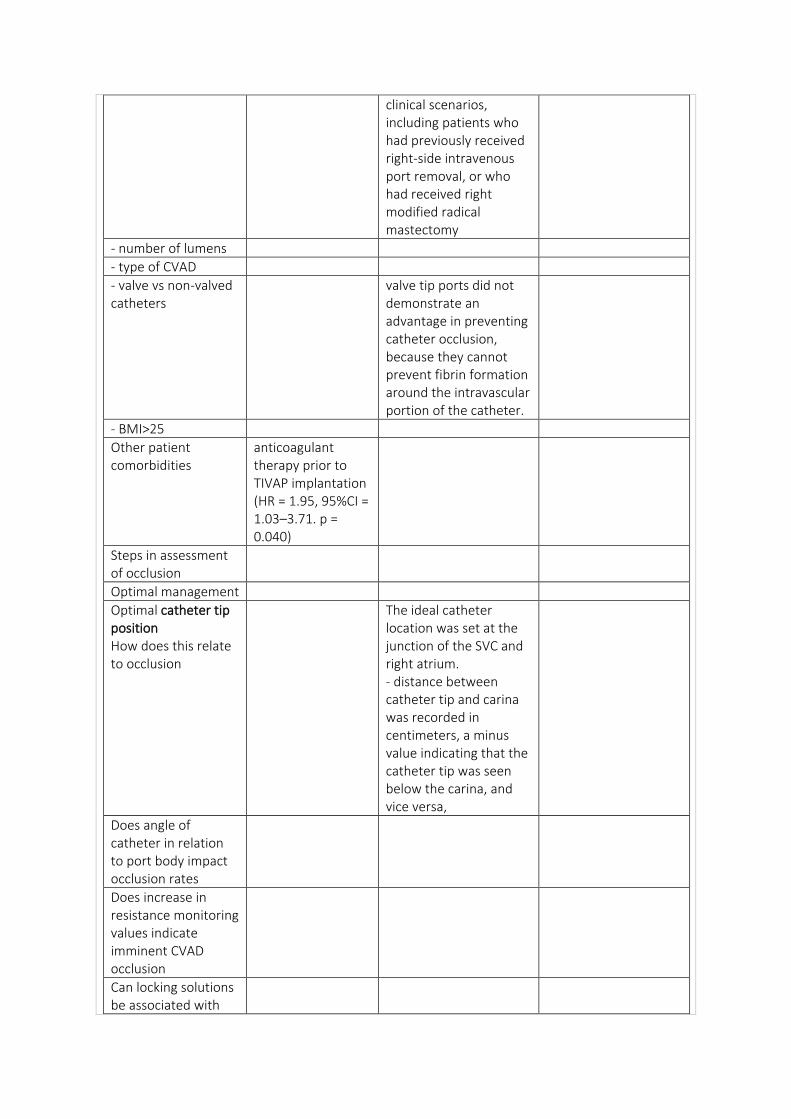
clinical scenarios, including patients who had previously received right-side intravenous port removal, or who had received right modified radical mastectomy
- number of lumens
- type of CVAD
- valve vs non-valved catheters
valve tip ports did not demonstrate an advantage in preventing catheter occlusion, because they cannot prevent fibrin formation around the intravascular portion of the catheter.
- BMI>25
Other patient comorbidities
anticoagulant therapy prior to TIVAP implantation (HR = 1.95, 95%CI = 1.03–3.71. p = 0.040)
Steps in assessment of occlusion
Optimal management
Optimal catheter tip position How does this relate to occlusion
The ideal catheter location was set at the junction of the SVC and right atrium. - distance between catheter tip and carina was recorded in centimeters, a minus value indicating that the catheter tip was seen below the carina, and vice versa,
Does angle of catheter in relation to port body impact occlusion rates
Does increase in resistance monitoring values indicate imminent CVAD occlusion
Can locking solutions be associated with
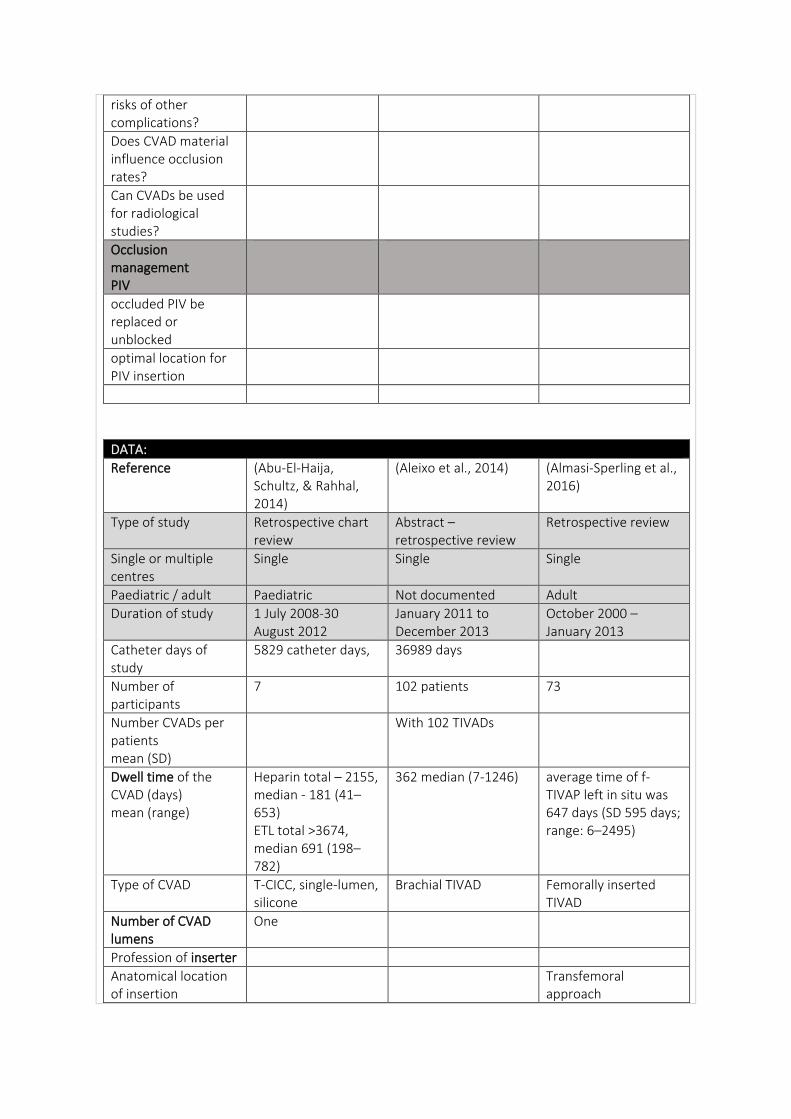
risks of other complications?
Does CVAD material influence occlusion rates?
Can CVADs be used for radiological studies?
Occlusion management PIV
occluded PIV be replaced or unblocked
optimal location for PIV insertion
DATA:
Reference (Abu-El-Haija, Schultz, & Rahhal, 2014)
(Aleixo et al., 2014) (Almasi-Sperling et al., 2016)
Type of study Retrospective chart review
Abstract – retrospective review
Retrospective review
Single or multiple centres
Single Single Single
Paediatric / adult Paediatric Not documented Adult
Duration of study 1 July 2008-30 August 2012
January 2011 to December 2013
October 2000 – January 2013
Catheter days of study
5829 catheter days,
36989 days
Number of participants
7 102 patients 73
Number CVADs per patients mean (SD)
With 102 TIVADs
Dwell time of the CVAD (days) mean (range)
Heparin total – 2155, median - 181 (41–653) ETL total >3674, median 691 (198–782)
362 median (7-1246) average time of f-TIVAP left in situ was 647 days (SD 595 days; range: 6–2495)
Type of CVAD T-CICC, single-lumen, silicone
Brachial TIVAD Femorally inserted TIVAD
Number of CVAD lumens
One
Profession of inserter
Anatomical location of insertion
Transfemoral approach
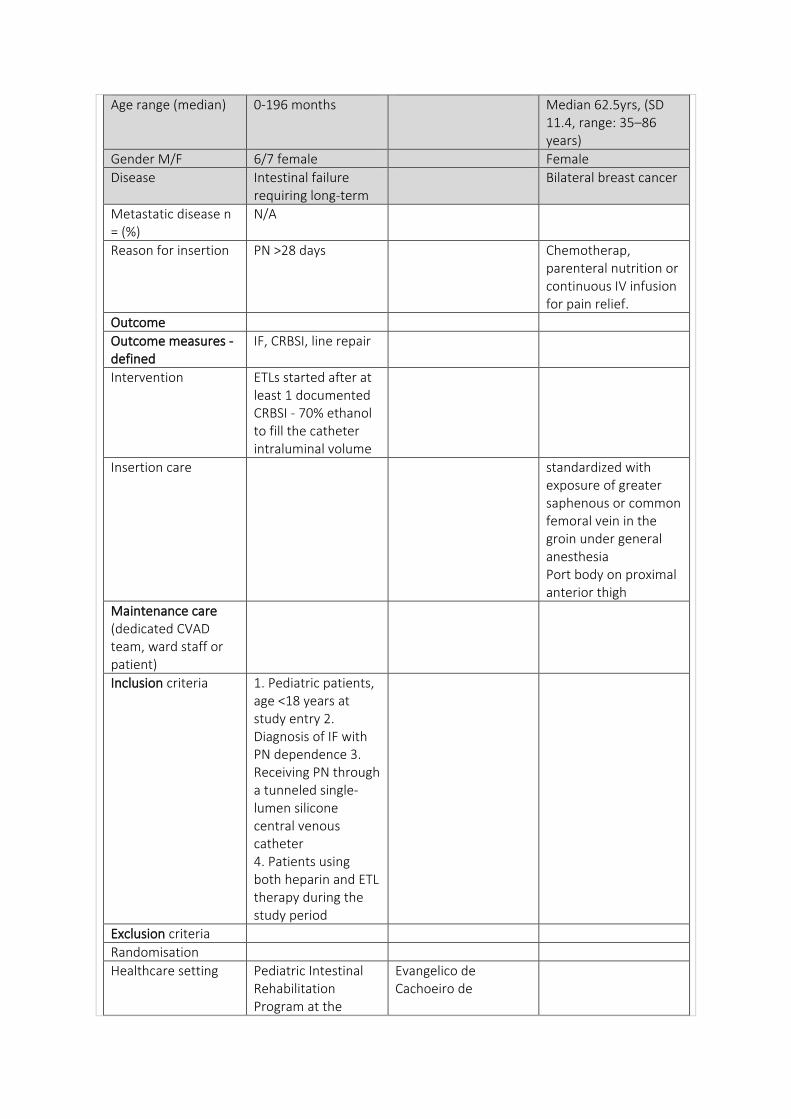
Age range (median) 0-196 months Median 62.5yrs, (SD 11.4, range: 35–86 years)
Gender M/F 6/7 female Female
Disease Intestinal failure requiring long-term
Bilateral breast cancer
Metastatic disease n = (%)
N/A
Reason for insertion PN >28 days Chemotherap, parenteral nutrition or continuous IV infusion for pain relief.
Outcome
Outcome measures - defined
IF, CRBSI, line repair
Intervention ETLs started after at least 1 documented CRBSI - 70% ethanol to fill the catheter intraluminal volume
Insertion care standardized with exposure of greater saphenous or common femoral vein in the groin under general anesthesia Port body on proximal anterior thigh
Maintenance care (dedicated CVAD team, ward staff or patient)
Inclusion criteria 1. Pediatric patients, age <18 years at study entry 2. Diagnosis of IF with PN dependence 3. Receiving PN through a tunneled single-lumen silicone central venous catheter 4. Patients using both heparin and ETL therapy during the study period
Exclusion criteria
Randomisation
Healthcare setting Pediatric Intestinal Rehabilitation Program at the
Evangelico de Cachoeiro de
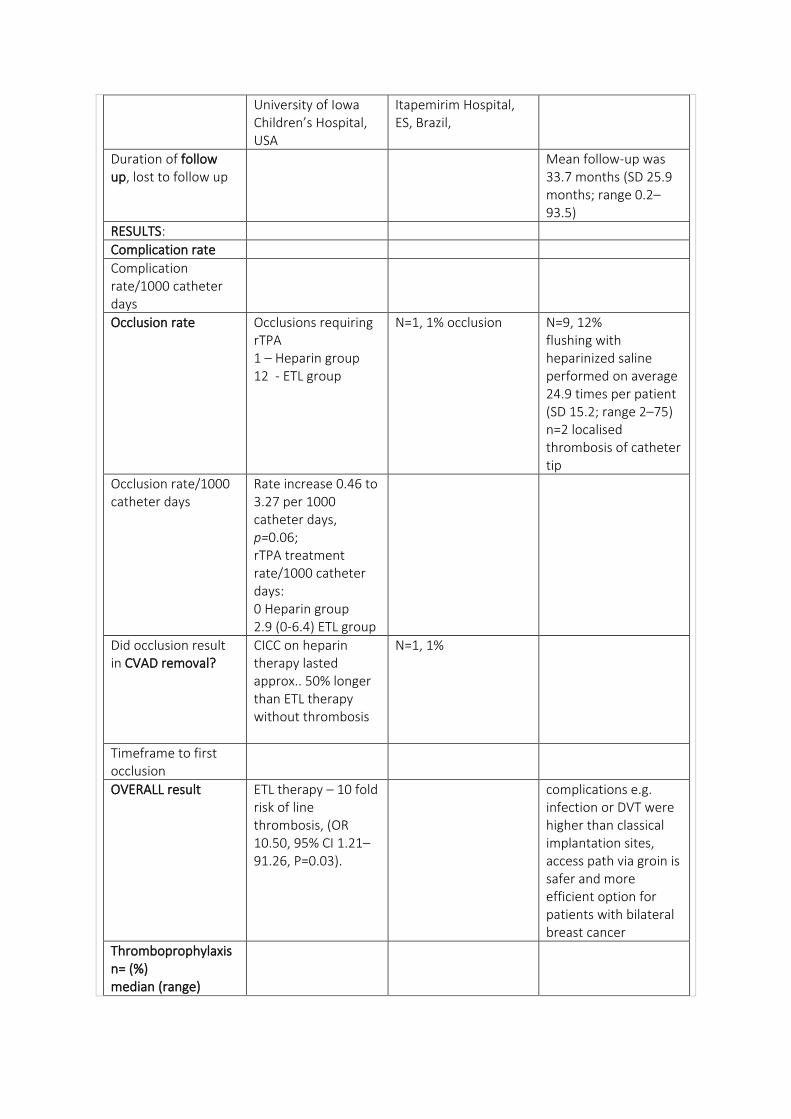
University of Iowa Children’s Hospital, USA
Itapemirim Hospital, ES, Brazil,
Duration of follow up, lost to follow up
Mean follow-up was 33.7 months (SD 25.9 months; range 0.2– 93.5)
RESULTS:
Complication rate
Complication rate/1000 catheter days
Occlusion rate Occlusions requiring rTPA 1 – Heparin group 12 - ETL group
N=1, 1% occlusion N=9, 12% flushing with heparinized saline performed on average 24.9 times per patient (SD 15.2; range 2–75) n=2 localised thrombosis of catheter tip
Occlusion rate/1000 catheter days
Rate increase 0.46 to 3.27 per 1000 catheter days, p=0.06; rTPA treatment rate/1000 catheter days: 0 Heparin group 2.9 (0-6.4) ETL group
Did occlusion result in CVAD removal?
CICC on heparin therapy lasted approx.. 50% longer than ETL therapy without thrombosis
N=1, 1%
Timeframe to first occlusion
OVERALL result ETL therapy – 10 fold risk of line thrombosis, (OR 10.50, 95% CI 1.21–91.26, P=0.03).
complications e.g. infection or DVT were higher than classical implantation sites, access path via groin is safer and more efficient option for patients with bilateral breast cancer
Thromboprophylaxis n= (%) median (range)
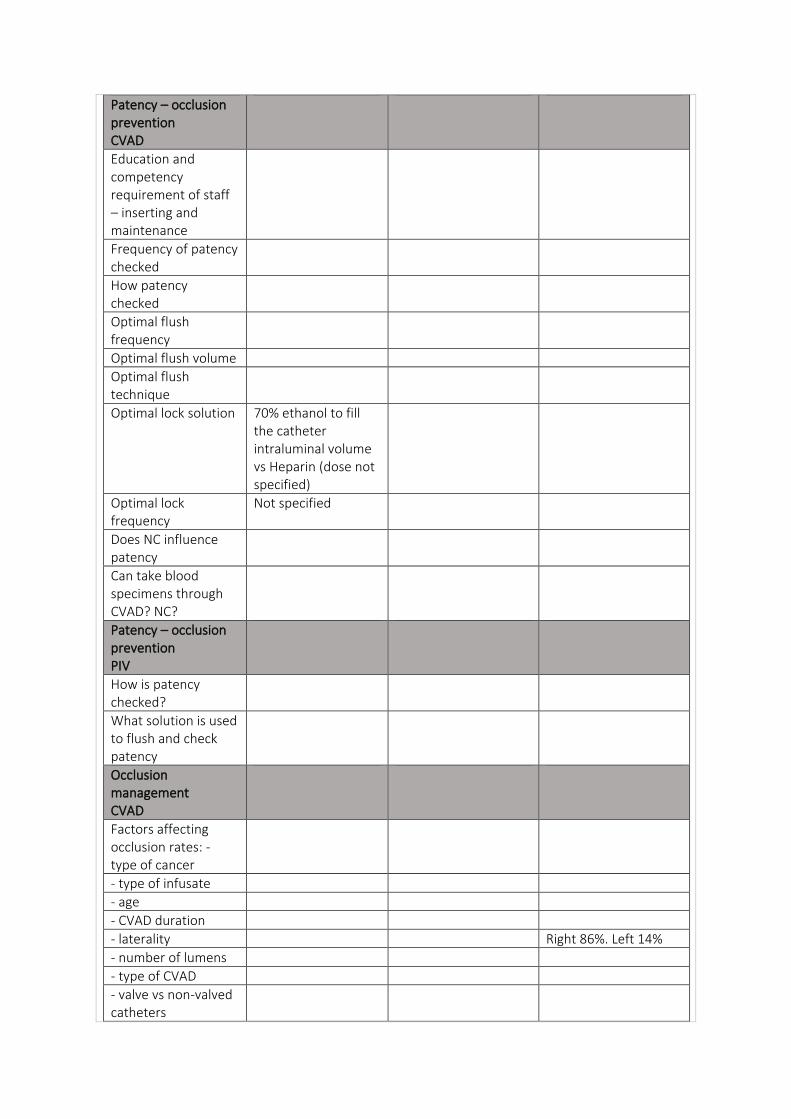
Patency – occlusion prevention CVAD
Education and competency requirement of staff – inserting and maintenance
Frequency of patency checked
How patency checked
Optimal flush frequency
Optimal flush volume
Optimal flush technique
Optimal lock solution 70% ethanol to fill the catheter intraluminal volume vs Heparin (dose not specified)
Optimal lock frequency
Not specified
Does NC influence patency
Can take blood specimens through CVAD? NC?
Patency – occlusion prevention PIV
How is patency checked?
What solution is used to flush and check patency
Occlusion management CVAD
Factors affecting occlusion rates: - type of cancer
- type of infusate
- age
- CVAD duration
- laterality Right 86%. Left 14%
- number of lumens
- type of CVAD
- valve vs non-valved catheters
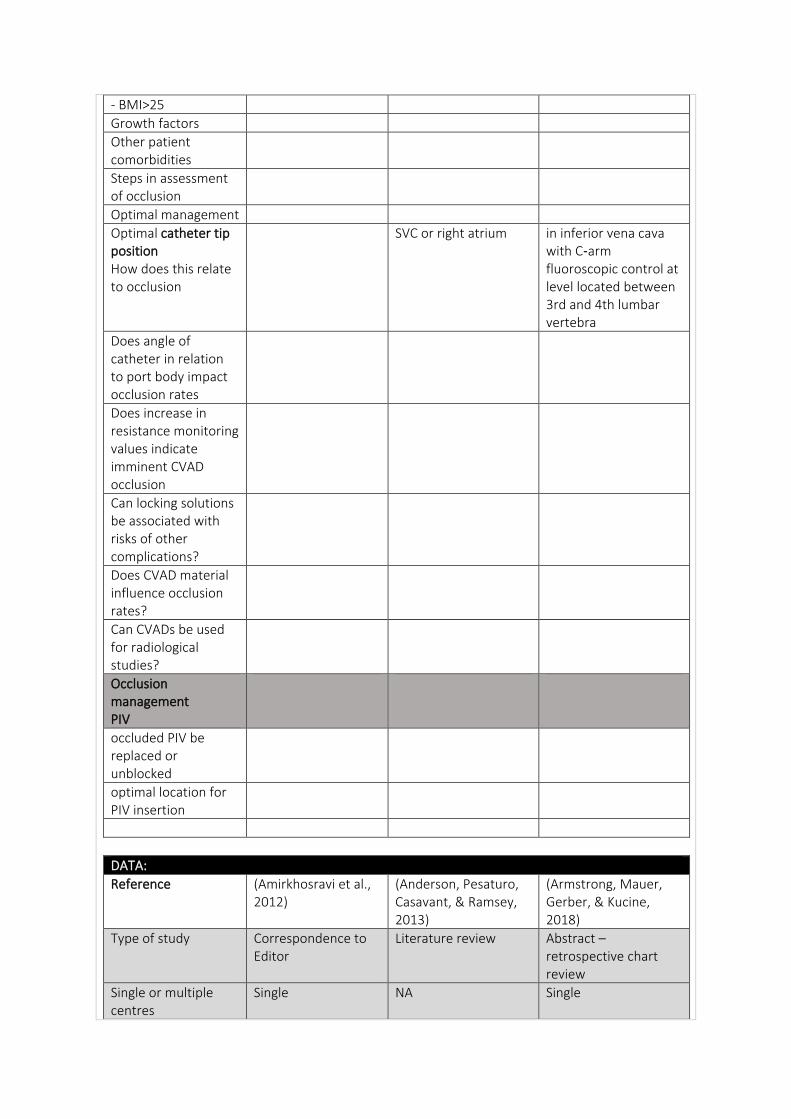
- BMI>25
Growth factors
Other patient comorbidities
Steps in assessment of occlusion
Optimal management
Optimal catheter tip position How does this relate to occlusion
SVC or right atrium in inferior vena cava with C‑arm fluoroscopic control at level located between 3rd and 4th lumbar vertebra
Does angle of catheter in relation to port body impact occlusion rates
Does increase in resistance monitoring values indicate imminent CVAD occlusion
Can locking solutions be associated with risks of other complications?
Does CVAD material influence occlusion rates?
Can CVADs be used for radiological studies?
Occlusion management PIV
occluded PIV be replaced or unblocked
optimal location for PIV insertion
DATA:
Reference (Amirkhosravi et al., 2012)
(Anderson, Pesaturo, Casavant, & Ramsey, 2013)
(Armstrong, Mauer, Gerber, & Kucine, 2018)
Type of study Correspondence to Editor
Literature review Abstract – retrospective chart review
Single or multiple centres
Single NA Single
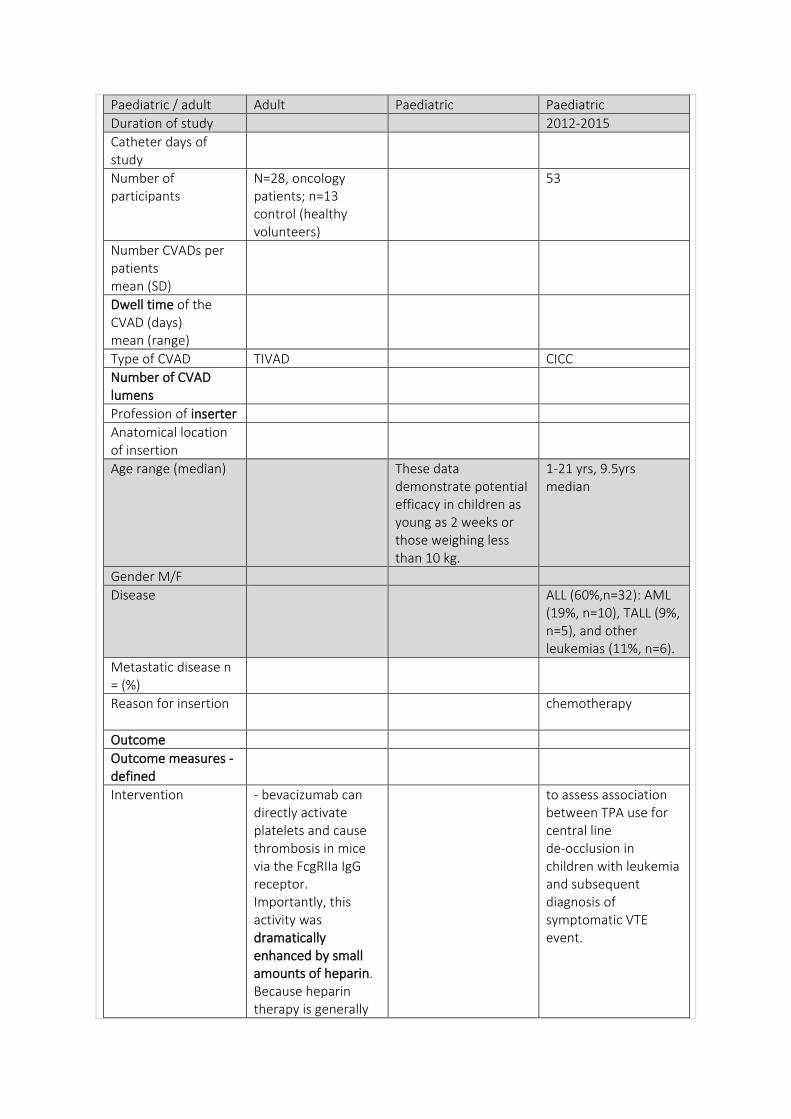
Paediatric / adult Adult Paediatric Paediatric
Duration of study 2012-2015
Catheter days of study
Number of participants
N=28, oncology patients; n=13 control (healthy volunteers)
53
Number CVADs per patients mean (SD)
Dwell time of the CVAD (days) mean (range)
Type of CVAD TIVAD CICC
Number of CVAD lumens
Profession of inserter
Anatomical location of insertion
Age range (median) These data demonstrate potential efficacy in children as young as 2 weeks or those weighing less than 10 kg.
1-21 yrs, 9.5yrs median
Gender M/F
Disease ALL (60%,n=32): AML (19%, n=10), TALL (9%, n=5), and other leukemias (11%, n=6).
Metastatic disease n = (%)
Reason for insertion chemotherapy
Outcome
Outcome measures - defined
Intervention - bevacizumab can directly activate platelets and cause thrombosis in mice via the FcgRIIa IgG receptor. Importantly, this activity was dramatically enhanced by small amounts of heparin. Because heparin therapy is generally
to assess association between TPA use for central line de-occlusion in children with leukemia and subsequent diagnosis of symptomatic VTE event.
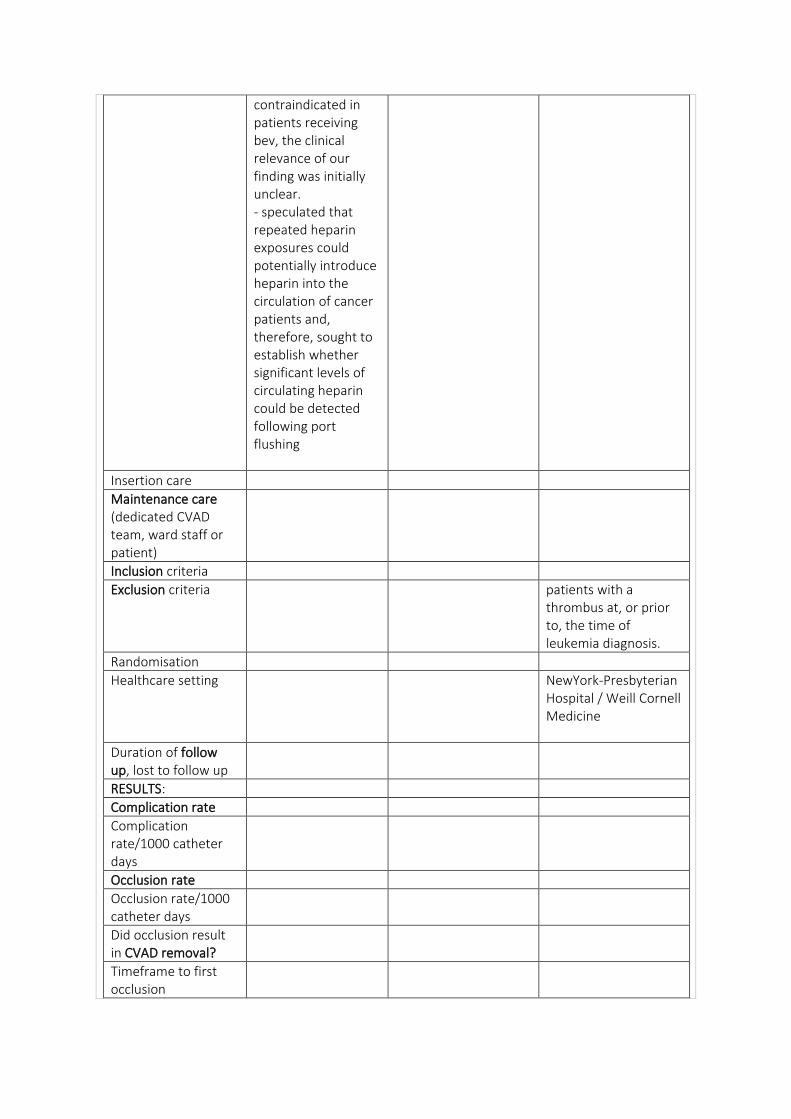
contraindicated in patients receiving bev, the clinical relevance of our finding was initially unclear. - speculated that repeated heparin exposures could potentially introduce heparin into the circulation of cancer patients and, therefore, sought to establish whether significant levels of circulating heparin could be detected following port flushing
Insertion care
Maintenance care (dedicated CVAD team, ward staff or patient)
Inclusion criteria
Exclusion criteria patients with a thrombus at, or prior to, the time of leukemia diagnosis.
Randomisation
Healthcare setting NewYork-Presbyterian Hospital / Weill Cornell Medicine
Duration of follow up, lost to follow up
RESULTS:
Complication rate
Complication rate/1000 catheter days
Occlusion rate
Occlusion rate/1000 catheter days
Did occlusion result in CVAD removal?
Timeframe to first occlusion
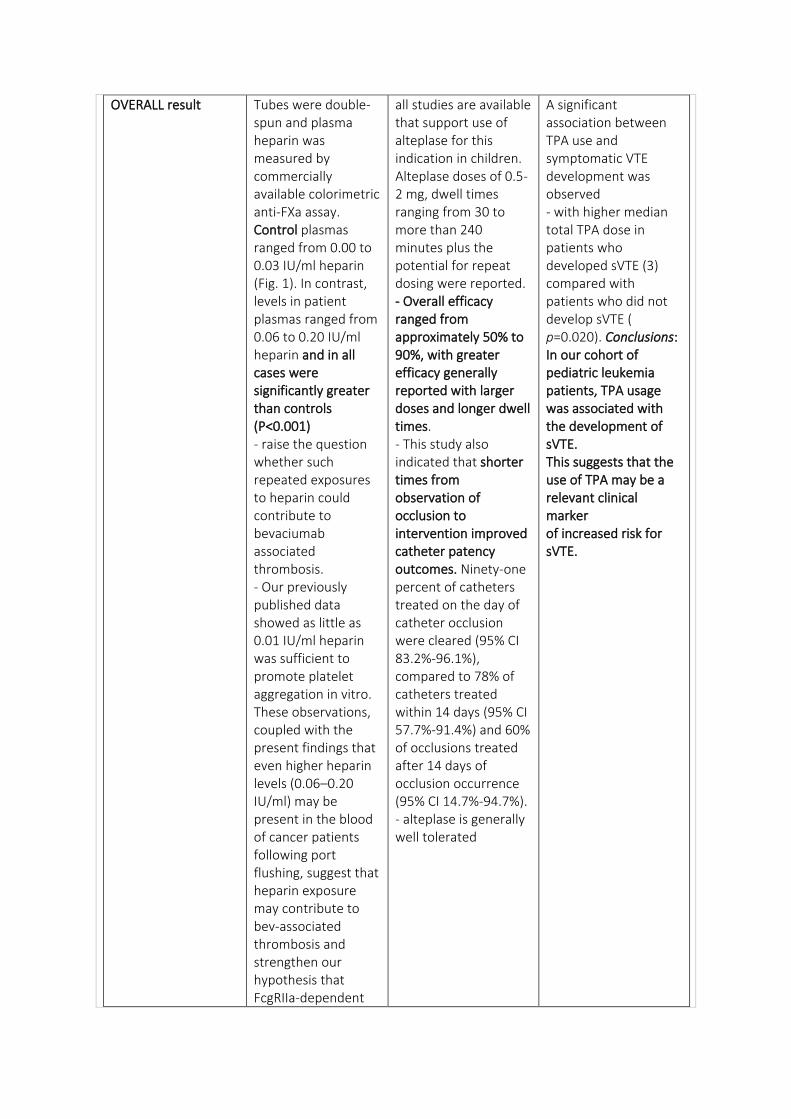
OVERALL result Tubes were double-spun and plasma heparin was measured by commercially available colorimetric anti-FXa assay. Control plasmas ranged from 0.00 to 0.03 IU/ml heparin (Fig. 1). In contrast, levels in patient plasmas ranged from 0.06 to 0.20 IU/ml heparin and in all cases were significantly greater than controls (P<0.001) - raise the question whether such repeated exposures to heparin could contribute to bevaciumab associated thrombosis. - Our previously published data showed as little as 0.01 IU/ml heparin was sufficient to promote platelet aggregation in vitro. These observations, coupled with the present findings that even higher heparin levels (0.06–0.20 IU/ml) may be present in the blood of cancer patients following port flushing, suggest that heparin exposure may contribute to bev-associated thrombosis and strengthen our hypothesis that FcgRIIa-dependent
all studies are available that support use of alteplase for this indication in children. Alteplase doses of 0.5-2 mg, dwell times ranging from 30 to more than 240 minutes plus the potential for repeat dosing were reported. - Overall efficacy ranged from approximately 50% to 90%, with greater efficacy generally reported with larger doses and longer dwell times. - This study also indicated that shorter times from observation of occlusion to intervention improved catheter patency outcomes. Ninety-one percent of catheters treated on the day of catheter occlusion were cleared (95% CI 83.2%-96.1%), compared to 78% of catheters treated within 14 days (95% CI 57.7%-91.4%) and 60% of occlusions treated after 14 days of occlusion occurrence (95% CI 14.7%-94.7%). - alteplase is generally well tolerated
A significant association between TPA use and symptomatic VTE development was observed - with higher median total TPA dose in patients who developed sVTE (3) compared with patients who did not develop sVTE ( p=0.020). Conclusions: In our cohort of pediatric leukemia patients, TPA usage was associated with the development of sVTE. This suggests that the use of TPA may be a relevant clinical marker of increased risk for sVTE.
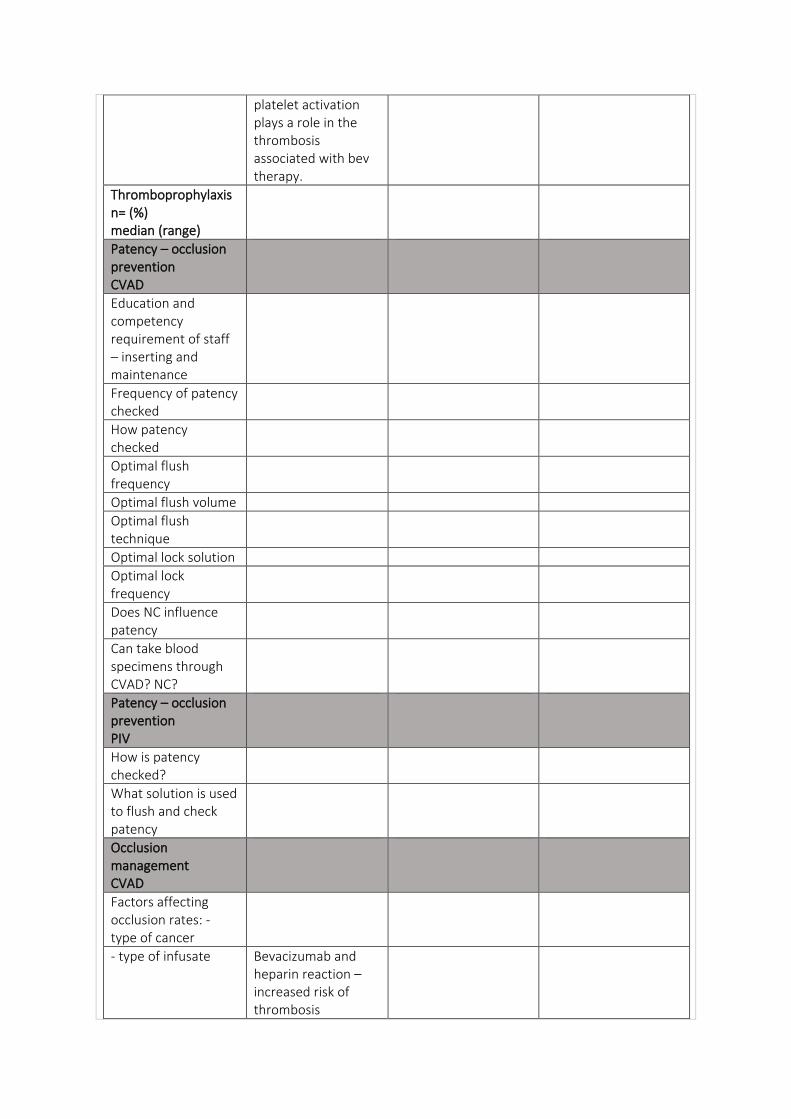
platelet activation plays a role in the thrombosis associated with bev therapy.
Thromboprophylaxis n= (%) median (range)
Patency – occlusion prevention CVAD
Education and competency requirement of staff – inserting and maintenance
Frequency of patency checked
How patency checked
Optimal flush frequency
Optimal flush volume
Optimal flush technique
Optimal lock solution
Optimal lock frequency
Does NC influence patency
Can take blood specimens through CVAD? NC?
Patency – occlusion prevention PIV
How is patency checked?
What solution is used to flush and check patency
Occlusion management CVAD
Factors affecting occlusion rates: - type of cancer
- type of infusate Bevacizumab and heparin reaction – increased risk of thrombosis
- age
- CVAD duration
- laterality
- number of lumens
- type of CVAD
- valve vs non-valved catheters
- BMI>25
Growth factors
Other patient comorbidities
All 7 patients who developed symptomatic VTE had received TPA prior. All pts who had TPA, had occlusion
Steps in assessment of occlusion
Optimal management Detailed process of occlusion management – Alteplase, then increase time, 2nd dose, then imaging -
Optimal catheter tip position How does this relate to occlusion
Does angle of catheter in relation to port body impact occlusion rates
Does increase in resistance monitoring values indicate imminent CVAD occlusion
Can locking solutions be associated with risks of other complications?
Does CVAD material influence occlusion rates?
Can CVADs be used for radiological studies?
Occlusion management PIV
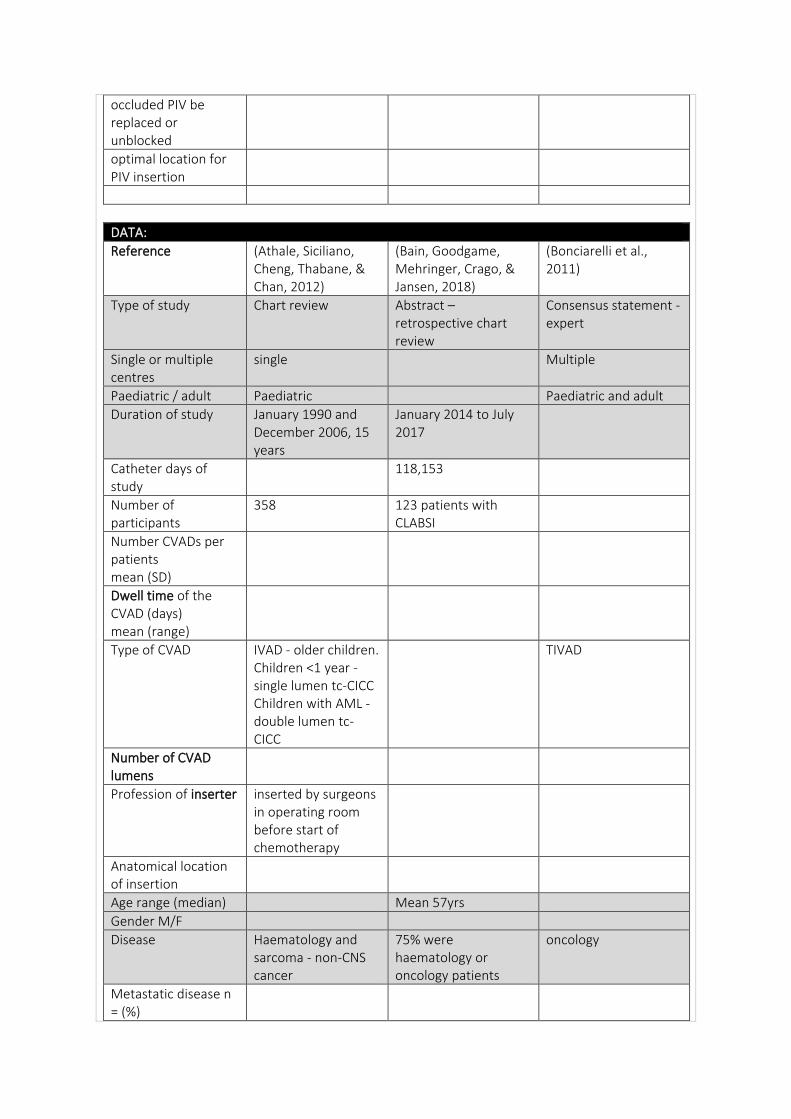
occluded PIV be replaced or unblocked
optimal location for PIV insertion
DATA:
Reference (Athale, Siciliano, Cheng, Thabane, & Chan, 2012)
(Bain, Goodgame, Mehringer, Crago, & Jansen, 2018)
(Bonciarelli et al., 2011)
Type of study Chart review Abstract – retrospective chart review
Consensus statement - expert
Single or multiple centres
single Multiple
Paediatric / adult Paediatric Paediatric and adult
Duration of study January 1990 and December 2006, 15 years
January 2014 to July 2017
Catheter days of study
118,153
Number of participants
358 123 patients with CLABSI
Number CVADs per patients mean (SD)
Dwell time of the CVAD (days) mean (range)
Type of CVAD IVAD - older children. Children <1 year - single lumen tc-CICC Children with AML - double lumen tc-CICC
TIVAD
Number of CVAD lumens
Profession of inserter inserted by surgeons in operating room before start of chemotherapy
Anatomical location of insertion
Age range (median) Mean 57yrs
Gender M/F
Disease Haematology and sarcoma - non-CNS cancer
75% were haematology or oncology patients
oncology
Metastatic disease n = (%)
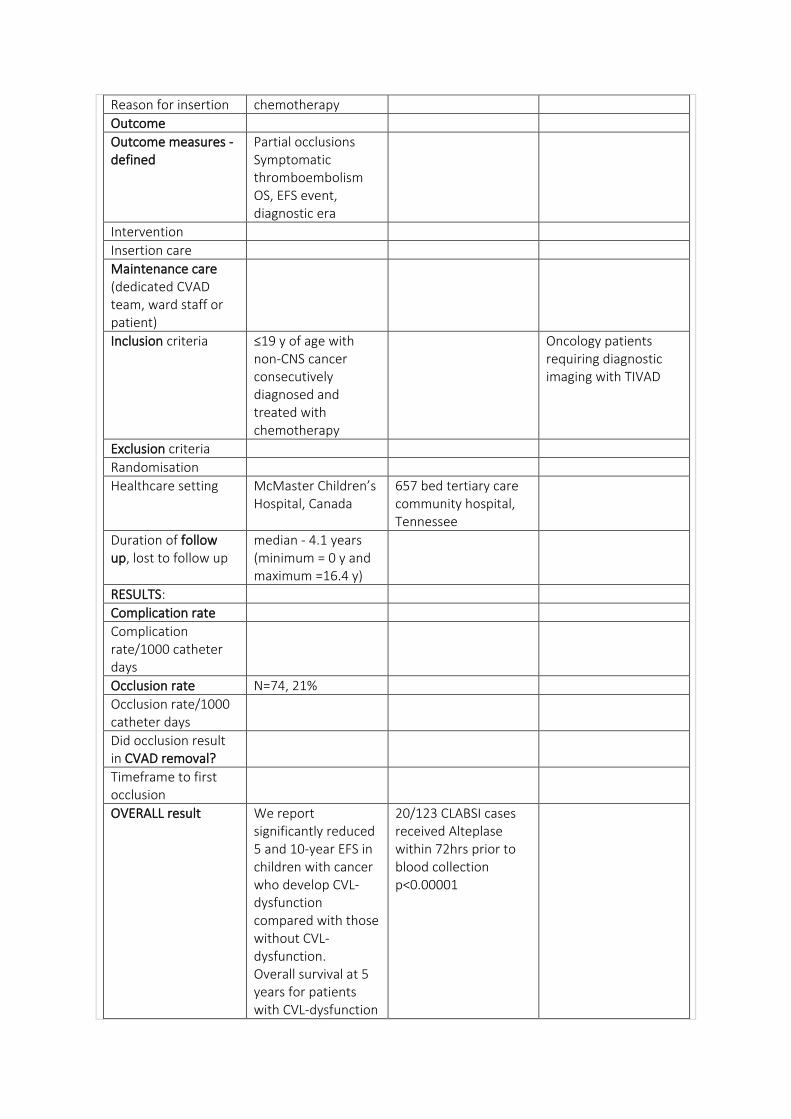
Reason for insertion chemotherapy
Outcome
Outcome measures - defined
Partial occlusions Symptomatic thromboembolism OS, EFS event, diagnostic era
Intervention
Insertion care
Maintenance care (dedicated CVAD team, ward staff or patient)
Inclusion criteria ≤19 y of age with non-CNS cancer consecutively diagnosed and treated with chemotherapy
Oncology patients requiring diagnostic imaging with TIVAD
Exclusion criteria
Randomisation
Healthcare setting McMaster Children’s Hospital, Canada
657 bed tertiary care community hospital, Tennessee
Duration of follow up, lost to follow up
median - 4.1 years (minimum = 0 y and maximum =16.4 y)
RESULTS:
Complication rate
Complication rate/1000 catheter days
Occlusion rate N=74, 21%
Occlusion rate/1000 catheter days
Did occlusion result in CVAD removal?
Timeframe to first occlusion
OVERALL result We report significantly reduced 5 and 10-year EFS in children with cancer who develop CVL-dysfunction compared with those without CVL-dysfunction. Overall survival at 5 years for patients with CVL-dysfunction
20/123 CLABSI cases received Alteplase within 72hrs prior to blood collection p<0.00001
was 70% compared with 82% for those without CVL-dysfunction
Thromboprophylaxis n= (%) median (range)
Patency – occlusion prevention CVAD
Education and competency requirement of staff – inserting and maintenance
- It is highly recommended that all radiological units using contrast infusion through venous ports should adopt specific prevention protocols (or “bundles”), and should implement an educational strategy including training courses for the health care personnel working with venous access devices. Operator education (medical, nursing, and technical staff) (cf. ePIC 2007: “Healthcare workers caring for a patient with a central venous access device should be trained and assessed as competent in using and consistently adhering to the infection prevention practices described in this guideline.” - Recommended - level of skill in use of implanted venous ports in radiology departments should be as high as in oncology departments – specific training, basic knowledge of proper maintenance
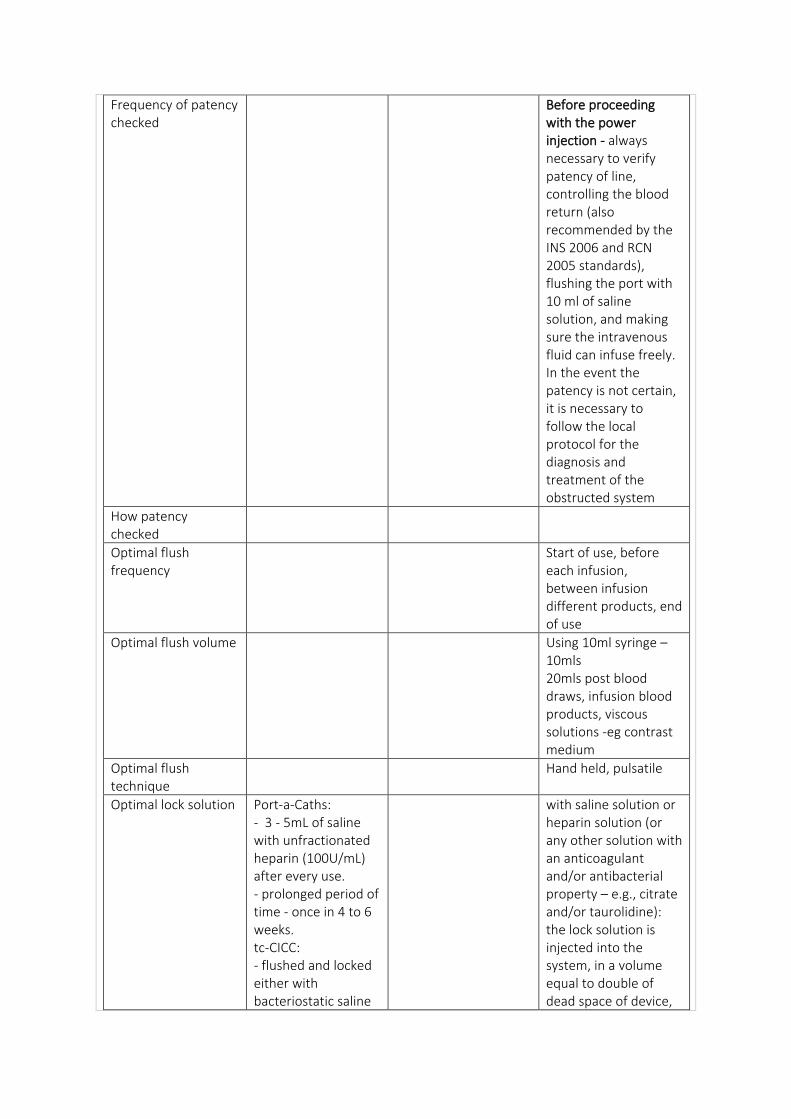
Frequency of patency checked
Before proceeding with the power injection - always necessary to verify patency of line, controlling the blood return (also recommended by the INS 2006 and RCN 2005 standards), flushing the port with 10 ml of saline solution, and making sure the intravenous fluid can infuse freely. In the event the patency is not certain, it is necessary to follow the local protocol for the diagnosis and treatment of the obstructed system
How patency checked
Optimal flush frequency
Start of use, before each infusion, between infusion different products, end of use
Optimal flush volume Using 10ml syringe – 10mls 20mls post blood draws, infusion blood products, viscous solutions -eg contrast medium
Optimal flush technique
Hand held, pulsatile
Optimal lock solution Port-a-Caths: - 3 - 5mL of saline with unfractionated heparin (100U/mL) after every use. - prolonged period of time - once in 4 to 6 weeks. tc-CICC: - flushed and locked either with bacteriostatic saline
with saline solution or heparin solution (or any other solution with an anticoagulant and/or antibacterial property – e.g., citrate and/or taurolidine): the lock solution is injected into the system, in a volume equal to double of dead space of device,
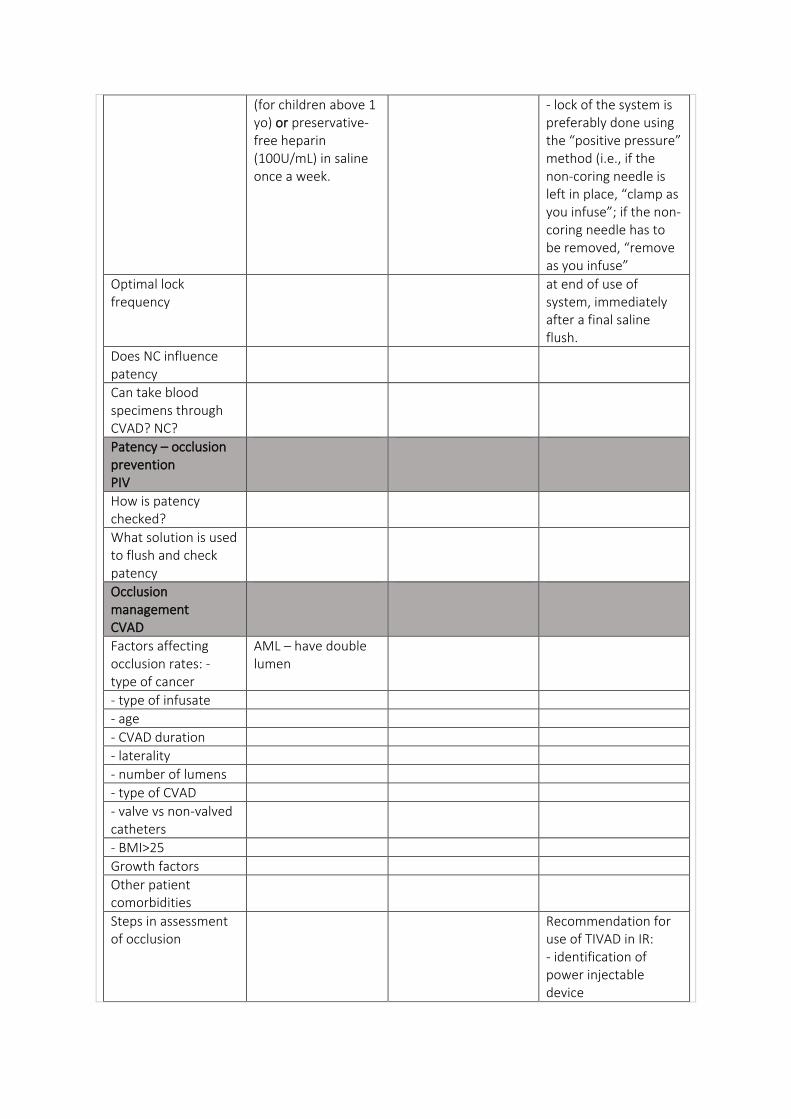
(for children above 1 yo) or preservative-free heparin (100U/mL) in saline once a week.
- lock of the system is preferably done using the “positive pressure” method (i.e., if the non-coring needle is left in place, “clamp as you infuse”; if the non-coring needle has to be removed, “remove as you infuse”
Optimal lock frequency
at end of use of system, immediately after a final saline flush.
Does NC influence patency
Can take blood specimens through CVAD? NC?
Patency – occlusion prevention PIV
How is patency checked?
What solution is used to flush and check patency
Occlusion management CVAD
Factors affecting occlusion rates: - type of cancer
AML – have double lumen
- type of infusate
- age
- CVAD duration
- laterality
- number of lumens
- type of CVAD
- valve vs non-valved catheters
- BMI>25
Growth factors
Other patient comorbidities
Steps in assessment of occlusion
Recommendation for use of TIVAD in IR: - identification of power injectable device
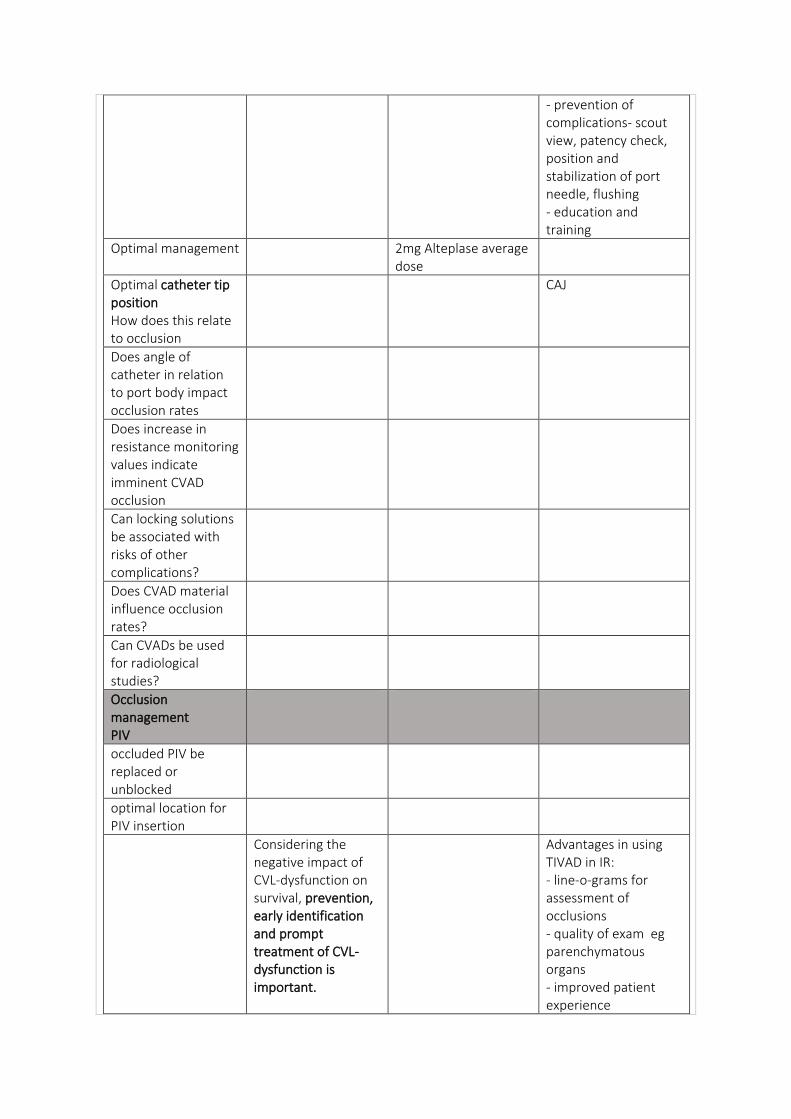
- prevention of complications- scout view, patency check, position and stabilization of port needle, flushing - education and training
Optimal management 2mg Alteplase average dose
Optimal catheter tip position How does this relate to occlusion
CAJ
Does angle of catheter in relation to port body impact occlusion rates
Does increase in resistance monitoring values indicate imminent CVAD occlusion
Can locking solutions be associated with risks of other complications?
Does CVAD material influence occlusion rates?
Can CVADs be used for radiological studies?
Occlusion management PIV
occluded PIV be replaced or unblocked
optimal location for PIV insertion
Considering the negative impact of CVL-dysfunction on survival, prevention, early identification and prompt treatment of CVL-dysfunction is important.
Advantages in using TIVAD in IR: - line-o-grams for assessment of occlusions - quality of exam eg parenchymatous organs - improved patient experience
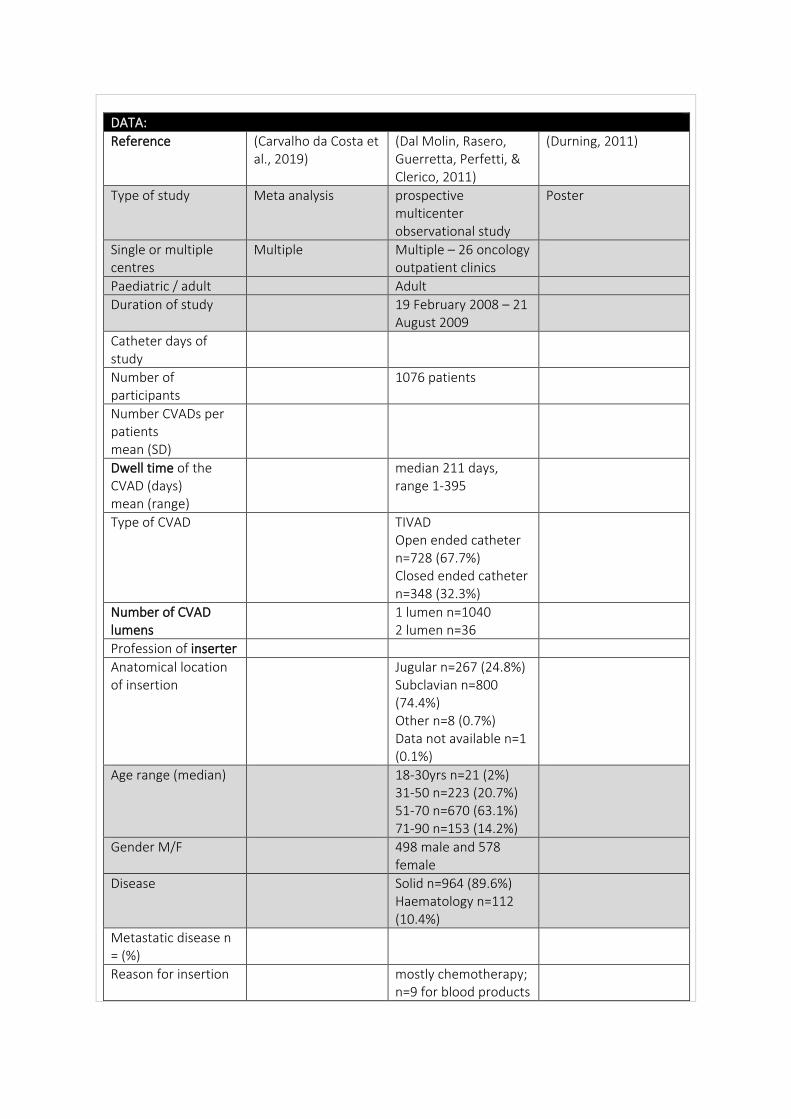
DATA:
Reference (Carvalho da Costa et al., 2019)
(Dal Molin, Rasero, Guerretta, Perfetti, & Clerico, 2011)
(Durning, 2011)
Type of study Meta analysis prospective multicenter observational study
Poster
Single or multiple centres
Multiple Multiple – 26 oncology outpatient clinics
Paediatric / adult Adult
Duration of study 19 February 2008 – 21 August 2009
Catheter days of study
Number of participants
1076 patients
Number CVADs per patients mean (SD)
Dwell time of the CVAD (days) mean (range)
median 211 days, range 1-395
Type of CVAD TIVAD Open ended catheter n=728 (67.7%) Closed ended catheter n=348 (32.3%)
Number of CVAD lumens
1 lumen n=1040 2 lumen n=36
Profession of inserter
Anatomical location of insertion
Jugular n=267 (24.8%) Subclavian n=800 (74.4%) Other n=8 (0.7%) Data not available n=1 (0.1%)
Age range (median) 18-30yrs n=21 (2%) 31-50 n=223 (20.7%) 51-70 n=670 (63.1%) 71-90 n=153 (14.2%)
Gender M/F 498 male and 578 female
Disease Solid n=964 (89.6%) Haematology n=112 (10.4%)
Metastatic disease n = (%)
Reason for insertion mostly chemotherapy; n=9 for blood products
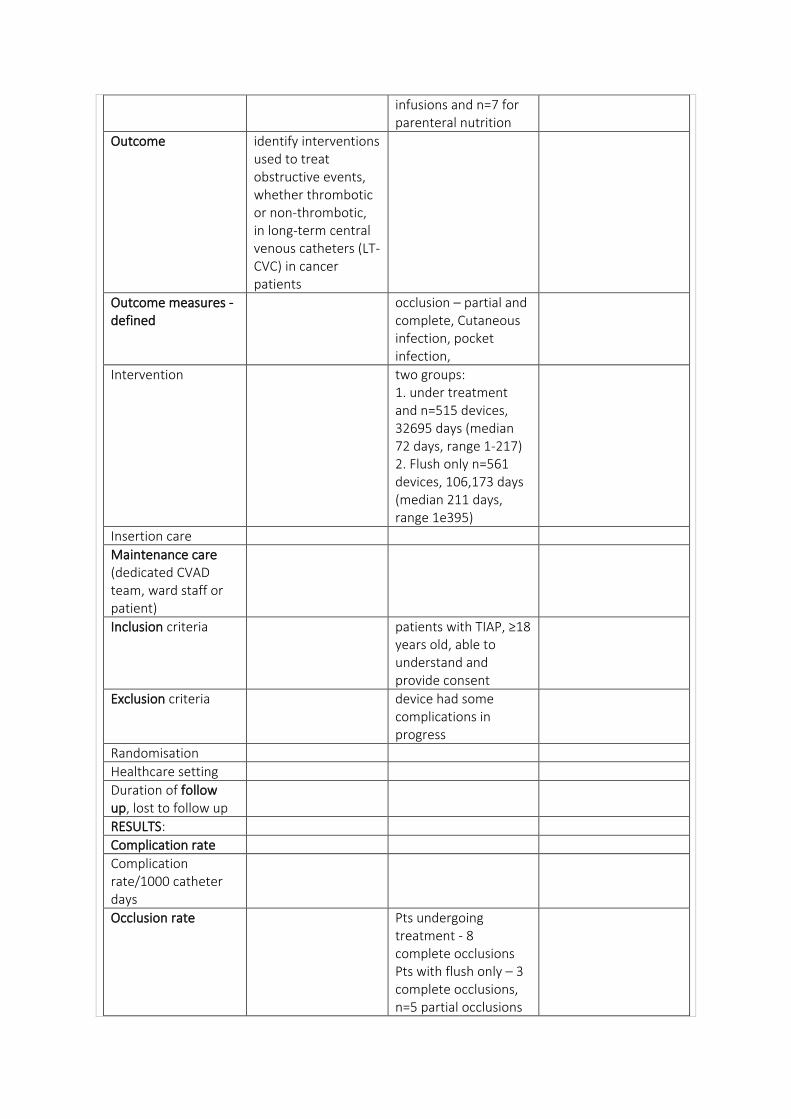
infusions and n=7 for parenteral nutrition
Outcome identify interventions used to treat obstructive events, whether thrombotic or non-thrombotic, in long-term central venous catheters (LT-CVC) in cancer patients
Outcome measures - defined
occlusion – partial and complete, Cutaneous infection, pocket infection,
Intervention two groups: 1. under treatment and n=515 devices, 32695 days (median 72 days, range 1-217) 2. Flush only n=561 devices, 106,173 days (median 211 days, range 1e395)
Insertion care
Maintenance care (dedicated CVAD team, ward staff or patient)
Inclusion criteria patients with TIAP, ≥18 years old, able to understand and provide consent
Exclusion criteria device had some complications in progress
Randomisation
Healthcare setting
Duration of follow up, lost to follow up
RESULTS:
Complication rate
Complication rate/1000 catheter days
Occlusion rate Pts undergoing treatment - 8 complete occlusions Pts with flush only – 3 complete occlusions, n=5 partial occlusions
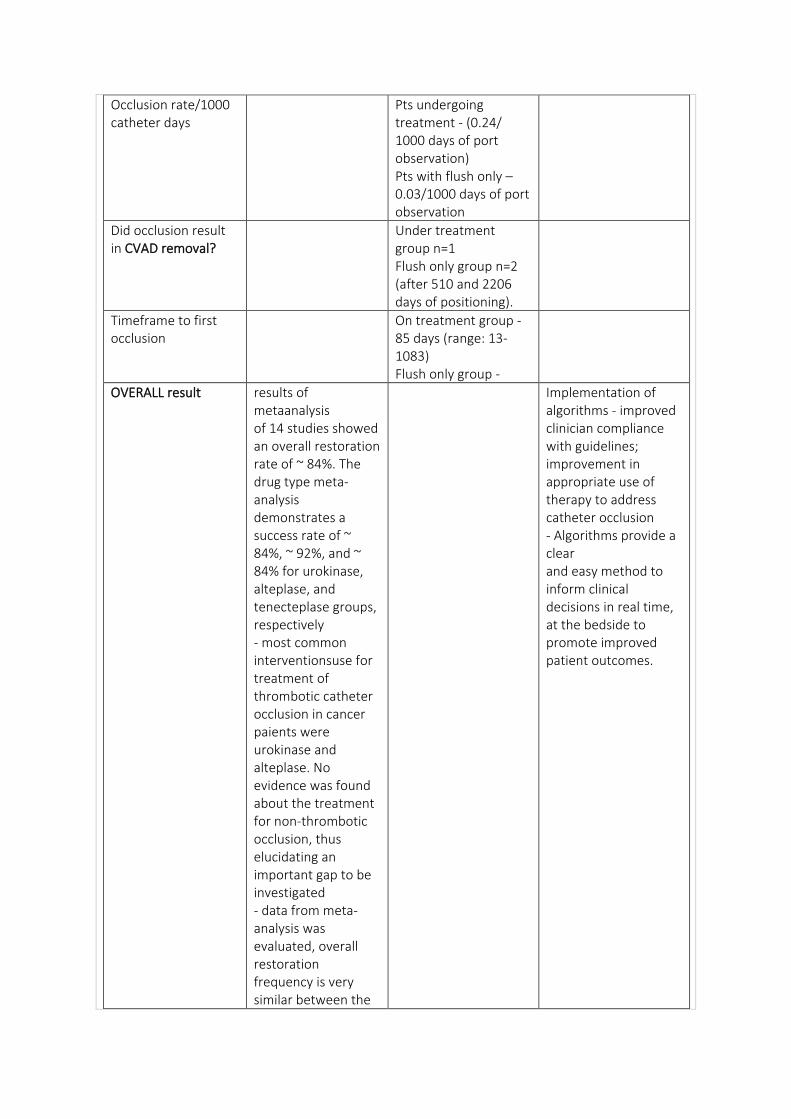
Occlusion rate/1000 catheter days
Pts undergoing treatment - (0.24/ 1000 days of port observation) Pts with flush only – 0.03/1000 days of port observation
Did occlusion result in CVAD removal?
Under treatment group n=1 Flush only group n=2 (after 510 and 2206 days of positioning).
Timeframe to first occlusion
On treatment group - 85 days (range: 13-1083) Flush only group -
OVERALL result results of metaanalysis of 14 studies showed an overall restoration rate of ~ 84%. The drug type meta-analysis demonstrates a success rate of ~ 84%, ~ 92%, and ~ 84% for urokinase, alteplase, and tenecteplase groups, respectively - most common interventionsuse for treatment of thrombotic catheter occlusion in cancer paients were urokinase and alteplase. No evidence was found about the treatment for non-thrombotic occlusion, thus elucidating an important gap to be investigated - data from meta-analysis was evaluated, overall restoration frequency is very similar between the
Implementation of algorithms - improved clinician compliance with guidelines; improvement in appropriate use of therapy to address catheter occlusion - Algorithms provide a clear and easy method to inform clinical decisions in real time, at the bedside to promote improved patient outcomes.
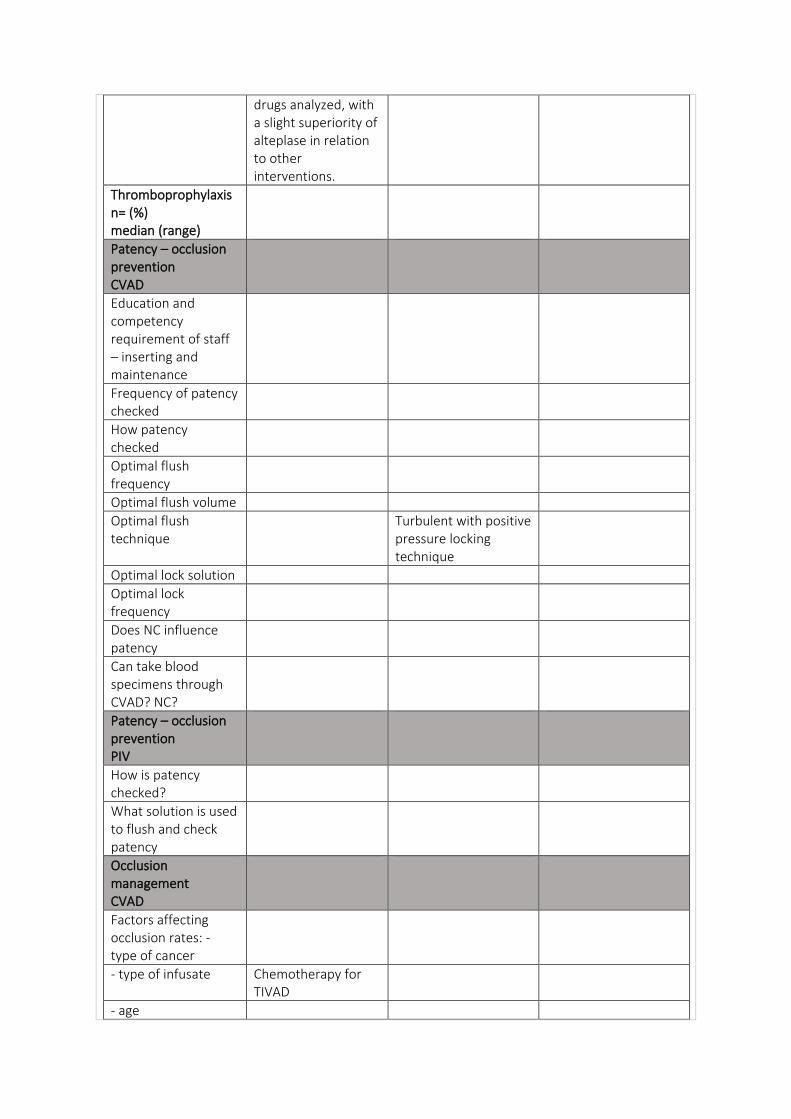
drugs analyzed, with a slight superiority of alteplase in relation to other interventions.
Thromboprophylaxis n= (%) median (range)
Patency – occlusion prevention CVAD
Education and competency requirement of staff – inserting and maintenance
Frequency of patency checked
How patency checked
Optimal flush frequency
Optimal flush volume
Optimal flush technique
Turbulent with positive pressure locking technique
Optimal lock solution
Optimal lock frequency
Does NC influence patency
Can take blood specimens through CVAD? NC?
Patency – occlusion prevention PIV
How is patency checked?
What solution is used to flush and check patency
Occlusion management CVAD
Factors affecting occlusion rates: - type of cancer
- type of infusate Chemotherapy for TIVAD
- age
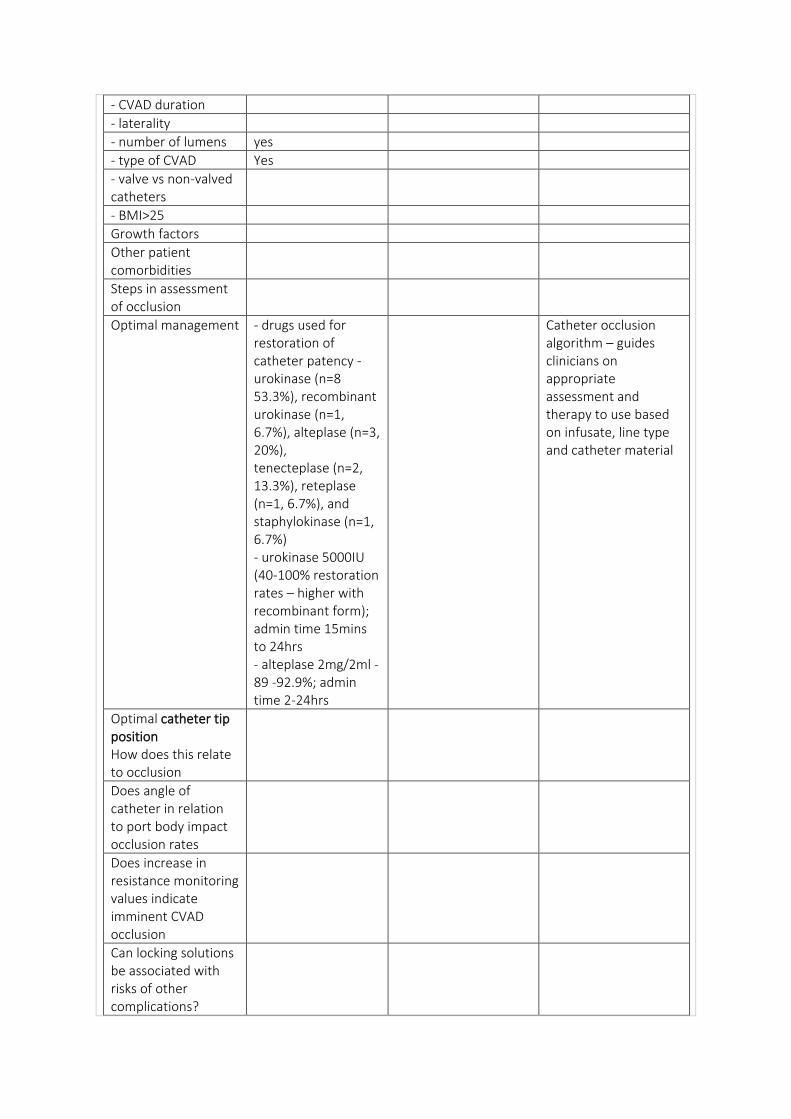
- CVAD duration
- laterality
- number of lumens yes
- type of CVAD Yes
- valve vs non-valved catheters
- BMI>25
Growth factors
Other patient comorbidities
Steps in assessment of occlusion
Optimal management - drugs used for restoration of catheter patency - urokinase (n=8 53.3%), recombinant urokinase (n=1, 6.7%), alteplase (n=3, 20%), tenecteplase (n=2, 13.3%), reteplase (n=1, 6.7%), and staphylokinase (n=1, 6.7%) - urokinase 5000IU (40-100% restoration rates – higher with recombinant form); admin time 15mins to 24hrs - alteplase 2mg/2ml - 89 -92.9%; admin time 2-24hrs
Catheter occlusion algorithm – guides clinicians on appropriate assessment and therapy to use based on infusate, line type and catheter material
Optimal catheter tip position How does this relate to occlusion
Does angle of catheter in relation to port body impact occlusion rates
Does increase in resistance monitoring values indicate imminent CVAD occlusion
Can locking solutions be associated with risks of other complications?
Does CVAD material influence occlusion rates?
Can CVADs be used for radiological studies?
Occlusion management PIV
occluded PIV be replaced or unblocked
optimal location for PIV insertion
In order to reduce complications, care of device is very important, and the role of nursing is crucial
DATA:
Reference (Fleury, Guignard, Fonzo-Christe, & Bonnabry, 2014)
(Forbrigger, Kuhle, Brown, Digout, & Kulkarni, 2018)
(Giordano et al., 2015)
Type of study Conference Abstract – literature review TIVAD and occlusions prevention and treatment
Poster abstract - population-based retrospective cohort study
Literature review for expert consensus for CVAD occlusion management
Single or multiple centres
multiple
Paediatric / adult paediatric Paediatric oncology
Duration of study 2000 - 2015 Lit search January 2000-January 2014
Catheter days of study
Number of participants
N=933
Number CVADs per patients mean (SD)
Dwell time of the CVAD (days) mean (range)
Type of CVAD TIVAD
Number of CVAD lumens
Profession of inserter
Anatomical location of insertion
Age range (median)
Gender M/F
Disease
Metastatic disease n = (%)
Reason for insertion
Outcome
Outcome measures - defined
Complete and partial occlusion. thrombosis
Intervention association between tPA and survival was examined
Insertion care
Maintenance care (dedicated CVAD team, ward staff or patient)
Inclusion criteria
Exclusion criteria
Randomisation
Healthcare setting Canadian Maritimes provinces of Nova Scotia, Prince Edward Island, and New Brunswick
Duration of follow up, lost to follow up
RESULTS:
Complication rate
Complication rate/1000 catheter days
Occlusion rate
Occlusion rate/1000 catheter days
Did occlusion result in CVAD removal?
Timeframe to first occlusion
OVERALL result n=190 (20%) received tPA: - n=93 (10%) patients received one dose of tPA - n=48 (5%) received two
- n=49 (5%) received ≥3 doses. Patients who received
≥1 doses of tPA had poorer survival than those who did not (HR 1.93, 95% CI 1.36-2.73). In the adjusted model, patients who received one (HR 1.73, 95% CI 1.08, 2.78) and two or more doses of tPA (HR 2.01, 95% CI 1.30-3.10) were more likely to die than patients who never received tPA - demonstrated a significantly poorer survival in pediatric cancer patients who received one or more doses of tPA
Thromboprophylaxis n= (%) median (range)
Patency – occlusion prevention CVAD
Education and competency requirement of staff – inserting and maintenance
Frequency of patency checked
How patency checked
Optimal flush frequency
Optimal flush volume minimum 10 ml syringe volume,
Optimal flush technique
using NS (normal saline) for flushing and positive pressure filling (pulsed flux technique)
Optimal lock solution
Optimal lock frequency
Does NC influence patency
Can take blood specimens through CVAD? NC?
Patency – occlusion prevention PIV
How is patency checked?
What solution is used to flush and check patency
Occlusion management CVAD
Factors affecting occlusion rates: - type of cancer
- type of infusate
- age
- CVAD duration
- laterality A lower thrombogenicity resulted from the insertion of the catheter from the right side
- number of lumens
- type of CVAD
- valve vs non-valved catheters
- BMI>25
Growth factors
Other patient comorbidities
positive family history of thrombosis was associated with the risk of occlusion of the CVC - significant association between the presence of CVC dysfunction and CVC-related thrombosis in children with cancer
Steps in assessment of occlusion
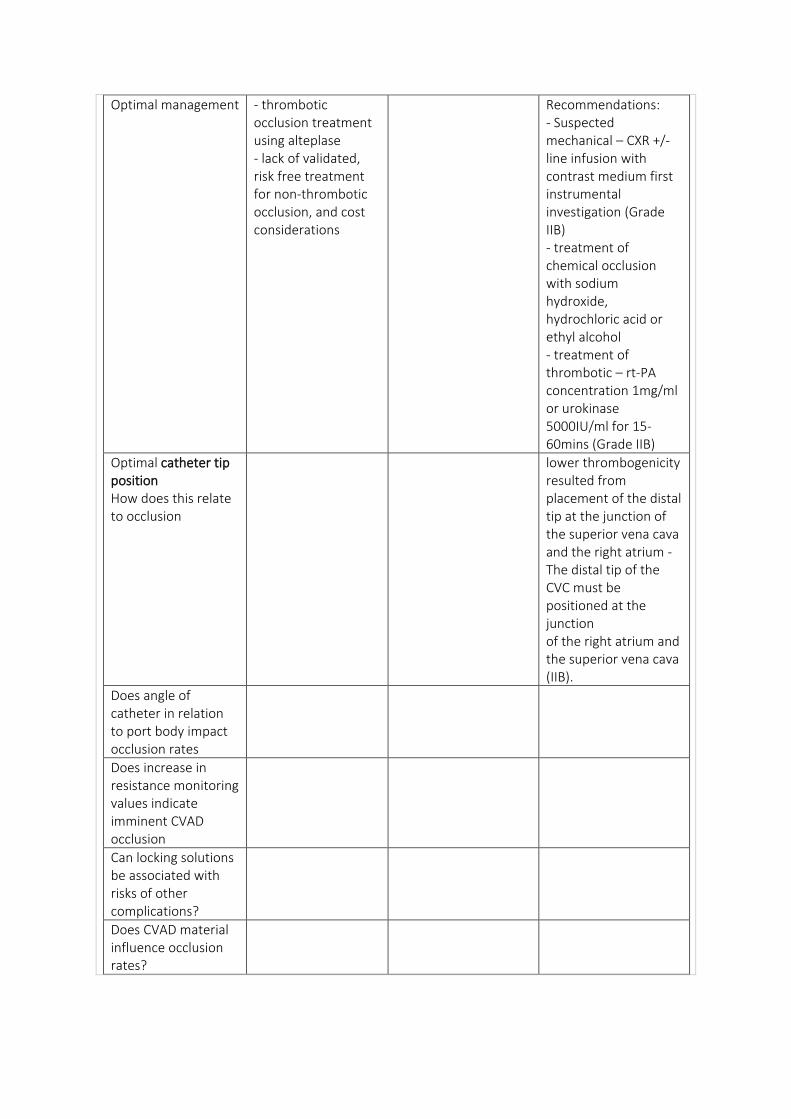
Optimal management - thrombotic occlusion treatment using alteplase - lack of validated, risk free treatment for non-thrombotic occlusion, and cost considerations
Recommendations: - Suspected mechanical – CXR +/- line infusion with contrast medium first instrumental investigation (Grade IIB) - treatment of chemical occlusion with sodium hydroxide, hydrochloric acid or ethyl alcohol - treatment of thrombotic – rt-PA concentration 1mg/ml or urokinase 5000IU/ml for 15-60mins (Grade IIB)
Optimal catheter tip position How does this relate to occlusion
lower thrombogenicity resulted from placement of the distal tip at the junction of the superior vena cava and the right atrium - The distal tip of the CVC must be positioned at the junction of the right atrium and the superior vena cava (IIB).
Does angle of catheter in relation to port body impact occlusion rates
Does increase in resistance monitoring values indicate imminent CVAD occlusion
Can locking solutions be associated with risks of other complications?
Does CVAD material influence occlusion rates?
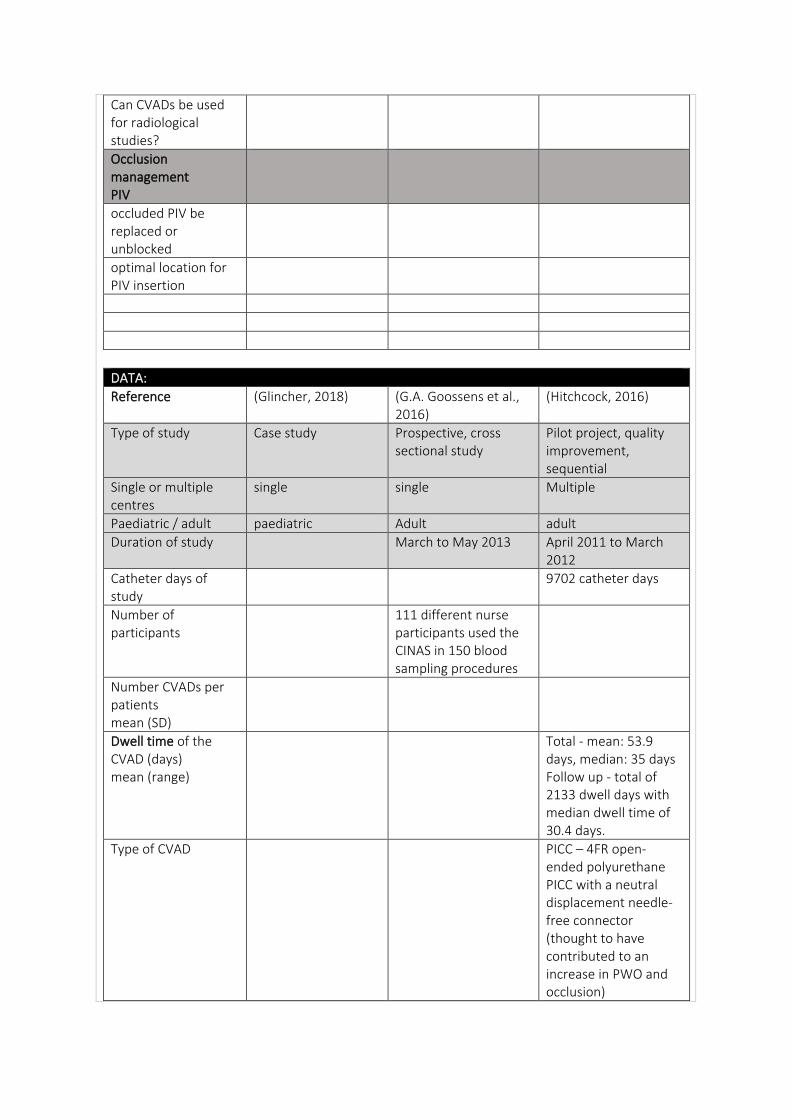
Can CVADs be used for radiological studies?
Occlusion management PIV
occluded PIV be replaced or unblocked
optimal location for PIV insertion
DATA:
Reference (Glincher, 2018) (G.A. Goossens et al., 2016)
(Hitchcock, 2016)
Type of study Case study Prospective, cross sectional study
Pilot project, quality improvement, sequential
Single or multiple centres
single single Multiple
Paediatric / adult paediatric Adult adult
Duration of study March to May 2013 April 2011 to March 2012
Catheter days of study
9702 catheter days
Number of participants
111 different nurse participants used the CINAS in 150 blood sampling procedures
Number CVADs per patients mean (SD)
Dwell time of the CVAD (days) mean (range)
Total - mean: 53.9 days, median: 35 days Follow up - total of 2133 dwell days with median dwell time of 30.4 days.
Type of CVAD PICC – 4FR open-ended polyurethane PICC with a neutral displacement needle-free connector (thought to have contributed to an increase in PWO and occlusion)
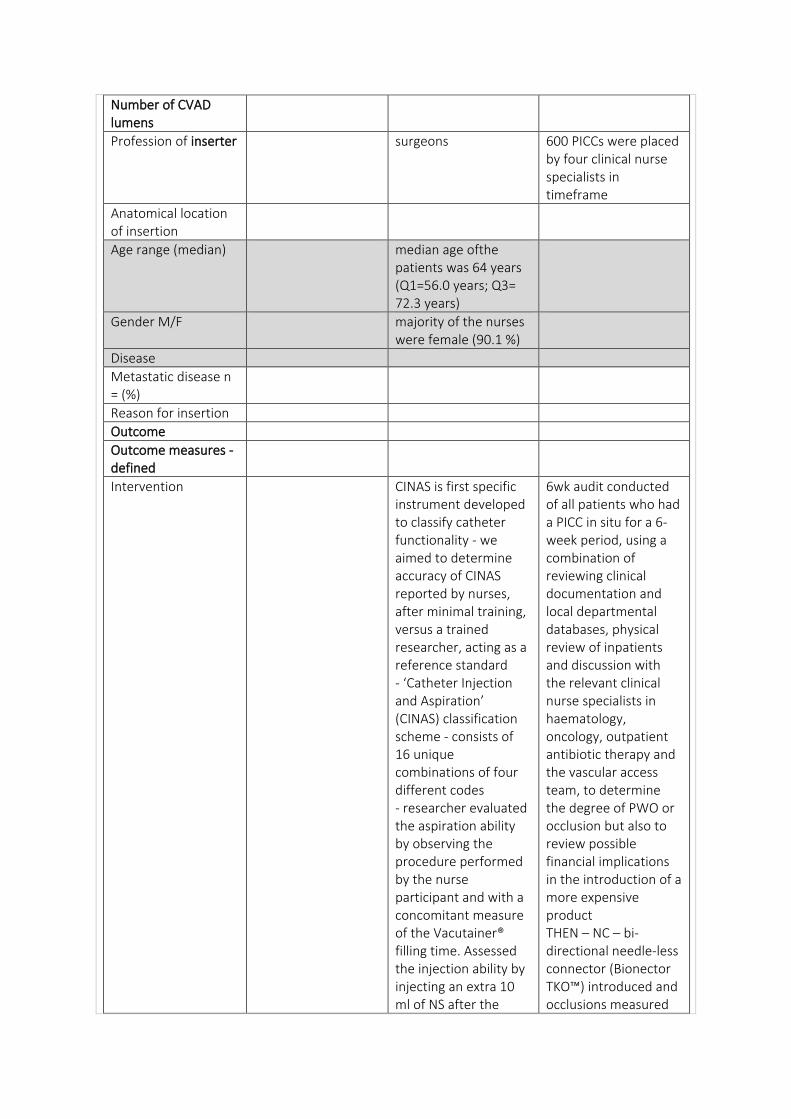
Number of CVAD lumens
Profession of inserter surgeons 600 PICCs were placed by four clinical nurse specialists in timeframe
Anatomical location of insertion
Age range (median) median age ofthe patients was 64 years (Q1=56.0 years; Q3= 72.3 years)
Gender M/F majority of the nurses were female (90.1 %)
Disease
Metastatic disease n = (%)
Reason for insertion
Outcome
Outcome measures - defined
Intervention CINAS is first specific instrument developed to classify catheter functionality - we aimed to determine accuracy of CINAS reported by nurses, after minimal training, versus a trained researcher, acting as a reference standard - ‘Catheter Injection and Aspiration’ (CINAS) classification scheme - consists of 16 unique combinations of four different codes - researcher evaluated the aspiration ability by observing the procedure performed by the nurse participant and with a concomitant measure of the Vacutainer® filling time. Assessed the injection ability by injecting an extra 10 ml of NS after the
6wk audit conducted of all patients who had a PICC in situ for a 6-week period, using a combination of reviewing clinical documentation and local departmental databases, physical review of inpatients and discussion with the relevant clinical nurse specialists in haematology, oncology, outpatient antibiotic therapy and the vascular access team, to determine the degree of PWO or occlusion but also to review possible financial implications in the introduction of a more expensive product THEN – NC – bi-directional needle-less connector (Bionector TKO™) introduced and occlusions measured
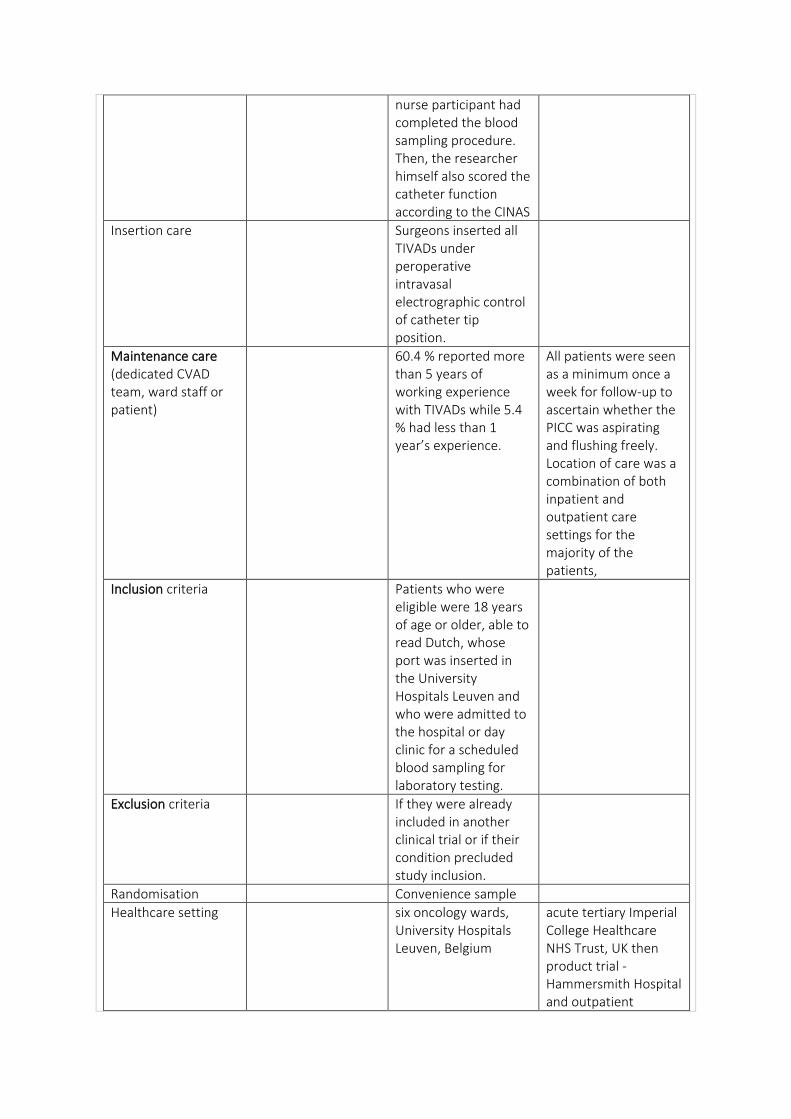
nurse participant had completed the blood sampling procedure. Then, the researcher himself also scored the catheter function according to the CINAS
Insertion care Surgeons inserted all TIVADs under peroperative intravasal electrographic control of catheter tip position.
Maintenance care (dedicated CVAD team, ward staff or patient)
60.4 % reported more than 5 years of working experience with TIVADs while 5.4 % had less than 1 year’s experience.
All patients were seen as a minimum once a week for follow-up to ascertain whether the PICC was aspirating and flushing freely. Location of care was a combination of both inpatient and outpatient care settings for the majority of the patients,
Inclusion criteria Patients who were eligible were 18 years of age or older, able to read Dutch, whose port was inserted in the University Hospitals Leuven and who were admitted to the hospital or day clinic for a scheduled blood sampling for laboratory testing.
Exclusion criteria If they were already included in another clinical trial or if their condition precluded study inclusion.
Randomisation Convenience sample
Healthcare setting six oncology wards, University Hospitals Leuven, Belgium
acute tertiary Imperial College Healthcare NHS Trust, UK then product trial - Hammersmith Hospital and outpatient
parenteral antibiotic therapy services at St Mary’s and Charing Cross Hospitals
Duration of follow up, lost to follow up
Seen weekly for 3-month evaluation of 70 patients with PICC insertion N=13 lost to follow-up (transfer to another institution or death)
RESULTS: A CINAS classification was possible in 100 % of catheter function assessments (n=150) for both the researcher, acting as a reference standard, and the nurse participants
Complication rate
Complication rate/1000 catheter days
Occlusion rate 65 patients (93%) had a fully functional PICC, that is, the PICC flushed and aspirated easily for the full duration of the required dwell time - n=13 (8%) had either PWO or complete occlusion; n=1 had two episodes of PWO, as the two episodes were 104 days apart they were treated as two different events in analysis, - n=1 oncology patient had complete luminal occlusion - vascular access team found Bionector TKO removed and replaced with standard NC (unknown reason); n=3 (4%) experienced PWO; n=1 patient was transferred within the
organisation to clinical area that did not recognise Bionector TKO and removed it, remaining two patients were haematology cohort and no explanation for PWO could be found.
Occlusion rate/1000 catheter days
- persistent withdrawal occlusion rate of 1/1000 catheter days - total occlusion rate of 0.4/1000 - n=14 patients; n= 9 - single-lumen 4 Fr PICC, n=5 - double-lumen 6 Fr power-injectable PICC
Did occlusion result in CVAD removal?
n=3 PICCs removed; n=2 cases treatment was complete, with the possible reason for occlusion being that the PICCs had not been used for 7 and 21 days respectively and n=1 pt with suspected neutropenic sepsis—as per organisational protocol all invasive devices were removed. The last patient with PWO had a double-lumen PICC in situ with one lumen not aspirating 20 days after insertion, this may have been due to the use of the PICC for aspirating blood from one lumen while delivering chemotherapy via the other lumen as a part of a research trial.
Timeframe to first occlusion
ranged from 9 to 144 days
Hitchcock:
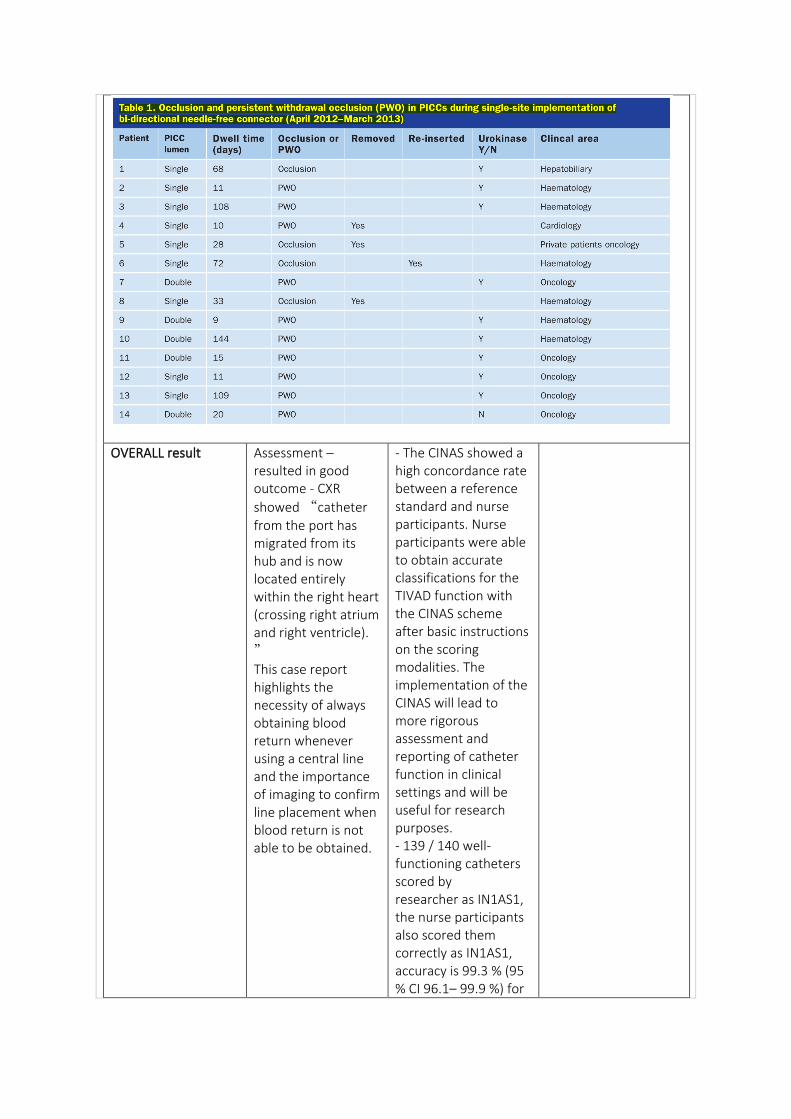
OVERALL result Assessment – resulted in good outcome - CXR
showed “catheter from the port has migrated from its hub and is now located entirely within the right heart (crossing right atrium and right ventricle).
” This case report highlights the necessity of always obtaining blood return whenever using a central line and the importance of imaging to confirm line placement when blood return is not able to be obtained.
- The CINAS showed a high concordance rate between a reference standard and nurse participants. Nurse participants were able to obtain accurate classifications for the TIVAD function with the CINAS scheme after basic instructions on the scoring modalities. The implementation of the CINAS will lead to more rigorous assessment and reporting of catheter function in clinical settings and will be useful for research purposes. - 139 / 140 well-functioning catheters scored by researcher as IN1AS1, the nurse participants also scored them correctly as IN1AS1, accuracy is 99.3 % (95 % CI 96.1– 99.9 %) for
classification of well-functioning catheters. - researcher classified 10 catheters as different from IN1AS1. Nine of these 10 or 90 % (95 % CI 55.5–98.3 %) were also classified as different from IN1AS1 by the nurse participants. Moreover, in 8 of 10 malfunctioning catheters (80 %, 95 % CI 44.4–97.5 %), the nurse participants attributed exactly the same score as the researcher. The overall accuracy of the CINAS scored by the nurse participants versus the researcher is (139+9) /150 or 98.7 % (CI 95.3–99.8 %).
Thromboprophylaxis n= (%) median (range)
Patency – occlusion prevention CVAD
Education and competency requirement of staff – inserting and maintenance
Frequency of patency checked
catheter function was evaluated using the institutional protocol to perform the blood sampling. Prior to blood sampling, the port is flushed with 10 ml of NS. This is followed by an aspiration of the first blood mixed with NS, using a 10-ml Vacutainer® tube, which is discarded. After collection of the
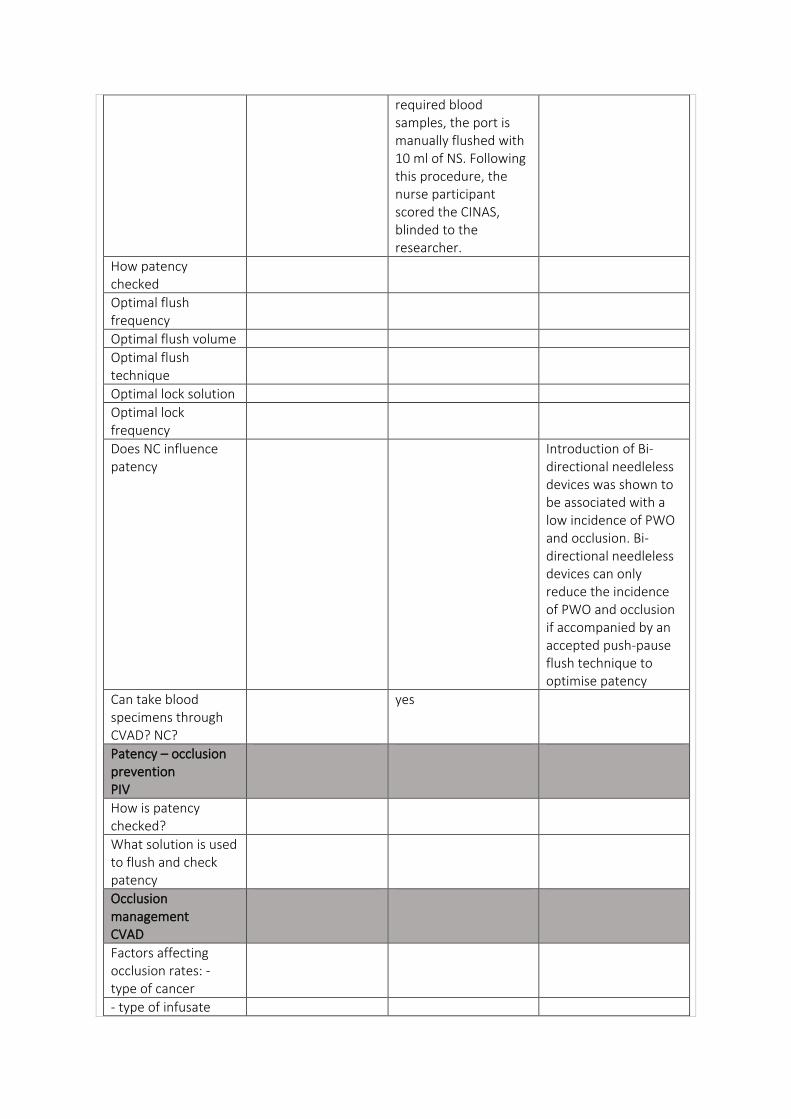
required blood samples, the port is manually flushed with 10 ml of NS. Following this procedure, the nurse participant scored the CINAS, blinded to the researcher.
How patency checked
Optimal flush frequency
Optimal flush volume
Optimal flush technique
Optimal lock solution
Optimal lock frequency
Does NC influence patency
Introduction of Bi-directional needleless devices was shown to be associated with a low incidence of PWO and occlusion. Bi-directional needleless devices can only reduce the incidence of PWO and occlusion if accompanied by an accepted push-pause flush technique to optimise patency
Can take blood specimens through CVAD? NC?
yes
Patency – occlusion prevention PIV
How is patency checked?
What solution is used to flush and check patency
Occlusion management CVAD
Factors affecting occlusion rates: - type of cancer
- type of infusate
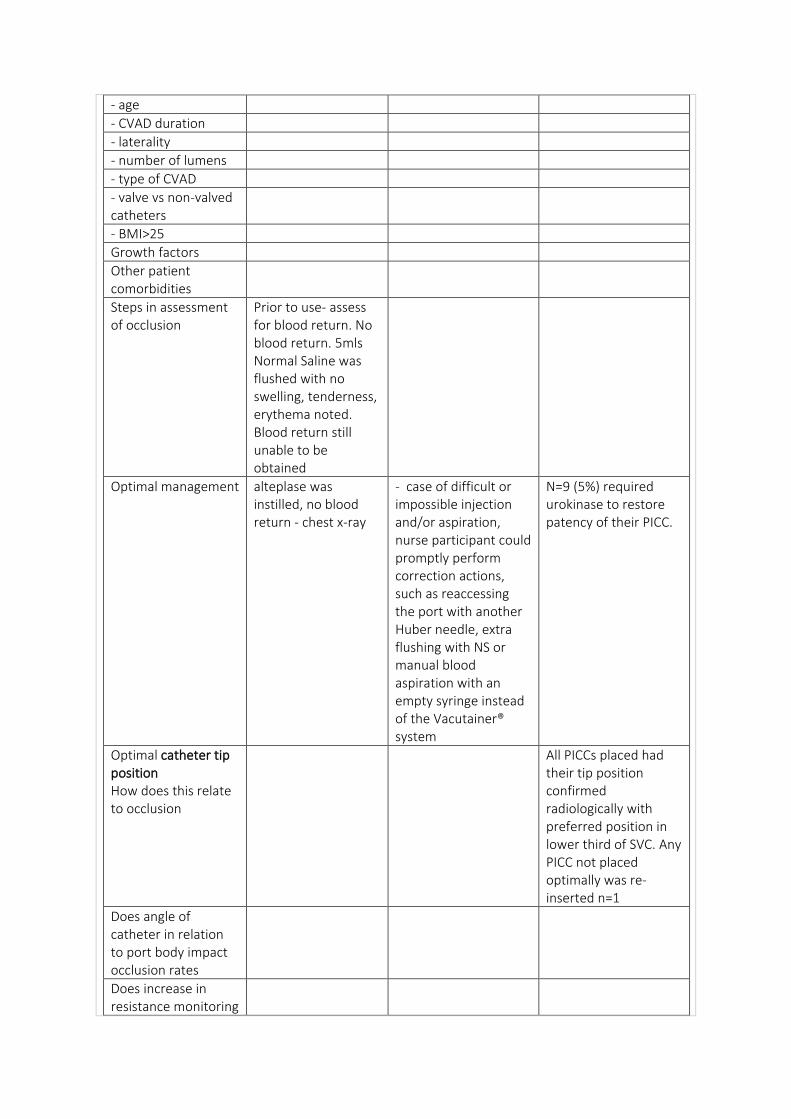
- age
- CVAD duration
- laterality
- number of lumens
- type of CVAD
- valve vs non-valved catheters
- BMI>25
Growth factors
Other patient comorbidities
Steps in assessment of occlusion
Prior to use- assess for blood return. No blood return. 5mls Normal Saline was flushed with no swelling, tenderness, erythema noted. Blood return still unable to be obtained
Optimal management alteplase was instilled, no blood return - chest x-ray
- case of difficult or impossible injection and/or aspiration, nurse participant could promptly perform correction actions, such as reaccessing the port with another Huber needle, extra flushing with NS or manual blood aspiration with an empty syringe instead of the Vacutainer® system
N=9 (5%) required urokinase to restore patency of their PICC.
Optimal catheter tip position How does this relate to occlusion
All PICCs placed had their tip position confirmed radiologically with preferred position in lower third of SVC. Any PICC not placed optimally was re-inserted n=1
Does angle of catheter in relation to port body impact occlusion rates
Does increase in resistance monitoring
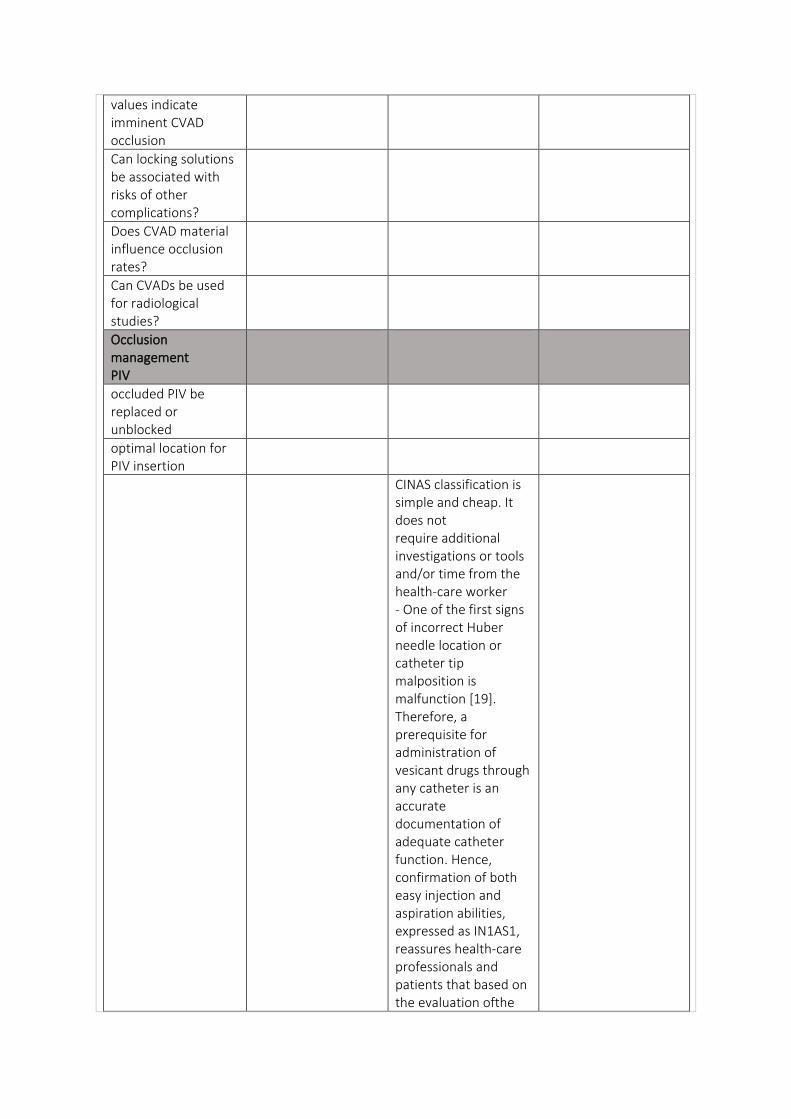
values indicate imminent CVAD occlusion
Can locking solutions be associated with risks of other complications?
Does CVAD material influence occlusion rates?
Can CVADs be used for radiological studies?
Occlusion management PIV
occluded PIV be replaced or unblocked
optimal location for PIV insertion
CINAS classification is simple and cheap. It does not require additional investigations or tools and/or time from the health-care worker - One of the first signs of incorrect Huber needle location or catheter tip malposition is malfunction [19]. Therefore, a prerequisite for administration of vesicant drugs through any catheter is an accurate documentation of adequate catheter function. Hence, confirmation of both easy injection and aspiration abilities, expressed as IN1AS1, reassures health-care professionals and patients that based on the evaluation ofthe
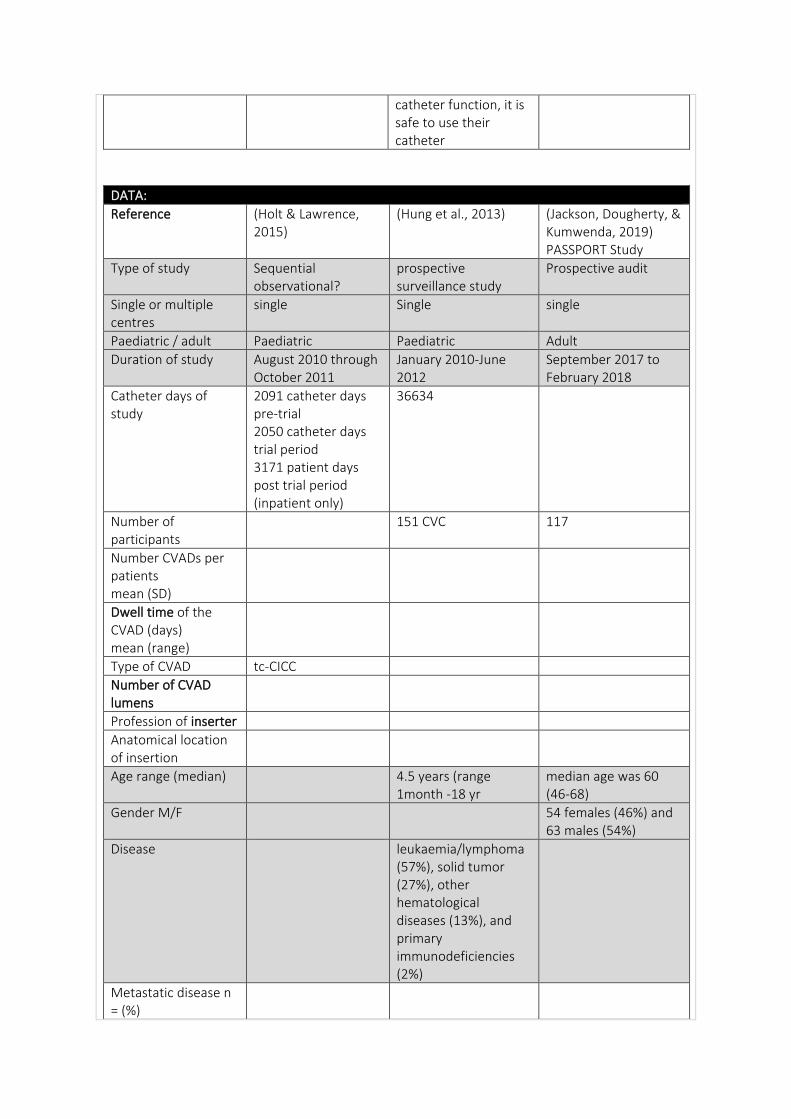
catheter function, it is safe to use their catheter
DATA:
Reference (Holt & Lawrence, 2015)
(Hung et al., 2013) (Jackson, Dougherty, & Kumwenda, 2019) PASSPORT Study
Type of study Sequential observational?
prospective surveillance study
Prospective audit
Single or multiple centres
single Single single
Paediatric / adult Paediatric Paediatric Adult
Duration of study August 2010 through October 2011
January 2010-June 2012
September 2017 to February 2018
Catheter days of study
2091 catheter days pre-trial 2050 catheter days trial period 3171 patient days post trial period (inpatient only)
36634
Number of participants
151 CVC 117
Number CVADs per patients mean (SD)
Dwell time of the CVAD (days) mean (range)
Type of CVAD tc-CICC
Number of CVAD lumens
Profession of inserter
Anatomical location of insertion
Age range (median) 4.5 years (range 1month -18 yr
median age was 60 (46-68)
Gender M/F 54 females (46%) and 63 males (54%)
Disease leukaemia/lymphoma (57%), solid tumor (27%), other hematological diseases (13%), and primary immunodeficiencies (2%)
Metastatic disease n = (%)
Reason for insertion
Outcome Baseline pre Neutron data collected
Catheter-associated infections and catheter blockage were the most frequent complications in our paediatric patients with CVC.
Treatment of occluded CVAD using standardised SynerKINASE dose regimens was safe and effective in restoring patency of CVAD.
Outcome measures - defined
total occlusive (TO) or b) Persistent Withdrawal Occlusion (PWO)
Intervention Change from MicroClave to Neutron bidirectional valve - focus to evaluate influence of the Neutron valve needleless device on the incidence of complete thrombotic intraluminal occlusions of CVCs
To determine the incidence of central venous catheter (CVC) complications in haematology-oncology paediatric patients.
Prospective audit of the management of occluded CVAD using standardised SynerKINASE (urokinase) dose algorithms
Insertion care
Maintenance care (dedicated CVAD team, ward staff or patient)
Inclusion criteria
Exclusion criteria device was not Broviac or Hickman, patient was not in Hem/Onc inpatient department or clinic when the occlusion occurred, the type of occlusion not documented, or if the t-PA dose was ordered but not given per the documentation. - Trial data exclude 2 occlusions treated during the Neutron device trial for which no data were available describing the nature of the occlusions.
Randomisation Data was collected anonymously using a web based platform.
Healthcare setting 38-bed inpatient hematology /oncology department and outpatient hematology/oncology clinic, Rady Children’s Hospital, San Diego California, USA
Queen Mary Hospital, Department of Paediatrics and Adolescent Medicine, Hong Kong, China
Duration of follow up, lost to follow up
RESULTS:
Complication rate 51 non-infective CVC complications
Complication rate/1000 catheter days
(0.14 per 1000 CVC days)
Occlusion rate total number of complete central line occlusions events from August to October 2010 (ie, the pretrial period) to September to October 2011 (during trial period) fell 74.3% - not included but noted - smaller (19.7%) reduction occurred with PICCs - At conclusion of initial trial period, ended in October 2011, Hem/Onc department continued to use Neutron device on all CVCs. During this time, data were collected from inpatient unit only and compared with patient-days rather than catheter-days for ease of ongoing assessment. Data from Nov. 2011 –
- blockage (56.9%) of the 51 non-infective CVC complications
first thrombolytic treatment with SynerKINASE, out of 53 CVAD with TO, patency was restored in 46 (87%) and out of 64 CVAD with POW patency was restored in 80%. The CVAD clearance rate was dose dependent, patency was restored in 82% of CVAD with 5000IU, 100% of CVAD with 10000IU and 90% of CVAD with the high dose of 25000IU. No adverse events were recorded in this audit.
Feb. 2012 - complete thrombotic occlusion of 1.58 per 1000 patient-days. It should be noted that during the 2-month period following the trial when the Neutron device was not used in our Hem/Onc inpatient unit, the complete thrombotic occlusion rate increased to 3.62 per 1000 patientdays. After resuming the use of the Neutron device in May 2012, the rate gradually fell again
Occlusion rate/1000 catheter days
Did occlusion result in CVAD removal?
29 CVC removed due to complications, 10% blockage
Timeframe to first occlusion
OVERALL result
Thromboprophylaxis n= (%) median (range)
Patency – occlusion prevention CVAD
Education and competency requirement of staff – inserting and maintenance
Frequency of patency checked
How patency checked
Optimal flush frequency
Optimal flush volume 2mls normal saline then heparin
Optimal flush technique
Optimal lock solution Before 2010 - 100 U/mL 3-5 April 2010 – changed to 10 U/mL heparin flush.
Optimal lock frequency
Does NC influence patency
Can take blood specimens through CVAD? NC?
Patency – occlusion prevention PIV
How is patency checked?
What solution is used to flush and check patency
Occlusion management CVAD
Factors affecting occlusion rates: - type of cancer
- type of infusate
- age
- CVAD duration
- laterality
- number of lumens
- type of CVAD
- valve vs non-valved catheters
- BMI>25
Growth factors
Other patient comorbidities
Steps in assessment of occlusion
Optimal management SynerKINASE doses administered ranged between 5000IU – 25000IU, the high dose of 25000IU has not been used previously in these centres. Additional doses of SynerKINASE were administered if
the first administration was unsuccessful.
Optimal catheter tip position How does this relate to occlusion
Does angle of catheter in relation to port body impact occlusion rates
Does increase in resistance monitoring values indicate imminent CVAD occlusion
Can locking solutions be associated with risks of other complications?
Does CVAD material influence occlusion rates?
Can CVADs be used for radiological studies?
Occlusion management PIV
occluded PIV be replaced or unblocked
optimal location for PIV insertion
Hem/Onc department continued to use the Neutron device on all CVCs, a housewide expansion to the hospital’s products committee during October 2012. Comparing 5 months of housewide occlusion data from June through October 2012 to the same time frame in 2013 demonstrated a 32.1% reduction in complete occlusions
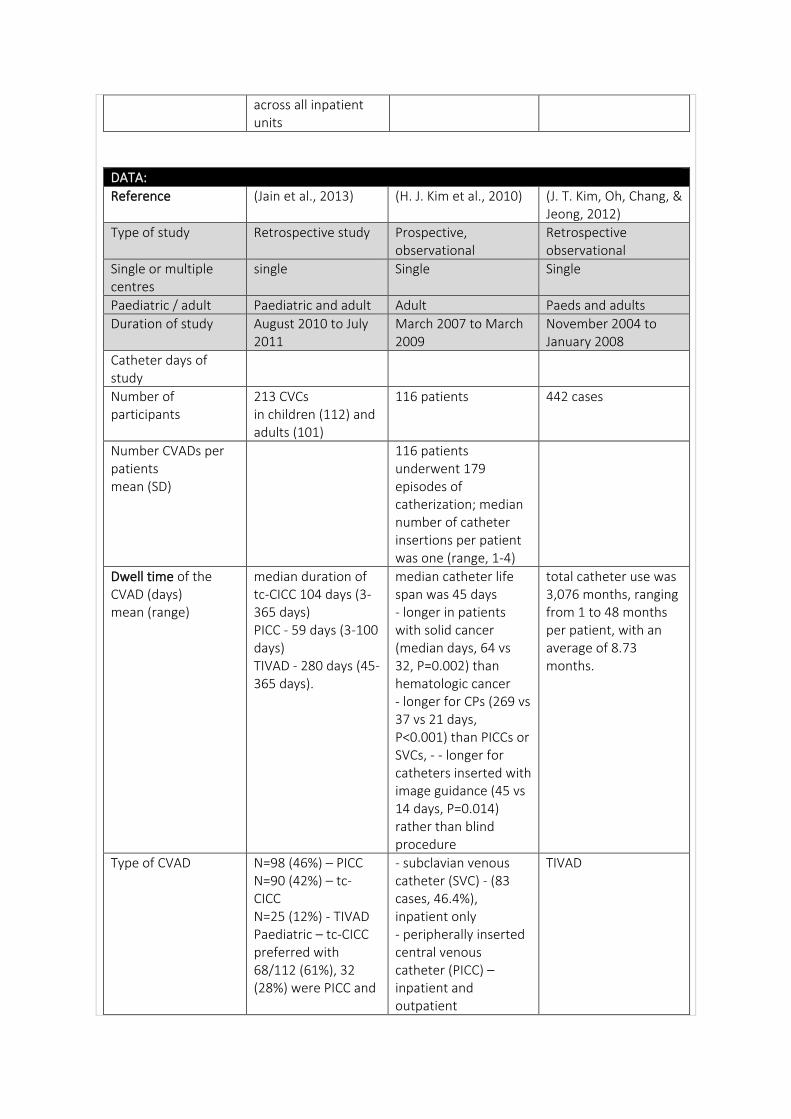
across all inpatient units
DATA:
Reference (Jain et al., 2013) (H. J. Kim et al., 2010) (J. T. Kim, Oh, Chang, & Jeong, 2012)
Type of study Retrospective study Prospective, observational
Retrospective observational
Single or multiple centres
single Single Single
Paediatric / adult Paediatric and adult Adult Paeds and adults
Duration of study August 2010 to July 2011
March 2007 to March 2009
November 2004 to January 2008
Catheter days of study
Number of participants
213 CVCs in children (112) and adults (101)
116 patients 442 cases
Number CVADs per patients mean (SD)
116 patients underwent 179 episodes of catherization; median number of catheter insertions per patient was one (range, 1-4)
Dwell time of the CVAD (days) mean (range)
median duration of tc-CICC 104 days (3-365 days) PICC - 59 days (3-100 days) TIVAD - 280 days (45-365 days).
median catheter life span was 45 days - longer in patients with solid cancer (median days, 64 vs 32, P=0.002) than hematologic cancer - longer for CPs (269 vs 37 vs 21 days, P<0.001) than PICCs or SVCs, - - longer for catheters inserted with image guidance (45 vs 14 days, P=0.014) rather than blind procedure
total catheter use was 3,076 months, ranging from 1 to 48 months per patient, with an average of 8.73 months.
Type of CVAD N=98 (46%) – PICC N=90 (42%) – tc- CICC N=25 (12%) - TIVAD Paediatric – tc-CICC preferred with 68/112 (61%), 32 (28%) were PICC and
- subclavian venous catheter (SVC) - (83 cases, 46.4%), inpatient only - peripherally inserted central venous catheter (PICC) – inpatient and outpatient
TIVAD
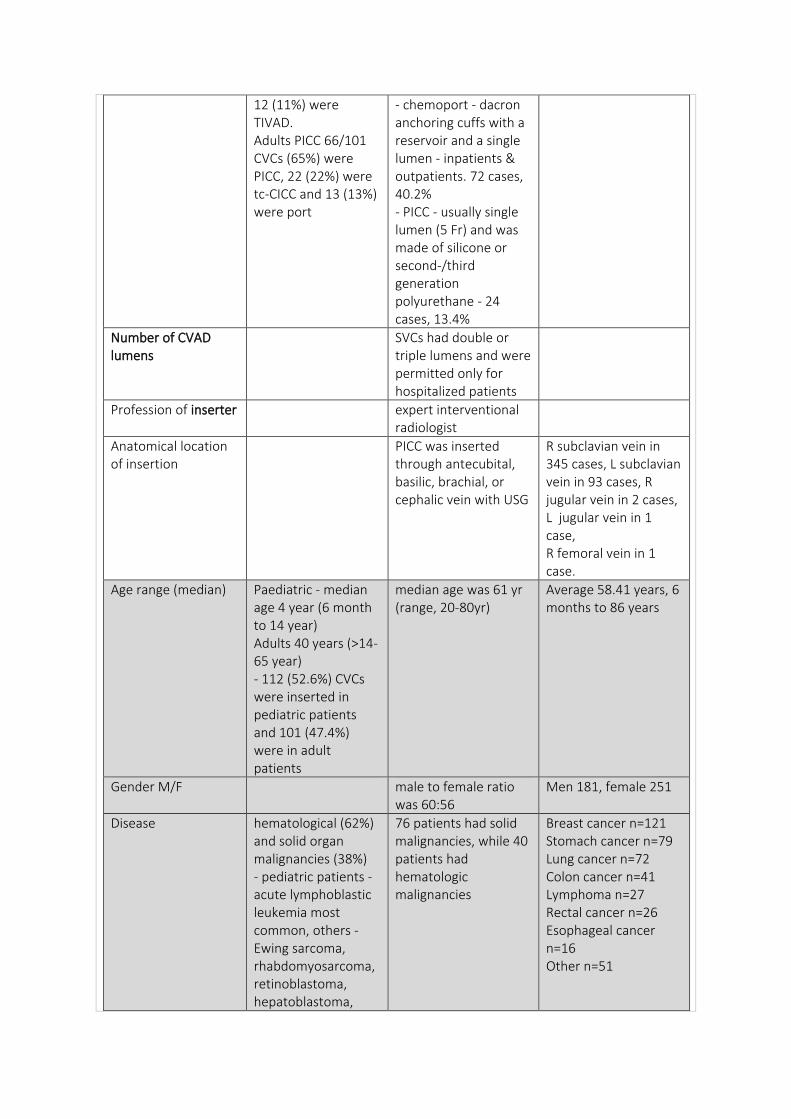
12 (11%) were TIVAD. Adults PICC 66/101 CVCs (65%) were PICC, 22 (22%) were tc-CICC and 13 (13%) were port
- chemoport - dacron anchoring cuffs with a reservoir and a single lumen - inpatients & outpatients. 72 cases, 40.2% - PICC - usually single lumen (5 Fr) and was made of silicone or second-/third generation polyurethane - 24 cases, 13.4%
Number of CVAD lumens
SVCs had double or triple lumens and were permitted only for hospitalized patients
Profession of inserter expert interventional radiologist
Anatomical location of insertion
PICC was inserted through antecubital, basilic, brachial, or cephalic vein with USG
R subclavian vein in 345 cases, L subclavian vein in 93 cases, R jugular vein in 2 cases, L jugular vein in 1 case, R femoral vein in 1 case.
Age range (median) Paediatric - median age 4 year (6 month to 14 year) Adults 40 years (>14-65 year) - 112 (52.6%) CVCs were inserted in pediatric patients and 101 (47.4%) were in adult patients
median age was 61 yr (range, 20-80yr)
Average 58.41 years, 6 months to 86 years
Gender M/F male to female ratio was 60:56
Men 181, female 251
Disease hematological (62%) and solid organ malignancies (38%) - pediatric patients - acute lymphoblastic leukemia most common, others - Ewing sarcoma, rhabdomyosarcoma, retinoblastoma, hepatoblastoma,
76 patients had solid malignancies, while 40 patients had hematologic malignancies
Breast cancer n=121 Stomach cancer n=79 Lung cancer n=72 Colon cancer n=41 Lymphoma n=27 Rectal cancer n=26 Esophageal cancer n=16 Other n=51
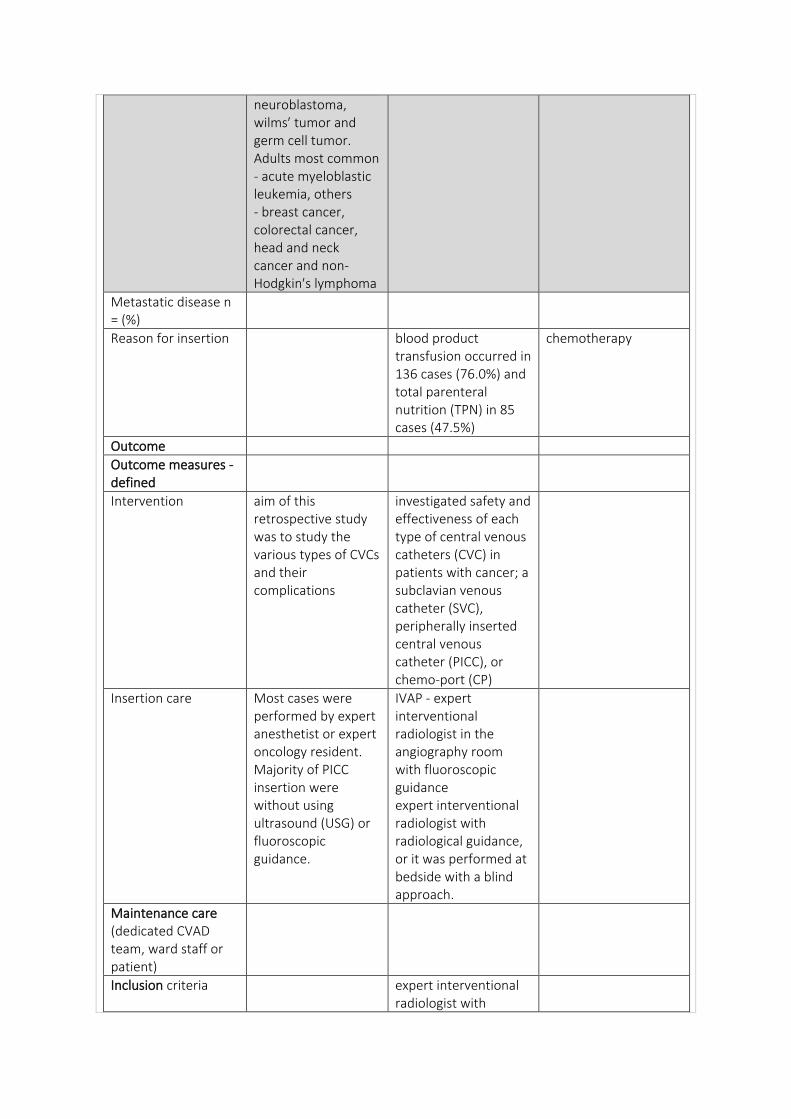
neuroblastoma, wilms′ tumor and germ cell tumor. Adults most common - acute myeloblastic leukemia, others - breast cancer, colorectal cancer, head and neck cancer and non-Hodgkin′s lymphoma
Metastatic disease n = (%)
Reason for insertion blood product transfusion occurred in 136 cases (76.0%) and total parenteral nutrition (TPN) in 85 cases (47.5%)
chemotherapy
Outcome
Outcome measures - defined
Intervention aim of this retrospective study was to study the various types of CVCs and their complications
investigated safety and effectiveness of each type of central venous catheters (CVC) in patients with cancer; a subclavian venous catheter (SVC), peripherally inserted central venous catheter (PICC), or chemo-port (CP)
Insertion care Most cases were performed by expert anesthetist or expert oncology resident. Majority of PICC insertion were without using ultrasound (USG) or fluoroscopic guidance.
IVAP - expert interventional radiologist in the angiography room with fluoroscopic guidance expert interventional radiologist with radiological guidance, or it was performed at bedside with a blind approach.
Maintenance care (dedicated CVAD team, ward staff or patient)
Inclusion criteria expert interventional radiologist with
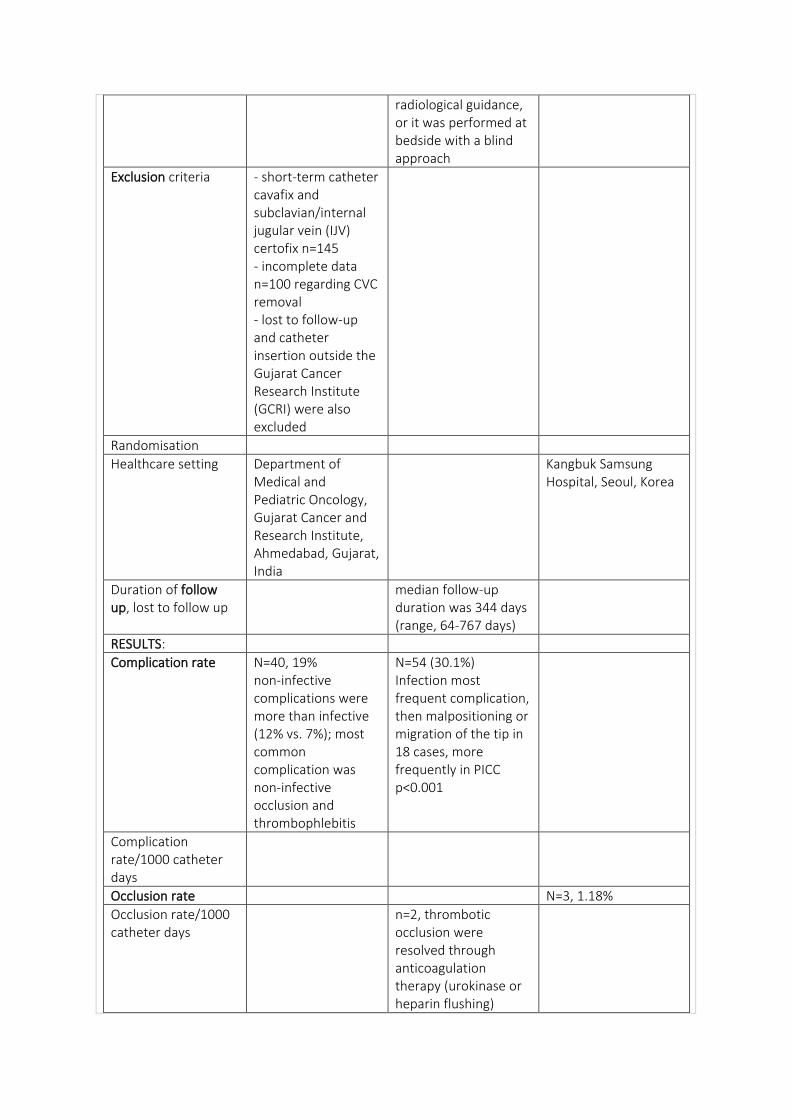
radiological guidance, or it was performed at bedside with a blind approach
Exclusion criteria - short-term catheter cavafix and subclavian/internal jugular vein (IJV) certofix n=145 - incomplete data n=100 regarding CVC removal - lost to follow-up and catheter insertion outside the Gujarat Cancer Research Institute (GCRI) were also excluded
Randomisation
Healthcare setting Department of Medical and Pediatric Oncology, Gujarat Cancer and Research Institute, Ahmedabad, Gujarat, India
Kangbuk Samsung Hospital, Seoul, Korea
Duration of follow up, lost to follow up
median follow-up duration was 344 days (range, 64-767 days)
RESULTS:
Complication rate N=40, 19% non-infective complications were more than infective (12% vs. 7%); most common complication was non-infective occlusion and thrombophlebitis
N=54 (30.1%) Infection most frequent complication, then malpositioning or migration of the tip in 18 cases, more frequently in PICC p<0.001
Complication rate/1000 catheter days
Occlusion rate N=3, 1.18%
Occlusion rate/1000 catheter days
n=2, thrombotic occlusion were resolved through anticoagulation therapy (urokinase or heparin flushing)
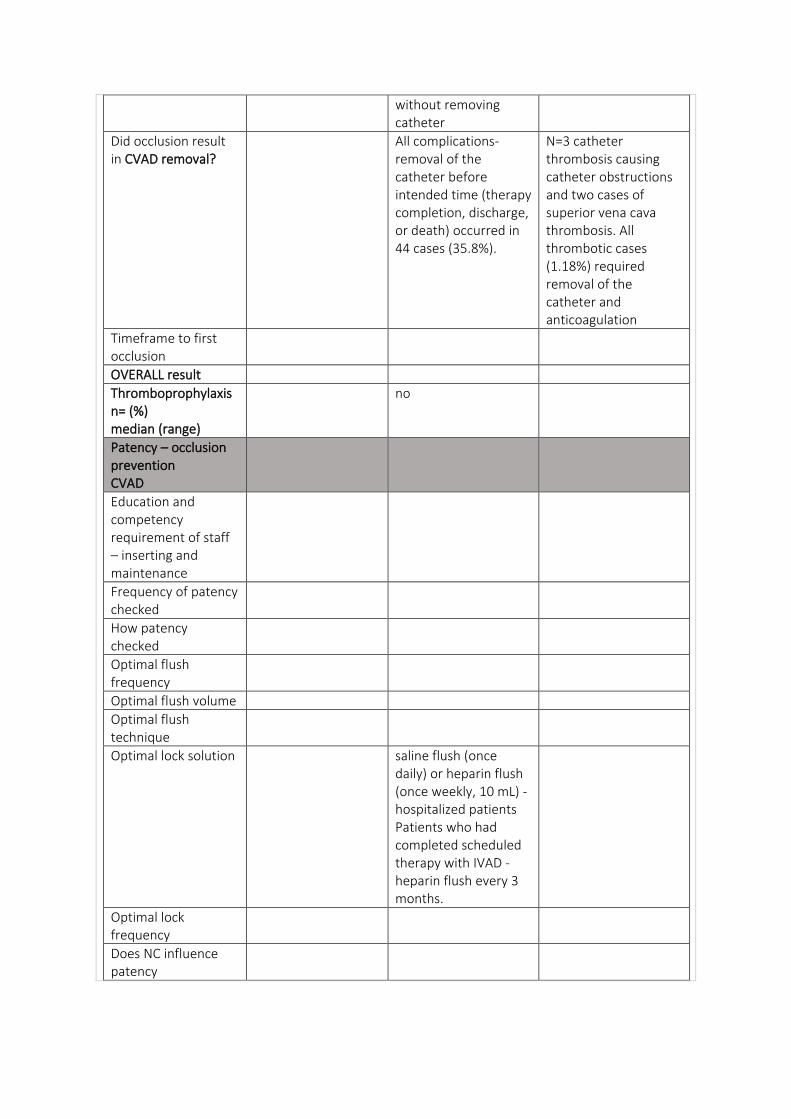
without removing catheter
Did occlusion result in CVAD removal?
All complications- removal of the catheter before intended time (therapy completion, discharge, or death) occurred in 44 cases (35.8%).
N=3 catheter thrombosis causing catheter obstructions and two cases of superior vena cava thrombosis. All thrombotic cases (1.18%) required removal of the catheter and anticoagulation
Timeframe to first occlusion
OVERALL result
Thromboprophylaxis n= (%) median (range)
no
Patency – occlusion prevention CVAD
Education and competency requirement of staff – inserting and maintenance
Frequency of patency checked
How patency checked
Optimal flush frequency
Optimal flush volume
Optimal flush technique
Optimal lock solution saline flush (once daily) or heparin flush (once weekly, 10 mL) - hospitalized patients Patients who had completed scheduled therapy with IVAD - heparin flush every 3 months.
Optimal lock frequency
Does NC influence patency
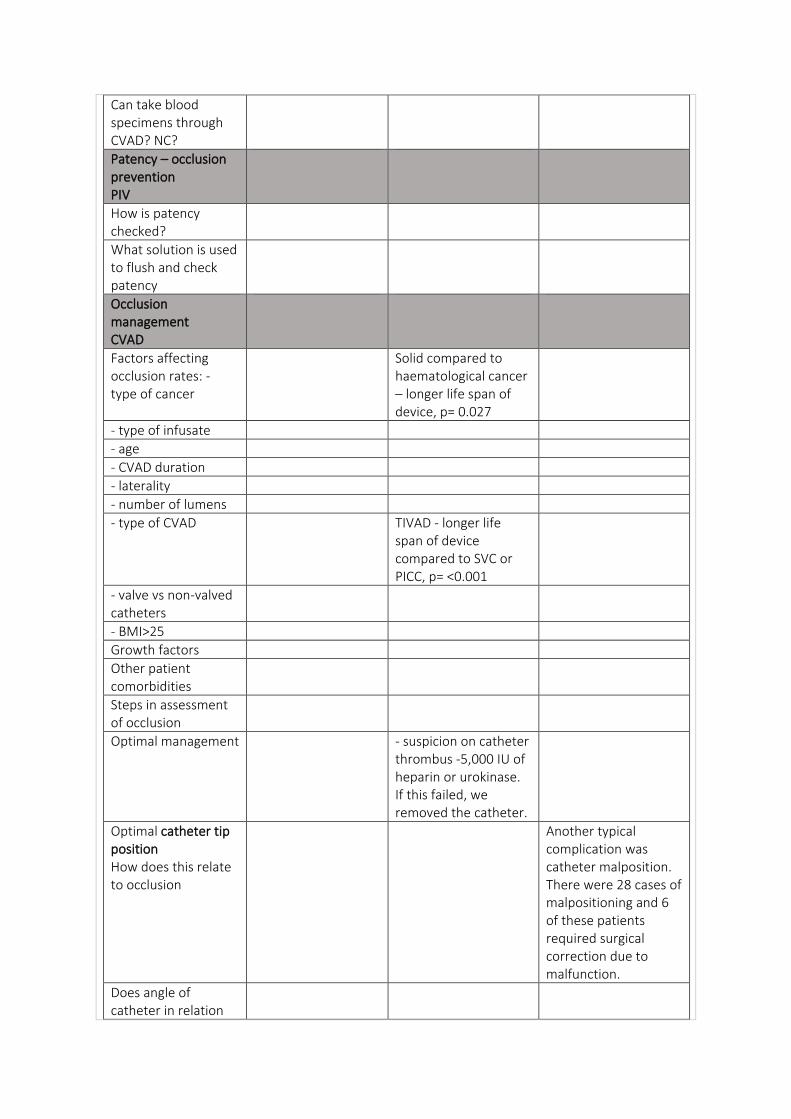
Can take blood specimens through CVAD? NC?
Patency – occlusion prevention PIV
How is patency checked?
What solution is used to flush and check patency
Occlusion management CVAD
Factors affecting occlusion rates: - type of cancer
Solid compared to haematological cancer – longer life span of device, p= 0.027
- type of infusate
- age
- CVAD duration
- laterality
- number of lumens
- type of CVAD TIVAD - longer life span of device compared to SVC or PICC, p= <0.001
- valve vs non-valved catheters
- BMI>25
Growth factors
Other patient comorbidities
Steps in assessment of occlusion
Optimal management - suspicion on catheter thrombus -5,000 IU of heparin or urokinase. If this failed, we removed the catheter.
Optimal catheter tip position How does this relate to occlusion
Another typical complication was catheter malposition. There were 28 cases of malpositioning and 6 of these patients required surgical correction due to malfunction.
Does angle of catheter in relation
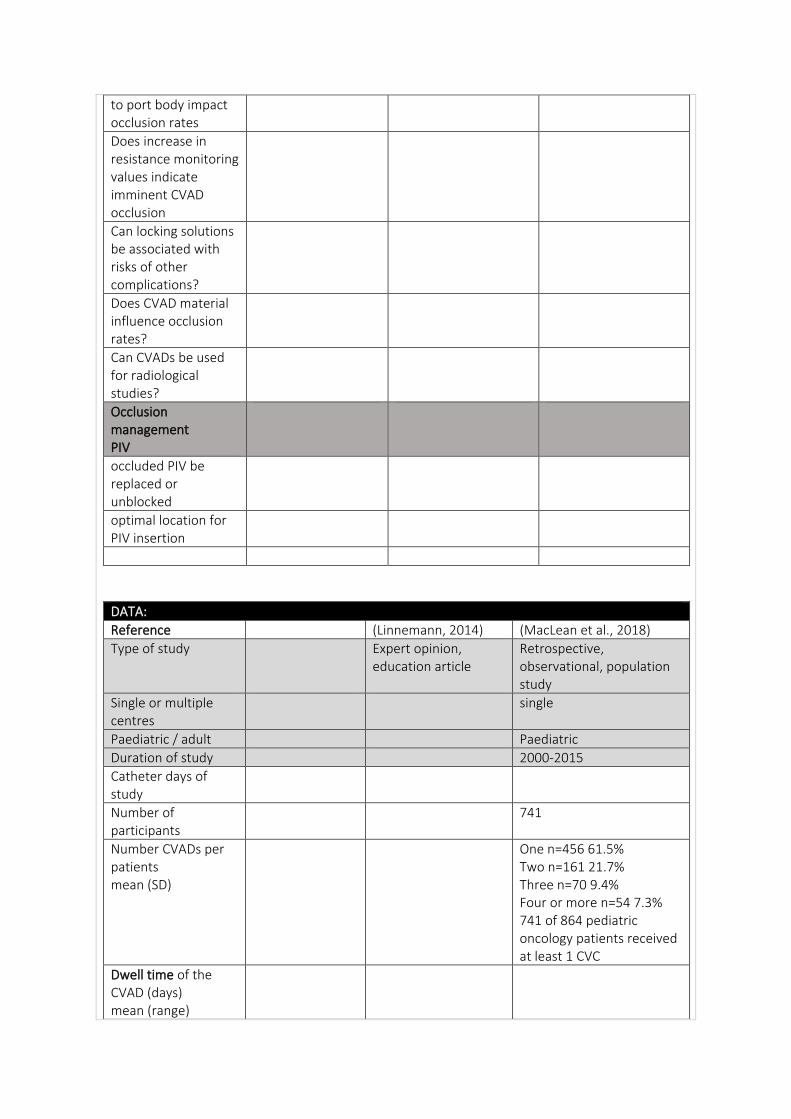
to port body impact occlusion rates
Does increase in resistance monitoring values indicate imminent CVAD occlusion
Can locking solutions be associated with risks of other complications?
Does CVAD material influence occlusion rates?
Can CVADs be used for radiological studies?
Occlusion management PIV
occluded PIV be replaced or unblocked
optimal location for PIV insertion
DATA:
Reference (Linnemann, 2014) (MacLean et al., 2018)
Type of study Expert opinion, education article
Retrospective, observational, population study
Single or multiple centres
single
Paediatric / adult Paediatric
Duration of study 2000-2015
Catheter days of study
Number of participants
741
Number CVADs per patients mean (SD)
One n=456 61.5% Two n=161 21.7% Three n=70 9.4% Four or more n=54 7.3% 741 of 864 pediatric oncology patients received at least 1 CVC
Dwell time of the CVAD (days) mean (range)
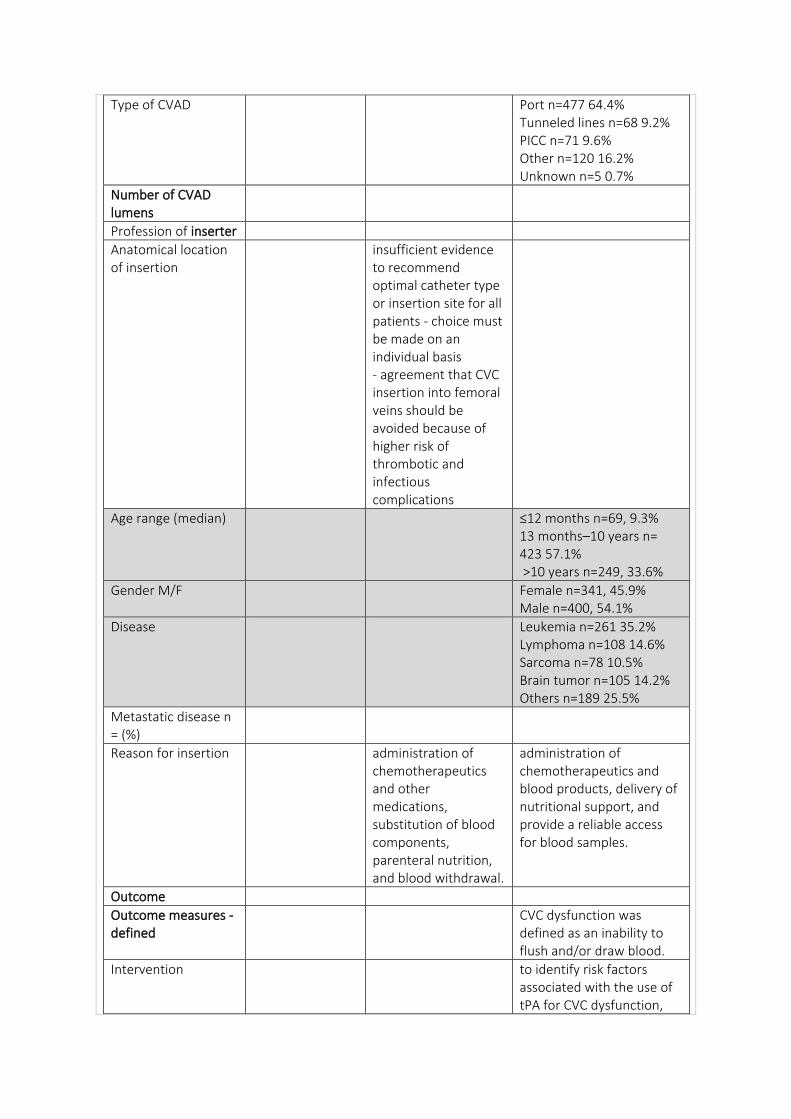
Type of CVAD Port n=477 64.4% Tunneled lines n=68 9.2% PICC n=71 9.6% Other n=120 16.2% Unknown n=5 0.7%
Number of CVAD lumens
Profession of inserter
Anatomical location of insertion
insufficient evidence to recommend optimal catheter type or insertion site for all patients - choice must be made on an individual basis - agreement that CVC insertion into femoral veins should be avoided because of higher risk of thrombotic and infectious complications
Age range (median) ≤12 months n=69, 9.3% 13 months–10 years n= 423 57.1% >10 years n=249, 33.6%
Gender M/F Female n=341, 45.9% Male n=400, 54.1%
Disease Leukemia n=261 35.2% Lymphoma n=108 14.6% Sarcoma n=78 10.5% Brain tumor n=105 14.2% Others n=189 25.5%
Metastatic disease n = (%)
Reason for insertion administration of chemotherapeutics and other medications, substitution of blood components, parenteral nutrition, and blood withdrawal.
administration of chemotherapeutics and blood products, delivery of nutritional support, and provide a reliable access for blood samples.
Outcome
Outcome measures - defined
CVC dysfunction was defined as an inability to flush and/or draw blood.
Intervention to identify risk factors associated with the use of tPA for CVC dysfunction,
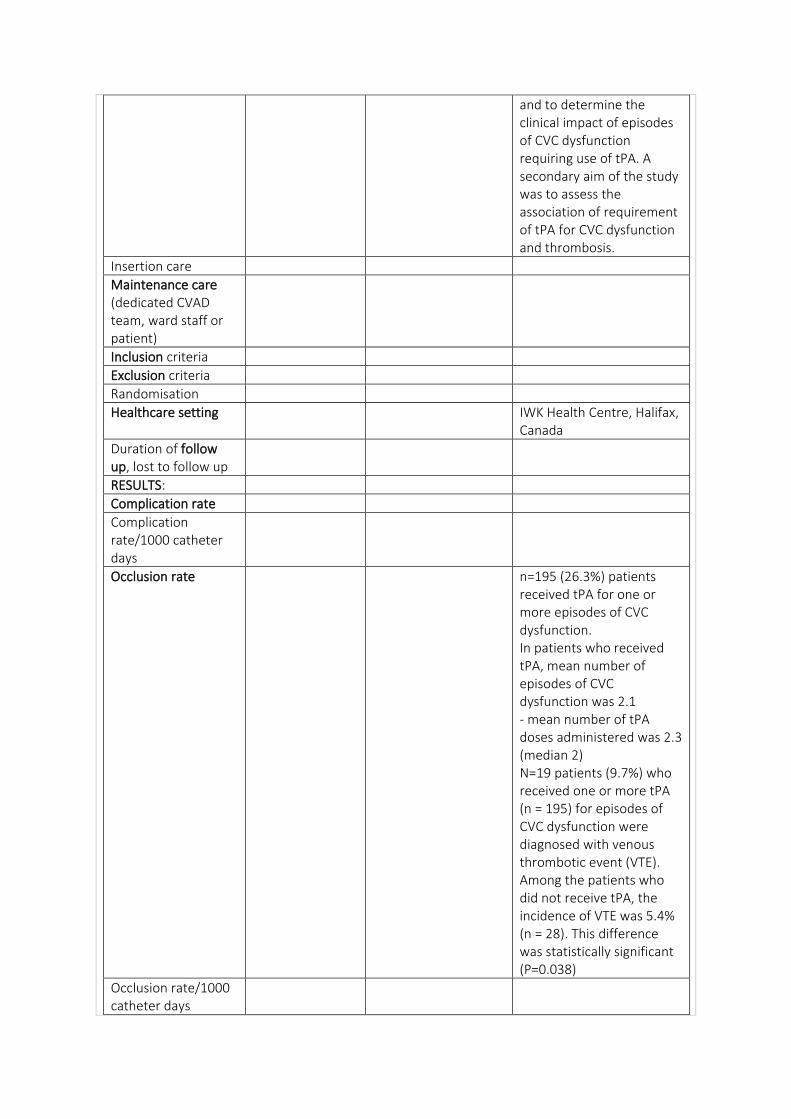
and to determine the clinical impact of episodes of CVC dysfunction requiring use of tPA. A secondary aim of the study was to assess the association of requirement of tPA for CVC dysfunction and thrombosis.
Insertion care
Maintenance care (dedicated CVAD team, ward staff or patient)
Inclusion criteria
Exclusion criteria
Randomisation
Healthcare setting IWK Health Centre, Halifax, Canada
Duration of follow up, lost to follow up
RESULTS:
Complication rate
Complication rate/1000 catheter days
Occlusion rate n=195 (26.3%) patients received tPA for one or more episodes of CVC dysfunction. In patients who received tPA, mean number of episodes of CVC dysfunction was 2.1 - mean number of tPA doses administered was 2.3 (median 2) N=19 patients (9.7%) who received one or more tPA (n = 195) for episodes of CVC dysfunction were diagnosed with venous thrombotic event (VTE). Among the patients who did not receive tPA, the incidence of VTE was 5.4% (n = 28). This difference was statistically significant (P=0.038)
Occlusion rate/1000 catheter days
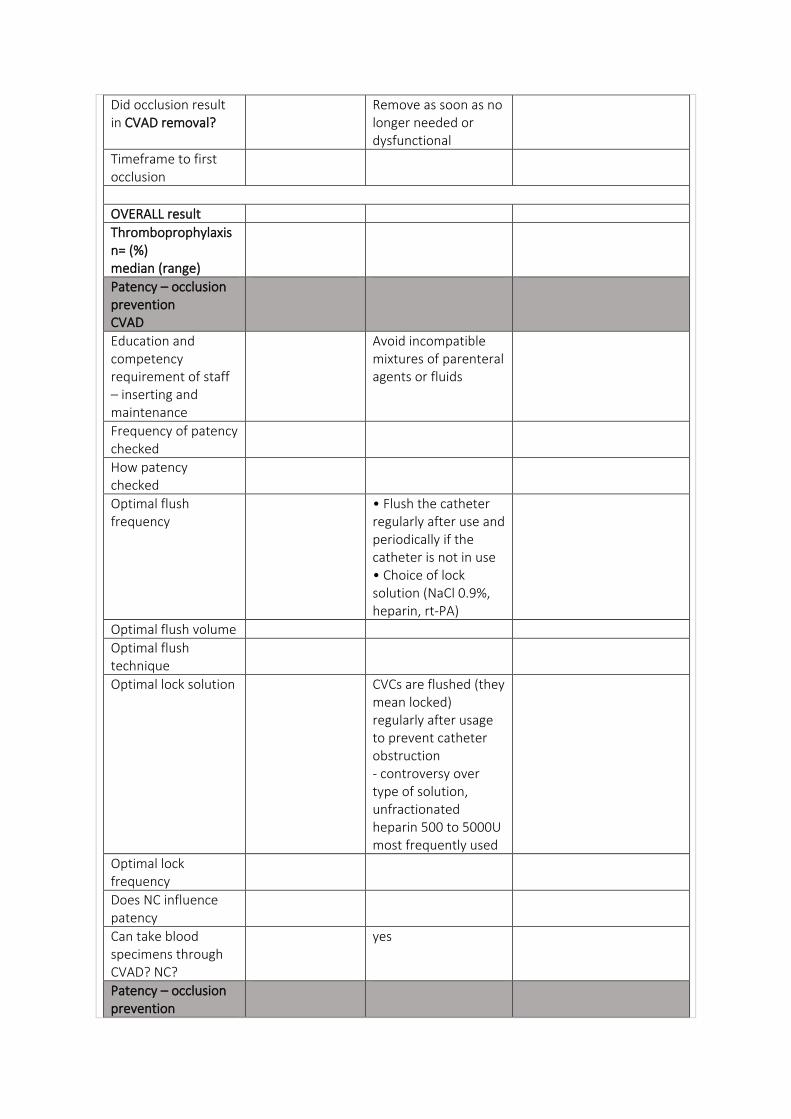
Did occlusion result in CVAD removal?
Remove as soon as no longer needed or dysfunctional
Timeframe to first occlusion
OVERALL result
Thromboprophylaxis n= (%) median (range)
Patency – occlusion prevention CVAD
Education and competency requirement of staff – inserting and maintenance
Avoid incompatible mixtures of parenteral agents or fluids
Frequency of patency checked
How patency checked
Optimal flush frequency
• Flush the catheter regularly after use and periodically if the catheter is not in use • Choice of lock solution (NaCl 0.9%, heparin, rt-PA)
Optimal flush volume
Optimal flush technique
Optimal lock solution CVCs are flushed (they mean locked) regularly after usage to prevent catheter obstruction - controversy over type of solution, unfractionated heparin 500 to 5000U most frequently used
Optimal lock frequency
Does NC influence patency
Can take blood specimens through CVAD? NC?
yes
Patency – occlusion prevention
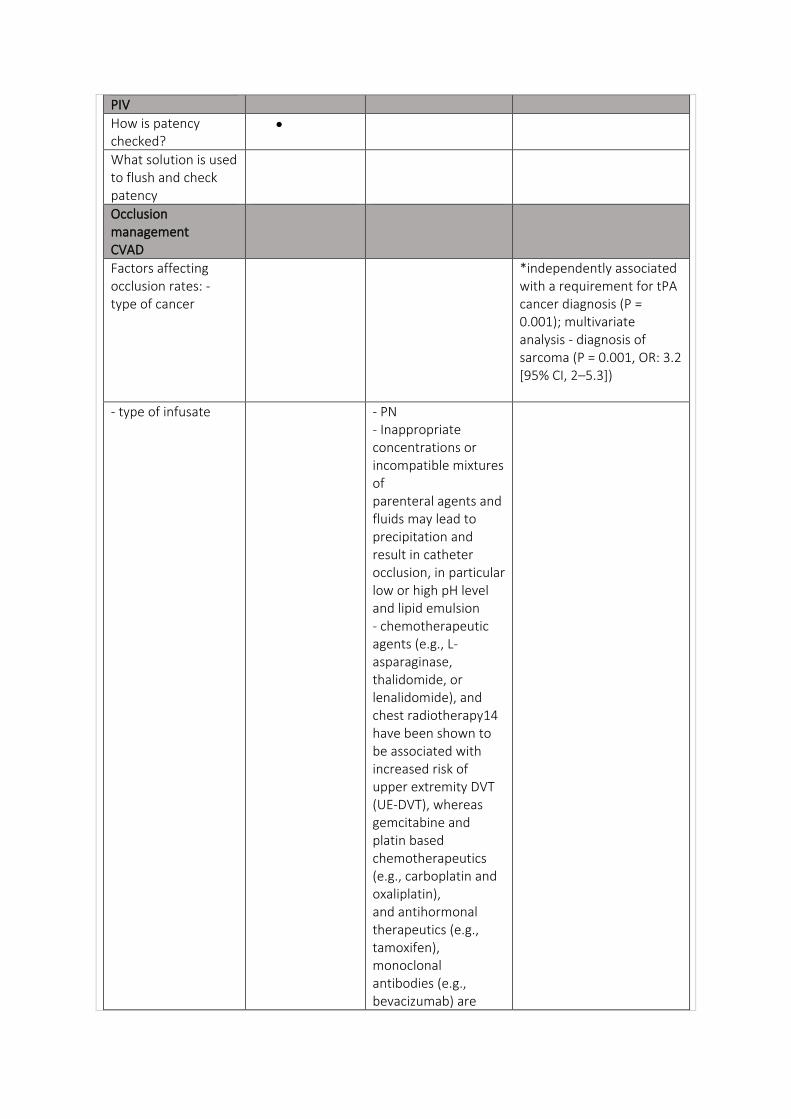
PIV
How is patency checked?
•
What solution is used to flush and check patency
Occlusion management CVAD
Factors affecting occlusion rates: - type of cancer
*independently associated with a requirement for tPA cancer diagnosis (P = 0.001); multivariate analysis - diagnosis of sarcoma (P = 0.001, OR: 3.2 [95% CI, 2–5.3])
- type of infusate - PN - Inappropriate concentrations or incompatible mixtures of parenteral agents and fluids may lead to precipitation and result in catheter occlusion, in particular low or high pH level and lipid emulsion - chemotherapeutic agents (e.g., L-asparaginase, thalidomide, or lenalidomide), and chest radiotherapy14 have been shown to be associated with increased risk of upper extremity DVT (UE-DVT), whereas gemcitabine and platin based chemotherapeutics (e.g., carboplatin and oxaliplatin), and antihormonal therapeutics (e.g., tamoxifen), monoclonal antibodies (e.g., bevacizumab) are
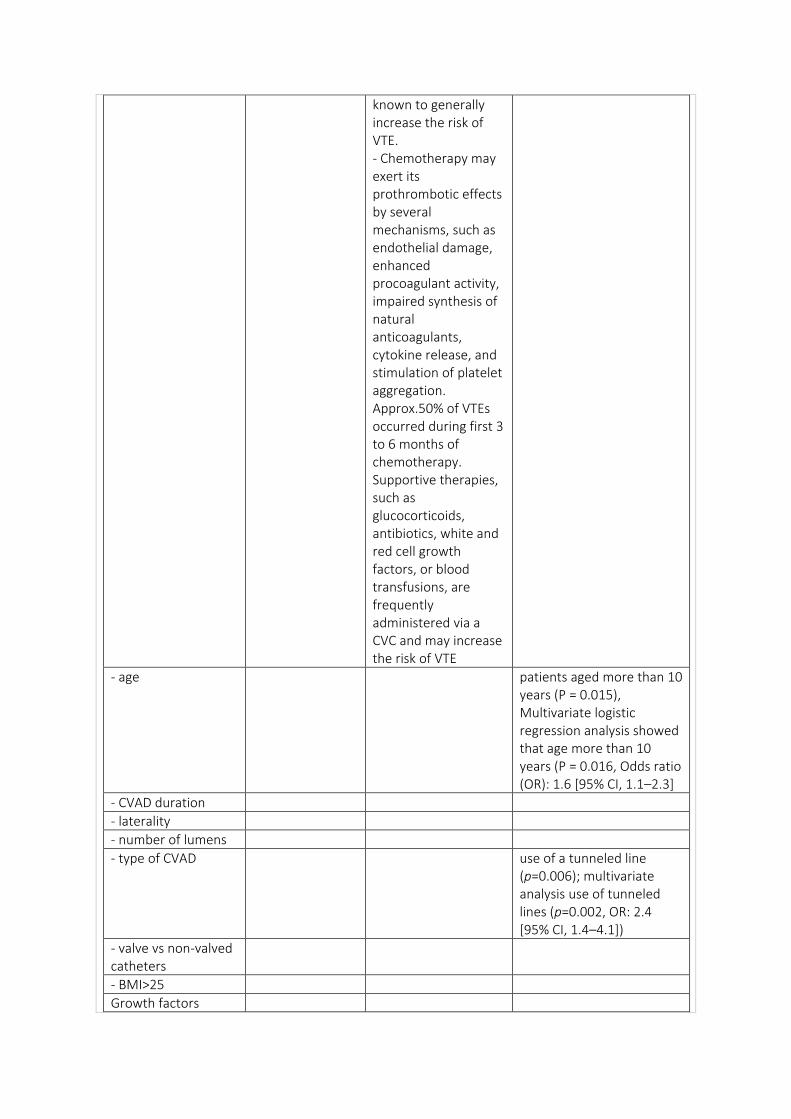
known to generally increase the risk of VTE. - Chemotherapy may exert its prothrombotic effects by several mechanisms, such as endothelial damage, enhanced procoagulant activity, impaired synthesis of natural anticoagulants, cytokine release, and stimulation of platelet aggregation. Approx.50% of VTEs occurred during first 3 to 6 months of chemotherapy. Supportive therapies, such as glucocorticoids, antibiotics, white and red cell growth factors, or blood transfusions, are frequently administered via a CVC and may increase the risk of VTE
- age patients aged more than 10 years (P = 0.015), Multivariate logistic regression analysis showed that age more than 10 years (P = 0.016, Odds ratio (OR): 1.6 [95% CI, 1.1–2.3]
- CVAD duration
- laterality
- number of lumens
- type of CVAD use of a tunneled line (p=0.006); multivariate analysis use of tunneled lines (p=0.002, OR: 2.4 [95% CI, 1.4–4.1])
- valve vs non-valved catheters
- BMI>25
Growth factors
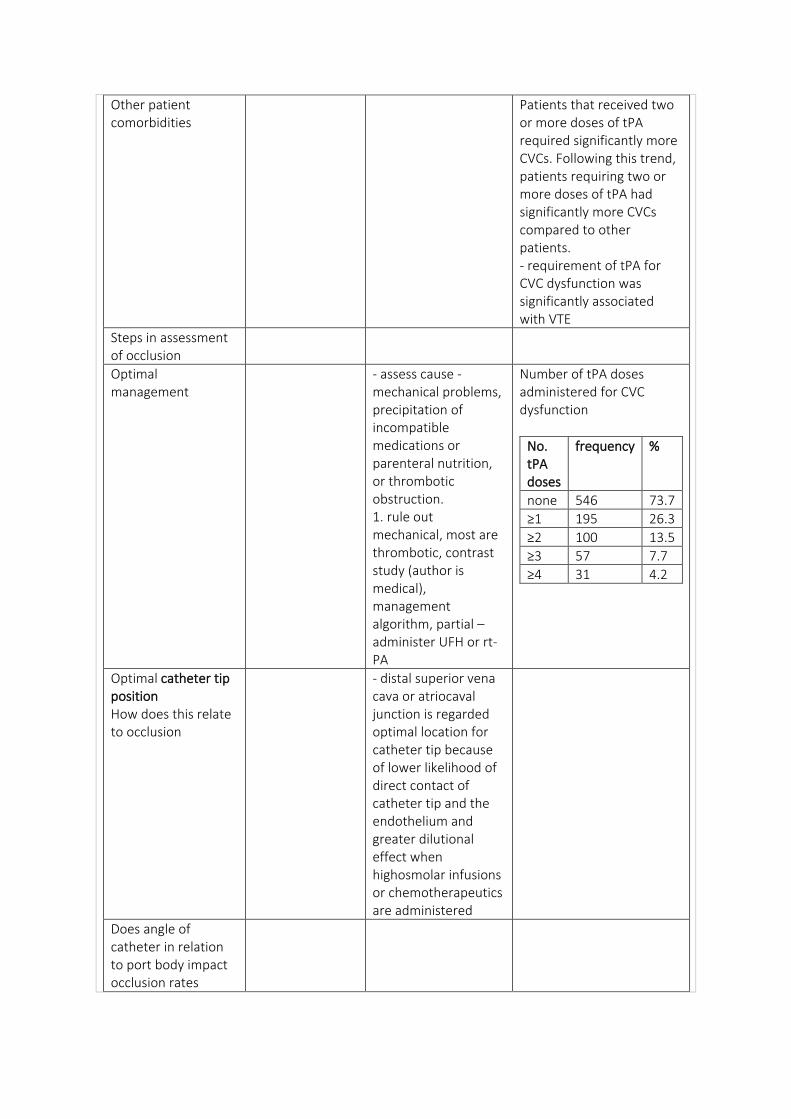
Other patient comorbidities
Patients that received two or more doses of tPA required significantly more CVCs. Following this trend, patients requiring two or more doses of tPA had significantly more CVCs compared to other patients. - requirement of tPA for CVC dysfunction was significantly associated with VTE
Steps in assessment of occlusion
Optimal management
- assess cause - mechanical problems, precipitation of incompatible medications or parenteral nutrition, or thrombotic obstruction. 1. rule out mechanical, most are thrombotic, contrast study (author is medical), management algorithm, partial – administer UFH or rt-PA
Number of tPA doses administered for CVC dysfunction
No. tPA doses
frequency %
none 546 73.7
≥1 195 26.3
≥2 100 13.5
≥3 57 7.7
≥4 31 4.2
Optimal catheter tip position How does this relate to occlusion
- distal superior vena cava or atriocaval junction is regarded optimal location for catheter tip because of lower likelihood of direct contact of catheter tip and the endothelium and greater dilutional effect when highosmolar infusions or chemotherapeutics are administered
Does angle of catheter in relation to port body impact occlusion rates
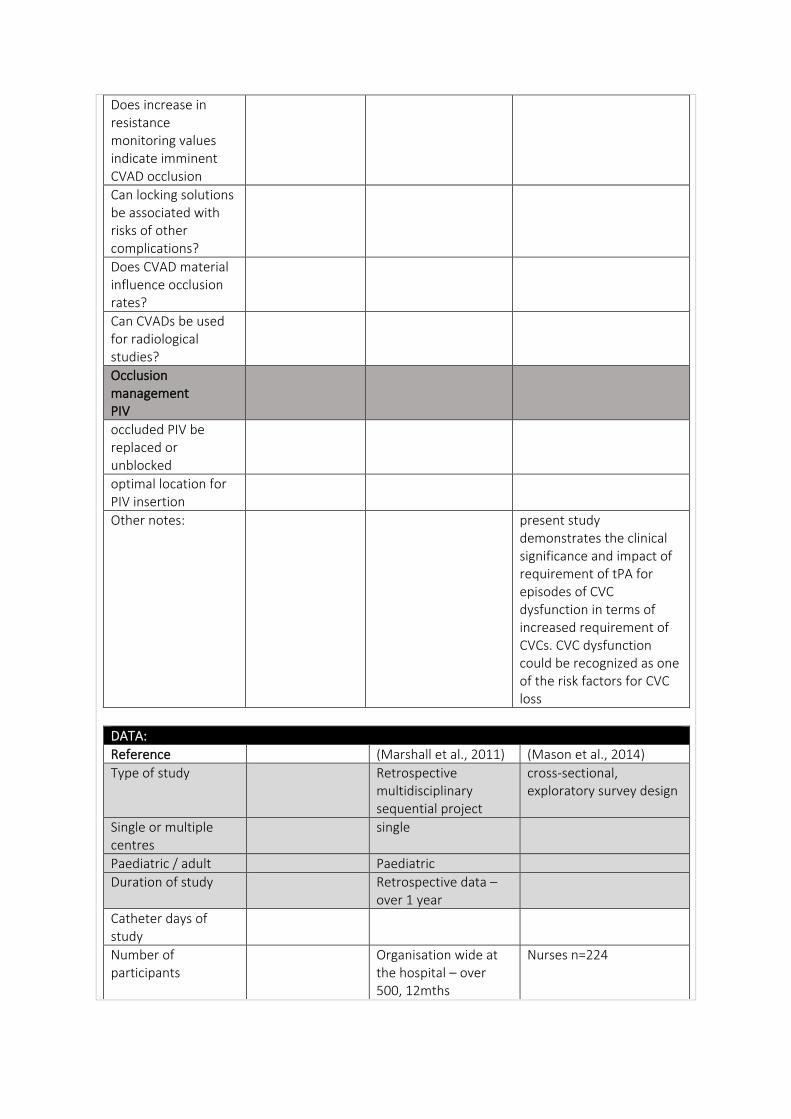
Does increase in resistance monitoring values indicate imminent CVAD occlusion
Can locking solutions be associated with risks of other complications?
Does CVAD material influence occlusion rates?
Can CVADs be used for radiological studies?
Occlusion management PIV
occluded PIV be replaced or unblocked
optimal location for PIV insertion
Other notes: present study demonstrates the clinical significance and impact of requirement of tPA for episodes of CVC dysfunction in terms of increased requirement of CVCs. CVC dysfunction could be recognized as one of the risk factors for CVC loss
DATA:
Reference (Marshall et al., 2011) (Mason et al., 2014)
Type of study Retrospective multidisciplinary sequential project
cross-sectional, exploratory survey design
Single or multiple centres
single
Paediatric / adult Paediatric
Duration of study Retrospective data – over 1 year
Catheter days of study
Number of participants
Organisation wide at the hospital – over 500, 12mths
Nurses n=224
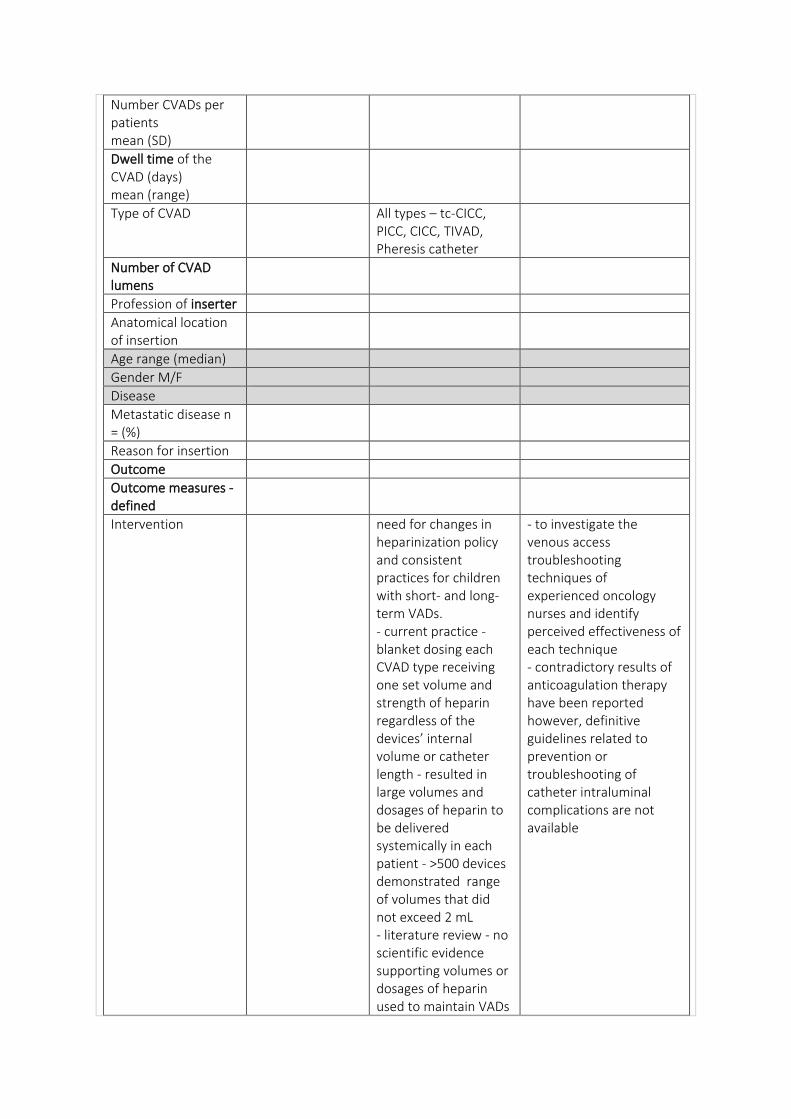
Number CVADs per patients mean (SD)
Dwell time of the CVAD (days) mean (range)
Type of CVAD All types – tc-CICC, PICC, CICC, TIVAD, Pheresis catheter
Number of CVAD lumens
Profession of inserter
Anatomical location of insertion
Age range (median)
Gender M/F
Disease
Metastatic disease n = (%)
Reason for insertion
Outcome
Outcome measures - defined
Intervention need for changes in heparinization policy and consistent practices for children with short- and long-term VADs. - current practice - blanket dosing each CVAD type receiving one set volume and strength of heparin regardless of the devices’ internal volume or catheter length - resulted in large volumes and dosages of heparin to be delivered systemically in each patient - >500 devices demonstrated range of volumes that did not exceed 2 mL - literature review - no scientific evidence supporting volumes or dosages of heparin used to maintain VADs
- to investigate the venous access troubleshooting techniques of experienced oncology nurses and identify perceived effectiveness of each technique - contradictory results of anticoagulation therapy have been reported however, definitive guidelines related to prevention or troubleshooting of catheter intraluminal complications are not available
- Group analysis of results was next phase of project - next task to look at current hospital policy to identify appropriate changes in heparinization - need for comprehensive education plan identified early – educational in-services with reference tables, change in policy at the same time
Insertion care
Maintenance care (dedicated CVAD team, ward staff or patient)
Inclusion criteria
Exclusion criteria
Randomisation
Healthcare setting Children’s Hospital of Michigan, USA
Duration of follow up, lost to follow up
RESULTS: benefits of nurse-driven collaborative and multidisciplinary project are many (standardization of hospital and home care protocols, cost savings in the reduction of heparin administered, etc), the most critical benefit is the decrease in risk to the patients
- nurses years in oncology 2-35yrs, average nearly 15yrs - pilot study done, no changes prior to survey - 14 questions and practice areas - n=224 responded, out of 4720, 2% - all or nearly all nurses asked pt to raise or move arm, cough, DB&C - instilling thrombolytic agent to be most effective technique - > half nurses (n = 123) used other techniques not mentioned in survey - n = 208/224 referred patients to another healthcare provider - radiology (n = 119), another nurse (n = 58), or
surgeon/ radiologist who placed the line (n = 39) - 67% of nurses reported a technique not expected to yield results - About 25% nurses used a contraindicated technique e.g. flushing rapidly against resistance.
Complication rate
Complication rate/1000 catheter days
Occlusion rate
Occlusion rate/1000 catheter days
Did occlusion result in CVAD removal?
Timeframe to first occlusion
OVERALL result
Thromboprophylaxis n= (%) median (range)
Patency – occlusion prevention CVAD
Education and competency requirement of staff – inserting and maintenance
Frequency of patency checked
How patency checked
Optimal flush frequency
Optimal flush volume
Optimal flush technique
Optimal lock solution
Optimal lock frequency
Does NC influence patency
Can take blood specimens through CVAD? NC?
Patency – occlusion prevention PIV
How is patency checked?
What solution is used to flush and check patency
Occlusion management CVAD
Factors affecting occlusion rates: - type of cancer
- type of infusate
- age
- CVAD duration
- laterality
- number of lumens
- type of CVAD
- valve vs non-valved catheters
- BMI>25
Growth factors
Other patient comorbidities
Steps in assessment of occlusion
Optimal management
Optimal catheter tip position How does this relate to occlusion
Does angle of catheter in relation to port body impact occlusion rates
Does increase in resistance monitoring values indicate imminent CVAD occlusion
Can locking solutions be associated with risks of other complications?
Does CVAD material influence occlusion rates?
Can CVADs be used for radiological studies?
Occlusion management PIV
occluded PIV be replaced or unblocked
optimal location for PIV insertion
DATA:
Reference (Matey & Camp-Sorrell, 2016)
(Muguet, Couraud, Perrot, Claer, & Souquet, 2012)
Type of study Expert opinion Retrospective observational
Single or multiple centres
Single
Paediatric / adult adult
Duration of study 12 months - 1 May 2010 and 31 April 2011
Catheter days of study
Number of participants
N=12
Number CVADs per patients mean (SD)
Dwell time of the CVAD (days) mean (range)
Type of CVAD TIVAD
Number of CVAD lumens
Profession of inserter
Anatomical location of insertion
Subclavian vein in 75% n=9
Age range (median) 46-72years, mean 63 yrs
Gender M/F 11 male, 1 female
Disease Lung cancer
Metastatic disease n = (%)
Reason for insertion
Outcome
Outcome measures - defined
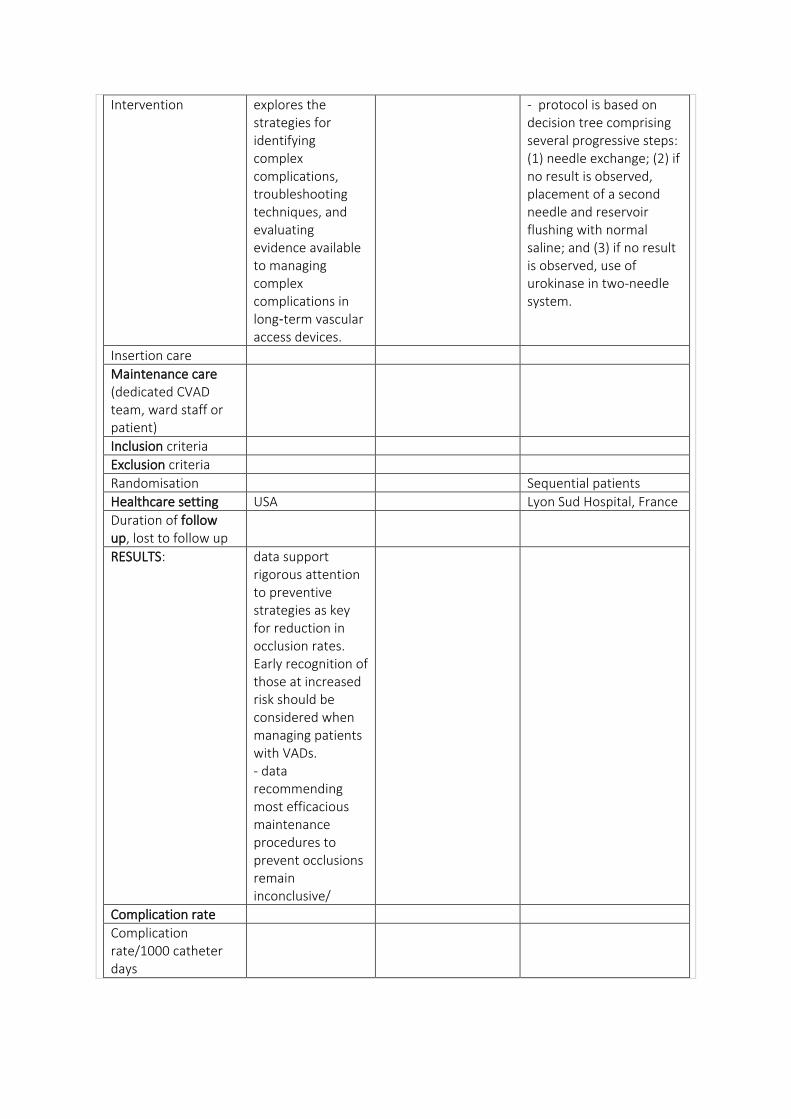
Intervention explores the strategies for identifying complex complications, troubleshooting techniques, and evaluating evidence available to managing complex complications in long‑term vascular access devices.
- protocol is based on decision tree comprising several progressive steps: (1) needle exchange; (2) if no result is observed, placement of a second needle and reservoir flushing with normal saline; and (3) if no result is observed, use of urokinase in two-needle system.
Insertion care
Maintenance care (dedicated CVAD team, ward staff or patient)
Inclusion criteria
Exclusion criteria
Randomisation Sequential patients
Healthcare setting USA Lyon Sud Hospital, France
Duration of follow up, lost to follow up
RESULTS: data support rigorous attention to preventive strategies as key for reduction in occlusion rates. Early recognition of those at increased risk should be considered when managing patients with VADs. - data recommending most efficacious maintenance procedures to prevent occlusions remain inconclusive/
Complication rate
Complication rate/1000 catheter days
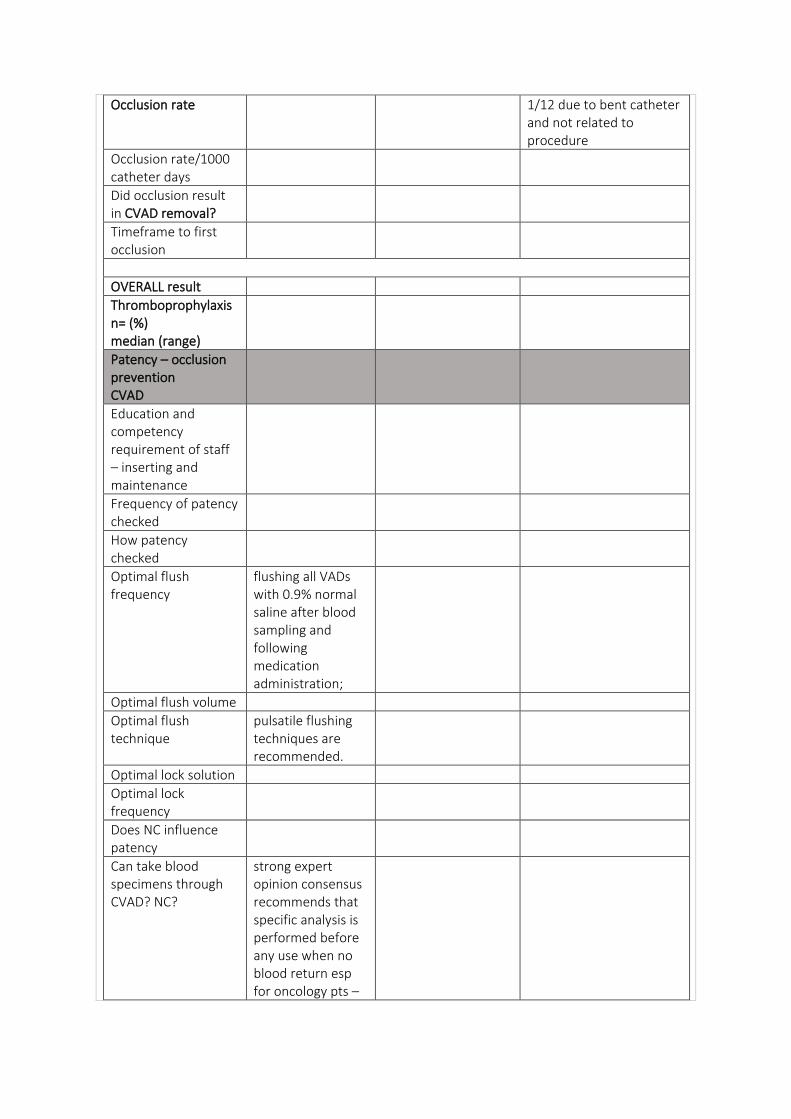
Occlusion rate 1/12 due to bent catheter and not related to procedure
Occlusion rate/1000 catheter days
Did occlusion result in CVAD removal?
Timeframe to first occlusion
OVERALL result
Thromboprophylaxis n= (%) median (range)
Patency – occlusion prevention CVAD
Education and competency requirement of staff – inserting and maintenance
Frequency of patency checked
How patency checked
Optimal flush frequency
flushing all VADs with 0.9% normal saline after blood sampling and following medication administration;
Optimal flush volume
Optimal flush technique
pulsatile flushing techniques are recommended.
Optimal lock solution
Optimal lock frequency
Does NC influence patency
Can take blood specimens through CVAD? NC?
strong expert opinion consensus recommends that specific analysis is performed before any use when no blood return esp for oncology pts –
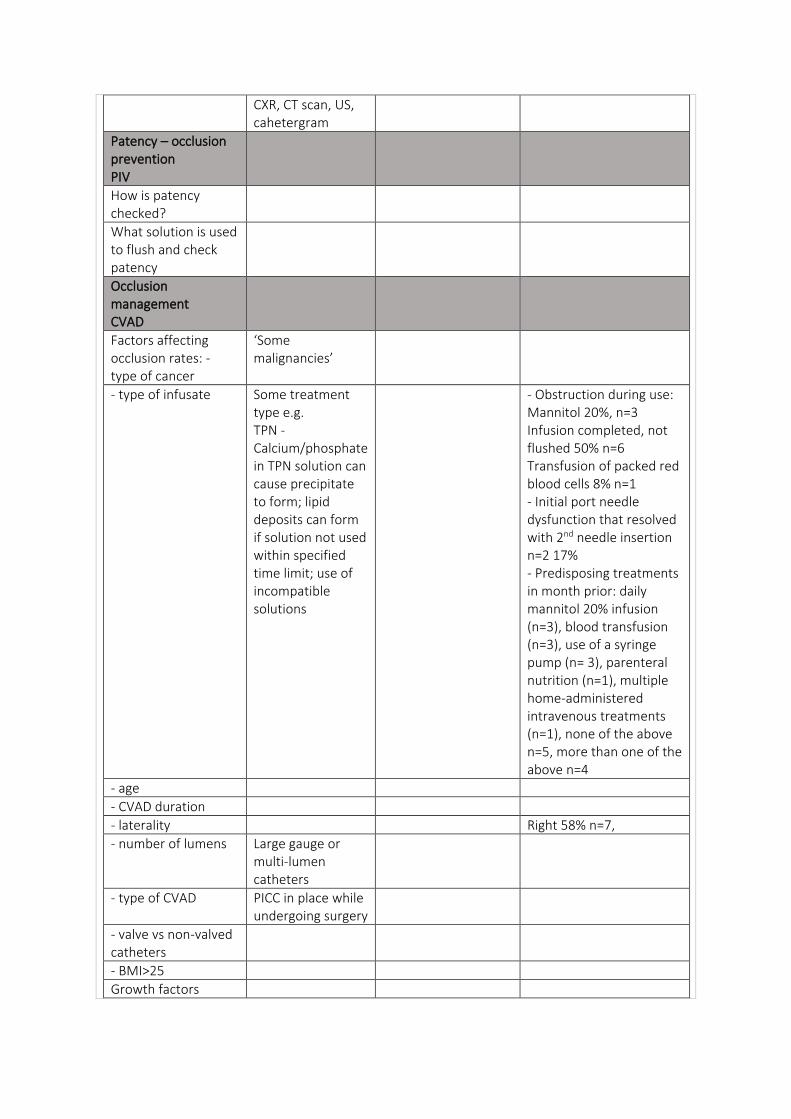
CXR, CT scan, US, cahetergram
Patency – occlusion prevention PIV
How is patency checked?
What solution is used to flush and check patency
Occlusion management CVAD
Factors affecting occlusion rates: - type of cancer
‘Some malignancies’
- type of infusate Some treatment type e.g. TPN - Calcium/phosphate in TPN solution can cause precipitate to form; lipid deposits can form if solution not used within specified time limit; use of incompatible solutions
- Obstruction during use: Mannitol 20%, n=3 Infusion completed, not flushed 50% n=6 Transfusion of packed red blood cells 8% n=1 - Initial port needle dysfunction that resolved with 2nd needle insertion n=2 17% - Predisposing treatments in month prior: daily mannitol 20% infusion (n=3), blood transfusion (n=3), use of a syringe pump (n= 3), parenteral nutrition (n=1), multiple home-administered intravenous treatments (n=1), none of the above n=5, more than one of the above n=4
- age
- CVAD duration
- laterality Right 58% n=7,
- number of lumens Large gauge or multi-lumen catheters
- type of CVAD PICC in place while undergoing surgery
- valve vs non-valved catheters
- BMI>25
Growth factors
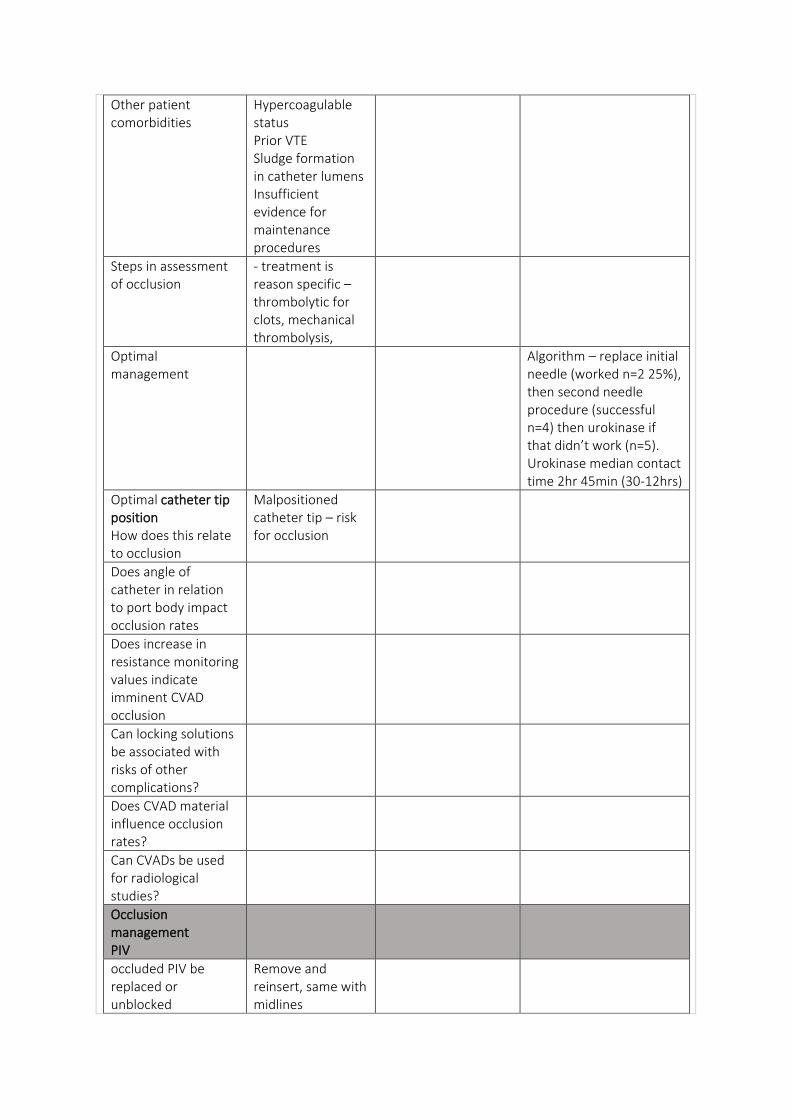
Other patient comorbidities
Hypercoagulable status Prior VTE Sludge formation in catheter lumens Insufficient evidence for maintenance procedures
Steps in assessment of occlusion
- treatment is reason specific – thrombolytic for clots, mechanical thrombolysis,
Optimal management
Algorithm – replace initial needle (worked n=2 25%), then second needle procedure (successful n=4) then urokinase if that didn’t work (n=5). Urokinase median contact time 2hr 45min (30-12hrs)
Optimal catheter tip position How does this relate to occlusion
Malpositioned catheter tip – risk for occlusion
Does angle of catheter in relation to port body impact occlusion rates
Does increase in resistance monitoring values indicate imminent CVAD occlusion
Can locking solutions be associated with risks of other complications?
Does CVAD material influence occlusion rates?
Can CVADs be used for radiological studies?
Occlusion management PIV
occluded PIV be replaced or unblocked
Remove and reinsert, same with midlines
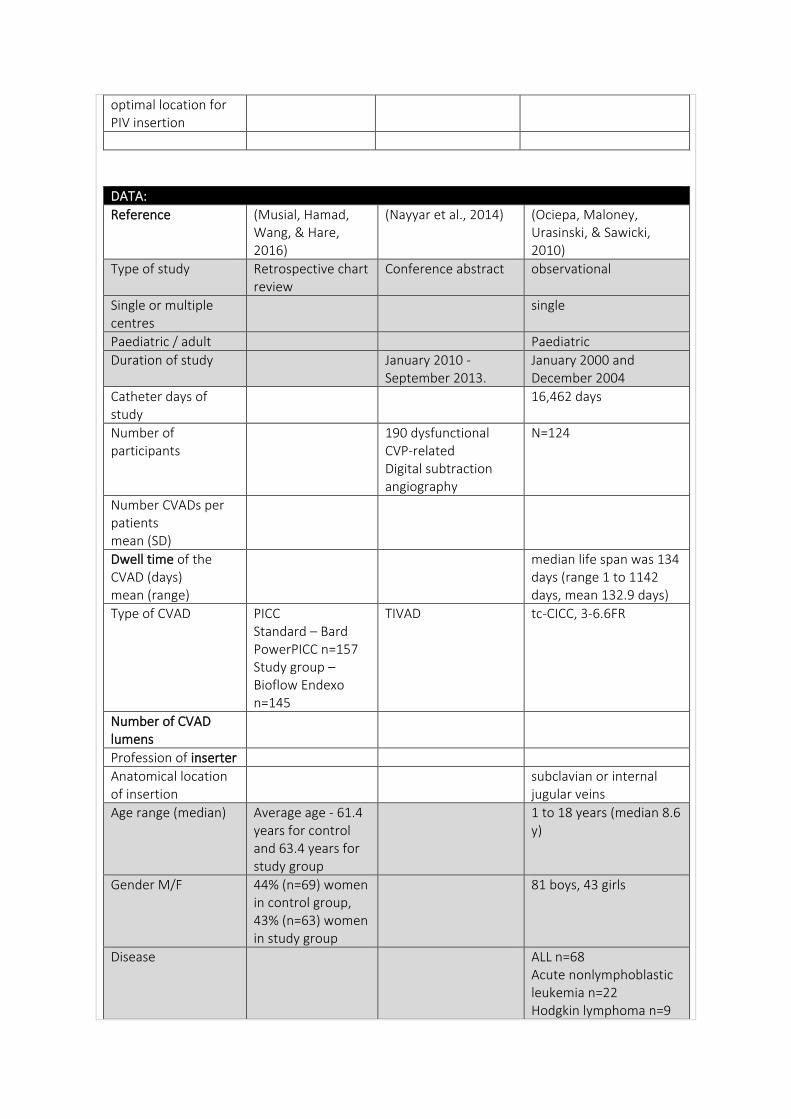
optimal location for PIV insertion
DATA:
Reference (Musial, Hamad, Wang, & Hare, 2016)
(Nayyar et al., 2014) (Ociepa, Maloney, Urasinski, & Sawicki, 2010)
Type of study Retrospective chart review
Conference abstract observational
Single or multiple centres
single
Paediatric / adult Paediatric
Duration of study January 2010 - September 2013.
January 2000 and December 2004
Catheter days of study
16,462 days
Number of participants
190 dysfunctional CVP-related Digital subtraction angiography
N=124
Number CVADs per patients mean (SD)
Dwell time of the CVAD (days) mean (range)
median life span was 134 days (range 1 to 1142 days, mean 132.9 days)
Type of CVAD PICC Standard – Bard PowerPICC n=157 Study group – Bioflow Endexo n=145
TIVAD tc-CICC, 3-6.6FR
Number of CVAD lumens
Profession of inserter
Anatomical location of insertion
subclavian or internal jugular veins
Age range (median) Average age - 61.4 years for control and 63.4 years for study group
1 to 18 years (median 8.6 y)
Gender M/F 44% (n=69) women in control group, 43% (n=63) women in study group
81 boys, 43 girls
Disease ALL n=68 Acute nonlymphoblastic leukemia n=22 Hodgkin lymphoma n=9
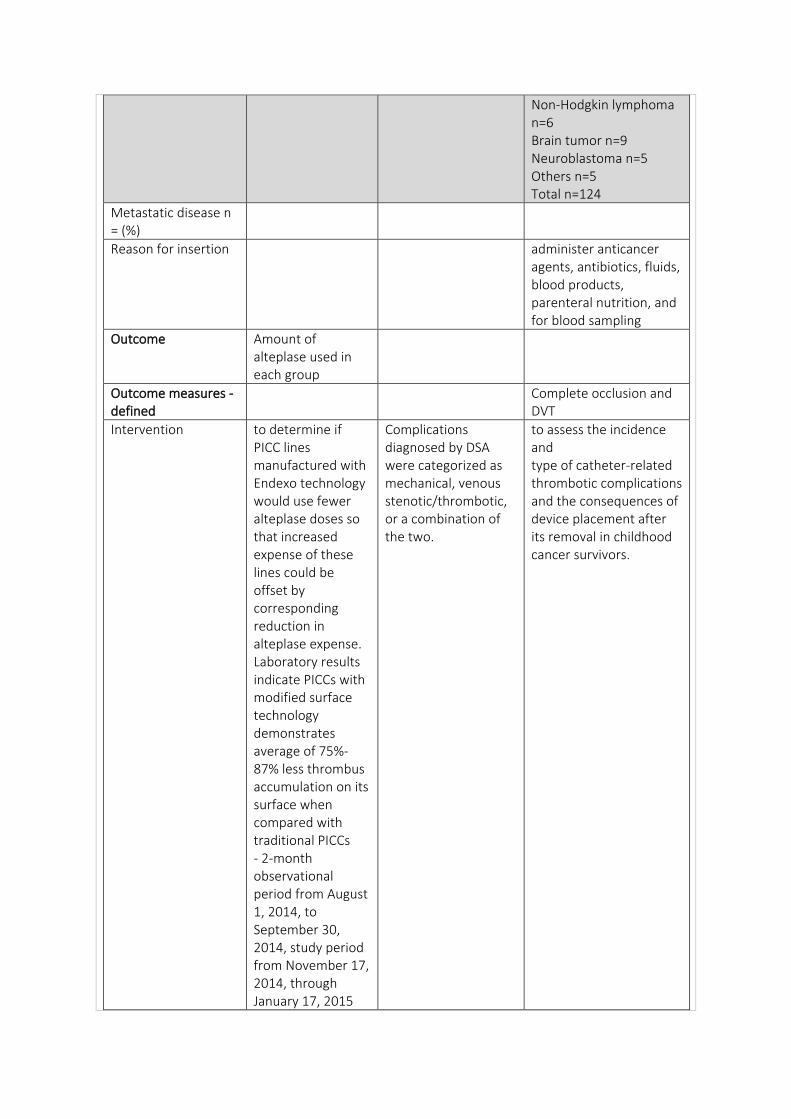
Non-Hodgkin lymphoma n=6 Brain tumor n=9 Neuroblastoma n=5 Others n=5 Total n=124
Metastatic disease n = (%)
Reason for insertion administer anticancer agents, antibiotics, fluids, blood products, parenteral nutrition, and for blood sampling
Outcome Amount of alteplase used in each group
Outcome measures - defined
Complete occlusion and DVT
Intervention to determine if PICC lines manufactured with Endexo technology would use fewer alteplase doses so that increased expense of these lines could be offset by corresponding reduction in alteplase expense. Laboratory results indicate PICCs with modified surface technology demonstrates average of 75%-87% less thrombus accumulation on its surface when compared with traditional PICCs - 2-month observational period from August 1, 2014, to September 30, 2014, study period from November 17, 2014, through January 17, 2015
Complications diagnosed by DSA were categorized as mechanical, venous stenotic/thrombotic, or a combination of the two.
to assess the incidence and type of catheter-related thrombotic complications and the consequences of device placement after its removal in childhood cancer survivors.
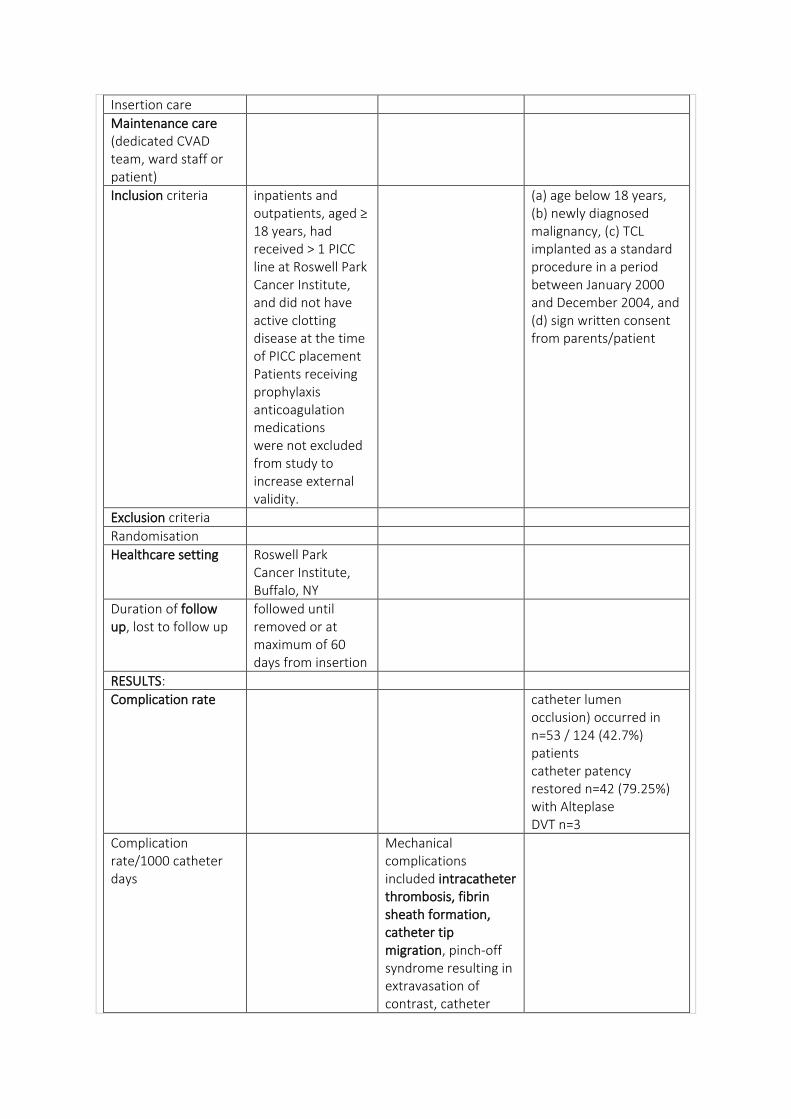
Insertion care
Maintenance care (dedicated CVAD team, ward staff or patient)
Inclusion criteria inpatients and outpatients, aged ≥ 18 years, had received > 1 PICC line at Roswell Park Cancer Institute, and did not have active clotting disease at the time of PICC placement Patients receiving prophylaxis anticoagulation medications were not excluded from study to increase external validity.
(a) age below 18 years, (b) newly diagnosed malignancy, (c) TCL implanted as a standard procedure in a period between January 2000 and December 2004, and (d) sign written consent from parents/patient
Exclusion criteria
Randomisation
Healthcare setting Roswell Park Cancer Institute, Buffalo, NY
Duration of follow up, lost to follow up
followed until removed or at maximum of 60 days from insertion
RESULTS:
Complication rate catheter lumen occlusion) occurred in n=53 / 124 (42.7%) patients catheter patency restored n=42 (79.25%) with Alteplase DVT n=3
Complication rate/1000 catheter days
Mechanical complications included intracatheter thrombosis, fibrin sheath formation, catheter tip migration, pinch-off syndrome resulting in extravasation of contrast, catheter
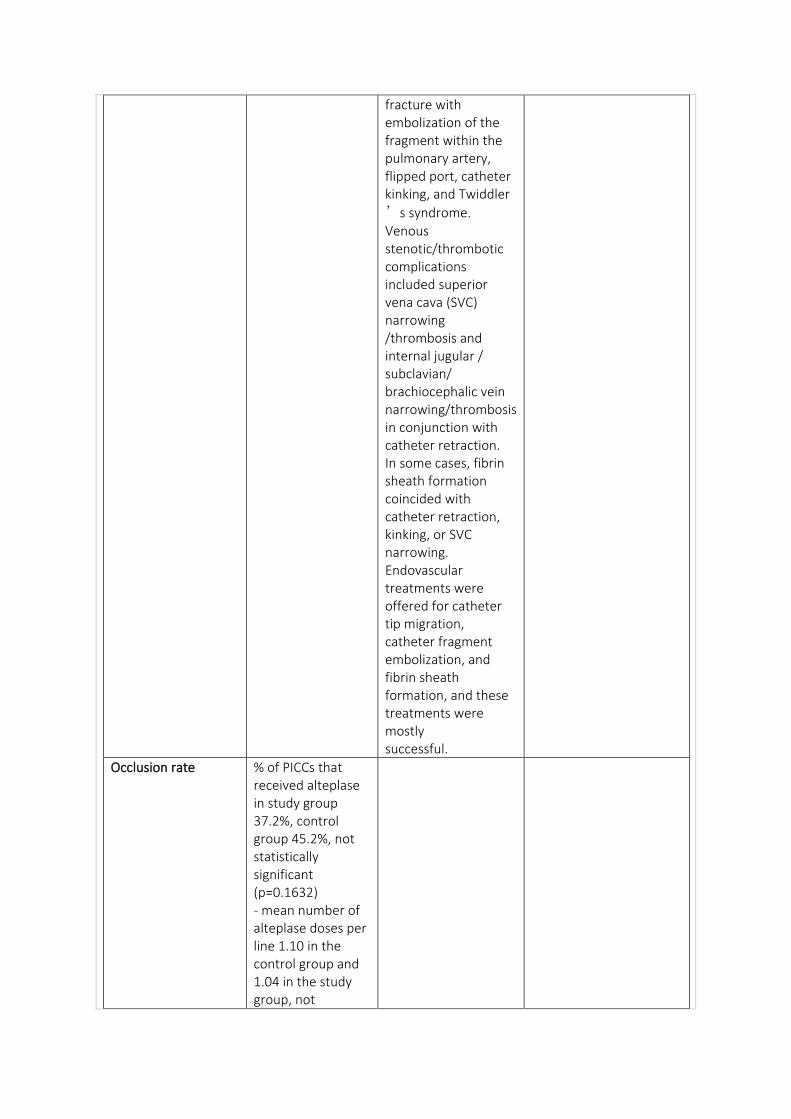
fracture with embolization of the fragment within the pulmonary artery, flipped port, catheter kinking, and Twiddler
’s syndrome. Venous stenotic/thrombotic complications included superior vena cava (SVC) narrowing /thrombosis and internal jugular / subclavian/ brachiocephalic vein narrowing/thrombosis in conjunction with catheter retraction. In some cases, fibrin sheath formation coincided with catheter retraction, kinking, or SVC narrowing. Endovascular treatments were offered for catheter tip migration, catheter fragment embolization, and fibrin sheath formation, and these treatments were mostly successful.
Occlusion rate % of PICCs that received alteplase in study group 37.2%, control group 45.2%, not statistically significant (p=0.1632) - mean number of alteplase doses per line 1.10 in the control group and 1.04 in the study group, not
statistically significant (p=.2776) - a significant association between total number of doses per line and baseline platelet count on day of PICC insertion (p= .0004) was observed after controlling for all related covariates
Occlusion rate/1000 catheter days
Did occlusion result in CVAD removal?
2/3 cases, 66% occlusion persisted so catheter removed
Timeframe to first occlusion
average time to first alteplase dose was approx. 2 days longer in the study group; however, average number of days from PICC placement to first alteplase dose did not differ significantly (p=.4258)
OVERALL result no statistical difference in average alteplase doses per line, number of PICCs requiring alteplase dose, or time to first dose of alteplase between study groups. economic analysis at our institution, adopting Endexo PICCs would result in increased expenses – per year $58,462 (alteplase use and new PICC)
DSA is useful tool in diagnosis of dysfunctional CVPs
- although heparin prophylaxis was used in all study patients, at least 1 thrombotic event was recorded in 45.2% of them, necessitating catheter removal in 23.2%. - The only conclusion regarding prophylaxis of catheter complications, which can be drawn from this study is that catheter flushing once weekly with unfractionated heparin is not a sufficient prophylactic method
- tPA effective in therapy of occluded lines, no side effects, even in patients with bleeding tendencies. The low tPA dosage (6 h of continuous infusion) was effective, resulting in restoration of CVC patency in 79.8% of patients. - frequency of TCL-related thrombotic events are underestimated
Thromboprophylaxis n= (%) median (range)
Patency – occlusion prevention CVAD
Education and competency requirement of staff – inserting and maintenance
Frequency of patency checked
How patency checked
Optimal flush frequency
Optimal flush volume
Optimal flush technique
Optimal lock solution 2mL of unfractionated heparin (50 U/mL) in every patient.
Optimal lock frequency
once weekly
Does NC influence patency
Can take blood specimens through CVAD? NC?
yes
Patency – occlusion prevention PIV
How is patency checked?
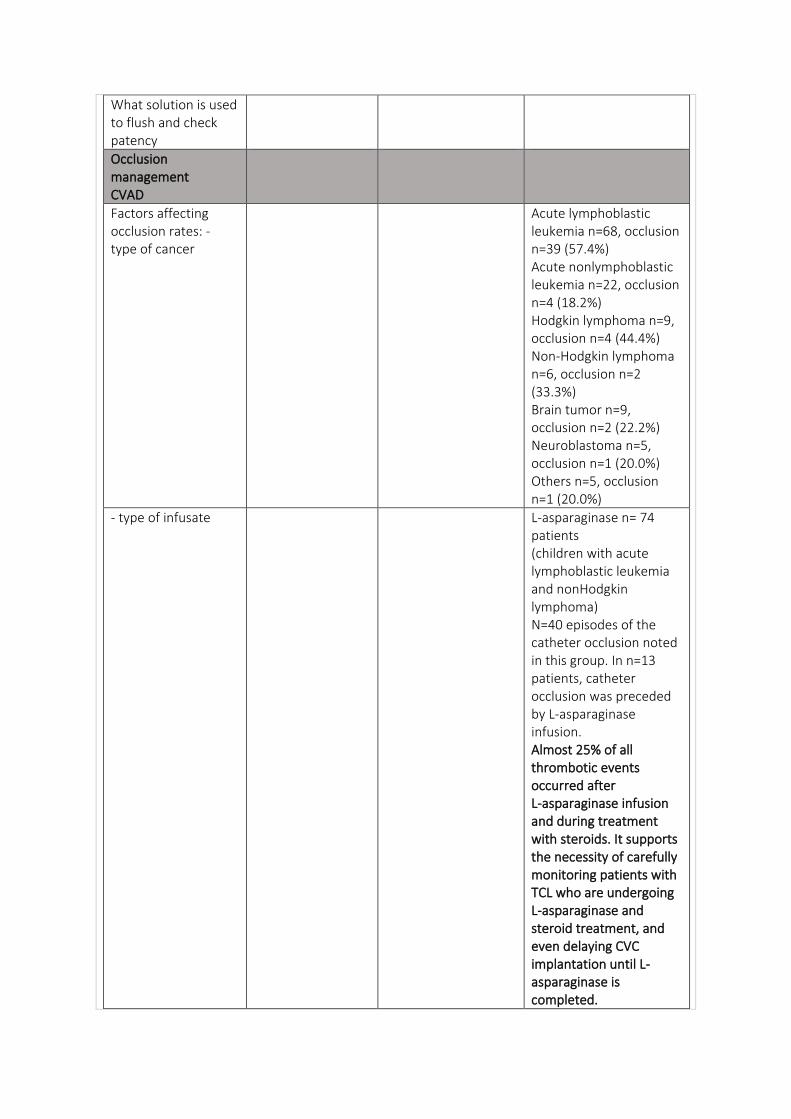
What solution is used to flush and check patency
Occlusion management CVAD
Factors affecting occlusion rates: - type of cancer
Acute lymphoblastic leukemia n=68, occlusion n=39 (57.4%) Acute nonlymphoblastic leukemia n=22, occlusion n=4 (18.2%) Hodgkin lymphoma n=9, occlusion n=4 (44.4%) Non-Hodgkin lymphoma n=6, occlusion n=2 (33.3%) Brain tumor n=9, occlusion n=2 (22.2%) Neuroblastoma n=5, occlusion n=1 (20.0%) Others n=5, occlusion n=1 (20.0%)
- type of infusate L-asparaginase n= 74 patients (children with acute lymphoblastic leukemia and nonHodgkin lymphoma) N=40 episodes of the catheter occlusion noted in this group. In n=13 patients, catheter occlusion was preceded by L-asparaginase infusion. Almost 25% of all thrombotic events occurred after L-asparaginase infusion and during treatment with steroids. It supports the necessity of carefully monitoring patients with TCL who are undergoing L-asparaginase and steroid treatment, and even delaying CVC implantation until L-asparaginase is completed.
- age
- CVAD duration
- laterality
- number of lumens
- type of CVAD
- valve vs non-valved catheters
- BMI>25
Growth factors
Other patient comorbidities
Steps in assessment of occlusion
Optimal management tPA continuous 6 hr infusion, 0.01mg/kg/hr
Optimal catheter tip position How does this relate to occlusion
Does angle of catheter in relation to port body impact occlusion rates
Does increase in resistance monitoring values indicate imminent CVAD occlusion
Can locking solutions be associated with risks of other complications?
Does CVAD material influence occlusion rates?
Can CVADs be used for radiological studies?
Occlusion management PIV
occluded PIV be replaced or unblocked
optimal location for PIV insertion
DATA:
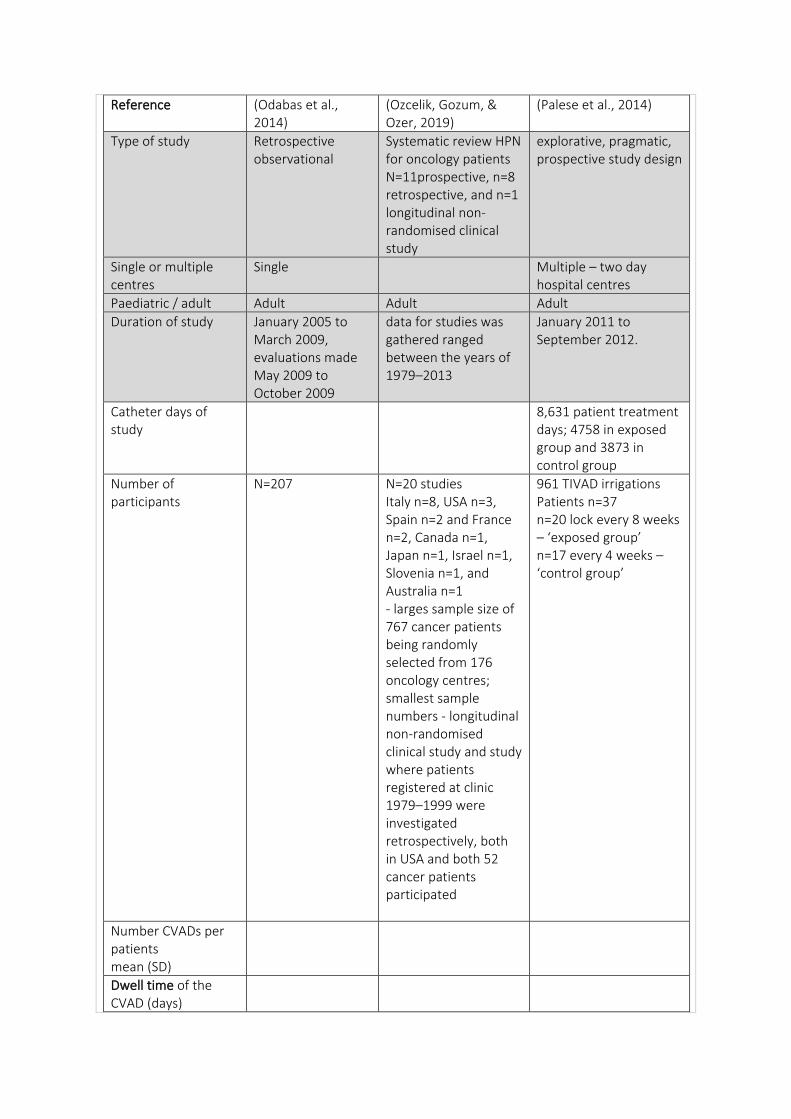
Reference (Odabas et al., 2014)
(Ozcelik, Gozum, & Ozer, 2019)
(Palese et al., 2014)
Type of study Retrospective observational
Systematic review HPN for oncology patients N=11prospective, n=8 retrospective, and n=1 longitudinal non-randomised clinical study
explorative, pragmatic, prospective study design
Single or multiple centres
Single Multiple – two day hospital centres
Paediatric / adult Adult Adult Adult
Duration of study January 2005 to March 2009, evaluations made May 2009 to October 2009
data for studies was gathered ranged between the years of 1979–2013
January 2011 to September 2012.
Catheter days of study
8,631 patient treatment days; 4758 in exposed group and 3873 in control group
Number of participants
N=207 N=20 studies Italy n=8, USA n=3, Spain n=2 and France n=2, Canada n=1, Japan n=1, Israel n=1, Slovenia n=1, and Australia n=1 - larges sample size of 767 cancer patients being randomly selected from 176 oncology centres; smallest sample numbers - longitudinal non-randomised clinical study and study where patients registered at clinic 1979–1999 were investigated retrospectively, both in USA and both 52 cancer patients participated
961 TIVAD irrigations Patients n=37 n=20 lock every 8 weeks – ‘exposed group’ n=17 every 4 weeks – ‘control group’
Number CVADs per patients mean (SD)
Dwell time of the CVAD (days)
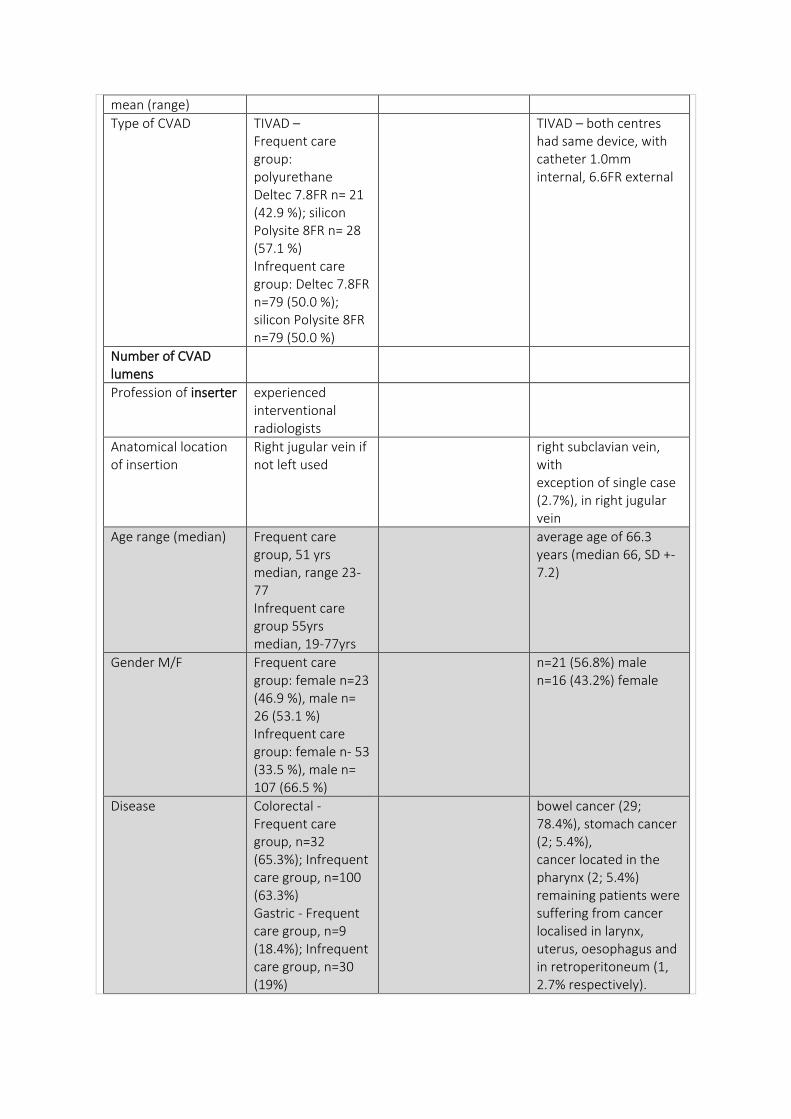
mean (range)
Type of CVAD TIVAD – Frequent care group: polyurethane Deltec 7.8FR n= 21 (42.9 %); silicon Polysite 8FR n= 28 (57.1 %) Infrequent care group: Deltec 7.8FR n=79 (50.0 %); silicon Polysite 8FR n=79 (50.0 %)
TIVAD – both centres had same device, with catheter 1.0mm internal, 6.6FR external
Number of CVAD lumens
Profession of inserter experienced interventional radiologists
Anatomical location of insertion
Right jugular vein if not left used
right subclavian vein, with exception of single case (2.7%), in right jugular vein
Age range (median) Frequent care group, 51 yrs median, range 23-77 Infrequent care group 55yrs median, 19-77yrs
average age of 66.3 years (median 66, SD +- 7.2)
Gender M/F Frequent care group: female n=23 (46.9 %), male n= 26 (53.1 %) Infrequent care group: female n- 53 (33.5 %), male n= 107 (66.5 %)
n=21 (56.8%) male n=16 (43.2%) female
Disease Colorectal - Frequent care group, n=32 (65.3%); Infrequent care group, n=100 (63.3%) Gastric - Frequent care group, n=9 (18.4%); Infrequent care group, n=30 (19%)
bowel cancer (29; 78.4%), stomach cancer (2; 5.4%), cancer located in the pharynx (2; 5.4%) remaining patients were suffering from cancer localised in larynx, uterus, oesophagus and in retroperitoneum (1, 2.7% respectively).
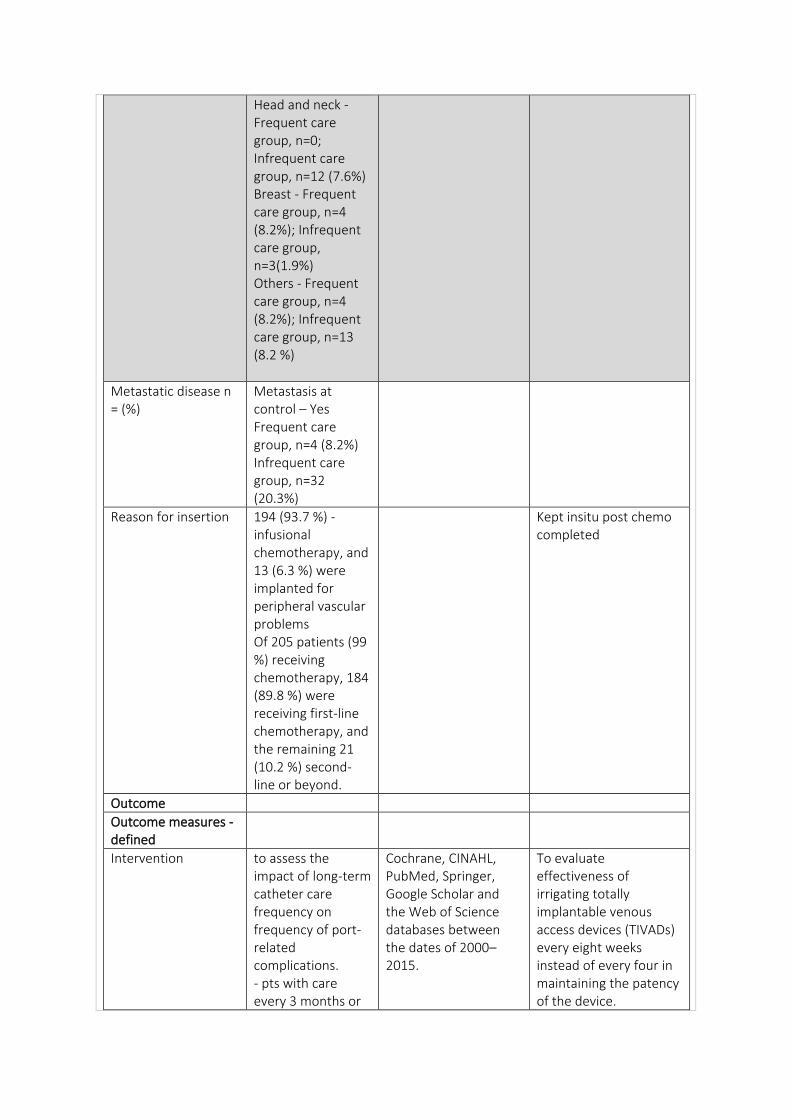
Head and neck - Frequent care group, n=0; Infrequent care group, n=12 (7.6%) Breast - Frequent care group, n=4 (8.2%); Infrequent care group, n=3(1.9%) Others - Frequent care group, n=4 (8.2%); Infrequent care group, n=13 (8.2 %)
Metastatic disease n = (%)
Metastasis at control – Yes Frequent care group, n=4 (8.2%) Infrequent care group, n=32 (20.3%)
Reason for insertion 194 (93.7 %) - infusional chemotherapy, and 13 (6.3 %) were implanted for peripheral vascular problems Of 205 patients (99 %) receiving chemotherapy, 184 (89.8 %) were receiving first-line chemotherapy, and the remaining 21 (10.2 %) second-line or beyond.
Kept insitu post chemo completed
Outcome
Outcome measures - defined
Intervention to assess the impact of long-term catheter care frequency on frequency of port-related complications. - pts with care every 3 months or
Cochrane, CINAHL, PubMed, Springer, Google Scholar and the Web of Science databases between the dates of 2000–2015.
To evaluate effectiveness of irrigating totally implantable venous access devices (TIVADs) every eight weeks instead of every four in maintaining the patency of the device.
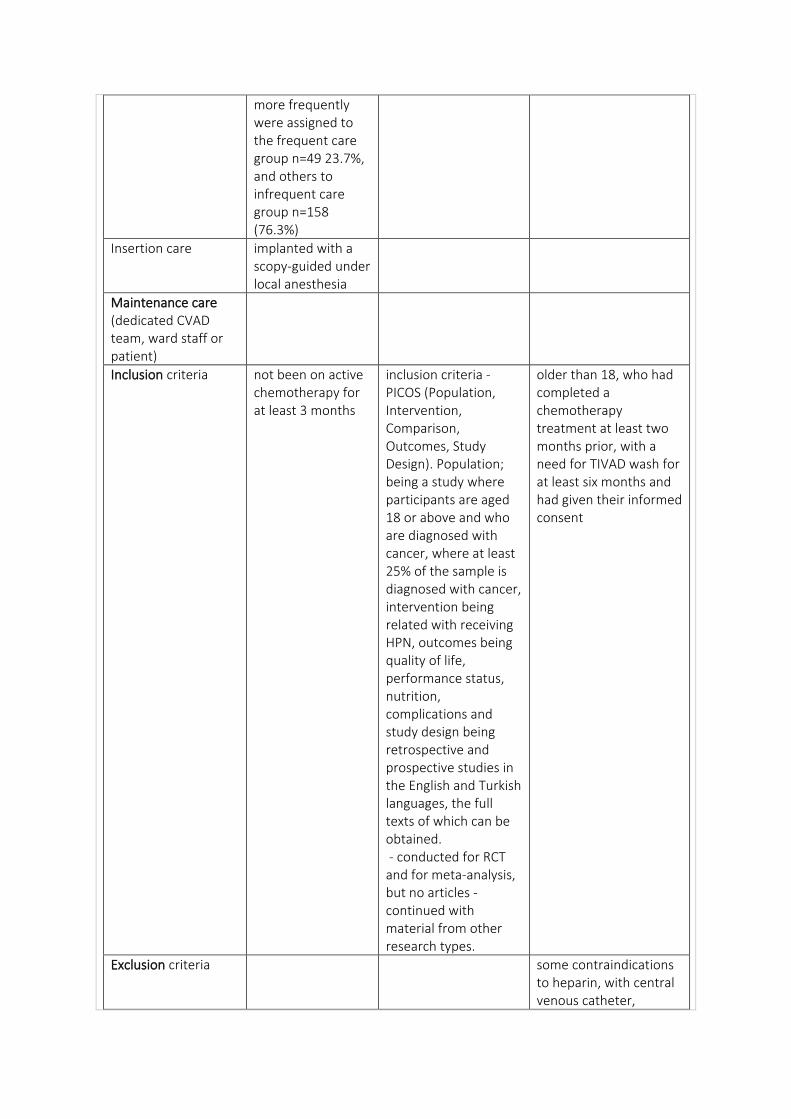
more frequently were assigned to the frequent care group n=49 23.7%, and others to infrequent care group n=158 (76.3%)
Insertion care implanted with a scopy-guided under local anesthesia
Maintenance care (dedicated CVAD team, ward staff or patient)
Inclusion criteria not been on active chemotherapy for at least 3 months
inclusion criteria - PICOS (Population, Intervention, Comparison, Outcomes, Study Design). Population; being a study where participants are aged 18 or above and who are diagnosed with cancer, where at least 25% of the sample is diagnosed with cancer, intervention being related with receiving HPN, outcomes being quality of life, performance status, nutrition, complications and study design being retrospective and prospective studies in the English and Turkish languages, the full texts of which can be obtained. - conducted for RCT and for meta‐analysis, but no articles - continued with material from other research types.
older than 18, who had completed a chemotherapy treatment at least two months prior, with a need for TIVAD wash for at least six months and had given their informed consent
Exclusion criteria some contraindications to heparin, with central venous catheter,
receiving parenteral nutrition or supportive care through the TIVAD, with infection manifested or suspected nd those reporting previous device infection(s) were excluded
Randomisation Consecutive sample
Healthcare setting Turkey two day hospital centres located in the northeast of Italy
Duration of follow up, lost to follow up
Median followup of all patients was 671 days (range 133–1712); Median frequency of port care in frequent care group was 90 days (range 30–90), 441.5 days in infrequent care group (range 91–1630)
consistent number of patients withdrew from their follow up care regimen for different reasons (removing TIVAD, restarting chemotherapy, or expiring). in the patients withdrawn from study, their TIVAD might have been occluded at the time of their exclusion: however, TIVAD was not evaluated for occlusion at the moment of the study withdrawal and these should be considered as a study limitation.
RESULTS:
Complication rate For each 1,000 HPN days, complications with a ratio of 3.58 were determined and for each 1,000 days with catheters, complications with a ratio of 1.3 were found - in four studies, stated differently with complications 2.2% - 45% being observed
Complication rate/1000 catheter days
Occlusion rate N=0 experienced port-related severe
For each 1,000 days with HPN or catheter-
6 occlusions in catheter that could be attributed
complications during follow-up time N=0 presented with port occlusion
mechanical problems in the interval of 0.07 and 2.13 Mechanical obstruction in catheter is another important problem – studies conducted in Japan, Slovenia, the USA, and Italy, mechanical problems with ratios of 5.9%, 19%, 1.6% and 3.9% occurred respectively, but are defined in different ways
to formation of fibrin plug in 6 pts, n=4 20% in exposed group, n=2 control group 11.7% - no statistically significant differences were observed in occurrence of occlusion between the groups (RR: 1.29, 95%CI: 0.67e2.50, p=0.49)
Occlusion rate/1000 catheter days
Did occlusion result in CVAD removal?
Timeframe to first occlusion
OVERALL result median interval of care in frequent care group was 90 days, and 441.5 days in infrequent care group - when routine care was performed with only 300 IU heparin, almost none of patients developed port occlusion.
- relative risk of occlusion was higher in exposed group receiving a wash every eight weeks compared to control group. This difference, however, was not statistically significant - among those exposed to irrigation every eight weeks, more occlusions were reported at end of the year. Therefore it might be suggested that flushing interval of TIVADs after 300 days ought to be reduced from eight weeks to four weeks - no statistically significant differences emerged in the occurrence of occlusion between TIVADs irrigated every four weeks rather than every eight weeks.
Reducing the number of accesses made to the device may reduce the risk of infection and patient discomfort. Within the limits of this study, it can be suggested that a prolongation of the wash interval to as long as eight weeks remains sufficient to maintain the patency of the device.
Thromboprophylaxis n= (%) median (range)
N0 N=1
Patency – occlusion prevention CVAD
Education and competency requirement of staff – inserting and maintenance
Frequency of patency checked
How patency checked
Optimal flush frequency
Optimal flush volume
Optimal flush technique
Optimal lock solution flushed with 10 mL 0.9 % saline solution then 3 mL of heparinized saline solution (100 IU heparin/ mL) = 300 IU
a positive pressure and pulsating flush procedure with 20 ml of normal saline, followed by 3ml of sodium heparin (250 IUs/ml 5) for a total of 150 UIs of heparin
Optimal lock frequency
Does NC influence patency
Can take blood specimens through CVAD? NC?
Patency – occlusion prevention
PIV
How is patency checked?
What solution is used to flush and check patency
Occlusion management CVAD
Factors affecting occlusion rates: - type of cancer
- type of infusate
- age
- CVAD duration
- laterality
- number of lumens
- type of CVAD When studies were investigated for mechanical complications, it was seen that in HPN applications, tunnelled catheters were superior when compared with PICC.
- valve vs non-valved catheters
- BMI>25
Growth factors
Other patient comorbidities
Steps in assessment of occlusion
Optimal management When occlusions occurred, it was not necessary to either remove the device or restore the patency of the device with the use of a fibrinolytic agent.
Optimal catheter tip position How does this relate to occlusion
Right atrium lower third of superior vena cava, in the atrio-caval junction, verified by CXR after placement
Does angle of catheter in relation to port body impact occlusion rates
Does increase in resistance monitoring
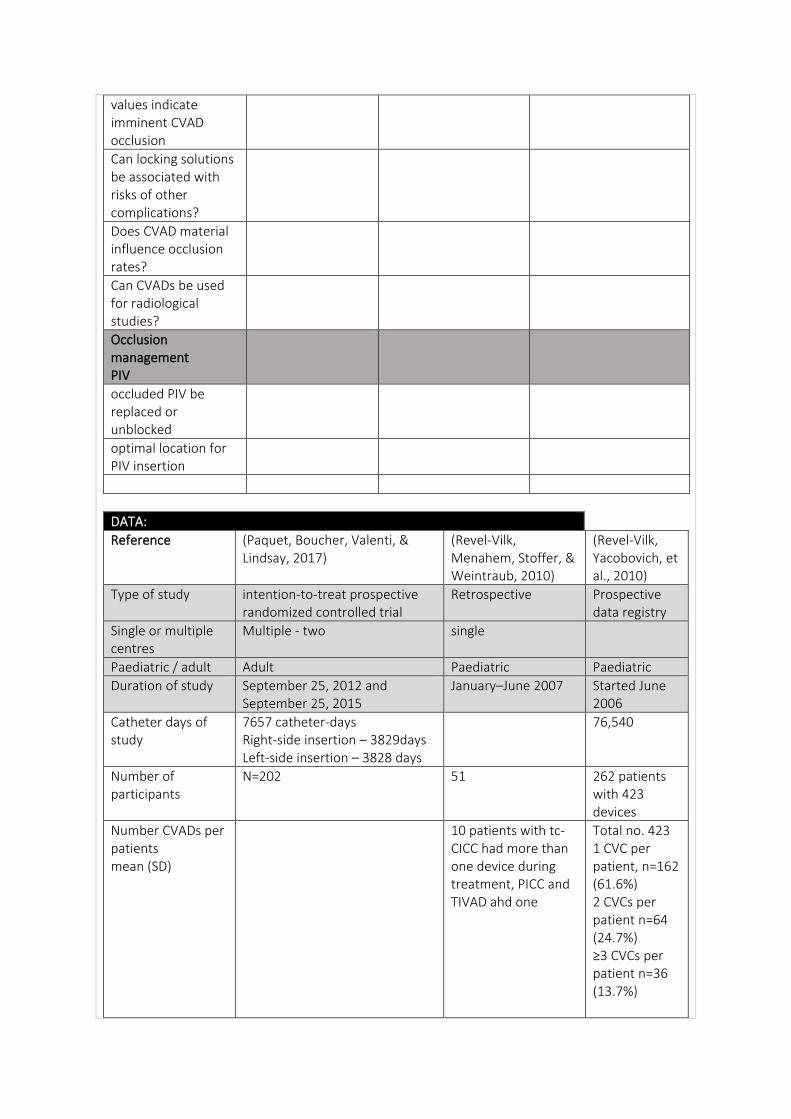
values indicate imminent CVAD occlusion
Can locking solutions be associated with risks of other complications?
Does CVAD material influence occlusion rates?
Can CVADs be used for radiological studies?
Occlusion management PIV
occluded PIV be replaced or unblocked
optimal location for PIV insertion
DATA:
Reference (Paquet, Boucher, Valenti, & Lindsay, 2017)
(Revel-Vilk, Menahem, Stoffer, & Weintraub, 2010)
(Revel-Vilk, Yacobovich, et al., 2010)
Type of study intention-to-treat prospective randomized controlled trial
Retrospective Prospective data registry
Single or multiple centres
Multiple - two single
Paediatric / adult Adult Paediatric Paediatric
Duration of study September 25, 2012 and September 25, 2015
January–June 2007 Started June 2006
Catheter days of study
7657 catheter-days Right-side insertion – 3829days Left-side insertion – 3828 days
76,540
Number of participants
N=202 51 262 patients with 423 devices
Number CVADs per patients mean (SD)
10 patients with tc-CICC had more than one device during treatment, PICC and TIVAD ahd one
Total no. 423 1 CVC per patient, n=162 (61.6%) 2 CVCs per patient n=64 (24.7%) ≥3 CVCs per patient n=36 (13.7%)
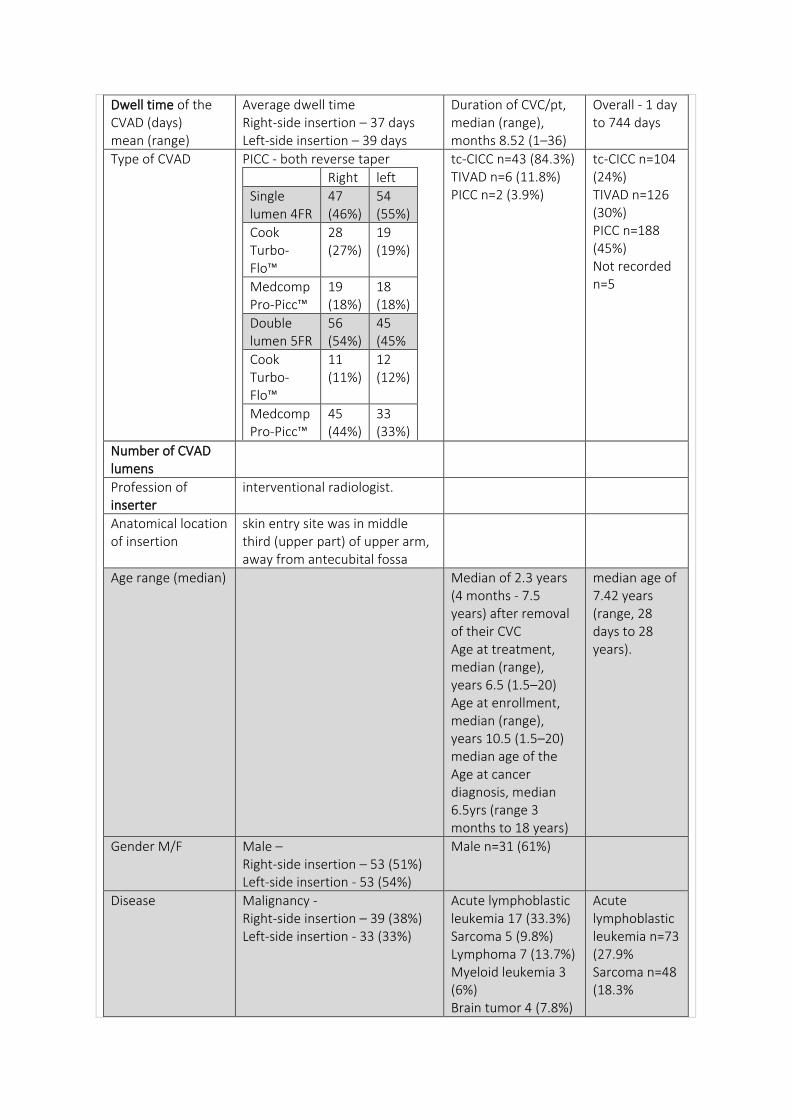
Dwell time of the CVAD (days) mean (range)
Average dwell time Right-side insertion – 37 days Left-side insertion – 39 days
Duration of CVC/pt, median (range), months 8.52 (1–36)
Overall - 1 day to 744 days
Type of CVAD PICC - both reverse taper
Right left
Single lumen 4FR
47 (46%)
54 (55%)
Cook Turbo-Flo™
28 (27%)
19 (19%)
Medcomp Pro-Picc™
19 (18%)
18 (18%)
Double lumen 5FR
56 (54%)
45 (45%
Cook Turbo-Flo™
11 (11%)
12 (12%)
Medcomp Pro-Picc™
45 (44%)
33 (33%)
tc-CICC n=43 (84.3%) TIVAD n=6 (11.8%) PICC n=2 (3.9%)
tc-CICC n=104 (24%) TIVAD n=126 (30%) PICC n=188 (45%) Not recorded n=5
Number of CVAD lumens
Profession of inserter
interventional radiologist.
Anatomical location of insertion
skin entry site was in middle third (upper part) of upper arm, away from antecubital fossa
Age range (median) Median of 2.3 years (4 months - 7.5 years) after removal of their CVC Age at treatment, median (range), years 6.5 (1.5–20) Age at enrollment, median (range), years 10.5 (1.5–20) median age of the Age at cancer diagnosis, median 6.5yrs (range 3 months to 18 years)
median age of 7.42 years (range, 28 days to 28 years).
Gender M/F Male – Right-side insertion – 53 (51%) Left-side insertion - 53 (54%)
Male n=31 (61%)
Disease Malignancy - Right-side insertion – 39 (38%) Left-side insertion - 33 (33%)
Acute lymphoblastic leukemia 17 (33.3%) Sarcoma 5 (9.8%) Lymphoma 7 (13.7%) Myeloid leukemia 3 (6%) Brain tumor 4 (7.8%)
Acute lymphoblastic leukemia n=73 (27.9% Sarcoma n=48 (18.3%
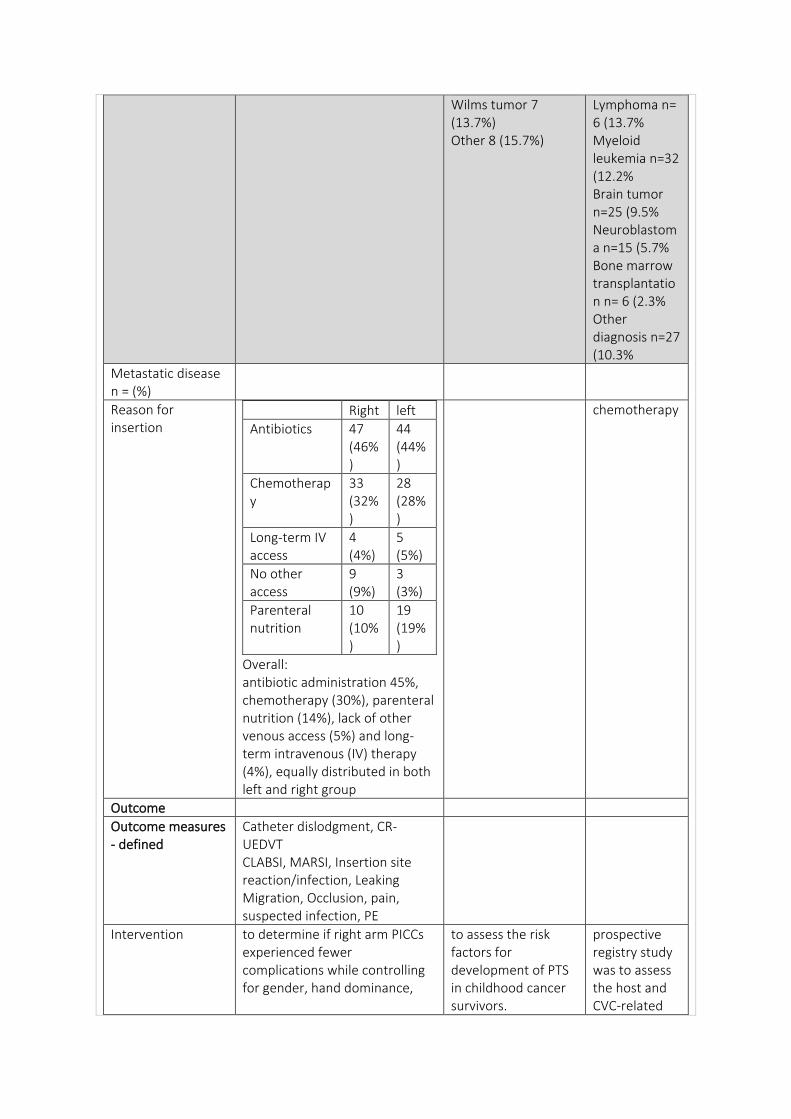
Wilms tumor 7 (13.7%) Other 8 (15.7%)
Lymphoma n= 6 (13.7% Myeloid leukemia n=32 (12.2% Brain tumor n=25 (9.5% Neuroblastoma n=15 (5.7% Bone marrow transplantation n= 6 (2.3% Other diagnosis n=27 (10.3%
Metastatic disease n = (%)
Reason for insertion
Right left
Antibiotics 47 (46%)
44 (44%)
Chemotherapy
33 (32%)
28 (28%)
Long-term IV access
4 (4%)
5 (5%)
No other access
9 (9%)
3 (3%)
Parenteral nutrition
10 (10%)
19 (19%)
Overall: antibiotic administration 45%, chemotherapy (30%), parenteral nutrition (14%), lack of other venous access (5%) and long-term intravenous (IV) therapy (4%), equally distributed in both left and right group
chemotherapy
Outcome
Outcome measures - defined
Catheter dislodgment, CR-UEDVT CLABSI, MARSI, Insertion site reaction/infection, Leaking Migration, Occlusion, pain, suspected infection, PE
Intervention to determine if right arm PICCs experienced fewer complications while controlling for gender, hand dominance,
to assess the risk factors for development of PTS in childhood cancer survivors.
prospective registry study was to assess the host and CVC-related
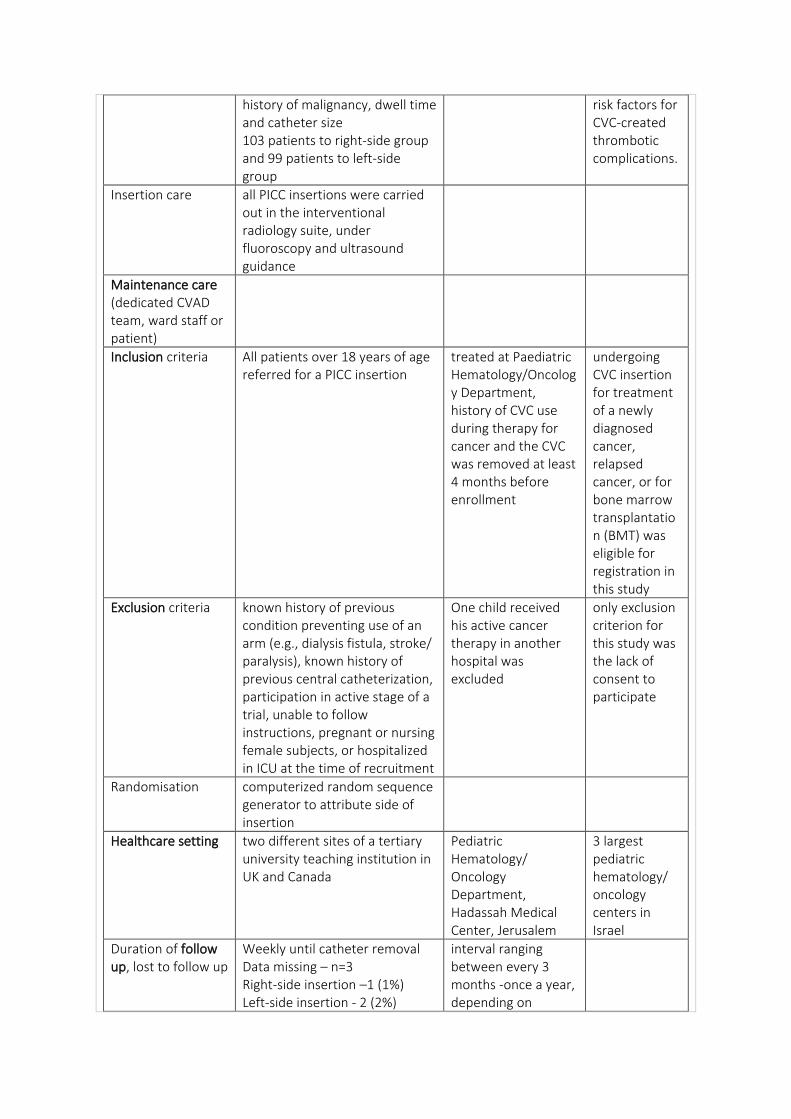
history of malignancy, dwell time and catheter size 103 patients to right-side group and 99 patients to left-side group
risk factors for CVC-created thrombotic complications.
Insertion care all PICC insertions were carried out in the interventional radiology suite, under fluoroscopy and ultrasound guidance
Maintenance care (dedicated CVAD team, ward staff or patient)
Inclusion criteria All patients over 18 years of age referred for a PICC insertion
treated at Paediatric Hematology/Oncology Department, history of CVC use during therapy for cancer and the CVC was removed at least 4 months before enrollment
undergoing CVC insertion for treatment of a newly diagnosed cancer, relapsed cancer, or for bone marrow transplantation (BMT) was eligible for registration in this study
Exclusion criteria known history of previous condition preventing use of an arm (e.g., dialysis fistula, stroke/ paralysis), known history of previous central catheterization, participation in active stage of a trial, unable to follow instructions, pregnant or nursing female subjects, or hospitalized in ICU at the time of recruitment
One child received his active cancer therapy in another hospital was excluded
only exclusion criterion for this study was the lack of consent to participate
Randomisation computerized random sequence generator to attribute side of insertion
Healthcare setting two different sites of a tertiary university teaching institution in UK and Canada
Pediatric Hematology/ Oncology Department, Hadassah Medical Center, Jerusalem
3 largest pediatric hematology/ oncology centers in Israel
Duration of follow up, lost to follow up
Weekly until catheter removal Data missing – n=3 Right-side insertion –1 (1%) Left-side insertion - 2 (2%)
interval ranging between every 3 months -once a year, depending on
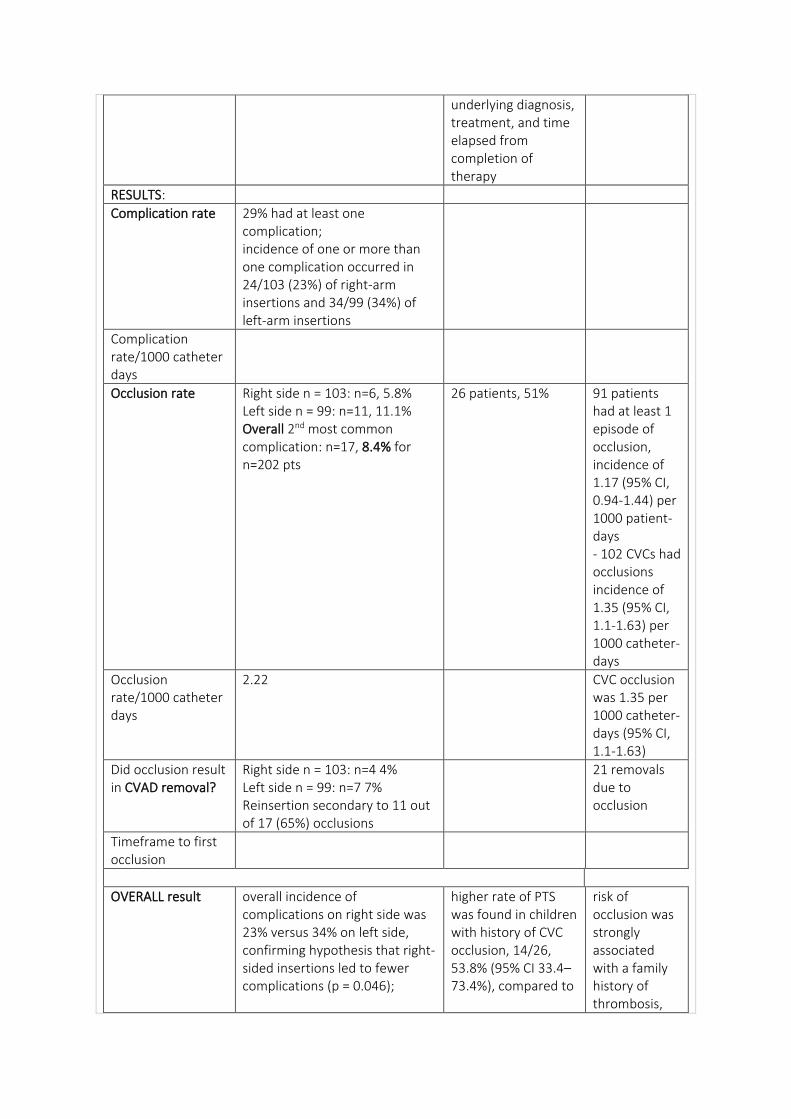
underlying diagnosis, treatment, and time elapsed from completion of therapy
RESULTS:
Complication rate 29% had at least one complication; incidence of one or more than one complication occurred in 24/103 (23%) of right-arm insertions and 34/99 (34%) of left-arm insertions
Complication rate/1000 catheter days
Occlusion rate Right side n = 103: n=6, 5.8% Left side n = 99: n=11, 11.1% Overall 2nd most common complication: n=17, 8.4% for n=202 pts
26 patients, 51% 91 patients had at least 1 episode of occlusion, incidence of 1.17 (95% CI, 0.94-1.44) per 1000 patient-days - 102 CVCs had occlusions incidence of 1.35 (95% CI, 1.1-1.63) per 1000 catheter-days
Occlusion rate/1000 catheter days
2.22 CVC occlusion was 1.35 per 1000 catheter-days (95% CI, 1.1-1.63)
Did occlusion result in CVAD removal?
Right side n = 103: n=4 4% Left side n = 99: n=7 7% Reinsertion secondary to 11 out of 17 (65%) occlusions
21 removals due to occlusion
Timeframe to first occlusion
OVERALL result overall incidence of complications on right side was 23% versus 34% on left side, confirming hypothesis that right-sided insertions led to fewer complications (p = 0.046);
higher rate of PTS was found in children with history of CVC occlusion, 14/26, 53.8% (95% CI 33.4–73.4%), compared to
risk of occlusion was strongly associated with a family history of thrombosis,
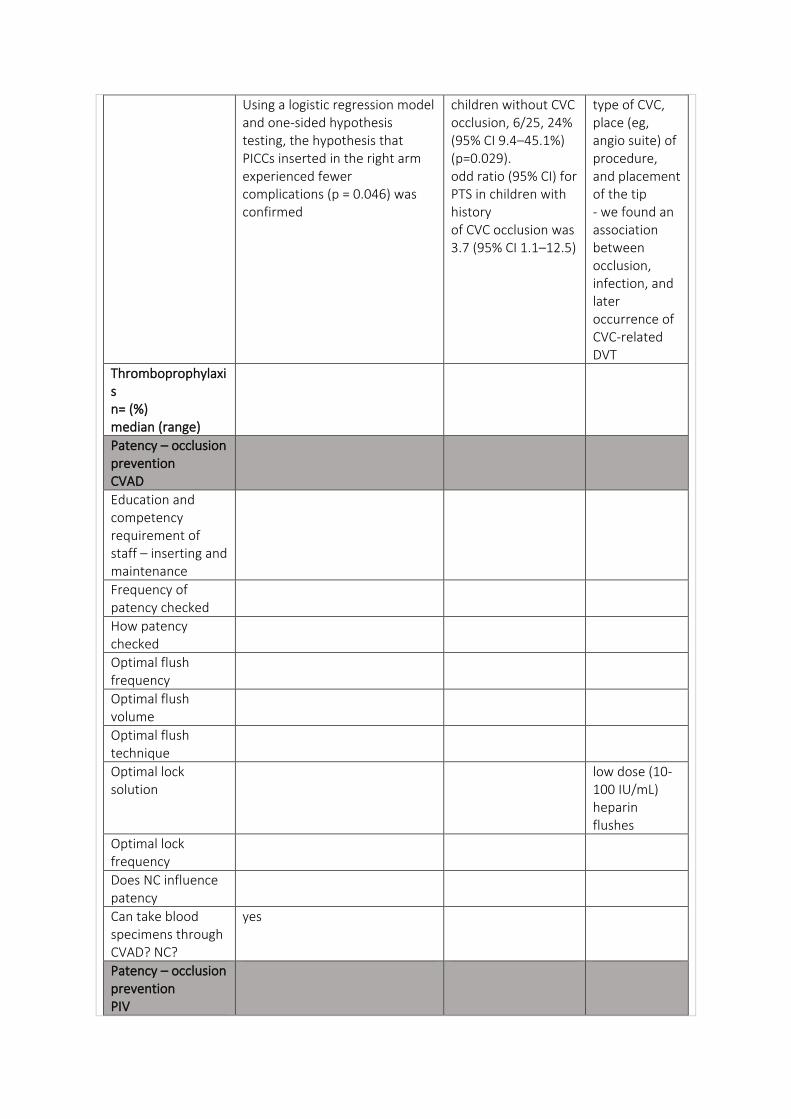
Using a logistic regression model and one-sided hypothesis testing, the hypothesis that PICCs inserted in the right arm experienced fewer complications (p = 0.046) was confirmed
children without CVC occlusion, 6/25, 24% (95% CI 9.4–45.1%) (p=0.029). odd ratio (95% CI) for PTS in children with history of CVC occlusion was 3.7 (95% CI 1.1–12.5)
type of CVC, place (eg, angio suite) of procedure, and placement of the tip - we found an association between occlusion, infection, and later occurrence of CVC-related DVT
Thromboprophylaxis n= (%) median (range)
Patency – occlusion prevention CVAD
Education and competency requirement of staff – inserting and maintenance
Frequency of patency checked
How patency checked
Optimal flush frequency
Optimal flush volume
Optimal flush technique
Optimal lock solution
low dose (10-100 IU/mL) heparin flushes
Optimal lock frequency
Does NC influence patency
Can take blood specimens through CVAD? NC?
yes
Patency – occlusion prevention PIV
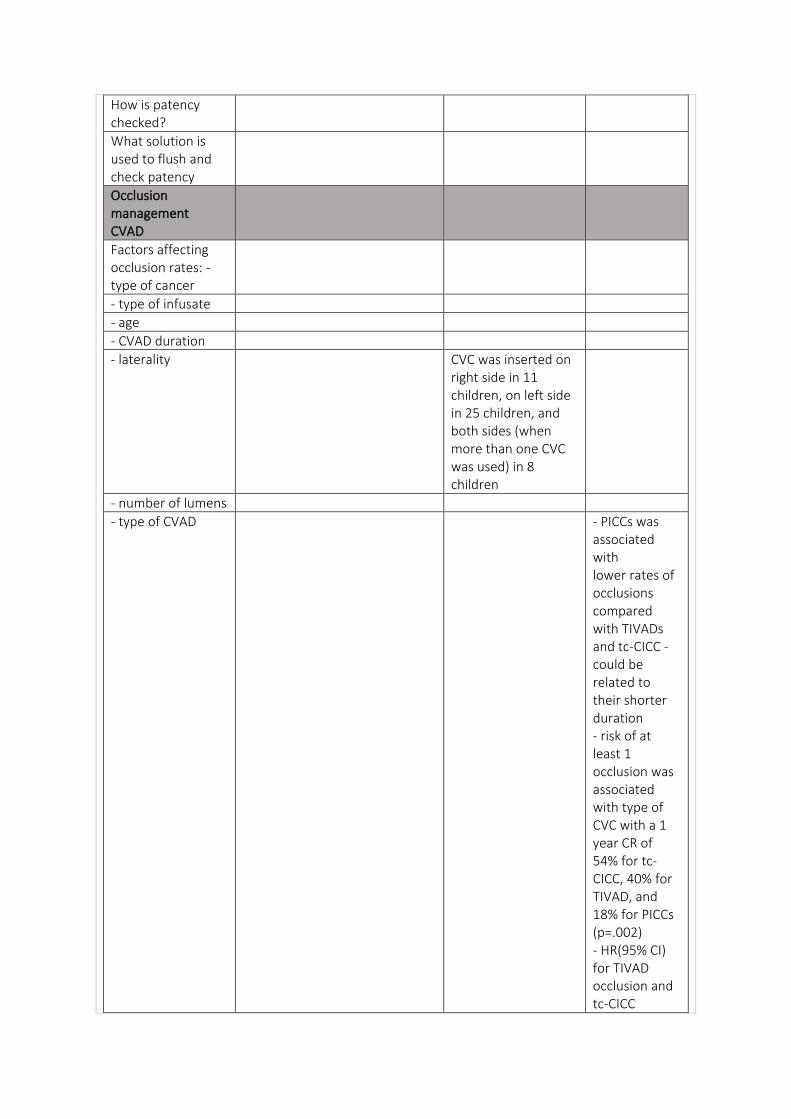
How is patency checked?
What solution is used to flush and check patency
Occlusion management CVAD
Factors affecting occlusion rates: - type of cancer
- type of infusate
- age
- CVAD duration
- laterality CVC was inserted on right side in 11 children, on left side in 25 children, and both sides (when more than one CVC was used) in 8 children
- number of lumens
- type of CVAD - PICCs was associated with lower rates of occlusions compared with TIVADs and tc-CICC - could be related to their shorter duration - risk of at least 1 occlusion was associated with type of CVC with a 1 year CR of 54% for tc-CICC, 40% for TIVAD, and 18% for PICCs (p=.002) - HR(95% CI) for TIVAD occlusion and tc-CICC
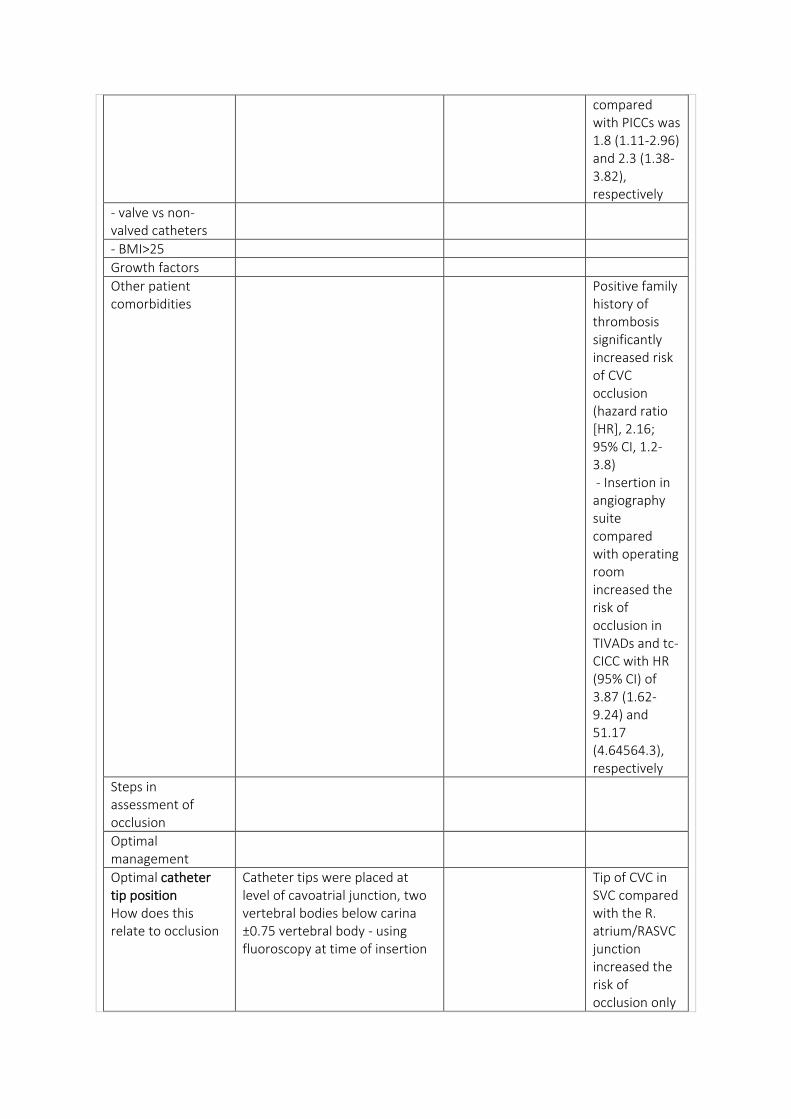
compared with PICCs was 1.8 (1.11-2.96) and 2.3 (1.38-3.82), respectively
- valve vs non-valved catheters
- BMI>25
Growth factors
Other patient comorbidities
Positive family history of thrombosis significantly increased risk of CVC occlusion (hazard ratio [HR], 2.16; 95% CI, 1.2-3.8) - Insertion in angiography suite compared with operating room increased the risk of occlusion in TIVADs and tc-CICC with HR (95% CI) of 3.87 (1.62-9.24) and 51.17 (4.64564.3), respectively
Steps in assessment of occlusion
Optimal management
Optimal catheter tip position How does this relate to occlusion
Catheter tips were placed at level of cavoatrial junction, two vertebral bodies below carina ±0.75 vertebral body - using fluoroscopy at time of insertion
Tip of CVC in SVC compared with the R. atrium/RASVC junction increased the risk of occlusion only
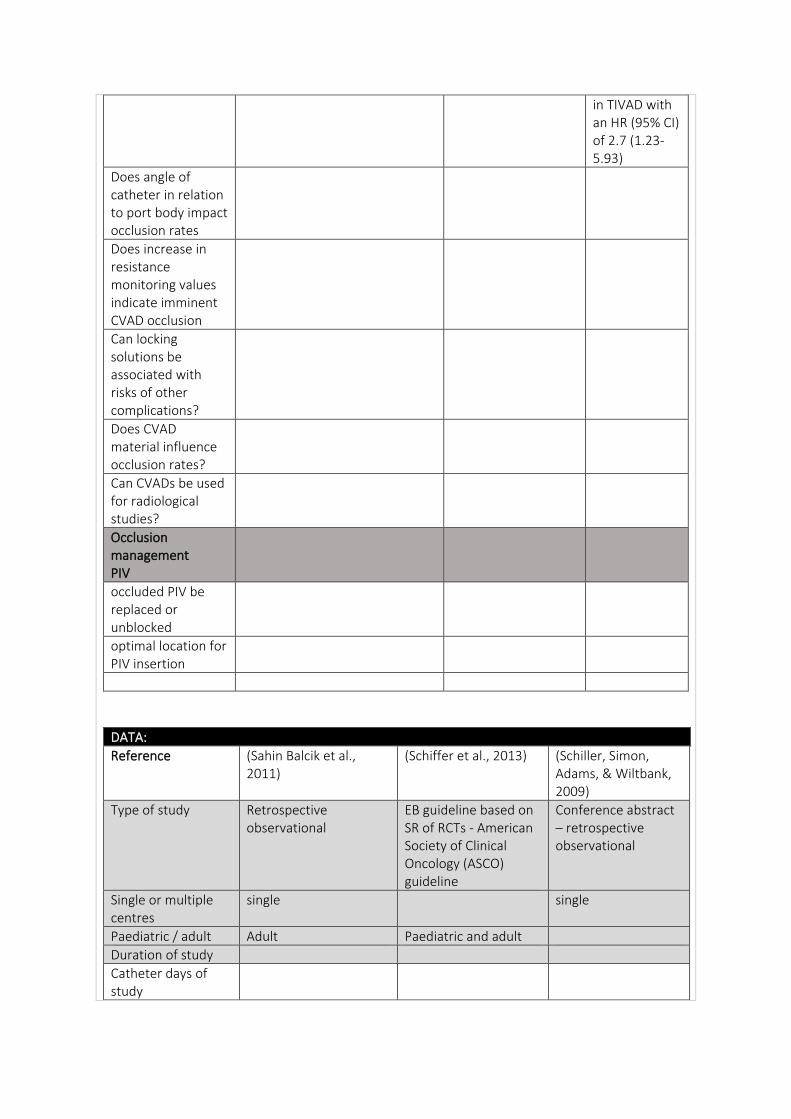
in TIVAD with an HR (95% CI) of 2.7 (1.23-5.93)
Does angle of catheter in relation to port body impact occlusion rates
Does increase in resistance monitoring values indicate imminent CVAD occlusion
Can locking solutions be associated with risks of other complications?
Does CVAD material influence occlusion rates?
Can CVADs be used for radiological studies?
Occlusion management PIV
occluded PIV be replaced or unblocked
optimal location for PIV insertion
DATA:
Reference (Sahin Balcik et al., 2011)
(Schiffer et al., 2013) (Schiller, Simon, Adams, & Wiltbank, 2009)
Type of study Retrospective observational
EB guideline based on SR of RCTs - American Society of Clinical Oncology (ASCO) guideline
Conference abstract – retrospective observational
Single or multiple centres
single single
Paediatric / adult Adult Paediatric and adult
Duration of study
Catheter days of study
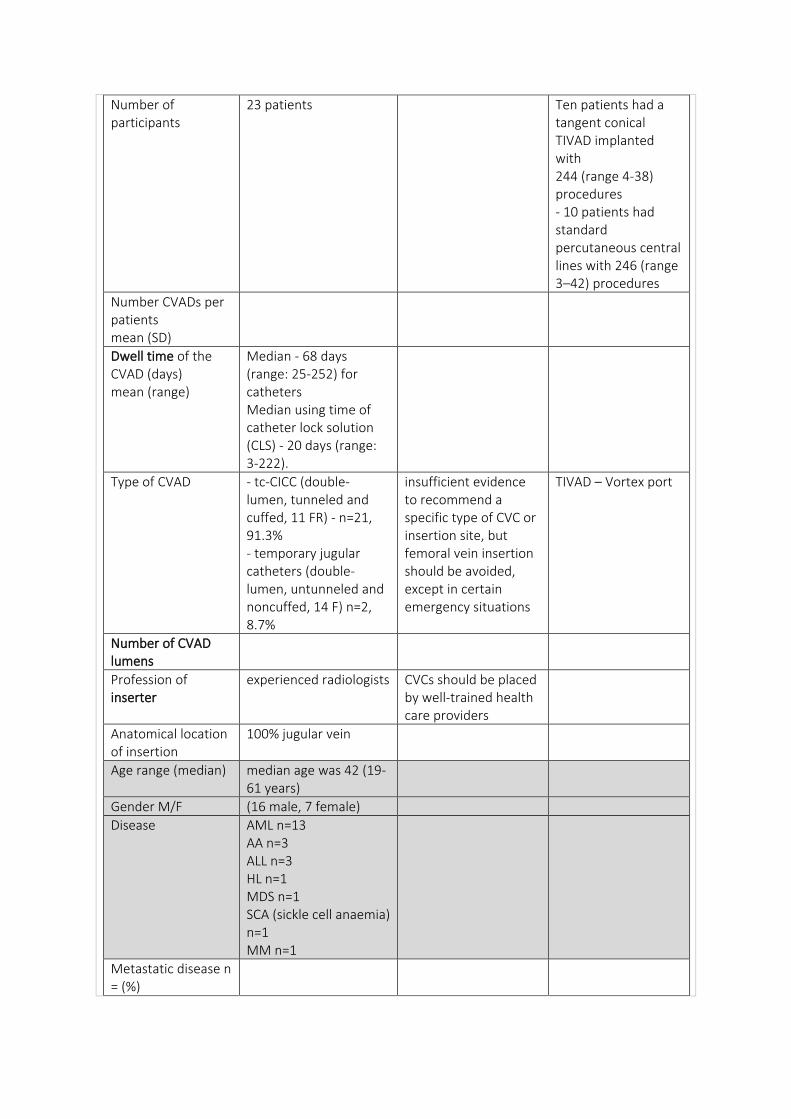
Number of participants
23 patients Ten patients had a tangent conical TIVAD implanted with 244 (range 4-38) procedures - 10 patients had standard percutaneous central lines with 246 (range 3–42) procedures
Number CVADs per patients mean (SD)
Dwell time of the CVAD (days) mean (range)
Median - 68 days (range: 25-252) for catheters Median using time of catheter lock solution (CLS) - 20 days (range: 3-222).
Type of CVAD - tc-CICC (double-lumen, tunneled and cuffed, 11 FR) - n=21, 91.3% - temporary jugular catheters (double-lumen, untunneled and noncuffed, 14 F) n=2, 8.7%
insufficient evidence to recommend a specific type of CVC or insertion site, but femoral vein insertion should be avoided, except in certain emergency situations
TIVAD – Vortex port
Number of CVAD lumens
Profession of inserter
experienced radiologists CVCs should be placed by well-trained health care providers
Anatomical location of insertion
100% jugular vein
Age range (median) median age was 42 (19-61 years)
Gender M/F (16 male, 7 female)
Disease AML n=13 AA n=3 ALL n=3 HL n=1 MDS n=1 SCA (sickle cell anaemia) n=1 MM n=1
Metastatic disease n = (%)
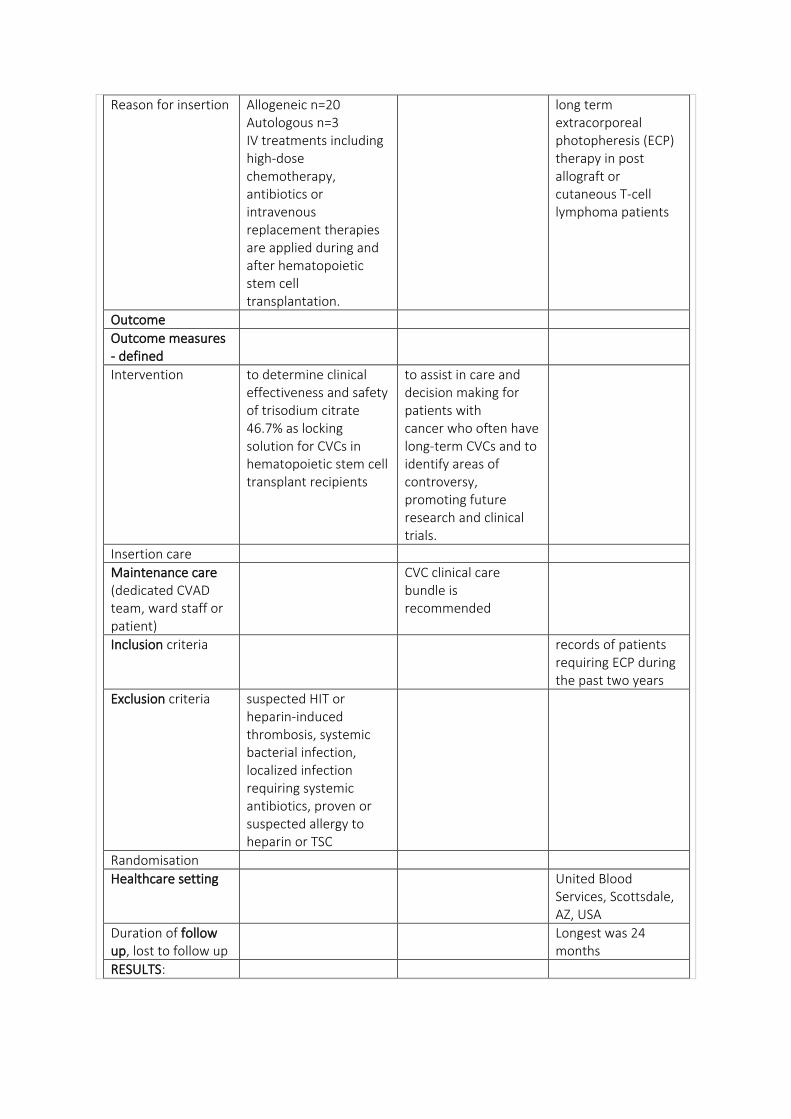
Reason for insertion Allogeneic n=20 Autologous n=3 IV treatments including high-dose chemotherapy, antibiotics or intravenous replacement therapies are applied during and after hematopoietic stem cell transplantation.
long term extracorporeal photopheresis (ECP) therapy in post allograft or cutaneous T-cell lymphoma patients
Outcome
Outcome measures - defined
Intervention to determine clinical effectiveness and safety of trisodium citrate 46.7% as locking solution for CVCs in hematopoietic stem cell transplant recipients
to assist in care and decision making for patients with cancer who often have long-term CVCs and to identify areas of controversy, promoting future research and clinical trials.
Insertion care
Maintenance care (dedicated CVAD team, ward staff or patient)
CVC clinical care bundle is recommended
Inclusion criteria records of patients requiring ECP during the past two years
Exclusion criteria suspected HIT or heparin-induced thrombosis, systemic bacterial infection, localized infection requiring systemic antibiotics, proven or suspected allergy to heparin or TSC
Randomisation
Healthcare setting United Blood Services, Scottsdale, AZ, USA
Duration of follow up, lost to follow up
Longest was 24 months
RESULTS:
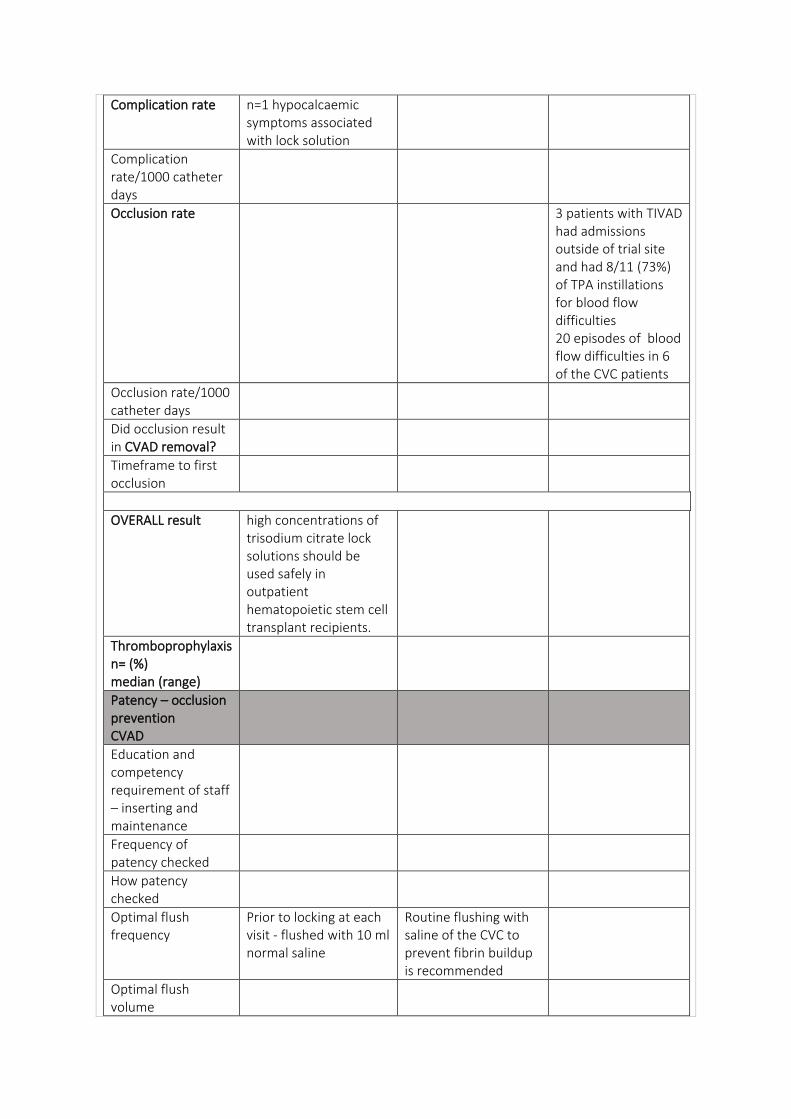
Complication rate n=1 hypocalcaemic symptoms associated with lock solution
Complication rate/1000 catheter days
Occlusion rate 3 patients with TIVAD had admissions outside of trial site and had 8/11 (73%) of TPA instillations for blood flow difficulties 20 episodes of blood flow difficulties in 6 of the CVC patients
Occlusion rate/1000 catheter days
Did occlusion result in CVAD removal?
Timeframe to first occlusion
OVERALL result high concentrations of trisodium citrate lock solutions should be used safely in outpatient hematopoietic stem cell transplant recipients.
Thromboprophylaxis n= (%) median (range)
Patency – occlusion prevention CVAD
Education and competency requirement of staff – inserting and maintenance
Frequency of patency checked
How patency checked
Optimal flush frequency
Prior to locking at each visit - flushed with 10 ml normal saline
Routine flushing with saline of the CVC to prevent fibrin buildup is recommended
Optimal flush volume
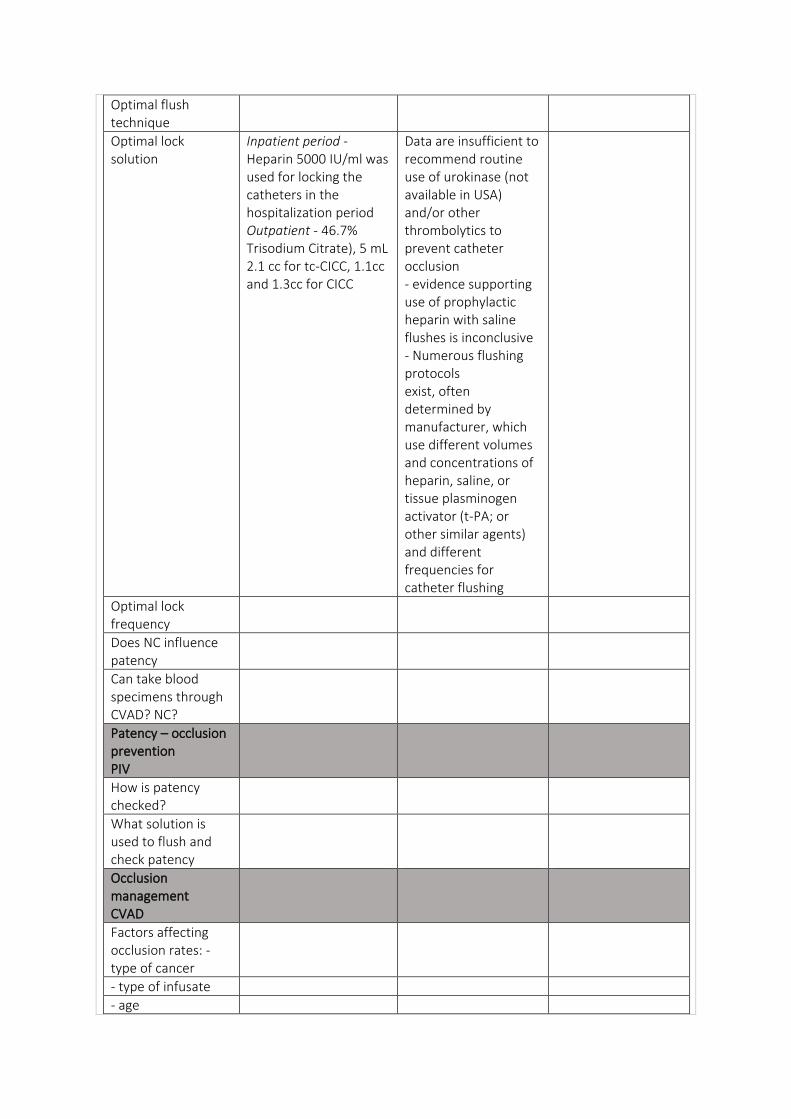
Optimal flush technique
Optimal lock solution
Inpatient period - Heparin 5000 IU/ml was used for locking the catheters in the hospitalization period Outpatient - 46.7% Trisodium Citrate), 5 mL 2.1 cc for tc-CICC, 1.1cc and 1.3cc for CICC
Data are insufficient to recommend routine use of urokinase (not available in USA) and/or other thrombolytics to prevent catheter occlusion - evidence supporting use of prophylactic heparin with saline flushes is inconclusive - Numerous flushing protocols exist, often determined by manufacturer, which use different volumes and concentrations of heparin, saline, or tissue plasminogen activator (t-PA; or other similar agents) and different frequencies for catheter flushing
Optimal lock frequency
Does NC influence patency
Can take blood specimens through CVAD? NC?
Patency – occlusion prevention PIV
How is patency checked?
What solution is used to flush and check patency
Occlusion management CVAD
Factors affecting occlusion rates: - type of cancer
- type of infusate
- age
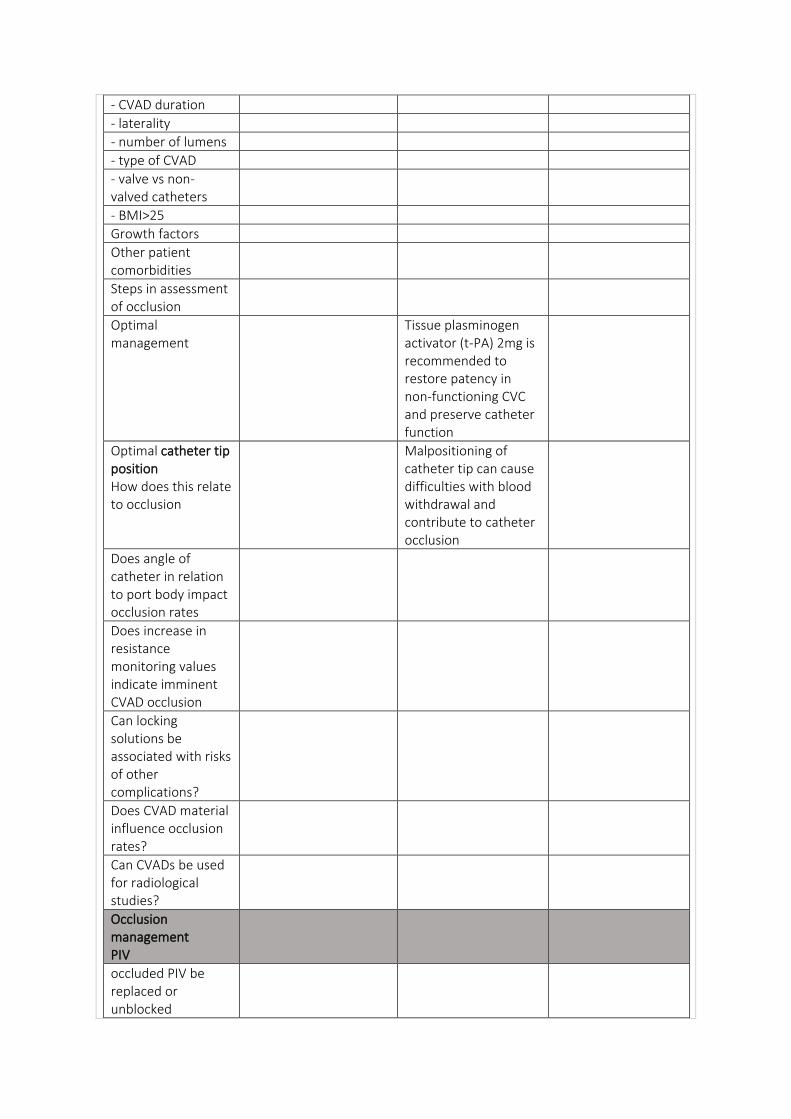
- CVAD duration
- laterality
- number of lumens
- type of CVAD
- valve vs non-valved catheters
- BMI>25
Growth factors
Other patient comorbidities
Steps in assessment of occlusion
Optimal management
Tissue plasminogen activator (t-PA) 2mg is recommended to restore patency in non-functioning CVC and preserve catheter function
Optimal catheter tip position How does this relate to occlusion
Malpositioning of catheter tip can cause difficulties with blood withdrawal and contribute to catheter occlusion
Does angle of catheter in relation to port body impact occlusion rates
Does increase in resistance monitoring values indicate imminent CVAD occlusion
Can locking solutions be associated with risks of other complications?
Does CVAD material influence occlusion rates?
Can CVADs be used for radiological studies?
Occlusion management PIV
occluded PIV be replaced or unblocked
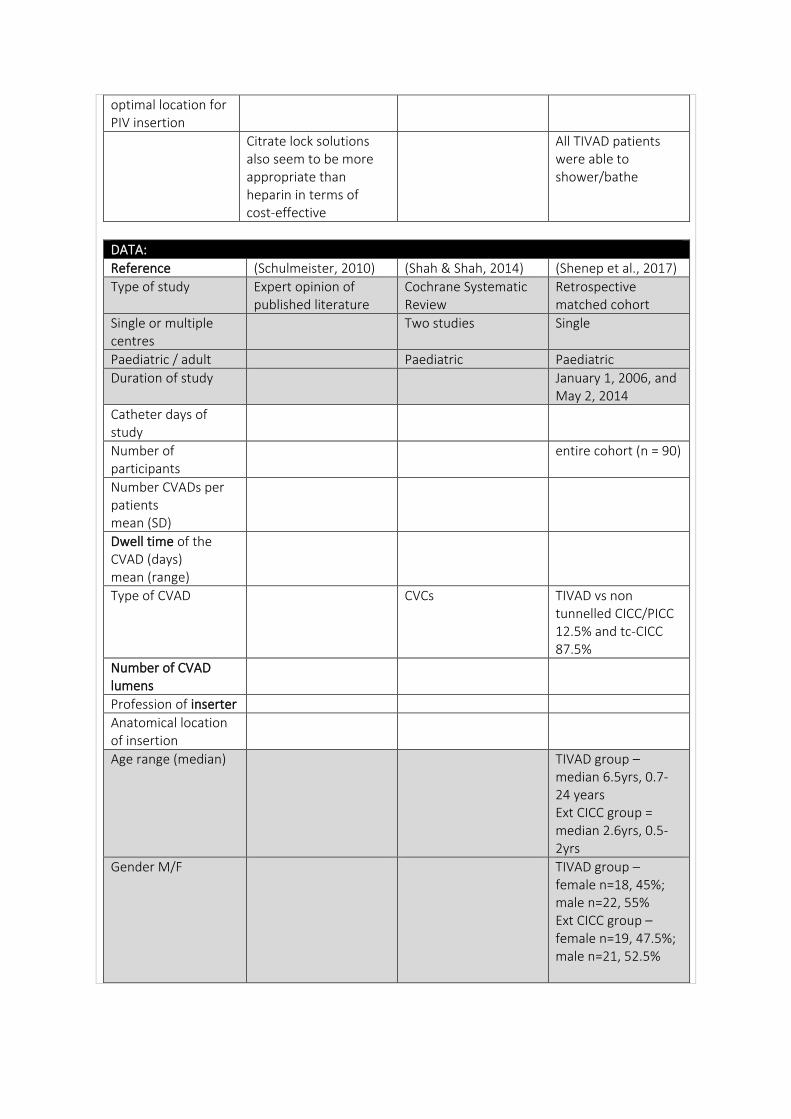
optimal location for PIV insertion
Citrate lock solutions also seem to be more appropriate than heparin in terms of cost-effective
All TIVAD patients were able to shower/bathe
DATA:
Reference (Schulmeister, 2010) (Shah & Shah, 2014) (Shenep et al., 2017)
Type of study Expert opinion of published literature
Cochrane Systematic Review
Retrospective matched cohort
Single or multiple centres
Two studies Single
Paediatric / adult Paediatric Paediatric
Duration of study January 1, 2006, and May 2, 2014
Catheter days of study
Number of participants
entire cohort (n = 90)
Number CVADs per patients mean (SD)
Dwell time of the CVAD (days) mean (range)
Type of CVAD CVCs TIVAD vs non tunnelled CICC/PICC 12.5% and tc-CICC 87.5%
Number of CVAD lumens
Profession of inserter
Anatomical location of insertion
Age range (median) TIVAD group – median 6.5yrs, 0.7-24 years Ext CICC group = median 2.6yrs, 0.5-2yrs
Gender M/F TIVAD group – female n=18, 45%; male n=22, 55% Ext CICC group – female n=19, 47.5%; male n=21, 52.5%
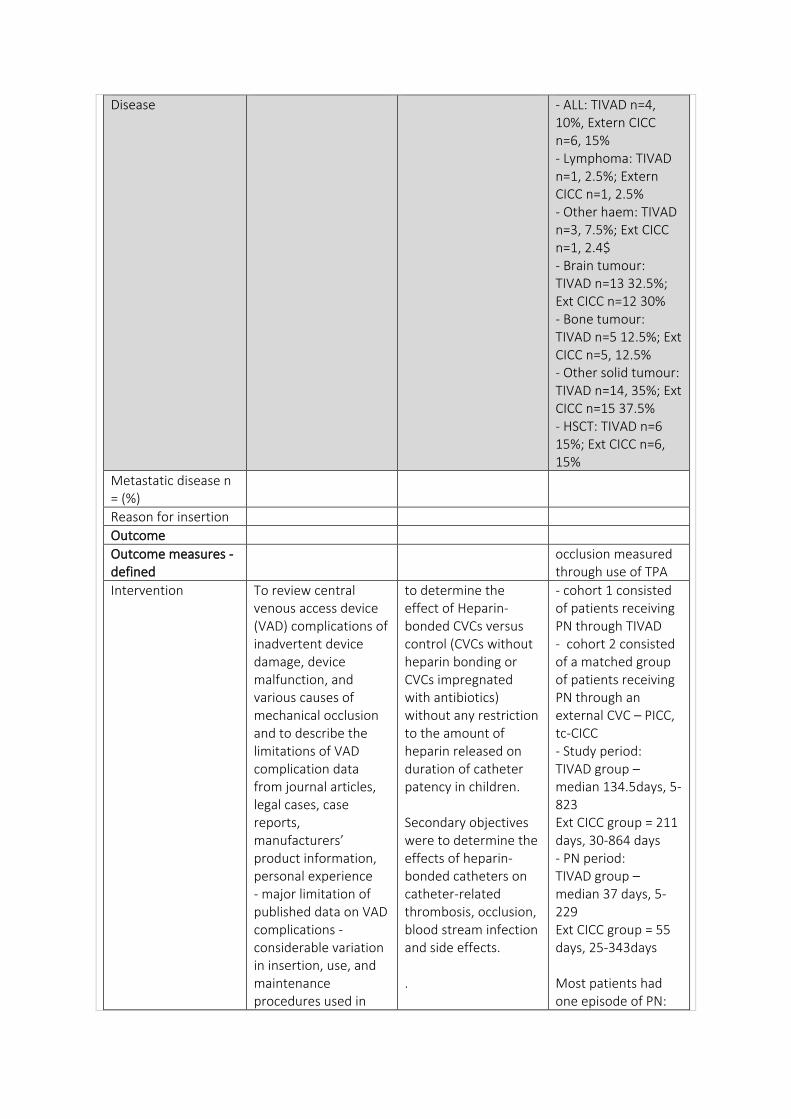
Disease - ALL: TIVAD n=4, 10%, Extern CICC n=6, 15% - Lymphoma: TIVAD n=1, 2.5%; Extern CICC n=1, 2.5% - Other haem: TIVAD n=3, 7.5%; Ext CICC n=1, 2.4$ - Brain tumour: TIVAD n=13 32.5%; Ext CICC n=12 30% - Bone tumour: TIVAD n=5 12.5%; Ext CICC n=5, 12.5% - Other solid tumour: TIVAD n=14, 35%; Ext CICC n=15 37.5% - HSCT: TIVAD n=6 15%; Ext CICC n=6, 15%
Metastatic disease n = (%)
Reason for insertion
Outcome
Outcome measures - defined
occlusion measured through use of TPA
Intervention To review central venous access device (VAD) complications of inadvertent device damage, device malfunction, and various causes of mechanical occlusion and to describe the limitations of VAD complication data from journal articles, legal cases, case reports, manufacturers’ product information, personal experience - major limitation of published data on VAD complications - considerable variation in insertion, use, and maintenance procedures used in
to determine the effect of Heparin-bonded CVCs versus control (CVCs without heparin bonding or CVCs impregnated with antibiotics) without any restriction to the amount of heparin released on duration of catheter patency in children. Secondary objectives were to determine the effects of heparin-bonded catheters on catheter-related thrombosis, occlusion, blood stream infection and side effects. .
- cohort 1 consisted of patients receiving PN through TIVAD - cohort 2 consisted of a matched group of patients receiving PN through an external CVC – PICC, tc-CICC - Study period: TIVAD group – median 134.5days, 5-823 Ext CICC group = 211 days, 30-864 days - PN period: TIVAD group – median 37 days, 5-229 Ext CICC group = 55 days, 25-343days Most patients had one episode of PN:
clinical practice. Another is that experiences have primarily been reported from a single or small number of institutions. Complication statistics also often include patients with diagnoses other than cancer. Therefore, findings cannot be generalized to all practice settings or oncology patient populations
TIVAD n=32, 80%; Ext CICC n=31, 77.5% Most pts had continuous PN: TIVAD 67.5%, Ext CICC 55%
Insertion care
Maintenance care (dedicated CVAD team, ward staff or patient)
Inclusion criteria Children (from birth to 18 years) who required CVCs. randomized and quasi-randomized controlled trials,
Exclusion criteria
Randomisation 50 consecutive individuals identified for cohort 1 (PN administered through TIVAD), and matched participants were sought by chart review to cohort 2 (PN administered through an external CVC), according to algorithm developed to identify a well-matched cohort-participants were matched on 1:1 basis.
Healthcare setting St. Jude Children’s Research Hospital, 68-bed pediatric oncology referral center, USA
Duration of follow up, lost to follow up
RESULTS:
Complication rate
Complication rate/1000 catheter days
Occlusion rate non-PN period - occlusion appeared to be less frequent in children with ports than those with external CVCs PN period - no significant difference in absolute complication rates according to CVC type because of markedly greater increase of risk in children with ports
Occlusion rate/1000 catheter days
One study - statistically significant reduction in risk of catheter occlusion after first week of catheter placement in the heparin-bonded catheter group compared to the non-heparin bonded catheter group, after ‘trend towards a reduction’ within one week of catheter placement - second study - a trend towards reduction in risk of catheter occlusion in heparin-bonded catheter group - Both studies were well-conducted with good rigor and low risks of bias, moderate to low for individual outcomes for grading
- TIVAD cohort - 50 participants -21 (42%) experienced at least 1 episode of occlusion; rate of occlusion significantly higher during PN period (RR = 10.0; 95% CI, 4.4– 22.8; 11.3 vs 0.6 events/1000 days) - external CVCs- increase in rate of occlusion (RR = 2.0; 95% CI, 1.0–4.1; 12.7 vs 3.7 events/1000 days) during the PN period
Did occlusion result in CVAD removal?
Timeframe to first occlusion
OVERALL result - no statistically significant difference in duration of catheter patency between heparin-bonded and non-heparin bonded catheters - due to variability in results, the findings of the studies, need to be confirmed in other studies before specific recommendations can be made
- This study confirms there is an increased risk of occlusion associated with PN. - relative increase in rate of occlusion during PN was significantly greater in children with ports than in those with CVCs (RR = 10.0 vs 2.0; RRR = 4.9; 95% CI, 1.6–14.5; p = .004). - important because occlusion events are associated with clinically significant adverse outcomes - up to 20% of occlusion events require CVC replacement, and attempts to clear obstruction can lead to CVC fracture or rupture
Thromboprophylaxis n= (%) median (range)
Patency – occlusion prevention CVAD
Education and competency requirement of staff – inserting and maintenance
Frequency of patency checked
How patency checked
Optimal flush frequency
appropriate and adequate VAD flushing’ between incompatible drugs/infusions
Optimal flush volume ‘
Optimal flush technique
Optimal lock solution
Optimal lock frequency
Does NC influence patency
Can take blood specimens through CVAD? NC?
Patency – occlusion prevention PIV
How is patency checked?
What solution is used to flush and check patency
Occlusion management CVAD
Factors affecting occlusion rates: - type of cancer
- type of infusate
- age
- CVAD duration
- laterality
- number of lumens
- type of CVAD
- valve vs non-valved catheters
- BMI>25
Growth factors
Other patient comorbidities
Steps in assessment of occlusion
Optimal management Chemical occlusions: agent to bring precipitate back to normal - High pH drug – sodium bicarbonate; low pH drug – hydrochloric acid; lipid esp with silicone (adheres to silicone) – ethyl alcohol
Optimal catheter tip position
Low in SVC
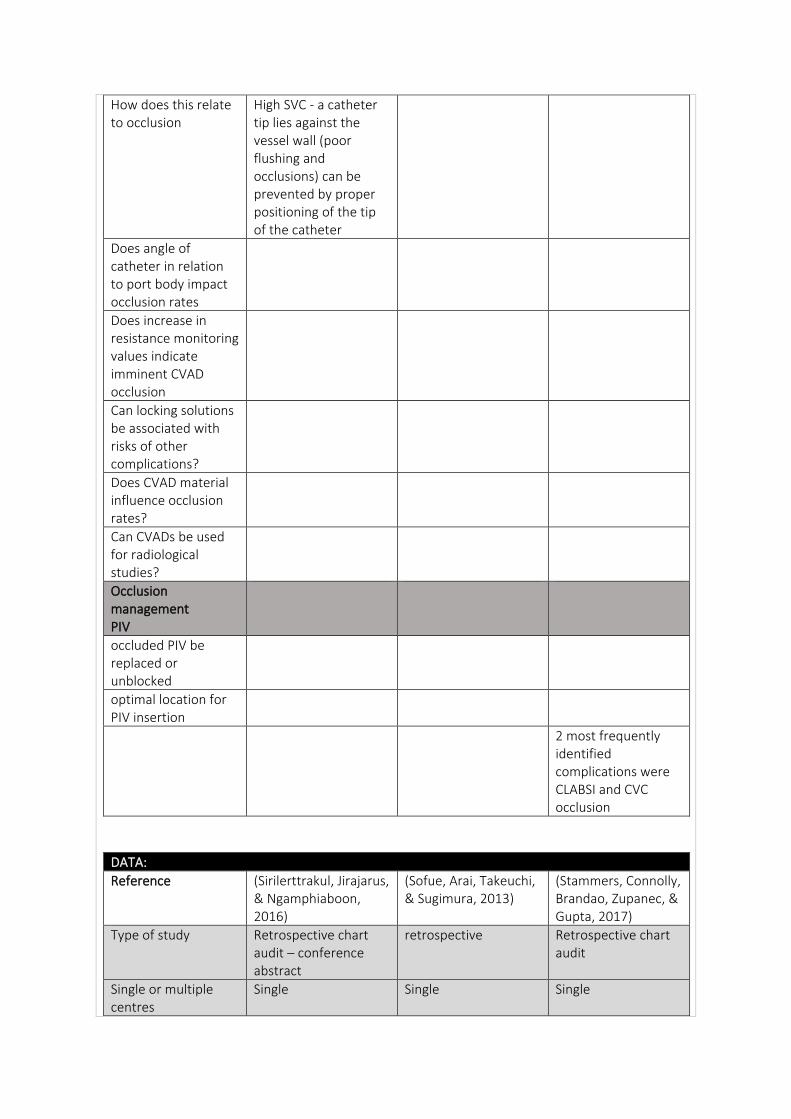
How does this relate to occlusion
High SVC - a catheter tip lies against the vessel wall (poor flushing and occlusions) can be prevented by proper positioning of the tip of the catheter
Does angle of catheter in relation to port body impact occlusion rates
Does increase in resistance monitoring values indicate imminent CVAD occlusion
Can locking solutions be associated with risks of other complications?
Does CVAD material influence occlusion rates?
Can CVADs be used for radiological studies?
Occlusion management PIV
occluded PIV be replaced or unblocked
optimal location for PIV insertion
2 most frequently identified complications were CLABSI and CVC occlusion
DATA:
Reference (Sirilerttrakul, Jirajarus, & Ngamphiaboon, 2016)
(Sofue, Arai, Takeuchi, & Sugimura, 2013)
(Stammers, Connolly, Brandao, Zupanec, & Gupta, 2017)
Type of study Retrospective chart audit – conference abstract
retrospective Retrospective chart audit
Single or multiple centres
Single Single Single
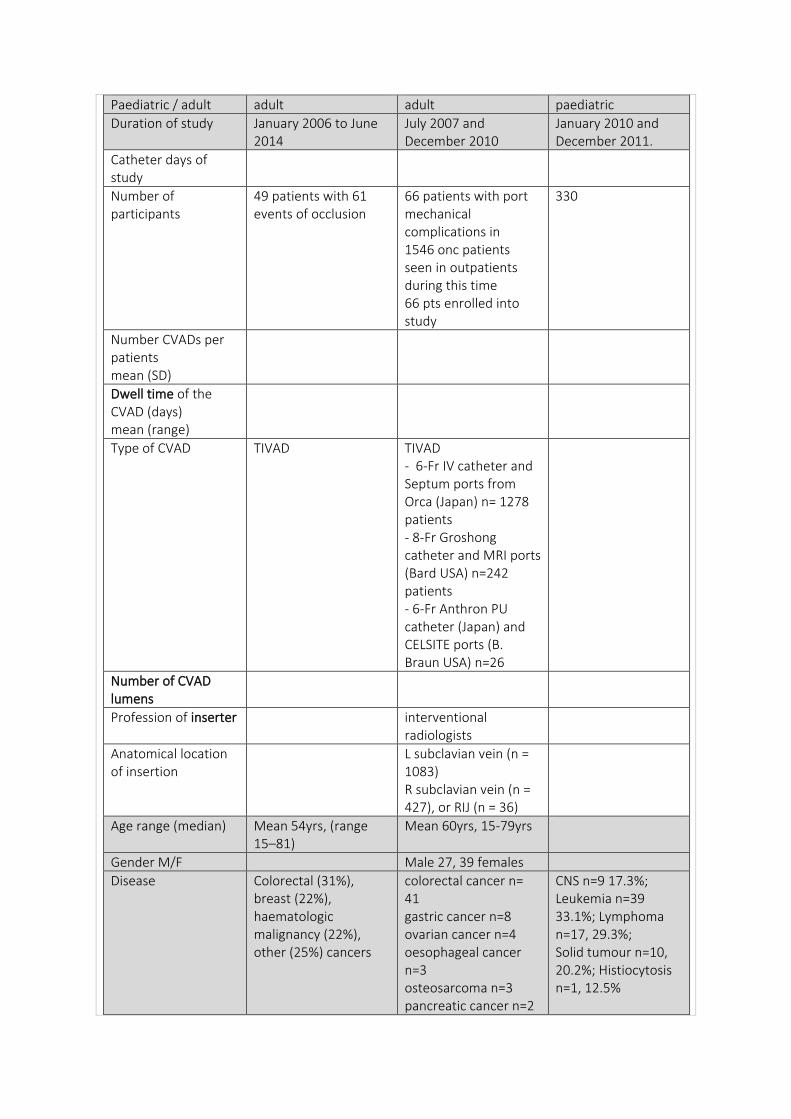
Paediatric / adult adult adult paediatric
Duration of study January 2006 to June 2014
July 2007 and December 2010
January 2010 and December 2011.
Catheter days of study
Number of participants
49 patients with 61 events of occlusion
66 patients with port mechanical complications in 1546 onc patients seen in outpatients during this time 66 pts enrolled into study
330
Number CVADs per patients mean (SD)
Dwell time of the CVAD (days) mean (range)
Type of CVAD TIVAD TIVAD - 6-Fr IV catheter and Septum ports from Orca (Japan) n= 1278 patients - 8-Fr Groshong catheter and MRI ports (Bard USA) n=242 patients - 6-Fr Anthron PU catheter (Japan) and CELSITE ports (B. Braun USA) n=26
Number of CVAD lumens
Profession of inserter interventional radiologists
Anatomical location of insertion
L subclavian vein (n = 1083) R subclavian vein (n = 427), or RIJ (n = 36)
Age range (median) Mean 54yrs, (range 15–81)
Mean 60yrs, 15-79yrs
Gender M/F Male 27, 39 females
Disease Colorectal (31%), breast (22%), haematologic malignancy (22%), other (25%) cancers
colorectal cancer n= 41 gastric cancer n=8 ovarian cancer n=4 oesophageal cancer n=3 osteosarcoma n=3 pancreatic cancer n=2
CNS n=9 17.3%; Leukemia n=39 33.1%; Lymphoma n=17, 29.3%; Solid tumour n=10, 20.2%; Histiocytosis n=1, 12.5%
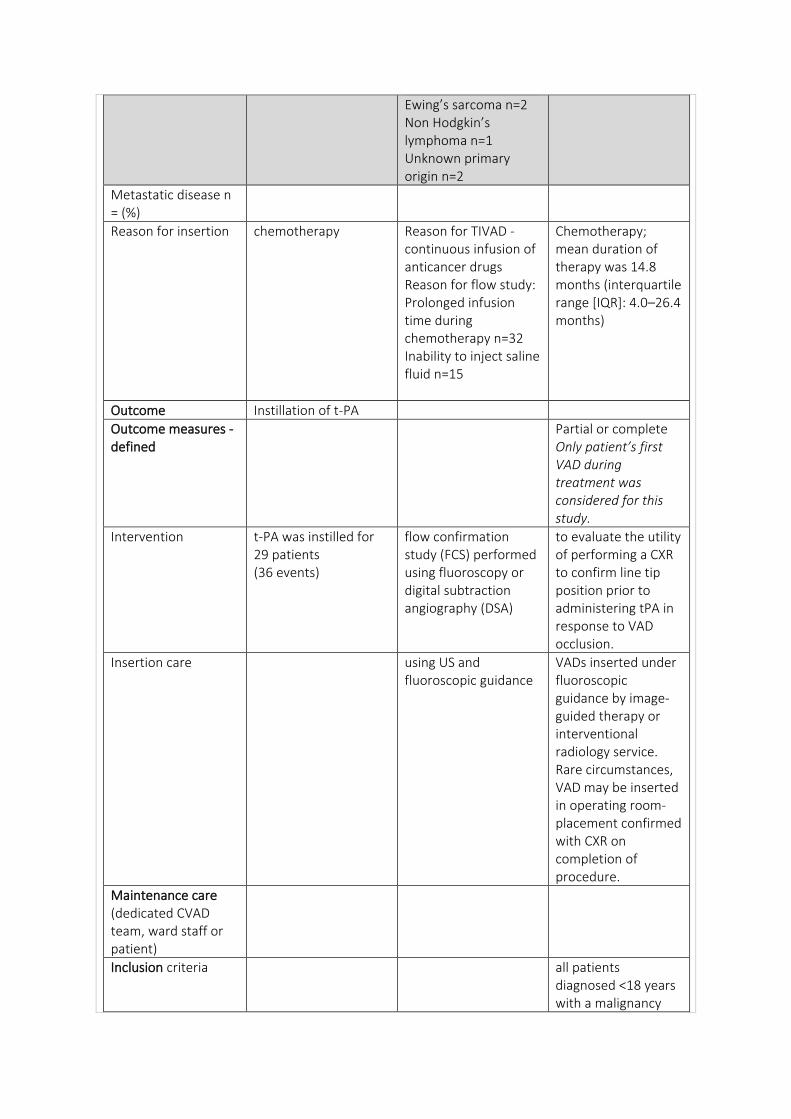
Ewing’s sarcoma n=2 Non Hodgkin’s lymphoma n=1 Unknown primary origin n=2
Metastatic disease n = (%)
Reason for insertion chemotherapy Reason for TIVAD - continuous infusion of anticancer drugs Reason for flow study: Prolonged infusion time during chemotherapy n=32 Inability to inject saline fluid n=15
Chemotherapy; mean duration of therapy was 14.8 months (interquartile range [IQR]: 4.0–26.4 months)
Outcome Instillation of t-PA
Outcome measures - defined
Partial or complete Only patient’s first VAD during treatment was considered for this study.
Intervention t-PA was instilled for 29 patients (36 events)
flow confirmation study (FCS) performed using fluoroscopy or digital subtraction angiography (DSA)
to evaluate the utility of performing a CXR to confirm line tip position prior to administering tPA in response to VAD occlusion.
Insertion care using US and fluoroscopic guidance
VADs inserted under fluoroscopic guidance by image-guided therapy or interventional radiology service. Rare circumstances, VAD may be inserted in operating room- placement confirmed with CXR on completion of procedure.
Maintenance care (dedicated CVAD team, ward staff or patient)
Inclusion criteria all patients diagnosed <18 years with a malignancy
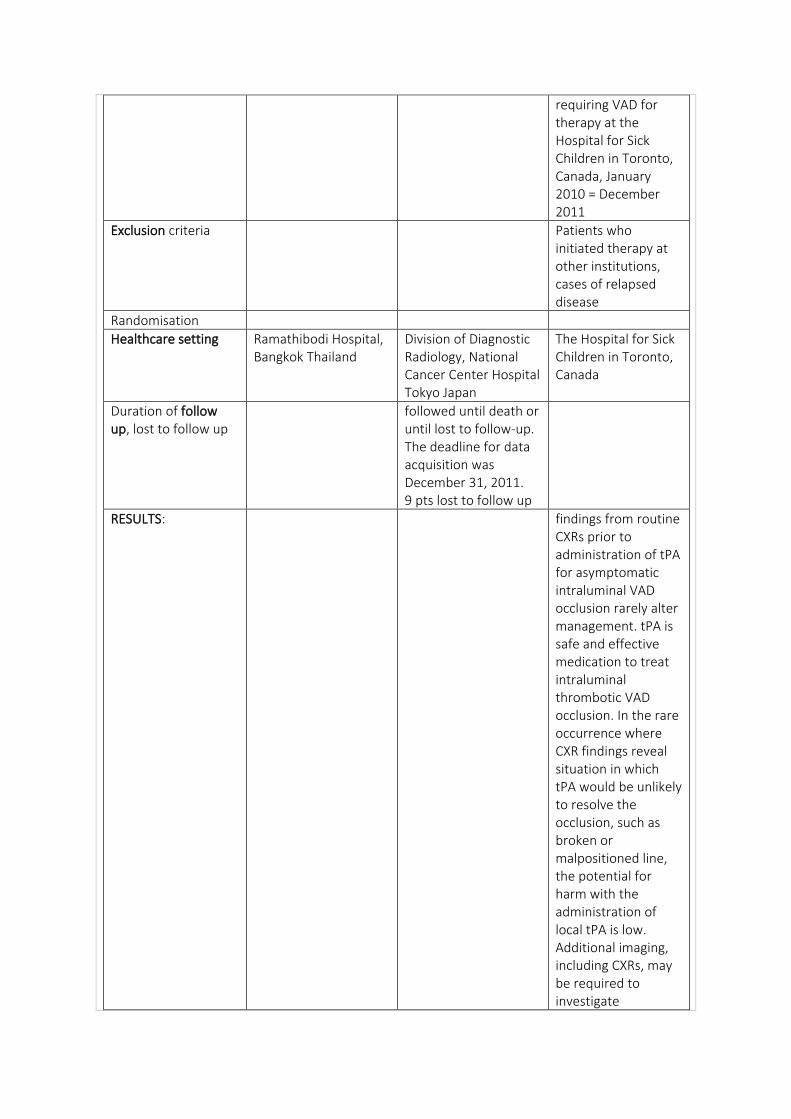
requiring VAD for therapy at the Hospital for Sick Children in Toronto, Canada, January 2010 = December 2011
Exclusion criteria Patients who initiated therapy at other institutions, cases of relapsed disease
Randomisation
Healthcare setting Ramathibodi Hospital, Bangkok Thailand
Division of Diagnostic Radiology, National Cancer Center Hospital Tokyo Japan
The Hospital for Sick Children in Toronto, Canada
Duration of follow up, lost to follow up
followed until death or until lost to follow-up. The deadline for data acquisition was December 31, 2011. 9 pts lost to follow up
RESULTS: findings from routine CXRs prior to administration of tPA for asymptomatic intraluminal VAD occlusion rarely alter management. tPA is safe and effective medication to treat intraluminal thrombotic VAD occlusion. In the rare occurrence where CXR findings reveal situation in which tPA would be unlikely to resolve the occlusion, such as broken or malpositioned line, the potential for harm with the administration of local tPA is low. Additional imaging, including CXRs, may be required to investigate
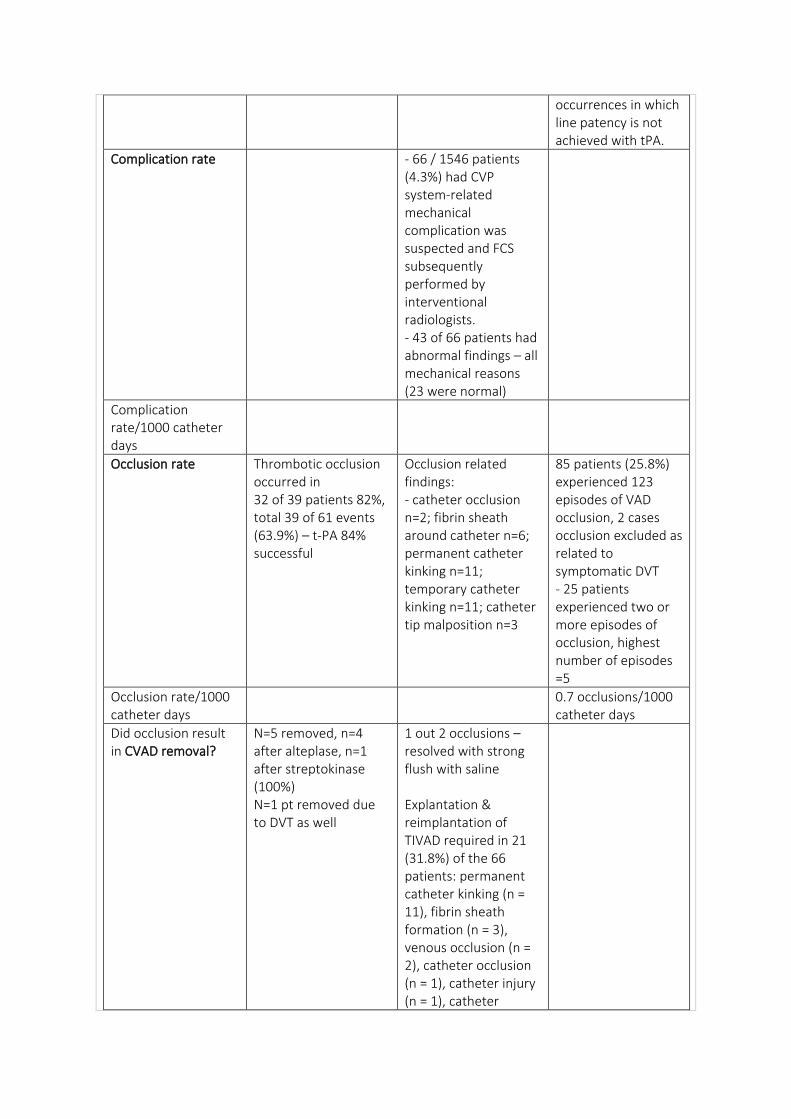
occurrences in which line patency is not achieved with tPA.
Complication rate - 66 / 1546 patients (4.3%) had CVP system-related mechanical complication was suspected and FCS subsequently performed by interventional radiologists. - 43 of 66 patients had abnormal findings – all mechanical reasons (23 were normal)
Complication rate/1000 catheter days
Occlusion rate Thrombotic occlusion occurred in 32 of 39 patients 82%, total 39 of 61 events (63.9%) – t-PA 84% successful
Occlusion related findings: - catheter occlusion n=2; fibrin sheath around catheter n=6; permanent catheter kinking n=11; temporary catheter kinking n=11; catheter tip malposition n=3
85 patients (25.8%) experienced 123 episodes of VAD occlusion, 2 cases occlusion excluded as related to symptomatic DVT - 25 patients experienced two or more episodes of occlusion, highest number of episodes =5
Occlusion rate/1000 catheter days
0.7 occlusions/1000 catheter days
Did occlusion result in CVAD removal?
N=5 removed, n=4 after alteplase, n=1 after streptokinase (100%) N=1 pt removed due to DVT as well
1 out 2 occlusions – resolved with strong flush with saline Explantation & reimplantation of TIVAD required in 21 (31.8%) of the 66 patients: permanent catheter kinking (n = 11), fibrin sheath formation (n = 3), venous occlusion (n = 2), catheter occlusion (n = 1), catheter injury (n = 1), catheter
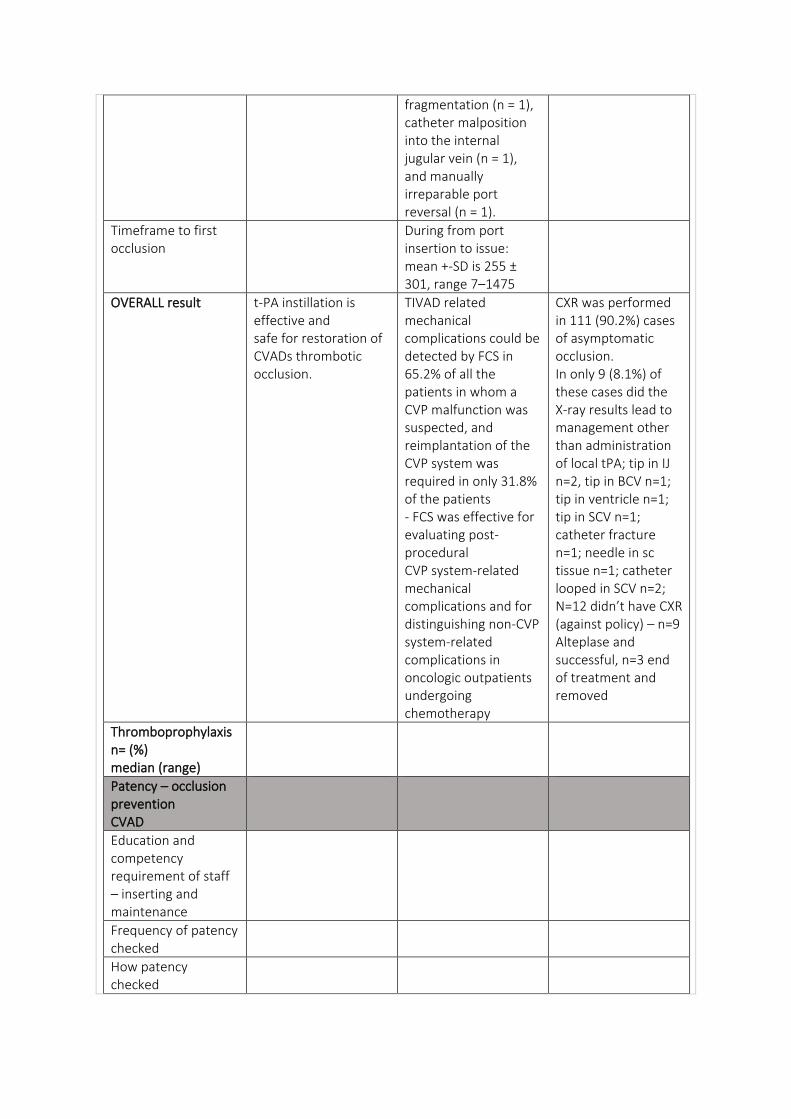
fragmentation (n = 1), catheter malposition into the internal jugular vein (n = 1), and manually irreparable port reversal (n = 1).
Timeframe to first occlusion
During from port insertion to issue: mean +-SD is 255 ± 301, range 7–1475
OVERALL result t-PA instillation is effective and safe for restoration of CVADs thrombotic occlusion.
TIVAD related mechanical complications could be detected by FCS in 65.2% of all the patients in whom a CVP malfunction was suspected, and reimplantation of the CVP system was required in only 31.8% of the patients - FCS was effective for evaluating post-procedural CVP system-related mechanical complications and for distinguishing non-CVP system-related complications in oncologic outpatients undergoing chemotherapy
CXR was performed in 111 (90.2%) cases of asymptomatic occlusion. In only 9 (8.1%) of these cases did the X-ray results lead to management other than administration of local tPA; tip in IJ n=2, tip in BCV n=1; tip in ventricle n=1; tip in SCV n=1; catheter fracture n=1; needle in sc tissue n=1; catheter looped in SCV n=2; N=12 didn’t have CXR (against policy) – n=9 Alteplase and successful, n=3 end of treatment and removed
Thromboprophylaxis n= (%) median (range)
Patency – occlusion prevention CVAD
Education and competency requirement of staff – inserting and maintenance
Frequency of patency checked
How patency checked
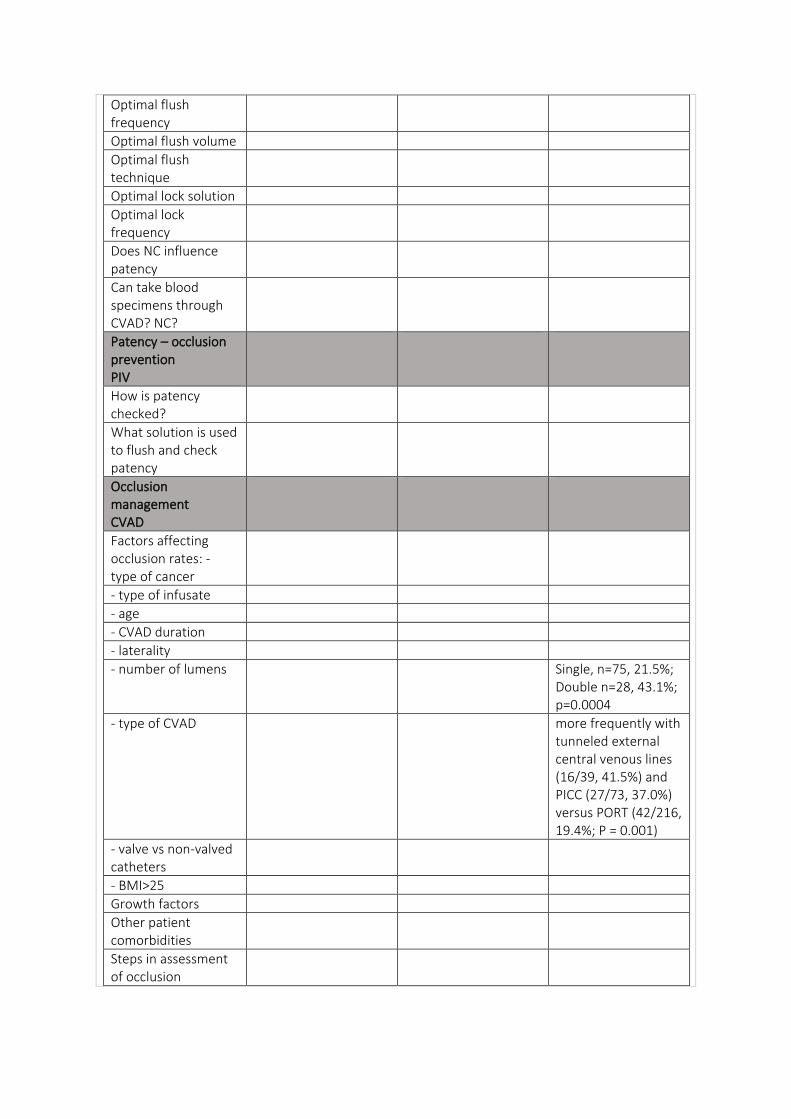
Optimal flush frequency
Optimal flush volume
Optimal flush technique
Optimal lock solution
Optimal lock frequency
Does NC influence patency
Can take blood specimens through CVAD? NC?
Patency – occlusion prevention PIV
How is patency checked?
What solution is used to flush and check patency
Occlusion management CVAD
Factors affecting occlusion rates: - type of cancer
- type of infusate
- age
- CVAD duration
- laterality
- number of lumens Single, n=75, 21.5%; Double n=28, 43.1%; p=0.0004
- type of CVAD more frequently with tunneled external central venous lines (16/39, 41.5%) and PICC (27/73, 37.0%) versus PORT (42/216, 19.4%; P = 0.001)
- valve vs non-valved catheters
- BMI>25
Growth factors
Other patient comorbidities
Steps in assessment of occlusion
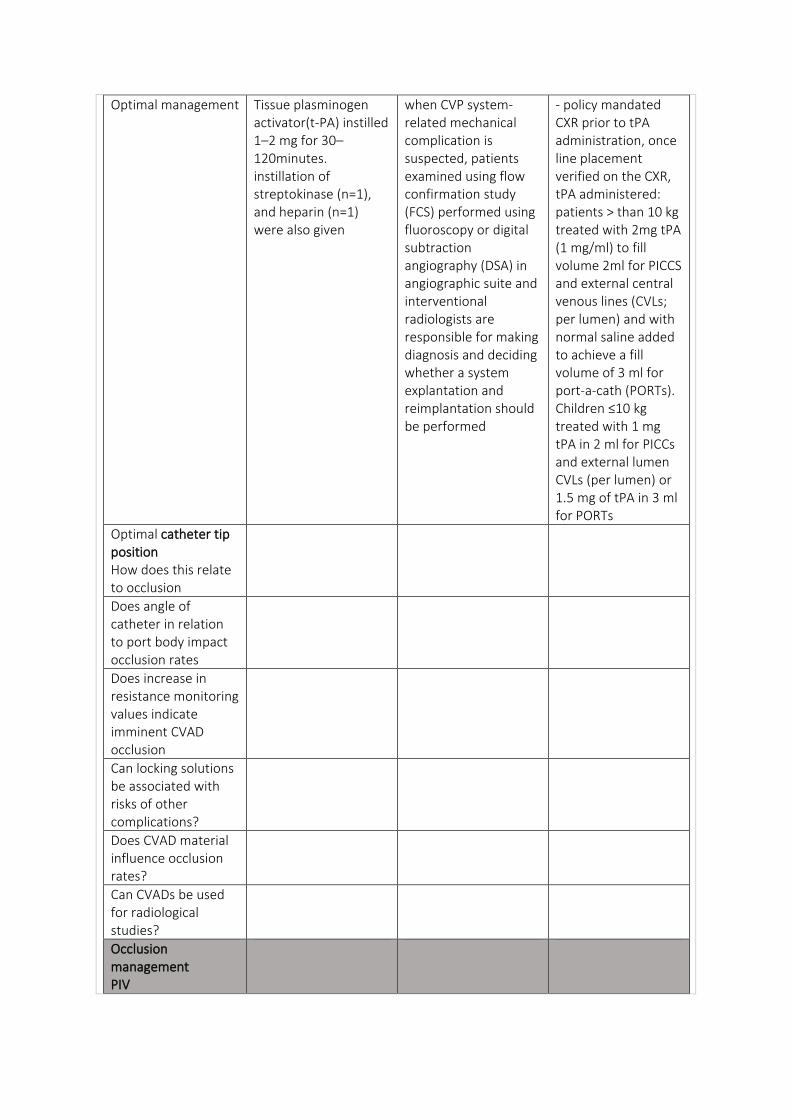
Optimal management Tissue plasminogen activator(t-PA) instilled 1–2 mg for 30–120minutes. instillation of streptokinase (n=1), and heparin (n=1) were also given
when CVP system-related mechanical complication is suspected, patients examined using flow confirmation study (FCS) performed using fluoroscopy or digital subtraction angiography (DSA) in angiographic suite and interventional radiologists are responsible for making diagnosis and deciding whether a system explantation and reimplantation should be performed
- policy mandated CXR prior to tPA administration, once line placement verified on the CXR, tPA administered: patients > than 10 kg treated with 2mg tPA (1 mg/ml) to fill volume 2ml for PICCS and external central venous lines (CVLs; per lumen) and with normal saline added to achieve a fill volume of 3 ml for port-a-cath (PORTs). Children ≤10 kg treated with 1 mg tPA in 2 ml for PICCs and external lumen CVLs (per lumen) or 1.5 mg of tPA in 3 ml for PORTs
Optimal catheter tip position How does this relate to occlusion
Does angle of catheter in relation to port body impact occlusion rates
Does increase in resistance monitoring values indicate imminent CVAD occlusion
Can locking solutions be associated with risks of other complications?
Does CVAD material influence occlusion rates?
Can CVADs be used for radiological studies?
Occlusion management PIV
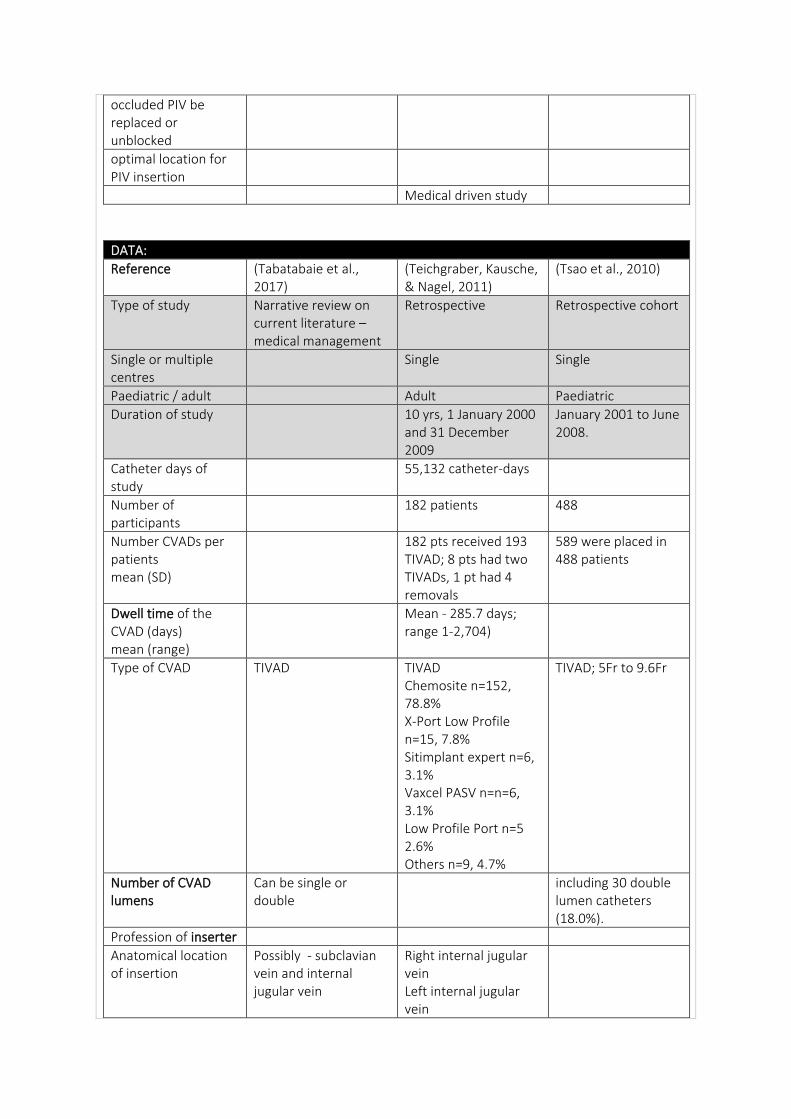
occluded PIV be replaced or unblocked
optimal location for PIV insertion
Medical driven study
DATA:
Reference (Tabatabaie et al., 2017)
(Teichgraber, Kausche, & Nagel, 2011)
(Tsao et al., 2010)
Type of study Narrative review on current literature – medical management
Retrospective Retrospective cohort
Single or multiple centres
Single Single
Paediatric / adult Adult Paediatric
Duration of study 10 yrs, 1 January 2000 and 31 December 2009
January 2001 to June 2008.
Catheter days of study
55,132 catheter-days
Number of participants
182 patients 488
Number CVADs per patients mean (SD)
182 pts received 193 TIVAD; 8 pts had two TIVADs, 1 pt had 4 removals
589 were placed in 488 patients
Dwell time of the CVAD (days) mean (range)
Mean - 285.7 days; range 1-2,704)
Type of CVAD TIVAD TIVAD Chemosite n=152, 78.8% X-Port Low Profile n=15, 7.8% Sitimplant expert n=6, 3.1% Vaxcel PASV n=n=6, 3.1% Low Profile Port n=5 2.6% Others n=9, 4.7%
TIVAD; 5Fr to 9.6Fr
Number of CVAD lumens
Can be single or double
including 30 double lumen catheters (18.0%).
Profession of inserter
Anatomical location of insertion
Possibly - subclavian vein and internal jugular vein
Right internal jugular vein Left internal jugular vein
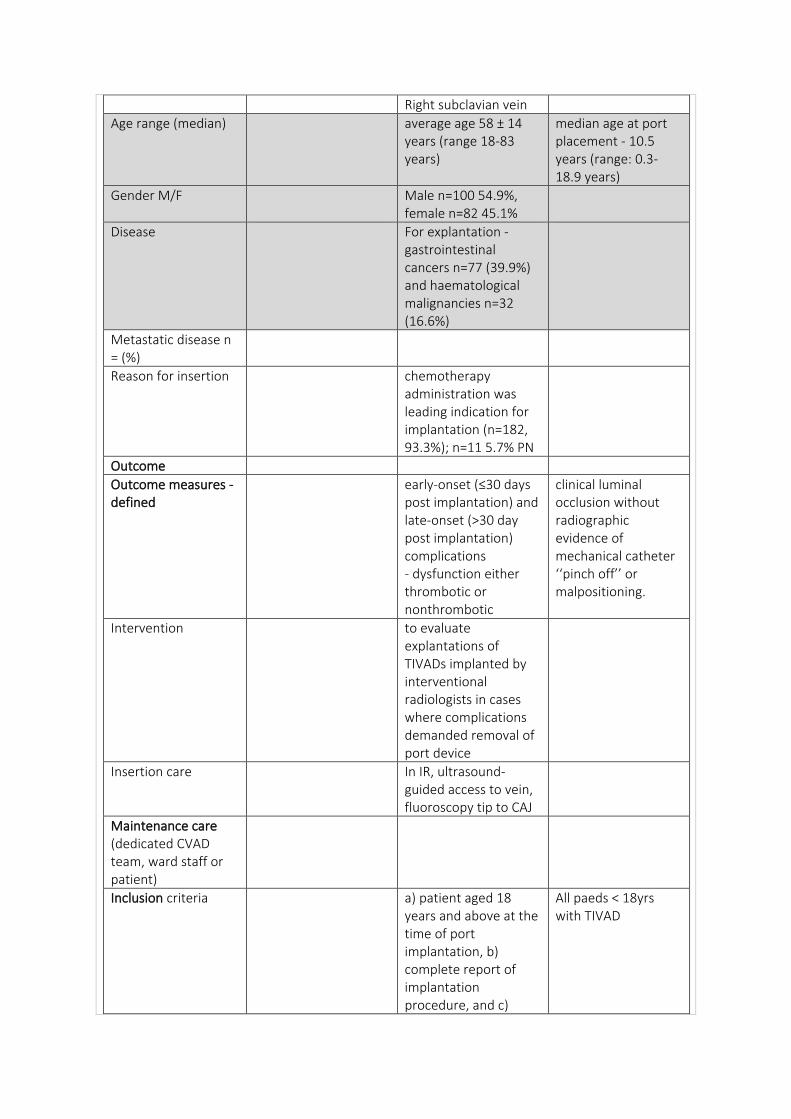
Right subclavian vein
Age range (median) average age 58 ± 14 years (range 18-83 years)
median age at port placement - 10.5 years (range: 0.3-18.9 years)
Gender M/F Male n=100 54.9%, female n=82 45.1%
Disease For explantation - gastrointestinal cancers n=77 (39.9%) and haematological malignancies n=32 (16.6%)
Metastatic disease n = (%)
Reason for insertion chemotherapy administration was leading indication for implantation (n=182, 93.3%); n=11 5.7% PN
Outcome
Outcome measures - defined
early-onset (≤30 days post implantation) and late-onset (>30 day post implantation) complications - dysfunction either thrombotic or nonthrombotic
clinical luminal occlusion without radiographic evidence of mechanical catheter ‘‘pinch off’’ or malpositioning.
Intervention to evaluate explantations of TIVADs implanted by interventional radiologists in cases where complications demanded removal of port device
Insertion care In IR, ultrasound-guided access to vein, fluoroscopy tip to CAJ
Maintenance care (dedicated CVAD team, ward staff or patient)
Inclusion criteria a) patient aged 18 years and above at the time of port implantation, b) complete report of implantation procedure, and c)
All paeds < 18yrs with TIVAD
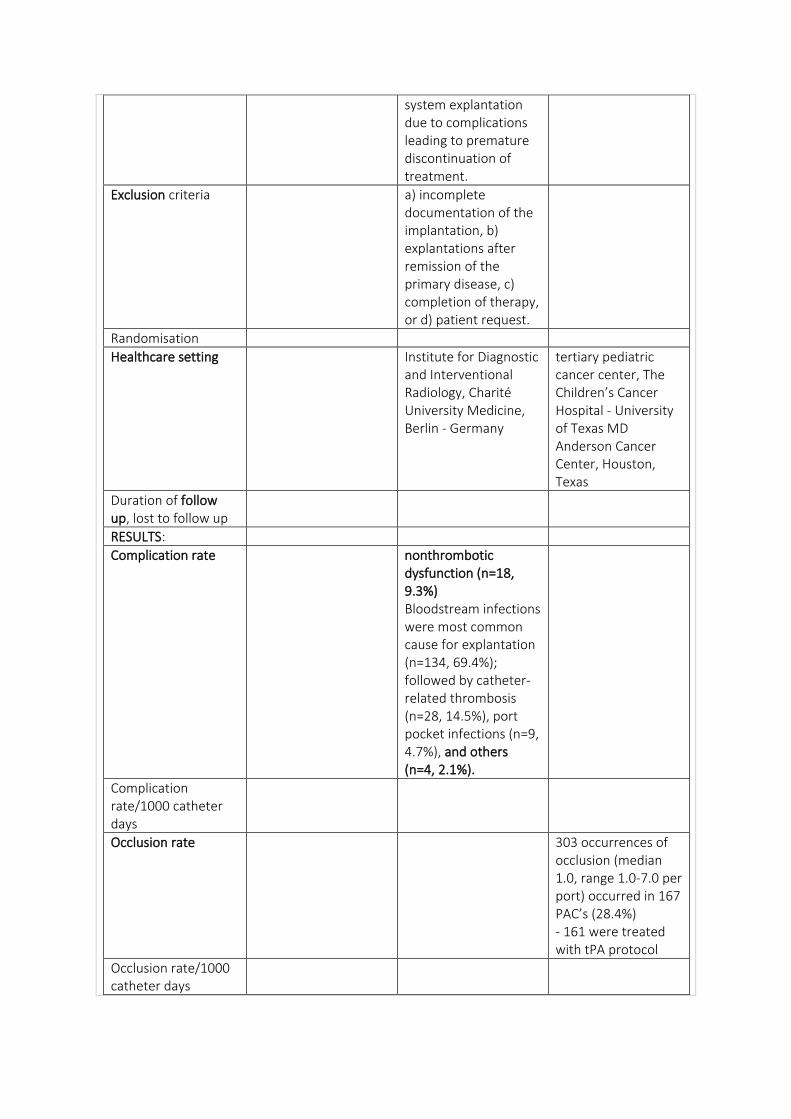
system explantation due to complications leading to premature discontinuation of treatment.
Exclusion criteria a) incomplete documentation of the implantation, b) explantations after remission of the primary disease, c) completion of therapy, or d) patient request.
Randomisation
Healthcare setting Institute for Diagnostic and Interventional Radiology, Charité University Medicine, Berlin - Germany
tertiary pediatric cancer center, The Children’s Cancer Hospital - University of Texas MD Anderson Cancer Center, Houston, Texas
Duration of follow up, lost to follow up
RESULTS:
Complication rate nonthrombotic dysfunction (n=18, 9.3%) Bloodstream infections were most common cause for explantation (n=134, 69.4%); followed by catheter-related thrombosis (n=28, 14.5%), port pocket infections (n=9, 4.7%), and others (n=4, 2.1%).
Complication rate/1000 catheter days
Occlusion rate 303 occurrences of occlusion (median 1.0, range 1.0-7.0 per port) occurred in 167 PAC’s (28.4%) - 161 were treated with tPA protocol
Occlusion rate/1000 catheter days
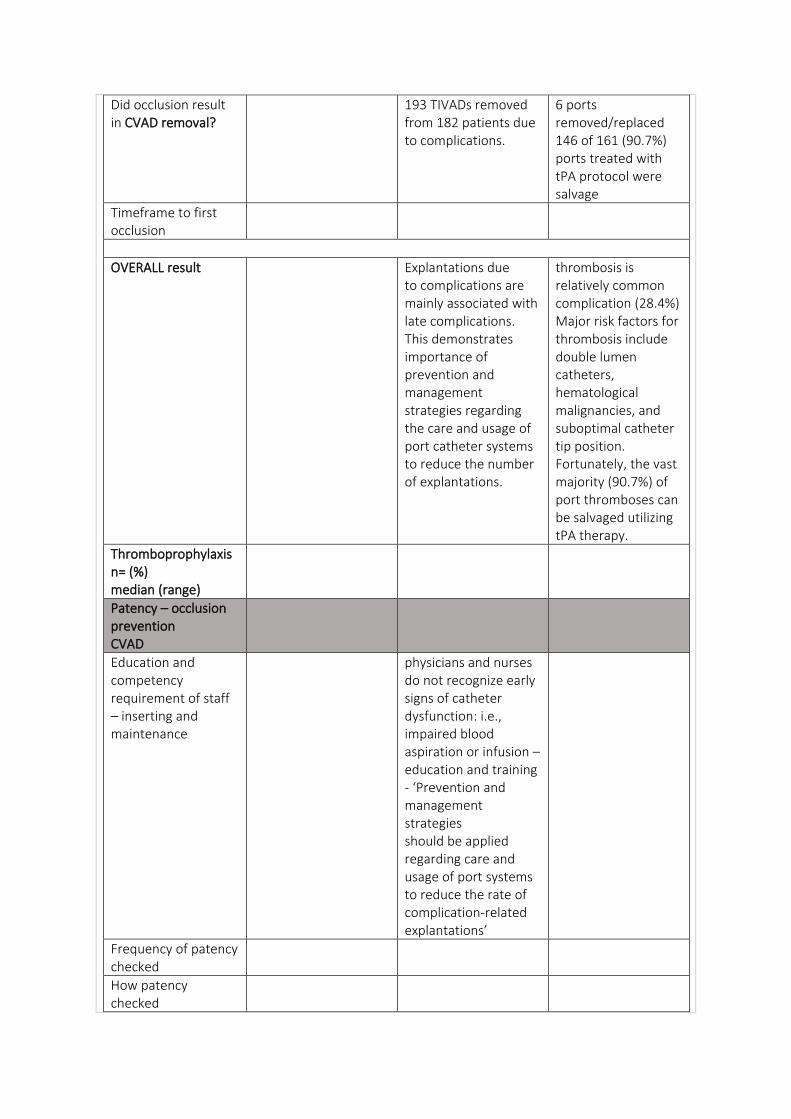
Did occlusion result in CVAD removal?
193 TIVADs removed from 182 patients due to complications.
6 ports removed/replaced 146 of 161 (90.7%) ports treated with tPA protocol were salvage
Timeframe to first occlusion
OVERALL result Explantations due to complications are mainly associated with late complications. This demonstrates importance of prevention and management strategies regarding the care and usage of port catheter systems to reduce the number of explantations.
thrombosis is relatively common complication (28.4%) Major risk factors for thrombosis include double lumen catheters, hematological malignancies, and suboptimal catheter tip position. Fortunately, the vast majority (90.7%) of port thromboses can be salvaged utilizing tPA therapy.
Thromboprophylaxis n= (%) median (range)
Patency – occlusion prevention CVAD
Education and competency requirement of staff – inserting and maintenance
physicians and nurses do not recognize early signs of catheter dysfunction: i.e., impaired blood aspiration or infusion – education and training - ‘Prevention and management strategies should be applied regarding care and usage of port systems to reduce the rate of complication-related explantations’
Frequency of patency checked
How patency checked
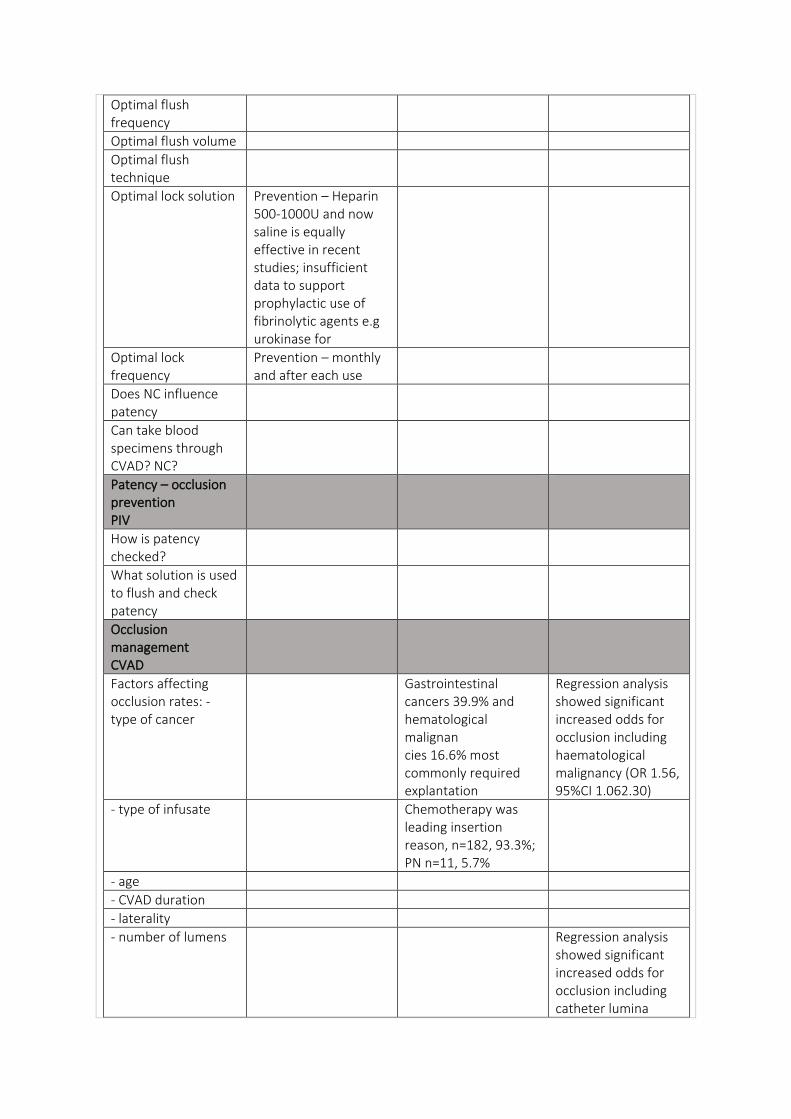
Optimal flush frequency
Optimal flush volume
Optimal flush technique
Optimal lock solution Prevention – Heparin 500-1000U and now saline is equally effective in recent studies; insufficient data to support prophylactic use of fibrinolytic agents e.g urokinase for
Optimal lock frequency
Prevention – monthly and after each use
Does NC influence patency
Can take blood specimens through CVAD? NC?
Patency – occlusion prevention PIV
How is patency checked?
What solution is used to flush and check patency
Occlusion management CVAD
Factors affecting occlusion rates: - type of cancer
Gastrointestinal cancers 39.9% and hematological malignan cies 16.6% most commonly required explantation
Regression analysis showed significant increased odds for occlusion including haematological malignancy (OR 1.56, 95%CI 1.062.30)
- type of infusate Chemotherapy was leading insertion reason, n=182, 93.3%; PN n=11, 5.7%
- age
- CVAD duration
- laterality
- number of lumens Regression analysis showed significant increased odds for occlusion including catheter lumina

(double lumen) - (OR 3.18, 95%CI 1.85-5.48)
- type of CVAD
- valve vs non-valved catheters
- BMI>25
Growth factors
Other patient comorbidities
RIJ (n=161, 83.4%), LIJ (n=29, 15.0%), or R SCV (n=3, 1.6%).
Steps in assessment of occlusion
Optimal management Successful management of port malfunction depends on accurate diagnosis of underlying mechanism – CXR to rule out mechanical, flow studies; solutions for drug precipitation - TPN solutions - 70% ethanol; hydrochloric acid (0.1 mol/L) - calcium phosphate crystals or acidic drug particles; Sodium hydroxide (0.1 mol/L) and sodium bicarbonate (1 mol/L) - alkaline drugs.
protocol utilizing tPA (2 mg/ml) with 30-60 minute dwell time (maximum 2 doses) was utilized.
Optimal catheter tip position How does this relate to occlusion
CAJ, final fluoroscopic image documented correct position of catheter tip at cavoatrial junction.
Regression analysis showed significant increased odds for occlusion including catheter tip malpositioning (OR 1.36, 95%CI 1.02-1.81).
Does angle of catheter in relation to port body impact occlusion rates
Does increase in resistance monitoring values indicate imminent CVAD occlusion
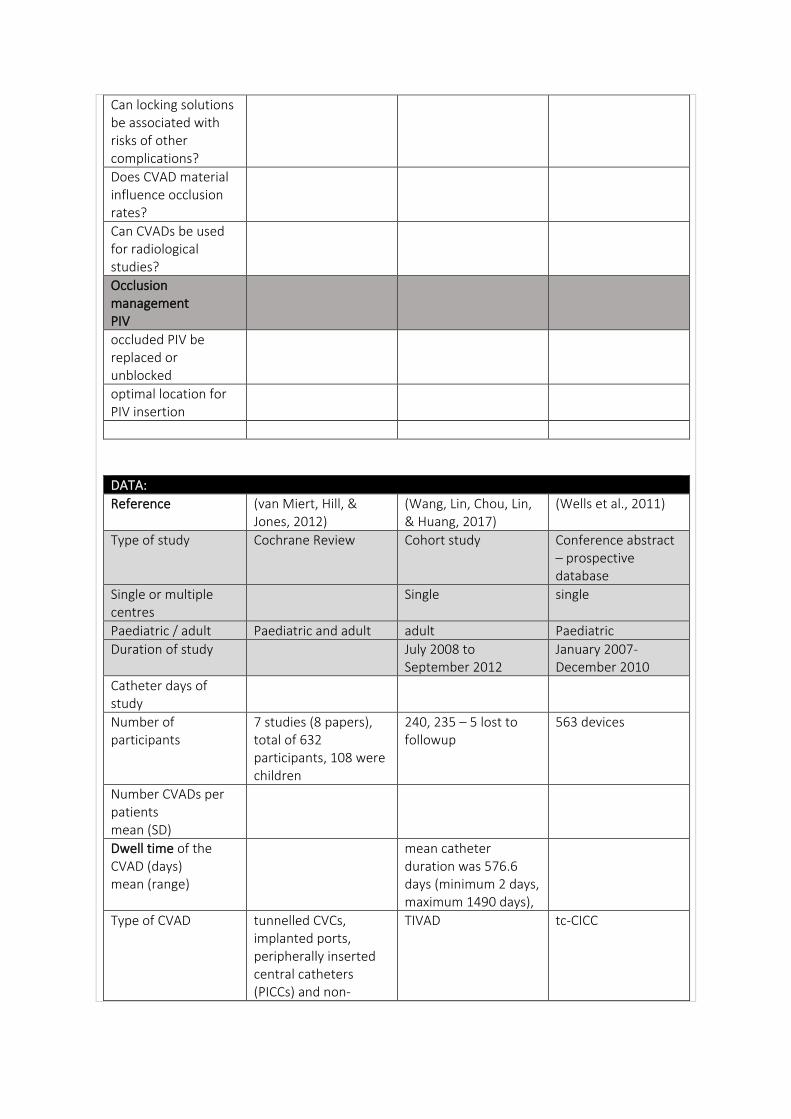
Can locking solutions be associated with risks of other complications?
Does CVAD material influence occlusion rates?
Can CVADs be used for radiological studies?
Occlusion management PIV
occluded PIV be replaced or unblocked
optimal location for PIV insertion
DATA:
Reference (van Miert, Hill, & Jones, 2012)
(Wang, Lin, Chou, Lin, & Huang, 2017)
(Wells et al., 2011)
Type of study Cochrane Review Cohort study Conference abstract – prospective database
Single or multiple centres
Single single
Paediatric / adult Paediatric and adult adult Paediatric
Duration of study July 2008 to September 2012
January 2007-December 2010
Catheter days of study
Number of participants
7 studies (8 papers), total of 632 participants, 108 were children
240, 235 – 5 lost to followup
563 devices
Number CVADs per patients mean (SD)
Dwell time of the CVAD (days) mean (range)
mean catheter duration was 576.6 days (minimum 2 days, maximum 1490 days),
Type of CVAD tunnelled CVCs, implanted ports, peripherally inserted central catheters (PICCs) and non-
TIVAD tc-CICC
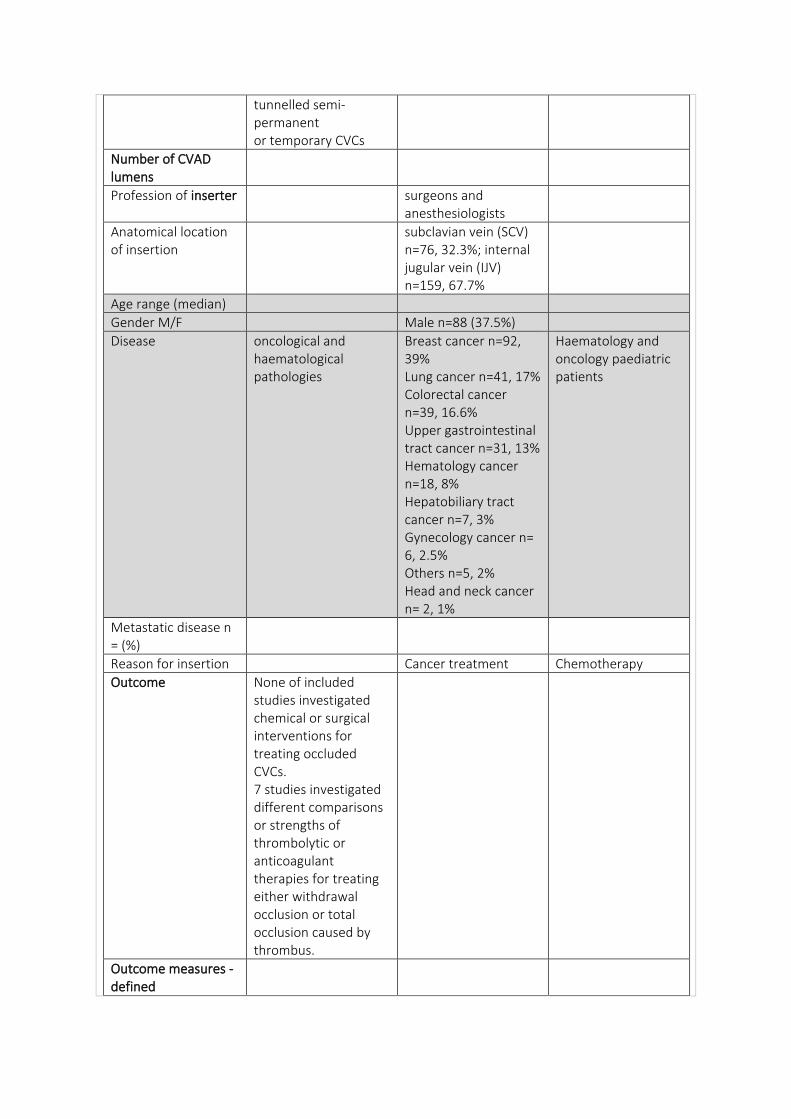
tunnelled semi-permanent or temporary CVCs
Number of CVAD lumens
Profession of inserter surgeons and anesthesiologists
Anatomical location of insertion
subclavian vein (SCV) n=76, 32.3%; internal jugular vein (IJV) n=159, 67.7%
Age range (median)
Gender M/F Male n=88 (37.5%)
Disease oncological and haematological pathologies
Breast cancer n=92, 39% Lung cancer n=41, 17% Colorectal cancer n=39, 16.6% Upper gastrointestinal tract cancer n=31, 13% Hematology cancer n=18, 8% Hepatobiliary tract cancer n=7, 3% Gynecology cancer n= 6, 2.5% Others n=5, 2% Head and neck cancer n= 2, 1%
Haematology and oncology paediatric patients
Metastatic disease n = (%)
Reason for insertion Cancer treatment Chemotherapy
Outcome None of included studies investigated chemical or surgical interventions for treating occluded CVCs. 7 studies investigated different comparisons or strengths of thrombolytic or anticoagulant therapies for treating either withdrawal occlusion or total occlusion caused by thrombus.
Outcome measures - defined
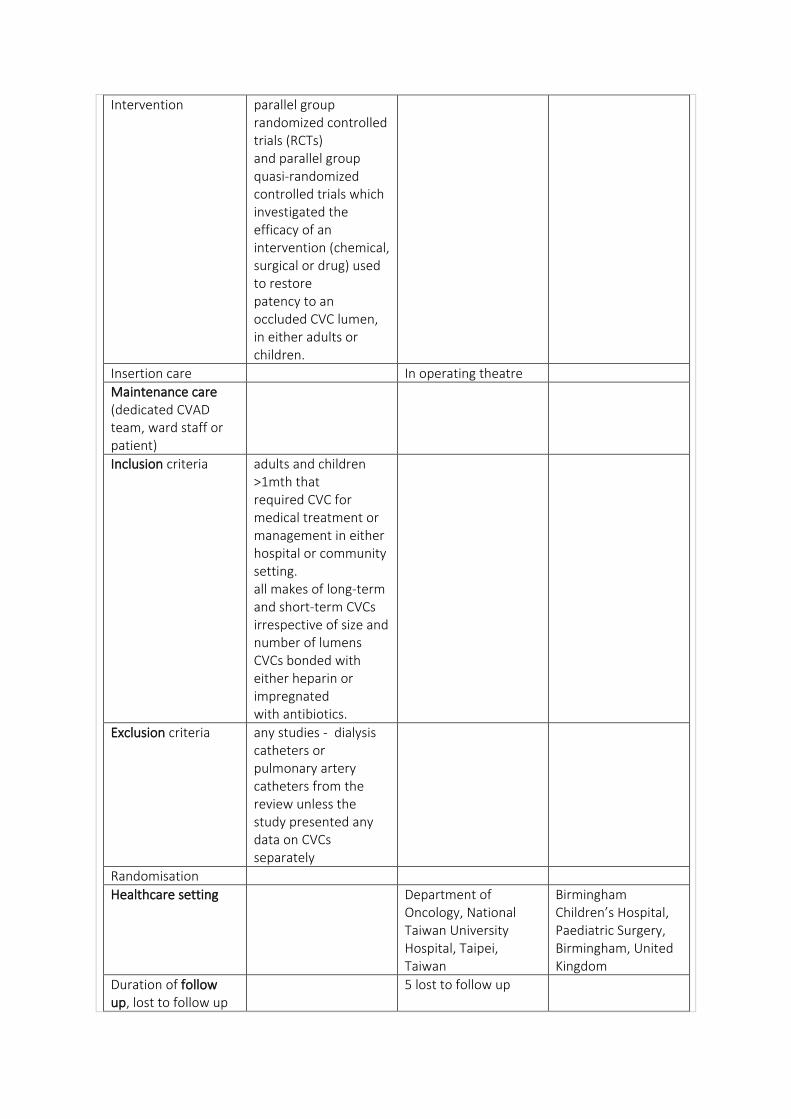
Intervention parallel group randomized controlled trials (RCTs) and parallel group quasi-randomized controlled trials which investigated the efficacy of an intervention (chemical, surgical or drug) used to restore patency to an occluded CVC lumen, in either adults or children.
Insertion care In operating theatre
Maintenance care (dedicated CVAD team, ward staff or patient)
Inclusion criteria adults and children >1mth that required CVC for medical treatment or management in either hospital or community setting. all makes of long-term and short-term CVCs irrespective of size and number of lumens CVCs bonded with either heparin or impregnated with antibiotics.
Exclusion criteria any studies - dialysis catheters or pulmonary artery catheters from the review unless the study presented any data on CVCs separately
Randomisation
Healthcare setting Department of Oncology, National Taiwan University Hospital, Taipei, Taiwan
Birmingham Children’s Hospital, Paediatric Surgery, Birmingham, United Kingdom
Duration of follow up, lost to follow up
5 lost to follow up
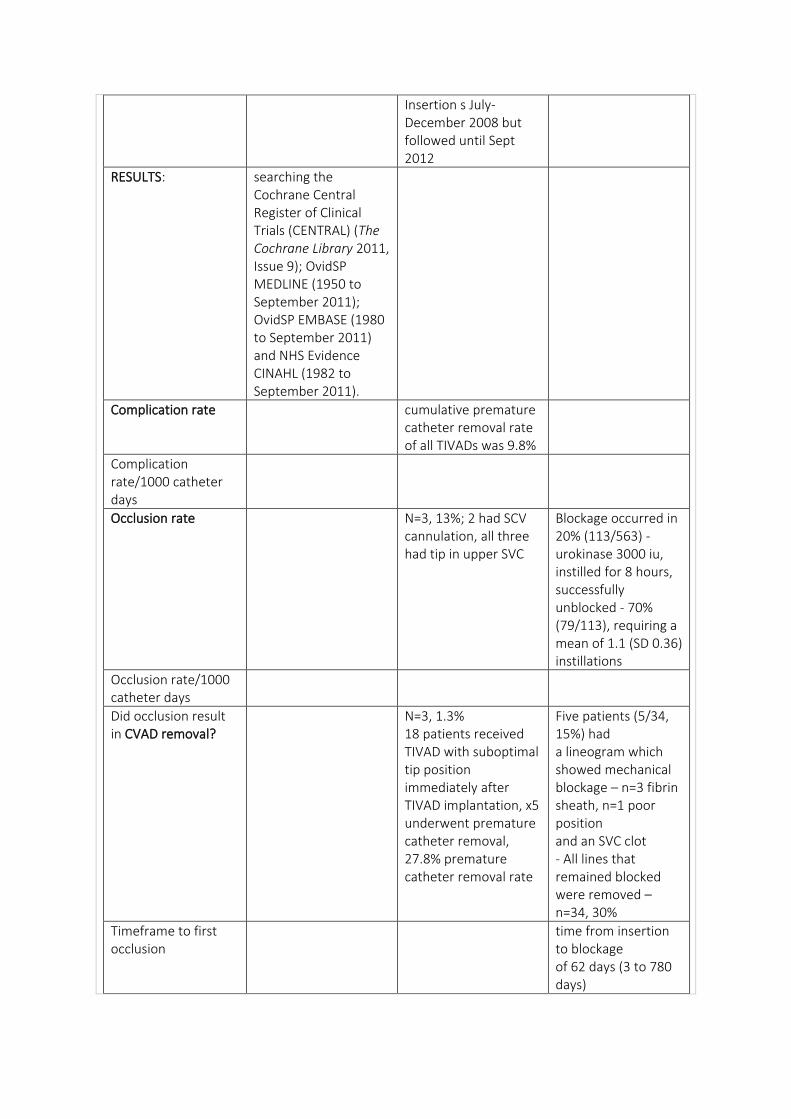
Insertion s July-December 2008 but followed until Sept 2012
RESULTS: searching the Cochrane Central Register of Clinical Trials (CENTRAL) (The Cochrane Library 2011, Issue 9); OvidSP MEDLINE (1950 to September 2011); OvidSP EMBASE (1980 to September 2011) and NHS Evidence CINAHL (1982 to September 2011).
Complication rate cumulative premature catheter removal rate of all TIVADs was 9.8%
Complication rate/1000 catheter days
Occlusion rate N=3, 13%; 2 had SCV cannulation, all three had tip in upper SVC
Blockage occurred in 20% (113/563) - urokinase 3000 iu, instilled for 8 hours, successfully unblocked - 70% (79/113), requiring a mean of 1.1 (SD 0.36) instillations
Occlusion rate/1000 catheter days
Did occlusion result in CVAD removal?
N=3, 1.3% 18 patients received TIVAD with suboptimal tip position immediately after TIVAD implantation, x5 underwent premature catheter removal, 27.8% premature catheter removal rate
Five patients (5/34, 15%) had a lineogram which showed mechanical blockage – n=3 fibrin sheath, n=1 poor position and an SVC clot - All lines that remained blocked were removed – n=34, 30%
Timeframe to first occlusion
time from insertion to blockage of 62 days (3 to 780 days)
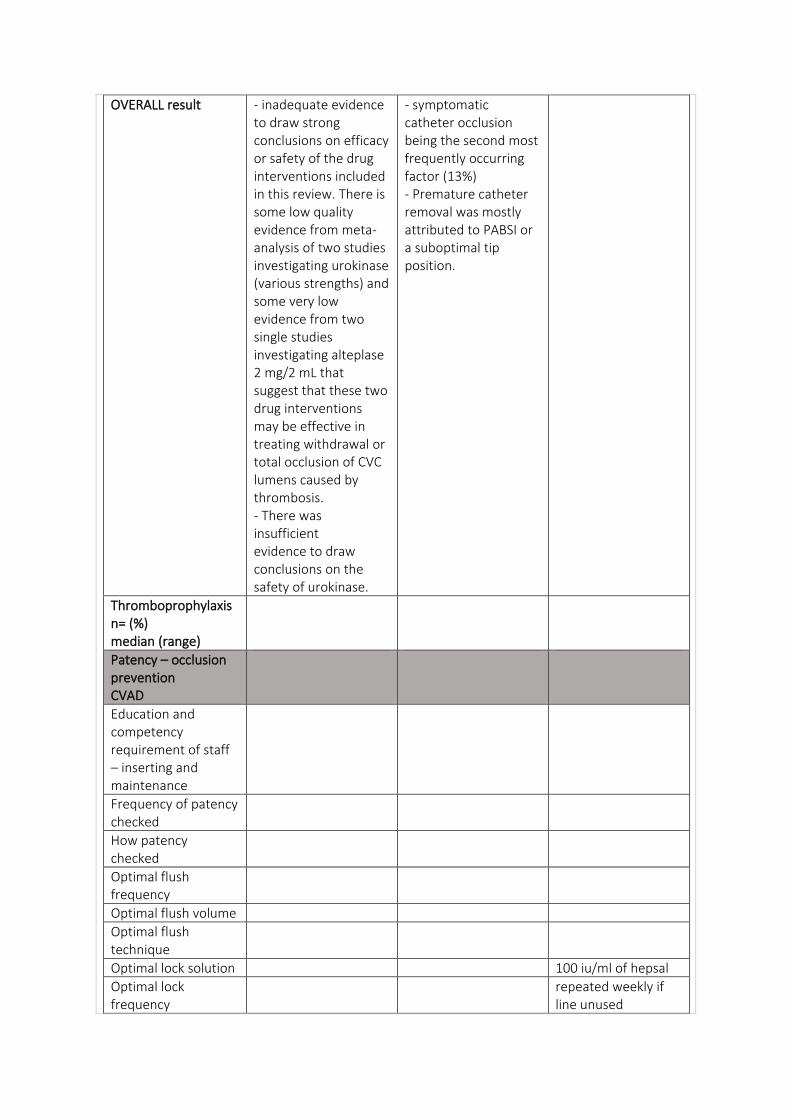
OVERALL result - inadequate evidence to draw strong conclusions on efficacy or safety of the drug interventions included in this review. There is some low quality evidence from meta-analysis of two studies investigating urokinase (various strengths) and some very low evidence from two single studies investigating alteplase 2 mg/2 mL that suggest that these two drug interventions may be effective in treating withdrawal or total occlusion of CVC lumens caused by thrombosis. - There was insufficient evidence to draw conclusions on the safety of urokinase.
- symptomatic catheter occlusion being the second most frequently occurring factor (13%) - Premature catheter removal was mostly attributed to PABSI or a suboptimal tip position.
Thromboprophylaxis n= (%) median (range)
Patency – occlusion prevention CVAD
Education and competency requirement of staff – inserting and maintenance
Frequency of patency checked
How patency checked
Optimal flush frequency
Optimal flush volume
Optimal flush technique
Optimal lock solution 100 iu/ml of hepsal
Optimal lock frequency
repeated weekly if line unused
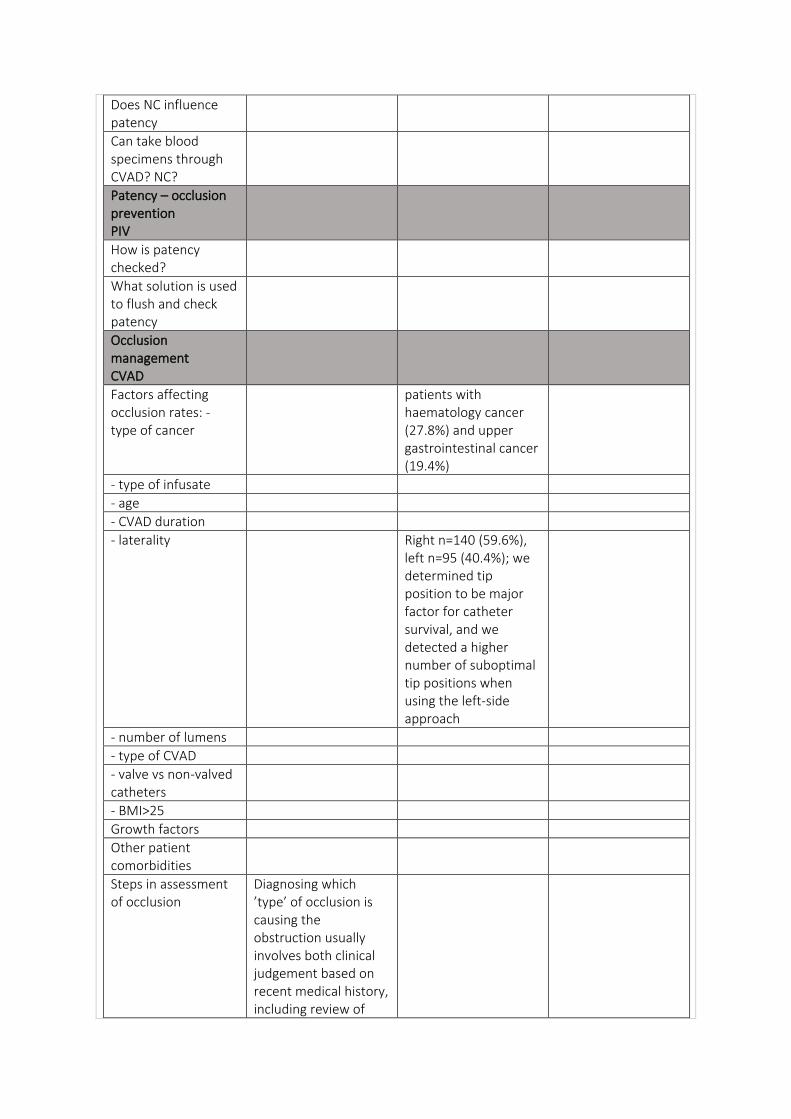
Does NC influence patency
Can take blood specimens through CVAD? NC?
Patency – occlusion prevention PIV
How is patency checked?
What solution is used to flush and check patency
Occlusion management CVAD
Factors affecting occlusion rates: - type of cancer
patients with haematology cancer (27.8%) and upper gastrointestinal cancer (19.4%)
- type of infusate
- age
- CVAD duration
- laterality Right n=140 (59.6%), left n=95 (40.4%); we determined tip position to be major factor for catheter survival, and we detected a higher number of suboptimal tip positions when using the left-side approach
- number of lumens
- type of CVAD
- valve vs non-valved catheters
- BMI>25
Growth factors
Other patient comorbidities
Steps in assessment of occlusion
Diagnosing which ’type’ of occlusion is causing the obstruction usually involves both clinical judgement based on recent medical history, including review of
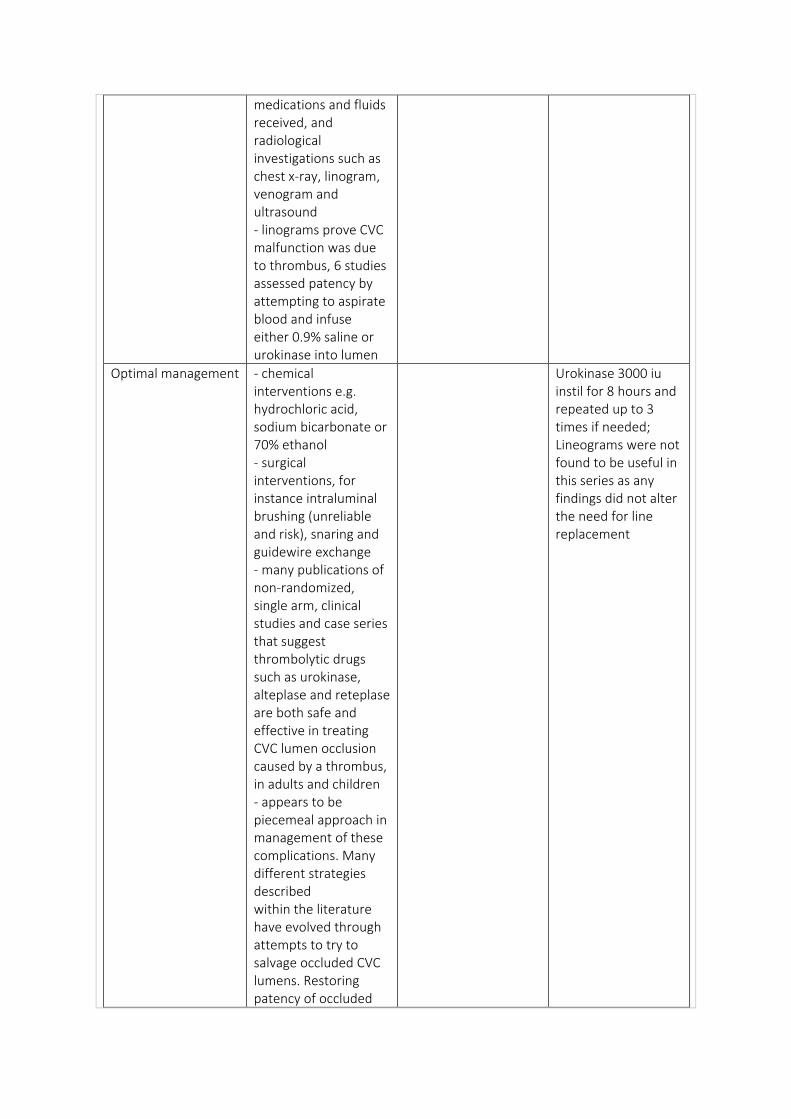
medications and fluids received, and radiological investigations such as chest x-ray, linogram, venogram and ultrasound - linograms prove CVC malfunction was due to thrombus, 6 studies assessed patency by attempting to aspirate blood and infuse either 0.9% saline or urokinase into lumen
Optimal management - chemical interventions e.g. hydrochloric acid, sodium bicarbonate or 70% ethanol - surgical interventions, for instance intraluminal brushing (unreliable and risk), snaring and guidewire exchange - many publications of non-randomized, single arm, clinical studies and case series that suggest thrombolytic drugs such as urokinase, alteplase and reteplase are both safe and effective in treating CVC lumen occlusion caused by a thrombus, in adults and children - appears to be piecemeal approach in management of these complications. Many different strategies described within the literature have evolved through attempts to try to salvage occluded CVC lumens. Restoring patency of occluded
Urokinase 3000 iu instil for 8 hours and repeated up to 3 times if needed; Lineograms were not found to be useful in this series as any findings did not alter the need for line replacement
CVC lumens does not appear to have been subjected to a comprehensive systematic review of the evidence to ascertain the safest and most effective method for treating each of the three types of CVC lumen occlusion in adults and children. - If lumen was found to have either withdrawal or total occlusion it was treated as thrombolytic occlusion. The types of thrombolytic therapy under investigation were urokinase, alteplase and alfimeprase, and the anticoagulant therapy was unfractionated heparin
Optimal catheter tip position How does this relate to occlusion
- distal one-third of the superior vena cava (SVC), the SVC-right atrial (RA) junction, and the upper half of the RA were recognized to be the optimal catheter tip positions - optimal position n=217, 92.3%; suboptimal n=18, 7.7% - Suboptimal tip position (HR 5.13, 95% confidence interval 1.73–15.21) was also risk factor for premature removal, and it was correlated with symptomatic TIVAD occlusion (p =0.0004).
Does angle of catheter in relation
to port body impact occlusion rates
Does increase in resistance monitoring values indicate imminent CVAD occlusion
Can locking solutions be associated with risks of other complications?
Does CVAD material influence occlusion rates?
Can CVADs be used for radiological studies?
Occlusion management PIV
occluded PIV be replaced or unblocked
optimal location for PIV insertion
CVC lumen occlusion can predispose the individual to further risk of morbidity and mortality due to delays in treatment regimens or nutritional support. Additionally, the patient may have to undergo further invasive surgical interventions to replace the CVC. CVC lumen occlusion, therefore, is not only disruptive to patients and their treatment regimens but also creates potential additional costs for the hospital. CVC occlusion can fall into the three distinct categories of drug precipitation or lipid
residue; anatomical or mechanical; and thrombotic. - overall quality of evidence is very low due to small sample sizes and significant methodological issues - evidence provided by meta-analysis of two studies comparing urokinase (various strengths) with placebo has been upgraded to low using the Grade system - Implications for practice There is inadequate evidence to draw strong conclusions on the efficacy or safety of the drug interventions included in this review. That said, there is some low quality evidence that appears to suggest that urokinase (various strengths) may be effective in treating withdrawal occlusion or total occlusion of either a semipermanent or temporary CVC caused by a thrombosis in adults and children with underlying medical conditions.
DATA:
Reference (Wolf et al., 2018) (Wolf et al., 2015) (Wolf, Shenep, Clifford, Curtis, & Flynn, 2013)
Type of study parallel-design, randomised, double-blind, placebo-
prospective ‘Review’ – expert opinion of current literature
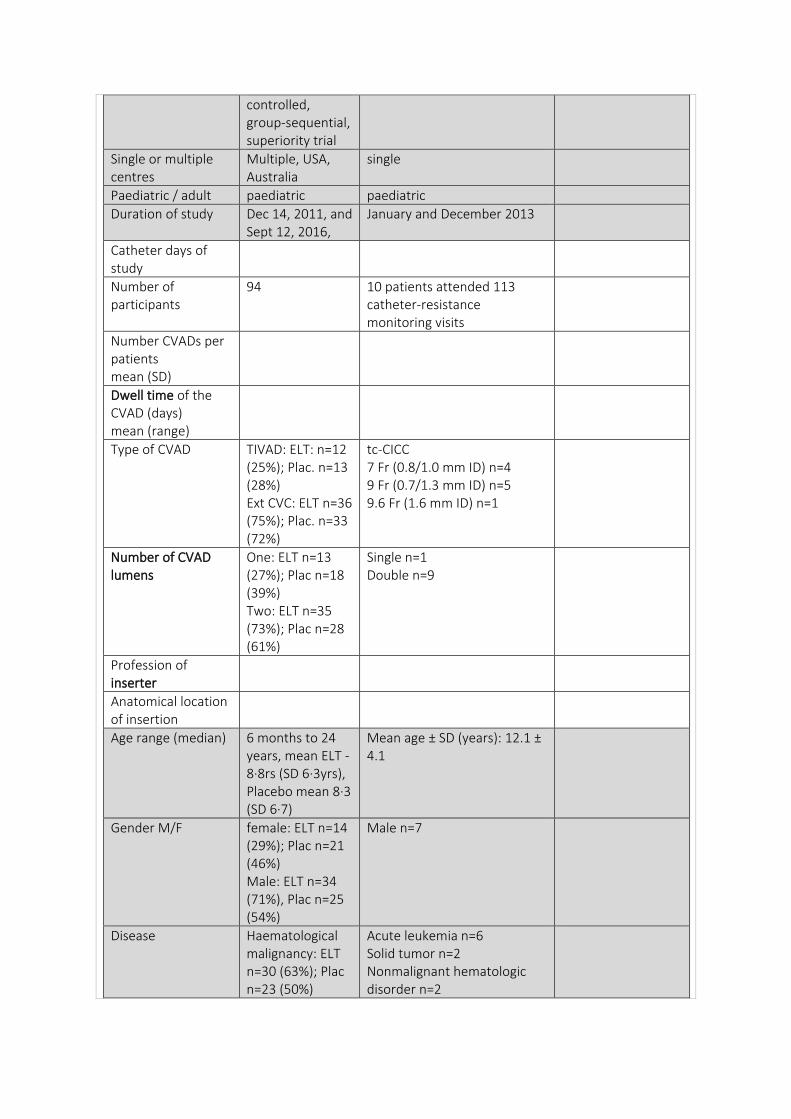
controlled, group-sequential, superiority trial
Single or multiple centres
Multiple, USA, Australia
single
Paediatric / adult paediatric paediatric
Duration of study Dec 14, 2011, and Sept 12, 2016,
January and December 2013
Catheter days of study
Number of participants
94 10 patients attended 113 catheter-resistance monitoring visits
Number CVADs per patients mean (SD)
Dwell time of the CVAD (days) mean (range)
Type of CVAD TIVAD: ELT: n=12 (25%); Plac. n=13 (28%) Ext CVC: ELT n=36 (75%); Plac. n=33 (72%)
tc-CICC 7 Fr (0.8/1.0 mm ID) n=4 9 Fr (0.7/1.3 mm ID) n=5 9.6 Fr (1.6 mm ID) n=1
Number of CVAD lumens
One: ELT n=13 (27%); Plac n=18 (39%) Two: ELT n=35 (73%); Plac n=28 (61%)
Single n=1 Double n=9
Profession of inserter
Anatomical location of insertion
Age range (median) 6 months to 24 years, mean ELT - 8·8rs (SD 6·3yrs), Placebo mean 8·3 (SD 6·7)
Mean age ± SD (years): 12.1 ± 4.1
Gender M/F female: ELT n=14 (29%); Plac n=21 (46%) Male: ELT n=34 (71%), Plac n=25 (54%)
Male n=7
Disease Haematological malignancy: ELT n=30 (63%); Plac n=23 (50%)
Acute leukemia n=6 Solid tumor n=2 Nonmalignant hematologic disorder n=2
Solid or brain tumour: ELT n=18 (38%); Plac n=20 (43%) Non-malignant haematological disorder: ELT n=0; Plac n-3, 7%
Metastatic disease n = (%)
Reason for insertion treatment for cancer or undergoing hematopoietic stem cell transplantation
Outcome
Outcome measures - defined
Intervention N=48 received ethanol lock therapy, n=46 received placebo.
determine the feasibility, acceptability, and efficacy of catheter-resistance monitoring - weekly catheter-resistance monitoring for up to 12 weeks, a novel approach to predicting central venous catheter occlusion in pediatric patients - Resistance was assess ed by measuring the inline pressure at multiple flow-rates via a syringe pump system fitted with a pressure-sensing transducer. When turbulent flow through the device was evident, resistance was not estimated, and the result was noted as “non-laminar.” - staff measured the inline pressure in the CVC twice at each of4 flow rates (typically 10, 50, 100, and 150 mL/h). Pressure was measured using a syringe pump with an incorporated pressure-sensing transducer, pressure sensor was placed below the estimated height of participant’s right atrium, with the participant lying at an angle of approximately 45°
Insertion care
Maintenance care (dedicated CVAD team, ward staff or patient)
Locks performed by nursing staff during inpatient stays or clinic visits At home - caregivers during outpatient care who had took training programme given by line-care nursing specialists and had to show proficiency before start of outpatient lock therapy.
CRM was performed weekly by trained study staff (medical doctor or registered nurse) for up to 12 weeks,
Inclusion criteria 6 months and 25 years and weighed at least 5 kg, were being treated for cancer or a haematological disorder or undergoing haemopoietic stem-cell transplantation, and had a new CLABSI (within 96 h of collection of the initial blood culture) related to a silicone tunnelled external CVC or port for which salvage therapy was planned
5 to 25 years who were receiving treatment that necessitated weekly hospital visits and had a tunnelled CVC (Hickman Catheter, Bard Access Systems, Salt Lake City, UT, USA), which was expected to remain in situ for at least 12 weeks
Exclusion criteria allergy to ethanol or heparin, concomitant use of disulfiram-like drugs, planned CVC removal or expected death within 6 days, continuous use or
28 visits were excluded: first visit (n = 10), previous visit R2 less than 85% (n = 7), TPA since previous visit (n = 10), and clinically abnormal CVC function (n = 1). Excluded CRM visits were termed “inconclusive”
occlusion of the CVC, pregnancy, recent ethanol lock therapy use, port pocket or tunnel tract infection, an alternative source of BSI, multiple long-term CVCs, and a polyurethane CVC Re-enrolment was not permitted.
Randomisation randomly assigned (1:1) by computerised stratified block randomisation, with a known block size of four, in the St Jude Pharmaceutical Services Department by pharmacists unmasked to the allocation.13 - stratification criteria were CVC type (port vs external CVC), absolute neutrophil count at enrolment (<500 cells per µL vs ≥500 cells per µL), presence of fungal bloodstream pathogen, and enrolling institution
Healthcare setting St Jude Children’s Research Hospital, which is a 69-bed paediatric oncology centre in Memphis, TN,
St. Jude Children’s Research Hospital, USA
USA, and at The Royal Children’s Hospital Melbourne, a 334-bed paediatric quaternary referral centre in Melbourne, VIC, Australia.
Duration of follow up, lost to follow up
10 participants discontinued ethanol lock therapy intervention: 7 with adverse events, 2 at patients’ request, and 1 due to study closure. Placebo group, 12 participants discontinued intervention: 5 because of adverse events, 2 because of death or palliative care, and 5 at patients’ request.
Ten participants followed for median of 15 weeks (range, 13–15 weeks). median number of CRM visits was 12 (range, 8–12). Two participants missed 1 or 2 visits, and 1 participant discontinued the study after 8 visits because displacement of the CVC necessitated its removal
RESULTS: primary outcome was proportion of treatment failures in ethanol lock therapy and placebo groups during the 5-day treatment phase and 24-week prophylaxis phase in the modified intention-to-treat population.
occlusion was more common (n = 33), as were occlusion events requiring TPA therapy (n = 17). Correlation between CRM and occlusion events was, therefore, further analyzed.
Complication rate
Complication rate/1000 catheter days
Occlusion rate Catheter occlusion requiring thrombolytic
Elevated catheter resistance (>8.8% increase) was strongly associated with subsequent development of acute
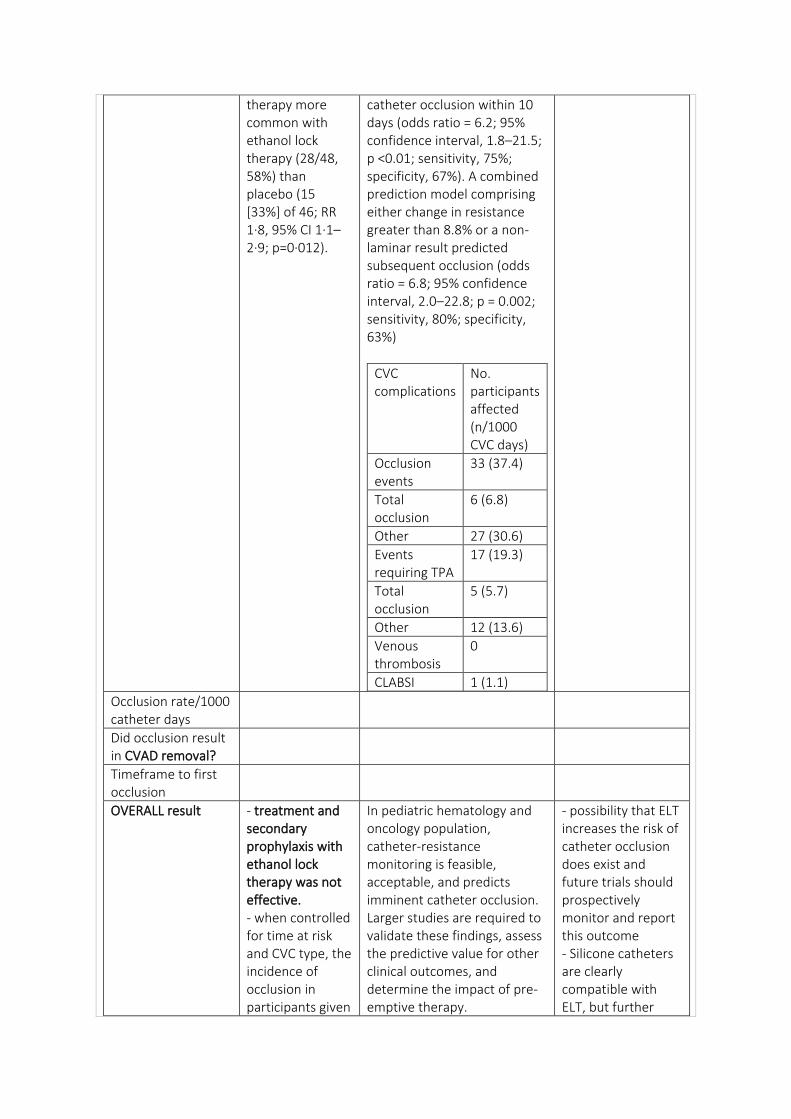
therapy more common with ethanol lock therapy (28/48, 58%) than placebo (15 [33%] of 46; RR 1·8, 95% CI 1·1–2·9; p=0·012).
catheter occlusion within 10 days (odds ratio = 6.2; 95% confidence interval, 1.8–21.5; p <0.01; sensitivity, 75%; specificity, 67%). A combined prediction model comprising either change in resistance greater than 8.8% or a non-laminar result predicted subsequent occlusion (odds ratio = 6.8; 95% confidence interval, 2.0–22.8; p = 0.002; sensitivity, 80%; specificity, 63%)
CVC complications
No. participants affected (n/1000 CVC days)
Occlusion events
33 (37.4)
Total occlusion
6 (6.8)
Other 27 (30.6)
Events requiring TPA
17 (19.3)
Total occlusion
5 (5.7)
Other 12 (13.6)
Venous thrombosis
0
CLABSI 1 (1.1)
Occlusion rate/1000 catheter days
Did occlusion result in CVAD removal?
Timeframe to first occlusion
OVERALL result - treatment and secondary prophylaxis with ethanol lock therapy was not effective. - when controlled for time at risk and CVC type, the incidence of occlusion in participants given
In pediatric hematology and oncology population, catheter-resistance monitoring is feasible, acceptable, and predicts imminent catheter occlusion. Larger studies are required to validate these findings, assess the predictive value for other clinical outcomes, and determine the impact of pre-emptive therapy.
- possibility that ELT increases the risk of catheter occlusion does exist and future trials should prospectively monitor and report this outcome - Silicone catheters are clearly compatible with ELT, but further
ethanol lock therapy was 2·5 times higher than those given placebo (95% CI 1·4–4·7; p=0·0038) - adverse events, including infusion reactions and catheter occlusion - more frequent in the ethanol lock therapy group - Discontinuation of lock therapy because of adverse effects or patient request occurred in a similar proportion of participants in the ethanol lock therapy group (nine [19%] of 48) and placebo (ten [22%] of 46; p=0·72). - Ethanol was not detected in any samples taken from participants who received placebo but was detected in 22 (54%) of 41 samples from the ethanol lock therapy group, with a level greater than 25 mg/dL, which is the maximum level recommended by the American Academy of Pediatrics, found in five samples (12%)
- risk of CVC occlusion within 10 days was significantly higher following a positive test (40.0% vs. 8.9%, p = 0.002). This model was the best predictor of CVC occlusion within 10 days (odds ratio = 6.8; 95% CI, 2.0–22.8; sensitivity, 80%; specificity, 63%).
study is required to determine the effect on polyurethane catheters.
- elevated risk of CVC occlusion is clinically important because occlusion can limit CVC use and cause drug extravasation or device fracture. In paediatric patients with cancer, occlusion independently predicts subsequent bloodstream infection, venous thrombosis, and overall mortality.
Thromboprophylaxis n= (%) median (range)
Patency – occlusion prevention CVAD
Education and competency requirement of staff – inserting and maintenance
Frequency of patency checked
How patency checked
Optimal flush frequency
Immediately before and after lock administration, CVC was flushed with 10 mL normal saline (1 mL/kg for children weighing <10 kg).
Optimal flush volume
Optimal flush technique
Optimal lock solution
lock therapy - ethanol (70%
ethanol in water) or placebo (heparin, 10 units per mL in normal saline) prescribed lock volume for each lumen was measured luminal volume plus 0·1 mL Heparinised saline flushes were used between each CVC access in both groups.
Optimal lock frequency
- given daily for first 5 days (treatment phase) then administered intermittently on up to 3 non-consecutive days per week for the next 24 weeks (prophylaxis phase). - injected into CVC, allowed to dwell for 2–4 h in each lumen on each intervention day, and subsequently aspirated
Does NC influence patency
Can take blood specimens through CVAD? NC?
Patency – occlusion prevention PIV
How is patency checked?
What solution is used to flush and check patency
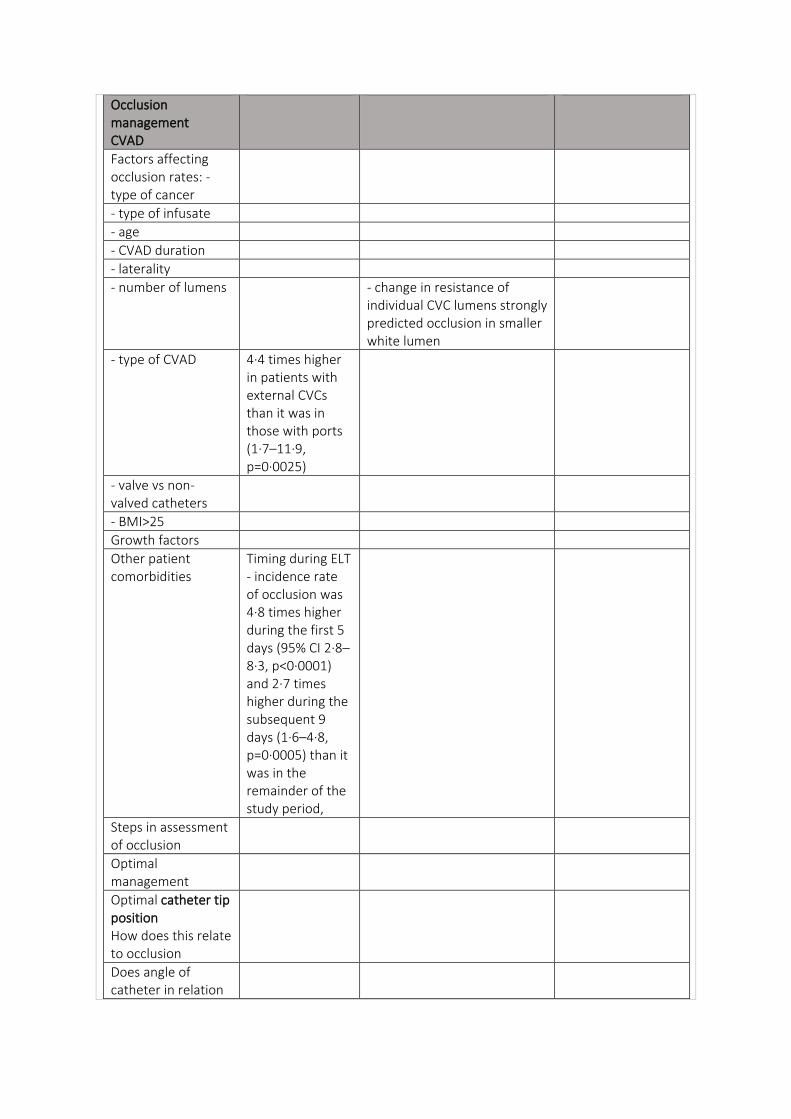
Occlusion management CVAD
Factors affecting occlusion rates: - type of cancer
- type of infusate
- age
- CVAD duration
- laterality
- number of lumens - change in resistance of individual CVC lumens strongly predicted occlusion in smaller white lumen
- type of CVAD 4·4 times higher in patients with external CVCs than it was in those with ports (1·7–11·9, p=0·0025)
- valve vs non-valved catheters
- BMI>25
Growth factors
Other patient comorbidities
Timing during ELT - incidence rate of occlusion was 4·8 times higher during the first 5 days (95% CI 2·8–8·3, p<0·0001) and 2·7 times higher during the subsequent 9 days (1·6–4·8, p=0·0005) than it was in the remainder of the study period,
Steps in assessment of occlusion
Optimal management
Optimal catheter tip position How does this relate to occlusion
Does angle of catheter in relation
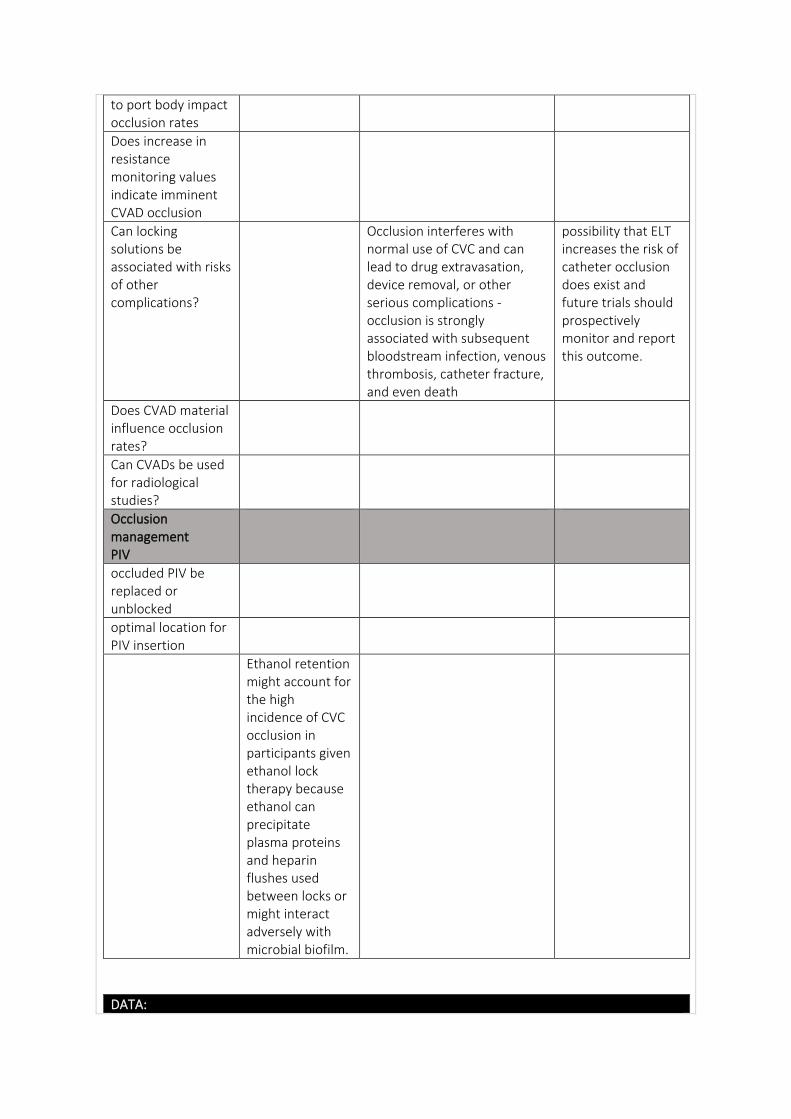
to port body impact occlusion rates
Does increase in resistance monitoring values indicate imminent CVAD occlusion
Can locking solutions be associated with risks of other complications?
Occlusion interferes with normal use of CVC and can lead to drug extravasation, device removal, or other serious complications - occlusion is strongly associated with subsequent bloodstream infection, venous thrombosis, catheter fracture, and even death
possibility that ELT increases the risk of catheter occlusion does exist and future trials should prospectively monitor and report this outcome.
Does CVAD material influence occlusion rates?
Can CVADs be used for radiological studies?
Occlusion management PIV
occluded PIV be replaced or unblocked
optimal location for PIV insertion
Ethanol retention might account for the high incidence of CVC occlusion in participants given ethanol lock therapy because ethanol can precipitate plasma proteins and heparin flushes used between locks or might interact adversely with microbial biofilm.
DATA:
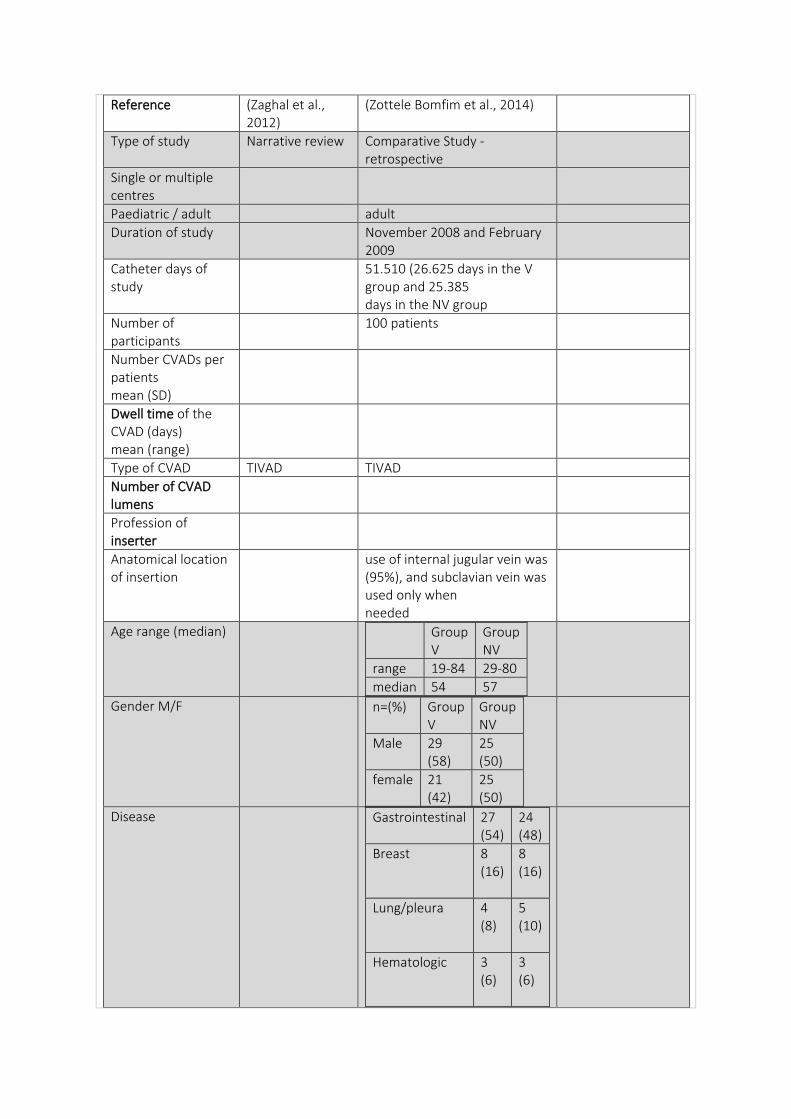
Reference (Zaghal et al., 2012)
(Zottele Bomfim et al., 2014)
Type of study Narrative review Comparative Study - retrospective
Single or multiple centres
Paediatric / adult adult
Duration of study November 2008 and February 2009
Catheter days of study
51.510 (26.625 days in the V group and 25.385 days in the NV group
Number of participants
100 patients
Number CVADs per patients mean (SD)
Dwell time of the CVAD (days) mean (range)
Type of CVAD TIVAD TIVAD
Number of CVAD lumens
Profession of inserter
Anatomical location of insertion
use of internal jugular vein was (95%), and subclavian vein was used only when needed
Age range (median) Group V
Group NV
range 19-84 29-80
median 54 57
Gender M/F n=(%) Group V
Group NV
Male 29 (58)
25 (50)
female 21 (42)
25 (50)
Disease Gastrointestinal
27 (54)
24 (48)
Breast 8 (16)
8 (16)
Lung/pleura 4 (8)
5 (10)
Hematologic 3 (6)
3 (6)
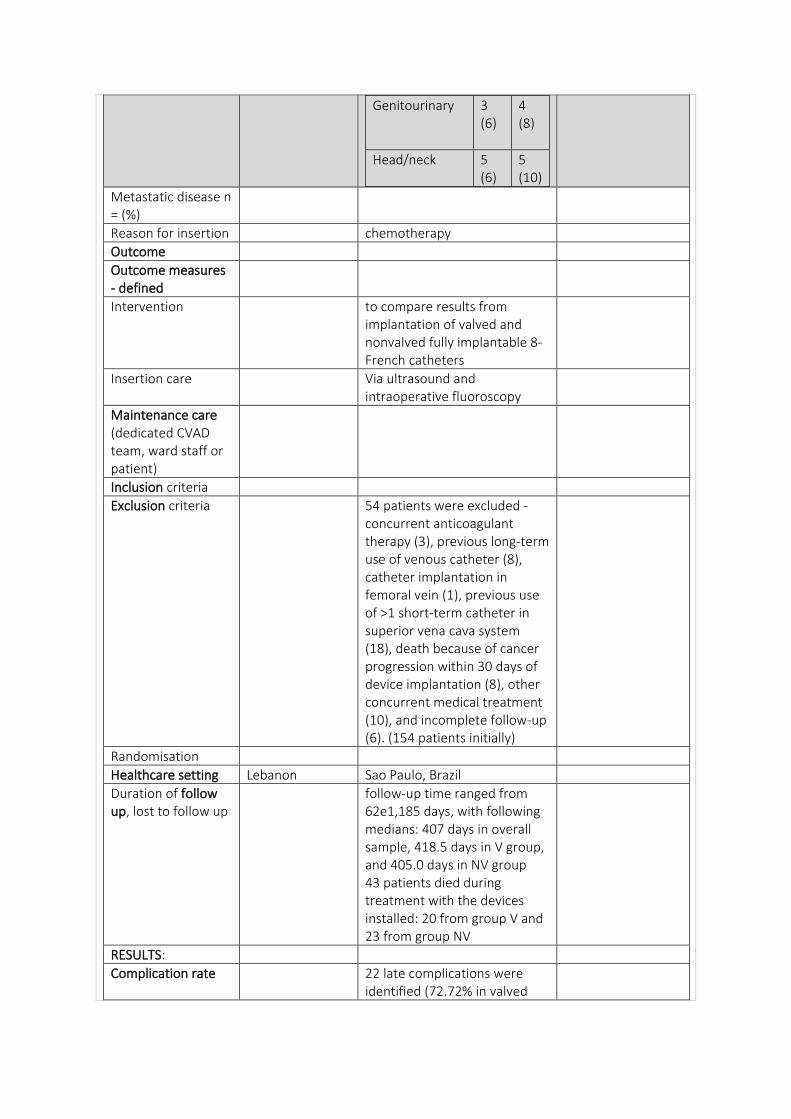
Genitourinary 3 (6)
4 (8)
Head/neck 5 (6)
5 (10)
Metastatic disease n = (%)
Reason for insertion chemotherapy
Outcome
Outcome measures - defined
Intervention to compare results from implantation of valved and nonvalved fully implantable 8-French catheters
Insertion care Via ultrasound and intraoperative fluoroscopy
Maintenance care (dedicated CVAD team, ward staff or patient)
Inclusion criteria
Exclusion criteria 54 patients were excluded - concurrent anticoagulant therapy (3), previous long-term use of venous catheter (8), catheter implantation in femoral vein (1), previous use of >1 short-term catheter in superior vena cava system (18), death because of cancer progression within 30 days of device implantation (8), other concurrent medical treatment (10), and incomplete follow-up (6). (154 patients initially)
Randomisation
Healthcare setting Lebanon Sao Paulo, Brazil
Duration of follow up, lost to follow up
follow-up time ranged from 62e1,185 days, with following medians: 407 days in overall sample, 418.5 days in V group, and 405.0 days in NV group 43 patients died during treatment with the devices installed: 20 from group V and 23 from group NV
RESULTS:
Complication rate 22 late complications were identified (72.72% in valved
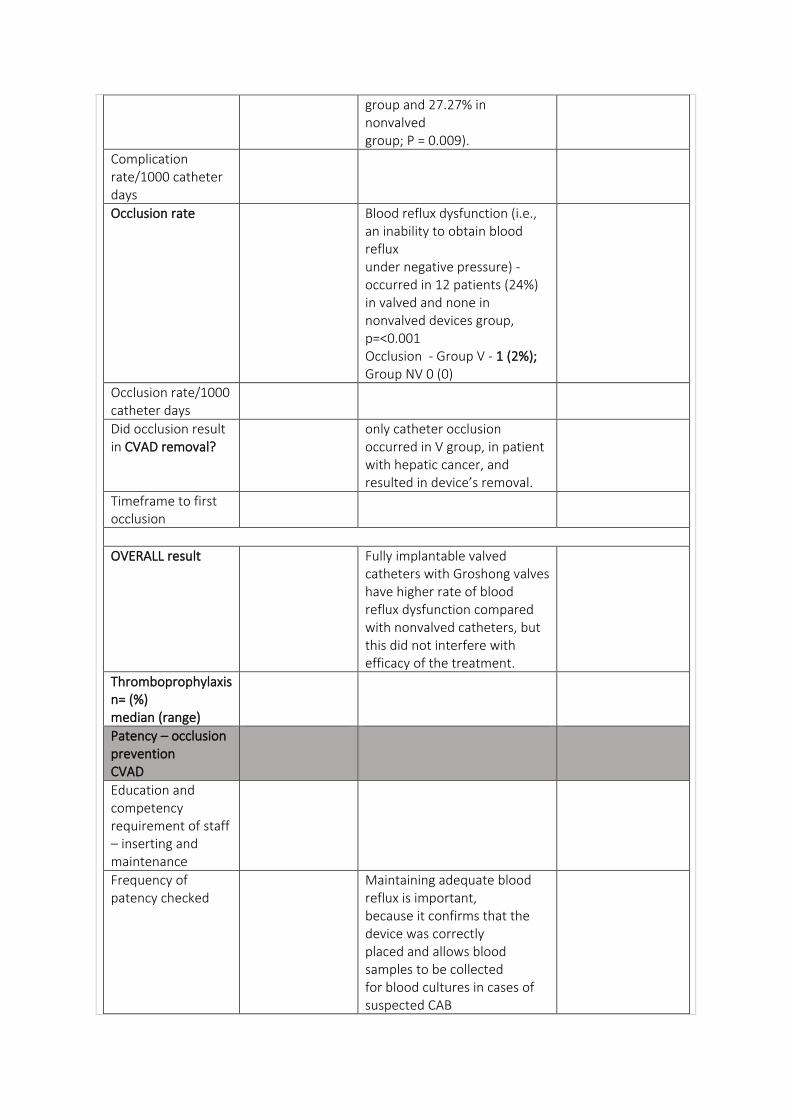
group and 27.27% in nonvalved group; P = 0.009).
Complication rate/1000 catheter days
Occlusion rate Blood reflux dysfunction (i.e., an inability to obtain blood reflux under negative pressure) - occurred in 12 patients (24%) in valved and none in nonvalved devices group, p=<0.001 Occlusion - Group V - 1 (2%); Group NV 0 (0)
Occlusion rate/1000 catheter days
Did occlusion result in CVAD removal?
only catheter occlusion occurred in V group, in patient with hepatic cancer, and resulted in device’s removal.
Timeframe to first occlusion
OVERALL result Fully implantable valved catheters with Groshong valves have higher rate of blood reflux dysfunction compared with nonvalved catheters, but this did not interfere with efficacy of the treatment.
Thromboprophylaxis n= (%) median (range)
Patency – occlusion prevention CVAD
Education and competency requirement of staff – inserting and maintenance
Frequency of patency checked
Maintaining adequate blood reflux is important, because it confirms that the device was correctly placed and allows blood samples to be collected for blood cultures in cases of suspected CAB
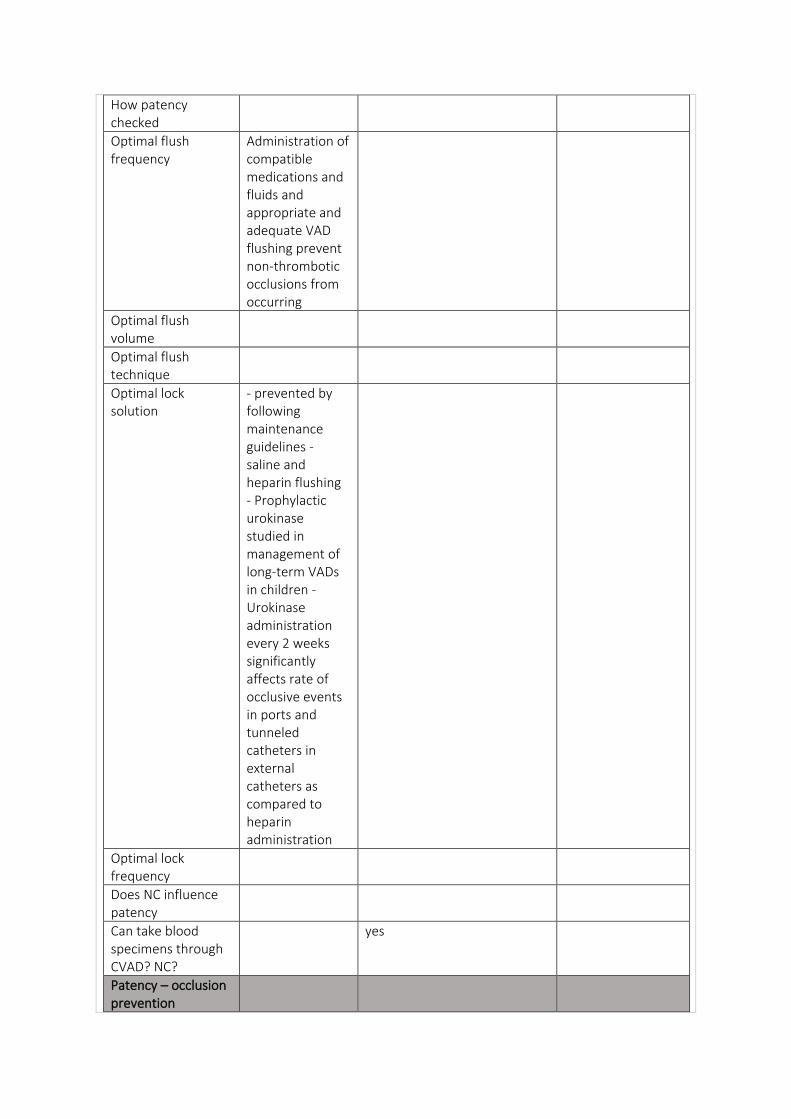
How patency checked
Optimal flush frequency
Administration of compatible medications and fluids and appropriate and adequate VAD flushing prevent non-thrombotic occlusions from occurring
Optimal flush volume
Optimal flush technique
Optimal lock solution
- prevented by following maintenance guidelines - saline and heparin flushing - Prophylactic urokinase studied in management of long-term VADs in children - Urokinase administration every 2 weeks significantly affects rate of occlusive events in ports and tunneled catheters in external catheters as compared to heparin administration
Optimal lock frequency
Does NC influence patency
Can take blood specimens through CVAD? NC?
yes
Patency – occlusion prevention
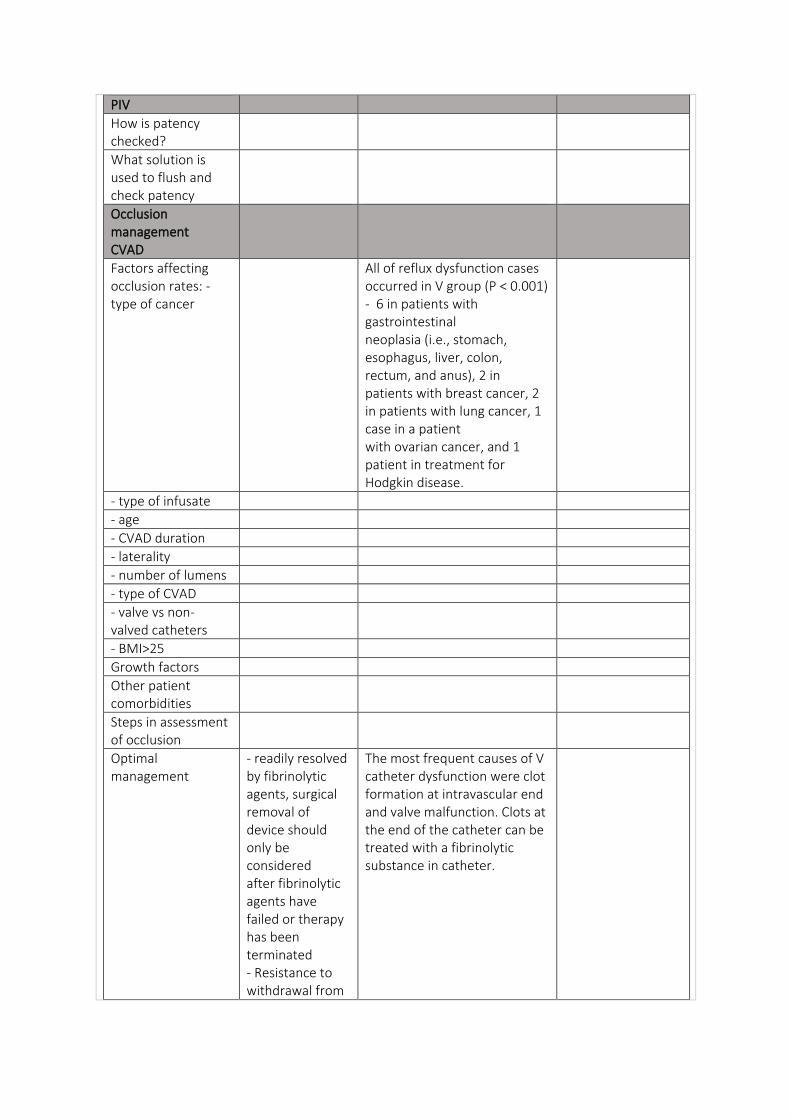
PIV
How is patency checked?
What solution is used to flush and check patency
Occlusion management CVAD
Factors affecting occlusion rates: - type of cancer
All of reflux dysfunction cases occurred in V group (P < 0.001) - 6 in patients with gastrointestinal neoplasia (i.e., stomach, esophagus, liver, colon, rectum, and anus), 2 in patients with breast cancer, 2 in patients with lung cancer, 1 case in a patient with ovarian cancer, and 1 patient in treatment for Hodgkin disease.
- type of infusate
- age
- CVAD duration
- laterality
- number of lumens
- type of CVAD
- valve vs non-valved catheters
- BMI>25
Growth factors
Other patient comorbidities
Steps in assessment of occlusion
Optimal management
- readily resolved by fibrinolytic agents, surgical removal of device should only be considered after fibrinolytic agents have failed or therapy has been terminated - Resistance to withdrawal from
The most frequent causes of V catheter dysfunction were clot formation at intravascular end and valve malfunction. Clots at the end of the catheter can be treated with a fibrinolytic substance in catheter.
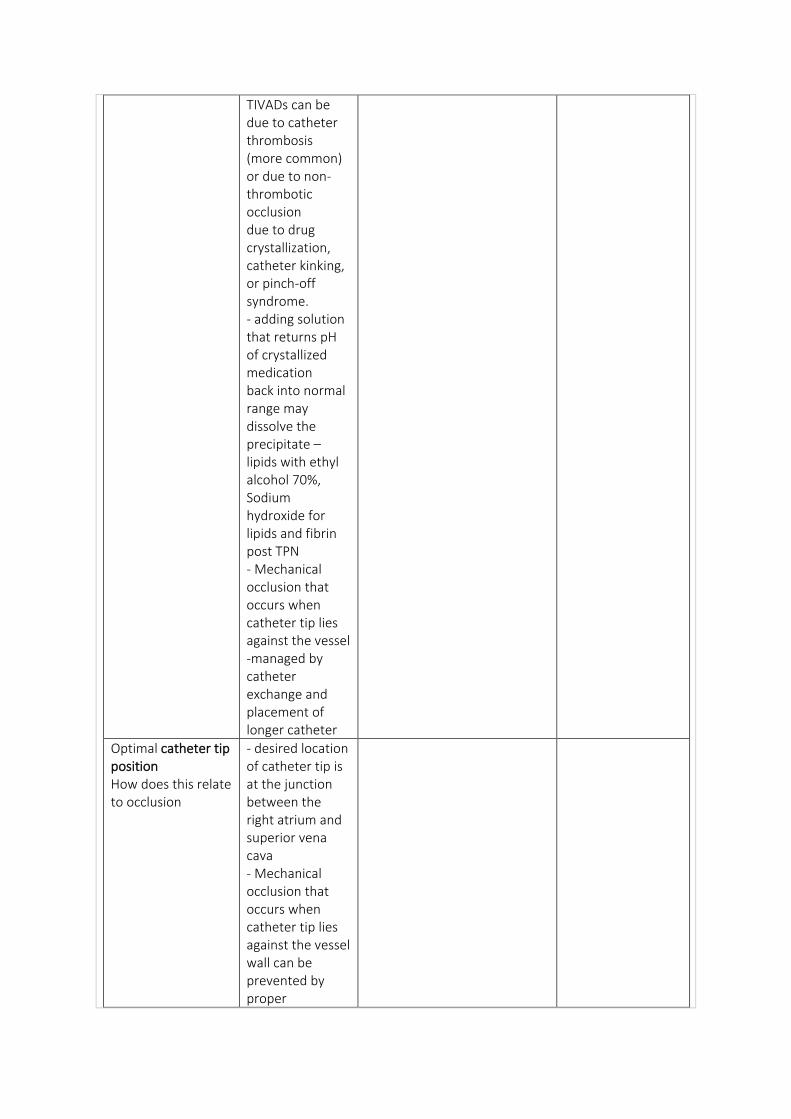
TIVADs can be due to catheter thrombosis (more common) or due to non-thrombotic occlusion due to drug crystallization, catheter kinking, or pinch-off syndrome. - adding solution that returns pH of crystallized medication back into normal range may dissolve the precipitate – lipids with ethyl alcohol 70%, Sodium hydroxide for lipids and fibrin post TPN - Mechanical occlusion that occurs when catheter tip lies against the vessel -managed by catheter exchange and placement of longer catheter
Optimal catheter tip position How does this relate to occlusion
- desired location of catheter tip is at the junction between the right atrium and superior vena cava - Mechanical occlusion that occurs when catheter tip lies against the vessel wall can be prevented by proper
positioning of the tip of the catheter
Does angle of catheter in relation to port body impact occlusion rates
Does increase in resistance monitoring values indicate imminent CVAD occlusion
Can locking solutions be associated with risks of other complications?
Does CVAD material influence occlusion rates?
Can CVADs be used for radiological studies?
Occlusion management PIV
occluded PIV be replaced or unblocked
optimal location for PIV insertion
Copyright © 2022 FDOKUMEN