
Protective Efficacy of N-(2-Hydroxyphenyl) Acetamide against Adjuvant-Induced Arthritis in Rats

Daily assessment of stressful events and coping amongpost-menopausal women with breast cancer treated withadjuvant chemotherapyecc_994 507..516
M. BROWALL, mnsc, doctoral student, The Sahlgrenska Academy at Göteborg University, Institute of Healthand Care Sciences, Göteborg, L.-O. PERSSON, associate professor, The Sahlgrenska Academy at GöteborgUniversity, Institute of Health and Care Sciences, Göteborg, K. AHLBERG, rn, phd, senior lecturer, TheSahlgrenska Academy at Göteborg University, Institute of Health and Care Sciences, Göteborg, and Departmentof Oncology, Sahlgrenska University Hospital, Division of Selected Clinical Specialties, Göteborg, P. KARLSSON,md, associate professor, Department of Oncology, Sahlgrenska University Hospital, Division of Selected ClinicalSpecialties, Göteborg, and Department of Oncology, Southern Älvsborg Hospital, Borås, & E. DANIELSON, phd,professor, The Sahlgrenska Academy at Göteborg University, Institute of Health and Care Sciences, Göteborg,and Department of Health Science, Mid Sweden University, Östersund, Sweden
BROWALL M., PERSSON L.-O., AHLBERG K., KARLSSON P. & DANIELSON E. (2009) European Journal ofCancer Care 18, 507–516Daily assessment of stressful events and coping among post-menopausal women with breast cancer treatedwith adjuvant chemotherapy
The purpose of the study was twofold: to examine what type of daily stressful events post-menopausal womanwith breast cancer experience during adjuvant chemotherapy and how bothersome these are and to identifycoping strategies used by these women used to manage such stressful events. The patient group comprised 75consecutively invited women (�55 years of age) at two university hospitals and one county hospital in Sweden.The Daily Coping Assessment was used to collect data over time. Data were analysed both qualitatively andquantitatively. Six categories of stressful events were identified: ‘nausea and vomiting’, ‘fatigue’, ‘othersymptoms’, ‘isolation and alienation’, ‘fear of the unknown’ and ‘being controlled by the treatment’. The firstthree categories were subsumed under the domain physical problems and the latter three under psychosocialproblems. Almost 30% of the diary entries recorded no stressful event. Physical problems were three times asfrequent as psychosocial problems. ‘Nausea/vomiting’ was the most frequently observed stressful event (21.6%).‘Isolation and alienation’ and ‘fear of the unknown’ were less frequent, but when they occurred they were ratedas the most distressing. Several coping strategies were used to manage each stressful event. The most commonstrategies were acceptance, relaxation and distraction. Religion was rarely used as a coping strategy.
Keywords: stressful events, coping, coping strategies, breast cancer, post-menopausal women.
INTRODUCTION
Approximately 6900 women developed breast cancer inSweden in 2004. About 65% of these women were post-menopausal and about 30% were aged 70 or older(National Board of Health and Welfare 2004). Adjuvantchemotherapy (CT) protocols used to treat women withbreast cancer have evolved over the last decade and have
Correspondence address: Maria Browall, The Sahlgrenska Academyat Göteborg University, Institute of Health and Care Sciences, Box 457,SE 405 30 Göteborg, Sweden (e-mail: [email protected]).
Accepted 23 June 2008DOI: 10.1111/j.1365-2354.2008.00994.x
European Journal of Cancer Care, 2009, 18, 507–516
Original article
© 2009 The AuthorsJournal compilation © 2009 Blackwell Publishing Ltd

extended survival for these women; however, such treat-ments and the disease itself may cause symptoms(Schreier & Williams 2004; Boehmke & Dickerson 2005;Miaskowski et al. 2006; Wood et al. 2006) and reducequality of life (QoL) (Given et al. 2001; Kurtz et al. 2001;De Jong et al. 2002; Ganz et al. 2003, 2004). Demographic,individual and disease characteristics are other factorsthat can influence patient experiences (Armstrong 2003;Kim et al. 2005). Although it is known that assessingsymptom distress helps to identify patients’ perceptions oftheir needs and problems (Rhodes et al. 2000), there is stilla lack of research that has explored the experience ofsymptom distress over time in breast cancer patientsundergoing treatment with chemotherapy (Cooley et al.2003).
According to Kornblith et al. (2001), the more stressbreast cancer patients must endure, the more likely theyare to have difficulty adjusting. The authors highlight theimportance of finding a link between the stressful eventsand the degree of distress they induce, and the need forthese women to have support systems in place before theevent occurs in order to facilitate adjustment. Hence, it isimportant that healthcare providers identify patients’particular stressors at an early stage, in order to be ableto target support needs early on and thereby help patientsto achieve optimal adjustment.
Lazarus and Folkman (1984) define coping as ‘constantlychanging cognitive and behavioral efforts to manage spe-cific external or internal demands that are appraised astaxing or exceeding the resources of a person’ (p. 141).Coping strategies have been shown to be associatedwith adjustment and QoL after breast cancer diagnosis(Epping-Jordan et al. 1999; Stanton et al. 2000; Avis et al.2005). A study by Manuel et al. (2007) found that effectiveadjustment may require that different coping strategies beimplemented for specific stressors and in relation to dif-ferent interventions. Some researchers have concludedthat different coping strategies are associated with differ-ent stressors, that is, symptom distress (Kuo & Ma 2002),age (Schnoll et al. 1998) or the diagnosis of cancer, whichin itself produces a great amount of distress (Shapiro et al.2001). A variety of determinants of coping strategies havebeen identified, or at least theorized in cancer patients.Nevertheless, according to Link et al. (2005), little isknown from the cancer patients’ own perspective regard-ing what factors contribute to the patients’ choice ofcoping strategy.
To be able to provide self-care management education,healthcare providers must have more knowledge abouthow well the patient is able to manage these stressfulevents (i.e. coping). In line with Lazarus’ definition of
coping, repeated assessments and a specification of thedemands are important to gain a more complete under-standing of the adjustment process (Stone & Neale 1984;Lazarus 1993). The Daily Coping Assessment (DCA)(Stone & Neale 1984; Porter & Stone 1996) was developedin accordance with these notions to enable detailedrecording of coping responses on a daily basis. The instru-ment is useful for eliciting stressful events as specifiedand described by the patient, as well as information aboutthe use of coping strategies in relation to those events.
The overall aim of the present study was to describestressful events experienced by post-menopausal womenwith breast cancer receiving adjuvant CT and how thesewomen handle these stressful events or situations. Thefollowing research questions were posed:
1 What types of daily stressful events (related or not to thecancer) do post-menopausal women with breast cancerexperience during adjuvant CT treatment and howbothersome are these?
2 What types of coping strategies do these women use tohandle these stressful events?
METHODS
Sample and setting
A consecutive series of newly-operated-upon, post-menopausal breast cancer patients scheduled for adjuvantCT at two university hospitals and one county hospital inSweden between November 2003 and November 2005were invited to participate. The inclusion criteria wereaged 55 years and older, newly diagnosed with histologicalconfirmed stage I to III a breast carcinomas, and able togive informed consent, to read and speak Swedish and tounderstand the purpose of the study. Age 55 years andabove was used to ensure that the women participatingin the study were homogeneous with respect to post-menopause.
The exclusion criteria were evidence of dementia,known history of psychiatric disorder and history of othercancers within the previous 5 years. Of 80 eligiblepatients, 75 patients agreed to participate. The age rangewas 55–77 years.
Procedure
This study was part of a larger study with the aim toinvestigate health-related QoL among post-menopausalwomen treated for breast cancer. Chemotherapy wasoffered to all patients with hormone receptor-negativebreast cancer and to high-risk hormone receptor-positive
BROWALL et al.
© 2009 The AuthorsJournal compilation © 2009 Blackwell Publishing Ltd
508

patients (i.e. tumour size > 50 mm and/or more than threepositive lymph nodes). The CT regimes were either flur-ouracil 600 mg/m2 intravenously, epirubicin 75 mg/m2
intravenously and cyclophosphamide 600 mg/m2 intrave-nously (FEC) every third week in a course of six treat-ments (n = 72) or cyclophosphamide 100 mg/m2 p.o. ondays 1–14 and methothrexate 40 mg/m2 intravenously andflurouracil 600 mg/m2 intravenously on days 1 and 8(CMF) in a course of six treatments (n = 3). Anti-emetictreatment was administered in accordance with localpractice. Generally, betametson 8 mg ¥ 1 intravenouslyand ondnsetron 8 mg ¥ 1 intravenously were given beforethe CT started. Subsequently, during days 1–4 ondanetron8 mg p.o. ¥ 2 was used together with a suppository meto-clopramid 20 mg on demand.
The first author contacted each woman interested inparticipating in the study. The women who agreed toparticipate were asked to complete a DCA diary for fiveconsecutive days starting on the treatment day of cycle 1(day 1) and after the third and last cycle of CT. Thus, eachpatient was requested to complete a total of 15 days. Theywere instructed to record all stressful events, the intensityof those events and the coping strategy used to managethem. The diary entries were mailed to the patients,together with a prepaid envelope and a letter explainingthe procedures and providing the telephone number of thefirst author.
A total of seven patients withdrew from adjuvant CTduring the six cycles due to various medical problems(diverticulitis, neutropenia, relapse, pulmonary embo-lism, neutropenia and heart conditions).
Measures
The DCA by Stone and Neale (1984) was developed spe-cifically for the daily recording of coping with everydaystressful events. Questions regarding the most stressfulevent of the day are completed once a day during fiveconsecutive days, where day 1 is the first day of treat-ment. The DCA contains four sections. The first sectionis a question to which the patients respond by describingthe most stressful event (illness related or not) in theirown words. The second section assesses the distressoccasioned by the stressful event. Scores range from 1(not at all bothersome) to 7 (extremely bothersome). Thethird section includes two questions concerning reac-tions to the stressful event: (1) how much control didyou have over its occurrence? (no control, some, quite alot); and (2) was it an expected stressful event or situa-tion? (completely unexpected, somewhat unexpected,somewhat anticipated, completely anticipated). The
fourth part includes eight categories of strategies formanaging the stressful event: distraction (thought aboutsomething else), situation redefinition (looked at theproblem in a different way), direct action (did somethingabout it), catharsis (expressed emotions), acceptance(accepted the problem), seeking social support (soughtsupport from others), relaxation (relaxed) and religion(sought spiritual support). The patients report whether ornot they use each of the strategies as a means of han-dling their recorded stressor for that day. The Swedishversion of the DCA was developed by Wasteson et al.(2002) and used for assessing patients with gastrointesti-nal cancer.
Analysis and reduction of qualitative data
A combination of qualitative and quantitative contentanalyses was conducted (Weber 1995). Qualitativecontent analysis was used to code and categorize patientresponses to the first question in the DCA, that is,descriptions of the most stressful events of the day. Alldiary entries were first read several times by the firstauthor (MB). The last author (ED) read a sample of thediary entries to obtain a sense of the whole. Texts thatwere relevant to the research question was then takenand compiled into a single text document. This textwas subsequently divided into units of meaning, whichwere then condensed into codes of stressful events.Identified codes were labelled to reflect the content ofthe categories.
All codes were cross-checked several times against theunits of meaning and entire diary text, and some wererevised. The codes were also compared for differencesand similarities with other codes, and tentative catego-ries were discussed and revised several times by three ofthe authors (MB, LP and ED), before they were finallysorted into six categories (Weber 1995). The categorieswere labelled ‘nausea and vomiting’, ‘fatigue’, ‘othersymptoms’, ‘isolation and alienation’, ‘fear of theunknown’ and ‘being controlled by the treatment’ andillustrated how the participants experienced the first 5days of adjuvant CT treatment at cycles 1, 3 and 6. Fromthese categories two major domains were observed:physical problems and psychosocial problems. Thedomain physical problems subsumed the categories‘nausea and vomiting’, ‘fatigue’ and ‘other symptoms’and the domain psychosocial problems consisted of ‘iso-lation and alienation’, ‘fear of the unknown’ and ‘beingcontrolled by the treatment’. Table 1 presents thederived categories and domains together with citationsfrom the diary to exemplify the categories.
Daily assessment of stressful events and coping
© 2009 The AuthorsJournal compilation © 2009 Blackwell Publishing Ltd
509

Tab
le1.
Dom
ain
san
dca
tego
ries
ofst
ress
ful
even
tsex
empl
ified
wit
hci
tati
ons
extr
acte
dfr
omth
edi
ary
entr
ies
Ph
ysic
alpr
oble
ms
Psy
chos
ocia
lpr
oble
ms
Nau
sea
and
vom
itin
gFa
tigu
eO
ther
sym
ptom
sIs
olat
ion
and
alie
nat
ion
Fear
ofth
eu
nk
now
nB
ein
gco
ntr
olle
dby
the
trea
tmen
t‘.
..fe
els
lik
eI
hav
ea
clu
mp
ofje
lly
inm
yst
omac
hth
atfi
lls
my
wh
ole
bell
yan
dsw
ays
back
and
fort
hI
wal
k’.
‘...
Dis
gust
ing
day,
the
wor
stin
alo
ng
tim
e.T
he
wor
stth
ing
abou
tta
kin
gan
ti-n
ause
api
lls
isth
atyo
ufe
eln
ause
ous
just
bylo
okin
gat
them
,it
’sa
litt
leof
avi
ciou
sci
rcle
’.
‘...
very
very
tire
d,a
grea
tw
eari
nes
s,..
.h
ardl
yab
leto
man
age
my
own
body
for
aco
upl
eof
hou
rs’.
‘...
that
you
’re
soti
red,
...w
ante
dto
doso
met
hin
gbu
tco
uld
n’t
man
age
to,
sad
tosa
y’.
‘...
har
dto
fin
da
bala
nce
betw
een
con
stip
atio
nan
ddi
arrh
oea,
...a
mso
afra
idof
beco
min
gco
nst
ipat
edth
atI
gulp
dow
nla
xati
ves’
.‘.
..h
eart
burn
,I
feel
lik
eI’
mbu
rnin
gu
p’.
‘Iw
asve
ryst
iff
inm
yar
mpi
tan
dab
ove
the
sore
,...
hav
ebe
com
em
ore
swol
len
,...
feel
sli
ke
Ih
ave
aw
eigh
ton
the
oper
ated
area
’.‘.
..ba
dta
ste
inm
ym
outh
’‘.
..bl
iste
rsin
my
mou
th’
‘Eve
nth
ough
Ih
ave
alo
tof
frie
nds
Ist
ill
feel
alon
ean
dem
pty’
.‘.
..a
feel
ing
ofir
revo
cabi
lity
and
hel
ples
snes
s’.
‘Ife
elou
tof
itan
dde
pres
sed.
Ita
ke
inev
eryt
hin
gfr
omth
eT
Van
dn
ewsp
aper
sth
at’s
abou
tbr
east
can
cer.
Ih
ave
anan
ger
insi
dem
ebe
cau
seI
hav
eca
nce
r’.
‘Ica
n’t
just
sit
and
talk
wit
hpe
ople
onth
eph
one,
...f
eels
lik
em
yso
ul
isou
tof
syn
cw
ith
my
body
,...
don
’tk
now
how
I’ll
man
age’
.‘A
sa
sin
gle
mot
her
ever
yday
life
has
togo
onas
usu
al,
even
ifI’
mn
otw
ell.
...fi
nd
out
wh
atyo
uca
nst
and
todo
and
beh
ave
acco
rdin
gly’
.‘I
feel
lik
eI’
min
agl
ass
jar
and
amse
ein
gth
ew
orld
thro
ugh
the
glas
s,cl
earl
yye
tre
mot
e.I
begi
nto
feel
ali
ttle
bett
erin
the
even
ing,
hop
efu
lly
the
wor
stis
over
’.
‘...
wor
ries
abou
tm
yfi
nan
cial
situ
atio
n,
my
purs
eis
shri
nk
ing’
.’T
his
ism
yla
stro
un
dof
trea
tmen
tsbu
tI
can
’tju
mp
for
joy,
Ik
eep
thin
kin
gan
dw
onde
rin
gif
the
can
cer
wil
lco
me
back
.Y
ouca
non
lyh
ope,
nev
erbe
sure
’.‘.
..w
orri
esan
dth
ough
tsab
out
illn
ess
and
can
cer,
abou
th
owit
affe
cts
oth
erth
ings
inli
fe,
such
asot
her
illn
esse
s’.
‘...
wor
ries
abou
th
owyo
u’l
lfe
elaf
ter
the
trea
tmen
t,n
otk
now
ing
duri
ng
the
trea
tmen
t,..
.im
agin
atio
nis
our
wor
stan
dgr
eate
sten
emy’
.‘.
..w
orri
esab
out
futu
repr
oble
m..
..I
hav
en’t
lost
any
hai
rye
t..
.it’
sa
pros
pect
that
both
ers
me
the
mos
t.So
far
no
prob
lem
s’.
‘My
life
isre
stri
cted
beca
use
the
trea
tmen
tst
eers
it.
It’s
har
d,I
was
supp
osed
togo
toa
birt
hda
ypa
rty’
.‘I
can
’tli
vea
nor
mal
life
,I
feel
con
trol
led,
it’s
hor
ribl
e’‘I
forg
otto
tak
eth
ean
ti-n
ause
api
llan
dh
adto
rush
hom
eto
tak
eit
...I
feel
con
trol
led,
it’s
apr
oble
m’.
BROWALL et al.
© 2009 The AuthorsJournal compilation © 2009 Blackwell Publishing Ltd
510
Ethics
The study was performed in accordance with the ethicalstandards of the Helsinki Declaration and Good ClinicalPractice guidelines (WMA 2000). The Ethics Committeesat Göteborgs University and Stockholm Universityapproved the study. All patients received oral and writteninformation and gave informed written consent beforeinclusion.
RESULTS
Socio-demographic and clinical characteristics
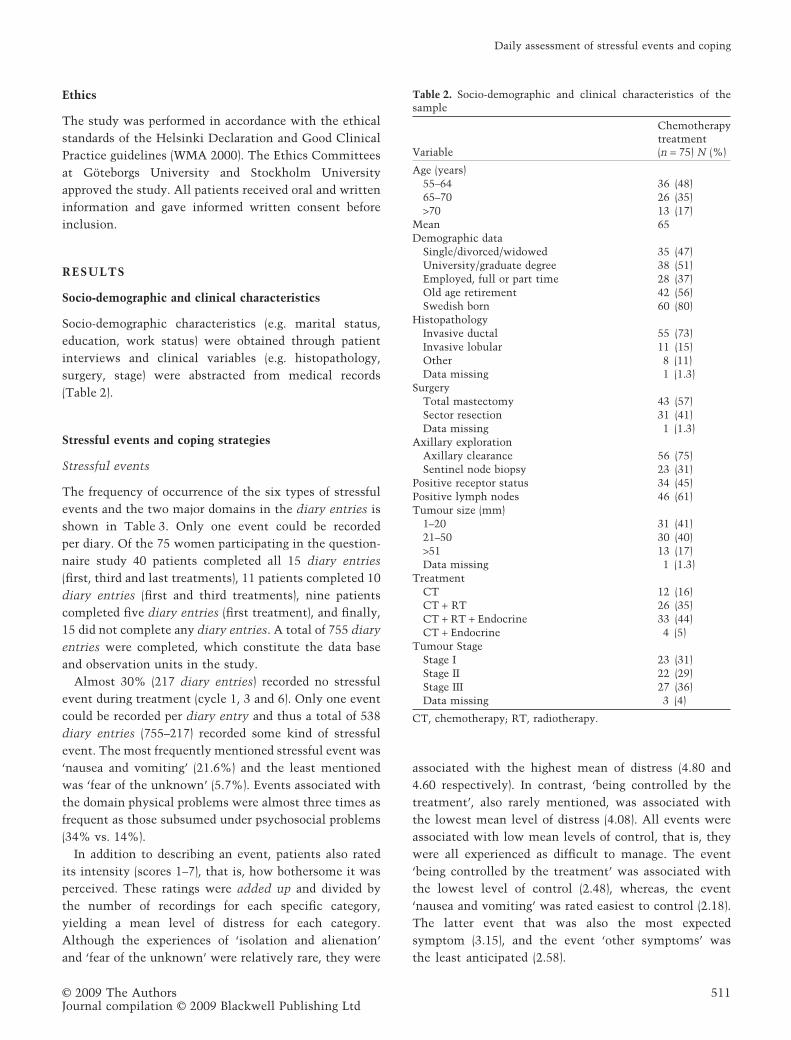
Socio-demographic characteristics (e.g. marital status,education, work status) were obtained through patientinterviews and clinical variables (e.g. histopathology,surgery, stage) were abstracted from medical records(Table 2).
Stressful events and coping strategies
Stressful events
The frequency of occurrence of the six types of stressfulevents and the two major domains in the diary entries isshown in Table 3. Only one event could be recordedper diary. Of the 75 women participating in the question-naire study 40 patients completed all 15 diary entries(first, third and last treatments), 11 patients completed 10diary entries (first and third treatments), nine patientscompleted five diary entries (first treatment), and finally,15 did not complete any diary entries. A total of 755 diaryentries were completed, which constitute the data baseand observation units in the study.
Almost 30% (217 diary entries) recorded no stressfulevent during treatment (cycle 1, 3 and 6). Only one eventcould be recorded per diary entry and thus a total of 538diary entries (755–217) recorded some kind of stressfulevent. The most frequently mentioned stressful event was‘nausea and vomiting’ (21.6%) and the least mentionedwas ‘fear of the unknown’ (5.7%). Events associated withthe domain physical problems were almost three times asfrequent as those subsumed under psychosocial problems(34% vs. 14%).
In addition to describing an event, patients also ratedits intensity (scores 1–7), that is, how bothersome it wasperceived. These ratings were added up and divided bythe number of recordings for each specific category,yielding a mean level of distress for each category.Although the experiences of ‘isolation and alienation’and ‘fear of the unknown’ were relatively rare, they were
associated with the highest mean of distress (4.80 and4.60 respectively). In contrast, ‘being controlled by thetreatment’, also rarely mentioned, was associated withthe lowest mean level of distress (4.08). All events wereassociated with low mean levels of control, that is, theywere all experienced as difficult to manage. The event‘being controlled by the treatment’ was associated withthe lowest level of control (2.48), whereas, the event‘nausea and vomiting’ was rated easiest to control (2.18).The latter event that was also the most expectedsymptom (3.15), and the event ‘other symptoms’ wasthe least anticipated (2.58).
Table 2. Socio-demographic and clinical characteristics of thesample
Variable
Chemotherapytreatment(n = 75) N (%)
Age (years)55–64 36 (48)65–70 26 (35)>70 13 (17)
Mean 65Demographic data
Single/divorced/widowed 35 (47)University/graduate degree 38 (51)Employed, full or part time 28 (37)Old age retirement 42 (56)Swedish born 60 (80)
HistopathologyInvasive ductal 55 (73)Invasive lobular 11 (15)Other 8 (11)Data missing 1 (1.3)
SurgeryTotal mastectomy 43 (57)Sector resection 31 (41)Data missing 1 (1.3)
Axillary explorationAxillary clearance 56 (75)Sentinel node biopsy 23 (31)
Positive receptor status 34 (45)Positive lymph nodes 46 (61)Tumour size (mm)
1–20 31 (41)21–50 30 (40)>51 13 (17)Data missing 1 (1.3)
TreatmentCT 12 (16)CT + RT 26 (35)CT + RT + Endocrine 33 (44)CT + Endocrine 4 (5)
Tumour StageStage I 23 (31)Stage II 22 (29)Stage III 27 (36)Data missing 3 (4)
CT, chemotherapy; RT, radiotherapy.
Daily assessment of stressful events and coping
© 2009 The AuthorsJournal compilation © 2009 Blackwell Publishing Ltd
511

Coping strategies
In total, 1790 coping strategies were reported in relation tothe 538 stressful events. Hence, several different copingstrategies were used to manage each stressful event, witha mean of 3.33 coping strategies per stressful event (1790/538). Table 4 presents the frequencies of reported copingstrategies. The most commonly used strategies wereacceptance (17.5%), relaxation (16.6%) and distraction(16.4%). The least used strategy was religion (1.7%).
Coping strategies in relation to stressful events
Table 5 shows the daily occurrence of each coping strategyfor each type of stressful event. Acceptance, relaxation,distraction and direct actions were commonly usedcoping strategies for all types of stress. Acceptance andrelaxation were particularly frequent in relation to theevents ‘fatigue’, ‘nausea and vomiting’ and ‘being con-trolled by the treatment’. Social support and situationredefinition were most commonly used to handle ‘fear ofthe unknown’. Situation redefinition was also commonly
used for ‘isolation and alienation’, ‘being controlled by thetreatment’ and ‘fatigue’. Religion was rarely used asa coping strategy, except in relation to ‘fear of theunknown’. Catharsis and social support also tended to beused in connection with this event. The greatest meannumber of coping strategies was used in relation to ‘fear ofthe unknown’ (3.95) and the least (2.80) for ‘other symp-toms’ (data not shown). Acceptance was the most fre-quently used coping strategy in the stress event domain‘physical problems’, whereas distraction was the mostfrequently used in the domain psychosocial problems.
DISCUSSION
Stressful events
Content analysis of a total of the 755 diary entries frompost-menopausal women undergoing adjuvant CT forbreast cancer yielded six categories of stressful eventswere over the treatment period.
A surprisingly high proportion (30%) of the diary entriesin this study recorded no stressful events during the adju-vant CT, which may suggest that the everyday life of thewomen in this study was not dominated by concerns,either related to the disease or unrelated to it. Among thewomen who experienced stressful events, more of theseevents were related to physical problems (34%) than topsychosocial problems (14%).
Nausea and vomiting was among the most frequentlyrecorded stressful events and also the most expected one.Many breast cancer studies report that despite advances inthe prevention and treatment of emesis, nausea and vom-iting is still considered to be among the most severe,feared and distressing symptoms of CT (Grunberg et al.2005; Lee et al. 2005; Booth et al. 2007), despite the wide-spread use of 5-HT3 antagonists (Lee et al. 2005). Most of
Table 3. Frequency of stressful events, mean levels of perceived distress, perceived control and perceived expectations
Stressful eventFrequency(%)
Level of distressM (SD)*
Level of controlM (SD)†
Level of expectationM (SD)‡
No stressful event 217 (28.7) – – –Nausea and vomiting 164 (21.6) 4.14 (1.8) 2.18 (0.6) 3.15 (0.8)Other symptoms 117 (15.5) 4.34 (1.7) 2.40 (0.6) 2.58 (1.1)Fatigue 99 (13.1) 4.30 (1.6) 2.37 (0.7) 2.92 (0.8)Isolation and alienation 66 (8.7) 4.80 (1.8) 2.29 (0.7) 2.64 (1.0)Being controlled by the treatment 49 (6.5) 4.08 (1.8) 2.48 (0.9) 2.65 (1.0)Fear of the unknown 43 (5.7) 4.60 (1.7) 2.26 (0.6) 2.95 (1.0)Physical problems 380 (33.8) 4.24 (1.7) 2.30 (0.6) 2.92 (0.9)Psychosocial problems 158 (14.0) 4.53 (1.8) 2.34 (0.7) 2.73 (1.0)Total (across all stressful events) 755 (100) 4.33 (1.8) 2.31 (0.7) 2.86 (0.9)
*High levels correspond to high distress (range 1–7).†High levels correspond to low control (range 1–3).‡High levels correspond to high expectation (range 1–4).
Table 4. Frequency (%) of use of the eight pre-defined copingstrategies
Coping strategies Frequency (%)
Acceptance 313 (17.5)Relaxation 297 (16.6)Distraction 293 (16.4)Direct action 279 (15.6)Situation redefinition 250 (14.0)Social support 186 (10.4)Catharsis 141 (7.9)Religion 31 (1.7)Total 1790 (100)
The patients could respond with more than one coping strategyfor each reported stressful event.
BROWALL et al.
© 2009 The AuthorsJournal compilation © 2009 Blackwell Publishing Ltd
512
the functional changes described in QoL studies have beenfound to be attributable to CT-induced nausea and vom-iting (Rusthoven et al. 1998; Bloechl-Daum et al. 2006). Arecent study by Dibble et al. (2003) reported that delayednausea is a significant problem in women with breastcancer that receive CT and experience nausea in stressfulsituations.
The fact that nausea and vomiting was the mostexpected stressful event in the present study reflects theinformation that is given by healthcare providers beforetreatment and what the general public knows about CTand its side effects. This finding also indicates that health-care providers still do not seem to know which pharma-cologic or non-pharmacologic treatments offer best relieffrom CT-induced nausea and vomiting. It also suggeststhe need for more research on this well-known symptom.
The patients’ experiences of isolation and alienationand fear of the unknown were rated as highly distressing,even though they were relatively rare. These stressfulevents may be likened to psychological distress (depres-sion and anxiety), which is a common symptom in rela-tion to the diagnosis of cancer and its treatment (Starket al. 2002; Kissane et al. 2004; Trask 2004; Sharpley &Christie 2007). Women with substantial symptoms ofdepression and anxiety often experience increased physi-cal side effects, as well as difficulty in managing these sideeffects. The symptoms may also lead to an experience ofoverall reduced QoL (De Jong et al. 2002; Badger et al.2004; Massie 2004; Schreier & Williams 2004). Symptomsof depression and anxiety also decrease the breast cancervictims’ ability to mobilize critical support when the needfor it is greatest (Manne et al. 2004). An interview studyby Browall et al. (2006) among women in breast cancerwith adjuvant treatment found that the treatment gavedistressing experiences with affect on both body andmind. The women received some positive support from
healthcare professionals. However, the women alsodescribed variations in professionals’ attitudes, knowledgeand empathy, and they were in need of more time forinformation including support. Healthcare providers needto learn more about these symptoms and how to best be ofhelp to the women.
Coping strategies
Acceptance, relaxation and distraction were the mostcommon coping strategies for managing all stressfulevents in this study. Correspondingly, they were also themost frequently used strategies to handle stressful eventsin patients with gastrointestinal cancer in a study byWasteson et al. (2002). The benefits of using these copingstrategies is also consistent with a recent study by Cohenand Fried (2007) in which relaxation and guided imageryshowed benefits in reducing fatigue. Relaxation therapyhas also been shown to improve QoL (Walker et al. 1999)and to reduce depressed mood, anxiety and pain(Hernandez-Reif et al. 2005) in women with breast cancer.Also, non-pharmacologic interventions such as self-hypnosis, relaxation and distraction have been shownto relieve CT-induced nausea (Roscoe et al. 2003; DeCarvalho et al. 2007).
The participants in this study recorded the use of avariety of coping strategies and used an average of 3.33different coping strategies per reported stressful event(1790/538). In other words, the women did not rely on asingle coping strategy but rather employed many differentcoping strategies to deal with the same stressful event.This has been confirmed by other studies of patients withdifferent cancer diagnoses. For example, Miedema et al.(2007) reported that young adults use various coping strat-egies to come to terms with the disease and its treatment.In an interview study by Link et al. (2005), it was found
Table 5. Coping strategies in relation to stressful events (per cent diary entries recording the use of the pre-defined coping strategies foreach of the ‘stressful events’)
Coping strategies
Nauseaandvomiting% (n)
Othersymptoms% (n)
Fatigue% (n)
Isolationandalienation% (n)
Beingcontrolledby thetreatment% (n)
Fearof theunknown% (n)
Physicalproblems% (n)
Psychosocialproblems% (n)
Acceptance 60.5 (98) 51.3 (60) 73.5 (72) 45.5 (30) 68.1 (32) 44.2 (19) 61.1 (231) 52.6 (82)Relaxation 58.6 (95) 45.3 (53) 72.4 (71) 45.5 (30) 57.4 (27) 48.8 (21) 57.9 (219) 50.0 (78)Distraction 59.9 (97) 47.9 (56) 52.6 (51) 57.6 (38) 51.1 (24) 62.8 (27) 53.9 (205) 57.1 (89)Direct action 54.3 (88) 49.6 (58) 54.1 (53) 57.6 (38) 40.4 (19) 53.5 (23) 52.6 (199) 51.3 (80)Situation redefinition 42.6 (69) 39.3 (46) 53.1 (52) 50.0 (33) 53.5 (25) 55.8 (24) 44.9 (168) 52.6 (82)Social support 30.9 (50) 24.8 (29) 39.8 (39) 45.5 (30) 27.7 (13) 55.8 (24) 31.5 (119) 42.9 (67)Catharsis 17.9 (29) 21.4 (25) 29.9 (29) 30.3 (20) 29.8 (14) 53.5 (23) 22.3 (84) 36.5 (57)Religion 6.2 (10) 0.9 (1) 5.2 (5) 6.1 (4) 4.1 (2) 20.9 (9) 4.3 (16) 9.7 (15)
Daily assessment of stressful events and coping
© 2009 The AuthorsJournal compilation © 2009 Blackwell Publishing Ltd
513

that cancer patients use many coping strategies and thatthose who thought of them as methods of control wereyounger, more confident of being cured and used moreproactive strategies (e.g. lifestyle changes). In anotherinterview study by Persson and Ryden (2006), it was sug-gested that well-adjusted persons with somatic disabilitiesand/or chronic illness use several types of coping strate-gies that complement each other.
METHODOLOGICAL CONSIDERATIONS
The strengths of the current study are the demographicand diagnostic homogeneity of the sample and the longi-tudinal design. Another strength may be that both quali-tative and quantitative methods were used to capture theexperience of patient-recorded stressful events and copingstrategies since coping processes are frequently assessedby means of quantitative standardized questionnairesalone (Lazarus 2006). Problems and health-related QoL areoften assessed at pre-defined time points, often in connec-tion with a visit at the clinic. Few studies have assessedpatient-reported problems on a daily basis and over time.Standardized questionnaires often ask about the mostcommonly occurring and/or typical problems during thepast week. In analysing such information it is difficult toknow how often the symptom is experienced during thatperiod. We wanted to describe the experiences of stressfulevents and the coping strategies that post-menopausalwomen use during the period of CT. Accordingly, webelieve that it is advantageous to let the patients them-selves specify their primary problems is during treatment.The use of a diary has the advantage of providing informa-tion regarding the frequency of occurrence of symptoms,which in turn gives a more comprehensive picture of howsymptoms change over time.
A weakness of this study may be the fact that the DCAdiary is not a well-known or established instrument. Inthe present study, the unit of observation was each diary.Consequently, individuals who submitted several diarieswere over-represented, while those submitting few wereunder-represented. It is thus possible that some of ourresults may be ‘biased’ due to the fact that a few individu-als may have reported the same stressful event and thesame type of coping in all their diary entries. To checkthis, we performed analyses with each individual as theunit of observation, for example, by examining the pro-portions of stressful events and coping strategies reportedby each individual. These analyses yielded roughly thesame results as those that are presented here.
Finally, there are some limitations to the generalizabil-ity of our findings. It is important to bear in mind that our
results are reported at the group level and cannot bedirectly translated to the level of the individual patient.Furthermore, this study was hospital-based with consecu-tively treated post-menopausal patients and hence we lackinformation about patients who were not referred for ornot offered adjuvant CT, as well as those who declinedparticipation.
CONCLUSIONS
Interestingly almost 30% of all diary entries recorded nostressful events during the CT treatment period. Nauseaand vomiting was the most frequently reported andmost expected stressful event. Curiously, although thissymptom is one of the most commonly known and widelystudied CT-induced symptoms and despite the availabil-ity of special anti-emetic medication programmes, it isstill a frequent problem.
The women used several coping strategies to managetheir stressful events during adjuvant CT. The most com-monly used strategies were acceptance, relaxation anddistraction, whereas religion was rarely used. Furtherresearch is needed to better understand the relationshipbetween stressful events and the different copingstrategies used by these women.
ACKNOWLEDGEMENTS
We are most grateful to all the women who took part inthe study. This study was funded and supported by theKing Gustav V Jubilee Clinic Cancer Research Founda-tion, Göteborg, and the Sahlgrenska Academy at GöteborgUniversity, Institute of Health and Care Sciences,Göteborg, Sweden.
REFERENCES
Armstrong T.S. (2003) Symptom experience: a concept analysis.Oncology Nursing Forum 30, 601–605.
Avis N.E., Crawford S. & Manuel J. (2005) Quality of life amongyounger women with breast cancer. Journal of Clinical Oncol-ogy 15, 3322–3330.
Badger T., Segrin C., Meek P., Lopez A.M. & Bonham E. (2004) Acase study of telephone interpersonal counseling for womenwith breast cancer and their partners. Oncology Nursing Forum31, 997–1003.
Bloechl-Daum B., Deuson R.R., Mavros P., Hansen M. &Herrstedt J. (2006) Delayed nausea and vomiting continue toreduce patients quality of life after highly and moderately eme-togenenic chemotherapy despite antiemetic treatment. Journalof Clinical Oncology 24, 4472–4478.
Boehmke M.M. & Dickerson S.S. (2005) Symptom, symptomexperiences, and symptom distress encountered by womenwith breast cancer undergoing current treatment modalities.Cancer Nursing 28, 382–389.
BROWALL et al.
© 2009 The AuthorsJournal compilation © 2009 Blackwell Publishing Ltd
514

Booth C.M., Clemon M., Dranitsaris G., Joy A., Young S., Cal-laghan W., Trudeau M. & Petrella T. (2007) Chemotherapy-induced nausea and vomiting in breast cancer patients: aprospective observational study. Journal of Support Oncology5, 374–380.
Browall M., Gaston-Johansson F. & Danielson E. (2006) Post-menopausal women with breast cancer: their experiences of thechemotherapy treatment period. Cancer Nursing 29, 34–42.
Cohen M. & Fried G. (2007) Comparing relaxation training andcognitive behavioral group therapy for women with breastcancer. Research on Social Work Practice 17, 313–323.
Cooley M.E., Short T.H. & Moriatary H.J. (2003) Symptom preva-lence, distress, and change over time in adults receiving treat-ment for lung cancer. Psycho-oncology 12, 694–708.
De Carvalho E.C., Martins F.T.M. & dos Santos C.B. (2007) Apilot study of a relaxation technique for management of nauseaand vomiting in patients receiving cancer chemotherapy.Cancer Nursing 30, 163–167.
De Jong N., Courtens A.M., Abu-Saad H.H. & Schouten H.C.(2002) Fatigue in patients with breast cancer receiving adjuvantchemotherapy: a review of the literature. Cancer Nursing 25,283–297.
Dibble S.L., Israel J., Nussey B., Casey K. & Luce J.L. (2003)Delayed chemotherapy-induced nausea in women treated forbreast cancer. Oncology Nursing Forum 30, 40–47.
Epping-Jordan J.E., Compas B.E., Osowiecki D.M., OppedisanoG., Gerhardt C., Primo K. & Krag D.N. (1999) Psychologicaladjustment to breast cancer: processes of emotional distress.Health Psychology 18, 315–326.
Ganz P.A., Guadagnoli E., Landrum M.B., Lash T.L., Radowski W.& Silliman R.A. (2003) Breast cancer in older women: quality oflife and psychosocial adjustments in the 15 months after diag-nosis. Journal of Clinical Oncology 21, 4027–4033.
Ganz P.A., Kwan L., Stanton A.L., Krupnick J.L., Rowland J.H.,Meyerowitz B.E., Bower J.E. & Belin T.R. (2004) Quality of lifeat the end of primary treatment of breast cancer: first resultsfrom the moving beyond cancer randomized trial. Journal ofNational Cancer Institute 96, 376–387.
Given C.W., Given B., Azzouz F., Kozachik S. & Stommel M.(2001) Predictors of pain and fatigue in the year following diag-nosis among elderly cancer patients. Journal of Pain andSymptom Management 21, 456–466.
Grunberg S.M., Osaba D., Hesketh P.J., Gralla R.J., Borjeson S.,Rapoport B.I., du Boris A. & Tonato M. (2005) Evaluation ofnew antiemetic agents and definition of antineoplastic agentemetogenicity – an update. Support Care Cancer 2, 80–84.
Hernandez-Reif M., Ironson G., Beutler J. & Vera Y. (2005)Natural killer cells and lymphocytes increase in women withbreast cancer following massage therapy. Internal Journal ofNeuroscience 115, 495–510.
Kim H.J., McGuire D.B., Tulman L. & Barsevick A.M. (2005)Symptom clusters: concept analysis and clinical implicationsfor cancer nursing. Cancer Nursing 28, 270–282.
Kissane D.W., Grabsch B., Love A., Clarke D.M., Bloch S. &Smith G.C. (2004) Psychiatric disorder in women with earlystage and advanced breast cancer: a comparative analysis.Australian New Zealand Journal of Psychiatry 38, 320–326.
Kornblith A.B., Herndon J.E., 2nd, Zuckerman E., Viscoli C.M.,Horwitz R.I., Cooper M.R., Harris L., Tkaczuk K.H., PerryM.C., Budman D., Norton C.C. & Holland J.; Cancer andLeukemia group B. (2001) Social support as a buffer to thepsychological impact of stressful life events in women withbreast cancer. Cancer 91, 443–454.
Kuo T. & Ma F. (2002) Symptom distress and coping strategies inpatients with non-small cell lung cancer. Cancer Nursing 25,309–317.
Kurtz M.C., Kurtz J.C., Stommel M., Given C.W. & Given B.(2001) Physical functioning and depression among olderpersons with cancer. Cancer Practice 9, 11–18.
Lazarus R.S. (1993) Coping theory and research: past, present, andfuture. Psychosomatic Medicine 55, 234–247.
Lazarus R.S. (2006) Emotions and interpersonal relationships:toward a person-centred conceptualization of emotions andcoping. Journal of Personality 74, 9–43.
Lazarus R.S. & Folkman S. (1984) Coping and adaptation. In: TheHandbook of Behavioural Medicine (ed. Gentry W.D.), pp. 282–325. Guilford, New York, USA.
Lee J., Dibble S.L., Pickett M. & Luce J. (2005) Chemotherapy-induced nausea/vomiting and functional status in womentreated for breast cancer. Cancer Nursing 28, 249–255.
Link L.B., Robbins S.L., Mancuso C.A. & Charlson M.E. (2005)How do cancer patients chose their coping strategies? Aqualitative study. Patient Education and Counseling 58,96–103.
Manne J., Sherman M., Ross S., Ostroff J., Heyman R.E. & Fox S.(2004) Couples support-related communication, psychologicaldistress, and relationship satisfaction among women with earlystage breast cancer. Journal of Consulting and Clinical Psy-chology 72, 660–670.
Manuel J.C., Burwell S.R., Crawford S.L., Lawrence R.H., FarmerD.F., Hege A., Phillips K. & Avis N.E. (2007) Younger women’sperceptions of coping with breast cancer. Cancer Nursing 30,85–94.
Massie M.J. (2004) Prevalence of depression in patients withcancer. Journal of the National Cancer Institute 32, 57–71.
Miaskowski C., Cooper B.A., Paul S.M., Dodd M., Lee K., Aouiz-erat B.E., West C., Cho M. & Bank A. (2006) Subgroups ofpatients with cancer with different symptom experiences andquality-of-life outcomes: a cluster analysis. Oncology NursingForum 33, E79–E89.
Miedema B., Hamilton R. & Easley J. (2007) From ‘invincibly’to ‘normalcy’. Coping strategies of young adults duringthe cancer journey. Palliative and Supportive Care 5, 41–49.
National Board of Health and Welfare (2004) Cancer Incidence inSweden. Socialstyrelsen, The National Board of Health andWelfare, Centre for Epidemiology, Official Statistics of Sweden,Stockholm, Sweden.
Persson L.-O. & Ryden A. (2006) Themes of effective coping inphysical disability: an interview study of 26 persons who havelearnt to live with their disability. Scandinavian Journal ofCaring Sciences 20, 355–363.
Porter L.S. & Stone A.A. (1996) An approach to assessing dailycoping. In: Handbook of Coping (eds. Zeidner M. & EndlerN.S.), pp. 133–150. John Wiley & Sons, New York, USA.
Rhodes V.A., McDaniel R.W., Homan S.S., Johnson M. & MadsenR. (2000) An instrument to measure symptom experience.Symptom occurrence and symptom distress. Cancer Nursing23, 49–54.
Roscoe J.A., Morrow G.R. & Hickok J.T. (2003) The efficacy ofacutpressure and acustimulation wrist bands for the reliefof chemotherapy- induced nausea and vomiting. A Universityof Rochester Cancer Center Community Clinical OncologyProgram multicenter study. Journal of Pain and SymptomManagement 26, 731–742.
Rusthoven J.J., Osaba D., Butts C.A., Yelle L., Findlay H. &Grenville A. (1998) The impact of post chemotherapy nauseaand vomiting on quality of life after moderately emetogenicchemotherapy. Support Care Cancer 6, 389–395.
Schnoll R.A., Harlow L.L., Stolbach L.L. & Brandt U. (1998) Astructural model of the relationship among stage of disease,
Daily assessment of stressful events and coping
© 2009 The AuthorsJournal compilation © 2009 Blackwell Publishing Ltd
515

age, coping, and psychological adjustments in women withbreast cancer. Psycho-oncology 7, 69–77.
Schreier A.M. & Williams S.A. (2004) Anxiety and quality of lifeof women who receive radiation or chemotherapy for breastcancer. Oncology Nursing Forum 31, 127–130.
Shapiro S.L., Lopez A.M., Schwartz G.E., Bootzin R., FigueredoA.J., Braden C.J., Sarah F. & Kurker S.F. (2001) Quality of lifeand breast cancer: relationship to psychosocial variables.Journal of Clinical Psychology 57, 501–519.
Sharpley C.F. & Christie D.R.H. (2007) How I was then and howI am now: current and retrospective self-reports of anxiety anddepression in Australian women with breast cancer. Psycho-oncology 16, 752–762.
Stanton A.L., Danoff-Burg S., Cameron C.L., Bishop M., CollinsC.A., Kirk S.B., Sworowski L.A. & Twillman R. (2000) Emo-tionally expressive coping predicts psychological and physicaladjustment to breast cancer. Journal of Consulting and ClinicalPsychology 68, 875–882.
Stark D., Kielyn W., Smith A., Velikova G., House A. & Selby P.(2002) Anxiety disorders in cancer patients: their nature, asso-ciations and relation to quality of life. Journal of ClinicalOncology 20, 3137–3148.
Stone A.A. & Neale J.M. (1984) New measure of daily coping:development and preliminary results. Journal of Personalityand Social Psychology 46, 892–906.
Trask P. (2004) Assessment of depression in cancer patients.Journal of the National Cancer Institute Monographs 32,80–92.
Walker L., Walker M., Ogston K., Heys S., Ah-See A., Miller I.,Hutcheon A., Sarkar T. & Eremin O. (1999) Psychological,clinical and pathological effects of relaxation training andguided imagery during primary chemotherapy. British Journalof Cancer 80, 262–268.
Wasteson E., Nordin K., Hoffman K., Glimelius B. & Sjöden P.-O.(2002) Daily assessment of coping in patients with gastrointes-tinal cancer. Psycho-oncology 11, 1–11.
Weber R.P. (1995) Basic content analysis. Series: quantitativeapplications in the social sciences. Sage University Paper.
WMA (2000) World Medical Association Declaration of Helsinki.Available at: http://www.wma.net/e/policy/b3htm
Wood L.J., Nail M., Gilster A., Winters K.A. & Elsea C.R. (2006)Cancer chemotherapy-related symptoms: evidence to suggest arole for proinflammatory cytokines. Oncology Nursing Forum33, 535–542.
BROWALL et al.
© 2009 The AuthorsJournal compilation © 2009 Blackwell Publishing Ltd
516
Copyright © 2022 FDOKUMEN




















![Poly[di(carboxylatophenoxy)phosphazene] is a potent adjuvant for intradermal immunization](https://static.fdokumen.com/doc/165x107/6335c6c4a1ced1126c0af097/polydicarboxylatophenoxyphosphazene-is-a-potent-adjuvant-for-intradermal-immunization.jpg)