CPME Info 141-2008
101
EUNetPaS Recommendation Patient safety EN Only 04/07/08 CPME Info 141-2008 Source EUNetPaS Object Recommendation Date of elaboration of the document 04/07/08 Date of transmission Object Patient safety, EUNetPaS Reference CPME 2008/118, CPME info 140-2008, CPME info 026-2008, CPME info 190-2007, CPME info 101-2007, CPME info 035-2007 Author Hanneke van der Wijngaart Rue Guimard, 15 - B-1040 Brussels - Belgium Tel. : +32 (0)2 732 72 02 - Fax : +32 (0)2 732 73 44 - E-mail : [email protected] - Web : http://www.cpme.eu
-
Upload
khangminh22 -
Category
Documents
-
view
2 -
download
0
Transcript of CPME Info 141-2008
EUNetPaS Recommendation Patient safety
EN Only
04/07/08
CPME Info 141-2008
Source EUNetPaS
Object Recommendation
Date of elaboration of the document
04/07/08
Date of transmission
Object Patient safety, EUNetPaS
Reference CPME 2008/118, CPME info 140-2008, CPME info 026-2008, CPME info 190-2007, CPME info 101-2007, CPME info 035-2007
Author Hanneke van der Wijngaart
Rue Guimard, 15 - B-1040 Brussels - Belgium Tel. : +32 (0)2 732 72 02 - Fax : +32 (0)2 732 73 44 - E-mail : [email protected] - Web : http://www.cpme.eu

1
ANNEX I DESCRIPTION OF THE ACTION
2
1. OVERVIEW........................................................................................................................................3
1.1. TITLE............................................................................................................................................3 1.2. PRIORITY AREA AND ACTION ........................................................................................................3 1.3. SUMMARY (OBJECTIVES, METHODS, EXPECTED RESULTS).............................................................3
2. OBJECTIVES .....................................................................................................................................4 2.1. GENERAL OBJECTIVE....................................................................................................................4 2.2. SPECIFIC OBJECTIVES....................................................................................................................4 2.3. INDICATORS CHOSEN: ...................................................................................................................6 2.4. RATIONALE AND RELATIVE MERITS OF THE PROJECT ....................................................................8
3. EXPECTED RESULTS....................................................................................................................10 3.1. OUTCOMES .................................................................................................................................10 3.2. DELIVERABLES...........................................................................................................................11
4. METHODOLOGY............................................................................................................................18 4.1. METHODS USED, REFERENCES ....................................................................................................18 4.2. ANALYSIS OF THE RISKS AND CONTINGENCY PLANNING .............................................................23 4.3. WORK PACKAGE OVERVIEW .......................................................................................................24 4.4. TIME SCHEDULE .........................................................................................................................27
5. WORK PACKAGES DECRIPTION..............................................................................................33 5.1. WORK PACKAGE N° 1: PATIENT SAFETY CULTURE.....................................................................33
5.1.1. List of partners involved .......................................................................................................33 5.1.2. Objectives .............................................................................................................................33 5.1.3. Description of the work.........................................................................................................33 5.1.4. Deliverables and links with other work packages ................................................................40
WORK PACKAGE N° 2: EDUCATION AND TRAINING...................................................................................44 5.1.5. List of partners involved .......................................................................................................44 5.1.6. Objectives .............................................................................................................................46 5.1.7. Description of the work.........................................................................................................46 5.1.8. Deliverables and links with other work packages ................................................................50
5.2. WORK PACKAGE N° 3: REPORTING AND LEARNING SYSTEMS....................................................53 5.2.1. List of partners involved .......................................................................................................53 5.2.2. Objectives .............................................................................................................................53 5.2.3. Description of the work.........................................................................................................53 5.2.4. Deliverables and links with other work packages ................................................................57
5.3. WORK PACKAGE N° 4: PILOT IMPLEMENTATION ON MEDICATION SAFETY ..................................61 5.3.1. List of partners involved .......................................................................................................61 5.3.2. Objectives .............................................................................................................................61 5.3.3. Description of the work.........................................................................................................61 5.3.4. Deliverables and links with other work packages ................................................................63
5.4. WORK PACKAGE N° 8: COORDINATION OF THE PROJECT.............................................................80 5.4.1. List of partners involved .......................................................................................................80 5.4.2. Description of the work.........................................................................................................80 5.4.3. Milestones .............................................................................................................................84 5.4.4. Deliverables..........................................................................................................................86
5.5. WORK PACKAGE N° 9: DISSEMINATION OF THE PROJECT............................................................87 5.5.1. Overall strategy and methods ...............................................................................................87 5.5.2. Objectives .............................................................................................................................88 5.5.3. Description of the dissemination work .................................................................................88 5.5.4. Milestones and deliverables..................................................................................................90 5.5.5. List of stakeholders ...............................................................................................................92
WORK PACKAGE N° 10: EVALUATION OF THE PROJECT.............................................................................94 5.5.6. List of parties involved..........................................................................................................94 5.5.7. Description of the work and methodologies .........................................................................94
6. MEASURES TO ENSURE VISIBILITY OF COMMUNITY CO-FUNDING...........................98
7. LIST OF COLLABORATING PARTNERS..................................................................................99

3
1. OVERVIEW
1.1. Title
European Union Network for Patient Safety (EUNetPaS)
1.2. Priority area and action
1. Health information (HI 2007) 1.7 Supporting the exchange of information and experience on good practice The primary targets of this project are Member State (MS) representatives (nodes) and relevant stakeholders: health administrations, professional organisations, patient associations, healthcare organisations (hospitals, primary healthcare centres, pharmacies…). Indirectly, however, the entire EU population is a potential target, in particular those individuals considered the most fragile who are in greatest need of medical care (women, children, the elderly and disabled).
1.3. Summary (objectives, methods, expected results)
Every tenth patient in EU hospitals suffers from an adverse event. A substantial number of these adverse events are preventable. Effective interventions can reduce their impact on morbidity and mortality.
General objective:
To establish an umbrella network to improve cooperation among MS (MS) in the field of Patient Safety (PS) (culture, reporting and learning systems, education) and thus avoid overlap and duplication of effort.
Methods and means:
EUNetPaS will provide a platform for collaboration and networking between MS, international organisations and stakeholders so that they can identify and exchange good practices. Different levels of involvement will be proposed:
1. Supervisory involvement in horizontal Work Packages (WP) to facilitate active participation of MS in the project and promote its achievements at both the EU and national levels:
a. Coordination of national network and participation in Steering Committee meetings;
b. Collection of information to complete mapping exercise via interviews of national stakeholders;
c. Dissemination via conferences or integration of EUNetPaS materials in national campaigns;
d. Impact assessment using EUNetPaS indicators.
2. Involvement in the medication safety pilot scheme (coordination in the field at MS level).
3. Proactive involvement: experts share their practical and theoretical experience in a mapping exercise, address barriers (e.g. legal) to dissemination of concepts, and prepare/ propose a repertoire of intervention strategies.

4
Expected outcomes:
- The integration of MS knowledge, experiences and expertise in order to develop PS programmes at MS level and establish a communality of shared principles.
- More efficient use of resources and support to countries less advanced in the field of PS.
- A European rapid response mechanism for sharing high priority PS issues or solutions among MS.
- The development of an EU community of healthcare organisations and national institutions involved in PS through a pilot scheme for medication error prevention.
- The production of guides for healthcare professionals on core competencies and the development of curricula for medical doctors and nurses to acquire competency.
- Support for raising awareness and developing a PS culture in MS. - The establishment, beyond the contract duration of a sustainable network of PS
involving all MS.
2. OBJECTIVES
2.1. General objective
The general objective of the project is to establish an umbrella network so that:
- Cooperation among MS and between MS and stakeholders is improved in the field of PS (culture, reporting and learning systems, education); overlap and duplication of effort are avoided and support is provided to countries less advanced countries.
- The development of PS programmes at MS level integrates knowledge, experiences and expertise from MS and shares common principles;
The lessons learnt from collaboration among MS within the network could also be shared with countries outside the EU via international organisations.
Moving the PS agenda forward could help increase the efficiency of healthcare in MS by reducing the costs due to medical errors.
2.2. Specific objectives
1. To develop an organisational framework for an EU network for Patient Safety (PS): this will entail setting up a supporting secretarial office and defining an internal communication strategy and appropriate tools.
2. To collect information regarding PS culture, reporting practices and indicators in MS building on the literature and on previous projects, notably the Council of Europe recommendation on Medication Safety and projects that were conducted under the aegis of the European Commission such as SIMPATIE and MARQUIS, and using the organizational framework of the network (national contact points coordinating national platforms) and the expertise of national agencies.
3. On the basis of the information collected, to define, test and validate an instrument for assessing PS culture in health care organizations of MS.
4. To promote PS education and training in MS, that are inspired by common principles and values through (i) building a platform for the mutual exchange of experience and knowledge on methods of planning and implementing sustainable learning interventions for healthcare professionals and of involving patients and

5
caregivers -through awareness and education programmes. (ii) reaching out to decision makers in Higher Education at national and European level to promote the integration of these learning methods and interventions in undergraduate and postgraduate medical and nursing curricula.
5. To analyze and share the information collected on reporting and learning systems and on their implementation in the EU MS, to identify commonalities and understand the pros and cons of the differences observed. A rapid alert mechanism will be proposed.
6. To identify good practices in reducing medication errors in hospitals, select a number of those and implement them in hospitals (2-3 hospitals in each of the 10 participating MS).
7. To create a community with those hospitals to exchange at the level of the health professionals directly involved in clinical care.
8. Patient safety awareness: to support MS’ actions in raising awareness on PS through conferences and to support visibility of their actions on PS.

6
2.3. Indicators chosen:
Title Description
Safety Culture
WP1
- By the end of month 12 of the project web based platform mapping agreed set of PS information in Europe will be launched, containing validated information from at least 90% of the member states involved as associated partners. (Specific Objective 2)
- By the end of month 22 of the project, a PS Culture
assessment instrument, that has been selected, tested in at least 3 countries and 15 hospitals will be offered to all MS national contact points (Specific Objective 3)
Education and Training
WP 2
- At M 20 at least 2 higher education institutions (one medical faculty and one nursing faculty) will accept to co-operate, jointly develop a fit-for-purpose PS learning intervention to be delivered within a specified time interval and return feed-back into the guidelines
- At least 95% acceptance of the guidelines for education in PS by the network (expressed as % positive votes)
- At least one publication in a peered reviewed journal and at least 3 presentations in international conferences
Reporting and Learning
WP3
- At least 70 % of the MS or institutions involved as associated partners in the project and participating to a national rapid alert system have accepted to participate to the EUNetPaS rapid alert system at in the rapid alert mechanism.(Specific Objective 5)
- By the end of the project all associated partners have sent at least 3 questions /answer for the " Frequently asked questions " of the library of methods for developing and implementing reporting and learning systems (Specific Objective 5)
Pilot in Medication Safety
WP4
- At least 90% of the Member States involved as associated partners in the WP 4 field testing have selected 3 hospitals, following the criteria established by WP 10 (Specific Objective 6).
- At least 70% of the hospitals having tested the Medication Safety recommendation have sent a positive feed back regarding its transferability at M 30 (Specific Objective 7)
Dissemination
WP9
- By the end of month 2 the professional part of the website (extranet) will be open
- At least 75% of the EU stakeholders involved in the project as associated partners have sent a

7
confirmation of the reception of the reports and guidelines at M32
Evaluation
WP 10
- At least 50% of the EU stakeholders involved as associated partners will be satisfied by the outcomes of the project at M 32. The satisfaction of the stakeholders will be evaluated, through network and impact assessment of the project
- 2 “meet the experts” meetings will be organized with representatives of the hospitals involved in the WP 4 filed testing. A satisfaction study via an evaluation questionnaire will be conducted.
8
2.4. Rationale and relative merits of the project
The evidence base is clearly stated in the “Recommendation on improving Patient Safety in the EU” that was endorsed by the High Level Group on Health Services and Medical Care:
Safety of health care services is valued highly by European citizens. According to the Eurobarometer survey published in January 2006, almost four in five European Union (EU) citizens (78%) consider medical errors as an important problem in their country.
PS is a major concern in Europe. The UK Department of Health, in its 2000 report, an organisation with a memory, estimated that adverse events occur in around 10% of hospital admissions or about 850,000 adverse events a year. A report by the Hospitals for Europe’s Working Party on Quality Care in Hospitals (HOPE) has also estimated that every tenth patient in hospitals in Europe suffers from preventable harm.
It is estimated that a substantial proportion of the adverse events which take place annually in health care settings in the EU are preventable and effective interventions can be made to reduce the effect of error on morbidity and mortality. However, it is difficult to obtain exact numbers because only a few MS have made in-depth studies into this. Nevertheless, it is evident that similar types of medical errors happen in all health care systems in spite of the differences in the way they are organised or financed.1
Under the High Level Group on Health Services and Medical Care, a specific Working Group brings together 27 MS, the key stakeholders and the main international organisations in this field. A European network for PS is one of the three main pillars of the framework on PS proposed by this working group.
Significances
EUNetPaS will provide a platform for collaboration and networking between MS, international organizations and stakeholders in the field of PS.
Added value at the MS level will be secured by ensuring synergies between national policies thus reducing overlap and duplication of effort for the mapping exercise and the identification, adaptation and testing of tools. At the EU level, added value will be obtained through the sharing of expertise, the transfer of knowledge, the coordination of MS efforts for PS and through the support of the Patient Safety Working Group Recommendation, as highlighted below:
1. Support development of national policies and programs (WP 1,2,3,4)
2. Empower citizens and patients (WP 2 and 9)
3. Develop positive PS cultures, leadership and clinical governance at the health care setting level (WP 1)
4. Education and training of health professionals and all other staff (WP 2)
5. Establish reporting and learning mechanisms (WP 3)
1 Recommendation on improving Patient Safety in the EU

9
6. Develop knowledge and evidence base for PS to implement change for safer care (WP 1,2,3,4)
7. Develop indicators for PS for different HC settings (WP 1)
8. Engage stakeholders (WP 3,4,9,10)
References 1. Adjeoda, K., Michel, P., de Sarasqueta A.M., Pohié, E., Quenon, J.L., Analyse approfondie
des causes d’évènements iatrogènes en milieu hospitalier, étude de la reproductibilité des analyses dans l’enquête ENEIS, Risque et qualité, 2004, 4: 9-15
2. Amalberti, R. Auroy, Y. Berwick, D., Barach, P. Five System Barriers To Achieving Ultrasafe Health Care, Ann Intern Med. 2005;142, 9: 756-764.
3. Baker, R., Norton, P., Flintoft, V., Blais, R., Brown, A., Cox, J., & al. The Canadian adverse events study: the incidence of adverse events among hospital patients in Canada. 2004, JMAC, 170(11), 1678-1686.
4. Bates, D., Cullen, D., Laird, N. & al. Incidence of adverse drug events and potential adverse drug events: implication for prevention. 1995, JAMA, 274, 29-34.
5. Bégaud, B., Martin, K. Haramburu, F., Moore, N. Rates of Spontaneous Reporting of Adverse Drug Reactions in France, 2002, JAMA, 288: 1588
6. Brennan T, Leape, L., Laird, N., Localio, A., Lawthers, A., Newhouse, J., & al. Incidence of adverse events and negligence in hospitalized patients: results of the Harvard medical practice survey study I. New England Journal Med. 1991; 324:370-376.
7. Carthey, J de Leval M R and Reason, J T Institutional resilience in healthcare systems Qual Saf Health Care 2001;10: 29-32
8. Davies, P., Lay-Yee, R., Briant, R., Shug, S., Scott, A., Johnson, S, et al. (2001). Adverse events in New Zealand public hospitals: principal findings from a national survey. Wellington: NZ ministery of Health.
9. European SIMPATIE project [Safety IMprovement for PATients In Europe]., 2006 10. JCAHO, National patient safety goals,
http://www.jointcommission.org/PatientSafety/NationalPatientSafetyGoals/. 11. Kohn, L., Corrigan, J., & Donaldson, M. (1999). To err is human - building a safer health
system. Committee on Quality in America. Washington DC: Institute of Medicine, National Academic Press.
12. Mohr JJ, Barach P, Cravero JP, Blike GT, Godfrey MM, Batalden PB, Nelson EC. Microsystems in health care: Designing patient safety into the microsystem. Jt Comm J Qual Saf. 2003 Aug;29(8):401-8.
13. OECD Quality Indicator Project: The Patient Safety Expert Panel, 2006, http://www.oecd.org/dataoecd
14. Ovretveit J. Which interventions are effective for improving patient safety: a review of reseach evidence. Stockholm: Karolinska Insitute, Medical Managment centre, 2005.
15. Philippe Michel, Jean Luc Quenon, Ahmed Djihoud, Sophie Tricaud-Vialle and Anne Marie de Sarasqueta French National survey of inpatient adverse events prospectively assessed with ward staff Qual. Saf. Health Care 2007;16;369-377
16. Seven Steps to Patient Safety. National Patient Safety Agency, 2004, found at www.npsa.nhs.uk/sevensteps
17. Weingart, S., Pagovitch, O., Sands, D., Li, J., Aronson, M., Davis, R., Bates, D., Phillips, R., What Can Hospitalized Patients Tell Us About Adverse Events? Learning from Patient-Reported Incidents, J Gen Int Med, 2005, 20 : 830
18. Vincent, C., Adams, S., & Stanhope, N. (1998). A framework for the analysis of risk and safety in medicine. BMJ 316, 1154-1157
19. World Alliance for Patient Safety, 2006, http://www.who.int/patientsafety/solutions/en/
10
20. Leape L, Brennan, T., Laird, N., Lawthers, A., Localio, A., Barnes, B., & al. The nature of adverse events and negligence in hospitalized patients: results of the Harvard medical practice survey study II. New England Journal Med. 1991; 324:377-384.
21. Michel, P., Quenon, J.L., de Sarasqueta, A.M., Scemama, O. Comparison of three methods for estimating rates of adverse events and rates of preventable adverse events in acute care hospitals. 2004. BMJ, 328, 1-5.
22. Michel P., Quenon, J.L., Djihoud, A., Tricuad-Vialle, S., de Sarasqueta, A.M. Domecq, S. Les évènements indésirables graves liés aux soins observés dans les établissmeents de santé: premiers résultats d’une étude nationale, Etudes et résultats (DRESS), 2005, 398:1-16
23. Schioler, T., Lipczac, H., Pedersen, B., et al. Incidence of adverse events in Hospitals. A retrospective study of medical records. 2003, Ugeskr Laeger, 163: 5370-5378.
24. Thomas, E., Studdert, L., Burstin, H.Orav, E., Zeena, T., Williams, J., & al. Incidence and types of Adverse events and negligent care in Utah and Colorado. Medical Care, 2000, 38(3), 261-271.
25. Vincent, C., Neale, G., Woloshynowych, M. Adverse events in British hospitals: preliminary retrospective record review. BMJ, 2001, 322: 517-519.
26. Wilson, R., Harrison, B., Gibberd, R., Hamilton, J. (1999). An analysis of the causes of adverse events from the quality in Australian Health Care Study. Medical Journal of Australia, 1999, 170(May): 411-15.
3. EXPECTED RESULTS
3.1. Outcomes
- The more efficient use of resources and support to countries less advanced in the field of PS through the exchange of information and best practices and by cooperation in the testing of common tools at the hospital level.
- The development of PS culture in MS through
o The integration of knowledge, experiences and expertise in HCOs of various MS;
o The involvement of decision makers in the development of coordinated PS programmes at MS level;
o The establishment of a recommendation of EU shared principles regarding PS.
- The production of guides for healthcare professionals on core competencies and the development of curricula for medical doctors and nurses to acquire competency.
- A European rapid alert mechanism for sharing high priority PS issues or solutions among MS.
- The testing of practices and tools to reduce medication errors in HCOs in various MS
- The development of an active EU community of hospitals and national institutions involved in PS through a pilot scheme for medication error prevention.

3.2. Deliverables
Deliverables identified in the following table shall be submitted within 1 month of the indicated delivery date
Deliverable Number
Deliverable Title Delivery Date
Nature ConfidentialityLevel
Stakeholders & Dissemination
D01 Kick-off meeting M 1 Coordinating meeting and WP meetings
Minutes of the meeting, with the list of all the participants
Partners Mail
D02 Initial Communication kit M 1 Logo, Graphical Chart, and design of the website (public / private areas) Leaflet presenting the network. Templates for EUNetPaS power point presentations and letters Standard acknowledgment sentences/ logos
Partners EUNetPaS partners, national contact points
D03 Global work plan ofEUNetPaS
M 2 Document Partners Intranet, EUNetPaS partners,
D04 Standard OperatingProcedures (SOP)
M 2 Document Partners Intranet, EUNetPaS partners
D05
Matrix for situation analysis M 3 Document providing a list of topics to be discussed in semi-directive interviews
Partners EUNetPaS partners, website intranet
D06
WP2 meeting M 4 WP meeting
Minutes of the meeting, with the list of all the participants
Partners Mail website
D07 WP 4 meeting M 5 WP meeting
Minutes of the meeting, with the list of all the participants
Draft guideline for selection of good practices to be
Core group (HOPE, PGEU, EFN, AT, BE, FI)
Mail website
11

implemented
Draft guideline for selection of hospitals
D08 Network of national contact points coordinating national PS platforms
M 6 List of institutions and contact persons with contact details:
National contact points in the 27 Member States
Coordinating secretariat
Partners Stakeholders, EUNetPaS partners Website, conferences, newsletters
D09 Dissemination plan M 6 Communication plan (to the professionals, policy makers and general public) with the exact plan and dates for every task/deliverable, including selection of 3 targeted events, 2 publications (M 15, M30) in peer-reviewed journals: for example, Quality and Safety in Health Care, International Journal of Quality in Health Care, Health Policy.
Partners EUNetPaS partners
D10 Specification of a Guidance document on PS education and Training
M 8 A communication specifying scope, intent, content of a guidance document of added value to the MS.
Public Stakeholders: EUNetPaS partners, healthcare professionals Available to partners on the website and presented at conferences
D11 WP 4 meeting (as part of the 2nd coordination meeting)
M 8 WP meeting
Minutes of the meeting, with the list and sign of all the participants
Guideline for selection of good practices to be implemented
Guideline for selection of hospitals
Partners Mail website
D12 Coordinating Meeting 22-23 September 08
M 8 Coordinating meeting, WP meetings
Minutes of the meeting, with the list of all the participants
Partners Mail
12
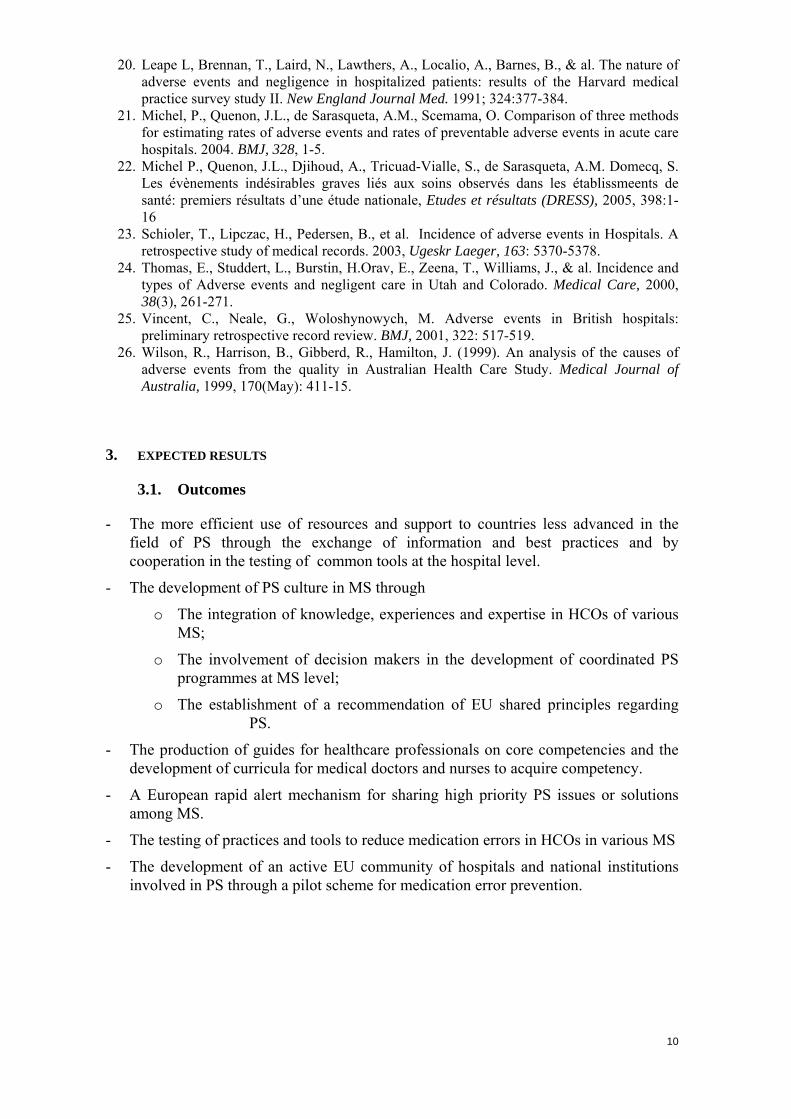
D13 Progress report M 8 Report Partners PHEA, partenrs
D14 WP 1 meeting M 9 Work package 1 meeting, Aarhus, Dk, report including minutes and list of participants
Partners Mail website
D15 Draft Compendium ofMedication safety good practices
M 9 Guideline proposed for implementation Partners Mail website
D16 WP 3 meeting M 11 WP3 meetings
Minutes of the meeting, with the list of all the participants
Partners Mail, website
D17
Situation analysis M 12 Web based platform / knowledge bank containing:
a) information on the context influencing PSC in MS, including legislative requirements, regulatory structures and key organizations;
b) previous and ongoing activities concerning PS culture, reporting systems, education and methods addressing medication errors incorporating mapping activities of other WPs in the project.
Standard information set will be collected from all member states and presented using the agreed framework. Country contact points will be in charge of collecting national information and validating it, as well as have the authority to update / change when necessary. Experts of WP (1-4) will review the information to ensure consistence.
CBO will coordinate and support the mapping exercise/ database. Data concerning current use of Culture surveys in network countries will be presented and structured according to criteria defined by a systematical critical literature review
Partners EUNetPaS Partners, website,conferences
This information will be available on the extranet
13

D18 PS Education and Training Knowledge Map
M 12 An information web space at the EUNetPaS website providing guided access to important documents relevant to WP2
Public Stakeholders: EUNetPaS partners, healthcare professionals Available to partners on the website and presented at conferences
D19 WP 4 meeting M 12 WP meetings
Minutes of the meeting, with the list and sign of all the participants
Compendium of good practices translated into implementation tools
Guideline for setting up a community of hospitals
Partners Mail website
D20 Compendium of Medication Safety implementation tools
M 14 Guideline for implementation and evaluation adapted to selected hospitals
Partners, hospitals involved in field testing
Training , meetings
Website.
D21 Coordinating meetingCopenhagen
M 16 Coordinating meeting and WP meetings
Minutes of the meeting, with the list of all the participants
Partners Mail, website
D22 Diversified teachingprograms for medical and nursing schools and Continuing Professional Development (CPD)
M 17 Course booklets for 4 teaching programs including target audiences, pre-requisites, list of learning objectives and topics, delivery details, and course documentation
Public Stakeholders: EUNetPaS partners, healthcare professionals Available to partners on the website and presented at conferences
D23 Technical and Financial Interim Reports
M 17 Report Confidential PHEA
14
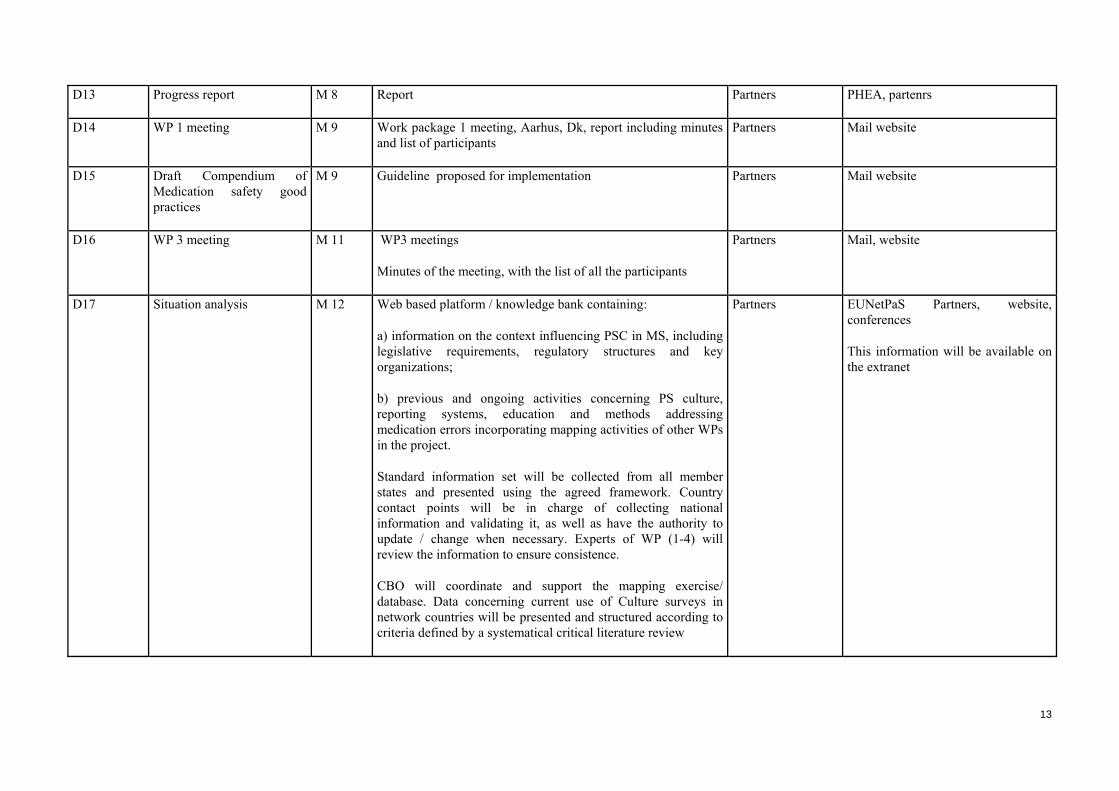
D24
Compendium of goodpractices and examples of regulation, legislation and organisation in patient safety (PS)
M 18 Web based addition to the mapping platform containing specific examples of good practice with the focus on PS culture, education, reporting systems and medication safety solutions. Information will be collected primarily from the countries that participate in respective WP and would include in depth description and experiences with relevant instruments. Information will be approved by the Steering Committee before web publication.
Public Stakeholders: EUNetPaS partners, national contact points, HCOs, healthcare professionals The compendium will be published, available on the website and presented at conferences
D25
WP 1 meeting M 22 Work package 1 meeting, Spain, report including minutes and list of participants
Partners Mail website
D26
PS Culture measurement tool
M 24 Validated and tested instrument to assess PS culture in health care organizations, including methodological background and implementation protocol. The questionnaire will be presented in English with a protocol describing translation-retranslation procedure, application (institutional level, subject characterisation, and minimum participation rate) and recommendations.
Public Stakeholders: EUNetPaS partners, national contact points, HCOs, healthcare professionals The instrument will be published, available on the website and presented at conferences
D27 Reporting and learningsystem data base
M 24 Web-based library of methods for reporting and implementing learning systems.
Partners Stakeholders: EUNetPaS partners, participating HCOs, healthcare professionals Available to partners on the extranet and presented at conferences
D28 Coordinating meetingAthens
M 24 Coordinating meeting and WP meetings
Minutes of the meeting, with the list of all the participants
Partners Mail website
D29 Progress report M 24 Report Partners PHEA, partners
D30 WP2 meeting M 25 WP meeting Partners Mail website
15
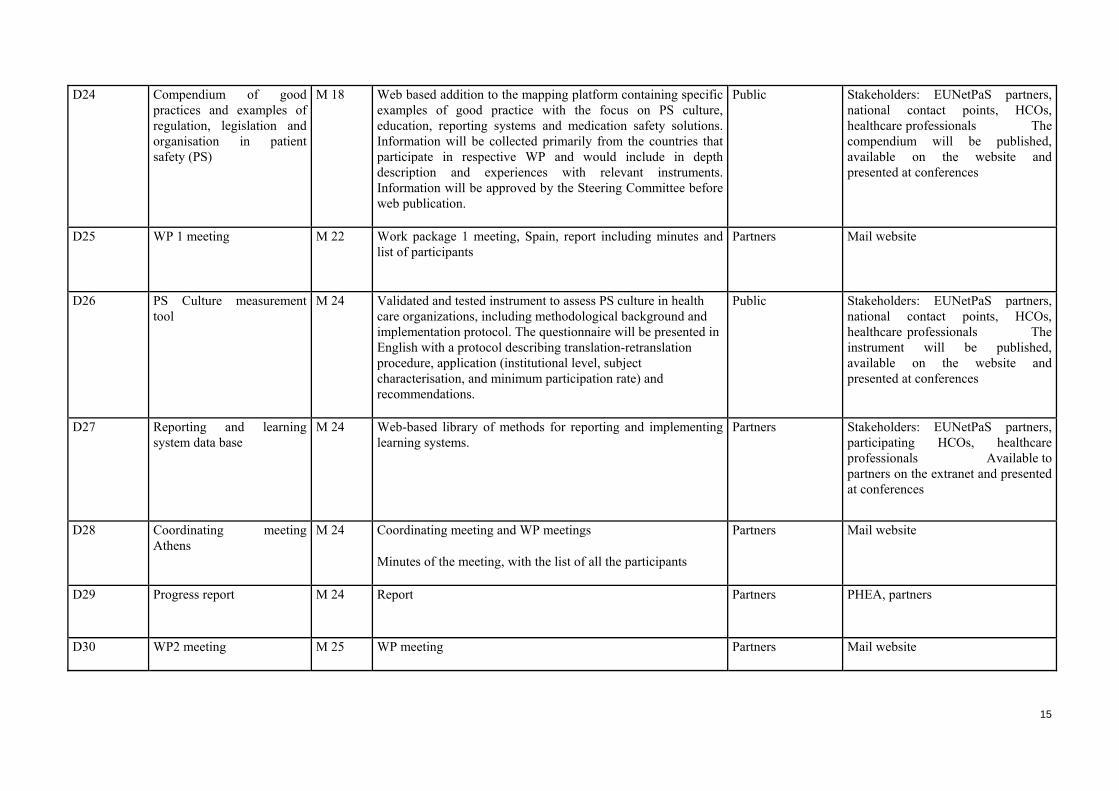
Minutes of the meeting, with the list of all the participants
D31 Guidelines for education in PS
M 25 Guidelines proposing core competencies and curricula for health professionals; guidance on patient and helpers education
Public Stakeholders: EUNetPaS partners, healthcare professionals Available to partners on the website and presented at conferences
D32 WP 3 meeting M 27 WP meetings
Minutes of the meeting, with the list of all the participants
Partners Mail website
D33 Coordinating final meeting Brussels
M 29 Coordinating meeting and WP meetings Partners Mail, website
D34 EU PS Rapid AlertMechanism
M 30 Web based electronic maintenance free program for sharing high priority PS issues or solutions among MS.
Monthly report
Partners onsubscription
extranet
D35 Medication Safetyrecommendation
M 30 Guideline Compendium presenting the results ofimplementation and proposing recommendations for further implementations
Public Stakeholders, EUNetPaS partners Website, conferences, newsletters
D36 EU community of Health Care Organisations and national institutions involved in PS
M 30 Document analysing the results of setting up a community of hospitals on the basis of pilot implementation of good practices and proposing recommendation for development and sustainability of such a community
Public Stakeholders: EUNetPaS partners, participating hospitals, healthcare professionals Available to participating hospitals and national institutions on the website and presented at conferences.
16

D37 Project’ impact assessment report
M 30 Report Using process indicators such as level of network use by MS, and the extent to which the network has aided and given new impetus to national PS initiative.
Public Stakeholders: PHEA, EUNetPaS partners, national contact points, healthcare professionals, general public Report sent to partners and relevant stakeholders (PSWG, PHEA…), open access to the report on the website
D38 Project evaluation report
M 30 Report. Give the results of an audit investigating whether the project objectives have been met and whether the deliverables in the work packages have been produced according to plan.
Partners Stakeholders: PHEA, EUNetPaS partners Report sent to partners and relevant stakeholders (PSWG, PHEA…)
D39 Technical and Financial Final Reports
M 32 Report
Minutes of the meeting, with the list of all the participants
Confidential PHEA
17

18
4. METHODOLOGY
4.1. Methods used, references
Methods used:
- Network development The development of the network will be based on the partners of the project representing the 27 MS. One partner in each Member State (generally a representative of the Ministry of Health: cf List of National Contact Points, below) will act as a national contact point. Most of these national representatives are members of the SANCO Patient Safety Working Group, therefore they are involved in PS both at national and EU level. They are also used to working together around PS issues. These national contact points will be involved in the information collection (cf WP 1,2,3,4), in the dissemination (cf WP 9) and in the evaluation of the project (cf WP 10). They will be strongly encouraged by project governance bodies (Steering Committee and Executive Board) to involve national stakeholders (health professionals’ representatives, patients’ representatives, decision makers) in these different tasks. The development of these national platforms will be also facilitated by the involvement in the project of the EU representatives of the main stakeholders (European Federation of Nurses, Standing Committee of European Doctors, European Patient Forum, Pharmaceutical Group of the European Union, European Federation of Hospitals). They will encourage the participation of their affiliates in these national PS platforms which should contribute to and enhance the impact of EUNetPaS. The management of the network will be facilitated by the coordinating secretariat including relevant communication platforms provided by the Main Partner (responsibilities and tasks are defined in the SOPs) but networking itself, ensuring the operational character of the Network will be promoted through the management of EUNetPaS activities including reporting, communication, evaluation…
List of National Contact Points:
Austria Federal Ministry of Health Family and Youth
Belgium FOD-DG1 : Ministry of Health
Bulgaria Ministry of Health
Cyprus Ministry of Health
Czech Republic Ministry of Health
Denmark SST : National Board of Health
Estonia Estonian Ministry of Social Affairs

19
Finland STM Finland : Ministry of Social Affairs and Health
France HAS : French National Authority for Health (Main Partner)
Germany GCPS : German Coalition for Patient Safety
Greece EKEVYL: Research Centre for Biomaterials
Hungary Alloy Consulting Informatikai és Tanacsado Kft.
Ireland HIQA : Health Information and Quality Authority of Ireland
Italy Ministry of Health
Latvia Ministry of Health
Lithuania StaHeCCA : State Health Care Accreditation Agency
Luxembourg Ministry of Health
Malta Ministry of Social Policy
Netherlands CBO : Dutch Institute for Healthcare Improvement
Poland CMJ : National Center for Quality Assessment in Health Care
Portugal DGS : Department of Health
Romania National School of Public Health and Health Services Management
Slovakia Ministry of Health
Slovenia Ministry of Health
Spain SMoH : Spanish Ministry of Health and Consumer Affairs
Sweden NBHW : The National Board of Health and Welfare
United Kingdom DoH : Department of Health, England
- Information collection:
Review of existing data: Sources of information will be based on the partners experience and knowledge in the field, they will select relevant data and studies especially in the so-called “grey literature” including national PS regulations and plans and circulate them among themselves. Available literature review on the subject (for example, Council of Europe Medication Safety recommendation) will be considered by the core WPs experts. This information will be updated during the project through systematic review of the main publications in the field: British Medical Journal, New England Journal of Medicine, Quality and Safety in Health Care, International Journal of Quality in Health Care, Health Policy.

20
Network mapping: Information collection framework (matrix), including key items that should be provided by all member states and protocol for information collection, will be developed by WP 1 with input from WP 2/3/4 on their respective subjects. The matrix and the information collection protocol will be approved by the Steering Committee. Through WP 8, national contact points will be approached with the request to collect the information through semi-structured interviews with representatives of relevant national organizations / institutions. Responses from countries, including the list of interviewed stakeholders will be collected through a web based tool and presented in the pre-defined framework. All countries are expected to provide core information set, including identification of the main stakeholders (decision makers as well as different categories of health care professionals and patients representatives) contacts / activities relevant for focus areas as PS culture, education, reporting and medication safety. The information will be validated by national contact points.
- Recommendation and tools proposals:
Once identified in each focus area, the main national stakeholders could be directly contacted by the relevant core WPs to be involved as outside experts groups. Discussions at the core WP level based on transfer of knowledge exchange of ideas, materials and best practices, will be organised to validate information to be included in the database (information focusing on PS Culture, PS Education, reporting and learning systems, medication safety) and to produce recommendations (reporting and learning systems, PS education, PS culture measurement tool, medication safety recommendation). A consensus among partners about the tools which could be promoted at the EU level will be reached during face to face meetings or E-meetings. Decision making will be based on Executive board proposals validated by Steering Committee as defined in the SOPs. Each WP involves a number of partners. They will validate the collected data and will propose methods and tools based on this information and on their own know-how. Different types of documents will be proposed: guidelines, compendium of good practices, evaluation questionnaires, recommendations. These documents will be tested and assessed by the network and the final versions will include this feedback and be validated by the Steering Committee. Recommendations will be provided with background information and evidence review according to the usual EBM practice and grading systems.
- Pilot testing:
Pilot testing will be used to test medication safety recommendation (WP4) and PS education programs (WP 2) in the MS with the objective of engaging the medical community (academics and practising healthcare professionals) in a practical exercise at the EU level.
For the WP4, 2-3 hospitals will be selected by the national contact points of the 10 participating MS (Finland, Belgium, Austria, France, Netherlands, Greece, Denmark, Ireland, Lithuania, Portugal). Selection criteria will be based on the involvement of the selected hospitals in PS. These criteria will be discussed at the WP4 level and formalised in a guideline (M8)
For the WP2, two (2) faculties of medicine and two (2) nursing schools will be selected by the national contact points on a voluntary basis. They will implement

21
the PS recommendation and conduct an evaluation based on a questionnaire developed by WP2 experts and on WP 10 relevant indicator (% of health care professionals who complete the recommended education program).
- External Coordination:
This project will and has already begun to coordinate its activities with EU, WHO and OECD projects through the involvement of the leaders of these projects in the network. Being involved as collaborating and for some of them as associated partners, they will attend steering comity meetings and take an active part in core work packages’ work to avoid duplication of work and ensure that the results of EU,WHO, CoE and OECD projects will be duly taken into consideration.
o HAS and CBO were involved in the SIMPATIE and MARQUIS projects and ESQH in SIMPATIE;
o The WHO Regional Office for Europe is a collaborating partner of EUNetPaS and will be specifically involved in WP 2 and 9;
o OECD is a collaborating partner of EUNetPaS and the contact person, N.Klazinga is also in charge of OECD health indicators program. He will be particularly involved in WP 1 and 10;
o CoE is a collaborating partner of EUNetPaS and P.Mierzewski who is the contact person was deeply involved in the CoE recommendation entitled: “Creation of a better medication safety culture in Europe: building up safe medication practices”. He will be particularly involved in WP 4
- Website development:
The interactive EUNetPaS website will be a major communication instrument ensuring both integration of the work programme communication (restricted access area of the website, with login and password for the partners) and dynamic communication window for the general and specialised public. This portal is crucial for the success of the project because it facilitates interaction between the partners and provides the tools to promote the EUNetPaS activities.
The public section of the EUNetPaS website will be regularly updated by the main partner thanks to Joomla technology, by informing on the network progress, announcing key events, etc. Topics and presentation will be adapted to the various visitors’ profiles: HC professionals, patients, general public, etc. Specific tools developed by the consortium will be progressively “grafted” onto the public site.
The EUNetPaS management extranet system with restricted access (password and login) will be developed using the PLONE open-source technology to create a flexible and easily accessible system for the dissemination and management of knowledge acting as a portal for all members. The resulting framework will be used to maintain a well-informed workforce, promote information exchange and increase efficiency, by creating an inclusive, comprehensive, and easily accessible organizational memory. The system will be accessible from the public section by entering login and password. The extranet represents the base of the collaborative platform and knowledge management system, it will contain at the
22
start all key documents related to the contract, project finances, and current work programme. It shall evolve our knowledge management through key steps:
• Acquiring complete sets of information on SOP, protocols and methods, and on the strategy of the project and supporting documentation;
• Ensuring that information is used strategically for sense-making, the creation of new knowledge, and in key decision making. This entails that participants will be kept constantly aware of all new developments within the project, including development of new skills, protocols and new data. A specific chat room platform will be proposed for the various WP activities, where members will be able to upload and download documents.
All information will be formatted into cross platform software documents and archived ensuring that all pertinent knowledge, past or present, generated inside or outside the project can easily be incorporated into any decision making. In addition to the generation of the knowledge database, all participants will be kept constantly updated on all information within the project through a monthly newsletter which will be electronically mailed to everybody.
Preliminary functional version of both the public and private sections of the EUNetPaS website will be ready for use by all partners at Month 1.
Sustainability:
- After the termination of the project, the website could be maintained to provide support to the Rapid Alert mechanism;
- It could provide a valuable communication tool for a future EU collaboration on PS,
to enhance the operational dimension of such collaboration; - The site could also provide a valuable communication tool to test the results of PS
research projects in the MS; - The public part of this website could also be used to relay future national or
international PS campaigns. - The sustainability of EUNetPaS will be discussed at the Patient Safety Working
Group level. If the added value of this Network is acknowledged by Member States and by the European Commission this point should be addressed in the future EC Patient Safety initiative
References
1) Ashcroft DM, Morecroft C, Parker D, Noyce PR. Safety culture assessment in community pharmacy: development, face validity, and feasibility of the Manchester Patient Safety Assessment Framework. Qual Saf Health Care 2005 Dec;14(6):417-21.
2) Jones J, Hunter D, Qualitative Research: Consensus methods for medical and health services research BMJ 1995;311:376-380

23
3) McGlynn EA, Kosecoff J, Brook RH. Format and conduct of consensus development conferences. International Journal of Technology Assessment in Health Care 1990;6:450-69. [Medline]
4) Pill J. The Delphi method: substance, context, a critique and an annotated bibliography. Socio-Economic Planning Science 1971;5:57-71.
5) Reason J, Wreathall J. Checklist for Assessing Institutional Resilience (CAIR). 2000.
6) Rowe G, Wright G, Bolger F. Delphi: a re-evaluation of research and theory. Technological Forecasting and Social Change 1991;39:235-51.
7) Sexton JB, Helmreich RL, Neilands TB, Rowan K, Vella K, Boyden J, et al. The Safety Attitudes Questionnaire: psychometric properties, benchmarking data, and emerging research. BMC Health Serv Res 2006 Apr 3;6(1):44.
8) Sexton JB, Helmreich RL, Pronovost P, Thomas EJ. Safety Climate Survey. 2004. IHI Institute for Healthcare Improvement (Books).
9) Sorra J, Nieva VF. Hospital Survey on Patient Safety Culture. AHRQ Publication no. 04 0041. September 2004. 2004. Rockville, MD: Agency for Healthcare Research and Quality.; 2006.
4.2. Analysis of the risks and contingency planning
Change in key personnel in the Associated Partners:
The handbook of Standing Operating Procedures (SOP) produced by the Coordinating Secretariat will facilitate the rapid information of new personnel on technical and administrative procedure and details of the project.
Delay in reporting by Associated Partners:
Early development of a strategy to require preliminary reporting 60 (or more) days prior to final reporting date.
Financial or management crises in one of the AP organisations:
Strong central coordination with assistance of WP Leaders, good internal communication and dispersion of tasks among partner organisations should contain the risk of WPs becoming diverted from their focus or timetable. WP 3 risk assessment and WP 1 risk management will be applied.
Major health emergencies affecting large populations:
Early development of an emergency plan by the Executive Committee and constant monitoring of the public health situation in order to allow priority to immediate public health intervention
24
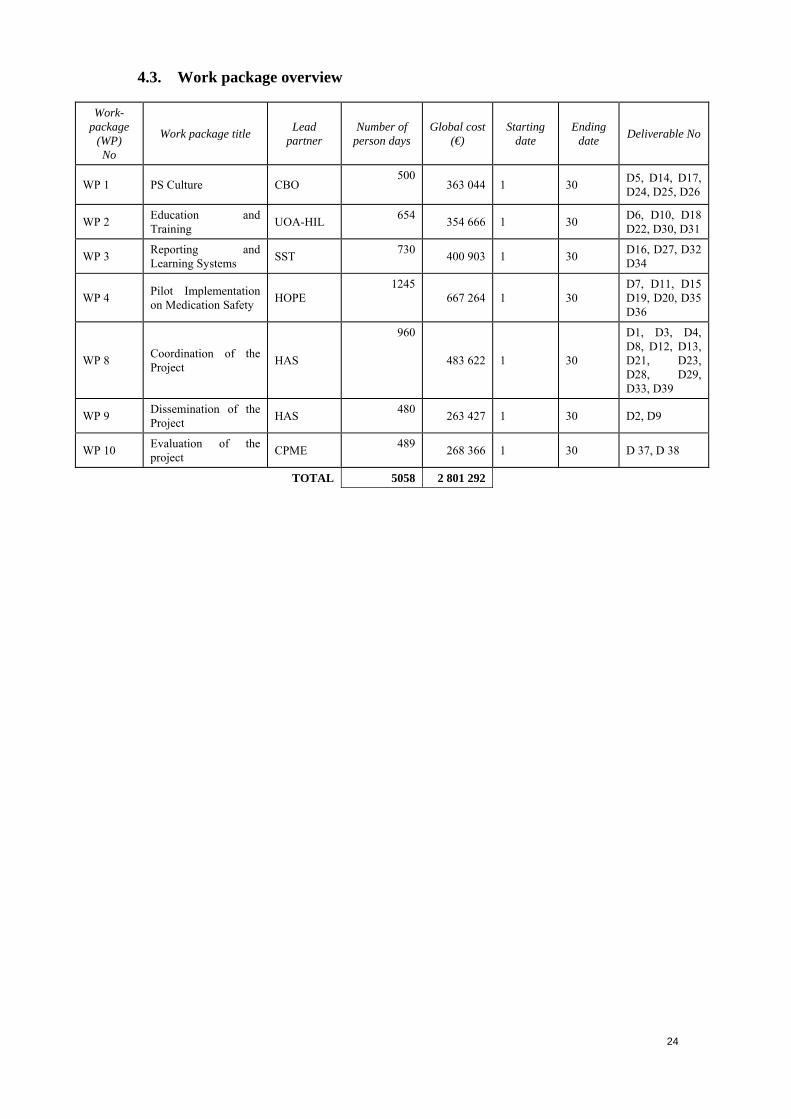
4.3. Work package overview
Work-package
(WP) No
Work package title Lead partner
Number of person days
Global cost (€)
Starting date
Ending date Deliverable No
WP 1 PS Culture CBO 500
363 044 1 30 D5, D14, D17,
D24, D25, D26
WP 2 Education and Training UOA-HIL 654 354 666 1 30 D6, D10, D18
D22, D30, D31
WP 3 Reporting and Learning Systems SST 730 400 903 1 30 D16, D27, D32
D34
WP 4 Pilot Implementation on Medication Safety HOPE
1245 667 264 1 30
D7, D11, D15 D19, D20, D35 D36
WP 8 Coordination of the Project HAS
960
483 622 1 30
D1, D3, D4, D8, D12, D13, D21, D23, D28, D29, D33, D39
WP 9 Dissemination of the Project HAS 480 263 427 1 30 D2, D9
WP 10 Evaluation of the project CPME 489 268 366 1 30 D 37, D 38
TOTAL 5058 2 801 292

Effort person/day
WP 1 WP 2 WP 3 WP 4 WP 8 WP 9 WP 10 Total Days 1 HAS 55 698 210 65 10282 CBO 170 10 55 2353 UOA-HIL 112 1124 SST 440 55 18 18 8 5395 HOPE 220 2206 STM-FIN 150 18 18 8 1947 CPME 60 18 18 160 2568 ESQH 150 1509 PGEU 95 18 18 8 13910 IPG 150 15011 SMOH 130 70 18 18 8 24412 HIQA 22 55 18 18 8 12113 GCPS 80 18 18 8 12414 FOD-DG1 150 18 18 8 19415 StaHeCCA 10 18 20 55 18 18 8 14716 NBHW 110 18 18 8 15417 DGS 110 55 18 18 8 20918 RUNMC 100 10019 EFN 40 60 95 18 18 43 27420 DOH 18 18 8 4421 EPF 25 10 18 25 7822 EKEVYL 207 40 55 18 18 8 347 TOTAL 500 654 730 1245 960 480 489 5058
*:subcontracting
25
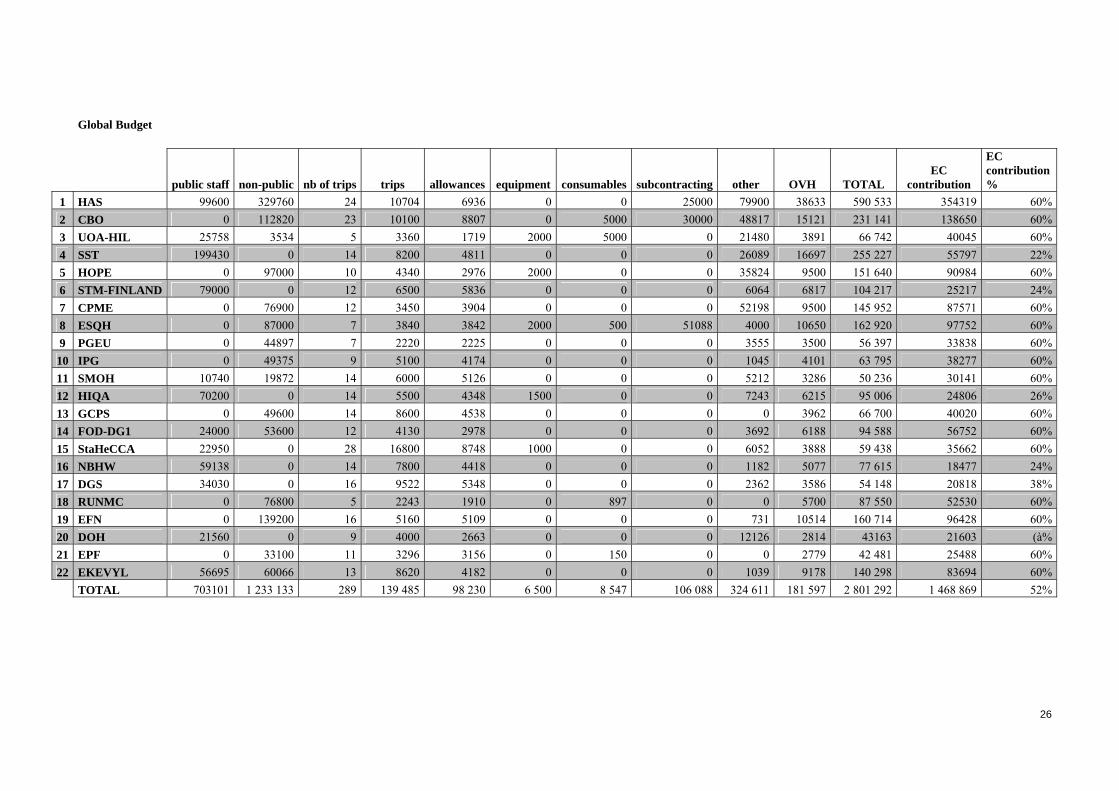
Global Budget
public staff non-public nb of trips trips allowances equipment consumables subcontracting other OVH TOTAL EC
contribution
EC contribution %
1 HAS 99600 329760 24 10704 6936 0 0 25000 79900 38633 590 533 354319 60%2 CBO 0 112820 23 10100 8807 0 5000 30000 48817 15121 231 141 138650 60% 3 UOA-HIL 25758 3534 5 3360 1719 2000 5000 0 21480 3891 66 742 40045 60%4 SST 199430 0 14 8200 4811 0 0 0 26089 16697 255 227 55797 22% 5 HOPE 0 97000 10 4340 2976 2000 0 0 35824 9500 151 640 90984 60%6 STM-FINLAND 79000 0 12 6500 5836 0 0 0 6064 6817 104 217 25217 24% 7 CPME 0 76900 12 3450 3904 0 0 0 52198 9500 145 952 87571 60%8 ESQH 0 87000 7 3840 3842 2000 500 51088 4000 10650 162 920 97752 60% 9 PGEU 0 44897 7 2220 2225 0 0 0 3555 3500 56 397 33838 60%10 IPG 0 49375 9 5100 4174 0 0 0 1045 4101 63 795 38277 60% 11 SMOH 10740 19872 14 6000 5126 0 0 0 5212 3286 50 236 30141 60%12 HIQA 70200 0 14 5500 4348 1500 0 0 7243 6215 95 006 24806 26% 13 GCPS 0 49600 14 8600 4538 0 0 0 0 3962 66 700 40020 60%14 FOD-DG1 24000 53600 12 4130 2978 0 0 0 3692 6188 94 588 56752 60% 15 StaHeCCA 22950 0 28 16800 8748 1000 0 0 6052 3888 59 438 35662 60%16 NBHW 59138 0 14 7800 4418 0 0 0 1182 5077 77 615 18477 24% 17 DGS 34030 0 16 9522 5348 0 0 0 2362 3586 54 148 20818 38%18 RUNMC 0 76800 5 2243 1910 0 897 0 0 5700 87 550 52530 60% 19 EFN 0 139200 16 5160 5109 0 0 0 731 10514 160 714 96428 60%20 DOH 21560 0 9 4000 2663 0 0 0 12126 2814 43163 21603 (à% 21 EPF 0 33100 11 3296 3156 0 150 0 0 2779 42 481 25488 60%22 EKEVYL 56695 60066 13 8620 4182 0 0 0 1039 9178 140 298 83694 60% TOTAL 703101 1 233 133 289 139 485 98 230 6 500 8 547 106 088 324 611 181 597 2 801 292 1 468 869 52%
26
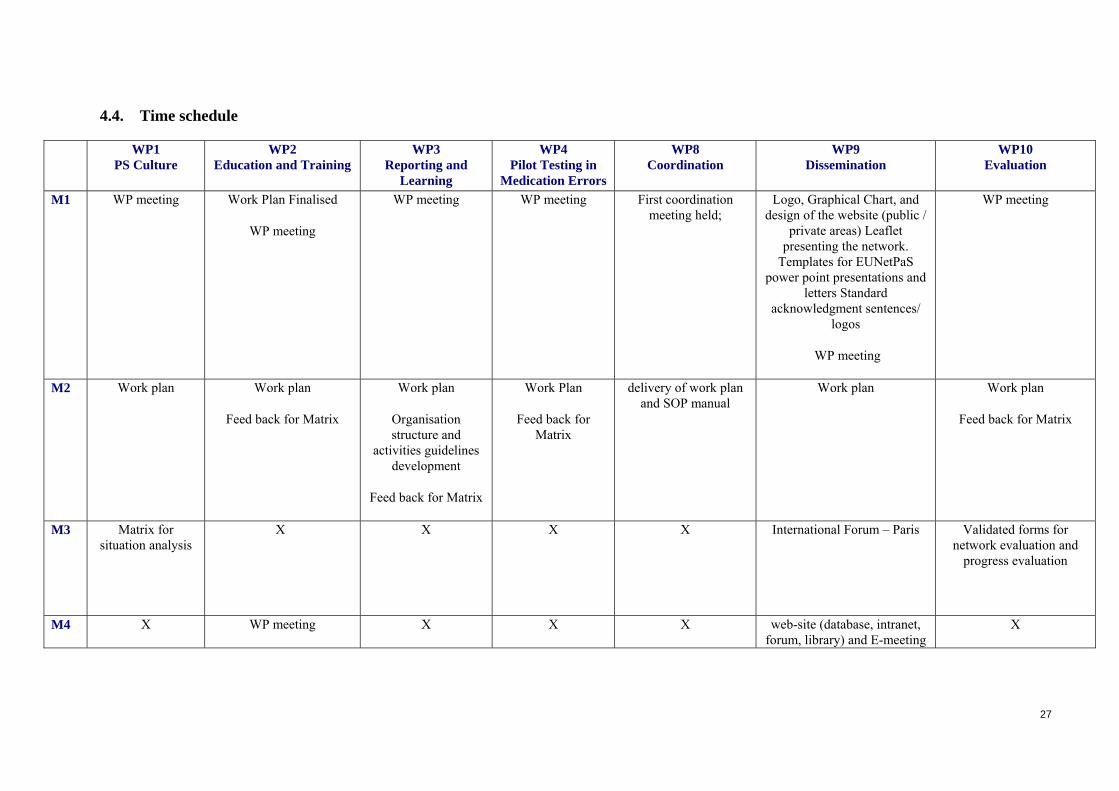
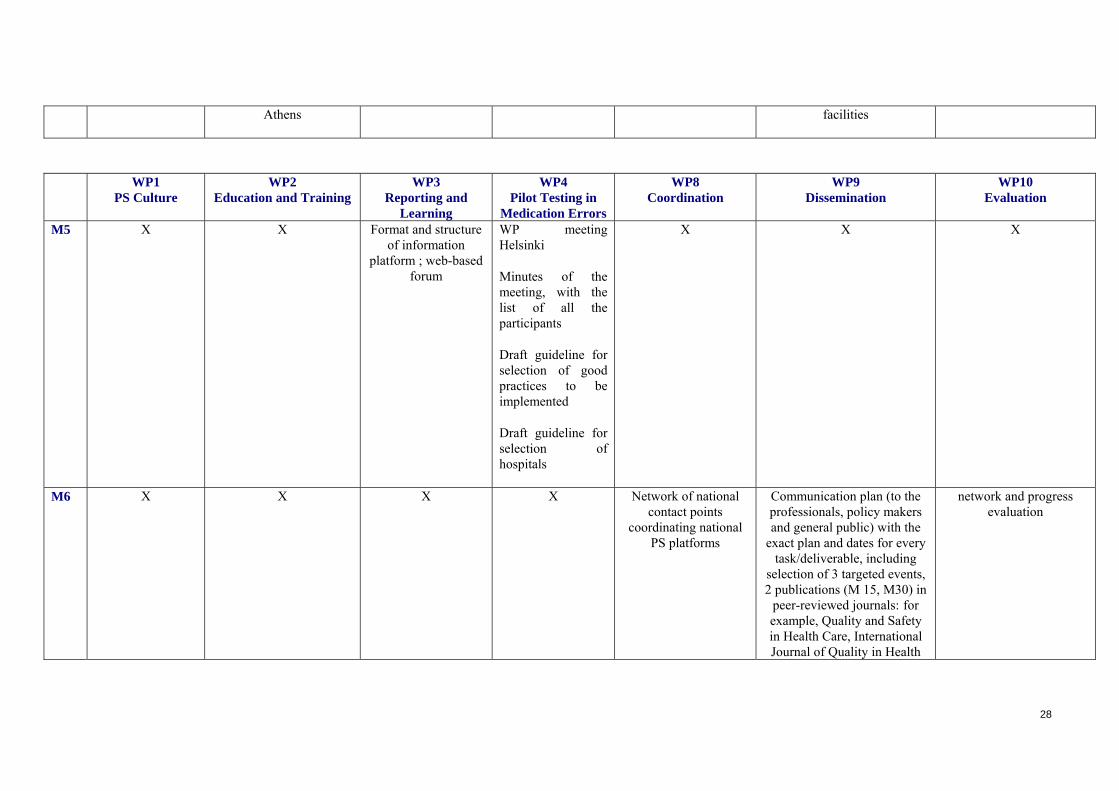
4.4. Time schedule
WP1PS Culture
WP2 Education and Training
WP3 Reporting and
Learning
WP4 Pilot Testing in
Medication Errors
WP8 Coordination
WP9 Dissemination
WP10 Evaluation
M1 WP meeting Work Plan Finalised
WP meeting
WP meeting WP meeting First coordination meeting held;
Logo, Graphical Chart, and design of the website (public /
private areas) Leaflet presenting the network.
Templates for EUNetPaS power point presentations and
letters Standard acknowledgment sentences/
logos
WP meeting
WP meeting
M2 Work plan Work plan
Feed back for Matrix
Work plan
Organisation structure and
activities guidelines development
Feed back for Matrix
Work Plan
Feed back for Matrix
delivery of work plan and SOP manual
Work plan Work plan
Feed back for Matrix
M3 Matrix for situation analysis
X X X X International Forum – Paris Validated forms for network evaluation and
progress evaluation
M4 X WP meeting X X X web-site (database, intranet, forum, library) and E-meeting
X
27
Athens facilities
WP1PS Culture
WP2 Education and Training
WP3 Reporting and
Learning
WP4 Pilot Testing in
Medication Errors
WP8 Coordination
WP9 Dissemination
WP10 Evaluation
M5 X X Format and structure of information
platform ; web-based forum
WP meeting Helsinki
Minutes of the meeting, with the list of all the participants
Draft guideline for selection of good practices to be implemented
Draft guideline for selection of hospitals
X X X
M6 X X X X Network of national contact points
coordinating national PS platforms
Communication plan (to the professionals, policy makers and general public) with the
exact plan and dates for every task/deliverable, including
selection of 3 targeted events, 2 publications (M 15, M30) in
peer-reviewed journals: for example, Quality and Safety in Health Care, International Journal of Quality in Health
network and progress evaluation
28

Care, Health Policy.
M7 X X X X X X X
M8 WP meeting WP meeting
Guidance document on PS education and
Training
WP meeting WP meeting
Paris
Guideline for selection of good practices to be implemented
Guideline for selection of hospitals
Second coordination meeting; feedback
from national contact points regarding situation analysis
Progress report
Open meeting in Paris (PFEU); European Health
Forum Gastein; 2009 timeframe of interventions
WP meeting
WP meeting
M9 WP meeting
Aarhus
X X Draft Compendiumof Medication safety good
practices
X ISQUA in Copenhagen X
M10 X X X X X X X
M11 X X WP meeting X X X X
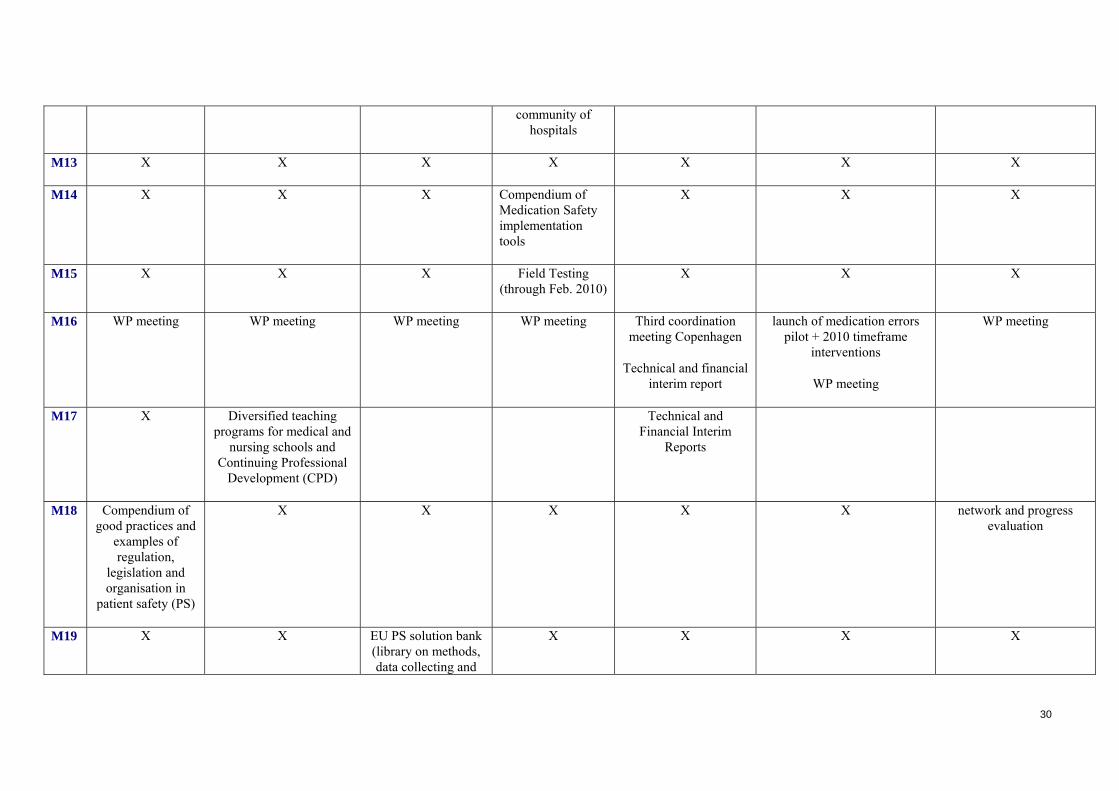
WP1PS Culture
WP2 Education and Training
WP3 Reporting and
Learning
WP4 Pilot Testing in
Medication Errors
WP8 Coordination
WP9 Dissemination
WP10 Evaluation
M12 Situation analysis PS Education and Training Knowledge Map
X WP meeting
Guideline for setting up a
X X network and progress evaluation
29
community of hospitals
M13 X X X X X X X
M14 X X X Compendium ofMedication Safety implementation tools
X X X
M15 X X X Field Testing(through Feb. 2010)
X X X
M16 WP meeting WP meeting
WP meeting WP meeting Third coordination meeting Copenhagen
Technical and financial interim report
launch of medication errors pilot + 2010 timeframe
interventions
WP meeting
WP meeting
M17 X Diversified teachingprograms for medical and
nursing schools and Continuing Professional
Development (CPD)
Technical andFinancial Interim
Reports
M18 Compendium of good practices and
examples of regulation,
legislation and organisation in
patient safety (PS)
X X X X X network and progress evaluation
M19 X X EU PS solution bank (library on methods, data collecting and
X X X X
30

analysing techniques)
WP1PS Culture
WP2 Education and Training
WP3 Reporting and
Learning
WP4 Pilot Testing in
Medication Errors
WP8 Coordination
WP9 Dissemination
WP10 Evaluation
M20 X X X X X X X
M21 X WP meeting X X X X X
M22 WP meeting
Madrid
X X X X X X
M23 X X X X X X X
M24 WP meeting
PS Culture measurement tool
WP meeting WP meeting
Reporting and learning system data
base
WP meeting
Fourth coordination meeting; Athens
Progress report
WP meeting first results of education pilot, launch of PS culture recommendation and library on reporting systems
WP meeting
network and progress evaluation
M25 WP2 meeting
Guidelines for education in PS
End of Field Testing
M26 X X X X X X X
M27 X X WP meeting
31
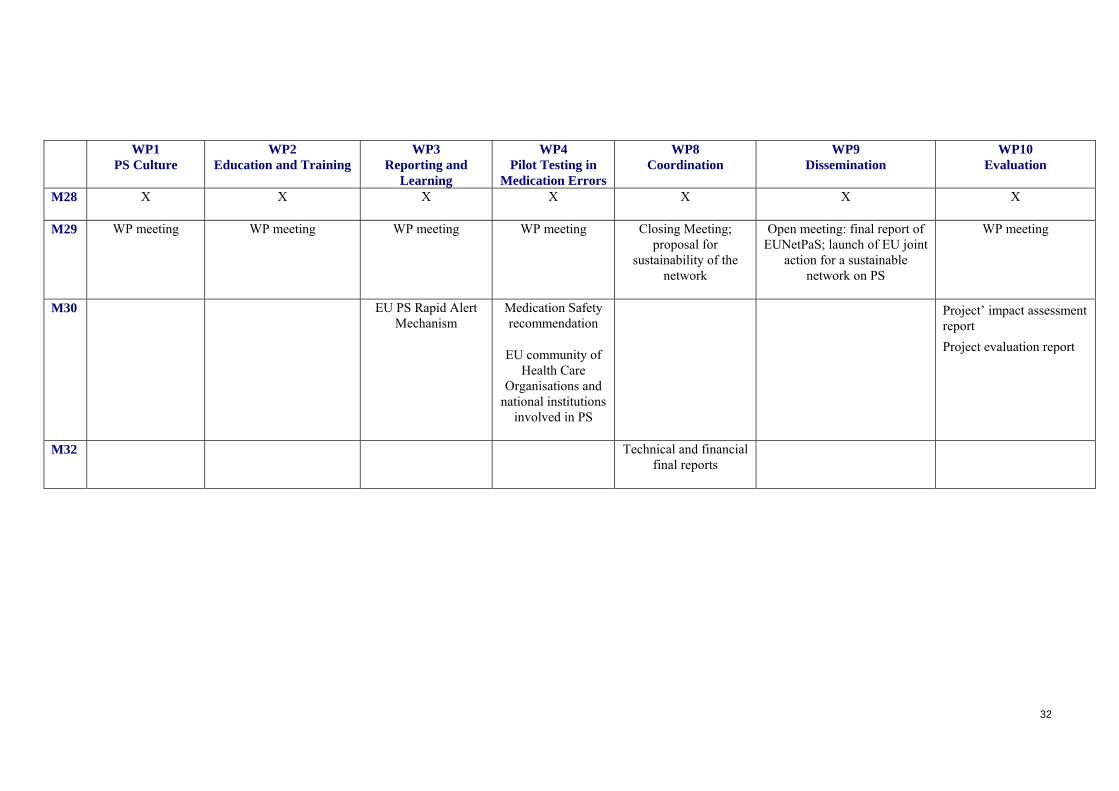
WP1PS Culture
WP2 Education and Training
WP3 Reporting and
Learning
WP4 Pilot Testing in
Medication Errors
WP8 Coordination
WP9 Dissemination
WP10 Evaluation
M28 X X X X X X X
M29 WP meeting WP meeting
WP meeting WP meeting
Closing Meeting; proposal for
sustainability of the network
Open meeting: final report of EUNetPaS; launch of EU joint
action for a sustainable network on PS
WP meeting
M30 EU PS Rapid Alert Mechanism
Medication Safety recommendation
EU community of Health Care
Organisations and national institutions
involved in PS
Project’ impact assessment report Project evaluation report
M32 Technical and financial final reports
32
33
5. WORK PACKAGES DECRIPTION
5.1. Work package n° 1: Patient Safety Culture
5.1.1. List of partners involved
CBO (Leader) 170 p/d will coordinate the WP situation analysis work (interview support, feedback from national contact points), the Patient Safety Culture (PSC) measurement tool ESQH 150 p/d indicator work, PSC measurement tool EFN 40 p/d PSC situation analysis (feed back from affiliates) SMoH 130 p/d PSC situation analysis, measurement tool StaHeCCA 10 p/d situation analysis
5.1.2. Objectives
Objective 2: Building on previous work (SIMPATIE, MARQUIS, WHO, OECD) and using the network, collect and exchange information regarding PS culture, practices and indicators in MS and make it accessible to stakeholders through web based systems to facilitate cross border care.
Objective 3 : Using the organizational framework of the network (national contact points coordinating national platforms) and the expertise of national agencies, define, test and validate an instrument for assessing PS culture in health care organizations of MS.
5.1.3. Description of the work
Situation analysis / mapping
WP 1 will coordinate the situation analysis for the whole project, including collection of the basic data set from all Member States. This will be done through WP 8 developed network of national contact points.
Information matrix
Months 0-3
WP 1 will coordinate the development of the information matrix focusing on the 4 EUNetPaS priorities: PS culture, reporting systems, education, medication safety. WP 2- 4 experts will collaborate to this development by submitting questions relevant to their respective WPs.
The matrix will include 4 series of questions focusing on the 4 EUNetPaS priorities. These questions will be based on the proposals developed in the respective WP, by their leaders, partners and other experts. WP 1 team will of course define the set of questions on PS Culture and the questions on legislative/regulatory/organizational context. In addition, a methodology for information collection will be developed and described in a protocol. Information collection methodology and the matrix, after input has been received by other wp, will be finalized by WP 1 and submitted to the Executive Board and the Steering committee for validation and final approval.

34
Information matrix depicts the basic data set that should be collected from all member states.
WP teams might contact identified organizations (especially in countries that are collaborating on the respective WPs) relevant for their work and obtain additional information and/or materials.
Data should identify/describe:
a) methods used in EU to assess/develop patient safety culture and information on the context influencing PSC in Member States, including legislative requirements, regulatory structures and key organizations,
b) previous and ongoing activities on PS culture, reporting systems, education and methods addressing medication safety incorporating mapping activities of other WPs in the project
Review of previous work /ICT design
Months 0-6
This work will be based on previous mapping exercises (SIMPATIE, MARQUIS, WHO, OECD) which will be integrated, structured and used as starting point in the EUNetPaS database.
Purposeful ICT application for situation analysis database will be developed by CBO and linked to EUNetPaS site. It will be based on the information matrix. The tool will be used both for information collection and presentation. Each country contact point will in essence have the `web-master’ authority over information from own country. CBO staff will act as administrator, with all open access publications being approved by the Project Steering Committee and the owner of the information (country contact).
Data collection:
Months 3-9
National representatives/experts will collaborate to create infrastructures for gathering information, validation and evaluation. They will use the matrix for the situation analysis, translating it if necessary. Common information collection protocol and suggested list of national contacts will help in increasing harmonization of data. Project governance bodies (coordination by WP 8, Steering committee and Executive Board) will support collection by strongly encouraging and facilitating involvement of national stakeholders (health professionals / providers representatives, patients, decision makers) in the collection exercise. EU representative organizations of the main stakeholders (European Federation of Nurses, Standing Committee of European Doctors, European Patient Forum, Pharmaceutical Group of the European Union, European Federation of Hospitals) are already involved in the project as partners / collaborators and are expected to encourage participation of their national affiliates. In addition they will provide experts to advise and review materials.
The national contact points will organize interviews (this may include but not be limited to: meetings, e-meetings, e-mail survey / call, telephone interviews etc) to collect available information from their respective countries. As mentioned, in WP1 developed

35
information matrix and data collection methodology (including definitions of items requested) will be available to help the process. Contact points are expected to structure responses according to the agreed matrix, validate information and send it to WP 1. Communication between WP 1 coordination and national contacts will include e-mail / telephone, and will make use of direct upload in the mapping data base. Documents and information can be submitted in English and national language(s), if latter an English summary will be appreciated.
Evaluation of situation analysis:
Months 9-12
WP 1 will send topic specific information to relevant WPs teams (education to WP 2, reporting and learning to WP 3, medication errors to WP 4) and will review Patient Safety Culture aspects. WP experts are expected to consolidate and structure mapped information focusing on the 4 priorities of EUNetPaS. WP 2, 3, 4 will then return evaluated information with their comments to WP1. WP 8 will coordinate this phase to ensure that the work plan is respected.
Publication mapping information and good practice compendium
Months 13-16
Consolidated situation analysis/ mapping will then be prepared for web publication by WP 1 and linked through WP 9 to the EUNetPaS website. After final approval of the whole by the project Steering Committee, web launch of the mapping is expected about months 15 of the project, followed by a compendium of examples of good practice a month later.
Patient Safety Culture
Gathering evidence Months 0-9
Phase 1: Systematic, critical literature review - focused on scope, evidence of psychometric validation, transnational application and relationships to 'objective' patient safety of current safety culture surveys. (Experts from ESQH Aarhus Office)
Phase 2: Identification of key institutions and experts involved in culture surveys in the network: Contact information via network nodes and mapping
Phase 3: Structured information gathering from network experts: Based on a protocol developed on the result of the literature review, structured telephone interviews will be performed with the identified experts/institution representatives with the purpose of mapping currently employed PS culture tools. The mapping will be presented in the structure defined by the review with added information on the duration and extent of application of the included surveys. These data can be presented on the website (Interviews performed by ESQH Aarhus Office expert - Data structured and presented by the Aarhus ESQH Office)

36
Phase 4: Rating and selection of appropriate PS culture survey(s) for application in the network: A structured mail-based Delphi process (according to SimPatie WP4 rating instrument) and based on phase 3 mapping information will be performed by an expert group (10-12 members). The expert group will be identified and selected via phase 3 interviews. (ESQH Aarhus Office)
Specific PS culture aspects (recommendations, measurement tools, indicators, campaigns) will be included in the situation analysis for information collection. Results will be evaluated and completed by a literature review and recommendations regarding safety culture.
Defining pilot
Months 9-15
WP1 experts will clarify the different methods used to assess PS culture in MS and will propose a number of tools suitable for assessing/developing PS culture, including (insofar applicable) PS indicators. Issues such as common standards for translation, modalities of implementation, evaluation of the relevance/appropriateness, validation and feasibility of the tools, use of results, spread/sharing of experiences and results across organizations will be addressed.
Examples of patient safety culture measurement tools which could be considered include but are not limited to the following: CAIR: Checklist for Assessing Institutional Resilience by the Psychological Department The University of Manchester and Cardiothoracic Unit, Hospital for Children NHS Trust, UK. HSPSC: The Hospital Survey on Patient Safety Culture by the Agency for Healthcare Research and Quality (AHRQ), USA. MaPSaF: Manchester Patient Safety Assessment Framework by the National Primary Care Research and Developmental Centre, University of Manchester, UK .SAQ: The Safety Attitudes Questionnaire by The University of Texas Center of excellence for Patient Safety Research and Practice. SCS: The Safety Climate Survey by the Institute of Healthcare Improvements, USA.
Feasibility testing selected instruments and validation
Months 15-20
In the second round, WP experts will contact directly national contact points / experts and collect information (results, evaluations) on the use of instruments selected. National (regional, local) experiences with use and validation would be analyzed and instruments prioritized.
Proposal for the PS Culture measurement tool with methodology for data collection will be submitted to the project Steering Committee and Board (M22) and published (M24).

Identifying a limited set of patient safety indicators:
Months 0-12
Phase 1: The indicators appropriate to WP 1-4 will be selected from existing, European updated patient safety indicator systems (SimPatie, OECD, PATH) by the ESQH Aarhus Office.
Phase 2: Alignment of the OECD, WHO-PATH, and Simpatie Indicator set in terms of data definitions, algorithms and application scope to create a common European Set of PSI's. (OECD; ESQH Aarhus Office)
Phase 3: Publication: Websites, Scientific journal, separate booklet (?)
Validation work is planned as a part of OECD-project.
Selected PS indicators will be tested by the hospitals participating in WP 4 as planed in the project’s implementation activities on medication errors
Mapping/Culture
year 2008 2009 Task
responsible months 02 03 04 05 06 07 08 09 10 11 12 01 02-08
Conc. framework
discussion
WP 1/ CBO/ SC
Meeting Utrecht
28
Conc. framework
WP consultation
WP 1/ CBO to WP 2,3,4
National Contact Points. WP8 /HAS
20
Draft framework
WP input
WP 2,3,4/ to WP1/CBO
National Contact Points. WP8 /HAS
X 15
Draft framework with
methodology/definitions
WP 1/ CBO to WP8/HAS
HAS to Steering Committee
X 30
Definite framework
Input Steering Committee
SC to WP 8/ HAS
HAS/ CBO edit
15
37

38
Definite framework
for information collection.
WP 8/HAS to NCP
CBO web tool
X X 30
Information collection
NCP interviews
NCP input in web tool
Support CBO
X X X 30
Information collection
initial review/structure
WP 1/CBO,
WP specific to 2,3,4, 8
X 30
Information review
comments/additional questions.
WP 1,2,3,4,8
Topic specific
X 15
Information review
draft mapping
WP 1/CBO to WP 8/Steering Committee
for approval
X 15
Mapping web launch WP 9/HAS and WP1/CBO
30
Announcement, update request, additional questions.
CBO to WP 8/ HAS
HAS to National Contact Points
February
Update, additional questions.
Information collection
National Contact Points input web tool
CBO web tool
February-
May
Update mapping
Good practice
WP 1/ CBO to WP2,3,4,8 comments/approval Steering Committee
June
Mapping and good practice update
WP9/HAS and WP1/CBO
Announcement, update request, additional questions.
WP 2,3,4 to WP 1/ CBO
CBO to HAS to National Contact Point

39
Update, additional questions.
Information collection
NCP input web tool
CBO web tool
Update mapping
Good practice
WP 1/ CBO to WP2,3,4,8 comments/approval Steering Committee
Mapping and good practice update
WP9/HAS and WP1/CBO
Culture survey
Systematic literature review
WP1/ESQH X X X X X X X X X
Identification of key experts and institutions performing PS Culture Surveys
WP1 CBO/National Contact Points
X X X X
Mapping of PS Culture survey use based on structured tele-interview of experts
WP1 ESQH X X X X
Selection of expert panel for rating of PS Culture Surveys
WP1 ESQH/National Contact Points
February
Rating Process, Tool selection
WP1 ESQH/Experts March-
Delivery of tool with protocol
WP1 ESQH –National Contact Points/WP 2-4
Indicator Update alignment
WP1 ESQH/OECD/(WHO)
X X X X X X
Publication: Indicator recommendation
WP1 ESQH/OECD – WP2-4
X
Culture survey
Systematic literature review
WP1/ESQH X X X X X X X X X

5.1.4. Deliverables and links with other work packages
Deliverable Number
Deliverable Title
Delivery Date
Nature Confidentiality Level
Stakeholders & Dissemination
D05 Matrix including core questions for the 4 core WP for situation analysis
M3 Document providing a list of topics to be discussed in semi-directive interviews
Partners EUNetPaS partners, website intranet
D14 WP 1 meeting M9 WP meeting Partners Mail website
D17 Situation analysis
M 12 Database providing: a) methods used in the EU to assess/develop patient safety culture (PSC) and information in the context of influencing PSC in MS, including legislative requirements, regulatory structures and key organizations, b) previous and ongoing activities concerning n PS culture, reporting systems, education and methods addressing medication errors incorporating mapping activities of other WPs in the project
Public EUNetPaS Partners, website, conferences
D24 Compendium of good practices and examples of regulation, legislation and organisation in patient safety (PS)
M16 Report: The focus will be on PS culture, education, reporting systems and medication safety solutions.
Public Stakeholders: EUNetPaS partners, national contact points, HCOs, healthcare professionals The compendium will be published, available on the website and presented at conferences
D25 WP 1 meeting M20 WP meeting Partners Mail website
D26 Patient Safety Culture measurement tool
M24 Validated questionnaire to measure PS culture in Hospitals through health care professionals working at the ward level
Public Stakeholders: EUNetPaS partners, national contact points, HCOs, healthcare professionals The instrument will be published, available on the website and
40
41
presented at conferences
Links with other WP:
Data collection will be conducted through national nodes (WP 8 coordination) and assessment of data will be conducted through WP 2, 3, 4 for their respective part. Database infrastructure will be provided by WP 8 and 9 as part of the website.
PS Culture Measurement tool will be assessed and promoted through national contact points
References: 1) Amalberti, R. Auroy, Y. Berwick, D., Barach, P. Five System Barriers To
Achieving Ultrasafe Health Care, Ann Intern Med. 2005;142, 9: 756-764.
2) Brennan TA et al. Accidental deaths saved lives and improved quality. N Engl J Med, 2005, 353, 13, 1405-9.
3) Caroll J, Quijada, M. Redirecting traditional professional values to
support safety: changing organisational culture in healthcare. Qual. Saf Health Care 2004(suppl II):ii16-ii21.
4) Carroll, J. Rudolph; J. Design of High reliability Organizations in
healthcare, Qual. Saf. Health Care e, Dec 2006; 15: i4 - i9
5) Carroll, J., Edmondson, A. leading organisational learning in healthcare, Qual. Saf. Health Care, 2002, 11:51-56.
6) Carthey, J de Leval M R and Reason, J T Institutional resilience in
healthcare systems Qual Saf Health Care 2001;10: 29-32
7) Edmondson, A. Learning from mistakes is easier said than done: group and organizational influences on the detection and correction of human error. J Appl Behav Sci,1996, 32, 5-28.
8) Firth-Cozens J. Barriers to incident reporting. Qual Saf Health Care
2002;11:7.
9) Grol R, Wensing, M. Adopting Best Evidence in Practice: What drives change?
10) Barriers to and incentives for achieving evidence-based practice. MJA
2004;180(6 Suppl):S57-S60.
11) Hart, E. Hazelgrove, J. Understanding the organisational context for adverse events in the heath services: the role of cultural censorship, Qual. Saf. Health Care, 2001, 10:257-262
42
12) JB Sexton (Texas), RL Helmreich, TB Neilands (un of California, San Francisco), K Rowan (UK), K Vella (UK), J Boyden (Cornwall), PR Roberts (NZ), EJ Thomas. The safety attitudes questionnaire: psychometric properties, benchmarking data, and emerging research. BMC Health services research 2006; 6: 44
13) Kaushal, R., Bates, D., Poon, E.,. et al Functional Gaps in Attaining a National Health Information Network,. Health Affairs, September/October 2005, 24 (5): 1281–89
14) Lawton, R. Parker, D. Barriers to incident reporting in a healthcare system, Qual.Saf.Health Care, 2002: 11:15-18
15) Leape, L, Berwick, D. Five Years After To Err Is Human: What Have We
Learned? Journal of the American Medical Association, May 18, 2005, 293 (19): 2384–90
16) MD Madsen, HB Andersen; K Itoh. Assessing safety culture in health
care. In: P Carayon, editor. Handbook of human factors and ergonomics in health care and patient safety. Mahwah: Lawrence Erlbaum Associated Inc Publishers; 200
17) ME Kho, JM Carbone, J Lucas. ( Canada) Safety climate survey : reliability of results from a multicenter ICU survey. Qual Saf Health Care 2005; 14: 273-278
18) P Pronovost, B Sexton. Assessing safety culture: guidelines and recommendations. Qual saf Health Care 2005; 14: 231-233
19) P Pronovost, CG Holzmueller, DM Needham, JB Sexton, M Miller, S Berenholtz, AW Wu, TM Perl, R Davis, D Baker, L Winner, L Morlock. How will we know patients are safer? An organisation-wide approach to measuring and improving safety. Crit Care Med 2006; 34: 1988-1995
20) Pauker S, Zane, E., Salem, D. Creating a safer health care system. JAMA 2005;294(14):2096-08
21) PJ Pronovost, B Weast, CG Holzmueller, BJ Rosenstein, RP Kidwell, KB
Haller, ER Feroli, JB Sexton, HR Rubin. Evaluation of the culture of safety : survey of clinicians and managers in an academic medical center. Qual Saf Halth Care 2003; 12: 405-410
22) SJ Singer, DM Gaba, JJ Geppert, AD Sinaiko, SK Howard, KC Park. The culture of safety: result of an organisation-wide survey in 15 California hospitals. Qual Saf Health care 2003; 12: 112-118
23) Sutcliffe K., (2004) Defining and classifying medical error: lessons for learning Qual. Saf. Health Care, 2004: 13:8-9
24) Vincent, C., Stanhope, N., Crowley-Murphy, M. Reasons for not reporting
adverse incidents: an empirical study, Journal of Evaluation in Clinical Practice, 5(1) : 13 - February 1999

43
25) Waring J. A qualitative study of the intra-hospital variations in incident
reporting International Journal for Quality in Health Care 2004 16(5):347-352
26) Zhan, C. Kelley, L., Yang, H., Keyes, M., Battles, J., Borotkanis,
R.Stryer, D. Medical Care. Health Care Quality and Disparities: Lessons from the First National Reports. 43(3) Supplement:I-42-I-47, March 2005.
__

44
Work package n° 2: Education and Training
5.1.5. List of partners involved
UOA-HIL (Leader), EKEVYL, 320 p/d WP coordination, situation analysis (edu), education pilot and education recommendation
EFN 60 p/d nursing school pilot
CPME 60 p/d medical school pilot
ESQH 60 p/d education guideline
EPF 25 p/d education guideline
DOH 80 p/d education guideline, situation analysis, pilot
GCPS 80 p/d education guideline, situation analysis, pilot CPD
SMoH 70 p/d education guideline, situation analysis, pilot
StaHeCCA 18 p/d situation analysis
HIQA 22 p/d situation analysis
Participant Tasks Total Person days/partner
ALL Partners
All partners will provide information on important national and international activities on PS Education and links to these activities. They will further review and comment on WP2 deliverables. Further to this, specific engagements are:
UOA-HIL/ EKEVYL
UOA-HIL will lead the WP and co-ordinate activities and meetings. As part of its co-ordination responsibilities Greece will manage integration activities and will draft the final guidance document, in a common structure. The co-ordinator will furthermore manage issues arising from sharing common information and will co-ordinate liaison with DG EDUCATION & CULTURE.
EKEVYL will host the WP2 specific meeting in Athens.
EKEVYL will lead the discussion on how collected WP2 related information should be classified and organized. Finally, UOA-HIL will participate in the nursing related activities in
320
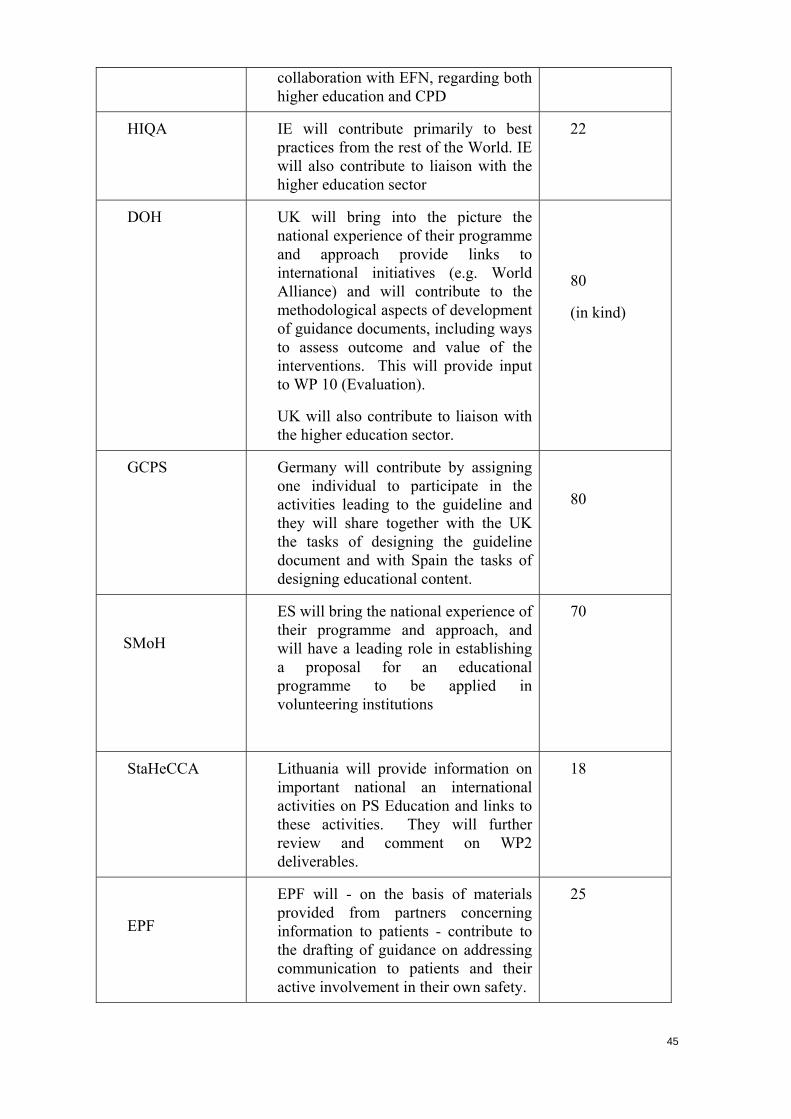
45
collaboration with EFN, regarding both higher education and CPD
HIQA IE will contribute primarily to best practices from the rest of the World. IE will also contribute to liaison with the higher education sector
22
DOH UK will bring into the picture the national experience of their programme and approach provide links to international initiatives (e.g. World Alliance) and will contribute to the methodological aspects of development of guidance documents, including ways to assess outcome and value of the interventions. This will provide input to WP 10 (Evaluation).
UK will also contribute to liaison with the higher education sector.
80
(in kind)
GCPS Germany will contribute by assigning one individual to participate in the activities leading to the guideline and they will share together with the UK the tasks of designing the guideline document and with Spain the tasks of designing educational content.
80
SMoH
ES will bring the national experience of their programme and approach, and will have a leading role in establishing a proposal for an educational programme to be applied in volunteering institutions
70
StaHeCCA Lithuania will provide information on important national an international activities on PS Education and links to these activities. They will further review and comment on WP2 deliverables.
18
EPF
EPF will - on the basis of materials provided from partners concerning information to patients - contribute to the drafting of guidance on addressing communication to patients and their active involvement in their own safety.
25

46
CPME
CPME will lead the discussion on the medical paradigm. CPME will contribute to this part of drafting the guideline and will perform specific work on medical curricula
60
ESQH ESQH will contribute to the drafting of the guideline for both professionals and patients and will particularly lead the discussion on requirements for competencies of management staff. This task is subcontracted by ESQH
60
EFN EFN will lead the discussion on the nursing paradigm, will contribute to this part of drafting the guideline and will perform specific work on nursing curricula.
60
5.1.6. Objectives
Objective 4: To promote PS education and training in MS, that are inspired by common principles and values through (i) building a platform for the mutual exchange of experience and knowledge on methods of planning and implementing sustainable learning interventions for healthcare professionals and of involving patients and caregivers -through awareness and education programmes. (ii) reaching out to decision makers in Higher Education at national and European level to promote the integration of these learning methods and interventions in undergraduate and postgraduate medical and nursing curricula.
5.1.7. Description of the work
Scope: Education should be targeted to specific audiences and purposes. Education related activities range from short, targeted actions aiming at creating visibility and awareness around issues to extended courses for in depth treatment of subjects aiming to build particular knowledge and skills. The full range of such activities will be necessary to support Patient Safety programmes during the whole cycle of a PS program. Patient Safety education activities in EUNETPAS will be considered:
- as part of CPD programmes for health care professionals.
- as actions aiming at patient empowerment
- as part of higher education programmes.

It is noted that the latter needs to be tackled in close liaison with the Education sector and involve also higher education institutions.
Approach: The overall approach is schematically depicted in figure 2.1. and it includes
(a) T.2.1. Information collection: i.e, an initial phase of information collection and organisation of “an inventory” of existing documented and validated experiences across the MS, which will provide the background for the next phases. Such documents will be in the form of approaches, methods, curricula, national CPD programmes, planning, assessment and accreditation frameworks, recommendations etc. This will be done according to a pre-defined “information matrix” shown in Table 2.1 which has been provisionally adopted and is to be further detailed, based on the collected information by M4, in Athens.. Collection of information will be performed by both the partners of WP2 with respect to own know-how and documentation and also in collaboration with WP1, through national contacts and for all MS. This information will also constitute WP2 specific starting situation for the impact assessment of WP10. Therefore the final information matrix will be also consolidated with relevant work in these WPs. The collected information will be thematically organised and made readily and effectively accessible through the project’s web tools to the interested parties in MS by M12.
Figure 2: WP2 Work flow diagram
(b) T.2.2. A Guidance Document: On the basis of the above, WP2 participants will explore the specific needs for practical supportive guidance for different levels of decision makers in MS and also the opportunities provided by exploiting the Network’s consolidated knowledge in order to propose the scope, intent, contents i,e., the specifications of a guidance document for Patient Safety Education and Training. Such a document is envisaged to provide a general framework for the development of core competencies in PS, according to associated roles and
47

responsibilities in the continuum of care processes. Appropriate delivery platforms i.e. courses, seminars, intensive courses, e-learning, self-education, workshops etc. will be considered. Accreditation and certification issues will be also addressed. Provisions for ensuring sustainability for such activities across the whole range from identifying new needs, updating contents, to assessment and accreditation of programmes and certification will be also proposed.
While it is recognised that competences and the needed learning interventions to build must be developed according to responsibilities rather than the professions, the content itself, e.g. in terms of use cases, practical work and projects etc, should be customised to different target groups. Considerations and specific guidance on how this may be done will also form part of the guidance document.
Network level consensus concerning guideline specification will be pursued in M8 in Paris.
Table 2.1. Information Collection Matrix
Higher Education
CPD/CME Awareness/ Foundation
organisation X X X
level X
Target groups X X X
Direct patient care X X X
People Care management
X X X
Patients /Carers X
Learning Intervention. profile
X X X
Learning objectives X X X
Delivery modes X X X
Assessment (competences, intervention)
X X X
Topics X X X
(c) T.2.3. Guidelines for PS Education and Training: An authoring group will be set up to draft the recommendation according to the adopted document specification. It is envisaged that sample learning interventions will be provided as appended materials and it is expected that they will be largely based on materials provided by the members of the network. These materials will be accompanied by a self assessment statement of the providing organisations as to their standing against the quality criteria that will be set forward in the guideline.
48
49
It is not the intention to validate such materials in the project, but rather to validate the concept that materials produced transparently and according to mutually accepted EUNetPaS criteria may become resources of the Network and as such they may be used and exploited by the whole Network membership. Obviously, such extended use of materials produced in one organisation will provide an excellent opportunity also for their validation, which however is regarded as an activity to be arranged between the provider and the user organisations and it is not part of the project.
A Network level consensus regarding the guideline and its implementation should be reached in M17 in Copenhagen.
(d) T 2.4. Diversification: Customisation of learning interventions will be performed in close collaboration of education and training organisations to specific needs: 4 working groups will be organised to deal with medical paradigm (lead: Standing Committee of EU Doctors), the nursing paradigm (lead: the European Federation of Nurses) and Continuous Professional Development (lead: the German Coalition for Patient Safety). Information and awareness of patients and care givers(lead by the European Patient Forum). The target would be to establish pilot programs (medical, nursing, Continuous Professional Development CPD and patient/caregiver) in at least 3 MS. D04 will be composed of 4 such “course books” one for each of the target audiences.
(e) T.2.5. Dissemination and pilots: The initiative will be promoted and disseminated through the network and the national contacts to the MS, with the objective to also identify institutions that would be prepared to include PS in their programs and to support them to deliver the learning interventions. Partners in WP2 have their own networks and through them they have already committed at least 4 candidate pilot sites for course delivery.
Such programs should be ready for implementation during at least the first semester of the academic year 2009-2010, in order to allow for collection of feedback into the recommendation document. Effort will be made to involve countries from Northern, Central and Southern Europe.
The delivery itself will not be part of the project. However the project will sponsor such initiatives by providing input and experts for setting up the programmes. It is not the intention to validate such learning interventions, but rather to validate the concept that learning interventions can in fact be produced in close collaboration between health care organisations and teaching institutions, according to mutually accepted EUNetPaS criteria (i.e. guidance). Agreement regarding the customized programs should be also reached during WP2 meeting scheduled in M17 in Copenhagen.
(f) T.2.6. Consultation: The draft guideline will be proposed on the website for public consultation. Feedback and comments will be considered to amend the draft. A consensus workshop will be organised in M25 in Athens.
(g) T.2.7. Liaison with other Initiatives: Links to the higher education sector will be pursued, nationally and through DG Education and Youth. The WP Management will also pursue linking this initiative to other national and international relevant education projects, disseminate the results and pursue their
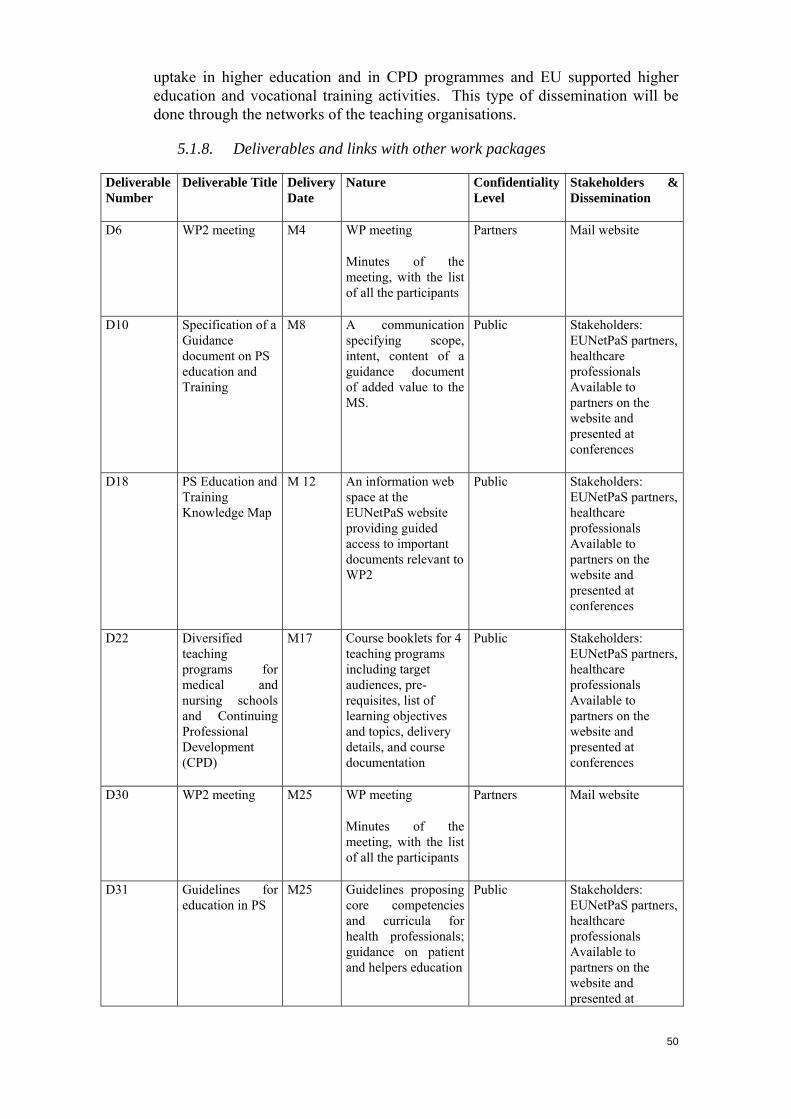
uptake in higher education and in CPD programmes and EU supported higher education and vocational training activities. This type of dissemination will be done through the networks of the teaching organisations.
5.1.8. Deliverables and links with other work packages
Deliverable Number
Deliverable Title Delivery Date
Nature Confidentiality Level
Stakeholders & Dissemination
D6 WP2 meeting M4 WP meeting
Minutes of the meeting, with the list of all the participants
Partners Mail website
D10 Specification of a Guidance document on PS education and Training
M8 A communication specifying scope, intent, content of a guidance document of added value to the MS.
Public Stakeholders: EUNetPaS partners, healthcare professionals Available to partners on the website and presented at conferences
D18 PS Education and Training Knowledge Map
M 12 An information web space at the EUNetPaS website providing guided access to important documents relevant to WP2
Public Stakeholders: EUNetPaS partners, healthcare professionals Available to partners on the website and presented at conferences
D22 Diversified teaching programs for medical and nursing schools and Continuing Professional Development (CPD)
M17 Course booklets for 4 teaching programs including target audiences, pre-requisites, list of learning objectives and topics, delivery details, and course documentation
Public Stakeholders: EUNetPaS partners, healthcare professionals Available to partners on the website and presented at conferences
D30 WP2 meeting M25 WP meeting
Minutes of the meeting, with the list of all the participants
Partners Mail website
D31 Guidelines for education in PS
M25 Guidelines proposing core competencies and curricula for health professionals; guidance on patient and helpers education
Public Stakeholders: EUNetPaS partners, healthcare professionals Available to partners on the website and presented at
50
51
conferences
Links with other WP: Participation to the situation analysis (WP1). Data collection will be conducted through national nodes (WP 8 coordination). Pilot implementation will be promoted through national contact points of interested MS. Special attention will be given to medication safety (WP4) to include educational topics in the field testing.
References:
1) Advisory Committee on Medical Training. Report and Recommendations on Undergraduate Medical Education. Doc. III/F/5127/3/92. Commission of the European Communities, Brussels, 1992.
2) American Medical Association. Future Directions for Medical Education. A Report of the Council on Medical Education. American Medical Association, Chicago, 1982.
3) Association of American Medical Colleges (AAMC). Physicians for the Twenty-First Century. Association of American Medical Colleges, Washington, 1984.
4) CME-Concept “Patient Safety” Identify errors Avoid incidents Correct consequences Learning from Errors –AZQ 2007
5) Course Material for B. Med. Year 5, 2006 , Faculty of Health, University of Newcastle
6) EMS Council (2005), An Outcome-based Core Curriculum In Patient Safety. Warsaw (Poland).
7) Frank JR. (Ed). 2005. The CanMEDS 2005 Physician competency framework. Better standards.
8) Panamerican Federation of Associations of Medical Schools. Medical Education in the Americas: Final Report of the EMA Project. PAFAMS, Caracas, 1990, 18. pp. 26-31
9) The Executive Council, The World Federation for Medical Education. International standards in medical education: assessment and accreditation of medical schools’ educational programmes. A WFME position paper. Medical Education 1998, 32, 549-58.
10) The Scottish Deans’ Medical Curriculum Group (2002). The Scottish Doctor - learning outcomes
11) WFME Task Force on Defining International Standards in Basic Medical Education. Report of the Working Party, Copenhagen, 14-16 October 1999. Medical Education, 2000, 34, 665-675.
12) WHO. Changing Medical Education: An Agenda for Action. Unpublished Document WHO/ EDUC/91.200, Geneva, 1991.
13) WHO. Doctors for Health. A WHO Global Strategy for Changing Medical Education and Medical Practice for Health for All. WHO, Geneva, 1996.
14) WHO. Priorities at the Interface of Health Care, Medical Practice and Medical Education: Report of the Global Conference on International Collaboration on Medical Education and Practice, 12-15 June 1994, Rockford, Illinois, USA. Unpublished Document,
15) World Federation for Medical Education The Edinburgh Declaration. Lancet 1988, 8068, 464.

52
16) World Federation for Medical Education, WFME Global Standards for Quality Improvement, Basic Medical Education / Postgraduate Medical Education / Continuing Professional Development (CPD) of Medical Doctors, Denmark 2003
17) World Federation for Medical Education. Proceedings of the World Summit on Medical Education. Medical Education 1994, 28 (Suppl.1).
18) World Health Assembly. Reorientation of Medical Education and Medical Practice for Health for All. WHA Resolution 48.8. WHO, Geneva, 1995.
19) World Health Assembly. WHA Resolution 42.38. WHO, Geneva, 1989. 20) World Healthcare Students’ Symposium (2005), Statement of Beliefs. Qawra
(Malta)
53
5.2. Work package n° 3: Reporting and Learning Systems
5.2.1. List of partners involved
SST (Leader) 440 p/d WP coordination situation analysis, reporting and learning systems database, rapid alert mechanism
DOH 110 p/d (in kind) situation analysis, database, rapid alert mechanism
NBHW 110 p/d situation analysis, database, rapid alert mechanism
StaHeCCA 20 p/d situation analysis
UOA-HIL, EKEVYL 40 p/d situation analysis
DGS 110 p/d situation analysis, database, rapid alert mechanism
CBO 10 p/d situation analysis
5.2.2. Objectives
Specific Objective number 5: To analyze and share the information collected on reporting and learning systems and on their implementation in the EU MS, to identify commonalities and understand the pros and cons of the differences observed. A rapid alert mechanism will be proposed.
5.2.3. Description of the work
Although relatively few MS have established national PS reporting systems there is a large amount of experience and knowledge on PS in EU as well as globally. In order to add value to European level activities in this field, this WP will identify, collect and structure this information in order to provide MS with a information and solution bank that they can draw upon in their own work with PS. This implies that WP3 will provide reliable, timely, transparent and transferable information on patient safety reporting and learning systems as input to decision-making in member states, and in the EU. The main methodology of this project consists in defining the right questions and in analysing and structuring the answers systematically following an agreed classification. This information will be available through a Web-based “library” of solutions including contact details for further information. This information will be provided to all the MS to draw upon, modify and use as they feel appropriate within their own healthcare system.
Literature Review & situation analysis: M1- M 11: SST, DOH, NBHW, DGS, StaHeCCA, CBO, UOA-HIL, EKEVYL
─ Existing patient safety reporting and learning Systems, as well as planned or already running pilot projects will be identified through contacts with national contact points coordinated by SST

54
─ The work package will therefore establish a list of contact persons contributing to the collective European expertise on reporting and learning Systems. These contacts will act as a information source on local systems and as sparing partner for the work package evaluating and giving feedback on the work (Expert group) .
─ On the basis of a Literature Review (see References) supplemented with information
from the expert group, SST will develop guidelines and protocols (including templates) for WP3 activities, including the collection of core information from national patient safety reporting and learning systems on subjects like legal framework, organisational structure (social, political, economic and health system), culture and data structure.
─ Situation analysis: WP 3 partners and the expert group will validate the list of topics
relevant to PS reporting and learning systems to be included in the situation analysis matrix. The WP3 partners are MS representatives involved in their respective national institutions in the implementation of such systems. Consolidated situation analysis will be included on the EUNetPaS Website (M12).
Time frame:
Date Nature Who
M01 Work plan All
M02 List of topics for the information matrix (WP1)
SST
M03 WP3 manual for activities SST
M03 Templates for WP3 activities
SST
M07 WP3 topics for Situation analysis matrix
All
M10 Data validation All
Web-based library of methods for implementing reporting and learning systems M15 – M24 SST, DOH, NBHW, DGS ─ An important task will be to relate the core information collected to
recommendations from international organisations like WHO and Council of Europe as well as to recommendations from health-related stakeholders. It will be important for this work package to engage with particularly WHO and work to build on rather than to duplicate work already in hand by the World Alliance for Patient Safety and the Council of Europe.
─ Web-based library of methods will be included on the EUNetPaS website (M24)
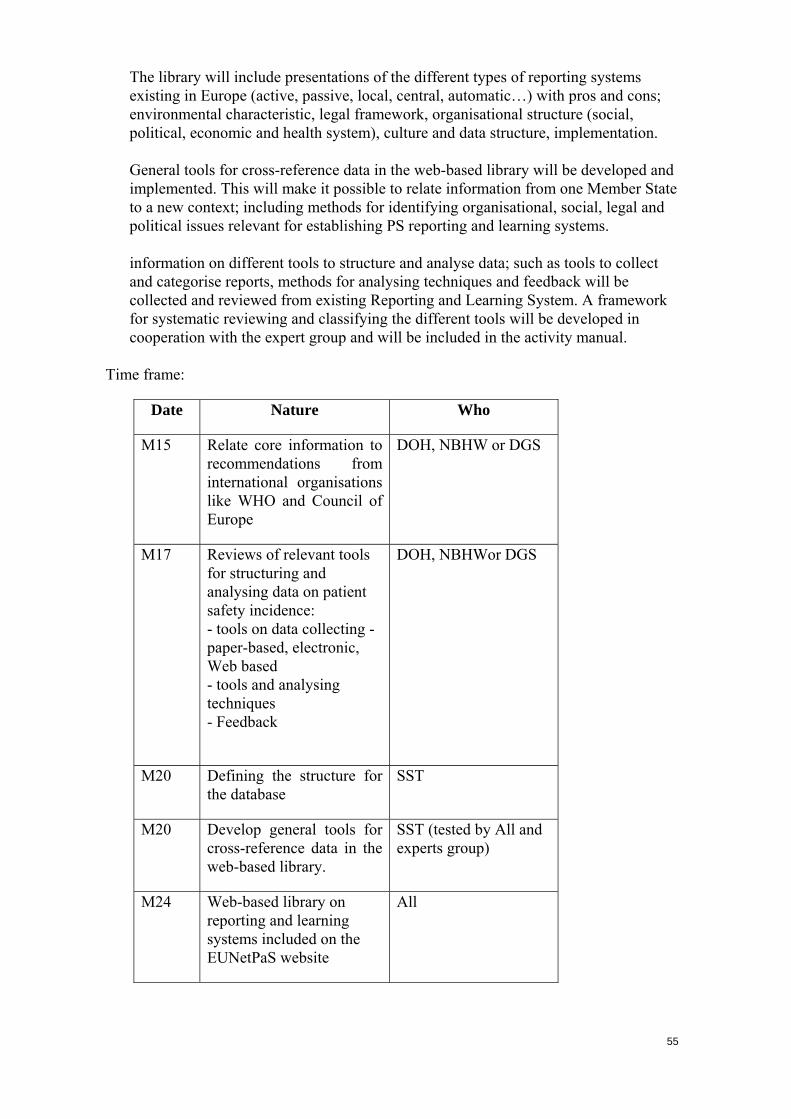
55
─ The library will include presentations of the different types of reporting systems existing in Europe (active, passive, local, central, automatic…) with pros and cons; environmental characteristic, legal framework, organisational structure (social, political, economic and health system), culture and data structure, implementation.
─ General tools for cross-reference data in the web-based library will be developed and implemented. This will make it possible to relate information from one Member State to a new context; including methods for identifying organisational, social, legal and political issues relevant for establishing PS reporting and learning systems.
─ information on different tools to structure and analyse data; such as tools to collect and categorise reports, methods for analysing techniques and feedback will be collected and reviewed from existing Reporting and Learning System. A framework for systematic reviewing and classifying the different tools will be developed in cooperation with the expert group and will be included in the activity manual.
Time frame:
Date Nature Who
M15 Relate core information to recommendations from international organisations like WHO and Council of Europe
DOH, NBHW or DGS
M17 Reviews of relevant tools for structuring and analysing data on patient safety incidence: - tools on data collecting - paper-based, electronic, Web based - tools and analysing techniques - Feedback
DOH, NBHWor DGS
M20 Defining the structure for the database
SST
M20 Develop general tools for cross-reference data in the web-based library.
SST (tested by All and experts group)
M24 Web-based library on reporting and learning systems included on the EUNetPaS website
All

56
Rapid alert mechanism: Establish a rapid alert mechanism for sharing high priority PS issue or solutions between all MS. M24 – M30 SST, DOH, NBHW, DGS Disseminating and sharing one country's own patient safety solutions with all MS. This area will consist of developing a rapid response mechanism for sharing high priority patient safety issues and other Patient Safety Solutions through a European solution bank, containing information based upon existing results from all relevant reporting systems in Europe. National alert mechanisms and programs in place will be identified through the expert group. Commitment by these national reporting organisations to make information available to all other MS will be sought by contacting the national authority responsible for the Reporting System. A common taxonomy for central elements of reported events will be proposed that will use information from existing Reporting and Leaning Systems. WHO’s International Classification on Patient Safety will be used as baseline for a common taxonomy. A function to convert existing taxonomy to WHO’s will be used until the WHO’s taxonomy is widely accepted. These recommendations will be reviewed by the expert group before being presented to the member states. A web based system allowing maintenance free and automatic information sharing from a supplier of information to a website and to a list of subscribers (standard software) will be proposed to partners before implemented on EUNetPaS website. The Rapid Alert Mechanism and the solution Bank will be implemented on EUNetPaS website on subscription (M30) Time frame:
Date Nature Who
M26 National alert mechanisms and programs in place will be identified
DOH, NBHW, DGS
M27 Commitment by these national reporting organisations to make information available to all other MS will be sought
SST
M27 A common taxonomy for central elements of reported events will be proposed
SST (Pilot tested by All and sub network)
M29 Internal evaluation report All
M30 The Rapid Alert Mechanism and the
All

solution Bank will be implemented on EUNetPaS website on subscription
5.2.4. Deliverables and links with other work packages
Deliverable Number
Deliverable Title
Delivery Date
Nature Confidentiality Level
Stakeholders & Dissemination
D16 WP 3 meeting
M11 WP3 meeting Partners Mail, website
D27 Reporting and learning system data base
M24 Web-based database of methods for reporting and implementing learning systems.
Partners Stakeholders: EUNetPaS partners, participating HCOs, healthcare professionals Available to partners on the website and presented at conferences
D32 WP 3 meeting
M27 WP meeting Partners Mail website
D34 EU PS Rapid Alert Mechanism
M30 Web based program for sharing high priority PS issues or solutions among MS.
Public Stakeholders: EUNetPaS partners, participating HCOs, healthcare professionals Available to partners on the website and presented at conferences
Links with other WP: Data collection will be coordinated by WP1 (situation analysis) conducted through national nodes (WP 8 coordination) and library development will be conducted through the web based infrastructure developed by WP 8 and 9. The rapid respond mechanism will developed considering input and needs of MS expressed by national contact points (WP 8). WP3 input relevant to medication safety will be proposed to WP4 for inclusion into the field testing
References:
1) ANAES-HAS Principes méthodologiques pour la gestion des risques en établissement de santé, Janvier 2003, http://www.anaes.fr
2) Aylin, P;, Tanna, S;, Bottle, A., Jarman, B. How often are adverse events reported in hospital statistics? BMJ, 2004, 329:369-70..
3) Barach P. The unintended consequences of Florida Medical liability Legislation. The law and patient safety. December 2005. http://www.webmm.ahrq.gov/perspectives.aspx
4) Beckmann, U., Bohringer, C., Carless, R., et al. Evaluation of two methods for quality improvement in intensive care: facilitated incident monitoring and retrospective medical chart review. Crit Care Med. 2003; 31(4):1006-1011.
57
5) Blendon RJ Views of practicing physicians and the public on medical errors. N Engl J Med, 2002, 347(24), 1933-40.
58
6) Chassin MR, Hannan EL, DeBuono BA .Benefits and Hazards of Reporting Medical Outcomes Publicly, N Engl J Med. 1996, Volume 334 (6):394-398
7) Cohen, M., Why error reporting system should be voluntary, BMJ, 2000, 320, 728-29 8) Cox JL, Zitner D, Courtney KD, MacDonald DL, Paterson G, Cochrane B, et al.
Undocumented patient information: an impediment to quality of care. American Journal of Medicine, 2003, 114(3):211-216
9) Cullen, D., Bates, D. Small,S. Cooper, J. Nemeskal, A Leape, L. The incident reporting system does not detect adverse drug events: a problem for quality improvement. J Qual Improv, 1995,21, 541-548.
10) Davies E. Cleary P. D. Hearing the Patient's Voice? Factors Affecting the Use of Patient Survey Data in Quality Improvement. Qual Saf Health Care 2005; 14(6):428–32..
11) Dovey S., Philipps R. What should we report to medical error reporting system? Qual. Saf. Health Care, 2004 13:322-3.
12) Egberts, T. Smulders M., de Koning, F., Meyboom, R., Leufkens, H. Can adverse drug reactions be detected earlier? A comparison of reports by patients and professionals, BMJ, 1996, 313:530-531
13) Entwistle, V.A., Mello, M., Troyen, M.P., Brennan, A. Advising Patients About Patient Safety: Current Initiatives Risk Shifting Responsibility, Joint Commission Journal on Quality and Patient Safety, September 2005, 31 (9): 483–94
14) European Health Committee. Prevention of adverse events in health care, a system approach (SP-SQS). Strasbourg: CDSP, 2004.
15) Florida patient safety network: Medical liability reform, Senate Bill 2-D 16) Flowers, L., Riley, T. State-based mandatory reporting system of medical errors : an
analysis of the legal and policy issues, March 2001, report of the National Academy for State Health Policy, Portland
17) Goldman, S., Kennedy, D., Graham, D., Gross T., Kapit R., Love L., White G.: The clinical impact of adverse event reporting, clinician Reviews 7 (7), 1997, 143 - 172
18) Griffen, F. IOM reports err regarding peer view confidentiality, Bull Am Coll Surg. 2003, 88, 8-11
19) GuidelineWorkingGroup. Updated guidelines for evaluation public health surveillance systems. Atlanta: US departement of health and human service, centers for disease Control and Prevention (CDC), 2001.
20) Guthrie P. US creates blame-free adverse event reporting. CMAJ 2006, 174(1):19 (news). 21) Hopkin Tanne, J. US doctors and public disagree over mandatory reporting of errors,
BMJ, 2002, 325 1055. 22) JCAHO (2000) Sentinel events; June 6, http://www.jcaho.org/sentinel/senvnt_frm.html 23) Jha, A. , Hupeerman, G., Teich, J., et al, Identyfing adverse drug events, 1998, JAMIA,
5 (3) : 305-14 24) Johnson C. Why did that happen? A brief explanation for the proliferation of barely
usable software in healthcare systems. 2nd US/UK patient safety research methodology workshop. AHRQ, Rockville, MD, September 23-24, 2003.
25) Johnson, C. Failure,in safety-critical systems: A handbook of incident and accident reporting, Glasgow University Press, 2003
26) Johnson,C.W. How Will We Get the Data and What Will We Do With It? Issues in the Reporting of Adverse Healthcare Events Quality and Safety in Health Care, 2003, 12 (2), 64-67.
27) Journal Officiel de la république française , ministère de la santé et des solidarités, arrêté du 25 avril 2006 relatif aux modalités de l’expérimentation de déclaration des évènements indésirables graves liés à des soins réalises lors d’investigations, de traitements, ou d’action de prévention autres que les infections nosocomiales
28) Kesselheim, A. , Ferris, T, Studdert, D. Will Physician-Level Measures of Clinical Performance Be Used in Medical Malpractice Litigation? Journal of the American Medical Association, April 19, 2006 295(15):1831–34
29) Leape LL. Reporting of adverse events. N Engl J Med 2002; 347(20): 1633-8. 30) Leape, L. Berwick, D. Safe system: are we up to it? BMJ, 2000, 725-726 31) Leape, L. reporting of medical errors: time for a reality check, Qual Saf. Health Care,
2000, 9, 144-45

59
32) Lewinson W. Physician patient communication. A key to malpractice prévention. JAMA 1994.272; 1619-20
33) Liang, B. The adverse event of unadressed medical error: identifying and filling the holes in the healthcare system. J law Med Ethics, 2001, 29, 346-348.
34) Marchev, M. Medical malpractice and medical errors, balancing facts and fears, December 2003, National Academy for State Affairs, Portland.
35) Murff, H., Patel,VL, Hripcsak, G., Bates, DW. Detecting adverse events for patient safety research: a review of current methodologies. J Biomed Inform., 2003, 36, 131-143.
36) National Patient Safety Agency: Delivering safer healthcare – a leadership checklist for NHS chief executives. NHS; 2004.
37) Osmon, S., Karn, C., Dunagan, C.., Prentice, D., Fraser, V., Kollef, M. , Reporting of medical errors : an intensive care unit experience, Critical care medicine, 2004, 32(3) 727-733
38) Ovretveit J. Which interventions are effective for improving patient safety: a review of reseach evidence. Stockholm: Karolinska Insitute, Medical Managment centre, 2005.
39) Phillips, R., Dovey, S., Hickner, J., Graham, D., Johnson, M. The AAFP Patient Safety reporting System : development and legal issues pertinent to medical error tracking and analysis, AHRQ chapter, Advances in Patient Safety, 2005, Vol 3:121-134
40) Posner, K., Geidushek, J., Haberkern, C, et al. Unexpected cardiac arrest among children during surgery: a North American registry to elucidate the incidence and causes of anesthesia related cardiac arrest. Qual. Saf Health care,2002, 11, 252-257.
41) Rajendran, P. Ethical Issues Involved in Disclosing Medical Errors. Medical Student JAMA. 286(9) 1079-83. September 5, 2001.
42) Ricci, M Goldman, A P de Leval, M R Cohen, G A Devaney F and J Carthey Pitfalls of adverse event reporting in paediatric cardiac intensive care , Archives of Disease in Childhood 2004;89:856-859.
43) Rosenthal, J., Booth, M., Defining reportable adverse events : a guide for states tracking medical errors, March 2003, National Academy for State Health Policy
44) Rosenthal, J.; Riley, T., Booth, M. State reporting of medical errors and adverse events, : results of a 50-state survey, April 2000, report of the National Academy for State Health Policy, Portland
45) Runciman, W., Lessons from the Australian patient safety foundation: setting up a national patient safety surveillance system – is this the right model? Qual Saf.Health Care, 2002, 11, 246-51
46) Runciman, W., Merry, A. (2003). Blame and the law in healthcare. Ann Intern Med. 2003; 138:974-9.
47) Safran D. G., Karp M., Coltin K. Measuring Patients' Experiences with Individual Primary Care Physicians: Results of a Statewide Demonstration Project. J Gen Int Med 2006 21(1):13-21.
48) Schmidek, J M, Weeks W B Relationship between tort claims and patient incident reports in the Veterans Health Administration Qual Saf Health Care 2005;14:117-122
49) Schneider, E., Lieberman, Publicly disclosed information about the quality of health care: response of the US public, Qual. Saf. Health Care, 2001, 10:96-103
50) Stanhope, N. Crowley-Murphy, M., Vincent, C. O’Connor A, Taylor-Adams S.: An evaluation of adverse incident reporting, Journal of evaluation in clinical practice, 5, 1, 1999, p 5 – 12
51) Suresh, G., Horbar, J., Plsek, P., et al, Voluntary anonymous reporting of medical errors for neonatal intensive care, Pediatrics, 2004 113, 1609-1618
52) Tamuz, M. Thomas, E; Franchois, K. Defining and classyfing medical errors, lessons from patient safety reporting system, Qual.Saf.Health Care, 2004: 13:13-20
53) Vaas, A. Patient Safety agency admits problems with it pilot scheme, BMJ, 2002, 432:1473
54) Volp, K. Grande, D., Residents’suggestions for reducing errors in teaching hospitals, New England J. Med. 2003, 27:348-9
55) Wald, H. Shojania, K. Incident reporting, In Making Health Care Safer : A Critical Analysis of Patient Safety Practices, Standford University, prepared for AHRQ, 2001, contract 290 chapter 4, Available at http://www.ahrq.gov/clinic/ptsafety/chap4.htm.

60
56) Walshe K (2000). Adverse events in health care: issues in measurement. Qual Saf Health Care 2000.9; 47-52.
57) Wanzel KR, Jamieson CG, Bohnen JMA. Complications on a General surgery service: incidence and reporting. Canadian Journal of Surgery, 2000, 43(2):113-117.
58) Weinberg, J. Medical Error and Patient Safety: Understanding Cultures in Conflict*. Law and Policy. 24(2): 93-113. April 2002
59) Weingart, S., Pagovitch, O., Sands, D., Li, J., Aronson, M., Davis, R., Bates, D., Phillips, R., What Can Hospitalized Patients Tell Us About Adverse Events? Learning from Patient-Reported Incidents, J Gen Int Med, Volume 20 Page 830 - September 2005
60) Wensing, M., Elwyn, G. Research on patients’views in the evaluation and improvement of quality of care, Qual Saf Health Care 2002, 11: 153-157
61) White, C. Doctors mistrust systems for reporting medical mistakes. BMJ 2004, 329; 12-3. 62) Wilson T, Pringle M, Sheikh A. Promoting patient safety in primary care. BMJ 2001;
323; 523-4. 63) World Alliance for Patient Safety. WHO draft guidelines for adverse event reporting and
learning systems. WHO 2005.
61
5.3. Work package n° 4: Pilot implementation on medication safety
5.3.1. List of partners involved
HOPE (Leader) 220 p/d WP coordination, situation analysis, medication safety good practices, pilot testing in medication safety
STM Finland 150 p/d situation analysis, medication safety recommendation, pilot testing
FOD-DG1 150 p/d situation analysis, medication safety recommendation, pilot testing
PGEU 95 p/d situation analysis, medication safety recommendation and pilot testing
IPG 150 p/d situation analysis, medication safety recommendation and pilot testing
EFN 95 p/d situation analysis, medication safety recommendation and pilot testing
HAS, CBO, UOA-HIL, EKEVYL, SST, HIQA, StaHeCCA, DGS 55 p/d each: pilot testing
5.3.2. Objectives
Objective 6: To identify good practices in reducing medication errors in hospitals, select a number of those and implement them in hospitals (2-3 hospitals in each of the 10 participating MS).
Objective 7: To create a community with those hospitals to exchange at the level of the health professionals directly involved in clinical care.
5.3.3. Description of the work
The different tasks will be based on collaboration between HOPE, organisations nominated by MS, European stakeholders and individual hospitals selected by MS. In each participating member state, a national contact point will be identified to liaise with HOPE central office and act as a coordinator at national level in the field-testing and implementation phase of the work package. Six partners constitute a core group with a stronger involvement in the activities of WP 4: (HOPE, AT, BE, FI, PGEU, EFN).
Collection and selection of good practices: M1- M 8: core group (HOPE, AT, BE, FI, PGEU, EFN). The first task will be to collect existing good practices to reduce medication errors that have been implemented at hospital level.
- Collection of good practices: all partners (national contact points) in EUNetPaS will be invited (M3 – M 7) to provide examples of good practices by filling up a template designed by the core group (sent on M 2) to be included in WP1 matrix for the situation analysis. This template will be simple to complete and will straight to the point presenting in general terms which sort of good practices should be collected. At this stage the selection criteria will not on purpose be ready. Setting criteria before collecting examples would be counterproductive by restraining proposals. Austria and Finland will present their respective experience in developing and implementing best practices in medication safety. HOPE, EFN and PGEU will seek

62
feed back from their respective national member. Practices identified by WP 1,2 and 3 that can contribute in a major way to medication safety will be considered.
- Literature Review: (please see 4 for the methodology) and the list of references for the type of documents which will be considered by the core group to complement to collection of good practices.
- Selection of good practices: the collected information will be assessed by the core group (M 8) based on a guideline. A first draft of guideline with criteria of selection of good practices for the pilot implementation will be produce by the core group before end of M 5 and submitted to the other 7 partners (national supervisors). Among other items to be identified in the meeting (M 5), the selection criteria will consider for each good practice collected: the evidence of significant reduction of medication error with the collected good practice; the possible implementation of this good practice in a foreign hospital setting.
Translation of good practices into implementation tools: M 8 – M 14 HOPE, Be, Fin, Aus, PGEU, EFN
- Once selected, the good practices will be translated into implementation tools. In a first phase the core group will work on a simplification of each good practice identified: what is the minimum to be implemented to reach the goal of reducing medication errors (M 8 – M 10). In a second phase the implementation tools will be submitted for correction to contact points in MS (national supervisor) involved in the field implementation, to take into account various aspects such as national environments (legal, organisational, medical), cultures, etc (M 11). In a third phase the implementation tools will be allocated to hospitals during the M 11 meeting involving all WP 4 partners (national supervisor) including hospitals (M 11). (M12-M13) Then the national supervisor and hospitals involved in the field implementation will be consulted for adaptation of the implementation tools to enhance transferability of the proposed recommendation.
- The two main factors are to make sure that the implementation can be adopted easily (acceptability), and is potentially useful and transferable in different national contexts (relevance).
Selection of participating hospitals M 6 – M10:
- Selection criteria will be defined by the core group (HOPE, Be, Fin, Aus, PGEU, EFN) to ensure a good level of commitment from the selected hospitals: commitment to PS and existing medication control organization will be considered (M 5) A guideline for selecting participating hospitals will be provided for comments to contact point in MS (national supervisor) (after end of M 5). Following an agreement on selection criteria in meeting (M 8) 20- 30 hospitals representing 10 MS will be selected by the corresponding contact points (national supervisor) (before end of M 10).
Field testing M 15- M 25
HOPE, Be, Fin, Aus, PGEU, EFN, HAS, CBO, UOA-HIL, EKEVYL, SST, HIQA, StaHeCCA, DGS

63
- A Guideline for implementation prepared by the core group and commented by the 7 other members (national contact point) will be provided to the MS involved (national contact point) and the selected hospitals before end of M 14.
- Implementation will then take place in the selected hospitals with the active contribution of national contact points relayed by the commitment of the national representatives of EU stakeholders (HOPE, EFN, PGEU) and a constant monitoring from HOPE central office.
- Under the supervision of national contact points, the hospitals will follow the guideline of implementation that will give them indications on how to implement the tool, this will integrate elements to evaluate the implementation. This guideline will also include evaluation tools (see data collection).
- Data collection (M15- M25): a grid will be designed by the core group to assess the level of implementation of the recommendation in the selected hospitals (number of participating wards, % of completed assessment grid) This document will be ready at M 14. It will provide elements for the evaluation of the implementation such as: to which condition the implementation was successful? For which reasons it was unsuccessful? etc
- Recommendation (M26 - M30): the evaluation of results will take place to propose recommendations to encourage implementation of the selected tool beyond the hospitals that did it, to which the associated partners will contribute. The hospitals selected for the field testing will form the back bone of an EU community of hospitals and national institutions involved in PS.
5.3.4. Deliverables and links with other work packages
D7 WP 4 meeting M5 WP meeting
Minutes of the meeting, with the list of all the participants
Draft guideline for selection of good practices to be implemented
Draft guideline for selection of hospitals
Core group (HOPE, PGEU, EFN, AT, BE, FI)
Mail website
D11
WP 4 meeting (as part of the 2nd coordination meeting)
M8 WP meeting
Minutes of the meeting, with the list and sign of all the participants
Guideline for selection of good practices to be implemented
Guideline for selection of hospitals
Partners Mail website
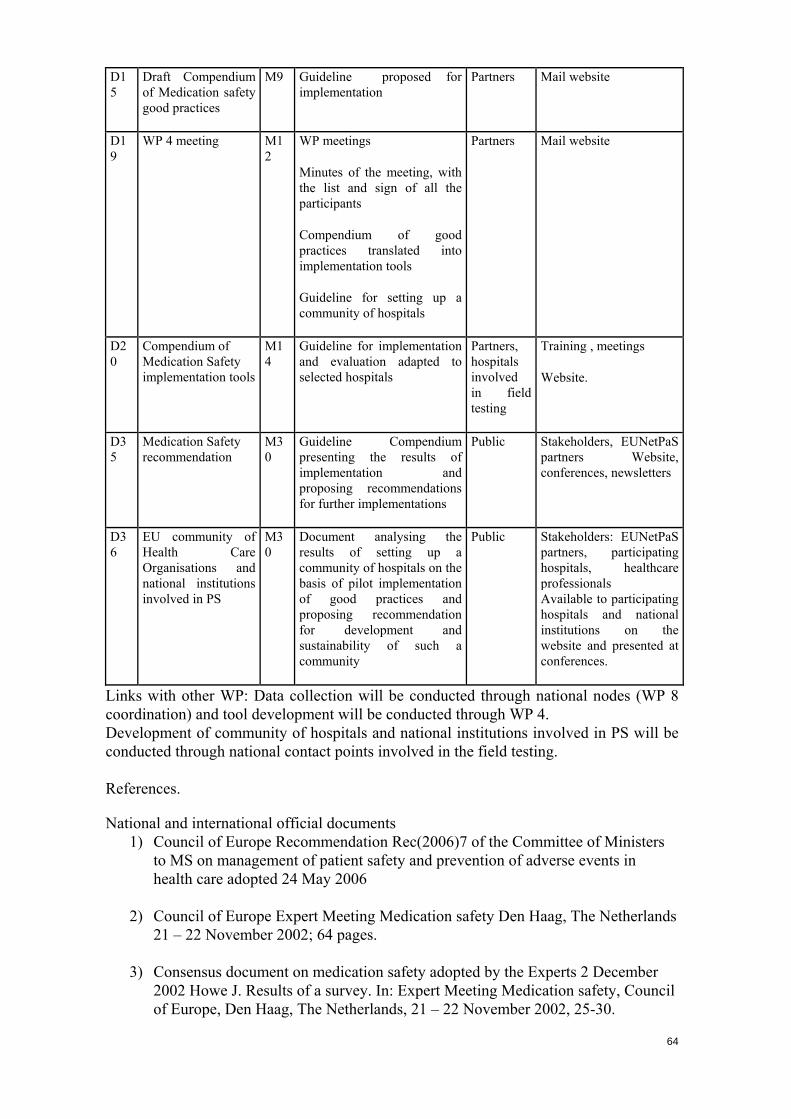
64
D15
Draft Compendium of Medication safety good practices
M9 Guideline proposed for implementation
Partners Mail website
D19
WP 4 meeting M12
WP meetings
Minutes of the meeting, with the list and sign of all the participants
Compendium of good practices translated into implementation tools
Guideline for setting up a community of hospitals
Partners Mail website
D20
Compendium of Medication Safety implementation tools
M14
Guideline for implementation and evaluation adapted to selected hospitals
Partners, hospitals involved in field testing
Training , meetings
Website.
D35
Medication Safety recommendation
M30
Guideline Compendium presenting the results of implementation and proposing recommendations for further implementations
Public Stakeholders, EUNetPaS partners Website, conferences, newsletters
D36
EU community of Health Care Organisations and national institutions involved in PS
M30
Document analysing the results of setting up a community of hospitals on the basis of pilot implementation of good practices and proposing recommendation for development and sustainability of such a community
Public Stakeholders: EUNetPaS partners, participating hospitals, healthcare professionals Available to participating hospitals and national institutions on the website and presented at conferences.
Links with other WP: Data collection will be conducted through national nodes (WP 8 coordination) and tool development will be conducted through WP 4. Development of community of hospitals and national institutions involved in PS will be conducted through national contact points involved in the field testing. References.
National and international official documents 1) Council of Europe Recommendation Rec(2006)7 of the Committee of Ministers
to MS on management of patient safety and prevention of adverse events in health care adopted 24 May 2006
2) Council of Europe Expert Meeting Medication safety Den Haag, The Netherlands
21 – 22 November 2002; 64 pages.
3) Consensus document on medication safety adopted by the Experts 2 December 2002 Howe J. Results of a survey. In: Expert Meeting Medication safety, Council of Europe, Den Haag, The Netherlands, 21 – 22 November 2002, 25-30.

65
4) Australian Council for Safety and Quality in Health Care. Second national report
on patient safety improving medication safety. Melbourne: Safety + Quality Council; 2002.
5) Canadian Coalition on Medication Incident Reporting and Prevention (CCMIRP)
A medication incident reporting and prevention system for Canada – Business plan. Otawa 20 March 2002; 69 pages.
. 6) Council of the European Communities Directive 2000/38/EC of 5 June 2000
amending Chapter V a (Pharmacovigilance) of Council Directive 75/319/EEC on the approximation of provisions laid down by law, Creation of a better medication safety culture in Europe: building up safe medication practices 260 regulation or administrative action relating to medicinal products Official Journal L 139 , 10/06/2000 P. 0028 –0030.
7) Dutch Institute for Health care Improvement CBO Safety improvement for
patients in Europe. Interim report SIMPATIE Project. Grant agreement n°2004108 May 2006: 54 pages. available at: http://ec.europa.eu/health/ph_projects/2004/action1/docs/action1_2004_inter_19_en.pdf
8) European Commission Luxembourg Declaration on Patient Safety: Patient Safety
– Making it happen! 5 April 2005; 2 pages. http://www.simpatie.org/Main/files/Luxembourg_Declaration_on_Patient_Safety_05042005.pdf/download http://www.simpatie.org/Main
9) European Commission. Guidance concerning “consultations with target patient groups” for the package leaflet. August 2005. Available at: http://pharmacos.eudra.org/F2/pharmacos/docs/Doc2005/08_05/USERTESTING
_20050817.pdf
10) European Medicines Agency (EMEA). Committee for Medicinal Products for Human Use. Guideline on risk management systems for medicinal products for human use. EMEA/CHMP/96268/2005 14 November 2005.
11) Health Canada. Drug Name Review: Look-alike Sound-alike (LA/SA) Health
Product Names . Revision 2005/08/03.
12) Helen Hamlyn Research Centre Information design for patient safety. NHS National Patient Safety Agency 2005; 115 pages.
13) NHS National Patient Safety Agency National reporting and learning system
service dataset – Acute/general hospital. 2003/04 Release 1.2.0 25p.
14) NHS National Patient Safety Agency Seven steps to patient safety : the full reference guide. London 2004; 188 pages.
15) NHS National Patient Safety Agency Building a memory: preventing harm,
reducing risks and improving patient safety. London July 2005; 62 pages.
66
16) NHS Scotland. Clinical Resource and Audit Centre. Good Practice Statement for the preparation of injections in nearpatient areas, including clinical and home environments. 2002; 32 pages.
17) Smith J Building a safer NHS for patients: Improving medication safety. UK
Department of Health 22 January 2004; 174 pages.
18) UK Department of Health. An organisation with a memory: report of an expert group on learning from adverse events in the NHS chaired by the Chief Medical Officer. Stationery Office, London; 2000. Report No.: ISBN 011 322441 9.
19) UK Department of Health and the Design Council. Design for patient safety.
2003.
20) World Alliance for Patient Safety WHO Draft guidelines for adverse event reporting and learning systems: from information to action. World Health Organization 2005; 77 pages.
Peer reviewed articles:
1) Ahscroft D, Morecroft C, Parker D, Noyce P. Patient safety on community pharmacy: understanding errors and managing risk. University of Manchester. 2005; 70 pages.
2) Allan EL, Barker KN. Fundamentals of medication error research. Am J Hosp
Pharm 1990; 47(3):555-571.
3) Alldred A. Purchasing safer medicines: a national risk assessment strategy. Hosp Pharmacist 2006; 13 (1): 17-19.
4) American Hospital Association (AHA), Health Research & Educational Trust
(HRET), and the Institute for Safe Medication Practices (ISMP) Pathways for medication safety. 2002
5) American Society of Consultant Pharmacists Guidelines for pharmacist
counseling of geriatric patients. 1998; 7 pages.
6) American Society of Hospital Pharmacists. ASHP guidelines on preventing medication errors in hospitals. Am J Hosp Pharm 1993; 50(2):305-314.
7) American Society of Health-System Pharmacists. ASHP guidelines on the
provision of medication information by pharmacists. Am J Health-Syst Pharm. 1996;53:1843–1845.
8) American Society of Health-System Pharmacists. ASHP Guidelines on
pharmacist-conducted patient education and counseling. Am J Health-Syst Pharm 1997;54:431-4.
9) Arce D. In defence of unit dose dispensing (Letter). Eur Hosp Pharm 1996;
2(5):222.

67
10) Barber N Should we consider non-compliance a medical error? Qual Saf Health Care 2002;11:81-84.
11) Baker GR, Norton PG, Flintoft V et al. The Canadian Adverse Events Study: the
incidence of adverse events among hospital patients in Canada. CMAJ 2004; 170(11):1678-1686.
12) Barker KN. The problems of detecting medication errors in hospitals. Am J Hosp
Pharm 1962; 19:361-369.
13) Barker KN. Experimental distribution system offers total drug control. Hospitals 1965; 39:142-155.
14) Barker KN, Mikeal RL, Pearson RE, Illig NA, Morse ML. Medication errors in
nursing homes and small hospitals. Am J Hosp Pharm 1982; 39(6):987-991.
15) Barker KN, Allan EL. Research on drug-use system errors. Am J Health Syst Pharm 1995; 52(4):400-403.
16) Barker KN, Flynn EA, Pepper GA, et al. Medication errors observed in 36 health
care facilities. Arch Intern Med 2002; 162: 1897-903.
17) Barker KN, Flynn EA, Pepper GA. Observation method of detecting medication errors. Am J Health Syst Pharm 2002; 59(23):2314-2316.5
18) Bates DW, Leape LL, Petrycki S. Incidence and preventability of adverse drug
events in hospitalized adults. J Gen Intern Med 1993; 8(6):289-294.
19) Bates DW, Cullen DJ, Laird N et al. Incidence of adverse drug events and potential adverse drug events. Implications for prevention. ADE Prevention Study Group. JAMA 1995; 274(1):29-34.
20) Bates DW, Spell N, Cullen DJ et al. The costs of adverse drug events in
hospitalized patients. Adverse Drug Events Prevention Study Group. JAMA 1997; 277(4):307-311.
21) Bates DW, Leape LL, Cullen DJ et al. Effect of computerized physician order
entry and a team intervention on prevention of serious medication errors. JAMA 1998; 280(15):1311-1316.
22) Bates DW, Teich JM, Lee J et al. The impact of computerized physician order
entry on medication error prevention. J Am Med Inform Assoc 1999; 6(4):313-321.
23) Bates, W. Using information technology to reduce rates of medication errors in
hospitals, BMJ, 2000, 320:788-91
24) Bates DW. Using information technology to screen for adverse drug events. Am J Health Syst Pharm 2002; 59(23):2317-2319.
25) Batty R, Barber ND. Ward pharmacy: a foundation for prescribing audit? Qual
Health Care 1992; 1(1):5-9.

68
26) Beaney AM, Black A, Dobson CR, Williamson S, Robinson M. Development and
application of a risk assessment tool to improve the safety of patients receiving injectable medicines. Hospital Pharmacist 2005; 12( 4):150-154.
27) Beijer HJ, de Blaey CJ. Hospitalisations caused by adverse drug reactions (ADR):
a meta-analysis of observational studies. Pharm World Sci 2002; 24(2):46-54.
28) Beso A, Franklin BD, Barber N. The frequency and potential causes of dispensing errors in a hospital pharmacy. Pharm World Sci 2005 ; 27 (3) : 182-190.
29) Bobb A, Gleason K, Husch M, Feinglass J, Yarnold PR, Noskin GA. The
epidemiology of prescribing errors: the potential impact of computerized prescriber order entry. Arch Intern Med 2004; 164(7):785-792.
30) Bond CA, Raehl CL, Franke T. Medication errors in United States hospitals.
Pharmacotherapy 2001; 21(9):1023-1036.
31) Boockvar K, Fishman E, Kyriacou CK, Monias A, Gavi S, Cortes T. Adverse events due to discontinuations in drug use and dose changes in patients transferred between acute and long-term care facilities. Arch Intern Med 2004; 164(5):545-550.
32) Brown S, Black K, Mrochek S, et al. RADARx: recognizing, assessing, and
documenting adverse Rx events. AMIA Annu Symp Proc 2000 : 101–5.
33) Cavell GF, Hughes DK. Does computerised prescribing improve the accuracy of drug administration? Pharm J 1997; 259: 782-784
34) Cavell GF. Medication incident reports — improving the quality of reporting.
Hospital Pharmacist 2006; 13( 2):53-55.
35) Chua SS, Wong IC, Edmondson H et al. A feasibility study for recording of dispensing errors and near misses' in four UK primary care pharmacies. Drug Saf 2003; 26(11):803-813.
36) Classen DC, Pestotnik SL, Evans RS, Burke JP. Computerized surveillance of
adverse drug events in hospital patients. JAMA 1991; 266(20):2847-2851.
37) Classen DC, Pestotnik SL, Evans RS, et al. Description of a computerized adverse drug event monitor using a hospital information system. Hosp Pharm 1992; 27: 774–83.
38) Classen DC, Metzger J. Improving medication safety: the measurement
conundrum and where to start. Int J Qual Health Care 2003; 15 Suppl 1:i41-i47.
39) Cohen MM, Kimmel NL, Benage MK et al. Medication safety programme reduces adverse drug events in a community hospital. Qual Saf Health Care 2005; 14(3):169-174.
69
40) Cohen MR. (Ed.) Medication errors. Washington (DC): American Pharmaceutical
Association . Washington (DC): 1999.
41) Cohen MR. Why error reporting systems should be voluntary. (Editorial). BMJ 2000; 320(7237):728-729.
42) Cohen MR. Trade name, INNs, and medication errors. Arch Intern Med 2002;
162: 2636-2637.
43) Colpaert K, Claus B, Somers A, Vandewoude K, Robays H, Decruyenaere J. Impact of computerized physician order entry on medication prescription errors in the intensive care unit: a controlled cross-sectional trial. Crit Care 2006; 10(1):R21.
44) Consejo General de Colegios Oficiales de Farmacéuticos e Instituto para el Uso
Seguro de los Medicamentos (ISMPSpain).Campaña de prevención de errores de medicación causados por similitud en los nombres de los
45) medicamentos. http://www.usal.es/ismp.
46) Cousins DH, Sabatier B, Begue D, Schmitt C, Hoppe-Tichy T. Medication errors in intravenous drug preparation andadministration: a multicentre audit in the UK, Germany and France. Qual Saf Health Care 2005; 14(3):190-195.
47) Cousins DH. International perspectives on patient safety. In Manasse HR and
Thompson KK. Medication safety: A guide for health care facilities. American Society of Health System Pharmacists. Bethesda. 2005; 327-350.
48) Cummings J, Bush P, Smith D, Matuszewski K. Bar-coding medication
administration overview and consensus recommendations. Am J Health Syst Pharm 2005; 62(24):2626-2629.
49) Dean BS, Allan EL, Barber ND, Barker KN. Comparison of medication errors in
an American and a British hospital. Am J Health Syst Pharm 1995; 52(22):2543-2549.
50) Dean B, Barber N, Schachter M. What is a prescribing error? Quality in Health
Care 2000; 9:232-237.
51) Dean B, Schachter M, Vincent C, Barber N. Prescribing errors in hospital inpatients: their incidence and clinical significance. Quality and Safety in Healthcare 2002; 11:340-344.
52) Dean FB, Vincent C, Schachter M, Barber N. The incidence of prescribing errors
in hospital inpatients: an overview of the research methods. Drug Saf 2005; 28(10):891-900.
53) Delgado SO, Escriva TA, Vilanova BM et al. Estudio comparativo de errores con
prescripción electrónica versus prescripción manual. Farm Hosp 2005; 29(4):228-235.
70
54) Einarson TR. Drug-related hospital admissions. Ann Pharmacother 1993; 27(7-8):832-840.
55) Estudio Nacional sobre los efectos adversos ligados a la hospitalización (ENEAS
2005). Informe. Febrero 2006. Ministerio de Sanidad y Consumo. Madrid 2006.
56) Evans RS, Classen DC, Stevens LE, et al. Using a hospital information system to assess the effects of adverse drug events. In: Safran C, editor. The Seventeenth Annual Symposium on Computer Applications in Medical Care. New York: McGraw-Hill Inc, 1994: 161-165.
57) Evans RS, Lloyd JF, Stoddard GJ, Nebeker JR, Samore MH. Risk factors for
adverse drug events: a 10-year analysis. Ann Pharmacother 2005; 39(7-8):1161-1168..
58) Fernando B, Savelyich BS, Avery AJ et al. Prescribing safety features of general
practice computer systems: evaluation using simulated test cases. BMJ 2004; 328(7449):1171 1172.
59) Ferner RE, Langford NJ, Anton C, Hutchings A, Bateman DN, Routledge PA.
Random and systematic medication errors in routine clinical practice: a multicentre study of infusions, using acetylcysteine as an example. Br J Clin Pharmacol 2001; 52(5):573-577.
60) Fertleman M, Barnett N and Patel T. Improving medication management for
patients: the effect of a pharmacist on post admission ward rounds. Qual Saf Health Care 2005; 14: 207-211.
61) Flynn EA, Barker KN, Pepper GA, Bates DW, Mikeal RL. Comparison of
methods for detecting medication errors in 36 hospitals and skilled-nursing facilities. Am J Health Syst Pharm 2002; 59(5):436-446..
62) Fontan JE, Maneglier V, Nguyen VX, Loirat C, Brion F. Medication errors in
hospitals: computerized unit dose drug dispensing system versus ward stock distribution system. Pharm World Sci 2003; 25(3):112-117.
63) Gandhi TK, Bates DW. Computer adverse drug event (ADE) detection and alerts.
In: Shojania KG, Duncan BW, McDonalds KM, Wachter RM, editors. Making Health Care Safer: A Critical Analysis of Patient Safety Practices Agency for Healthcare Research and Quality 2001; 79-85.
64) Gandhi SK, Shojania KG, Bates DW. Protocols for High-Risk Medicines:
Reducing Adverse Drug Events Related toAnticoagulants. In: Shojania KG, Duncan BW, McDonalds KM, Wachter RM, editors. Making Health Care Safer: A Critical Analysis of Patient Safety Practices Agency for Healthcare Research and Quality 2001; 87-100.
65) Gandhi TK, Weingart SN, Borus J et al. Adverse drug events in ambulatory care.
N Engl J Med 2003; 348(16):1556-1564.

71
66) Gandhi TK, Burstin HR, Cook EF, et al. Drug complications in outpatients. J Gen Intern Med 2000; 15: 149–54.
67) Gandhi TK, Seger DL, Bates DW. Identifying drug safety issues: from research to practice. Int J Qual Health Care 2000; 12: 69–76.
68) Garg AX, Adhikari NK, McDonald H et al. Effects of computerized clinical decision support systems on practitioner performance and patient outcomes: a systematic review. JAMA 2005; 293(10):1223-1238.
69) Gerety MB, Cornell JE, Plichta DT, Eimer M. Adverse events related to
medicines and drug withdrawal in nursing home residents. J Am Geriatr Soc 1993; 41(12):1326-1332.
70) Gosbee LL, Burkhardt ME. Application of human factors engineering in process
and equipment design. In: Manasse HR, Thompson KK, eds. Medication safety: a guide for health care facilities . Bethesda, MD: Am Soc Health-System Pharm, 2005: 201–26.
71) Grasela TH, Walawander CA, Kennedy DL, et al. Capability of hospital computer systems in performing drug-use evaluations and adverse drug event monitoring. Am J Hosp Pharm 1993; 50: 1889–95.
72) Greenall J, U D, Lam R. An effective tool to enhance a culture of patient safety
and assess the risks of medication usesystems. Healthcare Quaterly 2005; 8: 53-8.
73) Greengold NL, Shane R, Schneider P et al. The impact of dedicated medication nurses on the medication administration error rate: a randomized controlled trial. Arch Intern Med 2003; 163(19):2359-2367.
74) Han YY, Carcillo JA, Venkataraman ST et al. Unexpected increased mortality
after implementation of a commercially sold computerized physician order entry system. Pediatrics 2005; 116(6):1506-1512.
75) Hardmeier B, Braunschweig S, Cavallaro M et al. Adverse drug events caused by
medication errors in medical inpatients. Swiss Med Wkly 2004; 134(45-46):664-670.
76) Hartwig SC, Denger SD, Schneider PJ. Severity-indexed, incident report-based
medication error-reporting programme. Am J Hosp Pharm 1991; 48(12):2611-2616.
77) Hawkey CJ, Hodgson S, Norman A, Daneshmend TK, Garner ST. Effect of
reactive pharmacy intervention onquality of hospital prescribing. BMJ 1990; 300(6730):986-990.
78) Hidalgo Correas FJ, Bermejo VT, de Juana Velasco P, Garcia DB. Implantación
de un programmea de prescripción médica electrónica en un hospital del INSALUD. Farm Hosp 2002; 26(6):327-334.
79) Ho CYW, Dean BS, Barber ND. When do medication administration errors
happen to hospital inpatients? Int J Pharm Pract 1997; 5: 91-96.

72
80) Hoffman JM, Proulx SM. Medication errors caused by confusion if drug names.
Drug Saf 2003; 26: 445-52.
81) Honigman B, Lee J, Rothschild J et al. Using computerized data to identify adverse drug events in outpatients. J Am Med Inform Assoc 2001; 8(3):254-266.
82) Honigman B, Light P, Pulling RM, et al. A computerized method for identifying
incidents associated with adverse drug events in outpatients. Int J Med Informatics 2001; 61: 21–32.
83) Hoppes C, Holquist C, Phillips J. Generic name confusion. FDA Safety page.
Medicines Topics, October 6, 2003.
84) Ioannidis JP, Lau J. Evidence on interventions to reduce medical errors: an overview and recommendations for future research. J Gen Intern Med 2001; 16(5):325-334.
85) Institute for Safe Medication Practices. ISMP´s List of High-Alert Medications.
www.ismp.org
86) Institute for Safe Medication Practices. What´s in a name? Ways to prevent dispensing errors linked to name confusion. ISMP Medication Safety Alert! June 12, 2002.
87) Institute for Safe Medication Practices. A spectrum of problems with using color.
ISMP Medication Safety Alert! November 13, 2003.
88) Institute for Safe Medication Practices. High alert medication list. Available at: http://www.ismp.org/Tools/highalertmedications.pdf
89) Jha AK, Kuperman GJ, Teich JM, et al. Identifying adverse drug events:
development of a computer-based monitor and comparison with chart review and stimulated voluntary report. J Am Med Informatics Assoc 1998; 5: 305–14.
90) Kanjanarat P, Winterstein AG, Johns TE, Hatton RC, Gonzalez-Rothi R, Segal R.
Nature of preventable adverse drug events in hospitals: a literature review. Am J Health Syst Pharm 2003; 60(17):1750-1759.
91) Kaushal R, Bates DW, Landrigan C et al. Medication errors and adverse drug
events in pediatric inpatients. JAMA 2001; 285(16):2114-2120.
92) Kaushal R, Bates DW. Computerized Physician Order Entry (CPOE) with Clinical Decision Support Systems (CDSSs). In: Shojania KG, Duncan BW, McDonalds KM, Wachter RM, editors. Making Health Care Safer: A Critical Analysis of Patient Safety Practices Agency for Healthcare Research and Quality 2001: 59-69.
93) Kaushal R, Bates DW. The clinical pharmacist's role in preventing adverse drug
events. In: Shojania KG, Duncan BW, McDonalds KM, Wachter RM, editors.

73
Making Health Care Safer: A Critical Analysis of Patient Safety Practices Agency for Healthcare Research and Quality 2001; 71-77.
94) Kaushal R. Using chart review to screen for medication errors and adverse drug
events. Am J Health Syst Pharm 2002; 59(23):2323-2325.
95) Kaynes S. Negligence and the pharmacist: dispensing errors and prescribing errors Pharm J 1996; 257:32-5..
96) Klibanov OM, Eckel SF. Effects of automated dispensing on inventory control,
billing, workload, and potential for medication errors. Am J Health Syst Pharm 2003; 60(6):569-572.
97) Koppel R, Metlay JP, Cohen A et al. Role of computerized physician order entry
systems in facilitating medication errors. JAMA 2005; 293(10):1197-1203.
98) Kruse H, Johnson A, O’Connell D, Clarke T. Administering non-restricted medication in hospital. The implications and cost of using two nurses. Australian clinical review. 1992; 12: 77-83.
99) Kuyper AR. Patient counseling detects prescription errors. Hosp Pharm 1993;
28(12):1180-1189.
100) Lacasa C, Cot R, Roure C, et coll. Medication errors in a general hospital. Eur Hosp Pharm 1998; 4(2):35-40.
101) Lambert BL, Lin SJ, Tan H. Designing safe drug names. Drug Saf 2005; 28: 495-512.
102) Lankshear AJ, Sheldon TA, Lowson KV, Watt IS, Wright J. Evaluation of
the implementation of the alert issued by the UK National Patient Safety Agency on the storage and handling of potassium chloride concentrate solution. Qual Saf Health Care 2005; 14(3):196-201.
103) Lazarou J, Pomeranz BH, Corey PN. Incidence of adverse drug reactions
in hospitalized patients: a meta-analysis of prospective studies. JAMA 1998; 279(15):1200-1205.
104) Leape LL, Bates DW, Cullen DJ et al. Systems analysis of adverse drug
events. ADE Prevention Study Group. JAMA 1995; 274(1):35-43.
105) Leape LL, Kabcenell A, Berwick DM, Roessner J. Reducing adverse drug events. Institute for Healthcare Improvement, Boston; 1998.
106) Leape L. Statement concerning patient safety and medication errors
before the United States Senate. Subcommittee on Labor, Health and Human Services, and Education. January 25, 2000.
107) Lesar TS, Briceland L, Stein DS. Factors related to errors in medication
prescribing. JAMA 1997; 277(4):312-317.
74
108) Lesar TS, Briceland LL, Delcoure K, et al. Medication prescribing errors
in a teaching hospital. JAMA 1990; 263: 2329–34.
109) Lesar TS. Practitioner intervention-reporting systems for measuring the quality of drug use. Am J Health Syst Pharm2002; 59(23):2320-2322.
110) Lesar T, Mattis A, Anderson E, Avery J, Fields J, Gregoire J, Vaida A.
VHA New England Medication Error Prevention Initiative Collaborative. Using the ISMP Medication Safety Self-assessment to improve medication use process. Jt Comm J Qual Saf. 2003; 29:211-26
111) Letrilliart L, Hanslik T, Biour M, Fagot JP, Guiguet M, Flahault A.
Postdischarge adverse drug reactions in primary care originating from hospital care in France: a nationwide prospective study. Drug Saf 2001; 24(10):781-792.
112) Levy M, Azaz-Livshits T, Sadan B, et al. Computerized surveillance of
adverse drug reactions in hospital: implementation. Eur J Clin Pharm 1999; 54: 887–92.
113) McEvoy GK. Medicines information resources and medication safety. In
Manasse HR and Thompson KK. Medication safety: A guide for health care facilities. American Society of Health System Pharmacists. Bethesda.2005; 253-274.
114) McNeilly JL. Medication errors: a quality assurance tool. Nurs Manag
(Harrow) 1987; 18(12):53-58.
115) Michels RD, Meisel S. Programme using pharmacy technicians to obtain medication histories. Am J Health-Syst Pharm 2003; 60: 1982-1986.
116) Mille F, Bourdon O, Fontan JE, Brion F. Évaluation de la spécificité d’un
système de détection automatisé des interactions médicamenteuses. Act Pharm Biol Clin 2005; 12: 361-368.
117) Miller LK, Nelson MS et Spurlock BW A compendium of suggseted
practices for preventing and reducing medication errors. The California Institute for Health System Performance (CIHSP) November 2001; 80 pages.
118) Mirco A, Campos L, Falcao F, Nunes JS, Aleixo A. Medication errors in
an internal medicine department. Evaluation of a computerized prescription system. Pharm World Sci 2005; 27(4):351-352.
119) Morimoto T, Gandhi TK, Seger AC, Hsieh TC, Bates DW. Adverse drug
events and medication errors: detection and classification methods. Qual Saf Health Care 2004; 13(4):306-314.
120) Morris CJ, Rodgers S, Hammersley VS, Avery AJ, Cantrill JA. Indicators
for preventable drug related morbidity: application in primary care. Qual Saf Health Care 2004; 13(3):181-185.

75
121) Murff HJ, Patel VL, Hripcsak G, et al. Detecting adverse events for
patient safety research: a review of current methodologies. J Biomed Inform 2003; 36: 131–43.
122) Murray MD, Shojania KG. Unit dose drug distribution systems. In:
Shojania KG, Duncan BW, McDonalds KM,Wachter RM, editors. Making Health Care Safer: A Critical Analysis of Patient Safety Practices Agency for Healthcare Research and Quality 2001; 101-109.
123) Murray MD. Automated medication dispensing devices. In: Shojania KG,
Duncan BW, McDonalds KM, Wachter RM, editors. Making Health Care Safer: A Critical Analysis of Patient Safety Practices Agency for Healthcare Research and Quality 2001; 111-116.
124) Nadzam DM. A systems approach to medication use. In Cousins DD.
(Ed.) Medication use: a system approach to reducing errors. JCAHO, Joint Commission on Accreditation of Healthcare Organization, Oakbrook, IL 1998.
125) National Coordinating Council for Medication Error Reporting and
Prevention. NCCMERP Taxonomy of medicationerrors. 1998. 126) National Steering Committee on Patient Safety Building a Safer System:
A National Integrated Strategy for Improving Patient Safety in Canadian Health Care. Wade J (Ed.) September 2002; 48p.
127) Nebeker JR, Hoffman JM, Weir CR, Bennett CL, Hurdle JF. High rates of
adverse drug events in a highly computerized hospital. Arch Intern Med 2005; 165(10):1111-1116.
128) Nelson KM, Talbert RL. Drug-related hospital admissions.
Pharmacotherapy 1996; 16(4):701-707.
129) Neuenschwander M, Cohen MR, Vaida AJ, Patchett JA, Kelly J, Trohimovich B. Practical guide to bar coding for patient medication safety. Am J Health Syst Pharm 2003; 60: 768-79.
130) Ogden DA, Kinnear M, McArthur DM. A quantitative and qualitative
evaluation of medication error in hospital inpatients. Pharm J 1997;259: R19.
131) O’Neil AC, Petersen LA, Cook EF, et al. Physician reporting compared with medical-record review to identify adverse medical events. Ann Intern Med 1993; 119: 370–6.
132)
133) Oren E, Griffiths LP, Guglielmo BJ. Characteristics of antimicrobial overrides associated with automated dispensing machines. Am J Health Syst Pharm 2002; 59(15):1445-1448.
76
134) Oren E, Shaffer ER, Guglielmo BJ. Impact of emerging technologies on medication errors and adverse drug events. Am J Health Syst Pharm 2003; 60(14):1447-1458.
135) Orser BA Medication safety in anesthetic practice: first do no harm. Can J
Anaesth 2000; 47: 1051-1054.
136) Otero MJ, Dominguez-Gil A. Acontecimientos adversos por medicamentos: una patología emergente. Farmacia Hospitalaria 2000; 24(4):258-266.
137) Otero MJ, Martín R, Valverde MP, Domínguez-Gil A. Analysis of
preventable adverse drug events (ADEs) leadingto hospital admission: incidence, categorization and cost. 36th ASHP Midyear Clinical Meeting and Exhibits, New Orleans 2001.
138) Otero MJ, Codina C, Tamés MJ, Pérez M. Errores de medicación:
estandarización de la terminología y clasificación. Resultados de la Beca Ruiz-Jarabo 2000. Farmacia Hospitalaria 2003; 27(3):137-149.
139) Otero MJ. Errores de medicación y gestión de riesgos Rev Esp Salud
Pública 2003; 77: 527-540.
140) Otero MJ. El papel del farmacéutico en la prevención de los errores de medicación. En: Formación Continuada para Farmacéuticos de Hospital II. Módulo 3. Barcelona: Fundación Promedic 2004; 5-44.
141) Otero MJ. Nuevas iniciativas para mejorar la seguridad de la utilización
de los medicamentos en los hospitales. Rev Esp Salud Pública 2004; 78(3):323-339.
142) Otero MJ, Schmitt E. Clarifying terminology for adverse drug events. Ann
Intern Med 2005; 142(1):77-78.
143) Patterson ES, Rogers ML, Render ML. Fifteen best practice recommendations for bar-code medication administration in the Veterans Health Administration. Jt Comm J Qual Saf 2004; 30(7):355-365.
144) Paulino EI, Bouvy ML, Gastelurrutia MA, Guerreiro M, Buurma H. Drug
related problems identified in patientsdischarged from hospital. Pharm World Sci 2004; 26:353-60.
145) Payne TH, Savarino J, Marshall R, et al. Use of a clinical event monitor to
prevent and detect medication errors. AMIA Annu Symp Proc 2000 : 640–4.
146) Pirmohamed M, James S, Meakin S et al. Adverse drug reactions as cause of admission to hospital: prospective analysis of 18 820 patients. BMJ 2004; 329(7456):15-19.
147) Prescrire Editorial Staff Informed decisions: think of the INN Prescrire
International 2005;14(78):122.
77
148) Prescrire Editorial Staff A campaign to use International Nonproprietary
Names Prescrire International 2005;14(80):202.
149) Prescrire Editorial Staff. Health professionals and patients: adopt the INN! Prescrire International 2005; 14: 234-235.
150) Raschke RA, Gollihare B, Wunderlich TA et al. A computer alert system
to prevent injury from adverse drug events: development and evaluation in a community teaching hospital. JAMA 1998; 280(15):1317-1320.
151) Reason JT. Human error. Cambridge: Cambridge Univ.Press; 1990: 302
pages.
152) Reason JT. Human error: models and management. BMJ 2000; 320(7237):768-770.
153) Recio Blázquez ML, López Ruiz M, Arias Fernández L, Zamora Barrios
MD. Analysis of medication errors detected in the dispensing process by the unit dose system in a Spanish hospital. Eur J Hosp Pharm 2004;(1):20-25.
154) Resar RK, Rozich JD, Classen D. Methodology and rationale for the
measurement of harm with trigger tools. Qual Saf Health Care 2003; 12 Suppl 2:ii39-ii45.
155) Ridge KW, Jenkins DB, Noyce PR, Barber ND. Medication errors during
hospital ward rounds. Qual Health Care 1995; 4:240-243
156) Roughead EE, Gilbert AL, Primrose JG, Sansom LN. Drug-related hospital admissions: a review of Australian studies published 1988-1996. Med J Aust 1998; 168(8):405-408.
157) Rozich JD, Haraden CR, Resar RK. Adverse drug event trigger tool: a
practical methodology for measuring medication related harm. Qual Saf Health Care 2003; 12(3):194-200.
158) Savage SW, Schneider PJ, Pedersen CA. Utility of an online medication-
error-reporting system. Am.J.Health Syst.Pharm. 2005 ; 62 (21) : 2265-2270.
159) Schmitt E. Unit dose drug distribution systems: old-fashioned or safer ways for pharmaceutical care? Eur Hosp Pharm 2000; 6(1):4-12.
160) Schmitt E, Dufay E. Erreurs liées au conditionnement des médicaments:
quelles mesures prendre pour les réduire? Actu Pharm Hosp; 2005: 35-42.
161) Schnipper JL, Kirwin JL, Cotugno MC et al. Role of pharmacist counseling in preventing adverse drug events after hospitalization. Arch Intern Med 2006; 166(5):565-571.
162) Schnurrer JU, Stichtenoth DO, Frolich JC. Knowledge on drug dosages of
ward physicians. Eur J Clin Pharmacol 2002; 58(1):65-67.

78
163) Schwab M, Oetzel C, Morike K, Jagle C, Gleiter CH, Eichelbaum M. Using trade names: a risk factor for accidental drug overdose. Arch Intern Med 2002; 162: 1065-1066.
164) Seger AC, Gandhi TK, Hope C, et al. Development of a computerized adverse drug event (ADE) monitor in the outpatient setting. In: Henriksen K, Battles JB, Marks ES, et al., eds. Advances in patient safety: from research to implementation, Volume 2 . Rockville, MD: Agency for Healthcare Research and Quality, 2005: CD.
165) Shah SNH, Aslam M, Avery AJ. A survey of prescription errors in general practice. Pharm J 2002; 267: 860-862.
166) Smeaton L, Sheikh A, Avery A, Royal S, Hurwitz B, Dewey M.
Interventions for reducing preventable drug-related hospital admissions or preventable drug-related morbidity in primary care. Cochrane Database Syst Rev (protocol) 2002; Issue 4.
167) Smetzer JL, Vaida AJ, Cohen MR, Tranum D, Pittman MA, Armstrong
CW. Findings from the ISMP Medication Safety Self-assessment for hospitals. Jt Comm J Qual Saf. 2003; 29:586-97.
168) Spencer MG, Smith AP. A multidisciplinary study of dispensing errors in
British Hospitals. In J Pharm Pract 1993; 2: 142-6.
169) Sutter TL, Wellman GS, Mott DA, Schommer JC, Sherrin TP. Discrepancies with automated drug storage and distribution cabinets. Am J Health Syst Pharm 1998; 55(18):1924-1926.
170) Taxis K, Dean B, Barber N. Hospital drug distribution systems in the UK
and Germany--a study of medication errors. Pharm World Sci 1999; 21(1):25-31.
171) Taxis K, Barber N. Ethnographic study of incidence and severity of intravenous drug errors. BMJ 2003; 326(7391):684.
172) Thomas EJ, Studdert DM, Newhouse JP et al. Costs of medical injuries in
Utah and Colorado. Inquiry 1999; 36(3):255-264.
173) Thomas EJ, Studdert DM, Burstin HR, et al. Incidence and types of adverse events and negligent care in Utah and Colorado. Med Care 2000; 38: 261–71
174) van der Linden CM, Kerskes MC, Bijl AM, Maas HA, Egberts AC,
Jansen PA. Represcription after adverse drug reaction in the elderly: a descriptive study. Arch Intern Med 2006; 166(15):1666-1667.
175) van Gijssel-Wiersma DG, van den Bemt PM, Walenbergh-van Veen MC.
Influence of computerised medicationcharts on medication errors in a hospital. Drug Saf 2005; 28(12):1119-1129.
176) Vaida AJ, Cohen MR. Point-of-care bar-coded medication administration:
experience in the United States. Farm Hosp 2005; 29(3):151-152.

79
177) Vincent CA, Neale G, Woloshynowych M. Adverse events in British hospitals: preliminary retrospective record review. BMJ 2001; 322(7285):517-519.
178) von Laue NC, Schwappach DL, Koeck CM. The epidemiology of
preventable adverse drug events: a review of the literature. Wien Klin Wochenschr 2003; 115(12):407-415.
179) Warner A, Menachemi N, Brooks RG Health literacy, medication errors,
and health outcomes: is there a relationship? Hosp Pharm 2006;41(6):542-551.
180) Wasserfallen J, Livio F, Buclin T, Tillet L, Yersin B, Biollaz J. Rate, type, and cost of adverse drug reactions in emergency department admissions. Eur J Intern Med 2001; 12(5):442-447.
181) Wears RL. The science of safety. In: Zipperer L, Cushman S, (Eds.)
Lessons in patient safety. Chicago (IL): National Patient Safety Foundation; 2001; 1-6.
182) Weingart SN, Toth M, Sands DZ, Aronson MD, Davis RB, Phillips RS.
Physicians' decisions to override computerized drug alerts in primary care. Arch Intern Med 2003; 163(21):2625-2631.
183) Wiegman SA, Cohen MR. The patient’s role in preventing medication
errors. in Cohen MR (Ed.) Medication errors.American Pharmaceutical Association, Washington, 1999; 14.1-14.12.
184) Wilson RM, Runciman WB, Gibberd RW, Harrison BT, Newby L,
Hamilton JD. The Quality in Australian HealthCare Study. Med J Aust 1995; 163(9):458-471.
185) Winterstein AG, Sauer BC, Hepler CD, Poole C. Preventable drug-related
hospital admissions. Ann Pharmacother 2002; 36(7-8):1238-1248.
186) Wirtz V, Taxis K, Barber ND. An observational study of intravenous medication errors in the United Kingdom and in Germany. Pharm World Sci 2003; 25(3):104-111.

80
5.4. Work package n° 8: Coordination of the project
5.4.1. List of partners involved
HAS (Leader) 652 p/d management of the project, network coordination.
UOA-HIL, EKEVYL, SST, STM-Finland, CPME, PGEU, SMoH, HIQA, GCPS, FOD-DG1, StaHeCCA, NBHW, DGS, EFN, DOH 18 p/d each: national coordination or EU coordination (PGEU, CPME, EFN) collection of information through semi directive interviews
EPF 10 p/d collection of information
5.4.2. Description of the work
The development of the network is intimately linked to the management of the project as the network will be developed via the involvement of the partners in the EUNetPaS activities, specifically coordination, communication and evaluation. This activities will relayed by the national contact point at the national level with the help of the national representatives of EU stakeholders involved in the core activities of EUNetPaS.
- Management of the project:
o Governance: the decision making process is detailed in the Standard Operating Procedure (SOP) manual of EUNetPaS. The main partner (MP) will answer to the Steering Committee (SC) which is made up of one representative of each partner organisation (associated partners: AP and collaborating partners (CP)) and to the Executive Board (EB) which is made up of one representative for each of the work package (WP) leading organisation (lead partners: LP). Standard Operating Procedures project manual will be developed by the MP and made available to all APs after validation by the SC. SOP will identify every member of the SC and EB.
o Technical reporting; The Main Partner will collect all relevant material from LPs in due time to provide interim and final reports to the PHEA in accordance with the contract. MP will regularly check that milestones are reached and deliverables are delivered in conformity with the agreed work plans of the different WP and inform PHEA of any technical problems having potential consequences on the expected outcomes of the project. The MP will finalize the global work plan with the EB. The work plan will be approved by the SC during the kick off meeting. The main partner (MP) will also report to the Patient Safety Working Group (PSWG) of the High Level Group for Health Services and Medical Care. Each LP will be responsible for coordinating activities within their WP and will assist the MP with timely collection of reports from APs. The project’s work plan will be developed by the MP with the input of the EB. It will be validated by the SC after consultation of the PSWG.
o Administrative, legal reporting: MP will liaise with the PHEA to inform it of any changes occurring in the status of AP or affecting staff registered in annexe 2. MP will regularly update the documents listed in annex 3 to ensure the proper level of administrative control to the PHEA.

81
o Financial reporting: MP will provide AP with requested templates to monitor and report staff involvement in EUNetPaS activities (time shits) the eligible costs occurring during the contract, following the annex 2 budget allocation. MP will collect regularly the declaration of costs from AP to consolidate the requested interim and final financial reports to the PHEA in due time as agreed in the contract. MP will as the contact for the PHEA and for APs in procedural, administrative, and financial matters and for monitoring.
o Sustainability of the network: EUNetPaS has outlined the following five year goals: EUNetPaS would like to be:
Respected as an integrated European network of expertise, dedicated to the promotion of Patient Safety;
Recognised as a sustained and credible authority, promoting European standards and providing evidence based information and opinions on Patient Safety;
A best-practice network that will inspire other European health networks.
MP will ensure that the added value of EUNetPaS (situation analysis, recommendations, PS tools…) is adequately disseminated, as well as impact evaluation results. The network will be promoted by the MP as an implementation tool for future PS initiatives or research projects, ensuring an increasing level of EU harmonisation in the PS field.
- Network development coordination.
o MP will promote the development of the network. This network will be made of the partners of the project representing the 27 MS. One partner in each Member State (generally a representative of the Ministry of Health: cf the list below) will act as a national node. Most of these national representatives are members of the SANCO Patient Safety Working Group, therefore they are involved in PS both at national and EU level. They are also used to work together around PS issues. These national contact points or nodes will be involved in the information collection for the situation analysis (cf WP 1,2,3,4), in the dissemination (cf WP 9) and in the evaluation of the project (cf WP 10). They will be strongly encouraged by project governance bodies (Steering committee and Executive Board) to involve national stakeholders (health professionals representatives, patients representatives, decision makers) in these different tasks. The development of these national platforms will be also facilitated by the involvement in the project of the EU representatives of the main stakeholders (European Federation of Nurses, Standing Committee of European Doctors, European Patient Forum, Pharmaceutical Group of the European Union, European Federation of Hospitals). They will encourage the participation of their affiliates in these national PS platforms which should contribute to enhance EUNetPaS impact.
List of national contact points:
Austria Federal Ministry of Health Family and Youth
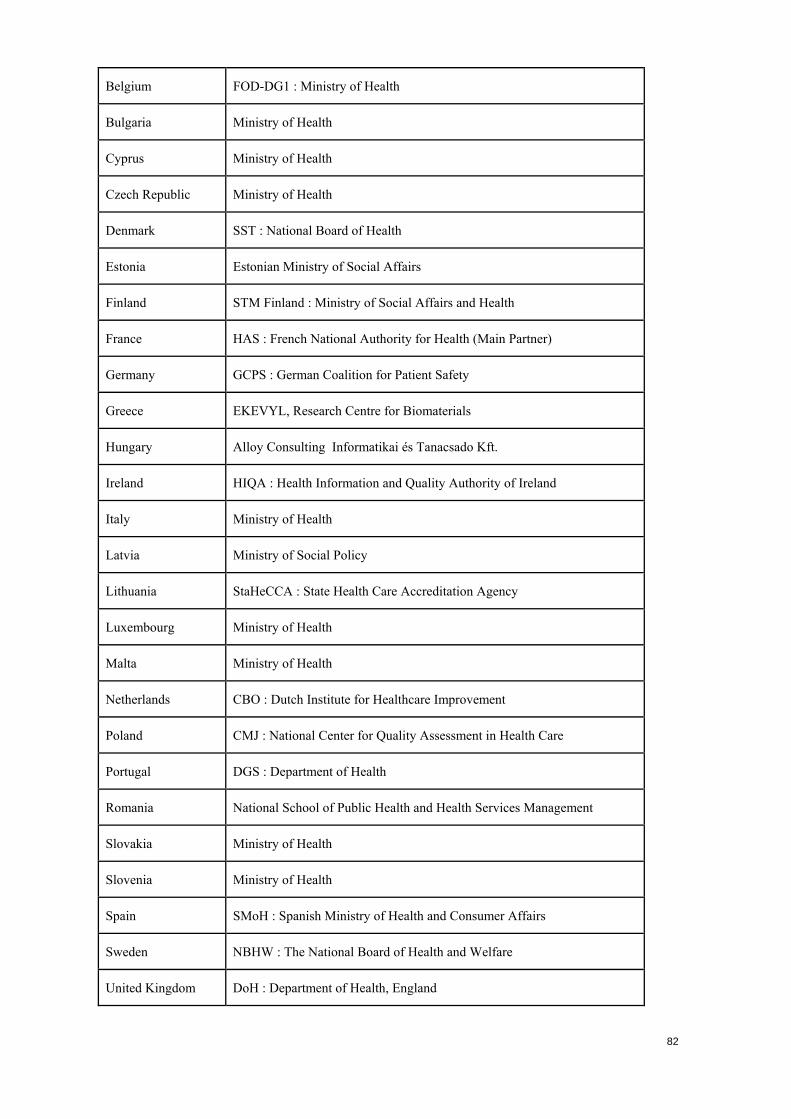
82
Belgium FOD-DG1 : Ministry of Health
Bulgaria Ministry of Health
Cyprus Ministry of Health
Czech Republic Ministry of Health
Denmark SST : National Board of Health
Estonia Estonian Ministry of Social Affairs
Finland STM Finland : Ministry of Social Affairs and Health
France HAS : French National Authority for Health (Main Partner)
Germany GCPS : German Coalition for Patient Safety
Greece EKEVYL, Research Centre for Biomaterials
Hungary Alloy Consulting Informatikai és Tanacsado Kft.
Ireland HIQA : Health Information and Quality Authority of Ireland
Italy Ministry of Health
Latvia Ministry of Social Policy
Lithuania StaHeCCA : State Health Care Accreditation Agency
Luxembourg Ministry of Health
Malta Ministry of Health
Netherlands CBO : Dutch Institute for Healthcare Improvement
Poland CMJ : National Center for Quality Assessment in Health Care
Portugal DGS : Department of Health
Romania National School of Public Health and Health Services Management
Slovakia Ministry of Health
Slovenia Ministry of Health
Spain SMoH : Spanish Ministry of Health and Consumer Affairs
Sweden NBHW : The National Board of Health and Welfare
United Kingdom DoH : Department of Health, England

83
o MP will ensure a secretariat for a sustainable network of “nodes” or national contact points, EU stakeholders and international organisations.
MP will provide the adequate communication tools (website intranet, address book, web based forum, E-meetings tool…) to ensure the adequate level of communication between the partners.
MP will act as a facilitator to ensure that transmission of information and involvement of partners are optimal. He will particularly pay attention to collaborating partners’ involvement in the network activities, including them in WP activities in accordance with their expressed wishes and their expertise. MS representatives will be involved in horizontal work packages to ensure a real EU coverage to EUNetPaS (coordination: aiming at developing national safety platform, communication: aiming at raising PS awareness and impact evaluation aiming at assessing the improvement of PS culture in their respective countries).
MP will check that the requested level of coordination with other international initiatives (WHO, IHI, High 5, World Alliance for PS, other ongoing EU projects…) will be provided. MP will perform a monthly surveillance of the corresponding websites and transfer information regarding these initiatives to EUNetPaS partners via EUNetPaS website. MP will represent EUNetPaS in these initiatives through participation to or information of corresponding advisory bodies.
MP will organize 5 coordinating meetings providing facilities to allow WP meetings in parallel sessions followed by governance body meetings to ensure efficient use of resources and fast activity progress validation (please see a generic agenda of coordinating meeting in 5.3.3 milestones). Specifically during the first part of the work plan, when the coordinated situation analysis and the planning of the field testing are due to take place. As member of the SC, one representative of each collaborating institution will be invited by the MP to the SC meetings (M1, M8, M30)
Each WP will organise two additional meetings allowing more flexibility to adapt timing to specific activities of each WP
- Progress reports (M12, M24) will be prepared by the MP to ensure rigorous quality assurance of the project and to prepare the interim and final report to the Commission (in coordination with WP evaluation).
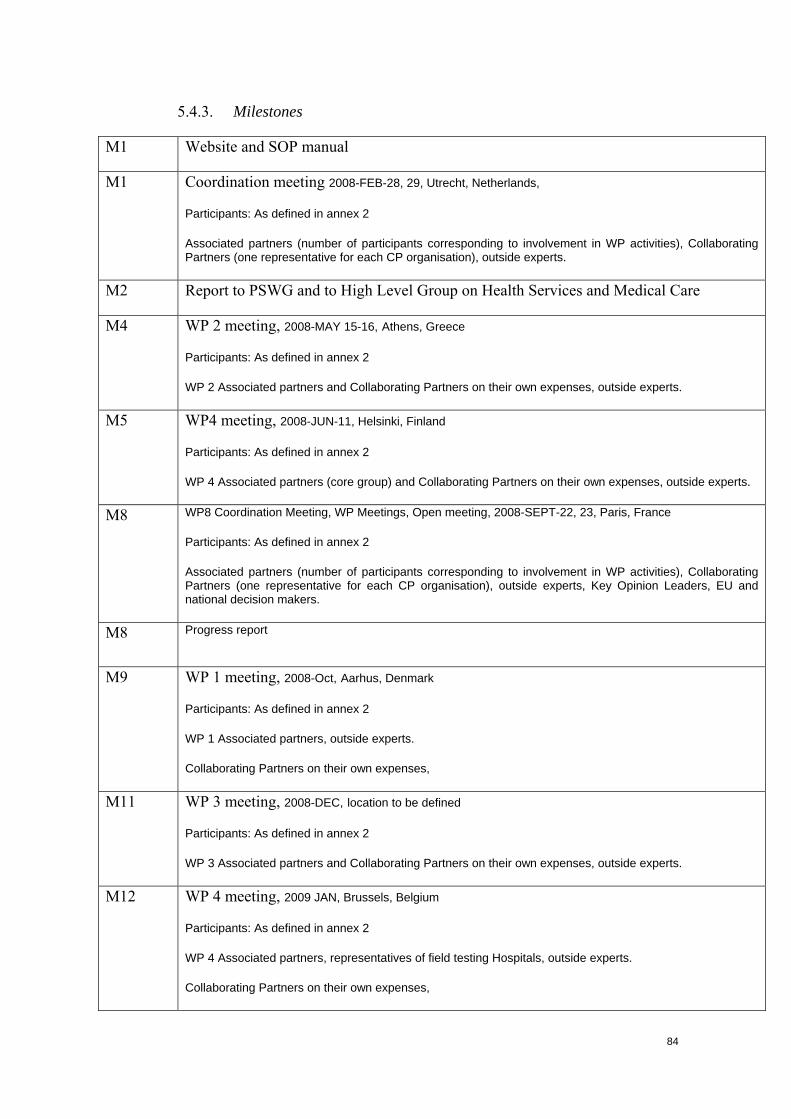
84
5.4.3. Milestones
M1 Website and SOP manual
M1 Coordination meeting 2008-FEB-28, 29, Utrecht, Netherlands,
Participants: As defined in annex 2
Associated partners (number of participants corresponding to involvement in WP activities), Collaborating Partners (one representative for each CP organisation), outside experts.
M2 Report to PSWG and to High Level Group on Health Services and Medical Care
M4 WP 2 meeting, 2008-MAY 15-16, Athens, Greece
Participants: As defined in annex 2
WP 2 Associated partners and Collaborating Partners on their own expenses, outside experts.
M5 WP4 meeting, 2008-JUN-11, Helsinki, Finland
Participants: As defined in annex 2
WP 4 Associated partners (core group) and Collaborating Partners on their own expenses, outside experts.
M8 WP8 Coordination Meeting, WP Meetings, Open meeting, 2008-SEPT-22, 23, Paris, France
Participants: As defined in annex 2
Associated partners (number of participants corresponding to involvement in WP activities), Collaborating Partners (one representative for each CP organisation), outside experts, Key Opinion Leaders, EU and national decision makers.
M8 Progress report
M9 WP 1 meeting, 2008-Oct, Aarhus, Denmark
Participants: As defined in annex 2
WP 1 Associated partners, outside experts.
Collaborating Partners on their own expenses,
M11 WP 3 meeting, 2008-DEC, location to be defined
Participants: As defined in annex 2
WP 3 Associated partners and Collaborating Partners on their own expenses, outside experts.
M12 WP 4 meeting, 2009 JAN, Brussels, Belgium
Participants: As defined in annex 2
WP 4 Associated partners, representatives of field testing Hospitals, outside experts.
Collaborating Partners on their own expenses,

85
M16 WP8 Coordination Meeting, WP Meetings, 2009-MAY, Copenhagen, Denmark
Participants: As defined in annex 2
Associated partners (number of participants corresponding to involvement in WP activities), outside experts.
Collaborating Partners on their own expenses,
M17 Technical and financial interim reports
M20 WP1 meeting, 2009-SEPT, Madrid, Spain
Participants: As defined in annex 2
WP1 Associated partners and outside experts.
Collaborating Partners on their own expenses,
M21 WP 2 meeting, 2009-OCT, Brussels, Belgium
Participants: As defined in annex 2
WP 2 Associated partners, outside experts.
Collaborating Partners on their own expenses,
M24 WP8 Coordination Meeting, WP Meetings, 2010-JAN, Athens, Greece
Participants: As defined in annex 2
Associated partners (number of participants corresponding to involvement in WP activities), representatives of field testing Hospitals, outside experts.
Collaborating partners on their own expenses
M24 Progress report
M27 WP3 meeting, 2010-APR, location TBD
Participants: As defined in annex 2
WP 2 Associated partners and Collaborating Partners on their own expenses, outside experts.
M29 WP8 Coordination Meeting, WP Meetings, Open meeting, 2010-JUN, Brussels, Belgium
Participants: As defined in annex 2
Associated partners (number of participants corresponding to involvement in WP activities), Collaborating Partners (one representative for each CP organisation), outside experts, Key Opinion Leaders, EU and national decision makers.
M32 Technical and financial final reports

5.4.4. Deliverables
Deliverable Number
Deliverable Title
Delivery Date
Nature Confidentiality Level
Stakeholders & Dissemination
D01 Kick-off meeting 28-29 Feb., Utrecht
M1 Coordinating meeting and WP meetings
Partners Mail
D03 Global work plan of EUNetPaS
M2 Document Partners Intranet, EUNetPaS partners,
D04 Standard Operating Procedure (SOP)
M2 Document Partners Intranet, EUNetPaS partners
D08 Network of national contact points coordinating national PS platforms
M6 List of institutions and contact persons. The network’s structure will be organised around national nodes or network coordinators, and have a supporting secretarial office and appropriate management tools.
Partners Stakeholders, EUNetPaS partners Website, conferences, newsletters
D12 Coordinating Meeting 22-23 September 08 Paris
M8 Coordinating meeting, WP meetings
Partners Mail
D13 Progress report M8 Report Partners PHEA, partenrs
D21 Coordinating meeting Copenhagen
M16 Coordinating meeting and WP meetings
Partners Mail, website
D23 Technical and Financial Interim Reports
M17 Report Confidential PHEA
D28 Coordinating meeting Athens
M24 Coordinating meeting and WP meetings
Partners Mail website
D29 Progress report M24 Report Partners PHEA, partners
D33 Coordinating final meeting Brussels
M29 Coordinating meeting and WP meetings
Partners Mail, website
D39 Technical and Financial Final Reports
M32 report Confidential PHEA
86

87
5.5. Work package n° 9: Dissemination of the Project
5.5.1. Overall strategy and methods
Tasks:
- To develop a communication strategy to raise and maintain awareness on Patient Safety (PS).
- To develop strategies for promoting the project’s objectives and informing on its achievements at EU, national and international levels via identified communication channels and the nodes and feedback from MS.
- To disseminate and handle information on national strategies and programmes on PS, key elements on PS culture, and performance indicators. This will facilitate coherent, effective and sustainable external and internal communication on the project and ensure that its aims, ongoing work, results and final products are known to all partners, identified stakeholders (decision makers, healthcare organisations, professionals and patient organisations) and target groups at EU and national levels.
Methods:
- The visual identity of the network (i.e. logo, graphical chart, banners, standard EC-grant acknowledgment sentence, etc.) will be designed and proposed by the main partner until approval by all partners at Month 1, prior the kick off meeting. Related basic communication tools will be then provided to all partners at Month 1 (it includes the EUNetPaS presentation leaflet (printed lots AND electronic version), EUNetPaS poster, templates for EUNetPaS slides and letters, etc.). The easily recognisable logo and graphical profile, common to all WPs and for use on all project-related documents, will be presented during the initial phase and will be a first step for guaranteeing cohesion of the network’s dissemination / communication strategy.
- SOP for “corporate” communication and dissemination will be proposed by the main partners, discussed and agreed by all partners during the kick off meeting (Month 1): it includes the definition of what will be considered as “EUNetPaS” official documents, the procedure for submission and endorsement of partners’ EUNetPaS articles by the Executive Board, timing for approval, rules for authorships and acknowledgment; etc.
- Secured efficient flow of information will be set up between MS and core WPs, as well as an interface between nodes and national networks, via the creation of a systematic e-mail/ postal address listing of the key MS contact points. The resulting address book will be then circulated inside the consortium.
An advocacy and communication strategy will be developed to promote PS and EUNetPaS results (networking activities). It will proceed first via the identification of all related international / national conferences and events over the contract period and selection of the key ones for presence / communication actions by EUNetPaS representatives, publications…). Same approach will be adopted for publications: listing of targeted journals (British Medical Journal, New England Journal of Medicine, American Journal of Medicine, Quality and Safety in Health Care, Journal of the American Medical Association), decision on the preparation of 2-3 major articles (ex:
88
press release on the launch of the network, one mid-term article on the general progress made at Month 15, one final article with presentation of the global achievements / conclusions and follow-up).
- Target groups will be identified in collaboration with partners and with PSWG.
- The EUNetPaS public website and restricted access platform (private extranet) will be accessible from the same internet home page. They will facilitate both communication and information exchange among network partners (extranet) and provide easy access to the project’s products and endorsed articles by external audiences.
5.5.2. Objectives
The development of a thorough and effective communication strategy, with the following goals:
- To increase awareness and understanding of EUNetPaS’s key offerings amongst internal and external target audiences
- To position EUNetPaS as the European primary network in information sharing, PS policy and research development and implementation
The EUNetPaS dissemination strategy will include, but not be limited to:
- The development of clear, focused messages to be used in all internal and external communications;
- The active promotion of the achievement of milestones and project successes.
5.5.3. Description of the dissemination work
Dissemination will be coordinated through multiple channels including: - The EUNetPaS website; The interactive EUNetPaS website managed by the main partner HAS and by selected partners (WP leaders) will be a major communication instrument ensuring both integration of the work programme communication (restricted access area of the website, with login and password for the partners) and dynamic communication window for the general and specialised public. This portal is crucial for the success of the project because it facilitates interaction between the partners and provides the tools to promote the EUNetPaS activities, recommendations and achievments.
The public section of the EUNetPaS website will be regularly updated by the main partner thanks to the Joomla technology, by informing on the network progress, announcing key events, posting job offers, etc. Topics and presentation will be adapted to the various visitors’ profiles with dedicated sections: HC professionals, patients, general public, etc. Specific tools developed by the consortium for external audiences will be progressively “grafted” onto the public site (ex: e-learning tools, educational material, etc.).

89
The EUNetPaS management extranet system with restricted access (password and login) will be developed using the PLONE technology creating a flexible and easily accessible system for the dissemination and management of knowledge acting as a portal for all members. The resultant knowledge management framework will be used to maintain a well-informed workforce, promote exchange and gain in efficiency, by creating an inclusive, comprehensive, and easily accessible organizational memory. In accordance with the internal resources in web design, it will be accessible from the public section by entering login and password. The extranet represents the base of the collaborative platform and knowledge management system, it will contain at the start all key documents related to the contract, consortium finances, and work programme. It shall evolve our knowledge management through key steps:
• Acquiring complete sets of information on SOP, protocols and methods, and on the strategy of the project and supporting documentation;
• Ensuring that information is used strategically for sense-making, the creation of new knowledge, and in key decision making. This entails that participants will be kept constantly aware of all new developments within the project, including development of new skills, protocols and new data. A specific chat room platform will be proposed for the various WP activities, where partners will be able to upload and download documents.
All information will be formatted into cross platform software documents and archived ensuring that all pertinent knowledge, past or present, generated inside or outside the project can easily be incorporated into any decision making. In addition to the generation of the knowledge database, all participants will be kept constantly updated on all information within the project through a monthly newsletter which will be electronically mailed to everybody.
- Targeted international events: Key events will be identified by the Executive Board and selected for presenting EUNetPaS. It could include among others:
o European Health Forum Gastein, o ISQUA, o International Forum on Quality and Safety in Health Care; o Inclusion of EUNetPaS presentation on EU presidency official
programmes (Slovenia, France, Czech Republic, Sweden, Belgium, Hungary, Spain)
o EUNetPaS follow-up at the Patient Safety Working group of the European Commission
o Coordination with various WHO programs, such as: World Alliance for Patient Safety Patients for Patient Safety Patient Safety Research. (WHO, DG RESEARCH)
- Presentation of the project at national level for example on the occasion of Safety and
Quality of Care national institutions (HAS, NICE, IQWIG…) annual events The dissemination strategy will consist of a two-pronged approach, that is, both an internal and external focus. To increase the efficacy of the EUNetPaS network, it will be necessary to clearly define the key stakeholders and create a database accessible to all participants;
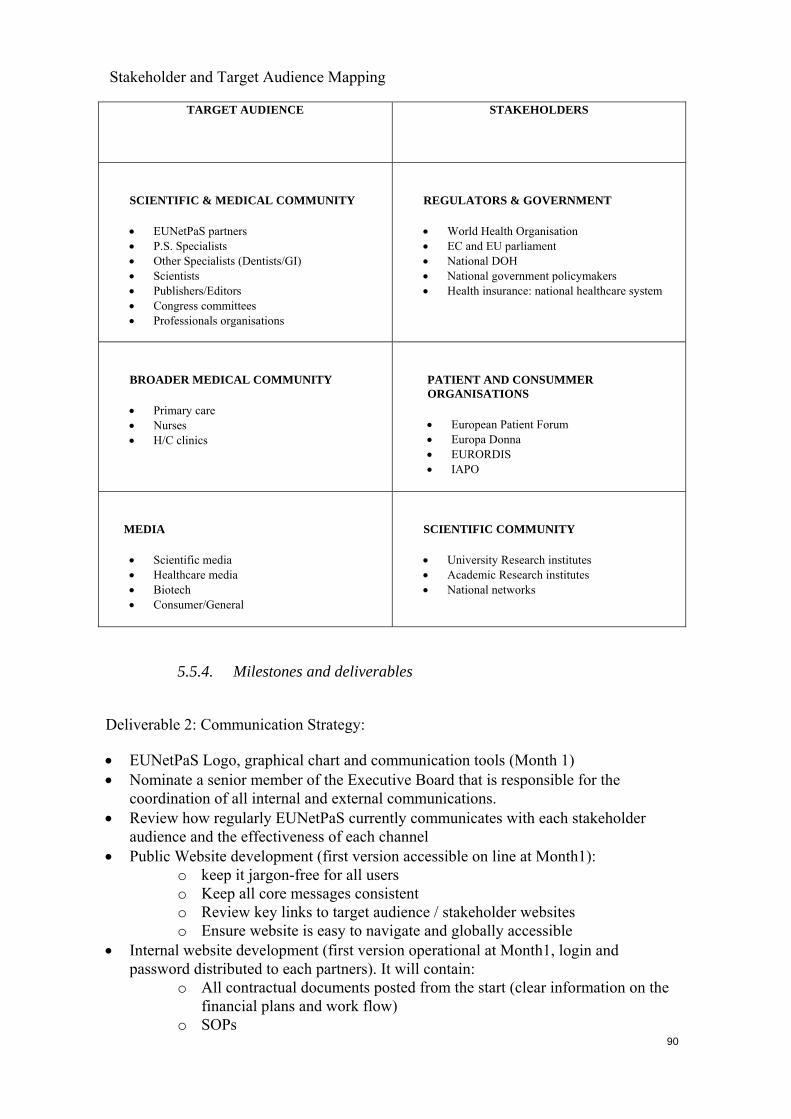
90
Stakeholder and Target Audience Mapping
TARGET AUDIENCE STAKEHOLDERS
SCIENTIFIC & MEDICAL COMMUNITY
• EUNetPaS partners • P.S. Specialists • Other Specialists (Dentists/GI) • Scientists • Publishers/Editors • Congress committees • Professionals organisations
REGULATORS & GOVERNMENT
• World Health Organisation • EC and EU parliament • National DOH • National government policymakers • Health insurance: national healthcare system
BROADER MEDICAL COMMUNITY
• Primary care • Nurses • H/C clinics
PATIENT AND CONSUMMER ORGANISATIONS
• European Patient Forum • Europa Donna • EURORDIS • IAPO
MEDIA
• Scientific media • Healthcare media • Biotech • Consumer/General
SCIENTIFIC COMMUNITY
• University Research institutes • Academic Research institutes • National networks
5.5.4. Milestones and deliverables
Deliverable 2: Communication Strategy:
• EUNetPaS Logo, graphical chart and communication tools (Month 1) • Nominate a senior member of the Executive Board that is responsible for the
coordination of all internal and external communications. • Review how regularly EUNetPaS currently communicates with each stakeholder
audience and the effectiveness of each channel • Public Website development (first version accessible on line at Month1):
o keep it jargon-free for all users o Keep all core messages consistent o Review key links to target audience / stakeholder websites o Ensure website is easy to navigate and globally accessible
• Internal website development (first version operational at Month1, login and password distributed to each partners). It will contain:
o All contractual documents posted from the start (clear information on the financial plans and work flow)
o SOPs

91
o Documentations for the partners (internal address book, newsletter, press articles, etc.)
o Internal communication platforms for each WP groups (chat rooms) o Agenda for internal meetings
• Create a simple and clear EUNetPaS information kit which can be used as content for internal and external communications. This will include the following documents:
o Network presentation leaflet, translated if necessary o Organisation fact sheet o Key milestones o Executive Board biographies o A short backgrounder on each of the 4 core WP (one paragraph
maximum). • Develop a monthly membership e-newsletter. This includes monthly highlights, key
updates from the steering committee on achieving annual business objectives, key project achievements, profile a key member and upcoming events.
• Meet with KOLs from relevant patient advocacy group (PAGs) and key stakeholders.
• Develop a target media list • Draft and distribute news releases on EUNetPaS milestones • International publications plan.
o Investigating and benchmarking relevant primary and secondary medical publications within the PS sector
o Compiling a EUNetPaS reference pack / bibliography based on a publications database
• Planned EUNetPaS presence at major national and international CME congresses would provide direct contact with key stakeholders
• Develop a target list and tier into three categories (1 being the most influential and relevant contacts)
o Conduct an ongoing relationship building programme of one-to-one briefings with tier 1 contacts.
o Invite key contacts to attend or participate in EUNetPaS’s annual symposia (Paris, Brussels)
Set-up a communication plan for the larger public (general, patient associations) outlining the communication channels and how they will be approached: ex: TV, radio broadcasts, daily newspapers. EUNetPaS poster for the hospitals/ GP waiting rooms, presenting in the local official language the network objectives and activities.
The EUNetPaS communications plan will be structured around the following six key questions: Objectives: What are we trying to communicate? Audience: Who do we want our message to reach? Messages: What do we need to tell our audience? Strategy: How can we most effectively communicate our message in order to reach
our targeted groups? Tactics: What will we do? Timeliness: What is the appropriate timeframe for communication?

Measuring Success
Output Impact Outcome
o How effectively were key messages disseminated?
o Build the EUNetPaS internal communication expertise and network
o Use internal opinion surveys to track effectiveness of internal communications channels
o Increase in media coverage
o Increase in stakeholder briefings
o Anecdotal feedback
o Semi-annually measure and compare awareness levels of EUNetPas’s offering and positioning amongst key stakeholders.
Deliverable Number
Deliverable Title
Delivery Date
Nature Confidentiality Level
Stakeholders & Dissemination
D02 Initial Communication kit
M 1 Logo, Graphical Chart, and design of the website (public / private areas) Leaflet presenting the network. Templates for EUNetPaS power point presentations and letters Standard acknowledgment sentences/ logos
Partners EUNetPaS partners, national contact points
D09 Dissemination plan
M 6 Communication plan (to the professionals, policy makers and general public) with the exact plan and dates for every task/deliverable, including selection of 3 targeted events, 2 publications (M 15, M30) in peer-reviewed journals: for example, Quality and Safety in Health Care, International Journal of Quality in Health Care, Health Policy.
Partners EUNetPaS partners
5.5.5. List of stakeholders
HAS (LEADER) 210 p/d development of communication strategy, website management, coordination of WP
92

93
UOA-HIL, EKEVYL, SST, STM-Finland, CPME, PGEU, SMoH, HIQA, GCPS, FOD-DG1, StaHeCCA, NBHW, DGS, EFN, DOH, EPF 18 p/d each: dissemination of EUNetPaS results at national level.
94
Work package n° 10: Evaluation of the project
5.5.6. List of parties involved
CPME (LEADER) 160 p/d coordination of the WP, project, network and impact assessment
RUNMC 100 p/d impact assessment
HAS 65 p/d project assessments,
EFN 43 p/d impact assessment at EU level
EPF 25 p/d impact assessment at EU level
UOA-HIL, EKEVYL, SST, STM-Finland, PGEU, SMoH, HIQA, GCPS, FOD-DG1, StaHeCCA, NBHW, DGS, DOH, 8 p/d impact assessment at national level
5.5.7. Description of the work and methodologies
Objectives: - Network evaluation will monitor
o Communication inside the network (electronic tools, data classification…) o Management of human resources (mobility programs, common
trainings…) o Network management (decisional framework, governing bodies
involvement) o Sustainability of the network (external funding, portfolio of projects…)
- Progress evaluation will monitor and provide an internal audit function to ensure the
production of the deliverables of each Work Package (WP) as defined in the project. - Impact evaluation of the project will measure the degree to which MS (MS) and
stakeholders have benefited from the network and ask them to what extent it has helped them move their Patient Safety (PS) agenda forward at national level.
Methods: - Network evaluation: milestones will be considered for each of the following aspects
of network evaluation: o Communication inside the network
Harmonisation of nomenclature Elaboration of a scheme for future common database Common database, accessible to all participants. Participation of partners in meetings, E-meetings, Tele
conferences
o Management of Human Resources, promotion of mobility programs and training
o Network Management
Setting up of the structure of governing bodies; Definition of frequency and agenda of governing bodies meetings

95
Effective and active participation of all participating organizations in the decision-making process
o “Insurance” of Continuation after the Conclusion of the Community’s
Funding Period
Portfolio of projects involving all the network’s participants; Search of external funding sources (both public and private);
- Progress evaluation:
Each WP will have its own milestones. Progress against milestones will be checked every 6 month. WP 10 will develop forms for this purpose. Special attention will be paid to deviations from plans, which will have to be explained (risk assessment and management). The evaluation will concern all APs. They will receive questionnaires relating to progress made in specific tasks, their opinion of EUNetPaS, and suggestions for improvement. All activities will be evaluated with regard to specific risks, planned impact and dissemination. The deliverables will be followed up.
- Impact evaluation:
EUNetPaS is expected to have an impact arising from core WP activities and from the dissemination of results and deliverables. The evaluation of the project’s impact will assess the extent to which specific EUNetPaS actions have contributed to the general and specific objectives of the project using the indicators defined below.
A questionnaire based on the selected indicators will be developed to assess to what extent the recommendations provided by EUNetPaS experts have impacted PS initiatives development in MS. This questionnaire will be used by national contact points and member associations of EU stakeholders to evaluate the project’s impact in EU MS through interviews of national stakeholders (healthcare organisations (HCOs), healthcare workers, patients’ representatives, decision makers…). These interviews will be conducted at the end (M28-M30) of the project to measure the impact of EUNetPaS in the different WP areas of intervention. The result of the impact evaluation will be presented at the closing conference where MS representatives, international organisations, national organisations, experts and other stakeholders will be asked to achieve a consensus on their engagement in the network and the project’s evaluation.
Indicators:
Title Description
Safety Culture
WP1
- By the end of month 12 of the project web based platform mapping agreed set of PS information in Europe will be launched, containing validated information from at least 90% of the member states involved as associated partners. (Specific Objective 2)
- By the end of month 22 of the project, a PS Culture
assessment instrument, that has been selected, tested in at least 3 countries and 15 hospitals will be offered

96
to all MS national contact points (Specific Objective 3)
Education and Training
WP 2
- At M 20 at least 2 higher education institutions (one medical faculty and one nursing faculty) will accept to co-operate, jointly develop a fit-for-purpose PS learning intervention to be delivered within a specified time interval and return feed-back into the guidelines
- At least 95% acceptance of the guidelines for education in PS by the network (expressed as % positive votes)
- At least one publication in a peered reviewed journal and at least 3 presentations in international conferences
Reporting and Learning
WP3
- At least 70 % of the MS or institutions involved as associated partners in the project and participating to a national rapid alert system have accepted to participate to the EUNetPaS rapid alert system at in the rapid alert mechanism.(Specific Objective 5)
- By the end of the project all associated partners have sent at least 3 questions /answer for the " Frequently asked questions " of the library of methods for developing and implementing reporting and learning systems (Specific Objective 5)
Pilot in Medication Safety
WP4
- At least 90% of the Member States involved as associated partners in the WP 4 field testing have selected 3 hospitals, following the criteria established by WP 10 (Specific Objective 6).
- At least 70% of the hospitals having tested the Medication Safety recommendation have sent a positive feed back regarding its transferability at M 30 (Specific Objective 7)
Dissemination
WP9
- By the end of month 2 the professional part of the website (extranet) will be open
- At least 75% of the EU stakeholders involved in the project as associated partners have sent a confirmation of the reception of the reports and guidelines at M32

97
Evaluation
WP 10
- At least 50% of the EU stakeholders involved as associated partners will be satisfied by the outcomes of the project at M 32. The satisfaction of the stakeholders will be evaluated, through network and impact assessment of the project
- 2 “meet the experts” meetings will be organized with representatives of the hospitals involved in the WP 4 filed testing. A satisfaction study via an evaluation questionnaire will be conducted.
Deliverables:
D37 impact assessment report
M30
Report Using process indicators such as level of network use by MS, and the extent to which the network has aided and given new impetus to national PS initiative.
Public Stakeholders: PHEA, EUNetPaS partners, national contact points, healthcare professionals, general public Report sent to partners and relevant stakeholders (PSWG, PHEA…), open access to the report on the website
D38 Project evaluation report
M30
Report. Give the results of an audit investigating whether the project objectives have been met and whether the deliverables in the work packages have been produced according to plan.
Partners
Stakeholders: PHEA, EUNetPaS partners Report sent to partners and relevant stakeholders (PSWG, PHEA…)
Evaluation is a critical element of all programmes, both in terms of achieving results and ensuring a continual improvement in the delivery of high quality programmes. To this end, EUNetPaS partners will work in collaboration to discuss and define the evaluation criteria from the beginning of the project, thus ensuring the cohesive integration of evaluation practices throughout the life of the project. The evaluation criteria will be approached through both strategic and tactical implementations and in order to ensure timely evaluation reporting, WP10 will work closely with all partners as well as with the other WPs to ensure that this task is completed as effectively and in as timely a manner as possible.

98
6. MEASURES TO ENSURE VISIBILITY OF COMMUNITY CO-FUNDING
The European Community co-funding will be acknowledged in all publications, website, and different types of communications (presentations at conferences, seminars, informal communications, etc.). The following wording will be printed on all EUNetPaS materials as listed above:
“This project stems from grant number N°A/ 100861 from the Public Health Executive Agency managing the Community's health programme 2003-2008”
The website will prominently display both the PHEA and EC logos.

7. LIST OF COLLABORATING PARTNERS
Collaborating organisation Contact person
Organisation Town / City Country Title / Function
Family name & First name Telephone No E-mail
Ministry of Health of Republic of Latvia
Riga Latvia DeputyHead
KLAVINA, Kristine 371 787 60 95 [email protected]
Ministerstvo zdravotnictví (Ministry of Health)
Prague Czech Republic DepartmentHead
KALVACHOVA, Milena
4202 24 97 23 61 [email protected]
Muenster University of Applied Sciences
Steinfurt Germany HOELSCHER, Uvo 49 251 83 62 603 [email protected]
Council of Europe Strasbourg France MIERZEWSKI, Piotr 33 3 88 41 30 04 [email protected]
World Health Organization Regional Office for Europe
Copenhagen Denmark HAFNER, Valentina 45 3917 1255 [email protected]
National Center for Quality Assessment in Health Care (NCQA)
Krakow Poland SeniorAdvisor
KUTRYBA, Barbara 48 12 423 20 88 [email protected]
Ministry of Health Sofia Bulgaria SPASSOVA, Svetlana 359 293 01 245 [email protected]
Estonian Ministry of Social Affairs Tallinn Estonia EERIKSOO, Hedy 37 26 26 91 39 [email protected]
ALLOY Consulting Informatikai és Tanácsadó Kft.
Budapest Hungary LáSZLó, Kulin 36 13 01 79 68 [email protected]
Federal Ministry of Health, Family and Youth
Vienna Austria WOSCHITZ-MERKAč, Maria
43 (171100) 4275 [email protected]
Ministère de la Santé et des Solidarités
Paris France BROYART, Anne 33 1 40 56 47 41 [email protected]
Ministry of Health Ljubljana Slovenia MOZINA, Martin 386 15 22 53 74 [email protected]
Page 99 of 101
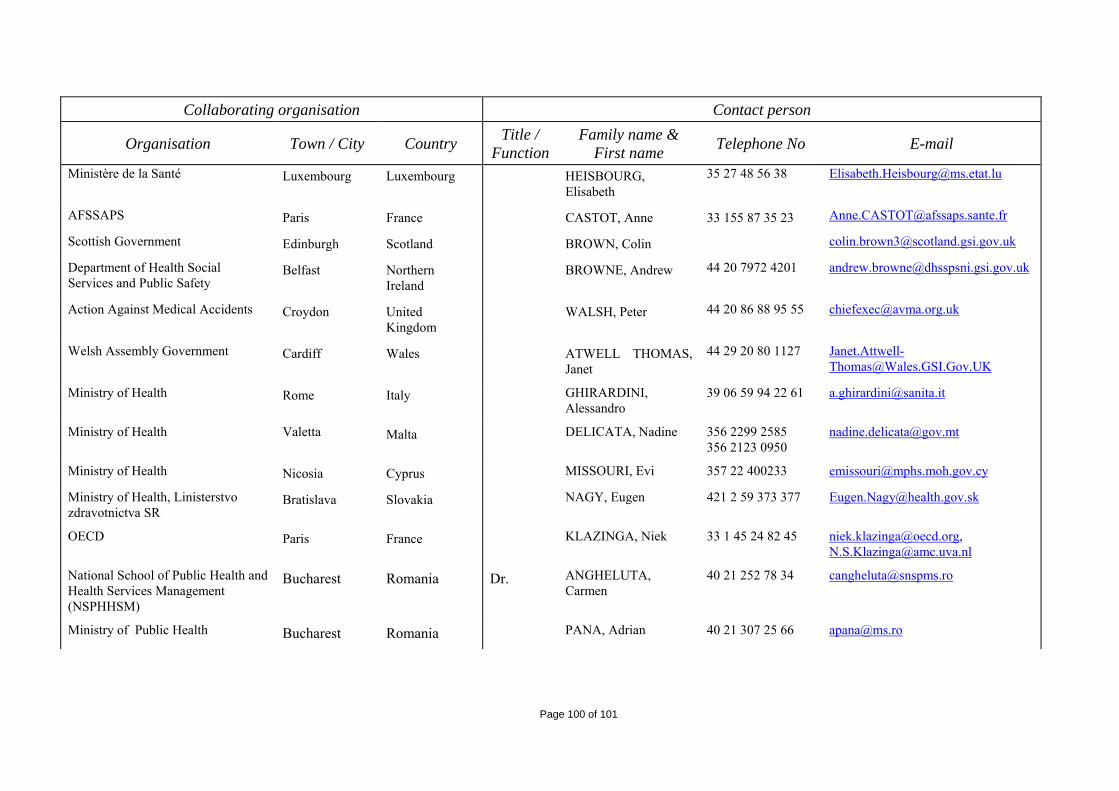
Collaborating organisation Contact person
Organisation Town / City Country Title / Function
Family name & First name Telephone No E-mail
Ministère de la Santé Luxembourg Luxembourg HEISBOURG,Elisabeth
35 27 48 56 38 [email protected]
AFSSAPS Paris France CASTOT, Anne 33 155 87 35 23 [email protected]
Scottish Government Edinburgh Scotland BROWN, Colin [email protected]
Department of Health Social Services and Public Safety
Belfast NorthernIreland
BROWNE, Andrew 44 20 7972 4201 [email protected]
Action Against Medical Accidents Croydon UnitedKingdom
WALSH, Peter 44 20 86 88 95 55 [email protected]
Welsh Assembly Government Cardiff Wales ATWELL THOMAS,Janet
44 29 20 80 1127 [email protected]
Ministry of Health Rome Italy GHIRARDINI, Alessandro
39 06 59 94 22 61 [email protected]
Ministry of Health Valetta Malta DELICATA, Nadine 356 2299 2585 356 2123 0950
Ministry of Health Nicosia Cyprus MISSOURI, Evi 357 22 400233 [email protected]
Ministry of Health, Linisterstvo zdravotnictva SR
Bratislava Slovakia NAGY, Eugen 421 2 59 373 377 [email protected]
OECD Paris France KLAZINGA, Niek 33 1 45 24 82 45 [email protected], [email protected]
National School of Public Health and Health Services Management (NSPHHSM)
Bucharest Romania Dr. ANGHELUTA, Carmen
40 21 252 78 34 [email protected]
Ministry of Public Health Bucharest Romania PANA, Adrian 40 21 307 25 66 [email protected]
Page 100 of 101