
Metacognitive and Nonmetacognitive Reliance on Affect as Information in Judgment
Upload
khangminh22Category
view
0download
0
UNIVERSITÄTSKLINIKUM HAMBURG-EPPENDORF
Klinik und Polyklinik für Psychiatrie und Psychotherapie
Arbeitsgruppe Neuropsychologie
Klinikdirektor Prof. Dr. Jürgen Gallinat
The role of cognitive and metacognitive maladaptive beliefs in the long-
term course of unipolar depression
Dissertation
zur Erlangung des Grades eines Doktors der Medizin /Zahnmedizin
an der Medizinischen Fakultät der Universität Hamburg.
vorgelegt von:
Mirjam Sophie Faissner
aus Heidelberg
Hamburg 2018

Angenommen von der
Medizinischen Fakultät der Universität Hamburg am: 22.01.2019
Veröffentlicht mit Genehmigung der
Medizinischen Fakultät der Universität Hamburg.
Prüfungsausschuss, die Vorsitzende: Prof. Dr. Lena Jelinek
Prüfungsausschuss, zweiter Gutachter: PD Dr. Levente Kriston
Dritter Gutachter: PD Dr. Philipp Klein

Für Lea, Simon, Angelika und Andreas

Table of Contents
Table of contents
Aims and hypotheses of the study ......................................................................................... 1
1. Introduction ....................................................................................................................... 2
2. Theoretical background ..................................................................................................... 3
2.1 Depressive disorders .................................................................................................... 3
2.1.1 Diagnostic criteria of depressive disorders according to DSM-IV ....................... 3
2.1.2 Epidemiology of depression .................................................................................. 4
2.1.3 Course and long-term remission rates in unipolar depression .............................. 7
2.1.4 Aetiology of depression ........................................................................................ 9
2.2 Cognition and metacognition in depression ............................................................... 15
2.2.1 Cognitive distortions in depression ..................................................................... 15
2.2.2 Metacognitive beliefs in depression .................................................................... 17
2.2.3 Empirical findings concerning maladaptive cognitive and metacognitive beliefs in
depression ..................................................................................................................... 20
2.3 Aims of the present study .......................................................................................... 43
3. Methods ........................................................................................................................... 45
3.1 Participants ................................................................................................................. 45
3.2 Procedure ................................................................................................................... 46
3.3 Measurements ............................................................................................................ 48
3.3.1 Sociodemographic variables ............................................................................... 48
3.3.1 Mini International Neuropsychiatric Interview ................................................... 48
3.3.2 Hamilton Depression Rating Scale ..................................................................... 48
3.3.3 Beck Depression Inventory ................................................................................. 49
3.3.4 Dysfunctional Attitude Scale .............................................................................. 49
3.3.5 Metacognitions Questionnaire 30........................................................................ 50
3.4 Data analysis .......................................................................................................... 51
4. Results ............................................................................................................................. 54

Table of Contents
4.1 Sample characteristics ................................................................................................ 54
4.2 Hypothesis 1 .............................................................................................................. 55
4.3 Hypothesis 2 .............................................................................................................. 56
4.4 Hypothesis 3a ............................................................................................................. 57
4.5 Hypothesis 3b ............................................................................................................ 58
4.6 Hypothesis 3c ............................................................................................................. 61
4.7 Hypothesis 4 .............................................................................................................. 62
5. Discussion ........................................................................................................................ 64
5.1 Summary of the aims and results of the study ........................................................... 64
5.2 Discussion of results concerning the long-term course of depression ....................... 65
5.3 Predicting the change of depression through cognitive and metacognitive maladaptive
beliefs ............................................................................................................................... 66
5.3.1 Cognitive maladaptive beliefs ............................................................................. 66
5.3.2 Metacognitive maladaptive beliefs...................................................................... 67
5.3.3 Further implications ............................................................................................ 69
5.4 The cognitive vulnerability model of depression ...................................................... 70
5.5 Limitations and strengths of the study ....................................................................... 71
5.6 Conclusions, further research requests and implications for clinical praxis .............. 74
6. Summary .......................................................................................................................... 77
7. Publication ....................................................................................................................... 79
8. List of abbreviations ........................................................................................................ 87
9. References ....................................................................................................................... 90
10. Acknowledgements ..................................................................................................... 108
11. CV ................................................................................................................................ 109
12. Eidesstattliche Erklärung ............................................................................................. 110
13. Appendix ..................................................................................................................... 111

List of Tables
List of tables
Table 1: Criteria for Major Depressive Episode according to DSM-IV ............................... 5
Table 2: Criteria for Dysthymic Disorder according to DSM-IV ........................................ 6
Table 3: Summary of methods and results of relevant studies concerning maladaptive
cognitive beliefs as vulnerability factors for depression ..................................................... 24
Table 4: Summary of methods and results of relevant studies concerning stability of
maladaptive cognitive beliefs .............................................................................................. 31
Table 5: Summary of methods and results of studies investigating metacognitive biases and
depression ............................................................................................................................ 38
Table 6: Sociodemographic characteristics at inclusion time point (t0) ............................. 45
Table 7: Sociodemographic characteristics at 3,5 years follow-up (t3) ............................. 54
Table 8: Sociodemographic characteristics at baseline assessment (t0) of t3 completers and
non-completers .................................................................................................................... 55
Table 9: Psychopharmacological data at 3,5 years follow-up (t3) ..................................... 56
Table 10: Initial status and change from t0 to t3 of self- and clinician assessed depression,
cognitive and metacognitive maladaptive beliefs ................................................................ 57
Table 11: Correlations of initial status and change from t0 to t3 of depression with initial
status and change from t0 to t3 of maladaptive cognitive and metacognitive beliefs, LGM
data ...................................................................................................................................... 58
Table 12: Model A1-3: Predictors of change of depressive symptoms (outcome: change of
HAMD (i.e. slope)) .............................................................................................................. 59
Table 13: Model B1-3: Predictors of change of depressive symptoms (outcome: change of
BDI (i.e. slope)) ................................................................................................................... 60
Table 14: Model A4: Predictors of change of depressive symptoms (outcome: change of
HAMD (i.e. slope)) .............................................................................................................. 61
Table 15: Model A4 Predictors of change of depressive symptoms (outcome: change of BDI
(i.e. slope)) ........................................................................................................................... 62
Table 16: Relative stability of the different constructs as measured by within-group effect
size d and test-retest correlation r ........................................................................................ 63
Table 17: Correlations of initial status and difference scores between t0 and t3 of depression
with initial status and difference scores between t0 and t3 of maladaptive cognitive and
metacognitive beliefs, using available data ....................................................................... 111
Table 18: Model A'1-3: Predictors of change of depressive symptoms (outcome: change of
HAMD (i.e. slope)) ............................................................................................................ 112

List of Tables
Table 19: Modell B'1-3: Predictors of change of depressive symptoms (outcome: change of
BDI (i.e. slope) ) ................................................................................................................ 113
Table 20: Correlation HAMD t0. t1. t2. t3 ........................................................................ 115
Table 21: Correlation BDI t0. t1. t2. t3 ............................................................................. 115
Table 22: Correlation DAS t0. t1. t2. t3 ............................................................................ 115
Table 23: Correlation PB t0. t1. t2. t3 ............................................................................... 116
Table 24: Correlation NB t0. t1. t2. t3 ............................................................................... 116
Table 25: Correlation NFC t0. t1. t2. t3 ............................................................................ 116

List of Figures
List of figures
Figure 1 Adaption of Wells’ metacognitive model of depression ...................................... 13
Figure 2 Flow of participants for the given study procedures and analysis. ....................... 47
Figure 3 Checking homoscedasticity of model A and B................................................... 114
Figure 4: Checking normality distribution of residuals of model A and B………………..114

Aims and Hypotheses of the Study
1
Aims and hypotheses of the study
Depression is a mental disorder with high prevalence, affecting up to one of ten people
worldwide. Extensive research has yielded considerable findings concerning the aetiology
of depression, but not all factors are fully understood. Maladaptive cognitive beliefs have
been shown to constitute an important vulnerability factor for depression. In addition, there
is evidence that maladaptive metacognitive beliefs are linked to depression and that they are
an important contributing factor in its development. However, it is unclear whether meta-
cognitive beliefs can add explanatory power to depression above and beyond maladaptive
cognitive beliefs. Also, the stability of metacognitive maladaptive beliefs as compared to the
stability of cognitive maladaptive beliefs and of depressive symptoms has not yet been in-
vestigated.
The aim of the present study is to investigate the course and stability of cognitive and
metacognitive maladaptive beliefs in the long-term course of depression.
Eighty-four patients with diagnosed depression are assessed with the Dysfunctional
Attitudes Scale (DAS) as a measure for cognitive maladaptive beliefs, three subscales of the
Metacognitive Questionnaire-30 (MCQ-30) as a measure for metacognitive maladaptive be-
liefs, the Hamilton Depression Rating Scale, and the Beck Depression Inventory at baseline.
They are reassessed after 4 weeks, 6 months and 3.5 years. The data is analyzed using a
longitudinal latent growths model approach.
The main hypothesis of the present study is that metacognitive maladaptive beliefs
explain additional variance of the change of depressive symptom severity from the baseline
assessment to the 3.5 years follow-up assessment above and beyond cognitive maladaptive
beliefs. In accordance with a vulnerability-stress model, it is postulated that the change of
depressive symptoms is predicted by the presence of a critical life event. Furthermore, it is
hypothesised that metacognitive maladaptive beliefs are more stable than cognitive mala-
daptive beliefs and more stable than depressive symptoms over the examination period.

Introduction
2
1. Introduction
Depression is one of the most prevalent mental disorders worldwide and is assumed to con-
cern up to one of ten individuals (World Health Organization, 2016). It contributes im-
portantly to the global burden of disease, ranging on the 5th place of leading causes of years
lived with disability worldwide, and on third place in high-income countries (Vos et al.,
2017). Because of high recurrence probability and high risk for chronicity, depression pro-
duces an important strain for concerned individuals (Bukh, Andersen, & Kessing, 2016;
Eaton et al., 2008).
Theoretical disease models are vital as they influence the development of therapeutic
approaches (Rose, 2003). Research has yielded remarkable findings concerning vulnerabil-
ity factors considered to play an important role in the aetiology of depression (Goh & Agius,
2010). Empirical investigations have shown that different cognitive vulnerability factors ex-
ist, one of them being cognitive maladaptive beliefs (Scher, Ingram, & Segal, 2005). It is
known that cognitive maladaptive beliefs are malleable and they constitute an important tar-
get in Cognitive Behavioural Therapy (CBT, Beck & Dozois, 2011). In spite of the efficacy
of established therapies such as CBT, amelioration of therapeutic interventions is needed, as
different challenges remain to be solved such as high recurrence rates (Eaton et al., 2008).
For that reason, there is need to amplify theoretical knowledge about depression in order to
improve the appropriateness of models. This, in turn, could lead to the enhancement of ther-
apies. It is suggested that metacognitive maladaptive beliefs could play an important role in
the aetiology of depression (Papageorgiou & Wells, 2001). However, the role of metacogni-
tive maladaptive beliefs and its interplay with cognitive maladaptive beliefs is not fully con-
clusive and until now, no longitudinal study with a clinical sample exists to elucidate this
interplay.
The present study examined the course and stability of cognitive and metacognitive
maladaptive beliefs and depressive symptoms in a longitudinal design with 3.5 years follow-
up in individuals with diagnosed depression. The aim was to investigate the effect of cogni-
tive and metacognitive maladaptive beliefs on the long-term course of depression. This work
starts with a presentation of symptomology, epidemiology, and aetiology of depression. This
is followed by an outline of the current state of research concerning cognition and metacog-
nition in depression, continuing with methods and results. Finally, results and conclusions
concerning underlying theoretical models of depression are discussed and possible conclu-
sions for therapeutic approaches are pointed out.

Theoretical Background – Depressive Disorder
3
2. Theoretical background
2.1 Depressive disorders
2.1.1 Diagnostic criteria of depressive disorders according to DSM-IV
This study applied the American Psychiatric Association’s (APA) definition of depressive
disorders (also referred to as “unipolar depression”) according to the Diagnostic and Statis-
tical Manual of Mental Disorders, Fourth Edition ( DSM-IV, APA, 2005) and description
will therefore be focused on this definition. The DSM-IV definition was used to achieve
consistency with baseline assessments. Nevertheless, it has to be noted that meanwhile, the
APA has published a new version of the DSM, the DSM-5 (APA, 2013) and important dif-
ferences to DSM-IV will be mentioned.
The DSM-IV integrates the category “depressive disorder”, which is subdivided in
“major depressive disorder”, “dysthymic disorder” and “depressive disorder not otherwise
specified”, in the section of “mood disorders” besides other disorders with mood disturb-
ances as their predominant features. “Depressive disorders” are to be distinguished from
“bipolar disorders” by the absence of maniac, mixed or hypomanic episodes in lifetime.1
According to DSM-IV, the major depressive disorder is classified as a clinical course with
at least one major depressive episode which is defined by the presence of either depressed
mood or the loss of interest or pleasure in nearly all activities for a period of at least two
weeks. Additionally, four further symptoms have to be present including somatic symptoms
such as weight loss or insomnia, or cognitive symptoms such as feeling of worthlessness or
guilt, concentration impairment, or suicidal ideation (see Table 1). The severity of major
depressive episodes can be rated as mild, moderate, and severe without or with psychotic
features. Diagnosis criteria do not differ significantly in DSM-5. A major depressive episode
is considered “in remission”, when the complete diagnostic criteria of a major depressive
episode have not been met for at least two consecutive months and “in partial remission” in
case when some criteria are still present, but do not conform with criteria for a major depres-
sive episode (APA, 2005). The term “full recovery” is defined as a symptom-free period for
six months after remission. The term “relapse” describes a return of depressive symptoms
before full recovery and “recurrence” the return of depressive symptoms after full recovery
(Berger, van Calker, Brakemeier, & Schramm, 2015).
1 The DSM-5 subclassifies the section of “mood disorders” into two distinct sections and classifies “major depressive disorder” in the section of “depressive disorders” (APA, 2013).

Theoretical Background – Depressive Disorder
4
A dysthymic disorder can be diagnosed if depressed mood is chronically present during two
years on more than half of the days and if the patient suffers of at least two further symptoms
such as poor appetite or loss of self-esteem (see Table 2). Symptom-free periods of two
consecutive months may not occur and criteria of a major depressive episode must not be
met. If a major depressive episode occurs on top of a dysthymic disorder, a double depression
can be diagnosed. The new diagnosis of persistent depressive disorder in DSM-5 includes
diagnostic criteria of both chronic major depression and dysthymia and criteria differ thus
from DSM-IV (APA, 2013).
2.1.2 Epidemiology of depression
According to the Word Health Organisation (WHO), depressive disorders are estimated to
be the most prevalent mental disorder across all regions and cultures, affecting up to one of
ten people worldwide (World Health Organization, 2016). Unipolar depressive disorders
contribute importantly to the global burden of disease. They are on 5th place of the leading
causes of burden of disease worldwide, measured in years lived with disability, and they
figure on the third place in high-income countries (Vos et al., 2017). In the United States of
America, major depressive episodes have a life-time prevalence of 17 % and a 12-months
prevalence of 9 % (Kessler, Petukhova, Sampson, Zaslavsky, & Wittchen, 2012). In Ger-
many, unipolar depression is estimated to have a 12-months prevalence of 8 % (Jacobi et al.,
2016). Prevalence of unipolar depression is about twice as high in women than in men (in
Germany, prevalence in women of 11 % and in men of 5 %; Jacobi et al., 2016). 12-months
prevalence for dysthymia is estimated 2 % in Germany of which 2 % for women and 1 %
for men (Jacobi et al., 2016). Data from the United States suggest that depression often re-
mains untreated or inadequately treated (Wang et al., 2005).
Depression might occur in people of all ages, but prevalence is significantly higher
in younger than in older individuals (Kessler et al., 2010). The peak of incidence appears to
be in the twenties with 50% of initial manifestations of depression occurring before the age
of 30, while onset of depression in older age remains possible (APA, 2013; Berger et al.,
2015). Recent data seem to suggest that the incidence of particularly mild depression in-
creases and that the age of the first manifestation drops which is referred to as the “cohort
effect” (Berger et al., 2015).

Theoretical Background – Depressive Disorder
5
Table 1: Criteria for Major Depressive Episode according to DSM-IV (APA, 2005): 327)
A. Five (or more) of the following symptoms have been present during the same 2-week period and
represent a change from previous functioning; at least one of the symptoms is either (1) depressed
mood or (2) loss of interest or pleasure.
Note: Do not include symptoms that are clearly due to a general medical condition, or mood-incon-
gruent delusions or hallucinations.
(1) Depressed mood most of the day, nearly every day, as indicated by either subjective
report (e.g., feels sad or empty) or observation made by others (e.g., appears tearful). Note:
In children and adolescents, can be irritable mood.
(2) Markedly diminished interest or pleasure in all, or almost all, activities most of the day,
nearly every day (as indicated by either subjective account or observation made by others)
(3) Significant weight loss when not dieting or weight gain (e.g., a change of more than 5%
of body weight in a month), or decrease or increase in appetite nearly every day. Note: In
children, consider failure to make expected weight gains.
(4) Insomnia or hypersomnia nearly every day
(5) Psychomotor agitation or retardation nearly every day (observable by others, not merely
subjective feelings of restlessness or being slowed down)
(6) Fatigue or loss of energy nearly every day
(7) Feelings of worthlessness or excessive or inappropriate guilt (which may be delusional)
nearly every day (not merely self-reproach or guilt about being sick)
(8) Diminished ability to think or concentrate, or indecisiveness, nearly every day (either by
subjective account or as observed by others)
(9) Recurrent thoughts of death (not just fear of dying), recurrent suicidal ideation without a
specific plan, or a suicide attempt or a specific plan for committing suicide
B. The symptoms do not meet criteria for a Mixed Episode.
C. The symptoms cause clinically significant distress or impairment in social, occupational, or other
important areas of functioning.
D. The symptoms are not due to the direct physiological effects of a substance (e.g., a drug of abuse,
a medication) or a general medical condition (e.g., hypothyroidism).
E. The symptoms are not better accounted for by Bereavement, i.e., after the loss of a loved one, the
symptoms persist for longer than 2 months or are characterized by marked functional impairment,
morbid preoccupation with worthlessness, suicidal ideation, psychotic symptoms, or psychomotor
retardation.

Theoretical Background – Depressive Disorder
6
Table 2: Criteria for Dysthymic Disorder according to DSM-IV (APA, 2005): 349)
A. Depressed mood for most of the day, for more days than not, as indicated either by subjective
account or observation by others, for at least 2 years. Note: In children and adolescents, mood can
be irritable and duration must be at least 1 year.
B. Presence, while depressed, of two (or more) of the following:
(1) poor appetite or overeating
(2) insomnia or hypersomnia
(3) low energy or fatigue
(4) low self-esteem
(5) poor concentration or difficulty making decisions
(6) feelings of hopelessness
C. During the 2-year period (1 year for children or adolescents) of the disturbance, the person has
never been without the symptoms in Criteria A and B for more than 2 months at a time.
D. No Major Depressive Episode has been present during the first 2 years of the disturbance (1
year for children and adolescents); i.e., the disturbance is not better accounted for by chronic Major
Depressive Disorder, or Major Depressive Disorder, In Partial Remission.
Note: There may have been a previous Major Depressive Episode provided there was a full re-
mission (no significant signs or symptoms for 2 months) before development of the Dysthymic
Disorder. In addition, after the initial 2 years (1 year in children or adolescents) of Dysthymic
Disorder, there may be superimposed episodes of Major Depressive Disorder, in which case both
diagnoses may be given when the criteria are met for a Major Depressive Episode.
E. There has never been a Manic Episode, a Mixed Episode, or a Hypomanic Episode, and criteria
have never been met for Cyclothymic Disorder.
F. The disturbance does not occur exclusively during the course of a chronic Psychotic Disorder,
such as Schizophrenia or Delusional Disorder.
G. The symptoms are not due to the direct physiological effects of a substance (e.g., a drug of
abuse, a medication) or a general medical condition (e.g., hypothyroidism).
H. The symptoms cause clinically significant distress or impairment in social, occupational, or
other important areas of functioning.

Theoretical Background – Depressive Disorder
7
While the DSM-IV states that prevalence of depression does not appear to be related to eth-
nicity, education, income or marital status (APA, 2005), the DSM-5 (APA, 2013) omits con-
clusions on this topic. Contrary from evidence from DSM-IV, recent studies indeed suggest
that a low socio-economic status measured by income, occupation and education is associ-
ated with a higher prevalence of depressive disorders (Busch, Maske, Ryl, Schlack, &
Hapke, 2013; Hoebel, Maske, Zeeb, & Lampert, 2017). Conclusively, low socio-economic
status rises the probability for the occurrence of depressive symptoms (Lampert, Kroll,
Lippe, Muters, & Stolzenberg, 2013).
Another important aspect of depression are psychiatric comorbidities because comor-
bid depression is often accompanied by an increased risk of suicide and chronification of
depression (Deutsche Gesellschaft für Psychiatrie, Psychotherapie und Nervenheilkunde &
Ärztliches Zentrum für Qualität in der Medizin, 2015). Depressed patients with axis-I-
comorbidities are more likely to have more severe depressive disorders with a higher mor-
bidity and a higher risk of chronification (Rush et al., 2005).2 Kessler et al. (2003) showed
in a large study conducted in the United States that about two thirds (64 %) of the participants
with a major depressive episode in the last 12 months had a psychiatric comorbidity, of
which anxiety disorders were leading with the list (58 %), followed by substance use (9 %)
and impulse control disorders (17 %).
2.1.3 Course and long-term remission rates in unipolar depression
This study examined the long-term course of depression. The course of depression varies
strongly among different individuals (APA, 2013). Depressive episodes can be self-limiting
and can recover spontaneously (Deutsche Gesellschaft für Psychiatrie, Psychotherapie und
Nervenheilkunde & Ärztliches Zentrum für Qualität in der Medizin, 2015). Before the in-
troduction of psychopharmacological therapies, the mean duration of depressive episodes
was about eight months (Berger et al., 2015). Nowadays, with new therapeutic possibilities,
mean episode duration is estimated to be around 16 weeks (Rovner & Casten, 2003).
Depression is a disorder with a high risk of recurrence (Solomon et al., 2000). Eaton
et al. (2008) conducted a prospective population-based cohort study with 23 years of follow-
up to investigate among others recurrence risk. 35% of the patients who had a first episode
of depression during the study also experienced recurrence and 85 % were in remission after
10 years irrespective of treatment. Similar data were reported in a prospective 5-year follow-
2 The term “axis-I-comorbidities” is used to denote all psychiatric diagnoses except for personality disorders as well as mental retardation.

Theoretical Background – Depressive Disorder
8
up study including patients with a first depressive episode and treated with antidepressant.
After a first depressive episode, 83.5% of the patients obtained remission after 5 years and
31.5% experienced recurrence. In addition, researchers found that after a first episode of
depression, about 50 - 65% of the patients suffer another depressive episode, and that 70 -
80% of the patients with a second episode suffered a third, and the risk of relapse after three
episodes might be around 90 % (Eaton et al., 2008; Katon et al., 2001). Moreover, the risk
of recurrence increases by 16% for each successive depressive episode (Solomon et al.,
2000). It was demonstrated that the increased risk of recurrence persists lifelong (Kessing,
Hansen, Andersen, & Angst, 2004). The likelihood of remission declines with increasing
duration of illness (Keller et al., 1992) and the risk of recurrence declines with increasing
duration of remission (Solomon et al., 2000). Hence, effective therapeutic approaches are
urgently needed to reduce the risk of long-lasting depressive periods with the ultimate goal
to avoid the risk of chronification.
In terms of therapeutic success, a meta-analysis including 25 studies examined the
efficacy of psychological interventions (cognitive behavioural therapy, mindfulness-based
cognitive therapy and interpersonal therapy) as compared to treatment as usual (routine clin-
ical management, assessments only, no treatment and waiting list) or antidepressant therapy
in the prevention of recurrence in depression (Biesheuvel-Leliefeld et al., 2015). The meta-
analysis found supporting evidence that psychological interventions prevent recurrence
more effectively than treatment as usual and antidepressant therapy. Another meta-analysis
supports that antidepressant therapy and psychotherapy are equivalent in short-term treat-
ment of depression, but that psychotherapy is superior in the longer-term management of
depression (Spielmans, Berman, & Usitalo, 2011). Furthermore, the favourable results of
recurrence reduction have been shown to remain stable in long-term follow-ups studies (Stei-
nert, Hofmann, Kruse, & Leichsenring, 2014), albeit the authors indicated that long-term
follow-up studies of psychotherapeutic interventions are rare and that their results are to be
evaluated with reservations.
Different hypotheses for the high recurrence rate in major depression have been pro-
posed (Bockting, Hollon, Jarrett, Kuyken, & Dobson, 2015). One is the “premorbid vulner-
ability thesis” according to which individuals with a high risk of recurrence have all the
characteristics which render them vulnerable to recurrent depression, most of them genetic,
even before their first episode (Burcusa & Iacono, 2007). Another hypothesis is the “scarring
hypothesis” which assumes that each episode leaves residual changes that subsequently in-
crease vulnerability for recurrence. Different types of changes have been proposed to be
Theoretical Background – Depressive Disorder
9
related to biological (Lok et al., 2013), cognitive (Elgersma, Glashouwer, Bockting, Pen-
ninx, & Jong, 2013), or stress-related mechanisms (Beshai, Dobson, Bockting, & Quigley,
2011). Even if mechanisms of vulnerability for recurrence and relapse remain controversial,
it can be concluded that recurrence in depression is frequent, that it is less likely to occur the
longer a person has recovered and that it is more likely to occur in patients with a history of
depression.
2.1.4 Aetiology of depression
Depression is a complex disorder and a variety of hypotheses on its aetiology have been
proposed (Hautzinger, 2010). Hypotheses concerning the aetiology of depression are in-
serted in distinct disease models that can usually be characterized either in biological or
psychological terms. As this work focuses on cognitive and metacognitive aspects of depres-
sion, psychosocial models on the aetiology of depression will be further explained in the
following. Important psychological models that will be presented are the behavioural model
after Lewinsohn (1974), Beck’s cognitive model (Beck, Hautzinger, & Bronder, 1992),
learned helplessness and attributional style according to Seligman (1976), and, more re-
cently, the metacognitive model as proposed by Wells (Wells & Schweiger, 2011).
Empirical data on biological influence provide sound support for the influence of
genetic factors (Lacerda-Pinheiro et al., 2014), epigenetic factors (Tsankova, Renthal, Ku-
mar, & Nestler, 2007), alteration of neurotransmitter systems (Werner & Coveñas, 2013),
alteration of intracellular signal transductor systems and neuroplasticity (Manji & Duman,
2001), altered sleep patterns (Modell, Ising, Holsboer, & Lauer, 2005), as well as alteration
of neuroendocrine systems (Arborelius, Owens, Plotsky, & Nemeroff, 1999; Binneman et
al., 2008).
In the light of the complexity of depressive syndromes, prevailing superordinate
models now integrate several disease models into multidimensional so-called “biopsychoso-
cial models” (Berger et al., 2015). One important superordinate model is the vulnerability-
stress model which was originally developed by Zubin & Spring (1977) for schizophrenia
and which is also applied to depression. According to this model, depression can be triggered
by stressful life events with the prerequisite that the individual is vulnerable for depression.
Vulnerability can be determined through multiple psychological, social and biological fac-
tors (Goh & Agius, 2010). Though a lot of research has been conducted in order to under-
stand the aetiology of depression, not all factors are fully explained and empirically proven

Theoretical Background – Depressive Disorder
10
and further research has to be pursued (Berger et al., 2015). In the following, psychosocial
models relevant to this work will be presented more closely.
2.1.4.1 The behavioural model
Lewinsohn (1974) developed an influential behavioural model of depression which states
that depression results from low levels of response-contingent positive reinforcement,
mainly in social interactions. The amount of positive reinforcement depends on three factors:
a) the number of events that potentially can be reinforcing for an individual, b) the availa-
bility of those events under defined circumstances, and c) the instrumental behavioural com-
petencies of the individual to provoke reinforcement from the environment (Dimidjian, Bar-
rera, Martell, Munoz, & Lewinsohn, 2011). Loss of positive reinforcement can result from
environmental change such as the loss of a loved person, severe physical illness, loss of
work, financial troubles or other important personal failures, as well as from personality
traits (Dimidjian et al., 2011). According to this model, loss of positive reinforcement sub-
sequently leads to depressed mood and resignation that, consequently, entail diminution of
behaviour likely to provoke alternative positive reinforcement. The patient shows depressed
behaviour. For the short term, the social environment usually reacts to depressive behaviour
with help offers and affective sympathy, which supports maintenance of depression and de-
pressed behaviour. Behaviour that usually led to positive reinforcement is prone to extinc-
tion. On the long term, though, the social environment often withdraws from the depressed
person which can lead to decreased activity and somatic as well as vegetative symptoms
(Dimidjian et al., 2011). Thus, according to the behavioural model, depression results from
the loss of positive reinforcement, the depressed individual’s reaction to that loss, and the
environmental reaction to the behavioural change. Several studies have found support for
Lewinsohns hypothesis (Gotlib, 1982; Youngren & Lewinsohn, 1980).
2.1.4.2 Learned helplessness and attributional style
Experimental studies on conditioned punishment in animals and humans repeatedly showed
that exposure to uncontrollable and unpleasant events can provoke uncertainty, anxiety, pas-
sivity, and apathy (Seligman, 1976). Importantly, if test persons were afterwards confronted
to controllable averse stimuli, they showed the same resigned behaviour (Seligman, 1976).
This led to the formulation of the model of learned helplessness to explain depression (Selig-
man, 1976). Helplessness is a psychological state that is often provoked if a person feels that
events are uncontrollable (Seligman & Rockstroh, 1979). According to this disease model,

Theoretical Background – Depressive Disorder
11
if a person is confronted to important life events that are experienced as aversive and uncon-
trollable, such as disabling disease or long-term unemployment, he/she shows similar be-
haviour, including passivity, apathy, and resignation. Seligman assumes that the mere con-
frontation to uncontrollable events is not sufficient for learned helplessness, the individual
needs to expect to be helpless. Seligman (1976) calls this the cognitive aspect of learned
helplessness. When confronted to uncontrollable life events or failures, individuals usually
try to understand the causes of those events. According to Seligman, that so-called attribu-
tional style can be characterised on three dimensions: internal – external, stable – unstable,
global – specific (Seligman, 1976). If individuals cognitively judge the cause of their failures
to be internal, stable and universal, they will expect to experience helplessness and failures
in future events and will be convinced that they will have no means to positively influence
the course of events. As per Seligman, this cognitive set will influence the affective, moti-
vational, cognitive, vegetative, and motoric reaction to events. For example, the individual
will show less motivation to react deliberately and will exhibit loss of appetite, loss of libido,
or endocrine disturbances (Seligman & Rockstroh, 1979). The model of learned helplessness
states that this behaviour leads to vulnerability for depression and maintenance of depressive
symptoms (Seligman, 1976). Empirical studies found support for the importance of the at-
tributional style (Raps, Peterson, Reinhard, Abramson, & Seligman, 1982). Furthermore, the
model of learned helplessness is of vital importance for biological research on depression.
A large number of animal models that investigate biological factors of depression are based
on the model of learned helplessness and those models are supposed to have excellent valid-
ity in mice and rats (Vollmayr & Gass, 2013).
2.1.4.3 Becks cognitive model
Beck developed a cognitive model of depression that tries to explain how cognitive factors
can lead to vulnerability for depression (Beck et al., 1992). The cognitive model acts on three
main concepts: 1) the cognitive triad, 2) cognitive schemata, and 3) cognitive distortions
(Beck et al., 1992). The cognitive triad consists of the cognitive patterns that determine how
a person perceives his-/herself, the world, and his/her future. According to Beck et al. (1992),
a depressed individual often describes his-/herself in a negative way and tends to explain
negative experiences with his/her own psychic, physical or moral defaults, showing low self-
esteem. The depressed person also interprets the world negatively, assuming that the world
is asking things he/she can’t achieve or is always placing obstacles in his/her way, hindering
thus his/her personal achievement. He/she expects that this won’t change in his/her future.

Theoretical Background – Depressive Disorder
12
Instead, he/she thinks that his/her future will be an interminable succession of failures, frus-
tration and disadvantages (Beck et al., 1992). The cognitive triad is based on negative cog-
nitive schemata. Beck understands “cognitive schemata” as stable cognitive patterns with
which an individual structures his/her experiences. Different schemata are developed in the
course of life and are applied in appropriate situations in order to sort and categorise different
competing stimuli. According to Becks disease model, vulnerability for depression can result
from early negative experiences that lead to the development of latent negative schemata. In
situations similar to the original one, those latent schemata are reactivated. Beck states that
whereas patients with mild depression can question their cognitive schemata, in severe de-
pression, negative schemata are activated in an increasing extend of situations until hyper-
active idiosyncratic schemata structure the individual’s complete cognitive organisation
(Beck et al., 1992). Finally, Beck (1979) identifies six systematic cognitive distortions that
lead to the maintenance of the negative schemata and stabilise vulnerability for depression.3
2.1.4.5 The metacognitive model according to Wells
Wells’ aetiological model of depression focuses on so-called “metacognitions” in depres-
sion, that are understood as a set of cognitions about one’s own beliefs that shape one’s
thinking style (Fisher & Wells, 2009). Wells states that when thinking about mental disor-
ders, it is important to investigate the cognitive processes and mechanisms that shape the
content of belief (Wells, 2001). For that reason, Wells developed a generic information pro-
cessing model, the Self-Regulatory Executive Function Model (S-REF model), which he
consecutively applied to different psychopathologies (Wells & Matthews, 1994). According
to the S-REF model, there are three interacting levels of cognition: 1) automatic stimulus-
driven processing that is highly reflexive, 2) controlled processing involved in conscious
appraisal of events and in conscious control of actions and thoughts and 3) self-knowledge
stored in long-term memory (Wells & Matthews, 1996). All emotional processing modes or
configurations available for any individual take place in this tripartite architecture of cogni-
tion. One specific emotional processing mode is the S-REF mode. Wells supposes that the
S-REF mode is the predominant mode in emotional disorders including depression. In this
mode, self-knowledge as stored in long-term memory directs the appraisal of external events
and body signs. Also, it regulates the appraisal of the significance of the own thoughts and
guides subsequent cognitions (Wells & Matthews, 1996). The S-REF mode contains two
3 For empirical support for the impact of cognitive distortions in depression and further information concerning the cognitive distortions, see 2.2.3.

Theoretical Background – Depressive Disorder
13
types of self-knowledge: declarative beliefs (e.g. “I am a failure”) and procedural beliefs on
general plans concerning processing and coping. The latter is metacognitive knowledge that
directs selective attention, memory retrieval and cognitive processing in response to external
stimuli (Wells & Matthews, 1996).
According to Wells, development and maintenance of depression is due to biased
metacognitions leading for example to inappropriate coping strategies or misguided atten-
tion. Wells supposes that in depression, metacognitive beliefs lead to a specific thinking style
in responding to negative thoughts, which Wells calls “cognitive attentional syndrome”,
CAS. The CAS consists of prolonged stable thinking in form of worry, rumination, focus on
threat, heightened self-focus, and counterproductive coping strategies (Fisher & Wells,
2009, 11). As to the metacognitive model of depression, if triggered by negative thoughts, a
depressed patient will first react with positive metacognitive beliefs about worry and rumi-
nation, such as: “My worrying helps me understand my sadness” (Wells & Schweiger,
Positive meta-cognitive beliefs
about rumination and worry
Trigger
Rumination
Negative metacognitive beliefs
about uncontrollability of negative
thoughts and rumination
Depression
Affect Behavoir Thoughts
Figure 1 Adaption of Wells’ metacognitive model of depression (2001, p. 47)

Theoretical Background – Depressive Disorder
14
2011). Thus, the patient considers rumination to be a good strategy to achieve a desired state,
for example alleviation of depressed feelings. In contrast, rumination will not give rise to
understanding the depressed mood and alleviation but will lead to a concentration on rumi-
nation itself. This, according to Wells, will entail negative metacognitive beliefs about the
uncontrollability of negative thoughts and rumination. The patient will then react with de-
pressed behaviour such as social withdrawal, reduced activity, and hopelessness. Wells
claims that constant rumination entails a loss of awareness for rumination so that the de-
pressed patients ability to interrupt his/her maladaptive thinking style is interfered (Fisher
& Wells, 2009). Thus, according to Wells, positive and negative metacognitive beliefs lead,
when triggered through negative events or emotions, to the development and maintenance
of depression. The metacognitive model of depression is summarised in figure 2.

Theoretical Background – Cognition and Metacognition in Depression
15
2.2 Cognition and metacognition in depression
2.2.1 Cognitive distortions in depression
Cognitive distortions are an important constituent of many cognitive approaches to depres-
sion and have been subject of a huge body of empirical investigations (Scher et al., 2005).
One can differentiate between cognitive maladaptive beliefs that concern salient, i.e. mean-
ingful and depression-specific content, and more general cognitive biases and impairment of
information processing that can occur in depression. Maladaptive cognitive beliefs refer to
“dysfunctional attitudes” and “cognitive errors” (Beck, 1979). Beck (1979) first described a
list of six maladaptive cognitive beliefs involved in onset, maintenance and recurrence of
depression which was subsequently expanded by Burns (1999), Freeman and DeWolf
(1992), and Freeman and Oster (1999).4 Examples for more general cognitive biases are
biased concentration and memory (Beblo, Sinnamon, & Baune, 2011), biased memory of
events and false memories (Gotlib & Joormann, 2010), as well as biased emotion recognition
(Liu, Huang, Wang, Gong, & Chan, 2012). As this work concentrated on the role of cognitive
maladaptive beliefs in comparison to the role of metacognitive maladaptive beliefs, cogni-
tive maladaptive beliefs will be described in more detail in the following.
Maladaptive cognitive beliefs are supposed to be developed as a consequence of la-
tent cognitive schemata (Hautzinger & Pössel, 2017). A widely accepted definition states
that cognitive schemata are constituted by “organized elements of past reactions and expe-
rience that form a relatively cohesive and persistent body of knowledge capable of guiding
subsequent perception and appraisals” (Segal, 1988, 147).5 A depressiogenic schema can be
activated either directly by situations similar to the early situations which led to the devel-
opment of the dysfunctional schema, or indirectly by fully active content-related schemata
(Scher et al., 2005). It is generally supposed that when activated, a schema induces mala-
daptive cognitive beliefs and leads via negative dysfunctional attitudes and automatic
thoughts to depressive symptoms (Hautzinger & Pössel, 2017). Hence, cognitive schemata,
maladaptive cognitive beliefs, and dysfunctional attitudes seem to play an important role in
the vulnerability for depression (Beck et al., 1992).
Labelling of maladaptive cognitive beliefs in depression is not consistent and de-
pends on the study design and on the employed instruments (Yurica & DiTomasso, 2005).
4 Cognitive distortions are common and can be found in different psychopathologies (Yurica and DiTomasso, 2005). This work focusses on the relevant cognitive and metacognitive distortions involved in onset, mainte-nance and recurrence of depression and will thus not address other cognitive distortions. 5 The origins of the cognitive vulnerability to depression have been the subject of a substantial body of empir-ical studies. For a detailed review, see Ingram (2003).

Theoretical Background – Cognition and Metacognition in Depression
16
Depression-specific maladaptive cognitive beliefs will briefly be introduced as they have
been established in CB-T (Hautzinger & Pössel, 2017).6 The first specific maladaptive cog-
nitive belief, “all-or-nothing-thinking”, describes the tendency to have absolute appraisals
and to think in black-and-white. This is to say, judgments are not differentiated and gradual.
For example, if a performance is not perfect, the exaggerated judgment “I am a total failure”
is rendered. Dichotomous thinking has been demonstrated to be in many cases present in
depression (Teasdale et al., 2001). Second, “overgeneralisation” refers to the maladaptive
cognitive belief according to which a negative event is interpreted as an example of an infi-
nite chain of negative events. A particularly extreme form of generalisation is so-called “la-
belling”. One’s own and other people’s acting is labelled in emotional and not precise terms.
For example, if an individual commits a minor misfortune, he/she is labelled a “complete
idiot”. Generalisation is connected to another specific maladaptive cognitive belief called
“mental filtering” according to which one negative detail will negatively influence the ap-
praisal of an event, tinting it in a negative way (Gotlib & Joormann, 2010). Another specific
maladaptive cognitive belief in depression is “disqualifying the positive”. This means that
positive experiences are refuted by insisting that they don’t count for any reason. Also,
“magnification and minimization” often occurs in depressed individuals. It means that one’s
own faults are exaggerated whereas one’s own achievements are minimized. On the oppo-
site, other people’s faults and achievements are evaluated the other way around. Effectively,
studies documented reduced reward-sensitivity in depressed individuals (Eshel & Roiser,
2010). In addition, “arbitrary inference” or “jumping to conclusion” is regularly performed
in depression. Negative assumptions are accepted on insufficient reasons. It includes “min-
dreading”, which means presuming that others think negatively about oneself, and wrong
predictions, which means evaluating events as predictors for negative future events and tak-
ing the predictions as facts. Pessimistic biases and predictions were shown to be common in
depression (Strunk & Adler, 2009). Another maladaptive cognitive belief is “emotional rea-
soning”. It describes the idea that emotions rather than objective facts will guide reasoning.
A depressed individual will assume that negative feelings depict the reality. Berle and
Moulds (2013) suppose that self-referent emotional reasoning might be associated with high
levels of dysphoric symptoms, although emotional reasoning in general was found to be
present in all individuals regardless of their level of depression.7 Furthermore, so-called
6 There is an abundance of empirical evidence for cognitive distortions in depression and exemplary studies will be cited subsequently. 7 Berle and Moulds (2013) conclude that further investigations are needed to analyze the association between depression and emotional reasoning.

Theoretical Background – Cognition and Metacognition in Depression
17
“should statements” have been identified as a typical maladaptive cognitive belief in depres-
sion. Statements on what one should, one must, or one must not, are employed as a means
of motivation. Often, they express a perfectionism that cannot be met. This can lead to res-
ignation and demotivation (for an overview concerning perfectionism as a risk factor for
depression, see Egan, Wade, & Shafran, 2011). Finally, “personalization” has been closely
connected to depression. It describes the fact that depressed individuals tend to feel respon-
sible for negative events even if they are not responsible. Indeed, it has been demonstrated
that depressed individuals tend to attribute negative events internally (Ball, McGuffin, &
Farmer, 2008).
2.2.2 Metacognitive beliefs in depression
After presenting the concept of cognitive maladaptive beliefs in depression, the focus will
now be turned to metacognitive maladaptive beliefs. Before stating most important findings
concerning metacognitive maladaptive beliefs in depression, the evolution of the term will
briefly be sketched.
High interest into metacognition is carried in different disciplines, including psychol-
ogy, philosophy or educational sciences (Dunlosky, 2009). In philosophy, the idea that self-
reflecting knowledge on one’s thinking processes is essential for cognition can be traced
back to antiquity (Dunlosky, 2009). Aristotle devotes important parts of De anime to the
question how human thinking and perceiving might function and proposes a first suggestion
of an architecture of mind (Caston, 2002). Nowadays, the concept of metacognition, its scope
and function, is at the heart of the debate about self-consciousness and the functioning of
mind (for an overview see Proust, 2010; van Gulick, 2017).
In the field of modern psychology, the idea was brought into focus by Flavell’s stud-
ies concerning the development of memory in children (Bayne, Cleeremans, & Wilken,
2009). Flavell states that for the development of memory, cognitive structures for the re-
trieval and storage of memories as well as knowledge about mnemonic strategies are neces-
sary: “It seems in large part to be the development of intelligent structuring and storage of
input, of intelligent search and retrieval operations, and of intelligent monitoring and
knowledge of these storage and retrieval operations – a kind of ‘meta-memory’ perhaps”
(Flavell, 1971, p. 277). Beyond the investigations concerning meta-memory, the idea of
meta-knowledge was expanded to different areas of cognitive processing (Flavell & Well-
man, 1977). Nisbett and Wilson (1977) published an influential review which questioned the

Theoretical Background – Cognition and Metacognition in Depression
18
capacity to gain real introspection into one’s own higher-order cognitive processes. There-
upon, empirical investigations have focussed on metacognition, aiming at understanding
three key-elements of metacognition: knowledge, control and monitoring of cognitions
(Bayne et al., 2009). A further cardinal point for psychology and cognitive sciences was the
introduction of a model of cognitive processing which involves two levels of processing,
object-level and meta-level, by Nelson (1990).
Because of the multidisciplinary interest devoted to metacognition, the concept is
complex and the term “metacognition” is not consistently defined (Semerari et al., 2012).
Different definitions have been proposed. Metacognition is most basically understood as
“thinking about one’s thinking” (Moritz, Veckenstedt, Bohn, Köther, & Woodward, 2013,
p. 359). Flavell defines metacognition as “knowledge and cognition about cognitive phe-
nomena” and distinguishes between two subtypes: “metacognitive knowledge” and “meta-
cognitive experiences” (Flavell, 1979, p. 906). Wells assumes that metacognition is “a multi-
faceted concept” which can be classified in three subtypes: metacognitive knowledge, met-
acognitive experiences and metacognitive control strategies (Wells, 2001, 7-9). So far, “met-
acognition” subsumes different cognitive functions associated with monitoring, acknowl-
edging, and controlling thoughts on the one hand and beliefs concerning those cognitive
functions on the other. The concept underlying this work is based on the broad definition
given by Flavell and Wellman (1977). The term ‘metacognition’ is understood as cognitions
about one’s own thinking processes (also see Moritz & Lysaker, 2018). Regarding depres-
sion, metacognitive maladaptive beliefs are defined through the instruments used to assess
them (see 2.3.5 Metacognitions Questionnaire-30).
There are further definitions to be noted. Koriat and Goldsmith (1998) stress the role
of metacognition for certainty of judgment in memory processing and information retrieval.
In agreement with that position, Moritz and Woodward (2006) assume that metacognition
plays an important role in the impairment of memory processing, including overconfidence
in memory errors as well as reduced confidence in correct memories. Gallo, Cramer, Wong,
and Bennett (2012) employ the concept of metacognition in Alzheimer’s research and use it
to describe the awareness of cognitive declines. Lysaker et al. (2013) hypothesize that met-
acognition has more accurately to be understood as a spectrum of activities ranging from
discrete activities to synthetic activities. Discrete activities are metacognitive processes al-
lowing for the awareness of one’s own experiences or of the accuracy of one’s own judge-
ments. Synthetic activities are involved in establishing complex representations of the own
self and about other persons by integrating multiple information. According to this model,

Theoretical Background – Cognition and Metacognition in Depression
19
discrete and synthetic activities are presumed to reciprocally influence one another (Aydin
et al., 2016). Gumley (2011) has argued that metacognition should be conceived in a trans-
diagnostic perspective, pointing to the close link between metacognition with social, affec-
tive, and interpersonal functioning in different psychopathological conditions. Pedone et al.
(2017) have proposed a concept called “Metacognitive Multi-Function Modell” that brings
together the concepts of metacognition, theory of mind, and mentalization.
Regarding depression, interest in metacognitions emanated from empirical findings
on the role of rumination in the onset and maintenance of depression. Nolen-Hoeksema hy-
pothesised that a ruminative response style to depressed mood which she defined as “behav-
iours and thoughts that focus one's attention on one's depressive symptoms and on the im-
plications of these symptoms” would influence the duration of depressive symptoms (Nolen-
Hoeksema, 1991, p. 569). In the past years, rumination has received increasing attention in
empirical investigations concerning depression (Papageorgiou & Wells, 2003c). Studies
supported that the induction of rumination in dysphoric patients would sustain depressed
mood, whereas distraction would improve mood (Huffziger & Kuehner, 2009; Singer &
Dobson, 2007). Sarin, Abela, and Auerbach (2005) demonstrated in a prospective study that
the tendency to ruminate as a response to depressed mood was associated with an increase
of depressive symptoms. An uncontrolled prospective study could find evidence that rumi-
nation predicted one-year relapse in depressed patients (Michalak, Hölz, & Teismann, 2011).
Figueroa et al. (2015) conducted a prospective cohort study that confirmed rumination as a
long-term relapse predictor in a 3.5 years interval. Rood, Roelofs, Bögels, Nolen-Hoeksema,
and Schouten (2009) summarised in a meta-review that in non-clinical youths, rumination
might be a vulnerability factor depression.
Wells and Matthews (1994) conjectured that a ruminative response style might be
due to positive and negative metacognitive beliefs about the function and consequences of
rumination when exposed to depressed mood. In an initial cross-sectional study, Papageor-
giou and Wells (2001) found first evidence for their hypothesis. They conducted semi-struc-
tured interviews about rumination with 75 patients with MDE and without psychiatric axis-
I-comorbidities. The interviews confirmed that all of the addressed patients shared the ex-
pected positive and negative metacognitive beliefs about rumination. As empirical findings
suggest, most relevant metacognitive beliefs in depression seem to be positive metacognitive
beliefs, negative metacognitive beliefs and metacognitive beliefs concerning need for con-
trol (Ruiz & Odriozola-Gonzalez, 2015). Positive metacognitive beliefs about worry and
rumination (positive beliefs, PB) are those that express positive beliefs about the function of

Theoretical Background – Cognition and Metacognition in Depression
20
worry and rumination as coping strategy in depressed mood. Examples would be: “Rumi-
nating about my problems helps me to focus on the most important things”, or “Ruminating
about my feelings helps me to recognize the triggers for my bad things that have happened
in the past” (Papageorgiou & Wells, 2003c, p. 14). Negative metacognitive beliefs (negative
beliefs, NB) concern the uncontrollability, danger and negative consequences of rumination,
for example: “It is impossible not to ruminate about the bad things that have happened in the
past”, “Ruminating will turn me into a failure”, or “Ruminating makes me physically ill”
(Papageorgiou & Wells, 2003c, p. 14). Metacognitive beliefs about the need for control
(NFC) express the conviction that the own negative thoughts should be controlled and that
it lays in one’s own responsibility to make sure that rumination does not occur. Examples
are: “I should be in control of my thoughts all of the time.”, “It is bad to think certain
thoughts”, or “If I could not control my thoughts, I would not be able to function.” (Cart-
wright-Hatton & Wells, 1997, p. 285). The findings led to the development of the Metacog-
nitions Questionnaire-30 (MCQ-30; Wells & Cartwright-Hatton, 2004) which aims at testing
the existence and intensity of metacognitive beliefs and comprises beyond the subscales for
PB, NB, and NFC two further subscales called “cognitive confidence” (CC) and “cognitive
self-consciousness” (CSC) (also see 2.3.5 Metacognitions Questionnaire-30). A presentation
of empirical findings concerning depression-specific maladaptive cognitive belief and met-
acognitive beliefs in depression will be given in the next section.
The concept underlying this work is based on the broad definition given by Flavell
and Wellman (1977). Regarding depression, metacognitive maladaptive beliefs are defined
through the instruments used to assess them (see 2.3.5 Metacognitions Questionnaire 30).
2.2.3 Empirical findings concerning maladaptive cognitive and metacognitive beliefs
in depression
2.2.3.1 Maladaptive cognitive beliefs in depression as vulnerability factors for depression
There is a huge body of empirical investigations concerning maladaptive cognitive beliefs
in depression, often assessed in terms of “dysfunctional attitudes” via the Dysfunctional At-
titudes Scale (DAS; Weissman & Beck, 1978, see 2.3.4 Dysfunctional Attitudes Scale). Sev-
eral longitudinal studies examined whether maladaptive cognitive beliefs predict onset or
return of depressive symptoms, thus focussing on dysfunctional attitudes as cognitive vul-
nerability factors for depression. Relevant studies are summarised in Table 3 and most im-
portant findings will be presented in the following.

Theoretical Background – Cognition and Metacognition in Depression
21
In a prospective 2.5 years follow-up study, Alloy et al. (2006) yielded evidence for the cog-
nitive vulnerability hypothesis of depression. In their study, cognitive vulnerability predicted
onset as well as recurrence of depressive symptoms over 2.5 years after controlling for age,
gender, initial score in Beck Depression Inventory (Beck, Steer, & Hautzinger, 1995, see
3.3.3) and former history of depression. The risk of onset of major depression was about 7
times greater among high cognitive risk participants and risk of onset of minor depression
was about 3.5 times greater. Negative life events have not, however, been considered in that
report. As they seem to play an important role in the onset of depression, this could entail an
important limitation of the study. Also, as high risk was defined as combination of dysfunc-
tional attitudes and attributional style, it remains elusive which factor plays a more important
role. Segal et al. (2006) conducted a longitudinal study where they followed-up patients with
MDE in remission over 18 months during which relapses was investigated on a bimonthly
basis. They found that dysfunctional attitudes were an important risk factor for relapse. As
limiting factor, the study only investigated dysfunctional attitudes in patients in remission
and did not include patients in their study that did not respond to therapy. Otto et al. (2007)
confirmed the results in a large three-year prospective study with 700 never-depressed, cur-
rently depressed and formerly depressed women. The DAS score significantly predicted de-
pressive episodes when controlling for the initial level of depression, but not when control-
ling for the former history of depression. Also, elevated DAS-sores were associated with a
former history of depression. As limiting factor, it has to be mentioned that only women
between 36 and 46 years of age where included in the study; hence generalisation might be
problematic. Iacoviello, Alloy, Abramson, Whitehouse, and Hogan (2006) corroborated that
maladaptive cognitive beliefs might play an important role in predicting the long-term course
of depression. They conducted a 2.5 years follow-up study with 159 initially non-depressed
individuals with whom diagnostic interviews and questionnaires were repeated every six
weeks. Patients were grouped as per their scores in DAS and in Cognitive Styles Question-
naire composite for negative events according to their cognitive vulnerability in high and
low risk groups. The high-risk group experienced more severe and more chronic courses of
depression than the low-risk group. Jarrett et al. (2012) tested in a prospective study if primed
or unprimed dysfunctional attitudes predict relapse in remitted patients with recurrent de-
pressive disorder. Patients who responded to an initial cognitive therapy were followed-up
during 24 months after 8 months of continuation therapy. The authors concluded that the
unprimed level of dysfunctional attitudes predicts the risk of relapse in the following 32
months. The results stayed significant after controlling for the level of depression before

Theoretical Background – Cognition and Metacognition in Depression
22
continuation therapy. Each additional point in the DAS score increased the risk of relapse
by 1 %. The limitation of the study is that only patients who had responded to the cognitive
therapy were included. Wang, Halvorsen, Eisemann, and Waterloo (2010) showed in a pro-
spective longitudinal study with nine-years follow-up with clinically depressed, formerly
depressed and never depressed individuals that early maladaptive schemata (during child-
hood developed body of coherent knowledge that guides appraisal and perception) are a
significant prediction factor for depression (see Table 4)
Struijs, Groenewold, Oude Voshaar, and Jonge (2013) examined cognitive vulnera-
bility in a large prospective study with one-year follow-up. Their data showed that cognitive
vulnerability predicts an increase of depressive symptoms. Negative life events moderated
this association. Kruijt et al. (2013) aimed to investigate the role of cognitive reactivity in
the onset of major depression. They conducted a prospective study with a two-year follow-
up including never depressed individuals. Their data support the hypothesis that cognitive
reactivity precedes and predicts a first episode of depression. A major limitation of the study
might be that the sample is recruited from a group at high risk for depression as they were
chosen from mainly depressed and anxious patients. For that reason, generalization might
be difficult. Importantly, Struijs et al. (2013) as well as Kruijt et al. (2013) did not measure
dysfunctional attitudes using the DAS, but tested cognitive reactivity using the Leiden Index
of Depression Sensitivity – revised (LEIDS-r). This might undermine comparability with the
other cited studies.
The results from Beevers, Keitner, Ryan, and Miller (2003) differed slightly from the
findings summarized until here. The authors examined in a prospective study with 121 de-
pressed individuals the relation between cognitive change and prediction of relapse during
one-year follow-up after hospitalization. A poor change of maladaptive cognitive beliefs
during hospitalization predicted a shorter period until return of depression, while total scores
of DAS after 6 months of outpatient treatment did not. As only severely depressed patients
who responded to therapy were included, the sample of 53 patients was relatively small and
generalisations are to be done with caution.
Moreover, there are two short-term prospective studies to be mentioned. Pedrelli,
Feldman, Vorono, Fava, and Petersen (2008) tested 117 depressed or dysthymic patients
who had responded to 8 weeks of pharmacotherapy after further 8 weeks. They confirmed
their hypothesis that the interaction of high level of dysfunctional attitudes and high level of
perceived stress would predict high level of depressive symptoms after therapy. Kuroda
(2016) investigated the association between maladaptive cognitive beliefs, subjective stress

Theoretical Background – Cognition and Metacognition in Depression
23
and depressive symptoms. Their findings suggest that maladaptive cognitive beliefs lead
only indirectly to depressive symptoms via subjective stress, but not directly. It must be
mentioned as limiting factors that 8 and 10 weeks are very short timeframes, which could
limit possible conclusions.
To summarize, cognitive maladaptive beliefs seem to contribute to cognitive vulner-
ability for depression, increasing the risk of the onset of depression, the risk of relapse in
remission and predict more severe and chronic courses. This effect could be moderated by a
stressful life event or perceived stress. Furthermore, not only the level, but also the change
of the level of maladaptive cognitive beliefs might play a role

Theoretical B
ackground – Cognition and M
etacognition in Depression
24
Author, year Sample Instruments Follow-up Main results Alloy et al., 2006 - n=347
- healthy first semes-ter students without psychiatric disorders - - cognitive high risk (HR, n=172) - cognitive low risk (LR, n=175)
- Cognitive Style Questionnaire (CSQ) - Dysfunctional Attitudes Scale (DAS) - Schedule for Affective Disor-ders and Schizophrenia—Life-time (SADS–L) - Beck Depression Inventory (BDI)
2.5 years follow-up
Initial score in BDI and past episodes of depression predicted further depres-sive episodes over 2.5 years follow-up. Cognitive risk significantly pre-dicted first onset as well as recurrences of depressive episode after controlling for gender, age, past history of depres-sion and initial BDI.
Beevers et al., 2003 - n=53 - depressed inpatients who responded to combined pharmaco-logical and psychoso-cial treatment
- Modified Hamilton Rating Scale for Depression (MHRSD) - Dysfunctional Attitudes Scale (DAS) - Extreme response style in DAS
- after treatment (t1) - after 6 months of continuation therapy (t2) - after 12 months (t3)
Poor change in dysfunctional attitudes and extreme response style was signif-icantly associated with short periods to symptom recurrence. The absolute level of DAS and number of extreme responses after continuation therapy were not significantly associated with time to symptom recurrence.
Cannon et al., 1999 - n=138 - clinical outpatients with major depression
- Beck Hopelessness Scale - Dysfunctional Attitude Scale (DAS) - Cognitions Questionnaire (CQ) - Problem Solving Inventory (PSI) - Hamilton Rating Scale for De-pression (HAMD-17)
None Higher scores in DAS and poor prob-lem solving significantly and non-re-dundantly predicted higher scores in hopelessness which seems to be asso-ciated to higher risk of suicidal tendendy in depression.
Table 3: Summary of methods and results of relevant studies concerning maladaptive cognitive beliefs as vulnerability factors for depression

Theoretical B
ackground – Cognition and M
etacognition in Depression
25
Author, year Sample Instruments Follow-up Main results Ebrahimi, Afshar, Doost, Mousavi, & Moolavi, 2012
- n=130 - patients with major depressive disorder or dysthymic disorder (n=65) - matched healthy controls (n=65)
- diagnosis via clinical interview - Dysfunctional Attitude Scale- 26-item (DAS-26) - General Health Questionnaire (GHQ-28)
None Higher score in DAS-26 increased risk of depression. Individuals could be grouped in low-risk and high-risk groups on basis of their cognitive vul-nerability. Likelihood of relapse in the high-risk group increased by 6.82 as compared to the low-risk group.
Halvorsen, Wang, Eisemann, & Water-loo, 2010
- n=149 - undergraduate stu-dents/ patients at GP: -clinically depressed (n=47) -formerly depressed (n=39) - never clinically de-pressed (n=29) -follow-up (n=115)
- Dysfunctional Attitude Scale (Form A) (DAS) - Young Schema Questionnaire (YSQ) - Beck Depression Inventory (BDI-I)
9 years follow-up
YSQ subscale “Undesirability” re-mained a significant predictor of de-pression 9 years later.
Iacoviello et al., 2006 - n=159 - initially not de-pressed participants who suffered a de-pressive episode dur-ing the study - grouped according to cognitive risk of de-veloping a depressive episode
- Cognitive Style Questionnaire (CSQ) - Dysfunctional Attitudes Scale (DAS) - expanded Schedule for Affec-tive Disorders and Schizophre-nia-Lifetimeinterview (SADS-L) - Beck Depression Inventory I (BDI I) - SADS-Change (SADS-C)
2,5 years follow-up
Patients with high cognitive vulnera-bility defined on the basis of high scores in DAS and negative events subscale of CSQ had more depressive episodes with higher severity and more chronicity of depression during 2.5 years of follow-up.

Theoretical B
ackground – Cognition and M
etacognition in Depression
26
Author, year Sample Instruments Follow-up Main results Jarrett et al., 2012 - n=523
- patients with recur-rent MDD without concurrent psychiatric axis-1 disorder - responders took part in phase (n=213)
- Visual Analog Scale (VAS) - Dysfunctional Attitudes Scale (DAS) - Hamilton Rating Scale for De-pression (HAMD) - Longitudinal Interval Follow-up Evaluation-Psychiatric Status Ratings (LIFE-PSR)
- 8-months fol-low-up (after continuation therapy, t1) - 24-months fol-low- up (t2)
Unprimed DAS score results predicted relapse in the 32 subsequent months. Unprimed DAS score continued to predict relapse after controlling for level of depression before continua-tion therapy.
Kuroda, 2016 - n=103 - undergraduate psy-chology students
- Depressive Schemas Scale (DSS) - A new scale measuring subjec-tive stress - Self-rating Depression Scale (SDS)
10 weeks fol-low-up
Dysfunctional attitudes at t0 led to de-pressive symptoms at t1 indirectly via subjective stress, but not directly.
Kruijt et al., 2013 - n=834 - Participants of Neth-erlands Study of De-pression and Anxiety (NESDA) without past history of major depression or dysthy-mia
- Composite International Diag-nostic Interview (CIDI) - Leiden Index of Depression Sensitivity – revised (LEIDS-r) - Implicit self-depressed associ-ations (ISDA) - Lifetime version 2.1 of the Composite International Diag-nostic Interview (CIDI) - Brugha Questionnaire - Inventory of Depression Symptomatology – Self Report (IDS-SR) - Neo five-factor inventory (NEO-FFI) on neuroticism
2 years follow-up
Cognitive reactivity was a significant predictor of incidence of depression, besides baseline depression and num-ber of negative life events between t0 and t1.

Theoretical B
ackground – Cognition and M
etacognition in Depression
27
Author, year Sample Instruments Follow-up Main results Otto et al., 2007 - n= 750
- never-depressed women (n=500) - women with past history of depression without dysthymia (n=230) - women with current depression (n=20)
- Structured Clinical Interview for DSM–IV Axis I Disorders (SCID) - Dysfunctional Attitudes Scale (DAS) - Life Experience Survey (LES) - Hamilton Rating Scale for De-pression (HAMD-17)
3 years follow-up
DAS scores at baseline assessment differed significantly between the groups with highest scores for cur-rently depressed and lowest scores for never depressed participants. DAS scores significantly predicted new ep-isodes of depression after controlling for initial levels of depression, but not when controlling for past history of depression.
Pedrelli et al., 2008 - n=117 - clinical patients with MDE and HAMD >15 who responded to pharmacotherapy with fluoxetine
- Dysfunctional Attitudes Scale (DAS) - Hamilton Rating Scale for De-pression (HAMD-17) - Perceived Stress Scale (PSS)
-Before treat-ment (t0) - after 8 weeks of pharmacother-apy (t2) - 8 weeks of fol-low-up with two-weekly as-sessments (t3-t6)
Perceived stress and dysfunctional at-titudes interacted significantly and predicted severity of depressive symp-toms after therapy. Dysfunctional atti-tudes at baseline were not a significant univariate predictor of depressive symptoms.
Segal et al., 2006 - n=301 - outpatients with MDE at t0 - patients with MDE in remission at t1 (n=99)
- Dysfunctional Attitudes Scale (DAS) - Beck Depression Inventory (BDI) - Hamilton Depression Rating Scale (HAMD-17) - Mood rating via visual ana-logue scale (VAS)
-posttreatment evaluation (t1) - 18-months fol-low-up (t2)
Higher dysfunctional attitudes at t1 in-creased risk of relapse of depression in the 18 months following remission. Cognitive reactivity predicted relapse, also after having controlled for the number of previous depressive epi-sodes.

Theoretical B
ackground – Cognition and M
etacognition in Depression
28
Author, year Sample Instruments Follow-up Main results Struijs et al., 2013 - n=2891
- patients with lifetime depressive and/or dys-thymic disorder (n=2329) - at follow-up (n= 2455)
- Inventory of Depressive Symptomatology Self Report (IDS-SR) - The Leiden Index of Depression Sensitivity-Re-vised (LEIDS-R) - Mastery Scale - Implicit Associations Test (IAT) - List of Threatening Experi-ences (LTE)
1-year follow-up Different factors of cognitive vulnera-bility (cognitive reactivity, external lo-cus of control, explicit self-depressive associations) differentially predicted increase of depressive symptoms over time. This association was moderated by negative life events.

Theoretical Background – Cognition and Metacognition in Depression
29
2.2.3.2 Stability of maladaptive cognitive beliefs
Several studies concerning the stability of cognitive maladaptive beliefs in depression exist.
One important question that those studies address is whether those attitudes are state-like
concomitants of depression or whether they are rather more stable trait-like vulnerability
factors for depression. Empirical findings relevant to this work are depicted in Table 4 and
the most important studies will be mentioned in what follows in more detail.
Zuroff, Blatt, Sanislow, Bondi, and Pilkonis (1999) conducted a prospective 18
months follow-up study with depressed patients. Their data, as analysed in three structural
equation models, support the idea that maladaptive cognitive beliefs show significant state-
dependency as well as significant stability during treatment period and follow-up time.
Beevers and Millers (2004) investigation support this hypothesis. They tested 121 patients
hospitalized for severe depression before inpatient therapy as well as 6 months and 18
months after admission. Their data provide support for the idea that maladaptive cognitive
beliefs have trait and state characteristics as mood change influenced them while they also
exposed underlying stability. The authors concluded that depressed individuals might have
stable negative cognition, but that accessibility to them might depend on sad mood. As a
limiting factor, a poor return rate of 65% after 18 months must be mentioned. Wang, Hal-
vorsen, Eisemann, and Waterloo (2010) yielded similar results in their prospective longitu-
dinal study with nine-years follow-up, showing that relative levels of dysfunctional attitudes
from baseline assessment to the nine years follow-up was significantly stable, also after con-
trolling for the level of depression at all assessments. Jarrett, Vittengl, Doyle, and Clark
(2007) also confirmed that DAS scores remained relatively stable during their 2 years fol-
low-up phase. A study from Hankin (2008) performed with children and adolescents aged
from 11 to 17 also partly supports this idea, but results are more ambiguous. The study design
comprised four follow-ups in 5 weeks. The mean-level stability of dysfunctional attitudes
was significant for the younger aged, whereas for the overall sample, maladaptive cognitive
beliefs showed mean-level change and increased over time. Test-retest correlation of dys-
functional attitudes was poor (r = .26), but the stability of maladaptive cognitive beliefs was
significant in their full model fit, but with poor fit in some subgroups. The authors suggest
that their data provide support for the idea that cognitive vulnerabilities exhibit trait as well
as state characteristics, but acknowledge that their results are not fully conclusive.
To sum up, the presented findings support the view that dysfunctional attitudes are
not a mere consequence of levels of depression, but have both state and trait characteristics.

Theoretical Background – Cognition and Metacognition in Depression
30
This suggests that dysfunctional attitudes could play an important role as vulnerability factor
for depression.

Theoretical B
ackground – Cognition and M
etacognition in Depression
31
Author, year Sample Instruments Follow-up Main results Beevers & Miller, 2004
- n=121 - inpatients with MDE - n=99 at t2 - n=92 at t2.
- Dysfunctional Attitudes Scale (DAS) - Cognitive Bias Questionnaire (CBQ) - Beck Depression Inventory (BDI)
- after treatment (t1) -6-months fol-low-up (t2) -18-months fol-low- up(t3)
Current levels of depression as well as prior levels of dysfunctional atti-tudes influenced the current level of dysfunctional attitudes. Dysfunc-tional attitudes showed moderate test-retest correlation from t0 to t1.
Halvorsen et al., 2010 - n=149 - undergraduate stu-dents/ patients at GP: -clinically depressed (n=47) -formerly depressed (n=39) - never clinically de-pressed (n=29) - 115 at follow-up
- Dysfunctional Attitude Scale (Form A) (DAS) - Young Schema Questionnaire (YSQ) - Beck Depression Inventory BD (I-I)
9-years follow-up
Data suggested that DAS score might be a trait vulnerability factor for depression.
Hankin, 2008 - n=350 - healthy pupils aged from 11-17
- Adolescent Cognitive Style Questionnaire (ACSQ) - Children’s Dysfunctional Atti-tudes Scale (CDAS) - Children’s Response Styles Questionnaire (CRSQ) - Children’s Depression Inven-tory (CDI)
5-months fol-low-up
Dysfunctional attitudes remained stable in the younger aged youths, but there were mean-level changes in the overall sample by increasing levels of dysfunctional attitudes over time.
Table 4: Summary of methods and results of relevant studies concerning stability of maladaptive cognitive beliefs

Theoretical B
ackground – Cognition and M
etacognition in Depression
32
Author, year Sample Instruments Follow-up Main results Jarrett et al., 2007 - n=156
- patients with non-psychotic, recurrent, major depressive dis-order and HDRS > 17 without concurrent medical disorders - ACT responders (n=84) - patients in follow-up phase (n=74)
- Structured Clinical Interview for DSM–III–R (SCID) -Inventory for Depressive Symptomatology, Clinician Version (IDSC) - Hamilton Rating Scale for De-pression (HAMD-17) - Beck Depression Inventory (BDI) - Inventory for Depressive Symptomatology, Self-Report Version (IDSR) - Attributional Style Question-naire (ASQ) - Dysfunctional Attitudes Scale (DAS) - Self-Efficacy Scale (SEF)
- after treatment (12-14 weeks of ACT, t1) - 8-months-fol-low-up (after continuation therapy or as-sessment only, t2) - 24-months fol-low-up (after 10 further sessions of CT or assess-ment only, t3)
The DAS score changed signifi-cantly during A-CT with Cohen’s d=1.05. Depressive symptoms also changed significantly during A-CT with Cohen’s d=1.55. Therapy-re-sponders did not differ at pre-A-CT assessment in DAS-scores, but dif-fered significantly from non-re-sponders in lower DAS-scores at session 9 and 17 and 20. Patients who improved more on the DAS improved more in depressive symptoms. Early change in DAS did not significantly predict later change in depressive symptoms. The mean DAS score remained rel-atively stable over follow-up phase.
Wang et al., 2010 - n=149 - undergraduate stu-dents and patients at GP: - clinically depressed (n=61) - formerly depressed (n=42) - never clinically de-pressed (n=46)
- Dysfunctional Attitude Scale (Form A) (DAS) - Young Schema Questionnaire (YSQ) - Beck Depression Inventory (BDI-I)
9-years follow-up
The authors found significant rela-tive stability of the dysfunctional attitudes level from baseline assess-ment to follow-up, also after con-trolling for level of depressive symptoms at both assess ments.

Theoretical B
ackground – Cognition and M
etacognition in Depression
33
Author, year Sample Instruments Follow-up Main results Zuroff et al., 1999 -n=250
- patients with depres-sive disorder -completed therapy (n=162) - complete data at t0 and t1 (n=154) - completed data at t3 (n=142)
- Dysfunctional Attitude Scale (DAS) - Beck Depression Inventory (BDI) - Depression subscale of Hop-kins Symptom Checklist - Schedule for Affective Disor-der and Schizophrenia- Change Version (SADS-C) - Hamilton Rating Depression Scale (HAMD-17)
- baseline assess-ment (t0) - post-treatment assessment (t1) - 6-months fol-low-up (t2) - 12-months fol-low-up (t3) - 18-months fol-low-up (t4)
After treatment, there were signifi-cant decreases in total the DAS-Score, in the subscale Need for Ap-proval and Perfectionism as well as in depressive symptoms. At t1 and t3, correlation between DAS and depression were significant and moderately large. Dysfunctional at-titudes showed relative stability from t0 to t1 with test-retest corre-lation .65 for Perfectionism, .56 for Need for Approval and. 65 for total DAS score. During follow-up, rela-tive stability was even higher. Also, dysfunctional attitudes showed sig-nificant state dependency as well as significant stability over treatment.

Theoretical Background – Cognition and metacognition in depression
34
2.2.3.3 Further relevant findings concerning maladaptive cognitive beliefs in depression
Concerning the mechanisms of change during therapy, a meta-analysis conducted by Garratt,
Ingram, Rand, and Sawalani (2007) found that according to the majority of analysed studies,
changes in cognition as function of cognitive therapies predicted a change in depression.
Jarrett et al. (2007) suppose that changes in dysfunctional attitudes are a product of changes
in depression, as their findings suggest that the change in depressive symptoms precedes the
change in cognitive content. In their prospective RCT with two-year follow-up, decrease in
DAS-score occurred early during acute phase cognitive therapy and remained stable during
two-year follow-up. Higher improvement in DAS-score was correlated to higher decrease of
depressive symptoms. To conclude, dysfunctional attitudes seem to be closely linked to de-
pressive symptoms and several studies seem to support the view that they might play a role
in the onset and recurrence of depression, but this role is not extensively understood.
Finally, some important meta-analyses should be mentioned. Scher et al. (2005) pre-
sented findings concerning cognitive distortions and depressogenic schemata as vulnerabil-
ity factors for depression. The authors first focussed on cross-sectional priming studies,
where the association between vulnerability, dysfunctional attitudes, negative mood induc-
tion and depressive symptoms was tested. The underlying hypothesis is that dysfunctional
attitudes are latent in vulnerable individuals and can be activated by emotional triggers such
as sad mood. This tendency to active dysfunctional attitudes when triggered is also called
“cognitive reactivity”. Vulnerability was mostly operationalized based on previous depres-
sive episodes. A great number of studies showed that an endorsement of dysfunctional atti-
tudes is associated with depressed mood states in individuals vulnerable for depression.
Priming effects were consistently found in different studies, vulnerable individuals showing
more dysfunctional attitudes in depressed mood states after having been primed. Next, Scher
et al. (2005) analysed longitudinal studies which examined whether stressful life events in
combination with vulnerability predicts depression over time. Several studies could show
that dysfunctional attitudes predicted depressive symptoms within a week after confrontation
to a stressful event. The results were more variable in studies where larger timeframes were
investigated. The authors concluded nevertheless that the vulnerability-stress model of cog-
nitive vulnerability based on dysfunctional cognitive attitudes is largely supported by evi-
dence.
Further evidence for the importance of cognitive distortions in depression can be
gained by the study corpus on cognitive behavioural therapy (CBT). CBT, which grounds

Theoretical Background – Cognition and metacognition in depression
35
on the above-discussed principles, has been demonstrated to be effective in depression (Beck
& Dozois, 2011; Butler, Chapman, Forman, & Beck, 2006; Clark & Beck, 2010).
2.2.3.4 Metacognitive maladaptive beliefs in depression
After describing the literature concerning cognitive maladaptive beliefs in depression, the
next section will focus on the research concerning metacognitive maladaptive beliefs in de-
pression. Cross-sectional studies provide evidence that maladaptive metacognitive beliefs
are linked to depression and suggest that they could play an important role in the onset,
maintenance and recurrence of depression. Most important findings are summarized in Table
5 and in the following paragraph. Maladaptive metacognitive beliefs were assessed with
Metacognitions Questionnaire 30 (MCQ-30; Wells & Cartwright-Hatton, 2004; see 2.3.5)
or with Positive Beliefs about Rumination Scale (PBRS; Papageorgiou & Wells, 2001) and
Negative Beliefs about Rumination Scale (NBRS, Papageorgiou & Wells, 2001). NBRS con-
tains two subscales: negative beliefs about the uncontrollability and harm of rumination
(NBRS 1) and negative beliefs about social and interpersonal consequences of ruminating
(NBRS 2). PBRS and NBRS correlate significantly and positively with subscales NB, PB,
CC and NFC of MCQ-30 with small to large effect sizes, where solely PBRS did not corre-
late significantly with CC (Roelofs, Huibers, Peeters, Arntz, & van Os, 2010). Roelofs et al.
(2010) assume construct validity because of significant and positive correlations between
PBRS and PB (r= .28), NBRS1 and NB and NFC (r= .61 and r=.48) as well as between
NBRS2 and NB and NFC (r= .39 and r= .55). Still, the discriminatory power and construct
validity of the different subscales can be questioned as PBRS also correlates significantly
with NFC (r= .34) and NBRS with PB (r= .31).
Importantly, out of 11 cross-sectional studies, only four tested depressed individuals
while the other studies assessed nonclinical participants. Generalizations to clinical individ-
uals from non-clinical samples should only be carried out with precaution because findings
can diverge as the Papageorgiou and Wells (2003b) study exemplifies. Cross-sectional stud-
ies with non-clinical participants established significant associations between metacognitive
beliefs, depressive symptoms and rumination (Huntley & Fisher, 2016; Papageorgiou
& Wells, 2003b; Roelofs et al., 2007; Solem, Hagen, Hoksnes, & Hjemdal, 2016) and a link
between the subscales of MCQ-30 and negative emotions (Tajrishi, Mohammadkhani, &
Jadidi, 2011). Yilmaz, Gençöz, and Wells (2015) concluded by means of their data that met-
acognitive beliefs are a better predictor of depression than dysfunctional schemata and cog-
nitive maladaptive beliefs.

Theoretical Background – Cognition and metacognition in depression
36
However, cross-sectional studies are certainly not appropriate for establishing causal rela-
tionships. Several longitudinal studies concerning the prediction of depression through met-
acognitive distortions exist that will be shortly presented in the following paragraph, all find-
ings are also depicted in Table 5. It should nevertheless be noted that none of the longitudinal
studies assessed clinical participants. Papageorgiou and Wells (2009) tested 164 nonclinical
university students in a prospective study with 3-months follow-up. Their data showed that
NB significantly predicted depressive symptoms 12 weeks later, after controlling for base-
line rumination and baseline level of depression. Limiting factors of the study is the short
follow-up and the young age of the participants (mean age 21.1 years; SD=4.2). It is not clear
whether their findings can be transferred to depressed individuals in general. Also, only neg-
ative beliefs concerning uncontrollability and harm and social consequences were investi-
gated which is only one of the assumed relevant metacognitions in depression. Yılmaz,
Gençöz, and Wells (2011) examined the prediction of depressive symptoms through mala-
daptive metacognitive beliefs in 161 nonclinical students and adults after 6 months. They
could show that metacognitions, particularly NB, predicted depressive symptoms after con-
trolling for stressful life events and demographic variables and consequently seem to consti-
tute an important vulnerability factor for depression. Nevertheless, because of low scores in
BDI (M=8.43, SD=6.42) at intake and follow-up (M =6.74, SD=5.47), it is uncertain whether
data apply for depressed individuals. Weber and Exner (2013) found in a prospective study
with two-months follow-up with 60 nonclinical students that PB had a significant effect on
rumination at follow-up after controlling for baseline rumination. Also, PB had an indirect
effect on depressive symptoms at follow-up that was mediated through rumination. A small
sample size, low age and the fact that only nonclinical students were tested are limiting fac-
tors of the findings. Ruiz and Odriozola-Gonzalez (2015) investigated in a prospective online
survey with 289 nonclinical participants the relation between psychological inflexibility (key
construct of Acceptance and Commitment Therapy), and maladaptive cognitive and meta-
cognitive beliefs over nine months. Their data suggest that psychological inflexibility sig-
nificantly mediated the longitudinal effect of metacognitive beliefs at baseline assessment,
particularly PB, NB, and NFC, on depressive symptoms at follow-up. Only 106 participants
(36,7%) completed both assessments and findings should thus be acknowledged with pre-
caution.
A meta-review conducted by Normann, van Emmerik, Arnold, and Morina (2014)
has analysed the efficacy of metacognitive therapy for depression as developed by Wells.
Their data, based on 16 published and nonpublished studies of which 9 were controlled trials,

Theoretical Background – Cognition and metacognition in depression
37
provided evidence for the efficacy of metacognitive therapy as compared to waitlist control
groups (between group Hedges g=1.81) and cognitive behavioural therapy (between group
Hedges g=0.97). Also, changes in metacognitions from pre- to post-treatment and follow-up
were large (in-group Hedges g=1.18 and 1.31).8 The efficacy of metacognitive therapy could
provide support the model on which it is based.
8 Changes in metacognition in patients after cognitive therapy were not investigated or reported.

Theoretical B
ackground – Cognition and m
etacognition in depression
38
Author (Year) Sample Instruments Follow-up Main results Halvorsen et al., 2015 - n=168
- currently depressed individuals (n=37) - previously depressed individuals (n=81) - never depressed indi-viduals (n=50)
- Structured Clinical Interview for DSM-IV, Axis I (SCID-I) - Beck Depression Inventory—Second Edition (BDI-II - The Beck Anxiety Inventory (BAI) - Metacognitions Questionnaire-30 (MCQ-30) - Thought Control Questionnaire (TCQ) - Ruminative Response Scale (RRS)
None A discriminant function analysis was conducted to analyse the best indica-tors for discrimination between the groups. Two functions were found. The best discriminators of the first function were rumination, MCQ NB, TCQ Worry, TCQ Punishment and TCQ Distraction. The second function was best correlated with MCQ NFC, MCQ, CC, TCQ Reappraisal and MCQ PB
Huntley & Fisher, 2016
- n=715 - non-clinical students
-Inventory of Depressive Sympto-matology-Self-Report (IDS-SR) -Ruminative Response Scale (RRS) - Dysfunctional Attitudes Scale (DAS) - Positive Beliefs about Rumina-tion Scale (PBRS) - Negative Beliefs about Rumina-tion Scale (NBRS): NBRS1: beliefs about the uncontrollability and harm, NBRS2: social and interpersonal consequences of ruminating
None The study found support that meta-cognitive beliefs explain additional variance in depressive symptoms above and beyond dysfunctional atti-tudes and rumination. It also showed that the relation between BP and de-pressive symptoms is fully mediated by rumination and that the relation be-tween NB and depressive symptoms was partially mediated by rumination. Negative beliefs about interpersonal and social consequences of rumina-tion did not predict depressive symp-toms.
Table 5: Summary of methods and results of studies investigating metacognitive biases and depression

Theoretical B
ackground – Cognition and m
etacognition in depression
39
Author (Year) Sample Instruments Follow-up Main results Papageorgiou & Wells, 2003b Study 1
- n=200 - adults with Major Depressive Disorder
-Inventory to Diagnose Depres-sion (IDD) - Ruminative Response Scale (RRS) - Positive Beliefs about Rumina-tion Scale (PBRS) - Negative Beliefs about Rumina-tion Scale subscales 1 and 2 (NBRS1+2) - Metacognitive Efficiency Sub-scale (MCQ3) of the Metacogni-tions Questionnaire
None The study showed a significant asso-ciation between depressive symp-toms, rumination, PB, NB, and meta-cognitive efficiency. The study also suggests that PB are linked to rumina-tion as a response to negative thoughts and mood. The relation between rumi-nation and depressive symptoms seemed to be mediated by NB.
Papageorgiou & Wells, 2003b Study 2
- n=200 - nonclinical graduate and nongraduate psy-chological students (MDE as exclusion cri-teria)
-Inventory to Diagnose Depres-sion (IDD) - Ruminative Response Scale (RRS) - Positive Beliefs about Rumina-tion Scale (PBRS) - Negative Beliefs about Rumina-tion Scale subscales 1 and 2 (NBRS1+2) - Cognitive Confidence Subscale (MCQ3) of the Metacognitions Questionnaire
None Results differed in comparison to study 1 (depressed sample). As in group 1, there was a significant corre-lation between depressive symptoms, rumination, PB and NB, but there was no significant correlation with CC.
Papageorgiou & Wells, 2009
- n=164 - nonclinical university students
-Inventory to Diagnose Depres-sion (IDD) - Ruminative Responses Scale (RRS) - Negative Beliefs about Rumina-tion Scale 1+2(NBRS 1+2)
3-months follow-up
NB were found to prospectively pre-dict depression when controlling for initial level of depression and rumina-tion.

Theoretical B
ackground – Cognition and m
etacognition in depression
40
Author (Year) Sample Instruments Follow-up Main results Roelofs et al., 2007 - n=196
- nonclinical under-graduates
- Quick Inventory of Depressive Symptomatology (QIDS) - Ruminative Response Scale (RRS) - Positive Beliefs about Rumina-tion Scale (PBRS) - Negative Beliefs about Rumina-tion (NBRS 1+2) -Miskimins Self-Goal Other Dis-crepancy Scale (MSGO)
None The study showed a direct and an in-direct link between rumination and depressive symptoms. NB mediated the indirect link. Also, a bidirectional link between rumination and NB was found.
Roelofs et al., 2010 - n=179 - patients with major depressive disorder
- inventory of depressive sympto-matology (IDS) - Structured Clinical Interview for DSM-IV axis I (SCID-I) - Beliefs about Rumination Scale (PBRS) - Negative Beliefs about Rumina-tion Scale 1+2(NBRS1, NBRS2) - Metacognitions Questionnaire-30 (MCQ-30), subscales 1,2,3,4 - Ruminative Response Scale (RRS) - Penn State Worry Questionnaire (PSWQ)
None Rumination had a direct association with depressive symptoms, NB were not significantly associated to depres-sive symptoms. Negative metacogni-tive beliefs concerning the interper-sonal and social consequences of ru-mination and uncontrollability and harm had a bidirectional relation with rumination. According to Roelofs et al., NB could contribute directly and indirectly (via rumination) to depres-sion.

Theoretical B
ackground – Cognition and m
etacognition in depression
41
Author (Year) Sample Instruments Follow-up Main results Ruiz & Odriozola-Gonzalez, 2015
- n=106 - nonclinical partici-pants, anonymous online survey
- Acceptance and Action Ques-tionnaire – II (AAQ-II) - Dysfunctional Attitude Scale – Revised (DAS-R) - Depression subscale of the De-pression Anxiety and Stress Scales-21 (DASS-21) - Metacognitions Questionnaire-30 (MCQ-30), subscales positive beliefs, negative beliefs, need for control.
9-months follow-up
Psychological inflexibility statisti-cally significantly mediated the rela-tion between PB, NB and NFC at t1 and depressive symptoms at t2.
Solem et al., 2016 - n=1433 - Norwayan nonclini-cal participants
- Positive Beliefs about Rumina-tion Scale (PBRS) - Ruminative Response Scale (RRS) - Negative Beliefs about Rumina-tion Scale 1+2 (NBRS 1+2) - Beck Depression Inventory (BDI)
None NBRS 1+2 and PBRS were all signif-icantly associated with depressive symptoms and rumination. Their data suggests that PB predicted rumination that predicted NB which, in turn, pre-dicted depressive symptoms.
Tajrishi et al., 2011 - n=300 - Iranian healthy stu-dents
- Metacognitions Questionnaire 30 (MCQ-30) - Hospital Anxiety And Depres-sion Scale (HADS)
None Four subscales of MCQ-30 were pos-itively correlated with negative emo-tions: PB, NB, NFC and CC.
Weber & Exner, 2013 - n=60 - non-clinical under-graduate and graduate university students
- Positive beliefs about rumination scale (PBRS) - Rumination response scale (RSQ) - Beck depression scale-II (BDI-II)
2-months follow-up
The study found that PB at t1 signifi-cantly explained additional variance of depressive symptoms at t2. Also, the study showed that rumination at t2 mediated the influence of PB at t1 on the level of depressive symptoms at t2.

Theoretical B
ackground – Cognition and m
etacognition in depression
42
Author (Year) Sample Instruments Follow-up Main results Yılmaz et al., 2011 - n=161
- non-clinical students and adults
- Meta-Cognitions Questionnaire-30 (MCQ-30) - Beck Anxiety Inventory (BAI) - Beck Depression Inventory (BDI) - Life Experiences Survey (LES) - Inventory of College Students’ Recent life Experiences (ICSRLE)
6-months follow-up
The study showed that a higher level of NB predicted the increase of de-pressive symptoms independently of demographic variables and stressful life events.
Yilmaz et al., 2015 - n=251 - non-clinical under-graduate and postgrad-uate university stu-dents
-Negative Beliefs About Rumina-tion Scale 1 and 2 (NBRS1 and NBRS2) -Positive Beliefs About Rumina-tion Scale (PBRS) - Dysfunctional Attitude Scale-24 (DAS-24) - Beck Depression Inventory (BDI) - Beck Anxiety Inventory (BAI)
None PB and NB explained a significant amount of variance in depressive symptoms above and beyond dysfunc-tional schemata. Higher levels of dys-functional attitudes were correlated to higher levels of depressive symptoms, too, but metacognitive beliefs showed higher predictive values for depres-sive symptoms than the set of dys-functional attitudes. They concluded that metacognitive beliefs make a greater contribution to depression than dysfunctional attitudes as measured by DAS.

Aims of the Present Study
43
2.3 Aims of the present study
As outlined in the introduction, depression is a chronic disease with a high recurrence prob-
ability. The present study examines a sample of initially depressed individuals over a period
of 3.5 years. First, it aims at replicating findings concerning the long-term course of depres-
sion. At baseline, the examined patients had already suffered 3 depressive episodes on aver-
age. For that reason, I conjecture that the data will yield a rate of patients with a recurrent
depressive disorder of around 70 - 90 % in accordance with studies in patients with a former
history of depression (i.e. Hypothesis 1, H1). Next, according to established aetiological
models, maladaptive cognitive beliefs are relevant in the aetiology of depression. Modifica-
tion of those content-related cognitive biases seems to reduce depressive symptoms, whereas
their stability seems to predict depressive symptoms. For that reason, maladaptive cognitive
beliefs are supposed to be important targets in the therapy of unipolar depression. Moreover,
empirical investigations have shown an association between maladaptive metacognitive be-
liefs and depressive symptoms. Still, only few studies concerning the association between
depression and cognitive and metacognitive maladaptive beliefs in the long-term course have
been published and the existing studies present limitations. Importantly, until now, no study
has directly compared cognitive and metacognitive maladaptive beliefs in depressed indi-
viduals in a longitudinal setting to investigate which of them is a better predicator of the
course of depressive symptoms. I conjecture that depressive symptoms and cognitive and
metacognitive maladaptive beliefs decrease from baseline to 3.5 years follow-up assessment
(H2). In light of the current state of empirical findings, I suppose that significant correlations
between the change of both cognitive and metacognitive maladaptive beliefs and the change
of depressive symptoms exist (H3a) and that metacognitive maladaptive beliefs explain ad-
ditional variance of the data above and beyond cognitive maladaptive beliefs (H3b). In ac-
cordance with vulnerability-stress models, I suppose that change of depressive symptoms is
also predicted by the presence of a critical life event (H3c).
Cognitive maladaptive beliefs have been shown to expose trait as well as state char-
acteristics, which means that they correlate with depressive symptom severity while showing
underlying stability. Long-term stability of maladaptive metacognitive beliefs has not yet
been exhaustively examined. As metacognitive maladaptive beliefs are conceptualized as
stable underlying cognitions on one’s own thinking style, emotions and behaviour, I hypoth-
esise that they are more stable than depressive symptoms as well as more stable than cogni-
tive maladaptive beliefs which have been shown to expose a certain dependency on sad mood
or stress (H4).

Aims of the Present Study
44
To sum up, the roles of cognitive and metacognitive maladaptive beliefs in long-term course
of depression remain elusive. Aim of the study was to examine the role of cognitive and
metacognitive maladaptive beliefs in depressed individuals over 3.5 years. The following
hypotheses are to be examined:
H1) The recurrence rate is between 70 and 90 %.
H2) Self- and clinician-assessed severity of depression (HAMD, BDI), level of cognitive
maladaptive beliefs (DAS) and level of metacognitive maladaptive beliefs (PB, NB,
NFC) decrease from baseline (t0) to 3,5 years follow-up (t3).
H3 a) There is a positive correlation between initial status and change of cognitive (DAS),
and metacognitive (BP, NB, NFC) maladaptive beliefs and initial status and change
of self- and clinician assessed severity of depression (HAMD, BDI).
H3 b) The initial status and change of cognitive (DAS) and metacognitive maladaptive be-
liefs (PB, NB, NFC) from t0 to t3 explain additional variance of the change of de-
pressive symptoms (DAS/BDI) from t0 to t3.
H3 c) The presence of a critical life event predicts the change of depressive symptoms from
t0 to t3.
H4) Maladaptive cognitive and metacognitive beliefs (DAS, NB, PB, NFC) are more sta-
ble than depressive symptoms (DAS/BDI) and maladaptive metacognitive beliefs
(NB, PB, NFC) are more stable than cognitive maladaptive beliefs (DAS) from t0 to
t3.

Methods
45
3. Methods
3.1 Participants
Participants were recruited after their admission to a psychosomatic outpatient day clinic
(RehaCentrum Hamburg). Psychologists and psychiatrists screened 171 patients shortly after
their admission and 93 of them were assessed at baseline. Eighty-four patients were included
in the study by previously defined in- and exclusion criteria. Inclusion criteria were the di-
agnosis of a depressive disorder (major depression or dysthymia) according to DSM IV and
age between 18 and 65 years. Exclusion criteria were the presence of lifetime maniac or
psychotic symptoms, suicidality (Suicidal Questionnaire Score Revised total score ≥ 7) or
intellectual disability (estimated IQ < 70). All patients gave a written informed consent after
trained staff had explained the aims of the study as well as the voluntariness of participation
and the confidentiality of data. At admission, of 84 patients, 36 (43%) were diagnosed with
a single episode of major depressive disorder, 47 (56%) with recurrent depression and 1
(1%) with dysthymia. Mean illness duration was 96 months (SD=104,96) and patients expe-
rienced on average a total of 3 depressive episodes (SD= 5,69) and were hospitalized for the
second time (SD=1,13). Of 84, more than half of the patients (n=43; 51%) suffered of at least
one comorbid psychiatric disorder, of which 38 (45%) met criteria for at least one comorbid
anxiety disorder, 4 (5%) fulfilled criteria for a substance abuse disorder, and one patient
(1%) met criteria for an eating disorder. At intake, 58 patients were medicated (antidepres-
sants n= 54, antipsychotics n= 2, combination n=2). Nearly half of the patients (n=35; 42%)
had received outpatient psychotherapeutic therapy prior to admission. Sociodemographic
characteristics of the sample at inclusion point (t0) are displayed in Table 6.
Table 6: Sociodemographic characteristics at inclusion time point (t0, Means (M) (standard
deviations (SD)) or frequencies (percentages).
Variable Sample (n=84)
Age (years) M=44.5 (SD=9,89)
Gender (female/male) 62 (74 %) / 22 (26 %)
Years of formal education M=10.61, SD=1.69
Job status (working/ sick leave/ unem-
ployed)
4 (5 %) / 47 (56 %) / 33 (39 %)

Methods
46
3.2 Procedure
We performed a parallel assessor-blind randomized clinical trial (RCT) about the efficacy
of Metacognitive Training in Depression (D-MCT). All patients participated in diagnostic
interviews including Mini International Neuropsychiatric Interview (M.I.N.I) and Hamilton
Depression Rating Scale (HAMD) at baseline (t0), conducted by examiners blind to the di-
agnostic status. Moreover, they completed various questionnaires, including Beck Depres-
sion Inventory (BDI), Dysfunctional Attitude Scale (DAS) and Metacognitive Questionnaire
30 (MCQ-30). Sociodemographic characteristics were investigated via a semi-structural in-
terview. All patients participated in a standard treatment outpatient program, 5 days a week
for 8 hours a day, which consisted of various psychological and physical interventions as
well as medication. After the baseline assessment, patients were allocated to two different
add-on therapies, D-MCT (experimental group) and health training (HT, active control
group) according to a fixed computer-generated randomization plan with a 1:1 allocation
ratio. After 4 weeks (post, t1) and 6 months (follow-up 1, t2), the same instruments were
administered except for M.I.N.I. and sociodemographic characteristics. Three years after
follow-up 1 (t3), all patients having participated in t0 were contacted by letter, email or via
phone and invited to participate in a long-term follow-up (follow-up 2, t3). All patients pro-
vided once again written informed consent prior to participation in t3. All instruments from
t1 were administered. Diagnostic interviews via phone were used to verify diagnostic status
including HAMD. The study was approved by the Ethics Committee of the German Psycho-
logical Association (JL-SM_102015_amd_102011). The first part of the study (t0, t1, t2)
was registered at the German Clinical Trials Register (No. DRKS00007907). The follow-up
study (t3) was registered on the database ClinicalTrials.gov provided by the U.S. National
Institutes of Health (No. NCT02771535). After having completed the follow-up 2 assess-
ment, all patients received 30 € compensation. Figure 1 summarizes the patient flow.

Methods
47
Assessed at 6-month follow-up, t2
(n=60)
Assessed at 3-year follow-up (n=60)
Patients screened after admission
(n=171)
Assessed at baseline, t0
(n=93)
Assessed at posttest, t1 (n=79)
Included, t0
(n=84)
78 declined participation · Time constraint (n=50) · Insufficient German (n=4) · No motivation (n=6) · Other reasons (n=18)
9 were excluded: · Bipolar (n=2) · No current or recurrent MDE (n=1) · SBQ-R 7 (n=2) · Assessment terminated due to distress (n=2) · 2 Withdrew consent (n=2)
Lost to posttest assessment (n=5)
Lost to 6-month follow-up assessment
(n=19)
Lost to 3-year follow-up assessment
(n=24)
Refused further participation: n=8
Could Not be reached: n=15
Dead: n=1
Analysis Excluded from analysis (n=0)
Complete cases (n=58)
Incomplete cases, only written participa-
tion (n=2)
Figure 2 Flow of participants for the given study procedures and analysis.

Methods
48
3.3 Measurements
3.3.1 Sociodemographic variables
Sociodemographic background characteristics were investigated via a semi-structural inter-
view. Obtained data included age, gender, educational background, drug abuse, smoking and
drinking habits as well as medication. Moreover, relapses of depressive symptoms, psychi-
atric admission and outpatient psychotherapies since t2 were retrieved at t3.
3.3.1 Mini International Neuropsychiatric Interview
The psychopathological status and psychiatric comorbidities were assessed using Mini In-
ternational Neuropsychiatric Interview (M.I.N.I.; Sheehan et al., 1998). The M.I.N.I. is a
brief structured diagnostic interview with an administration time of about 15 minutes used
to explore 15 axis-one disorders according to DSM-IV. The interview is structured in differ-
ent sections, each of them investigating a different disorder. For each disorder, one or two
screening questions are explored to rule out the diagnosis when negated. When answered
positively, further questions regarding the main symptoms follow. Sufficiency to the criteria
of good reliability and validity have been reported for the English and the French version,
further studies have confirmed the results for the Italian and the Japanese version (Lecrubier
et al., 1997; Rossi et al., 2004); Otsubo et al., 2005). In the present study, the German Version
5.0.0 was slightly modified in order to distinguish recurrent vs. single episode major depres-
sive disorder as well as double depression. Suicidality was explored using the Suicide Be-
haviours Questionnaire-Revised (SBQ-R; Osman et al., 2001), therefore the section C of the
M.I.N.I. which investigates suicidality was skipped.
3.3.2 Hamilton Depression Rating Scale
The severity of depression was measured using the 17-Item version of the Hamilton Depres-
sion Rating Scale (HAMD; Hamilton, 1960). The HAMD is a semi-structured interview
conducted by trained interviewers. The administration time is about 20 to 30 minutes. De-
pressive symptoms which had occurred in the last 7 days prior to examination are investi-
gated in 17 items. The items measure cognitive, affective, and somatic symptoms such as
mood, feelings of guilt, suicidal ideation, quality of sleep, anxiety, weight loss, loss of libido,
and hypochondriasis. A total score indicating the severity of depression is calculated by add-
ing the scores of each item. Severe depression is defined as a score ≥ 25, whereas scores ≤ 8

Methods
49
are considered as subclinical depressive symptoms according to the German National Guide-
lines (DGPPN, 2015). A meta-analysis documented adequate to good reliability and good
validity for the 17-version of the HAMD (Cronbach’s α between .46 and .97, test-retest re-
liability between .81 and .98; Bagby, Ryder, Schuller, & Marshall, 2004).
3.3.3 Beck Depression Inventory
I used the Beck Depression Inventory (BDI; Beck et al., 1995) as second instrument to meas-
ure the severity of depression. The BDI is a self-reported questionnaire consisting of 21
items with four scalings ranging from 0 to 3. The questionnaire is used to investigate depres-
sive symptoms that have occurred in the last 7 days prior to examination. It covers motiva-
tional, emotional, cognitive, and somatic symptoms matching the diagnosis criteria of major
depression according to the DSM-IV criteria. In order to estimate the severity of depression,
the scores of each item are added to a total score, where a total score of ≤ 10 is considered
as subclinical depressive symptoms, 11-19 as mild, 20-29 as moderate, and a score ≥ 30 as
indicator for clinically severe depressive symptoms according to the German National guide-
lines (DGPPN, 2015). In a meta-analysis, good reliability and validity were reported
(Cronbach’s α .86 for psychiatric patients; mean correlations of the BDI with HAMD .72;
Beck, Street, & Garbin, 1988).
3.3.4 Dysfunctional Attitude Scale
The Dysfunctional Attitude Scale, Form A (DAS; Weissman & Beck, 1978; German Ver-
sion: Hautzinger, Joormann, & Keller, 2005) was employed to assess dysfunctional cogni-
tive beliefs. The DAS is a self-reported questionnaire consisting of 40 items rated by partic-
ipants on a 7-point Likert scale (i.e., totally agree, agree very much, agree slightly, neutral,
disagree slightly, disagree very much, totally disagree). The items are expected to capture
the participant’s self-evaluation and negative attitudes concerning the self, the world, and
the future. Thus, they represent the content of typical dysfunctional cognitions in depression
such as need for social approval (e.g. “I cannot be happy unless most people I know admire
me”), perceived preconditions of happiness (e.g. “It is difficult to be happy unless one is
good looking, intelligent, rich, and creative”), or dysfunctional attitudes concerning personal
achievement or perfectionism (e.g. “If I fail partly, it is as bad as being a complete failure.”).
The score of each item is summed up to a total score indicating to which extent the partici-
pants’ thoughts are distorted, ranging from 40 to 280. Scores of 140 and higher are consid-
ered as clinically relevant, scores of 100 and lower as inconspicuous. The original version

Methods
50
of the DAS contained 100 items and has been subdivided by the authors to two 40-items
forms by a factor analysis. Consecutively, different factor analyses have been conducted
mostly identifying one to three factors, labelled for instance “Dependency”, “Achievement”
or “Perfectionism”, whereas no consent regarding the number and label of factors has been
achieved (Cane, Olinger, Gotlib, & Kuiper, 1986; Power et al., 1994; Floyd, Scogin, &
Chaplin, 2004; Beevers, Strong, Meyer, Pilkonis, & Miller, 2007; Moore, Fresco, Segal, &
Brown, 2014). Still, good reliability (internal reliability measured by Cronbach α between
.88 and .93 and test-retest reliability of .71; Weissman & Beck, 1978) and sufficient validity
(correlation with BDI of .65 and with the depression scale of Profile of Moods States of .76;
Weissman & Beck, 1978) have been reported for the 40-item version of the DAS.
3.3.5 Metacognitions Questionnaire-30
I employed three subscales of the Metacognitions Questionnaire-30 (MCQ-30; Wells
& Cartwright-Hatton, 2004) in order to assess metacognitive beliefs. The MCQ-30 is a 30-
item short form of the original MCQ which comprises 65 items (Cartwright-Hatton & Wells,
1997). It is a self-reported questionnaire rated by participants on a four-point Likert scale
(do not agree, agree slightly, agree moderately, agree very much). The MCQ-30 is com-
posed of five distinct subscales eliciting different conceptual scopes of metacognition sup-
posed to be relevant in the emergence and maintenance of different psychopathologies in-
cluding depression (Papageorgiou & Wells, 2003a). The authors labelled the five scales as
follows: (1) “positive beliefs about worry” (“positive beliefs”, PB, e.g. “Worrying helps me
to avoid problems in the future.”, six items), (2) “negative beliefs about thoughts concerning
uncontrollability and danger” (“negative beliefs”, NB, e.g. “My worrying is dangerous for
me.”, six items), (3) “cognitive confidence” (CC, e.g. “I have little confidence in my memory
for words and names”, six items), (4) “negative beliefs concerning the consequences of not
controlling thoughts” (“need for control”, NFC, e.g. “If I did not control a worrying thought,
and then it happens, it would be my fault.”, six items), and (5) “cognitive self-consciousness”
(CSC, e.g. “I think a lot about my thoughts.”, six items). In the present study, only subscales
(1), (2), and (4) were administered, as they were reported to be most related to depression
(Ruiz & Odriozola-Gonzalez, 2015). For each scale, a score ranging from 6 to 24 can be
calculated by adding the sums of the corresponding items. The higher the score, the higher
is the extent of metacognitive distortions regarding the concerned factor, although no cut-
off scores are defined. Good psychometric properties have been documented for the MCQ-
30, such as good internal consistency for each subscale (Cronbach α ranging from .72-.93),

Methods
51
as well as for the total scale (Cronbach α .93; (Wells & Cartwright-Hatton, 2004). Previous
studies showed good convergent validity, and acceptable to good test–retest reliability
(Wells & Cartwright-Hatton, 2004).
3.4 Data analysis
IBM SPSS 24.0 (IBM Corp., Armonk, New York, NY) software was used for all analyses.
Study completers and non-completers at t3 were compared concerning sociodemographic
and psychopathological features at t0. Group comparisons were executed via t-test and Chi²
test.
To test hypothesis one, recurrence data from patients participating in t3 assessment
was analyzed. In line with DSM-IV criteria (APA, 2005), the diagnosis of recurrent depres-
sion was given when patients had suffered two or more Major Depressive Episodes with an
interval of at least two consecutive months in which criteria for a Depressive Episode have
not been met. In accordance with Zimmerman et al. (2012), remission was defined as a
HAMD total score of 7 and below.
Subsequent data analysis was proceeded in two steps. First, latent growth curve mod-
els (LGMs) were calculated using Mplus (Muthén & Muthén, 2011). A latent growth model
was calculated for each outcome variable (HAMD, BDI) and each predictor construct in-
cluded in the theoretical model (DAS, PB, NB, NFC) to compute trajectories from baseline
assessment to 3.5 years follow-up after treatment. For each variable, an intercept, indicating
the status of the corresponding variable at baseline assessment, and a slope, specifying the
total change from baseline to long-term follow-up 3.5 years after treatment, was estimated.
The intercept was centered at baseline, the slope loading at baseline was fixed at zero, and
the slope loading at the last assessment was fixed at 1.0. In order to be able to capture non-
linear trajectories of change, the two intermediate slope loadings were freely estimated. Var-
iances of the intercept and slope were allowed to covariate, but residual variances were sup-
posed to be independent. A robust maximum likelihood was implemented to account for
possible non-normality. Data were supposed to be missing at random, conditional on infor-
mation in the model. The model fit was tested via goodness-of-fit indexes. The estimated
intercept and slope scores for each participant were saved and used for further analysis.
Regarding hypothesis 2, the means of the slopes were calculated and one-sample T-
tests were run to test whether the means of the relevant variables change significantly from
t0 to t3.

Methods
52
In terms of hypothesis 3, bivariate relations between self- and clinician-assessed severity of
depression (HAMD, BDI) and maladaptive cognitive (DAS) and metacognitive beliefs (PB,
NB, NFC) were examined by calculating Pearson’s correlations.
To test hypotheses 4, intercept and slope coefficients were used in multiple hierar-
chical regression models. First, assumptions for regression analyses were checked. Scatter-
plots showed linear relationships between predictor variables and outcome variable. Data
exposed homoscedasticity (see appendix, Figure 2) and the residuals of the regression lines
were normally distributed (see appendix, Figure 3). There was no perfect multicollinearity
(Durbin-Watson d = 2,4). Though, in model A and B, values of PB, NB and NFC showed
correlations between their respective slopes and intercepts (e.g. for model A: between inter-
cept and slope of BP, r = -.85, p < .001; between intercept and slope of NP r = -.76, p < .001;
between intercept and slope of NFC r = -.70, p < .001; correlations were similar for model
B) suggesting multicollinearity. Multicollinearity can produce untrustworthy unstandardized
regression coefficients b, because collinearity increases the standard error of b, it can limit
the size of R and R² and it renders it difficult to assess the importance of individual predictors
(Field, 2016). The variance inflation factor (VIF) as well as tolerance statistics (1/VIF) were
further used to check for multicollinearity. Multicollinearity is likely if the largest VIF is
larger than 5 or 10 and/or if tolerance is less than 0.2 or 0.1 (O’brien, 2007). In model A and
B, those criteria were not met (model A and B: largest VIF = 4.4, the lowest tolerance of
0.23). For that reason, sufficient independency of predictor variables was assumed.
Models A1-3 analysed the change of depressive symptoms over time. For that reason,
the slope of HAMD was entered as dependent variable. Preliminary regression analysis
tested the influence of the expected risk factors (age, gender, initial status of depression,
former history of depression). Significant risk factors were entered as first block predictors
(model A1), intercept and slope of DAS were included as second block predictors (model
A2), and intercepts and slopes of PB, NB and NFC were added as third block predictors
(model A3). Model B tested the model with slope and intercept of BDI as secondary outcome
parameter instead of HAMD.
To test hypothesis 5, further regression models were run to investigate whether crit-
ical life events predicted the association between vulnerability factors, i.e. cognitive and
metacognitive maladaptive beliefs (DAS, PB, NB, BFC), and depressive symptom severity.
To test the influence of a critical life event between t2 and t3, this variable was included in
the hierarchical regression as last step (models A4 and B4).

Methods
53
Finally, in order to test hypothesis 6, the relative stability of the relevant variables was com-
pared on the basis of the associated slopes and of the basis of the test-retest correlations. For
each construct, a standardized positively pooled within-group effect size d was calculated
by dividing the mean change from t0 to t3 assessment by the standard deviation of the base-
line measurements. This d can be used to assess a constructs stability relative to the other
constructs, as it measures mean change of a construct from t0 to t3: the higher d, the more
change has occurred from t0 to t3. Relative stability was compared to test-retest correlation
r between t0 and t3 of each construct.
Cohen's (1988) rules of thumb were applied to evaluate size of the measured effects.
Standardized regression weights (β) and correlation coefficients (r) of .1, .3, .5 were consid-
ered as weak, medium, and strong effects. Findings with p < .05 were considered statistically
significant.

Results
54
4. Results
4.1 Sample characteristics
The sociodemographic characteristics of the patients that completed t3 assessment are dis-
played in Table 7. For the sample characteristics at baseline assessment, see 3.1. Sample
characteristics at t1 and t2 have been described elsewhere (Jelinek et al., 2016). Completers
and non-completers did not differ statistically significantly regarding age (p = .45), years of
formal education (p = .97) gender (p = .35), intelligence as measured by MWTB 2 (p = .65)
at t0. Furthermore, they were statistically indistinguishable concerning their psychopatho-
logic status at t0: HAMD (p = .95), BDI (p = .59) comorbidities (p = .65). For a comparison
of t3 completers and non-completers at t0, see Table 8.
Table 7: Sociodemographic characteristics at 3,5 years follow-up (t3). Means (standard de-
viations) or frequencies (percentages)
Variable Sample
Age (years) n = 60 M=49.61 (SD=10,14)
Gender (female/male) n=60 47 (78 %) / 13 (22 %)
Years of formal education n=60 M=10.61, SD=1.69
Job status (employed/ edu-
cation / retired / unem-
ployed / housewife/ -hus-
band)
n=59 25 (42 %) / 1 (2 %) / 18 (31 %) / 10 (17 %) / 5 (9
%)
Critical life event between
t2 and t3
(yes / no)
n=58 41 (71 %) / 17 (29 %)

Results
55
Table 8: Sociodemographic characteristics at baseline assessment (t0) of t3 completers and
non-completers. Means (standard deviations) or frequencies (percentages)
T3 Completers T3 Non-Completers
Variable Sample Sample
Age n=60 M=45.98, SD=10.18 n=24 M=44.17, SD=8.80
Gender (female/male) n=60 46 (77 %) / 14 (23 %) n=24 16 (67 %) / 8 (33 %)
Years of formal educa-
tion
n=60 M=10.60, SD=1.73 n=24 M=10.62, SD=1.61
Intelligence (MWTB) n=60 M=52.52 SD=8.71 n=23 M=51.52, SD=8.70
HAMD n=60 M=15.46, SD=5.03 n=24 M=15.54, SD=5.71
BDI n=60 M=25.58, SD=10.88 n=23 M=26.93, SD=7.97
Comorbidities n=56 M=0.68 SD=0.79 n=23 M=1.00, SD=1.28
4.2 Hypothesis 1
Table 9 displays the psychopathological data of patients that completed the t3 assessment
including mean total score of HAMD, classification according to severity of depression via
HAMD, mean total score of BDI, classification according to severity of depression via BDI,
total number of stays and mean stay duration in psychiatry since t2, ambulant psychotherapy
since t2, current alcohol consume and current psychopharmacological medication. At t3, of
58 patients, 22 patients (38%) were diagnosed with an episode of major depressive disorder,
45 patients (78 %) met criteria for recurrent depression and 17 patients (29 %) for dysthy-
mia.9 Of 58, 13 patients (22 %) could be diagnosed with a double depression (i.e. major
depressive episode and dysthymia). At t3, the majority of the patients (n=47; 81 %) suffered
of either a recurrent depression or dysthymia or both. Patients experienced on average a total
of 17.26 depressive episodes (SD=23.97) in their lifetime. At t3, of 58, 27 patients (47 %)
had a HAMD ≤ 7 and can thus be considered in remission according to Zimmerman et al.
(2012). A recurrence rate of 78 % is in line with findings from literature that state a recur-
rence rate of 60 – 90 % in patients with a former history of depression. Hence, hypothesis 1
can be confirmed.
9 The diagnoses „major depressive disorder“, „recurrent depression“ and „dysthymia“ ca be given side by side. For that reason, the percentages add up to more than 100 %.
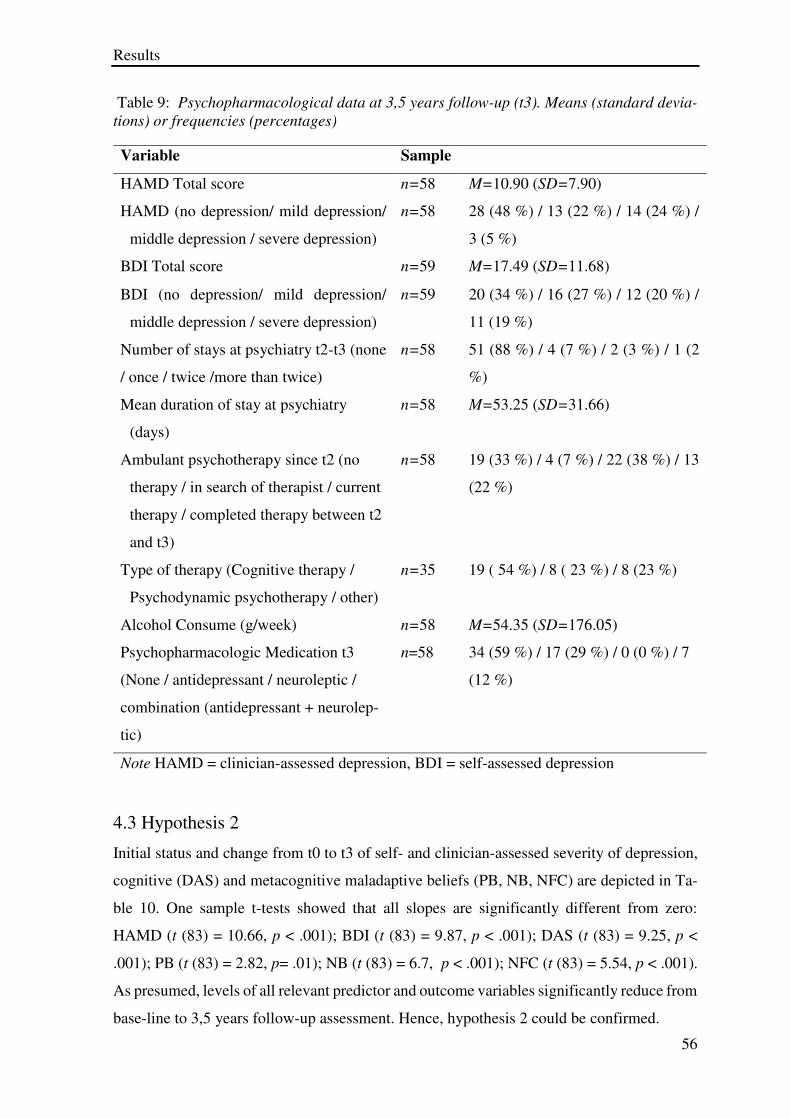
Results
56
Table 9: Psychopharmacological data at 3,5 years follow-up (t3). Means (standard devia-
tions) or frequencies (percentages)
4.3 Hypothesis 2
Initial status and change from t0 to t3 of self- and clinician-assessed severity of depression,
cognitive (DAS) and metacognitive maladaptive beliefs (PB, NB, NFC) are depicted in Ta-
ble 10. One sample t-tests showed that all slopes are significantly different from zero:
HAMD (t (83) = 10.66, p < .001); BDI (t (83) = 9.87, p < .001); DAS (t (83) = 9.25, p <
.001); PB (t (83) = 2.82, p= .01); NB (t (83) = 6.7, p < .001); NFC (t (83) = 5.54, p < .001).
As presumed, levels of all relevant predictor and outcome variables significantly reduce from
base-line to 3,5 years follow-up assessment. Hence, hypothesis 2 could be confirmed.
Variable Sample
HAMD Total score n=58 M=10.90 (SD=7.90)
HAMD (no depression/ mild depression/
middle depression / severe depression)
n=58 28 (48 %) / 13 (22 %) / 14 (24 %) /
3 (5 %)
BDI Total score n=59 M=17.49 (SD=11.68)
BDI (no depression/ mild depression/
middle depression / severe depression)
n=59 20 (34 %) / 16 (27 %) / 12 (20 %) /
11 (19 %)
Number of stays at psychiatry t2-t3 (none
/ once / twice /more than twice)
n=58 51 (88 %) / 4 (7 %) / 2 (3 %) / 1 (2
%)
Mean duration of stay at psychiatry
(days)
n=58 M=53.25 (SD=31.66)
Ambulant psychotherapy since t2 (no
therapy / in search of therapist / current
therapy / completed therapy between t2
and t3)
n=58 19 (33 %) / 4 (7 %) / 22 (38 %) / 13
(22 %)
Type of therapy (Cognitive therapy /
Psychodynamic psychotherapy / other)
n=35 19 ( 54 %) / 8 ( 23 %) / 8 (23 %)
Alcohol Consume (g/week) n=58 M=54.35 (SD=176.05)
Psychopharmacologic Medication t3
(None / antidepressant / neuroleptic /
combination (antidepressant + neurolep-
tic)
n=58 34 (59 %) / 17 (29 %) / 0 (0 %) / 7
(12 %)
Note HAMD = clinician-assessed depression, BDI = self-assessed depression

Results
57
Table 10: Initial status and change from t0 to t3 of self- and clinician assessed depression,
cognitive and metacognitive maladaptive beliefs
Note HAMD = clinician-assessed depression, BDI = self-assessed depression, DAS = cog-nitive maladaptive beliefs, PB = positive metacognitive beliefs, NB = negative metacogni-tive beliefs, NFC = metacognitive beliefs about the need for control
4.4 Hypothesis 3a
The correlations between the intercepts and slopes of self- and clinician-assessed depression
as well as the scores of cognitive and metacognitive maladaptive beliefs are displayed in
Table 11. The initial status of HAMD and BDI (i.e. intercepts) were significantly positively
correlated with the initial status of DAS, NB, NFC (i.e. intercepts) at small or medium effect
sizes. This means that the higher the initial severity of depression, the higher the initial score
in DAS, NB and NFC. Also, a change of HAMD (i.e. the slope) was positively associated at
medium effect sizes with changes of DAS and NB and at small effect size with change of
NFC (i.e. the slopes). A change of BDI was positively correlated at medium effect size with
changes of DAS, PB, NB, and NFC. Thus, a change of depressive symptoms was positively
correlated with a change of maladaptive cognitive beliefs and metacognitive beliefs and hy-
pothesis 3a could be confirmed. The correlations between initial scores and difference scores
between t0 and t3 of self- and clinician-assessed severity of depression, cognitive and met-
acognitive maladaptive beliefs with available data are depicted in the appendix (Table 17).
Variable Sample M SD
Initial status HAMD (intercept) n=84 15.53 4.49
Change of HAMD (slope) n=84 -4.86 4.18
Initial status BDI (intercept) n=84 25.86 10.11
Change of BDI (slope) n=84 -9.11 8.46
Initial status DAS (intercept) n=84 166.26 33.44
Change of DAS (slope) n=84 -20.93 20.73
Initial status PB (intercept) n=84 12.98 3.88
Change of PB (slope) n=84 -0.96 3.14
Initial status NB (intercept) n=84 17.89 3.51
Change of NB (slope) n=84 -2.79 3.82
Initial status NFC (intercept) n=84 13.78 3.99
Change of NFC (slope) n=84 -2.14 3.55

Results
58
The correlation Tables between the different testing times for each construct are shown in
the appendix (Tables 20-25) using available data.
Table 11: Correlations of initial status and change from t0 to t3 of depression with initial
status and change from t0 to t3 of maladaptive cognitive and metacognitive beliefs, LGM
data
4.5 Hypothesis 3b
To examine the effects of the initial status and the change of cognitive and metacognitive
maladaptive beliefs on the change of depression, multiple hierarchical regression analysis
was used. The assumptions for regression analysis were satisfied (see 3.4).
The results of the regression models A and B are depicted in Tables 12 and 13, model
A using change of clinician-assessed severity of depression as outcome variable (i.e. slope
of HAMD), while model B used change of self-assessed severity of depression as outcome
variable (i.e. slope of BDI). A preliminary regression analyses revealed that out of the ex-
pected risk factors (age, gender, initial status of depression, former history of depression),
only initial depressive symptoms had a significant effect on the change of depression and
was included in models A and B. The initial depression had a medium effect on the change
of depression in model A1 (HAMD) and strong effects in model B1 (BDI). Model A1 ex-
plained 18 % of the variance, model B1 could account for 30 % of variance of the outcome.
Initial status of DAS
Change of DAS
Initial status of PB
Change of PB
Initial status of NB
Change of NB
Initial status of NFC
Change of NFC
Initial status of HAMD
.36** .24* .03 .09 .25* -.12 .26* .00
Change of HAMD
-.15 .39** -.01 -.02 -.15 .34** -.08 .24*
Initial status of BDI
.49** .12 .20 -.13 .32** -.20 .39** -.19
Change of BDI
-.19 .41** -.20 .30** -.20 .47** -.18 .47**
Note Significant correlations (2-tailed) are flagged: ** = p < .01; * = p < .05. HAMD = cli-nician-assessed depression, BDI = self-assessed depression, DAS = cognitive maladaptive beliefs, PB = positive metacognitive beliefs, NB = negative metacognitive beliefs, NFC = metacognitive beliefs about the need for control.

Results
59
Table 12: Model A1-3: Predictors of change of depressive symptoms (outcome: change of
HAMD (i.e. slope) )
Models A2 and B2 included initial status and change of maladaptive cognitive beliefs (i.e.
intercept and slope of DAS) as possible predictors. In models A2 and B2, in addition to
initial status of depression, initial status of cognitive maladaptive beliefs predicted a change
of depression at small effect size and change of maladaptive cognitive beliefs at strong effect
size. The data suggest that high initial scores of DAS or a less beneficial change (i.e. a
smaller reduction or a higher increase) of the DAS from t0 to t3 were associated with a less
beneficial change of depressive symptoms from t0 to t3. Models A2 and B2 could explain
additional 29% of the variance of data in comparison to model A1 and B1.
b β p
Partial cor-
relation
Step 1 Model A1
Constant 1.24 .412
Initial Status of HAMD (intercept) -0.39 -0.42 < .001 -.42
Step 2 Model A2
Constant 2.761 .140
Initial Status of HAMD (intercept) -0.59 -0.63 < .001 -.60
Initial Status of DAS (intercept) 0.02 0.19 .043 .22
Change of DAS (slope) 0.12 0.58 < .001 .59
Step 3 Model A3
Constant 0.40 .890
Initial Status of HAMD (intercept) -0.57 -0.61 < .001 -.60
Initial Status of DAS (intercept) 0.01 0.07 .507 .08
Change of DAS (slope) 0.10 0.50 < .001 .48
Initial Status of PB (intercept) -0.30 -0.28 .095 -.19
Change of PB (slope) -0.38 -0.28 .089 -.20
Initial Status of NB (intercept) 0.38 0.31 .057 .22
Change of NB (slope) 0.44 0.40 .015 .28
Initial Status of NFC (intercept) 0.18 0.17 .281 .13
Change of NFC (slope) 0.03 0.03 .870 .02
Note R² = .18, F = 17.74 (p <.001) for step 1; ∆R² = .29, F = 23.35 ( p < .001) for step 2, ∆R²
= .06, F = 9.37 ( p < .001) for step 3. HAMD = clinician-assessed depression, DAS = cog-
nitive maladaptive beliefs, PB = positive metacognitive beliefs, NB = negative metacogni-
tive beliefs, NFC = metacognitive beliefs about the need for control, b = unstandardized
regression coefficient, β = standardized regression coefficient.

Results
60
Table 13: Model B1-3: Predictors of change of depressive symptoms (outcome: change of
BDI (i.e. slope))
Models A3 and B3 additionally include the slopes and the intercepts of PB, NB and NFC as
possible predictors. In model A3, only initial status of depression, change of DAS and
change of NB had a significant effect on the outcome variable. A less beneficial change of
DAS and NB were associated with a less beneficial change of depressive symptoms with
strong (change of DAS) and medium (change of NB) effect sizes. In model B3, initial status
of depression, change of DAS, initial status and change of NB, as well as initial status and
change of NFC emerged as predictors of the change of depression. High initial scores of NB
and NFC predicted a less beneficial change of depressive symptoms at medium effect size,
a less beneficial change in scores of DAS, NB and NFC predicted a less beneficial change
of depressive symptoms at medium effect sizes. Model A3 could significantly account for
additional 6% of variance of data in comparison to model A2, model B3 could significantly
explain additional 15 % as compared to model B2. In total, model A3 could explain 53 % of
variance of data and model B3 74 %. An exchange of the order of block 2 and 3 did not
b
β
p
Partial corre-
lation
Step 1 Model B1
Constant 2.82 .192
Initial Status of BDI (intercept) -0.46 -0.55 <.001 -.55
Step 2 Model B2
Constant 0.03 .991
Initial Status of BDI (intercept) -0.63 -0.76 < .001 -.71
Initial Status of DAS (intercept) 0.07 0.29 .001 .35
Change of DAS (slope) 0.23 0.56 < .001 .64
Step 3 Model B3
Constant -13.6 .002
Initial Status of BDI (intercept) -0.6 -0.72 < .001 -,75
Initial Status of DAS (intercept) 0.03 0.13 .101 .19
Change of DAS (slope) 0.12 0.30 < .001 .40
Initial Status of PB (intercept) -0.12 -0.06 .654 -.05
Change of PB (slope) 0.17 0.06 .611 .06
Initial Status of NB (intercept) 0.74 0.31 .011 .29
Change of NB (slope) 0.93 0.42 .001 .38
Initial Status of NFC (intercept) 0.70 0.33 .007 .31
Change of NFC (slope) 0.73 0.31 .013 .28
Note R² = .30, F = 35.7 ( p < .001) for step 1; ∆R² = .29, F = 38.7 ( p < .001) for step 2 ∆R²
= .15, F = 24,01 ( p < .001) for step 3. BDI = self-assessed depression, DAS = cognitive
maladaptive beliefs, PB = positive metacognitive beliefs, NB = negative metacognitive be-
liefs, NFC = metacognitive beliefs about the need for control, b = unstandardized regression
coefficient, β = standardized regression coefficient.

Results
61
essentially alter results (for models A’ and B’, see Tables 18 and 19 in the appendix). Hy-
pothesis 3b could be confirmed.
4.6 Hypothesis 3c
Models A4 and B4 additionally include the presence of a critical life event between t2 and
t3 as last step in the hierarchical regression analysis (see Tables 14 and 15). In model A4
(HAMD), a critical life event could explain additional 9 % of the variance of data. The pres-
ence of a critical life event between t2 and t3 significantly predicted less change in depressive
symptoms from t0 to t3 at medium effect size (β > .3). In model B4 (BDI), presence of a
critical life event did not emerge as significant predictor of the change of depression. Hy-
pothesis 6 can partially be confirmed.
Table 14: Model A4: Predictors of change of depressive symptoms (outcome: change of
HAMD (i.e. slope))
b
β
p
Partial cor-
relation
Step 4 Model A4
Constant -.25 .942 Initial Status of HAMD (intercept) -.59 -.61 < .001 -.58 Initial Status of DAS (intercept) .00 .02 .874 .02 Change of DAS (slope) .09 .44 .004 .41 Initial Status of PB (intercept) -.08 -.07 .722 -.05 Change of PB (slope) -.06 -.04 .840 -.03 Initial Status of NB (intercept) .02 .02 .924 .01 Change of NB (slope) .15 .14 .495 .10 Initial Status of NFC (intercept) .34 .31 .095 .24 Change of NFC (slope) -.03 -.02 .900 -.02 Presence of a Critical life event 3.37 .37 .004 .41
Note ∆R² = .09, F = 5.86 ( p =.004) for step 4; DAS = cognitive maladaptive beliefs, PB = positive metacognitive beliefs, NB = negative metacognitive beliefs, NFC = metacognitive beliefs about the need for control, b = unstandardized regression coefficient, β = standardized regression coefficient

Results
62
Table 15: Model A4 Predictors of change of depressive symptoms (outcome: change of BDI
(i.e. slope)
4.7 Hypothesis 4
Two measures were used to estimate stability: the standardized within-group effect size d
and the test-retest correlation from t0 to t3 r for each construct respectively. The results are
presented in Table 1. BDI, DAS, PB, and NFC showed significant positive test-retest corre-
lations at medium (PB) to large (BDI, DAS, NFC) effect sizes. This means that the mean
scores of BDI, DAS, PB, and NFC changed in the same way between t0 and t3.
The d-scores of HAMD, BDI, and DAS were numerically higher than the d-scores
of PB, NB and NFC, with the d-score of PB being the lowest. As high d values suggest
higher changes in mean scores than low d values, the results suggested that mean change
over 3.5 years of HAMD, BDI and DAS were higher than mean change over 3,5 years of
PB, NB and NFC. Hence, metacognitive maladaptive beliefs, particularly PB, appeared to
be more stable in long-term course than depressive symptoms and cognitive maladaptive
beliefs and hypothesis 5 could partially be confirmed.
b
β
p
Partial corre-
lation
Step 4 Model B4
Constant -14.38 .003 Initial Status of BDI (intercept) -.51 -.68 < .001 -.73 Initial Status of DAS (intercept) .01 .03 .708 .06 Change of DAS (slope) .10 .25 .017 .34 Initial Status of PB (intercept) .12 .05 .704 .06 Change of PB (slope) .16 .06 .671 .06 Initial Status of NB (intercept) .72 .32 .036 .30 Change of NB (slope) .82 .40 .009 .37 Initial Status of NFC (intercept) .69 .32 .017 .34 Change of NFC (slope) .86 .34 .013 .35
Presence of a Critical life event .26 .01 .869 .02
Note ∆R² = .00, F = 16.03 ( p < .001) for step 4; BDI = self-assessed depression, PB = positive metacognitive beliefs, NB = negative metacognitive beliefs, NFC = metacognitive beliefs about the need for control, b = unstandardized regression coefficient, β = standardized regression coefficient

Results
63
Table 16: Relative stability of the different constructs as measured by within-group effect
size d and test-retest correlation r
HAMD BDI DAS PB NB NFC
d 1.16 1.08 1.01 0.31 0.73 0.60
r t0 t3 .20 .40** .48** .27* .13 .37**
Note Significant correlations (2-tailed) are flagged: ** = p < .01; * = p < .05, HAMD = clinician-assessed depression, BDI = self-assessed depression, DAS = cognitive mala-daptive beliefs, PB = positive metacognitive beliefs, NB = negative metacognitive be-liefs, NFC = metacognitive beliefs about the need for control, diff t0t3 = Difference score between t0 and t3.

Discussion
64
5. Discussion
5.1 Summary of the aims and results of the study
The current study examined the role of cognitive and metacognitive maladaptive beliefs in
depression. It aimed at understanding the effect of cognitive versus metacognitive maladap-
tive beliefs on the long-term course of depressive symptoms using a latent growth model
approach. Cognitive maladaptive beliefs concern primarily the content of beliefs whereas
metacognitive maladaptive beliefs are roughly defined as thoughts about functions and con-
sequences of one’s own thinking. I assumed firstly that results concerning the long-term
course of depression regarding recurrence (about 70 - 90 % in literature, see 2.1.3) can be
replicated in this study. Furthermore, I hypothesised that initial status and change of meta-
cognitive maladaptive beliefs explain additional variance of the data in the prediction of
depressive symptoms above and beyond cognitive maladaptive beliefs. I also supposed that
change of depression could be predicted by a stressful life event that had occurred between
the 6 months and the 3.5 years follow-up assessment. I finally conjectured that metacognitive
maladaptive beliefs are more stable than depressive symptoms and more stable than cogni-
tive maladaptive beliefs and that they constitute a vulnerability factor for depression.
Regarding the long-term course of depression, at 3.5 years follow-up, 78 % of the
participants met criteria for a recurrent depressive disorder. Across all testing times, depres-
sive symptoms, cognitive and metacognitive maladaptive beliefs significantly decreased.
The change of depressive symptoms from baseline to 3.5 years follow-up assessment was
positively correlated with a change of cognitive and metacognitive maladaptive beliefs. Re-
gression analyses showed that out of the alleged risk factors and predictors, initial status of
depression, change of cognitive maladaptive beliefs and change of negative metacognitive
beliefs had a significant effect on the change of clinician-assessed symptom severity of de-
pression (primary outcome parameter, HAMD) with strong (change of DAS) and medium
(change of negative metacognitive beliefs) effect sizes. The final model could account for
53 % of the variance of the data. When repeating the analysis with the change of self-as-
sessed symptom severity of depression (secondary outcome parameter, BDI), the initial
scores of negative metacognitive beliefs and metacognitive beliefs about the need for con-
trol, as well as the change in cognitive maladaptive beliefs, in negative metacognitive beliefs,
and in metacognitive beliefs about the need for control predicted a less beneficial change of
depressive symptoms at medium effect sizes. This model could explain 74 % of variance of
data. Presence of a critical life event as a predictor of depression could be confirmed when

Discussion
65
analysis was conducted using HAMD, but not for BDI. Finally, our data showed that meta-
cognitive maladaptive beliefs, especially positive metacognitive beliefs, followed by nega-
tive metacognitive beliefs, and metacognitive beliefs about the need for control, appear to
be more stable in long-term course than depressive symptoms and cognitive maladaptive
beliefs.
5.2 Discussion of results concerning the long-term course of depression
Concerning the long-term recurrence rates, our results matched findings concerning recur-
rence in patients with a former history of depression (Eaton et al., 2008; Katon et al., 2001).
In our sample, only 46 % of the patients were estimated to be in remission according to the
HAMD at 3.5 years follow-up assessment. The high recurrence and low remission rate might
be due to the special sample structure examined in this study. The sample was composed of
patients in a psychosomatic clinic of whom more than half of the participants were already
diagnosed with a recurrent disorder at intake with 3 prior depressive episodes on average
and mean illness duration of 8 years. The probability of recurrence increases with each de-
pressive episode, with 50-65 % of the patients suffering a second episode after the first and
70-80 % of the patients who suffered a second episode suffering a third (Eaton et al., 2008;
Katon et al., 2001). Risk of recurrence increases by 16% for each successive depressive
episode (Solomon et al., 2000). For that reason, our sample was at high risk of recurrence
and the recurrence rate corresponds to the rate indicated in literature for individuals who had
already suffered two episodes. This could indicate that our findings cannot be transferred to
non-clinical samples without precaution, but our results should be valid for clinical samples
and individuals with former history of depression. As chronicity and recurrence is one of the
major problems of depression, our results can give valuable information about individuals
with courses of chronic depression. Also, our findings confirm the known fact that depres-
sion is a highly recurrent disorder and highlight the need to recognize and to treat depression
early in order to prevent severity and chronicity of depression.
Concerning comorbidities, our data match previous findings with 51 % of the patients
suffering a comorbid axis-one disorder at baseline assessment (as compared to 64 % in Kess-
ler et al., 2003), with anxiety disorders being the most frequent (in line with Kessler et al.,
2003).

Discussion
66
5.3 Predicting the change of depression through cognitive and metacognitive
maladaptive beliefs
In the regression analyses, out of the alleged predictors (gender, age, former history of de-
pression), only initial status of depression emerged as significant predictors of the change of
self- (HAMD) and clinician-assessed (BDI) symptom severity and was entered in the final
models as control variable. Models A1-4 used change of HAMD as primary outcome varia-
ble, while models B1-4 employed BDI as secondary outcome variable. In model A2 and B2,
initial status and change of maladaptive cognitive beliefs emerged as significant predictors
of the change of depression at high (change of cognitive maladaptive beliefs) and low (initial
status of cognitive maladaptive beliefs) effect sizes. High initial scores of cognitive mala-
daptive beliefs or low change of cognitive maladaptive beliefs from baseline to 3.5 years
follow-up assessment were associated with a low change of depressive symptoms. Model
A2 and B2 could explain additional 29% of variance. Inclusion of initial status and change
of positive metacognitive beliefs, negative metacognitive beliefs and metacognitive beliefs
about the need for control as possible predictors accounted for additional 6 % (model A3) or
15 % (model B3) of variance of data. In model A3, initial status of depression, change of
cognitive maladaptive beliefs, and change of negative metacognitive beliefs had a significant
effect on the outcome variable with strong (change of cognitive maladaptive beliefs) and
medium (change of negative metacognitive beliefs) effect sizes. In model B3, initial scores
of negative metacognitive beliefs and metacognitive beliefs about the need for control as
well as small change in cognitive maladaptive beliefs, negative metacognitive beliefs, and
metacognitive beliefs about the need for control predicted a less beneficial change (i.e. a
smaller reduction or a higher increase) of depressive symptoms at medium effect sizes. The
final model A3 could explain 53 % of variance of data and model B3 74 %.
5.3.1 Cognitive maladaptive beliefs
In terms of cognitive maladaptive beliefs in depression, our findings are in line with results
from various studies. When only initial status of depression, initial status and change of
cognitive maladaptive beliefs was integrated in the regression model (Model A2 and B2),
high initial status and less beneficial change in cognitive maladaptive beliefs predicted a less
beneficial change of depressive symptoms. Hence, the presence of cognitive maladaptive
beliefs appeared to contribute to depressive symptom severity. Prior studies confirmed that
the initial score of cognitive maladaptive beliefs is a vulnerability factor for the onset, recur-
rence, and severity of depression (Alloy et al., 2006; Iacoviello et al., 2006; Otto et al., 2007;

Discussion
67
Struijs et al., 2013). The fact that in the final models A3 and B3, only the change of cognitive
maladaptive beliefs emerged as predictor of the change of depression, while initial status of
DAS did not, is largely in line with findings from Beevers et al. (2003). They found that a
low reduction of maladaptive cognitive beliefs predicted shorter periods of time until relapse
in depression, while the total score of DAS did not. In combination with our finding, this
could mean that change in maladaptive cognitive beliefs is more important in the long-term
course of depression than initial scores. Thus, ongoing evaluation of maladaptive cognitive
beliefs during therapy as well as monitoring the targeted decrease is vital in the therapy of
depression.
5.3.2 Metacognitive maladaptive beliefs
Regarding metacognitive maladaptive beliefs, our results partly confirm prior findings, but
indicate that some assumptions may need to be revisited. First, the implementation of nega-
tive metacognitive beliefs and metacognitive beliefs about the need for control in the regres-
sion model could significantly explain an additional variance of the data (∆R² = .06 in model
A3 and ∆R² = .15 in model B3) in comparisons to models that only included initial status
and change of cognitive maladaptive beliefs. This suggests that metacognitive maladaptive
beliefs are not redundant with maladaptive cognitive beliefs and should be considered in the
theoretical background of depression. Thus, our findings can confirm the explanatory power
of metacognitive maladaptive beliefs in depression assumed by different cross-sectional
(Huntley & Fisher, 2016; Papageorgiou & Wells, 2003b; Roelofs et al., 2007; Tajrishi et al.,
2011, Yilmaz et al, 2015; Solem et al., 2016;) and one longitudinal study (Ruiz & Odriozola-
Gonzalez, 2015). Yilmaz et al. (2015) concluded that metacognitive maladaptive beliefs are
a better predictor of depression than cognitive maladaptive beliefs. In contrast, our data do
not confirm this conclusion, because in all models, integration of cognitive maladaptive be-
liefs explained more additional variance than integration of positive metacognitive beliefs,
negative metacognitive beliefs and metacognitive beliefs about the need for control, also
when swapping the order of the different steps in the regression analyses. For that reason,
our data indicates that although initial status and change of negative metacognitive beliefs
and metacognitive beliefs about the need for control are predictors of depression, the im-
portance of maladaptive cognitive beliefs in the course of depression could be confirmed.
Results can be discussed in the light of the different categories of metacognitive mal-
adaptive beliefs. Before discussing the results, it has to be remarked that in this study, sub-
scales of MCQ-30 were employed that are not fully congruent with PBRS and NBRS, often

Discussion
68
used in the cited studies (for example Papageorgiou & Wells, 2009; Roelofs et al., 2007;
Solem et al., 2016; Yilmaz et al., 2015) . This could limit the comparability of the results.
Nevertheless, as Roelofs et al. (2010) concluded that NBRS with positive metacognitive
beliefs and NBRS with negative metacognitive beliefs and metacognitive beliefs about the
need for control show construct validity, sufficient comparability of the different results can
be assumed.
Positive metacognitive beliefs have been considered to play an important role in the
onset of depression and several investigations support this hypothesis ( Weber & Exner,
2013; Halvorsen et al., 2015; Huntley & Fisher, 2016). In our study, however, neither initial
status nor change of positive metacognitive beliefs emerged as significant predictors of the
change of depression. When analysing and comparing the results with the literature in more
detail, this apparent incongruity can be explained. First, whereas Halvorsen et al. (2015)
identified positive metacognitive beliefs as a factor discriminating depressed from non-de-
pressed individuals, among the significant factors it was the least correlated. This is in ac-
cordance with our findings where change of positive beliefs was significantly correlated with
the change of BDI, but it was not significantly correlated with the change of HAMD. Second,
while discussing the results, it has to be considered that Weber and Exner (2013) and Huntley
and Fisher (2016) conducted their studies with non-clinical samples. They both found that
positive metacognitive beliefs had an indirect effect on depressive symptoms via rumination.
Nevertheless, as the Papageorgiou and Wells (2003b) study illustrates, findings can diverge
in clinical and non-clinical samples. For that reason, our results should preferentially be dis-
cussed in reference to studies that investigated clinical samples. Indeed, different studies are
available that investigated the relation between metacognitive beliefs, rumination and de-
pressive symptoms in clinical samples (Papageorgiou & Wells, 2003b; Roelofs et al., 2007).
In those clinical studies, instead of positive metacognitive beliefs, negative metacognitive
beliefs constituted the link between rumination and depressive symptoms. From this obser-
vation could follow that in clinical samples, negative metacognitive beliefs are more closely
linked to depression than positive metacognitive beliefs. This is consistent with our findings,
where neither initial status nor change of positive metacognitive beliefs emerged as predic-
tors of the change of depression. Moreover, in agreement with our results, negative meta-
cognitive beliefs emerged in several studies as predictors of depression. Two longitudinal
studies with non-clinical samples found negative metacognitive beliefs to be a predictor of
the course of depression (Papageorgiou & Wells, 2009; Yılmaz et al., 2011). Negative met-

Discussion
69
acognitive beliefs also emerged in one cross-sectional study with a clinical sample as dis-
criminating depressive and non-depressed individuals and was judged to be a vulnerability
factor for depression (Halvorsen et al., 2015). Thus, our data confirm the relevance of neg-
ative metacognitive beliefs in depression in a clinical sample with longitudinal study design.
Eventually, it has to be noted that our study is the only that investigated a clinical sample in
a longitudinal setting so that the interpretation and comparison of the cited studies is faced
to some restrictions that I tried to consider.
With regard to metacognitive beliefs about the need for control, in our sample, their
initial status and change predicted a change of depression only when analyses were per-
formed with BDI, but not with HAMD. Hence, the results concerning metacognitive beliefs
about the need for control are not fully conclusive. It is possible that the results were affected
by the modality of the administration of the measures, showing stronger associations when
the predictor and the outcome variable are both self-rated instruments (MCQ and BDI). In
addition, HAMD has been suggested to measure rather vegetative symptoms of depression
and to underrepresent cognitive symptoms, as worthlessness, hopelessness, and helpless-
ness, are not investigated (Zimmerman, Posternak, & Chelminski, 2005). BDI seems better
to address cognitive symptoms of depression: in a meta-analysis concerning the factor struc-
ture of BDI, it was presented that “negative attitudes” usually emerge as one of three highly
interrelated factors (Beck et al., 1988). This could also account for the greater explanation
of variance that was found when the regression analyses where computed with BDI. Our
results concerning beliefs about the need for control in relation to self-rated depressive symp-
toms are corroborated by findings from Halvorsen et al. (2015), were metacognitive mala-
daptive beliefs about the need for control were a constituent factor of a function discriminat-
ing never depressed, previously depressed and currently depressed individuals. Hence, de-
spite the discrepancy between our results with HAMD and BDI as outcome variable, the
results with BDI should be acknowledged and suggest that metacognitive beliefs about the
need for control do play a role in depression.
5.3.3 Further implications
Our results allow drawing some cautious conclusions regarding the aetiology of depression,
in particularly regarding the metacognitive model of depression (Wells & Schweiger, 2011),
while acknowledging that those conclusions cannot be but preliminary, as not all pathways
of the model have explicitly been tested. Positive metacognitive beliefs constitute an integral
part of the metacognitive model of depression which presumes that when triggered with sad

Discussion
70
mood, an individual is likely to react at first with positive metacognitive beliefs which, in
turn, could lead via rumination and negative metacognitive beliefs to depression (Wells
& Schweiger, 2011). This model assigns thus a predominant importance to both positive and
negative metacognitive beliefs, because it supposes that positive metacognitive beliefs lead
to unhelpful coping strategies while negative metacognitive beliefs entail beliefs about the
“uncontrollability of rumination and the meaning of depression” (Wells et al., 2012; Yilmaz
et al., 2015). The findings as discussed above could challenge the role of positive metacog-
nitive beliefs in the metacognitive model of depression, as neither initial status nor change
of positive metacognitive beliefs predicted depressive symptoms. While we could confirm
the importance of negative metacognitive beliefs and metacognitive beliefs about the need
for control in a longitudinal long-term study design with a clinical sample, our data could
not confirm the role of positive metacognitive beliefs in the onset, recurrence and mainte-
nance of depression as supposed by the metacognitive model. To conclude, our data suggest
that metacognitions do play an important role in the aetiology of depression, although it
seems that negative metacognitive beliefs and metacognitive beliefs about the need for con-
trol could be more important in clinical samples than positive metacognitive beliefs.
5.4 The cognitive vulnerability model of depression
This study moreover examined the relative stability of cognitive and metacognitive mala-
daptive beliefs in the long-term course of depression. Positive metacognitive beliefs seemed
to be the most stable, followed by negative metacognitive beliefs and metacognitive beliefs
about the need for control. Cognitive maladaptive beliefs seemed to be as stable as depres-
sive symptoms, both also significantly decreasing across all testing times. This suggests that
cognitive maladaptive beliefs might partly be concomitants of depression. Zuroff et al.
(1999), Beevers and Miller (2004) and Hankin (2008) all concluded that cognitive maladap-
tive beliefs might be state-dependent, while showing trait-like characteristics at the same
time. As I only examined relative stability, which is to say stability in relation to other meas-
ured constructs, our findings do not refute the thesis that cognitive maladaptive beliefs might
have trait characteristics, though our data can’t confirm it. But our data suggest that cognitive
maladaptive beliefs are less stable than metacognitive maladaptive beliefs. Until now, to the
best of our knowledge, no other studies have investigated the stability of metacognitive mal-
adaptive beliefs in a longitudinal study design. Our data lead to the conclusion that metacog-
nitive maladaptive beliefs might expose trait characteristics and that they might constitute
an important underlying vulnerability factor for depression. This hypothesis is in line with

Discussion
71
Halvorsen et al. (2015) who found in their cross-sectional comparison of never depressed,
previously depressed and currently depressed individuals that negative metacognitive beliefs
might have trait characteristics rendering individuals susceptible to depression or, alterna-
tively, that negative metacognitive beliefs might produce scar effects which make individu-
als who have experienced a depressive episode vulnerable to relapse.
The presence of a critical life event emerged as a predictor of the change of depres-
sive symptoms when introduced as last step in the regression model using HAMD. Our data
suggest that critical life events can provoke depression in individuals vulnerable for depres-
sion. The vulnerability hypothesis in terms of cognitive vulnerability because of cognitive
maladaptive beliefs is supported by findings from Struijs et al. (2013) and Scher et al. (2005).
To my knowledge, metacognitive maladaptive beliefs have not yet been examined as vul-
nerability factors in combination with critical life events. Our findings indicate that not only
cognitive maladaptive beliefs, but also metacognitive maladaptive beliefs (most notably neg-
ative metacognitive beliefs and metacognitive beliefs about the need for control) contribute
to cognitive vulnerability for depression. As limitation, the effect could not be reproduced
when using BDI. For that reason, and as the period between the critical life event and as-
sessment of depression could extend up to three years due to our study design, it seems
necessary to deepen vulnerability research in this regard. Taken together, the results show
that more research should be devoted to the issue of metacognitive maladaptive beliefs as
vulnerability factors for depression.
To conclude, our data are compatible with a vulnerability-stress model of depression
which includes cognitive as well as metacognitive maladaptive beliefs as vulnerability fac-
tors. Our findings are consistent with the idea of stable underlying cognitive assumptions
about the own thinking that, when triggered by a negative life event, lead to depressive
symptoms via cognitive maladaptive beliefs.
5.5 Limitations and strengths of the study
When interpreting the results, some limitations and strengths of the study should be kept in
mind. First, good to satisfying completion rates of the participants should be mentioned. The
response rate was very good at post (94 %) and satisfying at both follow-up assessments
(71% for t2 and t3). In comparable studies, return quote were of 82 % after three months
(Papageorgiou & Wells, 2009), 37% after nine months (Ruiz & Odriozola-Gonzalez, 2015),
77 % after nine years (Halvorsen, Wang, Eisemann, & Waterloo, 2010). Moreover, all parts
of the study were registered at trial register data-bases (German Clinical Trials Register for

Discussion
72
t0 to t2; ClinicalTrials.gov for t3). Registration contributes to increased transparency and
better access to clinical trials. As another strength of the study, the long investigation period
of 3,5 years has to be mentioned, since only few studies considering maladaptive metacog-
nitive beliefs in the long-term course of depression have been presented (Papageorgiou
& Wells, 2009; Ruiz & Odriozola-Gonzalez, 2015; Weber & Exner, 2013; Yılmaz et al.,
2011), of which none examined a clinical sample. However, the long interval of three years
without follow-up between 6 months and 3.5 years follow-up also could count as limiting
factor, although the course of depression, therapeutic interventions, critical life events and
stays in psychiatric departments between the two assessments were retrieved at 3.5 years
follow-up via a semi-structural interview. Since remission is defined by the APA (2013) as
a period of at least two consecutive months during which complete diagnostic criteria of a
major depressive episode have not been met, the choice of the follow-up intervals made it
impossible to assess remission at 3.5 years follow-up according to the official guidelines.
Consistent with other studies (see for example Zimmerman et al., 2012), HAMD score at 3.5
years follow-up was used to define remission which can be judged as satisfying.
Regarding the employed instruments, the study also has several strengths, though it
is not without limitations. The psychopathological status was investigated in detail at base-
line, using with M.I.N.I a highly standardized procedure, and examining not only depression,
but also other achsis-1 comorbidities. Furthermore, use of HAMD and BDI allowed for self-
assessment as well as external assessment of the severity of depressive symptoms. Use of
the HAMD as primary outcome measure could restrict findings. Though, the HAMD has
been criticized for poor interrater-reliability at individual item level, heterogeneity of item
description, overestimation of physical items and incomplete coverage of the symptom cri-
teria used to define major depression by the DSM-IV, such as worthlessness, indecisiveness
and concentration problems (Zimmerman et al., 2005). Still, as mainly one examiner con-
ducted the interviews at 3.5 years follow-up, the problem of poor interrater-reliability did
not occur at the long-term follow-up. Also, as mentioned, with BDI, a second measure of
depression was employed, balancing this limitation. Furthermore, the fact that only three
subscales of MCQ-30 were investigated could limit findings, even if the employed subscales
were reported to be closely linked to depression (Ruiz & Odriozola-Gonzalez, 2015; see
1.2.3.2). Because of the unclear role and status of metacognitive maladaptive beliefs in de-
pression, assessment of the subscales “cognitive confidence” and “cognitive self-conscious-
ness” could have been adequate for clarification. Furthermore, as rumination was found to
mediate the relation between positive metacognitive beliefs and depressive symptoms in

Discussion
73
non-clinical samples (Weber & Exner, 2013) and between negative metacognitive beliefs
and depressive symptoms in clinical samples (Papageorgiou & Wells, 2003b; Roelofs et al.,
2007), it seems to be disadvantageous that no instrument measuring rumination, such as
Ruminative Response Scale (RRS), was integrated in the study.
Finally, some particularities of the chosen sample have to be taken into account. First,
with mean HAMD 10.9 (SD = 7.9) and BDI of 17.49 (SD = 11.68) at inclusion assessment,
the sample seemed to show only mild depression which could imply that generalization to
more severely depressed individuals could be problematic. But, on the other hand, at intake,
patients had on average already suffered 3 depressive episodes with mean illness duration of
96 months. At long-term follow-up, 78% the collective were diagnosed with a recurrent de-
pression and 22% with a double depression, indicating the prevalence of chronic courses of
depression in our sample. Also, the fact that at long-term follow-up, out of 58, 60 % of the
patients (n=35) had underwent between 6 months and and 3.5 years follow-up or currently
followed outpatient psychotherapies and that 41 % of the patients (n=34) underwent current
antidepressant pharmacotherapy could explain the mean low scores in depression scales. In
addition, it has to be kept in mind that out of the 35 patients who underwent a psychotherapy,
54 % (n=19) followed a cognitive behavioural therapy (CBT) which is supposed to target
cognitive maladaptive beliefs, whereas metacognitive maladaptive beliefs are often not ad-
dressed in CBT. This fact could distort our results concerning the stability of cognitive and
metacognitive maladaptive beliefs. Nevertheless, it is ethically not justifiable to only assess
untreated depressed patients, so that limitations of that kind have to be accepted.
In terms of the data analysis, use of latent growths models (LGMs) can be judged as
another strength of the study. LGMs are established as statistical models used to analyse
univariate curves of longitudinal data (Muniz-Terrera et al., 2017). The analysis permits
flexible examination of change processes over time (Schmiedek & Wolff, 2010). As LGMs
are formulated under the structural equation model (SEM) frame, they can be utilized to
implement multivariate change processes and to establish relationships between them. More-
over, they are appropriate to test causal hypotheses via path models (Schmiedek & Wolff,
2010). With LGMs, mean as well as subject-specific trajectories can be estimated where
time invariant and time variant covariates may be included (Muniz-Terrera et al., 2017).
Also, LGMs allow for analyses of incomplete data, as analysis is not restricted to complete
cases, but all cases with data from at least one measure time can be included (Schmiedek
& Wolff, 2010).

Discussion
74
5.6 Conclusions, further research requests and implications for clinical praxis
Cognitive maladaptive beliefs are considered as confirmed vulnerability factors for depres-
sion and are integrated in aetiological models of depression. More recent findings suggest
that metacognitive maladaptive beliefs might in addition to or instead of cognitive maladap-
tive beliefs play an important role in the onset, maintenance, and recurrence of depression.
This study aimed to investigate the role of cognitive and metacognitive maladaptive beliefs
(positive metacognitive beliefs, negative metacognitive beliefs, and metacognitive beliefs
about the need for control) in the long-term course of depression. The results suggest that
maladaptive cognitive beliefs, negative metacognitive beliefs, and metacognitive beliefs
about the need for control, particularly their change, all significantly predict the change of
depressive symptom severity. Furthermore, metacognitive maladaptive beliefs seemed to be
more stable than cognitive maladaptive beliefs. Our data suggests that they could, besides
cognitive maladaptive beliefs, contribute to cognitive vulnerability for depression. As nega-
tive metacognitive beliefs and beliefs about the need for control explain additional variance
of the change of depressive symptoms, it seems necessary to implement these constructs in
the cognitive model of depression.
Nevertheless, the investigations concerning metacognitive maladaptive beliefs is fac-
ing serious problems because the term is not consistently used (Semerari et al., 2012). Defi-
nitions range from rather broad definitions as “thinking about one’s own thinking” (Moritz
et al., 2013, p. 359) to complex constructs subsuming different subtypes of metacognition
and implying different cognitive functions and cognitions about those functions (Wells,
2001). As outlined in the introduction (see 3.3.5), the concept of metacognition on which
this study is based, draws on the broad definition given by Flavell and Wellman (1977).
More precisely, metacognitive maladaptive beliefs assumed to be relevant in depression are
defined through the instruments used to assess them (see 2.3.5 Metacognitions Question-
naire 30). In this context, it has to be acknowledged that MCQ-30, MCQ65, PBRS and
NBRS, mainly employed to investigate metacognitive maladaptive beliefs in depression, are
not identical, even if the measured constructs overlap (for evaluation of MCQ-30 in com-
parison to MCQ65, see Wells & Cartwright-Hatton, 2004; for evaluation of PBRS and
NBRS in comparison to MCQ-30, see Roelofs et al., 2010). In line with Roelofs et al. (2010),
we may conclude that differences in results concerning the exact interplay of metacognitive
maladaptive beliefs and rumination in depression seem to be partly due to the differences of
the applied instruments. In addition, it is also possible that subscales of DAS and MCQ-30
partly measure the same constructs. When too many correlated variables are entered in a

Discussion
75
regression model, it becomes difficult to compare different predictors (Field, 2016). For that
reason, it could be necessary to investigate more profoundly inferences between DAS and
MCQ-30 before drawing final conclusions. In order to elucidate the exact role of the different
constructs, more research is warranted that illuminates the scope of the different instruments
and that elaborates a definition of metacognitive maladaptive beliefs which overlaps the dif-
ferent research approaches. Furthermore, research has suggested that metacognition is also
related to other constructs such as mindful attention awareness which has been suggested,
besides maladaptive metacognitions, to contribute to cognitive vulnerability (Solem et al.,
2015). This highlights the need to conduct more clinical studies that bring together different
constructs to create a complete model of the aetiology of depression. One attempt to integrate
different concepts has recently been proposed by Pedone et al. (2017) who suggest a model
integrating different theories such as theory of mind, metacognition and mentalization. Such
a model integrating and precisely defining distinct concepts that seem to be relevant in de-
pression would be very positive. The need for a clear concept of metacognition, metacogni-
tive processes and biases is reinforced by the emergence of a whole field of more experi-
mental research, dedicated for example to the link between physiological and metacognitive
processes (for example Capobianco, Morris, & Wells, 2018; Stange, Hamilton, Fresco, &
Alloy, 2017).
Depression is one of the most prevalent mental disorder world-wide and contributes
significantly to the burden of disease (World Health Organization, 2016). Early and effective
treatment of depression is crucial as it is known that longer and more sever episodes often
entail early relapses and reduce the likelihood of recovery (Keller et al., 1992). Although
different effective psychotherapeutic and pharmacologic therapies have been developed (for
an overview concerning the efficacy of different psychotherapies see Cuijpers, 2015), there
is still need to further improve established therapies. A study commissioned by the Bertels-
mann-Stiftung Germany found that in Germany, 50 % of patients with dysthymia, moderate
or severe depression received no or insufficient therapy (Bertelsmann Stiftung, 2014). But
even if therapy places were available for every patient, it is assumed that pharmacological
and psychotherapeutic therapies only would diminish about 30 % of the disease burden (An-
drews, Issakidis, Sanderson, Corry, & Lapsley, 2004) due to high drop-out rates (Swift &
Greenberg, 2012) and high recurrence probability (Eaton et al., 2008). This highlights that,
while so-called new wave therapies, such as Metacognitive Therapy as conceptualized by
Wells or Acceptance-And-Commitment-Therapy, seem, if at all, only slightly different from
established therapies such as CB-T in terms of efficacy (Cuijpers, 2015), there is need to

Discussion
76
ameliorate existing therapies. Our results support the idea that it could be beneficial for the
patients to implement strategies to modify metacognitive maladaptive beliefs in current ther-
apies. One example of this practice is the add-on therapy Metacognitive Training for De-
pression (D-MCT) which was developed by Jelinek, Hauschildt, and Moritz (2015) as group
intervention and which is fully compatible with CBT, while integrating a metacognitive
point of view. It yielded promising results in a feasibility study (Jelinek, Otte, Arlt, &
Hauschildt, 2013) and in a RCT with 6-months follow-up (Jelinek et al., 2016). Furthermore,
D-MCT also encountered high acceptance by patients (Jelinek, Moritz, & Hauschildt, 2017).
Also, depression is a frequent comorbidity that patients develop on the ground of
various medical condition (Kang et al., 2015). There is increasing evidence that metacogni-
tive maladaptive beliefs might contribute to distress or depression in Multiple Sklerosis
(Heffer-Rahn & Fisher, 2018), in Epilepsy (Fisher & Noble, 2017) and Diabetes (Purewal
& Fisher, 2018). Targeting metacognitive maladaptive beliefs in those medical conditions
might thus help to prevent comorbid depressive episodes. This is of vital importance, as
comorbid depression has been shown to impact the course of the diseases by deteriorating
quality of life, leading to increased impairment and a higher mortality (Kang et al., 2015).
To conclude, cognitive and metacognitive maladaptive beliefs play an important role
in onset, maintenance, and recurrence of depression. It seems vital to integrate the concept
of metacognitive maladaptive beliefs more stringently in therapeutic research and therapeu-
tic interventions.

Summary
77
6. Summary
Cognitive maladaptive beliefs (most commonly assessed using the Dysfunctional Attitudes
Scale [DAS]) have been shown to represent an important vulnerability factor in the onset,
relapse, and recurrence of depression. Besides, metacognitive maladaptive beliefs (as meas-
ured by the Metacognitive Questionnaire-30 [MCQ-30]) are also thought to contribute to
depression. However, the course and relationship of cognitive and metacognitive maladap-
tive beliefs in depressed individuals on the long-term has not been explored. Also, whereas
a extensive research concerning stability of cognitive maladaptive beliefs in depression has
been conducted, stability of metacognitive maladaptive beliefs has not been examined yet.
The aim of the present study was to investigate over a period of 3.5 years the role and sta-
bility of cognitive and metacognitive maladaptive beliefs in individuals with depression and
to elucidate whether cognitive or metacognitive maladaptive beliefs are a better predictor of
the course of depressive symptoms over this time span.
Eighty-four patients with depression were assessed with the DAS, three subscales of
the MCQ-30 (positive metacognitive beliefs, negative metacognitive beliefs, beliefs about
the need for control), the Hamilton Depression Rating Scale, and the Beck Depression In-
ventory at baseline and were reassessed after four weeks, 6 months and 3.5 years. Analyses
were carried using a longitudinal latent growth model approach.
Our data showed that change on the DAS and on the MCQ-30 subscale ‘negative
metacognitive beliefs’ significantly predicted the change in clinician-rated depressive symp-
tom severity over 3.5 years, and that change on the DAS and change and initial scores of the
MCQ-30 subscales ‘negative metacognitive beliefs’ and ‘need for control’ predicted change
in self-rated depressive symptom severity. Also, the presence of a critical life event signifi-
cantly predicted the change of clinician-rated depressive symptom severity. In all models,
maladaptive cognitive beliefs explained more additional variance than the MCQ-30 sub-
scales. In terms of stability, metacognitive maladaptive beliefs were more stable than cogni-
tive maladaptive beliefs.
Cognitive and metacognitive maladaptive beliefs were both predictors of depression,
with the DAS being a better predictor than the MCQ-30 subscales. As maladaptive meta-
cognitive beliefs were more stable than maladaptive cognitive beliefs, they should be con-
sidered an important underlying vulnerability factor for depression. In conclusion, both cog-
nitive and metacognitive maladaptive beliefs seem to contribute to depression and should be
considered as targets in the therapy of unipolar depression.

Summary
78
6. Zusammenfassung
Es konnte gezeigt werden, dass kognitive maladaptive Einstellungen (durch die Skala dys-
funktionaler Einstellungen [DAS] getestet), einen wichtigen Vulnerabilitätsfaktor für De-
pression darstellen. Daneben scheinen auch metakognitive maladaptive Einstellungen
(durch den Metakognitiven Fragebogen-30 [MCQ-30] getestet) zu Depression beizutragen.
Bisher wurde jedoch die Beziehung von kognitiven und metakognitiven maladaptiven Ein-
stellungen bei Personen mit Depression im Langzeitverlauf noch nicht untersucht. Während
bereits umfangreiche Forschung der Stabilität von kognitiven maladaptiven Einstellungen
gewidmet worden ist, wurde die Stabilität von metakognitiven maladaptiven Einstellungen
bislang noch nicht untersucht. Das Ziel der vorliegenden Studie war es, über einen Zeitraum
von 3.5 Jahren die Rolle und Stabilität von kognitiven und metakognitiven maladaptiven
Einstellungen bei depressiven Individuen zu untersuchen und zu klären, ob kognitive oder
metakognitive maladaptive Einstellungen einen besseren Prädiktor für den Verlauf depres-
siver Symptome darstellen.
Vierundachtzig Patient*innen mit Depression wurden bei Einschluss mittels der
DAS, drei Skalen des MCQ-30 (positive metakognitive Überzeugungen, negative metakog-
nitive Überzeugungen und Überzeugungen über das Bedürfnis nach Kontrolle), der Hamil-
ton Depression Skala und dem Beck-Depressions-Inventar untersucht. Follow-Up-Untersu-
chungen erfolgten nach vier Wochen, nach sechs Monaten und nach dreieinhalb Jahren. Die
Analysen wurden mithilfe eines latenten Wachstumsmodells ausgewertet.
Die Daten zeigten, dass eine Veränderung im DAS und in negativen metakognitiven
Überzeugungen signifikant die Veränderung in den durch eine*n Kliniker*in bewerteten de-
pressiven Symptome vorhersagte, und dass eine Veränderung im DAS und initialer Wert
und Veränderung in zwei MCQ-Subskalen den Verlauf der selbst-bewerteten depressiven
Symptome vorhersagten. Das Vorhandensein eines kritischen Lebensereignisses sagte de-
pressive Symptome voraus. In allen Modellen erklärten maladaptive kognitive Einstellungen
mehr Varianz als die MCQ-30 Subskalen. In Bezug auf die Stabilität zeigten sich metakog-
nitive maladaptive Einstellungen stabiler als kognitive maladaptive Einstellungen.
Sowohl kognitive als auch metakognitive maladaptive Einstellungen sagten den Ver-
lauf depressiver Symptome voraus, die DAS war dabei ein besserer Prädiktor als die MCQ-
30 Subskalen. Da metakognitive maladaptive Einstellungen stabiler als kognitive maladap-
tive Einstellungen waren, sollten sie als ein wichtiger zugrunde liegender Vulnerabilitäts-
faktor für Depression gewertet werden, deren Veränderung neben der kognitiver maladapti-
ver Einstellungen ein Ziel in der Therapie unipolarer Depression darstellen könnte.

Publication
79
7. Publication
Die Publikation ist nicht in der E-Dissertation enthalten. Sie ist verfügbar unter:
Faissner M, Kriston L, Moritz S, Jelinek L. Course and stability of cognitive and metacog-
nitive beliefs in depression. Depress Anxiety. 2018;1–8. https://doi.org/10.1002/da.22834.

Publication
80
Publication
81

Publication
82

Publication
83

Publication
84

Publication
85

Publication
86

List of Abbreviations
87
8. List of Abbreviations
AAQ-II Acceptance and Action Questionnaire – II
ACSQ Adolescent Cognitive Style Questionnaire
APA American Psychiatric Association
ASQ Attributional Style Questionnaire
BAI The Beck Anxiety Inventory
BDI Beck Depression Inventory, First Edition
BDI-II Beck Depression Inventory, Second Edition
CAS Cognitive attentional syndrome
CBT Cognitive Behavioural Therapy
CBQ Cognitive Bias Questionnaire
CC Cognitive Confidence
CDAS Children’s Dysfunctional Attitudes Scale
CDI Children’s Depression Inventory
CIDI Composite International Diagnostic Interview
CRSQ Children’s Response Styles Questionnaire
CSC Cognitive self-consciousness
CSQ Cognitive Style Questionnaire
CQ Cognitions Questionnaire
DAS Dysfunctional Attitude Scale
DAS-R Dysfunctional Attitude Scale – Revised
DASS-21 Depression subscale of the Depression Anxiety and Stress Scales-21
DAS-24 Dysfunctional Attitude Scale-24
D-MCT Metacognitive Training for Depression
DSS Depressive Schemas Scale
GHQ-28 General Health Questionnaire
GP General practitioner
H Hypothesis
HADS Hospital Anxiety And Depression Scale

List of Abbreviations
88
HAMD Hamilton Depression Rating Scale
HT Health Training
IAT Implicit Associations Test
ICSRLE Inventory of College Students’ Recent life Experiences
IDD Inventory to Diagnose Depression
IDSC Inventory for Depressive Symptomatology, Clinician Version
IDS-SR Inventory of Depression Symptomatology – Self Report
ISDA Implicit self-depressed associations
LEIDS-r Leiden Index of Depression Sensitivity – revised
LES Life Experience Survey
LIFE-PSR Longitudinal Interval Follow-up Evaluation-Psychiatric Status Ratings
LTE List of Threatening Experiences
M Mean
MCQ-30 Metacognitions Questionnaire-30
MDE Major Depressive Episode
MHRSD Modified Hamilton Rating Scale for Depression
M.I.N.I Mini International Neuropsychiatric Interview
MSGO Miskimins Self-Goal Other Discrepancy Scale
NB Negative metacognitive beliefs concerning uncontrollabil-ity, danger and negative consequences of rumination
NBRS1 Negative Beliefs about Rumination Scale: uncontrollability and harm
NBRS2 Negative Beliefs about Rumination Scale: Social and inter-personal consequences of ruminating
NEO-FFI Neo five-factor inventory
NFC Metacognitive beliefs about the need for control
PB Positive metacognitive beliefs about worry and rumination
PBRS Positive Beliefs about Rumination Scale
PSI Problem Solving Inventory

List of Abbreviations
89
PSS Perceived Stress Scale
PSWQ Penn State Worry Questionnaire
QIDS Quick Inventory of Depressive Symptomatology
RCT Randomized Controlled Study
RRS Ruminative Response Scale
RSQ Rumination response scale
SADS–L Schedule for Affective Disorders and Schizophrenia—Lifetime
SADS-C Schedule for Affective Disorder and Schizophrenia- Change Version
SBQ-R Suicide Behaviours Questionnaire-Revised
SCID Structured Clinical Interview for DSM–IV Axis I Disor-ders
SD Standard Deviation
SDS Self-rating Depression Scale
SEF Self-Efficacy Scale
SEM Structural Equation Model
S-REF Self-Regulatory Executive Function
TCQ Thought Control Questionnaire
VAS Visual Analog Scale
VIF Variance Indicator Factor
WHO Word Health Organisation
YSQ
Young Schema Questionnaire

References
90
9. References
Alloy, L. B., Abramson, L. Y., Whitehouse, W. G., Hogan, M. E., Panzarella, C., & Rose,
D. T. (2006). Prospective incidence of first onsets and recurrences of depression in indi-
viduals at high and low cognitive risk for depression. Journal of Abnormal Psychology,
115(1), 145–156. https://doi.org/10.1037/0021-843X.115.1.145
Andrews, G., Issakidis, C., Sanderson, K., Corry, J., & Lapsley, H. (2004). Utilising survey
data to inform public policy: Comparison of the cost-effectiveness of treatment of ten
mental disorders. The British Journal of Psychiatry : the Journal of Mental Science,
184(6), 526–533. https://doi.org/10.1192/bjp.184.6.526
APA. (2005). Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition (DSM-
IV) (4th ed.). Washington, DC: American Psychiatric Association.
APA. (2013). Diagnostic and statistical manual of mental disorders: DSM-5 (5. ed.). Wash-
ington, DC: American Psychiatric Publ.
Arborelius, L., Owens, M. J., Plotsky, P. M., & Nemeroff, C. B. (1999). The role of cortico-
tropin-releasing factor in depression and anxiety disorders. The Journal of Endocrinol-
ogy, 160(1), 1–12.
Aydin, O., Balikci, K., Tas, C., Aydin, P. U., Danaci, A. E., Brüne, M., & Lysaker, P. H.
(2016). The developmental origins of metacognitive deficits in schizophrenia. Psychiatry
Research, 245, 15–21. https://doi.org/10.1016/j.psychres.2016.08.012
Bagby, R. M., Ryder, A. G., Schuller, D. R., & Marshall, M. B. (2004). The Hamilton De-
pression Rating Scale: has the gold standard become a lead weight? The American Jour-
nal of Psychiatry, 161(12), 2163–2177. https://doi.org/10.1176/appi.ajp.161.12.2163
Ball, H. A., McGuffin, P., & Farmer, A. E. (2008). Attributional style and depression. The
British Journal of Psychiatry: the Journal of Mental Science, 192(4), 275–278.
https://doi.org/10.1192/bjp.bp.107.038711
Bayne, T., Cleeremans, A., & Wilken, P. (2009). The Oxford companion to consciousness.
[Oxford]: Oxford University Press.
Beblo, T., Sinnamon, G., & Baune, B. T. (2011). Specifying the neuropsychology of affec-
tive disorders: clinical, demographic and neurobiological factors. Neuropsychology Re-
view, 21(4), 337–359. https://doi.org/10.1007/s11065-011-9171-0
Beck, A. T. (1979). Cognitive Therapy of depression: Guilford Press. Retrieved from
https://books.google.de/books?id=L09cRS0xWj0C

References
91
Beck, A. T., & Dozois, D. J. A. (2011). Cognitive Therapy: Current status and future direc-
tions. Annual Review of Medicine, 62, 397–409. https://doi.org/10.1146/annurev-med-
052209-100032
Beck, A. T., Hautzinger, M., & Bronder, G. (1992). Kognitive Therapie der Depression (3.,
überarb. Aufl.). Weinheim: Psychologie-Verl.-Union.
Beck, A. T., Steer, R. A., & Hautzinger, M. (1995). Beck-Depressions-Inventar (BDI): Test-
handbuch (2., überarb. Aufl.). Bern: Huber.
Beck, A. T., Street, R. A., & Garbin, M. G. (1988). Psychometric properties of the Beck
Depression Inventory: Twenty-five years of evaluation. Clinical Psychology Review. (8),
77–100.
Beevers, C. G., Keitner, G. I., Ryan, C. E., & Miller, I. W. (2003). Cognitive predictors of
symptom return following depression treatment. Journal of Abnormal Psychology,
112(3), 488–496. https://doi.org/10.1037/0021-843X.112.3.488
Beevers, C. G., & Miller, I. W. (2004). Depression-related negative cognition: Mood-state
and trait dependent properties. Cognitive Therapy and Research, 28(3), 293–307.
https://doi.org/10.1023/B:COTR.0000031804.86353.d1
Beevers, C. G., Strong, D. R., Meyer, B., Pilkonis, P. A., & Miller, I. R. (2007). Efficiently
assessing negative cognition in depression: an item response theory analysis of the Dys-
functional Attitude Scale. Psychological Assessment, 19(2), 199–209.
https://doi.org/10.1037/1040-3590.19.2.199
Berger, M., van Calker, D., Brakemeier, E.-L., & Schramm, E. (2015). Affektive Störungen.
In M. Berger, H. Hecht, & A. Agyemang (Eds.), Psychische Erkrankungen: Klinik und
Therapie (5th ed., pp. 413–498). Munich: Urban & Fischer.
https://doi.org/10.1016/B978-3-437-22484-3.00011-6
Berle, D., & Moulds, M. L. (2013). Emotional reasoning processes and dysphoric mood:
cross-sectional and prospective relationships. PloS One, 8(6), e67359.
https://doi.org/10.1371/journal.pone.0067359
Bertelsmann Stiftung. (2014). Regionale Variation der Prävalenz und Behandlung von De-
pressionen - Ergebnisse des Faktencheck Depression: German Medical Science GMS
Publishing House; Düsseldorf.
Beshai, S., Dobson, K. S., Bockting, C. L. H., & Quigley, L. (2011). Relapse and recurrence
prevention in depression: current research and future prospects. Clinical Psychology Re-
view, 31(8), 1349–1360. https://doi.org/10.1016/j.cpr.2011.09.003

References
92
Biesheuvel-Leliefeld, K. E. M., Kok, G. D., Bockting, C. L. H., Cuijpers, P., Hollon, S. D.,
van Marwijk, H. W. J., & Smit, F. (2015). Effectiveness of psychological interventions
in preventing recurrence of depressive disorder: meta-analysis and meta-regression. Jour-
nal of Affective Disorders, 174, 400–410. https://doi.org/10.1016/j.jad.2014.12.016
Binneman, B., Feltner, D., Kolluri, S., Shi, Y., Qiu, R., & Stiger, T. (2008). A 6-week ran-
domized, placebo-controlled trial of CP-316,311 (a selective CRH1 antagonist) in the
treatment of major depression. The American Journal of Psychiatry, 165(5), 617–620.
https://doi.org/10.1176/appi.ajp.2008.07071199
Bockting, C. L., Hollon, S. D., Jarrett, R. B., Kuyken, W., & Dobson, K. (2015). A lifetime
approach to major depressive disorder: The contributions of psychological interventions
in preventing relapse and recurrence. Clinical Psychology Review, 41, 16–26.
https://doi.org/10.1016/j.cpr.2015.02.003
Bukh, J. D., Andersen, P. K., & Kessing, L. V. (2016). Rates and predictors of remission,
recurrence and conversion to bipolar disorder after the first lifetime episode of depres-
sion--a prospective 5-year follow-up study. Psychological Medicine, 46(6), 1151–1161.
https://doi.org/10.1017/S0033291715002676
Burcusa, S. L., & Iacono, W. G. (2007). Risk for recurrence in depression. Clinical Psychol-
ogy Review, 27(8), 959–985. https://doi.org/10.1016/j.cpr.2007.02.005
Burns, D. D. (1999). Feeling good: The new mood therapy (Revised and updated.). New
York: Avon.
Busch, M. A., Maske, U. E., Ryl, L., Schlack, R., & Hapke, U. (2013). Pravalenz von de-
pressiver Symptomatik und diagnostizierter Depression bei Erwachsenen in Deutschland:
Ergebnisse der Studie zur Gesundheit Erwachsener in Deutschland (DEGS1) [Prevalence
of depressive symptoms and diagnosed depression among adults in Germany: results of
the German Health Interview and Examination Survey for Adults (DEGS1)]. Bun-
desgesundheitsblatt, Gesundheitsforschung, Gesundheitsschutz, 56(5-6), 733–739.
https://doi.org/10.1007/s00103-013-1688-3
Butler, A. C., Chapman, J. E., Forman, E. M., & Beck, A. T. (2006). The empirical status of
cognitive-behavioral therapy: A review of meta-analyses. Clinical Psychology Review,
26(1), 17–31. https://doi.org/10.1016/j.cpr.2005.07.003
Cane, D. B., Olinger, L. J., Gotlib, I. H., & Kuiper, N. A. (1986). Factor structure of the
dysfunctional attitude scale in a student population. Journal of Clinical Psychology,

References
93
42(2), 307–309. https://doi.org/10.1002/1097-4679(198603)42:2<307:AID-
JCLP2270420213>3.0.CO;2-J
Capobianco, L., Morris, J. A., & Wells, A. (2018). Worry and rumination: Do they prolong
physiological and affective recovery from stress? Anxiety, Stress, and Coping, 31(3),
291–303. https://doi.org/10.1080/10615806.2018.1438723
Cartwright-Hatton, S., & Wells, A. (1997). Beliefs about worry and intrusions: The Meta-
Cognitions Questionnaire and its correlates: Journal of Anxiety Disorders, 11(3), 279–
296.
Caston, V. (2002). Aristotle on consciousness. Mind, 111(444), 751–815.
Clark, D. A., & Beck, A. T. (2010). Cognitive theory and therapy of anxiety and depression:
Convergence with neurobiological findings. Trends in Cognitive Sciences, 14(9), 418–
424. https://doi.org/10.1016/j.tics.2010.06.007
Cohen, J. W. (1988). Statistical power analysis for the behavioral sciences (2. ed.). Hills-
dale, NJ: Erlbaum.
Cuijpers, P. (2015). Psychotherapies for adult depression: Recent developments. Current
Opinion in Psychiatry, 28(1), 24–29. https://doi.org/10.1097/YCO.0000000000000121
Deutsche Gesellschaft für Psychiatrie, Psychotherapie und Nervenheilkunde, & Ärztliches
Zentrum für Qualität in der Medizin. (2015). S3-Leitlinie/Nationale VersorgungsLeitlinie
Unipolare Depression - Langfassung, 2. Auflage: Deutsche Gesellschaft für Psychiatrie,
Psychotherapie und Nervenheilkunde (DGPPN); Bundesärztekammer (BÄK); Kas-
senärztliche Bundesvereinigung (KBV); Arbeitsgemeinschaft der Wissenschaftlichen
Medizinischen Fachgesellschaften (AWMF).
DGPPN. (2015). Unipolare Depression: S3-Leitlinie/Nationale VersorgungsLeitlinie, 2.
Dimidjian, S., Barrera, M., JR, Martell, C., Munoz, R. F., & Lewinsohn, P. M. (2011). The
origins and current status of behavioral activation treatments for depression. Annual Re-
view of Clinical Psychology, 7, 1–38. https://doi.org/10.1146/annurev-clinpsy-032210-
104535
Dunlosky, J. (2009). Metacognition. Los Angeles: SAGE.
Eaton, W. W., Shao, H., Nestadt, G., Lee, H. B., Bienvenu, O. J., & Zandi, P. (2008). Popu-
lation-based study of first onset and chronicity in major depressive disorder. Archives of
General Psychiatry, 65(5), 513–520. https://doi.org/10.1001/archpsyc.65.5.513

References
94
Egan, S. J., Wade, T. D., & Shafran, R. (2011). Perfectionism as a transdiagnostic process:
a clinical review. Clinical Psychology Review, 31(2), 203–212.
https://doi.org/10.1016/j.cpr.2010.04.009
Elgersma, H. J., Glashouwer, K. A., Bockting, C. L. H., Penninx, B. W. J. H., & Jong, P. J.
de. (2013). Hidden scars in depression? Implicit and explicit self-associations following
recurrent depressive episodes. Journal of Abnormal Psychology, 122(4), 951–960.
https://doi.org/10.1037/a0034933
Eshel, N., & Roiser, J. P. (2010). Reward and punishment processing in depression. Biolog-
ical Psychiatry, 68(2), 118–124. https://doi.org/10.1016/j.biopsych.2010.01.027
Field, A. P. (2016). Discovering statistics using IBM SPSS statistics: And sex and drugs and
rock'n'roll (4th edition, [reprinted]). Los Angeles: Sage Publications.
Figueroa, C. A., Ruhé, H. G., Koeter, M. W., Spinhoven, P., van der Does, W., Bockting, C.
L., & Schene, A. H. (2015). Cognitive reactivity versus dysfunctional cognitions and the
prediction of relapse in recurrent major depressive disorder. The Journal of Clinical Psy-
chiatry, 76(10), e1306-12. https://doi.org/10.4088/JCP.14m09268
Fisher, P., & Wells, A. (2009). Metacognitive Therapy: Distinctive features. The CBT dis-
tinctive features series. London, New York: Routledge. Retrieved from http://sub-
hh.ciando.com/book/?bok_id=36070
Fisher, P. L., & Noble, A. J. (2017). Anxiety and depression in people with epilepsy: The
contribution of metacognitive beliefs. Seizure, 50, 153–159. https://doi.org/10.1016/j.sei-
zure.2017.06.012
Flavell, J. H. (1971). First Discussant's comments: what is memory development the devel-
opment of? Human Development, 14(4), 272–278. https://doi.org/10.1159/000271221
Flavell, J. H., & Wellman, H. M. (1977). Metamemory. In R. Kail, J. W. Hagen, & J. M.
Belmont (Eds.), Perspectives on the development of memory and cognition (pp. 3–30).
Hillsdale, NJ, New York [etc.]: Lawrence Erlbaum Associates; Wiley.
Flavell, J. H. (1979). Metacognition and cognitive monitoring: A new area of cognitive-
developmental inquiry. American Psychologist, 34(10), 906–911.
https://doi.org/10.1037/0003-066X.34.10.906
Floyd, M., Scogin, F., & Chaplin, W. F. (2004). The Dysfunctional Attitudes Scale: factor
structure, reliability, and validity with older adults. Aging & Mental Health, 8(2), 153–
160. https://doi.org/10.1080/13607860410001649572

References
95
Freeman, A., & Oster, C. (1999). Cognitive Behavior Therapy. In M. Hersen & A. S. Bellack
(Eds.), Handbook of comparative interventions for adult disorders (2nd ed., pp. 108–
138). New York: Wiley.
Freeman, A. M., & DeWolf, R. (1992). The 10 dumbest mistakes smart people make and
how to avoid them: Simple and sure techniques for gaining greater control of your life.
New York, NY: HarperPerennial.
Gallo, D. A., Cramer, S. J., Wong, J. T., & Bennett, D. A. (2012). Alzheimer's disease can
spare local metacognition despite global anosognosia: Revisiting the confidence-accuracy
relationship in episodic memory. Neuropsychologia, 50(9), 2356–2364.
https://doi.org/10.1016/j.neuropsychologia.2012.06.005
Garratt, G., Ingram, R. E., Rand, K. L., & Sawalani, G. (2007). Cognitive processes in cog-
nitive therapy: Evaluation of the mechanisms of change in the treatment of depression.
Clinical Psychology, 30(3), 224–239.
Goh, C., & Agius, M. (2010). The stress-vulnerability model: How does stress impact on
mental illness at the level of the brain and what are the consequences? Psychiatria Dan-
ubina, 22(2), 198–202.
Gotlib, I. H. (1982). Self-reinforcement and depression in interpersonal interaction: The role
of performance level. Journal of Abnormal Psychology, 91(1), 3–13.
Gotlib, I. H., & Joormann, J. (2010). Cognition and depression: Current status and future
directions. Annual Review of Clinical Psychology, 6, 285–312.
https://doi.org/10.1146/annurev.clinpsy.121208.131305
Gumley, A. (2011). Metacognition, affect regulation and symptom expression: a transdiag-
nostic perspective. Psychiatry Research, 190(1), 72–78. https://doi.org/10.1016/j.psy-
chres.2011.09.025
Halvorsen, M., Hagen, R., Hjemdal, O., Eriksen, M. S., Sorli, J., Waterloo, K., Wang, C. E.
A. (2015). Metacognitions and thought control strategies in unipolar major depression: A
comparison of currently depressed, previously depressed, and never-depressed individu-
als. Cognitive Therapy and Research, 39(1), 31–40. https://doi.org/10.1007/s10608-014-
9638-4
Halvorsen, M., Wang, C. E., Eisemann, M., & Waterloo, K. (2010). Dysfunctional attitudes
and early maladaptive schemas as predictors of depression: A 9-year follow-up study.
Cognitive Therapy and Research, 34(4), 368–379. https://doi.org/10.1007/s10608-009-
9259-5

References
96
Hamilton, M. (1960). A rating scale for depression. Journal of Neurology, Neurosurgery,
and, 23(1), 56–62.
Hankin, B. L. (2008). Stability of cognitive vulnerabilities to depression: A short-term pro-
spective multiwave study. Journal of Abnormal Psychology, 117(2), 324–333.
https://doi.org/10.1037/0021-843X.117.2.324
Hautzinger, M. (2010). Akute Depression. Fortschritte der Psychotherapie: Bd. 40. Göttin-
gen: Hogrefe.
Hautzinger, M., Joormann, J., & Keller, F. (2005). Skala dysfunktionaler Einstellungen: DAS
; Manual. Göttingen: Hogrefe.
Hautzinger, M., & Pössel, P. (2017). Kognitive Interventionen (1. Auflage 2017). Standards
der Psychotherapie: Vol. 1. Göttingen, Niedersachs: Hogrefe Verlag.
Heffer-Rahn, P., & Fisher, P. L. (2018). The clinical utility of metacognitive beliefs and
processes in emotional distress in people with multiple sclerosis. Journal of Psychoso-
matic Research, 104, 88–94. https://doi.org/10.1016/j.jpsychores.2017.11.014
Hoebel, J., Maske, U. E., Zeeb, H., & Lampert, T. (2017). Social inequalities and depressive
symptoms in adults: The role of objective and subjective socioeconomic status. PloS One,
12(1), e0169764. https://doi.org/10.1371/journal.pone.0169764
Huffziger, S., & Kuehner, C. (2009). Rumination, distraction, and mindful self-focus in de-
pressed patients. Behaviour Research and Therapy, 47(3), 224–230.
https://doi.org/10.1016/j.brat.2008.12.005
Huntley, C. D., & Fisher, P. L. (2016). Examining the role of positive and negative meta-
cognitive beliefs in depression. Scandinavian Journal of Psychology, 57(5), 446–452.
https://doi.org/10.1111/sjop.12306
Iacoviello, B. M., Alloy, L. B., Abramson, L. Y., Whitehouse, W. G., & Hogan, M. E.
(2006). The course of depression in individuals at high and low cognitive risk for depres-
sion: A prospective study. Journal of Affective Disorders, 93(1-3), 61–69.
https://doi.org/10.1016/j.jad.2006.02.012
Jacobi, F., Hofler, M., Strehle, J., Mack, S., Gerschler, A., Scholl, L., Wittchen, H.-U.
(2016). Erratum zu: Psychische Storungen in der Allgemeinbevolkerung. Studie zur Ge-
sundheit Erwachsener in Deutschland und ihr Zusatzmodul "Psychische Gesundheit"
(DEGS1-MH) [Erratum to: Mental disorders in the general population. Study on the
health of adults in Germany and the additional module mental health (DEGS1-MH)]. Der
Nervenarzt, 87(1), 88–90. https://doi.org/10.1007/s00115-015-4458-7

References
97
Jarrett, R. B., Minhajuddin, A., Borman, P. D., Dunlap, L., Segal, Z. V., Kidner, C. L., Thase,
M. E. (2012). Cognitive reactivity, dysfunctional attitudes, and depressive relapse and
recurrence in cognitive therapy responders. Behaviour Research and Therapy, 50(5),
280–286. https://doi.org/10.1016/j.brat.2012.01.008
Jarrett, R. B., Vittengl, J. R., Doyle, K., & Clark, L. A. (2007). Changes in cognitive content
during and following cognitive therapy for recurrent depression: Substantial and endur-
ing, but not predictive of change in depressive symptoms. Journal of Consulting and
Clinical Psychology, 75(3), 432–446. https://doi.org/10.1037/0022-006X.75.3.432
Jelinek, L., Hauschildt, M., & Moritz, S. (2015). Metakognitives Training bei Depression
(D-MKT): Mit Trainigsmaterial (1. Originalausgabe). Weinheim: Beltz.
Jelinek, L., Hauschildt, M., Wittekind, C. E., Schneider, B. C., Kriston, L., & Moritz, S.
(2016). Efficacy of Metacognitive Training for Depression: A randomized controlled
trial. Psychotherapy and Psychosomatics, 85(4), 231–234.
https://doi.org/10.1159/000443699
Jelinek, L., Moritz, S., & Hauschildt, M. (2017). Patients' perspectives on treatment with
Metacognitive Training for Depression (D-MCT): Results on acceptability. Journal of
Affective Disorders, 221, 17–24. https://doi.org/10.1016/j.jad.2017.06.003
Jelinek, L., Otte, C., Arlt, S., & Hauschildt, M. (2013). Denkverzerrungen erkennen und
korrigieren: Eine Machbarkeitsstudie zum Metakognitiven Training bei Depression (D-
MKT). Zeitschrift Für Psychiatrie, Psychologie Und Psychotherapie, 61(4), 247–254.
https://doi.org/10.1024/1661-4747/a000167
Kang, H.-J., Kim, S.-Y., Bae, K.-Y., Kim, S.-W., Shin, I.-S., Yoon, J.-S., & Kim, J.-M.
(2015). Comorbidity of depression with physical disorders: Research and clinical impli-
cations. Chonnam Medical Journal, 51(1), 8–18. https://doi.org/10.4068/cmj.2015.51.1.8
Katon, W., Rutter, C., Ludman, E. J., Korff, M. von, Lin, E., Simon, G., Unützer, J. (2001).
A randomized trial of relapse prevention of depression in primary care. Archives of Gen-
eral Psychiatry, 58(3), 241–247.
Keller, M. B., Lavori, P. W., Mueller, T. I., Endicott, J., Coryell, W., Hirschfeld, R. M., &
Shea, T. (1992). Time to recovery, chronicity, and levels of psychopathology in major
depression. A 5-year prospective follow-up of 431 subjects. Archives of General Psychi-
atry, 49(10), 809–816.

References
98
Kessing, L. V., Hansen, M. G., Andersen, P. K., & Angst, J. (2004). The predictive effect of
episodes on the risk of recurrence in depressive and bipolar disorders - a life-long per-
spective. Acta Psychiatrica Scandinavica, 109(5), 339–344.
https://doi.org/10.1046/j.1600-0447.2003.00266.x
Kessler, R. C., Berglund, P., Demler, O., Jin, R., Koretz, D., Merikangas, K. R., Wang, P. S.
(2003). The epidemiology of major depressive disorder: results from the National Comor-
bidity Survey Replication (NCS-R). JAMA, 289(23), 3095–3105.
https://doi.org/10.1001/jama.289.23.3095
Kessler, R. C., Birnbaum, H. G., Shahly, V., Bromet, E., Hwang, I., McLaughlin, K. A.,
Stein, D. J. (2010). Age differences in the prevalence and co-morbidity of DSM-IV major
depressive episodes: results from the WHO World Mental Health Survey Initiative. De-
pression and Anxiety, 27(4), 351–364. https://doi.org/10.1002/da.20634
Kessler, R. C., Petukhova, M., Sampson, N. A., Zaslavsky, A. M., & Wittchen, H.-U. (2012).
Twelve-month and lifetime prevalence and lifetime morbid risk of anxiety and mood dis-
orders in the United States. International Journal of Methods in Psychiatric Research,
21(3), 169–184. https://doi.org/10.1002/mpr.1359
Koriat, A., & Goldsmith, M. (1998). The role of metacognitive processes in the regulation
of memory performance. In G. Mazzoni (Ed.), Metacognition and cognitive neuropsy-
chology: Monitoring and control processes (pp. 97–118). Mahwah, NJ: L. Erlbaum.
Kruijt, A.-W., Antypa, N., Booij, L., Jong, P. J. de, Glashouwer, K., Penninx, B. W. J. H.,
& van der Does, W. (2013). Cognitive reactivity, implicit associations, and the incidence
of depression: A two-year prospective study. PloS One, 8(7), e70245.
https://doi.org/10.1371/journal.pone.0070245
Kuroda, Y. (2016). Dysfunctional attitudes lead to depressive symptoms by generating sub-
jective stress. The Journal of Psychology, 150(3), 358–370.
https://doi.org/10.1080/00223980.2015.1054335
Lacerda-Pinheiro, S. F., Pinheiro Junior, R. F. F., Pereira de Lima, M. A., Lima da Silva, C.
G., Vieira dos Santos, M. d. S., Teixeira Júnior, A. G., Bianco, B. A. V. (2014). Are there
depression and anxiety genetic markers and mutations? A systematic review. Journal of
Affective Disorders, 168, 387–398. https://doi.org/10.1016/j.jad.2014.07.016
Lampert, T., Kroll, L. E., Lippe, E. von der, Muters, S., & Stolzenberg, H. (2013).
Soziookonomischer Status und Gesundheit: Ergebnisse der Studie zur Gesundheit
Erwachsener in Deutschland (DEGS1) [Socioeconomic status and health: results of the

References
99
German Health Interview and Examination Survey for Adults (DEGS1)]. Bundesgesund-
heitsblatt, Gesundheitsforschung, Gesundheitsschutz, 56(5-6), 814–821.
https://doi.org/10.1007/s00103-013-1695-4
Lecrubier, Y., Sheehan, D. V., Weiller, E., Amorim, P., Bonora, I., Harnett Sheehan, K.,.
Dunbar, G. C. (1997). The Mini International Neuropsychiatric Interview (MINI). A short
diagnostic structured interview: Reliability and validity according to the CIDI. European
Psychiatry, 12(5), 224–231. https://doi.org/10.1016/S0924-9338(97)83296-8
Lewinsohn, P. M. (1974). A behavioral approach to depression. In R. J. Friedman & M. M.
Katz (Eds.), The psychology of depression: Contemporary theory and research (pp. 157–
185). New York: Wiley.
Liu, W.-h., Huang, J., Wang, L.-z., Gong, Q.-y., & Chan, R. C. K. (2012). Facial perception
bias in patients with major depression. Psychiatry Research, 197(3), 217–220.
https://doi.org/10.1016/j.psychres.2011.09.021
Lok, A., Bockting, C. L. H., Koeter, M. W. J., Snieder, H., Assies, J., Mocking, R. J. T.,
Schene, A. H. (2013). Interaction between the MTHFR C677T polymorphism and trau-
matic childhood events predicts depression. Translational Psychiatry, 3, e288.
https://doi.org/10.1038/tp.2013.60
Lysaker, P. H., Vohs, J. L., Ballard, R., Fogley, R., Salvatore, G., Popolo, R., & Dimaggio,
G. (2013). Metacognition, self-reflection and recovery in schizophrenia. Future Neurol-
ogy, 8(1), 103–115. https://doi.org/10.2217/fnl.12.78
Manji, H. K., & Duman, R. S. (2001). Impairments of neuroplasticity and cellular resilience
in severe mood disorders: implications for the development of novel therapeutics. Psy-
chopharmacology Bulletin, 35(2), 5–49.
Michalak, J., Hölz, A., & Teismann, T. (2011). Rumination as a predictor of relapse in mind-
fulness-based cognitive therapy for depression. Psychology and Psychotherapy, 84(2),
230–236. https://doi.org/10.1348/147608310X520166
Modell, S., Ising, M., Holsboer, F., & Lauer, C. J. (2005). The Munich vulnerability study
on affective disorders: premorbid polysomnographic profile of affected high-risk pro-
bands. Biological Psychiatry, 58(9), 694–699. https://doi.org/10.1016/j.bi-
opsych.2005.05.004
Moore, M. T., Fresco, D. M., Segal, Z. V., & Brown, T. A. (2014). An exploratory analysis
of the factor structure of the Dysfunctional Attitude Scale-Form A (DAS). Assessment,
21(5), 570–579. https://doi.org/10.1177/1073191114524272

References
100
Moritz, S., & Lysaker, P. H. (2018). Metacognition - What did James H. Flavell really say
and the implications for the conceptualization and design of metacognitive interventions.
Schizophrenia Research. Advance online publication.
https://doi.org/10.1016/j.schres.2018.06.001
Moritz, S., Veckenstedt, R., Bohn, F., Köther, U., & Woodward, T. S. (2013). Metacognitive
Training in schizophrenia: Theoretical rationale and administration. In D. L. Roberts &
D. L. Penn (Eds.), Social cognition in schizophrenia: From evidence to treatment
(pp. 358–383). Oxford: Oxford University Press USA.
Moritz, S., & Woodward, T. S. (2006). The contribution of metamemory deficits to schizo-
phrenia. Journal of Abnormal Psychology, 115(1), 15–25. https://doi.org/10.1037/0021-
843X.15.1.15
Muniz-Terrera, G., Robitaille, A., Kelly, A., Johansson, B., Hofer, S., & Piccinin, A. (2017).
Latent growth models matched to research questions to answer questions about dynamics
of change in multiple processes. Journal of Clinical Epidemiology, 82, 158–166.
https://doi.org/10.1016/j.jclinepi.2016.09.001
Muthén, L. K., & Muthén, B. O. (2011). Mplus: Statistical analysis with latent variables ;
user's guide (6. ed.). Los Angeles, Calif.: Muthén.
Nelson, T. O. (1990). Metamemory: A theoretical framework and new findings. In G. H.
Bower (Ed.), Psychology of Learning and Motivation: v. 26. The psychology of learning
and motivation: Advances in research and theory (Vol. 26, pp. 125–173). San Diego:
Academic Press. https://doi.org/10.1016/S0079-7421(08)60053-5
Nisbett, R. E., & Wilson, T. D. (1977). Telling more than we can know: Verbal reports on
mental processes. Psychological Review, 84(3), 231–259. https://doi.org/10.1037/0033-
295X.84.3.231
Nolen-Hoeksema, S. (1991). Responses to depression and their effects on the duration of
depressive episodes. Journal of Abnormal Psychology, 100(4), 569–582.
Normann, N., van Emmerik, Arnold A P, & Morina, N. (2014). The efficacy of metacogni-
tive therapy for anxiety and depression: a meta-analytic review. Depression and Anxiety,
31(5), 402–411. https://doi.org/10.1002/da.22273
O’brien, R. M. (2007). A caution regarding rules of thumb for variance inflation factors.
Quality & Quantity, 41(5), 673–690. https://doi.org/10.1007/s11135-006-9018-6

References
101
Osman, A., Bagge, C. L., Gutierrez, P. M., Konick, L. C., Kopper, B. A., & Barrios, F. X.
(2001). The Suicidal Behaviors Questionnaire-Revised (SBQ-R): validation with clinical
and nonclinical samples. Assessment, 8(4), 443–454.
Otsubo, T., Tanaka, K., Koda, R., Shinoda, J., Sano, N., Tanaka, S., Kamijima, K. (2005).
Reliability and validity of Japanese version of the Mini-International Neuropsychiatric
Interview. Psychiatry and Clinical Neurosciences, 59(5), 517–526.
https://doi.org/10.1111/j.1440-1819.2005.01408.x
Otto, M. W., Teachman, B. A., Cohen, L. S., Soares, C. N., Vitonis, A. F., & Harlow, B. L.
(2007). Dysfunctional attitudes and episodes of major depression: Predictive validity and
temporal stability in never-depressed, depressed, and recovered women. Journal of Ab-
normal Psychology, 116(3), 475–483. https://doi.org/10.1037/0021-843X.116.3.475
Papageorgiou, C., & Wells, A. (2001). Metacognitive beliefs about rumination in recurrent
major depression. Cognitive and Behavioral Practice, 8(2), 160–164.
https://doi.org/10.1016/S1077-7229(01)80021-3
Papageorgiou, C., & Wells, A. (2003a). An empirical test of a clinical metacognitive model
of rumination and depression. Cognitive Therapy and Research, 27(3), 261–273.
Papageorgiou, C., & Wells, A. (2003b). An empirical test of a clinical metacognitive model
of rumination and depression. Cognitive Therapy and Research, 27(3), 261–273.
https://doi.org/10.1023/A:1023962332399
Papageorgiou, C., & Wells, A. (2003c). Depressive rumination. Chichester, UK: John Wiley
& Sons Ltd.
Papageorgiou, C., & Wells, A. (2009). A prospective test of the clinical metacognitive model
of rumination and depression. International Journal of Cognitive Therapy, 2(2), 123–131.
https://doi.org/10.1521/ijct.2009.2.2.123
Pedone, R., Semerari, A., Riccardi, I., Procacci, M., Nicolo, G., & Carcione, A. (2017). De-
velopment of a self-report measure of metacognition: The matcognition self-assessment
scale (MSAS): Instrument description and factor structure. Clinical Neuropsychiatry,
14(3), 185–194.
Pedrelli, P., Feldman, G. C., Vorono, S., Fava, M., & Petersen, T. (2008). Dysfunctional
attitudes and perceived stress predict depressive symptoms severity following antidepres-
sant treatment in patients with chronic depression. Psychiatry Research, 161(3), 302–308.
https://doi.org/10.1016/j.psychres.2007.08.004

References
102
Power, M. J., Katz, R., McGuffin, P., Duggan, C. F., Lam, D., & Beck, A. T. (1994). The
Dysfunctional Attitude Scale (DAS). Journal of Research in Personality, 28(3), 263–276.
https://doi.org/10.1006/jrpe.1994.1019
Proust, J. (2010). Metacognition. Philosophy Compass, 5(11), 989–998.
https://doi.org/10.1111/j.1747-9991.2010.00340.x
Purewal, R., & Fisher, P. L. (2018). The contribution of illness perceptions and metacogni-
tive beliefs to anxiety and depression in adults with diabetes. Diabetes Research and
Clinical Practice, 136, 16–22. https://doi.org/10.1016/j.diabres.2017.11.029
Raps, C. S., Peterson, C., Reinhard, K. E., Abramson, L. Y., & Seligman, M. E. (1982).
Attributional style among depressed patients. Journal of Abnormal Psychology, 91(2),
102–108.
Roelofs, J., Huibers, M., Peeters, F., Arntz, A., & van Os, J. (2010). Positive and negative
beliefs about depressive rumination: A psychometric evaluation of two self-report scales
and a test of a clinical metacognitive model of rumination and depression. Cognitive Ther-
apy and Research, 34(2), 196–205. https://doi.org/10.1007/s10608-009-9244-z
Roelofs, J., Papageorgiou, C., Gerber, R. D., Huibers, M., Peeters, F., & Arntz, A. (2007).
On the links between self-discrepancies, rumination, metacognitions, and symptoms of
depression in undergraduates. Behaviour Research and Therapy, 45(6), 1295–1305.
https://doi.org/10.1016/j.brat.2006.10.005
Rood, L., Roelofs, J., Bögels, S. M., Nolen-Hoeksema, S., & Schouten, E. (2009). The in-
fluence of emotion-focused rumination and distraction on depressive symptoms in non-
clinical youth: A meta-analytic review. Clinical Psychology Review, 29(7), 607–616.
https://doi.org/10.1016/j.cpr.2009.07.001
Rose, N. (2003). Neurochemical selves. Society, 41(1), 46–59.
https://doi.org/10.1007/BF02688204
Rossi, A., Alberio, R., Porta, A., Sandri, M., Tansella, M., & Amaddeo, F. (2004). The reli-
ability of the Mini-International Neuropsychiatric Interview--Italian version. Journal of
Clinical Psychopharmacology, 24(5), 561–563.
Rovner, B., & Casten, R. (2003). The Epidemiology of Major Depressive Disorder. Evi-
dence–Based Eye Care, 4(4), 186–187. https://doi.org/10.1097/00132578-200310000-
00002

References
103
Ruiz, F. J., & Odriozola-Gonzalez, P. (2015). Comparing Cognitive, Metacognitive, and
Acceptance and Commitment Therapy models of depression: a longitudinal study survey.
The Spanish Journal of Psychology, 18, E39. https://doi.org/10.1017/sjp.2015.31
Rush, A. J., Zimmerman, M., Wisniewski, S. R., Fava, M., Hollon, S. D., Warden, D.,
Trivedi, M. H. (2005). Comorbid psychiatric disorders in depressed outpatients: demo-
graphic and clinical features. Journal of Affective Disorders, 87(1), 43–55.
https://doi.org/10.1016/j.jad.2005.03.005
Sarin, S., Abela, J., & Auerbach, R. (2005). The response styles theory of depression: A test
of specificity and causal mediation. Cognition & Emotion, 19(5), 751–761.
https://doi.org/10.1080/02699930441000463
Scher, C. D., Ingram, R. E., & Segal, Z. V. (2005). Cognitive reactivity and vulnerability:
empirical evaluation of construct activation and cognitive diatheses in unipolar depres-
sion. Clinical Psychology Review, 25(4), 487–510.
https://doi.org/10.1016/j.cpr.2005.01.005
Schmiedek, F., & Wolff, J. K. (2010). Latente Wachstumskurvenmodelle. In C. Wolf & H.
Best (Eds.), Handbuch der sozialwissenschaftlichen Datenanalyse (1st ed., pp. 1017–
1029). Wiesbaden: VS Verl. für Sozialwissenschaften.
Segal, Z. V. (1988). Appraisal of the self-schema construct in cognitive models of depres-
sion. Psychological Bulletin, 103(2), 147–162. https://doi.org/10.1037/0033-
2909.103.2.147
Segal, Z. V., Kennedy, S., Gemar, M., Hood, K., Pedersen, R., & Buis, T. (2006). Cognitive
reactivity to sad mood provocation and the prediction of depressive relapse. Archives of
General Psychiatry, 63(7), 749–755. https://doi.org/10.1001/archpsyc.63.7.749
Seligman, M. E. P. (1976). Learned helplessness and depression in animals and men. Uni-
versity programs modular studies. Morristown, NJ: General Learning Pr.
Seligman, M. E. P., & Rockstroh, B. (1979). Erlernte Hilflosigkeit. München: Urban &
Schwarzenberg.
Semerari, A., Cucchi, M., Dimaggio, G., Cavadini, D., Carcione, A., Battelli, V.,. Smeraldi,
E. (2012). The development of the Metacognition Assessment interview: Instrument de-
scription, factor structure and reliability in a non-clinical sample. Psychiatry Research,
200(2-3), 890–895. https://doi.org/10.1016/j.psychres.2012.07.015

References
104
Sheehan, D. V., Lecrubier, Y., Sheehan, K. H., Amorim, P., Janavs, J., Weiller, E., Dunbar,
G. C. (1998). The Mini-International Neuropsychiatric Interview (M.I.N.I.): the develop-
ment and validation of a structured diagnostic psychiatric interview for DSM-IV and
ICD-10. The Journal of Clinical Psychiatry, 59 Suppl 20, 22-33;quiz 34-57.
Singer, A. R., & Dobson, K. S. (2007). An experimental investigation of the cognitive vul-
nerability to depression. Behaviour Research and Therapy, 45(3), 563–575.
https://doi.org/10.1016/j.brat.2006.05.007
Solem, S., Hagen, R., Hoksnes, J. J., & Hjemdal, O. (2016). The metacognitive model of
depression: An empirical test in a large Norwegian sample. Psychiatry Research, 242,
171–173. https://doi.org/10.1016/j.psychres.2016.05.056
Solem, S., Hagen, R., Wang, C. E. A., Hjemdal, O., Waterloo, K., Eisemann, M., & Hal-
vorsen, M. (2015). Metacognitions and mindful attention awareness in depression: A
comparison of currently depressed, previously depressed and never depressed individu-
als. Clinical Psychology & Psychotherapy. Advance online publication.
https://doi.org/10.1002/cpp.1983
Solomon, D. A., Keller, M. B., Leon, A. C., Mueller, T. I., Lavori, P. W., Shea, M. T.,.
Endicott, J. (2000). Multiple recurrences of major depressive disorder. The American
Journal of Psychiatry, 157(2), 229–233. https://doi.org/10.1176/appi.ajp.157.2.229
Spielmans, G. I., Berman, M. I., & Usitalo, A. N. (2011). Psychotherapy versus second-
generation antidepressants in the treatment of depression: a meta-analysis. The Journal
of Nervous and Mental Disease, 199(3), 142–149.
https://doi.org/10.1097/NMD.0b013e31820caefb
Stange, J. P., Hamilton, J. L., Fresco, D. M., & Alloy, L. B. (2017). Perseverate or decenter?
Differential effects of metacognition on the relationship between parasympathetic inflex-
ibility and symptoms of depression in a multi-wave study. Behaviour Research and Ther-
apy, 97, 123–133. https://doi.org/10.1016/j.brat.2017.07.007
Steinert, C., Hofmann, M., Kruse, J., & Leichsenring, F. (2014). Relapse rates after psycho-
therapy for depression - stable long-term effects? A meta-analysis. Journal of Affective
Disorders, 168, 107–118. https://doi.org/10.1016/j.jad.2014.06.043
Struijs, S. Y., Groenewold, N. A., Oude Voshaar, R. C., & Jonge, P. de. (2013). Cognitive
vulnerability differentially predicts symptom dimensions of depression. Journal of Affec-
tive Disorders, 151(1), 92–99. https://doi.org/10.1016/j.jad.2013.05.057

References
105
Strunk, D. R., & Adler, A. D. (2009). Cognitive biases in three prediction tasks: a test of the
cognitive model of depression. Behaviour Research and Therapy, 47(1), 34–40.
https://doi.org/10.1016/j.brat.2008.10.008
Swift, J. K., & Greenberg, R. P. (2012). Premature discontinuation in adult psychotherapy:
a meta-analysis. Journal of Consulting and Clinical Psychology, 80(4), 547–559.
https://doi.org/10.1037/a0028226
Tajrishi, K. Z., Mohammadkhani, S., & Jadidi, F. (2011). Metacognitive beliefs and negative
emotions. Procedia - Social and Behavioral Sciences, 30, 530–533.
https://doi.org/10.1016/j.sbspro.2011.10.103
Teasdale, J. D., Scott, J., Moore, R. G., Hayhurst, H., Pope, M., & Paykel, E. S. (2001). How
does cognitive therapy prevent relapse in residual depression? Evidence from a controlled
trial. Journal of Consulting and Clinical Psychology, 69(3), 347–357.
https://doi.org/10.1037/0022-006X.69.3.347
Tsankova, N., Renthal, W., Kumar, A., & Nestler, E. J. (2007). Epigenetic regulation in
psychiatric disorders. Nature Reviews. Neuroscience, 8(5), 355–367.
https://doi.org/10.1038/nrn2132
Van Gulick, R. (2017). Consciousness. The Stanford Encyclopedia of Philosophy. Retrieved
from https://plato.stanford.edu/archives/sum2017/entries/consciousness/
Vollmayr, B., & Gass, P. (2013). Learned helplessness: unique features and translational
value of a cognitive depression model. Cell and Tissue Research, 354(1), 171–178.
https://doi.org/10.1007/s00441-013-1654-2
Vos, T., Abajobir, A. A., Abate, K. H., Abbafati, C., Abbas, K. M., Abd-Allah, F., Murray,
C. J. L. (2017). Global, regional, and national incidence, prevalence, and years lived with
disability for 328 diseases and injuries for 195 countries, 1990–2016: A systematic anal-
ysis for the Global Burden of Disease Study 2016. The Lancet, 390(10100), 1211–1259.
https://doi.org/10.1016/S0140-6736(17)32154-2
Wang, C. E. A., Halvorsen, M., Eisemann, M., & Waterloo, K. (2010). Stability of dysfunc-
tional attitudes and early maladaptive schemas: A 9-year follow-up study of clinically
depressed subjects. Journal of Behavior Therapy and Experimental Psychiatry, 41(4),
389–396. https://doi.org/10.1016/j.jbtep.2010.04.002

References
106
Wang, P. S., Lane, M., Olfson, M., Pincus, H. A., Wells, K. B., & Kessler, R. C. (2005).
Twelve-month use of mental health services in the United States: results from the Na-
tional Comorbidity Survey Replication. Archives of General Psychiatry, 62(6), 629–640.
https://doi.org/10.1001/archpsyc.62.6.629
Weber, F., & Exner, C. (2013). Metacognitive beliefs and rumination: A longitudinal study.
Cognitive Therapy and Research, 37(6), 1257–1261. https://doi.org/10.1007/s10608-
013-9555-y
Weissman, A. N., & Beck, A. T. (1978). Development and validation of the Dysfunctional
Attitude Scale: A preliminary investigation. Proceedings of the Annual Meeting of the
American Educational Research Association, 27–31. Retrieved from
http://files.eric.ed.gov/fulltext/ED167619.pdf
Wells, A. F., & Matthews, G. (1994). Attention and emotion: A clinical perspective. Hove:
Lawrence Erlbaum.
Wells, A. (2001). Emotional disorders and metacognition: Innovative Cognitive Therapy
(Repr. with corr). Chichester: Wiley.
Wells, A., & Cartwright-Hatton, S. (2004). A short form of the metacognitions question-
naire: Properties of the MCQ-30. Behaviour Research and Therapy, 42(4), 385–396.
https://doi.org/10.1016/S0005-7967(03)00147-5
Wells, A., Fisher, P., Myers, S., Wheatley, J., Patel, T., & Brewin, C. R. (2012). Metacog-
nitive Therapy in treatment-resistant depression: a platform trial. Behaviour Research and
Therapy, 50(6), 367–373. https://doi.org/10.1016/j.brat.2012.02.004
Wells, A., & Matthews, G. (1996). Modelling cognition in emotional disorder: The S-REF
model. Behaviour Research and Therapy, 34(11-12), 881–888.
https://doi.org/10.1016/S0005-7967(96)00050-2
Wells, A., & Schweiger, U. (2011). Metakognitive Therapie bei Angststörungen und De-
pression (1. Aufl.). Weinheim: Beltz.
Werner, F.-M., & Coveñas, R. (2013). Classical neurotransmitters and neuropeptides in-
volved in major depression in a multi-neurotransmitter system: A focus on antidepressant
drugs. Current Medicinal Chemistry, 20(38), 4853–4858.
World Health Organization. (2016). Monitoring health for the SDGs: Sustainable develop-
ment goals. World health statistics: Vol. 2016. Geneva: World Health Organization.

References
107
Yilmaz, A. E., Gençöz, T., & Wells, A. (2015). Unique contributions of metacognition and
cognition to depressive symptoms. The Journal of General Psychology, 142(1), 23–33.
https://doi.org/10.1080/00221309.2014.964658
Yılmaz, A. E., Gençöz, T., & Wells, A. (2011). The temporal precedence of metacognition
in the development of anxiety and depression symptoms in the context of life-stress: a
prospective study. Journal of Anxiety Disorders, 25(3), 389–396.
https://doi.org/10.1016/j.janxdis.2010.11.001
Youngren, M. A., & Lewinsohn, P. M. (1980). The functional relation between depression
and problematic interpersonal behavior. Journal of Abnormal Psychology, 89(3), 333–
341.
Yurica, C. L., & DiTomasso, R. A. (2005). Cognitive distortions. In A. Freeman, S. H.
Felgoise, A. M. Nezu, C. M. Nezu, & M. A. Reinecke (Eds.), Encyclopedia of Cognitive
Behavior Therapy (pp. 117–122). Boston, MA: Springer Science+Business Media Inc.
https://doi.org/10.1007/0-306-48581-8_36
Zimmerman, M., Martinez, J., Attiullah, N., Friedman, M., Toba, C., & Boerescu, D. A.
(2012). Symptom differences between depressed outpatients who are in remission accord-
ing to the Hamilton Depression Rating Scale who do and do not consider themselves to
be in remission. Journal of Affective Disorders, 142(1-3), 77–81.
https://doi.org/10.1016/j.jad.2012.03.044
Zimmerman, M., Posternak, M. A., & Chelminski, I. (2005). Is it time to replace the Ham-
ilton Depression Rating Scale as the primary outcome measure in treatment studies of
depression? Journal of Clinical Psychopharmacology, 25(2), 105–110.
https://doi.org/10.1097/01.jcp.0000155824.59585.46
Zubin, J., & Spring, B. (1977). Vulnerability: A new view of schizophrenia. Journal of Ab-
normal Psychology, 86(2), 103–126.
Zuroff, D. C., Blatt, S. J., Sanislow, C. A., Bondi, C. M., & Pilkonis, P. A. (1999). Vulnera-
bility to depression: reexamining state dependence and relative stability. Journal of Ab-
normal Psychology, 108(1), 76–89.

Acknowledgments
108
10. Acknowledgements
At the end of this thesis, I would like to thank several persons without whom this thesis
would not have been possible.
First, I would like to thank my supervisor Lena Jelinek for her advice, her motivation and
her immense knowledge she shared with me through all the stages of this work. Her contin-
uous and systematic guidance, support and encouragement helped me to engage in this re-
search and to accomplish this thesis.
Also, I deeply thank Levente Kriston who accepted to colecture the thesis. His advice and
constructive comments, especially in the analysis and interpretation of the data, have been a
great help.
I would like to express my gratitude to Steffen Moritz for giving me the opportunity to per-
form this research in his institute. I thank him for his support and helpful advice regarding
the publication of parts of this thesis.
Furthermore, I am grateful for the warm and good working atmosphere in the institute
“Klinische Neuropsychologie” at the University Clinical Centre Hamburg Eppendorf. I
thank all the members of the institute for their help in conducting this study. Especially, I
would like to thank Frederica Wallraff and Sabrina Michalski who worked with me in the
beginning of the follow-up study.
I acknowledge the financial support of the “Verein zur Förderung der Rehabilita-
tionsforschung in Hamburg, Mecklenburg-Vorpommern und Schleswig-Holstein” (vffr)
who funded this study.
Last but certainly not least, I would like to express my profound gratitude to my parents
Angelika and Andreas, to my sister Lea and to my brother Simon for their invaluable emo-
tional support in all situations. My heartfelt thanks goes to Paul Crone for his encourage-
ment, his honest feedback and his humour. I thank my friends for supporting and proofrea-
ding parts of this thesis.

CV
109
11. CV
Lebenslauf aus datenschutzrechtlichen Gründen nicht enthalten.

Erklärung
110
12. Eidesstattliche Erklärung
Ich versichere ausdrücklich, dass ich die Arbeit selbständig und ohne fremde Hilfe verfasst,
andere als die von mir angegebenen Quellen und Hilfsmittel nicht benutzt und die aus den
benutzten Werken wörtlich oder inhaltlich entnommenen Stellen einzeln nach Ausgabe
(Auflage und Jahr des Erscheinens), Band und Seite des benutzten Werkes kenntlich ge-
macht habe.
Ferner versichere ich, dass ich die Dissertation bisher nicht einem Fachvertreter an
einer anderen Hochschule zur Überprüfung vorgelegt oder mich anderweitig um Zulassung
zur Promotion beworben habe.
Ich erkläre mich einverstanden, dass meine Dissertation vom Dekanat der Medizini-
schen Fakultät mit einer gängigen Software zur Erkennung von Plagiaten überprüft werden
kann.
Unterschrift: .................................................................

Appendix
111
13. Appendix
Table 17: Correlations of initial status and difference scores between t0 and t3 of depression
with initial status and difference scores between t0 and t3 of maladaptive cognitive and met-
acognitive beliefs, using available data
DAS t0
DAS diff
t0t3 PB
PB diff
t0t3 NB t0
NB diff
t0t3 NFC t0
NFC diff
t0t3
HDRS t0 .33** -.09 .06 .08 .25* -.20 .25* -.03
HDRS
t0t3 -.25 .62** .00 .05 -.02 .30* .01 .32*
BDI t0 .50** -.07 .20 -.10 .31** -17 .39** -.17
BDI t0t3 -.44** .67** -.07 .21 -.15 .43** -.14 .52**
Note Significant correlations (2-tailed) are flagged: ** = p < .01; * = p < .05, HAMD = clinician-
assessed depression, BDI = self-assessed depression, DAS = cognitive maladaptive beliefs, PB =
positive metacognitive beliefs, NB = negative metacognitive beliefs, NFC = metacognitive be-
liefs about the need for control, diff t0t3 = Difference score between t0 and t3.

Appendix
112
Table 18: Model A'1-3: Predictors of change of depressive symptoms (outcome: change of HAMD
(i.e. slope))
b β p
Partial cor-
relation
Step 1 Model A'1
Constant 1.24 .412
Initial Status of HAMD (intercept) -0.39 -0.42 <.001 -.42
Step 2 Model A'2
Constant -3.85 0.193
Initial Status of HAMD (intercept) -0.47 -0.51 <.001 -.51
Initial Status of PB (intercept) -0.24 -0.23 .236 -.14
Change of PB (slope) -0.33 -0.25 .181 -.15
Initial Status of NB (intercept) 0.35 0.29 .107 .18
Change of NB (slope) 0.50 0.45 .013 .28
Initial Status of NFC (intercept) 0.38 0.36 .032 .24
Change of NFC (slope) 0.44 0.38 .026 .25
Step 3 Model A'3
Constant 0.40 .890
Initial Status of HAMD (intercept) -0.57 -0.61 <.001 -.60
Initial Status of PB (intercept) -0.30 -0.28 .095 -.19
Change of PB (slope) -0.38 -0.28 .089 -.20
Initial Status of NB (intercept) 0.37 0.31 .057 .22
Change of NB(slope) 0.44 0.40 .015 .28
Initial Status of NFC (intercept) 0.18 0.17 .281 .13
Change of NFC (slope) 0.03 0.03 .870 .02
Initial Status of DAS (intercept) 0.01 0.07 .507 .08
Change of DAS (slope) 0.10 0.50 <.001 .48
Note R² = .18, F = 17.74 ( p < .001) for step 1; ∆R² = .21, F = 6.92 (p = .001) for step 2, ∆R² = .15,
F = 9.37 ( p < .001) for step 3. HAMD = clinician-assessed depression, DAS = cognitive mala-
daptive beliefs, PB = positive metacognitive beliefs, NB = negative metacognitive beliefs, NFC =
metacognitive beliefs about the need for control, b = unstandardized regression coefficient, β = standardized regression coefficient.

Appendix
113
Table 19: Modell B'1-3: Predictors of change of depressive symptoms (outcome: change of BDI
(i.e. slope))
b β p
Partial cor-
relation
Step 1 Model B'1
Constant 2.82 .192
Initial Status of BDI (intercept) -0.46 -.55 <.001 -.55
Step 2
Constant -16.41 <.001
Initial Status of BDI (intercept) -0.53 -.63 <.001 -.71
Initial Status of PB (intercept) -0.03 -.01 .918 -.01
Change of PB (slope) 0.25 .09 .485 .08
Initial Status of NB (intercept) 0.73 .30 .020 .26
Change of NB (slope) 1.02 .46 <.001 .39
Initial Status of NFC (intercept) 1.02 .48 <.001 .42
Change of NFC (slope) 1.25 .52 <.001 .46
Step 3
Constant -13.60 .002
Initial Status of BDI (intercept) -0.60 -.72 <.001 -.75
Initial Status of PB (intercept) -0.12 -.06 .654 -.05
Change of PB (slope) 0.17 .06 .611 .06
Initial Status of NB (intercept) 0.74 .31 .011 .29
Change of NB(slope) 0.93 .42 <.001 .38
Initial Status of NFC (intercept) 0.70 .33 .007 .31
Change of NFC (slope) 0.73 .31 .013 .28
Initial Status of DAS (intercept) 0.03 .13 .101 .19
Change of DAS (slope) 0.12 .30 <.001 .40
Note R² = .30. F = 35.7 (p < .001) for step 1; ∆R² = .39. F = 24.68 ( p < .001) for step 2. ∆R² = .06.
F = 24.02 ( p < .001) for step 3. BDI = self-assessed depression. DAS = cognitive maladaptive
beliefs. PB = positive metacognitive beliefs. NB = negative metacognitive beliefs. NFC = meta-
cognitive beliefs about the need for control. b = unstandardized regression coefficient. β = stand-ardized regression coefficient.

Appendix
114
Figure 3 Checking homoscedasticity of model A and B
Figure 4 Checking normality distribution of residuals of model A and B

Appendix
115
Table 21: Correlation BDI t0. t1. t2. t3
BDI t0 BDI t1 BDI t2 BDI t3
BDI t0 1 .65** .57** .40**
BDI t1 .65** 1 .76** .53**
BDI t2 .57** .76** 1 .60**
BDI t3 .40** .53** .60** 1
Note Significant correlations (2-tailed) are flagged: **=p < .01; *=p < .05. BDI = self-assessed
depression.
Table 22: Correlation DAS t0. t1. t2. t3
DAS t0 DAS t1 DAS t2 DAS t3
DAS t0 1 .80** .64** .48**
DAS t1 .80** 1 .81** .50**
DAS t2 .64** .81** 1 .55**
DAS t3 .48** .50** .55** 1
Note Significant correlations (2-tailed) are flagged: **=p < .01; *=p < .05., DAS = cognitive mal-
adaptive beliefs.
Table 20: Correlation HAMD t0. t1. t2. t3
HAMD t0 HAMD t1 HAMD t2 HAMD t3
HAMD t0 1 .63** .51** .20
HAMD t1 .63** 1 .66** .38**
HAMD t2 .51** .66** 1 .43**
HAMD t3 .20 .38** .43** 1
Note Significant correlations (2-tailed) are flagged: **=p < .01; *=p < .05. HAMD = clinician-
assessed depression.

Appendix
116
Table 23: Correlation PB t0. t1. t2. t3
PB t0 PB t1 PB t2 PB t3
PB t0 1 .60** .39** .27*
PB t1 .60** 1 .53** .52**
PB t2 .39** .53** 1 .57**
PB t3 .27* .52** .57** 1
Note Significant correlations (2-tailed) are flagged: **=p< .01; *=p < .05. PB = positive metacog-
nitive beliefs.
Table 24: Correlation NB t0. t1. t2. t3
NB t0 NB t1 NB t2 NB t3
NB t0 1 .53** .32* .13
NB t1 .53** 1 .41** .55**
NB t2 .32* .41** 1 .37**
NB t3 .13 .55** .37** 1
Note Significant correlations (2-tailed) are flagged: **=p < .01; *=p < .05. NB = negative meta-
cognitive beliefs.
Table 25: Correlation NFC t0. t1. t2. t3
NFC t0 NFC t1 NFC t2 NFC t3
NFC t0 1 .66** .49** .37**
NFC t1 .66** 1 .67** .57**
NFC t2 .49** .67** 1 .64**
NFC t3 .37** .57** .64** 1
Note Significant correlations (2-tailed) are flagged: **=p < .01; *=p < .05. NFC = metacognitive
beliefs about the need for control.
Copyright © 2022 FDOKUMEN




















