
Copyright Undertaking - PolyU Electronic Theses
670
Copyright Undertaking This thesis is protected by copyright, with all rights reserved. By reading and using the thesis, the reader understands and agrees to the following terms: 1. The reader will abide by the rules and legal ordinances governing copyright regarding the use of the thesis. 2. The reader will use the thesis for the purpose of research or private study only and not for distribution or further reproduction or any other purpose. 3. The reader agrees to indemnify and hold the University harmless from and against any loss, damage, cost, liability or expenses arising from copyright infringement or unauthorized usage. IMPORTANT If you have reasons to believe that any materials in this thesis are deemed not suitable to be distributed in this form, or a copyright owner having difficulty with the material being included in our database, please contact [email protected] providing details. The Library will look into your claim and consider taking remedial action upon receipt of the written requests. Pao Yue-kong Library, The Hong Kong Polytechnic University, Hung Hom, Kowloon, Hong Kong http://www.lib.polyu.edu.hk
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of Copyright Undertaking - PolyU Electronic Theses

Copyright Undertaking
This thesis is protected by copyright, with all rights reserved.
By reading and using the thesis, the reader understands and agrees to the following terms:
1. The reader will abide by the rules and legal ordinances governing copyright regarding the use of the thesis.
2. The reader will use the thesis for the purpose of research or private study only and not for distribution or further reproduction or any other purpose.
3. The reader agrees to indemnify and hold the University harmless from and against any loss, damage, cost, liability or expenses arising from copyright infringement or unauthorized usage.
IMPORTANT
If you have reasons to believe that any materials in this thesis are deemed not suitable to be distributed in this form, or a copyright owner having difficulty with the material being included in our database, please contact [email protected] providing details. The Library will look into your claim and consider taking remedial action upon receipt of the written requests.
Pao Yue-kong Library, The Hong Kong Polytechnic University, Hung Hom, Kowloon, Hong Kong
http://www.lib.polyu.edu.hk

The Hong Kong Polytechnic University
School of Nursing
The Effects of a TTM-based Exercise Stage-Matched Intervention on
Patients with Coronary Heart Disease
Zhu Lixia
A thesis submitted in partial fulfillment of the requirements for the
degree of Doctor of Philosophy
December 2011
lbsys
Text Box
This thesis in electronic version is provided to the Library by the author. In the case where its contents is different from the printed version, the printed version shall prevail.


iii
ABSTRACT
Title: The effects of a TTM-based Exercise Stage-Matched Intervention (ESMI)
on patients with coronary heart disease
Background: Coronary heart disease (CHD) is a leading cause of death and disability
among adults worldwide. Regular exercise or exercise-based cardiac rehabilitation has
been shown to be beneficial to cardiac patients; however, participation and adherence
to exercise programmes is poor. The Transtheoretical Model (TTM) has been
demonstrated to be a successful model for changing exercise behaviour in various
populations from adolescents to the elderly. However, there have been few studies on
the use of the TTM for changing exercise behaviour among CHD patients.
Aim: To examine the effects of a TTM-based Exercise Stage-Matched Intervention
(ESMI) on sedentary patients with CHD. The primary outcome indicator is change in
exercise behaviour. The secondary outcome indicators are anginal attacks and quality
of life.
Methods: This study involved a randomized controlled trial using consecutive
sampling. A total of 196 subjects were recruited and randomly assigned to one of the
following three groups: the Conventional (C) Group (n = 67), the Patient Education
(PE) Group (n = 64), and the ESMI Group (n = 65). Outcome measures included
exercise stages of change, exercise self-efficacy, exercise decisional balance, exercise
duration per week, conditions of angina, and quality of life. Data collection was
carried out at baseline (T0), post-intervention (T1), at the 3-month follow-up period

iv
(T2), and at the 6-month follow-up period (T3). Data analysis was conducted based on
the intention-to-treat principle. Last observation carried forward (LOCF) was
employed to handle the missing data. One-way ANOVA, the Kruskal-Wallis test, and
Chi-square test were applied to analyze data among the three groups at each time
point. One-way repeated ANOVA, the Friedman test, and Cochran‘s Q test were used
to analyze data within groups over time.
Results: A total of 150 subjects completed the whole study. The findings showed that
significantly positive effects on changes in exercise behaviour were found in the
ESMI group, in terms of a more positive shift in the exercise stages of change (p <
0.001), higher exercise self-efficacy (p < 0.001), greater exercise benefits (p < 0.001),
fewer exercise barriers (p < 0.001), longer total exercise duration (minutes/week) (p <
0.001), and longer moderate exercise duration (minutes/week) (p < 0.001), after the
completion of the 8-week ESMI when compared with the C and PE groups. With
regard to anginal attacks, no significant differences in frequency, severity, and
duration of anginal attacks were found among the three groups at each time point. The
ESMI group demonstrated significantly better quality of life, in terms of
improvements in physical limitation (p < 0.01), treatment satisfaction (p < 0.001), and
disease perception (p < 0.001) of Seattle Angina Questionnaire (SAQ), and in physical
component summary (p < 0.01), mental component summary (p < 0.001), and
reported health transition (p < 0.05) of SF-36 after the completion of the 8-week
ESMI when compared with the C and PE groups. These significantly positive effects
were maintained at the 3- and 6-month follow-up periods, with the exception of those
for total exercise duration (minutes/week) and reported health transition, which had
disappeared at the 6-month follow-up period.

v
Conclusion: The TTM-based ESMI has significantly positive effects on changes in
exercise behaviour and quality of life in sedentary CHD patients. The findings
highlight the feasibility and importance of providing CHD patients with a structured
or formal patient education programme guided by the TTM.

vi
Publications arising from the thesis
1. Zhu, L.X., Ho, S.C., Ruan, G.Q., Xie, Q. & Sit, J.W.H. (2012). The effects of an
exercise stage-matched intervention on exercise behavior change in patients with
coronary heart disease - A randomized controlled trial. European Heart Journal,
14(suppl. A): A16.
2. Zhu, L.X., Ho, S.C. & Sit, J.W.H. (2012). The effects of an exercise stage-
matched intervention on quality of life in patients with coronary heart disease.
International Journal of Nursing Practice, 18(Suppl. 1): 30.
3. Zhu, L.X., Ho, S.C. & Sit, J.W.H. (2012). The experiences of Chinese patients
with coronary heart disease. Journal of Clinical Nursing, 21(3-4), 476-484.
4. Zhu, L.X., Ho, S.C. & Sit, J.W.H. (2011). The effects of exercise stage-matched
interventions on exercise behavior change among patients with coronary heart
disease - A pilot study. International Journal of Cardiology, 147(Suppl. 1): s11.
5. Zhu, L.X., Ho, S.C., Ruan, G.Q. & Sit, J.W.H. (under review). Can
TTM motivate CHD patients to do exercise? A report from a small-scaled
feasibility study in China. Applied Nursing Research.
6. Zhu, L.X., Ho, S.C. & Wong, T.K.S. (under review). Systematic review of the
effectiveness of health education programme on exercise behaviour change in
patients with heart disease. Patient Education and Counselling.
7. Zhu, L.X., Ho, S.C., Ruan, G.Q., Xie, Q., Zhu, H.H. & Sit, J.W.H. (under review).
Comparison of the demographic and clinical profile and outcome of dropouts and
completers in a randomized exercise trial among patients with coronary heart
disease. Journal of Clinical Rehabilitation.

vii
Conference presentations
1. Zhu, L.X., Ho, S.C., Ruan, G.Q., Xie, Q. & Sit, J.W.H. (2012). The effects of an
exercise stage-matched interventions on exercise behavior change in patients with
coronary heart disease - A randomized controlled trial. ICC 2012 International
Congress of Cardiology, Hong Kong, 24-26 February 2012, A16.
2. Zhu, L.X., Ho, S.C. & Sit, J.W.H. (2012). The effects of an exercise stage-
matched interventions on quality of life in patients with coronary heart disease.
The 15th
East Asian Forum of Nursing Scholars (EAFONS), Singapore, 22-23
February 2012, 30.
3. Zhu, L.X., Ho, S.C. & Sit, J.W.H. (2011). The effects of exercise stage-matched
interventions on exercise behavior change among patients with coronary heart
disease – A pilot study. CUHK-Mayo Clinic-Asia Cardiovascular Summit, Hong
Kong, 26-27 March 2011, s11.
4. Zhu, L.X., Ho, S.C. & Sit, J.W.H. (2010). The effects of exercise stage-matched
interventions on patients with coronary heart disease: A pilot study. Wuhan
International Conference 2010, Community Engagement Paving the Way to
Optimal Health, Wuhan, 3-4 April 2010, 80.
5. Zhu, L.X., Ho, S.C. & Sit, J.W.H. (2009). The experiences of Chinese patients
with coronary heart disease. The 12th East Asian Forum of Nursing Scholars
(EAFONS), Tokyo, Japan, 13-14 March 2009, 50.

viii
ACKNOWLEDGEMENTS
As a PhD student in the School of Nursing (SN), The Hong Kong Polytechnic
University, studying was a magnificent as well as a challenging experience for me. I
encountered difficulties and hardships. Nonetheless, these four years are also among
the happiest times of my life, and have provided me with some of my most precious
memories. Many people have directly or indirectly helped me to overcome my fear
and difficulties, enabling me to successfully complete my studies. I would like to
express my deepest gratitude to them here.
First of all, I sincerely thank my chief supervisor, Dr Jacqueline Ho, and my co-
supervisor, Dr Janet Sit, for their guidance and supervision throughout the whole
course of my doctoral studies. It would have been impossible for me to complete my
doctoral project without their kind support, encouragement, and help during these four
years. I would also like to take this opportunity to thank my two other co-supervisors,
Dr Guoqiang Ruan and Dr Qiang Xie, for their kind support and help during the data
collection process.
I also thank Miss Haihua ZHU for allowing me to collect data in the Xiamen Heart
Centre and giving me substantial support during the collecting of data. Many thanks
go to Dr Shuilong Chen, who offered me valuable assistance in screening patients and
prescribing exercises during the process of data collection. Special thanks go to Miss
Si Shi, who helped me to collect data for this study. Without their kind help and
support, it would have been impossible to complete the data collection process so
smoothly. I also wish to thank all of the nursing sisters in the cardiovascular ward of

ix
the Xiamen Heart Centre and The First Affiliated Hospital of Xiamen University for
their valuable assistance in many areas. In addition, I wish to thank all of the
participants in this study. Without their participation and full support, it would have
been impossible for me to conduct my research.
I would like to express my deepest appreciation to my family. I could have achieved
nothing without the support, love, and understanding of my husband, Haidong Yang,
throughout the whole study. I wish to express my special appreciation to my son,
Jingchen Yang. I would not have had the peace of mind to study without my son‘s
support. I also wish to express my deepest gratitude to my parents, Qingfu Zhu and
Jinyan Lin, who brought me up. I am especially grateful to my parents-in-law, Jinrui
Yang and Meipi Yang. I would not have been able to complete my studies without
their kind support and help in taking care of my son during the past four years. My
appreciation also is extended to other family members, Wenjin Yang, Guobao Zhu,
Liying Zhu, Yuanbao Zhu, and others, for their encouragement and support in the past
four years.

x
TABLE OF CONTENTS
Contents Page
Certificate of originality ……………………………………………………… ii
Abstract ……………………………………………………………………….. iii
Publications arising from the thesis …………………………………………. vi
Conference presentation ……………………………………………………... vii
Acknowledgement …………………………………………………………….. viii
Table of contents ……………………………………………………………… x
List of tables …………………………………………………………………... xiv
List of figures …………………………………………………………………. xvii
Chapter 1: Introduction ……………………………………………………… 1
1.1 Introduction …………………………………………………………….., 1
1.2 Background ……………………………………………………………… 1
1.3 Aim and Objectives ……………………………………………………... 7
1.4 Research questions ……………………………………………………… 7
1.5 Theoretical framework ………………………………………………….. 8
1.6 Significance of the study ……………………………………………….. 12
1.7 Thesis outline …………………………………………………………… 14
1.8 Summary ………………………………………………………………... 15
Chapter 2: Literature Review ……………………………………………….. 16
2.1 Introduction ……………………………………………………………... 16
2.2 Coronary heart disease (CHD) ………………………………………….. 16
2.2.1 Definition of coronary heart disease ………………………………. 16
2.2.2 Prevalence of coronary heart disease …………………………….... 17
2.2.3 Impact of coronary heart disease on patients …………………….... 21
2.3 Exercise and coronary heart disease …………………………………….. 34
2.3.1 Benefits of exercise for CHD patients …………………………….. 35
2.3.2 Hospital-based versus home-based exercise programmes ……….... 49
2.3.3 Cardiac rehabilitation programmes in China …………………….... 52
2.3.4 Safety of exercise for CHD patients ………………………………. 53
2.3.5 Poor attendance of exercise-based cardiac rehabilitation …………. 54
2.4 Patient education and exercise behaviour ……………………………….. 57

xi
2.4.1 Information needs of CHD patients ……………………………….. 57
2.4.2 Patient education on health promotion ……………………………. 61
2.4.3 Patient education and exercise behaviour …………………………. 66
2.4.4 Factors affecting the effectiveness of patient education …………... 95
2.4.5 Theoretical basis for patient education ……………………………. 98
2.5 The Transtheoretical Model (TTM) ……………………………………... 102
2.5.1 Overview of the TTM ……………………………………………... 103
2.5.2 The TTM and exercise behaviour………………………………….. 113
2.5.3 The TTM for changing exercise behaviour among patients with
heart disease ………………………………………………………...
131
2.6 Summary ……………………………………………………………….... 135
Chapter 3: Research Methodology ………………………………………….. 137
3.1 Introduction ……………………………………………………………... 137
3.2 Study design …………………………………………………………….. 137
3.3 Settings ………………………………………………………………….. 139
3.4 Sampling ………………………………………………………………… 139
3.5 Procedures ……………………………………………………………..... 142
3.6 Intervention ……………………………………………………………… 144
3.7 Instruments ……………………………………………………………… 153
3.8 Data collection …………………………………………………………... 170
3.9 Ethical considerations …………………………………………………… 171
3.10 Data analysis ………………………………………………………….... 172
3.11 Summary ……………………………………………………………….. 176
Chapter 4: The Pilot Study …………………………………………………... 177
4.1 Introduction ……………………………………………………………... 177
4.2 Aims …………………………………………………………………….. 177
4.3 Description of the setting………………………………………………… 177
4.4 Procedures ………………………………………………………………. 178
4.5 Results …………………………………………………………………... 180
4.5.1 Demographic and clinical characteristics …………………………. 183
4.5.2 Exercise stages of change …………………………………………. 186
4.5.3 Exercise self-efficacy ……………………………………………... 187
4.5.4 Exercise decisional balance ……………………………………….. 187

xii
4.5.5 Exercise …………………………………………………………… 189
4.5.6 Angina …………………………………………………………….. 190
4.5.7 Quality of life ……………………………………………………... 191
4.6 Implications for the main study …………………………………………. 195
4.7 Summary ……………………………………………………………….... 198
Chapter 5: Results ………………………………………………………......... 199
5.1 Introduction ……………………………………………………………... 199
5.2 Recruitment of patients ………………………………………………….. 199
5.3 Demographic and clinical characteristics of dropouts versus completers.. 202
5.4 Demographic and clinical characteristics of the patients ……………….. 205
5.5 Effects of the exercise stage-matched intervention (ESMI) …………….. 210
5.5.1 Exercise stages of change …………………………………………. 210
5.5.2 Exercise self-efficacy ……………………………………………... 218
5.5.3 Exercise decisional balance ……………………………………….. 222
5.5.4 Exercise …………………………………………………………… 228
5.5.5 Angina …………………………………………………………….. 234
5.5.6 Quality of life ……………………………………………………... 245
5.6 Summary ……………………………………………………………….... 273
Chapter 6: Discussion ………………………………………………………… 274
6.1 Introduction ……………………………………………………………... 274
6.2 High participation/completion rate ……………….................................... 274
6.3 The effects of the ESMI on CHD patients ………………………………. 276
6.3.1 Exercise behaviour …………………………………………........... 277
6.3.2 Health outcomes ……………………………………………........... 290
6.4 Tracking of the TTM-based ESMI on exercise behaviour …………….... 298
6.5 Limitations and controversies of the TTM ……………………………… 300
6.6 Nursing role of cardiac rehabilitation in mainland China ………………. 306
6.7 Summary ………………………………………………………………... 308
Chapter 7: Conclusions and Implications …………………………………... 310
7.1 Introduction ……………………………………………………………... 310
7.2 Conclusions from the findings …………………………………………... 310
7.3 Limitations of this study and recommendations for future research ……. 312
7.4 Implications ……………………………………………………………... 314

xiii
7.5 Summary ………………………………………………………………... 318
References ……………………………………………………………………... 319
Appendices ……………………………………………………………………. 365
Appendix I Contraindications for Exercise Training ……………………… 366
Appendix II Ethics Approval Letters ……………………………………… 368
Appendix III Access Approval Letters from the Hospitals …………........... 369
Appendix IV Screening Guidelines ………………………………………... 372
Appendix V Information Sheet ……………………………………………. 386
Appendix VI Consent Form ……………………………………………….. 388
Appendix VII Protocol of Weekly Patient Education Session …………….. 389
Appendix VIII Guidelines for Exercise Prescription ……………………… 390
Appendix IX Exercise Stage-Matched Pamphlets ……………..................... 397
Appendix X An Example of the TTM-based ESMI……………................... 444
Appendix XI Screening Form ……………………………………………… 446
Appendix XII Questionnaires ……………………………………………… 452
Appendix XIII Scoring Instructions ……………………………………….. 471
Appendix XIV Training Package ………………………………………….. 488
Appendix XV Status of Normal Distribution and Homogeneity of Variance
of Each Variable .......................................................................... 515
Appendix XVI The Results of the Baseline Outcome Comparisons ............. 516
Appendix III Access Approval Letters from the Hospitals - Chinese
Version ...................................................................................... ... 521
Appendix IV Screening Guidelines – Chinese Version……………………. 524
Appendix V Information Sheet – Chinese Version……………………….... 532
Appendix VI Consent Form – Chinese Version……………………………. 533
Appendix VII Protocol of Weekly Patient Education Session – Chinese
Version…...................................................................................... 534
Appendix VIII Guidelines for Exercise Prescription – Chinese Version ….. 535
Appendix IX Exercise Stage-Matched Pamphlets – Chinese Version…....... 541
Appendix XI Screening Form – Chinese Version .…………........................ 590
Appendix XII Questionnaires – Chinese Version …………......................... 596
Appendix XIII Scoring Instructions – Chinese Version …………................ 613
Appendix XIV Training Package – Chinese Version …………………….... 629
xiv
LIST OF TABLES
Table Page
Table 2.1 Studies on the effect of patient education on exercise behaviour …. 68
Table 2.2 Definitions of the processes of change for physical activity ……… 112
Table 2.3 The emphasis of different change processes according to stages of
change …………………………………………………………......
113
Table 3.1 Protocol of weekly exercise stage-matched intervention session ..... 148
Table 3.2 Guidelines of goal, processes, and strategies for changing exercise
behaviour in each stage ……………………………………............
149
Table 3.3 Outcome measurements …………………………………………… 157
Table 4.1 Demographic characteristics of the subjects ………………………. 184
Table 4.2 Clinical characteristics of the subjects …………………………….. 185
Table 4.3 Distribution of the exercise stages of change in the three groups …. 186
Table 4.4 Changes in the exercise stages of change in the three groups at T1 .. 186
Table 4.5 Changes in the mean scores of the exercise self-efficacy (ESE) in
the three groups ……………………………………………………
187
Table 4.6 Changes in the mean scores of the exercise benefits scale (EBS)
and exercise barriers scale (EBBS) in the three groups …………...
188
Table 4.7 Changes in the mean minutes of the total exercise duration and
moderate exercise duration per week in the three groups …………
189
Table 4.8 Changes in angina frequency, angina severity and angina duration
in the three groups ………………………………………................
190
Table 4.9 Changes in the mean scores of the five subscales of SAQ in the
three groups ………………………………………………………..
192
Table 4.10 Changes in the mean scores of the eight domains of SF-36 in the
three groups ………………………………………………………..
194
Table 5.1 Demographic characteristics of dropouts versus completers ……… 202
Table 5.2 Clinical characteristics of dropouts versus completers ……………. 204
Table 5.3 Demographic characteristics of the subjects ………………………. 206
Table 5.4 Clinical characteristics of the subjects …………………………….. 209
Table 5.5 Exercise stages of change at each time point ……………………… 212
Table 5.6 Comparisons of movement of exercise stages of change among

xv
groups at each time point …………………………………………. 215
Table 5.7 Comparisons of the mean change scores of the exercise stages of
change among groups at each time point ……………………….....
217
Table 5.8 Comparisons of exercise stages of change within each group across
time ………………………………………………………………...
218
Table 5.9 Mean and standard deviation of the exercise self-efficacy (ESE)
scale scores at each time point …………………………………….
219
Table 5.10 Comparisons of the mean change scores of the exercise self-
efficacy (ESE) scale among groups at each time point ……………
221
Table 5.11 Comparisons of exercise self-efficacy (ESE) within each group
across time …………………………………………………………
222
Table 5.12 Mean and standard deviation of the exercise benefits (EBS) scale
scores and exercise barriers scale (EBBS) scores at each time
point ………….................................................................................
224
Table 5.13 Comparisons of the mean change scores of the exercise benefits
scale (EBS) scores and exercise barriers scale (EBBS) scores
among groups at each time point ………………………………….
227
Table 5.14 Comparisons of the exercise benefits scale (EBS) scores and
exercise barriers scale (EBBS) scores within each group across
time ………………..........................................................................
228
Table 5.15 Mean and standard deviation of exercise duration (minutes/week)
at each time point ………………………………………………….
230
Table 5.16 Comparisons of the mean change minutes of exercise duration
(minutes/week) between groups at each time point ……………….
233
Table 5.17 Comparisons of exercise duration (minutes/week) within each
group across time ………………………………………………….
234
Table 5.18 Mean and standard deviation of angina frequency, angina severity
and angina duration at each time point ……………………………
237
Table 5.19 Comparisons of angina frequency, angina severity and angina
duration among groups at each time point ………………………...
240
Table 5.20 Comparisons of angina frequency, angina severity and angina
duration within each group across time ……………………………
242
Table 5.21 Comparisons of items on angina attack and anti-anginal drugs
xvi
taken in the past one week at each time point …………………….. 243
Table 5.22 Comparisons of anginal attack and anti-anginal drugs taken
within each group across time …………………………………......
245
Table 5.23 Mean and standard deviation of subscales of SAQ at each time
point ………………………………………………………………..
248
Table 5.24 Comparisons of mean change scores of subscales of SAQ among
groups at each time point ……………………………….................
253
Table 5.25 Comparisons of subscale scores of SAQ within each group across
time ………………………………………………………………...
255
Table 5.26 Mean and standard deviation of eight domains of SF-36 at each
time point …………………………………………………………..
258
Table 5.27 Comparisons of mean change scores of eight domains of SF-36
among groups at each time point ………………………………...
268
Table 5.28 Comparisons of eight domains of SF-36 within each group across
time ………………………………………………………………..
271
Table 6.1 The change in exercise stages of change in the ESMI group during
the intervention period .....................................................................
299

xvii
LIST OF FIGURES
Figure Page
Figure 1.1 Theoretical framework of the study …............................................. 11
Figure 2.1 The transtheoretical model of behaviour change …………………. 104
Figure 2.2 Relationship among stages of change, processes of change,
decisional balance and self-efficacy ……………………………….
105
Figure 3.1 Flowchart of the study design …………………………………….. 138
Figure 4.1 Flowchart of the pilot study ………………………………………. 182
Figure 5.1 Flowchart of the recruitment process....…………………………... 201
Figure 5.2 The number of patients in the action and maintenance stages at
each time point …………………………………………………….
213
Figure 5.3 The change in the exercise self-efficacy (ESE) scores throughout
the study …………………………………………………………...
220
Figure 5.4 The change in the exercise benefits scale (EBS) scores throughout
the study …………………………………………………………...
225
Figure 5.5 The change in the exercise barriers scale (EBBS) scores
throughout the study ……………………………………………….
225
Figure 5.6 The change in the total exercise duration (minute/week)
throughout the study ……………………………………………….
231
Figure 5.7 The change in the moderate exercise duration (minute/week)
throughout the study ……………………………………………….
231
Figure 5.8 The change in the angina frequency (episode/week) throughout
the study …………………………………………………………...
238
Figure 5.9 The change in the angina severity (0-10) throughout the study ….. 238
Figure 5.10 The change in the angina duration (minute/week) throughout the
study ……………………………………………………………….
239
Figure 5.11 The change in the physical limitation scores of SAQ throughout
the study …………………………………………………………...
249
Figure 5.12 The change in the angina stability scores of SAQ throughout the
study ……………………………………………………………….
249
Figure 5.13 The change in the angina frequency scores of SAQ throughout
the study …………………………………………………………...
250

xviii
Figure 5.14 The change in the treatment satisfaction scores of SAQ
throughout the study ……………………………………………….
250
Figure 5.15 The change in the disease perception scores of SAQ throughout
the study …………………………………………………………...
251
Figure 5.16 The change in the physical functioning scores of SF-36
throughout the study ………………………………………………
260
Figure 5.17 The change in the role-physical scores of SF-36 throughout the
study ……………………………………………………………….
260
Figure 5.18 The change in the bodily pain scores of SF-36 throughout the
study ……………………………………………………………….
261
Figure 5.19 The change of the general health scores of SF-36 throughout the
study ……………………………………………………………….
261
Figure 5.20 The change in the vitality scores of SF-36 throughout the study 262
Figure 5.21 The change in the social functioning scores of SF-36 throughout
the study …………………………………………………………...
262
Figure 5.22 The change in the role-emotional scores of SF-36 throughout the
study ……………………………………………………………….
263
Figure 5.23 The change in the mental health scores of SF-36 throughout the
study ……………………………………………………………….
263
Figure 5.24 The change in the physical component summary of SF-36
throughout the study ……………………………………………….
264
Figure 5.25 The change in the mental component summary of SF-36
throughout the study ……………………………………………….
264
Figure 5.26 The change in the reported health transition scores of SF-36
throughout the study ……………………………………………….
265

1
Chapter 1 Introduction
1.1 Introduction
This chapter presents an overview of this study and the reasons for conducting it. It
includes the background to the research problem, and the aims and objectives,
research questions, theoretical framework, and significance of the study.
1.2 Background
Although the World Health Organization (WHO) emphasizes primary and secondary
preventions of coronary heart disease (CHD), CHD is still a leading cause of death
and disability among adults worldwide (Lloyd-Jones, Adams, Brown et al., 2010).
The prevalence of CHD has increased rapidly over the past few decades in China
(Zhang, Lu & Liu, 2008). Around 652,000 people were diagnosed with CHD and
400,000 died of the disease in 2004, accounting for 22.0% of deaths from
cardiovascular disease and 9.0% of total deaths among the country‘s urban population
(Zhang, Lu & Liu, 2008). CHD has become the third leading cause of death among
Chinese adults (Health Statistics Information Centre of Ministry of Health, 2010). The
burden of caring for those with CHD has been growing in China and will become the
leading health care issue if methods of both primary and secondary prevention are not
addressed (Teo, Liu, Chow et al., 2009).
Exercise training alone or exercise-based cardiac rehabilitation has been shown to be
beneficial to CHD patients (Senuzun, Fadiloglu, Burke & Payzin, 2006; Taylor,

2
Brown, Ebrahim et al., 2004; Valkeinen, Analtonen & Kujala, 2010). The benefits
include a decrease in the frequency of anginal attacks and the number of sublingual
glyceryl trinitrate (GTN) tablets that need to be taken (Burke, Williams & Lockyer,
2002; Lewin, Furze, Robinson et al., 2002), a reduction in mortality rates, fatal
reinfarctions, and cardiac risk factors (e.g., lipid profiles and BMI) (Chair, Thompson,
Tang & Leung, 2007; Jolliffe, Rees, Taylor et al., 2001; Kelley, Kelley & Franklin,
2006; Taylor, Brown, Ebrahim et al., 2004), and improvements in physical
functioning (Brubaker, Witta & Angelopoulos, 2003; Franklin, Bonzheim, Warren et
al., 2002; Senuzun, Fadiloglu, Burke & Payzin, 2006), psychological well-being
(Arnold, Sewell & Singh, 2007; Burke, Williams & Lockyer, 2002; Lewin, Furze,
Robinson et al., 2002), and quality of life (Davies, Moxham, Rees et al., 2002; Hwang
& Marwick, 2009; Jeger, Jörg, Rickenbacher et al., 2007).
However, the participation rate in exercise training or exercise-based cardiac
rehabilitation programmes is low around the world despite convincing evidence of the
benefits of such programmes. In the United States, two large cohort reports on
Medicare patients showed that only 12.2% (N = 601,099) to 18.7% (N = 267,427) of
CHD patients attended at least one session of an outpatient cardiac rehabilitation
programme after being discharged from the hospital (Suaya, Shepard, Normand et al.,
2007; Suaya, Stason, Ades et al., 2009). In England, nationally, 29.0% of eligible
CHD patients attended cardiac rehabilitation programmes, with the proportion ranging
from 14.0% to 37.0% within regions (Bethell, Lewin, Evans et al., 2008). In Japan,
the national participation rate in outpatient cardiac rehabilitation programmes
following acute myocardial infarction was found to be only 3.8-7.6% (Goto, Saito,
Iwasaka et al., 2007). In Hong Kong, a study exploring the utilization of a 7-week
3
phase II outpatient cardiac rehabilitation programme showed that only 25.0% (37/145)
of the participants attended at least one session during the 6-month period following
their discharge from hospital and only 7.5% (11/145) completed the programme
(Chan, Chau & Chang, 2005). Although exercise-based cardiac rehabilitation has
been well developed in many countries, it is still underdeveloped in mainland China
(Thompson & Yu, 2007; Wang, Chair, Thompson & Twinn, 2009).
Of those who participated in cardiac rehabilitation programmes, the dropout rate is
high. In a randomized exercise trial, around 20.0% of patients following myocardial
infarction who participated in the exercise programme withdrew from it after two
months, and the dropout rate reached 45.0% during the first six months of the
programme (Dorn, Naughton, Imamura & Trevisan, 2001). Another study showed
that around 50.0% of women with CHD (107/228) failed to complete the prescribed
sessions (Sanderson & Bittner, 2005). Similar observations were made by Moore et al.
(2003), Sanderson et al. (2003), Sarrafzadegan et al. (2007), and Worcester et al.
(2004). Women, elderly persons or those with a low level of education, and those
suffering from depression or severe diseases were particularly prone to dropping out
of the programmes (Dorn, Naughton, Imamura & Trevisan, 2001; Suaya, Shepard,
Normand et al., 2007; Witt, Jacobsen, Weston et al., 2004). Given such discouraging
figures, interventions are needed to improve the uptake of exercise-based cardiac
rehabilitation programmes and adherence to them.
The possible reasons for the low attendance rates and poor adherence to exercise-
based cardiac rehabilitation programmes may be that CHD patients lack the interest or
motivation to attend the programmes (Evenson, Johnson & Aytur, 2006), or that they

4
lack the confidence to perform exercises, worry about the occurrence of angina, or
hold the misconception that physical activity may provoke an anginal attack
(Kristofferzon, Löfmark & Carlsson, 2007; Thompson & Lewin, 2000; Zhu, Ho & Sit,
2012). Our previous interview (Zhu, Ho & Sit, 2012) with 11 Chinese CHD patients
in mainland China shows that patients perceived CHD as a life-threatening illness
mostly related to chest pain and worries about the recurrence of heart attacks. Patients
often hold misconception that heart attacks are unpreventable and that physical
activity provokes chest pain. The result of these misconceptions is fewer changes in
behaviour and disengagement from physical activity. The use of action-oriented
interventions in cardiac rehabilitation programmes may also contribute to the low
attendance rates. This is because such interventions are typically designed for people
who are highly motivated and ready to change their behaviour. They are not effective
enough to motivate changes in behaviour among those who have no intention to
change or no interest in changing their behaviour (Marcus, Emmons, Simkin-
Slverman et al., 1998).
Health education is the most common intervention for increasing physical activity
among ageing adults (Conn, Valentine & Cooper, 2002). Having a theory/model to
guide health education is thought to be more effective in producing changes in
behaviour than having no theory/model (Painter, Borba, Hynes et al., 2008).
Numerous models and theories, such as the Transtheoretical Model (TTM), the Social
Cognitive Theory (SCT), the Health Belief Model (HBM), the Theory of Reasoned
Action (TRA), and the Theory of Planned Behaviour (TPB), have been used for
patient education to promote behavioural changes. Among these models/theories, the
TTM has been found to be effective on motivating changes in behaviour (Faghri,
5
Omokaro, Parker et al., 2008; Kim, 2007 & 2008; Lippke, Schwarzer, Ziegelmann et
al., 2010; Prochaska & DiClemente, 1983). The strength of the TTM is that it treats
behavioural change as a dynamic rather than an ―all or nothing‖ phenomenon
(Marshall & Biddle, 2001). The SCT, TPB, and HBM all focus on explaining a purely
behavioural criterion, namely, engaging in behaviour or not, whereas the TTM
explains a complex, mixed criterion that includes five stages of readiness for
behavioural change based on the cognitive, motivational, and behavioural aspects of
an individual (Courneya, 1995). The TTM allows practitioners to develop a stage-
matched intervention with reference to the stages of readiness for behavioural change.
For example, for an individual at the stages of precontemplation and contemplation,
no action-oriented intervention will be implemented because of the individual‘s lack
of intention or preparation to change his/her behaviour at these stages. Thus, the
employment of the TTM for changing exercise behaviour may be more appropriate
than mismatched or action-oriented interventions (Marcus, Emmons, Simkin-
Silverman et al., 1998).
A number of studies have illustrated that the TTM is an effective model for changing
exercise behaviour among various populations, from adolescents (Nigg & Courneya,
1998) to the elderly (Burbank, Reibe, Padula & Nigg, 2002; Findorff, Stock, Gross &
Wyman, 2007; Greaney, Riebe, Garber et al., 2008; Resnick & Nigg, 2003). Several
cross-sectional and longitudinal studies (Hellman, 1997; Jue & Cunningham, 1998)
showed that the application of the TTM for changing exercise behaviour could be
adopted for older adults with heart disease. Unfortunately, there have been few studies
examining the effects of the TTM-based intervention on changes in exercise
behaviour among heart disease patients. In our previous systematic review (Zhu, Ho

6
& Wong, unpublished), we found only three studies that used the TTM to motivate
heart disease patients to exercise. However, these three studies came to different
conclusions about adherence to exercise (Hughes, Gillies, Kirk et al., 2002; Hughes,
Mutrie & Maclntyre, 2007; Naser, Jafar, Kumar et al., 2008).
Despite these inconsistent results, all of these three studies recruited participants
immediately after the completion of the formal cardiac rehabilitation programme.
Clearly, all of the participants were in the preparation, action, or maintenance stages
at the time that they entered the study, which means that they were ready to change
their behaviour or already active at baseline. Based on the TTM, the strategies and
techniques (processes of change) used to motivate individuals in the precontemplation
or contemplation stages to change their behaviour are different from those in the
preparation, action, or maintenance stages because those in the precontemplation
stage usually have no intention or interest in changing their behaviour (Prochaska &
DiClemente, 1983). Individuals in the precontemplation stage tend to be defensive
and avoid changing their thinking and behaviour and to use fewer processes of change
than those in any other stage (Prochaska & DiClemente, 1983). Thus, whether the
TTM-based Exercise Stage-Matched Intervention (ESMI) is effective at motivating
sedentary patients with heart disease, who are in the precontemplation, contemplation,
and preparation stages, to engage in exercise is not clear.
In summary, regular exercise is beneficial for CHD patients. However, rates of
participation and adherence to exercise-based cardiac rehabilitation programmes are
unsatisfactory. The TTM is well known for motivating changes in behaviour; however,
it is seldom used to bring about changes in exercise behaviour among CHD patients.

7
Therefore, whether or not it can motivate sedentary CHD patients to engage in
exercise is unclear.
1.3 Aim and Objectives
The aim of this study is to evaluate the effects of a TTM-based Exercise Stage-
Matched Intervention (ESMI) on sedentary patients with CHD. The primary outcome
indicator is change in exercise behaviour in terms of exercise stages of change,
exercise self-efficacy, exercise decisional balance, and exercise duration per week.
The secondary outcome indicators are anginal attacks and quality of life. The
following objectives were set accordingly:
(1) To evaluate the effects of the TTM-based ESMI on changes in exercise
behaviour in CHD patients;
(2) To evaluate the effects of the TTM-based ESMI on anginal attacks in CHD
patients;
(3) To evaluate the effects of the TTM-based ESMI on the quality of life of CHD
patients.
1.4 Research questions
In accordance with the objectives of this study, the following research questions were
generated:

8
Will the CHD patients participating in the Exercise Stage-Matched Intervention
(ESMI) group:
(1) demonstrate a more positive shift in exercise stages of change than the
patients in the Patient Education (PE) group and the Conventional (C)
group?
(2) demonstrate higher exercise self-efficacy than the patients in the PE group
and the C group?
(3) demonstrate better exercise decisional balance in terms of greater exercise
benefits and fewer exercise barriers than the patients in the PE group and
the C group?
(4) demonstrate longer exercise duration (minutes/week) than the patients in
the PE group and the C group?
(5) demonstrate greater improvement in anginal attacks in terms of a reduction
in the frequency (episode/week), severity, and duration (minutes/week) of
angina and the number of anti-anginal drugs taken than the patients in the
PE group and the C group?
(6) demonstrate greater improvement in quality of life than the patients in the
PE group and the C group?
1.5 Theoretical Framework
In this study, the Exercise Stage-Matched Intervention (ESMI) was guided by the
TTM. The TTM consists of four constructs, including stages of change, processes of
change, self-efficacy for behavioural change, and decisional balance (Prochaska &
DiClemente, 1983). Based on the stages of change, individuals are divided into one of

9
the following five stages: precontemplation (no intention to start exercise in the next
six months), contemplation (being aware the problem exists and thinking about
starting exercise), preparation (currently engaging in some exercise, but not regularly),
action (successfully exercising regularly for less than six months), and maintenance
(exercising regularly for more than six months) (Marcus, Eaton, Rossi & Harlow,
1994; Prochaska & DiClemente, 1983). In this study, regular exercise is defined as
accumulating at least 30 minutes of moderate intensity physical activity throughout
the day for more than five days of the week (American College of Sports Medicine,
2006; Marcus, Forsyth & Blair, 2003).
The processes of change are covert and overt strategies and techniques that
individuals engage in when they attempt to modify their behaviours (Prochaska,
DiClemente & Norcross, 1992). There are ten processes, including consciousness
raising, dramatic relief, self-reevaluation, social liberation, environmental
reevaluation, helping relationships, counterconditioning, reinforcement management,
self-liberation, and stimulus control. Self-efficacy for behavioural change is an
important predictor of progress, with a linear increase from the precontemplation to
the maintenance stage. Higher self-efficacy means that individuals have a higher level
of confidence in their ability to engage in exercise. Decisional balance includes the
benefits and costs of performing a behavioural change, which vary across stages of
change. In the precontemplation stage, the benefits are meagre, with the costs
outweighing the benefits. By the contemplation or preparation stage, the benefits
increase to the same level as the costs, with the benefits eventually outweighing the
costs in the action and maintenance stages (Plotnikoff, Hotz, Birkett & Courneya,
2001).

10
The stages of change represent a temporal or developmental dimension that allows us
to understand when particular changes in attitudes, intentions, and behaviours occur,
while the processes of change enable us to understand how these changes occur
(Prochaska, DiClemente & Norcross, 1992). The TTM offers a promising approach to
integrating the stages and processes of change. Based on the stages of change,
researchers can develop stage-matched interventions. Individuals in different stages
use different processes of change to help them move on to a more advanced stage.
The processes of change are strategies and techniques used to motivate CHD patients
to change their exercise behaviour. For patients in different exercise stages of change,
different goals are set and different processes of change are used to enable them to
progress in stage. Subsequently, the ESMI improves individuals‘ exercise stages of
change, exercise self-efficacy, and exercise decisional balance (Kim, 2008; Marcus,
Emmons, Simkin-Silverman et al., 1998). Individuals with higher exercise self-
efficacy have more confidence about changing their exercise behaviour, which results
in a more positive shift in exercise stages of change. When the level of benefits of
changing one‘s exercise behaviour increase to the same level as the barriers,
individuals start to take action to change their exercise behaviour. When the benefits
outweigh the barriers, individuals are more likely to successfully adhere to exercise
behaviour, namely in the action and maintenance stages. The result is motivation to
engage in exercise.
After being motivated to exercise, individuals will tend to increase the duration of
their exercise, which is beneficial for CHD patients in terms of reducing anginal

11
attacks (Hambrecht, Walther, Möbius-Winkler et al., 2004) and improving their
quality of life (QoL) (Hwang & Marwick, 2009). A theoretical framework for the
ESMI is shown in Figure 1.1.
Processes of change
ESMI
Stages of
change
Decisional
balance
Self-efficacy
Exercise Motivation
Figure 1.1 Theoretical Framework of the Study
Reduce
Angina
Improve
Quality of Life
Increase
Exercise
Duration

12
1.6 Significance of the Study
The benefits of exercise-based cardiac rehabilitation programmes for cardiac patients
have been well documented. It is a worldwide problem that the participation and
adherence rates to the programmes are poor. The extent to which cardiac
rehabilitation services are effective depends on the patients‘ willingness and/or ability
to participate in and adhere to the recommended strategies necessary to achieve the
desired benefits (Sanderson & Bittner, 2005). Thus, how to motivate CHD patients to
exercise and/or how to improve the participation rate in exercise-based cardiac
rehabilitation programmes are global concerns. The TTM is an effective model for
bringing about changes in various behaviours, including exercise. Investigating the
effects of the TTM-based Exercise Stage-Matched Intervention (ESMI) on motivating
sedentary CHD patients to engage in exercise is timely, necessary, and important.
Although many studies regarding cardiac rehabilitation have been conducted in recent
years on patients with CHD, most of these were conducted in Western countries. Few
such studies have been conducted in China. Chen and Whitlock (2009) have pointed
out that more than 80.0% of deaths from cardiovascular disease are occurring in low-
and middle-income countries such as China, but most of the studies on this disease
have been conducted among populations in high-income countries. As a result, many
of the related clinical and public health policies being applied in lower-income
countries stem from studies carried out in high-income ones, and may therefore be
inappropriate given the substantially different physical, social, and economic
environments between the two types of countries. Thus, the findings from this study

13
should provide evidence for clinical practice and a foundation for further studies and
for the development of cardiac rehabilitation programmes in China.
Cardiac rehabilitation programmes have been well developed in many Western
countries. However, they are new to mainland China and are underdeveloped
(Thompson & Yu, 2007; Wang, Chair, Thompson & Twinn, 2009). Few hospitals in
China provide structured patient education programmes or formal cardiac
rehabilitation programmes for cardiac patients. Our previous qualitative study shows
that CHD patients eagerly sought information about cardiac rehabilitation and how to
prevent the recurrence of another heart attack, especially information about diet and
physical activity (Zhu, Ho & Sit, 2012). The findings from the qualitative study
highlight the need for health education to support CHD patients in mainland China.
There are no formal or structured patient education programmes in Xiamen City,
China, where the actual study was carried out. The introduction of a structured or
formal patient education programme supplemented with a booklet would be a great
improvement in the care of CHD patients. In addition, due to the increased prevalence
of chronic diseases, the Chinese government has been emphasizing primary and
secondary prevention of chronic diseases. Thus, together with the limited health care
resources, the paucity of rehabilitation facilities, and an underdeveloped
reimbursement system, the TTM-based ESMI may be a trend in the development of
cardiac rehabilitation programme in China. Home-based rehabilitation, one of the
characteristics of the TTM, should be a more practical and feasible approach to
helping Chinese CHD patients.

14
Regular exercise has been shown to be beneficial to patients with heart disease. It is
envisaged that the proposed health education programme based on the TTM will
motivate sedentary patients with coronary heart disease to engage in exercise and
consequently improve their angina and quality of life.
1.7 Thesis outline
This study consists of seven principal chapters, namely, the introduction, literature
review, research methodology, findings of the pilot study, results of the main study,
discussion, and conclusion and implications.
Chapter 1 starts with some relevant background information on the prevalence of
CHD and the benefits of exercise-based cardiac rehabilitation. Subsequently, the
problems and gaps in research, as well as the justification and significance of the
study are presented. The related aim, objectives, and research questions are then listed.
The theoretical framework of this study is provided. Lastly, this chapter provides an
outline summarizing the main contents of this thesis.
Chapter 2 contains a comprehensive review of the existing literature regarding the
research context and the main constructs under investigation, namely, coronary heart
disease, exercise, patient education, and the transtheoretical model of behaviour
change (TTM). Chapter 3 addresses the methodological issues of this study, namely,
the research design, sampling design, research procedures, detailed intervention,
outcome measurements, data collection, and data analysis.

15
Chapter 4 describes the findings from the pilot study and discusses the implications
for the main study. Chapter 5 presents the results of the main study. Chapter 6 fully
discusses the results of the main study by focusing on the research questions and
compares the findings with previous studies and the literature. Finally, Chapter 7
draws the conclusions of this study and discusses the implications for nursing practice,
as well as the limitations of the study and recommendations for future research.
1.8 Summary
Coronary heart disease is a leading cause of death and disability among adults
worldwide. Exercise-based cardiac rehabilitation programmes have been shown to
benefit patients with heart disease. However, rates of attendance in and adherence to
such programmes are poor. The TTM is a successful model for changing exercise
behaviour among various populations. Few studies have been conducted on the use of
the TTM for changing exercise behaviour in CHD patients. Therefore, whether or not
such a programme can motivate sedentary CHD patients to engage in exercise is
unclear. It is thus necessary to conduct a study to evaluate the effects of the TTM-
based Exercise Stage-Matched Intervention (ESMI) on changing the exercise
behaviour of sedentary CHD patients in China.

16
Chapter 2 Literature Review
2.1 Introduction
This chapter begins with a review of the literature on coronary heart disease (CHD),
including the prevalence of CHD and the impact of CHD on patients, followed by the
benefits and safety of exercise for CHD patients. Patient education and the
Transtheoretical Model (TTM) to promote exercise are presented as possible
approaches to address the low attendance rate in exercise-based cardiac rehabilitation
programmes. It is concluded that it is necessary to develop a patient education
programme based on the TTM to motivate sedentary CHD patients to engage in
exercise.
2.2 Coronary Heart Disease (CHD)
This section presents the definition and prevalence of CHD, and the impact of CHD
on patients, including physical, psychological, and social domains, and quality of life.
2.2.1 Definition of Coronary Heart Disease (CHD)
Coronary heart disease (CHD), also called ischemic heart disease, refers to coronary
circulation failure arising from a reduction or arrest of the blood supply to the
myocardium resulting from atherosclerosis of the coronary arteries and related
phenomena such as atheromatous plaque rupture and thrombosis (Khaw, 2005). CHD
manifests clinically as angina pectoris, myocardial infarction, cardiac failure,
17
arrhythmias and/or sudden death, usually related to acute arrhythmias. This study
focuses on patients with angina pectoris and/or myocardial infarction and those who
had undergone percutaneous coronary intervention (PCI).
2.2.2 Prevalence of Coronary Heart Disease (CHD)
This subsection presents the prevalence of CHD in foreign countries and China,
illustrating that the prevalence of CHD is high around the world.
Although the primary and secondary prevention of CHD is well developed, CHD is
still a leading cause of death and disability among adults worldwide. According to the
World Health Organization (WHO) (2008), an estimated 17.5 million people died of
cardiovascular disease (CVD) in 2005, representing 30.0% of all global deaths. Of
those deaths, 7.6 million were due to heart attacks and 5.7 million were due to strokes.
Around 82.0% of CVD deaths occurred in low and middle income countries (LMIC),
such as China. It was reported that, if appropriate action is not taken, an estimated
23.6 million people will die of CVD every year by 2030, mainly from coronary heart
disease and stroke (WHO, 2011).
According to the National Service Framework (2008), annually around 1.4 million
people suffer from angina and nearly 300,000 people suffer from myocardial
infarction (MI). In the United States, the prevalence of CHD was estimated to be 13
million (6.9% of the population) in 2002 (Bittner & Sanderson, 2006). Statistics from
the American Heart Association (2001) show that around 450,000 people die of CHD
each year. A recent report from the American Heart Association (Rosamond, Flegal,

18
Furie et al., 2008) shows that an estimated 600,000 new heart attacks and 320,000
recurrent attacks occur annually, and that CHD causes 20.0% of all deaths in the
United States. Rosamond et al. (2008) stated that 770,000 new heart attack cases
would be reported in America in 2008, and that nearly 430,000 would be potentially
recurrent attack cases. The prevalence of CHD was found to increase with age but to
decrease with rising educational levels (Rosamond, Flegal, Furie et al., 2008). It has
been reported that an estimated 30 million Americans will be diagnosed with CHD by
2050 (Foot, Lewis, Pearson & Beller, 2000).
In the United Kingdom, approximately two million people are suffering from angina
(Deaton & Namasivayam, 2004). The prevalence of angina was 5.0-10.0% in men
aged 40 to 60, with the incidence increasing with age (Bono, 1999). A recent cohort
study (Lampe, Morris & Walker, 2005), which followed up 7,735 men aged 40 to 59
from 1978 to 2000, showed that the rate of major coronary events fell substantially by
an average of 3.6% per year over the 20-year period, while the rate at which angina
pectoris was first diagnosed increased by an average of 2.6% per year. The findings
suggest that the number of survivors of CHD has increased.
In Finland, CHD causes approximately 14,000 deaths (7,500 men and 6,500 women)
every year in a population of about five million (Lukkarinen & Hentinen, 1997).
Approximately 50,000 people are diagnosed with coronary artery disease annually.
Cardiovascular disease is also the leading cause of morbidity and mortality in Ireland,
accounting for 39.0% of all deaths (Condon & McCarthy, 2006). In Sweden, it was
estimated that 90,000 people are being hospitalized annually due to MI.

19
Cardiovascular disease accounts for about 30.0% of all deaths in Sweden and 13.0%
of deaths are caused by MI (Bergman & Bertero, 2003).
In Hong Kong, heart disease has been the second leading cause of death since the
1960s (Department of Health, 2011), and more than 68.0% of all deaths from heart
disease are due to CHD (Hospital Authority, 2011). On average, CHD kills one Hong
Kong citizen every hour (Census and Statistics Department, 2011). Deaths from CHD
have increased in the period between 1981 and 2009, rising from 2,103 deaths in 1981
to 4,003 in 2005 and 4,360 in 2009 (Hospital Authority, 2011). Age standardized
CHD mortality rates in Hong Kong for those aged 35-64 were 44.3 (95% confidence
intervals (CI) 40.2-48.2) per 100,000 males and 14.1 (95% CI 11.6-16.6) per 100,000
females (Dwyer, Emmanuel, Janus, Wu, Hynes & Zhang, 2003). These figures
suggest that the mortality rate from CHD is high in Hong Kong. In short, the situation
regarding the prevalence of CHD in Hong Kong is also not promising.
The prevalence of CHD in China does not present an optimistic picture. It has
increased rapidly over the past few decades in China (Wu, 2003; Zhang, Lu & Liu,
2008) and has now become the third leading cause of death among Chinese adults
(Health Statistics Information Centre of Ministry of Health, 2010). The mortality rate
of CHD increased by 50.0% in men and by 27.0% in women aged 35 to 74 years in
Beijing between 1984 and 1999 (Critchley, Liu, Zhao, Wei & Capewell, 2004). From
1990 to 2000, the mortality rate of CHD has increased by 4.5% in urban areas and
4.1% in rural areas (Wu, 2003). Recent reports have shown that the morbidity rate of
CHD in China among those aged 35-74 years ranges from 2.0% to 6.0% (Chen, Meng
& Wei et al., 2007; Chen, Wei & Meng et al., 2005; Huang, Wang, Xu & Yin, 2002;

20
Li, Sun, Zheng et al., 2007; Yan, Zhang, Yang et al., 2004). Annually, there are 0.5
million new cases of MI and 3.0 million new cases of CHD (Yang, Yang & Liu,
2007). Around 652,000 people were diagnosed with CHD and 400,000 died of the
disease in 2004, accounting for 22.0% of deaths from cardiovascular disease and
9.0% of total deaths among the urban population (Zhang, Lu & Liu, 2008). According
to statistics from the WHO, in China, cardiovascular disease accounted for 33.0% of
all deaths in 2005 (WHO, 2005) and the estimated mortality of CHD was 7.3% of all
deaths in 2004 (WHO, 2004). The average mortality rate of CHD was 51.1 per
100,000 in China, ranging from 33.7 per 100,000 in rural areas to 74.1 per 100,000 in
urban areas in 2006 (Health Statistics Information Centre of Ministry of Health, 2007).
The report also illustrated that the mortality rate of CHD rises with age (2.1 per
100,000 in those aged 30-34 and 2454.8 per 100,000 in those aged 85 or above). The
latest report indicated that the mortality rate of heart disease was 128.8 per 100,000 in
cities in 2009, accounting for 20.8% of all deaths, and 112.9 per 100,000 in counties,
accounting for 17.2% of all deaths, with a rate of 118.3-133.2 per 100,000 males and
109.2-124.4 per 100,000 females in both the city and county (Health Statistics
Information Centre of Ministry of Health, 2010). The burden of caring for those with
CHD has been growing in China and will become the leading health care issue if
methods of both primary and secondary prevention are not addressed (Teo, Liu, Chow
et al., 2009).
The above review illustrates the globally high prevalence of CHD. CHD is a leading
cause of death and disability among adults globally. The prevalence of CHD has
grown quickly in recent decades in China to currently become the third leading cause
of death among adults in China.

21
2.2.3 Impact of Coronary Heart Disease on Patients
In view of the fact that CHD is one of the leading causes of death, it is important to
know about the impact of CHD on patients with respect to the physical, psychological,
emotional, and social aspects of their life, and their quality of life.
2.2.3.1 Physical Impact
The physical impact of CHD on patients can be illustrated in terms of symptoms
suffered by the patients, the limitations placed on their physical activities, or physical
disabilities.
2.2.3.1.1 Symptoms
Patients with CHD often experience a series of symptoms. Many qualitative studies
have demonstrated that the most common symptoms reported by CHD patients are
chest pain, breathlessness, and fatigue (Albarran, Clarke & Crawford, 2007;
Fitzsimons, Parahoo & Stringer, 2000; Jerlock, Gaston-Johansson & Danielson, 2005;
Johansson, Dahlberg & Ekebergh, 2003; McCormick, Naimark & Tate, 2002;
Roebuck, Furze & Thompson, 2001). Chest pain has been found to be the most severe
symptom and the most frequent reason cited by patients for why they were worried
about an impending heart attack (Roebuck, Furze & Thompson, 2001). Fitzsimons
and co-workers (2000) interviewed 70 patients waiting to undergo coronary artery
22
bypass graft (CABG) surgery. They found that the patients reported chest pain as an
experience that caused them to panic and that it was a major difficulty in their lives.
A number of quantitative studies also have indicated that CHD patients often
complain of chest pain, shortness of breath, and fatigue. A recent study in Pittsburgh
that recruited 116 black and 1,080 white CHD patients revealed that 73.8% of the
patients complained about shortness of breath, 71.8% reported experiencing chest
pain, and 5.9% reported fatigue (Hravnak, Whittle, Kellwy et al., 2007). Lindgren,
Fukuoka, Rankin and others (2008) questioned 247 elderly (age > 65 years) patients
with CHD about the symptoms they had experienced in the week before being
hospitalized. They found that fatigue was the most frequently reported symptom
(76.0%), followed by shortness of breath (62.0%) and chest pain (56.0%). These
studies have illustrated that CHD patients commonly suffer from chest pain,
breathlessness, and fatigue.
The influence of fatigue, usually raised as a complaint at the early stage of a post-MI
attack (Wiklund, Sanne, Elmfeldt et al., 1984), declines after the acute phase of MI
has passed (Hravnak, Whittle, Kellwy et al., 2007). Unlike fatigue, complaints of
chest pain and shortness of breath may last for a long time in the post-MI period. In
several large-scale cross-sectional studies, around 27.0% of patients complained of
angina one month after MI according to the Seattle Angina Questionnaire (SAQ),
24.0% six months after MI, and 20.0% 12 months after MI (Maddox, Reid, Spertus et
al., 2008; Plomondon, Magid, Masoudi et al., 2007; Spertus, Dawson, Masoudi et al.,
2006). Beinart et al. (2003) observed 1975 patients seven months after the onset of
acute coronary syndromes and found that appropriate 31.0% of the patients had

23
angina monthly, 25.0% had it weekly, and 8.7% experienced it daily. Around 50.0%
of CHD patients reported dyspnea one month after MI (Arnold, Spertus, Jones et al.,
2009). Near 40.0% of MI survivors reported chest pain and around 60.0% reported
dyspnea within five years following MI (Brown, Melville, Gray et al., 1999; Norekvål,
Wahl, Fridlund et al., 2007).) The dyspnea was strongly related to the severity of the
chest pain (Bengtson, Herlitz, Karlsson & Hjalmarson, 1996). These findings suggest
that angina and dyspnea are two common symptoms among patients with CHD, and
that these symptoms will persist for a long period of time.
Previous studies have indicated that symptoms of angina and/or dyspnea among
patients are strongly related to higher mortality (Arnold, Spertus, Jones et al., 2009;
Berecki-Gisolf, Humphreyes-Reid, Wilson & Dobson, 2009; Mozaffarian, Bryson,
Spertus et al., 2003), lower functional capacity (Scirica, 2009), a poorer quality of life
(Arnold, Spertus, Jones et al., 2009; Scirica, 2009), more frequent episodes of
rehospitalization (Arnold, Spertus, Jones et al., 2009), and lower treatment
satisfaction (Plomondon, Magid, Masoudi et al., 2007). The symptoms subsequently
influence the prognosis of CHD patients.
In a word, chest pain, shortness of breath, and fatigue were the most common
symptoms in CHD patients. Fatigue improved with time, while chest pain and
shortness of breath could have a prolonged impact on patients and were negatively
associated with survival rates, quality of life, rehospitalization, and treatment
satisfaction. Thus, interventions to improve anginal pain and shortness of breath are
critically important.

24
2.2.3.1.2 Physical Activity Limitations or Physical Disabilities
CHD patients have a lower exercise capacity than age-matched individuals without
CHD (Mital, Shrey, Govindaraju et al., 2000). As reported, heart disease has been
ranked as the third leading cause of activity limitations among those suffering from
chronic diseases (Pinsky, Jette, Branch et al., 1990). A cross-sectional study involving
4,286 women aged 60 - 79 years from 23 towns in England has shown that 37.2% of
the women experience limitations in locomotor activity and that CHD is the disease
with the second-strongest association with this limitation in activity (OR = 2.3)
(Adamson, Lawlor & Ebrahim, 2004). Following a heart attack, patients often
perceive some degree of disability or handicap. Near 90.0% of female MI survivors
(N = 145) reported that heart disease limited their daily activities during the first five
years of the post-MI period (Norekvål, Wahl, Fridlund et al., 2007). The Framingham
disability study (Pinsky, Jette, Branch et al., 1990) (N = 2576) found that disability is
is more prevalent in subjects with CHD than in those without CHD. Both
uncomplicated and complicated angina pectoris are strongly related to the degree of
disability in both men and women of all age groups. Similarly, MI patients are more
likely than those without MI to show a decline in physical functioning and social
functioning (Mendes de Leon, Krumholz, Vaccarino et al., 1998). Clearly, CHD
commonly has an impact on the daily activities of patients or results in physical
disability.
Limitations in physical activity are associated with symptoms, especially chest pain.
Kiessling and Henriksson (2007) assessed the prevalence and severity of chest pain
symptoms using the Canadian Cardiovascular Society Angina Classification in 253

25
Swedish patients with CHD. They found that 59.0% of the patients had slight to
severe chest pain limiting ordinary activities at baseline, 48.0% at the 1-year follow-
up period, and 49.0% at the 2-year follow-up period. Another study (Bengtson,
Herlitz, Karlsson & Hjalmarson, 1996), which involved 831 patients awaiting
revascularization, demonstrated that 88.0% of the patients reported chest pain that
limited their daily activities to some extent. Restricted physical activities were also
reported by CHD patients in several qualitative studies (Fitzsimons, Parahoo &
Stringer, 2000; Roebuck, Furze & Thompson, 2001). Thompson and Lewin (2000)
stated that CHD patients may lack the confidence to engage in exercise, worry about
the occurrence of angina, or hold the misconception that physical activity may
provoke an anginal attack, all of which will result in further physical deterioration.
Our preliminary qualitative study has also shown that CHD patients often stop
engaging in physical activity due to worries about provoking anginal pain (Zhu, Ho &
Sit, 2012).
Physical activity limitations or physical disability can have a further impact on the
rehabilitation of patients with CHD because physical activity or exercise is a core
component of cardiac rehabilitation programmes. Due to such limitations or
disabilities, CHD patients may stop participating in exercise-based cardiac
rehabilitation programmes. Previous studies have indicated that regular exercise or
involvement in an exercise-based cardiac rehabilitation programme significantly
increases the exercise capacity, physical fitness, and quality of life of CHD patients
(Ades, Pashkow, Fletcher et al., 2000; Bize, Johnson & Plotnikoff, 2007; Davies,
Moxham, Rees et al., 2010; Hwang & Marwick, 2009; Jeger, Jörg, Rickenbacher et al.,
2007) and reduced mortality, fatal reinfarction, and cardiac risk factors (e.g., lipid

26
profiles and BMI) (Jolliffe, Rees, Taylor et al., 2001; Kelley, Kelley & Franklin, 2006;
Taylor, Brown, Ebrahim et al., 2004). Consequently, physical limitations will delay a
patient‘s recovery.
To conclude, the most common symptoms experienced by CHD patients are chest
pain, shortness of breath, and fatigue. Patients with CHD often suffer from limitations
to their physical activities or physical disabilities to some degree. It is has been
reported that symptoms, especially chest pain, restrict their physical activities.
2.2.3.2 Psychological and Emotional Impact
The major forms of psychological and emotional distress that CHD patients complain
about are anxiety and depression, which may influence the prognosis of their disease.
This subsection presents a review of the above mentioned issues, so that the
psychological and emotional impact of CHD on patients can be addressed clearly.
2.2.3.2.1 Psychological and Emotional Distress
Owing to the high recurrence of heart attack and the high mortality rates of CHD,
patients often suffer from some kinds of psychological distress. The most common
forms of psychological distress in CHD patients are depression and anxiety. A
number of studies using various measuring instruments to examine the status of the
psychological health of CHD patients have indicated that the rate of depression
among such patients ranges from 28.4% to 78.6%, and the rate of anxiety ranges from
20.8% to 97.0% (Aben, Verhey, Strik et al., 2003; Chen, Gu, Lu & Yang, 1997; Cruz,

27
Fleck & Polanczyk, 2010; Du, Jiang, Yang et al., 2003; Hou, 2005; Jia & Shao, 2005;
Josephson, Casey, Waechter, Rosneck & Hughes, 2006; Long, Wang, Wang & Song,
2005; Todaro, Shen, Raffa et al., 2007; Wiklund, Sanne, Elmfeldt, Vedin &
Wilhelmsson, 1984; Zhang, Tang & Yu, 2005; Zhou & You, 2003). These findings
suggest that CHD patients have high morbidity rates from depression and anxiety.
When the Symptom Checklist 90 (SCL-90) was used to measure the psychological
health of CHD patients, the findings illustrated that the scores in all subscales of SCL-
90, especially in somatization, phobia, anxiety, and depression, were much higher for
CHD patients than for non-CHD patients (p < 0.05) (Aben, Verhey, Strik et al., 2003;
Huang & Zhang, 2004, Meng, Guo & Guo, 2004; Xu, 2004; Yue, 2004; Zhang,
Huang, Han & Li, 2004; Zhang, Wang & Zeng, 2004; Zhu, Lin, Huang et al., 2007).
These findings suggest that CHD patients have poor psychological health and are
prone to depression and anxiety.
When the relationship between emotional distress and cardiovascular symptoms (e.g.,
chest pain, fatigue, palpitations, presyncope, and dyspnea) was investigated, a strong
negative association was identified (Ketterer, Knysz, Keteyian et al., 2008). A
phenomenographic study (Johansson, Swahn & Strömberg, 2007) has revealed that a
patient‘s anxiety is mostly related to the nature of his/her physical symptoms. The
more severe the symptoms, the more likely anxiety is to emerge. A qualitative study
(White, Hunter & Holttum, 2007) with five newly diagnosed MI women has shown
that fear and anxiety are the most frequent emotional reactions to cardiac events.
Concerns about the future are one of main reasons for fear and anxiety. The patients
reported that they felt angry and frustrated by over-protectiveness, being told what to

28
do, and their restricted abilities. The perceived loss of their independence and the
existence of physical disabilities also made them feel sad.
Psychological and emotional distress in patients could last for a long period of time. A
study involving 201 MI patients has shown that 65.0% of the patients felt anxious and
depressed two months after MI (Wiklund, Sanne, Elmfeldt, Vedin & Wilhelmsson,
1984). More than half of the patients with acute coronary syndromes (N = 160)
reported anxiety and loss of confidence 3-12 months after hospitalization (Yuval,
Halon & Lewis, 2007). Almost one-fifth of the CHD patients failed to deal with their
emotional distress 3-5 years following the disease (Boersma, Maes & Joekes, 2005).
Younger patients are more likely than older ones to be suffering from psychological
distress. A study (Beckie, Fletcher, Beckstead et al., 2008) comparing the
psychological health of 92 younger (≤ 64 years) and 90 older (> 64 years) women
with CHD found that younger women had significantly worse psychosocial profiles
than older ones. Sixty-four per cent of younger women had depressive symptoms,
while the figure was 37.0% in older ones. Younger women also reported feeling
significantly more anxious than older ones (p < 0.001).
To conclude, anxiety and depression are common in CHD patients, especially
younger ones. Such feelings can persist for a long period of time.

29
2.2.3.2.2 Prognosis of CHD Patients with Psychological and Emotional
Symptoms
Previous studies (Albert, Chae, Rexrode et al., 2005; Ariyo, Haan, Tangen et al., 2000;
Gump, Matthews, Eberly & Chang, 2004) have demonstrated that levels of anxiety
and depression can predict the severity of CHD. The presence of depression and
anxiety is related to cardiac events, such as the recurrence of angina pectoris and
myocardial infarction, and sudden death (Frasure-Smith, Lesperance & Talajic, 1995;
Hemingway & Marmot, 1999; Lauzon, Beck, Huynh et al., 2003; Shen, Avivi, Todaro
et al., 2008). In a prospective cohort study (Rothenbacher, Hahmann, Wusten et al.,
2007), 1,052 patients with CHD aged 30-70 years were recruited. The results suggest
that anxiety might be a much stronger predictor than depression for subsequent
adverse cardiovascular events in patients with CHD. In another prospective study with
536 MI patients (Moser, Riegel, McKinley et al., 2007), the results indicated that
patients with a higher level of anxiety have significantly more episodes of
complications, such as ventricular tachycardia, ventricular fibrillation, reinfarction,
and ischemia in the acute stage, which influence a patient‘s prognosis. In addition,
CHD patients with anxiety or depression are less likely to adhere to medical advice
(Lauzon, Beck, Huynh et al., 2003; Thompson & Lewin, 2000; Ziegelstein, Fauerbach,
Stevens et al., 2000), less likely to return to work (So.dermana, Lisspersa & Sundinb,
2003; Thompson & Lewin, 2000), more likely to withdraw from cardiac rehabilitation
programmes (Josephson, Casey, Waechter, Rosneck & Hughes, 2006; Yohannes,
Yalfani, Doherty & Bundy, 2007), and more likely to have a poorer prognosis (Barth,
Schumacher & Herrmann-Lingen, 2004) as compared with CHD patients without
psychological distress.

30
The presence of anxiety and depression can also increase the mortality rate of CHD
patients. A recent meta-analysis (Barth, Schumacher & Herrmann-Lingen, 2004) has
shown that depressive symptoms increase the risk of mortality in CHD patients. The
death rate of patients with depression is double that of those without depression (OR =
2.2) within two years after the initial assessment. Even in the long term, the mortality
rate is still higher in CHD patients with depressive symptoms (OR = 1.8). The results
suggest that depression has to be considered as a relevant risk factor in patients with
CHD. Barefoot, Helms, Mark, and others (1996) examined the relationship between
depression and long-term mortality risk in patients with CHD for up to 19.4 years.
The results demonstrated that patients with moderate to severe depression have a
69.0% greater risk of cardiac death and a 78.0% greater risk of all-cause mortality
than non-depressed patients. The findings also showed that patients with moderate to
severe depression have an 84.0% greater risk of cardiac death 5-10 years later and a
72.0% greater risk after 10 years when compared with non-depressed patients. It is
concluded that depression may be persistent or frequently recurrent in CHD patients
and is associated with CHD progression, the triggering of acute events, or both.
Szekely, Balog, Benko, and others (2007) explored the long-term (four years) impact
of anxiety on mortality in 180 patients after cardiac surgery. They found that patients
with anxiety had a significantly higher mortality rate than those who did not suffer
from anxiety. A cohort study (Shibeshi, Yong-Xu & Blatt, 2007) with 516 CHD
patients over an average of 3.4 years illustrated that the risk of nonfatal MI or total
mortality rises with each unit of increase in the cumulative mean anxiety score.

31
Several studies have also shown that depression and/or anxiety are independent
factors associated with a worse quality of life, when the Medical Outcomes Study 36-
Item Short-Form (SF-36) was used to measure the quality of life of patients (Cruz,
Fleck & Polanczyk, 2010; Dickens, McGowan, Percival et al., 2006; Herry N,
Suryadipradja, Shatri & Prodjosudjadi, 2005; Lam, Chin, Lee et al., 2009). These
findings suggest that depression and/or anxiety predict the quality of life of patients.
In addition, patients with psychological problems have a higher consultation rate
(Lam, Chin, Lee et al., 2009), which implies that such patients add to the medical
burden.
To conclude, anxiety and depression are common in CHD patients. CHD patients with
such forms of psychological distresses as anxiety and depression have a poorer
prognosis than those who do not suffer from such distress. Depression and/or anxiety
also impair the quality of life of CHD patients. It is therefore important to identify
methods to improve the psychological health of CHD patients.
2.2.3.3 Social Impact
This subsection presents the impact of CHD on the social life of patients and the
burden on society of caring for CHD patients.
The physical activity of patients is strongly associated with social participation
(Adamson, Lawlor & Ebrahim, 2004). Previous studies have shown that the
proportion of adults returning to work after acute MI varies from 35.0% to 90.0%
(Cay, Vetter, Philip & Dugard, 1973; Earle, Ayanian & Heymann, 2006). Patients

32
with a higher socioeconomic status, a higher level of education, and who were
younger were more likely to resume work after acute MI. Patients with MI were
significantly less likely to return to work than patients with angina (56.0% versus
94.0%) (Earle, Ayanian & Heymann, 2006). Patients with a history of heart attack
tended to retire early, stop working, or look for a less demanding job. Those returning
to work experienced a considerable decrease in working efficiency. Symptoms such
as angina and breathlessness, together with emotional upset, and the attitude of
patients towards their physical disabilities were considered to be contributing factors.
Returning to work is a hallmark of recovery from CHD. Patients with limited physical
activities will reduce their social activities.
Apart from the social impact on individuals, the cost of CHD treatments is also a
burden. Bittner and Sanderson (2006) reported that over $100 billion is spent annually
on CHD in the United States in direct medical costs, disability payments, and lost
productivity. The estimated direct and indirect cost of CHD was $156.4 billion in
2008 in the United States (Rosamond, Flegal, Furie et al., 2008). The physical
limitations induced by CHD not only affect the social activity of patients, such as
their ability to return to work, but also increase the financial burden on society.
In a word, after MI patients are less likely to return to work and impose a heavy
burden on society. Thus, providing cardiac rehabilitation programmes to improve the
health of CHD patients, which consequently helps them return to work early and
reduces the social and financial burden of their illness, is meaningful.

33
2.2.3.4 Impact on Quality of Life (QoL)
Since CHD impairs the physical, psychological, and social health of patients, the
result is that they have a poor quality of life. Findings from a qualitative study showed
that MI leads to a variety of health-related problems that affect the quality of life of
patients (Roebuck, Furze & Thompson, 2001). Other studies have indicated that CHD
patients have a rather poor quality of life with respect to SF-36, with little
improvement found between admission and one month post discharge (Spiraki,
Kaitelidou, Papakonstantinou et al., 2008). Indeed, declines were observed in three of
the eight domains of SF-36 three months post discharge (Failde & Soto, 2006).
Around 25.0% of CHD patients had a poor quality of life (Zboralski, Galecki,
Wysokiński et al., 2009). Although many studies have shown that the quality of life of
CHD patients improves over time (Brink, Grankvist, Karlson et al., 2005;
Kristofferzon, Löfmark & Carlsson, 2005), patients following MI still had a clinically
poor health-related quality of life two years after acute MI (Bengtsson, Hagman,
Währborg & Wedel, 2004). When compared with an age- and sex-matched healthy
population, MI patients scored lower in most domains of SF-36 within a period of 2.5
years following MI (Alsén, Brink, Persson et al., 2010; Pettersen, Reikvam, Rollag &
Stavem, 2008; Sacker, Head & Bartley, 2008; Worcester, Murphy, Elliott et al., 2007;
Zboralski, Galecki, Wysokiński et al., 2009). These findings suggest that CHD
impairs the quality of life of patients. Patients with a poor quality of life suffered
significantly higher mortality in the 10 years following MI (Parakh, Bhat, Thombs et
al., 2010). Clearly, interventions to improve the quality of life of CHD patients are
necessary.

34
To sum up, CHD patients often experience a series of physical, psychological, and
emotional symptoms. The most common physical symptoms are chest pain,
breathlessness, and fatigue; the most common psychological and emotional symptoms
are anxiety and depression. These symptoms restrict patients‘ physical and social
activities. As a result, both the quality of life of the patients and society will be
affected.
2.3 Exercise and Coronary Heart Disease (CHD)
Physical activity refers to any bodily movement that is produced by the contraction of
skeletal muscles and that increases energy expenditure above the resting level.
Exercise is a subclass of physical activity and is defined as planned, structured, and
repetitive bodily movements performed specifically to improve or maintain physical
fitness (Fletcher & Braun, 2008).
Physical exercise is a core component of cardiac rehabilitation (Taylor, Brown,
Ebrahim et al., 2004), which has been shown to benefit the health of CHD patients
(Warburton, Katzmarzyk, Rhodes & Shephard, 2007). This section presents the
benefits of exercise for CHD patients, followed by similar effects contributed by
hospital/centre-based and home-based exercise programmes. The situation of cardiac
rehabilitation in China is then described and the safety of exercise for patients with
CHD is discussed. Finally, the poor attendance of exercise-based cardiac
rehabilitation programme is presented.
35
2.3.1 Benefits of Exercise for CHD Patients
This subsection reviewed the benefits of exercise for CHD patients in terms of lipid
indicators, heart rate (HR), blood pressure (BP), psychological well-being, angina,
coronary events, and quality of life.
2.3.1.1 Benefits of Exercise on Lipid Indicators
Lipid indicators, such as total cholesterol (TC), low-density lipoprotein cholesterol
(LDL-C), high-density lipoprotein cholesterol (HDL-C), and triglyceride (TG), are
related to the prognosis of CHD patients. The elevated levels of TC, LDL-C, or TG,
or lowered HDL-C increase the risks of reinfarction and mortality from CHD. A
number of studies have shown that regular exercise or exercise-based cardiac
rehabilitation leads to a significant reduction in body mass index (BMI), TC, LDL-C,
and TG levels, and significant increase in HDL-C levels (Asbury, Slattery, Grant et al.,
2008; Chair, Thompson, Tang & Leung, 2007; de Geus, van Hoof, Aerts & Meeusen,
2008; Franklin, Bonzheim, Warren et al., 2002; Jiang, Sit & Wong, 2007; Milani,
Lavie & Cassidy, 1996; Senuzun, Fadiloglu, Burke & Payzin, 2006). A decrease in
BMI would result in greater improvements in TC, LDL-C, and HDL-C in CHD
patients (Kelley, Kelley & Franklin, 2006).
Several meta-analyses have indicated that aerobic exercise or exercise-based cardiac
rehabilitation significantly increases HDL-C levels and decreases TC, LDL-C, and
TG levels in adults (Conn, Hafdahl, Cooper et al., 2009; Kelley, Kelley & Tran, 2005;
Kodama, Tanaka, Saito et al., 2007) and in CHD patients (Jolliffe, Rees, Taylor et al.,
36
2001; Kelley, Kelley & Franklin, 2006; Taylor, Brown, Ebrahim et al., 2004).
Kodama and others (2007) showed that every 10-minute prolongation of exercise per
session is associated with an approximately 1.4 mg/dl increase in HDL-C levels. This
finding suggests that exercise duration is very important because an increase in the
level of HDL-C is beneficial for CHD patients. These studies confirmed that regular
exercise or exercise-based cardiac rehabilitation benefits CHD patients in terms of
improving their lipid levels, consequently reducing their cardiac risk factors.
2.3.1.2 Benefits of Exercise on Heart Rate (HR) and Blood Pressure (BP)
Elevated HR is related to an increase in demand for oxygen, even when the heart
performed at a constant external work (Rosano, Vitale & Volterrrani, 2010).
Myocardial ischemia occurs from a mismatch between myocardial oxygen supply and
demand, both of which are influenced by HR. Elevated resting HR has long been
regarded as an independent predictor of cardiovascular and all-cause mortality in all
populations because high HR has direct detrimental effects not only on myocardial
ischemia but also on the progression of atherosclerosis, ventricular arrhythmias, and
left ventricular function (Batty, Shipley, Kivimaki et al., 2010; Rosano, Vitale &
Volterrrani, 2010). The risk increases when HR ≥ 70 bpm. A cohort study involving
9,580 subjects indicated that every 10 bpm increase in the resting HR was associated
with an 8.0% increase in major cardiovascular events in patients with stable CHD,
and a resting HR of ≥ 70 bpm was associated with a 40.0% increase in the risk of all-
cause mortality and more than double the risk of hospitalization due to heart failure
(Ho, Bittner, DeMicco et al., 2010).

37
A large-scale survey with 5,017 men and 5,607 women aged 30-69 years has
demonstrated an inverse dose-response relationship between self-reported leisure
physical activity and resting HR for both men and women (Emaus, Degerstrøm,
Wilsgaard et al., 2010). Aerobic exercise has been shown to lead to a significant
reduction in resting HR (Shiotani, Umegaki, Tanaka et al., 2009). Results from
several randomized controlled trials have also shown that exercise training or
exercise-based cardiac rehabilitation significantly increases maximal oxygen uptake
(Dressendorfer, Franklin, Cameron et al., 1995; Hambrecht, Walther, Mobius-Winkler,
et al., 2004; Hung, Daub, Black et al., 2004), and significantly reduces resting HR for
patients with CHD (Dressendorfer, Franklin, Cameron et al., 1995; Franklin,
Bonzheim, Warren et al., 2002). A meta-analysis has indicated that exercise training
significantly decreases resting HR in patients with heart disease (van Tol, Huijsmans,
Kroon et al., 2006). These findings suggest that exercise has the benefit of reducing
resting HR in patients with CHD.
Similar to HR, elevated BP increases risks for patients with CHD. Patients with CHD
have significantly higher systolic and diastolic BP as compared with those without
CHD (Kannel, Schwartz & McNamara, 1969). In a population-based prospective
study (Dorjgochoo, Shu, Zhang et al., 2009), the results showed that hypertension and
higher levels of individual BP parameters including systolic and diastolic BP, pulse
pressure, and mean arterial pressure were positively associated with mortality from all
causes, strokes, and CHD. Each five mmHg increment in systolic BP or mean arterial
pressure was associated with an increased risk of stroke mortality. In this study,
hypertension (all grades) accounted for 9.3% of all-cause, 25.5% of stroke-cause, and
21.7% of CHD-cause mortality.

38
Several studies have demonstrated an inverse relationship between physical activity
and BP (Fagard & Cornelissen, 2007; So, Sung, Li et al., 2010). One study on
Japanese male workers showed that subjects who walked > 8,000 steps/day or
exercised > 3 times/week had a significantly lower risk of developing hypertension as
compared with those who walked < 4,000 steps/day or exercised < 3 times/week
(Ishikawa-Takata, Tanaka, Nanbu & Ohta, 2010). Exercise training has a significant
effect on reducing BP (Cornelissen, Verheyden, Aubert & Fagard, 2010; Reboredo,
Henrique, Faria et al., 2010). Previous studies have shown that exercise training or
exercise-based cardiac rehabilitation has a significantly positive effect on reducing
systolic or diastolic BP among patients with CHD (Asbury, Slattery, Grant et al., 2008;
Franklin, Bonzheim, Warren et al., 2002; Jiang, Sit & Wong, 2007). Similar results
were found in two meta-analyses in patients with heart disease (Taylor, Brown,
Ebrahim et al., 2004; van Tol, Huijsmans, Kroon et al., 2006). These findings suggest
that exercise can decrease BP, which is beneficial for the prognosis of CHD patients.
2.3.1.3 Benefits of Exercise on Psychological Well-Being
CHD patients often experience some kinds of psychological distress, such as anxiety
and depression. Such distress can independently predict the poor prognosis of patients
with CHD, including the recurrence of angina pectoris and myocardial infarction, and
sudden death (Lauzon, Beck, Huynh et al., 2003; Rothenbacher, Hahmann, Wusten et
al., 2007; Shen, Avivi, Todaro et al., 2008).

39
Previous randomized controlled trials or quasi-experimental studies have shown that
exercise training or exercise-based cardiac rehabilitation led to significant
improvements in anxiety, depression, and other psychological symptoms (Arnold,
Sewell & Singh, 2007; Asbury, Slattery, Grant et al., 2008; Benzer, Platter, Oldridge
et al., 2007; Blumenthal, Sherwood, Babyak et al., 2005; Gary, 2006; Jolly, Taylor,
Lip et al., 2007; Josephson, Casey, Waechter, Rosneck & Hughes, 2006; Koukouvou,
Kouidi, Lacovides et al., 2004; Li, 2002; Milani, Lavie & Cassidy, 1996). A meta-
analysis with 19 trials showed that interventions to increase physical activity can
result in a decrease in anxiety symptoms among healthy adults (Conn, 2010). A
similar finding was found in another systematic review by Windle, Hughes, Linck,
and others (2010), who found that exercise is effective in promoting mental well-
being in older adults.
A reduction in anxiety or depression as a result of exercise is associated with an
improvement in fitness. One study (Milani & Lavie, 2007) showed that patients with
no improvement in exercise capacity attained no significant reduction in depressive
symptoms, whereas those who achieved a modest (1-10% increase in peak VO2) or
more robust (> 10% increase in peak VO2) enhancement in exercise capacity
experienced a reduction of more than 70.0% in the prevalence of depressive
symptoms. A meta-analysis examined the effects of the physical activity intervention
on psychological well-being in people with advanced age. The findings demonstrated
the benefits of aerobic exercise training for the psychological well-being of
individuals. Improvements in cardiovascular status, strength, and functional capacity
were associated with overall improvement in psychological well-being (Netz, Wu,
Becker & Tenenbaum, 2005). Clearly, the physical fitness of patients is linked to their
40
psychological well-being. Exercise training or exercise-based cardiac rehabilitation to
increase the physical fitness of CHD patients will ultimately improve their
psychological well-being. The inescapable conclusion is that exercise is beneficial for
the psychological well-being of CHD patients.
2.3.1.4 Benefits of Exercise on Angina
Exercise training alone or exercise-based cardiac rehabilitation can slow down, halt,
and even reverse the progression of atherosclerosis and reduce angina, exercise-
induced ischemic ST-segment depression, recurrent cardiac events, and a need for
coronary revascularization procedures (Franklin, Bonzheim, Warren et al., 2002).
Numerous studies have demonstrated that exercise or physical activity has promising
effects on the management of angina. A trial comparing the anti-anginal effects of
exercise with β-blockade has shown the benefits of exercise on anti-angina to be equal
to that of β-blockade (Todd & Ballantyne, 1990). Physical inactivity causes a
reduction in fitness, which may cause angina to be found at a lower exercise threshold
(Thompson & Lewin, 2000). When patients decrease in their level of activity, there
will be an increase in the rate of occurrence of angina. Such a feedback loop will go
on with the practice of inactivity (Furze, Bull, Lewin & Thompson, 2003). A
prospective survey involving 772 men with CHD indicated that physically inactive or
occasionally active men have the highest prevalence of breathlessness and chest pain
(Wannamethee, Shaper & Walker, 2000). This finding implies that physical activity
will reduce the prevalence of chest pain. A previous study demonstrated that CHD
patients who received a 12-month exercise training experienced an increase in

41
ischemic threshold by 30.0% when compared with the baseline (Hambrecht, Walther,
Mobius-Winkler et al., 2004). A single group pre-post study showed that exercise-
based cardiac rehabilitation reduced the frequency of anginal attacks and nitroglycerin
use (Smith, Layton, Newmark et al., 1987). A randomized controlled trial on 48 CHD
patients showed that 90.0% of the patients who received an intervention involving
exercise, stress management, smoking cessation, and a low-fat vegetarian diet,
reported a reduction in angina. Moreover, 82.0% of the patients in the intervention
group showed some degree of regression of coronary artery disease at the end of the
first year (Ornish, Brown, Scherwitz et al., 1990).
Cui, Ren, Wang, and others (2006) carried out a study to evaluate the effects of
exercise training on exercise tolerance in 57 patients following PCI. Patients in the
intervention group underwent exercise training 3 days/week for three months, with an
intensity of 50.0-80.0% of maximal HR according to the symptom limited exercise
test. The results showed that exercise training increased the patients‘ total exercise
time, the time to the appearance of ST-segment depression, and total exercise
tolerance, and decreased the incidence of exercise-induced angina. The findings
supported the view that exercise training could improve exercise tolerance and reduce
anginal attacks for patients who have undergone PCI.
The findings from the above studies suggest that exercise training or exercise-based
cardiac rehabilitation has a significant effect on reducing anginal attacks among
patients with CHD.

42
2.3.1.5 Benefits of Exercise on Coronary Events
Patients with CHD have a higher risk of coronary events, such as heart attacks, fatal
reinfarctions, and sudden death, than those without CHD. Physical activity or exercise
reduces the risk of coronary events (Scrutinio, Temporelli, Passantino & Giannuzzi,
2009). A prospective survey (Wannamethee, Shaper & Walker, 2000) included 772
men aged 52 to 73 years who were diagnosed with CHD. The findings indicated that
men who engaged in light to moderate intensity of activity showed a significant
reduction in the risk of total and cardiovascular mortality even after adjusting for age,
social class, smoking, obesity, history of MI, diabetes, stroke, and self-rated health
status. A longitudinal study over a 7-year period showed that individuals who
remained active or increased their level of physical activity following the first MI had
a lower risk of reinfarction or death due to all causes than those who remained
sedentary (Steffen-Batey, Nichaman, Goff et al., 2000). The findings from these
studies suggest that physical activity reduces the chances of coronary events in CHD
patients.
Previous studies have demonstrated that exercise-based cardiac rehabilitation
significantly reduces all-cause and cardiac-cause mortality, cardiovascular events,
restenosis, and fatal reinfarction (Goel, Lennon, Tilbury, Squires & Thomas, 2011;
Huang, Li, Mao et al., 2006; Huang, Mao, Deng et al., 2004; O‘Connor, Buring,
Yusuf et al., 1989). Exercise training was associated with a higher percentage of
event-free survivors (88.0%) (Hambrecht, Walther, Mobius-Winkler et al., 2004).
Exercise training or exercise-based cardiac rehabilitation may also reduce the rate of
hospitalization due to heart failure (Davies, Moxham, Rees et al., 2010; Hwang &

43
Marwick, 2009). These studies illustrate that exercise training or exercise-based
cardiac rehabilitation decreases the rate of occurrence of coronary events.
A meta-analysis with 33 observational cohort studies has revealed that individuals
who achieved 7.9 metabolic equivalents (METs) or more in maximal aerobic capacity
had a lower mortality and CHD risk than those whose aerobic capacity was less than
7.9 METs (Kodama, Saito, Tanaka et al., 2009). It was also found that a 1 -MET
increase in aerobic capacity was related to decreases of 13% and 15% in the risk of
all-cause mortality and CHD in healthy men and women, respectively (Kodama, Saito,
Tanaka et al., 2009). Another meta-analysis including 48 trials with a total of 8,940
CHD patients showed a reduction of 20.0% to 32.0% in all-cause mortality and
cardiac mortality among patients who attended an exercise-based rehabilitation
programme (Taylor, Brown, Ebrahim et al., 2004). Similar findings were reported by
another meta-analysis of CHD patients (Jolliffe, Rees, Taylor et al., 2001). The results
showed that exercise alone led to a 27.0% reduction in all-cause mortality and a
31.0% reduction in cardiac cause mortality. These two meta-analyses further confirm
the benefits of exercise for reducing mortality among populations with or without
CHD.
These findings suggest that exercise training or exercise-based cardiac rehabilitation
has beneficial effects on all-cause or cardiac-cause mortality, cardiovascular events,
and reinfarction for patients with CHD.

44
2.3.1.6 Quality of Life
Quality of life is considered an important indicator of the health of those with a
chronic disease, such as CHD (Wong & Chair, 2007) and has been used as an
endpoint in clinical trials and as a marker of health care quality (Dougherty, Dewhurst,
Nichol & Spertus, 1998). In this subsection, the benefits of exercise on quality of life
and the instruments used to measure it are reviewed.
2.3.1.6.1 Benefits of Exercise on Quality of Life
Since exercise training alone or exercise-based cardiac rehabilitation has beneficial
effects on both the physical and psychological health of patients with heart disease, it
will result in an improvement in their quality of life. A systematic review has
indicated that cross-sectional studies (n = 7) show a consistently moderate to strong
positive association between an individual‘s level of physical activity and his/her
health-related quality of life; and cohort studies (n = 2) and randomized controlled
studies (n = 4) tend to show that the level of physical activity has a positive effect on
health-related quality of life (Bize, Johnson & Plotnikoff, 2007). A number of
randomized controlled trials have demonstrated that exercise training alone or
exercise-based cardiac rehabilitation leads to a significant improvement in most
domains of health of SF-36, especially in physical functioning, bodily pain, general
health, role-physical, vitality, and mental health, among patients with heart disease
when compared with usual care (Arthur, Gunn, Thorpe et al., 2007; Arthur, Smith,
Kodis & McKelvie, 2002; Asbury, Slattery, Grant et al., 2008; Brubaker, Witta &
Angelopoulos, 2003; Dolansky & Moore, 2004; Elley, Kerse, Arroll & Robinson,

45
2003; Izawa, Hirano, Yamada et al., 2004; Jiang, Sit, Wong et al., 2004; Milani, Lavie
& Cassidy, 1996; Yonezawa, Masuda, Matsunage et al., 2009; Yu, Lau, Chau et al.,
2004).
A similar result was found when other quality of life scales (e.g., Seattle Angina
Questionnaires, Sickness Impact Profile and Minnessota Living with Heart Failure
Questionnaire) were used to measure the effects of exercise on patients with heart
disease (Arnold, Sewell & Singh, 2007; Benzer, Platter, Oldridge et al., 2007; Burke,
William & Lockyer, 2002; Franklin, Bonzheim, Warren et al., 2002; Gary, 2006;
Hung, Daub, Black et al., 2004; Koukouvou, Kouidi, Lacovides et al., 2004; Lewin,
Furze, Robinson et al., 2002; Marchionni, Fattirolli, Fumagalli et al., 2003; Senuzun,
Fadiloglu, Burke & Payzin, 2006). Several systematic reviews also have shown that
exercise training or exercise-based cardiac rehabilitation significantly improves
health-related quality of life in patients with heart disease (Davies, Moxham, Rees et
al., 2010; Hwang & Marwick, 2009; Taylor, Brown, Ebrahim et al., 2004). These
findings support the evidence that exercise training or exercise-based cardiac
rehabilitation benefits patients with heart disease by improving their quality of life.
2.3.1.6.2 Instruments for Measuring Quality of Life
Instruments developed to measure quality of life can be divided into two categories –
generic or disease specific. Generic tools provide a broad assessment of the health
status of an individual and allow comparisons of quality of life between groups of
patients with different conditions, while disease-specific instruments are designed to
measure quality of life by tapping those areas of life that may be affected by a specific
condition or illness (Dempster & Donnelly, 2000). Recently, many researchers have

46
recommended that both generic and disease-specific instruments should be used
together to evaluate quality of life (Arthur, Smith & Natarajan, 2008; Brodie, Inoue &
Shaw, 2008; Dempster & Donnelly, 2000; Lie, Arnesen, Sandvik, Hamilton & Bunch,
2009; McGillion, Watt-Watson, Stevens et al., 2008; Wong & Chair, 2007). The
benefits of using both generic and disease-specific instruments to measure quality of
life are: (i) to provide complementary information in clinical trials (Lie, Arnesen,
Sandvik, Hamilton & Bunch, 2009); (ii) to attain both sensitivity and specificity in
clinical change (Brodie, Inoue & Shaw, 2008); and (iii) to allow the results to be
compared with those for the general population, to make clinical interpretations more
meaningful (Arthur, Smith & Natarajan, 2008; Lie, Arnesen, Sandvik, Hamilton &
Bunch, 2009).
A systematic review (Dempster & Donnelly, 2000) of how the health-related quality
of life of patients with CHD is measured showed that the most commonly used
generic instruments are the Nottingham health profile (NHP), the SF-36, and the
sickness impact profile (SIP), and the main disease-specific instruments are the
quality of life after myocardial infarction (QLMI), the Seattle angina questionnaire
(SAQ), the quality of life index (QLI)-cardiac version, the angina pectoris quality of
life questionnaire (APQLQ), and the summary index. The NHP is a useful
measurement to assess whether or not patients have a severe health problem, but it
does not provide a comprehensive measure of quality of life, and it cannot
discriminate between the clinical classes of angina, and between people with heart
disease and healthy people (Dempster & Donnelly, 2000). The SF-36 is the most
well-known and widely used generic measure of health status. It consists of 36 items
under the following eight domains: physical functioning, bodily pain, role-physical,

47
general health, vitality, social functioning, role-emotional, and mental health. The
instrument has good psychometric properties but it cannot discriminate between
classes of angina (Dempster & Donnelly, 2000). The SIP consists of 136 items
grouped into 12 categories: sleep and rest, eating, work, home management,
recreation and pastimes, ambulation, mobility, body care and movement, social
interaction, alertness behaviour, emotional behaviour, and communication. The
instrument is too long and takes a great deal of time to administer. A comparison of
the three generic instruments reveals that the SF-36 and the NHP tend to have better
content validity in the field of heart disease than the SIP because they both cover the
areas of energy/vitality and bodily pain, while the SF-36 has higher internal
consistency coefficients and provides clearer evidence of discriminative validity than
the NHP. Thus, the SF-36 is the best generic instrument to use to measure quality of
life, and was the one selected and applied in this study.
With regard to disease-specific instruments, the QLMI consists of 26 items grouped
into five domains: symptoms, restriction, confidence, self esteem, and emotion. The
SAQ was developed to measure angina-related physical and emotional effects in CHD
patients and has been adapted cross-culturally for use in 13 countries, including China.
It consists of 19 items divided into five subscales: physical limitation, angina
frequency, angina stability, treatment satisfaction, and disease perception. All SAQ
domains show good reliability and validity, with the Cronbach α ranging from 0.67 to
0.91 (Kimble, Dunbar, Weintraub et al., 2002). The QLI was originally developed for
use on dialysis patients and was not commonly used on cardiac patients (Dempster &
Donnelly, 2000). The APQLQ consists of 22 items grouped into four domains:
physical activities, somatic symptoms, emotional distress, and life satisfaction. It has
48
good psychometric properties for discriminative purposes, but the responsiveness and
reliability of the instrument has been little examined (Dempster & Donnelly, 2000).
The summary index is a combination of the APQLQ, the angina impact questionnaire,
and the psychological general well-being scale to assess the health-related quality of
life of those with angina. However, it has received relatively little research attention.
The comparisons between the disease-specific instruments showed that the SAQ is
better at determining the impact of angina and more sensitive to clinical change than
the QLI (Dempster & Donnelly, 2000). Thus, the SAQ is the best disease-specific
instrument for measuring quality of life in CHD patients, as well as being simple and
easy to use.
Although the SF-36 can differentiate between patients with divergent medical,
psychiatric, and other serious medical conditions, there is some evidence to suggest
that it may inadequately distinguish between those with different severities of angina
as assessed by the Canadian Cardiovascular Society Angina Classification (Dougherty,
Dewhurst, Nichol & Spertus, 1998). The potential for the SF-36 to be insensitive to
changes in classes of angina necessitated the use of a second disease-specific
instrument, the SAQ to evaluate quality of life. Thus, in this study, both the SF-36 and
the SAQ were selected to measure the quality of life of CHD patients.
To sum up, exercise training alone or exercise-based cardiac rehabilitation can
improve the exercise capacity, psychological health, and quality of life of CHD
patients, and reduce risk factors and all-cause and cardiac-cause mortality.
Consequently, it will improve the prognosis of CHD patients. Thus, interventions to
motivate patients with heart disease to engage in exercise are very important and,
49
indeed, necessary. To catch the whole picture of the quality of life of CHD patients, it
is better to use both generic and disease-specific instruments together to assess the
quality of life of CHD patients. The commonly used generic and disease-specific
instruments for CHD patients are the SAQ and SF-36.
2.3.2 Hospital-based versus Home-based Exercise Programmes
Hospital-based cardiac rehabilitation programmes have been well developed in
Western countries. Most previous studies regarding exercise training programmes or
exercise-based cardiac rehabilitation interventions were hospital-based and lasted for
6-12 weeks. Despite the many known physical and psychosocial benefits of hospital-
based exercise programmes for patients with CHD, the low attendance rate of these
programmes is a widespread problem and is due to transport problems, cost, and
timetable conflicts involving family or work commitments (Chan, Chau & Chang,
2005; Evenson, Johnson & Aytur, 2006). Because it is safe for most cardiac patients
to engage in exercise and because of the results from the study of DeBusk and co-
workers (1990) indicating that accumulated physical activity (e.g., three 10-minute
bouts) of at least moderate intensity in one day produced similar improvements in
health-related outcomes to one longer exercise session (e.g., one 30-minute bout), a
home-based cardiac rehabilitation programme is an option for low-risk patients with
CHD.
Home-based rehabilitation increases uptake and adherence to rehabilitation
programmes (Jolly, Lip, Sandercock et al., 2003). Numerous studies have
demonstrated that patients who participated in a home-based cardiac rehabilitation

50
programme reported engaging in more exercise sessions per week throughout the
study (Arthur, Smith, Kodis & McKelvie, 2002) and scored higher scores in habitual
physical activity at the 12-month follow-up period when compared with those who
had attended a hospital-based cardiac rehabilitation programme (Smith, Arthur,
McKelvie & Kodis, 2004). A brief survey in the United Kingdom has shown that
patients aged > 60 years old and who were self-employed are more likely to prefer
home-based rehabilitation (Dalal & Evans, 2003). Thus, home-based cardiac
rehabilitation may improve uptake and exercise compliance among patients.
Several recent studies have demonstrated that home-based cardiac rehabilitation is as
effective as traditional hospital-based cardiac rehabilitation with respect to functional
capacity, heart rate recovery, lipid levels, anxiety and depression, and health-related
quality of life (HRQL) in patients with CHD (Arthur, Smith, Kodis & McKelvie,
2002; Dala, Evans, Campbell et al., 2007; Jolly, Taylor, Lip et al., 2007; Marchionni,
Fattirolli, Fumagalli et al., 2003; Oerkild, Frederiksen, Hansen et al., 2011; Smith,
Arthur, McKelvie & Kodis, 2004; Wu, Lin, Chen & Tsai, 2006), and risk factor
modification (e.g., aerobic exercise and a low-fat diet) (Yates, Heeren, Keller et al.,
2007). Two recent systematic reviews of home-based versus centre-based cardiac
rehabilitation involving 12 randomized controlled trials have indicated that there are
no differences in the outcomes of home- versus centre-based cardiac rehabilitation in
mortality, cardiac events, exercise capacity, BP, lipid profiles, and health-related
quality of life (Dalal, Zawada, Jolly, Moxham & Taylor, 2010; Taylor, Dalal, Jolly et
al., 2010), while home-based cardiac rehabilitation is superior to centre-based
rehabilitation in adherence to exercise (Dalal, Zawada, Jolly et al., 2010). These

51
studies suggest that home-based cardiac rehabilitation is as effective as centre-based
rehabilitation.
Previous studies have demonstrated that home-based cardiac rehabilitation has
positive effects on lipid levels, exercise capacity, peak oxygen consumption, exercise
duration on treadmill tests, distance of the 6-minute walk, psychological well-being,
and quality of life among patients with heart disease when compared with usual care
(Asbury, Slattery, Grant et al., 2008; Gary, 2006; Hwang & Marwick, 2009; Salvetti,
Oliveira Filho, Servantes & de Paola, 2008; Senuzun, Fadiloglu, Burke & Payzin,
2006). An additional positive effect on exercise self-efficacy was observed for
patients who attended a home-based cardiac rehabilitation programme (Senuzun,
Fadiloglu, Burke & Payzin, 2006; Sinclair, Conroy, Davies & Bayer, 2005). This
additional effect may be due to the fact that patients who attend home-based cardiac
rehabilitation need to monitor themselves during exercise. The self-monitoring of
exercise training might build their confidence in maintaining their level of exercise
and adhering to the exercise programme (Gary, 2006; Izawa, Watanabe, Omiya et al.,
2005). In addition, patients who participated in a home-based cardiac rehabilitation
programme perceived a higher level of social support when compared with those in
the hospital-based cardiac rehabilitation programme (Gary, 2006). This may be
because patients can obtain support from their family, friends or relatives when
exercising at home. Moreover, home-based cardiac rehabilitation is cost-effective for
low-risk patients (Marchionni, Fattirolli, Fumagalli et al., 2003; Salvetti, Oliveira
Filho, Servantes & de Paola, 2008).

52
To sum up, home-based cardiac rehabilitation is as effective as hospital-based cardiac
rehabilitation on mortality, risk factors, physical and psychological health, and quality
of life among patients with heart disease. Home-based cardiac rehabilitation has the
additional effect of increasing the exercise self-efficacy and social support of CHD
patients, improving exercise adherence, and being cost-effective. Thus, in this study
we selected a home-based cardiac rehabilitation programme for low-risk patients with
CHD.
2.3.3 Cardiac Rehabilitation Programmes in China
Few studies have been carried out in China on exercise training or exercise-based
cardiac rehabilitation for patients with heart disease. A limited number of studies have
shown that exercise training or exercise-based cardiac rehabilitation results in
significant improvements in lipid profiles (including TC, LDL-C, and TG) and BP
(Jiang, Sit & Wong, 2007), exercise capacity, angina, walking performance,
cardiovascular events, and daily activities (Cui, Ren, Wang et al., 2006; Huang, Mao,
Deng at al., 2004; Jiang, Sit & Wong, 2007; Li & Gao, 2007; Liu, Zhang, Yang, Yuan,
Yang & Brodie, 2007; Zhang, Li & Wang, 1999; Zhong, Lei, Qiao et al., 1999; Zhu,
2004), as well as quality of life (Huang, Li, Mao et al., 2006; Jiang, Sit, Wong et al.,
2004). Only one study (Li, 2002) evaluated the effect of exercise training on
psychological health, in which aerobic exercise training relieved the psychological
distress of CHD patients when SCL-90 was used to measure their psychological
health over six months.
53
Most of these studies were limited by their focus on PCI patients, the effectiveness of
their functional capacity, small sample sizes, and a non-RCT design. Little attention
was paid to the effects of exercise training or exercise-based cardiac rehabilitation on
self-efficacy, exercise adherence, psychological well-being, and quality of life. Thus,
studies with a high quality of design (e.g., RCT) and with a sample size of enough
power to evaluate the effects of exercise-based cardiac rehabilitation on exercise
adherence and quality of life are necessary in a Chinese CHD population.
2.3.4 Safety of Exercise for CHD Patients
Several studies have shown that it is safe for most cardiac patients to engage in
exercise training. Haskell (1994) reviewed the safety of cardiac exercise programmes
for cardiac patients. He suggested that high-risk patients should receive close
supervision when exercising for as long as required; low-risk patients should be
instructed to engage in unsupervised exercise at home; and moderate-risk patients
should begin with on-site supervision and proceed to nonmedical supervised or home-
based programmes as their clinical status improves. Pavy, Iliou, Meurin, and others
(2006) examined the rate of occurrence of complications during the performance of
exercise in the course of cardiac rehabilitation. A total of 25,420 cardiac patients were
recruited in the study. They underwent 42,419 exercise stress tests and performed
743,471 patient-hours of exercise training. Cardiovascular events were defined as
chest pain with typical ECG modifications, severe ventricular arrhythmias, syncope,
cardiopulmonary resuscitation, immediately transferring to a coronary care unit or
cardiac surgery, and using intravenous drugs. Any event that occurred during or up to
one hour after exercise stress testing or exercise training was considered a

54
cardiovascular complication resulting from exercise testing or training. The findings
showed that the rate of occurrence was 1 per 8,484 exercise stress tests and 1 per
49,565 patient-hours of exercise training. The cardiac arrest rate was 1.3 per million
patient-hours of exercise. There were no fatal complications and emergent
defibrillations in this study. In other words, it is suggested that exercise training or
exercise testing is safe for cardiac patients. The latest review (Audelin, Savage &
Ades, 2008) also suggests that exercise-based outpatient cardiac rehabilitation is safe
for very old patients (≥ 75 years). To sum up, exercise training is safe for most cardiac
patients.
2.3.5 Poor Attendance of Exercise-based Cardiac Rehabilitation
Despite the safety of exercising and the many known physical and psychosocial
benefits of exercise-based cardiac rehabilitation for CHD patients, the low attendant
rate of these programmes is a widespread problem that may be due to a lack of
motivation to engage in exercise (Evenson, Johnson & Aytur, 2006). Previous studies
(Burns, Camaione, Froman & Clark III, 1998; Franklin, Bonzheim, Warren et al.,
2002; Pell, Pell, Morrison et al., 1996) have shown that only 11.0 – 38.0% of patients
who suffered from MI or who had undergone CABG participated in formal cardiac
rehabilitation programmes after being discharged from hospital. This indicates that
these comprehensive services are vastly underutilized, especially by older adults and
women. In a cohort study in Victoria with 12,821 patients following acute MI, CABG,
or PCI, the findings demonstrated that rates of participation in at least one session of
an outpatient cardiac rehabilitation programme were only 15.0% for those with AMI,
37.0% for CABG, and 14.0% for PTCA (Sundararajan, Bunker, Begg et al., 2004). In

55
the United States, a large cohort study involving 267,427 Medicare CHD patients
showed that the overall participation rate was 18.7%, 13.9% for those following acute
MI and 31.0% for those had undergone CABG (Suaya, Shepard, Normand et al.,
2007). The latest cohort study with 601,099 Medicare patients revealed that only
12.2% of CHD patients attended at least one session of an outpatient cardiac
rehabilitation programme after being discharged from hospital (Suaya, Stason, Ades
et al., 2009). In England, nationally, 29.0% of eligible CHD patients attended cardiac
rehabilitation programmes, with the proportion ranging from 14.0% to 37.0% within
regions (Bethell, Lewin, Evans et al., 2008). In Japan, the national participation rate in
outpatient cardiac rehabilitation following acute MI was only 3.8-7.6% (Goto, Saito,
Iwasaka et al., 2007). These findings illustrate that participation rates in exercise-
based cardiac rehabilitation programmes are globally low.
Among those who participate in cardiac rehabilitation programmes, the dropout rate is
high. In a randomized exercise trial, around 20.0% of patients following MI who had
participated in the exercise programme withdrew from it after two months, and the
dropout rate reached 45.0% during the first six months of the programme (Dorn,
Naughton, Imamura & Trevisan, 2001). Another report showed that around 50.0% of
women with CHD (107/228) failed to complete the prescribed sessions of their
rehabilitation programme (Sanderson & Bittner, 2005). Similar observations were
made by Moore et al. (2003), Sanderson et al. (2003), Sarrafzadegan et al. (2007), and
Worcester et al. (2004). The situation was worse among women, elderly persons,
those with a low level of education, those suffering from depression, or those with
severe diseases (Dorn et al., 2001; Suaya, Shepard, Normand et al., 2007; Witt,
Jacobsen, Weston et al., 2004).

56
The attendance rate of cardiac rehabilitation programmes is similarly disappointing in
China. A study was conducted exploring the utilization of a 7-week phase II cardiac
rehabilitation outpatient programme in Hong Kong (Chan, Chau & Chang, 2005). The
programme consisting of education and exercise was scheduled weekly in the
afternoon on a particular weekday for two hours in the hospital. The results showed
that only 25.0% (37/145) of the participants attended at least one session during the 6-
month period following their discharge from hospital and only 7.5% (11/145) of these
attended and completed the 7-week cardiac rehabilitation programme, although 65.3%
(119/182) of them expressed an interest in or intention to attend the programme
before being discharged from the hospital (Chan, Chau & Chang, 2005). The main
reasons mentioned for not participating in the programme were: busy with work
(45.0%), forgetfulness (13.0%), too far away from home to the hospital (9.0%),
restricted by physical condition (4.0%), and no one to accompany oneself to the
hospital (4.0%). Another study had shown that more than 30.0% of CHD patients
engaged in no regular exercise at all (Chair, Lee, Lopez & Ling, 2007). These
findings suggest that another approach to delivering exercise-based cardiac
rehabilitation programmes and to increase uptake for low-risk patients is necessary,
and that, for those who are of low risk, home-based cardiac rehabilitation may be an
alternative to conventional programmes in encouraging them to engage in exercise.
Due to the low attendance rate of exercise-based cardiac rehabilitation programmes
for cardiac patients, interventions or strategies to motivate CHD patients to adopt
exercise is critically important and, indeed, necessary.

57
2.4 Patient Education and Exercise Behaviour
Patient education is one of the key components of cardiac rehabilitation for risk factor
modification. Patient education has been broadly defined as any planned activities that
include teaching, counselling, and behaviour modification, which could result in
changes in exercise behaviour (Conn, Hafdahl, Brown & Brown, 2008). This
subsection introduces the information needs of CHD patients. The effects of patient
education on promoting health and exercise behaviour are then presented. Finally,
factors affecting the effectiveness of patient education and strategies for patient
education are discussed.
2.4.1 Information Needs of CHD Patients
Many scholars (Hanssen, Nordrehaug & Hanestad, 2005; Stewart, Abbey, Shnek et al.,
2004; Tierney, Worth & Watson, 2000) have stated that patients with CHD have
unmet information needs after discharge, which may result in poorer treatment, less of
an ability to cope, and poorer psychological and physical well-being (Hanssen,
Nordrehaug & Hanestad, 2005). Findings from several qualitative studies (Thompson,
Ersser & Webster, 1995; Webster, Thompson & Mayou, 2002; Wang, Chair,
Thompson & Twinn, 2009) have shown that MI patients lack information and advice
about their condition, which influences their activities, lifestyle, and future plans.
These findings suggest that it is necessary for health professionals to provide
information to CHD patients. Previous studies have also shown that it is difficult for
patients to absorb the information during a hospital stay (Hanssen, Nordrehaug &

58
Hanestad, 2005; Turton, 1998). Hence, patient education for CHD patients after
discharge or community-based patient education is necessary.
In several qualitative studies (Jensen & Petersson, 2003; Thompson, Ersser &
Webster, 1995) MI patients expressed the need for knowledge and support after being
discharged from hospital. They sought information about how to deal with chest pain
and medication. A cross-sectional study demonstrated that more than 80.0% of
patients following PCI reported a need for information about heart disease and
lifestyle changes (Higgins, Murphy, Le Grande et al., 2005). Lifestyle changes, such
as following a healthy diet and ceasing to smoke, contributed to more than half of the
decline in the mortality rate from CHD between 1968 and 1976 (Goldman & Cook,
1984).
In a longitudinal study, Stewart and co-workers (2004) found that CHD patients
reported diet, dealing with high cholesterol, and exercise as their three top priorities.
A literature review (Duryée, 1992) showed that risk factors were viewed as a primary
patient concern in patients following MI. Medication, home activity, and symptom
management were also regarded as important needs. A meta-analysis (Scott &
Thompson, 2003) that included 14 trials, in which six trials used the same instrument
(the Cardiac Patient Learning Needs Inventory, CPLNI), was conducted to assess the
information needs of post-MI patients. The findings showed risk factors as being the
most important category of information needs, followed by information on cardiac
anatomy and physiology, medications, and physical activities.

59
A similar result was found when a modified CPLNI instrument was adopted to
measure the information needs of patients. A longitudinal study (Czar, MlittNsg &
Engler, 1997) using modified CPLNI to assess the learning needs of CHD patients
demonstrated that the top three-ranking categories were symptom recognition, cardiac
anatomy and physiology, and medications. Turton (1998) assessed the information
needs of post-MI patients and their spouse/partners using a modified CPLNI, in which
the term ‗risk factors‘ was replaced by the term ‗lifestyle factors‘ and the category
‗symptom management‘ was added to the inventory. The results showed that both
patients and their partners ranked symptom management and lifestyle factors as the
most important information needs. This suggests that post-MI patients and their
partners view practical information relating to survival as being of prime importance.
A number of studies have been conducted over the past decade in China to assess the
information needs of patients with CHD. The patients surveyed regarded information
about CHD, how to prevent recurrences of angina and heart attacks, diet and physical
activity, medication, self-monitoring and self-care, and how to deal with acute attacks
as their most important information needs (Chen & Jing, 2008; Du, Chen, & Liu,
2005; Hu, 2006; Jiang & Peng, 2005; Li & Liu, 2006; Li & Wang, 2006; Liu, 2005;
Wan & Wang, 2008).
Patients at different stages may have different kinds of information needs. On
admission, patients need information about their treatment regimen and the effects of
treatment, the current condition of their disease, and the significance of related body
examinations. During their stay in hospital, they need information about medication
and the skills of self-care. After discharge, they need information about risk factors
60
and how to prevent the recurrence of angina or heart attacks, and about the timetable
for further consultations with their doctor (He, Guo, & Guo, 2007). At the early stage
of convalescences, patients rank risk factors, medication, and anatomy and physiology
as the most important needs (Ashton, 1997; Chan, 1990). Another study by Larson
and co-workers (1996) to assess the information needs of 258 post-MI patients eight
weeks after discharge showed that, among the five top topics on which they needed
information, four were related to how to recognize and reduce the chances of getting
another heart attack. The findings further suggest that patients are concerned about
their survival and want to know how to reduce the chances of suffering from another
heart attack after discharge. In the long term, patients indicated that symptom
recognition, diet, and exercise were topics about which they considered it important to
receive information (Czar, MlittNsg & Engler, 1997; Stewart, Abbey, Shnek, Irvine &
Grace, 2004).
Our preliminary qualitative study (Zhu, Ho & Sit, 2012) with 11 CHD patients in
mainland China showed that most patients strongly expressed the need for
information pertinent to cardiac rehabilitation and preventing the recurrence of MI,
especially information regarding diet and physical activity. They wanted to know how
to adjust their lifestyle to prevent the illness from deterioration and how to reduce
their chances of suffering from another heart attack.
To sum up, patient education is important for CHD patients. They mainly need
information about symptom management, risk factors, the anatomy and physiology of
the heart, medications, lifestyle adjustment (diet and physical activity), and how to

61
reduce the chances of getting another heart attack. Therefore, all of these topics were
included in the patient education session in this study.
2.4.2 Patient Education on Health Promotion
Patient education can benefit CHD patients. The short-term effects of patient
education on the knowledge of individuals and changes in their behaviour have been
confirmed, while its long-term effects are as yet unclear. Many studies have
demonstrated that the effects of patient education on patients‘ knowledge about CHD,
diet, physical activity, and medication can be maintained for a short period of time
(Beckie, 1989; Fortmann, Williams, Hulley et al., 1982; Linde & Janz, 1979; Marshall,
Penckofer & Llewellyn, 1986; Meyer, Nash, McAlister & Maccoby, 1980; Plach,
Wierenga & Heidrich, 1996; Stern, Farquhar, Maccoby & Russell, 1976). In the
Stanford Three Community Study (Fortmann, Williams, Hulley et al., 1982; Meyer,
Nash, McAlister & Maccoby, 1980; Stern, Farquhar, Maccoby & Russell, 1976), it
was found that the effects of a mass-media community-wide patient education
campaign on the population‘s knowledge about healthy diets and physical activity
could last three years of the education campaign. However, one randomized
controlled trial (Elderen, Maes & Seegers, 1994) showed that the effects of an
inpatient education programme on the patients‘ knowledge about CHD could only be
sustained for four months. The effects disappeared one year after the implementation
of the programme.
It is known that increasing the knowledge of patients can promote related healthy
changes in behaviour and compliance with medication regimes (Campbell, Ritchie,

62
Thain et al., 1998; Hanssen, Nordrehaug, Eide & Hanestad, 2007; Linde & Janz, 1979;
Marshall, Penckofer & Llewellyn, 1986; Netto, McCloughan & Bhatnagar, 2007;
Plach, Wierenga & Heidrich, 1996). Many previous studies have shown that patient
education programmes promote changes in patients' behaviour, such as the adopting a
healthy diet, increasing exercise/physical activity, and quitting smoking (Aldana,
Greenlaw, Diehl et al., 2008; Campbell, Ritchie, Thain et al., 1998; Cupples &
McKnight, 1994; Fortmann, Williams, Hulley et al., 1982; Hanssen, Nordrehaug,
Eide & Hanestad, 2007; Mahler, Kulik & Tarazi, 1999; Meyer, Nash, McAlister &
Maccoby, 1980; Raleigh & Odtohan, 1987; Stern, Farquhar, Maccoby & Russell,
1976). Over time, these changes in behaviour resulted in a decrease in BMI, weight,
systolic and diastolic BP, resting HR, serum lipids, and blood glucose (Aldana,
Greenlaw, Diehl et al., 2008; Campbell, Ritchie, Thain et al., 1998; Giallauria, Lucci,
D‘Agostino et al., 2009; Jiang, Sit & Wong, 2007; Neubeck, Freedman, Briffa et al.,
2010; Redfern, Briffa, Ellis & Freedman, 2009), and a reduction in anginal pain and
rehospitalization due to angina (Cupples & McKnight, 1994; Hanssen, Nordrehaug,
Eide & Hanestad, 2009; Murchie, Campbell, Ritchie et al., 2004). Fuster (2007) stated
that patient education will increase the health awareness of patients and induce them
to modify their lifestyle. However, similar to knowledge, the long-term effects of
patient education on changes in behaviour are also not clear. One study indicated that
the effects of patient education on changes in behaviour were not maintained at the
one-year follow-up period (Elderen, Maes & Seegers, 1994). These findings may
suggest that patient education is beneficial for promoting the health of CHD patients,
while knowledge alone may not be enough for spur changes in behaviour, especially
over the long term.
63
A number of studies conducted in China on CHD patients have also demonstrated that
patient education programmes increased patients‘ knowledge about the disease (Fei,
You & Huang, 2007), improved compliance with medical regimens (Fei, You &
Huang, 2007; Luo, Chen, Meng & Ma, 2007), and reduced patients‘ anxiety and
depression and complications after PTCA (Hou, Zhou & Zhang, 2003). A home-based
cardiac rehabilitation programme that is mainly based on education and guidance led
to a significant decrease in hospital readmissions and significant improvements in
self-esteem and confidence in doing exercise among older cardiac patients (Sinclair,
Conroy, Davies & Bayer, 2005). These studies also suggest that patient education is
beneficial for promoting health in the Chinese CHD population.
Although patient education demonstrated a significant degree of effectiveness in
bringing about changes in knowledge and health behaviour, its effect on self-efficacy
for exercise compliance is not clear. Some studies indicated that patient education
improves patients‘ self-efficacy for low-fat diet compliance (Mahler, Kulik & Tarazi,
1999; Stewart, Abbey, Shnek, Irvine & Grace, 2004) and symptom management
(Kline, Scott & Britton, 2007). Higher cardiac self-efficacy is associated with better
health status after adjusting for CHD severity and depressive symptoms (Sarkar, Ali
& Whooley, 2007). According to Mahler et al. (1999), although patients who received
videotaped information at the point of discharge reported more engagement in
moderate and strenuous exercise one and three months after discharge than those in
the control group, no significant effect on self-efficacy for exercise compliance was
found. A randomized controlled trial on CHD patients indicated that patient education
significantly improves patients‘ knowledge, beliefs, and perceived level of control
when compared with the usual care (Tullmann, Haugh, Dracup & Bourguignon, 2007).

64
The findings imply that patient education may increase the confidence of patients to
change their behaviour. However, further research to confirm its effects on exercise
self-efficacy is necessary.
The effects of patient education on psychological distress are a subject of debate.
Some studies showed that patients receiving patient education had significantly lower
levels of anxiety than those receiving the usual care (Beckie, 1989; Raleigh &
Odtohan, 1987), while others revealed that patient education had no effect on
psychological distress (Dusseldorp, van Elderen, Maes et al., 1999; Elderen, Maes &
Seegers, 1994; Mahler, Kulik & Tarazi, 1999; Moore, 1996). Numerous studies have
indicated that patient education programmes only improve the physical health of
patients and have no effect on their psychological health when SF-36 (Hanssen,
Nordrehaug, Eide & Hanestad, 2007), the Profile of Mood States (PMS), and the
Sickness Impact Profile (SIP) (Moore, 1996) were used to measure outcomes. Thus,
studies to further examine the effect of patient education programmes on
psychological well-being are also essential.
A meta-analysis (Dusseldorp, van Elderen, Maes et al., 1999) that included 37
psychoeducational programmes involving patient education and stress management
was carried out. The findings indicated that such programmes led to a 34.0%
reduction in cardiac mortality and a 29.0% reduction in the recurrence of MI, and had
positive effects on BP, cholesterol, body weight, smoking cessation, exercise, and
dietary habits. The findings further suggest that the effects on cardiac mortality and
MI recurrence are associated with the successful control of BP, cholesterol levels,
body weight, smoking cessation, and exercise. Another large-scale RCT study also
65
showed that an intensive secondary prevention intervention led to decreases in
cardiovascular mortality, nonfatal MI, and stroke over three years (Giannuzzi,
Temporelli, Marchioli et al., 2008). Because of patient education brings about healthy
changes in behaviour, it improves the prognosis of patients. Several studies (Larson,
Nelson, Gustafson & Batalden, 1996; Stewart, Abbey, Shnek, Irvine & Grace, 2004)
have demonstrated that there is a link between meeting the needs of patients for
information about their illness and recovery and fewer depressive symptoms, greater
self-efficacy, better health care satisfaction, and healthier changes in behaviour such
as healthy dietary habits, exercise, and stress management, even after controlling for
the confounding factors (Larson, Nelson, Gustafson & Batalden, 1996; Stewart,
Abbey, Shnek, Irvine & Grace, 2004). Consequently, patient education improves the
quality of life of patients (Larson, Nelson, Gustafson & Batalden, 1996). These
studies also illustrated the benefits of patient education in bringing about changes in
behaviour on the part of patients and improvements in their health.
The effect of patient education on the quality of life of patients with heart disease has
also been the subject of debate. Several studies reported that patient education has a
short-term (≤ 6 months) effect on quality of life, whereas its long-term effect was not
clear. For example, results from two studies indicated that patient education led to a
significant improvement in the quality of life of patients with heart disease in the fifth
and sixth month when compared with the usual care (Brodie, Inoue & Shaw, 2008;
Hanssen, Nordrehaug, Eide & Hanestad, 2007). One study showed that counselling
patients on exercise significantly improved four of the eight SF-36 domains (role-
physical, bodily pain, general health, and vitality) over 12 months of general practice
(Elley, Kerse, Arroll & Robinson, 2003). However, Hanssen and others (2009) found

66
that, although patient education had a significant positive effect on quality of life
within six months, beyond six months there was no overall significant improvement
in the patients‘ physical or mental health as measured by SF-36. A similar result was
reported by Johnson, Lim, and Bowe (2009). Another study showed that patients
attending secondary prevention clinics demonstrated significant improvements in five
of the eight SF-36 domains (physical functioning, social functioning, role-physical,
bodily pain, and general health) at the 1-year follow-up period, while no significant
improvement in all domains was found in the intervention group at the 4-year follow-
up period when compared with the control group (Murchie, Campbell, Ritchie, Deans
& Thain, 2004). The discrepancy in the findings between these studies may be due to
the different research designs. Further studies to test the effects of patient education
on quality of life are clearly needed.
In conclusion, patients need information to improve their health. Patient education can
increase the knowledge of patients, which in turn induces changes in behaviour and
enhances self-efficacy. Consequently, the quality of life of the patients will improve.
However, the above-mentioned advantages were only illustrated by studies focusing
on the short-term (≤ 6 months) effects of patient education. For long-term (> 6 months)
effects, further studies are needed.
2.4.3 Patient Education and Exercise Behaviour
Patient education could improve the knowledge of individuals, which results in
behavioural changes. The positive effect of patient education on changes in exercise
behaviour was found in several studies. A recent meta-analysis conducted by Conn

67
and others (2008) demonstrated that patient education could significantly increase
physical activity among chronically ill adults when compared with the usual care. The
pooled effect size of this study was 0.45. The findings from another systematic review
showed that interventions mainly consisting of patient education significantly
increased the uptake of cardiac rehabilitation programmes (Davies, Taylor, Beswick
et al., 2010).
Our previous systematic review (Zhu, Ho & Wong, unpublished) included 37 RCT
studies to evaluate the effectiveness of patient education on changes in exercise
behaviour among patients with heart disease. The findings indicated that patient
education significantly improved individuals‘ adherence to exercise (the pooled risk
ratio was 1.48, 95% confidence intervals (CI) [1.32, 1.67]), exercise duration
(minutes/week) (the pooled standardized mean difference was 0.69, 95% CI [0.07,
1.31]), and exercise frequency (sessions/week) (the pooled mean difference was 1.46,
95% CI [0.43, 2.48]) immediately after the intervention. The significant positive
effect sizes declined at the follow-up period (≥ 6 months), with the exception of the
significant effect on exercise frequency, which disappeared altogether at the follow-
up period. No significant effects on exercise self-efficacy and exercise decisional
balance were found. Table 2.1 shows details of the 37 studies in our systematic review.
The findings suggest that patient education is effective at changing exercise behaviour
of patients with heart disease.

68
Table 2.1 Studies on the effect of patient education on exercise behaviour
Author
(year)
Country
Subjects
Mean
age
(years)
Sample
size
Theory/
model Interventions
Duration of
intervention Outcome measures Main results QS
Allen et al.
(2002)
USA
228 subjects (28% F, 72% M)
with hyper-
cholesterolemia
and coronary heart disease
were recruited
and included in
data analysis (IG=115,
CG=113).
60 228 No I: Patients received lipid management, including
individualized lifestyle
modification (step II diet
and home-based exercise program) and
pharmacologic
intervention, from a nurse
practitioner for 1 year after discharge in addition to
their usual care.
C: usual care
1 year Self-reported Physical Activity
Questionnaire at
baseline and at 12
months.
Physical activity (MET-hour/week
≥ 6 OR >30 min moderate
activity 3 times/week) [n(%)]:
1) baseline: IG 38/115(33%) vs 41/113(36.3%), p > 0.05;
2) 1-year: 46/115(40%) vs CG
29/113(26%), p = 0.02.
6
Allison &
Keller
(2004)
USA
108 subjects with coronary heart
disease were
recruited and 83
subjects (31% F, 69% M)
completed the
study (IG1=28,
IG2=27, CG=28).
72 83 Social-cognitive
theory
I1: The self-efficacy intervention based on
social-cognitive theory to
enhance confidence for
physical activity through a telephone intervention.
I2: A telephone follow up
protocol (a telephone call every 2 weeks) to report
their progress with the
physical activity and
exercise program prescribed in cardiac
rehabilitation, and
reminded to continue their
physical activity/exercise program.
C: usual care
12 weeks Physical Activity Scale for the Elderly
(PASE) and Self-
Efficacy Expectation
Scales (SES) at baseline, 6, and 12
weeks
(1) Self-reported physical activity (scores):
1) from baseline to the 6-week:
IG1 declined by 23.84% of
scores, IG2 declined by 18.86%, and CG declined by
28.82%, p > 0.05;
2) from 6 weeks to 12 weeks:
IG1 improved by 39.83% of scores, IG2 improved by
42.30%, and CG improved by
29.26%, p < 0.05.;
3) from baseline to 12 weeks: IG1 improved by 6.49%, IG2
by 15.46%, and CG by
-7.99%, p < 0.05.
4

69
Author
(year)
Country
Subjects
Mean
age
(years)
Sample
size
Theory/
model Interventions
Duration of
intervention Outcome measures Main results QS
Allison &
Keller
(2004)
USA
(2) Self-efficacy (mean scores):
1) baseline: similar among the
three groups;
2) from baseline to 6 weeks: IG1 increased 64.51% of mean
scores, IG2 increased
55.22%, and CG increased
42.70%, p > 0.05; 3) from 6 weeks to 12 weeks:
IG1 increased 9.81% of mean
scores, IG2 increased 6.68%,
and CG increased 7.67%, p > 0.05;
4) from baseline to 12 weeks:
IG1 increased 80.64% of
mean scores, IG2 increased 65.75%, and CG increased
53.64%, p > 0.05.
Arrigo et al.
(2008)
Switzerland
261 subjects with
heart disease were recruited
and 228 subjects
(14.5% F, 85.5%
M) completed the study (IG=105,
CG=123). 91%
with coronary
heart disease.
61 228 No I: Formal cardiac
rehabilitation included using a diary sheet for
physical activities and
taking part in a physician-
supervised group exercise session once every 3
months.
C: usual care
1 year Self-reported regular
physical activity (noticeably increase
pulse rate and
breathing ≥ 3 times
per week for ≥ 30 min) at baseline and
1 year.
Exercise adherence (moderately ≥
3 times per week for ≥ 30 minutes) [n (%)]:
1) baseline: no data available;
2) 1-year: IG 74/105 (70%) vs
CG 46/123 (37%), p < 0.0005.
4

70
Author
(year)
Country
Subjects
Mean
age
(years)
Sample
size
Theory/
model Interventions
Duration of
intervention Outcome measures Main results QS
Broadbent
et al.
(2009)
New
Zealand
103 MI patients
(12% F, 88% M)
were recruited,
96 completed 3-month follow up
(IG=50, CG=46),
and 79 completed
6-month follow up (IG=42,
CG=37).
55 79 No I: An illness perception
intervention which
consisted of three half-hour
individual patient sessions and one half-hour patient-
and-spouse session
delivered in hospital and
followed up to 6 months.
C: usual care.
During
hospitalizatio
n and 6
months' follow up
after
discharge
Self-reported
exercise (a single-
item scale from 0 to
10) at baseline, 3 and 6 months.
The amount of exercise (0-10):
1) baseline IG 3.40 vs CG 4.08,
p > 0.05;
2) 3-month: IG 4.32 vs CG 4.02, p > 0.05;
3) 6-month: IG 4.42 vs CG 4.14,
p > 0.05.
5
Brodie et al.
(2005, 2008)
UK
90 subjects (no
report about F &
M) with chronic
heart failure were recruited and 60
subjects
completed the
study (IG1=20, IG2=22,
CG=18).
79 60 Motivational
interviewing
I1: Standard care plus
motivational interviewing
programme on how to
increase energy expenditure by integration
of physical activities into
their daily routines.
I2: Motivational
interviewing only.
C: standard care
5 months The leisure-time
physical activity
questionnaire
(kcal/kg/day) and a 3-day physical
activity diary at
baseline and 5
months.
(1) Physical activities energy
expenditure (kcal/kg/day) [mean
(SD)]:
1) baseline: IG1 8.3 (2.5), IG2 6.6 (2.6) vs CG 9.7 (4.5), p >
0.05;
2) 5-month: IG1 10.5 (4.4), IG2
9.0 (3.3) vs CG 9.6 (4.3), p > 0.05.
(2) Leisure time activities
(kcal/kg/day) [mean (SD)]:
1) baseline: IG1 0, IG2 0.09 (4.3) vs CG 0.05 (2.4), p >
0.05;
2) 5-month: IG1 0.04 (0.1), IG2
0.16 (2.9) vs CG 0.08 (0.2), p > 0.05.
(3) Walking (kcal/kg/day) [mean
(SD)]:
1) baseline: IG1 1.2 (0.8), IG2 0.7 (0.4), CG 1.6 (1.2), p >
0.05;
2) 5-month: IG1 2.1 (1.1), IG2
1.7 (0.9) vs CG 1.9 (0.9), p > 0.05.
5

71
Author
(year)
Country
Subjects
Mean
age
(years)
Sample
size
Theory/
model Interventions
Duration of
intervention Outcome measures Main results QS
Butler et al.
(2009)
Australia
110 subjects
(24.5% F, 75.5%
M) with CABG,
PCI, MI, or ACS were recruited
(IG=55, CG=55)
and 98 subjects
completed the 6-week
intervention
(IG=48, CG=50)
and 90 subjects completed 6-
month follow up
(IG=44, CG=46).
64 98 No I: The 6-week intervention
included self-monitored
physical activity using a
pedometer and step calendar and 2 behavioural
counselling and goal-
setting sessions plus 2
generic physical activity information brochures.
C: usual care plus 2 generic
physical activity information brochures.
6 weeks and
6-month
follow up
Self-reported
physical activity
through Active
Australia Survey, Self-efficacy for
exercise scale, and
Outcome
expectancies for participation in
physical activity at
baseline, 6 weeks and
6 months.
(1) Total physical activity
(minute/week) [mean (SD)]:
1) baseline: IG 324.3(271.3) vs
CG 365.8 (272.6), p > 0.05; 2) 6-week: IG 410.9 (308.3) vs
CG 370.6 (309.6), p > 0.05;
3) 6-month: IG 455.5 (361.0) vs
355.2 (271.2), p < 0.05.
(2) Total physical activity
(session/week) [mean (SD)]:
1) baseline: IG 8.5 (5.1) vs CG 10.1 (6.5), p > 0.05;
2) 6-week: IG 11.4 (7.0) vs CG
9.2 (5.1), p < 0.05;
3) 6-month: IG 9.6 (5.8) vs 8.0 (4.4), p < 0.05.
(3) Walking (minute/week) [mean
(SD)]: 1) baseline: IG 227.7 (178.7) vs
CG 303.1 (232.4), p > 0.05;
2) 6-week: IG 308.4 (229.0) vs
CG 276.9 (229.9), p < 0.05; 3) 6-month: IG 262.5 (199.2) vs
CG 257.1 (214.3), p > 0.05.
(4) Walking (session/week) [mean (SD)]:
1) baseline: IG 7.1 (4.2) vs CG
8.8 (6.1), p > 0.05;
2) 6-week: IG 9.4 (5.6) vs CG 7.0 (4.2), p < 0.05;
3) 6-month: IG 7.3 (5.1) vs CG
6.5 (4.4), p < 0.05.
5

72
Author
(year)
Country
Subjects
Mean
age
(years)
Sample
size
Theory/
model Interventions
Duration of
intervention Outcome measures Main results QS
Campbell et
al.
(1998, 2003)
UK
1343 subjects
(42% F, 58% M)
with coronary
heart disease were recruited
and 1173
subjects
completed the study (IG=593,
CG=580).
66 1173 No I: Nurse run clinics
promoted medical and
lifestyle aspects of
secondary prevention and offered regular follow up
over one year.
C: usual care.
1 year and re-
assessed at 4
year (mean
follow up was at 4.7 years)
Health practices
index [Moderate
physical activity
(index of physical activity > 4)] at
baseline, 1 year and 4
years.
Moderate physical exercise [n
(%)]:
1) baseline: IG 221/587 (37.6%)
vs CG 183/568 (32.2%), p > 0.05;
2) 1-year: IG 247/587 (42.1%)
vs CG 177/568 (31.2%) (OR
= 1.67, 95% CI 1.23 to 2.26), p = 0.001;
3) 4-year: IG 171/494 (34.6%)
vs CG 128/455 (28.1%) (OR
= 1.26, 95% CI 0.88 to 1.81), p < 0.05.
6
Coull et al.
(2004)
UK
319 subjects
(40% F, 60% M)
with ischaemic
heart disease (IHD) were
recruited and 289
subjects
completed the study (IG=149,
CG=140).
67 289 No I: A mentor-led group,
through attending monthly
2 hour long meetings in
community facilities over a 1-year period.
C: usual care
One year Self-reported
physical activity in
previous week at
baseline and one year.
(1) Exercise (minute/week):
1) baseline: IG 697 vs CG 750;
2) 1-year: IG 843 vs CG 767,
difference +147 (95% CI -8 to +266), p > 0.05.
(2)Walking (minute/week):
1) baseline: IG 298 vs CG 303; 2) 1-year: IG 388 vs CG 320,
difference +73 (95%CI +1 to
+137), p < 0.05.
6

73
Author
(year)
Country
Subjects
Mean
age
(years)
Sample
size
Theory/
model Interventions
Duration of
intervention Outcome measures Main results QS
Cupples &
McKnight
(1994)
UK
688 subjects
(41% F, 59% M)
with angina were
recruited and 617 subjects
completed the
study (IG=317,
CG=300). 487 subjects
completed the 5-
year follow up
(IG=250, CG=237).
63 617 No I: Patients received
practical relevant advice
regarding cardiovascular
risk factors. They were reviewed at four monthly
intervals and given
appropriate health
education.
C: usual care.
2 years and 5
years' follow
up
Self-reported
exercise levels
(session/week for at
least 20 minutes per session) at baseline, 2
and 5 years.
(1) Physical exercise (≥ 5
sessions/week) [n (%)]:
1) baseline: IG 164/317 (51.7%)
vs CG 175/300 (58.3%), p > 0.05;
2-year: IG 194/317 (61.2%) vs CG
138/300 (46.0%), p < 0.01.
(2) Physical exercise [n (%)]:
compared to baseline, at 2 years
[IG 108 (34%) increased, 120
(38%) no changed, and 89 (28%) decreased] vs [CG 63 (21%)
increased, 74 (25%) no change,
and 163 (54%) decreased], p <
0.0001.
(3) Physical exercise (score based
on No of 20 minutes episodes per
week) (N=487) [mean, mean difference between groups (95%
CI)]:
1) baseline: IG 3.6 vs CG 3.8, -
0.2 (-0.5 to 0.1), p > 0.05; 2) 2-year: IG 4.0 vs 3.2, 0.7 (0.4
to 1.0), p < 0.05,
3) 5-year: IG 3.0 vs 2.8, 0.2 (-
0.2 to 0.5), p < 0.05.
6

74
Author
(year)
Country
Subjects
Mean
age
(years)
Sample
size
Theory/
model Interventions
Duration of
intervention Outcome measures Main results QS
Giallauria et
al.
(2009)
Italy
52 patients (15%
F, 85% M) after
acute MI were
recruited and included in data
analysis (IG=26,
CG=26).
58 52 No I: A multi-factorial,
educational and
behavioural intervention in
hospital once a month throughout the 24-month
follow up to receive dietary
advice, reinforcement on
maintaining a correct lifestyle, a session of
exercise training at the
follow up CPX, and a
booklet for exercise, diet, and smoking cessation.
C: usual care.
2 years Self-reported leisure
time physical
activities (LTPA)
questionnaire at the end of the initial 3-
month outpatient
cardiac rehabilitation
program and at 12-month and 24-month
follow up.
Exercise adherence (moderate to
high level of LTPA) [n (%)]:
1) 3-month: IG 23/26 (87%) vs
CG 23/26 (87%), p > 0.05; 2) 24-month: IG 15/26 (58%) vs
CG 7/26 (27%), p < 0.001.
6
Giannuzzi et
al.
(2008)
Italy
3241 subjects
(14% F, 86% M)
with recent MI
were recruited and included in
the data analysis
(IG=1620,
CG=1621).
58 3241 No I: A 3-year multifactorial
continued educational and
behavioural program
consisted of comprehensive cardiac rehabilitation
sessions with one-to-one
support monthly from
month 1 to month 6, then every 6 months for 3 years,
and a booklet. Each session
consisted of 30 minutes of
supervised aerobic exercise, plus lifestyle and
risk factor counselling
lasting at least 1 hour and
reinforcement of preventive interventions
lasting approximately 30
minutes.
C: usual care.
3 years Questionnaire on
leisure time physical
activity (3 items;
score range, 3 [most unfit] to 12 [≥ 3h/wk
of exercise]) at
baseline, 6, 12, 24
and 36 months.
Physical activity level (3.0-12.0
scores) [mean (SD)]:
1) baseline: IG 6.7 (2.5) vs CG
6.6 (2.4), p > 0.05; 2) 6-month: IG 7.5 (2.2) vs CG
7.1 (2.3), p = 0.005;
3) 12-month: IG 7.5 vs CG 7.2,
p = 0.20; 4) 24-month: IG 7.5 vs CG 7.1,
p = 0.01;
5) 36-month: IG 7.5 vs CG 7.1,
p = 0.01.
7

75
Author
(year)
Country
Subjects
Mean
age
(years)
Sample
size
Theory/
model Interventions
Duration of
intervention Outcome measures Main results QS
Gulanick et
al.
(1991)
USA
40 subjects (30%
F, 70% M) with
CHD were
recruited and 36 subjects
completed the
study (IG1=11,
IG2=13, CG=12). 55%
underwent
cardiac surgery.
58 36 No I1: Treadmill exercise
testing, teaching, and
exercise training (three
sessions weekly for 5 weeks);
I2: Treadmill exercise
testing and teaching, without exercise training.
C: usual care.
5 weeks Self-efficacy to
perform physical
activity and
performance of physical activity at
hospital discharge, 4
weeks after the
cardiac event, and 9 weeks recovery (after
the intervention).
(1) Self-efficacy for walking (1-25
scores) [mean (SD)]:
1) baseline: IG1 9.2 (2.8), IG2
8.6 (3.7) vs CG 11.4 (2.4), p > 0.05;
2) 4-week: IG1 16.8 (5.2), IG2
16.8 (5.2), vs CG 13.5 (4.3),
p > 0.05; 3) 9-week: IG1 21.1 (4.3), IG2
20.6 (3.0) vs CG 20.3 (3.8),
p > 0.05.
(2) Performance of walking (1-25
scores) [mean (SD)]:
1) baseline: IG1 12.5 (7.3), IG2
11.4 (5.3), vs CG 11.4 (4.8), p > 0.05;
2) 4-week: IG1 13.5 (4.9), IG2
11.0 (3.5) vs CG 10.3 (3.4),
p > 0.05; 3) 9-week: IG1 17.2 (4.4), IG2
14.6 (3.9) vs CG 15.8 (5.3),
p > 0.05.
4
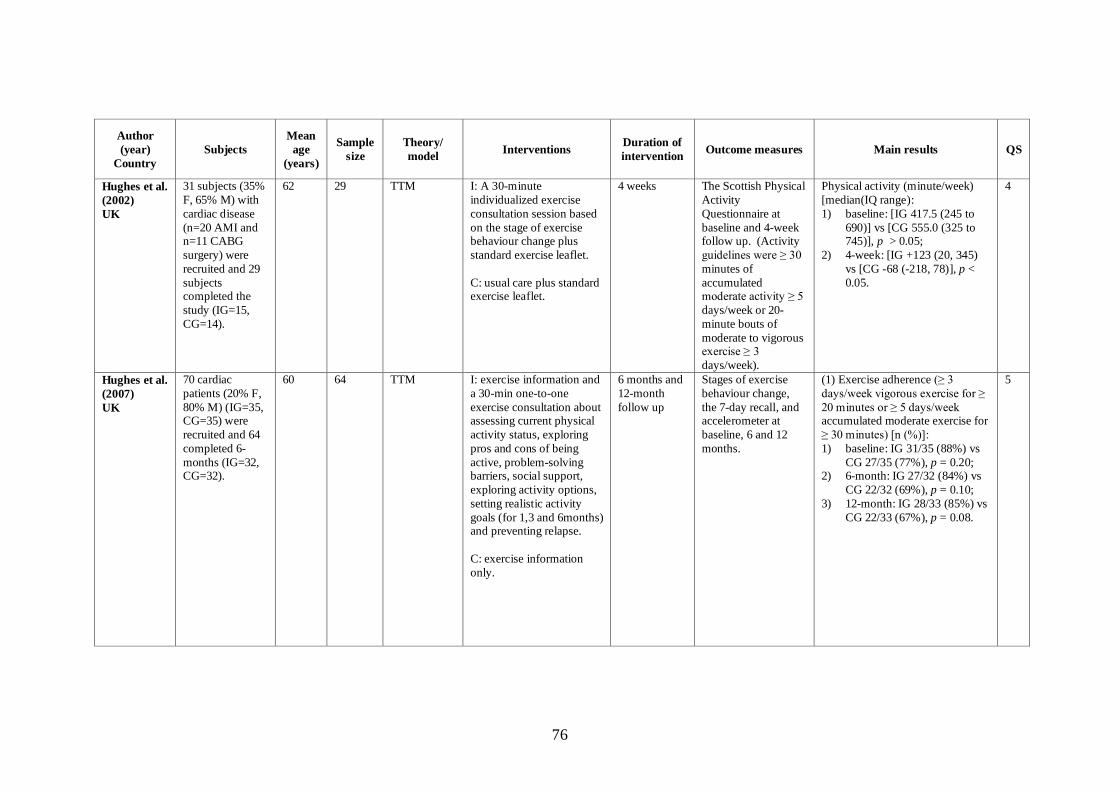
76
Author
(year)
Country
Subjects
Mean
age
(years)
Sample
size
Theory/
model Interventions
Duration of
intervention Outcome measures Main results QS
Hughes et al.
(2002)
UK
31 subjects (35%
F, 65% M) with
cardiac disease
(n=20 AMI and n=11 CABG
surgery) were
recruited and 29
subjects completed the
study (IG=15,
CG=14).
62 29 TTM I: A 30-minute
individualized exercise
consultation session based
on the stage of exercise behaviour change plus
standard exercise leaflet.
C: usual care plus standard exercise leaflet.
4 weeks The Scottish Physical
Activity
Questionnaire at
baseline and 4-week follow up. (Activity
guidelines were ≥ 30
minutes of
accumulated moderate activity ≥ 5
days/week or 20-
minute bouts of
moderate to vigorous exercise ≥ 3
days/week).
Physical activity (minute/week)
[median(IQ range):
1) baseline: [IG 417.5 (245 to
690)] vs [CG 555.0 (325 to 745)], p > 0.05;
2) 4-week: [IG +123 (20, 345)
vs [CG -68 (-218, 78)], p <
0.05.
4
Hughes et al.
(2007)
UK
70 cardiac
patients (20% F,
80% M) (IG=35, CG=35) were
recruited and 64
completed 6-
months (IG=32, CG=32).
60 64 TTM I: exercise information and
a 30-min one-to-one
exercise consultation about assessing current physical
activity status, exploring
pros and cons of being
active, problem-solving barriers, social support,
exploring activity options,
setting realistic activity
goals (for 1,3 and 6months) and preventing relapse.
C: exercise information
only.
6 months and
12-month
follow up
Stages of exercise
behaviour change,
the 7-day recall, and accelerometer at
baseline, 6 and 12
months.
(1) Exercise adherence (≥ 3
days/week vigorous exercise for ≥
20 minutes or ≥ 5 days/week accumulated moderate exercise for
≥ 30 minutes) [n (%)]:
1) baseline: IG 31/35 (88%) vs
CG 27/35 (77%), p = 0.20; 2) 6-month: IG 27/32 (84%) vs
CG 22/32 (69%), p = 0.10;
3) 12-month: IG 28/33 (85%) vs
CG 22/33 (67%), p = 0.08.
5

77
Author
(year)
Country
Subjects
Mean
age
(years)
Sample
size
Theory/
model Interventions
Duration of
intervention Outcome measures Main results QS
Hughes et al.
(2007)
UK
(2) Exercise (minute/week)
(median):
1) baseline: IG 300 vs CG 275,
p > 0.05; 2) IG: maintained from baseline
to 6 months (47min/week;
98%CI -43, 191) and 12
months (23min/week; 98% CI -63, 154);
3) CG: decreased by
115min/week from baseline
to 12 months (98% CI -228, -28) and 63min/week from 6
to 12 months (98% CI -126, -
5);
4) Significant difference for the change from baseline to 12
months (130min/week; 98%
CI -295, -20) between groups,
p < 0.05.
(3) Accelerometer (steps/week):
1) baseline: no available data;
2) IG: change from baseline to 6 months (98% CI -705 643,
860 599), and 12 months
(98% CI –381 927,504 719),
p > 0.05; 3) CG: from baseline to 6 month
decreased by 5.2% (98% CI–
215 141,4105 603), and 12
months decreased by 8% (98% CI -328 116, 4105 603);
p > 0.05.
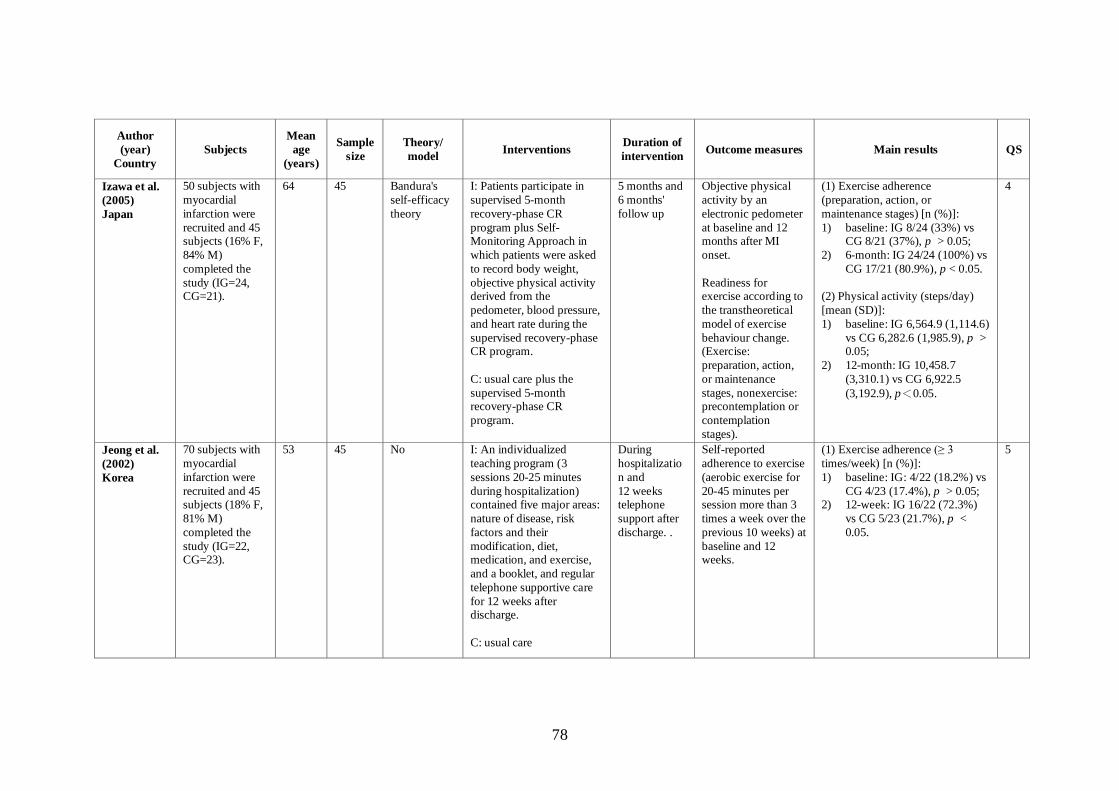
78
Author
(year)
Country
Subjects
Mean
age
(years)
Sample
size
Theory/
model Interventions
Duration of
intervention Outcome measures Main results QS
Izawa et al.
(2005)
Japan
50 subjects with
myocardial
infarction were
recruited and 45 subjects (16% F,
84% M)
completed the
study (IG=24, CG=21).
64 45 Bandura's
self-efficacy
theory
I: Patients participate in
supervised 5-month
recovery-phase CR
program plus Self-Monitoring Approach in
which patients were asked
to record body weight,
objective physical activity derived from the
pedometer, blood pressure,
and heart rate during the
supervised recovery-phase CR program.
C: usual care plus the
supervised 5-month recovery-phase CR
program.
5 months and
6 months'
follow up
Objective physical
activity by an
electronic pedometer
at baseline and 12 months after MI
onset.
Readiness for exercise according to
the transtheoretical
model of exercise
behaviour change. (Exercise:
preparation, action,
or maintenance
stages, nonexercise: precontemplation or
contemplation
stages).
(1) Exercise adherence
(preparation, action, or
maintenance stages) [n (%)]:
1) baseline: IG 8/24 (33%) vs CG 8/21 (37%), p > 0.05;
2) 6-month: IG 24/24 (100%) vs
CG 17/21 (80.9%), p < 0.05.
(2) Physical activity (steps/day)
[mean (SD)]:
1) baseline: IG 6,564.9 (1,114.6)
vs CG 6,282.6 (1,985.9), p > 0.05;
2) 12-month: IG 10,458.7
(3,310.1) vs CG 6,922.5
(3,192.9), p<0.05.
4
Jeong et al.
(2002)
Korea
70 subjects with
myocardial
infarction were
recruited and 45 subjects (18% F,
81% M)
completed the
study (IG=22, CG=23).
53 45 No I: An individualized
teaching program (3
sessions 20-25 minutes
during hospitalization) contained five major areas:
nature of disease, risk
factors and their
modification, diet, medication, and exercise,
and a booklet, and regular
telephone supportive care
for 12 weeks after discharge.
C: usual care
During
hospitalizatio
n and
12 weeks telephone
support after
discharge. .
Self-reported
adherence to exercise
(aerobic exercise for
20-45 minutes per session more than 3
times a week over the
previous 10 weeks) at
baseline and 12 weeks.
(1) Exercise adherence (≥ 3
times/week) [n (%)]:
1) baseline: IG: 4/22 (18.2%) vs
CG 4/23 (17.4%), p > 0.05; 2) 12-week: IG 16/22 (72.3%)
vs CG 5/23 (21.7%), p <
0.05.
5

79
Author
(year)
Country
Subjects
Mean
age
(years)
Sample
size
Theory/
model Interventions
Duration of
intervention Outcome measures Main results QS
Johnson et
al.
(2009)
Australia
154 women with
coronary heart
disease (AMI,
angina, PCI, or CABG) were
recruited and 144
subjects
completed the intervention
(IG=63, CG=81),
118 subjects at
the 3-month follow up
(IG=51, CG=67),
120 subjects at
the 6-month follow up
(IG=53, CG=67),
and 113 subjects
at the 12-month follow up
(IG=49, CG=64).
median
62-64
144 No I: Women were oriented to
the 12-week home walking
intervention and were
instructed to complete daily activity logs to
increase the likelihood of
adherence with physical
activity.
C: usual care.
12 weeks and
12 months'
follow up
Self-reported
maintenance of
physical activity (≥ 3
times/week) using the Stages of Change
model of exercise
behaviour at 3.6.and
12 months after outpatient cardiac
rehabilitation.
Regular physical activity ((≥ 3
times/week) [n (%)]:
1) 3-month: IG: 45/51 (90%) vs
CG 49/67 (74%), p = 0.03; 2) 6-month: IG 45/53 (87%) vs
CG 40/67 (61%), p = 0.003;
3) 12-month: 36/49 (77%) vs
CG 36/64 (56%), p = 0.03.
6

80
Author
(year)
Country
Subjects
Mean
age
(years)
Sample
size
Theory/
model Interventions
Duration of
intervention Outcome measures Main results QS
Lear et al.
(2001)
Canada
49 subjects (30%
F, 70% M) with
ischemic heart
disease (MI, a revascularization
procedure,
positive coronary
angiogram, or episodes of
angina) were
recruited and 36
subjects completed the
study (IG=17,
CG=19).
64 36 No I: A Lifestyle management
intervention (LMI) in
which patients received a
risk factor report (RFR) about their current and
previous lifestyle
behaviours (exercise, diet
and smoking sessions), six additional rehabilitation
sessions, two telephone
follow ups, and a full
lifestyle and risk factor assessment and counselling
session.
C: usual care
6 months A 4-week modified
version of the Leisure
Time Physical
Activity Questionnaire at
baseline and 6 month
after the intervention.
Physical activity (kcal/week)
[mean (SD)]:
1) baseline: IG 2175 (2107) vs
CG 3834 (3414), p < 0.05; 2) 6-month: IG 2458 (1169) vs
CG 2823 (1593), p > 0.05.
4
Lear et al.
(2002, 2003,
2006)
Canada
302 subjects
(18% F, 82% M)
with ischemic
heart disease (53% have had a
previous
myocardial
infarction and 73% have
undergone
previous
revascularization) were recruited
and included in
data analysis
(IG=151, CG=151)
64 302 TTM and
Social
Cognitive
Theory
I: An extensive lifestyle
management intervention
(ELMI) consists of cardiac
rehabilitation sessions, telephone follow ups and
lifestyle and risk factor
counselling sessions.
C: usual care.
4 years A 4-week modified
version of the Leisure
Time Physical
Activity Questionnaire.
General Self-efficacy
Scale and Exercise
Self-Efficacy Scale. Outcomes were
assessed at baseline,
1 and 4 years.
(1) Physical activity (kcal/week)
[mean (SD)]:
1) baseline: IG 3143 (2294) vs
CG 3022 (2308), p > 0.05; 2) 1-year: IG 2440 (1698) vs CG
2288 (1554), p > 0.05;
3) 4-year: IG 2099 (2074) vs CG
2349 (2018), p = 0.574.
(2) General Self-Efficacy (scores)
[mean (SD)]:
1) baseline: IG 43 (4) vs CG 42 (5), p > 0.05;
2) 1-year: IG 41 (5) vs CG 41
(5), p > 0.05;
3) 4-year: IG 42 (4) vs CG 42 (5), p = 0.885.
6

81
Author
(year)
Country
Subjects
Mean
age
(years)
Sample
size
Theory/
model Interventions
Duration of
intervention Outcome measures Main results QS
Lear et al.
(2002, 2003,
2006)
Canada
(3) Exercise Self-Efficacy (scores)
[mean (SD)]:
1) baseline: IG 67 (10) vs CG 65
(13), p > 0.05; 2) 1-year: IG 63 (15) vs CG 63
(16), p > 0.05;
3) 4-year: IG 63 (14) vs CG 62
(15), p = 0.457.
Lisspers et
al.
(1998, 1999,
2005)
Sweden
93 subjects with
coronary heart
disease recently
treated with PTCA were
recruited and 87
subjects (16% F,
84% M) completed the
study (IG=46,
CG=41).
53 87 No I: The residential
rehabilitation programme
had a 12-month period and
initiated by a 4-week residential stay at the
intervention unit which
consisted of intense health
education and activities promoting behavioural
changes and an 11-month
structured maintenance
program followed the in-patient phase.
C: usual care
1 year and 2
and 5 years'
follow up
Self-reported
questionnaire about
frequency of exercise
at baseline, 1, 2, 3 and 5 years.
An exercise session
was defined as effort corresponding to a
brisk walk for at least
20 min.
(1) Exercise (session/week):
1) Not reported (graphic display
only), p = 0.02.
(2) Exercise adherence (≥ 2
times/week) [n (%)]:
1) baseline: IG 13/46(28%) vs
CG 13/41(32%), p > 0.05; 2) 12-month: IG 26/46(56%) vs
CG 17/41(41%), p < 0.05.
(3) Exercise level (1-3 scores, the higher score the better exercise
level) [mean (SD)]:
1) baseline: no data available;
2) 12-month: IG 1.74 (1.33) vs CG 0.94 (1.13);
4

82
Author
(year)
Country
Subjects
Mean
age
(years)
Sample
size
Theory/
model Interventions
Duration of
intervention Outcome measures Main results QS
Lisspers et
al.
(1998, 1999,
2005)
Sweden
3) 24-month: IG 1.46 (1.37) vs
CG 0.82 (1.20);
4) 36-month: IG 1.35 (1.37) vs
CG 0.78 (1.23); 5) 60-month: IG 1.40 (1.30) vs
CG 1.00 (1.25).
Luszczynska
et al.
(2006)
UK
130 subjects after
uncomplicated
MI were
recruited and 114 subjects (36% F,
64% M)
completed the
study (IG=59, CG=55).
54 114 No I: An implementation
intention intervention on
behaviour change with the
use of a planning strategy. The intervention was given
on an individual basis and
lasted 10–15 min.
C: usual care after 2 weeks
short-term rehabilitation.
All patients received 2 weeks short-term
rehabilitation.
6 months Self-reported
physical activity
(Frequency of
moderate physical activity for ≥30 min)
at 4-10 days after MI,
the eighth week after
MI (2 weeks after a short-term
rehabilitation), and
eighth or ninth month
after MI (post- intervention).
(1) Physical activity (1-7, 1=
never, 2 = once in past two weeks,
3 = once/week, 4 = twice/week, 5
= three times/week, 6 = four times/week, 7 = five or more
times/week) [mean (SD)]:
1) baseline: IG 3.42 (2.14) vs
CG 4.23 (2.16), p > 0.05; 2) 8-week: IG 5.17 (1.59) vs CG
5.44 (1.10), p > 0.05;
3) 8-month: IG 4.75 (1.83) vs
CG 4.09 (1.69), p < 0.10.
4
Mildestvedt
et al.
(2008)
Norway
217 subjects with
coronary heart
disease were
recruited and 176 subjects (22% F,
78% M)
completed the
study (IG=90, CG=86).
56 176 No I: Standard rehabilitation
treatment plus an
additional individualized
self-efficacy and autonomy supportive intervention.
C: standard rehabilitation
treatment.
2 years Self-reported
exercise at baseline
and 6 and 24 months'
follow up.
(1) Exercise level (score 1-5, the
higher scores the better exercise
level) [mean (SD)]:
1) baseline: IG 3.3 (0.8) vs CG 3.2 (0.9), p = 0.49;
2) 6-month: IG 3.5 (0.7) vs CG
3.6 (0.7);
3) 24-month: IG 3.4 (0.8) vs CG 3.4 (0.8);
4) p(time) < 0.001, p(group) =
0.79, p(interaction) = 0.66.
5

83
Author
(year)
Country
Subjects
Mean
age
(years)
Sample
size
Theory/
model Interventions
Duration of
intervention Outcome measures Main results QS
Mildestvedt
et al.
(2008)
Norway
(2) Exercise self-efficacy [mean
(SD)]:
1) baseline: IG 3.9 (0.8) vs CG
4.0 (0.7), p = 0.48; 2) no detailed data available at 6
and 24 months, p > 0.05.
Moore et al.
(2006)
USA
273 subjects who
had a recent
cardiac event
(MI, CABG, and/or
angioplasty)
were recruited
and 250 subjects (38% F, 62% M)
completed the
study (IG=119,
CG=131).
81.2%
Caucasian.
51.6% MI, 54.8% CABG,
59.2%
Angioplasty.
62 250 Social
problem-
solving
model, self-efficacy
theory,
expectancy-
value theory, and relapse
prevention
theory.
I: ―Change Habits by
Applying New Goals and
Experiences‖ (CHANGE)
intervention consists of five small-group (6–8
people) 1½-hr counselling
and behaviour modification
sessions for self-efficacy enhancement, problem-
solving skills, and relapse
prevention strategies to
address their identified exercise maintenance
problems.
C: usual care after the completion of CRP
3 months and
1-year follow
up
Exercise adherence
(exercise ≥ 5
times/week for 30
min) through portable wristwatch HR
monitors (Polar
Vantage NV™, Polar
Electro, Kempele, Finland) and exercise
diaries; Exercise
Benefits/Barriers
Scale; Exercise Self-Efficacy by Exercise
Barriers and
Adherence Self-
Efficacy Scale at baseline, 3 months
and 1 year.
(1) Exercise adherence (moderate
exercise ≥ 150 minutes/week) [n
(%)]:
1) 3-month: IG 52/119 (43.8%) vs CG 45/131 (34.4%), p >
0.05;
2) 1-year: IG 34/119 (28.8%) vs
CG 35/131 (26.7%), p > 0.05. (2) Exercise adherence (moderate
exercise ≥ 5 times/week or 20
times/month) [n (%)]
1) 3-month: IG 19/119 (16.1%) vs CG 19/131 (14.8%), p >
0.05;
2) 1-year: IG 9/119 (7.5%) vs
CG 10/131 (8.1%), p > 0.05. (3) Exercise (hour/month) [mean
(SD)]:
1) 3-month: IG 9.5 (7.4) vs CG
8.5 (8.9), p > 0.05; 2) 1-year: IG 7.0 (7.2) vs CG 6.4
(9.2), p > 0.05.
(4) Exercise frequency
(session/month) [mean (SD)] 1) 3-month: IG 11.5 (7.8) vs CG
10.6 (9.2), p > 0.05;
2) 1-year: IG 7.6 (7.0) vs CG 7.1
(8.2), p > 0.05.
6

84
Author
(year)
Country
Subjects
Mean
age
(years)
Sample
size
Theory/
model Interventions
Duration of
intervention Outcome measures Main results QS
Moore et al.
(2006)
USA
(5) Exercise Benefits/Barriers
[mean (SD)]:
Benefits:
1) baseline: IG 90.4(10.6) vs CG 90.5(11.4), p > 0.05;
2) 3-month: IG 89.0(10.5) vs
CG 89.4(10.8), p > 0.05;
3) 1-year: IG 90.7(10.3) vs CG 90.5(9.8), p > 0.05.
Barriers:
1) baseline: IG 42.9(5.1) vs CG
42.3(5.4), p > 0.05; 2) 3-month: 42.4(5.3) vs CG
42.4(4.5), p > 0.05;
3) 1-year: 41.9(5.6) vs CG
41.9(4.8), p > 0.05.
(6) Exercise Self-Efficacy [mean
(SD)]:
Barriers: 1) baseline: IG 73.4(18.6) vs CG
72.1(20.6), p > 0.05;
2) 3-month: IG 71.6(19.6) vs
CG 71.1(21.8), p > 0.05; 3) 1-year: IG 72.0(21.9) vs CG
69.5(25.2), p > 0.05.
Adherence:
1) baseline: IG 91.8(14.7) vs CG 90.0(15.5), p > 0.05;
2) 3-month: IG 76.9(29.9) vs
76.5(30.3), p > 0.05;
3) 1-year: IG 69.4(37.0) vs CG 70.0(36.3), p > 0.05.

85
Author
(year)
Country
Subjects
Mean
age
(years)
Sample
size
Theory/
model Interventions
Duration of
intervention Outcome measures Main results QS
Mosca et al.
(2010)
USA
304 women with
coronary heart
disease were
recruited and 243 subjects
completed the
study (IG=121,
CG=122).
47.7% white,
33.6% black,
15.1% Hispanic.
62 243 Social
learning
theory
I: Education and
counselling during
hospitalization about
patients' adherence to secondary prevention goals
based on social learning
theory and the five A‘s
construct (ask, advise, agree, assist, arrange) and
receiving an educational
booklet.
C: usual care
During
hospitalizatio
n and
12 weeks postdischarge.
Follow up at
6 weeks and 6
months postdischarge.
Self-reported
adherence to physical
activity (at least 30
minutes three times per week or
enrollment in formal
cardiac
rehabilitation) at baseline, 6 weeks and
6 months after
postdischarge.
Exercise/cardiac rehabilitation
adherence (≥3 times/week) [n
(%)]:
1) baseline: IG 29/144 (20%) vs CG 29/148 (20%), p > 0.05;
2) 6 weeks: IG 27/119 (23%) vs
CG 27/121 (22%), p > 0.05;
3) 6 months: IG 41/108 (38%) vs CG 32/109 (29%), p >
0.05.
6
Naser et al.
(2008)
Iran
100 subjects
(16% F, 84% M)
with coronary
heart disease were recruited
and completed
the study (IG=50,
CG=50)
54 100 TTM I: An intensive
multifactorial lifestyle
modification program
(IMLM) based on the stages of change, which
was a 30-minute hospital-
based consultation along
with written guidelines and a two year post-hospital
intervention program
consisted of CRP exercise
sessions, lifestyle counselling and telephone
follow ups.
C: usual care
2 years Self-reported
questionnaire on type
of exercise (Not
described what kind of questionnaire) at
baseline and second
year.
Exercise adherence (vigorously 20
min 3 times/week) [n (%)]:
1) baseline: IG 10/50 (20%) vs
CG 11/50 (22%), p > 0.05; 2) 2-year: IG 44/50 (88%) vs
CG 10/50 (20%), p < 0.05.
6

86
Author
(year)
Country
Subjects
Mean
age
(years)
Sample
size
Theory/
model Interventions
Duration of
intervention Outcome measures Main results QS
Ornish et al.
(1990, 1998)
USA
48 subjects (9%
F, 91% M) with
moderate to
severe coronary heart disease
were recruited
and 37 subjects
completed the intervention
(IG=20, CG=17)
and 35 subjects
completed the 4-year follow up
(IG=20, CG=15).
56 35 No I: An intensive lifestyle
program included a week-
long residential retreat at
hotel followed by twice-weekly 4-h meetings. The
main contents of the
program included a 10%-
fat vegetarian diet, moderate aerobic exercise,
stress management
training, smoking
cessation, and group psychosocial support.
C: usual care
1 year and 5
years follow
up
Self-reported
exercise (frequency
and duration of
exercise) at baseline, 1-year and 5-year
follow up.
(1) Exercise frequency
(times/week) [mean (SD)]:
1) baseline: IG 2.66 (0.84) vs
CG 2.38 (0.77), p > 0.05; 2) 1-year: IG 4.97 (0.35) vs CG
2.87 (0.70), p = 0.06;
3) 5-year: IG 4.34 (0.49) vs CG:
3.57 (0.56), p = 0.64.
(2) Exercise (hours/week) [mean
(SD)]:
1) baseline: IG 2.26 (0.85) vs 2.42 (0.99), p > 0.05;
2) 1-year:IG 5.02 (0.61) vs
2.52 (0.70), p = 0.12; 3) 5-year: IG 3.56 (0.56) vs CG
2.90 (0.65), p = 0.50.
5
Redfern et
al.
(2008, 2009,
2010)
Australia
144 subjects
(25% F, 75% M)
after acute
coronary syndrome were
recruited and
included in data
analysis (IG=72, CG=72).
65 144 No I: The CHOICE
intervention included a 1
hour initial consultation
and multiple follow up phone calls over 3 months.
The programme was a
brief, patient-centred,
modular programme comprising a clinic visit
plus telephone support,
encompassing mandatory
cholesterol lowering and tailored preferential risk
modification.
C: usual care.
3 months and
1 and 4 years'
follow up
International Physical
Activity
Questionnaire
(IPAQ) score at baseline, 3 months,
and 1 and 4 years.
(1) Physical activity
(METS/kg/min) [mean (SD)]:
1) baseline: IG 314.7 (37.9) vs
CG 267.0 (31.6), p > 0.05; 2) 3-month: IG 1,186.6 (164.1)
vs CG 636.2 (115.4), p <
0.01;
3) 12-month: IG 1369.1(167.2) vs CG 715.1(103.5), p =
0.001);
4) 4-year: IG 1200 (209) vs CG
968 (196), p = 0.02. 5)
(2) Regular physical activity (≥ 5
days 30 minutes) [n (%)]:
1) baseline: IG 22/72 (31%) vs CG 17/72 (24%), p > 0.05;
7

87
Author
(year)
Country
Subjects
Mean
age
(years)
Sample
size
Theory/
model Interventions
Duration of
intervention Outcome measures Main results QS
Redfern et
al.
(2008, 2009,
2010)
Australia
2) 3-month: IG 56/72 (78%) vs
CG 23/72 (32%), p < 0.05;
3) 12-month: IG 47/67 (70%) vs
CG 21/69 (30%), p < 0.01]; 4) 4-year: IG 23/40 (57%) vs
CG 15/46 (33%), p = 0.01.
Salminen et
al.
(2005)
Finland
268 subjects with
coronary heart
disease were
recruited and 227 subjects (51% F,
49% M)
completed the
study (IG=118, CG=109).
74 227 No I: health advocacy,
counselling, and activation
program which consisted
of 16 lectures by experts, eight group discussions, six
group exercise sessions,
and three social activity
events.
C: usual care
2 years Self-reported
frequency of exercise
at baseline and 2
years.
There were no significant
differences in frequency of
exercise between two groups.
4
Senuzun et
al.
(2006)
USA
60 subjects (8%
F, 92% M) with
coronary heart
disease completed the
study (IG=30,
CG=30)
54 60 No I: The Phase II home-based
cardiac exercise program
included three 45–60-min
sessions per week for 12 weeks, and the
enhancement of self-
efficacy through
educational sessions and the use of goal setting,
modelling, and
physiological feedback
strategies.
C: usual care
12 weeks The cardiac exercise
self-efficacy index
(CESEI) at baseline
and 12 weeks.
Self-efficacy scores (mean):
1) baseline: IG 55.7 vs CG 55.7,
p = 0.695;
2) 12-week: IG 77.7 vs CG 60.6, p < 0.001.
4

88
Author
(year)
Country
Subjects
Mean
age
(years)
Sample
size
Theory/
model Interventions
Duration of
intervention Outcome measures Main results QS
Smeulders et
al.
(2006, 2009)
Netherlands
317 subjects
(27% F, 73% M)
with congestive
heart failure were recruited and
included in data
analysis
(IG=186, CG=131).
67 317 Bandura's
self-efficacy
theory
I: The 'Chronic Disease
Self-Management Program'
(CDSMP) consists of six
weekly group sessions to incorporate skills mastery,
reinterpretation of
symptoms, modelling, and
social persuasion to enhance self-efficacy
expectancies.
C: usual care
6 weeks and 6
and 12
months'
follow up
A modified version
of the 'Physical
activities scale'
comprised questions about the frequency
of the following three
categories: walking
for exercise, swimming, and
bicycling. Outcomes
were assessed at
baseline, 6 weeks, 6 and 12 months.
(1) Walking for exercise
(minute/month) [mean (SD)]:
1) baseline: IG 572.4 (791.0) vs
CG 563.3 (713.8), p = 0.877; 2) direct follow up (6 weeks):
IG 772.0 (998.0) vs CG 588.1
(681.7), p = 0.034;
3) 6-month: IG 753.3 (1050.1) vs CG 531.0 (780.4), p =
0.068;
4) 12-month: IG 628.2(762.7) vs
CG 552.8 (706.5), p = 0.269.
(2) Swimming (minute/month)
[mean (SD)]:
1) baseline: IG 22.2 (67.0) vs CG 41.7 (181.4), p = 0.258;
2) direct follow up: IG 33.8
(109.6) vs CG 30.1(141.8), p
= 0.331; 3) 6-month: IG 26.8 (86.5) vs
CG 52.8 (205.7), p = 0.217;
4) 12-month: IG 47.8 (181.5) vs
CG 51.1 (196.3), p = 0.991.
(3) Bicycling (minute/month)
[mean (SD)]:
1) baseline: IG 260.9 (526.0) vs CG 209.1 (423.0), p = 0.872;
2) direct follow up: IG 302.3
(520.4) vs CG 220.8 (382.8),
p = 0.176; 3) 6-month: IG 280.6 (604.2) vs
CG 228.5 (471.7), p = 0.675;
7
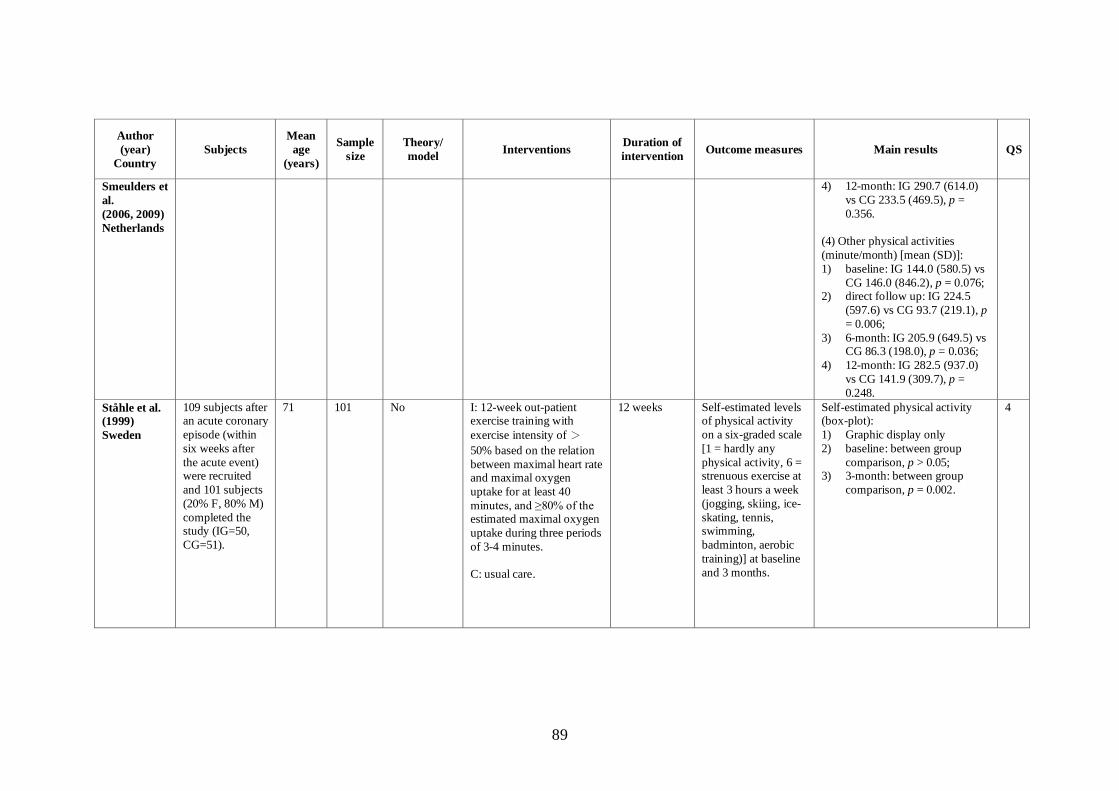
89
Author
(year)
Country
Subjects
Mean
age
(years)
Sample
size
Theory/
model Interventions
Duration of
intervention Outcome measures Main results QS
Smeulders et
al.
(2006, 2009)
Netherlands
4) 12-month: IG 290.7 (614.0)
vs CG 233.5 (469.5), p =
0.356.
(4) Other physical activities
(minute/month) [mean (SD)]:
1) baseline: IG 144.0 (580.5) vs
CG 146.0 (846.2), p = 0.076; 2) direct follow up: IG 224.5
(597.6) vs CG 93.7 (219.1), p
= 0.006;
3) 6-month: IG 205.9 (649.5) vs CG 86.3 (198.0), p = 0.036;
4) 12-month: IG 282.5 (937.0)
vs CG 141.9 (309.7), p =
0.248.
Ståhle et al.
(1999)
Sweden
109 subjects after an acute coronary
episode (within
six weeks after
the acute event) were recruited
and 101 subjects
(20% F, 80% M)
completed the study (IG=50,
CG=51).
71 101 No I: 12-week out-patient exercise training with
exercise intensity of >
50% based on the relation
between maximal heart rate and maximal oxygen
uptake for at least 40
minutes, and ≥80% of the estimated maximal oxygen
uptake during three periods
of 3-4 minutes.
C: usual care.
12 weeks Self-estimated levels of physical activity
on a six-graded scale
[1 = hardly any
physical activity, 6 = strenuous exercise at
least 3 hours a week
(jogging, skiing, ice-
skating, tennis, swimming,
badminton, aerobic
training)] at baseline
and 3 months.
Self-estimated physical activity (box-plot):
1) Graphic display only
2) baseline: between group
comparison, p > 0.05; 3) 3-month: between group
comparison, p = 0.002.
4

90
Author
(year)
Country
Subjects
Mean
age
(years)
Sample
size
Theory/
model Interventions
Duration of
intervention Outcome measures Main results QS
Stenlund et
al.
(2005)
Sweden
109 subjects 73
years or older
with coronary
heart disease were recruited
and 95 subjects
(30% F, 70% M)
completed the study (IG=48,
CG=47).
78 95 No I: Qi Gong and group
discussion which group
met weekly over 3 months
(a total of 12 group sessions). Each session
included 1h of Qi Gong
and 2h of discussions on
various themes.
C: usual care
3 months Self-reported current
level of physical
activity on a six-point
scale (‗1‘ corresponded to
sedentary and‗6‘ to
strenuous exercise) at
baseline and 3 months.
Physical activity level (score 1-6)
[mean (SD)]:
1) baseline: IG 3.4 (0.7) vs CG
3.6 (0.7), p > 0.05; 2) 3-month: IG 4.0 (0.7) vs CG
3.7 (0.7), p = 0.011.
4
The Vestfold
Heartcare
Study
Group
(2003)
Norway
Subjects (18% F,
82% M) with
stable CHD
(15.2%) or 5-39 days following
acute myocardial
infarction,
unstable angina pectoris, PCI or
CABG were
recruited and 191
completed 6-month follow up
(IG=95, CG=96)
and 182
completed 2-year follow up
(IG=91, CG=91).
55 191 No I: A comprehensive
lifestyle intervention
consisted of physical
exercise training and scheduled meeting
throughout the two-year
follow up period for a low
fat dietary advice, smoking cessation, physical activity
counselling, risk factor
management, psychosocial
support and health education related to
cardiovascular disease,
medication, reduction of
mental stress, relaxation and psychosocial factors.
C: usual care
6 weeks plus
9 weeks, 2
years
Self-reported
exercise and exercise
diaries at baseline, 6
months and 2 years.
Exercise adherence (≥ 60
minutes/week) (%):
1) baseline (similar between two
groups), p > 0.05; 2) 6-month: IG 88/95 (93%) vs
CG 69/96 (72%), p <0.001;
3) 2-year: IG 61/91 (67%) vs
CG 42/91 (46%), p <0.01.
5

91
Author
(year)
Country
Subjects
Mean
age
(years
Sample
size
Theory/
model Interventions
Duration of
intervention Outcome measures Main results QS
van Elderen-
van
Kemenade
et al.
(1994)
Netherlands
60 subjects after
acute myocardial
infarction were
recruited and 48 subjects (16% F,
84% M)
completed the
study (IG=22, CG=26).
57 48 No I: Two individual
counselling sessions and
two group health education
sessions (90 minutes/session) focusing
on medication, healthy
habits, anxiety and
depression during hospitalization and weekly
telephone calls for a period
of six weeks after
discharge from hospital.
C: usual care.
8 weeks and 1
year's follow
up
Self-reported
physical exercise:
spending more time,
the same amount of time or less time in
four areas of physical
activity: taking
walks, bicycling, participating in
organized sports
(e.g., tennis or
football and pursuing active hobbies) at
baseline, immediately
after the group
sessions prior to discharge, 8 weeks
after discharge, and 1
year after discharge.
Physical exercise (n):
(1)Taking walks:
1) baseline: no significant
difference between groups; 2) 8-week: (IG 15 more, 14
same, 1 less) vs (CG 11 more,
15 same, 4 less), p >
0.05; 3) 1-year: (IG 10 more, 2 same,
10 less) vs (CG 7 more, 7
same, 12 less), p > 0.05.
(2) Bicycling (n):
1) baseline: no significant
difference between groups;
2) 8-week: (IG 10 more, 18 same, 2 less) vs (CG 5 more,
16 same, 9 less), p < 0.05;
3) 1-year: (IG 8 more, 7 same, 7
less) vs (CG 8 more, 4 same, 14 less), p > 0.05.
(3) Active in organized sports (n):
1) baseline: no significant difference between groups;
2) 8-week: (IG 3 more, 27 same,
0 less) vs (CG 0 more, 26
same, 4 less), p < 0.05; 3) 1-year: (IG 6 more, 16 same,
0 less) vs (CG 12 more, 12
same, 2 less), p > 0.05.
(4) Pursuing active hobbies (n):
1) baseline: no significant
difference between groups;
2) 8-week: (IG 1 more, 24 same,

92
Author
(year)
Country
Subjects
Mean
age
(years)
Sample
size
Theory/
model Interventions
Duration of
intervention Outcome measures Main results QS
van
Elderen-van
Kemenade
(1994)
Netherlands
5 less) vs (CG 2 more, 23
same, 5 less), p > 0.05;
3) 1-year: (IG 9 more, 6 same, 7
less) vs (CG 8 more, 12 same, 6 less), p > 0.05.
Yates et al.
(2005)
USA
64 subjects (31% F, 69% M) who
had a recent
cardiac event
(MI, CABG, and/or PCI) were
recruited
(IG1=20, IG2=24, CG=20)
and 59 subjects
completed the
study (IG1=18, IG2=23,
CG=18).
97% white. 44 (69%) CABG
20 (31%) MI
and/or PCI.
67 59 Bandura's self-efficacy
theory
I1: Bandura's self-efficacy theory based booster
intervention by clinic.
I2: Bandura's self-efficacy
theory based booster intervention by telephone.
C: usual care
9 weeks and 3 and 6 months
after the
baseline
Self-reported exercise adherence
(aerobic activity
(brisk walking,
jogging, bicycling, or swimming) for more
than 20 min/session
and ≥ 3 times/week) at baseline, 3 and 6
months.
(1) Exercise adherence (≥ 3 times/week) [n (%)]:
1) 3-month: IG1 14/20 (70%)
(n=14), IG2 18/24 (75%) vs
CG 10/20 (50%), p > 0.05; 2) 6-month: IG1 8/20 (40%),
IG2 15/24 (63%) vs CG
10/20 (50%), p > 0.05. (2) Exercise frequency
(session/week)[mean(SD)]:
1) baseline: IG1 5.33(1.85), IG2
5.02(1.83) vs CG 5.70(1.78), p > 0.05;
2) 3-month: IG1 4.78(1.82), IG2
4.58(1.72) vs CG 4.03(1.62),
p > 0.05; 3) 6-month: IG1 4.65(1.82), IG2
3.67(1.96) vs CG 4.15(1.99);
p > 0.05.
(3) Exercise duration
(minute/session)[mean(SD)]:
1) baseline: IG1 31.45(1.85),
IG2 29.50(4.88) vs CG 31.45(4.99), p > 0.05;
2) 3-month: IG1 33.00(5.71),
IG2 29.71(6.23) vs CG
33.80(13.03), p > 0.05; 3) 6-month: IG1 30.10(11.08),
IG2 29.71(14.49) vs CG
27.55(13.12), p > 0.05.
4

93
Author
(year)
Country
Subjects
Mean
age
(years)
Sample
size
Theory/
model Interventions
Duration of
intervention Outcome measures Main results QS
Zhao &
Wong
(2009)
China
220 subjects with
myocardial
infarction or
angina pectoris were recruited
and 200 subjects
(51% F, 49% M)
completed the study (IG=100,
CG=100).
72 200 No I: The transitional care
programme (TCP)
consisted of pre-discharge
assessment, structured home visits and telephone
follow ups within four
weeks after discharge.
C: usual care
4 weeks and
8-week
follow up
Self-reported
physical exercise
adherence and a daily
record of exercise at baseline, 2 days, 4
and12 weeks after
discharge from
hospital.
Physical exercise adherence [n
(%)]:
1) baseline: [IG high 56(56%),
moderate 39(39%), low 5(5%)] vs [CG high 63(63%),
moderate 33(33%), low 4
(4%)], p = 0.600;
2) 2-day: [IG high 63(63%), moderate 34(34%), low
3(3%)] vs [CG high 63(63%),
moderate 33(33%), low 4
(4%)], p = 0.924; 3) 4-week: [IG high 74(74%),
moderate 23(23%), low
3(3%)] vs [CG high 62(62%),
moderate 32(32%), low 6(6%)], p = 0.171;
4) 12-week: [IG high 90(90%),
moderate 7(7%), low 3(3%)]
vs [CG high 62(62%), moderate 32(32%), low
6(6%)], p = 0.000.
5
Zwisler
(2008)
Denmark
770 subjects
(37% F, 63% M)
with congestive
heart failure (12%), ischemic
heart disease
(58%), or high
risk of ischemic heart disease
(30%) were
recruited and
completed the study (IG=380,
median
66
770 TTM and
self-efficacy
theory
I: Hospital-based
comprehensive cardiac
rehabilitation (6 weeks)
consisted of patient education, exercise
training, dietary
counselling, smoking
cessation, psychosocial support, and risk factor
management and clinical
assessment.
C: usual care
6-week and
12-month
follow up
interventions
Self-reported
adherence to the
advised increased
level of physical activity (from 4 hours
of moderate physical
activity a week to
>30 min/d) at baseline and 12
months.
(1) Community-based or private
services' physical exercise activity
[n (%)]:
1) no data available at baseline, p > 0.05;
2) 1-year: IG 125/380 (33%) vs
CG 23/390 (6%), p < 0.01.
6
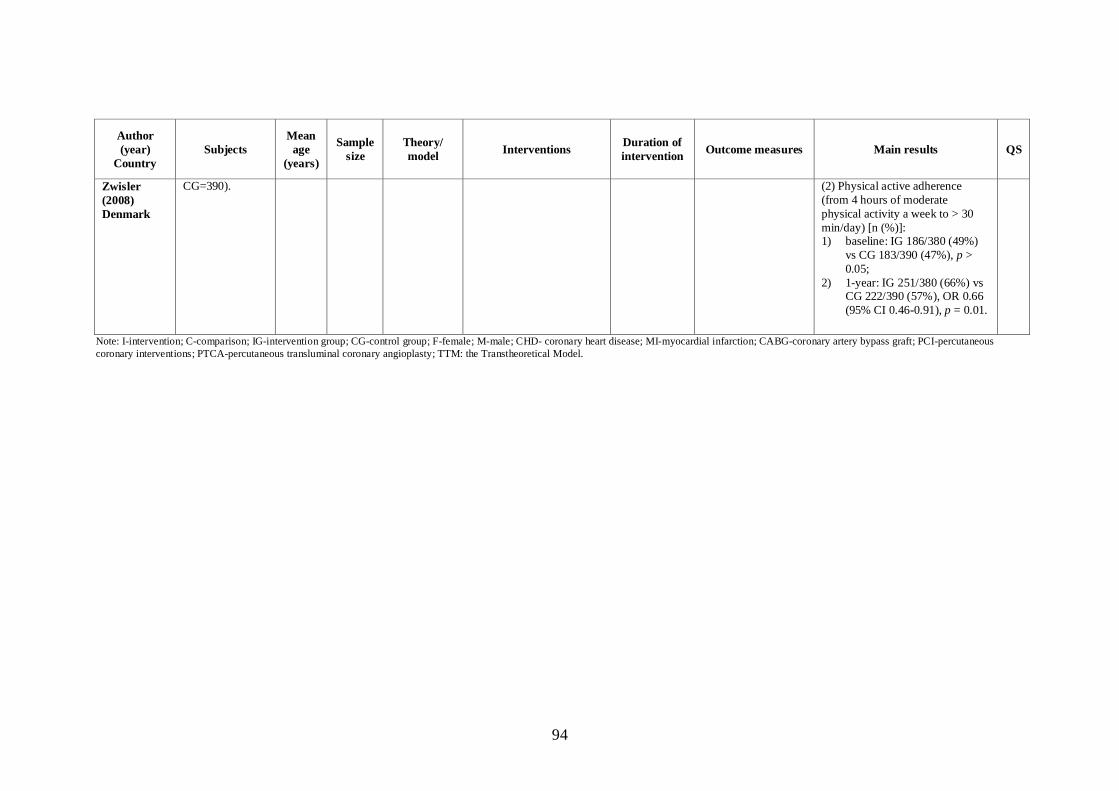
94
Author
(year)
Country
Subjects
Mean
age
(years)
Sample
size
Theory/
model Interventions
Duration of
intervention Outcome measures Main results QS
Zwisler
(2008)
Denmark
CG=390). (2) Physical active adherence
(from 4 hours of moderate
physical activity a week to > 30
min/day) [n (%)]: 1) baseline: IG 186/380 (49%)
vs CG 183/390 (47%), p >
0.05;
2) 1-year: IG 251/380 (66%) vs CG 222/390 (57%), OR 0.66
(95% CI 0.46-0.91), p = 0.01.
Note: I-intervention; C-comparison; IG-intervention group; CG-control group; F-female; M-male; CHD- coronary heart disease; MI-myocardial infarction; CABG-coronary artery bypass graft; PCI-percutaneous
coronary interventions; PTCA-percutaneous transluminal coronary angioplasty; TTM: the Transtheoretical Model.

95
2.4.4 Factors Affecting the Effectiveness of Patient Education
The effectiveness of patient education is determined by many factors. A number of
factors relate to difficulties in providing effective patient education, such as a
reduction in the time available for patient education due to shorter hospital stays, the
patient‘s physical and emotional status, the provision of non-tailored patient education,
and the shortage of nursing personnel (Padberg & Padberg, 1990). Kreuter and co-
workers (2000) suggest that for most patients, a tailored patient education is more
effective than a non-tailored one. Patients with high trait negative affectivity will tend
to show little change in health behaviour from participating in an education
programme following MI (Cameron, Petrie, Ellis et al., 2005). However, Duryée
(1992) found that, despite feeling anxious most patients were able to learn new
information, particularly information about the activities they should engage in after
being discharged. In China, An and others (2005) explored the factors affecting
patient education on lifestyle compliance among patients with CHD. They found that
many factors contribute to the effects of patient education on lifestyle compliance,
including gender (female patients are better than males at complying with a low-fat
diet), attitude, health beliefs, education levels (the higher the level of education, the
better the compliance), information sources, number and frequency of education
sessions, ability to receive health education, and living conditions (patients living in
cities show better compliance than those living in villages).
In a one-group pre-post intervention study (McPherson, Swenson, Pine & Leimer,
2002) with 436 patients, the findings illustrated that patients who were younger or
who were smokers were less likely to attend the programme than their older and

96
nonsmoking counterparts. The duration and frequency of the intervention, and the
design of the programme are predictors of its effects. In addition, the availability of
telephone calls or additional nurse visits during the follow-up period was also related
to the maintenance of healthy changes in behaviour and medical compliance. A
previous study also suggests that interactive intervention is more effective than non-
interactive intervention and stage-matched intervention is more effective than
mismatched intervention, especially in terms of long-term effects (Prochaska,
DiClemente, Velicer & Rossi, 1993).
Adherence to the programme is another factor contributing to its effectiveness.
Previous studies on the impact of gender differences on adherence to cardiac
rehabilitation programmes have produced inconsistent results (Leijon, Bendtsen,
Ståhle et al., 2010; Sarrafzadegan, Rabiei, Shirani et al., 2007; Taylor, Wilson &
Sharp, 2011). Some studies found no significant difference between men and women
in the dropout rate from such programmes (Cannistra, Balady, O‘Malley, Weiner &
Ryan, 1992; Leijon, Bendtsen, Ståhle et al., 2010), whereas other studies showed that
women are more likely than men to withdraw from such programmes (Halm, Penque,
Doll & Beahrs, 1999; Yohannes, Yalfani, Doherty & Bundy, 2007).
Marital status and other demographic and clinical characteristics may also influence
adherence. The findings from Ramm, Robinson and Sharpe (2001) indicated that
patients who are single or widowed, or living alone are more likely to withdraw from
cardiac rehabilitation programmes. Numerous studies have demonstrated that patients
who are younger, have lower levels of education, and are smokers are more likely to
withdraw from cardiac rehabilitation programmes (Dorn, Naughton, Imamura &
97
Trevisan, 2001; Leijon, Bendtsen, Ståhle et al., 2010; Moore, Dolansky, Ruland et al.,
2003; Ramm, Robinson & Sharpe, 2001; Sanderson, Phillips, Gerald, DiLillo, Bittner,
2003; Sarrafzadegan, Rabiei, Shirani et al., 2007; Taylor, Wilson & Sharp, 2011;
Worcester, Murphy, Mee, Roberts & Goble, 2004; Yohannes, Yalfani, Doherty &
Bundy, 2007). Several studies also showed that whether or not the patients had
financial problems and possessed medical insurance were also related to the uptake
and adherence to cardiac rehabilitation (Davies, Taylor, Beswick et al., 2010; Halm,
Penque, Doll & Beahrs, 1999; McCarthy, Dickson & Chyun, 2010; Mochari, Lee,
Kligfield & Mosca, 2006).
The mode of delivering patient education may also influence its effects. There are
many modalities for delivering patient education, including face-to-face sessions, the
telephone, written materials (e.g., handbooks and pamphlets), media-based education,
computer-tailored interventions, and internet-delivered interventions. Written material
is usually used as the basic mode in patient education. Face-to-face education with
written material has been widely used among CHD patients (Cupples & McKnight,
1994; Elderen, Maes & Seegers, 1994; Linde & Janz, 1979; Marshall, Penckofer &
Llewellyn, 1986). Face-to-face patient education followed by telephone consultations
is the most preferred approach for patients with CHD in China, (Chen & Jing, 2008;
Du, Chen, & Liu, 2005; Hu, 2006; Li & Liu, 2006; Li & Wang, 2006; Liu, 2005; Wan
& Wang, 2008). Hence, in this study written material was used as the basic mode,
with the addition of face-to-face patient education and telephone contact.
In summary, there are many factors that influence the effectiveness of patient
education. One of these factors is the method of delivering patient education. Since

98
the methods of face-to-face interaction together with telephone contact are preferred
by Chinese CHD patients, they were adopted in this study.
2.4.5 Theoretical Basis for Patient Education
Patient education is beneficial for CHD patients, yet several researchers have reported
that knowledge alone is not enough to induce patients to change their behaviour
(Chair, Thompson, Leung, Ng & Choi, 2011; Chair, Thompson, Tang & Leung, 2007;
Fortmann, Taylor, Folra & Winkleby, 1992; Johansson, Swahn & Strömberg, 2007).
In the Stanford Five-City Project, Fortmann and co-workers (1992) assessed the
effects of a patient education campaign on diet-related knowledge and behaviour and
cholesterol levels. They found that although community-based patient education
increased nutritional knowledge over time among both men and women in all cities, it
did not lead to changes in their behaviour with regard to the intake of dietary saturated
fats. They concluded that imparting knowledge alone might not be enough to promote
changes in dietary habits. A similar finding was reported by Ji, Huang, Chen, and
others (2005) on Chinese patients with diabetes mellitus. Scalzi, Burke, and
Greenland (1980) further showed that a structured inpatient education programme had
no effect on compliance with a low-fat, low-sodium diet when compared with the
usual care. Another study revealed that education and counselling during
hospitalization about patients‘ adherence to secondary prevention goals had no effect
on adherence to exercise (Mosca, Christian, Mochari-Greenberger et al., 2010). Hence,
patient education alone may not be enough to induce patients to modify their
behaviour.
99
The findings from a recent meta-analysis (Conn, Hafdahl, Brown & Brown, 2008)
showed that the effect of patient education on exercise behaviour was not related to
interventions tailored for the individual or to the mode of delivery of the intervention,
whereas it was associated with interventions based on different theoretical models.
Painter et al. (2008) stated that theory-based programmes on changing health
behaviour are regarded as more effective than those that do not use theory.
The Transtheoretical Model (TTM), Social Cognitive Theory (SCT), Health Belief
Model (HBM), the Theory of Reasoned Action (TRA), and the Theory of Planned
Behaviour (TPB) are most commonly used models and theories for patient education
concerned with bringing about changes in various behaviours (Painter, Borba, Hynes
et al., 2008). The social cognitive theory (SCT) was developed by Bandura from the
social learning theory in 1986 (Glanz, Rimer & Lewis, 2002). The SCT explains
human behaviour as a triadic, dynamic, and reciprocal model in which personal
factors (including cognition), behaviour, and environment influence each other. The
SCT includes numerous constructs, such as environments/situations, behavioural
capability, expectations, expectancies, self-control, observational learning,
reinforcements, self-efficacy, emotional coping responses, and reciprocal determinism.
Since it consists of so many constructs, some health educators and behavioural
scientists have complained that SCT is too comprehensive in its formulation (Glanz,
Rimer & Lewis, 2002) and too complicated for practitioners to use.
The HBM, developed in the 1950s, is one of the oldest models of health behaviour
and is a value-expectancy theory (Glanz, Rimer & Lewis, 2002). The main
components of the HBM are perceived threat and expectation. It postulates that the

100
likelihood of adopting behaviour appropriate to the prevention or control of some
disease depends on the individual‘s perception of a threat to personal health and a
conviction that the recommended action will reduce this threat (Burkholder & Nigg,
2002). However, according to the HBM, behavioural change is viewed as an ―all or
nothing‖ phenomenon (e.g., one either does or does not change one‘s behaviour). In
addition, although the HBM has been widely used to study behaviours involving risk
such as smoking and alcohol use, dental hygiene, contraceptive use, compliance with
medication for diabetes and hypertension, and dietary compliance, its use as a
theoretical framework for motivation to engage in exercise has been limited
(Burkholder & Nigg, 2002; Wood, 2008).
The Theory of Reasoned Action (TRA) and the Theory of Planned Behaviour (TPB),
developed in late 1960s, focus on theoretical constructs that are concerned with
individual motivational factors as determinants of the likelihood of performing a
specific behaviour (Glanz, Rimer & Lewis, 2002). The TRA comprises measures of
attitude and social normative perceptions that determine behavioural intention. The
TPB is an extension of the TRA and includes an additional construct on perceived
control over the performance of the behaviour. Both theories were developed to
understand the relationship between attitudes and behaviour. They assume a causal
chain that links behavioural beliefs and normative beliefs to behaviour through
attitudes and subjective norms. The most important predictor of behaviour in these
theories is intention, which includes attitude and subjective norms. Similar to the
HBM, both the TRA and TPB view behavioural change as an ―all or nothing‖
phenomenon.

101
The Transtheoretical Model (TTM) of behavioural change was developed by
Prochaska and DiClemente (1983) in the late 1970s and early 1980s. It is a model of
intentional behavioural change, originally designed for smoking cessation (Prochaska
& DiClemente, 1983 & 1984). Subsequently, the TTM has been expanded to cover
changes in various behaviour, including quitting cocaine, controlling weight,
following a low-fat diet, engaging in safe sex, using condoms, adopting exercise,
using sunscreen, and taking mammography screening (Prochaska & DiClemente,
1983; Prochaska & Velicer, 1997; Prochaska, Velicer, Rossi, Goldstein et al., 1994).
The TTM of behavioural change is an internationally recognized model that holds
much promise for changing health behaviour of all types, and can be used as a guide
for nurses in counselling individuals about exercise behaviour (Burbank, Reibe,
Padula & Nigg, 2002).
The strength of the TTM is that it treats behavioural change as dynamic, rather than as
an ―all or nothing‖ phenomenon (Marshall & Biddle, 2001). It allows practitioners to
treat individuals as they are – in different stages of readiness to make changes in
health behaviour (Glanz, Rimer & Lewis, 2002). The main difference between the
TTM and other theories/models, such as SCT, TPB, and HBM, is that the SCT, TPB,
and HBM were developed to explain a purely behavioural criterion using an all or
nothing phenomenon, that is, engaging in a behavioural change or not, whereas the
TTM attempts to explain a complex, mixed criterion in a dynamic sense. In addition,
the TTM allows practitioners to develop a stage-matched intervention with reference
to the stages of readiness for behavioural change.

102
Traditional interventions for encouraging the adoption and maintenance of an exercise
regime have been relatively ineffective. This may be due to the fact that providers
usually use action-oriented approaches, while most people who need to change their
behaviour are in the pre-action stages (precontemplation and contemplation) (Burbank,
Reibe, Padula & Nigg, 2002; Prochaska, DiClemente & Norcross, 1992).
Consequently, the programmes are not matched to their needs (Prochaska & Velicer,
1997). The TTM could be effectively used in tailoring treatment for these
―precontemplators‖ and ―contemplators‖ to encourage them to engage in exercise
(Marcus & Simkin, 1994). For individuals at the stages of precontemplation and
contemplation, no action-oriented intervention will be implemented because of the
lack of intention or preparation to change his/her behaviour at these stages. Thus, the
employment of the TTM to change exercise behaviour may outweigh the mismatched
or action-oriented interventions in effectiveness (Marcus, Emmons, Simkin-Silverman
et al., 1998). Therefore, in this study, the exercise stage-matched patient education
will be delivered based on the TTM.
2.5 The Transtheoretical Model (TTM)
In this section, the overview of the TTM is presented, followed by the effects of the
TTM-based Exercise Stage-Matched Intervention (ESMI) for changing exercise
behaviour, and the use of the TTM for changing exercise behaviour among patients
with heart disease.

103
2.5.1 Overview of the Transtheoretical Model (TTM)
The TTM consists of four core constructs: stages of change, self-efficacy, decisional
balance, and processes of change (Prochaska & DiClemente, 1983; Prochaska &
Velicer, 1997). The detailed contents of the TTM and the relationship between
constructs are shown in Figure 2.1 and Figure 2.2. A meta-analysis (Marshall &
Biddle, 2001) illustrates that different stages of change are related to different levels
of physical activity, self-efficacy, perceptions of the cons and pros of exercise, and
processes of change.

104
Consciousness raising
Dramatic relief
Environment reevaluation
Self-reevaluation
Social liberation
Processes of change
Counterconditioning
Helping relationships
Reinforcement management
Self-liberation
Stimulus control
Pros of behaviour
change
Decisional balance
Cons of behaviour change
1. Precontemplation
2. Contemplation
3. Preparation
Stages of change
4. Action
5. Maintenance
Confidence
Self-efficacy for
behaviour change
Temptation
Figure 2.1: The Transtheoretical Model of Behaviour Change (adapted from Burkholder & Nigg, 2002)
Experiential construct
Behaviouralconstruct

105
Precontemplation
Processes:
Consciousness
raising
Dramatic relief
Environmental
reevaluation
Decisional balance:
Pros << Cons
Self-efficacy (SE): Lowest SE
Contemplation
Processes:
Consciousness
raising
Self-reevaluation
Social liberation
Decisional balance:
Pros < Cons
Self-efficacy (SE):
Increasing SE
Preparation
Processes:
Self-reevaluation
Helping
relationships
Self-liberation
Decisional balance:
Pros ≤ Cons
Self-efficacy (SE):
Increasing SE
Action
Processes:
Reinforcement
management
Helping
relationships
Counter-
conditioning
Stimulus control
Decisional balance:
Pros > Cons
Self-efficacy (SE):
Increasing SE
Maintenance
Processes:
Reinforcement
management
Counter-
conditioning
Helping
relationships
Decisional balance:
Pros > Cons
Self-efficacy (SE):
Increasing SE
Figure 2.2: Relationship among stages of change, processes of change, decisional balance, and self-efficacy (Adapted from Burbank, Padula & Nigg, 2000; Burkholder & Nigg, 2002)

106
2.5.1.1 Stages of Change
Stages of change is a core construct of the TTM and is the most frequently applied
construct among the four constructs of the TTM (Buckworth & Wallace, 2002). Based
on the stages of change, individuals are classified into one of five stages, namely, the
precontemplation, contemplation, preparation, action, and maintenance stages
(Prochaska & DiClemente, 1983). The distinction between the different stages is
based on the behavioural change itself or the motivation to change one‘s behaviour.
Stages of change describes the temporal dimension of change as distinct stages based
on past behaviour and plans for future actions.
According to the TTM, people do not change all at once, but often move through a
series of stages toward changing their behaviour, (Burbank, Reibe, Padula & Nigg,
2002). People in the first stage of precontemplation have no intention of changing
their behaviour in the next six months. Contemplation is the stage at which
individuals are aware that a problem exists with their current behaviour and are
seriously thinking about overcoming it, to the point that they are thinking about
starting to exercise regularly in the next six months. In the preparation stage,
individuals are intending to take action to change their behaviour in the next 30 days,
or change their actions to some extent but not regularly. The next stage, action, is the
stage at which individuals have successfully changed their behaviour for less than six
months. Finally, in the maintenance stage, people have successfully sustained their
change in behaviour for six months or more (Nelson, 2000; Prochaska, DiClemente &
Norcross, 1992). Thus, individuals who are in the action and maintenance stages have
adopted a regular exercise regime. In this study, regular exercise is defined as
107
accumulating at least 30 minutes of moderately intense physical activity throughout
the day for more than five days of the week (American College of Sports Medicine,
2006; Marcus, Forsyth & Blair, 2003).
Movement through five stages does not always occur in a linear manner, but may also
be cyclical as many individuals must make several attempts at changing their
behaviour before they attain their goals (Marcus, Banspach, Lefebvre, Rossi, Carleton
& Abrams, 1992). Most people actually move through the stages of change in a spiral
pattern (Prochaska, DiClemente & Norcross, 1992). Individuals can also regress to
any previous stage, but learn from each attempt (Nigg, 2005). Individuals within the
same stage of changing their exercise behaviour hold similar beliefs about exercise
and use similar strategies and techniques to progress to the next stage. This implies
that interventionists could conduct stage-matched interventions based on the TTM to
encourage people to adopt and maintain regular physical activity or exercise
behaviour (Blissmer & McAuley, 2002).
2.5.1.2 Self-efficacy
Self-efficacy is a central construct of social learning theory (Bandura, 1997). This
construct involves two components: confidence and temptation. Confidence refers to
the level at which a person feels he/she can perform a specific action required to attain
a certain outcome (Bandura, 1986). It is the situation-specific confidence to
participate in behaviour with known outcomes (Buckworth & Wallace, 2002).
Temptation tempts individuals to engage in problematic behaviour in specific
situations (Prochaska & Marcus, 1995).

108
Self-efficacy is an important predictor of progress with a linear increase from the
precontemplation to the maintenance stage (Figure 2.2). In other words, it progresses
in stages, with individuals in the higher stages showing higher self-efficacy than those
in the lower stages (Plotnikoff, Hotz, Birkett & Courneya, 2001), while temptation
decreases across the stages (Prochaska & Marcus, 1995). A cross-sectional study
(Marcus, Pinto, Simkin, Audrain & Taylor, 1994) explored the utility of three
theoretical models, namely the stages of change model, self-efficacy theory, and the
decisional balance model, for understanding exercise behaviour among 431 employed
women averaging 41.1 years of age. The findings showed that women in the
precontemplation stage scored lowest in self-efficacy and those in the maintenance
stage scored highest. A longitudinal study (Marcus, Eaton, Rossi & Harlow, 1994),
suggests that self-efficacy is an important and strong predictor of current and future
exercise behaviour.
2.5.1.3 Decisional Balance
Decisional balance was originally based on Janis and Mann‘s theory of the decision-
making model (Janis & Mann, 1977, cited in Prochaska & Velicer, 1997), in which
decision making includes balancing eight central constructs: instrumental benefits for
self, instrumental benefits for others, instrumental costs to self, instrumental costs to
others, approval from self, approval from others, disapproval from self, and
disapproval from others. Prochaska further developed decision-making measures for
changing new behaviour in two constructs: the pros and cons of changing (Prochaska
& DiClemente, 1984; Prochaska, 2008; Prochaska, Velicer, Rossi et al., 1994). Two

109
main constructs of decisional balance, namely pros and cons, or benefits and costs of
performing behaviour, have been widely used in changing various types of behaviour,
including exercise behaviour (Marcus & Simkin, 1994; Prochaska, 2008). Prochaska
(2008) found that it is easier for most smokers to agree with the benefits of quitting
smoking than with the costs of quitting.
Decisional balance also varies across stages of change (Figure 2.2). In the
precontemplation stage, the pros are low, with cons outweighing pros. By the
contemplation or preparation stage, the pros increase to the same level as the cons,
with pros eventually outweighing cons in the action and maintenance stages
(Plotnikoff, Hotz, Birkett & Courneya, 2001). The results from 12 studies of problem
behaviour (Prochaska, Velicer, Rossi et al., 1994) have demonstrated that the cons of
changing the problem behaviours are higher than the pros for individuals who are in
the precontemplation stages. The opposite is true for individuals in the action stage in
11 of the 12 studies, with the exception of quitting cocaine. For most problem
behaviours, individuals need to perceive that the pros of changing the behaviour
outweigh the cons before they will take action to modify their behaviour (Prochaska,
Velicer, Rossi et al., 1994). Thus, in order to progress from the precontemplation to
the contemplation stage of changing behaviour, the pros of changing must increase;
whereas the cons of changing must decrease when individuals progress from the
contemplation to the action stage. Before progressing to the action stage, the pros and
cons will cross over, with the pros higher than the cons being a sign of being well
prepared for action (Prochaska & Velicer, 1997).

110
2.5.1.4 Processes of Change
The stages of change represent a temporal dimension that helps us to understand when
particular changes in attitudes, intentions, and behaviour occur, while the processes of
change are a second major dimension of the TTM that allow us to understand how
these changes occur (Prochaska, DiClemente & Norcross, 1992). Prochaska and
Velicer (1997) defined processes of change as covert and overt activities that people
use to progress through the stages.
Processes of change consist of two hierarchical constructs: experiential and
behavioural constructs. Each construct has five processes. These ten processes are
consciousness raising, dramatic relief, self-reevaluation, social liberation,
environmental reevaluation, helping relationships, counterconditioning, reinforcement
management, self-liberation, and stimulus control (see Table 2.2). Ten processes of
change have been identified as the strategies and techniques used most frequently and
successfully by people as they move through the stages (Burbank, Padula & Nigg,
2000). In a pre-post randomized control study, Woods, Mutrie, and Scott (2002)
examined the effectiveness of a stage-matched intervention for helping sedentary
young adults (precontemplators and contemplators) to initiate exercise. The results
demonstrate that stage improvers scored significantly higher on all of the behavioural
and four out of the five of the experiential processes of change. The findings suggest
that people used processes of change to assist their movement toward the next stage.
Numerous studies have illustrated that an integration of the stages and processes of
change can provide a useful guide for interventions (Burbank, Reibe, Padula & Nigg,

111
2002; Prochaska & Marcus, 1995). Once a particular individual‘s stage has been
assessed, interventionists have a better idea of which processes to emphasize in order
to help the individual progress to the next stages of change (Marcus & Simkin, 1994).
Subjects in different stages of change used the processes of change in significantly
different ways (Marcus, Rossi, Selby, Niaura & Abrams, 1992; Marcus & Simkin,
1994; Peterson & Aldana, 1999). For engagement in exercise, the precontemplators
used all ten processes significantly less than individuals in the other stages. Preparers
used behavioural processes more than contemplators, although they used the same
experiential processes. Subjects in the action stage used both experiential and
behavioural processes more than those in the preparation stage. Individuals in the
maintenance stage used experiential processes less and behavioural processes as often
as those in the action stage.
Prochaska and DiClemente (1983) suggested that, for smoking cessation based on the
TTM, individuals in the precontemplation stage use 8 of 10 processes significantly
less than any other group. Consciousness raising is emphasized most by people in the
contemplation stage. Self-reevaluation appears to bridge contemplation and
preparation because it is emphasized in both stages. Self-liberation is emphasized
when individuals prepare to take action. Helping relationships and reinforcement
management are emphasized when individuals take action. Counterconditioning and
stimulus control appear to bridge action and maintenance, since these two processes
are emphasized in both stages (see Table 2.3).

112
Table 2.2 Definitions of the processes of change for physical activity (Adapted
from Burbank, Padula & Nigg, 2000)
Processes of Change Definition
Experiential
Consciousness raising Efforts to seek new information and to gain
understanding and feedback about physical
activity
Dramatic relief Affective aspects of change involving
experiences and intense feelings about loss of
cardiovascular fitness due to inactivity
Self-reevaluation Emotional and cognitive reappraisal of values
regarding physical activity
Environmental reevaluation Consideration and assessment of how physical
inactivity affects the individual‘s physical and
social environment
Social liberation Developing awareness and acceptance of an
active lifestyle
Behavioural
Counterconditioning Substitution of alternative behaviours for
sedentary activities
Helping relationship Trusting, accepting, and using support from
others to be more active
Reinforcement management Changing the contingencies that control or
maintain physical inactivity and rewarding
physical activity
Self-liberation The individual‘s choice and commitment to
being more active, involving the belief that one
can change
Stimulus controls Control of situations and other causes that
trigger inactivity

113
Table 2.3 The emphasis of different processes of change according to stages of
change (Adapted from Prochaska, DiClemente & Norcross, 1992)
Stages of change
precontemplation contemplation preparation action maintenance
Processes Consciousness raising
Dramatic relief
Environmental reevaluation
Self-reevaluation
Self-liberation
Reinforcement management
Helping relationship
Counterconditioning
Stimulus control
2.5.2 The Transtheoretical Model (TTM) and Exercise Behaviour
Sonstroem first used the TTM to explain exercise behaviour at the University of
Rhode Island in the late 1980s (Prochaska & Marcus, 1995). In the early 1990s,
Marcus and colleagues first applied the TTM to change exercise behaviour in
worksite and community participants and the study showed promising result in
exercise behaviour (Marcus, Rossi, Selby, Niaura & Abrams, 1992; Marcus, Selby,
Niaura & Rossi, 1992; Marcus & Simkin, 1993). Subsequently, the TTM was widely
used for changing exercise behaviour in various populations from adolescents (Nigg
& Courneya, 1998) to the elderly (Burbank, Reibe, Padula & Nigg, 2002; Cardinal,
1997; Findorff, Stock, Gross & Wyman, 2007; Resnick & Nigg, 2003).

114
A number of studies have demonstrated that the exercise behaviour of individuals is
significantly associated with the constructs of the TTM, and that the TTM has good
internal and external validity for explaining exercise behaviour (Findorff, Stock,
Gross & Wyman 2007; Kim, 2007; Kim, Cardinal & Lee, 2006; Marcus, Rossi, Selby
et al., 1992; Nigg & Courneya, 1998). In a longitudinal study, Marcus, Eaton, Rossi,
and Harlow (1994) examined the stages of readiness to exercise and their relationship
to self-efficacy, the costs and benefits of exercise, and self-reported physical activity
among 698 employees in four Rhode Island worksites. The results demonstrated that
the level of physical activity of individuals could be predicted by knowing their stages
of readiness for exercise, their perceptions of the costs (cons) and benefits (pros) of
exercise, and their self-efficacy for exercise. The results also indicated that the TTM
could successfully predict exercise behaviour six months later, with no exercise
intervention during the 6-month period.
Although the TTM has been widely used in the past decade for explaining exercise
behaviour, most studies used cross-sectional design and few experimental studies
were carried out. A meta-analysis (Marshall & Biddle, 2001) of 71 studies examined
the applications of the TTM in the domain of physical activity and exercise. Of these
studies, 54 were cross-sectional, six were longitudinal, ten were quasi-experimental,
and only one was a randomized controlled trial. Due to the limitations of the cross-
sectional design, experimental studies need to be conducted to determine the
relationship of cause and effect between the TTM and exercise behaviour.
As stated by Burbank, Reiba, Padula, and Nigg (2002), the TTM can be used as a
guide for nurses in counselling individuals to motivate changes in their exercise
115
behaviour. Based on an individual‘s stages of change, a stage-matched intervention
can be developed. The stage-matched intervention refers to the use of different
strategies and techniques (processes of change) matched to an individual‘s stage of
readiness to change his/her behaviour according to the TTM to bring about changes in
behaviour (Kim, 2008). Similarly, the exercise stage-matched intervention refers to
strategies and techniques that are matched to the individual‘s current stage of
readiness to change his/her exercise behaviour (Kim, 2008). The effects of the TTM-
based Exercise Stage-Matched Intervention (ESMI) for changing exercise behaviour
are thoroughly reviewed below.
2.5.2.1 Effects of the ESMI on Exercise Stages of Change (ESC)
Previous studies have shown that the TTM-based ESMI had a significantly positive
effect on changing exercise behaviour in various populations, with respect to the
exercise stages of change scale. Marcus, Banspach, Lefebvre, and others (1992) first
used the TTM as a framework for encouraging the adoption of an exercise regime
among 610 community participants aged 18 to 82 years in early 1990s. A 6-week
intervention programme included written materials targeted at an individual‘s specific
stage of readiness to exercise, such as weekly ―fun walks‖, and an ―activity night‖.
The results indicated that most subjects progressed in their stage of exercise adoption
after the 6-week stage-matched intervention. Nevertheless, the lack of a control group
in this study induced uncertainties in the results.
Several studies have demonstrated that 4-10 weeks of the TTM-based ESMI using
self-help stage-matched manuals or internet-based motivational messages had a

116
significantly positive effect on exercise stages of change in a worksite setting when
compared with the generic intervention or usual care (Ishii, Nakiri, Nagatomi et al.,
2007; Marcus, Emmons, Simkin-Silverman et al., 1998; Peterson & Aldana, 1999).
Another single group pre-post test also showed similar results in worksites (Faghri,
Omokaro, Parker et al., 2008). Consistent with these studies, similar results with
respect to exercise stages of change were found when the ESMI was adopted among
university students over an 8-week to 6-month intervention period (Huang, Hung,
Chang & Chang, 2009; Ma, Ma & Zhu, 2006; Woods, Mutrie & Scott, 2002; Kim,
2008), among young to middle-aged women over an 8-12 week intervention period
(Fahrenwald, Atwood, Walker et al., 2004; Shirazi, Wallace, Niknami et al., 2007),
and among the general population through a website over a five week period (Lippke,
Schwarzer, Ziegelmann et al., 2010) when compared with the stage-mismatched
intervention group or control group.
In a series of PACE (the Patient-Centered Assessment and Counseling for Exercise)
studies, non-randomized controlled trials were conducted using a brief intervention
(3-5 minutes of counselling based on the TTM) and a booster phone call to patients
two weeks after they had received counselling from a physician. The findings showed
that the intervention significantly improved the exercise stages of change of healthy,
sedentary adults over the six-week intervention period (Calfas, Long, Sallis et al.,
1996; Purath, Miller, McCabe & Wilbur, 2004). In another series of PACE studies
involving non-randomized controlled trials, a 12-week exercise promotion
intervention based on the TTM led to a significant improvement in exercise stages of
change among adults with chronic disease (Shin, Yun, Jang & Lim, 2006) and among
resident physicians of internal medicine (Rogers, Gutin, Humphries et al., 2005).

117
Burbank et al. (2002) found that the TTM can be used as a framework for changing
exercise behaviour among the elderly. Several single-group design studies have
demonstrated that the stage-based intervention resulted in a significant improvement
in exercise stages of change among the elderly after the intervention as compared with
the baseline (Märki, Bauer, Angst et al., 2006; Märki, Bauer, Nigg et al., 2006). A
number of randomized controlled trials have also indicated that the exercise stage-
matched intervention significantly improved the exercise stages of change among
elderly people when compared with the comparison group (Findorff, Stock, Gross &
Wyman, 2007; Greaney, Riebe, Garber et al., 2008; Resnick & Nigg, 2003). Greaney
and others (2008) found that significant effect on exercise stages of change was
detected when the individuals who were in the maintenance stage at baseline were
excluded, whereas no significant difference in stage progression was identified if
those in the maintenance stage were not excluded. This finding suggests that there is a
ceiling effect on exercise stages of change if individuals in the maintenance stage at
baseline are recruited in the study.
A number of studies also showed that a 20-30 minute counselling session based on the
TTM or a tailored leaflet-based physical activity intervention based on the TTM could
significantly improved exercise stages of change among diabetes patients after the 4-
week to 6-month intervention (Dutton, Provost, Tan & Smith, 2008; Jackson,
Asimakopoulou & Scammell, 2007; Kirk, Higgins, Hughes et al., 2001; Kirk,
MacIntyre, Mutrie & Fisher, 2003). The positive effect on exercise stages of change
was maintained at the 12-month follow-up period (Kirk, Mutrie, MacIntyre & Fisher,
2004). Similar results for the TTM-based ESMI on exercise stages of change were

118
found in studies of diabetes patients (Huang & Tang, 1996; Zhu & Chen, 2007),
breast cancer patients who received 12 weekly phone calls (Pinto, Frierson, Rabin et
al., 2005; Pinto, Rabin & Dunsiger, 2009), patients with chronic disease over a 12-
week intervention period (Shin, Yun, Jang & Lim, 2006), and adults at increased risk
of developing coronary heart disease (Steptoe, Kerry, Rink & Hilton, 2001). These
studies indicate that the TTM-based ESMI is effective at motivating various
populations to engage in exercise or maintain their adherence to regular exercise.
However, the long-term (> 6 months) effect of the TTM-based exercise stage-matched
intervention on exercise stages of change was not clear. Several studies showed that
the TTM-based exercise intervention had a significantly positive effect on exercise
stages of change at the 12-month follow-up period (Kirk, Mutrie, MacIntyre & Fisher,
2004; Märki, Bauer, Nigg et al., 2006) and that this effect was maintained at the 24-
month follow-up period (Greaney, Riebe, Garber et al., 2008). However, findings
from some studies revealed that the positive effect of the TTM-based physical activity
intervention on exercise stages of change had disappeared at the 6-8 month follow-up
period (Goldstein, Pinto, Marcus et al., 1999; Pinto, Friedman, Marcus et al., 2002).
Although positive effects were found, a number of negative findings relating to the
stage-matched intervention have also been reported. In one study (Naylor, Simmonds,
Riddoch et al., 1999), a single-contact counselling session (of approximately five
minutes) based on the stages of change model for exercise adoption was carried out in
four primary care centres. Two hundred and ninety-four subjects were recruited and
randomly allocated to one of four groups, which respectively received the following:
stage-oriented exercise materials with counselling (stage plus counselling), stage-
119
oriented materials without counselling (stage no counselling), non-staged materials
with counselling (counselling only), and the current level of advice. The results
showed that there was no significant group or interaction effect for exercise stages of
change after controlling for baseline differences in self-efficacy, age, and gender. The
authors concluded that the stage-based interventions were not superior to the other
interventions. However, these results require further examination because the attrition
rate was high in this study, 39.0% at eight weeks and 54.0% at 24 weeks. The
distribution of the subjects across the stages of change at baseline was higher in the
preparation and maintenance stages than in the precontemplation, contemplation, and
action stages. There was a ceiling effect for those in the maintenance stage. The
intervention only consisted of a single contact (lasting appropriately five minutes). A
longer contact session and interactive counselling may produce more obvious effects.
Thus, the results might not be reliable.
Griffin-Blake and DeJoy (2006) compared the effectiveness of stage-matched
interventions with social-cognitive physical activity interventions in a study involving
208 employees in two academic colleges in the USA. Participants were randomly
allocated to either a stage-matched self-help intervention group or a social-cognitive
self-help intervention group. The findings showed that the two interventions were
equally effective in increasing exercise stages of change (34.9% versus 33.9%). This
finding may be jeopardized by the unsatisfactory sampling at baseline. Only a few
participants (about 1.0%) in the precontemplation stage were found in both groups at
baseline and nearly half of the participants were in the maintenance stage. Such a
sampling may explain why the social-cognitive physical activity intervention
produced the same effect as the stage-matched intervention in this study. One session

120
of motivation based on the TTM for physical activity in 38 obese patients also showed
no significant effect in motivational stages of change, although the intervention group
demonstrated a significant improvement in minutes of physical activity engaged in
weekly (Schelling, Munsch, Meyer et al., 2009). Similarly, negative results were
found in the studies of van Sluijs and others (2005) and Jimmy and Martin (2005), in
which the results of the TTM-based intervention group were not superior in exercise
stages of change when compared with those of the control group.
Nelson (2000) compared the effects of the stage-matched intervention on physical
activity with the exercise prescription in military primary care. The results indicated
that the stage-matched intervention led to no significant improvements in motivation
and exercise stages of change, although positive trends for these parameters were
found and the participants in the stage-matched group tended to engage in more daily
physical activity. In sum, the data in this study was inconclusive because post hoc
power analysis was low. Thus, further studies are recommended.
A critical review was carried out by Adams and White (2003) of 26 papers
documenting 16 intervention programmes based on the TTM. Of these programmes,
seven used TTM-based counselling, four used TTM-based written materials only, and
five used a mixture of TTM-based counselling and written information. They found
that TTM-based activity promotion interventions were effective in promoting the
adoption of activity in the short term (≤ 6 months), while the long-term (> 6 months)
adherence was disappointing. Adams and White (2005) addressed some possible
reasons for why stage-based activity promotion interventions are less effective than
originally proposed. These reasons are that: (a) exercise behaviour is a more complex

121
behaviour than currently recognized; (b) many algorithms for determining current
exercise stages of change have not been validated; (c) exercise behaviour is
determined by stage-based interventions; and (d) truly stage-based interventions are
highly complex requiring more than one level of development and evaluation. A
systematic review (van Sluijs, van Poppel & van Mechelen, 2004) of 13 studies on
physical activity interventions showed that the methodology of these studies varied
widely and the results were inconsistent. The authors of the review concluded that no
evidence was found for the effects on stages of change and actual levels of physical
activity during the short-, medium, and long-term follow-up periods.
A recent systematic review (Hutchison, Breckon & Johnston, 2009) showed numerous
inconsistencies involving the development and implementation/application of TTM-
based interventions. The majority of interventions reported to be based on the TTM
failed to accurately present all constructs of the model. This systematic review also
indicated that, of the seven studies that employed interventions that had been
developed using all four constructs of the TTM, six revealed statistically significant
short-term findings, and one demonstrated significant short- and long-term findings,
while of the 17 studies using interventions had not been tailored to all four constructs
of the TTM, 12 reported significant short-term findings, and one revealed significant
short- and long-term findings. These findings suggest that interventions tailored to the
four constructs of the TTM are more likely to show positive results.
In summary, the effect of the TTM-based ESMI on exercise stages of change is
inconclusive. Further studies to examine its effect on exercise stages of change are
necessary. Interventions based on four constructs of the TTM are superior to those

122
that are not based on all four constructs of the TTM. A further discussion regarding
the effects of the TTM-based ESMI on exercise behaviour in patients with heart
disease will be presented in section 2.5.3.
2.5.2.2 Effects of the ESMI on Exercise Self-Efficacy (ESE)
Exercise self-efficacy is an important predictor of progress, with linear increases from
the precontemplation stage to the maintenance stage (Plotnikoff, Hotz, Birkett &
Courneya, 2001). Thus, the levels of exercise self-efficacy predict progress in the
exercise stages of change (Marcus, Eaton, Rossi & Harlow, 1994; Tung & Hsu, 2009).
There have been few studies examining the effect of the TTM-based ESMI on
exercise self-efficacy in various populations. Previous studies have come to
inconsistent conclusions. A randomized controlled study demonstrated that the 8-
week TTM-based ESMI significantly increased the exercise self-efficacy of the
participants, who were university students (Kim, 2008). A similar result was found
when a web-based ESMI based on the TTM was designed to promote physical
activity among Taiwanese female freshmen in a university (Huang, Hung, Chang &
Chang, 2009). Another randomized pilot test of ―Moms on the Move‖ (Fahrenwald,
Atwood, Walker, Johnson & Berg, 2004) showed that an 8-week TTM-based
intervention delivered in the form of four structured, biweekly, provider-delivered
telephone contacts supplemented with an interactive brochure, led to significant
improvements in all TTM constructs including exercise self-efficacy when compared
with the results for the control group. A quasi-experimental study also indicated that a
5-month TTM-based intervention led to significant improvement in exercise self-

123
efficacy among 193 telecom workers in Taiwan (Kao, Lu & Huang, 2002). Another
study (Blisser, 2000) to examine the effects of stage-matched, stage-mismatched, and
standard care among 288 university staff members also revealed that the stage-
matched intervention was more effective at increasing exercise self-efficacy than the
stage-mismatched intervention and standard care.
However, several studies showed inconsistent results. Naylor et al. (1999) found that
with respect to exercise self-efficacy the use of stage-oriented exercise materials with
counselling did not produce superior results to those seen among the group that
received non-staged materials with counselling or the control group. The limitation of
their study was that the use of a single-contact counselling session (of approximately
five minutes) and the high dropout rate (39.0% at 8 weeks and 54.0% at 24 weeks),
which may contribute to the negative results. In a non-randomized controlled study
(Shin, Yun, Jang & Lim, 2006), a tailored stage-matched intervention based on the
TTM had no significant effect on exercise self-efficacy among Korean adults with
chronic diseases, although the intervention showed potential for promoting progress
in the exercise stages of change. A similar result was found in the study of Nelson
(2000), in which the exercise stage-matched intervention led to no significant
improvement in exercise self-efficacy when compared with the exercise prescription
in military primary care. However, this study had low power analysis. Thus, the
author stated that caution is needed in interpreting the results and that further studies
are needed.

124
Due to the limited number of studies evaluating the effect of the TTM-based ESMI on
exercise self-efficacy, and the inconsistent conclusions from the previous studies,
further studies are necessary.
2.5.2.3 Effects of the ESMI on Exercise Decisional Balance
Exercise decisional balance includes exercise benefits and exercise barriers. There
have been few studies on the TTM-based exercise interventions that have evaluated
its effect on exercise benefits or exercise barriers (Hutchison, Breckon & Johnston,
2009). Previous studies regarding TTM-based interventions to increase exercise have
shown inconsistent results with respect to the exercise decisional balance. Some
studies have shown that the TTM-based ESMI significantly increased the pros of
exercising and decreased the cons of exercising in the view of the participants, when
compared with the results seen among the control group (Fahrenwald, Atwood,
Walker, Johnson & Berg, 2004; Kao, Lu & Huang, 2002; Kim, 2008). However, other
studies showed no significant effects on the exercise decisional balance when the
TTM-based ESMI was used to promote changes in exercise behaviour (Griffin-Blake
& DeJoy, 2006; Nelson, 2000). These negative results may be due to the
unsatisfactory sampling at baseline. Only 1.0% of the participants were in the
precontemplation stage and nearly half of them were in the maintenance stage at
baseline (Griffin-Blake & DeJoy, 2006). Another possible reason for the negative
results may be low power analysis (Nelson, 2000). Thus, further studies to examine
the effect of the TTM-based ESMI on exercise decisional balance are recommended.

125
2.5.2.4 Effects of the ESMI on Exercise
Previous studies have shown that the TTM-based ESMI had significantly positive
effects on exercise duration, steps taken per week, or daily energy expenditure in
various populations. Several single-group design studies showed that the TTM-based
exercise intervention significantly increased the duration of moderate exercise per
week or steps taken during planned exercise when compared with the baseline data in
various populations (Faghri, Omokaro, Parker et al., 2008; Märker, Bauer, Angst et al.,
2006; Märker, Bauer, Nigg et al., 2006; Pinto, Rabin & Dunsiger, 2009). Some quasi-
experimental trials also indicated that the TTM-based exercise stage-matched
intervention significantly improved the duration of moderate exercise engaged in by
the participants per week over a 4-6 week intervention when compared with the
control group (Calfas, Long, Sallis et al., 1996; Ishii, Nakiri, Nagatomi et al., 2007).
A number of randomized controlled trials demonstrated that the TTM-based exercise
stage-matched intervention had significant effects on both total and moderate exercise
duration per week, activity counts, and daily energy expenditure when compared with
the stage-mismatched intervention group or the control group among patients with
type 2 diabetes mellitus (Jackson, Asimakopoulou & Scammell, 2007; Kirk, Higgins,
Hughes et al., 2001; Kirk, MacIntyre, Mutrie & Fisher, 2003; Kirk, Mutrie, MacIntyre
& Fisher, 2004), young to middle-aged women (Fahrenwald, Atwood, Walker et al.,
2004; Huang, Hung, Chang & Chang, 2009; Purath, Miller, McCabe & Wilbur, 2004;
Shirazi, Wallace, Niknami et al., 2007), obese patients (Schelling, Munsch, Meyer et
al., 2009), sedentary adults (Pinto, Friedman, Marcus et al., 2002), breast cancer
patients (Pinto, Frierson, Rabin et al., 2005), adults at increased risk of developing

126
CHD (Steptoe, Doherty, Rink et al., 1999), and patients with heart disease (Hughes,
Gillies, Kirk et al., 2002; Hughes, Mutrie & MacIntyre, 2007; Naser, Jafar, Kumar et
al., 2008).
The first multiple behaviour intervention study, including exercise behaviour
(Johnson, Paiva, Cummins et al., 2008), used TTM as a framework for weight
management among a population of overweight and obese adults (BMI 25-39.9; N =
1277). Participants were randomly assigned into either a no-treatment control or
home-based, stage-matched multiple behaviour interventions (n = 628) for up to three
behaviours based on the assessments at baseline, three, six, and nine months. The
authors of the study found that the participants in the intervention group showed
significant positive effects on weight lost, healthy eating (47.5% versus 34.3%),
exercise (44.9% versus 38.1%), managing emotional distress (49.7% versus 30.3%),
and intake of untreated fruits and vegetables (48.5% versus 39.0%). Such positive
effects continued to progress to the action/maintenance stage at 24 months. The
findings from two systematic reviews have demonstrated that interventions focusing
on a single exercise behaviour have a better effect on exercise than multiple behaviour
interventions among cardiac patients (Conn, Hafdahl, Moore et al., 2009) and
European teenagers (De Meester, van Lenthe, Spittaels et al., 2009). These studies
suggest that the TTM-based exercise staged-matched intervention has a positive effect
on increasing engagement in exercise among various populations.
However, most of these studies focused on the short-term (≤ 6 months) effect of the
TTM-based ESMI on exercise duration per week or step counts. The long-term (> 6
month) effect was not clear. As Pinto, Friedman, Marcus, and others (2002) reported,

127
the significant effects of the exercise intervention based on the TTM and social
cognitive theory on the duration of moderate exercise were found immediately after
the 3-month intervention, while the significantly positive effects were not maintained
at the 6-month follow-up period. A similar result was seen in Huang, Hung, Chang
and, Chang‘s (2009) study, in which they found that the effect did not persist in the
follow-up period.
The negative effect of the TTM-based ESMI on the duration of moderate exercise was
also found in some studies (Dutton, Provost, Tan & Smith, 2008; Goldstein, Pinto,
Marcus et al., 1999; Griffin-Blake & DeJoy, 2006; Jimmy & Martin, 2005; Kosma,
Cardinal & Mccubbin, 2005; Naylor, Simmonds, Riddoch et al., 1999; Taylor,
Demoor, Smith et al., 2006; van Sluijs, van Poppel, Twisk et al., 2005; Wanner,
Martin-Diener, Braun-Fahrlander et al., 2009). These studies found that the TTM-
based exercise intervention was not superior to standard or generic education or usual
care with regard to the duration of moderate exercise. Although several studies have
shown that the TTM-based exercise intervention progressed participants‘ exercise
stages of change, no significant effect on moderate exercise duration was detected
(Dutton, Provost, Tan & Smith, 2008; Goldstein, Pinto, Marcus et al., 1999; Kim,
2008).
However, these negative results required further examination because most of these
studies used a single-contact counselling or brief counselling session (of
approximately five minutes) (Goldstein, Pinto, Marcus et al., 1999; Naylor,
Simmonds, Riddoch, Velleman & Turton, 1999), had a high attrition rate (39.0% at
eight weeks and 54.0% at 24 weeks) (Naylor et al., 1999), a small sample size (N=75)

128
(Kosma, Cardinal & Mccubbin, 2005), and had a large number of participants in the
preparation or maintenance stages at baseline (Goldstein, Pinto, Marcus et al., 1999;
Griffin-Blake & DeJoy, 2006), all of which contributed to the negative results. Thus,
further studies with longer counselling contacts, a larger sample size, and the
recruitment of sedentary participants (namely, individuals in the precontemplation,
contemplation, and preparation stages) may result in positive effects when the TTM-
based ESMI is used to promote exercise.
2.5.2.5 Other Effects of the ESMI
In addition to the effects of the TTM-based ESMI on the exercise stages of change,
exercise self-efficacy, exercise decisional balance, and physical exercise levels or
exercise duration, the stage-matched intervention can increase the uptake of
programmes (Prochaska, DiClemente & Norcross, 1992; Prochaska & Velicer, 1997)
and reduce dropout rates (Schelling, Munsch, Meyer et al., 2009). As reported by
Rakowski, Ehrich, Goldstein, and others (1998), a TTM-based stage-matched
intervention led to a significant increase in the uptake of screening mammography
among women aged 40-74. Peterson and Aldana (1999) also found that participants
who had received the stage-matched information were more likely to report having
read the information sent to them than those who had received generic information.
Beckie and Beckstead (2010) reported that women in the stage-matched programme
attended significantly more sessions of the prescribed exercise (90% versus 77%)
when compared with women in the traditional cardiac rehabilitation programme.
These findings suggest that the TTM-based ESMI could increase the uptake of such
programmes and decrease the dropout rates.

129
Since the TTM-based exercise intervention could motivate individuals to adopt an
exercise regime and previous studies have shown that regular exercise could increase
the ischemia threshold, exercise tolerance, physical fitness, and quality of life of CHD
patients (Bize, Johnson & Plotnikoff, 2007; Cui, Ren, Wang et al., 2006; Hambrecht,
Walther, Mobius-Winkler et al., 2004), the TTM-based ESMI may reduce their
anginal pain and yield a better quality of life. However, few studies have been carried
out to evaluate the instrument‘s effects on anginal pain and quality of life.
The results from the previous studies regarding the effects of the TTM-based ESMI
quality of life have led to inconsistent conclusions. Some studies demonstrated
positive effects on quality of life when the TTM was applied to exercise interventions
(Beckie & Beckstead, 2011; Kirk, Higgins, Hughes, et al., 2001). Beckie and
Beckstead (2010 & 2011) focused on multiple behavioural changes, such as healthy
eating, engagement in physical activity, and stress management, based on the TTM.
They found a significantly positive impact on quality of life as assessed by the SF-36,
the Multiple Discrepancies Theory questionnaire (MDT), and the Self-Anchoring
Striving Scale (SASS). Kirk et al. (2001) examined the effect of a 30-minute TTM-
based one-to-one exercise consultation on the promotion of physical activity among
patients with type II diabetes. They found that the patients who had received the
exercise consultation significantly increased their exercise stages of change, physical
activity counts, and minutes of physical activity per week, and significantly improved
their quality of life with respect to SF-36 as compared with those who received the
care accorded to the control group.

130
On the other hand, other studies have found negative results with regard to quality of
life. Taylor and others (2006) reported that a lifestyle physical activity programme
based on the TTM and social cognitive theory led to no significant improvements in
quality of life with respect to the SF-36 immediately after the 6-month intervention
for patients with prostate cancer. The authors explained that the lack of significant
differences may be due to the limited power of their study, because they did not reach
their projected sample size. Another studies conducted by Hughes and others (2007)
also revealed that a TTM-based exercise consultation programme led to no significant
change in all domains of SF-36 after the 6-month intervention. The authors explained
that this result was due to the high scores of all domains of SF-36 at baseline.
To conclude, TTM as a framework for changing exercise behaviour was found to be
more effective in inducing changes in behaviour in various populations when
compared with action-oriented interventions or the usual care. When employing TTM,
an interactive intervention is preferred. The intervention period varied from a few
days during the period of hospitalization to two years. The desirable implementation
period ranged from 6 to 12 weeks. Thus, an 8-week intervention period was designed
for this study.
Previous studies regarding the effects of the TTM-based ESMI on the exercise stages
of change, exercise self-efficacy, exercise decisional balance, and exercise duration
were inconclusive. Most studies have shown positive effects on these parameters in
the short term (≤ 6 months). The long-term (> 6 months) effects were not clear. The
negative results of the TTM-based ESMI on these parameters may be due to a poor
research design, a relatively short or brief counseling period, a high attrition rate, a

131
small sample size, and large number of participants in the preparation, action, or
maintenance stages at baseline. Thus, future studies regarding the effects of the TTM-
based ESMI should use more counselling contacts and a sufficiently large sample size,
reduce the dropout rate, and recruit sedentary participants (i.e., exclude those who are
in the action or maintenance stages). In addition, few studies have been conducted to
test the effects of the TTM-based ESMI on anginal pain and quality of life, with the
previous studies having shown discrepancies in their findings on quality of life. Thus,
future research to examine the effect of the instrument on anginal pain and quality of
life is necessary.
2.5.3 The TTM for Changing Exercise Behaviour among Patients with Heart
Disease
Several cross-sectional and longitudinal studies (Hellman, 1997; Jue & Cunningham,
1998; Kanning, 2010) have shown that the TTM could be applied for changing
exercise behaviour among adults with heart disease. Paradis, Cossette, Frasure-Smith,
Heppell, and Guertin (2010) examined the preliminary effects of a motivational
nursing intervention based on the stages of change model in heart failure patients (n =
30). They included multiple behavioural changes, such as the restriction of fluids,
following a low-salt diet, daily measurements of weight, exercise, and medication.
The study focused on self-care in relation to heart failure. A positive trend was found
in the intervention group, while the outcome measure did not include changes in
exercise behaviour. Beckie (2006) utilized the TTM and motivational interviewing to
guide the stage-matched intervention to promote multiple behavioural changes (e.g.,
healthy eating, physical activity, and stress management) for women with CHD. The

132
clinical nurse specialist carried out three 1-hour individualized motivational
interviews with each participant based on stage assessments carried out over 12 weeks.
However, the outcome measurements focused on psychological well-being and
quality of life (Beckie & Beckstead, 2011; Beckie, Beckstead & Schocken, 2011).
Exercise behaviour was not assessed at post-intervention or in the follow-up period,
and this study only focused on women with CHD.
There have been few studies examining the effects of the TTM-based interventions on
changes in exercise behaviour among patients with heart disease. Our previous
systematic review (Zhu, Ho & Wong, unpublished) found that only three studies used
the TTM as a framework for changing exercise behaviour in heart disease patients.
The findings from these three studies showed inconsistent conclusions in exercise
adherence (Hughes, Gillies, Kirk et al., 2002; Hughes, Mutrie & Maclntyre, 2007;
Naser, Jafar, Kumar et al., 2008). Naser and others (2008) conducted an intensive
multifactorial lifestyle modification programme (IMLM) based on the TTM over two
years in 100 CHD patients. The findings demonstrated a significant effect on
adherence to regular exercise based on a self-reported questionnaire on type of
exercise. Hughes and others (2002) recruited 31 cardiac patients and delivered a 30-
minute individualized exercise consultation session based on the TTM over four
weeks. The results showed a significant increase in exercise duration per week
(minutes/week) after the intervention based on the Scottish physical activity
questionnaire. Another study by Hughes and others (2007) also recruited 70 cardiac
patients and delivered a 30-minute individualized exercise consultation session based
on the TTM with regular follow-ups for six months. Although a significant effect on
exercise duration per week was found based on the 7-day recall, no significant effects

133
were detected in accelerometer counts/week and adherence to regular exercise both
immediately after the intervention and at the follow-up period.
Despite these inconsistent results, all of the participants in these three studies were
recruited after the completion of the formal cardiac rehabilitation programme. Thus,
all of the participants in these three studies were in the preparation, action, or
maintenance stages at the start of the study, which means that they were ready to
change their exercise behaviour or were already active at baseline. Based on the TTM,
the strategies and techniques (processes of change) used to motivate individuals in the
precontemplation or contemplation stage to change their behaviour differ from those
in the preparation, action, or maintenance stage because individuals in the
precontemplation stage may have no intention or interest in changing their behaviour
(Prochaska & DiClemente, 1983). It may be much easier to motivate individuals in
the preparation or action stage to adopt or maintain changes in behaviour than to
persuade those in the precontemplation or contemplation stage to change their
behaviour. This is because those in the preparation stage are ready to change their
behaviour and those in the action or maintenance stage have already changed their
behaviour, while those in the precontemplation stage tend to be defensive and avoid
changing their thinking and behaviour and tend to make use of fewer processes of
change than those in any of the other stages (Prochaska & DiClemente, 1983).
Cardiac rehabilitation services in China are poor and underdeveloped (Wang, Chair,
Thompson & Twinn, 2009). Few hospitals in China provide cardiac rehabilitation
programmes. It is much more important to use the TTM to motivate sedentary
individuals to adopt exercise than active individuals. In addition, these three studies
did not assess the outcomes on exercise stages of change, exercise self-efficacy, and
134
exercise decisional balance. Thus, it is necessary and important to conduct a study
recruiting sedentary CHD patients to motivate them to change their exercise
behaviour.
Only one randomized controlled trial claiming to use the TTM as a theoretical
framework was conducted in China with 45 patients who had undergone PCI (Kang,
Li, Liang et al., 2006). Although the researchers stated that the study used the TTM as
a framework, the intervention did not match the stage that each patient was in. All of
the patients in the intervention group received the same intervention, one-session
group intervention including one 30-minute education session, a 20-minute video
about exercise rehabilitation, one 25-minute session of supervised exercise training
during hospitalization, and two telephone calls after their discharge from hospital to
check their exercise compliance. The whole intervention lasted for four weeks. Data
collection was conducted at pre- and post-intervention. The results showed that
patients who had received the intervention significantly improved in activity capacity,
activity adherence, and exercise self-efficacy (confidence), and significantly reduced
levels of depression as compared with those in the control group, while no difference
in quality of life (SF-36) was found between the two groups. Since this study did not
deliver stage-matched interventions, no information relating to the assessment of
stages of change was available. In addition, the study only focused on the patients
following PCI. Thus, there have in fact been no studies conducted in China guided by
the TTM to motivate CHD patients to engage in exercise.
To sum up, few studies have been carried out to examine the effects of the TTM-
based ESMI on changes in exercise behaviour among patients with heart disease.

135
Findings from previous studies have come to inconsistent conclusions and all of the
three studies that were found only recruited patients in the preparation, action, and
maintenance stages at baseline. Due to the limited number of RCT studies employing
TTM with exercise stage-matched interventions for changing exercise behaviour in
CHD patients, inconsistent conclusions, and active participants at the start of the study,
further studies are required. Moreover, there were no studies examining the effects of
the TTM-based ESMI on changes in exercise behaviour and quality of life among
sedentary CHD patients (namely, patients that are in the precontemplation,
contemplation, and preparation stages). This is the first study to evaluate the effects of
the instrument on sedentary CHD patients. Thus, in this study, we focused on
evaluating the effects of the TTM-based ESMI on changes in exercise behaviour,
anginal attacks and quality of life among sedentary CHD patients using a randomized
controlled study design.
2.6 Summary
CHD is a leading cause of death and disability among adults worldwide. It impacts
the health of individuals in many ways. Physical activity or exercise has been proven
to be of great benefit to CHD patients, so it is included as a core component of cardiac
rehabilitation programmes (Taylor, Brown, Ebrahim et al., 2004). However, poor
attendance and adherence to exercise-based cardiac rehabilitation programmes is a
worldwide problem. The Transtheoretical Model (TTM) for behavioural change has
been shown to be an effective model for changing exercise behaviour among various
populations. For cardiac patients, however, there have been few studies on cardiac
rehabilitation programmes using the TTM as a framework. Thus, in this study, the

136
Exercise Stage-Matched Intervention (ESMI) to increase the adoption of an exercise
regime among sedentary CHD patients according to the TTM was developed.
The failure of patients to improve after training has been provided may be related to
the strategy used to implement the cardiac rehabilitation programme. An action-
oriented intervention is not useful for people who have no intention or interest in
changing their behaviour (e.g., precontemplators or contemplators). A stage-matched
intervention that attempts to change behaviour based on an individual‘s current stages
of change may have more promising results than general patient education or
conventional care.
Based on the literature review regarding the TTM, an ESMI lasting a total of eight
weeks and delivered through face-to-face or telephone contacts plus exercise stage-
matched pamphlets were utilized in this study. The participants were followed up for
six months with an assessment every 3 months. This study aims to evaluate if the
TTM-based ESMI is effective in motivating sedentary CHD patients to change their
exercise behaviour, and subsequently improving their angina and quality of life.

137
Chapter 3 Research Methodology
3.1 Introduction
This study aims to examine the effects of the TTM-based Exercise Stage-Matched
Intervention (ESMI) on sedentary patients with coronary heart disease (CHD) in
China. This chapter describes the study design that was adopted to evaluate the effects
of the interventions. Details of the selection criteria, procedures, instruments, data
analysis, and ethical considerations are explained.
3.2 Study Design
This is an experimental study with consecutive sampling. Eligible patients were
randomly assigned to either the control groups or the experimental group, taking
stage-matching (the precontemplation, contemplation, and preparation stages) into
consideration by using a random number table. There were three groups in this study:
the control group (Conventional, C, group), in which patients received conventional
care; the ―sham‖ group (Patient Education, PE, group), in which patients received
conventional care, one 2-hour session of patient education about CHD and a booklet,
and eight weekly sessions of general patient education about exercise; and the
experimental group (Exercise Stage-Matched Intervention, ESMI, group), in which
patients received conventional care, one 2-hour session of patient education about
CHD and the booklet (the same as that of the PE group), and eight weekly sessions of
ESMI together with exercise stage-matched pamphlets. This intervention was carried
out with reference to the Transtheoretical Model (TTM) (Prochaska & DiClemente,

138
1983). To investigate the effects of the intervention, the collecting of data was
conducted at T0 (immediately before the commencement of the experiment), T1 (after
the completion of the 8-week ESMI), T2 (three months after T1), and T3 (six months
after T1). Figure 3.1 is the flowchart of the study design.
Note: C group: Conventional group; PE group: Patient Education group; ESMI group: Exercise Stage-
Matched Intervention group.
Patients were randomly assigned to one of the following groups taking into consideration their exercise stages
Subject Recruitment
- Screening assessment
- Sign consent form
T0: Baseline Measurements
C Group PE Group ESMI Group
One 2-hour patient education session on CHD
T2: 3 months after T1 (5 months after T0)
T3: 6 months after T1 (8 months after T0)
Figure 3.1 Flowchart of the study design
T1: after the completion of the 8-week ESMI (2 months after T0)
8 weekly sessions
of ESMI
8 weekly sessions of
general PE about exercise

139
3.3 Settings
The patients were recruited from three medical institutions in Xiamen City: The
Xiamen Heart Centre, the Cardiac Unit of the First Affiliated Hospital of Xiamen
University, and The Medical Service Centre of Lujiang Community, Xiamen City,
China. The Xiamen Heart Centre is the largest cardiac unit and the only heart centre
in Xiamen City. The centre has 100 beds and around 200-300 cardiovascular patients
visit the cardiac clinic every day. The First Affiliated Hospital of Xiamen University
is a teaching hospital of Xiamen University and is the largest comprehensive hospital
with a cardiac unit in Xiamen City. This cardiac unit has 60 beds and the cardiac
clinic receives about 100-200 cardiovascular patients a day. These two institutions
treat most cardiovascular patients in Xiamen City. The Medical Service Centre of
Lujiang Community is one of the medical service centres in Xiamen City. The
conventional care given in these three hospitals is similar. It consists of simple and
unstructured patient education about diet, exercise, and medication of relevance to
cardiac patients. All these three hospitals had no structured or formal patient
education programme or cardiac rehabilitation programme for cardiac patients.
3.4 Sampling
Consecutive sampling was used to recruit patients from September 2009 to January
2011 for this study.

140
3.4.1 Selection Criteria
3.4.1.1 Inclusion Criteria
The inclusion criteria were:
patients who were medically stable as determined by the cardiologist;
patients who had been diagnosed with angina pectoris, myocardial infarction, or
had undergone Percutaneous Transluminal Coronary Angioplasty (PTCA) or
Percutaneous Coronary Intervention (PCI) for at least three months;
patients who were sedentary according to the exercise stages of change scale – that
is, patients in the precontemplation, contemplation, and preparation stages
(Marcus et al., 1994);
patients who were 18 years old or above;
patients who were able to communicate and read in Chinese;
patients who were living in Xiamen City, Fujian Province, and who could be
contacted by telephone.
3.4.1.2 Exclusion Criteria
The exclusion criteria were set with reference to the guidelines for cardiac
rehabilitation (Wenger, Smith, Froelicher & Comoss, 1999) and the contraindications
of exercise from the expert working group of the National Heart Foundation of
Australia (Briffa, Maiorana, Sheerin et al., 2006). The details of the guidelines and the
contraindications of exercise are shown in Appendix I.
141
The exclusion criteria were:
patients who had previously participated in any cardiac rehabilitation programme;
patients who had cognitive impairment (e.g., dementia) or who had been diagnosed
with a psychiatric illness (e.g., psychosis);
patients who had depression that might influence their participation in or adherence
to the exercise programme – that is, their scores on the Hospital Depression
Subscale (HADS-D) were equal to or higher than 11;
patients who had unstable angina (Briffa et al., 2006; Wenger, Smith, Froelicher &
Comoss, 1999);
patients who had critical aortic stenosis (Briffa et al., 2006; Wenger, Smith,
Froelicher & Comoss, 1999);
patients who had uncontrolled symptomatic heart failure (e.g., NYHA III/IV),
diabetes with poor blood glucose control (e.g., fasting blood glucose > 15 mmol/L),
or uncontrolled atrial or ventricular arrhythmias (e.g., resting heart rate > 120bpm,
atrial fibrillation, third-degree AV block) (Briffa et al., 2006; Wenger, Smith,
Froelicher & Comoss, 1999);
patients who had a resting SBP > 180 mmHg or resting DBP > 110 mmHg (Briffa
et al., 2006);
patients who had acute myocarditis or pericarditis that could be worsened by
exercise;
patients who had suffered embolism during the previous three months;
patients who had an acute noncardiac disorder that could affect their performance of
exercise or be aggravated by exercise (e.g., infection, renal failure, thyrotoxicosis).

142
3.4.2 Sample Size
The researcher used the keywords to search for relevant articles in the MEDLINE and
CINAHL databases. There are no similar experimental studies using TTM on patients
with heart disease. The sample size of this study could not be calculated with
reference to previous studies. It was calculated based on the conventional method of
power analysis by using a medium effect size of 0.25 for an ANOVA analysis (Cohen,
1988), a power of 0.80, three groups (u = 2), and a significance level of 0.05. The plan
was to recruit 156 participants, with 52 in each group, according to the power table
(Cohen, 1988). In the pilot study, the dropout rate was 16.0%. With reference to a
cardiac rehabilitation study in mainland China (Jiang, 2005), the dropout rate was set
as 20.0%. Thus, the size of the sample in this study was amended to 63 patients in
each group. As a result, the total number of patients recruited was 189.
3.5 Procedures
Before the commencement of the study, ethical approval (Appendix II) was granted
from the Human Ethics Committee of The Hong Kong Polytechnic University and
access approvals (Appendix III) were obtained from the hospitals. The cardiologists in
each hospital were responsible for screening patients in accordance with the screening
guidelines (Appendix IV). Patients who met the selection criteria were recruited from
the outpatient cardiac clinics. The purpose and procedures of the study were explained
to them by the researcher (ZLX) using an information sheet (Appendix V) and they
were asked to sign a consent form (Appendix VI) to indicate that they were willing to
participate in the study. After being recruited, each patient received a gift (around
143
HKD 20) as a token of thanks for their participation. Before the group allocation, a
registered nurse (RN) who was blinded to the study design collected the baseline data
(T0): exercise stages of change, exercise self-efficacy, exercise decisional balance,
exercise duration, conditions of angina, and quality of life. Taking into consideration
their exercise stages of change, the patients were randomly allocated by the researcher
(ZLX) using a random number table to one of the following three groups: the
Conventional (C) Group, the Patient Education (PE) Group, and the Exercise Stage-
Matched Intervention (ESMI) Group.
After the group allocation, patients in the C group (control group) received
conventional care only; patients in the PE group (―sham‖ group) received
conventional care, one 2-hour session of patient education about CHD and the booklet,
and eight weekly sessions of general patient education about exercise; patients in the
ESMI group (experimental group) received the same interventions as the PE group
except that the eight weekly sessions were focused on the ESMI together with the
exercise stage-matched pamphlets. Data collection was conducted by the RN
immediately after the completion of the 8-week ESMI (T1), three months after T1 (T2),
and six months after T1 (T3).
To minimize cross contamination among the C, PE, and ESMI groups, appointments
for face-to-face contacts or data collection were scheduled in different time slots for
patients in the different groups. For example, patients in the ESMI group were invited
to come to the hospital on Mondays, Wednesdays, and Fridays, and those in the PE
group were scheduled to come to the hospital on Tuesdays, Thursdays, and Saturdays
for a face-to-face consultation.

144
3.6 Intervention
The details of the intervention received by each group are described in this section.
3.6.1 Conventional (C) Group
All of the patients in this study received conventional care, which consisted of simple
and unstructured patient education about diet, exercise, and medication suited to
cardiac patients. Patients in the C group received conventional care only. Since the
booklet about cardiac rehabilitation (which had been developed by the Hong Kong
Cardiac Rehabilitation and Prevention Centre of Tung Wah Hospital and the
organization Care for Your Heart) that was used in the PE and ESMI groups is
beneficial to CHD patients, it was also provided to the patients in the C group after
the completion of the study.
3.6.2 Patient Education (PE) Group
Patients in the PE group received conventional care, one 2-hour patient education
session and the booklet about cardiac rehabilitation, and eight weekly sessions of
general patient education about exercise. The contents of the 2-hour patient education
session were: (i) an introduction to the heart, including the anatomy and physiology of
heart; (ii) an introduction to CHD; (iii) the risk factors of CHD; (iv) the diagnostic
investigation and treatment of CHD; (v) dietary principles for patients with heart
disease; and (vi) exercise for patients with CHD. Patient education was delivered in
groups. There were 6-10 patients in each group. The booklet was given to the patients

145
immediately after the 2-hour patient education session. The eight weekly sessions of
general patient education on exercise were delivered after the one 2-hour session of
patient education in the mode of face-to-face or telephone contacts. Each patient
received at least two sessions of face-to-face contact. Each session of face-to-face
contact lasted about 30 minutes, while each telephone contact lasted 5-10 minutes.
The contents of the 8-week period of patient education included compliance checking
and the delivery of information related to the benefits and importance of regular
exercise (Appendix VII).
3.6.3 Exercise Stage-Matched Intervention (ESMI) Group
Similar to the PE group, patients in the ESMI group received conventional care, one
2-hour session of patient education including the booklet, and eight weekly sessions
of ESMI together with the exercise stage-matched pamphlets. The ESMI was
implemented according to the Transtheoretical Model (TTM), taking the factors of
coronary heart disease and Chinese culture into consideration. The intervention was a
collaboration between the researcher (ZLX) and the cardiologists. The researcher was
responsible for the patient education session, the weekly assessment of the patients'
exercise stages of change, and the delivery of strategies and techniques to the patients
according to the TTM. The cardiologists were responsible for the assessment of the
patients' physical condition and for prescribing exercise for those at the stage of
preparation with reference to Appendix VIII. To facilitate the implementation of
ESMI in Chinese patients, some examples of exercises popular among the Chinese
(e.g., Taichi and the Twist) were included in the recommendations.

146
3.6.3.1 Exercise Stage-Matched Intervention (ESMI)
According to the TTM, behavioural changes can be divided into five stages, namely,
precontemplation, contemplation, preparation, action, and maintenance (Prochaska &
DiClemente, 1983). Stage-matched intervention refers to the intervention that is
matched to the individual‘s current stage of behavioural change. In this study, the
Exercise Stage-Matched Intervention (ESMI) refers to strategies and techniques that
are matched to the individual‘s current stage of readiness for changes in exercise
behaviour as described by the TTM (Kim, 2008).
In this study, the ESMI was implemented weekly for eight weeks in the form of either
face-to-face or telephone contacts. An 8-week period was selected because the period
for inducing changes in exercise behaviour by using the TTM-based stage-matched
intervention ranges from one week to two years (Blissmer, 2000; de Vet, de Nooijer,
de Vries & Brug, 2008; Kim, 2008; Marcus, Banspach, Lefebvre, Ross et al., 1992;
Naser, Jafar, Kumar et al., 2008; Peterson & Aldana, 1999), with most interventions
lasting 6-12 weeks (Blissmer & McAuley, 2002; Kim, 2008; Marcus, Banspach,
Lefebvre, Ross et al., 1992; Peterson & Aldana, 1999). Therefore, the Exercise Stage-
Matched Intervention was scheduled for eight weeks in this study.
The ESMI was carried out weekly over an 8-week period after the one 2-hour session
of patient education. The stage-matched intervention together with the assessment of
the patient‘s exercise stage of readiness for change according to the exercise stages of
change scale (Marcus, Rossi, Selby, Niaura & Abrams, 1992) was delivered through
face-to-face or telephone contacts. The form of contact was determined by the

147
availability of the patients, but each patient must receive at least two sessions of face-
to-face contact over the eight weeks. Each session of face-to-face contact lasted about
30 minutes, while each telephone contact lasted 5-15 minutes.
During the 8-week intervention period, the researcher assessed each patient‘s exercise
stages of change weekly according to the exercise stages of change scale before
delivering the ESMI. The detailed protocol of the ESMI that was delivered weekly is
shown in Table 3.1. In formulating the ESMI, the guidelines (Table 3.2), such as
goals, processes of change, and strategies and techniques for changing exercise
behaviour in each stage, were set with reference to those developed by Burbank,
Reibe, Padula, and Nigg (2002) to motivate the elderly to engage in exercise. When
the patient was in the preparation stage and prepared to engage in exercise, a physical
examination for prescribing exercise was scheduled. The cardiologists assessed the
patient to ensure that it was safe for him/her to engage in exercise. Exercise was then
prescribed by the cardiologists in accordance with the patient‘s physical condition and
the guidelines for prescribing exercise (Appendix VIII).
With regard to the implementation of ESMI, the researcher (ZLX) and the patient
discussed the matter with reference to the guidelines developed by Burbank and co-
workers (2002) (Table 3.2). Different strategies and techniques were used for patients
at different stages of change. A Chinese version of the exercise stage-matched
pamphlet (Appendix IX) was prepared to reinforce the strategies and techniques being
implemented in each stage. The original English version of the pamphlet was
designed by Blissmer (2000). The Chinese version was prepared with reference to the
one designed by Blissmer (2000), and taking into account the factor of coronary heart

148
disease, and the guidelines of the ESMI (Table 3.2). A case to illustrate the details of
the 8-week TTM-based ESMI is shown in Appendix X.
Table 3.1 Protocol of the weekly exercise stage-matched intervention session
(I) Checking for Compliance
1. Did you perform exercise in the past one week?
2. What kind of exercise did you perform?
3. How many days did you perform it in the past one week?
4. How long did you perform it per day?
5. What was/were the RPE score(s) that you recorded on the exercise log sheet?
6. How did you feel during the exercise? Did you experience any increase in
respiratory rate? Any sweating?
7. Did you experience any discomfort during the exercise?
8. Did you take any anti-anginal medication because of exercise in the past one
week? If yes, how many pills did you take?
(II) Exercise Stage-Matched Intervention
1. Check the exercise stages of change.
2. Individual stage-matched discussion between patients and the researcher (30
minutes for face-to-face contact and 5-15 minutes for telephone contact)
according to the guidelines of the ESMI (Table 3.2).
3. Stage-matched pamphlet for home-based reinforcement and/or exercise
prescription.

149
Table 3.2 Guidelines of goals, processes, and strategies for changing exercise behaviour in each stage
Stage Goal Processes Strategies
Precontemplation Increase awareness
of the need to
change
Consciousness raising
Dramatic relief
Environmental
reevaluation
Self-reevaluation
Provide education about the risks of not exercising
Provide information on the benefits of physical activity
Give personalized feedback about the risks of the current behaviour (e.g.,
physical deconditioning, recurrent MI, and so on)
Discuss feelings and perceptions of active/inactive behaviour
Discuss how a sedentary lifestyle affects role implementation and social
activities
Encourage thinking about the benefits of physical activity for oneself
Encourage thinking about change
Contemplation
Increase
motivation and
confidence in the
ability to change
Consciousness raising
Dramatic relief
Self-reevaluation
Social liberation
Identify questions about exercise and continue to provide education about
the personal risks of inactivity and the benefits of physical activity
Discuss feelings and perceptions about loss of cardiovascular fitness due to
inactivity
Find out what is stopping the individual from engaging in physical activity
Decrease the barriers to physical activity
Encourage reflection on the ways in which inactivity affects their life
Point out people who included regular physical activity in their lives
Increase awareness of opportunities that exist to encourage regular physical
activity

150
Stage Goal Processes Strategies
Preparation Negotiate a plan
for exercising
Consciousness raising
Self-reevaluation
Helping relationships
Self-liberation
Further provide information about the benefits of physical activity and the
personal risks of physical inactivity.
Create a new self-image as an exerciser
Make a public commitment to exercise
Identify alternatives to exercising
Make a plan for engaging in exercise or regular physical activity
Gather support from others
Encourage a component of behavioural change where they can experience
success
Discuss the safety of exercise/physical activity, including an exercise
prescription by a cardiologist
Action Reaffirm
commitment and
follow up
Reinforcement
management
Helping relationships
Counterconditioning
Stimulus control
Frequent positive reinforcement with rewards for exercising regularly
Find exercise buddies
Mobilization of social support to participate in the process or reinforce the
process
Introduce additional exercise alternatives
Check off each time you exercise
Plan for resisting the temptation to skip exercise sessions

151
3.6.3.2 The Relevance and Validity of the ESMI for Use in the Chinese Context
The TTM has been applied to Chinese people. Most such studies were of a cross-
sectional design to test the application of the TTM, involving physical activity among
family caregivers in Taiwan (Tung & Gillett, 2005; Tung, Gillett & Pattillo, 2005),
general health promotion activities among Hong Kong Chinese adults (Lam, Chan,
Ho & Chan, 2004), and physical activity among students in mainland China (Fang,
Sun & Zhao, 2006; Ma, Wang & Li, 2008; Sun, Zhang, Liu & Wang, 2008). The
findings from these studies show that the TTM can be utilized in Chinese populations
to explain exercise behaviour. One case study using the TTM to change behaviour
relating to physical activity (Huang & Tang, 1996) among patients with diabetes
mellitus in Taiwan showed a significant increase in physical activity. Ma, Ma, and
Zhu (2006) evaluated the effectiveness of a stage-matched intervention on physical
activity in 426 university students. The results indicated that the stage-matched
intervention significantly increases the adoption of exercise and progress in exercising.
These studies suggest that the TTM as a framework is effective in inducing changes in
exercise behaviour among Chinese populations.
Before the commencement of the study, five local health professionals, who are
cardiologists, reviewed the intervention programme for its validity according to the
research aim and expected outcomes for CHD patients. All of them agreed that the
intervention programme was valid and feasible in terms of aim and expected
outcomes.

152
After the completion of the pilot study, eight CHD patients who had completed the
eight sessions of ESMI were invited to evaluate the intervention programme (both the
contacts and the format of the delivery) in terms of the relevance, appropriateness,
and feasibility of the intervention for CHD patients. Seven of them expressed the view
that the contents and the delivery format of the intervention were useful, appropriate,
and acceptable for CHD patients. Their views also suggest that the ESMI is valid and
feasible for use among CHD patients in Xiamen City, China.
3.6.3.3 Fidelity of the Intervention
The fidelity of the intervention refers to the demonstration that the delivery of the
intervention was the same across participants throughout the study (Dumas, Lynch,
Laughlin, Smith & Prinz, 2001). This section presents the fidelity of the intervention
in this study.
3.6.3.3.1 Consistency in the Delivery of the Intervention
The intervention was delivered by only one person, the researcher (ZLX), who
designed the entire study and the protocol of this study and who is familiar with the
TTM. The TTM is a user-friendly model that is simple, straight forward, and easy to
use. The researcher delivered the intervention following the protocol and the
guidelines of the TTM-based ESMI (Table 3.2) throughout the study. During the
intervention period, the details of the stage assessment, the goal, processes, strategies,
and techniques delivered to each patient for motivating exercise behaviour were
recorded. An example was illustrated in Appendix X. In addition, the delivery of the

153
intervention, the cases, and the use of the protocol were reported to the supervisors
biweekly during the intervention period. The consistency in delivering the
intervention was closely monitored.
3.6.3.3.2 The Patients' Adherence to the Intervention
This study focused on home-based exercise and the researcher could not monitor the
patients' exercise at home day by day. Thus, to ensure that the patients adhered to the
intervention, a log book was used to record their exercise at home. The patients were
asked to record the details of their daily exercise in the log book (Appendix XII), such
as the type of exercise that they had engaged in, the frequency, intensity, and duration
of each episode of exercise, whether they had experienced angina, and the taking of
any anti-anginal drugs as a result of the exercise. The log book could serve as a
motivator for patients to engage in exercise at home. With the help of the log book,
the patients could also be monitored on whether or not they had adhered to the
intervention at home. During the 8-week intervention period, the patients' adherence
to the intervention was monitored by cross-checking the weekly compliance records
and the log book information through either face-to-face or telephone contacts (Table
3.1).
3.7 Instruments
In accordance with the objectives of this study, several instruments were employed to
screen subjects or measure outcomes.

154
3.7.1 Screening Assessment
In the screening assessment, demographic and clinical data were collected from the
patients‘ medical records. The emotional state of the patients in terms of whether they
suffered from depression was assessed according to the Hospital Depression Subscale
(HADS-D). The details of the screening guidelines are shown in Appendix IV.
3.7.1.1 Demographic Data
To better understand the patients‘ demographic information, the following
demographic data were collected, including the patients‘ gender, age, marital status,
educational level, employment status, occupation, religious belief, family income,
type of medical payment, and habitation (Appendix XI).
3.7.1.2 Clinical Data
The clinical data collected in this study included the patients‘ medical diagnosis,
family history related to CHD, PCI/Stent treatment, smoking status, alcohol
consumption, chronic illnesses such as diabetes mellitus and hypertension, and
medication taken (Appendix XI).
3.7.1.3 Hospital Depression Subscale (HADS-D)
The Hospital Anxiety and Depression Scale (HADS) was developed by Zigmond and
Snaith in 1983. It is a widely used self-reported instrument for anxiety and depression

155
in non-psychiatric populations (Martin & Thompson, 2000). The HADS has been
used extensively in studies of cardiac patients (Barth & Martin, 2005; Furze, Bull,
Lewin & Thompson, 2003; Lewin, Furze, Robinson et al., 2002; Martin & Thompson,
2000) and its psychometric properties are well established (Martin & Thompson, 2000;
Stafford, Berk & Jackson, 2007). The scale is comprised of two parts – depression
and anxiety. The Hospital Depression Subscale (HADS-D) (Appendix XI) was used
in this study for screening. The reliability of the HADS-D was tested by Marin and
Thompson (2000) on 194 patients with coronary heart disease. The Cronbach alpha
coefficient was 0.72. A systematic review of its validity ranged from 0.67 to 0.90
(mean = 0.82) (Bjelland, Dahl, Haug & Neckelmann, 2002). The HADS-D has been
shown to be strongly correlated with the Beck Depression Inventory (BDI), with the
correlations between BDI and HADS-D ranging from 0.62 to 0.73 (Bjelland, Dahl,
Haug & Neckelmann, 2002).
HADS-D can reveal an individual‘s emotional state during the past week. There are
seven questions in HADS-D, with the score for each question ranging from zero to
three. A score of seven or less indicates a non-depression case, 8-10 a borderline case
of depression, and 11 or above a definite case of depression (Arving, Glimelius &
Brandberg, 2008; Zhang, 2005). The reliability and validity of the Chinese version of
HADS (Ye & Xu, 1993) were tested on 287 pregnant women. For the Chinese version
HADS-D (Appendix XI), the Cronbach alpha coefficient was 0.82 and the half
reliability was 0.82. The cut-off point for depression is similar to that in the original
version, with a score of 11 or above indicating depression (Xia, 2006).

156
The HADS-D was selected to screen the emotional state of patients because it is a
simple and easy scale to administer, has a clear cut-off point for depression, and has
good reliability and validity.
3.7.1.4 Screening Form
To facilitate the screening assessment of the potential subjects, a screening form
(Appendix XI) was drawn up with reference to the selection criteria. Guidelines for
screening were prepared (Appendix IV) so that the cardiologists could screen each
patient in accordance with these guidelines.
3.7.2 Outcome Measurements
Based on the objectives of this study, the outcome measurements included exercise
stages of change, exercise self-efficacy, exercise decisional balance, exercise duration
(minute/week), conditions of angina, and quality of life. The primary outcome
indicators are exercise stages of change, exercise self-efficacy, exercise decisional
balance, and exercise duration (minute/week). The secondary outcome indicators are
angina and quality of life. The data were recorded at different periods of time (Table
3.3).

157
Table 3.3 Outcome measurements
Items Baseline
measurements (T0)
After the completion
of the 8-week ESMI
(T1)
3 months after T1 (T2) 6 months after T1 (T3)
Exercise Stages of Change
Exercise Stages of Change Scale
Exercise Self-Efficacy
Exercise Self-Efficacy Scale
Exercise Decisional Balance
Exercise Benefits Scale
Exercise Barriers Scale
Exercise
Frequency (sessions/week)
Intensity (RPE 6-20)
Duration (minutes/week)
Angina occurred during exercise (yes / no)
Anti-anginal drugs (additional number of
tablets taken per week)
Angina
Frequency of angina (episodes/week)
Severity of angina (0-10)
Duration of angina (minutes)
Anti-anginal drugs (total number of tablets
taken/week)
Quality of Life
Seattle Angina Questionnaire (SAQ)
Short Form 36-item Health Survey (SF-36)

158
3.7.2.1 Exercise Stages of Change Scale
The Exercise Stages of Change Scale (Marcus, Selby, Niaura & Rossi, 1992) was
developed from the original stages of change scale for smoking cessation (Prochaska
& DiClemente, 1983) with five questions to identify the stages. The test-retest
reliability of the stages of change for smoking cessation was 0.72 (Donovan, Jones,
Holman & Corti, 1998).
The statements specific to the exercise stages of change scale were formulated
accordingly: (a) precontemplation: ―I currently do not exercise, and I do not intend to
start exercising in the next six months‖; (b) contemplation: ―I currently do not engage
in exercise, but I am thinking about starting to exercise in the next six months‖; (c)
preparation: ―I currently exercise some, but not regularly‖; (d) action: ―I currently
exercise regularly, but I have only begun doing so within the last six months‖; and (d)
maintenance: ―I currently exercise regularly, and have done so for longer than six
months‖. Patients were required to mark only one stage that best describes their
current state of readiness for regular exercise. Courneya (1995) further modified the
scale into a form consisting of one item (e.g., Do you engage in exercise regularly?)
with five statements representing each stage (Appendix XII). The five statements, one
based on each stage of change, are described and the patients are asked to select one
of the five statements that best describes their current level of exercise. The five
statements are arranged from the precontemplation to the maintenance stages as
follows: (i) ―No, and I do not intend to in the next six months‖ means that the
individual is in the precontemplation stage; (ii) ―No, but I intend to in the next six
months‖ means that the individual is in the contemplation stage; (iii) ―No, but I intend

159
to in the next 30 days‖ means that the individual is in the preparation stage; (iv) ―Yes,
I have been for less than six months‖ means that the individual is in the action stage;
and (v) ―Yes, I have been for more than six months‖ means that the individual is in
the maintenance stage. This modified version has been widely used by many scholars
in many studies (Burbank, Reibe, Padula & Nigg, 2002; Nigg, 2001; Nigg &
Courneya, 1998; Tung, 2003). Thus, it is employed in this study.
The original scale has been tested and found to have good reliability. As reported, the
Kappa index of reliability for this scale over a two-week period was 0.78 (n = 20)
(Marcus, Selby, Niaura & Rossi, 1992). The two-week test-retest reliability
coefficient of the modified version is 0.79, obtained from the 148 patients (Courneya,
1995). In addition, the scale has been shown to be significantly associated with
exercise with respect to the 7-Day Recall Exercise Questionnaire (Marcus & Simkin,
1994). Hellsten, Nigg, Norman and others (2008) conducted a study to accumulate
evidence of behavioural validity for exercise stages of change scale, which examined
nine studies. The findings showed that the exercise stages of change scale was
behaviourally valid, as evidenced by self-reported physical activity, self-reported
exercise, self-reported sedentary behaviours, pedometers, and physical functioning.
The original English version of this modified scale was first translated into Chinese
by Tung (2003) using a two-part method: translation by a committee and back-
translation. Both the committee members and translators were bilingual persons who
were fluent in both Chinese and English. After the completion of the original and
back-translation processes, a panel of three professional nursing experts from Taiwan
reviewed the clarity and linguistic appropriateness of the Chinese version. This

160
Chinese version of the exercise stages of change was adopted in this study (Appendix
XII).
3.7.2.2 Exercise Self-efficacy Scale
The Exercise Self-Efficacy Scale (Appendix XII) was developed by Bandura (1997)
to measure the degree of confidence in one‘s ability to perform exercise under
specific situations. This scale contains 18 items covering different situations.
Individuals mark their degree of confidence on a 100-point scale in 10-unit intervals
ranging from 0 (cannot do) through intermediate degrees of assurance such as 50
(moderately certain can do) to complete assurance, 100 (certainly can do), with the
higher score showing more confidence to execute regular physical activity (Bandura,
1997; Shin, Jang & Pender, 2001; Tung, 2003).
The original version of this scale was translated into Chinese by Tung (2003)
(Appendix XII). This translated version has been back-translated and reviewed for
clarity and linguistic appropriateness by three nursing experts. It has a high degree of
internal consistency as shown by its Cronbach‘s alpha coefficient of 0.96 (Tung,
2003). This translated version had also been used in mainland China on 46 patients
who had undergone percutaneous coronary intervention (PCI) and was shown to be
valid and reliable for Chinese populations (Kang, Li, Liang et al., 2006). This Chinese
version of exercise self-efficacy scale was adopted in this study.
161
3.7.2.3 Exercise Decisional Balance
Two scales are utilized to determine exercise decisional balance: the Exercise
Benefits Scale and the Exercise Barriers Scale (Appendix XII), which were developed
by Sechrist, Walker, and Pender (1987) to assess the benefits of and barriers to
exercise as perceived by individuals. The Exercise Benefits Scale consists of 29 items
and the Exercise Barrier Scale consists of 14 items. Patients were asked to rate the
items using a 4-point Likert scale, with one being strongly disagree to four being
strongly agree with each statement. The instrument, which includes the two scales,
can be used as a whole (43 items) with the reversed score of the barriers scale, or the
two scales can be used separately. The possible range of scores on the whole
instrument is 43-172, with the range for the benefits scale being 29-116 and that for
the barriers scale being 14-56. The higher scores on the exercise benefits scale show
that the patients perceived there to be greater benefits to exercise, while the lower
scores on the exercise barriers scale show that patients perceived there to be fewer
barriers to exercise.
Sechrist, Walker, and Pender (1987) conducted a psychometric evaluation of the
exercise benefits and barriers scale on 650 adults and found that the instrument has
good internal consistency. The whole instrument (43 items) achieved a standardized
Cronbach‘s alpha coefficient of 0.95. The benefits scale (29 items) achieved a
standardized alpha coefficient of 0.95 while the figure for the barriers scale (14 items)
was 0.87. The test-retest reliability was also measured on a sample of 63 individuals
recruited from the community, at intervals of two weeks. The correlation coefficients

162
were 0.89 for the whole instrument, 0.89 for the benefits scale, and 0.77 for the
barriers scale (Sechrist, Walker & Pender, 1987).
Tung (2003) translated the original English version of the Exercise Benefits/Barriers
Scales into Chinese (Appendix XII). This translated version has been back-translated
and reviewed for clarity and linguistic appropriateness by three nursing experts. It was
then revised after a pilot test involving eight Taiwanese students (Tung, 2003). Its
reliability was tested on a sample of 108 Taiwanese family caregivers. The Chinese
version of these two scales has a high degree of internal consistency, with Cronbach‘s
alpha coefficients of 0.97 and 0.93, respectively (Tung, 2003). Thus, the Chinese
version of these two scales was used in this study.
3.7.2.4 Exercise
To record the details of the patients‘ daily exercise conditions, a log book (Appendix
XII) was designed to record the type of exercise, the frequency, intensity and duration
of each episode of exercise, whether angina occurred, and the number of additional
anti-anginal medicine tablets/pills taken due to exercise. The intensity of exercise was
assessed by Borg‘s Rating of Perceived Exertion (RPE) Scale, which ranged from 6 to
20, with 6 being very, very light (rest) and 20 being a level of exercise leading to
exhaustion.
The RPE is an easy and reliable tool for both the assessment and prescription of
exercise (Carvalho, Bocchi & Guimaraes, 2009; Eston & Thompson, 1997; Okura &
Tanaka, 2001). It is a reliable method for quantifying exercise of various levels of

163
intensity (Day, McGuigan, Brice & Foster, 2004; Minganti, Capranica, Meeusen,
Amici & Piacentini, 2010; Wallace, Slattery & Coutts, 2009). It is also an important
tool for self-monitoring and self-regulating the exercise engaged in by patients with
heart disease (Carvalho, Bocchi & Guimaraes, 2009). The RPE was found to be
significantly correlated with the method based on HR (r = 0.55-0.94) (Borresen &
Lambert, 2008; Minganti, Capranica, Meeusen, Amici & Piacentini, 2010; Wallace,
Slattery & Coutts, 2009), distances measures (r = 0.37-0.81) (Wallace, Slattery &
Coutts, 2009), maximal oxygen uptake (VO2max), and oxygen uptake at the anaerobic
threshold (VO2AT) (r= 0.89 and r = 0.87, respectively) (Okura & Tanaka, 2001). A
Chinese version of RPE was tested for validity and reliability among 54 Hong Kong
adults by Leung, Leung, and Chung (2004). The findings demonstrated that the RPE
was significantly correlated with heart rate (r ≥ 0.73), power output (r ≥ 0.69), and
oxygen consumption (r ≥ 0.68). The overall test-retest intraclass correlation
coefficient (ICC) was 0.92, which suggests that the scale is reliable.
3.7.2.5 Angina
The log book (Appendix XII) recorded the details of the patients‘ daily angina. The
information recorded included the frequency, severity, and duration of each episode
of angina, and the frequency and number of anti-anginal medicine tablets/pills taken
per week. The patients were told to rate each episode of angina for severity on a
Chinese Pain Intensity Verbal Rating Scale (C-PIVRS), which was developed by Liu,
Chung, and Wong (2003). It has been shown to have good reliability and validity in
Chinese populations, with the intraclass correlation coefficient (ICC) ranging from
0.78 to 0.90 (Liu, Chung & Wong, 2003). The test-retest correlation coefficients

164
between the C-PIVRS and the visual analog scale (VAS) are r = 0.92 and 0.91,
respectively. The scale is rated from 0 to 10, with 0 being no pain, 5 being very
painful, and 10 being ‗crucifying pain‘. The patients were also required to rate the
duration of the episode of angina in minutes, and the number of tablets/pills of anti-
anginal medicine taken per day.
3.7.2.6 Quality of life
The Seattle Angina Questionnaire and the Medical Outcomes Study 36-Item Short-
Form (SF-36) were employed to assess the quality of life of the patients in this study.
3.7.2.6.1 Seattle Angina Questionnaire (SAQ)
The Seattle Angina Questionnaire (SAQ) (Appendix XII) is a disease-specific self-
administered instrument for patients with CHD, which was developed by Spertus et al.
(1995). It was used to assess the patients‘ quality of life in the past four weeks.
Previous studies have demonstrated that the SAQ is valid, reproducible, and sensitive
to clinical change (Dougherty, Dewhurst, Nichol & Spertus, 1998; Kimble, Dunbar,
Weintraub, et al., 2002; Spertus, Winder, Dewhurst et al., 1995; Spertus, Jones,
McDonell et al., 2002). This scale has been adapted cross-culturally in more than 13
countries, including China (Schroter & Lamping, 2006).
The SAQ was developed to quantify the physical and emotional effects of CHD. It
consists of a 19-item questionnaire with five subscales that measure clinically relevant
domains of CHD, including physical limitations, angina stability, angina frequency,

165
treatment satisfaction, and disease perception. The physical limitation subscale
measures how daily activities are limited by symptoms of CHD. The angina stability
subscale assesses change over time in the frequency of angina at the patient‘s most
strenuous level of activity, whereas the angina frequency subscale quantifies the
number of impacts CHD has on his or her health-related quality of life (HRQL). The
treatment satisfaction subscale quantifies satisfaction with the current treatment of
angina. The disease perception subscale characterizes the patient‘s perception of the
impact of CHD on their quality of life (Dougherty, Dewhurst, Nichol & Spertus,
1998).
Each subscale of the SAQ has been independently validated and demonstrated to be
reliable and responsive to clinical change. As tested on 107 patients with chronic
stable angina pectoris, the internal consistency reliability (Cronbach‘s alpha) of the
SAQ of each subscale ranged from 0.66 to 0.89, and the 2-week intraclass correlation
coefficients (r) of physical limitations, angina frequency, angina stability, treatment
satisfaction, and disease perception were 0.72, 0.80, 0.33, 0.58 and 0.67, respectively
(Dougherty, Dewhurst, Nichol & Spertus, 1998). The SAQ takes less than five
minutes to complete and is brief and easily self-administrated.
The Chinese version of the SAQ (Rao & Yuan, 1996) (Appendix XII) was employed
in this study to investigate the quality of life of CHD patients. Liu (2003) tested its
reliability and validity on 35 CHD patients. The results showed that the 2-week test-
retest reliability coefficients for physical limitations, angina stability, angina
frequency, treatment satisfaction, and disease perception were 0.99, 0.58, 0.97, 0.98,
and 0.94 respectively and the total Cronbach‘s alpha coefficient was 0.76. The

166
findings suggest that the Chinese version of the SAQ has good reliability and validity
and can be used for Chinese CHD patients.
The SAQ is scored by assigning an ordinal value to each response and summing up
the scores of items within each of the five subscales. The scoring instructions were
published by Cardiovascular Outcomes Inc. (2010), which was developed by Spertus
and colleagues (Appendix XIII). The possible range of scores for each subscale is
from 0 to 100, with higher scores indicating better levels of functioning.
3.7.2.6.2 SF-36
SF-36 (Appendix XII) was developed by Ware and colleagues (McHorney, Ware &
Raczek, 1993; Ware & Sherbourne, 1992). It is used to measure changes in the
previous four weeks and is also the most convenient instrument for assessing health-
related quality of life (HRQL) changes (Kiebzak, Pierson, Campbell & Cook, 2002).
The SF-36 is a generic and comprehensive instrument used to measure health-related
quality of life in all social and demographic groups, regardless of age, disease, or
treatment condition (Corcoran & Durham, 2000).
Compared with other generic instruments, such as the Nottingham Health Profile
(NHP) and the Sickness Impact Profile (SIP), the SF-36 achieves the best results
(Thompson & Roebuck, 2001). It has few floor or ceiling effects, good internal
consistency, and high test-retest reliability (sensitivity to change) (Thompson &
Roebuck, 2001). As reported, the internal consistency of the SF-36, the Cronbach‘s
alpha coefficient, ranges from 0.65 to 0.96 (Dougherty, Dewhurst, Nichol & Spertus,

167
1998; Failde & Ramos, 2000). Compared with WHO100, the SF-36 is simple and
easy to administer. The SF-36 is self-administered and takes around ten minutes to
complete. Thus, the SF-36 was selected in this study to measure the quality of life of
CHD patients.
The SF-36 measures eight domains of health: physical functioning (PF), role
limitations as a result of physical problems (RP), bodily pain (BP), general health
perception (GH), vitality (VT), social functioning (SF), mental health (MH), and role
limitations as a result of emotional problems (RE). Physical functioning (10 items)
refers to the extent to which health limits physical activities such as self-care, walking,
climbing stairs, bending, lifting, and moderate and vigorous activities. Role limitation
- physical (4 items) refers to the extent to which physical health interferes with work
or other daily activities, including accomplishing less than wanted, limitations in the
kinds of activities engaged in, and having difficulty in carrying out one‘s role. Bodily
pain (2 items) refers to the intensity of pain and the effect of pain on normal work,
both inside and outside the house. General health perception (5 items) refers to
personal evaluations of health, including current health, health outlook, and resistance
to illness. Vitality (4 items) refers to feeling energetic and full of pep versus feeling
tired and worn out. Social functioning (2 items) refers to the extent to which physical
health or emotional problems interfere with normal social activities. Mental health (5
items) refers to general mental health, including depression, anxiety, behavioural-
emotional control, and general positive affect. Role limitation - emotional (3 items)
refers to the extent to which emotional problems interfere with work or other daily
activities, including a decrease in the amount of time spent on work, accomplishing
less than wanted, and failing to work as carefully as usual. The SF-36 can be grouped

168
into two summary dimensions: the physical component summary (PCS) and the
mental component summary (MCS). The physical component summary includes four
domains of health, such as physical functioning, role limitation - physical, bodily pain,
and general health perception. The mental component summary (MCS) includes
another four domains of health: vitality, social functioning, mental health, and role
limitation - emotional. The SF-36 includes another one item - reported health
transition (HT) which refers to the perception of health conditions as compared with
the previous one year.
The Chinese version of the SF-36 Health Survey (Chinese Version SF-36) (Appendix
XII), which was translated by Fang (2005), was employed in this study to measure
quality of life. According to the study by Zhang, Xu, Huang, and Li (2004), the split -
half reliability coefficient of the Chinese Version of the SF-36 was 0.94 and test-retest
reliability coefficients for most subscales ranged from 0.60 to 0.90 when tested on
167 elderly adults. Liu, Li, Ren and others (2001) tested its reliability on various
groups in China. They found that the internal consistency reliability coefficient alpha
of the Chinese version of the SF-36 ranged from 0.62 to 0.94 when tested on 1,603
rural residents, 0.68 to 0.82 on 646 urban residents, 0.79 to 0.95 on 122 patients with
osteoporosis, and 0.78 to 0.95 on 150 stroke patients. Jiang, Sit, Wong, and others
(2004) also tested it on 167 patients with CHD. They found that the internal consistent
reliability coefficient alpha values for general health, physical functioning, role
physical, role emotional, social functioning, bodily pain, vitality, and mental health at
the two assessment times were 0.84 and 0.77, 0.91 and 0.90, 0.90 and 0.63, 0.85 and
0.85, 0.79 and 0.67, 0.81 and 0.81, 0.67 and 0.68, and 0.69 and 0.70, respectively; the
corresponding test-retest reliability coefficients for these eight scales were 0.76, 0.79,

169
0.63, 0.66, 0.67, 0.66, 0.62, and 0.65. To prepare the data for analysis, the raw scores
obtained from each SF-36 domain were finally transformed in a 0 to 100 scale based
on the transformation formula recommended by Fang (2005). Scores for all areas
were calculated using the medical outcomes study (MOS) scoring system (Fang, 2005)
(Appendix XIII). Each subscale was computed to give a scaled score from 0 (lowest
well-being) to 100 (highest well-being).
The SAQ is a disease-specific questionnaire for CHD patients. It was developed to
assess the quality of life of CHD patients in relation to angina. The SF-36 is a generic
health survey scale and is widely used to assess the quality of life of people in China
and other countries. It includes both physical and mental components. In recent years,
many researchers have recommended that both the generic and disease-specific
instruments should be used together to evaluate quality of life (Arthur, Smith &
Natarajan, 2008; Brodie, Inoue & Shaw, 2008; Dempster & Donnelly, 2000; Lie,
Arnesen, Sandvik, Hamilton & Bunch, 2009; McGillion, Watt-Watson, Stevens et al.,
2008; Wong & Chair, 2007). The combination of both the generic and disease-
specific instruments to measure quality of life provides complementary information
(Lie, Arnesen, Sandvik, Hamilton & Bunch, 2009) to obtain both sensitivity and
specificity in clinical change (Brodie, Inoue & Shaw, 2008); and allows comparison
of the results with both the general population and CHD patients, making clinical
interpretation more meaningful (Arthur, Smith & Natarajan, 2008; Lie, Arnesen,
Sandvik, Hamilton & Bunch, 2009). In addition, although the SF-36 is a
comprehensive instrument to measure health-related quality of life and can
discriminate between patients with divergent medical, psychiatric, and other serious
medical conditions, some evidence suggests that it may inadequately discriminate

170
between those with different severities of angina as assessed by the Canadian
Cardiovascular Society Classification (Dougherty, Dewhurst, Nichol & Spertus,
1998). The potential for the SF-36 to be insensitive to changes in angina class
necessitated the use of a disease-specific instrument, the SAQ, to evaluate quality of
life. Thus, both the SAQ and SF-36 were used to assess the quality of life of CHD
patients in this study.
3.8 Data collection
Data collection was done at four time points by the RN (Figure 3.1). The first (T0)
round of data collection was conducted after the patients were recruited and before the
group assignment. The second (T1) round of data collection was conducted
immediately after the completion of the 8-week ESMI. The third (T2) round of data
collection was conducted three months after the completion of the intervention. The
final (T3) round of data collection was conducted six months after the intervention.
Before the commencement of data collection, the RN underwent training on how to
collect data. To set clear guidelines for the nurse, a training package (Appendix XIV)
was prepared for her. The RN was blind to the group assignment, research design,
research hypotheses, and the interventions in order to prevent any subjective bias
from occurring, so that a single-blind condition could be achieved.

171
3.9 Ethical Considerations
Ethical approval (Appendix II) was granted from the Human Subjects Ethics
Committee of The Hong Kong Polytechnic University and access approvals
(Appendix III) were obtained from the Xiamen Heart Centre, the First Affiliated
Hospital of Xiamen University, and the Medical Service Centre of Lujiang
Community. The study was explained to each patient using a written information
sheet (Appendix V). Written consent (Appendix VI) was obtained from each patient
before he/she participated in the study. Patients were allowed to withdraw from the
study at any time and for any reason, with no penalty. A code number was assigned to
each patient. All of the information provided by the patients was kept confidential and
anonymous. Only the members of the research team could access the data. Since it
was believed that the booklet provided in the patient education session would be of
benefit to all patients, patients in the Conventional group also received the booklet
after the completion of the study.
Regular exercise/physical activity has been shown to be beneficial to cardiac patients.
This study aims to motivate CHD patients to engage in exercise, so the study is
believed to benefit them. Some patients might experience mild chest discomfort while
exercising. To minimize the risk to the patient, cardiologists assessed the physical,
psychological, and emotional status of each patient according to the screening
guidelines (Appendix IV) before referring him/her to this study. During the
intervention, when the patients were in the preparation stage and ready to engage in
exercise, the cardiologists assessed them again and prescribed exercise according to
the guidelines for exercise prescription (Appendix VIII). Each patient‘s progress in

172
exercise intensity and exercise duration was monitored weekly so that he or she would
not be overloaded by the prescribed exercise. Each patient was instructed to contact
the researcher at any time by phone if he/she experienced any discomfort during the
intervention.
The researcher contacted each patient in the intervention groups weekly during the 8-
week intervention period to check whether he/she was experiencing any discomfort
while exercising. If the patients were experiencing discomfort, they would be
instructed to cut down on the intensity and duration of the exercise or to stop
exercising altogether, and were again assessed by the cardiologists on their exercise
prescription.
Clear guidelines for the termination of exercise done at home were given to each
patient in both the PE and ESMI groups, with reference to the recommendations from
the expert working group of the National Heart Foundation of Australia (Briffa,
Maiorana, Sheerin et al., 2006) (Appendix VIII).
3.10 Data Analysis
Data analyses were carried out based on the intention-to-treat principle of analysis.
Last observation carried forward (LOCF) was used to handle missing data. The data
analyses were conducted using the Statistical Package for the Social Sciences, version
17.0 (SPSS Inc., Chicago, II USA). Data analyses include both descriptive and
inferential statistical analyses. Descriptive statistics such as frequencies, means,
standard deviations, and percentages were used to describe the demographic and

173
clinical data and to outline outcome measures at different time points. A further
selection of inferential statistics for between- and within-group comparisons was
based on the data as well as on the normality and homogeneity of variance tests. For
data that are intervals or ratio data, normally distributed and insignificant on the
homogeneity of variance test, parametric inferential statistics were used. Otherwise,
non-parametric tests were applied.
The baseline demographic and clinical data, with the exception of level of education,
age, and depression, were treated as nominal data. Data on levels of education and
exercise stages of change were treated as ordinal data. Data on age, depression,
exercise self-efficacy, exercise benefits, exercise barriers, exercise duration per week,
angina frequency, angina severity, angina duration per week, and quality of life on
both SAQ and SF-36 were treated as interval data.
After conducting the normality and homogeneity tests, only data on exercise self-
efficacy was normally distributed. Data on age, depression, exercise benefits, exercise
barriers, exercise duration per week, angina frequency, angina severity, angina
duration per week, and quality of life on both SAQ and SF-36 were not normally
distributed and the related homogeneity of variance among the three groups was
violated.
Regarding the nominal and ordinal demographic and clinical data, such as gender,
marital status, current employment status, and occupation, a Chi-square test was used
to compare the differences among the C, PE, and ESMI groups. For the interval and

174
ratio demographic data, such as depression, the Kruskal-Wallis test was used to
compare the differences among the three groups.
Data on the exercise stages of change were treated as ordinal data. The Kruskal-
Wallis Test was used to examine the differences in the mean change values among the
C, PE, and ESMI groups at T0, T1, T2, and T3, respectively. Compared to the baseline,
the patients were also classified into progressed, stable, and regressed cases based on
the exercise stages of change scale at T1, T2, and T3, respectively. All of these data
were viewed as nominal data. The Chi-square test was used to analyze such data
among the C, PE, and ESMI groups at T1, T2, and T3, respectively. The Friedman test
was applied to examine the differences within groups across time from T0 to T3.
Since data on the exercise self-efficacy scale were normally distributed and the related
homogeneity of variance was achieved, one way ANOVA was applied to examine the
differences in the mean change values among the C, PE, and ESMI groups at T0, T1,
T2, and T3, respectively. One way repeated ANOVA was applied to examine the
differences within groups across time from T0 to T3.
Since data on exercise benefits, exercise barriers, exercise duration per week, angina
frequency, angina severity, angina duration per week, and quality of life on both SAQ
and SF-36 are not normally distributed and the related homogeneity of variance
among the three groups was violated, a non-parametric test was applied. The Kruskal-
Wallis Test was used to examine the differences in the mean change values of these
variables among the C, PE, and ESMI groups at T0, T1, T2, and T3, respectively. The

175
Friedman test was applied to examine the differences within groups across time from
T0 to T3.
Data in the log book on whether patients experienced angina and whether they took
anti-anginal drugs in the past one week were viewed as nominal and binary data. The
Chi-square test was used to analyze the data among the C, PE, and ESMI groups at T0,
T1, T2, and T3, respectively. The Cochran‘s Q test was then applied to examine the
differences within each group across time from T0 to T3.
Intention-to-treat analysis was employed in this study because the availability of the
patients to attend patient education sessions and their willingness to spend time on
patient education were the key factors affecting the accuracy of the findings. In
addition, intention-to-treat analysis was used to maintain the benefits of
randomization. Last observation carried forward (LOCF) is one of the commonly used
ways of handling missing data for intention-to-treat analysis, especially when a
variable is assessed at multiple time points for each patient (Barnes, Mallinckrodt,
Lindborg & Carter, 2008; Elobeid, Padilla, McVie et al., 2009; Herman, Botser,
Tenenbaum & Chechick, 2009; Yan, Lee & Li, 2009). In the LOCF analysis, a
subject‘s last available assessment is imputed for all remaining unobserved response
measurements. In this study, most of the dropouts in the PE and ESMI groups
withdrew from the study before the completion of the 8-week period of ESMI (Figure
5.1). Thus, with the use of LOCF to handle missing data, most of the missing data in
the experimental group is replaced by the baseline data, which may well result in a
conservative estimate of the effects of treatment (Barnes, Mallinckrodt, Lindborg &

176
Carter, 2008; Boers, 2008). Thus, the LOCF was employed to analyze the data in this
study. The significance level, p value, was set at 0.05 with two tails.
3.11 Summary
This chapter described the methods used in this study. An experimental design was
applied in this study. The sampling, procedure, data collection, data analyses, and
ethical considerations were also introduced in this chapter.

177
Chapter 4 The Pilot Study
4.1 Introduction
This chapter presents the results of the pilot study. The pilot study is a trial run of the
main study. This chapter includes a discussion of the aims of the study, the
characteristics of the subjects, the procedures of the study, the preliminary results, and
the implications for the main study.
4.2 Aims
Since there is no formal or structured patient education programme for CHD patients
in China, the aims of the pilot study can be set as follows: (1) to test whether it is
feasible to implement a formal patient education programme in Xiamen City, China;
and (2) to examine the preliminary effects of the TTM-based Exercise Stage-Matched
Intervention (ESMI) on patients with coronary heart disease (CHD).
4.3 Description of the setting
The pilot study was conducted from May 2009 to August 2009 in the Medical Service
Centre of Gulangyu Community, Xiamen City, China. The Gulangyu community is
located on Gulangyu Island, Xiamen City. There are no cars or bicycles on the island.
To reach Gulangyu, people need to take a 5-minute ferry ride from the centre of
Xiamen City. Due to the inconvenient transportation arrangements, many people
move away from Gulangyu Island. There are only around 16,000 permanent residents

178
on this island and most of them are elderly or children. Around 25% of the population
are more than 60 years old. According to the database of the medical records of the
community hospital, the mean age of CHD patients in the hospital is 71.8 years and
most have suffered from the illness for around 10 years.
4.4 Procedures
Before conducting the pilot study, ethical approval was obtained from the Human
Ethics Committee of The Hong Kong Polytechnic University. Access approval was
also obtained from the Medical Service Centre of the Gulangyu Community. The
criteria for screening patients for the pilot study were the same as those for the main
study, except that patients in the action and maintenance stages were also recruited in
the pilot study.
Potential patients were identified from the medical records of the Medical Service
Centre of the Gulangyu Community. They were invited to attend the screening
assessment in the hospital and were given a verbal explanation by phone of the
purposes of the study with reference to the information sheet. They were promised
that there would be no penalty if they refused to participate in or withdrew from the
study during the study period. A cardiologist screened patients according to the
screening guidelines (Appendix IV).
Eligible patients were labelled in accordance with the exercise stages of change scale.
Those labelled as being at the Pre-action level were in the precontemplation,
contemplation, and preparation stages. When patients were in the action and
179
maintenance stages, they were labelled as being at the Action level. Using a random
number table, patients of each level were then randomly allocated to one of the
following three groups: the Conventional (C) Group, the Patient Education (PE)
Group, and the Exercise Stage-Matched Intervention (ESMI) Group. In the original
research proposal, eligible patients were to be randomly allocated to one of the three
groups according to the random number table with reference to a five-stage match
(precontemplation, contemplation, preparation, action, and maintenance) based on the
exercise stages of change scale. The randomization of patients with reference to a pre-
action or action level match instead of a five-stage match is due to the small size of
the sample in the pilot study.
Patients in the C group received the conventional care, consisting of a simple and
unstructured patient education session that included information about diet, exercise,
and medications for CHD patients. Patients in the PE group received the conventional
care, one 2-hour session of patient education about CHD, and a booklet developed by
the Hong Kong Cardiac Rehabilitation and Prevention Centre of Tung Wah Hospital
and the organization Care for Your Heart. The content of the one 2-hour session of
patient education was the same as the one proposed for the main study. Patients in the
ESMI group received the conventional care, one 2-hour session of patient education
about CHD and the booklet (the same as that given to the PE group), eight weekly
ESMI sessions, and a stage-matched pamphlet, as proposed for the main study.
Patient education was delivered in groups. The size of each group ranged from 4 to 8
patients.

180
Data was collected at two time points: before the commencement of any interventions
(T0) and after the completion of the 8-week ESMI (T1) by an RN who was blinded to
the study design and the group allocation. Data collection at the 3-month follow up
(T2) and the 6-month follow-up period (T3) were not conducted due to time
constraints. In addition, the purposes of this pilot study were to test the feasibility of
implementing a patient education programme and to examine the preliminary effects
of the TTM-based ESMI in the patient education programme on CHD patients. After
the completion of the 8-week ESMI sessions, the researcher would have a good idea
of whether or not it would be feasible to implement the patient education programme
in Xiamen City. Comparison of the net changes in each outcome variable among the
three groups after the implementation of the interventions could indicate the trend of
the effects of the TTM-based ESMI on CHD patients. Thus, post-test data collection
was only conducted immediately after the completion of the 8-week ESMI.
After the completion of the pilot study, eight CHD patients who had received and
completed the eight sessions of ESMI were invited to discuss the intervention
programme in terms of both the contacts and the format of the delivery of the
intervention. The purpose of the discussion was to evaluate the relevance,
appropriateness, and feasibility of the intervention for CHD patients.
4.5 Results
Fifty-five patients were contacted for screening. Twenty-five CHD patients, who met
the selection criteria, were recruited in this study. Before the commencement of any
interventions, four patients withdrew from the study for the reasons listed in Figure

181
4.1. In the end, 21 patients completed the study. In this study, patients who did not
attend the one 2-hour patient education session about CHD, did not receive at least
two face-to-face contacts over the eight weeks, did not attend at least four of the eight
ESMI sessions, or did not complete the data collection procedures were viewed as
having dropped out of the study.
An intention-to-treat analysis was performed in this study. The missing data were
replaced by the baseline data. The Chi-square test and Kruskal-Wallis test were
applied for comparisons of the demographic and clinical data and net changes in the
outcome variables after the implementation of the interventions among the three
groups.
This pilot study went smoothly. The screening guidelines for the cardiologist to
screen patients were clear and appropriate. Most patients attended the patient
education programme and completed the study. No cardiac events or angina attacks
occurred during the time that the patients were engaged in exercise. These results
suggest that it is feasible to carry out the patient education programme based on the
TTM for CHD patients in Xiamen City, China.
Most of the patients who had received the 8-week TTM-based ESMI said that the
contents and the delivery format of the intervention were useful, appropriate, and
acceptable for CHD patients. Their views suggest that the ESMI is valid and feasible
for use among CHD patients in Xiamen City, China.

182
55 patients participated in screening
30 were excluded from the study according to the selection criteria
25 eligible subjects signed the written consent form
C group (n=8) PE group (n=8) ESMI group (n=9)
T0: Baseline data collection
3 dropouts (One was visiting her son and
looking after her grandson in
other city; one felt it was too
time-consuming and was
reluctant to participate in the
study; the remaining one was
away for a few days.)
1 dropout (The patient complained of
discomfort and received an
IV infusion immediately in
the out-patient
department.)
C group (n=8) PE group (n=5) ESMI group (n=8)
Randomization with reference to exercise level (pre-action or action)
T1: Outcomes measured immediately after the intervention (n=21)
Figure 4.1 Flowchart of the pilot study
Note: C group: the Conventional group; PE group: the Patient Education group; ESMI group: the
Exercise-Stage-Matched Intervention group.

183
4.5.1 Demographic and clinical characteristics
Of the 25 eligible patients, one patient had been diagnosed with myocardial infarction
(MI) and 24 had been diagnosed with angina pectoris. Age ranged from 55 to 83 years,
with the mean age being 67.4 ± 6.6 years. In each group, over 75.0% of the patients
were married and living with their spouse. All of the patients were retired and
currently not working. The details of the characteristics of the patients are shown in
Tables 4.1 and 4.2. The Chi-square test and Kruskal-Wallis test were used to compare
the demographic and clinical data among the three groups. No statistically significant
difference was found among the three groups (Tables 4.1 & 4.2).

184
Table 4.1 Demographic Characteristics of the Subjects
C group
(n = 8)
n (%)
PE group
(n = 8)
n (%)
ESMI group
(n = 9)
n (%)
Chi-square test
χ2 p
Age [mean (SD)] year a 67.0 (7.0) 66.6 (8.1) 68.3 (5.2) 0.529a 0.768a
Gender
Male
Female
3 (37.5)
5 (62.5)
2 (25.0)
6 (75.0)
2 (22.2)
7 (77.8)
0.543 0.762
Marital status
Single/Widow
Married
2 (25.0)
6 (75.0)
0 (0.0)
8 (100)
2 (22.2)
7 (77.8)
2.265 0.322
Education
Elementary School
High School
College or above
1 (12.5)
7 (87.5)
0 (0.0)
1 (12.5)
6 (75.0)
1 (12.5)
1 (11.1)
4 (44.4)
4 (44.4)
5.763 0.218
Occupation before
retirement
Manual labour
Technical
Clerical
Managerial
Professional
Other
2 (25.0)
2 (25.0)
1 (12.5)
1 (12.5)
2 (25.0)
0 (0.0)
2 (25.0)
1 (12.5)
1 (12.5)
2 (25.0)
1 (12.5)
1 (12.5)
0 (0.0)
1 (11.1)
2 (22.2)
3 (33.3)
3 (33.3)
0 (0.0)
6.858 0.739
Religious beliefs
Yes
No
3 (37.5)
5 (62.5)
4 (50.0)
4 (50.0)
3 (33.3)
6 (66.7)
0.521 0.771
Family income
(per month)
≤ ¥5,000
≥ ¥5,001
4 (50.0)
4 (50.0)
3 (37.5)
5 (62.5)
5 (55.6)
4 (44.4)
0.572 0.751
Medical payments
Totally reimbursed
Partially reimbursed
Totally self-paid
0 (0.0)
7 (87.5)
1 (12.5)
1 (12.5)
6 (75.0)
1 (12.5)
0 (0.0)
9 (100)
0 (0.0)
3.551 0.470
Living conditions
Living alone
Living with spouse/
children
1 (12.5)
7 (87.5)
0 (0.0)
8 (100)
2 (22.2)
7 (77.8)
1.983 0.318
a: Kruskal-Wallis test

185
Table 4.2 Clinical Characteristics of the Subjects
C
(n=8)
n (%)
PE
(n=8)
n (%)
ESMI
(n=9)
n (%)
Chi-square test
χ2 p
Diagnosis 2.214 0.331
Angina pectoris 8 (100) 7 (87.5) 9 (100)
MI 0 (0.0) 1 (12.5) 0 (0.0)
PCI/stent 0.405 0.817
Yes 1 (12.5) 1 (12.5) 2 (22.2)
No 7 (87.5) 7 (87.5) 7 (77.8)
CHD family history 3.230 0.199
Yes 4 (50.0) 2 (25.0) 1 (11.1)
No 4 (50.0) 6 (75.0) 8 (88.9)
Diagnosed with DM 0.011 0.995
Yes 1 (12.5) 1 (12.5) 1 (11.1)
No 7 (87.5) 7 (87.5) 8 (88.9)
Diagnosed with hypertension 3.222 0.200
Yes 7 (87.5) 7 (87.5) 5 (55.6)
No 1 (12.5) 1 (12.5) 4 (44.4)
Smoking status 2.249 0.690
Never smoking 6 (75.0) 7 (87.5) 8 (88.9)
Once smoking 1 (12.5) 1 (12.5) 1 (11.1)
Current smoking 1 (12.5) 0 (0.0) 0 (0.0)
Alcohol drinking status 2.214 0.331
Never drinking 7 (87.5) 8 (100) 9 (100)
Once drinking 1 (12.5) 0 (0.0) 0 (0.0)
Current drinking 0 (0.0) 0 (0.0) 0 (0.0)
Current medications
Nitrates 0 (0.0) 1 (12.5) 1 (11.1) 1.034 0.596
Beta-blockers 3 (37.5) 2 (25.0) 1 (11.1) 1.623 0.444
ACE inhibitors 3 (37.5) 2 (25.0) 2 (22.2) 0.543 0.762
Calcium antagonists 3 (37.5) 4 (50.0) 2 (22.2) 1.430 0.489
Anti-platelets 2 (25.0) 2 (25.0) 0 (0.0) 2.679 0.262
Lipid-lowering drugs 1 (12.5) 0 (0.0) 1 (11.1) 1.034 0.596
Others# 1 (12.5) 4 (50.0) 4 (44.4) 2.877 0.237
Depression score [Mean (SD)]a 3.9 (3.8) 3.5 (3.0) 3.1 (2.2) 0.066a 0.967a
a: Kruskal-Wallis test; #: ―Others‖ refers to traditional Chinese anti-anginal medicines, such as the
Suxiaojiuxin pill (速效救心丸), the Shexiangbaoxin pill (麝香保心丸), and the Danshen pill (丹参滴
丸).

186
4.5.2 Exercise Stages of Change (ESC)
As shown in Tables 4.3 and 4.4, more patients in the ESMI group progressed in their
exercise stages of change than those in both the C and PE groups, and patients in the
PE group were more likely to progress in their exercise stages of change than those in
the C group, although no significant difference in changes in exercise stages of
change was detected among the three groups (Table 4.4).
Table 4.3 Distribution of the Exercise Stages of Change (ESC) in the Three Groups
ESC
C group
(n=8)
PE group
(n=8)
ESMI group
(n=9)
T0
n (%)
T1
n (%)
T0
n (%)
T1
n (%)
T0
n (%)
T1
n (%)
Precontemplation 1(12.5) 1(12.5) 0(0.0) 0(0.0) 2(22.2) 0(0.0)
Contemplation 1(12.5) 1(12.5) 0(0.0) 0(0.0) 1(11.1) 1(11.1)
Preparation 3(37.5) 3(37.5) 6(75.0) 2(25.0) 4(44.4) 1(11.1)
Action 1(12.5) 0(0.0) 0(0.0) 4(50.0) 0(0.0) 5(55.6)
Maintenance 2(25.0) 3(37.5) 2(25.0) 2(25.0) 2(22.2) 2(22.2)
T0: baseline data; T1: data immediately after the completion of the 8-week ESMI.
Table 4.4 Changes in the Exercise Stages of Change (ESC) in the Three Groups at T1
ESC
C group
(n=8)
n (%)
PE group
(n=8)
n (%)
ESMI group
(n=9)
n (%)
Chi-square test
χ2 p
Progressed 1 (12.5) 4 (50.0) 6 (67.7) 5.215 0.074
Stable 7 (87.5) 4 (50.0) 3 (33.3)
Progressed: patients moved forward by at least one stage as compared with the baseline; Stable:
patients did not move and there was no change as compared with the baseline.

187
4.5.3 Exercise Self-Efficacy (ESE)
After the interventions were implemented, the mean scores of ESE decreased in both
the C and PE groups, while they increased substantially in the ESMI group (Table
4.5). When the mean change scores of ESE were compared, a significant difference
was found among the three groups (mean rank: ESMI group = 16.4, PE group = 13.3,
C group = 8.9, p = 0.013). Patients in the ESMI group were more confident about
their ability to perform exercise than those in the C and PE groups.
Table 4.5 Changes in the Mean Scores of Exercise Self-Efficacy (ESE) in the Three
Groups
T0 T1 T1 - T0
pa
C
(n=8)
mean
(SD)
PE
(n=8)
mean
(SD)
ESMI
(n=9)
mean
(SD)
C
(n=8)
mean
(SD)
PE
(n=8)
mean
(SD)
ESMI
(n=9)
mean
(SD)
C
(n=8)
mean
(SD)
PE
(n=8)
mean
(SD)
ESMI
(n=9)
mean
(SD)
ESE 1127.5
(322.3)
1075.0
(471.5)
843.3
(208.8)
1058.8
(356.2)
1068.8
(406.8)
1319.4
(319.5)
-68.8
(468.1)
-6.3
(243.0)
476.1
(338.6)
0.013*
a: Kruskal-Wallis Test; T0: baseline data; T1: data immediately after the completion of the 8-week
ESMI; The ESE scores range from 0 to 1,800, with the higher scores indicating greater confidence in
engaging in exercise; * p < 0.05.
4.5.4 Exercise Decisional Balance
There were two scales to determine the exercise decisional balance of the patients: the
Exercise Benefits Scale (EBS) and the Exercise Barriers Scale (EBBS). The higher
the scores of the EBS were, the greater the perception of the benefits of engaging in
exercise. However, when the scores were higher, patients would also have the

188
perception that the barriers to engaging in exercise were greater, in accordance with
the EBBS.
Table 4.6 shows the changes in exercise decisional balance among the three groups.
An increase in the mean scores of EBS at T1 was seen for all of the groups. The
participants perceived exercise to be beneficial to them regardless of any interventions
that were being implemented. No significant differences in the mean change scores of
EBS were detected among the three groups (Table 4.6). All of the groups saw a
decrease in the mean scores of EBBS at T1. They perceived fewer barriers to engaging
in exercise, regardless of any interventions that were being implemented. Significant
differences in the mean change scores of EBBS were identified among the three
groups (mean rank: ESMI group = 9.3, PE group = 18.6, C group = 11.6, p = 0.027),
with the ESMI group demonstrating the greatest reduction in the mean change score
for EBBS, followed by the C group, and the PE group.
Table 4.6 Changes in the Mean Scores of the Exercise Benefits Scale (EBS) and Exercise
Barriers Scale (EBBS) in the three groups
T0 T1 T1 - T0
pa
C
(n=8)
mean
(SD)
PE
(n=8)
mean
(SD)
ESMI
(n=9)
mean
(SD)
C
(n=8)
mean
(SD)
PE
(n=8)
mean
(SD)
ESMI
(n=9)
mean
(SD)
C
(n=8)
mean
(SD)
PE
(n=8)
mean
(SD)
ESMI
(n=9)
mean
(SD)
EBS 81.6
(11.8)
84.3
(8.1)
87.7
(9.0)
87.3
(13.5)
89.9
(9.5)
90.0
(8.6)
5.6
(7.5)
5.6
(6.1)
2.3
(5.3)
0.512
EBBS 29.6
(7.5)
23.3
(6.1)
28.9
(4.5)
24.0
(8.0)
22.8
(5.3)
20.8
(6.2)
-5.6
(5.4)
-0.5
(2.8)
-8.1
(6.2)
0.027*
a: Kruskal-Wallis Test; T0: baseline data; T1: data immediately after the completion of the 8-week
ESMI; The EBS scores range from 29 to 116, with the higher scores indicating greater benefits from
engaging in exercise; The EBBS scores range from 14 to 56, with the lower scores indicating fewer
barriers to engaging in exercise; * p < 0.05.

189
4.5.5 Exercise
Changes in the exercise duration (minutes/week) were investigated. As shown in
Table 4.7, the duration of both total and moderate exercise (minutes/week) increased
among all three groups after the intervention was implemented. The ESMI group
showed the greatest increase in both total and moderate exercise duration per week
among the three groups after the interventions were implemented, while the C group
demonstrated the least improvement in exercise duration. Significant differences in
the mean change of the total exercise duration (minutes/week) were found among the
three groups (mean rank: ESMI group = 17.1, PE group = 13.5, C group = 7.9, p =
0.037) (Table 4.7).
Table 4.7 Changes in the Mean Minutes of the Total Exercise Duration (TED) and
Moderate Exercise Duration (MED) per week in the Three Groups
T0 T1 T1 - T0
pa
C
(n=8)
mean
(SD)
PE
(n=8)
mean
(SD)
ESMI
(n=9)
mean
(SD)
C
(n=8)
mean
(SD)
PE
(n=8)
mean
(SD)
ESMI
(n=9)
mean
(SD)
C
(n=8)
mean
(SD)
PE
(n=8)
mean
(SD)
ESMI
(n=9)
mean
(SD)
TED 421.4
(318.2)
203.8
(276.3)
176.7
(202.0)
423.8
(200.5)
441.3
(252.6)
571.1
(346.4)
2.5
(196.7)
237.5
(274.0)
394.4
(383.5)
0.037*
MED 245.0
(272.6)
136.3
(144.2)
158.3
(198.7)
246.3
(251.1)
271.3
(185.7)
423.3
(280.2)
1.3
(86.6)
135.0
(211.0)
265.0
(265.5)
0.114
a: Kruskal-Wallis Test; T0: baseline data; T1: data immediately after the completion of the 8-week
ESMI.

190
4.5.6 Angina
As shown in Table 4.8, no significant differences in the mean change of angina
frequency (episodes/week), angina severity, and angina duration (minutes/week) were
found among the three groups. Due to the fact that most patients prefer to take
traditional Chinese anti-anginal medications, such as the heart-protecting musk pill
(Shexiangbaoxin pill), the Danshen pill, and the Suxiaojiuxin pill instead of nitrates,
the number of sublingual glyceryl trinitrate (GTN) used per week was not calculated.
Table 4.8 Changes in Angina Frequency (AF), Angina Severity (AS), and Angina
Duration (AD) in the Three Groups
T0 T1 T1 - T0
pa
C
(n=8)
mean
(SD)
PE
(n=8)
mean
(SD)
ESMI
(n=9)
mean
(SD)
C
(n=8)
mean
(SD)
PE
(n=8)
mean
(SD)
ESMI
(n=9)
mean
(SD)
C
(n=8)
mean
(SD)
PE
(n=8)
mean
(SD)
ESMI
(n=9)
mean
(SD)
AF 0.6
(0.5)
0.8
(0.7)
1.8
(3.0)
0.6
(0.9)
0.6
(0.7)
1.1
(2.3)
0.0
(0.9)
-0.1
(0.4)
-0.6
(2.1)
0.909
AS 1.9
(1.8)
1.3
(1.3)
1.1
(1.5)
1.1
(2.4)
0.8
(1.0)
0.9
(1.3)
-0.8
(2.2)
-0.5
(1.1)
-0.2
(1.5)
0.690
AD 3.1
(3.5)
1.4
(1.7)
1.2
(1.6)
10.8
(20.8)
1.4
(1.8)
4.4
(9.8)
7.6
(21.7)
0.0
(0.5)
3.2
(9.5)
0.876
a: Kruskal-Wallis Test; AF: Angina Frequency (episodes/week); AS: Angina Severity (0-10), with the
higher scores indicating more serious angina; AD: Angina Duration (minutes/week); T0: baseline data;
T1: data immediately after the completion of the 8-week ESMI.
191
4.5.7 Quality of life
In this study, the patients‘ quality of life was measured using the Seattle Angina
Questionnaire (SAQ) and the Medical Outcomes Study 36-Item Short-Form (SF-36).
4.5.7.1 Seattle Angina Questionnaire (SAQ)
The SAQ consists of the following five subscales: physical limitation, angina stability,
angina frequency, treatment satisfaction, and disease perception. Table 4.9 shows that,
after the interventions were implemented, the mean scores of five subscales of SAQ
increased for both the PE and ESMI groups while the mean scores of angina stability,
treatment satisfaction, and disease perception decreased for the C group. Significant
differences in the mean change scores of angina stability were identified among the
three groups (mean rank: PE group = 17.2, ESMI group = 14.4, C group = 7.3, p =
0.014), with the C group having the lowest scores.

192
Table 4.9 Changes in the Mean Scores of the Five Subscales of SAQ in the Three Groups
T0 T1 T1 - T0
pa
C
(n=8)
mean
(SD)
PE
(n=8)
mean
(SD)
ESMI
(n=9)
mean
(SD)
C
(n=8)
mean
(SD)
PE
(n=8)
mean
(SD)
ESMI
(n=9)
mean
(SD)
C
(n=8)
mean
(SD)
PE
(n=8)
mean
(SD)
ESMI
(n=9)
mean
(SD)
Physical
limitations
75.7
(19.5)
72.9
(18.2)
73.8
(16.7)
82.1
(16.5)
81.3
(9.6)
83.6
(11.4)
6.4
(25.4)
8.3
(12.9)
9.9
(12.9)
0.511
Angina
stability
65.6
(18.6)
50.0
(18.9)
61.1
(22.1)
37.5
(13.4)
59.4
(12.9)
61.1
(13.2)
-28.1
(20.9)
9.4
(22.9)
0.0
(25.0)
0.014*
Angina
frequency
85.0
(14.1)
76.3
(21.3)
82.2
(26.8)
87.5
(14.9)
87.5
(14.9)
84.4
(17.4)
2.5
(19.8)
11.3
(21.0)
2.2
(17.2)
0.652
Treatment
satisfaction
78.1
(12.5)
79.7
(16.3)
62.5
(23.4)
76.6
(22.1)
82.0
(8.5)
74.3
(25.1)
-1.6
(22.8)
2.3
(13.7)
11.8
(23.9)
0.425
Disease
perception
64.6
(22.6)
61.5
(17.2)
66.7
(18.6)
61.5
(23.1)
66.7
(17.8)
72.2
(20.4)
-3.1
(24.8)
5.2
(12.5)
5.6
(22.8)
0.643
a: Kruskal-Wallis Test; T0: baseline data; T1: data immediately after the completion of the 8-week
ESMI; The scores of each subscale of SAQ range from 0 to 100, with the higher scores indicating a
better quality of life.
4.5.7.2 SF-36
As shown in Table 4.10, after the interventions were implemented, for all three groups,
the mean scores of physical functioning, role-physical, social functioning, role-
emotional, physical component summary, and mental component summary increased,
and the mean score for reported health transition decreased. In addition, higher mean
change scores of vitality and mental health were seen for the ESMI group as
compared with those for the C and PE groups. When the mean change scores of the
eight domains, the physical component summary, mental component summary, and

193
reported health transition of SF-36 were compared among the three groups, no
significant differences were identified among them (Table 4.10).

194
Table 4.10 Changes in the Mean Scores of the Eight Domains of SF-36 in the Three
Groups
T0 T1 T1 - T0
pa
C
(n=8)
mean
(SD)
PE
(n=8)
mean
(SD)
ESMI
(n=9)
mean
(SD)
C
(n=8)
mean
(SD)
PE
(n=8)
mean
(SD)
ESMI
(n=9)
mean
(SD)
C
(n=8)
mean
(SD)
PE
(n=8)
mean
(SD)
ESMI
(n=9)
mean
(SD)
Physical
functioning
82.5
(9.3)
82.5
(11.0)
79.4
(13.8)
86.3
(11.9)
88.8
(6.4)
87.8
(6.7)
3.8
(12.5)
6.3
(8.3)
8.3
(16.4)
0.668
Role-
physical
50.0
(32.7)
84.4
(35.2)
61.1
(48.6)
75.0
(46.3)
90.6
(18.6)
75.0
(33.1)
25.0
(50.0)
6.3
(41.7)
13.9
(39.7)
0.789
Bodily pain 66.4
(21.9)
66.9
(5.5)
69.9
(23.6)
65.4
(16.4)
71.5
(21.7)
60.3
(17.3)
-1.0
(14.1)
4.6
(21.6)
-9.6
(19.6)
0.477
General
health
37.1
(28.8)
60.4
(18.6)
58.4
(22.5)
42.5
(29.6)
66.9
(13.2)
57.3
(18.1)
5.4
(9.3)
6.5
(13.7)
-1.1
(11.9)
0.425
Vitality
64.4
(20.1)
73.8
(20.7)
60.6
(21.4)
61.3
(23.9)
77.5
(13.1)
78.3
(13.9)
-3.1
(19.4)
3.8
(17.1)
17.8
(13.7)
0.056
Social
functioning
70.3
(25.8)
76.6
(15.6)
70.8
(16.5)
71.9
(26.5)
84.4
(18.6)
84.7
(13.7)
1.6
(35.6)
7.8
(13.3)
13.9
(17.1)
0.631
Role-
Emotional
50.0
(47.1)
70.8
(41.6)
74.1
(43.4)
79.2
(39.6)
83.3
(35.6)
88.9
(33.3)
29.2
(45.2)
12.5
(35.4)
14.8
(33.8)
0.610
Mental
health
56.5
(17.4)
67.5
(5.8)
57.3
(13.4)
55.0
(18.1)
65.5
(8.0)
65.8
(2.9)
-1.5
(7.7)
-2.0
(10.7)
8.4
(13.0)
0.316
PCS 236.0
(73.3)
294.1
(52.1)
268.9
(86.2)
269.1
(89.1)
317.8
(49.6)
280.4
(47.5)
33.1
(58.1)
23.6
(48.8)
11.6
(68.1)
0.772
MCS 241.2
(91.7)
288.7
(75.0)
262.8
(77.3)
267.3
(80.5)
310.7
(57.9)
317.7
(50.3)
26.1
(71.7)
22.1
(61.7)
54.9
(39.0)
0.281
HT 3.8
(0.9)
3.1
(1.3)
3.4
(0.7)
3.3
(0.5)
2.6
(1.4)
2.7
(0.5)
-0.5
(0.5)
-0.5
(0.9)
-0.8
(0.8)
0.628
a: Kruskal-Wallis Test; The scores of each domain range from 0 to 100, with the higher scores
indicating better health in each domain; PCS: Physical Component Summary (PF + RP + BP + GH);
MCS: Mental Component Summary (VT + SF + RE + MH); HT: Reported Health Transition, the
scores range from 1 to 5, with the lower scores indicating better health conditions; T0: baseline data; T1:
data immediately after the completion of the 8-week ESMI.

195
4.6 Implications for the main study
On the whole, the pilot study went smoothly. The main aims of the pilot study were to
test the feasibility of implementing the patient education programme in China and to
examine the preliminary effects of the TTM-based ESMI on patients with coronary
heart disease. These aims were achieved in the pilot study. The results from the pilot
study showed that the TTM-based ESMI had potentially positive effects on changing
exercise behaviour in terms of exercise stages of change, exercise self-efficacy,
exercise barriers, and exercise duration per week, and quality of life in terms of some
subscales of the SAQ and SF-36. Due to the small sample size, non-parametric tests
were conducted to analyze the data.
Based on the preliminary results, the proposed method and procedures can be
implemented for the main study with the following minor modifications:
4.6.1 Research Setting
Due to the special environment on Gulangyu Island, individuals living in this area are
expected to engage much more actively in physical activities than those living in other
communities in Xiamen City. Therefore, the effects of the TTM-based ESMI on one‘s
exercise behaviour may be minimized. In addition, according to the medical records
of the Medical Service Centre of Gulangyu Community, the mean age of all CHD
patients was 71.8 years old. Thus, it is suggested that the main study should be
conducted in other hospitals in Xiamen City in order to obtain more sedentary and
younger subjects.

196
4.6.2 Selection Criteria
One of the primary outcome variables in this study was the exercise stages of change.
The inclusion of individuals in the action and maintenance stages would result in a
ceiling effect in the exercise stages of change. The possible explanation for why the
TTM-based ESMI did not seem to demonstrate any significant effects on the exercise
stages of change in this pilot study is that patients in the action and maintenance
stages were also recruited in the pilot study, which resulted in a ceiling effect. In order
to avoid the ceiling effect with regard to the exercise stages of change, patients in the
action and maintenance stages will not be recruited in the main study because there is
no room for those who are in the maintenance stage to improve. In addition,
individuals in the action and maintenance stages are already exercising regularly. It is
more significant and meaningful to motivate sedentary CHD patients to change their
exercise behaviour than active ones. Thus, the actual study would only recruit
sedentary CHD patients who are in the precontemplation, contemplation, and
preparation stages according to the exercise stages of change scale. Those who are in
the action or maintenance stage will not be recruited in the main study.
4.6.3 Intervention
In this pilot study, patients in the PE group only received one 2-hour session of patient
education about CHD and the booklet, whereas patients in the ESMI group received
eight weekly sessions of ESMI through face-to-face or telephone contact in addition
to the one 2-hour session of patient education about CHD and the booklet. These

197
different frequencies of contact between the PE and ESMI groups may have
contributed to the better effects of the ESMI on exercise behaviour as compared with
the PE. To make the interventions of the ESMI and PE groups more comparable in
terms of contacts between the researcher and the patients, those in the PE group will
also receive eight weekly contacts face-to-face or over the telephone, the same as
designated for the ESMI group. They will receive at least two sessions of face-to-face
contacts over eight weeks. The contents of the eight weekly contacts will include
checking for compliance with the exercise regime and delivering information
regarding the importance and benefits of regular exercise.
4.6.4 Outcome measurements
Patients in the pilot study preferred to take traditional Chinese anti-anginal drugs,
such as the heart-protecting musk pill (Shexiangbaoxin pill), the Danshen pill, and the
Suxiaojiuxin pill, instead of nitrates when they experience anginal pain or chest
discomfort. Thus, in both the daily angina and daily physical activity records, patients
should record the type and number of any anti-anginalists taken, not only the number
of nitrates taken. In addition, the assessment of angina frequency regarding the taking
of nitrates in the SAQ (i.e., SAQ4: Over the past four week, on average, how many
times have you had to take nitros (nitroglycerin tablets) for your chest pain, chest
tightness, or angina) was changed to all anti-anginal drugs taken for chest pain, chest
tightness, or angina in the past four weeks.

198
4.7 Summary
This chapter presents the results of the pilot study and the implications for the main
study. The pilot study went smoothly, with no cardiac events or angina attacks
occurring during the time that the patients were engaged in exercise. The results
showed that the TTM-based ESMI had potentially positive effects on changing
exercise behaviour and on some domains of quality of life with respect to the SAQ
and SF-36. These findings suggest that it is feasible and effective to implement the
TTM-based ESMI in the patient education programme for CHD patients in Xiamen
City, China.

199
Chapter 5 Results
5.1 Introduction
This chapter presents the results of patient recruitment, the characteristics of the
patients, a comparison of patient characteristics between dropouts and completers of
the study, and the results, which address the research questions.
5.2 Recruitment of patients
A total of 1,140 patients were contacted for screening. Eight hundred and seventy-
seven patients were excluded according to the selection criteria and 67 patients
refused to participate in this study for the following three main reasons: (i) taking care
of grandchildren and have no time to participate in the programme (n = 27); (ii)
feeling that it takes too much time and so refuse to join the programme (n = 24); and
(iii) feel that my current health condition is good and that I do not need to join it (n =
16). Therefore, a total of 944 patients were not recruited in this study.
A total of 196 patients who met the selection criteria were recruited in this study.
They were classified according to the following three exercise stages of change:
precontemplation stage (n = 38), contemplation stage (n = 35), and preparation stage
(n = 123). They were then randomly allocated to one of the following three groups:
the C group (n = 67), the PE group (n = 64), and the ESMI group (n = 65). A total of
46 patients (23.5%) [17 patients in the C group (25.4%), 17 patients in the PE group
(26.6%), and 12 patients in the ESMI group (18.5%)] withdrew from the study during

200
the study period. In this study, dropouts were defined as: (i) patients who did not
attend one 2-hour patient education session about CHD; (ii) patients who did not
receive at least two face-to-face contacts over the eight weeks; (iii) patients who did
not attend at least four of the eight ESMI sessions (50%); or (iv) patients who did not
complete the data collection exercise at each time point. The reasons for the dropouts
are listed in Figure 5.1. The most common reasons were as follows: (i) the patient had
left Xiamen City (e.g., visiting children in another city, returning to the country side,
or going to a foreign country) during the study period; (ii) the patient refused to come
to the hospital due to the bad weather (e.g., too cold in winter or too hot in summer);
and (iii) the patient was busy with work or other tasks such as taking care of
grandchildren. In the end, a total of 150 patients completed the study. The overall
completion rate was 76.5%. The average participation rate of the eight ESMI sessions
was 85.2%. Intention-to-treat (ITT) analysis was employed in this study. Last
Observation Carried Forward (LOCF) was used to handle the missing data.

201
Screening (N=1140)
- Excluded by selection
criteria (n=877)
- Refusal (n=67)
T0: Baseline data collection (N=196)
Randomization with reference to the exercise stages of change
C group (n=67) PE group (n=64) ESMI group (n=65)
4 dropouts - Diagnosed with lung
cancer (1)
- Too busy to take care of
her husband who was
diagnosed with gastric
cancer (1)
- Left Xiamen City (1)
- Refusal (1)
11 dropouts - Diagnosed with lung
cancer (1)
- Too busy to take care of
grandchild (2)
- Left Xiamen City (2)
- Refusal (6)
C group (n=63) T1 PE group (n=53) ESMI group (n=56)
1 dropout - Left Xiamen City (1)
1 dropout - Felt uncomfortable (1)
C group (n=55) PE group (n=52) ESMI group (n=55) T2
C group (n=50) T3 PE group (n=47)
ESMI group (n=53)
5 dropouts - Left Xiamen City (2)
- Not contactable (1)
- Refusal (2)
9 dropouts - Left Xiamen City (3)
- Hospitalized (1)
- Refusal (5)
8 dropouts - Got sick (1)
- Left Xiamen City (2)
- Refusal (5)
5 dropouts - Hospitalized (1)
- Left Xiamen City (2)
- Not contactable (1)
- Refusal (1)
2 dropouts - Refusal (2)
Figure 5.1 Flowchart of the recruitment process

202
5.3 Demographic and clinical characteristics of dropouts versus completers
This section compared the demographic and clinical characteristics of the dropouts
from the study and those who completed the study. Tables 5.1 and 5.2 show that
significant differences between the dropouts and completers were detected in gender,
marital status, type of medical payment, and anti-platelets taken. Dropouts were more
likely to be female, single or widowed, and have to pay for the entire amount of their
medical treatment themselves. Conversely, males, those were married, and those who
received partial reimbursement of their medical expenses (e.g., medical insurance)
were more likely to complete the study. The patients who completed the study were
more likely to take anti-platelets.
Table 5.1 Demographic Characteristics of Dropouts versus Completers
Dropouts
(n=46)
n (%)
Completers
(n=150)
n (%)
χ2 p
Age [mean (SD)] 64.4(11.0) 63.6(9.2) 0.522 a 0.603
Gender 6.198 0.013*
Male 27(58.7) 116(77.3)
Female 19(41.3) 34(22.7)
Marital status 4.866 0.027*
Single/widowed 7(15.2) 8(5.4)
Married 39(84.8) 142(94.7)
Living conditions 0.165 0.544
Living alone 1(2.2) 2(1.3)
Living with spouse and/or
children
45(97.8) 148(98.7)
a t-test;
b Fisher‘s exact test; * p < 0.05;
** p < 0.01.

203
Table 5.1 Continued
Dropouts
(n=46)
n (%)
Completers
(n=150)
n (%)
χ2 p
Education 3.310 0.346
No formal education 3(6.5) 6(4.0)
Elementary school 11(23.9) 21(14.0)
High school 22(47.8) 86(57.3)
College or above 10(21.7) 37(24.7)
Current employment status 3.382 0.184
Not working 41(89.1) 115(76.7)
Part-time work 1(2.2) 6(4.0)
Full-time work 4(8.7) 29(19.3)
Occupation before retirement 4.758 0.446
Manual labour 18(39.1) 40(26.7)
Technical 4(8.7) 21(14.0)
Clerical 6(13.0) 32(21.3)
Managerial 8(17.4) 31(20.7)
Professional 4(8.7) 13(8.7)
Business/Commercial 6(13.0) 13(8.7)
Religious beliefs 2.566 0.277
No belief 28(60.9) 103(68.7)
Buddhism 13(28.3) 40(26.7)
Christianity 5(10.9) 7(4.7)
Family income per month 8.906 0.113
≤ $1,000 RMB 5(10.9) 11(7.3)
$1,001-3,000 RMB 18(39.1) 31(20.7)
$3,001-5,000 RMB 11(23.9) 57(38.0)
$5,001-7,000 RMB 4(8.7) 16(10.7)
$7,001-10,000 RMB 3(6.5) 20(13.3)
≥ $10,001 RMB 5(10.9) 15(10.0)
Type of medical payment 15.079 0.001**
Totally reimbursed 1(2.2) 2(1.3) 0.165 b 0.554
Partially reimbursed 35(76.1) 142(94.7) 13.882 b 0.001**
Totally self-paid 10(21.7) 6(4.0) 14.777 b 0.001**
a t-test;
b Fisher‘s exact test; * p < 0.05;
** p < 0.01.

204
Table 5.2 Clinical Characteristics of dropouts versus completers
Dropouts
(n=46)
n (%)
Completers
(n=150)
n (%)
χ2 p
Diagnosis 0.00 0.997
Angina pectoris 27(58.7) 88(58.7)
MI 19(41.3) 62(41.3)
PCI/stent 3.186 0.074
Yes 25(54.3) 103(68.7)
No 21(45.7) 47(31.3)
CHD family history 0.949 0.330
Yes 6(13.0) 29(19.3)
No 40(87.0) 121(80.7)
Diagnosed with DM 1.562 0.211
Yes 18(39.1) 44(29.3)
No 28(60.9) 106(70.7)
Diagnosed with hypertension 0.003 0.957
Yes 33(71.7) 107(71.3)
No 13(28.3) 43(28.7)
Smoking status 1.378 0.502
Never smoking 26(56.5) 70(46.7)
Quit smoking 13(28.3) 51(34.0)
Current smoking 7(15.2) 29(19.3)
Alcohol drinking status 1.279 0.528
Never drinking 38(82.6) 120(80.0)
Quit drinking 6(13.0) 16(10.7)
Current drinking 2(4.3) 14(9.3)
Current medications
Nitrates 8(17.4) 47(31.3) 3.390 0.066
ß-blockers 31(67.4) 112(74.7) 0.945 0.331
ACE inhibitors 13(28.3) 49(32.7) 0.316 0.574
Calcium antagonists 11(23.9) 55(36.7) 2.564 0.109
Anti-platelets 38(82.6) 139(92.7) 4.068 0.044*
Lipid-lowering drugs 32(69.6) 124(82.7) 3.720 0.054
HADS-D scores [mean (SD)] 2.3(2.3) 2.5(2.3) -0.435 a 0.664
a: t-test; HADS-D: Depression Subscale of the Hospital Anxiety and Depression Scale; * p < 0.05.

205
5.4 Demographic and clinical characteristics of the patients
This section describes and compares the demographic and clinical characteristics of
the three groups of patients to determine whether the random assignment produced
equivalent groups. Table 5.3 shows the demographic characteristics of the patients in
this study. The mean age of the patients was 63.8 years, with a range from 26 to 82
years. More than 70% of the patients were male. The overwhelming majority (92.3%)
of the patients were married and living with family members. More than 70% of the
patients had a high school level of education or above. Nearly 80% of the patients
were retired or not currently working. Before retirement, patients mainly worked as
manual labourers (29.6%) or in clerical (19.4%) and managerial (19.9%) jobs. More
than 60% of the patients had no religious beliefs. Regarding family income per month,
about 70% of the patients had a family income ranging from RMB 1,001- 5,000 per
month. About 80% of the patients had medical insurance. No statistically significant
differences in demographic data were identified among the C, PE, and ESMI groups
as confirmed by the Chi-square test, one-way ANOVA, or the Kruskal-Wallis test
(Table 5.3).

206
Table 5.3 Demographic Characteristics of the Subjects
Total
(N=196)
n (%)
C
(n=67)
n (%)
PE
(n=64)
n (%)
ESMI
(n=65)
n (%)
χ2 p
Age [mean (SD)] year 63.8(9.6) 65.8(10.1) 63.5(8.9) 61.9(9.5) 2.805 a 0.063
≤ 60 years 60(30.6) 14(20.9) 21(32.8) 25(38.5) 9.060 0.060
61-70 years 88(44.9) 29(43.3) 30(46.9) 29(44.6)
> 70 years 48(24.5) 24(35.8) 13(20.3) 11(16.9)
Gender 0.880 0.644
Male 143(73.0) 49(73.1) 49(76.6) 45(69.2)
Female 53(27.0) 18(26.9) 15(23.4) 20(30.8)
Marital status 2.746 0.253
Single/widowed 15(7.6) 8(11.9) 3(4.7) 4(6.2)
Married 181(92.3) 59(88.1) 61(95.3) 61(93.8)
Education 0.293b 0.864
No formal education 9(4.6) 5(7.5) 2(3.1) 2(3.1)
Elementary school 32(16.3) 7(10.4) 14(21.9) 11(16.9)
High school 108(55.1) 38(56.7) 31(48.4) 39(60.0)
College or above 47(24.0) 17(25.4) 17(26.6) 13(20.0)
Current employment
status
3.314 0.507
Not working 156(79.6) 56(83.6) 52(81.3) 48(73.8)
Part-time work 7(3.6) 3(4.5) 1(1.6) 3(4.6)
Full-time work 33(16.8) 8(11.9) 11(17.2) 14(21.5)
Occupation before
retirement
15.635 0.111
Manual labour 58(29.6) 21(31.3) 21(32.8) 16(24.6)
Technical 25(12.8) 9(13.4) 7(10.9) 9(13.8)
Clerical 38(19.4) 15(22.4) 12(18.8) 11(16.9)
Managerial 39(19.9) 17(25.4) 11(17.2) 11(16.9)
Professional 17(8.7) 2(3.0) 9(14.1) 6(9.2)
Business/Commercial 19(9.7) 3(4.5) 4(6.3) 12(18.5)
Religious beliefs 6.150 0.188
No belief 131(66.8) 50(74.6) 43(67.2) 38(58.5)
Buddhism 53(27.0) 12(17.9) 17(26.6) 24(36.9)
Christianity 12(6.1) 5(7.5) 4(6.3) 3(4.6)
a: one-way ANOVA; b: Kruskal-Wallis Test.
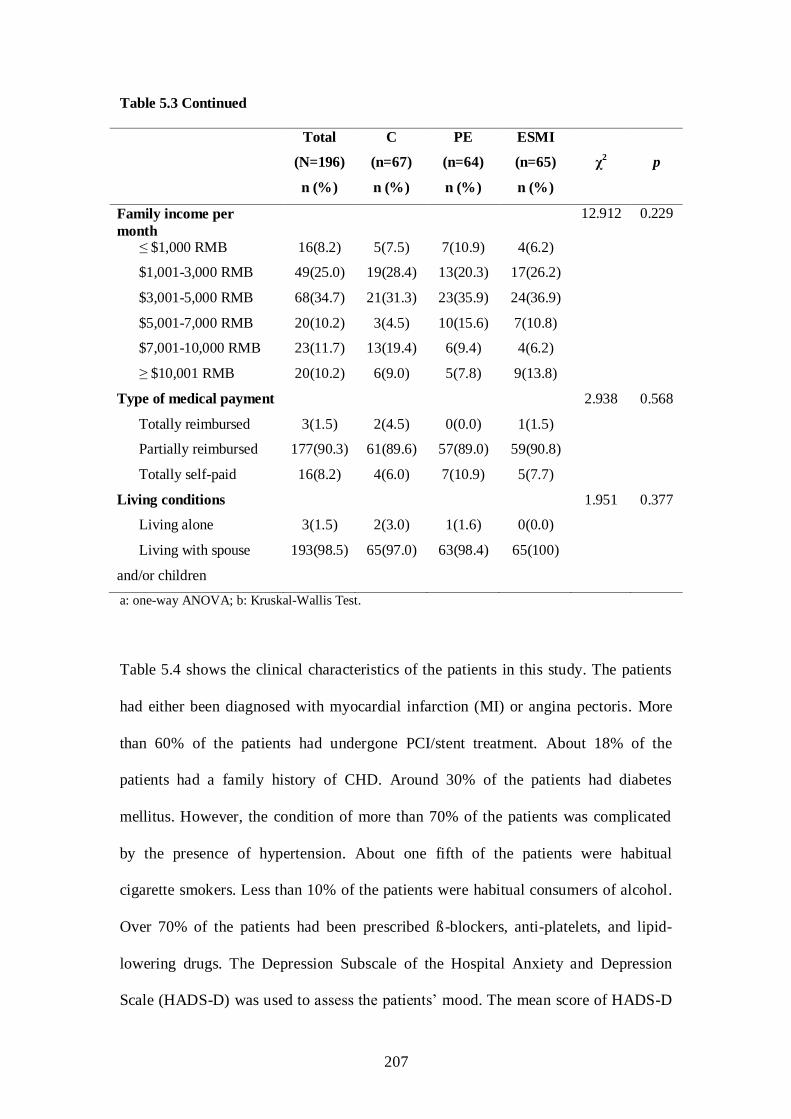
207
Table 5.3 Continued
Total
(N=196)
n (%)
C
(n=67)
n (%)
PE
(n=64)
n (%)
ESMI
(n=65)
n (%)
χ2 p
Family income per
month
12.912 0.229
≤ $1,000 RMB 16(8.2) 5(7.5) 7(10.9) 4(6.2)
$1,001-3,000 RMB 49(25.0) 19(28.4) 13(20.3) 17(26.2)
$3,001-5,000 RMB 68(34.7) 21(31.3) 23(35.9) 24(36.9)
$5,001-7,000 RMB 20(10.2) 3(4.5) 10(15.6) 7(10.8)
$7,001-10,000 RMB 23(11.7) 13(19.4) 6(9.4) 4(6.2)
≥ $10,001 RMB 20(10.2) 6(9.0) 5(7.8) 9(13.8)
Type of medical payment 2.938 0.568
Totally reimbursed 3(1.5) 2(4.5) 0(0.0) 1(1.5)
Partially reimbursed 177(90.3) 61(89.6) 57(89.0) 59(90.8)
Totally self-paid 16(8.2) 4(6.0) 7(10.9) 5(7.7)
Living conditions 1.951 0.377
Living alone 3(1.5) 2(3.0) 1(1.6) 0(0.0)
Living with spouse
and/or children
193(98.5) 65(97.0) 63(98.4) 65(100)
a: one-way ANOVA; b: Kruskal-Wallis Test.
Table 5.4 shows the clinical characteristics of the patients in this study. The patients
had either been diagnosed with myocardial infarction (MI) or angina pectoris. More
than 60% of the patients had undergone PCI/stent treatment. About 18% of the
patients had a family history of CHD. Around 30% of the patients had diabetes
mellitus. However, the condition of more than 70% of the patients was complicated
by the presence of hypertension. About one fifth of the patients were habitual
cigarette smokers. Less than 10% of the patients were habitual consumers of alcohol.
Over 70% of the patients had been prescribed ß-blockers, anti-platelets, and lipid-
lowering drugs. The Depression Subscale of the Hospital Anxiety and Depression
Scale (HADS-D) was used to assess the patients‘ mood. The mean score of HADS-D

208
was 2.5, which showed that the patients in this study were not suffering from
depression. The Kruskal-Wallis test was used to analyze the scores because the scores
were not normally distributed. When using the Chi-square test or the Kruskal-Wallis
test to analyze the clinical data of the C, PE, and ESMI groups, no statistically
significant differences among them were found (Table 5.4).

209
Table 5.4 Clinical Characteristics of the Subjects
Total
(N=196)
n (%)
C
(n=67)
n (%)
PE
(n=64)
n (%)
ESMI
(n=65)
n (%)
χ2 p
Diagnosis 3.249 0.197
Angina pectoris 115(58.7) 34(50.7) 38(59.4) 43(66.2)
MI 81(41.3) 33(49.3) 26(40.6) 22(33.8)
PCI/stent 0.688 0.709
Yes 128(65.3) 42(62.7) 41(64.1) 45(69.2)
No 68(34.7) 25(37.3) 23(35.9) 20(30.8)
CHD family history 2.507 0.286
Yes 35(17.9) 8(11.9) 14(21.9) 13(20.0)
No 161(82.1) 59(88.1) 50(78.1) 52(80.0)
Diagnosed with DM 0.153 0.926
Yes 62(31.6) 20(29.9) 21(32.8) 21(32.3)
No 134(68.4) 47(70.1) 43(67.2) 44(67.7)
Diagnosed with
hypertension
3.650 0.161
Yes 140(71.4) 53(79.1) 41(64.1) 46(70.8)
No 56(28.6) 14(20.9) 23(35.9) 19(29.2)
Smoking status 1.762 0.779
Never smoking 96(49.0) 31(46.3) 30(46.9) 35(53.8)
Quit smoking 64(32.7) 23(34.3) 20(31.3) 21(32.3)
Current smoking 36(18.4) 13(19.4) 14(21.9) 9(13.8)
Alcohol drinking status 3.157 0.532
Never drinking 158(80.6) 55(82.1) 53(82.8) 50(76.9)
Quit drinking 22(11.2) 9(13.4) 6(9.4) 7(10.8)
Current drinking 16(8.2) 3(4.5) 5(7.8) 8(12.3)
Current medications
Nitrates 55(28.1) 20(29.9) 18(28.1) 17(26.2) 0.224 0.894
ß-blockers 143(73.0) 53(79.1) 46(71.9) 44(67.7) 2.235 0.327
ACE inhibitors 62(31.6) 20(29.9) 19(29.7) 23(35.4) 0.633 0.729
Calcium antagonists 66(33.7) 26(38.8) 15(23.4) 25(38.5) 4.460 0.108
Anti-platelets 177(90.3) 58(86.6) 59(92.2) 60(92.3) 1.626 0.443
Lipid-lowering drugs 156(79.6) 53(79.1) 49(76.6) 54(83.1) 0.857 0.651
HADS-D scores [mean (SD)]
2.5(2.3) 2.2(2.3) 2.8(2.4) 2.4(2.0) 3.420 a 0.181
a: Kruskal-Wallis test; HADS-D: Depression Subscale of the Hospital Anxiety and Depression Scale.

210
5.5 Effects of the Exercise Stage-Matched Intervention (ESMI)
Before the data analysis, skewness, kurtosis, the Kolmogorov-Smirnov test, and Q-Q
plot were employed to explore whether the data were normally distributed. The
Levene's test was used to explore the homogeneity of variance among the three
groups for each piece of data at each time point. The results showed that only the
scores of the exercise self-efficacy scale were normally distributed, and the related
homogeneity of variance was achieved at each time point (Appendix XV). Thus,
parametric tests were employed for the analyses of the data on exercise self-efficacy.
Non-parametric tests were applied for other data.
5.5.1 Exercise Stages of Change
Exercise stages of change is a core construct of the TTM. There are five stages,
namely, the precontemplation, contemplation, preparation, action, and maintenance
stages. The higher the stage, the better the exercise behaviour. In this section, the
effects of the TTM-based ESMI on exercise stages of change were presented as the
following research question:
Q1: Will the CHD patients who participated in the Exercise Stage-Matched
Intervention (ESMI) group demonstrate a more positive shift in exercise stages
of change than the patients in the Patient Education (PE) group and the
Conventional (C) group?

211
Table 5.5 and Figure 5.2 show the shifts in the exercise stages of change among the
three groups throughout the study. All of the CHD patients in the three groups were
motivated to engage in exercise after the intervention. More patients in the ESMI
group were in the action and maintenance stages than those in the PE and C groups
from T1 to T3. Slightly more than 60% (40/65) of the patients in the ESMI group were
in the action/maintenance stage immediately after the 8-week intervention (T1),
around 55% (36/65) at the 3-month follow up (T2), and over 40% (27/65) at the 6-
month follow up (T3). A trend of a reduction in the proportion of those in the
action/maintenance stage in the ESMI group was observed during the follow-up
period. In the PE group, around 17% (11/64) of the patients were in the
action/maintenance stage immediately after the 8-week intervention (T1), nearly 30%
(19/64) at the 3-month follow up (T2), and over 20% (14/64) at the 6-month follow up
(T3). For the C group, 4.5% (3/67) of the patients were in the action/maintenance
stage immediately after the 8-week intervention (T1), 7.5% (5/67) at the 3-month
follow up (T2), and 12% (8/67) at the 6-month follow up (T3).

212
Table 5.5 Exercise Stages of Change at Each Time Point
C group
(n=67)
n (%)
PE group
(n=64)
n (%)
ESMI group
(n=65)
n (%)
T0 Precontemplation 10(14.9) 17(26.6) 11(16.9)
Contemplation 9(13.4) 9(14.1) 17(26.2)
Preparation 48(71.6) 38(59.4) 37(56.9)
T1 Precontemplation 11(16.4) 9(14.1) 2(3.1)
Contemplation 9(13.4) 5(7.8) 2(3.1)
Preparation 44(65.7) 39(60.9) 21(32.3)
Action 3(4.5) 11(17.2) 40(61.5)
T2 Precontemplation 13(19.4) 9(14.1) 2(3.1)
Contemplation 3(4.5) 7(10.9) 3(4.6)
Preparation 46(68.7) 29(45.3) 24(36.9)
Action 5(7.5) 19(29.7) 36(55.4)
T3 Precontemplation 6(9.0) 8(12.5) 2(3.1)
Contemplation 6(9.0) 5(7.8) 5(7.7)
Preparation 47(70.1) 37(57.8) 31(47.7)
Action 4(6.0) 6(9.4) 5(7.7)
Maintenance 4(6.0) 8(12.5) 22(33.8)
T0: baseline data; T1: data immediately after the completion of the 8-week intervention; T2: data at the
3-month follow up; T3: data at the 6-month follow up.

213
Figure 5.2 The Number of Patients in the Action and Maintenance
Stages at Each Time Point
03
58
0
11
19
14
0
40
36
27
0
5
10
15
20
25
30
35
40
45
T0 T1 T2 T3
Time
Nu
mb
er o
f P
ati
ents
in
th
e A
ctio
n a
nd
Ma
inte
na
nce
Sta
ges
C
PE
ESMI
Patients were divided into the categories of progressed, stable, and regressed after the
8-week intervention when compared to their baseline exercise stages of change. When
compared with the baseline, patients who progressed or moved forward at least one
stage higher were classified as progressed; patients who did not make any movement
in their exercise stages of change were classified as stable; and those who had
regressed or moved backward at least one stage lower were classified as regressed. As
shown in Table 5.6, in the ESMI group, more than 75% of the patients progressed in
their exercise stages of change immediately after the completion of the 8-week
intervention (T1) as compared with the baseline, slightly over 70% at the 3-month
follow up (T2), and more than 60% at the 6-month follow up (T3); in the PE group,
nearly 40% of the patients progressed in their exercise stages of change immediately
after the completion of the 8-week intervention (T1) as compared with the baseline,

214
and over 40% at both the 3- and 6-month follow up (T2 & T3); in the C group, slightly
over 10% of the patients progressed in their exercise stages of change immediately
after the completion of the 8-week intervention (T1), 18% at the 3-month follow up
(T2), and around 25% at the 6-month follow up (T3). No significant differences in
exercise stages of change among the three groups were detected at baseline (T0) (p =
0.199) (Appendix XVI). Significant differences in the movement of the exercise
stages of change were identified among the three groups at T1 (p < 0.01), T2 (p < 0.01)
and T3 (p < 0.01), when the Chi-square test was adopted to analyze the data (Table
5.6). These findings suggest that the patients in the ESMI group were more likely to
progress in their exercise stages of change after the completion of the 8-week
intervention and during the 6-month follow-up period as compared with those in the
PE and C groups.
The effect sizes (odd ratio, OR) of the ESMI on progression ranged from 5.2 to 24.6
immediately after the 8-week intervention as compared with the PE and C group,
respectively. This finding suggests that the patients in the ESMI group were 5.2 and
24.6 times more likely to progress in their exercise stages of change immediately after
the completion of the 8-week intervention as compared with those in the PE and C
group, respectively. The OR ranged from 2.1 to 3.1 and from 4.4 to 11.1 at the 3 - and
6-month follow-up, which suggests that the patients who participated in the ESMI
group were 2.1-3.1 and 4.4 -11.1 times more likely to progress their exercise stages of
change than those in the PE and C groups, respectively, during the 3- and 6-month
follow-up period. These findings reveal that the patients who participated in the ESMI
group demonstrated a more positive shift in exercise stages of change than those in
the PE and C groups.

215
Table 5.6 Comparisons of Movement of Exercise Stages of Change among Groups at
Each Time Point
C group
(n=67)
n (%)
PE group
(n=64)
n (%)
ESMI group
(n=65)
n (%)
χ2 p
Effect size
ORa OR
b
T1 Progressed 8(11.9) 25(39.1) 50(76.9) 59.151 0.000** 24.6 5.2
Stable 52(77.6) 36(56.3) 15(23.1)
Regressed 7(10.4) 3(4.7) 0(0)
T2 Progressed 12(17.9) 28(43.8) 46(70.8) 39.743 0.000** 11.1 3.1
Stable 47(70.1) 32(50.0) 19(29.2)
Regressed 8(11.9) 4(6.3) 0(0)
T3 Progressed 18(26.9) 28(43.8) 40(61.5) 16.787 0.002** 4.4 2.1
Stable 44(65.7) 34(53.1) 23(35.4)
Regressed 5(7.5) 2(3.1) 2(3.1)
Progressed: patients move forward at least one stage higher as compared to the baseline; Stable:
patients do not move any stage as compared to the baseline; Regressed: patients move backward at
least one stage lower as compared to the baseline; T1: data immediately after the completion of the 8-
week intervention; T2: data at the 3-month follow up; T3: data at the 6-month follow up; ** p < 0.01; a:
calculated OR as compared with the C group; b: calculated OR as compared with the PE group.
A recommended alternative approach to conceptualizing stage progression as a
trichotomous variable would be to count the number of stages progressed as the outcome
variable (Nigg, 2002). For example, an individual progressing a single stage (e.g.,
progress from the precontemplation to the contemplation stage, or progress from the
preparation to the action stage) would receive a score of 1, while an individual
progressing two stages would receive a score of 2 (e.g., progress from the contemplation
to the action stage), and so on. Regression to an earlier stage would be assigned negative
scores. For example, the subjects regressing a single stage (e.g., regress from the

216
contemplation to the precontemplation stage) would receive a negative score of 1; the
subjects regressing two stages would receive a negative score of 2, and so on. Then, the
mean scores of the exercise stages of change in each group were calculated at T1, T2, and
T3. As shown in Table 5.7, all of the three groups demonstrated an increase in the mean
scores of the exercise stages of change from T1 to T3, and the ESMI group demonstrated
higher mean scores of the exercise stages of change than did the PE and C groups.
Significant differences in the mean scores of the exercise stages of change were detected
among the three groups at T1 (mean rank: ESMI group = 134.0, PE group = 95.3, and
C group = 67.2, p < 0.01), T2 (mean rank: ESMI group = 127.0, PE group = 98.5, and
C group = 70.9, p < 0.01) and T3 (mean rank: ESMI group = 119.5, PE group = 96.6,
and C group = 80.0, p < 0.01), when the Kruskal-Wallis test was applied to analyze
the data (Table 5.7).
The effect size (r) of the TTM-based ESMI on the exercise stages of change ranged
from 0.3 to 0.5. According to Cohen (1988), this would be considered a medium (0.25)
to large effect (0.40) for an ANOVA analysis (Table 5.7). Clearly, the patients who
participated in the ESMI group demonstrated a more positive shift in the exercise
stages of change than those in the PE and C groups.

217
Table 5.7 Comparisons of the Mean Change Scores of the Exercise Stages of Change
among Groups at Each Time Point
C group
(n=67)
mean(SD)
PE group
(n=64)
mean(SD)
ESMI group
(n=65)
mean(SD)
Kruskal-Wallis test Effect
size
(r) χ
2 p
T1 - T0 0.0(0.7) 0.5(0.8) 1.1(0.9) 55.461 0.000** 0.5
T2 - T0 0.1(0.8) 0.6(0.9) 1.1(0.9) 37.992 0.000** 0.4
T3 - T0 0.3(0.9) 0.7(1.0) 1.2(1.3) 18.995 0.000** 0.3
** p < 0.01.
When the within-group comparisons were made using the Friedman test, significant
differences in the exercise stages of change were found among all of the three groups
from T0 to T3 (mean rank: C group: T0 = 2.4, T1 = 2.4, T2 = 2.5, T3 = 2.8, p < 0.01; PE
group: T0 = 1.9, T1 = 2.6, T2 = 2.7, T3 = 2.8, p < 0.01; ESMI group: T0 = 1.5, T1 = 2.9,
T2 = 2.7, T3 = 2.9, p < 0.01) (Table 5.8). This finding suggests that all of the three
groups progressed in their exercise stages of change over time.

218
Table 5.8 Comparisons of Exercise Stages of Change within Each Group across Time
Group Variable
T0
n (%)
T1
n (%)
T2
n (%)
T3
n (%)
Friedman test
χ2 p
C
group
Precontemplation 10(14.9) 11(16.4) 13(19.4) 6(9.0) 13.299 0.004**
Contemplation 9(13.4) 9(13.4) 3(4.5) 6(9.0)
Preparation 48(71.6) 44(65.7) 46(68.7) 47(70.1)
Action 0 3(4.5) 5(7.5) 4(6.0)
Maintenance 0 0 0 4(6.0)
PE
group
Precontemplation 17(26.6) 9(14.1) 9(14.1) 8(12.5) 36.364 0.000**
Contemplation 9(14.1) 5(7.8) 7(10.9) 5(7.8)
Preparation 38(59.4) 39(60.9) 29(45.3) 37(57.8)
Action 0 11(17.2) 19(29.7) 6(9.4)
Maintenance 0 0 0 8(12.5)
ESMI
group
Precontemplation 11(16.9) 2(3.1) 2(3.1) 2(3.1) 83.966 0.000**
Contemplation 17(26.2) 2(3.1) 3(4.6) 5(7.7)
Preparation 37(56.9) 21(32.3) 24(36.9) 31(47.7)
Action 0 40(61.5) 36(55.4) 5(7.7)
Maintenance 0 0 0 22(33.8)
T0: baseline data; T1: data immediately after the completion of the 8-week intervention; T2: data at the
3-month follow up; T3: data at the 6-month follow up; ** p < 0.01.
5.5.2 Exercise Self-Efficacy (ESE)
Exercise self-efficacy is one of the main constructs of the TTM. It predicts the change
in exercise behaviour with a linear increase from the precontemplation to the
maintenance stage. The higher scores of the exercise self-efficacy scale indicate more
confidence in engaging in exercise. This section examined the following research
question:

219
Q2: Will the CHD patients who participated in the Exercise Stage-Matched
Intervention (ESMI) group demonstrate higher exercise self-efficacy than the
patients in the Patient Education (PE) group and the Conventional (C) group?
Referring to Table 5.9 and Figure 5.3, the mean scores of the exercise self-efficacy
scale in the ESMI group sharply increased during the period of the implementation of
the intervention (T0) and slowly decreased from T1 to T3, with the mean scores still
higher than the baseline; in the PE group, the mean scores rose steadily during the
period of the implementation of the intervention, and kept rising from T1 to T3; in the
case of the C group, the mean scores slightly declined during the period of the
implementation of the intervention (T1) and then rose from T1 to T3, with the mean
scores higher than the baseline. As a whole, the mean scores of the exercise self-
efficacy scale for the ESMI group were higher than those for the PE and C groups,
and those for the PE group were higher than those for the C group from T1 to T3.
Table 5.9 Mean and Standard Deviations of the Exercise Self-Efficacy (ESE) Scale
Scores at Each Time Point
ESE
C group
(n=67)
mean(SD)
PE group
(n=64)
mean(SD)
ESMI group
(n=65)
mean(SD)
T0 843.3(305.0) 809.5(307.6) 800.5(294.8)
T1 820.1(329.6) 936.9(345.3) 1183.8(360.3)
T2 869.6(344.7) 971.7(371.5) 1158.7(386.1)
T3 977.8(374.5) 1022.8(383.5) 1127.2(395.9)
T0: baseline data; T1: data immediately after the completion of the 8-week intervention; T2: data at the
3-month follow up; T3: data at the 6-month follow up; The scores range from 0 to 1,800 with the higher
scores indicating greater confidence in engaging in exercise.

220
Since the data on exercise self-efficacy were normally distributed and the related
homogeneity of variances among the three groups was achieved (Appendix XV), one-
way ANOVA was applied. At baseline, no significant differences in the mean scores
of the exercise self-efficacy scale were detected among the three groups (p = 0.692)
(Appendix XVI). After the completion of the 8-week intervention, the mean change
scores of the exercise self-efficacy scale were much higher for the ESMI group than
for the PE and C groups, and the mean change scores for the PE group were higher
than those for the C group at T1, T2, and T3 (Table 10). Significant differences in the
mean change scores of the exercise self-efficacy scale were found among the three
groups at T1 (F (2, 193) = 35.9, p < 0.01), T2 (F (2, 193) = 17.6, p < 0.01), and T3 (F (2,
193) = 4.8, p < 0.01) (Table 5.10).

221
The effect size (r) of the TTM-based ESMI on the exercise self-efficacy was 0.5
immediately after the completion of the 8-week intervention (T1) and ranged from 0.2
to 0.4 during the 6-month follow-up period (Table 5.10). This would be viewed as a
medium (0.25) to large effect (0.40) for an ANOVA analysis based on Cohen‘s (1988)
terms. These findings suggest that the patients who participated in the ESMI group
demonstrated higher exercise self-efficacy than those in the PE and C groups. In other
words, the patients who participated in the ESMI group showed greater confidence
about engaging in exercise than those in the PE and C groups.
Table 5.10 Comparisons of the Mean Change Scores of the Exercise Self-Efficacy (ESE)
Scale among Groups at Each Time Point
C group
(n=67)
mean(SD)
PE group
(n=64)
mean(SD)
ESMI group
(n=65)
mean(SD)
One-way ANOVA Effect
size
(r) F p
T1 - T0 -23.2(225.1) 127.3(271.1) 383.4(329.8) 35.936 0.000** 0.5
T2 - T0 26.3(286.9) 162.2(328.1) 358.2(351.2) 17.599 0.000** 0.4
T3 - T0 134.5(335.9) 213.3(372.3) 326.7(364.5) 4.808 0.009** 0.2
** p < 0.01.
For the within-group comparisons of the mean scores of the exercise self-efficacy
scale, the one-way repeated ANOVA was performed. Significant differences were
seen for all three groups in the mean scores of the exercise self-efficacy scale from T0
to T3 (C group: F(2.5, 66) = 7.6, p < 0.01; PE group: F(2.3, 63) = 11.8, p < 0.01;
ESMI group: F(2.3, 64) = 47.1, p < 0.01) (Table 5.11). This finding suggests that
over time the patients in all of the three groups became more confident about
engaging in exercise.
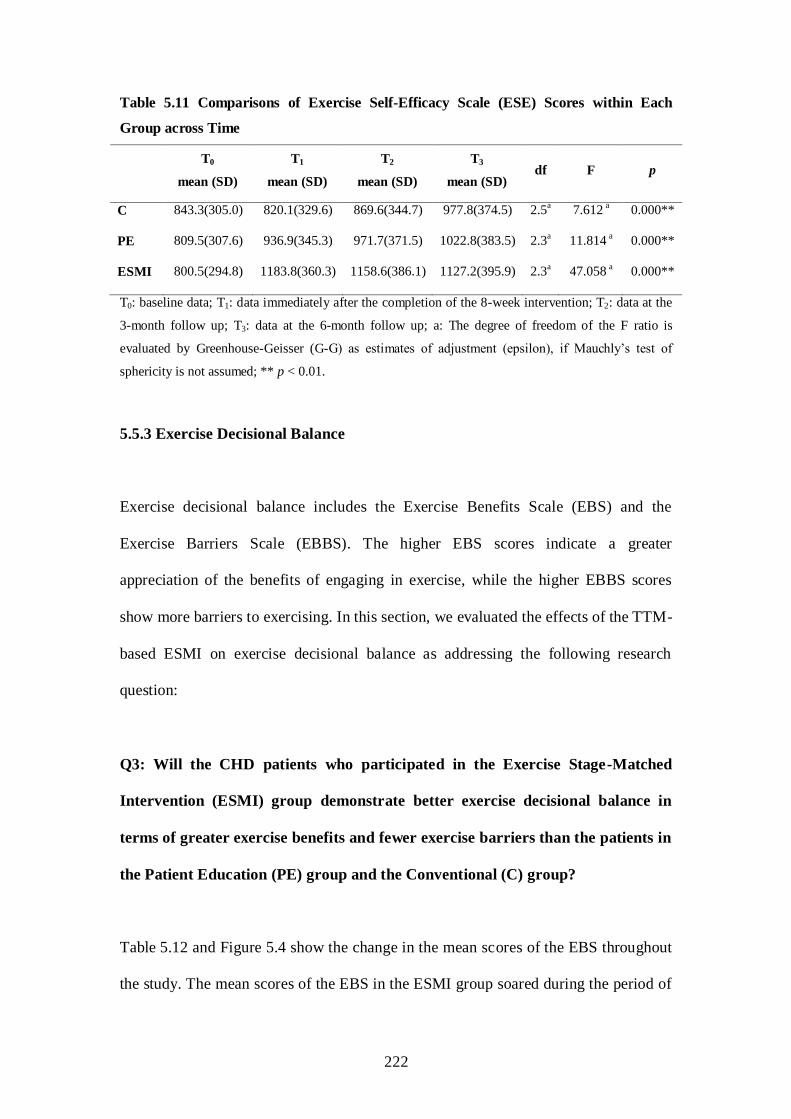
222
Table 5.11 Comparisons of Exercise Self-Efficacy Scale (ESE) Scores within Each
Group across Time
T0
mean (SD)
T1
mean (SD)
T2
mean (SD)
T3
mean (SD) df F p
C 843.3(305.0) 820.1(329.6) 869.6(344.7) 977.8(374.5) 2.5a 7.612
a 0.000**
PE 809.5(307.6) 936.9(345.3) 971.7(371.5) 1022.8(383.5) 2.3a 11.814
a 0.000**
ESMI 800.5(294.8) 1183.8(360.3) 1158.6(386.1) 1127.2(395.9) 2.3a 47.058
a 0.000**
T0: baseline data; T1: data immediately after the completion of the 8-week intervention; T2: data at the
3-month follow up; T3: data at the 6-month follow up; a: The degree of freedom of the F ratio is
evaluated by Greenhouse-Geisser (G-G) as estimates of adjustment (epsilon), if Mauchly‘s test of
sphericity is not assumed; ** p < 0.01.
5.5.3 Exercise Decisional Balance
Exercise decisional balance includes the Exercise Benefits Scale (EBS) and the
Exercise Barriers Scale (EBBS). The higher EBS scores indicate a greater
appreciation of the benefits of engaging in exercise, while the higher EBBS scores
show more barriers to exercising. In this section, we evaluated the effects of the TTM-
based ESMI on exercise decisional balance as addressing the following research
question:
Q3: Will the CHD patients who participated in the Exercise Stage-Matched
Intervention (ESMI) group demonstrate better exercise decisional balance in
terms of greater exercise benefits and fewer exercise barriers than the patients in
the Patient Education (PE) group and the Conventional (C) group?
Table 5.12 and Figure 5.4 show the change in the mean scores of the EBS throughout
the study. The mean scores of the EBS in the ESMI group soared during the period of

223
the implementation of the intervention (T1), kept rising from T1 to T2, and then
dropped slightly from T2 to T3, with the mean scores much higher than the baseline.
For the PE group, the mean scores were stable during the period of the
implementation of the intervention (T1) and then increased steadily from T1 to T3. In
the C group, the mean scores decreased slightly during the period of the
implementation of the intervention (T1), and then increased steadily from T1 to T3,
with the mean scores much higher than the baseline. The mean scores of the EBS
were higher for the ESMI group than for the PE and C groups, and those for the PE
group were higher than those for the C group from T1 to T3.
Referring to Table 5.12 and Figure 5.5, in the ESMI group, the mean scores of the
EBBS plummeted during the period of the implementation of the intervention (T1),
and then increased steadily from T1 to T3, with the mean scores lower than the
baseline; the mean scores in the PE group slowly and steadily declined during the
period of the implementation of the intervention (T1), remained stable from T1 to T2,
and increased slightly again from T2 to T3, with the mean scores lower than the
baseline; for the C group, the mean scores dropped slightly during the period of the
implementation of the intervention (T1), remained stable from T1 to T2 , and decreased
slightly again from T2 to T3.

224
Table 5.12 Mean and Standard Deviations of the Exercise Benefits Scale (EBS) Scores
and the Exercise Barriers Scale (EBBS) Scores at Each Time Point
Variable C group
(n=67)
mean (SD)
PE group
(n=64)
mean (SD)
ESMI group
(n=65)
mean (SD)
EBS
T0 82.5(7.6) 83.7(8.0) 82.6(7.0)
T1 80.7(6.8) 83.6(8.4) 88.6(9.3)
T2 83.9(6.4) 88.7(10.5) 93.0(11.9)
T3 85.7(9.2) 90.6(12.2) 92.1(10.7)
EBBS
T0 29.1(2.8) 29.0(3.8) 29.5(2.8)
T1 28.4(2.3) 27.6(4.9) 23.2(6.0)
T2 28.4(2.2) 27.5(4.5) 24.6(5.4)
T3 27.8(3.2) 28.0(3.5) 25.8(4.7)
T0: baseline data; T1: data immediately after the completion of the 8-week intervention; T2: data at the
3-month follow up; T3: data at the 6-month follow up; The scores of the EBS range from 0 to 116, with
the higher scores indicating greater benefits from engaging in exercise; The scores of the EBBS range
from 0 to 56, with the lower scores indicating fewer barriers to engaging in exercise.

225

226
Because the data on both the EBS and EBBS were not normally distributed and the
related homogeneity of variance among the three groups was not achieved in the data
for both (Appendix XV), non-parametric tests were applied to analyze this data. At
baseline, there were no significant differences in the mean scores of the EBS (p =
0.984) and EBBS (p = 0.916) among the three groups as confirmed by the Kruskal-
Wallis test (Appendix XVI). After the completion of the 8-week intervention, higher
mean change scores of the EBS and lower mean change scores of the EBBS were
seen for the ESMI group than for the PE and C groups, and higher mean change
scores of the EBS and lower mean change scores of the EBBS were noted for the PE
group than for the C group. When the three groups were compared, significant
differences in both the mean change scores of the EBS and EBBS were revealed at T1
(mean rank: benefits: ESMI group = 129.7, PE group = 91.1, C group = 75.3, p < 0.01;
barriers: ESMI group = 67.8, PE group = 110.7, C group = 116.6, p < 0.01), T2 (mean
rank: benefits: ESMI group = 124.2, PE group = 96.4, C group = 75.6, p < 0.01;
barriers: ESMI group = 74.2, PE group = 109.5, C group = 111.6, p < 0.01), and T3
(mean rank: benefits: ESMI group = 116.4, PE group = 97.6, C group = 82.0, p < 0.01;
barriers: ESMI group = 81.0, PE group = 111.7, C group = 102.9, p < 0.01) (Table
5.13).
The effect size (r) of the TTM-based ESMI ranged from 0.3 to 0.4 on the EBS and
from 0.3 to 0.5 on the EBBS from T1 to T3, which in Cohen‘s (1988) terms, would be
considered between medium (0.25) and large effects (0.40) for an ANOVA analysis.
Thus, these findings suggest that the patients who participated in the ESMI group
experienced greater benefits from exercise and encountered lower barriers to exercise
than those in the PE and C groups. In other words, the patients who participated in the

227
ESMI group perceived there to be greater benefits and fewer barriers to engaging in
exercise than those in the PE and C groups.
Table 5.13 Comparisons of the Mean Change Scores of the Exercise Benefits Scale (EBS)
and the Exercise Barriers Scale (EBBS) among Groups at Each Time Point
Variable
C group
(n=67)
mean (SD)
PE group
(n=64)
mean (SD)
ESMI group
(n=65)
mean (SD)
Kruskal-Wallis test Effect
size (r) χ2 p
EBS
T1 - T0 -1.7(6.8) -0.1(7.5) 6.0(9.0) 32.156 0.000** 0.4
T2 - T0 1.5(7.5) 5.0(9.6) 10.4(10.0) 24.527 0.000** 0.4
T3 - T0 3.2(8.1) 7.0(12.0) 9.5(10.2) 12.264 0.002** 0.3
EBBS
T1 - T0 -0.8(2.8) -1.4(4.5) -6.2(6.0) 29.445 0.000** 0.5
T2 - T0 -0.8(2.8) -1.6(4.5) -4.8(5.6) 18.547 0.000** 0.4
T3 - T0 -1.4(3.3) -1.1(4.1) -3.7(5.0) 10.388 0.006** 0.3
** p < 0.01.
For the within-group comparisons of the mean scores of the EBS and the EBBS, the
Friedman test was performed. Significant differences in the mean scores of the EBS
were detected in all of the three groups from T0 to T3 (mean rank: C group: T0 = 2.5,
T1 = 1.8, T2 = 2.8, T3 = 2.9, p < 0.01; PE group: T0 = 2.1, T1 = 1.9, T2 = 2.9, T3 = 3.1,
p < 0.01; ESMI group: T0 = 1.6, T1 = 2.4, T2 = 3.1, T3 = 3.0, p < 0.01) (Table 5.14).
Both the C and ESMI groups revealed significant differences in the mean scores of
the EBBS from T0 to T3 (mean rank: C group: T0 = 2.9, T1 = 2.5, T2 = 2.4, T3 = 2.2, p
< 0.01; ESMI group: T0 = 3.3, T1 = 2.0, T2 = 2.3, T3 = 2.4, p < 0.01) (Table 5.14). No
significant difference in the mean scores of the EBBS was found in the PE group over
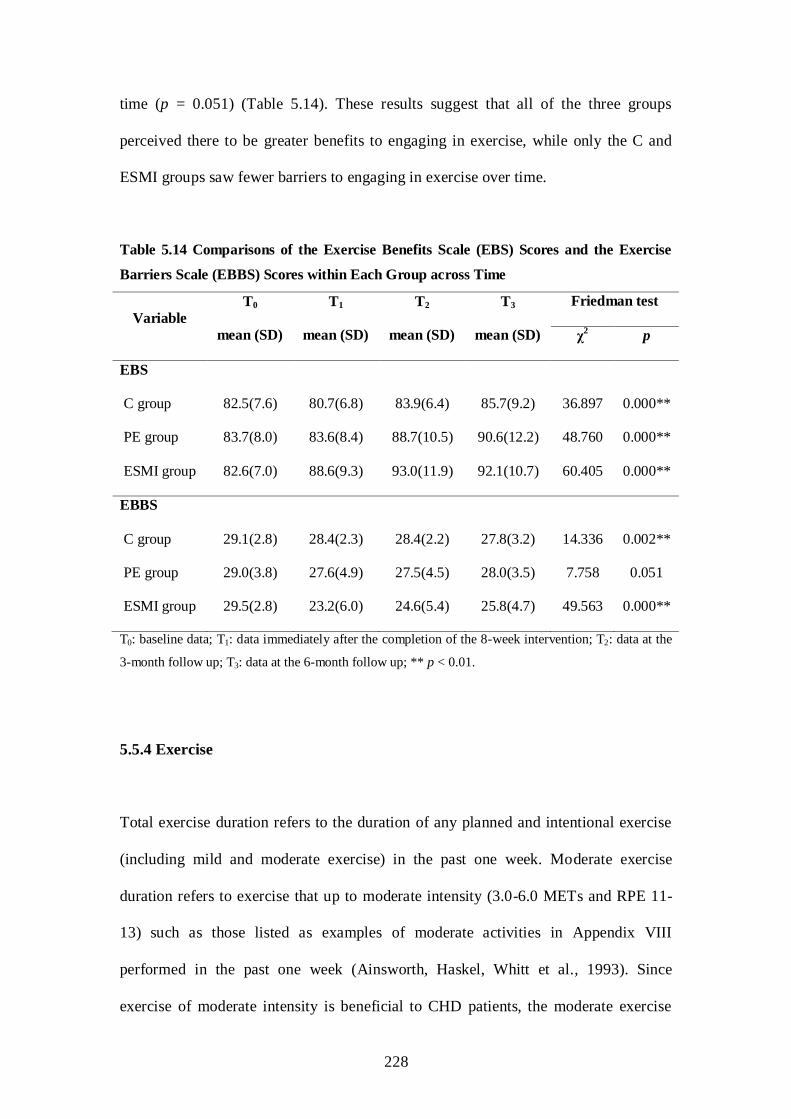
228
time (p = 0.051) (Table 5.14). These results suggest that all of the three groups
perceived there to be greater benefits to engaging in exercise, while only the C and
ESMI groups saw fewer barriers to engaging in exercise over time.
Table 5.14 Comparisons of the Exercise Benefits Scale (EBS) Scores and the Exercise
Barriers Scale (EBBS) Scores within Each Group across Time
Variable
T0
mean (SD)
T1
mean (SD)
T2
mean (SD)
T3
mean (SD)
Friedman test
χ2 p
EBS
C group 82.5(7.6) 80.7(6.8) 83.9(6.4) 85.7(9.2) 36.897 0.000**
PE group 83.7(8.0) 83.6(8.4) 88.7(10.5) 90.6(12.2) 48.760 0.000**
ESMI group 82.6(7.0) 88.6(9.3) 93.0(11.9) 92.1(10.7) 60.405 0.000**
EBBS
C group 29.1(2.8) 28.4(2.3) 28.4(2.2) 27.8(3.2) 14.336 0.002**
PE group 29.0(3.8) 27.6(4.9) 27.5(4.5) 28.0(3.5) 7.758 0.051
ESMI group 29.5(2.8) 23.2(6.0) 24.6(5.4) 25.8(4.7) 49.563 0.000**
T0: baseline data; T1: data immediately after the completion of the 8-week intervention; T2: data at the
3-month follow up; T3: data at the 6-month follow up; ** p < 0.01.
5.5.4 Exercise
Total exercise duration refers to the duration of any planned and intentional exercise
(including mild and moderate exercise) in the past one week. Moderate exercise
duration refers to exercise that up to moderate intensity (3.0-6.0 METs and RPE 11-
13) such as those listed as examples of moderate activities in Appendix VIII
performed in the past one week (Ainsworth, Haskel, Whitt et al., 1993). Since
exercise of moderate intensity is beneficial to CHD patients, the moderate exercise

229
duration was calculated according to the self-reports and log records of the patients.
This section examined the effects of the TTM-based ESMI on exercise duration
(minutes/week) as the following research question:
Q4: Will the CHD patients who participated in the Exercise Stage-Matched
Intervention (ESMI) group demonstrate longer exercise duration (minutes/week)
than the patients in the Patient Education (PE) group and the Conventional (C)
group?
The changes in the total exercise duration (minutes/week) throughout the study were
shown in Table 5.15 and Figure 5.6. In the ESMI group, the mean minutes of the total
exercise duration per week increased sharply during the period of the implementation
of the intervention (T1) and decreased steadily from T1 to T3, with the mean length
still longer than the baseline; the mean minutes of the total exercise duration per week
in the PE group rose rapidly during the period of the implementation of the
intervention (T1), dropped slightly from T1 to T2, and rose steadily again from T2 to T3,
with the mean length slightly shorter than that in the ESMI group at T3; for the C
group, the mean minutes of the total exercise duration per week rose slowly and
steadily from T0 to T3, with the mean minutes about the same as in the ESMI group at
T3.
Table 5.15 and Figure 5.7 show the changes in the moderate exercise duration
(minutes/week) throughout the study. Regarding the ESMI group, the mean minutes
of the moderate exercise duration per week soared during the period of the
implementation of the intervention (T1), decreased slightly from T1 to T2, and dropped
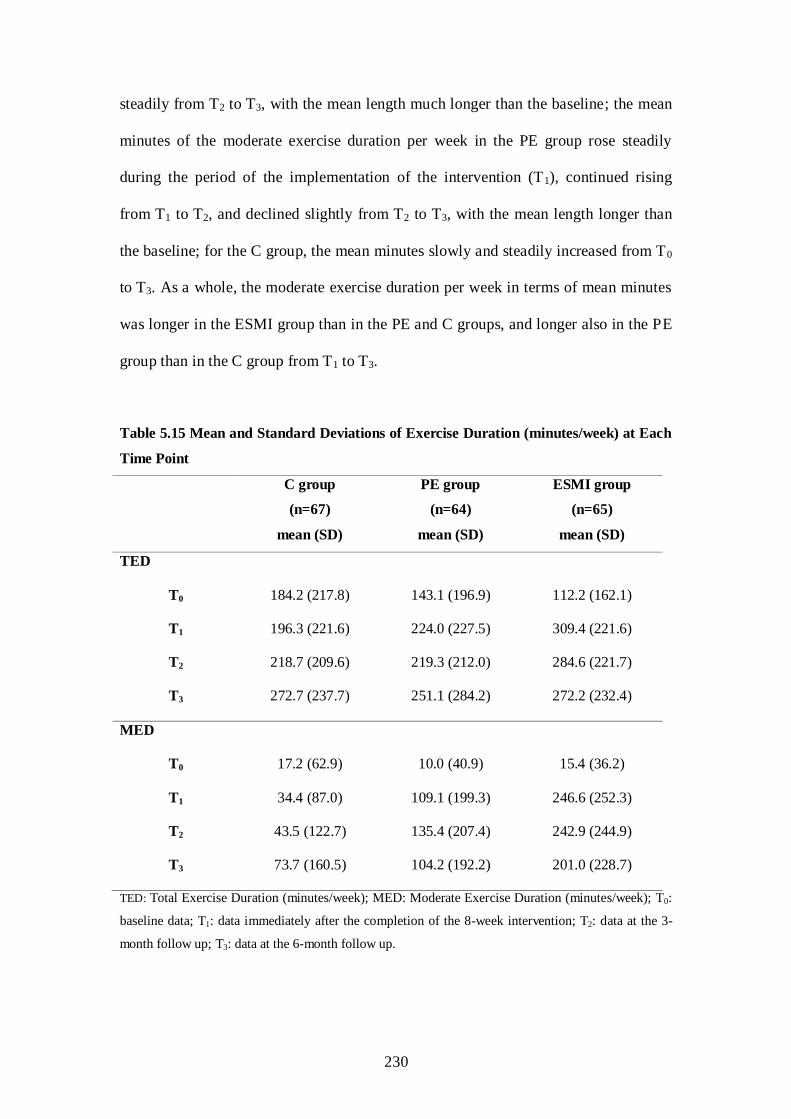
230
steadily from T2 to T3, with the mean length much longer than the baseline; the mean
minutes of the moderate exercise duration per week in the PE group rose steadily
during the period of the implementation of the intervention (T1), continued rising
from T1 to T2, and declined slightly from T2 to T3, with the mean length longer than
the baseline; for the C group, the mean minutes slowly and steadily increased from T0
to T3. As a whole, the moderate exercise duration per week in terms of mean minutes
was longer in the ESMI group than in the PE and C groups, and longer also in the PE
group than in the C group from T1 to T3.
Table 5.15 Mean and Standard Deviations of Exercise Duration (minutes/week) at Each
Time Point
C group
(n=67)
mean (SD)
PE group
(n=64)
mean (SD)
ESMI group
(n=65)
mean (SD)
TED
T0 184.2 (217.8) 143.1 (196.9) 112.2 (162.1)
T1 196.3 (221.6) 224.0 (227.5) 309.4 (221.6)
T2 218.7 (209.6) 219.3 (212.0) 284.6 (221.7)
T3 272.7 (237.7) 251.1 (284.2) 272.2 (232.4)
MED
T0 17.2 (62.9) 10.0 (40.9) 15.4 (36.2)
T1 34.4 (87.0) 109.1 (199.3) 246.6 (252.3)
T2 43.5 (122.7) 135.4 (207.4) 242.9 (244.9)
T3 73.7 (160.5) 104.2 (192.2) 201.0 (228.7)
TED: Total Exercise Duration (minutes/week); MED: Moderate Exercise Duration (minutes/week); T0:
baseline data; T1: data immediately after the completion of the 8-week intervention; T2: data at the 3-
month follow up; T3: data at the 6-month follow up.

231

232
As the data on the total exercise duration (minutes/week) and moderate exercise
duration (minutes/week) were not normally distributed and the related homogeneity of
variance among the three groups was violated in the data for both (Appendix XV),
non-parametric tests were performed to analyze them. At baseline, no significant
differences in the mean minutes of both the total (p = 0.145) and moderate exercise
duration (p = 0.314) (minutes/week) were found among the three groups when the
Kruskal-Wallis test was applied (Appendix XVI). After the completion of the 8-week
intervention, the mean minutes of both the total and moderate exercise duration
(minutes/week) for all three groups increased as compared with the baseline (Table
5.16). The mean change in minutes in both the total and moderate exercise duration
per week was longer for the ESMI group than for the PE and C groups, and longer for
the PE group than for the C group. When the three groups were compared, significant
differences in the mean change in minutes of the total exercise duration per week
were detected at T1 (mean rank: ESMI group = 128.0, PE group = 92.9, C group =
75.3, p < 0.01) and T2 (mean rank: ESMI group = 115.2, PE group = 92.8, C group =
87.7, p < 0.05), while significant differences in the mean change in minutes of the
moderate exercise duration per week were found at T1 (mean rank: ESMI group =
129.0, PE group = 93.5, C group = 73.7, p < 0.01), T2 (mean rank: ESMI group =
122.0, PE group = 100.9, C group = 73.5, p < 0.01), and T3 (mean rank: ESMI group
= 118.9, PE group = 93.4, C group = 83.6, p < 0.01) (Table 5.16).
The effect size (r) of the TTM-based ESMI varied from 0.1 to 0.4 on the total exercise
duration (minutes/week) and from 0.3 to 0.5 on the moderate exercise duration
(minutes/week) from T1 to T3 (Table 5.16), which would be viewed as a small (0.10)
to large effect (0.40) on the total exercise duration per week, and a medium (0.25) to

233
large effect (0.40) on the moderate exercise duration per week for an ANOVA
analysis according to Cohen‘s (1988) terms. Thus, these findings suggest that the
patients who participated in the ESMI group exercised for a longer duration
(minutes/week) than those in the PE and C groups.
Table 5.16 Comparisons of Mean Change in Minutes of Exercise Duration
(minutes/week) among Groups at Each Time Point
C group
(n=67)
mean (SD)
PE group
(n=64)
mean (SD)
ESMI group
(n=65)
mean (SD)
Kruskal-Wallis test Effect
size
(r) χ
2 p
TED
T1 - T0 12.2 (220.1) 80.9 (164.3) 197.2 (198.6) 30.411 0.000** 0.4
T2 - T0 34.6 (236.9) 76.2 (177.2) 172.5 (226.1) 8.928 0.012* 0.3
T3 - T0 88.5 (255.4) 108.0 (230.5) 160.0 (218.7) 3.363 0.186 0.1
MED
T1 - T0 17.2 (89.3) 99.1 (194.7) 231.2 (251.9) 41.043 0.000** 0.5
T2 - T0 26.3 (111.8) 125.4 (199.4) 227.5 (251.8) 29.677 0.000** 0.4
T3 - T0 56.5 (133.6) 94.2 (189.5) 185.6 (227.7) 17.515 0.000** 0.3
TED: Total Exercise Duration (minutes/week); MED: Moderate Exercise Duration (minutes/week).
*p < 0.05; **p < 0.01.
For the within-group comparisons of the mean minutes of the total exercise duration
per week and moderate exercise duration per week, the Friedman test was performed.
Significant differences were seen in all the three groups in the mean minutes of the
total exercise duration per week from T0 to T3 (mean rank: C group: T0 = 2.2, T1 = 2.4,
T2 = 2.5, T3 = 2.9, p < 0.01; PE group: T0 = 2.0, T1 = 2.6, T2 = 2.6, T3 = 2.8, p < 0.01;
ESMI group: T0 = 1.6, T1 = 3.1, T2 = 2.7, T3 = 2.6, p < 0.01) and moderate exercise
duration per week from T0 to T3 (mean rank: C group: T0 = 2.3, T1 = 2.5, T2 = 2.5, T3

234
= 2.7, p < 0.01; PE group: T0 = 2.0, T1 = 2.6, T2 = 2.8, T3 = 2.6, p < 0.01; ESMI group:
T0 = 1.6, T1 = 3.0, T2 = 2.8, T3 = 2.6, p < 0.01) (Table 5.17). These results suggest that
patients in all the three groups increased their exercise duration (minutes/week) over
time.
Table 5.17 Comparisons of Exercise Duration (minutes/week) within Each Group across
Time
T0
mean (SD)
T1
mean (SD)
T2
mean (SD)
T3
mean (SD)
Friedman test
χ2 p
TED
C group 184.2(217.8) 196.3(221.6) 218.7(209.6) 272.7(237.7) 13.356 0.004**
PE group 143.1(196.9) 224.0(227.5) 219.3(212.0) 251.1(284.2) 19.972 0.000**
ESMI group 112.2(162.1) 309.4(221.6) 284.6(221.7) 272.2(232.4) 57.956 0.000**
MED
C group 17.2(62.9) 34.4(87.0) 43.5(122.7) 73.7(160.5) 12.049 0.007**
PE group 10.0(40.9) 109.1(199.3) 135.4(207.4) 104.2(192.2) 27.914 0.000**
ESMI group 15.4(36.2) 246.6(252.3) 242.9(244.9) 201.0(228.7) 65.021 0.000**
TED: Total Exercise Duration (minutes/week); MED: Moderate Exercise Duration (minutes/week); T0:
baseline data; T1: data immediately after the completion of the 8-week intervention; T2: data at the 3-
month follow up; T3: data at the 6-month follow up; ** p < 0.01.
5.5.5 Angina
This section compared anginal pain in the three groups in terms of angina frequency
(episodes/week), angina severity, and angina duration (minutes/week), whether
anginal attacks occurred, and whether or not the patients took anti-anginal drugs, as
addressed in the following research question:

235
Q5: Will the CHD patients who participated in the Exercise Stage-Matched
Intervention (ESMI) group demonstrate a greater reduction in angina in terms
of angina frequency, angina severity, angina duration (minutes/week), anginal
attacks, and anti-anginal drugs taken than the patients in the Patient Education
(PE) group and the Conventional (C) group?
As shown in Table 5.18, according to the self-reports and log records of patients, the
average angina frequency (episodes/week) is around 1.0 per week with very slight
pain (the average severity of an episode of angina is less than 1.0), and the average
duration of an anginal attack is mostly less than 10 minutes per week in all the three
groups. Referring to Table 5.18 and Figure 5.8, the mean episodes of angina per week
among patients in the ESMI group decreased substantially during the period of the
implementation of the intervention (T1), remained stable from T1 to T2, and rose
slightly from T2 to T3, with the mean episodes being fewer than the baseline; stability
in angina frequency, in terms of the mean episodes of angina per week, was seen
among patients in the PE group during the period of the implementation of the
intervention (T1), a slight decrease was noted from T1 to T2, and a slight increase from
T2 to T3, with the mean episodes slightly fewer than the baseline; a rapid drop in
angina frequency, in terms of the mean episodes of angina per week, was noted
among patients in the C group during the period of the implementation of the
intervention (T1), and a steady rise from T1 to T3, with the mean episodes slightly
fewer than the baseline. On the whole, episodes of angina were less frequent in the
ESMI group than in the PE and C groups, and less frequent in the PE group than in
the C group from T1 to T3.

236
As shown in Table 5.18 and Figure 5.9, in the ESMI group, the mean angina severity
obviously declined during the period of the implementation of the intervention (T1),
remained stable from T1 to T2, and slightly increased from T2 to T3, with the mean
angina severity lower than the baseline at T3; in the PE group, the mean angina
severity decreased steadily from T0 to T3, with the mean angina severity still higher
than in the ESMI group at T3; in the C group, the mean angina severity decreased
rapidly during the period of the implementation of the intervention (T1), rose slightly
from T1 to T2, and decreased steadily again from T2 to T3, with the mean angina
severity much lower than the baseline. On the whole, the mean angina severity in the
ESMI group is lower than that in the PE and C groups, and that in the PE group is
lower than that in the C group from T1 to T3.
As shown in Table 5.18 and Figure 5.10, the mean angina duration (minutes/week) in
the ESMI group decreased rapidly during the period of the implementation of the
intervention (T1) and increased slightly from T1 to T3, with the mean angina duration
shorter than the baseline at T3; the mean angina duration in the PE group obviously
decreased during the period of the implementation of the intervention (T1) and rose
slightly from T1 to T3, and was one minute shorter than the baseline at T3; the mean
angina duration in the C group decreased from T0 to T3, and was still longer than in
the ESMI group but shorter than in the PE group at T3. On the whole, the mean angina
duration in the ESMI group is shorter than that in the PE and C groups from T1 to T3,
and that in the PE group is shorter than that in the C group from T1 to T2.

237
Table 5.18 Mean and Standard Deviations of Angina Frequency (AF), Angina Severity
(AS), and Angina Duration (AD) at Each Time Point
C group
(n=67)
mean (SD)
PE group
(n=64)
mean (SD)
ESMI group
(n=65)
mean (SD)
AF
T0 1.4 (3.1) 1.1 (2.8) 0.9 (1.4)
T1 1.0 (1.6) 1.1 (2.9) 0.4 (0.9)
T2 1.0 (2.0) 0.9 (2.9) 0.4 (0.9)
T3 1.2 (2.8) 1.0 (3.1) 0.6 (2.1)
AS
T0 0.7 (1.2) 0.7 (1.1) 0.5 (0.7)
T1 0.4 (0.7) 0.5 (1.0) 0.2 (0.5)
T2 0.5 (0.8) 0.4 (0.9) 0.2 (0.5)
T3 0.3 (0.5) 0.4 (0.9) 0.3 (0.7)
AD
T0 13.4 (33.0) 9.8 (23.0) 9.3 (29.4)
T1 10.6 (45.2) 6.3 (16.6) 2.0 (6.4)
T2 10.0 (24.9) 7.0 (21.2) 2.2 (6.9)
T3 6.3 (14.0) 8.8 (30.2) 3.5 (12.5)
AF: Angina Frequency (episodes/week); AS: Angina Severity (0-10); AD: Angina Duration
(minutes/week); T0: baseline data; T1: data immediately after the completion of the 8-week intervention;
T2: data at the 3-month follow up; T3: data at the 6-month follow up.

238

239
Because the data on angina frequency (episodes/week), angina severity (0-10), and
angina duration (minutes/week) were not normally distributed and the related
homogeneity of variance among the three groups was not achieved in each variable
(Appendix XV), non-parametric tests were applied. No significant differences were
found in the mean episodes of angina frequency per week (p = 0.887), mean angina
severity (p = 0.891), and mean minutes of angina duration (p = 0.829) among the
three groups at baseline (Appendix XVI). Reductions in angina frequency
(episodes/week), angina severity, and angina duration (minutes/week) were observed
in all three groups after the completion of the 8-week intervention as compared with
the baseline (Table 5.19). No significant differences in the mean change of angina
frequency (episodes/week), angina severity, and angina duration (minutes/week) were

240
detected among the three groups at each time point when the Kruskal-Wallis test was
applied to analyze the data (Table 5.19).
The effect sizes of the TTM-based ESMI on the angina frequency (episodes/week),
angina severity and angina duration (minutes/week) ranged from 0.0 to 0.1 (Table
5.19), which was a small effect (0.10) for an ANOVA analysis according to Cohen
(1988). Thus, these findings suggest that the patients who participated in the ESMI
group did not experience a greater reduction in angina frequency (episodes/week),
angina severity, and angina duration (minutes/week) than those in the PE and C
groups.
Table 5.19 Comparisons of Angina Frequency (AF), Angina Severity (AS), and Angina
Duration (AD) among Groups at Each Time Point
C group
(n=67)
mean (SD)
PE group
(n=64)
mean (SD)
ESMI group
(n=65)
mean (SD)
Kruskal-Wallis test Effect
size
(r) χ
2 p
AF
T1 - T0 -0.5(3.0) -0.0(1.1) -0.5(1.4) 2.149 0.341 0.1
T2 - T0 -0.4(2.4) -0.2(1.1) -0.5(1.4) 0.383 0.826 0.1
T3 - T0 -0.3(2.4) -0.1(1.4) -0.3(2.5) 2.015 0.365 0.0
AS
T1 - T0 -0.3(1.0) -0.2(1.0) -0.3(0.8) 0.906 0.636 0.1
T2 - T0 -0.2(1.2) -0.3(1.0) -0.3(0.8) 0.444 0.801 0.0
T3 - T0 -0.4(1.1) -0.3(0.8) -0.2(1.0) 0.388 0.824 0.1
AD
T1 - T0 -2.8(56.5) -3.5(20.6) -7.3(29.2) 1.794 0.408 0.1
T2 - T0 -3.3(40.3) -2.8(23.8) -7.1(29.0) 0.734 0.693 0.1
T3 - T0 -7.1(33.6) -0.9(31.8) -5.8(31.4) 1.160 0.560 0.1
AF: Angina Frequency (episodes/week); AS: Angina Severity (0-10); AD: Angina Duration
(minutes/week).

241
The Friedman test was applied for within-group comparisons of angina frequency
(episodes/week), angina severity, and angina duration (minutes/week). No significant
differences in angina frequency (episodes/week), angina severity, and angina duration
(minutes/week) were identified in the C group over time (Table 5.20). Significant
differences in angina severity (mean rank: T0 = 2.7, T1 = 2.5, T2 = 2.4, T3 = 2.4, p <
0.05) and angina duration (minutes/week) (mean rank: T0 = 2.7, T1 = 2.6, T2 = 2.4, T3
= 2.4, p < 0.05) were detected in the PE group over time (Table 5.20). Significant
differences in angina frequency (episodes/week) (mean rank: T0 = 2.8, T1 = 2.5, T2 =
2.4, T3 = 2.4, p < 0.01), angina severity (mean rank: T0 = 2.8, T1 = 2.5, T2 = 2.4, T3 =
2.4, p < 0.01), and angina duration (minutes/week) (mean rank: T0 = 2.8, T1 = 2.4, T2
= 2.4, T3 = 2.3, p < 0.01) were found in the ESMI group over time (Table 5.20). These
findings suggest that the patients who participated in both the PE and ESMI groups
experienced a reduction in the severity and duration (minutes/week) of their anginal
attacks over time, with those in the ESMI group also experienced a decline in the
frequency (episodes/week) of angina over time.

242
Table 5.20 Comparisons of Angina Frequency (AF), Angina Severity (AS), and Angina
Duration (AD) within Each Group across Time
T0
mean (SD)
T1
mean (SD)
T2
mean (SD)
T3
mean (SD)
Friedman test
χ2 p
AF
C group 1.4(3.1) 1.0(1.6) 1.0(2.0) 1.2(2.7) 3.370 0.338
PE group 1.1(2.8) 1.1(2.9) 0.9(2.9) 1.0(3.1) 5.440 0.142
ESMI group 0.9(1.4) 0.4(0.9) 0.4(0.9) 0.6(2.1) 14.591 0.002**
AS
C group 0.7(1.2) 0.4(0.7) 0.5(0.8) 0.3(0.5) 6.759 0.080
PE group 0.7(1.1) 0.5(1.0) 0.4(0.9) 0.4(0.9) 9.232 0.026*
ESMI group 0.5(0.7) 0.2(0.5) 0.2(0.5) 0.3(0.7) 15.448 0.001**
AD
C group 13.4(33.0) 10.6(45.2) 10.0(24.9) 6.3(14.0) 3.140 0.370
PE group 9.8(23.0) 6.3(16.6) 7.0(21.2) 8.8(30.2) 8.903 0.031*
ESMI group 9.3(29.4) 2.0(6.4) 2.2(6.9) 3.5(12.5) 18.717 0.000**
AF: Angina Frequency (episodes/week); AS: Angina Severity (0-10); AD: Angina Duration
(minutes/week); T0: baseline data; T1: data immediately after the completion of the 8-week intervention;
T2: data at the 3-month follow up; T3: data at the 6-month follow up; *p < 0.05; ** p < 0.01.
Table 5.21 shows changes in the occurrence of anginal attacks and in the taking of
anti-anginal drugs in the past one week throughout the study. Since the data on the
anginal attacks and anti-anginal drugs are binary data, a Chi-square test was
performed. A trend towards a reduction in the occurrence of anginal attacks was
observed in both the PE and ESMI group from T0 to T3. However, no significant
differences in the occurrence of anginal attacks and taking of anti-anginal drugs were
detected among the three groups at each time point (Table 5.21). These results suggest
that the patients who participated in the ESMI group did not experience a greater

243
reduction in the occurrence of anginal attacks and in the amount of anti-anginal drugs
taken per week.
Table 5.21 Comparisons of Items on the Occurrence of Anginal Attacks and Anti-
Anginal Drugs taken in the Past One Week among Groups at Each Time Point
Variable
C group
(n=67)
n (%)
PE group
(n=64)
n (%)
ESMI group
(n=65)
n (%)
χ2 p
T0 Anginal attack 0.049 0.976
Yes 27(40.3) 25(39.1) 25(38.5)
No 40(59.7) 39(60.9) 40(61.5)
Anti-anginal
drugs taken
1.223 0.543
Yes 17(25.4) 12(18.8) 12(18.5)
No 50(74.6) 52(81.2) 53(81.5)
T1 Anginal attack 2.042 0.360
Yes 23(34.3) 19(29.7) 15(23.1)
No 44(65.7) 45(70.3) 50(76.9)
Anti-anginal
drugs taken
1.878 0.391
Yes 12(17.9) 12(18.8) 7(10.8)
No 55(82.1) 52(81.2) 58(89.2)
T2 Anginal attack 5.638 0.060
Yes 25(37.3) 15(23.4) 13(20.0)
No 42(62.7) 49(76.6) 52(80.0)
Anti-anginal
drugs taken
3.352 0.187
Yes 14(20.9) 6(9.4) 10(15.4)
No 53(79.1) 58(90.6) 55(84.6)
T3 Anginal attack 5.820 0.054
Yes 21(31.3) 14(21.9) 9(13.8)
No 46(68.7) 50(78.1) 56(86.2)
Anti-anginal
drugs taken
1.516 0.469
Yes 12(17.9) 7(10.9) 8(12.3)
No 55(82.1) 57(89.1) 57(87.7)
T0: baseline data; T1: data immediately after the completion of the 8-week intervention; T2: data at the
3-month follow up; T3: data at the 6-month follow up.

244
For the within-group comparisons of the occurrence of anginal attacks and anti-
anginal drugs taken in the past one week, Cochran‘s Q was performed because the
data was binary. As shown in Table 5.22, no significant differences in the occurrence
of angina attacks and anti-anginal drugs taken were identified in the C group over
time; significant differences in both the occurrence of anginal attacks (p < 0.05) and
anti-anginal drugs taken (p < 0.05) were found in the PE group over time; and a
significant difference in the occurrence of anginal attacks (p < 0.01) was detected in
the ESMI group over time. These results suggest that, over time, the patients in both
the PE and ESMI groups experienced a reduction in the occurrence of anginal attacks,
with those in the PE group also decreasing the amount of the anti-anginal drugs that
they were taking.

245
Table 5.22 Comparisons of the Occurrence of Angina Attacks and Anti-Anginal Drugs
taken within Each Group across Time
Group T0
n (%)
T1
n (%)
T2
n (%)
T3
n (%)
Cochran’s
Q p
Anginal attack
C group Yes 27(40.3) 23(34.3) 25(37.3) 21(31.3) 2.353 0.502
No 40(59.7) 44(65.7) 42(62.7) 46(68.7)
PE group Yes 25(39.1) 19(29.7) 15(23.4) 14(21.9) 9.857 0.020*
No 39(60.9) 45(70.3) 49(76.6) 50(78.1)
ESMI group Yes 25(38.5) 15(23.1) 13(20.0) 9(13.8) 18.130 0.000**
No 40(61.5) 50(76.9) 52(80.0) 56(86.2)
Anti-anginal
drugs taken
C group Yes 17(25.4) 12(17.9) 14(20.9) 12(17.9) 2.680 0.444
No 50(74.6) 55(82.1) 53(79.1) 55(82.1)
PE group Yes 12(18.8) 12(18.8) 6(9.4) 7(10.9) 7.851 0.049*
No 52(81.3) 52(81.3) 58(90.6) 57(89.1)
ESMI group Yes 12(18.5) 7(10.8) 10(15.4) 8(12.3) 3.612 0.306
No 53(81.5) 58(89.2) 55(84.6) 57(87.7)
T0: baseline data; T1: data immediately after the completion of the 8-week intervention; T2: data at the
3-month follow up; T3: data at the 6-month follow up; *p < 0.05; ** p < 0.01.
5.4.6 Quality of life
In this study, quality of life was assessed using both the Seattle Angina Questionnaire
(SAQ) and the Medical Outcomes Study 36-Item Short-Form (SF-36). This section
tested the effects of the TTM-based ESMI on quality of life in terms of the SAQ and
SF-36 to address the following research question:

246
Q6: Will the CHD patients who participated in the Exercise Stage-Matched
Intervention (ESMI) group demonstrate greater improvement in quality of life
than the patients in the Patient Education (PE) group and the Conventional (C)
group?
5.6.1 Seattle Angina Questionnaire (SAQ)
The SAQ consists of the following five subscales: physical limitations, angina
stability, angina frequency, treatment satisfaction, and disease perception. The scores
of each subscale range from 0 to 100, with the higher scores indicating better health
conditions or quality of life.
Table 5.23 and Figures 5.11 to 5.15 show the change in the mean scores of the five
subscales of SAQ in each group from the baseline (T0) to the 6-month follow-up
period (T3). In the ESMI group, the mean scores for physical limitations, angina
frequency, treatment satisfaction, and disease perception increased sharply during the
period of the implementation of the intervention (T1) and remained stable from T1 to
T3, with the mean scores of these four subscales being much higher than the baseline,
while the mean scores for angina stability increased steadily during the period of the
implementation of the intervention (T1), continued to rise from T1 to T2, and then
dropped sharply from T2 to T3, with the mean scores lower than the baseline (T0). In
the PE group, the mean scores for angina stability, angina frequency, treatment
satisfaction, and disease perception climbed steadily from the baseline (T0) to the 3-
month follow up (T2), then fell from T2 to T3, with the exception of the mean scores
for treatment satisfaction, which kept rising from T2 to T3. The rising slope of these

247
subscales in the PE group was much smaller than in the ESMI group. The mean
scores for angina frequency, treatment satisfaction, and disease perception in the PE
group at the 6-month follow-up (T3) were higher than the baseline, while the mean
scores for angina stability at the 6-month follow-up (T3) were lower than the baseline.
The mean scores for physical limitations in the PE group declined slightly during the
period of the implementation of the intervention (T1), went up to a little higher than
the baseline from T1 to T2, and then decreased slightly again from T2 to T3, with the
mean scores slightly higher than the baseline (T0). In the C group, the mean scores for
physical limitations and treatment satisfaction plunged during the period of the
implementation of the intervention (T1) while the mean scores for physical limitations
remained stable from T1 to T3, and those for treatment satisfaction continued to
decline from T1 to T2, before rising again from T2 to T3, with the mean scores higher
than the baseline. The mean scores for angina stability, angina frequency, and disease
perception in the C group increased slightly or remained stable from T0 to T2 and
continued to rise from T2 to T3, with the exception of the mean scores for angina
stability, which decreased from T2 to T3. Higher mean scores for all five subscales of
SAQ from T1 to T3 were observed in the ESMI group than in the C and PE groups,
while higher mean scores for all five subscales of SAQ from T1 to T3 were seen in the
PE group than in the C group.

248
Table 5.23 Mean and Standard Deviations of the Subscales of SAQ at Each Time Point
C group
(n=67)
mean (SD)
PE group
(n=64)
mean (SD)
ESMI group
(n=65)
mean (SD)
Physical limitations
T0 85.5(13.1) 85.9(13.0) 82.0(12.9)
T1 80.3(15.0) 83.8(12.5) 90.3(10.7)
T2 81.2(14.7) 87.2(12.6) 89.4(11.2)
T3 80.8(14.3) 86.3(11.1) 90.2(10.2)
Angina stability
T0 47.0(20.7) 50.8(20.4) 51.5(20.7)
T1 47.4(17.5) 51.6(19.4) 55.0(19.9)
T2 49.3(16.8) 52.0(16.2) 56.2(20.7)
T3 47.8(12.1) 46.9(14.4) 49.6(16.2)
Angina frequency
T0 83.3(18.1) 84.1(19.7) 83.5(17.6)
T1 84.8(18.6) 85.9(18.7) 91.4(12.9)
T2 84.6(19.3) 89.8(15.6) 91.8(13.2)
T3 86.4(20.6) 88.1(19.3) 91.2(18.8)
Treatment satisfaction
T0 69.9(20.1) 68.8(18.5) 66.9(17.5)
T1 67.5(18.4) 73.5(16.5) 84.7(15.1)
T2 66.0(16.7) 76.1(16.2) 84.3(16.4)
T3 73.5(17.4) 77.2(17.1) 84.3(18.0)
Disease perception
T0 71.1(21.9) 69.8(21.8) 68.1(17.7)
T1 71.4(20.0) 75.8(17.9) 84.2(17.7)
T2 71.0(20.8) 80.1(17.5) 85.0(18.2)
T3 76.6(19.4) 79.7(18.3) 84.5(20.3)
The scores of each subscale of SAQ range from 0 to 100, with the higher scores indicating better health
conditions; T0: baseline data; T1: data immediately after the completion of the 8-week intervention; T2:
data at the 3-month follow up; T3: data at the 6-month follow up.

249

250

251
Since the data of each subscale of SAQ were not normally distributed and the related
homogeneity of variance among the three groups was not achieved in most data
(Appendix XV), non-parametric tests were employed to analyze them. At baseline, no
significant differences were detected in the mean scores of the five subscales of SAQ
among the three groups when the Kruskal-Wallis test was performed (p > 0.05)
(Appendix XVI). Higher mean change scores for each subscale of SAQ were
observed in the ESMI group than in the C and PE groups from T1 to T3 (Table 5.24).
Significant differences were found among the C, PE, and ESMI groups in the mean
change scores for physical limitations (mean rank: T1 - T0: ESMI group = 131.0, PE
group = 88.0, and C group = 76.9, p = 0.000; T2 - T0: ESMI group = 123.0, PE group
= 95.6, and C group = 77.6, p = 0.000; T3 - T0: ESMI group = 125.1, PE group = 93.0,
and C group = 78.1, p = 0.000), treatment satisfaction (mean rank: T1 - T0: ESMI

252
group = 130.2, PE group = 93.1, and C group = 72.9, p = 0.000; T2 - T0: ESMI group
= 126.7, PE group = 98.2, and C group = 71.4, p = 0.000; T3 - T0: ESMI group =
121.0, PE group = 93.2, and C group = 81.7, p = 0.000), and disease perception (mean
rank: T1 - T0: ESMI group = 125.9, PE group = 95.8, and C group = 74.5, p = 0.000;
T2 - T0: ESMI group = 122.4, PE group = 99.8, and C group = 74.1, p = 0.000; T3 - T0:
ESMI group = 118.0, PE group = 95.0, and C group = 83.0, p = 0.001) of SAQ at T1,
T2, and T3 (Table 5.24). No significant differences in the mean change scores for
angina stability and angina frequency were identified among the three groups at each
time point.
The effect size (r) of the TTM-based ESMI on the five subscales of the SAQ varied
from 0.1 to 0.4 (Table 24), which in Cohen‘s (1988) terms would be considered a
small (0.10) to large effect (0.40) for an ANOVA analysis. Clearly, the patients who
participated in the ESMI group demonstrated greater improvement in quality of life in
terms of the SAQ, especially with regard to physical limitations, treatment satisfaction,
and disease perception than those in the PE and C groups.
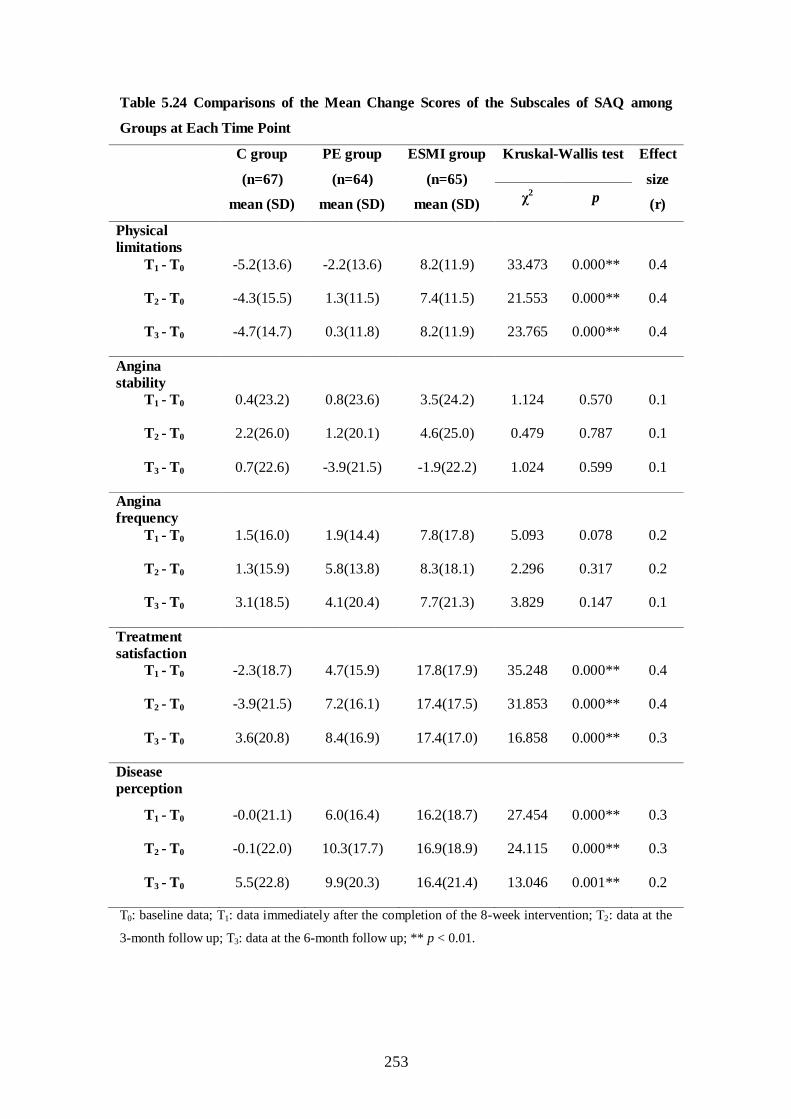
253
Table 5.24 Comparisons of the Mean Change Scores of the Subscales of SAQ among
Groups at Each Time Point
C group
(n=67)
mean (SD)
PE group
(n=64)
mean (SD)
ESMI group
(n=65)
mean (SD)
Kruskal-Wallis test Effect
size
(r) χ
2 p
Physical
limitations
T1 - T0 -5.2(13.6) -2.2(13.6) 8.2(11.9) 33.473 0.000** 0.4
T2 - T0 -4.3(15.5) 1.3(11.5) 7.4(11.5) 21.553 0.000** 0.4
T3 - T0 -4.7(14.7) 0.3(11.8) 8.2(11.9) 23.765 0.000** 0.4
Angina
stability
T1 - T0 0.4(23.2) 0.8(23.6) 3.5(24.2) 1.124 0.570 0.1
T2 - T0 2.2(26.0) 1.2(20.1) 4.6(25.0) 0.479 0.787 0.1
T3 - T0 0.7(22.6) -3.9(21.5) -1.9(22.2) 1.024 0.599 0.1
Angina
frequency
T1 - T0 1.5(16.0) 1.9(14.4) 7.8(17.8) 5.093 0.078 0.2
T2 - T0 1.3(15.9) 5.8(13.8) 8.3(18.1) 2.296 0.317 0.2
T3 - T0 3.1(18.5) 4.1(20.4) 7.7(21.3) 3.829 0.147 0.1
Treatment
satisfaction
T1 - T0 -2.3(18.7) 4.7(15.9) 17.8(17.9) 35.248 0.000** 0.4
T2 - T0 -3.9(21.5) 7.2(16.1) 17.4(17.5) 31.853 0.000** 0.4
T3 - T0 3.6(20.8) 8.4(16.9) 17.4(17.0) 16.858 0.000** 0.3
Disease
perception
T1 - T0 -0.0(21.1) 6.0(16.4) 16.2(18.7) 27.454 0.000** 0.3
T2 - T0 -0.1(22.0) 10.3(17.7) 16.9(18.9) 24.115 0.000** 0.3
T3 - T0 5.5(22.8) 9.9(20.3) 16.4(21.4) 13.046 0.001** 0.2
T0: baseline data; T1: data immediately after the completion of the 8-week intervention; T2: data at the
3-month follow up; T3: data at the 6-month follow up; ** p < 0.01.

254
For within-group comparisons of each subscale of SAQ, the Friedman test was
performed. The C group showed significant differences in the mean scores for angina
frequency (mean rank: T0 = 2.3, T1 = 2.4, T2 = 2.6, T3 = 2.8, p < 0.05) and disease
perception (mean rank: T0 = 2.5, T1 = 2.3, T2 = 2.4, T3 = 2.9, p < 0.05) from T0 to T3.
The PE group revealed significant differences in the mean scores for angina frequency
(mean rank: T0 = 2.2, T1 = 2.5, T2 = 2.6, T3 = 2.7, p < 0.05), treatment satisfaction
(mean rank: T0 = 2.1, T1 = 2.4, T2 = 2.8, T3 = 2.8, p < 0.01), and disease perception
(mean rank: T0 = 2.0, T1 = 2.4, T2 = 2.7, T3 = 2.9, p < 0.01) from T0 to T3. The ESMI
group demonstrated significant differences in the mean scores for physical limitations
(mean rank: T0 = 1.9, T1 = 2.7, T2 = 2.7, T3 = 2.7, p < 0.01), angina frequency (mean
rank: T0 = 2.0, T1 = 2.6, T2 = 2.7, T3 = 2.8, p < 0.01), treatment satisfaction (mean
rank: T0 = 1.5, T1 = 2.8, T2 = 2.8, T3 = 2.9, p < 0.01), and disease perception (mean
rank: T0 = 1.6, T1 = 2.7, T2 = 2.9, T3 = 2.8, p < 0.01) from T0 to T3 (Table 5.25). No
significant differences in the mean scores for angina stability were detected in any of
the three groups over time (Table 5.25).

255
Table 5.25 Comparison of the Subscale Scores of SAQ within Each Group across Time
Group
T0
mean (SD)
T1
mean (SD)
T2
mean (SD)
T3
mean (SD)
Friedman test
χ2 p
Physical
limitations
C group 85.5(13.1) 80.3(15.0) 81.2(14.7) 80.8(14.3) 7.764 0.051
PE group 85.9(13.0) 83.8(12.5) 87.2(12.6) 86.3(11.1) 4.927 0.177
ESMI group 82.0(12.9) 90.3(10.7) 89.4(11.2) 90.2(10.2) 29.950 0.000**
Angina
stability
C group 47.0(20.7) 47.4(17.5) 49.3(16.8) 47.8(12.1) 0.095 0.992
PE group 50.8(20.4) 51.6(19.4) 52.0(16.2) 46.9(14.4) 5.527 0.137
ESMI group 51.5(20.7) 55.0(19.9) 56.2(20.7) 49.6(16.2) 7.092 0.069
Angina
frequency
C group 83.3(18.1) 84.8(18.6) 84.6(19.3) 86.4(20.6) 9.836 0.020*
PE group 84.1(19.7) 85.9(18.7) 89.8(15.6) 88.1(19.3) 9.539 0.023*
ESMI group 83.5(17.6) 91.4(12.9) 91.8(13.2) 91.2(18.8) 28.798 0.000**
Treatment
satisfaction
C group 69.9(20.1) 67.5(18.4) 66.0(16.7) 73.5(17.4) 7.469 0.058
PE group 68.8(18.5) 73.5(16.5) 76.1(16.2) 77.2(17.1) 17.790 0.000**
ESMI group 66.9(17.5) 84.7(15.1) 84.3(16.4) 84.3(18.0) 64.141 0.000**
Disease
perception
C group 71.1(21.9) 71.1(20.0) 71.0(20.8) 76.6(19.4) 10.606 0.014*
PE group 69.8(21.8) 75.8(17.9) 80.1(17.5) 79.7(18.3) 24.862 0.000**
ESMI group 68.1(17.7) 84.2(17.7) 85.0(18.2) 84.5(20.3) 61.018 0.000**
The scores of each subscale of SAQ range from 0 to 100, with the higher scores indicating better health
conditions; T0: baseline data; T1: data immediately after the completion of the 8-week intervention; T2:
data at the 3-month follow up; T3: data at the 6-month follow up; *p < 0.05; ** p < 0.01.

256
5.4.6.2 SF-36
The SF-36 includes the following eight domains: Physical Functioning (PF), Role-
Physical (RP), Bodily Pain (BP), General Health (GH), Vitality (VT), Social
Functioning (SF); Role-Emotional (RE), and Mental Health (MH). These eight
domains are classified into two components: Physical Component Summary (PCS, PF
+ RP + BP + GH), and Mental Component Summary (MCS, VT + SF + RE + MH).
The higher scores of these domains indicate better health functioning. In addition, SF-
36 has another item: Reported Health Transition (HT). The lower scores of this item
indicate better health conditions.
Table 5.26 and Figures 5.16-5.25 show the changes in the mean scores of the above
mentioned eight domains of the SF-36, the physical component summary, mental
component summary, and reported health transition throughout the study. For the
ESMI group, the mean scores of all eight domains, and the PCS and MCS of SF-36,
increased sharply during the period of the implementation of the intervention (T1),
and remained stable or kept rising from T1 to T3. However, the mean scores for role-
physical, role-emotional, and mental health declined from T1 to T2, then rose slightly
again from T2 to T3. Meanwhile, the mean scores for mental health continued to fall
from T2 to T3, with the mean scores still higher than the baseline (T0). All of the mean
scores at T1, T2, and T3 were higher than the baseline (T0).
In the PE group, the mean scores of all eight domains, and the PCS and MCS of SF-
36, went up slightly or remained stable during the period of the implementation of the
intervention (T1); the mean scores for physical functioning, vitality, social functioning,

257
and mental health continued to increase steadily from T1 to T3, while the mean scores
for role-physical, bodily pain, role-emotional, PCS and MCS, declined from T1 to T2,
and remained stable or declined from T2 to T3. However, the mean scores for bodily
pain and MCS rebounded slightly from T2 to T3. Meanwhile, the mean scores for
general health were stable from T1 to T2, before falling slightly from T2 to T3. All of
the mean scores at T1, T2, and T3 were higher than the baseline (T0), with the
exception of the mean scores for role-physical at T3 and role-emotional at T2 and T3,
which were lower than the baseline (T0).
For the C group, the mean scores for physical functioning, general health, vitality,
social functioning, and the MCS of SF-36 dropped slightly during the period of the
implementation of the intervention (T1) and rose steadily from T1 to T3. However, the
mean scores for vitality remained stable from T1 to T2, then rose from T2 to T3, with
the mean scores equalling the baseline (T0). The mean scores for role-physical, bodily
pain, and PCS rose rapidly during the period of the implementation of the intervention
(T1) and declined steadily from T1 to T3, except that the mean scores for PCS
increased slightly again from T2 to T3. The mean scores for role-emotional remained
stable during the period of the implementation of the intervention (T1), slowly went
up from T1 to T2, and fell from T2 to T3. The mean scores for role-physical, social
functioning, role-emotional, mental health, and MCS at T3 were lower than the
baseline (T0).
Figure 5.26 shows the changes in the mean scores for reported health transition
throughout the study. The mean scores for reported health transition in all three
groups declined substantially from T0 to T3. The decrease slope was largest in the

258
ESMI group, followed by the PE group, and last by the C group. As a whole, higher
mean scores for all eight domains, PCS, and MCS, and lower mean scores for
reported health transition were seen for the ESMI group than for the C and PE groups
from T0 to T3.
Table 5.26 Mean and Standard Deviations of Eight Domains of SF-36 at Each Time
Point
C group
(n=67)
mean (SD)
PE group
(n=64)
mean (SD)
ESMI group
(n=65)
mean (SD)
Physical functioning (PF)
T0 81.4(13.6) 82.3(9.7) 78.8(16.2)
T1 80.6(12.6) 82.7(11.4) 86.4(13.7)
T2 83.3(11.3) 85.2(11.0) 87.5(13.8)
T3 84.8(12.8) 87.3(9.3) 88.7(13.4)
Role-physical (RP)
T0 72.0(40.0) 63.7(39.6) 67.3(39.3)
T1 79.9(35.9) 74.2(38.3) 86.2(26.5)
T2 72.0(40.7) 69.1(41.0) 80.0(33.7)
T3 69.0(43.8) 64.1(42.2) 81.5(35.4)
Bodily pain (BP)
T0 73.7(24.8) 75.4(22.1) 75.4(22.9)
T1 82.2(22.2) 79.9(22.4) 87.7(16.7)
T2 76.5(23.2) 76.2(23.5) 87.6(17.1)
T3 74.9(24.8) 79.5(21.7) 85.3(20.8)
General health (GH)
T0 57.4(22.8) 55.4(22.3) 57.9(23.4)
T1 56.0(23.7) 64.2(20.8) 71.8(21.0)
T2 57.3(25.7) 64.6(21.3) 73.5(20.0)
T3 63.8(25.5) 62.7(23.0) 71.8(25.0)
Vitality (VT)
T0 72.5(17.6) 70.9(17.1) 68.8(18.8)
T1 68.3(19.2) 70.9(16.9) 80.2(15.1)
T2 68.4(18.0) 71.7(16.2) 79.8(14.1)
T3 72.5(17.0) 74.3(14.1) 82.0(13.0)

259
Table 5.26 Continued
C group
(n=67)
mean (SD)
PE group
(n=64)
mean (SD)
ESMI group
(n=65)
mean (SD)
Social functioning (SF)
T0 84.5(22.1) 79.3(23.8) 80.6(21.7)
T1 82.8(22.4) 81.6(22.7) 90.0(17.6)
T2 83.6(22.3) 83.4(19.9) 91.9(16.5)
T3 84.1(22.1) 85.9(21.1) 91.2(17.5)
Role-emotional (RE)
T0 80.6(34.9) 84.9(27.8) 79.0(36.1)
T1 80.6(38.1) 87.0(28.9) 92.3(24.8)
T2 83.1(35.0) 81.8(34.1) 86.2(33.3)
T3 79.6(37.6) 82.3(33.6) 89.2(31.2)
Mental health (MH)
T0 83.0(13.9) 80.4(10.4) 80.4(12.8)
T1 80.6(14.5) 80.9(11.7) 88.9(10.3)
T2 81.6(13.9) 82.8(9.7) 87.3(10.8)
T3 82.3(14.1) 82.9(10.1) 85.8(13.3)
Physical component
summary (PCS)
T0 284.5(76.9) 276.8(65.1) 279.5(75.8)
T1 298.7(77.7) 301.1(64.5) 332.1(57.9)
T2 289.1(79.2) 295.2(70.2) 328.5(65.5)
T3 292.5(90.1) 293.6(69.8) 327.3(77.2)
Mental component
summary (MCS)
T0 320.6(67.6) 315.6(59.0) 308.8(72.2)
T1 312.3(79.9) 320.5(60.7) 351.4(58.6)
T2 316.7(76.8) 319.6(60.1) 345.1(62.4)
T3 318.5(76.8) 325.5(60.0) 348.2(64.6)
Reported health transition
(HT)
T0 3.3(1.1) 3.1(1.3) 3.3(1.1)
T1 3.3(1.0) 2.8(1.1) 2.7(1.1)
T2 3.1(0.9) 2.7(1.1) 2.6(1.2)
T3 2.9(1.0) 2.5(1.1) 2.5(1.2)
The scores of each domain range from 0 to 100, with the higher scores indicating better health
functioning; The scores of HT range from 1 to 5, with the lower scores indicating better health
conditions; PCS = PF + RP + BP + GH; MCS = VT + SF + RE + MH.
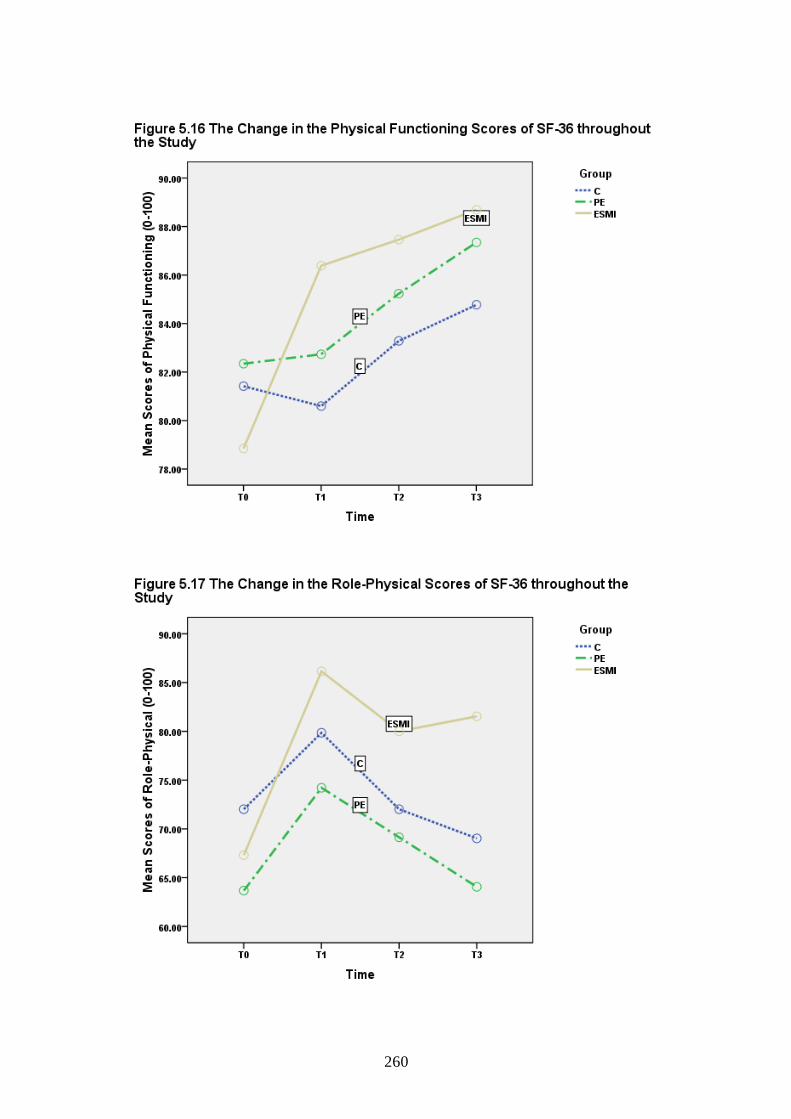
260

261

262

263

264

265
Since the data on the eight domains of SF-36, physical component summary, mental
component summary, and reported health transition were not normally distributed and
the related homogeneity of variance among the three groups was not achieved in most
data (Appendix XV), non-parametric tests were used to analyze them. At baseline, no
significant differences were found in the mean scores of the eight domains, the
physical component summary, mental component summary, and reported health
transition among the three groups, as confirmed by the Kruskal-Wallis test (Appendix
XVI). After the completion of the 8-week intervention, higher mean change scores for
all eight domains, the physical component summary and mental component summary,
and a larger reduction in the mean scores for reported health transition were observed
in the ESMI than in the PE and C groups at T1, T2, and T3 (Table 5.27). Significant
differences were identified in the mean change scores for physical functioning (mean

266
rank: T1 - T0: ESMI group = 125.0, PE group = 88.3, C group = 82.6, p < 0.01; T2 - T0:
ESMI group = 121.2, PE group = 93.4, C group = 81.4, p < 0.01; T3 - T0: ESMI group
= 117.4, PE group = 94.1, C group = 84.4, p < 0.01), vitality (mean rank: T1 - T0:
ESMI group = 128.6, PE group = 88.9, C group = 78.5, p < 0.01; T2 - T0: ESMI group
= 127.2, PE group = 90.8, C group = 78.1, p < 0.01; T3 - T0: ESMI group = 127.8, PE
group = 88.1, C group = 80.0, p < 0.01), social functioning (mean rank: T1 - T0: ESMI
group = 113.0, PE group = 97.7, C group = 85.2, p < 0.05; T2 - T0: ESMI group =
112.9, PE group = 97.1, C group = 85.9, p < 0.05; T3 - T0: ESMI group = 109.8, PE
group = 102.4, C group = 83.8, p < 0.05), mental health (mean rank: T1 - T0: ESMI
group = 129.6, PE group = 91.1, C group = 75.4, p < 0.01; T2 - T0: ESMI group =
119.1, PE group = 100.5, C group = 76.6, p < 0.01; T3 - T0: ESMI group = 117.3, PE
group = 98.6, C group = 80.2, p < 0.01), physical component summary (mean rank: T1
- T0: ESMI group = 118.0, PE group = 93.3, C group = 84.6, p < 0.01; T2 - T0: ESMI
group = 117.7, PE group = 92.5, C group = 85.6, p < 0.01; T3 - T0: ESMI group =
114.1, PE group = 92.7, C group = 88.9, p < 0.05), and mental component summary
(mean rank: T1 - T0: ESMI group = 127.0, PE group = 92.2, C group = 76.9, p < 0.01;
T2 - T0: ESMI group = 121.7, PE group = 89.9, C group = 84.2, p < 0.01; T3 - T0:
ESMI group = 117.4, PE group = 95.5, C group = 83.1, p < 0.01) among the three
groups at T1, T2, and T3 (Table 5.27). Significant differences in the mean change
scores for general health (mean rank: T1 - T0: ESMI group = 128.6, PE group = 88.9,
C group = 78.5, p < 0.01; T2 - T0: ESMI group = 119.3, PE group = 98.8, C group =
78.0, p < 0.01) and reported health transition (mean rank: T1 - T0: ESMI group = 84.6,
PE group = 100.2, C group = 110.3, p < 0.05; T2 - T0: ESMI group = 85.4, PE group =
100.6, C group = 109.2, p < 0.05) were also found among the three groups at T1 and
T2, but the effects disappeared at T3 (Table 5.27). In addition, significant differences

267
in the mean change scores for bodily pain (mean rank: T2 - T0: ESMI group = 113.4,
PE group = 90.6, C group = 91.7, p < 0.05) were detected among the three groups at
T2, while no significant differences were found at T1 and T3 (Table 5.27).
The effect sizes of the TTM-based ESMI on the eight domains, PCS, MCS, and
reported health transition of the SF-36 ranged from 0.1 to 0.4 (Table 5.27), which
would be between a small (0.10) and large (0.40) effect for an ANOVA analysis
based on Cohen‘s (1988) terms. These findings suggest that the patients who
participated in the ESMI group experienced a better quality of life in terms of the SF-
36, especially with regard to physical functioning, vitality, social functioning, mental
health, PCS, and MCS than those in the PE and C groups.

268
Table 5.27 Comparisons of the Mean Change Scores of Eight Domains of SF-36 among
Groups at Each Time Point
C group
(n=67)
mean (SD)
PE group
(n=64)
mean (SD)
ESMI group
(n=65)
mean (SD)
Kruskal-Wallis test Effect
size
(r) χ
2 p
PF
T1 - T0 -0.8(11.5) 0.4(9.1) 7.5(10.8) 22.983 0.000** 0.3
T2 - T0 1.9(11.4) 2.9(8.7) 8.6(11.3) 17.855 0.000** 0.3
T3 - T0 3.4(12.2) 5.0(9.5) 9.8(11.8) 12.288 0.002** 0.2
RP
T1 - T0 7.8(37.5) 10.5(40.3) 18.8(38.8) 3.075 0.215 0.1
T2 - T0 0.0(47.9) 5.5(42.4) 12.7(41.7) 2.226 0.329 0.1
T3 - T0 -3.0(53.9) 0.4(43.5) 14.2(39.5) 4.495 0.106 0.2
BP
T1 - T0 8.5(23.4) 4.5(19.9) 12.3(24.7) 4.531 0.104 0.1
T2 - T0 2.8(25.6) 0.8(22.2) 12.1(25.8) 6.976 0.031* 0.2
T3 - T0 1.2(29.1) 4.1(22.7) 9.8(29.1) 4.016 0.134 0.1
GH
T1 - T0 -1.4(20.3) 8.8(20.7) 14.0(24.7) 19.907 0.000** 0.3
T2 - T0 -0.0(22.3) 9.2(23.5) 15.6(20.1) 17.683 0.000** 0.3
T3 - T0 6.4(23.8) 7.3(21.6) 14.0(24.9) 4.512 0.105 0.1
VT
T1 - T0 -4.2(15.7) 0.0(15.4) 11.3(17.8) 28.906 0.000** 0.4
T2 - T0 -4.0(18.8) 0.8(17.0) 10.9(15.0) 26.834 0.000** 0.4
T3 - T0 0.0(16.5) 3.4(13.4) 13.2(15.4) 27.130 0.000** 0.4
SF
T1 - T0 -1.7(25.0) 2.3(23.6) 9.4(22.1) 9.071 0.011** 0.2
T2 - T0 -0.9(22.9) 4.1(24.5) 11.3(22.1) 8.409 0.015* 0.2
T3 - T0 -0.4(24.1) 6.6(23.1) 10.6(21.7) 8.456 0.015* 0.2

269
Table 5.27 Continued
C group
(n=67)
mean (SD)
PE group
(n=64)
mean (SD)
ESMI group
(n=65)
mean (SD)
Kruskal-Wallis test Effect
size
(r) χ
2 p
RE
T1 - T0 -0.0(33.8) 2.1(33.5) 13.3(31.6) 5.217 0.074 0.2
T2 - T0 2.5(37.3) -3.1(29.5) 7.2(40.2) 1.215 0.545 0.1
T3 - T0 -1.0(44.6) -2.6(33.2) 10.3(35.8) 4.312 0.116 0.2
MH
T1 - T0 -2.4(13.3) 0.5(10.7) 8.5(12.6) 32.569 0.000** 0.4
T2 - T0 -1.5(14.0) 2.3(11.0) 6.8(10.8) 19.093 0.000** 0.3
T3 - T0 -0.7(14.2) 2.5(11.3) 5.4(10.3) 14.460 0.001** 0.2
PCS
T1 - T0 14.2(63.8) 24.3(60.7) 52.7(70.5) 12.311 0.002** 0.2
T2 - T0 4.6(71.8) 18.4(63.0) 49.0(69.5) 11.672 0.003** 0.3
T3 - T0 8.0(86.9) 16.8(67.0) 47.9(81.6) 7.554 0.023* 0.2
MCS
T1 - T0 -8.3(62.7) 4.9(56.9) 42.6(69.4) 26.947 0.000** 0.3
T2 - T0 -4.0(69.0) 4.1(53.1) 36.3(70.0) 16.667 0.000** 0.3
T3 - T0 -2.1(72.5) 9.9(56.1) 39.3(65.6) 12.392 0.002** 0.3
HT
T1 - T0 -0.0(1.1) -0.2(1.3) -0.6(1.3) 7.493 0.024* 0.2
T2 - T0 -0.2(1.2) -0.4(1.4) -0.8(1.3) 6.562 0.038* 0.2
T3 - T0 -0.4(1.2) -0.5(1.4) -0.9(1.3) 5.269 0.072 0.2
PF: Physical Functioning; RP: Role-Physical; BP: Bodily Pain; GH: General Health; VT: Vitality; SF:
Social Functioning; RE: Role-Emotional; MH: Mental Health; PCS: Physical Component Summary
(PF + RP + BP + GH); MCS: Mental Component Summary (VT + SF + RE + MH); HT: Reported
Health Transition; *p < 0.05; ** p < 0.01.

270
For within-group comparisons of eight domains, the physical component summary,
mental component summary, and reported health transition of SF-36, the Friedman
test was applied. The C group showed significant differences in the mean scores for
physical functioning (mean rank: T0 = 2.4, T1 = 2.3, T2 = 2.5, T3 = 2.9, p < 0.01) and
general health (mean rank: T0 = 2.5, T1 = 2.2, T2 = 2.4, T3 = 2.9, p < 0.01) over time
(Table 5.28). The PE group demonstrated significant differences in the mean scores
for physical functioning (mean rank: T0 = 2.2, T1 = 2.1, T2 = 2.8, T3 = 2.9, p < 0.01),
general health (mean rank: T0 = 2.1, T1 = 2.6, T2 = 2.7, T3 = 2.7, p < 0.01), social
functioning (mean rank: T0 = 2.3, T1 = 2.5, T2 = 2.5, T3 = 2.8, p < 0.05), physical
component summary (mean rank: T0 = 2.1, T1 = 2.6, T2 = 2.7, T3 = 2.6, p < 0.05), and
reported health transition (mean rank: T0 = 2.8, T1 = 2.5, T2 = 2.4, T3 = 2.3, p < 0.05)
over time (Table 5.28). The ESMI group revealed significant differences in all eight
domains, such as physical functioning (mean rank: T0 = 1.6, T1 = 2.5, T2 = 2.8, T3 =
3.1, p < 0.01), role-physical (mean rank: T0 = 2.2, T1 = 2.7, T2 = 2.5, T3 = 2.6, p <
0.01), bodily pain (mean rank: T0 = 2.1, T1 = 2.7, T2 = 2.6, T3 = 2.6, p < 0.01), general
health (mean rank: T0 = 1.7, T1 = 2.7, T2 = 2.8, T3 = 2.8, p < 0.01), vitality (mean rank:
T0 = 1.7, T1 = 2.8, T2 = 2.6, T3 = 2.9, p < 0.01), social functioning (mean rank: T0 =
2.1, T1 = 2.6, T2 = 2.7, T3 = 2.7, p < 0.01), role-emotional (mean rank: T0 = 2.3, T1 =
2.6, T2 = 2.5, T3 = 2.6, p < 0.01), mental health (mean rank: T0 = 1.7, T1 = 3.0, T2 =
2.6, T3 = 2.7, p < 0.01), physical component summary (mean rank: T0 = 1.7, T1 = 2.7,
T2 = 2.8, T3 = 2.8, p < 0.01), mental component summary (mean rank: T0 = 1.7, T1 =
2.9, T2 = 2.6, T3 = 2.8, p < 0.01), and reported health transition (mean rank: T0 = 3.1,
T1 = 2.4, T2 = 2.3, T3 = 2.2, p < 0.01) over time (Table 5.28).

271
Table 5.28 Comparisons of Eight Domains of SF-36 within Each Group across Time
T0
mean (SD)
T1
mean (SD)
T2
mean (SD)
T3
mean (SD)
Friedman test
χ2 p
PF
C group 81.4(13.6) 80.6(12.6) 83.3(11.3) 84.8(12.8) 14.487 0.002**
PE group 82.3(9.7) 82.7(11.4) 85.2(11.0) 87.3(9.3) 31.233 0.000**
ESMI group 78.8(16.2) 86.4(13.7) 87.5(13.8) 88.7(13.4) 76.073 0.000**
RP
C group 72.0(40.0) 79.9(35.9) 72.0(40.7) 69.0(43.8) 2.991 0.393
PE group 63.7(39.6) 74.2(38.3) 69.1(41.0) 64.1(42.2) 5.283 0.152
ESMI group 67.3(39.3) 86.2(26.5) 80.0(33.7) 81.5(35.4) 13.627 0.003**
BP
C group 73.7(24.8) 82.2(22.2) 76.5(23.2) 74.9(24.8) 6.894 0.075
PE group 75.4(22.1) 79.9(22.4) 76.2(23.5) 79.5(21.7) 4.363 0.225
ESMI group 75.4(22.9) 87.7(16.7) 87.6(17.1) 85.3(20.8) 17.067 0.001**
GH
C group 57.4(22.8) 56.0(23.7) 57.3(25.7) 63.8(25.5) 13.297 0.004**
PE group 55.4(22.3) 64.2(20.8) 64.6(21.3) 62.7(23.0) 12.586 0.006**
ESMI group 57.9(23.4) 71.8(21.0) 73.5(20.0) 71.8(25.0) 41.915 0.000**
VT
C group 72.5(17.6) 68.3(19.2) 68.4(18.0) 72.5(17.0) 6.889 0.076
PE group 70.9(17.1) 70.9(16.9) 71.7(16.2) 74.3(14.1) 2.589 0.459
ESMI group 68.8(18.7) 80.15(15.1) 79.8(14.1) 82.0(13.0) 51.881 0.000**
SF
C group 84.5(22.1) 82.8(22.4) 83.6(22.3) 84.1(22.1) 1.492 0.684
PE group 79.3(23.8) 81.6(22.7) 83.4(19.9) 85.9(21.1) 8.339 0.040*
ESMI group 80.6(21.7) 90.0(17.6) 91.9(16.5) 91.2(17.5) 25.930 0.000**
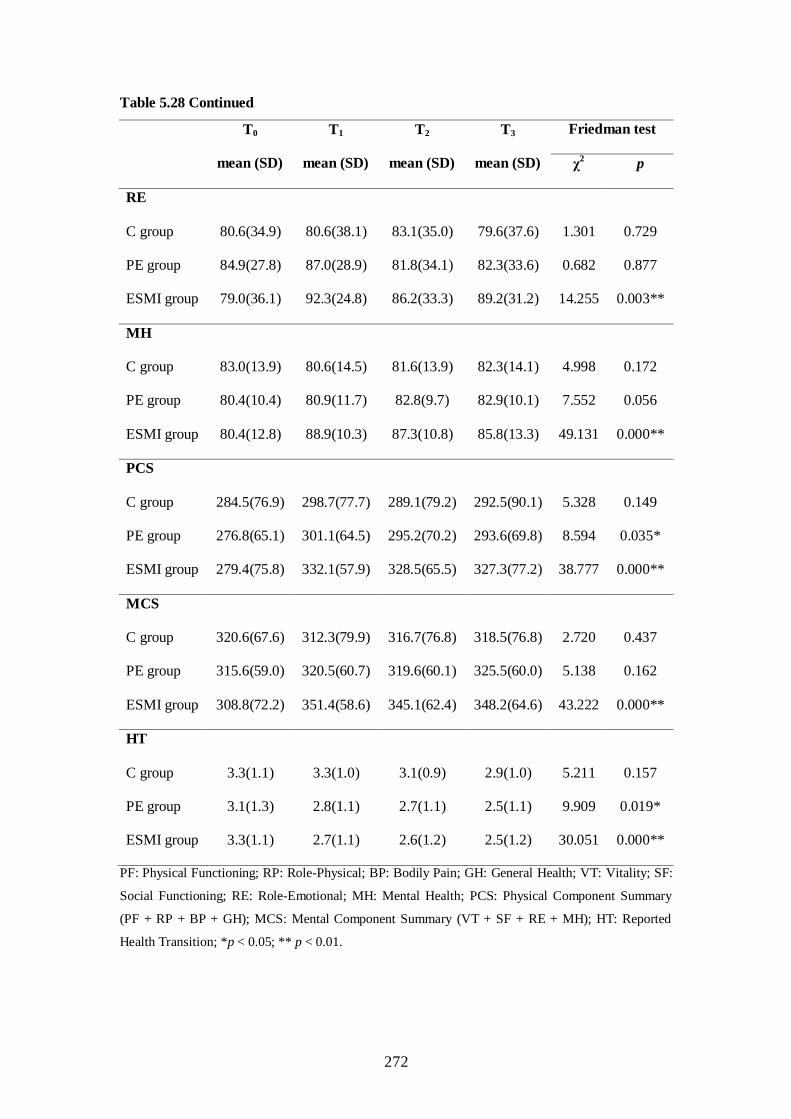
272
Table 5.28 Continued
T0
mean (SD)
T1
mean (SD)
T2
mean (SD)
T3
mean (SD)
Friedman test
χ2 p
RE
C group 80.6(34.9) 80.6(38.1) 83.1(35.0) 79.6(37.6) 1.301 0.729
PE group 84.9(27.8) 87.0(28.9) 81.8(34.1) 82.3(33.6) 0.682 0.877
ESMI group 79.0(36.1) 92.3(24.8) 86.2(33.3) 89.2(31.2) 14.255 0.003**
MH
C group 83.0(13.9) 80.6(14.5) 81.6(13.9) 82.3(14.1) 4.998 0.172
PE group 80.4(10.4) 80.9(11.7) 82.8(9.7) 82.9(10.1) 7.552 0.056
ESMI group 80.4(12.8) 88.9(10.3) 87.3(10.8) 85.8(13.3) 49.131 0.000**
PCS
C group 284.5(76.9) 298.7(77.7) 289.1(79.2) 292.5(90.1) 5.328 0.149
PE group 276.8(65.1) 301.1(64.5) 295.2(70.2) 293.6(69.8) 8.594 0.035*
ESMI group 279.4(75.8) 332.1(57.9) 328.5(65.5) 327.3(77.2) 38.777 0.000**
MCS
C group 320.6(67.6) 312.3(79.9) 316.7(76.8) 318.5(76.8) 2.720 0.437
PE group 315.6(59.0) 320.5(60.7) 319.6(60.1) 325.5(60.0) 5.138 0.162
ESMI group 308.8(72.2) 351.4(58.6) 345.1(62.4) 348.2(64.6) 43.222 0.000**
HT
C group 3.3(1.1) 3.3(1.0) 3.1(0.9) 2.9(1.0) 5.211 0.157
PE group 3.1(1.3) 2.8(1.1) 2.7(1.1) 2.5(1.1) 9.909 0.019*
ESMI group 3.3(1.1) 2.7(1.1) 2.6(1.2) 2.5(1.2) 30.051 0.000**
PF: Physical Functioning; RP: Role-Physical; BP: Bodily Pain; GH: General Health; VT: Vitality; SF:
Social Functioning; RE: Role-Emotional; MH: Mental Health; PCS: Physical Component Summary
(PF + RP + BP + GH); MCS: Mental Component Summary (VT + SF + RE + MH); HT: Reported
Health Transition; *p < 0.05; ** p < 0.01.

273
5.7 Summary
This chapter presented the recruitment of the participants in this study, their
characteristics, a comparison of their exercise stages of change, exercise self-efficacy,
exercise benefits and barriers, exercise duration per week, angina, and quality of life
within and between the patients in the C, PE, and ESMI groups at each time point (T0,
T1, T2 and, T3). The findings showed a significantly more positive shift in the exercise
stages of change, higher exercise self-efficacy, greater exercise benefits, fewer
exercise barriers, longer exercise duration per week, and better quality of life in terms
of the SAQ and SF-36 in the ESMI group than in the C and PE groups immediately
after the 8-week intervention and at the 3- and 6-month follow-up period. These
findings suggest that the TTM-based ESMI has significantly positive effects on
changing exercise behaviour and improving quality of life in sedentary CHD patients
in China. However, in this study it was also observed during the follow-up period that
the effects on these variables tended to fade away.

274
Chapter 6 Discussion
6.1 Introduction
This chapter discusses the results of the study based on the research questions, in
order to determine whether the aims of the study had been achieved. It also compares
the findings with other related studies. This chapter includes a discussion of the high
participation/completion rate in this study; the effects of the TTM-based ESMI on
changing exercise behaviour and improving health outcomes in terms of reducing
anginal attacks and improving quality of life; and the tracking of the TTM-based
ESMI on exercise behaviour.
6.2 High Participation/Completion Rate
A total of 196 sedentary CHD patients were recruited in this study, of whom 150
completed the whole study. The completion rate in this study was 76.5% (150/196) –
much higher than that in previous studies of exercise-based cardiac rehabilitation
programmes, in which the participation/completion rate during the first six months
was about 50% (Dorn, Naughton, Imamura & Trevisan, 2001; Moore, Dolansky,
Ruland, Pashkow & Blackburn, 2003; Sanderson & Bittner, 2005; Sanderson, Phillips,
Gerald, DiLillo & Bittner, 2003; Sarrafzadegan, Rabiei, Shirani et al., 2007;
Worcester, Murphy, Mee, Roberts & Goble, 2004). Previous studies have shown that
the participation rate decreases over time, particularly six months into a programme
(Dorn, Naughton, Imamura & Trevisan, 2001; Touillet, Guesdon, Bosser, Beis &
Paysant, 2010). The finding from this study also showed that the average participation
275
rate in the eight weekly ESMI sessions was 85.2%. The high participation and
completion rates in this study substantiate the view that the implementation of the
TTM-based ESMI in cardiac rehabilitation programmes is suitable for sedentary CHD
patients in China.
The following two factors may have contributed to the high participation/completion
rate in this study. First, the delivery of a client-centred intervention may have been a
contributor. The characteristic of the TTM-based ESMI is the delivery of strategies or
techniques matched to the client's current stage of behavioural change (Burbank,
Padula & Nigg, 2000; Prochaska, DiClemente & Norcross, 1992), which may meet
the client's most needs (Prochaska & Velicer, 1997). Thus, a stage-specific
intervention can be delivered according to the TTM. Previous studies have
demonstrated that a TTM-based stage-matched intervention can increase the uptake of
programmes (Prochaska, DiClemente & Norcross, 1992; Prochaska & Velicer, 1997;
Rakowski, Ehrich, Goldstein et al., 1998) and reduce dropout rates (Beckie &
Beckstead, 2010; Schelling, Munsch, Meyer et al., 2009). In addition, in this study the
eight weekly ESMI sessions were delivered through either face-to-face or telephone
contacts. These modes of contact are the approaches most preferred by CHD patients
in China (Chen & Jing, 2008; Du, Chen, & Liu, 2005; Hu, 2006; Li & Liu, 2006; Li &
Wang, 2006; Liu, 2005; Wan & Wang, 2008) because these both forms of contact are
interactive in nature. Moreover, in this study the face-to-face or telephone contacts
between the researcher and the patients were scheduled according to the time that the
patients were available regardless of whether this was in the evenings or at weekends.
This kind of client-centred contact schedule may have contributed to the high
participation rate in the eight weekly ESMI sessions in this study (85.2%).

276
Second, the fact that there were no reports of exercise-induced adverse effects (e.g.,
heart attacks due to exercise) may have been another contributor to the high
participation/completion rate in this study. Previous studies have indicated that CHD
patients often lack the confidence to perform exercises because they worry about the
occurrence of angina or hold the misconception that physical activity may provoke an
anginal attack (Kristofferzon, Löfmark & Carlsson, 2007; Thompson & Lewin, 2000;
Zhu, Ho & Sit, 2012). Our previous interviews (Zhu, Ho & Sit, 2012) with 11 Chinese
CHD patients in mainland China also showed that the patients perceived CHD to be a
life-threatening illness mostly related to chest pain and worried about the recurrence
of heart attacks. Patients often hold the misconception that heart attacks cannot be
prevented and that physical activity provokes chest pain. The result of these
misconceptions is fewer changes in behaviour and even disengagement from physical
activity. During the whole study period, there were no reports of exercise-induced
adverse effects, which may have helped the patients to build up their confidence
(exercise self-efficacy) to engage in exercise and correct their misconception that
physical activity would provoke anginal attacks. Correcting their misconceptions may
have further enhanced their confidence to change exercise behaviour. Thus, the fact
that no exercise-induced adverse effects occurred during the study period may have
been a factor contributing to the high participation/completion rate in this study.
6.3 The Effects of the TTM-based ESMI on CHD Patients
In this randomized controlled trial, eligible patients were randomly allocated to one of
the following three groups: the Conventional (C) group, the Patient Education (PE)

277
group, and the Exercise Stage-Matched Intervention (ESMI) group. The aim of this
study was to evaluate whether sedentary CHD patients who participated in the ESMI
group had better results in exercise behaviour and health outcomes in terms of anginal
attacks and quality of life than those in the C and PE groups. Accordingly, in this
section, the effects of the TTM-based ESMI on these two areas are thoroughly
discussed.
6.3.1 Exercise Behaviour
This is the first study to examine the effects of the TTM-based ESMI on exercise
behaviour among sedentary CHD patients in China. In this study, exercise behaviour
was evaluated by exercise stages of change, exercise self-efficacy, exercise decisional
balance, and exercise duration per week. In this subsection, changes in the exercise
behaviour of each group were discussed thoroughly.
6.3.1.1 Exercise behaviour of the Conventional (C) Group
The findings from this study showed that the patients in all the three groups improved
their exercise behaviour after the interventions. This finding showed that patients in
the C group could also be motivated to change their exercise behaviour over time,
namely, they showed significant progress in exercise stages of change, exercise self-
efficacy, exercise benefits, and exercise duration per week, and a decrease in exercise
barriers over time. Possible explanations for the improvements noted in the C group
may be the content of conventional care, normal recovery, and measurement effects.
Patients in the C group only received conventional care, which is simple and

278
unstructured patient education on diet, exercise, and medications related to CHD.
Casually delivering information to them about the benefits of exercise and the risks of
physical inactivity may also have improved their knowledge of exercise and increased
their awareness of the importance of engaging in exercise, which resulted in a change
in their behaviour. Another possible reason for the progress in exercise behaviour
seen in the C group over time may be that it was due to the normal process of
recovery. Near half of the patients who participated in this study had been diagnosed
with coronary heart disease (myocardial infarction, angina pectoris, or had undergone
PTCA/PCI) for around three months. As they recovered from their illness, they may
have naturally increased the level of their physical activities or exercise. A previous
study has shown that self-efficacy increased over time, as patients had an opportunity
to gain confidence as they succeeded in adapting to lifestyle changes (Barnason,
Zimmerman, Nieween et al., 2003). With physical recovery over time, patients may
have accordingly become more confident about their ability to engage in exercise.
Finally, measurement effects may be another contributor to the changes in exercise
behaviour seen in the C group. A positive measurement effect has been observed in
randomized controlled trials promoting regular exercise (van Sluijs, van Poppel,
Twisk et al., 2005; van Sluijs, van Poppel, Twisk & van Mechelen, 2006). In these
studies, statistically significant measurement effects were found in self-reported
exercise, self-efficacy for resisting relapse, and knowledge and awareness, although
there were no significant differences in exercise stages of change and accelerometer
data (i.e., counts per minute). Van Sluijs et al. (2006) stated that measurements of
exercise or physical activity influence patients‘ exercise behaviour, possibly triggered
by a raised awareness, because awareness of one‘s own behaviour is an important

279
starting point for behavioural change. They explained that the content of the
measurements might have triggered this awareness because when patients were asked
about their level of exercise in detail, they were given the opportunity to create an
overview of their exercise pattern during a normal week. All of the patients in this
study underwent outcome measurements four times, which may have resulted in the
measurement effects that possibly contributed to the effects found in the C group.
However, all of the three groups were administered the same time-point outcome
measurements. The measurement effects were evenly distributed in all three groups.
Thus, measurement effects did not contribute to the findings from the comparisons
between the groups, which instead can be attributed to the effects of the intervention.
6.3.1.2 Exercise behaviour of the Patient Education (PE) Group
In this study, patients in the PE group demonstrated better effects on exercise
behaviour in terms of a more positive shift in exercise stages of change, higher
exercise self-efficacy, greater exercise benefits, fewer exercise barriers and longer
moderate exercise duration per week as compared with those in the C group. These
findings suggest that general patient education about CHD and exercise also has a
positive impact on changing exercise behaviour in sedentary CHD patients. The
finding of the positive effect on exercise behaviour is similar to the results from
previous systematic reviews of chronically ill patients (Conn, Hafdahl, Brown &
Brown, 2008) and heart disease patients (Zhu, Ho & Wong, unpublished), which
showed that patient education has a positive effect on changing exercise behaviour.

280
Patients in the PE group received conventional care, one 2-hour patient education
session and a booklet about cardiac rehabilitation, and eight weekly sessions of
general patient education about the importance and benefits of regular exercise. Thus,
one possible explanation for the finding in the PE group is that patient education
improved the patients‘ knowledge of CHD and exercise. Knowledge about the risk
factors for CHD is related to compliance with lifestyle changes (e.g., physical activity)
(Alm-Roijer, Stagmo, Udén & Erhardt, 2004). Previous studies have demonstrated
that patient education can increase the patients‘ knowledge and promote related
healthy behavioural changes (e.g., exercise) (Aldana, Greenlaw, Diehl et al., 2008;
Fuster, 2007; Hogan & Neill, 1982; Netto, McCloughan & Bhatnagar, 2007; Plach,
Wierenga & Heidrich, 1996). In addition, simply providing educational information
about CHD and exercise can also be viewed as a process of change according to
Prochaska and DiClemente (1983), who pointed out that consciousness raising (e.g.,
seeking new information and gaining understanding and feedback about exercise)
helps individuals to move from one motivational stage to another (Schelling, Munsch,
Meyer et al., 2009). Another possible explanation for this finding may be that most
patients (more than 60%) were at the preparation stage at baseline in this study, which
implies that most of the patients were ready to change their exercise behaviour at the
start of the study. The general patient education about the importance and benefits of
exercise was sufficient to motivate those who were already ready to begin to change
their exercise behaviour. The findings of this study suggest that general patient
education regarding CHD and the importance and benefits of exercise will also have a
positive impact on motivating sedentary CHD patients to engage in exercise.

281
Although few studies have evaluated the effect of generic patient education on
changing exercise behaviour with respect to exercise stages of change, exercise self-
efficacy, and exercise decisional balance, a number of studies have shown that patient
education may have a significantly positive effect on exercise adherence, with
participants who exercised regularly reaching the required guidelines (Allen,
Blumenthal, Margolis et al., 2002; Arrigo, Brunner-LaRocca, Lefkovits et al., 2008;
Cupples & McKnight, 1994; Giallauria, Lucci, D‘Agostino, Vitelli et al., 2009; Jeong,
Chae, Moon & Yoo, 2002; Johnson, Lim & Bowe, 2009; Murchie, Campbell, Ritchie
et al., 2003; Redfern, Briffa, Ellis & Freedman, 2008; The Vestfold Heartcare Group,
2003). These studies also indicate the importance of providing knowledge and giving
general information on cardiac rehabilitation and exercise for CHD patients to
motivate them to engage in exercise.
6.3.1.3 Exercise behaviour of the Exercise Stage-Matched Intervention (ESMI)
Group
Among the patients in the ESMI group, a significantly positive effect was observed
with regard to changes in exercise behaviour in terms of a more positive shift in the
exercise stages of change (p < 0.001), higher exercise self-efficacy (p < 0.001),
greater exercise benefits (p < 0.001), fewer exercise barriers (p < 0.001), and longer
moderate exercise duration per week (p < 0.001) than those in the C and PE groups.
These significantly positive effects persisted at the 3- and 6-month follow-up periods.
These findings suggest that using the 8-week TTM-based ESMI through face-to-face
and telephone contacts is effective at motivating sedentary CHD patients to engage in
exercise.

282
The positive effect of the TTM-based ESMI on changing exercise behaviour is
consistent with the results of previous studies that used the TTM to change exercise
behaviour among people in the community (Marcus, Banspach, Lefebvre et al., 1992)
and in worksite settings (Cardinal & Sachs, 1996; Faghri, Omokaro, Parker et al.,
2008; Ishii, Nakiri, Nagatomi et al., 2007; Peterson & Aldana, 1999; Purath, Miller,
McCabe & Wilbur, 2004), among adolescents (Nigg & Courneya, 1998), university
students (Huang, Hung, Chang & Chang, 2009; Kim, 2007 & 2008; Woods, Mutrie &
Scott, 2002), young to middle-aged women (Fahrenwald, Atwood, Walker, Johnson
& Berg, 2004; Shirazi, Wallace, Niknami et al., 2007), the elderly (Burbank, Reibe,
Padula & Nigg, 2002; Findorff, Stock, Gross & Wyman, 2007; Greaney, Riebe,
Garber et al., 2008; Märki, Bauer, Angst et al., 2006; Märki, Bauer, Nigg et al., 2006;
Resnick & Nigg, 2003), the general population (Bock, Marcus, Pinto & Forsyth, 2001;
Calfas, Long, Sallis et al., 1996; Lippke, Schwarzer, Ziegelmann et al., 2010),
physicians (Rogers, Gutin, Humphries et al., 2005), diabetes patients (Huang & Tang,
1996; Jackson, Asimakopoulou & Scammell, 2007; Kirk, Higgins, Hughes et al.,
2001; Kirk, MacIntyre, Mutrie & Fisher, 2003; Kirk, Mutrie, MacIntyre & Fisher,
2004; Zhu & Chen, 2007), breast cancer patients (Pinto, Frierson, Rabin et al., 2005),
patients with chronic disease (Shin, Yun, Jang & Lim, 2006), adults at increased risk
of developing coronary heart disease (Steptoe, Kerry, Rink & Hilton, 2001), and
patients with heart disease (Hughes, Gillies, Kirk et al., 2002; Hughes, Mutrie &
Maclntyre, 2007; Naser, Jafar, Kumar et al., 2008). These studies have shown that the
TTM-based ESMI is effective at motivating various populations to start exercising or
to maintain regular adherence to exercise. However, previous studies did not address
the issue of the effectiveness of the TTM-based ESMI on the exercise behaviour of

283
sedentary CHD patients. The findings from this study add evidence to support the
argument that the TTM-based ESMI is effective at changing the exercise behaviour of
sedentary CHD patients.
On the other hand, the findings in this study of the effect of the TTM-based ESMI on
changing exercise behaviour were inconsistent with those of other studies, which
found no significant effect on exercise behaviour from exercise consultations based
on the TTM as compared with generic patient education or the usual care (Dutton,
Provost, Tan & Smith, 2008; Goldstein, Pinto, Marcus et al., 1999; Jimmy & Martin,
2005; Kosma, Cardinal & Mccubbin, 2005; Pinto, Friedman, Marcus et al., 2002;
Taylor, Demoor, Smith et al., 2006; Wanner, Martin-Diener, Braun-Fahrländer et al.,
2009). The exception was one study that showed that the TTM-based exercise
intervention had a significant effect on exercise behaviour (increasing moderate
exercise duration per week) immediately after the intervention, although the effect
disappeared at the 6-month follow-up period (Pinto, Friedman, Marcus et al., 2002).
The discrepancies in the results on exercise behaviour between these studies and this
study may be attributed to the limited power reported by the authors of those studies
to detect the differences between the experimental and control groups (Goldstein,
Pinto, Marcus et al., 1999; Taylor, Demoor, Smith et al., 2006), the different research
designs (e.g., web-based intervention delivery) (Kosma, Cardinal & Mccubbin, 2005;
Wanner, Martin-Diener, Braun-Fahrländer et al., 2009), the involvement of
participants with physical disabilities (Kosma, Cardinal & Mccubbin, 2005), and the
recruitment of active participants at baseline (participants who performed around 130
minutes of moderate exercise per week at baseline), which resulted in little room for
further improvements (Dutton, Provost, Tan & Smith, 2008).

284
In this study, the patients in the ESMI group received conventional care, one 2-hour
session of patient education and a booklet regarding cardiac rehabilitation, and eight
weekly ESMI sessions and exercise stage-matched pamphlets. Three possible
explanations can be put forward for the positive effects of the TTM-based ESMI on
exercise behaviour. First, the characteristics of the TTM-based ESMI may be a main
contributor. The TTM-based ESMI is a client-centred and stage-specific intervention
for behavioural change, in which the strategies and techniques that are delivered are
matched to the individual's current stage of behavioural change. For patients in
different stages, different goals were set, and different processes of change or
strategies/techniques were used to motivate them to move to a more advanced stage.
This differed from the general patient education delivered to the PE group, in which
all of the participants received the same intervention on CHD and the same
information on the importance and benefits of exercise, without taking into
consideration their attitudes, intentions, and changes in their behaviour, namely, the
intervention was delivered without considering their exercise stages of change.
Previous studies have also demonstrated that a stage-matched intervention has a better
effect on behavioural change than a mismatched or non-matched one (Marcus,
Emmons, Simkin-Silverman et al., 1998; Prochaska, DiClemente, Velicer & Rossi,
1993). This is because a stage-specific and stage-matched intervention encourages
individuals to change their behaviour, since the delivery of the intervention occurs at a
time when the patients are most open to considering the particular changes suitable to
their condition at the time. For example, for those in the precontemplation or
contemplation stage, general patient education may not be effective at motivating
them to engage in exercise because such an intervention is typically designed for

285
people who are highly motivated and ready to begin to change their behaviour. It is
not effective enough to motivate a change in behaviour among those who have no
intention or interest in changing their behaviour (Marcus, Emmons, Simkin-Slverman
et al., 1998). In contrast, according to the TTM-based ESMI, only experiential
strategies or techniques, such as delivering information on the benefits of physical
activity (consciousness raising) and the personal risks of physical inactivity (dramatic
relief), uncovering the barriers to exercise, and encouraging thoughts about changing
one‘s sedentary lifestyle, were provided for those in the precontemplation or
contemplation stage and no action-oriented interventions were offered to them. On the
other hand, with respect to those in the action or maintenance stage, general patient
education may be not sufficient to help such participants overcome obstacles and
solve problems that they have encountered to maintain or adhere to regular exercise,
while the TTM-based ESMI providing problem-solving skills (e.g.,
counterconditioning, stimulus control, and reinforcement management) and the skills
to seek social support (e.g., helping relationships) may help them to overcome
obstacles, solve problems and resist relapsing into physical inactivity. Thus, providing
the TTM-based ESMI for patients could lead to better results in changing exercise
behaviour than general patient education and conventional care, as seen in this study.
This can explain why the patients in the ESMI group had better outcomes in exercise
behaviour than those in the C and PE groups in this study.
In addition, only sedentary CHD patients were recruited in this study. Thus, the
movement across the various stages of change, patients in the ESMI group not only
received information on the importance and benefits of exercise (e.g., consciousness
raising), but also received information about the risks of physical inactivity (e.g.,

286
dramatic relief), about self-reevaluation, environmental reevaluation, social liberation,
self-liberation to exercise, and about the skills of problem-solving (e.g.,
counterconditioning), overcoming barriers (e.g., stimulus control), and rewarding
oneself for physical activity (e.g., reinforcement management). The skills of problem-
solving, overcoming barriers, and rewarding oneself for physical activity were
provided especially for those in the action stage (starting to take action to engage in
regular exercise). In addition, all of the patients in the ESMI group were encouraged
to seek social support (e.g., helping relationships) as much as possible, which may
also have helped them to conquer barriers to engaging in exercise and to increase their
confidence in and perceptions of the benefits of exercise. Previous studies have
demonstrated that social support is a very important factor for attendance in a cardiac
rehabilitation programme (Hagan, Botti & Watts, 2007) and a predictor of a cardiac
patient‘s adherence to an exercise regime (Davies, Taylor, Beswick et al., 2010;
Moore, Dolansky, Ruland, Pashkow & Blackburn, 2003).
In this study, changes in exercise behaviour were measured using the exercise stages
of change scale (Marcus, Selby, Niaura & Rossi, 1992) and a log book. A log book
can facilitate accurate assessments of a patient‘s exercise behaviour, so that the most
appropriate and stage-specific intervention can be provided for that person. Keeping a
log book is also intended to motivate patients to engage in exercise.
Second, offering patients in this study a booklet and pamphlet may also have had a
positive effect on changing their exercise behaviour. The patients received a booklet
about cardiac rehabilitation immediately after completing the one 2-hour session of
patient education. The booklet is printed in colour, contains pictures, and is easy for

287
CHD patients to understand. Therefore, the information delivered in the patient
education session can be enhanced. A series of exercise stage-matched pamphlets in
simplified Chinese was also provided to patients in the ESMI group. Therefore, the
strategies and techniques employed to motivate changes in exercise behaviour can be
reinforced, namely by reinforcing participation at home. Thus, this multi-faceted
intervention (face-to-face and telephone contacts together with written materials) may
be credited for the positive results in exercise behaviour.
Third, home-based exercise may be another factor in the positive effect of the TTM-
based ESMI on exercise behaviour. In this study, the implementation of the TTM-
based ESMI was in a home-based mode. Patients in the ESMI group were encouraged
to start exercising at home and to incorporate exercise into their daily life, such as by
climbing the stairs instead of taking a lift, and by walking to the supermarket instead
of taking a bus. These skills would help them to start adopting exercise at home and to
develope the habit of exercising. Although patients in the PE group were also
encouraged to engage in exercise at home, they did not receive coaching on the
strategies or skills to incorporate exercise into their daily life. This may be one
possible explanation for why patients in the ESMI group demonstrated better results
in exercise behaviour than those in the PE group. The home-based exercise allowed
the patients to monitor themselves during the exercise session. Previous studies have
revealed that patients who attended home-based cardiac rehabilitation programmes
could significantly improve their exercise self-efficacy (Senuzun, Fadiloglu, Burke &
Payzin, 2006; Sinclair, Conroy, Davies & Bayer, 2005) because they needed to
monitor themselves at home during exercise. This training in self-monitoring their
exercise could help the patients build up their confidence (self-efficacy) in exercising

288
to a level sufficient to cause them to develop an exercise regime and to adhere to it
(Gary, 2006; Izawa, Watanabe, Omiya et al. 2005). In addition, patients who attended
a home-based cardiac rehabilitation programme perceived a higher level of social
support as compared with those in a hospital-based cardiac rehabilitation programme
(Gary, 2006). Social support is very important for attendance in or adherence to
cardiac rehabilitation programmes (Davies, Taylor, Beswick et al., 2010; Hagan, Botti
& Watts, 2007; Moore, Dolansky, Ruland, Pashkow & Blackburn, 2003). Obtaining
social support is itself also a process of change (e.g., helping relationships) for
behavioural change, which further enhances the individual's participation in exercise.
Thus, home-based exercise may have contributed to the positive effect of the TTM-
based ESMI on exercise behaviour that was observed in this study.
In this study, the most common reasons that the patients gave for dropping out of the
study were that they were leaving Xiamen City, busy with caring for grandchildren or
family members, and bad weather (e.g., too cold or hot). The findings suggest that it is
more appropriate to provide a home-based exercise programme for CHD patients in
Xiamen City than a centre-based one because of the former‘s convenience, cost-
effectiveness, high accessibility, and the much greater opportunity that patients have
to participate in it. Previous studies have also suggested that patients are more likely
to adhere to a home-based exercise programme than to a centre-based one (Arthur,
Smith, Kodis & McKelvie, 2002; Dalal, Zawada, Jolly et al., 2010; Leijon, Bendtsen,
Ståhle et al., 2010). Thus, the positive results on exercise behaviour in this study may
be attributed to the provision of support for home-based exercise. It may be a trend to
develop home-based exercise programmes for cardiac patients. This idea is consistent

289
with Thompson's (2007) hybrid mode of cardiac rehabilitation care – combining both
centre- and home-based rehabilitation cares.
Although the significant positive effects of the TTM-based ESMI on exercise
behaviour in terms of exercise stages of change, exercise self-efficacy, exercise
decisional balance, and exercise duration per week were sustained at the 6-month
follow-up period, a fading away of these effects was also found in the ESMI group
during the follow-up period. Due to time constraints, the longer follow-up effect of
the TTM-based ESMI on exercise behaviour was not evaluated in this study. Thus,
whether or not the positive effect of the TTM-based ESMI on exercise behaviour
would persist longer than six months remains unclear. Further studies over a longer
duration are needed to clarify this issue.
The trend of a reduction during the follow-up period may also suggest that the one 2-
hour session of patient education and a booklet, plus an 8-week TTM-based ESMI
and exercise stage-matched pamphlets, may not be enough to maintain the positive
impact on exercise behaviour in the long-term follow-up period (> 6 months). As
Adams and White (2005) argued, while the TTM-based stage-matched interventions
appear more likely to induce short-term changes in behaviour, they are not superior to
non-staged interventions in inducing long-term changes in behaviour. The effective
promotion of longer-term physical activity requires longer-lasting interventions that
may need to go beyond health education, incorporating environmental change
strategies to improve opportunities for physical activity and/or other strategies (e.g.,
social support) to maintain or adhere to regular physical activity (Brug, Conner, Harré,
Kremers, McKellar & Whitelaw, 2005). Thus, additional strategies or techniques

290
should be explored and added to improve the long-term effects of the intervention. A
booster intervention for the TTM-based ESMI may be a solution. A further study
featuring the addition of a booster intervention around the 6-month follow-up period
is suggested. Having a support group consisting of the patient‘s spouse or other family
members participating in the programme together with the patient may be another
way to encourage the patient to maintain long-term adherence to the exercise regime.
A further study focusing on this aspect is suggested.
6.3.2 Health Outcomes
This study focused on the effect of the TTM-based ESMI on health outcomes in terms
of anginal attacks and quality of life. A larger decline in angina frequency, angina
severity, angina duration, and anti-anginal drugs taken after the 8-week intervention
was found in the ESMI group than in the PE and C groups. However, no significant
differences in these variables were found among the three groups in this study. This
finding suggests that the TTM-based ESMI had no significant effect on anginal
attacks. The possible improvement in the ESMI group with regard to angina may be
due to the normal process of recovery from their illness. Nearly 50% of the patients in
this study were recruited immediately after the 3-month diagnosis of CHD (following
MI or PCI). Thus, they were still in the recovery stage. Another possible explanation
for the insignificant differences in angina variables among the three groups may be
due to the fact that the patients in this study experienced few episodes of angina
(around one episode/week), low angina severity (0-1, from no to slight pain), short
angina duration (about 10 minutes/week), and few anginal attacks and anti-anginal
drugs taken. Clearly, patients in this study only perceived mild angina. There may

291
have been little room for further improvements to begin with. In addition, the TTM is
targeted at motivating sedentary CHD patients to change their exercise behaviour.
Exercise-induced physiological changes may require some time to bring about.
Therefore, a longer intervention period is needed to achieve a significant reduction in
angina.
Regarding the quality of life, the results from this study showed that patients in the C
group improved in some domains of quality of life, especially in angina frequency and
disease perception of SAQ, and in physical functioning and general health of SF-36
over time. This improvement in the quality of life in the C group may have been due
to the normal recovery process and may have been a result of an increase in
engagement in exercise over time.
This study also showed that patients in the PE group had a better quality of life,
especially in angina frequency, treatment satisfaction, and disease perception of SAQ,
and in physical functioning, general health, social functioning, physical components
summary, and reported health transition of SF-36, than those in the C group. These
findings suggest that the structured patient education also had positive effects on the
quality of life of sedentary CHD patients. Several studies on controlling angina,
mainly through patient education, exercise training, and printed materials, have shown
that these approaches led to a significant improvement in quality of life with regard to
the SAQ (Burke, Williams & Lockyer, 2002; Lewin, Cay, Todd et al., 1995; Lewin,
Furze, Robinson et al., 2002), which is consistent with the findings of this study. A
number of randomized controlled trials also have revealed that cardiac rehabilitation
programmes or secondary prevention programmes, mainly including patient education

292
and exercise training, significantly improved the quality of life of CHD patients with
regard to SF-36 (Hanssen, Nordrehaug, Eide & Hanestad, 2007; Jiang, Sit, Wong,
Cheng & Li, 2004; McHugh, Lindsay, Hanlon et al., 2001; Murchie, Campbell,
Ritchie et al., 2004; Yu, Lau, Chau et al., 2004). A similar result was also reported in
several non-RCT studies (Izawa, Hirano, Yamada et al., 2004; Yonezawa, Masuda,
Matsunaga et al., 2009). These studies also suggest that the PE has a positive impact
on the quality of life of CHD patients with regard to both the SAQ and SF-36.
The greater improvement in quality of life in the PE group as compared with the C
group in this study may be a result of the increase in total and moderate exercise
duration per week and the contents of patient education. First, an increase in the
number of minutes of both total and moderate exercise duration per week may be a
factor. More patients in the action and maintenance stages (adopting regular exercise)
and a longer duration of moderate exercise were found in the PE group as compared
with the C group, which may explain why patients in the PE group showed a greater
improvement in quality of life than those in the C group. Second, patients in the PE
group received one 2-hour session of patient education related to CHD, including
information on the risk factors of CHD, healthy diets, and exercise, while those in the
C group only received conventional care. Health education can increase the patients‘
knowledge and promote related healthy changes in behavioiur or compliance with
lifestyle changes (Aldana, Greenlaw, Diehl et al., 2008; Alm-Roijer, Stagmo, Udén &
Erhardt, 2004; Fuster, 2007; Netto, McCloughan & Bhatnagar, 2007; Plach, Wierenga
& Heidrich, 1996). Such risk factor modifications and a healthy diet may also
contribute to an improvement in quality of life over time. This study focused on
changes in exercise behaviour and did not evaluate the results of diet and other risk

293
factor modifications. Thus, it is not clear whether patients modified these risk factors
and changed their diet after receiving one 2-hour session of patient education and the
booklet about cardiac rehabilitation. Further studies are recommended to clarify this
issue. Moreover, as with the ESMI group, the eight weekly sessions of general patient
education through face-to-face or telephone contacts, may have helped CHD patients
to learn more about angina and CHD, which may also have contributed to the
improvements seen in their treatment satisfaction and quality of life.
The findings from this study showed that patients in the ESMI group demonstrated
significantly greater improvements in three of the five subscales (namely, physical
limitations, treatment satisfaction, and disease perception) of SAQ, in five of the eight
domains of SF-36 (namely, physical functioning, general health, vitality, social
functioning, and mental health), the physical components summary, mental
components summary, and reported health transition of SF-36 as compared with those
in the C and PE groups. These significantly positive effects were maintained at the 3-
and 6-month follow-up periods, with the exception of those for general health and
reported health transition, which had disappeared by the 6-month follow-up period.
These findings suggest that the TTM-based ESMI could significantly improve the
quality of life of CHD patients, as measured using both disease-specific and generic
instruments.
This is the first study to use both the SAQ and SF-36 to evaluate the effect of the
TTM-based ESMI on quality of life. The limited number of studies on the effects of
the TTM-based stage-matched intervention on quality of life usually used the SF-36
to measure such effects. The positive findings on quality of life with regard to the SF-

294
36 are similar to the results of other studies, which found that a stage-matched
intervention resulted in significantly greater improvements in quality of life
immediately after the intervention according to the SF-36 (Beckie & Beckstead, 2011;
Kirk, Higgins, Hughes et al., 2001). However, these studies did not evaluate the
effects of the intervention during the follow-up period. On the other hand, the findings
of this study are inconsistent with those of Taylor and colleagues (2006), who found
that a lifestyle physical activity programme based on the TTM and social cognitive
theory resulted in no significant improvements in quality of life with respect to the
SF-36 six months after the intervention for patients with prostate cancer. The authors
explained that the lack of significant differences could have been due to the limited
power of the study, because they did not attain their projected sample size. Another
study conducted by Hughes, Mutrie, and Maclntyre (2007) also revealed that an
exercise consultation programme based on the TTM indicated no significant change
in all domains of SF-36 after the 6-month intervention. The authors explained that this
result was due to the high scores in all domains of SF-36 at baseline.
One possible reason for the observed improvements in quality of life in this study may
be that the TTM-based ESMI motivated sedentary CHD patients to change their
exercise behaviour and significantly increased their moderate exercise duration per
week, which subsequently improved their quality of life. In this study, 61.5% of the
patients in the ESMI group were in the action and maintenance stages (regularly
engaging in moderate exercise) immediately after the 8-week intervention, 55.4% at
the 3-month follow-up period, and 41.5% at the 6-month follow-up period as
compared with 4.5%, 7.5%, and 12.0% in the C group, and 17.2%, 29.7%, and 21.9%
in the PE group, respectively. The findings also showed that patients in the ESMI

295
group increased their moderate exercise per week to 231.2 minutes immediately after
the 8-week intervention, 227.5 minutes at the 3-month follow-up period, and 185.6
minutes at the 6-month follow-up period; while the figures were only 17.2, 26.3, and
56.5 minutes for the C group, and 99.1, 125.4, and 94.2 minutes for the PE group. The
significantly more patients in the action and maintenance stages and with a longer
moderate exercise duration per week in the ESMI group as compared with the C and
PE groups may explain why patients in the ESMI group demonstrated better quality
of life with regard to both the SAQ and SF-36, especially in the areas of physical
limitations, treatment satisfaction, disease perception, physical components summary,
and mental components summary, than those in the C and PE groups.
Increasing the duration of exercise per week has been shown to be beneficial to
reducing angina in CHD patients and improving their quality of life with respect to
the SAQ (Burke, Williams & Lockyer, 2002; Franklin, Bonzheim, Warren, Sue, Byl
& Gordon, 2002; Lewin, Furze, Robinson et al., 2002; Senuzun, Fadiloglu, Burke &
Payzin, 2006). Previous studies have demonstrated that regular exercise or physical
activity could increase the ischemic threshold and exercise tolerance of CHD patients
(Cui, Ren, Wang et al., 2006; Hambrecht, Walther, Mobius-Winkler et al., 2004), and
reduce exercise-induced angina (Cui, Ren, Wang et al., 2006), which may explain
why patients in the ESMI group demonstrated greater improvement in physical
limitations as compared with those in the C and PE groups. Previous studies have
shown an inverse relationship between the manifestation of symptoms of angina in
patients and treatment satisfaction and quality of life (Longmore, Spertus, Alexander
et al., 2011; Plomondon, Magid, Masoudi et al., 2007; Scirica, 2009).
296
A number of studies have also demonstrated that regular exercise or exercise-based
cardiac rehabilitation improved the exercise capacity, physical performance, and
quality of life of cardiac patients with respect to the SF-36 (Ades, Pashkow, Fletcher
et al., 2000; Bize, Johnson & Plotnikoff, 2007; Davies, Moxham, Rees et al., 2010;
Hwang & Marwick, 2009; Jeger, Jörg, Rickenbacher et al., 2007; Jiang, Sit, Wong et
al., 2004; Salvetti, Oliveira, Servantes & de Paola, 2008; van Tol, Huijsmans, Kroon
et al., 2006; Willmer & Waite, 2009). This may explain the positive findings for the
ESMI group in the present study, especially with regard to the physical components
summary.
The significantly positive effect on the mental components summary in the ESMI
group suggests that the TTM-based ESMI can improve the psychological well-being
of CHD patients. A previous study has shown that there is a link between exercise
capacity and the mental well-being of CHD patients (Milani & Lavie, 2007). Thus,
increased exercise can yield improvements in the mental well-being of CHD patients,
as has been shown in a number of systematic reviews (Netz, Wu, Becker &
Tenenbaum, 2005; Windle, Hughes, Linck et al., 2010). In this study, the TTM-based
ESMI motivated the sedentary CHD patients to engage in exercise and significantly
increased their exercise duration per week, which may have contributed to its positive
effect on the mental components summary as seen in this study.
However, no significant differences in angina stability and angina frequency were
found among the three groups at each time point. These results are similar to the
findings on angina conditions as mentioned in the patients‘ log records. No significant
differences in angina stability were also seen across time in all three groups. However,

297
a substantial reduction in angina stability was observed in all three groups at the 6-
month follow-up period, especially for the PE and ESMI groups. This phenomenon
was also in line with the angina conditions as reported in the patients‘ log records.
Possible explanations for this phenomenon are that the patients in both the PE and
ESMI groups were motivated and encouraged to engage in exercise. Thus, they may
have increased the intensity of their exercise after the intervention, while those in the
C group maintained their usual level of exercise intensity. The increase in exercise
intensity would result in a greater risk of suffering from angina, which may have
diluted the differences in angina stability and angina frequency between the groups.
However, that no significant differences in angina stability were noted in both the
between and within group comparisons suggests that the current exercise prescription
is safe for CHD patients.
No significant effects of the TTM-based ESMI on bodily pain, role-physical, and role
emotional aspects were found in this study. This finding was similar to the study of
Beckie and Beckstead (2011), who found that a TTM-based cardiac rehabilitation
programme significantly improved the general health, social functioning, vitality, and
mental health of women with CHD with regard to SF-36, while no significant effect
was detected on physical functioning, bodily pain, role-physical, and role-emotional
aspects. These findings suggest that it may be more difficult to bring about changes in
the domains of physiological and mental well-being than in other domains affecting
the functioning of CHD patients. Further research is needed to confirm this claim.
298
6.4 Tracking of the TTM-based ESMI on Exercise Behaviour
In order to determine changes in the trend of exercise behaviour during the 8-week
intervention period, the TTM-based ESMI was tracked with regard to exercise
behaviour. The results are presented and discussed in this section. As shown in Table
6.1, during the 8-week intervention period, the percentage of patients who progressed
to the action stage (engaging in regular exercise) increased over time. Delivering only
one session of the TTM-based ESMI could motivate CHD patients to at least,
consider to engaging in exercise (Contemplation stage) (Table 6.1). In fact, all of the
patients in the ESMI group started to exercise (Preparation and Action stages) at the
fifth week and over 50% of them were motivated to engage in regular exercise
(Action stage) (Table 6.1). The largest percentage of the patients who were motivated
to engage in regular exercise was by the eighth week, with over 70% of the patients in
the action stage (Table 6.1). This finding indicates that the TTM-based ESMI has a
dose-effect on changing exercise behaviour in sedentary CHD patients in China, i.e.,
an increase in the length of the intervention period will lead to an increase in the
number of patients who have progressed to the action stages (Table 6.1). The finding
also suggests that a longer intervention design or a booster intervention during the
follow-up period may improve on or maintain the positive effect on exercise
behaviour in the long-term follow-up period. The finding of the dose-effect on
exercise behaviour in this study is consistent with the results from a systematic review
(Thompson, Chair, Chan, Astin, Davidson & Ski, 2011), which also showed that
effectiveness improves with increased intensity (number and length of contacts).

299
In addition, the finding also showed the dynamic nature of exercise behaviour, in that
patients may move forward or backward in exercise stages of change during the
whole study period. This phenomenon echoes the TTM in that behavioural change is
dynamic and would move forward or backward during the whole process (Prochaska
& DiClemente, 1983; Prochaska & Velicer, 1997). The movement through five stages
does not always occur in a linear manner, but may also be cyclical, as many
individuals must make several attempts at changing their behaviour before they attain
their goals (Marcus, Banspach, Lefebvre, Rossi, Carleton & Abrams, 1992). Thus, it
is very important to assess an individual‘s exercise stages of change each time before
delivering the intervention. This will guarantee the delivery of the most appropriate
and stage-matched intervention for the patient. It is also very important to identify an
individual‘s barriers to exercise and explore ways of overcoming these obstacles so
that the patients will maintain their adherence to an exercise regime for as long as
possible.
Table 6.1 The changes in exercise stages of change in the ESMI group during the
intervention period
wk1
(n=57)
n(%)
wk2
(n=57)
n(%)
wk3
(n=56)
n(%)
wk4
(n=56)
n(%)
wk5
(n=55)
n(%)
wk6
(n=56)
n(%)
wk7
(n=55)
n(%)
wk8
(n=56)
n(%)
PC 6(10.5) 0 0 0 0 0 0 0
C 16(24.6) 4(7.0) 5(8.9) 2(3.6) 0 0 2(3.6) 1(1.8)
P 35(53.8) 39(68.4) 35(62.5) 29(51.8) 25(45.5) 26(46.4) 21(38.2) 15(26.8)
A 0 14(24.6) 16(28.6) 25(44.6) 30(54.5) 30(53.6) 32(58.2) 40(71.4)
PC: Precontemplation; C: Contemplation; P: Preparation; A: Action

300
6.5 Limitations and Controversies of the TTM
Although the Transtheoretical Model (TTM) of behavioural change has been widely
used to bring about changes in various behaviours, including exercise behaviour, and
has demonstrated promising results, it should also be noted that the TTM has a
number of limitations and that there are some controversies surrounding the TTM. In
this section, critiques of the TTM are discussed, and the strategies for dealing with
these critiques are explained. For example, the technique of motivational interviewing
is cited to enhance the validity of the categorisation of stages.
6.5.1 Validity of the categorisation of stages
The TTM emphasizes that behavioural change is a progression through a series of five
stages, namely precontemplation, contemplation, preparation, action, and maintenance
(Prochaska & DiClemente, 1983). The classification of these stages may violate the
assumptions of "qualitative transformations" (Bandura, 1997), especially with regard
to the action and maintenance stages because these two stages only differ in the
duration of behavioural adoption rather than in kind.
The specific problem associated with the categorisation of stages for exercise
behaviour may be due to the potential mismatch between a person's perceived and
actual exercise behaviour according to the TTM. A more specific kind of behaviour
and having a clearer goal or criterion for a specific change in behaviour would enable
people to evaluate their behaviour more accurately and reduce the discrepancy
between subjective assessment and actual exercise behaviour (Povey, Conner, Sparks,

301
James & Shepherd, 1999). It was suggested in a previous study (Reed, Velicer,
Prochaska, Rossi & Marcus, 1997) that clearly describing the stages of change and
using a complete definition of exercise that includes frequency, duration, and intensity,
would increase the validity and reliability of stage categorisation.
During our pilot study, we did encounter the problem of how to accurately categorize
individuals into different stages of change. Thus, after the pilot study, we set a clear
description of the five stages of change and a complete definition of regular exercise
with details on frequency, duration, and intensity, as follows: (i) precontemplation:
individuals are currently not doing exercise and have no intention to start exercising
in the next six months; (ii) contemplation: individuals are aware that a problem exists
with sedentary behaviour and they are seriously thinking about starting to exercise in
the next six months; (iii) preparation: individuals are currently engaging in some
exercise, but not regularly; (iv) action: individuals have been successfully exercising
regularly for less than six months; and (v) maintenance: individuals have been
exercising regularly for more than six months (Marcus, Eaton, Rossi & Harlow, 1994;
Prochaska & DiClemente, 1983). In this study, regular exercise is defined as
accumulating at least 30 minutes (at bouts of at least 10 minutes) of moderate
intensity of physical activity (3-6 METs, RPE 11-13, see examples of moderate
intensity of physical activity in Appendix XII) throughout the day for more than five
days of the week (American College of Sports Medicine, 2006; Marcus, Forsyth &
Blair, 2003).
According to the definition of five stages of change in the present study, the first two
stages are differences in degree of intention (precontemplators have no intention of

302
changing, and the contemplators have some intention of changing in the near future)
which is an important, though not sufficient, condition for behavioural change (Brug,
Conner, Harré, Kremers, McKellar & Whitelaw, 2005). The difference between the
stages of contemplation and preparation is that those in the stage of preparation have
taken some action to change their behaviour, such as engaging in some exercise, but
not regularly. The difference between the stages of preparation and action is that those
in the stage of action engage in regular exercise. The difference between the last two
stages is a difference in duration of behavioural adoption, with six months as a cut-off
point. Considering that the stage of maintenance may be viewed as an extension of the
action stage (Bandura, 1997; Povey et al., 1999), in our actual study we only focused
on the first three stages of the model. This was because, first, we could concentrate on
the motivational nature of the model; and, second, concerns about the validity of the
categorisation of stages could be minimized.
6.5.2 Behavioural change is "nonreversible"
According to the TTM, behavioural change is temporal and dynamic in nature
(Prochaska & DiClemente, 1983). Individuals move forward or backward during the
whole process. Relapse or regression is a common construct used to represent such
reversals (Prochaska & Velicer, 1997). In a genuine stage theory, a change in stage is
nonreversible (Bandura, 1997). However, behavioural change is different from
biological change. It includes relapse and recovery (Bandura, 1997). The findings
from this study showed that CHD patients progressed or regressed in their exercise
stages of change during the whole study period, which is consistent with the argument
that behavioural change is dynamic and will move forward or backward during the

303
whole process, as mentioned by Prochaska and DiClemente (1983) and Prochaska and
Velicer (1997). In a number of studies using the TTM as a framework to motivate
individuals to adopt exercise, this phenomenon was also observed during the process
of change in exercise behaviour (Bock, Marcus & Pinto, 2001; Dutton, Provost, Tan
& Smith, 2008; Kirk, Higgins, Hughes et al., 2001; Marcus, Emmons, Simkin-
Silverman et al., 1998; Purath, Miller, McCabe & Wilbur, 2004). The findings from
these studies also support the reversibility of behavioural change over time. The
phenomenon of the reversibility of behavioural change suggests that health care
professionals should assess an individual's stages of change in specific behaviour each
time before delivering a stage-matched intervention. This phenomenon also suggests
that health care professionals may need to provide support or a booster intervention
during the follow-up period to maintain the healthy change in behaviour over the long
term.
6.5.3 Complexity of physical activity
Physical activity is not a single behaviour, but a complex category of different
specific actions, such as transport behaviours, work-related physical activities, home-
making activities, gardening, and other leisure-time activities, including sports (Brug,
Conner, Harré, Kremers, McKellar & Whitelaw, 2005). Therefore, it is understood
that it is difficult to establish the validity of the TTM for complex health behaviours
(Brug et al., 2005). To deal with this inadequacy in the model, a clear definition of
physical activity was provided in this study. Physical activity refers to any planned
physical activity performed to increase physical fitness (Appendix XII). A complete
definition of regular exercise was also put forward in this study. As reported, using a

304
clear, commonly known, stable goal makes the process of applying the model of
behavioural change more concrete and certainly less difficult (Povey, Conner, Sparks,
James & Shepherd, 1999).
In this study, physical activity was defined as a planned behaviour, different from
addictive behaviours, that is the goal or end-point of behavioural change. In this study,
the goal was to motivate sedentary CHD patients to change their exercise behaviour.
This difference may cause problems for the model, which was originally based on
addictive behaviours (Povey, Conner, Sparks, James & Shepherd, 1999). There may
be many factors, such as environment, gender, age, and socioeconomic position, that
influence exercise behaviour, the motivation to participate in physical activity, and
exercise stages of change (Adams & White, 2005). These factors may be beyond the
scope of the TTM. As such, we once again acknowledge the inadequacy of the TTM
in this aspect. However, we would like to highlight the value of the TTM in
motivating changes in exercise behaviour in sedentary CHD patients. It has ignited a
spark in changing exercise behaviour, which is a critical step in promoting health.
6.5.4 Clinical application of the TTM
The findings from this study indicate that the 8-week TTM-based exercise stage-
matched intervention could set off a spark in sedentary CHD patients to change their
exercise behaviour. We believe that the TTM should play a role in changing health
behaviour. However, we agree that the model takes time to understand. As mentioned,
we experienced difficulties in applying it in the pilot study. To strengthen the clinical
applicability of the TTM, we have used a clear description of the five stages and a

305
complete definition of specific behaviour (e.g., exercise), and set a clear goal and
―end-point‖ of behavioural change in our actual study. These measures can enhance
the validity of stage categorisation and reduce the difficulty of using the model in
clinical practice (Povey, Conner, Sparks, James & Shepherd, 1999; Reed, Velicer,
Prochaska, Rossi & Marcus, 1997).
In addition, we suggest exploring the inclusion of motivational interviewing in future
clinical applications of TTM. Motivational interviewing (Miller & Rollnick, 2002;
Rollnick & Miller, 1995) is a client-centred method of communication that is focused
on enhancing the intrinsic motivation for change. A systematic review was conducted
to examine the related research findings, with specific comments on cardiovascular
health (Thompson, Chair, Chan, Astin, Davidson & Ski, 2011). The conclusion of this
review is that motivational interviewing is a practical front-line approach to
behavioural change. We wonder whether the inclusion of motivational interviewing
will augment the effects of TTM-based exercise stage-matched interventions. Further
studies focusing on this aspect are suggested.
In summary, while the TTM has a couple of limitations and controversies, especially
regarding the validity of stage categorisation and the complexity of physical activity,
the TTM-based ESMI is an effective approach to motivating sedentary CHD patients
to change their exercise behaviour and it is useful for clinical practice. Using a clear
description of five stages and a complete definition of specific behaviour (e.g.,
exercise) could increase the validity of stage categorisation and reduce the difficulty
of using the model in clinical practice. It is suggested that motivational interviewing

306
be included in the clinical application of the TTM. Further studies are recommended
to explore the related effects.
6.6 Role of Nurses in Cardiac Rehabilitation in Mainland China
Cardiac rehabilitation is defined as "the sum of activities required to influence
favourably the underlying causes of cardiac disease, as well as to ensure patients the
best possible physical, mental and social conditions so that they may, by their own
efforts, preserve or resume when lost, as normal a place as possible in the life of the
community" (p. 5) (WHO, 1993). Cardiac rehabilitation consists mainly of patient
education, exercise training, risk factor management, and behavioural change. Cardiac
rehabilitation is usually provided by a multidisciplinary team that includes nurses,
physiotherapists, medical staff, dietitians, psychologists, pharmacists, occupational
therapists, and social workers (Brown, 2009). Thus, cardiac rehabilitation is a
multifactorial, multidisciplinary activity, in which nurses should play a pivotal role in
prevention, education, and the delivery of health care (Stokes, 2000). In the UK, over
80.0% of cardiac rehabilitation programmes are coordinated by nurses (Stokes, 2000).
Nurses are members of the team, but the role of nurses in cardiac rehabilitation has
not been clearly defined both internationally and nationally (Pellatt, 2003). Fridlund
(2002) stated that the role of nurses in cardiac rehabilitation is to act as a container, a
counsellor, a coach, and an educator. As identified by Burton (2000), the nature of a
nurse‘s role in rehabilitation is to be a caregiver, a facilitator of personal recovery, and
a case manager. Smith (1999) found six key roles for nurses in the rehabilitation of an
adult, namely, to act as a technical expert and provider of care, to provide

307
psychological support, and to be an educator, coordinator, team worker, and evaluator.
Another report indicated the following eight categories of roles in rehabilitation
nursing: essential nursing skills, therapeutic practice, coordination, education,
empowerment and advocacy, political awareness, advice and counselling, and clinical
governance (Hawkey & Williams, 2007). A large part of the role of nurses in cardiac
rehabilitation is to provide opportune education in relation to cardiac disease,
cardiovascular risk factors, cardiac misconceptions, vocational and psychosocial
issues, and the secondary prevention of CHD (Brown, 2009).
Although cardiac rehabilitation programmes are well developed in Western countries,
such programmes are new and still underdeveloped in mainland China (Thompson &
Yu, 2007; Wang, Chair, Thompson & Twinn, 2009). Therefore, the role of nurses in
cardiac rehabilitation is also not well developed in mainland China. There is no
―blueprint‖ for nursing education, nor for the quality of nursing education with regard
to cardiac rehabilitation in China. Thus, a clear definition of the role of nurses and
regulations/guidelines regarding their role in cardiac rehabilitation are required to
standardize the role, as well as education requirements, competency standards, and
outcome measurements (Lowe, Plummer, O'Brien & Boyd, 2012; Wang & Xu, 2010).
The development of the field of cardiac rehabilitation requires that a greater emphasis
be placed on training and education for nurses in mainland China. Thus, providing
adequate education and training programmes is essential to strengthening their role in
cardiac rehabilitation (Stokes, 2000). For example, it is recommended that post-
registration training in cardiac rehabilitation be provided for nurses to enhance their
knowledge related to cardiac rehabilitation, their skills on how to provide patient

308
education programmes for CHD patients, and their skills on assessing exercise
behaviour.
The present study showed better changes in exercise behaviour and greater
improvements in the quality of life of CHD patients in both the PE and ESMI groups
as compared with those in the C group. These findings suggest that providing a
patient education programme guided by the TTM or a generic patient education
programme could have positive effects on Chinese CHD patients. Health care
professionals in mainland China could provide this kind of patient education
programme for CHD patients. The role of nurses in this study was to provide patient
education for CHD patients, assess their exercise stages of change, and deliver ESMI
or generic PE through either face-to-face or telephone contacts. The patient education
programme in this study is very simple and easy for nurses to perform. It is estimated
that a nurse with a bachelor‘s degree in nursing education and at least two years of
working experience in cardiovascular disease can provide such a patient education
programme from assessment to evaluation for CHD patients in mainland China.
6.7 Summary
This chapter thoroughly discussed and compared the high participation/completion
rate in this study with that of other studies, the effects of the TTM-based ESMI on the
exercise behaviour and health outcomes of patients with coronary heart disease, and
also discussed the tracking of the TTM-based ESMI on exercise behaviour. The
findings showed that the 8-week TTM-based ESMI was effective at changing exercise
behaviour and improving the quality of life of sedentary patients with CHD. These

309
positive effects of the TTM-based ESMI were maintained nearly to the point of the 6-
month follow-up period, while fading away effects on exercise behaviour were also
observed in this study. The findings suggest that introducing a booster intervention at
around the 6-month follow-up period or adding a support group (e.g., the spouse) to
maintain these positive effects may be considered. Better effects on exercise
behaviour and some domains of quality of life with regard to the SAQ and SF-36 after
the 8-week interventions were observed in the PE group as compared with the C
group, but these results lagged behind those for the ESMI group. These findings
suggest that the structured patient education on cardiac knowledge and exercise is
very important in motivating sedentary CHD patients to change their exercise
behaviour, while general patient education alone may be insufficient to do so. In order
to achieve desirable outcomes in exercise behaviour, the TTM-based ESMI may be a
solution. However, it should also be noted that the TTM has several limitations and
controversies. The findings of this study support the view that nurses have a role to
play in cardiac rehabilitation. Suggestions were made on the development of this role
in cardiac rehabilitation.

310
Chapter 7 Conclusions and Implications
7.1 Introduction
The aim of this study was to examine the effects of the TTM-based ESMI on
sedentary patients with CHD. This chapter contains a discussion of the conclusions
that can be drawn from the findings in this study, an examination of the limitations of
this study, and recommendations for future research. The implications of this study in
relation to clinical practice, nursing education, and the development of health care
policies are also presented.
7.2 Conclusions from the Findings
The TTM-based ESMI has shown itself to be an effective method for bringing about
changes in exercise behaviour in sedentary CHD patients and, consequently,
improving their quality of life. Below are the conclusions that can be drawn from this
study.
7.2.1 Changing Exercise Behaviour
In this study, the ESMI group showed a more positive shift in exercise stages of
change (p < 0.001) and higher exercise self-efficacy (p < 0.001) when compared with
the C and PE groups. The ESMI group also showed better decisional balance in terms
of higher exercise benefits scores (p < 0.001) and lower exercise barriers scores (p <
0.001) than the C and PE groups. Patients in the ESMI group engaged in exercise for

311
a longer duration (minutes/week) (p < 0.001) than the other two groups. To sum up,
the TTM-based ESMI could motivate sedentary CHD patients to engage in exercise.
7.2.5 Reducing Angina
After the TTM-based ESMI was implemented, there was an improvement in anginal
attacks in terms of a significant reduction in frequency (episodes/week) (p < 0.01),
severity (p < 0.01), and duration (minutes/week) (p < 0.001) as compared with the
baseline. No significant differences in these variables were detected among the three
groups at each time point. These findings suggest that the TTM-based ESMI has no
significantly positive effects on reducing anginal attacks in sedentary patients with
CHD.
7.2.6 Improving Quality of Life
The findings from this study have revealed that the ESMI group demonstrated
significantly better quality of life, in terms of improvements in physical limitations (p
< 0.01), treatment satisfaction (p < 0.001), and disease perception (p < 0.001) of SAQ,
and in physical component summary (p < 0.01), mental component summary (p <
0.001), and reported health transition (p < 0.05) of SF-36 in sedentary CHD patients
when compared with the C and PE groups. These findings suggest that the TTM-
based ESMI is an effective method for improving the quality of life of CHD patients,
as seen when both specific and general measurements were used to measure quality of
life.

312
7.3 Limitations of This Study and Recommendations for Future Research
Although this study was conducted based on the evidence of the systematic review,
and employed a high-quality study design, a pilot study, and main study, there were
still several limitations to the study. The findings from this study should be interpreted
with caution due to the following limitations, which future studies should strive to
overcome.
7.3.1 Self-reported Outcome Measurements
In this study, outcome variables were measured based on self-reports. This kind of
outcome measurement may have been affected by social desirability or poor recall,
especially with regard to levels of exercise (Davies, Taylor, Beswick et al., 2010).
Thus, the use of objective measurements, such as pedometers and heart monitors, to
validate self-reported exercise behaviour in such research would be desirable (Davies,
Taylor, Beswick et al., 2010) and is recommended in future studies. In this study, a
log book was used to record the patients‘ engagement in exercise in the past one week.
This could verify the results of self-reported exercise and minimize the possibility of
bias.
7.3.2 Exclusion of Depressive Patients
Patients with depression were not recruited in this study. In this study, the primary
outcome measurement is exercise behaviour. Previous studies have shown that
individuals with depression were less likely to participate in and more likely to

313
withdraw from cardiac rehabilitation programmes than those without depression
(Dorn, Naughton, Imamura & Trevisan, 2001; Taylor, Wilson & Sharp, 2011) and
had poor medical compliance (Lauzon, Beck, Huynh et al., 2003; Thompson & Lewin,
2000; Ziegelstein, Fauerbach, Stevens et al., 2000). In order to avoid bias in the
outcome measurements for changing exercise behaviour, patients with depression
were excluded from this study. This study focused on motivating sedentary CHD
patients to engage in exercise and was not particularly designed for those with
depression. Thus, coming up with an intervention to motivate those with depression to
engage in exercise is another area of future research interest.
7.3.3 No Long-term Follow up
In this study, the effects of the TTM-based ESMI on CHD patients were evaluated
immediately after the completion of the 8-week interventions and at the 3- and 6-
month follow-up periods. Since the long-term (> 6 months) effects of the TTM-based
ESMI could not be confirmed and there was fade away trend, the introduction of a
support group - inviting the patient's spouse or other family members to participating
in the programme together, as a method of maintaining exercise behaviour could be
considered. Adding a booster intervention around the 6-month follow-up period, or
additional strategies or techniques could be adopted for CHD patients to maintain the
positive effects of the intervention in long-term follow-up period. A further study
focusing on these aspects would be of value.
314
7.4 Implications
This discussion on the implications of this study focuses specifically on clinical
practice, nursing education, and policy development.
7.4.1 Implications for Clinical Practice
7.4.1.1 Patient education is an essential part of rehabilitation care
Patient education is an essential part of cardiac rehabilitation. Patients in China lack
knowledge on cardiac rehabilitation (Wong, Chair, Thompson & Twinn, 2009). They
seek information about cardiac rehabilitation and about preventing the recurrence of
MI, especially information about diet and physical activity (Zhu, Ho & Sit, 2012).
Patients in both the PE and ESMI groups received one 2-hour session of patient
education about coronary heart disease. This study showed that patients in both the PE
and ESMI groups were more ready to engage in exercise when compared with the C
group. This finding suggests a need to provide a structured or formal patient education
programme for CHD patients in China.
7.4.1.2 The TTM-based ESMI is an effective way to change exercise behaviour in
CHD patients
The aim of this study was to examine the effects of the TTM-based ESMI on patients
with CHD. The effects on patients with regard to exercise stages of change, exercise
self-efficacy, exercise decisional balance, and exercise duration per week were

315
significantly more positive for those in the ESMI group than for those in the PE and C
groups. This result suggests that the TTM-based ESMI is useful and effective for
encouraging sedentary CHD patients to change their exercise behaviour.
The number of people with CHD in China is growing (Health Statistics Information
Centre of Ministry of Health, 2010; Zhang, Lu & Liu, 2008) and there are multiple
obstacles to developing cardiac rehabilitation programmes in China, including limited
medical resources, the low administrative priority accorded to such programmes,
staffing and time pressures, insufficient knowledge and competence to run such
programmes, and an underdeveloped reimbursement system (Thompson & Yu, 2007;
Wang, Chair, Thompson & Twinn, 2009). An innovative and cost-effective
programme is needed to meet the requirements of the increasing number of people
with CHD. The TTM-based ESMI is a simple, economical, and effective way of
motivating CHD patients to begin exercising and improving their quality of life. The
positive findings in this study can facilitate the introduction of the TTM-based ESMI
to China.
A series of pamphlets for different exercise stages of change was developed in this
study. These exercise stage-matched pamphlets, which motivate patients to engage in
exercise, were tailor-made for Xiamen patients. The strategies and techniques to
motivate Xiamen‘s CHD patients to change their exercise behaviour were identified
in this study. They will play an important role in the development of TTM-based
cardiac rehabilitation programmes for CHD patients in that city. This study also sets
an excellent example for health professionals in the other parts of China to develop
their own set of TTM-based ESMI pamphlets and cardiac rehabilitation programmes.

316
7.4.1.3 Home-based exercise programmes are suitable for Chinese CHD patients
Due to the limited medical resources and underdeveloped reimbursement system in
mainland China, researchers have tried to come up with a cost-effective cardiac
rehabilitation programme for CHD patients. In this study, the TTM-based ESMI,
which can facilitate home-based cardiac rehabilitation, has been shown to be an
effective intervention for motivating sedentary CHD patient to adopt exercise and
improve their quality of life. This kind of home-based exercise programme meets the
rehabilitation care needs of CHD patients through education, face-to-face and
telephone contacts, and an emphasis on patient self-monitoring of an exercise regime
prescribed by a cardiologist. Home-based rehabilitation is well known for its
convenience, cost-effectiveness, high accessibility, and great opportunity for patients
to participate in cardiac rehabilitation. Taking into account the current conditions in
China, the approach of home-based cardiac rehabilitation should be most suitable for
Chinese CHD patients, as well as for those suffering from chronic illnesses.
In addition, Thompson (2007) has pointed out that the trend of the cardiac
rehabilitation development would be a ―hybrid‖ mode, that is, combining both centre-
and home-based rehabilitation care. In this study, patients in the ESMI group received
general patient education at a hospital and were instructed to engage in exercise at
home through face-to-face or telephone contacts. The findings from this study echo
Thompson‘s argument by showing the feasibility of implementing this hybrid mode
of rehabilitation.

317
7.4.2 Implications for nursing education
Nurses form the bulk of the health care workforce in China. Because nurses have the
most contact, and most continuous contact, with patients at all stages of recovery, they
are in a good position to take on responsibilities relating to rehabilitation care (Jiang,
2005). Education is a key strategy for nursing development. A multifaceted and
comprehensive cardiac rehabilitation requires nurses equipped with a wide range of
knowledge and skills. However, little formal education or training is offered to nurses
in China. Several reports have also stated that Chinese health professionals have
insufficient knowledge and competence to run cardiac rehabilitation programmes
(Thompson & Yu, 2007; Wang, Chair, Thompson & Twinn, 2009). Therefore, to
promote the development of cardiac rehabilitation, efforts should be devoted to
educating or training nurses. As Jiang (2005) stated, hospitals can offer rehabilitation
services for cardiac patients by equipping more nurses with knowledge and practical
skills on cardiac rehabilitation.
7.4.3 Implications for health care policy
Most studies on exercise-based cardiac rehabilitation or exercise behaviour have been
conducted in high-income countries. As a result, many of the related clinical and
public health policies being applied in lower-income countries (e.g., China) arise from
studies carried out in high-income regions. There are no existing policies developed
by professional nursing organizations about the roles and responsibilities of nurses in
cardiac rehabilitation in China. This study has shown that patient education plus the
TTM-based ESMI delivered by nurses through face-to-face and telephone contacts is

318
effective at motivating CHD patients to engage in exercise, consequently improving
their quality of life. Policies and guidelines on the role and responsibilities of nurses
in cardiac rehabilitation programmes should be established to guide professional
practice in the domain of cardiac rehabilitation and secondary prevention.
7.5 Summary
The TTM-based ESMI is effective at motivating sedentary CHD patients to engage in
exercise and improve their quality of life. Despite its limitations, this study has
important implications for the field of heath care and health care policy in China, and
has provided numerous useful suggestions for discussion and implementation.
319
References
Aben, I., Verhey, F., Strik, J., Lousberg, R., Lodder, J. & Honig, A. (2003). A
comparative study into the one year cumulative incidence of depression after
stroke and myocardial infarction. Journal of Neurology Neurosurgery and
Psychiatry, 74, 581-585.
Adams, J. & White, M. (2003). Are activity promotion interventions based on the
transtheoretical model effective? A critical review. British Journal of Sports
Medicine, 37, 106-114.
Adams, J. & White, M. (2005). Why don‘t stage-based activity promotion
interventions work? Health Education Research, 20(2), 237-243.
Adamson, J., Lawlor, D.A. & Ebrahim, S. (2004). Chronic diseases, locomotor
activity limitation and social participation in older women: cross sectional survey
of British women‘s heart and health study. Age and Ageing, 33, 293-298.
Ades, P.A., Pashkow, F.J., Fletcher, G., Pina, I.L., Zohman, L.R. & Nestor, J.R.
(2000). A controlled trial of cardiac rehabilitation in the home setting using
electrocardiographic and voice transtelephonic monitoring. American Heart
Journal, 139, 543-548.
Ainsworth, B.E., Haskell, W.L., Whitt, M.C., Irwin M.L., Swartz A.M., Strath S.J. et
al. (1993). Compendium of physical activities: an update of activity codes and
MET intensities. Medicine and Science in Sports and Exercise, 32(9), s498-s516.
Albarran, J.W., Clarke, B.A. & Crawford, J. (2007). Women‘s experiences of
myocardial infarction were described in terms of gradual onset, not having chest
pain, and responding to symptoms. Journal of Clinical Nursing, 16, 1292-1301.
Albert, C.M., Chae, C.U., Rexrode, K.M., Manson, J.E. & Kawachi, I. (2005).
Phobic anxiety and risk of coronary heart disease and sudden cardiac death
among women. Circulation, 111, 480-487.
Aldana, S.G., Greenlaw, R.L., Diehl, H.A., Merrill, R.M., Salberg, A. & Englert, H.
(2008). A video-based lifestyle intervention and changes in coronary risk. Health
Education Research, 23(1), 115-124.
Allen, J. K., Blumenthal, R. S., Margolis, S., Young, D. R., Miller, E. R. & Kelly, K.
(2002). Nurse case management of hypercholesterolemia in patients with
coronary heart disease: results of a randomized clinical trial. American Heart
Journal, 144, 678-686.
Allison, M.J. & Keller, C. (2004). Self-efficacy intervention effect on physical
activity in older adults. Western Journal of Nursing Research, 26, 31-46.
Alm-Roijer, C., Stagmo, M., Udén, G. & Erhardt, L. (2004). Better knowledge
improves adherence to lifestyle changes and medication in patients with coronary
heart disease. European Journal of Cardiovascular Nursing, 3, 321-330.

320
Alsén, P., Brink, E., Persson, L.O., Brändström, Y. & Karlson, B.W. (2010). Illness
perceptions after myocardial infarction: Relations to fatigue, emotional distress,
and health-related quality of life. Journal of Cardiovascular Nursing, 25(2), E1-
E10.
American College of Sports Medicine. (2006). ACSM’s guidelines for exercise testing
and prescription. Philadelphia: Lippincott Williams & Wilkins.
American Heart Association. (2001). Statistics. Available at
http://www.americanheart.org/presenter.jhtml?identifier=1200026
An, L.J., Wu, AP., Du, Y.Y., Ba, J.P., Wang, M., Qi, Y.H., Zhang, Z. & Yuan, B.
(2005). The effects of health instruction and danger awareness‘s patient
education on lifestyle compliance in patients with coronary heart disease.
Chinese Journal of Practical Nursing, 21(11A), 51-52.
Ariyo, A.A., Haan, M., Tangen, C.M., Furberg, C.D., Rutledge, J.C., Cushman, M. &
Dobs, A. (2000). Depression symptoms and risks of coronary heart disease and
mortality in elderly Americans. Circulation, 102, 1773-1779.
Arnold, H.J, Sewell, L. & Singh, S.J. (2007). A comparison of once-versus twice-
weekly supervised phase III cardiac rehabilitation. British Journal of Cardiology,
14(1), 45-48.
Arnold, S.V., Spertus, J.A., Jones, P.G., Xiao, L. & Cohen, D.J. (2009). The impact of
dyspnea on health-related quality of life in patients with coronary artery disease:
Results from the PREMIER registry. American Heart Journal, 157, 1042-1049,
e1.
Arrigo, I., Brunner-LaRocca, H., Lefkovits, M., Pfisterer, M. & Hoffmann, A. (2008).
Comparative outcome one year after formal cardiac rehabilitation: the effects of
a randomized intervention to improve exercise adherence. European Journal of
Cardiovascular Prevention and Rehabilitation, 15, 306-311.
Arthur, H.M., Gunn, E., Thorpe, K.E., Ginis, K.M., Mataseje, L., McCartney, N. &
McKelvie, R.S. (2007). Effect of aerobic vs combined aerobic-strength training
on 1-year, post-cardiac rehabilitation outcomes in women after a cardiac event.
Journal of Rehabilitation Medicine, 39, 730-735.
Arthur, H.M., Smith, K.M., Kodis, J. & McKelvie, R. (2002). A controlled trial of
hospital versus home-based exercise in cardiac patients. Medicine and Science in
Sports and Exercise, 34(10), 1544-1550.
Arthur, H.M., Smith, K.M. & Natarajan, M.K. (2008). Quality of life at referral
predicts outcome of elective coronary artery angiogram. International Journal of
Cardiology, 126, 32-36.

321
Arving, C., Glimelius, B. & Brandberg, Y. (2008). Four weeks of daily assessments
of anxiety, depression and activity compared to a point assessment with the
hospital anxiety and depression scale. Quality Life Research, 17, 95-104.
Asbury, E.A, Slattery, C., Grant, A., Evans, L., Barbir, M. & Collins. P. (2008).
Cardiac rehabilitation for the treatment of women with chest pain and normal
coronary arteries. Journal of the North American Menopause Society, 15(3), 1-7.
Ashton, K.C. (1997). Perceived learning needs of men and women after myocardial
infarction. Journal Cardiovascular Nursing, 12(1), 93-100.
Audelin, M.C., Savage, P.D. & Ades, P.A. (2008). Exercise-based cardiac
rehabilitation for very old patients (≥ 75 years): Focus on physical function.
Journal of Cardiopulmonary Rehabilitation and Prevention, 28, 163-173.
Bandura, A. (1986). Social Foundations of Thought and Action: A Cognitive Social
Theory. Englewood Cliffs, NJ, Prentice Hall.
Bandura, A. (1997) Self-efficacy: The exercise of control. New York: Freeman & Co.
Bandura, A. (1997). The anatomy of stages of change. American Journal of Health
Promotion, 12(1), 8-10.
Barefoot, J.C., Helms, M.J., Mark, D.B., Blumenthal, J.A., Califf, R.M., Haney, T.L.
et al. (1996). Depression and long-term mortality risk in patients with coronary
artery disease. American Journal of Cardiology, 78, 613-617.
Barnason, S., Zimmerman, L., Nieveen, J., Schmaderer, M., Carranza, B. & Reilly, S.
(2003). Impact of a home communication intervention for coronary artery bypass
graft patients with ischemic heart failure on self-efficacy, coronary disease risk
factor modification, and functioning. Heart and Lung, 32, 147-158.
Barnes, S.A., Mallinckrodt, C.H., Lindborg, S.R. & Carter, M.K. (2008). The impact
of missing data and how it is handled on the rate of false-positive results in drug
development. Pharmaceutical Statistics, 7, 215-225.
Barth, J. & Martin, C.R. (2005). Factor structure of the hospital anxiety and
depression scale (HADS) in German coronary heart disease patients. Health and
Quality of Life Outcome, 3, 1-9.
Barth, J., Schumacher, M. & Herrmann-Lingen, C. (2004). Depression as a risk factor
for mortality in patients with coronary heart disease: a meta-analysis.
Psychosomatic Medicine, 66, 802-813.
Batty, G.D., Shipley, M.J., Kivimaki, M., Marmot, M. & Smith, G.D. (2010).
Walking pace, leisure time physical activity, and resting heart rate in relation to
disease-specific mortality in London: 40 years follow-up of the original
Whitehall study. An update of our work with Professor Jerry N. Morris (1910-
2009). Annals of Epidemiology, 20, 661-669.

322
Beckie, T.M. (1989). A supportive-educative telephone programme: impact on
knowledge and anxiety after coronary artery bypass graft surgery. Heart and
Lung, 18(1), 46-55.
Beckie, T.M. (2006). A behaviour change intervention for women in cardiac
rehabilitation. Journal of Cardiovascular Nursing, 21(2), 146-153.
Beckie, T.M. & Beckstead, J.W. (2010). Predicting cardiac rehabilitation attendance
in a gender-tailored randomized clinical trial. Journal of Cardiopulmonary
Rehabilitation and Prevention, 30, 147-156.
Beckie, T.M. & Beckstead, J.W. (2010). The effects of a cardiac rehabilitation
program tailored for women on global quality of life: A randomized clinical trial.
Journal of Women's Health, 19(11), 1977-1985.
Beckie, T.M. & Beckstead, J.W. (2011). The effects of a cardiac rehabilitation
program tailored for women on their perceptions of health: A randomized
clinical trial. Journal of Cardiopulmonary Rehabilitation and Prevention, 31, 25-
34.
Beckie, T.M., Beckstead, J.W. & Schocken, D.D. (2011). The effects of a tailored
cardiac rehabilitation program on depressive symptoms in women: A
randomized clinical trial. International Journal of Nursing Studies, 48, 3-12.
Beckie, T.M., Fletcher, G.F., Beckstead, J.W., Schocken, D.D. & Evans, M.E. (2008).
Adverse baseline physiological and psychosocial profiles of women enrolled in a
cardiac rehabilitation clinical trial. Journal of Cardiopulmonary Rehabilitation
and Prevention, 28, 52-60.
Beinart, S.C., Sales, A.E., Spertus, J.A., Plomondon, M.E., Every, N.R. & Rumsfeld,
J.S. (2003). Impact of angina burden and other factors on treatment satisfaction
after acute coronary syndromes. American Heart Journal, 146, 646-652.
Bengtson, A., Herlitz, J., Karlsson, T. & Hjalmarson, A. (1996). Distress correlates
with the degree of chest pain: a description of patients awaiting revascularisation.
Heart, 75, 257-260.
Bengtsson, I., Hagman, M., Währborg, P. & Wedel, H. (2004). Lasting impact on
health-related quality of life after a first myocardial infarction. International
Journal of Cardiology, 97, 509-516.
Benzer, W., Platter, M., Oldridge, N.B., Schwann, H., Machreich, K., Kullich, W.,
Mayr, K., Philippi, A., Dörler, J. & Höfer, S. (2007). Short-term patient-reported
outcomes after different exercise-based cardiac rehabilitation programmes.
European Journal of Cardiovascular Prevention and Rehabilitation, 14, 441-447.
Berecki-Gisolf, J., Humphreyes-Reid, L., Wilson, A. & Dobson, A. (2009). Angina
symptoms are associated with mortality in older women with ischemic heart
disease. Circulation, 120, 2330-2336.
323
Bergman, E. & Bertero, C. (2003). 'Grasp life again'. A qualitative study of the
motive power in myocardial infarction patients. European Journal of
Cardiovascular Nursing, 2, 303-310.
Bethell, H., Lewin, R., Evans, J., Turner, S., Allender, S. & Petersen, S. (2008).
Outpatient cardiac rehabilitation attendance in England: variability by region and
clinical characteristics. Journal of Cardiopulmonary Rehabilitation and
Prevention, 28, 386-391.
Bittner, V. & Sanderson, B. (2006). Cardiac rehabilitation as secondary prevention
center. Coronary Artery Disease, 17, 211-218.
Bize, R., Johnson, J.A. & Plotnikoff, R.C. (2007). Physical activity level and health-
related quality of life in the general adult population: a systematic review.
Preventive Medicine, 45, 401-415.
Bjelland, I., Dahl, A.A., Haug, T.T. & Neckelmann, D. (2002). The validity of the
Hospital Anxiety and Depression Scale: An updated literature review. Journal of
Psychosomatic Research. 52, 69-77.
Blissmer, B.J. (2000). Integrating the theory of planned behaviour and the
transtheoretical model: a prospective study of lifestyle activity. Dissertation:
University of Illinois at Urbana-Champaign.
Blissmer, B. & McAuley, E. (2002). Testing the requirements of stages of physical
activity among adults: the comparative effectiveness of stage-matched,
mismatched, standard care, and control interventions. Annals of Behavioral
Medicine, 24(3), 181-189.
Blumenthal, J.A., Sherwood, A., Babyak, M.A., Watkins, L.L., Waugh, R.,
Georgiades, A., Bacon, S.L., Hayano, J., Coleman, R.E. & Hinderliter, A. (2005).
Effects of exercise and stress management training on markers of cardiovascular
risk in patients with ischemic heart disease: a randomized controlled trial.
Journal of the American Medical Association, 293(13), 1626-1634.
Bock, B.C., Marcus, B.H., Pinto, B.M. & Forsyth, L.H. (2001). Maintenance of
physical activity following an individualized motivationally tailored intervention.
Annals of Behavioral Medicine, 23(2), 79-87.
Boers, M. (2008). Missing data in trials: Do we have to keep carrying the last
observation forward? Arthritis and Rheumatism (Arthritis Care and Research),
59(1), 2-3.
Boersma, S.N., Maes, S. & Joekes, K. (2005). Goal disturbance in relation to anxiety,
depression, and health-related quality of life after myocardial infarction. Quality
of Life Research, 14, 2265-2275.
Bono, D.D. (1999). Investigation and management of stable angina: revised
guidelines 1998. Heart, 81, 546-555.

324
Borresen, J. & Lambert, M.I. (2008). Quantifying training load: a comparison of
subjective and objective methods. International Journal of Sports Physiology
Performance, 3(1), 16-30.
Briffa, T.G., Maiorana, A., Sheerin, N.J., Stubbs, A.G., Oldenburg, B.F., Sammel,
N.L. & Allan, R.M. (2006). Physical activity for people with cardiovascular
disease: recommendations of the National Heart Foundation of Australia.
Medical Journal of Australia, 184(2), 71-75.
Brink, E., Grankvist, G., Karlson, B.W. & Hallberg, L.R.M. (2005). Health-related
quality of life in women and men one year after acute myocardial infarction.
Quality of Life Research, 14, 749-757.
Broadbent, E., Ellis, C.J., Thomas, J., Gamble, G. & Petrie, K.J. (2009). Further
development of an illness perception intervention for myocardial infarction
patients: A randomized controlled trial. Journal of Psychosomatic Research, 67,
17-23.
Brodie, D. A. & Inoue, A. (2005). Motivational interviewing to promote physical
activity for people with chronic heart failure. Journal of Advanced Nursing,
50(5), 518-527.
Brodie, D.A., Inoue, A. & Shaw, D.G. (2008). Motivational interviewing to change
quality of life for people with chronic heart failure: A randomised controlled trial.
International Journal of Nursing Studies, 45, 489-500.
Brown, A. (2009). The role of a cardiac rehabilitation specialist nurse. British Journal
of Cardiac Nursing, 4(5), 230-232.
Brown, N., Melville, M., Gray, D., Young, T., Munro, J., Skene, A.M. & Hampton,
J.R. (1999). Quality of life four years after acute myocardial infarction: short
form 36 scores compared with a normal population. Heart, 81(4), 352-358.
Brubaker, C., Witta, E.L. & Angelopoulos, T.J. (2003). Maintaining exercise
tolerance and quality of life by long-term participation in a hospital-based
wellness programme for individuals with congestive heart failure. Journal of
Cardiopulmonary Rehabilitation, 23, 352-356.
Brug, J., Conner, M., Harré, N., Kremers, S., McKellar, S. & Whitelaw, S. (2005).
The Transtheoretical model and stages of change: a critique observations by five
commentators on the paper by Adams, J. And White, M. (2004) Why don't stage-
based activity promotion interventions work? Health Education Research, 20(2),
244-258.
Buckworth, J. & Wallace, L.S. (2002). Application of the transtheoretical model to
physically active adults. Journal of Sports Medicine and Physical Fitness, 42,
360-367.
Burbank, P.M., Padula, C.A. & Nigg, C.R. (2000). Changing health behaviours of
older adults. Journal of Gerontological Nursing, 26(3), 26-33.

325
Burbank, P.M., Reibe, D., Padula, C.A. & Nigg, C. (2002). Exercise and older adults:
changing behaviour with the transtheoretical model. Orthopaedic Nursing, 21(4),
51-63.
Burke, D., Williams, A. & Lockyer, L. (2002). The development of a nurse-led angina
management programme. Professional Nurse, 18(2), 86-90.
Burkholder, G.J. & Nigg, C.C. (2002). Overview of the Transtheoretical Model. In P.
M. Burbank & D. Riebe (Eds). Promoting exercise and behaviour change in
older adults. Interventions with the Transtheoretical Model. New York: Springer
Publishing Company, Inc.
Burns, K.J., Camaione, D.N., Froman, R. & Clark III, B.A. (1998). Predictors of
referral to cardiac rehabilitation and cardiac exercise self-efficacy. Clinical
Nursing Research, 7(2), 147-163.
Burton, C.R. (2000). A description of the nursing role in stroke rehabilitation. Journal
of Advanced Nursing, 32(1), 174-181.
Butler, L., Furber, S., Phongsavan, P., Mark, A. & Bauman, A. (2009). Effects of a
pedometer-based intervention on physical activity levels after cardiac
rehabilitation: A randomized controlled trial. Journal of Cardiopulmonary
Rehabilitation and Prevention, 29, 105-114.
Calfas, K.J., Long, B.J., Sallis, J.F., Wooten, W.J., Pratt, M. & Patrick, K. (1996). A
controlled trial of physician counselling to promote the adoption of physical
activity. Preventive Medicine, 25, 225-233.
Cameron, L.D., Petrie, K.J., Ellis, C.J., Buick, D. & Weinman, J.A. (2005). Trait
negative affectivity and responses to a patient education intervention for
myocardial infarction patients. Psychology and Health, 20(1), 1-18.
Campbell, N. C., Ritchie, L. D., Thain, J., Deans, H. G., Rawles, J. M. & Squair, J. L.
(1998). Secondary prevention in coronary heart disease: a randomised trial of
nurse led clinics in primary care. Heart, 80, 447-452.
Cannistra, L.B., Balady, G.J., O‘Malley, C.J., Weiner, D.A. & Ryan, T.J. (1992).
Comparison of the clinical profile and outcome of women and men in cardiac
rehabilitation. American Journal of Cardiology, 69, 1274-1279.
Cardinal, B.J. (1997). Construct validity of stages of change for exercise behaviour.
American Journal of Health Promotion, 12(1), 68-74.
Cardinal, B.J. & Sachs, M.L. (1996). Effects of mail-mediated, stage-matched
exercise behavior change strategies on female adults ‗leisure-time‘ exercise
behavior. Journal of Sports Medicine and Physical Fitness, 36(2), 100-107.
Cardiovascular Outcomes Inc. Scoring instruction for Seattle Angina Questionnaire -
2010 update. Available at: http://cvoutcomes.org/licenses/4008.

326
Carvalho, V.O., Bocchi, E.A. & Guimarães, G.V. (2009). The Borg Scale as an
important tool of Self-monitoring and self-regulation of exercise prescription in
heart failure patients during hydrotherapy: A randomized blinded controlled trial.
Circulation Journal, 73, 1871-1876.
Cay, E.L., Vetter, N., Philip, A. & Dugard, P. (1973). Return to work after a heart
attack. Journal of Psychosomatic Research, 17, 231-243.
Census and Statistics Department. (2011). Hong Kong Annual Digest of Statistics.
Government Printer, Hong Kong.
Chan, D.S.K., Chau, J.P.C. & Chang, A.M. (2005). Acute coronary syndromes:
cardiac rehabilitation programmes and quality of life. Journal of Advanced
Nursing, 49(6), 591-599.
Chan, V. (1990). Content areas for cardiac teaching: patients‘ perceptions of the
importance of teaching content after myocardial infarction. Journal of Advanced
Nursing, 15, 1139-1145.
Chair, S.Y., Chan, S.W.C., Thompson, D.R., Leung, K.P., Ng, S.K.C. & Choi, K.C.
(2011). Short-term effect of motivational interviewing on clinical and
psychological outcomes and health-related quality of life in cardiac rehabilitation
patients with poor motivation in Hong Kong: a randomized controlled trial.
European Journal of Cardiovascular Prevention & Rehabilitation, 0(00), 1-10.
Chair, S.Y., Lee, S.F., Lopez, V. & Ling, E.M. (2007). Risk factors of Hong Kong
Chinese patients with coronary heart disease. Journal of Clinical Nursing, 16,
1278-1284.
Chair, S.Y., Thompson, D.R., Tang, S.W. & Leung, K.P. (2007). The effect of cardiac
rehabilitation on changing patients' clinical outcomes. British Journal of Cardiac
Nursing, 2(4), 198-202.
Chen, J.P., Gu, W.P., Lu, E.B. & Yang, L.C. (1997). A survey of emotional disorder
in patients with coronary heart disease. Chinese Journal of Mental Health, 11(3),
143-144.
Chen, N.Y., Meng, X.Y., Wei, B., Zhang, Y. & Feng, Q.M. (2007). Epidemiological
features of coronary heart disease in urban residents of Guangxi province.
Practical Preventive Medicine, 14(5), 1384-1386.
Chen, N.Y., Wei, B., Meng, X.Y., Wu, G.W., Wang, F., Xie, Y.H. & Zhang, Y.
(2005). Epidemiologycial survey and analysis of coronary heart disease from
urban residents in Gungxi. Guangxi Preventive Medicine, 11(2), 65-67.
Chen, W. & Jing, N.L. (2008). An investigation and analysis of educational needs of
patients with coronary heart disease. Family Nurse, 6(1A), 16.
327
Chen, Z.M. & Whitlock, G. (2009). Unveiling the causes of heart disease in China.
Heart, 95(22), 1818-1819.
Cohen, J. (1988). Statistical power analysis for the behavioural sciences. New Jersey:
Lawrence Erlbaum Associate, Inc.
Condon, C. & McCarthy, G. (2006). Lifestyle changes following acute myocardial
infarction: Patients perspectives. European Journal of Cardiovascular Nursing, 5,
37 - 44.
Conn, V.S. (2010). Anxiety outcomes after physical activity interventions: meta-
analysis findings. Nursing Research, 59(3), 224-231.
Conn, V.S., Hafdahl, A.R., Brown, S.A. & Brown, L.M. (2008). Meta-analysis of
patient education interventions to increase physical activity among chronically ill
adults. Patient Education and Counselling, 70(2), 157-172.
Conn, V.S., Hafdahl, A.R., Cooper, P.S., Brown, L.M. & Lusk, S.L. (2009). Meta-
analysis of workplace physical activity interventions. American Journal of
Preventive Medicine, 37(4), 330-339.
Conn VS, Valentine JC, Cooper HM. (2002). Interventions to increase physical
activity among aging adults: A meta-analysis. Annals of Behavioral Medicine,
24(3), 190-200.
Corcoran, W.E. & Durham, C.F. (2000). Quality of life as an outcome-based
evaluation of coronary artery bypass graft critical paths using the SF-36. Quality
Management in Health Care, 8(2), 72-81.
Cornelissen, V.A., Verheyden, B., Aubert, A.E. & Fagard, R.H. (2010). Effects of
aerobic training intensity on resting, exercise and post-exercise blood pressure,
heart rate and heart-rate variability. Journal of Human Hypertension, 24, 175-
182.
Coull, A. J., Taylor, V. H., Elton, R., Murdoch, P. S. & Hargreaves, A. D. (2004). A
randomised controlled trial of senior Lay Health Mentoring in older people with
ischaemic heart disease: The Braveheart Project. Age and Ageing, 33, 348-354.
Courneya, K.S. (1995). Understanding readiness for regular physical activity in older
individuals: an application of the Theory of Planned Behaviour. Health
Psychology, 14(1), 80-87.
Critchley, J., Liu, J., Zhao, D., Wei, W. & Capewell, S. (2004). Explaining the
increase in coronary heart disease mortality in Beijing between 1984 and 1999.
Circulation, 110, 1236-1244.
Cruz, L.N., Fleck, M.P.d.A. & Polanczyk, C.A. (2010). Depression as a determinant
of quality of life in patients with chronic disease: data from Brazil. Social
Psychiatry and Psychiatric Epidemiology, 45, 953-961.

328
Cui, F., Ren, Y.S., Wang, H.F., Li, L., Mu, X. & Ma, H. (2006). Effects of
rehabilitation training on exercise tolerance of patients with coronary heart
disease after percutaneous coronary intervention. Chinese Journal of Physical
Medical Rehabilitation, 28(3), 177-179.
Cupples, M.E. & McKnight, A. (1994). Randomised controlled trial of health
promotion in general practice for patients at high cardiovascular risk. British
Medical Journal, 309(6960), 993-996.
Czar, M.L., MlittNsg, E. & Engler, M.M. (1997). Perceived learning needs of patients
with coronary artery disease using a questionnaire assessment tool. Journal of
Acute and Critical Care, 26(2), 109-117.
Dalal, H.M. & Evans, P.H. (2003). Achieving national service framework standards
for cardiac rehabilitation and secondary prevention. British Medical Journal, 326,
481-484.
Dalal, H.M., Evans, P.H., Campbell, J.L., Taylor, R.S., Watt, A., Read, K.L.Q.,
Mourant, A.J., Wingham, J., Thompson, D.R. & Pereira Gray, D.J. (2007).
Home-based versus hospital-based rehabilitation after myocardial infarction: a
randomized trial with preference arms – Cornwall Heart Attack Rehabilitation
Management Study (CHARMS). International Journal of Cardiology, 119, 202-
211.
Dalal, H.M., Zawada, A., Jolly, K., Moxham, T. & Taylor, R.S. (2010). Home based
versus centre based cardiac rehabilitation: Cochrane systematic review and meta-
analysis. British Medical Journal, 340, bs631. doi:10.1136/bmj.b5631.
Davies, E.J., Moxham, T., Rees, K., Singh, S., Coats, A.J.S., Ebrahim, S., Lough, F.
& Taylor, R.S. (2010). Exercise based rehabilitation for heart failure. Cochrane
Database of Systematic Reviews, Issue 4. Art No.: CD003331. DOI:
10.1002/14651858. CD003331. pub3.
Davies, P., Taylor, F., Beswick, A., Wise, F., Moxham, T., Rees, K. & Ebrahim, S.
(2010). Promoting patient uptake and adherence in cardiac rehabilitation.
Cochrane Database of Systematic Reviews, Issue 7. Art. No.: CD007131. DOI:
10.1002/14651858.CD007131.pub2.
Day, M.L., McGuigan, M.R., Brice, G. & Foster, C. (2004). Monitoring exercise
intensity during resistance training using the session RPE scale. Journal of
Strength and Conditioning Research, 18(2), 353-358.
de Geus, B., van Hoof, E., Aerts, I. & Meeusen, R. (2008). Cycling to work: influence
on indexes of health in untrained men and women in Flanders. Coronary heart
disease and quality of life. Scandinavian Journal of Medicine and Science in
Sports, 18, 498-510.
De Meester, F., van Lenthe, F.J., Spittaels, H., Lien, N. & De Bourdeaudhuij, I.
(2009). Interventions for promoting physical activity among European teenagers:

329
a systematic review. International Journal of Behavioral Nutrition and Physical
Activity, 6, 82.
de Vet, E., de Nooijer, J., de Vries, N.K. & Brug, J. (2008). Testing the
transtheoretical model for fruit intake: comparing web-based tailored stage-
matched and stage-mismatched feedback. Health Education Research, 23(2),
218-227.
Deaton, C. & Namasivayam, S. (2004). Nursing outcomes in coronary heart disease.
Journal of Cardiovascular Nursing, 19(5), 308-315.
DeBusk, R.F., Stenestrand, U., Sheehan, M. & Haskell, W.L. (1990). Training effects
of long versus short bouts of exercise in healthy subjects. American Journal of
Cardiology, 65, 1010-1013.
Department of Health. (2011). Department of Health Annual Report 2010/2011.
Government Printer, Hong Kong.
Dempster, M. & Donnelly, M. (2000). Measuring the health related quality of life of
people with ischemic heart disease. Heart, 83, 641-644.
Dickens, C.M., McGowan, L., Percival, C., Tomenson, B., Cotter, L., Heagerty, A. &
Creed, F.H. (2006). Contribution of depression and anxiety to impaired health-
related quality of life following first myocardial infarction. British Journal of
Psychiatry, 189, 367-372.
Dolansky, M.A. & Moore, S.M. (2004). Effects of cardiac rehabilitation on the
recovery outcomes of older adults after coronary artery bypass surgery. Journal
of Cardiopulmonary rehabilitation, 24, 236-244.
Donovan, R.J., Jones, S., Holman, C.D.A. & Corti, B. (1998) Assessing the reliability
of a stage of change scale. Health Education Research, 13(2), 285-291.
Dorjgochoo, T., Shu, X.O., Zhang, X.G., Li, H.L., Yang, G., Gao, L.F., Cai, H., Gao,
Y.T. & Zheng, W. (2009). Relation of blood pressure components and categories
and all-cause, stroke and coronary heart disease mortality in urban Chinese
women: a population-based prospective study. Journal of Hypertension, 27, 468-
475.
Dorn, J., Naughton, J., Imamura, D. & Trevisan, M. (2001). Correlates of compliance
in a randomized exercise trial in myocardial infarction patients. Medicine and
Science in Sports and Exercise, 33(7), 1081-1089.
Dougherty, C.M, Dewhurst, T., Nichol, W.P. & Spertus, J. (1998). Comparison of
three quality of life instruments in stable angina pectoris: Seattle Angina
Questionnaire, Short Form Health Survey (SF-36), and Quality of Life Index-
Cardiac Version III. Journal of Clinical Epidemiology, 51(7), 569-575.
Dressendorfer, R.H., Franklin, B.A., Cameron, J.L., Trahan, K.J., Gordon, S. &
Timmis, G.C. (1995). Exercise training frequency in early post-infarction cardiac

330
rehabilitation: Influence on aerobic conditioning. Journal of Cardiopulmonary
Rehabilitation, 15, 269-276.
Du, C.L., Chen, Z.Y. & Liu, S.Q. (2005). Investigation and analysis of educational
needs and strategies in patients with coronary heart disease. Journal of North
China Coal Medical College, 7(1), 87-88.
Du, X.L., Jiang, Y.F., Yang, H.M., Ai, H. & Gu, X.F. (2003). Analysis of depression
mood and related factors of hospitalized patients with coronary heart disease.
Chinese Journal of Nursing, 38(10), 761-764.
Dumas, J.E., Lynch, A.M., Laughlin, J.E., Smith, E.P. & Prinz, R.J. (2001).
Promoting intervention fidelity: Conceptual issues, methods, and preliminary
results from the EARLY ALLIANCE prevention trial. American Journal of
Preventive Medicine, 20(1S), 38-47.
Duryée, R. (1992). The efficacy of inpatient education after myocardial infarction.
Heart and Lung, 21(3), 217-225.
Dusseldorp, E., van Elderen, T., Maes, S., Meulman, J. & Kraaij, V. (1999). A meta-
analysis of psychoeducational programmes for coronary heart disease patients.
Health Psychology, 18(5), 506-519.
Dutton, G.R., Provost, B.C., Tan, F. & Smith, D. (2008). A tailored print-based
physical activity intervention for patients with type 2 diabetes. Preventive
Medicine, 47, 409-411.
Dwyer, T., Emmanuel, S.C., Janus, E.D., Wu, Z., Hynes, K.L. & Zhang, C. (2003).
The emergence of coronary heart disease in populations of Chinese descent.
Atherosclerosis, 67, 303-310.
Earle, A., Ayanian, J.Z. & Heymann, J. (2006). Work resumption after newly
diagnosed coronary heart disease: findings on the importance of paid leave.
Journal of Women’s Health, 15(4), 430-441.
Elderen, T.V., Maes, S. & Seegers, G. (1994). Effects of a post-hospitalization group
patient education programme for patients with coronary heart disease.
Psychology and Health, 9, 317-330.
Elley, C.R., Kerse, N., Arroll, B. & Robinson, E. (2003). Effectiveness of counselling
patients on physical activity in general practice: cluster randomised controlled
trial. British Medical Journal, 326, 1-6.
Elobeid, M.A., Padilla, M.A., McVie, T., Thomas, O., Brock, D.W., Musser, B., et al.
(2009). Missing data in randomized clinical trials for weight loss: scope of the
problem, state of the field, and performance of statistical methods. PloS ONE,
4(8), e6624. doi:10.1371/journal.pone.0006624.
Emaus, A., Degerstrøm, J., Wilsgaard, T., Hansen, B.H., Dieli-Conwright, C.M.,
Furberg, A.S., Pettersen, S.A., Andersen, L.B., Eggen, A.E., Bernstein, L. &

331
Thune, I. (2010). Does a variation in self-reported physical activity reflect
variation in objectively measured physical activity, resting heart rate, and
physical fitness? Results from the Tromsø study. Scandinavian Journal of Public
Health, 38, 105-118.
Eston, R.G. & Thompson M. (1997) Use of ratings of perceived exertion for
predicting maximal work rate and prescribing exercise intensity in patients
taking atenolol. British Journal of Sports Medicine, 31, 114-119.
Evenson, K.R., Johnson, A. & Aytur, S.A. (2006). Five-year changes in North
Carolina outpatient cardiac rehabilitation. Journal of Cardiopulmonary
Rehabilitation, 26, 366-376.
Fagard, R.H. & Cornelissen, V.A. (2007). Effect of exercise on blood pressure control
in hypertensive patients. European Journal of Cardiovascular Prevention and
Rehabilitation, 14(1), 12-17.
Faghri, P.D., Omokaro, C., Parker, C., Nichols, E., Gustavesen, S. & Blozie, E.
(2008). E-technology and pedometer walking program to increase physical
activity at work. Journal of Primary Prevention, 29, 73-91.
Fahrenwald, N.L., Atwood, J.R., Walker, S.N., Johnson, D.R. & Berg, K. (2004). A
randomized pilot test of ―Moms on the Move‖: A physical activity intervention
for WIC mothers. Annals of Behavioral Medicine, 27(2), 82-90.
Failde, I. & Ramos, I. (2000). Validity and reliability of the SF-36 health survey
questionnaire in patients with coronary artery disease. Journal of Clinical
Epidemiology, 53, 359-365.
Failde, I.I. & Soto, M.M. (2006). Changes in health related quality of life 3 months
after an acute coronary syndrome. BMC Public Health, 6, 18.
Fang, J.Q. (2005). Short form 36 health survey questionnaire, SF-36. In Z.J. Zhang
(Ed). A handbook of behavioural medical scale. Beijing: Chinese Medical
Electronic Audio-Video Publishing House.
Fang, M., Sun, Y. & Zhao, J.H. (2006). Research on stage of changes model of
exercise behaviour among adolescents. Chinese Journal of Public Health, 22(8),
209-210.
Fei, X., You, G.Y. & Huang, Y. (2007). The effects of patient education through
nursing process on compliance in patients with coronary heart disease. Modern
Preventive Medicine, 34(10), 1949-1951.
Findorff, M.J., Stock, H.H., Gross, C.R. & Wyman, J.F. (2007). Does the
transtheoretical mode (TTM) explain exercise behaviour in a community-based
sample of older women? Journal of Aging Health, 19, 985-1003.

332
Fitzsimons, D., Parahoo, K. & Stringer, M. (2000). Waiting for coronary artery
bypass surgery: a qualitative analysis. Journal of Advanced Nursing, 32(5),
1243-1252.
Fletcher, B. & Braun, L.T. (2008). Sedentary Lifestyle. In Moser, D.K. & Riegel, B.
(Ed). Cardiac Nursing: A Companion to Braunwald’s Heart Disease. USA:
Saunders Elserier Inc. 2008. p485.
Foot, D.K., Lewis, R.P., Pearson, T.A. & Beller, G.A. (2000). Demographics and
cardiology, 1950-2050. Journal of the American College of Cardiology, 35(5,
suppl B), 66B-80B
Fortmann, S.P., Taylor, C.B., Folra, J.A. & Winkleby, M.A. (1992). Effect of
community patient education on plasma cholesterol levels and diet: the Stanford
Five-City Project. American Journal of Epidemiology, 137, 1039-1055.
Fortmann, S.P., Williams, P.T., Hulley, S.B., Maccoby, N. & Farquhar, J.W. (1982).
Does dietary patient education reach only the privileged? The Stanford Three
Community Study. Circulation, 66(1), 77-82.
Franklin, B.A., Bonzheim, K., Warren, J., Sue, H., Byl, N. & Gordon, N. (2002).
Effects of a contemporary, exercise-based rehabilitation and cardiovascular risk-
reduction programme on coronary patients with abnormal baseline risk factors.
Chest, 122(1), 338-343.
Frasure-smith, N., Lesperance, F. & Talajic, M. (1995). The impact of negative
emotions on prognosis following myocardial infarction: is it more than
depression? Health Psychology, 14(5), 388-398.
Fridlund, B. (2002). The role of the nurse in cardiac rehabilitation programmes.
European Journal of Cardiovascular Nursing, 1(1), 15-18.
Furze, G., Bull, P., Lewin, R.J., & Thompson, D.R. (2003). Development of the york
angina beliefs questionnaire. Journal of Health Psychology, 8, 307-314.
Fuster, V. (2007). A new perspective on non-prescription statins: an opportunity for
patient education and involvement. American Journal of Cardiology, 100, 907-
910.
Gary, R. (2006). Exercise self-efficacy in older women with diastolic heart failure.
Journal of Gerontological Nursing, 31-39.
Giallauria, F., Lucci, R., D‘Agostino, M., Vitelli, A., Maresca, L., Mancini, M., et al.
(2009). Two-year multicomprehensive secondary prevention program: favorable
effects on cardiovascular functional capacity and coronary risk profile after acute
myocardial infarction. Journal of Cardiovascular Medicine, 10, 772-780.
Giannuzzi, P., Temporelli, P.L., Marchioli, R., Maggioni, A.P., Balestroni, G., Ceci,
V., Chieffo, C., Gattone, M., Griffo, R., Schweiger, C., Tavazzi, L., Urbinati, S.,
Valagussa, F. & Vanuzzo, D. (2008). Global secondary prevention strategies to

333
limit event recurrence after myocardial infarction. Archives of Internal Medicine,
168(20), 2194-2204.
Glanz, K., Rimer, B.K. & Lewis, F.M. (Ed). (2002). Health behaviour and health
education: theory, research, and practice. San Francisco: Jossey-Bass, c2002.
Goel, K., Lennon, R.J., Tilbury, T., Squires, R.W. & Thomas, R.J. (2011). Impact of
cardiac rehabilitation on mortality and cardiovascular events after percutanesous
coronary intervention in the community. Circulation, 123, 2344-2352.
Goldman, L. & Cook, E.F. (1984). The decline in ischemic heart disease mortality
rates: An analysis of the comparative effects of medical interventions and
changes in lifestyle. Annals of Internal Medicine, 101, 825-836.
Goldstein, M.G., Pinto, B.M., Marcus, B.H., Lynn, H., Jette, A.M., Rakowski, W.,
McDermott, S., DePue, J.D., Milan, F.B., Dubé, C. & Tennstedt, S. (1999).
Physician-based physical activity counselling for middle-aged and older adults:
A randomized trial. Annals of Behavioral Medicine, 21(1), 40-47.
Goto, Y., Saito, M., Iwasaka, T., Daida, H., Kohzuki, M., Ueshima, K., Makita, S.,
Adachi, H., Yokoi, H., Omiya, K., Mikouchi, H. & Yokoyama, H. (2007). Poor
implementation of cardiac rehabilitation despite broad dissemination of coronary
interventions for acute myocardial infarction in Japan: a nationwide survey.
Circulation Journal, 71(2), 173-179.
Greaney, M.L., Riebe, D., Garber, C.E., Rossi, J.S., Lees, F.D., Burbank, P.A., Nigg,
C.R., Ferrone, C.L. & Clark, P.G. (2008). Long-term effects of a stage-based
intervention for changing exercise intentions and behaviour in older adults. The
Gerontologist, 48(3), 358-367.
Griffin-Blake, C.S. & DeJoy, D.M. (2006). Evaluation of social-cognitive versus
stage-matched, self-help physical activity interventions at the workplace.
American Journal of Health Promotion, 20(3), 200-209.
Gulanick, M. (1991). Is phase 2 cardiac rehabilitation necessary for early recovery of
patients with cardiac disease? A randomized, controlled study. Heart and Lung,
20, 9-15.
Gump, B.B., Matthews, K.A., Eberly, L.E. & Chang, Y. (2004). Depression
symptoms and mortality in men: results from the multiple risk factor intervention
trial. Stroke, 36, 98-102.
Hagan, N.A., Botti, M.A. & Watts, R.J. (2007). Financial, family, and social factors
impacting on cardiac rehabilitation attendance. Heart and Lung, 36, 105-113.
Halm, M., Penque, S., Doll, N. & Beahrs, M. (1999). Women and cardiac
rehabilitation: referral and compliance patters. Journal of Cardiovascular
Nursing, 13(3), 83-92.

334
Hambrecht, R., Walther, C., Möbius-Winkler, S., Gielen, S., Linke, A., Conradi, K.,
Erbs, S., Kluge, R., Kendziorra, K., Sabri, O., Sick, P. & Schuler, G. (2004).
Percutaneous coronary angioplasty compared with exercise training in patients
with stable coronary artery disease: A randomized trial. Circulation, 109, 1371-
1378.
Hanssen, T.A., Nordrehaug, J.E., Eide, G.E. & Hanestad, B.R. (2007). Improving
outcomes after myocardial infarction: a randomized controlled trial evaluating
effects of a telephone follow-up intervention. European Journal of
Cardiovascular Prevention and Rehabilitation, 14(3), 429-437.
Hanssen, T.A., Nordrehaug, J.E., Eide, G.E. & Hanestad, B.R. (2009). Does a
telephone follow-up intervention for patients discharged with acute myocardial
infarction have long-term effects on health-related quality of life? A randomised
controlled trial. Journal of Clinical Nursing, 18, 1334-1345.
Hanssen, T.A., Nordrehaug, J.E. & Hanestad, B.R. (2005). A qualitative study of the
information needs of acute myocardial infarction patients, and their preferences
for follow-up contact after discharge. European Journal of Cardiovascular
Nursing, 4, 37- 44.
Haskell, W.L. (1994). The efficacy and safety of exercise programmes in cardiac
rehabilitation. Medicine and Science in Sports and Exercise, 26(7), 815-823.
Hawkey, B. & Williams, J. (2007). Role of the rehabilitation nurse. London: the
Royal College of Nursing, 20 Cavendish Square, London, W1G0RN.
He, X.L., Guo, C.X. & Guo, Y.Y. (2007). Investigation of demands of coronary heart
disease patients at different phases for patient education. Journal of Nursing,
14(3), 23-25.
Health Statistics Information Centre of the Ministry of Health, P.R.China. (2007). An
Annual Report of Chinese Health Statistic - 2007. Available at:
http://www.moh.gov.cn/publicfiles (accessed 1 October, 2007)
Health Statistics Information Centre of the Ministry of Health, P.R.China. (2010). An
Annual Report of Chinese Health Statistic - 2010. Available at:
http://www.moh.gov.cn/publicfiles (accessed 12 April 2011).
Hellman, E.A. (1997). Use of the stages of change in exercise adherence model
among older adults with a cardiac diagnosis. Journal of Cardiopulmonary
Rehabilitation, 17(3), 145-155.
Hellsten, L., Nigg, C., Norman, G., Burbank, P., Braun, L., Breger, R., Coday, M.,
Elliot, D., Garber, C., Greaney, M., Lees, F., Matthews, C., Moe, E., Resnick, B.,
Riebe, D., Rossi, J., Toobert, D. & Wang, T. (2008). Accumulation of
behavioural validation evidence for physical activity stage of change. Health
Psychology, 27(Supple. 1), s43-s53.

335
Hemingway, H. & Marmot, M. (1999). Evidence based cardiology: psychosocial
factors in the aetiology and prognosis of coronary heart disease: systematic
review of prospective cohort studies. British Medical Journal. 318, 1460-1467.
Herman, A., Botser, I.B., Tenenbaum, S. & Chechick, A. (2009) Intention-to-treat
analysis and accounting for missing data in orthopaedic randomized clinical
trials. Journal of Bone and Joint Surgery, 91, 2137-2143.
Herry N, H.R.K., Suryadipradja, H.R.M., Shatri, H. & Prodjosudjadi, W. (2005). The
influence of depression on the quality of life of male patients post acute
myocardial infarct. Acta Medicine Indones – Indones Journal of Internal
Medicine, 37(2), 71-78.
Higgins, R.O., Murphy, B.M., Le Grande, M.R., Parkinson, A., Worcester, M.U.C., &
Goble, A.J. (2005). Expressed preferences for patient education of patients after
percutaneous coronary intervention. European Journal of Cardiovascular
Prevention and Rehabilitation, 12, 572-579.
Ho, J.E., Bittner, V., DeMicco, D.A., Breazna, A., Deedwania, P.C. & Waters, D.D.
(2010). Usefulness of heart rate at rest as a predictor of mortality, hospitalization
for heart failure, myocardial infarction, and stroke in patients with stable
coronary heart disease (data from the Treating to New Targets [TNT] Trial).
American Journal of Cardiology, 105, 905-911.
Hofman-Bang, C., Lisspers, J., Nordlander, R., Nygren, A., Sundin, O., Öhman, A. &
Rydén, L. (1999). Two-year results of a controlled study of residential
rehabilitation for patients treated with percutaneous transluminal coronary
angioplasty. A randomized study of a multifactorial programme. European Heart
Journal, 20, 1465-1474.
Hogan, C.A. & Neill, W.A. (1982). Effects of a teaching program on knowledge,
physical activity, and socialization in patients disabled by stable angina pectoris.
Journal of Cardiac Rehabilitation, 2(5), 379-385.
Hospital Authority. (2009/2010). Hospital Authority Statistical Report: Hong Kong,
China: Hong Kong Hospital Authority.
Hou, D.X. (2005). An investigation on psycho-problems of middle-aged in-patients
with coronary heart disease. Journal of Clinical Psychosomatic Disease, 11(1),
48-49.
Hou, Y.F., Zhou, F.C. & Zhang, X.H. (2003). The effects of patient education on
patients‘ early post-operative complication following percutaneous coronary
intervention. Shandong Medical Journal, 43(8), 57.
Hravnak, M., Whittle, J., Kellwy, M.E., Sereika, S., Good, C.B., Lbraim, S.A. &
Conigliaro, J. (2007). Symptom expression in coronary heart disease and
revascularization recommendations for Black and White patients. American
Journal of Public Health. 97(9), 1701-1708.

336
Hu, L.Q. (2006). Investigation of educational needs and strategies in patients with
coronary heart disease. Journal of Nurses Training, 21(1), 74-75.
Huang, F.G., Wang, Q.P., Xu, F. & Yin, X.M. (2002). The epidemiological
distributing character and hazards analysis of coronary heart disease from Jiaoou
district in Nanjing. Theory and Practice of Chinese Medicine, 2002(9), 1277.
Huang, F.L. & Zhang, W. (2004). Investigation and analysis of mental health level
and correlative factors of patients with coronary heart disease. Health
Psychology Journal, 12(3), 188-190.
Huang, K.M., Li, M.H., Mao, C.H., Deng, M., Zhang, G.X., Li, Y.X. & Chen, Y.Y.
(2006). Effect of rehabilitation nursing on the quality of life and complications in
patients with coronary heart disease undergoing PTCA and stent. Chinese
Journal of Rehabilitation Medicine, 21(5), 451-453.
Huang, K.M., Mao, C.H., Deng, M., Li, M.H., Zhang, G.X., Liang, J.Q. & Liu, H.C.
(2004). Effect of rehabilitation nursing on the recovery and restenosis of patients
with coronary heart disease undergoing PTCA and stent. Chinese Journal of
Cardiovascular Rehabilitation, 14(2), 101-103.
Huang, Q.L. & Tang, S.M. (1996). An experience using the transtheoretical model of
health behaviour change to promote exercise in a type 2 diabetes patient. Journal
of Nursing, 54(5), 99-103.
Huang, S.J., Hung, W.C., Chang, M. & Chang, J. (2009). The effect of an internet-
based, stage-matched message intervention on young Taiwanese women‘s
physical activity. Journal of Health Communication, 14(3), 210-227.
Hughes, A.R., Gillies, F., Kirk, A.F., Mutrie, N., Hillis, W.S. & Maclntyre, P.D.
(2002). Exercise consultation improves short-term adherence to exercise during
phase IV cardiac rehabilitation. Journal of Cardiopulmonary Rehabilitation, 22,
421-425.
Hughes, A.R., Mutrie, N. & Maclntyre, P.D. (2007). Effect of an exercise consultation
on maintenance of physical activity after completion of phase III exercise-based
cardiac rehabilitation. European Journal of Cardiovascular Prevention and
Rehabilitation, 14, 114-121.
Hung, C., Daub, B., Black, B., Welsh, R., Quinney, A. & Haykowsky M. (2004).
Exercise training improves overall physical fitness and quality of life in older
women with coronary artery disease. Chest, 126, 1026-1031.
Hutchison, A.J., Breckon, J.D. & Johnston, L.H. (2009). Physical activity behaviour
change interventions based on the Transtheoretical Model: A systematic review.
Health Education and Behavior, 36, 829-845.
Hwang, R. & Marwick, T. (2009). Efficacy of home-based exercise programmes for
people with chronic heart failure: a meta-analysis. European Journal of
Cardiovascular Prevention and Rehabilitation, 16, 527-535.

337
Ishii, A., Nakiri, M., Nagatomi, K., Tsuji, Y., Hoshiko, M., Yamaguchi, Y.,
Muramoto, J. & Ishitake, T. (2007). Effect of a physical activity improvement
program using the Transtheoretical Model at a small-scale company. Kurume
Medical Journal, 54, 1-8.
Ishikawa-Takata, K., Tanaka, H., Nanbu, K. & Ohta, T. (2010). Beneficial effect of
physical activity on blood pressure and blood glucose among Japanese male
workers. Diabetes Research and Clinical Practice, 87, 394-400.
Izawa, K., Hirano, Y., Yamada, S., Oka, K., Omiya, K. & Iijima, S. (2004).
Improvement in physiological outcomes and health-related quality of life
following cardiac rehabilitation in patients with acute myocardial infarction.
Circulation Journal, 68, 315-320.
Izawa, K.P., Watanabe, S., Omiya, K., Hirano, Y., Oka, K., Osada, N., et al. (2005).
Effect of the self-monitoring approach on exercise maintenance during cardiac
rehabilitation: A randomized, controlled trial. American Journal of Physical
Medicine and Rehabilitation, 84, 313-321.
Jackson, R., Asimakopoulou, K. & Scammell, A. (2007). Assessment of the
transtheoretical model as used by dietitians in promoting physical activity in
people with type 2 diabetes. Journal of Human Nutrition and Dietetics, 20, 27-36.
Jeger, R.V., Jörg, L., Rickenbacher, P., Pfisterer, M.E. & Hoffmann, A. (2007).
Benefit of outpatient cardiac rehabilitation in under-represended patient
subgroup. Journal of Rehabilitation Medicine, 39, 246-251.
Jensen, B.O. & Petersson, K. (2003). The illness experiences of patients after a first
time myocardial infarction. Patient Education and Counselling, 51, 123-131.
Jeong, H.S., Chae, J.S., Moon, J.S. & Yoo, Y.S. (2002). An individualized teaching
program for atherosclerotic risk factor reduction in patients with myocardial
infarction. Yonsei Medical Journal, 43(1), 93-100.
Jerlock, M., Gaston-Johansson, F. & Danielson, E. (2005). Living with unexplained
chest pain. Journal of Clinical Nursing, 14, 956-964.
Ji, W.Y., Huang, Z.H., Chen, S.R., Zheng, A.Y. & Wu, Y.D. (2005). Investigation of
community patient education and lifestyle change intervention in patients with
diabetes mellitus. Journal of Nurses Training, 20(8), 696-698.
Jia, Y. & Shao, X. (2005). A survey of mental status of coronary artery disease
inpatients and its influencing factors. Chinese Nursing Research, 19(9A), 1714-
1716.
Jiang, G.W. & Peng, F. (2005). Investigation of educational needs of patients with
coronary heart disease. Modern Medicine and Health, 21(18), 2530-2531.

338
Jiang, X.L. (2005). The effects of a nurse-led cardiac rehabilitation programme on
patients with coronary heart disease in Chengdu, China. Dissertation: The Hong
Kong Polytechnic University.
Jiang, X.L. Sit, J.W. & Wong, T.K.S. (2007). A nurse-led cardiac rehabilitation
programme improves health behaviours and cardiac physiological risk
parameters: evidence from Chengdu, China. Journal of Clinical Nursing, 16,
1886-1897.
Jiang, X.L. Sit, J.W. & Wong, T.K.S., Cheng, Y.J. & Li, J.P. (2004). Effect of a
cardiac rehabilitation programme on the quality of life of patients with coronary
heart disease. Chinese Journal of Evidence-Based Medicine, 4(12), 852-858.
Jimmy, G. & Martin, B.W. (2005). Implementation and effectiveness of a primary
care based physical activity counselling scheme. Patient Education and
Counseling, 56: 323-331.
Johansson, A., Dahlberg, K. & Ekebergh, M. (2003). Living with experiences
following a myocardial infarction. European Journal of Cardiovascular Nursing,
2, 229-236.
Johansson, I., Swahn, E. & Strömberg, A. (2007). Manageability, vulnerability and
interaction: A qualitative analysis of acute myocardial infarction patients'
conceptions of the event. European Journal of Cardiovascular Nursing, 6, 184–
191.
Johnson, N.A., Lim, L.L. & Bowe, S.J. (2009). Multicenter randomized controlled
trial of a home walking intervention after outpatient cardiac rehabilitation on
health-related quality of life in women. European Journal of Cardiovascular
Prevention and Rehabilitation, 16, 633-637.
Johnson, S.S. Paiva, A.L., Cummins, C.O., Johnson, J.L., Dyment, S.J., Wright, J.A.,
Prochaska, J.O., Prochaska, J.M. & Sherman, K. (2008). Transtheoretical model-
based multiple behaviour intervention for weight management: effectiveness on
a population basis. Preventive Medicine, 46, 238-246.
Jolliffe, J.A., Rees, K., Taylor, R.S., Thompson, D., Oldridge, N. & Ebrahim, S.
(2001). Exercise-based rehabilitation for coronary heart disease. Cochrane
Database of Systematic Review, Issue 1, Art. No.: CD001800. DOI:
10.1002/14651858. CD001800.
Jolly, K., Lip, G.Y.H., Sandercock, J., Greenfield, S.M., Raftery, J.P., Mant, J., Taylor,
R., Lane, D., Lee, K.W. & Stevens, A.J. (2003). Home-based versus hospital-
based cardiac rehabilitation after myocardial infarction or revascularisation:
design and rationale of the Birmingham Rehabilitation Uptake Maximisation
Study (BRUM): a randomised controlled trial. BMC Cardiovascular Disorders,
3, 10.
Jolly, K., Taylor, R., Lip, G.Y.H., Greenfield, S., Raftery, J., Mant, J., Lane, D., Jones,
M, Lee, K.W. & Stevens, A. (2007). The Birmingham Rehabilitation Uptake

339
Maximisation Study (BRUM). Home-based compared with hospital-based
cardiac rehabilitation in a multi-ethnic population: cost-effectiveness and patient
adherence. Health Technology Assessment, 11(35), 1-118.
Josephson, E.A., Casey, E.C., Waechter, D., Rosneck, J. & Hughes, J.W. (2006)
Gender and depression symptoms in cardiac rehabilitation. Journal of
Cardiopulmonary Rehabilitation, 26, 160-163.
Jue, N.H. & Cunningham, S.L. (1998). Stages of exercise behaviour change at two
time periods following coronary artery bypass graft surgery. Progress in
Cardiovascular Nursing, 13(1), 23-33.
Kang, X.F., Li, Z., Liang, T., Chen, Y.D., Zhang, X.M., Gao, R.X. & Zang, X.H.
(2006). The effect of exercise-base rehabilitation on patients underwent
percutaneous transluminal coronary intervention. Chinese Journal of Nursing,
41(4), 315-317.
Kannel, W.B., Schwartz, M.J. & McNamara, P.M. (1969). Blood pressure and risk of
coronary heart disease: The Framingham Study. Disease Chest, 56, 43-52.
Kanning, M. (2010). Physically active patients with coronary artery disease: a
longitudinal investigation of the processes of exercise behaviour change. British
Journal of Health Psychology, 15, 583-597.
Kao, Y.H., Lu, C.M. & Huang, Y.C. (2002). Impact of a transtheoretical model on the
psychosocial factors affecting exercise among workers. Journal of Nursing
Research, 10(4), 303-309.
Kelley, G.A., Kelley, K.S. & Franklin, B. (2006). Aerobic exercise and lipids and
lipoproteins in patients with cardiovascular disease. Journal of Cardiopulmonary
Rehabilitation, 26, 131-139.
Kelley, G.A., Kelley, K.S. & Tran, Z.V. (2005). Exercise, lipids, and lipoproteins in
older adults: a meta-analysis. Preventive Cardiology, 8, 206-214.
Ketterer, M.W., Knysz, W., Keteyian, S.J., Schairer, J., Jafri, S., Alam, M., Farha, A.J.
& Deveshwar, S. (2008). Cardiovascular symptoms in coronary artery disease
patients are strongly correlated with emotional distress. Psychosomatics, 49, 230-
234.
Khaw, K.T. (2005). Epidemiology of coronary heart disease in women. In Wenger,
Nanette Kass & Collins, Peter (Ed). Women and Heart Disease. London and
New York: Taylor & Francis, 2005, 2nd
edition.
Kiebzak, G.M., Pierson, L.M., Campbell, M. & Cook, J.W. (2002). Use of the SF36
general health status survey to document health-related quality of life in patients
with coronary artery disease: effect of disease and response to coronary artery
bypass graft surgery. Heart and Lung, 31, 207-213.

340
Kiessling, A. & Henriksson, P. (2007). Time trends of chest pain symptoms and
health related quality of life in coronary artery disease. Health and Quality of
Life Outcomes, 5(13), 1-10.
Kim, Y.H. (2007). Application of the transtheoretical model to identify psychological
constructs influencing exercise behaviour: a questionnaire survey. International
Journal of Nursing Studies, 44, 936-944.
Kim, Y.H. (2008). A stage-matched intervention for exercise behaviour change based
on the transtheoretical model. Psychological Reports, 102, 939-950.
Kim, Y.H., Cardinal, B.J. & Lee, J.Y. (2006). Understanding exercise behaviour
among Korean adults: a test of the Transtheoretical model. International Journal
of Behavioural Medicine, 13(4), 295-303.
Kimble, L.P, Dunbar, S.B, Weintraub, W.S, McGuire, D.B, Fazio, S., De, A.K. &
Strickland, O. (2002). The seattle angina questionnaire: Reliability and validity
in women with chronic stable angina. Heart Disease, 4, 206-211.
Kirk, A.F., Higgins, L.A., Hughes, A.R., Fisher, B.M., Hillis, S. & MacIntyre, P.D.
(2001). A randomized, controlled trial to study the effect of exercise
counsultation on the promotion of physical activity in people with type 2
diabetes: a pilot study. Diabetic Medicine, 18, 877-882.
Kirk, A.F., MacIntyre, P., Mutrie, N. & Fisher, M. (2003). Increasing physical activity
in people with type 2 diabetes. Diabetes Care, 26, 1186-1192.
Kirk, A.F., Mutrie, N., MacIntyre, P.D. & Fisher, M.B. (2004). Promoting and
maintaining physical activity in people with type 2 diabetes. American Journal of
Preventive Medicine, 27(4), 289-296.
Kline, K.S., Scott, L.D. & Britton, A.S. (2007). The use of supportive-educative and
mutual goal-setting strategies to improve self-management for patients with heart
failure. Home Healthcare Nurse, 25(8), 502-510.
Kodama, S., Saito, K., Tanaka, S., Maki, M., Yachi, Y., Asumi, M., Sugawara, A.,
Totsuka, K., Shimano, H., Ohashi, Y., Yamada, N. & Sone, H. (2009).
Cardiorespiratory fitness as a quantitative predictor of all-cause mortality and
cardiovascular events in healthy men and women. Journal of the American
Medical Association, 301, 2024-2035.
Kodama, S., Tanaka, S., Saito, K., Shu, M., Sone, Y., Onitake, F., Suzuki, E.,
Shimano, H., Yamamoto, S., Kondo, K., Ohashi, Y., Yamada, N. & Sone, H.
(2007). Effect of aerobic exercise training on serum levels of high-density
lipoprotein cholesterol: a meta-analysis. Archives of Internal Medicine, 167, 999-
1008.
Kosma, M., Cardinal, B.J. & Mccubbin, J.A. (2005). A pilot study of a web-based
physical activity motivational program for adults with physical disabilities.
Disability and Rehabilitation, 27(23), 1435-1442.
341
Koukouvou, G., Kouidi, E., Lacovides, A., Konstantinidou, E., Kaprinis, G., &
Deligiannis, A. (2004). Quality of life, psychological and physiological changes
following exercise training in patients with chronic heart failure. Journal
Rehabilitation Medicine, 36, 36-41.
Kreuter, M.W., Oswald, D.L., Bull, F.C. & Clark, E.M. (2000). Are tailored health
education materials always more effective than non-tailored materials? Health
Education Research, 15(3), 305-315.
Kristofferzon, M.L., Löfmark, R. & Carlsson, M. (2005). Coping, social support and
quality of life over time after myocardial infarction. Journal of Advanced
Nursing, 52(2), 113-124.
Kristofferzon, M.L., Löfmark, R. & Carlsson, M. (2007). Striving for balance in daily
life: experiences of Swedish women and men shortly after a myocardial
infarction. Journal of Clinical Nursing, 16, 391-401.
Lam, C.L.K., Chin, W.Y., Lee, P.W.H., Lo, Y.Y.C., Fong, D.Y.T. & Lam, T.P.
(2009). Unrecognised psychological problems impair quality of life and increase
consultation rates in Chinese elderly patients. International Journal of Geriatric
Psychiatry, 24, 979-989.
Lam, T.H., Chan, B., Ho, S.Y. & Chan, W.M. (2004). Stage of change for general
health promotion action and health-related lifestyle practices in Chinese adults.
Preventive Medicine, 38, 302-308.
Lampe, F.C., Morris, R.W. & Walker, M. (2005). Trends in rates of different forms of
diagnosed coronary heart disease, 1978 to 2000: prospective, population based
study of British men. British Medical Journal, 330, 1-5.
Larson, C.O., Nelson, E.C., Gustafson, D. & Batalden, P.B. (1996). The relationship
between meeting patients‘ information needs and their satisfaction with hospital
care and general health status outcomes. International Journal for Quality in
Health Care, 8(5), 447-456.
Lauzon, C., Beck, C.A., Huynh, T., Dion, D., Racine, N., Carignan, S., Diodati, J.G.,
Charbonneau, F., Dupuis, R. & Pilote, L. (2003). Depression and prognosis
following hospital admission because of acute myocardial infarction. Canadian
Medical Association Journal, 168, 547-552.
Lear, S. A., Ignaszewski, A., Laquer, E. A., Pritchard, P. H. & Frohlich, J. J. (2001).
Extensive lifestyle management intervention following cardiac rehabilitation:
pilot study. Rehabilitation Nursing, 26(6), 227-232.
Lear, S.A., Ignaszewski, A., Linden, W., Brozic, A., Kiess, M., Spinelli, J.J., Pritchard,
P.H. & Frohlich, J.J. (2002). A randomized controlled trial of an extensive
lifestyle management intervention (ELMI) following cardiac rehabilitation: study
design and baseline data. Current Controlled Trials in Cardiovascular Medicine,
3, 9.

342
Lear, S.A., Ignaszewski, A., Linden, W., Brozic, A., Kiess, M., Spinelli, J.J., Pritchard,
P.H. & Frohlich, J.J. (2003). The Extensive Lifestyle Management Intervention
(ELMI) following cardiac rehabilitation trial. European Heart Journal, 24, 1920-
1927.
Lear, S.A., Spinelli, J.J., Linden, W., Brozic, A., Kiess, M., Frohlich, J.J. &
Ignaszewski, A. (2006). The Extensive Lifestyle Management Intervention
(ELMI) after cardiac rehabilitation: a 4-year randomized controlled trial.
American Heart Journal, 152, 333-339.
Leijon, M.E., Bendtsen, P., Ståhle, A., Ekberg, K., Festin, K. & Nilsen, P. (2010).
Factors associated with patients self-reported adherence to prescribed physical
activity in routine primary health care. BMC Family Practice, 11, 38.
http://www.biomedcentral.com/1471-2296/11/38.
Leung, R.W., Leung, M.L. & Chung, P.K. (2004). Validity and reliability of a
Cantonese-translated rating of perceived exertion scale among Hong Kong adults.
Perceptual and Motor Skills, 98(2), 725-735.
Lewin, B., Cay, E.L., Todd, I., Soryal, I., Goodfield, N., Bloomfield, P. & Elton, R.
(1995). The angina management programme: a rehabilitation treatment. Journal
of British Cardiology, 1, 221-226.
Lewin, R.J., Furze, G., Robinson, J., Griffith, K., Wiseman, S., Pye, M. & Boyle, R.
(2002). A randomized controlled trial of a self-management plan for patients
with newly diagnosed angina. British Journal of General Practice, 52, 194-201.
Li, H. (2002). The application of aerobics in psychology recover of coronary heart
disease patients. Chinese Journal of Clinical Rehabilitation, 6(11), 1638.
Li, J. & Gao, Z.Y. (2007). The effect of exercise training on heart function in patients
with coronary heart disease. World Health Digest, 4(7), 162-163.
Li, S.B. & Wang, D. (2006). Investigation and analysis of educational needs on
patients with coronary heart disease. China Medical Herald, 3(30), 146.
Li, X.J., Sun, Z.Q., Zheng, L.Q., Feng, L., Zhang, X.Z., Zhang, X.G., et al. (2007)
Correlative risk factors and epidemic characteristics of coronary heart disease
among rural adult groups in North of China. Journal of Shanxi Medical
University, 38(2), 139-142.
Li, X.L. & Liu, C.L. (2006). An investigation of educational needs of patients with
coronary heart disease. International Journal of Nursing, 25(2), 126-127.
Liang, Q. & Ma, H. (2001). A status of quality of life on patients with coronary heart
disease. Chinese Journal of Internal Medicince, 40(3), 212-213.
Lie, I., Arnesen, H., Sandvik, L., Hamilton, G. & Bunch, E.H. (2009). Health-related
quality of life after coronary artery bypass grafting. The impact of a randomised

343
controlled home-based intervention program. Quality of Life Research, 18, 201-
207.
Linde, B.J. & Janz, N.M. (1979). Effect of a teaching programme on knowledge and
compliance of cardiac patients. Nursing Research, 28(5), 282-286.
Lindgren, T.G., Fukuoka, Y., Rankin, S.H., Cooper, B.A., Carroll, D. & Munn, Y.
(2008). Cluster analysis of elderly cardiac patients‘ prehospital symptomatology.
Nursing Research, 57(1), 14-23.
Lippke, S., Schwarzer, R., Ziegelmann, J.P., Scholz, U. & Schüz, B. (2010). Testing
stage-specific effects of a stage-matched intervention: A randomized controlled
trial targeting physical exercise and its predictors. Health Education and
Behavior, 37, 533-546.
Lisspers, J., Sundin, Ö., Hofman-Bang, C., Nordlander, R., Nygren, A., Rydén, L. &
Öhman, A. (1998). Behavioral effects of a comprehensive, multifactorial
program for lifestyle change after percutaneous transluminal coronary
angioplasty: A prospective, randomized, controlled study. Journal of
Psychosomatic Research, 46(2), 143-154.
Lisspers, J., Sundin, Ö., Öhman, A., Hofman-Bang, C., Rydén, L. & Nygren, A.
(2005). Long-term effects of lifestyle behavior change in coronary artery disease:
effects on recurrent coronary events after percutaneous coronary intervention.
Health Psychology, 24(1), 41-48.
Liu, C.J., Li, N.X., Ren, X.H., Li, J., Zhang, J. & Sun, D. (2001). Feasibility of using
short form 36 in Chinese population. Journal of West China University Medical
Science, 32(1), 39-42.
Liu, J.Y.W., Chung, J.W.Y. & Wong, T.K.S. (2003). The psychometric properties of
Chinese pain intensity verbal rating scale. Acta Anaesthesiologica Scandinavica,
47, 1013-1019.
Liu, S.H. (2003). The Evaluation of the Reliability and Validity of SAQ Applied in a
Group of Chinese Patients with CHD. Thesis for Master Degree: Tianjin Medical
University.
Liu, X., Zhang, W., Yang, X.L., Yuan, X.J., Yang, F.Y. & Brodie, D.A. (2007).
Change of aerobic working capacity and myocardial oxygen supply of coronary
heart disease patients after cardiac rehabilitation. China Sport Science, 27(6), 35-
38.
Liu, Y. (2005). A survey of demands for patient education in patients with coronary
heart disease. Chinese Nursing Research, 19(1), 115-116.
Lloyd-Jones, D., Adams, R., Brown, T.M., Carnethon, M., Dai, S., De Simone, G.,
Ferguson, T.B., Ford, E., Furie, K., Gillespie, C., Go, A., Greenlund, K., Haase,
N., Hailpern, S., Ho, P.M., Howard, V., Kissela, B., Kittner, S., Lackland, D.,
Lisabeth, L., Marelli, A., McDermott, MM., Meigs, J., Mozaffarian, D.,

344
Mussolino, M., Nichol, G., Roger, V.L., Rosamond, W., Sacco, R., Sorlie, P.,
Stafford, R., Thom, T., Wasserthiel-Smoller, S., Wong, N. & Wylie-Rosett, J.
(2010). Heart Disease and Stroke Statistics— 2010 Update: a report from the
American Heart Association. Circulation, 121(7), 948-954.
Long, J.L., Wang, H.Y., Wang, Y.X. & Song, X.J. (2005). Comparisons of
psychosocial factors of patients with coronary heart disease. Journal of Clinical
Psychosomatic Disease, 11(2), 140-145.
Longmore, R.B., Spertus, J.A., Alexander, K.P., Gosch, K., Reid, K.J., Masoudi, F.A.,
Krumholz, H.M. & Rich, M.W. (2011). Angina frequency after myocardial
infarction and quality of life in older versus younger adults: the prospective
registry evaluating myocardial infarction: event and recovery study. American
Heart Journal, 16(3), 631-638.
Lowe, G., Plummer, V., O'Brien, A.P. & Boyd, L. (2012). Time to clarify - the value
of advanced practice nursing roles in health care. Journal of Advanced Nursing,
68(3), 677-685.
Lukkarinen, H. & Hentinen, M. (1997). Assessment of quality of life with the
Nottingham Health Profile among patients with coronary heart disease. Journal
of Advanced Nursing, 26(1), 73-84.
Luo, X.H., Chen, W.P., Meng, W.Y. & Ma, Y. (2007). The effects of patient
education on treatment attitude, medical compliance, and recurrence of
depression on coronary heart disease patients with depression. Chinese Journal
of Gerontology, 27, 1086-1087.
Luszczynska, A. (2006). An implementation intentions intervention, the use of a
planning strategy, and physical activity after myocardial infarction. Social
Science and Medicine, 62: 900-908.
Ma, S., Ma, Y.X. & Zhu, W. (2006). A dynamic observational study on effect of
intervention by stages on university students‘ exercise behaviour. Chinese
Journal of Behavioural Medical Science, 15(12), 1106-1108.
Ma, S., Wang, B.S. & Li, J.Z. (2008). The application of the transtheoretical model:
an intervention on exercise behaviour among University students. Chinese
Journal of Sports and Medicine, 27(2), 235-237.
Maddox, T.M., Reid, K.J., Spertus, J.A., Mittleman, M., Krumholz, H.M., Parashar,
S., Ho, M. & Rumsfeld, J.S. (2008). Angina at 1 year after myocardial infarction:
prevalence and associated findings. Archives of International Medicine, 168(12),
1310-1316.
Mahler, H.I.M., Kulik, J.A. & Tarazi, R.Y. (1999). Effects of a videotape information
intervention at discharge on diet and exercise compliance after coronary bypass
surgery. Journal of Cardiac Rehabilitation, 19(3), 170-177.

345
Marchionni, N., Fattirolli, F., Fumagalli, S., Oldridge, N., Lungo, F.D., Morosi, L.,
Burgisser, C. & Masotti, G. (2003). Improved exercise tolerance and quality of
life with cardiac rehabilitation of older patients after myocardial infarction:
Results of a randomized, controlled trial. Circulation, 107(17), 2201-2206.
Marcus, B.H., Banspach, S.W., Lefebvre, R.C., Rossi, J.S., Carleton, R.A. & Abrams,
D.B. (1992). Using the stages of change model to increase the adoption of
physical activity among community patients. American Journal of Health
Promotion, 6(6), 424-429.
Marcus, B.H., Eaton, C.A., Rossi, J.S. & Harlow, L.L. (1994). Self-efficacy, decision-
making, and stages of change: an integrative model of physical exercise. Journal
of Applied Social Psychology, 24(6), 489-508.
Marcus, B.H., Emmons, K.M., Simkin-Silverman, L.R., Linnan, L.A., Taylor, E.R.,
Bock, B.C., Roberts, M.B., Rossi, J.S. & Abrams, D.B. (1998). Evaluation of
motivationally tailored vs. standard self-help physical activity interventions at
the workplace. American Journal of Health Promotion, 12(4), 246-253.
Marcus, B.H., Forsyth, L.H. & Blair, S. (Ed). (2003). Motivating people to be
physically active. USA: Human Kinetics.
Marcus, B.H., Pinto, B.M., Simkin, L.R., Audrain, J.E. & Taylor, E.R. (1994).
Application of Theoretical models to exercise behavior among employed women.
American Journal of Health Promotion, 9(1), 49-55.
Marcus, B.H., Rossi, J.S., Selby, V.C., Niaura, R.S. & Abrams, D.B. (1992). The
stages and processes of exercise adoption and maintenance in a worksite sample.
Health Psychology, 11(6), 386-395.
Marcus, B.H., Selby, V.C., Niaura, R.S. & Rossi, J.S. (1992). Self-efficacy and the
stages of exercise behaviour change. Research Quarterly for Exercise and Sport,
63(1), 60-66.
Marcus, B.H. & Simkin, L.R. (1993). The stages of exercise behaviour. Journal of
Sports Medicine and Physical Fitness, 33(1), 83-89.
Marcus, B.H. & Simkin, L.R. (1994). The transtheoretical model: applications to
exercise behaviour. Medicine and Science in Sports and Exercise, 26(11), 1400-
1404.
Märki, A., Bauer, B., Angst, F., Nigg, C.R., Gillmann, G. & Gebring, T.M. (2006).
Systematic counselling by general practitioners for promoting physical activity
in elderly patients: a feasibility study. Swiss Medical Weekly, 136, 482-488.
Märki, A., Bauer, G.F., Nigg, C.R., Conca-Zeller, A. & Gebring, T.M. (2006).
Transtheoretical model-based exercise counselling for older adults in
Switzerland: quantitative results over a 1-year period. Soz Preventive Medicine,
51, 273-280.

346
Marshall, J., Penckofer, S. & Llewellyn, J. (1986). Structured postoperative teaching
and knowledge and compliance of patients who had coronary artery bypass
surgery. Heart and Lung, 15(1), 76-82.
Marshall, S.J. & Biddle, S.J.H. (2001). The transtheoretical model of behaviour
change: a meta-analysis of applications to physical activity and exercise. Annals
of Behavioral Medecine, 23(4), 229-246.
Martin, C.R. & Thompson, D.R. (2000). A psychometric evaluation of the hospital
anxiety and depression scale in coronary care patients following acute
myocardial infarction. Psychology, Health and Medicine, 5(2), 193-201.
Mayoux-Benhamou, A., Giraudet-Le Quintrec, J.S., Ravaud, P., Champion, K.,
Dernis, E., Zerkak, D., Roy, C., Kahan, A., Revel, M. & Dougados, M. (2008).
Influence of patient education on exercise compliance in rheumatoid arthritis: a
prospective 12-month randomized controlled trial. Journal of Rheumatology,
35(2), 216-223.
McCarthy, M.M., Dickson, V.V. & Chyun, D. (2010). Barriers to cardiac
rehabilitation in women with cardiovascular disease: an integrative review.
Journal of Cardiovascular Nursing, 00(0), 1-10.
McCormick, K.M., Naimark, B.J. & Tate, R.B. (2002). Symptoms and distress in
patients awaiting coronary artery bypass surgery. Canadian Journal of Nursing
Research. 34(4), 95-105.
McGillion, M.H., Watt-Watson, J., Stevens, B., LeFort, S.M., Coyte, P. & Graham, A.
(2008). Randomized controlled trial of a psychoeducation program for the self-
management of chronic cardiac pain. Journal of Pain and Symptom Management,
36(2), 126-140.
McHorney, C.A., Ware, J.E. & Raczek, A.E. (1993). The MOS 36-item short form
health survey (SF-36): II. Psychometric and clinical tests of validity in measuring
physical and mental health constructs. Medical Care, 31(3), 247-263.
McHugh, F., Lindsay, G.M., Hanlon, P., Hutton, I., Brown, M.R., Morrison, C. &
Wheatley, D.J. (2001). Nurse led shared care for patients on the waiting list for
coronary artery bypass surgery: a randomised controlled trial. Heart, 86, 317-323.
McPherson, C.P., Swenson, K.K., Pine, D.A. & Leimer, L. (2002). A nurse-based
pilot programme to reduce cardiovascular risk factors in a primary care setting.
American Journal of Management Care, 8, 543-555.
Mendes de Leon, C.F., Krumholz, H.M., Vaccarino, V., Williams, C.S., Glass, T.A.,
Berkman, L.F. & Kas, S.V. (1998). A population-based perspective of changes in
health-related quality of life after myocardial infarction in older men and women.
Journal of Clinical Epidemiology, 51(7), 609-616.

347
Meng, T.Y., Guo, H. & Guo, P. (2004). Correlative study of life quality and mental
health in senile patients with coronary heart disease. Journal of Clinical
Psychosomatic Disease, 10(2), 116-118.
Meyer, A.J., Nash, J.D., McAlister, A.L. & Maccoby, N. (1980). Skills training in a
cardiovascular patient education campaign. Journal of Consulting and Clinical
Psychology, 48(2), 129-142.
Milani, R.V. & Lavie, C.J. (2007). Impact of cardiac rehabilitation on depression and
its associated mortality. The American Journal of Medicine, 120, 799-806.
Milani, R.V., Lavie, C.J. & Cassidy, M.M. (1996). Effects of cardiac rehabilitation
and exercise training programmes on depression in patients after major coronary
events. American Heart Journal. 132, 726-732.
Mildestvedt, T., Meland, E. & Eide, G.E. (2008). How important are individual
counselling, expectancy beliefs and autonomy for the maintenance of exercise
after cardiac rehabilitation? Scandinavian Journal of Public Health, 36, 832-840.
Miller, W.R. & Rollnick, S. (2002). Motivational interviewing: Preparing people for
change. New York: Guilford Press.
Minganti, C., Capranica, L., Meeusen, R., Amici, S. & Piacentini, M.F. (2010). The
validity of session-rating of perceived exertion method for quantifying training
load in teamgym. Journal of Strength and Conditioning Research, 24(11), 3063-
3068.
Mital, A., Shrey, D.E., Govindaraju, M., Broderick, T.M., Colon-Brown, K. & Gustin,
B.W. (2000). Accelerating the return to work (RTW) chances of coronary heart
disease (CHD) patients: part 1 – development and validation of a training
programme. Disability and Rehabilitation, 22(13/14), 604-620.
Mochari, H., Lee, J.R., Kligfield, P. & Mosca, L. (2006). Ethnic differences in
barriers and referral to cardiac rehabilitation among women hospitalized with
coronary heart disease. Preventive Cardiology, 9, 8-13.
Moore, S.M. (1996). The effects of a discharge information intervention on recovery
outcomes following coronary artery bypass surgery. International Journal of
Nursing Studies, 33(2), 181-189.
Moore, S.M. & Charvat, J.M. (2002). Using the CHANGE intervention to enhance
long-term exercise. Nursing Clinics of North America, 37, 273-283.
Moore, S.M., Charvat, J.M., Gordon, N.H., Pashkow, F., Ribisl, P., Roberts, B.L. &
Rocco, M. (2006). Effects of a CHANGE intervention to increase exercise
maintenance following cardiac events. Annals of Behavioral Medicine, 31(1), 53-
62.

348
Moore, S.M., Dolansky, M.A., Ruland, C.M., Pashkow, F.J. & Blackburn, G.G.
(2003). Predictors of women‘s exercise maintenance after cardiac rehabilitation.
Journal of Cardiopulmonary Rehabilitation, 23, 40-49.
Mosca, L., Christian, A.H., Mochari-Greenberger, H., Kligfield, P. & Smith, S.C.Jr.
(2010). A randomized clinical trial of secondary prevention among women
hospitalized with coronary heart disease. Journal of Women’s Health, 19(2),
195-202.
Moser, D.K., Riegel, B., McKinley, S., Doering, L.V., An, K. & Sheahan, S. (2007).
Impact of anxiety and perceived control on in-hospital complications after acute
myocardial infarction. Psychosomatic Medicine, 69, 10-16.
Mozaffarian, D., Bryson, C.L., Spertus, J.A., McDonell, M.B. & Fihn, S.D. (2003).
Anginal symptoms consistently predict total mortality among outpatients with
coronary artery disease. American Heart Journal, 146, 1015-1022.
Murchie, P., Campbell, N. C., Ritchie L.D., Simpson, J.A. & Thain, J. (2003).
Secondary prevention clinics for coronary heart disease: four year follow up of a
randomised controlled trial in primary care. British Medical Journal, 326, 1-6.
Murchie, P., Campbell, N.C., Ritchie, L.D., Deans, H.G. & Thain, J. (2004). Effects
of secondary prevention clinics on health status in patients with coronary heart
disease: 4 year follow-up of a randomized trial in primary care. Family Practice,
21, 567-574.
Naser, A., Jafar, S., Kumar, G.V., Daga M.K., Hadi, H.S., Saeed, D., Mohamadreza, S.
& Hossein, M.A. (2008). Cardiac risk factor changes through an intensive
multifactorial life style modification program in CHD patients: Results from a
two year follow up. Journal of Biological Sciences, 8(2), 248-257.
National Service Framework. (2008). Coronary Heart Disease. From
http://www.dh.gov.uk/en/Healthcare/NationalServiceFramworks/Coronaryheartd
isease/index.htm
Naylor, P.J., Simmonds, G., Riddoch, C., Velleman, G. & Turton, P. (1999).
Comparison of stage-matched and unmatched interventions to promote exercise
behaviour in the primary care setting. Health Education Research, 14(5), 653-
666.
Nelson, M.S. (2000). A stage matched physical activity intervention in military
primary care. University of Maryland, Dissertation.
Netto, G., McCloughan, L. & Bhatnagar, A. (2007). Effective heart disease
prevention: Lessons from a qualitative study of user perspectives in Bangladeshi,
Indian and Pakistani communities. Public Health, 121, 177-186.
Netz, Y., Wu, M.J., Becker, B.J. & Tenenbaum, G. (2005). Physical activity and
psychological well-being in advanced age: a meta-analysis of intervention
studies. Psychology and Aging, 20(2), 272-284.
349
Neubeck, L., Freedman, S.B., Briffa, T. Bauman, A. & Redfern, J. (2010). Four-year
follow-up of the choice of health options in prevention of cardiovascular events
randomized controlled trial. European Journal of Cardiovascular Prevention
and Rehabilitation, 00(00), 1-8.
Nigg, C.R. (2001). Explaining adolescent exercise behaviour change: a longitudinal
application of the transtheoretical model. Annals Behavioral Medicine, 23(1), 11-
20.
Nigg, C.R. (2002). Physical Activity Assessment Issues in Population Based
Interventions: A Stage Approach. In: Welk GJ, eds. Physical Activity
Assessments for Health-Related Research. Champaign, IL: Human Kinetics.
Nigg, C.R. (2005). There is more to stages of exercise than just exercise. Exercise and
Sport Science Reviews, 33(1), 32-35.
Nigg, C.R. & Courneya, K.S. (1998). Transtheoretical model: examining adolescent
exercise behaviour. Journal of Adolescent Health, 22, 214-224.
Norekvål, T.M., Wahl, A.K., Fridlund, B., Nordrehaug, J.E. Wentzel-Larsen, T. &
Hanestad, B.R. (2007). Quality of life in female myocardial infarction survivors:
a comparative study with a randomly selected general female population cohort.
Health and Quality of Life Outcomes, 5, 58-68.
O‘Connor, G.T., Buring, J.E., Yusuf, S., Goldhaber, S.Z., Olmstead, E.M.,
Paffenbarger, R.S. & Hennekens, C.H. (1989). An overview of randomized trial
of rehabilitation with exercise after myocardial infarction. Circulation, 80, 234-
244.
Oerkild, B., Frederiksen, M., Hansen, J.F., Simonsen, L., Skowgaard, L.T. & Prescott,
E. (2011). Home-based cardiac rehabilitation is as effective as centre-based
cardiac rehabilitation among elderly with coronary heart disease: results from a
randomised clinical trial. Age and Aging, 40, 78-85.
Okura, T. & Tanaka, K. (2001). A unique method for predicting cardiorespiratory
fitness using rating of perceived exertion. Journal of Physiological Anthropology,
20(5), 255-261.
Ornish, D., Brown, S.E., Scherwitz, L.W., Billings, J.H., Armstrong, W.T., Ports,
T.A., McLanahan, S.M., Kirdeeide, R.L., Brand, R.J. & Gould, K.L. (1990). Can
lifestyle changes reverse coronary heart disease? The Lifestyle Heart Trial.
Lancet, 336(8708), 129-133.
Ornish, D., Scherwitz, L. W., Billings, J. H., et al. (1998). Intensive lifestyle changes
for reversal of coronary heart disease. Journal of the American Medical
Association, 280(23), 2001-2007.

350
Padberg, R.M. & Padberg, L.F. (1990). Strengthening the effectiveness of patient
education: applying principles of adult education. Oncology Nursing Forum,
17(1), 65-69.
Painter, J.E., Borba, C.P.C., Hynes, M., Mays, D. & Glanz, K. (2008). The use of
theory in health behaviour research from 2000 to 2005: a systematic review.
Annals of Behavioral Medicine, 35, 358-362.
Paradis, V., Cossette, S., Frasure-Smith, N., Heppell, S. & Guertin, M.C. (2010). The
efficacy of a motivational nursing intervention based on the stages of change on
self-care in heart failure patients. Journal of Cardiovascular Nursing, 25(2), 130-
141.
Parakh, K., Bhat, U., Thombs, B., Fauerbach, J.A., Bush, D.E. & Ziegelstein, R.C.
(2010). Self-assessed physical health predicts 10-year mortality after myocardial
infarction. Journal of Cardiopulmonary Rehabilitation and Prevention, 30, 35-
39.
Pavy, B., Iliou, M.C., Meurin, P., Tabet, J.Y. & Corone, S. (2006). Safety of exercise
training for cardiac patients. Results of the French registry of complications
during cardiac rehabilitation. Archives of Internal Medicine, 166, 2329-2334.
Pell, J., Pell, A., Morrison, C., Blatchford, O. & Dargie, H. (1996). Retrospective
study of influence of deprivation on uptake of cardiac rehabilitation. British
Medical Journal, 313, 267.
Pellatt, G.C. (2003). Perceptions of the nursing role in spinal cord injury rehabilitation.
British Journal of Nursing, 12(5), 292-299.
Peterson, T. & Aldana, S.G. (1999). Improving exercise behaviour: an application of
the stages of change model in a worksite setting. American Journal of Health
Promotion, 13(4), 229-232.
Pettersen, K.I., Reikvam, A., Rollag, A. & Stavem, K. (2008). Understanding sex
differences in health-related quality of life following myocardial infarction.
International Journal of Cardiology, 130, 449-456.
Pinsky, J.L., Jette, A.M., Branch, L.G., Kannel, W.B. & Feinleib, M. (1990). The
Framingham Disability Study: relationship of various coronary heart disease
manifestations to disability in older persons living in the community. American
Journal of Public Health, 80(11), 1363-1367.
Pinto, B.M., Friedman, R. Marcus, B.H., Kelley, H., Tennstedt, S. & Gillman, M.W.
(2002). Effects of a computer-based, telephone-counseling system on physical
activity. American Journal of Preventive Medicine, 23(2), 113-120.
Pinto, B.M., Frierson, G.M., Rabin, C., Trunzo, J.J. & Marcus, B.H. (2005). Home-
based physical activity intervention for breast cancer patients. Journal of Clinical
Oncology, 23(15), 3577-3587.

351
Pinto, B.M., Rabin, C. & Dunsiger, S. (2009). Home-based exercise among cancer
survivors: adherence and its predictors. Psycho-Oncology, 18, 369-376.
Plach, S., Wierenga, M.E. & Heidrich, S.M. (1996). Effect of a postdischarge
education class on coronary artery disease knowledge and self-reported health-
promoting behaviours. Heart and Lung, 25, 367-372.
Plomondon, M.E., Magid, D.J., Masoudi, F.A., Jones, P.G., Havranek, E., Peterson,
E.D., Krumholz, H.M., Spertus, J.A. & Rumsfeld, J.S. (2007). Association
between angina and treatment satisfaction after myocardial infarction. Journal of
General Internal Medicine, 23(11), 1-6.
Plotnikoff, R.C., Hotz, S.B., Birkett, N.J. & Courneya, K.S. (2001). Exercise and the
transtheoretical model: a longitudinal test of a population sample. Preventive
Medicine, 33, 441-452.
Povey, R., Conner, M., Sparks, P., James, R. & Shepherd, R. (1999). A critical
examination of the application of the Transtheoretical model's stages of change
to dietary behaviors. Health Education Research, 14(5), 641-651.
Prochaska, J.O. (2008). Decision making in the Transtheoretical model of behaviour
change. Medical Decision Making, 28, 845-849.
Prochaska, J.O. & DiClemente, C.C. (1983). Stages and processes of self-change of
smoking: toward an integrative model of change. Journal of Consulting and
Clinical Psychology, 51(3), 390-395.
Prochaska, J.O. & DiClemente, C.C. (1984). Self change processes, self efficacy and
decisional balance across five stages of smoking cessation. Progress in Clinical
Biochemistry and Medicine, 156, 131-140.
Prochaska, J.O. DiClemente, C.C. & Norcross, J.C. (1992). In search of how people
change: applications to addictive behaviours. American Psychologist, 47(9),
1102-1114.
Prochaska, J.O., DiClemente, C.C., Velicer, W.F. & Rossi, J.S. (1993). Standardized,
individualized, interactive, and personalized self-help programmes for smoking
cessation. Health Psychology, 12(5), 399-405.
Prochaska, J. O. & Marcus, B. H. (1995). The transtheoretical model: Applications to
exercise. Exercise Adherence II. R. Dishman. Illinois, Human Kinetics Press.
Prochaska, J.O. & Velicer, W.F. (1997). The transtheoretical model of health behavior
change. American Journal of Health Promotion, 12(1), 38-48.
Prochaska, J.O., Velicer, W.F., Rossi, J.S., Goldstein, M.G., Marcus, B.H., Rakowski,
W., Fiore, C., Harlow, L.L., Redding, C.A., Rosenbloom, D. & Rossi, S.R.
(1994). Stages of change and decisional balance for 12 problem behaviours.
Health Psychology, 13(1), 39-46.

352
Purath, J., Miller, A.M., McCabe, G. & Wilbur, J. (2004). A brief intervention to
increase physical activity in sedentary working women. Canadian Journal of
Nursing Research, 26(1), 76-91.
Rakowski, W., Ehrich, B., Goldstein, M.G., Rimer, B.K., Pearlman, D.N., Clark,
M.A., Velicer, W.F. & Woolverton, H. (1998). Increasing mammography among
women aged 40-74 by use of a stage-matched, tailored intervention. Preventive
Medicine, 27, 748-756.
Raleigh, E.H. & Odtohan, B.C. (1987). The effect of a cardiac teaching programme
on patient rehabilitation. Heart and Lung, 16(3), 311-317.
Ramm, C., Robinson, S. & Sharpe, N. (2001). Factors determining non-attendance at
a cardiac rehabilitation programme following myocardial infarction. New
Zealand Medical Journal, 114, 227-229.
Rao, Z.H. & Yuan, Z.M. (1996). An new questionnaire to evaluate physical functional
status on patients with coronary heart disease. International Journal of
Geriatrics, 17(1), 14-16.
Reboredo, M.M., Henrique, D.M.N., Faria, R.D.S., Chaoubah, A., Bastos, M.G. &
Paula, R.B.D. (2010). Exercise training during hemodialysis reduces blood
pressure and increases physical functioning and quality of life. Artificial Organs,
34(7), 586-593.
Redfern, J., Briffa, T., Ellis, E. & Freedman, S.B. (2008). Patient-centered modular
secondary prevention following acute coronary syndrom. Journal of
Cardiopulmonary Rehabilitation and Prevention, 28, 107-115.
Redfern, J., Briffa, T., Ellis, E. & Frredman, S.B. (2009). Choice of secondary
prevention improves risk factors after acute coronary syndrome: 1-year follow-
up of the CHOICE (Choice of Health Options In prevention of Cardiovascular
Events) randomized controlled trial. Heart, 95, 468-475.
Reed, G.R., Velicer, W.F., Prochaska, J.O., Rossi, J.S. & Marcus, B.H. (1997). What
makes a good staging algorithm: examples from regular exercise. American
Journal of Health Promotion, 12(1), 57-66.
Resnick, B. & Nigg, C. (2003). Testing a theoretical model of exercise behaviour for
older adults. Nursing Research, 52(2), 80-88.
Roebuck, A., Furze, G. & Thompson, D.R. (2001). Health-related quality of life after
myocardial infarction: an interview study. Journal of Advanced Nursing, 34(6),
787-794.
Rogers, L.Q., Gutin, B., Humphries, M.C., Lemmon, C.R., Waller, J.L., Baranowski,
T. & Saunders, R. (2005). A physician fitness program: enhancing the physician
as an ―exercise‖ role model for patients. Teaching and Learning in Medicine,
17(1), 27-35.

353
Rollnick, S. & Miller, W.R. (1995). What is motivational interviewing? Behavioural
and Cognitive Psychotherapy, 23, 325-334.
Rosamond, W., Flegal, K., Furie, K., Go, A., Greenlund, K., Haase, N., Hailpern,
S.M., Ho, M., Howard, V., Kissela, B., Kittner, S., Lloyd-Jones, D., McDermott,
M., Meigs, J., Moy, C., Nichol, G., O‘Donnell, C., Roger, V., Sorlie, P.,
Steinberger, J., Thom, T., Wilson, M., Hong, Y., American Heart Association
Statistics Committee & Stroke Statistics Subcommittee. (2008). Heart disease
and stroke statistics 2008 update: a report from the American Heart Association
statistics committee and stroke statistics subcommittee. Circulation, 117, e25-
e146.
Rosano, G.M.C., Vitale, C. & Volterrani, M. (2010). Heart rate in ischemic heart
disease. The innovation of ivabradine: more than pure heart rate reduction.
Advances in Therapy, 27(4), 202-210.
Rothenbacher, D., Hahmann, H., Wusten, B., Koenig, W. & Brenner, H. (2007).
Symptoms of anxiety and depression in patients with stable coronary heart
disease: prognostic value and consideration of pathogenetic links. European
Journal of Cardiovascular Prevention and Rehabilitation, 14, 547-554.
Sacker, A. Head, J. & Bartley, M. (2008). Impact of coronary heart disease on health
functioning in an aging population: are there differences according to
socioeconomic position? Psychosomatic Medicine, 70, 133-140.
Salminen, M., Isoaho, R., Vahlberg, T., Ojanlatva, A., Irjala, K. & Kivelä S.L. (2005).
Effects of health advocacy, counseling, and activation among older coronary
heart disease (CHD) patients. Aging Clinical and Experimental Research, 17,
472-478.
Salvetti, X.M., Oliveira, J.A., Servantes, D.M. & de Paola, A.A.V. (2008). How much
do the benefits cost? Effects of a home-based training programme on
cardiovascular fitness, quality of life, programme cost and adherence for patients
with coronary disease. Clinical Rehabilitation, 22, 987-996.
Sanderson, B.K. & Bittner, V. (2005). Women in cardiac rehabilitation: outcomes and
identifying risk for dropout. American Heart Journal, 150, 1052-1058.
Sanderson, B.K., Phillips, M.M., Gerald, L., DiLillo, V. & Bittner, V. (2003). Factors
associated with the failure of patients to complete cardiac rehabilitation for
medical and nonmedical reasons. Journal of Cardiopulmonary Rehabilitation, 23,
281-289.
Sarkar, U., Ali, S. & Whooley, M.A. (2007). Self-efficacy and health status in patients
with coronary heart disease: findings from the Heart and Soul study.
Psychosomatic Medicine, 69, 306-312.
Sarrafzadegan, N., Rabiei, K., Shirani, S., Kabir, A., Mohammadifard, N. & Roohafza,
H. (2007). Drop-out predictors in cardiac rehabilitation programmes and the

354
impact of sex differences among coronary heart disease patients in Iranian
sample: a cohort study. Clinical Rehabilitation, 21, 362-372.
Scalzi, C.C., Burke, L.E. & Greenland, S. (1980). Evaluation of an inpatient
educational programme for coronary patients. Heart and Lung, 9, 846-853.
Schelling, S., Munsch, S., Meyer, A.H., Newark, P., Biedert, E. & Margraf, J. (2009).
Increasing the motivation for physical activity in obese patients. International
Journal of Eating Disorders, 42, 130-138.
Schroter, S. & Lamping, D.L. (2006). Responsiveness of the coronary
revascularization outcome questionnaire compared with the SF-36 and Seattle
Angina Questionnaire. Quality of Life Research, 15, 1069-1078.
Scirica, B.M. (2009). Chronic angina: definition, prevalence, and implications for
quality of life. Reviews in Cardiovascular Medicine, 10(Suppl 1), S3-S10.
Scott, J.T. & Thompson, D.R. (2003). Assessing the information needs of post-
myocardial infarction patients: a systematic review. Patient Education and
Counseling, 50, 167-177.
Scrutinio, D., Temporelli, P.L., Passantino, A. & Giannuzzi, P. (2009). Long-term
secondary prevention programs after cardiac rehabilitation for the reduction of
future cardiovascular events: focus on regular physical activity. Future
Cardiology, 5(3), 297-314.
Sechrist, K.R., Walker, S.N. & Pender, N.J. (1987) Development and psychometric
evaluation of the exercise benefits/barriers scale. Research in Nursing and
Health, 10, 357-365.
Senuzun, F., Fadiloglu, C., Burke, L. E. & Payzin, S. (2006). Effects of home-based
cardiac exercise program on the exercise tolerance, serum lipid values and self-
efficacy of coronary patients. European Journal of Cardiovascular Prevention
and Rehabilitation, 13, 640-645.
Shen, B.J., Avivi, Y.E., Todaro, J.F., Spiro III, A., Laurenceau, J.P., Ward, K.D. &
Niaura, R. (2008). Anxiety characteristics independently and prospectively
predict myocardial infarction in men. Journal of the American College of
Cardiology. 51, 113-119.
Shibeshi, W.A., Young-Xu, Y. & Blatt, C.M. (2007). Anxiety worsens prognosis in
patients with coronary artery disease. Journal of the American College of
Cardiology, 49(20), 2021-2027.
Shin, Y.H., Jang, H.J. & Pender, N.J. (2001). Psychometric evaluation of the exercise
self-efficacy scale among Korean adults with chronic disease. Research in
Nursing and Health, 24, 68-76.
355
Shin, Y.H., Yun, S.K., Jang, H.J. & Lim, J.H. (2006). A tailored program for the
promotion of physical exercise among Korean adults with chronic diseases.
Applied Nursing Research, 19, 88-94.
Shiotani, H., Umegaki, Y., Tanaka, M., Kimura, M. & Ando, H. (2009). Effects of
aerobic exercise on the circadian rhythm of heart rate and blood pressure.
Chronobiology International, 26(8), 1636-1646.
Shirazi, K.K., Wallace, L.M., Niknami, S., Hidarnia, A., Torkaman, G., Gilchrist, M.
& Faghihzadeh, S. (2007). A home-based, transtheoretical change model
designed strength training intervention to increase exercise to prevent
osteoporosis in Iranian women aged 40-65 years: a randomized controlled trial.
Health Education Research, 22(3), 305-317.
Sinclair, A.J., Conroy, S.P., Davies, M. & Bayer, A.J. (2005). Post-discharge home-
based support for older cardiac patients: a randomized controlled trial. Age and
Ageing, 34, 338-343.
Smeulders, E. S., van Haastregt, J. C., Ambergen, T., Janssen-Boyne, J. J., van Eijk, J.
T. & Kempen, G. I. (2009). The impact of a self-management group programme
on health behaviour and healthcare utilization among congestive heart failure
patients. European Journal of Heart Failure, 11, 609-616.
Smeulders, E. S., van Haastregt, J. C., van Hoef, E.F., van Eijk, J. T. & Kempen, G. I.
(2006). Evaluation of a self-management programme for congestive heart failure
patients: design of a randomised controlled trial. BMC Health Services Research,
6, 91.
Smith, K.M., Arthur, H.M., McKelvie, R.C. & Kodis, J. (2004). Differences in
sustainability of exercise and health-related quality of life outcomes following
home or hospital-based cardiac rehabilitation. European Journal of
Cardiovascular Prevention and Rehabilitation, 11, 313-319.
Smith, L.K., Layton, K., Newmark, J.L. & Diethrich, E.B. (1987). An intensive
cardiovascular rehabilitation program for patients with disabling angina and
diffuse coronary artery disease. Journal of Cardiopulmonary Rehabilitation, 7,
425-429.
Smith, M. (1999). Nursing and rehabilitation. In: Smith, M. (ed). Rehabilitation in
Adult Nursing Practice. Edinburgh: Churchill Livingstone, 31-52.
So, H.K., Sung, R.Y.T., Li, A.M., Choi, K.C., Nelson, E.A.S., Yin, J., Ng, P.C. & Fok,
T.F. (2010). Higher exercise frequency associated with lower blood pressure in
Hong Kong adolescents: a population-based study. Journal of Human
Hypertension, 24, 646-651.
So.dermana, E., Lisspersa, J. & Sundinb, O. (2003). Depression as a predictor of
return to work in patients with coronary artery disease. Social Science and
Medicine, 56, 193–202.

356
Spertus, J.A., Dawson, J., Masoudi, F.A., Krumholz, H.M., Reid, K.J., Peterson, E.D.
& Rumsfeld, J.S. (2006). Prevalence and predictors of angina pectoris one month
after myocardial infarction. American Journal of Cardiology, 98, 282-288.
Spertus, J.A., Jones, P., McDonell, M., Fan, V. & Fihn, S.D. (2002). Health status
predicts long-term outcome in outpatients with coronary disease. Circulation,
106, 43-49.
Spertus, J.A., Winder, J.A., Dewhurst, T.A., Dewhurst, T.A., Prodzinski, J.,
McDonell, M. & Fihn, S.D. (1995). Development and evaluation of the Seattle
angina questionnaire: A new functional status measure for coronary artery
disease. Journal of the American College of Cardiology, 25(2), 333-341.
Spiraki, C., Kaitelidou, D., Papakonstantinou, V., Prezerakos, P. & Maniadakis, N.
(2008). Health-related quality of life measurement in patients admitted with
coronary heart disease and heart failure to a cardiology department of a
secondary urban hospital in Greece. Hellenic Journal of Cardiology, 49, 241-247.
Stafford, L., Berk, M. & Jackson, H.J. (2007). Validity of the hospital anxiety and
depression scale and patient health questionnaire-9 to screen for depression in
patients with coronary heart disease. General Hospital Psychiatry, 29, 417-424.
Stähle, A., Nordlander, N., Rydén, L. & Mattsson, E. (1999). Effects of organized
aerobic group training in elderly patients discharged after an acute coronary
syndrome. A randomized controlled study. Scandinavian Journal of
Rehabilitation Medicine, 31, 101-107.
Steffen-Batey, L., Nichaman, M.Z., Goff, D.C., Frankowski, R.F., Hanis, C.L.,
Ramsey, D.J. & Labarthe, D.R. (2000). Change in level of physical activity and
risk of all-cause mortality or reinfarction: the Corpus Christi Heart Project.
Circulation, 102, 2204-2209.
Stenlund, T., Lindström, B., Granlund, M. & Burell, G. (2005). Cardiac rehabilitation
for the elderly: Qi Gong and group discussions. European Journal of
Cardiovascular Prevention and Rehabilitation, 12, 5-11.
Steptoe, A., Doherty, S., Rink, E., Kerry, S., Kendrick, T. & Hilton, S. (1999).
Behavioural counselling in general practice for the promotion of healthy
behaviour among adults at increased risk of coronary heart disease: randomised
trial. British Medical Journal, 319, 943-948.
Steptoe, A., Kerry, S., Rink, E. & Hilton, S. (2001). The impact of behavioural
counselling on stage of change in fat intake, physical activity, and cigarette
smoking in adults at increased risk of coronary heart disease. American Journal
of Public Health, 91(2), 265-269.
Stern, M.P. & Farquhar, J.W., Maccoby, N. & Russell, S.H. (1976). Results of a two-
year patient education campaign on dietary behaviour: The Stanford Three
Community Study. Circulation, 54(5), 826-832.

357
Stewart, D.E., Abbey, S.E., Shnek, Z.M., Irvine, J. & Grace, S.L. (2004). Gender
differences in health information needs and decisional preferences in patients
recovering from an acute ischemic coronary event. Psychosomatic Medicine, 66,
42-48.
Stokes, H.C. (2000). Education and training towards competency for cardiac
rehabilitation nurses in the United Kingdom. Journal of Clinical Nursing, 9, 411-
419.
Suaya, J.A., Shepard, D.S., Normand, S.L.T., Ades, P.A., Prottas, J. & Stason, W.B.
(2007). Use of cardiac rehabilitation by medicare beneficiaries after myocardial
infarction or coronary bypass surgery. Circulation, 116, 1653-1662.
Suaya, J.A., Stason, W.B., Ades, P.A., Normand, S.L.T. & Shepard, D.S. (2009).
Cardiac rehabilitation and survival in older coronary patients. Journal of the
American College of Cardiology, 54, 25-33.
Sun, F.C., Zhang, X., Liu, X.L. & Wang, L.Q. (2008). Study on Guidance of TTM in
college students sports exercise after class. Journal of Nanjing Institute of
Physical Education, 22(4), 77-78, 88, 98.
Sundararajan, V., Bunker, S.J., Begg, S., Marshall, R. & McBurney, H. (2004).
Attendance rates and outcomes of cardiac rehabilitation in Victoria, 1998.
Medical Journal of Australia, 180, 268-271.
Szekely, A., Balog, P., Benko, E., Breuer, T., Szekely, J., Kertai, M.D., Horkay, F.,
Kopp, M.S. & Thayer, J.F. (2007). Anxiety predicts mortality and morbidity
after coronary artery and valve surgery – a 4-year follow-up study.
Psychosomatic Medicine, 69, 625-631.
Taylor, C.C., Demoor, C., Smith, M.A., Dunn, A.L., Basen-Engquist, K., Nielsen, I.,
Pettaway, C., Sellin, R., Massey, P. & Gritz, E.R. (2006). Active for life after
cancer: a randomized trial examining a lifestyle physical activity program for
prostate cancer patients. Psycho-Oncology, 15, 847-862.
Taylor, G.H., Wilson, S.L. & Sharp, J. (2011). Medical, psychological, and
sociodemographic factors associated with adherence to cardiac rehabilitation
programs: A systematic review. Journal of Cardiovascular Nursing, 26(3), 202-
209.
Taylor, R.S., Brown, A., Ebrahim, S., Jolliffe, J., Noorani, H., Rees, K., Skidmore, B.,
Stone, J.A., Thompson, A.R. & Oldridge, N. (2004). Exercise-based
rehabilitation for patients with coronary heart disease: systematic review and
meta-analysis of randomized controlled trials. American Journal of Medicine,
116, 682-692.
Taylor, R.S., Dalal, H., Jolly, K., Moxham, T. & Zawada, A. (2010). Home-based
versus centre-based cardiac rehabilitation. Cochrane Database of Systematic
Reviews, Issue 1. Art. No.: CD007130. DOI: 10. 1002/14651858. CD007130.
pub2.

358
Teo, K.K, Liu, L., Chow, C.K., Wang, X., Islam, S., Jiang, L., Sanderson, J.E.,
Rangarajan, S. & Yusuf, S. (2009). Potentially modifiable risk factors associated
with myocardial infarction in China: the INTERHEART China study. Heart, 95,
1857-1864.
The Vestfold Heartcare Study Group. (2003). Influence on lifestyle measures and
five-year coronary risk by a comprehensive lifestyle intervention programme in
patients with coronary heart disease. European Journal of Cardiovascular
Prevention and Rehabilitation, 10, 429-437.
Thompson, D.R. (2007). Role of nurse-led, clinic and home-based intervention on
chronic heart failure patients. Journal of the Hong Kong College of Cardiology,
15 (Suppl 1), A66.
Thompson, D.R., Chair, S.Y., Chan, S.W., Astin, F., Davidson, P.M. & Ski, C.F.
(2011). Motivational interviewing: a useful approach to improving
cardiovascular health? Journal of Clinical Nursing, 20, 1236-1244.
Thompson, D.R. & Lewin, R.P. (2000). Management of the post-myocardial
infarction patient: rehabilitation and cardiac neurosis. Heart, 84, 101-105.
Thompson, D.R. & Roebuck, A. (2001). The measurement of health-related quality of
life in patients with coronary heart disease. Journal of Cardiological Nursing,
16(1), 28-33.
Thompson, D.R., Ersser, S.J., & Webster, R.A. (1995). The experiences of patients
and their partners 1 month after a heart attack. Journal of Advanced Nursing, 22,
707-714.
Thompson, D.R. & Yu, C.M. (2007). Cardiac rehabilitation: China. In J. Perk, P.
Mathes, H. Gohlke, C. Monpere, I. Hellemans, H. McGee, P. Sellier & H. Saner
(Ed). Cardiovascular prevention and rehabilitation. Lodon: Springer.com.
Tierney, A.J, Worth, A. & Watson, N. (2000). Meeting patients' information needs
before and after discharge from hospital. Journal of Clinical Nursing, 9, 859-860.
Todaro, J.F., Shen, B.J., Raffa, S.D., Tilkemeier, P.L. & Niaura, R. (2007).
Prevalence of anxiety disorders in men and women with established coronary
heart disease. Journal of Cardiopulmonary Rehabilitation and Prevention, 27,
86-91.
Todd, I.C. & Ballantyne, D. (1990). Antianginal efficacy of exercise training: a
comparison with β-blockade. Heart, 64, 14-19.
Touillet, A., Guesdon, H., Bosser, G., Beis, J.M. & Paysant, J. (2010). Assessment of
compliance with prescribed activity by hemiplegic stroke patients after an
exercise programme and physical activity education. Annals of Physical &
Rehabilitation Medicine, 53, 250-265.

359
Tullmann, D.F., Haugh, K.H., Dracup, K.A. & Bourguignon, C. (2007). A
Randomized Controlled Trial to Reduce Delay in Older Adults Seeking Help for
Symptoms of Acute Myocardial Infarction. Research in Nursing and Health, 30,
485-497.
Tung, W.C. (2003). Examination of the transtheoretical model and physical activity
in family caregivers in Taiwan. Dissertation: The University of Utah.
Tung, W.C. & Gillett, P.A. (2005). Stages of change for physical activity among
family caregivers. Journal of Advanced Nursing, 49(5), 513-521.
Tung, W.C., Gillett, P.A. & Pattillo, R.E. (2005). Application the transtheoretical
model to physical activity in family caregivers in Taiwan. Public Health Nursing,
22(4), 299-310.
Tung, W.C. & Hsu, C.H. (2009). Assessing transcultural validity of the
transtheoretical model with Chinese Americans and physical activity. Journal of
Transcultural Nursing, 20, 286-295.
Turton, J. (1998). Importance of information following myocardial infarction: a study
of the self-perceived information needs of patients and their spouse/partner
compared with the perceptions of nursing staff. Journal of Advanced Nursing,
27,770-778.
Valkeinen, H., Aaltonen, S. & Kujala, M. (2010). Effects of exercise training on
oxygen uptake in coronary heart disease: a systematic review and meta-analysis.
Scandinavian Journal of Medicine and Science in Sports, 20, 545-555.
van Elderen-van Kemenade, T.E., Maes, S. & van den Broek, Y. (1994). Effects of a
health education programme with telephone follow-up during cardiac
rehabilitation. British Journal of Clinical Psychology, 33, 367-378.
van Sluijs, E.M.F., van Poppel, M.N.M., Twisk, J.W.R. & van Mechelen, W. (2006).
Physical activity measurements affected participants‘ behaviour in a randomized
controlled trial. Journal of Clinical Epidemiology, 59, 404-411.
van Sluijs, E.M.F., van Poppel, M.N.M., Twisk, J.W.R., Chin A Paw, M.J., Calfas,
K.J. & van Mechelen, W. (2005). Effect of a tailored physical activity
intervention delivered in general practice settings: results of a randomized
controlled trial. American Journal of Public Health, 95(10), 1825-1831.
van Sluijs, EMF., van Poppel MNM. & van Mechelen W. (2004). Stage-based
lifestyle interventions in primary care: are they effective? American Journal of
Preventive Medicine, 26(4), 330-343.
van Tol, B.A.F., Huijsmans, R.J., Kroon, D.W., Schothorst, M. & Kwakkel, G. (2006).
Effects of exercise training on cardiac performance, exercise capacity and quality
of life in patients with heart failure: a meta-analysis. European Journal of Heart
Failure, 8, 841-850.

360
Wallace, L.K., Slattery, K.M. & Coutts, A.J. (2009). The ecological validity ad
application of the seesion-RPE method for quantifying training loads in
swimming. International Journal of Nursing Studies, 23(1), 33-38.
Wan, G.S. & Wang, X.Y. (2008). Investigation and analysis of teaching needs on
patients with coronary heart disease. Chinese Journal of Modern Drug
Application, 2(5), 111-113.
Wang, X.L & Xu, L.H. (2010). Critical review of cardiac rehabilitation and nursing
research in patients with coronary heart disease. Shanghai Nursing, 10(2), 69-71.
Wang, W.R., Chair, S.Y., Thompson, D.R. & Twinn, S.F. (2009). Health care
professionals‘ perceptions of hospital-based cardiac rehabilitation in mainland
China: an exploratory study. Journal of Clinical Nursing, 18, 3401-3408.
Wannamethee, G.S., Shaper, A.G. & Walker, M. (2000). Physical activity and
mortality in older men with diagnosed coronary heart disease. Circulation, 102,
1358-1363.
Wanner, M., Martin-Diener, E., Braun-Fahrländer, C., Bauer, G. & Martin, B.W.
(2009). Effectiveness of active-online, an individually tailored physical activity
intervention, in a real-life setting: randomized controlled trial. Journal of
Medical Internet Research, 11(3), e23.
Warburton, D.E.R., Katzmarzyk, P.T., Rhodes, R.E. & Shephard, R.J. (2007).
Evidence-informed physical activity guidelines for Canadian adults. Applied
Physiology, Nutrition, and Metabolism, 32, s16-s68.
Ware, J.E. & Sherbourne, C.D. (1992). The MOS 36-item short-form health survey
(SF-36). I. Conceptual framework and item selection. Medical Care, 30(6), 473-
483.
Webster, R.A., Thompson, D.R. & Mayou, R.A. (2002). The experiences and needs
of Gujarati Hindu patients and partners in the first month after a myocardial
infarction. European Journal of Cardiovascular Nursing, 69-76.
Wenger, N.K., Smith, L.K., Froelicher, E.S., Comoss, P.M. (Ed). (1999). Cardiac
rehabilitation: a guide to practice in the 21st century. New York, NY: Marcel
Dekker. 70.
White, J., Hunter, M. & Holttum, S. (2007). How do women experience myocardial
infarction? A qualitative exploration of illness perceptions, adjustments and
coping. Psychology, Health and Medicine. 12(3), 278-288.
Wiklund, I., Sanne, H., Elmfeldt, D., Vedin, A. & Wilhelmsson, C. (1984). Emotional
reaction, health preoccupation and sexual activity two months after a myocardial
infarction. Scandinavian Journal of Rehabilitation Medicine. 16(2), 47-56.
361
Willmer, K.A. & Waite, M. (2009). Long-term benefits of cardiac rehabilitation: a
five-year follow-up of community-based phase 4 programmes. British Journal of
Cardiology, 16, 73-77.
Windle, G., Hughes, D., Linck, P., Russell, I. & Woods, B. (2010). Is exercise
effective in promoting mental well-being in older age? A systematic review.
Aging and Mental Health, 14(6), 652-669.
Witt, B.J., Jacobsen, S.J., Weston, S.A., Killian, J.M., Meverden, R.A., Allison, T.G.,
Reeder, G.S. & Roger, V.L. (2004). Cardiac rehabilitation after myocardial
infarction in the Community. Journal of the American College of Cardiology, 44,
988-996.
Wong, M.S. & Chair, S.Y. (2007). Changes in health-related quality of life following
percutaneous coronary intervention: a longitudinal study. International Journal
of Nursing Studies, 44, 1334-1342.
Wood, M.E. (2008). Theoretical framework to study exercise motivation for breast
cancer risk reduction. Oncology Nursing Forum, 35(1), 89-95.
Woods, C., Mutrie, N. & Scott, M. (2002). Physical activity intervention: a
transtheoretical model-based intervention designed to help sedentary young
adults become active. Health Education Research, 17(4), 451-460.
Worcester, M.U.C., Murphy, B.M., Elliott, P.C., Le Grande, M.R., Higgins, R.O.,
Goble, A.J. & Roberts, S.B. (2007). Trajectories of recovery of quality of life in
women after an acute cardiac event. British Journal of Health Psychology, 12, 1-
15.
Worcester, M.U.C., Murphy, B.M., Mee, V.K., Roberts, S.B. & Goble, A.J. (2004).
Cardiac rehabilitation programmes: predictors of non-attendance and drop-out.
European Journal of Cardiovascular Prevention and Rehabilitation, 11, 328-335.
World Health Organization. (1993). Needs and action priorities in cardiac
rehabilitation and secondary prevention in patients with coronary heart disease.
Copenhagen: WHO.
World Health Organization (WHO). (2004). Information database - 2004 (accessed
12 April 2011). Available at: https://apps.who.int/infobase/Mortality.
World Health Organization (WHO). (2005). The Impact of Chronic Disease in China
- 2005 (accessed 12 April 2011). Available at: http://
www.who.int/chp/chronic_disease_report/media/china.
World Health Organization (WHO). (2008). Cardiovascular Disease - 2008 (accessed
10 January 2009). Available at: http://www.who.int/cardiovascular_disease.
World Health Organization (WHO). (2011). Cardiovascular Disease - 2011 (accessed
12 April 2011). Available at: http:// www.who.int./cardiovascular_disease.
362
Wu, S.K., Lin, Y.W., Chen, C.L. & Tsai, S.W. (2006). Cardiac rehabilitation vs.
home exercise after coronary artery bypass graft surgery. American Journal of
Physical Medicine and Rehabilitation, 85, 711-717.
Wu, X.G. (2003). An epidemiological status and trends of coronary heart disease in
Chinese population. Chinese Journal of Prevention and Control of Chronic Non-
communicable Disease, 11(4), 190-191.
Xia, Y.T. (2006). The analysis of reliability and validity of the hospital anxiety and
depression scale for pregnant women. Journal of Nursing (China), 13(11), 62-63.
Xu, L. (2004). Investigation and study of the personality, mentality and quality of life
in patients with coronary heart disease. Health Psychology Journal, 12(3), 178-
183.
Yan, X., Lee, S. & Li, N. (2009) Missing data handling methods in medical device
clinical trials. Journal of Biopharmaceutical Statistics, 19, 1085-1098.
Yan, Z.M., Zhang, M.R., Yang, Z., Li, Y.T. & Gong, H.Q. (2004). Epidemiological
survey and analysis of coronary heart disease from residents in Kunming. Soft
Science of Health, 18(6), 334-336
Yang, M., Yang, S. & Liu, X.H. (2007). A review of psychological assessment and
interventions on patient with coronary heart disease. Chinese Journal of
Practical Nursing, 23(8), 73-74.
Yates, B. C., Anderson, T., Hertzog, M., Ott, C. & Williams, J. (2005). Effectiveness
of follow-up booster sessions in improving physical status after cardiac
rehabilitation: health, behavioral, and clinical outcomes. Applied Nursing
Research, 18, 59-62.
Yates, B.C., Heeren, B.M., Keller, S.M., Agrawal, S., Stoner, J.A. & Ott, C. (2007).
Comparing two methods of rehabilitation for risk factor modification after a
cardiac event. Rehabilitation Nursing, 32(1), 15-22.
Ye, W.F. & Xu, J.M. (1993). The application and evaluation of hospital anxiety and
depression scale with patients in general hospital. Chinese Journal of Behaviour
Science, 2(3), 17-19.
Yohannes, A.M., Yalfani, A., Doherty, P. & Bundy, C. (2007). Predictors of drop-out
from an outpatient cardiac rehabilitation programme. Clinical Rehabilitation, 21,
222-229.
Yonezawa, R., Masuda, T., Matsunaga, A., Takahashi, Y., Saitoh, M., Ishii, A.,
Kutsuna, T., Matsumoto, T., Yamamoto, K., Aiba, N., Hara, M. & Izumi, T.
(2009). Effects of phase II cardiac rehabilitation on job stress and health-related
quality of life after return to work in middle-aged patients with acute myocardial
infarction. International Heart Journal, 50, 279-290.

363
Yu, C.M., Lau, C.P., Chau, J., McGhee, S., Kong, S.L., Cheung, B.M.Y. & Li, L.S.W.
(2004). A short course of cardiac rehabilitation program is highly cost effective
in improving long-term quality of life in patients with recent myocardial
infarction or percutaneous coronary intervention. Archives of Physical Medicine
& Rehabilitation, 85, 1915-1922.
Yue, L.P. (2004). Psychological analysis of 84 patients with coronary heart disease.
Chinese Journal of Health Psychology, 12(6), 429-430.
Yuval, R., Halon, D.A. & Lewis, B.S. (2007). Perceived disability and lifestyle
modification following hospitalization for non-ST elevation versus ST elevation
acute coronary symdromes: the patients‘ point of view. European Journal of
Cardiovascular Nursing, 6, 287-292.
Zboralski, K., Galecki, P., Wysokiński, A., Orzechowska, A. & Talarowska, M.
(2009). Quality of life and emotional functioning in selected cardiovascular
diseases. Kardiologia Polska, 67(11), 1228-1234.
Zhang, B.H., Li, X.W. & Wang, X.H. (1999). The effects of rehabilitation exercise on
the aerobic capacity of the patients with CHD post intervention therapy. Chinese
Journal of Cardiovascular Rehabilitation Medicine, 8(4), 3-5.
Zhang, H.S., Wang, X.M. & Zeng, D.Y. (2004). Clinical features of psychological
status in patients with coronary heart disease. Chinese Journal of Clinical
Rehabilitation, 8(15), 2806-2807.
Zhang, J.P., Tang, Y. & Yu, X.P. (2005). Investigation on mental status in patients
with coronary heart disease. Journal of Nursing Science, 20(15), 43-45.
Zhang, L., Xu, D.Z., Huang, J.Y. & Li, L.S. (2004). Study on the application of the
Chinese version of SF-36 scales and selection of interceptive cents for its grade
range. Chinese Journal of Epidemiology, 25(1), 69-73.
Zhang, X.H., Lu, Z.L. & Liu, L. (2008). Coronary heart disease in China. Heart, 94,
1126-1131.
Zhang, Y.C., Huang, C.S., Han, L. & Li, S.M. (2004). Analysis of clinical characters
and psychosocial factors in patients with coronary heart disease. Nervous
Diseases and Mental Health, 4(5), 364-365.
Zhang, Z.J. (Ed). (2005). A handbook of behavioural medical scale. Beijing: Chinese
Medical Electronic Audio-Video Publishing House.
Zhao, Y. & Wong, F.K.Y. (2009). Effects of a postdischarge transitional care
programme for patients with coronary heart disease in China: A randomised
controlled trial. Journal of Clinical Nursing, 18, 2444-2455.
Zhong B., Lei Y., Qiao SB., Zhang WC., Liu YN. & Liu Y. (1999). Contrast study on
exercise rehabilitation in patients with angina of coronary heart disease. Chinese
Journal of Cardiovascular Rehabilitation Medicine, 8(4), 11-13.

364
Zhou, Y. & You, L.M. (2003). Psychological status and psychological care of the
patients with coronary heart disease. Chinese Journal of Nursing, 38(11), 836-
838.
Zhu, F. & Chen, Y.J. (2007). The effect of transtheoretical model for patient
education to the behavioural changes of diabetic patients. Zhejiang Preventive
Medicine, 19(8), 31, 41, 61.
Zhu, L.X., Ho, S.C. & Sit, W.H.J. (2012). The experiences of Chinese patients with
coronary heart disease. Journal of Clinical Nursing, 21(3-4), 476-484.
Zhu, L.X., Ho, S.C. & Wong, T.K.S. (unpublished). The effectiveness of health
education on exercise behaviour of patients with heart disease.
Zhu, L.X., Lin, B.L., Huang, L.P., Dai, X.Y., Chen, S.Z. & Song, M.Y. (2007).
Correlation about psychological condition and social supports for patients with
coronary heart disease. Chinese Journal of Practical Nursing, 23(12), 55-58.
Zhu, Y.J. (2004). Evaluation of 4-week exercise therapy on the amelioration of left
heart function and activities of daily living in patients with acute myocardial
infarction accompanied by left heart failure. Chinese Journal of Clinical
Rehabilitation, 8(27), 5788-5789.
Ziegelstein, R.C., Fauerbach, J.A., Stevens, S.S., Romanelli, J., Richter, D.P. & Bush,
D.E. (2000). Patients with depression are less likely to follow recommendations
to reduce cardiac risk during recovery from a myocardial infarction. Archives of
Internal Medicine, 160, 1818-1823.
Zwisler, A.D., Soja, A. M., Rasmussen, S., Frederiksen, M., Abadini, S., Appel, J.,
Rasmussen, H., Gluud, C., Iversen, L., Sigurd, B., Madsen, M. & Fischer-
Hansen, J. (2008). Hospital-based comprehensive cardiac rehabilitation versus
usual care among patients with congestive heart failure, ischemic heart disease,
or high risk of ischemic heart disease: 12-month results of a randomized clinical
trial. American Heart Journal, 155, 1106-1113.

365
Appendices

366
Appendix I Contraindications for Exercise Training
Contraindications for Exercise Training
According to Wenger, Smith, Froelicher, Comoss (1999) and the expert work group
of the National Heart Foundation of Australia (Briffa, Maiorana, Sheerin, Stubbs &
Oldenburg et al., 2006), people with the following contraindications should not
engage in outpatient cardiac rehabilitation exercise training or physical activity:-
Table I Contraindications for exercise training
Wenger et al. (1999) Briffa et al. (2006)
Unstable angina;
Resting SBP > 200 mmHg or resting
DBP > 110 mmHg;
Orthostatic blood pressure drop of >
20mmHg with symptoms;
Critical aorthic stenosis (peak systolic
pressure gradient > 50 mmHg with
aortic valve orifice area < 0.75 cm2 in
average size adult);
Acute systematic illness or fever;
Uncontrolled atrial or ventricular
arrhythmias;
Uncontrolled sinus tachycardia (> 120
beats/min);
Uncompensated CHF;
Third degree AV block (without
pacemaker);
Active pericarditis or myocarditis;
Recent embolism;
Thrombophlebitis;
Unstable angina;
Uncontrolled hypertension or with
grade 3 (severe) hypertension e.g.,
SBP ≥ 180 and DBP ≥ 110
mmHg;
Symptomatic hypotension < 90/60
mmHg;
Severe aortic stenosis;
Symptoms such as chest
discomfort and shortness of breath
on low activity;
Resting tachycardia or
arrhythmias;
Acute infection or fever, or are
feeling unwell (including acute
myocarditis or pericarditis);
Uncontrolled cardiac failure;
Diabetes with poor blood glucose
control, e.g., blood glucose level
< 6 mmol/L or > 15 mmol/L

367
Table I Contraindications for exercise training (Continue)
Wenger et al. (1999) Briffa et al. (2006)
Resting ST segment displacement
(>2mm);
Uncontrolled diabetes (resting blood
glucose > 400 mg/dL);
Severe orthopaedic problems that
would prohibit exercise;
Other metabolic problems, such as
acute thyroiditis, hypo- or
hyperkalemia, hypovolemia, etc.

368
Appendix II Ethics Approval Letters




372
Appendix IV Screening Guidelines
Screening Guidelines
The following guidelines are provided for the cardiologists to screen each potential
patient and to decide whether the patient is suitable for participating in this study or
not, that is an exercise stage-matched intervention. According to the following
guidelines, if the patient does not meet any one item of the requirements, the patient
will not be invited to participate in the study.
1.Age__________years
Suitable:age ≥ 18 years old。
Unsuitable:age < 18 years old。
2. Is the patient living in Xiamen City?
Suitable:The patient is living in Xiamen City and can be contacted by telephone.
Living Address:____________________________________________
Telephone:______________________________________________
Unsuitable:The patient is not living in Xiamen City or cannot be contacted by
telephone.
3.Does patient be able to communicate in mandarin and read in Chinese?
Suitable:The patient is able to communicate in mandarin and read in Chinese.
Unsuitable:The patient has difficulties/obstacles in communicating in mandarin
or reading in Chinese.
Note:
(1) Communicate ability refers to the patient can understand the communication
contents and can communicate to each other using precise words.
(2) Communication difficulties / obstacles of communication refer to that the patient
is unable to understand the contents, can not convey the meaning of words, or

373
can not communicate to each other.
(3) Reading ability refers to the patient can read and understand Chinese
(4) Reading difficulties refer to the patient can not read in Chinese.
4.Disease diagnosis: angina pectoris, myocardial infarction, PCI
Suitable:The patient has been diagnosed with angina pectoris or myocardial
infarction or has undergone PCI for at least three months.
Unsuitable:The patient has been diagnosed with angina pectoris or myocardial
infarction or has undergone PCI for less than three months.
Note:
A.Angina pectoris ,date of diagnosis_________(month/year)
Diagnosis:According to the diagnostic criteria from the International Society of
Cardiology and the World Health Organization in 1979:
1)Medical history:Have a medical history of typical angina, that is the chest
discomfort is induced by the exertion or emotional excitement, usually lasting 1-
15 minutes, may radiate to the jaw, throat, shoulder, back, left arm or wrist, and
can be relieved by rest or sublingual nitroglycerin in a few minutes.
2)Men over the age of 40 years and women over the age of 45; the resting ECG
shows a significant myocardial ischemia; or the exercise test shows positive
results, without any other causes (e.g., a variety of heart disease, autonomic
dysfunction, significant anemia, COPD, taking digitalis, and electrolyte
imbalance), and has two of the following three items: hypertension, high blood
cholesterol and diabetes.
3)The patient was confirmed by the coronary angiography with the luminal
diameter stenosis 70% or more.
B. Myocardial infarction (___time), date of diagnosis_______(month/year)
Diagnosis:According to the revised diagnostic criteria from the National Integrative
control of coronary heart disease, angina, cardiac arrhythmia research symposium (in
Shanghai) in 1979.
I. Meet two of the following three items,the patient can be diagnosed with acute
myocardial infarction:

374
1)Typical clinical symptoms: A typical history of a serious and persistent chest
pain;
2)Abnormal Q spread or ST-T segment on ECG as the evolution of myocardial
infarction;
3)Increased serum enzyme as the process of myocardial infarction.
II. Certainly information (e.g., ECG or serum enzyme) confirmed that the patient had
suffered from myocardial infarction.
C. PCI (______time),date of PCI_________(month/year)
Diagnosis : PCI Includes percutaneous coronary angioplasty (PTCA), coronary
stenting, rotational atherectomy of coronary artery plaque, laser angioplasty
techniques.
5.Is patient medically stable?
Suitable:The patient is medically stable.
Unsuitable:The patient is not medically stable。
Note:
Whether the patient is medically stable or not is judged by the cardiologists.
References are as follows:
① Patients with stable vital signs, that is breathing, pulse, blood pressure and body
temperature within normal limits (see below for specific measurements); no fever
(oral temperature below 37.5 ℃ ); no manifestation of unstable angina or acute
myocardial infarction.
6.Does patient have unstable angina?
Suitable:Patient has no unstable angina.
Unsuitable:Patient has unstable angina.
Note:
(1)Stable angina: Patient has a stable condition. Stable angina is characterized by a
deep, poorly localized chest or arm discomfort that is reproducibly associated with

375
physical exertion or emotional stress and relieved within 5-15 minutes by rest
and/or sublingual nitroglycerin. Most patients can predict under what conditions
(such as how far, how fast, and how many steps to go, and so on) will occur angina
pain.
(2)Unstable angina:The unstable angina are classified as five types:
1)New angina: Individuals have never experienced angina before and suddenly
occurred frequent angina after physical exertion in the recent one month. It
can be deteriorated into myocardial infarction.
2)Worsening angina: Individuals have a history of angina, but the onset of
angina become more frequent and the pain become more serious recently,
which often last more than 15 minutes and can not be relieved by
nitroglycerin.
3)Resting angina: Angina occurs at rest or sleep with severe pain and individuals
are often forced to sit or stand.
4)Variant angina: The clinical manifestations are similar to the resting angina,
but ST-segment elevation on ECG during angina attack, which is due to the
sudden coronary artery spasm. The patient will suffer from myocardial
infarction sooner or later.
5)Post-infarction angina: Recurrent angina one month after the acute myocardial
infarction. This suggests that there may be a recurrence of myocardial
infarction.
7.Has patient participate in any cardiac rehabilitation programme?
Suitable:The patient has never participated in any cardiac rehabilitation
programme.
Unsuitable:The patient has participated in any related cardiac rehabilitation
programme.
Note:
(1) The related cardiac rehabilitation programme refers to structure patient
education regarding coronary heart disease, organized exercise training, or
instructions for cardiac rehabilitation and risk factor control.

376
8.Does patient have any cognitive impairment?
Suitable:The patient has no cognitive impairment.
Unsuitable:The patient has cognitive impairment.
Note:
( 1 ) Meet any one following item, the patient is thought to have cognitive
impairment:
1)Has been diagnosed with psychosis.
2)Has been diagnosed with dementia.
3)Has been diagnosed with mental retardation.
4)Suffered from aphasia or agnosia after stroke or traumatic brain injury.
9.Does patient have depression?
Suitable:The patient has no depression.
Unsuitable:The patient has depression.
Note:
(1) In this study, the depression is diagnosed based on that the scores are equal to 11
or more on the Hospital Anxiety and Depression Scale – Depression Subscale.
10.Does patient have critical aortic stenosis?
Suitable:The patient has no critical aortic stenosis.
Unsuitable:The patient has been diagnosed with critical aortic stenosis.
Note:
(1) Aortic valve stenosis is narrowing of the orifice between the left ventricle and
the aorta. Normal aortic valve area is 3.0cm2 or more. When the valve area is
reduced to 1.5cm2, it is the mild stenosis; when the valve area becomes
1.0cm2, there is a significant pressure gradient and is classified as moderate
stenosis; when the valve area is < 0.75cm2, it can appear clinical symptoms
and is classified as severe stenosis.

377
(2) The common etiologies of the aortic valve stenosis are inflammatory
rheumatic valvular, congenital malformations and degenerative.
(3) The characteristic symptoms of critical aortic stenosis include chest pain,
syncope, heart failure or sudden death. Once the symptoms appeared, it often
has a progressive deterioration. If the patients do not receive treatment with
surgery, they will die within an average of 2-3 years. The typical signs of
aortic valve stenosis are a loud, rough systolic murmur which is most obvious
at the right edge of the second intercostals sternum and left sternal border of
the third and fourth intercostals, increased with the inhalation of amyl nitrite
or supine posture and weakened with the application of vasopressors or
standing. Generally, the more severe aortic stenosis, the stronger systolic
murmur. The intensity level of murmur is up to 3-4/6 grade and it is
accompanied with tremors and may radiate into the carotid arteries and to the
apex of the left ventricle.
(4) Laboratory tests: X-ray examination shows expansion after aortic stenosis and
calcification of aortic valve in most cases; ECG shows that around 85% of the
patients have left ventricular hypertrophy; echocardiography shows that the
aortic opening is smaller than 15 mm, the open speed slows down, and the
valve leaflets become thickening; Doppler ultrasound can measure blood
velocity in the heart and intravascular, calculate the maximum pressure
gradient across the valve by measuring aortic blood flow velocity, and also
can calculate the aortic valve area; cardiac catheterization is a golden method
for the diagnosis of aortic stenosis and the judgments of its severity. Since the
examination is invasive way, it is not use as a routine examination.
(5) According to the patient‘s medical history, typical symptoms and signs, and
laboratory tests (X-ray, electrocardiogram and echocardiography), it can be
generally made a diagnosis.
11.Heart function according to the New York Heart Functional Classification
(NYHA):
Suitable:According to the NYHA classification, the patient‘s heart function is
I/II grade.
378
Unsuitable:According to the NYHA classification, the patient‘s heart function
is III/IV grade.
Note:
① I:No limitation of physical activity. Ordinary physical activity does not cause
undue fatigue, palpitation, or dyspnea (shortness of breath).
② II:Slight limitation of physical activity. Comfortable at rest, but ordinary physical
activity results in fatigue, palpitation, or dyspnea.
③ III :Marked limitation of physical activity. Comfortable at rest, but less than
ordinary activity causes fatigue, palpitation, or dyspnea.
④ IV:Unable to carry out any physical activity without discomfort. Symptoms of
cardiac insufficiency at rest. If any physical activity is undertaken, discomfort
is increased.
12.Diabetes mellitus (DM)
Suitable: The patient has no diabetes mellitus, or the patient has been diagnosed
with diabetes mellitus, but the blood glucose is controlled in the optical levels (fasting
blood glucose <15 mmol/L).
Unsuitable: If the patient uses hypoglycaemic drugs in the normal case, the
current blood glucose levels ≥ 15mmol/L.
Note:
(1) Diagnosis of diabetes: morning fasting blood glucose level ≥ 7.0mmol/L, or
the blood glucose in any time or the OGTT ≥ 11.1mmol/L.
(2) The blood glucose is measured using a blood glucose meter to measure the
blood at the end of the capillary blood on the left ring finger.
13.Hypertension
Suitable: The patient has no hypertension, or the patient has been diagnosed with
hypertension, but the blood pressure is well controlled, in the case of taking anti-

379
hypertensive drugs, the current systolic BP < 23.94kPa (180mmHg) or diastolic BP <
14.67 kPa (110mmHg).
Unsuitable: The patient has high blood pressure, taking anti-hypertensive drugs,
the current systolic BP ≥ 23.94kPa (180mmHg) or diastolic BP ≥ 14.67kPa
(110mmHg).
Note:
(1) Diagnosis of hypertension: Using the criteria published by the U.S. National
Joint Committee on Hypertension in 1997, that is the patient can be diagnosed
with hypertension if the resting systolic BP ≥ 18.6kPa (140mmHg) or resting
diastolic blood pressure ≥ 12.0 kPa (90mmHg).
(2) The guidelines for measuring blood pressure:
1)Using mercury sphygmomanometer to measure blood pressure on the right
brachial artery.
2)The patient should be emotionally stable, taking 15-minute break before the
measurement of blood pressure. If any following accidences occur, such as
smoking, exercise, mood changes, the patient should rest for 20-30 minutes
before the measurement.
3)The patient takes sitting position with the arm (brachial artery) at the same
level of the fourth rib.
4)The lower edge of the cuff is 2-3cm above the cubital fossa. An appropriate
tightness is able to insert a finger.
5)When a stethoscope appears the first pulse tone, the scale value of the mercury
column is the systolic BP; when the pulse sound suddenly become weak or
disappeared, the scale value of the mercury column is the diastolic BP.
14.Does patient has arrhythmias? Heart rate_________bpm.
Suitable:The patient‘s heart rhythm is regular with the pulse rate of 60-100
bpm.
Unsuitable:The patient has sinus tachycardia (pulse rate ≥ 120 bpm).

380
Note:
(1)Use pulse rate to show heart rate. The measurements of pulse rate are presented
as follows:
1)Measure the pulse rate on the right radial artery.
2)Patient preparation: Take sitting posture with stable mood and take 15-minute
break before the measurement. If the patient performs the following activities,
such as strenuous exercise, stress, fear, etc, he/she should rest for 20-30
minutes before the measurement.
3)The measurer uses the index, middle and ring fingers to press on the patient‘s
radial artery to measure it.
4)Use the second hand watch to measure the pulse for 30 seconds and multiply it
by 2.
15.Does patient have atrial fibrillation?
Suitable:The patient has no atrial fibrillation.
Unsuitable:The patient has atrial fibrillation.
Note:
(1)The clinical manifestations of the atrial fibrillation: Cardiac auscultation shows
that the intensity of the first heart sound is volatile and the heart rhythm is irregular.
When the ventricular rate is rapid, it will occur pulse shortage, that is the pulse rate is
less than heart rate.
16.Does patient have ventricular arrhythmias?
Suitable:The patient‘s heart rhythm is regular without ventricular arrhythmias.
Unsuitable : The patient is suffering from frequent premature ventricular
contractions (≥ 5 bpm), paired premature ventricular contractions or ventricular
tachycardia (pulse rate ≥ 120 bpm), ventricular flutter or ventricular fibrillation.

381
Note:
(1) Ventricular arrhythmias: The most common one is the premature ventricular
contractions. The premature ventricular contractions often have no direct
related symptoms. Patients may feel palpitations, a sense of weightlessness
like rapid movements of the elevator, or a strong heart beat after compensatory
pause. Cardiac auscultation shows that there is a long stop after the premature
ventricular contraction, the intensity of the second heart sound of premature
ventricular contraction decreased, and only can hear the first heart sound.
Radial artery pulse is weakened or disappeared.
17.Does patient have third-degree AV block?
Suitable:The patient has no third-degree AV block.
Unsuitable:The patient has the third-degree AV block.
Note:The features of the third-degree AV block as follows:
(1) The activities of atrial and ventricular are separative and unrelated;
(2) The atrial rate is higher than the ventricular rate. The atrial impulse comes
from the sinus node or ectopic atrial rhythm (atrial tachycardia, flutter or
fibrillation);
(3) The ventricular pacemaker usually located at slightly below the block part.
18.Does patient have acute myocarditis?
Suitable:The patient has no acute myocarditis.
Unsuitable:The patient has acute myocarditis.
Note:
(1) Acute myocarditis refers to the recent onset of disease. The clinical
manifestations, such as chest discomfort, rapid heart rate, chest tightness,
palpitations, and tachycardia, are obvious and changeable. Laboratory tests
show elevated myocardial enzymes, ST segment elevation or depression, T

382
wave inversion and arrhythmia on the ECG, and the cardiac ultrasound shows
the reduction of diffuse or localized left ventricular wall contraction. The
disease history is within six months. The most common one is viral
myocarditis.
(2) Diagnosis of viral myocarditis: Currently, the method used to isolate virus for
the diagnosis of viral myocarditis is only conducted in few hospitals. Most
hospitals diagnose with the disease only based on the clinical manifestations,
ECG and the results of enzyme investigation.
19.Does patient have acute pericarditis?
Suitable:The patient has no acute pericarditis.
Unsuitable:The patient has acute pericarditis.
Note:
(1) Pericarditis refers to an inflammation of the pericardium, the membranous sac
enveloping the heart.
(2) Symptoms of acute pericarditis:
1) Chest pain: The most characteristic symptom of pericarditis is chest pain. The
pain may worsen with deep inspiration, coughing, swallowing and when lying
down or turning.
2) Symptoms of cardiac tamponade: It may appear dyspnea, paleness, irritability,
cyanosis, fatigue, upper abdominal pain, swelling or shock.
3) Symptoms of pericardial effusion pressure on adjacent organs: dyspnea,
coughing or hoarseness or swallowing difficulties.
4) Other symptoms: Chills, fever, palpitations, sweating and fatigue.
(3) Signs of acute pericarditis:
1)Pericardial friction rub: The most characteristic sign of pericarditis is a creaky
or scratchy friction rub heard most clearly at the left lower sternal border.
2)Signs of pericardial effusion:
• Cardiac signs: The heart beat becomes weakened or disappeared, or appears at

383
the inside left edge of the cardiac dullness. The cardiac dullness expands to
both sides of the heart and the relative dullness is disappeared. When the
patient change position from sitting to supine, the second and third intercostals
cardiac dullness becomes widened. Heart sound is light and distant.
• Signs of oppression left lung: When there is a large pericardial effusion, the
heart shifts backward which results in oppression of the left lung and can
cause the atelectasis of the left lung lower lobe. Under the left shoulder area,
there is a dullness area, the fremitus is enhanced and the bronchial breath
sounds can be heard (E wart sign).
• Signs of cardiac oppression: The tachycardia is obvious. Venous pressure is
increased seriously and can be expanded with heart beat and inspiration. It
also appears the manifestations of circulation congestion, such as
hepatomegaly with tenderness, ascites, subcutaneous edema and the positive
signs of liver-jugular reflux. The systolic blood pressure becomes lower, the
pulse pressure decreases, the pulse becomes thin and may appear paradoxical
pulse.
20.Does patient have embolism during the previous three months?
Suitable:The patient has no embolism during the previous three months。
Unsuitable:The patient has suffered from an embolism within the recent three
months.
Note:
(1) Thromboembolic disease includes myocardial infarction, cerebrovascular
disease, pulmonary thromboembolism, deep vein thrombosis, DIC and other
diseases.
21.Does patient have any acute noncardiac disorder that may affect exercise
performance or be aggravated by exercise (e.g., infection, renal failure,
thyrotoxicosis)?

384
Suitable:The patient has no acute noncardiac disorder that may affect exercise
performance or be aggravated by exercise (e.g., infection, renal failure,
thyrotoxicosis).
Unsuitable:The patient has acute noncardiac disorder that may affect exercise
performance or be aggravated by exercise (e.g., infection, renal failure,
thyrotoxicosis).
Note:
I.Acute infection
(1)Infection: When the on-site measurement of patients‘ oral temperature is ≥
37.5℃,the patients are viewed as infection ( body temperature______℃).
(2)The measurement of temperature:
1)Use mercury thermometer to measure the oral temperature.
2)The patients take a comfortable position and the mood is stable. If the patients
do any the following activities before measurement, such as exercise, eating,
hot or cold drink, cold or hot compress, bath, hip bath, enema, etc, they should
rest for 30 minutes before measurement.
3)The mercury thermometer is below 35℃.
4)Diagonally put the mercury side of the oral thermometer at the sublingual nest
and close moth for 3 minutes.
II.Acute and chronic renal failure
1) Acute renal failure (ARF) is a reversible clinical syndrome where there is a
sudden and almost complete loss of kidney function (decreased GFR) over a
period of hours to days with failure to excrete nitrogenous waste products and
to maintain fluid and electrolyte homestasis. The main manifestation of the
ARF is an increase in serum creatinine (Cr) and BUN. Urine volume is often
changed, including oliguria (less than 400 ml/day) and anuria (less than 50
ml/day).
2) Diagnosis of acute renal failure is based on the changes of the absolute or
relative value of serum creatinine (Cr), such as the absolute value of the Cr
increases average of 44.2umol/L or 88.4umol/L per day, or the relative value
385
of the Cr increases 25%~100% within 24~72 hours.
3) Chronic renal failure (CRF) is a progressive, irreversible deterioration in renal
function in which the body‘s ability to maintain metabolic and fluid and
electrolyte balance fails, resulting in uremia or azotemia.
4) Diagnosis of chronic renal failure is based on the medical history, signs and
laboratory tests.
III.Hyperthyroidism
(1)Diagnosis of hyperthyroidism: If the patient meets the following three items,
the diagnosis is confirmed.
1)High metabolic symptoms and signs
2)Goiter
3)Increase in serum TT4 and FT4 and decrease in TSH

386
Appendix V Information Sheet
INFORMATION SHEET
The effects of an exercise stage-matched intervention on patients with coronary
heart disease (CHD)
You are invited to participate in a study supervised by Dr Jacqueline Ho, Dr Janet Sit,
Dr. Guoqiang Ruan (a cardiologist) and Dr Qiang Xie (a cardiologist), and conducted
by Lixia Zhu, who is the student of the School of Nursing, The Hong Kong
Polytechnic University.
This study is aimed to evaluate the effects of an exercise stage-matched intervention
on patients with coronary heart disease (CHD). You will be randomly allocated to
different groups of interventions. The interventions include conventional service, one
2-hour health education session, and 8-week exercise stage-matched intervention
sessions. For the 8-week intervention sessions, they will be run weekly for 8 weeks
with 15-30 minutes per session. Regardless of which group you are, you have to
complete some questionnaires at four different time points: before you receive any
service/intervention from us, 8 weeks after the completion of the service/intervention,
3 and 6 months after the completion of the service/intervention.
The regular exercise/physical activity has been shown to be beneficial to patients with
heart disease. Thus, the exercise stage-matched intervention, which aims to motivate
CHD patients to do exercise, will benefit patients in this study. However, mild chest
discomfort may be found during exercise. To minimize the effects of chest discomfort
on you, a cardiologist will assess your physical, psychological and emotional status
before you are allowed to join this study. In addition, the cardiologist will prescribe
your dose of exercise and monitor the whole progress of the intervention. If you
experience any discomfort during the intervention, you can contact Lixia ZHU at any
time for help.
387
You have rights to withdraw from the study at any time during the study without any
penalty. All information related to you will be kept confidential by assigning a code
number for you. The raw data can only be accessed by the research team members.
If you have any complaints about the conduct of this research study, please do not
hesitate to contact Ms. Kath Lui, Secretary of the Human Subjects Ethics Sub-
Committee of The Hong Kong Polytechnic University in person or in writing (c/o
Research Office in Room M502 of the University). If you would like more
information about this study, please contact Lixia Zhu or her supervisor Dr Jacqueline
Ho.
Thank you for participating in this study.
Principal Investigator
Zhu Lixia

388
Appendix VI Consent Form
CONSENT TO PARTICIPATE IN RESEARCH
The effects of an exercise stage-matched intervention on patients
with coronary heart disease (CHD)
I _______________________ hereby consent to participate in the captioned research
supervised by Dr Jacqueline Ho, Dr Janet Sit, Dr Guoqiang Ruan (cardiologist) and
Dr Qiang Xie (cardiologist) and conducted by Lixia Zhu.
I understand that information obtained from this research may be used in future
research and published. However, my right to privacy will be retained, i.e., my
personal details will not be revealed.
The procedure as set out in the attached information sheet has been fully explained. I
understand the benefits and risks involved. My participation in the project is voluntary.
I acknowledge that I have the right to question any part of the procedure and can
withdraw at any time without penalty of any kind.
Name of participant
Signature of participant
Name of Parent or Guardian (if applicable)
Signature of Parent or Guardian (if applicable)
Name of researcher Zhu Lixia
Signature of researcher
Date

389
Appendix VII Protocol of Weekly Patient Education Session
Protocol for the Weekly Patient Education Informing Session
(I) Checking for Compliance
1. Did you perform exercise in the past one week?
2. What kind of exercise did you perform?
3. How many days did you perform it in the past one week?
4. How long did you perform it per day?
5. What was/were the RPE score(s) that you recorded on the exercise log sheet?
6. How did you feel during the exercise? Did you experience any increase in
respiratory rate? Any sweating?
7. Did you experience any discomfort during the exercise?
8. Did you take any anti-anginal medication because of exercise in the past one week?
If yes, how many pills did you take?
(II) Patient Education Informing
1. Inform the benefits and importance of regular exercise

390
Appendix VIII Guidelines for Exercise Prescription
Guidelines for Exercise Prescription
A. General rules when prescribing exercise to cardiac patients (Exercise
prescription website, 2009)
Recommendations
Exercise
mode
o Any form of physical activity which uses large muscle groups.
o Examples: walking (3.0-4.0 mph), cycling (8-11.9 mph), etc.
(see the examples of moderate intensity of physical activity)
Exercise
intensity
o Moderate intensity (activities equal to 3-6 METs).
o Initial exercise intensity is generally lower than that
recommended for healthy persons.
Exercise
duration
o Generally longer than that for healthy persons.
o 30-60 minutes of continuous or accumulated exercise for each
day (at least 10 minutes per bout).
Exercise
frequency
o Generally higher than that for healthy persons.
o At least 5 days per week is desirable, and preferably daily.
Progression o Generally slower than that for healthy persons.
o Depends on each person‘s specific abilities, goals and
preferences.
o A specific goal should be to increase aerobic capacity and
reduce submaximal myocardial oxygen demands.
(connect next page)

391
Recommendations
Special
considerations
o The prescribed activity should address the individual's goals.
o The activity should be enjoyable and easy to perform.
o Factors including medications, meal schedules, associated
complications/ disabilities/ impairments/ risk factors and
subclinical health problems which may be exaggerated by
exercise, etc should be carefully assessed and considered when
prescribing exercise.
o Monitor for abnormal signs and symptoms (e.g., chest pain, light
headedness, arrhythmias, etc) which can guide us to amend the
prescription.
o Increasing muscular strength is an important complement to an
aerobic training programme.
o Clients with low level of fitness are advised to start exercise
programme at lower intensities.
o Hypoglycaemia may occur several hours after exercise.

392
B. Exercise prescription for CHD patients (Exercise prescription website, 2009)
Function Improve heart function, reduce angina pain and MI recurrence,
improve quality of life
Exercise mode Aerobic activity such as walking (3.0-4.0 mph) (for detail see the
examples of moderate intensity of physical activity)
Select one or two interest exercises with examples of moderate
intensity of physical activity as reference and perform it.
Exercise
intensity
Moderate intensity (activities equal to 3-6 METs) (see Examples
of Moderate Intensity Level of Physical Activities).
Use Borg‘s scale (RPE) to monitor your exercise intensity. You
are recommended to exercise at 11-13 level on 6-20 Borg‘s scale.
Exercise
duration
30-60 minutes of continuous or accumulated exercise for each day
(at least 10 minutes per bout).
Exercise
frequency
At least 5 days per week is desirable, and preferably daily.
Termination Guidelines for termination of physical activity (Briffa, Maiorana,
Sheerin et al., 2006):
• Typical cardiac pain or discomfort in the chest and/or
radiation to the shoulders, neck, jaw or arms, or other
symptoms reminiscent of previous myocardial ischaemia;
• Dizziness, light headedness or feeling faint;
• Difficulty breathing or undue shortness of breath;
• Nausea;
• Uncharacteristic excessive sweating;
• Palpitations associated with feeling unwell;
• Undue fatigue;
• Leg ache that curtails function;
• Physical inability to continue.
Special
considerations
The prescribed activity should address the individual's goals,
characteristics, preference and medication.
Contact If you have any discomfort during exercise, you can contact the
researcher at any time.

393
Examples of moderate intensity level of physical activities
(adapted from Ainsworth, Haskell, Whitt et al., 1993)
Specific
activity
METs Moderate activities (3-6 METs)
Sports 3.3-5.0 Walking, 3.0-4.0mph or 4.8-6.4 km/h, level, firm surface
4.5 Badminton, social singles and doubles, general
6.0 Basketball, non-game, general
3.0 Bowling
4.0 Table tennis, ping pong
4.0 Tai chi
5.0 Tennis, doubles
3.0 Volleyball, non-competitive, 6-9 member team, general
5.0 Softball or baseball, fast or slow pitch, general
6.0 Swimming at lake, ocean or river, leisurely, not lap
swimming, general
4.0-6.0 Bicycling, 8-11.9mph, leisure, slow, light effort
3.0-5.5 Bicycling, stationary, 50-100 watts, light effort
6.0 Hiking, cross country
Dancing
and
conditioning
exercise
3.5 Callisthenics, home exercise, light or moderate effort,
general (example: back exercise)
4.0 Gymnastics, general
4.8 Twist , jazz, tap, jitterbug
3.0-4.5
fast (disco, folk, square), slow (e.g., waltz, slow dancing),
tango
4.0 Drums
Home
activities
3.5 Mopping
3.0-3.5 Downstairs, going up & down from floor
4.0-5.0 Walk/run – playing with child(ren) – only active periods
3.0-4.5 Walking, 2.5-3.5mph slowly and carrying objects less than
25 pounds

394
C. Physical Screening Item Form before Action
The following items were used to help the cardiologist to understand patients‘ health
status and to make sure whether they were suitable to start exercise or not before they
took action to exercise, action stage. If the patient was suitable to exercise, the
cardiologist would prescribe an exercise prescription to him/her according to the
guidelines for exercise prescription. In addition, it would help patients to monitor
themselves at home during exercise.
1. Blood pressure ________mmHg
2. Heart rate/pulse rate__________ bpm
3. Is patient medically stable? ① Yes ② No
4. Does patient have unstable angina? ① Yes ② No
5. Heart function according to the New York Heart Functional Classification:
① I: No limitation of physical activity. Ordinary physical activity does not cause
undue fatigue, palpitation, or dyspnea (shortness of breath).
② II: Slight limitation of physical activity. Comfortable at rest, but ordinary
physical activity results in fatigue, palpitation, or dyspnea.
③ III: Marked limitation of physical activity. Comfortable at rest, but less than
ordinary activity causes fatigue, palpitation, or dyspnea.
③ VI: Unable to carry out any physical activity without discomfort. Symptoms of
cardiac insufficiency at rest. If any physical activity is undertaken, discomfort
is increased.
6. Does patient have resting heart rate > 120 bpm? ① Yes ② No
7. Does patient have atrial fibrillation? ① Yes ② No
8. Does patient have ventricular arrhythmias? ① Yes ② No
9. Does patient have third-degree AV block? ① Yes ② No
10. Does patient have critical aortic stenosis? ① Yes ② No
11. Does patient have acute myocarditis? ① Yes ② No
12. Does patient have acute pericarditis? ① Yes ② No
13. Has patient had embolism during the previous three months? ① Yes ② No

395
14. Does patient have any acute noncardiac disorder that may affect exercise
performance or be aggravated by exercise (e.g., infection, renal failure,
thyrotoxicosis)? ① Yes ② No
Result of screening:
Is patient suitable for exercise? ① Yes ② No
Signature of cardiologist: ___________________________________
Date: ___________________________________________________
References
Ainsworth, B.E., Haskell, W.L., Whitt, M.C., Irwin M.L., Swartz A.M., Strath S.J. et
al. (1993). Compendium of physical activities: an update of activity codes and
MET intensities. Medicine & Science in Sports & Exercise, 32(9), s498-s516.
Exercise prescription website. (2009). Prescription guidelines. Available at:
http://exerciserx.cheu.gov.hk/html/eng/index.asp?n=sec2_Guidelines (accessed
April 2009).
Briffa, T.G., Maiorana, A., Sheerin, N.J., Stubbs, A.G., Oldenburg, B.F., Sammel,
N.L. & Allan, R.M. (2006). Physical activity for people with cardiovascular
disease: recommendations of the National Heart Foundation of Australia. Medical
Journal of Australia, 184(2), 71-75.
396
D. Form of Exercise Prescription
Recommended
mode of exercise
Exercise duration
(minutes/day)
Exercise intensity
(RPE)
Exercise frequency
(sessions/day)
Exercise progress
Rate of Perceived Exertion (RPE)
Signature of cardiologist: _______________ Date: ______________
Very
light
Fairly
light
Some-
what
hard
Hard Very
hard
Very,
very
hard
Very,
very
light

397
Appendix IX Exercise Stage-Matched Pamphlets
Pre-Contemplation Pamphlet

398
Lear more about:
Why Should I Exercise?
How Can I Become more Active?
Keys to an Active Lifestyle
Recall the successful experiences in behaviour change
The Saga of Lifestyle Linda
Physical Activity: What‟s in it for Me?
“… to gain the benefits of
regular activity you do not
have to go out and kill
yourself at the gym for hours”

399
The large number of reasons why you should exercise actually makes this a difficult
question to answer. All individuals exercise for their own reasons that can range from
how they feel when they exercise and look after a few months to the long-term health
and longevity benefits.
The long-term benefits of regular physical activity are probably pretty familiar to you
by now. Everyone knows that being physically active can help reduce your risk for
heart disease, diabetes, and even cancer. Not surprisingly given the many health
benefits, regular activity can even increase your life expectancy. There are also
numerous psychological benefits that you may experience with regular activity
including reductions in depression and stress and increased cognitive function, well-
being, and quality of life.
Although these long-term benefits are certainly important, you probably want to know
what being active can do for you right now. Being physically active can help you
improve heart and lung function and cardiovascular circulation, control your weight
and blood pressure, reduce chest discomfort and angina pain (see The Saga of
Lifestyle Linda), decrease your blood ―bad cholesterol‖ (low density lipoprotein
cholesterol) level and increase your blood ―good cholesterol‖ (high density
lipoprotein cholesterol) level. A number of studies have shown that being physically
active can delay or improve atherosclerosis or even reduce the atherosclerotic plaque
which results in reducing myocardial infarction rate, extending you life-span, and
improving your quality of life. In addition, being physically active can improve the
establishment of coronary collateral circulation and blood supply to the heart.
Consequently, it is beneficial for the recovery of coronary heart disease and the
reduction in the frequency of angina pain and re-infarction. Being physically active
can improve your flexibility, and your ability to perform everyday tasks with less
effort and pain. You can experience an afternoon of playing with your child without
the soreness you typically experience the next day. Being physically active also can
Why should I Exercise?

400
improve your sleep and appetite, and help you to establish healthy image and increase
your confidence.
These things may all sound great, but you still may lack confidence to perform
exercise/physical activity. You may think that people with coronary heart disease can
not exercise, and that exercise will add burden to heart which will provoke anginal
pain or hart attack. Actually, numerous studies have illustrated that low to moderate
intensity physical activity is not harmful to coronary heart disease, while it is
beneficial to the recovery of the disease, reduction in frequency of anginal pain or
heart attack. These things may all sound great, but you still may think that being
physically active will be boring and painful. Believe it or not, to gain the benefits of
regular activity you do not have to go out and kill yourself at the gym for hours. You
can incorporate activity into your everyday life at a moderate intensity (see Keys to a
Physically Active Lifestyle). After you have been active for a while you will find
yourself enjoying activity more and more and you will even begin to seek out more
demanding activities.
You must first realize that shifting from a sedentary to an active lifestyle is not going
to happen overnight. Below are just a couple of strategies that you can use to help you
get ready to begin your active lifestyle.
1) Learn More About Physical Activity
So you‘re not really ready to commit to a program of regular physical activity.
However, if you pay attention to the message all around you all day you may be
surprised at what you‘ll learn.
- Talk to friends, family members, and co-workers about why they exercise
- Talk to your physician to get his/her perspective on the link between your
health and physical activity
How Can I Become More Active?

401
- Watch for information in the newspaper about physical activity and its
benefits
- Look for positive examples of physical activity in the media
2) Focus on the Benefits of Activity
Often before we begin a new activity all we do is think about reasons for not changing
our behavior. I am sure you can list a number of reasons why you can‘t really begin a
more active lifestyle right now.
However, you should not focus on those negative aspects, instead think again about
all of the reasons you should be active.
To help you get started thinking about all of the benefits that you can get from being
active try completing the following list. To help you get started some of the common
benefits of activity have already been filled in, but remember, everyone has his or her
own goals and reasons for being active. Write down the benefits that being regularly
active will have for you.
Benefits of Regular Activity
Focus on why you should be more active rather than on reasons not to be active
1. I can control my weight
2. I can control my blood pressure
3. I can do more activities easier
4.___________________________________
5.___________________________________
6.___________________________________
7.___________________________________
8.___________________________________
9.___________________________________
10.__________________________________

402
Active Opportunities are All Around You - Just move!
Believe it or not, you have a number of chances to be active throughout your day. Try
to take advantage of those opportunities during your day to help make physical
activity a part of your everyday life. Recent research has indicated that even the
accumulation of activity over the course of your day can have significant health
benefits. You can divide 30-60 minutes physical activities into 2-3 times to complete
it, with more than 10 minutes per time. The accumulated 30-60 minutes‘ exercise in
one day has the same benefits as the continuous 30-60 minutes‘ exercise.
Use the Stairs
Using the stairs instead of the elevator can be an easy way to work some extra activity
into your day. You should be an ―Elevoider‖ that chooses to climb the flights of stairs.
If the floor you are going to is too high (generally not an issue in Champaign-Urbana)
take the stairs the first few flights and the elevator the rest of the way. For example,
Ms Ma, 41 years old, is working in a company. She had myocardial infarction half
year ago and underwent emergency PCI treatment. She doesn‘t dare to perform
exercise after discharging from the hospital. She perceives physical weakness and is
easy to get cold. After instructions from the health professionals, she knows that
exercise is very important for disease recovery. After that, Ms Ma decides to exercise
30 minutes per day. Due to the tight working schedule, she has no time to exercise in
a gym. She decides to use stairs instead of elevator everyday. Interestingly, her health
condition becomes better and feels much easier to walk.
Walk as much as Possible
Why not get off the bus a stop or two earlier and walk the rest of the way to your
building to get in a 5-10 minute walk?
Keys to a Physically Active Lifestyle

403
Take a 10-15 minute walk during your lunch break. This is a good way to gain a new
perspective on your day thus far and the day ahead. Walking with colleagues also
offers a way to socialize. If you had been retired, walking with your family members
after dinner can enhance family feelings.
Of course you feel great when you get that spot in the front of the parking lot, but if
you think about it you‘ll feel bad for circling the lot in your car when you could have
just parked in the back and walked a couple of minutes more. You may even save
some time!
Participate in Planned Physical Activities
Although there are a number of benefits associated with lifestyle activity that you
accumulate during the day, that doesn‘t mean you shouldn‘t try and schedule in some
regular, more strenuous activity, especially if you have weight loss or fitness goals.
Try to plan a visit to the gym or a more strenuous walk after dinner.
404
I believe that you can successfully change the sedentary behaviour. In order to let you
be confident to become an active exerciser, please spend a few minutes to fill in the
following form regarding your ―past successful record‖. Think about the behaviours
that you have successfully changed. This will help you to find back your confidence.
A. Behaviours that I have successfully changed
1. ___________________________________________________________________
2. ___________________________________________________________________
3. ___________________________________________________________________
B. Factors that help to successfully change the behaviours
1. ___________________________________________________________________
2. ___________________________________________________________________
3. ___________________________________________________________________
C. Factors that stop from change
1. ___________________________________________________________________
2. ___________________________________________________________________
3. ___________________________________________________________________
Recall the successful experiences in behaviour change
405
Becoming more physically active is by no means an easy matter. Lifestyle Linda
thought that it would be impossible to ever become physically active. At the age of 45,
she weighed over 200 pounds, had high blood pressure, and had coronary heart
disease. She perceived chest tightness occasionally and the ECG manifestations show
ischemia myocardial.
While on a trip to Washington, D.C. with her family last summer Linda had trouble
walking up the steps of the Lincoln Memorial and huffed and puffed her way up to the
top. It was at that moment that Linda decided to begin incorporating more activity
into her lifestyle. Over one year later Linda has succeeded in becoming more active
on a regular basis and actually chooses to climb the stairs instead of using the elevator.
After talking to her doctor Linda had begun to take a 5-10 minute walk after dinner
every night. It wasn‘t easy, but she was determined to never feel embarrassed when
doing a simple physical activity.
After those first few weeks she began to take a walk after lunch at work and then
extended her after dinner walks to 20 minutes. She feels great and enjoys her walks.
She never thought she would get there, but she has succeeded in making physical
activity a part of her day. She enjoys various benefits from the regular physical
activity everyday, especially in physical fitness, walking much easier, and more
reduction in the frequency of anginal pain.
You are on your way to making
activity a part of your lifestyle!
You can do it!
The Saga of Lifestyle Linda

406
Appendix IX Exercise Stage-Matched Pamphlets
Contemplation Pamphlet

407
Learn More About:
I’m Ready to Commit!
Nix the Negatives
What Benefits can I Get from Exercise?
Why not Take Action?
“Active” Learning
Becoming an Active Person
What if I Stay Inactive?
Stepping to Success
“While you are wondering
if it can be done, someone
is already doing it.”
Physical Activity: I‟m Ready to Go!
408
As you seriously consider beginning to increase your level of physical activity, you
have taken a very important step on the path to successfully incorporating physical
activity into your everyday life.
There are several more important steps that you need to take before you will truly
experience an active lifestyle, but there are several proven strategies that you can
employ to help you on your way.
In this newsletter are several strategies you can use to help you solidify our
commitment to make regular activity a part of your life.
The changes that you are thinking about making are important and can have a number
of beneficial consequences in your health and life. Get ready to make the commitment
to a healthy active life!
The more you consider beginning a program of regular activity, the more likely you
are convinced of the benefits of regular activity. However, you probably still have
lingering doubts about our abilities and focus many of your thoughts on the
drawbacks of regular activity.
The negative aspects of exercise such as the time it takes to be active, the energy it
will require and use and the soreness you may feel afterwards probably all weigh
heavily on your mind. However, before you are ready to really commit to a program
of regular activity you need to get control over the negative aspects that you perceive
as the drawbacks of being physically active.
Nix the Negatives
I’m Ready to Commit!

409
One strategy is to think of the negative aspects such as a perceived lack of time
simply as a barrier that you have to overcome. You do not have to schedule an hour or
two block of time to go to the gym to work out, you may simply begin by
incorporating activity into your day by walking places, taking the stairs, etc.
Another strategy is to realize that although it may seem difficult first, incorporating
behaviors into your life can be accomplished without much difficulty. Think about
how habituated brushing your teeth has become. You were willing to incorporate that
activity into your daily life, can you not do the same for a habit that will have so many
physical and mental benefits?
Being regular active is very important for your disease recovery. It can bring you
many benefits as follows:
1. Improve your heart and lung function
2. Improve the establishment of coronary collateral circulation
3. Reduce anginal pain and dyspnea
4. Prevent stent restenosis or re-infarction
5. Control blood lipoprotein
6. Decrease stress
7. Control weight
8. Decrease blood pressure
9. Enhance physical function
10. Help sleep
11. Establish healthy image and increase your confidence
12. __________________________________________
Wow, there are so many benefits. Let‘s take action!
What Benefits can I Get from Exercise?

410
Although you know that there are many benefits of being regular active and you may
also want to perform physical activity, you still did not take action. What are barriers
that stop from your action? In order to help you better resolve the barriers of physical
activity, please write down the barriers of physical activity. To help you get started,
some of the common barriers of activity have already been filled in, but remember,
everyone has his or her own barriers for being active. Write down the barriers that
will stop you from activity.
1. Too many works
2. Worry about the heart attack
3. It is boring
4. ______________________________________
5. ______________________________________
6. ______________________________________
7. ______________________________________
8. ______________________________________
9. ______________________________________
10. _____________________________________
Based on the list of barriers for your activity, you should think about how to resolve
the barriers? If you have no time to exercise due to many works, you can think about
that being regular active does not mean that you should spent numerous hours to go
out and in the gym. You can simply incorporate activities into your daily life, such as
walking to supermarket to buy something or to somewhere to do business, or using
stairs instead of taking elevator. Accumulating activities have the same benefits.
Think about that a ten minutes episode is very quick. If you worry about the heart
attack provoking from physical activity, you can consult with a cardiologist to make
sure whether you could exercise? Talk about the benefits for exercise for you? I guess
that the doctor will tell you that appropriate regular active is beneficial for preventing
Why not Take Action?
-- Barriers of Physical Activity

411
heart attack. If you think that exercise is very boring, you can think about how
benefits of exercise for your recovery. If you….
As you begin to minimize what you think are the negative consequences or barriers
to activity, you should still be attempting to learn more about activity and adding to
your list of the benefits regular activity can have in your life.
In an effort t to learn more about physical activity you need to move from a passive
learner to an ―active‖ learner that is constantly seeking out new knowledge and
sources of information about physical activity. This type of learning involves you
asking questions about activity.
You may ask yourself, how much activity do I need to do? Some of this information
may be found in the newsletters you receive, but you can look for answers in
newspaper articles about activity. If you hear about a study on the news you can try
and locate the source and read it for yourself. You need to seek out your own answers.
You may also wonder about what activities are best for you. Your best source of
information may be asking others around you what they do and enjoy. Try out some
of these activities and decide for yourself. The ideal activity is the one that you enjoy
doing. Think about things you enjoy and try to figure out if you can be active while
doing that activity. If you enjoy nature, walk outside. If you like to ready, try reading
while riding a stationary bike. If you enjoy team activities, find a community league
that you can join.
You may also wonder about the psychological benefits of being regularly active. Ask
people you know that are active what they get out of it. Do they feel better after they
exercise? Does it help clear their heads? Does it relieve some of the stress in their
lives?
“Active” Learning for an Active Lifestyle

412
Develop your own set of questions that you want to answer and ―actively‖ seek out
those answers. You need to constantly learn more about physical activity and what it
will do for you in particular. As your list of positives grows and negatives shrink, you
will be on your way to committing to activity.
One of the biggest steps you can take towards making regular activity a part of your
life is to learn to identify yourself as an exerciser or active person. How you envision
yourself goes a long way towards determining your behaviors.
Imagine that you consider yourself to be a kind, compassionate person. You will go
out of your way to help others and listen to their problems. Now imagine that you are
an active person. Think about what behaviors should go along with such a label.
You will also need to spend some time thinking about how your current behaviors
help define you as an individual. Do you immediately come home and plop on the
couch and turn on the television? Think about why you do this. Ask yourself, what an
active person would do? Maybe instead of sitting at the table and discussing your day
with your spouse you can go for a walk together and talk about your day.
When you realize that you can help shape your identity by the behaviors you engage
in, you can start to do the behaviors that help make you into the person you want to be.
Think about how you would like to feel and look and then honestly ask yourself if
your current habits and behaviors are making you that person. If the answer is no then
you need to change your behaviors and remold your self-image.
Becoming an Active Person

413
Another important step you can take in affirming your desire and commitment to
being active is to imagine what your life might be like if you were to remain inactive.
Although these might not be pleasant thoughts, they should help motivate you to
make that change.
The consequences of inactivity are not very pleasant. Imagine how you would feel if
you were morbidly obese. Imagine how you would feel if you become weak day by
day. Imagine how you would feel if the blood lipoprotein and cholesterol is increasing.
Imagine the feelings of heart attack. Imagine the feelings of your family and friends if
you die young from a heart attack. Do you feel guilty about just sitting around ever
evening after work? Is a lifestyle of inactivity acting just life a bomb that is waiting to
explode its negative consequences throughout your life and the lives of those around
you?
All of these negative feelings that you imagine when you think about remaining
inactive can be a powerful tool in helping you realize why you need to be active.
These are all situations that you do not want to come to pass. Luckily the decision is
yours, you can be active and do everything in your power to prevent these negative
feelings, or you can be sedentary and passive and let them happen to you.
You are the only one that has the power to make these changes in your life. Others
can offer you help and guidance, but you need to commit to those behaviors.
What if I Stay Inactive?
--Toward healthy lifestyle

414
Making a significant change in your lifestyle is not an easy task. You need to begin by
taking some small steps in the right direction.
You could finish reading this and make a commitment to yourself to go for a brisk 5
minute walk today. Work you way up to your activity goals.
Current recommendations are that you walk approximately 10,000 steps a day, but as
cliché as it may be, you have to start the journey with a few small steps.
Today you just walk not jog. Only 5 minutes, no more. When you complete 5-minute
walk, how is your feelings? Does 5 minutes pass quickly?
Start from 5 minutes, then 10 minutes, and realize your activity goal step by step.
Let‘s start walk today1
Stepping to Success

415
Appendix IX Exercise Stage-Matched Pamphlets
Preparation Pamphlet

416
Learn More About:
Ready, Set, Let’s Go!
Formalize your Commitment
Everyone Needs a Hand
Realize Your Ideals
What Activities Should I Do?
What should I Pay Attention to during the Exercise?
Developing Your Activity Goals
My Activity Goal Worksheet
“Always remember that it
is you that is making this
commitment to yourself
and your health”
Physical Activity: I‟m On My Way!

417
You are ready to begin making physical activity a part of your life. You may have
already begun to increase your activity levels and look for ways to incorporate
physical activity into your lifestyle. Congratulations!
Now as you prepare to take you activity to the next level, there are several strategies
that you may employ to help you begin a lifestyle of regular activity. There are
several key strategies to help you formalize your commitment to activity, learn how to
set reasonable activity goals, find out how to get others to help you be active, and
further develop your self-image as an active individual.
You are well on your way to being regularly active. Using the strategies discussed in
this newsletter you can succeed in making activity a part of your life.
As you prepare to get, and stay, active on a regular basis, one approach that you can
take to strengthen your commitment is to make your goals and plans formal.
We all like to make up ―to do‖ lists and check off our accomplishments (at least we
hope to get to them all) at the end of each day. In much the same way, by making
your commitment to be regularly active known, you can enhance your pride as you
reach your exercise goals.
However, in order for this strategy to be successful you need to develop realistic
activity goals for yourself. Make sure to read the section on developing your activity
goals for more information about proper goal setting.
Formalize your Commitment
Ready, Set, Let’s Go!

418
After you have developed your own activity goals you need to formalize these goals.
When your goals are written down or you tell others about them you eliminate your
ability to ignore those goals. You no longer can say to yourself that you‘ll do them
next time or that is not what you really expected to do. You are responsible for your
own action or inaction.
In order to help you make your goals formal, we have provided you with a personal
activity goal sheet attached as the last page of this newsletter. Take the time to fill it
out and then place it somewhere you‘ll see it. Better yet, post it where others can see
it. Always remember that it is you that is making this commitment to yourself and
your health.
A great way to help you reach your activity goals is to find a friend or buddy that can
support your efforts. This person can either be a cheerleader who offers you
encouragement, a watchdog that reminds you when you are slipping, or someone
making the change with you. Ideally your buddy will be a combination each of these
three aspects.
Your buddy must be aware of your goals and told how they can best help you. The aid
that you receive should always be positive. Criticism and yelling will not help
motivate you to stick with your activity program.
Your buddy may be your spouse or co-worker. Even your children can act as buddies
to help support you on your way to becoming more active. The key is to get a
supportive buddy that wants to help you make the change. For example, Mr Chen, 57
years old, has been diagnosed with coronary heart disease for two years. He was
inactive after he got the disease, so he often feels chest discomfort. After he received
instructions from the health professional, he knows that being physical active is
beneficial for his disease recovery. In order to help himself start and maintain to
Everyone Needs a Hand

419
exercise, he committed to perform regular exercise to his family members and to
obtain their supports and help. After that, when the time is up, his daughter would
remind him ―It is time to exercise‖. His daughter also asked her son to accompany Mr
Chen to play basketball 2-3 times per week. Not surprising, Mr Chen successfully
changes exercise behaviour and maintains regular exercise. After being regular
exercise for four weeks, Mr Chen felt more and more comfortable, much easier to
walk, and less anginal pain. Since he experiences the benefits from the physical
activity, he becomes more and more like to exercise. After half year, regular exercise
becomes an interest of his life.
As you continue on your path to making physical activity a habit in your life, you
need to work on continuing to redefine yourself as an active individual. By this point
in your life you already have a well established sense of who you are and you now
need to think of yourself as someone that is active on a regular basis.
You are defined by the roles in your life, whether they be at your job or in your family.
The behaviors you engage in are often the best reflection of who you are. To help you
become the more active individual that you want to be you need to continue to let
your actions speak for themselves and be more active.
You need to let go of any behaviors from your past that may have been keeping you
from being active. It may be comforting to know that every evening you will go home,
eat dinner, and then sit down to ―Must See TV‖. However, the pleasure that you
receive from this may largely be the comfort you associate with that habituated
behavior. You defend the behavior by saying that it is just what you do everyday, it is
a part of who you are.
However, the only reason you feel such comfort in this behavior is because that it is
what you have been doing for so long. Changing your behaviors and habits may be
Realize Your Ideals

420
stressful, but realize that with a little time and effort, physical activity may be a good
habit in your life. Taking a walk after work will then be what you are comfortable
doing everyday. You need to be patient with yourself as you attempt to redefine what
you do. Keep in mind all that you are doing for yourself by being more active and
remember that you are worth the effort.
In order to receive the benefits of regular activity, recent scientific research has
recognized that you do not have to work out hard at the gym for over 30 minutes
nearly everyday as we used to believe. Health benefits can be found simply by
accumulating 30 minutes of moderate intensity activity on most days of the week.
This means that you can incorporate several bouts of activity into your day in order to
reach your activity goals. You now have several choices for meeting your exercise
goals that can range from getting in several 10 minutes at a greater level of intensity.
This flexibility in activity choices should make it easier for you to match your activity
desires to your own lifestyle and situational demands.
Moderate Activity – What is It?
You may very well wonder how hard you have to be working to do moderate activity.
A classic example is walking briskly. Wandering around the mall window shopping
will not qualify as brisk walking, you need to be walking ―with a purpose‖. The
notion of lifestyle activity is that it is activity that you can incorporate into your life.
However, it would be a mistake to simply assume that you are getting enough activity
in your life. Wandering around the office or puttering around in the garden will not be
enough, you need to get your heart rate up about its normal daily level. If the exercise
what you were performing can not make you feel mild asthma, it can not strength
your heart and lung. This is why a busy work can not reach the exercise effects.
What Activities Should I Do?

421
In reality no one can dictate a certain speed in miles per hour that you need to walk or
bike, the best judge of moderate activity is yourself. You need to learn to pay
attention to your body. You can tell when our heart rate is elevated and you are
breathing more heavily. These are the keys to understanding your moderate level of
activity. Depending on your initial fitness level you will need to do work at different
absolute loads to work at a relatively moderate intensity. Learn to take and monitor
your pulse to help get an idea of how what you feel translates into beats per minute.
An important thing to remember is that moderate intensity activity should not be
painful. If you are in pain or just cannot go on anymore, then you should stop because
you have over-stepped your abilities. You should be able to maintain this moderate
level of activity for a long period of time.
The signs of appropriate exercise load are: when you are exercising, you have a little
sweating and mild breathing but does not affect your speech, feel comfortable in the
morning after getting up, no sleepy or any discomfort; after the exercise, feel light,
good appetite and good sleep. If you feel dizziness, chest tightness, palpitations,
shortness of breath, loss of appetite, poor sleep and heavy fatigue indicating that the
exercise is over load.
Once you are comfortable being more active, you should still consider incorporating
some more intense activities into your life. This may mean you make a visit to the
gym, swim some laps at the pool, go to an aerobics class or begin to jog some while
you walk. These more intense activities will really begin to improve your fitness.
Common Examples of Moderate Activities
For patients with coronary heart disease, the best moderate exercise is brisk walk (80-
100 meters/minute). The following examples are equal to moderate intensity activities.
Home activities
o Mopping
o Downstairs, going up and down from floor

422
o Walk/run – playing with child(ren) – only active periods
o Walking, 2.5-3.5 mph slowly and carrying objects less than 25 pounds.
Sports
o Walking, 3.0-4.0 mph level, firm surface
o Badminton, social singles and doubles, general
o Basketball, non-game, general
o Bowling
o Table tennis, ping pong
o Tai chi
o Tennis, doubles
o Volleyball, non-competitive, 6-9 member team, general
o Softball or baseball, fast or slow pitch, general
o Swimming at lake, ocean or river, leisurely, not lap swimming, general
o Bicycling, 8.0-11.9 mph, leisure, slow, light effort
o Bicycling, stationary, 50-100 watts, light effort
o Hiking, cross country
Conditioning exercise
o Fitness club sports
o Calisthenics, home exercise, light or moderate effort, general (example: back
exercise)
o Gymnastics, general
o Weight loss calisthenics
Dancing
o Twist, jazz, tap, jitterbug
o Fast (disco, folk, square), slow (e.g., waltz, slow dancing), tango
o Drums

423
Exercise is safe for most patients with coronary heart disease. In order to avoid any
accidence, patients with coronary heart disease should pay attention to the following
issues when they are doing exercise:
o Before start regular exercise, take physical examination and have exercise
prescription from the cardiologist;
o Carry nitroglycerin pills or other anti-angina drugs when performing exercise,
such as shexiangbaoxin pills, suxiaojiuxin pills or danshendiwan, to prepare
for chest pain, which are placed under the tongue;
o Warm up before the exercise and cooling down after the exercise. Usually, use
walk or calisthenics for 5-10 minutes. Insufficient preparation of warm up and
cooling down is the most common reason caused accidence;
o Avoid to do exercise when you are too hungry or full, too cold or hot
environment, physical fatigue, and angry or poor emotion. Start exercise 2
hours after meal and avoid to entering places with too much different
temperature.
o Avoid hot shower immediately after exercise. It is better to take shower half
hour after exercise to reduce the impact on the heart and prevent suddenly die
after exercise.
o Avoid lifting heavy objects. If necessary, keep breathing smoothly and should
not hold your breath.
o Note that the air flows and pay attention to whether your heart rate is
excessive speed or irregular.
o Avoid competitive sport and accelerating movement too fast, e.g., race of
climbing stairs fast.
o Restart exercise 2 days after disappearing the symptoms and signs of cold or
fever.
o Low temperatures in early morning which is not suitable for patients with
heart disease to exercise, so it is best to exercise in the morning or evening.
What should I Pay Attention to during Exercise?

424
Indications to terminate exercise/activity
o Typical cardiac pain or discomfort in the chest and/or radiation to the
shoulders, neck, jaw or arms, or other symptoms reminiscent of previous
myocardial ischaemia;
o Dizziness, light headedness or feeling faint;
o Difficulty breathing or undue shortness of breath;
o Nausea;
o Uncharacteristic excessive sweating;
o Palpitations associated with feeling unwell;
o Undue fatigue;
o Leg ache that curtails function
o Physical inability to continue.
Other points should also be remembered
o If you are unable to breath and speech during exercise, you should take rest
until only a slight breather before continuing.
o If you feel chest pain, rest until the pain disappears. If the chest pain appeared
regularly, you should tell the cardiologist. If you have anginal pain, take
medicine and then continue to exercise.
o Doing exercise according to the plan. Do not do exercise too much in the short
term which will delay your recovery and even dangerous. Haste makes waste.
o If you feel discomfort one day during exercise, do not worry. Everyone may
encounter this condition. Ask yourself whether you have too large exercise
than the past few days, which may explain why you feel a bit tired.

425
In order to experience success in achieving your activity goals you need to learn to set
proper goals. This involves forming realistic expectations about changing your
behavior. The focus of your goals in the beginning should be on how short-term goals
or behaviors can help lead to the long-term benefits you are seeking.
Becoming active on a regular basis is not going to happen overnight. If you have been
inactive for a while you will need to ease into this new lifestyle. Before you know it,
being active will be second nature, but that can only come with time. You also cannot
expect a dramatic weight loss without engaging in more vigorous activity and
incorporating dietary modifications into your new, healthy lifestyle. For now, you
should just concentrate on developing some short-range goals to increase our activity
level.
The last page of this newsletter offers you a chance to develop some activity
commitments of your own. You can make an initial commitment to walk after lunch
and dinner everyday for 10 minutes, you can agree to use the stairs, and you can also
set your own specific goals. Remember that it is you who is making this change, what
do you hope to get out of it and how can you best help to make that happen? Write in
your own specific activity goals.
After filling in your goals, sign and date your commitment. Then place this sheet
somewhere you (and others) will see it on a daily basis. Whenever you look at this
sheet, you should check off those behaviors that you are doing, if you are not meeting
all your goals, don‘t despair. The average individual will make the same New Years
Resolution 3 times before they successfully change their behavior. Using the
strategies in the newsletters you receive should help you make the change, but expect
some setbacks. The key is to make sure that the goals are reasonable, focus on what
you have accomplished so far, and then redouble your efforts to meet the goals.
Developing Your Activity Goals

426
My Activity Goal Worksheet
I will walk _________ minutes a day.
I will climb stairs when possible.
I will __________________________
I will do my best to make activity a part of my life.
I can and will be an active individual
Signed ______________________
Date________________________

427
Appendix IX Exercise Stage-Matched Pamphlets
Action Pamphlet

428
Learn More About:
Moving Towards an Active Lifestyle
Make Healthy Substitutions
Reward Yourself – You’re Doing a Good Thing
Spice Up Your Activity Routine
Inactivity – Just Don’t Do it!
The art of Problem Solving
“Keep on „Moving‟
towards your activity
goals!”
Physical Activity: I‟m “Moving” Along!

429
You should be proud of yourself and all that you are doing to improve your life. As
you are well aware, regular physical activity can have numerous mental and physical
health benefits. The key for you is to continue to incorporate physical activity into
your life.
There may be minor setbacks along the way, but in the articles in this pamphlet you
will find a number of strategies designed to keep you moving towards your physical
activity goals.
As you strive to maintain a lifestyle that includes regular physical activity, you need
to learn how to avoid those situations that may foster inactivity, learn to refocus your
thoughts about your behavior, and develop your own reward structure. It will also be
important for you to continue to add some variety to your activity choices. Doing the
same activities day in and day out can lead to boredom and reduced motivation.
Congratulations, you are well on your way to an active lifestyle. Now just keep on
moving!
As you continue to make physical activity an everyday part of your life, you will be
tempted from time to time to slip back into your bad habit of being inactive. Think of
all the ―bad‖ things you let yourself get away with during the holiday season. You
need to recognize when you are slipping and attempt to refocus on your goals.
When you begin to revert back to a sedentary lifestyle you may begin to think of all
the reasons why you should not be active. This is when you need to have a dialogue
Make Healthy Substitutions
Moving Towards an Active Lifestyle

430
with yourself. If you think being active takes too much time remind yourself of how
quickly 10 minutes at a time can add up! If you are focusing on how activity makes
you sweaty, remind yourself about how good you feel after you exercise.
Think of all the opportunities that are available for you to incorporate physical
activity into your lifestyle to replace your old inactive habits. If you are someone that
needs to watch television, then find exercises that you can do in your home while
watching television such as walking on a treadmill or riding a stationary bike. If you
like to sit around and talk with your co-workers after you eat lunch, try to get them to
take a walk with you so that you can talk and get some activity at the same time.
You will be tempted to slip back into old habits, but you need to plan for those times
and find ways to continue to make activity a part of your life.
As you continue to reach your physical activity goals, you are probably feeling better
about yourself and your health. That in and of itself may be reward enough for many,
however, you really should take the time to congratulate yourself on a good job.
Being physically active is not necessarily an easy thing although the more you do it,
the more it becomes a part of your life.
There are several ways that you can ―reward‖ yourself for your efforts to help keep up
your motivation for physical activity. Assuming that you have a set of activity goals
written down (if you don‘t go ahead and write out how you intend to incorporate
activity into your day), a simple reward may be to check off those goals that you have
reached or are reaching. The simple act of checking off a ―to do‖ can often be a great
reward and boost to your confidence. If you aren‘t reaching some goals yet, think of
how good you‘ll feel when you can check those off as well.
Reward Yourself – You’re Doing a Good Thing

431
When you successfully avoid a situation that may lead to inactivity, reward yourself
with a verbal pat on the back. Positive words and thoughts such as ―Good going!‖ and
―I can do it‖ can act as great motivators. You can be your own cheering section. If
you are exhibiting good behaviors then you have every right to feel good about
yourself. Go ahead, ―keep it up‖!
If you don‘t want to act as your own cheerleader, you should enlist the aid of others
around you. They can help encourage you if they know your physical activity goals.
Having your family, friends, and co-workers offer you encouragement can make you
realize that your efforts are not going unnoticed.
A final reward strategy is to set up a behavioral contract with yourself. You can
choose a specific reward that you will receive if you are able to successfully meet a
particularly challenging goal.
However, do not reward your activity with inactivity. If you plan to take a special trip
or vacation, make sure that it is one that would allow you to continue to make activity
a part of your day. Let the new scenery at your vacation site be the reward for you as
you take a long walk.
A very important aspect to making physical activity an everyday part of your life is to
make sure that it does not become boring. Although this may seem at odds with the
suggestion that you make regular activity a habit, you need to include activities or
settings that you enjoy.
If you are meeting your activity goals by taking a walk, try a new route around that
campus or your neighborhood. New scenery or a more challenging route can add
some variety to your routine and give you something to look forward to in your next
Spice Up Your Activity Routine

432
walk. A habit does not have to become boring if you can keep adding different aspects.
Use new activities and settings to add some ―spice‖ to your activity goals.
Another great way of helping you continue to meet your activity goals is to try more
challenging tasks. If you have been walking for a mile every evening, try to make it a
mile and a half or set a goal to walk it faster than you did last week. As you become
more and more active you will find that what you did when you made the switch from
a sedentary lifestyle now seems rather easy. To keep your motivation high you need
to provide yourself with goals that are challenging enough that you feel a sense of
accomplishment when you reach them.
You may also want to try a totally different activity. As long as you are careful not to
over-exert yourself, you can try and get involved in some competitive sports. Try
playing racquetball or a get involved in a departmental game of basketball or softball.
You can also try a new piece of equipment at the gym. If you have been eyeing that
new cardiovascular machine, go ahead and give it a try. You may find it to be an
activity that you really enjoy.
The key is to make sure that your activity patterns are constantly changing so that you
are not stuck in a ―rut‖ of activity that you decide to break by revering to a sedentary
lifestyle. Keep it different, new and challenging and before long you‘ll be amazed at
the wide variety of physical activities in which you participate on a regular basis.
One of the major obstacles that you will face in your efforts to be an active individual
will occur when you face those situations that tempt you to be inactive. With poor
weather such as rain, snow, and cold it can be very tempting to stay inside and do
nothing. Unfortunately, you cannot afford to do nothing. To stay active you need to
start by understanding which situations will offer the most challenges to you meeting
your activity goals.
Inactivity – Just Don’t Do it!
433
The following list contains several common barriers that individuals encounter when
they attempt to be active on a regular basis. Review the list and add a few of your own
at the bottom.
IT’S HARD TO EXERCSIE…
1) During poor weather
2) When on vacation or holiday season
3) When a visitor at home
4) When there are too many things to do at home
5) When you face a deadline at work
6) When you feel tired
7) When your ―buddy‖ can not be active with you
8) ________________________________________
9) ________________________________________
10) _______________________________________
Looking at this list you may feel over-whelmed and wonder how you can even
continue to be active on a regular basis. However, by examining when you are
tempted to be sedentary you have taken an important first step to continuing your
active lifestyle.
Now that you have acknowledged situations that may lead to inactivity, one key is to
try and avoid those situations or create plans to help you deal with them when they
occur.
For example, when the weather prevents you from taking a walk outside, try going for
a walk in the Armory or around the local mall, or doing calisthenics or marking time
at home. Develop your own weather contingency plans so that when poor weather hits
you already know how you are going to continue with your planned activity.
Likewise, during the stressful time of the holiday season, rather than limit your
activity, you should take extra care to find the time to be active. The time you

434
spending being active may give you a chance to clear your head and do something
nice for yourself rather than focusing on others all the time.
When there is a visitor at home, you can try to take a walk with the visitor after the
dinner, so you can exercise while chatting, which serves two purposes, rather than sit
there and talk. If there are too many things to do at home, you can incorporate your
exercise in your daily life, or seek help from your family members to reach your
exercise goal.
For each of these situations, you need to be prepared to overcome the barrier and
continue to meet your exercise goals. Another way that you can help meet your goals
is to leave reminders around your home or office to encourage you to be active. You
can leave post-it notes around, mail yourself a postcard reminding you to be active,
send yourself a reminder through campus mail or even leave your work-out shoes in
front of your door. You can also set a clock in you mobile phone to remind you
exercise everyday. The key is to surround yourself with enough positive messages
that you are able to overcome those negative situations that encourage you to be
inactive.
A final way to combat the temptation to be sedentary is to continue to make and
revise ―activity to do‖ lists. By having a set of specific plans and goals for each day
you are able to foresee any obstacles or barriers and plan accordingly. Having a
number of activity options will allow you to choose the one best suited for meeting
your goals on that day depending on the weather or your time commitments.
You are well on your way to making physical activity a part of your life. The
continued effort that prevents you from reverting to a sedentary lifestyle is well worth
that effort. Think of all the positive benefits that being physically active is having in
your life. Keep on moving towards your goals!

435
Using IDEA form
I – Identify a barrier that keeps you from being active.
_____________________________________________________________________
_____________________________________________________________________
_____________________________________________________________________
D – Develop a few creative solutions (the more the merrier)
_____________________________________________________________________
_____________________________________________________________________
_____________________________________________________________________
E – Evaluate your list of solutions. In the following space, write the solution you are
wiling to try. While you‘re at it, write down precisely when you will put it into action.
_____________________________________________________________________
_____________________________________________________________________
_____________________________________________________________________
A – Analyze how well your plan worked and revise it if necessary. If your plan
worked well, give it five stars. If it only deserves two stars, write down how it could
become a five-star plan. If your plan bombed completely, look back at your list of
solutions and try again. (remember, a plan that doesn‘t work isn‘t a complete failure.
It often points toward the solution that will work. The only failure is giving up.)
_____________________________________________________________________
_____________________________________________________________________
____________________________________________________________________
The Art of Problem Solving

436
Appendix IX Exercise Stage-Matched Pamphlets
Maintenance Pamphlet

437
Learn More About:
Maintaining an Active Lifestyle
How to Maintain Regular Exercise Habit?
It’s Not the End of the World
It’s Your Lifestyle – Take Charge
Help Make Change Happen
“You are doing a great job!
Physical activity is a part of
your lifestyle!”
Physical Activity: Doing it for a Lifetime!

438
You have managed to make physical activity a regular part of your life and should be
commended for your commitment. You are doing a great deal to help enhance your
physical and mental health. Admit it, you feel great that physical activity is a part of
your life.
Although you have succeeded in meeting the activity goals that you set for yourself,
now is not the time to relax. The physical activity ―habit‖ that you have acquired is
beneficial, but you still need to be wary of any setbacks that may land you right back
in your Lay-Z-Boy.
The best way to ensure that you can remain active is to learn how to effectively
manage the setbacks that you will eventually encounter, to continue to plan for times
when staying active becomes difficult, and to enhance your identity as an active
individual by serving as a role model for change.
You should select exercise as……
o Interesting……
It is very hard to maintain a sport if you don‘t like it. If you have done sports, such as
bicycling, walking, swimming, dancing, and playing bowling and badminton, you try
to start these sports.
How to Maintain Regular Exercise Habit?
Maintaining an Active Lifestyle

439
o Regular……
If you cannot properly adhere to exercise, you can participate in organized sports,
such as exercise classes. If the weather is bad, you can do some sports that you can.
Swimming is a special good exercise because you can do it the whole year. If you
cannot swim, you can participate a swimming training.
o Diversified……
Do several sports, so when you feel tired of a sport, you can make other activities.
o Nearby……
Travel is costly and time-consuming, you may give it up easily. If there are no places
that you can go in your area, you can use rowing machine or a bicycle stationary at
home, or marking walk/run at hall or balcony. These activities may be tedious, so you
can exercise while watching TV.
o Incorporating in your daily life……
Make exercise as part of your life. Try to walk or bike to work or shopping.
It is going to happen. It is inevitable. Eventually you will slip and fail to meet your
activity goals. It may be a run of terrible weather, excessive demands at your job, or
the pressures of the holiday season. No matter how it occurs, you need to be ready to
deal with the time when you must get back on the right track towards a healthy active
lifestyle.
It’s Not the End of the World

440
You need to realize that you are not failure, that this is not the end of the world.
Setbacks are a part of everything we do in our lives, what separates individuals is their
ability to successfully cope with these setbacks.
There a few strategies that you can use to get back into the activity habit. First, you
need to get back into your activity routine as quickly as possible. Don‘t waste your
time lamenting the missed opportunities, get back to being active. Your relapse is not
permanent and you are in charge of deciding how long it will last. Make sure your slip
back into your sedentary lifestyle a short stay.
You also need to stay positive and focused. All your work is not wasted when you fail
to meet your goals. Remember all that you have accomplished, it did not happen
overnight and neither will your transition to a sedentary lifestyle. With a positive
attitude you will be active again.
The challenges of a lifetime of activity mean that you will slop at one point. When
that occurs make sure you stay positive and get back into action as soon as possible.
You are an active individual!
Making physical activity a continuing part of your life may not be necessarily easy,
but is something that you can do. You should be congratulated for your efforts so far
and with some of these strategies you will be active for decades to come and enjoy the
benefits of activity the entire time.
You are at your greatest risk for relapse when you encounter unusual situations. If you
are unprepared you may be likely to revert to an old habit as a way of coping with a
novel or particularly stressing event. These urges to revert to your prior behaviors can
be surprisingly strong, however, with proper planning you can deal with these
situations as they arise.
It’s Your Lifestyle – Take Charge

441
You need to make sure that you plan ahead when unusual circumstances may keep
you from your typical activity routine. If you are on vacation, then make sure you
bring along your exercise clothes and investigate if where you are staying has fitness
facilities or a recommended route for a walk or run.
When events occur unexpectedly, you need to take a moment to two to re-examine
your activity goals and why you are committed to those goals. Reviewing your goals
will give you an opportunity to plan how you will continue your activity or deal with
your relapse if being inactive is inevitable.
You also need to make sure that you occasionally take the time to remind yourself
why you are active. Watch the television and news for reports on the benefits of
activity and congratulate yourself on your behavior. For every hassle or obstacle that
you can think of why you should not be active, challenge yourself to think of 4 or 5
reasons why you should be active.
Now that you are active, you may forget why you even began your activity in the first
place. Occasionally reminding yourself of the benefits you have received from your
active lifestyle can act as a great motivational tool for your continued good behavior.
Another tool for meeting the challenges of a lifetime of physical activity is to make it
a habituated part of your day. Just like showering in the morning, you may eventually
get to the point where you don‘t feel like yourself until you have gone for a 20 minute
walk.
This habituation of activity is an important step in ensuring that you are making a
lifetime commitment to activity that you will be able to maintain.

442
As someone that is physically active and enjoying the benefits of a program of regular
activity, you need to realize your potential to encourage change in those around you.
Serving as an example or role model can be a great way for you to continue to
develop your own identity as an active individual as well as serve as a motivational
tool against relapsing to a sedentary lifestyle.
What does it mean to be a role model? Acting as an ―Activity Cop‖ certainly will
offend more people than it will encourage to becoming active. People will simply
avoid you. What you can do is make sure that you take the stairs when they take the
elevators. If they ask why you are doing it, you can share your experiences with them
and they may choose to join you next time. You can also invite people along for your
daily walks. If someone wants to join you, you should share your knowledge with
them to help them begin to make activity a part of their life.
The benefits of regular activity in your life should be evident enough that individuals
seek you out on their own. You role is to help facilitate change in those individuals
that seek you out and to serve as an example of the positive efforts of regular physical
activity.
As an active individual you are the example that many people around you will use
when they consider making activity a part of their life. This responsibility should help
encourage you to minimize any relapses that occur as well as focus on the positive
aspects of activity. If someone that is regularly active is constantly complaining about
time constraints and fatigue, that will not encourage others.
You should be proud of your accomplishments, but with those accomplishments you
need to realize that you now have some responsibilities. The best way to meet those
responsibilities is to maintain your healthy, active lifestyle with a positive outlook.
Help Make Change Happen

443
References
Blair, S.N., Dunn, A.L., Marcus, B.H., Carpenter, R.A., & Jaret, P. (2001). Active
living every day. Champaign, IL: Human Kinetics.
Blissmer, B.J. (2000). Integrating the theory of planned behaviour and the
transtheoretical model: a prospective study of lifestyle activity. Dissertation:
University of Illinois at Urbana-Champaign.
Briffa, T.G., Maiorana, A., Sheerin, N.J., Stubbs, A.G., Oldenburg, B.F., Sammel,
N.L. & Allan, R.M. (2006). Physical activity for people with cardiovascular disease:
recommendations of the National Heart Foundation of Australia. Medical Journal of
Australia, 184(2), 71-75.
Marcus, B.H., Forsyth, L.H. & Blair S. (2003). Motivating people to be physically
active. United States: Human Kinetics.
Tung, W.C. (2003). Examination of the transtheoretical model and physical activity
in family caregivers in Taiwan. Dissertation: The University of Utah.
Self-help cardiac rehabilitation handbook. (unpublish). School of Nursing, The Hong
Kong Polytechnic University, The Chinese University of Hong Kong, and Peking
Union Medical College (Ed), 2009.

444
Appendix X An Example of the TTM-based ESMI
An example of the TTM-based Exercise Stage-Matched Intervention (ESMI)
Mr Wang received one 2-hour session of patient education and a booklet about cardiac rehabilitation.
Immediately after receiving the education session, he was booked an appointment for face-to-face
consultation at the hospital next week.
week1 Face-to-face contact at hospital:
• Assessment of exercise stages of change (Appendix XIV): After receiving the one 2-hour session of
patient education, Mr Wang knew that exercise is beneficial to his illness recovery and started to
thinking about it, but he did not take any action yet. Thus, he was in the contemplation stage.
• Delivering ESMI (Table 3.2): The goal of increasing motivation and confidence in the ability to
change was set and the following strategies were provided: ① Delivering the information about the
benefits of physical activity (consciousness raising) and the risks of physical inactivity (dramatic
relief); ② Finding out his barriers to engaging in physical activity (The main barrier stopping him
from engaging in exercise was that he thought that exercise would increase his heart load which was harmful to heart because he had suffered from MI.) (Giving related information to correct his
misconception); ③ Pointing out people who included regular exercise in their lives and now are
obtaining benefits from exercise (social liberation); ④ Increasing awareness of opportunities that exist
to encourage regular exercise; ⑤ Encouraging him to think about change.
• ESMI pamphlet (Appendix IX): Contemplation pamphlet was given to him.
week2 Telephone follow-up:
• Compliance checking (Table 3.1): In the past one week, he took jogging 15 minutes per day on 7
days. During the exercise, he had mild sweating, felt a little fast breathing, perceived light exertion (RPE 12), and did not experience any discomfort or take any anti-angina drugs.
• Assessment of exercise stages of change (Appendix XIV): He exercised some, but not up to the
accumulated 30 minutes per day on at least five days per week. Thus, he was in the preparation stage.
• Delivering ESMI (Table 3.2): Congratulation to him because he had moved forward one stage. The
goal of negotiating a plan for exercising was set and the following strategies were provided: ① Further
providing information about the benefits of physical activity and the personal risks of physical
inactivity; ② Discussing the safety of exercise and attentions should be paid during exercise
(Introducing guidelines for termination of physical activity. Advise him to call the researcher at any
time if he experienced any discomfort due to exercise); ③ Finding out difficulties encountered in
exercising (He experienced no difficulty in exercising); ④ Encouraging him to obtain social support
from his family members to support his engagement in exercise (helping relationships); ⑤ Invite him
to come to the hospital for exercise prescription by the cardiologist next week.
week3 Face-to-face contact at hospital:
• Compliance checking (Table 3.1): In the past one week, he continued to take jogging 15 minutes per
day on 7 days. During the exercise, he had mild sweating and a little fast breathing, perceived exertion
fairly light (RPE 11), and did not experience any discomfort or take any anti-angina drugs.
• Assessment of exercise stages of change (Appendix XIV): He was in the preparation stage.
• Exercise prescription (Appendix VIII): The cardiologist examined his physical conditions and prescribed exercise prescription for him (He is fit for exercise of moderate intensity). Show the
examples of moderate intensity of level of physical activity to him (He likes walking, jogging and
hiking). The exercise prescription was that he could take walking or jogging (5 km/h) 20 minutes/day
with the progression of 5 minutes/day per 2-4 weeks up to jogging (5-6 km/h) at least 30 minutes/day.
• Delivering ESMI (Table 3.2): The goal of negotiating a plan for exercising was set and the following
strategies were provided: ① Encouraging him to create a new self-image as an exerciser (self-
reevaluation); ② Encouraging him to make a public commitment to exercise (Encourage the patient to
inform his family members that exercise is beneficial to him and he start to engaging in exercise) (self-
liberation); ③ Making a plan for engaging in exercise; ④ Encouraging him to obtain social support to
participate in exercise.
• ESMI pamphlet (Appendix IX): Preparation pamphlet was given to him.
week4 Telephone follow-up:
• Compliance checking (Table 3.1): In the past one week, he took jogging 20 minutes per day on 7
days. During the exercise, he had mild sweating, felt a little fast breathing and perceived exertion fairly
light (RPE 11), and did not experience any discomfort or take any anti-angina drugs.
• Assessment of exercise stages of change (Appendix XIV): He was in the preparation stage.
• Delivering ESMI (Table 3.2): The goal of negotiating a plan for exercising was set and the following
strategies were provided: ① Further discussing the safety of exercise and attentions should be paid
during exercise; ② Finding out whether he encountered any difficulties in maintaining regular
exercise? (He experienced no difficulty in it); ③Telling him that accumulated exercise (e.g., three 10-
minute bouts) of moderate intensity in one day produced similar benefits to one longer exercise session
(e.g., one 30-minute bout); ④ Encouraging him to find exercise buddies (helping relationships).

445
An example of the TTM-based Exercise Stage-Matched Intervention (ESMI) (Continue)
week5 Telephone follow-up:
• Compliance checking (Table 3.1): In the past one week, he took jogging 15 minutes per session, two
sessions per day on 7 days. During the exercise, he had mild sweating, felt a little fast breathing and
perceived fairly light (RPE 11), and did not experience any discomfort or take any anti-angina drugs.
• Assessment of exercise stages of change (Appendix XIV): He was in the action stage.
• Delivering ESMI (Table 3.2): Congratulation to him because he had moved forward one stage. The goal of reaffirming commitment and following up was set and the following strategies were provided:
① Encouraging him to reward himself for exercise regularly (reinforcement management); ② Finding
out whether he encountered any difficulties in maintaining regular exercise? (He experienced no
difficulty in it); ③ Introducing additional exercise alternatives, such as hiking on the weekend; ④
Encouraging him to find exercise buddies (helping relationships); ⑤ Encouraging him to check off
each time when he exercised (reinforcement management).
week6 Telephone follow-up:
• Compliance checking (Table 3.1): In the past one week, he took jogging 15-20 minutes per session,
two sessions per day on 7 days. During the exercise, he had mild sweating, felt a little fast breathing and perceived fairly light (RPE 11), and did not experience any chest discomfort or take any anti-
angina drugs.
• Assessment of exercise stages of change (Appendix XIV): He was in the action stage.
• Delivering ESMI (Table 3.2): The goal of reaffirming commitment and following up was set and the
following strategies were provided: ① Further encouraging him to reward himself for exercise
regularly (e.g., buy a special gift or a coat to reward himself) (reinforcement management); ② Finding
out whether he encountered any difficulties in maintaining regular exercise; ③ Introducing additional
exercise alternatives, such as bicycling; ④ Encouraging him to find exercise buddies (Invite his wife to
exercise together) (helping relationships); ⑤ Encouraging him to maintain regular exercise.
week7 Telephone follow-up:
• Compliance checking (Table 3.1): In the past one week, he only took jogging 20 minutes per day on
2 days. During the exercise, he had mild sweating, felt a little fast breathing and perceived fairly light (RPE 11), and did not experience any discomfort or take any anti-angina drugs.
• Assessment of exercise stages of change (Appendix XIV): He was in the preparation stage.
• Delivering ESMI (Table 3.2): The goal of negotiating a plan for exercising was set and the following
strategies were provided: ① Finding out why he cut down exercise in the past one week? (He said that
the main reason to cut down the exercise was due to the bad weather (raining in most days of the past one week)). (According to his situation, suggest him to do indoor exercise when it is raining.) (stimulus
control); ② Introducing additional exercise alternatives, such as calisthenics and/or marking run at
home (counterconditioning); ③ Encouraging him to think about the benefits of exercise and good
health conditions due to engaging in regular exercise recently; ④ Encouraging him to maintain regular
exercise.
• Make an appointment for face-to-face consultation at the hospital next week.
week8 Face-to-face contact at hospital:
• Compliance checking (Table 3.1): In the past one week, he took jogging around 20 minutes per session, two sessions per days on 7 days. During the exercise, he had mild sweating, felt a little fast
breathing and perceived fairly light (RPE 11), and did not experience any discomfort or take any anti-
angina drugs.
• Assessment of exercise stages of change (Appendix XIV): He was in the action stage.
• Delivering ESMI (Table 3.2): The goal of reaffirming commitment and following up was set and the
following strategies were provided: ① Further encouraging him to reward himself for exercise
regularly (e.g., buy a special gift to reward himself) (Reinforcement management); ② Finding out
whether he encountered any difficulties in maintaining regular exercise (He said that, usually, there were no difficulties in maintaining regular exercise, except that he travels on business). Encourage him
to bring exercise suits together when he is traveling on business and encourage him to do some
exercises inside of hotel or take walking around hotel (stimulus control); ③ Introducing additional
exercise alternatives, such as calisthenics, Taichi and home exercise (counterconditioning); ④
Encouraging him to find exercise buddies (Join a community fitness club sports) (helping
relationships); ⑤Encouraging him to obtain social support to participate in exercise or maintain
regular exercise; ⑥Planning for resisting the temptation to skip exercise, such as bad weather,
holidays/vocations (e.g., Lunar New Year), and traveling on business (stimulus control); ⑦Encouraging him to maintain regular exercise.
• ESMI pamphlet (Appendix IX): Action pamphlet was given to him.

446
Appendix XI Screening Form
Part I Demographic Data
1. Gender
① Male ② Female
2. Age __________years old
3. Marital status
① Single ② Married ③ Divorced ④ Separated ⑤ Widowed
4. Education level (circle the highest level that you have completed)
① No formal education ② Elementary school
③ Junior high school ④ Senior high school
⑤ Associate degree ⑥ Baccalaureate degree or above
5. Current employment status
① Not working
② Working on a part-time basis
③ Working on a full-time basis
6. Occupation before retirement
① Manual labour ② Technical ③ Clerical
④ Managenal ⑤ Professional ⑥ Business/Commercial
⑦ Other, please specify_________________________
7. Religious belief
① No belief ② Buddhism ③ Christianism
④ Islamism ⑤ Catholicism ⑥ Taoism
⑦ Other, please specify_________________________

447
8. Family income per month
① Less than ¥1,000 ②¥1,001-3,000 ③¥3,001-5,000
④¥5,001-7,000 ⑤¥7,001-10,000 ⑥¥More than 10,001
9. Type of medical payment
① Totally reimbursed ② Partially reimbursed
③ Medical insurance ④ Totally self-paid
10. Living condition
① Living alone ② Living with friend ③ Living with spouse
④ Living with children ⑤ Living with spouse and children
Part II Clinical Data
1. Diagnosis
① Angina pectoris ② Myocardial infarction
2. PCI/Stent intervention
① No ② Yes
3. CHD family history (occurring at age < 50)
① No ② Yes
4. Diagnosed with diabetes mellitus (DM)
① No ② Yes
5. Diagnosed with hypertension
① No ② Yes (________mmHg)
448
6. Smoking (use of cigarettes, cigars, cigarillos, pipe tobacco, or any other form of
tobacco)
① Never smoking
② Once smoking (average_____/day), now quit smoking.
③ Current smoking (average _____/day).
7. Alcohol drinking
① Never drinking
② Once drinking (average ___kg/week), now quit drinking.
③ Current drinking (average ____kg/week).
8. Current medication
8.1 Nitrates_______________________________________________________
8.2 Beta-blockers___________________________________________________
8.3 ACE inhibitors__________________________________________________
8.4 Calcium antagonists______________________________________________
8.5 Lipid-lowering drugs_____________________________________________
8.6 Antiplatelets____________________________________________________
8.7 Others_________________________________________________________
Part III Hospital Anxiety and Depression Scale – Depression
Subscale (HADS-D)
Doctors are aware that emotions play an important part in most illness. If your doctor
knows about these feelings he will be able to help you more. This questionnaire is
designed to help your doctor to know how you feel. Read each item and mark a
number in the right column opposite the reply which comes closest to how you have
been feeling in the past week. Don‘t take too long over your replies: your immediate
reaction to each item will probably be more accurate than a long thought-out response.

449
Sub-
scale
Items Answer Score
1 I still enjoy the things I used to
enjoy
Definitely as much
Not quite so much
Only a little
Hardly at all
0
1
2
3
2 I can laugh and see the funny
side of things
As much as I always could
Not quite so much now
Definitely not so much now
Not at all
0
1
2
3
3 I feel cheerful
Not at all
Not often
Sometimes
Most of the time
3
2
1
0
4 I feel as if I am slowed down Nearly all the time
Very often
Sometimes
Not at all
3
2
1
0
5 I have lost interest in my
appearance
Definitely
I don‘t take so much care as I should
I may not take quite as much care
I take just as much care as ever
3
2
1
0
6 I look forward with enjoyment
to things
As much as I ever did
Rather less than I used to
Definitely less than I used to
Hardly at all
0
1
2
3
7 I can enjoy a good book or TV
programme
Often
Sometimes
Not often
Very seldom
0
1
2
3
Total scores: _______________

450
Part IV Screening Item Form
The following items were used to help cardiologist to screen patients according to the
screening guidelines based on the selection criteria and to decide whether they were
suitable to participate in the project, the exercise stage-matched intervention. Patients
would not be recommended to participate in the project if they did not meet any one
of the following items.
1. Age ________years
① Less than 18 years old ② Equal to or more than 18 years old
2. Whether is patient living in Xiamen City?
① Yes, address______________________________________________
Contact telephone No.:______________________________________
② No
3. Patient‘s ability of communication in mandarin and reading in Chinese
(1) The ability of communication in mandarin ① Yes ② No
(2) The ability of reading in Chinese ① Yes ② No
4. Disease diagnosis
① Angina pectoris, date of diagnosis ____________month/year;
② Myocardial infarction, date of diagnosis________month/year;
③ PCI/Stent treatment, date of treatment__________month/year.
5. Is patient medically stable? ① Yes ② No
6. Does patient have unstable angina? ① Yes ② No
7. Has patient participate any cardiac rehabilitation programme?
① Yes ② No
8. Does patient have any cognitive impairment or diagnose with any psychiatric
illnesses such as psychosis and dementia? ① Yes ② No
9. Does patient have depression? ① Yes ② No
10. Has patient have critical aortic stenosis? ① Yes ② No
11. Heart function according to the New York Hear Functional Classification:

451
① I: No limitation of physical activity. Ordinary physical activity does not cause
undue fatigue, palpitation, or dyspnea (shortness of breath).
② II: Slight limitation of physical activity. Comfortable at rest, but ordinary
physical activity results in fatigue, palpitation, or dyspnea.
③ III: Marked limitation of physical activity. Comfortable at rest, but less than
ordinary activity causes fatigue, palpitation, or dyspnea.
③ VI: Unable to carry out any physical activity without discomfort. Symptoms of
cardiac insufficiency at rest. If any physical activity is undertaken, discomfort
is increased.
12. Diabetes mellitus (DM)
① No ② Yes (resting blood glucose _______________)
13. Hypertension
① No ② Yes (blood pressure___________mmHg)
14. Hear rate/pulse rate _________bpm
15. Does patient have resting heart rate > 120 bpm? ① Yes ② No
16. Does patient have atrial fibrillation? ① Yes ② No
17. Does patient have ventricular arrhythmias? ① Yes ② No
18. Does patient have third-degree AV block? ① Yes ② No
19. Does patient have resting SBP > 180mmHg or resting DBP > 110mmHg?
① Yes ② No
20. Does patient have acute myocarditis? ① Yes ② No
21. Does patient have acute pericarditis? ① Yes ② No
22. Has patient have embolism during the previous three months?
① Yes ② No
23. Does patient have any acute noncardiac disorder that may affect exercise
performance or be aggravated by exercise (e.g., infection, renal failure,
thyrotoxicosis)? ① Yes ② No
Result of screening: ① Recommend ② Not recommend
Name of cardiologist: ______________________________________
Signature of cardiologist: ___________________________________
Date: ___________________________________________________
452
Appendix XII Questionnaires
Part I Exercise Stages of Change
DIRECTIONS: Regular physical activity is any planned physical activity (e.g., tai
chi, brisk walking, bicycling, swimming) performed to increase physical fitness. Such
activity should accumulate at least 30 minutes of moderate intensity physical activity
throughout the day for more than 5 days of the week (see EXAMPLES OF
MODERATE ACTIVITIES). It is not necessary to perform activity all in one
session. Several 10-min sessions can be just as effective. Moderate intensity physical
activity dose not have to be painful but to be effective. It should be done at a level that
increases your breathing rate and causes you to break a sweat.
Do you exercise regularly according to the definition above? Please mark only
ONE of five statements:
1._____ No, and I do NOT intend to in the next 6 months.
2._____ No, but I intend to in the next 6 months.
3._____ No, but I intend to in the next 30 days.
4._____ Yes, I have been for LESS than 6 months.
5._____ Yes, I have been for MORE than 6 months.
Scoring:
Item 1 = Precontemplation
Item 2 = Contemplation
Item 3 = Preparation
Item 4 = Action
Item 5 = Maintenance

453
Examples of moderate intensity level of physical activities
(adapted from Ainsworth, Haskell, Whitt et al., 1993)
Specific
activity
METs Moderate activities (3-6 METs)
Sports 3.3-5.0 Walking, 3.0-4.0mph or 4.8-6.4 km/h, level, firm surface
4.5 Badminton, social singles and doubles, general
6.0 Basketball, non-game, general
3.0 Bowling
4.0 Table tennis, ping pong
4.0 Tai chi
5.0 Tennis, doubles
3.0 Volleyball, non-competitive, 6-9 member team, general
5.0 Softball or baseball, fast or slow pitch, general
6.0 Swimming at lake, ocean or river, leisurely, not lap
swimming, general
4.0-6.0 Bicycling, 8-11.9mph, leisure, slow, light effort
3.0-5.5 Bicycling, stationary, 50-100 watts, light effort
6.0 Hiking, cross country
Dancing
and
conditioning
exercise
3.5 Callisthenics, home exercise, light or moderate effort,
general (example: back exercise)
4.0 Gymnastics, general
4.8 Twist , jazz, tap, jitterbug
3.0-4.5
fast (disco, folk, square), slow (e.g., waltz, slow dancing),
tango
4.0 Drums
Home
activities
3.5 Mopping
3.0-3.5 Downstairs, going up & down from floor
4.0-5.0 Walk/run – playing with child(ren) – only active periods
3.0-4.5 Walking, 2.5-3.5mph slowly and carrying objects less than
25 pounds
Others 3.0-6.0

454
Part II Exercise Self-Efficacy Scale (ESES)
DIRECTIONS: A number of situations are described below that can make it hard to
stick to physical activity regularly. On the items below, please rate your degree of
confidence that you can perform physical activity on a regular basis by recording in
each of the blank spaces a number from 0 to 100 using the scale below.
0 10 20 30 40 50 60 70 80 90 100
Cannot Moderately Certain
do at all certain can do can do
(0-100)
1. When I am feeling tired.
2. When I am feeling under pressure from work.
3. During bad weather
4. After recovering from an injury that caused me to stop exercising.
5. During or after experiencing personal problems.
6. When I am feeling depressed.
7. When I am feeling anxious.
8. After recovering from an illness that caused me to stop exercising.
9. When I feel physical discomfort when I exercise.
10. After a vacation.
11. When I have too much work to do at home.
12. When visitors are present.
13. When there are other interesting things to do.
14. If I don‘t reach my exercise goals.
15. Without support from my family or friends.
16. During a vacation
17. When I have other time commitments.
18. After experiencing family problems.

455
Part III Exercise Benefits and Barriers
Exercise Benefits Scale
INSTRUCTIONS: Below are statements that relate to ideas about exercise. Please
indicate the degree to which you agree or disagree with the statements by circling:
1=Strongly Disagree (SD)
2=Disagree (D)
3=Agree (A)
4=Strongly Agree (SA)
SD D A SA
1. I enjoy exercise. 1 2 3 4
2. Exercise decrease feelings of stress and tension for me. 1 2 3 4
3. Exercise improves my mental health. 1 2 3 4
4. I will prevent heart attacks by exercising. 1 2 3 4
5. Exercise increases my muscle strength. 1 2 3 4
6. Exercise gives a sense of personal accomplishment. 1 2 3 4
7. Exercising makes me feel relaxed. 1 2 3 4
8. Exercising lets me have contact with friends and
persons I enjoy.
1 2 3 4
9. Exercising will keep me from having high blood
pressure.
1 2 3 4
10. Exercising improves the level of my physical fitness. 1 2 3 4
11. Exercising improves functioning of my cardiovascular
system.
1 2 3 4
12. My muscle tone is improved with exercise. 1 2 3 4
13. I have improved feelings of well-being from exercise. 1 2 3 4
14. Exercising increases my stamina. 1 2 3 4
15. Exercising improves my flexibility. 1 2 3 4
16. My disposition is improved with exercise. 1 2 3 4
17. Exercising helps me sleep better at night. 1 2 3 4
18. I will live longer if I exercise. 1 2 3 4

456
19. Exercising helps me decrease fatigue. 1 2 3 4
20. Exercising is a good way for me to meet with new
people.
1 2 3 4
21. My physical endurance is improved by exercising. 1 2 3 4
22. Exercising improves my self-concept. 1 2 3 4
23. Exercising increases my mental alertness. 1 2 3 4
24. Exercise allows me to carry out normal activities
without tiredness.
1 2 3 4
25. Exercise improves the quality of my work. 1 2 3 4
26. Exercise is good entertainment. 1 2 3 4
27. Exercise increases my acceptance by others. 1 2 3 4
28. Exercise improves overall body functioning for me. 1 2 3 4
29. Exercise improves the way my body looks. 1 2 3 4
Copyright © Sechrist, K.R., Walker, S.N., & Pender, N.J. (1987)

457
Exercise Barriers Scale
INSTRUCTIONS: Below are statements that relate to ideas about exercise. Please
indicate the degree to which you agree or disagree with the statements by circling:
1=Strongly Disagree (SD)
2=Disagree (D)
3=Agree (A)
4=Strongly Agree (SA)
SD D A SA
1. Exercising takes too much of my time. 1 2 3 4
2. Exercise tires me. 1 2 3 4
3. Places for me to exercise are too far away. 1 2 3 4
4. I am too embarrassed to exercise. 1 2 3 4
5. It costs too much to exercise. 1 2 3 4
6. Exercise facilities do not have convenient schedules for me. 1 2 3 4
7. I am fatigued by exercise. 1 2 3 4
8. My spouse (or significant other) does not encourage
exercising.
1 2 3 4
9. Exercise takes too much time from family responsibilities. 1 2 3 4
10. I think people in exercise clothes look funny. 1 2 3 4
11. My family members do not encourage me to exercise. 1 2 3 4
12. Exercise takes too much time from family relationships. 1 2 3 4
13. Exercise is hard work for me. 1 2 3 4
14. There are too few places for me to exercise. 1 2 3 4
Copyright © Sechrist, K.R., Walker, S.N., & Pender, N.J. (1987)

458
Part IV Log Book for Patients’ Self-reporting and Self-evaluation of
Physical Activity
DIRECTIONS: This is a log book for recording the details of your daily physical
activity performed, including the mode (see the examples of moderate activities),
frequency, intensity and duration of each session of physical activity, whether it occur
angina and the additional number of short-acting sublingual trinitrate (GTN) or any
other anti-anginal drug tablets taken during the physical activity. The intensity of
physical activity was assessed by rating Borg‘s Rate of Perceived Exertion (RPE)
from 6 to 20, with 6 being very, very light (rest) and 20 being exhaustion. Level of
exercise, please rate the number from 6 to 20 to represent your perceived exertion.
Please also record the mode, frequency, and duration of each session of physical
activity, and the occurrence of anginal pain and the additional number of GTN tablets
or any other anti-anginal drugs taken when angina occurs due to the physical activity.
Rate of Perceived Exertion (RPE)
Very
light
Fairly
light
Some-
what
hard
Hard Very
hard
Very,
very
hard
Very,
very
light

459
Date
Physical activity
Total
Mon Tues Wed Thurs Fri Sat Sun
Mode
Frequency
Intensity (RPE: 6-20)
Duration (minute)
Angina occurs?
No
Yes
Take additional number
of GTN or any other
anti-anginal drugs
because of physical
activity (number)

460
Part V Log Book for Patients’ Self-reporting and Self-evaluation of
Angina
DIRECTIONS: This is a log book for recording the details of your daily angina,
including the frequency, severity and duration of each episode of angina, and the total
number of short-acting sublingual trinitrate (GTN) and any other anti-anginal drugs
tablets taken each day. Each episode of angina for severity was rated by a following
visual scale from 0 to 10, with 0 being no pain and 10 being ‗Crucifying pain‘, 5
being very painful. Please rate the number from 0 to 10 to represent your perceived
severity of angina and document the duration of each episode in minutes, and the total
number of GTN and any other anti-anginal drugs tablets taken each day.
10
Crucifying pain
9
Crushing the heart and lungs
8
Excruciating pain
7
Unbearable
6
Indescribable
5
Very painful
4
Painful
3
Bearable
2
Quite painful
1
Slight pain
0 No pain

461
Date
Angina
Total*
Mon Tues Wed Thu Fri Sat Sun
Frequency of angina
Severity of angina (0-10)
Duration of each episode of
angina (min)
Total number of GTN and any
other anti-anginal drugs taken
each day
*For the total of ―severity of angina‖, calculate its average value.

462
Part VI Quality of Life
Seattle Angina Questionnaire (SAQ)
1. The following is a list of activities that people often do during the week. Although
for some people with several medical problems it is difficult to determine what it is
that limits them, please go over the activities listed below and indicate how much
limitation you have had due to chest pain, chest tightness, or angina over the past 4
weeks. (Place an ―√ ‖ in one box on each line).
Activity Severely
limited
Moderately
limited
Somewhat
limited
A little
limited
Not
limited
Limited,
or did
not do
for other
reasons
Dressing
yourself □ □ □ □ □ □
Walking indoors
on level ground □ □ □ □ □ □
Showering □ □ □ □ □ □
Climbing a hill
or a flight of
stairs without
stopping
□ □ □ □ □ □
Gardening,
vaccuming, or
carrying
groceries
□ □ □ □ □ □
Walking more
than a block at a
brisk pace
□ □ □ □ □ □

463
Activity Severely
limited
Moderately
limited
Somewhat
limited
A little
limited
Not
limited
Limited,
or did
not do
for other
reasons
Running or
jogging □ □ □ □ □ □
Lifting or
moving heavy
objects (e.g.,
furniture,
children)
□ □ □ □ □ □
Participating in
strenuous sports
(e.g., swimming,
tennis)
□ □ □ □ □ □
2. Compared with 4 weeks ago, how often do you have chest pain, chest tightness, or
angina when doing your most strenuous level of activity?
I have had chest pain, chest tightness, or angina……
Much
more often
Slightly
more often
About the
same
Slightly
less often
Much less
often
I‘ve had no chest
pain over the last 4
weeks
□ □ □ □ □ □
3. Over the past 4 weeks, on average, how many times have you had chest pain, chest
tightness, or angina?

464
I get chest pain, chest tightness, or angina……
4 or more
times per
day
1-3 times
per day
3 or more
times per
week but not
every day
1-2 times
per week
Less than
once a
week
None over
the past 4
weeks
□ □ □ □ □ □
4. Over the past 4 weeks, on average, how many times have you had to take nitros
(nitroglycerin tablets) for your chest pain, chest tightness, or angina?
4 or more
times per
day
1-3 times
per day
3 or more times
per week but not
every day
1-2 times
per week
Less than
once a
week
None over
the past 4
weeks
□ □ □ □ □ □
5. How bothersome is it for you to take your pills for chest pain, chest tightness or
angina as prescribed?
Very
bothersome
Moderately
bothersome
Somewhat
bothersome
A little
bothersome
Not
bothersome
at all
My doctor
has not
prescribed
pills
□ □ □ □ □ □

465
6. How satisfied are you that everything possible is being done to treat your chest pain,
chest tightness, or angina?
Not satisfied
at all
Mostly
dissatisfied
Somewhat
satisfied
Mostly
satisfied
Highly
satisfied
□ □ □ □ □
7. How satisfied are you with the explanations your doctor has given you about your
chest pain, chest tightness, or angina?
Not satisfied
at all
Mostly
dissatisfied
Somewhat
satisfied
Mostly
satisfied
Highly
satisfied
□ □ □ □ □
8. Overall, how satisfied are you with the current treatment of your chest pain,
tightness, or angina?
Not satisfied
at all
Mostly
dissatisfied
Somewhat
satisfied
Mostly
satisfied
Highly
satisfied
□ □ □ □ □
9. Over the past 4 weeks, how much has your chest pain, chest tightness, or angina
interfered with your enjoyment of life?
It has severely
limited my
enjoyment of
life
It has
moderately
limited my
enjoyment of
life
It has slightly
limited my
enjoyment of
life
It has barely
limited my
enjoyment of
life
It has not
limited my
enjoyment of
life
□ □ □ □ □
466
10. If you had to spend the rest of your life with your chest pain, chest tightness, or
angina the way it is right now, how would you feel about this?
Not satisfied
at all
Mostly
dissatisfied
Somewhat
satisfied
Mostly
satisfied
Highly
satisfied
□ □ □ □ □
11. How often do you worry that you may have a heart attack or die suddenly?
I can‘t stop
worrying
about it
I often think
or worry
about it
I
occasionally
worry about
it
I rarely
think or
worry
about it
I never
think or
worry
about it
□ □ □ □ □

467
Short Form 36 Health Survey Questionnaire (SF-36)
The following questions are to assess your opinion, feeling and ability to perform
daily activities. Please choose the answer that is closest to your condition for each
question.
1. In general, would you say your health is:
Excellent
Very good
Good
Fair
Poor
2. Compared to one year ago, how would you rate your health in general now?
Much better now than one year ago
Somewhat better now than one year ago
About the same as one year ago
Somewhat worse now than one year ago
Much worse now than one year ago
3. The following items about activities you might do during a typical day. Does your
health now limit you in these activities? If so, how much?
Limited a
lot
Limited a
little
Not
limited
Vigorous activities, such as running, lifting heavy
objects, participating in strenuous sports
Moderate activities, such as moving a table,
cleaning the floor
Lifting or carrying groceries
Climbing several flights of stairs
Climbing one flight of stairs

468
Bending, kneeling, or stooping
Walking 1500 meters
Walking 800 meters
Walking 100 meters
Bathing or dressing yourself
4. During the past four weeks, have you had any of the following problems with your
work or other regular activities as a result of your physical health?
Yes No
Cut down on the amount of time you spent on work or other
activities
Accomplished less than you would like
Were limited in the kind of work or other activities
Had difficulty performing the work or other activities (for
example, it took extra effort)
5. During the past four weeks, have you had any of the following problems with your
work or other regular daily activities as a result of any emotional problems (such as
feeling depressed or anxious)?
Yes No
Cut down on the amount of time you spent on work or other
activities
Accomplished less than you would like
Did work or other activities less carefully than usual
6. During the past four weeks, to what extent has your physical health or emotional
problems interfered with your normal social activities with family, friends, neighbors,
or groups?

469
Not at all
Slightly
Moderately
Quite a bit
Extremely
7. How much bodily pain have you had during the past four weeks?
None
Very mild
Mild
Moderate
Severe
Very severe
8. During the past four weeks, how much did pain interfere with your normal work,
including work outside the home and housework?
Not at all
A little bit
Moderately
Quite a bit
Extremely
9. The next set of questions is about how you feel and how things have been with you
during the past four weeks. For each question, please give the one answer that comes
closest to the way you have been feeling.
How much of the time during the past
four weeks
All
the
time
Most
of
the
time
A
good
bit of
the
time
Some
of
the
time
A
little
of
the
time
None
of
time
Did you feel full of pep?
Have you been a very nervous person?
Have you felt so down in the dumps that

470
nothing could cheer you up?
Have you felt calm and peaceful?
Did you have a lot of energy?
Have you felt downhearted and blue?
Did you feel worn out?
Have you been a happy person?
Did you feel tired?
Has your physical health or emotional
problems interfered with your social
activities like visiting friends, relatives,
etc.
10. How true or false is each of the following statements for you?
Definitely
true
Mostly
true
Don‘t
know
Mostly
false
Definitely
false
I seem to get sick a little easier
than other people
I am as healthy as anybody I
know
I expect my health to get worse
My health is excellent

471
Appendix XIII Scoring Instructions
Part I Scoring instructions and data analyses of the exercise stages of
change
There are three ways to handle with data of exercise stages of change: ① At every
outcome measure point (e.g., T0, T1, T2 and T3), the count of distribution of each stage
and proportion could be employed to show data. The exercise stages of change
contain five stages, such as precontemplation, contemplation, preparation, action and
maintenance stages. Since these five stages are ordinal data and there are three groups
in this study, Kruskal-Wallis test could be used to compare the difference in the
exercise stages of change among the three groups at each time point and Friedman test
could be used for within group comparison from T0 to T3. ② An approach to
conceptualizing stage progression as a trichotomous variable (progression, stable and
regression) would be to count the number of stages progressed, stable or regressed as the
outcome variable. For example, compared to the baseline exercise stages of change, an
individual progresses at least one single stage (e.g., progress from precontemplation to
contemplation stage or to action stage) would be viewed as progression. An individual
regresses at least one earlier stage (e.g., regress from contemplation to precontemplation
stage) would be assigned as regression. An individual has no movement of exercise
stages of change before and after the intervention would be viewed as stable. The count
and proportion of each label could be employed to show data. Kruskal-Wallis test could
be used to compare the difference in the exercise stages of change among the three
groups at each time point and Friedman test could be used for within group
comparison from T0 to T3. ③ A recommended alternative approach to conceptualizing
stage progression as a trichotomous variable would be to count the number of stages
progressed as the outcome variable. For example, an individual progressing a single
stage (e.g., progress from precontemplation to contemplation stage, or progress from
contemplation to action stage) would receive a score of 1, while an individual
progressing two stages would receive a score of 2 (e.g., progress from precontemplation
to action stage), and so on. Regression to an earlier stage would be assigned negative
scores. For example, the subjects regressing a single stage (e.g., regress from
contemplation to precontemplation stage) would receive a negative score of 1; the

472
subjects regressing two stages would receive a negative score of 2, and so on. Then we
can calculate the mean scores of exercise stages change in each group. For the scores of
each point (e.g., T1, T2 and T3), one way ANOVA or Kruskal-Wallis test (if data is not
normally distributed and/or the related homogeneity of variance was not achieved) could
be used to analyze the data. Within each group, one-way repeated ANOVA or Friedman
test would be used to analyze the data. (Nigg, 2002, cited in G.J. Welk (Ed)).
Part II Scoring instructions and data analyses of the exercise self-
efficacy scale
The exercise self-efficacy scale consists of 18 items. The scores of each item ranges
from 0 (can not do at all) to 100 (certainly can do). The instrument may be scored and
used in its entirely. The total scores can be calculated to add scores of each item.
Scores on the total instrument can range from 0 to 1800. The higher scores mean the
higher degree of confidence to perform physical activity on a regular basis. The data
are scale data. We can calculate the mean scores of each group and then use two-way
repeated ANOVA to analyze the groups, time and interactive effects. For the scores of
each point (e.g., T0, T1, T2 and T3), one way ANOVA or Kruskal-Wallis test (if data is
not normally distributed and/or the related homogeneity of variance was not achieved)
could be used to analyze the data. Within each group, one-way repeated ANOVA or
Friedman test would be used to analyze the data.
Part III Scoring instructions and data analyses of the exercise
benefits and barriers scale
The instrument can be scored and used in its entirely or as two separate scales, such as
the exercise benefits scale and the exercise barriers scale. The instrument has a four-
response, force-choice Liker-type format with responses ranging from 4 (strongly
agree) to 1 (strongly disagree). Barrier Scale items are reverse-scored.

473
Missing data can be handled in one of the two ways. If more than five percent of the
items are unanswered, it is recommended that the response be discarded. If the
missing item response rate is less than five percent, median substitution prevents
falsely low scores.
Scores on the total instrument can range from 43 to 172. The higher the score, the
more positively the individual perceives exercise. When the Benefits Scale is used
alone, the score range is between 29 and 116. When the Barriers Scale is used alone,
scores range between 14 and 56. If used alone, the Barriers Scale does not need to be
reverse-scored. In this instance, the higher the score on the Exercise Barriers Scale,
the greater the perception of barriers to exercise.
In this study, we used the instrument as two separate scales. The scores of exercise
benefits scale and exercise barriers scale were calculated separately. The data are
scale data. We can calculate the mean scores of each group and then use two-way
repeated ANOVA to analyze the groups, time and interactive effects. For the scores of
each point (e.g., T0, T1, T2 and T3), one way ANOVA or Kruskal-Wallis test (if data is
not normally distributed and/or the related homogeneity of variance was not achieved)
could be used to analyze the data. Within each group, one-way repeated ANOVA or
Friedman test would be used to analyze the data.
Part IV Scoring instructions and data analyses of Patients’ Self-
reporting and Self-evaluation of Physical activity
1. Duration of physical activity: Calculate the duration of any planned and/or
intentional physical activities and moderate physical activities performed for
physical fitness in the past one week. The moderate physical activities duration
was calculated based on the moderate physical activities according to the form of
examples of moderate physical activities.The data are ratio data. We can calculate
the mean scores of each group and then use two-way repeated ANOVA to analyze
the groups, time and interactive effects. For the scores of each point (e.g., T0, T1, T2
and T3), one way ANOVA or Kruskal-Wallis test (if data is not normally distributed
474
and/or the related homogeneity of variance was not achieved) could be used to
analyze the data. Within each group, one-way repeated ANOVA or Friedman test
would be used to analyze the data.
2. The number of anti-anginal drugs taken: Calculate the number of any anti-anginal
drugs taken in the past one week due to the chest pain, chest tightness or angina
induced by physical activities. The anti-anginal drugs include short-acting
sublingual trinitrate, shexiangbaoxin pill, danshendiwan and suxiaojiuxin pill.
Thus, calculate the number of these anti-anginal drugs taken in the past one week.
Although these anti-anginal drugs have similar effect on anti-anginal pain, they
have different taking ways and doses. We cannot simply compare the number of
each anti-anginal drugs taken. Based on whether patient took the anti-anginal
drugs during exercise session in the past one week, the data were viewed as
nominal data. The count of and proportion of whether patient took anti-anginal
drug could be employed to show data. Chi-square test could be used to analyze
data at each time point among the three groups and Cochran‘s Q test could be
used to analyze data within each group from T0 to T3.
Part V Scoring instructions and data analyses of Patients’ Self-
reporting and Self-evaluation of Angina
1. Angina frequency (episodes/week): Calculate the total episodes of angina attack in
the past one week. The data are scale data. We can calculate the mean scores of
each group and then use two-way repeated ANOVA to analyze the groups, time
and interactive effects. For the scores of each point (e.g., T0, T1, T2 and T3), one
way ANOVA or Kruskal-Wallis test (if data is not normally distributed and/or the
related homogeneity of variance was not achieved) could be used to analyze the data.
Within each group, one-way repeated ANOVA or Friedman test would be used to
analyze the data.
2. Angina severity (0-10): The severity of each episode of angina was rated by a
visual scale ranged from 0 to 10, with 0 being no pain and 10 being ‗Crucifying
pain‘, 5 being very painful. Patients rate the number from 0 to 10 to represent their
perceived severity of angina. Calculate the average severity of angina in the past

475
one week. The data are ratio data. We can calculate the mean scores of each group
and then use two-way repeated ANOVA to analyze the groups, time and
interactive effects. For the scores of each point (e.g., T0, T1, T2 and T3), one way
ANOVA or Kruskal-Wallis test (if data is not normally distributed and/or the related
homogeneity of variance was not achieved) could be used to analyze the data. Within
each group, one-way repeated ANOVA or Friedman test would be used to analyze
the data.
3. Angina duration (minutes/week): Calculate the total minutes of angina duration in
the past one week. The data are ratio data. We can calculate the mean scores of
each group and then use two-way repeated ANOVA to analyze the groups, time
and interactive effects. For the scores of each point (e.g., T0, T1, T2 and T3), one
way ANOVA or Kruskal-Wallis test (if data is not normally distributed and/or the
related homogeneity of variance was not achieved) could be used to analyze the data.
Within each group, one-way repeated ANOVA or Friedman test would be used to
analyze the data.
4. Based on whether patient experienced angina in the past one week, the data was
viewed as a nominal data. The count of and proportion of whether patient
experienced angina could be employed to show data. Chi-square test could be
used to analyze data at each time point among the three groups and Cochran‘s Q
test could be used to analyze data within each group from T0 to T3.
5. Anti-anginal drugs taken: Calculate the number of any anti-anginal drugs taken in
the past one week, such as short-acting sublingual trinitrate, shexiangbaoxin pill,
danshendiwan and suxiaojiuxin pill. Thus, calculate the number of these anti-
anginal drugs taken in the past one week. Although these anti-anginal drugs have
similar effect on anti-anginal pain, they have different taking ways and doses. We
cannot simply compare the number of each anti-anginal drug taken. Based on
whether patient took the anti-anginal drugs in the past one week, the data were
viewed as nominal data. The count of and proportion of whether patient took anti-
anginal drugs could be employed to show data. Chi-square test could be used to
analyze data at each time point among the three groups and Cochran‘s Q test
could be used to analyze data within each group from T0 to T3.

476
Part VI Scoring and Interpreting the SAQ
There are 5 summary scores within the SAQ, which are calculated as follows:
A. The Physical Limitation scale
The Physical Limitation score corresponds to questions 1a through 1i. Responses to
questions 1a through 1i should be coded numerically as follows:
1 = Extremely Limited
2 = Quite a bit Limited
3 = Moderately Limited
4 = Slightly Limited
5 = Not at all Limited
6 = Limited for other reasons or did not do the activity
If the responses to questions 1a through 1i are not 1, 2, 3, 4 or 5 then the response is
set to missing. Note that a response of 6 is treated as a missing value. Missing values
are assigned the average score for that level of activity. Activities are grouped into 3
levels of exertional requirements. The lowest level includes dressing, walking and
showering (1a, 1b and 1c); the middle level is climbing, gardening, and walking more
than a block (1d, 1e and 1f); the highest level includes running, lifting, and sports (1g,
1h and 1i). If any one item in a group is missing, then assign the average value of the
other group items to the missing item. If all items in the lowest or the highest level are
missing, then assign each item the mean of the items in the middle level. If all items
in the middle level are missing, then assign each item the average of the means of the
lowest and highest levels. If more than 4 items are missing in this scale then no
reasonable score for this dimension can be calculated. After accounting for any
missing items the physical limitation score is computed by standardizing the mean
response of all nine items as follows:
Physical Limitation = 100*(Mean Response – 1)/4

477
B. The Angina Stability scale
The Angina Stability score corresponds to question 2. Responses to question 2 should
be coded numerically as follows:
1 = Much more often
2 = Slightly more often
3 = About the same
4 = Slightly less often
5 = Much less often
6 = I‘ve had no chest pain over the last 4 weeks
If the response is 6 (no chest pain over last 4 weeks) then set the response to 3 (about
the same). If the response is missing then angina stability cannot be computed and
will be missing. Otherwise, the angina stability score is computed by standardizing
the result as follows:
Angina Stability = 100*(Response – 1)/4
C. The Angina Frequency scale
The Angina Frequency score corresponds to questions 3 and 4. Responses should be
coded sequentially 1 to 6 in order of increasing health status, with 1 denoting the
response associated with the lowest health status. If at least one question response is
present then the angina frequency is computed by standardizing the mean response as
follows:
Angina Frequency = 100*(Mean Response – 1)/5
D. The Treatment Satisfaction scale
The Treatment Satisfaction score corresponds to questions 5, 6, 7 and 8. Responses
should be coded sequentially (1, 2, 3…) in order of increasing health status, with 1

478
denoting the response associated with the lowest health status. If responses to
questions 5, 6, 7 and 8 are not values 1, 2, 3, 4, or 5 then the response is set to missing.
Note that a response of 6 for question 5 is treated as a missing value. If at least two
responses are present then the treatment satisfaction score is computed by calculating
the mean response and standardizing the result as follows:
Treatment Satisfaction = 100*(Mean Response – 1)/4
E. The Quality of Life scale
The Quality of Life score corresponds to questions 9, 10 and 11. Responses should be
coded sequentially 1 to 5 in order of increasing health status, with 1 denoting the
response associated with the lowest health status. If the responses to questions 9, 10
and 11 are not values 1, 2, 3, 4 or 5 then the response is set to missing. If at least two
responses are present then the Quality of Life score may be computed by
standardizing the mean response as follows:
Quality of Life = 100*(Mean Response – 1)/4
Part VII Scoring instructions of MOS SF-36
1. The contents and structure of MOS SF-36
The MOS SF-36 is a generic health survey questionnaire and was developed by the
American Boston Institute of Health. It was widely used to assess quality of life in
general population, clinical trials and health policy evaluation. The SF-36 includes
eight domains, such as physical functioning (PF), role-physical (RP), bodily pain (BP),
general health (GH), vitality (VT), social functioning (SF), role-emotional (RE), and
mental health (MH), and one item, reported health transition (HT).

479
2. Scoring instruction of MOS SF-36
2.1 Basic steps
First, coding each item of MOS SF-36
Second, scoring of each item
Third, calculate the scores of each domain. The basic formula for scoring as follow:
Scores of each
domain =
Real scores – possible lowest scores of this domain
Possible highest scores – possible lowest scores
2.2 Handle with missing data: Sometime responders do not response to all the items
of each domain. The items that are not answered are viewed as missing data. If more
than half of the items of each domain are answered, we should calculate the scores of
this domain. The missing data is replaced with mean scores.
2.3 Scores of each domain and calculation
2.3.1 PF:Physical Functioning
Item:3
(1) Vigorous activities, such as running, lifting heavy objects, participating in
strenuous sports
(2) Moderate activities, such as moving a table, cleaning the floor
(3) Lifting or carrying groceries
(4) Climbing several flights of stairs
(5) Climbing one flight of stairs
(6) Bending, kneeling, or stooping
(7) Walking 1500 meters
(8) Walking 800 meters
(9) Walking 100 meters
(10) Bathing or dressing yourself
Coding and scoring

480
Answer Coding Scoring
Limited a lot
Limited a little
Not limited
1
2
3
1
2
3
Scoring and calculation
Add all scores of each item of this domain and calculate the final scores of PF. The
higher scores of PE, the better health status.
PF Real scores -10
20
2.3.2 RP:Role-Physical
Item:4
(1) Cut down on the amount of time you spent on work or other activities
(2) Accomplished less than you would like
(3) Were limited in the kind of work or other activities
(4) Had difficulty performing the work or other activities (for example, it took extra
effort)
Coding and scoring
Answer Coding Scoring
Yes
No
1
2
1
2
Scoring and calculation
Add all scores of each item of this domain and calculate the final scores of RP. The
higher scores of RP, the better health status.
RP = Real scores - 4
4

481
2.3.3 BP:Bodily Pain
Item:7,8
7. How much bodily pain have you had during the past four weeks?
8. During the past four weeks, how much did pain interfere with your normal work,
including work outside the home and housework?
Coding and scoring of item 7
Answer Coding Scoring
None
Very mild
Mild
Moderate
Severe
Very severe
1
2
3
4
5
6
6.0
5.4
4.2
3.1
2.2
1.0
Coding and scoring of item 7 - if individual answered both item 7 and item 8
Answer Code of item 8 Code of item 7 Scores of item 8
Not at all 1 1 6
Not at all 1 2 - 6 5
A little bit 2 1 - 6 4
Moderately 3 1 - 6 3
Quite a bit 4 1 - 6 2
Extremely 5 1 - 6 1
Coding and scoring of item 7 - if no response to item 7
Answer Coding Scoring
Not at all 1 6.0
A little bit 2 4.75
Moderately 3 3.5
Quite a bit 4 2.25
Extremely 5 1.0
Scoring and calculation
Add all scores of each item of this domain and calculate the final scores of BP. The

482
higher scores of BP, the better health status.
BP = Real scores - 2
10
2.3.4 GH:General Health
Item:1,10
1. In general, would you say your health is:
10.1 I seem to get sick a little easier than other people
10.2 I am as healthy as anybody I know
10.3 I expect my health to get worse
10.4 My health is excellent
Coding and scoring of item 1&10.1-10.4
Item 1 Answer Coding Scoring
Excellent 1 5.0
Very good 2 4.4
Good 3 3.4
Fair 4 2.0
Poor 5 1.0
Item 10.1,10.3 Answer Coding Scoring
Definitely true 1 1
Mostly true 2 2
Don‘t know 3 3
Mostly false 4 4
Definitely false 5 5
Item 10.2,10.4 Answer Coding Scoring
Definitely true 1 5
Mostly true 2 4
Don‘t know 3 3

483
Mostly false 4 2
Definitely false 5 1
Scoring and calculation
Add all scores of each item of this domain and calculate the final scores of GH. The
higher scores of GH, the better health status.
GH = Real scores - 5
20
2.3.5 VT:Vitality
Item:9.1,9.5,9.7,9.9
9.1 Did you feel full of pep?
9.5 Did you have a lot of energy?
9.7 Did you feel worn out?
9.9 Did you feel tired?
Coding and scoring
Item 9.1,9.5 Answer Coding Scoring
All the time 1 6
Most of the time 2 5
A good bit of the time 3 4
Some of the time 4 3
A little of the time 5 2
None of time 6 1
Item 9.7,9.9 Answer Coding Scoring
All the time 1 1
Most of the time 2 2
A good bit of the time 3 3
Some of the time 4 4

484
A little of the time 5 5
None of time 6 6
Scoring and calculation
Add all scores of each item of this domain and calculate the final scores of VT. The
higher scores of VT, the better health status.
VT = Real scores - 4
20
2.3.6 SF:Social Functioning
Item:6,9.10
6. During the past four weeks, to what extent has your physical health or emotional
problems interfered with your normal social activities with family, friends, neighbors,
or groups?
9.10 Has your physical health or emotional problems interfered with your social
activities like visiting friends, relatives, etc.
Coding and scoring
Item 6 Answer Coding Scoring
Not at all 1 5
Slightly 2 4
Moderately 3 3
Quite a bit 4 2
Extremely 5 1
Item 9.10 Answer Coding Scoring
All the time 1 1
Most of the time 2 2
A good bit of the time 3 3
Some of the time 3 3
A little of the time 4 4

485
None of time 5 5
Scoring and calculation
Add all scores of each item of this domain and calculate the final scores of SF. The
higher scores of SF, the better health status.
SF = Real scores - 2
8
2.3.7 RE:Role-Emotional
Item:5
(1) Cut down on the amount of time you spent on work or other activities
(2) Accomplished less than you would like
(3) Did work or other activities less carefully than usual
Coding and scoring
Answer Coding Scoring
Yes 1 1
No 2 2
Scoring and calculation
Add all scores of each item of this domain and calculate the final scores of RE. The
higher scores of RE, the better health status.
RE = Real scores - 3
3

486
2.3.8 MH:Mental Health
Item:9.2,9.3,9.4,9.6,9.8
9.2 Have you been a very nervous person?
9.3 Have you felt so down in the dumps that nothing could cheer you up?
9.4 Have you felt calm and peaceful?
9.6 Have you felt downhearted and blue?
9.8 Have you been a happy person?
Coding and scoring
Item 9.2,9.3,
9.6
Answer Coding Scoring
All the time 1 1
Most of the time 2 2
A good bit of the time 3 3
Some of the time 4 4
A little of the time 5 5
None of time 6 6
Item 9.4,9.8 Answer Coding Scoring
All the time 1 6
Most of the time 2 5
A good bit of the time 3 4
Some of the time 4 3
A little of the time 5 2
None of time 6 1
Scoring and calculation
Add all scores of each item of this domain and calculate the final scores of MH. The
higher scores of MH, the better health status.

487
MH = Real scores - 5
25
2.3.9 HT:Reported Health Transition
Item:2
2. Compared to one year ago, how would you rate your health in general now?
Code and scoring
Answer Code
Much better now than one year ago 1
Somewhat better now than one year ago 2
About the same as one year ago 3
Somewhat worse now than one year ago 4
Much worse now than one year ago 5
(Statistics department, Public Health College, Zhongshan Medical University, Fang
Ji-Qian & Hao Yuan-Tao, 2009)

488
Appendix XIV Training Package
Training Package
This trainer package introduced how to train a registered nurse (RN) to collect data. It
included two parts (1) Researcher went through each item with the RN to help her
understand the meaning of each item, and then guide the RN how to use instructions
to help patients better understand and fill in the questionnaires; (2) Role play: Select
1-2 persons to play as patients and the researcher played as an audience, the RN
collected data one by one item according to the questionnaires. The researcher
corrected and explained timely if there was any wrong or inconsistence in order to
guaranteeing using the same instructions to collect data to each patient.
First of all, the data collector should understand the purpose of each questionnaire and
the meaning of each item of each questionnaire and how to use it.

489
Part I Exercise Stages of Change Scale
Instructions
The exercise stages of change is used to assess patient‘s current exercise stage.
1. Moderate intensity physical activity refers to any physical activity up to 3-6 METs,
such as fishing from river bank, walking or standing (3.5 METs) (see examples of
moderate activities for details).
2. Regular physical activity is any planned or intentional physical activity (e.g., tai chi,
brisk walking, bicycling, swimming) performed to increase physical fitness. Such
activity should accumulate at least 30 minutes of moderate intensity physical activity
throughout the day for more than 5 days of the week. Several 10-min sessions can be
just as effective.
3. Definition of different exercise stages
(1) Precontemplation is the stage at which individuals are currently not doing
exercise and have no intention to start exercise in the next 6 months.
(2) Contemplation is the stage at which individuals are aware that a problem exists
with sedentary behaviour and they are seriously thinking about starting to exercise in
the next 6 months.
(3) Preparation is the stage at which individuals are intending to take action to
change sedentary habits in the next 30 days or those who currently exercise some, but
not regularly.
(4) Action is the stage at which individuals modify their behaviour, experiences, or
environment to overcome their problems; they have successfully exercised regularly
for less than 6 months.

490
(5) Maintenance is the stage at which individuals have exercised regularly for more
than 6 months.
4. Item 1 = Precontemplation; Item 2 = Contemplation; Item 3 = Preparation; Item 4 =
Action; Item 5 = Maintenance.
5. The way to determine patient‘s exercise stages of change (Figure 1).
The RN used the following flowchart to assess patient‘s current exercise stages of
change. The RN should show the patient the table of examples of moderate activities
when she was asking ―Are you accumulating at least 30 minutes of moderate-intensity
physical activity on most (five or more) days of the week?‖ and asked him/her
whether he/she had done any equal activities as the examples of moderate activities?
One thing should be noted that any physical activities that patient performed was to
increase his/her physical fitness. It would not be counted if the activity was done for
housework or job. We focused on leisure time physical activities. Additionally, the
physical activity should accumulate at least 30 minutes of moderate intensity physical
activity throughout the day for more than 5 days of the week and continuing at least
10 minutes per episode.

491
Readiness to change
Are you accumulating at least 30 minutes of
moderate-intensity physical activity on most
(five or more) days of the week?
Are you accumulating at least 30
minutes of moderate-intensity
physical activity each week?
Have you been active on a
regular basis for the last six
months?
Do you intend to
increase your
physical activity?
If you are doing
physical activity
infrequently, you are in stage 3.
If you are active
consistently but for
less than six months, you are in stage 4.
If you have
maintained the new
habit for six months
or more, you are in stage 5 If you are not
even thinking
about it, you are in stage 1.
If you are giving it a
thought now and then
but not doing activity, you are in stage 2.
No Yes
Yes
Yes
Yes
No
No
No
Figure 1 Flow chart for determining the stages of change
(Marcus, Forsyth & Blair, 2003)

492
Part II Exercise Self-Efficacy Scale (ESES)
Instructions
1. Since a number of situations can make it hard to stick to physical activity regularly,
the exercise self-efficacy scale is used to measure the degree of confidence to perform
physical activity on a regular basis if you encountered the following 18 situations.
Zero means that you cannot do at all, 100 mean that you certainly can do, and 50
means that you moderately certain can do. Please record in each of the blank spaces a
number from 0 to 100 using the scale below.
0 10 20 30 40 50 60 70 80 90 100
Cannot Moderately Certain
do at all certain can do can do
2. Instructions for each item.
(1) When I am feeling tired. How many confidences do you have to perform
physical activity on a regular basis when you are feeling tired? Please select a number
from 0 to 100 to show your degree of confidence. Zero means that you cannot do at
all and 100 mean that you certainly can do it.
(2) When I am feeling under pressure from work. How many confidences do you
have to perform physical activity on a regular basis when you are feeling under
pressure from work? Please select a number from 0 to 100 to show your degree of
confidence.
(3) During bad weather. How many confidences do you have to perform physical
activity on a regular basis during bad weather? Please select a number from 0 to 100
to show your degree of confidence.
(4) After recovering from an injury that caused me to stop exercising. How many
confidences do you have to perform physical activity on a regular basis after
recovering from an injury that caused you to stop exercising? Please select a number
from 0 to 100 to show your degree of confidence.

493
(5) During or after experiencing personal problems. How many confidences do
you have to perform physical activity on a regular basis during or after experiencing
personal problems? Please select a number from 0 to 100 to show your degree of
confidence.
(6) When I am feeling depressed. How many confidences do you have to perform
physical activity on a regular basis when you are feeling depressed? Please select a
number from 0 to 100 to show your degree of confidence.
(7) When I am feeling anxious. How many confidences do you have to perform
physical activity on a regular basis when you are feeling anxious? Please select a
number from 0 to 100 to show your degree of confidence.
(8) After recovering from an illness that caused me to stop exercising. How many
confidences do you have to perform physical activity on a regular basis after
recovering from an illness that caused you to stop exercising? Please select a number
from 0 to 100 to show your degree of confidence.
(9) When I feel physical discomfort when I exercise. How many confidences do
you have to perform physical activity on a regular basis when you feel physical
discomfort when you exercise? Please select a number from 0 to 100 to show your
degree of confidence.
(10) After a vacation. How many confidences do you have to perform physical
activity on a regular basis after a vacation? Please select a number from 0 to 100 to
show your degree of confidence.
(11) When I have too much work to do at home. How many confidences do you
have to perform physical activity on a regular basis when you have too much work to
do at home? Please select a number from 0 to 100 to show your degree of confidence.
(12) When visitors are present. How many confidences do you have to perform
physical activity on a regular basis when visitors are present? Please select a number
from 0 to 100 to show your degree of confidence.
(13) When there are other interesting things to do. How many confidences do you
have to perform physical activity on a regular basis when there are other interesting
things to do? Please select a number from 0 to 100 to show your degree of confidence.
(14) If I don’t reach my exercise goals. How many confidences do you have to
perform physical activity on a regular basis if you don‘t reach your exercise goals?
Please select a number from 0 to 100 to show your degree of confidence.

494
(15) Without support from my family or friends. How many confidences do you
have to perform physical activity on a regular without support from your family or
friends? Please select a number from 0 to 100 to show your degree of confidence.
(16) During a vacation. How many confidences do you have to perform physical
activity on a regular basis during a vacation? Please select a number from 0 to 100 to
show your degree of confidence.
(17) When I have other time commitments. How many confidences do you have to
perform physical activity on a regular basis when you have other time commitments?
Please select a number from 0 to 100 to show your degree of confidence.
(18) After experiencing family problems. How many confidences do you have to
perform physical activity on a regular basis after experiencing family problems?
Please select a number from 0 to 100 to show your degree of confidence.
Part III Exercise Benefits and Barriers Scales
Exercise Benefits Scale (EBS)
1. Directions
The exercise benefits scale is used to measure the degree to which patients feel the
benefits of exercise. Below are statements that relate to ideas about exercise benefits.
Asking patient whether he/she agree or disagree with each statement and the degree to
which he/she you agree or disagree with each statement by circling: 1=Strongly
Disagree (SD), 2=Disagree (D), 3=Agree (A), and 4=Strongly Agree (SA).
2. Instructions of each item
(1) I enjoy exercise. Whether do you agree that you enjoy exercise? Do you strongly
agree (disagree) or only agree (disagree)?
(2) Exercise decrease feelings of stress and tension for me. Whether do you agree
that exercise decrease feelings of stress and tension for you? Do you strongly agree
(disagree) or only agree (disagree)?
495
(3) Exercise improves my mental health. Whether do you agree that exercise
improves your mental health? Do you strongly agree (disagree) or only agree
(disagree)?
(4) I will prevent heart attacks by exercising. Whether do you agree that you will
prevent heart attacks by exercising? Do you strongly agree (disagree) or only agree
(disagree)?
(5) Exercise increases my muscle strength. Whether do you agree that exercise
increases your muscle strength? Do you strongly agree (disagree) or only agree
(disagree)?
(6) Exercise gives a sense of personal accomplishment. Whether do you agree that
exercise gives a sense of personal accomplishment? Do you strongly agree (disagree)
or only agree (disagree)?
(7) Exercising makes me feel relaxed. Whether do you agree that exercising makes
you feel relaxed? Do you strongly agree (disagree) or only agree (disagree)?
(8) Exercising lets me have contact with friends and persons I enjoy. Whether do
you agree that exercising lets you have contact with friends and persons you enjoy?
Do you strongly agree (disagree) or only agree (disagree)?
(9) Exercising will keep me from having high blood pressure. Whether do you
agree that exercising will keep you from having high blood pressure? Do you strongly
agree (disagree) or only agree (disagree)?
(10) Exercising improves the level of my physical fitness. Whether do you agree
that exercising improves the level of your physical fitness? Do you strongly agree
(disagree) or only agree (disagree)?
(11) Exercising improves functioning of my cardiovascular system. Whether do
you agree that exercising improves functioning of your cardiovascular system? Do
you strongly agree (disagree) or only agree (disagree)?
(12) My muscle tone is improved with exercise. Whether do you agree that your
muscle tone is improved with exercise? Do you strongly agree (disagree) or only
agree (disagree)?
(13) I have improved feelings of well-being from exercise. Whether do you agree
that you have improved feelings of well-being from exercise? Do you strongly agree
(disagree) or only agree (disagree)?
(14) Exercising increases my stamina. Whether do you agree that exercising
increases your stamina? Do you strongly agree (disagree) or only agree (disagree)?

496
(15) Exercising improves my flexibility. Whether do you agree that exercising
improves your flexibility? Do you strongly agree (disagree) or only agree (disagree)?
(16) My disposition is improved with exercise. Whether do you agree that your
disposition is improved with exercise? Do you strongly agree (disagree) or only agree
(disagree)?
(17) Exercising helps me sleep better at night. Whether do you agree that exercising
helps you sleep better at night? Do you strongly agree (disagree) or only agree
(disagree)?
(18) I will live longer if I exercise. Whether do you agree that you will live longer if
you exercise? Do you strongly agree (disagree) or only agree (disagree)?
(19) Exercising helps me decrease fatigue. Whether do you agree that exercising
helps you decrease fatigue? Do you strongly agree (disagree) or only agree (disagree)?
(20) Exercising is a good way for me to meet with new people. Whether do you
agree that exercising is a good way for you to meet with new people? Do you strongly
agree (disagree) or only agree (disagree)?
(21) My physical endurance is improved by exercising. Whether do you agree that
your physical endurance is improved by exercising? Do you strongly agree (disagree)
or only agree (disagree)?
(22) Exercising improves my self-concept. Whether do you agree that exercising
improves your self-concept? Do you strongly agree (disagree) or only agree (disagree)?
(23) Exercising increases my mental alertness. Whether do you agree that
exercising increases your mental alertness? Do you strongly agree (disagree) or only
agree (disagree)?
(24) Exercise allows me to carry out normal activities without tiredness. Whether
do you agree that exercise allows you to carry out normal activities without tiredness?
Do you strongly agree (disagree) or only agree (disagree)?
(25) Exercise improves the quality of my work. Whether do you agree that exercise
improves the quality of your work? Do you strongly agree (disagree) or only agree
(disagree)?
(26) Exercise is good entertainment. Whether do you agree that exercise is good
entertainment? Do you strongly agree (disagree) or only agree (disagree)?
(27) Exercise increases my acceptance by others. Whether do you agree that
exercise increases your acceptance by others? Do you strongly agree (disagree) or
only agree (disagree)?

497
(28) Exercise improves overall body functioning for me. Whether do you agree that
exercise improves overall body functioning for you? Do you strongly agree (disagree)
or only agree (disagree)?
(29) Exercise improves the way my body looks. Whether do you agree that exercise
improves the way your body looks? Do you strongly agree (disagree) or only agree
(disagree)?
Exercise Barriers Scale (EBBS)
1. Directions
The exercise barriers scale is used to measure the degree to which patients feel
barriers to perform regular exercise. Below are statements that relate to ideas about
exercise barriers. Asking patient whether he/she agree or disagree with the following
each statement and the degree to which he/she you agree or disagree with each
statement by circling: 1=Strongly Disagree (SD), 2=Disagree (D), 3=Agree (A), and
4=Strongly Agree (SA).
2. Instructions of each item
(1) Exercising takes too much of my time. Whether do you agree that exercising
takes too much of your time? Do you strongly agree (disagree) or only agree
(disagree)?
(2) Exercise tires me. Whether do you agree that exercise tires you? Do you strongly
agree (disagree) or only agree (disagree)?
(3) Places for me to exercise are too far away. Whether do you agree that places for
you to exercise are too far away? Do you strongly agree (disagree) or only agree
(disagree)?
(4) I am too embarrassed to exercise. Whether do you agree that you are too
embarrassed to exercise? Do you strongly agree (disagree) or only agree (disagree)?
(5) It costs too much to exercise. Whether do you agree that it costs too much to
exercise? Do you strongly agree (disagree) or only agree (disagree)?

498
(6) Exercise facilities do not have convenient schedules for me. Whether do you
agree that exercise facilities do not have convenient schedules for you? Do you
strongly agree (disagree) or only agree (disagree)?
(7) I am fatigued by exercise. Whether do you agree that you are fatigued by
exercise? Do you strongly agree (disagree) or only agree (disagree)?
(8) My spouse (or significant other) does not encourage exercising. Whether do
you agree that your spouse (or significant other) does not encourage exercising? Do
you strongly agree (disagree) or only agree (disagree)?
(9) Exercise takes too much time from family responsibilities. Whether do you
agree that exercise takes too much time from family responsibilities? Do you strongly
agree (disagree) or only agree (disagree)?
(10) I think people in exercise clothes look funny. Whether do you agree that you
think people in exercise clothes look funny? Do you strongly agree (disagree) or only
agree (disagree)?
(11) My family members do not encourage me to exercise. Whether do you agree
that your family members do not encourage you to exercise? Do you strongly agree
(disagree) or only agree (disagree)?
(12) Exercise takes too much time from family relationships. Whether do you
agree that exercise takes too much time from family relationships? Do you strongly
agree (disagree) or only agree (disagree)?
(13) Exercise is hard work for me. Whether do you agree that exercise is hard work
for you? Do you strongly agree (disagree) or only agree (disagree)?
(14) There are too few places for me to exercise. Whether do you agree that there
are too few places for you to exercise? Do you strongly agree (disagree) or only agree
(disagree)?

499
Part IV Log Book for Patients’ Self-reporting and Self-evaluation of
Physical activity
Instructions
1. This is the log book for recording the details of patients‘ moderate physical activity
performed in the past one week, including the mode (see the examples of moderate
activities), frequency, intensity and duration of each session of physical activity,
whether it occur angina and the additional number of short-acting sublingual trinitrate
(GTN) or any other anti-anginal drugs tablets taken during the physical activity.
2. The RN should show the form of examples of moderate activities to each patient
and then ask him/her what kind of activities he/she had performed in the past one
week? Please record the frequency (episodes) and duration (minutes) of physical
activities in the past one week in the form with the references of the patient‘s records.
3. The intensity of physical activity was assessed by rating Borg‘s Rate of Perceived
Exertion (RPE) from 6 to 20, with 6 being very, very light (rest) and 20 being
exhaustion. Please ask each patient to recall and rate the number from 6 to 20 to
represent their perceived physical exertion.
4. Please also ask each patient to recall the mode, frequency, and duration of each
session of physical activity, and whether it occur anginal pain and the additional
number of GTN tablets or any other anti-anginal drugs taken when feeling angina
because of physical activity.
Rate of Perceived Exertion (RPE)
Very
light
Fairly
light
Some-
what
hard
Hard Very
hard
Very,
very
hard
Very,
very
light

500
Part V Log Book for Patients’ Self-reporting and Self-evaluation of
Angina
Instructions
1. This is the log book for recalling the details of patients‘ angina in the past one week,
including frequency, severity, and duration of angina, and the number of short-acting
sublingual trinitrate (GTN) and any other anti-anginal drugs tablets taken each day.
2. Please ask each patient to recall the details of frequency of angina, severity and
duration of each episode of angina in the past one week, and the total number of
short-acting sublingual trinitrate (GTN) and any other anti-anginal drugs tablets taken
each day. Please record this information in the form with reference to the patient‘s
records.
3. The severity of each episode of angina for was rated by a following visual scale
from 0 to 10, with 0 being no pain and 10 being ‗Crucifying pain‘, 5 being very
painful. Please ask patients to rate the number from 0 to 10 to represent your
perceived severity of angina.
4. Please also ask each patient recall and to rate the duration of each episode in
minutes and the total number of GTN and any other anti-anginal tablets taken each
day.

501
10
Crucifying pain
9
Crushing the heart and lungs
8
Excruciating pain
7
Unbearable
6
Indescribable
5
Very painful
4
Painful
3
Bearable
2
Quite painful
1
Slight pain
0 No pain

502
Part VI Quality of Life
Seattle Angina Questionnaire (SAQ)
Instructions
1. The Seattle Angina Questionnaire (SAQ) is a specific quality of life scale to
measure CHD patients‘ degree of physical limitation by angina, angina frequency,
angina stability, treatment satisfaction and disease perception in the past four weeks.
2. Instructions of each item
(1) The following is a list of activities that people often do during the week. Although
for some people with several medical problems it is difficult to determine what it is
that limits them, please go over the activities listed below and indicate how much
limitation you have had due to chest pain, chest tightness, or angina over the past 4
weeks.
a. Dressing yourself: In the past 4 weeks, whether did you have any chest pain, chest
tightness, or angina limited you to dress yourself? If you didn‘t have any limitation,
please place the ―√ ‖in the corresponding box of not limited. If you had any limitation,
please indicate how much limitation you have due to chest pain, chest tightness, or
angina: severely limited, moderately limited, somewhat limited, or a little limited.
Please select one choice which most expresses your feeling and place the ―√ ‖ in the
corresponding box. If you were Limited, or did not do for other reasons, please place
the ―√ ‖ in the box of Limited, or did not do for other reasons.
b. Walking indoors on level ground: In the past 4 weeks, whether did you have any
chest pain, chest tightness, or angina limited you to walk indoors on level ground? If
you didn‘t have any limitation, please place the ―√ ‖in the corresponding box of not
limited. If you had any limitation, please indicate how much limitation you have due
to chest pain, chest tightness, or angina: severely limited, moderately limited,
somewhat limited, or a little limited. Please select one choice which most expresses
your feeling and place the ―√ ‖ in the corresponding box. If you were Limited, or did

503
not do for other reasons, please place the ―√ ‖ in the box of Limited, or did not do for
other reasons.
c. Showering: In the past 4 weeks, whether did you have any chest pain, chest
tightness, or angina limited your showering? If you didn‘t have any limitation, please
place the ―√ ‖in the corresponding box of not limited. If you had any limitation,
please indicate how much limitation you have due to chest pain, chest tightness, or
angina: severely limited, moderately limited, somewhat limited, or a little limited.
Please select one choice which most expresses your feeling and place the ―√ ‖ in the
corresponding box. If you were Limited, or did not do for other reasons, please place
the ―√ ‖ in the box of Limited, or did not do for other reasons.
d. Climbing a hill or a flight of stairs without stopping: In the past 4 weeks,
whether did you have any chest pain, chest tightness, or angina limited you to climb a
hill or a flight of stairs without stopping? If you didn‘t have any limitation, please
place the ―√ ‖in the corresponding box of not limited. If you had any limitation,
please indicate how much limitation you have due to chest pain, chest tightness, or
angina: severely limited, moderately limited, somewhat limited, or a little limited.
Please select one choice which most expresses your feeling and place the ―√ ‖ in the
corresponding box. If you were Limited, or did not do for other reasons, please place
the ―√ ‖ in the box of Limited, or did not do for other reasons.
e. Gardening, vaccuming, or carrying groceries: In the past 4 weeks, whether did
you have any chest pain, chest tightness, or angina limited your gardening, vaccuming
or carrying groceries? If you didn‘t have any limitation, please place the ―√ ‖in the
corresponding box of not limited. If you had any limitation, please indicate how much
limitation you have due to chest pain, chest tightness, or angina: severely limited,
moderately limited, somewhat limited, or a little limited. Please select one choice
which most expresses your feeling and place the ―√ ‖ in the corresponding box. If you
were Limited, or did not do for other reasons, please place the ―√ ‖ in the box of
Limited, or did not do for other reasons.
f. Walking more than a block at a brisk pace: In the past 4 weeks, whether did you
have any chest pain, chest tightness, or angina limited you to walk more than a block

504
at a brisk pace? If you didn‘t have any limitation, please place the ―√ ‖in the
corresponding box of not limited. If you had any limitation, please indicate how much
limitation you have due to chest pain, chest tightness, or angina: severely limited,
moderately limited, somewhat limited, or a little limited. Please select one choice
which most expresses your feeling and place the ―√ ‖ in the corresponding box. If you
were Limited, or did not do for other reasons, please place the ―√ ‖ in the box of
Limited, or did not do for other reasons.
g. Running or jogging: In the past 4 weeks, whether did you have any chest pain,
chest tightness, or angina limited you to run or jog? If you didn‘t have any limitation,
please place the ―√ ‖in the corresponding box of not limited. If you had any limitation,
please indicate how much limitation you have due to chest pain, chest tightness, or
angina: severely limited, moderately limited, somewhat limited, or a little limited.
Please select one choice which most expresses your feeling and place the ―√ ‖ in the
corresponding box. If you were Limited, or did not do for other reasons, please place
the ―√ ‖ in the box of Limited, or did not do for other reasons.
h. Lifting or moving heavy objects (e.g., furniture, children): In the past 4 weeks,
whether did you have any chest pain, chest tightness, or angina limited you to lift or
move heavy objects (e.g., furniture, children)? If you didn‘t have any limitation,
please place the ―√ ‖in the corresponding box of not limited. If you had any limitation,
please indicate how much limitation you have due to chest pain, chest tightness, or
angina: severely limited, moderately limited, somewhat limited, or a little limited.
Please select one choice which most expresses your feeling and place the ―√ ‖ in the
corresponding box. If you were Limited, or did not do for other reasons, please place
the ―√ ‖ in the box of Limited, or did not do for other reasons.
i. Participating in strenuous sports (e.g., swimming, tennis): In the past 4 weeks,
whether did you have any chest pain, chest tightness, or angina limited you to
participate in strenuous sports (e.g., swimming, tennis)? If you didn‘t have any
limitation, please place the ―√ ‖in the corresponding box of not limited. If you had
any limitation, please indicate how much limitation you have due to chest pain, chest
tightness, or angina: severely limited, moderately limited, somewhat limited, or a little
limited. Please select one choice which most expresses your feeling and place the ―√ ‖

505
in the corresponding box. If you were Limited, or did not do for other reasons, please
place the ―√ ‖ in the box of Limited, or did not do for other reasons.
(2) Compared with 4 weeks ago, how often do you have chest pain, chest tightness, or
angina when doing your most strenuous level of activity?
I have had chest pain, chest tightness, or angina……
How often do you have chest pain, chest tightness, or angina when doing your most
strenuous level of activity in the latest 4 weeks? Compared with 4 weeks ago, do you
have chest pain, chest tightness, or angina much more often, slightly more often,
about the same, slightly less often, much less often, or you have had no chest pain
over the past 4 weeks?
(3) Over the past 4 weeks, on average, how many times have you had chest pain,
chest tightness, or angina?
I get chest pain, chest tightness, or angina……
4 or more
times per
day
1-3 times
per day
3 or more
times per
week but not
every day
1-2 times
per week
Less than
once a
week
None over
the past 4
weeks
4. Over the past 4 weeks, on average, how many times have you had to take nitros
(nitroglycerin tablets) for your chest pain, chest tightness, or angina?
4 or more
times per
day
1-3 times
per day
3 or more times
per week but not
every day
1-2 times
per week
Less than
once a
week
None over
the past 4
weeks

506
5. How bothersome is it for you to take your pills for chest pain, chest tightness or
angina as prescribed?
Very
bothersome
Moderately
bothersome
Somewhat
bothersome
A little
bothersome
Not
bothersome
at all
My doctor
has not
prescribed
pills
6. How satisfied are you that everything possible is being done to treat your chest pain,
chest tightness, or angina?
Not satisfied
at all
Mostly
dissatisfied
Somewhat
satisfied
Mostly
satisfied
Highly
satisfied
7. How satisfied are you with the explanations your doctor has given you about your
chest pain, chest tightness, or angina?
Not satisfied
at all
Mostly
dissatisfied
Somewhat
satisfied
Mostly
satisfied
Highly
satisfied
8. Overall, how satisfied are you with the current treatment of your chest pain,
tightness, or angina?
Not satisfied
at all
Mostly
dissatisfied
Somewhat
satisfied
Mostly
satisfied
Highly
satisfied
9. Over the past 4 weeks, how much has your chest pain, chest tightness, or angina
interfered with your enjoyment of life?

507
It has severely
limited my
enjoyment of
life
It has
moderately
limited my
enjoyment of
life
It has slightly
limited my
enjoyment of
life
It has barely
limited my
enjoyment of
life
It has not
limited my
enjoyment of
life
10. If you had to spend the rest of your life with your chest pain, chest tightness, or
angina the way it is right now, how would you feel about this?
Not satisfied
at all
Mostly
dissatisfied
Somewhat
satisfied
Mostly
satisfied
Highly
satisfied
11. How often do you worry that you may have a heart attack or die suddenly?
I can‘t stop
worrying
about it
I often think
or worry
about it
I
occasionally
worry about
it
I rarely
think or
worry
about it
I never
think or
worry
about it
508
Short Form 36 Health Survey Questionnaire (SF-36)
The following questions are to assess your opinion, feeling and ability to perform
daily activities. Please choose the answer that is closest to your condition for each
question.
1. In general, would you say your health is:
Excellent
Very good
Good
Fair
Poor
2. Compared to one year ago, how would you rate your health in general now?
Much better now than one year ago
Somewhat better now than one year ago
About the same as one year ago
Somewhat worse now than one year ago
Much worse now than one year ago
3. The following items about activities you might do during a typical day. Does your
health now limit you in these activities? If so, how much?
Limited a
lot
Limited a
little
Not
limited
Vigorous activities, such as running, lifting heavy
objects, participating in strenuous sports
Moderate activities, such as moving a table,
cleaning the floor
Lifting or carrying groceries
Climbing several flights of stairs
Climbing one flight of stairs
Bending, kneeling, or stooping

509
Walking 1500 meters
Walking 800 meters
Walking 100 meters
Bathing or dressing yourself
(1) Vigorous activities, such as running, lifting heavy objects, participating in
strenuous sports: Does your health now limit you in vigorous activities, such as
running, lifting heavy objects, participating in strenuous sports? If so, how much? Is it
limited a lot or a little?
(2) Moderate activities, such as moving a table, cleaning the floor: Does your
health now limit you in moderate activities, such as moving a table, cleaning the floor?
If so, how much? Is it limited a lot or a little?
(3) Lifting or carrying groceries: Does your health now limit you in lifting or
carrying groceries? If so, how much? Is it limited a lot or a little?
(4) Climbing several flights of stairs: Does your health now limit you in climbing
several flights of stairs? If so, how much? Is it limited a lot or a little?
(5) Climbing one flight of stairs: Does your health now limit you in climbing one
flight of stairs? If so, how much? Is it limited a lot or a little?
(6) Bending, kneeling, or stooping: Does your health now limit you in bending,
kneeling, or stooping? If so, how much? Is it limited a lot or a little?
(7) Walking 1500 meters: Does your health now limit you in walking 1500 meters?
If so, how much? Is it limited a lot or a little?
(8) Walking 800 meters: Does your health now limit you in walking 800 meters? If
so, how much? Is it limited a lot or a little?
(9) Walking 100 meters: Does your health now limit you in walking 100 meters? If
so, how much? Is it limited a lot or a little?
(10) Bathing or dressing yourself: Does your health now limit you in bathing or
dressing yourself? If so, how much? Is it limited a lot or a little?
4. During the past four weeks, have you had any of the following problems with your
work or other regular activities as a result of your physical health?

510
Yes No
Cut down on the amount of time you spent on work or other
activities
Accomplished less than you would like
Were limited in the kind of work or other activities
Had difficulty performing the work or other activities (for
example, it took extra effort)
(1) Cut down on the amount of time you spent on work or other activities: During
the past four weeks, have you had any of the problems with cutting down on the
amount of time you spent on work or other activities as a result of your physical
health?
(2) Accomplished less than you would like: During the past four weeks, have you
had any of the problems with accomplishing less than you would like on work or
other activities as a result of your physical health?
(3) Were limited in the kind of work or other activities: During the past four weeks,
have you had any of the problems with limiting in the kind of work or other activities
as a result of your physical health?
(4) Had difficulty performing the work or other activities (for example, it took
extra effort): During the past four weeks, have you had difficulty performing the
work or other activities (for example, it took extra effort) as a result of your physical
health?
5. During the past four weeks, have you had any of the following problems with your
work or other regular daily activities as a result of any emotional problems (such as
feeling depressed or anxious)?
Yes No
Cut down on the amount of time you spent on work or other
activities
Accomplished less than you would like
Did work or other activities less carefully than usual

511
(1) Cut down on the amount of time you spent on work or other activities: During
the past four weeks, have you had any of the problems with cutting down on the
amount of time you spent on work or other activities as a result of any emotional
problems (such as feeling depressed or anxious)?
(2) Accomplished less than you would like: During the past four weeks, have you
had any of the problems with accomplishing less than you would like on work or
other activities as a result of any emotional problems (such as feeling depressed or
anxious)?
(3) Did work or other activities less carefully than usual: During the past four
weeks, have you had any of the problems with work or other activities less carefully
than usual as a result of any emotional problems (such as feeling depressed or
anxious)?
6. During the past four weeks, to what extent has your physical health or emotional
problems interfered with your normal social activities with family, friends, neighbors,
or groups?
Not at all
Slightly
Moderately
Quite a bit
Extremely
7. How much bodily pain have you had during the past four weeks?
None
Very mild
Mild
Moderate
Severe
Very severe
8. During the past four weeks, how much did pain interfere with your normal work,
including work outside the home and housework?
Not at all

512
A little bit
Moderately
Quite a bit
Extremely
9. The net set of questions is about how you feel and how things have been with you
during the past four weeks. For each question, please give the one answer that comes
closest to the way you have been feeling.
How much of the time during the past
four weeks
All
the
time
Most
of
the
time
A
good
bit of
the
time
Some
of
the
time
A
little
of
the
time
None
of
time
Did you feel full of pep?
Have you been a very nervous person?
Have you felt so down in the dumps that
nothing could cheer you up?
Have you felt calm and peaceful?
Did you have a lot of energy?
Have you felt downhearted and blue?
Did you feel worn out?
Have you been a happy person?
Did you feel tired?
Has your physical health or emotional
problems interfered with your social
activities like visiting friends, relatives,
etc.
(1) Did you feel full of pep? During the past four weeks, how much of the time did
you feel full of pep? All the time, most of the time, a good bit of the time, some of the
time, a little of the time, or none of time?
(2) Have you been a very nervous person? During the past four weeks, how much
of the time have you been a very nervous person? All the time, most of the time, a
good bit of the time, some of the time, a little of the time, or none of time?

513
(3) Have you felt so down in the dumps that nothing could cheer you up? During
the past four weeks, how much of the time have you felt so down in the dumps that
nothing could cheer you up? All the time, most of the time, a good bit of the time,
some of the time, a little of the time, or none of time?
(4) Have you felt calm and peaceful? During the past four weeks, how much of the
time have you felt calm and peaceful? All the time, most of the time, a good bit of the
time, some of the time, a little of the time, or none of time?
(5) Did you have a lot of energy? During the past four weeks, how much of the time
did you have a lot of energy? All the time, most of the time, a good bit of the time,
some of the time, a little of the time, or none of time?
(6) Have you felt downhearted and blue? During the past four weeks, how much of
the time have you felt downhearted and blue? All the time, most of the time, a good
bit of the time, some of the time, a little of the time, or none of time?
(7) Did you feel worn out? During the past four weeks, how much of the time did
you feel worn out? All the time, most of the time, a good bit of the time, some of the
time, a little of the time, or none of time?
(8) Have you been a happy person? During the past four weeks, how much of the
time have you been a happy person? All the time, most of the time, a good bit of the
time, some of the time, a little of the time, or none of time?
(9) Did you feel tired? During the past four weeks, how much of the time did you
feel tired? All the time, most of the time, a good bit of the time, some of the time, a
little of the time, or none of time?
(10) Has your physical health or emotional problems interfered with your social
activities like visiting friends, relatives, etc. During the past four weeks, how much
of the time has your physical health or emotional problems interfered with your social
activities like visiting friends, relatives, etc. All the time, most of the time, a good bit
of the time, some of the time, a little of the time, or none of time?

514
10. How true or false is each of the following statements for you?
Definitely
true
Mostly
true
Don‘t
know
Mostly
false
Definitely
false
I seem to get sick a little easier
than other people
I am as healthy as anybody I
know
I expect my health to get worse
My health is excellent
(1) I seem to get sick a little easier than other people: Do you feel that you seem to
get sick a little easier than other people? Definitely true, mostly true, don‘t know,
mostly false, or definitely false?
(2) I am as healthy as anybody I know: Do you feel that you are as healthy as
anybody you know? Definitely true, mostly true, don‘t know, mostly false, or
definitely false?
(3) I expect my health to get worse: Do you feel that you expect your health to get
worse? Definitely true, mostly true, don‘t know, mostly false, or definitely false?
(4) My health is excellent: Do you feel that your health is excellent? Definitely true,
mostly true, don‘t know, mostly false, or definitely false?
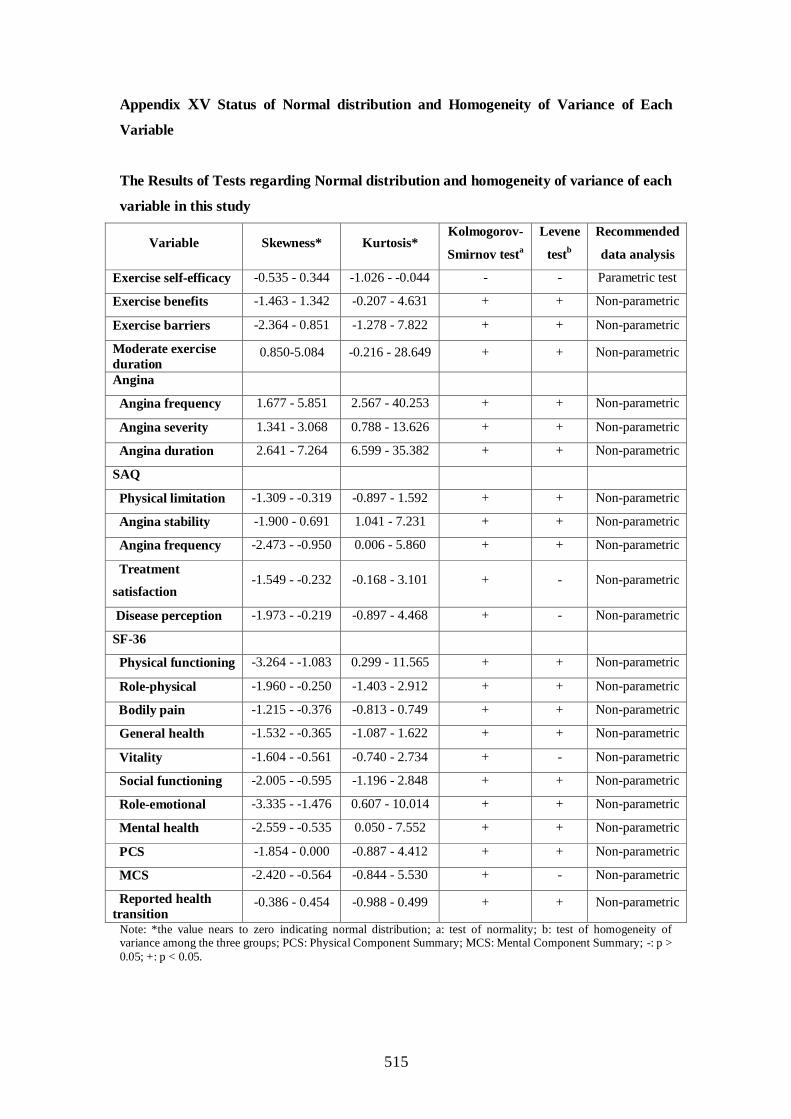
515
Appendix XV Status of Normal distribution and Homogeneity of Variance of Each
Variable
The Results of Tests regarding Normal distribution and homogeneity of variance of each
variable in this study
Variable Skewness* Kurtosis* Kolmogorov-
Smirnov testa
Levene
testb
Recommended
data analysis
Exercise self-efficacy -0.535 - 0.344 -1.026 - -0.044 - - Parametric test
Exercise benefits -1.463 - 1.342 -0.207 - 4.631 + + Non-parametric
Exercise barriers -2.364 - 0.851 -1.278 - 7.822 + + Non-parametric
Moderate exercise
duration 0.850-5.084 -0.216 - 28.649 + + Non-parametric
Angina
Angina frequency 1.677 - 5.851 2.567 - 40.253 + + Non-parametric
Angina severity 1.341 - 3.068 0.788 - 13.626 + + Non-parametric
Angina duration 2.641 - 7.264 6.599 - 35.382 + + Non-parametric
SAQ
Physical limitation -1.309 - -0.319 -0.897 - 1.592 + + Non-parametric
Angina stability -1.900 - 0.691 1.041 - 7.231 + + Non-parametric
Angina frequency -2.473 - -0.950 0.006 - 5.860 + + Non-parametric
Treatment
satisfaction -1.549 - -0.232 -0.168 - 3.101 + - Non-parametric
Disease perception -1.973 - -0.219 -0.897 - 4.468 + - Non-parametric
SF-36
Physical functioning -3.264 - -1.083 0.299 - 11.565 + + Non-parametric
Role-physical -1.960 - -0.250 -1.403 - 2.912 + + Non-parametric
Bodily pain -1.215 - -0.376 -0.813 - 0.749 + + Non-parametric
General health -1.532 - -0.365 -1.087 - 1.622 + + Non-parametric
Vitality -1.604 - -0.561 -0.740 - 2.734 + - Non-parametric
Social functioning -2.005 - -0.595 -1.196 - 2.848 + + Non-parametric
Role-emotional -3.335 - -1.476 0.607 - 10.014 + + Non-parametric
Mental health -2.559 - -0.535 0.050 - 7.552 + + Non-parametric
PCS -1.854 - 0.000 -0.887 - 4.412 + + Non-parametric
MCS -2.420 - -0.564 -0.844 - 5.530 + - Non-parametric
Reported health
transition -0.386 - 0.454 -0.988 - 0.499 + + Non-parametric
Note: *the value nears to zero indicating normal distribution; a: test of normality; b: test of homogeneity of variance among the three groups; PCS: Physical Component Summary; MCS: Mental Component Summary; -: p >
0.05; +: p < 0.05.

516
Appendix XVI – The results of the baseline outcome comparisons
1. Exercise Stages of Change
Table 1 shows that there is no significant difference in the distribution of exercise
stages of change among the C, PE and ESMI groups at baseline (T0).
Table 1 Distribution of exercise stages of change at T0
C
(n=67)
n (%)
PE
(n=64)
n (%)
ESMI
(n=65)
n (%)
Kruskal-Wallis test
χ2 p
Precontemplation 10(14.9) 17(26.6) 11(16.9) 3.233 0.199
Contemplation 9(13.4) 9(14.1) 17(26.2)
Preparation 48(71.6) 38(59.4) 37(56.9)
2. Exercise Self-Efficacy (ESE)
Table 2 shows that no significant difference in exercise self-efficacy scores was found
among the three groups at baseline (T0).
Table 2 Exercise Self-Efficacy (ESE) at T0
C
(n=67)
mean(SD)
PE
(n=64)
mean(SD)
ESMI
(n=65)
mean(SD)
One-way ANOVA
F p
ESE 843.3(305.0) 809.5(307.6) 800.5(294.8) 0.368 0.692

517
3. Exercise Decisional Balance
Exercise decisional balance includes Exercise Benefits Scale (EBS) and Exercise
Barriers Scale (EBBS). As shown in Table 3, no significant differences were found in
exercise benefits and barriers scales among the three groups at baseline (T0).
Table 3 Exercise Benefits Scale (EBS) Scores and Exercise Barriers Scale (EBBS) Scores
at T0
C group
(n=67)
mean (SD)
PE group
(n=64)
mean (SD)
ESMI group
(n=65)
mean (SD)
df
Kruskal-Wallis test
χ2 p
EBS 82.5(7.6) 83.7(8.0) 82.6(7.0) 2 0.032 0.984
EBBS 29.1(2.8) 29.0(3.8) 29.5(2.8) 2 0.175 0.916
4. Exercise
Table 4 shows that no significant difference was detected in both the total exercise
duration (minute/week) and moderate exercise duration (minute/week) among the
three groups at baseline (T0).
Table 4 Exercise Duration (minutes/week) at T0
C group
(n=67)
mean (SD)
PE group
(n=64)
mean (SD)
ESMI group
(n=65)
mean (SD)
df
Kruskal-Wallis test
χ2 p
TED 184.2(217.8) 143.1(196.9) 112.2(162.1) 2 3.858 0.145
MED 17.2(62.9) 10.0(40.9) 15.4(36.2) 2 2.320 0.314
Note: TED: Total Exercise Duration (minute/week); MED: Moderate Exercise Duration (minute/week).

518
5. Angina
Tables 5and 6 show that no significant difference was found in the angina frequency
(episode/week), angina severity, angina duration (minute/week), angina attack, and
anti-anginal drugs taken among the three groups at baseline (T0).
Table 5 Angina Frequency, Angina Severity and Angina Duration at T0
C group
(n=67)
mean (SD)
PE group
(n=64)
mean (SD)
ESMI group
(n=65)
mean (SD)
df
Kruskal-Wallis test
χ2 p
AF 1.4(3.1) 1.1(2.8) 0.9(1.4) 2 0.240 0.887
AS 0.7(1.2) 0.7(1.1) 0.5(0.7) 2 0.232 0.891
AD 13.4(33.0) 9.8(23.0) 9.3(29.4) 2 0.374 0.829
Note: AF: Angina Frequency (episodes/week); AS: Angina Severity (0-10); AD: Angina Duration
(minutes/week).
Table 6 Items on whether patients have angina attack and anti-anginal drugs taken in
the past one week at T0
C group
(n=67)
n (%)
PE group
(n=64)
n (%)
ESMI group
(n=65)
n (%)
Chi-square test
χ2 p
Angina
attack
Yes 27(40.3) 25(39.1) 25(38.5) 0.049 0.976
No 40(59.7) 39(60.9) 40(61.5)
Anti-anginal
drugs taken
Yes 17(25.4) 12(18.8) 12(18.5) 1.223 0.543
No 50(74.6) 52(81.2) 53(81.5)

519
6. Quality of life
In this study, quality of life was assessed by using Seattle Angina Questionnaire (SAQ)
and SF-36.
6.1 Seattle Angina Questionnaire (SAQ)
As shown in Table 7, no significant difference was found in each subscale scores of
SAQ among the three groups at T0.
Table 7 Subscale Scores of SAQ at T0
C group
(n=67)
mean (SD)
PE group
(n=64)
mean (SD)
ESMI group
(n=65)
mean (SD)
df
Kruskal-Wallis test
χ2 p
Physical
limitation 85.5(13.1) 85.9(13.0) 82.0(12.9) 2 4.453 0.108
Angina
stability 47.0(20.7) 50.8(20.4) 51.5(20.7) 2 2.092 0.351
Angina
frequency 83.3(18.1) 84.1(19.7) 83.5(17.6) 2 0.472 0.790
Treatment
satisfaction 69.9(20.1) 68.8(18.5) 66.9(17.5) 2 1.328 0.515
Disease
perception 71.1(21.9) 69.8(21.8) 68.1(17.7) 2 1.499 0.473
6.2 SF-36
As shown in Table 8, no significant difference was found in each subscale scores and
total scores of SF-36 among the three groups at T0.

520
Table 5.15 Subscale Scores of SF-36 at T0
C group
(n=67)
mean (SD)
PE group
(n=64)
mean (SD)
ESMI group
(n=65)
mean (SD)
df
Kruskal-Wallis test
χ2 p
PF 81.4(13.6) 82.3(9.7) 78.8(16.2) 2 0.418 0.811
RP 72.0(40.0) 63.7(39.6) 67.3(39.3) 2 1.955 0.376
BP 73.7(24.8) 75.4(22.1) 75.4(22.9) 2 0.155 0.925
GH 57.4(22.8) 55.4(22.3) 57.9(23.4) 2 0.615 0.735
VT 72.5(17.6) 70.9(17.1) 68.8(18.8) 2 1.052 0.591
SF 84.5(22.1) 79.3(23.8) 80.6(21.7) 2 2.110 0.348
RE 80.6(34.9) 84.9(27.8) 79.0(36.1) 2 0.351 0.839
MH 83.0(13.9) 80.4(10.4) 80.4(12.8) 2 4.911 0.086
PCS 284.5(76.9) 276.8(65.1) 279.5(75.8) 2 1.236 0.539
MCS 320.6(67.6) 315.6(59.0) 308.8(72.2) 2 1.072 0.585
TS 605.1(124.4) 592.3(112.2) 588.3(136.1) 2 1.014 0.602
HT 3.3(1.1) 3.1(1.3) 3.3(1.1) 2 1.697 0.428
PF: Physical Functioning; RP: Role-Physical; BP: Bodily Pain; GH: General Health; VT: Vitality; SF:
Social Functioning; RE: Role-Emotional; MH: Mental Health; PCS: Physical Component Summary
(PF + RP + BP + GH); MCS: Mental Component Summary (VT + SF + RE + MH); TS: Total Scores
of SF-36 (PF + RP + BP + GH + VT + SF + RE + MH); HT: Reported Health Transition.




524
Appendix IV Screening Guidelines – Chinese Version
筛查标准指引
以下是一些条目帮助心血管医生了解每位病人是否适合参与本研究项目,
即时期匹配运动干预的项目。如果以下条目中,病人有一项不符合标准,则不
建议参与本研究。
1.年龄__________岁
符合:年龄 ≥ 18 岁。
不符合:年龄 < 18 岁。
2. 是否居住在厦门
符合:病人居住在厦门并有联系电话。
居住地址:______________________________________________
联系电话:______________________________________________
不符合:病人没有居住在厦门或没有联系电话。
3.病人的沟通和阅读汉字的能力:
符合:病人能进行沟通并有阅读能力。
不符合:病人沟通困难或沟通障碍,或病人有阅读困难。
注释:
① 能进行沟通:是指病人能明白沟通内容,可以互相沟通,语言表达准确。
② 沟通困难/沟通障碍:是指病人不能明白沟通内容,词不达意或不能沟
通。
③ 有阅读能力:是指病人能看懂基本的汉字并明白其意思。
④ 阅读困难:是指病人一点都看不懂汉字。
4.疾病诊断:心绞痛、心肌梗塞、冠状动脉介入治疗术后
符合:病人被诊断为心绞痛或心肌梗塞三个月以上,或经皮冠状动脉介入
治疗术后三个月以上。
不符合:病人被诊断为心绞痛或心肌梗塞三个月以内,或经皮冠状动脉介
入治疗术后三个月以内。
525
注释:
A.心绞痛 ,诊断时间_________(月/年)
诊断依据: 根据 1979 年国际心脏病学会和协会及世界卫生组织的诊断标准:
1) 病史:有典型心绞痛发作病史,即由劳累或情绪激动诱发胸部不适,通常
持续 1-15 分钟,可放射至下颌、咽喉、肩、背、左臂或腕部,休息或舌下
含化硝酸甘油数分钟即可缓解。
2) 男性 40 岁、女性 45 岁以上的病人,休息时心电图有明显心肌缺血表现,
或心电图运动试验阳性,无其它原因(各种心脏病、植物神经功能失调、
显著贫血、阻塞性肺气肿、服用洋地黄、电解质紊乱)可查,并有下列三
项中的两项者:高血压、高胆固醇血症、糖尿病。
3) 或经冠状动脉造影确诊的患者,即管腔直径狭窄 70%以上。
B. 心肌梗塞 (_______次),诊断时间_________(月/年)
诊断依据:根据 1979 年全国中西医结合防治冠心病、心绞痛、心律失常研究座
谈会(于上海)修订的诊断标准:
I.有下列三项之二,可诊断为急性心肌梗塞:
1) 临床症状典型:典型的病史是出现严重而持久的胸痛;
2) 心电图有异常 Q 波及/或 ST-T 有符合心肌梗塞的衍变;
3) 血清酶增高,符合心肌梗塞的过程者。
II. 有肯定资料(如心电图或血清酶)证明以往患过心肌梗塞
C.冠状动脉介入治疗术后(______次),介入治疗时间_________(月/年)
诊断依据:包括经皮冠状动脉成型术(PTCA)、冠状动脉支架置入术、冠状动脉
斑块旋磨术、激光血管成型术等技术。
5.是否病情稳定
符合:病人病情稳定。
不符合:病人病情不稳定。
注释:
病人的病情稳定与否,由心血管医生判断决定。参考指标如下:
① 病情稳定:病人生命体征平稳,即呼吸、脉搏、血压和体温基本在正常范围
内(具体测量方法参见下文);没有发烧(口腔温度低于 37.5℃);没有不稳
定型心绞痛或急性心肌梗塞表现。
6.是否有不稳定型心绞痛
符合:病人没有不稳定型心绞痛。
不符合:病人有不稳定型心绞痛。
注释:
(1)稳定型心绞痛:病人病情稳定,在近三个月时间内,心绞痛发作的频度、
诱因、疼痛的部位、性质及持续时间(3-5 分钟/次)大致相同。多数病人能
预知在什么情况下(如走多远、走多快、上多少台阶等)会发生心绞痛。
(2)不稳定型心绞痛:主要包括 5 种类型
6)初发性心绞痛:指病人过去从未发生过心绞痛,近 1 个月内突然出现频

526
繁的劳累后心绞痛,可恶化发展成心肌梗死。
7)恶化性心绞痛:病人原有心绞痛病史,近来突然发作更频繁,疼痛程度
加重,常持续 15 分钟以上,用硝酸甘油效果不明显。
8)静息性心绞痛:心绞痛发作在卧位或休息睡眠时,疼痛剧烈,常被迫坐
起或站立。
9)变异性心绞痛:临床表现与静息性心绞痛相似,但发作时心电图有关导
联 ST 段抬高,为冠状动脉突然痉挛所致,病人迟早会发生心肌梗死。
10) 梗死后心绞痛:在急性心肌梗死 1 个月后又反复发作心绞痛,提
示有可能再次发生心肌梗死。
7.是否曾经参加过任何有关心脏康复的项目
符合:病人没有参加过任何有关心脏康复的项目。
不符合:病人曾经参加过任何有关心脏康复的项目。
注释:
(2) 参加有关心脏康复的项目:是指参加过任何系统的冠心病健康教育、有
组织的运动训练、或心脏康复指导及危险因素的控制等活动项目。
8.是否有认知功能障碍
符合:病人没有认知功能障碍。
不符合:病人有认知功能障碍。
注释:
(1)有下列一项,可认为病人有认知功能障碍:
5)被诊断有精神疾病
6)被诊断有老年痴呆症
7)被诊断有智力低下
8)脑中风或脑外伤后出现失语或失认现象
9.是否有精神抑郁症
符合:病人没有精神抑郁症。
不符合:病人有精神抑郁症。
注释:
(1) 在本研究中,精神抑郁症是指根据医院焦虑和抑郁量表-抑郁分量表
(HADS-D)得分在 11 分以上者。
10.重度主动脉瓣狭窄
符合:病人没有重度主动脉瓣狭窄。
不符合:病人曾经被诊断为重度主动脉瓣狭窄。
注释:
(6) 正常主动脉瓣口面积 在 3.0cm2 以上。当瓣口面积减小为 1.5cm
2 时为轻
度狭窄;1.0cm2 时即可产生明显压力阶差,为中度狭窄;< 0.75cm
2 时可

527
出现临床症状,为重度狭窄。
(7) 主动脉狭窄的常见病因为风湿性瓣膜炎、先天性畸形和老年退行性改变
所致。
(8) 重度主动脉狭窄的特征性症状包括心绞痛、晕厥、心衰或猝死,且一旦
出现症状常呈进行性恶化,如不进行手术治疗,平均 2-3 年内死亡。典
型的体征是收缩期杂音以胸骨右缘第二肋间和胸骨左缘第 3、第 4 肋间
最明显,在吸入亚硝酸异戊酯或平卧时增强,在应用升压药或站立时减
弱。一般主动脉狭窄越重,杂音越强,强度达 3-4/6 级多伴有震颤,且向
颈部、锁骨上窝及心尖区传导。
(9) 实验室检查:多数病例 X 线检查可见主动脉狭窄后扩张、主动脉瓣钙
化;心电图检查约 85%患者示左室肥厚;超声心动图检查可显示主动脉
开放幅度小于 15mm,开放速度减慢,瓣叶增厚;Doppler 超声可测定心
脏及血管内的血流速度,通过测定主动脉瓣血流速度可计算出最大跨瓣
压力阶差,亦可计算出主动脉瓣口面积;心导管检查是肯定主动脉瓣狭
窄诊断,且对其严重度作出判断,由于此检查是创伤性检查,一般不作
为常规检查。
(10)根据病人的病史、典型症状和体征以及实验室检查(X 线、心电图和超
声心动图),一般可以做出诊断。
11.心功能状况 ,按纽约心脏病学会(NYHA)心功能分级:
符合:按 NYHA 心功能分级,病人心功能状况为 I 或 II 级。
不符合:按 NYHA 心功能分级,病人心功能状况为 III 或 IV 级。
注释:
① I 级:活动量不受限制
② II 级:活动量轻度受限制,重体力活动时,患者出现疲乏、心悸、呼吸困难
或心绞痛。
③ III 级:活动量重度受限制,轻度体力活动时,患者出现疲乏、心悸、呼吸困
难或心绞痛。
④ IV级:患者不能从事体力活动,休息状态下亦有疲乏、心悸、呼吸困难或心
绞痛。
12.糖尿病
符合:病人没有糖尿病,或病人有糖尿病,但血糖控制在理想水平(空腹
血糖在 15mmol/L 以下)。
不符合:若在正常使用降血糖药情况下,目前病人血糖水平 ≥ 15mmol/L。
注释:
(3) 糖尿病诊断依据:早晨空腹血糖水平 ≥ 7.0mmol/L、任意时间 或 OGTT
中 2 小时血糖 ≥ 11.1mmol/L 均可诊断为糖尿病。
(4) 血糖的测量以左侧无名指末端的毛细血管血,用血糖测量仪测得血糖值
为准。

528
13.高血压
符合:病人没有高血压,或病人有高血压,但血压控制较好,在服用抗高
血压药情况下,目前收缩压 < 23.94kPa (180mmHg)或舒张压 < 14.67 kPa
(110mmHg)。
不符合:病人有高血压,在服用抗高血压药情况下,目前收缩压 ≥
23.94kPa (180mmHg)或舒张压 ≥ 14.67 kPa (110mmHg)。
注释:
(3) 高血压诊断依据:采用 1997 年美国高血压全国联合委员会发表的高血压
判断标准,即安静休息状态下,收缩压 ≥ 18.6kPa (140mmHg)或舒张压 ≥
12.0 kPa (90mmHg)均可诊断为高血压。
(4) 血压测量的标准:
6)应用水银血压计测量右侧肱动脉的血压;
7)病人测量血压前应情绪稳定, 测量前休息 15 分钟。若测量前有下列情
况发生:吸烟、运动、情绪变化等,应休息 20-30 分钟后再测量。
8)病人取坐位,手臂(肱动脉)位置与心脏在同一水平,平第四肋。
9)袖带下缘距肘窝 2-3cm,松紧以能插入一指为宜。
10) 当听诊器中出现第一声搏动,此时水银柱所指的刻度,即为收缩
压;当搏动声突然变弱或消失,此时水银柱所指的刻度即为舒张压。
14.是否有心律失常。 心率_________次/分钟
符合:病人心律规则,脉率在 60-100 次/分钟 。
不符合:病人有窦性心动过速(脉率 ≥ 120 次/分钟)。
注释:
(1)用脉率表示心率,脉搏测量的方法如下:
5)测量右侧桡动脉的脉率
6)病人准备:取坐位,情绪稳定, 测量前休息 15 分钟。若测量前有下列
活动:剧烈运动、紧张、恐惧等,应休息 20-30 分钟后再测量。
7)测量者以示指、中指、无名指的指端按压在患者桡动脉处测量。
8)使用有秒针的表,测脉搏 30 秒,乘以 2。
15.是否有心房颤动
符合:病人没有心房颤动。
不符合:病人有心房颤动。
注释:
(1)心房颤动的临床表现:心脏听诊第一心音强度变化不定,心律极不规则。
当心室率快时可发生脉搏短绌,即脉率小于心率。
16.是否有室性心律不齐
符合:病人心律规则,没有出现室性心律不齐。

529
不符合:病人出现频发室性期前收缩(≥ 5 次/分钟)、成对室性期前收缩
或室性心动过速(脉率 ≥ 120 次/分钟)、心室扑动或心室颤动的患者。
注释:
(2) 室性心律不齐:最常见的是室性期前收缩。室性期前收缩常无与之直接
相关的症状。患者可感到心悸,类似电梯快速升降的失重感或代偿间歇
后有力的心脏搏动。听诊时,室性期前收缩后出现较长的停歇,室性期
前收缩之第二心音强度减弱,仅能听到第一心音。桡动脉搏动减弱或消
失。
17.是否有三度房室传导阻滞
符合:病人没有三度房室传导阻滞。
不符合:病人有三度房室传导阻滞。
注释:三度房室传导阻滞的特征如下:
(4) 心房与心室活动各自独立、互不相关;
(5) 心房率大于心室率,心房冲动来自窦房结或异位心房节律(房性心动
过速、扑动或颤动);
(6) 心室起搏点通常在阻滞部位稍下方。
18.是否有急性心肌炎
符合:病人没有急性心肌炎。
不符合:病人有急性心肌炎。
注释:
(3) 急性心肌炎:指新近发病,临床症状如心前区不适、心率增快、胸闷、
心悸、心动过速等明显且多变,实验室检查如心肌酶谱升高,心电图示
ST 段抬高或压低和 T 波倒置、心律失常,心脏超声有左心室壁弥漫性或
局限性收缩幅度减低等变化,病程多在 6 个月以内。多数以病毒性心肌
炎为常见。
(4) 病毒性心肌炎的诊断:目前分离出病毒以确诊为病毒性心肌炎的方法只
有在少数医院采用,大多数医院的诊断仅仅是通过临床症状、心电图及
酶学检查的结果推测出来的。
19.是否有急性心包炎
符合:病人没有急性心包炎。
不符合:病人有急性心包炎。
注释:
(1)急性心包炎的症状:
1) 心前区疼痛:心前区疼痛常于体位改变、深呼吸、咳嗽、吞咽、卧位尤
其当抬腿或左侧卧位时加剧,坐位或前倾位时减轻;

530
2) 心脏压塞的症状:可出现呼吸困难、面色苍白、烦躁不安、紫绀、乏
力、上腹部疼痛、浮肿、甚至休克;
3) 心包积液对邻近器官压迫的症状:呼吸困难、咳嗽或声音嘶哑、或咽下
困难等;
4) 全身症状:发冷、发热、心悸、出汗、乏力等症状,与原发疾病的症状
常难以区分。
(2)急性心包炎的体征:
1)心包摩擦音
2)心包积液的体征:
• 心脏体征:心尖搏动减弱、消失或出现于心浊音界左缘内侧处。心浊音
界向两侧扩大、相对浊音区消失,患者由坐位转变为卧位时第二、三肋
间的心浊音界增宽。心音轻而远,心率快。少数患者在胸骨左缘第三、
四肋间可听得舒张早期额外者(心包叩击音),呈拍击样。
• 左肺受压迫的征象:有大量心包渗液时,心脏向后移位,压迫左侧肺
部,可引起左肺下叶不张。左肩胛肩下常有浊音区,语颤增强,并可听
到支气管呼吸音(E wart 征)。
• 心脏压寒的征象:出现明显的心动过速,静脉压显著升高,可产生颈静
脉怒张,搏动和吸气时扩张,肝肿大伴触痛,腹水,皮下水肿和肝-颈静
脉反流征阳性等体循环淤血表现。动脉收缩压降低,脉压减小,脉搏细
弱,可出现奇脉。
20.近三个月有血栓栓塞史
符合:病人近三个月没有血栓栓塞史。
不符合:病人近三个月有血栓栓塞史。
注释:
(2) 血栓栓塞性疾病:包括心肌梗死、脑血管病、肺血栓栓塞、深静脉血
栓、弥漫性血管内凝血(DIC)及其他多种疾病。
21.是否有影响运动或由于运动而病情加重的急性非心脏性疾病,如感染、肾
功能衰竭、甲亢等
符合:病人没有影响运动或由于运动而病情加重的急性非心脏性疾病,如
感染、肾功能衰竭、甲亢等。
不符合:病人有影响运动或由于运动而病情加重的急性非心脏性疾病,如
感染、肾功能衰竭、甲亢等。
注释:
I.急性感染
(1)感染:病人现场测量口腔温度 ≥ 37.5℃,则认为病人有感染(体温
______℃)
(2)体温测量方法:
5)应用水银体温计测量口温
6)病人取舒适体位,情绪稳定。测量体温前若有下列活动,如运动、进
食、冷热饮、冷热敷、洗澡、坐浴、灌肠等,应休息30分钟后再测量。
531
7)将水银体温计甩至35℃以下
8)将口表水银端斜放于舌下热窝处闭口,测量3分钟。
II.急慢性肾功能衰竭
5) 急性肾功能衰竭:是由各种原因引起的肾功能在短时间内(几小时至几
周)突然下降而出现的氮质废物滞留和尿量减少综合征。主要表现为氮
质废物血肌酐(Cr)和尿素氮(BUN)升高,水、电解质和酸碱平衡紊
乱,及全身各系统并发症。常伴有少尿(< 400ml/d),但也可以无少尿表
现。
6) 急性肾功能衰竭的诊断一般是基于血肌酐的绝对或相对值的变化来诊
断,如血肌酐绝对值每日平均增加44.2umol/L或88.4umol/L;或在24~72
小时内血肌酐值相对增加25%~100%。
7) 慢性肾功能衰竭:是指慢性肾脏病引起的肾小球滤过率(GFR)下降及
与此相关的代谢紊乱和临床症状组成的综合征。
8) 慢性肾功能衰竭的诊断,根据病史、体征和实验室检查即可做出诊断。
III.甲状腺功能亢进症(甲亢)
(1)甲亢的诊断:具备以下三项,诊断即可成立。
4)高代谢症状和体征
5)甲状腺肿大
6)血清TT4 、FT4增高,TSH减低。

532
Appendix V Information Sheet – Chinese Version
有关资料
时期匹配运动干预对冠心病患者的效果研究
诚邀您参加由何淑贞博士、薛咏红博士、阮国强副主任医师(心脏病专科医师)
和谢强主任医师(心脏病专科医师)负责监督,朱丽霞同志负责执行的研究计
划。朱同志是香港理工大学护理学院学生。
这项研究的目的是评估时期匹配运动干预对冠心病患者的效果。根据随
机分配的原则,您可能会参与不同的研究组别。研究活动包括如常的护
理服务或 2 小时的健康教育±为期 8 周的时期匹配运动行为干预活
动。这 8 周的干预是要每周进行 1 次 1 5 -3 0 分钟的干预活动。无论您
是属于那一组别,您都要在干预开始之前、干预结束时和干预结束后 3
个月和 6 个月填写一些问卷。
规律运动已被证实对心脏病患者有益 ,所以时期匹配运动干预旨在引导
冠心病患者运动将会对参与本研究的患者有益。然而,在运动期间,您
可能会出现轻微的胸部不适。为减少可能出现的胸部不适,在您参与研
究之前 , 一名心脏专科医生将评估您的身体和心理精神状况、开具运动
剂量和监督您的运动进度。如果在运动过程中有出现任何不适,可以随
时与朱丽霞同志联络 ,寻求帮助。
您享有充分的权利在研究开始之前或之后决定退出这项研究,而不会受到任何
对您不正常的待遇或被追究责任。凡有关您的资料将会保密及加上编码。所有
资料,只有研究人员得悉。
如果您对这项研究有任何的不满,可随时与香港理工大学人类实验对象操守小
组委员会秘书吕小姐联络(地址:香港理工大学研究事务处 M502 室转交)。如果
您想获得更多有关这项研究的资料,请与朱丽霞同志联络,或联络她的导师何
淑贞博士。
谢谢您参与这项研究
主要研究员(PI)
朱丽霞

533
Appendix VI Consent Form – Chinese Version
参 与 研 究 同 意 书
时期匹配运动干预对冠心病患者的效果研究
本人____________同意参加由何淑贞博士、薛詠红博士、阮国强副主任医师和
谢强主任医师负责监督,朱丽霞同志执 行 的 研 究 项 目
我 理 解 此 研 究 所 获 得 的 资 料 可 用 于 未 来 的 研 究 和 学 术 交 流 然 而
我 有 权 保 护 自 己 的 隐 私 , 我 的 个 人 资 料 将 不 能 泄 漏
我 对 所 附 资 料 的 有 关 步 骤 已 经 得 到 充 分 的 解 释 我 理 解 可 能 会 出
现 的 风 险 我 是 自 愿 参 与 这 项 研 究
我 理 解 我 有 权 在 研 究 过 程 中 提 出 问 题, 并 在 任 何 时 候 决 定 退 出 研
究 而 不 会 受 到 任 何 不 正 常 的 待 遇 或 被 追 究 责 任
参 加 者 姓 名:
参 加 者 签 名:
父 母 姓 名 或 监 护 人 姓 名 : (如 需 要)
父 母 或 监 护 人 签 名: (如 需 要)
研 究 人员 姓 名: 朱丽霞
研 究 人员 签 名:
日 期:

534
Appendix VII Protocol of Weekly Patient Education Session – Chinese Version
每周健康教育的协议书
(I)核对依从性
1. 在过去的一周里,您做运动了吗?
2. 做了什么运动?
3. 在过去的一周里,您做了几天运动?
4. 每天做多久运动?
5. 您的活动日志上记录的自我辛苦评估指数是多少?
6. 运动时您有什么感觉?是否呼吸增快?是否出汗?
7. 运动过程中有什么不舒服吗?
8. 是否因为运动服用了抗心绞痛药物?若有,那服用了多少片/粒?
(II)健康教育
1. 讲解规律运动的益处和重要性。

535
Appendix VIII Guidelines for Exercise Prescription – Chinese Version
冠心病病人的运动处方
A. 运动处方时应注意的一般规则 (运动处方网站,2009)
建议
运动模式 • 任何使用大肌群的身体活动
• 例如:步行(3.0-4.0 英里/小时,相当于 4.8-6.4 公里/小
时)、慢骑自行车(13-19 公里/小时)等 [参见中等强度活
动的例子]
运动强度 • 中等剧烈程度 (3-6METs 的活动)[参见中等强度活动的
例子]
• 起始强度一般较健康人士的建议强度为低
运动所需时
间
• 通常较健康人士长
• 每天连续或累积进行 30-60 分钟运动(每次至少 10 分钟)
运动次数 • 通常较健康人士多
• 以一周最少五天较为合适,每天进行更佳
运动进度 • 通常较健康人士缓慢
• 根据每人的能力、目标与喜好而定
• 目标之一应该是增加带氧能力及减低最大心肌氧气的需求
(submaximal myocardial oxygen demands)。
特别考虑 • 处方的活动须切合个人目标。
• 活动须有趣及易于进行。
• 於开具运动处方时,应小心评估及考虑所服药物、进餐时
间、相关并发症/缺陷/损伤/风险等因素,以及所有可
能因运动而恶化,但无明显临床病征的健康问题。
• 留意各种异常症状(如胸痛、头晕、心律不正常等),以
便对运动处方作出适当的修正。
• 体适能水平较低的病人,其运动计划应以较低强度起首。
• 运动后数小时可能出现血糖过低的情况。

536
B. 冠心病病人的运动处方方案 (运动处方网站,2009)
基本作用 增强心脏功能,减少心绞痛和心梗的发生率,提高生活质量
运动模式 带氧运动为主, 如:步行(4.8-6.4 公里/小时) [具体参
见中等强度活动的例子]
参考中等强度活动的例子,选择一项或几项您感兴趣的活
动来执行
运动强度 中等强度运动(3-6 METs)
活动必须达到一定的强度才有效果,对冠心病患者来说,
活动达到中等强度为宜。您可以应用自我辛苦评估指数
(RPE)来判断您的活动水平。您的活动必须达到 RPE
11-13,即感觉轻松至有点辛苦为准。
运动所需时间 每天 30-60 分钟,每次至少 10 分钟
运动次数 一周至少五天
运动停止指征 若出现以下的症状或体征,马上停止运动 (Briffa, Maiorana,
Sheerin et al., 2006):
• 典型的胸痛或胸部不适,或放射到肩部、下颌部、颈
部或手臂;或感受到以前心肌梗塞的症状;
• 眩晕、头晕或身体虚弱;
• 呼吸困难或气喘
• 不典型出汗
• 过度疲倦
• 腿痛限制其功能
• 身体无法继续运动
特别考虑 应结合考虑病人的健康状况、性格、喜好和服药情况等开运
动处方
联络方式 若运动过程中出现任何不适,可随时与研究者联系。

537
中等强度活动的例子(3-6 METs)
(摘自 Ainsworth, Haskell, Whitt et al., 1993)
活动类型 METs 中等强度的活动例子
运动 3.3-5.0 散步(4.8-6.4 公里/小时)
4.5 打羽毛球(非竞赛性的)
6.0 篮球(非竞赛性的)
3.0 保龄球
4.0 乒乓球
4.0 太极拳
5.0 双打网球
3.0 排球(非竞赛性的)
5.0 垒球或棒球
6.0 游泳(非竞赛性的)
4.0-6.0 慢骑自行车(13-19 公里/小时)
3.0-5.5 踏固定脚踏车(50-100 瓦)
6.0 郊游(徒步),爬山
保健操和跳
舞
3.5 健身操(一般的,家里运动,如:背部运动)
4.0 体操(一般的)
4.8 跳扭秧歌、爵士舞、吉特巴舞
3.0-4.5
迪斯科、民族舞、广场舞、华尔兹舞、慢舞或探戈
舞
4.0 打鼓(腰鼓)
日常活动 3.5 拖地板
3.0-3.5 爬楼梯(上下楼梯)
4.0-5.0 走/跑:与小孩一起玩(仅活动期间)
3.0-4.5 走路(4.0-5.6 公里/小时,手提少于 22.5 斤的物
品)
Reference
Ainsworth, B.E., Haskell, W.L., Whitt, M.C., Irwin M.L., Swartz A.M., Strath S.J. et
al. (1993). Compendium of physical activities: an update of activity codes and
MET intensities. Medicine & Science in Sports & Exercise, 32(9), s498-s516.
Exercise prescription website. (2009). Prescription guidelines. Available at:
http://exerciserx.cheu.gov.hk/html/eng/index.asp?n=sec2_Guidelines (accessed
April 2009).
Briffa, T.G., Maiorana, A., Sheerin, N.J., Stubbs, A.G., Oldenburg, B.F., Sammel,
N.L. & Allan, R.M. (2006). Physical activity for people with cardiovascular
disease: recommendations of the National Heart Foundation of Australia.
Medical Journal of Australia, 184(2), 71-75.

538
C. 行动前身体状况记录
一名心血管医生评估病人身体状况。以下是一些条目帮助心血管医生了解
每位病人的身体状况,以便了解该病人是否适合开始运动,即进入行动阶段。
如果该病人可以进入行动阶段,则医生将帮助病人开出运动处方,确保病人运
动安全。同时,帮助病人在家里运动时可以自行监测。
1.血压_________毫米汞柱
2.心率/脉率_________次/分钟
3.是否病情稳定 ① 是 ② 否
4.是否有不稳定型心绞痛 ① 是 ② 否
5.心功能状况 ,按纽约心脏病学会(NYHA)心功能分级:
① I 级:活动量不受限制
② II 级:活动量轻度受限制,重体力活动时患者出现疲乏、心悸、呼吸困难
或心绞痛。
③ III 级:活动量重度受限制,轻度体力活动时患者出现疲乏、心悸、呼吸
困难或心绞痛。
④ IV 级:患者不能从事体力活动,休息状态下亦有疲乏、心悸、呼吸困难
或心绞痛。
6.是否有窦性心动过速(> 120 次/分) ①是 ② 否
7.是否有心房颤动 ①是 ② 否
8.是否有室性心律不齐 ①是 ② 否
9.是否有三度房室传导阻滞 ①是 ② 否
10.是否有重度主动脉瓣狭窄 ①是 ② 否
11.是否有急性心肌炎 ①是 ② 否
12.是否有急性心内膜炎 ①是 ② 否

539
13.近三个月有栓塞史 ①是 ② 否
14.是否有影响运动或由于运动而病情加重的急性非心脏性疾病,如感染、肾
功能衰竭、甲亢等 ①是 ② 否
评估结果:该病人是否可以进行运动 ①可以 ②不可以
心血管医生签名: ____________________
日期: ______________________________

540
D. 运动处方记录表
建议的运动形式
运动时间(分/天)
运动强度(RPE)
运动次数(次/周)
运动的进度
自我辛苦评估指数(RPE)
心血管医生签名: ________________ 日期: ________________
很
轻
松
轻松
有
点
辛
苦
辛苦
很
辛
苦
非
常
辛
苦
非
常
轻
松

541
Appendix IX Exercise Stage-Matched Pamphlets – Chinese Version
香港理工大学护理学院
意向前期小册子

542
内容提要:
我为什么要运动?
我如何才能变得更积极
积极生活方式的要点
回忆我曾经成功改变的习惯
琳达的传奇故事
运动:它能给我什么?
「。。。获得规律运动的好
处,您不一定要走出去或花
几个小时在健身房里」

543
有许多的理由可以问答这个难题——您为什么要运动?每个人都有自己的
理由去参与运动,从运动后的良好感觉到期待几个月甚至长期的健康和长寿等
益处都是您需要运动的理由。
规律运动的长期好处您可能很熟悉了。每个人都知道运动可以降低患冠心
病、糖尿病、甚至癌症的危险。不要惊讶于运动带来这么多健康的益处,规律
的运动还可以延长您的寿命。运动也有许多心理方面的好处。您可能能感觉
到,规律运动可以减少抑郁和压力,并提高认识能力、健康和生活质量。
尽管这些长期益处很重要,您可能想知道积极的运动对您目前有什么好
处?规律运动可以增强您的心肺功能、促进全身血液循环、降低您的体重和血
压、减少胸部不适和疼痛(参阅琳达的传奇故事)、降低您体内「坏胆固醇」
(低密度脂蛋白胆固醇)并增加您体内「好胆固醇」(高密度脂蛋白胆固醇)
水平。大量的研究已表明,规律的运动可以延缓或改善动脉粥样硬化,甚至缩
小粥样硬化的斑块,减少心肌梗塞的发生率,从而延长您的寿命和提高您的生
活质量。同时,规律运动能促进冠状动脉侧支循环的建立,改善心脏的血液供
应,有利于冠心病的康复,也能降低心绞痛发作的次数和心肌梗塞的复发率。
规律运动还能增加您的动作的灵活度和日常的活动能力。也许,在某天下午,
您能感受到您和您的孙子或儿子一起游玩,而没有以前感受到的那种胸部不
适。此外,规律运动还可以改善您的睡眠、增强您的食欲,并有助于您建立健
康形象及增强自信心。
这些事情听起来感觉很好,但您可能仍然没有信心,认为得了冠心病后不
能运动。您可能认为运动会增加心脏的负担,导致心绞痛或心脏病的发作。其
实许多的研究均已证实,适当的低-中强度的运动不但对冠心病没有害处,反而
有利于冠心病的康复,减少心绞痛或心脏病发作的次数。尽管如此,您可能仍
然认为运动是很无聊和痛苦的事。不管您相信与否,规律运动不一定要到室外
或花几个小时在健身房里运动。您可以将运动纳入到您的日常生活活动中,在
中等强度运动水平即可(参阅积极生活方式的要点)。运动一段时间之后,您
将会发现您越来越喜欢运动,并寻求更多的运动。
我为什么要运动?

544
首先,您必须知道从不运动到运动的生活方式转变不是一夜之间就能完成
的事。以下是一些策略,可帮助您准备成为积极的生活方式:
1. 学习更多有关运动的知识
虽然您还没准备好参加规律的运动,但是,如果您每天关注一下您身边的
所有信息,您会惊讶于您所学到的知识。
- 跟您的朋友、家人和同事交谈为什么他们要运动?
- 跟您的医生交谈,看他/她是如何看待健康和运动?
- 阅读报子上有关运动和运动益处的信息。
- 寻找媒体上有关运动的正面例子
2. 着眼于运动的好处
在我们开始一种新的行为之前,我们经常所想的往往都是那些不改变我
们原来行为的各种理由。我相信您现在就可以列出许多为什么您不能进行积极
生活方式的理由。然而,您不能着眼于这些负面的因素。相反,您应该想想您
必须运动的各种理由。
为了帮助您开始思考运动能给您带来的各种好处,请试着完成下列的表
格。我们已经帮您填好几个常见的运动好处。但是,您要记住,每个人都有自
己的目标和运动的理由。写下您将获得的规律运动的好处。
我如何才能变得更积极

545
规律运动的好处
着眼于为什么您必须运动,而不是不运动的理由:
1. 我可以控制体重
2. 我可以降低血压
3. 我可以更轻松地完成更多的活动
4. ___________________________________________
5. ___________________________________________
6. ___________________________________________
7. ___________________________________________
8. ___________________________________________
9. ___________________________________________
10. ___________________________________________

546
运动机会就在您的身边——只要动,就行
不管您相信与否,您每天有很多的机会可以运动。尽量利用这些机会,使
运动成为您生活的一部分。近来的研究表明,一天中积累的运动同样对您的健
康非常有益。您可以将一天 30-60 分钟的运动,分成 2-3 次来完成,每次运动
十几分钟。这样一天中累积的运动与一次性完成的运动同样有效。
使用楼梯
用爬楼梯代替乘电梯来增加您每天的运动量是一种简便易行的方式。选择
爬楼梯,您将成为「不用电梯者」。假如您要去的地方楼层太高,您可以先爬
几层,然后再乘电梯。例如,马女士,41 岁,上班族,半年前突发心肌梗塞,
急诊进行经皮冠状动脉支架植入术,出院后不敢运动,病后自感体质虚弱,容
易感冒。经过医务人员指导后,知道运动对冠心病康复的重要性。此后,马女
士决定每天锻炼 30 分钟。由于上班比较忙,没有时间去健身房,所以她决定利
用每天上下班和办事时爬楼梯(16 层)代替乘电梯来锻炼身体。果然,两个月
后,马女士的身体状况改善很多,走起路来也轻松多了。
尽可能的走路
为什么不提前下公共汽车一两站,然后走路到您要去的地方?这样您可以
散步 10-15 分钟。
在午餐休息期间,散步 10-15 分钟,这是一个非常好的方式。不仅可以运
动,还可以给您时间,对前一天和今天所做的工作进行一个新的回顾。此外,
餐后和同事一起散步也提供了一个社交机会。如果您已经退休,每天餐后和家
人一起散步,可增进家人感情。
毫无疑问,当您想泊车时,发现前面有一停车场时,您肯定会很高兴。但
是,想想您必须绕停车场一圈去停车,这会使您觉得很扫兴,尤其是您就近有
积极生活方式的要点

547
一个停车位。如果您就近泊车,只要多走几分钟的路,而不需要绕一圈,这样
也可以节省时间。多好!
参加计划运动
尽管一天中累积起来的运动有很多好处,但这并不意味着您不需要尝试或
安排一些规律的、更大强度的运动,尤其是您想强健您的心脏、减轻体重或达
到健身的目的。试着计划去健身房,或餐后更大强度的散步。

548
我相信您可以成功地改变这种静坐的生活方式。为了让您有信心改变成积
极的运动者,请您花几分钟时间填写以下表格,有关您「过去成功的记录」。
想想您曾经成功地改变了哪些习惯,这样会让您找回信心。
A. 我曾经改变的习惯
1. __________________________________________________________________
2. __________________________________________________________________
3. __________________________________________________________________
B. 帮助我成功改变这些习惯的因素
1.___________________________________________________________________
2.___________________________________________________________________
3.___________________________________________________________________
C. 阻碍我改变的因素
1.___________________________________________________________________
2.___________________________________________________________________
3.___________________________________________________________________
回忆我曾经成功改变的习惯

549
开始更多的运动决不是件容易的事。琳达曾认为,她绝不可能成为一名积
极的运动者。在她 50 岁时,她的体重是 90 公斤(200 磅),有高血压和冠心
病。偶有胸闷,并且心电图检查有心肌缺血的表现。
退休前,琳达忙于工作和家务,觉得没有时间运动。去年夏天,琳达与家
人一起去华盛顿旅游,她一路非常困难的爬上林肯纪念堂,一路上呼吸困难和
气喘。也就在那个时候,琳达决定开始每天多参与运动。一年后,琳达成功地
成为规律的运动者。胸闷的次数减少,并且心电图也恢复正常了。她每天选择
爬楼梯代替乘电梯。跟她的医生交谈后,琳达开始每天晚餐后散步 5-10 分钟。
虽然这很不容易,但她决定再也不要因为进行一些简单的运动而感到尴尬。
这样运动几个星期后,她开始每天午餐后散步,并逐渐扩展到晚餐后也散
步,每天散步 20 分钟。她感觉这样很好,并慢慢喜欢散步。当她丈夫称赞她是
「运动者」,她特别高兴。她从来没有想到自己能达到这种境界,但她成功地
做到将运动成为生活的一部分。她现在每天都能享受规律运动给她带来的各种
好处,特别是身体强壮了,走起路来轻松多了,胸闷的次数越来越少了。
琳达的传奇故事

550
香港理工大学护理学院
意向期小册子

551
内容提要:
我准备好要开始运动了
拒绝负面的影响
运动能给我什么好处?
为什么没有行动?
「主动」学习积极的生活方式
成为一个积极的人
如果我没有运动会怎样?
迈向成功
「当您在想是否可以做时,
一些人早已开始做了」
运动:我准备运动了

552
当您真的开始考虑增加您的活动量水平时,这表明您已经跨出了很关键的
一步,即您已经成功地迈向将运动纳入到您的日常生活之中的非常关键的一
步。
在您真正体验到一种积极的生活方式之前,您还需要迈出几个关键的步
伐。有几个可靠的策略,您可以用来帮助您上路。
在这份小册子里,有几种策略您可以用来帮助您巩固您的承诺——使运动
成为您生活的一部分。
您现在正在考虑的生活方式的改变很重要,并且能给您的健康和生命带来
很多好处。准备好承诺拥有一个健康、积极的生活!
我准备好要开始运动了

553
您考虑越多关于开始规律的运动,您就会越相信规律运动的益处。然而,
您可能仍然怀疑您的能力,并只关注许多规律运动的坏处。
运动的负面因素,如花时间、需要能量、和可能感觉疼痛等。所有这些沉
重的思想负担都会影响您的行动。然而,在您准备好真正开始规律运动之前,
您必须要控制那些您认为规律运动不好的负面因素。
方法之一:您将这些负面的因素(如没有时间),简单地当作您必须克服
的障碍物。您不要特意安排一个小时或走几段路程的时间到室外运动,您可以
简单地将这些运动纳入到您的日常生活中,如步行去某个地方办事而不需要等
公共汽车,或选择爬楼梯而不要每次乘电梯等。
方法之二:尽管刚开始时可能会有困难,一旦您学会将运动纳入到您的日
常生活中,您会轻松地完成所要达到的运动水平。想想您是如何形成每天刷牙
的习惯?您也可以将运动形成您生活的一部分。难道您不可以形成一种类似刷
牙的习惯?而且这种习惯对您的生理和精神都有很多好处。
拒绝负面的影响

554
适量的规律运动对于冠心病患者的康复是非常重要的。它可以给您带来许
多好处:
有助于强健您的心肺功能
有助于冠状动脉侧支循环的建立
有助于减少胸痛和呼吸困难
有助于预防支架再狭窄或心梗再发作
有助于降低血脂
有助于减轻压力
有助于控制体重
有助于减低血压
有助于增强体能
有助于睡眠
有助于建立健康形象及增强自信心
__________________________________________
__________________________________________
__________________________________________
哇,运动原来有这么多的好处,赶紧行动吧!
运动能给我什么好处?

555
——参加规律运动的难处?
尽管您知道规律运动有许多的好处,您可能也想运动,但您可能仍然没
办法行动起来。到底是什么原因阻碍您的行动?为了更好的帮您解决阻碍您行
动的难处,请写下您认为参加规律运动的坏处或难处。我们已经帮您填好几个
常见的运动坏处或难处。写下您将参加规律运动的坏处或难处。
1. 太多工作
2. 害怕心脏病发作
3. 无聊
4.________________________________________________
5.________________________________________________
6.________________________________________________
7.________________________________________________
8.________________________________________________
9.________________________________________________
10._______________________________________________
根据您所写下的执行运动的难处,想想您如何克服这些困难?如果您是
因为有太多工作而没时间运动,那么您就想想其实运动不一定要花很多时间特
意到室外或健身房去运动,您可以简单地将运动纳入到您的日常生活中,如走
路去菜市场买菜、走路去某个地方办事、或平常利用爬楼梯代替乘电梯等。一
天中累积的运动也同样有效。想想一次十几分钟是不是很快? 如果担心运动会
诱发心脏病发作,那么您可以先跟心血管医生咨询,谈谈您是否可以运动?谈
谈运动对您是否有好处?我想医生会告诉您,适当的规律运动对预防心脏病发
作有帮助。如果您认为运动很无聊,那么您就多想想运动对您疾病的康复有多
么重要。如果。。。。。。
为什么没有行动?

556
当您开始尽量少去思考运动的不良后果或运动的难处时,您仍然应该努力
学习有关运动的信息,并在规律运动的益处表格中,增加规律运动对您生活的
好处的点子。努力学习更多有关运动的知识,您需要从一个被动学习者变成一
个主动的学习者。主动的学习者是不断地寻求运动的新知识和信息来源。这种
学习方式包括您询问有关运动的问题。
您可能会自问:我需要做多少的运动?您可能会在这份小册子中获得一些
这方面的信息,但您也可以在报纸上有关运动的栏目里找到答案。假如您听说
在某份报纸上有一则关于运动方面的研究,您可以试着去找出这份报纸,然后
念给自己听。您需要自己去寻找您想要的答案。
您也许也想知道什么运动对您最好?最好的方法是问您身边的人,看他们
做什么运动或喜欢什么运动?尝试几种运动,然后自己决定看要做哪种运动?
最好的运动是您喜欢的运动。想想您喜欢什么,然后想想做这种运动是否可以
使您成为更积极。假如您喜欢自然,那么到室外散步;假如您喜欢看书,那么
您可以一边脚踏固定自行车,一边看书;假如您喜欢集体活动,您可以加入一
个社区联盟。
您也许也想知道规律运动对您的心理健康有什么好处?询问那些您认识的
积极运动的人,问他们运动给他们带来什么好处?问他们运动后是否感觉好多
了?是否运动后头脑更清醒?是否运动后缓解他们生活中的压力?
形成自己的一套问题,这些问题是您想要回答的,然后积极去寻找它们的
答案。您需要不断地学习有关运动的知识,了解运动会对您有什么特别的好
处?当有关运动的好处不断增加,同时坏处不断减少时,您将开始运动了。
「主动」学习积极的生活
方式

557
使规律运动成为您生活的一部分,最重要的一步是学会确认自己是否是积
极的人。您如何想象自己,将决定您的行为。
假如您认为自己是一个善良、有激情的人,您将会主动帮助别人,倾听他
们的困难在哪里?假如您认为自己是一个积极的人,想想这种人该拥有哪些行
为?
您需要花点时间思考,您目前的行为如何帮助您定义您自己。如果您回家
后马上扑通一声坐到沙发上,然后打开电视,您是什么想的?想想您为什么这
样做?问问您自己,一个积极的人应该做什么?积极的人,不是坐在餐桌前与
您爱人谈论您今天是怎样过,而是一边散步一边谈论您今天的事。
当您认识到改变一些行为可以改变您的个性时,您可以开始改变一些行为
来帮助您成为您想要的那种人。想想成为您想要的那种人后,您会是什么感
觉?然后坦诚地问自己,您目前的习惯和行为是否能使您成为那种人?
假如答案是否定的话,那么您应该改变您的行为,改造您的自我形象。
成为一个积极的人

558
——朝着健康的生活方式前进
另一种很重要的方法使您增加运动的欲望,是想象一下如果不运动,您的
生活会是怎样?尽管这种想象过程并不好受,但可以促使您想改变这种生活方
式。
不活动的结果是很不好的。想想发胖时您会有什么感觉?想想一天比一天
虚弱时您会有什么感觉?想想血脂和胆固醇增高时会怎样?想想心绞痛发作时
您会有什么感受?想想由于心脏病发作而死,您的家人和朋友会有什么感受?
每天晚上吃饭后只是坐在那里,您是否感到羞愧?不活动的生活方式就像一颗
炸弹,随时都可能爆发。它的不良后果会影响您的一生和您身边的人。
当您想保持这种不活动状态时,回想这些不活动的不良感觉会有效的帮助
您认识到为什么您需要运动。那些情景您都不想去体验。幸运的是,决定权在
于您自己手中。您可以积极运动,做任何事情去预防这些不良事件的发生,或
者您可以不活动,被动地等待他们的来临。
您是唯一一个具有能力改变您自己生活的人。其他人只能给您提供帮助或
指导,但您必须执行那些行为。
如果我没有运动会怎样?

559
改变一种生活方式不是一件容易的事,您应该朝正确的方向,每次迈出几
小步。
当您读完这份小册子时,您应该对自己承诺:今天快速行走 5 分钟。然后
逐渐实现您的运动目标。
如果说,目前建议您每天走路 10 000 步左右,这是不现实的,您必须从
每天几小步开始。要知道「千里之行始于足下」。
今天只要散步,不要跑步。只要 5 分钟,不要多。当您完成 5 分钟散步,
您有什么感觉?5 分钟是不是过得很快?
从 5 分钟开始,然后 10 分钟,逐渐实现您的运动目标。
现在开始散步吧!
迈向成功
560
香港理工大学护理学院
准备期小册子

561
内容提要:
准备,出发
使您的承诺正式化
每个人都需要帮助
认识您的理想
我应该做哪些运动?
运动时,我应该注意什么?
形成您的运动目标
我的运动目标表
运动:我正在路上
「要记住,是您使这一承诺变
成有益于您自己和您的健康」
562
您开始准备将运动成为您生活的一部分。也许您早已开始增加您的活动量
水平,正在寻找如何将运动纳入到您的生活中。恭喜您!
现在是准备将您的运动上升到更高一个水平。有几种方法,您可以用来帮
助您开始规律运动的生活方式。有几个重要的方法帮助您使您的承诺正式化,
如:学习如何建立合理的运动目标;学习如何寻求别人的帮助,使您成为积极
的人;进一步发展成为一个积极人的自我形象。
您已经很好地朝规律运动的方向前进。使用这份小册子中谈到的方法,您
可以成功地将运动成为您生活的一部分。
准备,出发

563
正如您准备成为积极的规律运动者,有一种方法您可以用来增强您的承
诺,那就是设定您的运动目标,并形成正式的计划书。
我们都喜欢拟一份「要做」的表,然后每天核对是否完成(至少我们希望
每一项都完成)。同样的方法可以用来实现您规律运动的承诺。当您实现您的
目标时,您会增加自信和自豪感。
但是为了使您的方法有效,您要为自己设定一个实际可行的运动目标。要
想知道有关设定合适的运动目标的详细信息,您一定要阅读「形成您的运动目
标」那一栏的内容。
设定好您个人的运动目标后,您需要将这些目标正式化。当您将这些目标
写下来或告诉别人您要达到的运动目标,会减少您忽略这些目标。这样,您就
不会说「我下次再做或这不是您真正想做的」。您要对自己的行动或不行动负
责。
为帮助您形成正式的目标,我们提供给您个人的运动目标表,附在这份小
册子的最后一页。请花点时间,将这个表格给填了,然后贴在您容易看到的地
方。最好是每个地方都能看到它。要记住,是您使这一承诺变成有益于您自己
和您的健康。
使您的承诺正式化

564
帮助您实现运动目标,一种很好的方法是寻找一个会支持您运动的朋友或
伙伴。这个人可以是一个啦啦队队长,鼓励您运动;也可以是监视器,当您不
想运动时提醒您;或是一个人与您一块改变运动行为。您的理想伙伴是拥有这
三个特点。
您的伙伴应该知道您的运动目标,您要告诉他如何更好的帮助您。您得到
的帮助一定是积极、正面的帮助。任何批判和大喊大叫都不利于刺激您坚持您
的运动方案。
您的伙伴可以是您的爱人或同事,甚至您的孩子或孙子也可以作为您的伙
伴来支持您运动。关键的是得到一个支持的伙伴,帮助您改变您的生活方式。
给您举个例子,陈 XX,男,57 岁,诊断冠心病 2 年,患病后不敢运动,经常
感觉胸闷。经医务人员的指导后,知道运动对他的疾病康复有好处。为了让自
己能坚持运动,他向家人宣布自己要坚持运动,并获得家人的支持。此后,每
天运动时间一到,家人都会提醒他「时间到了,要开始运动了」。他的女儿还
会特意叫儿子(即陈 XX 的孙子)陪爷爷一起打球。这样,陈 XX 成功地坚持
了规律运动。经过 4 周的规律运动后,陈 XX 明显地感觉到人越来越舒服,走
路越来越轻松,胸闷的情况也逐渐减少。由于陈 XX 享受到运动的益处,自然
越来越喜欢运动了。半年后,运动已成为他生活的一种乐趣。
每个人都需要帮助

565
当您继续努力使运动在您的生活中成为一种习惯,您需要继续定义您自己
是一个积极生活的人。这样,在您的生活中,您已经成功地建立一种您是谁的
感觉。现在,您需要继续让您的行动证实您是一个比较积极的人。
过去的任何会妨碍您成为积极人的行为,您都要将它们放弃。 知道每天
晚上都可以回家吃饭,然后坐下来看「必须要看的电视节目」,您可能很开
心。然而,这种开心多数是因为您规律运动使您的身体舒适所带来的。您可能
会反驳说,这只是您每天做的事情或是您性格的一部分。
但是,您感觉舒适的唯一理由,是因为长期以来您一直这么做。改变您的
行为和习惯是很痛苦的事,但是只要您认识到只要花一点点时间和精力,运动
就会成为您生活的一部分。餐后或工作后散步一会儿,将成为您每天很舒适的
活动。当您重新定位您要做什么时,您要对自己有耐心。记住您所作的一切是
为您自己成为一个比较积极的人,并记住这值得您去努力。
认识您的理想

566
近来的科学研究已经表明,获得规律运动的益处,不要象您以前所认为的
那样,必须几乎每天在健身房里剧烈运动 30 分钟。其实,一周中多数时间里,
进行中等强度的运动,每天累积 30 分钟以上,同样可以获得健康的益处。这意
味着,您可以将几次运动纳入到您的日常生活中,来达到运动的目的。您现在
有几种选择来达到运动的目的,从参加几个十分钟的运动课程,一次 30 分钟的
运动课程,或室外在要求的运动强度下运动 20-30 分钟。这种富有弹性的运动
选择方式将使您更容易地将运动的目的和您的生活以及情境需求融入一起。
中等强度的运动——那是什么?
您可能很想知道,到底您应该做多大强度的运动,才算是中等强度的运
动?最经典的中等强度的运动方式是快步行走!在商场里闲逛不属于快步行
走。您必须带有「目的」的散步。生活式运动的概念是您可以将运动纳入到您
的生活之中的运动。 但是,您可能会误认为您生活中已经有足够的活动。您要
知道,在办公室游荡或在花园里走走,这是不够的。您必须使您的心率和呼吸
比平常加快,这样的运动才有效。如果您所进行的锻炼不能使您轻微的气喘,
那么它就无法使您的心肺强健。这也是为什么从事一份忙碌的工作却无法达到
锻炼作用的原因。
在现实生活中,没有人能够控制每个小时固定走路或骑车几公里或几千
米。最好判断中等运动强度的是您自己。您要学会留心观察您的身体。您要知
道什么时候心率加快和呼吸加速。由于每个人的基础健康状况不同,每个人达
到中等强度的运动量会不一样。学会测量和监测您的脉搏,帮助您感觉如何转
化为每分钟的心跳。
您要记住的是,中等强度的运动是没有疼痛或痛苦的运动。如果您感觉到
疼痛或无法继续运动,您必须停止运动,这表明您已经运动过量了。中等强度
的运动是您能维持这种运动,并能持续一段较长时间。
我应该做哪些运动?

567
合适运动量的标志是:运动时稍出汗,轻度呼吸加快但不影响讲话,早晨
起床时感觉舒适,无疲劳感或其他不适感。运动后如感到轻快,食欲、睡眠较
好,表明运动量适宜。如果运动后头晕、胸闷、心悸、气短、食欲减退、睡眠
不佳、明显疲乏,说明运动量过大。
假如您增加活动量后没有感觉不适,您可以考虑在您的生活中增加一些更
大强度的运动。这表明您可以去健身房,游泳池游几个来回,参加有氧运动班
或散步后慢跑一会儿。这些比较大强度的运动将真正改善您的健康。
常见的中等强度活动的例子
对于冠心病患者来说,其实最好的中度运动是快速行走(80-100 米 /分
钟)。以下是一些相当于中等强度活动的例子。
日常活动
用手拖地板
爬楼梯(上下楼梯)
走/跑: 与小孩一起玩(仅活动期间)
走路(4.0-5.6 公里/小时,手提少于 22.5 公斤的物品)
运动
散步 (4.8-6.4 公里/小时)
打太极拳
双打网球
乒乓球
羽毛球(非竞赛性的)
排球(非竞赛性的)
篮球(非竞赛性的)
保龄球
垒球或棒球
慢骑自行车(13-19 公里/小时)
踏固定脚踏车(50-100 瓦)
游泳
郊游(徒步)、爬山

568
保健操
健身操(一般的、家里运动,如:背部运动)
体操(一般的)
减肥体操
跳舞
跳扭扭舞、扭秧歌、 爵士舞、吉特巴舞
迪斯科、民族舞、广场舞、华尔兹舞、慢舞或探戈舞
打鼓(腰鼓)

569
对大多数冠心病患者来说,适量的运动是安全的。为预防意外,冠心病患
者进行运动时应注意以下一些事项:
运动前要先有心血管医生的检查及对运动量的推荐。
冠心病病人应随身携带硝酸甘油丸或其它抗心绞痛药物,如麝香保心
丸、速效救心丸或丹参滴丸等,以备胸口痛时放在舌下。
运动前应做准备活动(热身运动),运动后应做整理运动。一般采用散
步、体操等活动,分别是 5-10 分钟。准备活动和整理活动不充分是造成
锻炼意外的最常见原因。
在太饿或太饱、太冷或太热的环境、身体疲劳、盛怒及心情太差时,都
应避免运动。饱餐后休息 2 小时才做运动。避免出入温差太大的场所。
运动后切忌马上进行热水澡,最好是运动后半小时再洗澡,以减低对心
脏的冲击及预防运动后的暴毙。
避免推举重物等用力的工作,如需要时,保持呼吸畅顺,切忌忍气。
注意空气流通,注意心跳是否过度加快或不规律。
要避免竞技性运动,避免加速过急的运动,如快速地爬楼梯竞赛。
感冒或发热后要在症状和体征消失 2 天以上才能恢复运动。
清晨气温较低,不适宜心脏病患者进行锻炼,因此最好是上午或傍晚出
去锻炼。
运动停止指征
若出现以下的症状或体征,应马上停止运动:
• 典型的胸痛或胸部不适,或放射到肩部、下颌部、颈部或手臂;或感受
到以前心肌梗塞的症状;
• 眩晕、头晕或身体虚弱;
• 呼吸困难或气喘
• 不典型出汗
运动时,我应该注意什么?

570
• 过度疲倦
• 腿痛限制其功能
• 身体无法继续运动
运动时还需要记住的要点
如果运动时您喘不过气以至无法说话,休息,直到仅有轻微的喘息再继
续。
如果您感觉胸痛,休息直至疼痛消失。如果胸痛规律发生,则需要告知医
生。如果您有心绞痛则服药后再继续锻炼。
按计划进行,不要在短期内做过量的运动,这会延缓您的康复,甚至发生
危险。欲速则不达。
如果您某天锻炼时感觉不好,不要因此而烦恼,每个人都可能发生这种情
况。问问自己是否已经比过去的几天运动量大了些,这可以解释为什么您
感觉有点疲劳。

571
为了体验您实现运动目标时的成功感觉,您要学会设定合适的目标,包括
形成现实可行的改变您行为的期望。开始时,您的目标,重点是如何使短期的
目标或行为帮助您实现您要追求的长期效益。
形成规律的运动不是一夜之间就能实现的。假如您已经不活动一段时间,
您需要慢慢进入这一新的生活方式。您知道,形成积极的运动习惯是第二自
然,但这种自然只能慢慢来。就象减肥一样,您不能奢望在没有参加积极的活
动和将饮食改变纳入到新的健康的生活方式之中,会迅速地减轻体重。现在,
您集中精力形成一些短期的目标,然后慢慢增加您的活动量。
这份小册子的最后一页是提供给您一次机会,让您设定一些您自己可执行
的运动目标。刚开始时,您可以每天在午餐和晚餐后散步 10 分钟;您可以爬楼
梯;也可以设定具体的目标。要记住,是您使这些改变发生,是您希望从运动
中得到什么好处,也是您如何更好地帮助这些好处发生?
填好您的目标、签名和执行日期,然后将这份表格放在您和别人都可以看
到的地方。每当您看到这份表格,您都要核对一下您是否完成那些行为?如果
您没有实现您的目标,不要气馁。一般人在成功地改变行为之前,需要相同的
「新年改革」3 次。使用这份小册子中介绍的方法帮助您改变行为,但要预见
一些挫折或困难。关键是确信目标是可行的、合理的。着眼于您完成了哪些行
为,然后加倍努力实现目标。
形成您的运动目标

572
我将每天散步________分钟
我将尽可能地爬楼梯
我将______________________________
我将尽最大努力使运动成为我生活的一部分
我能并将成为一个积极运动的人
签名___________________
日期___________________
我的运动目标

573
香港理工大学护理学院
行动期小册子

574
内容提要:
朝着积极的生活方式前进
发展健康的替代方法
奖励您自己——您做了一件好事
润色您的日常活动
不活动——千万不能不活动
问题解决的艺术——IDEA 表格
运动:我正在「动」
「朝着您的目标前进」

575
您应该为自己感到自豪,您所作的一切都是有益于您的健康。只要您留
意,规律的运动会给您的精神和生理健康带来许多好处。关键在于您要坚持将
运动纳入到您的生活中。
坚持规律的运动可能会遇到一些小的挫折,但是在这份小册子中,您会发
现许多方法,可以帮助您朝向您的运动目标前进。
当您努力保持一种规律运动的健康生活方式时,您要学会如何避免那些可
能使您不运动的情况,学会巩固您运动行为的思想,以及形成您自己的奖励方
式。不断地增加您运动选择的多样化也是很重要的。每天重复同样的运动会很
烦并且会减少动力。
恭喜您!您已经很好地朝着积极的生活方式前进。现在只要继续前进就
行!
朝着积极的生活方式前进

576
当您不断地努力使运动成为您每天生活的一部分,您会不时地被诱惑返回
到您以前不运动的坏生活习惯中。想想所有可能让您在节假日里逃脱运动的
「坏」情况。您要知道您在什么情况下或什么时候不想运动,然后努力去重新
调整您的运动目标。
当您不幸回复到原来静坐的生活方式时,您可以想象为什么您不能活动的
所有理由?这时候需要您和您自己进行对话。假如您认为运动会花费太多时
间,提醒您自己每次 10 分钟很快,每次运动可以累加起来。如果您认为运动会
出很多汗,提醒您自己运动后感觉多好。
想想所有您可能得到的将运动纳入您生活中的机会,来代替旧的、不活动
的习惯。假如您喜欢看电视,那就找些可以在家里做的运动,如:在跑步机上
走或在固定自行车上踏,这样您可以一边看电视一边运动。假如家里没有跑步
机或固定自行车,您可以在大厅或阳台进行原地踏步走/跑,或做做体操。假如
您喜欢散步,可以试着每天走路或骑自行车去菜市场买菜,而不用去挤公共汽
车。假如您喜欢午餐后坐在那里和您同事聊天,可以试着叫他们一块散步,这
样您们可以边谈话边活动。
您有可能会被诱惑回复到原来旧的生活习惯轨道上,您应该提前计划如何
避免这些情况发生,使您一直保持运动是生活的一部分。
发展健康的替代方法

577
当您不断地实现您的运动目标时,您可能对自己和您的健康感觉越来越
好。不断的进步,本身就是一种奖励,但是您还是需要花点时间庆祝自己的进
步。形成规律的运动不是一件容易的事,虽然您做得越多,运动越会成为您生
活的一部分。
有几种方式可以奖励您自己,奖励您努力保持运动。假如您有一套的运
动目标(如果您没法坚持运动,您就列出您如何想将运动成为生活的一部
分),简单的奖励方式是在那些您已经实现或正要实现的目标上打「√」。这
种简单的「已做」的核对方式经常是一个很大的奖励,能增加您的自信。假如
您没有达到一些目标,那么想想目标实现后,打「√」的感觉多好。
当您成功地避免一些可能使您不运动的情景时,奖励自己一个背上有文
字的牌子。鼓励的话或想法,如:「做得好!」或「我能做到」。这些都能给
您带来很大的动力。您可以自己给自己助威。如果您表现好的行为,那么您有
权利对自己感觉好点。干吧! 「继续下去」。
如果您不想自己担任啦啦队队长,您可以招募您身边的人来帮助您。如
果他们知道您的运动目标,他们会帮助并鼓励您。让您的家人、朋友、或同事
来鼓励您,使您实现您的目标,这样您的努力就不会被人忽视。
最后一种奖励方式,是给自己建立一个行为协议。如果您能顺利地实现
这个特别的、有挑战性的目标时,您可以选择一种特别的奖励方式。但是千万
不要奖励您不运动。假如您计划一个特别的旅行或假期,要保证这种旅行或假
期能将运动成为您每天的活动之一。让您假期里的新风景作为您的奖励,只要
您走一段路程就有一个风景。
奖励您自己——您做了一件好事

578
要使运动成为您每天生活的一部分,很重要的一点是您不要对运动感到
无聊。这看起来好像与建议您使规律运动成为一种习惯相矛盾,您要参加一些
您喜欢的运动或在您喜欢的环境下运动。
就拿散步来说,假如您要实现您的运动目标,您可以在校园周围或邻近
地区找一条新的可以散步的路线。新的风景或更多富有挑战性的路线会增加您
运动路线的多样化,并给您一些期望继续走下去。只要您不断增添一些不同的
运动方式,习惯就不会变的无聊。使用新的运动和环境来增加一些「香料」,
从而实现您的运动目标。
另一种帮助您不断实现您的运动目标的方法,是尝试更富有挑战性的任
务。如果您每天晚上散步一英里(1.6 公里),试着一公里或一半或设定一个目
标,使走的速度比上周快一点。当您越来越积极运动时,您会发现您所做的努
力使静坐的生活变成运动的生活方式越来越容易。为使您保持较高的动力,您
要给自己一个有足够挑战性的目标,这样当您实现目标时,会有一种成就感。
您可能也想尝试完全不同的运动。只要您小心不要过量,您可以试着进
行一些新的运动。打壁球或参加一篮球队或垒球队。您也可以在健身房尝试一
些新的设备。假如您已经瞄准那个新的运动仪器,干吧,试一下。您可能会发
现那种活动您很喜欢。
关键是要确信您的运动方式不断变化,这样您就不会停滞不前,去改变
那种您决定改变的静坐生活方式。保持不同、新颖、和挑战性,不久您就会惊
讶于有这么多种的运动。参加这些运动可以形成规律运动的习惯。
润色您的日常活动

579
在您努力成为积极运动的人的过程中,您将面对的最主要的障碍之一,是
那些诱惑您不活动的情景。不好的天气,如:下雨、下雪、或寒冷,这会使人
很想待在室内,什么都不想做。不幸的是,您不能什么都不做。为保持积极运
动,您要开始明白在哪些情景下,对您实现运动目标最有挑战性。
下列单子包含每个人努力成为规律运动者可能遭遇的几个常见阻碍,回顾
这个单子,在底下增加一些您自己的阻碍因素。
很难运动。。。。
1. 在恶劣的天气里
2. 在休假中或假期里
3. 当家里有客人来访时
4. 当家里有太多事要做时
5. 当您面对工作的最后期限时
6. 当您感觉累时
7. 当您的伙伴不能陪您一块运动时
8. _____________________________________
9. _____________________________________
10. ____________________________________
看看这个单子,您可能会有一种想战胜的感觉,或想如何保持规律的运
动。知道自己什么时候或在什么情况下会被诱惑不运动,是您保持积极生活方
式的关键一步。
既然您承认在某些情况下会导致您不想运动,关键是努力避免这些情景,
或设定计划帮助您应对这些情况的发生。
不活动——千万不能不活动

580
例如,当天气不允许您外出散步,您可以试着在屋里或在附近的购物中心
散步,如可以在室内做体操或原地踏步走/跑。形成您自己的天气管理计划,这
样当恶劣天气来临时,您已经知道如何继续您的运动计划。
同样,在节假日紧张的时间里,不是限制您的活动,而是应该更加留意寻
找时间来运动。运动的时候,可能会给您一个机会清理一下您的头脑。努力做
一些对您有益的事,而不是总在想那些苦恼的事。
如果家里有客人来访,您可以试着餐后与客人一起出去散散步,这样您们
可以一边聊天一边锻炼,一举两得,而不是坐在那里聊。如果家里有太多的事
要做时,您可以尽量将运动纳入到您的日常活动中,也可以寻求家人的帮助来
完成您的运动目标。
对于每种这样的情景,您都要准备好如何克服这些阻碍因素,然后继续实
现您的运动目标。另一种可以帮助您实现您的目标的方法是,在您家里或办公
室里放置一些提醒物来提醒和鼓励您运动。您可以在周边放置便利贴(百事
贴)、寄给自己一张明信片提醒您去运动、给自己寄一种提醒物、或在您家门
口放置一双运动鞋等提醒您去运动。您也可以给自己的手机设定一个闹钟,每
天提醒自己要锻炼。总之,关键是在您周围给您足够的正面信息,这样您可以
克服那些负面的情景来鼓励您坚持运动。
最后一种战胜那些使您不运动的诱惑的方法,是坚持制定或「修改」活动
表。通过每天制定一套的特定计划和目标,这些目标您可以预见可能遇到的阻
碍或困难,然后制定相应的计划。多样的运动选择方式,会允许您根据当天的
天气或您的时间,选择最合适的运动方式来实现您的目标。
您已经很好地将运动成为您生活的一部分。接下来的努力是防止您返回到
原来静坐的生活方式,这是非常值得努力的事。想想运动给您生活带来所有有
益的事。继续沿着您的目标前进!

581
使用 IDEA 表格
I——发现阻碍您运动的困难
_____________________________________________________________________
_____________________________________________________________________
_____________________________________________________________________
D——形成解决问题的方法(越具体越好)
_____________________________________________________________________
_____________________________________________________________________
_____________________________________________________________________
E——评估这些方法。在下面的空白处,写下您要尝试的方法。当您写计划
时,您要写下执行的具体时间.
_____________________________________________________________________
_____________________________________________________________________
_____________________________________________________________________
A——分析计划是否有效?如果有需要,请修订计划。假如您的计划执行很
好,给五个星星。假如计划执行不好,只有两个星星,那您写下如何使它变成
五个星星的计划?假如您的计划完全泡汤,请重新回顾一下您上面列出的解决
方法的单子,重新再试一下。(记住,计划效果不好不等于完全失败。计划朝
向解决问题的方向,一般都会有效。只有放弃才是真正的失败)
_____________________________________________________________________
_____________________________________________________________________
_____________________________________________________________________
问题解决的艺术
582
香港理工大学护理学院
维持期小册子

583
内容提要
维持积极的生活方式
如何维持运动的习惯?
不是世界末日
是您的生活方式——要负责
帮助发生变化
「您做得很好!运动是您
生活的一部分」
运动:我一辈子做运动!

584
您已经努力使运动成为您生活的一部分,您必须执行您的承诺。您已经做
了很多有助于增强您躯体和精神健康的工作。相信运动成为您生活的一部分会
让您感觉很好。
尽管您已经成功地实现您为自己所设定的运动目标,但现在不是说可以放
松了。您已经形成的运动习惯对您非常有益,但您仍然需要警惕任何可能倒退
的现象,这会让您返回到原来不运动的状态。
确保您坚持运动的最好方式,是学会如何有效的管理您可能碰到的各种倒
退现象;当坚持运动有困难时,您要像以前一样计划时间;加强认同做一个积
极的人,把她作为您行为改变的模范。
维持积极的生活方式

585
您应该选择的运动是。。。。。
感兴趣的。。。
如果您并不喜欢这项运动就很难坚持。如果您过去进行过骑单车、散步、
游泳、跳舞、打保龄球、羽毛球等运动,那么尝试重新开始这些项目。
规律的。。。
如果您不能很好地坚持,可以参加一些有组织的运动,如运动课程。如果
天气不好,做些您能做的事情,游泳是特别好的运动项目,因为您全年都可以
进行,如果您不会游泳,可以参加游泳培训班。
多样化的。。。
多进行几种运动,以便当您对一项运动感觉厌烦时,可以进行其他的运
动。
就近的。。。
旅行花费高且耗时,您很容易放弃。如果在您居住地区附近没有什么可去
的地方,您可在家使用划船机或脚踏车运动机,也可以在家里大厅或阳台进行
原地踏步跑,这些运动可能很乏味,所以您可以边运动边看电视节目。
融入生活的。。。
使运动成为您生活的一部分,尽量步行或骑自行车上班或购物。
如何维持运动的习惯?

586
要发生的总会发生。最终您可能倒退或没有实现您的运动目标,这可能是
由于恶劣的天气、工作的额外需求、或假期的压力等造成的。但不管是什么原
因引起的,您都要准备好应对这些情况,以使您回到朝向健康的运动生活方
式。
您要知道,您不是失败了,这也不是世界末日。倒退现象是我们生活中做
每件事情都会碰到的情况。人与人的区别在于他们对付倒退的能力。
有一些方法可以使您恢复积极运动的习惯。第一,您要尽可能地恢复规律
运动。不要浪费时间哀叹您丢失的运动机会,恢复积极的运动状态。倒退不是
永久的,并且您有能力决定倒退时间的长短,尽可能使您返回的静坐生活方式
短些。
您要保持积极和有目标。即使您没有达到您的目标,您所做的工作也没有
浪费。记住,您要实现的事情不是一夜之间就能做到的。暂时的倒退,也不会
使您重新回到静坐的生活方式。只要有积极的态度,您就会重新积极起来。
一辈子运动的挑战是您可能在某一时间会倒退,当倒退时,要保证尽可能
的积极和重新恢复积极的运动方式。因为您是一个积极生活的人!
不是世界末日

587
使运动一直成为您生活的一部分可能不容易,但您能做到。您要庆祝自己
一直以来的努力。使用一些策略,您可以在以后的十几年里,保持积极运动状
态,然后一生享受运动带来的好处。
当您遇到不寻常的情况时,是您发生倒退的最危险的时刻。如果您没有准
备好如何应对这种新的或特别的压力事件,您可能会返回到原来的旧习惯中,
即静坐的生活方式。这些刺激会非常强烈地诱惑您返回到以前的行为中,但是
只要有合适的计划,当这些情况发生时,您可以应付自如。
您要确信提前计划这些可能妨碍您常规运动的不寻常情况。假如您在休
假,那么要保证您随身携带运动服,并了解您去的地方是否有健身设施或可以
散步和慢跑的场所。
当事情意外地发生时,您要花点时间重新审核您的运动目标,然后回答为
什么您要执行这些目标。回顾您的运动目标,会给您一个机会去计划如何坚持
运动,或如何应对可能出现的不运动现象。
您也需要偶尔花点时间提醒自己为什么要运动。观看运动有益的电视节目
或新闻报道,祝贺自己的行为。对每个麻烦或障碍,您都能想想为什么您不运
动,挑战自己想出 4 到 5 个为什么您要运动的理由。
虽然您现在是积极的运动者,但您可能忘记您是怎样开始运动的。偶尔提
醒自己从积极运动中得到的好处,这会给您坚持运动带来很大的动力。
另一个满足您一辈子运动的挑战,是使运动成为一种习惯,成为您每天生
活的一部分。就像每天洗澡,最后您可能养成每天运动的习惯,至感觉不太像
您自己的程度,直到您每天坚持散步 30 分钟。
这种运动的习惯,是保证您一辈子运动的关键一步,它会让您坚持运动。
是您的生活方式——您要负责

588
假如您身边有人每天运动,然后正在享受规律运动带来的各种好处,那么
您要意识到这些人可能会帮助您发生变化。把他们作为榜样或模范,这会帮助
您建立自己作为一个积极的人的形象,防止返回到静坐的生活方式中的有力武
器。
模范是什么意思?将模范作为「活动刑警」会得罪很多人,这会比鼓励成
为积极的人更多。人们会简单地回避您。您所要做的是当他们乘电梯时,您爬
楼梯。假如他们问为什么您要爬楼梯,那么您就与他们分享您的体验和感受,
也许他们下次会选择加入您的队伍,一起爬楼梯。您也可以邀请别人每天一起
散步。假如有人想跟您一起散步,您应该与他们分享您的知识来帮助他们养成
运动是生活一部分的习惯。
规律运动对您一生的好处已很明显了,所以别人找您作为他们的模范,您
的职责是帮助他们发生变化,帮助那些将您作为规律运动正面效益的榜样的人
发生变化。
您要为您的成就感到自豪。但是除了成就感外,您要知道您还有一些责
任。完成责任的最好方法是维持您健康的和积极的生活方式以及乐观的生活态
度。
帮助发生变化
589
References
Blair, S.N., Dunn, A.L., Marcus, B.H., Carpenter, R.A., & Jaret, P. (2001). Active
living every day. Champaign, IL: Human Kinetics.
Blissmer, B.J. (2000). Integrating the theory of planned behaviour and the
transtheoretical model: a prospective study of lifestyle activity. Dissertation:
University of Illinois at Urbana-Champaign.
Briffa, T.G., Maiorana, A., Sheerin, N.J., Stubbs, A.G., Oldenburg, B.F., Sammel,
N.L. & Allan, R.M. (2006). Physical activity for people with cardiovascular disease:
recommendations of the National Heart Foundation of Australia. Medical Journal of
Australia, 184(2), 71-75.
Marcus, B.H., Forsyth, L.H. & Blair S. (2003). Motivating people to be physically
active. United States: Human Kinetics.
Tung, W.C. (2003). Examination of the transtheoretical model and physical activity
in family caregivers in Taiwan. Dissertation: The University of Utah.
院外自助式心脏康复手册(未出版). 香港理工大学护理学院,香港中文大学护
理学院和中国协和医科大学护理学院编制。

590
Appendix XI Screening Form – Chinese Version
第一部份 个人资料
1.性别: ①男 ② 女
2.年龄:________岁
3.婚姻状况:
①未婚 ②已婚 ③离婚 ④分居 ⑤丧偶
4.教育程度
①没有正规教育 ②小学 ③初中 ④高中/中专
⑤大学专科 ⑥大学本科及以上
5.目前就业状况
①没有工作 ②兼职 ③ 全职
6.职业(退休前)
①体力劳动者 ② 技术人员 ③ 文职人员 ④ 管理人员
⑤专业人员 ⑥经商人员 ⑦其他_____________
7.宗教信仰
① 没有 ②佛教 ③基督教 ④ 伊斯兰教 ⑤天主教
⑥道教 ⑦其他_____________
8.家庭每月收入
①¥1000 以下 ②¥1001-3000 ③¥3001-5000 ④¥5001-7000
⑤¥7001-10000 ⑥¥10001 以上
9.医疗费用支付方式
①公费 ② 部分公费 ③ 医保 ④全部自费
10.居住情况
① 独居 ② 与朋友同居 ③与配偶同居
④与子女同居 ⑤与配偶和子女同居
591
第二部份 临床资料
1.诊断
①心绞痛 ② 心肌梗塞
2.冠状动脉介入治疗
①无 ② 有
3.冠心病家族史(50 岁前发病)
①无 ② 有
4.糖尿病 ① 无 ② 有
5.高血压 ① 无 ②有 (血压_________毫米汞柱)
6.吸烟状况(使用香烟、雪茄、小雪娇、烟斗烟草、或任何其它形式的烟草)
①从未吸烟
②以前吸烟(平均每天吸____支/天),现已戒烟。
③目前吸烟 (平均每天吸____支/天)
7.饮酒状况
①从未饮酒
②以前饮酒(饮酒量______克/周),现已戒酒。
③目前饮酒(饮酒量______克/周)
8.目前口服药物
8.1 硝酸酯类_________________________________________________________
8.2 β-阻滞剂__________________________________________________________
8.3 血管紧张素转换酶抑制剂____________________________________________
8.4 钙通道阻滞剂______________________________________________________
8.5 降脂药____________________________________________________________
8.6 抗血小板药_______________________________________________________
8.7 其他______________________________________________________________

592
第三部分 综合性医院抑郁量表
情绪在大多数疾病中起着重要作用,如果医生了解你的情绪变化,他们就能
给你更多的帮助。这个测定表是专门设计帮助医生了解你的情绪,请你阅读以
下各个项目,在其中最符合你上个月以来的情绪的答案下划一条线。对这些问
题的回答不要作过多的考虑,对每个问题立即作出回答比考虑后再回答更为正
确。
类别 问题 回答 评分
D1 我对以往感兴趣的事情还是有兴
趣
肯定一样
不像以往那样多
只有一点儿
基本上没有了
0
1
2
3
D2 我能够哈哈大笑,并看到事物好
的一面
我经常这样
现在已经不大这样了
现在肯定是不太多了
根本没有
0
1
2
3
D3 我感到愉快 根本没有
并不经常
有时
大多数时间
3
2
1
0
D4 我对自己的仪容(打扮自己)失
去兴趣
肯定
并不像我应该做到的那样关心
我可能不是非常关心
我仍像以往一样关心
3
2
1
0
D5 我对一切都是乐观地向前看 差不多是这样做的
并不完全是这样做的
很少这样做
几乎从来不这样做
0
1
2
3

593
D6 我好像感到情绪在渐渐低落 几乎所有的时间
很经常
有时
根本没有
3
2
1
0
D7 我能欣赏一本好书或一项好的广
播或电视节目
常常
有时
并非经常
很少
0
1
2
3
总分______________
第四部分 筛查项目
以下是一些条目帮助心血管医生了解每位病人是否适合参与本研究,即时期
匹配运动行为干预的项目。如果以下条目中,病人有一项不符合标准,则不建
议参与本研究。
1.年龄__________岁
① 小于 18 岁 ② 大于等于 18 岁
2.是否居住在厦门
① 是,地址___________________________________________________
联系电话:_________________________________________________
② 否
3.病人的沟通和阅读汉字的能力:
1)语言沟通能力 ① 能进行沟通 ② 沟通困难/沟通障碍
2)阅读汉语的能力 ① 有阅读能力 ② 阅读困难

594
4.疾病诊断:心绞痛 心肌梗塞
① 心绞痛 ,诊断时间_________(月/年)
② 心肌梗塞,诊断时间_________(月/年)
③ 冠状动脉介入治疗术后,介入治疗时间_________(月/年)
5.是否病情稳定 ① 是 ② 否
6.是否有不稳定型心绞痛 ① 是 ② 否
7.是否曾经参加过任何有关心脏康复的项目 ① 是 ② 否
8.是否有认知功能障碍 ① 是 ② 否
9.是否有精神抑郁症 ① 是 ② 否
10.是否有重度主动脉狭窄 ① 是 ② 否
11.心功能状况 ,按纽约心脏病学会(NYHA)心功能分级:
① I 级:活动量不受限制
② II 级:活动量轻度受限制,重体力活动时患者出现疲乏、心悸、呼吸困难
或心绞痛。
③ III 级:活动量重度受限制,轻度体力活动时患者出现疲乏、心悸、呼吸
困难或心绞痛。
④ IV 级:患者不能从事体力活动,休息状态下亦有疲乏、心悸、呼吸困难
或心绞痛。
12.糖尿病
① 无
② 有,空腹血糖______________

595
13.高血压
① 无
② 有 (血压_________毫米汞柱)
14.心率/脉率_________次/分钟
15.是否有窦性心动过速(> 120 次/分) ①是 ② 否
16.是否有心房颤动 ①是 ② 否
17.是否有室性心律不齐 ①是 ② 否
18.是否有三度房室传导阻滞 ①是 ② 否
19.是否有收缩压大于 180mmHg 或舒张压大于 110mmHg ①是 ② 否
20.是否有急性心肌炎 ①是 ② 否
21.是否有急性心内膜炎 ①是 ② 否
22.近三个月有栓塞史 ①是 ② 否
23.是否有影响运动或由于运动而病情加重的急性非心脏性疾病,如感染、肾
功能衰竭、甲亢等 ①是 ② 否
筛选结果: ① 推荐 ② 不推荐
心血管医生姓名: _______________ 签名: _________________
日期: _________________

596
Appendix XII Questionnaires – Chinese Version
第一部分 活动之变动时期问卷
说明:规律的身体活动是指任何有计划的身体活动〈如太极拳,快步行走,骑
脚踏车,游泳等〉,用以增加身体体能。这样的活动应该累积每天至少 30 分钟
(每次至少 10 分钟)的中度身体活动,每星期多于五天〈参见中等强度活动的
例子〉。执行这样的活动不需要一次做完,几次十几分钟的活动时间也能够有
效。身体活动不需要痛苦才会有效,但应该做到增加您的呼吸速率和引起您流
汗的程度。
问题:
按照以上定义,您是否从事于规律的身体活动?(选一个答案)
1 = 没有,而且我不打算在未来的六个月内去做。
2 = 没有,但我打算在未来的六个月内去做。
3 = 没有,但我打算在未来的 30 天内去做。
4 = 是,我已经从事于规律的身体活动少于六个月。
5 = 是,我已经从事于规律的身体活动多于六个月。
1 = 前意向期
2 = 意向期
3 = 准备期
4 = 行动期
5 = 维持期

597
中等强度活动的例子
(摘自 Ainsworth, Haskell, Whitt et al., 1993)
活动类型 METs 中等强度的活动
运动 3.3-
5.0 散步(4.8-6.4 公里/小时)
4.5 羽毛球(非竞赛性的)
4.0 乒乓球
4.0 太极拳
3.0 保龄球
5.0 双打网球
3.0 排球(非竞赛性的)
6.0 篮球(非竞赛性的)
5.0 垒球或棒球
6.0 游泳(非竞赛性的)
4.0-
6.0 慢骑自行车(13-19 公里/小时)
3.0-
5.5 踏固定脚踏车(50-100 瓦)
6.0 郊游(徒步),爬山
保健操和跳
舞
3.5 健身操(一般的,家里运动,如:背部运动)
4.0 体操(一般的)
4.8 跳扭秧歌、爵士舞、吉特巴舞
3.0-
4.5
舞厅(如:迪斯科、民族舞、广场舞、华尔兹舞、慢舞
或探戈舞)
4.0 打鼓(腰鼓)
日常活动 3.5 拖地板
3.0-
3.5 爬楼梯(上下楼梯)
4.0-
5.0 走/跑:与小孩一起玩(仅活动期间)
3.0-
4.5 走路(4.0-5.6 公里/小时,手提少于 22.5 斤的物品)
其它(具
体)
3.0-
6.0

598
第二部分 运动自我效能量表
以下所描述的许多状况会影响规律的身体活动(每周五次或五次以上),
根据下面的问题,估计您能执行规律运动的自信程度,从 0 到 100 分,将符合
您情况的数值填在横线上。
0 10 20 30 40 50 60 70 80 90 100
完全不能做 中度肯定能做 肯定能做
(0-100)
1.当我觉得疲劳时 ___________
2.当我觉得工作有压力时 ___________
3.天气不好时 ___________
4.因受伤停止了运动,等损伤愈合后 ___________
5.正在经历或刚经历了个人问题后 ___________
6.当我觉得沮丧时 ___________
7. 当我觉得焦虑时 ___________
8.因疾病而使我停止运动康复后 ___________
9. 当我运动觉得不舒服时 ___________
10.在假期后 ___________
11.当我在家里有太多工作要做时 ___________
12.当有客人来访时 ___________
13.当有其他有趣的事情要做时 ___________
14.如果我没有达到自己的运动目标时 ___________
15.没有我的家人和朋友的支持时 ___________

599
16.在假期中 ___________
17.当我有其他的事情约定时 ___________
18.在经历家庭事件后 ___________
总分 ___________
第三部分 运动益处和阻碍量表
运动益处量表
说明:以下叙述是关于运动的一些想法,请用圈选的方式,指出您对每个叙述
同意或不同意的程度。
1 = 强烈不同意
2 = 不同意
3 = 同意
4 = 强烈同意
1. 我从运动得到乐趣。 1 2 3 4
2. 运动减少我紧张和压力的感觉。 1 2 3 4
3. 运动增进我的心理健康。 1 2 3 4
4. 运动将预防我发生心脏病。 1 2 3 4
5. 运动会增强我的肌肉力量。 1 2 3 4
6. 运动给予我个人成就感。 1 2 3 4
7. 运动使我觉得放松。 1 2 3 4
8. 运动让我和我喜欢的朋友及人们有联系。 1 2 3 4
9. 运动将使我远离高血压。 1 2 3 4
10.运动改善我的心脏血管系统功能。 1 2 3 4
11.运动增进我的身体体能的强度。 1 2 3 4
12.运动增进我的肌肉结实。 1 2 3 4
13.因为运动,我感觉自己比较健康。 1 2 3 4

600
14.运动增进我的耐力。 1 2 3 4
15.运动增进我的柔软度。 1 2 3 4
16.运动改善我的脾气。 1 2 3 4
17.运动帮助我晚上睡的较好。 1 2 3 4
18.假如我做运动,我将会活的久一点。 1 2 3 4
19.运动帮助我减少疲劳。 1 2 3 4
20.运动是让我遇见新朋友的好方法。 1 2 3 4
21.运动改善我的身体持久力。 1 2 3 4
22.运动改善我对自己的想法。 1 2 3 4
23.运动增加我心理上的警觉性。 1 2 3 4
24.运动可使我做正常活动(如煮饭、购物、
园艺、清洁等)时不会觉得疲倦。 1 2 3 4
25.运动改善我的工作品质。 1 2 3 4
26.运动是好的娱乐。 1 2 3 4
27.运动增加其它人对我的接受度(如较喜
欢与我相处、较接受我的想法等)。 1 2 3 4
28.运动增进我整体的身体功能。 1 2 3 4
29.运动改善我身体的外观(如看起来较健康、
较年轻等)。 1 2 3 4

601
运动阻碍量表
说明:以下叙述是关于运动的一些想法,请用圈选的方式,指出您对每个叙述
同意或不同意的程度。
1 = 强烈不同意
2 = 不同意
3 = 同意
4 = 强烈同意
1.运动用掉太多我的时间。 1 2 3 4
2.运动让我疲倦。 1 2 3 4
3.做运动的地方离我太远。 1 2 3 4
4.我觉得很不自在去做运动。 1 2 3 4
5.运动要花太多的钱。 1 2 3 4
6.做运动场所的时间表对我是不方便的。 1 2 3 4
7.运动使我觉得疲惫不堪。 1 2 3 4
8.我的配偶(或其它重要的人)不鼓励运动。 1 2 3 4
9.运动用掉太多家庭责任的时间(如做家务、
农务、照顾生病的家人等)。 1 2 3 4
10.我觉得人们做运动时的衣服看起来可笑。 1 2 3 4
11.我的家人不鼓励我去做运动。 1 2 3 4
12.运动用掉太多家庭互动的时间(如与家人
相处、家庭聚会等)。 1 2 3 4
13.对我而言,做运动是困难的事情。 1 2 3 4
14.我能做运动的场所太少了。 1 2 3 4

602
第四部分 身体活动自我报告与自我评价表
指导语:该表格用于记录您每天进行中等强度体力活动的情况,包括体力活动
的种类(参见中等强度活动的例子)、次数、强度、持续时间、是否发生心绞
痛以及因为体力活动额外服用抗心绞痛药物的情况?体力活动的强度用 Borg 自
我辛苦评估指数(RPE),从 6 至 20。6 表示非常轻松(安静休息时感觉),
20 表示精疲力竭。请记录您每次体力活动时感觉到的辛苦程度,请选择从 6 到
20 的数字表示您的体力活动强度。同时,记录每次体力活动的种类、次数、持
续的时间(分钟)、运动时是否发生心绞痛以及因为运动需要额外服用硝酸甘
油或其它抗心绞痛药物使用的片数(即扣除平时常规服用的片数)。
自我辛苦评估指数
非
常
轻松
很
轻
松
轻
松
有
点
辛苦
辛
苦
很
辛
苦
非
常
辛苦
非
常
轻松

603
日期
体力活动情况
合计
星期一 星期二 星期三 星期四 星期五 星期六 星期日
体力活动的种类
体力活动的次数
体力活动的强度 (RPE: 6-20)
体力活动的持续时间(分钟)
体力活动时是否发生
心绞痛
无
有
因为体力活动需要额外服用硝
酸甘油类或其它抗心绞痛药物
(片数)

604
第五部分 心绞痛自我报告与自我评价表
指导语:该表格用以记录您每天心绞痛发生的情况。请详细记录您出现心绞痛
的次数、每次疼痛的强度、持续时间、及每天服用抗心绞痛药物使用的片数。
心绞痛疼痛的强度用下列的疼痛评估量表从 0 至 10 表示,0 表示您没有疼痛,5
表示有十分痛,10 表示痛到死,依据您感受的疼痛情况选择从 0 到 10 的数字表
示您的疼痛强度。请您记录每次心绞痛发作持续的时间(分钟)和每天硝酸甘
油或其它抗心绞痛药物使用的次数及数量(片/粒数)。
10
痛到死
9
痛摧肺腑
8
剧痛
7
不可忍受
6
难以形容
5
十分痛
4
好痛
3
可以忍受
2
颇痛
1
微痛
0 不痛
605
日期
心绞痛情况
合计*
星期一 星期二 星期三 星期四 星期五 星期六 星期日
心绞痛发作次数
心绞痛的强度 (0-10)
每次心绞痛发作持续
的时间(分钟)
每天含服硝酸甘油或
其它抗心绞痛药物的
片数
注释:*合计时心绞痛的强度算平均每次心绞痛疼痛的强度

606
第六部分 生活质量调查问卷
西雅图心绞痛问卷
1.下列是一般人在一周当中经常进行的活动。虽然对某些有严重疾病的患者,
他们的日常活动受到限制的原因很难确定,请就下列的活动,指出您在过去 4
星期中,因为胸痛、胸闷、或心绞痛而受到限制的程度 。
(请在每一行相应的□内打“√”)
有极
大限
制
有较
大限
制
有一
些限
制
有很
少限
制
没有
任何
限制
因其他原因受限
制或没有进行此
活动
自己穿衣服 □ □ □ □ □ □
在室内的平地行走 □ □ □ □ □ □
淋浴 □ □ □ □ □ □
上小山坡或上一层楼梯
而中途不休息 □ □ □ □ □ □
整理花园、吸尘或提携
杂物 □ □ □ □ □ □
快速地走一个街口以上 □ □ □ □ □ □
跑步或慢跑 □ □ □ □ □ □
提起或移动重物(如家
具、小孩) □ □ □ □ □ □
参与激烈运动(如游泳
和打网球) □ □ □ □ □ □
2.与 4 星期前比较,当您进行最激烈的活动时,胸痛、胸闷或心绞痛等情形有
多常发生?
更常发生 较常发生 大致一样 较少发生 更少发生 过去四星期中从
未发生胸痛
□ □ □ □ □ □

607
3.在过去 4 星期中,平均而言,您曾发生过几次胸痛、胸闷或心绞痛?
我发生过胸痛、胸闷或心绞痛„„
每天 4 次
或以上
每天
1-3 次
每星期 3 次或以
上,但不是每天
发生
每星期
1-2 次
每星期少
于 1 次
过去四星期
中从未发生
□ □ □ □ □ □
4.在过去 4 星期中,平均而言,您曾因胸痛、胸闷或心绞痛而服用过几次舌下
含片(如硝化甘油粒或救心药)或其它抗心绞痛药物?
我曾服用过几次舌下含片„„
每天 4 次
或以上
每天
1-3 次
每星期 3 次或以
上,但不是每天
服用
每星期
1-2 次
每星期少
于 1 次
过去四星期
中从未服用
□ □ □ □ □ □
5. 服用医生所开给您治疗胸痛、胸闷或心绞痛的药物会对您造成多少困扰?
有极大困
扰
有较大困
扰
有一些困
扰
有很少困
扰
没有任何
困扰
医生没开
处方
□ □ □ □ □ □
6.对于您的胸痛、胸闷或心绞痛的所有治疗,您的满意度如何?
完全不满意 大多不满意 有些满意 大多满意 非常满意
□ □ □ □ □

608
7.对于您的医生曾向您解释说明有关您的胸痛、胸闷或心绞痛情形,您的满意
度如何?
完全不满意 大多不满意 有些满意 大多满意 非常满意
□ □ □ □ □
8.总的来说,对于目前您胸痛、胸闷或心绞痛等的治疗情形,您的满意度如
何?
完全不满意 大多不满意 有些满意 大多满意 非常满意
□ □ □ □ □
9.过去 4 星期中,因为胸痛、胸闷或心绞痛而影响您享受生活的程度有多大?
极大影响
我的生活享受
较大影响
我的生活享受
有一些影响
我的生活享受
很少影响
我的生活享受
没有任何影响
我的生活享受
□ □ □ □ □
10.假如在您今后的生活中胸痛、胸闷或心绞痛的状况与现在一样,您对此的
感觉如何?
完全不满意 大多不满意 有些满意 大多满意 非常满意
□ □ □ □ □
11.您有多常想到或担心您可能会心脏病发作和突然死亡?
我无法停止想
到或担心
我经常想到
或担心
我有时会想
到或担心
我很少想
到或担心
我从未想到
或担心
□ □ □ □ □

609
健康状况调查问卷 (SF-36)
下面的问题是询问您对自己健康状况的看法、您的感觉如何以及您进行日常活
动的能力如何。如果您没有把握如何回答问题,尽量作一个最好的答案,并在
您认为最适合您的答案上打一个“√”。
1. 总体来讲,您目前的健康状况是:
非常好
很好
好
一般
差
2.跟一年前相比,您觉得您现在的健康状况是:
比一年前好多了
比一年前好一些
和一年前差不多
比一年前差一些
比一年前差多了
健康和日常活动
3.以下这些问题都与日常活动有关。您目前的健康状况是否限制了这些活动?
如果有限制,程度如何?
有很多
限制
有一点
限制
根本没
限制
⑴重体力活动(如跑步、搬重物、激烈活动等)
⑵一般体力活动(如移桌子、扫地、做操等)
⑶手提日杂用品(如买菜、购物等)
⑷上几层楼梯
610
⑸上一层楼梯
⑹弯腰、屈膝、下蹲
⑺步行 1500 米左右的路程
⑻步行 800 米左右的路程
⑼步行约 100 米的路程
⑽自己洗澡、穿衣
4.在过去四个星期里,您的工作和日常活动有没有因为身体健康的原因而出现
以下这些问题?
有 没有
⑴减少了工作或其他活动的时间
⑵本来想要做的事情只能完成一部分
⑶想要做的工作与活动的种类受到限制
⑷完成工作或其他活动有困难(比如:感到格外吃力)
5.在过去四个星期里,您的工作和日常活动有没有因为情绪问题(如感到消沉
或者忧虑)的原因而出现以下问题?
有 没有
⑴减少了工作或其他活动的时间
⑵本来想要做的事情只能完成一部分
⑶工作或从事其他活动时不如平时仔细
6.在过去四个星期里,您的身体健康状况或情绪不好在多大程度上影响了您与
家人、朋友、邻居或单位同事的正常社交活动?
根本没有影响
很少有影响
有中度影响
有较大影响
有极大影响

611
7.在过去四个星期里,您有身体上的疼痛吗?
根本没有疼痛
有很轻微疼痛
有轻微疼痛
有中度疼痛
有严重疼痛
有很严重疼痛
8.在过去四个星期里,您身体上的疼痛影响您的正常工作吗?(包括上班和家
务活动等)?
根本没有影响
有一点影响
有中度影响
有较大影响
有极大影响
您的感觉
9.以下这些问题有关过去一个月里您的感觉如何以及您的情况如何。(对每一
条问题,请钩出最接近您的感觉的那个答案)
在过去一个月里持续的时间 所有的
时间
绝大部
分时间
比较多
时间
一部分
时间
小部分
时间
没有此
感觉
⑴您觉得生活充实吗?
⑵您感到精神紧张吗?
⑶您感到垂头丧气,什么事
情都不能使您振作起来吗?
⑷您感到心平气和吗?
⑸您感到精力充沛吗?
⑹您感到情绪低落吗?
⑺您感到精疲力竭吗?

612
⑻您感到快乐吗?
⑼您感到疲乏吗?
⑽您的健康限制了您的社交
活动(如走亲访友)吗?
10.请对下面的每一句话,选出最符合您情况的答案?
(每一横行只打一个钩)
绝对
正确
部分
正确
不能
肯定
大部分
错误
绝对
错误
⑴我好像比别人容易生病
⑵我和我认识的人一样健康
⑶我感到我的健康状况在变坏
⑷我的健康状况非常好

613
Appendix XIII Scoring Instructions – Chinese Version
第一部分 规律身体活动之变动时期问卷计分和统计说明
规律身体活动之变动时期问卷可以用三种统计方法来处理:① 在每个数
据收集的阶段(如:T0, T1, T2 和 T3),对每个规律身体活动之变动时期的分布
情况,可以用频数进行统计。由于五个时期(前意向期、意向期、准备期、行
动期和维持期)之间是等级资料,本研究中有三个组(对照组、一般健康教育
组和时期匹配运动干预组),所以组间比较可以应用秩和检验(K-W test)进
行分析,组内比较可以用 M 检验(Friedman test)进行分析。② 将干预后或随
访时的规律身体活动之变动时期的变动情况与干预前比较,将其数据看成是计
数资料,即如果个体干预后向前移动一个时期或以上(如:从前意向期向意向
期移动或行动期移动)则为进步;如果个体干预后向后或倒退一个时期或以上
(如:从意向期向前意向期移动或行动期向前意向期移动)则为退步;如果个
体干预后运动时期没有改变则为稳定。可以用频数进行统计,然后组间比较可
以应用秩和检验(K-W test)进行分析,组内比较可以用 M 检验(Friedman
test)进行分析。 ③ 干预前后的规律身体活动之变动时期的效果变成计量资料
来分析,即如果个体干预后向前移动一个时期(如:从前意向期向意向期移动
或意向期向行动期移动)得 1 分;如果个体干预后向前移动两个时期(如:从
前意向期向行动期移动)得 2 分,以此类推。如果个体干预后向后或倒退一个
时期(如:从意向期向前意向期移动或行动期向意向期移动)得负 1 分;如果
倒退两个时期(如:从行动期向前意向期移动)得负 2 分,以此类推。最后可
以做均数分析。对 T1 (T1-T0), T2 (T2-T0) 和 T3 (T3-T0) 的得分,用单因素方差分
析或 K-W 非参数检验(如果数据不呈正态分布或方差齐性不齐)。组内不同时
间点的比较可用重复测量的方差分析或 M 检验(Friedman test)进行分析。
(Nigg, 2002, cited in G.J. Welk (Ed)).

614
第二部分 运动自我效能量表计分和统计说明
运动自我效能量表包括 18 条条目,每条条目的得分介于 0 分(完全不能
做)至 100 分(肯定能做)之间。可以将运动自我效能量表中每一条条目所得
分数相加,求得总分。总分范围是 0 分至 1800 分。分数越高说明越有信心执行
规律的身体活动。该数据是计量资料,可以求得均分,然后应用双因素重复测
量的方差分析进行检验组内和组间得分的差异。如果数据呈正态分布并且方差
齐性检验齐的话,每个时间点的组间之间比较用单因素方差分析(如 T0, T1, T2
和 T3),每个组内不同时间点的比较可用重复测量的方差分析。如果数据不呈
正态分布或方差齐性检验不齐的话,则每个时间点的组间之间比较用非参数的
秩和检验(K-W test),每个组内不同时间点的比较可用 M 检验 (Friedman test)。
第三部分 运动益处和障碍量表计分和统计说明
运动益处和障碍量表可以作为一个总量表或分成两个次量表,即运动益
处量表和运动障碍量表。该量表的每条条目有四个等级的答案,即从非常同意
(4)至非常不同意(1)。如果该量表作为一个总量表来看,则运动障碍量表
条目的计分是反向得分,即非常同意得 1 分,非常不同意得 4 分。
丢失数据可以有两种方法处理:如果超过 5%的条目没有回答,则建议将
这份问卷丢弃;如果少于 5%的条目没有回答,则用中位数代替丢失的数据以防
错误的低得分。
该量表总体得分介于 43 至 172 分之间。分数越高说明个体越感觉运动有
好处。当两个量表单独使用时,运动益处量表的得分介于 29 至 116 分之间,运
动障碍量表的得分介于 14 至 56 分之间。如果两个量表单独使用,运动障碍量
表的计分不需要反向计分,这时,运动障碍量表的分数越高,说明个体感受到
的运动障碍越大。
在本研究中,运动益处和障碍量表作为两个次量表来用。两个次量表的
得分分开来计算。该数据是计量资料,可以求得均分,然后应用双因素重复测
量的方差分析进行检验组内和组间得分的差异。如果数据呈正态分布并且方差
615
齐性检验齐的话,每个时间点的组间之间比较用单因素方差分析(如 T0, T1, T2
和 T3),每个组内不同时间点的比较可用重复测量的方差分析。如果数据不呈
正态分布或方差齐性检验不齐的话,则每个时间点的组间之间比较用非参数的
秩和检验(K-W test),每个组内不同时间点的比较可用 M 检验 (Friedman test)。
第四部分 身体活动自我报告与自我评价日志计分和统计说明
1.身体活动时间:计算在过去一周里,进行任何有计划/有目的(为增强健康
而进行的)的活动时间和中等强度活动的时间。中等强度活动的时间是依据
病人进行中等强度活动例子表格中活动的时间来算。该数据是计量资料,可
以求得均分,然后应用双因素重复测量的方差分析进行检验组内和组间得分
的差异。如果数据呈正态分布并且方差齐性检验齐的话,每个时间点的组间
之间比较用单因素方差分析(如 T0, T1, T2 和 T3),每个组内不同时间点的
比较可用重复测量的方差分析。如果数据不呈正态分布或方差齐性检验不齐
的话,则每个时间点的组间之间比较用非参数的秩和检验(K-W test),每个
组内不同时间点的比较可用 M 检验 (Friedman test)。
2.抗心绞痛药物使用的次数和片数或粒数:计算在过去一周里,因为运动或身
体活动出现胸痛、胸闷或心绞痛而服用任何抗心绞痛药物的次数和数量(片
/粒),例如:硝酸甘油、麝香保心丸、丹参滴丸或速效救心丸的次数和片/
粒数。虽然这几种药物都具有抗心绞痛作用,但这几种药物的服用方法的和
使用剂量不同,不能进行简单的服用片数或粒数进行比较。根据病人是否服
用抗心绞痛的药物,可将数据视为分类资料。进行频数统计,然后用卡方检
验进行统计分析。对于抗心绞痛药物使用的次数可视为计量资料,根据数据
是否呈正态分布和方差齐性与否,每个时间点(如 T0, T1, T2 和 T3)的组间
之间比较用单因素方差分析或用非参数的秩和检验(K-W test),每个组内不
同时间点的比较用重复测量的方差分析或 M 检验 (Friedman test)。
非
常
轻
松

616
第五部分 心绞痛自我报告和自我评价日志计分和统计说明
1.心绞痛发作次数(次数/周):计算在过去的一周里,病人心绞痛发作的次
数。该数据是计量资料,根据数据是否呈正态分布和方差齐性与否,每个时
间点(如 T0, T1, T2 和 T3)的组间之间比较用单因素方差分析或用非参数的
秩和检验(K-W test),每个组内不同时间点的比较用重复测量的方差分析或
M 检验 (Friedman test)。
2.心绞痛的强度(0-10):根据疼痛评估量表,心绞痛疼痛的强度用从 0 至 10
表示,0 表示您没有疼痛,5 表示有十分痛,10 表示痛到死。如果患者选微
痛,计 1 分;选颇痛计 2 分;依此类推。计算在过去的一周里,平均每次心
绞痛疼痛的强度。该数据是计量资料,根据数据是否呈正态分布和方差齐性
与否,每个时间点(如 T0, T1, T2 和 T3)的组间之间比较用单因素方差分析
或用非参数的秩和检验(K-W test),每个组内不同时间点的比较用重复测量
的方差分析或 M 检验 (Friedman test)。
3.心绞痛发作的时间(分钟/周):计算在过去的一周里,心绞痛发作的总的
时间,即一周内每次心绞痛发作时间的总和。该数据是计量资料,根据数据
是否呈正态分布和方差齐性与否,每个时间点(如 T0, T1, T2 和 T3)的组间
之间比较用单因素方差分析或用非参数的秩和检验(K-W test),每个组内不
同时间点的比较用重复测量的方差分析或 M 检验 (Friedman test)。
4.根据病人是否出现心绞痛,可将数据视为分类资料。进行频数统计,然后用
卡方检验进行各个时间点(如 T0, T1, T2 和 T3)组间统计分析,用 Cochran‘s
Q 检验进行组内比较。
5.抗心绞痛药物的使用:计算在过去的一周里,使用抗心绞痛药物的片数或粒
数。例如:硝酸甘油、麝香保心丸、丹参滴丸或速效救心丸的次数和片/粒
数。虽然这几种药物都具有抗心绞痛作用,但这几种药物的服用方法的和使
用剂量不同,不能进行简单的服用片数或粒数进行比较。根据病人是否服用
抗心绞痛的药物,可将数据视为分类资料。进行频数统计,然后用卡方检验
进行各个时间点(如 T0, T1, T2 和 T3)组间统计分析,用 Cochran‘s Q 检验进
行组内比较。

617
第六部分 西雅图心绞痛问卷计分说明
西雅图心绞痛问卷包括以下五个部分:
A. 躯体受限
躯体受限次量表的得分是对应问题1a 至 1i 。1a 至1i 答案数字编码如下:
1 = 有极大限制
2 = 有较大限制
3 = 有一些限制
4 = 有很少限制
5 = 没有任何限制
6 = 因其他原因受限制或没有进行此活动
如果1a 至1i 的回答不是1、2、3、4或5,那么该条目被当作丢失。值得
一提的是,当回答是6时也被认为是丢失。丢失的数据用该活动水平的平均值来
代替。活动被分为三层活动水平。最低层包括穿衣、走路和淋浴(1a, 1b 和
1c);中间层是爬坡或爬楼梯、整理花园和快速地走一个街口以上(1d, 1e 和
1f); 最高层是慢跑、提重物和激烈运动(1g, 1h 和1i)。如果一组中任何一条
条目丢失,那么用该组中其它条目的均值来代替。如果所以最低或最高层的条
目都丢失,则用中间层的均数值来代替。如果中间层的所以条目都丢失,则用
最高层和最低层和的均数值来代替。如果该躯体受限次量表中有4条以上的条目
的数字丢失,那么就没有合理的计算方法来代替丢失值。计算丢失值以后,躯
体受限次量表的得分为标准化的9条条目平均值,计算方式如下:
躯体受限 = 100*(平均值 – 1)/4
B. 心绞痛稳定性
心绞痛稳定性的得分对应于问题2。问题2的答案数字编码如下:
1 = 更常发生

618
2 = 较常发生
3 = 大致一样
4 = 较少发生
5 = 更少发生
6 = 过去四星期中从未发生胸痛
如果答案为6(过去四星期中从未发生胸痛)则设置为答案3(大致一
样)相同。假如没有回答,那心绞痛的稳定性则无法计算,将被认为是丢失。
否则,心绞痛稳定性的标化计算方式如下:
心绞痛稳定性 = 100*(答案的相应编码 – 1)/4
C. 心绞痛频率
心绞痛频率得分对应于问题3和4。根据健康状况的改善,答案按顺序相
应地被编码为1至6,1为健康状况最差。如果至少有一条条目回答,则心绞痛的
频率标化计算方式如下:
心绞痛频率 = 100*(平均值 – 1)/5
D. 治疗满意度
治疗满意度的得分对应于问题5、6、7和8。根据健康状况的改善,答案
按顺序相应地被编码为1至6,1为健康状况最差。如果问题5、6、7和8的回答不
是1、2、3、4或5,那么该问题视为丢失。值得注意的是,如果问题5的回答是
6,那么也被视为丢失。假如至少有两个条目有回答,那么治疗满意度的标化计
算方式如下:
治疗满意度 = 100*(平均值 – 1)/4
619
E. 生活质量
生活质量的得分对应于问题9、10和11。根据健康状况的改善,答案按顺
序相应地被编码为1至5,1为健康状况最差。如果问题9、10和11的回答不是1、
2、3、4或5,则被认为是丢失。假如至少有两个条目有回答,那么生活质量的
标化计算方式如下:
生活治疗 = 100*(平均值 – 1)/4
第七部分 SF-36计分说明
1. SF-36的内容与结构
2. SF-36计分方法:
2.1 基本步骤
2.2 关于缺失值的处理
2.3 健康状况各方面得分及换算
1. SF-36的内容与结构
SF-36 是美国波士顿健康研究所研制的简明健康调查问卷,被广泛应用
于普通人群的生存质量测定、临床试验效果评价以及卫生政策评估等领域。SF-
36 作为简明健康调查问卷,它从生理机能、生理职能、躯体疼痛、一般健康状
况、精力、社会功能、情感职能以及精神健康等8 个方面全面概括了被调查者
的生存质量。
1.1 生理机能(PF:Physical Functioning):测量健康状况是否妨碍了正常的生
理活动。用第3 个问题来询问PF。
1.2 生理职能(RP:Role-Physical):测量由于生理健康问题所造成的职能限
制。
1.3 躯体疼痛(BP:Bodily Pain):测量疼痛程度以及疼痛对日常活动的影响。

620
1.4 一般健康状况(GH:General Health):测量个体对自身健康状况及其发展
趋势的评价。
1.5 精力(VT:Vitality):测量个体对自身精力和疲劳程度的主观感受。
1.6 社会功能(SF:Social Functioning):测量生理和心理问题对社会活动的数
量和质量所造成的影响,用于评价健康对社会活动的效应。
1.7 情感职能(RE:Role-Emotional):测量由于情感问题所造成的职能限制。
1.8 精神健康(MH:Mental Health):测量四类精神健康项目,包括激励、压
抑、行为或情感失控、心理主观感受。
除了以上8个方面外,SF-36 还包含另一项健康指标:健康变化(HT:Reported
HealthTransition),用于评价过去一年内健康状况的总体变化情况。
2. SF-36计分方法:
2.1 基本步骤:第一步,量表条目编码;
第二步,量表条目计分;
第三步,量表健康状况各个方面计分及得分换算。得分换算的基本公式
为:
换算得分 = 实际得分 - 该方面的可能的最低得分
.100 该方面的可能的最高得分与最低得分之差
2.2 关于缺失值的处理:有时应答者没有完全回答量表中所有的问题条目,我们
把没有答案的问题条目视为缺失。我们建议在健康状况的各个方面所包含的多
个问题条目中,如果应答者回答了至少一半的问题条目,就应该计算该方面的
得分。缺失条目的得分用其所属方面的平均分代替。
2.3 健康状况各方面得分及换算:

621
2.3.1 生理机能(PF:Physical Functioning)
问题条目:3
(1) 重体力活动(如跑步、举重物、激烈运动等)
(2) 适度活动(如移桌子、扫地、做操等)
(3) 手提日杂用品(如买菜、购物等)
(4) 上几层楼梯
(5) 上一层楼梯
(6) 弯腰、曲膝、下蹲
(7) 步行1500米左右的路程
(8) 步行800米左右的路程
(9) 步行约100米的路程
(10) 自己洗澡、穿衣
条目编码及计分
答案 条目编码 条目计分
有很多限制
有一点限制
根本没限制
1
2
3
1
2
3
方面计分及换算
将各个条目得分相加得实际得分,再按下式算得最终得分PF。PF得分越高,健
康状况越好。
PF = 实际得分-10
.100 20
2.3.2 生理职能(RP:Role-Physical)
问题条目:4
(1) 减少了工作或其他活动的时间
(2) 本来想要做的事情只能完成一部分

622
(3) 想要做的工作或活动的种类受到限制
(4) 完成工作或其他活动有困难 (比如,需要额外的努力)
条目编码及计分
答案 条目编码 条目计分
有
没有
1
2
1
2
方面计分及换算
将各个条目得分相加得实际得分,再按下式算得最终得分RP。RP 得分越高,
健康状况越好。
RP = 实际得分-4
.100 4
2.3.3 躯体疼痛(BP:Bodily Pain)
问题条目:7,8
7. 在过去四个星期里, 您有身体上的疼痛吗?
8. 在过去四个星期里, 身体上的疼痛影响您的正常工作吗(包括上班工作和家务
活动)?
条目7的编码及计分
答案 条目编码 条目计分
根本没有疼痛
有很轻微疼痛
有轻微疼痛
有中度疼痛
有严重疼痛
有很严重疼痛
1
2
3
4
5
6
6.0
5.4
4.2
3.1
2.2
1.0
条目8的编码及计分-----如果对条目7和8均做了回答

623
答案 如果条目8的编码为 且 条目7的编码为 那么 条目8的计
分为
根本没有影响 1 1 6
根本没有影响 1 2 至 6 5
有一点影响 2 1 至 6 4
有中度影响 3 1 至 6 3
有较大影响 4 1 至 6 2
有极大影响 5 1 至 6 1
条目8的编码及计分-----如果对条目7没有做回答
答案 条目编码 条目计分
根本没有影响 1 6.0
有一点影响 2 4.75
有中度影响 3 3.5
有较大影响 4 2.25
有极大影响 5 1.0
方面计分及换算
将各个条目得分相加得实际得分,再按下式算得最终得分BP。BP 得分越高,
健康状况越好。
BP = 实际得分-2
.100 10
2.3.4 一般健康状况(GH:General Health)
问题条目:1,10
1. 总体来讲, 您的健康状况是
10.1 我好象比别人容易生病
10.2 我跟我认识的人一样健康
10.3 我认为我的健康状况在变坏

624
10.4 我的健康状况非常好
条目1&10.1-10.4的编码及计分
问题条目1 答案 条目编码 条目计分
非常好 1 5.0
很好 2 4.4
好 3 3.4
一般 4 2.0
差 5 1.0
问题条目10.1,
10.3 答案 条目编码 条目计分
绝对正确 1 1
大部分正确 2 2
不能肯定 3 3
大部分错误 4 4
绝对错误 5 5
问题条目10.2,
10.4 答案 条目编码 条目计分
绝对正确 1 5
大部分正确 2 4
不能肯定 3 3
大部分错误 4 2
绝对错误 5 1
方面计分及换算
将各个条目得分相加得实际得分,再按下式算得最终得分GH。GH 得分越高,
健康状况越好。
GH = 实际得分-5
.100 20

625
2.3.5 精力(VT:Vitality)
问题条目:9.1,9.5,9.7,9.9
9.1 您觉得生活充实吗?
9.5 您精力充沛吗?
9.7 您觉得筋疲力尽吗?
9.9 您感觉疲劳吗?
条目的编码及计分
问题条目9.1,9.5 答案 条目编码 条目计分
所有的时间 1 6
大部分时间 2 5
比较多时间 3 4
一部分时间 4 3
小部分时间 5 2
没有此感觉 6 1
问题条目9.7,9.9 答案 条目编码 条目计分
所有的时间 1 1
大部分时间 2 2
比较多时间 3 3
一部分时间 4 4
小部分时间 5 5
没有此感觉 6 6
方面计分及换算
将各个条目得分相加得实际得分,再按下式算得最终得分VT。VT得分越高,
健康状况越好。
VT = 实际得分-4
.100 20

626
2.3.6 社会功能(SF:Social Functioning)
问题条目:6,9.10
6. 在过去的四个星期里, 您的身体健康或情绪不好在多大程度上影响了您与家
人、朋友、邻居或集体的正常社交活动?
9.10 您的健康限制了您的社交活动(如走亲访友)吗?
条目的编码及计分
问题条目6 答案 条目编码 条目计分
根本没有影响 1 5
很少有影响 2 4
有中度影响 3 3
有较大影响 4 2
有极大影响 5 1
问题条目9.10 答案 条目编码 条目计分
所有的时间 1 1
大部分时间 2 2
比较多时间 3 3
一部分时间 3 3
小部分时间 4 4
没有此感觉 5 5
方面计分及换算
将各个条目得分相加得实际得分,再按下式算得最终得分SF。SF得分越高,健
康状况越好。
SF = 实际得分-2
.100 8

627
2.3.7 情感职能(RE:Role-Emotional)
问题条目:5
(1) 减少了工作或其它活动的时间
(2) 本来想要做的事情只能完成一部分
(3) 做工作或其它活动不如平时仔细
条目的编码及计分
答案 条目编码 条目计分
有 1 1
没有 2 2
方面计分及换算
将各个条目得分相加得实际得分,再按下式算得最终得分RE。RE 得分越高,
健康状况越好。
RE = 实际得分-3
.100 3
2.3.8 精神健康(MH:Mental Health)
问题条目:9.2,9.3,9.4,9.6,9.8
9.2 您是一个精神紧张的人吗?
9.3 您感到垂头丧气,什么事都不能使您振作起来吗?
9.4 您觉得平静吗?
9.6 您的情绪低落吗?
9.8 您是个快乐的人吗?
条目的编码及计分
问题条目9.2,
9.3,9.6 答案 条目编码 条目计分
所有的时间 1 1
大部分时间 2 2

628
比较多时间 3 3
一部分时间 4 4
小部分时间 5 5
没有此感觉 6 6
问题条目9.4,9.8 答案 条目编码 条目计分
所有的时间 1 6
大部分时间 2 5
比较多时间 3 4
一部分时间 4 3
小部分时间 5 2
没有此感觉 6 1
方面计分及换算
将各个条目得分相加得实际得分,再按下式算得最终得分MH。MH得分越高,
健康状况越好。
MH = 实际得分-5
.100 25
2.3.9 健康变化(HT:Reported Health Transition)
问题条目:2
2. 跟一年前相比, 您觉得您现在的健康状况是:
条目的编码及计分
答案 条目编码
比一年前好多了 1
比一年前好一些 2
和一年前差不多 3
比一年前差一些 4
比一年前差多了 5
(中山医科大学公共卫生学院卫生统计学教研室 方积乾、郝元涛, 2009)

629
Appendix XIV Training Package – Chinese Version
教练包
这个教练包是介绍如何训练研究助理收集数据。主要包括两个步骤:(1)研究
者和研究助理一起过目每一个条目,并解释每个条目的意思和如何使用指导
语,以便研究对象能更好的理解和填写问卷;(2)角色扮演:选择 1-2 个人扮
演病人,研究者作为观众,研究助理根据问卷上的条目一一询问“病人”来收
集数据。对有异议的地方,研究者及时给以更正和解释,以确保每条条目尽量
使用统一的指导语。
首先,作为数据收集者必须明白每个量表使用的目的、每个量表中每条条目的
意思以及每个量表使用的注意事项。以下我们一一来介绍每个量表。
630
第一部分 规律身体活动之变动时期问卷
说明:
规律身体活动之变动时期问卷是用来评估病人目前的运动行为处于哪个
时期。其中:
1.中等强度身体活动:是指代谢当量为3-6代谢当量(MET)的活动,如:站在
河边钓鱼(3.5MET)(具体参见中等强度活动的例子)。
2.规律的身体活动:是指任何有计划/有目的(为增强健康而进行的)的活
动。这种活动必须累积每天至少30分钟(每次至少10分钟)的中等强度身体活
动,每星期至少五天。
3.不同运动时期的定义
(1) 意向前期:是指个体目前没有进行任何运动,并且不打算在未来的六个
月里开始运动。
(2) 意向期:是指个体已经意识到久坐行为是有问题的,而且他/她认真地考
虑在未来的六个月里开始运动。
(3) 准备期:是指个体打算在未来的30天里采取行动,改变静坐的习惯,或
个体已经开始一些运动,但不规律。
(4) 行动期:是指个体改变他(她)的行为、体验或环境来克服他的问题;
他已经成功地进行规律运动少于6个月。
(5) 维持期:是指个体已经维持规律运动6个月以上。
4. 问卷中:1 =意向前期,2 = 意向期,3 = 准备期,4 = 行动期,5 = 维持期
5.决定运动/身体活动变化之时期的方法 (见图 1)
研究助理用图 1 的流程图来评估病人目前的运动时期。当问到“您是否每周绝
大多数时间(5 天或以上)累积做每天至少 30 分钟的中等强度活动?”时,研
究助理要出示中等强度活动例子的表格给病人,问他/她是否进行表格中所列的
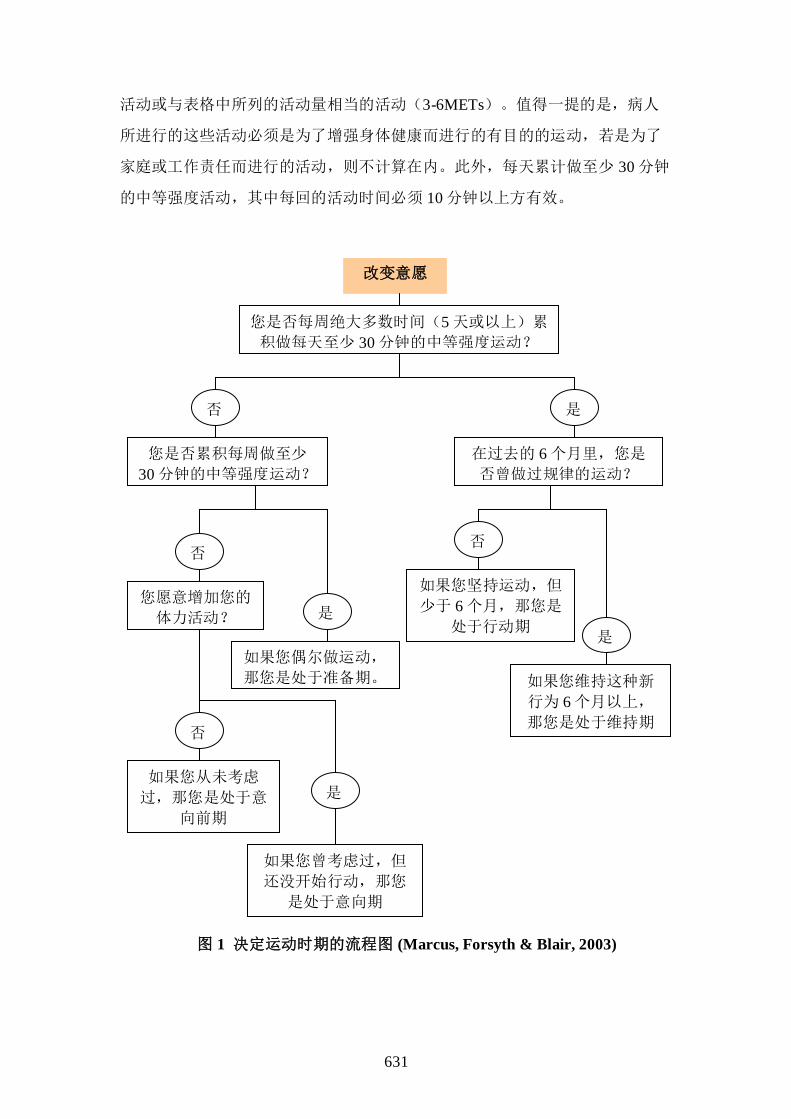
631
活动或与表格中所列的活动量相当的活动(3-6METs)。值得一提的是,病人
所进行的这些活动必须是为了增强身体健康而进行的有目的的运动,若是为了
家庭或工作责任而进行的活动,则不计算在内。此外,每天累计做至少 30 分钟
的中等强度活动,其中每回的活动时间必须 10 分钟以上方有效。
改变意愿
您是否每周绝大多数时间(5 天或以上)累
积做每天至少 30 分钟的中等强度运动?
您是否累积每周做至少
30 分钟的中等强度运动?
在过去的 6 个月里,您是
否曾做过规律的运动?
您愿意增加您的
体力活动?
如果您偶尔做运动,
那您是处于准备期。
如果您坚持运动,但
少于 6 个月,那您是
处于行动期
如果您维持这种新
行为 6 个月以上,
那您是处于维持期
如果您从未考虑
过,那您是处于意
向前期
如果您曾考虑过,但
还没开始行动,那您
是处于意向期
否 是
是
是
是
否 否
否
图 1 决定运动时期的流程图 (Marcus, Forsyth & Blair, 2003)

632
第二部分 运动自我效能量表
说明:
1.由于很多状况可能会影响您维持或进行规律的身体活动,运动自我效能量表
是用来测量假设您遇到以下 18 种情况(量表的内容)时,您有多少信心执行规
律的身体活动。0 表示完全不能做或完全没有信心做,100 表示肯定能做或肯定
有信心做,50 表示中度肯定能做(如下刻度)。从 0 到 100 分,将符合您情况
的数值填在横线上。
0 10 20 30 40 50 60 70 80 90 100
完全不能做 中度肯定能做 肯定能做
2.量表上每个指标使用的指导语
(1)当我觉得疲劳时:当您觉得疲劳时,您有多少信心完成每周五次或五次以
上的规律身体活动?从 0 至 100 分选一个数字表示您能执行的信心程度。
0 表示完全不能做或完全没有信心做,100 表示肯定能做或肯定有信心
做。
(2)当我觉得工作有压力时:当您觉得工作上有压力时,您有多少信心完成每
周五次或五次以上的规律身体活动?从 0 至 100 分选一个数字表示您能执
行的信心程度。
(3)天气不好时:当天气不好时(如下雨、太冷或太热),您有多少信心完成
每周五次或五次以上的规律身体活动?从 0 至 100 分选一个数字表示您能
执行的信心程度。
(4)因受伤停止了运动,等损伤愈合后:如果您因为身体受伤停止了运动,那
损伤愈合后,您有多少信心完成每周五次或五次以上的规律身体活动?从
0 至 100 分选一个数字表示您能执行的信心程度。
(5)正在经历或刚经历了个人问题后:如果您正在经历或刚经历了个人问题
(如:感情或婚姻问题)之后,您有多少信心完成每周五次或五次以上的
规律身体活动?从 0 至 100 分选一个数字表示您能执行的信心程度。

633
(6)当我觉得沮丧时:当您觉得沮丧(灰心失望)时,您有多少信心完成每周
五次或五次以上的规律身体活动?从 0 至 100 分选一个数字表示您能执行
的信心程度。
(7)当我觉得焦虑时:当您觉得焦虑时,您有多少信心完成每周五次或五次以
上的规律身体活动?从 0 至 100 分选一个数字表示您能执行的信心程度。
(8)因疾病而使我停止运动康复后:如果您因为疾病(如:感冒)而停止运动
(或规律身体活动),等疾病康复后, 您有多少信心完成每周五次或五
次以上的规律身体活动?从 0 至 100 分选一个数字表示您能执行的信心程
度。
(9)当我运动觉得不舒服时:当您运动(或规律身体活动)觉得不舒服时,您
有多少信心完成每周五次或五次以上的规律身体活动?从 0 至 100 分选一
个数字表示您能执行的信心程度。
(10)在假期后:在假期(如度假、节假日、过年、过节)后,您有多少信心
完成每周五次或五次以上的规律身体活动?从 0 至 100 分选一个数字表示
您能执行的信心程度。
(11)当我在家里有太多工作要做时:当您在家里有太多工作(或事情)要做
时,您有多少信心完成每周五次或五次以上的规律身体活动?从 0 至 100
分选一个数字表示您能执行的信心程度。
(12)当有客人来访时:当您家里有客人来访时,您有多少信心完成每周五次
或五次以上的规律身体活动?从 0 至 100 分选一个数字表示您能执行的信
心程度。
(13)当有其他有趣的事情要做时:当您有其他有趣的事情(您感兴趣的事
情,如:看电视节目)要做时,您有多少信心完成每周五次或五次以上的
规律身体活动?从 0 至 100 分选一个数字表示您能执行的信心程度。
(14)如果我没有达到自己的运动目标时:如果您没有达到自己的运动目标
(每周至少五次以上的运动)时,您有多少信心完成每周五次或五次以上
的规律身体活动?从 0 至 100 分选一个数字表示您能执行的信心程度。
(15)没有我的家人和朋友的支持时:如果您的家人和朋友都不支持时,您有
多少信心完成每周五次或五次以上的规律身体活动?从 0 至 100 分选一个
数字表示您能执行的信心程度。

634
(16)在假期中:如果您正在度假(如,旅游、出游等)或正在节假日、过年
过节中,您有多少信心完成每周五次或五次以上的规律身体活动?从 0 至
100 分选一个数字表示您能执行的信心程度。
(17)当我有其他的事情约定时:当您有其他的事情约定时,您有多少信心完
成每周五次或五次以上的规律身体活动?从 0 至 100 分选一个数字表示您
能执行的信心程度。
(18)在经历家庭事件后:如果在您经历家庭事件(如:重大的家庭经济问题
或亲人去世等)后,您有多少信心完成每周五次或五次以上的规律身体活
动?从 0 至 100 分选一个数字表示您能执行的信心程度。
第三部分 运动益处和阻碍量表
运动益处量表
说明:
1.运动益处量表是用来测量病人认为运动有什么好处。研究助理可以针对每条
叙述问病人是否同意该叙述,以及同意或不同意的程度。如果病人强烈不同意
该叙述则选 1,只是不同意选 2,同意选 3,强烈同意则选 4。
2.量表上每个指标使用的指导语
(1) 我从运动得到乐趣:您是否同意您从运动中得到乐趣?是强烈(不)同
意或只是(不)同意?
(2) 运动减少我紧张和压力的感觉:您是否同意运动减少您紧张和压力的感
觉?是强烈(不)同意或只是(不)同意?
(3) 运动增进我的心理健康:您是否同意运动增进您的心理健康?是强烈
(不)同意或只是(不)同意?
(4) 运动将预防我发生心脏病:您是否同意运动将预防您发生心脏病?是强
烈(不)同意或只是(不)同意?
(5) 运动会增强我的肌肉力量:您是否同意运动会增强您的肌肉力量?是强
烈(不)同意或只是(不)同意?

635
(6) 运动给予我个人成就感:您是否同意运动给予您个人成就感?是强烈
(不)同意或只是(不)同意?
(7) 运动使我觉得放松:您是否同意运动使您觉得放松?是强烈(不)同意
或只是(不)同意?
(8) 运动让我和我喜欢的朋友及人们有联系:您是否同意运动让您和您喜欢
的朋友及人们有联系?是强烈(不)同意或只是(不)同意?
(9) 运动将使我远离高血压:您是否同意运动将使您远离高血压?是强烈
(不)同意或只是(不)同意?
(10)运动改善我的心脏血管系统功能:您是否同意运动改善您的心脏血管系
统功能(如增强心脏功能)?是强烈(不)同意或只是(不)同意?
(11)运动增进我的身体体能的强度:您是否同意运动增进您的身体体能的强
度(如:增强体质)?是强烈(不)同意或只是(不)同意?
(12)运动增进我的肌肉结实:您是否同意运动可以增进您的肌肉结实?是强
烈(不)同意或只是(不)同意?
(13)因为运动,我感觉自己比较健康:您是否同意因为运动,您感觉自己比
较健康?是强烈(不)同意或只是(不)同意?
(14)运动增进我的耐力:您是否同意运动可以增进您的耐力(即您做同一强
度的活动,可以活动的更久一点或活动的强度更大一点)?是强烈
(不)同意或只是(不)同意?
(15)运动增进我的柔软度:您是否同意运动可以增进您的柔软度(如:活动
更灵活)?是强烈(不)同意或只是(不)同意?
(16)运动改善我的脾气:您是否同意运动可以改善您的脾气?是强烈(不)
同意或只是(不)同意?
(17)运动帮助我晚上睡的较好:您是否同意运动帮助您晚上睡的更好?是强
烈(不)同意或只是(不)同意?
(18)假如我做运动,我将会活的久一点:您是否同意假如您做运动,您将会
活的久一点?是强烈(不)同意或只是(不)同意?
(19)运动帮助我减少疲劳:您是否同意运动帮助您减少疲劳?是强烈(不)
同意或只是(不)同意?
(20)运动是让我遇见新朋友的好方法:您是否同意运动是让您遇见新朋友的

636
好方法?是强烈(不)同意或只是(不)同意?
(21)运动改善我的身体持久力:您是否同意运动改善您的身体持久力(即您
做同一强度的活动,可以活动的更久一点)?是强烈(不)同意或只是
(不)同意?
(22)运动改善我对自己的想法:您是否同意运动改善您对自己的想法(改善
对自己的看法,如: 因为运动,您认为自己是一个积极者)?是强烈
(不)同意或只是(不)同意?
(23)运动增加我心理上的警觉性:您是否同意运动增加您心理上的警觉性
(反应灵敏)?是强烈(不)同意或只是(不)同意?
(24)运动可使我做正常活动(如煮饭,购物,园艺,清洁等)时不会觉得疲
倦:您是否同意运动可使您做正常活动(如煮饭,购物,园艺,清洁等)
时不会觉得疲倦?是强烈(不)同意或只是(不)同意?
(25)运动改善我的工作品质:您是否同意运动改善您的工作品质(工作质
量)?是强烈(不)同意或只是(不)同意?
(26)运动是好的娱乐:您是否同意运动是好的娱乐?是强烈(不)同意或只
是(不)同意?
(27)运动增加其它人对我的接受度(如较喜欢与我相处,较接受我的想法
等):您是否同意运动增加其它人对您的接受度(如较喜欢与我相处,较
接受您的想法等)?是强烈(不)同意或只是(不)同意?
(28)运动增进我整体的身体功能:您是否同意运动增进您整体的身体功能?
是强烈(不)同意或只是(不)同意?
(29)运动改善我身体的外观(如看起来较健康,较年轻等):您是否同意运动
改善我身体的外观(如看起来较健康,较年轻等)?是强烈(不)同意或
只是(不)同意?

637
运动阻碍量表
说明:
1.运动阻碍量表是用来评估哪些因素阻碍病人进行运动。你可以针对每个叙述
问病人是否同意该叙述,以及同意或不同意的程度。如果病人强烈不同意该叙
述则选 1,只是不同意选 2,同意选 3,强烈同意则选 4。
2.量表上每个指标使用的指导语
(1) 运动用掉太多我的时间:您是否同意运动会用掉太多您的时间?是强烈
(不)同意或只是(不)同意?
(2) 运动让我疲倦:您是否同意运动会使您疲倦?是强烈(不)同意或只是
(不)同意?
(3) 做运动的地方离我太远:您是否同意做运动的地方离您太远?是强烈
(不)同意或只是(不)同意?
(4) 我觉得很不自在去做运动:您是否同意您觉得很不自在去做运动?是强
烈(不)同意或只是(不)同意?
(5) 运动要花太多的钱:您是否同意运动要花太多的钱?是强烈(不)同意
或只是(不)同意?
(6) 做运动场所的时间表对我是不方便的:您是否同意做运动场所的时间表
对您是不方便的?是强烈(不)同意或只是(不)同意?
(7) 运动使我觉得疲惫不堪:您是否同意运动使您觉得疲惫不堪?是强烈
(不)同意或只是(不)同意?
(8) 我的配偶(或其它重要的人)不鼓励运动:您是否同意您的配偶(或其它重
要的人)不鼓励您去运动?是强烈(不)同意或只是(不)同意?
(9) 运动用掉太多家庭责任的时间(如做家务, 农务,照顾生病的家人等)
:您是否同意运动用掉太多您家庭责任的时间(如做家务, 农
务,照顾生病的家人等)?是强烈(不)同意或只是(不)同意?
(10)我觉得人们做运动时的衣服看起来可笑:您是否同意您觉得人们做运动
时的衣服看起来可笑?是强烈(不)同意或只是(不)同意?
(11)我的家人不鼓励我去做运动:您是否同意您的家人不鼓励您去做运动?

638
是强烈(不)同意或只是(不)同意?
(12)运动用掉太多家庭互动的时间(如与家人相处,家庭聚会等):您是否同
意运动用掉太多家庭互动的时间(如与家人相处,家庭聚会等)?是强烈
(不)同意或只是(不)同意?
(13)对我而言,做运动是困难的事情:您是否同意对您来说,做运动是困难
的事情?是强烈(不)同意或只是(不)同意?
(14)我能做运动的场所太少了:您是否同意您能做运动的场所太少了?是强
烈(不)同意或只是(不)同意?
第四部分 身体活动自我报告与自我评价表
说明:
(1) 该表格用于记录研究对象在过去一周里进行中等强度体力活动的情况,
包括体力活动的种类、次数、强度、持续时间、是否发生心绞痛以及因
为体力活动额外服用抗心绞痛药物的情况?
(2) 您(研究助理)可以出示中等强度活动的例子的表格给病人,问病人在
过去一周里进行了哪些体力活动?结合研究对象自我记录的身体活动情
况,将在过去一周中每天身体活动的次数,每次活动持续的时间(用分
钟表示),填写在相应的表格里。
(3) 每次体力活动的强度用 Borg 自我辛苦评估指数(RPE),从 6 至 20 表
示。6 表示非常轻松(安静休息时感觉),20 表示精疲力竭。请研究对
象回忆在过去的一周里,您每次进行体力活动时感觉到的辛苦程度,选
择从 6 到 20 的数字表示您的体力活动强度,并将数字填写在相应的表格
里。
(4) 同时,请研究对象回忆每次活动(运动)时是否发生心绞痛以及因为活
动(运动)需要额外服用硝酸甘油或其它抗心绞痛药物使用的片数(即
扣除平时常规服用的片数)。

639
自我辛苦评估指数
第五部分 心绞痛自我报告与自我评价表
说明:
(1) 该表格记录研究对象在过去一周里心绞痛发生的情况,包括心绞痛的次
数、每次疼痛的强度、持续时间、及每天服用抗心绞痛药物使用的片
数。
(2) 请您(研究对象)详细回忆在过去一周里,您出现心绞痛的次数、每次
疼痛的强度、持续时间、及每天服用抗心绞痛药物使用的片数。结合研
究对象记录的情况,将这些指标记录在相应的表格里。
(3) 心绞痛疼痛的强度用下列的疼痛评估量表从 0 至 10 表示,0 表示您没有
疼痛,5 表示有十分痛,10 表示痛到死,依据您感受的疼痛情况选择从
0 到 10 的数字表示您每次的疼痛强度,并填写在相应的表格里。
(4) 请研究对象回忆每次心绞痛发作持续的时间(分钟)和每天硝酸甘油或
其它抗心绞痛药物使用的次数及数量(片/粒数)(每天的总片/粒数)。
很
轻
松
轻松
有
点
辛苦
辛苦
很
辛
苦
非
常
辛苦
非
常
轻松
640
10
痛到死
9
痛摧肺腑
8
剧痛
7
不可忍受
6
难以形容
5
十分痛
4
好痛
3
可以忍受
2
颇痛
1
微痛
0 不痛
第六部分 生活质量调查问卷
西雅图心绞痛量表
说明:
1.西雅图心绞痛量表是冠心病特异生活质量量表,用来测量冠心病病人在过去
4 个星期中,因为心绞痛日常活动受限制的程度、心绞痛发生的频率、心绞痛
的稳定性、治疗满意度以及疾病感知的情况。
2.量表上每个指标使用的指导语
(1) 下列是一般人在一周当中经常进行的活动,指出您在过去 4 星期中,因
为胸痛、胸闷、或心绞痛而活动受到限制的程度 。针对每一项活动,在
每一行相应的有极大限制、有较大限制、有一些限制、有很少限制、没
有任何限制、或因其他原因受限制或没有进行此活动的□内打「√」。

641
(请在每一行相应的□内打「√」)
有极
大限
制
有较
大限
制
有一
些限
制
有很
少限
制
没有
任何
限制
因其他原因受限
制或没有进行此
活动
自己穿衣服 □ □ □ □ □ □
在室内的平地行走 □ □ □ □ □ □
淋浴 □ □ □ □ □ □
上小山坡或上一层楼梯
而中途不休息 □ □ □ □ □ □
整理花园、吸尘或提携
杂物 □ □ □ □ □ □
快速地走一个街口以上 □ □ □ □ □ □
跑步或慢跑 □ □ □ □ □ □
提起或移动重物(如家
具、小孩) □ □ □ □ □ □
参与激烈运动(如游泳
和打网球) □ □ □ □ □ □
指导语:
a. 自己穿衣服:在过去的 4 星期中,您是否有因为胸痛、胸闷、或心绞
痛而影响您自己穿衣服,若没有任何限制,则在此相应的□内打
「√」;若有受限制,那受限制的程度怎样:有极大限制、有较大限
制、有一些限制、有很少限制、或因其他原因受限制或没有进行此活
动?请选一项符合您自己的情况并在相应的□内打「√」。
b. 在室内的平地行走:在过去的 4 星期中,您是否有因为胸痛、胸闷、
或心绞痛而限制您在室内的平地行走,若没有任何限制,则在其相应
的□内打“√”;若有受限制,那受限制的程度怎样:有极大限制、
有较大限制、有一些限制、有很少限制、或因其他原因受限制或没有
进行此活动?请选一项符合您自己的情况并在相应的□内打「√」。
c. 淋浴:在过去的 4 星期中,您是否有因为胸痛、胸闷、或心绞痛而限
制您淋浴,若没有任何限制,则在其相应的□内打「√」;若有受限

642
制,那受限制的程度怎样:有极大限制、有较大限制、有一些限制、
有很少限制、或因其他原因受限制或没有进行此活动?请选一项符合
您自己的情况并在相应的□内打「√」。
d. 上小山坡或上一层楼梯而中途不休息:在过去的 4 星期中,您是否有
因为胸痛、胸闷、或心绞痛而限制您上小山坡或上一层楼梯而中途不
休息,若没有任何限制,则在其相应的□内打「√」;若有受限制,
那受限制的程度怎样:有极大限制、有较大限制、有一些限制、有很
少限制、或因其他原因受限制或没有进行此活动?请选一项符合您自
己的情况并在相应的□内打「√」。
e. 整理花园、吸尘或提携杂物:在过去的 4 星期中,您是否有因为胸
痛、胸闷、或心绞痛而限制您整理花园、吸尘或提携杂物,若没有任
何限制,则在其相应的□内打「√」;若有受限制,那受限制的程度
怎样:有极大限制、有较大限制、有一些限制、有很少限制、或因其
他原因受限制或没有进行此活动?请选一项符合您自己的情况并在相
应的□内打「√」。
f. 快速地走一个街口以上: 在过去的 4 星期中,您是否有因为胸痛、胸
闷、或心绞痛而限制您快速地走一个街口以上,若没有任何限制,则
在其相应的□内打「√」;若有受限制,那受限制的程度怎样:有极
大限制、有较大限制、有一些限制、有很少限制、或因其他原因受限
制或没有进行此活动?请选一项符合您自己的情况并在相应的□内打
「√」。
g. 跑步或慢跑: 在过去的 4 星期中,您是否有因为胸痛、胸闷、或心绞
痛而限制您跑步或慢跑,若没有任何限制,则在其相应的□内打
「√」;若有受限制,那受限制的程度怎样:有极大限制、有较大限
制、有一些限制、有很少限制、或因其他原因受限制或没有进行此活
动?请选一项符合您自己的情况并在相应的□内打「√」。
h. 提起或移动重物(如家具、小孩): 在过去的 4 星期中,您是否有因
为胸痛、胸闷、或心绞痛而限制提起或移动重物(如家具、小孩),
若没有任何限制,则在其相应的□内打「√」;若有受限制,那受限
制的程度怎样:有极大限制、有较大限制、有一些限制、有很少限
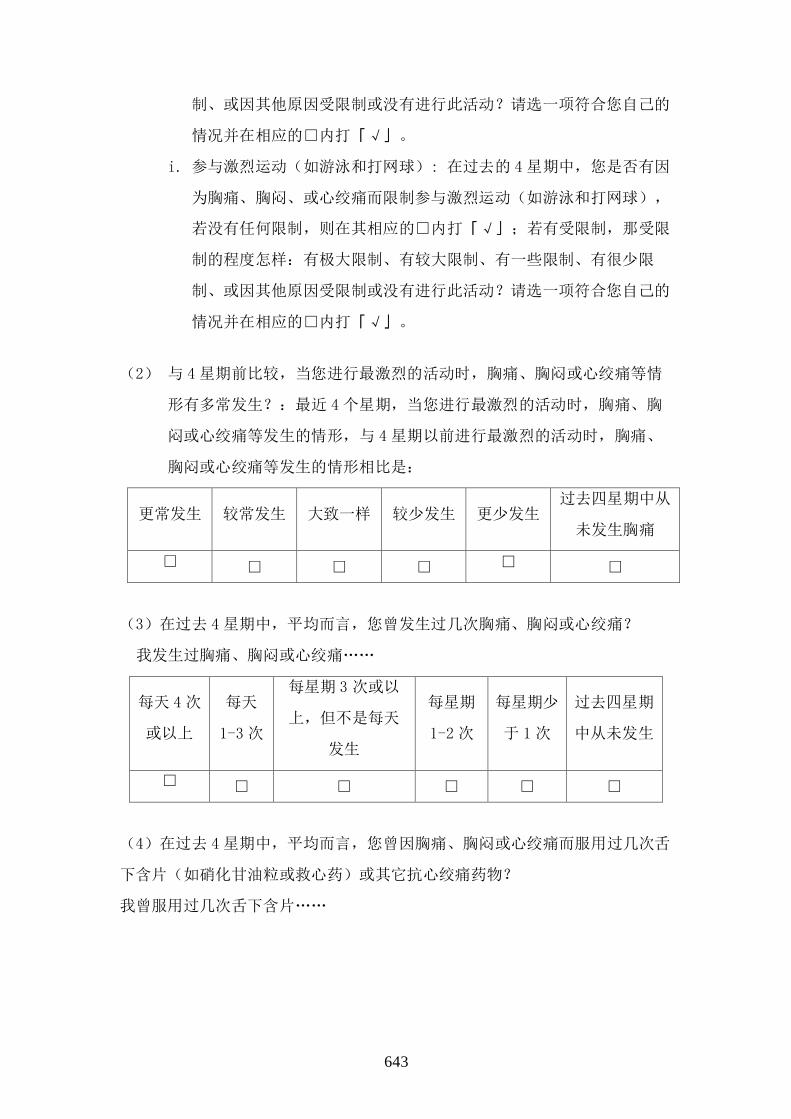
643
制、或因其他原因受限制或没有进行此活动?请选一项符合您自己的
情况并在相应的□内打「√」。
i. 参与激烈运动(如游泳和打网球): 在过去的 4 星期中,您是否有因
为胸痛、胸闷、或心绞痛而限制参与激烈运动(如游泳和打网球),
若没有任何限制,则在其相应的□内打「√」;若有受限制,那受限
制的程度怎样:有极大限制、有较大限制、有一些限制、有很少限
制、或因其他原因受限制或没有进行此活动?请选一项符合您自己的
情况并在相应的□内打「√」。
(2) 与 4 星期前比较,当您进行最激烈的活动时,胸痛、胸闷或心绞痛等情
形有多常发生?:最近 4 个星期,当您进行最激烈的活动时,胸痛、胸
闷或心绞痛等发生的情形,与 4 星期以前进行最激烈的活动时,胸痛、
胸闷或心绞痛等发生的情形相比是:
更常发生 较常发生 大致一样 较少发生 更少发生 过去四星期中从
未发生胸痛
□ □ □ □ □ □
(3)在过去 4 星期中,平均而言,您曾发生过几次胸痛、胸闷或心绞痛?
我发生过胸痛、胸闷或心绞痛„„
每天 4 次
或以上
每天
1-3 次
每星期 3 次或以
上,但不是每天
发生
每星期
1-2 次
每星期少
于 1 次
过去四星期
中从未发生
□ □ □ □ □ □
(4)在过去 4 星期中,平均而言,您曾因胸痛、胸闷或心绞痛而服用过几次舌
下含片(如硝化甘油粒或救心药)或其它抗心绞痛药物?
我曾服用过几次舌下含片„„

644
每天 4 次
或以上
每天
1-3 次
每星期 3 次或以
上,但不是每天
服用
每星期
1-2 次
每星期少
于 1 次
过去四星期
中从未服用
□ □ □ □ □ □
(5) 服用医生所开给您治疗胸痛、胸闷或心绞痛的药物会对您造成多少困
扰?
有极大困
扰
有较大困
扰
有一些困
扰
有很少困
扰
没有任何
困扰
医生没开
处方
□ □ □ □ □ □
(6)对于您的胸痛、胸闷或心绞痛的所有治疗,您的满意度如何?
完全不满意 大多不满意 有些满意 大多满意 非常满意
□ □ □ □ □
(7)对于您的医生曾向您解释说明有关您的胸痛、胸闷或心绞痛情形,您的满
意度如何?
完全不满意 大多不满意 有些满意 大多满意 非常满意
□ □ □ □ □
(8)总的来说,对于目前您胸痛、胸闷或心绞痛等的治疗情形,您的满意度如
何?
完全不满意 大多不满意 有些满意 大多满意 非常满意
□ □ □ □ □
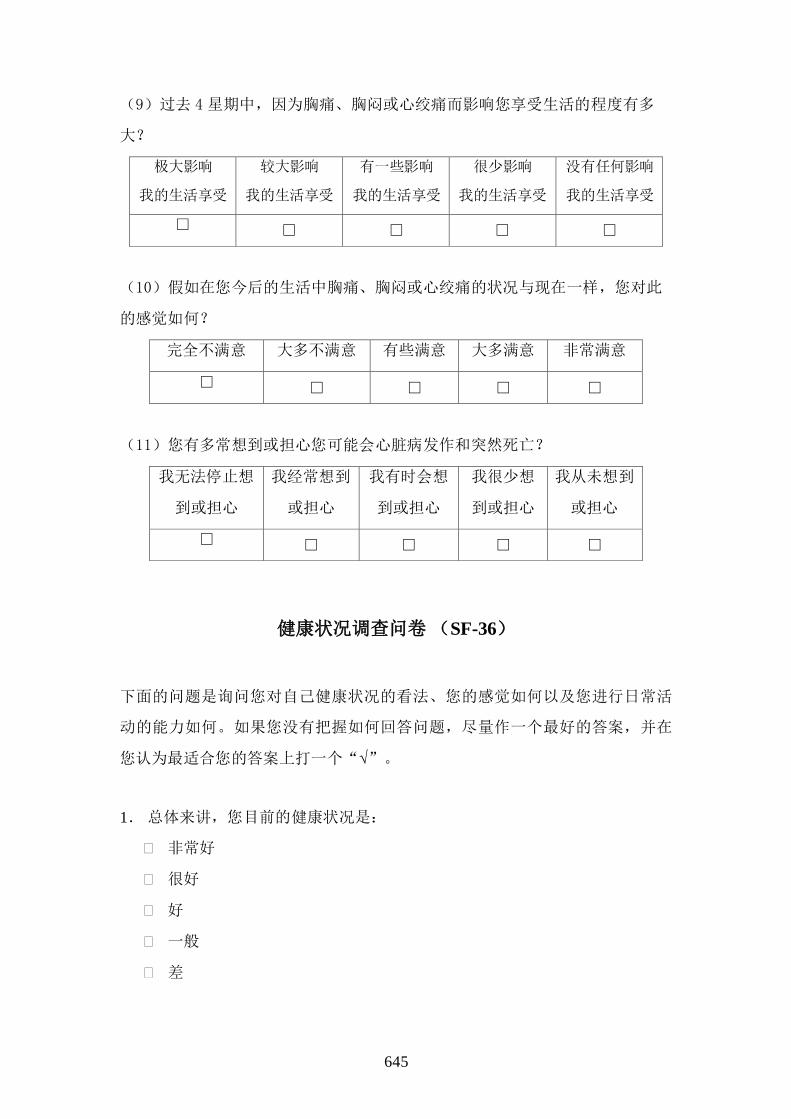
645
(9)过去 4 星期中,因为胸痛、胸闷或心绞痛而影响您享受生活的程度有多
大?
极大影响
我的生活享受
较大影响
我的生活享受
有一些影响
我的生活享受
很少影响
我的生活享受
没有任何影响
我的生活享受
□ □ □ □ □
(10)假如在您今后的生活中胸痛、胸闷或心绞痛的状况与现在一样,您对此
的感觉如何?
完全不满意 大多不满意 有些满意 大多满意 非常满意
□ □ □ □ □
(11)您有多常想到或担心您可能会心脏病发作和突然死亡?
我无法停止想
到或担心
我经常想到
或担心
我有时会想
到或担心
我很少想
到或担心
我从未想到
或担心
□ □ □ □ □
健康状况调查问卷 (SF-36)
下面的问题是询问您对自己健康状况的看法、您的感觉如何以及您进行日常活
动的能力如何。如果您没有把握如何回答问题,尽量作一个最好的答案,并在
您认为最适合您的答案上打一个“√”。
1. 总体来讲,您目前的健康状况是:
非常好
很好
好
一般
差

646
2.跟一年前相比,您觉得您现在的健康状况是:
比一年前好多了
比一年前好一些
和一年前差不多
比一年前差一些
比一年前差多了
健康和日常活动
3.以下这些问题都与日常活动有关。您目前的健康状况是否限制了这些活动?
如果有限制,程度如何?
有很多
限制
有一点
限制
根本没
限制
⑴重体力活动(如跑步、搬重物、激烈活动等)
⑵一般体力活动(如移桌子、扫地、做操等)
⑶手提日杂用品(如买菜、购物等)
⑷上几层楼梯
⑸上一层楼梯
⑹弯腰、屈膝、下蹲
⑺步行 1500 米左右的路程
⑻步行 800 米左右的路程
⑼步行约 100 米的路程
⑽自己洗澡、穿衣
指导语:
(1) 重体力活动(如跑步、搬重物、激烈活动等):您目前的健康状况是否
限制了您的重体力活动(如跑步、搬重物、激烈活动等)?如果有限
制,程度如何?是有很多限制还是有一点限制?
(2) 一般体力活动(如移桌子、扫地、做操等):您目前的健康状况是否限
制了您的一般体力活动(如移桌子、扫地、做操等)?如果有限制,程
度如何?是有很多限制还是有一点限制?

647
(3) 手提日杂用品(如买菜、购物等):您目前的健康状况是否限制了您手
提日杂用品(如买菜、购物等)?如果有限制,程度如何?是有很多限
制还是有一点限制?
(4) 上几层楼梯:您目前的健康状况是否限制了您上几层楼梯(两层以上,
不停)?如果有限制,程度如何?是有很多限制还是有一点限制?
(5) 上一层楼梯:您目前的健康状况是否限制了您上一层楼梯?如果有限
制,程度如何?是有很多限制还是有一点限制?
(6) 弯腰、屈膝、下蹲:您目前的健康状况是否限制了您弯腰、屈膝、下
蹲?如果有限制,程度如何?是有很多限制还是有一点限制?
(7) 步行 1500 米左右的路程:您目前的健康状况是否限制了您步行 1500 米
左右的路程?如果有限制,程度如何?是有很多限制还是有一点限制?
(8) 步行 800 米左右的路程:您目前的健康状况是否限制了您步行 800 米左
右的路程?如果有限制,程度如何?是有很多限制还是有一点限制?
(9) 步行约 100 米的路程:您目前的健康状况是否限制了您步行约 100 米的
路程?如果有限制,程度如何?是有很多限制还是有一点限制?
(10)自己洗澡、穿衣:您目前的健康状况是否限制了您自己洗澡、穿衣?如
果有限制,程度如何?是有很多限制还是有一点限制?
4.在过去四个星期里,您的工作和日常活动有没有因为身体健康的原因而出现
以下这些问题?
有 没有
⑴减少了工作或其他活动的时间
⑵本来想要做的事情只能完成一部分
⑶想要做的工作与活动的种类受到限制
⑷完成工作或其他活动有困难(比如:感到格外吃力)
指导语:
(1) 在过去四个星期里,您的工作和日常活动有没有因为身体健康的原因而
出现减少了工作或其他活动的时间。
(2) 在过去四个星期里,您的工作和日常活动有没有因为身体健康的原因而
出现本来想要做的事情只能完成一部分。

648
(3) 在过去四个星期里,您的工作和日常活动有没有因为身体健康的原因而
出现想要做的工作与活动的种类受到限制
(4) 在过去四个星期里,您的工作和日常活动有没有因为身体健康的原因而
出现完成工作或其他活动有困难(比如:感到格外吃力)
5.在过去四个星期里,您的工作和日常活动有没有因为情绪问题(如感到消沉
或者忧虑)的原因而出现以下问题?
有 没有
⑴减少了工作或其他活动的时间
⑵本来想要做的事情只能完成一部分
⑶工作或从事其他活动时不如平时仔细
指导语:
(1) 在过去四个星期里,您的工作和日常活动有没有因为情绪问题(如感到
消沉或者忧虑)的原因而出现减少了工作或其他活动的时间。
(2) 在过去四个星期里,您的工作和日常活动有没有因为情绪问题(如感到
消沉或者忧虑)的原因而出现本来想要做的事情只能完成一部分。
(3) 在过去四个星期里,您的工作和日常活动有没有因为情绪问题(如感到
消沉或者忧虑)的原因而出现工作或从事其他活动时不如平时仔细。
6.在过去四个星期里,您的身体健康状况或情绪不好在多大程度上影响了您与
家人、朋友、邻居或单位同事的正常社交活动?
根本没有影响
很少有影响
有中度影响
有较大影响
有极大影响
7.在过去四个星期里,您有身体上的疼痛吗?如果有,疼痛的程度?
根本没有疼痛
有很轻微疼痛

649
有轻微疼痛
有中度疼痛
有严重疼痛
有很严重疼痛
8.在过去四个星期里,您身体上的疼痛影响您的正常工作吗?(包括上班和家
务活动等)?
根本没有影响
有一点影响
有中度影响
有较大影响
有极大影响
您的感觉
9.以下这些问题有关过去一个月里您的感觉如何以及您的情况如何。(对每一
条问题,请钩出最接近您的感觉的那个答案)
在过去一个月里持续的时间 所有的
时间
绝大部
分时间
比较多
时间
一部分
时间
小部分
时间
没有此
感觉
⑴您觉得生活充实吗?
⑵您感到精神紧张吗?
⑶您感到垂头丧气,什么事
情都不能使您振作起来吗?
⑷您感到心平气和吗?
⑸您感到精力充沛吗?
⑹您感到情绪低落吗?
⑺您感到精疲力竭吗?
⑻您感到快乐吗?
⑼您感到疲乏吗?
⑽您的健康限制了您的社交
活动(如走亲访友)吗?

650
指导语:
(1) 在过去一个月里,您觉得生活充实吗?如果有,有多少时间觉得生活充
实?
(2) 在过去一个月里,您感到精神紧张吗?如果有,有多少时间感到精神紧
张?
(3) 在过去一个月里,您感到垂头丧气,什么事情都不能使您振作起来吗?
如果有,有多少时间感到垂头丧气,什么事情都不能使您振作起来?
(4) 在过去一个月里,您感到心平气和吗?如果有,有多少时间感到心平气
和?
(5) 在过去一个月里,您感到精力充沛吗?如果有,有多少时间感到精力充
沛?
(6) 在过去一个月里,您感到情绪低落吗?如果有,有多少时间感到情绪低
落?
(7) 在过去一个月里,您感到精疲力竭吗?如果有,有多少时间感到精疲力
竭?
(8) 在过去一个月里,您感到快乐吗?如果有,有多少时间感到快乐?
(9) 在过去一个月里,您感到疲乏吗?如果有,有多少时间感到疲乏?
(10)在过去一个月里,您觉得您的健康限制了您的社交活动(如走亲访友)
吗?如果有,有多少时间觉得您的健康限制了您的社交活动(如走亲访
友)?
10.请对下面的每一句话,选出最符合您情况的答案?
(每一横行只打一个钩)
绝对
正确
部分
正确
不能
肯定
大部分
错误
绝对
错误
⑴我好像比别人容易生病
⑵我和我认识的人一样健康
⑶我感到我的健康状况在变坏
⑷我的健康状况非常好

651
指导语:
(1) 您是否觉得您好像比别人容易生病?正确、错误或不能肯定?绝对正确
或绝对错误?
(2) 您是否觉得您和您认识的人一样健康?正确、错误或不能肯定?绝对正
确或绝对错误?
(3) 您是否感到您的健康状况在变坏?正确、错误或不能肯定?绝对正确或
绝对错误?
(4) 您是否觉得您的健康状况非常好?正确、错误或不能肯定?绝对正确或
绝对错误?




















