
Contracted Birth: Limited Agency, Authoritative Knowledge, and Modern Meanings of Choice in American...
86
Contracted Birth: Limited Agency, Authoritative Knowledge, and Modern Meanings of Choice in American Reproduction Jessalyn Ballerano April 1, 2011 In Partial Fulfillment of the Department of Anthropology Honors Curriculum Prof. Ayala Emmett University of Rochester
Transcript of Contracted Birth: Limited Agency, Authoritative Knowledge, and Modern Meanings of Choice in American...

Contracted Birth: Limited Agency, Authoritative Knowledge, and Modern Meanings of
Choice in American Reproduction
Jessalyn Ballerano April 1, 2011
In Partial Fulfillment of the Department of Anthropology
Honors Curriculum Prof. Ayala Emmett
University of Rochester
For my Mama, Momeé, and all the other mothers in my life - past, present and future.
Table of Contents
I. Introduction…………………………………………………………………………1-3 II. Theory and Method………………………………………………………………..4-10 III. Analysis and Discussion of American Birth Practices…………………………...10-63
i. The American Conceptualization of Birth…………………………………....10-16 ii. Preparation for Birth………………………………………………………….17-21 iii. Attendants and Support Systems……………………………………………..21-34 iv. Birth Territory………………………………………………………………...34-42 v. The Use of Medication in Childbirth…………………………………………42-48 vi. The Technology of Birth……………………………………………………..48-56 vii. The Locus of Decision-Making………………………………………………56-63
IV. Resistance, Change and the Future of American Birth…………………………..63-75 V. Appendix A- Glossary………………..…………………………………………..76-77 VI. Appendix B- Statistics………………………………………..…………………..78-79 V. Bibliography and Suggested Resources………………………………..………...80-83
Ballerano 2011
1
Introduction
In September 2010, I joined the research mailing list of the International Confederation of
Midwives. It consists of practitioners, midwifery students and teachers, and scholars, and serves
as a distribution point for a wide array of information concerning the world of midwifery:
discussions of health topics, announcements of events, conferences and job openings, question-
and-responses based on individual inquiry, debate over political/legal processes around
reproductive health, and dissemination of research, statistics, and academic projects. This list,
populated by mostly non-American users, was my starting point. Was my intuition that
something was lacking in American childbirth worth pursuing? Had the women’s movement of
the 1970s manifested in optimal reproductive care, not only for childless women (another matter
entirely), but for mothers as well?
I wanted to see whether women’s experiences were in line with the reproduction
narratives of internet discourse, television and news media: everything from orgasmic home
births and breastfeeding lawsuits to botched surgeries, murdered abortion providers, post-partum
depression on the rise, and a soaring Cesarean section rate.1 Out of the seemingly overwhelming
array of birth options and styles, were American women and families receiving care that aligned
with their individual needs, values and choices? Could a mostly-foreign network of actively
engaged, formally recognized, and evidentially successful “alternative” care providers signal
limitations to what “normal birth” means in the U.S.? In a country that claims so many resources,
embodies so many cultures, and prides itself in modern medical innovation, could everyday
behavior and attitudes towards pregnancy, labor and delivery reveal a health system that is
nonetheless entrenched in insensitivity, misinformation and inequality?
1 Traceable in Time Magazine, as well as news publications, film and television programming. http://healthland.time.com/ category/medicine/reproductive-health-medicine/ and http://healthland.time.com/ category/love-family/pregnancy .
Ballerano 2011
2
The amount of general material on birth and labor is vast, and relevant scholarship in
both the social and medical sciences has been consistently produced since the late 1800s. And
yet there seems to be a glaring disparity between what Americans claim to know and believe
about birth and how they actually do it. Birth is a human’s first cultural act, and yet when I
proposed my research I was told by a male scholar- “It’s such a female issue.” Don’t we all hold
stake in reproduction and how society manages pregnancy and birth? Rejecting its dismissal as a
“women’s issue”, I argue that the need for comprehensive, universally accessible information on
childbirth, and the ability to apply that information as practical knowledge in the birth event, is
very much a human rights issue.
Despite elite medical training, innovations in technology, and claims of equality and
patients’ rights, the state of maternal and prenatal care in the U.S. is less than optimal. Fifty
countries had lower national maternal mortality rates in 2008, and American infant mortality
rates suffer similarly (WHO 2008). Subjectively, too many women are going into the birth
process with too little knowledge of their choices, too little agency, and not enough trust in their
own bodies and natural capabilities. Even those with correct information face obstacles in
utilizing it to control their birth experience. Those sound like value-laden assumptions, but they
are daily evidenced when birth participants are pressured by insurance companies and hospitals
to follow a “technocratic birth” procedure that is high in costs and medical risks, but valued by
those in the business of birth for its efficiency and profitability (Davis-Floyd 1993; Epstein,
2008). The result is unnecessary interventions, which are riskier than commonly perceived, and
perhaps more importantly, a sense of dissatisfaction and even trauma in mothers who experience
the standard biomedical model.2
2 See Appendix B for rates of U.S. intervention use based on scientific evidence, obstetric practice, and midwifery practice.
Ballerano 2011
3
Is this level of medical intervention into a natural biological process necessary? Years of
research from both supporters of physician-led birth and the natural birth community have shown
alternative models of care, specifically those provided by midwives, to create better outcomes for
mother and baby (Gaskin 2002: 456-60). “Healthy outcomes”, as well as other aims (a sense of
pride and accomplishment, family bonding, and embodied empowerment), are attainable in the
biomedical birth model, but I will show how the institutionalization of birth and contemporary
women’s experiences reveal the limitations of a tradition that systemically pathologies
pregnancy and disables women’s agency in controlling their birth settings, decisions, and overall
experience. This is not to say that aspects of the biomedical model are not valuable and at times
essential to women and infants lives. But beyond “surviving”, birth that is peaceful, natural, and
even pleasurable is becoming an ever-more sought out experience for women everywhere.
At the same time, popular media advertising and the broader health system perpetuate
patients’ ignorance and unquestioning trust in the authority of doctors, making “actively
managed” birth, in which doctors use multiple medicines and machines to control the process, a
still-growing reality for today’s mothers and, potentially, generations to come. How are women
negotiating the spectrum of health care? In what ways are they empowering themselves or
submitting to systemic expectations? How can care-providers adequately provide a healthy birth
experience while allowing patients to make choices that align with their personal and cultural
values? I hope to reveal not only the tensions that currently define American birth practices, but
also to ease them, with considerations of how to fit “the most natural thing in the world” into a
modern society, without sacrificing dignity, agency, and happiness.
~
Ballerano 2011
4
Theory and Method
Brigitte Jordan’s 1978 biosocial comparative framework allows for understanding
contemporary American birth practice as one of many locally shaped and globally situated birth
cultures. Conceptualizing the United States as a fluid, cyclic, and increasingly complex society, I
will compare current birth practices to those of the American past, and to those of international
peers. The true investigation is internal and familiar- what has or has not changed in the past
thirty years? How are American citizens living up to their expectations to be the most educated,
the best cared for, and the most free? How are they manifesting traditional values of
individualism, progress, and family in the provision of health care? What kind of power is
expressed in the interactions and experiences that shape, and are shaped by, those values?
Along with my own ethnographic work, I attempt to account for the significance of social
science in influencing discourse and, potentially, agency within the realm of childbirth. A
number of social scientists, including Emily Martin, Robbie Davis-Floyd, Crista Craven, Carolyn
F. Sargent, and Ellen Lazarus, followed in Jordan’s wake and today continue to explore
reproductive practices. Martin in particular has been essential to me in addressing feminist and
Marxist perspectives on women’s health care. The most contemporary of these anthropologists
discuss the implications of global neoliberal capitalism as a driving force of self-perception and
individual behavior, how consumerism defines healthcare, and forms of diversity and resistance
to these patterns.
I make my analysis based on various routes of information. Statistics, stories, and
examples are drawn from anthropological research, historical accounts and media
representations. In traditional ethnographic form, I carried out a number of in-depth interviews
and attempted different instances of participant-observation. My primary informants were those
Ballerano 2011
5
with whom I conducted the interviews. A young female doctor, completing her residency in
upstate New York, answered my questions about biomedical interventions and the hospital
setting for birth and C-section deliveries. She also helped me gain access to one of the hospitals
she worked in, where I shadowed her for a day of deliveries. I was able to observe and at times
assist in three births over a 12-hour period, the average weekday shift for a resident. This “mini-
immersion” served to confirm, update, and fine-tune the understanding I had gained from other
anthropologists and my interviewees.3
I had known this informant since childhood and was close to her family. She had
apprenticed with doulas (trained non-medical birthing attendants) and was herself delivered by a
midwife. Because of her background, Dr. B4 made for an excellent key informant; while she was
educated for, worked within, and for the most part subscribed to the biomedical model of care,
she was aware of, and incorporated whenever possible, alternative methods and attitudes for
antenatal care. She herself expressed an awareness of her unique attitude and a concern that she
would lose the ability to manifest it, as she would presumably became more jaded from work
experiences that revealed systemic obstacles to non-conformity. She also serves as a
representative of more recent generations of obstetricians; whereas women composed only 9% of
U.S. obstetrics and gynecology students in 1970, in 2001 they made up 45.7% of students and a
majority 71.8% of resident physicians (Johnson, et. al 2005).
While her characteristics do not necessarily make her a more “marginal” character, she
and her female colleagues certainly stand apart from the prototypical male-physician role
described by historians and anthropologists up until today (McGregor 1998: 74-5). Current
feminist critiques can no longer belabor an all-male physician workforce, a major game changer
3 A number of works, particularly those of Brigitte Jordan, contain more in-depth studies of hospital-setting births, and serve as valuable lenses into the structural relationships and power dynamics of the scene. 4 All names have been changed.
Ballerano 2011
6
for discourse long-concerned with the patriarchy and sexism of medicine and the professional
world. That is not to say that elements of that dynamic do not linger or hold influence, but the
state of women in healthcare is more complex than numbers can communicate; on the one hand,
Dr. B’s very existence stands as proof of a shift in gender expectations and female power in the
medical world; at the same time, however, her gender might not stop her from repeating the same
patronizing doctor-patient interactions identified as symptomatic of a hierarchical care system
that is rooted in inequality and patriarchal hegemony.
I conducted two other long interviews with mothers. One was Megan, a 27-year-old
mother, student and waitress from upstate New York who delivered her son in a hospital under
the care of the same male physician that attended to her mother and grandmother in the past. I
also interviewed my own mother, Chrys, who was also 27 when she delivered me in a hospital
under the care of a female midwife and male doctor, after attempting a home birth. These two
women turned out to represent similar statuses and backgrounds of identity, although decades
apart. Both women had unplanned pregnancies, worked to support themselves, and remained
unmarried as of our interviews. Both came from Italian American families in New York State,
and both had been educated, my mother through a state university and Megan through
professional training and some college. These similarities illuminate how other factors, like
historical context, personal beliefs, family influence, and type of education can determine a
woman’s unique experience of birth. That is not to say that all the women of one group or status
behave in one way, but ethnographers like Christa Craven (2007) and Ellen Lazarus (1994) did
find class trends between groups of women in terms of what and why they expected certain
birthing outcomes and prenatal care models.
Ballerano 2011
7
Coming from a working class family but having received a college degree and studied
women’s issues extensively, my mother fell into a muddled category. Like some women of the
current natural birth movement, many of whom are wealthier, she was ideologically drawn to the
midwifery model of care- she appreciated the natural, woman-centered, non-interventionist
system that home delivery offered. At the same time, she was not financially successful in her
twenties, and like many lower-income women considered in anthropological literature, relied on
state-run healthcare at the time of her pregnancy, which covers hospital births. State law did not
allow home birth deliveries with lay-midwives at the time, but she still chose to attempt what
was essentially an illegal birth. This is a strange case compared to many of the others I had read.
Most women were either philosophically drawn to midwifery and could afford it out-of-pocket,
or were forced into using a midwife because they did not have insurance. She embodied a
spectrum of these rationales, although I would say the ideological factor was stronger.
My mother decided she did not want the hospital birth experienced by my grandmother
and 99% of American women, and so some of her expectations were reactionarily developed to
avoid one (Block 2007). I, on the other hand, love hearing about the day I was born, and look
forward to attempting a midwife-supported birth when I chose to have a child, just as she did. By
including our personal story, I am attempting not only to be reflexive and subjective in my
research, although that is what I have come to expect of modern ethnography. It also serves to
highlight one position of my generation of American women- a community of so many mixed
experiences, ideologies, ethnicities and childhood understandings of birth. I am a cultural
informant of this generation and also of the digital age, having grown up alongside personal
computation and the World Wide Web. The options and information available to young women
Ballerano 2011
8
today are a flurry of facts, controversy, prejudices, and misinformation, all available at the click
of a mouse or the tap of a touchpad.
In addition to the long interviews with Megan and Chrys, I collected multiple other birth
stories to gain a sense of the variety of women’s experiences. Some were five minute
conversations with acquaintances and peers, and others were found in popular publications, on
advocacy websites, virtual discussions, and, surprisingly, the free video uploading network,
YouTube.com. Without regular access to live homebirths, these home videos and the writings of
midwives made up the majority of home birth stories I considered. I also occasionally watched
the popular program “A Baby Story”, broadcast by the TLC network, for a sense of what anyone
with cable might come across concerning birth.5 The majority of the births on this program are
in-hospital, but rarely do they go smoothly; whether or not they are realistic was another question
I considered while shadowing Dr. B.
As scholar and potential consumer, I paid attention to the myriad websites of midwifery
service providers, journals and blogs, advocates, and regulatory organizations. Many resources
were for people who were unhappy with their initial birth experiences, and looking for
something different. The Internet, in fact, was my entry point into learning about mainstream and
alternative antenatal care, midwifery, and home birthing. As a medium of knowledge and
community, the virtual sphere presents its own questions: Will mother-centered, culturally
sensitive, evidence-based care manifest via virtual discourse? Will new media, transnational
sharing, and heightened visibility create a new narrative for the participants of modern childbirth
to claim as their own?
5 A running daily series in which each hour-long episode features two different families, the final weeks of the mother’s pregnancy, and the actual labor and delivery of the baby.
Ballerano 2011
9
Considering that Jordan’s Birth in Four Cultures is only a generation old speaks to the
relevance of this topic, not only for anthropological studies but also for public knowledge and
health. This is apparent in the fact that many of her (and her contemporaries’) observations and
critiques of U.S. birthing “norms” are still valid- while some details of obstetric and
gynecological care standards have changed, the fundamental dynamics of reproductive care, and
the power at stake, is much the same. While insurance and health companies can now be added
to the medical community of those with control over care practices, it is still the patients, in this
case laboring women, who are subject to the authoritative decisions of others.
As Jordan outlined, understanding the “doing of birth” in the U.S. is one perspective into
how humans across and within cultures share universal traits of physiology, but behave around
those traits according to different beliefs and legitimized authoritative knowledge. By identifying
certain components that are common to all birth processes, Jordan was able to systematize birth
cross-culturally. Functionally, birth inherently requires certain events and resources, and so
Jordan constructed the following categories, which I will use to frame contemporary American
birth practices (1983: 34- 63):
i. Definition or Conceptualization of the Event……………………………………10 ii. Preparation for Birth…………………………………………………………….17 iii. Attendants and Support Systems…………………………………………………21 iv. Birth Territory……………………………………………………………………34 v. The Use of Medication in Childbirth…………………………………………….42 vi. The Technology of Birth………………………………………………………….48 vii. The Locus of Decision-Making..............................................................................56
For each appropriate section, I will discuss: a) directly observed hospital births, b) the
experiences of informants (including my own interviewees as well as other ethnographic
subjects, c) the alternatives offered by the midwifery model of care (according to ethnographic
accounts, self-reporting of midwifery advocates, and publicly available home-videos), d) basic
Ballerano 2011
10
historical context, and e) the theoretical implications of these realities and interactions. These
different sections flow into and influence one another, and so it is not my intention simplify any
one detail as belonging completely to one category or another. Rather, I hope that this scheme
will provide both a detailed understanding of the complex, multiple and flexible realities of
contemporary birth in the U.S. as well as a cross-chronological illustration of the phenomena’s
discursive and transformative nature, from the early twentieth century to the present.
Analysis and Discussion of American Birth Practices
I. The American Conceptualization of Birth
The ways in which birth is defined in American culture weigh heavily on the
establishment of particular practices, behaviors, and expectations as “normal”. As Jordan points
out, the universal physiology of birth is socially interpreted and given meaning in various ways,
resulting in different justifications for different behaviors around the event (1983: 34-5). Once a
certain cultural understanding is institutionalized, such as the authority of scientific knowledge in
Western societies, all are subject to its power, albeit in different ways. Women, in particular,
must share in negotiating and interacting with a specifically scientific and medical understanding
of their own bodily processes, from menstruation to menopause (Martin 1987: 5). Childbirth has
a unique place in the minds of Americans in that it is at once medical and natural. In accordance
with Jordan’s “biosocial” model, there is certainly a sense that becoming a mother is a social act
(a rite of passage, a test, a life crisis, etc.), but the actual “doing” of that transformation, birth, is
considered a medical event in the U.S. (1983: 1-2, 9).
Ballerano 2011
11
The strictly medical definition of parturition6, which has structured modern perinatal7
care over the last century, is a relatively recent development. J. Marion Sims, a controversial
practitioner considered the “father of gynecology”, did not start experimenting with alternatives
to the traditional methods of women healers until the mid 1800s (McGregor 1998: 3-7). Today,
most people have an understanding of the process at something that occurs naturally but
demands medical attention. Even delineating what is “natural” and what is “medical” about birth
is difficult. For example, some might consider “natural birth” to mean non-surgical, i.e. vaginal,
delivery. Others might expect “natural birth” to include minimal intervention and medication, or
consider any hospital birth to be “medical” because it is attended by physicians, even if no
technology or drugs are used.8 This tension of meaning is thematic to modern anthropology
studies- inherently “natural” processes can become socialized and are then considered “cultural”,
leading to questions of what makes something “unnatural” and how much a cultural definition
overwhelms or shares space with a natural one.
The difficulty in identifying the somewhat ambiguous concepts of natural and medical
birth is reflected in the inconsistency expressed by some women in their descriptions of their
birth experiences. In our interviews, spoken descriptions of expectations, decisions in the labor
process, and justifications for those moments alternated between “natural” and “medical”
language, as did the women’s behavior. Megan, for example, came from a family of women who
had all had Cesarean sections. She went into her pregnancy hoping not to need one, but having
6 Also “birth” or “childbirth”;; the process of bringing forth a child from the uterus, ending pregnancy (Encylopedia Britannica) 7 The weeks before, during, and immediately after childbirth. 8 I will use the term “natural” to refer to a birth that does not include pain medication or technological intervention, including induction or fetal heart rate monitoring. I will use “vaginal birth” to refer to births that are not surgical, but may include other interventions, such as epidurals, morphine, fetal heart rate monitoring, and induction. Finally, “surgical birth” refers to delivery by C-section, vacuum or forceps. Please note that these are my distinctions and the word choices of some of my subjects may not follow them.
Ballerano 2011
12
been told “You’re probably more likely gonna have a C-section, just because, if you’re built that
way…” She intended to avoid a surgical birth (author’s voice in italics):
I wanted to do it really just, just do it the natural way, if I could. For a lot of reasons, for recovery time, and for being put out, I just wasn’t a big…I don’t know I didn’t want to do that. Did your doctor go into the details of your different options with you? Nu-uh, not really. They just said that like, it pretty much was up to me…It’s not…It’s a lot different than it used to be, because before C-sections were so much more common, and now, they try to like…make you do as natural as possible. I think it depends a lot on the person. It depends a lot on the risk. Megan. Personal Interview. January 2011
Megan simultaneously defines her expectations to do birth “the natural way” and places her
experience in the medicalized context of the doctor’s suggestions. She also mentions the “risk”
factor in birth, a medical category that could have limited her choice to do a vaginal birth. At the
same time, many of her reasons for trying a vaginal delivery were to avoid the risks- recovery
time, pain, anesthesia- of surgical birth.
Her experience illustrates how even with an understanding that she could do a natural
birth, that capability was dependent on the approval and supervision of a medical authority (her
family OB/GYN). Megan did deliver her son vaginally, but only after being induced and
receiving an epidural. Whether or not she still considered the intervened experience “natural” is
unclear. The phrase “as natural as possible” suggests an understanding that there is a spectrum of
options and behaviors she considers natural, and others, such as surgery, that are distinctly
medical. This is illustrative of many women’s experiences in contemporary birthing- an
amalgam of decisions, objects, and relationships that make the entire process a true integration of
scientific, natural, and cultural components. Megan also repeatedly attributed a positive
significance to the experience of natural birth, saying “…I thought it would be good, just to go
through the experience. I think everyone should experience it…I think that every woman…you
Ballerano 2011
13
should try, at least give it a shot.” She felt proud and independent for having a different
experience than her female relatives, a social aspect of empowerment through biological
processes worth considering (2011).
Even having chosen a vaginal birth, a healthy, confident woman like Megan was
expected to rely on her doctor for a successful outcome. Western medicine has turned pregnancy
into a “condition” and the expectant mother into a “patient”. While such labels may seem
obvious and mundane, especially in a society where everything from nutrition to libido or
learning can be overseen by a doctor, they are powerful ways of shaping cultural expectations of
reproduction. A “patient” is usually considered weakened in some way, in need of supervision or
help, and unable to contribute to society except marginally (Jordan, 1983: 35). By grouping
birthing women in with those who are ill, wounded, and in pain, medical institutions assert their
role a source of treatment, solutions, and relief. Indeed without the conception of pregnant and
laboring women as vulnerable or in need of management, there would be no place for them in a
hospital.9 In particular, pain management has a major role in care given during labor, and
understandably so. “I think overall people underestimated how much pain they are going to be
in,” explained Dr. B in a phone interview. “In society today we aren’t ever in pain. Nobody is
ever prepared for pain- you know you get a headache you take something for it. So this is
certainly something new to them,” (November 2010). But whereas some may expect and view
pain as a natural and temporary part of the birthing process, the American mentality seems to be
that pain is a problem that needs to be solved in order to have a successful delivery.
9 It is significant that much early obstetrical specialization among physicians was focused around relieving the pain of childbirth and other genital/reproductive processes. More on this will be discussed in Section V on Medication. For an in-depth history, see From Midwives to Medicine: The Birth of American Gynecology, by Deborah Kuhn McGregor (1998).
Ballerano 2011
14
This stands in stark contrast to the mentality behind perinatal care in places like Holland.
Jordan’s own 1978 observations of Dutch midwife-based care system, which was and still is
covered by insurance providers, is still valid- the 2008 documentary Pregnant In America: A
Nation’s Miscarriage takes a look at current Dutch midwifery and home birthing practices there
in an effort to frame such alternatives as safe, accessible and viable for modern women (Jordan
1983: 32, 36-7). What stands out in the film is the practitioner’s sense of service and assistance
to the mother, rather than management and manipulation. Tom Kreuning, a Dutch male midwife
who has delivered over 3,000 home births, explains:
“We don’t see it as where you go with your car to the garage, and you fix something. Because usually nothing is broken or nothing is damaged. We do not take patients; we take clients, because they are not ill. You coach them through pregnancy and delivery and you have to do that really well, because they don’t forget you, for their lifetime.”
Buonaugurio 2008, 22:50 Kreuning’s attitude, and those of his patients, is that women are capable, healthy people going
through a natural process that may or may not need medical attention, but should not be viewed
as a problem or something to be feared. Rather, birth is a meaningful experience that care-
providers like Kreuning are invested in personally and honored to assist.
American expectations that women cannot self-manage their pain, and that removing the
physical discomfort from the labor process will make it work better, are based in fear and, even
more so, ignorance of how the body and mind are designed to work through such physiological
processes. Martin posits that the repeated existential separation of the woman from her body and
baby is a symptom of this; the idea that labor and birth is something that “happens” to a women,
and not something she “does”, can limit her sense of agency or control, making women feel
fearful or hesitant and resulting in passive acceptance of management by others (1987: 86-90).
Hence, when doctors unassumingly ask patients what they are considering for pain management,
Ballerano 2011
15
something I saw repeatedly in my hospital observations, women are likely to accept that they
will indeed need pain management and do not question the doctor’s assumption, because their
body is framed as an independent source of pain or distress, out of their control. In describing his
European patients’ attitudes, Kreuning illustrates the seeming irrationality of this attitude. “They
know it hurts but it’s only for a short period of time,” he explains, “And well, ‘My mother did it
and my grandmother did it, so I can do it’…and of course there are millions of other women in
the world who did it,” (Buonagurio 2008: 23:26). But fear, rather than confidence, is a defining
factor of birth in America and comes hand-in-hand with its medicalized representation. With
medicine comes pathology: risk, abnormality, side effects, infection and complications, all of
which are seen as the dangers of childbirth which make the pregnant woman so vulnerable and
delicate if not outright ill. Add to this the modern innovations that allow for prenatal testing of
disease and disability, and the number of threats that could potentially be feared by an expectant
parent are manifold. The need for medicine implies a problem, and so reproductive processes
have become something scary to many women.
Even healthy, knowledgeable moms can become fearful when their labor is placed in a
pathological context or they recognize a part of the process as something medical, as opposed to
natural. Chrys, who was confident going into her at-home labor despite the fact she does not
“handle pain very well”, became tense when her cervix, becoming irritated after hours of waiting
and checking, started to bleed a small amount. “I’m just such a non-medical person that I was
freaked out by the blood, I thought ‘Oh my God the baby’s in trouble!” (2010). Here, a woman
who identifies childbirth as natural and knows full well that bodily fluids are involved became
frightened at an aspect of the process she considered unfamiliar and unknown, i.e. “trouble” for a
“medical person” to understand. Ideologically, Chrys had chosen a natural homebirth because
Ballerano 2011
16
she did not want to rely on the biomedical model experienced by her mother, a model which
scared her:
Well my attitude towards pregnancy and having a baby when I was in my early 20s was to not do that and not to have a child ever, until I saw my friend experience a homebirth with her first son, and I realized that birth didn’t have to be as horribly scary as I had imagined it would be from the stories I heard as a kid. And that’s what first got me thinking about having a child, was the fact that I could see it being done in a loving way. Chrys. Personal Interview. December 2010
Despite seeing birth in a new way, through the midwifery care model, Chrys still considered her
body and the labor process through the lens of medical knowledge, the same knowledge that
defines the very institutionalized care she feared (emphasis added) :
Maybe part of it was that as much as I wanted to have a home birth and I feared the medical model, I also feared that something would go wrong at home and we wouldn’t be equipped to deal with it, so it might be that I felt safer in the hospital in so far as I knew I was doing everything I was supposed to be doing…(2010)
Here, Chrys explicitly reveals anxiety about a problem occurring and not having the tools to
fix it, because she didn’t follow the rules. This is the very language that Martin and other
feminists, (including Chrys) have used as an indicator in their critique of childbirth practices and
women’s health care in general (Martin 1987: 20). The argument that male-dominated
institutions have historically viewed women in mechanical terms, as inefficient machines in need
of male use/ management/ improvement, is nothing new. What is interesting is that this mother, a
self-proclaimed feminist and college-educated scholar of these very ideas, in describing and
justifying her own birth experiences, utilizes the same language that she and her contemporaries
(Martin published in 1987, Chrys birthed in 1988) point to as indication of the dehumanizing,
alienated character of techno-medical health care. Clearly, there is a complex relationship
between the institutionalized aspects of childbirth, the means that define those institutions, and
Ballerano 2011
17
the fear that surrounds medicine. In Section VII, I discuss further the implications of this
hegemonic phenomenon, an intersection of power, authoritative knowledge, gender, and control.
II. Preparation for Birth
The nine months of pregnancy leading up to parturition are as essential to mothers’ and
babies’ well-being as the moments of labor and delivery.10 There are a myriad of philosophies on
what kinds of activities, nutrition, and emotional behavior are beneficial or detrimental, healthy
or not. But the actual level of care that women receive- from gynecological exams and
ultrasounds to nutritional counseling and birthing classes, varies greatly across socio-economic
class, ethnic and cultural context, and personal beliefs. As may seem obvious, the more money
and education a woman has, the more options she has for such care, and the more likely she is
able to pursue them actively. In her interviews with women about their bodies and health care,
Martin found “class refracted through concerns about health”. She points out that wealthier and
middle-class women with expendable resources are more likely to look outside of the home or
family for care of all kinds, whereas working class women are more dependent on kinship and
neighborhood support,” (1987: 6).
For perinatal care, these distinctions are essential to understanding how women view
pregnancy and their role in the process of reproduction. It is important to note that women do not
all want and expect the same things out of pregnancy and birth. Ellen Lazarus draws connections
between the desire for knowledge about birth and how it manifests in her examination of class in
relation to choices and control for birthing women (1994). She describes how all classes of
10 Pregnancy’s three trimesters mark the physiology of fetal growth and do not conform to specific lengths of time, but they are conventionally broken up into three month segments. Starting from “presumed conception” date, the third semester starts at 28 weeks. Stoppard, Dr. Miriam. Pregnancy, Conception and Birth. 1993. Dorling Kindersley: London, England and New York, NY.
Ballerano 2011
18
women were more concerned with quality of care- good hospitals, good technology, and caring
medical providers, whereas middle and upper-class women were more concerned with issues of
control and choice in their births than their working-class peers (1994: 26-29). Differences in
these groups’ access to knowledge- of pregnancy, of the medical system, of their own bodies-
influenced their desires and expectations, which were not always met as they had hoped.
It is also essential to understand just how much financial costs and insurance limitations
affect the prenatal care choices of women. “Feminists thought that information would give
women control over choices, thereby empowering them,” Lazarus explains (1994: 28). But what
if the choices highlighted by education are only available to some? Poorer women,
“overwhelmed with social and economic problems”, may not be able to choose certain types of
care even if they are aware of them (Lazarus 1994: 26). Take Megan’s choice not to attend
birthing classes as an example. She was working full-time as a hair-dresser during her pregnancy
and, as with the lower-income women Lazarus cites, was unmarried and had an unplanned
pregnancy at a relatively earlier age (Lazarus 1994: 26, Ballerano 2011:1, 8). (Author’s voice in
italics):
I didn’t take birthing classes. I didn’t want to, I was like you know I’m not gonna spend $300, cause the class was like $250, you know? They just said, push like you’re going to the bathroom... So I was like, my body is either gonna know, that I’m able to do it or I’m not gonna be able to do it. Taking a birthing class gets you kind of, you know, aware of whats gonna happen, but…It might make you nervous. Cause you watch videos on labor, and I don’t wanna see someone… The last thing you wanna do is watch some horrible video, like the worst situation possible. “This could happen to you.” I just wanna go in…(2011)
Megan is clearly aware that birthing classes exist in her area, and seems to think she
knows what they consist of, but because of the cost, relies on her own intuitive knowledge and
that of the medical team to deliver her son. Her expressions of fear at what the class might reveal
Ballerano 2011
19
is indicative of the mentality described earlier, even though going into labor without preparation
could very well be more frightening. I saw this played out in person during my hospital
observations, when a young African-American mother was delivering her second child, attended
by a physician and nurse. Despite having labored before, she was panicky and nervous, unsure of
what to do and confused by the doctor’s directions to push. “How? How do I push?” she
exclaimed, and, as with Megan, she was instructed to push as if making a bowel movement. In
another delivery, a mother’s first, attended by a nurse-midwife, the woman had read up on
laboring techniques and, despite being somewhat frightened by the pure physical difficulty of it,
knew exactly how to follow her contractions, breathe accordingly, and use her muscles to bear
down when the midwife instructed her to. A major difference between these women’s
experiences and the varying degree of confidence they expressed was their mental and physical
preparation for birth.
Whatever the educational aspect of preparation, the actual pre-natal care women receive
is largely dependent on their financial resources and insurance, and can vary in quality and
continuity. This is a major issue for women who rely on public institutions for their health
concerns. Chrys, although working with a midwife, went to a physician for basic check-ups, in
part because her Medicaid covered such care. Most of these visits were actually carried out by
nursing staff, who became friendly with her and many of whom were present later during the
delivery. Megan, on the other hand, had monthly visits with the same physician her mother,
aunts and grandmother had used in the past- he was personally present for her check-ups and had
a deeper understanding of her family and background than a public medic may have had.
Unfortunately, many women do not receive pre-natal care from the same person throughout their
pregnancy, and a large number of poorer or uninsured women receive no pre-natal care at all. A
Ballerano 2011
20
good number of the women I saw at the upstate New York hospital I visited came into the
delivery ward having received their pre-natal care at a different location. The young African-
American woman mentioned above could not even remember who her doctor was. This
discontinuity of care for lower income women is problematic for ensuring emotional support and
quality of treatment. Lazarus points out that the structure of the clinics utilized by lower-income
women is a major factor in limiting optimal care- understaffing, shifting schedules, and a
insurance system that puts paperwork and purse before people make for less-than-optimal results
(emphasis added):
…Poor women saw many different people: nurses, aides, clerks, nutritionists, and social workers, over the course of their pregnancies. Such organization hindered developing a relationship between a supportive caregiver and a pregnant woman. Because medical personnel continuously shifted, there was no single care giver to transmit information. Contradictory explanations led to unnecessary tests. At other times, women were not told why they were having tests nor were they informed about test results. The medical record became the chief link from one visit to the next. (Lazarus 1994: 33)
Even when women do receive continuous care, the physicality of pre-natal care has its
own implications. For any woman who has received a gynecological exam, it is not difficult to
imagine why having monthly check-ups could be unpleasant. That is not to say that all such care
is bad or unnecessary, but the very structure of obstetrics lends itself to discomfort,
depersonalization, and distorted self-image. Internal examinations using a speculum, a plastic or
metal vice-like tool, can be painful and are always intrusive, but rely heavily on the personal
touch and consideration of the examiner. Most of the women I observed expressed pain during
these examinations and would even yell “Ouch!” or “That hurts!”. Of course, when the
examination was required, the attending physician could do nothing but apologize and continue.
Another major aspect of pre-natal care is actual check-ups on the infant, something that has
always been practiced but the method for which has changed over the years. While traditional
Ballerano 2011
21
midwives may feel for the baby’s position and check its heartbeat, it was not until the
introduction of the sonogram into prenatal care that the baby could be seen and the heartbeat
amplified for anyone to hear. There are a number of implications for fetal heart rate monitoring
and ultrasounds that I will discuss in Section V on Technology, but in terms of pre-natal care this
technology has certainly had a profound effect. Modern couples can choose to find out the sex of
their child, and certainly some risk factors are more easily identifiable now because of the
images provided by ultrasounds. How this affects parents’ views of the child and the pregnancy
is questionable and certainly controversial. Even today, the technology is less than perfect, and
indications of fetal stress and malpresentation can lead to unnecessary worry for low-risk moms.
In other cases, of course, such checks can lead to life-saving decisions and appropriate
preparations for higher-risk births. Clearly, this type of care should be accessible, especially
considering that many lower-income women also suffer from health problems (such as
malnutrition, diabetes, family history of alcoholism and addiction, and obesity) that make
identifying high-risk pregnancies all that much more important. And yet, it is these very women
who need it the most that are least likely to receive continuous quality pre-natal care. I suspect
that an in-depth examination of discrepancies in pre-natal services would reveal larger trends of
class and race in relation to infant and maternal mortality, difficult or high-risk births, and
overall dissatisfaction with the pregnancy and birth experience.
III. Attendants and Support Systems
The participants in the birth process are not limited to the mother and baby. Care-providers,
family members, friends and sometimes strangers have all attended births in various settings
across and within cultures. The first well-known ethnography I read as a student of anthropology
Ballerano 2011
22
depicted a !Kung woman of the Kalahari Desert quietly delivering a baby all alone, hiding in the
brush near her home. In the historical novel The Red Tent, Jewish scholar Anita Diamant
describes how women of the immediate and extended family gathered in the women’s tent
during ancient childbirth, to provide direct and indirect physical and emotional support to the
laboring mother.11 Historically, most cultures have placed childbirth in the realm of women and
the domestic- midwives have traditionally been the main attendants of birth, as well as other life
stages and events, and were communally valued for their skills (Cassidy 2006: 27; Hachey 2004:
16). It wasn’t until male physicians started to specialize in techniques and tools for relieving the
pain of childbirth that women, mostly upper-class, started to look to these men for products that
midwives could not offer (Hachey 2004: 15-19).12 Today, most of the births depicted in
American television and movies show a birth scene in which a mother is attended by one or two
nurses, a physician, her mother, a nervous husband, and perhaps a medical student.
This scenario almost exactly replicates what I actually witnessed in an upstate-New York
teaching hospital- the two vaginal deliveries I was allowed to observe were attended by the
father-to-be, the woman’s mother, a primary care provider (in one case a physician, in the other,
a nurse-midwife), and an attending nurse. The presence of the father is a development from the
work of Dr. Robert Bradley (“the Bradley Method”) in the 1960s- until then Western delivery
rooms were closed to fathers for justifications ranging from modesty to sterility, to the simple
lack of knowledge a man might have about birth (Block 2007: 155; Cassidy 2006: 198-9;
McGregor 1998: 48-9). Supposedly, there is an official limit of three non-medical people in the
11 While Diamant claims she did not find any direct evidence of menstrual tents in ancient Iraq/Israel (circa 1500 BCE), she justifies her fictional creation on the basis that such tents were a common feature of “pre-modern cultures” worldwide. See FAQs at www.anitadiamant.com. 12 For more on the transition from midwifery to obstetrics, I suggest McGregor and the work of medical historian and anthropologist Paul Starr, whose influence can be found in most social science discussions of maternal health care.
Ballerano 2011
23
room during labor and deliver, friends or family. Dr. B explained that this was to minimize
confusion, allow the smooth movement of equipment, bodies, and lighting when necessary, and
because “once there is more than three, with all of us, it’s just impossible,” (2010). “All of us”
refers to the seemingly unlimited amount of medical personnel allowed in the delivery room.
The very organization of many hospitals, particularly teaching hospitals like this one, create a
flow of people that is difficult to control. Weekday shifts for residents here are usually 12 hours,
extended to 24 hours on weekends (yes, that is 24 hours of medical work without rest). Dr. B
estimated that there are usually about 10 nurses on duty at a given time, with 4 residents on
during the week and 3 on weekends. During my 12 weekend hours at the hospital, there were
anywhere from 5 to 15 women being monitored and cared for simultaneously- ideally, this
averages out to about a 1:1 nurse-to-patient ratio and a 1:3 doctor-to-patient ratio, but from what
I saw, nurses were usually assigned to multiple patients and doctors oversaw a large number of
them. Because the length of labor and delivery varies so much from woman to woman, it is
likely she will be cared for by multiple shifts or start care with one doctor and end it with
another. Add to this the other patients wandering around, families awaiting news, and the
occasional lost person looking for the nursery, and the mix of people potentially present for
supposedly private moments is something of a crowd.
In the birth attended by a resident obstetrician, there was also a male medical student and two
male physicians who stood, arms crossed, next to me while directing the attending resident,
mother, and student. Considering the above discussion of problems in continuity of care, it is
important to note that this woman was not able to remember who her doctor was. The resident
announced that Dr. __ would be arriving soon, and when the woman asked who that was, the
resident had to explain, “Remember? Your doctor? He has a beard?” The description didn’t seem
Ballerano 2011
24
to help, and as the physician, once he arrived, stood by me, feet away from the laboring woman,
speaking encouragement but doing nothing, I don’t know if it mattered.
Everyone but the family members and one of the physicians wore scrubs, myself included.
The uniform helps identify medical personnel (I was “one of them”), but it is distinct from
“scrubbing in”, the sterilization process and outfitting that is required in a surgical setting.
Sterility, in fact, has little to do with current restrictions on birth attendees, and as shown in
Section IV, hospital sterility is misunderstood. Even wearing the scrub uniform, however, I felt
embarrassed at my presence, like an intruder, assumed to be a medical student- I could play no
active role and had nothing to contribute but my gaze, and so found myself looking around
nervously and trying to stay out of everyone’s way.13 Unless you have witnessed someone’s
personal health care as a stranger, it is hard to understand the sense of discomfort and even guilt I
felt at having gained entrance into these very private moments of women’s lives.
An exchange I had upon entrance into one of the other delivery rooms illustrates why this can
feel uncomfortable for the researcher trained in social and feminist theory. I was lucky enough to
discover a British-trained nurse-midwife (“Mary”) working in the hospital, who had delivered
over 3,000 babies in her 25-year career and had a patient that was expected to deliver while I was
there. Sure enough, a few hours after speaking to the midwife, Dr. B told me I could follow her
because she was about to deliver her patient. Mary walked into the room first (the expectant
father and the woman’s mother were already inside with a nurse) and asked, as the physician
had, “I have a student with me, can she come in?” She motioned and I walked in, timidly, as I
was no longer with the doctor I knew and wanted to be sure I was following polite protocol:
13 Although I went through the formal paperwork and was introduced to the medical staff Dr. B, there was a general misunderstanding of what I was doing at the hospital. The staff repeatedly assumed I was a medical student until I explained otherwise. The patients were told I was a student but there was an unspoken sense that I should play the part of medical student (i.e. not anthropologist) unless directed otherwise, probably for the comfort of the patients who were, in general, vulnerable to the authority and directions of the medical staff.
Ballerano 2011
25
Close the door, close the curtain, turn and smile and thank the woman for allowing me to be
present. Her response, at once casual and somewhat wistful, struck me: “I’ve had so many
female problems that I don’t care who sees me.”
I was pained at the implications of her statement. For one, here was a woman who had
had enough reproductive health issues that she had become adjusted to the medical gaze on her
genitals and most private processes, a gaze intended for fixing and learning. While a certain level
of comfort is certainly admirable in such situations, to my ears, this was surely objectification, at
once subtle and drastic. Her reproductive processes and organs had been pathologized by
continuous need for medical attention, and so her problem was compartmentalized as female
(whether she had other, non-reproductive/genital health issues I do not know). Because her
health care had consisted of attention from multiple care givers (much like in the case of the
women coming to deliver after having received treatment at a public clinic), this woman had
come to see another pair of eyes, or hands, or advice, as just another consequence of having
“female problems” that must be fixed and/or learned from. Her body many times been an object
of examination and display, and now she no longer cared for whom (although I am sure my
scrubs and clipboard assured her of the appropriateness of my presence). Also interesting is her
equating “sees me” with “seeing my medical problems”. She had come to associate her own
body with a medical failure to function as a healthy female, and so she equated seeing her
genitals, her femaleness, with seeing her, as if, in the hospital setting, her reproductive parts were
what defined her. Perhaps the most important question here was if she considered labor and birth
another “female problem”. Was she actually grouping childbirth with whatever illness or
difficulties she had suffered in the past? Or was she simply justifying my (supposedly medical)
Ballerano 2011
26
presence by the fact that she had been viewed medically so many times before, and one more
gaze would not make a difference?
This woman, “Venus”, who had had so many problems she associated with being female, had
a relatively quick, easy delivery. She had been induced but was using no pain medication. “Good
woman, what a good woman,” the Mary would purr, while gently massaging the base of Venus’
vagina to allow the baby’s head to ease out gradually. She had read about birthing and breathing
and pushing, and with each contraction gave it her all. I found myself, at the nurse’s suggestion,
holding Venus’ foot and leg, nodding in encouragement and trying to hold her gaze when she
looked at me. After the delivery, I thanked her again and told her I was honored to assist. She
seemed to think nothing of it- after all, I was just another medical person. The experience was
undeniably moving for me, and yet, here I was, a complete stranger with minimal medical
training, assisting a woman give birth in a hospital setting where the crisis-like perception of the
event was ever-present with the constant beeping of monitors and array of tools and drugs
available at every turn. Where was the line drawn for appropriate attendees? How is it decided
which people will provide support and which are to be restricted? Coming from within the
scientific establishment, I and anyone else with the appropriate clothes, nametag or forms, could
attend a birth. But the very relatives of the mother and child, who had a vested personal interest
in the goings-on and outcome of the birth, were limited to a few.
One might assume from this analysis that hospitals are focused on control in a way that the
major alternative, home birth, is not, but that would assume a limited view of what control
means. While biomedical attendees aim to control bodily processes with drugs, chemicals and
tools, the midwifery model of care also aims for a sense of control, but not over the body. Rather,
midwives encourage women to let their intuition and body control the dynamics, from people to
Ballerano 2011
27
pillows, of their births, rather than a set of institutionalized standards. For many women, home
birth is an appealing alternative to hospitals because it allows them control over participation that
would otherwise be dictated by protocol. Home birthers do not have strangers wandering around
outside their door, and can have as many relatives and friends around as they like. For example,
in the majority of home birth videos I watched on Youtube.com, children were present. My
brother and I were able to attend our youngest sibling’s birth in the center my stepmother labored
at, but in most hospitals, including the one I visited, children are not allowed in the delivery
room. “That partly has to do with that it would take away focus from the mom,” explained Dr. B
when I initially interviewed her. But what if the mother wants her children to share in what is
essentially a familial experience, or learn about “the miracle of life” as my stepmother wanted
me to? It seems more likely that disallowing children is more convenient for physicians who are
trying to control the birth process as much as possible in accordance with what they have learned
works best- a mother taking time to comfort a child or answer a question is not focusing on the
doctor and their instructions. And since the hospital system assumes instruction and intervention
by a doctor is what makes birth “work better”, anything that interferes with the doctor’s practice
is considered an obstacle to management and efficiency, even if the mother finds it supportive or
beneficial. This does not mean that having the whole family over is necessarily the best way to
give birth, but what is evident is that birth companions and attendees, and the emotion and action
they bring with them, can provide significant support, or not, to a woman’s birth experience.
Who those people are should be, except in emergency circumstances of need, up to her.
It is not just midwives who are aware of the significance of such dynamics. “Lots of
people can be in the room during the labor, which can be very stressful or a very supportive
environment,” Dr. B said, referring to the large number of medical personnel that can add up,
Ballerano 2011
28
along with the mother’s chosen companions. But even intimate companions can have unintended
influence; Chrys experienced this dynamic not in a hospital but in her three days of laboring at
home. She had, along with my father and midwife, a number of female friends from a women’s
group, who constantly brought food, gave massages and took photos. It sounds idyllic, but in
reality Chrys thinks it may have contributed a slow progression of labor. When she started to
become stressed, her midwife suggested switching to the hospital:
She advised [moving] because I was not relaxed anymore- and I think that part of it was that I had too many women in my circle that were checking on me and giving me different vibes- I probably should have only had moms, experienced moms, in the circle. Being that I was not experienced. I think it’s different if you already are experienced to have novices there, so you can maybe mentor them a little bit. But I don’t think that should’ve been my role, but I didn’t know. I was ignorant. I didn’t realize that all those vibes from all those different women- some of whom didn’t get along as well as I had thought they did- interacted with my energy. And I think that was why[...]as soon as I got in my midwife’s car and we drove not even all the way around the corner of the street, my water broke. It was like I needed a change of environment. (2010)
Clearly, the presence of multiple people creates a social, even emotional, dynamic that
can affect the mother’s state of mind, and, in turn, her body. The support Chrys thought having
her friends around would provide turned out to be a stress factor. At the same time, being able to
work with her boyfriend and actually use his body for physical support- “I think I had exhausted
him”- was essential to her continued comfort as well as their personal bond. The dual emotional-
physical nature of the support women need in labor makes it difficult to go into labor knowing
what kind of support systems will be best. Both people and objects make up an environment that
is potentially beneficial or detrimental to the mother’s progress. For example, once Chrys left her
home for the hospital, she was able to use provided props like a bar to lean on, making it easier
for her to attain a comfortable position without exhausting her partner. Even if she had known
ahead of time that such furniture would be helpful, and outfitted her home with such structures, it
Ballerano 2011
29
would have been hard to predict that her friend’s attitudes would affect her so negatively. This
speaks to the variability and individuality of every woman’s birthing experience- the only thing
one can say for sure is that the unexpected may occur. This is why it is so important to leave as
many options available to women as possible- restricting her choices of companions, positions,
and emotional support, and denying her the option to change her mind, only restricts the
potential for her to connect with her body in such as way as to best facilitate delivery.
While I cannot speak for every hospital or midwife in America, I think it is important at
this point to note the different emotional roles I observed between different types of attendants,
roles that have been reinforced by other’s ethnography and even carry a hint of cultural
stereotype in them. The fact that nurses, valued for their bedside manner, doctors, expected to act
professionally yet patiently, and alternative providers, such as midwives and doulas, all
potentially interact together in a hospital setting makes for an interesting point of comparison. A
moment of crisis I observed illustrates the differences between the general approaches between
these different “characters” of the maternal care system. At the hospital, while Dr. B was tending
to a patient elsewhere and I was chatting with nurses at one of the stations, a woman in a nearby
room started to scream, “What does that mean? What does that mean?” Her water had broken
very early in her pregnancy and she had been expected to miscarry weeks ago, but for some
reason never did and was now in the hospital hoping to deliver her baby, albeit prematurely. She
was yelling because her umbilical cord had dropped, a sign that her infant was dead, and a few
minutes later she delivered a stillborn. In the few moments following her shouts, I witnessed
upwards of 10 people run into her room, yelling directions while an emergency announcement
rang over the intercom. Doctors, nurses and residents, some of which I hadn’t seen until this
moment, crowded in and out of the door, having been sitting just a moment ago, shopping online
Ballerano 2011
30
and sipping coffee. I cannot imagine the bustle and stares of so many people was any comfort to
the woman, who I could not see but was surely upset. And there was no way that there was
anything so many people could do, physically, to improve the situation. While I’m sure
everyone’s intentions were to help, witnessing the mad rush to the crisis was akin to watching
school children gather around a playground confrontation.
Following the event, the attitudes and reactions of the different care providers were
perfect prototypes of the sentimental nurse and the stoic physician. The woman’s attending
nurse, Sandy (who I would later work with in the operating room), who had been quite friendly
and was regularly cracking jokes throughout my time there, collapsed into tears after leaving the
room where the stillborn had been born. “It’s just so unfair,” she sobbed, as Mary rubbed her
back, and she commented on how “it’s always the nicest people” who suffer such tragedies, and
that she would pray for them. While this was happening, Dr. B, who had not been present when
the crisis occurred, was going through the case file of another patient. She made a small facial
movement with her eyebrows, as if to say “ah well, c’est la vie”, and continued on to working
with the patient at hand. She could not afford to become emotionally invested in such cases-
there are too many and she works too many hours- allowing herself to get upset would just
exhaust her and affect her performance. Dr. B is not an inconsiderate or dispassionate person, but
her role as leader of the nursing team and the person responsible for all the other patients in labor
necessitated that she remain calm, unaffected even, during the moment of difficulty.
I cry almost every time I see a birth, even when it’s on video. Dr. B did not, nor did any
of the other medical professionals I witnessed. “You’re so calm!” I exclaimed, and “you get used
to it,” was her response. On the other hand, when I explained my inability to remain stoic to
Mary, the nurse-midwife, she smiled and responded, “It’s supposed to make you cry,” affirming
Ballerano 2011
31
the seeming strangeness of the other staff’s lack of emotion. Hours later, near ten in the evening,
I did not cry when I witnessed a Cesarean delivery14. The surgery was successful, but the
emotional aspect of seeing the mother struggle, and her relief at the delivery, was not a part of
the surgical birth. The two surgeons, behind a blue curtain blocking the mother’s upper half,
made small talk about the airport and cracked jokes while cutting through inches of fat, muscle,
and uterus to retrieve the baby. Some of the jokes were at the expense of the mother, who was
obese and taking a long time to cut through because of the large amount of fat on her abdomen.
The same nurse who had been crying earlier in the day was now also making jokes, miming to
me the girth of an imaginary belly and rolling her eyes when the mother, oblivious on the other
side, would innocently ask, “How’s it going? Are you almost done?” This explicit isolation of
the mother from the actual process and from the other participants was probably necessary for a
smooth operation- I can’t imagine seeing the surgery would have been a pleasant experience for
her- but the disregard for her dignity was not. Tennessee midwife, educator and author Ina May
Gaskin comments on this lack of compassion in a story she tells in the 2002 edition of Spiritual
Midwifery, originally published in 1975:
…The mother had fallen asleep while her incision was being closed, and while her belly was still open about an inch deep, the doctor put his hands on either side of the incision and, moving the wound as if it were a puppet mouth, said, “Hi, Steve,” to the young intern across the operating table from him. The remark was intended to be funny but wasn’t… (2002: 466)
14 There was more confusion about my role in the surgery room. I was surprised and excited that my presence had been approved and even encouraged by Dr. B and the two attending surgeons, although no one bothered to ask the mother for her permission. Part-way through the surgery, a nurse recording the participants asked me to spell my name and then asked “And you’re a third year medical student?” I stammered- I didn’t want to lie but I didn’t know if announcing that I was not a medical person would be wise when the mother, feet away from us, could hear. She asked me again, and in desperation I looked at Sandy, who knew who I actually was. “Yes, she’s a third-year,” Sandy said, and then whispered, “Explain later.” While I had followed the protocol, and presented no real risk to the mother by being there, it was understood by everyone in the room that the mother did not, and should not, know that a non-medical person was involved in her surgery, over which she had no control.
Ballerano 2011
32
This scenario highlights the different attitudes that color biomedical maternity care.
While serious, beautiful, funny, and sad moments occur daily in delivery and labor rooms, the
participants process and cope with those moments differently. The casual nonchalance of the
physicians stands in stark contrast to the calm but connected support of the midwife and the
sentimental antics of the nurse. I think these behaviors are manifestations of different ideologies
that instruct each participants understanding of their role. The midwife sees herself as a support
to the woman, who does the actual birthing and is capable of physiological birth with the
midwife’s guidance and preparation. The nurses are trained to be efficient yet personal, showing
emotions that empathize with whoever they are serving, be it patient or physician, while
facilitating the use of tools and timing in accordance with hospital standards. The doctors,
ironically, seem the most disconnected from the intrapersonal aspect of labor and childbirth; they
are the deliverers, the mechanical experts, and the overseeing authority in a birth community that
looks to them for safe outcomes and timeliness.
Negotiating these different roles and attitudes can be difficult for the mother who
envisions a specific birth experience for herself. Choosing between the different “birthing styles”
provided by various providers is especially difficult when clients don’t understand the different
ideological training that comes with each type. A professor told me about a friend who was
feeling confused, oppressed even, by the barrage of suggestions and insistence of friends
directing her to which type of birth she should have, and who could best provide it. The trend in
the use of doulas, trained non-medical labor coaches, is a reflection of modern women’s needs to
articulate their desires in the face of a system that is inherently contradictory. For example, going
to a highly-recommended hospital obstetrician for perinatal care may preclude the option of a
medication free labor and delivery, even if the woman is capable of delivering without drugs.
Ballerano 2011
33
Likewise, a birthing tub may be accessible and viable for some deliveries, but expecting to labor
in water while working with a doctor that insists on continuous monitoring may be next to
impossible. Even choosing a midwife can be difficult, considering that some are more “purist”
than others and may be less willing to accommodate interventions or medication that mother
decides she wants. Having a doula who knows beforehand what her expectations are, and which
support systems are the most important, can be essential to the laboring mother whose
exhaustion, hormones, and medication may make it difficult for her to communicate those
wishes at critical junctures.
Even well-designed selection of attendees may not provide the support a woman needs.
When my mother arrived at the hospital, she was close to delivering me and explained her
situation to the nursing staff, who were soon replaced by the morning shift. Once delivered,
when she found that the new shift was not as compliant with her demands (not immediately
taking the baby to be measured, not giving the baby a vitamin shot that Chrys had arranged to
have later with her doctor), she found herself and her partner unsupported by their midwife, who
was, ironically, negotiating the legal and political pressures bearing down on her profession at
the time:
The unfortunate thing was that [the midwife] and her assistant left. To go talk with the doctor. Over coffee… about his decision to no longer back her up for these types of things. And that was when I needed them the most. I needed someone there to support Phil and I in our protocol, and what we didn’t want the hospital intervening in, and there was no one there to remind the hospital that when we got there we had…this paper plan, which had suddenly disappeared because the shift changed. So I was upset. (2010)
Evidently, just having a “birth plan” does not guarantee it will be followed. Dr. B
expressed frustration at the expectation for everything to go as planned , “which is a terrible idea
because it never works the way they want it to. They expect certain people to be there but then
Ballerano 2011
34
they aren’t. I think having a general idea of what you want is a good thing, and to be clear,”
(2010). Again, knowing how variable birth can be, expecting an exact process according to your
ideal may be unrealistic, but mightn’t birth plans be a “terrible idea” because the hospital system
does not accommodate the mother’s voice? Where is the support for the mother who does not
want to utilize the standard technobirth procedures? Why is the continuity for the mother whose
labor is treated by a stranger? My mother continued:
…They were just trying to do their jobs and Phil and I were exhausted… [we] had been up for three days… The other thing is you are all pumped up almost like you’re on drugs when you have all those hormones flying through you, so it was hard to articulate in a timely way, that’s why you supposed to have it in writing, and unfortunately the paperwork didn’t follow me from shift to shift.(2010)
Dr. B expressed the need “to be clear” but dismisses a written birth plan as unrealistic;; and yet, a
woman in the throes of physiological changes, “hormones flying”, may have no other way of
defining her expectations. Support systems that integrate the woman’s needs with the capabilities
of the care providers can only be achieved when there is clear communication of what each
parties expectations are. Overall, if a mother’s expectations cannot be met, or are refused, by her
attendees, then perhaps other attendees, who are willing to accommodate her values and desires,
should be made available. Unfortunately this is not the case in hospitals, where the biomedical
model of efficiency and standardization dominates the roles of the participants.
IV. Birth Territory
“We pretty much took over the whole apartment,” says my mother. She is describing the
three days of labor that preceded my birth in a nearby hospital. “I was singing, I took baths, I
walked around, I went outside with the cat,” (2011). These are the freedoms of being at home.
To wear what one pleases, or nothing at all, and to move, eat, and make noise without fear of
Ballerano 2011
35
disturbing another patient or being reprimanded by a nurse for eating. Women who choose home
births do so for these options, and also for the convenience and familiarity of home. “I’m very
comfortable to just be here. Have your own things and your own bed,” explains one of the Dutch
home birthers in Pregnant in America (2008: 22:20). Every woman’s home is different, and so it
is impossible to describe the space of home birth, but what can be said is that all of the woman’s
personal belongings, those that serve her functionally and emotionally, are available. The
products potentially needed to monitor a normal, low-risk birth are either provided by a midwife
or available to order online; you can rent a birthing pool for your living room if you like.
Certified and nurse-midwives are authorized to dispense specific medications and trained to use
specific tools. Also belonging to the mother and her family are all the airborne germs and
bacteria that are present in the home. Ironically, these pathogens are far less dangerous than the
ones to which women can be exposed to in hospitals. They are already familiar to the
inhabitants’ immune systems, if not products of their own bodies, and so are less likely to cause
infection, let alone be deadly or as varied as those among the sick and dying of public health
institutions.
Anthropology has continually pointed to the significance of space in shaping cultural
experiences. Brigitte Jordan extended this idea to the observation that the location of birth,
seemingly trivial at first glance, is also a specific territory. The relationships that come with
territorial understandings of space are powerful and affect the interactions that take place there.
Jordan also distinguishes the spaces in which birth occurs as either marked or unmarked-that is,
specified as a special location for the doing of childbirth (i.e. a hospital), or unspecified and
considered a part of the woman’s normal realm of existence (i.e. her bedroom) (1983: 48). This
distinction also separates expectations of who will attend the birth- whereas the domestic sphere
Ballerano 2011
36
allows for routine, unspecialized participants, such as the father, a space that is specialized
necessitates particular people as well. A birthing system’s choice of location “assigns
responsibility for the course of labor and credit for its outcome,” (1983: 50-1). The fact that the
historical shift of American childbirth from the home (private) to the hospital (public) was
preceded by a shift in the attendants of birth, from female midwife to male physician, adds a
strong element of patriarchal responsibility to the space equation. When space carries with it
gendered power, its significance is only more marked and influential.
While the majority of American births today are in –hospital, most of history has
witnessed home birthing as the norm. While a growing number of modern families are choosing
birth centers and their own homes for birthing, this is a small enough community that they are
often misunderstood if not downright demonized in the public sphere; many of the home births
are unaccounted for because of legal, financial, and political obstacles that force them to occur
under the radar. However, celebrity support and “new age” trends towards preferences for
“natural” services, products, and ideas have given home birthing a solid base of advocates and
consumers- contemporary research like Christa Craven’s Pushing for Midwifery (2010) provide
anthropological understandings of this community’s efforts to receive validation and increase
access to alternative birthing options on a social, economic, and political level. While this
movement personally interests me, in order to understand how the majority of Americans are
birthing, a discussion of the hospital setting is more fitting, although home births make for
illustrative comparisons.
The Labor and Delivery (D&L) floor I observed was in the shape of a giant U. In the
center of either side is a nurse station, with long desks lining the walls and a number of desktop
computers. Between the two stations, inside the U, is an elevator lobby; patients and visitors can
Ballerano 2011
37
go to either side of the lobby, where they are greeted by a reception desk that blocks the monitors
from view and separates the staff from the laypeople. Each station also has a back room where
staff belongings, administrative announcements and meals are out of the way. Along the rest of
the hallways are a few bathrooms, patients’ rooms, two small kitchens, more computer cubbies,
and closets. At the crest of the U is another long desk, behind which is a glass window looking
into what looks like an abandoned nursery. A sign on the door says “Parents: Please check in to
pick up your baby!” Another sign, at the opposite end of the floor, reads “Physicians Lounge”
but is taped over by a picture of Einstein sticking his tongue out, with the type “Lounge of
Knowledge”.
There are 21 rooms scattered around the U, and two main meeting spaces for the staff. As
noted above, changes in shifts and responsibilities mean that multiple staff must regularly
communicate and act on the status of multiple patients. The most striking result of this structural
difficulty is something I noticed immediately upon arriving and being shown the nurse’s station.
Behind the reception desk, two large monitors are set on the wall above two desktop computers
with the same images. One is a color coded table of each patient, her attending nurse, her stats
(including the number of pregnancies and births she’s had, how many centimeters dilated she is,
and what medications she is using), the stage and status of her labor (i.e. Delivered, In Labor,
Scheduled C-section), and her room number. That same room number also titles one of 16 boxes
on the second monitor, each of which show a fetal heart rate monitor strip and a graph strip of
the woman’s contractions. The result of this very efficient and easily understandable system is
that the room number, not the woman’s name, because the main identifier between the multiple
staff on her “case”. Because of the flow of patients and staff across an entire labor and delivery
floor, using a number instead of a name to communicate the needs and changes of each “case” is
Ballerano 2011
38
the only way to guarantee that the intended provider or care will end up with the right patient.
For example, Dr. B might ask “Has anyone checked on 21?”, and a nurse may respond, “Yes, I
did, but 16 needs you.”
While at first I was dismayed at this seemingly insensitive means of communicating about
people, I soon realized that it really was the only viable way to ensure timeliness and consistency
in such a setting. Clearly, such treatment is less than optimal, but in a space so large, with so
many people and so many complicated variables (one woman’s medicine could be another’s
lethal allergen), it would have been difficult for the busy physicians and nurses to effectively
communicate to one another and carry out care provision. What is problematic is that the hospital
system necessitates a need for such measures; a smaller capacity, continuous perinatal care from
the same person or people, and less complicated interventions would make it much easier to
attend to laboring women and their needs. Birth centers, which are basically buildings equipped
with all the medical and technological interventions of hospitals but aimed specifically around
pregnancy and birth, could better allow for this kind of personalization and sensitivity to the
individual experiences of women and families. But, as Block points out, hospitals are used to
“ordering chaos”, and such elements of control become necessary when a large number of
variables could have a negative effect (2007: 5).
Going into one of the empty patient rooms reveals a private one-bed room akin to the
hotel-like aesthetic portrayed on television. The bed is raised on an adjustable platform and
accompanied by various monitors and machines to the side, some of which are one wheels. The
only time I saw a mother out of bed was when some women would walk back and forth around
the hall with a companion, usually to facilitate labor starting. A particularly large digital clock
with a red read-out is posted to the side of the bed, at eye-height. This is the giant counter that
Ballerano 2011
39
attendees use to document the “progress” of dilatation, measure contractions, and to emphasize
the importance of time in this setting. Awareness of time’s passing becomes particularly
important once drugs are introduced, because their efficacy is based in speeding up or slowing
down labor. There is also a television installed above and in front of the bed, the way screens are
installed in the peripheries of sports bar patrons. The hospital provides this for the long hours of
waiting that labor often entails- and I did see a mother watching TV while she ate- but Dr. B
claims that if attendants, especially fathers, are watching during the actual birth, “we give them
dirty looks”.15 A small table for holding belongings and two comfortable chairs are against the
wall, and a small plastic adult-sized potty against the other. I did not see any additional props,
stools, or tubs that are available in some hospitals and birthing centers.
While there are no shared rooms here, the public nature of the space is undeniable. This is
a difference between contemporary understandings of privacy and the past, in which peoples of
many cultures traditionally separated laboring women and their helpers from the rest of the
community (although often still in the domestic space), in huts, barnyards, or bushes- this has as
much to do with safety and privacy as the popular notion that women’s bodies and the products
of birth (feces, blood, urine, mucus) were contaminating to others (Cassidy 2006: 50-1).
Paradoxically, hospitals both separate pregnant women from the general community while
including them in the community of the sick, those who actually are contaminating. The shared
hallways allow for private moments to be audible and sometimes visible for other patients,
visitors and staff to witness. And so despite superficial attempts at creating a home-like
atmosphere- wooden rather than industrial cabinets, patterned curtains instead of hospital-blue
plastic dividers, lighting with dimmers instead of fluorescent tubing- a sense that this is familiar
15 There was a basketball game playing the entire time Dr. B worked with the laboring African-American mother. No one turned it off and on multiple occasions, when I felt nervous or unsure of what else to do, I looked up at it rather than face the woman.
Ballerano 2011
40
territory is conspicuously absent. The conformity of the rooms negates any possibility of
individuality, and their arrangement, one after another, makes it clear that each patient is only
one of many, marked only by a number. Because of the structural design of the hospital
environment, and because of the communication system that design requires, being heard as an
individual is difficult. As a result, gaining any semblance of control as a patient becomes
impossible in a space that is already controlled by the standards of others.
As mentioned above, the notion that hospitals have everything “under control” and that
this makes them safer is false. While many of the features are designed to regulate people’s
interactions and manage their physical freedom, a hospital is an unpredictable and sometimes
dangerous place. This is simply because it is a place for the diseased and dying. Emotions of
families can run high, mistakes can have catastrophic results, and the vast amount of expensive
and powerful drugs, sophisticated equipment, and germs create a potential pool of corruption,
accidents and infection waiting to happen. It is surprising how many people think these spaces
are sterile- ion Dr. B’s words, “hospitals are friggin’ germ buckets,” (2010). In fact, the risk of
infection in a hospital is much higher to mother and baby compared to the home atmosphere,
where most of the germs or bacteria present are already familiar to the family’s immune systems.
Even medical staff are at risk here-immunizations and protective gear are a must for people
working with the sick and dying.16 Historically, the “lying-in” hospitals and maternity wards of
the mid-nineteenth century were rampant with disease, infested by rats, and pregnant shared
space, and even beds, with sick people. Doctor’s spread infections by moving from person to
person, with perhaps a corpse in between, not washing their hands before performing vaginal
16 I was required to provide extensive immunization records to the Education Department of the hospital I visited before gaining permission to shadow Dr. B. I had to receive two shots- one for tetanus testing and the other for the annual flu vaccine, which I otherwise would have not chosen to receive.
Ballerano 2011
41
exams or deliveries (Cassidy 2006: 54-7).17 Standards of cleanliness and care are much improved
since then, but it is no wonder that hospitals were once places for the poorest and least powerful
of society. Upper-class women were still having home births when these early hospitals were
developing, and the poor women who came to them were often subject to medical
experimentation and the worst of iatrogenic mishaps.
Those experiments- and failures- are what led the current model of hospitals and the care
received there. A legacy of butchered, diseased, and complicated births has led to a space that is
much cleaner, with many more rules and a more logical separation of different kinds of patients.
But the dangers of hospitals still exist, and it is in the operating room that the highest standards
of protection are expected. Multiple heavy doors, marked as restricted zones, section of the OR
from the rest of the L&D ward- the space is limited to those with specialized knowledge and
authority. A scrub space and hallway with equipment, blankets, and sterile uniforms and masks
lead to a very bright OR that is also full of equipment, adjustable fluorescent lights shining down
from all angles. It is difficult to know what time of day it is as there are no windows or inklings
of the outside world. A tray of surgery tools lies next to a table where the woman receiving a C-
section lies. Extenders on either side accommodate larger patients, and most of the machines- IV
drips, heart rate monitors, ultrasounds- are on wheels for easy re-arrangement and access. In the
middle of all of this, the operating team, myself included, stands around the mother, who lies
with her lower half accessible to the surgeons and her upper half isolated by a blue curtain. The
physical separation of the mother from the surgery space- both by visual impairment and
anesthesia- was the most explicit removal of the birth process from the mother I have seen; her
body may as well have been separate from her head. The OR is almost esoteric in its isolation
17 Male physicians also regularly used forceps until (date), as it was considered immodest for their male hands to enter the woman’s vagina to turn or assist the baby’s emergence. Jordan’s data on 1970s Yucatan Mayan births described midwives who similarly refrained from touching the mother’s genitals (1983: 22)
Ballerano 2011
42
from the rest of the hospital and its sterility requirements. It clearly belongs to the skilled
surgeon, the obstetrician in need of absolute control if s/he is to perform a major invasive
surgery. It is distinctly not a place for physiological birth- there is no vagina, no contractions,
and no breathing exercises. The woman’s body itself, numb and immobilized, transforms into a
part of the room, an object from which the fetus must be distracted. The fragmentation of the
space translates into the fragmentation of the woman’s body, from herself and from her infant,
and puts all the pieces into the hands of the obstetrician, via restricted access and restricted
knowledge.
V. Use of Medication
Brigitte Jordan’s defines medication as “any substance introduced into the woman’s body for
one or both of two purposes: to affect the course of labor (speeding it up or slowing it down) or
to provide pain relief for the woman,” (1983: 54). When people need relief or time is essential, it
is certainly understandable to want to provide solutions- it is no crime of medicine to ease
suffering. But when medication carries its own risks and is applied under the assumption that a
woman will be unable to deliver a child without it, especially when those risks are not fully
explained, its use can have both iatrogenic and psycho-social effects.
In particular, providing pain management has a major role in care given during labor, and
understandably so. “I think overall people underestimated how much pain they are going to be
in,” explained Dr. B in a phone interview. “In society today we aren’t ever in pain. Nobody is
ever prepared for pain- you know you get a headache you take something for it. So this is
certainly something new to them,” (2010). But whereas some may expect and view pain as a
natural and temporary part of the birthing process, the American mentality seems to be that pain
Ballerano 2011
43
is a problem that needs to be solved in order to have a successful delivery. As discussed in
Section I, the placement of labor and the body as alien to the woman makes her subject to the
external burden of reproduction, turning her into a victim that is, as a patient, suffering. Hence,
when doctors unassumingly ask patients, “Have you been thinking about pain management?”,
something I saw repeatedly in my hospital observations, women are likely to accept that they
will indeed need pain management and do not question the doctor’s assumption, because their
body is framed as an independent source of pain or distress, out of their control. In describing his
European clients’ attitudes, Kreuning illustrates the seeming irrationality of this assumption.
“They know it hurts but it’s only for a short period of time,” he explains, “And well, ‘My mother
did it and my grandmother did it, so I can do it’…and of course there are millions of other
women in the world who did it,” (Buonagurio 2008: 23:26).
What’s frustrating is not so much the expectancy of pain management, but the type of
management utilized. The epidural and other options, such as morphine, are based on methods
that were developed for whole body relief or, as in the “twilight sleeps” of the 1950s-1960s, to
completely separate the mother from the birth experience by making her unconscious. Today,
every anesthesiologist has a signature combination of anesthetic and narcotic- the recipients
safety and comfort is dependent on their recipe and correct application (Block 2007: 24). Despite
its world-class training and development of anesthesiology, the U.S. has yet to develop an
effective way of numbing only the back pain and pressure of contractions, without affecting the
rest of the body and the mother’s ability to function normally. Even American practitioners who
are keen to calm their patients see the problems this presents to normal physiological birth:
When I first came in I was trying to get women to walk around, or take a bath, try other ways of doing pain control. But now I see the women who get the epidural are so much happier. Otherwise they are freaking out because they can’t handle the pain. My big problem with it is you can’t move. I think one of
Ballerano 2011
44
the biggest risks of a hospital birth is that your labor can’t progress. You lie there and stay there. I always encourage them to get up and move around. (2010)
Since movement is the main natural for facilitating the baby’s progress down the birth canal,
as well as making the mother more comfortable, pain medication can actually have a delaying
effect on labor. When women started lying down for birth in the 1800s, both because of
anesthesia’s debilitating effects and because modesty required it in the presence of male doctors,
they began obstructing the natural mechanics of upright mammalian birth (Block 2007: 23;
Buonagurio 2008).
In the case of induction, even the evidence of medical research suggests that it is applied far
too often and for unjustified reasons. Induction, often taken for granted as a convenient way to
schedule a delivery or end a long and exhausting pregnancy, is actually an object of much debate
within the maternal care community. While some doctors and even midwives induce by
manually stripping the cervical membranes, a method that is “less” of an intervention but can
still have unwanted consequences, most inductions are done chemically. To start, a pill is placed
in the vagina to loosen the tissue and relax the muscles. Cytotec, a drug that is not FDA-
approved and has actually been shown to increase the risk of uterine rupture and other
complications in pregnant women, is commonly used for this purpose.18 Hours later the patient
receives Pitocin, a synthetic imitation of the hormone oxytocin, which causes uterine
contractions. A laboring woman is dosed via IV drip, and the range of sensitivity to the drug
varies greatly. Once the drip is started, the Pitocin starts to cause contractions at a faster and
stronger rate then what would occur naturally. Each contraction constricts the oxygen supply to
the baby, and while natural ones that are gradual and more spread out are tolerable to the fetus,
induced contractions leave little recovery time in between. This can be dangerous to the baby and 18 Buonagurio 2008 and a follow-up e-mail with Dr. B, March 2011
Ballerano 2011
45
create more pain for the mother. Megan recalls how her contractions started to come on 10
minutes after the Pitocin was started:
I was like “Ok I’m gonna see how long I can go before I get… an epidural,” cause I wanted to see if I could handle it. And I couldn’t. So I ended up getting an epidural. Probably like an hour and a half after I got the Pitocin...Oh it was horrible it was really bad, I couldn’t even move. I was in the fetal position. I had severe back pain…I was like “This is gonna be so much tension on the baby, it’s not gonna be good for him, it’s not gonna be good for me. I’m not gonna be able to relax, and like concentrate on what I’m doing. (2011)
Remembering that Megan had originally wanted as natural a childbirth as possible, one has to
wonder how much each intervention contributed to her experiencing pretty much every
biomedical intervention except for surgery. Critics from within and outside of the biomedical
system complain of the “chain of intervention” that leads to unnecessary costs and, sometimes,
iatrogenic problems such as uterine rupture, the need for an episiotomy, and the risk of Cesarean
section (Epstein 2008). Megan, for example, waited for her labor to start naturally.19 When she
went a week past her due date, her doctor decided to induce her, even though there is evidence to
suggest that waiting, rather than inducing, can pose less risks and result in a healthy outcome
(Block 2007: 274). Since she was induced, her contractions came on stronger and faster than
they normally would and were thus more painful. She may not have chosen to get an epidural,
had the increased pain of induced contractions not been so strong:
The pain was, especially being induced, you don’t gradually get into it, you get right into, like, the last stages of labor, the intense pain…some people, their water breaks and they gradually start to feel the pain and they can build their pain tolerance up to it. And me I was just like thrown right into full-blown, intense pain labor. (2011)
Megan was able to continue laboring, and with pain relief got enough rest to deliver
vaginally a short while later. She was able to feel the pressure of when to push and her baby was 19 She had already lost her mucus plug, or “bloody show”, but labor may take anywhere from hours to weeks after this bacteria-fighting cervical barrier descends. (Gaskin 2002: 232)
Ballerano 2011
46
ready to come out. Had she not progressed after the epidural, however, she probably would have
received a Cesarean section, like the woman whose surgery I attended. When the integrated use
of Pitocin and the epidural (which can lower blood pressure) cause a) distress to baby and b) the
inability of the mother to feel and react to her baby’s movements, a delayed labor is the result,
which is often solved by surgery (Interview with Dr. B, 2010).
Megan was happy she got the epidural, and so are many women who choose this pain
relief; the point is not to criticize pain relief in and of itself. Neither is induction always
unnecessary, but patients need to know the truth about the medicines they are being offered.
“The risk of induction is a 50% increased risk of Cesarean section,” explains Dr. B. “We induce
for health reasons, like diabetes or pre-eclempsia…Induction equals an increased risk of
malpresentation, babies in the wrong position at start of labor;; there’s an increased risk of C-
section but women don’t seem to understand why that’s a risk,”(2010). When a professional
warns you about the risks of their specialty, it may be a good time to listen.
At the same time, obstetricians’ ability to provide pain medication was the early basis of
their existence as a career profession (Hachey 2004: 20). And women, perhaps not understanding
the risks of what felt like relief, had a role in making those careers. Upper class women seeking
control of the childbirth experience, a goal that could be considered an expression of first-wave
feminism, felt that painless childbirth was the solution, and these wealthy drug consumers of the
time are those who gave physicians a material role that midwifery could not fill. Their desire for
numbness and even unconsciousness makes sense considering the Victorian context of these
women’s reproduction- a demand for large families, a prudish public sphere, corseted waists and
the expectation of inactivity among women all could have contributed to making childbirth a
especially difficult, embarrassing, mysterious and frightening experience (Block 2007: 23-4).
Ballerano 2011
47
The fact that OB/GYN practice emerged out of this state of women’s culture says a lot about its
perspective on pregnancy and birth as problematic medical events in need of fixing. For women
whose experience of birth was already so far out of their control, maximum removal from the
process, be it by pain relief or heavy narcotics, became the ideal.
Fortunately for today’s women, there was resistance to this model, although women
didn’t start visibly reclaiming birth until the natural birth movement of the 1960s and 1970s.
Despite their systematic devaluation by the medical profession, starting at the turn of the
twentieth century, a few individual midwives continued to practice under the radar and were
available, albeit scarce, to share their methods for natural birth when women again started to
demand it. They were backed by new access to nurse training (hence the distinction between lay-
midwife and nurse-midwife) and a generation of women looking for a “gentler birth experience”
than the bed restrictions and episiotomies of hospital birth (Cassidy 2006: 44-45). The women-
centered philosophies of natural care-providers made pain less of an issue for women who
wanted to be empowered by their birth experience. This ideology was what eventually inspired
Chrys to have a natural childbirth in 1988:
I’m not really big on the whole allopathic medicine thing because I do think the body does know how to do these things. And I think our own ability to create our brain chemicals that help us along the process…the pain, its not just that I don’t remember how bad the pain might have been during that last stage of delivery. I do remember enough of it to feel like…it was almost ecstatic, even though I’d had such a long, tiresome labor. I didn’t quite have the orgasm or orgasmic experience that I’d read about in Spiritual Midwifery…I think that the brain releases enough endorphins and opiates by itself and all different stress hormones, whatever it is that keeps us from…I think we need to trust the body more. (2010)
Author of Spiritual Midwifery Ina May Gaskin was on the road in the 1970s to spread a
spiritually conscious lifestyle, and began delivering babies in the buses of a caravan that became
the Tennessee commune The Farm (Cassidy 2006: 45; Gaskin 2002: 15-19). And so while
Ballerano 2011
48
physicians had capitalized on earlier American women’s fears and demands for pain control,
those fears started to turn into confidence and a form of pain management that involved working
with the body rather than inundating it with potentially risky medications. The movement for
natural childbirth continues today, but obstetric control of most pregnancies means that most
women are being subjected to (potentially unnecessary) highly medicated birth, sometimes
without them knowing it.
VI. The Technology of Birth
In addition to medicinal interventions, technology is a major factor in American birth
practices, as it is in many cultures. While “tools” have been used by healers and midwives
throughout history, in various forms (plants as medicine, bricks as supports, ropes as props, ritual
objects for protection), the very technological character of todays obstetric tools makes them
more complicated and specialized than ever (Jordan 1983: 58-60) . As tools have advanced,
incorporating scientific innovations like x-rays, computers and chemical compounds, the
knowledge of how to use those tools has become increasingly esoteric. As a result, there are less
people who are able to use them, more need for medical specialization, and more utilization of
robotic and computerized systems of care. As pharmaceuticals advanced with increasing demand
for pain relief, obstetric technology has rapidly evolved to meet time-obsessed neoliberal
demands for efficiency, speed and control.
Marxist critiques like Martin’s compare this streamlining of birth to the streamlining of
the industrial process, in which productivity is based on the number of products (i.e. babies)
produced (delivered) in a given workday (hospital shift) by unskilled laborers (women) and their
managers or owners (doctors) (1987: 57, 61). Mothers are told they are having “efficient or
Ballerano 2011
49
inefficient contractions” and are measured as progressing, or not (called dystocia, which
originally signaled only the mechanical failure of the infant to descend), in specific periods of
time for each stage of labor (Martin 1987: 59; Block 2007: 19). The birth system has become an
industry in which all stakeholders are struggling to balance their demanding roles and badly
founded expectations with the natural obstacles to controlling major physiological events. The
implications of the “political economy” of maternal and perinatal care are far-reaching; when
obstetricians are paid on a case-by-case basis, each of which has different needs and
complications, but are also expected to treat non-maternal and non-laboring women in their
private practice, while simultaneously having their own family and health to care for, the need
for efficacy and control seems justified. The attitudes and potential for mistreatment that result
from such a high-pressure system are a matter of course. “It is no surprise that patients are
neglected in a system where an obstetrician tries to be all thing to all women…no other specialist
anywhere in health care tries to maintain competence in so many areas,” (Wagner 2006: 6).
Whether or not obstetrics’ unique difficulties stem from an unrealistic obsession of
industrial and Victorian-era men to control and perfect the female body, as I suspect¸ the result
of that singular focus is that “obstetricians plates are full to overflowing” (Wagner 2006: 6).
Because they are unable to meet the varied demands of maternal, infant, family planning and
women’s health care, they have come to rely on “perverse” applications of productive means
(Martin 1987: 67). To start, the application of pain medication and induction drugs via IV drip or
injection can be considered a technological coping mechanism for what would otherwise be
treated with patience, plants, massage, and other naturalistic means of relief or induction, like
movement, deep breathing, or even induced vomiting. Because a computer can control both pain
and induction medication, and because nurses are trained to administer such technology, doctors
Ballerano 2011
50
need not even be present to use them and need only to direct someone else in their application,
which is ideal for saving time spent moving between patients or locations.
As discussed above, the careless application of such technology for the convenience of
the doctor can have iatrogenic effects on the women in his or her care, even when its use is
framed as being beneficial to the mother (Block 14). This has been criticized even from within
the obstetric community;; in light of Jordan’s observation that a given cultural system is least
likely to change from within, these criticisms speak volumes about how badly maternal care has
deteriorated in recent years (Jordan 1983: 2, 8). Inductions, which significantly increase the risk
of C-section (among other complications), were practiced in 44% of U.S. labors in 2002; the
evidence-based suggestion, internationally, is 10%. Current national Cesarean rates are upwards
of 34%, whereas the World Health Organization and evidence-based research suggests 10-
15%.20 The inclination to blame this on physicians schedules is based on the admission from the
medical community that “attending” obstetricians are rarely present for the actual birth of their
patients, and that, more shockingly, the hours from midnight to 6a.m. see a significant jump in
neonatal infant mortality (Wagner 2006: 5). That implies that obstetricians are pushing more and
more deliveries into the regular shift hours of 9am to 5pm with inductions and surgeries, while
providing significantly less quality care (if any) to mothers and babies that fall outside of the
most comfortable time frame for working. The births I attended were, except for surgery,
attended y residents or nurse-midwives, not by fully trained obstetricians. Most of the care up to
the delivery was, as Wagner suggests, done by nurses, who have no other obligations other than
to care for their ward patients (2006: 6).
What I did see a lot of was conversations over the phone between nurses, lower-ranking
resident OB/GYNs, and the head obstetricians. Jordan goes so far as to call nurses the “liaison” 20 See Appendix B, Table 1.
Ballerano 2011
51
between the patient and her doctor;; they are under pressure to make judgments on the patients’
statuses “within a small range of error” (hence the continuous use of electronic monitoring) so as
to best decide when the doctor is actually needed (Jordan 1997: 63). Patient’s were regularly
discussed between Dr. B and her department chair over the phone, even though he was in the
hospital and most likely sitting at his laptop in the “Lounge of Knowledge” down the hall. These
conversations often contained elements of persuasion, justification, and even resistance to the
physician’s decisions. At one point, the other resident, a woman, complimented Dr. B on her
ability to negotiate diagnosis and treatments with their department chair over the phone. When
those who are removed from the patients are eager to progress the labor and make interventions,
often unnecessarily, it is up to the person with more personal experience of the patient to defend
a different or less intrusive solution. Because of the remote monitors that screened and displayed
every patient’s status continually, it was relatively easy to communicate essential updates
without actual continuous face-to-face contact, between doctors and even between doctors and
patients. The result- that women are left alone, hooked up to machines, while their care is
managed from a separate room- is yet another dehumanizing and uncompassionate regularity of
the hospital system.
One of the machines yet to be discussed is the electronic fetal monitor. The straps that
pick up on the infant’s heart beat and broadcast them into the room immobilize the mother, as
does the IV drip she may be attached to. She likely is, as monitors are only deemed necessary
once medication has been administered. They are used without medication too, which can cause
unnecessary monitoring of the fetus that has been argued to cause stress, bad judgments, and
overreactions on the parts of patients and doctors alike (Block 2007: 33-5). Nonetheless, the
product exploded after it was released in 1969 and saw revenue increases of nearly 1000%, even
Ballerano 2011
52
though it was only intended for use in high-risk pregnancies (32). Now, Block suggests, EFM
use has become a primary means of negotiating litigation- the heart rate strip serves as evidence
of proper (or improper) care in court (33-4).
While the benefits of EFM in more complicated pregnancies are obvious, the need to track
the infant’s heart rate otherwise is debatable. In terms of birthing environment, the loud presence
of the fetal heart beat can be strange and even stressful. Of course, hearing a future child’s
heartbeat can be a beautiful moment, as heralded by media depictions of expectant couples, but it
can also be overwhelming and even frightening. Martin’s fieldwork illustrates the disconcerting
nature of the experience for some of the women she interviewed. “…My doctor gave me the
heartbeat,” reflects one woman, “It’s like he took it away from me because he said ‘Here’s the
heartbeat,’” (1987: 72). While the reality of a pulse certainly defines the existence of the fetus,
the raw biology of it can be disturbing, especially in the vulnerable moments leading up to
delivery. While observing in the hospital I realized a few hours into my experience that there was
almost constantly an audible heartbeat in every room, and if not a constant beeping reminding us
the machine was there. It made it much easier for women and doctors to “hear” when a
contraction was coming (because each contraction causes an increased heart rate in the fetus),
but also sounded almost threatening, as if reminding us of the fragility of life and the constant
possibility of danger.
Culturally, the heartbeat has been regularly utilized as a symbol of fear- adrenaline pumping
during a chase scene, a slowing pulse at the moment of death, a young person’s first realization
of their own mortality. In watching an advertisement for a recent new television program called
“One Born Every Second”, I initially thought I was watching the trailer of a horror movie. A
steady heartbeat played against a white background, and as the beats increased in intensity and
Ballerano 2011
53
speed, so did the background noise of medical personnel ordering each other around, yelling for
equipment. Suddenly, right when the heartbeat seems so fast it might explode, the white light
fades to the title and a baby’s cry is heard. In this example of popular media, the heartbeat is
used to imply a sense of panic, urgency, and fear, not comfort, knowledge, and stability. While
making rounds with Dr. B, I could not help but think of this chaotic vision of childbirth every
time an infant’s heartbeat was broadcast across the room for all of us to hear.
When the fetal heart rate does show signs of distress, most obstetricians turn to the epitome
of modern maternal care technology- the Cesarean section. History accounts for births by surgery
as early as 320 B.C., when a royal advisor in India decided to rescue an infant prince from a
dying queen. Surgical births were practiced around the world, and it even became Roman law
(hence the name) that infants be cut from the womb of a dead mother, as it was taboo to be
buried pregnant. Surgeries were also performed on women while they were still alive, but a
mother’s survival wasn’t recorded until the end of the 16th century, when a Swiss pig farmer
successfully operated on his wife without butchering her fatally (Ballerano 2010).
Of course, we’ve gotten better at medicine since the 1500s, but it’s easy to see why, as with
any other surgery, Cesareans are dangerous procedures and are traditionally used as a last resort.
In some cases, surgical birth is truly necessary, as when doctors discovered a fibroid growth in
Charlene, a mother who had already birthed a large boy before becoming pregnant with her
daughter 6 years later. “I sort of assumed it would be another vaginal birth,” says Charlene, “It
was daunting to be split wide open.” In some ways, it was nice to know exactly when she was
due, and her doctors were informative and reassuring. “I never felt like they were pushing for
anything, and in some ways recovery was easier than from the regular birth,” she says.
Compared to her first labor, which took so long she found herself doing taxes between
Ballerano 2011
54
contractions, the surgery, which usually lasts about 40 minutes, was quick and painless
(Interview, November 2010).
While Charlene’s case illustrates why such technological interventions can be life-saving, it
is the constant over-application of such means that creates additional risk and trauma to
otherwise healthy moms. Cesareans are major intrusive surgeries that carry the risks of internal
bleeding, infection, damage to other organs, infertility and even death. And yet, as Dr. B
observes, “too many women think that a C-section is a totally benign thing,” (2010). Even if
physically successful, the psychological and developmental effects of surgery can be detrimental
to the family. The mother needs weeks to heal, which can hinder her ability to care for a child.
The infant is almost immediately removed from the room post-surgery (restricting immediate
mother-baby bonding); surgically delivered babies are less likely to breastfeed, and there are
links between post-partum depression and Cesarean sections (Block 2007: 27, 145-7).
“Post-traumatic stress disorder”, also common among soldiers and survivors of domestic
violence or natural disaster, has been identified in up to 6% of mothers, who experienced some
kind of “birth trauma” (Block 2007: 145). What’s interesting is that it is not just the physical
trauma that can cause later emotional distress, but the “how” of the birth process-the attitudes of
the doctors, the atmosphere, the amount of attention paid to the mother’s needs. Consider the
casual atmosphere of the operating room described above. The mother was not only completely
powerless and unable to participate in the birth, but the staff repeatedly made jokes at her
expense and ignored her requests for information on the progress of the surgery. This is not to
dismiss the purely physical extremity of such interventions. In the surgery I attended the
surgeons and nurse gave me small responsibilities to assist. As I held a retractor in one hand (a
tool akin to a bent metal spatula) to hold back layers of fat and muscle, and suctioned spraying
Ballerano 2011
55
blood and the smoke off of sutured veins with a tube in my other hand, I was a loss for how
people could consider such a process harmless and convenient.
Martin, Jordan and others pinpoint the over-dependency on technology as a major
contributing factor to such trauma. While doing rounds with Dr. B, I noticed how everyone in the
room was constantly checking the screens of the various monitors, rather than looking directly at
the patient- it was the technology that drew the attention of the participants, including those who
were untrained receive or interpret any information from the screens (Jordan 1997: 63). Where is
the human connection that makes birth a personal achievement when all the activity, and much
of the credit, is based around the use of highly complicated equipment to which regular women
have no access? The loss of control that women experience in surgery is “an intense experience
of fragmentation” that is augmented by the fact that more people, more tools, and more
procedures are necessary to carry out this type of birth (Martin 1987: 82). The surgery I attended
required 2 surgeons, an assisting nurse, myself, an anesthesiologist, a second nurse who stood by
the mother, the mother’s companion, and two more scrub nurses who assisted in dressing us in
sterile garments and keeping track of the over 30 bloody rags and multiple instruments that were
used during the procedure.
Recall the chain of interventions discussed above, in which pre-emptive induction and
pressures to deliver according to doctors’ schedules lead to unnecessary surgery. Why is it that,
even with myriads of stories from traumatized women and piles of research evidence pointing to
the increased risk of such measures, hospitals continue to subject births to extreme technological
intervention?21 Martin blames to obstetrics’ mechanical view of the female body and the
resulting expectation of perfected efficiency (1987:27-65). This techno-view of the body
21 For more stories and discussions of surgical experiences, see Pushed by Jennifer Block and Born In the USA, by Marsden Wagner.
Ballerano 2011
56
originated in seventeenth-century French descriptions of the uterus as a “mechanical pump”, and
was furthered by the replacement of midwives hands with male hands using tools in the name of
modesty (54). Once obstetricians set out to “supplement and anticipate the efforts of nature”,
devices originally intended to treat “abnormal, critical cases” became standard tools for men who
were unable or unwilling to utilize the wisdom of traditional female midwives, the very group
their profession needed to marginalize in order to become the dominant birth authorities. As a
result, doctors and patients have come to expect technology to perform the processes that once
belonged solely to the mother and her trusted female companions.
VII. Locus of Decision Making
What all the preceding discussion amounts to is that the decision-making process of
American childbirth is not a simple matter of right or wrong, yes or no. The complex interaction
of people, spaces, and tools create a “culture of birth” in which choice does not belong to one
person and manifests in a plurality of ways. Even when the mother, doctor and other participants
go into the birth process knowing what they expect, and even when the condition of the
pregnancy is well understood, the unexpected nature of physiological processes along with the
far-reaching consequences of even minor decisions make for a complicated route from the
earliest stages of labor to the delivery and recovery of the mother and baby.
When the metaphor of “productive means” is applied to hospital childbirth, in which the
doctor manages the labor of the mother, the bureaucratic nature of the biomedical system is
revealed. While small choices are made at each level, this framework reveals how no one
decision is completely owned by the mother, the actual “doer” of birth. Unfortunately, it places
the mother at the bottom of the chain, as the unskilled laborer who, without active management,
Ballerano 2011
57
is inefficient- this is due in part to mechanistic views of the female body but also the entrenched
understanding of pregnant women as vulnerable and inexpert in the processes of birth.
Supervising her labor is the nurse, who serves as an intermediary between the woman’s body, the
machines that measure her “performance”, and the upper management- she is the supervisor who
must ensure things “run smoothly” and that directions are followed. 22
The division line to the next rank of participants- nurse practitioners, nurse-midwives, and
resident physicians or medical students- is more fuzzy. Each have different qualifications,
restrictions, and ideological roles to embody. They must negotiate between their personal
experiences with patients and expected protocol, like the nurses, but also between the need to
validate their authority via the approval of head physicians and the risk of taking full
responsibility for birth outcomes. At this point in the chain of command it is easy to see why
even small mistakes create recipients of blame for bad outcomes- the pressure to provide care in
line with the standard techno-medical model is high. And doctors are aware of the magnitude of
their responsibility “The decision to go to a C-section is my most difficult decision every time
and it makes me very upset,” said Dr. B on the phone. “I hate it.” The middle level of
management, students and residents in particular, consistently turn to the in-house obstetricians
for advice. Confirmations and corrections from the highest ranked physicians perhaps lend some
ease to the ethical and emotional difficulty of essentially controlling people’s physical well-
being.23 This was evidenced in the frequent phone calls Dr. B had to make to her chair when
22 As with so many processes of daily life, the language of industrial production and mechanical function permeate the way we describe even the most human of activities. 23 Even though physicians, objectively, cannot control “everything” about physiological processes, they are perceived as being capable of doing so because they have the tools of science and knowledge of medicine. Americans expect “modern medicine” to solve all ills when, in reality, there have always been mistakes, morbidity, and fatality in the hands of those who claim to augment or control natural processes. Hasn’t medicine always been a means of fighting nature and the mortality of living things? If patients with unrealistic expectations of their doctors powers are continually disappointed with their services, they must change their expectations or change their
Ballerano 2011
58
deciding how to handle a case. These physicians, established surgeons who may have a private
practice in addition to their hospital patients, are akin to upper management or, depending on
their role in the hospital, the owner class.
They call major decisions and tirelessly oversee everyone’s performance and are
considered responsible for the success of the team, i.e. the delivery of a healthy product. They
are also the final “expert” in complicated situations- if their knowledge does not cure the
problem, then their elite skill with the scalpel blade will (Martin 1987: 19). In controlling the
most dangerous tools (i.e. surgery) and dictating the use of machines and medications, physicians
most visibly manifest their power throughout the birth process. Despite being the face of
obstetric care- a woman who chooses a specific doctor does so in the expectation that her care
will meet that doctor’s standard- they are the most removed from labor and birth process, often
right up until the delivery, when they can catch the infant and proclaim the outcome a success.
Like the owner of a restaurant, they are given credit for the efficient work of a larger team and
the pleasing final product, or blamed for disastrous service and results. For this reason, and in
contradiction to their seeming removal from the process, they hold much stake in childbirth
outcomes.
That investment is guided and threatened by the final player in this scenario- the
insurance companies. The actual patient’s insurance dictates not only which types of care and
medicine are available to each mother, but how much of that care is paid for. They interact
cyclically with demands of consumers and supply of pharmaceutical/technology companies.
They also hold unspoken power in the services they choose, or don’t choose to provide; as
insurance groups are understood as managers of risk, their perspective on what care if
services. In the case of maternal care, it would seem that better services can exist and expectations need to be realigned.
Ballerano 2011
59
good/beneficial and what care is “risky” is given undue weight from their customers. Likewise
the doctor’s malpractice insurers, supposedly protecting the legal and financial interests of
physicians, dictate to practitioners which types of care are risky or not. In the face of current
lawsuit-happy society, physicians and hospitals have a vested interest in taking precautions to
protect themselves- hence continuous monitoring, reliance on the “guaranteed outcome” of
surgery, and repeated oppression of patient’s unique or less traditional birth demands.
Whether we frame them as the CEOs or the stockbrokers of birth production, it is
insurance companies who, explicitly removed from the physio-social reality of birth, set the
initial scope of possible decisions for all parties involved. Moving back down the ranks, each
party is necessarily limited to fewer decisions by the restrictions imposed by entity above it, be it
person or company. In this way, choice becomes exponentially smaller for the mother who
chooses, or is forced into, a hospital birth process. The implication of this is that, once the
hospital’s “means of production” are applied to reproduction, the knowledge and agency of the
mother stops being what “counts”, and is superseded by the authority and knowledge of first
care-providers but ultimately firms and corporations.
This is the phenomenon of authoritative knowledge (AK), as described by Brigitte Jordan
(1993) and expanded on by social scientists ever since (Davis-Floyd and Sargent 1997). AK
must be understood as one type of knowledge that exists and interacts with others (Jordan 1997:
56). What distinguishes AK from “information” is that it “counts” in a way so as to justify
behavior, frame judgments, and create beliefs. Most important to understand is that the weight of
AK does not mean that it is correct, only that it is valued by participants in its sharing and use
(58). But, as in the case of medical knowledge (which is assumed to be based in scientific
knowledge), once a kind of knowledge becomes the legitimate measure of truth within a
Ballerano 2011
60
community, alternative forms of knowledge that may have once coexisted with this AK become
devalued or even dismissed altogether (56). Jordan illustrates this with a realistic example I can
confirm as standard practice today. In the hospital setting, whether or not a woman believes she
is ready to push and deliver her infant, and however many vaginal exams by nurses and students
have seen that she is fully dilated and effaced, it takes a final examination and confirmation by a
physician for the pushing stage to move forward. That is, the fact that the woman is ready (as
evidenced by her body), although available to all participants, is not considered reality until it is
validated by a doctor (66). This evidences what Foucault proposed- while knowledge itself is
usually considered powerful, it is actually the purveyor of that knowledge who defines its power.
The status of the “voice” of the knowledge dictates whether it is to be valued as “true” or not,
and so the same information may not carry equal weight across multiple sources (57-8).
To what extent science has become women’s “common sense”;; how much have patients
come to rely on physicians in knowing the reality of their labor and birth process? Assuming
Gramsci’s definition of hegemony, in which an “entire [permeating] system of values, attitudes,
beliefs, morality, etc.” becomes internalized by society through popular and scholastic assertion
and reinforcement, Martin and Jordan posit that institutionalized biomedical authority is what
subtly and explicitly defines the “truth” about childbirth, delineating the intuitive/body wisdom
of women and alternative care-providers (Martin 1987: 23, 62-3; Jordan 1993: 57, 59). I expand
that claim to the observation that the U.S., with a highly privatized insurance industry and no
universal healthcare, has created a biomedical system in which it is industry standards that set the
framework of authoritative truth for the lived experiences of all patients, not just laboring
mothers. In the context of childbirth, this means that women’s self-knowledge and intuitive
understanding of the birth process, as well as the knowledge of midwives who support her
Ballerano 2011
61
natural wisdom, is marginalized in favor of the norms of the medical establishment, even when
those norms are not based in scientific evidence.
Jordan argues that institutionalized medicine has becomes so entrenched as authoritative
in part because of the active, conscious reinforcement of physician power over patient agency.
She refers to the directed pushing, or the delay of pushing, between nurses and laboring mothers
as evidence of this- whether or not a woman feels she must push, a nurse will tell her to wait or
start depending on the doctor’s preference and presence (1993: 67). While I am sure some care
providers consciously accept the hegemony of AK, I think that modern stakeholders in the birth
process are actually more likely to negotiate between types of knowledge, in part due to litigation
risk but also in recognition of the diverse ideologies, cultural values, and subjective
embodiments of reproduction that women bring to childbirth. This implies both increased
sensitivity to the weaknesses of obstetric science and resistance on the part of women and
providers who are aware AK’s undue influence.24
For example, I listened to a physician counsel a woman in early labor as to whether or not
she should attempt a VBAC (vaginal birth after Cesarean) or schedule a surgical birth. She gave
a thorough and balanced description of the risks of each and was honest about the inaccuracy of
the ultrasound off of which she was basing the baby’s size. She left it up to the parents to decide
what they wanted to do, but when we left the room she admitted that she had really wanted to
push for the Cesarean because she felt comfortable about its potential outcome; she was clearly
empathizing with the woman’s excitement about doing a vaginal birth, however, and was
hesitant to push the family towards one decision or another. They had a successful VBAC later
that weekend. This example stands in sharp contrast to the many hospitals that do not even offer
24 Bourdieu and Passeron (1977) describe the acceptance of AK and its power structures as “natural, legitimate, and in the best interest of all parties”, rather than as “socially constructed, relative, and often coercive”, as “misrecognition” (Jordan 1997: 57).
Ballerano 2011
62
VBACs, the women forced to travel interstate or birth at home to have one and, at the most
extreme, women who are court-ordered to undergo Cesarean sections against their will.25
The informed consent of this couple is the ideal of all health care and assumed to give
patients decision-making power that in reality is very dependent on the individual doctor and
specific insurance that participants utilize. Patients’ rights advocate argue that patients should be
able to provide informed consent or dissent but that their capability to do so is dependent on the
thoroughness and competency of their expert care providers. It is much easier to follow “doctor’s
orders” than to justify resistance behavior, like Chrys did when she left the hospital “against”
those orders only hours after giving birth (her doctor actually allowed her to leave but had to
official document that he had advised her to stay). And yet, perhaps because they do not trust the
competency of their providers, mothers resist hospitals’ AK regularly, from sneaking in and out
of hospitals, to hiding their labor so as to avoid medical control, to using underground lay
midwives when no one else will provide a VBAC or breech vaginal delivery (Block 2007: 94-
101).
It all comes down to different forms of authoritative knowledge- who are the voices and
what are the ways of knowing that we trust and submit our bodies to? To which knowledge, and
to which speakers of knowledge, do we give power? The midwife (“with woman”) works with
experiential knowledge and intuitional knowledge of the mother, and supports the woman’s
doing of birth (Davis-Floyd and Davis 1996). Her priority to help the mother only when she is
needed can provide empowered, healthy outcomes. The physician’s knowledge comes from a
tradition of removing woman from the birth process, in exchange for the man’s doing of birth.
25 “Malpractice insurers and hospital attorneys have concluded that offering VBAC is not a sound business decision,” - Dr. Mark Landon of Ohio State University College of Medicine. Despite the lack of evidence, maternal care systems have “distorted the risk” of VBACs to the point that they are difficult to attain and legally dangerous to physicians. Block, Jennifer. Pushed. 2007: 87-91.
Ballerano 2011
63
Originally, this also created healthier outcomes, considering that obstetric practice was
developed when there were a lot of unhealthy outcomes and general sexual and reproductive
ignorance in society (i.e. Victorian times).26 But the theoretical benefits of biomedicine have
started to outweigh its practical benefits, in the name of science, industry, and priorities of
efficiency and pathological relief;; the result is that misconceived “truths” about childbirth are
utilized by the decision-makers, that is, insurance and medical technology companies, who shape
the U.S. healthcare system with profit and litigation power. And now, it no longer matters
whether a male or female is voicing the knowledge that has come to be considered the best: even
female practitioners have the power to reinforce, consciously or not, a biomedical view of the
female body, and of all patients, that necessitates management which may, in fact, be a detriment
to their overall experience or health.
Resistance, Change and the Future of American Birth
Months after joining the research mailing list for the International Confederation of
Midwives, I joined a U.S.-based virtual forum, based on a popular e-mail and search engine,
which claimed to serve as a network for shareholders in birth, specifically parents. I found it
disappointing- there were few members, even fewer authors, a lack of variety of posts, and many
of them treated issues not directly birth-related, such as parenting in general or post-partum
depression. These issues are worthy of consideration, but the low activity level made it difficult
to ascertain any pattern or definitive community from this group.
I would later find that there were plenty more active groups that suggest the Internet may
be accomplishing something for women and care-providers, in terms of disseminating
26 Indeed it was one of the first American female physicians who pointed to the corset as a probably cause of the reproductive difficulties of late nine-teenth century women. “The corset should not be worn for two hundred years before pregnancy takes place.”-Alice B. Stockham, in Tokology, 1883. 167-8. Block 2007
Ballerano 2011
64
information and articulating supportive communities; women I corresponded with via e-mail
expressed gratitude and enthusiasm for being able to share their stories. Birth-specific search
engines, if you can find them, allow users to find the information and even ratings of physicians,
hospitals and midwives. And research-based non-profit activist groups like Childbirth
Connection, most visible through their websites, appear to prioritize the experiences of women
as evidence of what is working, or not, in the national maternity care system.27 These seem like
the tools for change- awareness and education are the first steps towards collective, conscious
action, and yet every year, millions of American women and babies continue to experience birth
as determined by a model that has proven to be flawed.
In 1987 Emily Martin described childbirth activist groups and subtle forms of resistance
among women as a “defense” of natural birth (139). Whereas midwives, as the main providers of
alternative perinatal care, were once isolated from one another by language, ethnicity, and
varying traditions of practice, the internet has provided a space for solidarity. The research list I
joined at the beginning of this project was a space not just for communication of research and
events, but served to self-validate the midwifery profession and affirm its presence in the global
scholastic sphere. Likewise, accreditation organizations and informational resources like the
American College of Midwifery and the North American Midwives Alliance have used virtual
presence to disseminate accurate information about their practices and display efforts to
standardize and improve their training to the expectations of the biomedical tradition.
At the same time, opposing views and the strength of the technobirth model also hold
ground in the virtual sphere, and so negotiating the reality of birth there can be just as complex
and challenging of a process as it is for women in “real life”. Anti-choice bloggers, multiple and
27 Childbirth Connection’s Listening to Mothers Initiative, in partnership with Lamaze International, collected women’s childbearing stories in 2002 and 2006, for the purpose of analysis, outreach and education towards improved outcomes for mother and baby. www.childbirthconnection.org
Ballerano 2011
65
varied sources of medical “fact”, and lobbying and marketing on the part of the medical
establishment present equally persuasive sources of “truth” for women deciding what they want
out of childbirth. Reflecting the attitudes of practice in the hospital setting, websites like those of
the American College of Obstetrics are didactic, self-righteous and backed up by years of
standardizing “normal” birth- it is what most women find familiar and have come to expect. It is
these authoritative voices – of the medical establishment, of high-gloss self-diagnosis tools, of
mainstream media- that shape the assumptions of consumers and their care providers.
The plurality of information and discourse within the virtual public sphere paradoxically
threatens the potential power of the Internet for empowerment and connection. Its multiplicity
devalues the Internet as a reliable source, for the very reason that there is so much information
from so many sources. As Megan said when I asked her if she did any pre-labor research, “I
didn’t go online that much cause, you know, you don’t know what’s true and what’s not,”
(2011). Which knowledge is authoritative when the true identities, language, and intentions of its
sources are masked by the multitudes of the virtual forum? And even when a patient succeeds in
finding valuable information, how is she expected to apply it in a setting that devalues her
knowledge and individual preference in the face of legal and financial barriers? Those who are
able to evade this pattern tend to have other advantages, such as wealth, the ability to travel to
escape legal limitations, or insider knowledge of the health care system. These discrepancies
speak to the role technological resources, education, and money play in determining conscious
consideration and activity around pregnancy and birth.
The Internet highlights the unreasonable gap between those who have and those who do
not- be it a virtual connection, a comprehensive insurance policy, or a compassionate birth
attendant. The proof of the variability of childbirth is strewn across the virtual sphere- home
Ballerano 2011
66
videos, story forums, therapy groups, and public reports all reveal the array of what is possible
for women. And yet my observations suggest that these options, so easily accessible at the click
of a mouse, are not attainable for the majority of laboring mothers. Feminist scholar Gillian
Youngs reminds us of the dangers of investing false hope in “virtual utopias” when non-virtual
conditions are what actually influence daily reality of health (2007).
The U.S. appears to have attained a level of awareness in which alternative knowledge of
birth is “out there” but has not yet manifested as authoritative acknowledgement of birth as
anything but a hospital event. On the one hand, more information really may help women to
know the facts about their birthing options, and on a logistical level the internet makes it easier to
find diverse care providers and better understand the legal and political implications of one’s
choices. But any patient or health consumer needs outside information before being able to
browse selectively enough to discriminate quality sources. For the medical community, the
“mutual accommodation” of diverse health systems, suggested by Brigitte Jordan in 1983, is far
more attainable when globally networked professionals can organize, educate, and evolve via the
Internet, with fewer barriers of geography, language and class. Alternatively, the stagnancy of
conversation that is never carried into action may very well threaten the momentum of any
movement for change. If health advocates are content to discuss their problems and share stories,
rather than taking political action, their goals will never manifest as real changes in the lived
experiences of patients.
My own interest in childbirth was sparked by early exposure to the successes and
challenges of midwifery- a care system that directly opposes such hierarchal controls of
individual health. I tried to be aware of this throughout my research, although at times I found
the experiences of women going through the hospital to seem not only more painful than others
Ballerano 2011
67
but sometimes downright horrendous. While I cannot judge what kind of birth, be it by surgery,
bathtub, or hospital bed, is “right” or “wrong”, I do believe that I can advocate for more
awareness about women’s actual choices. Whatever a woman’s preference, be it induction and
epidural or squatting in her own bedroom, she deserves respect, information, and appropriate
care that optimizes her and her infant’s potential well-being.
In watching an interview with reproductive anthropologist Robbie Davis-Floyd, I felt a
rush of affirmation when she started to cry and admitted that, not as an anthropologist, but as a
mother, she could say that home birthing her ten-pound baby was one of the most empowering
experiences in her life. Considering that what seems to be lacking most among women is their
own authoritative knowledge, I think it is important for scholars to advocate more strongly by
creating culturally-sensitive, accurate and accessible ways to reclaim health care in general. It is
anthropologists who are able to help articulate the intricacies and varieties of childbearing and
other biosocial experiences, not just doctors and lawmakers. Why can’t we use our
comprehensive methods, along with the multiple functions of modern communication
technology, to become the channels of knowledge that women so clearly need? In identifying as
a feminist, an anthropologist, and a child of “alternative birth”, I find it completely acceptable
and ethical to consider action and education a part of my role as a scholar, and more importantly,
my role as a stakeholder in reproduction.
While as of yet the Internet has not overturned the entrenched power of corporations, the
moneyed interests of the medical establishment, or the divisions of gender, race and class that
define American health care, I have hope for the future of birthing mothers. The dissemination of
information and experiences via the Web does not directly change the experiences of patients
and doctors restricted by their contracts with insurance agencies, but the virtual community can
Ballerano 2011
68
be a starting point for restructuring power dynamics. It will take legislative leaps, an overhauling
of the health care system in general, and a reintegration of individualism into Western medicine
as we know it for the experience of childbirth to reach its full potential in the U.S., none of which
are simple or easy feats. But if the questions of agency and knowledge portrayed by Brigitte
Jordan and Emily Martin decades ago continue to persist for today’s laboring mothers- isn’t it
time that social scientists turned their words into actions?
The power to make health care decisions has continually shifted, from women to men to
doctors to companies. It is time that those of us with a vested interest in the rights of all people,
not just women, shift our powers as well. The Internet tells a birth story of freedom, diversity,
and choice that has yet to become a reality for American women. But rather than remaining
complicit with this illusion, perhaps anthropologists can act upon it, to create a new birth
narrative and, possibly, a new birth reality. Change in the hospital will not come about by simply
writing journal articles, posting the evidence-based research, or discussing personal experiences.
But it can occur when enough people challenge the power of corporate entities through mass
protest, convince their communities to question assumptions of gender and race-based
inequalities, and demand, as citizens and patients, comprehensive and dignified health care
standards. These interactions can start with the click of a mouse, and I believe that up-and-
coming anthropologists, coming from a disciplinary investment in social justice and armed with
technology that has brought down dictators and defined a new generation, are the people to
initiate them.
The increasing availability of birth, (real and representational), and a more open model of
communal participation in the actual processes (i.e. allowing fathers to be present) allows non-
traditional participants and laypeople to now see themselves as potential stake-holders in the
Ballerano 2011
69
“doing of birth”. Advocates for more birth options and the use of evidence-based care have
identified with different causes and aims throughout recent history. Understanding how and in
what context these participants view themselves is significant for understanding the current
tension in the spectrum of beliefs about what American birth should be and how previous
discourse has shaped the variable and dynamic experiences of today. The ways in which mothers
across American history have negotiated birth has contributed in paradoxical ways to the current
state of perinatal care. As feminists and, more recently, as consumers, women have identified
different problems, and very different solutions, in how to create a satisfactory birth experience.
Wealthy Victorian consumers of physician’s treatments looked for pain relief and viewed
physio-mental removal from labor as a form of gaining control over reproduction that, in all
other senses, belonged to men. It was consumer demand for medication and “modern” tools of
surgery that pushed midwifery practices into the marginalized communities of the poor and
multi-ethnic masses. It also put less-privileged women into the experimenting hands of
obstetricians who needed to practice gynecological surgeries, often without the use of pain
medication and sometimes against their will (McGregor 1998).
Post-industrial Americans who valued efficiency and high-tech innovation further looked to
machines and intervention to manipulate the time requirements of natural labor, while lauding
painless labor as a woman’s right. In the mid-twentieth century, that right was expanded to
include more naturalistic methods of control (such as Lamaze breathing), and was accompanied
by the growth of both the midwifery/homebirth community and the continued plethora of
technological techniques and products. Today, all birthing options imaginable up to this point
exist somewhere for some people, but the overwhelming majority of Americans experience
hospital birth that is highly structured, highly technological, and highly priced.
Ballerano 2011
70
The tension between women’s natural physiological processes and the efforts of biomedical
practice has been a constant theme throughout this trajectory, but what has changed is the way in
which the participants identify. What is most apparent is that, while both “women’s right’s” and
“consumer choice” rhetoric and justifications have continually influenced the standard of health
care, a shift has occurred. Since the second wave of feminism that peaked in the 1970s, women
have identified more and more as consumers and less as feminists. The neoliberal capitalist
policies of U.S. government and service providers have created a culture in which spending
power, not citizenship or human rights, define what is important and what is not. Indeed it is the
“stuff” of birth- machines, anesthesia products, baby clothes, formula, vaccines, parenting
magazines- that makes up most women’s understanding of the birth process;; for the most part
they choose between products rather than philosophies of birth.
This is problematic for feminists like Chrys who had to study hard, navigate institutionalized
restrictions, and justify themselves against public opinion in order to get the birth experience
they wanted. She explains why it was so important to her to claim her own birth process and pass
that experience on to me:
Some of us got educated and sought that education, and went out of our way to get that information. And once you have information that you have to go after, I think you have an instinct for wanting to pass it on. It’s like “I had to hunt for this shit, I don’t know if she’ll find it if I don’t hand it to her.” And that’s probably what it was;; trying to be protective of you as a female and saying, “Look don’t take for granted that you’re gonna be just fine if you do x y and z like all the other girls, because that’s not just fine. We don’t live in a “just fine” society. (2010)
For women like her, the standard system of birth presented challenges to feminist values of
independence, strength, and resistance to the oppression of a patriarchal history. Today’s
feminist, where she can be found, must argue that yes, the quantitative power of women has
improved dramatically (i.e. more women in medical schools), but the qualitative experiences of
Ballerano 2011
71
women are still mediated by a hierarchy of class and gender inequalities that are rooted in the
patronizing beginnings of the medical establishment. But what does it mean when people have
stopped identifying with values as feminists and started identifying with the power, elitism and
conformity of consumerism?
The popular “right to choose” rhetoric of the abortion movement was also applied in the
natural birth movement, in which women from the 1970s and onward argued that they should, as
the people actually carrying out pregnancies and mothering infants, have the right to choose
when, where, and how they delivered babies. While the familiar feminist argument for birthing
options still applies, in truth it seems that many of the changes made in perinatal care, including
those towards the male-dominated biomedical model, were as much a matter of wealth as
gender. Ironically, the class of women that once demanded these changes is now the class
demanding changes again- that is, it is women with higher incomes and more education that are
demanding the availability of midwifery and home birthing options- the very care systems their
predecessors were disengaging themselves from a century ago (Hachey 2004).
It is still those with money that have the power to influence the care systems available. The
fact that women who can afford private insurance and selective doctors are demanding
alternative options as consumers has problematic implications for the U.S. birthing system as a
whole, strategically beneficial as it may be. Aside from the difficulties this movement presents to
those with less money and fewer insurance options, the very identification of what was once a
women’s movement as a consumer movement weighs a heavy influence on how such care will
develop in years to come. As with any regulation, the legitimization of midwifery could certainly
make it more available to those who have the insurance to cover it, but at the same time the large
segments of the population that rely on such “alternative” care because they have no other
Ballerano 2011
72
choice- i.e. have no insurance or find that their public options are less than satisfactory- may find
themselves in need of options that, because they have been mainstreamed and commoditized, are
no longer available to them (Craven 2007: 705-9) .
This is not to say that legitimizing midwifery in and of itself is a threat to these women,
but if it is done by identifying it as a consumer issue, I suggest that the sustainability of such a
change is questionable. The use of a consumer movement, by both mothers and care-providers,
implies variable depths of awareness of not only the national health care system but society at
large. Where consumer identity is used consciously as a strategy to further the midwifery cause
(as opposed to feminist or patient identity), it assumes a neoliberal, free-market society for the
future. That is to say, if advocates are framing their demands for alternative care availability as a
need for consumers, it is because they believe that consumer, i.e. monetary, power will reign as
strongly in future negotiations as it does now.
The fact that legislation rarely changes unless challenged reinforces this, and the current
administrations’ difficulties in re-organizing national healthcare policy have shown just how
strongly divides of wealth, class and reproductive values influence such changes. Policies made
to satisfy the demands of people who can spend money will probably continue to benefit those
who can spend money, often at the expense of those who cannot, as they have less political sway.
This is problematic not just in terms of inequality, but because the socio-structural future of the
U.S. is anything but definite and knowable. How would the demands of wealthier consumers fare
in a system that utilized universal health care? If change came about from the demands of
citizens-as-patients, and not consumers, the permanence of that progress would be more likely-
just as the civil and women’s rights movements implemented changes that remained and
progressed for the benefit of their respective groups. Consumers, on the other hand, are fluid,
Ballerano 2011
73
even fickle, in their expectations, desires, and ideals, and therefore so are the actions they
demand from business and government.
I think many advocates are aware that framing their movement as one of “consumers” is
just a smart way of working within the system, especially those who have been a part of the birth
movement since its inception. The Internet, as a means of communication, lends itself to this
neoliberal strategizing- the virtual sphere is one in which serious scholastic material shares space
with flashing coupon codes and video ads. But activists’ willingness to play the money game, in
combination with those advocates who ideologically subscribe to the importance of consumer
rights without an acknowledgement of the civil/gender rights that preceded them, reinforces
neoliberal mentalities in the present.
“Consumer demand”, as framed by movement strategists, and actual consumer demand
from women who truly identify as consumers, i.e. believe they should be heard because they
have spending power, combine into one movement with many meanings but one implication: it
is those who will meet that demand, i.e. pharmaceutical/medical technology companies,
insurance groups, and legislators, who will ultimately control the options. These three groups, by
appearing to produce health care options, restrictions, requirements, provisions, and promotions
as demanded by “consumers”, may in fact contribute to limiting women’s options because those
very options have been identified as consumer rights. If it is simply money that will determine
influence over private and state entities managing U.S. healthcare, than future money, i.e. future
consumer movements, will just as easily alter the system, for better or for worse. If midwifery
advocates want sustained progress and the continued availability of multiple birth options for the
majority of women, it is as patients they are likely to achieve such ends.
Ballerano 2011
74
What is truly surprising to me is how long the “consumer identity” has been utilized by
reproductive care advocates. Even Brigitte Jordan, observing in the late 1970s, identified
resistance to the biomedical model as a consumer movement (1983: iii). Perhaps this suggests
that feminists and human rights activists of the time were ahead of the curve, estimating the
neoliberal appeal of identifying as consumers and the durability of such identification for future
progress. In this context, it makes sense to identify as consumers because, as Jordan suggests,
“any given controversy is decided not on the basis of the kind of evidence that is produced…but
rather its status will depend on how well it fits with the socio-political realities and the
ideological belief system of its time and place,” (74). Years of research have been illustrative of
problems with the biomedical model of birth care, and yet it continues to define the status quo
(61, 69-74).
If contemporary Americans identify with “free-market choice” and “consumer rights”,
and if those working within the birthing system (i.e. doctors, hospitals, insurance providers), are
also subject to the neoliberal paradigm, than it may only be as consumers of medicine that
advocates can influence change. Less contemporary identifications, such as feminism or
citizenship, are not conceptually or practically familiar to those within a health care system so
heavily dependent on fiscal power, insurance-based decisions, and temporal and economic
efficiency. In a neoliberal capitalist context then, the biomedical model cannot initially be
challenged or improved upon on the basis of women’s rights or even citizens rights because it is
not defined by its benefits to women or, like countries with socialized medicine, its benefits for
all citizens, regardless of gender, race or class.
Whichever identifications are chosen by those who hold stake in women’s health, the
narrative of reproductive choice is an ongoing development in contemporary American society.
Ballerano 2011
75
My research suggests that the challenges once faced by Victorian wives and their 1970s feminist
descendents are still of utmost importance in the experiences of contemporary women- how
much do their own voices and knowledge count in the production of reproduction? While many
of the quantitative measures of equality have improved, the experiential evidence suggests that
they count for very little. The number of choices highlighted by the virtual sphere and seemingly
available to women and families qua consumers distracts from the reality of very limited choices
once they enter the hospital qua patients. Those who are satisfied with the services and products
of this system may very well continue to utilize them, but women looking for alternatives or
rejecting standard practice are continually challenged, restricted, and at times coerced into
processes in which they do not wish to partake. Even when a woman has the information and
resources to know what she wants out of childbirth, her ability to manifest that knowledge as
power over the process is dependent on such external aspects to her person as her wealth, her
profession, her support people, and her ability to negotiate the rules of the hospital and insurance
systems. Feminists of the last half-century bemoaned this stipulation as symptomatic of a sexist
system. Now, a result of yet another ideological shift in power, the problem of patient agency
continues despite fewer limitations of gendered dynamics; the authoritative decisions of the
doctor, male or female, are now systematically restricted to the profit-motivated strategies of
pharmaceutical and insurance corporations, contracting the voices of birthing women into
silence.
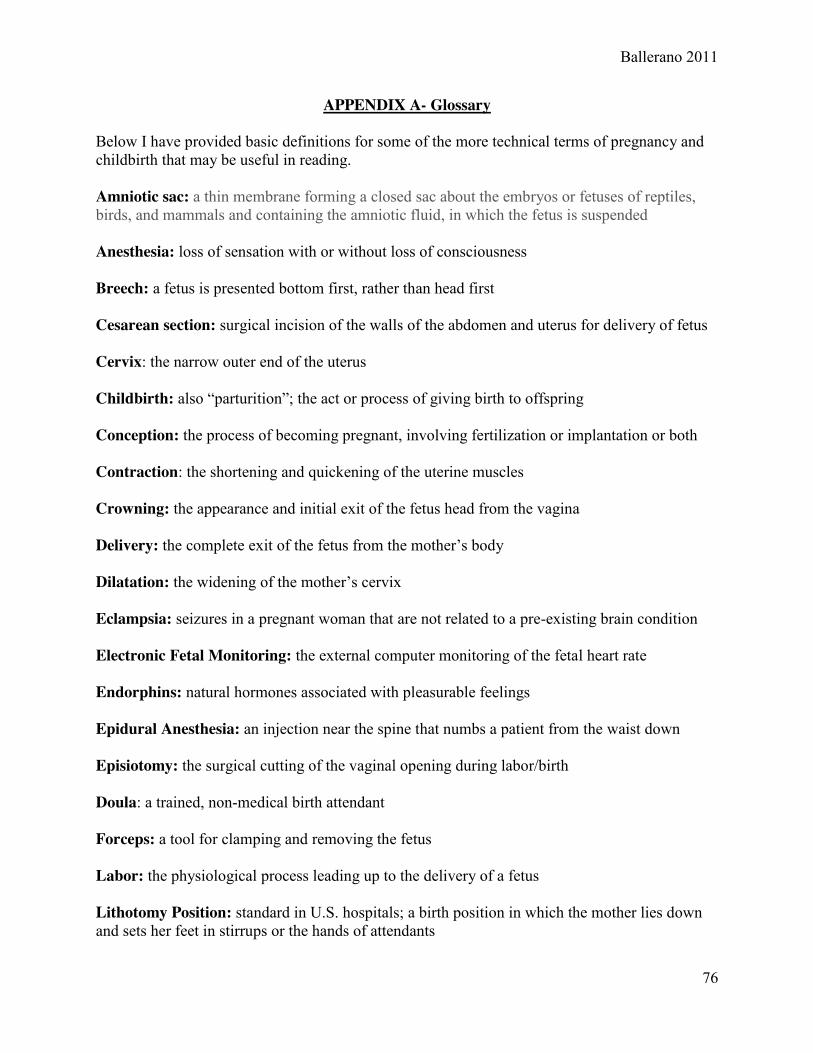
Ballerano 2011
76
APPENDIX A- Glossary
Below I have provided basic definitions for some of the more technical terms of pregnancy and childbirth that may be useful in reading. Amniotic sac: a thin membrane forming a closed sac about the embryos or fetuses of reptiles, birds, and mammals and containing the amniotic fluid, in which the fetus is suspended Anesthesia: loss of sensation with or without loss of consciousness Breech: a fetus is presented bottom first, rather than head first Cesarean section: surgical incision of the walls of the abdomen and uterus for delivery of fetus Cervix: the narrow outer end of the uterus Childbirth: also “parturition”;; the act or process of giving birth to offspring Conception: the process of becoming pregnant, involving fertilization or implantation or both Contraction: the shortening and quickening of the uterine muscles Crowning: the appearance and initial exit of the fetus head from the vagina Delivery: the complete exit of the fetus from the mother’s body Dilatation: the widening of the mother’s cervix Eclampsia: seizures in a pregnant woman that are not related to a pre-existing brain condition Electronic Fetal Monitoring: the external computer monitoring of the fetal heart rate Endorphins: natural hormones associated with pleasurable feelings Epidural Anesthesia: an injection near the spine that numbs a patient from the waist down Episiotomy: the surgical cutting of the vaginal opening during labor/birth Doula: a trained, non-medical birth attendant Forceps: a tool for clamping and removing the fetus Labor: the physiological process leading up to the delivery of a fetus Lithotomy Position: standard in U.S. hospitals; a birth position in which the mother lies down and sets her feet in stirrups or the hands of attendants
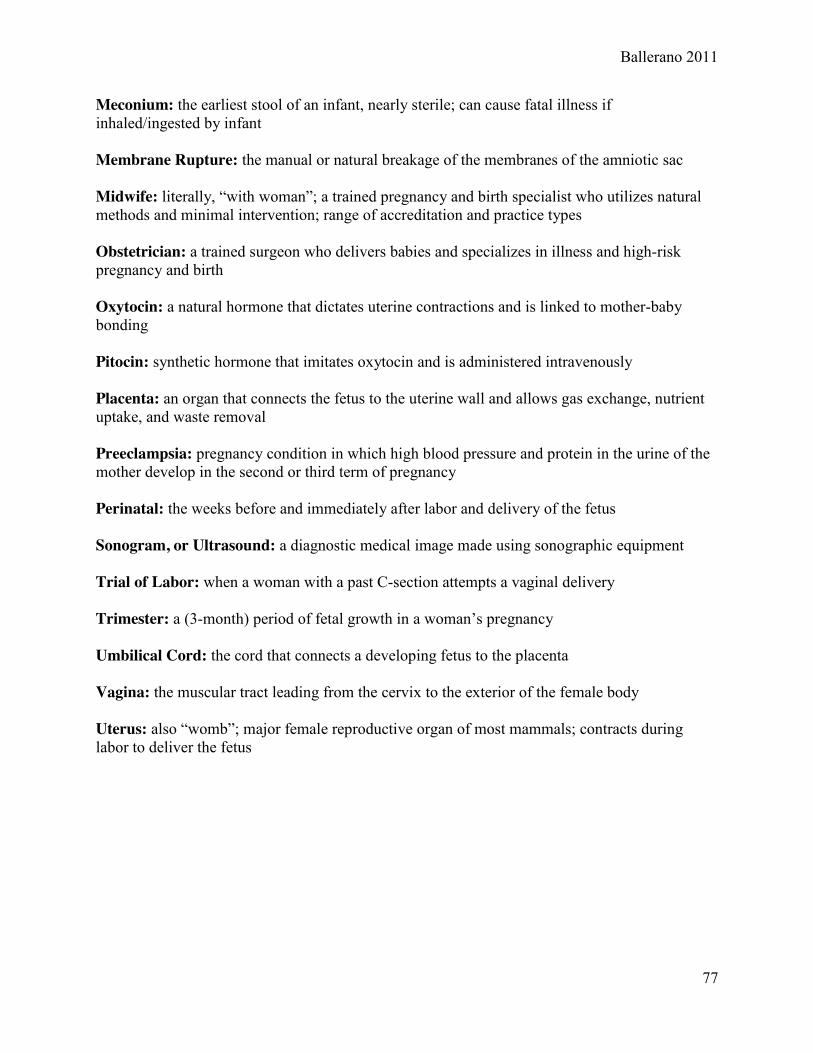
Ballerano 2011
77
Meconium: the earliest stool of an infant, nearly sterile; can cause fatal illness if inhaled/ingested by infant Membrane Rupture: the manual or natural breakage of the membranes of the amniotic sac Midwife: literally, “with woman”;; a trained pregnancy and birth specialist who utilizes natural methods and minimal intervention; range of accreditation and practice types Obstetrician: a trained surgeon who delivers babies and specializes in illness and high-risk pregnancy and birth Oxytocin: a natural hormone that dictates uterine contractions and is linked to mother-baby bonding Pitocin: synthetic hormone that imitates oxytocin and is administered intravenously Placenta: an organ that connects the fetus to the uterine wall and allows gas exchange, nutrient uptake, and waste removal Preeclampsia: pregnancy condition in which high blood pressure and protein in the urine of the mother develop in the second or third term of pregnancy Perinatal: the weeks before and immediately after labor and delivery of the fetus Sonogram, or Ultrasound: a diagnostic medical image made using sonographic equipment Trial of Labor: when a woman with a past C-section attempts a vaginal delivery Trimester: a (3-month) period of fetal growth in a woman’s pregnancy Umbilical Cord: the cord that connects a developing fetus to the placenta Vagina: the muscular tract leading from the cervix to the exterior of the female body Uterus: also “womb”;; major female reproductive organ of most mammals; contracts during labor to deliver the fetus
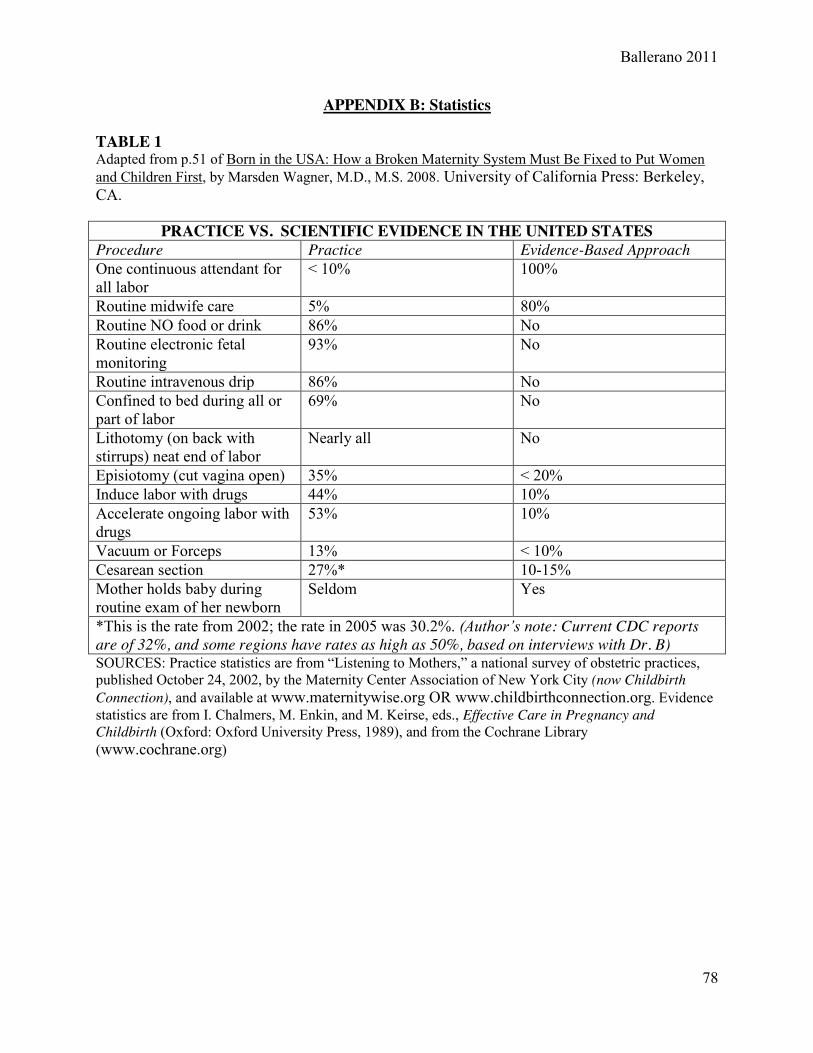
Ballerano 2011
78
APPENDIX B: Statistics TABLE 1 Adapted from p.51 of Born in the USA: How a Broken Maternity System Must Be Fixed to Put Women and Children First, by Marsden Wagner, M.D., M.S. 2008. University of California Press: Berkeley, CA.
PRACTICE VS. SCIENTIFIC EVIDENCE IN THE UNITED STATES Procedure Practice Evidence-Based Approach One continuous attendant for all labor
< 10% 100%
Routine midwife care 5% 80% Routine NO food or drink 86% No Routine electronic fetal monitoring
93% No
Routine intravenous drip 86% No Confined to bed during all or part of labor
69% No
Lithotomy (on back with stirrups) neat end of labor
Nearly all No
Episiotomy (cut vagina open) 35% < 20% Induce labor with drugs 44% 10% Accelerate ongoing labor with drugs
53% 10%
Vacuum or Forceps 13% < 10% Cesarean section 27%* 10-15% Mother holds baby during routine exam of her newborn
Seldom Yes
*This is the rate from 2002; the rate in 2005 was 30.2%. (Author’s note: Current CDC reports are of 32%, and some regions have rates as high as 50%, based on interviews with Dr. B) SOURCES: Practice statistics are from “Listening to Mothers,” a national survey of obstetric practices, published October 24, 2002, by the Maternity Center Association of New York City (now Childbirth Connection), and available at www.maternitywise.org OR www.childbirthconnection.org. Evidence statistics are from I. Chalmers, M. Enkin, and M. Keirse, eds., Effective Care in Pregnancy and Childbirth (Oxford: Oxford University Press, 1989), and from the Cochrane Library (www.cochrane.org)
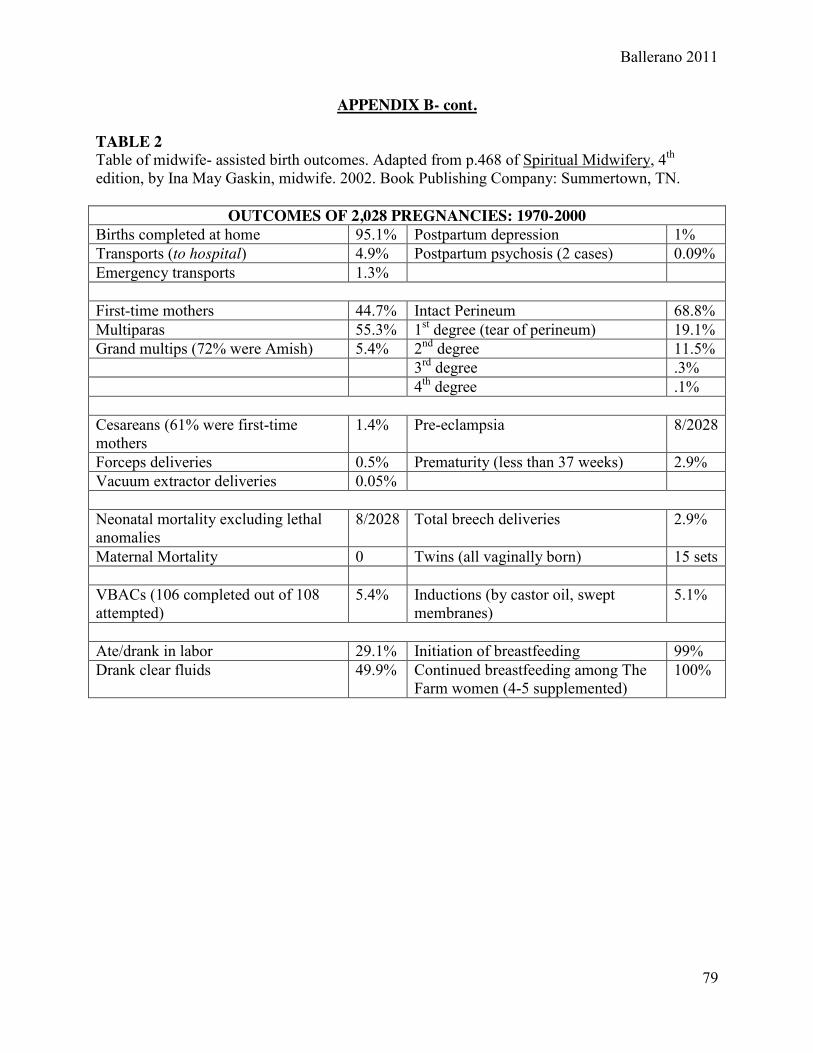
Ballerano 2011
79
APPENDIX B- cont. TABLE 2 Table of midwife- assisted birth outcomes. Adapted from p.468 of Spiritual Midwifery, 4th edition, by Ina May Gaskin, midwife. 2002. Book Publishing Company: Summertown, TN.
OUTCOMES OF 2,028 PREGNANCIES: 1970-2000 Births completed at home 95.1% Postpartum depression 1% Transports (to hospital) 4.9% Postpartum psychosis (2 cases) 0.09% Emergency transports 1.3% First-time mothers 44.7% Intact Perineum 68.8% Multiparas 55.3% 1st degree (tear of perineum) 19.1% Grand multips (72% were Amish) 5.4% 2nd degree 11.5% 3rd degree .3% 4th degree .1% Cesareans (61% were first-time mothers
1.4% Pre-eclampsia 8/2028
Forceps deliveries 0.5% Prematurity (less than 37 weeks) 2.9% Vacuum extractor deliveries 0.05% Neonatal mortality excluding lethal anomalies
8/2028 Total breech deliveries 2.9%
Maternal Mortality 0 Twins (all vaginally born) 15 sets VBACs (106 completed out of 108 attempted)
5.4% Inductions (by castor oil, swept membranes)
5.1%
Ate/drank in labor 29.1% Initiation of breastfeeding 99% Drank clear fluids 49.9% Continued breastfeeding among The
Farm women (4-5 supplemented) 100%
Ballerano 2011
80
Bibliography and Suggested Resources
“A Baby Story”. A production of TLC via the Discovery Network. Various episodes. 2010-2011.
Block, Jennifer. Pushed: The Painful Truth about Childbirth and Modern Maternity Care. 2007.
De Capo Press, Cambridge, MA.
Bogdan-Lovis, Elizabeth A. Review of Birth by Design: Pregnancy, Maternity Care, and
Midwifery in North America and Europe, by Raymond DeVries, Cecilia Benoit, Edwin
R. Van Teijlingen, and Sirpa Wrede, eds. Medical Anthropology Quarterly 17.4 (2003):
514-15.
Browner, Carole. "The Social Formation of Childbirth”. A Review of Recent Research: The First
Birth: A Family Turning Point , by Doris R. Entwisle and Susan G. Doering.;
Anthropology of Human Birth, by Margarita Artschwager Kay.; Ethnography of Fertility
and Birth, by Carol P. MacCormack.; Childbirth: Alternatives to Medical Control, by
Shelly Romalis." Medical Anthropology Newsletter 14.1 (1982): 1+.
The Business of Being Born. Directed by Abby Epstein, Produced by Ricki Lake. DVD. 2008.
Cassidy, Tina. Birth: The Surprising History of How We Are Born. 2006. Grove Press. New
York, NY.
The Center for Disease Control. National Vital Statistics Program, US Dept of Health and
Human Resources. National Center for Health Statistics.
<http://205.207.175.93/VitalStats/TableViewer/tableView.aspx? ReportId=15101>;
<http://www.cdc.gov/nchs/data/databriefs/db35.htm>;
<http://www.childtrendsdatabank.org/?q=node/214>.
“Chrys”. Personal Interview conducted by Jessalyn Ballerano. December 2010.
Ballerano 2011
81
Citizens for Midwifery. New York Legal Status of Direct Entry Midwives
<http://cfmidwifery.org/states/states.aspx?ST=NY>.
Cockrell, Dawn, and Jordan Beal. "Dawn Cockrell, 39 Midwife." Texas Monthly: The Working
Life Sept. 2009: 26-28. Web.
Craven, Christa. "A “Consumer’s Right” to Choose a Midwife: Shifting Meanings for
Reproductive Rights under Neoliberalism." American Anthropologist 4th ser. 109 (2007):
701-12.
Davis-Floyd, Robbie, and Elizabeth Davis. "Intuition as Authoritative Knowledge in Midwifery
and Homebirth." Medical Anthropology Quarterly 10.2 (1996): 237-69.
Davis-Floyd, Robbie, and Carolyn Sargent. "Introduction." Medical Anthropology Quarterly
10.2 (1996): 111-20.
Davis-Floyd, Robbie E. and Carolyn F. Sargent, eds. Childbirth and Authoritative
Knowledge: Cross-Cultural Perspectives. 1997. University of California Press. Berkeley
and Los Angeles, CA.
Gaskin, Ina May. "Intuition and the Emergence of Midwifery as Authoritative Knowledge."
Medical Anthropology Quarterly 10.2 (1996): 295-98.
Gaskin, Ina May. Spiritual Midwifery. 4th Ed. 2002. Book Publishing Company. Summertown,
TN.
Hachey, Marguerite Rice. “Childbirth in the Twentieth Century: Shifting Cultural Meanings of
Childbirth from the Rise of the Hospital System through Contemporary Medical
Revolutions.” Honors Thesis, Union College, 2004.
Ballerano 2011
82
International Confederation of Midwives: Midwifery and Reproductive Health Research
Electronic Mailing List. September 2010-2011
Johnson AM, Schnatz PF, Kelsey AM, Ohannessian CM. “Do women prefer care from female or
male obstetrician-gynecologists? A study of patient gender preference”. J Am Osteopath
Assoc. 2005 Aug;105(8):369-79. Johns Hopkins University School of Medicine,
Baltimore, MD.USA. Accessed: February 23, 2011.
Jordan, Brigitte. Birth in Four Cultures: A Crosscultural Investigation of Childbirth in
Yucatan,Holland, Sweden and the United States. 1983 Eden Press, Montreal Quebec.
Jordan, Brigitte. “Authoritative Knowledge and its Construction”. From Childbirth and
Authoritative Knowledge: Cross-Cultural Perspectives. 1997:56.
Laboring Under an Illusion: Mass Media Childbirth vs. the Real Thing. Produced by Vicki
Elson, MA, CCE. DVD. 2009.
Lazarus, Ellen S. "What Do Women Want?: Issues of Choice, Control, and Class in Pregnancy
and Childbirth." Medical Anthropology Quarterly 8.1 (1994): 25-46.
Martin, Emily. The Woman in the Body. 1986. Beacon Press. Boston, MA.
McGregor, Deborah Kuhn. From Midwives to Medicine: The Birth of American Gynecology.
1998. Rutgers University Press. Piscataway, NJ.
“Megan”. Personal Interview conducted by Jessalyn Ballerano. January 2011.
“The Mother-Friendly Childbirth Initiative”: The First Consensus Initiative of the Coalition for
Improving Maternity Services (CIMS). Found in pp. 456-60 of Spiritual Midwifery, by
Ina May Gaskin, 2002.
Ballerano 2011
83
Pregnant In America. Directed by Steve Buonaugurio. Bella Media Productions. DVD. 2008.
Sargent, Carolyn, and Grace Bascope. "Ways of Knowing about Birth in Three Cultures."
Medical Anthropology Quarterly 10.2 (1996): 213-36.
Stoppard, Dr. Miriam. Conception, Pregnancy and Birth. 1993 Dorling Kindersley, Inc: New
York, NY
Time Magazine. http://healthland.time.com/ category/medicine/reproductive-health-medicine/
and http://healthland.time.com/ category/love-family/pregnancy .
Wagner, Marsden, M.D., MS. Born in the USA: How a Broken Maternity Care System Must Be
Fixed to Put Women and Children First. 2006. University of California Press. Berkeley,
CA.
World Health Organization. Maternal Health: Maternal mortality ratio, 2008.
http://gamapserver.who.int/gho/ interactive_charts/mdg5_mm/atlas.html.
Youngs, Gillian. “Making the Virtual Real: Feminist Challenges in the 21st Century”. From
Blogging Feminism: (Web)Sites of Resistance in The Scholar and Feminist Online. Issue
5.2. (2007). Barnard Center for Research on Women. www.barnard.edu/sfonline/blogs.




















