Contents - UNHCR data portal
42
....................................................................................................................................... Jordan 70 Contents Field Articles 71 Evolution of WFP’s food assistance programme for Syrian refugees in Jordan 74 Meeting nutritional needs of Syrian refugee children and women in Jordan 76 UNHCR cash programming in emergencies – implementation and coordination experience during the Syrian refugee response in Jordan 78 Aid effectiveness: determining vulnerability among Syrian refugees in Jordan 82 Responding to nutrition gaps in Jordan in the Syrian Refugee Crisis: Infant and Young Child Feeding education and malnutrition treatment 85 Managing infant and young child feeding in refugee camps in Jordan 89 Postscript 90 The situation of older refugees and refugees with disabilities, injuries, and chronic diseases in the Syria crisis 93 Experiences of emergency nutrition programming in Jordan 97 Women’s protection and empowerment programming for Syrian refugees in urban Jordan: challenges and lessons learned Research 101 The social life of nutrition among Syrian refugees in Jordan Views 105 UN and INGO experiences of coordination in Jordan News 107 Experiences on Nutrition in Emergencies Training for Syrian refugees response in Jordan Agency Profile 108 Jordan Health Aid Society (JHAS) 110 Jordan Hashemite Charity Organisation (JHCO) A Syrian refugee, with her family in Ramtha, Jordan; UNHCR / J. Kohler / February 2014
-
Upload
khangminh22 -
Category
Documents
-
view
3 -
download
0
Transcript of Contents - UNHCR data portal

. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Jordan
70
ContentsField Articles71 Evolution of WFP’s food assistance
programme for Syrian refugees in Jordan
74 Meeting nutritional needs of Syrian refugeechildren and women in Jordan
76 UNHCR cash programming in emergencies –implementation and coordination experience during the Syrian refugee response in Jordan
78 Aid effectiveness: determining vulnerabilityamong Syrian refugees in Jordan
82 Responding to nutrition gaps in Jordan in the Syrian Refugee Crisis: Infant and Young Child Feeding education and malnutrition treatment
85 Managing infant and young child feeding inrefugee camps in Jordan
89 Postscript
90 The situation of older refugees and refugeeswith disabilities, injuries, and chronic diseases in the Syria crisis
93 Experiences of emergency nutrition programming in Jordan
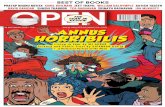
97 Women’s protection and empowerment programming for Syrian refugees in urban Jordan: challenges and lessons learned
Research101 The social life of nutrition among Syrian
refugees in Jordan
Views105 UN and INGO experiences of coordination
in Jordan
News107 Experiences on Nutrition in Emergencies
Training for Syrian refugees response in Jordan
Agency Profile108 Jordan Health Aid Society (JHAS)
110 Jordan Hashemite Charity Organisation (JHCO)
A Syrian refugee, with her family in Ramtha, Jordan; UNHCR / J. Kohler / February 2014

Figure 1: Number of WFP beneficiaries in camps and communities (Jan 2013-July 2014)
71
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Evolution ofWFP’s foodassistanceprogrammefor Syrianrefugees inJordanBy Edgar Luce
For the past twoyears, Edgar Lucehas been working forWFP Jordan as aProgramme Officerby monitoringoperations, writing
reports and acting as the VAM(Vulnerability Assessment and Mapping)focal point. He has more than five years ofinternational experience in agriculturaldevelopment and humanitarian reliefworking with NGOs prior to the UN.
Thanks to Henry Sebuliba, WFP for helpingcoordinate inputs, reviews and approvalsin the article’s development.
WFP assistanceSince the onset of the Syrian refugee crisis inmid-2012, WFP has been providing food as-sistance to Syrian refugees in Jordan in anumber of ways. WFP began providing foodassistance through the provision of hot mealsin Zaatari refugee camp when it first openedin July 2012. WFP transitioned to take homerations of dry ingredients by October 2012;this was followed by the provision of paperfood vouchers that refugees can redeem inshops from September 2013 including thelarge supermarkets which opened in January2014. In non-camp settings, assistance beganwith hot meals to a few hundred families intransit centres, followed by the introductionof paper vouchers in August 2012. In January2014, the transition to e-vouchers began incommunities and all UNHCR registered Syrianrefugees should have an e-card by the end ofAugust 2014. WFP’s voucher programme inJordan is implemented through three estab-lished cooperating partners (Islamic ReliefWorldwide, Human Relief Foundation andSave the Children International), and a fourthrecent addition, ACTED, in the newly openedAzraq camp. is article describes the differenttypes of assistance, how and why they evolved.
Food distributions in Zaatari refugeecampFollowing the opening of Zaatari refugeecamp in July 2012, WFP distributed hot mealsfrom local restaurants to camp residents twicea day, typically consisting of rice, a proteinsource such as chicken or meat, together withbread, fruit and a vegetable. is was notsustainable for the rapid influx of refugeesthat followed (rising from 3,685 individuals
in August 2012 to 129,756 in April 2013).us, WFP transitioned to the distributionof dry rations in October 2012, once kitchenswith cooking facilities were available for camprefugees to use. e rations, consisting ofrice, lentils, bulgur wheat, pasta, oil, sugarand salt, were distributed from dedicated dis-tribution sites to all residents every two weeks.Together with the daily distribution of bread,this provided 2,100 kcal per person per day.UNHCR also provided additional comple-mentary food normally consisting of cannedtomatoes, tomato paste, tuna, canned beansand tea through the same distributions.
Paper voucher assistance e paper voucher modality was introducedfor the registered refugees living amongst thehost community (August 2012 – 19,000 ben-eficiaries) and later in Zaatari camp (September2013 – 104,000 beneficiaries). e introductionof the voucher programme helped bring asense of normalcy to Syrian refugees allowingthem to shop in regular supermarkets fortheir preferred foods. e vouchers alsooffered access to a greater diversity of foodswith higher nutritional value, including freshfruits, dairy products, meat, chicken, fish andvegetables. is programme also led to jobsfor nearly 400 Jordanians in WFP’s partnershops where refugees used their vouchers;more than $229 million has been injectedinto the local economy since its launch throughtill July 20141.
500,000450,000400,000350,000300,000250,000200,000150,000100,000
50,0000
Jan-
13
Feb-
13
Mar
-13
Apr
-13
May
-13
Jun-
13
Jul-1
3
Aug
-13
Sep-
13
Oct
-13
Nov
-13
Dec
-13
Jan-
14
Feb-
14
Mar
-14
Apr
-14
May
-14
Jun-
14
July
-14
Community Camps
1 Economic impact study: Direct and indirect impact of the WFP food voucher programme in Jordan, April2014.
WFP
Field Articles ...................................................
WFP
Jord
an

72
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Field ArticleIn Zaatari camp, vouchers were initially re-
deemed in shops run by 16 partner communi-ty-based organisations (CBOs). In January 2014,WFP established two supermarkets in Zaataricamp allowing camp based refugees’ food needsto be met entirely through vouchers. WFP grad-ually decreased the distributions of dry foodrations while increasing the value of the vouchers.Now that food assistance has shied completelyto vouchers in camps aside from the daily dis-tribution of bread (due to concerns over thegovernment bread subsidy), each refugee receivesWFP monthly vouchers valued at 20JD(US$28.20). In communities refugees receivethe full voucher value of 24JD (US$33.84) perperson per month. is amount is based on thecost of a basic food basket which provides ap-proximately 2,100 kcals per person daily. Ongoingmonthly price monitoring conducted by WFPand its partners has shown that food prices inparticipating shops are similar, and oen cheaper,than those in the non-participating stores2. SinceJanuary 2013, WFP has kept the voucher valueconstant at JOD24 (US$33.84) per person permonth as food prices have remained relativelyconstant, even decreasing in some areas ofJordan.3
In April 2014, for the first time in the historyof humanitarian assistance, Azraq refugee campopened with a fully-fledged WFP supermarketalong with WFP food vouchers. is meant that
all refugees arriving in the camp could startpurchasing their own food immediately.
e number of beneficiaries of WFP’s voucherprogramme increased steadily from 67,500 in-dividuals in January 2013 to 537,000 individualsby February 2014. All registered Syrian refugeesliving in host communities have been able toredeem their vouchers in 77 designated shopsin 12 governorates (July 2014). Shops are con-tracted by WFP’s partners and are located inareas with a significant concentration of refugees.In these communities, the head of the householdreceives two paper vouchers every month. Eachvoucher is valid for two weeks and will expire ifnot used during the validity period. e vouchervalue varies according to the household size, aseach individual receives the equivalent of 24JD(US$33.84) monthly.
E-voucher programme WFP assistance to Syrian refugees living amongstthe host population in Jordan is now carriedout through electronic food vouchers. is pro-gramme is implemented through a partnershipwith MasterCard and a local bank, Jordan AhliBank (JAB), under its Corporate Social Respon-sibility (CSR) programme. E-vouchers functionlike a pre-paid debit card, with WFP transferringthe voucher value directly to the e-voucher on amonthly basis through the partner bank (seeFigure 1). WFP has now transferred almost allrefugee households to electronic vouchers in
the host communities and started to pilot thisapproach in camps as well. E-vouchers allowthe beneficiaries to spend their entitlements inmultiple visits to the shops and are also morediscreet and therefore less stigmatising. As thecards are recharged automatically through thepartner bank, beneficiaries are no longer requiredto travel to monthly distributions to receivetheir food assistance. When making a purchasein the supermarket, refugees must present theire-vouchers together with their matching UNHCRrefugee identification card and input their fourdigit security code – the same process used forregular credit and debit cards.
Key findings and lessons learnede paper voucher system was introduced asassessments showed that Jordan has a fully in-tegrated market structure with the necessarycommercial and physical infrastructure to meetincreased consumer demand without affectingits current supply lines and price levels. Fur-thermore, since Syrian families are accustomedto shopping for their food, vouchers allowedthem to continue their regular approach to pur-
2 For example, in April 2014, a standard food basket cost JOD21.60 (US$30.24) in participating stores and JOD21.80 (US$30.52) in the non-participating outlets. Source: Economic impact study: Direct and indirect impact of the WFP food voucher programme in Jordan, April 2014.
3 Food basket is composed of rice, bulgur wheat, pasta, pulses, sugar, vegetable oil, salt and canned meat.

73
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Field Articlechasing food, helping to return a sense of nor-mality to their lives while enabling them toselect their preferred food items and meet theirindividual consumption and dietary needs. WFPkeeps an open policy regarding what food itemsare selected; beneficiaries are able to purchaseall food items except soda, chips and candy.
e WFP food voucher programme buildslinkages between refugees and host communitiesand helps to stimulate local economies throughthe promotion of local production and sales.Findings from a recent WFP Economic ImpactStudy4 show that WFP assistance will equate to0.7% of the Jordanian GDP through the voucherprogramme in 2014. e voucher programmehas already led to some US$2.5 million investmentin physical infrastructure by the participatingretailers, created nearly 400 jobs in the foodretail sector and generated almost US$6 millionin additional tax receipts for the Jordanian gov-ernment.
e gradual shi to e-cards brings severalimportant benefits to both Syrian refugees andWFP. ese include allowing refugees to spendtheir monthly entitlements in multiple visits tothe shops (paper vouchers have to be spent inone go and only allow two shopping visits permonth). is is useful for refugees who havelimited storage facilities especially during thehot summer months or limited access to trans-portation. It also is a much more discreet assis-tance modality, which is important when livingin host communities where tensions are increasingover time. While vouchers in general are morecostly than the purchase of bulk commodities,given the transfer value of vouchers has to coverretail prices and is therefore higher per personthan the cost of bulk food purchases, much lessis also spent on administrative and logisticalcosts. us, with vouchers more total value istransferred to beneficiaries. Similarly, it is im-possible to cost the added value for refugees in
making their own household food decisions.With vouchers WFP was able to scale up quicklyand absorb the high number of refugees crossingon a daily basis. us, vouchers are by far thepreferred mode of assistance when comparedwith in-kind food in Jordan. E-vouchers areeven more efficient given WFP does not needto print hundreds of thousands of paper vouchersevery month, sort and distribute them throughpartners, then reconcile all redeemed vouchers.As part of the partner bank’s CSR programme,most services are provided to WFP free ofcharge, including the printing of all cards,loading of the monthly assistance and trackingand reporting.
WFP has a robust monitoring system thatcovers all activities such as e-cards, paper vouch-ers, school feeding in camps, nutrition activities.WFP monitors all partner shops, shop owners,prices in both partner and non-partner shopsfor comparison purposes, beneficiary perceptions,distribution sites and household food securityinformation, such as food consumption scoresand coping strategies on a regular basis. BecauseWFP assists nearly all registered Syrian refugeesin Jordan, the prevalence of food insecurityamongst Syrian refugees is relatively low at 6%in communities5. Furthermore, food consumptionis also high, as 90% have an acceptable foodconsumption score with only 8% classified bor-derline and 2% poor.
Initial monitoring findings of the e-cardmodality showed many Syrian refugees in Jordanare illiterate and thus unable to read and fullyunderstand the voucher programme. In response,WFP created communication materials with il-lustrated explanations of the e-card process.Monitoring has also shown that shop ownersare more satisfied with the e-card modalitygiven they are paid much faster and do notneed to track thousands of paper vouchers.Lastly, beneficiaries have explained their content
with the voucher programme in general as theyare more able to cover family members withspecific dietary needs compared to the receiptof in-kind food.
JAB, WFP’s partner bank, is responsible forsetting up, maintaining and managing a safe,effective and efficient mechanism for the elec-tronic voucher system though prepaid cards.e bank has established procedures for thecontrol, oversight, monitoring and accountingof the prepaid card system and is responsiblefor providing, installing and maintaining point-of-sale machines in all selected retailers. ebank is also responsible, if necessary, for estab-lishing bank accounts for all WFP retailers andfor producing prepaid cards for each beneficiaryhousehold. It is also the role of the partner bankto provide comprehensive and timely reportingon beneficiaries’ card use and subaccount activity.e bank has designated an experienced customersupport focal team for project implementation,monitoring, facilitation and coordination, whileproviding WFP and cooperating partners withremote web access for card maintenance andaccount/transactions information. Lastly, thebank is providing facilities such as help desks,call centres and help lines as well as systemtraining to WFP, cooperating partners and re-tailers in addition to financial literacy trainingfor beneficiaries.
In addition to the WFP hotline hosted bythe bank, all partners have hotlines as an effectivebeneficiary feedback mechanism - answeringquestions on locations of distributions andshops, referring beneficiaries to other agencyhotlines for non-food related issues, relayinglost e-card or forgotten pin numbers to thebank and counseling beneficiaries on how touse the e-card. On average, WFP receives morethan 1,500 calls per month through its hotlines.All partners are also required to operate hotlinesas well.
Sustainable funding, including ensuring thetiming of donations to meet cash flow require-ments, continues to pose challenges for futurefood assistance. Maintaining the cash flow andensuring contingency stocks are ready to assista possible large influx of refugees is extremelychallenging when working with a funding horizonof one month. Given the fiscal costs of currentrefugee operations around Syria, WFP is workingwith sister agencies and host governments todevise a more mid-term approach to affordingSyrian refugees the ability to provide for them-selves even in a time of crisis.
For more information, contact: Dina Elkassa-by, Press Information Officer – WFP Syria Re-gional Emergency, email:[email protected],
4 Economic impact study: Direct and indirect impact of the WFP food voucher programme in Jordan, April 2014.
5 Findings from the Comprehensive Food Security Monitoring Exercise (CFSME) conducted in January 2014, report released July 2014. http://documents.wfp.org/stellent/groups/public/ documents/ep/wfp266893.pdfRe
in S
kulle
rud/
WFP

. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
74
Field Article
BackgroundDue to the prolonged and evolving nature ofthe crisis in Syria many Syrians have soughtand continue to seek refuge in neighbouringcountries such as Lebanon, Turkey, Iraq,Egypt and Jordan. According to the populationfigures of the United Nations High Commis-sioner for Refugees (UNHCR), there are618,086 registered Syrian refugees in Jordanas of 18 September 20141. Approximately85% of Syrian refugees in Jordan live withinthe community, mainly in the governoratesof Amman, Mafraq, Irbid and Zarqa. e re-maining 15% of the refugee community livein Za’atri and Azraq camps.
Pre crisis data on Syrian refugees indicateda poor nutrition level for children under 5(CU5) according to World Health Organisa-tion’s thresholds, with an estimated 9.3%wasted, 10.3% underweight and 23% stunted2.Micronutrient deficiencies were also foundto be common -(anaemia prevalence was es-timated at 29.2%), presenting a risk for sub-optimal growth among CU53.
In order to assess the needs of Syrianrefugees in Jordan, WFP and the United Na-tions Children Fund (UNICEF) conductedthe Inter-Agency Nutrition Assessment inNovember 2012 with the participation of Jor-dan’s Ministry of Health (MoH), the Depart-ment of Statistics (DOS), UNHCR, WHO,the United Nations Population Fund (UNFPA),Save the Children International (SCI) as wellas other NGOs. e assessment evaluatedthe nutrition and food security level of Syrianrefugees living in both urban/rural areas andcamp settings.
According to the assessment’s findings,Global Acute Malnutrition (GAM or wasting)prevalence rates were found to be 5.8% incamp settings and 5.1% among refugees re-siding in urban communities4. e assessmentalso found that 4% of Syrian CU5 and 6.3%of pregnant and nursing women and girlswere moderately malnourished and recom-mended the provision of targeted supple-mentary feeding support for this category.Consistent with the pre-crisis data the as-sessment also revealed sub-optimal Infantand Young Child Feeding (IYCF) practicesamong the refugee community in Jordan;just under half of children below 2 years old(49.6% in the camp and 42.7% in the localcommunity) continued to be breastfed.
Programme plan andimplementationAs per the recommendations of the 2012Joint Nutrition Assessment, WFP introduceda Targeted Supplementary Feeding Programme(TSFP) to treat moderately malnourished
Syrian children and women both in campsand in urban communities. is was basedon the Memorandum of Understanding be-tween WFP and UNHCR in Jordan whichstipulates that WFP is responsible for themanagement and treatment of moderate acutemalnutrition (MAM), while UNHCR is re-sponsible for the management of Severe AcuteMalnutrition (SAM).
In addition, distribution of SuperCerealPlus was launched in Zaatari camp for childrenaged 6-23 months to ensure they had accessto age-appropriate food considering they arenot readily available in Zaatari camp and canonly be purchased in pharmacies.
In June 2013, UNHCR started blanket dis-tribution of a locally procured fortified blendedfood (Sahaa) to all children aged 6-23 months.is was distributed over a period of threemonths5. In addition, treatment of MAMcommenced using the same product untilFebruary 2014 when transition to the use ofSuperCereal Plus began.
Targeted Supplementary FeedingProgramme (TSFP) Since February 2014, WFP in partnershipwith Medair, Save the Children Jordan (SCJ)and ACTED have been distributing SuperCe-real Plus as part of WFP’s TSFP to treat mod-erately malnourished CU5 and pregnant andnursing women and girls in both the localcommunities and camp settings. In February2014, before the launch of the TSFP pro-gramme, SCJ conducted a comprehensiveMid Upper Arm Circumference (MUAC)screening of all CU5 and pregnant and nursingwomen and girls in Zaatari camp. It took 12days to complete and a total of 13,009 CU5were screened, amongst whom 27 SAM casesand 164 MAM cases were found.
In addition, a total of 2,515 pregnant andnursing women and girls were screened, ofwhom 51 were found to be malnourished.Identified cases were contacted prior to theTSFP enrolment days, however SCJ facedchallenges in following up on some of thecases due to redundant mobile phone contactsprovided by the beneficiaries. In Zaatari camp,SCJ has also recruited communitymobilisers/volunteers who are responsible
Meetingnutritionalneeds ofSyrian refugeechildren andwomen inJordanBy Henry Sebuliba and Farah El-Zubi
Henry Sebuliba is aNutrition ProgrammeOfficer at the World FoodProgramme RegionalEmergency CoordinationUnit in Amman, Jordan. APublic Health nutritionist,
he has more than 10 years of internationalexperience in nutrition programming in Africa,Asia and the Middle East.
Farah El-Zubi is theNutrition ProgrammeOfficer at the World FoodProgramme’s JordanEmergency OperationsUnit in Amman, Jordan.Farah also supports
coordination of the Food Security Sector inJordan in addition to managing protection-related matters, and has former experienceworking with the World Health Organisation’sIraq Country Office for four years.
1 Source: http://data.unhcr.org/syrianrefugees/country .php?id=107
2 Syrian Family Health Survey (2009)3 MOH, Nutrition Surveillance System Report 20114 Inter- Agency Nutrition assessment Syrian refugees in
Jordan host communities and Zaatri camp, 20125 It was distributed as a blanket for 3 months but a
reduced ration for the third month. See article by Save the Children Jordan that describes this support in more detail.
WFP complementary foodassistance in Zaatari Camp
WFP
, Jor
dan,
201
4
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .

75
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
5 It was distributed as a blanket for 3 months but a reduced ration for the third month. See article by Save the Children Jordan that describes this support in more detail.
6 See field article in this edition of Field Exchange (48) describing JHAS programming in Jordan
7 See field article in this edition of Field Exchange (48) describing Medair’s programming in Jordan
8 See field articles by both Medair and Save the Children Jordan explaining aspects of this programme.
TSFP follow up indowntown Amman
Din
a_El
-Kas
saby
/WFP
, Jor
dan,
201
4
for conducting routine MUAC screenings. CU5and pregnant and nursing women and girls di-agnosed with MAM are issued referral tokenswhich they presented at MAM treatment sitesand have their anthropometric measurementstaken to confirm if they are eligible for enrolmentto the TSFP programme.
Moderately malnourished CU5 meeting an-thropometric admission criteria (MUAC <125mm and >= 115mm and no oedema) andpregnant and nursing women and girls withMUAC < 230mm are admitted to the programme.Beneficiaries are provided with a two weeksration of SuperCereal Plus. Children are providedwith a daily ration of 200g/day while pregnantand nursing women and girls receive 250g/day.Follow up visits are conducted every two weeksto replenish SuperCereal Plus supplies, and forbeneficiary medical review as well as provisionof systematic treatment at health clinics run bythe Jordan Health Aid Society (JHAS).
By the end of May 2014, three months fol-lowing the roll-out of the WFP nutrition pro-gramme, SCJ had reached 223 beneficiaries inZaatari camp (168 CU5 and 55 pregnant andnursing women and girls) out of the targeted1,510 beneficiaries (1,154 CU5 and 356 pregnantand nursing women and girls).
Estimation of the targets was based on the2012 nutrition survey findings however it appearsthat nutrition levels had improved. Consequentlyfewer children with MAM were been identifiedby WFP partners. Analysis of the performanceindicators in the camp reveal that 68% of thetarget population have been cured, 23% defaultedand 9% transferred to Outpatient erapeuticCare (OTP).
In both Zaatari and Azraq camps, sensitisationactivities are carried out by community volunteersand cooperating partners’ staff prior to distri-bution of SuperCereal Plus and during follow-up visits, in addition to nutrition education ses-sions conducted at health clinics in the camps.
WFP supports TSFP implementation in thelocal community through a partnership with
Medair which operates in coordination withthe Jordanian Health Aid Society (JHAS) tomanage the community component of the pro-gramme. Management of acute malnutrition isconducted in each of the six available JHAShealth clinics in Amman, Jerash, Ajloun Zarqa,Mafraq and Irbid. e Medair outreach andmobile teams are responsible for screening andreferring malnourished children and pregnantand nursing women and girls in the communityto JHAS clinics for treatment6. Routine sensiti-sation of the refugee population is conducted byMedair outreach volunteer teams and throughthe JHAS clinics7. A total of 215 beneficiaries in-cluding 79 children and 140 pregnant and nursingwomen and girls have been reached to date (June2014) and out of these 71% have been cured,22% defaulted and 7% were non responders.
Blanket age-appropriate foodassistanceAge-appropriate food support is provided tochildren aged 6-23 months in the camps. Eachchild is provided with 100g/day of SuperCerealPlus on a monthly basis. A total of 8,258 CU5in Zaatari camp received SuperCereal Plus underthis programme in May 2014 (target 13,000).WFP, in partnership with ACTED, are also pro-viding supplementary food to all CU5 in Azraqcamp. In May 2014, about 456 newly arrivedchildren were reached. is is lower than thetarget figure of (1266) as a larger case load ofnew arrivals was anticipated.
Decision-making regarding approachIn Jordan, Syrian refugees receive their food as-sistance in the form of vouchers provided byWFP which beneficiaries can redeem in WFP’ssupermarkets in the camps. However, accordingto Jordanian law, specialised weaning-foods foryoung children can only be obtained from phar-macies. is means, that nutritious age-appro-priate foods are not available in WFP super-markets in the camps where beneficiaries redeemtheir vouchers. erefore, distribution of Su-perCereal Plus rather than food voucher/cashwas used for provision of age-appropriate foodin camps.
Implementation challengesSome of the main challenges confronting theimplementation of the programmes were relatedto Syrian refugee children and women’s tasteacceptance of SuperCereal Plus. is was aproduct that they had not used or eaten before.However WFP partners (SCJ, Medair/JHAS andACTED) addressed this concern by holdingsensitisation sessions and awareness campaignsabout the use and benefits of SuperCereal Plus.is includes carrying out cooking demonstra-tions, as well as encouraging beneficiaries toadd condiments such as honey, fruits, sugarand salt to make the product tastier. As a result,acceptability increased significantly8.
Ensuring follow-up of moderately acute mal-nourished children and women, especially inthe community, has proven difficult as theycannot be easily traced through mobile phones,either because they have changed their numbersor are no longer in the country and this hascontributed to the observed high default rates.
Conclusion Preliminary results of the follow-up nutritionsurvey conducted in refugees living in Zaataricamp and the local community between Apriland May 2014 are suggesting an improvementin acute malnutrition prevalence rates amongSyrian refugees community in Jordan. e 2014survey findings revealed that GAM rates are at1.2% in Za’atri camp and 0.8% in the local com-munity, a clear improvement in comparison tothe 2012 findings. However, it also showed thatmicronutrient deficiencies have persisted amongSyrian refugees, especially those living in camps.Results showed that anaemia prevalence was at48.7% among CU5 and as high as 64% amongchildren under 2 years. Anaemia levels remainhigh in girls and women of reproductive age,standing at 44.7%. ese results indicate thatanaemia prevalence is critically high and aserious public health concern.
Given the low prevalence of acute malnutritionamong Syrian refugees in Jordan, there has beena shi in focus to promote optimal nutritionand integrating cultural practices in comple-mentary nutrition support as well as stepstowards integrating malnutrition within the na-tional health system. In any case, it will beessential for nutrition stakeholders in Jordan tocontinue to monitor the nutrition status ofSyrian refugees in Jordan as long as the Syriacrisis persists.
For more information, contact: ShadaMoghraby, WFP Public Information Officer,email: [email protected]
Field Article

76
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
How did we get here?Over the last decade, two distinct trends havepushed cash-based interventions1 to the fore ofinternational refugee response operations. efirst one is the phenomenon of urban refugeesand the second one is the maturity and acceptancethat cash assistance has reached of late. Urbanrefugees, which is an amorphous category mostlydescribing refugees who do not live in designatedcamps or sites, have certainly come back intofocus with the Iraqi refugee crisis and the Syrianrefugee crisis2. Historically, urban refugees havealways been the core of UNHCR’s work, but aerdecades of resource-intensive and headline-grab-bing camp-based responses, this focus needed tobe strengthened.3 Currently, UNHCR runs sig-nificant urban responses in the Americas, in theMiddle East and in Asia and for some years,UNHCR has been working on refining its policyand operations to adapt to these new settings.4
Jordan provides a particular example of anurban refugee context as it has been generouslyhosting both Iraqi and Syrian refugees in largenumbers. UNHCR in Jordan was one of thefirst operations implementing a large-scale cashassistance programme during the Iraqi influx,which is why the operation was able to leveragethe existing system swily to respond to theSyrian influx. Although Jordan is home to thevery large well-known refugee camp of Zaatari,urban refugees make up over 80% of the refugeepopulation in the Hashemite Kingdom.
e maturation and increased acceptance ofcash assistance is probably best understoodthrough literature review and the swathes of
publications on cash assistance in the last fiveyears.5 e period of expansion can be placedsomewhere around 2006 when only six donorsfunded cash assistance, and 2011 when 41 donorswere involved in cash assistance (largely in thecontext of humanitarian programming). Anothermanifestation of this trend is the creation of theCash Learning Partnership (CaLP) initiative(www.cashlearning.org), which should be un-derstood as a successful attempt to promotecash-based assistance through capacity building,research, advocacy and information sharing.
Cash-based interventions run byUNHCR in JordanDrawing on the increased acceptance and so-phistication of cash-based assistance systems,UNHCR in Jordan has been able to develop astate-of-the-art cash assistance system, which isfully secured through biometric identity verifi-cation to prevent fraud. It is unrivalled in termsof cost-effectiveness and efficiency in UNHCR’scurrent operations worldwide.
Despite the fact that there are more thanhalf a million registered refugees dispersedacross Jordan, UNHCR in close collaborationwith its partner International Relief and Devel-opment (IRD), has managed to conduct indi-vidual assessments based on home visits for allcases. Between 2012 and September 2014 over170,000 visits were undertaken6. is wealth ofinformation is then used by a case managementcommittee to determine eligibility based on pre-defined criteria. Eligibility is re-assessed atregular intervals (12 months at the most) and
process and impact are continuously measuredby quarterly post-distribution monitoring (PDM)exercises.
e delivery mechanism is the ATM networkof UNHCR’s partner Cairo Amman Bank. esystem does not require any card or PIN code;instead the beneficiary has their iris scanned atthe ATM itself, which validates the identity andauthorises the pay-out without requiring anyfurther action. e system has been widely rec-ognized as cutting-edge and has not had a singlefail in trillions of transactions across all accountsat Cairo Amman Bank. As a result, UNHCRhas been able to transfer over $50 million USDto the most vulnerable Syrian refugees in Jordanover a two year period starting in mid-2012.Disbursements have been above $30 millionUSD in 2014 alone. Cash transfers allow UNHCRto implement directly rather than to sub-contractwork, which means that the programme is oneof the most cost-effective models of deliveringassistance to refugees at less than three per centoverhead. us, not only is it ensured that over$97 USD of every $100 USD donated goesdirectly to the refugees, but the system set up byUNHCR in Jordan ensures that it also goes tothose in need – due to the individual assessments– and reaches them without fail – due to thebiometrics component of the delivery mechanism.
By Volker Schimmel
Volker Schimmel is UNHCR’s Head of Field Office Ammanand manages the agency’s cash assistance programme inJordan. He has worked in refugee and displacementsituations with UNHCR, UNRWA and OCHA.
1 Organisations use different terms for cash assistance. The most commonly used term is cash transfer programmes (CTP), but cash assistance (CA) and cash based interventions (CBI) are also regularly found.
2 See for example: http://www.unhcr.org/516d658c9.html3 Merrill Smith. Warehousing Refugees: A Denial of Rights, a
Waste of Humanity. World Refugee Survey 20044 See for example UNHCR’s Alternative to Camps Policy:
http://www.unhcr.org/5422b8f09.html5 DfID Literature Review: http://r4d.dfid.gov.uk/PDF/Articles/
cash-transfers-literature-review.pdf6 Syrian refugees living outside camps in Jordan. Home visit
data findings, 2013. Available at: www.unhcr.org/urban
As of October 2014, UNHCR Jordan was assisting 22,692 families (20,492 Syrian and 2,200 orIRQ, SUD and SOM nationality) with monthly cash assistance. The level of assistance rangesfrom 7$5 USD to $400 USD depending on family size and vulnerability. In 2014, UNHCR wasresponsible for 75% of the cash transfer volume in Jordan. The total amount transferred torefugees in October 2014 was $3.1 million USD.
UNHCR cash programmingin emergencies –implementation andcoordination experienceduring the Syrian refugeeresponse in Jordan
UNHCR staff assisting Syrian refugee withtheir first-time access to cash assistance
through iris scanning, Mafraq, Jordan.
Jare
d Ko
hler
/ U
NH
CR 2
013
Field Article

77
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Process and impact monitoring also corrob-orate this. Moreover, customer satisfaction ishigh. Refugees consistently report that at a rateof around 95% that the service had functionedwithout any disruptions or problems. Moreover,if level of assistance is carefully calibrated toensure that cash assistance is a cash complement,the appropriate usage of cash assistance is high.UNHCR PDMs show that 98% of the assistanceis spent on basic needs ranging from rent (84%)to children’s needs (8%) to food and health (8%).
In March 2014, UNHCR teamed up withthe World Bank for a pilot on welfare modelling7,which also included an impact assessment ofthe cash assistance programme using re-assess-ment data from follow-up home visits. It producedtwo important findings. Firstly, the exclusionerror of the case management system comparedwith a welfare modelling system was 1%, whereasthe inclusion error was 4.7% for a welfare basedapproach. Secondly, UNHCR’s cash assistancewas able to reduce the number of refugees livingbelow the poverty line by 10% across Jordanand in certain Governorates, such as Amman,by up to 15%. e emphasis on the assistanceitself oen overlooks the additional benefits ofthis type of programme that is achieved at thesame time, in terms of protection of refugees.An interesting study in 2012, which includedJordan, showed how critical cash assistance isin order to enhance the protection of refugees,particularly in non-camp settings.8 Protectionis first and foremost ensured by not stigmatisingthe refugee through, for example, distributionof in-kind assistance at designated centres. Sinceurban refugees are rarely assisted with shelter
support, contrary to refugees in camp settings,cash assistance enables them to secure theirdwelling and household and avoid exploitation.Cash assistance effectively makes any refugee acustomer and participant in a market, who isable to act and make decisions as any othercitizen of their country of refugee would.
Certainly, cash assistance projects – even ifthey are as advanced as UNHCR’s Jordan pro-gramme – can always be improved. One avenuethat is currently being worked on by UNHCRin close collaboration with the World Bank is tomove away from the resource-intensive casemanagement approach of the decision-makingand to apply instead a system of modelling withsafeguards. is would ensure good targetingbased on minimal information that can be col-lected during registration with UNHCR, whichincludes biodata, information about the familycomposition, professional, educational and socialbackground as well as current location. It wouldeliminate the need for, and overhead of, a homevisit – and mitigate any exclusion errors throughsafeguards (including a home visit) and anappeals system. An extension and roll out ofthis is through the inter-agency vulnerabilityframework (or VAF) which is currently beingelaborated in Jordan. e framework combinesmodelling and criteria-based decision makingelaborated by key partners in the refugee response,including UN agencies, international non-gov-ernmental organisations, donors and refugees.
e second area of innovation is the plan toconnect the payment system in a highly securedand encrypted manner to UNHCR’s registrationdatabase, which is also based on the same systemfor biometric identity verification. Once thisconnection is in place, it will allow any partnerin the refugee response to deliver cash assistancethrough the bank whilst always relying on themost recent registration information as updatedby UNHCR. is will eliminate the problem ofoutdated data being used by partner organisations,who only collect the information during the as-sessment stage, but are oen not able to respondto changes in registration status over time,thereby at times serving refugees who are nolonger registered.
Coordinating cash assistance in arefugee responseere is an emerging body of literature on co-ordination of cash interventions in humanitariansettings.9 e case of Jordan is no exception.
e so-called Cash Working Group was one ofthe first coordination groups to be created in2012 in order to harmonise the refugee responsein Jordan. Over the course of the next two years,important strides forward were made. e Work-ing Group elaborated common criteria for eli-gibility, a joint PDM system, a referral mechanism,a system to check against and prevent cases ofduplicate assistance, as well as a Minimum Ex-penditure Basket. It also set out a strategic work-plan, defined levels of vulnerability across thepopulation and developed the broader targetingmethodology under the VAF. However, manychallenges for coordination remain – partly dueto the fact that cash provision as a responsemodality has been used to provide support formultiple sectors in Jordan over the course ofthe crisis. In response, any conditional cash as-sistance was managed not through the CashWorking Group, but the working group coveringthe ‘conditionality’. As such, cash for rent, forexample, started to be managed by the ShelterWorking Group from 2013. is means that thevalue and raison d’etre of a Cash Working Grouphas been gradually diminishing. Furthermore,it is still a formidable obstacle to align levels ofassistance, which is partly due to the fact thatprojects are usually defined by the budgets firstand by the coordination standards second. isissue can and should also be explored furtherfrom a Good Humanitarian Donorship (GHD)perspective10.
Overall, however, the cash coordinationsystem in Jordan should be considered a success,as it has managed to create a baseline, shi theinter-agency operation towards an evidence-based way of programming and created standardsfor each stakeholder – including donors – tofollow and enforce in order to ensure an equitableand predictable assistance system putting theprotection and needs of refugees first.
ConclusionIn a context of large-scale urban refugee response,cash as a modality is here to stay. It is not only avery fast and cost-effective way to deliver assis-tance, but, if designed well, also ensures veryefficient use of humanitarian funding. UNHCR’sJordan operation has in many ways proven thisand set a standard for future implementation,whilst emphasising the need to continuouslyinnovate and iterate in order to maximise cost-effectiveness and efficiency of protection andassistance delivery to refugees across the globe.
For more information, contact: Volker Schimmel,email: [email protected]
7 Modelling means applying econometric and statistical methods in order to arrive at ways of predicting the welfare of a family through proxy means testing. It uses a sample of households and detailed information of their vulnerability and then tests for the strongest predictors of poverty. Thesecould be family size, size of the dwelling, single parent households, etc.
8 www.cashlearning.org/downloads/EXAMINING-PROTECTION-AND-GENDER-IN-CASH-AND-VOUCHER-TRANSFERS_Summary_March2013.pdf
9 See for example: http://www.cashlearning.org/downloads/ 120618%20Groupe%20URD_Cash%20coordination _comparative%20study_Final.pdf
10 http://www.goodhumanitariandonorship.org/
Bank employee assisting Syrianrefugee in their first withdrawal ofcash assistance, Amman, Jordan.
Jare
d Ko
hler
/ U
NH
CR 2
014
Jare
d Ko
hler
/ U
NH
CR 2
014
Syrian refugee using iris scantechnology to withdraw monthlycash assistance, Amman, Jordan.
Field Article. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .

78
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Aid effectivenessand VulnerabilityAssessmentFramework:determiningvulnerabilityamong Syrianrefugees in Jordan
The conflict in Syria, which beganin 2011, has continued to createa worsening refugee situation.ere is currently a growing pop-
ulation of 3,033,9721 registered refugees insurrounding countries and the region.Re-alising the challenges that this number ofrefugees posed combined with the need tobe more effective, UNHCR’s Field Infor-mation Support Servicessection launcheda project entitled ‘Design and implementa-tion of the framework for humanitarianaid effectiveness. ’e main objective ofthis UNHCR initiative is to improve aideffectiveness, by ensuring a needs-basedand principled approach to humanitarianresponse. In order to achieve this objective,UNHCR and its partners needed to worktogether, at country level, to agree on andput in place mechanisms for:
a) Definition of vulnerable groups/households in need of assistance, and agree-ment on minimum sectoral data to inform this definition with partners
b) Identification of vulnerable householdsc) Development of shared tools (database
and data entry form) for the tracking of assistance provided by UNHCR and partners, agreement on data consolida-tion, and protection, data ownership, sharing/access agreement with partners
e process was driven by two factors. First,an interest in providing the right supportto vulnerable people; for example, was itenough to provide the same support to alldisabled people when their vulnerabilitiesmay actually have required some differen-tiation in the type of support they received?Second, it was highly likely that there wouldbe a reduction in resources available as thecrisis continued and other crises aroundthe world emerged; a better targeting mech-anism would be needed to determine eligi-bility for limited aid.
The project approachIn order to test the concept of a vulnerabilityanalysis framework, piloting was undertakenin Jordan in both the refugee camp context(specifically Zaatari camp) and with refugeesin urban areas of the country. e pilot fo-cused on health and cash assistance. eproject was planned in three phases. esewere:
Phase 1: Scoping and coordination:Identification and engagement of key stake-holders, review of existing vulnerability as-sessment methods, set up and meeting ofsteering group.
Phase 2: Facilitation and design:Support to sector leads to develop a vul-nerability assessment strategy, database anddata entry tool design
Phase 3: Lessons learned and recommendations:Document a lessons learned exercise UN-HCR approached ACAPS2 to support theprojectas a non-operational entity in theregion, i.e. without any assistance program-ming. Furthermore, ACAPS have specificassessment expertise and experience andhad enjoyed previous successful partnershipswith UNHCR. Support by ACAPS includedthe deployment of an assessment expert towork in country with UNHCR and all rele-vant partners in a collaborative manner todefine vulnerability based on emergencylife-saving needs, and specifically to define
By Hisham Khogali, Lynnette Larsen, KateWashington and Yara Romariz Maasri
Hisham Khogali is anindependent consultant with19 years of experience in arange of humanitariancontexts. Hisham has an MSc.in Human Nutrition fromLSHTM and has worked for
NGO’s, the Red Cross Movement and various UNagencies. In Jordan, he worked for the AssessmentCapacities Project (ACAPS).
Lynnette Larsen is a humanitarian informationmanagement specialist who has managedHumanitarian Information Centres in Kosovo, Iraqand Liberia and similar IM efforts in the 2005Pakistan earthquake, 2008 Cyclone Nargis (Burma)and 2010 Haiti earthquake responses. She co-ledimplementation of the OCHA’s IM capacitybuilding strategy and developed an IM strategywithin the Cluster approach.
Kate Washington is the lead facilitator for the VulnerabilityAssessment Frameworkdevelopment with UNHCR.Previously, she worked for 5years with CARE Internationalin Jordan and has over 13 years
of regional experience across Syria, Lebanon andJordan. She holds a Master of Sciences degree inDevelopment Studies from SOAS, University ofLondon.
Yara Romariz Maasri is anAssociate Coordination Officerwith UNHCR Jordan and hasbeen supporting theVulnerability AssessmentFramework since November2013. She previously worked in
refugee resettlement for over four years inLebanon, Kenya and Cameroon, and was co-editorof the Fahamu Refugee Legal Aid Newsletter forthree years. She holds a Master of Science inForced Migration from the Refugee Studies Centre,University of Oxford.
The current VAF development team consists ofKate Washington, Harry Brown, Marco Santacroceand Carolyn Davis. The work of the VAF team hasbeen overseen and supported by Alex Tyler andVolker Schimmel of UNHCR. WFP and UNICEF havealso provided essential support throughout thedevelopment process.
1 As of 17 November 2014, http://data.unhcr.org/syrianrefugees/regional.php
2 ACAPS is the Assessment Capacities Project: it supports and strengthens humanitarian capacities to carry out coordinated assessments before, during and after crises. Through development and provision of innovative tools, know-how, training and deployment of assessment specialists, ACAPS aims to contribute towards a change in the humanitarian system’s current practice with respect to needs assessments.
Syrian children in their newhousing unit in Irbid, Jordan
Georg Schaumberger/NRC

79
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
eligibility criteria for refugees receiving assistance,in the health and cash assistance sectors (as astarting point).
Phase 1: Scoping and coordinationis phase took place in the second half of2013. UNHCR has an established methodologyfor assessing vulnerability. is method, usingthe Specific Needs codes3, was applied in theSyrian refugee context as in other contexts whereUNHCR works. is ‘group’ approach has anumber of key weaknesses including:
• Generalisations about vulnerable groups tend to exclude those that are generally not thought of as vulnerable, e.g. at a workshop in Zaatari camp, the issue of men being vulnerable particularly to violence, but also their potential to commit violent acts due to unemployment, was raised. In addition, in the context of Jordan, adolescent girls areparticularly vulnerable (e.g. to becoming child brides). Yet neither unemployed men nor adolescent girls are included in the specific needs codes of UNHCR.
• Generalisations about vulnerable groups also fail to recognise that not everyone in a vulnerable group is equally vulnerable (UNHCR addresses this through exclusion criteriain the cash programme).
• A group approach is one dimensional and cannot capture the fact that a household or individual can be in more than one disad-vantaged group at a time, i.e. potentially having greater vulnerability.
• A group approach also does not explain why someone is disadvantaged; an elderly person is not vulnerable because they are old, but perhaps because they are isolated
or lack resources to maintain themselves.• e approach also does not take account of
the temporal and spatial aspects of vulnera-bility; people can move in and out of vul-nerability, e.g. a Syrian refugee who gains employment becomes less vulnerable, or refugees with proximity to services may be less vulnerable than those further away.
Initial reviews of secondary data and meetingswith partners of UNHCR, both in health andcash assistance, revealed that different systemswere being used for identifying vulnerability.is was particularly true in the case of cash as-sistance where a number of partners had adopteda scorecard approach.However, different score-cards were used by different partners.e scorecard approach provided a more transparent ap-proach to determining vulnerability and enableda multi-dimensional approach that incorporatedboth vulnerable groups and potential copingstrategies/vulnerabilities. However, the scoringof cards created divisions amongst partners forwhom there was no standard scoring mechanism4.is difficulty in agreeing scoring may havebeen exacerbated by organisational mandates5.It is also important to recognise that differentorganisations had different objectives for theircash assistance programmes, with some adoptinga one off emergency assistance approach andothers (e.g. UNHCR) adopting a three month(renewable) cycle approach. Cash assistancemay be conditional or unconditional.Scorecardsalso rarely took into account access to servicesas a key vulnerability determinant.
In order to ensure a common understandingof vulnerability, the following three characteristicsof vulnerability were proposed and agreed ininitial meetings/workshops with partners. Namelythat vulnerability is:• multi-dimensional and differential (varies
across physical space and among and within social groups)
• scale dependent (with regard to time, space and units of analysis such as individual, household, region, system)
• dynamic (the characteristics and driving forces of vulnerability change over time).
ese principles underpinned Phase 2: the fa-cilitation and design of a vulnerability analysissystem.
Phase 2: Vulnerability AnalysisFramework: developing an inter-agency approachAer a two-month hiatus during the developmentof the annual Refugee Response Plan (RRP 6),work on the Vulnerability Analysis Frameworkproject resumed in mid-November of 2013.Meetings with UNICEF and WFP led to a deci-sion to broaden the scope of the project beyondthe Cash Assistance working group and invitethe participation of a wider range of stakeholdersin its development. Following informal presen-tations of a proposed approach to groups ofUnited Nations (UN) agencies, internationalnon-governmental organisations (INGOs) anddonors, an inter-agency steering committee,(consisting of five UN agencies, five INGOs andtwo donors) was established to guide furtherdevelopment of an assessment methodologyand implementation6.
roughout discussions with potential newpartners, the key objective of the project remainedthe development of a standardised approach toassessing household vulnerability to supportequitable programmatic decisions. A standardlist of approximately 10-15 household indicatorsof vulnerability, developed by the humanitariancommunity through existing sector and inter-sector coordination mechanisms, would be usedby UNHCR and other agencies in determiningeligibility for assistance. However, it was stressedthat while a household vulnerability ‘score’ couldbe used as a factor in decision-making, it shouldnot be the sole criterion used in decision-making.Furthermore, the final decision on allocatingany assistance would always rest with the indi-vidual agency responsible for managing the par-ticular intervention. Because vulnerability isnot a static concept, the frequency with which are-assessment would be carried out was identifiedas one of the critical considerations in opera-tionalising the exercise. Additional risk analysiswould be carried out throughout the project
3 The UNHCR Specific Needs Codes categorise refugees into groups such as unaccompanied minors, disabled etc.
4 More specifically the weighting of scorecards was different.5 Organisations weight vulnerabilities based on the
objectives or specific persons of concern that they wish to target.
6 Steering Committee Members: CARE, Danish Refugee Council, Handicap International/Help Age, Première Urgence - Aide Médicale Internationale, Reach, WFP, WHO, UNICEF, WHO and, UN Women.
A Syrian refugee family tells a UNHCR staffmember about life in a tented settlement.
UN
HCR
/J. K
ohle
r/Fe
brua
ry 2
014
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Abu Khaled shows the well his familyuses for non-potable water in Irbid.
UN
HCR
/J. K
ohle
r/Fe
brua
ry 2
014

80
development process to identify any potentialharmful impacts of the assessment on households,for example, the potential impact on marginalpopulations who fail to qualify as the least vul-nerable but for whom assistance may be a criticalfactor in preventing a deterioration in circum-stances over time.
Generating a relative household vulnerability‘score’ would be done through a mix of sector-based and cross-cutting quantitative and quali-tative indicators. Linking to location data foreach household would enable agencies to analysethe data by vulnerability level, programmingsector and geographic areas. It was proposed tostart with data collection through the UNHCRregistration and re-registration process andhome visit data, with an eventual expansion ofthe collection process to, for example, selectedNGOs, in order to speed up the development ofa significant body of information. e projectwould also focus initially on refugee householdsoutside the established refugee camps becauseof both the larger size of the target populationand high levels of assistance still being providedin the camp setting. e data would be centrallystored and made available to participating agen-cies subject to normal concerns for privacy andsensitivity of data. Linking the data to UNHCR’sRefugee Assistance Information System (RAIS)would eventually enable analysis of humanitarianassistance effectiveness in reducing or preventingvulnerability by establishing a household recordof assistance to be matched against a vulnerabilityprofile.
Developing ‘indicators’ of vulnerability To increase awareness of the project and initiatethe development of vulnerability indicators, aday-long workshop in February 2014 broughttogether representatives of sectors and sub-sectors to dra list of approximately 25 indicatorsfrom which a final (shorter) list would be culled.Although the seriousness with which all theparticipants approached the work was impressive,the groups achieved varying degrees of successin fleshing out indicators. Some groups wereable to reach a more detailed articulation whileothers struggled to move beyond the discussionphase. Although most participants felt the taskwas a challenging one, comments from severalparticipants indicated appreciation for the con-sultative approach chosen. e exercise, in ad-dition to providing an important first step inthe development of indicators, also helped to
solidify the image of the project as an inter-agency initiative and one that would provideuseful tools and information for a broad rangeof humanitarian actors.
Definition of vulnerability andframework outcomese February workshop also established a work-ing definition of vulnerability for the SyrianRefugee Crisis in Urban areas of Jordan: “therisk of exposure of Syrian refugee householdsto harm, primarily in relation to protectionthreats, inability to meet basic needs, limitedaccess to basic services, food insecurity, and theability of the population to cope with the con-sequences of this harm”. Using this as a basis fordefining the scope of the Vulnerability AssessmentFramework (VAF) that is being developed, theVAF inter-agency steering committee is over-seeing the VAF development process which willhave the following outcomes:
• Data against VAF indicators are collected atthe registration stage by UNHCR and duringhome visits by UN agencies and NGOs, andare uploaded into a central database.
• With the data regularly updated, the database will generate a ‘vulnerability profile’ for each refugee household, based on thresholds of ‘extremely vulnerable, very vulnerable’, etc.
• Partners are able to access the database and conduct queries, while ensuring that confi-dentiality and protection rules are respected,e.g. query: percentage or number of ex-tremely vulnerable refugee households in Irbid governorate, or a district of Irbid.
• Partners will be able to conduct sector-specific queries, to help them better target
their assistance by geographical area and household level, prompting further technicalassessments.
• Partners who have identified beneficiaries for individual household assistance are ableto check the ‘vulnerability profile’ of that household against the database, by upload-ing a list of unique identifiers (e.g. UNHCRor Ministry of Interior registration number).ey may then be able to modify their deci-sion of whom to assist, based on the vulner-ability profile.
• e VAF should reduce duplication of assistance. Partners are encouraged to log assistance they have provided to a refugee household in the database. If partners are systematic in this entry, other partners can then see which households have already been assisted in the database, when search-ing for the unique identifiers.
• rough periodic reports, the humanitarian community will be able to monitor trendsin vulnerability by geographical area, in-forming broader strategic processes, such as the Regional Response Plan.
Ultimately, VAF data will provide a compre-hensive picture of vulnerability among refugeesthat may be used for advocacy purposes andfor planning and prioritising of aid interventions.
Progress to datee VAF process is multifaceted and a numberof key components have been developed, pilotedand rolled out, these include:
• In March 2014, an inter-agency participatoryassessment was conducted with Syrian refugees, through 70 focus groups, with responses disaggregated by age, gender and disability. e VAF indicators were includedin the discussions of refugee priorities/key concerns, and perceptions of their own or their community’s vulnerabilities.
• An assessment tool was designed using the VAF indicators identified in the February workshop.
• A World Bank team has conducted a detailed analysis of indicators used by
7 UNHCR’s registration software programme (database application) used in more than 70 countries, see: http://www.unhcr.org/pages/49c3646cf5.html
8 A software development phase when software features are complete.
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
The Saudi Relief Committee and Campaigns packed Ramadanfood parcels daily and transported them to Zaatari camp.
WFP
/Din
a El
kass
aby
ECHO and WFP provide food vouchers toSyrian refugees in Jordan, Save the Childrenmanages distribution at Zaatari camp.
WFP
/Din
a El
kass
aby
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .

81
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
UNHCR for Cash Assistance decisions, using proGres7 and Home Visit data. From a welfare perspective, this provides an objective validation of many of the VAF indicators.
• Standard Operating Procedures (SOPs) on how the tool could be applied have been draed by the VAF team.
• A Communication strategy for both partnersand beneficiaries has been developed, and aCommunications Specialist was brought onboard to implement the initial phase.
• e VAF data collection tool was piloted androlled out in June with over 15,000 house-holds having been interviewed to date.
roughout July-September, building on thework of the World Bank, econometric analysisof the VAF data was conducted and a VAFWelfare model that identifies the characteristicsof vulnerable householdswas developed. ismodel uses predicted expenditure as a proxyfor welfare and provides a mapping of the vul-nerability spread across those households thathave been interviewed. Data collection is ongoingwith UNHCR, through implementing partnerInternational Relief and Development (IRD),interviewing approximately 5000 new householdsa month.
In August an inter-agency appeals mechanismworkshop was held and an appeal mechanismand interface designed. is appeals mechanismis now being piloted in cooperation with theWFP. Refugees can appeal for re-instatement inthe WFP food assistance programme, followingcuts made to the beneficiary list based on criteriadeveloped as a result of the WFP ComprehensiveFood Security Monitoring Exercise conductedin December 2013/January 2014. In October,an appeals database in RAIS was developed byUNHCR and launched in beta version8 to assistin the process.
A user interface module in the RAIS is beingdeveloped by UNHCR, to allow updating ofvulnerability scoring at the household level,access to interested partners to inform assistancedecisions, and from which vulnerability trendsanalysis can be extracted.
e VAF team also facilitated an additionalparticipatory interagency inter-sectoral workshopin October 2014 to elaborate Sector Based Vul-nerability Assessment Rules that will complementthe Welfare/Vulnerability Assessment model.e workshop built on work conducted inLebanon to define sector level vulnerability de-cision trees. Each sector was tasked with lookingat the multiple data points available from theVAF questionnaire and UNHCR home visitform in order to identify and then articulatesector specific indices of vulnerability and developweights for each, which allow a sector level cal-culation of vulnerability. is sector level scoringis still under review but will allow for a morenuanced picture of household vulnerability. Forexample, VAF partners will be able to access in-formation that tells them a household’s overallvulnerability score but also a breakdown ofrelative vulnerabilities by sector. is shouldallow for programmatic decisions to be madeon the most appropriate types of interventionand acknowledges the holistic and interlinkednature of vulnerability.
Risks and safeguardsGiven the impact that the household vulnerabilityscore could potentially have on the assistancereceived by a household, it is important that thenature and limitations of the data are clearlyunderstood by all actors and that safeguardsare included in the framework to minimise therisk that data are misused. Discussions with theProtection Unit in UNHCR have also takenplace throughout the process.
e assessment process needs to be carefullyconsidered to minimise exclusion risk, i.e. therisk that households or segments of the refugeepopulation are excluded from the process ortheir level of vulnerability is incorrectly cate-gorised and they are excluded from receivingassistance. One example of a mitigating actionwhich has been developed and is being piloted(see above) is an appeals process by whichhouseholds can contest any changes in the pro-vision of assistance based on VAF vulnerabilityscores. is will continue to be articulated at asector level as the VAF is rolled out.
Additionally, there is a risk that refugeesthose without support, may eventually becomevulnerable so that there is a need for periodicre-assessment or other means by which toidentify changing household circumstances.
As stated above, the VAF process minimizesrisk of exclusion for refugees through 1) appeals process, or fast-tracked reassessment
for border line cases 2) periodic update of vulnerability status3) quality assurance of data collectors and
database.
It is important to highlight that the VAF willnot replace the need for sector-specific detailedneeds assessments, but will assist in streamliningplanning of such assessments and/or program-matic interventions by, for example, identifyinggeographical areas where a large number ofcases with a sector-specific ‘flag’ are located.
VAF validation plan and roll outFinally, the VAF steering committee is now ar-ticulating a validation plan that will review andvalidate the different components of theWelfare/Vulnerability model and the SectorLevel rules before the VAF is fully rolled out topartner organisations. e validation plan willuse a participatory and inter-agency/inter-sectorapproach. Further consultations with refugeesto review vulnerability indicators and indiceswill be conducted. Additionally, multifunctionteams will conduct ‘blind’ visits to a randomisedselection of households (across the vulnerabilitythresholds) that have undergone VAF interviewsand scoring to assess the accuracy of the modelsand rules. On the basis of the results of thesevalidation activities, the steering committee anda peer review committee of other vulnerabilityspecialists from the region will sign off on theVAF models and the full set of VAF tools willbe made available to partners.
Currently, the VAF aims to be fully operationaland launched in January 2015. During an initialsix month period there will be a VAF oversightcommittee who will monitor the use of VAFtools and VAF data by partners. By June 2015,Phase 3 of the process will be conducted with afull review of the process to date, revision of themodels or rules as necessary and the documen-tation of lessons learnt and recommendations.
For more information, contact: Kate Washington,email: [email protected]
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Abu Nasser and his family having fled Syria, livesin a single room near Jordan's southern city ofKarak. About half of the Syrian refugees in Karakreport not having adequate water and sanitation.
UN
HCR
/J. K
ohle
r/Fe
brua
ry 2
014
Refugees can cook dry food rations inone of 250 communal kitchens set upby UNHCR in Zaatari camp.
WFP
/Din
a El
kass
aby

82
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Field Article
Responding tonutrition gapsin Jordan in theSyrian RefugeeCrisis: Infantand YoungChild Feedingeducation andmalnutritiontreatmentBy Gabriele Fänder and Megan Frega
Gabriele Fänder is theRegional Health andNutrition Advisor withMedair in the Syria CrisisResponse Programme,based in Amman.Previous work
experience in various roles inSomalia/Somaliland, Afghanistan and India.
Megan Frega is theRegionalCommunication Officerfor the Medair SyriaCrisis Programme.Megan is based in Beirutand is the media liaison
and external communication focal point. [email protected]
This project is supported through generousfunding from UNICEF and WFP.
BackgroundAt the start of 2012, there were only a handfulof Syrian families who had taken refuge inJordan. By September of the same year, thenumber of refugees had increased to about45,000; one year later, it had grown by half amillion. Conflict and violence in Syria drovehundreds of thousands into neighbouringnations, without resources or means to survive.e sudden population influx and need forbasic items, food, shelter, and health care forover half a million people exacerbated theexisting problems of scare resources.
Prior to the Syrian crisis, infant and youngchild feeding (IYCF) practices were poor inthe region evidenced by low exclusive breast-feeding prevalence for infants less than 6months1 and high anaemia prevalence rateamong children of toddler age.2 Accordingto FAO (2011)3, early initiation of breastfeedingamongst mothers in Syria was very low at32%, while reports on the national levelindicate a prevalence of 46%4. e most recentfigures report exclusive breastfeeding preva-lence at 42.6%5 and only 37% of children 6-9months of age had been introduced to com-plementary foods6. Early initiation of breast-feeding and exclusive breastfeeding amongstinfants less than 6 months of age is significantlylower in Jordan, at 39% and 22% respectively7.ese findings suggest inadequate pre-existinghealth and nutrition preventive behaviours,especially poor infant and young child feedingpractices, amongst both the refugee and hostpopulations.
Breastfeeding practices need to be protectedduring emergencies; it is well known that in-fants who are not breastfed are at a manifoldhigher risk of morbidity and mortality thanbreastfed children8. Breastfeeding is emo-tionally and psychologically restorative towomen under stress. A woman’s body is de-signed to feed and nurture her child evenunder difficult circumstances. In emergencysituations, appropriate and safe IYCF practicesare less likely than under stable conditions.Bottle feeding comes with increased risks;poor water quality, an inability to sterilisethe bottle/nipple, artificial ingredients inbreastmilk substitutes (BMS), and lack ofsustainability, can all contribute to poor nu-trition and health in infants dependent onBMS.
Early IYCF assessmentMedair arrived in Jordan at the start of theSyrian crisis in 2012, to respond to the growingpublic health and shelter needs. From thestart, IYCF and nutrition were identified as alarge public health need that was not beingcovered by other agencies. Medair chose tofocus efforts on IYCF to prevent a rise inmalnutrition as the crisis deepened. At thebeginning of the IYCF project, Medair explored
IYCF practices among Syrian refugee mothersthrough individual interviews and focus groupdiscussions in November 2012 to probe com-munity perceptions and practices. An assess-ment in November 2012 set a baseline forIYCF indicators to monitor the project.
e November 2012 assessment foundthat Jordanians and Syrians had similar mis-conceptions surrounding breastfeeding. Fewmothers or caretakers understood the benefitsor importance of exclusive breastfeeding forinfants for the first six months. Refugees oenreported they exclusively breastfed but onprobing, were found to give other fluids totheir infants. Another common misconceptionwas that bottle feeding was preferable, andthat stress on a woman’s body prevents herfrom breastfeeding. Older generations withpoor education on the benefits of breastfeedingoen counsel younger women to give BMS,and younger women almost exclusively followthis advice. Misconceptions amongst caregiversand mothers during the discussions includedpoor advice, telling women to “give waterand herbs,” or that “breastmilk alone is in-sufficient for infants,” and “traditional ap-proaches are preferred.”
Additional assessments found that medicalstaff in local clinics and hospitals oen gavewrong or conflicting advice about breastfeedingto caretakers, contributing to poorer nutritionand breastfeeding practices. Many hospitalsand clinics oen did not emphasise the im-portance and nutritional benefits of colostrum9
aer delivery. Some doctors advised womenthat breastmilk alone was not sufficient, de-pending on the women’s diet or personal nu-trition.
IYCF programmeIn 2012, Medair began the IYCF projectthrough a partnership with the Jordan HealthAid Society (JHAS), a national NGO10. epurpose of the project is to protect childrenunder five years and pregnant and lactatingwomen (PLW) by screening for malnutritionand educating caregivers about IYCF practices.e project focuses on education on exclusivebreastfeeding for expectant mothers, targets
1 UNICEF http://www.unicef.org/infobycountry/syria _statistics.html, http://www.unicef.org/infoby country/ jordan_statistics.html
2 WHO http://who.int/vmnis/anaemia/data/ database/countries/jor_ida.pdf
3 WHO, Nutrition Country Profile, http://apps.who.int/nutrition/landscape/report.aspx?iso=SYR&rid=161 &template=nutrition&goButton=Go
4 http://www.unicef.org/infobycountry/syria_ statistics.html
5 http://www.unicef.org/infobycountry/syria_ statistics.html
6 International Baby Food Action Network, 20117 http://www.unicef.org/infobycountry/syria
_statistics.html
Refugee women in thenorth of Jordan

83
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Field Article
mothers with infants less than 6 months of ageto encourage exclusive breastfeeding, and targetsmothers with children less than 2 years to en-courage the correct and timely introduction ofcomplementary food.
Working in collaboration with JHAS in north-ern Jordan, Medair began education and pro-motion groups in JHAS clinics and in mobileclinics in the surrounding areas. Each of the sixfixed clinics and one mobile clinic are staffedwith a nutrition officer who is responsible forIYCF promotion and breastfeeding counsellingand oversees the management of acute malnu-trition in the related health clinic. During 10months of project implementation, 4,690 PLWreceived IYCF education and 919 mothers en-gaged in breastfeeding counselling sessions.Medair also delivered training on IYCF, malnu-trition screening and malnutrition treatment tohealth staff, doctors, technicians and nursesfrom six JHAS clinics outside Zaatari camp,one JHAS clinic inside Zaatari camp and onemobile clinic. e partner clinics are located inAmman (2), Zarqa, Mafraq, Ramtha and Irbid.e mobile clinic covers the South of Jordan(Karak, Madaba, Tafila, Ma’an, Aqaba).
Community networkingIn 2013, Medair incorporated a community net-working component into the programme thatemployed volunteers to educate the refugeecommunity on IYCF practices and to screen formalnutrition. Many of the Jordanian volunteerseducating the refugee communities were equallyunaware of the importance of exclusive breast-feeding, and appreciated the training for theirown families. Training took place in the JHAStraining centre in Amman or in the Medairoffice in Mafraq (North Jordan). Communityvolunteers initially received three days of trainingon IYCF, nutrition including acute malnutrition,BCC (Behaviour Change Communication) andgeneral health and hygiene topics, specificallypreventable communicable diseases. Every month,community volunteers gather in their relevantservice area and receive refresher training onthese topics.
e community component involves 35Medair volunteers who conduct house-to-housevisits with stand-up education presentations to
teach and train entire families. Community vol-unteers include Syrian and Jordanian men andwomen, who work to a weekly target of 50-58household visits. All volunteers receive a weeklyincentive and transportation costs upon sub-mitting a weekly work report. e programmecoverage area is the six northern governoratesof Jordan (Amman, Zarqa, Mafraq, Irbid, Jerashand Ajloun). Over the course of 10 months,4,977 PLW received IYCF education, and 31,485caregivers were reached with IYCF and healthpromotion education through the communityproject. Each family is taught and counselleddepending on the ages of their children, somothers receive advice on complementary feed-ing, breastfeeding, and infant nutrition as ap-propriate. Families also receive information onwhere to go for additional services, where toget food vouchers, how to enrol in cash-assistanceprogrammes, and were to find additional healthservices.
Medair also establishes small, individualsupport groups, so that mothers have the oppor-tunity to sit together and learn from one another.At this point, only two regular mother supportgroups are fully functioning in Zarqa Governorate.Other groups meet sporadically in all programmeareas. e interest to meet and participate inmother groups is very high; sometimes up to 50women try to participate in one gathering. Oneof the recommendations emerging from theMedair programme will be to scale up mothersupport groups in terms of enabling regularmeetings of the same small group, to betterfacilitate learning and influence behaviour change.
Mothers who are unable to breastfeed arereferred to Medair partner clinics for professionalsupport. A qualified midwife or an obstetrician/gynaecologist specialist checks mothers to es-tablish reasons for not breastfeeding. Motherswho are willing to re-lactate receive relevantbreastfeeding support. Unfortunately, for thosemothers who cannot or do not want to breastfeed,there is no support for BMS supply facilitatedby any health facility outside Zaatari camp. Se-curity issues surrounding BMS targeted distri-bution in the camp (see below) have dissuadedcommunity service providers from getting in-volved in BMS distributions. Infant formula isexpensive; a 250g tin costs 5 JOD (7USD) andlasts 4-5 days. As a result, many mothers usecheaper milk powder instead.
Programme coverage and impactSince the inception of the programme, com-munities in general, including males and fathers,have been receptive and open to education andlearning. Many families have requested additionalinformation about IYCF from volunteers andare eager to learn more. Medair’s project covers60% of the refugee population in the northerngovernorates, where, as shown earlier, over30,000 mothers and caregivers have receivedpromotion and counselling on IYCF (averagecontacts to May 201411).
A follow up Medair survey was carried outin March 2014 to examine project impact. e
sampling frames involved:• 31,485 caregivers who were visited by the
Medair IYCF volunteers between November2013 and April 2014 and had received breastfeeding education.
• 128 caregivers with infants less than 6 months were included in a 24 hour dietary recall to assess breastfeeding status.
e survey showed an increase in breastfeedingknowledge but not an improvement in breast-feeding practice. Knowledge amongst mothersof at least two benefits of breastfeeding had in-creased from 49.5% (November 2013) to 71%in the community and 91.2% in the healthfacility setting (March 2014). However, exclusivebreastfeeding practice among the mothers whoknew about breastfeeding recommendationsshowed no change (24.2% community surveyand 25% health facility based, March 2014) andin fact, was worse than the pre-crisis nationalprevalence in Syria (42.6%12). ese findingsshow that while a large percentage of familiesin Jordan have been successfully educated onthe benefits of breastfeeding, more time andother measures to address social and culturalbarriers are needed actually to effect nutritionbehaviour changes.
Among the 91 mothers of infants less than 6months who were not exclusively breastfeeding,more than half (64.8%, n=59) fed their babywith infant formula, followed by other liquidsincluding water (20%), traditional soup andliquid (16.5%), and raw milk (15.4%). Datafrom one health facility showed similar results,finding that 44.4% of caregivers who were notexclusively breastfeeding fed their baby infantformula.
Treatment of moderate acutemalnutrition (MAM)To treat MAM in children below 5 years of ageand PLW, as implementing partner for WFP,Medair has been distributing Super Cereal Plusin a targeted supplementary feeding programme(TSFP)13. Mothers were initially reluctant to eatthis food or give it to their malnourished child,thinking it might cause them harm. However,Medair began cooking demonstrations duringdistributions at local clinics to show the womenhow to prepare the food, even eating some withthem. e demonstrations have helped removethe stigma of this ‘refugee food’. As soon as theSuper Cereal Plus was cooked during demon-strations, children would start eating it, finishingthe whole test portion in no time at all. esame applied for reluctant PLW, once they tried
8 Bahi R, et al. Bull of WHO 2005;83 (6):418-4269 Colostrum is the breastmilk produced during
pregnancy and immediately after birth. It is low in fat, and high in carbohydrates, protein, and antibodies. It is low in volume and provides concentrated, highly digestible nutrition to the newborn.
10 See profile of JHAS in this edition of Field Exchange11 Mothers with breast feeding difficulties, with sick
children and with malnourished children have received several follow up visits during the programme period. This also includes mothers who are malnourished
12 UNICEF, http://www.unicef.org/infobycountry/syria_statistics.html
Male focus groupM
egan
Fre
ya/M
edai
r, Jo
rdan
, 201
3

84
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Field Article
the cooked food they all agreed it was quitepossible to eat it. However, everyone unanimouslyagreed it needed sugar to improve the taste.During cooking demonstrations, beneficiariesthemselves who had recovered through eatingthe product, advocated for its use and gave tipson how to improve its taste.
Acute malnutrition screeningSince 2012, screening for acute malnutritionhas been undertaken by Medair and communityworkers, targeting PLW and children under fiveyears. e number of children with acute mal-nutrition identified through screening is verylow, much lower than the expected rate accordingto the nutrition survey findings in 2012. Out of46,383 children screened in clinics and com-munities during the 11 months project period,only 69 severe acute malnutrition (SAM) casesand 124 MAM cases were identified. Out of10,088 PLW screened during the 11 monthsproject period, 457 were identified as acutelymalnourished.
ChallengesBMS donations and suppliese culture of bottle feeding in Syria and Jordanwas perpetuated through the untargeted distri-bution of breastmilk substitutes (BMS) in theearly days of the response and the concept thatpoor diet among lactating women negativelyimpacted on their ability to breastfeed. Especiallyduring the first phase of the influx of refugeesinto Jordan (end of 2012 and through the firsthalf of 2013), many non-governmental organi-sations (NGOs), community-based organisationsand well-meaning donors from Gulf countriesdistributed huge amounts of BMS to refugeesin camps and host communities. BMS productswere not distributed according to assessed needs,for example to mothers who were unable tobreastfeed. BMS were usually included as ageneral item in food baskets distributed torefugee families. ose distributions were ingeneral ‘once-off’ distributions with no provisionfor sustained supply to infants established onthese products.
In order to regulate these BMS distributions,the Nutrition Working Group in Jordan developedStandard Operating Procedures on Distributionand Procurement of Infant Formula and InfantFeeding Equipment14. ose guidelines were pro-
moted within the wider NGO community andto donors. From that point onwards, donationswere streamlined through UNHCR and all BMSdonations stored in a warehouse in NorthernJordan. Managing donations created a largeamount of work for the Nutrition Working Groupwho had to decide what to do with the donations,which far exceeded the need for BMS. At onepoint, the Nutrition Working Group had to decidewhat to do with thousands of boxes of differentBMS types and milk powder in storage.
For Zaatari camp, to meet the needs of non-breastfed infants, clear protocols were developedfor the supply of BMS. Mothers are individuallyassessed by a qualified midwife from an appointedclinic (run by the national NGO, Jordan HealthAid Society (JHAS)15. Where BMS supply is in-dicated, the mother obtains a written prescriptionfor BMS, which is supplied at designated distri-bution points. Outside the camp, managing BMShas proven to be more complicated. Refugeesare widespread across all six northern governoratesand it is more difficult to find specialised clinicsacross those Governorates who not only havethe expertise to qualify mothers for BMS distri-bution, but also to facilitate supply. Experiencerelated to riots and attacks on distribution pointsin the camp related to BMS16 have preventedclinics outside the camp agreeing to store BMSproducts and be part of a BMS distribution.
Expectations of aidOne of the challenges Medair faces in program-ming is the need to distribute physical aid alongwith education. Refugees oen expect physicalaid - cash, hygiene items, kitchen equipment,etc. - and struggle to see the importance of edu-cation without accompanying in-kind assistance.Community volunteers are received with suspi-cion if they come to “only talk”. Initially, familiesdon’t see the importance of education and pro-motion related to IYCF. To respond to this de-mand, volunteers have begun to distributespoons, cups, and breastfeeding shawls to womenwith children under 6 months of age, as well ashygiene kits to mothers with children under 2years. Beneficiaries put the need for cash aboveall other needs, sometimes failing to recognisethe importance of other initiatives. Donors,stakeholders, and medical staff also typicallysee IYCF support approach as a ‘so’ approachwithout much impact.
e timeline for aid delivery is a challenge.In emergencies, short intervention timelinesand quick impact programmes are preferred.As reflected earlier, behaviour change requiresa longer term approach.
Discussion and recommendationsTo tackle social and cultural barriers and increaseeffectiveness of IYCF promotion in Jordan, ad-ditional mother support groups and learninggroups need to be incorporated into the educationprocess. Community led and sponsored supportgroups with cooking demonstrations, continuallearning discussions, and referral informationshould be held regularly.
Doctors and health staff must be targeted asthey are the primary source of information forrefugees. Doctors must encourage breastfeedingamong patients and hospitals must have deliverystaff who promote good feeding practices. Moth-ers must also be informed through antenatalcare visits about the importance of exclusivebreastfeeding and the benefits of breastmilkversus infant formula. e Jordanian Ministryof Health is a critical partner to champion keyIYCF messages within the country. Messagingthrough radio, television and newspapers abouthealth and hygiene practices must permeateboth the Jordanian population and the refugeecommunity. Hygiene materials should be dis-tributed along with messaging to enable long-term behaviour change.
UNICEF has requested that Medair begin tochampion their baby friendly hospitals initiative(BFHI), which will seek to train health workerson the importance of immediate breastfeedingaer delivery. None of the clinics which Medairsupports has BFHI status, however, this isplanned in the next stage of programming.
With regard to the needs of non-breastfedinfants, the provision of targeted supplies ofBMS in the community setting is a particularchallenge and remains an outstanding gap.
During every training session, whether withcommunities, volunteers or medical staff, Medairhave found that participants are excited to learnabout how important IYCF practices are andwant to learn more. Technical support materialin Arabic tailored to the context of the MiddleEast would greatly help training delivery.
For long-term change to happen, the approachmust continue to be community led and focusedon the needs of poor, vulnerable families. Physicalaid should accompany health messaging andeducation. Prevention programmes over curativeinterventions should lead the response.
For more information, contact Gabriele Fän-der, email: [email protected], tel(Jordan): +962 (0)796 294628
13 See article by WFP for more details on the TSFP.14 Available from: http://data.unhcr.org/ syrianrefugees/
regional.php15 See article by JHAS and profile of the agency in this edition
of Field Exchange.16 See the article by Save the Children Jordan that elaborates
on these BMS problems in Zaatari camp.Education on the use
of Super Cereal Plus. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .H
eba
Sede
r/M
edai
r, Jo
rdan
, 201
4

85
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Field Article
Since the beginning of the emergency inSyria, over 500,000 Syrians have crossedthe borders into Jordan and are eitherhosted by the Jordanian community or
residing in refugee camps. e first refugeecamp in Jordan was Zaatari, administered bythe Government of Jordan-appointed SyrianRefugee Camp Directorate (SRCD), with thesupport of UNHCR. More than 350,000 Syrianshave been registered in Zaatari camp since itsopening in July 2012. A large number of refugeeshave subsequently le Zaatari camp to urbanand rural areas in Jordan.
At the beginning of the emergency, a numberof assessments were conducted to determinethe health and nutrition needs of the refugees,including e Inter-Agency Nutrition Assessmentconducted in November 20121. is recom-mended strengthening the awareness, promotion,and protection of optimal infant and youngchild feeding (IYCF) practices through preventiveand nutrition promoting services.
Prior to the crisis, IYCF practices were alreadypoor in Syria. According to the MICS2 surveyof 2006, the prevalence of early initiation ofbreastfeeding was 46%, and the prevalence ofexclusive breastfeeding in infants under 6 monthsof age was only 43%. IYCF indicators were notfavourable in Jordan either; the 2012 DHS3
showed that in the past few years, exclusivebreastfeeding rates have dropped from 27% to23%. In Zaatari camp in Jordan, there was ahigh demand for infant formula early in thecrisis response. Whilst only a small percentageof women requesting supplies were physiologically
unable to breastfeed, common use of infant for-mula pre-crisis among the Syrian refugees, cou-pled with untargeted and unsolicited distributionof infant formula in the early humanitarian re-sponse and high levels of stress and anxietyamong women, fuelled this demand.
In late 2012, a Nutrition sub-working group(Nutrition SWG) was established as a sub-groupof the Health Working Group, initially chairedby UNHCR and co-chaired by Save the ChildrenJordan (SCJ) from November 2013. Initial ad-vocacy and response initiatives involved the de-velopment and sharing of two key guiding doc-uments through the Nutrition SWG, namely:• Guidance Note on Appropriate Infant and
Young Child Feeding Practices in the Current Refugee Emergency in Jordan (26th of November 2012)4.
• Standardised Operating Procedures (SOPs) on Donations, Distribution and Procurementof Infant Formula and Infant Feeding Equipment in the Current Refugee Emergency in Jordan (26th of November 2012)5.
Save the Children Jordan programmeBreastfeeding in an emergency is known to bethe safest way to protect infants and young chil-dren from an increased risk of infection andfrom becoming malnourished. Breastfeedingsupport was a key recommendation of Inter-Agency Nutrition Assessment (as above). Giventhis, SCJ launched the Infant and Young ChildFeeding in Emergencies (IYCF-E) programmein Zaatari camp in December 2012, aer com-pleting a technical training supported by Save
the Children US. e programme was fundedby OCHA, Save the Children US, UKAid andthe German Cooperation-Save Germany. Itaimed to reach 90% of pregnant and lactatingwomen (PLWs) and children under 5 years inthe camp. At the time (November 2012), thecamp population was estimated to be 45,0006.
e programme’s main goal was to promote,protect, and support appropriate IYCF practices,including early initiation of breastfeeding within1 hour of birth, exclusive breastfeeding forinfants under 6 months, and appropriate andtimely introduction of complementary foodalong with breastfeeding aer 6 months.
Mother-baby friendly spacese IYCF programme started with the estab-lishment of the first of three caravans serving asa mother-baby friendly space (safe haven). ecaravan engaged a team of five trained IYCFcounsellors responsible for individual counsellingsessions and follow up, five educators responsiblefor group education sessions and 10 supportingSyrian community mobilisers.
By Sura Alsamman
Managing infant and young childfeeding in refugee camps in Jordan
1 Inter-agency nutrition assessment Syrian refugees in Jordan host communities and Za-atari camp. Final report. January 2013
2 Multiple Indicator Cluster Survey (MICS), Syrian Arab Republic, 2006 http://www.childinfo.org/files/MICS3_Syria _FinalReport_2006_Eng.pdf
3 Demographic and Health Surveys (DHS) for Jordan, 2012. http://dhsprogram.com/what-we-do/survey/survey-display-403.cfm
4 Available at http://data.unhcr.org/syrianrefugees/ regional.php
5 Available at http://data.unhcr.org/syrianrefugees/ regional.php
6 Current estimates of Zaatari camp population are around 90,000 people (June 2014)
A group teaching sessionin the IYCF caravan
Save
the
Child
ren
Jord
an, 2
013
Sura Alsamman is nutrition supervisor atSave the Children Jordan, responsible forthe overall all coordination of the IYCFtechnical functions and activities incamps and south of Jordan. Previouslyshe worked in various maternal and childnutrition programmes.
Save the Children Jordan (SCJ) is a registered Jordanian NGO established in1974, with Her Royal Highness, Princess Basma Bint Talal as the Chairperson ofthe Board. SCJ is part of and the only Arab member of the 30 Save the Childrenorganisation members operating in 120 countries worldwide. In Jordan, SCJdevelops much needed national programmes that focus on creating sustainableresults where every child attains the right to survival, protection, developmentand participation.

86
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Field Article
A simple rapid assessment was conducted inthe first few days of operation in Zaatari camp,to explore the prevailing infant feeding practicesand challenges faced by PLWs and caregivers.is exercise allowed SCJ to better design thecounselling and education sessions in the pro-gramme; it was not intended to provide a fulldataset or statistical analysis. e assessmenthighlighted many misconceptions among mothersincluding mothers believing they don’t haveenough breastmilk/mothers convinced thatbreastmilk is drying up due to stress/mothersbelieving that breastmilk is not enough forinfants in the first few days of life. e rapid as-sessment indicated the need to emphasise theimportance of exclusive breastfeeding and thecorrect timing of starting complementary feeding.
e assessment also identified cases of breast-feeding difficulties, like engorgement and mastitis,which counsellors started following up with im-mediately.
As the camp population rapidly increased,and in partnership with UNICEF, two new IYCFcaravans were established to cover all 12 districtsin the camp. Eight new staff members joinedthe team to support in following up with mothers.e IYCF caravans are located in districts 3, 4and 8, next to the three main schools in thecamp. Based on the camp population distribution,those caravans are reachable to most mothers.Each caravan currently has an educator and aSyrian caravan assistant on a daily basis, alongwith the counsellor and community mobiliser
assigned for each district. On average, 120-150mothers visit the three IYCF caravans on a dailybasis. Some mothers attend daily, others weeklyas they wish. On average, there are 150 newvisits to the caravans per week.
e caravan is promoted as a safe space forbreastfeeding, where privacy and support isprovided for all pregnant women and motherswith children under 5 years. Education sessionsare held in the caravan on a daily basis from9:00am till 3:00pm covering topics such as nu-trition for PLW, the importance of breastfeeding,complementary feeding, and feeding during ill-ness. Initially, infants who were using infantformula attended the paediatrician, but noware directed to the IYCF caravan also. A nutrientdense snack (high energy biscuit) and a bottleof water are provided to mothers as incentivesto visit the caravan and to highlight the impor-tance of nutrition and fluids for breastfeedingmothers. Breastfeeding shawls for privacy (pro-vided by UNHCR as a gi in kind) were alsodistributed to lactating mothers. A bottle/cupamnesty activity also operates in the caravan,where mothers are encouraged to exchange anyfeeding bottle they have for a measured cupwhich is considered safer, more hygienic andeasier to clean.
In order to respond to mothers concerns,IYCF educators follow up with the various healthissues arising in the camp. For example, foodsafety and hygiene was emphasised when diar-rhoea cases increased and the importance ofearly initiation of breastfeeding was emphasisedwhen cases of jaundice were identified in new-borns. In addition, the IYCF educators participateactively in the sensitisation and mobilisationfor the different immunisation campaigns.
Over 18 months of operation (Dec 2012 toMay 2014), the programme has reached 15,600mothers through the caravan and tent counsellingsessions in Zaatari camp. Non-breastfed infantsare supported through individual counsellingsessions. A high proportion of the mothersattend with children under 2 years of age.
Community mobilisersFrom the early stages of implementation, com-munity mobilisation was identified as one ofthe main components of the programme. It wasagreed that each Jordanian staff (counsellor/ed-ucator) would closely work with a Syrian mo-biliser who was chosen based on their background(nurses, college graduates) and how well theyknew the camp community. e mobilisers mainresponsibilities are to identify mothers whoneed breastfeeding support and help in spreadingthe IYCF messages. If they encounter mothersusing infant formula, they direct them to theIYCF caravans, or refer to a counsellor to inves-tigate relactation, or at a minimum, ensure thatare preparing infant formula as hygienically aspossible. It is clear that having Syrian mothersas part of the team and communicating thesame messages makes it much easier to com-municate with the refugees and discuss theirbeliefs and misconceptions around infant feeding
Sara is one of the community mobilisers working with the IYCF team in Zaatari camp. Sara decidedto join the team after her successful experience in breastfeeding her youngest child and seeinghow this affected his health compared to his four older sisters.
Travelling with her four daughters, Sara arrived at the camp in the heat and dust of July 2012. Asthe days passed, Sara gradually settled in, amongst relatives and neighbours. She learned to copein a difficult environment, with insufficient food supplies and inadequate accommodationconditions. Sara first visited us one cold December morning in 2012, as a result of an outreachcampaign we conducted in the camp. She was pregnant with her fifth child. When she first came,she expressed her concern regarding sanitation in the camp and access to clean water. She didnot possess sufficient knowledge about the benefits of breastfeeding her child. This applied toboth her and the community as a whole.
With her delivery date approaching, the IYCF counsellors’ visits to Sara increased. She was taughtthe different positions for breastfeeding, the signs of proper breast attachment, the importance ofcolostrum (the first milk produced by a mother on giving birth), as it is rich in immunologicallyactive cells, antibodies, Vitamin A and other protective proteins, and much more. After Sara’sdischarge from the hospital on giving birth, IYCF counsellors from SCJ continued to visit her on aweekly basis to monitor the progress of the baby’s health and weight, provide emotional supportfor her, and answer any questions or address concerns she may have.
“For the first six months, I exclusively breastfed Tamer, as I had been advised; he is the only child Iexclusively breastfed and I can clearly see the difference in comparison to his four older sisters. Heis more resistant to diseases and infections, and is more alert and active. In addition, I myselfexperience great joy when I breastfeed him, I tend to transition into a state of serenity, tranquillityand bliss. A state that in a camp environment is unattainable.”
Even as Tamer grew, Sara continued to visit the IYCF caravan as often as possible. She would relateher story to other pregnant and lactating mothers and her enthusiasm was infectious. Sara hasbecome our ambassador in Zaatari Camp. She is such a strong advocate of breastfeeding and sowe are happy to have her among our team of Syrian camp mobilisers.
Save
the
Child
ren
Jord
an, 2
013
An individual teaching session
Box 1 Community mobiliser – success story

87
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Field Article
practices. Difficulty following up with motherswas one of the major challenges we faced at thebeginning; families were constantly changingtheir locations in the camp (moving to a higherarea, closer to the market, next to new arrivingrelatives). With no contact information otherthan the address given in the initial visit, it wasvery difficult to reach the mother again. However,with the help of the community mobilisers teamand their connections with street leaders, theteam were able to reach many of these cases. Acase study regarding one community mobiliser’sexperiences is included in Box 1.
Coordination with partners and health fa-cilities in the camp has also played a key role indisseminating IYCF messages. rough agree-ments and Memoranda of Understanding(MOUs) with different partners, IYCF educatorshave the opportunity to reach mothers and con-duct sessions in clinics and women/youth centres.Recognising that contact with mothers imme-diately aer birth increases the possibility ofexclusive breastfeeding and early initiation, IYCFcounsellors provide counselling sessions on adaily basis in the two health facilities providingdelivery services in the camp.
Acknowledging the impact of the messagescommunicated by health providers, and noticingsome cases of misinformation from health staffin the field clinics, it was crucial to ensure thatunified IYCF messages were delivered by alldoctors, midwives and nurses. Key informationincludes the importance of colostrum and earlyinitiation of breastfeeding, duration of exclusivebreastfeeding, timely introduction of comple-mentary feeding, and indications for prescriptionof infant formula (medical indications and whereinfants are not breastfed, see below). To addressthese issues, an orientation session was conductedfor all health providers on IYCF; key messageswere also circulated through the health coordi-nation meeting. Due to the high staff turnoverin such situations, continuous follow up remainsa necessity to ensure a unified message.
e difficulties in managing infantformulaMonitoring infant formula prescription and dis-pensing has been a major challenge from thebeginning of the crisis response in Jordan. Char-acteristics of optimal IYCF practices and theprovisions of the International Code of Marketingof Breastmilk substitutes (BMS) were relatively
unknown. Controlling BMS (typically infantformula) supply was a new concept among na-tional health staff and caregivers, especiallygiven that infant formula use was the norm forthe Syrian community pre-crisis. Hence mostof the caregivers argued it should be part of theration or distributed for every family withchildren under 2 years of age. Field hospitalsreceived donations of infant formula, bottlesand teats and were distributing them for allmothers.
Infant formula prices are relatively high.Many mothers who received it opted to sell it inthe camp streets or sent it outside to be sold inthe community (it was clearly seen for sale inthe camp market).To reduce distribution channelsand ensure targeted distribution, UNHCR fol-lowed up on this issue. A series of meetingswere held with different health providers toensure that there was a system in place tomanage the process of supply provision of infantformula. It was agreed that only one healthfacility would be responsible for dispensinginfant formula and a protocol was establishedregarding individual assessment of need andsupply method (see Box 1). It was very importantfor SCJ to make sure that IYCF caravans werenot involved with any kind of BMS prescriptionor dispensing. Within a few days of starting thenew process, however, it was clear that the refugeeswere not happy with it. Angry men would gatherat the health facility and demand infant formula.In addition, they restrained their wives fromtaking the physical examinations. Many infantformula packs were taken by force and the midwifereceived several threats of attack.
Sensitisation was critical for calming the sit-uation. Mothers and caregivers were referred tothe IYCF caravan for education sessions on theimportance of controlling this prescriptionprocess and the dangers of artificial feeding inemergencies. IYCF educators were present on adaily basis in the health clinic explaining theimportance of breastfeeding and superiority ofbreastmilk. But it was also clear that further se-curity precautions needed to be in place. It wasdecided to have the prescription and dispensingin two different locations - the examination andprescription undertaken in the health clinic andthe distribution at another more secure location.Once both locations were identified (this tooksome time), it was agreed that an IYCF staffmember would be present in each facility tosupport and monitor the process. A databasewas developed to keep track of mothers receivinginfant formula (names, ages, ration card number)to avoid duplication, to allow regular follow upto ensure hygienic and correct preparation ofthe infant formula and to explore the possibilityof re-lactation. Even with the strict prescriptioncriteria, infant formula tins were being sold inthe camp market. us it was agreed with staffbased in the dispensing site to open each tin
Infant formula is prescribed based on any of the medical indications for infant formula use asrecommended by WHO7 or when physical examination of the mother finds there is no breastmilksupply.
All mothers requesting infant formula are required to undergo a physical examination by a midwifeto determine if there is breastmilk supply. This includes mothers who have never breastfed. If themidwife determines that there is no breastmilk supply, the mother is prescribed infant formula. Ifthe mother is found to be able to breastfeed based on physical examination and is found to havegood milk supply, then she is not supplied with infant formula. In practice, in most cases wheremothers are already using infant formula, there is not a ‘good’ supply of breastmilk, and thesemothers are generally prescribed formula.
If the mother is interested in relactation, the counsellor follows up with her regularly and graduallydecrease the quantity of infant formula provided. If the mother does not have breastmilk supplyand is not interested in relactation, then she keeps visiting the midwife on a monthly basis toreceive the infant formula prescription.
Infant formula is provided for infants until 12 months only.
Weighing infants on a monthly basis would be a useful additional indicator to inform and monitorinfant formula prescription. Unfortunately growth monitoring is not yet in place, but itsimplementation is under discussion.
7 Acceptable medical reasons for use of breast-milk substitutes. WHO/NMH/NHD/09.01. WHO/FCH/CAH/09.01. http://www.who.int/maternal_child_adolescent/documents/WHO_FCH_CAH_09.01/en/
Save
the
Child
ren
Jord
an, 2
013
One of the IYCF caravans in Zaatari camp
Box 1 Community mobiliser – success story

88
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Field Article
once the mother received it. is mechanismworked well, as no one was then willing to buyan already opened tin of infant formula.
Infant formula donations and their untargeteddistribution remain a challenge. Although theSOPs (see earlier) have been circulated, sharedand discussed with all partners, individual do-nations of infant formula still find their way tothe camp. It is worth noting that many mothersare refusing the donations or returning anyquantities they receive as they are exclusivelybreastfeeding. Street leaders from the communityapproached the clinic a few months ago withquantities of donated formula; they wanted toleave it with the midwife as she would knowwho actually needs to receive it, which showsthat the community is now aware of the risks ofsuch distributions. An average of 10 new mothersis prescribed formula on a weekly basis. Withthe opening of a new refugee camp (Azraq camp)in Jordan in April 2014, many lessons have beenapplied from the experiences in Zaatari camp. Asystem for infant formula provision has been inplace from the beginning. Upon prescription,mothers are given specific dates to go and receivethe infant formula, the dispensing takes placetwice a week, and a list is communicated eachtime from the prescription to the dispensingsite to avoid any confusion. As of September2014, 226 mothers are prescribed infant formulain Zaatari camp (camp population 79,708), 28mothers in Asraq camp (approx. 13,000 popula-tion) and 7 mothers in Emarati Jordanian camp(EJC) (about 4000 population) (see below).
Complementary feedingDuring the early days in Za’atri camp, the foodration was provided by WFP along with a com-plementary ration by UNHCR. People com-plained about lack of diversity, but the mainconcern from a nutritional point of view wasmeeting the needs of children aged 6-23 months.Mothers were constantly complaining that theration didn’t include anything adequate for thisage group, and not everyone in the camp hadthe ability to buy fruit and vegetables.
e need for a fortified food suitable forchildren 6-23 months was agreed and WFPsought procurement of international supply ofSuper Cereal Plus. Due to complications in pro-curement that delayed supplies by seven months(see below), UNHCR, UNICEF and SCJ stop-
gapped with an intended short term (4 month)blanket distribution of a local fortified porridge,targeting children 6-23 months (March – June2013). Four packs of 250g each were providedfor each child on monthly basis. Special cases,such as cerebral palsy children, were also includedin the distribution. e distribution itself was achallenge as many security concerns were raisedregarding families with older children whowould not receive the product. Careful sensiti-sation was undertaken to inform the communityand explain to them the importance and rationaleof the product for this specific age group. elocal complementary food was well received byfamilies but was expensive. It was not availableto purchase in the camp markets. ree cycleswere completed but the fourth did not happendue to inadequate funds.
Referral and management of acutemalnutrition casesA mid upper arm circumference (MUAC) screen-ing conducted by the SCJ team during the com-plementary food distribution period found aglobal acute malnutrition rate (GAM) rate of2.6%. Since malnutrition was not a major concernin Jordan pre-crisis, there were no clear nationalprotocols or referral pathways. e NutritionSWG developed a national protocol, which waslater adopted by the Ministry of Health, anddraed a letter requesting permission to importRUTF (Plumpy’nut) and fortified blended food(Super Cereal Plus). In reality, product approvalsand releasing of the products from customstook more than six months. us the identifiedcases had to be managed using other interven-tions. Severe acute malnutrition (SAM) caseswere referred to the MSF hospital inside thecamp and moderate acute malnutrition (MAM)cases were provided with the locally procuredfortified food porridge and followed up by IYCFcounsellors. e local fortified had a very goodnutritional profile, and mothers were constantlyinstructed on preparation methods and numberof meals to offer per day.
Eventually in January 2014, Super CerealPlus was officially approved by the Jordan Foodand Drug Administration (JFDA) and in part-nership with WFP, SCJ launched the Supple-mentary Feeding Programme (SFP) in Zaataricamp. A blanket distribution for children 6-23months is currently taking place on a monthlybasis, and a targeted distribution with regular
follow up is conducted for MAM cases twice amonth. e Super Cereal Plus is not well acceptedby the children compared to the local fortifiedporridge that was initially provided.
Outside Zaatri campAs of July 2013, the SCJ IYCF programme wasalso providing services to the Emarati Jordaniancamp (EJC) and to the host community. EJC isa relatively small camp compared to Zaatariwith a population of only 3,600 refugees. eprocess of monitoring infant formula was alsodifficult at the beginning, as the clinic was pro-viding infant formula on a weekly basis to allfamilies with infants under 1 year of age. It tooka while to convince the management and thehealth providers of the need to control this, andthe adverse effect it could have on infant’s health.e IYCF midwife is now responsible for pre-scribing the infant formula and only sevenmothers are now receiving supplies on medicalgrounds. Given the small camp population, SCJis able to follow up with all infants under 1 yearin the camp. Overall, 30-40 mothers receiveIYCF counselling on a daily basis in the IYCFcaravan. By working closely with the clinic, SCJensure that each infant below 6 months is beingfollowed up by the IYCF counsellor in the camp.
DiscussionAer 16 months of implementing IYCF in thecamps and host community, we have successfullyreached 29,000 PLW (new visits or first coun-selling contacts) and 40,000 children under 5years (total contacts). More than 47,000 benefi-ciaries (mothers, fathers, and grandmothers)have attended the IYCF sessions conducted indifferent partner’s locations.
It is becoming clear that building capacityand cooperation with health providers on com-municating a unified IYCF message plays acrucial role in convincing mothers of the im-portance of breastfeeding and early breastfeedinginitiation. Higher rates of exclusive breastfeedingare noticed among mothers who are regularlyfollowed up by IYCF counsellors, and anecdotally,many are noticing the lower incidence of diar-rhoea and respiratory infections compared toother non-breastfed infants.
In terms of meeting the needs of infants de-pendent on infant formula, greater control onthe implementation of the International Codeof Marketing of BMS by the Ministry of Healthwould have been very helpful. Uncontrolleddistribution of infant formula early in the crisiswas a great cause of tension with the community;if the community had been informed of theprocedures and guidelines from the beginning,we could have avoided many problems. is iswhat is currently being done in Azraq campand there have been no problems. Now, in Zaatricamp, the needs of formula fed infants are beingmet - supplies are always available, there is aclear referral pathway and system in place formothers who need formula and there is followup of infants.
For more information, contact: Sura Alsamman,email: [email protected]
Save
the
Child
ren
Jord
an, 2
013
Cup for bottle exchange in the IYCF caravan

89
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
The articles by Medair and Save the Childrenhighlight the challenges in protecting andpromoting sound infant and young childfeeding (IYCF) practices in a humanitarianemergency. Much of the guidance on IYCF hasbeen developed for resource poor settings.Infants in these settings who are not breastfedhave a much higher risk of dying. This risk isexacerbated by the upheaval generated byemergency settings. There have been fewarticles published on experiences of IYCF inemergencies in low to middle income countries,such as Jordan. Acute malnutrition prevalenceamongst Syrian refugees in Jordan is low andnot considered a public health problem, andmortality rates are low and stable; regardlessthere is always an important need to promotesound IYCF practices for optimal infant andyoung child health outcomes.
Alsamman and Fander et al highlight the poorIYCF practices both in Syria and in the refugeehosting country, Jordan, prior to the refugeeinflux. Though it is critical to try and protectbreastfeeding throughout all stages of therefugee programming, this has been mademuch harder by the poor practices pre-conflict,the low level of knowledge amongst manyhumanitarian actors, including medical andnursing staff, and the misconceptions aroundbreastfeeding. There were many non-traditionalactors involved in the response most of whomhad not been exposed to the Code or theOperational Guidance on IYCF in Emergencies(IYCF-E). Though health and nutritionprogramme managers from internationalorganisations were well-versed in the currentrecommendations about the use of breastmilksubstitutes (BMS), doctors and midwivesproviding services were not generally verysupportive of breastfeeding or easilysuccumbed to pressure from mothers andfamily members to provide infant formula.Practices surrounding delivery were also notconducive to early initiation, with the infantoften separated from the mother and started onother liquids. This highlights the need to notonly target humanitarian service providers withtraining in key beneficial IYCF practices but also,in the medium to longer term, to strengthenthe IYCF component of medical and nursingschool curricula and revitalise the Baby FriendlyHospital Initiative.
Unsolicited donations of BMS continue at thetime of writing. Fortunately, the StandardOperating Procedures on Distribution andProcurement of Infant Formula and InfantFeeding Equipment1 put in place in November2012 by the Nutrition Sub-working Group (andupdated in May 2014) meant that manydonations came to the attention of the nutrition
actors and measures could be taken tominimise the risks associated with suchdonations. However, as pointed out by Flanderset al, this was very time consuming at a timewhen there were many other pressing priorities.Furthermore, if the NWG had been consultedprior to the donation, a request would havebeen made for other food or non-food items,such as age appropriate complementary food inplace of infant formula.
There were many donations and distributions ofBMS outside of the health system demonstratingthat advocacy and training needs to also targetother sectoral actors in addition to thoseworking in health and nutrition. Non-traditionalactors, especially the military and emerginghumanitarian actors, also need to be madeaware. As these actors expand their geographicalscope into other crisis-affected parts of theworld - many of which have considerably highermalnutrition rates and poorer hygiene andsanitation situations – the effects ofindiscriminate use of BMS on infant morbidityand mortality would be much more severe.
Another key challenge in the Syrian situationand detailed by these two articles is how tosupport non-breastfed infants and theirmothers to ensure optimal growth andwellbeing but without undermining keymessages in support of breastfeeding. Much ofthe focus of IYCF programming has beensupport to breastfeeding mothers orrelactation. Alsamman has outlined the supportin camp settings in Jordan to non-breastfedinfants. In non-camp settings, this has beenvery difficult to put in place. Most refugeesaccess Ministry of Health services and apartfrom ad hoc support to some women, non-governmental organisation (NGO) serviceproviders are not in a position to meet thedemand for infant formula which would entailassessment of women for their ability tobreastfeed, prescription and dispensing whenindicated and support to non–breastfed infants.Their reluctance to get involved has also beeninfluenced by security concerns based on theexperiences in Zaatri Camp outlined byAlsamman. In Jordan, infant formula is onlyavailable through pharmacies and is thereforenot available through the WFP-supported foodvoucher schemes, which has also limitedformula use in out-of-camp settings.Recognising that there are mothers who willnot be able to breastfeed and who will havedifficulties affording formula, the NutritionWorking Group is exploring the option ofreferring mothers who are unable to breastfeed(after assessment by a midwife trained in IYCF)for cash assistance so that they can purchaseformula themselves. This would be combined
with the additional support and follow upneeded for non-breastfed infants but willreduce the likelihood of the potential problemsassociated with actual formula distribution. Thedifferent approaches in the camp and non-camp settings in Jordan have resulted informula feeding being considerably morecommon in out-of-camp infant refugeescompared to those living in the camp (16.1 % ofthose 23 months and under had receivedformula in the preceding 24 hours versus 9.8%respectively). 2 Though the more restrictedaccess in the camp to BMS and the IYCFprogramming are no doubt significant factors,more research is needed on the determinants ofinfant feeding choices in displaced populations.Are displaced women choosing to breastfeedbecause of economic necessity as well asconvenience and if so how can these factors beused to promote breastfeeding in similarsituations?
Lastly, more consideration needs to be given tothe question of informed choice in infantfeeding practices and to what extenthumanitarian actors should withhold supportfor formula feeding in women who have made atruly informed choice. Are humanitarian actorsprepared to support this approach in settingswhere the choice to formula feed - though notoptimal - does not carry the same healthconsequences as in other settings? Eventhough the Operational Guidance on IYCF-Epromotes the minimisation of the risks ofartificial feeding, this is not always given theattention it needs in IYCF programming.Furthermore, the tendency is to focus onmothers who cannot breastfeed and not thosewho choose to not breastfeed. The economicconsiderations of an informed choice approachare also considerable. Infant formula is anexpensive commodity and it is unlikely thatlimited humanitarian funds could be used tosupport provision of formula in a situationwhere a woman has chosen to formula feed.Indiscriminate distribution of BMS andunsolicited donations should still be managedas per the Operational Guidance on IYCF-E butshould a harm minimisation approach beconsidered in some settings? The Syrian refugeesituation, with most refugees fleeing to low -middle income countries, has raised thesequestions and is challenging actors to reviewthinking on this issue.
For more information, contact: Ann Burton,email:[email protected]
Commentary on experiences of IYCF support in the Jordan responsePostscriptBy Ann Burton, Senior Public Health Officer UNHCR Jordan
1 Available at the UNHCR Syria response, portal: visit http://data.unhcr.org/syrianrefugees/regional.php
2 Preliminary findings Interagency Nutrition Survey of Refugees in Zaatri and Out-of-Camp settings, May 2014 (unpublished)
Postscript

90
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Assisting the most vulnerable in theSyria crisise conflict in Syria was triggered by protestsin mid-March 2011. Now, three years later, ithas evolved into a complex and protracted hu-manitarian crisis, spilling into neighbouringcountries and the wider Middle East region.Nearly three million people have fled Syria andan estimated 9.3 million people are in need ofhumanitarian assistance across the region. Mostrefugees live outside of camps in different urbanand rural settings. e scale of the Syria crisis isstretching the capacity of humanitarian actorsto ensure and maintain standard quality assistancethat address specific vulnerabilities and needs.A global partnership between HelpAge Inter-national and Handicap International led to adecision to address this recurrent issue by initi-ating a Syrian crisis-focused inclusion pro-gramme. e programme is aimed at facilitatingthe implementation of a principled, inclusiveand accessible humanitarian response for themost vulnerable, especially older refugees andrefugees with disabilities.
e inclusion team consist of three experts:one Inclusion Advisor in both Jordan andLebanon and a Programme Manager at regionallevel. eir inclusion mainstreaming work focuseson:• Capacity building of humanitarian actors to
design and implement programmes and activities that are inclusive towards older refugees and refugees with disabilities.
• Providing technical support to humanitarian actors on age and disability inclusion.
• Advocacy and awareness raising on inclusion issues with the coordination structures (working groups, task forces, coordination meetings) and towards donorsand authorities.
• Leading coordination on age and disability related issues through the Disability & OlderAge Working Group in Lebanon, and the Age & Disability Task Force in Zaatari camp (Jordan).
e main aim of inclusion mainstreaming workis to enhance inclusiveness of the overall responsetowards the most vulnerable groups, i.e. thepersons excluded from services or response andmore specifically, older refugees and refugeesaffected by an injury, disability or chronic con-dition – as these groups of individuals are mostlikely to be excluded or invisible. Rather thancreating parallel targeted activities and services,the programme seeks the integration of age anddisability considerations into the programmingof all responding actors.
Vulnerability assessment approachAt the operational level, Handicap Internationalhas a distinct approach toward targeting themost vulnerable among the refugee populationin Jordan and Lebanon. Using its trademarkDisability and Vulnerability Focal Point mecha-nism (DVFP), the organisation effectively reachesout to refugees at community level and seeks toaddress the gaps which lead to a lack of accessto, or exclusion from, services, which could fur-ther lead to increased vulnerability. First, mappingof the context – including available services – isdone. Based on that mapping, vulnerability pro-files are determined for the different contexts.Both the vulnerability of the household and in-dividuals are taken into account. Subsequently,there are four entry points for new cases to beassessed by Handicap International: via a hotline,through fixed point (Handicap Internationalcentre established within community facilities),
through referral from outside (including com-munity focal persons), and on-the-spot identi-fication by outreach teams.
For assessing the vulnerability, Handicap In-ternational looks at the interaction betweenpersonal factors (such as age, gender or disability)and environmental factors (such as access toservices or the availability of an assistive devicewhen required). Handicap International assessesbasic needs (food, shelter, water, sanitation andhygiene (WASH), health, household essentialitems, education) as well as specific needs (phys-ical and functional rehabilitation, psychosocialsupport). Once the person is assessed, the Hand-icap International referral focal point decideson possible internal and/or external referrals.As much as possible, Handicap Internationaltries to refer to the services that already exist, toavoid duplication. However, whenever the serviceis not available or is of insufficient quality, Hand-icap International can provide complementarydirect services (see below) which vary dependingon the context and the identified gaps. Referralsnot only provide information but also establisha connection between the individual or householdand the external actor receiving the referral.
Handicap International can directly provideidentified beneficiaries with physical and func-tional rehabilitation and psychosocial supportservices, as well as with emergency livelihoodsupport such as cash assistance. e cash assis-tance is unconditional, to support the most vul-nerable households to meet their basic needs,including food and shelter. In the Bekaa regionof Lebanon, Handicap International also providesnewcomers – refugees who have been in thecountry less than 30 days – with essential house-
By Lydia de Leeuw
Lydia de Leeuw is the Regional Inclusion Programme Manager for bothHelpAge International and Handicap International in the Syria crisis.She has extensive experience in the Middle East working on refugeeprotection, rights based advocacy, research, and project management,and holds a BSc and MSc in Criminology.
Thanks to Becky Achan, Technical Advisor on Inclusion with Handicap International andHelpAge International in Jordan, who helped conceptualise and develop the article outline.
The situation of older refugeesand refugees with disabilities,injuries, and chronic diseasesin the Syria crisis
Field Article

91
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Hameeda Salamat (65) sits in the family's apartment in Irbid. “I have diabetes and highblood pressure,” explains Hameeda. “I didn’t receive any medication here in Jordan so wehave been buying medicine with our own money. But the new medicines I received weredifferent and made me sick.” Saadiyeh recalls: “She was very sick for a week. Then thehospital made sure she got back to using her old medication, which she had been usingfor seven years already. After that she became better.” Despite being registered withUNCHR, the family was not aware that they are entitled to get the medication for free,using the proof of their UNHCR registration. The Handicap International mobile teamprovided the family with information regarding their access to free medication.
Ahmad KhairBirjawi (67) takes a rest after doing rehabilitation exercises with a HandicapInternational physiotherapist (Abu Samra, Tripoli, Lebanon). Ahmed suffers from diabetesand cardiovascular disease. Complications of his diabetes led to the amputation of hislower right leg in 2006. Because of the fighting in his hometown, he and his family wereforced to flee to Lebanon. Even though the sun is shining outside, their place is cold andhumid. Ahmed doesn’t go outside much. As the family lives on the second floor, it isextremely difficult to carry Ahmed down the stairs, so he normally doesn’t get to leavethe building. A small plateau outside the front door of the apartment is the only outsidespace that is accessible for Ahmed.“We are looking for another place to live, somewherewhere there is an equal bottom floor so that he can go outside,” says his wife, Ilham.
Salem Kasha (35) with his wife and children live in a small apartment in El Mina, Tripoli,Lebanon. Salem was injured in a bombing close to his family home in Aleppo. He is nowreceiving rehabilitative care for his injuries, provided by Handicap International. Stillfaced with pain and limited mobility, Salem is unable to work. The lack of an income is anincreasing problem for his family. “I have problems moving my right hand. Now I cannotwork because of my hand, and I don’t know what to do anymore. I feel desperate. Wehave registered ourselves as refugees, but do not receive any support.” Without anincome, the family’s financial reserves have finished, and paying the rent has becomeimpossible. “I am asking the landlord to wait for the next payment,” says Salem.
1 Hidden victims of the Syrian crisis: disabled, injured and older refugees. Jointly published by HelpAge International and Handicap International. 2014
©L. de Leeuw /Handicap International – HelpAge International, Irbid, Jordan, 2014
©L. de Leeuw /Handicap International – HelpAge International, Tripoli, Lebanon, 2014
©L. de Leeuw /Handicap International – HelpAge International, Tripoli, Lebanon, 2014
hold items. is in kind support for newcomers is har-monised throughout Lebanon. e package is comprisedof a hygiene kit, a kitchen kit, a baby kit (if needed), mat-tresses and blankets. e World Food Programme (WFP)complements all Handicap International’s Household Es-sential Items kits in Bekaa with a food parcel.
Hidden victims of the Syria crisisExtensive operational experience of Handicap Internationaland HelpAge International has shown that people withdisabilities and older people are oen overlooked incrises. Due to a variety of obstacles they oen faceparticular difficulty in accessing humanitarian assistance,especially when the available services or facilities are notadapted and not accessible or suitable for them. At thesame time, due to their age, serious medical conditionand/or disability, these groups are oen disproportionallyaffected by crisis and displacement. Mainstream healthresponses in humanitarian crises largely fail to addressthe needs of those with manageable chronic health con-ditions. People living with non-communicable diseasesmay face limited access to care and interruption of theirtreatment. e subsequent interruptions in their treatmentcan result in severe complications, including stroke (dueto hypertension) and gangrene foot or blindness (due tocomplications of diabetes), which inevitably leads to in-creasing levels of morbidity, disability, and mortality.During displacement, people – in particular older people– who have specific nutritional needs may face challengesin accessing the food they need. is can lead to bothqualitative and quantitative malnutrition. Refugees livingwith a disability can face protection risks and increasedvulnerability due to lack of physically accessible emergencyservices, breakdown in their support system, or the lossof assistive device(s).
As in many other crises, the Syria crisis response washampered by a lack of disaggregated data on olderrefugees, and refugees living with a disabilities, injury, orchronic disease. erefore, in late 2013, HelpAge Inter-national and Handicap International undertook a studyin Jordan and Lebanon aimed at creating robust evidenceand data on the numbers and basic and specific needs ofolder refugees and refugees living with an injury, im-pairment or chronic condition1. e study also comparedthe needs of these oen marginalised groups to the needsof the wider refugee population in these countries.
For the data collection, 3,202 refugees were surveyedin seven governorates in Jordan and Lebanon. All membersof households were enumerated, interviewed and screened.Older people were identified as those aged 60 years andabove. e survey found that 22% were affected by animpairment, of which 6% were affected by a severe im-pairment. One in five surveyed refugees was living withmore than one impairment. Older people were dispro-portionately affected by impairments, with a staggering70% of those aged above 60 years presenting with at leastone impairment. Older people were also almost twice aslikely as children to present with intellectual impairments.In the study it was found that of the surveyed refugees,15.6% were affected by chronic disease. An age analysisshowed there are three main profiles affected: peopleaged up to 30 years, of whom 10% are affected by chronicdiseases; those aged 30-50 years, of whom 30% areaffected; and those aged 50 years or over, of whom half
Field Article. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .

92
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Saadiyah (47) is working on a dress in Irbid, Jordan
©L.
de
Leeu
w /H
andi
cap
Inte
rnat
iona
l – H
elpA
ge In
tern
atio
nal,
Irbid
, Jor
dan,
201
4are affected. is profile of different age groupsand prevalence of chronic conditions can be in-strumental to inform the design and delivery ofhealth services in the Syria response.
e Syrian conflict has been noted for itshighly disabling impact on the Syrian populationdue to the levels of conflict related injuries. iswas confirmed by this study in which 5.7% ofsurveyed refugees have a significant injury, i.e.one that has an impact on body function andhence a potentially disabling effect. e over-whelming majority – 4 out of 5 injuries – wasdirectly caused by the conflict. is means thatin Jordan, 1 in 15 Syrian refugees have been in-jured as a result of the war. In Lebanon this is 1in 30 refugees. Consistent with the nature ofthe conflict, bombing, shrapnel wounds andgunshots account for a large proportion ofinjuries (58%). Additionally, of those reportinginjury, 25% resulted from accidents such as fallsand burns – accidents that become more commonby living in homes damaged by the conflict orfleeing attack.
Humanitarian implications of theexisting needse prevalence of chronic diseases among Syrianrefugees in Jordan and Lebanon (15.6%) tells ushow widespread the needs in this regard are. InJordan and Lebanon, the three most commonreasons for refugees seeking healthcare resultfrom chronic conditions, specifically diabetes,cardiovascular conditions and lung disease. De-spite this priority need, many refugees face in-surmountable challenges in covering the costof accessing health services. In Lebanon, somerefugees stated that they were unable to affordthe cost of transport to health centres, let alonethe required 25% contribution to their hospitalbills. Several chronic conditions also imply day-to-day expenses, such as the cost of needles,blood glucose test strips or syringes.
Besides the financial barrier, there is also agap in the quality of the management of chronicdiseases in Jordan and Lebanon. A health as-
sessment carried out by HelpAge Internationalfound there was almost no health education forpatients, there was limited capacity among healthstaff to assess patients with chronic diseasesproperly, limited services available to supportearly screening for chronic diseases such as di-abetes and hypertension, and no proper moni-toring with laboratory tests or follow up. Finally,there is a gap in terms of prevention; muchmore can be done to raise awareness aroundhealthy living and diet. HelpAge Internationaland Handicap International are working withlocal partners to improve prevention, as well asidentification and referral of those with non-communicable disease, and to support the na-tional health systems to improve levels of care.
With regard to the humanitarian implicationsof injuries among Syrian refugees, it is clearthat the need for care and assistance reaches farbeyond the emergency response. Many injuredrefugees are struggling to find long-term physicalrehabilitation care, as well as post-operativecare. ere is a lack of complete post-operativecare. Handicap International’s intervention, pro-viding physical rehabilitation services, is notenough without other actors helping. e limitedavailability of physical rehabilitation support isa worrying issue. Where physical rehabilitationcare can mitigate the development of potentiallypermanent disability, the lack thereof can leadto the worsening of existing injury-related healthconditions. Handicap International’s interventionshave revealed high numbers of injuries leadingto amputation, as well as spinal cord injuriescaused by shelling and gunshots, which result inserious and sometimes permanent impairments.Beyond immediate health care, these complexinjuries require long term physical rehabilitation,psychological support, and for those with per-manent impairments, sometimes lifelong care.
Recommendations Humanitarian actors and national systems strug-gle to cope with the high numbers of injuries,chronic conditions and impairments, and the
continuous influx of new refugees. e mid andlong term implications of injuries among Syrianrefugees require that national and internationalhealth care providers work together in a collab-orative effort to address the current needs ofthis population, but also prepare for the longerterm financial and human resource requirementsneeded to prepare health systems, families andcommunities to ensure adequate support. Inparticular, all stakeholders need to prioritiselong-term physical rehabilitation care and post-surgical care adequately, according to the preva-lence and types of injuries inflicted.
Furthermore, it is critical that long termhealth planning in Jordan and Lebanon takesaccount of the need for prevention, monitoringand regular treatment for non-communicablediseases to avoid heightened levels of both im-pairment requiring further care, and ultimatelyto reduce levels of morbidity and mortality. iscould be done through awareness raising aroundhealthy living and diet, health education for pa-tients, capacity building among health staff toproperly assess patients with chronic diseases,increased early screening or monitoring ofchronic diseases such as diabetes and hyperten-sion, with laboratory tests or follow up.
Current and past experiences indicate thatoverall, a ‘twin-track’ approach to addressingbasic and specific needs of refugees affected byinjury, impairment or chronic disease, providesthe best safeguard for equal access to servicesfor all. In a twin track approach, actors ensurethat – on the one hand – they integrate refugeeswith specific needs into their mainstream pro-gramming to the largest extent possible and –on the other hand – where necessary, activitiesare designed to target people with specific needsseparately. For example, a refugee in a wheelchairshould be able to access latrines in a camp likeeveryone else (accessible WASH design – main-stream approach) but might also require physicalrehabilitation support for his legs amputation(targeted activity by a specialised agency). Bothtargeted and mainstream activities are essentialto ensure the full integration of refugees withspecific needs in the overall humanitarian re-sponse. In the Syria response there have beenmany good examples of both targeted and main-stream responses. However, with the currentneeds, a continuation and expansion of both isrequired.
For more information, contact: Regional: Lydia de Leeuw, email: [email protected], tel: +962 789226128Jordan: Becky Achan, email: [email protected], tel: +962 788858651Lebanon: Boram Lee, email: [email protected], tel: +961 76993330
For questions regarding Handicap Internation-al’s operational response in the region, contact:Anne Garella, Regional Emergency Represen-tative, [email protected]
Field Article

93
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
The founding team of the JordanHealth Aid Society (JHAS) in 2005comprised Jordanians keen to en-force local leadership in order to
respond effectively to humanitarian needs ofvulnerable population groups (see a profileon JHAS in this edition of Field Exchange).One of the earliest humanitarian calls towhich JHAS responded was the Iraqi crisis.Since then, JHAS has increased its experience,expertise and collaborative working relation-ships to respond to different humanitarianemergencies in the Middle East and NorthAfrica (MENA) region. JHAS missions haveincluded emergency response teams com-prising experienced medical and non-medicalsupporting staff deployed to the Gaza strip,South Sudan, Yemen and Libya.
Over the years, JHAS had established asolid network of primary static and mobilehealth care clinics in Jordan where differentprimary medical and health services havebeen incorporated. With the onset of theSyrian crisis in March 2011, humanitarianand health aid responses in Jordan began anew chapter. In the earliest stages of theSyrian crisis, humanitarian aid was providedto assemble refugee camps and to supportemergency/life-saving aid. However, accessto quality nutrition among refugees with spe-cific nutritional requirements, such as pregnantand lactating women (PLW) and infants andyoung children, was limited since only generalfood rations were provided. At the same time,food insecurity due to social, health and pro-tection issues was an identified problem butremained unresolved. e situation becameeven more complicated with refugees’ urban-isation, as resources like food coupons hadto be exchanged for shelter and other basicsurvival needs. According to UNHCR regis-tration records, the total number of Syrianrefugees in Jordan had reached 597, 328 byJune 2014 of which only 16.26% are hostedin refugee camps. e remainder of Syrianrefugees have settled within host communities.1
With the escalation of the Syrian crisis,agencies with experience of humanitariannutrition programme implementation, suchas MEDAIR and Médecins Sans Frontières(MSF), pointed out critical issues that couldaggravate the already complex and challengingnutritional situation of the refugee population,such as poor shelter conditions, limited generalfood rations, cold winters and very poor hy-giene conditions, which commonly predisposeto impaired health status. Appropriate nu-trition programming during the early stagesof the Syrian crisis was constrained by a lackof updated data on malnutrition prevalenceamongst the Syrian refugees. National pre-crisis data from Syria (2009) recorded a preva-
lence of 12% wasting, 10% underweight and28% stunting which while not ideal, were notat emergency levels. However, given the un-folding situation, it was clear that there was aneed for an up-to-date nutrition survey forthis refugee population.
In November 2012, a nutrition survey ofSyrian refugees in Jordan found a 5.1% preva-lence of wasting2 among children under fiveyears in host communities and 5.8% in Zaataricamp (the main camp for Syrian refugees inJordan), 8.2% stunting in host communitiesand 15.9% in Zaatari camp, and 2% under-weight in host communities and 6.3% in Za-atari camp3. Although these results were nota trigger for ‘emergency’ nutrition interven-tions, they did raise concerns amongst thenutrition group of humanitarian agenciesworking in Jordan, about the need to maintainsystematic screening and surveillance, espe-cially for vulnerable population groups suchas children and PLW. is was especially aconcern as refugees continued to arrive inJordan in ever increasing numbers. In linewith this thinking, integration of medical nu-trition services into primary health careseemed a sound approach to facilitate earlydiagnosis of malnutrition, thereby helpingprevent an increased prevalence of acute mal-nutrition.
Programming through partnershipJHAS and MEDAIR partnered in 2013 to im-plement a comprehensive programme onCommunity-based Management of AcuteMalnutrition (CMAM) and Infant and YoungChild Feeding (IYCF) practices. Initially, theJHAS-MEDAIR partnership introducedscreening for acute malnutrition indicatorsto the primary medical practice within JHASclinics in January 2013. is was preceded bya comprehensive IYCF/ CMAM training inDecember 2012 of selected staff (medicaldoctors, nurses, midwives, health educatorsand community outreach workers). FromJanuary to October 2013, MUAC only wasused in screening. Weight for height (WFH)was added to screening in October 2013 inpreparation for implementing the outpatienttherapeutic programme (OTP) and the sup-plementary feeding programme (SFP), sinceboth use WFH as an admission criterion andfor follow-up. JHAS, with technical supportfrom MEDAIR , has become a lead agency inJordan with capacity to implement this typeof programme.
Experiencesof emergencynutritionprogrammingin JordanBy Ruba Ahmad Abu-Taleb
Ruba Ahmad Abu-Talebis Nutrition coordinatorat Jordan Health AidSociety (JHAS). Sheliaises between nationaland international NGOsand JHAS relating to all
nutrition activities and oversees theimplementation of all nutrition and healtheducation related activities within JHAS clinicsand outreach structures.
The author gratefully acknowledges the workand support of Dr Ann Burton, HealthUnit/UNHCR, and Gabriele Fänder, RegionalHealth and Nutrition Advisor for MEDAIR. Theauthor would sincerely like to acknowledgecontinual technical support and adviceoffered by UNHCR and MEDAIR to integratenutrition services into primary health servicesof JHAS clinics and for integrating nutritionprofessionals into JHAS clinic teams. Theauthor would also like to express profoundgratitude and deep regards to the continualguidance and support of JHAS founder (Dr.Yaroup Al-Ajlouni) and JHAS projects manager(Nicola Dababneh). Sincere thanks also go tothe various departments of JHAS for their kindcooperation and valuable insights.
1 Source: data.unhcr.org, 20142 Based on weight-for height (WFH)3 Inter-agency nutrition assessment Syrian refugees in
Jordan host communities and Zaatari camp. Final report.January 2013. Available from UNHCR Syria response online portal at http://data.unhcr.org/syrianrefugees/ country.php?id=107
Field Article
Preparing for a Super CerealPlus porridge demonstration
JHA
S, Jo
rdan
, 201
4
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .

94
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
partnership between UNHCR and JHAS hasfurther strengthened the capacity of JHAS tobecome the first line healthcare provider forthe Syrian refugees in Jordan. JHAS staff haveregularly attended national health sector meet-ings and sub-working groups, which has al-lowed JHAS to participate in identifying keystrategic areas for humanitarian interventionsin health and nutrition.
e credibility of JHAS has been enhancedby participation in a number of trainings.MEDAIR has conducted trainings on CMAMand IYCF for health workers in JHAS on aregular basis. At Nutrition Working Grouplevel, JHAS attended training on SFP imple-mentation organised by WFP for partneragencies. At the regional level, selected JHASstaff attended a Middle East and North Africa(MENA) Region Nutrition in Emergenciestraining. While these trainings have beentechnical in nature, they have also equippedtrainees with an understanding of the pro-tection rights of refugees, as well as the needto be considerate of specific social, culturaland psychological characteristics of those ac-cessing services.
Implementation of the nutritionprogrammes Guidance developmentAlthough prevalence of acute malnutritionhas been low, the Nutrition Working Group5
advocated for preparedness measures, suchas draing context-specific guidelines andstandard operating protocols for the treatmentof acute malnutrition and anaemia. e Nu-trition Working Group assembled a task forceconsisting of JHAS, MEDAIR and Save theChildren Jordan (SCJ) to dra operationalguidelines for the integrated management ofacute malnutrition and management of irondeficiency anaemia in pregnancy.
e CMAM programme Syrian refugee children and PLW have beenregarded as the most vulnerable populationgroup and therefore, are the primary targetgroup in the CMAM programme. e pro-
Table 1: Preliminary results* of blood Hbstatus survey in targeted groupswithin camp and urban settings
Zaatari Camp Non-camp (urban)settings
Women 15-49years
45.0 % 31.0 %
Children under5 years
49.0 % 25.9%
Table 2: Admission and discharge criteria toinpatient care (SAM with medicalcomplications)
Admission criteria Transfer toOTP/SFP
Children6-59months
Medicalcomplicationsstabilised
Successfulappetite test
Children transferto either OTP orSFP dependingon theiranthropometricstatus
Bilateral pitting oedema++ or any grade ofbilateral pitting oedemawith severe wasting.
Table 3: Admission and discharge criteriafor OTP (SAM without medicalcomplications)
Admissioncriteria
Discharge criteria
Children6-59months
WFH lessthan -3 zscoresand/orMUAC of lessthan11.5cms
Bilateralpittingoedema +and ++
Dischargedfrominpatientcare
Anthropometric dischargecriteria as above
WFH < -3 z score orMUAC< 11.5 cm PLUSany of the followingmedical complications:• Anorexia• Intractable vomiting• Convulsions• Lethargy, not alert• Unconscious• Lower respiratory
tract infection• High fever• Severe dehydration• Severe anaemia• Hypoglycaemia• Hypothermia
Children are dischargedaccording to their admissioncriteria:• WFH greater than -3 z
scores at two consecutive visits and/or
• MUAC greater than or equal to 11.5 cm at two consecutive visits
• 15% weight gain (from admission weight when free of oedema)
• No oedema for two consecutive weeks
• Clinically well and alert
*Reported figures in the table are preliminary and final resultsare yet to be officially reported.
A number of agencies, including UNHCR,UNICEF, WFP and Centres for Disease Con-trol and Prevention (CDC), collaborated toplan and implement another nutrition surveyin April 2014. JHAS, in partnership withMEDAIR, participated in supervising surveyteams and in the data collection component.e survey targeted Syrian refugee children(0-5 years old) and women of child bearingage ((CBA); 15-49 years old). e surveymeasured MUAC, WFH and blood haemo-globin (Hb) status. In addition, respondentswere asked questions about food securitystatus, water, sanitation and hygiene (WASH)conditions of refugee families, as well as polioand measles vaccination coverage. Preliminaryresults4 indicate alarming levels of iron defi-ciency anaemia among women and childrenwithin both camps and urban settings (seeTable 1). Global acute malnutrition (GAM)rates were relatively low: GAM (MUAC based)prevalence was 1.5% inside Zaatari camp and0.4% outside the camp (urban setting). How-ever, findings for many other indicators thatdirectly or indirectly impact on nutrition –anaemia prevalence, compromised food se-curity, IYCF practices, shelter and WASHconditions – all confirmed concerns of a riskof a worsening nutritional status of the Syrianrefugee population. us, the nutrition sub-working group is currently looking for op-portunities to scale up nutrition programmesand introduce other potentially needed in-terventions.
Aer almost 18 months since JHAS startedapplying malnutrition screening in clinics,JHAS has become the sole agency in Jordanto implement SFPs within urban settings anda comprehensive OTP within camps andurban settings, with ongoing technical supportfrom UNHCR and MEDAIR. e SFP beganas a targeted programme (malnourished chil-dren under 5 years and PLW) and in June2014, was expanded to both blanket and tar-geted programming (through the addition ofall children less than 5 years in JHAS clinicand outreach settings).
Capacity developmentOver 100 national and international non-governmental organisations (NGO) and part-ners of UN agencies have been working inJordan in response to the Syria crisis. e
Table 4: Admission and discharge criteria for SFP (MAM cases)
Admission criteria Discharge criteria
Children6-59months
WFH less than -2 z scores and greater than -3 z scores WFH greater than -2 z scores at two consecutive visits
MUAC less than 12.5cm and greater than or equal to 11.5cm MUAC greater than or equal to 12.5 cm at two consecutive visits
Discharged from OTP Children discharged from OTP should stay in the SFP for a minimum of 2 months
Discharged from inpatient care Children discharged from inpatient care* should stay in the SFP for a minimum of 2 months
PLWs MUAC less than 23cm for pregnant woman in second orthird trimester
MUAC greater than or equal to 23 cm at two consecutive visits or when the infant becomes6 months**Infants aged 6 months and older should be assessed by MUAC and referred appropriately
MUAC less than 23cm for lactating women with infantsyounger than 6 months
* Children stay in inpatient care until their medical condition has stabilised. Afterwards are discharged into OTP or SFP according to their anthropometric (MUAC/WFH) indicators.**If a mother is compliant with the programme but has remained malnourished for more than 4 months, complicating medical conditions or social aspects are investigated and necessary support provided.
4 Results pending (June 2014). Check for updated availability at http://data.unhcr.org/syrianrefugees/regional.php
5 Nutrition is covered in a sub-working group of the Health Working Group. It is co-chaired by UNHCR and Save the Children Jordan.
Field Article. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .

Field Article
95
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
gramme has focused on community mobilisationto maximise coverage, access and compliance.JHAS clinics and outreach settings have beenable to integrate management of acute malnu-trition into their daily working schemes.
e four main elements of the CMAM pro-gramme are management of moderate acutemalnutrition (MAM/SFP), management of severeacute malnutrition (SAM/OTP), inpatient man-agement for severe acute malnutrition withmedical complications (SAM/SC) and communityoutreach. Admission and discharge criteria arereported in Tables 2, 3 and 4.
SFPs and OTPs operate in both Zaatari campand urban settings. In Zaatari camp, JHAS/UN-HCR supports the OTP while SCJ/WFP supportsthe SFP. Outside the camp setting, mobile JHASclinics are employed for remote areas or wheretransport for patients is unavailable, throughwhich CMAM services are made available oraccessed (see Box 1). Within urban settings,JHAS in collaboration with UNHCR andMEDAIR, support nine OTP/SFP sites. iscomprises six JHAS static clinics, one MMU,and two OTP/SFP sites in Jerash and Ajlounimplemented by local community based organ-isations (CBOs) (therapeutic and supplementaryfood provision happens once weekly at eachCBO site). Other mobile services screen formalnutrition using MUAC tapes and refer tothe nearest JHAS clinics.
Both WFH and MUAC criteria are used toassess children and a thorough medical evaluationis conducted on admission. Medication andOTP/SFP foods (Ready to Use erapeutic Food(RUTF) for SAM children and Super CerealPlus for MAM children and PLW’s) are prescribed
according to standard protocols. erapeuticand supplementary food commodities have beenapproved for use in both camp and non-campsettings, which has made it possible to facilitateintegrated CMAM programmes in both con-texts.
For SAM children in particular, physical ex-amination also aims to identify acute medicalconditions requiring hospitalisation. Where suchcases are identified, JHAS facilitates the referralprocess through an established network withaffiliated MoH hospitals. JHAS focal points ineach hospital follow up with admitted cases andprovide timely feedback. Malnourished SAMor MAM children with chronic illnesses aretreated as outpatients, in close cooperation withJHAS nutritionists for potential nutritional sup-port needed. Anthropometric evaluation andmonitoring of PLW’s is conducted solely throughMUAC measurements.
In all urban JHAS clinics and in Zaataricamp, a specific day of the week has beenassigned for OTP/SFP RUTF prescription/RUSFprovision. However if a SAM child is identifiedwithin the week, s/he receives medical and nu-tritional assessment and a RUTF ration untilthe nominated attendance day. On attendance,patients are followed up and monitored andthere are Super Cereal cooking demonstrationsessions. It appears that the exchange of experi-ences between SFP and OTP clients has improvedSFP compliance, i.e. reduced defaulting.
Management of iron deficiency anaemiain pregnancyAs part of standard antenatal care visits, pregnantwomen in JHAS clinics are screened for theirblood Hb status. A blood Hb level less than 11
• One fixed mobile medical unit (MMU) with scheduled trips within southern governorates of Jordan (Tafilah, Kerak, Ma’an, Aqaba, Qatranah and Madaba). This unit provides primary medical care and facilitates secondary referrals through defined local stations in southern governorates. CMAM services are completely supported through the MMU.
• One community outreach team consisting of 10 community health workers, responsible for liaising between refugee population and JHAS in terms of health care services’ provision and UNHCR registration issues.
• One medical team deployed once weekly to remote areas of Jordan (those not covered by the MMU schedule). This team responds torequests from local communities to implement a ‘Free Medical Day6.’
Box 1 Mobile JHAS clinic services
g/dl is classified as moderate anaemia, whereas,a blood Hb status less than 7.9 g/dl is classifiedas severe anaemia. In the latter case, a pregnantwoman will be directly referred for urgentmedical care through JHAS affiliated hospitals.According to operational guidelines developedby the Nutrition Working Group, pregnantwomen receiving antenatal care within JHASclinics receive supplementary doses of iron andfolic acid starting from the second trimester ofpregnancy until 6 months postpartum (see Table5). Pregnant women remain under close medicalsupervision, in case dosage alterations are needed.To date, there has been no specific programmeregarding anaemia in children less than 5 years,however this has been integrated into the Nu-trition Working Group strategy for 2014.
Programme figuresA relatively low number of children have beendiagnosed with SAM or MAM in 2014 in bothurban JHAS clinics and Zaatari camp (see Tables6 and 7). is accords with the 2014 nutritionsurvey data. Given the relatively low caseloadin Zaatari camp, JHAS in coordination withSCJ have had capacity to conduct regular coun-selling visits for SAM patients, especially thosemissing their distributions. is has allowedcaregivers to discuss any constraints they havein programme participation with JHAS staff.
Interestingly, PLW’s have so far representedthe majority of SFP beneficiaries. is has raisedseveral questions around food security and pro-tection issues. is relatively high caseload ofmalnutrition amongst PLW is mirrored in their6 A free medical day is a term used to describe the activity of
providing primary medical care free of charge. This term is used by different community based organisations in Jordan.
Table 5: Guidelines for iron supplementation topregnant women
AgeGroups
Indications forsupplementation
Dosageschedule
Duration
Pregnantwomen
Universalsupplementation
Iron: 60 mg/day Folic acid: 400 μg/day
6 months inpregnancy
Lactatingwomen
Where anaemiaprevalence isabove 40%
Iron: 60 mg/day Folic acid: 400 g/day
6 months inpregnancy, andcontinuing to 3monthspostpartum
Table 6: Malnourished children and PLW’senrolled in urban programmes
Indications for supplementationAccumulative 2014 (week 25, June2014)
Children withMAM
56 children still in SFP
Children withSAM
6 boys in OTP
2 girls in OTP
MalnourishedPLW
88 pregnant women and 78 lactatingwomen in SFPTP6 boys in OTP
Table 7: SAM children enrolledin OTP* within Zaataricamp
Accumulative 2014(week 25, June 2014)
Numberof SAMchildrenin Zaataricamp
23 boys in OTP
23 girls in OTP
*JHAS only implements OTP in Zaatari camp.The SFP is implemented by SCJ, hencefigures are not presented here
Breastfeeding support inan urban clinic in Amman
JHA
S, Jo
rdan
, 201
4
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .

96
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
blood Hb status. e prevalence of iron deficiencyanaemia (IDA) among pregnant women screenedfor their blood Hb status within JHAS clinics in2014 is reported to be 43.16%. e culturalpropensity to early marriage may be partiallycontributing to compromised maternal health,as a pregnant teenager faces increased demandfor nutrients to support both foetal growth andadult maturation.
Challenges and observationsA number of challenges were encountered asMUAC screening was rolled out amongst JHAShealth workers in JHAS clinics and outreach set-tings. Both health practitioners and beneficiarieswere unfamiliar with MUAC measurement, re-sulting in poor MUAC measuring accuracy. iswas oen compounded by caretakers havingdifficulty in calming the child or getting the childto expose the whole of their arm, especially incold weather conditions. In addition, given thevery low initial caseload, some practitioners ques-tioned the value of MUAC as an accurate indicatorof malnutrition, especially when some childrenwho looked pale, weak or detached were foundto have a normal MUAC measurement.
Another challenge faced by JHAS teams wasfostering sufficient understanding of CMAM/IYCF concepts, especially when there was a sig-nificant delay in getting the therapeutic and sup-plementary foods approved and released in Jordan.e first step in procuring the therapeutic andsupplemental food commodities was to decide,at Nutrition Working Group level, which productswere needed. Procurement of Super Cereal Plus(for SFP) and Ready to Use erapeutic Food7
(RUTF) (for OTP) was agreed. WFP was re-sponsible for securing MoH approval to procureSuper Cereal Plus. Although MoH approvalswere granted later than expected, the considerabledelay in launching the SFP was largely due to de-layed custom’s release of Super Cereal Plus andtime taken to secure the necessary Jordan Foodand Drug Administration (JFDA) approvals. Asa learned lesson, the Nutrition Working Groupcontacted all authorities prior to internationalprocurement of RUTF in order to avoid anyfurther delay in implementing the OTP. As aresult, RUTF procurement and JFDA’s approvalsall went smoothly without significant delays.
e delays in SFP and OTP programmingdue to supply issues required stop-gapping at
an operational level. e majority of childrenand PLWs identified as malnourished were reg-ular patients at JHAS clinics so that retrievingtheir records and getting in contact with themwas possible once therapeutic and supplementaryfoods had become available. Although JHASteams were able to overcome the problem ofrefugees changing residence by referring to thenearest JHAS clinic and exchanging patient data,a few patients were untraceable and thereforedropped out because of disconnected phonenumbers.
A challenging part of outreach work hasbeen trying to support young mothers aroundbreastfeeding. Given the cultural norms inSyria, girls become mothers at a very young ageand are usually put under pressure to weanfemale infants to increase the chance of becomingpregnant, hoping that the next child will be aboy. Community outreach workers also reportthat refugees’ interest in, and acceptance of, nu-trition education is compromised. is is par-ticularly the case in refugee extended familycontexts, where cash and shelter needs are pri-oritised over other needs including health andnutrition.
Lessons learnede partnerships with UNHCR and MEDAIRhave given JHAS a wealth of expertise to investin future sustainable national action plans forthe management of acute malnutrition. However,the skills of health and nutrition professionalsat JHAS still need to be strengthened to meetthe needs of different targeted populations.
As JHAS had taken the lead role in screeningfor malnutrition within urban settings, refreshertrainings and frequent supervision visits tohealth workers has provided strong motivationfor JHAS staff.
Although screening and health educationhas gradually been improving, patient compliancewith the SFP/OTP programmes has been difficultto achieve. JHAS nutritionists working in clinicshave therefore linked each patient with MEDAIRcommunity outreach volunteers. is has allowedfor follow up and communication beyond theclinic setting and contributed to better under-standing amongst mothers and caretakers ofthe underlying causes of malnutrition and howto address them.
Other efforts to improve SFP and OTP per-formance have included caretakers’ focus groupdiscussions and cooking sessions in JHAS clinicsto demonstrate optimal Super Cereal cookingmethods and recommended consistency. Mothersused to undercook the Super Cereal Plus whichnegatively affected its taste; satisfaction of mothersand children with Super Cereal Plus has nowimproved. In Zaatari camp, focus group discus-sions and linkages with outreach workers havehugely improved caretakers’ compliance withSAM treatment programmes. Caretakers areasked to return empty RUTF/Super Cereal Pluspackets as one marker of compliance. is has,in turn, been reflected in improvement in thehealth status of SAM children and an increasednumbers of caretakers presenting to JHAS clinicsasking to have their children screened for mal-nutrition.
e low caseload of acute malnutrition inJordan in camps and urban settings has providedroom for gradual capacity building of JHAShealth and nutrition professionals. e experiencefrom this relatively small scale CMAM will be asolid base for JHAS to scale up programmingfor any nutrition emergency.
For more information, contact: Ruba AhmadAbu-Taleb, email: [email protected]: +962 77 7466 610 Web: www.jordanhealthaid.org
7 Plumpy’nut
Field Article
JHA
S, Jo
rdan
, 201
4
JHA
S, Jo
rdan
, 201
4
An urban clinic in Amman
Teaching how to prepare SuperCereal Plus in an Amman clinic
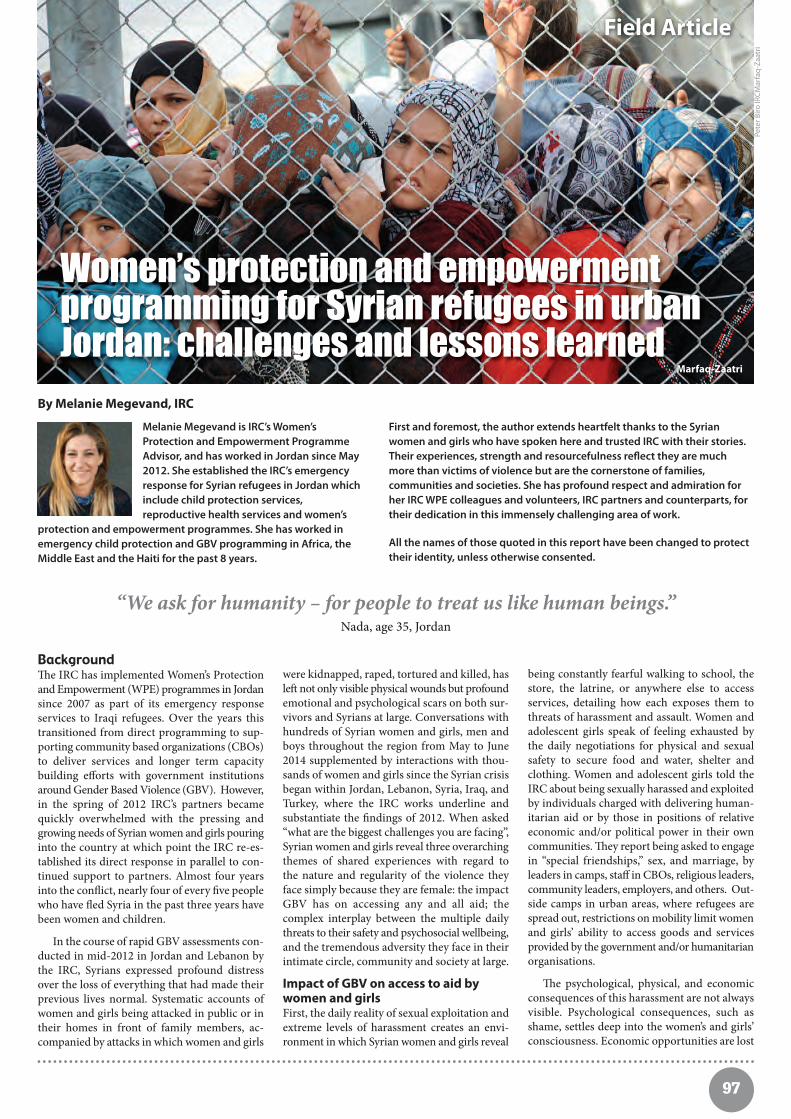
97
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Backgrounde IRC has implemented Women’s Protectionand Empowerment (WPE) programmes in Jordansince 2007 as part of its emergency responseservices to Iraqi refugees. Over the years thistransitioned from direct programming to sup-porting community based organizations (CBOs)to deliver services and longer term capacitybuilding efforts with government institutionsaround Gender Based Violence (GBV). However,in the spring of 2012 IRC’s partners becamequickly overwhelmed with the pressing andgrowing needs of Syrian women and girls pouringinto the country at which point the IRC re-es-tablished its direct response in parallel to con-tinued support to partners. Almost four yearsinto the conflict, nearly four of every five peoplewho have fled Syria in the past three years havebeen women and children.
In the course of rapid GBV assessments con-ducted in mid-2012 in Jordan and Lebanon bythe IRC, Syrians expressed profound distressover the loss of everything that had made theirprevious lives normal. Systematic accounts ofwomen and girls being attacked in public or intheir homes in front of family members, ac-companied by attacks in which women and girls
were kidnapped, raped, tortured and killed, hasle not only visible physical wounds but profoundemotional and psychological scars on both sur-vivors and Syrians at large. Conversations withhundreds of Syrian women and girls, men andboys throughout the region from May to June2014 supplemented by interactions with thou-sands of women and girls since the Syrian crisisbegan within Jordan, Lebanon, Syria, Iraq, andTurkey, where the IRC works underline andsubstantiate the findings of 2012. When asked“what are the biggest challenges you are facing”,Syrian women and girls reveal three overarchingthemes of shared experiences with regard tothe nature and regularity of the violence theyface simply because they are female: the impactGBV has on accessing any and all aid; thecomplex interplay between the multiple dailythreats to their safety and psychosocial wellbeing,and the tremendous adversity they face in theirintimate circle, community and society at large.
Impact of GBV on access to aid bywomen and girlsFirst, the daily reality of sexual exploitation andextreme levels of harassment creates an envi-ronment in which Syrian women and girls reveal
being constantly fearful walking to school, thestore, the latrine, or anywhere else to accessservices, detailing how each exposes them tothreats of harassment and assault. Women andadolescent girls speak of feeling exhausted bythe daily negotiations for physical and sexualsafety to secure food and water, shelter andclothing. Women and adolescent girls told theIRC about being sexually harassed and exploitedby individuals charged with delivering human-itarian aid or by those in positions of relativeeconomic and/or political power in their owncommunities. ey report being asked to engagein “special friendships,” sex, and marriage, byleaders in camps, staff in CBOs, religious leaders,community leaders, employers, and others. Out-side camps in urban areas, where refugees arespread out, restrictions on mobility limit womenand girls’ ability to access goods and servicesprovided by the government and/or humanitarianorganisations.
e psychological, physical, and economicconsequences of this harassment are not alwaysvisible. Psychological consequences, such asshame, settles deep into the women’s and girls’consciousness. Economic opportunities are lost
Women’s protection and empowermentprogramming for Syrian refugees in urbanJordan: challenges and lessons learned
By Melanie Megevand, IRC
Melanie Megevand is IRC’s Women’sProtection and Empowerment ProgrammeAdvisor, and has worked in Jordan since May2012. She established the IRC’s emergencyresponse for Syrian refugees in Jordan whichinclude child protection services,reproductive health services and women’s
protection and empowerment programmes. She has worked inemergency child protection and GBV programming in Africa, theMiddle East and the Haiti for the past 8 years.
“We ask for humanity – for people to treat us like human beings.”Nada, age 35, Jordan
Field Article
Pete
r Biro
IRCM
arfa
q-Za
atri
Marfaq-Zaatri
First and foremost, the author extends heartfelt thanks to the Syrianwomen and girls who have spoken here and trusted IRC with their stories.Their experiences, strength and resourcefulness reflect they are muchmore than victims of violence but are the cornerstone of families,communities and societies. She has profound respect and admiration forher IRC WPE colleagues and volunteers, IRC partners and counterparts, fortheir dedication in this immensely challenging area of work.
All the names of those quoted in this report have been changed to protecttheir identity, unless otherwise consented.

98
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
because women and adolescent girls must curtailactivities outside the home to protect themselvesfrom additional abuse. As the internationalcommunity fails to ensure that all services takeinto account the specific needs and challengeswomen and girls face in accessing services, theyhave developed coping mechanisms respondingto harassment by changing their behaviour,opting to stay home instead of leaving theirhouse or tent, further disenfranchising themfrom access to services. While freedom ofmobility was somewhat limited for many womenand girls prior to displacement, they are unani-mous in saying that increased fear of sexualassault and harassment has placed even furtherrestrictions on displaced women and girls astraditional norms place a heavy and potentiallydangerous responsibility for family honour onwomen and girls. Men and boys we spoke with
concur, explaining that they are raised with theunderstanding that it is their duty to defend thehonour of their families even when it can resultin severe and fatal repercussions for womenand girls, as the mere suggestion of impugningthat honour permits men to commit so-calledhonour crimes. A recent report commissionedby UNHCR which surveyed 135 female headsof households taking refuge in Egypt, Jordan,and Lebanon showed that approximately halfof the women interviewed le the house less intheir host country than when they were living inSyria.1 Women reported feeling isolated and im-prisoned in their own homes.2 Further, 60% ofwomen expressed feelings of insecurity, and onein three women stated that they felt too scaredor overwhelmed to leave their homes at all.3
e vast majority of women and girls are re-luctant to seek help when harassed, fearing fortheir safety or the safety of their families, aswell as possible deportation or retaliation bytheir host community. For those abused by land-lords or employers, their greatest fear was losingtheir income or their home. As a response tothese threats, their world becomes smaller andlonelier, but not necessarily safer.
Domestic violenceSecond, women and girls shared with us thattheir homes are not places of refuge and theyspeak of increased incidents of domestic violence.Indeed, over the past year in both Jordan andLebanon, more than 70% of violent incidentsreported to IRC WPE staff happened in refugees’homes. Of those incidents, 80% were perpetratedby an intimate partner or someone known tothe victim.4 Women and adolescent girls sharewith us their perception of increased physicaland emotional violence from their husbandssince fleeing Syria attributing this “yelling andbeating” as men’s way of coping with the stressof trauma and of being a refugee. One womantold the IRC:
“My husband beats me, and I think this stemsfrom a psychological problem…he is relieving
the stress because he is beating me.” Mona, age 21, Lebanon.
Other women speak about the lack of employ-ment opportunities available for their husbands,resulting in their inability to fulfil their traditionalrole as the family provider:
“Men are becoming angry – they can’t providefor their family. My husband wasn’t a smoker –now he is. He is extremely irritated all the time
and takes it out on the kids. He is violenttowards the kids; he is violent towards me.”
Farah, age 38, Jordan.
Others perceive causes of the increased physicaland emotional abuse due to the fact that
“when a woman goes out to do the shopping or get coupons, he isn’t grateful. No, he is the opposite. He gets angrier, making commentslike: “You didn’t cook; you didn’t work today.
His anger increases.”Haifa, age 41, Jordan.
Women also mention other refugee realities: menbeing frustrated by the lack of privacy to engagein sexual relations with their wives, a sense ofhopelessness regarding the future, and constantconcern over meeting basic needs for the household(i.e., rent, food, water, shelter, clothing, and healthcare costs). One woman noted:
“I have to think with my husband how to paythe rent…we are always fighting, especially
because of these living conditions.” Samira, Age 19, Turkey.
e physical and emotional toll of this violenceon women and adolescent girls impacts everyaspect of their lives keeping them isolated, afraidand dependent on those who abuse them. Despitethe stark impact of domestic violence, the hu-manitarian community has been reluctant toaddress it, seeing such violence as a privatematter outside the scope of traditional aid man-dates. is hesitancy must stop. Aid is system-atically organized and filtered through heads ofhouseholds (who are almost always male). Yetwomen and girls repeatedly disclose incidents ofdomestic violence citing leverage and control ofaccess to services as part of their abusers’ tactics.
Women need programmes that confront thisreality. is in turn requires a change in both
Zaeemah, age 34, Jordan “I want my voice to be heard everywhere– so that everyone can feel with us.”
In late 2013, I fled Syria aer myhusband was briefly detained. In Jordan,our once loving relationship quickly grewtense and my husband became moreviolent. It is illegal for him to work andgrowing frustrated with his inability toprovide for their family, he began hittingme and our children. I’ve lost all respectfor him because of how he treats ourchildren. I have so much love for mychildren – they have missed out on a lotof things, and I blame him for not beingable to help them and not treating themwell. When he is hitting me or them I justcry a lot - I try not to, but I do. “Despitetaking contraceptives, I recently learnedthat I am pregnant. I feel suffocated. Myhusband can’t handle any more kids. Weboth felt that we did not want to haveanother child with each other. I’ve triedto get an abortion, but here it isn’tallowed. I see similar situationshappening with my neighbours andrelatives. I still have hope – everymoment I feel guilty that I can’t help myhusband and I know deep down I stilllove him, but for now…the world is dark.”
IRC
1 We Just Keep Silent – Gender-based violence amongst Syrian refugees in the Kurdistan Region of Iraq, UN WOMEN (April 2014) http://uniraq.org/images/documents/ We%20 Just%20Keep%20Silent%20final%20English.pdf
2 See the Syria Regional Refugee Response Inter-Agency Regional Sharing Portal. http://data.unhcr.org/syrianrefugees/settlement.php?id=176&country=107®ion=77
3 We Just Keep Silent – Gender-based violence amongst Syrian refugees in the Kurdistan Region of Iraq, UN WOMEN (April 2014) http://uniraq.org/images/documents/We%20 Just%20Keep%20Silent%20final%20English.pdf
4 This information comes from the Gender-based Violence IMS using the Gender-based Violence IMS Classification Tool, which consists of six types of gender-based violence, their definitions, and a standardized approach for classifying incidents.
Field Article
IRC women’s center
Mer
edith
Hut
chis
on/IR
C

99
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
the scale of programming and the approachesbeing used. On-going domestic violence cannotbe addressed by programmes that treat violenceagainst women and girls as a one-time occurrence,with discrete one-off interventions to heal woundsor prosecute perpetrators. All sectors of aidmust take stock of the hostile dynamics thatfuel domestic violence when aid remains headof household centric.
Early and forced marriagesird, Syrian women and girls talk about earlyand forced marriage in the specific context ofconflict, displacement and dwindling resources.While acknowledging that early marriage is acustomary practice in Syria, Syrian adolescentgirls explain that the way in which marriage iscarried out has changed since the conflict asthey are forced to marry at younger ages, mar-
rying men who in other circumstances wouldnot have been considered suitable, are exposedto more violence in and out of the home, andfind it increasingly difficult to access servicessuch as healthcare and education once married.
“In my case, I got married really young [at 13].It’s very hard for me to get pregnant. It was
really hard to get a child; I had 5 miscarriages.I am now in debt because I paid for the
injection to get pregnant...My husband wantsto divorce me.”
Zain, age 18, Lebanon.
Fear for refugee girls’ safety exacerbated byovercrowding in homes and tents, financial con-siderations, and questions parents and girls haveabout the utility of girls attending school in thehost country strongly influence the justificationfor early marriage. Women and adolescent girls,and in some cases men as well, said if therewere other options available, these early andforced marriages would not take place or atleast be delayed.
ere can be no question that displacementfrom Syria, compounded by obstacles to educa-tion, contributes to early marriages and doublesthe threat for adolescent girls already experiencingdangerously challenged lives. Yet, the conse-quences of early and forced marriage are notonly are traumatising; they can be fatal. enewly married girl faces a host of challenges in-cluding ongoing displacement, difficulties indealing with the responsibilities of marriageand taking care of the household, physical andemotional abuse inflicted by their husband orhusband’s family, and difficulty conceiving orexperiencing health complications associatedwith adolescent pregnancy. Pregnancy is con-sistently among the leading causes of death forgirls aged 15 to 19 worldwide,5 and girls youngerthan fieen are five times more likely to die inchildbirth than women in their twenties.6 Inaddition, domestic violence poses a significantdanger for married adolescent girls. In manyinstances, married women and adolescent girlsreport that these challenges become groundsfor divorce. Because divorce represents a stainon the sense of family honour, violence againstthe woman or girl may increase and her socialmobility is further restricted.
“My father does not allow me to go outbecause I’m divorced and I need to protect my honour. Neighbours look at me when I[do] go out, even to a close place, as if I’m
eccentric. I always hear that they talk badlyabout me. My eldest brother hits and insults
me if I insist on going out.”Haya, age 16, Syria
IRC Women’s Protection andEmpowerment programme Syrian women share with us their fear for thesafety of their daughters and oen make choicesmeant to protect them in the short term, knowingthese decisions could harm them in the longterm. e reality is these women do not haveclear or easy choices to make for themselves orfor their children. e IRC Women’s Protection
and Empowerment programme provides servicesto an average of 2000 women every month inJordan. Its design combines prevention, em-powerment, response and coordination activities,guided by the use and triangulation of multipleassessment tools including safety audits, servicemappings, community mappings, focus groupdiscussions and individual interviews. Primarilyconducted with Syrian women and girls (althoughmen and boys are also consulted) the tools arespecifically tailored to outline the main needs,challenges and barriers in availability and accessto services, as well as dynamics of GBV thatwomen and girls face. e IRC plays an activecoordination role working with national andsub-national working groups, governmental de-partments, as well as local and internationalhumanitarian organisations to ensure womenand girls’ needs are taken into account acrosshumanitarian sectors, and that services for GBVsurvivors are comprehensive.
Providing quality survivor-centred servicesincluding case management, and psychologicalsupport is the bedrock of IRC programming.ese confidential services were initially em-bedded in amongst the first fully female staffedprimary and reproductive health clinics inRamtha and Mafraq and continue to be at thecore of our programming in 2014. As we gainedthe valuable trust of the Jordanian and Syriancommunities, we were able to expand our servicesat the request of women and girls within theurban communities of Irbid, Rmatha and Mafraqthrough the establishment of women centresthat serve as “safe spaces” where both refugeeand host country women and girls can attend.
Sabeen, age 15, Lebanon
One day I came home to my fatherarguing with my mother, saying it wastime for me to get married. He wanted toarrange a match with my cousin, puttingme under a man’s protection andreducing the family’s financial burden. Itold my father that I didn’t want to getmarried – that I didn’t love this man,and my mother said she thought I wastoo young. However, less than a weeklater I was called into the house andfound a Sheikh waiting with my fatherand future husband. We were wed rightthere and then – it was a total shock forme, but I wasn’t able to do anything tostop it. I had such big dreams – I wantedto be a fashion designer, but now I’mtrapped in this marriage-which for me islike a prison. I am not allowed to go toschool, I feel depressed. I used to ignorewhat is happening inside me, but all ofthese feelings are accumulating, and Iam afraid I will explode.”
IRC
5 See International Centre for Research on Women. Child Marriage Facts and Figures. http://www.icrw.org/child-marriage-facts-and-figures
6 See International Centre for Research on Women. Child Marriage Facts and Figures. http://www.icrw.org/child-marriage-facts-and-figures
A Syrian woman and her niecein a refugee camp in Jordan
Mer
edith
Hut
chis
on/IR
C
Field Article

100
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
e IRC was subsequently asked to lead similarprogramming in Za’atari camp for women andgirls. Women and girls have told us that withoutthese spaces, many women and girls would notbe allowed to go anywhere. e IRC Centresfocus on strengthening informal support networksamong women and girls to promote copingwith the trauma of displacement, and buildingon the resilience of women and girls to supportcommunity-based protection mechanisms. eIRC supports a broad range of group psychosocialactivities in the form of skills trainings, infor-mation sessions, non-formal education, repro-ductive health classes and other trainings thatare designed, informed, and led by women andgirls in the safe space. ese Women Centresserve as entry points for survivors of physicaland sexual violence where they will not face thestigma attached to being a survivor of violenceand by extension, promoting help-seeking be-haviour. Survivors can report incidents confi-dentially, and access services including counsellingand healthcare. Age-appropriate services andsupport in the same centre are available. InJordan over 11,000 women and girls have takenpart in healing activities or services at IRC-supported centres in 2013 and more than 6,000women and girls have received psychosocialsupport from IRC psychologists.
Cash assistance to mitigate risksSexual exploitation, early and forced marriagesand unprecedented levels of domestic violencewere identified by women and girls, as well asmen and boys, as triggered by lack of economicmeans and opportunities for women and girls.In response and following IRC safety audits andcommunity based safety planning, cash assistancewas identified as a response to reduce multiplerisks for women and girls. IRCs cash assistanceprogramme, which uses ATM bankcards, providesfamilies up to 120 Jordanian Dinars per month(about USD $180) for six months. It has benefittedover 2,400 refugee families to date. In addition,over 13,400 “dignity kits” consisting of sanitarynapkins, soap and other essential items havebeen distributed to women and girls of repro-ductive age. During the winter months, special-
ized kits are provided to help vulnerable familiesmake it through sub-zero temperatures.
Supporting and increasing women and girls’decision-making power and their access to, andcontrol over, economic resources are a key aspectof IRC’s prevention efforts particularly in urbansettings. is material and financial supportmitigates and aims to contribute to reducingthe risk of domestic violence, sexual and otherforms of exploitation as well as other harmfulcoping mechanisms. Given the current challengesfacing Syrian women and girls economic activitiesalone – without giving due attention to protectivemechanisms – can create additional violence ifmen feel threatened by women’s new economicstatus, and if women are expected to managesums of money that may put them at risk in thecommunity without support on how to safelydo so. Supporting women to access and controlmoney therefore provides an important partsafety measure and the experience shows riskscan be addressed through partnership withwomen and informed programmes.7 Participatingin social and economic activities creates protectivemechanisms for women and girls – allowingthem to rebuild social connections and networks
that have been severed because of conflict.Women and girls networks gives them a rarespace and opportunity to talk amongst themselves– without supervision or control from others intheir lives – about their specific issues and prob-lems, and oen serves as a place of support andhealing. In addition, expanding economic op-portunities can be a protective factor as it allowswomen and girls to avoid harmful economicactivities leading to sexual exploitation.
Conclusionse international community has been promisingfor years to bring the interests of women andgirls from the margins of service provision tothe mainstream of humanitarian programming.An apparent and understandable sense of hope-lessness is setting in for many Syrian womenand girls as we fail to act. Critically, for womenand girls the need is for immediate action notonly to make women and girls safe from ex-ploitation and abuse, but empowered to beactive participants in their homes, communitiesand their own lives. e humanitarian commu-nity’s will to prioritize the needs of women andgirls in both word and deed is the most criticalkey to success as we are all accountable forbringing women and girls from the margins ofservice provision to the mainstream of human-itarian programming. Women and girls’ voicesmust be a key force in driving humanitarian ac-tion. UN agencies, non-governmental organi-sations, host and donor governments must seekout and value women and girls’ perspectivesacross all services and be held accountable forapplying the minimum standards as laid out inthe Interagency Guidelines for the Preventionand Response to GBV.
For more information, contact: Melanie Megevand, email: [email protected]
7 IRC Gender discussion research brief http://gbvresponders. org/empowerment/eae-evidence/ Economic household discussion group tools: http://gbvresponders.org/ empowerment/eae-tools-resources/ IRC Gender discussion research brief: http://gbvresponders.org/empowerment/eae-evidence/ and Economic household discussion group tools: http://gbvresponders.org/empowerment/eae-tools-resources/
Ned
Col
t /IR
C
IRC volunteer Rania speaks with a Syrian refugee at a refugee camp in Jordan.Rania is a Syrian refugee who meets with as many as 50 families per week toinform them about available programming and support in the camp.
Field Article
A Syrian refugee girl paints at achildren’s play area at an IRC
women’s center at Zaatari camp.
Mer
edith
Hut
chis
on /
IRC

101
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
By Luigi Achilli and Raymond Apthorpe
Luigi Achilli is research associateat the Institut Français du Proche-Orient (IFPO) in Amman. He holdsan M.A. and a Ph.D. in politicalanthropology from the School ofOriental and African Studies(SOAS). His research and writing
focus on everyday forms of political engagement anddisengagements, political identity, nationalism,Palestinian issues, refugees and refugee camps, and thepolitics of space. He is currently working on thereverberation of the Arab Spring in Jordan.
Raymond Apthorpe is ananthropologist specialising inapplied humanitarian anddevelopment aid studies. He iscurrently the Vice President ofCouncil of the RoyalAnthropological Institute,
London. Currently Raymond is a Visiting Professor-elect,London School Economics and Political Science; and aprofessorial research associate at School of Oriental andAfrican Studies, University of London. He undertook thiswork with ENN on a voluntary basis.
Luigi and Raymond extend sincere thanks extendsincere thanks to UPP, UNHCR, Medair, Save the ChildrenJordan; many other humanitarian agencies’ staff,national and international, who helped us in variousways; the individual scholars and other professionalswho shared insights with us and at times accompaniedus, and Tara Shoham (ENN volunteer) for setting upmost of our meetings and taking part in them.
J700
Methode collection of data relied mainly on40 individual interviews and two focusgroup discussions held over a period of20 days in February 2014. e interviewsof refugees, aid personnel, scholars andothers on which this paper is based wereplanned in advance where possible andbased on a schedule of questions coveringkey thematic areas of interest as developedwith input from ENN and the nutritionsub-working group in Jordan. Neverthe-less, in the event much depended on thevagaries of chance and access, and who,when it came to an actual meeting, werewilling to make themselves available tous, and how far they would go in ad-dressing what turned out to include somehighly controversial issues. e researchwas carried out in various parts of thecountry. Our interviews involved severalvisits to non-governmental organisation(NGO) field offices in Amman, Karakand the Jordan Valley, one visit to Zaataricamp and two visits in two informaltented settlements (ITS) - Deir ‘Alla andMafraq respectively. Of course, for aproperly social anthropological study(that would be based more on social ob-servation, participant involvement, andgenerally ‘being indeed living there’ thanreliance on interviewing), a much longertime for fieldwork is needed, besidestime to access all the available literaturethat directly or indirectly could be ofhelp to this type of study. e analyticalperspective we designed emerged as ourobservations proceeded.
Setting the scene is special edition of Field Exchangecontains descriptions of the different sit-uations of Syrian refugees in Jordan.Some live in official camps, others donot; some did, but many have movedout since. rough our research we weretold of a number who were in ‘informaltented settlements’ (ITS) who chose orin instances, were moved1 to campswhether they originated there or not;most ITS dwellers we heard about, fornow anyway, remain in these largely serv-ice-less places. Some Syrians fled to Jordanat the very outset of the conflict, othersare still coming. In addition, while thetotal number of Syrian refugees in Jordan(and elsewhere) is very high, those whoalready resided in Jordan prior to thecivil war should also be taken into account.An added complication is that whilemany refugees have registered with theUNHCR, many others have not, or mustmanage while their re-registration is stillpending. e vast majority of Syrianrefugees we met by most accounts aretotally or only partly unaware of whatrelief services there are for refugees, whilethose that are – and have registered – arenot all accessing them2. Furthermore,from our inquiries, it appears some Syriansdo not register, either as refugees orasylum seekers, as they consider them-selves in transit and en route to anothercountry. ey believe that having thelabel ‘refugee’ would only hinder that.In one informal tented settlement we
The social life ofnutrition amongSyrian refugeesin Jordan
Saka
h M
alka
wi/W
FP, J
orda
n, 2
014
ResearchAs the ENN embarked on developing this special edition of Field Exchange inSeptember 2013, it was clear that most of the articles would describe theexperiences of programming staff. We wished to redress the balance a little byfeaturing refugee and host population social experiences of the multi-faceted areaof nutrition. Given very limited resources, this capture could only extend to thecollation of a small number of individual refugee experiences in Jordan. Weengaged two enthusiastic anthropologists, Luigi and Raymond, and an equallyenthused volunteer graduate, Tara, to undertake this work and add a freshperspective. is article shares what they found and their personal reflections onwhat they saw and heard in the process.
As the authors state at the outset, this is not a study of a representative sample ofaffected refugees and no conclusions should be drawn regarding the nature andimpact of the response in Jordan; there is extensive work on this that can beaccessed at the UNHCR Syria response portal(http://data.unhcr.org/syrianrefugees/regional.php).
1 “On Sunday 5 January, residents of Informal Tented Settlements around Greater Mafraq municipality were evicted and forced to move.” See minutes Informal Tented Settlements Taskforce Meeting(meeting date: 9 January 2014). Also, during the researchers field visit in the Jordan valley, a former site was pointed out to us, with the information from the Jordanian Women’s Union (JWU) that its former occupants had been relocated.
2 It is important to note that UNHCR evidence shows
that 96% of registered refugees have access to MoH services. In a UNHCR supported survey of registeredrefugees, nearly all households (91.7%) knew refugeechildren younger than 5 years have free access to vaccination, and 96.3% knew that all UNHCR registered refugees have free access to governmentalservices at primary health centres and hospitals. Only 65.8% were aware that refugees who can't access governmental health services could seek services at UNHCR-supported health facilities.
.............................................................

102
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Fatima is a 25 year old woman from Homs. On the 20th July 2013, she left Syria and crossedthe border into Jordan with her husband and her two children aged 8 and 10 years. They spentone night in Zaatari Camp for registration purposes; the following day, the whole familymoved to Karak, where they are now living.
Fatima works part time for Save the Children Jordan for 10 JOD per day, three days per week.She is the only one to work: her children are too young and her husband is disabled – his rightarm was severely injured by a bomb in Syria. The work is regular but the salary too meagre tocope with the daily expenses. To pay the rent of the house, the family sell their monthly foodvouchers. The voucher value is 96 JOD, but they sell it only for 60 JOD.
The family would like to have different types of food, but they cannot afford to. They eatpotatoes almost every day, only on Friday can they afford to have meat, generally poultry. Fatima laments her incapacity to feed her children and husband with a more varied andbalanced diet, especially meat and vegetables. However, she also claims that her first prioritywould be to give her children sweets. She comments: “you know, if I could buy food, the firstfood I would buy is chocolate for my children. At the school, (Jordanian) children make fun ofthem. All the other children have snacks, but they don’t have anything but bread. They mockthem calling ‘Syrian dogs6’ because they are different. I’m afraid; I don’t want my childrengrowing up thieves because of the hardships that they have to endure!”
Umm Khalil lives in Zaatari Camp. She left Syria with her two children in 2012 to join herhusband who was already living in the camp. The husband had left Syria one month earlierafter deserting the regular army.
The woman does not work. Her two grown up children and her husband are not in steadyemployment; they alternated between petty jobs and long periods of economic inactivity.Like many other refugees in and outside Zaatari Camp, the family sells the food vouchers thatit receives periodically from the WFP to afford diverse types of food such as dairy products andfresh meat.
Umm Khalil says that they cannot afford healthy complementary foods such as fruit andvegetables as the voucher will not cover this price. She also blames the family’s poor diet onthe logic of “wasta” that relegates them to the margins of refugees’ political economy. The term“wasta” indicates the use of family connections and relationships of patronage that are centralin the search of jobs, credit, and favours in the region. Umm Khalil claims that access to regularjobs, and hence to better food, in the camp’s informal market is determined by a smallcommunity of Syrian refugees originating from a specific part of the Syrian governorate ofDara’a. Being one of the first communities of Syrians to settle down in the camp, they have hadthe time to consolidate their power over the newcomers. According to Umm Khalili, “there ismafia in the camp! These people are generally related through kinship. This means that theydecide who can work and who cannot work. They are also those who can decide who can selltheir vouchers and who cannot. Others decide what kind of food can be bought, and theyhave access to better food because they have money.”
were told that no one had registered as a refugee be-cause of fear of their information being made knownto Syrian officials or because they saw no benefit toregistration since they normally moved in search ofwork (see Box 1). So, simply what a ‘refugee’ isexactly – or inexactly – can be a puzzle. Equally im-portant, forced migration may be due to a numberof different factors – social, economic, and political.Any overall nutritional profiling must allow for thiscomplex picture.
As two social anthropologists, the ENN asked us toponder and probe some of the social – and human –aspects of emergency nutrition for the Syrian refugeesin Jordan as a contribution to this special issue ofField Exchange. On the basis of a month’s ‘fieldwork’in Jordan (March 2014 plus a few days reflecting andwriting, in April), what we could aim to do was ofcourse limited, but threefold: (a) to model the socialside of nutrition arranged and integrated with thebio-medical side and bring it to the fore as ‘the sociallife of nutrition’; (b) to rehearse something of what a‘beneficiaries’-oriented study of the social aspects ofnutrition in a refugee population should aim to con-sider4, and why; (c) to interview as many refugeehouseholds or household members and ‘focus groups’as possible in the circumstances as to their nutritionalstatus and issues, and report briefly our findings.
Nutrition as a social as well as a bio-medical processNutrition is integral to and arranged as part of thesocial life of people. It has social, economic andpolitical pre-conditions, dimensions, and aspects.Refugees’ social lives, like other peoples’, affect andare affected by their nutrition and malnutrition (seeBox 2). at refugees do have social lives of theirown, despite being treated by relief agencies for ad-ministrative purposes just as displaced demographiccategories – such as ‘refugee women’, ‘refugee men’,‘refugee infants and children’, and such – must itselfbe a major point to make at the outset of this analysis.Refugees should be studied as people as well asrefugees. Besides their refugee needs and concerns,they have everyday agendas of their own about theirnon-refugee ordinary lives5, whether or not theseagendas are known to the authorities.
By way of introduction, three points are highlightedto begin with. First, we soon found that for all kindsand categories of refugees in Jordan we met, ‘foodsecurity’ is the overriding issue in their estimation.Second, the overwhelming household priority forthose who do not live in refugee camps and settlements– generally said to amount to some 80 per cent of thetotal – is somehow to meet the high rent that landlords
Box 2 What type of nutrition?
Box 3 Political economy
Research
We visited a Jordanian Women’s Union (JWU) centre in the Jordan valley region, opened in2007 by a former school teacher, followed by two nearby ITSs. The JWU runs social,educational, awareness raising and vocational activities, as well as occasionally providingmedical services by visiting doctors in at least one of the ITSs. Many in the medical tents are illdue to exposure to the pesticides they use in the greenhouses where they work3 , moreoverthere are no facilities in the tented settlements to wash, go to the toilet, and no clean water.“The poverty is taking away our children’s childhood” someone said. Households pay 25JD permonth to have a tent on the land where they work. Syrian refugees work alongside Egyptianrefugees but earn less money: Syrians - 1JD per hour, Egyptians - 1 ½ JD per hour.
It is mainly the women who work in the greenhouses, and sometimes the children. Thenorthern Syrian’s have brought this culture here. Southern Syrian men do work (especially ifthey are educated). Their diet is poor in protein. They receive some vegetables, as well as pay,but they sell them for extra income. Their e-cards, which are not exchangeable for cash, are forpurchasing food and other items for up to 24JD per month (12 JD every two weeks) per family.It costs however 1JD to go to the mall in Salt to use them. The e -card was introduced to stoprefugees selling their vouchers – agency staff considered that, assuming the proceeds wouldnot be spent on food, this would inevitably negatively affect refugees’ diet. However, as mostpeople in the tents don’t register as refugees, they are not entitled to receive e-vouchers.Interviewees gave two reasons behind this decision: first, they are too afraid, thinking thattheir information might be given to the secret police who will then send them back to Syriaand secondly, many have a very nomadic style of life, moving from one work place to another,so it is not beneficial for them to register.
Box 1 e-voucher and the issue of registration
3 This is based on reports from the refugees and staff from the JWU4 What are generally termed ‘beneficiary’ studies tend to focus on
selected target groups or supposed representatives of these at a particular point – or points – in time. Loose use of the ‘beneficiary’ word – such as ‘we have served 10s of 1000s of beneficiaries’ – is practically meaningless sociologically as well as administratively. Cf. Raymond Apthorpe. 2012. Effective aid: the poetics of some aidworkers’ angles on how humanitarian aid ‘works’. Third World Quarterly. Special Issue, Vol 33, No 8.
5 Cf. Achilli, L. Palestinian refugees and identity: nationalism, politics,and the everyday, I.B.Tauris. Forthcoming.
6 The researchers felt it important to cite the exact words used and not sanitize others’ statements. However in doing so, it is equally important to reinforce the point that the opinion expressed reflects the experience of a single person and, as such, should not be extended to the totality of Syrian refugees’ experience.

103
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
demand for basement accommodation space.7
ird, food has not only nutritional values butit is also politically, socially, and culturallydefined.
During our fieldwork we could observe, forexample, how refugees’ political economy andinstitutions shape and limit individual andhousehold choice over what to eat and when(see Box 3). Likewise, individual tastes arestrictly intertwined with cultural preference; allaffect people’s nutritional patterns. Virtuallyeverywhere we went we were told no one likedthe taste of the World Food Programme (WFP)supplied Super Cereal relief ration food. Ap-parently, unless you were in a position to affordto find and add sugar, no one would want to eatit (see Box 4). Neither, again according to whatwe saw or heard practically everywhere we went,would refugees eat frozen meat or fish, evenwhere it was available and affordable. Some saidit had a bad taste, others doubted that the use-by dates on frozen food were reliable (given thecommon practice in some stores of switchingoff power at night to economise on costs). Yetothers said that “though those who travel andare modern eat frozen food, we [ordinary folk]do not” (see Box 5). Regarding dairy products,in Zaatari camp and elsewhere, people told usthat while at home in Syria these were availableand affordable, they had do without them inJordan and use only powered milk; an inferiorsubstitute, as they saw it, which again theywould avoid.
All in all, to what extent, even in extremitiesof situations, people, refugees included, will orwill not change their cultural values and prefer-ences and for example, accept to eat whateverthey can get simply to survive, remains to besocially researched as a matter of refugees’knowledge, attitudes, and practices anywhere,let alone in Jordan specifically. Our impressionsare that perhaps even in emergencies, culturalpreferences may tend to harden. Despite thepopular idea that in emergencies and otherstressful times there is nothing but social break-down, our fieldwork and other accounts docu-ment the extents to which ordinary social insti-tutions and practices continue to be part of thesocial scene despite disruptions and otherchanges. Refugee camp, and non-camp, life isno exception. at in some extremities suchavoidances and indeed other social and culturalpractices do change and perhaps break down is
another scenario – but under what kinds ofpressures, against which alternatives, at whatthresholds, and with what outcomes?
Nutrition is already an inter-sectorNutrition is not just one thing, with sharply de-fined boundaries, but many things, itself an in-ter-sector. Towards better addressing ‘nutrition’amongst Syrian refugees in Jordan, it must beremembered that nutritional status depends onmany things at once, not on diet and food intakealone.
To begin with, it is worth noting how ‘shelter’and ‘health’ are part and parcel of refugees’ nu-trition issues. For example, chronic health con-ditions can have a big impact on all age categories.At the same time, extremes of climate andweather as in Jordan can mean that poor sheltercan be deleterious, especially in the winter, tohealth and nutrition. Similarly, all of our in-formants – either development and humanitarianaid agency staff or Syrian refugees – appreciated
the many contributing factors to malnutrition.None pointed to material shortage of food toexplain the cases of undernutrition among them.
Another consideration is the new policy inJordan of cash aid that has gained ground inthe form of ordinary vouchers and, more recently,e-vouchers. Indications from our work are thatvouchers for food items are actively traded by arange of purchasers. Social protection, in thesense of household socio-economic-health se-curity, may involve a family selling its vouchersfor a much lower price than its value (oen at aloss to the seller of 12 per cent) in order to sup-plement a meagre family budget. As to whomsuch vouchers are sold, it is to other refugees, tothe host population, and sometimes even toaid-workers, as for instance in the Zaatari camp(where there are currently an estimated 3,000aid staff). Needless to say, these transactionsare detrimental to refugees’ ‘proper’ nutrition.
Abu Omar spent two weeks in Zaatari Camp before moving to Deir Alla in the Jordan Valley. He leftthe camp because one of his children was very sick, and he knew a Syrian doctor who lived in theJordan Valley. He rented a house in Deir Alla where he now lives whit his wife and children.
Abu Omar used to be a teacher in Syria but is now a plasterer/decorator. He is earning 7JOD perday. Despite living in hardships with a salary that barely covers the rent of his flat, the man claims tobe in a far better situation of those Syrian refugees who live in ITSs near his house. These peoplehave established their settlements on the very lands where they work. Households rely primarily onagricultural waged labour - an unsteady source of income that tends to vanish as the winterapproaches.
Abu Omar has a fridge and, with that, a far richer diet than his country mates who leave just nearbyin the ITS, who relay mostly on tinned/boxed foods. He and his family can afford to eat cheese,olives, olive oil, rice, lentils, beans, vegetable and eggs.
However, despite the “luxury” of owning a fridge, like people living in the ITS, Abu Omar does noteat meat. The WFP voucher allows him to buy only frozen meat. Frozen meat, however, is widelybelieved among Syrian refugees to be poisonous and toxic. Dishonest sellers are rumored tochange the ‘use by’ date on the packaging of the meat or turn of the fridges at night – to saveelectricity – and then refreeze the meat. As Abu Omar put it, “people who travel might eat it, but itis not good, it tastes different. We don’t even know whether is halal [‘permissible’ under Islamicdietary guidelines]”.
7 See http://data.unhcr.org/syrianrefugees/country.php?id=107.Din
a_El
-Kas
saby
/WFP
, Jor
dan,
201
4
Box 5 “Dangerous” food
Research
Shadi and his wife, a young couple in their early twenties, have a 2 year old daughter and anotherchild, only days from birth, when we met them. They came to Jordan partly because they felt unsafein Syria. They spent 15 days in Zaatari camp and then left because of its poor conditions, to join anaunt who was living nearby.
Shadi farmed sheep in Syria and is now doing the same for a Jordanian employer. They do not payrent for their accommodation in season, only out of the season, but they have to travel far into thecentre of the city to buy the food with the vouchers provided by WFP, which is expensive. They seekto buy the same food that they bought in Syria, but lament the lack of sheep’s milk and cheese. Theydo not like the meat which they could buy with the WFP voucher as it is frozen and so, they claim,unhealthy.
Shadi’s wife was identified as moderately malnourished during screening, on account of inadequatecalorie intake during her pregnancy. She is, however, suspicious of the WFP’s specialised SuperCereal Plus for the treatment and prevention of moderate acute malnutrition among Syrian refugeewomen and children with which she has been supplied. It tastes wrong, she claims, the procedure tocook it is too complicated, and as we observed, there is not always agreement on how to prepare it(the international aid worker, and the national nutrition staffer, robustly disagreed as to exactly whatquantities to mix). Social protection in the sense of household socio-economic-health security mayinvolve a family selling its WFP-supplied Super Cereal Plus at the roadside for a much lower pricethan its value to supplement a meagre family budget.
Box 4 Super Cereal Plus
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .

104
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
From our discussions, we cannot judge whatoverall difference the introduction of vouchershas made to nutrition amongst those we spoketo and certainly not in the refugee populationat large, What we can reflect is that much islikely to depend on specifics, such as whatfood/non-food items, if available, vouchers canbe spent on; where, at what time intervals; andas a market in vouchers develops (including inZaatari camp) precisely who sells and who buys,why and what then is done with the proceeds.
In this context, nutrition’s social protectiondimension is also evident in several regards.Violent social relations among refugees and be-tween them and/or the host community may bedirectly or indirectly interconnected with nutritionin various ways. For example, most of the casesof malnutrition reported to us were amongstSyrian refugees living in the ITS. It is likely thatsub-standard living conditions and inadequateWASH contributed to the poor nutrition situationthat we observed. Yet, ITS have increasingly be-come a default option for those refugees – mostlycoming from the governorates of Aleppo, Hama,and Rural Damascus – who le Zaatari also be-cause of the inter-community tensions withinthe camp as well as issues like lack of privacy andfreedom of movement, feelings of being impris-oned, and humiliation. Another example ofrefugee host population tensions surfacing occursin relation to the strong dislike of the taste ofWFP-supplied relief food – one refugee interviewedwondered whether it might be poisonous, giventhat it was not also made available to their poorJordanian neighbours!
Finally, in this short listing of essential in-fluences, household social-time managementneeds to be taken into account towards under-standing refugees’ decision-making about nu-trition. For example, on being told by a refugeethat she “had not enough time” to take bestcare of the nutrition of her infants, it turnedout this was because of the elderly and infirmshe had to care for too. Since she was largelyconfined to her home space, she was not able toget about much – for example, to the clinic tohave her children screened, vaccinated or lookedaer when ill. She had become socially isolatedcompared with her life before and as a result,not able to cope and manage well. e nutritionand health of her children suffered as a result.
Nutrition and humanitarian reliefNutrition is intimately linked with personalmatters of health, individual and household in-come and a whole range of issues important forsocial policy and administration – such as vul-nerability criteria, ease of access, and effectivetargeting.
For Syrian refugees in Jordan, access needsto be considered in terms of access on the partof the relief agencies to their target populations,and access on the part of these populations tothe agencies (see Box 6). is dichotomy hasobvious implications. For example, internationalagencies’ views on who are the most vulnerableand in greatest need may differ considerablyfrom those of the refugees themselves. In addition,
NGO and UN vulnerability criteria tend tochange over time. In the short time we had forthis research and with the resources available tous, we were unable to track such changes andcome to any conclusion about overall outcomesand impacts.
A further complication is that straightforwardemergency response is rarely unbound fromwhat we consider a developmental agenda or atleast a longer term strategy. Nutrition as wehave seen is itself inter-sectoral. Like otheremergency assistance provision, a nutritionalprogramme may also be, besides one of targetedrelief, a project of selective nutritional reform.A case in point is, for example, what cameacross to us as an “educational war” in Jordanbetween, on the one side, the advocates of breast-feeding and, on the other, users of infant formula.If such a war is indeed being waged, it is hard totell which side is losing or winning – and atwhat costs. Organisations such as Save theChildren Jordan (SCJ) strongly advocate breast-feeding support as do international agenciessuch as Medair who kindly invited us to seesome of their work first hand. SCJ’s Coordinatorfor Nutrition - who co-chairs with UNHCR theNutrition Working Group for the Syrian refugees- showed us in Zaatari camp how SCJ provideseducation and skilled support on optimal breast-feeding practices9. e challenge for SCJ andsimilar agencies is that most Syrian refugees inZaatari are from rural areas in Syria whereinfant formula is commonly used to feed infants.For those we interviewed, this is because, besidesthe convenience offered through formula feeding,“it is also the modern way to go”. For us thisraises some questions we found impossible toanswer, such as what level of compromise is ap-propriate between an aid agency’s public healthinterest approach and the individuals own choice,which in turn, is a function of their own valuesand responses to their circumstances and con-ditions. And furthermore, to what length shouldthe aid response go to, to achieve behaviouraland social chance in an emergency context?
As we see it, a relief organisation that embarkson this type of social and nutritional re-educationin the context of a relief programme, sometimesusing the same programme and staff, has bothemergency relief and development objectivesin that they are relying on behaviour changes in
an emergency context that may take some time.A question this poses for us (and perhaps re-search) is whether what may be best for thehealth of the population at large is difficult forthe individual to accept and accommodate andconsequently gives the agency a bad name inthe eyes of its intended target population. isis a complex matter to resolve.
Conclusion: The complex socialrelations of nutritione social relations of nutrition are to be soughtin its sociography, that is who knows and inter-relates with who, as well as its social and culturalinstitutions at large, such as what and whoseknowledge, attitudes and customary, seasonalpractices prevail with regard to food, health,nutrition, domestic and political economy andso forth. Hence, as our fieldwork illustrates,there is need for a household and communitysocial context-informed approach to the man-agement of aid programmes and their implan-tation and evaluation. Refugees are people, notswarms of atoms. eir affairs are not simply‘spontaneous’ or automatic ‘reflex’ reactions tochallenges and opportunities. Rather actualhealth and nutritional outcomes are beyond thebio-medical. ey are underpinned by social,political, economic and security variables. eyare therefore informed by patterns of commu-nication and choices whether in the circumstancesthey can be well-informed or not.
Unfortunately, rarely in emergency reliefstudies do the social relations and social issuesin refugees’ everyday lives that affect their nu-trition and health, and indeed all aspects oftheir lives, get the attention they deserve.
For more information, contact: Luigi Achilli,email: [email protected] and RaymondApthorpe, email:[email protected]
Nadia is a 43 year old woman, from a village near Damascus. In May 2013, she crossed into Jordanwith her four children aged between 6 – 15 years. Her husband remained in Syria. She went directlyto Karak by-passing Zaatari Camp, choosing that destination because a relative who moved toJordan before the war would help them settle. Nadia youngest son is very sick, diagnosed with arare chromosome disorder, “he looks 3 years old but is already 6”. An expensive private doctor sheconsulted prescribed a diet rich in protein, however she said she can only afford to buy potatoes.She does not work. Her two eldest children carry out occasional jobs, but irregularly and withoutearning enough to cover even food costs.
Nadia is not enrolled in any programme of assistance. She said that she was never contacted by anyhumanitarian organisation. She had received cash assistance just once, from Save the ChildrenInternational, she said, but since then nothing, no assistance of any kind from any organisation. Itappears that like Nadia, there are numerous other refugees who are unaware of the servicesavailable and/or the criteria of access.
8 Information note from ENN: The supplementary feeding programme only targeted Syrian refugees given their higher vulnerability. Recognising the population’s negative experiences around Super Cereal Plus, considerable work has been done since its introduction to sensitise the population to its value and how it should be prepared. Satisfaction has increased as a result (see articles by Save the Children Jordan and Medair in this 48th edition of Field Exchange).
9 Save the Children Jordan and UNHCR also support targeted provision of infant formula to infants who are not breastfed in Zaatari camp. This aspect of the programming was not encountered by the researchers.
Box 6 A special diet
Research
105
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Views
As of July 2014, there are now over600,000 Syrian refugees in Jordan;with up to 80,000 in camps, and520,000 in urban and rural areas.
e Government of Jordan, civil society andthe international community have all steppedup to meet the enormous needs, both of refugeesand of the Jordanian communities1 affected bythe crisis. e Jordan Refugee Response is thebroad frame for these.
Under the leadership of the Government ofJordan and coordinated by UNHCR, the JordanRefugee Response is a collaborative effort betweenthe donor community, United Nations (UN)agencies, international and national non-gov-ernmental organisations (NGOs), community-based organisations, refugees and Jordaniancommunities.
All levels of the Government of Jordan areengaged in the response, from the Office of thePrime Minister, the Ministry of Foreign Affairs,the Ministry of Interior and the Ministry ofPlanning and International Cooperation(MOPIC), to the line ministries working witheach of the sectors, and the governorates andmunicipalities in refugee-affected areas. In 2014,the Ministry of Interior created the SyrianRefugee Assistance Directorate (SRAD), whichis the primary government entity for the coor-dination of refugee issues in the country.
From an inter-agency perspective, the mainstrategic framework for the response is the
Jordan chapter of the Regional Response Plan(RRP)2. In 2014, 64 partners have appealed fora total of USD 1 Billion through the RRP.Delivery is organised through eight sectors—Cash, Education, Food Security, Health, Non-Food Items (NFIs), Protection, Shelter, andWater, Sanitation and Hygiene (WASH). esectors are linked through an Inter-Sector Work-ing Group (ISWG) – a meeting of sector chairswith the aim to encourage synergies betweensectors – which in turn reports up to the headsof UN and NGOs who meet together in the In-ter-Agency Task Force (IATF). Nutrition, togetherwith Reproductive Health and Mental Healthand Psychosocial Support Services (MHPSS),are sub-sectors of Health.
Complementary yet independent from thesestructures, the International NGO (INGO)Forum sets common policies and pursues ad-vocacy initiatives, based on consensus amongthe NGO community. ere are currently 53INGOs signed up to the INGO Forum.
e scale of the refugee response and themyriad of partners and structures involved pro-vide a glimpse into the complexities and chal-lenges faced in achieving effective coordination.is is a massive operation, with staffing numberswell into the thousands. Each organisation hasalso experienced a significant expansion in staffcompared to two years ago. UNHCR alone hasgrown from around 100 staff in 2012 to now al-most 700 staff by mid-2014.
Refugee Coordination pre-dates the Trans-formative Agenda3 and is distinct from theCluster system. More recently it has been reaf-firmed at the global level through the RefugeeCoordination Model4. In short, in collaborationwith the Government of Jordan and mandatedby the UN General Assembly, UNHCR remainsthe coordinating organisation for the entire re-sponse. e time-line for UNHCR’s engagementstretches well beyond the emergency phase. Italso includes longer term care and maintenance,as well as the pursuit of durable solutions,through voluntary repatriation, local reintegrationor resettlement to a third country.
At the same time, there are many parallelswith the Cluster system. Key operational UNagencies – especially WFP, UNICEF, WHO andUNFPA – manage sectors in which they havespecific expertise. While UNHCR remains overallthe ‘agency of last resort’, other UN agencies arecommitted to delivery in their sectors, boththrough their own mandates and through a
By Alex Tyler and Jack Byrne
Alex Tyler is Inter-Sector Coordinator for UNHCR Jordan
Jack Byrne is Country Director for IRC and Chair of the INGO Forum for Jordan
1 The response to vulnerable Jordanian populations is built into every project approved by the Government of Jordan; it is mandated that each project responding to refugees must respond to vulnerable host populations. In recognitionof the need to ensure Jordanian communities are effectivelyassisted, both the RRP strategies in 2013 and 2014 have explicitly targeted host communities. In 2014, over 700,000 Jordanians are benefiting from the RRP.
2 Available at http://www.unhcr.org/syriarrp63 For more information, see www.humanitarianinfo.org 4 UNHCR, Refugee Coordination Model, November 2013,
available at http://www.unhcr.org/53679e2c9.pdf
UN and INGO experiencesof coordination in Jordan
WFP
-Jon
atha
n D
umon
t
...........................................................................

106
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
series of global and national memoranda of un-derstanding with UNHCR. International andnational NGOs are crucial at all levels of the re-sponse – from strategic leadership down to thedaily delivery of protection and assistance torefugees and Jordanian communities.
e Cluster system has also set the tone forwhat is expected from coordination; in manyrespects contributing to the professionalisationof coordination as a function within aid work.e efforts of Global Clusters and the Inter-Agency Standing Committee (IASC) have definedstandards and guidelines, many of which areapplicable in refugee situations. ey have alsotried and tested coordination structures andappeal mechanisms – developing best practicesthat have also been adapted by UNHCR andpartners across the region affected by the Syriacrisis.
For instance, adapting best practices, theprocess resulting in Jordan’s RRP has beenrobust. ree months of inclusive planning atthe strategic and sector levels resulted in a clearstrategy, peer-reviewed by sector chairs, andbuilt on over 1,200 projects or activities of the64 appealing partners.
Professionalising coordination clearly hasmany benefits – more efficient systems, reducingduplication and better serving partners’ infor-mation needs. It also brings some risks. WhileUNHCR and many other organisations nowhave dedicated coordination staff in Jordan, thedanger is that coordination structures becomeheavy, overbearing on organisations’ independ-ence and, at worst, self-serving and dislocatedfrom the realities faced by staff at field level andfrom the people we are trying to help. e pro-liferation of coordination structures – the ‘taskforce disease’ – can itself be counter-productive.Too many meetings are particularly onerous onthe smaller international and national NGOs,who do not have the staffing levels necessary toattend them all. One risk is that some partnersopt-out of these meetings, or send junior staff.is can result in actual decision making beingfurther skewed towards the larger organisations.
In Jordan, we have an o repeated mantra tokeep coordination to the “minimum necessaryto facilitate collective action”, and that each newstructure or process proposed needs to demon-strate a clear added value. We have tried variousways to meet this standard. First, regular anony-mous surveys are conducted with sector membersto canvass opinion on the performance of thesectors in general, and also to elicit feedbackfrom sector members on how coordinationstructures can be improved or streamlined5.Secondly, the INGO forum has a seat on the In-ter-Sector Working Group, and is consulted ondesign of these structures. e recent roll out ofcoordination fora in three governorates ofMafraq, Irbid and Amman only went aheadaer extensive discussions with and within theINGO forum. It has to be said that we are notthere yet, and oen find ourselves well beyond
the line of ‘the minimum necessary’, but will gothrough regular ‘retrenchment’ of meetings tokeep this under control.
Investing in Information Management as acoordination service has been important, bothto facilitate planning and implementation bypartners, and to shi coordination meetingsfrom long, round-the-table sessions, to beingmore focused on both strategy developmentand problem-solving. e Jordan response usesa number of portals and platforms to keep part-ners updated. An example is ActivityInfo6 – anonline platform for planning activities and re-porting achievements against pre-defined indi-cators. Originally developed by UNICEF in theDemocratic Republic of the Congo (DRC), Ac-tivityInfo allows partners to log their own ac-tivities and check what everyone else is doingand where7. Used well it is a transparent systemdesigned to empower partners, enabling themto conduct simple gap analysis, generating mapsand charts for their activities and for a geo-graphical area or for the sector as a whole. UN-HCR is aware that partners need some initialsupport and training to be able to use its fullpotential. With high staff turnover this can be achallenge in itself.
From the INGO perspectivee Jordan INGO Forum came together as aninformal group of the handful of organisationsthat had been operating in Jordan before theonset of the Syrian crisis. It has gradually playeda much larger role in overall crisis coordinationas more and more INGOs established themselvesin Amman – with the largest INGOs establishingboth a country and regional offices in the capitalcity. Establishment of the Forum was not at thebehest of donors or UN agencies but rather wasan organic process to meet the needs of members,at first around safety, security, advocacy and in-formation sharing, and then to be importantstakeholders at the table with the UN, the gov-ernment of Jordan, and with donors. e thirteenlargest INGOs operating in Jordan programmewell over $100 million in humanitarian activitiesto aid refugees and vulnerable Jordanians andare some of the most operational actors in thecrisis.
Forum leadership and representation wentthrough a number of iterations, from an informalChair and Co-Chair that facilitated monthlymeetings, to its present structure of a Chair andfour Steering Committee members. At the strate-gic levels, these five people represent INGOs onthe Inter-Agency Task Force, the HumanitarianCountry Team, the Inter-Sector working Groups,monthly meetings with donors, and with thegovernment of Jordan, mainly through interactionwith the MOPIC.
Despite having a legitimate place at the table,achieving meaningful INGO representationwithin existing and new coordination structuresremains a challenge. Some INGOs manage largerbudgets and certainly have greater operationalcapacity than many of the smaller UN agencies.
Conversely, many INGOs are short-term re-sponders with rapid staff turnover, and do nothave the resources to dedicate to the Forum orto the multitude of coordination meetings thattake place on a daily basis. A particular challengefor INGOs and the UN alike are new coordinationmechanisms underway from various stakeholders,which tend to hinder implementation of whathas already been agreed to and blur the linesaround who is doing what. Additional layers ofcoordination need strong justification and buy-in from all involved; otherwise there is the riskof alienating donor agencies who fund thesemechanisms and of driing farther from thereal purpose of our collective response, whichis to assist those affected by the crisis.
It is widely acknowledged among the hu-manitarian community that in Jordan, coordi-nation and communication between and amongINGOs and their counterparts in the UN workswell relative to coordination structures in othercountries in the region. It is critical that INGOscontinue to advocate for issues that affect theirability to operate with neutrality, to choose well-informed representatives to speak for the col-lective, and to engage actively with the UN andthe government of Jordan to protect humanitarianspace in the face of concerns over safety and se-curity, which, while unarguable, will have negativeeffects for Syrians seeking refuge in Jordan andfor Syrians already here.
To conclude, there are traditional rivalriesbetween some organisations – both at the UNlevel and among INGOs. Organisations do com-pete for funds and for responsibilities overdifferent sectors. While organisations do ofcourse recognise that pursuing common goalscollectively is the most effective way to serverefugees’ needs, there is an ever present jostlingfor space between the partners. Coordinationcannot be blind to this, or the pursuit of theoverall goals may be negatively affected. It iskey that structures are balanced, built on mutualrespect, consultative and do provide space forvisibility and independence of organisations.At the same time, no one organisation can go italone, and expect to deliver an impact beyondtheir own project. e strength of the JordanRefugee Response is that it recognises greaterbenefits come from collective action of all theorganisations involved, each bringing to thetable their own skills and expertise in a genuinelyinclusive manner.
More information on refugee coordination inJordan can be found through the Jordan country pages at http://data.unhcr.org/syrian-refugees/country.php?id=107 and in the draCoordination Briefing Kit at http://data.un-hcr.org/syrianrefugees/download.php?id=6379
5 See the latest survey results at http://data.unhcr.org/ syrianrefugees/download.php?id=6158
6 For Jordan, Activityinfo is accessed through the URL www.syrianrefugeeresponse.org
7 See Claire Barnhoorn (2014). Spreading around the globe: ActivityInfo. Field Exchange 47, April 2014. p51. www.ennonline.net/fex/47/spreading
Views

107
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
With funding from UNHCR, In-ternational Medical Corps (IMC)developed and conducted a fivedays Nutrition in Emergencies
(NiE) training course in Arabic, adapted to theSyrian refugee context in Jordan, for 23 healthproviders from national and international non-governmental organisations (NGOs) and UnitedNations (UN) agencies assisting Syrian refugeesliving in Zaatari camp and in host communities.e five days NiE training was conducted fromDecember 16-20, 2012 in Irbid, Jordan. ecourse focused on infant and young child feedingin emergencies (IYCF-E); maternal nutritionand anaemia; chronic diseases and nutrition inemergency context; as well as coordination andnutrition assessments.
Lessons learnt from previous NiE trainingsconducted in Lebanon by the American Uni-versity in Beirut1 (AUB) and the InternationalOrthodox Christian Charities (IOCC)2, discus-sions with UNHCR at field and Geneva level,and information gathered from health providersproviding services to Syrian refuges in Lebanon,Jordan, and Turkey and to Syrians in Syria,were used to develop the Jordan NiE training.All of the above showed that IYCF; micronutrientdeficiencies especially anaemia in women andchildren; maternal nutrition and chronic diseasewere critical contextual issues to address in thetraining. Health care providers and social workersneeded the tools and knowledge to counsel Syr-ians on exclusive breastfeeding and appropriatecomplementary feeding; nutrition interventionfor chronic diseases such as diabetes, heartdisease, hypertension, and obesity; preventionand treatment of anaemia and adequate maternalnutrition; and assessment of nutritional status.
e curriculum for the Jordan NiE was basedon the IASC Harmonised Training Package(HTP)3 developed under the umbrella of theGlobal Nutrition Cluster, which was used todevelop the two previous NiE Arabic trainings
in Lebanon. However, the HTP and the NiEArabic curriculum that already existed did notinclude a module on chronic diseases and theirnutrition intervention in emergencies. Addi-tionally, the HTP did not include a specificmodule on maternal nutrition, but rather hadsome relevant information scattered in the differ-ent modules that needed to be collated. Moreover,the team developed case studies relevant to theSyrian refugee situation in Jordan (camp andnon-camp refugees) which differs from the sit-uation in Lebanon (non-camp refugee setting).
For the chronic diseases presentation, edu-cation materials that had been developed byIMC and AUB for the Iraqi refugees in Lebanonwere used and provided to the Jordan trainees.On one side of the materials there are picturesof what is acceptable and not acceptable to eataccording to the chronic disease diet. On theother side, there is written guidance that thehealth or social worker can provide to the patient.ese materials were felt to be adequate to usefor the Syrian refugees since the pictures wereregion appropriate and the Arabic was the officialArabic that is read in all the Middle East.
On day one of the training, the focus was onthe causes and types of malnutrition in emer-gencies and appropriate nutrition interventionsin emergencies. On day two, the focus was onassessment in emergencies, assessing nutritionstatus and needs of at-risk populations, moni-toring of nutrition interventions, and micronu-trient deficiencies and interventions in emer-gencies. On day three, the focus was on addressingthe needs of pregnant and lactating women inemergencies; common chronic nutrition diseasesand their nutritional management, and consid-erations for chronic disease management in anemergency.
Days four and five, focused on IYCF includingan introduction on IYCF-E, guidance on IYCF- getting to know the Code, and optimal IYCF:
recommendations for breastfeeding and com-plementary feeding guidance and support, breast-feeding mother support, counselling and edu-cation, and operational guidance on IYCF forcommunity health workers, assessment and casemanagement.
Coordination between the sectors, as well asbetween different players providing assistance,was woven into all the presentations. e trainersdrove home the concept that the preventionand treatment of malnutrition requires a multi-sectoral approach and close coordination betweenNGOs, UN agencies, Ministry of Health (MoH),and affected populations. e cluster approachwas mentioned but not detailed since this is arefugee crisis and so coordination is within UN-HCR’s mandate for response.
Daily feedback was solicited from the par-ticipants and an end of training evaluation wasalso conducted. e participants felt that thetraining was of great value to them. ey learntnew skills that will help them improve thequality of their work. ey also appreciated theinteractive format of the training, that the ex-amples and case studies were reality based fromthe Syrian context and that they were providedwith tools to solve current issues that they facein their day to day work.
e main conclusions from this training wasthat there is need to develop an HTP moduleon maternal nutrition and one on chronicdiseases in emergencies as these two are currentlynot fully covered in the HTP modules. Inaddition, there is need for a critical mass oftrained responders to the Syrian crisis on NiE.
For more information, contact: CarolineAbla, email: [email protected]
Experiences on Nutrition in Emergencies Trainingfor Syrian refugees response in Jordan
By Caroline Abla
Caroline Abla is the Director of the Nutrition and Food SecurityDepartment at International Medical Corps. Caroline has over 22years of international experience in managing nutrition and publichealth programmes both in the field and at headquarters. She hasimplemented programmes in Somalia, Rwanda, Burundi, andKenya and has responded to humanitarian emergencies includingnutrition crises in Ethiopia, Niger, Kenya, Darfur, and Haiti.
International Medical Corps would like to acknowledge UNHCR for funding this NiEtraining.
News
1 Source: Dr. Hala Ghattas, American University of Beirut2 Source: Linda Shaker-Berbari, International Orthodox
Christian Charities (IOCC)3 Available at: http://www.ennonline.net/htpversion2/modules
Participants in the NIE training in Jordan in 2012
Caro
line
Abl
a/IM
C, Jo
rdan
, 201
3
...........................................................................
108
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Agency Profile
Name: Jordan Health Aid Society (JHAS)
Address: Um Mutawe Alaslameah Street, Jandweel,building number 69, Amman, Jordan
Phone: +962 795640906
Email: [email protected]
Website: http://www.jordanhealthaid.org/
Year founded: 2005
CEO/President: Dr. Yaroup Al-Ajlouni
No. of HQ staff: 70
No. of staff in Jordan (not HQ): 535
No of staff outside Jordan: 290
In April 2014, the ENN interviewed Ruba Abu Taleb,Nutrition Coordinator with JHAS, about the agency. Rubajoined JHAS in January 2013 as a nutrition coordinatorfor the JHAS/Medair CMAM/IYCF1 programme. She is a
Jordanian national and has a degree in Human Nutrition andDietetics. You can read about JHAS’s nutrition programming inthis edition of Field Exchange.
When was JHAS set up, by whom and why?JHAS is a national non-profit, non-governmental organisation(NGO) serving and supporting the local community in Jordanand the Middle East and North Africa (MENA) region. It wasfounded July 20th, 2005 by a medical doctor who was experiencedin humanitarian work. It was established not due to a specificcrisis situation but to provide medical and health services todisadvantaged population groups in Jordan and the MENAregion. is includes spreading awareness on healthy living anddisease prevention. e main sectors we work in are health,non-food items sector and shelter.
How does JHAS operate?JHAS provides humanitarian services through partnership agree-ments with different United Nations (UN) agencies and otherinternational agencies. For example, through UNHCR, JHASprovides primary health care and facilitates secondary life-saving health care and health services to refugees in Jordan. ewell-established JHAS/UNHCR system is the only referral systemfor secondary health care for the Syrian refugees in Jordan. Itcomprises a central referral hub and an affiliated network ofhospitals. In practice, JHAS liaises with around 17 agenciesworking in primary health care seeking hospital case referrals.As needed, additional funding support is sought from the Emer-gency Relief Fund (ERF)/OCHA to support the capacity of theexisting JHAS/UNHCR system
Interview by Tara Shoham, ENN volunteer
1 Community based management of acute malnutrition/Infant and young child feeding
JHAS supported clinic in Amman
JHA
S, Jo
rdan
, 201
4............................................

109
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
A key partner of JHAS on nutrition in the Syria response isthe NGO MEDAIR; JHAS implements the technical planprovided by MEDAIR to provide nutrition services to vulnerablepopulation groups in Jordan. JHAS is the implementing partnerfor MEDAIR on UNICEF and WFP programmes of work,specifically IYCF and supplementary feeding programming.JHAS is also an implementing partner of both InternationalMedical Corps and Johanniter International, which activitiesinclude medical evacuation of refugees and distribution ofnon-food items.
How is JHAS funded?JHAS does not receive public donations; international agenciesprovide JHAS with implementation plans and associatedfunding, and JHAS provides the space and the staff for the im-plementation of those programmes. JHAS also directly solicitsfunding from the ERF in response to calls for proposals.
How many and what is the professional mix of JHASstaff?JHAS has more than 1,000 employees distributed throughoutdifferent JHAS centres. Staff include medical doctors, generalpractitioners and specialists, pharmacists, nutritionists, nurses,psychotherapists, and other non-medical staff who supportmanagement and information exchange, logistics, reportingand patient registration issues. At JHAS, staff s are classified asmanagement (logistics, finance, and human resources) or pro-grammes (implementation and direct management).
Does JHAS operate outside Jordan?Under its emergency response mandate, JHAS is present withinSyria providing emergency, primary and secondary medicalcare. JHAS is also registered and approved in Egypt and Dubai.JHAS had completed emergency deployments in the Gazastrip, Libya and Darfur at the time of those conflicts. Withinthese countries, JHAS provided medical support through fieldhospitals and assisted in building the capacity of local healthworkers to launch health aid response for their countries.
Has JHAS grown in size since the influx of Syrianrefugees?Since 2009, JHAS has had a partnership agreement withUNHCR for the provision of primary and secondary healthaid to Iraqi refugees in Jordan. However, in partnership andwith continual technical support from UNHCR, JHAS staffinghas increased significantly by several hundred in 2011 inorder to respond adequately to the Syrian crisis. Even beforeZaatari camp opened, Syrians had started to cross over intoJordan. Ever since the JHAS/UNHCR Syrian response pro-gramme was launched, JHAS has provided primary healthcarevia static and mobile clinics and facilitated referral for advancedmedical care for the Syrian refugees in Jordan. Static JHASclinics have always been (then and now) located at vital pointsin different governorates, e.g. Irbid, Mafraq and Amman.JHAS also has mobile medical units which ‘wander’ throughoutsouthern areas of Jordan.
With the opening of Azraq camp (April 2014); there havebeen calls at health sector level in Jordan for contingency plansto deal with an expected large influx of refugees to the camp.Due to the success of the JHAS/UNHCR system in managingpatients’ referral for advanced medical care, it is also thedesignated system for managing Azraq patients’ referrals.
Did JHAS’ nutrition work only begin with the influx ofrefugees from Syria?e JHAS nutrition programme comprising CMAM and IYCFsupport was launched in January 2013. Before that, health andnutrition education messaging was the extent of our nutritionwork with those attending JHAS clinics. rough 2013, thenutrition component of JHAS health services became betterdefined and gradually other programmes have been developedand integrated into the services, such as management of severeacute malnutrition (SAM) (partnered with UNHCR), managementof MAM (MEDAIR-WFP), and management of iron deficiencyanaemia in pregnancy. is has been established alongside theongoing IYCF programme (MEDAIR-UNICEF). Most recently,JHAS participated in the nutrition survey involving UNHCR,UNICEF, WFP, Centres for Disease Control & Prevention (CDC)and implemented by MEDAIR in partnership with JHAS. JHASparticipated in supervising teams and the data collection componentof the survey. At the Nutrition Working Group level, JHAS hasalso participated in draing the operational guidelines for CMAMand for anaemia management.
How did JHAS become the implementing partner on acutemalnutrition in the Jordan response?rough our participation in national health sector meetings andour awareness of all health sector activities, JHAS proposed toimplement the CMAM/IYCF programme in 2012. Since then,JHAS and MEDAIR have worked jointly to support different nu-trition activities.
How would you describe the culture of the organisation?As can be seen from the mission statement, the inherent cultureof JHAS is to provide medical and health services to vulnerablepopulation groups with non-profit aims. JHAS therefore continuouslysearches for opportunities for national and international cooperationwith different NGO’s and UN agencies.
JHAS staff remain in need of further capacity building andtechnical support, especially in relation to adapting to particularcontexts where there is a need to provide health support andadhere to strict humanitarian guidelines. erefore, training hasbeen regarded as an integral part of the JHAS’ recruitment andemployee evaluation process.
How would you describe the culture of the internationalorganisations that have ‘arrived’ in response to the crisis?Are there any challenges to working with theinternational agencies or knowing what is going on?Currently in Jordan there are many different agencies workingand responding to the Syrian crisis. A challenging feature of thecurrent situation is the rapidly increasing demand of healthfacilities and health workers themselves. Once JHAS and otheragencies agreed on unified working schemes, the challengesremained purely technical and these were always quickly resolved.
International agencies acknowledge the fact that they haveaccess to educated staff to work with in Jordan. In many othercountries, they have had to implement programmes themselvesbut in Jordan they are able just to participate in recruiting keylocal staff to oversee programmes. ere have occasionally beencultural differences. For example, the IYCF programme prompteddisagreements regarding how acceptable it is to have a mother ona poster exposing a large area of her breast while breastfeeding.On the whole however, international agencies have worked con-structively and productively with JHAS.
Agency Profile

110
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
During the ENN’s visit to Jordan in March 2014, wehad the opportunity to meet with Marwan I. Al-Hennawy, Head of the Division of Coordination,Communication and programmes at Jordan
Hashemite Charity Organisation (JHCO), and gain an insightinto this national agency that has been at the forefront of hu-manitarian assistance in Jordan.
When was JHCO founded and how did it come about?JHCO was founded in 1990. It is a not-for-profit, non-politicalorganisation. It grew out of an initiative by the Government ofJordan and Prince Al Hasan, Crown Prince at that time, to helpthe Sudanese people during the dry season. When the Iraqicrisis unfolded, the initiative was formulated into JHCO, andbecame a non-governmental organisation (NGO) registeredwith the Ministry of Social Affairs. JHCO went on to work as aninternational NGO, reaching more than 36 countries. JHCO isthe biggest ‘on the ground’ national agency in Jordan, delegatedby the Jordanian government as the operational partner forcountries wishing to present aid to Jordan or other affectedcountries. ere are about 70 staff, all based in Jordan.
What was JHCO’s role in the early Syria response inJordan?At the beginning of the Syria crisis response, the governmentappointed JHCO as the coordinating partner for assistance toSyrian refugees. Many INGOs and United Nations (UN) agenciestherefore work with JHCO.
JHCO put in great effort in the early days of the Syria crisisresponse. “We were almost alone with UNHCR at the very be-ginning, before Zaatari camp was established. e influx happenedso quickly, no one could image the large number of arrivals wewould see per day”. In February 2012, around 50,000 Syrianrefugees crossed the border placing a huge burden on the gov-ernment, UNHCR and JHCO successfully united efforts toestablish a decent life in the camp. JHCO was involved in settingup tents, the registration system and a welcome meal. Many or-ganisations coordinated with JHCO for delivery of aid. Later,JHCO coordinated, with the help of donations, to replace morethan 5,000 tents with prefabricated units to help refugees copewith the approaching winter.
Name: Jordan Hashemite Charity Organisation (JHCO)
Address: Sa'eed Bino St, Khalda, Amman, Jordan
Phone: + 962 6 5523190
Email: [email protected]
Website: www.jhco.org.jo
Year founded: 1990
President: Ayman Reyadd Almefleh
No. of HQ staff: 70
No of staff worldwide: 0
Agency Profile
Interview by Marie McGrath, Field Exchange Editor
WFP
/Jon
atha
n D
umon
t

111
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
What are your current areas of operation?
More than three-quarters of Syrian refugees live outside a campsetting. JHCO now focuses on those living outside the camp,given their high proportion and also because the governmenthas appointed a Syrian Refugees Affairs Department, headed bythe Public Security Directorate, whose focus is to assist camprefugees.
Could you describe the close working relationship youhave with the Jordanian government?
Any NGO in Jordan (whether local or international) must applyto the Ministry of Planning and International Cooperation forapproval of any proposed programme of work. Where appropriate,the Ministry will request that the agency coordinate with JHCOon programming. JHCO’s operational focus is on in-kinddonations and cash assistance. If the proposed work involvesanother operational sector, then other ministries are involved.For example, if it involves education services, the agency mustcoordinate with the Ministry of Education. If it involves health,then the Ministry of Health must be consulted.
If an NGO gets the approval of the Ministry of Planning andInternational Cooperation, then “we work together as a team”.One of JHCO’s strengths is logistics and distribution capacitythroughout Jordan. JHCO has central warehouses in every gov-ernorate. If NGOs need to store items until a distribution plan isdrawn up, these facilities can be used. JHCO provides help withfood and winterisation projects, such as clothes and cashassistance, as well as helping with identification of and access tobeneficiaries. JHCO has a database of Syrian refugees in Jordan.e organisation jointly plans with agencies who should betargeted across all governorates and effects distribution throughJHCO staff, volunteers and community based organisations(CBOs).
Which agencies have you worked with?
JHCO partners include but are not exclusive to the LutheranWorld Federation (LWF), Danish Refugee Council (DRC), In-ternational Orthodox Christian Charities (IOCC), World Visionand Islamic Relief. JHCO co-chairs the food sector with WFPand enjoys good relations with UNHCR, regularly attendingmeetings of the food sector, cash sector and non-food items(NFI) sector.
What other areas of humanitarian assistance are youinvolved with?
A large component of JHCO’s humanitarian assistance is distri-bution of in-kind donations. Many NGOs operating outsideJordan do not have a national branch. Also, there are oen indi-vidual efforts to collect materials for refugees in emergencies;JHCO facilitates the collection and distribution of these donations.For example, in February 2014, JHCO received an IFAD1 donation(Rome) and were asked to distribute on their behalf. e distri-bution plan was sent by JHCO for approval to IFAD, followed indue course by evidence of the distribution. e donations JHCOreceive depend on the season, e.g. in winter, blankets, carpets,clothes and food are common. In summer, food and cash ismore typical. Donated food usually takes account of culturalpreferences and typically includes rice, sugar, canned foods, tea,tahini, beans, pasta and oil.
JHCO are also involved in supporting cash programming,implemented in an agreement with a local bank. Cash payments 1 International Fund for Agricultural Development
Agency Profile
Refugee home north of Jordan
Gab
riele
Fän
der/
Med
air,
Jord
an, 2
014
are made on a monthly basis using an ATM card. JHCO help tofinalise the beneficiaries list and to contact the beneficiaries.Islamic Relief and DRC are two of the agencies JHCO collaboratewith on cash assistance.
Do you provide assistance outside Jordan?
JHCO has been involved in many international responses, suchas the Iraqi crisis, Gaza crisis in 2008 and 2010, and now theSyrian crisis. JHCO do not have an operational presence outsideJordan but typically provide in-kind donations that are distributedby contacts in the affected country. “We never reject any kindof request for assistance”. Requests may come through JHCO’swebsite or through diplomatic channels. For example, the gov-ernment of affected countries may contact the Jordanian gov-ernment via their embassy with a request for assistance. egovernment of Jordan then contacts JHCO. e Jordanianpeople are generous and respond to international disasters withmonetary or in-kind donations to JHCO. Sometimes JHCOcontact local NGOs in Jordan and organise a campaign forurgent assistance for a particular crisis; they usually “comerunning to help”. For international assistance, the governmentof Jordan may provide transport, e.g. a plane, to deliver thedonated supplies.
How are you funded?
JHCO funding mostly comes from the private sector, e.g. privatebanks, individual business owners, universities and individuals –especially those working in the private sector who may donateany annual benefit/bonus to JHCO.
Do you have any final words on the Syrian crisis fromyour perspective?
e Syrian crisis is a huge refugee crisis. Unlike many otherlarge scale disasters in the world, e.g. Haiti 2010 or floods inPakistan, it is not short lived but looks like it will continue.Syrian refugees continue to cross the border into Jordan. Hu-manitarian assistance is a permanent fixture for the foreseeablefuture, as politically there is no cause for optimism regarding asolution in the near future.