Contents lists available at ScienceDirect The Journal of Supercritical Fluids
10
J. of Supercritical Fluids 83 (2013) 47–56 Contents lists available at ScienceDirect The Journal of Supercritical Fluids jou rn al hom epage: www.elsevier.com/locate/supflu Modeling the inactivation of Staphylococcus aureus and Serratia marcescens in clinical solid waste using supercritical fluid carbon dioxide Md. Sohrab Hossain a , Venugopal Balakrishnan b , Nik Norulaini Nik Ab Rahman c , Zainul Ahmad Rajion d , Mohd Omar Ab Kadir a,∗ a Division of Environmental Technology, School of Industrial Technology, Universiti Sains Malaysia, 11800 Penang, Malaysia b Institute for Research in Molecular Medicine, Universiti Sains Malaysia, 11800, Penang, Malaysia c School of Distance Education, Universiti Sains Malaysia, 11800 Penang, Malaysia d School of Dental Science, Universiti Sains Malaysia, 16150 Kubang Kerian, Kelantan, Malaysia a r t i c l e i n f o Article history: Received 26 June 2013 Received in revised form 24 August 2013 Accepted 24 August 2013 Keywords: Clinical solid waste Inactivation modeling Pathogenic bacteria Regrowth Supercritical carbon dioxide Waste management a b s t r a c t The aim of the present study was to determine an effective sterilization method for safe handling and recycle-reuse of clinical solid waste materials. Supercritical fluid carbon dioxide (SC-CO 2 ) was applied in the inactivation of gram positive Staphylococcus aureus (S. aureus) and gram negative Serratia marcencens (S. marcescens) in clinical solid waste. The colony forming activity of the bacteria was completely lost at pressures 10–40 MPa, temperatures 35–80 ◦ C and treatment period between 5 and 120 min. An increase in pressure at constant temperature and vice versa with the increasing treatment time enhanced the SC- CO 2 inactivation efficiency. The inactivation process was illustrated by the modified Gompertz equation. The SC-CO 2 inactivation of bacteria was compared with the steam autoclaved bacteria. Regrowth of the bacteria was observed in the autoclaved sample while no re-growth was detected in the SC-CO 2 treated clinical solid waste. Results from SEM image analysis, cellular protein and enzymatic activity of untreated, autoclaved and SC-CO 2 treated S. marcescens and S. aureus cells confirmed that SC-CO 2 is an effective sterilization method. © 2013 Elsevier B.V. All rights reserved. 1. Introduction Clinical solid waste is considered as the most hazardous and potentially infectious among all types of waste generated in a com- munity. The technologies used at present to dispose the clinical solid waste is not environmentally friendly and do not cope with clinical solid waste in a safe manner [1–4]. Many studies have been documented to determine a safer clinical waste management practice within an affordable cost by the healthcare facilities. Clini- cal solid waste contains enormous volumes of recyclable materials [5,6]. The development of recycling clinical solid waste can serve as a means of reducing rising quantities of clinical solid waste gen- eration and its treatment cost [1,5–8]. Lee et al. [5] reported that clinical solid waste must be free from infectious agent prior to conducted recycling program. Marinkovi ´ c et al. [6] declared that sterilization using a mobile device at its source is the most accept- able solution to prevent infectious risks and to minimize the clinical ∗ Corresponding author. Tel.: +60 4 653 5206; fax: +60 4 658 5435. E-mail addresses: [email protected], sohrab [email protected] (M.O.A. Kadir). waste generation. Sawalem et al. [4] suggested adopting a low oper- ating cost, easily implementable, and low maintenance sterilization method in clinical waste management to prevent contamination. Sterilization of clinical solid waste presents a challenge to cur- rent sterilization technology due to the major portions of clinical solid waste are heat sensitive plastic or polymer materials. In med- ical practice, the most common sterilization techniques used are steam autoclaving, ethylene oxide, and gamma-radiation [9,10]. Though, all these methods assure a satisfactory microbial inactiva- tion, there still exists a number of limitations [11,12]. Supercritical fluid carbon dioxide (SC-CO 2 ) is effective in sterilization agent and has notable benefits over the existing sterilization method. SC-CO 2 has been proven to be effective against any sort of microorgan- isms, as it impacts the target microorganisms both physically and chemically [11,13,14]. SC-CO 2 technology sterilizes the heat sensi- tive biomedical device without any damage and lowering its quality [10,14]. Bacteria are cellular microorganisms, able to re-grow and mul- tiply under favorable nutrient requirements [15,16]. It must be ensured the complete inactivation of the bacteria in the cellu- lar level in order to avoid unexpected re-growth of bacteria prior to decide any sterilization technology [17]. The mechanisms of 0896-8446/$ – see front matter © 2013 Elsevier B.V. All rights reserved. http://dx.doi.org/10.1016/j.supflu.2013.08.011
-
Upload
independent -
Category
Documents
-
view
1 -
download
0
Transcript of Contents lists available at ScienceDirect The Journal of Supercritical Fluids

Mmd
MZa
b
c
d
a
ARRA
KCIPRSW
1
pmscbpc[aeccsa
(
0h
J. of Supercritical Fluids 83 (2013) 47– 56
Contents lists available at ScienceDirect
The Journal of Supercritical Fluids
jou rn al hom epage: www.elsev ier .com/ locate /supf lu
odeling the inactivation of Staphylococcus aureus and Serratiaarcescens in clinical solid waste using supercritical fluid carbonioxide
d. Sohrab Hossaina, Venugopal Balakrishnanb, Nik Norulaini Nik Ab Rahmanc,ainul Ahmad Rajiond, Mohd Omar Ab Kadira,∗
Division of Environmental Technology, School of Industrial Technology, Universiti Sains Malaysia, 11800 Penang, MalaysiaInstitute for Research in Molecular Medicine, Universiti Sains Malaysia, 11800, Penang, MalaysiaSchool of Distance Education, Universiti Sains Malaysia, 11800 Penang, MalaysiaSchool of Dental Science, Universiti Sains Malaysia, 16150 Kubang Kerian, Kelantan, Malaysia
r t i c l e i n f o
rticle history:eceived 26 June 2013eceived in revised form 24 August 2013ccepted 24 August 2013
eywords:linical solid waste
a b s t r a c t
The aim of the present study was to determine an effective sterilization method for safe handling andrecycle-reuse of clinical solid waste materials. Supercritical fluid carbon dioxide (SC-CO2) was applied inthe inactivation of gram positive Staphylococcus aureus (S. aureus) and gram negative Serratia marcencens(S. marcescens) in clinical solid waste. The colony forming activity of the bacteria was completely lost atpressures 10–40 MPa, temperatures 35–80 ◦C and treatment period between 5 and 120 min. An increasein pressure at constant temperature and vice versa with the increasing treatment time enhanced the SC-
nactivation modelingathogenic bacteriaegrowthupercritical carbon dioxideaste management
CO2 inactivation efficiency. The inactivation process was illustrated by the modified Gompertz equation.The SC-CO2 inactivation of bacteria was compared with the steam autoclaved bacteria. Regrowth ofthe bacteria was observed in the autoclaved sample while no re-growth was detected in the SC-CO2
treated clinical solid waste. Results from SEM image analysis, cellular protein and enzymatic activity ofuntreated, autoclaved and SC-CO2 treated S. marcescens and S. aureus cells confirmed that SC-CO2 is aneffective sterilization method.
. Introduction
Clinical solid waste is considered as the most hazardous andotentially infectious among all types of waste generated in a com-unity. The technologies used at present to dispose the clinical
olid waste is not environmentally friendly and do not cope withlinical solid waste in a safe manner [1–4]. Many studies haveeen documented to determine a safer clinical waste managementractice within an affordable cost by the healthcare facilities. Clini-al solid waste contains enormous volumes of recyclable materials5,6]. The development of recycling clinical solid waste can serves a means of reducing rising quantities of clinical solid waste gen-ration and its treatment cost [1,5–8]. Lee et al. [5] reported thatlinical solid waste must be free from infectious agent prior to
onducted recycling program. Marinkovic et al. [6] declared thatterilization using a mobile device at its source is the most accept-ble solution to prevent infectious risks and to minimize the clinical∗ Corresponding author. Tel.: +60 4 653 5206; fax: +60 4 658 5435.E-mail addresses: [email protected], sohrab [email protected]
M.O.A. Kadir).
896-8446/$ – see front matter © 2013 Elsevier B.V. All rights reserved.ttp://dx.doi.org/10.1016/j.supflu.2013.08.011
© 2013 Elsevier B.V. All rights reserved.
waste generation. Sawalem et al. [4] suggested adopting a low oper-ating cost, easily implementable, and low maintenance sterilizationmethod in clinical waste management to prevent contamination.
Sterilization of clinical solid waste presents a challenge to cur-rent sterilization technology due to the major portions of clinicalsolid waste are heat sensitive plastic or polymer materials. In med-ical practice, the most common sterilization techniques used aresteam autoclaving, ethylene oxide, and gamma-radiation [9,10].Though, all these methods assure a satisfactory microbial inactiva-tion, there still exists a number of limitations [11,12]. Supercriticalfluid carbon dioxide (SC-CO2) is effective in sterilization agent andhas notable benefits over the existing sterilization method. SC-CO2has been proven to be effective against any sort of microorgan-isms, as it impacts the target microorganisms both physically andchemically [11,13,14]. SC-CO2 technology sterilizes the heat sensi-tive biomedical device without any damage and lowering its quality[10,14].
Bacteria are cellular microorganisms, able to re-grow and mul-
tiply under favorable nutrient requirements [15,16]. It must beensured the complete inactivation of the bacteria in the cellu-lar level in order to avoid unexpected re-growth of bacteria priorto decide any sterilization technology [17]. The mechanisms of
48 Md.S. Hossain et al. / J. of Supercr
Table 1Gravimetric composition of clinical solid wastes used in the study.
Material % by mass (dry basis)
Hard plastic 30Broken glass 25Fabric 15Metal 20
SiSceooeas
iomrtssccbiercuemcsr
2
2
cfsht(btsm2i
iwmcm
Rubber 10
Total 100
C-CO2 on the inactivation of bacteria are yet to be confirmedn the literature. Several inactivation mechanisms of bacteria inC-CO2 sterilization have been proposed. While, there are someommon features and there are also points of disagreement. Sev-ral hypotheses have been proposed as the inactivation mechanismf bacteria in SC-CO2 sterilization, including cell rupture, changesf protein, loss of enzymatic activities, to name a few [14,18]. How-ver, there is limited evidence available in literature to clarify thembiguity on the inactivation mechanism of bacteria in SC-CO2terilization.
The purpose of the present study was to determine the feasibil-ty of the clinical solid waste sterilization causing the inactivationf Staphylococcus aureus (S. aureus) and Serratia marcencens (S.arcescens) using SC-CO2. S. aureus is the most common cause of
espiratory diseases, skin infection and food poisoning. This bac-erium is capable of causing life-threatening infectious diseasesuch as pneumonia, meningitis, osteomyelitis, endocarditis, toxichock syndrome, bacteremia, and sepsis [18]. Serratia marcescensauses endemic and epidemic nosocomial infections and known toause infections of the respiratory tract, urinary tract, wounds, andloodstream [19]. Both S. aureus and S. marcescens were detected
n clinical solid waste [20]. In addition, the SC-CO2 sterilizationfficiency was evaluated based on the re-growth potential of bacte-ia in sterilized waste. The SC-CO2 sterilization efficiency wasompared with the steam autoclave, which is most commonlysed sterilization method in clinical solid waste management. Sev-ral analytical methods were utilized to elucidate the inactivationechanisms of the bacteria subjected to SC-CO2 and steam auto-
lave treatment of clinical solid waste. The finding of the presenttudy would be useful for determining a safe disposal and resource-ecovery clinical solid waste management practice.
. Materials and methods
.1. Sample preparation
The clinical solid waste materials used in this study wereollected from Hospital Lam Wah Ee, one of specialized healthcareacilities in Penang Island, Malaysia. The collected samples wereterilized in an autoclave (121 ◦C for 15 min) to ensure the safeandling. Later, the sterilized waste was dried in air at roomemperature until the moisture content reduced to about 5%w/w.). Heat resistant waste materials (i.e., hard plastic materials,roken glass, textile, metals, etc.) were manually separated fromhe sterilized waste. No tissue waste was used in the present study,ince the tissue waste is not heat resistant. Later the selected wasteaterials were manually cut to the desired size between 1.27 and
.54 cm. The gravimetric composition of clinical solid wastes usedn this study is presented in Table 1.
S. aureus and S. marcescens used in the present study weresolated from the clinical solid waste [20]. The bacteria isolated
ere stored in a freezer at −80 ◦C in bacterial glycerol stock. Theicroorganisms were re-cultured in selective media to obtain fresh
ultures (i.e., blood agar media for S. auerus and MacConkey agaredia for S. marcescens). From the culture growth, a single isolated
itical Fluids 83 (2013) 47– 56
colony was transferred to nutrient broth (NB) agar and incubatedat 37 ◦C for 24 h. 20 mL of bacterial solution was prepared using5 mL of bacterial Nutrient broth, 5 mL of sterile glycerol and 10 mLsterile 0.9% saline solution. The glycerol was used as surfactantfor the homogeneous distribution of bacteria in the sample. Thebacteria mixture was then added to 0.25 kg of waste dropwise andmixed vigorously using a glass rod. Subsequently, the mixture ofthe clinical solid waste was placed in the SC-CO2 1.2 L sterilizationvessel.
2.2. SC-CO2 treatment
The supercritical sterilization reactor system was used to ster-ilize the clinical solid waste is shown in Fig. 1. After placing thesample in the SC-CO2 sterilization vessel, the vessel was tightlyclosed. The sensitivity of bacteria to the SC-CO2 treatment wasperformed with varying pressure (10–40 MPa) and temperature(35–80 ◦C) at different duration of treatment time (5, 15, 30, 45,60, 90 and 120 min). When the temperature of the SC-CO2 sys-tem reached the set temperature, the connecting valve (V01) wasopened and the decompression valves (V02 and V03) were closed.The liquid CO2 (95% purity), contained in a siphoned cylinder, wasthen pumped into the treatment vessel until the desired pressurewas achieved. The connecting valve (V01) was opened through-out the entire treatment. The pressure loading times were 0.93,4.03, 5.17 and 5.85 min for the pressure 10, 20, 30 and 40 MPa,respectively. After the desired treatment duration had elapsed, theconnecting valve (V01) was closed and the vessel was depressur-ized by slowly opening the decompression valves (V02 and V03).Later, the SC-CO2 treated sample was collected for the enumera-tion of viable colony. Triplicate experiments were conducted andthe results are expressed as means ± standard errors.
2.3. Enumeration of viable colony
The number of viable colonies in the sample was determinedbefore treatment and after the treatment (at the time t min) usinga pour-plate method. For the bacteria colony counting, sterilizeddistilled water was added to the bacteria-contaminated sample ina ratio of 1:5 g mL−1. Next, 1 mL of the contaminated distilled waterwas taken in the eight fold serial dilution, from which 0.1 mL aliquotwas removed for seeding on Petri dishes containing nutrient agarmedia using a sterile Drigalski spatula. The dishes with the cul-ture medium were labeled and incubated at 37 ◦C for 48 h prior tocounting. The initial concentrations of the bacteria were found tobe 7.7 ± 0.2 log CFU g−1 and 7.8 ± 0.2 log CFU g−1 for S. aureus and S.marcescens, respectively. This procedure was carried out in dupli-cate to determine the average bacterial colony concentration inwaste. Results were expressed as the logarithm of surviving colonyforming units per gram of waste (log CFU g−1). It should be notedthat any bacterial colony that did not grow on the surface of theagar plate from the treated sample, would lead to overestimation ofthe degree of inactivation. However, if there is no bacterial colonyrecovery from the treated sample, the total bacterial colony wasconsidered as one colony due to the logarithmic study.
The amount of bacterial colonies was calculated by the numberof individual colonies that formed on the surface of agar plates. Thenumber of colony forming units per gram of waste was calculatedusing the following equation:CFU
g= Number of bacterial colonies
Agar plating volume× 1
dilution factor
× volume of contaminatemass of waste
(1)
The log survival ratio of the number of viable colonies in agram sample was calculated as number of survival colonies after

Md.S. Hossain et al. / J. of Supercritical Fluids 83 (2013) 47– 56 49
F n presc
s(
L
2S
mpm
l
w(itdta
t
mtGtribetbxata
2s
wsa
ig. 1. Supercritical fluid carbon dioxide sterilization system. V: valve, DP: desigontroller.
terilization (N) to the number of viable colonies before treatmentN0), as shown in Eq. (2).
og survival ratio = LogN
N0(2)
.4. Mathematical model for inactivation of bacteria usingC-CO2
The modified Gompertz equation was used to describe the sig-oidal curve for the bacterial inactivation, which includes lag
hase, exponential inactivation phase and asymptotic phase. Theodified Gompertz equation is expressed as follows [21]:
ogN
N0= A · exp
[− exp
{−kdme
A(� − t) + 1
}](3)
here, log N/N0 is the logarithmic ratio of viable cell count. A−log Nmax) is the lower asymptote value, kdm is the maximumnactivation rate (min−1), � is the time for lag phase and t is thereatment time. The time length for the complete inactivation isefined by tt. At complete inactivation time, log N/N0 = A, with theangent through the inflection point. Thus, the tt can be calculateds:
t = � + A
kdm(4)
The biological parameters (A, �, kdm) of the modified Gompertzodel were determined using the experimental data. Whereas,
he tt value was determined according to Eq. (4). The modifiedompertz equation (Eq. (3)) is a nonlinear equation; thereafter
he bacteria cell inactivation data were fitted through non-linearegression with Levenberg–Marquardt algorithm in order to min-mize the residual sum of the squares (RSS) of the differenceetween the predicted and observed value. Keleida Graph 4 (Syn-rgy software ver., 2007; Pennsylvania, USA) was used to calculatehe starting values by searching of the steepest ascent of the curveetween the datum points (estimation of kdm), the line with the-axis (estimation of �), and final datum point as the estimation forsymptote (A). The fitting goodness of the model was assessed usinghe regression coefficients (R2) and RSS values of the experimentalnd the predicted values at their 95% confidence level.
.5. Re-growth of S. aureus and S. marcescens in sterilized clinicalolid waste
Mixture of the bacterial solution containing 5 mL Nutrient Brothith bacteria, 20 mL of sterilized glycerol and 25 mL sterilized 0.9%
aline solution, was added into 0.5 kg of clinical solid waste samplend mixed vigorously using a glass rod. The contaminated clinical
sure, DT: design temperature. kcal/h: kilocalorie per hour, ALC: automatic level
solid waste was then sterilized using the optimized experimentalcondition of autoclave and SC-CO2. The experimental conditionswere optimized in the preliminary studies of the current research,and these were temperature 121 ◦C, time 60 min for steam auto-clave treatment [17], and pressure 20 MPa, temperature 60 ◦C andtreatment time 60 min for SC-CO2 [22]. After sterilization, the sam-ple was placed in biohazard bin with addition of 250 mL sterilizeddistilled water and mixed vigorously using a glass rod. Then, thesample was stored at room temperature (25 ± 1 ◦C) to determinethe re-growth of bacteria at every 24 h interval for 10 days. For theobservation of S. aureus and S. marcescens re-growth, 1 mL of thecontaminated distilled water was taken to culture on agar media.Blood and MacKonkey agar media was used to culture S. aureus andS. marcescens, respectively.
2.6. Scanning electron microscope image analysis of bacteria
Scanning electron microscope (SEM) image was taken of auto-clave treated, SC-CO2 treated and untreated S. auerus and S.marcescens, in clinical solid waste. 10 g clinical solid waste wastaken into 50 mL distilled water and the contaminate sample wasshaken vigorously for 10 min. Later, the clinical solid waste wasseparated through filtration and the supernatant was collected. Thesupernatant was centrifuged at 2000 × g for 15 min and the pellet ofbacteria was collected. The collected pellet was resuspended withMcDowell-Trump fixative for 2 h, which contains 4% formaldehydeand 1% glutaraldehyde in 0.1 M sodium phosphate buffer at pH 7.2.The cell was then resuspended 3 times using 0.1 M sodium phos-phate buffer with gentle agitation for 10 min each. The suspendedcells were then placed in 1% Osmium tetra-oxide for 1 h. The cellswere rinsed 3 times using 0.1 M sodium phosphate buffer for 10 mineach. The rinsed cells were dehydrated using a series of ethanolsolution for 10 min each, starting with 50% ethanol and continuethrough 75% and 95%. Subsequently, the cells were rinsed 2 timeswith 100% ethanol for 10 min each; then rinsed with Hexamethyl-disiazane 2 times for 10 min each, and placed in the Dessicator inorder to air dry at room temperature. The dried cells were thenmounted into the SEM stub, coated with gold powder with doubleside carbon tape, and viewed using scanning electron microscope(VeriosTM XHR-450, Japan).
2.7. Analysis of the cellular protein of the bacteria
To investigate the effect of autoclave and SC-CO2 on the cellu-
lar protein, the protein degradation of autoclave treated, SC-CO2treated and untreated S. auerus and S. marcescens in clinical solidwaste were observed using sodium dodecyl sulphate polyacrylam-ide gel electrophoresis (SDS-PAGE). 50 mL sterile distilled water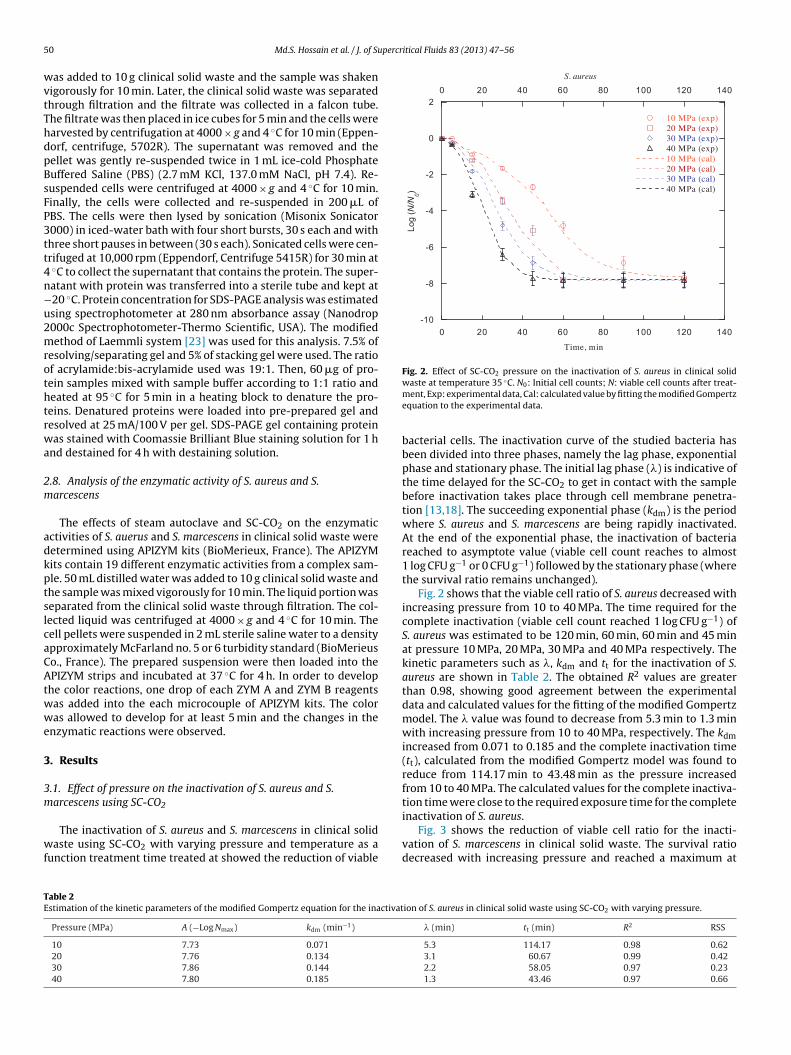
5 percritical Fluids 83 (2013) 47– 56
wvtThdpBsFP3tt4n−u2mrothtrwa
2m
adkptslcaCAtwwe
3
3m
wf
-10
-8
-6
-4
-2
0
2
0 20 40 60 80 100 120 140
S. aureus
10 MPa (exp)20 MPa (exp)30 MPa (exp)40 MPa (exp)10 MPa (cal)20 MPa (cal)30 MPa (cal)40 MPa (cal)
0 20 40 60 80 100 120 140
Log
(N/N0)
Time, min
Fig. 2. Effect of SC-CO2 pressure on the inactivation of S. aureus in clinical solid◦
TE
0 Md.S. Hossain et al. / J. of Su
as added to 10 g clinical solid waste and the sample was shakenigorously for 10 min. Later, the clinical solid waste was separatedhrough filtration and the filtrate was collected in a falcon tube.he filtrate was then placed in ice cubes for 5 min and the cells werearvested by centrifugation at 4000 × g and 4 ◦C for 10 min (Eppen-orf, centrifuge, 5702R). The supernatant was removed and theellet was gently re-suspended twice in 1 mL ice-cold Phosphateuffered Saline (PBS) (2.7 mM KCl, 137.0 mM NaCl, pH 7.4). Re-uspended cells were centrifuged at 4000 × g and 4 ◦C for 10 min.inally, the cells were collected and re-suspended in 200 �L ofBS. The cells were then lysed by sonication (Misonix Sonicator000) in iced-water bath with four short bursts, 30 s each and withhree short pauses in between (30 s each). Sonicated cells were cen-rifuged at 10,000 rpm (Eppendorf, Centrifuge 5415R) for 30 min at◦C to collect the supernatant that contains the protein. The super-atant with protein was transferred into a sterile tube and kept at20 ◦C. Protein concentration for SDS-PAGE analysis was estimatedsing spectrophotometer at 280 nm absorbance assay (Nanodrop000c Spectrophotometer-Thermo Scientific, USA). The modifiedethod of Laemmli system [23] was used for this analysis. 7.5% of
esolving/separating gel and 5% of stacking gel were used. The ratiof acrylamide:bis-acrylamide used was 19:1. Then, 60 �g of pro-ein samples mixed with sample buffer according to 1:1 ratio andeated at 95 ◦C for 5 min in a heating block to denature the pro-eins. Denatured proteins were loaded into pre-prepared gel andesolved at 25 mA/100 V per gel. SDS-PAGE gel containing proteinas stained with Coomassie Brilliant Blue staining solution for 1 h
nd destained for 4 h with destaining solution.
.8. Analysis of the enzymatic activity of S. aureus and S.arcescens
The effects of steam autoclave and SC-CO2 on the enzymaticctivities of S. auerus and S. marcescens in clinical solid waste wereetermined using APIZYM kits (BioMerieux, France). The APIZYMits contain 19 different enzymatic activities from a complex sam-le. 50 mL distilled water was added to 10 g clinical solid waste andhe sample was mixed vigorously for 10 min. The liquid portion waseparated from the clinical solid waste through filtration. The col-ected liquid was centrifuged at 4000 × g and 4 ◦C for 10 min. Theell pellets were suspended in 2 mL sterile saline water to a densitypproximately McFarland no. 5 or 6 turbidity standard (BioMerieuso., France). The prepared suspension were then loaded into thePIZYM strips and incubated at 37 ◦C for 4 h. In order to develop
he color reactions, one drop of each ZYM A and ZYM B reagentsas added into the each microcouple of APIZYM kits. The coloras allowed to develop for at least 5 min and the changes in the
nzymatic reactions were observed.
. Results
.1. Effect of pressure on the inactivation of S. aureus and S.arcescens using SC-CO2
The inactivation of S. aureus and S. marcescens in clinical solidaste using SC-CO2 with varying pressure and temperature as a
unction treatment time treated at showed the reduction of viable
able 2stimation of the kinetic parameters of the modified Gompertz equation for the inactivat
Pressure (MPa) A (−Log Nmax) kdm (min−1)
10 7.73 0.071
20 7.76 0.134
30 7.86 0.144
40 7.80 0.185
waste at temperature 35 C. N0: Initial cell counts; N: viable cell counts after treat-ment, Exp: experimental data, Cal: calculated value by fitting the modified Gompertzequation to the experimental data.
bacterial cells. The inactivation curve of the studied bacteria hasbeen divided into three phases, namely the lag phase, exponentialphase and stationary phase. The initial lag phase (�) is indicative ofthe time delayed for the SC-CO2 to get in contact with the samplebefore inactivation takes place through cell membrane penetra-tion [13,18]. The succeeding exponential phase (kdm) is the periodwhere S. aureus and S. marcescens are being rapidly inactivated.At the end of the exponential phase, the inactivation of bacteriareached to asymptote value (viable cell count reaches to almost1 log CFU g−1 or 0 CFU g−1) followed by the stationary phase (wherethe survival ratio remains unchanged).
Fig. 2 shows that the viable cell ratio of S. aureus decreased withincreasing pressure from 10 to 40 MPa. The time required for thecomplete inactivation (viable cell count reached 1 log CFU g−1) ofS. aureus was estimated to be 120 min, 60 min, 60 min and 45 minat pressure 10 MPa, 20 MPa, 30 MPa and 40 MPa respectively. Thekinetic parameters such as �, kdm and tt for the inactivation of S.aureus are shown in Table 2. The obtained R2 values are greaterthan 0.98, showing good agreement between the experimentaldata and calculated values for the fitting of the modified Gompertzmodel. The � value was found to decrease from 5.3 min to 1.3 minwith increasing pressure from 10 to 40 MPa, respectively. The kdmincreased from 0.071 to 0.185 and the complete inactivation time(tt), calculated from the modified Gompertz model was found toreduce from 114.17 min to 43.48 min as the pressure increasedfrom 10 to 40 MPa. The calculated values for the complete inactiva-tion time were close to the required exposure time for the complete
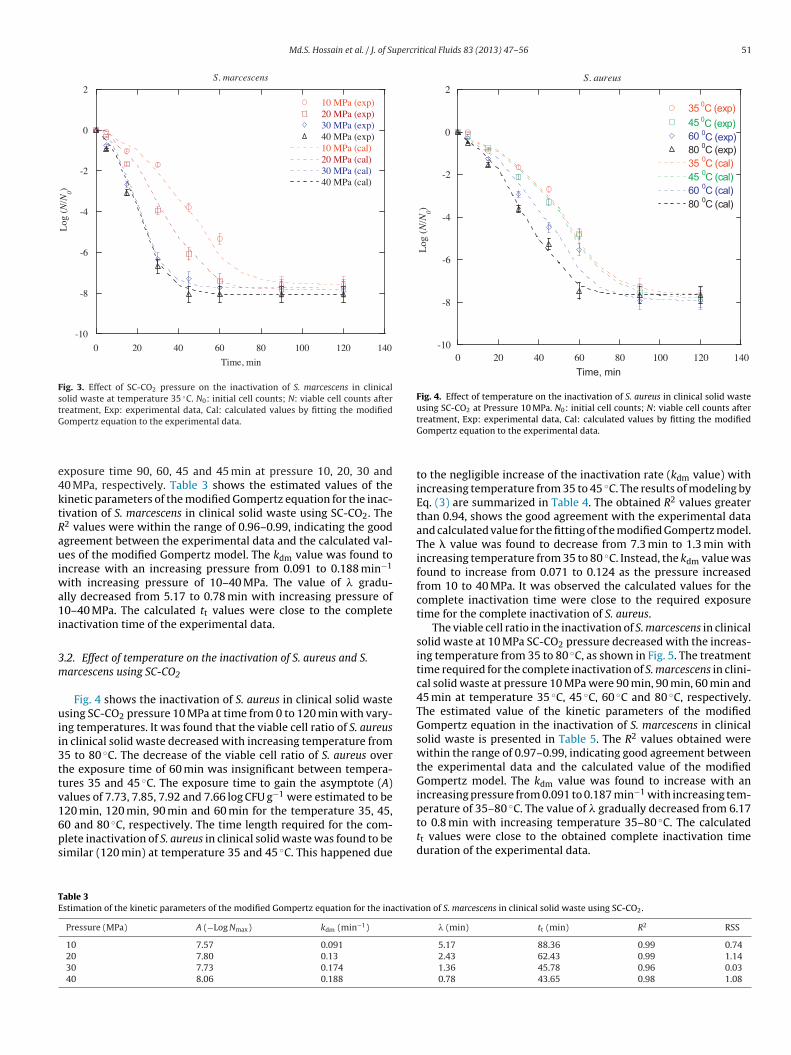
inactivation of S. aureus.Fig. 3 shows the reduction of viable cell ratio for the inacti-vation of S. marcescens in clinical solid waste. The survival ratiodecreased with increasing pressure and reached a maximum at
ion of S. aureus in clinical solid waste using SC-CO2 with varying pressure.
� (min) tt (min) R2 RSS
5.3 114.17 0.98 0.623.1 60.67 0.99 0.422.2 58.05 0.97 0.231.3 43.46 0.97 0.66
Md.S. Hossain et al. / J. of Supercritical Fluids 83 (2013) 47– 56 51
-10
-8
-6
-4
-2
0
2
0 20 40 60 80 100 12 0 140
S. marcescens
10 MPa (exp)20 MPa (exp)30 MPa (exp)40 MPa (exp)10 MPa (cal)20 MPa (cal)30 MPa (cal)40 MPa (cal)
Log
(N
/N0)
Time , min
Fig. 3. Effect of SC-CO2 pressure on the inactivation of S. marcescens in clinicalsolid waste at temperature 35 ◦C. N0: initial cell counts; N: viable cell counts aftertreatment, Exp: experimental data, Cal: calculated values by fitting the modifiedG
e4ktRauiwa1i
3m
uii3ttv16ps
-10
-8
-6
-4
-2
0
2
140120100806040200
S. aureus
3545608035456080
Log
(N
/N0)
Time, min
0C (exp)0C (exp)0C (exp)0C (exp)0C (cal)0C (cal)0C (cal)0C (cal)
Fig. 4. Effect of temperature on the inactivation of S. aureus in clinical solid wasteusing SC-CO2 at Pressure 10 MPa. N0: initial cell counts; N: viable cell counts after
TE
ompertz equation to the experimental data.
xposure time 90, 60, 45 and 45 min at pressure 10, 20, 30 and0 MPa, respectively. Table 3 shows the estimated values of theinetic parameters of the modified Gompertz equation for the inac-ivation of S. marcescens in clinical solid waste using SC-CO2. The2 values were within the range of 0.96–0.99, indicating the goodgreement between the experimental data and the calculated val-es of the modified Gompertz model. The kdm value was found to
ncrease with an increasing pressure from 0.091 to 0.188 min−1
ith increasing pressure of 10–40 MPa. The value of � gradu-lly decreased from 5.17 to 0.78 min with increasing pressure of0–40 MPa. The calculated tt values were close to the complete
nactivation time of the experimental data.
.2. Effect of temperature on the inactivation of S. aureus and S.arcescens using SC-CO2
Fig. 4 shows the inactivation of S. aureus in clinical solid wastesing SC-CO2 pressure 10 MPa at time from 0 to 120 min with vary-
ng temperatures. It was found that the viable cell ratio of S. aureusn clinical solid waste decreased with increasing temperature from5 to 80 ◦C. The decrease of the viable cell ratio of S. aureus overhe exposure time of 60 min was insignificant between tempera-ures 35 and 45 ◦C. The exposure time to gain the asymptote (A)alues of 7.73, 7.85, 7.92 and 7.66 log CFU g−1 were estimated to be
20 min, 120 min, 90 min and 60 min for the temperature 35, 45,0 and 80 ◦C, respectively. The time length required for the com-lete inactivation of S. aureus in clinical solid waste was found to beimilar (120 min) at temperature 35 and 45 ◦C. This happened dueable 3stimation of the kinetic parameters of the modified Gompertz equation for the inactivat
Pressure (MPa) A (−Log Nmax) kdm (min−1)
10 7.57 0.091
20 7.80 0.13
30 7.73 0.174
40 8.06 0.188
treatment, Exp: experimental data, Cal: calculated values by fitting the modifiedGompertz equation to the experimental data.
to the negligible increase of the inactivation rate (kdm value) withincreasing temperature from 35 to 45 ◦C. The results of modeling byEq. (3) are summarized in Table 4. The obtained R2 values greaterthan 0.94, shows the good agreement with the experimental dataand calculated value for the fitting of the modified Gompertz model.The � value was found to decrease from 7.3 min to 1.3 min withincreasing temperature from 35 to 80 ◦C. Instead, the kdm value wasfound to increase from 0.071 to 0.124 as the pressure increasedfrom 10 to 40 MPa. It was observed the calculated values for thecomplete inactivation time were close to the required exposuretime for the complete inactivation of S. aureus.
The viable cell ratio in the inactivation of S. marcescens in clinicalsolid waste at 10 MPa SC-CO2 pressure decreased with the increas-ing temperature from 35 to 80 ◦C, as shown in Fig. 5. The treatmenttime required for the complete inactivation of S. marcescens in clini-cal solid waste at pressure 10 MPa were 90 min, 90 min, 60 min and45 min at temperature 35 ◦C, 45 ◦C, 60 ◦C and 80 ◦C, respectively.The estimated value of the kinetic parameters of the modifiedGompertz equation in the inactivation of S. marcescens in clinicalsolid waste is presented in Table 5. The R2 values obtained werewithin the range of 0.97–0.99, indicating good agreement betweenthe experimental data and the calculated value of the modifiedGompertz model. The kdm value was found to increase with anincreasing pressure from 0.091 to 0.187 min−1 with increasing tem-perature of 35–80 ◦C. The value of � gradually decreased from 6.17
to 0.8 min with increasing temperature 35–80 ◦C. The calculatedtt values were close to the obtained complete inactivation timeduration of the experimental data.ion of S. marcescens in clinical solid waste using SC-CO2.
� (min) tt (min) R2 RSS
5.17 88.36 0.99 0.742.43 62.43 0.99 1.141.36 45.78 0.96 0.030.78 43.65 0.98 1.08

52 Md.S. Hossain et al. / J. of Supercritical Fluids 83 (2013) 47– 56
Table 4Estimation of the kinetic parameters of the modified Gompertz equation for the inactivation of S. aureus in clinical solid waste using SC-CO2 with varying temperature.
Temperature (◦C) A (−Log Nmax) kdm (min−1) � (min) tt min R2 RSS
35 7.73 0.071 7.3 116.17 0.98 0.6245 7.85 0.073 5.5 113.03 0.94 1.1360 7.92 0.090 2.1 89.71 0.99 0.5180 7.66 0.124 1.1 62.87 0.99 0.95
Table 5Estimation of the kinetic parameters of the modified Gompertz equation for the inactivation of S. marcescens in clinical solid waste using SC-CO2 with varying temperature.
Temperature (◦C) A (−Log Nmax) kdm (min−1) � (min) tt min R2 RSS
35 7.57 0.091 6.17 89.36 0.99 0.74
3m
1
k
l
wpbt1sstta1
Fwafi
45 7.67 0.092
60 7.61 0.13580 8.02 0.187
.3. Analysis of dependence on temperature by the Arrheniusodel
The effects of temperature (35, 45, 60 and 80 ◦C) on kdm at0 MPa were analyzed using the following equations [21]:
dm = a · e−Ed/RT (5.18)
n kdm = ln a +(−Ed
R
) (1T
)(5.19)
here, kdm is the inactivation rate of the bacteria (min−1), a is are exponential factor (min−1), Ed is the activation energy of theacteria inactivation (kJ mol−1), which might be calculated fromhe slope and the intercept of the straight line of the plot of ln kdm vs/T (where T is the absolute temperature), and R is the ideal gas con-tant (8.314 J mole−1 K−1). The activation energy (Ed) exposes theensitivity of S. aureus and S. marcescens, to the SC-CO2 treatment
emperature. Fig. 6 shows the temperature dependence inactiva-ion rate obtained via Arrhenius plot for the inactivation of S. aureusnd S. marcescens in clinical solid waste at SC-CO2 pressure of0 MPa. According to the linear regression graph shown in Fig. 6,-10
-8
-6
-4
-2
0
2
140120100806040200
S. marcescens
35 C (exp)45 C (exp)60 C (exp)80 C (exp)35 C (cal)45 C (cal)60 C (cal)80 C (cal)
Log
(N
/N0)
Time, min
0
0
0
0
0
0
0
0
ig. 5. Effect of temperature on the inactivation of S. marcescens in clinical solidaste using SC-CO2 at pressure 10 MPa. N0: initial cell counts; N: viable cell counts
fter treatment, Exp: experimental data, Cal: calculated values by fitting the modi-ed Gompertz equation to the experimental data.
4.6 87.97 0.97 0.721.3 57.67 0.99 0.210.8 43.69 0.99 0.39
the Ed value for the inactivation of S. aureus and S. marcescens were11.61 kJ mol−1 and 15.03 kJ mol−1, respectively.
3.4. Re-growth of S. aureus and S. marcescens in SC-CO2 andautoclave treated clinical solid waste
Determination of the re-growth potential of S. aureus and S.marcescens was done by assessing the bacterial cultures of sam-ples post treated with SC-CO2 and autoclave for signs of cultureviability. The initial concentrations of S. aureus and S. marcescensin pre-sterilized clinical solid waste were 7.41 log CFU g−1 and7.26 log CFU g−1, respectively. S. aureus and S. marcescens con-taminated clinical solid waste was sterilized using optimizedexperimental conditions of steam autoclave (i.e., temperature121 ◦C for 60 min) and SC-CO2 (i.e., pressure 20 MPa, temperature60 ◦C and treatment time 60 min). The results obtained are pre-sented in Table 6. The absence of re-growth in cultures from SC-CO2treated clinical solid waste was evident from day 0 to day 10. Con-versely, S. aureus and S. marcescens demonstrated re-growth inautoclaved clinical solid waste cultures. The S. aureus appeared tohave started to re-grow at 4 days post sterilization and S. marcescens
took a day longer at 5 days post sterilization. Once S. aureus andS. marcescens were started to re-grow in autoclave treated clinicalsolid waste, both bacteria were found to continuously re-grow untilthe maximum observation time of day 10.Fig. 6. Temperature dependence of the inactivation rate for the inactivation of S.aureus, and S. marcescens in clinical solid waste at 10 MPa SC-CO2 pressure.

Md.S. Hossain et al. / J. of Supercritical Fluids 83 (2013) 47– 56 53
Table 6Re-growth S. aureus and S. marcescens in sterilized clinical solid waste.
Treatment Name of bacteriaTime, day
0 1 2 3 4 5 6 7 8 9 10
Autoclave S. aureus × × × × √ √ √ √ √ √ √S. marcescens × × × × × √ √ √ √ √ √
SC-CO S. aureus × × × × × × × × × × ××
×
3a
adsSmStSd
Fuc6
2
S. marcescens × × ×
: re-growth negative;√
: re-growth positive.
.5. Morphological alterations of SC-CO2 and autoclaved S.ureus and S. marcescens
The morphological changes on S. aureus and S. marcescens inutoclaved and SC-CO2 treated clinical solid waste were markedlyepicted in the scanning electron micrographs (Figs. 7 and 8). Theamples autoclaved at temperature 121 ◦C and 60 min, and theC-CO2 treated at pressure 20 MPa, temperature 60 ◦C and treat-ent time 60 min revealed distinct differences. The cell walls of
. aureus and S. marcescens remained unchanged before and afterhe autoclave treatment. In other words, autoclaved S. aureus and. marcescens cells maintained the outer smooth structure. Obviousifferences in the morphological changes were observed between
ig. 7. Scanning electron micrographs indicating cell wall ruptures of S. aureus. A:ntreated, B: autoclaved treated, C: SC-CO2 treated. Experimental conditions, auto-lave: temperature 121 ◦C and time 60 min; SC-CO2: pressure 20 MPa, temperature0 ◦C and treatment time 60 min.
× × × × × × ×
the SEM images of untreated and SC-CO2 treated S. aureus and S.Marcescens cells present in the clinical solid waste. Fig. 8 reflects theSEM image of the SC-CO2 treated S. marcescens which reveal brokencell walls, exposure of cells, cell rupture, cell distortion, puncturedholes and disintegration of the cellular membrane. The partial cellwall damage was observed in the SC-CO2 treated gram positivebacteria of S. aureus, as shown in Fig. 7.
3.6. Effect of autoclave and SC-CO2 treatment on the cellularprotein of S. aureus and S. marcescens
Due to the penetration of the CO2 into the sterilized bacteriacell, the cytoplasmic substance might be extracted by the CO2. Itwas analyzed the degradation of the cellular protein in treated
and untreated bacteria cell, which is one of the major cytoplas-mic materials of the bacterial cell. The degradation of the cellularprotein of untreated, autoclaved and SC-CO2 treated S. aureus andS. marcescens was carried out using spectrophotometer at 280 nmFig. 8. Scanning electron micrographs of S. marcescens. A: untreated, B: autoclavedtreated, C: SC-CO2 treated. Experimental conditions, autoclave: temperature 121 ◦Cand time 60 min; SC-CO2: pressure 20 MPa, temperature 60 ◦C and treatment time60 min.
54 Md.S. Hossain et al. / J. of Supercr
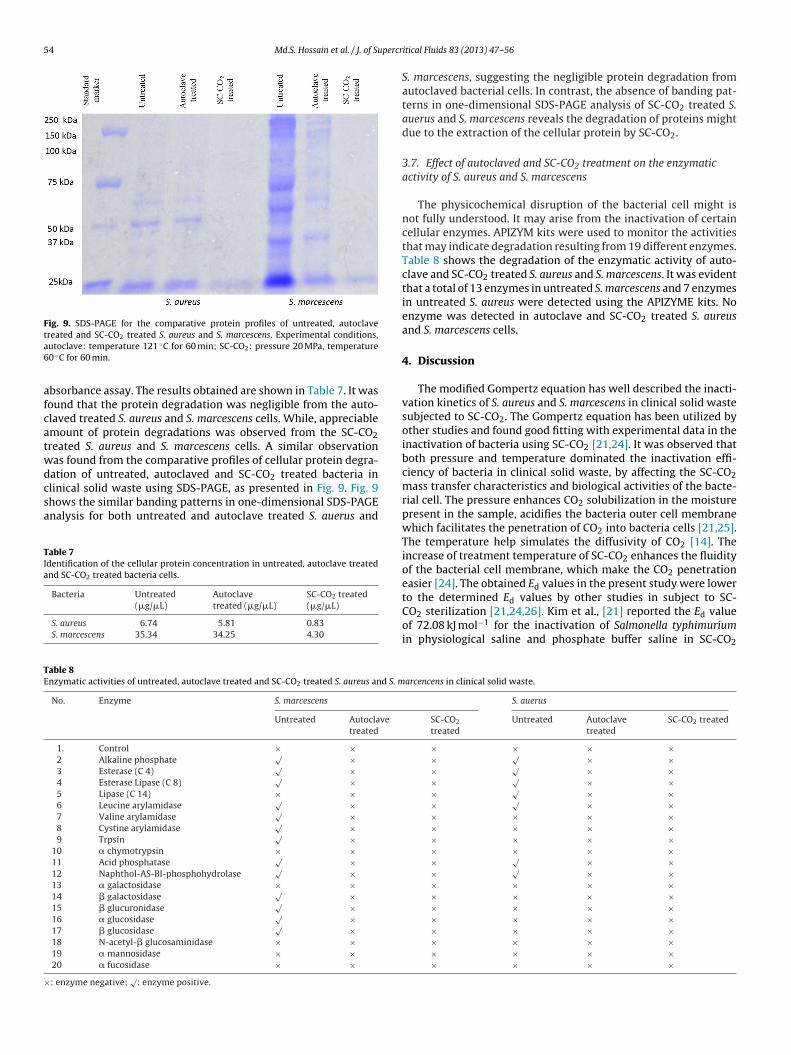
Fig. 9. SDS-PAGE for the comparative protein profiles of untreated, autoclaveta6
afcatwdcsa
TIa
TE
×
reated and SC-CO2 treated S. aureus and S. marcescens. Experimental conditions,utoclave: temperature 121 ◦C for 60 min; SC-CO2: pressure 20 MPa, temperature0 ◦C for 60 min.
bsorbance assay. The results obtained are shown in Table 7. It wasound that the protein degradation was negligible from the auto-laved treated S. aureus and S. marcescens cells. While, appreciablemount of protein degradations was observed from the SC-CO2reated S. aureus and S. marcescens cells. A similar observationas found from the comparative profiles of cellular protein degra-ation of untreated, autoclaved and SC-CO2 treated bacteria in
linical solid waste using SDS-PAGE, as presented in Fig. 9. Fig. 9hows the similar banding patterns in one-dimensional SDS-PAGEnalysis for both untreated and autoclave treated S. auerus andable 7dentification of the cellular protein concentration in untreated, autoclave treatednd SC-CO2 treated bacteria cells.
Bacteria Untreated(�g/�L)
Autoclavetreated (�g/�L)
SC-CO2 treated(�g/�L)
S. aureus 6.74 5.81 0.83S. marcescens 35.34 34.25 4.30
able 8nzymatic activities of untreated, autoclave treated and SC-CO2 treated S. aureus and S. m
No. Enzyme S. marcescens
Untreated Autoclavetreated
1. Control × ×
2 Alkaline phosphate√ ×
3 Esterase (C 4)√ ×
4 Esterase Lipase (C 8)√ ×
5 Lipase (C 14) × ×
6 Leucine arylamidase√ ×
7 Valine arylamidase√ ×
8 Cystine arylamidase√ ×
9 Trpsin√ ×
10 � chymotrypsin × ×
11 Acid phosphatase√ ×
12 Naphthol-AS-BI-phosphohydrolase√ ×
13 � galactosidase × ×
14 � galactosidase√ ×
15 � glucuronidase√ ×
16 � glucosidase√ ×
17 � glucosidase√ ×
18 N-acetyl-� glucosaminidase × ×
19 � mannosidase × ×
20 � fucosidase × ×
: enzyme negative;√
: enzyme positive.
itical Fluids 83 (2013) 47– 56
S. marcescens, suggesting the negligible protein degradation fromautoclaved bacterial cells. In contrast, the absence of banding pat-terns in one-dimensional SDS-PAGE analysis of SC-CO2 treated S.auerus and S. marcescens reveals the degradation of proteins mightdue to the extraction of the cellular protein by SC-CO2.
3.7. Effect of autoclaved and SC-CO2 treatment on the enzymaticactivity of S. aureus and S. marcescens
The physicochemical disruption of the bacterial cell might isnot fully understood. It may arise from the inactivation of certaincellular enzymes. APIZYM kits were used to monitor the activitiesthat may indicate degradation resulting from 19 different enzymes.Table 8 shows the degradation of the enzymatic activity of auto-clave and SC-CO2 treated S. aureus and S. marcescens. It was evidentthat a total of 13 enzymes in untreated S. marcescens and 7 enzymesin untreated S. aureus were detected using the APIZYME kits. Noenzyme was detected in autoclave and SC-CO2 treated S. aureusand S. marcescens cells.
4. Discussion
The modified Gompertz equation has well described the inacti-vation kinetics of S. aureus and S. marcescens in clinical solid wastesubjected to SC-CO2. The Gompertz equation has been utilized byother studies and found good fitting with experimental data in theinactivation of bacteria using SC-CO2 [21,24]. It was observed thatboth pressure and temperature dominated the inactivation effi-ciency of bacteria in clinical solid waste, by affecting the SC-CO2mass transfer characteristics and biological activities of the bacte-rial cell. The pressure enhances CO2 solubilization in the moisturepresent in the sample, acidifies the bacteria outer cell membranewhich facilitates the penetration of CO2 into bacteria cells [21,25].The temperature help simulates the diffusivity of CO2 [14]. Theincrease of treatment temperature of SC-CO2 enhances the fluidityof the bacterial cell membrane, which make the CO2 penetrationeasier [24]. The obtained Ed values in the present study were lower
to the determined Ed values by other studies in subject to SC-CO2 sterilization [21,24,26]. Kim et al., [21] reported the Ed valueof 72.08 kJ mol−1 for the inactivation of Salmonella typhimuriumin physiological saline and phosphate buffer saline in SC-CO2arcencens in clinical solid waste.
S. auerus
SC-CO2
treatedUntreated Autoclave
treatedSC-CO2 treated
× × × ×× √ × ×× √ × ×× √ × ×× √ × ×× √ × ×× × × ×× × × ×× × × ×× × × ×× √ × ×× √ × ×× × × ×× × × ×× × × ×× × × ×× × × ×× × × ×× × × ×× × × ×

percr
toi[S1rraotbiti
srafwtcmitardictwbps
imcnSrpiDirtawErpitt
bTmeebac
Md.S. Hossain et al. / J. of Su
reatment at pressure 10 MPa. Kim et al., [26] obtained the Ed valuef 84 kJ mol−1for E. coli O157:H7 and 110 kJ mol−1 for generic E. colin physiological saline subjected to SC-CO2 sterilization. Liao et al.,24] determined the Ed value of 20.64 kJ mol−in the inactivation ofalmonella typhimurium in carrot juice using a SC-CO2 pressure of0 MPa. Thus, it can be postulated that the Ed values of the bacte-ia inactivation might depend on the variation of bacteria species,ange of the temperature and the types of sample studied. Shulernd Kargi [27] obtained the Ed value for the thermal sterilizationf E. coli about 532 kJ mol−1. The minimal Ed values compared tohermal sterilization process is implying that the inactivation ofacteria using SC-CO2 does not occur as results of heat during the
nactivation process. Although, temperature is an important fac-or for the inactivation bacteria in SC-CO2 sterilization, it is not asmportant as in the thermal sterilization [21].
The re-growth bacteria was found in autoclave treated clinicalolid waste might be due to the incomplete destruction of the bacte-ial cell during sterilization the clinical solid waste. In other words,utoclave treated the bacteria physically, using heat that producedrom the saturated steam. The sterilization efficiency of autoclaveas highly dependents on the homogeneous heat penetration into
he waste [28]. Due to the low moisture content present in clini-al solid waste, the heat penetration into the clinical solid wasteight be heterogeneous resulting in minor injury and incomplete
nactivation of bacteria cell. The presence of sufficient nutrients inhe nutritious clinical solid waste at room temperature, would give
potential for the injured bacteria cell to re-grow. Earlier studieseported that the SC-CO2 prevents the growth of microorganismsue to the loss of cellular metabolisms [9,21,29]. SC-CO2 steril-
zation inactivates the bacteria both physically (by pressure) andhemically (the fluid CO2 extracts the cellular materials). Despitehe presence of nutritious nutrient in the sterilized clinical solidaste, the likelihood that two regrow is minimal due to the com-
ined effect of double effect SC-CO2 treatment. The analysis of SEMhotograph, protein and enzymatic activity of bacteria in SC-CO2terilized clinical solid waste confirmed the resulting effects.
Examination of the scanning electron micrographs did notndicate any morphological changes on autoclaved treated S.
arcescens and S. aureus cells. A differing effect with completeell wall destruction was observed in the SC-CO2 treated gramegative S. marcescens. Partial cell wall damage was observed inC-CO2 treated gram positive bacteria of S. aureus. These bacte-ia showed ruptures on the surface as a consequent of SC-CO2ressure and the penetration of the fluid CO2 into the cells dur-
ng the SC-CO2 sterilization (Fig. 7). In comparison to the work ofillow et al., [14], who observed that the SC-CO2 treated gram pos-
tive S. aureus and gram negative E. coli cells in the SEM imagesemained largely intact. These bacteria were isolated from SC-CO2reated biodegradable polymers at pressure 20.5 MPa and temper-ture 34 ◦C for 45 min. This is unlike the findings by Kim et al., [26]ho made the observation that the ofSC-CO2 treated and untreated
. coli O157:H7 at pressure 10 MPa, temperature 35 ◦C for 30 minemained practically the same. In contrast to the significant mor-hological structural changes of SC-CO2 treated bacteria observed
n the present study which might be due to higher experimen-al conditions (pressure 20 MPa, temperature 60 ◦C and treatmentime 60 min).
The outer surface remained smooth and intact, and negligi-le protein degradation was observed in autoclaved bacteria cells.his is unlike to the obvious protein degradation observed in S.arcescens and S. aureus exposed to SC-CO2 (Table 7). The loss of
nzymatic activity in bacteria occur either via the inactivation of
nzymes themselves or by the physicochemical disruption of theacteria cells [26,30]. In this study the loss of the cellular enzymaticctivity in autoclaved S. marcescens, S. aureus might be due to theoagulation of the cellular enzyme by the saturated steam heat.itical Fluids 83 (2013) 47– 56 55
While in SC-CO2 sterilization, the loss of the enzymatic activity ofS. marcescens, S. aureus cells could be due to the physicochemicaldisruption of the bacteria cells.
In essence, the inactivation of S. aureus and S. marcescens insteam autoclave treated clinical waste might be due to the lossof cellular enzymatic activities of the bacteria. The heat from thesaturated steam during autoclave treatment denatured the cellularenzyme thus losing the activity. This observation was found similarto the proposed deactivation mechanism of bacteria in the steamautoclave treatment by Rutala [31]. Examination of the SEM images,conclusions from cellular protein and enzymatic activity tests of SC-CO2 treated S. marcescens and S. aureus cells suggest that the SC-CO2inactivates the bacteria both physically and chemically. The pres-sure causes the rupture and penetration of the SC-CO2 into the cellwall, which results in cell wall damage or formation of fissures onthe cell wall and, loss of outer membrane. The fluid CO2 could havedissolved cellular materials and extracted out with the SC-CO2. Thefindings of the present study is in congruent with the proposedinactivation mechanisms of bacteria in the SC-CO2 treatment byLin et al., [32] and Zhang et al., [10]. The inactivation mechanismof bacteria in SC-CO2 sterilized clinical solid waste were consid-ered to be consistent with results of mathematical analysis usingGompertz modified equation. In the lag phase, SC-CO2 were in con-tact with the bacterial cell present in the waste, and simultaneouslypenetrated and dissolved the cellular materials of bacteria. The dis-solution and extraction of the cellular materials of the bacteria mostlikely to have occurred at the exponential phase.
5. Conclusion
The modified Gompertz equation was well described the SC-CO2inactivation kinetics of S. aureus and S. marcescens in clinical solidwaste. The Arrhenius plot for the inactivation of S. aureus and S.marcescens in clinical solid waste revealed the inactivation of bacte-ria in SC-CO2 was not only the physical effect by the high pressure ofSC-CO2, but the combination of the physical and chemical effects ofSC-CO2. The bacterial re-growth in autoclave treated clinical solidwaste reveals that the steam autoclave is an ineffective method fortreating clinical solid waste. Analysis of SEM images, cellular pro-tein, enzymatic activity and the absence of re-growth of bacteria inSC-CO2 sterilized in clinical solid waste indicated that the SC-CO2 isan effective method for the inactivation of bacteria in clinical solidwaste.
Acknowledgements
This work was supported by the Research University grantof Universiti Sains Malaysia (1001/PTEKIND/811185). One of theauthors, gratefully acknowledges the Institute for Post GraduateStudies, Universiti Sains Malaysia for providing a post graduateresearch fellowship as financial support.
References
[1] M.S. Hossain, A. Santhanam, N.A. Nik Norulaini, A.K. Mohd Omar, Clinicalsolid waste management practices and its impact on human health andenvironment—a review, Waste Management 31 (2011) 754–766.
[2] A. Bdour, B. Altrabsheh, N. Hadadin, M. Al-Shareif, Assessment of medicalwastes management practice: a case study of the northern part of Jordan, WasteManagement 27 (2007) 746–759.
[3] A.Z. Alagöz, G. Kocasoy, Determination of the best appropriate managementmethods for the health-care wastes in Istanbul, Waste Management 28 (2008)1227–1235.
[4] M. Sawalem, E. Selic, J.D. Herbell, Hospital waste management in Libya: a casestudy, Waste Management 29 (2009) 1370–1375.
[5] B.-K. Lee, M.J. Ellenbecker, R. Moure-Ersaso, Alternatives for treatment anddisposal cost reduction of regulated medical wastes, Waste Management 24(2004) 143–151.
5 percr
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
6 Md.S. Hossain et al. / J. of Su
[6] N. Marinkovic, K. Vitale, N.J. Holcer, A. Dzakula, T. Pavic, Management of haz-ardous medical waste in Croatia, Waste Management 28 (2008) 1049–1056.
[7] M. Tsakona, E. Anagnostopoulou, E. Gidarakos, Hospital waste managementand toxicity evaluation: a case study, Waste Management 27 (2007) 912–920.
[8] T.L. Tudor, Towards the development of a standardised measurement unit forhealthcare waste generation, Resources, Conservation and Recycling 50 (2007)319–333.
[9] A. White, D. Burns, T.W. Christensen, Effective terminal sterilization usingsupercritical carbon dioxide, Journal of Biotechnology 123 (2006) 504–515.
10] J. Zhang, T.A. Davis, M.A. Matthews, M.J. Drews, M. LaBerge, Y.H. An, Sterilizationusing high-pressure carbon dioxide, Journal of Supercritical Fluids 38 (2006)354–372.
11] N.A. Nik Norulaini, A. Ahmad, F.M. Omar, A.A.S. Banana, I.S.Md. Zaidul, M.O.Ab.Kadir, Sterilization and extraction of palm oil from screw pressed palm fruitfiber using supercritical carbon dioxide, Separation and Purification Technology60 (2008) 272–277.
12] S. Spilimbergo, A. Bertucco, F.M. Lauro, G. Bertoloni, Inactivation of Bacillus sub-tilis spores by supercritical CO2 treatment, Innovative Food Science & EmergingTechnologies 4 (2003) 161–165.
13] S.R. Kim, H.T. Kim, H.J. Park, S. Kim, H.J. Choi, G.-S. Hwang, J.H. Yi, D.H. Ryu, K.H.Kim, Fatty acid profiling and proteomic analysis of Salmonella enterica serotypeTyphimurium inactivated with supercritical carbon dioxide, International Jour-nal of Food Microbiology 134 (2009) 190–195.
14] A.K. Dillow, F. Dehghani, J.S. Hrkach, N.R. Foster, R. Langer, Bacterial inactivationby using near- and supercritical carbon dioxide, Proceedings of the NationalAcademy of Sciences of the United States of America 96 (1999) 10344–10348.
15] M.N. Chong, B. Jin, H. Zhu, C. Saint, Bacterial inactivation kinetics, regrowth andsynergistic competition in a photocatalytic disinfection system using anatasetitanate nanofiber catalyst, Journal of Photochemistry and Photobiology A:Chemistry 214 (2010) 1–9.
16] P. Rusin, J. Rose, C. Haas, C. Gerba, Risk assessment of opportunistic bacte-rial pathogens in drinking water, in: G. Ware (Ed.), Reviews of EnvironmentalContamination and Toxicology, Springer, New York, 1997, pp. 57–83.
17] M.S. Hossain, V. Balakrishnan, N.N.N.A. Rahman, M.Z.I. Sarker, M.O.A. Kadir,Treatment of clinical solid waste using a steam autoclave as a possible alter-native technology to incineration, International Journal of EnvironmentalResearch and Public Health 9 (2012) 855–867.
18] (a) H. Liao, X. Hu, X. Liao, F. Chen, J. Wu, Inactivation of Escherichia coli inoculatedinto cloudy apple juice exposed to dense phase carbon dioxide, InternationalJournal of Food Microbiology 118 (2007) 126–131;(b) Y.-W. Tang, C.W. Stratton, Staphylococcus aureus: an old pathogen with newweapons, Clinics in Laboratory Medicine 30 (2010) 179–208.
[
[
itical Fluids 83 (2013) 47– 56
19] A.A. Bremer, R.O. Darouiche, Ventriculoperitoneal shunt infection due to Ser-ratia marcescens, Journal of Infection 50 (2005) 138–141.
20] M.S. Hossain, N.A. Nik Norulaini, V. Balakrishnan, V. Puvanesuaran, M. Sarker,A.K. Mohd Kadir, Infectious risk assessment of unsafe handling practices andmanagement of clinical solid waste, International Journal of EnvironmentalResearch and Public Health 10 (2013) 556–567.
21] S.R. Kim, M.S. Rhee, B.C. Kim, H. Lee, K.H. Kim, Modeling of the inactivation ofSalmonella typhimurium by supercritical carbon dioxide in physiological salineand phosphate-buffered saline, Journal of Microbiological Methods 70 (2007)132–141.
22] S. Hossain, Supercritical Cabon Dioxide sterilization of Clinical Solid Waste,School of Industrial Technology, Universiti Sains Malaysia, Penang, Malaysia,2013, pp. 245.
23] U.K. Laemmli, Cleavage of structural proteins during the assembly of the headof bacteriophage T4, Nature 227 (1970) 680–685.
24] H. Liao, X. Kong, Z. Zhang, X. Liao, X. Hu, Modeling the inactivation of Salmonellatyphimurium by dense phase carbon dioxide in carrot juice, Food Microbiology27 (2010) 94–100.
25] L. Garcia-Gonzalez, A.H. Geeraerd, J. Mast, Y. Briers, K. Elst, L. Van Ginneken,J.F. Van Impe, F. Devlieghere, Membrane permeabilization and cellular death ofEscherichia coli, Listeria monocytogenes and Saccharomyces cerevisiae as inducedby high pressure carbon dioxide treatment, Food Microbiology 27 (2010)541–549.
26] S.R. Kim, M.S. Rhee, B.C. Kim, K.H. Kim, Modeling the inactivation ofEscherichia coli O157:H7 and generic Escherichia coli by supercritical carbondioxide, International Journal of Food Microbiology 118 (2007) 52–61.
27] M.L. Shuler, F. Kargi, Bioprocess Engineering: Basic Concepts, Prentice Hall, NewJersey, USA, 2002.
28] J.L. Lauer, D.R. Battles, D. Vesley, Decontaminating infectious laboratorywaste by autoclaving, Applied and Environmental Microbiology 44 (1982)690–694.
29] F. Dehghani, N. Annabi, M. Titus, P. Valtchev, A. Tumilar, Sterilization of gin-seng using a high pressure CO2 at moderate temperatures, Biotechnology andBioengineering 102 (2009) 569–576.
30] S.-I. Hong, Y.-R. Pyun, Membrane damage and enzyme inactivation of Lacto-bacillus plantarum by high pressure CO2 treatment, International Journal ofFood Microbiology 63 (2001) 19–28.
31] W.A. Rutala, Disinfection and sterilization of patient-care items, Infection con-trol and Hospital Epidemiology 17 (1996) 377–384.
32] H.-M. Lin, Z. Yang, L.-F. Chen, Inactivation of Saccharomyces cerevisiae bysupercritical and subcritical carbon dioxide, Biotechnology Progress 8 (1992)458–461.