
Congenital Intraspinal Lipomas: Histological Analysis of 234 Cases and Review of the Literature
7
Congenital Intraspinal Lipomas: Histological Analysis of 234 Cases and Review of the Literature ARIELLE LELLOUCH-T UBIANA, 1 *MICHEL ZERAH, 2 MARTIN CATALA, 3 NICOLE BROUSSE, 1 AND ALAIN-PIERRE KAHN 2 1 Laboratoire d’Anatomie Pathologique, Ho ˆ pital Necker-Enfants Malades, 149 rue de Se ` vres, 75015 Paris, France 2 Service de Neurochirurgie Pe ´ diatrique, Ho ˆ pital Necker-Enfants Malades, 149 rue de Se ` vres, 75015 Paris, France 3 Laboratoire d’Histologie-Embryologie, Ho ˆ pital Pitie ´ -Salpe ˆ trie ` re, Paris, URA CNRS 2115, 75013 Paris, France Received November 28, 1997; accepted September 4, 1998. ABSTRACT The clinical, radiologic, and pathologic data from a series of 234 patients hospitalized in the Pediatric Neuro- surgical Department of the Necker–Enfants Malades Hospital, Paris, for congenital intraspinal lipomas and operated on from 1976 to 1995 were examined. Histologi- cal studies showed that these lesions may be simple lipomas, similar to those developing elsewhere in the body, or they may be more complex forms including in addition to the lipomatous component a variety of unusual ectopic tissues of ectodermal, mesodermal, and/or endodermal origin. These complex forms indica te the malformative nature of these tumors. When they contain elements that are truly foreign to the region, the possibility of teratoma with a tumoral potential should be considered. Data found in the literature and from Necker–Enfants Malades Hospital are dis- cussed. Key words: congenital intraspinal lipoma, dysraphia, teratoma INTRODUCTION Congenital intraspinal lipomas are a rare form of spinal dysraphism in children. They can be defined as a mass of adiposal tissue coming in contact with the medullary nervous tissue. Intraspinal lipomas involve mainly the lower extremity of the spinal canal: they may involve the filum or, more often, the conus. Lipomas of the cord are exceptional, and are mostly thoracic. The incidence of the malformation, calcu- lated from two French regional registers, was found to be 4 to 8.5/100,000. This estimate, however, is certainly low, because the number of symptomless intraspinal lipomas is unknown. In all series, the two main clinical features leading to diagnosis were cutaneous stigmata on the lower back and neurological disturbances that are mainly neuro- orthopedic and sphincter-related. These presum- ably stable lesions can grow in some cases. Surgical indications are controversial in asymptomatic pa- tients and pathogenesis is still a matter of debate. Using the series of 234 intraspinal lipomas oper- ated on in the Pediatric Neurosurgical Department of the Ho ˆ pital des Enfants Malades in Paris, we describe here the histological findings of these rare lesions and discuss their anatomic, clinical, embryo- logic, and pathologic features. METHODS The study was carried out retrospectively, using data from 234 patients who had congenital intraspi- *Corresponding author Pediatric and Developmental Pathology 2, 346–352, 1999 Pediatric and Developmental Pathology r 1999 Society for Pediatric Pathology
-
Upload
univ-paris5 -
Category
Documents
-
view
0 -
download
0
Transcript of Congenital Intraspinal Lipomas: Histological Analysis of 234 Cases and Review of the Literature
Congenital Intraspinal Lipomas:Histological Analysis of 234 Casesand Review of the Literature
ARIELLE LELLOUCH-TUBIANA,1* MICHEL ZERAH,2 MARTIN CATALA,3NICOLE BROUSSE,1 AND ALAIN-PIERRE KAHN2
1Laboratoire d’Anatomie Pathologique, Hopital Necker-Enfants Malades, 149 rue de Sevres, 75015 Paris, France2Service de Neurochirurgie Pediatrique, Hopital Necker-Enfants Malades, 149 rue de Sevres, 75015 Paris, France3Laboratoire d’Histologie-Embryologie, Hopital Pitie-Salpetriere, Paris, URA CNRS 2115, 75013 Paris, France
Received November 28, 1997; accepted September 4, 1998.
ABSTRACTThe clinical, radiologic, and pathologic data from aseries of 234 patients hospitalized in the Pediatric Neuro-surgical Department of the Necker–Enfants MaladesHospital, Paris, for congenital intraspinal lipomas andoperated on from 1976 to 1995 were examined. Histologi-cal studies showed that these lesions may be simplelipomas, similar to those developing elsewhere in thebody, or they may be more complex forms including inaddition to the lipomatous component a variety ofunusual ectopic tissues of ectodermal, mesodermal,and/or endodermal origin. These complex forms indicate the malformative nature of these tumors. When theycontain elements that are truly foreign to the region,the possibility of teratoma with a tumoral potentialshould be considered. Data found in the literatureand from Necker–Enfants Malades Hospital are dis-cussed.
Key words: congenital intraspinal lipoma, dysraphia,teratoma
INTRODUCTIONCongenital intraspinal lipomas are a rare form ofspinal dysraphism in children. They can be definedas a mass of adiposal tissue coming in contact withthe medullary nervous tissue. Intraspinal lipomas
involve mainly the lower extremity of the spinal
canal: they may involve the filum or, more often,
the conus. Lipomas of the cord are exceptional, and
are mostly thoracic.
The incidence of the malformation, calcu-
lated from two French regional registers, was found
to be 4 to 8.5/100,000. This estimate, however, is
certainly low, because the number of symptomless
intraspinal lipomas is unknown. In all series, the
two main clinical features leading to diagnosis
were cutaneous stigmata on the lower back and
neurological disturbances that are mainly neuro-
orthopedic and sphincter-related. These presum-
ably stable lesions can grow in some cases. Surgical
indications are controversial in asymptomatic pa-
tients and pathogenesis is still a matter of debate.
Using the series of 234 intraspinal lipomas oper-
ated on in the Pediatric Neurosurgical Department
of the Hopital des Enfants Malades in Paris, we
describe here the histological findings of these rare
lesions and discuss their anatomic, clinical, embryo-
logic, and pathologic features.
METHODSThe study was carried out retrospectively, using
data from 234 patients who had congenital intraspi-*Corresponding author
Pediatric and Developmental Pathology 2, 346–352, 1999 Pediatric and Developmental Pathology
r1999 Society for Pediatric Pathology

nal lipomas and were operated on at the Necker–Enfants Malades Hospital in Paris from 1976 to1995.
The mean age of the patients at the time ofsurgery was 6 years, 4 months. The lipomas in-volved almost exclusively the conus. Rare cases of
lipomas of the filum were included in this study. Allsurgical specimens were examined histologically.The samples were fixed by immersion in 10%formaldehyde, dehydrated, and embedded in paraf-fin, then sectioned and stained with hematoxylin-eosin-safranin and Masson’s trichrome.
Figure 1. Macroscopy of a spinal lipoma, showing agreasy surface.
Figure 2. Photomicrograph of the lipoma. The tumor iscomposed of well-differentiated adipose tissue. Fibroussepta divide the fatty mass into a multilobular pattern.Hematoxylin-eosin, 3100.
Figure 3. Intralipomatous Vater-Pacini neurosensorialcorpuscle. Hematoxylin-eosin, 3400.
Figure 4. Intralipomatous glial tissue surrounded bydense fibrosis. Hematoxylin-eosin, 3200.
Figure 5. Photomicrograph of a lipoma showing afibrous nodule containing an ependymal-lined canalsurrounded by arachnoidal tissue. Hematoxylin-eosin,3180.
Figure 6. Photomicrograph of a squamous epithelialtissue.
CONGENITAL INTRASPINAL LIPOMAS 347

RESULTSClinically in our series there was a significantfemale preponderance (F/M: 1.6/1). The averageage at diagnosis was 6.4 years. The malformationwas diagnosed earlier in the presence of cutaneousstigma as well as more recently. From 1990 to 1994,the average age at diagnosis was 9 months, withpatients showing skin abnormality. Cutaneousanomalies were present in 89.4% of our patients.The most frequent of these skin anomalies was asubcutaneous lump located at the midline of thelower back. Neurological deficits affected 56.7% ofour patients; these were predominantly sphincterdisturbances (42%) and motor deficits (31%). In allseries, vesical sphincter dysfunctions were the mostfrequent deficit. They affected more than half ofour patients and included incontinence, dysuria/retention, and infection. Bowel dysfunction con-sisted of constipation, sometimes severe, and stoolleakage. A neuro-orthopedic syndrome was presentin 31% of our patients and affected the lower limbs:40% of our patients had a club foot, often with anequinovarus deformity with clawing of the toes,36% had muscular atrophia of the leg, 21% hadhypotrophia of the leg or foot, and 27.6% hadsuperficial hypoesthesia. At examination, 34% ofpatients had a central motor neuron syndrome.
Associated spinal malformations occurredmostly as spina bifida occulta, which was presentin 91% of our patients. Associated visceral malfor-mations were found in 27% of patients in our series(Table 1). Uroanogenital malformations were themost frequent. Eighty percent of intraspinal lipo-mas in this series involved the conus, and 20%, thefilum. In 23% of cases histological examinationshowed lipomas similar to subcutaneous lipomasdeveloping elsewhere in the body (Fig. 1). Theywere made of mature adiposal cells, arranged inlobules with a striking amount of fibrous tissue
interspersed between the adiposal lobules (Fig. 2).In 77% of cases lipomas appeared more complex,containing a wide variety of ectopic tissues ofectodermal, mesodermal, or endodermal origin(Tables 2 and 3). Indeed, careful examination of thelipomas showed associated tissues. In our series,the more frequent tissues encountered were stri-ated muscular tissue (37%), nerves (63%), andsensory nerve corpuscles, such as Vater-Pacini (Fig.3) or end-bulb of Krause (21%). All these tissueswere intralipomatous, surrounded by a dense fibro-sis, and were part of the lesion. In 18% of cases glialor neuroglial tissue, surrounded by fibrous tissue,was observed, without an association of myelome-ningocele (Fig. 4). In 7% of cases arachnoid tissuewas found associated with glial tissue or isolated ina fibrous strand. Ependymal structures, arrangedas ependymal cells lining canals of irregular out-lines, and sometimes surrounded by glial tissue,were present in 5% of cases (Fig. 5). Other tissueswere more rarely observed in association with thefatty cells of the lipoma. In our series we foundsquamous epithelial tissue (2%) (Fig. 6), often
Table 1. Visceral associated malformations
Malformations n %
Anorectal 15 6.4
Genital 9 3.8
Urinary 14 6
Cardiac 5 2.1
Other 21 8.9
Total 64 27
Table 2. Type of tissues found in lipomas
n %
Tissues normally presentin sacrococcygeal region
Skeletal muscle 87 37
Sensory nerve corpuscles 50 21
Neuroglial tissue 37 18
Ependymal tissue 10 5
Meningeal tissue 14 7
Skin 5 2
Bone 8 3
Cartilage 15 6
Smooth muscle 15 6
Autonomic ganglia 11 5
Ganglion cells 3 1
Lymph nodes 8 3
Tissues foreign to sacrococcygeal region
Homologous
Cerebellar tissue 1 ,1
Immature neural tissue 5 2
Heterologous
Renal 2 1
Respiratory 2 1
Digestive 2 1
348 A. LELLOUCH-TUBIANA ET AL.

lining dermoid or epidermoid cysts, cartilaginousnodules (6%), bone tissue (3%), lymph nodes (3%),and autonomic ganglia (5%), as well as capillaryangiomas included in the lipomatous mass (4%)(Fig. 7). Finally, other tissue patterns foreign to thelumbosacral region were present in our series:smooth muscular tissue (6%), and respiratory ordigestive epithelia lining cysts (2%). Some epithe-lial cysts were lined by ciliated cells and had asmooth muscle muscularis in their walls and con-tained seromucous glands, suggesting bronchialwalls. We also found renal corpuscles (1%) (Fig. 8)and cerebellar tissue (,1%) (Fig. 9).
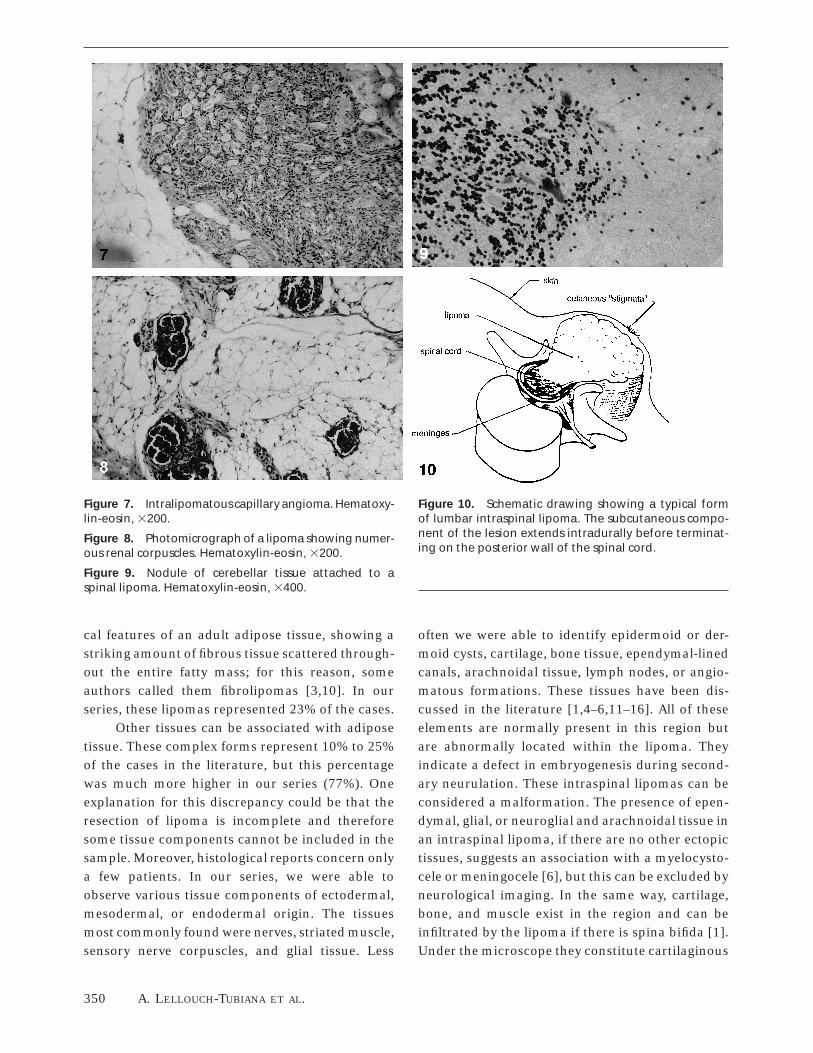
DISCUSSIONCongenital intraspinal lipomas are well-known le-sions that have been reported on numerous occa-sions, but only few reports have included histologi-cal study [1–6]. Anatomically, intraspinal lipomasare distributed on both sides of a spina bifida—onone side in the subcutaneous tissue, without de-fined outlines and along with the normal adiposetissue, and on the other side intradurally in thesubarachnoid spaces before terminating on theposterior face of the spinal cord (Fig. 10). Thespinal cord is exceptionally normal and its termina-tion is usually low lying, under the second lumbarvertebra, which is considered the normal inferiorlevel. Anomalies of the spinal cord include cavita-tion, torsion, duplication, and rarely, segmentar
agenesis. Hydromyelia is the anomaly most fre-quently observed; it is usually terminal, and rarelyextends to thoracic or cervical segments. The rootsgenerally show abnormal direction, conformation,or distribution.
Embryologically, the tail bud is formed afterthe end of primary or classic neurulation. Afterclosure of the posterior neuropore, all the tissueslying caudally to the already formed neural tubeaggregate to form a mass of cells, the so-called tailbud. This mass grows and yields a solid cellularcylinder, the medullary cord. This cavitates andcoalesces with all the cavities that ultimately form acentral canal, prolonging that which was formedduring primary neurulation. The tail bud is thusresponsible for development of the caudal part ofthe spinal cord. This type of neurulation proceed-ing cavitation has been termed secondary neurula-tion [7].
In our series, as in most others in the litera-ture, there was a significant female preponderance.The average age at diagnosis in our series was 6.4years, similar to that reported in the literature (7.1years). In all series, the two main clinical featuresleading to diagnosis were cutaneous stigmata onthe lower back and neurological disturbances, thatare mainly neuro-orthopedic and sphincter-related.The concept that intraspinal lipomas cause neuro-logical symptoms by ‘‘tethering’’ the spinal cord inthe growing child has gained wide acceptance [8,9],although this does not necessarily exclude thecompression effect that is restricted to a few caseswith larger lesions or with unstable lesions mani-festing growth.
In all series, 90.5% of the patients had skinstigmata and neurologic deficits affected .58% ofpatients, predominantly sphincter disturbances(61%) and motor deficits (39%). Overall, vesicalsphincter dysfunctions were the most frequentdeficit. They affected more than half of our pa-tients. Associated visceral malformations were re-ported in 16% of the published cases and 27% inour series.
The consensus in the literature on surgicalindications in symptomatic children is that earlysurgery is favored. Surgery for asymptomatic pa-tients, however, is still debated. There are very fewhistopathological studies of these congenital intra-spinal lipomas. Some of them report the histologi-
Table 3. Quantity of tissues present in lipomas
n %
Fat alone (pure lipomas) 54 23
Regional tissues other than fat
1 Tissue 56 24
2 Tissues 35 15
3 Tissues 10 4.27
4 Tissues 4 1.7
5 Tissues 1 ,1
Tissues not normally present in region
Renal only 1 ,1
Respiratory only 1 ,1
Digestive only 2 1
Cerebellar 1 ,1
Immature neural tissue 5 2
Renal 1 respiratory 1 ,1
CONGENITAL INTRASPINAL LIPOMAS 349
cal features of an adult adipose tissue, showing astriking amount of fibrous tissue scattered through-out the entire fatty mass; for this reason, someauthors called them fibrolipomas [3,10]. In ourseries, these lipomas represented 23% of the cases.
Other tissues can be associated with adiposetissue. These complex forms represent 10% to 25%of the cases in the literature, but this percentagewas much more higher in our series (77%). Oneexplanation for this discrepancy could be that theresection of lipoma is incomplete and thereforesome tissue components cannot be included in thesample. Moreover, histological reports concern onlya few patients. In our series, we were able toobserve various tissue components of ectodermal,mesodermal, or endodermal origin. The tissuesmost commonly found were nerves, striated muscle,sensory nerve corpuscles, and glial tissue. Less
often we were able to identify epidermoid or der-moid cysts, cartilage, bone tissue, ependymal-linedcanals, arachnoidal tissue, lymph nodes, or angio-matous formations. These tissues have been dis-cussed in the literature [1,4–6,11–16]. All of theseelements are normally present in this region butare abnormally located within the lipoma. Theyindicate a defect in embryogenesis during second-ary neurulation. These intraspinal lipomas can beconsidered a malformation. The presence of epen-dymal, glial, or neuroglial and arachnoidal tissue inan intraspinal lipoma, if there are no other ectopictissues, suggests an association with a myelocysto-cele or meningocele [6], but this can be excluded byneurological imaging. In the same way, cartilage,bone, and muscle exist in the region and can beinfiltrated by the lipoma if there is spina bifida [1].Under the microscope they constitute cartilaginous
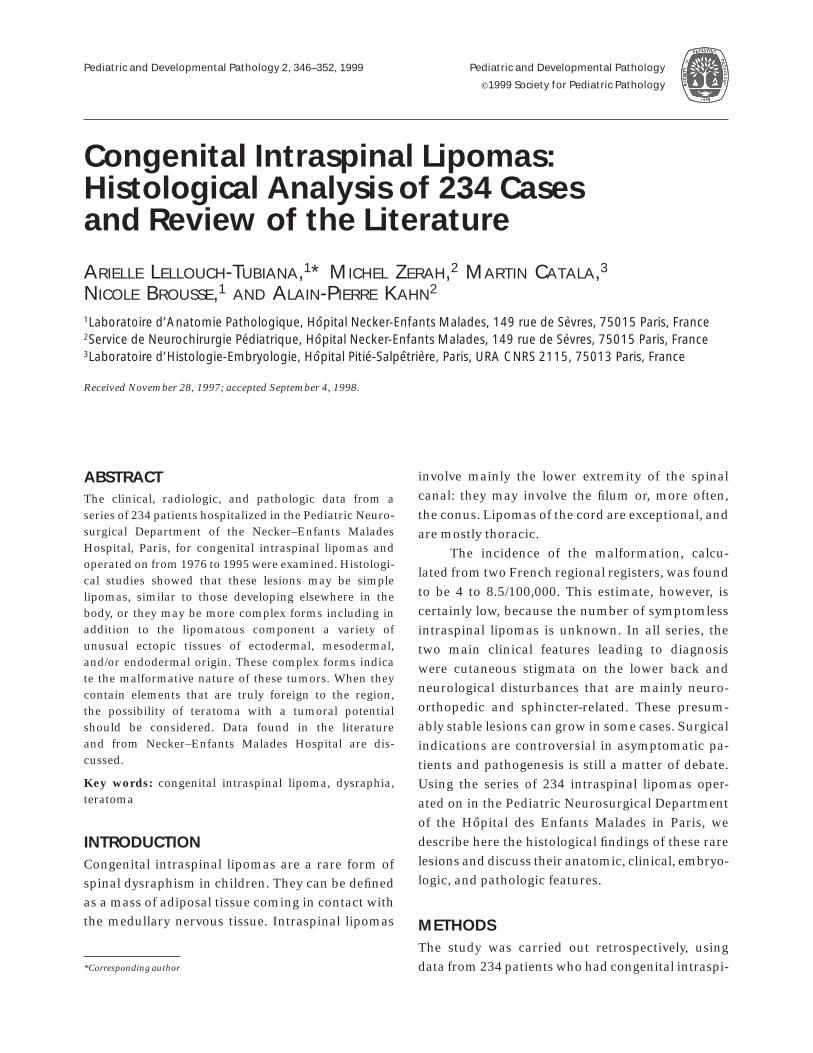
Figure 7. Intralipomatous capillary angioma. Hematoxy-lin-eosin, 3200.
Figure 8. Photomicrograph of a lipoma showing numer-ous renal corpuscles. Hematoxylin-eosin, 3200.
Figure 9. Nodule of cerebellar tissue attached to aspinal lipoma. Hematoxylin-eosin, 3400.
Figure 10. Schematic drawing showing a typical formof lumbar intraspinal lipoma. The subcutaneous compo-nent of the lesion extends intradurally before terminat-ing on the posterior wall of the spinal cord.
350 A. LELLOUCH-TUBIANA ET AL.

or bony nodules and muscular fascicles included
within the lipoma, far from the surrounding tissue.
Small intralipomatous angiomatous formations
were found in our series. These lesions have
been reported in the literature as angiolipomas
[17–21].
Much more rarely, ectopic tissues that are
never encountered in the region have been ob-
served in the lipoma. We have identified renal
corpuscles, cysts lined by a respiratory or digestive
epithelium, and even a nodule of cerebellar paren-
chyma attached to the lipoma. Occasionally one
finds bits of cerebellum free in the spinal subarach-
noid space because of herniation, but usually they
are necrotic. Endometrial tissue has been reported
in the literature in two observations [8,9], and
occasional lipomas have been associated with het-
erotopic thyroid tissue [10]. The presence of only
one ectopic mature tissue can be considered a
malformative heterotopia (choristoma). However,
if more than one heterotopic tissue type that is
totally foreign to the region, of ectodermal, endoder-
mal, and mesodermal origin, and at different stages
of maturation—from the embryonal stage to adult
tissue—is present within the lipoma, the possibility
of teratoma with a tumoral potential should be
considered. These are mostly benign teratomas,
and are pluritissular and mature. Individual cases
of malignant degeneration of these teratomas have
been described [22,23]. Delayed malignant transfor-
mation took the form of anaplastic carcinoma. The
presence of embryonal tissue components in the
teratoma, generally immature nervous tissue, sug-
gests an immature teratoma, which classically has
a bad prognosis. For Lemire and Beckwith [6], the
immaturity of a teratoma must be correlated with
the patient’s age and in a very young child, doesn’t
necessarily indicate a bad prognosis, in contrast to
an adult. For these authors, malignancy rarely
occurs in the form of a yolk sac tumor. This raises
the question as to whether these complex lipomas
can behave like a tumor. It is widely accepted that
congenital intraspinal lipomas are anatomically
stable lesions [24]. Nevertheless, growth has been
reported when obesity occurs [13,25]. Rarely,
growth of complex teratomas may result from
malignant degeneration [22,23].
In conclusion, congenital lumbosacral lipo-
mas are often complex lesions in which adiposal
tissue is associated with a variety of tissue patterns.
In most cases, they are malformative lesions or
hamartomas. But when they contain tissues totally
foreign to the region, the possibility of teratoma
with a tumoral potential should be considered, and
may explain their behavior.
REFERENCES
1. Bale PM. Sacrococcygeal developmental abnormalities andtumors in children. Perspect Pediatr Pathol 1984;1:9–56.
2. Kernohan JW, Woltman HW, Adson AW. Intramedullarytumors of the spinal cord: a review of fifty-one cases, withan attempt at histologic classification. Arch Neurol Psychia-try 1931;25:679–701.
3. Ehni G, Love JG. Intraspinal lipomas. Arch Neurol Psychia-try 1945;53:1–28.
4. Bouton JM, Martin CH, Rickham PP. Hamartoma andspina bifida. J Pediatr Surg 1966;1:559–565.
5. Walsh JW, Markesbery WR. Histological features of con-genital lipomas of the lower spinal canal. J Neurosurg1980;52:564–569.
6. Lemire RJ, Beckwith JB. Pathogenesis of congenital tu-mors and malformations of the sacrococcygeal region.Teratology 1982;25:201–213.
7. Catala M, Teillet MA, Le Douarin NM. Organization anddevelopment of the tail bud analyzed with the quail-chickchimaera system. Mech Dev 1995;51:51–65.
8. Molleston MC, Roth KA, Wippold FJ, Grubb RL. Tetheredcord syndrome from a choristoma of mullerian origin. JNeurosurg 1991;74:497–500.
9. Rougier A, Vital C, Caillaud P. Uterus-like mass of theconus medullaris with associated tethered cord. Neurosur-gery 1993;33:328–331.
10. Emery JC, Lenden RG. Lipomas of the cauda equina andother fatty tumors related to neurospinal dysraphism. DevMed Child Neurol 1969;20:62–70.
11. Stookey B. Intradural spinal lipoma. Arch Neurol Psychia-try 1927;18:16–43.
12. Taniguchi T, Mufson JA. Intradural lipoma of the spinalcord. J Neurosurg 1950;10:584–586.
13. Bassett RC. The neurologic deficit associated with lipomasof the cauda equina. Ann Surg 1950;13:109–116.
14. Derek AB, Bruce MB, Sutton LN. Management of the childwith a lipomyelomeningocele. Clin Neurosurg 1981;30:464–476.
15. Gowers WR. Myolipoma of spinal cord. Trans Pathol SocLond 1876;27:19–22.
16. Sachs E, Fincher EF. Intramedullary lipoma of the spinalcord. Arch Surg 1928;17:829–833.
17. Anson JA, Cybulski GR, Reyes M. Spinal extradural angio-lipoma: a report of two cases and review of the literature.Surg Neurol 1990;34:173–178.
18. Kuroda S, Abe H, Akino M, Iwasaki Y, Nagashima K.Infiltrating spinal angiolipoma causing myelopathy: casereport. Neurosurgery 1990;27:315–318.
19. Miki T, Oka M, Shima M, Hirofuji E, Tanaka S. Spinalangiolipoma. A case report. Acta Neurochirurg 1981;58:115–119.
CONGENITAL INTRASPINAL LIPOMAS 351

20. Pagni CA, Canavero S. Spinal epidural angiolipoma: rareor unreported? Neurosurgery 1992;31:758–764.
21. Preul MC, Leblanc R, Tampieri D, Robitaille Y, Pokrupa R.Spinal angiolipomas. J Neurosurg 1993;78:280–286.
22. Love JG. Delayed malignant development of a con-genital teratoma with spina bifida. J Neurosurg 1968;29:532–533.
23. Mickle JP, Mc Lennan JE. Malignant teratoma arisingwithin a lipomeningocele. J Neurosurg 1975;43:761–763.
24. Swanson HS, Barnett JC. Intradural lipomas in children.Pediatrics 1962;29:911–926.
25. Aoki N. Rapid growth of intraspinal lipoma demonstratedby magnetic resonance imaging. Surg Neurol 1990;34:107–110.
352 A. LELLOUCH-TUBIANA ET AL.




















